User login
Jennifer Smith is the editor of Oncology Practice, part of MDedge Hematology/Oncology. She was previously the editor of Hematology Times, an editor at Principal Investigators Association, and a reporter at The Oneida Daily Dispatch. She has a BS in journalism.
Transient opioid use linked to COPD exacerbation
according to a study of Medicaid claims data.
The data showed that opioid exposure in the prior 7 days was significantly associated with acute respiratory exacerbation. The odds of exacerbation increased as the morphine-equivalent daily dose increased and as the exposure window decreased.
These results “underline the immediacy of the risk of opioid use,” according to Yiran Rong of the department of pharmacy administration at the University of Mississippi in University and colleagues. Ms. Rong and colleagues reported their findings in the American Journal of Epidemiology.
The researchers analyzed Mississippi Medicaid administrative claims data from 2013-2017, which included 1,354 beneficiaries with 1,972 exacerbation events. The beneficiaries had a mean age of 53.11 years, 69.9% were female, and 59.7% were white. The patients had an average of 1.46 exacerbation events, and 62.27% of these events occurred in patients who had an opioid prescription filled in the previous 7 days.
The researchers compared the frequency and dose of opioid exposure in the 7 days before an exacerbation to the opioid exposure in 10 control periods, each 7 days long.
Opioid exposure in the prior 7 days was associated with an 80.8% increase in the odds of exacerbation. The odds ratio, adjusted for exposure to bronchodilators, corticosteroids, benzodiazepines, and beta-blockers, was 1.81 (95% confidence interval, 1.60-2.05).
Opioid exposure was associated with exacerbation in patients with a single exacerbation event (OR, 1.91; 95% CI, 1.61, 2.27), multiple events (OR, 1.71; 95% CI, 1.45-2.01), events recorded in the emergency department (OR, 2.01; 95% CI, 1.71-2.35), and events recorded in the hospital (OR, 1.47; 95% CI, 1.21-1.79).
The odds of exacerbation increased as the morphine-equivalent daily dose increased. Each 25-mg increase in morphine-equivalent daily dose was associated with an 11.2% increase in the odds of exacerbation (OR, 1.11; 95% CI, 1.04-1.20).
“This dose-response relationship is consistent with previously established evidence … and is indicative of the need for caution in prescribing high doses of opioids to COPD patients,” the researchers wrote.
They also found the odds of exacerbation increased as the exposure window decreased. The OR was 1.74 (95% CI, 1.54-1.97) for opioid exposure in an 8-day window before exacerbation and 2.00 (95% CI, 1.73-2.30) for opioid exposure in a 5-day window before exacerbation.
This suggests that “opioid-induced respiratory depression has a very short-term onset,” according to the researchers.
The team noted that this study has limitations, including its retrospective, observational nature, but the results suggest transient opioid use is associated with acute respiratory exacerbation of COPD.
There was no funding for this study, and none of the researchers declared conflicts of interest.
SOURCE: Rong Y et al. Am J Epidemiol. 2019 Jul 30. doi: 10.1093/aje/kwz169.
according to a study of Medicaid claims data.
The data showed that opioid exposure in the prior 7 days was significantly associated with acute respiratory exacerbation. The odds of exacerbation increased as the morphine-equivalent daily dose increased and as the exposure window decreased.
These results “underline the immediacy of the risk of opioid use,” according to Yiran Rong of the department of pharmacy administration at the University of Mississippi in University and colleagues. Ms. Rong and colleagues reported their findings in the American Journal of Epidemiology.
The researchers analyzed Mississippi Medicaid administrative claims data from 2013-2017, which included 1,354 beneficiaries with 1,972 exacerbation events. The beneficiaries had a mean age of 53.11 years, 69.9% were female, and 59.7% were white. The patients had an average of 1.46 exacerbation events, and 62.27% of these events occurred in patients who had an opioid prescription filled in the previous 7 days.
The researchers compared the frequency and dose of opioid exposure in the 7 days before an exacerbation to the opioid exposure in 10 control periods, each 7 days long.
Opioid exposure in the prior 7 days was associated with an 80.8% increase in the odds of exacerbation. The odds ratio, adjusted for exposure to bronchodilators, corticosteroids, benzodiazepines, and beta-blockers, was 1.81 (95% confidence interval, 1.60-2.05).
Opioid exposure was associated with exacerbation in patients with a single exacerbation event (OR, 1.91; 95% CI, 1.61, 2.27), multiple events (OR, 1.71; 95% CI, 1.45-2.01), events recorded in the emergency department (OR, 2.01; 95% CI, 1.71-2.35), and events recorded in the hospital (OR, 1.47; 95% CI, 1.21-1.79).
The odds of exacerbation increased as the morphine-equivalent daily dose increased. Each 25-mg increase in morphine-equivalent daily dose was associated with an 11.2% increase in the odds of exacerbation (OR, 1.11; 95% CI, 1.04-1.20).
“This dose-response relationship is consistent with previously established evidence … and is indicative of the need for caution in prescribing high doses of opioids to COPD patients,” the researchers wrote.
They also found the odds of exacerbation increased as the exposure window decreased. The OR was 1.74 (95% CI, 1.54-1.97) for opioid exposure in an 8-day window before exacerbation and 2.00 (95% CI, 1.73-2.30) for opioid exposure in a 5-day window before exacerbation.
This suggests that “opioid-induced respiratory depression has a very short-term onset,” according to the researchers.
The team noted that this study has limitations, including its retrospective, observational nature, but the results suggest transient opioid use is associated with acute respiratory exacerbation of COPD.
There was no funding for this study, and none of the researchers declared conflicts of interest.
SOURCE: Rong Y et al. Am J Epidemiol. 2019 Jul 30. doi: 10.1093/aje/kwz169.
according to a study of Medicaid claims data.
The data showed that opioid exposure in the prior 7 days was significantly associated with acute respiratory exacerbation. The odds of exacerbation increased as the morphine-equivalent daily dose increased and as the exposure window decreased.
These results “underline the immediacy of the risk of opioid use,” according to Yiran Rong of the department of pharmacy administration at the University of Mississippi in University and colleagues. Ms. Rong and colleagues reported their findings in the American Journal of Epidemiology.
The researchers analyzed Mississippi Medicaid administrative claims data from 2013-2017, which included 1,354 beneficiaries with 1,972 exacerbation events. The beneficiaries had a mean age of 53.11 years, 69.9% were female, and 59.7% were white. The patients had an average of 1.46 exacerbation events, and 62.27% of these events occurred in patients who had an opioid prescription filled in the previous 7 days.
The researchers compared the frequency and dose of opioid exposure in the 7 days before an exacerbation to the opioid exposure in 10 control periods, each 7 days long.
Opioid exposure in the prior 7 days was associated with an 80.8% increase in the odds of exacerbation. The odds ratio, adjusted for exposure to bronchodilators, corticosteroids, benzodiazepines, and beta-blockers, was 1.81 (95% confidence interval, 1.60-2.05).
Opioid exposure was associated with exacerbation in patients with a single exacerbation event (OR, 1.91; 95% CI, 1.61, 2.27), multiple events (OR, 1.71; 95% CI, 1.45-2.01), events recorded in the emergency department (OR, 2.01; 95% CI, 1.71-2.35), and events recorded in the hospital (OR, 1.47; 95% CI, 1.21-1.79).
The odds of exacerbation increased as the morphine-equivalent daily dose increased. Each 25-mg increase in morphine-equivalent daily dose was associated with an 11.2% increase in the odds of exacerbation (OR, 1.11; 95% CI, 1.04-1.20).
“This dose-response relationship is consistent with previously established evidence … and is indicative of the need for caution in prescribing high doses of opioids to COPD patients,” the researchers wrote.
They also found the odds of exacerbation increased as the exposure window decreased. The OR was 1.74 (95% CI, 1.54-1.97) for opioid exposure in an 8-day window before exacerbation and 2.00 (95% CI, 1.73-2.30) for opioid exposure in a 5-day window before exacerbation.
This suggests that “opioid-induced respiratory depression has a very short-term onset,” according to the researchers.
The team noted that this study has limitations, including its retrospective, observational nature, but the results suggest transient opioid use is associated with acute respiratory exacerbation of COPD.
There was no funding for this study, and none of the researchers declared conflicts of interest.
SOURCE: Rong Y et al. Am J Epidemiol. 2019 Jul 30. doi: 10.1093/aje/kwz169.
FROM THE AMERICAN JOURNAL OF EPIDEMIOLOGY
Timing, volume of transfusion may not matter in children with severe anemia
Trial results suggest African children with uncomplicated, severe anemia may not require immediate blood transfusion, and the volume of transfusion may only matter in the context of fever.

The TRACT trial showed no significant differences in 28-day mortality or other clinical outcomes between children who received immediate transfusions and those who did not.
Similarly, there was no significant difference in 28-day mortality among children who received transfusions of 20 mL/kg and those who received transfusions of 30 mL/kg. There was evidence to suggest a higher transfusion volume may benefit children without fevers, but this was an exploratory endpoint. The findings were published in the New England Journal of Medicine.
These results suggest “there is no credible reason to transfuse immediately or to transfuse a higher volume of blood, at least in pediatric populations in regions such as these two sub-Saharan countries [Uganda and Malawi],” Julie R. Ingelfinger, MD, of Massachusetts General Hospital in Boston, wrote in an accompanying editorial, also published in the New England Journal of Medicine (2019;381:475-6).
“The possible effect of higher volume transfusion in patients with fever may trigger additional and potentially useful studies,” she added.
Immediate transfusion
One goal of the TRACT trial was to determine if blood transfusion is the best treatment for children with severe anemia. With this in mind, Kathryn Maitland, MD, PhD, of Imperial College London and colleagues evaluated 1,565 Ugandan and Malawian children with uncomplicated, severe anemia. The patients’ median age was 26 months, and 984 (62.9%) had malaria.
The children were randomized to immediate transfusion (n = 778) or no immediate transfusion (n = 787). Children who did not have an immediate transfusion (control group) could receive a transfusion if they exhibited new signs of clinical severity or had their hemoglobin decrease to below 4 g/dL.
All children in the immediate-transfusion group received a transfusion, as did 386 (49.0%) in the control group. The median time to transfusion was 1.3 hours in the immediate group and 24.9 hours in the control group. The mean total blood volume transfused per child was 314 plus or minus 228 mL and 142 plus or minus 224, respectively. The follow-up period was 180 days, and 4.5% of patients (n = 71) were lost to follow-up.
The researchers found no significant difference between the treatment groups with regard to mortality, other clinical outcomes, or the cost of care.
The 28-day mortality rate was 0.9% in the immediate-transfusion group and 1.7% in the control group (hazard ratio, 0.54; 95% confidence interval, 0.22-1.36; P = .19). The 180-day mortality was 4.5% and 6.0%, respectively (HR, 0.75; 95% CI, 0.48-1.15).
Transfusion volume
To assess the effects of transfusion volume, Dr. Maitland and colleagues evaluated 3,196 Ugandan and Malawian children with severe anemia. The median age of the children was 37 months, and 2,050 (64.1%) had malaria.
The children received a transfusion of 30 mL/kg (n = 1,592) or 20 mL/kg (n = 1,596) at a median of 1.2 hours after randomization. Some children – 197 in the 30-mL/kg group and 300 in the 20-mL/kg group – received additional transfusions. The mean volume of total blood transfused per child was 475 plus or minus 385 mL, and 353 plus or minus 348 mL, respectively.
Overall, there was no significant between-group difference with regard to mortality. The 28-day mortality rate was 3.4% in the 30 mL/kg group and 4.5% in the 20 mL/kg group (HR = 0.76; 95% CI, 0.54 to 1.08; P = .12).
However, the 28-day mortality rate did differ according to the presence of fever at screening. The mortality rate was lower in the 30 mL/kg group for children without fevers (HR = 0.43; 95% CI, 0.27 to 0.69) but higher in the 30 mL/kg group for febrile children (HR = 1.91; 95% CI, 1.04 to 3.49).
For other outcomes, including readmissions and serious adverse events, the researchers found no significant between-group differences.
This trial was supported by a grant from the United Kingdom Medical Research Council through a concordat with the Department for International Development. One researcher has a Wellcome Senior Research Fellowship, and another is a National Institute for Health Research Senior Investigator. Dr. Ingelfinger is a deputy editor at the New England Journal of Medicine. No other relevant conflicts of interest were reported.
SOURCES: Maitland K et al. N Engl J Med. 2019;381:407-19. Maitland K et al. N Engl J Med. 2019;381:420-31.
Trial results suggest African children with uncomplicated, severe anemia may not require immediate blood transfusion, and the volume of transfusion may only matter in the context of fever.
The TRACT trial showed no significant differences in 28-day mortality or other clinical outcomes between children who received immediate transfusions and those who did not.
Similarly, there was no significant difference in 28-day mortality among children who received transfusions of 20 mL/kg and those who received transfusions of 30 mL/kg. There was evidence to suggest a higher transfusion volume may benefit children without fevers, but this was an exploratory endpoint. The findings were published in the New England Journal of Medicine.
These results suggest “there is no credible reason to transfuse immediately or to transfuse a higher volume of blood, at least in pediatric populations in regions such as these two sub-Saharan countries [Uganda and Malawi],” Julie R. Ingelfinger, MD, of Massachusetts General Hospital in Boston, wrote in an accompanying editorial, also published in the New England Journal of Medicine (2019;381:475-6).
“The possible effect of higher volume transfusion in patients with fever may trigger additional and potentially useful studies,” she added.
Immediate transfusion
One goal of the TRACT trial was to determine if blood transfusion is the best treatment for children with severe anemia. With this in mind, Kathryn Maitland, MD, PhD, of Imperial College London and colleagues evaluated 1,565 Ugandan and Malawian children with uncomplicated, severe anemia. The patients’ median age was 26 months, and 984 (62.9%) had malaria.
The children were randomized to immediate transfusion (n = 778) or no immediate transfusion (n = 787). Children who did not have an immediate transfusion (control group) could receive a transfusion if they exhibited new signs of clinical severity or had their hemoglobin decrease to below 4 g/dL.
All children in the immediate-transfusion group received a transfusion, as did 386 (49.0%) in the control group. The median time to transfusion was 1.3 hours in the immediate group and 24.9 hours in the control group. The mean total blood volume transfused per child was 314 plus or minus 228 mL and 142 plus or minus 224, respectively. The follow-up period was 180 days, and 4.5% of patients (n = 71) were lost to follow-up.
The researchers found no significant difference between the treatment groups with regard to mortality, other clinical outcomes, or the cost of care.
The 28-day mortality rate was 0.9% in the immediate-transfusion group and 1.7% in the control group (hazard ratio, 0.54; 95% confidence interval, 0.22-1.36; P = .19). The 180-day mortality was 4.5% and 6.0%, respectively (HR, 0.75; 95% CI, 0.48-1.15).
Transfusion volume
To assess the effects of transfusion volume, Dr. Maitland and colleagues evaluated 3,196 Ugandan and Malawian children with severe anemia. The median age of the children was 37 months, and 2,050 (64.1%) had malaria.
The children received a transfusion of 30 mL/kg (n = 1,592) or 20 mL/kg (n = 1,596) at a median of 1.2 hours after randomization. Some children – 197 in the 30-mL/kg group and 300 in the 20-mL/kg group – received additional transfusions. The mean volume of total blood transfused per child was 475 plus or minus 385 mL, and 353 plus or minus 348 mL, respectively.
Overall, there was no significant between-group difference with regard to mortality. The 28-day mortality rate was 3.4% in the 30 mL/kg group and 4.5% in the 20 mL/kg group (HR = 0.76; 95% CI, 0.54 to 1.08; P = .12).
However, the 28-day mortality rate did differ according to the presence of fever at screening. The mortality rate was lower in the 30 mL/kg group for children without fevers (HR = 0.43; 95% CI, 0.27 to 0.69) but higher in the 30 mL/kg group for febrile children (HR = 1.91; 95% CI, 1.04 to 3.49).
For other outcomes, including readmissions and serious adverse events, the researchers found no significant between-group differences.
This trial was supported by a grant from the United Kingdom Medical Research Council through a concordat with the Department for International Development. One researcher has a Wellcome Senior Research Fellowship, and another is a National Institute for Health Research Senior Investigator. Dr. Ingelfinger is a deputy editor at the New England Journal of Medicine. No other relevant conflicts of interest were reported.
SOURCES: Maitland K et al. N Engl J Med. 2019;381:407-19. Maitland K et al. N Engl J Med. 2019;381:420-31.
Trial results suggest African children with uncomplicated, severe anemia may not require immediate blood transfusion, and the volume of transfusion may only matter in the context of fever.
The TRACT trial showed no significant differences in 28-day mortality or other clinical outcomes between children who received immediate transfusions and those who did not.
Similarly, there was no significant difference in 28-day mortality among children who received transfusions of 20 mL/kg and those who received transfusions of 30 mL/kg. There was evidence to suggest a higher transfusion volume may benefit children without fevers, but this was an exploratory endpoint. The findings were published in the New England Journal of Medicine.
These results suggest “there is no credible reason to transfuse immediately or to transfuse a higher volume of blood, at least in pediatric populations in regions such as these two sub-Saharan countries [Uganda and Malawi],” Julie R. Ingelfinger, MD, of Massachusetts General Hospital in Boston, wrote in an accompanying editorial, also published in the New England Journal of Medicine (2019;381:475-6).
“The possible effect of higher volume transfusion in patients with fever may trigger additional and potentially useful studies,” she added.
Immediate transfusion
One goal of the TRACT trial was to determine if blood transfusion is the best treatment for children with severe anemia. With this in mind, Kathryn Maitland, MD, PhD, of Imperial College London and colleagues evaluated 1,565 Ugandan and Malawian children with uncomplicated, severe anemia. The patients’ median age was 26 months, and 984 (62.9%) had malaria.
The children were randomized to immediate transfusion (n = 778) or no immediate transfusion (n = 787). Children who did not have an immediate transfusion (control group) could receive a transfusion if they exhibited new signs of clinical severity or had their hemoglobin decrease to below 4 g/dL.
All children in the immediate-transfusion group received a transfusion, as did 386 (49.0%) in the control group. The median time to transfusion was 1.3 hours in the immediate group and 24.9 hours in the control group. The mean total blood volume transfused per child was 314 plus or minus 228 mL and 142 plus or minus 224, respectively. The follow-up period was 180 days, and 4.5% of patients (n = 71) were lost to follow-up.
The researchers found no significant difference between the treatment groups with regard to mortality, other clinical outcomes, or the cost of care.
The 28-day mortality rate was 0.9% in the immediate-transfusion group and 1.7% in the control group (hazard ratio, 0.54; 95% confidence interval, 0.22-1.36; P = .19). The 180-day mortality was 4.5% and 6.0%, respectively (HR, 0.75; 95% CI, 0.48-1.15).
Transfusion volume
To assess the effects of transfusion volume, Dr. Maitland and colleagues evaluated 3,196 Ugandan and Malawian children with severe anemia. The median age of the children was 37 months, and 2,050 (64.1%) had malaria.
The children received a transfusion of 30 mL/kg (n = 1,592) or 20 mL/kg (n = 1,596) at a median of 1.2 hours after randomization. Some children – 197 in the 30-mL/kg group and 300 in the 20-mL/kg group – received additional transfusions. The mean volume of total blood transfused per child was 475 plus or minus 385 mL, and 353 plus or minus 348 mL, respectively.
Overall, there was no significant between-group difference with regard to mortality. The 28-day mortality rate was 3.4% in the 30 mL/kg group and 4.5% in the 20 mL/kg group (HR = 0.76; 95% CI, 0.54 to 1.08; P = .12).
However, the 28-day mortality rate did differ according to the presence of fever at screening. The mortality rate was lower in the 30 mL/kg group for children without fevers (HR = 0.43; 95% CI, 0.27 to 0.69) but higher in the 30 mL/kg group for febrile children (HR = 1.91; 95% CI, 1.04 to 3.49).
For other outcomes, including readmissions and serious adverse events, the researchers found no significant between-group differences.
This trial was supported by a grant from the United Kingdom Medical Research Council through a concordat with the Department for International Development. One researcher has a Wellcome Senior Research Fellowship, and another is a National Institute for Health Research Senior Investigator. Dr. Ingelfinger is a deputy editor at the New England Journal of Medicine. No other relevant conflicts of interest were reported.
SOURCES: Maitland K et al. N Engl J Med. 2019;381:407-19. Maitland K et al. N Engl J Med. 2019;381:420-31.
FROM NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point:
Major finding: The 28-day mortality was 0.9% in patients who had immediate transfusions and 1.7% in those who did not (hazard ratio, 0.54; P = .19). The 28-day mortality rate was 3.4% in patients who received transfusions of 30 mL/kg and 4.5% in those who received transfusions of 20 mL/kg (HR, 0.76; P = .12). However, the mortality rate was lower in the 30-mL/kg group for children without fevers (HR, 0.43) and higher in the 30-mL/kg group for febrile children (HR, 1.91).
Study details: A phase 3 trial of African children with severe anemia who were randomized to immediate transfusion (n = 778) or no immediate transfusion (n = 787) and transfusions of 30 mL/kg (n = 1,592) or 20 mL/kg (n = 1,596)
Disclosures: The trial was supported by a grant from the United Kingdom Medical Research Council through a concordat with the Department for International Development. One researcher has a Wellcome Senior Research Fellowship, and another is a National Institute for Health Research Senior Investigator.
Sources: Maitland K et al. N Engl J Med. 2019;381:407-19. Maitland K et al. N Engl J Med. 2019;381:420-31.
ASTRO announces new president-elect, board members
The American Society for Radiation Oncology (ASTRO) has elected a new president-elect and three new officers to its board of directors.

The incoming president-elect is Laura Dawson, MD, of Princess Margaret Cancer Centre and University of Toronto. Dr. Dawson is a professor and radiation oncologist specializing in gastrointestinal malignancies with a focus on hepatobiliary carcinoma and liver metastases, stereotactic body radiation therapy, image-guided radiation therapy, and normal tissue radiation toxicity.
Dr. Dawson will begin her term in September 2019 during ASTRO’s 61st annual meeting. She will serve a 1-year term as president-elect, a 1-year term as president, and a 1-year term as chair of the ASTRO board. During her tenure, Dr. Dawson plans to address issues such as physician burnout, restrictive prior authorization practices, and diversity in the workforce.
Neha Vapiwala, MD, is ASTRO’s new secretary/treasurer-elect. Dr. Vapiwala is an associate professor, vice-chair of education in the department of radiation oncology, and dean of admissions at the Perelman School of Medicine at the University of Pennsylvania in Philadelphia.

She specializes in the management of patients with genitourinary cancers, and her research is focused on improving the delivery of photon- and proton-based radiation.
Dr. Vapiwala will serve a 1-year term as ASTRO’s secretary/treasurer-elect followed by a 3-year term as secretary/treasurer. In these roles, she plans to address challenges in health care economics and assess the role of artificial intelligence and other new technologies in radiation oncology.
Constantine Mantz, MD, is ASTRO’s new Health Policy Council vice-chair. Dr. Mantz is chief policy officer and a radiation oncologist at 21st Century Oncology in Ft. Meyers, Fla.

He specializes in head and neck, prostate, breast, lung, and colorectal cancers.
Dr. Mantz will serve a 2-year term as vice-chair of the Health Policy Council followed by a 2-year term as chair. Dr. Mantz plans to address payment reform issues, including the implementation of an alternative payment model for radiation oncology.
Brian Marples, PhD, is ASTRO’s new Science Council vice-chair. Dr. Marples is a research professor and director of radiobiology in the department of radiation oncology at the University of Miami Miller School of Medicine. His research is focused on maximizing a tumor’s response to radiation while minimizing damage to normal tissue.

Dr. Marples will serve a 2-year term as vice-chair of the Science Council, followed by a 2-year term as chair. He plans to engage the medical community and the public in radiation oncology innovations, such as new technologies that combine radiation and immunotherapy.
Movers in Medicine highlights career moves and personal achievements by hematologists and oncologists. Did you switch jobs, take on a new role, climb a mountain? Tell us all about it at [email protected], and you could be featured in Movers in Medicine.
The American Society for Radiation Oncology (ASTRO) has elected a new president-elect and three new officers to its board of directors.
The incoming president-elect is Laura Dawson, MD, of Princess Margaret Cancer Centre and University of Toronto. Dr. Dawson is a professor and radiation oncologist specializing in gastrointestinal malignancies with a focus on hepatobiliary carcinoma and liver metastases, stereotactic body radiation therapy, image-guided radiation therapy, and normal tissue radiation toxicity.
Dr. Dawson will begin her term in September 2019 during ASTRO’s 61st annual meeting. She will serve a 1-year term as president-elect, a 1-year term as president, and a 1-year term as chair of the ASTRO board. During her tenure, Dr. Dawson plans to address issues such as physician burnout, restrictive prior authorization practices, and diversity in the workforce.
Neha Vapiwala, MD, is ASTRO’s new secretary/treasurer-elect. Dr. Vapiwala is an associate professor, vice-chair of education in the department of radiation oncology, and dean of admissions at the Perelman School of Medicine at the University of Pennsylvania in Philadelphia.
She specializes in the management of patients with genitourinary cancers, and her research is focused on improving the delivery of photon- and proton-based radiation.
Dr. Vapiwala will serve a 1-year term as ASTRO’s secretary/treasurer-elect followed by a 3-year term as secretary/treasurer. In these roles, she plans to address challenges in health care economics and assess the role of artificial intelligence and other new technologies in radiation oncology.
Constantine Mantz, MD, is ASTRO’s new Health Policy Council vice-chair. Dr. Mantz is chief policy officer and a radiation oncologist at 21st Century Oncology in Ft. Meyers, Fla.
He specializes in head and neck, prostate, breast, lung, and colorectal cancers.
Dr. Mantz will serve a 2-year term as vice-chair of the Health Policy Council followed by a 2-year term as chair. Dr. Mantz plans to address payment reform issues, including the implementation of an alternative payment model for radiation oncology.
Brian Marples, PhD, is ASTRO’s new Science Council vice-chair. Dr. Marples is a research professor and director of radiobiology in the department of radiation oncology at the University of Miami Miller School of Medicine. His research is focused on maximizing a tumor’s response to radiation while minimizing damage to normal tissue.
Dr. Marples will serve a 2-year term as vice-chair of the Science Council, followed by a 2-year term as chair. He plans to engage the medical community and the public in radiation oncology innovations, such as new technologies that combine radiation and immunotherapy.
Movers in Medicine highlights career moves and personal achievements by hematologists and oncologists. Did you switch jobs, take on a new role, climb a mountain? Tell us all about it at [email protected], and you could be featured in Movers in Medicine.
The American Society for Radiation Oncology (ASTRO) has elected a new president-elect and three new officers to its board of directors.
The incoming president-elect is Laura Dawson, MD, of Princess Margaret Cancer Centre and University of Toronto. Dr. Dawson is a professor and radiation oncologist specializing in gastrointestinal malignancies with a focus on hepatobiliary carcinoma and liver metastases, stereotactic body radiation therapy, image-guided radiation therapy, and normal tissue radiation toxicity.
Dr. Dawson will begin her term in September 2019 during ASTRO’s 61st annual meeting. She will serve a 1-year term as president-elect, a 1-year term as president, and a 1-year term as chair of the ASTRO board. During her tenure, Dr. Dawson plans to address issues such as physician burnout, restrictive prior authorization practices, and diversity in the workforce.
Neha Vapiwala, MD, is ASTRO’s new secretary/treasurer-elect. Dr. Vapiwala is an associate professor, vice-chair of education in the department of radiation oncology, and dean of admissions at the Perelman School of Medicine at the University of Pennsylvania in Philadelphia.
She specializes in the management of patients with genitourinary cancers, and her research is focused on improving the delivery of photon- and proton-based radiation.
Dr. Vapiwala will serve a 1-year term as ASTRO’s secretary/treasurer-elect followed by a 3-year term as secretary/treasurer. In these roles, she plans to address challenges in health care economics and assess the role of artificial intelligence and other new technologies in radiation oncology.
Constantine Mantz, MD, is ASTRO’s new Health Policy Council vice-chair. Dr. Mantz is chief policy officer and a radiation oncologist at 21st Century Oncology in Ft. Meyers, Fla.
He specializes in head and neck, prostate, breast, lung, and colorectal cancers.
Dr. Mantz will serve a 2-year term as vice-chair of the Health Policy Council followed by a 2-year term as chair. Dr. Mantz plans to address payment reform issues, including the implementation of an alternative payment model for radiation oncology.
Brian Marples, PhD, is ASTRO’s new Science Council vice-chair. Dr. Marples is a research professor and director of radiobiology in the department of radiation oncology at the University of Miami Miller School of Medicine. His research is focused on maximizing a tumor’s response to radiation while minimizing damage to normal tissue.
Dr. Marples will serve a 2-year term as vice-chair of the Science Council, followed by a 2-year term as chair. He plans to engage the medical community and the public in radiation oncology innovations, such as new technologies that combine radiation and immunotherapy.
Movers in Medicine highlights career moves and personal achievements by hematologists and oncologists. Did you switch jobs, take on a new role, climb a mountain? Tell us all about it at [email protected], and you could be featured in Movers in Medicine.
U.S. fertility rate, teen births are on the decline
The general fertility rate in the United States decreased 2% between 2017 and 2018, according to a report from the Centers for Disease Control and Prevention.

Fertility rates, defined as births per 1,000 women aged 15-44 years, declined for all racial/ethnic groups studied.
Teen birth rates, or births among girls aged 15-19 years, declined from 2017 to 2018 as well.
These data come from the National Vital Statistics System’s Natality Data File, which includes information from birth certificates for all births in the United States.
The data show a decline in the general fertility rate from 60.3 per 1,000 women in 2017 to 59.1 per 1,000 women in 2018, a significant decrease (P less than .05).
Fertility rates declined across the three largest racial/ethnic groups studied, decreasing:
- 3% in Hispanic women, from 67.6 to 65.9 per 1,000.
- 2% in non-Hispanic black women, from 63.1 to 62.0 per 1,000.
- 2% in non-Hispanic white women, from 57.2 to 56.3 per 1,000.
Similarly, teen birth rates declined 7% from 2017 to 2018, decreasing from 18.8 to 17.4 births per 1,000 girls aged 15-19 years (P less than .05). Rates decreased:
- 8% in Hispanic teens, from 28.9 to 26.7 per 1,000.
- 4% in non-Hispanic black teens, from 27.5 to 26.3 per 1,000.
- 8% in non-Hispanic white teens, from 13.2 to 12.1 per 1,000.
The data also show an increase in the rate of vaginal births after previous cesarean (VBAC) delivery. The percentage of VBAC deliveries increased from 12.8% in 2017 to 13.3% in 2018 (P less than .05).
VBAC delivery rates increased across all racial/ethnic groups studied, although the increase among non-Hispanic back women was not significant.
Finally, the report shows an increase in preterm and early term births from 2017 to 2018. Preterm deliveries (less than 37 weeks of gestation) increased from 9.93% to 10.02%, and early term deliveries (37-38 weeks) increased from 26.00% to 26.53% (P less than .05).
At the same time, full-term births (39-40 weeks) decreased from 57.49% to 57.24%, and late- and post-term births (41 weeks or more) decreased from 6.58 % to 6.20% (P less than .05). These findings were consistent across the racial/ethnic groups studied.
SOURCE: Martin JA et al. NCHS Data Brief. 2019 July; no 346.
The general fertility rate in the United States decreased 2% between 2017 and 2018, according to a report from the Centers for Disease Control and Prevention.
Fertility rates, defined as births per 1,000 women aged 15-44 years, declined for all racial/ethnic groups studied.
Teen birth rates, or births among girls aged 15-19 years, declined from 2017 to 2018 as well.
These data come from the National Vital Statistics System’s Natality Data File, which includes information from birth certificates for all births in the United States.
The data show a decline in the general fertility rate from 60.3 per 1,000 women in 2017 to 59.1 per 1,000 women in 2018, a significant decrease (P less than .05).
Fertility rates declined across the three largest racial/ethnic groups studied, decreasing:
- 3% in Hispanic women, from 67.6 to 65.9 per 1,000.
- 2% in non-Hispanic black women, from 63.1 to 62.0 per 1,000.
- 2% in non-Hispanic white women, from 57.2 to 56.3 per 1,000.
Similarly, teen birth rates declined 7% from 2017 to 2018, decreasing from 18.8 to 17.4 births per 1,000 girls aged 15-19 years (P less than .05). Rates decreased:
- 8% in Hispanic teens, from 28.9 to 26.7 per 1,000.
- 4% in non-Hispanic black teens, from 27.5 to 26.3 per 1,000.
- 8% in non-Hispanic white teens, from 13.2 to 12.1 per 1,000.
The data also show an increase in the rate of vaginal births after previous cesarean (VBAC) delivery. The percentage of VBAC deliveries increased from 12.8% in 2017 to 13.3% in 2018 (P less than .05).
VBAC delivery rates increased across all racial/ethnic groups studied, although the increase among non-Hispanic back women was not significant.
Finally, the report shows an increase in preterm and early term births from 2017 to 2018. Preterm deliveries (less than 37 weeks of gestation) increased from 9.93% to 10.02%, and early term deliveries (37-38 weeks) increased from 26.00% to 26.53% (P less than .05).
At the same time, full-term births (39-40 weeks) decreased from 57.49% to 57.24%, and late- and post-term births (41 weeks or more) decreased from 6.58 % to 6.20% (P less than .05). These findings were consistent across the racial/ethnic groups studied.
SOURCE: Martin JA et al. NCHS Data Brief. 2019 July; no 346.
The general fertility rate in the United States decreased 2% between 2017 and 2018, according to a report from the Centers for Disease Control and Prevention.
Fertility rates, defined as births per 1,000 women aged 15-44 years, declined for all racial/ethnic groups studied.
Teen birth rates, or births among girls aged 15-19 years, declined from 2017 to 2018 as well.
These data come from the National Vital Statistics System’s Natality Data File, which includes information from birth certificates for all births in the United States.
The data show a decline in the general fertility rate from 60.3 per 1,000 women in 2017 to 59.1 per 1,000 women in 2018, a significant decrease (P less than .05).
Fertility rates declined across the three largest racial/ethnic groups studied, decreasing:
- 3% in Hispanic women, from 67.6 to 65.9 per 1,000.
- 2% in non-Hispanic black women, from 63.1 to 62.0 per 1,000.
- 2% in non-Hispanic white women, from 57.2 to 56.3 per 1,000.
Similarly, teen birth rates declined 7% from 2017 to 2018, decreasing from 18.8 to 17.4 births per 1,000 girls aged 15-19 years (P less than .05). Rates decreased:
- 8% in Hispanic teens, from 28.9 to 26.7 per 1,000.
- 4% in non-Hispanic black teens, from 27.5 to 26.3 per 1,000.
- 8% in non-Hispanic white teens, from 13.2 to 12.1 per 1,000.
The data also show an increase in the rate of vaginal births after previous cesarean (VBAC) delivery. The percentage of VBAC deliveries increased from 12.8% in 2017 to 13.3% in 2018 (P less than .05).
VBAC delivery rates increased across all racial/ethnic groups studied, although the increase among non-Hispanic back women was not significant.
Finally, the report shows an increase in preterm and early term births from 2017 to 2018. Preterm deliveries (less than 37 weeks of gestation) increased from 9.93% to 10.02%, and early term deliveries (37-38 weeks) increased from 26.00% to 26.53% (P less than .05).
At the same time, full-term births (39-40 weeks) decreased from 57.49% to 57.24%, and late- and post-term births (41 weeks or more) decreased from 6.58 % to 6.20% (P less than .05). These findings were consistent across the racial/ethnic groups studied.
SOURCE: Martin JA et al. NCHS Data Brief. 2019 July; no 346.
Results support first-line T-DM1 in HER2+ breast cancer
Trastuzumab emtansine (T-DM1) is a suitable first-line therapy for patients with HER2-positive, advanced breast cancer who cannot receive taxane-based therapy, according to researchers.
Final results from the phase 3 MARIANNE trial revealed similar overall survival (OS) in patients who received T-DM1, T-DM1 plus pertuzumab, or trastuzumab plus a taxane (HT). All three regimens resulted in a median OS exceeding 50 months.
The incidence of grade 3 or higher adverse events (AEs) was highest in patients who received HT.
Edith A. Perez, MD, of Mayo Clinic Cancer Center in Jacksonville, Fla., and colleagues reported these results in Cancer.
The MARIANNE trial (NCT01120184) enrolled 1,095 adults with HER2-positive, advanced breast cancer. They were randomized to receive HT, T-DM1, or T-DM1 plus pertuzumab. Patients in the HT arm received trastuzumab plus paclitaxel or docetaxel according to the investigator’s discretion.
In all, 352 patients received HT (257 on docetaxel and 96 on paclitaxel), 361 patients received T-DM1 plus placebo, and 366 received T-DM1 plus pertuzumab.
Response and OS
In the primary analysis, the median OS was not reached in any treatment arm at a median follow-up of 35 months. The rate of objective response was 67.9% in the HT arm, 64.2% in the T-DM1 plus pertuzumab arm, and 59.7% in the T-DM1 arm. The median duration of response was 12.5 months, 21.2 months, and 20.7 months, respectively.
For the final OS analysis, the median duration of follow-up was 54 months. Roughly 70% of patients in each arm had received at least one treatment regimen during follow-up.
The final median OS was similar across the treatment arms – 50.9 months in the HT arm, 53.7 months in the T-DM1 arm, and 51.8 months in the T-DM1 plus pertuzumab arm. With the HT arm as a reference, the stratified hazard ratio was 0.93 for the T-DM1 arm and 0.86 for the T-DM1 plus pertuzumab arm.
OS results were consistent across subgroups. Although there were some differences in hazard ratios, “none of the examined subgroups showed a clear benefit with one treatment regimen in comparison with the others,” the researchers wrote.
The researchers also analyzed OS by response status at 6.5 months after randomization. Among nonresponders, the median OS was 41.9 months in the T-DM1 plus pertuzumab arm, 45.7 months in the T-DM1 arm, and 48.1 months in the HT arm. Among responders, the median OS was not reached in the T-DM1 plus pertuzumab arm, 64.4 months, and 56.3 months, respectively.
There were no baseline characteristics or biomarkers that were strongly associated with response by treatment group. However, in the HT and T-DM1 arms, patients with above-median HER2 messenger RNA expression were more likely to respond.
Safety
Rates of grade 3 or higher AEs were 55.8% in the HT arm, 47.1% in the T-DM1 arm, and 48.6% in the T-DM1 plus pertuzumab arm. The most common grade 3 or higher AEs were as follows:
- HT arm – neutropenia (19.3%), febrile neutropenia (6.5%), and diarrhea (4.2%).
- T-DM1 arm – increased aspartate aminotransferase (6.9%), thrombocytopenia (6.6%), and anemia (5.0%).
- T-DM1 plus pertuzumab arm – thrombocytopenia (9.0%), anemia (7.1%), and increased alanine aminotransferase (6.0%).
Rates of AE-related treatment discontinuation were 20.8% in the T-DM1 arm, 23.0% in the T-DM1 plus pertuzumab arm, and 30.6% in the HT arm. Rates of AE-related death were 1.4%, 1.9%, and 2.0%, respectively.
This study was funded by F. Hoffmann–La Roche. Dr. Perez was previously employed by Genentech/Roche. Her fellow authors disclosed relationships with Roche and many other companies.
SOURCE: Perez EA et al. Cancer. 2019 Jul 18. doi: 10.1002/cncr.32392.
Trastuzumab emtansine (T-DM1) is a suitable first-line therapy for patients with HER2-positive, advanced breast cancer who cannot receive taxane-based therapy, according to researchers.
Final results from the phase 3 MARIANNE trial revealed similar overall survival (OS) in patients who received T-DM1, T-DM1 plus pertuzumab, or trastuzumab plus a taxane (HT). All three regimens resulted in a median OS exceeding 50 months.
The incidence of grade 3 or higher adverse events (AEs) was highest in patients who received HT.
Edith A. Perez, MD, of Mayo Clinic Cancer Center in Jacksonville, Fla., and colleagues reported these results in Cancer.
The MARIANNE trial (NCT01120184) enrolled 1,095 adults with HER2-positive, advanced breast cancer. They were randomized to receive HT, T-DM1, or T-DM1 plus pertuzumab. Patients in the HT arm received trastuzumab plus paclitaxel or docetaxel according to the investigator’s discretion.
In all, 352 patients received HT (257 on docetaxel and 96 on paclitaxel), 361 patients received T-DM1 plus placebo, and 366 received T-DM1 plus pertuzumab.
Response and OS
In the primary analysis, the median OS was not reached in any treatment arm at a median follow-up of 35 months. The rate of objective response was 67.9% in the HT arm, 64.2% in the T-DM1 plus pertuzumab arm, and 59.7% in the T-DM1 arm. The median duration of response was 12.5 months, 21.2 months, and 20.7 months, respectively.
For the final OS analysis, the median duration of follow-up was 54 months. Roughly 70% of patients in each arm had received at least one treatment regimen during follow-up.
The final median OS was similar across the treatment arms – 50.9 months in the HT arm, 53.7 months in the T-DM1 arm, and 51.8 months in the T-DM1 plus pertuzumab arm. With the HT arm as a reference, the stratified hazard ratio was 0.93 for the T-DM1 arm and 0.86 for the T-DM1 plus pertuzumab arm.
OS results were consistent across subgroups. Although there were some differences in hazard ratios, “none of the examined subgroups showed a clear benefit with one treatment regimen in comparison with the others,” the researchers wrote.
The researchers also analyzed OS by response status at 6.5 months after randomization. Among nonresponders, the median OS was 41.9 months in the T-DM1 plus pertuzumab arm, 45.7 months in the T-DM1 arm, and 48.1 months in the HT arm. Among responders, the median OS was not reached in the T-DM1 plus pertuzumab arm, 64.4 months, and 56.3 months, respectively.
There were no baseline characteristics or biomarkers that were strongly associated with response by treatment group. However, in the HT and T-DM1 arms, patients with above-median HER2 messenger RNA expression were more likely to respond.
Safety
Rates of grade 3 or higher AEs were 55.8% in the HT arm, 47.1% in the T-DM1 arm, and 48.6% in the T-DM1 plus pertuzumab arm. The most common grade 3 or higher AEs were as follows:
- HT arm – neutropenia (19.3%), febrile neutropenia (6.5%), and diarrhea (4.2%).
- T-DM1 arm – increased aspartate aminotransferase (6.9%), thrombocytopenia (6.6%), and anemia (5.0%).
- T-DM1 plus pertuzumab arm – thrombocytopenia (9.0%), anemia (7.1%), and increased alanine aminotransferase (6.0%).
Rates of AE-related treatment discontinuation were 20.8% in the T-DM1 arm, 23.0% in the T-DM1 plus pertuzumab arm, and 30.6% in the HT arm. Rates of AE-related death were 1.4%, 1.9%, and 2.0%, respectively.
This study was funded by F. Hoffmann–La Roche. Dr. Perez was previously employed by Genentech/Roche. Her fellow authors disclosed relationships with Roche and many other companies.
SOURCE: Perez EA et al. Cancer. 2019 Jul 18. doi: 10.1002/cncr.32392.
Trastuzumab emtansine (T-DM1) is a suitable first-line therapy for patients with HER2-positive, advanced breast cancer who cannot receive taxane-based therapy, according to researchers.
Final results from the phase 3 MARIANNE trial revealed similar overall survival (OS) in patients who received T-DM1, T-DM1 plus pertuzumab, or trastuzumab plus a taxane (HT). All three regimens resulted in a median OS exceeding 50 months.
The incidence of grade 3 or higher adverse events (AEs) was highest in patients who received HT.
Edith A. Perez, MD, of Mayo Clinic Cancer Center in Jacksonville, Fla., and colleagues reported these results in Cancer.
The MARIANNE trial (NCT01120184) enrolled 1,095 adults with HER2-positive, advanced breast cancer. They were randomized to receive HT, T-DM1, or T-DM1 plus pertuzumab. Patients in the HT arm received trastuzumab plus paclitaxel or docetaxel according to the investigator’s discretion.
In all, 352 patients received HT (257 on docetaxel and 96 on paclitaxel), 361 patients received T-DM1 plus placebo, and 366 received T-DM1 plus pertuzumab.
Response and OS
In the primary analysis, the median OS was not reached in any treatment arm at a median follow-up of 35 months. The rate of objective response was 67.9% in the HT arm, 64.2% in the T-DM1 plus pertuzumab arm, and 59.7% in the T-DM1 arm. The median duration of response was 12.5 months, 21.2 months, and 20.7 months, respectively.
For the final OS analysis, the median duration of follow-up was 54 months. Roughly 70% of patients in each arm had received at least one treatment regimen during follow-up.
The final median OS was similar across the treatment arms – 50.9 months in the HT arm, 53.7 months in the T-DM1 arm, and 51.8 months in the T-DM1 plus pertuzumab arm. With the HT arm as a reference, the stratified hazard ratio was 0.93 for the T-DM1 arm and 0.86 for the T-DM1 plus pertuzumab arm.
OS results were consistent across subgroups. Although there were some differences in hazard ratios, “none of the examined subgroups showed a clear benefit with one treatment regimen in comparison with the others,” the researchers wrote.
The researchers also analyzed OS by response status at 6.5 months after randomization. Among nonresponders, the median OS was 41.9 months in the T-DM1 plus pertuzumab arm, 45.7 months in the T-DM1 arm, and 48.1 months in the HT arm. Among responders, the median OS was not reached in the T-DM1 plus pertuzumab arm, 64.4 months, and 56.3 months, respectively.
There were no baseline characteristics or biomarkers that were strongly associated with response by treatment group. However, in the HT and T-DM1 arms, patients with above-median HER2 messenger RNA expression were more likely to respond.
Safety
Rates of grade 3 or higher AEs were 55.8% in the HT arm, 47.1% in the T-DM1 arm, and 48.6% in the T-DM1 plus pertuzumab arm. The most common grade 3 or higher AEs were as follows:
- HT arm – neutropenia (19.3%), febrile neutropenia (6.5%), and diarrhea (4.2%).
- T-DM1 arm – increased aspartate aminotransferase (6.9%), thrombocytopenia (6.6%), and anemia (5.0%).
- T-DM1 plus pertuzumab arm – thrombocytopenia (9.0%), anemia (7.1%), and increased alanine aminotransferase (6.0%).
Rates of AE-related treatment discontinuation were 20.8% in the T-DM1 arm, 23.0% in the T-DM1 plus pertuzumab arm, and 30.6% in the HT arm. Rates of AE-related death were 1.4%, 1.9%, and 2.0%, respectively.
This study was funded by F. Hoffmann–La Roche. Dr. Perez was previously employed by Genentech/Roche. Her fellow authors disclosed relationships with Roche and many other companies.
SOURCE: Perez EA et al. Cancer. 2019 Jul 18. doi: 10.1002/cncr.32392.
FROM CANCER
BTK mutations linked to CLL progression on ibrutinib
Mutations in Bruton’s tyrosine kinase (BTK) are associated with progression of chronic lymphocytic leukemia (CLL) in patients taking ibrutinib, according to a new study.

Researchers analyzed a “real-life” cohort of CLL patients taking ibrutinib for about 3 years and found that patients with BTK mutations were significantly more likely to progress (P = .0005).
“Our findings support that mutational analysis should be considered in patients receiving ibrutinib who have residual clonal lymphocytosis, and that clinical trials are needed to evaluate whether patients with a BTK mutation may benefit from an early switch to another treatment,” wrote Anne Quinquenel, MD, PhD, of Hôpital Robert Debré, Université Reims (France) Champagne-Ardenne, and colleagues. Their report is in Blood.
The researchers studied 57 CLL patients who were still on ibrutinib after at least 3 years and provided fresh blood samples. The median time between the start of ibrutinib and sample collection was 3.5 years.
All 57 patients had minimal residual disease at baseline. Of the 55 patients with response data available, 48 had a partial response, and 7 had a partial response with lymphocytosis.
Mutational profiling was possible in 30 patients who had a CLL clone greater than or equal to 0.5 x 109/L.
BTK mutations were present in 17 of the 30 patients (57%). There were 20 BTK mutations in total, all were at C481, and 14 were at C481S.
The researchers also identified 15 patients with TP53 mutations and 4 patients with phospholipase Cg2 (PLCG2) mutations. All 4 patients with PLCG2 mutations also had a BTK mutation and a TP53 mutation.
However, there were no significant associations between BTK mutations and other mutations. BTK mutations were not associated with the number of previous therapies a patient received or the need for ibrutinib dose interruptions or reductions.
The researchers assessed CLL progression at median of 8.5 months from sample collection and found the presence of a BTK mutation was significantly associated with progression (P = .0005).
Of the 17 patients with a BTK mutation, 14 progressed with one case of Richter’s syndrome. Three patients who progressed were still on ibrutinib, nine patients received venetoclax, and two patients died without further treatment.
Of the 13 patients without BTK mutations, just two patients progressed. One patient died without further treatment, and the other received venetoclax.
The event-free survival was significantly shorter in patients with a BTK mutation than in those without (P = .0380), but there was no significant difference in overall survival.
This research was supported by Sunesis Pharmaceuticals and the Force Hemato (fonds de recherche clinique en hématologie) foundation. The researchers reported relationships with Janssen, Gilead, Roche, and AbbVie.
SOURCE: Quinquenel A et al. Blood. 2019 Jun 26. doi: 10.1182/blood.2019000854.
Mutations in Bruton’s tyrosine kinase (BTK) are associated with progression of chronic lymphocytic leukemia (CLL) in patients taking ibrutinib, according to a new study.
Researchers analyzed a “real-life” cohort of CLL patients taking ibrutinib for about 3 years and found that patients with BTK mutations were significantly more likely to progress (P = .0005).
“Our findings support that mutational analysis should be considered in patients receiving ibrutinib who have residual clonal lymphocytosis, and that clinical trials are needed to evaluate whether patients with a BTK mutation may benefit from an early switch to another treatment,” wrote Anne Quinquenel, MD, PhD, of Hôpital Robert Debré, Université Reims (France) Champagne-Ardenne, and colleagues. Their report is in Blood.
The researchers studied 57 CLL patients who were still on ibrutinib after at least 3 years and provided fresh blood samples. The median time between the start of ibrutinib and sample collection was 3.5 years.
All 57 patients had minimal residual disease at baseline. Of the 55 patients with response data available, 48 had a partial response, and 7 had a partial response with lymphocytosis.
Mutational profiling was possible in 30 patients who had a CLL clone greater than or equal to 0.5 x 109/L.
BTK mutations were present in 17 of the 30 patients (57%). There were 20 BTK mutations in total, all were at C481, and 14 were at C481S.
The researchers also identified 15 patients with TP53 mutations and 4 patients with phospholipase Cg2 (PLCG2) mutations. All 4 patients with PLCG2 mutations also had a BTK mutation and a TP53 mutation.
However, there were no significant associations between BTK mutations and other mutations. BTK mutations were not associated with the number of previous therapies a patient received or the need for ibrutinib dose interruptions or reductions.
The researchers assessed CLL progression at median of 8.5 months from sample collection and found the presence of a BTK mutation was significantly associated with progression (P = .0005).
Of the 17 patients with a BTK mutation, 14 progressed with one case of Richter’s syndrome. Three patients who progressed were still on ibrutinib, nine patients received venetoclax, and two patients died without further treatment.
Of the 13 patients without BTK mutations, just two patients progressed. One patient died without further treatment, and the other received venetoclax.
The event-free survival was significantly shorter in patients with a BTK mutation than in those without (P = .0380), but there was no significant difference in overall survival.
This research was supported by Sunesis Pharmaceuticals and the Force Hemato (fonds de recherche clinique en hématologie) foundation. The researchers reported relationships with Janssen, Gilead, Roche, and AbbVie.
SOURCE: Quinquenel A et al. Blood. 2019 Jun 26. doi: 10.1182/blood.2019000854.
Mutations in Bruton’s tyrosine kinase (BTK) are associated with progression of chronic lymphocytic leukemia (CLL) in patients taking ibrutinib, according to a new study.
Researchers analyzed a “real-life” cohort of CLL patients taking ibrutinib for about 3 years and found that patients with BTK mutations were significantly more likely to progress (P = .0005).
“Our findings support that mutational analysis should be considered in patients receiving ibrutinib who have residual clonal lymphocytosis, and that clinical trials are needed to evaluate whether patients with a BTK mutation may benefit from an early switch to another treatment,” wrote Anne Quinquenel, MD, PhD, of Hôpital Robert Debré, Université Reims (France) Champagne-Ardenne, and colleagues. Their report is in Blood.
The researchers studied 57 CLL patients who were still on ibrutinib after at least 3 years and provided fresh blood samples. The median time between the start of ibrutinib and sample collection was 3.5 years.
All 57 patients had minimal residual disease at baseline. Of the 55 patients with response data available, 48 had a partial response, and 7 had a partial response with lymphocytosis.
Mutational profiling was possible in 30 patients who had a CLL clone greater than or equal to 0.5 x 109/L.
BTK mutations were present in 17 of the 30 patients (57%). There were 20 BTK mutations in total, all were at C481, and 14 were at C481S.
The researchers also identified 15 patients with TP53 mutations and 4 patients with phospholipase Cg2 (PLCG2) mutations. All 4 patients with PLCG2 mutations also had a BTK mutation and a TP53 mutation.
However, there were no significant associations between BTK mutations and other mutations. BTK mutations were not associated with the number of previous therapies a patient received or the need for ibrutinib dose interruptions or reductions.
The researchers assessed CLL progression at median of 8.5 months from sample collection and found the presence of a BTK mutation was significantly associated with progression (P = .0005).
Of the 17 patients with a BTK mutation, 14 progressed with one case of Richter’s syndrome. Three patients who progressed were still on ibrutinib, nine patients received venetoclax, and two patients died without further treatment.
Of the 13 patients without BTK mutations, just two patients progressed. One patient died without further treatment, and the other received venetoclax.
The event-free survival was significantly shorter in patients with a BTK mutation than in those without (P = .0380), but there was no significant difference in overall survival.
This research was supported by Sunesis Pharmaceuticals and the Force Hemato (fonds de recherche clinique en hématologie) foundation. The researchers reported relationships with Janssen, Gilead, Roche, and AbbVie.
SOURCE: Quinquenel A et al. Blood. 2019 Jun 26. doi: 10.1182/blood.2019000854.
FROM BLOOD
CAR T-cell therapy less effective in transformed follicular lymphoma
All complete responders with FL were still in remission at a median follow-up of 24 months, but the median duration of response was 10.2 months for patients with tFL.
Alexandre V. Hirayama, MD, of the Fred Hutchinson Cancer Research Center in Seattle, and colleagues reported these results in Blood.
The trial enrolled 21 adults with relapsed/refractory CD19+ B-cell malignancies, including 8 patients with FL and 13 with tFL. At baseline, the FL/tFL patients had a median age of 56 years (range, 51-62), and 67% were male. Most patients (n = 19) had stage III/IV disease, 17 had extranodal disease, 8 had bulky disease, and 6 had bone marrow involvement. The patients had received a median of 5 prior therapies (range, 2-8), and 13 had received a transplant.
In this study, patients received a lymphodepleting regimen of cyclophosphamide and fludarabine, followed by 2 x 106 CD19 CAR T cells/kg. Five patients (one with FL and four with tFL) also received bridging chemotherapy between leukapheresis and lymphodepletion.
Grade 1-2 cytokine release syndrome occurred in 50% of FL patients and 39% of tFL patients (P = .35). Grade 1-2 neurotoxicity occurred in 50% and 23%, respectively (P = .67). There were no cases of grade 3 or higher cytokine release syndrome or neurotoxicity.
Most FL patients (7 of 8; 88%) achieved a complete response (CR) to treatment, and all of these patients were still in CR at a median follow-up of 24 months (range, 5-37 months). One FL patient received a transplant while in CR.
Six of 13 tFL patients (46%) achieved a CR. At a median follow-up of 38 months (range, 3-39 months), the median duration of response was 10.2 months. The median progression-free survival was 11.2 months in patients who achieved a CR and 1.4 months in all tFL patients.
The researchers noted that peak CAR T-cell counts and the duration of CAR T-cell detection were similar between FL and tFL patients. However, tFL patients had higher serum interleukin-8 concentrations and higher lactate dehydrogenase levels before treatment.
Past research suggested that IL-8 mediates the recruitment of tumor-associated neutrophils, promotes diffuse large B-cell lymphoma progression, and can contribute to local immune suppression. Other studies have linked elevated lactate dehydrogenase to aggressive disease and a more immunosuppressive tumor microenvironment.
“Although these data raise the possibility that differences in the tumor microenvironment may, in part, contribute to differences in outcomes after CAR T-cell immunotherapy in FL and tFL patients, additional studies are required,” the researchers wrote.
This research was supported by the National Institutes of Health, the Life Science Discovery Fund, the Bezos family, the University of British Columbia Clinician Investigator Program, the Fred Hutchinson Cancer Research Center’s Immunotherapy Integrated Research Center, and Juno Therapeutics/Celgene.
The researchers disclosed relationships with Celgene, Juno Therapeutics, Lyell Immunopharma, Adaptive Biotechnologies, Nohla, Kite Pharma, Gilead, Genentech, Novartis, Eureka Therapeutics, Nektar Therapeutics, Caribou Biosciences, Precision Biosciences, Aptevo, Humanigen, and Allogene.
SOURCE: Hirayama AV et al. Blood. 2019 Jun 26. doi: 10.1182/blood.2019000905
All complete responders with FL were still in remission at a median follow-up of 24 months, but the median duration of response was 10.2 months for patients with tFL.
Alexandre V. Hirayama, MD, of the Fred Hutchinson Cancer Research Center in Seattle, and colleagues reported these results in Blood.
The trial enrolled 21 adults with relapsed/refractory CD19+ B-cell malignancies, including 8 patients with FL and 13 with tFL. At baseline, the FL/tFL patients had a median age of 56 years (range, 51-62), and 67% were male. Most patients (n = 19) had stage III/IV disease, 17 had extranodal disease, 8 had bulky disease, and 6 had bone marrow involvement. The patients had received a median of 5 prior therapies (range, 2-8), and 13 had received a transplant.
In this study, patients received a lymphodepleting regimen of cyclophosphamide and fludarabine, followed by 2 x 106 CD19 CAR T cells/kg. Five patients (one with FL and four with tFL) also received bridging chemotherapy between leukapheresis and lymphodepletion.
Grade 1-2 cytokine release syndrome occurred in 50% of FL patients and 39% of tFL patients (P = .35). Grade 1-2 neurotoxicity occurred in 50% and 23%, respectively (P = .67). There were no cases of grade 3 or higher cytokine release syndrome or neurotoxicity.
Most FL patients (7 of 8; 88%) achieved a complete response (CR) to treatment, and all of these patients were still in CR at a median follow-up of 24 months (range, 5-37 months). One FL patient received a transplant while in CR.
Six of 13 tFL patients (46%) achieved a CR. At a median follow-up of 38 months (range, 3-39 months), the median duration of response was 10.2 months. The median progression-free survival was 11.2 months in patients who achieved a CR and 1.4 months in all tFL patients.
The researchers noted that peak CAR T-cell counts and the duration of CAR T-cell detection were similar between FL and tFL patients. However, tFL patients had higher serum interleukin-8 concentrations and higher lactate dehydrogenase levels before treatment.
Past research suggested that IL-8 mediates the recruitment of tumor-associated neutrophils, promotes diffuse large B-cell lymphoma progression, and can contribute to local immune suppression. Other studies have linked elevated lactate dehydrogenase to aggressive disease and a more immunosuppressive tumor microenvironment.
“Although these data raise the possibility that differences in the tumor microenvironment may, in part, contribute to differences in outcomes after CAR T-cell immunotherapy in FL and tFL patients, additional studies are required,” the researchers wrote.
This research was supported by the National Institutes of Health, the Life Science Discovery Fund, the Bezos family, the University of British Columbia Clinician Investigator Program, the Fred Hutchinson Cancer Research Center’s Immunotherapy Integrated Research Center, and Juno Therapeutics/Celgene.
The researchers disclosed relationships with Celgene, Juno Therapeutics, Lyell Immunopharma, Adaptive Biotechnologies, Nohla, Kite Pharma, Gilead, Genentech, Novartis, Eureka Therapeutics, Nektar Therapeutics, Caribou Biosciences, Precision Biosciences, Aptevo, Humanigen, and Allogene.
SOURCE: Hirayama AV et al. Blood. 2019 Jun 26. doi: 10.1182/blood.2019000905
All complete responders with FL were still in remission at a median follow-up of 24 months, but the median duration of response was 10.2 months for patients with tFL.
Alexandre V. Hirayama, MD, of the Fred Hutchinson Cancer Research Center in Seattle, and colleagues reported these results in Blood.
The trial enrolled 21 adults with relapsed/refractory CD19+ B-cell malignancies, including 8 patients with FL and 13 with tFL. At baseline, the FL/tFL patients had a median age of 56 years (range, 51-62), and 67% were male. Most patients (n = 19) had stage III/IV disease, 17 had extranodal disease, 8 had bulky disease, and 6 had bone marrow involvement. The patients had received a median of 5 prior therapies (range, 2-8), and 13 had received a transplant.
In this study, patients received a lymphodepleting regimen of cyclophosphamide and fludarabine, followed by 2 x 106 CD19 CAR T cells/kg. Five patients (one with FL and four with tFL) also received bridging chemotherapy between leukapheresis and lymphodepletion.
Grade 1-2 cytokine release syndrome occurred in 50% of FL patients and 39% of tFL patients (P = .35). Grade 1-2 neurotoxicity occurred in 50% and 23%, respectively (P = .67). There were no cases of grade 3 or higher cytokine release syndrome or neurotoxicity.
Most FL patients (7 of 8; 88%) achieved a complete response (CR) to treatment, and all of these patients were still in CR at a median follow-up of 24 months (range, 5-37 months). One FL patient received a transplant while in CR.
Six of 13 tFL patients (46%) achieved a CR. At a median follow-up of 38 months (range, 3-39 months), the median duration of response was 10.2 months. The median progression-free survival was 11.2 months in patients who achieved a CR and 1.4 months in all tFL patients.
The researchers noted that peak CAR T-cell counts and the duration of CAR T-cell detection were similar between FL and tFL patients. However, tFL patients had higher serum interleukin-8 concentrations and higher lactate dehydrogenase levels before treatment.
Past research suggested that IL-8 mediates the recruitment of tumor-associated neutrophils, promotes diffuse large B-cell lymphoma progression, and can contribute to local immune suppression. Other studies have linked elevated lactate dehydrogenase to aggressive disease and a more immunosuppressive tumor microenvironment.
“Although these data raise the possibility that differences in the tumor microenvironment may, in part, contribute to differences in outcomes after CAR T-cell immunotherapy in FL and tFL patients, additional studies are required,” the researchers wrote.
This research was supported by the National Institutes of Health, the Life Science Discovery Fund, the Bezos family, the University of British Columbia Clinician Investigator Program, the Fred Hutchinson Cancer Research Center’s Immunotherapy Integrated Research Center, and Juno Therapeutics/Celgene.
The researchers disclosed relationships with Celgene, Juno Therapeutics, Lyell Immunopharma, Adaptive Biotechnologies, Nohla, Kite Pharma, Gilead, Genentech, Novartis, Eureka Therapeutics, Nektar Therapeutics, Caribou Biosciences, Precision Biosciences, Aptevo, Humanigen, and Allogene.
SOURCE: Hirayama AV et al. Blood. 2019 Jun 26. doi: 10.1182/blood.2019000905
FROM BLOOD
Guidelines update donor selection criteria for HSCT
Newly updated guidelines can inform the selection of adult donors and cord blood units for allogeneic hematopoietic stem cell transplant.
The evidence-based guidelines suggest high-resolution human leukocyte antigen (HLA) matching and donor age are important when selecting adult donors, while HLA matching, cell dose, and banking practices should be considered when selecting cord blood units.
The guidelines were developed by the National Marrow Donor Program (NMDP) and Center for International Blood and Marrow Transplant Research (CIBMTR) and were recently published in Blood.
Adult donors
The guidelines recommend high-resolution HLA typing for adult donors and patients. This means typing for HLA-A, -B, -C, and -DRB1, at minimum. Typing at other loci – DPB1, DQB1, DRB3/4/5, DQA1, and DPA1 – is “optional but often helpful.”
An 8/8 HLA-matched donor is considered optimal. If only 7/8-matched donors are available, select a donor with a single allele mismatched at the patient’s homozygous locus if possible, and select an HLA-C*03:03 mismatch over an HLA-C*03:04 mismatch where applicable.
For both 8/8- and 7/8-matched donors, try to avoid mismatches at DQB1 and DRB3/4/5, and select DPB1 mismatches based on the DPB1 T-cell epitope algorithm. Mismatches of allotypes targeted by donor-specific HLA antibodies (DSA), including DQA1 and DPA1, should be avoided.
The guidelines recommend pursuing multiple donors because not all potential donors will be available. Younger donors should be prioritized over older donors. Other factors – such as sex or cytomegalovirus serostatus – should not affect donor selection.
Cord blood
For cord blood donations, testing attached segment identity is mandatory, red blood cell–replete units are not recommended, and both unit cryovolume and year of cryopreservation should be taken into consideration. The guidelines note that “some expert centers” favor red blood cell–depleted units with a postcryopreservation volume of about 25 ml/bag, and units banked more recently “may be linked to optimal banking practices.”
The guidelines recommend a minimum of eight high-resolution HLA typing for cord blood units and patients. A 4/6 match (HLA-A, -B, -DRB1) is acceptable, as is a 4/8 match (HLA-A, -B, -C, and -DRB1) or greater. In the case of a double-unit transplant, there is no need to match the units to each other.
“DSA must be considered on a case-by-case basis,” according to the guidelines. The patient’s diagnosis, prior immunosuppressive therapy, planned conditioning regimen, and DSA number/titer/specificity/complement fixation should be taken into consideration. DSA-targeted units should be avoided in patients with nonmalignant conditions and used with caution in patients with hematologic malignancies.
For single–cord blood units, the total nucleated cell dose should be at least 2.5 x 107/kg, and the number of CD34+ cells should be at least 1.5 x 105/kg. For double-unit transplants, the total nucleated cell dose should be at least 1.5 x 107/kg for each unit, and the number of CD34+ cells should be at least 1.0 x 105/kg for each unit.
The guidelines note that additional research is needed to inform how to balance cell dose against HLA match. However, cell dose should often take priority over HLA match for adults and larger pediatric patients, and HLA match can take priority in children, smaller adults, or patients with common HLA typing who have multiple units with a high cell dose.
The guidelines’ authors reported relationships with MolMed, NexImmune, AbbVie, Bellicum, Incyte, Medigene, Merck, Nektar, Novartis, Servier, Miltenyi, and the U.S. government/military.
SOURCE: Dehn J et al. Blood. 2019 Jul 10. doi: 10.1182/blood.2019001212.
Newly updated guidelines can inform the selection of adult donors and cord blood units for allogeneic hematopoietic stem cell transplant.
The evidence-based guidelines suggest high-resolution human leukocyte antigen (HLA) matching and donor age are important when selecting adult donors, while HLA matching, cell dose, and banking practices should be considered when selecting cord blood units.
The guidelines were developed by the National Marrow Donor Program (NMDP) and Center for International Blood and Marrow Transplant Research (CIBMTR) and were recently published in Blood.
Adult donors
The guidelines recommend high-resolution HLA typing for adult donors and patients. This means typing for HLA-A, -B, -C, and -DRB1, at minimum. Typing at other loci – DPB1, DQB1, DRB3/4/5, DQA1, and DPA1 – is “optional but often helpful.”
An 8/8 HLA-matched donor is considered optimal. If only 7/8-matched donors are available, select a donor with a single allele mismatched at the patient’s homozygous locus if possible, and select an HLA-C*03:03 mismatch over an HLA-C*03:04 mismatch where applicable.
For both 8/8- and 7/8-matched donors, try to avoid mismatches at DQB1 and DRB3/4/5, and select DPB1 mismatches based on the DPB1 T-cell epitope algorithm. Mismatches of allotypes targeted by donor-specific HLA antibodies (DSA), including DQA1 and DPA1, should be avoided.
The guidelines recommend pursuing multiple donors because not all potential donors will be available. Younger donors should be prioritized over older donors. Other factors – such as sex or cytomegalovirus serostatus – should not affect donor selection.
Cord blood
For cord blood donations, testing attached segment identity is mandatory, red blood cell–replete units are not recommended, and both unit cryovolume and year of cryopreservation should be taken into consideration. The guidelines note that “some expert centers” favor red blood cell–depleted units with a postcryopreservation volume of about 25 ml/bag, and units banked more recently “may be linked to optimal banking practices.”
The guidelines recommend a minimum of eight high-resolution HLA typing for cord blood units and patients. A 4/6 match (HLA-A, -B, -DRB1) is acceptable, as is a 4/8 match (HLA-A, -B, -C, and -DRB1) or greater. In the case of a double-unit transplant, there is no need to match the units to each other.
“DSA must be considered on a case-by-case basis,” according to the guidelines. The patient’s diagnosis, prior immunosuppressive therapy, planned conditioning regimen, and DSA number/titer/specificity/complement fixation should be taken into consideration. DSA-targeted units should be avoided in patients with nonmalignant conditions and used with caution in patients with hematologic malignancies.
For single–cord blood units, the total nucleated cell dose should be at least 2.5 x 107/kg, and the number of CD34+ cells should be at least 1.5 x 105/kg. For double-unit transplants, the total nucleated cell dose should be at least 1.5 x 107/kg for each unit, and the number of CD34+ cells should be at least 1.0 x 105/kg for each unit.
The guidelines note that additional research is needed to inform how to balance cell dose against HLA match. However, cell dose should often take priority over HLA match for adults and larger pediatric patients, and HLA match can take priority in children, smaller adults, or patients with common HLA typing who have multiple units with a high cell dose.
The guidelines’ authors reported relationships with MolMed, NexImmune, AbbVie, Bellicum, Incyte, Medigene, Merck, Nektar, Novartis, Servier, Miltenyi, and the U.S. government/military.
SOURCE: Dehn J et al. Blood. 2019 Jul 10. doi: 10.1182/blood.2019001212.
Newly updated guidelines can inform the selection of adult donors and cord blood units for allogeneic hematopoietic stem cell transplant.
The evidence-based guidelines suggest high-resolution human leukocyte antigen (HLA) matching and donor age are important when selecting adult donors, while HLA matching, cell dose, and banking practices should be considered when selecting cord blood units.
The guidelines were developed by the National Marrow Donor Program (NMDP) and Center for International Blood and Marrow Transplant Research (CIBMTR) and were recently published in Blood.
Adult donors
The guidelines recommend high-resolution HLA typing for adult donors and patients. This means typing for HLA-A, -B, -C, and -DRB1, at minimum. Typing at other loci – DPB1, DQB1, DRB3/4/5, DQA1, and DPA1 – is “optional but often helpful.”
An 8/8 HLA-matched donor is considered optimal. If only 7/8-matched donors are available, select a donor with a single allele mismatched at the patient’s homozygous locus if possible, and select an HLA-C*03:03 mismatch over an HLA-C*03:04 mismatch where applicable.
For both 8/8- and 7/8-matched donors, try to avoid mismatches at DQB1 and DRB3/4/5, and select DPB1 mismatches based on the DPB1 T-cell epitope algorithm. Mismatches of allotypes targeted by donor-specific HLA antibodies (DSA), including DQA1 and DPA1, should be avoided.
The guidelines recommend pursuing multiple donors because not all potential donors will be available. Younger donors should be prioritized over older donors. Other factors – such as sex or cytomegalovirus serostatus – should not affect donor selection.
Cord blood
For cord blood donations, testing attached segment identity is mandatory, red blood cell–replete units are not recommended, and both unit cryovolume and year of cryopreservation should be taken into consideration. The guidelines note that “some expert centers” favor red blood cell–depleted units with a postcryopreservation volume of about 25 ml/bag, and units banked more recently “may be linked to optimal banking practices.”
The guidelines recommend a minimum of eight high-resolution HLA typing for cord blood units and patients. A 4/6 match (HLA-A, -B, -DRB1) is acceptable, as is a 4/8 match (HLA-A, -B, -C, and -DRB1) or greater. In the case of a double-unit transplant, there is no need to match the units to each other.
“DSA must be considered on a case-by-case basis,” according to the guidelines. The patient’s diagnosis, prior immunosuppressive therapy, planned conditioning regimen, and DSA number/titer/specificity/complement fixation should be taken into consideration. DSA-targeted units should be avoided in patients with nonmalignant conditions and used with caution in patients with hematologic malignancies.
For single–cord blood units, the total nucleated cell dose should be at least 2.5 x 107/kg, and the number of CD34+ cells should be at least 1.5 x 105/kg. For double-unit transplants, the total nucleated cell dose should be at least 1.5 x 107/kg for each unit, and the number of CD34+ cells should be at least 1.0 x 105/kg for each unit.
The guidelines note that additional research is needed to inform how to balance cell dose against HLA match. However, cell dose should often take priority over HLA match for adults and larger pediatric patients, and HLA match can take priority in children, smaller adults, or patients with common HLA typing who have multiple units with a high cell dose.
The guidelines’ authors reported relationships with MolMed, NexImmune, AbbVie, Bellicum, Incyte, Medigene, Merck, Nektar, Novartis, Servier, Miltenyi, and the U.S. government/military.
SOURCE: Dehn J et al. Blood. 2019 Jul 10. doi: 10.1182/blood.2019001212.
FROM BLOOD
Large genetic cohort supports NfL as Alzheimer’s biomarker
LOS ANGELES – Neurofilament light, or NfL, is an increasingly studied biomarker of axonal damage across a range of neurodegenerative diseases, including Alzheimer’s disease. And because it is a biomarker that can be measured in blood, it is a less invasive measure of disease progression in Alzheimer’s than cerebrospinal fluid markers.
At the Alzheimer’s Association International Conference, scientists studying the world’s largest cohort of early-onset Alzheimer’s families presented results from a cross-sectional and longitudinal study of more than 2,000 carriers and noncarriers of a single Alzheimer’s-causing mutation (Presenilin 1 E280A) that occurs in an extended Colombian family.
While previous studies have also looked at NfL in cohorts of autosomal dominant mutation carriers, this study strengthens evidence for NfL as an Alzheimer’s biomarker in the largest single-mutation cohort to date.
Yakeel Quiroz, PhD, of Harvard University in Boston and colleagues reported that, in a cross-sectional study of 1,070 mutation carriers and 1,074 noncarriers aged 8-75 years (mean age, 29-30 years; 46% male), mean plasma NfL levels were elevated in cognitively unimpaired carriers (18.08 pg/mL), compared with noncarriers (9.09 pg/mL; P less than .0001).
Longitudinal data from 504 of those carriers and noncarriers showed that NfL levels begin to diverge significantly between the groups at age 22, more than 2 decades before the mean onset of mild cognitive impairment for this cohort (44 years). The between-group differences in NfL continued to widen with advancing age.
“At approximately age 22, the axons, the neurons are already changing, and this measure serves as an early sign of degeneration,” Dr. Quiroz said in an interview. “This is really telling us about neurodegeneration related to Alzheimer’s disease because these are people destined to develop Alzheimer’s dementia later in life and have no age-related comorbidities that could cause elevation in NfL.”
A study published early this year in a different cohort of about 400 autosomal dominant Alzheimer’s disease mutation carriers and noncarriers found that the longitudinal rate of change of serum NfL could discriminate carriers from noncarriers almost a decade earlier than cross-sectional absolute NfL levels – at 16 years and 7 years, respectively, before expected onset of symptoms (Nat Med. 2019 Feb;25[2]:277–83).
In Dr. Quiroz and colleagues’ study, both cross-sectional and longitudinal findings showed carriers to significantly differ from noncarriers by age 22 years. “We’re seeing differences between groups that reach statistical significance earlier” – decades, in this case, before onset of symptoms, Dr. Quiroz said. The current study is distinguished by its exceptional power, she said: “No one has done this with such a large number of carriers with a single genetic mutation.”

Eric Reiman, MD, of Banner Alzheimer’s Institute in Phoenix, the coauthor on the study who presented the findings to the conference, commented in an interview that they illustrate “the opportunity for fluid biomarkers to be used in trials.”
Dr. Reiman cautioned, however, that the NfL measurements are likely a more useful measure of preclinical neurodegeneration in genetic early-onset Alzheimer’s than in late-onset or sporadic disease, which represents the lion’s share of Alzheimer’s cases.
“In autosomal dominant Alzheimer’s disease, these [NfL] changes really go up – probably more so than in late onset,” he said.
Dr. Reiman said these cohort findings add to growing interest in less-invasive biomarkers for Alzheimer’s, both in research and clinical practice. “If NfL is already elevated as a marker of active neurodegeneration, in early phase trials you might think about looking to it as a proof of concept – so where in 6-12 months you can see reductions [in NfL].”
Dr. Reiman added that “there will be other fluid biomarkers coming down the pike that will be exciting as well, and which people will learn a lot more about in the next few months.”
Dr. Quiroz had no disclosures related to her findings. Other authors on the study, including Dr. Reiman, have received research support and/or consulting fees from pharmaceutical manufacturers.
LOS ANGELES – Neurofilament light, or NfL, is an increasingly studied biomarker of axonal damage across a range of neurodegenerative diseases, including Alzheimer’s disease. And because it is a biomarker that can be measured in blood, it is a less invasive measure of disease progression in Alzheimer’s than cerebrospinal fluid markers.
At the Alzheimer’s Association International Conference, scientists studying the world’s largest cohort of early-onset Alzheimer’s families presented results from a cross-sectional and longitudinal study of more than 2,000 carriers and noncarriers of a single Alzheimer’s-causing mutation (Presenilin 1 E280A) that occurs in an extended Colombian family.
While previous studies have also looked at NfL in cohorts of autosomal dominant mutation carriers, this study strengthens evidence for NfL as an Alzheimer’s biomarker in the largest single-mutation cohort to date.
Yakeel Quiroz, PhD, of Harvard University in Boston and colleagues reported that, in a cross-sectional study of 1,070 mutation carriers and 1,074 noncarriers aged 8-75 years (mean age, 29-30 years; 46% male), mean plasma NfL levels were elevated in cognitively unimpaired carriers (18.08 pg/mL), compared with noncarriers (9.09 pg/mL; P less than .0001).
Longitudinal data from 504 of those carriers and noncarriers showed that NfL levels begin to diverge significantly between the groups at age 22, more than 2 decades before the mean onset of mild cognitive impairment for this cohort (44 years). The between-group differences in NfL continued to widen with advancing age.
“At approximately age 22, the axons, the neurons are already changing, and this measure serves as an early sign of degeneration,” Dr. Quiroz said in an interview. “This is really telling us about neurodegeneration related to Alzheimer’s disease because these are people destined to develop Alzheimer’s dementia later in life and have no age-related comorbidities that could cause elevation in NfL.”
A study published early this year in a different cohort of about 400 autosomal dominant Alzheimer’s disease mutation carriers and noncarriers found that the longitudinal rate of change of serum NfL could discriminate carriers from noncarriers almost a decade earlier than cross-sectional absolute NfL levels – at 16 years and 7 years, respectively, before expected onset of symptoms (Nat Med. 2019 Feb;25[2]:277–83).
In Dr. Quiroz and colleagues’ study, both cross-sectional and longitudinal findings showed carriers to significantly differ from noncarriers by age 22 years. “We’re seeing differences between groups that reach statistical significance earlier” – decades, in this case, before onset of symptoms, Dr. Quiroz said. The current study is distinguished by its exceptional power, she said: “No one has done this with such a large number of carriers with a single genetic mutation.”
Eric Reiman, MD, of Banner Alzheimer’s Institute in Phoenix, the coauthor on the study who presented the findings to the conference, commented in an interview that they illustrate “the opportunity for fluid biomarkers to be used in trials.”
Dr. Reiman cautioned, however, that the NfL measurements are likely a more useful measure of preclinical neurodegeneration in genetic early-onset Alzheimer’s than in late-onset or sporadic disease, which represents the lion’s share of Alzheimer’s cases.
“In autosomal dominant Alzheimer’s disease, these [NfL] changes really go up – probably more so than in late onset,” he said.
Dr. Reiman said these cohort findings add to growing interest in less-invasive biomarkers for Alzheimer’s, both in research and clinical practice. “If NfL is already elevated as a marker of active neurodegeneration, in early phase trials you might think about looking to it as a proof of concept – so where in 6-12 months you can see reductions [in NfL].”
Dr. Reiman added that “there will be other fluid biomarkers coming down the pike that will be exciting as well, and which people will learn a lot more about in the next few months.”
Dr. Quiroz had no disclosures related to her findings. Other authors on the study, including Dr. Reiman, have received research support and/or consulting fees from pharmaceutical manufacturers.
LOS ANGELES – Neurofilament light, or NfL, is an increasingly studied biomarker of axonal damage across a range of neurodegenerative diseases, including Alzheimer’s disease. And because it is a biomarker that can be measured in blood, it is a less invasive measure of disease progression in Alzheimer’s than cerebrospinal fluid markers.
At the Alzheimer’s Association International Conference, scientists studying the world’s largest cohort of early-onset Alzheimer’s families presented results from a cross-sectional and longitudinal study of more than 2,000 carriers and noncarriers of a single Alzheimer’s-causing mutation (Presenilin 1 E280A) that occurs in an extended Colombian family.
While previous studies have also looked at NfL in cohorts of autosomal dominant mutation carriers, this study strengthens evidence for NfL as an Alzheimer’s biomarker in the largest single-mutation cohort to date.
Yakeel Quiroz, PhD, of Harvard University in Boston and colleagues reported that, in a cross-sectional study of 1,070 mutation carriers and 1,074 noncarriers aged 8-75 years (mean age, 29-30 years; 46% male), mean plasma NfL levels were elevated in cognitively unimpaired carriers (18.08 pg/mL), compared with noncarriers (9.09 pg/mL; P less than .0001).
Longitudinal data from 504 of those carriers and noncarriers showed that NfL levels begin to diverge significantly between the groups at age 22, more than 2 decades before the mean onset of mild cognitive impairment for this cohort (44 years). The between-group differences in NfL continued to widen with advancing age.
“At approximately age 22, the axons, the neurons are already changing, and this measure serves as an early sign of degeneration,” Dr. Quiroz said in an interview. “This is really telling us about neurodegeneration related to Alzheimer’s disease because these are people destined to develop Alzheimer’s dementia later in life and have no age-related comorbidities that could cause elevation in NfL.”
A study published early this year in a different cohort of about 400 autosomal dominant Alzheimer’s disease mutation carriers and noncarriers found that the longitudinal rate of change of serum NfL could discriminate carriers from noncarriers almost a decade earlier than cross-sectional absolute NfL levels – at 16 years and 7 years, respectively, before expected onset of symptoms (Nat Med. 2019 Feb;25[2]:277–83).
In Dr. Quiroz and colleagues’ study, both cross-sectional and longitudinal findings showed carriers to significantly differ from noncarriers by age 22 years. “We’re seeing differences between groups that reach statistical significance earlier” – decades, in this case, before onset of symptoms, Dr. Quiroz said. The current study is distinguished by its exceptional power, she said: “No one has done this with such a large number of carriers with a single genetic mutation.”
Eric Reiman, MD, of Banner Alzheimer’s Institute in Phoenix, the coauthor on the study who presented the findings to the conference, commented in an interview that they illustrate “the opportunity for fluid biomarkers to be used in trials.”
Dr. Reiman cautioned, however, that the NfL measurements are likely a more useful measure of preclinical neurodegeneration in genetic early-onset Alzheimer’s than in late-onset or sporadic disease, which represents the lion’s share of Alzheimer’s cases.
“In autosomal dominant Alzheimer’s disease, these [NfL] changes really go up – probably more so than in late onset,” he said.
Dr. Reiman said these cohort findings add to growing interest in less-invasive biomarkers for Alzheimer’s, both in research and clinical practice. “If NfL is already elevated as a marker of active neurodegeneration, in early phase trials you might think about looking to it as a proof of concept – so where in 6-12 months you can see reductions [in NfL].”
Dr. Reiman added that “there will be other fluid biomarkers coming down the pike that will be exciting as well, and which people will learn a lot more about in the next few months.”
Dr. Quiroz had no disclosures related to her findings. Other authors on the study, including Dr. Reiman, have received research support and/or consulting fees from pharmaceutical manufacturers.
REPORTING FROM AAIC 2019
Test could inform care of patients with pancreatic cysts
A newly developed test could help clinicians more accurately identify which patients with pancreatic cysts require surgery, according to researchers.
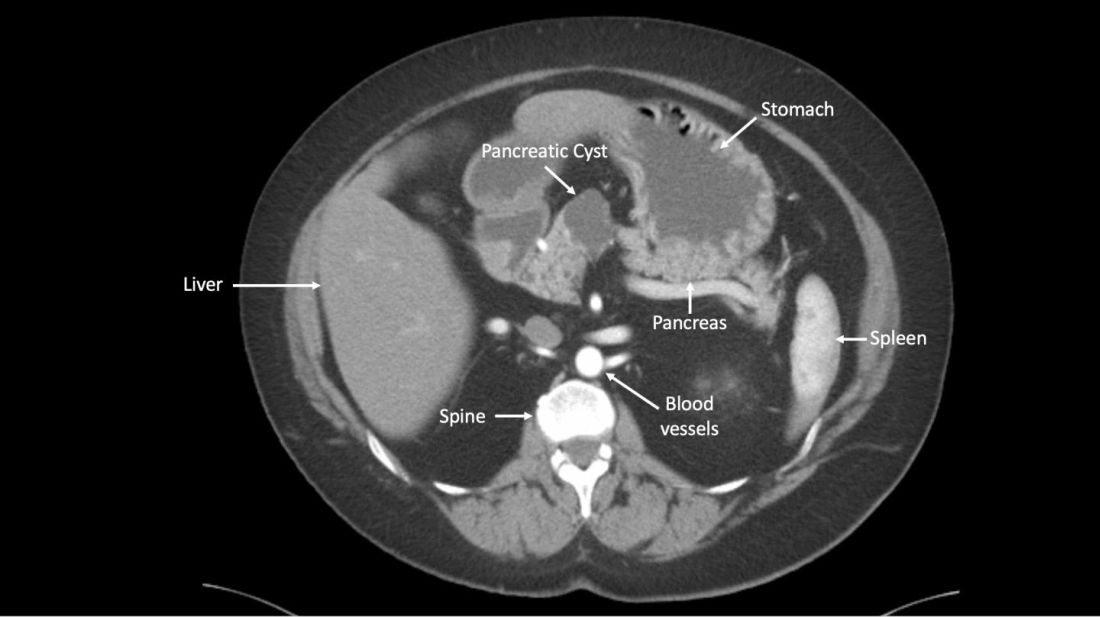
The test, CompCyst, incorporates clinical and imaging data as well as data on genetic and biochemical markers associated with pancreatic cancer.
CompCyst proved more effective than standard practice in estimating the risk of cancer so as to differentiate patients who should undergo surgery from patients who require monitoring and those who need no additional care.
Simeon Springer, PhD, of Ring Therapeutics in Cambridge, Mass., and colleagues described the development and testing of CompCyst in Science Translational Medicine.
The researchers collected data from 875 patients who had undergone surgical resection of pancreatic cysts. The team used clinical, imaging, and molecular data from 436 of those patients to train CompCyst to classify patients into three categories.
- Patients with benign, nonmucin-producing cysts who do not require surgery or monitoring
- Patients who require monitoring because they have mucin-producing cysts with low- or intermediate-grade dysplasia
- Patients who have invasive cancer or high-grade dysplasia and require surgery.
The researchers then tested CompCyst in the remaining 426 patients (the validation cohort), comparing CompCyst with standard practice, which involves use of clinical and imaging criteria only.
“Our aim [in developing CompCyst] was not to replace current knowledge derived from clinical data and imaging characteristics with molecular testing but, rather, to integrate all these aspects together,” study author Marco Dal Molin, MD, of Johns Hopkins University, Baltimore, said in a press conference.
“An important aspect of this paper is the comparison between the performance of our test and current clinical practice. Because the histopathology of all cysts was known from surgical specimens, we could determine, in retrospect, what the optimal treatment should have been.”
Histopathology showed that 53 patients in the validation cohort had a benign, nonmucin-producing cyst and did not require any additional intervention. Standard practice correctly identified 19% (n =10) of these patients, while CompCyst correctly identified 60% (n = 32).
There were 140 patients who had mucin-producing cysts with low- or intermediate-grade dysplasia. Standard practice correctly identified 34% (n = 48) of these patients, while CompCyst correctly identified 49% (n = 68).
“Overall, the use of CompCyst would have avoided unnecessary surgery in 60% of the patients in this study,” Dr. Dal Molin said.
Surgery was needed in 152 patients in the validation cohort. Standard practice correctly identified 89% (n = 135) of these patients, while CompCyst correctly identified 91% (n = 138). Neither method would have recommended discharge for any patient who actually required surgery, the researchers noted.
Based on these results, the researchers are hoping to make CompCyst available to patients at Johns Hopkins within the next 6-12 months.
“In the long term, we hope that a new, prospective study will be carried out, which will gain approval of this test by the FDA [Food and Drug Administration],” study author Bert Vogelstein, MD, of Johns Hopkins, said at the press conference.
“Then, at that point, we hope the technology can be commercialized and offered to the public through a company called Thrive [Earlier Detection], which has licensed the technology from Johns Hopkins.”
This research was supported by the Lustgarten Foundation for Pancreatic Cancer Research, the Virginia and D.K. Ludwig Fund for Cancer Research, the Sol Goldman Pancreatic Cancer Research Center, the Michael Rolfe Pancreatic Cancer Foundation, the Benjamin Baker Scholarship, and the National Institutes of Health. The researchers reported relationships with Thrive Earlier Detection, Personal Genome Diagnostics, Eisai-Morphotek, Sysmex Inostics, Nexus Strategy (Camden Partners), NeoPhore, and CAGE.
SOURCE: Springer S et al. Sci Transl Med. 2019 Jul 17. doi: 10.1126/scitranslmed.aav477.
A newly developed test could help clinicians more accurately identify which patients with pancreatic cysts require surgery, according to researchers.
The test, CompCyst, incorporates clinical and imaging data as well as data on genetic and biochemical markers associated with pancreatic cancer.
CompCyst proved more effective than standard practice in estimating the risk of cancer so as to differentiate patients who should undergo surgery from patients who require monitoring and those who need no additional care.
Simeon Springer, PhD, of Ring Therapeutics in Cambridge, Mass., and colleagues described the development and testing of CompCyst in Science Translational Medicine.
The researchers collected data from 875 patients who had undergone surgical resection of pancreatic cysts. The team used clinical, imaging, and molecular data from 436 of those patients to train CompCyst to classify patients into three categories.
- Patients with benign, nonmucin-producing cysts who do not require surgery or monitoring
- Patients who require monitoring because they have mucin-producing cysts with low- or intermediate-grade dysplasia
- Patients who have invasive cancer or high-grade dysplasia and require surgery.
The researchers then tested CompCyst in the remaining 426 patients (the validation cohort), comparing CompCyst with standard practice, which involves use of clinical and imaging criteria only.
“Our aim [in developing CompCyst] was not to replace current knowledge derived from clinical data and imaging characteristics with molecular testing but, rather, to integrate all these aspects together,” study author Marco Dal Molin, MD, of Johns Hopkins University, Baltimore, said in a press conference.
“An important aspect of this paper is the comparison between the performance of our test and current clinical practice. Because the histopathology of all cysts was known from surgical specimens, we could determine, in retrospect, what the optimal treatment should have been.”
Histopathology showed that 53 patients in the validation cohort had a benign, nonmucin-producing cyst and did not require any additional intervention. Standard practice correctly identified 19% (n =10) of these patients, while CompCyst correctly identified 60% (n = 32).
There were 140 patients who had mucin-producing cysts with low- or intermediate-grade dysplasia. Standard practice correctly identified 34% (n = 48) of these patients, while CompCyst correctly identified 49% (n = 68).
“Overall, the use of CompCyst would have avoided unnecessary surgery in 60% of the patients in this study,” Dr. Dal Molin said.
Surgery was needed in 152 patients in the validation cohort. Standard practice correctly identified 89% (n = 135) of these patients, while CompCyst correctly identified 91% (n = 138). Neither method would have recommended discharge for any patient who actually required surgery, the researchers noted.
Based on these results, the researchers are hoping to make CompCyst available to patients at Johns Hopkins within the next 6-12 months.
“In the long term, we hope that a new, prospective study will be carried out, which will gain approval of this test by the FDA [Food and Drug Administration],” study author Bert Vogelstein, MD, of Johns Hopkins, said at the press conference.
“Then, at that point, we hope the technology can be commercialized and offered to the public through a company called Thrive [Earlier Detection], which has licensed the technology from Johns Hopkins.”
This research was supported by the Lustgarten Foundation for Pancreatic Cancer Research, the Virginia and D.K. Ludwig Fund for Cancer Research, the Sol Goldman Pancreatic Cancer Research Center, the Michael Rolfe Pancreatic Cancer Foundation, the Benjamin Baker Scholarship, and the National Institutes of Health. The researchers reported relationships with Thrive Earlier Detection, Personal Genome Diagnostics, Eisai-Morphotek, Sysmex Inostics, Nexus Strategy (Camden Partners), NeoPhore, and CAGE.
SOURCE: Springer S et al. Sci Transl Med. 2019 Jul 17. doi: 10.1126/scitranslmed.aav477.
A newly developed test could help clinicians more accurately identify which patients with pancreatic cysts require surgery, according to researchers.
The test, CompCyst, incorporates clinical and imaging data as well as data on genetic and biochemical markers associated with pancreatic cancer.
CompCyst proved more effective than standard practice in estimating the risk of cancer so as to differentiate patients who should undergo surgery from patients who require monitoring and those who need no additional care.
Simeon Springer, PhD, of Ring Therapeutics in Cambridge, Mass., and colleagues described the development and testing of CompCyst in Science Translational Medicine.
The researchers collected data from 875 patients who had undergone surgical resection of pancreatic cysts. The team used clinical, imaging, and molecular data from 436 of those patients to train CompCyst to classify patients into three categories.
- Patients with benign, nonmucin-producing cysts who do not require surgery or monitoring
- Patients who require monitoring because they have mucin-producing cysts with low- or intermediate-grade dysplasia
- Patients who have invasive cancer or high-grade dysplasia and require surgery.
The researchers then tested CompCyst in the remaining 426 patients (the validation cohort), comparing CompCyst with standard practice, which involves use of clinical and imaging criteria only.
“Our aim [in developing CompCyst] was not to replace current knowledge derived from clinical data and imaging characteristics with molecular testing but, rather, to integrate all these aspects together,” study author Marco Dal Molin, MD, of Johns Hopkins University, Baltimore, said in a press conference.
“An important aspect of this paper is the comparison between the performance of our test and current clinical practice. Because the histopathology of all cysts was known from surgical specimens, we could determine, in retrospect, what the optimal treatment should have been.”
Histopathology showed that 53 patients in the validation cohort had a benign, nonmucin-producing cyst and did not require any additional intervention. Standard practice correctly identified 19% (n =10) of these patients, while CompCyst correctly identified 60% (n = 32).
There were 140 patients who had mucin-producing cysts with low- or intermediate-grade dysplasia. Standard practice correctly identified 34% (n = 48) of these patients, while CompCyst correctly identified 49% (n = 68).
“Overall, the use of CompCyst would have avoided unnecessary surgery in 60% of the patients in this study,” Dr. Dal Molin said.
Surgery was needed in 152 patients in the validation cohort. Standard practice correctly identified 89% (n = 135) of these patients, while CompCyst correctly identified 91% (n = 138). Neither method would have recommended discharge for any patient who actually required surgery, the researchers noted.
Based on these results, the researchers are hoping to make CompCyst available to patients at Johns Hopkins within the next 6-12 months.
“In the long term, we hope that a new, prospective study will be carried out, which will gain approval of this test by the FDA [Food and Drug Administration],” study author Bert Vogelstein, MD, of Johns Hopkins, said at the press conference.
“Then, at that point, we hope the technology can be commercialized and offered to the public through a company called Thrive [Earlier Detection], which has licensed the technology from Johns Hopkins.”
This research was supported by the Lustgarten Foundation for Pancreatic Cancer Research, the Virginia and D.K. Ludwig Fund for Cancer Research, the Sol Goldman Pancreatic Cancer Research Center, the Michael Rolfe Pancreatic Cancer Foundation, the Benjamin Baker Scholarship, and the National Institutes of Health. The researchers reported relationships with Thrive Earlier Detection, Personal Genome Diagnostics, Eisai-Morphotek, Sysmex Inostics, Nexus Strategy (Camden Partners), NeoPhore, and CAGE.
SOURCE: Springer S et al. Sci Transl Med. 2019 Jul 17. doi: 10.1126/scitranslmed.aav477.
FROM SCIENCE TRANSLATIONAL MEDICINE
Key clinical point: A test called CompCyst could help clinicians more accurately identify which patients with pancreatic cysts require surgery.
Major finding: CompCyst correctly identified 91% of patients who required surgery, 49% of those who required monitoring, and 60% of patients who required no further care.
Study details: A retrospective analysis of 875 patients with pancreatic cysts
Disclosures: The research was supported by the Lustgarten Foundation for Pancreatic Cancer Research, the Virginia and D.K. Ludwig Fund for Cancer Research, the Sol Goldman Pancreatic Cancer Research Center, the Michael Rolfe Pancreatic Cancer Foundation, the Benjamin Baker Scholarship, and the National Institutes of Health. The researchers reported relationships with Thrive Earlier Detection, Personal Genome Diagnostics, Eisai-Morphotek, Sysmex Inostics, Nexus Strategy (Camden Partners), NeoPhore, and CAGE.
Source: Springer S et al. Sci Transl Med. 2019 Jul 17. doi: 10.1126/scitranslmed.aav477.