User login
Almost 2 million try to quit smoking in wake of CDC campaign
Almost 2 million Americans tried to quit smoking in the wake of a 2012 government educational campaign, and at least 100,000 of them have quit permanently.
That’s according to an analysis of the Centers for Disease Control and Prevention’s (CDC’s) Tips From Former Smokers campaign that was published online in the Lancet on Sept. 9 (doi: 10.1016/S0140-6736(13)61686-4). The analysis by CDC officials estimates that 1.6 million Americans tried to quit after the campaign’s launch in March 2012. By June 2012, when it ended, at least 100,000 of them could be defined as having permanently quit.
"These are really minimal estimates," said Dr. Thomas Frieden, director of the CDC, in a briefing with reporters. "We think the actual impact may have been even larger than this."

The Tips From Former Smokers campaign was made possible by a $54 million grant from the Affordable Care Act’s Public Health and Prevention Fund. Print ads featured graphic photos of former smokers with stomas, or scars from open heart surgery. Former smokers also described tobacco’s toll on their health in broadcast and radio ads and videos posted to the CDC website. The TV ads directed viewers to the 1-800-QUIT-NOW quit line or to the National Cancer Institute’s quit assistance website, www.smokefree.gov.
A testimonial from former smoker Terrie Hall has been the most-visited page on the entire CDC site, receiving 2.5 million hits so far, Dr. Frieden said. In it, Ms. Hall tells smokers: "Record your voice for loved ones while you still can." Ms. Hall was diagnosed with throat cancer, had her larynx removed, and now speaks with the aid of an artificial voice box.
Overall, the tips campaign was seen by four out of five smokers, the Lancet report estimated.
To assess how well the campaign worked, the CDC used a nationally representative online survey. Current smokers – those who had smoked at least 100 cigarettes in their lifetime and now smoked every day or some days – and nonsmokers (all others) were compared. There was a baseline survey before the campaign started and another immediately after the campaign ended.
Of the invited smokers, 70% (4,108) responded, and 58% (3,000) of the invited nonsmokers responded to the baseline survey. After the campaign ended, 74% (3,058) of the smokers and 74% (2,220) of the nonsmokers responded. About 75% of the smokers and nonsmokers said they recalled seeing at least one tips ad.
The prevalence of smokers who tried to quit in the past 3 months increased from 31% before the tips campaign to 35% after the campaign. At the end of the 12-week campaign, 13% of smokers who tried to quit said they had not smoked again.
After stratifying the results of the overall response to the campaign, the CDC researchers found that there were more quit attempts among younger smokers, lighter smokers, African American smokers, and smokers with less education.
Calls to the 1-800-QUIT-NOW line increased 132% during the 12-week campaign, 200,000 more calls than during the same period the previous year. There were also 500,000 unique visitors to the www.smokefree.gov website.
The analysis showed that the campaign spurred a large number of nonsmokers to talk to their friends or family about the dangers of smoking and quitting. Applying the findings to the U.S. population, the researchers reported that almost 5 million nonsmokers recommended a smoking cessation service to a friend or family member, and 6 million discussed the dangers of smoking.
Lisha Hancock was one of those smokers who heard from a family member about quitting, but she also said that she was influenced greatly by Terrie Hall’s story. Ms. Hancock told reporters that she smoked for 17 years, starting at age 21. Family and peer pressure did not motivate her to quit. But her 5-year-old son’s questions and response to Ms. Hall’s ads, along with her own impressions from Ms. Hall’s testimonial, moved her. "You can see the regret and sadness in her eyes," said Ms. Hancock, in a conference call.
After seeing the ads and online testimonials, Ms. Hancock decided to make a plan, made some diet and exercise changes, and used nicotine lozenges to help her quit. She has gone about 6 months without smoking, she said.
The CDC report found that thanks to more people quitting, the campaign may have added 500,000 quality-adjusted life-years to the U.S. population, which suggests a cost per life-year saved of less than $200. That ranks the campaign "among the most cost-effective preventive interventions," said the CDC authors.

Meanwhile, the $54 million spent on the campaign is less than what the tobacco industry spends for 3 days of marketing, according to the report. The industry’s $8 billion in annual spending far outweighs the federal government’s capabilities, but Dr. Frieden said he was optimistic. "We’re going to win that David and Goliath battle," he told reporters.
Dr. Frieden said that the study results validated a large, national educational antismoking campaign. The CDC will continue to find ways to alert the public to the dangers of smoking, he said. The agency ran additional Tips From Former Smokers ads between March and June this year. That campaign included exhortations for smokers to talk to their physicians about quitting.
The authors reported having no financial disclosures.
On Twitter @aliciaault
Almost 2 million Americans tried to quit smoking in the wake of a 2012 government educational campaign, and at least 100,000 of them have quit permanently.
That’s according to an analysis of the Centers for Disease Control and Prevention’s (CDC’s) Tips From Former Smokers campaign that was published online in the Lancet on Sept. 9 (doi: 10.1016/S0140-6736(13)61686-4). The analysis by CDC officials estimates that 1.6 million Americans tried to quit after the campaign’s launch in March 2012. By June 2012, when it ended, at least 100,000 of them could be defined as having permanently quit.
"These are really minimal estimates," said Dr. Thomas Frieden, director of the CDC, in a briefing with reporters. "We think the actual impact may have been even larger than this."
The Tips From Former Smokers campaign was made possible by a $54 million grant from the Affordable Care Act’s Public Health and Prevention Fund. Print ads featured graphic photos of former smokers with stomas, or scars from open heart surgery. Former smokers also described tobacco’s toll on their health in broadcast and radio ads and videos posted to the CDC website. The TV ads directed viewers to the 1-800-QUIT-NOW quit line or to the National Cancer Institute’s quit assistance website, www.smokefree.gov.
A testimonial from former smoker Terrie Hall has been the most-visited page on the entire CDC site, receiving 2.5 million hits so far, Dr. Frieden said. In it, Ms. Hall tells smokers: "Record your voice for loved ones while you still can." Ms. Hall was diagnosed with throat cancer, had her larynx removed, and now speaks with the aid of an artificial voice box.
Overall, the tips campaign was seen by four out of five smokers, the Lancet report estimated.
To assess how well the campaign worked, the CDC used a nationally representative online survey. Current smokers – those who had smoked at least 100 cigarettes in their lifetime and now smoked every day or some days – and nonsmokers (all others) were compared. There was a baseline survey before the campaign started and another immediately after the campaign ended.
Of the invited smokers, 70% (4,108) responded, and 58% (3,000) of the invited nonsmokers responded to the baseline survey. After the campaign ended, 74% (3,058) of the smokers and 74% (2,220) of the nonsmokers responded. About 75% of the smokers and nonsmokers said they recalled seeing at least one tips ad.
The prevalence of smokers who tried to quit in the past 3 months increased from 31% before the tips campaign to 35% after the campaign. At the end of the 12-week campaign, 13% of smokers who tried to quit said they had not smoked again.
After stratifying the results of the overall response to the campaign, the CDC researchers found that there were more quit attempts among younger smokers, lighter smokers, African American smokers, and smokers with less education.
Calls to the 1-800-QUIT-NOW line increased 132% during the 12-week campaign, 200,000 more calls than during the same period the previous year. There were also 500,000 unique visitors to the www.smokefree.gov website.
The analysis showed that the campaign spurred a large number of nonsmokers to talk to their friends or family about the dangers of smoking and quitting. Applying the findings to the U.S. population, the researchers reported that almost 5 million nonsmokers recommended a smoking cessation service to a friend or family member, and 6 million discussed the dangers of smoking.
Lisha Hancock was one of those smokers who heard from a family member about quitting, but she also said that she was influenced greatly by Terrie Hall’s story. Ms. Hancock told reporters that she smoked for 17 years, starting at age 21. Family and peer pressure did not motivate her to quit. But her 5-year-old son’s questions and response to Ms. Hall’s ads, along with her own impressions from Ms. Hall’s testimonial, moved her. "You can see the regret and sadness in her eyes," said Ms. Hancock, in a conference call.
After seeing the ads and online testimonials, Ms. Hancock decided to make a plan, made some diet and exercise changes, and used nicotine lozenges to help her quit. She has gone about 6 months without smoking, she said.
The CDC report found that thanks to more people quitting, the campaign may have added 500,000 quality-adjusted life-years to the U.S. population, which suggests a cost per life-year saved of less than $200. That ranks the campaign "among the most cost-effective preventive interventions," said the CDC authors.
Meanwhile, the $54 million spent on the campaign is less than what the tobacco industry spends for 3 days of marketing, according to the report. The industry’s $8 billion in annual spending far outweighs the federal government’s capabilities, but Dr. Frieden said he was optimistic. "We’re going to win that David and Goliath battle," he told reporters.
Dr. Frieden said that the study results validated a large, national educational antismoking campaign. The CDC will continue to find ways to alert the public to the dangers of smoking, he said. The agency ran additional Tips From Former Smokers ads between March and June this year. That campaign included exhortations for smokers to talk to their physicians about quitting.
The authors reported having no financial disclosures.
On Twitter @aliciaault
Almost 2 million Americans tried to quit smoking in the wake of a 2012 government educational campaign, and at least 100,000 of them have quit permanently.
That’s according to an analysis of the Centers for Disease Control and Prevention’s (CDC’s) Tips From Former Smokers campaign that was published online in the Lancet on Sept. 9 (doi: 10.1016/S0140-6736(13)61686-4). The analysis by CDC officials estimates that 1.6 million Americans tried to quit after the campaign’s launch in March 2012. By June 2012, when it ended, at least 100,000 of them could be defined as having permanently quit.
"These are really minimal estimates," said Dr. Thomas Frieden, director of the CDC, in a briefing with reporters. "We think the actual impact may have been even larger than this."
The Tips From Former Smokers campaign was made possible by a $54 million grant from the Affordable Care Act’s Public Health and Prevention Fund. Print ads featured graphic photos of former smokers with stomas, or scars from open heart surgery. Former smokers also described tobacco’s toll on their health in broadcast and radio ads and videos posted to the CDC website. The TV ads directed viewers to the 1-800-QUIT-NOW quit line or to the National Cancer Institute’s quit assistance website, www.smokefree.gov.
A testimonial from former smoker Terrie Hall has been the most-visited page on the entire CDC site, receiving 2.5 million hits so far, Dr. Frieden said. In it, Ms. Hall tells smokers: "Record your voice for loved ones while you still can." Ms. Hall was diagnosed with throat cancer, had her larynx removed, and now speaks with the aid of an artificial voice box.
Overall, the tips campaign was seen by four out of five smokers, the Lancet report estimated.
To assess how well the campaign worked, the CDC used a nationally representative online survey. Current smokers – those who had smoked at least 100 cigarettes in their lifetime and now smoked every day or some days – and nonsmokers (all others) were compared. There was a baseline survey before the campaign started and another immediately after the campaign ended.
Of the invited smokers, 70% (4,108) responded, and 58% (3,000) of the invited nonsmokers responded to the baseline survey. After the campaign ended, 74% (3,058) of the smokers and 74% (2,220) of the nonsmokers responded. About 75% of the smokers and nonsmokers said they recalled seeing at least one tips ad.
The prevalence of smokers who tried to quit in the past 3 months increased from 31% before the tips campaign to 35% after the campaign. At the end of the 12-week campaign, 13% of smokers who tried to quit said they had not smoked again.
After stratifying the results of the overall response to the campaign, the CDC researchers found that there were more quit attempts among younger smokers, lighter smokers, African American smokers, and smokers with less education.
Calls to the 1-800-QUIT-NOW line increased 132% during the 12-week campaign, 200,000 more calls than during the same period the previous year. There were also 500,000 unique visitors to the www.smokefree.gov website.
The analysis showed that the campaign spurred a large number of nonsmokers to talk to their friends or family about the dangers of smoking and quitting. Applying the findings to the U.S. population, the researchers reported that almost 5 million nonsmokers recommended a smoking cessation service to a friend or family member, and 6 million discussed the dangers of smoking.
Lisha Hancock was one of those smokers who heard from a family member about quitting, but she also said that she was influenced greatly by Terrie Hall’s story. Ms. Hancock told reporters that she smoked for 17 years, starting at age 21. Family and peer pressure did not motivate her to quit. But her 5-year-old son’s questions and response to Ms. Hall’s ads, along with her own impressions from Ms. Hall’s testimonial, moved her. "You can see the regret and sadness in her eyes," said Ms. Hancock, in a conference call.
After seeing the ads and online testimonials, Ms. Hancock decided to make a plan, made some diet and exercise changes, and used nicotine lozenges to help her quit. She has gone about 6 months without smoking, she said.
The CDC report found that thanks to more people quitting, the campaign may have added 500,000 quality-adjusted life-years to the U.S. population, which suggests a cost per life-year saved of less than $200. That ranks the campaign "among the most cost-effective preventive interventions," said the CDC authors.
Meanwhile, the $54 million spent on the campaign is less than what the tobacco industry spends for 3 days of marketing, according to the report. The industry’s $8 billion in annual spending far outweighs the federal government’s capabilities, but Dr. Frieden said he was optimistic. "We’re going to win that David and Goliath battle," he told reporters.
Dr. Frieden said that the study results validated a large, national educational antismoking campaign. The CDC will continue to find ways to alert the public to the dangers of smoking, he said. The agency ran additional Tips From Former Smokers ads between March and June this year. That campaign included exhortations for smokers to talk to their physicians about quitting.
The authors reported having no financial disclosures.
On Twitter @aliciaault
FROM THE LANCET
Major finding: About 2 million Americans tried to quit in March 2012, and by June 2012 at least 100,000 remained abstinent following a public education campaign.
Data source: Data compiled from a baseline and follow-up survey of nationally representative samples of adult smokers and nonsmokers.
Disclosures: The authors reported having no financial disclosures.

Teen drug and alcohol use decline, but more adults using marijuana
Teens are drinking less, seem to be responding to messages to stay away from nonmedical use of prescription drugs, and are slightly curbing marijuana use. For adults, however, the story is slightly different. Marijuana use is increasing, especially in those aged 18 to 25, and overall illicit drug use is growing in the 50- to 64-year-old segment.
That’s according to the latest data from the annual National Survey on Drug Use and Health (NSDUH), which is sponsored by the Substance Abuse and Mental Health Services Administration (SAMHSA), and tracks the illicit use of substances in the U.S. population. The 2012 NSDUH report screened almost 70,000 people aged 12 and over between January through December 2012.
"These findings show that while we have made progress in preventing some aspects of substance abuse, we must redouble our efforts to reduce and eliminate all forms of it throughout our nation," said SAMHSA Administrator Pamela S. Hyde, in a statement.
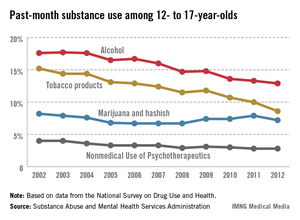
Marijuana is by far the most popular illicit drug in America. Overall, 7% of survey respondents were current marijuana users in 2012. Past-month use rose in almost every age group from 2007 to 2012. A quarter of 18- to-20-year-olds and 17% of 21- to-25-year-olds were past-month users, and a third of each group had used in the past year.
Rates declined very slightly for 12- to-17-year olds, from 7.9% in 2011 to 7.2% in 2012. But the proportion who said smoking marijuana once or twice a week was risky decreased from 55% in 2007 to 44% in 2012. A similar slight decline in use, but a larger decline in perception of risk also was seen in the Monitoring the Future survey released in December, which is sponsored by the National Institute on Drug Abuse.

The decreased perception of harm is particularly dangerous, because it can lead to higher usage rates, said Dr. Sharon Levy, director of the Adolescent Substance Abuse Program at Children’s Hospital, Boston, in an interview. The edging up of marijuana use among older adolescents is likely attributable to an ever-present and growing national conversation that marijuana is safe, said Dr. Levy, who also serves as chair of the American Academy of Pediatrics’ Committee on Substance Abuse.
She said that while cannabinoids might end up being useful from a medical standpoint, marijuana itself is associated with harms in children and adolescents, including an increase in mental health disorders and decline in motivation, and potentially, a higher risk of cognitive decline.
The AAP’s most-recent statement on substance abuse intervention and treatment (Pediatrics 2011;128:e1330) recommends that clinicians start screening children for substance abuse at age 12 years. By that time, it’s likely that they’ve heard of marijuana, Dr. Levy said. Children expect health advice from their pediatrician; the aim is to keep the information both medically and personally relevant as much as possible, she said. Athletes can be told that smoking will affect their lungs, for instance.
More positively, the SAMHSA data showed a stabilization of nonmedical use of prescription drugs, such as narcotics, among young adults aged 18-25 years. In 2012, 5% of that age cohort admitted to past-month use, which was similar to rates in 2010 and 2011, but lower than the 6.4% reported in 2009.
Past-month drinking, binge drinking, and heavy drinking among adolescents aged 12-17 years also stabilized, and rates were lower than previous high points of 2002 and 2009.
About half of Americans over the age of 12 years say they are current drinkers. About a quarter in 2012 identified as binge drinkers, which is five or more drinks on one occasion at least 1 day in the past month. That’s the same rate as in 2011. Heavy drinking stayed the same also, for all age groups.
The declines in alcohol, tobacco, and nonmedical prescription drug use among children were encouraging, and indicate that government and physician-led efforts "are having an impact," Dr. Levy said.
"We’re never going to eliminate all use, but we can continue to push it down," Dr. Levy said.
R. Gil Kerlikowske, director of the Office of National Drug Control Policy, agreed that campaigns focusing on prescription drug use had had some effect. "For the first time in a decade, we are seeing real and significant reductions in the abuse of prescription drugs in America, proving that a more comprehensive response to our drug problem can make a real difference in making our nation healthier and safer," he said in a statement.
One area of concern: an upward trend in heroin use. In 2012, 669,000 Americans said they’d used heroin in the past year, compared with 373,000 in 2007. There’s been a small uptick in heroin users aged 18-25 years. And there’s been a big increase over the last decade in the number of Americans who would be classified under the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) as having heroin dependence, according to the report. In 2012, 467,000 people would be labeled dependent, compared with 214,000 in 2002. Last year, 450,000 Americans received treatment for heroin abuse.
Overall, 4 million Americans over the age of 12 (1.5% of the population) received alcohol or illicit drug use treatment. That number and percentage have basically stayed the same since 2002. In 2012, the largest number of those who received treatment – 2.4 million – reported receiving treatment for alcohol use. Next came treatment for pain relievers (973,000), and third was marijuana use (957,000).
An estimated 23 million Americans (8% of the nation) needed treatment; 2.5 million received care in a specialized facility. Of the 21 million who did not get care, only 1 million said they felt that they actually needed treatment, according to SAMHSA. In that group, some 31% said they’d made an effort but could not get into a program. The primary reason was "a lack of insurance coverage and inability to pay the cost," said the SAMHSA report.
"Expanding prevention, treatment, and support for people in recovery for substance use disorders will be our guide as we work to address other emerging challenges, including the recent uptick in heroin use shown in this survey," Mr. Kerlikowske said.
On Twitter @aliciaault
Teens are drinking less, seem to be responding to messages to stay away from nonmedical use of prescription drugs, and are slightly curbing marijuana use. For adults, however, the story is slightly different. Marijuana use is increasing, especially in those aged 18 to 25, and overall illicit drug use is growing in the 50- to 64-year-old segment.
That’s according to the latest data from the annual National Survey on Drug Use and Health (NSDUH), which is sponsored by the Substance Abuse and Mental Health Services Administration (SAMHSA), and tracks the illicit use of substances in the U.S. population. The 2012 NSDUH report screened almost 70,000 people aged 12 and over between January through December 2012.
"These findings show that while we have made progress in preventing some aspects of substance abuse, we must redouble our efforts to reduce and eliminate all forms of it throughout our nation," said SAMHSA Administrator Pamela S. Hyde, in a statement.
Marijuana is by far the most popular illicit drug in America. Overall, 7% of survey respondents were current marijuana users in 2012. Past-month use rose in almost every age group from 2007 to 2012. A quarter of 18- to-20-year-olds and 17% of 21- to-25-year-olds were past-month users, and a third of each group had used in the past year.
Rates declined very slightly for 12- to-17-year olds, from 7.9% in 2011 to 7.2% in 2012. But the proportion who said smoking marijuana once or twice a week was risky decreased from 55% in 2007 to 44% in 2012. A similar slight decline in use, but a larger decline in perception of risk also was seen in the Monitoring the Future survey released in December, which is sponsored by the National Institute on Drug Abuse.
The decreased perception of harm is particularly dangerous, because it can lead to higher usage rates, said Dr. Sharon Levy, director of the Adolescent Substance Abuse Program at Children’s Hospital, Boston, in an interview. The edging up of marijuana use among older adolescents is likely attributable to an ever-present and growing national conversation that marijuana is safe, said Dr. Levy, who also serves as chair of the American Academy of Pediatrics’ Committee on Substance Abuse.
She said that while cannabinoids might end up being useful from a medical standpoint, marijuana itself is associated with harms in children and adolescents, including an increase in mental health disorders and decline in motivation, and potentially, a higher risk of cognitive decline.
The AAP’s most-recent statement on substance abuse intervention and treatment (Pediatrics 2011;128:e1330) recommends that clinicians start screening children for substance abuse at age 12 years. By that time, it’s likely that they’ve heard of marijuana, Dr. Levy said. Children expect health advice from their pediatrician; the aim is to keep the information both medically and personally relevant as much as possible, she said. Athletes can be told that smoking will affect their lungs, for instance.
More positively, the SAMHSA data showed a stabilization of nonmedical use of prescription drugs, such as narcotics, among young adults aged 18-25 years. In 2012, 5% of that age cohort admitted to past-month use, which was similar to rates in 2010 and 2011, but lower than the 6.4% reported in 2009.
Past-month drinking, binge drinking, and heavy drinking among adolescents aged 12-17 years also stabilized, and rates were lower than previous high points of 2002 and 2009.
About half of Americans over the age of 12 years say they are current drinkers. About a quarter in 2012 identified as binge drinkers, which is five or more drinks on one occasion at least 1 day in the past month. That’s the same rate as in 2011. Heavy drinking stayed the same also, for all age groups.
The declines in alcohol, tobacco, and nonmedical prescription drug use among children were encouraging, and indicate that government and physician-led efforts "are having an impact," Dr. Levy said.
"We’re never going to eliminate all use, but we can continue to push it down," Dr. Levy said.
R. Gil Kerlikowske, director of the Office of National Drug Control Policy, agreed that campaigns focusing on prescription drug use had had some effect. "For the first time in a decade, we are seeing real and significant reductions in the abuse of prescription drugs in America, proving that a more comprehensive response to our drug problem can make a real difference in making our nation healthier and safer," he said in a statement.
One area of concern: an upward trend in heroin use. In 2012, 669,000 Americans said they’d used heroin in the past year, compared with 373,000 in 2007. There’s been a small uptick in heroin users aged 18-25 years. And there’s been a big increase over the last decade in the number of Americans who would be classified under the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) as having heroin dependence, according to the report. In 2012, 467,000 people would be labeled dependent, compared with 214,000 in 2002. Last year, 450,000 Americans received treatment for heroin abuse.
Overall, 4 million Americans over the age of 12 (1.5% of the population) received alcohol or illicit drug use treatment. That number and percentage have basically stayed the same since 2002. In 2012, the largest number of those who received treatment – 2.4 million – reported receiving treatment for alcohol use. Next came treatment for pain relievers (973,000), and third was marijuana use (957,000).
An estimated 23 million Americans (8% of the nation) needed treatment; 2.5 million received care in a specialized facility. Of the 21 million who did not get care, only 1 million said they felt that they actually needed treatment, according to SAMHSA. In that group, some 31% said they’d made an effort but could not get into a program. The primary reason was "a lack of insurance coverage and inability to pay the cost," said the SAMHSA report.
"Expanding prevention, treatment, and support for people in recovery for substance use disorders will be our guide as we work to address other emerging challenges, including the recent uptick in heroin use shown in this survey," Mr. Kerlikowske said.
On Twitter @aliciaault
Teens are drinking less, seem to be responding to messages to stay away from nonmedical use of prescription drugs, and are slightly curbing marijuana use. For adults, however, the story is slightly different. Marijuana use is increasing, especially in those aged 18 to 25, and overall illicit drug use is growing in the 50- to 64-year-old segment.
That’s according to the latest data from the annual National Survey on Drug Use and Health (NSDUH), which is sponsored by the Substance Abuse and Mental Health Services Administration (SAMHSA), and tracks the illicit use of substances in the U.S. population. The 2012 NSDUH report screened almost 70,000 people aged 12 and over between January through December 2012.
"These findings show that while we have made progress in preventing some aspects of substance abuse, we must redouble our efforts to reduce and eliminate all forms of it throughout our nation," said SAMHSA Administrator Pamela S. Hyde, in a statement.
Marijuana is by far the most popular illicit drug in America. Overall, 7% of survey respondents were current marijuana users in 2012. Past-month use rose in almost every age group from 2007 to 2012. A quarter of 18- to-20-year-olds and 17% of 21- to-25-year-olds were past-month users, and a third of each group had used in the past year.
Rates declined very slightly for 12- to-17-year olds, from 7.9% in 2011 to 7.2% in 2012. But the proportion who said smoking marijuana once or twice a week was risky decreased from 55% in 2007 to 44% in 2012. A similar slight decline in use, but a larger decline in perception of risk also was seen in the Monitoring the Future survey released in December, which is sponsored by the National Institute on Drug Abuse.
The decreased perception of harm is particularly dangerous, because it can lead to higher usage rates, said Dr. Sharon Levy, director of the Adolescent Substance Abuse Program at Children’s Hospital, Boston, in an interview. The edging up of marijuana use among older adolescents is likely attributable to an ever-present and growing national conversation that marijuana is safe, said Dr. Levy, who also serves as chair of the American Academy of Pediatrics’ Committee on Substance Abuse.
She said that while cannabinoids might end up being useful from a medical standpoint, marijuana itself is associated with harms in children and adolescents, including an increase in mental health disorders and decline in motivation, and potentially, a higher risk of cognitive decline.
The AAP’s most-recent statement on substance abuse intervention and treatment (Pediatrics 2011;128:e1330) recommends that clinicians start screening children for substance abuse at age 12 years. By that time, it’s likely that they’ve heard of marijuana, Dr. Levy said. Children expect health advice from their pediatrician; the aim is to keep the information both medically and personally relevant as much as possible, she said. Athletes can be told that smoking will affect their lungs, for instance.
More positively, the SAMHSA data showed a stabilization of nonmedical use of prescription drugs, such as narcotics, among young adults aged 18-25 years. In 2012, 5% of that age cohort admitted to past-month use, which was similar to rates in 2010 and 2011, but lower than the 6.4% reported in 2009.
Past-month drinking, binge drinking, and heavy drinking among adolescents aged 12-17 years also stabilized, and rates were lower than previous high points of 2002 and 2009.
About half of Americans over the age of 12 years say they are current drinkers. About a quarter in 2012 identified as binge drinkers, which is five or more drinks on one occasion at least 1 day in the past month. That’s the same rate as in 2011. Heavy drinking stayed the same also, for all age groups.
The declines in alcohol, tobacco, and nonmedical prescription drug use among children were encouraging, and indicate that government and physician-led efforts "are having an impact," Dr. Levy said.
"We’re never going to eliminate all use, but we can continue to push it down," Dr. Levy said.
R. Gil Kerlikowske, director of the Office of National Drug Control Policy, agreed that campaigns focusing on prescription drug use had had some effect. "For the first time in a decade, we are seeing real and significant reductions in the abuse of prescription drugs in America, proving that a more comprehensive response to our drug problem can make a real difference in making our nation healthier and safer," he said in a statement.
One area of concern: an upward trend in heroin use. In 2012, 669,000 Americans said they’d used heroin in the past year, compared with 373,000 in 2007. There’s been a small uptick in heroin users aged 18-25 years. And there’s been a big increase over the last decade in the number of Americans who would be classified under the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) as having heroin dependence, according to the report. In 2012, 467,000 people would be labeled dependent, compared with 214,000 in 2002. Last year, 450,000 Americans received treatment for heroin abuse.
Overall, 4 million Americans over the age of 12 (1.5% of the population) received alcohol or illicit drug use treatment. That number and percentage have basically stayed the same since 2002. In 2012, the largest number of those who received treatment – 2.4 million – reported receiving treatment for alcohol use. Next came treatment for pain relievers (973,000), and third was marijuana use (957,000).
An estimated 23 million Americans (8% of the nation) needed treatment; 2.5 million received care in a specialized facility. Of the 21 million who did not get care, only 1 million said they felt that they actually needed treatment, according to SAMHSA. In that group, some 31% said they’d made an effort but could not get into a program. The primary reason was "a lack of insurance coverage and inability to pay the cost," said the SAMHSA report.
"Expanding prevention, treatment, and support for people in recovery for substance use disorders will be our guide as we work to address other emerging challenges, including the recent uptick in heroin use shown in this survey," Mr. Kerlikowske said.
On Twitter @aliciaault

AGA shines light on gut microbiome on Capitol Hill
Scientific advisers from the AGA’s Center for Gut Microbiome Research and Education went to Capitol Hill in late July to make a pitch for increased research funding, including for the National Institutes of Health’s Human Microbiome Project.
The advisers – Rob Knight, Ph.D., Dr. Martin J. Blaser, and Dr. Gary D. Wu – along with AGA President Loren A. Laine, briefed congressional staff on the science of the gut microbiome and the importance of delving further into its workings.
"There’s no question that understanding and manipulating the gut microbiome will be very important in attacking diseases, and how we take care of patients’ diseases in the future," said Dr. Laine.

Dr. Knight, an associate professor of chemistry at the University of Colorado, Boulder, and a career scientist with the Howard Hughes Medical Institute, gave an overview of the field, focusing on what’s been collected so far by the Human Microbiome Project. The HMP, begun in 2007, aims to characterize the healthy human microbiome by sampling 300 subjects (from 15 body sites on men and 18 sites on women).
So far, the HMP data have shown that humans have unique microbiome "fingerprints." We are 90% different, with microbes differing according to age, sex, and geographic area – and possibly by other parameters, as well. Getting the genomic fingerprint of the microbiome is important because microbes can help determine, for instance, whether certain drugs might cause liver toxicity or make a person more attractive to mosquitoes, said Mr. Knight. The HMP, however, is limited to studying healthy Western adults.
Dr. Knight is a collaborator on the American Gut Project, which is using crowd-sourced samples to further examine the makeup of the gut microbiome. So far, several thousand people from around the world have participated. It is funded by $99 "donations," from each participant, which cover the cost of the sampling kit. The donations go to the Biofrontiers Institute at the University of Colorado, Boulder, and the Earth Microbiome Project.
There is a need for faster DNA sequencing, databases of normal and abnormal microbiomes to provide a baseline, and research into how the microbiome affects health, including longitudinal studies to predict and monitor health changes, and animal models to help establish causality, said Dr. Knight.
Dr. Blaser, professor of microbiology and director of the Human Microbiome Program at the New York University Langone Medical Center, said findings so far had stimulated interest in researching the identity of various microbes, their activities, how the human host responds to microbes, the forces that maintain equilibrium in the host, and the unique characteristics of each individual’s microbiome. He and others have been looking into how antibiotic use in childhood might be affecting obesity. Studies have shown a correlation between heavy antibiotic use in certain areas of the country and greater rates of obesity in those same areas, said Dr. Blaser.
Antibiotic use may also be leading to less diversity in the guts of American adults, he said. There is a need for more research on the consequences of antibiotic use, and to help produce better diagnostics and therapies that are more narrowly targeted, he said. It would also be useful to examine the potential for both prebiotic and probiotic therapies, Dr. Blaser said.
Dr. Wu, professor of medicine at the University of Pennsylvania, Philadelphia, briefed the attendees on the success of fecal transplants to treat Clostridium difficile. So far, the procedure has offered proof of principle that human microbiota can be modified to treat disease, said Dr. Wu. It also has provided a window into the biology of the gut microbiome.
But "we must be very cautious," said Dr. Wu, noting that there are no data on short-term or long-term consequences of fecal transplant. The gut includes bacteria, fungi, and viruses, many of which have not been fully characterized yet, and is a "dynamic and living consortium that can change over time in ways that scientists cannot fully predict," said Dr. Wu.
He noted that clinicians had accidentally infected a generation of patients with hepatitis C through blood transfusions, because hepatitis C virus had not been discovered yet.
In the future, the aim is to standardize the process – both in creating the material to be transplanted and the conditions under which it is given, said Dr. Wu. There is also a need for functional studies in humans, to determine how the transplants work. Finally, he said, "it’s of tremendous importance that there be a register so people can be tracked for short- and long-term safety."
With potentially thousands of people getting fecal transplants in the near future, education of the lay public and clinicians is also crucial, said Dr. Wu.
The AGA’s Center for Gut Microbiome Research and Education will help fulfill that role. Started in March, its mission is to advance research and education. The advisory board will make recommendations to the AGA Governing Board on policy and research strategies.
Danone Inc. is a founding supporter of the center.
On Twitter @aliciaault
Scientific advisers from the AGA’s Center for Gut Microbiome Research and Education went to Capitol Hill in late July to make a pitch for increased research funding, including for the National Institutes of Health’s Human Microbiome Project.
The advisers – Rob Knight, Ph.D., Dr. Martin J. Blaser, and Dr. Gary D. Wu – along with AGA President Loren A. Laine, briefed congressional staff on the science of the gut microbiome and the importance of delving further into its workings.
"There’s no question that understanding and manipulating the gut microbiome will be very important in attacking diseases, and how we take care of patients’ diseases in the future," said Dr. Laine.
Dr. Knight, an associate professor of chemistry at the University of Colorado, Boulder, and a career scientist with the Howard Hughes Medical Institute, gave an overview of the field, focusing on what’s been collected so far by the Human Microbiome Project. The HMP, begun in 2007, aims to characterize the healthy human microbiome by sampling 300 subjects (from 15 body sites on men and 18 sites on women).
So far, the HMP data have shown that humans have unique microbiome "fingerprints." We are 90% different, with microbes differing according to age, sex, and geographic area – and possibly by other parameters, as well. Getting the genomic fingerprint of the microbiome is important because microbes can help determine, for instance, whether certain drugs might cause liver toxicity or make a person more attractive to mosquitoes, said Mr. Knight. The HMP, however, is limited to studying healthy Western adults.
Dr. Knight is a collaborator on the American Gut Project, which is using crowd-sourced samples to further examine the makeup of the gut microbiome. So far, several thousand people from around the world have participated. It is funded by $99 "donations," from each participant, which cover the cost of the sampling kit. The donations go to the Biofrontiers Institute at the University of Colorado, Boulder, and the Earth Microbiome Project.
There is a need for faster DNA sequencing, databases of normal and abnormal microbiomes to provide a baseline, and research into how the microbiome affects health, including longitudinal studies to predict and monitor health changes, and animal models to help establish causality, said Dr. Knight.
Dr. Blaser, professor of microbiology and director of the Human Microbiome Program at the New York University Langone Medical Center, said findings so far had stimulated interest in researching the identity of various microbes, their activities, how the human host responds to microbes, the forces that maintain equilibrium in the host, and the unique characteristics of each individual’s microbiome. He and others have been looking into how antibiotic use in childhood might be affecting obesity. Studies have shown a correlation between heavy antibiotic use in certain areas of the country and greater rates of obesity in those same areas, said Dr. Blaser.
Antibiotic use may also be leading to less diversity in the guts of American adults, he said. There is a need for more research on the consequences of antibiotic use, and to help produce better diagnostics and therapies that are more narrowly targeted, he said. It would also be useful to examine the potential for both prebiotic and probiotic therapies, Dr. Blaser said.
Dr. Wu, professor of medicine at the University of Pennsylvania, Philadelphia, briefed the attendees on the success of fecal transplants to treat Clostridium difficile. So far, the procedure has offered proof of principle that human microbiota can be modified to treat disease, said Dr. Wu. It also has provided a window into the biology of the gut microbiome.
But "we must be very cautious," said Dr. Wu, noting that there are no data on short-term or long-term consequences of fecal transplant. The gut includes bacteria, fungi, and viruses, many of which have not been fully characterized yet, and is a "dynamic and living consortium that can change over time in ways that scientists cannot fully predict," said Dr. Wu.
He noted that clinicians had accidentally infected a generation of patients with hepatitis C through blood transfusions, because hepatitis C virus had not been discovered yet.
In the future, the aim is to standardize the process – both in creating the material to be transplanted and the conditions under which it is given, said Dr. Wu. There is also a need for functional studies in humans, to determine how the transplants work. Finally, he said, "it’s of tremendous importance that there be a register so people can be tracked for short- and long-term safety."
With potentially thousands of people getting fecal transplants in the near future, education of the lay public and clinicians is also crucial, said Dr. Wu.
The AGA’s Center for Gut Microbiome Research and Education will help fulfill that role. Started in March, its mission is to advance research and education. The advisory board will make recommendations to the AGA Governing Board on policy and research strategies.
Danone Inc. is a founding supporter of the center.
On Twitter @aliciaault
Scientific advisers from the AGA’s Center for Gut Microbiome Research and Education went to Capitol Hill in late July to make a pitch for increased research funding, including for the National Institutes of Health’s Human Microbiome Project.
The advisers – Rob Knight, Ph.D., Dr. Martin J. Blaser, and Dr. Gary D. Wu – along with AGA President Loren A. Laine, briefed congressional staff on the science of the gut microbiome and the importance of delving further into its workings.
"There’s no question that understanding and manipulating the gut microbiome will be very important in attacking diseases, and how we take care of patients’ diseases in the future," said Dr. Laine.
Dr. Knight, an associate professor of chemistry at the University of Colorado, Boulder, and a career scientist with the Howard Hughes Medical Institute, gave an overview of the field, focusing on what’s been collected so far by the Human Microbiome Project. The HMP, begun in 2007, aims to characterize the healthy human microbiome by sampling 300 subjects (from 15 body sites on men and 18 sites on women).
So far, the HMP data have shown that humans have unique microbiome "fingerprints." We are 90% different, with microbes differing according to age, sex, and geographic area – and possibly by other parameters, as well. Getting the genomic fingerprint of the microbiome is important because microbes can help determine, for instance, whether certain drugs might cause liver toxicity or make a person more attractive to mosquitoes, said Mr. Knight. The HMP, however, is limited to studying healthy Western adults.
Dr. Knight is a collaborator on the American Gut Project, which is using crowd-sourced samples to further examine the makeup of the gut microbiome. So far, several thousand people from around the world have participated. It is funded by $99 "donations," from each participant, which cover the cost of the sampling kit. The donations go to the Biofrontiers Institute at the University of Colorado, Boulder, and the Earth Microbiome Project.
There is a need for faster DNA sequencing, databases of normal and abnormal microbiomes to provide a baseline, and research into how the microbiome affects health, including longitudinal studies to predict and monitor health changes, and animal models to help establish causality, said Dr. Knight.
Dr. Blaser, professor of microbiology and director of the Human Microbiome Program at the New York University Langone Medical Center, said findings so far had stimulated interest in researching the identity of various microbes, their activities, how the human host responds to microbes, the forces that maintain equilibrium in the host, and the unique characteristics of each individual’s microbiome. He and others have been looking into how antibiotic use in childhood might be affecting obesity. Studies have shown a correlation between heavy antibiotic use in certain areas of the country and greater rates of obesity in those same areas, said Dr. Blaser.
Antibiotic use may also be leading to less diversity in the guts of American adults, he said. There is a need for more research on the consequences of antibiotic use, and to help produce better diagnostics and therapies that are more narrowly targeted, he said. It would also be useful to examine the potential for both prebiotic and probiotic therapies, Dr. Blaser said.
Dr. Wu, professor of medicine at the University of Pennsylvania, Philadelphia, briefed the attendees on the success of fecal transplants to treat Clostridium difficile. So far, the procedure has offered proof of principle that human microbiota can be modified to treat disease, said Dr. Wu. It also has provided a window into the biology of the gut microbiome.
But "we must be very cautious," said Dr. Wu, noting that there are no data on short-term or long-term consequences of fecal transplant. The gut includes bacteria, fungi, and viruses, many of which have not been fully characterized yet, and is a "dynamic and living consortium that can change over time in ways that scientists cannot fully predict," said Dr. Wu.
He noted that clinicians had accidentally infected a generation of patients with hepatitis C through blood transfusions, because hepatitis C virus had not been discovered yet.
In the future, the aim is to standardize the process – both in creating the material to be transplanted and the conditions under which it is given, said Dr. Wu. There is also a need for functional studies in humans, to determine how the transplants work. Finally, he said, "it’s of tremendous importance that there be a register so people can be tracked for short- and long-term safety."
With potentially thousands of people getting fecal transplants in the near future, education of the lay public and clinicians is also crucial, said Dr. Wu.
The AGA’s Center for Gut Microbiome Research and Education will help fulfill that role. Started in March, its mission is to advance research and education. The advisory board will make recommendations to the AGA Governing Board on policy and research strategies.
Danone Inc. is a founding supporter of the center.
On Twitter @aliciaault

ACO spillover effect: Lower spending for all
Implementing the requirements of an accountable care organization for one group of patients may lower costs and improve care for every patient seen in a physician’s practice, according to a study published online Aug. 27 in JAMA.
Dr. J. Michael McWilliams of Harvard Medical School, Boston, and his colleagues looked at whether the Blue Cross Blue Shield of Massachusetts’ Alternative Quality Contract (ACQ), a successful ACO started in 2009, was associated with changes in spending or quality of care for Medicare beneficiaries who were not part of the ACO.
In the AQC, physicians and other providers assumed financial risk if they spent more than a global budget, but shared savings with the insurer if spending was under budget. Physicians could also receive bonuses for meeting quality targets.

The investigators compared total quarterly medical spending per beneficiary between two groups: beneficiaries who received care through the AQC in 2009 or 2010 (1.7 million person-years) and controls who received care from other providers (JAMA 2013;310:829-836).
Quarterly spending per beneficiary in 2007 and 2008 (prior to the AQC contracts) was $150 higher for the AQC group than the control group. Two years after the ACQ contracts went into effect, the difference was $51 per quarter. The biggest reduction in spending was for beneficiaries with five or more conditions, and in spending on outpatient care. Spending was significantly reduced for office visits, emergency department visits, minor procedures, imaging, and lab tests.
Some improvement was seen on quality measures. The number of beneficiaries tested for low-density lipoprotein levels increased. Prior to the AQC, LDL testing rates for diabetic beneficiaries in the AQC group were 2.2% higher than for controls. By the second year, the testing rate was 5.2% higher for those in the AQC. LDL testing rates also improved for cardiovascular disease patients in the AQC.
No improvement was seen on other quality measures, including hospitalization for an ambulatory care–sensitive condition related to cardiovascular disease or diabetes; readmission within 30 days of discharge; screening mammography for women aged 65-69 years; LDL testing for beneficiaries with a history of ischemic heart disease, myocardial infarction, or stroke; and hemoglobin A1c testing and retinal exams for beneficiaries with diabetes.
"These findings suggest that global payment incentives in the AQC elicited responses from participating organizations that extended beyond targeted case management of BCBS enrollees," the authors wrote.
Overall, the study "suggests that organizations in Massachusetts willing to assume greater financial risk were capable of achieving modest reductions in spending for Medicare beneficiaries without compromising quality of care," wrote Dr. McWilliams and his colleagues.
The study also showed that physicians and provider organizations who see spillover effects from one ACO contract might be willing "to enter similar contracts with additional insurers."
But there is a potential downside to the spillover effect, according to the authors: Because cost and quality may be improved overall, "competing insurers with similar provider networks could offer lower premiums without incurring the costs of managing an ACO."
The study was supported by grants from the National Institute on Aging, the American Federation for Aging Research, the Doris Duke Charitable Foundation, and the Commonwealth Fund. The investigators reported no relevant conflicts of interest.
On Twitter @aliciaault
Implementing the requirements of an accountable care organization for one group of patients may lower costs and improve care for every patient seen in a physician’s practice, according to a study published online Aug. 27 in JAMA.
Dr. J. Michael McWilliams of Harvard Medical School, Boston, and his colleagues looked at whether the Blue Cross Blue Shield of Massachusetts’ Alternative Quality Contract (ACQ), a successful ACO started in 2009, was associated with changes in spending or quality of care for Medicare beneficiaries who were not part of the ACO.
In the AQC, physicians and other providers assumed financial risk if they spent more than a global budget, but shared savings with the insurer if spending was under budget. Physicians could also receive bonuses for meeting quality targets.
The investigators compared total quarterly medical spending per beneficiary between two groups: beneficiaries who received care through the AQC in 2009 or 2010 (1.7 million person-years) and controls who received care from other providers (JAMA 2013;310:829-836).
Quarterly spending per beneficiary in 2007 and 2008 (prior to the AQC contracts) was $150 higher for the AQC group than the control group. Two years after the ACQ contracts went into effect, the difference was $51 per quarter. The biggest reduction in spending was for beneficiaries with five or more conditions, and in spending on outpatient care. Spending was significantly reduced for office visits, emergency department visits, minor procedures, imaging, and lab tests.
Some improvement was seen on quality measures. The number of beneficiaries tested for low-density lipoprotein levels increased. Prior to the AQC, LDL testing rates for diabetic beneficiaries in the AQC group were 2.2% higher than for controls. By the second year, the testing rate was 5.2% higher for those in the AQC. LDL testing rates also improved for cardiovascular disease patients in the AQC.
No improvement was seen on other quality measures, including hospitalization for an ambulatory care–sensitive condition related to cardiovascular disease or diabetes; readmission within 30 days of discharge; screening mammography for women aged 65-69 years; LDL testing for beneficiaries with a history of ischemic heart disease, myocardial infarction, or stroke; and hemoglobin A1c testing and retinal exams for beneficiaries with diabetes.
"These findings suggest that global payment incentives in the AQC elicited responses from participating organizations that extended beyond targeted case management of BCBS enrollees," the authors wrote.
Overall, the study "suggests that organizations in Massachusetts willing to assume greater financial risk were capable of achieving modest reductions in spending for Medicare beneficiaries without compromising quality of care," wrote Dr. McWilliams and his colleagues.
The study also showed that physicians and provider organizations who see spillover effects from one ACO contract might be willing "to enter similar contracts with additional insurers."
But there is a potential downside to the spillover effect, according to the authors: Because cost and quality may be improved overall, "competing insurers with similar provider networks could offer lower premiums without incurring the costs of managing an ACO."
The study was supported by grants from the National Institute on Aging, the American Federation for Aging Research, the Doris Duke Charitable Foundation, and the Commonwealth Fund. The investigators reported no relevant conflicts of interest.
On Twitter @aliciaault
Implementing the requirements of an accountable care organization for one group of patients may lower costs and improve care for every patient seen in a physician’s practice, according to a study published online Aug. 27 in JAMA.
Dr. J. Michael McWilliams of Harvard Medical School, Boston, and his colleagues looked at whether the Blue Cross Blue Shield of Massachusetts’ Alternative Quality Contract (ACQ), a successful ACO started in 2009, was associated with changes in spending or quality of care for Medicare beneficiaries who were not part of the ACO.
In the AQC, physicians and other providers assumed financial risk if they spent more than a global budget, but shared savings with the insurer if spending was under budget. Physicians could also receive bonuses for meeting quality targets.
The investigators compared total quarterly medical spending per beneficiary between two groups: beneficiaries who received care through the AQC in 2009 or 2010 (1.7 million person-years) and controls who received care from other providers (JAMA 2013;310:829-836).
Quarterly spending per beneficiary in 2007 and 2008 (prior to the AQC contracts) was $150 higher for the AQC group than the control group. Two years after the ACQ contracts went into effect, the difference was $51 per quarter. The biggest reduction in spending was for beneficiaries with five or more conditions, and in spending on outpatient care. Spending was significantly reduced for office visits, emergency department visits, minor procedures, imaging, and lab tests.
Some improvement was seen on quality measures. The number of beneficiaries tested for low-density lipoprotein levels increased. Prior to the AQC, LDL testing rates for diabetic beneficiaries in the AQC group were 2.2% higher than for controls. By the second year, the testing rate was 5.2% higher for those in the AQC. LDL testing rates also improved for cardiovascular disease patients in the AQC.
No improvement was seen on other quality measures, including hospitalization for an ambulatory care–sensitive condition related to cardiovascular disease or diabetes; readmission within 30 days of discharge; screening mammography for women aged 65-69 years; LDL testing for beneficiaries with a history of ischemic heart disease, myocardial infarction, or stroke; and hemoglobin A1c testing and retinal exams for beneficiaries with diabetes.
"These findings suggest that global payment incentives in the AQC elicited responses from participating organizations that extended beyond targeted case management of BCBS enrollees," the authors wrote.
Overall, the study "suggests that organizations in Massachusetts willing to assume greater financial risk were capable of achieving modest reductions in spending for Medicare beneficiaries without compromising quality of care," wrote Dr. McWilliams and his colleagues.
The study also showed that physicians and provider organizations who see spillover effects from one ACO contract might be willing "to enter similar contracts with additional insurers."
But there is a potential downside to the spillover effect, according to the authors: Because cost and quality may be improved overall, "competing insurers with similar provider networks could offer lower premiums without incurring the costs of managing an ACO."
The study was supported by grants from the National Institute on Aging, the American Federation for Aging Research, the Doris Duke Charitable Foundation, and the Commonwealth Fund. The investigators reported no relevant conflicts of interest.
On Twitter @aliciaault
FROM JAMA
Major finding: Quarterly spending per Medicare beneficiary was reduced by about $100 for those who were receiving care in a practice that had a contract with Blues Cross Blue Shield of Massachusetts’ Alternative Quality Contract.
Data source: Quasi-experimental comparisons from 2007-2010 of Medicare beneficiaries served by 11 provider organizations who entered the AQC in 2009 or 2010, compared to those served by other providers.
Disclosures: The study was supported by grants from the National Institute on Aging, the American Federation for Aging Research, the Doris Duke Charitable Foundation, and the Commonwealth Fund. The investigators reported no relevant conflicts of interest.

Bipartisan support is one key to getting SGR fixed, AMA president says
WASHINGTON – Congress appears to be on the brink of reforming the Medicare Sustainable Growth Rate formula after many years of temporary payment updates that physicians say undermine the stability of their practices and of the federal health program, as well.
Dr. Ardis Dee Hoven, president of the American Medical Association, discusses why Congress is so much closer to solving the Medicare physician payment puzzle this year. She also weighs in on prospects for action in the House and Senate when lawmakers return from their summer recess in September and what the practice world might look like after the SGR disappears.
On Twitter @aliciaault
WASHINGTON – Congress appears to be on the brink of reforming the Medicare Sustainable Growth Rate formula after many years of temporary payment updates that physicians say undermine the stability of their practices and of the federal health program, as well.
Dr. Ardis Dee Hoven, president of the American Medical Association, discusses why Congress is so much closer to solving the Medicare physician payment puzzle this year. She also weighs in on prospects for action in the House and Senate when lawmakers return from their summer recess in September and what the practice world might look like after the SGR disappears.
On Twitter @aliciaault
WASHINGTON – Congress appears to be on the brink of reforming the Medicare Sustainable Growth Rate formula after many years of temporary payment updates that physicians say undermine the stability of their practices and of the federal health program, as well.
Dr. Ardis Dee Hoven, president of the American Medical Association, discusses why Congress is so much closer to solving the Medicare physician payment puzzle this year. She also weighs in on prospects for action in the House and Senate when lawmakers return from their summer recess in September and what the practice world might look like after the SGR disappears.
On Twitter @aliciaault

Doctors seek halt on meaningful use stage 2 penalties
The Medical Group Management Association wants an indefinite hold on penalties to be levied on physicians who cannot move on to the next stage of meaningful use of electronic health records.
In an Aug. 21 letter to the Health and Human Services (HHS) department, Dr. Susan Turney, MGMA president and chief executive officer, said that physicians who have already met requirements for stage 1 meaningful use should not be penalized if they can’t meet the requirements for stage 2.

Physicians have been receiving incentive payments to become meaningful users of EHRs under the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009. Those payments continue through 2014. But stage 2 starts in 2014, and physicians will be penalized in 2015 if they can’t meet the goals.
Dr. Turney noted that while there are 2,200 products and 1,400 complete EHRs that are certified by the government for stage 1, so far, there are only 75 products and 21 complete EHRs that are certified for stage 2.
That dearth of certified technology does not give physicians enough time to upgrade their systems or acquire new technology to allow them to be ready to participate in stage 2, Dr. Turney said.
Physicians not only are waiting on vendors to upgrade their products, but have to consider whether they can afford to invest in new technology. And, if they do, staff will have to be trained, which can take a year or more, she noted.
In addition to indefinitely delaying penalties on physicians who have achieved stage 1 but not stage 2, the MGMA recommended that HHS also extend the reporting period for stage 2 for at least a year. "This extra year would provide additional time for vendors to upgrade their software, certify for the stage 2 criteria, and install the products," Dr. Turney wrote.
HHS also should extend the reporting period for stage 1 so that providers who have attested for stage 1 and whose EHR has not been recertified by January 2015 can continue to report on stage 1 during 2014.
The MGMA is also concerned about the stage 2 criteria that would require physicians to give at least 5% of their patients the ability to view, download, and transmit their health information online within 4 days of it being posted. That requirement should be closely monitored and potentially adjusted, according to the MGMA letter.
The MGMA represents 22,500 leaders at 13,200 organizations that in turn employ or are affiliated with 280,000 physicians.
[email protected]
On Twitter @aliciaault
The Medical Group Management Association wants an indefinite hold on penalties to be levied on physicians who cannot move on to the next stage of meaningful use of electronic health records.
In an Aug. 21 letter to the Health and Human Services (HHS) department, Dr. Susan Turney, MGMA president and chief executive officer, said that physicians who have already met requirements for stage 1 meaningful use should not be penalized if they can’t meet the requirements for stage 2.
Physicians have been receiving incentive payments to become meaningful users of EHRs under the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009. Those payments continue through 2014. But stage 2 starts in 2014, and physicians will be penalized in 2015 if they can’t meet the goals.
Dr. Turney noted that while there are 2,200 products and 1,400 complete EHRs that are certified by the government for stage 1, so far, there are only 75 products and 21 complete EHRs that are certified for stage 2.
That dearth of certified technology does not give physicians enough time to upgrade their systems or acquire new technology to allow them to be ready to participate in stage 2, Dr. Turney said.
Physicians not only are waiting on vendors to upgrade their products, but have to consider whether they can afford to invest in new technology. And, if they do, staff will have to be trained, which can take a year or more, she noted.
In addition to indefinitely delaying penalties on physicians who have achieved stage 1 but not stage 2, the MGMA recommended that HHS also extend the reporting period for stage 2 for at least a year. "This extra year would provide additional time for vendors to upgrade their software, certify for the stage 2 criteria, and install the products," Dr. Turney wrote.
HHS also should extend the reporting period for stage 1 so that providers who have attested for stage 1 and whose EHR has not been recertified by January 2015 can continue to report on stage 1 during 2014.
The MGMA is also concerned about the stage 2 criteria that would require physicians to give at least 5% of their patients the ability to view, download, and transmit their health information online within 4 days of it being posted. That requirement should be closely monitored and potentially adjusted, according to the MGMA letter.
The MGMA represents 22,500 leaders at 13,200 organizations that in turn employ or are affiliated with 280,000 physicians.
[email protected]
On Twitter @aliciaault
The Medical Group Management Association wants an indefinite hold on penalties to be levied on physicians who cannot move on to the next stage of meaningful use of electronic health records.
In an Aug. 21 letter to the Health and Human Services (HHS) department, Dr. Susan Turney, MGMA president and chief executive officer, said that physicians who have already met requirements for stage 1 meaningful use should not be penalized if they can’t meet the requirements for stage 2.
Physicians have been receiving incentive payments to become meaningful users of EHRs under the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009. Those payments continue through 2014. But stage 2 starts in 2014, and physicians will be penalized in 2015 if they can’t meet the goals.
Dr. Turney noted that while there are 2,200 products and 1,400 complete EHRs that are certified by the government for stage 1, so far, there are only 75 products and 21 complete EHRs that are certified for stage 2.
That dearth of certified technology does not give physicians enough time to upgrade their systems or acquire new technology to allow them to be ready to participate in stage 2, Dr. Turney said.
Physicians not only are waiting on vendors to upgrade their products, but have to consider whether they can afford to invest in new technology. And, if they do, staff will have to be trained, which can take a year or more, she noted.
In addition to indefinitely delaying penalties on physicians who have achieved stage 1 but not stage 2, the MGMA recommended that HHS also extend the reporting period for stage 2 for at least a year. "This extra year would provide additional time for vendors to upgrade their software, certify for the stage 2 criteria, and install the products," Dr. Turney wrote.
HHS also should extend the reporting period for stage 1 so that providers who have attested for stage 1 and whose EHR has not been recertified by January 2015 can continue to report on stage 1 during 2014.
The MGMA is also concerned about the stage 2 criteria that would require physicians to give at least 5% of their patients the ability to view, download, and transmit their health information online within 4 days of it being posted. That requirement should be closely monitored and potentially adjusted, according to the MGMA letter.
The MGMA represents 22,500 leaders at 13,200 organizations that in turn employ or are affiliated with 280,000 physicians.
[email protected]
On Twitter @aliciaault

House committee unanimously passes SGR replacement
The demise of the Medicare Sustainable Growth Rate formula is a step closer to reality as the House Energy and Commerce Committee voted unanimously July 31 in favor of legislation that would remove the formula.
Both Democrats and Republicans on the committee supported the Medicare Patient Access and Quality Improvement Act of 2013 in a 51-0 vote. The legislation, H.R. 2810, was authored by Rep. Michael Burgess (R-Tex.), and developed with input from physician organizations.
If enacted, the legislation would replace the SGR with a 0.5% payment increase for physicians from 2014 through 2018. It would continue to support fee-for-service medicine, but also encourage the formation of new delivery models and reward reporting of quality data.

"In harnessing the ideas of the medical profession, and working as a team with Energy and Commerce Democrats as well as Ways and Means Republicans, we have crafted a policy that will not only get out of committee but has the merits to make it to the president’s desk," Rep. Fred Upton (R-Mich.), chairman of the Energy and Commerce Committee, said in a statement.
Rep. Henry Waxman (D-Calif.), the committee’s ranking minority member, said, "What is obvious today is that we have a bipartisan commitment to try to solve this problem. And that when we decide to work together, we can achieve positive results." He also noted that "in more than a decade of saying something needs to be done, I’m pleased that this committee is the first to act to bring this issue to the forefront."
The American College of Physicians said it was mostly pleased with the legislation and its progress. In addition to rewarding physician efficiency, "the bill promises to accelerate the growth of patient-centered medical homes, an innovative primary care delivery model that has been shown to improve outcomes and lower the costs of care for patients across the country," said Dr. Molly Cooke, ACP president, in a statement.
The college "looks forward to continuing to work with the House and Senate on a bipartisan basis to get legislation enacted this year that includes these and other key elements of the House Energy and Commerce Committee bill, plus additional improvements needed to accelerate the movement toward high-value, patient-centered health care."
The American Medical Association and the American Academy of Family Physicians also support the legislation. When the bill was approved by the Energy and Commerce Health Subcommittee, the AAFP said it was disappointed that the bill did not have higher payments for primary care.
During those deliberations, the AMA, AAFP, ACP, and some state medical societies also told the committee that a provision addressing misvalued codes could end up cutting physician pay. They’ve asked the committee to consider an amendment that would remove the misvalued code provisions from the bill; such an amendment was not considered by the committee.
The introduction of the legislation also represents several months of collaboration among physician stakeholders like the American Gastroenterological Association and the congressional committees. The AGA was pleased that the committee worked with the physician community and incorporated many of our suggestions into the legislation. The AGA, and the Alliance of Specialty Medicine, conveyed our views to the committee and believe that the legislation moves physicians in the right direction and gives physicians opportunity to develop new payment models and quality indicators meaningful to their specialty.
The legislation still has a long path to passage. The House Ways and Means Committee and the Senate Finance Committee have also been working on legislation to replace the SGR. And so far, legislators in both houses have not addressed how to pay for an SGR fix.
Several Energy and Commerce Committee members acknowledged the looming financial reality during deliberations.
"One of the largest hurdles to overcome will be how to pay for the cost associated with fixing the SGR," said Rep. Eliot Engel (D-N.Y.). He urged his colleagues to continue the spirit of bipartisanship when figuring out the cost of replacement.
"We know that the work is not done," said Rep. Phil Gingrey (R-Ga.). "Any fiscally responsible bill in today’s budgetary environment must be paid for. I look forward to finding offsets that do not impact the practice of medicine but instead focus on good governance and combating waste," said the congressman, who is also an ob.gyn.
That work will likely come in September, when Congress returns from its summer recess.
On Twitter @aliciaault
The demise of the Medicare Sustainable Growth Rate formula is a step closer to reality as the House Energy and Commerce Committee voted unanimously July 31 in favor of legislation that would remove the formula.
Both Democrats and Republicans on the committee supported the Medicare Patient Access and Quality Improvement Act of 2013 in a 51-0 vote. The legislation, H.R. 2810, was authored by Rep. Michael Burgess (R-Tex.), and developed with input from physician organizations.
If enacted, the legislation would replace the SGR with a 0.5% payment increase for physicians from 2014 through 2018. It would continue to support fee-for-service medicine, but also encourage the formation of new delivery models and reward reporting of quality data.
"In harnessing the ideas of the medical profession, and working as a team with Energy and Commerce Democrats as well as Ways and Means Republicans, we have crafted a policy that will not only get out of committee but has the merits to make it to the president’s desk," Rep. Fred Upton (R-Mich.), chairman of the Energy and Commerce Committee, said in a statement.
Rep. Henry Waxman (D-Calif.), the committee’s ranking minority member, said, "What is obvious today is that we have a bipartisan commitment to try to solve this problem. And that when we decide to work together, we can achieve positive results." He also noted that "in more than a decade of saying something needs to be done, I’m pleased that this committee is the first to act to bring this issue to the forefront."
The American College of Physicians said it was mostly pleased with the legislation and its progress. In addition to rewarding physician efficiency, "the bill promises to accelerate the growth of patient-centered medical homes, an innovative primary care delivery model that has been shown to improve outcomes and lower the costs of care for patients across the country," said Dr. Molly Cooke, ACP president, in a statement.
The college "looks forward to continuing to work with the House and Senate on a bipartisan basis to get legislation enacted this year that includes these and other key elements of the House Energy and Commerce Committee bill, plus additional improvements needed to accelerate the movement toward high-value, patient-centered health care."
The American Medical Association and the American Academy of Family Physicians also support the legislation. When the bill was approved by the Energy and Commerce Health Subcommittee, the AAFP said it was disappointed that the bill did not have higher payments for primary care.
During those deliberations, the AMA, AAFP, ACP, and some state medical societies also told the committee that a provision addressing misvalued codes could end up cutting physician pay. They’ve asked the committee to consider an amendment that would remove the misvalued code provisions from the bill; such an amendment was not considered by the committee.
The introduction of the legislation also represents several months of collaboration among physician stakeholders like the American Gastroenterological Association and the congressional committees. The AGA was pleased that the committee worked with the physician community and incorporated many of our suggestions into the legislation. The AGA, and the Alliance of Specialty Medicine, conveyed our views to the committee and believe that the legislation moves physicians in the right direction and gives physicians opportunity to develop new payment models and quality indicators meaningful to their specialty.
The legislation still has a long path to passage. The House Ways and Means Committee and the Senate Finance Committee have also been working on legislation to replace the SGR. And so far, legislators in both houses have not addressed how to pay for an SGR fix.
Several Energy and Commerce Committee members acknowledged the looming financial reality during deliberations.
"One of the largest hurdles to overcome will be how to pay for the cost associated with fixing the SGR," said Rep. Eliot Engel (D-N.Y.). He urged his colleagues to continue the spirit of bipartisanship when figuring out the cost of replacement.
"We know that the work is not done," said Rep. Phil Gingrey (R-Ga.). "Any fiscally responsible bill in today’s budgetary environment must be paid for. I look forward to finding offsets that do not impact the practice of medicine but instead focus on good governance and combating waste," said the congressman, who is also an ob.gyn.
That work will likely come in September, when Congress returns from its summer recess.
On Twitter @aliciaault
The demise of the Medicare Sustainable Growth Rate formula is a step closer to reality as the House Energy and Commerce Committee voted unanimously July 31 in favor of legislation that would remove the formula.
Both Democrats and Republicans on the committee supported the Medicare Patient Access and Quality Improvement Act of 2013 in a 51-0 vote. The legislation, H.R. 2810, was authored by Rep. Michael Burgess (R-Tex.), and developed with input from physician organizations.
If enacted, the legislation would replace the SGR with a 0.5% payment increase for physicians from 2014 through 2018. It would continue to support fee-for-service medicine, but also encourage the formation of new delivery models and reward reporting of quality data.
"In harnessing the ideas of the medical profession, and working as a team with Energy and Commerce Democrats as well as Ways and Means Republicans, we have crafted a policy that will not only get out of committee but has the merits to make it to the president’s desk," Rep. Fred Upton (R-Mich.), chairman of the Energy and Commerce Committee, said in a statement.
Rep. Henry Waxman (D-Calif.), the committee’s ranking minority member, said, "What is obvious today is that we have a bipartisan commitment to try to solve this problem. And that when we decide to work together, we can achieve positive results." He also noted that "in more than a decade of saying something needs to be done, I’m pleased that this committee is the first to act to bring this issue to the forefront."
The American College of Physicians said it was mostly pleased with the legislation and its progress. In addition to rewarding physician efficiency, "the bill promises to accelerate the growth of patient-centered medical homes, an innovative primary care delivery model that has been shown to improve outcomes and lower the costs of care for patients across the country," said Dr. Molly Cooke, ACP president, in a statement.
The college "looks forward to continuing to work with the House and Senate on a bipartisan basis to get legislation enacted this year that includes these and other key elements of the House Energy and Commerce Committee bill, plus additional improvements needed to accelerate the movement toward high-value, patient-centered health care."
The American Medical Association and the American Academy of Family Physicians also support the legislation. When the bill was approved by the Energy and Commerce Health Subcommittee, the AAFP said it was disappointed that the bill did not have higher payments for primary care.
During those deliberations, the AMA, AAFP, ACP, and some state medical societies also told the committee that a provision addressing misvalued codes could end up cutting physician pay. They’ve asked the committee to consider an amendment that would remove the misvalued code provisions from the bill; such an amendment was not considered by the committee.
The introduction of the legislation also represents several months of collaboration among physician stakeholders like the American Gastroenterological Association and the congressional committees. The AGA was pleased that the committee worked with the physician community and incorporated many of our suggestions into the legislation. The AGA, and the Alliance of Specialty Medicine, conveyed our views to the committee and believe that the legislation moves physicians in the right direction and gives physicians opportunity to develop new payment models and quality indicators meaningful to their specialty.
The legislation still has a long path to passage. The House Ways and Means Committee and the Senate Finance Committee have also been working on legislation to replace the SGR. And so far, legislators in both houses have not addressed how to pay for an SGR fix.
Several Energy and Commerce Committee members acknowledged the looming financial reality during deliberations.
"One of the largest hurdles to overcome will be how to pay for the cost associated with fixing the SGR," said Rep. Eliot Engel (D-N.Y.). He urged his colleagues to continue the spirit of bipartisanship when figuring out the cost of replacement.
"We know that the work is not done," said Rep. Phil Gingrey (R-Ga.). "Any fiscally responsible bill in today’s budgetary environment must be paid for. I look forward to finding offsets that do not impact the practice of medicine but instead focus on good governance and combating waste," said the congressman, who is also an ob.gyn.
That work will likely come in September, when Congress returns from its summer recess.
On Twitter @aliciaault

Money is key barrier to health insurance for young adults
Affordability, not perceived lack of need, is the major barrier to health insurance coverage for many young adults, according to a survey from the Commonwealth Fund.
"There is a stereotype that young adults believe they are ‘invincible’ and don’t want or need health insurance," Commonwealth Fund vice president Sara Collins, the study’s lead author, said at a briefing. "This survey shows that is a myth. A typical uninsured young adult is from a low- or middle-income family and works a low-wage job. In general, young adults value health insurance but cannot afford it."
Fewer 19- to-25-year-olds are uninsured this year – 34% vs. 43% in 2011 – mostly due to Affordable Care Act provisions that allow them to stay on their parents’ insurance plans until age 26.

However, these young adults have little overall awareness of the health insurance exchanges and options they will offer. At the time of the survey (March 2013), only 27% of young adults knew health insurance exchanges would open Oct. 1.
The survey, which compared results against a 2011 survey, also found that in states that are not expanding their Medicaid programs, low-income young adults may fall through the coverage cracks.
When offered coverage through an employer, 67% of young adults surveyed said they signed up. Among the third who did not, 36% were covered by their parents’ policy, 22% said it was too expensive, 19% were covered by a spouse or partner’s insurance, 4% had purchased coverage on their own, and 13% had other reasons. Only 5% said they did not want or need insurance; the remainder did not answer.
These young adults are viewed as key to making the ACA’s health insurance exchanges work. Generally healthier, they will help spread risk and keep premiums lower for all participants in the exchanges.
But the Commonwealth Fund survey found that states and the federal government have much work ahead of them to increase knowledge of exchanges in this age group, especially among those who have been recently uninsured or who have lower incomes.
Seventy-nine percent of those with incomes below 133% of the federal poverty line responded that they had not heard of the health insurance exchanges. The exchanges will be required to offer coverage to people with incomes up to that level, and subsidies will be available for buyers who are at 100%-400% of the poverty line.
The Commonwealth Fund estimated that 82% of young adults who have spent some time being uninsured would be eligible for those subsidies.
The Commonwealth Fund Health Insurance Tracking Survey of Young Adults was conducted by an online research firm in 2011 and 2013, among a representative sample of young adults. In 2011, 3,438 adults aged 19-29 were randomly sampled; 1,863 responded (54%). In 2013, 3,530 young adults were surveyed; 1,885 responded (53.4%). Just over 1,000 responded in both years.
On Twitter @aliciaault
Affordability, not perceived lack of need, is the major barrier to health insurance coverage for many young adults, according to a survey from the Commonwealth Fund.
"There is a stereotype that young adults believe they are ‘invincible’ and don’t want or need health insurance," Commonwealth Fund vice president Sara Collins, the study’s lead author, said at a briefing. "This survey shows that is a myth. A typical uninsured young adult is from a low- or middle-income family and works a low-wage job. In general, young adults value health insurance but cannot afford it."
Fewer 19- to-25-year-olds are uninsured this year – 34% vs. 43% in 2011 – mostly due to Affordable Care Act provisions that allow them to stay on their parents’ insurance plans until age 26.
However, these young adults have little overall awareness of the health insurance exchanges and options they will offer. At the time of the survey (March 2013), only 27% of young adults knew health insurance exchanges would open Oct. 1.
The survey, which compared results against a 2011 survey, also found that in states that are not expanding their Medicaid programs, low-income young adults may fall through the coverage cracks.
When offered coverage through an employer, 67% of young adults surveyed said they signed up. Among the third who did not, 36% were covered by their parents’ policy, 22% said it was too expensive, 19% were covered by a spouse or partner’s insurance, 4% had purchased coverage on their own, and 13% had other reasons. Only 5% said they did not want or need insurance; the remainder did not answer.
These young adults are viewed as key to making the ACA’s health insurance exchanges work. Generally healthier, they will help spread risk and keep premiums lower for all participants in the exchanges.
But the Commonwealth Fund survey found that states and the federal government have much work ahead of them to increase knowledge of exchanges in this age group, especially among those who have been recently uninsured or who have lower incomes.
Seventy-nine percent of those with incomes below 133% of the federal poverty line responded that they had not heard of the health insurance exchanges. The exchanges will be required to offer coverage to people with incomes up to that level, and subsidies will be available for buyers who are at 100%-400% of the poverty line.
The Commonwealth Fund estimated that 82% of young adults who have spent some time being uninsured would be eligible for those subsidies.
The Commonwealth Fund Health Insurance Tracking Survey of Young Adults was conducted by an online research firm in 2011 and 2013, among a representative sample of young adults. In 2011, 3,438 adults aged 19-29 were randomly sampled; 1,863 responded (54%). In 2013, 3,530 young adults were surveyed; 1,885 responded (53.4%). Just over 1,000 responded in both years.
On Twitter @aliciaault
Affordability, not perceived lack of need, is the major barrier to health insurance coverage for many young adults, according to a survey from the Commonwealth Fund.
"There is a stereotype that young adults believe they are ‘invincible’ and don’t want or need health insurance," Commonwealth Fund vice president Sara Collins, the study’s lead author, said at a briefing. "This survey shows that is a myth. A typical uninsured young adult is from a low- or middle-income family and works a low-wage job. In general, young adults value health insurance but cannot afford it."
Fewer 19- to-25-year-olds are uninsured this year – 34% vs. 43% in 2011 – mostly due to Affordable Care Act provisions that allow them to stay on their parents’ insurance plans until age 26.
However, these young adults have little overall awareness of the health insurance exchanges and options they will offer. At the time of the survey (March 2013), only 27% of young adults knew health insurance exchanges would open Oct. 1.
The survey, which compared results against a 2011 survey, also found that in states that are not expanding their Medicaid programs, low-income young adults may fall through the coverage cracks.
When offered coverage through an employer, 67% of young adults surveyed said they signed up. Among the third who did not, 36% were covered by their parents’ policy, 22% said it was too expensive, 19% were covered by a spouse or partner’s insurance, 4% had purchased coverage on their own, and 13% had other reasons. Only 5% said they did not want or need insurance; the remainder did not answer.
These young adults are viewed as key to making the ACA’s health insurance exchanges work. Generally healthier, they will help spread risk and keep premiums lower for all participants in the exchanges.
But the Commonwealth Fund survey found that states and the federal government have much work ahead of them to increase knowledge of exchanges in this age group, especially among those who have been recently uninsured or who have lower incomes.
Seventy-nine percent of those with incomes below 133% of the federal poverty line responded that they had not heard of the health insurance exchanges. The exchanges will be required to offer coverage to people with incomes up to that level, and subsidies will be available for buyers who are at 100%-400% of the poverty line.
The Commonwealth Fund estimated that 82% of young adults who have spent some time being uninsured would be eligible for those subsidies.
The Commonwealth Fund Health Insurance Tracking Survey of Young Adults was conducted by an online research firm in 2011 and 2013, among a representative sample of young adults. In 2011, 3,438 adults aged 19-29 were randomly sampled; 1,863 responded (54%). In 2013, 3,530 young adults were surveyed; 1,885 responded (53.4%). Just over 1,000 responded in both years.
On Twitter @aliciaault

Sunshine apps track industry payments
Two new smartphone apps aim to help log drug, device, and diagnostic manufacturer payments to doctors and health care providers, as called for by the Affordable Care Act.
To promote transparency in relationships between providers and industry, the ACA requires that manufacturers track and report payments for consulting, honoraria, and more.

Originally known as the Sunshine Act, the effort is now called the Open Payments Program by the Centers for Medicare and Medicaid Services (CMS).
While physicians are not required to inventory anything of value they receive from manufacturers, CMS and many medical professional societies advise that they do so.
The app for physicians – Open Payments for Physicians – is designed to help doctors keep tabs on all their transactions in real time. Users can manually enter all the information regarding a particular transaction, for example, the receipt of a grant payment or a gift that’s worth more than $10.
The app is free and can be downloaded from the iTunes App Store or from Google Play.
CMS also created an app for industry representatives to use (Open Payments for Industry).
Industry users and physician users can exchange information with their apps. By using a built-in QR (quick response) code reader, the manufacturer can transfer a record of a transaction to the physician for review, according to the agency.
In a blog post, CMS Program Integrity Director Dr. Peter Budetti said the agency’s "foray into mobile technology is about providing user-friendly tools for doctors, manufacturers, and others in the health care industry to use in working with us to implement the law in a smart way."
The idea is that physicians can use the records contained in the app to compare what’s reported by manufacturers to CMS. There is a 45-day lag between when the data are reported to CMS and posted publicly. Physicians have that window to challenge the reports before they are posted on the Open Payments website. Corrections can be made later, but the erroneous data will likely stay public for awhile.
The first year of the program will be a little bit more forgiving. Data collected beginning Aug. 1 won’t be publicly reported until September 2014.
The apps can’t be used to directly transfer data to CMS, said the agency, which added that although it developed the apps, it will not "validate the accuracy of data stored in the apps, nor will it be responsible for protecting data stored in the apps."
[email protected]
On Twitter @aliciaault
Two new smartphone apps aim to help log drug, device, and diagnostic manufacturer payments to doctors and health care providers, as called for by the Affordable Care Act.
To promote transparency in relationships between providers and industry, the ACA requires that manufacturers track and report payments for consulting, honoraria, and more.
Originally known as the Sunshine Act, the effort is now called the Open Payments Program by the Centers for Medicare and Medicaid Services (CMS).
While physicians are not required to inventory anything of value they receive from manufacturers, CMS and many medical professional societies advise that they do so.
The app for physicians – Open Payments for Physicians – is designed to help doctors keep tabs on all their transactions in real time. Users can manually enter all the information regarding a particular transaction, for example, the receipt of a grant payment or a gift that’s worth more than $10.
The app is free and can be downloaded from the iTunes App Store or from Google Play.
CMS also created an app for industry representatives to use (Open Payments for Industry).
Industry users and physician users can exchange information with their apps. By using a built-in QR (quick response) code reader, the manufacturer can transfer a record of a transaction to the physician for review, according to the agency.
In a blog post, CMS Program Integrity Director Dr. Peter Budetti said the agency’s "foray into mobile technology is about providing user-friendly tools for doctors, manufacturers, and others in the health care industry to use in working with us to implement the law in a smart way."
The idea is that physicians can use the records contained in the app to compare what’s reported by manufacturers to CMS. There is a 45-day lag between when the data are reported to CMS and posted publicly. Physicians have that window to challenge the reports before they are posted on the Open Payments website. Corrections can be made later, but the erroneous data will likely stay public for awhile.
The first year of the program will be a little bit more forgiving. Data collected beginning Aug. 1 won’t be publicly reported until September 2014.
The apps can’t be used to directly transfer data to CMS, said the agency, which added that although it developed the apps, it will not "validate the accuracy of data stored in the apps, nor will it be responsible for protecting data stored in the apps."
[email protected]
On Twitter @aliciaault
Two new smartphone apps aim to help log drug, device, and diagnostic manufacturer payments to doctors and health care providers, as called for by the Affordable Care Act.
To promote transparency in relationships between providers and industry, the ACA requires that manufacturers track and report payments for consulting, honoraria, and more.
Originally known as the Sunshine Act, the effort is now called the Open Payments Program by the Centers for Medicare and Medicaid Services (CMS).
While physicians are not required to inventory anything of value they receive from manufacturers, CMS and many medical professional societies advise that they do so.
The app for physicians – Open Payments for Physicians – is designed to help doctors keep tabs on all their transactions in real time. Users can manually enter all the information regarding a particular transaction, for example, the receipt of a grant payment or a gift that’s worth more than $10.
The app is free and can be downloaded from the iTunes App Store or from Google Play.
CMS also created an app for industry representatives to use (Open Payments for Industry).
Industry users and physician users can exchange information with their apps. By using a built-in QR (quick response) code reader, the manufacturer can transfer a record of a transaction to the physician for review, according to the agency.
In a blog post, CMS Program Integrity Director Dr. Peter Budetti said the agency’s "foray into mobile technology is about providing user-friendly tools for doctors, manufacturers, and others in the health care industry to use in working with us to implement the law in a smart way."
The idea is that physicians can use the records contained in the app to compare what’s reported by manufacturers to CMS. There is a 45-day lag between when the data are reported to CMS and posted publicly. Physicians have that window to challenge the reports before they are posted on the Open Payments website. Corrections can be made later, but the erroneous data will likely stay public for awhile.
The first year of the program will be a little bit more forgiving. Data collected beginning Aug. 1 won’t be publicly reported until September 2014.
The apps can’t be used to directly transfer data to CMS, said the agency, which added that although it developed the apps, it will not "validate the accuracy of data stored in the apps, nor will it be responsible for protecting data stored in the apps."
[email protected]
On Twitter @aliciaault

Cost of health insurance moderates, but workers pay more
The rise in the cost of employer-sponsored health insurance has ameliorated in the past year, continuing a flattening trend, but patients continue to be asked to pay a bigger share.
That’s the conclusion of the 13th annual survey of nonfederal private and public employers with three or more workers conducted by the Kaiser Family Foundation and the Health Research & Educational Trust, and published Aug. 20 in the journal Health Affairs (doi: 10.1377/hlthaff.2013.0644).
Kaiser and HRET estimate that in 2013, 149 million nonelderly people receive coverage through employer-sponsored insurance, with 57% of U.S. firms offering health benefits – a statistically insignificant change from 61% in 2012 and 60% in 2011. But smaller companies and those with many low-wage workers do not offer benefits as frequently.
In 2013, the average annual premiums for employer-sponsored health insurance rose 5% to $5,884 for single coverage and 4% to $16,351 for family coverage from 2012. This continues the pattern seen over the past few years, with relatively small premium increases.
Workers on average pay 18% of the premium for single coverage and 29% for family coverage, again, similar to the two previous years. "We are in a prolonged period of moderation in premiums, which should create some breathing room for the private sector to try to reduce costs without cutting back benefits for workers," said Kaiser President and CEO Drew Altman, in a statement.
But workers are still struggling to cover health costs. During the same period (2012-2013), wages increased 1.8% and inflation increased 1.1%. And since 2003, the average premium for family coverage has increased 80%, and the average worker contribution has risen 89%.
Employers continue to cost-shift. Seventy-eight percent of covered workers have a deductible, with the average for single coverage running about $1,100 (largely unchanged from 2012). But big deductibles are getting to be more common. Firms with less than 200 employees generally charged more than $1,000, and the number doing that rose from 49% of all such firms in 2012 to 58% in 2013.
Three-quarters of workers have a fixed copayment for office visits with primary care physicians and specialists. That copay averages $23 for primary care and $35 for specialty care for in-network physicians. Out-of-network amounts were not covered in the survey, but Kaiser assumes that patients bear a greater cost for those visits. About 20% of workers pay a percent of the visit (coinsurance) for primary care and the same amount for specialty care. They pay an average 18% of the visit.
The survey found that preferred provider organization (PPO) plans are the most common, enrolling 57% of covered workers in 2013. High-deductible health plans, also known as catastrophic plans, are the next most popular, with 20% of covered workers. Deductibles in those plans range from around $2,000 for single coverage to $4,000 for family coverage, with some much higher.
Only 14% of workers are enrolled in health maintenance organizations (HMOs), 9% in a point-of-service (POS) plan, and less than 1% in a conventional fee-for-service plan. High-deductible plans have grown exponentially since first coming on the scene – going from 8% in 2009 to 17% in 2011 – but have plateaued in the last few years, according to the report.
Also of interest to physicians:
• 23% of employers offering benefits have high performance or tiered networks in their largest health plan. The programs help steer patients to providers who have been identified as being more efficient or giving higher-quality care.
• 56% cover services provided by retail health clinics. Among firms covering services in these settings, 17% provide a financial incentive to receive services in a retail clinic instead of a physician’s office.
• Almost all employers with more than 200 workers and most smaller employers offer at least one wellness program. The majority offer at least one of the following in 2013: weight loss programs, gym membership discounts or on-site exercise facilities, biometric screening, smoking cessation, personal health coaching, health and nutrition education, web-based resources, flu shots or vaccinations, employee assistance programs (EAPs), or a wellness newsletter. Thirty-six percent of large firms and 8% of smaller firms offer employees a financial incentive to participate.
The growth in wellness programs "will be an important issue to watch next year, as employers will have more flexibility and could ask workers to pay more because of their lifestyles and health conditions," said Kaiser Vice President Gary Claxton, the study’s lead investigator and director of the Foundation’s Health Care Marketplace Project.
Mr. Claxton and his colleagues found that an increasing number of employees are likely to be subject to the Affordable Care Act’s various provisions. Thirty-six percent of covered workers are in "grandfathered" plans – that is, they are exempt from the law – down from 48% in 2012 and 56% in 2011.
The authors reported no disclosures.
[email protected]
On Twitter @aliciaault
The rise in the cost of employer-sponsored health insurance has ameliorated in the past year, continuing a flattening trend, but patients continue to be asked to pay a bigger share.
That’s the conclusion of the 13th annual survey of nonfederal private and public employers with three or more workers conducted by the Kaiser Family Foundation and the Health Research & Educational Trust, and published Aug. 20 in the journal Health Affairs (doi: 10.1377/hlthaff.2013.0644).
Kaiser and HRET estimate that in 2013, 149 million nonelderly people receive coverage through employer-sponsored insurance, with 57% of U.S. firms offering health benefits – a statistically insignificant change from 61% in 2012 and 60% in 2011. But smaller companies and those with many low-wage workers do not offer benefits as frequently.
In 2013, the average annual premiums for employer-sponsored health insurance rose 5% to $5,884 for single coverage and 4% to $16,351 for family coverage from 2012. This continues the pattern seen over the past few years, with relatively small premium increases.
Workers on average pay 18% of the premium for single coverage and 29% for family coverage, again, similar to the two previous years. "We are in a prolonged period of moderation in premiums, which should create some breathing room for the private sector to try to reduce costs without cutting back benefits for workers," said Kaiser President and CEO Drew Altman, in a statement.
But workers are still struggling to cover health costs. During the same period (2012-2013), wages increased 1.8% and inflation increased 1.1%. And since 2003, the average premium for family coverage has increased 80%, and the average worker contribution has risen 89%.
Employers continue to cost-shift. Seventy-eight percent of covered workers have a deductible, with the average for single coverage running about $1,100 (largely unchanged from 2012). But big deductibles are getting to be more common. Firms with less than 200 employees generally charged more than $1,000, and the number doing that rose from 49% of all such firms in 2012 to 58% in 2013.
Three-quarters of workers have a fixed copayment for office visits with primary care physicians and specialists. That copay averages $23 for primary care and $35 for specialty care for in-network physicians. Out-of-network amounts were not covered in the survey, but Kaiser assumes that patients bear a greater cost for those visits. About 20% of workers pay a percent of the visit (coinsurance) for primary care and the same amount for specialty care. They pay an average 18% of the visit.
The survey found that preferred provider organization (PPO) plans are the most common, enrolling 57% of covered workers in 2013. High-deductible health plans, also known as catastrophic plans, are the next most popular, with 20% of covered workers. Deductibles in those plans range from around $2,000 for single coverage to $4,000 for family coverage, with some much higher.
Only 14% of workers are enrolled in health maintenance organizations (HMOs), 9% in a point-of-service (POS) plan, and less than 1% in a conventional fee-for-service plan. High-deductible plans have grown exponentially since first coming on the scene – going from 8% in 2009 to 17% in 2011 – but have plateaued in the last few years, according to the report.
Also of interest to physicians:
• 23% of employers offering benefits have high performance or tiered networks in their largest health plan. The programs help steer patients to providers who have been identified as being more efficient or giving higher-quality care.
• 56% cover services provided by retail health clinics. Among firms covering services in these settings, 17% provide a financial incentive to receive services in a retail clinic instead of a physician’s office.
• Almost all employers with more than 200 workers and most smaller employers offer at least one wellness program. The majority offer at least one of the following in 2013: weight loss programs, gym membership discounts or on-site exercise facilities, biometric screening, smoking cessation, personal health coaching, health and nutrition education, web-based resources, flu shots or vaccinations, employee assistance programs (EAPs), or a wellness newsletter. Thirty-six percent of large firms and 8% of smaller firms offer employees a financial incentive to participate.
The growth in wellness programs "will be an important issue to watch next year, as employers will have more flexibility and could ask workers to pay more because of their lifestyles and health conditions," said Kaiser Vice President Gary Claxton, the study’s lead investigator and director of the Foundation’s Health Care Marketplace Project.
Mr. Claxton and his colleagues found that an increasing number of employees are likely to be subject to the Affordable Care Act’s various provisions. Thirty-six percent of covered workers are in "grandfathered" plans – that is, they are exempt from the law – down from 48% in 2012 and 56% in 2011.
The authors reported no disclosures.
[email protected]
On Twitter @aliciaault
The rise in the cost of employer-sponsored health insurance has ameliorated in the past year, continuing a flattening trend, but patients continue to be asked to pay a bigger share.
That’s the conclusion of the 13th annual survey of nonfederal private and public employers with three or more workers conducted by the Kaiser Family Foundation and the Health Research & Educational Trust, and published Aug. 20 in the journal Health Affairs (doi: 10.1377/hlthaff.2013.0644).
Kaiser and HRET estimate that in 2013, 149 million nonelderly people receive coverage through employer-sponsored insurance, with 57% of U.S. firms offering health benefits – a statistically insignificant change from 61% in 2012 and 60% in 2011. But smaller companies and those with many low-wage workers do not offer benefits as frequently.
In 2013, the average annual premiums for employer-sponsored health insurance rose 5% to $5,884 for single coverage and 4% to $16,351 for family coverage from 2012. This continues the pattern seen over the past few years, with relatively small premium increases.
Workers on average pay 18% of the premium for single coverage and 29% for family coverage, again, similar to the two previous years. "We are in a prolonged period of moderation in premiums, which should create some breathing room for the private sector to try to reduce costs without cutting back benefits for workers," said Kaiser President and CEO Drew Altman, in a statement.
But workers are still struggling to cover health costs. During the same period (2012-2013), wages increased 1.8% and inflation increased 1.1%. And since 2003, the average premium for family coverage has increased 80%, and the average worker contribution has risen 89%.
Employers continue to cost-shift. Seventy-eight percent of covered workers have a deductible, with the average for single coverage running about $1,100 (largely unchanged from 2012). But big deductibles are getting to be more common. Firms with less than 200 employees generally charged more than $1,000, and the number doing that rose from 49% of all such firms in 2012 to 58% in 2013.
Three-quarters of workers have a fixed copayment for office visits with primary care physicians and specialists. That copay averages $23 for primary care and $35 for specialty care for in-network physicians. Out-of-network amounts were not covered in the survey, but Kaiser assumes that patients bear a greater cost for those visits. About 20% of workers pay a percent of the visit (coinsurance) for primary care and the same amount for specialty care. They pay an average 18% of the visit.
The survey found that preferred provider organization (PPO) plans are the most common, enrolling 57% of covered workers in 2013. High-deductible health plans, also known as catastrophic plans, are the next most popular, with 20% of covered workers. Deductibles in those plans range from around $2,000 for single coverage to $4,000 for family coverage, with some much higher.
Only 14% of workers are enrolled in health maintenance organizations (HMOs), 9% in a point-of-service (POS) plan, and less than 1% in a conventional fee-for-service plan. High-deductible plans have grown exponentially since first coming on the scene – going from 8% in 2009 to 17% in 2011 – but have plateaued in the last few years, according to the report.
Also of interest to physicians:
• 23% of employers offering benefits have high performance or tiered networks in their largest health plan. The programs help steer patients to providers who have been identified as being more efficient or giving higher-quality care.
• 56% cover services provided by retail health clinics. Among firms covering services in these settings, 17% provide a financial incentive to receive services in a retail clinic instead of a physician’s office.
• Almost all employers with more than 200 workers and most smaller employers offer at least one wellness program. The majority offer at least one of the following in 2013: weight loss programs, gym membership discounts or on-site exercise facilities, biometric screening, smoking cessation, personal health coaching, health and nutrition education, web-based resources, flu shots or vaccinations, employee assistance programs (EAPs), or a wellness newsletter. Thirty-six percent of large firms and 8% of smaller firms offer employees a financial incentive to participate.
The growth in wellness programs "will be an important issue to watch next year, as employers will have more flexibility and could ask workers to pay more because of their lifestyles and health conditions," said Kaiser Vice President Gary Claxton, the study’s lead investigator and director of the Foundation’s Health Care Marketplace Project.
Mr. Claxton and his colleagues found that an increasing number of employees are likely to be subject to the Affordable Care Act’s various provisions. Thirty-six percent of covered workers are in "grandfathered" plans – that is, they are exempt from the law – down from 48% in 2012 and 56% in 2011.
The authors reported no disclosures.
[email protected]
On Twitter @aliciaault
FROM HEALTH AFFAIRS
Major finding: Employer-sponsored health insurance premiums rose 4% for family coverage and 5% for single coverage in 2013; deductibles, coinsurance, and other out-of-pocket costs also continued to rise for workers.
Data source: Survey of more than 2,000 nonfederal private and public employers with three or more workers.
Disclosures: The authors reported no disclosures.