User login
What can we offer patients with mild cognitive impairment?
We can promote healthy nutrition, physical activity, socialization, and mental activity. These interventions help stabilize and even improve cognition, as well as enhance quality of life and mood, delay institutionalization, and reduce disruptive behaviors. However, no medication is approved by the US Food and Drug Administration for treating mild cognitive impairment (MCI).
WHAT IS MILD COGNITIVE IMPAIRMENT?
MCI is a dynamic stage between normal aging and dementia. It is diagnosed in patients with an objective cognitive deficit but preserved function.
Population-based studies have found a wide range of rates of MCI incidence (21.5–71.3 per 1,000 person-years) and prevalence (3%–42%).1 The risk of progression from MCI to dementia ranges from 5% to 25% per year and is highest with MCI that involves memory loss (amnestic MCI).2,3
MCI can be regarded as a syndrome that is often associated with Alzheimer pathology and that has variable outcomes. In MCI due to Alzheimer disease, the primary complaint is short-term memory loss.4 Patients who have multiple impaired cognitive domains with prominent deficits in attention and executive function and relatively unimpaired short-term memory (nonamnestic MCI) are more likely to have vascular or Lewy body pathologies.5 Although distinctions between amnestic and nonamnestic MCI can be useful for counseling patients, both subtypes have similar proportions of “pure” Alzheimer disease pathology, vascular infarcts, and other pathologies at autopsy.5,6
GENERAL MANAGEMENT—IMPROVE OVERALL HEALTH
Primary management of MCI should focus on improving lifestyle factors and treating comorbid conditions that can affect cognition (eg, depression, nutritional deficiencies).
An important goal of management is to preserve working memory, ie, the ability to maintain and manipulate information while ignoring distractions. Preservation of working memory but not short-term memory is associated with slower functional decline in MCI and early Alzheimer disease.7 Lifestyle factors including sleep, stress, and exercise affect working memory performance and, thus, functional ability.
Minimizing the risk of traumatic brain injury by reducing the risk of falling is also important. Although the role of alcohol consumption as it relates to cognition is controversial, physicians may counsel older adults with MCI to reduce their alcohol consumption even if they are consuming no more than one standard drink in a 24-hour period, in order to reduce the risk of falls and their sequelae.
Optimally controlling blood pressure, lipids, and blood sugar can reduce cardiovascular risk and may slow progression of MCI to dementia.2
Smoking should be stopped and polypharmacy avoided, with particular emphasis on eliminating medications included in the Beers criteria.8
A HEALTHY DIET MAY HELP
Although evidence supporting the benefits of various diets for MCI remains scarce with mixed results, a healthy diet may favorably affect cognition. A 2009 systematic review found that observational studies showed that long-chain omega-3 fatty acids had a positive influence on cognition, but results from clinical trials were equivocal.9 Studies investigating the impact on cognition of the Mediterranean diet—rich in vegetables, fruits, whole grains, lean protein, and olive oil—remain mixed (possibly because of dietary and cognitive measurement variations between studies) but suggest that it promotes slower cognitive decline.10
PHYSICAL ACTIVITY HAS MULTIPLE BENEFITS
Physical activity has many health benefits in the elderly: it reduces muscle loss, increases functional capacity, and decreases the risk of falls.11 Several randomized controlled trials have explored the relationship between physical activity and cognition in patients with varying degrees of cognitive impairment. Although the optimal type and duration of exercise needed to achieve a specific benefit remains unclear, physical activity has been found to be helpful in more studies than not.12 Baker et al13 found that 45 to 60 minutes of high-intensity aerobic activity 4 days a week for 6 months improved executive function.
MAINTAIN SOCIAL ACTIVITIES
Social engagement—which can include a range of activities from conversation to structured group activities—is important for maintaining cognitive function.
A prospective cohort study14 that followed participants for 1 to 3 years after MCI diagnosis found that those who progressed from mild to severe cognitive impairment were less likely to attend a place of worship, work, or volunteer.
A longitudinal study of 89 elderly people without known dementia evaluated measures of socialization, global cognitive function, and Alzheimer disease pathology seen on brain autopsy. Lower cognitive function was associated with more disease pathology, but social network size modified this relationship: cognitive function was less impaired than expected for those with a large social network, even for those with a high burden of brain pathology.15
ENCOURAGE BRAIN EXERCISE
Activities can include “cognitive hobbies” such as playing board games, reading, playing a musical instrument, and doing crossword puzzles. Specific cognitive training strategies (eg, mnemonics, calligraphy therapy, computer-based interventions) have shown benefits, although it is unclear if some interventions are more effective than others.12
MULTIMODAL STRATEGIES
There are no data supporting strategies that combine multiple interventions compared with a single intervention on cognitive outcome. However, most single interventions likely contain socialization as an unstated intervention. For example, group settings for a cognitive or physical activity may include interactions with an instructor and interactions with other participants. It is thus difficult to identify truly unimodal interventions.
An example of a multimodal approach for cognitive impairment is tai chi. Physical activity in tai chi is used for coordinated movements and balance; attention, visual imagery, and memory provide cognitive stimulation; and it is frequently performed in a group setting or with an instructor. A 1-year trial in 389 MCI patients found that those who practiced tai chi had lower clinical dementia rating scale scores than the control group who participated in stretching and toning exercises.16
Table 1 summarizes recommendations for patients with MCI. In addition, referral to a geriatrician should be considered for assistance with evaluation and management, particularly if the patient lacks a capable caregiver or if the caregiver is under stress.
- Ward A, Arrighi HM, Michels S, Cedarbaum JM. Mild cognitive impairment: disparity of incidence and prevalence estimates. Alzheimers Dement 2012; 8:14–21.
- Mariani E, Monastero R, Mecocci P. Mild cognitive impairment: a systematic review. J Alzheimers Dis 2007; 12:23–35.
- Jean L, Bergeron ME, Thivierge S, Simard M. Cognitive intervention programs for individuals with mild cognitive impairment: systematic review of the literature. Am J Geriatr Psychiatry 2010; 18:281–296.
- Petersen RC, Parisi JE, Dickson DW, et al. Neuropathologic features of amnestic mild cognitive impairment. Arch Neurol 2006; 63:665–672.
- Schneider JA, Arvanitakis Z, Leurgans SE, Bennett DA. The neuropathology of probable Alzheimer disease and mild cognitive impairment. Ann Neurol 2009; 66:200–208.
- Ferman TJ, Smith GE, Kantarci K, et al. Nonamnestic mild cognitive impairment progresses to dementia with Lewy bodies. Neurology 2013; 81:2032–2038.
- Pillai JA, Bonner-Jackson A, Walker E, Mourany L, Cummings JL. Higher working memory predicts slower functional decline in autopsy-confirmed Alzheimer’s disease. Dement Geriatr Cogn Disord 2014; 38:224–233.
- American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2012; 60:616–631.
- Fotuhi M, Mohassel P, Yaffe K. Fish consumption, long-chain omega-3 fatty acids and risk of cognitive decline or Alzheimer disease: a complex association. Nat Clin Pract Neurol 2009; 5:140–152.
- Kuczmarski MF, Allegro D, Stave E. The association of healthful diets and cognitive function: a review. J Nutr Gerontol Geriatr 2014; 33:69–90.
- Heyn P, Abreu BC, Ottenbacher KJ. The effects of exercise training on elderly persons with cognitive impairment and dementia: a meta-analysis. Arch Phys Med Rehabil 2004; 85:1694–1704.
- Horr T, Messinger-Rapport B, Pillai JA. Systematic review of strengths and limitations of randomized controlled trials for non-pharmacological interventions in mild cognitive impairment: focus on Alzheimer’s disease. J Nutr Health Aging 2015; 19:141–153.
- Baker LD, Frank LL, Foster-Schubert K, et al. Effects of aerobic exercise on mild cognitive impairment: a controlled trial. Arch Neurol 2010; 67:71-79.
- Hughes TF, Flatt JD, Fu B, Chang CC, Ganguli M. Engagement in social activities and progression from mild to severe cognitive impairment: the MYHAT study. Int Psychogeriatr 2013; 25:587–595.
- Bennett DA, Schneider JA, Tang Y, Arnold SE, Wilson RS. The effect of social networks on the relation between Alzheimer’s disease pathology and level of cognitive function in old people: a longitudinal cohort study. Lancet Neurol 2006; 5:406–412.
- Lam LC, Chau RC, Wong BM, et al. A 1-year randomized controlled trial comparing mind body exercise (tai chi) with stretching and toning exercise on cognitive function in older Chinese adults at risk of cognitive decline. J Am Med Dir Assoc 2012; 13:568.e15–568.e20.
We can promote healthy nutrition, physical activity, socialization, and mental activity. These interventions help stabilize and even improve cognition, as well as enhance quality of life and mood, delay institutionalization, and reduce disruptive behaviors. However, no medication is approved by the US Food and Drug Administration for treating mild cognitive impairment (MCI).
WHAT IS MILD COGNITIVE IMPAIRMENT?
MCI is a dynamic stage between normal aging and dementia. It is diagnosed in patients with an objective cognitive deficit but preserved function.
Population-based studies have found a wide range of rates of MCI incidence (21.5–71.3 per 1,000 person-years) and prevalence (3%–42%).1 The risk of progression from MCI to dementia ranges from 5% to 25% per year and is highest with MCI that involves memory loss (amnestic MCI).2,3
MCI can be regarded as a syndrome that is often associated with Alzheimer pathology and that has variable outcomes. In MCI due to Alzheimer disease, the primary complaint is short-term memory loss.4 Patients who have multiple impaired cognitive domains with prominent deficits in attention and executive function and relatively unimpaired short-term memory (nonamnestic MCI) are more likely to have vascular or Lewy body pathologies.5 Although distinctions between amnestic and nonamnestic MCI can be useful for counseling patients, both subtypes have similar proportions of “pure” Alzheimer disease pathology, vascular infarcts, and other pathologies at autopsy.5,6
GENERAL MANAGEMENT—IMPROVE OVERALL HEALTH
Primary management of MCI should focus on improving lifestyle factors and treating comorbid conditions that can affect cognition (eg, depression, nutritional deficiencies).
An important goal of management is to preserve working memory, ie, the ability to maintain and manipulate information while ignoring distractions. Preservation of working memory but not short-term memory is associated with slower functional decline in MCI and early Alzheimer disease.7 Lifestyle factors including sleep, stress, and exercise affect working memory performance and, thus, functional ability.
Minimizing the risk of traumatic brain injury by reducing the risk of falling is also important. Although the role of alcohol consumption as it relates to cognition is controversial, physicians may counsel older adults with MCI to reduce their alcohol consumption even if they are consuming no more than one standard drink in a 24-hour period, in order to reduce the risk of falls and their sequelae.
Optimally controlling blood pressure, lipids, and blood sugar can reduce cardiovascular risk and may slow progression of MCI to dementia.2
Smoking should be stopped and polypharmacy avoided, with particular emphasis on eliminating medications included in the Beers criteria.8
A HEALTHY DIET MAY HELP
Although evidence supporting the benefits of various diets for MCI remains scarce with mixed results, a healthy diet may favorably affect cognition. A 2009 systematic review found that observational studies showed that long-chain omega-3 fatty acids had a positive influence on cognition, but results from clinical trials were equivocal.9 Studies investigating the impact on cognition of the Mediterranean diet—rich in vegetables, fruits, whole grains, lean protein, and olive oil—remain mixed (possibly because of dietary and cognitive measurement variations between studies) but suggest that it promotes slower cognitive decline.10
PHYSICAL ACTIVITY HAS MULTIPLE BENEFITS
Physical activity has many health benefits in the elderly: it reduces muscle loss, increases functional capacity, and decreases the risk of falls.11 Several randomized controlled trials have explored the relationship between physical activity and cognition in patients with varying degrees of cognitive impairment. Although the optimal type and duration of exercise needed to achieve a specific benefit remains unclear, physical activity has been found to be helpful in more studies than not.12 Baker et al13 found that 45 to 60 minutes of high-intensity aerobic activity 4 days a week for 6 months improved executive function.
MAINTAIN SOCIAL ACTIVITIES
Social engagement—which can include a range of activities from conversation to structured group activities—is important for maintaining cognitive function.
A prospective cohort study14 that followed participants for 1 to 3 years after MCI diagnosis found that those who progressed from mild to severe cognitive impairment were less likely to attend a place of worship, work, or volunteer.
A longitudinal study of 89 elderly people without known dementia evaluated measures of socialization, global cognitive function, and Alzheimer disease pathology seen on brain autopsy. Lower cognitive function was associated with more disease pathology, but social network size modified this relationship: cognitive function was less impaired than expected for those with a large social network, even for those with a high burden of brain pathology.15
ENCOURAGE BRAIN EXERCISE
Activities can include “cognitive hobbies” such as playing board games, reading, playing a musical instrument, and doing crossword puzzles. Specific cognitive training strategies (eg, mnemonics, calligraphy therapy, computer-based interventions) have shown benefits, although it is unclear if some interventions are more effective than others.12
MULTIMODAL STRATEGIES
There are no data supporting strategies that combine multiple interventions compared with a single intervention on cognitive outcome. However, most single interventions likely contain socialization as an unstated intervention. For example, group settings for a cognitive or physical activity may include interactions with an instructor and interactions with other participants. It is thus difficult to identify truly unimodal interventions.
An example of a multimodal approach for cognitive impairment is tai chi. Physical activity in tai chi is used for coordinated movements and balance; attention, visual imagery, and memory provide cognitive stimulation; and it is frequently performed in a group setting or with an instructor. A 1-year trial in 389 MCI patients found that those who practiced tai chi had lower clinical dementia rating scale scores than the control group who participated in stretching and toning exercises.16
Table 1 summarizes recommendations for patients with MCI. In addition, referral to a geriatrician should be considered for assistance with evaluation and management, particularly if the patient lacks a capable caregiver or if the caregiver is under stress.
We can promote healthy nutrition, physical activity, socialization, and mental activity. These interventions help stabilize and even improve cognition, as well as enhance quality of life and mood, delay institutionalization, and reduce disruptive behaviors. However, no medication is approved by the US Food and Drug Administration for treating mild cognitive impairment (MCI).
WHAT IS MILD COGNITIVE IMPAIRMENT?
MCI is a dynamic stage between normal aging and dementia. It is diagnosed in patients with an objective cognitive deficit but preserved function.
Population-based studies have found a wide range of rates of MCI incidence (21.5–71.3 per 1,000 person-years) and prevalence (3%–42%).1 The risk of progression from MCI to dementia ranges from 5% to 25% per year and is highest with MCI that involves memory loss (amnestic MCI).2,3
MCI can be regarded as a syndrome that is often associated with Alzheimer pathology and that has variable outcomes. In MCI due to Alzheimer disease, the primary complaint is short-term memory loss.4 Patients who have multiple impaired cognitive domains with prominent deficits in attention and executive function and relatively unimpaired short-term memory (nonamnestic MCI) are more likely to have vascular or Lewy body pathologies.5 Although distinctions between amnestic and nonamnestic MCI can be useful for counseling patients, both subtypes have similar proportions of “pure” Alzheimer disease pathology, vascular infarcts, and other pathologies at autopsy.5,6
GENERAL MANAGEMENT—IMPROVE OVERALL HEALTH
Primary management of MCI should focus on improving lifestyle factors and treating comorbid conditions that can affect cognition (eg, depression, nutritional deficiencies).
An important goal of management is to preserve working memory, ie, the ability to maintain and manipulate information while ignoring distractions. Preservation of working memory but not short-term memory is associated with slower functional decline in MCI and early Alzheimer disease.7 Lifestyle factors including sleep, stress, and exercise affect working memory performance and, thus, functional ability.
Minimizing the risk of traumatic brain injury by reducing the risk of falling is also important. Although the role of alcohol consumption as it relates to cognition is controversial, physicians may counsel older adults with MCI to reduce their alcohol consumption even if they are consuming no more than one standard drink in a 24-hour period, in order to reduce the risk of falls and their sequelae.
Optimally controlling blood pressure, lipids, and blood sugar can reduce cardiovascular risk and may slow progression of MCI to dementia.2
Smoking should be stopped and polypharmacy avoided, with particular emphasis on eliminating medications included in the Beers criteria.8
A HEALTHY DIET MAY HELP
Although evidence supporting the benefits of various diets for MCI remains scarce with mixed results, a healthy diet may favorably affect cognition. A 2009 systematic review found that observational studies showed that long-chain omega-3 fatty acids had a positive influence on cognition, but results from clinical trials were equivocal.9 Studies investigating the impact on cognition of the Mediterranean diet—rich in vegetables, fruits, whole grains, lean protein, and olive oil—remain mixed (possibly because of dietary and cognitive measurement variations between studies) but suggest that it promotes slower cognitive decline.10
PHYSICAL ACTIVITY HAS MULTIPLE BENEFITS
Physical activity has many health benefits in the elderly: it reduces muscle loss, increases functional capacity, and decreases the risk of falls.11 Several randomized controlled trials have explored the relationship between physical activity and cognition in patients with varying degrees of cognitive impairment. Although the optimal type and duration of exercise needed to achieve a specific benefit remains unclear, physical activity has been found to be helpful in more studies than not.12 Baker et al13 found that 45 to 60 minutes of high-intensity aerobic activity 4 days a week for 6 months improved executive function.
MAINTAIN SOCIAL ACTIVITIES
Social engagement—which can include a range of activities from conversation to structured group activities—is important for maintaining cognitive function.
A prospective cohort study14 that followed participants for 1 to 3 years after MCI diagnosis found that those who progressed from mild to severe cognitive impairment were less likely to attend a place of worship, work, or volunteer.
A longitudinal study of 89 elderly people without known dementia evaluated measures of socialization, global cognitive function, and Alzheimer disease pathology seen on brain autopsy. Lower cognitive function was associated with more disease pathology, but social network size modified this relationship: cognitive function was less impaired than expected for those with a large social network, even for those with a high burden of brain pathology.15
ENCOURAGE BRAIN EXERCISE
Activities can include “cognitive hobbies” such as playing board games, reading, playing a musical instrument, and doing crossword puzzles. Specific cognitive training strategies (eg, mnemonics, calligraphy therapy, computer-based interventions) have shown benefits, although it is unclear if some interventions are more effective than others.12
MULTIMODAL STRATEGIES
There are no data supporting strategies that combine multiple interventions compared with a single intervention on cognitive outcome. However, most single interventions likely contain socialization as an unstated intervention. For example, group settings for a cognitive or physical activity may include interactions with an instructor and interactions with other participants. It is thus difficult to identify truly unimodal interventions.
An example of a multimodal approach for cognitive impairment is tai chi. Physical activity in tai chi is used for coordinated movements and balance; attention, visual imagery, and memory provide cognitive stimulation; and it is frequently performed in a group setting or with an instructor. A 1-year trial in 389 MCI patients found that those who practiced tai chi had lower clinical dementia rating scale scores than the control group who participated in stretching and toning exercises.16
Table 1 summarizes recommendations for patients with MCI. In addition, referral to a geriatrician should be considered for assistance with evaluation and management, particularly if the patient lacks a capable caregiver or if the caregiver is under stress.
- Ward A, Arrighi HM, Michels S, Cedarbaum JM. Mild cognitive impairment: disparity of incidence and prevalence estimates. Alzheimers Dement 2012; 8:14–21.
- Mariani E, Monastero R, Mecocci P. Mild cognitive impairment: a systematic review. J Alzheimers Dis 2007; 12:23–35.
- Jean L, Bergeron ME, Thivierge S, Simard M. Cognitive intervention programs for individuals with mild cognitive impairment: systematic review of the literature. Am J Geriatr Psychiatry 2010; 18:281–296.
- Petersen RC, Parisi JE, Dickson DW, et al. Neuropathologic features of amnestic mild cognitive impairment. Arch Neurol 2006; 63:665–672.
- Schneider JA, Arvanitakis Z, Leurgans SE, Bennett DA. The neuropathology of probable Alzheimer disease and mild cognitive impairment. Ann Neurol 2009; 66:200–208.
- Ferman TJ, Smith GE, Kantarci K, et al. Nonamnestic mild cognitive impairment progresses to dementia with Lewy bodies. Neurology 2013; 81:2032–2038.
- Pillai JA, Bonner-Jackson A, Walker E, Mourany L, Cummings JL. Higher working memory predicts slower functional decline in autopsy-confirmed Alzheimer’s disease. Dement Geriatr Cogn Disord 2014; 38:224–233.
- American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2012; 60:616–631.
- Fotuhi M, Mohassel P, Yaffe K. Fish consumption, long-chain omega-3 fatty acids and risk of cognitive decline or Alzheimer disease: a complex association. Nat Clin Pract Neurol 2009; 5:140–152.
- Kuczmarski MF, Allegro D, Stave E. The association of healthful diets and cognitive function: a review. J Nutr Gerontol Geriatr 2014; 33:69–90.
- Heyn P, Abreu BC, Ottenbacher KJ. The effects of exercise training on elderly persons with cognitive impairment and dementia: a meta-analysis. Arch Phys Med Rehabil 2004; 85:1694–1704.
- Horr T, Messinger-Rapport B, Pillai JA. Systematic review of strengths and limitations of randomized controlled trials for non-pharmacological interventions in mild cognitive impairment: focus on Alzheimer’s disease. J Nutr Health Aging 2015; 19:141–153.
- Baker LD, Frank LL, Foster-Schubert K, et al. Effects of aerobic exercise on mild cognitive impairment: a controlled trial. Arch Neurol 2010; 67:71-79.
- Hughes TF, Flatt JD, Fu B, Chang CC, Ganguli M. Engagement in social activities and progression from mild to severe cognitive impairment: the MYHAT study. Int Psychogeriatr 2013; 25:587–595.
- Bennett DA, Schneider JA, Tang Y, Arnold SE, Wilson RS. The effect of social networks on the relation between Alzheimer’s disease pathology and level of cognitive function in old people: a longitudinal cohort study. Lancet Neurol 2006; 5:406–412.
- Lam LC, Chau RC, Wong BM, et al. A 1-year randomized controlled trial comparing mind body exercise (tai chi) with stretching and toning exercise on cognitive function in older Chinese adults at risk of cognitive decline. J Am Med Dir Assoc 2012; 13:568.e15–568.e20.
- Ward A, Arrighi HM, Michels S, Cedarbaum JM. Mild cognitive impairment: disparity of incidence and prevalence estimates. Alzheimers Dement 2012; 8:14–21.
- Mariani E, Monastero R, Mecocci P. Mild cognitive impairment: a systematic review. J Alzheimers Dis 2007; 12:23–35.
- Jean L, Bergeron ME, Thivierge S, Simard M. Cognitive intervention programs for individuals with mild cognitive impairment: systematic review of the literature. Am J Geriatr Psychiatry 2010; 18:281–296.
- Petersen RC, Parisi JE, Dickson DW, et al. Neuropathologic features of amnestic mild cognitive impairment. Arch Neurol 2006; 63:665–672.
- Schneider JA, Arvanitakis Z, Leurgans SE, Bennett DA. The neuropathology of probable Alzheimer disease and mild cognitive impairment. Ann Neurol 2009; 66:200–208.
- Ferman TJ, Smith GE, Kantarci K, et al. Nonamnestic mild cognitive impairment progresses to dementia with Lewy bodies. Neurology 2013; 81:2032–2038.
- Pillai JA, Bonner-Jackson A, Walker E, Mourany L, Cummings JL. Higher working memory predicts slower functional decline in autopsy-confirmed Alzheimer’s disease. Dement Geriatr Cogn Disord 2014; 38:224–233.
- American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2012; 60:616–631.
- Fotuhi M, Mohassel P, Yaffe K. Fish consumption, long-chain omega-3 fatty acids and risk of cognitive decline or Alzheimer disease: a complex association. Nat Clin Pract Neurol 2009; 5:140–152.
- Kuczmarski MF, Allegro D, Stave E. The association of healthful diets and cognitive function: a review. J Nutr Gerontol Geriatr 2014; 33:69–90.
- Heyn P, Abreu BC, Ottenbacher KJ. The effects of exercise training on elderly persons with cognitive impairment and dementia: a meta-analysis. Arch Phys Med Rehabil 2004; 85:1694–1704.
- Horr T, Messinger-Rapport B, Pillai JA. Systematic review of strengths and limitations of randomized controlled trials for non-pharmacological interventions in mild cognitive impairment: focus on Alzheimer’s disease. J Nutr Health Aging 2015; 19:141–153.
- Baker LD, Frank LL, Foster-Schubert K, et al. Effects of aerobic exercise on mild cognitive impairment: a controlled trial. Arch Neurol 2010; 67:71-79.
- Hughes TF, Flatt JD, Fu B, Chang CC, Ganguli M. Engagement in social activities and progression from mild to severe cognitive impairment: the MYHAT study. Int Psychogeriatr 2013; 25:587–595.
- Bennett DA, Schneider JA, Tang Y, Arnold SE, Wilson RS. The effect of social networks on the relation between Alzheimer’s disease pathology and level of cognitive function in old people: a longitudinal cohort study. Lancet Neurol 2006; 5:406–412.
- Lam LC, Chau RC, Wong BM, et al. A 1-year randomized controlled trial comparing mind body exercise (tai chi) with stretching and toning exercise on cognitive function in older Chinese adults at risk of cognitive decline. J Am Med Dir Assoc 2012; 13:568.e15–568.e20.

In reply: Risk of falls
In Reply: The query regarding bicycle helmet use as a preventive measure in elderly people at high risk of recurrent falls is interesting. Prior to our article going to press, we reviewed the literature and found no quality studies of helmet use in preventing brain injury at home or in residential facilities. The few studies of helmet use vs no helmet use focused on sports and suggested that the benefit of current helmet design may be more limited than previously thought. Although sports helmets reduce the risk of linear impact causing death, major injury, skull fracture, and (if a facial portion is present) facial injury, there is little protection against injury from rotational forces. Concussion, a form of mild brain injury, does not appear to be reduced by helmet use in sports.1 Additionally, 77% of soldiers hospitalized with traumatic brain injury were wearing a helmet at the time of injury.2
In addition to questioning the effectiveness of helmets in recurrent fallers, one has to consider the ability of a helmet to be fitted properly (for example, the fit will change after a haircut or change in hairstyle), the willingness of the individual to wear it, the ability of the patient or caregiver to attach it, and the impact of wearing a helmet on psychosocial interactions. Helmet use in a recurrent faller would have to be considered an individualized intervention amenable to caregiver and patient but without proven benefit.
- Benson BW, Hamilton GM, Meeuwisse WH, McCrory P, Dvorak J. Is protective equipment useful in preventing concussion? A systematic review of the literature. Br J Sports Med 2009; 43:i56–i67.
- Wojcik BE, Stein CR, Bagg K, Humphrey RJ, Orosco J. Traumatic brain injury hospitalizations of US army soldiers deployed to Afghanistan and Iraq. Am J Prev Med 2010; 38:S108–S116.
In Reply: The query regarding bicycle helmet use as a preventive measure in elderly people at high risk of recurrent falls is interesting. Prior to our article going to press, we reviewed the literature and found no quality studies of helmet use in preventing brain injury at home or in residential facilities. The few studies of helmet use vs no helmet use focused on sports and suggested that the benefit of current helmet design may be more limited than previously thought. Although sports helmets reduce the risk of linear impact causing death, major injury, skull fracture, and (if a facial portion is present) facial injury, there is little protection against injury from rotational forces. Concussion, a form of mild brain injury, does not appear to be reduced by helmet use in sports.1 Additionally, 77% of soldiers hospitalized with traumatic brain injury were wearing a helmet at the time of injury.2
In addition to questioning the effectiveness of helmets in recurrent fallers, one has to consider the ability of a helmet to be fitted properly (for example, the fit will change after a haircut or change in hairstyle), the willingness of the individual to wear it, the ability of the patient or caregiver to attach it, and the impact of wearing a helmet on psychosocial interactions. Helmet use in a recurrent faller would have to be considered an individualized intervention amenable to caregiver and patient but without proven benefit.
In Reply: The query regarding bicycle helmet use as a preventive measure in elderly people at high risk of recurrent falls is interesting. Prior to our article going to press, we reviewed the literature and found no quality studies of helmet use in preventing brain injury at home or in residential facilities. The few studies of helmet use vs no helmet use focused on sports and suggested that the benefit of current helmet design may be more limited than previously thought. Although sports helmets reduce the risk of linear impact causing death, major injury, skull fracture, and (if a facial portion is present) facial injury, there is little protection against injury from rotational forces. Concussion, a form of mild brain injury, does not appear to be reduced by helmet use in sports.1 Additionally, 77% of soldiers hospitalized with traumatic brain injury were wearing a helmet at the time of injury.2
In addition to questioning the effectiveness of helmets in recurrent fallers, one has to consider the ability of a helmet to be fitted properly (for example, the fit will change after a haircut or change in hairstyle), the willingness of the individual to wear it, the ability of the patient or caregiver to attach it, and the impact of wearing a helmet on psychosocial interactions. Helmet use in a recurrent faller would have to be considered an individualized intervention amenable to caregiver and patient but without proven benefit.
- Benson BW, Hamilton GM, Meeuwisse WH, McCrory P, Dvorak J. Is protective equipment useful in preventing concussion? A systematic review of the literature. Br J Sports Med 2009; 43:i56–i67.
- Wojcik BE, Stein CR, Bagg K, Humphrey RJ, Orosco J. Traumatic brain injury hospitalizations of US army soldiers deployed to Afghanistan and Iraq. Am J Prev Med 2010; 38:S108–S116.
- Benson BW, Hamilton GM, Meeuwisse WH, McCrory P, Dvorak J. Is protective equipment useful in preventing concussion? A systematic review of the literature. Br J Sports Med 2009; 43:i56–i67.
- Wojcik BE, Stein CR, Bagg K, Humphrey RJ, Orosco J. Traumatic brain injury hospitalizations of US army soldiers deployed to Afghanistan and Iraq. Am J Prev Med 2010; 38:S108–S116.
Stand by me! Reducing the risk of injurious falls in older adults
Falls and fall-related injuries are common in older adults Every year, 30% of those who are 65 and older fall,1 and the consequences are potentially serious. Falls are the primary cause of hip fracture, which requires an extensive period of rehabilitation. However, rehabilitation does not always restore the older adult to his or her preinjury functional state. In fact, at 6 to 12 months after a hip fracture, 22% to 75% of elderly patients have not recovered their prefracture ambulatory or functional status.2
Falls are also the most common cause of traumatic brain injury in older adults,3 often resulting in long-term cognitive and emotional problems and pain that compromise quality of life. Falls can be fatal and in fact are the leading cause of death from injury in older adults.4
Practitioners can reduce fall-related injury5 and potentially improve quality of life by screening older adults yearly, performing a focused history and examination when necessary, and implementing evidence-based interventions.
RISK FACTORS
A single identifiable factor may account for only a small portion of the fall risk. Falls in older adults are, in general, multifactorial and can be caused by medical conditions (eg, sarcopenia, particularly of the lower limbs, vision loss, urinary incontinence, neuropathies), cognitive impairment, medications such as psychotropic drugs, and home hazards such as area rugs, extension cords, and dimly lit stairways.
The strongest predictors of falls are a recent fall and the presence of a gait or balance disorder.6
SCREENING TESTS
Joint guidelines from the American Geriatrics Society and British Geriatrics Society,7 published in 2011, recommend that practitioners screen older adults yearly for fall risk by asking two questions: “Have you fallen in the past year?” and “Are you having difficulty with gait or balance?” A negative response to both questions suggests a low risk of falling in the near future. Patients with two or more falls, a balance or gait problem (subjective or objective), or history of a fall requiring medical attention should undergo a focused history and physical examination plus a multifactorial risk assessment.
A report of one fall without injury should prompt a simple office-based test of balance. Examples of tests include the Get Up and Go, the Timed Up and Go, and the One-Legged Stance (the Unipedal Stance).
In the Get Up and Go test, patients sit comfortably in a chair with a straight back. They rise from the chair, stand still, walk a short distance (about 3 meters), turn around, walk back to the chair, and sit down.8 The clinician notes any deviation from a confident, smooth performance.
In the Timed Up and Go test, the clinician records the time it takes for the patient to rise from a hardback chair, walk 10 feet (3 meters), turn, return to the chair, and sit down.9 Most older adults complete this test in less than 10 seconds. Taking longer than 14 seconds is associated with a high risk of falls.10
For the One-Legged Stance test, the clinician asks the patient to stand on one leg. A patient without significant balance issues is able to stand for at least 5 seconds.11
Figure 1 summarizes the approach for a community-dwelling patient who presents to the outpatient setting. A complete multifactorial risk assessment may require a dedicated appointment or referral to a specialist such as a geriatrician, physiatrist, or neurologist.
WHAT INFORMATION DOES A FOCUSED HISTORY INCLUDE?
The fall-focused history includes:
A detailed description of the circumstances of the fall or falls, symptoms (such as dizziness), and injuries or other consequences of the fall.7
A medication review. Table 1 includes commonly prescribed drug classes associated with increased fall risk.12 Be especially vigilant for eyedrops used to treat glaucoma (some can potentiate bradycardia) and for psychotropic drugs.
Drug regimens with a high psychotropic burden can be identified with the Drug Burden Index13 or the Anticholinergic Risk Scale,14 but these scales are cumbersome and are usually used only as part of a research study. The updated Beers criteria15 and use of a structured medication review such as the START and STOPP algorithms16 can help prune unnecessary, inappropriate, and high-risk medications such as:
- Selective serotonin reuptake inhibitors in the absence of current major depression. These drugs increase the risk of falls and decrease bone density.17
- Proton pump inhibitors in the absence of a true indication for this drug class to treat reflux. Drugs in this class reduce bone density and increase the risk of hip fracture after 1 year of continuous use18
- Cholinesterase inhibitors in the absence of demonstrated benefit to dementia symptoms for the particular patient. Drugs in this class are associated with falls, hip fracture, bradycardia, and possible need for pacemaker placement.19
Review of activities of daily living (ADLs). A functional assessment of the patient’s ability to complete ADLs helps identify targets for therapy. Assess whether the patient is afraid of falling and, if so, what impact this fear has on ADLs. This can help determine whether the fear protects the patient from performing risky tasks, or harms the patient by contributing to deconditioning.
Medical conditions. Consider chronic conditions that can impair mobility and increase fall risk. These include urinary incontinence, cognitive impairment (eg, dementia), neuropathy, degenerative neurologic conditions such as Parkinson disease, and degenerative arthritis. Osteoporosis increases the risk of fracture in a fall. Vitamin D deficiency increases both fall and fracture risk.20
PHYSICAL EXAMINATION FINDINGS
Assess the patient’s vision, proprioception, reflexes, and cortical, extrapyramidal, and cerebellar function.7
Perform a detailed assessment of the patient’s gait, balance, and mobility. Assess the lower extremities for joint and nerve function, muscle strength, and range of motion.7 The use of brain imaging, if appropriate, is guided by gait abnormalities. Unexpected findings such as neuropathy may require referrals for further evaluation.
Examine the patient’s feet and footwear for signs of poor fit and for styles that may be inappropriate for someone at risk of falling, such as high heels.
Conduct a cardiovascular examination. In addition to assessing heart rate and rhythm and checking for heart murmurs, evaluate the patient for postural changes in heart rate and blood pressure. Wait at least 2 minutes before asking the patient to change position from supine to seated and from seated to standing. A longer interval (3 to 5 minutes) can be used depending on the patient’s history. For example, an older adult reporting a syncopal episode standing by the kitchen sink may need a longer standing interval prior to blood pressure measurement than an older adult who falls right after standing up from a chair.
If there is a strong suspicion that an orthostatic condition contributed to a fall but it is not possible to elicit orthostasis in the office, it may be necessary to refer the patient for tilt-table testing. If the circumstances suggest that pressure along the neck, or turning the neck, contributed to a fall, referral for carotid sinus stimulation may be appropriate. If there is a concern that a brady- or tachyarrhythmia contributed to the fall, a referral for 24- or 48-hour Holter monitoring or a 30-day loop monitor may be indicated.
Assess the patient’s mental status. Cognitive impairment itself is an independent predictor of falls7 because it can reduce processing speed and impair executive function.21 Executive dysfunction may contribute to falls by causing problems with multitasking, drug compliance, and judgment. The presence and severity of cognitive impairment may affect recommendation options (see below), so the assessment should include a screening test. Consider using the Mini-Cog, which requires the patient to recall three words and draw an analog clock (Figure 2).22
Some cognitive screening tests validated for use in the general older population include the General Practitioner Assessment of Cognition and the Memory Impairment Screen.23 More involved cognitive testing such as the Folstein Mini-Mental State Examination, Montreal Cognitive Assessment, and the Saint Louis University Mental Status Examination are routinely performed in a geriatric or neurologic setting. The Folstein is a proprietary test; the other two are not.
Conditions such as circulatory disease, chronic obstructive pulmonary disease, depression, and arthritis are associated with a higher risk of falling, even with adjustment for drug use and other potential confounding factors.24
A brief mood assessment is part of the multifactorial assessment because mood disorders in older adults can lead to deconditioning, drug noncompliance, and other conditions that lead to falls and fall-related injuries. Options for screening include the Geriatric Depression Scale (15 or 30 questions) and the Patient Health Questionnaire (the PHQ-2 or the PHQ-9).7
WHAT ARE THE EVIDENCE-BASED INTERVENTIONS?
In general, interventions are chosen according to the risks identified by the assessment; multiple interventions are usually necessary. It is ineffective to identify risk factors without providing intervention.25
Specific interventions with recommendation levels A and B are listed in Table 2.7 Level A interventions are specifically supported by strong evidence and should be recommended. Of note, although vitamin D3 may not be bioequivalent to vitamin D2, studies in older adults have not consistently found a clinically different outcome, and either may be supplemented in the community-dwelling elderly. Except for vitamin D, these interventions target community-dwelling older adults who are cognitively intact.
Home assessments are effective in high-risk patients, such as those with poor vision and those who were recently hospitalized. The goal is to improve safety, particularly during patient transfers, with education and training provided by an occupational or physical therapist or other geriatric specialist. The benefit of home assessment and environmental modification is greater when combined with other strategies and in general should not be implemented alone.
Exercise is an important intervention. The number needed to treat (NNT) to prevent one fall in older people over the course of at least 12 weeks is 16.26 This compares favorably with interventions that are commonly used in the general population, such as aspirin therapy as secondary prevention for cardiovascular disease (NNT for 1 year = 50)27 and statin therapy to prevent one death from a cardiovascular event over 5 years in people with known heart disease (NNT = 83).28
Exercise recommendations should be customized to the patient. The amount and type of exercise depends on the patient’s baseline physical activity, medication use including antiplatelet and anticoagulant therapy, home environment, cardiac and pulmonary reserve, vision and hearing deficits, and comorbidities including neuropathy and arthritis.
The well-known risks associated with exercise include myocardial infarction and cardiac arrest, as well as falls and fractures. However, the benefits extend beyond fall risk and include improvements in physical function, glycemic control, cardiopulmonary reserve, bone density, arthritic pain, mood, and cognition. Exercise can also help manage weight, reduce sarcopenia, and increase opportunities for socialization. In most positive trials, the exercise interventions lasted longer than 12 weeks, had variable intensity, and occurred 1 to 3 times per week.
The American College of Sports Medicine recommends that older adults perform aerobic exercise 3 to 5 times per week, 20 to 60 minutes per session (the lower ranges are for frail elderly patients).29 It also recommends resistance training 2 to 4 days per week, 20 to 45 minutes per session, depending on the patient’s level of frailty and conditioning.30 Most older adults do not exercise enough.
Interventions listed at the bottom of Table 2 do not, in general, have enough evidence to support or discourage their use; these are level C recommendations. However, these interventions may be considered for certain individuals. For example, older adults with diabetic neuropathy are often unaware of their foot position when they walk. Additionally, those with diabetic neuropathy may have slower generation of ankle and knee strength compared with age-matched controls. These patients may benefit from targeted physical therapy to strengthen ankle and knee extensors and to retrain stride and speed to improve both gait and safety awareness.
Patients who wear shoes that fit poorly, have high heels, or are not laced or buckled have a higher risk of falls.31 Consider recommending footwear that has a firm, low, rubber heel and a sole with a large surface contact area, which may help reduce the risk of falling.32 Advise patients to wear shoes when they are at home and to avoid using slippers and going barefoot.33
Cataract surgery, another level C intervention, is associated with fewer fall-related injuries, particularly hip fracture.34 Noncataract vision interventions (such as exchanging progressive or bifocal lenses for single-lens glasses) may be effective in select patients if distorted vision in the lower fields of view increases the risk of falling, particularly outdoors.35
INTERVENTIONS FOR SPECIAL POPULATIONS
Falls occur more frequently in mobile residents of long-term care facilities than in community-dwelling adults.7 Institutional residents are older and more frail, have more cognitive impairment, and are prescribed more medications. Half of long-term care residents fall at least once a year.7
The data support giving combined calcium and vitamin D supplementation to older adults in long-term care facilities to reduce fracture rates.36 The NNT to prevent one hip fracture is about 111.37 Hip protectors in this setting may reduce the risk of a hip fracture but also may increase the risk of a pelvic fracture. They do not alter the risk of falling.38
Collaborative interventions can help reduce the fall risk in older adults in the nursing home.39 Input from medical, psychosocial, nursing, podiatric, dietary, and therapy services can be solicited and incorporated into an individualized fall prevention program. The program can also include modifications in the environment to improve safety and reduce fall risk.
The benefits of exercise in reducing injurious falls in long-term care is less clear than in the community, likely because of the heterogeneity of both the long-term care population and the studied interventions. Exercise has other benefits, however. It maintains a person’s ability to complete ADLs, improves mood, reduces hyperglycemia, and improves quality of life. Some studies have found a greater risk of falling with exercise therapy as independence increased.40 However, a meta-analysis in 2013 found that exercise interventions, ranging from 3 to 24 months and consisting mainly of balance and resistance training, reduced the risk of falls by 23%.41 Mixing several types of exercises was helpful. Studies of a longer duration with exercise sessions at least 2 to 3 times per week demonstrated the most benefit.41 There was no statistically significant reduction in fracture risk in this meta-analysis,41 although, possibly, more participants would have been needed for a longer period to demonstrate a benefit. Additionally, no study combined osteoporosis treatment with exercise interventions.
WHAT EVIDENCE EXISTS FOR PATIENTS WITH COGNITIVE IMPAIRMENT?
Currently, there are no specific evidence-based recommendations for fall prevention in community-dwelling older adults with cognitive impairment and dementia.7 Cognitively impaired adults are typically excluded from community studies of fall prevention. The one study that specifically investigated community-dwelling adults with cognitive impairment was not able to demonstrate a fall reduction with multifactorial intervention.42
PREVENTING FALLS IN ELDERLY PATIENTS WHO RECENTLY HAD A STROKE
Falls are common in patients who have had a cerebrovascular event. Up to 7% of patients fall in the first week after a stroke. In the year after a stroke, 55% to 75% of patients experience a fall.43 Falls account for the most common medical complication after a stroke.44
Several small studies found that vitamin D supplementation after a stroke reduced both the rate of falls and the number of people who fall.45 Additional interventions such as exercise, medication, and visual aids have been studied, but there is little evidence to support their use. Mobile patients who have lower-extremity hemiparesis after a stroke may develop osteoporosis in the affected limb, so evaluation and appropriate pharmacologic therapy may be considered.
- Tromp AM, Pluijm SM, Smit JH, Deeg DJ, Bouter LM, Lips P. Fall-risk screening test: a prospective study on predictors for falls in community-dwelling elderly. J Clin Epidemiol 2001; 54:837–844.
- Binder EF, Brown M, Sinacore DR, Steger-May K, Yarasheski KE, Schechtman KB. Effects of extended outpatient rehabilitation after hip fracture: a randomized controlled trial. JAMA 2004; 292:837–846.
- Sterling DA, O’Connor JA, Bonadies J. Geriatric falls: injury severity is high and disproportionate to mechanism. J Trauma 2001; 50:116–119.
- Centers for Disease Control and Prevention (CDC). Web-based Injury Statistics Query and Reporting System (WISQARSTM). www.cdc.gov/injury/wisqars. Accessed April 8, 2015.
- Tinetti ME, Baker DI, King M, et al. Effect of dissemination of evidence in reducing injuries from falls. N Engl J Med 2008; 359:252–261.
- Ganz DA, Bao Y, Shekelle PG, Rubenstein LZ. Will my patient fall? JAMA 2007; 297:77–86.
- Panel on Prevention of Falls in Older Persons, American Geriatrics Society and British Geriatrics Society. Summary of the Updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc 2011; 59:148–157.
- Mathias S, Nayak US, Isaacs B. Balance in elderly patients: the “get-up and go” test. Arch Phys Med Rehabil 1986; 67:387–389.
- Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 1991; 39:142–148.
- Shumway-Cook A, Brauer S, Woollacott M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Phys Ther 2000; 80:896–903.
- Springer BA, Marin R, Cyhan T, Roberts H, Gill NW. Normative values for the unipedal stance test with eyes open and closed. J Geriatr Phys Ther 2007; 30:8–15.
- Leipzig RM, Cumming RG, Tinetti ME. Drugs and falls in older people: a systematic review and meta-analysis: I. Psychotropic drugs. J Am Geriatr Soc 1999; 47:30–39.
- Hilmer SN, Mager DE, Simonsick EM, et al. A drug burden index to define the functional burden of medications in older people. Arch Intern Med 2007; 167:781–787.
- Rudolph JL, Salow MJ, Angelini MC, McGlinchey RE. The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch Intern Med 2008; 168:508–513.
- American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2012; 60:616–631.
- Gallagher P, Ryan C, Byrne S, Kennedy J, O’Mahony D. STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Ther 2008; 46:72–83.
- Sterke CS, Ziere G, van Beeck EF, Looman CW, van der Cammen TJ. Dose-response relationship between selective serotonin re-uptake inhibitors and injurious falls: a study in nursing home residents with dementia. Br J Clin Pharmacol 2012; 73:812–820.
- Khalili H, Huang ES, Jacobson BC, Camargo CA Jr, Feskanich D, Chan AT. Use of proton pump inhibitors and risk of hip fracture in relation to dietary and lifestyle factors: a prospective cohort study. BMJ 2012; 344:e372.
- Gill SS, Anderson GM, Fischer HD, et al. Syncope and its consequences in patients with dementia receiving cholinesterase inhibitors: a population-based cohort study. Arch Intern Med 2009; 169:867–873.
- Janssen HC, Samson MM, Verhaar HJ. Vitamin D deficiency, muscle function, and falls in elderly people. Am J Clin Nutr 2002; 75:611–615.
- Muir SW, Gopaul K, Montero Odasso MM. The role of cognitive impairment in fall risk among older adults: a systematic review and meta-analysis. Age Ageing 2012; 41:299–308.
- Borson S, Scanlan J, Brush M, Vitaliano P, Dokmak A. The Mini-Cog: a cognitive ‘vital signs’ measure for dementia screening in multi-lingual elderly. Int J Geriatr Psychiatry 2000; 15:1021–1027.
- Cordell CB, Borson S, Boustani M, et al; Medicare Detection of Cognitive Impairment Workgroup. Alzheimer’s Association recommendations for operationalizing the detection of cognitive impairment during the Medicare Annual Wellness Visit in a primary care setting. Alzheimers Dement 2013; 9:141–150.
- Lawlor DA, Patel R, Ebrahim S. Association between falls in elderly women and chronic diseases and drug use: cross sectional study. BMJ 2003; 327:712–717.
- Day L, Fildes B, Gordon I, Fitzharris M, Flamer H, Lord S. Randomised factorial trial of falls prevention among older people living in their own homes. BMJ 2002; 325:128.
- Chang JT, Morton SC, Rubenstein LZ, et al. Interventions for the prevention of falls in older adults: systematic review and meta-analysis of randomised clinical trials. BMJ 2004; 328:680.
- Antithrombotic Trialists’ (ATT) Collaboration; Baigent C, Blackwell L, Collins R, et al. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet 2009; 373:1849–1860.
- Baigent C, Keech A, Kearney PM, et al; Cholesterol Treatment Trialists’ (CTT) Collaborators. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005; 366:1267–1278.
- Mazzeo RS; American College of Sports Medicine (ACSM). Exercise and the older adult. ACSM Current Comment. www.acsm.org/docs/current-comments/exerciseandtheolderadult.pdf. Accessed April 8, 2015.
- Willoughby DS; American College of Sports Medicine (ACSM). Resistance training and the older adult. ACSM Current Comment. www.acsm.org/docs/current-comments/resistancetrainingandtheoa.pdf. Accessed April 8, 2015.
- Tencer AF, Koepsell TD, Wolf ME, et al. Biomechanical properties of shoes and risk of falls in older adults. J Am Geriatr Soc 2004; 52:1840–1846.
- Lord SR, Bashford GM. Shoe characteristics and balance in older women. J Am Geriatr Soc 1996; 44:429–433.
- Kelsey JL, Procter-Gray E, Nguyen US, Li W, Kiel DP, Hannan MT. Footwear and falls in the home among older individuals in the MOBILIZE Boston Study. Footwear Sci 2010; 2:123–129.
- Tseng VL, Yu F, Lum F, Coleman AL. Risk of fractures following cataract surgery in Medicare beneficiaries. JAMA 2012; 308:493–501.
- Cumming RG, Ivers R, Clemson L, et al. Improving vision to prevent falls in frail older people: a randomized trial. J Am Geriatr Soc 2007; 55:175–181.
- Bischoff-Ferrari HA, Dawson-Hughes B, Willett WC, et al. Effect of vitamin D on falls: a meta-analysis. JAMA 2004; 291:1999–2006.
- Avenell A, Mak JCS, O’Connell D. Vitamin D and vitamin D analogues for preventing fractures in postmenopausal women and older men. Cochrane Database Syst Rev 2014; 4:CD000227.
- Santesso N, Carrasco-Labra A, Brignardello-Petersen R. Hip protectors for preventing hip fractures in older people. Cochrane Database Syst Rev 2014; 3:CD001255.
- Messinger-Rapport B, Dumas LG. Falls in the nursing home: a collaborative approach. Nurs Clin North Am 2009; 44:187–195.
- Faber MJ, Bosscher RJ, Chin A, Paw MJ, van Wieringen PC. Effects of exercise programs on falls and mobility in frail and pre-frail older adults: a multicenter randomized controlled trial. Arch Phys Med Rehabil 2006; 87:885–896.
- Silva RB, Eslick GD, Duque G. Exercise for falls and fracture prevention in long term care facilities: a systematic review and meta-analysis. J Am Med Dir Assoc 2013; 14:685–689.e2.
- Shaw FE, Bond J, Richardson DA, et al. Multifactorial intervention after a fall in older people with cognitive impairment and dementia presenting to the accident and emergency department: randomised controlled trial. BMJ 2003; 326:73.
- Ashburn A, Hyndman D, Pickering R, Yardley L, Harris S. Predicting people with stroke at risk of falls. Age Ageing 2008; 37:270–276.
- Davenport RJ, Dennis MS, Wellwood I, Warlow CP. Complications after acute stroke. Stroke 1996; 27:415–420.
- Verheyden GS, Weerdesteyn V, Pickering RM, et al. Interventions for preventing falls in people after stroke. Cochrane Database Syst Rev 2013; 5:CD008728.
Falls and fall-related injuries are common in older adults Every year, 30% of those who are 65 and older fall,1 and the consequences are potentially serious. Falls are the primary cause of hip fracture, which requires an extensive period of rehabilitation. However, rehabilitation does not always restore the older adult to his or her preinjury functional state. In fact, at 6 to 12 months after a hip fracture, 22% to 75% of elderly patients have not recovered their prefracture ambulatory or functional status.2
Falls are also the most common cause of traumatic brain injury in older adults,3 often resulting in long-term cognitive and emotional problems and pain that compromise quality of life. Falls can be fatal and in fact are the leading cause of death from injury in older adults.4
Practitioners can reduce fall-related injury5 and potentially improve quality of life by screening older adults yearly, performing a focused history and examination when necessary, and implementing evidence-based interventions.
RISK FACTORS
A single identifiable factor may account for only a small portion of the fall risk. Falls in older adults are, in general, multifactorial and can be caused by medical conditions (eg, sarcopenia, particularly of the lower limbs, vision loss, urinary incontinence, neuropathies), cognitive impairment, medications such as psychotropic drugs, and home hazards such as area rugs, extension cords, and dimly lit stairways.
The strongest predictors of falls are a recent fall and the presence of a gait or balance disorder.6
SCREENING TESTS
Joint guidelines from the American Geriatrics Society and British Geriatrics Society,7 published in 2011, recommend that practitioners screen older adults yearly for fall risk by asking two questions: “Have you fallen in the past year?” and “Are you having difficulty with gait or balance?” A negative response to both questions suggests a low risk of falling in the near future. Patients with two or more falls, a balance or gait problem (subjective or objective), or history of a fall requiring medical attention should undergo a focused history and physical examination plus a multifactorial risk assessment.
A report of one fall without injury should prompt a simple office-based test of balance. Examples of tests include the Get Up and Go, the Timed Up and Go, and the One-Legged Stance (the Unipedal Stance).
In the Get Up and Go test, patients sit comfortably in a chair with a straight back. They rise from the chair, stand still, walk a short distance (about 3 meters), turn around, walk back to the chair, and sit down.8 The clinician notes any deviation from a confident, smooth performance.
In the Timed Up and Go test, the clinician records the time it takes for the patient to rise from a hardback chair, walk 10 feet (3 meters), turn, return to the chair, and sit down.9 Most older adults complete this test in less than 10 seconds. Taking longer than 14 seconds is associated with a high risk of falls.10
For the One-Legged Stance test, the clinician asks the patient to stand on one leg. A patient without significant balance issues is able to stand for at least 5 seconds.11
Figure 1 summarizes the approach for a community-dwelling patient who presents to the outpatient setting. A complete multifactorial risk assessment may require a dedicated appointment or referral to a specialist such as a geriatrician, physiatrist, or neurologist.
WHAT INFORMATION DOES A FOCUSED HISTORY INCLUDE?
The fall-focused history includes:
A detailed description of the circumstances of the fall or falls, symptoms (such as dizziness), and injuries or other consequences of the fall.7
A medication review. Table 1 includes commonly prescribed drug classes associated with increased fall risk.12 Be especially vigilant for eyedrops used to treat glaucoma (some can potentiate bradycardia) and for psychotropic drugs.
Drug regimens with a high psychotropic burden can be identified with the Drug Burden Index13 or the Anticholinergic Risk Scale,14 but these scales are cumbersome and are usually used only as part of a research study. The updated Beers criteria15 and use of a structured medication review such as the START and STOPP algorithms16 can help prune unnecessary, inappropriate, and high-risk medications such as:
- Selective serotonin reuptake inhibitors in the absence of current major depression. These drugs increase the risk of falls and decrease bone density.17
- Proton pump inhibitors in the absence of a true indication for this drug class to treat reflux. Drugs in this class reduce bone density and increase the risk of hip fracture after 1 year of continuous use18
- Cholinesterase inhibitors in the absence of demonstrated benefit to dementia symptoms for the particular patient. Drugs in this class are associated with falls, hip fracture, bradycardia, and possible need for pacemaker placement.19
Review of activities of daily living (ADLs). A functional assessment of the patient’s ability to complete ADLs helps identify targets for therapy. Assess whether the patient is afraid of falling and, if so, what impact this fear has on ADLs. This can help determine whether the fear protects the patient from performing risky tasks, or harms the patient by contributing to deconditioning.
Medical conditions. Consider chronic conditions that can impair mobility and increase fall risk. These include urinary incontinence, cognitive impairment (eg, dementia), neuropathy, degenerative neurologic conditions such as Parkinson disease, and degenerative arthritis. Osteoporosis increases the risk of fracture in a fall. Vitamin D deficiency increases both fall and fracture risk.20
PHYSICAL EXAMINATION FINDINGS
Assess the patient’s vision, proprioception, reflexes, and cortical, extrapyramidal, and cerebellar function.7
Perform a detailed assessment of the patient’s gait, balance, and mobility. Assess the lower extremities for joint and nerve function, muscle strength, and range of motion.7 The use of brain imaging, if appropriate, is guided by gait abnormalities. Unexpected findings such as neuropathy may require referrals for further evaluation.
Examine the patient’s feet and footwear for signs of poor fit and for styles that may be inappropriate for someone at risk of falling, such as high heels.
Conduct a cardiovascular examination. In addition to assessing heart rate and rhythm and checking for heart murmurs, evaluate the patient for postural changes in heart rate and blood pressure. Wait at least 2 minutes before asking the patient to change position from supine to seated and from seated to standing. A longer interval (3 to 5 minutes) can be used depending on the patient’s history. For example, an older adult reporting a syncopal episode standing by the kitchen sink may need a longer standing interval prior to blood pressure measurement than an older adult who falls right after standing up from a chair.
If there is a strong suspicion that an orthostatic condition contributed to a fall but it is not possible to elicit orthostasis in the office, it may be necessary to refer the patient for tilt-table testing. If the circumstances suggest that pressure along the neck, or turning the neck, contributed to a fall, referral for carotid sinus stimulation may be appropriate. If there is a concern that a brady- or tachyarrhythmia contributed to the fall, a referral for 24- or 48-hour Holter monitoring or a 30-day loop monitor may be indicated.
Assess the patient’s mental status. Cognitive impairment itself is an independent predictor of falls7 because it can reduce processing speed and impair executive function.21 Executive dysfunction may contribute to falls by causing problems with multitasking, drug compliance, and judgment. The presence and severity of cognitive impairment may affect recommendation options (see below), so the assessment should include a screening test. Consider using the Mini-Cog, which requires the patient to recall three words and draw an analog clock (Figure 2).22
Some cognitive screening tests validated for use in the general older population include the General Practitioner Assessment of Cognition and the Memory Impairment Screen.23 More involved cognitive testing such as the Folstein Mini-Mental State Examination, Montreal Cognitive Assessment, and the Saint Louis University Mental Status Examination are routinely performed in a geriatric or neurologic setting. The Folstein is a proprietary test; the other two are not.
Conditions such as circulatory disease, chronic obstructive pulmonary disease, depression, and arthritis are associated with a higher risk of falling, even with adjustment for drug use and other potential confounding factors.24
A brief mood assessment is part of the multifactorial assessment because mood disorders in older adults can lead to deconditioning, drug noncompliance, and other conditions that lead to falls and fall-related injuries. Options for screening include the Geriatric Depression Scale (15 or 30 questions) and the Patient Health Questionnaire (the PHQ-2 or the PHQ-9).7
WHAT ARE THE EVIDENCE-BASED INTERVENTIONS?
In general, interventions are chosen according to the risks identified by the assessment; multiple interventions are usually necessary. It is ineffective to identify risk factors without providing intervention.25
Specific interventions with recommendation levels A and B are listed in Table 2.7 Level A interventions are specifically supported by strong evidence and should be recommended. Of note, although vitamin D3 may not be bioequivalent to vitamin D2, studies in older adults have not consistently found a clinically different outcome, and either may be supplemented in the community-dwelling elderly. Except for vitamin D, these interventions target community-dwelling older adults who are cognitively intact.
Home assessments are effective in high-risk patients, such as those with poor vision and those who were recently hospitalized. The goal is to improve safety, particularly during patient transfers, with education and training provided by an occupational or physical therapist or other geriatric specialist. The benefit of home assessment and environmental modification is greater when combined with other strategies and in general should not be implemented alone.
Exercise is an important intervention. The number needed to treat (NNT) to prevent one fall in older people over the course of at least 12 weeks is 16.26 This compares favorably with interventions that are commonly used in the general population, such as aspirin therapy as secondary prevention for cardiovascular disease (NNT for 1 year = 50)27 and statin therapy to prevent one death from a cardiovascular event over 5 years in people with known heart disease (NNT = 83).28
Exercise recommendations should be customized to the patient. The amount and type of exercise depends on the patient’s baseline physical activity, medication use including antiplatelet and anticoagulant therapy, home environment, cardiac and pulmonary reserve, vision and hearing deficits, and comorbidities including neuropathy and arthritis.
The well-known risks associated with exercise include myocardial infarction and cardiac arrest, as well as falls and fractures. However, the benefits extend beyond fall risk and include improvements in physical function, glycemic control, cardiopulmonary reserve, bone density, arthritic pain, mood, and cognition. Exercise can also help manage weight, reduce sarcopenia, and increase opportunities for socialization. In most positive trials, the exercise interventions lasted longer than 12 weeks, had variable intensity, and occurred 1 to 3 times per week.
The American College of Sports Medicine recommends that older adults perform aerobic exercise 3 to 5 times per week, 20 to 60 minutes per session (the lower ranges are for frail elderly patients).29 It also recommends resistance training 2 to 4 days per week, 20 to 45 minutes per session, depending on the patient’s level of frailty and conditioning.30 Most older adults do not exercise enough.
Interventions listed at the bottom of Table 2 do not, in general, have enough evidence to support or discourage their use; these are level C recommendations. However, these interventions may be considered for certain individuals. For example, older adults with diabetic neuropathy are often unaware of their foot position when they walk. Additionally, those with diabetic neuropathy may have slower generation of ankle and knee strength compared with age-matched controls. These patients may benefit from targeted physical therapy to strengthen ankle and knee extensors and to retrain stride and speed to improve both gait and safety awareness.
Patients who wear shoes that fit poorly, have high heels, or are not laced or buckled have a higher risk of falls.31 Consider recommending footwear that has a firm, low, rubber heel and a sole with a large surface contact area, which may help reduce the risk of falling.32 Advise patients to wear shoes when they are at home and to avoid using slippers and going barefoot.33
Cataract surgery, another level C intervention, is associated with fewer fall-related injuries, particularly hip fracture.34 Noncataract vision interventions (such as exchanging progressive or bifocal lenses for single-lens glasses) may be effective in select patients if distorted vision in the lower fields of view increases the risk of falling, particularly outdoors.35
INTERVENTIONS FOR SPECIAL POPULATIONS
Falls occur more frequently in mobile residents of long-term care facilities than in community-dwelling adults.7 Institutional residents are older and more frail, have more cognitive impairment, and are prescribed more medications. Half of long-term care residents fall at least once a year.7
The data support giving combined calcium and vitamin D supplementation to older adults in long-term care facilities to reduce fracture rates.36 The NNT to prevent one hip fracture is about 111.37 Hip protectors in this setting may reduce the risk of a hip fracture but also may increase the risk of a pelvic fracture. They do not alter the risk of falling.38
Collaborative interventions can help reduce the fall risk in older adults in the nursing home.39 Input from medical, psychosocial, nursing, podiatric, dietary, and therapy services can be solicited and incorporated into an individualized fall prevention program. The program can also include modifications in the environment to improve safety and reduce fall risk.
The benefits of exercise in reducing injurious falls in long-term care is less clear than in the community, likely because of the heterogeneity of both the long-term care population and the studied interventions. Exercise has other benefits, however. It maintains a person’s ability to complete ADLs, improves mood, reduces hyperglycemia, and improves quality of life. Some studies have found a greater risk of falling with exercise therapy as independence increased.40 However, a meta-analysis in 2013 found that exercise interventions, ranging from 3 to 24 months and consisting mainly of balance and resistance training, reduced the risk of falls by 23%.41 Mixing several types of exercises was helpful. Studies of a longer duration with exercise sessions at least 2 to 3 times per week demonstrated the most benefit.41 There was no statistically significant reduction in fracture risk in this meta-analysis,41 although, possibly, more participants would have been needed for a longer period to demonstrate a benefit. Additionally, no study combined osteoporosis treatment with exercise interventions.
WHAT EVIDENCE EXISTS FOR PATIENTS WITH COGNITIVE IMPAIRMENT?
Currently, there are no specific evidence-based recommendations for fall prevention in community-dwelling older adults with cognitive impairment and dementia.7 Cognitively impaired adults are typically excluded from community studies of fall prevention. The one study that specifically investigated community-dwelling adults with cognitive impairment was not able to demonstrate a fall reduction with multifactorial intervention.42
PREVENTING FALLS IN ELDERLY PATIENTS WHO RECENTLY HAD A STROKE
Falls are common in patients who have had a cerebrovascular event. Up to 7% of patients fall in the first week after a stroke. In the year after a stroke, 55% to 75% of patients experience a fall.43 Falls account for the most common medical complication after a stroke.44
Several small studies found that vitamin D supplementation after a stroke reduced both the rate of falls and the number of people who fall.45 Additional interventions such as exercise, medication, and visual aids have been studied, but there is little evidence to support their use. Mobile patients who have lower-extremity hemiparesis after a stroke may develop osteoporosis in the affected limb, so evaluation and appropriate pharmacologic therapy may be considered.
Falls and fall-related injuries are common in older adults Every year, 30% of those who are 65 and older fall,1 and the consequences are potentially serious. Falls are the primary cause of hip fracture, which requires an extensive period of rehabilitation. However, rehabilitation does not always restore the older adult to his or her preinjury functional state. In fact, at 6 to 12 months after a hip fracture, 22% to 75% of elderly patients have not recovered their prefracture ambulatory or functional status.2
Falls are also the most common cause of traumatic brain injury in older adults,3 often resulting in long-term cognitive and emotional problems and pain that compromise quality of life. Falls can be fatal and in fact are the leading cause of death from injury in older adults.4
Practitioners can reduce fall-related injury5 and potentially improve quality of life by screening older adults yearly, performing a focused history and examination when necessary, and implementing evidence-based interventions.
RISK FACTORS
A single identifiable factor may account for only a small portion of the fall risk. Falls in older adults are, in general, multifactorial and can be caused by medical conditions (eg, sarcopenia, particularly of the lower limbs, vision loss, urinary incontinence, neuropathies), cognitive impairment, medications such as psychotropic drugs, and home hazards such as area rugs, extension cords, and dimly lit stairways.
The strongest predictors of falls are a recent fall and the presence of a gait or balance disorder.6
SCREENING TESTS
Joint guidelines from the American Geriatrics Society and British Geriatrics Society,7 published in 2011, recommend that practitioners screen older adults yearly for fall risk by asking two questions: “Have you fallen in the past year?” and “Are you having difficulty with gait or balance?” A negative response to both questions suggests a low risk of falling in the near future. Patients with two or more falls, a balance or gait problem (subjective or objective), or history of a fall requiring medical attention should undergo a focused history and physical examination plus a multifactorial risk assessment.
A report of one fall without injury should prompt a simple office-based test of balance. Examples of tests include the Get Up and Go, the Timed Up and Go, and the One-Legged Stance (the Unipedal Stance).
In the Get Up and Go test, patients sit comfortably in a chair with a straight back. They rise from the chair, stand still, walk a short distance (about 3 meters), turn around, walk back to the chair, and sit down.8 The clinician notes any deviation from a confident, smooth performance.
In the Timed Up and Go test, the clinician records the time it takes for the patient to rise from a hardback chair, walk 10 feet (3 meters), turn, return to the chair, and sit down.9 Most older adults complete this test in less than 10 seconds. Taking longer than 14 seconds is associated with a high risk of falls.10
For the One-Legged Stance test, the clinician asks the patient to stand on one leg. A patient without significant balance issues is able to stand for at least 5 seconds.11
Figure 1 summarizes the approach for a community-dwelling patient who presents to the outpatient setting. A complete multifactorial risk assessment may require a dedicated appointment or referral to a specialist such as a geriatrician, physiatrist, or neurologist.
WHAT INFORMATION DOES A FOCUSED HISTORY INCLUDE?
The fall-focused history includes:
A detailed description of the circumstances of the fall or falls, symptoms (such as dizziness), and injuries or other consequences of the fall.7
A medication review. Table 1 includes commonly prescribed drug classes associated with increased fall risk.12 Be especially vigilant for eyedrops used to treat glaucoma (some can potentiate bradycardia) and for psychotropic drugs.
Drug regimens with a high psychotropic burden can be identified with the Drug Burden Index13 or the Anticholinergic Risk Scale,14 but these scales are cumbersome and are usually used only as part of a research study. The updated Beers criteria15 and use of a structured medication review such as the START and STOPP algorithms16 can help prune unnecessary, inappropriate, and high-risk medications such as:
- Selective serotonin reuptake inhibitors in the absence of current major depression. These drugs increase the risk of falls and decrease bone density.17
- Proton pump inhibitors in the absence of a true indication for this drug class to treat reflux. Drugs in this class reduce bone density and increase the risk of hip fracture after 1 year of continuous use18
- Cholinesterase inhibitors in the absence of demonstrated benefit to dementia symptoms for the particular patient. Drugs in this class are associated with falls, hip fracture, bradycardia, and possible need for pacemaker placement.19
Review of activities of daily living (ADLs). A functional assessment of the patient’s ability to complete ADLs helps identify targets for therapy. Assess whether the patient is afraid of falling and, if so, what impact this fear has on ADLs. This can help determine whether the fear protects the patient from performing risky tasks, or harms the patient by contributing to deconditioning.
Medical conditions. Consider chronic conditions that can impair mobility and increase fall risk. These include urinary incontinence, cognitive impairment (eg, dementia), neuropathy, degenerative neurologic conditions such as Parkinson disease, and degenerative arthritis. Osteoporosis increases the risk of fracture in a fall. Vitamin D deficiency increases both fall and fracture risk.20
PHYSICAL EXAMINATION FINDINGS
Assess the patient’s vision, proprioception, reflexes, and cortical, extrapyramidal, and cerebellar function.7
Perform a detailed assessment of the patient’s gait, balance, and mobility. Assess the lower extremities for joint and nerve function, muscle strength, and range of motion.7 The use of brain imaging, if appropriate, is guided by gait abnormalities. Unexpected findings such as neuropathy may require referrals for further evaluation.
Examine the patient’s feet and footwear for signs of poor fit and for styles that may be inappropriate for someone at risk of falling, such as high heels.
Conduct a cardiovascular examination. In addition to assessing heart rate and rhythm and checking for heart murmurs, evaluate the patient for postural changes in heart rate and blood pressure. Wait at least 2 minutes before asking the patient to change position from supine to seated and from seated to standing. A longer interval (3 to 5 minutes) can be used depending on the patient’s history. For example, an older adult reporting a syncopal episode standing by the kitchen sink may need a longer standing interval prior to blood pressure measurement than an older adult who falls right after standing up from a chair.
If there is a strong suspicion that an orthostatic condition contributed to a fall but it is not possible to elicit orthostasis in the office, it may be necessary to refer the patient for tilt-table testing. If the circumstances suggest that pressure along the neck, or turning the neck, contributed to a fall, referral for carotid sinus stimulation may be appropriate. If there is a concern that a brady- or tachyarrhythmia contributed to the fall, a referral for 24- or 48-hour Holter monitoring or a 30-day loop monitor may be indicated.
Assess the patient’s mental status. Cognitive impairment itself is an independent predictor of falls7 because it can reduce processing speed and impair executive function.21 Executive dysfunction may contribute to falls by causing problems with multitasking, drug compliance, and judgment. The presence and severity of cognitive impairment may affect recommendation options (see below), so the assessment should include a screening test. Consider using the Mini-Cog, which requires the patient to recall three words and draw an analog clock (Figure 2).22
Some cognitive screening tests validated for use in the general older population include the General Practitioner Assessment of Cognition and the Memory Impairment Screen.23 More involved cognitive testing such as the Folstein Mini-Mental State Examination, Montreal Cognitive Assessment, and the Saint Louis University Mental Status Examination are routinely performed in a geriatric or neurologic setting. The Folstein is a proprietary test; the other two are not.
Conditions such as circulatory disease, chronic obstructive pulmonary disease, depression, and arthritis are associated with a higher risk of falling, even with adjustment for drug use and other potential confounding factors.24
A brief mood assessment is part of the multifactorial assessment because mood disorders in older adults can lead to deconditioning, drug noncompliance, and other conditions that lead to falls and fall-related injuries. Options for screening include the Geriatric Depression Scale (15 or 30 questions) and the Patient Health Questionnaire (the PHQ-2 or the PHQ-9).7
WHAT ARE THE EVIDENCE-BASED INTERVENTIONS?
In general, interventions are chosen according to the risks identified by the assessment; multiple interventions are usually necessary. It is ineffective to identify risk factors without providing intervention.25
Specific interventions with recommendation levels A and B are listed in Table 2.7 Level A interventions are specifically supported by strong evidence and should be recommended. Of note, although vitamin D3 may not be bioequivalent to vitamin D2, studies in older adults have not consistently found a clinically different outcome, and either may be supplemented in the community-dwelling elderly. Except for vitamin D, these interventions target community-dwelling older adults who are cognitively intact.
Home assessments are effective in high-risk patients, such as those with poor vision and those who were recently hospitalized. The goal is to improve safety, particularly during patient transfers, with education and training provided by an occupational or physical therapist or other geriatric specialist. The benefit of home assessment and environmental modification is greater when combined with other strategies and in general should not be implemented alone.
Exercise is an important intervention. The number needed to treat (NNT) to prevent one fall in older people over the course of at least 12 weeks is 16.26 This compares favorably with interventions that are commonly used in the general population, such as aspirin therapy as secondary prevention for cardiovascular disease (NNT for 1 year = 50)27 and statin therapy to prevent one death from a cardiovascular event over 5 years in people with known heart disease (NNT = 83).28
Exercise recommendations should be customized to the patient. The amount and type of exercise depends on the patient’s baseline physical activity, medication use including antiplatelet and anticoagulant therapy, home environment, cardiac and pulmonary reserve, vision and hearing deficits, and comorbidities including neuropathy and arthritis.
The well-known risks associated with exercise include myocardial infarction and cardiac arrest, as well as falls and fractures. However, the benefits extend beyond fall risk and include improvements in physical function, glycemic control, cardiopulmonary reserve, bone density, arthritic pain, mood, and cognition. Exercise can also help manage weight, reduce sarcopenia, and increase opportunities for socialization. In most positive trials, the exercise interventions lasted longer than 12 weeks, had variable intensity, and occurred 1 to 3 times per week.
The American College of Sports Medicine recommends that older adults perform aerobic exercise 3 to 5 times per week, 20 to 60 minutes per session (the lower ranges are for frail elderly patients).29 It also recommends resistance training 2 to 4 days per week, 20 to 45 minutes per session, depending on the patient’s level of frailty and conditioning.30 Most older adults do not exercise enough.
Interventions listed at the bottom of Table 2 do not, in general, have enough evidence to support or discourage their use; these are level C recommendations. However, these interventions may be considered for certain individuals. For example, older adults with diabetic neuropathy are often unaware of their foot position when they walk. Additionally, those with diabetic neuropathy may have slower generation of ankle and knee strength compared with age-matched controls. These patients may benefit from targeted physical therapy to strengthen ankle and knee extensors and to retrain stride and speed to improve both gait and safety awareness.
Patients who wear shoes that fit poorly, have high heels, or are not laced or buckled have a higher risk of falls.31 Consider recommending footwear that has a firm, low, rubber heel and a sole with a large surface contact area, which may help reduce the risk of falling.32 Advise patients to wear shoes when they are at home and to avoid using slippers and going barefoot.33
Cataract surgery, another level C intervention, is associated with fewer fall-related injuries, particularly hip fracture.34 Noncataract vision interventions (such as exchanging progressive or bifocal lenses for single-lens glasses) may be effective in select patients if distorted vision in the lower fields of view increases the risk of falling, particularly outdoors.35
INTERVENTIONS FOR SPECIAL POPULATIONS
Falls occur more frequently in mobile residents of long-term care facilities than in community-dwelling adults.7 Institutional residents are older and more frail, have more cognitive impairment, and are prescribed more medications. Half of long-term care residents fall at least once a year.7
The data support giving combined calcium and vitamin D supplementation to older adults in long-term care facilities to reduce fracture rates.36 The NNT to prevent one hip fracture is about 111.37 Hip protectors in this setting may reduce the risk of a hip fracture but also may increase the risk of a pelvic fracture. They do not alter the risk of falling.38
Collaborative interventions can help reduce the fall risk in older adults in the nursing home.39 Input from medical, psychosocial, nursing, podiatric, dietary, and therapy services can be solicited and incorporated into an individualized fall prevention program. The program can also include modifications in the environment to improve safety and reduce fall risk.
The benefits of exercise in reducing injurious falls in long-term care is less clear than in the community, likely because of the heterogeneity of both the long-term care population and the studied interventions. Exercise has other benefits, however. It maintains a person’s ability to complete ADLs, improves mood, reduces hyperglycemia, and improves quality of life. Some studies have found a greater risk of falling with exercise therapy as independence increased.40 However, a meta-analysis in 2013 found that exercise interventions, ranging from 3 to 24 months and consisting mainly of balance and resistance training, reduced the risk of falls by 23%.41 Mixing several types of exercises was helpful. Studies of a longer duration with exercise sessions at least 2 to 3 times per week demonstrated the most benefit.41 There was no statistically significant reduction in fracture risk in this meta-analysis,41 although, possibly, more participants would have been needed for a longer period to demonstrate a benefit. Additionally, no study combined osteoporosis treatment with exercise interventions.
WHAT EVIDENCE EXISTS FOR PATIENTS WITH COGNITIVE IMPAIRMENT?
Currently, there are no specific evidence-based recommendations for fall prevention in community-dwelling older adults with cognitive impairment and dementia.7 Cognitively impaired adults are typically excluded from community studies of fall prevention. The one study that specifically investigated community-dwelling adults with cognitive impairment was not able to demonstrate a fall reduction with multifactorial intervention.42
PREVENTING FALLS IN ELDERLY PATIENTS WHO RECENTLY HAD A STROKE
Falls are common in patients who have had a cerebrovascular event. Up to 7% of patients fall in the first week after a stroke. In the year after a stroke, 55% to 75% of patients experience a fall.43 Falls account for the most common medical complication after a stroke.44
Several small studies found that vitamin D supplementation after a stroke reduced both the rate of falls and the number of people who fall.45 Additional interventions such as exercise, medication, and visual aids have been studied, but there is little evidence to support their use. Mobile patients who have lower-extremity hemiparesis after a stroke may develop osteoporosis in the affected limb, so evaluation and appropriate pharmacologic therapy may be considered.
- Tromp AM, Pluijm SM, Smit JH, Deeg DJ, Bouter LM, Lips P. Fall-risk screening test: a prospective study on predictors for falls in community-dwelling elderly. J Clin Epidemiol 2001; 54:837–844.
- Binder EF, Brown M, Sinacore DR, Steger-May K, Yarasheski KE, Schechtman KB. Effects of extended outpatient rehabilitation after hip fracture: a randomized controlled trial. JAMA 2004; 292:837–846.
- Sterling DA, O’Connor JA, Bonadies J. Geriatric falls: injury severity is high and disproportionate to mechanism. J Trauma 2001; 50:116–119.
- Centers for Disease Control and Prevention (CDC). Web-based Injury Statistics Query and Reporting System (WISQARSTM). www.cdc.gov/injury/wisqars. Accessed April 8, 2015.
- Tinetti ME, Baker DI, King M, et al. Effect of dissemination of evidence in reducing injuries from falls. N Engl J Med 2008; 359:252–261.
- Ganz DA, Bao Y, Shekelle PG, Rubenstein LZ. Will my patient fall? JAMA 2007; 297:77–86.
- Panel on Prevention of Falls in Older Persons, American Geriatrics Society and British Geriatrics Society. Summary of the Updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc 2011; 59:148–157.
- Mathias S, Nayak US, Isaacs B. Balance in elderly patients: the “get-up and go” test. Arch Phys Med Rehabil 1986; 67:387–389.
- Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 1991; 39:142–148.
- Shumway-Cook A, Brauer S, Woollacott M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Phys Ther 2000; 80:896–903.
- Springer BA, Marin R, Cyhan T, Roberts H, Gill NW. Normative values for the unipedal stance test with eyes open and closed. J Geriatr Phys Ther 2007; 30:8–15.
- Leipzig RM, Cumming RG, Tinetti ME. Drugs and falls in older people: a systematic review and meta-analysis: I. Psychotropic drugs. J Am Geriatr Soc 1999; 47:30–39.
- Hilmer SN, Mager DE, Simonsick EM, et al. A drug burden index to define the functional burden of medications in older people. Arch Intern Med 2007; 167:781–787.
- Rudolph JL, Salow MJ, Angelini MC, McGlinchey RE. The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch Intern Med 2008; 168:508–513.
- American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2012; 60:616–631.
- Gallagher P, Ryan C, Byrne S, Kennedy J, O’Mahony D. STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Ther 2008; 46:72–83.
- Sterke CS, Ziere G, van Beeck EF, Looman CW, van der Cammen TJ. Dose-response relationship between selective serotonin re-uptake inhibitors and injurious falls: a study in nursing home residents with dementia. Br J Clin Pharmacol 2012; 73:812–820.
- Khalili H, Huang ES, Jacobson BC, Camargo CA Jr, Feskanich D, Chan AT. Use of proton pump inhibitors and risk of hip fracture in relation to dietary and lifestyle factors: a prospective cohort study. BMJ 2012; 344:e372.
- Gill SS, Anderson GM, Fischer HD, et al. Syncope and its consequences in patients with dementia receiving cholinesterase inhibitors: a population-based cohort study. Arch Intern Med 2009; 169:867–873.
- Janssen HC, Samson MM, Verhaar HJ. Vitamin D deficiency, muscle function, and falls in elderly people. Am J Clin Nutr 2002; 75:611–615.
- Muir SW, Gopaul K, Montero Odasso MM. The role of cognitive impairment in fall risk among older adults: a systematic review and meta-analysis. Age Ageing 2012; 41:299–308.
- Borson S, Scanlan J, Brush M, Vitaliano P, Dokmak A. The Mini-Cog: a cognitive ‘vital signs’ measure for dementia screening in multi-lingual elderly. Int J Geriatr Psychiatry 2000; 15:1021–1027.
- Cordell CB, Borson S, Boustani M, et al; Medicare Detection of Cognitive Impairment Workgroup. Alzheimer’s Association recommendations for operationalizing the detection of cognitive impairment during the Medicare Annual Wellness Visit in a primary care setting. Alzheimers Dement 2013; 9:141–150.
- Lawlor DA, Patel R, Ebrahim S. Association between falls in elderly women and chronic diseases and drug use: cross sectional study. BMJ 2003; 327:712–717.
- Day L, Fildes B, Gordon I, Fitzharris M, Flamer H, Lord S. Randomised factorial trial of falls prevention among older people living in their own homes. BMJ 2002; 325:128.
- Chang JT, Morton SC, Rubenstein LZ, et al. Interventions for the prevention of falls in older adults: systematic review and meta-analysis of randomised clinical trials. BMJ 2004; 328:680.
- Antithrombotic Trialists’ (ATT) Collaboration; Baigent C, Blackwell L, Collins R, et al. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet 2009; 373:1849–1860.
- Baigent C, Keech A, Kearney PM, et al; Cholesterol Treatment Trialists’ (CTT) Collaborators. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005; 366:1267–1278.
- Mazzeo RS; American College of Sports Medicine (ACSM). Exercise and the older adult. ACSM Current Comment. www.acsm.org/docs/current-comments/exerciseandtheolderadult.pdf. Accessed April 8, 2015.
- Willoughby DS; American College of Sports Medicine (ACSM). Resistance training and the older adult. ACSM Current Comment. www.acsm.org/docs/current-comments/resistancetrainingandtheoa.pdf. Accessed April 8, 2015.
- Tencer AF, Koepsell TD, Wolf ME, et al. Biomechanical properties of shoes and risk of falls in older adults. J Am Geriatr Soc 2004; 52:1840–1846.
- Lord SR, Bashford GM. Shoe characteristics and balance in older women. J Am Geriatr Soc 1996; 44:429–433.
- Kelsey JL, Procter-Gray E, Nguyen US, Li W, Kiel DP, Hannan MT. Footwear and falls in the home among older individuals in the MOBILIZE Boston Study. Footwear Sci 2010; 2:123–129.
- Tseng VL, Yu F, Lum F, Coleman AL. Risk of fractures following cataract surgery in Medicare beneficiaries. JAMA 2012; 308:493–501.
- Cumming RG, Ivers R, Clemson L, et al. Improving vision to prevent falls in frail older people: a randomized trial. J Am Geriatr Soc 2007; 55:175–181.
- Bischoff-Ferrari HA, Dawson-Hughes B, Willett WC, et al. Effect of vitamin D on falls: a meta-analysis. JAMA 2004; 291:1999–2006.
- Avenell A, Mak JCS, O’Connell D. Vitamin D and vitamin D analogues for preventing fractures in postmenopausal women and older men. Cochrane Database Syst Rev 2014; 4:CD000227.
- Santesso N, Carrasco-Labra A, Brignardello-Petersen R. Hip protectors for preventing hip fractures in older people. Cochrane Database Syst Rev 2014; 3:CD001255.
- Messinger-Rapport B, Dumas LG. Falls in the nursing home: a collaborative approach. Nurs Clin North Am 2009; 44:187–195.
- Faber MJ, Bosscher RJ, Chin A, Paw MJ, van Wieringen PC. Effects of exercise programs on falls and mobility in frail and pre-frail older adults: a multicenter randomized controlled trial. Arch Phys Med Rehabil 2006; 87:885–896.
- Silva RB, Eslick GD, Duque G. Exercise for falls and fracture prevention in long term care facilities: a systematic review and meta-analysis. J Am Med Dir Assoc 2013; 14:685–689.e2.
- Shaw FE, Bond J, Richardson DA, et al. Multifactorial intervention after a fall in older people with cognitive impairment and dementia presenting to the accident and emergency department: randomised controlled trial. BMJ 2003; 326:73.
- Ashburn A, Hyndman D, Pickering R, Yardley L, Harris S. Predicting people with stroke at risk of falls. Age Ageing 2008; 37:270–276.
- Davenport RJ, Dennis MS, Wellwood I, Warlow CP. Complications after acute stroke. Stroke 1996; 27:415–420.
- Verheyden GS, Weerdesteyn V, Pickering RM, et al. Interventions for preventing falls in people after stroke. Cochrane Database Syst Rev 2013; 5:CD008728.
- Tromp AM, Pluijm SM, Smit JH, Deeg DJ, Bouter LM, Lips P. Fall-risk screening test: a prospective study on predictors for falls in community-dwelling elderly. J Clin Epidemiol 2001; 54:837–844.
- Binder EF, Brown M, Sinacore DR, Steger-May K, Yarasheski KE, Schechtman KB. Effects of extended outpatient rehabilitation after hip fracture: a randomized controlled trial. JAMA 2004; 292:837–846.
- Sterling DA, O’Connor JA, Bonadies J. Geriatric falls: injury severity is high and disproportionate to mechanism. J Trauma 2001; 50:116–119.
- Centers for Disease Control and Prevention (CDC). Web-based Injury Statistics Query and Reporting System (WISQARSTM). www.cdc.gov/injury/wisqars. Accessed April 8, 2015.
- Tinetti ME, Baker DI, King M, et al. Effect of dissemination of evidence in reducing injuries from falls. N Engl J Med 2008; 359:252–261.
- Ganz DA, Bao Y, Shekelle PG, Rubenstein LZ. Will my patient fall? JAMA 2007; 297:77–86.
- Panel on Prevention of Falls in Older Persons, American Geriatrics Society and British Geriatrics Society. Summary of the Updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc 2011; 59:148–157.
- Mathias S, Nayak US, Isaacs B. Balance in elderly patients: the “get-up and go” test. Arch Phys Med Rehabil 1986; 67:387–389.
- Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 1991; 39:142–148.
- Shumway-Cook A, Brauer S, Woollacott M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Phys Ther 2000; 80:896–903.
- Springer BA, Marin R, Cyhan T, Roberts H, Gill NW. Normative values for the unipedal stance test with eyes open and closed. J Geriatr Phys Ther 2007; 30:8–15.
- Leipzig RM, Cumming RG, Tinetti ME. Drugs and falls in older people: a systematic review and meta-analysis: I. Psychotropic drugs. J Am Geriatr Soc 1999; 47:30–39.
- Hilmer SN, Mager DE, Simonsick EM, et al. A drug burden index to define the functional burden of medications in older people. Arch Intern Med 2007; 167:781–787.
- Rudolph JL, Salow MJ, Angelini MC, McGlinchey RE. The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch Intern Med 2008; 168:508–513.
- American Geriatrics Society 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2012; 60:616–631.
- Gallagher P, Ryan C, Byrne S, Kennedy J, O’Mahony D. STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Ther 2008; 46:72–83.
- Sterke CS, Ziere G, van Beeck EF, Looman CW, van der Cammen TJ. Dose-response relationship between selective serotonin re-uptake inhibitors and injurious falls: a study in nursing home residents with dementia. Br J Clin Pharmacol 2012; 73:812–820.
- Khalili H, Huang ES, Jacobson BC, Camargo CA Jr, Feskanich D, Chan AT. Use of proton pump inhibitors and risk of hip fracture in relation to dietary and lifestyle factors: a prospective cohort study. BMJ 2012; 344:e372.
- Gill SS, Anderson GM, Fischer HD, et al. Syncope and its consequences in patients with dementia receiving cholinesterase inhibitors: a population-based cohort study. Arch Intern Med 2009; 169:867–873.
- Janssen HC, Samson MM, Verhaar HJ. Vitamin D deficiency, muscle function, and falls in elderly people. Am J Clin Nutr 2002; 75:611–615.
- Muir SW, Gopaul K, Montero Odasso MM. The role of cognitive impairment in fall risk among older adults: a systematic review and meta-analysis. Age Ageing 2012; 41:299–308.
- Borson S, Scanlan J, Brush M, Vitaliano P, Dokmak A. The Mini-Cog: a cognitive ‘vital signs’ measure for dementia screening in multi-lingual elderly. Int J Geriatr Psychiatry 2000; 15:1021–1027.
- Cordell CB, Borson S, Boustani M, et al; Medicare Detection of Cognitive Impairment Workgroup. Alzheimer’s Association recommendations for operationalizing the detection of cognitive impairment during the Medicare Annual Wellness Visit in a primary care setting. Alzheimers Dement 2013; 9:141–150.
- Lawlor DA, Patel R, Ebrahim S. Association between falls in elderly women and chronic diseases and drug use: cross sectional study. BMJ 2003; 327:712–717.
- Day L, Fildes B, Gordon I, Fitzharris M, Flamer H, Lord S. Randomised factorial trial of falls prevention among older people living in their own homes. BMJ 2002; 325:128.
- Chang JT, Morton SC, Rubenstein LZ, et al. Interventions for the prevention of falls in older adults: systematic review and meta-analysis of randomised clinical trials. BMJ 2004; 328:680.
- Antithrombotic Trialists’ (ATT) Collaboration; Baigent C, Blackwell L, Collins R, et al. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet 2009; 373:1849–1860.
- Baigent C, Keech A, Kearney PM, et al; Cholesterol Treatment Trialists’ (CTT) Collaborators. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005; 366:1267–1278.
- Mazzeo RS; American College of Sports Medicine (ACSM). Exercise and the older adult. ACSM Current Comment. www.acsm.org/docs/current-comments/exerciseandtheolderadult.pdf. Accessed April 8, 2015.
- Willoughby DS; American College of Sports Medicine (ACSM). Resistance training and the older adult. ACSM Current Comment. www.acsm.org/docs/current-comments/resistancetrainingandtheoa.pdf. Accessed April 8, 2015.
- Tencer AF, Koepsell TD, Wolf ME, et al. Biomechanical properties of shoes and risk of falls in older adults. J Am Geriatr Soc 2004; 52:1840–1846.
- Lord SR, Bashford GM. Shoe characteristics and balance in older women. J Am Geriatr Soc 1996; 44:429–433.
- Kelsey JL, Procter-Gray E, Nguyen US, Li W, Kiel DP, Hannan MT. Footwear and falls in the home among older individuals in the MOBILIZE Boston Study. Footwear Sci 2010; 2:123–129.
- Tseng VL, Yu F, Lum F, Coleman AL. Risk of fractures following cataract surgery in Medicare beneficiaries. JAMA 2012; 308:493–501.
- Cumming RG, Ivers R, Clemson L, et al. Improving vision to prevent falls in frail older people: a randomized trial. J Am Geriatr Soc 2007; 55:175–181.
- Bischoff-Ferrari HA, Dawson-Hughes B, Willett WC, et al. Effect of vitamin D on falls: a meta-analysis. JAMA 2004; 291:1999–2006.
- Avenell A, Mak JCS, O’Connell D. Vitamin D and vitamin D analogues for preventing fractures in postmenopausal women and older men. Cochrane Database Syst Rev 2014; 4:CD000227.
- Santesso N, Carrasco-Labra A, Brignardello-Petersen R. Hip protectors for preventing hip fractures in older people. Cochrane Database Syst Rev 2014; 3:CD001255.
- Messinger-Rapport B, Dumas LG. Falls in the nursing home: a collaborative approach. Nurs Clin North Am 2009; 44:187–195.
- Faber MJ, Bosscher RJ, Chin A, Paw MJ, van Wieringen PC. Effects of exercise programs on falls and mobility in frail and pre-frail older adults: a multicenter randomized controlled trial. Arch Phys Med Rehabil 2006; 87:885–896.
- Silva RB, Eslick GD, Duque G. Exercise for falls and fracture prevention in long term care facilities: a systematic review and meta-analysis. J Am Med Dir Assoc 2013; 14:685–689.e2.
- Shaw FE, Bond J, Richardson DA, et al. Multifactorial intervention after a fall in older people with cognitive impairment and dementia presenting to the accident and emergency department: randomised controlled trial. BMJ 2003; 326:73.
- Ashburn A, Hyndman D, Pickering R, Yardley L, Harris S. Predicting people with stroke at risk of falls. Age Ageing 2008; 37:270–276.
- Davenport RJ, Dennis MS, Wellwood I, Warlow CP. Complications after acute stroke. Stroke 1996; 27:415–420.
- Verheyden GS, Weerdesteyn V, Pickering RM, et al. Interventions for preventing falls in people after stroke. Cochrane Database Syst Rev 2013; 5:CD008728.
KEY POINTS
- Practitioners can reduce fall-related injury by screening older adults yearly with questions about problems with balance and gait, performing a focused history and examination when necessary, and implementing evidence-based interventions.
- Cognitive impairment itself is an independent predictor of falls because it can reduce processing speed and impair executive function.
- An exercise program with resistance, balance, and gait training is usually prescribed to patients at high risk, along with a home assessment and withdrawal or minimization of psychoactive and antipsychotic medications.
- Combined calcium and vitamin D supplements should be given to most older adults in long-term care facilities to reduce fracture rates.
- There are no specific evidence-based recommendations for fall prevention in community-living older adults with cognitive impairment or dementia.
When should I discuss driving with my older patients?
Most older drivers are safe drivers and are less likely than younger people to drive recklessly, at high speeds, or under the influence of alcohol.1 However, motor vehicle injuries are the second leading cause of injury-related deaths among older adults. Very old adults (80 years and over) have higher rates of fatality and injury in motor vehicle crashes per million miles driven than any other age group except for teenagers.1 Therefore, consider safety screening of all very old drivers plus any older adult with certain high-risk medical conditions, including the following.
NEUROCOGNITIVE DISORDERS
Drivers with Alzheimer disease—the most common type of major neurocognitive disorder (dementia) in older adults in the United States—are at high risk for adverse driving events due to impaired memory, attentiveness, problem-solving skills, multitasking, orientation, judgment, and reaction speed. Even in amnesic mild cognitive impairment—a mild neurocognitive disorder without functional decline—driving skills such as lane control may be impaired.2
Frontotemporal dementia, a less common cause of dementia in older adults, is associated with profound impairments in reasoning, task flexibility, planning, and execution. Persons with frontotemporal dementia are more likely to speed, run stop signs, and suffer more off-road crashes and collisions.3
The diagnosis of dementia, however, is less predictive of driving risk than the stage of dementia. The American Academy of Neurology recommends that health care providers clinically “stage” all demented individuals using a validated tool at diagnosis and periodically afterwards. The Clinical Dementia Rating (CDR) scale is appropriate for staging dementia in the office. The CDR has also been shown to identify people with dementia who are at an increased risk of unsafe driving, with strong evidence (level of evidence A) relating dementia stage to driving risk.4 The CDR assigns a score of 1 for mild dementia (function impaired in at least one complex activity); 2 for moderate dementia (function impaired in at least one basic activity); and 3 for severe dementia. Individuals with a CDR score of 2 or higher are considered to be at very high risk if still driving. These persons should be encouraged to surrender their driving privileges.4 Even with mild dementia (CDR score of 1), as few as 41% of drivers may drive safely.4 Most persons with mild cognitive impairment (CDR score of 0.5) are safe drivers.
Patients often have poor insight into their driving safety. However, a caregiver’s rating of driving skills as marginal or unsafe is useful in identifying unsafe drivers (level of evidence B) and can be considered a red flag.4 Predictors with less support in the literature (level of evidence C) include recent traffic citations, motor vehicle accidents, and self-reported situational avoidance, such as limiting driving to familiar roadways. Additional predictors include Mini-Mental State Examination scores of 24 or less, and/or the emergence of an aggressive or impulsive personality (Table 1). A driver evaluation is helpful when there is mild cognitive impairment or mild dementia with at least one red flag.
Clinicians who are not comfortable with staging dementia as mild, moderate, or severe may consider referring to a neurologist or geriatrician.
There is no evidence to support or refute the benefit of interventional strategies such as driver rehabilitation for drivers with dementia.
PARKINSON DISEASE
Individuals with mild motor disability from Parkinson disease may be fit drivers. As the disease progresses, drivers with Parkinson disease may make more errors than healthy elders in visual scanning, signaling, vehicle positioning, and velocity regulation (eg, traveling so slowly that it may be unsafe).5 Clinicians can consider referring a patient with Parkinson disease for a baseline driving evaluation upon diagnosis, and then every 1 to 2 years for reassessment. Alternate transportation should be arranged as the disease progresses.
EPISODIC INCAPACITATION
Approximately 1% to 3% of all motor vehicle accidents are due to sudden incapacitation of an otherwise safe driver.
Syncope. Neurally mediated (vasovagal) syncope accounts for 30% to 35% of syncopal episodes while driving.6 Cardiac arrhythmias are the next most common cause and include bradyarrhythmias (7%), supraventricular tachyarrhythmias (2%–15%), and ventricular tachyarrhythmias (5%–17%). Because neurocardiogenic syncope often recurs, consider restricting driving for those with recurrent or severe neurocardiogenic syncopal episodes until symptoms are controlled.
Arrhythmias. Driving recommendations for various arrhythmias7,8 are listed in Table 2.
Many patients who have an implantable cardioverter-defibrillator (ICD) device experience an unexpected shock. For individuals with a history of ventricular tachycardia or fibrillation, the 5-year actuarial incidence of appropriate ICD shocks ranges between 55% and 70%. However, data indicate that 90% to 100% of drivers who received ICD discharges while driving continued to drive without causing motor vehicle accidents.9,10
Seizures. States differ in their rules for reporting drivers who have epilepsy or breakthrough seizures. Physicians should refer to their state regulations when counseling these patients.
POLYPHARMACY
Polypharmacy is common in older adults. Many take psychoactive drugs that can impair tracking, alertness, coordination, and reaction time. With the “Roadwise Rx” tool (www.roadwiserx.com), health care providers and patients can enter the names of medicines to check if they affect driving ability. Nonproprietary on-line tools such as “START” (Screening Tool to Alert doctors to Right Treatment) and “STOPP” (Screening Tool of Older Persons’ Potentially Inappropriate Prescriptions) can be used to prune medication lists.
DRIVING EVALUATION
America is a nation of highways overflowing with cars. Cars provide transportation but also reflect wealth and personality, particularly for men. Practically, the ability to drive a car allows older men and women to socialize in the community, shop for essentials, and take care of themselves without being a burden. Driving cessation can cause social isolation and depressive symptoms and can strain caregiver resources.
It is therefore understandable for health care providers to feel reluctant or uncomfortable counseling older adults to give up their driving privileges. A health care provider who identifies driving safety concerns can refer a patient to a geriatrician for further risk assessment or to a certified driver rehabilitation specialist (CDRS) for a driving evaluation. A CDRS will also offer the patient and caregiver information on local resources for transportation alternatives. A list of local CDRSs can be found on the Association for Driver Rehabilitation Specialists website (www.aded.net). Many hospitals have occupational therapists who are CDRSs.
The evaluation typically involves an assessment of the driver’s knowledge of traffic signs and laws, a cognitive assessment, possibly a simulation, and finally an on-road driving evaluation if deemed appropriate. Medicare coverage depends on diagnosis and the state carrier.
- Williams AF. Teenage drivers: patterns of risk. J Safety Res 2003; 34:5–15.
- Griffith HR, Okonkwo OC, Stewart CC, et al. Lower hippocampal volume predicts decrements in lane control among drivers with amnestic mild cognitive impairment. J Geriatr Psychiatry Neurol 2013; 26:259–266.
- de Simone V, Kaplan L, Patronas N, Wassermann EM, Grafman J. Driving abilities in frontotemporal dementia patients. Dement Geriatr Cogn Disord 2007; 23:1–7.
- Iverson DJ, Gronseth GS, Reger MA, Classen S, Dubinsky RM, Rizzo M; Quality Standards Subcomittee of the American Academy of Neurology. Practice parameter update: evaluation and management of driving risk in dementia: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2010; 74:1316–1324.
- Classen S, Brumback B, Monahan M, et al. Driving errors in Parkinson’s disease: moving closer to predicting on-road outcomes. Am J Occup Ther 2014; 68:77–85.
- Blitzer ML, Saliba BC, Ghantous AE, Marieb MA, Schoenfeld MH. Causes of impaired consciousness while driving a motorized vehicle. Am J Cardiol 2003; 91:1373–1374.
- Sorajja D, Shen WK. Driving guidelines and restrictions in patients with a history of cardiac arrhythmias, syncope,or implantable devices. Curr Treat Options Cardiovasc Med 2010; 12:443–456.
- Task force members; Vijgen J, Botto G, Camm J, et al. Consensus statement of the European Heart Rhythm Association: updated recommendations for driving by patients with implantable cardioverter defibrillators. Europace 2009; 11:1097–1107.
- Conti JB, Woodard DA, Tucker KJ, Bryant B, King LC, Curtis AB. Modification of patient driving behavior after implantation of a cardioverter defibrillator. Pacing Clin Electrophysiol 1997; 20:2200–2204.
- Lerecouvreux M, Aït Saïd M, Paziaud O, et al. Automobile driving and implantable defibrillators. Arch Mal Coeur Vaiss 2005; 98:288–293. Article in French.
Most older drivers are safe drivers and are less likely than younger people to drive recklessly, at high speeds, or under the influence of alcohol.1 However, motor vehicle injuries are the second leading cause of injury-related deaths among older adults. Very old adults (80 years and over) have higher rates of fatality and injury in motor vehicle crashes per million miles driven than any other age group except for teenagers.1 Therefore, consider safety screening of all very old drivers plus any older adult with certain high-risk medical conditions, including the following.
NEUROCOGNITIVE DISORDERS
Drivers with Alzheimer disease—the most common type of major neurocognitive disorder (dementia) in older adults in the United States—are at high risk for adverse driving events due to impaired memory, attentiveness, problem-solving skills, multitasking, orientation, judgment, and reaction speed. Even in amnesic mild cognitive impairment—a mild neurocognitive disorder without functional decline—driving skills such as lane control may be impaired.2
Frontotemporal dementia, a less common cause of dementia in older adults, is associated with profound impairments in reasoning, task flexibility, planning, and execution. Persons with frontotemporal dementia are more likely to speed, run stop signs, and suffer more off-road crashes and collisions.3
The diagnosis of dementia, however, is less predictive of driving risk than the stage of dementia. The American Academy of Neurology recommends that health care providers clinically “stage” all demented individuals using a validated tool at diagnosis and periodically afterwards. The Clinical Dementia Rating (CDR) scale is appropriate for staging dementia in the office. The CDR has also been shown to identify people with dementia who are at an increased risk of unsafe driving, with strong evidence (level of evidence A) relating dementia stage to driving risk.4 The CDR assigns a score of 1 for mild dementia (function impaired in at least one complex activity); 2 for moderate dementia (function impaired in at least one basic activity); and 3 for severe dementia. Individuals with a CDR score of 2 or higher are considered to be at very high risk if still driving. These persons should be encouraged to surrender their driving privileges.4 Even with mild dementia (CDR score of 1), as few as 41% of drivers may drive safely.4 Most persons with mild cognitive impairment (CDR score of 0.5) are safe drivers.
Patients often have poor insight into their driving safety. However, a caregiver’s rating of driving skills as marginal or unsafe is useful in identifying unsafe drivers (level of evidence B) and can be considered a red flag.4 Predictors with less support in the literature (level of evidence C) include recent traffic citations, motor vehicle accidents, and self-reported situational avoidance, such as limiting driving to familiar roadways. Additional predictors include Mini-Mental State Examination scores of 24 or less, and/or the emergence of an aggressive or impulsive personality (Table 1). A driver evaluation is helpful when there is mild cognitive impairment or mild dementia with at least one red flag.
Clinicians who are not comfortable with staging dementia as mild, moderate, or severe may consider referring to a neurologist or geriatrician.
There is no evidence to support or refute the benefit of interventional strategies such as driver rehabilitation for drivers with dementia.
PARKINSON DISEASE
Individuals with mild motor disability from Parkinson disease may be fit drivers. As the disease progresses, drivers with Parkinson disease may make more errors than healthy elders in visual scanning, signaling, vehicle positioning, and velocity regulation (eg, traveling so slowly that it may be unsafe).5 Clinicians can consider referring a patient with Parkinson disease for a baseline driving evaluation upon diagnosis, and then every 1 to 2 years for reassessment. Alternate transportation should be arranged as the disease progresses.
EPISODIC INCAPACITATION
Approximately 1% to 3% of all motor vehicle accidents are due to sudden incapacitation of an otherwise safe driver.
Syncope. Neurally mediated (vasovagal) syncope accounts for 30% to 35% of syncopal episodes while driving.6 Cardiac arrhythmias are the next most common cause and include bradyarrhythmias (7%), supraventricular tachyarrhythmias (2%–15%), and ventricular tachyarrhythmias (5%–17%). Because neurocardiogenic syncope often recurs, consider restricting driving for those with recurrent or severe neurocardiogenic syncopal episodes until symptoms are controlled.
Arrhythmias. Driving recommendations for various arrhythmias7,8 are listed in Table 2.
Many patients who have an implantable cardioverter-defibrillator (ICD) device experience an unexpected shock. For individuals with a history of ventricular tachycardia or fibrillation, the 5-year actuarial incidence of appropriate ICD shocks ranges between 55% and 70%. However, data indicate that 90% to 100% of drivers who received ICD discharges while driving continued to drive without causing motor vehicle accidents.9,10
Seizures. States differ in their rules for reporting drivers who have epilepsy or breakthrough seizures. Physicians should refer to their state regulations when counseling these patients.
POLYPHARMACY
Polypharmacy is common in older adults. Many take psychoactive drugs that can impair tracking, alertness, coordination, and reaction time. With the “Roadwise Rx” tool (www.roadwiserx.com), health care providers and patients can enter the names of medicines to check if they affect driving ability. Nonproprietary on-line tools such as “START” (Screening Tool to Alert doctors to Right Treatment) and “STOPP” (Screening Tool of Older Persons’ Potentially Inappropriate Prescriptions) can be used to prune medication lists.
DRIVING EVALUATION
America is a nation of highways overflowing with cars. Cars provide transportation but also reflect wealth and personality, particularly for men. Practically, the ability to drive a car allows older men and women to socialize in the community, shop for essentials, and take care of themselves without being a burden. Driving cessation can cause social isolation and depressive symptoms and can strain caregiver resources.
It is therefore understandable for health care providers to feel reluctant or uncomfortable counseling older adults to give up their driving privileges. A health care provider who identifies driving safety concerns can refer a patient to a geriatrician for further risk assessment or to a certified driver rehabilitation specialist (CDRS) for a driving evaluation. A CDRS will also offer the patient and caregiver information on local resources for transportation alternatives. A list of local CDRSs can be found on the Association for Driver Rehabilitation Specialists website (www.aded.net). Many hospitals have occupational therapists who are CDRSs.
The evaluation typically involves an assessment of the driver’s knowledge of traffic signs and laws, a cognitive assessment, possibly a simulation, and finally an on-road driving evaluation if deemed appropriate. Medicare coverage depends on diagnosis and the state carrier.
Most older drivers are safe drivers and are less likely than younger people to drive recklessly, at high speeds, or under the influence of alcohol.1 However, motor vehicle injuries are the second leading cause of injury-related deaths among older adults. Very old adults (80 years and over) have higher rates of fatality and injury in motor vehicle crashes per million miles driven than any other age group except for teenagers.1 Therefore, consider safety screening of all very old drivers plus any older adult with certain high-risk medical conditions, including the following.
NEUROCOGNITIVE DISORDERS
Drivers with Alzheimer disease—the most common type of major neurocognitive disorder (dementia) in older adults in the United States—are at high risk for adverse driving events due to impaired memory, attentiveness, problem-solving skills, multitasking, orientation, judgment, and reaction speed. Even in amnesic mild cognitive impairment—a mild neurocognitive disorder without functional decline—driving skills such as lane control may be impaired.2
Frontotemporal dementia, a less common cause of dementia in older adults, is associated with profound impairments in reasoning, task flexibility, planning, and execution. Persons with frontotemporal dementia are more likely to speed, run stop signs, and suffer more off-road crashes and collisions.3
The diagnosis of dementia, however, is less predictive of driving risk than the stage of dementia. The American Academy of Neurology recommends that health care providers clinically “stage” all demented individuals using a validated tool at diagnosis and periodically afterwards. The Clinical Dementia Rating (CDR) scale is appropriate for staging dementia in the office. The CDR has also been shown to identify people with dementia who are at an increased risk of unsafe driving, with strong evidence (level of evidence A) relating dementia stage to driving risk.4 The CDR assigns a score of 1 for mild dementia (function impaired in at least one complex activity); 2 for moderate dementia (function impaired in at least one basic activity); and 3 for severe dementia. Individuals with a CDR score of 2 or higher are considered to be at very high risk if still driving. These persons should be encouraged to surrender their driving privileges.4 Even with mild dementia (CDR score of 1), as few as 41% of drivers may drive safely.4 Most persons with mild cognitive impairment (CDR score of 0.5) are safe drivers.
Patients often have poor insight into their driving safety. However, a caregiver’s rating of driving skills as marginal or unsafe is useful in identifying unsafe drivers (level of evidence B) and can be considered a red flag.4 Predictors with less support in the literature (level of evidence C) include recent traffic citations, motor vehicle accidents, and self-reported situational avoidance, such as limiting driving to familiar roadways. Additional predictors include Mini-Mental State Examination scores of 24 or less, and/or the emergence of an aggressive or impulsive personality (Table 1). A driver evaluation is helpful when there is mild cognitive impairment or mild dementia with at least one red flag.
Clinicians who are not comfortable with staging dementia as mild, moderate, or severe may consider referring to a neurologist or geriatrician.
There is no evidence to support or refute the benefit of interventional strategies such as driver rehabilitation for drivers with dementia.
PARKINSON DISEASE
Individuals with mild motor disability from Parkinson disease may be fit drivers. As the disease progresses, drivers with Parkinson disease may make more errors than healthy elders in visual scanning, signaling, vehicle positioning, and velocity regulation (eg, traveling so slowly that it may be unsafe).5 Clinicians can consider referring a patient with Parkinson disease for a baseline driving evaluation upon diagnosis, and then every 1 to 2 years for reassessment. Alternate transportation should be arranged as the disease progresses.
EPISODIC INCAPACITATION
Approximately 1% to 3% of all motor vehicle accidents are due to sudden incapacitation of an otherwise safe driver.
Syncope. Neurally mediated (vasovagal) syncope accounts for 30% to 35% of syncopal episodes while driving.6 Cardiac arrhythmias are the next most common cause and include bradyarrhythmias (7%), supraventricular tachyarrhythmias (2%–15%), and ventricular tachyarrhythmias (5%–17%). Because neurocardiogenic syncope often recurs, consider restricting driving for those with recurrent or severe neurocardiogenic syncopal episodes until symptoms are controlled.
Arrhythmias. Driving recommendations for various arrhythmias7,8 are listed in Table 2.
Many patients who have an implantable cardioverter-defibrillator (ICD) device experience an unexpected shock. For individuals with a history of ventricular tachycardia or fibrillation, the 5-year actuarial incidence of appropriate ICD shocks ranges between 55% and 70%. However, data indicate that 90% to 100% of drivers who received ICD discharges while driving continued to drive without causing motor vehicle accidents.9,10
Seizures. States differ in their rules for reporting drivers who have epilepsy or breakthrough seizures. Physicians should refer to their state regulations when counseling these patients.
POLYPHARMACY
Polypharmacy is common in older adults. Many take psychoactive drugs that can impair tracking, alertness, coordination, and reaction time. With the “Roadwise Rx” tool (www.roadwiserx.com), health care providers and patients can enter the names of medicines to check if they affect driving ability. Nonproprietary on-line tools such as “START” (Screening Tool to Alert doctors to Right Treatment) and “STOPP” (Screening Tool of Older Persons’ Potentially Inappropriate Prescriptions) can be used to prune medication lists.
DRIVING EVALUATION
America is a nation of highways overflowing with cars. Cars provide transportation but also reflect wealth and personality, particularly for men. Practically, the ability to drive a car allows older men and women to socialize in the community, shop for essentials, and take care of themselves without being a burden. Driving cessation can cause social isolation and depressive symptoms and can strain caregiver resources.
It is therefore understandable for health care providers to feel reluctant or uncomfortable counseling older adults to give up their driving privileges. A health care provider who identifies driving safety concerns can refer a patient to a geriatrician for further risk assessment or to a certified driver rehabilitation specialist (CDRS) for a driving evaluation. A CDRS will also offer the patient and caregiver information on local resources for transportation alternatives. A list of local CDRSs can be found on the Association for Driver Rehabilitation Specialists website (www.aded.net). Many hospitals have occupational therapists who are CDRSs.
The evaluation typically involves an assessment of the driver’s knowledge of traffic signs and laws, a cognitive assessment, possibly a simulation, and finally an on-road driving evaluation if deemed appropriate. Medicare coverage depends on diagnosis and the state carrier.
- Williams AF. Teenage drivers: patterns of risk. J Safety Res 2003; 34:5–15.
- Griffith HR, Okonkwo OC, Stewart CC, et al. Lower hippocampal volume predicts decrements in lane control among drivers with amnestic mild cognitive impairment. J Geriatr Psychiatry Neurol 2013; 26:259–266.
- de Simone V, Kaplan L, Patronas N, Wassermann EM, Grafman J. Driving abilities in frontotemporal dementia patients. Dement Geriatr Cogn Disord 2007; 23:1–7.
- Iverson DJ, Gronseth GS, Reger MA, Classen S, Dubinsky RM, Rizzo M; Quality Standards Subcomittee of the American Academy of Neurology. Practice parameter update: evaluation and management of driving risk in dementia: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2010; 74:1316–1324.
- Classen S, Brumback B, Monahan M, et al. Driving errors in Parkinson’s disease: moving closer to predicting on-road outcomes. Am J Occup Ther 2014; 68:77–85.
- Blitzer ML, Saliba BC, Ghantous AE, Marieb MA, Schoenfeld MH. Causes of impaired consciousness while driving a motorized vehicle. Am J Cardiol 2003; 91:1373–1374.
- Sorajja D, Shen WK. Driving guidelines and restrictions in patients with a history of cardiac arrhythmias, syncope,or implantable devices. Curr Treat Options Cardiovasc Med 2010; 12:443–456.
- Task force members; Vijgen J, Botto G, Camm J, et al. Consensus statement of the European Heart Rhythm Association: updated recommendations for driving by patients with implantable cardioverter defibrillators. Europace 2009; 11:1097–1107.
- Conti JB, Woodard DA, Tucker KJ, Bryant B, King LC, Curtis AB. Modification of patient driving behavior after implantation of a cardioverter defibrillator. Pacing Clin Electrophysiol 1997; 20:2200–2204.
- Lerecouvreux M, Aït Saïd M, Paziaud O, et al. Automobile driving and implantable defibrillators. Arch Mal Coeur Vaiss 2005; 98:288–293. Article in French.
- Williams AF. Teenage drivers: patterns of risk. J Safety Res 2003; 34:5–15.
- Griffith HR, Okonkwo OC, Stewart CC, et al. Lower hippocampal volume predicts decrements in lane control among drivers with amnestic mild cognitive impairment. J Geriatr Psychiatry Neurol 2013; 26:259–266.
- de Simone V, Kaplan L, Patronas N, Wassermann EM, Grafman J. Driving abilities in frontotemporal dementia patients. Dement Geriatr Cogn Disord 2007; 23:1–7.
- Iverson DJ, Gronseth GS, Reger MA, Classen S, Dubinsky RM, Rizzo M; Quality Standards Subcomittee of the American Academy of Neurology. Practice parameter update: evaluation and management of driving risk in dementia: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2010; 74:1316–1324.
- Classen S, Brumback B, Monahan M, et al. Driving errors in Parkinson’s disease: moving closer to predicting on-road outcomes. Am J Occup Ther 2014; 68:77–85.
- Blitzer ML, Saliba BC, Ghantous AE, Marieb MA, Schoenfeld MH. Causes of impaired consciousness while driving a motorized vehicle. Am J Cardiol 2003; 91:1373–1374.
- Sorajja D, Shen WK. Driving guidelines and restrictions in patients with a history of cardiac arrhythmias, syncope,or implantable devices. Curr Treat Options Cardiovasc Med 2010; 12:443–456.
- Task force members; Vijgen J, Botto G, Camm J, et al. Consensus statement of the European Heart Rhythm Association: updated recommendations for driving by patients with implantable cardioverter defibrillators. Europace 2009; 11:1097–1107.
- Conti JB, Woodard DA, Tucker KJ, Bryant B, King LC, Curtis AB. Modification of patient driving behavior after implantation of a cardioverter defibrillator. Pacing Clin Electrophysiol 1997; 20:2200–2204.
- Lerecouvreux M, Aït Saïd M, Paziaud O, et al. Automobile driving and implantable defibrillators. Arch Mal Coeur Vaiss 2005; 98:288–293. Article in French.

Advance care planning: Beyond the living will
Mr. B., an 82-year-old retired accountant with hypertension, was diagnosed with early Alzheimer disease 6 years ago. He now needs supervision with bathing and dressing and no longer consistently recognizes family members. You are seeing him in the office today after a hospitalization for aspiration pneumonia, his second in the past 6 months.
In the hospital, a brain scan showed that atrophy had progressed and white-matter disease was more extensive than 3 years earlier. A barium swallow study showed esophageal dysmotility and aspiration. He was prescribed a “dysphagia diet,”1 which he dislikes.
Since returning home, he has been disoriented, he has been wandering about the house, and he has fallen several times. He has lost 10 pounds in 6 months. Because of his confusion, his wife cannot take him out, and she is exhausted caring for him.
Reviewing his medical record, you note that 10 years ago, Mr. B. completed a living will and designated his wife as his proxy decision-maker via a medical power of attorney document.
PLANNING IS OFTEN NEGLECTED
Many clinicians and older patients feel a strong need to document, in advance, the patient’s wishes regarding medical care in the event the patient becomes seriously ill and unable to participate in treatment decisions. Professional societies such as the American Geriatrics Society promote advance care planning,2 and some indices of the quality of medical care include whether advance directives have been discussed and completed.3
Yet, despite the high profile of advance care planning,4 few patients actually fill out advance directives,5 with completion rates that vary widely,6–8 sometimes by ethnicity and sex.9,10 Furthermore, in a crisis, these directives are seldom followed.11
In this paper, we recommend an approach to advance care planning for older adults that redirects the focus from “signing away” interventions such as dialysis, mechanical ventilation, and tube feeding. Instead, the focus is on the goals of care. We also advocate naming a surrogate decision-maker, since the medical power of attorney is more flexible and more widely applicable than the living will.
START BY LISTENING
A change in function resulting from disease progression, hospitalization, trauma, or other reasons is an ideal opportunity to introduce the process of advance care planning.
The first step is to find out how well the patient and family understand the patient’s relevant medical conditions, and what their expectations, hopes, and concerns are. This listening phase can provide insight into the patient’s values and goals and how much the patient and family want to engage in these discussions.
In matters of health behavior (such as advance care planning), people change only when they are ready to change.12,13 Thus, we advise physicians to defer extensive discussions of values and goals of care until patients and families are ready to listen, hear, and talk about these topics (often, after a change for the worse in prognosis).
And it is a process. Advance care directives are most likely to be set up and followed if the patient and doctor discuss this issue during multiple visits, rather than if the physician merely hands the patient a packet of forms and information.14–16
CASE CONTINUED: A PEG TUBE REFUSED
Mrs. B. says that Mr. B. is in good health except for his memory: he does not have a serious condition such as diabetes, heart failure, or cancer. While Mr. B. was in the hospital, the hospitalist recommended placing a percutaneous endoscopic gastrostomy (PEG) tube, but Mrs. B. declined the recommendation because her husband had a living will that specified “no artificially or technologically supplied nutrition or hydration.”
At this point, Mrs. B. begins to cry. She has slept poorly because of his wandering. Also, her two daughters do not support her refusal of the PEG tube.
Comment. This brief conversation illuminates knowledge deficits in Mrs. B.’s understanding of Alzheimer disease and the circumstances in which the living will applies. Although one could argue that Mr. B.’s Alzheimer disease has advanced to the point that he is likely to die of a complication of that condition, he is not likely to die in the near future. If he is not considered by law and his physician to be terminally ill or permanently unconscious, a living will likely does not offer guidance about artificial feeding.
LIMITATIONS OF A LIVING WILL
A living will, a commonly used advance directive, states that the patient does not wish to receive life-sustaining treatment in the event that he or she suffers an incurable, irreversible disease and cannot give informed consent, and it often lists specific treatments that the patient does not want. However, we believe that approaching the patient with a list of life-sustaining measures to accept or reject, before discussing goals of care and prognosis, puts the cart before the horse. This approach threatens to distract from the need to ascertain values and offer appropriate care. Additionally, a living will is active only within a very limited scenario and does not address relatively routine but important decisions in a person’s care.
All ‘terminal illness’ isn’t the same
A living will goes into effect only if the patient either enters a permanent vegetative state following an event such as cardiac arrest or severe brain trauma, or is diagnosed with a terminal illness such as metastatic cancer, and lacks decision-making capacity.
But what is terminal illness? The definition differs from state to state, but it is generally defined as an irreversible condition leading to death in a relatively short time. The time may not be specified, as in Florida statute 765. In contrast, Ohio Revised Code 2133.01(AA) uses the phrase “relatively short,” while other states specify a time, such as within 6 months (Texas Health and Safety Code 166.002). The Medicare hospice benefit also carries a short time limit, usually less than 6 months.
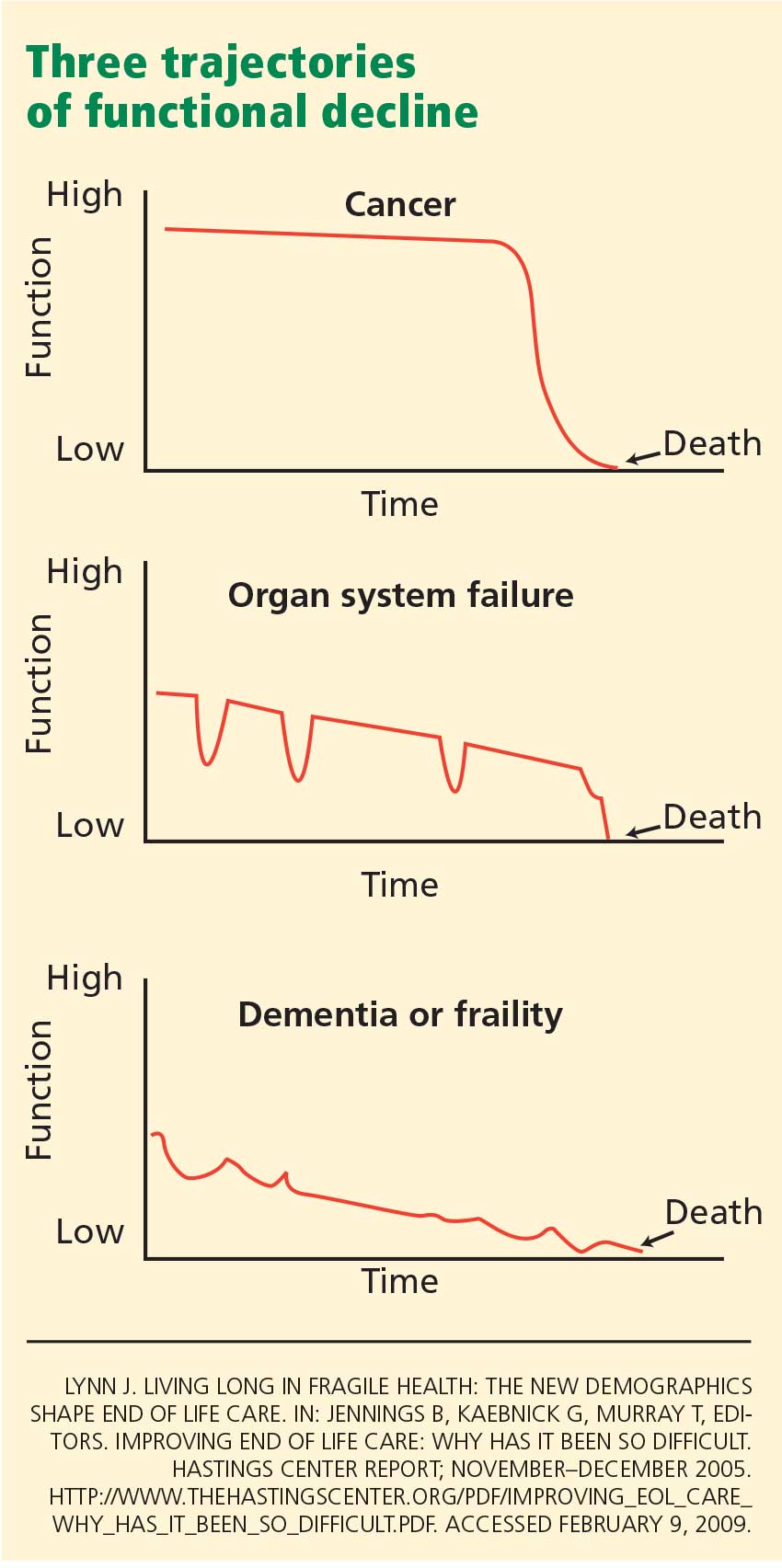
The middle panel in Figure 1 depicts a more typical decline from serial organ insults such as stroke followed by infection from aspiration or followed by falls. Older adults with dementia or with multiple progressive diseases such as heart failure, diabetes, hypertension, or cancer decline in a trajectory such as in the bottom panel of Figure 1.
A living will might not be activated in the latter two scenarios until years into the condition because the patient would not be considered terminally ill—by state law, by the health care provider, or even by the patient.
The living will does not address routine interventions
In most states, living wills address only life-sustaining treatments such as dialysis, mechanical ventilation, and medically supplied nutrition and hydration. Living wills do not address relatively common diseases in older adults that could cause severe debility, such as a major stroke or advanced dementia.
If an older patient has dementia, a living will is unlikely to provide guidance about interventions such as intubation to get through an episode of potentially reversible respiratory failure, a feeding tube to correct weight loss, or cardiac catheterization or bypass surgery to treat angina. Yet these important decisions often arise as function declines and comorbidities progress.
Patients may change their minds
Many older adults are reluctant to sign documents to “micromanage” their future care if they should become ill.19 Many people change their mind as the situation changes.11,20,21 Although few claim they would want burdensome interventions if they had dementia22 or if their prognosis were poor,23 patients may tolerate more burdensome interventions if they are already receiving treatments for chronic illnesses such as end-stage renal disease.24
Thus, a living will may help if unexpected trauma occurs in a healthy person, but not so much if chronic illness progresses over a period of years.
Advance directives may not be honored
Even if completed, written advance directives may not be followed, for a variety of reasons. Physicians may not know the patient has a living will, and fewer than one-third of people who actually complete an advance directive have discussed its content with a physician.25 The people named as surrogate decision-makers may not know the patient’s wishes. Family members may disagree with the goals and plan of care and may interfere with implementation of the advance care plan. A patient may see multiple physicians at different institutions who may not communicate with each other about the patient’s wishes. Also, physicians and patients may interpret terms such as “terminally ill” differently, making it difficult to translate the documents into an action plan.
CASE CONTINUED: RELIEVING CAREGIVER STRESS
Returning to Mr. B., your first goal is to address care issues, including caregiver stress. Skilled services in the home are appropriate for him at this time (and Medicare will pay for them) because he is still homebound. These services could include physical therapy, occupational therapy, and speech (swallowing) therapy. A home care agency may also provide an aide for a few weeks to assist with bathing and other personal needs.
You strongly recommend that the family (including both daughters) participate in the Alzheimer’s Association educational programs. You recommend that Mrs. B. locate an adult day care program now so that when Mr. B. completes his home therapy course and is no longer homebound, he may attend. Day care would provide a therapeutic environment for him and respite for her.
You request that the home care agency provide a social worker to advise her on community resources. Meta-analysis suggests that structured, multicomponent interventions with caregivers of demented patients reduce several types of caregiver burden and delay institutionalization.26
He improves with conservative measures
Three weeks later, Mr. B. is sleeping better and has stopped wandering. However, he dislikes the thickened liquids required by the dysphagia diet and has lost another 2 pounds. If his beverages are not thickened, he coughs profusely when he swallows. His daughters are still pressuring Mrs. B. for a PEG tube; one of them has angrily asserted that the doctors are going to allow her father to die.
You explain the burdens of PEG tubes: surgical risks, continued aspiration, disrupted bowel habits, the risk of the tube being accidentally or intentionally dislodged by the patient, and special binders (which may be uncomfortable) or restraints (which may cause further functional decline) that may be necessary to prevent this complication.
You request that the speech therapist work with the patient more aggressively in the use of swallowing techniques such as the chin tuck, which may be at least as effective as thickeners in preventing both aspiration pneumonia and dehydration.27 The therapist will need to include Mrs. B. in these sessions, since she will be Mr. B.’s coach at mealtime.
With more aggressive speech therapy, the patient’s weight stabilizes over the next 4 weeks. He is in day care 3 days a week, and Mrs. B. is more rested and relaxed.
Cardiopulmonary resuscitation
You continue the advance care planning discussion and suggest that if Mr. B. aspirates, is hospitalized again, and declines further care, it would be helpful to delineate instructions for resuscitation. Right now, although his Alzheimer disease is advanced, he is not clearly terminal. Thus, his living will does not strictly apply and provides limited guidance about intubation, cardiopulmonary resuscitation (CPR), or medically supplied nutrition and hydration. However, because Mrs. B. is his agent in the medical power of attorney, this document enables her to make a wide spectrum of treatment decisions on his behalf.
Mrs. B. asks about her husband’s prognosis and why CPR would not be helpful.
Comment. Further discussion with her could be guided by an estimate of Mr. B.’s prognosis. Function-based tools28,29 may also be useful. For example,28,30 an 80-year-old man with high functional status might have a life expectancy of more than 10 years. Mr. B., with multiple medical problems and declining function, would have an estimated life expectancy of approximately 3 years. Even without specifically categorizing function, impaired cognition by itself predicted a shorter life expectancy in population-based studies.31,32
Regarding CPR, patients and families may overestimate successful outcomes. A recent study33 of 10 years of outcomes of in-hospital cardiac arrest found that only 6.6% of patients survived to discharge. The average age of the survivors was 59 years, and fewer than half of them survived 3 years after cardiac arrest. In eight studies of CPR outcomes in nursing homes,34 three studies had no survivors, and all but one study had a survival rate below 5%.
PROVIDING APPROPRIATE CARE, NOT LIMITING TREATMENTS
In the case of Mr. B., as in many situations encountered with older patients, written advance directives provide little help or guidance. Instead, we recommend a model of advance care planning that takes place during multiple office visits over time, and that maintains a focus on providing appropriate care rather than on limiting life-sustaining treatments. We recommend providing estimates of prognosis and CPR outcomes when the family appeares ready to hear them. This approach should result in a care-oriented process while moving the family towards decisions regarding artificial feeding and CPR.
All patients, particularly those unwilling or unable to participate in advance care planning, are encouraged to identify one or more surrogate decision-makers and articulate how much flexibility that person should be given in important health care decisions. The medical power of attorney can be activated any time the patient lacks decision-making capacity and deactivated when decision-making capacity returns.38,39
As in the case of Mr. B., a tailored approach to advance care planning requires clinicians to estimate life expectancy (more than 5 years, less than 5 years, or less than 1 year) and to determine the patient’s and the family’s readiness to focus on a values-oriented and goal-oriented care plan. Some patients are not receptive to advance care planning, and clinical time and effort are optimized by providing the right amount of information to patients when they are ready to receive it.
For relatively healthy older adults
Figure 2 is the algorithm for older patients who are expected to live at least 5 years, ie, who are relatively healthy and functional. Patients with little or no interest in advance care planning can be asked about it annually, or sooner if their medical condition changes. Patients with limited interest can be given written information, specifically living will and medical power of attorney documents recognized in their state. Patients more open to advance care planning can be offered a values history form (Table 1), Web sites, and educational materials, with a plan to discuss them at future appointments.
Periodic reevaluation of values and goals of care is important. Patients may assert that particular interventions (eg, a PEG tube or dialysis) are “worse than death” when they are healthy, but they may change their views over time.21 Additionally, although a recent hospitalization or a decline in function may predispose patients to want to limit life-sustaining treatments, they may return to their earlier values and wishes a few months later, particularly if their medical condition stabilizes. 20 Values and decisions should be reassessed not only when medical conditions deteriorate, but also when they improve.
For chronically ill patients
Caregiver stress is important to identify and address, since caregivers often neglect themselves.40–42
For terminally ill patients
In this situation, patients and families need information about community resources that can assist them in the home. Some older adults with cognitive impairment may be exploited or neglect themselves, and referral to an adult protective services agency may be needed.
Treatment burden, particularly due to multiple prescribed medications, may be high and should be reassessed in light of the goals of treatment. Polypharmacy reduction is especially important at this stage in the illness, since the goals of care may be different than when the medications were prescribed.
Physical or psychosocial symptoms may be the cue to bring up the topic of palliative care. If the patient is expected to live less than 6 months, hospice referral is appropriate. With either palliative care or hospice, the focus of attention shifts explicitly from curing the disease to managing symptoms, and from the patient to the patient-family dyad. Interventions such as CPR and ventilatory support should be discussed and information from Table 2 provided to the patient and family.
Complete advance care planning incorporates taking a values history, estimating life expectancy, determining physical, psychosocial and spiritual needs, clarifying treatment goals, and estimating manageable treatment burden. Offering statistics on CPR and providing state-specific living will and medical power of attorney documents are important but are only one facet of effective advance care planning. In fact, shifting the emphasis of advance care planning from statistics and forms to values and goals of care may help in developing a more comprehensive care plan.
Goals of care range from curing the disease (with aggressive therapy, which may be burdensome) to simply improving function or decreasing pain. In the latter case, one may be able to discontinue some of the patient’s drugs, utilize medical and community resources more effectively, and better meet the patient’s needs.
Woven through all these discussions should be reassurance that the plan can be revisited and possibly revised, and that the physician will be there to help with those decisions.
For acutely ill patients in the hospital
Episodic, staged advance care planning is appropriate not only in the office but also in other settings such as assisted living and nursing facilities.
In the hospital, however, a different approach is needed, since patients are usually admitted because of an acute illness or sudden functional decline, or both. Decisions about technological interventions such as CPR, mechanical ventilation, or dialysis may be needed urgently. Often, patients are unable to provide guidance to physicians during acute illness because of delirium and other impediments. Developing a plan for care in the hospital may require urgent family meetings. However, if a surrogate decision-maker is in place, and if the patient has already participated in some form of advance care planning as an outpatient, the values and goals of care previously identified can contribute to decision-making during hospitalization.
As mentioned above, fragmentation of health care across providers and health care systems may limit the effectiveness of office-based advance care planning. It may be reasonable to train office staff to place advance care planning documentation in easily accessible sections of the patient’s medical record and to forward these to specialists involved in a patient’s care.
The patient and family should be encouraged and empowered to help with this process and should have updated advance care planning documentation readily available. In some states, comprehensive medical order sets, especially for end-of-life care, are portable across care settings and address CPR, medically supplied nutrition, hospital transfer, and antibiotic treatment.43
Research suggests that health care systems are more likely to comply with patients’ end-of-life preferences when portable medical order forms are developed and disseminated.44–44 Ultimately, major changes in health care delivery, including universal electronic health records, may be needed to implement and communicate patients’ advance care planning preferences across settings.
- National Dysphagia Diet Task Force. National Dysphagia Diet: Standardization for Optimal Care. Chicago, IL: American Dietetic Association, 2002.
- Nusbaum N, Goldstein M. American Geriatrics Society. The Patient Education Forum. Advance Directives, 2008. www.americangeriatrics.org/education/forum/advance_dir.shtml. Accessed March 9, 2009.
- Wenger NS, Roth CP, Shekelle PA; COVE Investigators. Introduction to the assessing care of vulnerable elders–3 quality indicator measurement set. J Am Geriatr Soc 2007; 55(suppl 2):S247–S252.
- Emanuel LL, Danis M, Pearlman RA, Singer PA. Advance care planning as a process: structuring the discussions in practice. J Am Geriatr Soc 1995; 43:440–446.
- Teno J, Lynn J, Wenger N, et al. Advance directives for seriously ill hospitalized patients: effectiveness with the patient self-determination act and the SUPPORT intervention. SUPPORT Investigators. Study to Understand Prognoses and P for Outcomes and Risks of Treatment. J Am Geriatr Soc 1997; 45:500–507.
- Hammes BJ, Rooney BL. Death and end-of-life planning in one midwestern community. Arch Intern Med 1998; 158:383–390.
- Gordon NP, Shade SB. Advance directives are more likely among seniors asked about end-of-life care p. Arch Intern Med 1999; 159:701–704.
- Morrison RS, Meier DE. High rates of advance care planning in New York City’s elderly population. Arch Intern Med 2004; 164:2421–2426.
- Perkins HS, Geppert CMA, Gonzales A, Cortez JD, Hazuda HP. Cross-cultural similarities and differences in attitudes about advance care planning. J Gen Intern Med 2002; 17:48–57.
- Perkins HS, Cortez JD, Hazuda HP. Advance care planning: does patient gender make a difference? Am J Med Sci 2004; 327:25–32.
- The SUPPORT Principal Investigators. A controlled trial to improve care for seriously ill hospitalized patients. Study to Understand Prognoses and P for Outcomes and Risks of Treatments (SUPPORT). JAMA 1995; 274:1591–1598.
- Prochaska JO, DiClemente CC, Norcross JC. In search of how people change. Applications to addictive behaviors. Am Psychol 1992; 47:1102–1114.
- Nigg CR, Burbank PM, Padula C, et al. Stages of change across ten health risk behaviors for older adults. Gerontologist 1999; 39:473–482.
- Patel RV, Sinuff T, Cook DJ. Influencing advance directive completion rates in non-terminally ill patients: a systematic review. J Crit Care 2004; 19:1–9.
- Hanson LC, Earp JA, Garrett J, Menon M, Danis M. Community physicians who provide terminal care. Arch Intern Med 1999; 159:1133–1138.
- Ramsaroop SD, Reid MC, Adelman RD. Completing an advance directive in the primary care setting: what do we need for success? J Am Geriatr Soc 2007; 55:277–283.
- Lynn J. Living long in fragile health: the new demographics shape end of life care. In:Jennings B, Kaebnick G, Murray T, editors. Improving End of Life Care: Why Has It Been So Difficult. Hastings Center Report November–December 2005: Special No:S14–S18.
- Beaumont JG, Kenealy PM. Incidence and prevalence of the vegetative and minimally conscious states. Neuropsychol Rehabil 2005; 15:184–189.
- Hawkins NA, Ditto PH, Danks JH, Smucker WD. Micromanaging death: process p, values, and goals in end-of-life medical decision making. Gerontologist 2005; 45:107–117.
- Ditto PH, Jacobson JA, Smucker WD, Danks JH, Fagerlin A. Context changes choices: a prospective study of the effects of hospitalization on life-sustaining treatment p. Med Decis Making 2006; 26:313–322.
- Lockhart LK, Ditto PH, Danks JH, Coppola KM, Smucker WD. The stability of older adults’ judgments of fates better and worse than death. Death Stud 2001; 25:299–317.
- Gjerdingen DK, Neff JA, Wang M, Chaloner K. Older persons’ opinions about life-sustaining procedures in the face of dementia. Arch Fam Med 1999; 8:421–425.
- Heap MJ, Munglani R, Klinck JR, Males AG. Elderly patients’ p concerning life-support treatment. Anaesthesia 1993; 48:1027–1033.
- Singer PA, Thiel EC, Naylor CD, et al. Life-sustaining treatment p of hemodialysis patients: implications for advance directives. J Am Soc Nephrol 1995; 6:1410–1417.
- Hofmann JC, Wenger NS, Davis RB, et al. Patient p for communication with physicians about end-of-life decisions. SUPPORT Investigators. Study to Understand Prognoses and Preference for Outcomes and Risks of Treatment. Ann Intern Med 1997; 127:1–12.
- Pinquart M, Sorensen S. Helping caregivers of persons with dementia: which interventions work and how large are their effects? Int Psychogeriatr 2006; 18:577–595.
- Robbins J, Gensler G, Hind J, et al. Comparison of 2 Interventions for liquid aspiration on pneumonia incidence: a randomized trial. Ann Intern Med 2008; 148:509–518.
- Walter LC, Covinsky KE. Cancer screening in elderly patients: a framework for individualized decision making. JAMA 2001; 285:2750–2756.
- Lee SJ, Lindquist K, Segal MR, Covinsky KE. Development and validation of a prognostic index for 4-year mortality in older adults. JAMA 2006; 295:801–808.
- Losey R, Messinger-Rapport BJ. At what age should we discontinue colon cancer screening in the elderly? Cleve Clin J Med 2007; 74:269–272.
- Larson EB, Shadlen MF, Wang L, et al. Survival after initial diagnosis of Alzheimer disease. Ann Intern Med 2004; 140:501–509.
- Suthers K, Kim JK, Crimmins E. Life expectancy with cognitive impairment in the older population of the United States. J Gerontol B Psychol Sci Soc Sci 2003; 58:S179–S186.
- Bloom HL, Shukrullah I, Cuellar JR, Lloyd MS, Dudley SC, Zafari AM. Long-term survival after successful inhospital cardiac arrest resuscitation. Am Heart J 2007; 153:831–836.
- Finucane TE, Harper GM. Attempting resuscitation in nursing homes: policy considerations. J Am Geriatr Soc 1999; 47:1261–1264.
- Pearlman R, Startks H, Cain K, Cole W, Rosengren D, Patrick D. Your Life, Your Choices. 2nd ed. Department of Veterans Affairs, National Center for Ethics in Health Care, 2007.
- Molloy DW. Let Me Decide. Hamilton, Ontario: Newgrange Press, 1996.
- Dunn PM, Schmidt TA, Carley MM, Donius M, Weinstein MA, Dull VT. A method to communicate patient p about medically indicated life-sustaining treatment in the out-of-hospital setting. J Am Geriatr Soc 1996; 44:785–791.
- Fried TR, O’Leary J, Van Ness P, Fraenkel L. Inconsistency over time in the p of older persons with advanced illness for life-sustaining treatment. J Am Geriatr Soc 2007; 55:1007–1014.
- Fried TR, Van Ness PH, Byers AL, Towle VR, O’Leary JR, Dubin JA. Changes in p for life-sustaining treatment among older persons with advanced illness. J Gen Intern Med 2007; 22:495–501.
- Diwan S, Hougham GW, Sachs GA. Strain experienced by caregivers of dementia patients receiving palliative care: findings from the Palliative Excellence in Alzheimer Care Efforts (PEACE) Program. J Palliat Med 2004; 7:797–807.
- Covinsky KE, Yaffe K. Dementia, prognosis, and the needs of patients and caregivers. Ann Intern Med 2004; 140:573–574.
- Shega JW, Levin A, Hougham GW, et al. Palliative Excellence in Alzheimer Care Efforts (PEACE): a program description. J Palliat Med 2003; 6:315–320.
- Center for Ethics in Health Care. Physician orders for life-sustaining treatment paradigm. www.ohsu.edu/ethics/polst/. Accessed March 9, 2009.
- Lee MA, Brummel-Smith K, Meyer J, Drew N, London MR. Physician orders for life-sustaining treatment (POLST): outcomes in a PACE program. Program of All-Inclusive Care for the Elderly. J Am Geriatr Soc 2000; 48:1219–1225.
- Meyers JL, Moore C, McGrory A, Sparr J, Ahern M. Physician orders for life-sustaining treatment form: honoring end-of-life directives for nursing home residents. J Gerontol Nurs 2004; 30:37–46.
- Tolle SW, Tilden VP, Nelson CA, Dunn PM. A prospective study of the efficacy of the physician order form for life-sustaining treatment. J Am Geriatr Soc 1998; 46:1097–1102.
- Cantor MD, Pearlman RA. Advance care planning in long-term care facilities. J Am Med Dir Assoc 2004; 5(suppl 2):S72–S80.
Mr. B., an 82-year-old retired accountant with hypertension, was diagnosed with early Alzheimer disease 6 years ago. He now needs supervision with bathing and dressing and no longer consistently recognizes family members. You are seeing him in the office today after a hospitalization for aspiration pneumonia, his second in the past 6 months.
In the hospital, a brain scan showed that atrophy had progressed and white-matter disease was more extensive than 3 years earlier. A barium swallow study showed esophageal dysmotility and aspiration. He was prescribed a “dysphagia diet,”1 which he dislikes.
Since returning home, he has been disoriented, he has been wandering about the house, and he has fallen several times. He has lost 10 pounds in 6 months. Because of his confusion, his wife cannot take him out, and she is exhausted caring for him.
Reviewing his medical record, you note that 10 years ago, Mr. B. completed a living will and designated his wife as his proxy decision-maker via a medical power of attorney document.
PLANNING IS OFTEN NEGLECTED
Many clinicians and older patients feel a strong need to document, in advance, the patient’s wishes regarding medical care in the event the patient becomes seriously ill and unable to participate in treatment decisions. Professional societies such as the American Geriatrics Society promote advance care planning,2 and some indices of the quality of medical care include whether advance directives have been discussed and completed.3
Yet, despite the high profile of advance care planning,4 few patients actually fill out advance directives,5 with completion rates that vary widely,6–8 sometimes by ethnicity and sex.9,10 Furthermore, in a crisis, these directives are seldom followed.11
In this paper, we recommend an approach to advance care planning for older adults that redirects the focus from “signing away” interventions such as dialysis, mechanical ventilation, and tube feeding. Instead, the focus is on the goals of care. We also advocate naming a surrogate decision-maker, since the medical power of attorney is more flexible and more widely applicable than the living will.
START BY LISTENING
A change in function resulting from disease progression, hospitalization, trauma, or other reasons is an ideal opportunity to introduce the process of advance care planning.
The first step is to find out how well the patient and family understand the patient’s relevant medical conditions, and what their expectations, hopes, and concerns are. This listening phase can provide insight into the patient’s values and goals and how much the patient and family want to engage in these discussions.
In matters of health behavior (such as advance care planning), people change only when they are ready to change.12,13 Thus, we advise physicians to defer extensive discussions of values and goals of care until patients and families are ready to listen, hear, and talk about these topics (often, after a change for the worse in prognosis).
And it is a process. Advance care directives are most likely to be set up and followed if the patient and doctor discuss this issue during multiple visits, rather than if the physician merely hands the patient a packet of forms and information.14–16
CASE CONTINUED: A PEG TUBE REFUSED
Mrs. B. says that Mr. B. is in good health except for his memory: he does not have a serious condition such as diabetes, heart failure, or cancer. While Mr. B. was in the hospital, the hospitalist recommended placing a percutaneous endoscopic gastrostomy (PEG) tube, but Mrs. B. declined the recommendation because her husband had a living will that specified “no artificially or technologically supplied nutrition or hydration.”
At this point, Mrs. B. begins to cry. She has slept poorly because of his wandering. Also, her two daughters do not support her refusal of the PEG tube.
Comment. This brief conversation illuminates knowledge deficits in Mrs. B.’s understanding of Alzheimer disease and the circumstances in which the living will applies. Although one could argue that Mr. B.’s Alzheimer disease has advanced to the point that he is likely to die of a complication of that condition, he is not likely to die in the near future. If he is not considered by law and his physician to be terminally ill or permanently unconscious, a living will likely does not offer guidance about artificial feeding.
LIMITATIONS OF A LIVING WILL
A living will, a commonly used advance directive, states that the patient does not wish to receive life-sustaining treatment in the event that he or she suffers an incurable, irreversible disease and cannot give informed consent, and it often lists specific treatments that the patient does not want. However, we believe that approaching the patient with a list of life-sustaining measures to accept or reject, before discussing goals of care and prognosis, puts the cart before the horse. This approach threatens to distract from the need to ascertain values and offer appropriate care. Additionally, a living will is active only within a very limited scenario and does not address relatively routine but important decisions in a person’s care.
All ‘terminal illness’ isn’t the same
A living will goes into effect only if the patient either enters a permanent vegetative state following an event such as cardiac arrest or severe brain trauma, or is diagnosed with a terminal illness such as metastatic cancer, and lacks decision-making capacity.
But what is terminal illness? The definition differs from state to state, but it is generally defined as an irreversible condition leading to death in a relatively short time. The time may not be specified, as in Florida statute 765. In contrast, Ohio Revised Code 2133.01(AA) uses the phrase “relatively short,” while other states specify a time, such as within 6 months (Texas Health and Safety Code 166.002). The Medicare hospice benefit also carries a short time limit, usually less than 6 months.
The middle panel in Figure 1 depicts a more typical decline from serial organ insults such as stroke followed by infection from aspiration or followed by falls. Older adults with dementia or with multiple progressive diseases such as heart failure, diabetes, hypertension, or cancer decline in a trajectory such as in the bottom panel of Figure 1.
A living will might not be activated in the latter two scenarios until years into the condition because the patient would not be considered terminally ill—by state law, by the health care provider, or even by the patient.
The living will does not address routine interventions
In most states, living wills address only life-sustaining treatments such as dialysis, mechanical ventilation, and medically supplied nutrition and hydration. Living wills do not address relatively common diseases in older adults that could cause severe debility, such as a major stroke or advanced dementia.
If an older patient has dementia, a living will is unlikely to provide guidance about interventions such as intubation to get through an episode of potentially reversible respiratory failure, a feeding tube to correct weight loss, or cardiac catheterization or bypass surgery to treat angina. Yet these important decisions often arise as function declines and comorbidities progress.
Patients may change their minds
Many older adults are reluctant to sign documents to “micromanage” their future care if they should become ill.19 Many people change their mind as the situation changes.11,20,21 Although few claim they would want burdensome interventions if they had dementia22 or if their prognosis were poor,23 patients may tolerate more burdensome interventions if they are already receiving treatments for chronic illnesses such as end-stage renal disease.24
Thus, a living will may help if unexpected trauma occurs in a healthy person, but not so much if chronic illness progresses over a period of years.
Advance directives may not be honored
Even if completed, written advance directives may not be followed, for a variety of reasons. Physicians may not know the patient has a living will, and fewer than one-third of people who actually complete an advance directive have discussed its content with a physician.25 The people named as surrogate decision-makers may not know the patient’s wishes. Family members may disagree with the goals and plan of care and may interfere with implementation of the advance care plan. A patient may see multiple physicians at different institutions who may not communicate with each other about the patient’s wishes. Also, physicians and patients may interpret terms such as “terminally ill” differently, making it difficult to translate the documents into an action plan.
CASE CONTINUED: RELIEVING CAREGIVER STRESS
Returning to Mr. B., your first goal is to address care issues, including caregiver stress. Skilled services in the home are appropriate for him at this time (and Medicare will pay for them) because he is still homebound. These services could include physical therapy, occupational therapy, and speech (swallowing) therapy. A home care agency may also provide an aide for a few weeks to assist with bathing and other personal needs.
You strongly recommend that the family (including both daughters) participate in the Alzheimer’s Association educational programs. You recommend that Mrs. B. locate an adult day care program now so that when Mr. B. completes his home therapy course and is no longer homebound, he may attend. Day care would provide a therapeutic environment for him and respite for her.
You request that the home care agency provide a social worker to advise her on community resources. Meta-analysis suggests that structured, multicomponent interventions with caregivers of demented patients reduce several types of caregiver burden and delay institutionalization.26
He improves with conservative measures
Three weeks later, Mr. B. is sleeping better and has stopped wandering. However, he dislikes the thickened liquids required by the dysphagia diet and has lost another 2 pounds. If his beverages are not thickened, he coughs profusely when he swallows. His daughters are still pressuring Mrs. B. for a PEG tube; one of them has angrily asserted that the doctors are going to allow her father to die.
You explain the burdens of PEG tubes: surgical risks, continued aspiration, disrupted bowel habits, the risk of the tube being accidentally or intentionally dislodged by the patient, and special binders (which may be uncomfortable) or restraints (which may cause further functional decline) that may be necessary to prevent this complication.
You request that the speech therapist work with the patient more aggressively in the use of swallowing techniques such as the chin tuck, which may be at least as effective as thickeners in preventing both aspiration pneumonia and dehydration.27 The therapist will need to include Mrs. B. in these sessions, since she will be Mr. B.’s coach at mealtime.
With more aggressive speech therapy, the patient’s weight stabilizes over the next 4 weeks. He is in day care 3 days a week, and Mrs. B. is more rested and relaxed.
Cardiopulmonary resuscitation
You continue the advance care planning discussion and suggest that if Mr. B. aspirates, is hospitalized again, and declines further care, it would be helpful to delineate instructions for resuscitation. Right now, although his Alzheimer disease is advanced, he is not clearly terminal. Thus, his living will does not strictly apply and provides limited guidance about intubation, cardiopulmonary resuscitation (CPR), or medically supplied nutrition and hydration. However, because Mrs. B. is his agent in the medical power of attorney, this document enables her to make a wide spectrum of treatment decisions on his behalf.
Mrs. B. asks about her husband’s prognosis and why CPR would not be helpful.
Comment. Further discussion with her could be guided by an estimate of Mr. B.’s prognosis. Function-based tools28,29 may also be useful. For example,28,30 an 80-year-old man with high functional status might have a life expectancy of more than 10 years. Mr. B., with multiple medical problems and declining function, would have an estimated life expectancy of approximately 3 years. Even without specifically categorizing function, impaired cognition by itself predicted a shorter life expectancy in population-based studies.31,32
Regarding CPR, patients and families may overestimate successful outcomes. A recent study33 of 10 years of outcomes of in-hospital cardiac arrest found that only 6.6% of patients survived to discharge. The average age of the survivors was 59 years, and fewer than half of them survived 3 years after cardiac arrest. In eight studies of CPR outcomes in nursing homes,34 three studies had no survivors, and all but one study had a survival rate below 5%.
PROVIDING APPROPRIATE CARE, NOT LIMITING TREATMENTS
In the case of Mr. B., as in many situations encountered with older patients, written advance directives provide little help or guidance. Instead, we recommend a model of advance care planning that takes place during multiple office visits over time, and that maintains a focus on providing appropriate care rather than on limiting life-sustaining treatments. We recommend providing estimates of prognosis and CPR outcomes when the family appeares ready to hear them. This approach should result in a care-oriented process while moving the family towards decisions regarding artificial feeding and CPR.
All patients, particularly those unwilling or unable to participate in advance care planning, are encouraged to identify one or more surrogate decision-makers and articulate how much flexibility that person should be given in important health care decisions. The medical power of attorney can be activated any time the patient lacks decision-making capacity and deactivated when decision-making capacity returns.38,39
As in the case of Mr. B., a tailored approach to advance care planning requires clinicians to estimate life expectancy (more than 5 years, less than 5 years, or less than 1 year) and to determine the patient’s and the family’s readiness to focus on a values-oriented and goal-oriented care plan. Some patients are not receptive to advance care planning, and clinical time and effort are optimized by providing the right amount of information to patients when they are ready to receive it.
For relatively healthy older adults
Figure 2 is the algorithm for older patients who are expected to live at least 5 years, ie, who are relatively healthy and functional. Patients with little or no interest in advance care planning can be asked about it annually, or sooner if their medical condition changes. Patients with limited interest can be given written information, specifically living will and medical power of attorney documents recognized in their state. Patients more open to advance care planning can be offered a values history form (Table 1), Web sites, and educational materials, with a plan to discuss them at future appointments.
Periodic reevaluation of values and goals of care is important. Patients may assert that particular interventions (eg, a PEG tube or dialysis) are “worse than death” when they are healthy, but they may change their views over time.21 Additionally, although a recent hospitalization or a decline in function may predispose patients to want to limit life-sustaining treatments, they may return to their earlier values and wishes a few months later, particularly if their medical condition stabilizes. 20 Values and decisions should be reassessed not only when medical conditions deteriorate, but also when they improve.
For chronically ill patients
Caregiver stress is important to identify and address, since caregivers often neglect themselves.40–42
For terminally ill patients
In this situation, patients and families need information about community resources that can assist them in the home. Some older adults with cognitive impairment may be exploited or neglect themselves, and referral to an adult protective services agency may be needed.
Treatment burden, particularly due to multiple prescribed medications, may be high and should be reassessed in light of the goals of treatment. Polypharmacy reduction is especially important at this stage in the illness, since the goals of care may be different than when the medications were prescribed.
Physical or psychosocial symptoms may be the cue to bring up the topic of palliative care. If the patient is expected to live less than 6 months, hospice referral is appropriate. With either palliative care or hospice, the focus of attention shifts explicitly from curing the disease to managing symptoms, and from the patient to the patient-family dyad. Interventions such as CPR and ventilatory support should be discussed and information from Table 2 provided to the patient and family.
Complete advance care planning incorporates taking a values history, estimating life expectancy, determining physical, psychosocial and spiritual needs, clarifying treatment goals, and estimating manageable treatment burden. Offering statistics on CPR and providing state-specific living will and medical power of attorney documents are important but are only one facet of effective advance care planning. In fact, shifting the emphasis of advance care planning from statistics and forms to values and goals of care may help in developing a more comprehensive care plan.
Goals of care range from curing the disease (with aggressive therapy, which may be burdensome) to simply improving function or decreasing pain. In the latter case, one may be able to discontinue some of the patient’s drugs, utilize medical and community resources more effectively, and better meet the patient’s needs.
Woven through all these discussions should be reassurance that the plan can be revisited and possibly revised, and that the physician will be there to help with those decisions.
For acutely ill patients in the hospital
Episodic, staged advance care planning is appropriate not only in the office but also in other settings such as assisted living and nursing facilities.
In the hospital, however, a different approach is needed, since patients are usually admitted because of an acute illness or sudden functional decline, or both. Decisions about technological interventions such as CPR, mechanical ventilation, or dialysis may be needed urgently. Often, patients are unable to provide guidance to physicians during acute illness because of delirium and other impediments. Developing a plan for care in the hospital may require urgent family meetings. However, if a surrogate decision-maker is in place, and if the patient has already participated in some form of advance care planning as an outpatient, the values and goals of care previously identified can contribute to decision-making during hospitalization.
As mentioned above, fragmentation of health care across providers and health care systems may limit the effectiveness of office-based advance care planning. It may be reasonable to train office staff to place advance care planning documentation in easily accessible sections of the patient’s medical record and to forward these to specialists involved in a patient’s care.
The patient and family should be encouraged and empowered to help with this process and should have updated advance care planning documentation readily available. In some states, comprehensive medical order sets, especially for end-of-life care, are portable across care settings and address CPR, medically supplied nutrition, hospital transfer, and antibiotic treatment.43
Research suggests that health care systems are more likely to comply with patients’ end-of-life preferences when portable medical order forms are developed and disseminated.44–44 Ultimately, major changes in health care delivery, including universal electronic health records, may be needed to implement and communicate patients’ advance care planning preferences across settings.
Mr. B., an 82-year-old retired accountant with hypertension, was diagnosed with early Alzheimer disease 6 years ago. He now needs supervision with bathing and dressing and no longer consistently recognizes family members. You are seeing him in the office today after a hospitalization for aspiration pneumonia, his second in the past 6 months.
In the hospital, a brain scan showed that atrophy had progressed and white-matter disease was more extensive than 3 years earlier. A barium swallow study showed esophageal dysmotility and aspiration. He was prescribed a “dysphagia diet,”1 which he dislikes.
Since returning home, he has been disoriented, he has been wandering about the house, and he has fallen several times. He has lost 10 pounds in 6 months. Because of his confusion, his wife cannot take him out, and she is exhausted caring for him.
Reviewing his medical record, you note that 10 years ago, Mr. B. completed a living will and designated his wife as his proxy decision-maker via a medical power of attorney document.
PLANNING IS OFTEN NEGLECTED
Many clinicians and older patients feel a strong need to document, in advance, the patient’s wishes regarding medical care in the event the patient becomes seriously ill and unable to participate in treatment decisions. Professional societies such as the American Geriatrics Society promote advance care planning,2 and some indices of the quality of medical care include whether advance directives have been discussed and completed.3
Yet, despite the high profile of advance care planning,4 few patients actually fill out advance directives,5 with completion rates that vary widely,6–8 sometimes by ethnicity and sex.9,10 Furthermore, in a crisis, these directives are seldom followed.11
In this paper, we recommend an approach to advance care planning for older adults that redirects the focus from “signing away” interventions such as dialysis, mechanical ventilation, and tube feeding. Instead, the focus is on the goals of care. We also advocate naming a surrogate decision-maker, since the medical power of attorney is more flexible and more widely applicable than the living will.
START BY LISTENING
A change in function resulting from disease progression, hospitalization, trauma, or other reasons is an ideal opportunity to introduce the process of advance care planning.
The first step is to find out how well the patient and family understand the patient’s relevant medical conditions, and what their expectations, hopes, and concerns are. This listening phase can provide insight into the patient’s values and goals and how much the patient and family want to engage in these discussions.
In matters of health behavior (such as advance care planning), people change only when they are ready to change.12,13 Thus, we advise physicians to defer extensive discussions of values and goals of care until patients and families are ready to listen, hear, and talk about these topics (often, after a change for the worse in prognosis).
And it is a process. Advance care directives are most likely to be set up and followed if the patient and doctor discuss this issue during multiple visits, rather than if the physician merely hands the patient a packet of forms and information.14–16
CASE CONTINUED: A PEG TUBE REFUSED
Mrs. B. says that Mr. B. is in good health except for his memory: he does not have a serious condition such as diabetes, heart failure, or cancer. While Mr. B. was in the hospital, the hospitalist recommended placing a percutaneous endoscopic gastrostomy (PEG) tube, but Mrs. B. declined the recommendation because her husband had a living will that specified “no artificially or technologically supplied nutrition or hydration.”
At this point, Mrs. B. begins to cry. She has slept poorly because of his wandering. Also, her two daughters do not support her refusal of the PEG tube.
Comment. This brief conversation illuminates knowledge deficits in Mrs. B.’s understanding of Alzheimer disease and the circumstances in which the living will applies. Although one could argue that Mr. B.’s Alzheimer disease has advanced to the point that he is likely to die of a complication of that condition, he is not likely to die in the near future. If he is not considered by law and his physician to be terminally ill or permanently unconscious, a living will likely does not offer guidance about artificial feeding.
LIMITATIONS OF A LIVING WILL
A living will, a commonly used advance directive, states that the patient does not wish to receive life-sustaining treatment in the event that he or she suffers an incurable, irreversible disease and cannot give informed consent, and it often lists specific treatments that the patient does not want. However, we believe that approaching the patient with a list of life-sustaining measures to accept or reject, before discussing goals of care and prognosis, puts the cart before the horse. This approach threatens to distract from the need to ascertain values and offer appropriate care. Additionally, a living will is active only within a very limited scenario and does not address relatively routine but important decisions in a person’s care.
All ‘terminal illness’ isn’t the same
A living will goes into effect only if the patient either enters a permanent vegetative state following an event such as cardiac arrest or severe brain trauma, or is diagnosed with a terminal illness such as metastatic cancer, and lacks decision-making capacity.
But what is terminal illness? The definition differs from state to state, but it is generally defined as an irreversible condition leading to death in a relatively short time. The time may not be specified, as in Florida statute 765. In contrast, Ohio Revised Code 2133.01(AA) uses the phrase “relatively short,” while other states specify a time, such as within 6 months (Texas Health and Safety Code 166.002). The Medicare hospice benefit also carries a short time limit, usually less than 6 months.
The middle panel in Figure 1 depicts a more typical decline from serial organ insults such as stroke followed by infection from aspiration or followed by falls. Older adults with dementia or with multiple progressive diseases such as heart failure, diabetes, hypertension, or cancer decline in a trajectory such as in the bottom panel of Figure 1.
A living will might not be activated in the latter two scenarios until years into the condition because the patient would not be considered terminally ill—by state law, by the health care provider, or even by the patient.
The living will does not address routine interventions
In most states, living wills address only life-sustaining treatments such as dialysis, mechanical ventilation, and medically supplied nutrition and hydration. Living wills do not address relatively common diseases in older adults that could cause severe debility, such as a major stroke or advanced dementia.
If an older patient has dementia, a living will is unlikely to provide guidance about interventions such as intubation to get through an episode of potentially reversible respiratory failure, a feeding tube to correct weight loss, or cardiac catheterization or bypass surgery to treat angina. Yet these important decisions often arise as function declines and comorbidities progress.
Patients may change their minds
Many older adults are reluctant to sign documents to “micromanage” their future care if they should become ill.19 Many people change their mind as the situation changes.11,20,21 Although few claim they would want burdensome interventions if they had dementia22 or if their prognosis were poor,23 patients may tolerate more burdensome interventions if they are already receiving treatments for chronic illnesses such as end-stage renal disease.24
Thus, a living will may help if unexpected trauma occurs in a healthy person, but not so much if chronic illness progresses over a period of years.
Advance directives may not be honored
Even if completed, written advance directives may not be followed, for a variety of reasons. Physicians may not know the patient has a living will, and fewer than one-third of people who actually complete an advance directive have discussed its content with a physician.25 The people named as surrogate decision-makers may not know the patient’s wishes. Family members may disagree with the goals and plan of care and may interfere with implementation of the advance care plan. A patient may see multiple physicians at different institutions who may not communicate with each other about the patient’s wishes. Also, physicians and patients may interpret terms such as “terminally ill” differently, making it difficult to translate the documents into an action plan.
CASE CONTINUED: RELIEVING CAREGIVER STRESS
Returning to Mr. B., your first goal is to address care issues, including caregiver stress. Skilled services in the home are appropriate for him at this time (and Medicare will pay for them) because he is still homebound. These services could include physical therapy, occupational therapy, and speech (swallowing) therapy. A home care agency may also provide an aide for a few weeks to assist with bathing and other personal needs.
You strongly recommend that the family (including both daughters) participate in the Alzheimer’s Association educational programs. You recommend that Mrs. B. locate an adult day care program now so that when Mr. B. completes his home therapy course and is no longer homebound, he may attend. Day care would provide a therapeutic environment for him and respite for her.
You request that the home care agency provide a social worker to advise her on community resources. Meta-analysis suggests that structured, multicomponent interventions with caregivers of demented patients reduce several types of caregiver burden and delay institutionalization.26
He improves with conservative measures
Three weeks later, Mr. B. is sleeping better and has stopped wandering. However, he dislikes the thickened liquids required by the dysphagia diet and has lost another 2 pounds. If his beverages are not thickened, he coughs profusely when he swallows. His daughters are still pressuring Mrs. B. for a PEG tube; one of them has angrily asserted that the doctors are going to allow her father to die.
You explain the burdens of PEG tubes: surgical risks, continued aspiration, disrupted bowel habits, the risk of the tube being accidentally or intentionally dislodged by the patient, and special binders (which may be uncomfortable) or restraints (which may cause further functional decline) that may be necessary to prevent this complication.
You request that the speech therapist work with the patient more aggressively in the use of swallowing techniques such as the chin tuck, which may be at least as effective as thickeners in preventing both aspiration pneumonia and dehydration.27 The therapist will need to include Mrs. B. in these sessions, since she will be Mr. B.’s coach at mealtime.
With more aggressive speech therapy, the patient’s weight stabilizes over the next 4 weeks. He is in day care 3 days a week, and Mrs. B. is more rested and relaxed.
Cardiopulmonary resuscitation
You continue the advance care planning discussion and suggest that if Mr. B. aspirates, is hospitalized again, and declines further care, it would be helpful to delineate instructions for resuscitation. Right now, although his Alzheimer disease is advanced, he is not clearly terminal. Thus, his living will does not strictly apply and provides limited guidance about intubation, cardiopulmonary resuscitation (CPR), or medically supplied nutrition and hydration. However, because Mrs. B. is his agent in the medical power of attorney, this document enables her to make a wide spectrum of treatment decisions on his behalf.
Mrs. B. asks about her husband’s prognosis and why CPR would not be helpful.
Comment. Further discussion with her could be guided by an estimate of Mr. B.’s prognosis. Function-based tools28,29 may also be useful. For example,28,30 an 80-year-old man with high functional status might have a life expectancy of more than 10 years. Mr. B., with multiple medical problems and declining function, would have an estimated life expectancy of approximately 3 years. Even without specifically categorizing function, impaired cognition by itself predicted a shorter life expectancy in population-based studies.31,32
Regarding CPR, patients and families may overestimate successful outcomes. A recent study33 of 10 years of outcomes of in-hospital cardiac arrest found that only 6.6% of patients survived to discharge. The average age of the survivors was 59 years, and fewer than half of them survived 3 years after cardiac arrest. In eight studies of CPR outcomes in nursing homes,34 three studies had no survivors, and all but one study had a survival rate below 5%.
PROVIDING APPROPRIATE CARE, NOT LIMITING TREATMENTS
In the case of Mr. B., as in many situations encountered with older patients, written advance directives provide little help or guidance. Instead, we recommend a model of advance care planning that takes place during multiple office visits over time, and that maintains a focus on providing appropriate care rather than on limiting life-sustaining treatments. We recommend providing estimates of prognosis and CPR outcomes when the family appeares ready to hear them. This approach should result in a care-oriented process while moving the family towards decisions regarding artificial feeding and CPR.
All patients, particularly those unwilling or unable to participate in advance care planning, are encouraged to identify one or more surrogate decision-makers and articulate how much flexibility that person should be given in important health care decisions. The medical power of attorney can be activated any time the patient lacks decision-making capacity and deactivated when decision-making capacity returns.38,39
As in the case of Mr. B., a tailored approach to advance care planning requires clinicians to estimate life expectancy (more than 5 years, less than 5 years, or less than 1 year) and to determine the patient’s and the family’s readiness to focus on a values-oriented and goal-oriented care plan. Some patients are not receptive to advance care planning, and clinical time and effort are optimized by providing the right amount of information to patients when they are ready to receive it.
For relatively healthy older adults
Figure 2 is the algorithm for older patients who are expected to live at least 5 years, ie, who are relatively healthy and functional. Patients with little or no interest in advance care planning can be asked about it annually, or sooner if their medical condition changes. Patients with limited interest can be given written information, specifically living will and medical power of attorney documents recognized in their state. Patients more open to advance care planning can be offered a values history form (Table 1), Web sites, and educational materials, with a plan to discuss them at future appointments.
Periodic reevaluation of values and goals of care is important. Patients may assert that particular interventions (eg, a PEG tube or dialysis) are “worse than death” when they are healthy, but they may change their views over time.21 Additionally, although a recent hospitalization or a decline in function may predispose patients to want to limit life-sustaining treatments, they may return to their earlier values and wishes a few months later, particularly if their medical condition stabilizes. 20 Values and decisions should be reassessed not only when medical conditions deteriorate, but also when they improve.
For chronically ill patients
Caregiver stress is important to identify and address, since caregivers often neglect themselves.40–42
For terminally ill patients
In this situation, patients and families need information about community resources that can assist them in the home. Some older adults with cognitive impairment may be exploited or neglect themselves, and referral to an adult protective services agency may be needed.
Treatment burden, particularly due to multiple prescribed medications, may be high and should be reassessed in light of the goals of treatment. Polypharmacy reduction is especially important at this stage in the illness, since the goals of care may be different than when the medications were prescribed.
Physical or psychosocial symptoms may be the cue to bring up the topic of palliative care. If the patient is expected to live less than 6 months, hospice referral is appropriate. With either palliative care or hospice, the focus of attention shifts explicitly from curing the disease to managing symptoms, and from the patient to the patient-family dyad. Interventions such as CPR and ventilatory support should be discussed and information from Table 2 provided to the patient and family.
Complete advance care planning incorporates taking a values history, estimating life expectancy, determining physical, psychosocial and spiritual needs, clarifying treatment goals, and estimating manageable treatment burden. Offering statistics on CPR and providing state-specific living will and medical power of attorney documents are important but are only one facet of effective advance care planning. In fact, shifting the emphasis of advance care planning from statistics and forms to values and goals of care may help in developing a more comprehensive care plan.
Goals of care range from curing the disease (with aggressive therapy, which may be burdensome) to simply improving function or decreasing pain. In the latter case, one may be able to discontinue some of the patient’s drugs, utilize medical and community resources more effectively, and better meet the patient’s needs.
Woven through all these discussions should be reassurance that the plan can be revisited and possibly revised, and that the physician will be there to help with those decisions.
For acutely ill patients in the hospital
Episodic, staged advance care planning is appropriate not only in the office but also in other settings such as assisted living and nursing facilities.
In the hospital, however, a different approach is needed, since patients are usually admitted because of an acute illness or sudden functional decline, or both. Decisions about technological interventions such as CPR, mechanical ventilation, or dialysis may be needed urgently. Often, patients are unable to provide guidance to physicians during acute illness because of delirium and other impediments. Developing a plan for care in the hospital may require urgent family meetings. However, if a surrogate decision-maker is in place, and if the patient has already participated in some form of advance care planning as an outpatient, the values and goals of care previously identified can contribute to decision-making during hospitalization.
As mentioned above, fragmentation of health care across providers and health care systems may limit the effectiveness of office-based advance care planning. It may be reasonable to train office staff to place advance care planning documentation in easily accessible sections of the patient’s medical record and to forward these to specialists involved in a patient’s care.
The patient and family should be encouraged and empowered to help with this process and should have updated advance care planning documentation readily available. In some states, comprehensive medical order sets, especially for end-of-life care, are portable across care settings and address CPR, medically supplied nutrition, hospital transfer, and antibiotic treatment.43
Research suggests that health care systems are more likely to comply with patients’ end-of-life preferences when portable medical order forms are developed and disseminated.44–44 Ultimately, major changes in health care delivery, including universal electronic health records, may be needed to implement and communicate patients’ advance care planning preferences across settings.
- National Dysphagia Diet Task Force. National Dysphagia Diet: Standardization for Optimal Care. Chicago, IL: American Dietetic Association, 2002.
- Nusbaum N, Goldstein M. American Geriatrics Society. The Patient Education Forum. Advance Directives, 2008. www.americangeriatrics.org/education/forum/advance_dir.shtml. Accessed March 9, 2009.
- Wenger NS, Roth CP, Shekelle PA; COVE Investigators. Introduction to the assessing care of vulnerable elders–3 quality indicator measurement set. J Am Geriatr Soc 2007; 55(suppl 2):S247–S252.
- Emanuel LL, Danis M, Pearlman RA, Singer PA. Advance care planning as a process: structuring the discussions in practice. J Am Geriatr Soc 1995; 43:440–446.
- Teno J, Lynn J, Wenger N, et al. Advance directives for seriously ill hospitalized patients: effectiveness with the patient self-determination act and the SUPPORT intervention. SUPPORT Investigators. Study to Understand Prognoses and P for Outcomes and Risks of Treatment. J Am Geriatr Soc 1997; 45:500–507.
- Hammes BJ, Rooney BL. Death and end-of-life planning in one midwestern community. Arch Intern Med 1998; 158:383–390.
- Gordon NP, Shade SB. Advance directives are more likely among seniors asked about end-of-life care p. Arch Intern Med 1999; 159:701–704.
- Morrison RS, Meier DE. High rates of advance care planning in New York City’s elderly population. Arch Intern Med 2004; 164:2421–2426.
- Perkins HS, Geppert CMA, Gonzales A, Cortez JD, Hazuda HP. Cross-cultural similarities and differences in attitudes about advance care planning. J Gen Intern Med 2002; 17:48–57.
- Perkins HS, Cortez JD, Hazuda HP. Advance care planning: does patient gender make a difference? Am J Med Sci 2004; 327:25–32.
- The SUPPORT Principal Investigators. A controlled trial to improve care for seriously ill hospitalized patients. Study to Understand Prognoses and P for Outcomes and Risks of Treatments (SUPPORT). JAMA 1995; 274:1591–1598.
- Prochaska JO, DiClemente CC, Norcross JC. In search of how people change. Applications to addictive behaviors. Am Psychol 1992; 47:1102–1114.
- Nigg CR, Burbank PM, Padula C, et al. Stages of change across ten health risk behaviors for older adults. Gerontologist 1999; 39:473–482.
- Patel RV, Sinuff T, Cook DJ. Influencing advance directive completion rates in non-terminally ill patients: a systematic review. J Crit Care 2004; 19:1–9.
- Hanson LC, Earp JA, Garrett J, Menon M, Danis M. Community physicians who provide terminal care. Arch Intern Med 1999; 159:1133–1138.
- Ramsaroop SD, Reid MC, Adelman RD. Completing an advance directive in the primary care setting: what do we need for success? J Am Geriatr Soc 2007; 55:277–283.
- Lynn J. Living long in fragile health: the new demographics shape end of life care. In:Jennings B, Kaebnick G, Murray T, editors. Improving End of Life Care: Why Has It Been So Difficult. Hastings Center Report November–December 2005: Special No:S14–S18.
- Beaumont JG, Kenealy PM. Incidence and prevalence of the vegetative and minimally conscious states. Neuropsychol Rehabil 2005; 15:184–189.
- Hawkins NA, Ditto PH, Danks JH, Smucker WD. Micromanaging death: process p, values, and goals in end-of-life medical decision making. Gerontologist 2005; 45:107–117.
- Ditto PH, Jacobson JA, Smucker WD, Danks JH, Fagerlin A. Context changes choices: a prospective study of the effects of hospitalization on life-sustaining treatment p. Med Decis Making 2006; 26:313–322.
- Lockhart LK, Ditto PH, Danks JH, Coppola KM, Smucker WD. The stability of older adults’ judgments of fates better and worse than death. Death Stud 2001; 25:299–317.
- Gjerdingen DK, Neff JA, Wang M, Chaloner K. Older persons’ opinions about life-sustaining procedures in the face of dementia. Arch Fam Med 1999; 8:421–425.
- Heap MJ, Munglani R, Klinck JR, Males AG. Elderly patients’ p concerning life-support treatment. Anaesthesia 1993; 48:1027–1033.
- Singer PA, Thiel EC, Naylor CD, et al. Life-sustaining treatment p of hemodialysis patients: implications for advance directives. J Am Soc Nephrol 1995; 6:1410–1417.
- Hofmann JC, Wenger NS, Davis RB, et al. Patient p for communication with physicians about end-of-life decisions. SUPPORT Investigators. Study to Understand Prognoses and Preference for Outcomes and Risks of Treatment. Ann Intern Med 1997; 127:1–12.
- Pinquart M, Sorensen S. Helping caregivers of persons with dementia: which interventions work and how large are their effects? Int Psychogeriatr 2006; 18:577–595.
- Robbins J, Gensler G, Hind J, et al. Comparison of 2 Interventions for liquid aspiration on pneumonia incidence: a randomized trial. Ann Intern Med 2008; 148:509–518.
- Walter LC, Covinsky KE. Cancer screening in elderly patients: a framework for individualized decision making. JAMA 2001; 285:2750–2756.
- Lee SJ, Lindquist K, Segal MR, Covinsky KE. Development and validation of a prognostic index for 4-year mortality in older adults. JAMA 2006; 295:801–808.
- Losey R, Messinger-Rapport BJ. At what age should we discontinue colon cancer screening in the elderly? Cleve Clin J Med 2007; 74:269–272.
- Larson EB, Shadlen MF, Wang L, et al. Survival after initial diagnosis of Alzheimer disease. Ann Intern Med 2004; 140:501–509.
- Suthers K, Kim JK, Crimmins E. Life expectancy with cognitive impairment in the older population of the United States. J Gerontol B Psychol Sci Soc Sci 2003; 58:S179–S186.
- Bloom HL, Shukrullah I, Cuellar JR, Lloyd MS, Dudley SC, Zafari AM. Long-term survival after successful inhospital cardiac arrest resuscitation. Am Heart J 2007; 153:831–836.
- Finucane TE, Harper GM. Attempting resuscitation in nursing homes: policy considerations. J Am Geriatr Soc 1999; 47:1261–1264.
- Pearlman R, Startks H, Cain K, Cole W, Rosengren D, Patrick D. Your Life, Your Choices. 2nd ed. Department of Veterans Affairs, National Center for Ethics in Health Care, 2007.
- Molloy DW. Let Me Decide. Hamilton, Ontario: Newgrange Press, 1996.
- Dunn PM, Schmidt TA, Carley MM, Donius M, Weinstein MA, Dull VT. A method to communicate patient p about medically indicated life-sustaining treatment in the out-of-hospital setting. J Am Geriatr Soc 1996; 44:785–791.
- Fried TR, O’Leary J, Van Ness P, Fraenkel L. Inconsistency over time in the p of older persons with advanced illness for life-sustaining treatment. J Am Geriatr Soc 2007; 55:1007–1014.
- Fried TR, Van Ness PH, Byers AL, Towle VR, O’Leary JR, Dubin JA. Changes in p for life-sustaining treatment among older persons with advanced illness. J Gen Intern Med 2007; 22:495–501.
- Diwan S, Hougham GW, Sachs GA. Strain experienced by caregivers of dementia patients receiving palliative care: findings from the Palliative Excellence in Alzheimer Care Efforts (PEACE) Program. J Palliat Med 2004; 7:797–807.
- Covinsky KE, Yaffe K. Dementia, prognosis, and the needs of patients and caregivers. Ann Intern Med 2004; 140:573–574.
- Shega JW, Levin A, Hougham GW, et al. Palliative Excellence in Alzheimer Care Efforts (PEACE): a program description. J Palliat Med 2003; 6:315–320.
- Center for Ethics in Health Care. Physician orders for life-sustaining treatment paradigm. www.ohsu.edu/ethics/polst/. Accessed March 9, 2009.
- Lee MA, Brummel-Smith K, Meyer J, Drew N, London MR. Physician orders for life-sustaining treatment (POLST): outcomes in a PACE program. Program of All-Inclusive Care for the Elderly. J Am Geriatr Soc 2000; 48:1219–1225.
- Meyers JL, Moore C, McGrory A, Sparr J, Ahern M. Physician orders for life-sustaining treatment form: honoring end-of-life directives for nursing home residents. J Gerontol Nurs 2004; 30:37–46.
- Tolle SW, Tilden VP, Nelson CA, Dunn PM. A prospective study of the efficacy of the physician order form for life-sustaining treatment. J Am Geriatr Soc 1998; 46:1097–1102.
- Cantor MD, Pearlman RA. Advance care planning in long-term care facilities. J Am Med Dir Assoc 2004; 5(suppl 2):S72–S80.
- National Dysphagia Diet Task Force. National Dysphagia Diet: Standardization for Optimal Care. Chicago, IL: American Dietetic Association, 2002.
- Nusbaum N, Goldstein M. American Geriatrics Society. The Patient Education Forum. Advance Directives, 2008. www.americangeriatrics.org/education/forum/advance_dir.shtml. Accessed March 9, 2009.
- Wenger NS, Roth CP, Shekelle PA; COVE Investigators. Introduction to the assessing care of vulnerable elders–3 quality indicator measurement set. J Am Geriatr Soc 2007; 55(suppl 2):S247–S252.
- Emanuel LL, Danis M, Pearlman RA, Singer PA. Advance care planning as a process: structuring the discussions in practice. J Am Geriatr Soc 1995; 43:440–446.
- Teno J, Lynn J, Wenger N, et al. Advance directives for seriously ill hospitalized patients: effectiveness with the patient self-determination act and the SUPPORT intervention. SUPPORT Investigators. Study to Understand Prognoses and P for Outcomes and Risks of Treatment. J Am Geriatr Soc 1997; 45:500–507.
- Hammes BJ, Rooney BL. Death and end-of-life planning in one midwestern community. Arch Intern Med 1998; 158:383–390.
- Gordon NP, Shade SB. Advance directives are more likely among seniors asked about end-of-life care p. Arch Intern Med 1999; 159:701–704.
- Morrison RS, Meier DE. High rates of advance care planning in New York City’s elderly population. Arch Intern Med 2004; 164:2421–2426.
- Perkins HS, Geppert CMA, Gonzales A, Cortez JD, Hazuda HP. Cross-cultural similarities and differences in attitudes about advance care planning. J Gen Intern Med 2002; 17:48–57.
- Perkins HS, Cortez JD, Hazuda HP. Advance care planning: does patient gender make a difference? Am J Med Sci 2004; 327:25–32.
- The SUPPORT Principal Investigators. A controlled trial to improve care for seriously ill hospitalized patients. Study to Understand Prognoses and P for Outcomes and Risks of Treatments (SUPPORT). JAMA 1995; 274:1591–1598.
- Prochaska JO, DiClemente CC, Norcross JC. In search of how people change. Applications to addictive behaviors. Am Psychol 1992; 47:1102–1114.
- Nigg CR, Burbank PM, Padula C, et al. Stages of change across ten health risk behaviors for older adults. Gerontologist 1999; 39:473–482.
- Patel RV, Sinuff T, Cook DJ. Influencing advance directive completion rates in non-terminally ill patients: a systematic review. J Crit Care 2004; 19:1–9.
- Hanson LC, Earp JA, Garrett J, Menon M, Danis M. Community physicians who provide terminal care. Arch Intern Med 1999; 159:1133–1138.
- Ramsaroop SD, Reid MC, Adelman RD. Completing an advance directive in the primary care setting: what do we need for success? J Am Geriatr Soc 2007; 55:277–283.
- Lynn J. Living long in fragile health: the new demographics shape end of life care. In:Jennings B, Kaebnick G, Murray T, editors. Improving End of Life Care: Why Has It Been So Difficult. Hastings Center Report November–December 2005: Special No:S14–S18.
- Beaumont JG, Kenealy PM. Incidence and prevalence of the vegetative and minimally conscious states. Neuropsychol Rehabil 2005; 15:184–189.
- Hawkins NA, Ditto PH, Danks JH, Smucker WD. Micromanaging death: process p, values, and goals in end-of-life medical decision making. Gerontologist 2005; 45:107–117.
- Ditto PH, Jacobson JA, Smucker WD, Danks JH, Fagerlin A. Context changes choices: a prospective study of the effects of hospitalization on life-sustaining treatment p. Med Decis Making 2006; 26:313–322.
- Lockhart LK, Ditto PH, Danks JH, Coppola KM, Smucker WD. The stability of older adults’ judgments of fates better and worse than death. Death Stud 2001; 25:299–317.
- Gjerdingen DK, Neff JA, Wang M, Chaloner K. Older persons’ opinions about life-sustaining procedures in the face of dementia. Arch Fam Med 1999; 8:421–425.
- Heap MJ, Munglani R, Klinck JR, Males AG. Elderly patients’ p concerning life-support treatment. Anaesthesia 1993; 48:1027–1033.
- Singer PA, Thiel EC, Naylor CD, et al. Life-sustaining treatment p of hemodialysis patients: implications for advance directives. J Am Soc Nephrol 1995; 6:1410–1417.
- Hofmann JC, Wenger NS, Davis RB, et al. Patient p for communication with physicians about end-of-life decisions. SUPPORT Investigators. Study to Understand Prognoses and Preference for Outcomes and Risks of Treatment. Ann Intern Med 1997; 127:1–12.
- Pinquart M, Sorensen S. Helping caregivers of persons with dementia: which interventions work and how large are their effects? Int Psychogeriatr 2006; 18:577–595.
- Robbins J, Gensler G, Hind J, et al. Comparison of 2 Interventions for liquid aspiration on pneumonia incidence: a randomized trial. Ann Intern Med 2008; 148:509–518.
- Walter LC, Covinsky KE. Cancer screening in elderly patients: a framework for individualized decision making. JAMA 2001; 285:2750–2756.
- Lee SJ, Lindquist K, Segal MR, Covinsky KE. Development and validation of a prognostic index for 4-year mortality in older adults. JAMA 2006; 295:801–808.
- Losey R, Messinger-Rapport BJ. At what age should we discontinue colon cancer screening in the elderly? Cleve Clin J Med 2007; 74:269–272.
- Larson EB, Shadlen MF, Wang L, et al. Survival after initial diagnosis of Alzheimer disease. Ann Intern Med 2004; 140:501–509.
- Suthers K, Kim JK, Crimmins E. Life expectancy with cognitive impairment in the older population of the United States. J Gerontol B Psychol Sci Soc Sci 2003; 58:S179–S186.
- Bloom HL, Shukrullah I, Cuellar JR, Lloyd MS, Dudley SC, Zafari AM. Long-term survival after successful inhospital cardiac arrest resuscitation. Am Heart J 2007; 153:831–836.
- Finucane TE, Harper GM. Attempting resuscitation in nursing homes: policy considerations. J Am Geriatr Soc 1999; 47:1261–1264.
- Pearlman R, Startks H, Cain K, Cole W, Rosengren D, Patrick D. Your Life, Your Choices. 2nd ed. Department of Veterans Affairs, National Center for Ethics in Health Care, 2007.
- Molloy DW. Let Me Decide. Hamilton, Ontario: Newgrange Press, 1996.
- Dunn PM, Schmidt TA, Carley MM, Donius M, Weinstein MA, Dull VT. A method to communicate patient p about medically indicated life-sustaining treatment in the out-of-hospital setting. J Am Geriatr Soc 1996; 44:785–791.
- Fried TR, O’Leary J, Van Ness P, Fraenkel L. Inconsistency over time in the p of older persons with advanced illness for life-sustaining treatment. J Am Geriatr Soc 2007; 55:1007–1014.
- Fried TR, Van Ness PH, Byers AL, Towle VR, O’Leary JR, Dubin JA. Changes in p for life-sustaining treatment among older persons with advanced illness. J Gen Intern Med 2007; 22:495–501.
- Diwan S, Hougham GW, Sachs GA. Strain experienced by caregivers of dementia patients receiving palliative care: findings from the Palliative Excellence in Alzheimer Care Efforts (PEACE) Program. J Palliat Med 2004; 7:797–807.
- Covinsky KE, Yaffe K. Dementia, prognosis, and the needs of patients and caregivers. Ann Intern Med 2004; 140:573–574.
- Shega JW, Levin A, Hougham GW, et al. Palliative Excellence in Alzheimer Care Efforts (PEACE): a program description. J Palliat Med 2003; 6:315–320.
- Center for Ethics in Health Care. Physician orders for life-sustaining treatment paradigm. www.ohsu.edu/ethics/polst/. Accessed March 9, 2009.
- Lee MA, Brummel-Smith K, Meyer J, Drew N, London MR. Physician orders for life-sustaining treatment (POLST): outcomes in a PACE program. Program of All-Inclusive Care for the Elderly. J Am Geriatr Soc 2000; 48:1219–1225.
- Meyers JL, Moore C, McGrory A, Sparr J, Ahern M. Physician orders for life-sustaining treatment form: honoring end-of-life directives for nursing home residents. J Gerontol Nurs 2004; 30:37–46.
- Tolle SW, Tilden VP, Nelson CA, Dunn PM. A prospective study of the efficacy of the physician order form for life-sustaining treatment. J Am Geriatr Soc 1998; 46:1097–1102.
- Cantor MD, Pearlman RA. Advance care planning in long-term care facilities. J Am Med Dir Assoc 2004; 5(suppl 2):S72–S80.
KEY POINTS
- In the ambulatory setting, start by assessing the patient’s prognosis and his or her receptiveness to advance care planning.
- For a patient in declining health who is willing to participate in the care planning process, it may be useful to take a full values history and to review the goals of care.
- For a patient with advanced disease who is unable or unwilling to participate in advance care planning, a limited approach may be appropriate, ie, identifying a surrogate decision-maker and ascertaining how much flexibility the surrogate should have with health care decisions.
- Whatever the patient’s life expectancy and level of receptivity, brief, episodic discussions are more useful than a one-time description of available written advance directives.