User login
Shades of SARS? New Virus Took Root in Pneumonia Patient
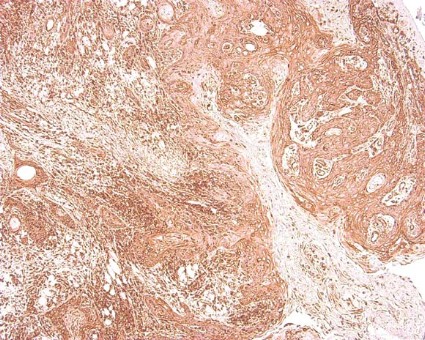
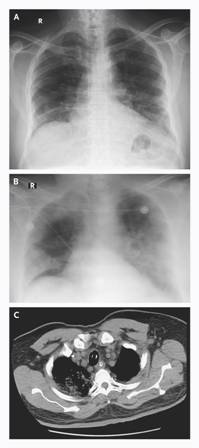
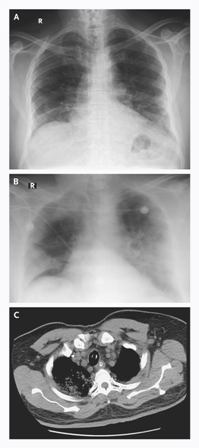
A novel coronavirus has been identified in a 60-year-old man with acute pneumonia who died of progressive respiratory and renal failure 11 days after hospital admission, according to a report in the New England Journal of Medicine that was published online on Oct. 17.
The virus, known as HCoV-EMC, is a previously unknown betacoronavirus species. The closest known relatives are two bat coronaviruses: HKU4 and HKU5.
"The clinical picture was remarkably similar to that of the severe acute respiratory distress syndrome [(SARS)] outbreak in 2003 and reminds us that animal coronaviruses can cause severe disease in humans," said lead author Dr. Ali Moh Zaki of the Dr. Soliman Fakeeh Hospital in Jeddah, Saudi Arabia, and his colleagues.
The patient was a 60-year-old Saudi man who first presented with a 7-day history of fever, cough, expectoration, and shortness of breath, the researchers said (N. Engl. J. Med. 2012 [doi:10.1056/NEJMoa211721]). He had no history of heart or kidney disease, did not smoke, and took no medications chronically.
The researchers tested a sputum sample when the patient was admitted to the hospital, and the results suggested that the virus was replicating. Tests of infected cell cultures with indirect immunofluorescence assays were negative for likely viruses including influenza A and B, respiratory syncytial virus, adenovirus, and parainfluenza viruses types 1 to 3. But serum samples collected at 10 and 11 days after the patient was hospitalized "reacted strongly when dilutions of 1:20 were tested on immunofluorescence assay specific for IgG antibodies," the researchers noted. By contrast, 2,400 control samples from other patients at the same hospital between 2010 and 2012 were negative, suggesting that the patient had developed antibodies to a previously unknown virus.
Genetic sequencing of the new virus linked it to a Betacoronavirus genus and set it apart from known human coronaviruses, which belong to the Alphacoronavirus genus, the researchers explained.
At the time of hospital admission, the patient’s body mass index was 35 kg/m2, his blood pressure was 140/80 mm Hg, his pulse was 117 beats per minute, and his temperature was 38.3 C. The patient was initially treated with oseltamivir, levofloxacin, piperacillin-tazobactam, and micafungin; meropenem was started on day 4.
"No symptoms were observed in the hospital among doctors and nurses caring for the patient, which suggests that the disease did not spread readily," the researchers said. However, the more thorough epidemiologic investigations can be conducted with the completion of the genomic sequencing of HCoV-EMC and the development of virus-specific rapid diagnostic tests, they added.
The Center for Infectious Disease Research and Policy at the University of Minnesota (CIDRAP) reported on the gene sequencing and testing methods used to identify the virus, and on the status of a second infected patient – a 49-year-old man from Qatar – who presented with similar symptoms and was last reported to be in stable condition.
"Although HCoV-EMC does not have many of the worrisome characteristics of SARS-CoV, we should take notice of the valuable lessons learned during the 2003 SARS outbreak with respect to outbreak investigations and management," the researchers said.
The study was supported in part by the European Commission Seventh Framework Program for Research and Technology Development Project EMPERIE.
Lead author Dr. Zaki had no financial conflicts to disclose. Several of the study coauthors have financial interest in Viroclinics Biosciences B.V. through a holding company administered by Erasmus Medical Center in Rotterdam, the Netherlands. Viroclinics and Erasmus Medical Center have jointly filed a patent on the new virus genome.
A novel coronavirus has been identified in a 60-year-old man with acute pneumonia who died of progressive respiratory and renal failure 11 days after hospital admission, according to a report in the New England Journal of Medicine that was published online on Oct. 17.
The virus, known as HCoV-EMC, is a previously unknown betacoronavirus species. The closest known relatives are two bat coronaviruses: HKU4 and HKU5.
"The clinical picture was remarkably similar to that of the severe acute respiratory distress syndrome [(SARS)] outbreak in 2003 and reminds us that animal coronaviruses can cause severe disease in humans," said lead author Dr. Ali Moh Zaki of the Dr. Soliman Fakeeh Hospital in Jeddah, Saudi Arabia, and his colleagues.
The patient was a 60-year-old Saudi man who first presented with a 7-day history of fever, cough, expectoration, and shortness of breath, the researchers said (N. Engl. J. Med. 2012 [doi:10.1056/NEJMoa211721]). He had no history of heart or kidney disease, did not smoke, and took no medications chronically.
The researchers tested a sputum sample when the patient was admitted to the hospital, and the results suggested that the virus was replicating. Tests of infected cell cultures with indirect immunofluorescence assays were negative for likely viruses including influenza A and B, respiratory syncytial virus, adenovirus, and parainfluenza viruses types 1 to 3. But serum samples collected at 10 and 11 days after the patient was hospitalized "reacted strongly when dilutions of 1:20 were tested on immunofluorescence assay specific for IgG antibodies," the researchers noted. By contrast, 2,400 control samples from other patients at the same hospital between 2010 and 2012 were negative, suggesting that the patient had developed antibodies to a previously unknown virus.
Genetic sequencing of the new virus linked it to a Betacoronavirus genus and set it apart from known human coronaviruses, which belong to the Alphacoronavirus genus, the researchers explained.
At the time of hospital admission, the patient’s body mass index was 35 kg/m2, his blood pressure was 140/80 mm Hg, his pulse was 117 beats per minute, and his temperature was 38.3 C. The patient was initially treated with oseltamivir, levofloxacin, piperacillin-tazobactam, and micafungin; meropenem was started on day 4.
"No symptoms were observed in the hospital among doctors and nurses caring for the patient, which suggests that the disease did not spread readily," the researchers said. However, the more thorough epidemiologic investigations can be conducted with the completion of the genomic sequencing of HCoV-EMC and the development of virus-specific rapid diagnostic tests, they added.
The Center for Infectious Disease Research and Policy at the University of Minnesota (CIDRAP) reported on the gene sequencing and testing methods used to identify the virus, and on the status of a second infected patient – a 49-year-old man from Qatar – who presented with similar symptoms and was last reported to be in stable condition.
"Although HCoV-EMC does not have many of the worrisome characteristics of SARS-CoV, we should take notice of the valuable lessons learned during the 2003 SARS outbreak with respect to outbreak investigations and management," the researchers said.
The study was supported in part by the European Commission Seventh Framework Program for Research and Technology Development Project EMPERIE.
Lead author Dr. Zaki had no financial conflicts to disclose. Several of the study coauthors have financial interest in Viroclinics Biosciences B.V. through a holding company administered by Erasmus Medical Center in Rotterdam, the Netherlands. Viroclinics and Erasmus Medical Center have jointly filed a patent on the new virus genome.
A novel coronavirus has been identified in a 60-year-old man with acute pneumonia who died of progressive respiratory and renal failure 11 days after hospital admission, according to a report in the New England Journal of Medicine that was published online on Oct. 17.
The virus, known as HCoV-EMC, is a previously unknown betacoronavirus species. The closest known relatives are two bat coronaviruses: HKU4 and HKU5.
"The clinical picture was remarkably similar to that of the severe acute respiratory distress syndrome [(SARS)] outbreak in 2003 and reminds us that animal coronaviruses can cause severe disease in humans," said lead author Dr. Ali Moh Zaki of the Dr. Soliman Fakeeh Hospital in Jeddah, Saudi Arabia, and his colleagues.
The patient was a 60-year-old Saudi man who first presented with a 7-day history of fever, cough, expectoration, and shortness of breath, the researchers said (N. Engl. J. Med. 2012 [doi:10.1056/NEJMoa211721]). He had no history of heart or kidney disease, did not smoke, and took no medications chronically.
The researchers tested a sputum sample when the patient was admitted to the hospital, and the results suggested that the virus was replicating. Tests of infected cell cultures with indirect immunofluorescence assays were negative for likely viruses including influenza A and B, respiratory syncytial virus, adenovirus, and parainfluenza viruses types 1 to 3. But serum samples collected at 10 and 11 days after the patient was hospitalized "reacted strongly when dilutions of 1:20 were tested on immunofluorescence assay specific for IgG antibodies," the researchers noted. By contrast, 2,400 control samples from other patients at the same hospital between 2010 and 2012 were negative, suggesting that the patient had developed antibodies to a previously unknown virus.
Genetic sequencing of the new virus linked it to a Betacoronavirus genus and set it apart from known human coronaviruses, which belong to the Alphacoronavirus genus, the researchers explained.
At the time of hospital admission, the patient’s body mass index was 35 kg/m2, his blood pressure was 140/80 mm Hg, his pulse was 117 beats per minute, and his temperature was 38.3 C. The patient was initially treated with oseltamivir, levofloxacin, piperacillin-tazobactam, and micafungin; meropenem was started on day 4.
"No symptoms were observed in the hospital among doctors and nurses caring for the patient, which suggests that the disease did not spread readily," the researchers said. However, the more thorough epidemiologic investigations can be conducted with the completion of the genomic sequencing of HCoV-EMC and the development of virus-specific rapid diagnostic tests, they added.
The Center for Infectious Disease Research and Policy at the University of Minnesota (CIDRAP) reported on the gene sequencing and testing methods used to identify the virus, and on the status of a second infected patient – a 49-year-old man from Qatar – who presented with similar symptoms and was last reported to be in stable condition.
"Although HCoV-EMC does not have many of the worrisome characteristics of SARS-CoV, we should take notice of the valuable lessons learned during the 2003 SARS outbreak with respect to outbreak investigations and management," the researchers said.
The study was supported in part by the European Commission Seventh Framework Program for Research and Technology Development Project EMPERIE.
Lead author Dr. Zaki had no financial conflicts to disclose. Several of the study coauthors have financial interest in Viroclinics Biosciences B.V. through a holding company administered by Erasmus Medical Center in Rotterdam, the Netherlands. Viroclinics and Erasmus Medical Center have jointly filed a patent on the new virus genome.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Less Irrigation May Reduce Abscesses After Appendectomy
CHICAGO – High-volume intra-abdominal irrigation significantly increased the risk of postoperative abscess in a study of 327 appendectomy patients and led investigators to conclude that use of irrigation should be limited in these patients.
The classical thinking that irrigation during appendectomies washes away bacteria is changing, as additional data suggest that irrigation might create pockets of fluid that can lead to the formation of abscesses, Dr. Esteban Gnass said at the annual clinical congress of the American College of Surgeons.
Previous studies have shown that postoperative abscess (POA) formation significantly increases the length of a patient’s hospital stay and hospital costs, said Dr. Gnass of Riverside County Regional Medical Center in Moreno Valley, Calif.
To determine the association between irrigation during surgery and POA formation, he and his colleagues reviewed data from 265 laparoscopic and 62 open procedures conducted between January 2009 and June 2011. There were no significant demographic differences between patients in the two procedure groups. Patients also were subdivided according to perforated vs. nonperforated and irrigated vs. nonirrigated.
A total of 17 postoperative abscesses were observed, all of which occurred in irrigated patients. In addition, 88% of the postoperative abscess cases involved at least 500 mL of irrigation. "Large irrigation volumes carried a higher risk of POA," Dr. Gnass said.
After controlling for multiple variables, the investigators found that both irrigation volume and perforation were significantly associated with abscess formation.
In both the laparoscopic and open groups, 100% of perforated patients received at least 500 mL of irrigation, compared with 75% of the nonperforated patients in the laparoscopy group and 0% of nonperforated patients in the open group.
POA rates and perforation rates were not significantly different between laparoscopic and open groups (5% vs. 4%, and 25% vs. 37%, respectively).
On further analysis of the POA cases only, perforation rates were not significantly different between laparoscopic and open groups (72% vs. 67%).
"Surgical technique was not associated with abscess formation," Dr. Gnass noted.
Among the perforated cases only, postoperative abscesses developed in 18% of those who received at least 500 mL of irrigation and in none of those who received less than 500 mL of irrigation.
More research in the form of a prospective, randomized trial is needed to confirm the results, but based on the current findings, "we can suggest limiting the use of irrigation to 500 cc or less" in appendectomy procedures, Dr. Gnass said.
He reported having no relevant financial disclosures.
CHICAGO – High-volume intra-abdominal irrigation significantly increased the risk of postoperative abscess in a study of 327 appendectomy patients and led investigators to conclude that use of irrigation should be limited in these patients.
The classical thinking that irrigation during appendectomies washes away bacteria is changing, as additional data suggest that irrigation might create pockets of fluid that can lead to the formation of abscesses, Dr. Esteban Gnass said at the annual clinical congress of the American College of Surgeons.
Previous studies have shown that postoperative abscess (POA) formation significantly increases the length of a patient’s hospital stay and hospital costs, said Dr. Gnass of Riverside County Regional Medical Center in Moreno Valley, Calif.
To determine the association between irrigation during surgery and POA formation, he and his colleagues reviewed data from 265 laparoscopic and 62 open procedures conducted between January 2009 and June 2011. There were no significant demographic differences between patients in the two procedure groups. Patients also were subdivided according to perforated vs. nonperforated and irrigated vs. nonirrigated.
A total of 17 postoperative abscesses were observed, all of which occurred in irrigated patients. In addition, 88% of the postoperative abscess cases involved at least 500 mL of irrigation. "Large irrigation volumes carried a higher risk of POA," Dr. Gnass said.
After controlling for multiple variables, the investigators found that both irrigation volume and perforation were significantly associated with abscess formation.
In both the laparoscopic and open groups, 100% of perforated patients received at least 500 mL of irrigation, compared with 75% of the nonperforated patients in the laparoscopy group and 0% of nonperforated patients in the open group.
POA rates and perforation rates were not significantly different between laparoscopic and open groups (5% vs. 4%, and 25% vs. 37%, respectively).
On further analysis of the POA cases only, perforation rates were not significantly different between laparoscopic and open groups (72% vs. 67%).
"Surgical technique was not associated with abscess formation," Dr. Gnass noted.
Among the perforated cases only, postoperative abscesses developed in 18% of those who received at least 500 mL of irrigation and in none of those who received less than 500 mL of irrigation.
More research in the form of a prospective, randomized trial is needed to confirm the results, but based on the current findings, "we can suggest limiting the use of irrigation to 500 cc or less" in appendectomy procedures, Dr. Gnass said.
He reported having no relevant financial disclosures.
CHICAGO – High-volume intra-abdominal irrigation significantly increased the risk of postoperative abscess in a study of 327 appendectomy patients and led investigators to conclude that use of irrigation should be limited in these patients.
The classical thinking that irrigation during appendectomies washes away bacteria is changing, as additional data suggest that irrigation might create pockets of fluid that can lead to the formation of abscesses, Dr. Esteban Gnass said at the annual clinical congress of the American College of Surgeons.
Previous studies have shown that postoperative abscess (POA) formation significantly increases the length of a patient’s hospital stay and hospital costs, said Dr. Gnass of Riverside County Regional Medical Center in Moreno Valley, Calif.
To determine the association between irrigation during surgery and POA formation, he and his colleagues reviewed data from 265 laparoscopic and 62 open procedures conducted between January 2009 and June 2011. There were no significant demographic differences between patients in the two procedure groups. Patients also were subdivided according to perforated vs. nonperforated and irrigated vs. nonirrigated.
A total of 17 postoperative abscesses were observed, all of which occurred in irrigated patients. In addition, 88% of the postoperative abscess cases involved at least 500 mL of irrigation. "Large irrigation volumes carried a higher risk of POA," Dr. Gnass said.
After controlling for multiple variables, the investigators found that both irrigation volume and perforation were significantly associated with abscess formation.
In both the laparoscopic and open groups, 100% of perforated patients received at least 500 mL of irrigation, compared with 75% of the nonperforated patients in the laparoscopy group and 0% of nonperforated patients in the open group.
POA rates and perforation rates were not significantly different between laparoscopic and open groups (5% vs. 4%, and 25% vs. 37%, respectively).
On further analysis of the POA cases only, perforation rates were not significantly different between laparoscopic and open groups (72% vs. 67%).
"Surgical technique was not associated with abscess formation," Dr. Gnass noted.
Among the perforated cases only, postoperative abscesses developed in 18% of those who received at least 500 mL of irrigation and in none of those who received less than 500 mL of irrigation.
More research in the form of a prospective, randomized trial is needed to confirm the results, but based on the current findings, "we can suggest limiting the use of irrigation to 500 cc or less" in appendectomy procedures, Dr. Gnass said.
He reported having no relevant financial disclosures.
AT THE ANNUAL CLINICAL CONGRESS OF THE AMERICAN COLLEGE OF SURGEONS
Male Gender, Length of Stay Raise Readmission Risk
CHICAGO – Approximately half of hospital readmissions are surgery related and one-third of these are due to infections, data from nearly 3,000 Medicare patients indicated.
Risk factors for readmission included male gender, higher ASA (American Society of Anesthesiologists) class, and longer hospital stay, Dr. Shanu N. Kothari said at the annual clinical congress of the American College of Surgeons.
Recent health care reform initiatives include a proposal to reduce reimbursement for certain 30-day hospital readmissions among Medicare patients, he noted.
Dr. Kothari of Gundersen Lutheran Health System in La Crosse, Wis., and his colleagues reviewed data from 2,865 Medicare patients who had surgery at their institution between Jan. 1, 2010, and May 16, 2011. A readmission was defined as any patient who was readmitted within 30 days of initial surgery. Patients with incomplete follow-up data and those who died within 30 days were excluded.
The overall 30-day readmission rate was 7%. Readmitted patients were significantly more likely to be male compared with nonreadmitted patients (54% vs. 44%) and significantly more likely to have an ASA class of 3 or greater (84% vs. 66%). There were no significant differences in age or body mass index between readmitted and nonreadmitted patients.
In addition, the average length of stay and operative times were significantly longer for readmitted patients vs. nonreadmitted patients (4.8 days vs. 2.8 days and 123 minutes vs. 98 minutes).
A majority of the procedures were general and orthopedic, and 77% were elective.
Of the readmitted patients, "84% had at least one chronic condition, and patients with cardiac disease, renal disease, and diabetes had higher readmission rates," Dr. Kothari said.
The reasons for readmission were divided into four categories: surgery related (53%), not related to the surgical procedure (35%), planned (7%), and patient related (5%).
The most common surgery-related reasons for readmission were infections (32%), medication side effects (12%), or pulmonary complications (9%), Dr. Kothari noted.
Most of the readmissions unrelated to the index surgical procedure were exacerbations of underlying conditions, such as renal failure or heart failure. Patient-related reasons for readmission included noncompliance with discharge instructions or medications, as well as psychological issues.
"Further study is needed to address reasons for readmission on a multicenter level," said Dr. Kothari. "Decreased reimbursement should be discouraged for readmissions directly related to patient noncompliance."
Dr. Kothari said he had no relevant financial disclosures.
CHICAGO – Approximately half of hospital readmissions are surgery related and one-third of these are due to infections, data from nearly 3,000 Medicare patients indicated.
Risk factors for readmission included male gender, higher ASA (American Society of Anesthesiologists) class, and longer hospital stay, Dr. Shanu N. Kothari said at the annual clinical congress of the American College of Surgeons.
Recent health care reform initiatives include a proposal to reduce reimbursement for certain 30-day hospital readmissions among Medicare patients, he noted.
Dr. Kothari of Gundersen Lutheran Health System in La Crosse, Wis., and his colleagues reviewed data from 2,865 Medicare patients who had surgery at their institution between Jan. 1, 2010, and May 16, 2011. A readmission was defined as any patient who was readmitted within 30 days of initial surgery. Patients with incomplete follow-up data and those who died within 30 days were excluded.
The overall 30-day readmission rate was 7%. Readmitted patients were significantly more likely to be male compared with nonreadmitted patients (54% vs. 44%) and significantly more likely to have an ASA class of 3 or greater (84% vs. 66%). There were no significant differences in age or body mass index between readmitted and nonreadmitted patients.
In addition, the average length of stay and operative times were significantly longer for readmitted patients vs. nonreadmitted patients (4.8 days vs. 2.8 days and 123 minutes vs. 98 minutes).
A majority of the procedures were general and orthopedic, and 77% were elective.
Of the readmitted patients, "84% had at least one chronic condition, and patients with cardiac disease, renal disease, and diabetes had higher readmission rates," Dr. Kothari said.
The reasons for readmission were divided into four categories: surgery related (53%), not related to the surgical procedure (35%), planned (7%), and patient related (5%).
The most common surgery-related reasons for readmission were infections (32%), medication side effects (12%), or pulmonary complications (9%), Dr. Kothari noted.
Most of the readmissions unrelated to the index surgical procedure were exacerbations of underlying conditions, such as renal failure or heart failure. Patient-related reasons for readmission included noncompliance with discharge instructions or medications, as well as psychological issues.
"Further study is needed to address reasons for readmission on a multicenter level," said Dr. Kothari. "Decreased reimbursement should be discouraged for readmissions directly related to patient noncompliance."
Dr. Kothari said he had no relevant financial disclosures.
CHICAGO – Approximately half of hospital readmissions are surgery related and one-third of these are due to infections, data from nearly 3,000 Medicare patients indicated.
Risk factors for readmission included male gender, higher ASA (American Society of Anesthesiologists) class, and longer hospital stay, Dr. Shanu N. Kothari said at the annual clinical congress of the American College of Surgeons.
Recent health care reform initiatives include a proposal to reduce reimbursement for certain 30-day hospital readmissions among Medicare patients, he noted.
Dr. Kothari of Gundersen Lutheran Health System in La Crosse, Wis., and his colleagues reviewed data from 2,865 Medicare patients who had surgery at their institution between Jan. 1, 2010, and May 16, 2011. A readmission was defined as any patient who was readmitted within 30 days of initial surgery. Patients with incomplete follow-up data and those who died within 30 days were excluded.
The overall 30-day readmission rate was 7%. Readmitted patients were significantly more likely to be male compared with nonreadmitted patients (54% vs. 44%) and significantly more likely to have an ASA class of 3 or greater (84% vs. 66%). There were no significant differences in age or body mass index between readmitted and nonreadmitted patients.
In addition, the average length of stay and operative times were significantly longer for readmitted patients vs. nonreadmitted patients (4.8 days vs. 2.8 days and 123 minutes vs. 98 minutes).
A majority of the procedures were general and orthopedic, and 77% were elective.
Of the readmitted patients, "84% had at least one chronic condition, and patients with cardiac disease, renal disease, and diabetes had higher readmission rates," Dr. Kothari said.
The reasons for readmission were divided into four categories: surgery related (53%), not related to the surgical procedure (35%), planned (7%), and patient related (5%).
The most common surgery-related reasons for readmission were infections (32%), medication side effects (12%), or pulmonary complications (9%), Dr. Kothari noted.
Most of the readmissions unrelated to the index surgical procedure were exacerbations of underlying conditions, such as renal failure or heart failure. Patient-related reasons for readmission included noncompliance with discharge instructions or medications, as well as psychological issues.
"Further study is needed to address reasons for readmission on a multicenter level," said Dr. Kothari. "Decreased reimbursement should be discouraged for readmissions directly related to patient noncompliance."
Dr. Kothari said he had no relevant financial disclosures.
AT THE ANNUAL CLINICAL CONGRESS OF THE AMERICAN COLLEGE OF SURGEONS
Major Finding: A total of 53% of 30-day readmissions at a single institution were surgically related, and 32% of these were due to infections.
Data Source: The data come from a retrospective study of 2,865 Medicare patients who underwent surgery at a single institution between Jan. 1, 2010, and May 16, 2011.
Disclosures: Dr. Kothari said he had no relevant financial disclosures.
One-Third of Postop Problems Arise After Discharge
CHICAGO – Approximately one-third of surgical complications were diagnosed after patients left the hospital, based on data from nearly 60,000 procedures performed at 112 hospitals.
Reporting postoperative complications, including surgical site infections, has become a mandatory quality reporting initiative for hospitals, and the Affordable Care Act requires reporting of readmissions, said Dr. Melanie Morris of the University of Alabama at Birmingham.
"Some postoperative complications may lead to readmissions, but this may not tell the whole story," she noted at the annual clinical congress of the American College of Surgeons.
To determine the timing of postoperative complications and the nature of readmissions, Dr. Morris and her colleagues reviewed Veterans Affairs data from the noncardiac Surgical Care Improvement Project (SCIP) cohort from 2005 to 2009 for 59,464 surgical procedures in which there was at least one complication.
"It’s very important that patients are accurately educated on the signs and symptoms of complications so they know to seek timely care after discharge."
Surgical cases were classified by specialty into gastrointestinal, gynecologic, orthopedic, and vascular. Complications were grouped into organ-based systems. For example, urinary complications included renal failure, renal insufficiency, and urinary tract infections; respiratory complications included failure to wean, pneumonia, and reintubation; and surgical site infections (SSIs) included both deep and superficial wounds.
The overall complication rate was approximately 15%, and 32% of complications were diagnosed after hospital discharge, Dr. Morris said. More than half (56%) of all SSIs were diagnosed after discharge, she added.
A statistically significant difference appeared in postdischarge complications by surgical specialty. The SSI rate was 5.4%, followed by respiratory complications (5.0%), urinary tract infection (4.9%), cardiac complications (3.2%), and venous thromboembolism (1.2%).
"Our GI surgical patients had the highest overall complication rate," Dr. Morris noted. Among GI patients, colectomy patients had the highest SSI rate (11%), and 23% of the GI complications were diagnosed after hospital discharge.
In addition, 78% of SSIs in orthopedic patients were diagnosed after discharge, as were 39% of SSIs in GI patients, 77% of SSIs in vascular surgery patients, and 95% of SSIs in gynecologic patients, said Dr. Morris.
There were no significant differences in length of hospital stay based on complications, Dr. Morris said.
The overall readmission rate was 11.9%, and 70% of these patients had no identifiable postoperative complication. Of those who did have an identifiable postop complication, 72% were diagnosed before discharge from the hospital.
The probability of being readmitted to the hospital over time was highest in patients with a postdischarge diagnosis of a complication. The overall length of stay was 5 days, and the average length of stay for patients with any complication was 9 days.
Patient-specific factors associated with an increased risk of readmission included a history of heart failure, renal failure, diabetes, weight loss, and smoking. Procedure-specific factors associated with an increased risk of readmission included a longer operating time, a more contaminated wound, and a higher ASA (American Society of Anesthesiologists) class.
Length of stay was slightly protective for readmission, and the presence of any complication was associated with a high risk of readmission.
"It’s very important that patients are accurately educated on the signs and symptoms of complications so they know to seek timely care after discharge," said Dr. Morris. "Postoperative complications must be measured beyond hospital discharge to capture the whole story.
"Systematic collection of postoperative complications must include postdischarge data as well as readmissions to accurately measure quality," she said.
Dr. Morris said she had no relevant financial disclosures.
CHICAGO – Approximately one-third of surgical complications were diagnosed after patients left the hospital, based on data from nearly 60,000 procedures performed at 112 hospitals.
Reporting postoperative complications, including surgical site infections, has become a mandatory quality reporting initiative for hospitals, and the Affordable Care Act requires reporting of readmissions, said Dr. Melanie Morris of the University of Alabama at Birmingham.
"Some postoperative complications may lead to readmissions, but this may not tell the whole story," she noted at the annual clinical congress of the American College of Surgeons.
To determine the timing of postoperative complications and the nature of readmissions, Dr. Morris and her colleagues reviewed Veterans Affairs data from the noncardiac Surgical Care Improvement Project (SCIP) cohort from 2005 to 2009 for 59,464 surgical procedures in which there was at least one complication.
"It’s very important that patients are accurately educated on the signs and symptoms of complications so they know to seek timely care after discharge."
Surgical cases were classified by specialty into gastrointestinal, gynecologic, orthopedic, and vascular. Complications were grouped into organ-based systems. For example, urinary complications included renal failure, renal insufficiency, and urinary tract infections; respiratory complications included failure to wean, pneumonia, and reintubation; and surgical site infections (SSIs) included both deep and superficial wounds.
The overall complication rate was approximately 15%, and 32% of complications were diagnosed after hospital discharge, Dr. Morris said. More than half (56%) of all SSIs were diagnosed after discharge, she added.
A statistically significant difference appeared in postdischarge complications by surgical specialty. The SSI rate was 5.4%, followed by respiratory complications (5.0%), urinary tract infection (4.9%), cardiac complications (3.2%), and venous thromboembolism (1.2%).
"Our GI surgical patients had the highest overall complication rate," Dr. Morris noted. Among GI patients, colectomy patients had the highest SSI rate (11%), and 23% of the GI complications were diagnosed after hospital discharge.
In addition, 78% of SSIs in orthopedic patients were diagnosed after discharge, as were 39% of SSIs in GI patients, 77% of SSIs in vascular surgery patients, and 95% of SSIs in gynecologic patients, said Dr. Morris.
There were no significant differences in length of hospital stay based on complications, Dr. Morris said.
The overall readmission rate was 11.9%, and 70% of these patients had no identifiable postoperative complication. Of those who did have an identifiable postop complication, 72% were diagnosed before discharge from the hospital.
The probability of being readmitted to the hospital over time was highest in patients with a postdischarge diagnosis of a complication. The overall length of stay was 5 days, and the average length of stay for patients with any complication was 9 days.
Patient-specific factors associated with an increased risk of readmission included a history of heart failure, renal failure, diabetes, weight loss, and smoking. Procedure-specific factors associated with an increased risk of readmission included a longer operating time, a more contaminated wound, and a higher ASA (American Society of Anesthesiologists) class.
Length of stay was slightly protective for readmission, and the presence of any complication was associated with a high risk of readmission.
"It’s very important that patients are accurately educated on the signs and symptoms of complications so they know to seek timely care after discharge," said Dr. Morris. "Postoperative complications must be measured beyond hospital discharge to capture the whole story.
"Systematic collection of postoperative complications must include postdischarge data as well as readmissions to accurately measure quality," she said.
Dr. Morris said she had no relevant financial disclosures.
CHICAGO – Approximately one-third of surgical complications were diagnosed after patients left the hospital, based on data from nearly 60,000 procedures performed at 112 hospitals.
Reporting postoperative complications, including surgical site infections, has become a mandatory quality reporting initiative for hospitals, and the Affordable Care Act requires reporting of readmissions, said Dr. Melanie Morris of the University of Alabama at Birmingham.
"Some postoperative complications may lead to readmissions, but this may not tell the whole story," she noted at the annual clinical congress of the American College of Surgeons.
To determine the timing of postoperative complications and the nature of readmissions, Dr. Morris and her colleagues reviewed Veterans Affairs data from the noncardiac Surgical Care Improvement Project (SCIP) cohort from 2005 to 2009 for 59,464 surgical procedures in which there was at least one complication.
"It’s very important that patients are accurately educated on the signs and symptoms of complications so they know to seek timely care after discharge."
Surgical cases were classified by specialty into gastrointestinal, gynecologic, orthopedic, and vascular. Complications were grouped into organ-based systems. For example, urinary complications included renal failure, renal insufficiency, and urinary tract infections; respiratory complications included failure to wean, pneumonia, and reintubation; and surgical site infections (SSIs) included both deep and superficial wounds.
The overall complication rate was approximately 15%, and 32% of complications were diagnosed after hospital discharge, Dr. Morris said. More than half (56%) of all SSIs were diagnosed after discharge, she added.
A statistically significant difference appeared in postdischarge complications by surgical specialty. The SSI rate was 5.4%, followed by respiratory complications (5.0%), urinary tract infection (4.9%), cardiac complications (3.2%), and venous thromboembolism (1.2%).
"Our GI surgical patients had the highest overall complication rate," Dr. Morris noted. Among GI patients, colectomy patients had the highest SSI rate (11%), and 23% of the GI complications were diagnosed after hospital discharge.
In addition, 78% of SSIs in orthopedic patients were diagnosed after discharge, as were 39% of SSIs in GI patients, 77% of SSIs in vascular surgery patients, and 95% of SSIs in gynecologic patients, said Dr. Morris.
There were no significant differences in length of hospital stay based on complications, Dr. Morris said.
The overall readmission rate was 11.9%, and 70% of these patients had no identifiable postoperative complication. Of those who did have an identifiable postop complication, 72% were diagnosed before discharge from the hospital.
The probability of being readmitted to the hospital over time was highest in patients with a postdischarge diagnosis of a complication. The overall length of stay was 5 days, and the average length of stay for patients with any complication was 9 days.
Patient-specific factors associated with an increased risk of readmission included a history of heart failure, renal failure, diabetes, weight loss, and smoking. Procedure-specific factors associated with an increased risk of readmission included a longer operating time, a more contaminated wound, and a higher ASA (American Society of Anesthesiologists) class.
Length of stay was slightly protective for readmission, and the presence of any complication was associated with a high risk of readmission.
"It’s very important that patients are accurately educated on the signs and symptoms of complications so they know to seek timely care after discharge," said Dr. Morris. "Postoperative complications must be measured beyond hospital discharge to capture the whole story.
"Systematic collection of postoperative complications must include postdischarge data as well as readmissions to accurately measure quality," she said.
Dr. Morris said she had no relevant financial disclosures.
AT THE ANNUAL CLINICAL CONGRESS OF THE AMERICAN COLLEGE OF SURGEONS
Major Finding: Approximately 32% of surgical complications, including 56% of surgical site infections, were diagnosed after patients were discharged from the hospital.
Data Source: The data come from a review of 59,464 surgical procedures performed at 112 VA hospitals.
Disclosures: Dr. Morris said she had no relevant financial disclosures.
Robotic Surgery Beneficial in HPV-, Non-HPV-Related Oral Cancer
WASHINGTON – Oropharyngeal squamous cell cancer patients who underwent transoral robotic surgery had an overall 2-year survival rate of 87%, with no significant differences between patients who were positive vs. negative for the human papillomavirus, based on data from 52 patients.
HPV is associated with 45%-70% of cases of oropharyngeal squamous cell carcinoma (OPSCCa), said Dr. Kiran Kakarala, who conducted the study at Ohio State University in Columbus.
Previous studies have shown a significant difference in survival rates for patients with HPV-positive tumors, compared with those with negative tumors, Dr. Kakarala said. However, other studies have suggested that the use of transoral robotic surgery (TORS) for OPSCCa patients could narrow the gap in survival based on HPV status.
Dr. Kakarala and his colleagues reviewed data from 52 patients who underwent TORS with neck dissection and postoperative adjuvant treatment for previously untreated OPSCCa. The patients were part of a prospective single-arm cohort study at a single academic medical center.
HPV status was available for 42 patients; 36 were positive and 6 were negative. Demographic characteristics were not significantly different between the HPV-positive and negative patients. The mean age of the HPV-positive patients was 59 years, and the mean age of the negative patients was 57 years. The tonsil was the primary tumor site in 89% of the positive patients and 83% of the negative patients; the base of the tongue was the primary site in 11% of the positive patients and 17% of the negative patients.
HPV-positive patients had significantly higher N classifications based on the TNM Classification of Malignant Tumors, compared with HPV-negative patients (P = .015), and a significantly higher stage (P = .017). No significant differences were found in the number of HPV-positive vs. negative patients who received postoperative radiation or chemotherapy.
The 2-year survival rate was 87% for all 52 patients, 92% for HPV-positive patients, and 75% for HPV-negative patients. Two-year disease-specific survival rates were 92%, 92%, and 75%, respectively. Two-year disease-free survival rates were 86%, 97%, and 50%, respectively.
"The 2-year overall survival and disease-specific survival were not statistically different between HPV-positive and negative patients treated with TORS followed by radiation with or without chemotherapy as indicated," Dr. Kakarala said.
The study was limited by its small size and retrospective design, but the findings suggest a role for minimally invasive TORS in OPSCCa patients, he said.
"Randomized trials incorporating minimally invasive transoral surgical procedures with radiation therapy and chemotherapy, and comparing survival, quality of life, and cost outcomes between these treatment modalities, are indicated," he added.
The findings were presented at the annual meeting of the American Academy of Otolaryngology–Head and Neck Surgery Foundation.
Dr. Kakarala had no financial conflicts to disclose.
WASHINGTON – Oropharyngeal squamous cell cancer patients who underwent transoral robotic surgery had an overall 2-year survival rate of 87%, with no significant differences between patients who were positive vs. negative for the human papillomavirus, based on data from 52 patients.
HPV is associated with 45%-70% of cases of oropharyngeal squamous cell carcinoma (OPSCCa), said Dr. Kiran Kakarala, who conducted the study at Ohio State University in Columbus.
Previous studies have shown a significant difference in survival rates for patients with HPV-positive tumors, compared with those with negative tumors, Dr. Kakarala said. However, other studies have suggested that the use of transoral robotic surgery (TORS) for OPSCCa patients could narrow the gap in survival based on HPV status.
Dr. Kakarala and his colleagues reviewed data from 52 patients who underwent TORS with neck dissection and postoperative adjuvant treatment for previously untreated OPSCCa. The patients were part of a prospective single-arm cohort study at a single academic medical center.
HPV status was available for 42 patients; 36 were positive and 6 were negative. Demographic characteristics were not significantly different between the HPV-positive and negative patients. The mean age of the HPV-positive patients was 59 years, and the mean age of the negative patients was 57 years. The tonsil was the primary tumor site in 89% of the positive patients and 83% of the negative patients; the base of the tongue was the primary site in 11% of the positive patients and 17% of the negative patients.
HPV-positive patients had significantly higher N classifications based on the TNM Classification of Malignant Tumors, compared with HPV-negative patients (P = .015), and a significantly higher stage (P = .017). No significant differences were found in the number of HPV-positive vs. negative patients who received postoperative radiation or chemotherapy.
The 2-year survival rate was 87% for all 52 patients, 92% for HPV-positive patients, and 75% for HPV-negative patients. Two-year disease-specific survival rates were 92%, 92%, and 75%, respectively. Two-year disease-free survival rates were 86%, 97%, and 50%, respectively.
"The 2-year overall survival and disease-specific survival were not statistically different between HPV-positive and negative patients treated with TORS followed by radiation with or without chemotherapy as indicated," Dr. Kakarala said.
The study was limited by its small size and retrospective design, but the findings suggest a role for minimally invasive TORS in OPSCCa patients, he said.
"Randomized trials incorporating minimally invasive transoral surgical procedures with radiation therapy and chemotherapy, and comparing survival, quality of life, and cost outcomes between these treatment modalities, are indicated," he added.
The findings were presented at the annual meeting of the American Academy of Otolaryngology–Head and Neck Surgery Foundation.
Dr. Kakarala had no financial conflicts to disclose.
WASHINGTON – Oropharyngeal squamous cell cancer patients who underwent transoral robotic surgery had an overall 2-year survival rate of 87%, with no significant differences between patients who were positive vs. negative for the human papillomavirus, based on data from 52 patients.
HPV is associated with 45%-70% of cases of oropharyngeal squamous cell carcinoma (OPSCCa), said Dr. Kiran Kakarala, who conducted the study at Ohio State University in Columbus.
Previous studies have shown a significant difference in survival rates for patients with HPV-positive tumors, compared with those with negative tumors, Dr. Kakarala said. However, other studies have suggested that the use of transoral robotic surgery (TORS) for OPSCCa patients could narrow the gap in survival based on HPV status.
Dr. Kakarala and his colleagues reviewed data from 52 patients who underwent TORS with neck dissection and postoperative adjuvant treatment for previously untreated OPSCCa. The patients were part of a prospective single-arm cohort study at a single academic medical center.
HPV status was available for 42 patients; 36 were positive and 6 were negative. Demographic characteristics were not significantly different between the HPV-positive and negative patients. The mean age of the HPV-positive patients was 59 years, and the mean age of the negative patients was 57 years. The tonsil was the primary tumor site in 89% of the positive patients and 83% of the negative patients; the base of the tongue was the primary site in 11% of the positive patients and 17% of the negative patients.
HPV-positive patients had significantly higher N classifications based on the TNM Classification of Malignant Tumors, compared with HPV-negative patients (P = .015), and a significantly higher stage (P = .017). No significant differences were found in the number of HPV-positive vs. negative patients who received postoperative radiation or chemotherapy.
The 2-year survival rate was 87% for all 52 patients, 92% for HPV-positive patients, and 75% for HPV-negative patients. Two-year disease-specific survival rates were 92%, 92%, and 75%, respectively. Two-year disease-free survival rates were 86%, 97%, and 50%, respectively.
"The 2-year overall survival and disease-specific survival were not statistically different between HPV-positive and negative patients treated with TORS followed by radiation with or without chemotherapy as indicated," Dr. Kakarala said.
The study was limited by its small size and retrospective design, but the findings suggest a role for minimally invasive TORS in OPSCCa patients, he said.
"Randomized trials incorporating minimally invasive transoral surgical procedures with radiation therapy and chemotherapy, and comparing survival, quality of life, and cost outcomes between these treatment modalities, are indicated," he added.
The findings were presented at the annual meeting of the American Academy of Otolaryngology–Head and Neck Surgery Foundation.
Dr. Kakarala had no financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF OTOLARYNGOLOGY – HEAD AND NECK SURGERY FOUNDATION
Major Finding: Oropharyngeal squamous cell carcinoma patients who underwent robotic surgery had a 2-year survival rate of 87%, with 92% survival for HPV-positive patients and 75% for HPV-negative patients.
Data Source: The data come from a review of 52 patients.
Disclosures: Dr. Kakarala had no financial conflicts to disclose.
Adenotonsillectomy Dries Up Some Bed-Wetting
WASHINGTON – Adenotonsillectomy reduced obstructive sleep apnea and bed-wetting in half of 35 children diagnosed with both conditions.
The study was limited by its small size, but the findings suggest that children with severe obstructive sleep apnea and nocturnal enuresis might benefit on both counts with adenotonsillectomy, said Dr. Prasad Thottam of Children’s Hospital of Michigan, Detroit.
The average age of the children studied was 8 years, 60% were male, and their average body mass index was 24 kg/m2. Proper bladder function was documented in all of the children, and none had chronic conditions such as cerebral palsy, severe asthma, or morbid obesity. All experienced bed-wetting more than 3 nights per week. Any medications taken for nocturnal enuresis were discontinued for 1 month prior to surgery.
Four children had adenoidectomies, two had tonsillectomies, and 29 had adenotonsillectomies. After an average of 10 weeks post surgery, 51% of the children had reductions in bed-wetting, said Dr. Thottam. The reductions were most notable in children with a higher BMI and worse apnea characteristics on polysomnography.
Girls were five times more likely than were boys to have bed-wetting resolve after surgery. Children with prolonged stage 2 sleep were eight times more likely than were those with a normal duration of stage 2 sleep to have bed-wetting resolve.
In addition, when comparing the sleep architecture of the patients to established normal levels, an apnea-hypopnea index greater than 10 was associated with a higher rate of resolution of bed-wetting compared with the rest of the population.
The findings were presented at the annual meeting of the American Academy for Otolaryngology – Head and Neck Surgery Foundation. Dr. Thottam had no financial conflicts to disclose.
WASHINGTON – Adenotonsillectomy reduced obstructive sleep apnea and bed-wetting in half of 35 children diagnosed with both conditions.
The study was limited by its small size, but the findings suggest that children with severe obstructive sleep apnea and nocturnal enuresis might benefit on both counts with adenotonsillectomy, said Dr. Prasad Thottam of Children’s Hospital of Michigan, Detroit.
The average age of the children studied was 8 years, 60% were male, and their average body mass index was 24 kg/m2. Proper bladder function was documented in all of the children, and none had chronic conditions such as cerebral palsy, severe asthma, or morbid obesity. All experienced bed-wetting more than 3 nights per week. Any medications taken for nocturnal enuresis were discontinued for 1 month prior to surgery.
Four children had adenoidectomies, two had tonsillectomies, and 29 had adenotonsillectomies. After an average of 10 weeks post surgery, 51% of the children had reductions in bed-wetting, said Dr. Thottam. The reductions were most notable in children with a higher BMI and worse apnea characteristics on polysomnography.
Girls were five times more likely than were boys to have bed-wetting resolve after surgery. Children with prolonged stage 2 sleep were eight times more likely than were those with a normal duration of stage 2 sleep to have bed-wetting resolve.
In addition, when comparing the sleep architecture of the patients to established normal levels, an apnea-hypopnea index greater than 10 was associated with a higher rate of resolution of bed-wetting compared with the rest of the population.
The findings were presented at the annual meeting of the American Academy for Otolaryngology – Head and Neck Surgery Foundation. Dr. Thottam had no financial conflicts to disclose.
WASHINGTON – Adenotonsillectomy reduced obstructive sleep apnea and bed-wetting in half of 35 children diagnosed with both conditions.
The study was limited by its small size, but the findings suggest that children with severe obstructive sleep apnea and nocturnal enuresis might benefit on both counts with adenotonsillectomy, said Dr. Prasad Thottam of Children’s Hospital of Michigan, Detroit.
The average age of the children studied was 8 years, 60% were male, and their average body mass index was 24 kg/m2. Proper bladder function was documented in all of the children, and none had chronic conditions such as cerebral palsy, severe asthma, or morbid obesity. All experienced bed-wetting more than 3 nights per week. Any medications taken for nocturnal enuresis were discontinued for 1 month prior to surgery.
Four children had adenoidectomies, two had tonsillectomies, and 29 had adenotonsillectomies. After an average of 10 weeks post surgery, 51% of the children had reductions in bed-wetting, said Dr. Thottam. The reductions were most notable in children with a higher BMI and worse apnea characteristics on polysomnography.
Girls were five times more likely than were boys to have bed-wetting resolve after surgery. Children with prolonged stage 2 sleep were eight times more likely than were those with a normal duration of stage 2 sleep to have bed-wetting resolve.
In addition, when comparing the sleep architecture of the patients to established normal levels, an apnea-hypopnea index greater than 10 was associated with a higher rate of resolution of bed-wetting compared with the rest of the population.
The findings were presented at the annual meeting of the American Academy for Otolaryngology – Head and Neck Surgery Foundation. Dr. Thottam had no financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF OTOLARYNGOLOGY - HEAD AND NECK SURGERY FOUNDATION
Major Finding: Adenotonsillectomy reduced bed-wetting and obstructive sleep apnea in 51% of children with both conditions.
Data Source: The data come from a prospective study of 35 children with nighttime enuresis and obstructive sleep apnea.
Disclosures: Dr. Thottam had no financial conflicts to disclose.
Antipsychotic Use Spikes in Medicaid-Enrolled Children
Antipsychotic use in children aged 3-18 years increased by 62% between 2002 and 2007, according to Medicaid data from about 15 million children in the United States.
Although the use of second-generation antipsychotics (SGAs) in children has grown in recent decades, evidence supporting their effectiveness for many conditions is limited, said Meredith Matone of the Children’s Hospital of Philadelphia and her colleagues, including Dr. David M. Rubin, codirector of policy lab at the hospital and an associate professor of pediatrics at the University of Pennsylvania, Philadelphia.
"In light of recent research indicating rising use of antipsychotics in children coupled with concurrent research demonstrating significant side effects of these medications, it felt like a critical next step to understand who the populations of users were and how this population may have changed over the course of the last decade," she said in an interview. The findings were published online (Health Services Research Sept. 5 [doi:10.1111/j.1475-6773.2012.01461.x]).
To examine the relationship between diagnosis and prescription of SGAs, the researchers reviewed Medicaid data from children in 50 states and the District of Columbia between 2002 and 2007.
Overall, 354,000 children were using SGAs in 2007. Of these, 39% were diagnosed with attention-deficit/hyperactivity disorder (ADHD), 11% with bipolar disorder, 12% with ADHD and bipolar, and 38% with other conditions.
In 2007, 50% of children taking antipsychotics had a diagnosis of ADHD, and in 14%, ADHD was their only mental health diagnosis. Approximately two-thirds (65%) of the antipsychotic prescriptions for children were for off-label use of the drugs. "The lack of safety and efficacy data is especially significant given a growing body of research indicating serious adverse side effects of antipsychotics in children," the researchers noted.
The study points out that neither the American Academy of Child and Adolescent Psychiatry nor the American Academy of Pediatrics recommends second-generation antipsychotics for ADHD management.
Ms. Matone and her colleagues said they had expected to see use of the medications for diagnoses associated with diagnoses such as ADHD and conduct disorder – despite the lack of Food and Drug Administration approval of the drugs for those indications. "However, the size of this population of off-label users and its growth over time was surprising," Ms. Matone said.
"For clinicians, these findings reinforce the importance of both understanding safety concerns associated with pediatric antipsychotic use and being informed about the efficacy and availability of alternative non-pharmacologic treatment therapies.
"There is also a need for information sharing with parents about treatment decisions involving off-label medication use, safety concerns, and alternative treatment approaches," she said.
In addition, further research is needed to explore the indication for antipsychotic use in patients with behavioral problems such as ADHD, the researchers noted.
The study was supported by the Agency for Healthcare Research and Quality and by a fellowship from the Stoneleigh Foundation to Dr. Rubin.
Antipsychotic use in children aged 3-18 years increased by 62% between 2002 and 2007, according to Medicaid data from about 15 million children in the United States.
Although the use of second-generation antipsychotics (SGAs) in children has grown in recent decades, evidence supporting their effectiveness for many conditions is limited, said Meredith Matone of the Children’s Hospital of Philadelphia and her colleagues, including Dr. David M. Rubin, codirector of policy lab at the hospital and an associate professor of pediatrics at the University of Pennsylvania, Philadelphia.
"In light of recent research indicating rising use of antipsychotics in children coupled with concurrent research demonstrating significant side effects of these medications, it felt like a critical next step to understand who the populations of users were and how this population may have changed over the course of the last decade," she said in an interview. The findings were published online (Health Services Research Sept. 5 [doi:10.1111/j.1475-6773.2012.01461.x]).
To examine the relationship between diagnosis and prescription of SGAs, the researchers reviewed Medicaid data from children in 50 states and the District of Columbia between 2002 and 2007.
Overall, 354,000 children were using SGAs in 2007. Of these, 39% were diagnosed with attention-deficit/hyperactivity disorder (ADHD), 11% with bipolar disorder, 12% with ADHD and bipolar, and 38% with other conditions.
In 2007, 50% of children taking antipsychotics had a diagnosis of ADHD, and in 14%, ADHD was their only mental health diagnosis. Approximately two-thirds (65%) of the antipsychotic prescriptions for children were for off-label use of the drugs. "The lack of safety and efficacy data is especially significant given a growing body of research indicating serious adverse side effects of antipsychotics in children," the researchers noted.
The study points out that neither the American Academy of Child and Adolescent Psychiatry nor the American Academy of Pediatrics recommends second-generation antipsychotics for ADHD management.
Ms. Matone and her colleagues said they had expected to see use of the medications for diagnoses associated with diagnoses such as ADHD and conduct disorder – despite the lack of Food and Drug Administration approval of the drugs for those indications. "However, the size of this population of off-label users and its growth over time was surprising," Ms. Matone said.
"For clinicians, these findings reinforce the importance of both understanding safety concerns associated with pediatric antipsychotic use and being informed about the efficacy and availability of alternative non-pharmacologic treatment therapies.
"There is also a need for information sharing with parents about treatment decisions involving off-label medication use, safety concerns, and alternative treatment approaches," she said.
In addition, further research is needed to explore the indication for antipsychotic use in patients with behavioral problems such as ADHD, the researchers noted.
The study was supported by the Agency for Healthcare Research and Quality and by a fellowship from the Stoneleigh Foundation to Dr. Rubin.
Antipsychotic use in children aged 3-18 years increased by 62% between 2002 and 2007, according to Medicaid data from about 15 million children in the United States.
Although the use of second-generation antipsychotics (SGAs) in children has grown in recent decades, evidence supporting their effectiveness for many conditions is limited, said Meredith Matone of the Children’s Hospital of Philadelphia and her colleagues, including Dr. David M. Rubin, codirector of policy lab at the hospital and an associate professor of pediatrics at the University of Pennsylvania, Philadelphia.
"In light of recent research indicating rising use of antipsychotics in children coupled with concurrent research demonstrating significant side effects of these medications, it felt like a critical next step to understand who the populations of users were and how this population may have changed over the course of the last decade," she said in an interview. The findings were published online (Health Services Research Sept. 5 [doi:10.1111/j.1475-6773.2012.01461.x]).
To examine the relationship between diagnosis and prescription of SGAs, the researchers reviewed Medicaid data from children in 50 states and the District of Columbia between 2002 and 2007.
Overall, 354,000 children were using SGAs in 2007. Of these, 39% were diagnosed with attention-deficit/hyperactivity disorder (ADHD), 11% with bipolar disorder, 12% with ADHD and bipolar, and 38% with other conditions.
In 2007, 50% of children taking antipsychotics had a diagnosis of ADHD, and in 14%, ADHD was their only mental health diagnosis. Approximately two-thirds (65%) of the antipsychotic prescriptions for children were for off-label use of the drugs. "The lack of safety and efficacy data is especially significant given a growing body of research indicating serious adverse side effects of antipsychotics in children," the researchers noted.
The study points out that neither the American Academy of Child and Adolescent Psychiatry nor the American Academy of Pediatrics recommends second-generation antipsychotics for ADHD management.
Ms. Matone and her colleagues said they had expected to see use of the medications for diagnoses associated with diagnoses such as ADHD and conduct disorder – despite the lack of Food and Drug Administration approval of the drugs for those indications. "However, the size of this population of off-label users and its growth over time was surprising," Ms. Matone said.
"For clinicians, these findings reinforce the importance of both understanding safety concerns associated with pediatric antipsychotic use and being informed about the efficacy and availability of alternative non-pharmacologic treatment therapies.
"There is also a need for information sharing with parents about treatment decisions involving off-label medication use, safety concerns, and alternative treatment approaches," she said.
In addition, further research is needed to explore the indication for antipsychotic use in patients with behavioral problems such as ADHD, the researchers noted.
The study was supported by the Agency for Healthcare Research and Quality and by a fellowship from the Stoneleigh Foundation to Dr. Rubin.
FROM HEALTH SERVICES RESEARCH
Major Finding: In 2007, 50% of children taking antipsychotics had a diagnosis of attention-deficit/hyperactivity disorder.
Data Source: The findings are based on Medicaid data from about 15 million children in 50 states and the District of Columbia between 2002 and 2007.
Disclosures: The study was supported by the Agency for Healthcare Research and Quality and by a fellowship from the Stoneleigh Foundation to coauthor Dr. Rubin.
Flu Vaccination Called an 'Ethical and Professional Responsibility'
WASHINGTON – Approximately 42% of the U.S. population and 67% of health care workers received influenza vaccinations last year, according to data from the Centers for Disease Control and Prevention.
Since the CDC’s 2010 recommendation for universal flu vaccination for everyone aged 6 months and older, "we seem to be on track in protecting the nation against influenza," Dr. William Schaffner, past president of the National Foundation for Infectious Diseases, said at a press conference.

But there is room for improvement, and clinicians play a key role, said Dr. Schaffner, who also serves as a professor and chair of preventive medicine at Vanderbilt University in Nashville, Tenn.
"I believe that the immunization of the health care provider community is both an ethical and professional responsibility," he said. "It is for two reasons: The first and most important is a patient safety issue, so we do not transmit our influenza infection to our patients."
"The other reason is, when influenza strikes, we need to be vertical, not horizontal," he continued. "We need to be ready to provide health care during that period of great community stress."
"There are many factors that make it easier than ever for everyone to receive flu vaccination," including a plentiful vaccine supply and a variety of venues, including workplaces, where individuals can be vaccinated, said Dr. Schaffner. Proper handwashing, cough and sneeze etiquette, and the prompt use of antivirals also are important to prevent and limit the spread of the flu.
"A physician’s recommendation can be the deciding factor for patients who are sitting on the fence" about getting a flu vaccination, said Litjen Tan, Ph.D., director of medicine and public health for the American Medical Association.
Recent CDC data indicate that pregnant women whose doctors recommended flu vaccination were five times as likely to get a vaccination, and 44% of adults above age 65 who didn’t intend to get vaccinated did so when a doctor recommended it, Dr. Tan said.
"Every physician has an opportunity this flu season to remind their patients to get vaccinated," he said. "Physicians such as cardiologists, obstetricians and gynecologists, pulmonologists, and endocrinologists, who all have high-risk patients, should encourage their patients to seek influenza vaccinations as soon as they are available."
Approximately 85 million doses of flu vaccine have been distributed so far this season, with more on the way, for a total of about 135 million doses, said Dr. Daniel Jernigan, deputy director of the influenza division in the CDC’s National Center for Immunization and Respiratory Diseases.
"The best time to get vaccinated is before the flu season starts," he said. "It is hard to know when the flu will start and where it will start," but vaccination is still recommended throughout the flu season.
This year's vaccine contains a new A virus and a new B virus.
"The few strains we have seen so far match what’s in the vaccine," Dr. Jernigan said.
Although last year’s flu season was the mildest since 1982, clinicians should not be complacent about vaccination for themselves and their patients, said Dr. Howard Koh, assistant secretary for health at the U.S. Department of Health and Human Services.
"The last few years have demonstrated that the flu is predictably unpredictable," Dr. Koh said. The flu pandemic of 2009-2010 was followed by an unusually mild flu season in 2011-2012, but flu-related hospitalizations and deaths occur every year.
"We can’t look to the past to predict the future," he emphasized.
Dr. Koh highlighted data on the recent progress in vaccination coverage, which appeared in Morbidity and Mortality Weekly Report online Sept. 27 (2012;61:753-63).
Overall, 52% of children aged 6 months to 17 years were vaccinated during the 2011-2012 season, approximately the same rate as the previous year, with a rate of 75% among children aged 6 months to 23 months.
However, vaccination of adolescents remains a challenge; 34% of children aged 13-17 years were vaccinated, said Dr. Koh. Adults aged 65 years and older had a 65% vaccination rate last year, but this was a drop from 74% in 2008-2009.
Vaccination coverage among pregnant women was consistent with the previous year, at 47%, remaining significantly higher than the 30% rate before the 2008-2009 flu season.
For the second year in a row, no racial or ethnic disparities were seen in vaccination rates for children, although these disparities persist among adults, Dr. Koh said.
The press conference was sponsored by the National Foundation for Infectious Diseases. For the complete report on flu vaccination in health care personnel and in pregnant women, visit the MMWR website here.
WASHINGTON – Approximately 42% of the U.S. population and 67% of health care workers received influenza vaccinations last year, according to data from the Centers for Disease Control and Prevention.
Since the CDC’s 2010 recommendation for universal flu vaccination for everyone aged 6 months and older, "we seem to be on track in protecting the nation against influenza," Dr. William Schaffner, past president of the National Foundation for Infectious Diseases, said at a press conference.
But there is room for improvement, and clinicians play a key role, said Dr. Schaffner, who also serves as a professor and chair of preventive medicine at Vanderbilt University in Nashville, Tenn.
"I believe that the immunization of the health care provider community is both an ethical and professional responsibility," he said. "It is for two reasons: The first and most important is a patient safety issue, so we do not transmit our influenza infection to our patients."
"The other reason is, when influenza strikes, we need to be vertical, not horizontal," he continued. "We need to be ready to provide health care during that period of great community stress."
"There are many factors that make it easier than ever for everyone to receive flu vaccination," including a plentiful vaccine supply and a variety of venues, including workplaces, where individuals can be vaccinated, said Dr. Schaffner. Proper handwashing, cough and sneeze etiquette, and the prompt use of antivirals also are important to prevent and limit the spread of the flu.
"A physician’s recommendation can be the deciding factor for patients who are sitting on the fence" about getting a flu vaccination, said Litjen Tan, Ph.D., director of medicine and public health for the American Medical Association.
Recent CDC data indicate that pregnant women whose doctors recommended flu vaccination were five times as likely to get a vaccination, and 44% of adults above age 65 who didn’t intend to get vaccinated did so when a doctor recommended it, Dr. Tan said.
"Every physician has an opportunity this flu season to remind their patients to get vaccinated," he said. "Physicians such as cardiologists, obstetricians and gynecologists, pulmonologists, and endocrinologists, who all have high-risk patients, should encourage their patients to seek influenza vaccinations as soon as they are available."
Approximately 85 million doses of flu vaccine have been distributed so far this season, with more on the way, for a total of about 135 million doses, said Dr. Daniel Jernigan, deputy director of the influenza division in the CDC’s National Center for Immunization and Respiratory Diseases.
"The best time to get vaccinated is before the flu season starts," he said. "It is hard to know when the flu will start and where it will start," but vaccination is still recommended throughout the flu season.
This year's vaccine contains a new A virus and a new B virus.
"The few strains we have seen so far match what’s in the vaccine," Dr. Jernigan said.
Although last year’s flu season was the mildest since 1982, clinicians should not be complacent about vaccination for themselves and their patients, said Dr. Howard Koh, assistant secretary for health at the U.S. Department of Health and Human Services.
"The last few years have demonstrated that the flu is predictably unpredictable," Dr. Koh said. The flu pandemic of 2009-2010 was followed by an unusually mild flu season in 2011-2012, but flu-related hospitalizations and deaths occur every year.
"We can’t look to the past to predict the future," he emphasized.
Dr. Koh highlighted data on the recent progress in vaccination coverage, which appeared in Morbidity and Mortality Weekly Report online Sept. 27 (2012;61:753-63).
Overall, 52% of children aged 6 months to 17 years were vaccinated during the 2011-2012 season, approximately the same rate as the previous year, with a rate of 75% among children aged 6 months to 23 months.
However, vaccination of adolescents remains a challenge; 34% of children aged 13-17 years were vaccinated, said Dr. Koh. Adults aged 65 years and older had a 65% vaccination rate last year, but this was a drop from 74% in 2008-2009.
Vaccination coverage among pregnant women was consistent with the previous year, at 47%, remaining significantly higher than the 30% rate before the 2008-2009 flu season.
For the second year in a row, no racial or ethnic disparities were seen in vaccination rates for children, although these disparities persist among adults, Dr. Koh said.
The press conference was sponsored by the National Foundation for Infectious Diseases. For the complete report on flu vaccination in health care personnel and in pregnant women, visit the MMWR website here.
WASHINGTON – Approximately 42% of the U.S. population and 67% of health care workers received influenza vaccinations last year, according to data from the Centers for Disease Control and Prevention.
Since the CDC’s 2010 recommendation for universal flu vaccination for everyone aged 6 months and older, "we seem to be on track in protecting the nation against influenza," Dr. William Schaffner, past president of the National Foundation for Infectious Diseases, said at a press conference.
But there is room for improvement, and clinicians play a key role, said Dr. Schaffner, who also serves as a professor and chair of preventive medicine at Vanderbilt University in Nashville, Tenn.
"I believe that the immunization of the health care provider community is both an ethical and professional responsibility," he said. "It is for two reasons: The first and most important is a patient safety issue, so we do not transmit our influenza infection to our patients."
"The other reason is, when influenza strikes, we need to be vertical, not horizontal," he continued. "We need to be ready to provide health care during that period of great community stress."
"There are many factors that make it easier than ever for everyone to receive flu vaccination," including a plentiful vaccine supply and a variety of venues, including workplaces, where individuals can be vaccinated, said Dr. Schaffner. Proper handwashing, cough and sneeze etiquette, and the prompt use of antivirals also are important to prevent and limit the spread of the flu.
"A physician’s recommendation can be the deciding factor for patients who are sitting on the fence" about getting a flu vaccination, said Litjen Tan, Ph.D., director of medicine and public health for the American Medical Association.
Recent CDC data indicate that pregnant women whose doctors recommended flu vaccination were five times as likely to get a vaccination, and 44% of adults above age 65 who didn’t intend to get vaccinated did so when a doctor recommended it, Dr. Tan said.
"Every physician has an opportunity this flu season to remind their patients to get vaccinated," he said. "Physicians such as cardiologists, obstetricians and gynecologists, pulmonologists, and endocrinologists, who all have high-risk patients, should encourage their patients to seek influenza vaccinations as soon as they are available."
Approximately 85 million doses of flu vaccine have been distributed so far this season, with more on the way, for a total of about 135 million doses, said Dr. Daniel Jernigan, deputy director of the influenza division in the CDC’s National Center for Immunization and Respiratory Diseases.
"The best time to get vaccinated is before the flu season starts," he said. "It is hard to know when the flu will start and where it will start," but vaccination is still recommended throughout the flu season.
This year's vaccine contains a new A virus and a new B virus.
"The few strains we have seen so far match what’s in the vaccine," Dr. Jernigan said.
Although last year’s flu season was the mildest since 1982, clinicians should not be complacent about vaccination for themselves and their patients, said Dr. Howard Koh, assistant secretary for health at the U.S. Department of Health and Human Services.
"The last few years have demonstrated that the flu is predictably unpredictable," Dr. Koh said. The flu pandemic of 2009-2010 was followed by an unusually mild flu season in 2011-2012, but flu-related hospitalizations and deaths occur every year.
"We can’t look to the past to predict the future," he emphasized.
Dr. Koh highlighted data on the recent progress in vaccination coverage, which appeared in Morbidity and Mortality Weekly Report online Sept. 27 (2012;61:753-63).
Overall, 52% of children aged 6 months to 17 years were vaccinated during the 2011-2012 season, approximately the same rate as the previous year, with a rate of 75% among children aged 6 months to 23 months.
However, vaccination of adolescents remains a challenge; 34% of children aged 13-17 years were vaccinated, said Dr. Koh. Adults aged 65 years and older had a 65% vaccination rate last year, but this was a drop from 74% in 2008-2009.
Vaccination coverage among pregnant women was consistent with the previous year, at 47%, remaining significantly higher than the 30% rate before the 2008-2009 flu season.
For the second year in a row, no racial or ethnic disparities were seen in vaccination rates for children, although these disparities persist among adults, Dr. Koh said.
The press conference was sponsored by the National Foundation for Infectious Diseases. For the complete report on flu vaccination in health care personnel and in pregnant women, visit the MMWR website here.
FROM A NATIONAL FOUNDATION FOR INFECTIOUS DISEASES INFLUENZA PRESS CONFERENCE

Don't Rush to Intervene in Pediatric Epiglottitis
WASHINGTON – Managing pediatric epiglottitis without intervention resulted in significantly shortened hospital stays and lower costs, based on data from 820 children.
"Due to the increasing rarity of this disease, suspicion for the diagnosis must remain high for prompt recognition and treatment," said Dr. Marci J. Neidich of Cincinnati Children’s Hospital Medical Center. The use of intubation and tracheotomy to treat epiglottitis in children continues to decline, with a trend toward conservative management, she noted at the annual meeting of the American Academy of Otolaryngology – Head and Neck Surgery Foundation.
To assess the predictive factors for intervention, Dr. Neidich and her colleagues reviewed data from 820 patients in the Kids’ Inpatient Databases for 2006 and 2009 who were treated for acute epiglottitis with and without obstruction.
Overall, 705 children (86%) were managed conservatively and 115 (14%) required intervention (defined as either a tracheotomy or intubation).
Conservative management of epiglottitis in children resulted in a significantly shorter length of hospital stay compared with intervention (an average of 4 days vs. 11 days). The average cost was significantly lower as well ($18,487 vs. $83,037).
Patients were significantly more likely to be managed conservatively in urgent admission compared with emergent cases, and in urban nonteaching hospitals compared with urban teaching hospitals.
Other significant predictors of conservative management included being in a hospital not primarily for children versus a children’s unit or children’s hospital, and being in a small or medium-sized hospital compared with a large hospital.
There were no significant differences in age, race, or sex between the nonintervention and intervention groups. Approximately one-third were female, and approximately 42% were white. The average age was 6 years in the intervention group and 8 years in the nonintervention group. Mortality was less than 10 patients.
The results suggest that most children with epiglottitis can be managed conservatively for a lower cost and with shorter hospital stays and lower mortality rates, said Dr. Neidich. However, additional studies are needed to investigate which patients would be appropriate for intervention versus conservative management, she said.
Dr. Neidich reported having no relevant financial conflicts.
WASHINGTON – Managing pediatric epiglottitis without intervention resulted in significantly shortened hospital stays and lower costs, based on data from 820 children.
"Due to the increasing rarity of this disease, suspicion for the diagnosis must remain high for prompt recognition and treatment," said Dr. Marci J. Neidich of Cincinnati Children’s Hospital Medical Center. The use of intubation and tracheotomy to treat epiglottitis in children continues to decline, with a trend toward conservative management, she noted at the annual meeting of the American Academy of Otolaryngology – Head and Neck Surgery Foundation.
To assess the predictive factors for intervention, Dr. Neidich and her colleagues reviewed data from 820 patients in the Kids’ Inpatient Databases for 2006 and 2009 who were treated for acute epiglottitis with and without obstruction.
Overall, 705 children (86%) were managed conservatively and 115 (14%) required intervention (defined as either a tracheotomy or intubation).
Conservative management of epiglottitis in children resulted in a significantly shorter length of hospital stay compared with intervention (an average of 4 days vs. 11 days). The average cost was significantly lower as well ($18,487 vs. $83,037).
Patients were significantly more likely to be managed conservatively in urgent admission compared with emergent cases, and in urban nonteaching hospitals compared with urban teaching hospitals.
Other significant predictors of conservative management included being in a hospital not primarily for children versus a children’s unit or children’s hospital, and being in a small or medium-sized hospital compared with a large hospital.
There were no significant differences in age, race, or sex between the nonintervention and intervention groups. Approximately one-third were female, and approximately 42% were white. The average age was 6 years in the intervention group and 8 years in the nonintervention group. Mortality was less than 10 patients.
The results suggest that most children with epiglottitis can be managed conservatively for a lower cost and with shorter hospital stays and lower mortality rates, said Dr. Neidich. However, additional studies are needed to investigate which patients would be appropriate for intervention versus conservative management, she said.
Dr. Neidich reported having no relevant financial conflicts.
WASHINGTON – Managing pediatric epiglottitis without intervention resulted in significantly shortened hospital stays and lower costs, based on data from 820 children.
"Due to the increasing rarity of this disease, suspicion for the diagnosis must remain high for prompt recognition and treatment," said Dr. Marci J. Neidich of Cincinnati Children’s Hospital Medical Center. The use of intubation and tracheotomy to treat epiglottitis in children continues to decline, with a trend toward conservative management, she noted at the annual meeting of the American Academy of Otolaryngology – Head and Neck Surgery Foundation.
To assess the predictive factors for intervention, Dr. Neidich and her colleagues reviewed data from 820 patients in the Kids’ Inpatient Databases for 2006 and 2009 who were treated for acute epiglottitis with and without obstruction.
Overall, 705 children (86%) were managed conservatively and 115 (14%) required intervention (defined as either a tracheotomy or intubation).
Conservative management of epiglottitis in children resulted in a significantly shorter length of hospital stay compared with intervention (an average of 4 days vs. 11 days). The average cost was significantly lower as well ($18,487 vs. $83,037).
Patients were significantly more likely to be managed conservatively in urgent admission compared with emergent cases, and in urban nonteaching hospitals compared with urban teaching hospitals.
Other significant predictors of conservative management included being in a hospital not primarily for children versus a children’s unit or children’s hospital, and being in a small or medium-sized hospital compared with a large hospital.
There were no significant differences in age, race, or sex between the nonintervention and intervention groups. Approximately one-third were female, and approximately 42% were white. The average age was 6 years in the intervention group and 8 years in the nonintervention group. Mortality was less than 10 patients.
The results suggest that most children with epiglottitis can be managed conservatively for a lower cost and with shorter hospital stays and lower mortality rates, said Dr. Neidich. However, additional studies are needed to investigate which patients would be appropriate for intervention versus conservative management, she said.
Dr. Neidich reported having no relevant financial conflicts.
AT THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF OTOLARYNGOLOGY - HEAD AND NECK SURGERY FOUNDATION
Major Finding: Managing pediatric epiglottitis without intervention significantly shortened hospital stays (4 days vs. 11 days) and cut costs ($18,487 vs. $83,037) compared with intervention.
Data Source: The data come from a review of 820 patients in the Kids’ Inpatient Databases for 2006 and 2009 who were treated for acute epiglottitis with and without obstruction.
Disclosures: Dr. Neidich said she had no relevant financial conflicts.
CCR7 Predicts Cervical Metastasis in Oral Cancer
WASHINGTON – Chemokine receptor CCR7 expression is a significant predictor of cervical metastases in patients with squamous cell carcinoma in the oral cavity, based on data from 60 adults.
Metastatic spread of squamous cell carcinoma (SCC) is common, but the mechanisms behind the spread remain unclear, said Dr. Levi G. Ledgerwood of the University of California, Davis. "There has been a great deal of work that has looked at lymphocyte entry into lymphatics," he said at the annual meeting of the American Academy of Otolaryngology-Head and Neck Surgery Foundation.
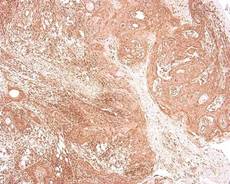
Recent research has focused on the chemokine receptor CCR7, a cell-surface molecule that is required for T-cell entry from the bloodstream and peripheral tissues into lymphatics, he noted. Data from previous studies suggest that CCR7 might play a role in various cancers in the metastases of the lymph nodes.
Dr. Ledgerwood and his colleagues reviewed tissue samples from primary tumors in 60 oral SCC patients who underwent surgical resection at a single center between 2006 and 2011. The study included 30 samples from patients with metastases and 30 samples from patients without metastases. There were no significant demographic differences between the groups, although each group had more male than female patients, Dr. Ledgerwood noted. A total of 30 patients were node positive, and 30 were node negative.
Overall, patients with cervical metastases showed significantly higher CCR7 expression than those without cervical metastases (P less than .001). A total of 97% of node-positive patients were positive for CCR7 expression, but only 43% of patients without cervical metastases were positive for CCR7.
When the lymph nodes of the samples from metastatic cancer patients were examined, all 30 node-positive patients showed expression of CCR7, Dr. Ledgerwood added.
Although the study was limited by its small size, the results suggest a possible role for CCR7 in T-cell access to lymphatics, said Dr. Ledgerwood.
"This is a preliminary study, but we feel that this receptor could provide a very interesting target for future drug therapies and could also help in predicting the behavior of tumors," he said.
Dr. Ledgerwood had no financial conflicts to disclose.
WASHINGTON – Chemokine receptor CCR7 expression is a significant predictor of cervical metastases in patients with squamous cell carcinoma in the oral cavity, based on data from 60 adults.
Metastatic spread of squamous cell carcinoma (SCC) is common, but the mechanisms behind the spread remain unclear, said Dr. Levi G. Ledgerwood of the University of California, Davis. "There has been a great deal of work that has looked at lymphocyte entry into lymphatics," he said at the annual meeting of the American Academy of Otolaryngology-Head and Neck Surgery Foundation.
Recent research has focused on the chemokine receptor CCR7, a cell-surface molecule that is required for T-cell entry from the bloodstream and peripheral tissues into lymphatics, he noted. Data from previous studies suggest that CCR7 might play a role in various cancers in the metastases of the lymph nodes.
Dr. Ledgerwood and his colleagues reviewed tissue samples from primary tumors in 60 oral SCC patients who underwent surgical resection at a single center between 2006 and 2011. The study included 30 samples from patients with metastases and 30 samples from patients without metastases. There were no significant demographic differences between the groups, although each group had more male than female patients, Dr. Ledgerwood noted. A total of 30 patients were node positive, and 30 were node negative.
Overall, patients with cervical metastases showed significantly higher CCR7 expression than those without cervical metastases (P less than .001). A total of 97% of node-positive patients were positive for CCR7 expression, but only 43% of patients without cervical metastases were positive for CCR7.
When the lymph nodes of the samples from metastatic cancer patients were examined, all 30 node-positive patients showed expression of CCR7, Dr. Ledgerwood added.
Although the study was limited by its small size, the results suggest a possible role for CCR7 in T-cell access to lymphatics, said Dr. Ledgerwood.
"This is a preliminary study, but we feel that this receptor could provide a very interesting target for future drug therapies and could also help in predicting the behavior of tumors," he said.
Dr. Ledgerwood had no financial conflicts to disclose.
WASHINGTON – Chemokine receptor CCR7 expression is a significant predictor of cervical metastases in patients with squamous cell carcinoma in the oral cavity, based on data from 60 adults.
Metastatic spread of squamous cell carcinoma (SCC) is common, but the mechanisms behind the spread remain unclear, said Dr. Levi G. Ledgerwood of the University of California, Davis. "There has been a great deal of work that has looked at lymphocyte entry into lymphatics," he said at the annual meeting of the American Academy of Otolaryngology-Head and Neck Surgery Foundation.
Recent research has focused on the chemokine receptor CCR7, a cell-surface molecule that is required for T-cell entry from the bloodstream and peripheral tissues into lymphatics, he noted. Data from previous studies suggest that CCR7 might play a role in various cancers in the metastases of the lymph nodes.
Dr. Ledgerwood and his colleagues reviewed tissue samples from primary tumors in 60 oral SCC patients who underwent surgical resection at a single center between 2006 and 2011. The study included 30 samples from patients with metastases and 30 samples from patients without metastases. There were no significant demographic differences between the groups, although each group had more male than female patients, Dr. Ledgerwood noted. A total of 30 patients were node positive, and 30 were node negative.
Overall, patients with cervical metastases showed significantly higher CCR7 expression than those without cervical metastases (P less than .001). A total of 97% of node-positive patients were positive for CCR7 expression, but only 43% of patients without cervical metastases were positive for CCR7.
When the lymph nodes of the samples from metastatic cancer patients were examined, all 30 node-positive patients showed expression of CCR7, Dr. Ledgerwood added.
Although the study was limited by its small size, the results suggest a possible role for CCR7 in T-cell access to lymphatics, said Dr. Ledgerwood.
"This is a preliminary study, but we feel that this receptor could provide a very interesting target for future drug therapies and could also help in predicting the behavior of tumors," he said.
Dr. Ledgerwood had no financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF OTOLARYNGOLOGY-HEAD AND NECK SURGERY FOUNDATION