User login
FDA panel rejects implanted GLP1-RA dosing device for T2D
Sept. 21 from an advisory committee of the Food and Drug Administration.
The 19 voting panel members mostly cited concerning signals of both renal toxicity in the form of excess episodes of acute kidney injury (AKI) as well as increased cardiovascular events compared with placebo as their main reasons for voting that the developing company, Intarcia Therapeutics, had not shown adequate evidence that the benefits of the drug-device combination, known as ITCA 650, outweighed its risks for treating people with type 2 diabetes.
“I’m quite uncomfortable with the AKI safety,” said panel member Erica Brittain, PhD, deputy chief of the Biostatistics Research Branch of the National Institute of Allergy and Infectious Diseases in Bethesda, Md.
The case that ITCA 650 is ready for routine use was also undermined by uncertainty documented by FDA staff about the uniformity and reliability of exenatide delivery by the DUROS device, a matchstick-sized reservoir that’s placed subcutaneously and designed to deliver exenatide continuously for 6 months at a time, noted Cecilia C. Low Wang, MD, chair of the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee.
“No evidence of improved adherence”
Another shortcoming was no data on the impact that this form of drug delivery, first developed and FDA approved to treat patients with prostate cancer with leuprolide acetate, really accomplished its goal of improving adherence to a glycemic-control agent. Intarcia Therapeutics presented “no evidence of improved adherence,” said Dr. Low Wang, director of the Glucose Management Team at the University of Colorado Hospital.
However, she and several other panel members acknowledged the compelling comments from several patients and health care professionals experienced in using or administering the device who, during the public comment period, voiced anecdotal testimonials to its positive impact on treatment compliance.
Seven years of FDA review
This review of ITCA 650 capped a nearly 7-year effort by Intarcia Therapeutics to receive marketing approval for ITCA 650 from the FDA, which began with an application filed in November 2016 (and denied by the agency in September 2017). Intarcia resubmitted an amended application in 2019 that the FDA again rejected in 2020. The company’s persistence following that led to the current panel meeting, the first time the ITCA 650 evidence came before an advisory panel.
Committee members in general praised the concept of managing blood glucose by continuous release of a medication 6 months at a time. They also offered ideas on a path forward, such as a study that used an active competitor. Ideally, that could be another agent from the same class of GLP-1 receptor agonists such as Bydureon, an injected formulation of exenatide administered by subcutaneous injection once a week.
But the key, agreed panel members, was to bulk up the evidence that ITCA 650 is safe. “The data show concerning safety signals that need further investigation,” summed up Dr. Low Wong. “There are concerns about overall safety, all-cause mortality, AKI, cardiovascular events, and glycemic excursions.”
All voting members of the advisory committee met the FDA’s standard for having no relevant financial relationships.
A version of this article appeared on Medscape.com.
Sept. 21 from an advisory committee of the Food and Drug Administration.
The 19 voting panel members mostly cited concerning signals of both renal toxicity in the form of excess episodes of acute kidney injury (AKI) as well as increased cardiovascular events compared with placebo as their main reasons for voting that the developing company, Intarcia Therapeutics, had not shown adequate evidence that the benefits of the drug-device combination, known as ITCA 650, outweighed its risks for treating people with type 2 diabetes.
“I’m quite uncomfortable with the AKI safety,” said panel member Erica Brittain, PhD, deputy chief of the Biostatistics Research Branch of the National Institute of Allergy and Infectious Diseases in Bethesda, Md.
The case that ITCA 650 is ready for routine use was also undermined by uncertainty documented by FDA staff about the uniformity and reliability of exenatide delivery by the DUROS device, a matchstick-sized reservoir that’s placed subcutaneously and designed to deliver exenatide continuously for 6 months at a time, noted Cecilia C. Low Wang, MD, chair of the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee.
“No evidence of improved adherence”
Another shortcoming was no data on the impact that this form of drug delivery, first developed and FDA approved to treat patients with prostate cancer with leuprolide acetate, really accomplished its goal of improving adherence to a glycemic-control agent. Intarcia Therapeutics presented “no evidence of improved adherence,” said Dr. Low Wang, director of the Glucose Management Team at the University of Colorado Hospital.
However, she and several other panel members acknowledged the compelling comments from several patients and health care professionals experienced in using or administering the device who, during the public comment period, voiced anecdotal testimonials to its positive impact on treatment compliance.
Seven years of FDA review
This review of ITCA 650 capped a nearly 7-year effort by Intarcia Therapeutics to receive marketing approval for ITCA 650 from the FDA, which began with an application filed in November 2016 (and denied by the agency in September 2017). Intarcia resubmitted an amended application in 2019 that the FDA again rejected in 2020. The company’s persistence following that led to the current panel meeting, the first time the ITCA 650 evidence came before an advisory panel.
Committee members in general praised the concept of managing blood glucose by continuous release of a medication 6 months at a time. They also offered ideas on a path forward, such as a study that used an active competitor. Ideally, that could be another agent from the same class of GLP-1 receptor agonists such as Bydureon, an injected formulation of exenatide administered by subcutaneous injection once a week.
But the key, agreed panel members, was to bulk up the evidence that ITCA 650 is safe. “The data show concerning safety signals that need further investigation,” summed up Dr. Low Wong. “There are concerns about overall safety, all-cause mortality, AKI, cardiovascular events, and glycemic excursions.”
All voting members of the advisory committee met the FDA’s standard for having no relevant financial relationships.
A version of this article appeared on Medscape.com.
Sept. 21 from an advisory committee of the Food and Drug Administration.
The 19 voting panel members mostly cited concerning signals of both renal toxicity in the form of excess episodes of acute kidney injury (AKI) as well as increased cardiovascular events compared with placebo as their main reasons for voting that the developing company, Intarcia Therapeutics, had not shown adequate evidence that the benefits of the drug-device combination, known as ITCA 650, outweighed its risks for treating people with type 2 diabetes.
“I’m quite uncomfortable with the AKI safety,” said panel member Erica Brittain, PhD, deputy chief of the Biostatistics Research Branch of the National Institute of Allergy and Infectious Diseases in Bethesda, Md.
The case that ITCA 650 is ready for routine use was also undermined by uncertainty documented by FDA staff about the uniformity and reliability of exenatide delivery by the DUROS device, a matchstick-sized reservoir that’s placed subcutaneously and designed to deliver exenatide continuously for 6 months at a time, noted Cecilia C. Low Wang, MD, chair of the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee.
“No evidence of improved adherence”
Another shortcoming was no data on the impact that this form of drug delivery, first developed and FDA approved to treat patients with prostate cancer with leuprolide acetate, really accomplished its goal of improving adherence to a glycemic-control agent. Intarcia Therapeutics presented “no evidence of improved adherence,” said Dr. Low Wang, director of the Glucose Management Team at the University of Colorado Hospital.
However, she and several other panel members acknowledged the compelling comments from several patients and health care professionals experienced in using or administering the device who, during the public comment period, voiced anecdotal testimonials to its positive impact on treatment compliance.
Seven years of FDA review
This review of ITCA 650 capped a nearly 7-year effort by Intarcia Therapeutics to receive marketing approval for ITCA 650 from the FDA, which began with an application filed in November 2016 (and denied by the agency in September 2017). Intarcia resubmitted an amended application in 2019 that the FDA again rejected in 2020. The company’s persistence following that led to the current panel meeting, the first time the ITCA 650 evidence came before an advisory panel.
Committee members in general praised the concept of managing blood glucose by continuous release of a medication 6 months at a time. They also offered ideas on a path forward, such as a study that used an active competitor. Ideally, that could be another agent from the same class of GLP-1 receptor agonists such as Bydureon, an injected formulation of exenatide administered by subcutaneous injection once a week.
But the key, agreed panel members, was to bulk up the evidence that ITCA 650 is safe. “The data show concerning safety signals that need further investigation,” summed up Dr. Low Wong. “There are concerns about overall safety, all-cause mortality, AKI, cardiovascular events, and glycemic excursions.”
All voting members of the advisory committee met the FDA’s standard for having no relevant financial relationships.
A version of this article appeared on Medscape.com.
Exercise timing may dictate obesity, type 2 diabetes risk
Tongyu Ma, PhD, research assistant professor with the Health Sciences Department, Franklin Pierce University, Rindge, N.H., and colleagues studied data on almost 5,300 individuals, finding a strong association between moderate to vigorous physical activity (MVPA) and obesity.
The research, published in Obesity, showed that people who exercised in the morning had a lower body mass index than that of those who exercised at other times, even though they were more sedentary.
For the second study, Chirag J. Patel, PhD, associate professor of biomedical informatics at Harvard Medical School, Boston, and colleagues examined more than 93,000 individuals and found that morning and afternoon, but not evening, exercise reduced the risk for type 2 diabetes.
However, the results, published in Diabetologia, also indicated that people who undertook at least MVPA were protected against developing type 2 diabetes no matter what time of day they exercised.
Along with considering the timing of exercise, the authors suggest that it is “helpful to include some higher intensity activity to help reduce the risk of developing diabetes and other cardiovascular disease.”
Morning exercisers perform less physical activity
Dr. Ma and colleagues noted that “although a beneficial association among the levels of physical activity with obesity has been frequently reported, the optimal timing of physical activity for decreasing obesity remains controversial.”
The researchers analyzed data from the National Health and Nutrition Examination Survey for the 2003-2004 and 2005-2006 cycles, because accelerometry was implemented in those periods.
They included 5,285 individuals aged ≥ 20 years who had physical activity measured via an accelerometer worn on the right hip during waking hours for 7 consecutive days.
The diurnal pattern of MVPA was classified into three clusters by the established technique of K-means clustering analysis: morning (n = 642), midday (n = 2,456), and evening (n = 2,187).
The association between MVPA, diurnal pattern, and obesity was then assessed in linear regression models taking into account a range of potential confounding factors.
Overall, participants in the morning cluster were older and more likely to be female than those in the other clusters (P < .001 for both). They were also more likely to be nonsmokers (P = .007) and to have less than high school education (P = .0041).
Morning cluster individuals performed less physical activity and were more sedentary than those in the midday and evening groups (P < .001 for both), although they were more likely to be healthy eaters (P = .004), with a lower calorie intake (P < .001).
Individuals in the morning cluster had, on average, a lower body mass index than those in other clusters, at 27.4 vs. 28.4 in the midday cluster and 28.2 in the evening cluster (P for interaction = .02).
Morning cluster participants also had a lower waist circumference than participants in the midday or evening cluster: 95.9 cm, 97.9 cm, and 97.3 cm, respectively (P for interaction = .06).
The team reported that there was a strong linear association between MVPA and obesity in the morning cluster, whereas there was a weaker curvilinear association in the midday and evening clusters.
“This is exciting new research that is consistent with a common tip for meeting exercise goals – that is, schedule exercise in the morning before emails, phone calls, or meetings that might distract you,” Rebecca Krukowski, PhD, professor, public health sciences, University of Virginia, Charlottesville, said in a release.
However, she noted that the cross-sectional nature of the study means that it is “not known whether people who exercise consistently in the morning may be systematically different from those who exercise at other times, in ways that were not measured in this study.
“For example, people who exercise regularly in the morning could have more predictable schedules, such as being less likely to be shift workers or less likely to have caregiving responsibilities that impede morning exercise,” said Dr. Krukowski, who was not involved in the study.
No association between evening activity and type 2 diabetes risk
In the second study, the team studied 93,095 persons in the UK Biobank, with a mean age of 62 years and no history of type 2 diabetes, who wore a wrist accelerometer for 1 week.
The movement data were used to estimate the metabolic equivalent of task, which was then summed into the total physical activity completed in the morning, afternoon, and evening and linked to the development of incident type 2 diabetes.
After adjustment for potential confounding factors, both morning and afternoon physical activity were associated with a reduced risk of developing type 2 diabetes, at hazard ratios of 0.90 (P = 7 × 10-8) and 0.91 (P = 1 × 10-5), respectively.
However, there was no association between evening activity and the risk for type 2 diabetes, at a hazard ratio of 0.95 (P = .07).
The team found, however, that MVPA and vigorous physical activity were associated with a reduced risk for type 2 diabetes at all times of day.
Dr. Patel’s study was supported in part by National Institutes of Health grants. No other funding was declared. No relevant financial relationships were declared.
A version of this article appeared on Medscape.com.
Tongyu Ma, PhD, research assistant professor with the Health Sciences Department, Franklin Pierce University, Rindge, N.H., and colleagues studied data on almost 5,300 individuals, finding a strong association between moderate to vigorous physical activity (MVPA) and obesity.
The research, published in Obesity, showed that people who exercised in the morning had a lower body mass index than that of those who exercised at other times, even though they were more sedentary.
For the second study, Chirag J. Patel, PhD, associate professor of biomedical informatics at Harvard Medical School, Boston, and colleagues examined more than 93,000 individuals and found that morning and afternoon, but not evening, exercise reduced the risk for type 2 diabetes.
However, the results, published in Diabetologia, also indicated that people who undertook at least MVPA were protected against developing type 2 diabetes no matter what time of day they exercised.
Along with considering the timing of exercise, the authors suggest that it is “helpful to include some higher intensity activity to help reduce the risk of developing diabetes and other cardiovascular disease.”
Morning exercisers perform less physical activity
Dr. Ma and colleagues noted that “although a beneficial association among the levels of physical activity with obesity has been frequently reported, the optimal timing of physical activity for decreasing obesity remains controversial.”
The researchers analyzed data from the National Health and Nutrition Examination Survey for the 2003-2004 and 2005-2006 cycles, because accelerometry was implemented in those periods.
They included 5,285 individuals aged ≥ 20 years who had physical activity measured via an accelerometer worn on the right hip during waking hours for 7 consecutive days.
The diurnal pattern of MVPA was classified into three clusters by the established technique of K-means clustering analysis: morning (n = 642), midday (n = 2,456), and evening (n = 2,187).
The association between MVPA, diurnal pattern, and obesity was then assessed in linear regression models taking into account a range of potential confounding factors.
Overall, participants in the morning cluster were older and more likely to be female than those in the other clusters (P < .001 for both). They were also more likely to be nonsmokers (P = .007) and to have less than high school education (P = .0041).
Morning cluster individuals performed less physical activity and were more sedentary than those in the midday and evening groups (P < .001 for both), although they were more likely to be healthy eaters (P = .004), with a lower calorie intake (P < .001).
Individuals in the morning cluster had, on average, a lower body mass index than those in other clusters, at 27.4 vs. 28.4 in the midday cluster and 28.2 in the evening cluster (P for interaction = .02).
Morning cluster participants also had a lower waist circumference than participants in the midday or evening cluster: 95.9 cm, 97.9 cm, and 97.3 cm, respectively (P for interaction = .06).
The team reported that there was a strong linear association between MVPA and obesity in the morning cluster, whereas there was a weaker curvilinear association in the midday and evening clusters.
“This is exciting new research that is consistent with a common tip for meeting exercise goals – that is, schedule exercise in the morning before emails, phone calls, or meetings that might distract you,” Rebecca Krukowski, PhD, professor, public health sciences, University of Virginia, Charlottesville, said in a release.
However, she noted that the cross-sectional nature of the study means that it is “not known whether people who exercise consistently in the morning may be systematically different from those who exercise at other times, in ways that were not measured in this study.
“For example, people who exercise regularly in the morning could have more predictable schedules, such as being less likely to be shift workers or less likely to have caregiving responsibilities that impede morning exercise,” said Dr. Krukowski, who was not involved in the study.
No association between evening activity and type 2 diabetes risk
In the second study, the team studied 93,095 persons in the UK Biobank, with a mean age of 62 years and no history of type 2 diabetes, who wore a wrist accelerometer for 1 week.
The movement data were used to estimate the metabolic equivalent of task, which was then summed into the total physical activity completed in the morning, afternoon, and evening and linked to the development of incident type 2 diabetes.
After adjustment for potential confounding factors, both morning and afternoon physical activity were associated with a reduced risk of developing type 2 diabetes, at hazard ratios of 0.90 (P = 7 × 10-8) and 0.91 (P = 1 × 10-5), respectively.
However, there was no association between evening activity and the risk for type 2 diabetes, at a hazard ratio of 0.95 (P = .07).
The team found, however, that MVPA and vigorous physical activity were associated with a reduced risk for type 2 diabetes at all times of day.
Dr. Patel’s study was supported in part by National Institutes of Health grants. No other funding was declared. No relevant financial relationships were declared.
A version of this article appeared on Medscape.com.
Tongyu Ma, PhD, research assistant professor with the Health Sciences Department, Franklin Pierce University, Rindge, N.H., and colleagues studied data on almost 5,300 individuals, finding a strong association between moderate to vigorous physical activity (MVPA) and obesity.
The research, published in Obesity, showed that people who exercised in the morning had a lower body mass index than that of those who exercised at other times, even though they were more sedentary.
For the second study, Chirag J. Patel, PhD, associate professor of biomedical informatics at Harvard Medical School, Boston, and colleagues examined more than 93,000 individuals and found that morning and afternoon, but not evening, exercise reduced the risk for type 2 diabetes.
However, the results, published in Diabetologia, also indicated that people who undertook at least MVPA were protected against developing type 2 diabetes no matter what time of day they exercised.
Along with considering the timing of exercise, the authors suggest that it is “helpful to include some higher intensity activity to help reduce the risk of developing diabetes and other cardiovascular disease.”
Morning exercisers perform less physical activity
Dr. Ma and colleagues noted that “although a beneficial association among the levels of physical activity with obesity has been frequently reported, the optimal timing of physical activity for decreasing obesity remains controversial.”
The researchers analyzed data from the National Health and Nutrition Examination Survey for the 2003-2004 and 2005-2006 cycles, because accelerometry was implemented in those periods.
They included 5,285 individuals aged ≥ 20 years who had physical activity measured via an accelerometer worn on the right hip during waking hours for 7 consecutive days.
The diurnal pattern of MVPA was classified into three clusters by the established technique of K-means clustering analysis: morning (n = 642), midday (n = 2,456), and evening (n = 2,187).
The association between MVPA, diurnal pattern, and obesity was then assessed in linear regression models taking into account a range of potential confounding factors.
Overall, participants in the morning cluster were older and more likely to be female than those in the other clusters (P < .001 for both). They were also more likely to be nonsmokers (P = .007) and to have less than high school education (P = .0041).
Morning cluster individuals performed less physical activity and were more sedentary than those in the midday and evening groups (P < .001 for both), although they were more likely to be healthy eaters (P = .004), with a lower calorie intake (P < .001).
Individuals in the morning cluster had, on average, a lower body mass index than those in other clusters, at 27.4 vs. 28.4 in the midday cluster and 28.2 in the evening cluster (P for interaction = .02).
Morning cluster participants also had a lower waist circumference than participants in the midday or evening cluster: 95.9 cm, 97.9 cm, and 97.3 cm, respectively (P for interaction = .06).
The team reported that there was a strong linear association between MVPA and obesity in the morning cluster, whereas there was a weaker curvilinear association in the midday and evening clusters.
“This is exciting new research that is consistent with a common tip for meeting exercise goals – that is, schedule exercise in the morning before emails, phone calls, or meetings that might distract you,” Rebecca Krukowski, PhD, professor, public health sciences, University of Virginia, Charlottesville, said in a release.
However, she noted that the cross-sectional nature of the study means that it is “not known whether people who exercise consistently in the morning may be systematically different from those who exercise at other times, in ways that were not measured in this study.
“For example, people who exercise regularly in the morning could have more predictable schedules, such as being less likely to be shift workers or less likely to have caregiving responsibilities that impede morning exercise,” said Dr. Krukowski, who was not involved in the study.
No association between evening activity and type 2 diabetes risk
In the second study, the team studied 93,095 persons in the UK Biobank, with a mean age of 62 years and no history of type 2 diabetes, who wore a wrist accelerometer for 1 week.
The movement data were used to estimate the metabolic equivalent of task, which was then summed into the total physical activity completed in the morning, afternoon, and evening and linked to the development of incident type 2 diabetes.
After adjustment for potential confounding factors, both morning and afternoon physical activity were associated with a reduced risk of developing type 2 diabetes, at hazard ratios of 0.90 (P = 7 × 10-8) and 0.91 (P = 1 × 10-5), respectively.
However, there was no association between evening activity and the risk for type 2 diabetes, at a hazard ratio of 0.95 (P = .07).
The team found, however, that MVPA and vigorous physical activity were associated with a reduced risk for type 2 diabetes at all times of day.
Dr. Patel’s study was supported in part by National Institutes of Health grants. No other funding was declared. No relevant financial relationships were declared.
A version of this article appeared on Medscape.com.
AAP advises against low-carb diets for children with diabetes
according to a new clinical report.
Citing a lack of high-quality data and potential for adverse effects with carbohydrate restriction among younger individuals, lead author Anna Neyman, MD, of Indiana University, Indianapolis, and colleagues suggested that pediatric patients with type 2 diabetes should focus on reducing nutrient-poor carbohydrate intake, while those with type 1 diabetes should only pursue broader carbohydrate restriction under close medical supervision.
“There are no guidelines for restricting dietary carbohydrate consumption to reduce risk for diabetes or improve diabetes outcomes in youth,” the investigators wrote in Pediatrics. “Thus, there is a need to provide practical recommendations for pediatricians regarding the use of low-carbohydrate diets in patients who elect to follow these diets, including those with type 1 diabetes and for patients with obesity, prediabetes, and type 2 diabetes.”
Their new report includes a summary of the various types of carbohydrate-restricted diets, a review of available evidence for these diets among pediatric patients with type 1 and type 2 diabetes, and several practical recommendations based on their findings.
Dr. Neyman and colleagues first noted a lack of standardization in describing the various tiers of carbohydrate restriction; however, they offered some rough guidelines. Compared with a typical, balanced diet, which includes 45%-65% of calories from carbohydrates, a moderately restrictive diet includes 26%-44% of calories from carbohydrates, while a low-carb diet includes less than 26% of calories from carbs. Further down the scale, very low-carb diets and ketogenic diets call for 20-50 g of carbs per day or less than 20 g of carbs per day, respectively.
“There is evidence from adult studies that these diets can be associated with significant weight loss, reduction in insulin levels or insulin requirements, and improvement in glucose control,” the investigators noted. “Nevertheless, there is a lack of long-term safety and efficacy outcomes in youth.”
They went on to cite a range of safety concerns, including “growth deceleration, nutritional deficiencies, poor bone health, nutritional ketosis that cannot be distinguished from ketosis resulting from insulin deficiency, and disordered eating behaviors.”
“Body dissatisfaction associated with restrictive dieting practices places children and adolescents at risk for inadequate dietary intake, excessive weight gain resulting from binge-eating after restricting food intake, and use of harmful weight-control strategies,” the investigators wrote. “Moreover, restrictive dieting practices may negatively impact mental health and self-concept and are directly associated with decreased mood and increased feelings of anxiety.”
Until more evidence is available, Dr. Neyman and colleagues advised adherence to a balanced diet, including increased dietary fiber and reduced consumption of ultra-processed carbohydrates.
“Eliminating sugary beverages and juices significantly improves blood glucose and weight management in children and adolescents,” they noted.
For pediatric patients with type 1 diabetes, the investigators suggested that low-carb and very low-carb diets should only be pursued “under close diabetes care team supervision utilizing safety guidelines.”
Lack of evidence is the problem
David Ludwig, MD, PhD, codirector of the New Balance Foundation Obesity Prevention Center, Boston Children’s Hospital, and professor of pediatrics at Harvard Medical School, also in Boston, said the review is “rather general” and “reiterates common, although not always fair, concerns about carbohydrate restriction.”

“The main issue they highlight is the lack of evidence, especially from clinical trials, for a low-carbohydrate diet in children, as related to diabetes,” Dr. Ludwig said in a written comment, noting that this is indeed an issue. “However, what needs to be recognized is that a conventional high-carbohydrate diet has never been shown to be superior in adults or children for diabetes. Furthermore, whereas a poorly formulated low-carb diet may have adverse effects and risks (e.g., nutrient deficiencies), so can a high-carbohydrate diet – including an increase in triglycerides and other risk factors comprising metabolic syndrome.”
He said that the “main challenge in diabetes is to control blood glucose after eating,” and a high-carb makes this more difficult, as it requires more insulin after a meal than a low-carb meal would require, and increases risk of subsequent hypoglycemia.
For those interested in an alternative perspective to the AAP clinical report, Dr. Ludwig recommended two of his recent review articles, including one published in the Journal of Nutrition and another from the Journal of Clinical Investigation. In both, notes the long history of carbohydrate restriction for patients with diabetes, with usage dating back to the 1700s. Although the diet fell out of favor with the introduction of insulin, Dr. Ludwig believes that it needs to be reconsidered, and is more than a passing fad.
“Preliminary research suggests that this dietary approach might transform clinical management and perhaps normalize HbA1c for many people with diabetes, at substantially reduced treatment costs,” Dr. Ludwig and colleagues wrote in the JCI review. “High-quality randomized controlled trials, with intensive support for behavior changes, will be needed to address this possibility and assess long-term safety and sustainability. With total medical costs of diabetes in the United States approaching $1 billion a day, this research must assume high priority.”
This clinical report was commissioned by the AAP. Dr. Ludwig received royalties for books that recommend a carbohydrate-modified diet.
This article was updated 9/20/23.
according to a new clinical report.
Citing a lack of high-quality data and potential for adverse effects with carbohydrate restriction among younger individuals, lead author Anna Neyman, MD, of Indiana University, Indianapolis, and colleagues suggested that pediatric patients with type 2 diabetes should focus on reducing nutrient-poor carbohydrate intake, while those with type 1 diabetes should only pursue broader carbohydrate restriction under close medical supervision.
“There are no guidelines for restricting dietary carbohydrate consumption to reduce risk for diabetes or improve diabetes outcomes in youth,” the investigators wrote in Pediatrics. “Thus, there is a need to provide practical recommendations for pediatricians regarding the use of low-carbohydrate diets in patients who elect to follow these diets, including those with type 1 diabetes and for patients with obesity, prediabetes, and type 2 diabetes.”
Their new report includes a summary of the various types of carbohydrate-restricted diets, a review of available evidence for these diets among pediatric patients with type 1 and type 2 diabetes, and several practical recommendations based on their findings.
Dr. Neyman and colleagues first noted a lack of standardization in describing the various tiers of carbohydrate restriction; however, they offered some rough guidelines. Compared with a typical, balanced diet, which includes 45%-65% of calories from carbohydrates, a moderately restrictive diet includes 26%-44% of calories from carbohydrates, while a low-carb diet includes less than 26% of calories from carbs. Further down the scale, very low-carb diets and ketogenic diets call for 20-50 g of carbs per day or less than 20 g of carbs per day, respectively.
“There is evidence from adult studies that these diets can be associated with significant weight loss, reduction in insulin levels or insulin requirements, and improvement in glucose control,” the investigators noted. “Nevertheless, there is a lack of long-term safety and efficacy outcomes in youth.”
They went on to cite a range of safety concerns, including “growth deceleration, nutritional deficiencies, poor bone health, nutritional ketosis that cannot be distinguished from ketosis resulting from insulin deficiency, and disordered eating behaviors.”
“Body dissatisfaction associated with restrictive dieting practices places children and adolescents at risk for inadequate dietary intake, excessive weight gain resulting from binge-eating after restricting food intake, and use of harmful weight-control strategies,” the investigators wrote. “Moreover, restrictive dieting practices may negatively impact mental health and self-concept and are directly associated with decreased mood and increased feelings of anxiety.”
Until more evidence is available, Dr. Neyman and colleagues advised adherence to a balanced diet, including increased dietary fiber and reduced consumption of ultra-processed carbohydrates.
“Eliminating sugary beverages and juices significantly improves blood glucose and weight management in children and adolescents,” they noted.
For pediatric patients with type 1 diabetes, the investigators suggested that low-carb and very low-carb diets should only be pursued “under close diabetes care team supervision utilizing safety guidelines.”
Lack of evidence is the problem
David Ludwig, MD, PhD, codirector of the New Balance Foundation Obesity Prevention Center, Boston Children’s Hospital, and professor of pediatrics at Harvard Medical School, also in Boston, said the review is “rather general” and “reiterates common, although not always fair, concerns about carbohydrate restriction.”
“The main issue they highlight is the lack of evidence, especially from clinical trials, for a low-carbohydrate diet in children, as related to diabetes,” Dr. Ludwig said in a written comment, noting that this is indeed an issue. “However, what needs to be recognized is that a conventional high-carbohydrate diet has never been shown to be superior in adults or children for diabetes. Furthermore, whereas a poorly formulated low-carb diet may have adverse effects and risks (e.g., nutrient deficiencies), so can a high-carbohydrate diet – including an increase in triglycerides and other risk factors comprising metabolic syndrome.”
He said that the “main challenge in diabetes is to control blood glucose after eating,” and a high-carb makes this more difficult, as it requires more insulin after a meal than a low-carb meal would require, and increases risk of subsequent hypoglycemia.
For those interested in an alternative perspective to the AAP clinical report, Dr. Ludwig recommended two of his recent review articles, including one published in the Journal of Nutrition and another from the Journal of Clinical Investigation. In both, notes the long history of carbohydrate restriction for patients with diabetes, with usage dating back to the 1700s. Although the diet fell out of favor with the introduction of insulin, Dr. Ludwig believes that it needs to be reconsidered, and is more than a passing fad.
“Preliminary research suggests that this dietary approach might transform clinical management and perhaps normalize HbA1c for many people with diabetes, at substantially reduced treatment costs,” Dr. Ludwig and colleagues wrote in the JCI review. “High-quality randomized controlled trials, with intensive support for behavior changes, will be needed to address this possibility and assess long-term safety and sustainability. With total medical costs of diabetes in the United States approaching $1 billion a day, this research must assume high priority.”
This clinical report was commissioned by the AAP. Dr. Ludwig received royalties for books that recommend a carbohydrate-modified diet.
This article was updated 9/20/23.
according to a new clinical report.
Citing a lack of high-quality data and potential for adverse effects with carbohydrate restriction among younger individuals, lead author Anna Neyman, MD, of Indiana University, Indianapolis, and colleagues suggested that pediatric patients with type 2 diabetes should focus on reducing nutrient-poor carbohydrate intake, while those with type 1 diabetes should only pursue broader carbohydrate restriction under close medical supervision.
“There are no guidelines for restricting dietary carbohydrate consumption to reduce risk for diabetes or improve diabetes outcomes in youth,” the investigators wrote in Pediatrics. “Thus, there is a need to provide practical recommendations for pediatricians regarding the use of low-carbohydrate diets in patients who elect to follow these diets, including those with type 1 diabetes and for patients with obesity, prediabetes, and type 2 diabetes.”
Their new report includes a summary of the various types of carbohydrate-restricted diets, a review of available evidence for these diets among pediatric patients with type 1 and type 2 diabetes, and several practical recommendations based on their findings.
Dr. Neyman and colleagues first noted a lack of standardization in describing the various tiers of carbohydrate restriction; however, they offered some rough guidelines. Compared with a typical, balanced diet, which includes 45%-65% of calories from carbohydrates, a moderately restrictive diet includes 26%-44% of calories from carbohydrates, while a low-carb diet includes less than 26% of calories from carbs. Further down the scale, very low-carb diets and ketogenic diets call for 20-50 g of carbs per day or less than 20 g of carbs per day, respectively.
“There is evidence from adult studies that these diets can be associated with significant weight loss, reduction in insulin levels or insulin requirements, and improvement in glucose control,” the investigators noted. “Nevertheless, there is a lack of long-term safety and efficacy outcomes in youth.”
They went on to cite a range of safety concerns, including “growth deceleration, nutritional deficiencies, poor bone health, nutritional ketosis that cannot be distinguished from ketosis resulting from insulin deficiency, and disordered eating behaviors.”
“Body dissatisfaction associated with restrictive dieting practices places children and adolescents at risk for inadequate dietary intake, excessive weight gain resulting from binge-eating after restricting food intake, and use of harmful weight-control strategies,” the investigators wrote. “Moreover, restrictive dieting practices may negatively impact mental health and self-concept and are directly associated with decreased mood and increased feelings of anxiety.”
Until more evidence is available, Dr. Neyman and colleagues advised adherence to a balanced diet, including increased dietary fiber and reduced consumption of ultra-processed carbohydrates.
“Eliminating sugary beverages and juices significantly improves blood glucose and weight management in children and adolescents,” they noted.
For pediatric patients with type 1 diabetes, the investigators suggested that low-carb and very low-carb diets should only be pursued “under close diabetes care team supervision utilizing safety guidelines.”
Lack of evidence is the problem
David Ludwig, MD, PhD, codirector of the New Balance Foundation Obesity Prevention Center, Boston Children’s Hospital, and professor of pediatrics at Harvard Medical School, also in Boston, said the review is “rather general” and “reiterates common, although not always fair, concerns about carbohydrate restriction.”
“The main issue they highlight is the lack of evidence, especially from clinical trials, for a low-carbohydrate diet in children, as related to diabetes,” Dr. Ludwig said in a written comment, noting that this is indeed an issue. “However, what needs to be recognized is that a conventional high-carbohydrate diet has never been shown to be superior in adults or children for diabetes. Furthermore, whereas a poorly formulated low-carb diet may have adverse effects and risks (e.g., nutrient deficiencies), so can a high-carbohydrate diet – including an increase in triglycerides and other risk factors comprising metabolic syndrome.”
He said that the “main challenge in diabetes is to control blood glucose after eating,” and a high-carb makes this more difficult, as it requires more insulin after a meal than a low-carb meal would require, and increases risk of subsequent hypoglycemia.
For those interested in an alternative perspective to the AAP clinical report, Dr. Ludwig recommended two of his recent review articles, including one published in the Journal of Nutrition and another from the Journal of Clinical Investigation. In both, notes the long history of carbohydrate restriction for patients with diabetes, with usage dating back to the 1700s. Although the diet fell out of favor with the introduction of insulin, Dr. Ludwig believes that it needs to be reconsidered, and is more than a passing fad.
“Preliminary research suggests that this dietary approach might transform clinical management and perhaps normalize HbA1c for many people with diabetes, at substantially reduced treatment costs,” Dr. Ludwig and colleagues wrote in the JCI review. “High-quality randomized controlled trials, with intensive support for behavior changes, will be needed to address this possibility and assess long-term safety and sustainability. With total medical costs of diabetes in the United States approaching $1 billion a day, this research must assume high priority.”
This clinical report was commissioned by the AAP. Dr. Ludwig received royalties for books that recommend a carbohydrate-modified diet.
This article was updated 9/20/23.
FROM PEDIATRICS
Screening finds high rates of CVD in diabetes, COPD patients
AMSTERDAM – , compared with usual care, in a Dutch study involving more than 1,200 people and 25 primary care practices.
Scaling up this program to larger populations could potentially uncover huge numbers of currently unrecognized people with CVD given the large number of adults with type 2 diabetes plus those with COPD, Amy Groenewegen, MD, said at the annual congress of the European Society of Cardiology.
“I think this screening is ready for routine use, but it could be followed by prospective studies that investigate whether it produces more benefits in patient-centered outcomes,” Dr. Groenewegen said in a press briefing. She stressed that it has not yet been clearly proven that patients with these chronic diseases are better off long term when their CVD is detected sooner using the tested approach.
“We need simple ways to identify relevant patients for additional screening and potential treatment” of CVD, commented Lars Kober, MD, designated discussant at the Congress and a cardiologist and professor at Rigshospitalet, Copenhagen University Hospital.
A ‘very simple’ symptom questionnaire
The study is important because it tested a “very simple” symptom questionnaire as the initial screening phase, yet resulted in a CVD diagnostic rate that was two- to threefold higher than in the control patients managed with usual care, Dr. Kober noted.
The Reviving the Early Diagnosis of CVD (RED-CVD) trial randomized 14 primary care practices in the Netherlands to apply a structured screening protocol to adults with type 2 diabetes or COPD, and another 11 practices that served as controls and provided their patients with usual care.
The study included 624 people in the screening arm and 592 in the usual-care arm. Their average age was about 68 years. In the screening arm, 87% had type 2 diabetes and 20% had COPD, including 6.3% with both. In the usual-care arm, 86% had type 2 diabetes, 21% had COPD, with 7.4% having both.
About a quarter of the study cohort had a history of a CVD diagnosis, but they were included for their potential for developing another form of CVD. The study considered three types of CVD: coronary artery disease, heart failure, and atrial fibrillation.
The CVD screening protocol began with an 11-question survey, completed by patients, that asked about their symptoms. The survey was devised by a research team at the University Medical Center Groningen, the Netherlands, who collaborated on the study.
The second phase for people who had suggestive symptoms was a physical examination, measurement of serum N-terminal pro-brain natriuretic peptide (elevated levels signal incident heart failure), and an ECG. People who continued to show findings consistent with CVD in this phase were then referred on a discretionary basis by the attending physician to a specialist.
More than doubling the CVD diagnosis rate
The screening program produced a total of 50 new CVD diagnoses in the screening cohort (8%) and 18 in the control, usual-care arm (3%), for the study’s primary endpoint. The greatest number of events involved heart failure, followed by coronary disease.
The screening questionnaire identified 70% of the people who completed it with suggestive symptoms, such as shortness of breath, claudication, or palpitations. The follow-up assessments of phase two narrowed the group with possible new CVD down to 44% of the people in this arm, and the participating physicians referred 39% to a specialist.
An analysis that adjusted for several demographic and clinical variables and excluded nonobstructive coronary disease as a new CVD diagnosis showed that the systematic screening approach resulted in 2.4-fold more new diagnoses than usual care, reported Dr. Groenewegen, an epidemiologist at University Medical Center Utrecht, the Netherlands.
RED-CVD received no commercial funding. Dr. Groenewegen disclosed no relevant financial relationships. Dr. Kober has received honoraria from AstraZeneca, Bayer, Boehringer Ingelheim, Novartis, and Novo Nordisk.
A version of this article first appeared on Medscape.com.
AMSTERDAM – , compared with usual care, in a Dutch study involving more than 1,200 people and 25 primary care practices.
Scaling up this program to larger populations could potentially uncover huge numbers of currently unrecognized people with CVD given the large number of adults with type 2 diabetes plus those with COPD, Amy Groenewegen, MD, said at the annual congress of the European Society of Cardiology.
“I think this screening is ready for routine use, but it could be followed by prospective studies that investigate whether it produces more benefits in patient-centered outcomes,” Dr. Groenewegen said in a press briefing. She stressed that it has not yet been clearly proven that patients with these chronic diseases are better off long term when their CVD is detected sooner using the tested approach.
“We need simple ways to identify relevant patients for additional screening and potential treatment” of CVD, commented Lars Kober, MD, designated discussant at the Congress and a cardiologist and professor at Rigshospitalet, Copenhagen University Hospital.
A ‘very simple’ symptom questionnaire
The study is important because it tested a “very simple” symptom questionnaire as the initial screening phase, yet resulted in a CVD diagnostic rate that was two- to threefold higher than in the control patients managed with usual care, Dr. Kober noted.
The Reviving the Early Diagnosis of CVD (RED-CVD) trial randomized 14 primary care practices in the Netherlands to apply a structured screening protocol to adults with type 2 diabetes or COPD, and another 11 practices that served as controls and provided their patients with usual care.
The study included 624 people in the screening arm and 592 in the usual-care arm. Their average age was about 68 years. In the screening arm, 87% had type 2 diabetes and 20% had COPD, including 6.3% with both. In the usual-care arm, 86% had type 2 diabetes, 21% had COPD, with 7.4% having both.
About a quarter of the study cohort had a history of a CVD diagnosis, but they were included for their potential for developing another form of CVD. The study considered three types of CVD: coronary artery disease, heart failure, and atrial fibrillation.
The CVD screening protocol began with an 11-question survey, completed by patients, that asked about their symptoms. The survey was devised by a research team at the University Medical Center Groningen, the Netherlands, who collaborated on the study.
The second phase for people who had suggestive symptoms was a physical examination, measurement of serum N-terminal pro-brain natriuretic peptide (elevated levels signal incident heart failure), and an ECG. People who continued to show findings consistent with CVD in this phase were then referred on a discretionary basis by the attending physician to a specialist.
More than doubling the CVD diagnosis rate
The screening program produced a total of 50 new CVD diagnoses in the screening cohort (8%) and 18 in the control, usual-care arm (3%), for the study’s primary endpoint. The greatest number of events involved heart failure, followed by coronary disease.
The screening questionnaire identified 70% of the people who completed it with suggestive symptoms, such as shortness of breath, claudication, or palpitations. The follow-up assessments of phase two narrowed the group with possible new CVD down to 44% of the people in this arm, and the participating physicians referred 39% to a specialist.
An analysis that adjusted for several demographic and clinical variables and excluded nonobstructive coronary disease as a new CVD diagnosis showed that the systematic screening approach resulted in 2.4-fold more new diagnoses than usual care, reported Dr. Groenewegen, an epidemiologist at University Medical Center Utrecht, the Netherlands.
RED-CVD received no commercial funding. Dr. Groenewegen disclosed no relevant financial relationships. Dr. Kober has received honoraria from AstraZeneca, Bayer, Boehringer Ingelheim, Novartis, and Novo Nordisk.
A version of this article first appeared on Medscape.com.
AMSTERDAM – , compared with usual care, in a Dutch study involving more than 1,200 people and 25 primary care practices.
Scaling up this program to larger populations could potentially uncover huge numbers of currently unrecognized people with CVD given the large number of adults with type 2 diabetes plus those with COPD, Amy Groenewegen, MD, said at the annual congress of the European Society of Cardiology.
“I think this screening is ready for routine use, but it could be followed by prospective studies that investigate whether it produces more benefits in patient-centered outcomes,” Dr. Groenewegen said in a press briefing. She stressed that it has not yet been clearly proven that patients with these chronic diseases are better off long term when their CVD is detected sooner using the tested approach.
“We need simple ways to identify relevant patients for additional screening and potential treatment” of CVD, commented Lars Kober, MD, designated discussant at the Congress and a cardiologist and professor at Rigshospitalet, Copenhagen University Hospital.
A ‘very simple’ symptom questionnaire
The study is important because it tested a “very simple” symptom questionnaire as the initial screening phase, yet resulted in a CVD diagnostic rate that was two- to threefold higher than in the control patients managed with usual care, Dr. Kober noted.
The Reviving the Early Diagnosis of CVD (RED-CVD) trial randomized 14 primary care practices in the Netherlands to apply a structured screening protocol to adults with type 2 diabetes or COPD, and another 11 practices that served as controls and provided their patients with usual care.
The study included 624 people in the screening arm and 592 in the usual-care arm. Their average age was about 68 years. In the screening arm, 87% had type 2 diabetes and 20% had COPD, including 6.3% with both. In the usual-care arm, 86% had type 2 diabetes, 21% had COPD, with 7.4% having both.
About a quarter of the study cohort had a history of a CVD diagnosis, but they were included for their potential for developing another form of CVD. The study considered three types of CVD: coronary artery disease, heart failure, and atrial fibrillation.
The CVD screening protocol began with an 11-question survey, completed by patients, that asked about their symptoms. The survey was devised by a research team at the University Medical Center Groningen, the Netherlands, who collaborated on the study.
The second phase for people who had suggestive symptoms was a physical examination, measurement of serum N-terminal pro-brain natriuretic peptide (elevated levels signal incident heart failure), and an ECG. People who continued to show findings consistent with CVD in this phase were then referred on a discretionary basis by the attending physician to a specialist.
More than doubling the CVD diagnosis rate
The screening program produced a total of 50 new CVD diagnoses in the screening cohort (8%) and 18 in the control, usual-care arm (3%), for the study’s primary endpoint. The greatest number of events involved heart failure, followed by coronary disease.
The screening questionnaire identified 70% of the people who completed it with suggestive symptoms, such as shortness of breath, claudication, or palpitations. The follow-up assessments of phase two narrowed the group with possible new CVD down to 44% of the people in this arm, and the participating physicians referred 39% to a specialist.
An analysis that adjusted for several demographic and clinical variables and excluded nonobstructive coronary disease as a new CVD diagnosis showed that the systematic screening approach resulted in 2.4-fold more new diagnoses than usual care, reported Dr. Groenewegen, an epidemiologist at University Medical Center Utrecht, the Netherlands.
RED-CVD received no commercial funding. Dr. Groenewegen disclosed no relevant financial relationships. Dr. Kober has received honoraria from AstraZeneca, Bayer, Boehringer Ingelheim, Novartis, and Novo Nordisk.
A version of this article first appeared on Medscape.com.
AT ESC CONGRESS 2023
FDA clears new capabilities for diabetes app BlueStar
The latest clearance, announced on Aug. 23, enables the app-based platform to provide bolus insulin dose recommendations that are based on glucose and trend data from a compatible continuous glucose monitoring (CGM) device. On Aug. 15, the FDA cleared the BlueStar to use connected insulin dosing data in personalized bolus insulin dosing recommendations.
“Welldoc is the first company to receive clearance for a CGM-informed bolus calculator specifically designed for adults who manage their diabetes with multiple daily injections of insulin,” according to a company statement.
“With this clearance, Welldoc is filling a significant gap for people who require complex insulin regimens. By connecting directly with CGM data and using both glucose values and trend arrows, the BlueStar solution will provide precise and in-the-moment insulin dosing guidance directly to individuals, helping them reach their glucose targets,” endocrinologist Grazia Aleppo, MD, of Northwestern University, Chicago, said in the statement.
The new features extend the platform’s existing digital diet and lifestyle coaching capabilities. Previous FDA clearances included expansions to use most types of available insulins, including bolus and premixed insulin titration for patients with type 2 diabetes, in September 2021 and for basal insulin adjustment in June 2020.
Dr. Aleppo was a principal investigator in Welldoc’s clinical validation study for BlueStar.
A version of this article first appeared on Medscape.com.
The latest clearance, announced on Aug. 23, enables the app-based platform to provide bolus insulin dose recommendations that are based on glucose and trend data from a compatible continuous glucose monitoring (CGM) device. On Aug. 15, the FDA cleared the BlueStar to use connected insulin dosing data in personalized bolus insulin dosing recommendations.
“Welldoc is the first company to receive clearance for a CGM-informed bolus calculator specifically designed for adults who manage their diabetes with multiple daily injections of insulin,” according to a company statement.
“With this clearance, Welldoc is filling a significant gap for people who require complex insulin regimens. By connecting directly with CGM data and using both glucose values and trend arrows, the BlueStar solution will provide precise and in-the-moment insulin dosing guidance directly to individuals, helping them reach their glucose targets,” endocrinologist Grazia Aleppo, MD, of Northwestern University, Chicago, said in the statement.
The new features extend the platform’s existing digital diet and lifestyle coaching capabilities. Previous FDA clearances included expansions to use most types of available insulins, including bolus and premixed insulin titration for patients with type 2 diabetes, in September 2021 and for basal insulin adjustment in June 2020.
Dr. Aleppo was a principal investigator in Welldoc’s clinical validation study for BlueStar.
A version of this article first appeared on Medscape.com.
The latest clearance, announced on Aug. 23, enables the app-based platform to provide bolus insulin dose recommendations that are based on glucose and trend data from a compatible continuous glucose monitoring (CGM) device. On Aug. 15, the FDA cleared the BlueStar to use connected insulin dosing data in personalized bolus insulin dosing recommendations.
“Welldoc is the first company to receive clearance for a CGM-informed bolus calculator specifically designed for adults who manage their diabetes with multiple daily injections of insulin,” according to a company statement.
“With this clearance, Welldoc is filling a significant gap for people who require complex insulin regimens. By connecting directly with CGM data and using both glucose values and trend arrows, the BlueStar solution will provide precise and in-the-moment insulin dosing guidance directly to individuals, helping them reach their glucose targets,” endocrinologist Grazia Aleppo, MD, of Northwestern University, Chicago, said in the statement.
The new features extend the platform’s existing digital diet and lifestyle coaching capabilities. Previous FDA clearances included expansions to use most types of available insulins, including bolus and premixed insulin titration for patients with type 2 diabetes, in September 2021 and for basal insulin adjustment in June 2020.
Dr. Aleppo was a principal investigator in Welldoc’s clinical validation study for BlueStar.
A version of this article first appeared on Medscape.com.
Even an hour’s walk a week lowers risk in type 2 diabetes
although the impact on retinopathy is weaker, reveals a cohort study of U.K. individuals.
The research, based on data from more than 18,000 participants in the U.K. Biobank, suggests that the minimal level of self-reported activity to reduce the risk for both neuropathy and nephropathy may be the equivalent of less than 1.5 hours of walking per week.
The results are “encouraging and reassuring for both physicians and patients,” lead author Frederik P.B. Kristensen, MSc, PhD student, department of clinical epidemiology, Aarhus (Denmark) University, said in an interview.

“Our findings are particularly promising for neuropathy since, currently, no disease-modifying treatment exists, and there are limited preventive strategies available.”
Mr. Kristensen highlighted that “most diabetes research has focused on all-cause mortality and macrovascular complications. In the current study, we also found the same pattern for microvascular complications: Even small amounts of physical activity will benefit your health status.”
The minimal level of activity they identified, he said, is also an “achievable [goal] for most type 2 diabetes patients.”
Mr. Kristensen added, however, that the study was limited by excluding individuals with limited mobility and those living in temporary accommodation or care homes.
And prospective studies are required to determine the dose-response relationship between total, not just leisure-time, activity – ideally measured objectively – and risk for microvascular complications, he observed.
The research was published recently in Diabetes Care.
Impact of exercise on microvascular complications in T2D has been uncertain
The authors point out that microvascular complications – such as nerve damage (neuropathy), kidney problems (nephropathy), and eye complications (retinopathy) – occur in more than 50% of individuals with type 2 diabetes and have a “substantial impact” on quality of life, on top of the impact of macrovascular complications (such as cardiovascular disease), disability, and mortality.
Although physical activity is seen as a “cornerstone in the multifactorial management of type 2 diabetes because of its beneficial effects on metabolic risk factors,” the impact on microvascular complications is “uncertain” and the evidence is limited and “conflicting.”
The researchers therefore sought to examine the dose-response association, including the minimal effective level, between leisure-time physical activity and neuropathy, nephropathy, and retinopathy.
They conducted a cohort study of individuals aged 37-82 years from the U.K. Biobank who had type 2 diabetes, which was identified using the Eastwood algorithm and/or an A1c greater than or equal to 48 mmol/mol (6.5%).
Individuals with type 1 diabetes or gestational diabetes were excluded, as were those with major disabling somatic disorders, neurodegenerative diseases, and mental disorders, among others.
Leisure-time physical activity was based on the self-reported frequency, duration, and types of physical activities and was combined to calculate the total leisure time activity in MET-hours per week.
Using the American Diabetes Association/World Health Organization recommendations of 150-300 minutes of moderate to vigorous leisure-time physical activity per week, the researchers determined the recommended moderate activity level to be 150 minutes, (equivalent to 2.5 hours, or 7.5 MET-hours per week).
In all, 18,092 individuals with type 2 diabetes were included in the analysis, of whom 37% were women. The mean age was 60 years.
Ten percent of participants performed no leisure-time physical activity, 38% performed activity below the threshold for moderate activity, 20% performed at the recommended level, and 32% were more active.
Those performing no physical activity were more likely to be women, to be younger, to have a higher body mass index, and to have a greater average A1c, as well as have a more unfavorable sociodemographic and behavioral profile.
Over a median follow-up of 12.1 years, 3.7% of the participants were diagnosed with neuropathy, 10.2% with nephropathy, and 11.7% with retinopathy, equating to an incidence per 1,000 person-years of 3.5, 9,8, and 11.4, respectively.
The researchers found that any level of physical activity was associated with an approximate reduction in the risk for neuropathy and nephropathy.
Multivariate analysis indicated that, compared with no physical activity, activity below the recommended level was associated with an adjusted hazard ratio (aHR) for neuropathy of 0.71, whereas the aHR for activity at the recommended level was 0.73 and that for activity above the recommended level was 0.67.
The aHR for nephropathy, compared with no physical activity, was 0.79 for activity below the recommended level, 0.80 for activity at the recommended level, and 0.80 for activity above the recommended level.
The association between physical activity and retinopathy was weaker, however, at aHRs of 0.91, 0.91, and 0.98 for activity below, at, and above the recommended level, respectively.
The researchers suggest that this lower association could be due to differences in the etiology of the different forms of microvascular complications.
Hyperglycemia is the key driver in the development of retinopathy, they note, whereas other metabolic risk factors, such as obesity, insulin resistance, inflammation, dyslipidemia, and hypertension, play a role in neuropathy and nephropathy.
The associations were also less pronounced in women.
Mr. Kristensen said that this is “an important area that needs to be addressed.”
“While different rates between men and women regarding incidence of type 2 diabetes, metabolic risk factors, complications, and the initiation of, and adherence to, therapy have been found,” he continued, “the exact mechanisms remain unclear. We need a further understanding of sex-differences in metabolic regulation, as well as in material living conditions, social and psychological factors, and access to health care, which may influence the risk of complications.”
Mr. Kristensen added, “Sex differences may be present in more areas than we are aware.”
Mr. Kristensen is supported by a PhD grant from Aarhus University. Other authors received funding from the Danish Diabetes Association, the Australian National Health and Medical Research Council, the New South Wales Government, the Spanish Ministry of Universities, the European Union NextGenerationEU/PRTR (Plan de Recuperación) through a Margarita Salas contract of the University of Vigo, and the Government of Andalusia, Research Talent Recruitment Programme. No relevant financial relationships were declared.
A version of this article appeared on Medscape.com.
although the impact on retinopathy is weaker, reveals a cohort study of U.K. individuals.
The research, based on data from more than 18,000 participants in the U.K. Biobank, suggests that the minimal level of self-reported activity to reduce the risk for both neuropathy and nephropathy may be the equivalent of less than 1.5 hours of walking per week.
The results are “encouraging and reassuring for both physicians and patients,” lead author Frederik P.B. Kristensen, MSc, PhD student, department of clinical epidemiology, Aarhus (Denmark) University, said in an interview.
“Our findings are particularly promising for neuropathy since, currently, no disease-modifying treatment exists, and there are limited preventive strategies available.”
Mr. Kristensen highlighted that “most diabetes research has focused on all-cause mortality and macrovascular complications. In the current study, we also found the same pattern for microvascular complications: Even small amounts of physical activity will benefit your health status.”
The minimal level of activity they identified, he said, is also an “achievable [goal] for most type 2 diabetes patients.”
Mr. Kristensen added, however, that the study was limited by excluding individuals with limited mobility and those living in temporary accommodation or care homes.
And prospective studies are required to determine the dose-response relationship between total, not just leisure-time, activity – ideally measured objectively – and risk for microvascular complications, he observed.
The research was published recently in Diabetes Care.
Impact of exercise on microvascular complications in T2D has been uncertain
The authors point out that microvascular complications – such as nerve damage (neuropathy), kidney problems (nephropathy), and eye complications (retinopathy) – occur in more than 50% of individuals with type 2 diabetes and have a “substantial impact” on quality of life, on top of the impact of macrovascular complications (such as cardiovascular disease), disability, and mortality.
Although physical activity is seen as a “cornerstone in the multifactorial management of type 2 diabetes because of its beneficial effects on metabolic risk factors,” the impact on microvascular complications is “uncertain” and the evidence is limited and “conflicting.”
The researchers therefore sought to examine the dose-response association, including the minimal effective level, between leisure-time physical activity and neuropathy, nephropathy, and retinopathy.
They conducted a cohort study of individuals aged 37-82 years from the U.K. Biobank who had type 2 diabetes, which was identified using the Eastwood algorithm and/or an A1c greater than or equal to 48 mmol/mol (6.5%).
Individuals with type 1 diabetes or gestational diabetes were excluded, as were those with major disabling somatic disorders, neurodegenerative diseases, and mental disorders, among others.
Leisure-time physical activity was based on the self-reported frequency, duration, and types of physical activities and was combined to calculate the total leisure time activity in MET-hours per week.
Using the American Diabetes Association/World Health Organization recommendations of 150-300 minutes of moderate to vigorous leisure-time physical activity per week, the researchers determined the recommended moderate activity level to be 150 minutes, (equivalent to 2.5 hours, or 7.5 MET-hours per week).
In all, 18,092 individuals with type 2 diabetes were included in the analysis, of whom 37% were women. The mean age was 60 years.
Ten percent of participants performed no leisure-time physical activity, 38% performed activity below the threshold for moderate activity, 20% performed at the recommended level, and 32% were more active.
Those performing no physical activity were more likely to be women, to be younger, to have a higher body mass index, and to have a greater average A1c, as well as have a more unfavorable sociodemographic and behavioral profile.
Over a median follow-up of 12.1 years, 3.7% of the participants were diagnosed with neuropathy, 10.2% with nephropathy, and 11.7% with retinopathy, equating to an incidence per 1,000 person-years of 3.5, 9,8, and 11.4, respectively.
The researchers found that any level of physical activity was associated with an approximate reduction in the risk for neuropathy and nephropathy.
Multivariate analysis indicated that, compared with no physical activity, activity below the recommended level was associated with an adjusted hazard ratio (aHR) for neuropathy of 0.71, whereas the aHR for activity at the recommended level was 0.73 and that for activity above the recommended level was 0.67.
The aHR for nephropathy, compared with no physical activity, was 0.79 for activity below the recommended level, 0.80 for activity at the recommended level, and 0.80 for activity above the recommended level.
The association between physical activity and retinopathy was weaker, however, at aHRs of 0.91, 0.91, and 0.98 for activity below, at, and above the recommended level, respectively.
The researchers suggest that this lower association could be due to differences in the etiology of the different forms of microvascular complications.
Hyperglycemia is the key driver in the development of retinopathy, they note, whereas other metabolic risk factors, such as obesity, insulin resistance, inflammation, dyslipidemia, and hypertension, play a role in neuropathy and nephropathy.
The associations were also less pronounced in women.
Mr. Kristensen said that this is “an important area that needs to be addressed.”
“While different rates between men and women regarding incidence of type 2 diabetes, metabolic risk factors, complications, and the initiation of, and adherence to, therapy have been found,” he continued, “the exact mechanisms remain unclear. We need a further understanding of sex-differences in metabolic regulation, as well as in material living conditions, social and psychological factors, and access to health care, which may influence the risk of complications.”
Mr. Kristensen added, “Sex differences may be present in more areas than we are aware.”
Mr. Kristensen is supported by a PhD grant from Aarhus University. Other authors received funding from the Danish Diabetes Association, the Australian National Health and Medical Research Council, the New South Wales Government, the Spanish Ministry of Universities, the European Union NextGenerationEU/PRTR (Plan de Recuperación) through a Margarita Salas contract of the University of Vigo, and the Government of Andalusia, Research Talent Recruitment Programme. No relevant financial relationships were declared.
A version of this article appeared on Medscape.com.
although the impact on retinopathy is weaker, reveals a cohort study of U.K. individuals.
The research, based on data from more than 18,000 participants in the U.K. Biobank, suggests that the minimal level of self-reported activity to reduce the risk for both neuropathy and nephropathy may be the equivalent of less than 1.5 hours of walking per week.
The results are “encouraging and reassuring for both physicians and patients,” lead author Frederik P.B. Kristensen, MSc, PhD student, department of clinical epidemiology, Aarhus (Denmark) University, said in an interview.
“Our findings are particularly promising for neuropathy since, currently, no disease-modifying treatment exists, and there are limited preventive strategies available.”
Mr. Kristensen highlighted that “most diabetes research has focused on all-cause mortality and macrovascular complications. In the current study, we also found the same pattern for microvascular complications: Even small amounts of physical activity will benefit your health status.”
The minimal level of activity they identified, he said, is also an “achievable [goal] for most type 2 diabetes patients.”
Mr. Kristensen added, however, that the study was limited by excluding individuals with limited mobility and those living in temporary accommodation or care homes.
And prospective studies are required to determine the dose-response relationship between total, not just leisure-time, activity – ideally measured objectively – and risk for microvascular complications, he observed.
The research was published recently in Diabetes Care.
Impact of exercise on microvascular complications in T2D has been uncertain
The authors point out that microvascular complications – such as nerve damage (neuropathy), kidney problems (nephropathy), and eye complications (retinopathy) – occur in more than 50% of individuals with type 2 diabetes and have a “substantial impact” on quality of life, on top of the impact of macrovascular complications (such as cardiovascular disease), disability, and mortality.
Although physical activity is seen as a “cornerstone in the multifactorial management of type 2 diabetes because of its beneficial effects on metabolic risk factors,” the impact on microvascular complications is “uncertain” and the evidence is limited and “conflicting.”
The researchers therefore sought to examine the dose-response association, including the minimal effective level, between leisure-time physical activity and neuropathy, nephropathy, and retinopathy.
They conducted a cohort study of individuals aged 37-82 years from the U.K. Biobank who had type 2 diabetes, which was identified using the Eastwood algorithm and/or an A1c greater than or equal to 48 mmol/mol (6.5%).
Individuals with type 1 diabetes or gestational diabetes were excluded, as were those with major disabling somatic disorders, neurodegenerative diseases, and mental disorders, among others.
Leisure-time physical activity was based on the self-reported frequency, duration, and types of physical activities and was combined to calculate the total leisure time activity in MET-hours per week.
Using the American Diabetes Association/World Health Organization recommendations of 150-300 minutes of moderate to vigorous leisure-time physical activity per week, the researchers determined the recommended moderate activity level to be 150 minutes, (equivalent to 2.5 hours, or 7.5 MET-hours per week).
In all, 18,092 individuals with type 2 diabetes were included in the analysis, of whom 37% were women. The mean age was 60 years.
Ten percent of participants performed no leisure-time physical activity, 38% performed activity below the threshold for moderate activity, 20% performed at the recommended level, and 32% were more active.
Those performing no physical activity were more likely to be women, to be younger, to have a higher body mass index, and to have a greater average A1c, as well as have a more unfavorable sociodemographic and behavioral profile.
Over a median follow-up of 12.1 years, 3.7% of the participants were diagnosed with neuropathy, 10.2% with nephropathy, and 11.7% with retinopathy, equating to an incidence per 1,000 person-years of 3.5, 9,8, and 11.4, respectively.
The researchers found that any level of physical activity was associated with an approximate reduction in the risk for neuropathy and nephropathy.
Multivariate analysis indicated that, compared with no physical activity, activity below the recommended level was associated with an adjusted hazard ratio (aHR) for neuropathy of 0.71, whereas the aHR for activity at the recommended level was 0.73 and that for activity above the recommended level was 0.67.
The aHR for nephropathy, compared with no physical activity, was 0.79 for activity below the recommended level, 0.80 for activity at the recommended level, and 0.80 for activity above the recommended level.
The association between physical activity and retinopathy was weaker, however, at aHRs of 0.91, 0.91, and 0.98 for activity below, at, and above the recommended level, respectively.
The researchers suggest that this lower association could be due to differences in the etiology of the different forms of microvascular complications.
Hyperglycemia is the key driver in the development of retinopathy, they note, whereas other metabolic risk factors, such as obesity, insulin resistance, inflammation, dyslipidemia, and hypertension, play a role in neuropathy and nephropathy.
The associations were also less pronounced in women.
Mr. Kristensen said that this is “an important area that needs to be addressed.”
“While different rates between men and women regarding incidence of type 2 diabetes, metabolic risk factors, complications, and the initiation of, and adherence to, therapy have been found,” he continued, “the exact mechanisms remain unclear. We need a further understanding of sex-differences in metabolic regulation, as well as in material living conditions, social and psychological factors, and access to health care, which may influence the risk of complications.”
Mr. Kristensen added, “Sex differences may be present in more areas than we are aware.”
Mr. Kristensen is supported by a PhD grant from Aarhus University. Other authors received funding from the Danish Diabetes Association, the Australian National Health and Medical Research Council, the New South Wales Government, the Spanish Ministry of Universities, the European Union NextGenerationEU/PRTR (Plan de Recuperación) through a Margarita Salas contract of the University of Vigo, and the Government of Andalusia, Research Talent Recruitment Programme. No relevant financial relationships were declared.
A version of this article appeared on Medscape.com.
FROM DIABETES CARE
ESC backs SGLT2 inhibitor plus GLP-1 in diabetes with high CVD risk
AMSTERDAM – The era of guidelines that recommended treatment with either a sodium-glucose cotransporter-2 (SGLT-2) inhibitor or a glucagonlike peptide-1 (GLP-1) receptor agonist in people with type 2 diabetes mellitus and established cardiovascular disease (CVD) ended with new recommendations from the European Society of Cardiology that call for starting both classes simultaneously.
said Darren K. McGuire, MD, at the annual congress of the European Society of Cardiology.
The society’s new guidelines for managing CVD in patients with diabetes, released on Aug. 25 and presented in several sessions at the Congress, also break with the past by calling for starting treatment with both an SGLT-2 inhibitor and a GLP-1 receptor agonist without regard to a person’s existing level of glucose control, including their current and target hemoglobin A1c levels, and regardless of background therapy, added Dr. McGuire, a cardiologist and professor at the UT Southwestern Medical Center in Dallas and a member of the ESC panel that wrote the new guidelines.
Instead, the new guidance calls for starting both drug classes promptly in people diagnosed with type 2 diabetes and established atherosclerotic CVD.
Both the previous ESC guidelines from 2019 as well as the current Standards of Care for 2023 document from the American Diabetes Association call for using one class or the other, but they hedge on combined treatment as discretionary.
Different mechanisms mean additive benefits
“With increasing numbers of patients with type 2 diabetes in trials for SGLT-2 inhibitors or GLP-1 receptor agonists who were also on the other drug class, we’ve done large, stratified analyses that suggest no treatment-effect modification” when people received agents from both drug classes, Dr. McGuire explained in an interview. “While we don’t understand the mechanisms of action of these drugs for CVD, we’ve become very confident that they use different mechanisms” that appear to have at least partially additive effects.
“Their benefits for CVD risk reduction are completely independent of their glucose effects. They are cardiology drugs,” Dr. McGuire added.
The new ESC guidelines highlight two other clinical settings where people with type 2 diabetes should receive an SGLT-2 inhibitor regardless of their existing level of glucose control and any other medical treatment: people with heart failure and people with chronic kidney disease (CKD) based on a depressed estimated glomerular filtration rate and an elevated urine albumin-to-creatinine ratio.
Nephropathy was considered by the ESC’s guideline panel to confer risk that is similar to that of established atherosclerotic CVD, Dr. McGuire said.
The guidelines also, for the first time for ESC recommendations, made treatment with finerenone (Kerendia, Bayer) a class 1 level A recommendation for people with type 2 diabetes and CKD.
SCORE2-Diabetes risk estimator
Another major change in the new ESC guideline revision is introduction of a CVD risk calculator intended to estimate the risk among people with type 2 diabetes but without established CVD, heart failure, or CKD.
Called the SCORE2-Diabetes risk estimator, it calculates a person’s 10-year risk for CVD and includes adjustment based on the European region where a person lives; it also tallies different risk levels for women and for men.
The researchers who developed the SCORE2-Diabetes calculator used data from nearly 230,000 people to devise the tool and then validated it with data from an additional 217,000 Europeans with type 2 diabetes.
Key features of the calculator include its use of routinely collected clinical values, such as age, sex, systolic blood pressure, smoking status, serum cholesterol levels, age at diabetes diagnosis, hemoglobin A1c level, and estimated glomerular filtration rate.
“For the first time we have a clear score to categorize risk” in people with type 2 diabetes and identify who needs more aggressive treatment to prevent CVD development,” said Emanuele Di Angelantonio, MD, PhD, deputy director of the cardiovascular epidemiology unit at the University of Cambridge (England).
The guidelines say that people who have a low (< 5%) or moderate (5%-9%) 10-year risk for CVD are possible candidates for metformin treatment. Those with high (10%-19%) or very high (≥ 20%) risk are possible candidates for treatment with metformin and/or an SGLT-2 inhibitor and/or a GLP-1 receptor agonist, said Dr. Di Angelantonio during his talk at the congress on the new risk score.
“The risk score is a good addition” because it estimates future CVD risk better and more systematically than usual practice, which generally relies on no systematic tool, said Naveed Sattar, PhD, professor of metabolic medicine at the University of Glasgow (Scotland) and also a member of the guideline-writing panel.
The new risk score “is a reasonable way” to identify people without CVD but at elevated risk who might benefit from treatment with a relatively expensive drug, such as an SGLT-2 inhibitor, Dr. Sattar said in an interview. “It doesn’t rely on any fancy biomarkers or imaging, and it takes about 30 seconds to calculate. It’s not perfect, but it gets the job done,” and it will increase the number of people with type 2 diabetes who will receive an SGLT-2 inhibitor, he predicted.
Dr. McGuire has been a consultant to Altimmune, Applied Therapeutics, AstraZeneca, Bayer, Boehringer-Ingelheim, Intercept, Lexion, Lilly, Merck, New Amsterdam, and Pfizer. Dr. Di Angelantonio had no disclosures. Dr. Sattar has been a consultant to Abbott, Amgen, AstraZeneca, Boehringer Ingelheim, Lilly, Novartis, Novo Nordisk, Pfizer, and Roche Diagnostics.
A version of this article appeared on Medscape.com.
AMSTERDAM – The era of guidelines that recommended treatment with either a sodium-glucose cotransporter-2 (SGLT-2) inhibitor or a glucagonlike peptide-1 (GLP-1) receptor agonist in people with type 2 diabetes mellitus and established cardiovascular disease (CVD) ended with new recommendations from the European Society of Cardiology that call for starting both classes simultaneously.
said Darren K. McGuire, MD, at the annual congress of the European Society of Cardiology.
The society’s new guidelines for managing CVD in patients with diabetes, released on Aug. 25 and presented in several sessions at the Congress, also break with the past by calling for starting treatment with both an SGLT-2 inhibitor and a GLP-1 receptor agonist without regard to a person’s existing level of glucose control, including their current and target hemoglobin A1c levels, and regardless of background therapy, added Dr. McGuire, a cardiologist and professor at the UT Southwestern Medical Center in Dallas and a member of the ESC panel that wrote the new guidelines.
Instead, the new guidance calls for starting both drug classes promptly in people diagnosed with type 2 diabetes and established atherosclerotic CVD.
Both the previous ESC guidelines from 2019 as well as the current Standards of Care for 2023 document from the American Diabetes Association call for using one class or the other, but they hedge on combined treatment as discretionary.
Different mechanisms mean additive benefits
“With increasing numbers of patients with type 2 diabetes in trials for SGLT-2 inhibitors or GLP-1 receptor agonists who were also on the other drug class, we’ve done large, stratified analyses that suggest no treatment-effect modification” when people received agents from both drug classes, Dr. McGuire explained in an interview. “While we don’t understand the mechanisms of action of these drugs for CVD, we’ve become very confident that they use different mechanisms” that appear to have at least partially additive effects.
“Their benefits for CVD risk reduction are completely independent of their glucose effects. They are cardiology drugs,” Dr. McGuire added.
The new ESC guidelines highlight two other clinical settings where people with type 2 diabetes should receive an SGLT-2 inhibitor regardless of their existing level of glucose control and any other medical treatment: people with heart failure and people with chronic kidney disease (CKD) based on a depressed estimated glomerular filtration rate and an elevated urine albumin-to-creatinine ratio.
Nephropathy was considered by the ESC’s guideline panel to confer risk that is similar to that of established atherosclerotic CVD, Dr. McGuire said.
The guidelines also, for the first time for ESC recommendations, made treatment with finerenone (Kerendia, Bayer) a class 1 level A recommendation for people with type 2 diabetes and CKD.
SCORE2-Diabetes risk estimator
Another major change in the new ESC guideline revision is introduction of a CVD risk calculator intended to estimate the risk among people with type 2 diabetes but without established CVD, heart failure, or CKD.
Called the SCORE2-Diabetes risk estimator, it calculates a person’s 10-year risk for CVD and includes adjustment based on the European region where a person lives; it also tallies different risk levels for women and for men.
The researchers who developed the SCORE2-Diabetes calculator used data from nearly 230,000 people to devise the tool and then validated it with data from an additional 217,000 Europeans with type 2 diabetes.
Key features of the calculator include its use of routinely collected clinical values, such as age, sex, systolic blood pressure, smoking status, serum cholesterol levels, age at diabetes diagnosis, hemoglobin A1c level, and estimated glomerular filtration rate.
“For the first time we have a clear score to categorize risk” in people with type 2 diabetes and identify who needs more aggressive treatment to prevent CVD development,” said Emanuele Di Angelantonio, MD, PhD, deputy director of the cardiovascular epidemiology unit at the University of Cambridge (England).
The guidelines say that people who have a low (< 5%) or moderate (5%-9%) 10-year risk for CVD are possible candidates for metformin treatment. Those with high (10%-19%) or very high (≥ 20%) risk are possible candidates for treatment with metformin and/or an SGLT-2 inhibitor and/or a GLP-1 receptor agonist, said Dr. Di Angelantonio during his talk at the congress on the new risk score.
“The risk score is a good addition” because it estimates future CVD risk better and more systematically than usual practice, which generally relies on no systematic tool, said Naveed Sattar, PhD, professor of metabolic medicine at the University of Glasgow (Scotland) and also a member of the guideline-writing panel.
The new risk score “is a reasonable way” to identify people without CVD but at elevated risk who might benefit from treatment with a relatively expensive drug, such as an SGLT-2 inhibitor, Dr. Sattar said in an interview. “It doesn’t rely on any fancy biomarkers or imaging, and it takes about 30 seconds to calculate. It’s not perfect, but it gets the job done,” and it will increase the number of people with type 2 diabetes who will receive an SGLT-2 inhibitor, he predicted.
Dr. McGuire has been a consultant to Altimmune, Applied Therapeutics, AstraZeneca, Bayer, Boehringer-Ingelheim, Intercept, Lexion, Lilly, Merck, New Amsterdam, and Pfizer. Dr. Di Angelantonio had no disclosures. Dr. Sattar has been a consultant to Abbott, Amgen, AstraZeneca, Boehringer Ingelheim, Lilly, Novartis, Novo Nordisk, Pfizer, and Roche Diagnostics.
A version of this article appeared on Medscape.com.
AMSTERDAM – The era of guidelines that recommended treatment with either a sodium-glucose cotransporter-2 (SGLT-2) inhibitor or a glucagonlike peptide-1 (GLP-1) receptor agonist in people with type 2 diabetes mellitus and established cardiovascular disease (CVD) ended with new recommendations from the European Society of Cardiology that call for starting both classes simultaneously.
said Darren K. McGuire, MD, at the annual congress of the European Society of Cardiology.
The society’s new guidelines for managing CVD in patients with diabetes, released on Aug. 25 and presented in several sessions at the Congress, also break with the past by calling for starting treatment with both an SGLT-2 inhibitor and a GLP-1 receptor agonist without regard to a person’s existing level of glucose control, including their current and target hemoglobin A1c levels, and regardless of background therapy, added Dr. McGuire, a cardiologist and professor at the UT Southwestern Medical Center in Dallas and a member of the ESC panel that wrote the new guidelines.
Instead, the new guidance calls for starting both drug classes promptly in people diagnosed with type 2 diabetes and established atherosclerotic CVD.
Both the previous ESC guidelines from 2019 as well as the current Standards of Care for 2023 document from the American Diabetes Association call for using one class or the other, but they hedge on combined treatment as discretionary.
Different mechanisms mean additive benefits
“With increasing numbers of patients with type 2 diabetes in trials for SGLT-2 inhibitors or GLP-1 receptor agonists who were also on the other drug class, we’ve done large, stratified analyses that suggest no treatment-effect modification” when people received agents from both drug classes, Dr. McGuire explained in an interview. “While we don’t understand the mechanisms of action of these drugs for CVD, we’ve become very confident that they use different mechanisms” that appear to have at least partially additive effects.
“Their benefits for CVD risk reduction are completely independent of their glucose effects. They are cardiology drugs,” Dr. McGuire added.
The new ESC guidelines highlight two other clinical settings where people with type 2 diabetes should receive an SGLT-2 inhibitor regardless of their existing level of glucose control and any other medical treatment: people with heart failure and people with chronic kidney disease (CKD) based on a depressed estimated glomerular filtration rate and an elevated urine albumin-to-creatinine ratio.
Nephropathy was considered by the ESC’s guideline panel to confer risk that is similar to that of established atherosclerotic CVD, Dr. McGuire said.
The guidelines also, for the first time for ESC recommendations, made treatment with finerenone (Kerendia, Bayer) a class 1 level A recommendation for people with type 2 diabetes and CKD.
SCORE2-Diabetes risk estimator
Another major change in the new ESC guideline revision is introduction of a CVD risk calculator intended to estimate the risk among people with type 2 diabetes but without established CVD, heart failure, or CKD.
Called the SCORE2-Diabetes risk estimator, it calculates a person’s 10-year risk for CVD and includes adjustment based on the European region where a person lives; it also tallies different risk levels for women and for men.
The researchers who developed the SCORE2-Diabetes calculator used data from nearly 230,000 people to devise the tool and then validated it with data from an additional 217,000 Europeans with type 2 diabetes.
Key features of the calculator include its use of routinely collected clinical values, such as age, sex, systolic blood pressure, smoking status, serum cholesterol levels, age at diabetes diagnosis, hemoglobin A1c level, and estimated glomerular filtration rate.
“For the first time we have a clear score to categorize risk” in people with type 2 diabetes and identify who needs more aggressive treatment to prevent CVD development,” said Emanuele Di Angelantonio, MD, PhD, deputy director of the cardiovascular epidemiology unit at the University of Cambridge (England).
The guidelines say that people who have a low (< 5%) or moderate (5%-9%) 10-year risk for CVD are possible candidates for metformin treatment. Those with high (10%-19%) or very high (≥ 20%) risk are possible candidates for treatment with metformin and/or an SGLT-2 inhibitor and/or a GLP-1 receptor agonist, said Dr. Di Angelantonio during his talk at the congress on the new risk score.
“The risk score is a good addition” because it estimates future CVD risk better and more systematically than usual practice, which generally relies on no systematic tool, said Naveed Sattar, PhD, professor of metabolic medicine at the University of Glasgow (Scotland) and also a member of the guideline-writing panel.
The new risk score “is a reasonable way” to identify people without CVD but at elevated risk who might benefit from treatment with a relatively expensive drug, such as an SGLT-2 inhibitor, Dr. Sattar said in an interview. “It doesn’t rely on any fancy biomarkers or imaging, and it takes about 30 seconds to calculate. It’s not perfect, but it gets the job done,” and it will increase the number of people with type 2 diabetes who will receive an SGLT-2 inhibitor, he predicted.
Dr. McGuire has been a consultant to Altimmune, Applied Therapeutics, AstraZeneca, Bayer, Boehringer-Ingelheim, Intercept, Lexion, Lilly, Merck, New Amsterdam, and Pfizer. Dr. Di Angelantonio had no disclosures. Dr. Sattar has been a consultant to Abbott, Amgen, AstraZeneca, Boehringer Ingelheim, Lilly, Novartis, Novo Nordisk, Pfizer, and Roche Diagnostics.
A version of this article appeared on Medscape.com.
AT ESC CONGRESS 2023
Liraglutide fixes learning limit tied to insulin resistance
A single injection of the GLP-1 receptor agonist liraglutide led to short-term normalization of associative learning in people with obesity and insulin resistance, a finding that suggests say the authors of a recent report in Nature Metabolism.
“We demonstrated that dopamine-driven associative learning about external sensory cues crucially depends on metabolic signaling,” said Marc Tittgemeyer, PhD, professor at the Max Planck Institute for Metabolism Research in Cologne, Germany, and senior author of the study. Study participants with impaired insulin sensitivity “exhibited a reduced amplitude of behavioral updating that was normalized” by a single subcutaneous injection of 0.6 mg of liraglutide (the starting daily dose for liraglutide for weight loss, available as Saxenda, Novo Nordisk) given the evening before testing.
The findings, from 30 adults with normal insulin sensitivity and normal weight and 24 adults with impaired insulin sensitivity and obesity, suggest that metabolic signals, particularly ones that promote energy restoration in a setting of energy deprivation caused by insulin or a glucagon-like peptide-1 (GLP-1) receptor agonist, “profoundly influence neuronal processing,” said Dr. Tittgemeyer. The findings suggest that impaired metabolic signaling such as occurs with insulin resistance in people with obesity can cause deficiencies in associative learning.
‘Liraglutide can normalize learning of associations’
“We show that in people with obesity, disrupted circuit mechanisms lead to impaired learning about sensory associations,” Dr. Tittgemeyer said in an interview. “The information provided by sensory systems that the brain must interpret to select a behavioral response are ‘off tune’ ” in these individuals.
“This is rather consequential for understanding food-intake behaviors. Modern obesity treatments, such as liraglutide, can normalize learning of associations and thereby render people susceptible again for sensory signals and make them more prone to react to subliminal interactions, such as weight-normalizing diets and conscious eating,” he added.
The normalization in associative learning that one dose of liraglutide produced in people with obesity “fits with studies showing that these drugs restore a normal feeling of satiety, causing people to eat less and therefore lose weight,” he explained.
Dr. Tittgemeyer noted that this effect is likely shared by other agents in the GLP-1 receptor agonist class, such as semaglutide (Ozempic, Wegovy, Novo Nordisk) but is likely not an effect when agents agonize receptors to other nutrient-stimulated hormones such as glucagon and the glucose-dependent insulinotropic polypeptide.
The findings “show that liraglutide restores associative learning in participants with greater insulin resistance,” a “highly relevant” discovery, commented Nils B. Kroemer, PhD, head of the section of medical psychology at the University of Bonn, Germany, who was not involved with this research, in a written statement.
The study run by Dr. Tittgemeyer and his associates included 54 healthy adult volunteers whom they assessed for insulin sensitivity with their homeostasis model assessment of insulin resistance. The researchers divided the cohort into groups; one group included 24 people with impaired insulin sensitivity, and one included 30 with normal insulin sensitivity. The average body mass index (BMI) of the normal sensitivity group was about 24 kg/m2; in the insulin-resistant subgroup, BMI averaged about 33 kg/m2.
The associative learning task tested the ability of participants to learn associations between auditory cues (a high or low tone) and a subsequent visual outcome (a picture of a face or a house). During each associative learning session, participants also underwent functional MRI of the brain.
Liraglutide treatment leveled learning
The results showed that the learning rate was significantly lower in the subgroup with impaired insulin sensitivity, compared with those with normal insulin sensitivity following treatment with a placebo injection. This indicates a decreased adaptation of learning to predictability variations in individuals with impaired insulin sensitivity.
In contrast, treatment with a single dose of liraglutide significantly enhanced the learning rate in the group with impaired insulin sensitivity but significantly reduced the learning rate in the group with normal insulin sensitivity. Liraglutide’s effect was twice as large in the group with impaired insulin sensitivity than in the group with normal insulin sensitivity, and these opposing effects of liraglutide resulted in a convergence of the two groups’ adaptive learning rates so that there wasn’t any significant between-group difference following liraglutide treatment.
After analyzing the functional MRI data along with the learning results, the researchers concluded that liraglutide normalized learning in individuals with impaired insulin sensitivity by enhancing adaptive prediction error encoding in the brain’s ventral striatum and mesocortical projection sites.
This apparent ability of GLP-1 analogues to correct this learning deficit in people with impaired insulin sensitivity and obesity has implications regarding potential benefit for people with other pathologies characterized by impaired dopaminergic function and associated with metabolic impairments, such as psychosis, Parkinson’s disease, and depression, the researchers say.
“The fascinating thing about GLP-1 receptor agonists is that they have an additional mechanism that relates to anti-inflammatory effects, especially for alleviating cell stress,” said Dr. Tittgemeyer. “Many ongoing clinical trials are assessing their effects in neuropsychiatric diseases,” he noted.
The study received no commercial funding. Dr. Tittgemyer and most of his coauthors had no disclosures. One coauthor had several disclosures, which are detailed in the report. Dr. Kroemer had no disclosures.
A version of this article first appeared on Medscape.com.
A single injection of the GLP-1 receptor agonist liraglutide led to short-term normalization of associative learning in people with obesity and insulin resistance, a finding that suggests say the authors of a recent report in Nature Metabolism.
“We demonstrated that dopamine-driven associative learning about external sensory cues crucially depends on metabolic signaling,” said Marc Tittgemeyer, PhD, professor at the Max Planck Institute for Metabolism Research in Cologne, Germany, and senior author of the study. Study participants with impaired insulin sensitivity “exhibited a reduced amplitude of behavioral updating that was normalized” by a single subcutaneous injection of 0.6 mg of liraglutide (the starting daily dose for liraglutide for weight loss, available as Saxenda, Novo Nordisk) given the evening before testing.
The findings, from 30 adults with normal insulin sensitivity and normal weight and 24 adults with impaired insulin sensitivity and obesity, suggest that metabolic signals, particularly ones that promote energy restoration in a setting of energy deprivation caused by insulin or a glucagon-like peptide-1 (GLP-1) receptor agonist, “profoundly influence neuronal processing,” said Dr. Tittgemeyer. The findings suggest that impaired metabolic signaling such as occurs with insulin resistance in people with obesity can cause deficiencies in associative learning.
‘Liraglutide can normalize learning of associations’
“We show that in people with obesity, disrupted circuit mechanisms lead to impaired learning about sensory associations,” Dr. Tittgemeyer said in an interview. “The information provided by sensory systems that the brain must interpret to select a behavioral response are ‘off tune’ ” in these individuals.
“This is rather consequential for understanding food-intake behaviors. Modern obesity treatments, such as liraglutide, can normalize learning of associations and thereby render people susceptible again for sensory signals and make them more prone to react to subliminal interactions, such as weight-normalizing diets and conscious eating,” he added.
The normalization in associative learning that one dose of liraglutide produced in people with obesity “fits with studies showing that these drugs restore a normal feeling of satiety, causing people to eat less and therefore lose weight,” he explained.
Dr. Tittgemeyer noted that this effect is likely shared by other agents in the GLP-1 receptor agonist class, such as semaglutide (Ozempic, Wegovy, Novo Nordisk) but is likely not an effect when agents agonize receptors to other nutrient-stimulated hormones such as glucagon and the glucose-dependent insulinotropic polypeptide.
The findings “show that liraglutide restores associative learning in participants with greater insulin resistance,” a “highly relevant” discovery, commented Nils B. Kroemer, PhD, head of the section of medical psychology at the University of Bonn, Germany, who was not involved with this research, in a written statement.
The study run by Dr. Tittgemeyer and his associates included 54 healthy adult volunteers whom they assessed for insulin sensitivity with their homeostasis model assessment of insulin resistance. The researchers divided the cohort into groups; one group included 24 people with impaired insulin sensitivity, and one included 30 with normal insulin sensitivity. The average body mass index (BMI) of the normal sensitivity group was about 24 kg/m2; in the insulin-resistant subgroup, BMI averaged about 33 kg/m2.
The associative learning task tested the ability of participants to learn associations between auditory cues (a high or low tone) and a subsequent visual outcome (a picture of a face or a house). During each associative learning session, participants also underwent functional MRI of the brain.
Liraglutide treatment leveled learning
The results showed that the learning rate was significantly lower in the subgroup with impaired insulin sensitivity, compared with those with normal insulin sensitivity following treatment with a placebo injection. This indicates a decreased adaptation of learning to predictability variations in individuals with impaired insulin sensitivity.
In contrast, treatment with a single dose of liraglutide significantly enhanced the learning rate in the group with impaired insulin sensitivity but significantly reduced the learning rate in the group with normal insulin sensitivity. Liraglutide’s effect was twice as large in the group with impaired insulin sensitivity than in the group with normal insulin sensitivity, and these opposing effects of liraglutide resulted in a convergence of the two groups’ adaptive learning rates so that there wasn’t any significant between-group difference following liraglutide treatment.
After analyzing the functional MRI data along with the learning results, the researchers concluded that liraglutide normalized learning in individuals with impaired insulin sensitivity by enhancing adaptive prediction error encoding in the brain’s ventral striatum and mesocortical projection sites.
This apparent ability of GLP-1 analogues to correct this learning deficit in people with impaired insulin sensitivity and obesity has implications regarding potential benefit for people with other pathologies characterized by impaired dopaminergic function and associated with metabolic impairments, such as psychosis, Parkinson’s disease, and depression, the researchers say.
“The fascinating thing about GLP-1 receptor agonists is that they have an additional mechanism that relates to anti-inflammatory effects, especially for alleviating cell stress,” said Dr. Tittgemeyer. “Many ongoing clinical trials are assessing their effects in neuropsychiatric diseases,” he noted.
The study received no commercial funding. Dr. Tittgemyer and most of his coauthors had no disclosures. One coauthor had several disclosures, which are detailed in the report. Dr. Kroemer had no disclosures.
A version of this article first appeared on Medscape.com.
A single injection of the GLP-1 receptor agonist liraglutide led to short-term normalization of associative learning in people with obesity and insulin resistance, a finding that suggests say the authors of a recent report in Nature Metabolism.
“We demonstrated that dopamine-driven associative learning about external sensory cues crucially depends on metabolic signaling,” said Marc Tittgemeyer, PhD, professor at the Max Planck Institute for Metabolism Research in Cologne, Germany, and senior author of the study. Study participants with impaired insulin sensitivity “exhibited a reduced amplitude of behavioral updating that was normalized” by a single subcutaneous injection of 0.6 mg of liraglutide (the starting daily dose for liraglutide for weight loss, available as Saxenda, Novo Nordisk) given the evening before testing.
The findings, from 30 adults with normal insulin sensitivity and normal weight and 24 adults with impaired insulin sensitivity and obesity, suggest that metabolic signals, particularly ones that promote energy restoration in a setting of energy deprivation caused by insulin or a glucagon-like peptide-1 (GLP-1) receptor agonist, “profoundly influence neuronal processing,” said Dr. Tittgemeyer. The findings suggest that impaired metabolic signaling such as occurs with insulin resistance in people with obesity can cause deficiencies in associative learning.
‘Liraglutide can normalize learning of associations’
“We show that in people with obesity, disrupted circuit mechanisms lead to impaired learning about sensory associations,” Dr. Tittgemeyer said in an interview. “The information provided by sensory systems that the brain must interpret to select a behavioral response are ‘off tune’ ” in these individuals.
“This is rather consequential for understanding food-intake behaviors. Modern obesity treatments, such as liraglutide, can normalize learning of associations and thereby render people susceptible again for sensory signals and make them more prone to react to subliminal interactions, such as weight-normalizing diets and conscious eating,” he added.
The normalization in associative learning that one dose of liraglutide produced in people with obesity “fits with studies showing that these drugs restore a normal feeling of satiety, causing people to eat less and therefore lose weight,” he explained.
Dr. Tittgemeyer noted that this effect is likely shared by other agents in the GLP-1 receptor agonist class, such as semaglutide (Ozempic, Wegovy, Novo Nordisk) but is likely not an effect when agents agonize receptors to other nutrient-stimulated hormones such as glucagon and the glucose-dependent insulinotropic polypeptide.
The findings “show that liraglutide restores associative learning in participants with greater insulin resistance,” a “highly relevant” discovery, commented Nils B. Kroemer, PhD, head of the section of medical psychology at the University of Bonn, Germany, who was not involved with this research, in a written statement.
The study run by Dr. Tittgemeyer and his associates included 54 healthy adult volunteers whom they assessed for insulin sensitivity with their homeostasis model assessment of insulin resistance. The researchers divided the cohort into groups; one group included 24 people with impaired insulin sensitivity, and one included 30 with normal insulin sensitivity. The average body mass index (BMI) of the normal sensitivity group was about 24 kg/m2; in the insulin-resistant subgroup, BMI averaged about 33 kg/m2.
The associative learning task tested the ability of participants to learn associations between auditory cues (a high or low tone) and a subsequent visual outcome (a picture of a face or a house). During each associative learning session, participants also underwent functional MRI of the brain.
Liraglutide treatment leveled learning
The results showed that the learning rate was significantly lower in the subgroup with impaired insulin sensitivity, compared with those with normal insulin sensitivity following treatment with a placebo injection. This indicates a decreased adaptation of learning to predictability variations in individuals with impaired insulin sensitivity.
In contrast, treatment with a single dose of liraglutide significantly enhanced the learning rate in the group with impaired insulin sensitivity but significantly reduced the learning rate in the group with normal insulin sensitivity. Liraglutide’s effect was twice as large in the group with impaired insulin sensitivity than in the group with normal insulin sensitivity, and these opposing effects of liraglutide resulted in a convergence of the two groups’ adaptive learning rates so that there wasn’t any significant between-group difference following liraglutide treatment.
After analyzing the functional MRI data along with the learning results, the researchers concluded that liraglutide normalized learning in individuals with impaired insulin sensitivity by enhancing adaptive prediction error encoding in the brain’s ventral striatum and mesocortical projection sites.
This apparent ability of GLP-1 analogues to correct this learning deficit in people with impaired insulin sensitivity and obesity has implications regarding potential benefit for people with other pathologies characterized by impaired dopaminergic function and associated with metabolic impairments, such as psychosis, Parkinson’s disease, and depression, the researchers say.
“The fascinating thing about GLP-1 receptor agonists is that they have an additional mechanism that relates to anti-inflammatory effects, especially for alleviating cell stress,” said Dr. Tittgemeyer. “Many ongoing clinical trials are assessing their effects in neuropsychiatric diseases,” he noted.
The study received no commercial funding. Dr. Tittgemyer and most of his coauthors had no disclosures. One coauthor had several disclosures, which are detailed in the report. Dr. Kroemer had no disclosures.
A version of this article first appeared on Medscape.com.
FROM NATURE METABOLISM
Apple cider vinegar, fenugreek best herbal remedies for T2D: Review
The review included 44 randomized clinical trials with more than 3,000 participants using six herbal remedies: apple cider vinegar, cinnamon, curcumin, fenugreek seeds, ginger, and saffron.
Apple cider vinegar, fenugreek seeds, curcumin (turmeric), and cinnamon resulted in statistically significant reductions in fasting blood glucose, compared with the control groups in the clinical trials. Out of all the remedies, the authors found apple cider vinegar to be the most effective for lowering fasting blood glucose levels.
The review also found that apple cider vinegar and fenugreek seeds had a statistically significant effect on reducing A1c, compared with the control groups. The authors found the herbal remedies made no difference to insulin level or homeostatic model assessment for insulin resistance (HOMA-IR).
The results are published online in Diabetes & Metabolic Syndrome: Clinical Research & Reviews. The authors said they hoped the review would help medical professionals and people with type 2 diabetes understand the effectiveness of different herbal remedies and consider incorporating these remedies into standard care.
“Some people use curcumin, some use ginger, some use apple cider [vinegar], but it’s not clear which is better,” said Shiv Mudgal, PhD, corresponding author of the paper and an associate professor in nursing at the All India Institute of Medical Sciences in Deoghar, India.
“We thought it would be nice to get some idea about how they work and how they compete with each other,” said Subodh Kumar, MD, the first author and an associate professor in pharmacology at the All India Institute of Medical Sciences in Deoghar, India.
They wanted to understand how the herbal remedies worked by including insulin level and HOMA-IR as measurable outcomes but found nothing conclusive. Instead, they speculated that the effect of apple cider vinegar and fenugreek seeds on blood glucose and A1c could be related to delayed gastric emptying, among other mechanisms.
However, the results should be interpreted with caution, said Dr. Kumar.
Apple cider vinegar had three clinical trials to back the finding, and fenugreek seeds had four studies supporting the results – fewer than the other included remedies. The authors also identified risks of bias from the randomization process and the allocation concealment process in several of the included trials.
Most of the studies included only short follow-up periods, meaning that the long-term effects of using these herbal remedies to help manage type 2 diabetes remain unclear.
The six herbal remedies included in the study were chosen out of dozens of popular complementary medicines for the strength and number of clinical trials backing their use.
The limited number included in the review is a drawback, according to Merlin Willcox, DPhil, a clinical lecturer in general practice at the University of Southampton, England, who was not involved in the research.
“It means they’ve left out stuff that’s potentially effective,” Dr. Willcox said in an interview.
Dr. Willcox, who has coauthored a review of herbal remedies for glycemic control in type 2 diabetes, said he was surprised that apple cider vinegar came out on top in this analysis.
His review concluded that aloe vera leaf gel, psyllium fiber, and fenugreek seeds appeared to be the most effective at reducing A1c, compared with the control groups of the included trials, out of 18 plant-based remedies.
There were no adverse effects associated with the herbal remedies, according to Dr. Mudgal. However, the evidence for the herbal remedies included in their review also lacked substantial follow-up periods assessing their long-term effects.
“You need to look at the evidence for each individual remedy; it’s not just about what plant it is, but it’s about what preparation, what dose. All of that comes into play,” Dr. Willcox said.
Up to 3.6 million people use herbal remedies to manage type 2 diabetes in the United States, according to a 2014 study cited by the review authors. The number is much higher elsewhere: As many as two-thirds of patients with diabetes in India and Saudi Arabia incorporate herbal remedies to help manage symptoms, whereas about half of patients with diabetes in the United Kingdom use herbal medicines.
Experts warn of the risks associated with using herbal medicines to complement traditional therapies.
“I caution my patients about dietary supplements and herbals because of the lack of high-quality data demonstrating efficacy and safety,” Katherine H. Saunders, MD, DABOM, cofounder of Intellihealth and clinical assistant professor of medicine at Weill Cornell Medicine, New York, said in an interview.
For Dr. Willcox, the risks relate to where patients get their information from. Many patients with type 2 diabetes are too scared to talk to their doctor about herbal medicines.
“They think their doctor is going to be negative or dismissive,” Dr. Willcox said. “So patients are getting their information from family and friends or from the Internet, which is not necessarily the most reliable, evidence-based source of information.”
The authors have reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
The review included 44 randomized clinical trials with more than 3,000 participants using six herbal remedies: apple cider vinegar, cinnamon, curcumin, fenugreek seeds, ginger, and saffron.
Apple cider vinegar, fenugreek seeds, curcumin (turmeric), and cinnamon resulted in statistically significant reductions in fasting blood glucose, compared with the control groups in the clinical trials. Out of all the remedies, the authors found apple cider vinegar to be the most effective for lowering fasting blood glucose levels.
The review also found that apple cider vinegar and fenugreek seeds had a statistically significant effect on reducing A1c, compared with the control groups. The authors found the herbal remedies made no difference to insulin level or homeostatic model assessment for insulin resistance (HOMA-IR).
The results are published online in Diabetes & Metabolic Syndrome: Clinical Research & Reviews. The authors said they hoped the review would help medical professionals and people with type 2 diabetes understand the effectiveness of different herbal remedies and consider incorporating these remedies into standard care.
“Some people use curcumin, some use ginger, some use apple cider [vinegar], but it’s not clear which is better,” said Shiv Mudgal, PhD, corresponding author of the paper and an associate professor in nursing at the All India Institute of Medical Sciences in Deoghar, India.
“We thought it would be nice to get some idea about how they work and how they compete with each other,” said Subodh Kumar, MD, the first author and an associate professor in pharmacology at the All India Institute of Medical Sciences in Deoghar, India.
They wanted to understand how the herbal remedies worked by including insulin level and HOMA-IR as measurable outcomes but found nothing conclusive. Instead, they speculated that the effect of apple cider vinegar and fenugreek seeds on blood glucose and A1c could be related to delayed gastric emptying, among other mechanisms.
However, the results should be interpreted with caution, said Dr. Kumar.
Apple cider vinegar had three clinical trials to back the finding, and fenugreek seeds had four studies supporting the results – fewer than the other included remedies. The authors also identified risks of bias from the randomization process and the allocation concealment process in several of the included trials.
Most of the studies included only short follow-up periods, meaning that the long-term effects of using these herbal remedies to help manage type 2 diabetes remain unclear.
The six herbal remedies included in the study were chosen out of dozens of popular complementary medicines for the strength and number of clinical trials backing their use.
The limited number included in the review is a drawback, according to Merlin Willcox, DPhil, a clinical lecturer in general practice at the University of Southampton, England, who was not involved in the research.
“It means they’ve left out stuff that’s potentially effective,” Dr. Willcox said in an interview.
Dr. Willcox, who has coauthored a review of herbal remedies for glycemic control in type 2 diabetes, said he was surprised that apple cider vinegar came out on top in this analysis.
His review concluded that aloe vera leaf gel, psyllium fiber, and fenugreek seeds appeared to be the most effective at reducing A1c, compared with the control groups of the included trials, out of 18 plant-based remedies.
There were no adverse effects associated with the herbal remedies, according to Dr. Mudgal. However, the evidence for the herbal remedies included in their review also lacked substantial follow-up periods assessing their long-term effects.
“You need to look at the evidence for each individual remedy; it’s not just about what plant it is, but it’s about what preparation, what dose. All of that comes into play,” Dr. Willcox said.
Up to 3.6 million people use herbal remedies to manage type 2 diabetes in the United States, according to a 2014 study cited by the review authors. The number is much higher elsewhere: As many as two-thirds of patients with diabetes in India and Saudi Arabia incorporate herbal remedies to help manage symptoms, whereas about half of patients with diabetes in the United Kingdom use herbal medicines.
Experts warn of the risks associated with using herbal medicines to complement traditional therapies.
“I caution my patients about dietary supplements and herbals because of the lack of high-quality data demonstrating efficacy and safety,” Katherine H. Saunders, MD, DABOM, cofounder of Intellihealth and clinical assistant professor of medicine at Weill Cornell Medicine, New York, said in an interview.
For Dr. Willcox, the risks relate to where patients get their information from. Many patients with type 2 diabetes are too scared to talk to their doctor about herbal medicines.
“They think their doctor is going to be negative or dismissive,” Dr. Willcox said. “So patients are getting their information from family and friends or from the Internet, which is not necessarily the most reliable, evidence-based source of information.”
The authors have reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
The review included 44 randomized clinical trials with more than 3,000 participants using six herbal remedies: apple cider vinegar, cinnamon, curcumin, fenugreek seeds, ginger, and saffron.
Apple cider vinegar, fenugreek seeds, curcumin (turmeric), and cinnamon resulted in statistically significant reductions in fasting blood glucose, compared with the control groups in the clinical trials. Out of all the remedies, the authors found apple cider vinegar to be the most effective for lowering fasting blood glucose levels.
The review also found that apple cider vinegar and fenugreek seeds had a statistically significant effect on reducing A1c, compared with the control groups. The authors found the herbal remedies made no difference to insulin level or homeostatic model assessment for insulin resistance (HOMA-IR).
The results are published online in Diabetes & Metabolic Syndrome: Clinical Research & Reviews. The authors said they hoped the review would help medical professionals and people with type 2 diabetes understand the effectiveness of different herbal remedies and consider incorporating these remedies into standard care.
“Some people use curcumin, some use ginger, some use apple cider [vinegar], but it’s not clear which is better,” said Shiv Mudgal, PhD, corresponding author of the paper and an associate professor in nursing at the All India Institute of Medical Sciences in Deoghar, India.
“We thought it would be nice to get some idea about how they work and how they compete with each other,” said Subodh Kumar, MD, the first author and an associate professor in pharmacology at the All India Institute of Medical Sciences in Deoghar, India.
They wanted to understand how the herbal remedies worked by including insulin level and HOMA-IR as measurable outcomes but found nothing conclusive. Instead, they speculated that the effect of apple cider vinegar and fenugreek seeds on blood glucose and A1c could be related to delayed gastric emptying, among other mechanisms.
However, the results should be interpreted with caution, said Dr. Kumar.
Apple cider vinegar had three clinical trials to back the finding, and fenugreek seeds had four studies supporting the results – fewer than the other included remedies. The authors also identified risks of bias from the randomization process and the allocation concealment process in several of the included trials.
Most of the studies included only short follow-up periods, meaning that the long-term effects of using these herbal remedies to help manage type 2 diabetes remain unclear.
The six herbal remedies included in the study were chosen out of dozens of popular complementary medicines for the strength and number of clinical trials backing their use.
The limited number included in the review is a drawback, according to Merlin Willcox, DPhil, a clinical lecturer in general practice at the University of Southampton, England, who was not involved in the research.
“It means they’ve left out stuff that’s potentially effective,” Dr. Willcox said in an interview.
Dr. Willcox, who has coauthored a review of herbal remedies for glycemic control in type 2 diabetes, said he was surprised that apple cider vinegar came out on top in this analysis.
His review concluded that aloe vera leaf gel, psyllium fiber, and fenugreek seeds appeared to be the most effective at reducing A1c, compared with the control groups of the included trials, out of 18 plant-based remedies.
There were no adverse effects associated with the herbal remedies, according to Dr. Mudgal. However, the evidence for the herbal remedies included in their review also lacked substantial follow-up periods assessing their long-term effects.
“You need to look at the evidence for each individual remedy; it’s not just about what plant it is, but it’s about what preparation, what dose. All of that comes into play,” Dr. Willcox said.
Up to 3.6 million people use herbal remedies to manage type 2 diabetes in the United States, according to a 2014 study cited by the review authors. The number is much higher elsewhere: As many as two-thirds of patients with diabetes in India and Saudi Arabia incorporate herbal remedies to help manage symptoms, whereas about half of patients with diabetes in the United Kingdom use herbal medicines.
Experts warn of the risks associated with using herbal medicines to complement traditional therapies.
“I caution my patients about dietary supplements and herbals because of the lack of high-quality data demonstrating efficacy and safety,” Katherine H. Saunders, MD, DABOM, cofounder of Intellihealth and clinical assistant professor of medicine at Weill Cornell Medicine, New York, said in an interview.
For Dr. Willcox, the risks relate to where patients get their information from. Many patients with type 2 diabetes are too scared to talk to their doctor about herbal medicines.
“They think their doctor is going to be negative or dismissive,” Dr. Willcox said. “So patients are getting their information from family and friends or from the Internet, which is not necessarily the most reliable, evidence-based source of information.”
The authors have reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM DIABETES & METABOLIC SYNDROME: CLINICAL RESEARCH & REVIEWS
Human frailty is a cash cow
Doctor, if you are caring for patients with diabetes, I sure hope you know more about it than I do. The longer I live, it seems, the less I understand.
In a free society, people can do what they want, and that’s great except when it isn’t. That’s why societies develop ethics and even public laws if ethics are not strong enough to protect us from ourselves and others.
Sugar, sugar
When I was growing up in small-town Alabama during the Depression and World War II, we called it sugar diabetes. Eat too much sugar, you got fat; your blood sugar went up, and you spilled sugar into your urine. Diabetes was fairly rare, and so was obesity. Doctors treated it by limiting the intake of sugar (and various sweet foods), along with attempting weight loss. If that didn’t do the trick, insulin injections.
From then until now, note these trends.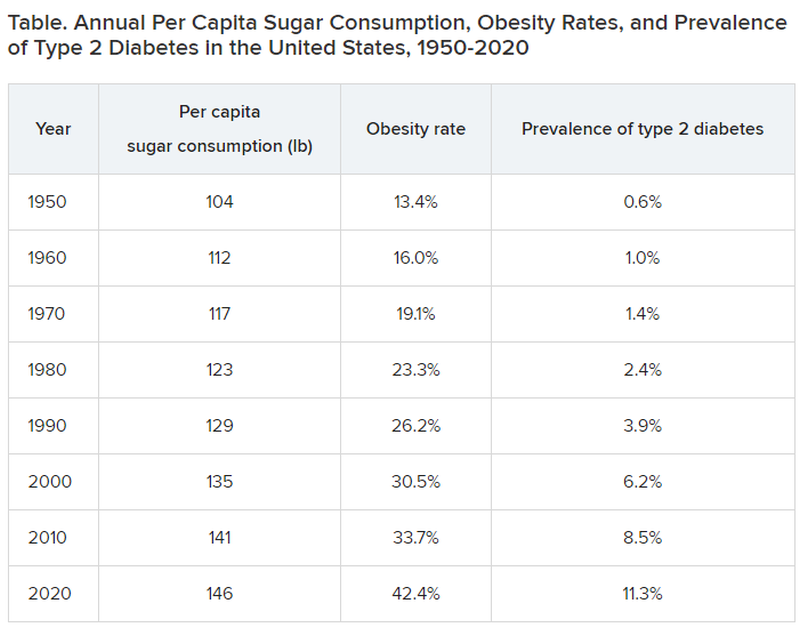
Type 2 diabetes was diagnosed even more infrequently before 1950:
- 1920: 0.2% of the population
- 1930: 0.3% of the population
- 1940: 0.4% of the population
In 2020, although 11.3% of the population was diagnosed with type 2 diabetes, the unknown undiagnosed proportion could be much higher.
Notice a correlation between sugar consumption and prevalence of diabetes? Of course, correlation is not causation, but at the same time, it sure as hell is not negation. Such concordance can be considered hypothesis generating. It may not be true causation, but it’s a good bet when 89% of people with diabetes have overweight or obesity.
What did the entire medical, public health, government, agriculture, nursing, food manufacturing, marketing, advertising, restaurant, and education constituencies do about this as it was happening? They observed, documented, gave lip service, and wrung their hands in public a bit. I do not believe that this is an organized active conspiracy; it would take too many players cooperating over too long a period of time. But it certainly may be a passive conspiracy, and primary care physicians and their patients are trapped.
The proper daily practice of medicine consists of one patient, one physician, one moment, and one decision. Let it be a shared decision, informed by the best evidence and taking cost into consideration. That encounter represents an opportunity, a responsibility, and a conundrum.
Individual health is subsumed under the collective health of the public. As such, a patient’s health is out of the control of both physician and patient; instead, patients are the beneficiaries or victims of the “marketplace.” Humans are frail and easily taken advantage of by the brilliant and highly motivated strategic planning and execution of Big Agriculture, Big Food, Big Pharma, Big Marketing, and Big Money-Driven Medicine and generally failed by Big Government, Big Public Health, Big Education, Big Psychology, and Big Religion.
Rethinking diabetes
Consider diabetes as one of many examples. What a terrific deal for capitalism. then it discovers (invents) long-term, very expensive, compelling treatments to slim us down, with no end in sight, and still without ever understanding the true nature of diabetes.
Gary Taubes’s great new book, “Rethinking Diabetes: What Science Reveals About Diet, Insulin, and Successful Treatments,” is being published by Alfred A. Knopf in early 2024.
It is 404 pages of (dense) text, with 401 numbered references and footnotes, a bibliography of 790 references, alphabetically arranged for easy cross-checking, and a 25-page index.
Remember Mr. Taubes’s earlier definitive historical treatises: “Good Calories, Bad Calories” (2007), “Why We Get Fat” (2010), “The Case Against Sugar” (2016), and “The Case for Keto” (2020)?
This new book is more like “Good Calories, Bad Calories”: long, dense, detailed, definitive, and of great historical reference value, including original research information from other countries in other languages. The author told me that the many early research reference sources were available only in German and that his use of generative artificial intelligence as an assistant researcher was of great value.
Nonphysician author Mr. Taubes uses his deep understanding of science and history to inform his long-honed talents of impartial investigative journalism as he attempts to understand and then explain why after all these years, the medical scientific community still does not have a sound consensus about the essence of diabetes, diet, insulin, and proper prevention and treatment at a level that is actually effective – amazing and so sad.
To signal these evolved and evolving conflicts, the book includes the following chapters:
- “Rise of the Carbohydrate-Rich and Very-Low-Carbohydrate Diets”
- “The Fear of Fat and High-Fat Diets”
- “Insulin and The End of Carbohydrate Restriction and Low Blood Sugar”
Yes, it is difficult. Imagine the bookend segments: “The Nature of Medical Knowledge” and “The Conflicts of Evidence-Based Medicine.” There is also a detailed discussion of good versus bad science spanning three long chapters.
If all that reads like a greatly confused mess to you then you’re beginning to understand. If you are a fan of an unbiased explication of the evolution of understanding the ins and outs of scientific history in richly documented detail, this is a book for you. It’s not a quick nor easy read. And don’t expect to discover whether the newest wonder drugs for weight loss and control of diabetes will be the long-term solution for people with obesity and diabetes worldwide.
Obesity and overweight are major risk factors for type 2 diabetes. About 90% of patients with diabetes have either overweight or obesity. Thus, the complications of these two conditions, which largely overlap, include atherosclerotic cardiovascular disease; myocardial infarction; stroke; hypertension; metabolic syndrome; lower-extremity gangrene; chronic kidney disease; retinopathy; glaucoma; cataracts; disabling osteoarthritis; breast, endometrial, colon, and other cancers; fatty liver; sleep apnea; and peripheral neuropathy. These diseases create a major lucrative business for a wide swathe of medical and surgical specialties, plus hospital, clinic, device, pharmaceutical, and food industries.
In summary, we’ve just been through 40 years of failure to recognize the sugar-elephant in the room and intervene with serious preventive efforts. Forty years of fleshing out both the populace and the American medical-industrial complex (AMIC). Talk about a sweet spot. The only successful long-term treatment of obesity (and with it, diabetes) is prevention. Don’t emphasize losing weight. Focus on preventing excessive weight gain, right now, for the population, beginning with yourselves. Otherwise, we continue openly to perpetuate a terrific deal for the AMIC, a travesty for everyone else. Time for some industrial grade penance and a course correction.
Meanwhile, here we are living out Big Pharma’s dream of a big populace, produced by the agriculture and food industries, enjoyed by capitalism after failures of education, medicine, and public health: a seemingly endless supply of people living with big complications who are ready for big (expensive, new) medications to fix the world’s big health problems.
Dr. Lundberg is editor in chief, Cancer Commons. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Doctor, if you are caring for patients with diabetes, I sure hope you know more about it than I do. The longer I live, it seems, the less I understand.
In a free society, people can do what they want, and that’s great except when it isn’t. That’s why societies develop ethics and even public laws if ethics are not strong enough to protect us from ourselves and others.
Sugar, sugar
When I was growing up in small-town Alabama during the Depression and World War II, we called it sugar diabetes. Eat too much sugar, you got fat; your blood sugar went up, and you spilled sugar into your urine. Diabetes was fairly rare, and so was obesity. Doctors treated it by limiting the intake of sugar (and various sweet foods), along with attempting weight loss. If that didn’t do the trick, insulin injections.
From then until now, note these trends.
Type 2 diabetes was diagnosed even more infrequently before 1950:
- 1920: 0.2% of the population
- 1930: 0.3% of the population
- 1940: 0.4% of the population
In 2020, although 11.3% of the population was diagnosed with type 2 diabetes, the unknown undiagnosed proportion could be much higher.
Notice a correlation between sugar consumption and prevalence of diabetes? Of course, correlation is not causation, but at the same time, it sure as hell is not negation. Such concordance can be considered hypothesis generating. It may not be true causation, but it’s a good bet when 89% of people with diabetes have overweight or obesity.
What did the entire medical, public health, government, agriculture, nursing, food manufacturing, marketing, advertising, restaurant, and education constituencies do about this as it was happening? They observed, documented, gave lip service, and wrung their hands in public a bit. I do not believe that this is an organized active conspiracy; it would take too many players cooperating over too long a period of time. But it certainly may be a passive conspiracy, and primary care physicians and their patients are trapped.
The proper daily practice of medicine consists of one patient, one physician, one moment, and one decision. Let it be a shared decision, informed by the best evidence and taking cost into consideration. That encounter represents an opportunity, a responsibility, and a conundrum.
Individual health is subsumed under the collective health of the public. As such, a patient’s health is out of the control of both physician and patient; instead, patients are the beneficiaries or victims of the “marketplace.” Humans are frail and easily taken advantage of by the brilliant and highly motivated strategic planning and execution of Big Agriculture, Big Food, Big Pharma, Big Marketing, and Big Money-Driven Medicine and generally failed by Big Government, Big Public Health, Big Education, Big Psychology, and Big Religion.
Rethinking diabetes
Consider diabetes as one of many examples. What a terrific deal for capitalism. then it discovers (invents) long-term, very expensive, compelling treatments to slim us down, with no end in sight, and still without ever understanding the true nature of diabetes.
Gary Taubes’s great new book, “Rethinking Diabetes: What Science Reveals About Diet, Insulin, and Successful Treatments,” is being published by Alfred A. Knopf in early 2024.
It is 404 pages of (dense) text, with 401 numbered references and footnotes, a bibliography of 790 references, alphabetically arranged for easy cross-checking, and a 25-page index.
Remember Mr. Taubes’s earlier definitive historical treatises: “Good Calories, Bad Calories” (2007), “Why We Get Fat” (2010), “The Case Against Sugar” (2016), and “The Case for Keto” (2020)?
This new book is more like “Good Calories, Bad Calories”: long, dense, detailed, definitive, and of great historical reference value, including original research information from other countries in other languages. The author told me that the many early research reference sources were available only in German and that his use of generative artificial intelligence as an assistant researcher was of great value.
Nonphysician author Mr. Taubes uses his deep understanding of science and history to inform his long-honed talents of impartial investigative journalism as he attempts to understand and then explain why after all these years, the medical scientific community still does not have a sound consensus about the essence of diabetes, diet, insulin, and proper prevention and treatment at a level that is actually effective – amazing and so sad.
To signal these evolved and evolving conflicts, the book includes the following chapters:
- “Rise of the Carbohydrate-Rich and Very-Low-Carbohydrate Diets”
- “The Fear of Fat and High-Fat Diets”
- “Insulin and The End of Carbohydrate Restriction and Low Blood Sugar”
Yes, it is difficult. Imagine the bookend segments: “The Nature of Medical Knowledge” and “The Conflicts of Evidence-Based Medicine.” There is also a detailed discussion of good versus bad science spanning three long chapters.
If all that reads like a greatly confused mess to you then you’re beginning to understand. If you are a fan of an unbiased explication of the evolution of understanding the ins and outs of scientific history in richly documented detail, this is a book for you. It’s not a quick nor easy read. And don’t expect to discover whether the newest wonder drugs for weight loss and control of diabetes will be the long-term solution for people with obesity and diabetes worldwide.
Obesity and overweight are major risk factors for type 2 diabetes. About 90% of patients with diabetes have either overweight or obesity. Thus, the complications of these two conditions, which largely overlap, include atherosclerotic cardiovascular disease; myocardial infarction; stroke; hypertension; metabolic syndrome; lower-extremity gangrene; chronic kidney disease; retinopathy; glaucoma; cataracts; disabling osteoarthritis; breast, endometrial, colon, and other cancers; fatty liver; sleep apnea; and peripheral neuropathy. These diseases create a major lucrative business for a wide swathe of medical and surgical specialties, plus hospital, clinic, device, pharmaceutical, and food industries.
In summary, we’ve just been through 40 years of failure to recognize the sugar-elephant in the room and intervene with serious preventive efforts. Forty years of fleshing out both the populace and the American medical-industrial complex (AMIC). Talk about a sweet spot. The only successful long-term treatment of obesity (and with it, diabetes) is prevention. Don’t emphasize losing weight. Focus on preventing excessive weight gain, right now, for the population, beginning with yourselves. Otherwise, we continue openly to perpetuate a terrific deal for the AMIC, a travesty for everyone else. Time for some industrial grade penance and a course correction.
Meanwhile, here we are living out Big Pharma’s dream of a big populace, produced by the agriculture and food industries, enjoyed by capitalism after failures of education, medicine, and public health: a seemingly endless supply of people living with big complications who are ready for big (expensive, new) medications to fix the world’s big health problems.
Dr. Lundberg is editor in chief, Cancer Commons. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Doctor, if you are caring for patients with diabetes, I sure hope you know more about it than I do. The longer I live, it seems, the less I understand.
In a free society, people can do what they want, and that’s great except when it isn’t. That’s why societies develop ethics and even public laws if ethics are not strong enough to protect us from ourselves and others.
Sugar, sugar
When I was growing up in small-town Alabama during the Depression and World War II, we called it sugar diabetes. Eat too much sugar, you got fat; your blood sugar went up, and you spilled sugar into your urine. Diabetes was fairly rare, and so was obesity. Doctors treated it by limiting the intake of sugar (and various sweet foods), along with attempting weight loss. If that didn’t do the trick, insulin injections.
From then until now, note these trends.
Type 2 diabetes was diagnosed even more infrequently before 1950:
- 1920: 0.2% of the population
- 1930: 0.3% of the population
- 1940: 0.4% of the population
In 2020, although 11.3% of the population was diagnosed with type 2 diabetes, the unknown undiagnosed proportion could be much higher.
Notice a correlation between sugar consumption and prevalence of diabetes? Of course, correlation is not causation, but at the same time, it sure as hell is not negation. Such concordance can be considered hypothesis generating. It may not be true causation, but it’s a good bet when 89% of people with diabetes have overweight or obesity.
What did the entire medical, public health, government, agriculture, nursing, food manufacturing, marketing, advertising, restaurant, and education constituencies do about this as it was happening? They observed, documented, gave lip service, and wrung their hands in public a bit. I do not believe that this is an organized active conspiracy; it would take too many players cooperating over too long a period of time. But it certainly may be a passive conspiracy, and primary care physicians and their patients are trapped.
The proper daily practice of medicine consists of one patient, one physician, one moment, and one decision. Let it be a shared decision, informed by the best evidence and taking cost into consideration. That encounter represents an opportunity, a responsibility, and a conundrum.
Individual health is subsumed under the collective health of the public. As such, a patient’s health is out of the control of both physician and patient; instead, patients are the beneficiaries or victims of the “marketplace.” Humans are frail and easily taken advantage of by the brilliant and highly motivated strategic planning and execution of Big Agriculture, Big Food, Big Pharma, Big Marketing, and Big Money-Driven Medicine and generally failed by Big Government, Big Public Health, Big Education, Big Psychology, and Big Religion.
Rethinking diabetes
Consider diabetes as one of many examples. What a terrific deal for capitalism. then it discovers (invents) long-term, very expensive, compelling treatments to slim us down, with no end in sight, and still without ever understanding the true nature of diabetes.
Gary Taubes’s great new book, “Rethinking Diabetes: What Science Reveals About Diet, Insulin, and Successful Treatments,” is being published by Alfred A. Knopf in early 2024.
It is 404 pages of (dense) text, with 401 numbered references and footnotes, a bibliography of 790 references, alphabetically arranged for easy cross-checking, and a 25-page index.
Remember Mr. Taubes’s earlier definitive historical treatises: “Good Calories, Bad Calories” (2007), “Why We Get Fat” (2010), “The Case Against Sugar” (2016), and “The Case for Keto” (2020)?
This new book is more like “Good Calories, Bad Calories”: long, dense, detailed, definitive, and of great historical reference value, including original research information from other countries in other languages. The author told me that the many early research reference sources were available only in German and that his use of generative artificial intelligence as an assistant researcher was of great value.
Nonphysician author Mr. Taubes uses his deep understanding of science and history to inform his long-honed talents of impartial investigative journalism as he attempts to understand and then explain why after all these years, the medical scientific community still does not have a sound consensus about the essence of diabetes, diet, insulin, and proper prevention and treatment at a level that is actually effective – amazing and so sad.
To signal these evolved and evolving conflicts, the book includes the following chapters:
- “Rise of the Carbohydrate-Rich and Very-Low-Carbohydrate Diets”
- “The Fear of Fat and High-Fat Diets”
- “Insulin and The End of Carbohydrate Restriction and Low Blood Sugar”
Yes, it is difficult. Imagine the bookend segments: “The Nature of Medical Knowledge” and “The Conflicts of Evidence-Based Medicine.” There is also a detailed discussion of good versus bad science spanning three long chapters.
If all that reads like a greatly confused mess to you then you’re beginning to understand. If you are a fan of an unbiased explication of the evolution of understanding the ins and outs of scientific history in richly documented detail, this is a book for you. It’s not a quick nor easy read. And don’t expect to discover whether the newest wonder drugs for weight loss and control of diabetes will be the long-term solution for people with obesity and diabetes worldwide.
Obesity and overweight are major risk factors for type 2 diabetes. About 90% of patients with diabetes have either overweight or obesity. Thus, the complications of these two conditions, which largely overlap, include atherosclerotic cardiovascular disease; myocardial infarction; stroke; hypertension; metabolic syndrome; lower-extremity gangrene; chronic kidney disease; retinopathy; glaucoma; cataracts; disabling osteoarthritis; breast, endometrial, colon, and other cancers; fatty liver; sleep apnea; and peripheral neuropathy. These diseases create a major lucrative business for a wide swathe of medical and surgical specialties, plus hospital, clinic, device, pharmaceutical, and food industries.
In summary, we’ve just been through 40 years of failure to recognize the sugar-elephant in the room and intervene with serious preventive efforts. Forty years of fleshing out both the populace and the American medical-industrial complex (AMIC). Talk about a sweet spot. The only successful long-term treatment of obesity (and with it, diabetes) is prevention. Don’t emphasize losing weight. Focus on preventing excessive weight gain, right now, for the population, beginning with yourselves. Otherwise, we continue openly to perpetuate a terrific deal for the AMIC, a travesty for everyone else. Time for some industrial grade penance and a course correction.
Meanwhile, here we are living out Big Pharma’s dream of a big populace, produced by the agriculture and food industries, enjoyed by capitalism after failures of education, medicine, and public health: a seemingly endless supply of people living with big complications who are ready for big (expensive, new) medications to fix the world’s big health problems.
Dr. Lundberg is editor in chief, Cancer Commons. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.