User login
Should patients with acute DVT limit activity?
PROBABLY NOT. Ambulation, combined with compression of the affected extremity, appears to be safe for medically stable patients with deep venous thromboses (DVT) (strength of recommendation [SOR]: A, consistent randomized controlled trials [RCTs]). Leg compression and ambulation, compared with bed rest without compression, can effectively decrease swelling and pain (SOR: A, consistent RCTs).
Only weak data exist to suggest that early ambulation can reduce mortality (SOR: C, cohort studies with historical controls).
Evidence summary
Patients with acute DVT have traditionally been treated with immobilization and bed rest, combined with anticoagulation, for days. This approach is motivated by fear of dislodging an unstable thrombus and causing a pulmonary embolism (PE) and by the belief that inactivity relieves local pain and swelling. On the other hand, bed rest promotes stasis, an element in Virchow’s triad.
Early ambulation doesn’t raise risk of PE
We performed a structured literature review, which found 6 RCTs and 3 cohort studies that address this problem. All 6 RCTs included patients with acute DVT but without life-threatening conditions.1-6 They assessed various outcomes, including incidence of new PE, change in leg circumference, leg pain, patient well-being, and progression of DVT.
The studies consistently found that early ambulation, along with compression, is safe when compared with bed rest ( TABLE ). Although the sample size of all the RCTs was small, the RCTs showed consistent trends in favor of ambulation and compression.
A prospective cohort study of new PE in patients treated with ambulation and compression plus anticoagulation found that the incidence of PE was significantly lower than historical incidence rates in patients managed with bed rest.7
Another study using the RIETE registry, a Spanish registry of consecutively enrolled patients with objectively confirmed acute DVT or PE, found no significant difference in occurrence of new PE between immobilized and mobilized patients.8 Patients with DVT who were immobilized were generally sicker, more likely to have PaO2 <60, and more likely to have received lower doses of low-molecular-weight heparin (LMWH) compared with the group that walked (P<.005).
TABLE
Early ambulation and compression: What RCTs show
| Subjects | Study groups | Results |
|---|---|---|
| 129 patients with DVT, treated with LMWH1 | Strict immobilization for 4 days Ambulation for ≥4 h/d, along with compression for 4 days or until swelling subsided | At 4 days: No difference in PE, leg pain, leg size, mortality At 3 months: No difference in PE, mortality |
| 146 patients with DVT, all anticoagulated5 | Hospital treatment with 5 days of bed rest Home care with early walking and compression stockings | No difference in occurrence of new PE after 10 days |
| 126 patients with DVT, treated with LMWH, compression6 | Strict bed rest for 8 days with leg elevation Began full ambulation on day 2 | No difference in PE |
| 102 patients with DVT, treated with LMWH, compression4 | Bed rest for 5 days Ambulation | No differences in PE, thrombus progression, serious adverse events, or leg pain Study didn’t recruit expected number of patients Study showed a trend toward benefit from ambulation |
| 53 patients with DVT2,7 | Ambulation and use of firm, inelastic Unna boot bandages Ambulation and elastic compression stockings Strict bed rest for 9 days and no compression | No difference in quality of life or PE DVT-related symptoms, leg pain, and circumference improved in compression/ambulation groups No changes noted at 2 years |
| 72 patients with DVT, treated with anticoagulation and compression3 | Daily walking exercise and weekly group exercise Control group | No difference in DVT, PE, phlebography results, or calf circumference |
| DVT, deep vein thrombosis; LMWH, low-molecular-weight heparin; PE, pulmonary embolism. | ||
Does ambulation affect thrombus propagation?
A multicenter RCT showed that thrombus progression occurred more often in patients who were treated with bed rest compared with patients treated with ambulation and compression (P<.01).2
Another RCT revealed a similar trend, though the difference didn’t reach statistical significance because of small sample size.4 The clinical importance of these phlebographic studies isn’t clear.
Is it the walking, or compression, that works?
RCTs have shown that ambulation with leg compression, compared with bed rest without compression, can effectively decrease leg swelling and pain1,2,4 The difference was detectable 2 years after DVT.7
In contrast, RCTs in which both ambulating and resting patients received compression therapy showed no significant difference in leg circumference at 1 or 6 months.3 This finding suggests that the benefit on local symptoms may result from compression rather than ambulation.
Reduced mortality? Evidence is weak
Estimates of the possible effect on mortality of ambulation compared with bed rest are based on cohort studies. A cohort study in which 691 patients were kept walking with compression therapy reported a mortality rate of 0.2%.9 In another cohort, the mortality rate was also 0.2%, and all deaths occurred in patients older than 70 years.10
This rate is lower than rates reported in the historic literature, which typically are 1% among patients treated with unfractionated heparin and bed rest.9,10 A retrospective, multicenter cohort of 1647 patients treated with unfractionated heparin and bed rest in different German hospitals reported a rate of fatal PE of 2.33%.11
Data from the RIETE registry indicated that overall mortality was significantly higher in immobilized patients with a PE (3.6% vs 0.5% in mobile patients; P=.01).8 Notably, immobilized patients with a PE were more likely to be hypoxic and also tended to receive lower doses of LMWH. No differences were found in outcomes for patients with DVT.
Recommendations
The American College of Chest Physicians (ACCP) doesn’t recommend bed rest in its guidelines for treating acute venous thromboembolism, but rather ambulation as tolerated after starting anticoagulation. Patients who are not hemodynamically stable should be stabilized first.
The ACCP also recommends wearing an elastic compression stocking with a pressure of 30 to 40 mm Hg at the ankle for 2 years after an episode of DVT and a course of intermittent pneumatic compression for patients with severe edema of the leg resulting from post-thrombotic syndrome.12
A joint guideline from the American College of Physicians and the American Academy of Family Physicians doesn’t make recommendations about ambulation for therapy of DVT and PE.13
1. Aschwanden M, Labs KH, Engel H, et al. Acute deep vein thrombosis: early mobilization does not increase the frequency of pulmonary embolism. Thromb Haemost. 2001;85:42-46.
2. Blattler W, Partsch H. Leg compression and ambulation is better than bed rest for the treatment of acute deep venous thrombosis. Int Angiol. 2003;22:393-400.
3. Isma N, Johanssson E, Bjork A, et al. Does supervised exercise after deep venous thrombosis improve recanalization of occluded vein segments? A randomized study. J Thromb Thrombolysis. 2007;23:25-30.
4. Junger M, Diehm C, Storiko H, et al. Mobilization versus immobilization in the treatment of acute proximal deep venous thrombosis: a prospective, randomized, open, multicentre trial. Curr Med Res Opin. 2006;22:593-602.
5. Romera A, Vila R, Perez-Piqueras A, et al. Early mobilization in patients with acute deep vein thrombosis: does it increase the incidence of symptomatic pulmonary embolism? Phlebology. 2005;20:141.-
6. Schellong SM, Schwarz T, Kropp J, et al. Bed rest in deep vein thrombosis and the incidence of scintigraphic pulmonary embolism. Thromb Haemost. 1999;82(suppl 1):127-129.
7. Partsch H, Kaulich M, Mayer W. Immediate mobilisation in acute vein thrombosis reduces post-thrombotic syndrome. Int Angiol. 2004;23:206-212.
8. Trujillo-Santos J, Perea-Milla E, Jimenez-Puente A, et al. Bed rest or ambulation in the initial treatment of patients with acute deep vein thrombosis or pulmonary embolism: findings from the RIETE registry. Chest. 2005;127:1631-1636.
9. Partsch H, Kechavarz B, Kohn H, et al. The effect of mobilisation of patients during treatment of thromboembolic disorders with low-molecular-weight heparin. Int Angiol. 1997;16:189-192.
10. Partsch H. Therapy of deep vein thrombosis with low molecular weight heparin, leg compression and immediate ambulation. Vasa. 2001;30:195-204.
11. Martin M. PHLECO: a multicenter study of the fate of 1647 hospital patients treated conservatively without fibrinolysis and surgery. Clin Invest. 1993;71:471-477.
12. Buller HR, Agnelli G, Hull RD, et al. Antithrombotic therapy for venous thromboembolic disease: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126 (suppl 3):401S-428S.
13. Snow V, Qaseem A, Barry P, et al. Management of venous thromboembolism: a clinical practice guideline from the American College of Physicians and the American Academy of Family Physicians. Ann Intern Med. 2007;146:204-210.
PROBABLY NOT. Ambulation, combined with compression of the affected extremity, appears to be safe for medically stable patients with deep venous thromboses (DVT) (strength of recommendation [SOR]: A, consistent randomized controlled trials [RCTs]). Leg compression and ambulation, compared with bed rest without compression, can effectively decrease swelling and pain (SOR: A, consistent RCTs).
Only weak data exist to suggest that early ambulation can reduce mortality (SOR: C, cohort studies with historical controls).
Evidence summary
Patients with acute DVT have traditionally been treated with immobilization and bed rest, combined with anticoagulation, for days. This approach is motivated by fear of dislodging an unstable thrombus and causing a pulmonary embolism (PE) and by the belief that inactivity relieves local pain and swelling. On the other hand, bed rest promotes stasis, an element in Virchow’s triad.
Early ambulation doesn’t raise risk of PE
We performed a structured literature review, which found 6 RCTs and 3 cohort studies that address this problem. All 6 RCTs included patients with acute DVT but without life-threatening conditions.1-6 They assessed various outcomes, including incidence of new PE, change in leg circumference, leg pain, patient well-being, and progression of DVT.
The studies consistently found that early ambulation, along with compression, is safe when compared with bed rest ( TABLE ). Although the sample size of all the RCTs was small, the RCTs showed consistent trends in favor of ambulation and compression.
A prospective cohort study of new PE in patients treated with ambulation and compression plus anticoagulation found that the incidence of PE was significantly lower than historical incidence rates in patients managed with bed rest.7
Another study using the RIETE registry, a Spanish registry of consecutively enrolled patients with objectively confirmed acute DVT or PE, found no significant difference in occurrence of new PE between immobilized and mobilized patients.8 Patients with DVT who were immobilized were generally sicker, more likely to have PaO2 <60, and more likely to have received lower doses of low-molecular-weight heparin (LMWH) compared with the group that walked (P<.005).
TABLE
Early ambulation and compression: What RCTs show
| Subjects | Study groups | Results |
|---|---|---|
| 129 patients with DVT, treated with LMWH1 | Strict immobilization for 4 days Ambulation for ≥4 h/d, along with compression for 4 days or until swelling subsided | At 4 days: No difference in PE, leg pain, leg size, mortality At 3 months: No difference in PE, mortality |
| 146 patients with DVT, all anticoagulated5 | Hospital treatment with 5 days of bed rest Home care with early walking and compression stockings | No difference in occurrence of new PE after 10 days |
| 126 patients with DVT, treated with LMWH, compression6 | Strict bed rest for 8 days with leg elevation Began full ambulation on day 2 | No difference in PE |
| 102 patients with DVT, treated with LMWH, compression4 | Bed rest for 5 days Ambulation | No differences in PE, thrombus progression, serious adverse events, or leg pain Study didn’t recruit expected number of patients Study showed a trend toward benefit from ambulation |
| 53 patients with DVT2,7 | Ambulation and use of firm, inelastic Unna boot bandages Ambulation and elastic compression stockings Strict bed rest for 9 days and no compression | No difference in quality of life or PE DVT-related symptoms, leg pain, and circumference improved in compression/ambulation groups No changes noted at 2 years |
| 72 patients with DVT, treated with anticoagulation and compression3 | Daily walking exercise and weekly group exercise Control group | No difference in DVT, PE, phlebography results, or calf circumference |
| DVT, deep vein thrombosis; LMWH, low-molecular-weight heparin; PE, pulmonary embolism. | ||
Does ambulation affect thrombus propagation?
A multicenter RCT showed that thrombus progression occurred more often in patients who were treated with bed rest compared with patients treated with ambulation and compression (P<.01).2
Another RCT revealed a similar trend, though the difference didn’t reach statistical significance because of small sample size.4 The clinical importance of these phlebographic studies isn’t clear.
Is it the walking, or compression, that works?
RCTs have shown that ambulation with leg compression, compared with bed rest without compression, can effectively decrease leg swelling and pain1,2,4 The difference was detectable 2 years after DVT.7
In contrast, RCTs in which both ambulating and resting patients received compression therapy showed no significant difference in leg circumference at 1 or 6 months.3 This finding suggests that the benefit on local symptoms may result from compression rather than ambulation.
Reduced mortality? Evidence is weak
Estimates of the possible effect on mortality of ambulation compared with bed rest are based on cohort studies. A cohort study in which 691 patients were kept walking with compression therapy reported a mortality rate of 0.2%.9 In another cohort, the mortality rate was also 0.2%, and all deaths occurred in patients older than 70 years.10
This rate is lower than rates reported in the historic literature, which typically are 1% among patients treated with unfractionated heparin and bed rest.9,10 A retrospective, multicenter cohort of 1647 patients treated with unfractionated heparin and bed rest in different German hospitals reported a rate of fatal PE of 2.33%.11
Data from the RIETE registry indicated that overall mortality was significantly higher in immobilized patients with a PE (3.6% vs 0.5% in mobile patients; P=.01).8 Notably, immobilized patients with a PE were more likely to be hypoxic and also tended to receive lower doses of LMWH. No differences were found in outcomes for patients with DVT.
Recommendations
The American College of Chest Physicians (ACCP) doesn’t recommend bed rest in its guidelines for treating acute venous thromboembolism, but rather ambulation as tolerated after starting anticoagulation. Patients who are not hemodynamically stable should be stabilized first.
The ACCP also recommends wearing an elastic compression stocking with a pressure of 30 to 40 mm Hg at the ankle for 2 years after an episode of DVT and a course of intermittent pneumatic compression for patients with severe edema of the leg resulting from post-thrombotic syndrome.12
A joint guideline from the American College of Physicians and the American Academy of Family Physicians doesn’t make recommendations about ambulation for therapy of DVT and PE.13
PROBABLY NOT. Ambulation, combined with compression of the affected extremity, appears to be safe for medically stable patients with deep venous thromboses (DVT) (strength of recommendation [SOR]: A, consistent randomized controlled trials [RCTs]). Leg compression and ambulation, compared with bed rest without compression, can effectively decrease swelling and pain (SOR: A, consistent RCTs).
Only weak data exist to suggest that early ambulation can reduce mortality (SOR: C, cohort studies with historical controls).
Evidence summary
Patients with acute DVT have traditionally been treated with immobilization and bed rest, combined with anticoagulation, for days. This approach is motivated by fear of dislodging an unstable thrombus and causing a pulmonary embolism (PE) and by the belief that inactivity relieves local pain and swelling. On the other hand, bed rest promotes stasis, an element in Virchow’s triad.
Early ambulation doesn’t raise risk of PE
We performed a structured literature review, which found 6 RCTs and 3 cohort studies that address this problem. All 6 RCTs included patients with acute DVT but without life-threatening conditions.1-6 They assessed various outcomes, including incidence of new PE, change in leg circumference, leg pain, patient well-being, and progression of DVT.
The studies consistently found that early ambulation, along with compression, is safe when compared with bed rest ( TABLE ). Although the sample size of all the RCTs was small, the RCTs showed consistent trends in favor of ambulation and compression.
A prospective cohort study of new PE in patients treated with ambulation and compression plus anticoagulation found that the incidence of PE was significantly lower than historical incidence rates in patients managed with bed rest.7
Another study using the RIETE registry, a Spanish registry of consecutively enrolled patients with objectively confirmed acute DVT or PE, found no significant difference in occurrence of new PE between immobilized and mobilized patients.8 Patients with DVT who were immobilized were generally sicker, more likely to have PaO2 <60, and more likely to have received lower doses of low-molecular-weight heparin (LMWH) compared with the group that walked (P<.005).
TABLE
Early ambulation and compression: What RCTs show
| Subjects | Study groups | Results |
|---|---|---|
| 129 patients with DVT, treated with LMWH1 | Strict immobilization for 4 days Ambulation for ≥4 h/d, along with compression for 4 days or until swelling subsided | At 4 days: No difference in PE, leg pain, leg size, mortality At 3 months: No difference in PE, mortality |
| 146 patients with DVT, all anticoagulated5 | Hospital treatment with 5 days of bed rest Home care with early walking and compression stockings | No difference in occurrence of new PE after 10 days |
| 126 patients with DVT, treated with LMWH, compression6 | Strict bed rest for 8 days with leg elevation Began full ambulation on day 2 | No difference in PE |
| 102 patients with DVT, treated with LMWH, compression4 | Bed rest for 5 days Ambulation | No differences in PE, thrombus progression, serious adverse events, or leg pain Study didn’t recruit expected number of patients Study showed a trend toward benefit from ambulation |
| 53 patients with DVT2,7 | Ambulation and use of firm, inelastic Unna boot bandages Ambulation and elastic compression stockings Strict bed rest for 9 days and no compression | No difference in quality of life or PE DVT-related symptoms, leg pain, and circumference improved in compression/ambulation groups No changes noted at 2 years |
| 72 patients with DVT, treated with anticoagulation and compression3 | Daily walking exercise and weekly group exercise Control group | No difference in DVT, PE, phlebography results, or calf circumference |
| DVT, deep vein thrombosis; LMWH, low-molecular-weight heparin; PE, pulmonary embolism. | ||
Does ambulation affect thrombus propagation?
A multicenter RCT showed that thrombus progression occurred more often in patients who were treated with bed rest compared with patients treated with ambulation and compression (P<.01).2
Another RCT revealed a similar trend, though the difference didn’t reach statistical significance because of small sample size.4 The clinical importance of these phlebographic studies isn’t clear.
Is it the walking, or compression, that works?
RCTs have shown that ambulation with leg compression, compared with bed rest without compression, can effectively decrease leg swelling and pain1,2,4 The difference was detectable 2 years after DVT.7
In contrast, RCTs in which both ambulating and resting patients received compression therapy showed no significant difference in leg circumference at 1 or 6 months.3 This finding suggests that the benefit on local symptoms may result from compression rather than ambulation.
Reduced mortality? Evidence is weak
Estimates of the possible effect on mortality of ambulation compared with bed rest are based on cohort studies. A cohort study in which 691 patients were kept walking with compression therapy reported a mortality rate of 0.2%.9 In another cohort, the mortality rate was also 0.2%, and all deaths occurred in patients older than 70 years.10
This rate is lower than rates reported in the historic literature, which typically are 1% among patients treated with unfractionated heparin and bed rest.9,10 A retrospective, multicenter cohort of 1647 patients treated with unfractionated heparin and bed rest in different German hospitals reported a rate of fatal PE of 2.33%.11
Data from the RIETE registry indicated that overall mortality was significantly higher in immobilized patients with a PE (3.6% vs 0.5% in mobile patients; P=.01).8 Notably, immobilized patients with a PE were more likely to be hypoxic and also tended to receive lower doses of LMWH. No differences were found in outcomes for patients with DVT.
Recommendations
The American College of Chest Physicians (ACCP) doesn’t recommend bed rest in its guidelines for treating acute venous thromboembolism, but rather ambulation as tolerated after starting anticoagulation. Patients who are not hemodynamically stable should be stabilized first.
The ACCP also recommends wearing an elastic compression stocking with a pressure of 30 to 40 mm Hg at the ankle for 2 years after an episode of DVT and a course of intermittent pneumatic compression for patients with severe edema of the leg resulting from post-thrombotic syndrome.12
A joint guideline from the American College of Physicians and the American Academy of Family Physicians doesn’t make recommendations about ambulation for therapy of DVT and PE.13
1. Aschwanden M, Labs KH, Engel H, et al. Acute deep vein thrombosis: early mobilization does not increase the frequency of pulmonary embolism. Thromb Haemost. 2001;85:42-46.
2. Blattler W, Partsch H. Leg compression and ambulation is better than bed rest for the treatment of acute deep venous thrombosis. Int Angiol. 2003;22:393-400.
3. Isma N, Johanssson E, Bjork A, et al. Does supervised exercise after deep venous thrombosis improve recanalization of occluded vein segments? A randomized study. J Thromb Thrombolysis. 2007;23:25-30.
4. Junger M, Diehm C, Storiko H, et al. Mobilization versus immobilization in the treatment of acute proximal deep venous thrombosis: a prospective, randomized, open, multicentre trial. Curr Med Res Opin. 2006;22:593-602.
5. Romera A, Vila R, Perez-Piqueras A, et al. Early mobilization in patients with acute deep vein thrombosis: does it increase the incidence of symptomatic pulmonary embolism? Phlebology. 2005;20:141.-
6. Schellong SM, Schwarz T, Kropp J, et al. Bed rest in deep vein thrombosis and the incidence of scintigraphic pulmonary embolism. Thromb Haemost. 1999;82(suppl 1):127-129.
7. Partsch H, Kaulich M, Mayer W. Immediate mobilisation in acute vein thrombosis reduces post-thrombotic syndrome. Int Angiol. 2004;23:206-212.
8. Trujillo-Santos J, Perea-Milla E, Jimenez-Puente A, et al. Bed rest or ambulation in the initial treatment of patients with acute deep vein thrombosis or pulmonary embolism: findings from the RIETE registry. Chest. 2005;127:1631-1636.
9. Partsch H, Kechavarz B, Kohn H, et al. The effect of mobilisation of patients during treatment of thromboembolic disorders with low-molecular-weight heparin. Int Angiol. 1997;16:189-192.
10. Partsch H. Therapy of deep vein thrombosis with low molecular weight heparin, leg compression and immediate ambulation. Vasa. 2001;30:195-204.
11. Martin M. PHLECO: a multicenter study of the fate of 1647 hospital patients treated conservatively without fibrinolysis and surgery. Clin Invest. 1993;71:471-477.
12. Buller HR, Agnelli G, Hull RD, et al. Antithrombotic therapy for venous thromboembolic disease: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126 (suppl 3):401S-428S.
13. Snow V, Qaseem A, Barry P, et al. Management of venous thromboembolism: a clinical practice guideline from the American College of Physicians and the American Academy of Family Physicians. Ann Intern Med. 2007;146:204-210.
1. Aschwanden M, Labs KH, Engel H, et al. Acute deep vein thrombosis: early mobilization does not increase the frequency of pulmonary embolism. Thromb Haemost. 2001;85:42-46.
2. Blattler W, Partsch H. Leg compression and ambulation is better than bed rest for the treatment of acute deep venous thrombosis. Int Angiol. 2003;22:393-400.
3. Isma N, Johanssson E, Bjork A, et al. Does supervised exercise after deep venous thrombosis improve recanalization of occluded vein segments? A randomized study. J Thromb Thrombolysis. 2007;23:25-30.
4. Junger M, Diehm C, Storiko H, et al. Mobilization versus immobilization in the treatment of acute proximal deep venous thrombosis: a prospective, randomized, open, multicentre trial. Curr Med Res Opin. 2006;22:593-602.
5. Romera A, Vila R, Perez-Piqueras A, et al. Early mobilization in patients with acute deep vein thrombosis: does it increase the incidence of symptomatic pulmonary embolism? Phlebology. 2005;20:141.-
6. Schellong SM, Schwarz T, Kropp J, et al. Bed rest in deep vein thrombosis and the incidence of scintigraphic pulmonary embolism. Thromb Haemost. 1999;82(suppl 1):127-129.
7. Partsch H, Kaulich M, Mayer W. Immediate mobilisation in acute vein thrombosis reduces post-thrombotic syndrome. Int Angiol. 2004;23:206-212.
8. Trujillo-Santos J, Perea-Milla E, Jimenez-Puente A, et al. Bed rest or ambulation in the initial treatment of patients with acute deep vein thrombosis or pulmonary embolism: findings from the RIETE registry. Chest. 2005;127:1631-1636.
9. Partsch H, Kechavarz B, Kohn H, et al. The effect of mobilisation of patients during treatment of thromboembolic disorders with low-molecular-weight heparin. Int Angiol. 1997;16:189-192.
10. Partsch H. Therapy of deep vein thrombosis with low molecular weight heparin, leg compression and immediate ambulation. Vasa. 2001;30:195-204.
11. Martin M. PHLECO: a multicenter study of the fate of 1647 hospital patients treated conservatively without fibrinolysis and surgery. Clin Invest. 1993;71:471-477.
12. Buller HR, Agnelli G, Hull RD, et al. Antithrombotic therapy for venous thromboembolic disease: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126 (suppl 3):401S-428S.
13. Snow V, Qaseem A, Barry P, et al. Management of venous thromboembolism: a clinical practice guideline from the American College of Physicians and the American Academy of Family Physicians. Ann Intern Med. 2007;146:204-210.
Evidence-based answers from the Family Physicians Inquiries Network
When should COX-2 selective NSAIDs be used for osteoarthritis and rheumatoid arthritis?
Cyclo-oxygenase-2 (COX-2) selective nonsteroidal anti-inflammatory drugs (NSAIDs) are as effective as acetaminophen and nonselective NSAIDs in treating of osteoarthritis, and are equally effective in reducing pain and inflammation and improving of joint function for patients with rheumatoid arthritis, when compared with nonselective NSAIDs. The COX-2 selective NSAIDs also have a better gastrointestinal safety profile in short-term (6–12 month) treatment (strength of recommendation [SOR]: A, based on meta-analysis of randomized controlled trials with patient-oriented outcomes).
However, with recent growing concern of the cardiovascular safety of COX-2 selective NSAIDs, it is imperative to select appropriate patients by considering benefit vs risks, which include serious gastrointestinal bleeding (TABLE 1), history of intolerance to nonselective NSAID, cardiovascular disease or associated risks, renal disease, patient’s preference, and cost.
Nonselective NSAIDs with misoprostol or a PPI instead of COX-2 inhibitor is a reasonable strategy
Joseph Saseen, PharmD, FCCP, BCPS
University of Colorado at Denver and Health Sciences Center, Denver, Colo
Although celecoxib is an effective NSAID, rofecoxib and lumericoxib are the only COX-2 selective inhibitors that definitively reduce gastrointestinal (GI) ulcerations/complications compared with nonselective NSAID therapy.1,2 However, neither of these are on the market. Data from the CLASS study showed no reduced risk of GI ulcerations/complications with celecoxib vs ibuprofen or diclofenac among patients receiving low-dose aspirin.3 Low-dose aspirin reduces cardiovascular events for patients with moderate or high cardiovascular risk (Framingham scores ≥10%). Therefore, using nonselective NSAID therapy in combination with either misoprostol or a proton pump inhibitor (eg, omeprazole) instead of celecoxib, is a reasonable and proven strategy to provide NSAID therapy for patients on low-dose aspirin who are at high risk for NSAID-associated gastropathy.
Evidence summary
A Cochrane review4 (6 randomized controlled trials, N=1689, mean duration 5.8 weeks) assessed the efficacy and safety of acetaminophen in the management of osteoarthritis, comparing it with placebo and NSAIDs. Acetaminophen was superior to placebo in pain reduction and global assessment (number needed to treat [NNT]=2) with a similar safety profile. NSAIDs were better than acetaminophen in pain reduction, patient (NNT=6) and physician global assessment (NNT=17), but no better for functional improvement. Compared with nonselective NSAIDs, acetaminophen led to fewer withdrawals (number needed to harm [NNH]=20) and fewer GI adverse events (NNH=9), but there was no statistical difference when compared with COX-2 selective NSAIDs.
Another Cochrane review5 (26 randomized controlled trials) found that rofecoxib (Vioxx) was more effective than placebo (NNT=5), and equally effective with other NSAIDs in the management of osteoarthritis. They reported fewer GI adverse events (endoscopically observed gastric erosion and ulcers) with rofecoxib than with other NSAIDs—naproxen (Naprosyn), ibuprofen (Motrin), diclofenac (Cataflam), nabumetone (Relafen), diclofenac/misoprostol (Arthrotec), and nimesulide. However, the withdrawal rate due to adverse events and the increase in blood pressure and edema were significantly greater with rofecoxib than placebo at 6 weeks.
Two Cochrane reviews6-7 confirmed the efficacy of celecoxib (Celebrex) and rofecoxib in treating of rheumatoid arthritis. One review included 2 RCTs (N=8734) with a placebo arm (8 weeks) and naproxen arm (9 months).7 The rofecoxib groups (25 mg, 50 mg) had more responders than the placebo group (NNT=8 and 6 respectively). Compared with naproxen (1 g), no difference was seen in efficacy in the OMERACT outcomes (Outcome Measures for Rheumatoid Arthritis Clinical Trials), but all combined GI adverse events (perforation, ulcer, obstruction, bleeding, and all episodes of GI bleeding) were significantly reduced at 9 months (NNH=20). The withdrawals were the same in the 3 groups. Compared with placebo, the rofecoxib groups had similar incidence of elevated blood pressure and edema (NNH=50 and 100, respectively). Compared with the naproxen group, no difference was seen in renal adverse events, but total cardiovascular thrombotic events (NNH=200) and nonfatal MI (NNH=300) increased at 9 months in the 50 mg rofecoxib group.
Similar cardiovascular adverse events were reported in the APPROVE trial.9 In this study, patients taking rofecoxib 25 mg daily for 18 months had increased total thrombotic events (MI, stroke, peripheral arterial and venous thrombosis, and pulmonary embolism) when compared with placebo (NNH=63). A recent study also raised the same concern of increased cardiovascular adverse events with celecoxib.10 This study demonstrated an increase risk of cardiovascular events (combined death, myocardial infarction, stroke, and heart failure) for patients taking celecoxib 200 mg twice a day (NNH=77) or 400 mg twice a day (NNH=42).
Many patients taking low-dose aspirin for cardioprotection also frequently require treatment of pain and inflammation with a NSAID. Even low-dose aspirin (75 mg/d) is known to be associated with increased GI toxicity (ulcers and hemorrhages).11 A recent double-blind, randomized placebo-controlled trial found that 12 weeks of treatment with a combination of low-dose aspirin and a COX-2 selective NSAID (rofecoxib) had more than twice the incidence of endoscopically confirmed gastric and duodenal ulcers, compared with aspirin alone, and no difference with a nonselective NSAID.12 This has raised the safety concern of concomitant use of a COX-2 selective NSAID with low-dose aspirin.
TABLE 1
Prediction of serious gastrointestinal bleeding
| RISK FACTORS PRESENT | RISK OF GI BLEEDING |
|---|---|
| 0 factor | 0.4 % |
| Any 1 factor | 1.0 % |
| All 4 factors | 9.0 % |
| Risk factors include age >75 years, history of peptic ulcer disease, history of gastrointestinal bleeding, history of cardiovascular disease | |
| Source: Silverstein et al, Ann Intern Med 1995.8 | |
Recommendations from others
The American Pain Society recommends that for patients with osteoarthritis, acetaminophen is the drug of choice for mild pain.13 For moderate to severe pain and or inflammation, a COX-2 selective NSAID is the first choice, unless the patient is at significant risk for hypertension or renal disorder. For patients with active rheumatoid arthritis and moderate to severe pain with or without inflammation, a COX-2 selective NSAID should be used concomitantly with a disease-modifying antirheumatic drug (DMARD), unless contraindicated by existing uncontrolled hypertension and renal disease. It further recommends that for a person who is at risk for a cardiovascular event, an aspirin (75–160 mg/d), should be given along with a COX-2 selective NSAID.
The American College of Rheumatology recommends that a COX-2 selective NSAID should be considered for a person with osteoarthritis and pain not relieved by an adequate dose of acetaminophen (not to exceed 4 g/d).14,15 The COX-2 selective NSAID is particularly advantageous for those who have higher risk factors for adverse GI events (TABLE 2). For a person with rheumatoid arthritis, in addition to DMARDs, NSAIDs (salicylates, nonselective NSAID, or COX-2 selective NSAID) should be used to reduce joint pain and swelling and improve joint function. Patients with additional risks for cardiovascular events should be cautioned about use of a COX-2 selective NSAID.
A recent AHRQ report on managing osteoarthritis underscores the importance of physician-patient partnership and patient’s self management of osteoarthritis, and recommends acetaminophen (up to 4 g/day) as the drug of choice.16 It further cautions the injudicious use of NSAIDs because of its greater GI toxicity when compared with acetaminophen, and its higher medical costs.
TABLE 2
Risk factors for upper gastrointestinal adverse events
| Age ≥65 years |
| Comorbid medical conditions |
| Oral glucocorticoids |
| History of peptic ulcer disease |
| History of upper gastrointestinal bleeding |
| Anticoagulants |
| Source: American College of Rheumatology, Arthritis Rheum 2000.12 |
1. Bombardier C, Laine L, Reicin A, et al. Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. N Engl J Med 2000;343:1520-1528.
2. Schnitzer TJ, Burmester GR, Mysler E, et al. Comparison of lumiracoxib with naproxen and ibuprofen in the Therapeutic Arthritis Research and Gastrointestinal Event Trial (TARGET), reduction in ulcer complications: randomised controlled trial. Lancet 2004;364:665-674.
3. Silverstein FE, Faich G, Goldstein JL, et al. Gastrointestinal toxicity with celecoxib vs nonsteroidal anti-inflammatory drugs for osteoarthritis and rheumatoid arthritis: the CLASS study: A randomized controlled trial. Celecoxib Long-term Arthritis Safety Study. JAMA 2000;284:1247-1255.
4. Towheed TE, Judd MG, Hochberg MC, Wells G. Acetaminophen for osteoarthritis. Cochrane Database Syst Rev 2003;(2):CD004257.-
5. Garner SE, Fidan DD, Frankish RR, Maxwell LJ. Rofecoxib for osteoarthritis. Cochrane Database Syst Rev 2005;(1):CD005115.-
6. Garner S, Fidan D, Frankish R, et al. Celecoxib for rheumatoid arthritis. Cochrane Database Syst Rev 2002;(4):CD003831.-
7. Garner SE, Fidan DD, Frankish RR, et al. Rofecoxib for rheumatoid arthritis. Cochrane Database Syst Rev 2005;(1):CD003685.-
8. Silverstein FE, Graham DY, Senior JR, et al. Misoprostol reduced serious gastrointestinal complications in patients with rheumatoid arthritis receiving nonsteroidal anti-inflammatory drugs. A randomized, double-blind, placebo-controlled trial. Ann Intern Med 1995;123:241-249.
9. Bresalier RS, Sandler RS, Quan H, et al. Cardiovascular events associated with rofecoxib in a colorectal adenoma chemoprevention trial. N Engl J Med 2005;352:1092-1102.
10. Solomon SD, McMurray JJ, Pfeffer MA, et al. Cardiovascular risk associated with celecoxib in clinical trial for colorectal adenoma prevention. N Engl J Med 2005;352:1071-1080.
11. Derry S, Loke YK. Risk of gastrointestinal haemorrhage with long term use of aspirin: meta-analysis. BMJ 2000;321:1183-1187.
12. Laine L, Maller ES, Yu C, Quan H, Simon T. Ulcer formation with low-dose enteric-coated aspirin and the effect of COX-2 selective inhibition: A double-blind trial. Gastroenterology 2004;127:395-402.
13. Simon LS, Lipman AG, Jacox AK, et al. Pain in Osteoarthritis, Rheumatoid Arthritis and Juvenile Chronic Arthritis. 2nd ed. Glenview, Ill: American Pain Society; 2002.
14. American College of Rheumatology (ACR) Subcommittee on Osteoarthritis Guidelines. Recommendations for the medical management of osteoarthritis of the hip and knee: 2000 update. American College of Rheumatology Subcommittee on Osteoarthritis Guidelines. Arthritis Rheum 2000;43:1905-1915.
15. American College of Rheumatology Subcommittee on Rheumatoid Arthritis Guidelines. Guidelines for the management of rheumatoid arthritis: 2002 Update. Arthritis Rheum 2002;46:328-346.
16. Managing Osteoarthritis: Helping the Elderly Maintain Function and Mobility. Issue 4, AHRQ Pub. No 02-0023, May 2002. Agency for Healthcare Research and Quality. Available at: www.ahrq.gov/research/osteoria/osteoria.htm#self-manage.
Cyclo-oxygenase-2 (COX-2) selective nonsteroidal anti-inflammatory drugs (NSAIDs) are as effective as acetaminophen and nonselective NSAIDs in treating of osteoarthritis, and are equally effective in reducing pain and inflammation and improving of joint function for patients with rheumatoid arthritis, when compared with nonselective NSAIDs. The COX-2 selective NSAIDs also have a better gastrointestinal safety profile in short-term (6–12 month) treatment (strength of recommendation [SOR]: A, based on meta-analysis of randomized controlled trials with patient-oriented outcomes).
However, with recent growing concern of the cardiovascular safety of COX-2 selective NSAIDs, it is imperative to select appropriate patients by considering benefit vs risks, which include serious gastrointestinal bleeding (TABLE 1), history of intolerance to nonselective NSAID, cardiovascular disease or associated risks, renal disease, patient’s preference, and cost.
Nonselective NSAIDs with misoprostol or a PPI instead of COX-2 inhibitor is a reasonable strategy
Joseph Saseen, PharmD, FCCP, BCPS
University of Colorado at Denver and Health Sciences Center, Denver, Colo
Although celecoxib is an effective NSAID, rofecoxib and lumericoxib are the only COX-2 selective inhibitors that definitively reduce gastrointestinal (GI) ulcerations/complications compared with nonselective NSAID therapy.1,2 However, neither of these are on the market. Data from the CLASS study showed no reduced risk of GI ulcerations/complications with celecoxib vs ibuprofen or diclofenac among patients receiving low-dose aspirin.3 Low-dose aspirin reduces cardiovascular events for patients with moderate or high cardiovascular risk (Framingham scores ≥10%). Therefore, using nonselective NSAID therapy in combination with either misoprostol or a proton pump inhibitor (eg, omeprazole) instead of celecoxib, is a reasonable and proven strategy to provide NSAID therapy for patients on low-dose aspirin who are at high risk for NSAID-associated gastropathy.
Evidence summary
A Cochrane review4 (6 randomized controlled trials, N=1689, mean duration 5.8 weeks) assessed the efficacy and safety of acetaminophen in the management of osteoarthritis, comparing it with placebo and NSAIDs. Acetaminophen was superior to placebo in pain reduction and global assessment (number needed to treat [NNT]=2) with a similar safety profile. NSAIDs were better than acetaminophen in pain reduction, patient (NNT=6) and physician global assessment (NNT=17), but no better for functional improvement. Compared with nonselective NSAIDs, acetaminophen led to fewer withdrawals (number needed to harm [NNH]=20) and fewer GI adverse events (NNH=9), but there was no statistical difference when compared with COX-2 selective NSAIDs.
Another Cochrane review5 (26 randomized controlled trials) found that rofecoxib (Vioxx) was more effective than placebo (NNT=5), and equally effective with other NSAIDs in the management of osteoarthritis. They reported fewer GI adverse events (endoscopically observed gastric erosion and ulcers) with rofecoxib than with other NSAIDs—naproxen (Naprosyn), ibuprofen (Motrin), diclofenac (Cataflam), nabumetone (Relafen), diclofenac/misoprostol (Arthrotec), and nimesulide. However, the withdrawal rate due to adverse events and the increase in blood pressure and edema were significantly greater with rofecoxib than placebo at 6 weeks.
Two Cochrane reviews6-7 confirmed the efficacy of celecoxib (Celebrex) and rofecoxib in treating of rheumatoid arthritis. One review included 2 RCTs (N=8734) with a placebo arm (8 weeks) and naproxen arm (9 months).7 The rofecoxib groups (25 mg, 50 mg) had more responders than the placebo group (NNT=8 and 6 respectively). Compared with naproxen (1 g), no difference was seen in efficacy in the OMERACT outcomes (Outcome Measures for Rheumatoid Arthritis Clinical Trials), but all combined GI adverse events (perforation, ulcer, obstruction, bleeding, and all episodes of GI bleeding) were significantly reduced at 9 months (NNH=20). The withdrawals were the same in the 3 groups. Compared with placebo, the rofecoxib groups had similar incidence of elevated blood pressure and edema (NNH=50 and 100, respectively). Compared with the naproxen group, no difference was seen in renal adverse events, but total cardiovascular thrombotic events (NNH=200) and nonfatal MI (NNH=300) increased at 9 months in the 50 mg rofecoxib group.
Similar cardiovascular adverse events were reported in the APPROVE trial.9 In this study, patients taking rofecoxib 25 mg daily for 18 months had increased total thrombotic events (MI, stroke, peripheral arterial and venous thrombosis, and pulmonary embolism) when compared with placebo (NNH=63). A recent study also raised the same concern of increased cardiovascular adverse events with celecoxib.10 This study demonstrated an increase risk of cardiovascular events (combined death, myocardial infarction, stroke, and heart failure) for patients taking celecoxib 200 mg twice a day (NNH=77) or 400 mg twice a day (NNH=42).
Many patients taking low-dose aspirin for cardioprotection also frequently require treatment of pain and inflammation with a NSAID. Even low-dose aspirin (75 mg/d) is known to be associated with increased GI toxicity (ulcers and hemorrhages).11 A recent double-blind, randomized placebo-controlled trial found that 12 weeks of treatment with a combination of low-dose aspirin and a COX-2 selective NSAID (rofecoxib) had more than twice the incidence of endoscopically confirmed gastric and duodenal ulcers, compared with aspirin alone, and no difference with a nonselective NSAID.12 This has raised the safety concern of concomitant use of a COX-2 selective NSAID with low-dose aspirin.
TABLE 1
Prediction of serious gastrointestinal bleeding
| RISK FACTORS PRESENT | RISK OF GI BLEEDING |
|---|---|
| 0 factor | 0.4 % |
| Any 1 factor | 1.0 % |
| All 4 factors | 9.0 % |
| Risk factors include age >75 years, history of peptic ulcer disease, history of gastrointestinal bleeding, history of cardiovascular disease | |
| Source: Silverstein et al, Ann Intern Med 1995.8 | |
Recommendations from others
The American Pain Society recommends that for patients with osteoarthritis, acetaminophen is the drug of choice for mild pain.13 For moderate to severe pain and or inflammation, a COX-2 selective NSAID is the first choice, unless the patient is at significant risk for hypertension or renal disorder. For patients with active rheumatoid arthritis and moderate to severe pain with or without inflammation, a COX-2 selective NSAID should be used concomitantly with a disease-modifying antirheumatic drug (DMARD), unless contraindicated by existing uncontrolled hypertension and renal disease. It further recommends that for a person who is at risk for a cardiovascular event, an aspirin (75–160 mg/d), should be given along with a COX-2 selective NSAID.
The American College of Rheumatology recommends that a COX-2 selective NSAID should be considered for a person with osteoarthritis and pain not relieved by an adequate dose of acetaminophen (not to exceed 4 g/d).14,15 The COX-2 selective NSAID is particularly advantageous for those who have higher risk factors for adverse GI events (TABLE 2). For a person with rheumatoid arthritis, in addition to DMARDs, NSAIDs (salicylates, nonselective NSAID, or COX-2 selective NSAID) should be used to reduce joint pain and swelling and improve joint function. Patients with additional risks for cardiovascular events should be cautioned about use of a COX-2 selective NSAID.
A recent AHRQ report on managing osteoarthritis underscores the importance of physician-patient partnership and patient’s self management of osteoarthritis, and recommends acetaminophen (up to 4 g/day) as the drug of choice.16 It further cautions the injudicious use of NSAIDs because of its greater GI toxicity when compared with acetaminophen, and its higher medical costs.
TABLE 2
Risk factors for upper gastrointestinal adverse events
| Age ≥65 years |
| Comorbid medical conditions |
| Oral glucocorticoids |
| History of peptic ulcer disease |
| History of upper gastrointestinal bleeding |
| Anticoagulants |
| Source: American College of Rheumatology, Arthritis Rheum 2000.12 |
Cyclo-oxygenase-2 (COX-2) selective nonsteroidal anti-inflammatory drugs (NSAIDs) are as effective as acetaminophen and nonselective NSAIDs in treating of osteoarthritis, and are equally effective in reducing pain and inflammation and improving of joint function for patients with rheumatoid arthritis, when compared with nonselective NSAIDs. The COX-2 selective NSAIDs also have a better gastrointestinal safety profile in short-term (6–12 month) treatment (strength of recommendation [SOR]: A, based on meta-analysis of randomized controlled trials with patient-oriented outcomes).
However, with recent growing concern of the cardiovascular safety of COX-2 selective NSAIDs, it is imperative to select appropriate patients by considering benefit vs risks, which include serious gastrointestinal bleeding (TABLE 1), history of intolerance to nonselective NSAID, cardiovascular disease or associated risks, renal disease, patient’s preference, and cost.
Nonselective NSAIDs with misoprostol or a PPI instead of COX-2 inhibitor is a reasonable strategy
Joseph Saseen, PharmD, FCCP, BCPS
University of Colorado at Denver and Health Sciences Center, Denver, Colo
Although celecoxib is an effective NSAID, rofecoxib and lumericoxib are the only COX-2 selective inhibitors that definitively reduce gastrointestinal (GI) ulcerations/complications compared with nonselective NSAID therapy.1,2 However, neither of these are on the market. Data from the CLASS study showed no reduced risk of GI ulcerations/complications with celecoxib vs ibuprofen or diclofenac among patients receiving low-dose aspirin.3 Low-dose aspirin reduces cardiovascular events for patients with moderate or high cardiovascular risk (Framingham scores ≥10%). Therefore, using nonselective NSAID therapy in combination with either misoprostol or a proton pump inhibitor (eg, omeprazole) instead of celecoxib, is a reasonable and proven strategy to provide NSAID therapy for patients on low-dose aspirin who are at high risk for NSAID-associated gastropathy.
Evidence summary
A Cochrane review4 (6 randomized controlled trials, N=1689, mean duration 5.8 weeks) assessed the efficacy and safety of acetaminophen in the management of osteoarthritis, comparing it with placebo and NSAIDs. Acetaminophen was superior to placebo in pain reduction and global assessment (number needed to treat [NNT]=2) with a similar safety profile. NSAIDs were better than acetaminophen in pain reduction, patient (NNT=6) and physician global assessment (NNT=17), but no better for functional improvement. Compared with nonselective NSAIDs, acetaminophen led to fewer withdrawals (number needed to harm [NNH]=20) and fewer GI adverse events (NNH=9), but there was no statistical difference when compared with COX-2 selective NSAIDs.
Another Cochrane review5 (26 randomized controlled trials) found that rofecoxib (Vioxx) was more effective than placebo (NNT=5), and equally effective with other NSAIDs in the management of osteoarthritis. They reported fewer GI adverse events (endoscopically observed gastric erosion and ulcers) with rofecoxib than with other NSAIDs—naproxen (Naprosyn), ibuprofen (Motrin), diclofenac (Cataflam), nabumetone (Relafen), diclofenac/misoprostol (Arthrotec), and nimesulide. However, the withdrawal rate due to adverse events and the increase in blood pressure and edema were significantly greater with rofecoxib than placebo at 6 weeks.
Two Cochrane reviews6-7 confirmed the efficacy of celecoxib (Celebrex) and rofecoxib in treating of rheumatoid arthritis. One review included 2 RCTs (N=8734) with a placebo arm (8 weeks) and naproxen arm (9 months).7 The rofecoxib groups (25 mg, 50 mg) had more responders than the placebo group (NNT=8 and 6 respectively). Compared with naproxen (1 g), no difference was seen in efficacy in the OMERACT outcomes (Outcome Measures for Rheumatoid Arthritis Clinical Trials), but all combined GI adverse events (perforation, ulcer, obstruction, bleeding, and all episodes of GI bleeding) were significantly reduced at 9 months (NNH=20). The withdrawals were the same in the 3 groups. Compared with placebo, the rofecoxib groups had similar incidence of elevated blood pressure and edema (NNH=50 and 100, respectively). Compared with the naproxen group, no difference was seen in renal adverse events, but total cardiovascular thrombotic events (NNH=200) and nonfatal MI (NNH=300) increased at 9 months in the 50 mg rofecoxib group.
Similar cardiovascular adverse events were reported in the APPROVE trial.9 In this study, patients taking rofecoxib 25 mg daily for 18 months had increased total thrombotic events (MI, stroke, peripheral arterial and venous thrombosis, and pulmonary embolism) when compared with placebo (NNH=63). A recent study also raised the same concern of increased cardiovascular adverse events with celecoxib.10 This study demonstrated an increase risk of cardiovascular events (combined death, myocardial infarction, stroke, and heart failure) for patients taking celecoxib 200 mg twice a day (NNH=77) or 400 mg twice a day (NNH=42).
Many patients taking low-dose aspirin for cardioprotection also frequently require treatment of pain and inflammation with a NSAID. Even low-dose aspirin (75 mg/d) is known to be associated with increased GI toxicity (ulcers and hemorrhages).11 A recent double-blind, randomized placebo-controlled trial found that 12 weeks of treatment with a combination of low-dose aspirin and a COX-2 selective NSAID (rofecoxib) had more than twice the incidence of endoscopically confirmed gastric and duodenal ulcers, compared with aspirin alone, and no difference with a nonselective NSAID.12 This has raised the safety concern of concomitant use of a COX-2 selective NSAID with low-dose aspirin.
TABLE 1
Prediction of serious gastrointestinal bleeding
| RISK FACTORS PRESENT | RISK OF GI BLEEDING |
|---|---|
| 0 factor | 0.4 % |
| Any 1 factor | 1.0 % |
| All 4 factors | 9.0 % |
| Risk factors include age >75 years, history of peptic ulcer disease, history of gastrointestinal bleeding, history of cardiovascular disease | |
| Source: Silverstein et al, Ann Intern Med 1995.8 | |
Recommendations from others
The American Pain Society recommends that for patients with osteoarthritis, acetaminophen is the drug of choice for mild pain.13 For moderate to severe pain and or inflammation, a COX-2 selective NSAID is the first choice, unless the patient is at significant risk for hypertension or renal disorder. For patients with active rheumatoid arthritis and moderate to severe pain with or without inflammation, a COX-2 selective NSAID should be used concomitantly with a disease-modifying antirheumatic drug (DMARD), unless contraindicated by existing uncontrolled hypertension and renal disease. It further recommends that for a person who is at risk for a cardiovascular event, an aspirin (75–160 mg/d), should be given along with a COX-2 selective NSAID.
The American College of Rheumatology recommends that a COX-2 selective NSAID should be considered for a person with osteoarthritis and pain not relieved by an adequate dose of acetaminophen (not to exceed 4 g/d).14,15 The COX-2 selective NSAID is particularly advantageous for those who have higher risk factors for adverse GI events (TABLE 2). For a person with rheumatoid arthritis, in addition to DMARDs, NSAIDs (salicylates, nonselective NSAID, or COX-2 selective NSAID) should be used to reduce joint pain and swelling and improve joint function. Patients with additional risks for cardiovascular events should be cautioned about use of a COX-2 selective NSAID.
A recent AHRQ report on managing osteoarthritis underscores the importance of physician-patient partnership and patient’s self management of osteoarthritis, and recommends acetaminophen (up to 4 g/day) as the drug of choice.16 It further cautions the injudicious use of NSAIDs because of its greater GI toxicity when compared with acetaminophen, and its higher medical costs.
TABLE 2
Risk factors for upper gastrointestinal adverse events
| Age ≥65 years |
| Comorbid medical conditions |
| Oral glucocorticoids |
| History of peptic ulcer disease |
| History of upper gastrointestinal bleeding |
| Anticoagulants |
| Source: American College of Rheumatology, Arthritis Rheum 2000.12 |
1. Bombardier C, Laine L, Reicin A, et al. Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. N Engl J Med 2000;343:1520-1528.
2. Schnitzer TJ, Burmester GR, Mysler E, et al. Comparison of lumiracoxib with naproxen and ibuprofen in the Therapeutic Arthritis Research and Gastrointestinal Event Trial (TARGET), reduction in ulcer complications: randomised controlled trial. Lancet 2004;364:665-674.
3. Silverstein FE, Faich G, Goldstein JL, et al. Gastrointestinal toxicity with celecoxib vs nonsteroidal anti-inflammatory drugs for osteoarthritis and rheumatoid arthritis: the CLASS study: A randomized controlled trial. Celecoxib Long-term Arthritis Safety Study. JAMA 2000;284:1247-1255.
4. Towheed TE, Judd MG, Hochberg MC, Wells G. Acetaminophen for osteoarthritis. Cochrane Database Syst Rev 2003;(2):CD004257.-
5. Garner SE, Fidan DD, Frankish RR, Maxwell LJ. Rofecoxib for osteoarthritis. Cochrane Database Syst Rev 2005;(1):CD005115.-
6. Garner S, Fidan D, Frankish R, et al. Celecoxib for rheumatoid arthritis. Cochrane Database Syst Rev 2002;(4):CD003831.-
7. Garner SE, Fidan DD, Frankish RR, et al. Rofecoxib for rheumatoid arthritis. Cochrane Database Syst Rev 2005;(1):CD003685.-
8. Silverstein FE, Graham DY, Senior JR, et al. Misoprostol reduced serious gastrointestinal complications in patients with rheumatoid arthritis receiving nonsteroidal anti-inflammatory drugs. A randomized, double-blind, placebo-controlled trial. Ann Intern Med 1995;123:241-249.
9. Bresalier RS, Sandler RS, Quan H, et al. Cardiovascular events associated with rofecoxib in a colorectal adenoma chemoprevention trial. N Engl J Med 2005;352:1092-1102.
10. Solomon SD, McMurray JJ, Pfeffer MA, et al. Cardiovascular risk associated with celecoxib in clinical trial for colorectal adenoma prevention. N Engl J Med 2005;352:1071-1080.
11. Derry S, Loke YK. Risk of gastrointestinal haemorrhage with long term use of aspirin: meta-analysis. BMJ 2000;321:1183-1187.
12. Laine L, Maller ES, Yu C, Quan H, Simon T. Ulcer formation with low-dose enteric-coated aspirin and the effect of COX-2 selective inhibition: A double-blind trial. Gastroenterology 2004;127:395-402.
13. Simon LS, Lipman AG, Jacox AK, et al. Pain in Osteoarthritis, Rheumatoid Arthritis and Juvenile Chronic Arthritis. 2nd ed. Glenview, Ill: American Pain Society; 2002.
14. American College of Rheumatology (ACR) Subcommittee on Osteoarthritis Guidelines. Recommendations for the medical management of osteoarthritis of the hip and knee: 2000 update. American College of Rheumatology Subcommittee on Osteoarthritis Guidelines. Arthritis Rheum 2000;43:1905-1915.
15. American College of Rheumatology Subcommittee on Rheumatoid Arthritis Guidelines. Guidelines for the management of rheumatoid arthritis: 2002 Update. Arthritis Rheum 2002;46:328-346.
16. Managing Osteoarthritis: Helping the Elderly Maintain Function and Mobility. Issue 4, AHRQ Pub. No 02-0023, May 2002. Agency for Healthcare Research and Quality. Available at: www.ahrq.gov/research/osteoria/osteoria.htm#self-manage.
1. Bombardier C, Laine L, Reicin A, et al. Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. N Engl J Med 2000;343:1520-1528.
2. Schnitzer TJ, Burmester GR, Mysler E, et al. Comparison of lumiracoxib with naproxen and ibuprofen in the Therapeutic Arthritis Research and Gastrointestinal Event Trial (TARGET), reduction in ulcer complications: randomised controlled trial. Lancet 2004;364:665-674.
3. Silverstein FE, Faich G, Goldstein JL, et al. Gastrointestinal toxicity with celecoxib vs nonsteroidal anti-inflammatory drugs for osteoarthritis and rheumatoid arthritis: the CLASS study: A randomized controlled trial. Celecoxib Long-term Arthritis Safety Study. JAMA 2000;284:1247-1255.
4. Towheed TE, Judd MG, Hochberg MC, Wells G. Acetaminophen for osteoarthritis. Cochrane Database Syst Rev 2003;(2):CD004257.-
5. Garner SE, Fidan DD, Frankish RR, Maxwell LJ. Rofecoxib for osteoarthritis. Cochrane Database Syst Rev 2005;(1):CD005115.-
6. Garner S, Fidan D, Frankish R, et al. Celecoxib for rheumatoid arthritis. Cochrane Database Syst Rev 2002;(4):CD003831.-
7. Garner SE, Fidan DD, Frankish RR, et al. Rofecoxib for rheumatoid arthritis. Cochrane Database Syst Rev 2005;(1):CD003685.-
8. Silverstein FE, Graham DY, Senior JR, et al. Misoprostol reduced serious gastrointestinal complications in patients with rheumatoid arthritis receiving nonsteroidal anti-inflammatory drugs. A randomized, double-blind, placebo-controlled trial. Ann Intern Med 1995;123:241-249.
9. Bresalier RS, Sandler RS, Quan H, et al. Cardiovascular events associated with rofecoxib in a colorectal adenoma chemoprevention trial. N Engl J Med 2005;352:1092-1102.
10. Solomon SD, McMurray JJ, Pfeffer MA, et al. Cardiovascular risk associated with celecoxib in clinical trial for colorectal adenoma prevention. N Engl J Med 2005;352:1071-1080.
11. Derry S, Loke YK. Risk of gastrointestinal haemorrhage with long term use of aspirin: meta-analysis. BMJ 2000;321:1183-1187.
12. Laine L, Maller ES, Yu C, Quan H, Simon T. Ulcer formation with low-dose enteric-coated aspirin and the effect of COX-2 selective inhibition: A double-blind trial. Gastroenterology 2004;127:395-402.
13. Simon LS, Lipman AG, Jacox AK, et al. Pain in Osteoarthritis, Rheumatoid Arthritis and Juvenile Chronic Arthritis. 2nd ed. Glenview, Ill: American Pain Society; 2002.
14. American College of Rheumatology (ACR) Subcommittee on Osteoarthritis Guidelines. Recommendations for the medical management of osteoarthritis of the hip and knee: 2000 update. American College of Rheumatology Subcommittee on Osteoarthritis Guidelines. Arthritis Rheum 2000;43:1905-1915.
15. American College of Rheumatology Subcommittee on Rheumatoid Arthritis Guidelines. Guidelines for the management of rheumatoid arthritis: 2002 Update. Arthritis Rheum 2002;46:328-346.
16. Managing Osteoarthritis: Helping the Elderly Maintain Function and Mobility. Issue 4, AHRQ Pub. No 02-0023, May 2002. Agency for Healthcare Research and Quality. Available at: www.ahrq.gov/research/osteoria/osteoria.htm#self-manage.
Evidence-based answers from the Family Physicians Inquiries Network
What are effective therapies for Clostridium difficile-associated diarrhea?
Oral metronidazole and oral vancomycin are equally effective treatments for Clostridium difficile–associated diarrhea (CDAD) (strength of recommendation [SOR]: A, based on randomized trials). Oral vancomycin is considerably more expensive and may select for colonization with vancomycin-resistant enterococci, leading the American College of Gastroenterology to recommend oral metronidazole as preferred therapy (SOR: C, expert opinion). They recommend therapy with vancomycin for those who are pregnant, breast feeding, less than 10 years old, nonresponders to metronidazole, critically ill, or allergic or intolerant to metronidazole (SOR: C, expert opinion).
Treat first recurrences the same as primary infection. In persons with recurrent infection, addition of the probiotic agent Saccharomyces boulardii. reduces the risk of further recurrences (SOR: B, single RCT). Little other evidence exists to guide therapy for subsequent recurrences.
Evidence summary
Two randomized controlled trials have compared the efficacy of oral metronidazole and oral vancomycin for treatment of CDAD.1,2 Both studies demonstrated statistically equivalent cure rates exceeding 90%, with relapse rates of 10% to 20% for each drug. These small trials lacked the power to detect small but potentially significant differences in treatment response.
No published data exist indicating that vancomycin is more effective than metronidazole in any clinical setting. A dose-range study showed that 125 mg of oral vancomycin 4 times a day is as effective as higher doses.3 Patients who cannot take medication by mouth should receive intravenous metronidazole, 500 mg 4 times per day. Unlike vancomycin, metronidazole achieves potentially effective concentrations in the intestinal lumen following intravenous administration.4
Treatment of first recurrences of infection with metronidazole or vancomycin produces response rates similar to treatment of initial infections.5 A minority of patients suffers multiple relapses of infection, and there are few data to guide therapy in this setting.
A randomized, double-blinded, placebocontrolled study evaluated the impact of adding the probiotic agent Saccharomyces boulardii. to either metronidazole or vancomycin.6 For persons with recurrent infection, addition of S boulardii. led to a 30% decrease in the absolute risk of relapse (64% relapse vs 34%; number needed to treat=3; P.<.05). There was also a nonsignificant trend toward reduced recurrences in the treatment of primary infections. The 2 minor side effects noted with this treatment were dry mouth (number needed to harm [NNH]=11) and constipation (NNH=9). S boulardii. capsules are available from health food stores and via the Internet. Several published case series describe various additional approaches to therapy of recurrent CDAD (Table).
TABLE
Medical treatment of C difficile–.associated diarrhea
| Indication | Treatment |
|---|---|
| First episode of C difficile.–associated diarrhea (SOR: A; SOR: C for preference over vancomycin) | Metronidazole, 500 mg orally 3 times daily for 10 days |
| First episode, allergy, or intolerance to metronidazole, pregnant, breast feeding, or age <10 years (SOR: A; SOR: C for preference over metronidazole) | Vancomycin, 125 mg orally 4 times daily for 10 days |
| Unable to take oral medication (SOR: C) | Metronidazole 500 mg IV 4 times daily |
| First recurrence (SOR: C) | As for first episode or Option #1 below |
| Second or greater recurrence: | |
| Option #1 (SOR: B, single RCT) | Metronidazole or vancomycin, plus S boulardii. (500 mg twice daily [3 x 1010 CFUs]) |
| Option #2 (SOR: C) | Vancomycin or metronidazole plus rifampin 300 mg oral twice daily for 10 days |
| Option #3 (SOR: C) | Vancomycin tapered dose: |
| 125 mg orally 4 times daily for 7 days | |
| 125 mg orally twice daily for 7 days | |
| 125 mg orally once daily for 7 days | |
| 125 mg orally every other day for 7 days | |
| 125 mg orally every 3 days for 14 days | |
| Option #4 (SOR: C) | Vancomycin plus cholestyramine 4 g twice daily for 10 days |
Recommendations from others
The American College of Gastroenterology and the American College of Physicians treatment guidelines for CDAD both call for treatment with oral metronidazole 250 mg 4 times daily or 500 mg 3 times daily.7,8 The American College of Gastroenterology recommends vancomycin (125 mg orally 4 times daily) when there is an intolerance or confirmed resistance to metronidazole, failure of response, when the patient is pregnant, breast feeding, or under 10 years of age, critically ill from colitis, or when the diarrhea could be related to Staphylococcus aureus.. In milder cases, treatment may involve only discontinuation of antibiotics and supportive therapy with observation. Opiates and antispasmodics should be avoided. These guidelines do not recommend any treatment over another for therapy of multiple recurrences.
Discontinue the offending antibiotic and treat the infection; prevent outbreaks via patient-to-patient transmission
Joe Tribuna, MD
Kimdary Chek, MD, MDH
Most cases of Clostridium difficile–.associated diarrhea are caused by antibiotic use; it is therefore one of the most common nosocomial infections. In addition to discontinuing use of the offending antibiotic and treating the infection, it is also important to prevent further outbreaks via patient-to-patient transmission. In our hospital, once a patient is diagnosed with C difficile., contact precautions are instituted. If the patient is incontinent, isolation in a single room is required. If the patient is continent
1. Teasley DG, Gerding DN, Olson MM, et al. Prospective randomised trial of metronidazole versus vancomycin for Clostridium-difficile-associated diarrhoea and colitis. Lancet 1983;2:1043-1046.
2. Wenisch C, Parschalk B, Hasenhundl M, Hirschl AM, Graninger W. Comparison of vancomycin, teicoplanin, metronidazole, and fusidic acid for the treatment of Clostridium difficile-associated diarrhea. Clin Infect Dis 1996;22:813-818.
3. Fekety R, Silva J, Kauffman C, Buggy B, Deery HG. Treatment of antibiotic-associated Clostridium difficile colitis with oral vancomycin: comparison of two dosage regimens. Am J Med 1989;86:15-19.
4. Bolton RP, Culshaw MA. Faecal metronidazole concentrations during oral and intravenous therapy for antibiotic associated colitis due to Clostridium difficile. Gut 1986;27:1169-1172.
5. Bartlett JG, Tedesco FJ, Shull S, Lowe B, Chang T. Symptomatic relapse after oral vancomycin therapy of antibiotic-associated pseudomembranous colitis. Gastroenterology 1980;78:431-434.
6. McFarland LV, Surawicz CM, Greenberg RN, Fekety R, Elmer GW, Moyer KA, et al. A randomized placebo-controlled trial of Saccharomyces boulardii in combination with standard antibiotics for Clostridium difficile disease. JAMA 1994;271:1913-1918.
7. Fekety R. Guidelines for the diagnosis and management of Clostridium difficile-associated diarrhea and colitis. American College of Gastroenterology, Practice Parameters Committee. Am J Gastroenterol 1997;92:739-750.
8. Hurley B.W., Nguyen C. C. Drug therapy: use of antimicrobial agents as first-line drug therapy for CDAD. PIER: Clinical Guidance from ACP, 2004. Available at: pier.acponline.org/physicians/diseases/d320/d320.html. Accessed on July 14, 2004.
Oral metronidazole and oral vancomycin are equally effective treatments for Clostridium difficile–associated diarrhea (CDAD) (strength of recommendation [SOR]: A, based on randomized trials). Oral vancomycin is considerably more expensive and may select for colonization with vancomycin-resistant enterococci, leading the American College of Gastroenterology to recommend oral metronidazole as preferred therapy (SOR: C, expert opinion). They recommend therapy with vancomycin for those who are pregnant, breast feeding, less than 10 years old, nonresponders to metronidazole, critically ill, or allergic or intolerant to metronidazole (SOR: C, expert opinion).
Treat first recurrences the same as primary infection. In persons with recurrent infection, addition of the probiotic agent Saccharomyces boulardii. reduces the risk of further recurrences (SOR: B, single RCT). Little other evidence exists to guide therapy for subsequent recurrences.
Evidence summary
Two randomized controlled trials have compared the efficacy of oral metronidazole and oral vancomycin for treatment of CDAD.1,2 Both studies demonstrated statistically equivalent cure rates exceeding 90%, with relapse rates of 10% to 20% for each drug. These small trials lacked the power to detect small but potentially significant differences in treatment response.
No published data exist indicating that vancomycin is more effective than metronidazole in any clinical setting. A dose-range study showed that 125 mg of oral vancomycin 4 times a day is as effective as higher doses.3 Patients who cannot take medication by mouth should receive intravenous metronidazole, 500 mg 4 times per day. Unlike vancomycin, metronidazole achieves potentially effective concentrations in the intestinal lumen following intravenous administration.4
Treatment of first recurrences of infection with metronidazole or vancomycin produces response rates similar to treatment of initial infections.5 A minority of patients suffers multiple relapses of infection, and there are few data to guide therapy in this setting.
A randomized, double-blinded, placebocontrolled study evaluated the impact of adding the probiotic agent Saccharomyces boulardii. to either metronidazole or vancomycin.6 For persons with recurrent infection, addition of S boulardii. led to a 30% decrease in the absolute risk of relapse (64% relapse vs 34%; number needed to treat=3; P.<.05). There was also a nonsignificant trend toward reduced recurrences in the treatment of primary infections. The 2 minor side effects noted with this treatment were dry mouth (number needed to harm [NNH]=11) and constipation (NNH=9). S boulardii. capsules are available from health food stores and via the Internet. Several published case series describe various additional approaches to therapy of recurrent CDAD (Table).
TABLE
Medical treatment of C difficile–.associated diarrhea
| Indication | Treatment |
|---|---|
| First episode of C difficile.–associated diarrhea (SOR: A; SOR: C for preference over vancomycin) | Metronidazole, 500 mg orally 3 times daily for 10 days |
| First episode, allergy, or intolerance to metronidazole, pregnant, breast feeding, or age <10 years (SOR: A; SOR: C for preference over metronidazole) | Vancomycin, 125 mg orally 4 times daily for 10 days |
| Unable to take oral medication (SOR: C) | Metronidazole 500 mg IV 4 times daily |
| First recurrence (SOR: C) | As for first episode or Option #1 below |
| Second or greater recurrence: | |
| Option #1 (SOR: B, single RCT) | Metronidazole or vancomycin, plus S boulardii. (500 mg twice daily [3 x 1010 CFUs]) |
| Option #2 (SOR: C) | Vancomycin or metronidazole plus rifampin 300 mg oral twice daily for 10 days |
| Option #3 (SOR: C) | Vancomycin tapered dose: |
| 125 mg orally 4 times daily for 7 days | |
| 125 mg orally twice daily for 7 days | |
| 125 mg orally once daily for 7 days | |
| 125 mg orally every other day for 7 days | |
| 125 mg orally every 3 days for 14 days | |
| Option #4 (SOR: C) | Vancomycin plus cholestyramine 4 g twice daily for 10 days |
Recommendations from others
The American College of Gastroenterology and the American College of Physicians treatment guidelines for CDAD both call for treatment with oral metronidazole 250 mg 4 times daily or 500 mg 3 times daily.7,8 The American College of Gastroenterology recommends vancomycin (125 mg orally 4 times daily) when there is an intolerance or confirmed resistance to metronidazole, failure of response, when the patient is pregnant, breast feeding, or under 10 years of age, critically ill from colitis, or when the diarrhea could be related to Staphylococcus aureus.. In milder cases, treatment may involve only discontinuation of antibiotics and supportive therapy with observation. Opiates and antispasmodics should be avoided. These guidelines do not recommend any treatment over another for therapy of multiple recurrences.
Discontinue the offending antibiotic and treat the infection; prevent outbreaks via patient-to-patient transmission
Joe Tribuna, MD
Kimdary Chek, MD, MDH
Most cases of Clostridium difficile–.associated diarrhea are caused by antibiotic use; it is therefore one of the most common nosocomial infections. In addition to discontinuing use of the offending antibiotic and treating the infection, it is also important to prevent further outbreaks via patient-to-patient transmission. In our hospital, once a patient is diagnosed with C difficile., contact precautions are instituted. If the patient is incontinent, isolation in a single room is required. If the patient is continent
Oral metronidazole and oral vancomycin are equally effective treatments for Clostridium difficile–associated diarrhea (CDAD) (strength of recommendation [SOR]: A, based on randomized trials). Oral vancomycin is considerably more expensive and may select for colonization with vancomycin-resistant enterococci, leading the American College of Gastroenterology to recommend oral metronidazole as preferred therapy (SOR: C, expert opinion). They recommend therapy with vancomycin for those who are pregnant, breast feeding, less than 10 years old, nonresponders to metronidazole, critically ill, or allergic or intolerant to metronidazole (SOR: C, expert opinion).
Treat first recurrences the same as primary infection. In persons with recurrent infection, addition of the probiotic agent Saccharomyces boulardii. reduces the risk of further recurrences (SOR: B, single RCT). Little other evidence exists to guide therapy for subsequent recurrences.
Evidence summary
Two randomized controlled trials have compared the efficacy of oral metronidazole and oral vancomycin for treatment of CDAD.1,2 Both studies demonstrated statistically equivalent cure rates exceeding 90%, with relapse rates of 10% to 20% for each drug. These small trials lacked the power to detect small but potentially significant differences in treatment response.
No published data exist indicating that vancomycin is more effective than metronidazole in any clinical setting. A dose-range study showed that 125 mg of oral vancomycin 4 times a day is as effective as higher doses.3 Patients who cannot take medication by mouth should receive intravenous metronidazole, 500 mg 4 times per day. Unlike vancomycin, metronidazole achieves potentially effective concentrations in the intestinal lumen following intravenous administration.4
Treatment of first recurrences of infection with metronidazole or vancomycin produces response rates similar to treatment of initial infections.5 A minority of patients suffers multiple relapses of infection, and there are few data to guide therapy in this setting.
A randomized, double-blinded, placebocontrolled study evaluated the impact of adding the probiotic agent Saccharomyces boulardii. to either metronidazole or vancomycin.6 For persons with recurrent infection, addition of S boulardii. led to a 30% decrease in the absolute risk of relapse (64% relapse vs 34%; number needed to treat=3; P.<.05). There was also a nonsignificant trend toward reduced recurrences in the treatment of primary infections. The 2 minor side effects noted with this treatment were dry mouth (number needed to harm [NNH]=11) and constipation (NNH=9). S boulardii. capsules are available from health food stores and via the Internet. Several published case series describe various additional approaches to therapy of recurrent CDAD (Table).
TABLE
Medical treatment of C difficile–.associated diarrhea
| Indication | Treatment |
|---|---|
| First episode of C difficile.–associated diarrhea (SOR: A; SOR: C for preference over vancomycin) | Metronidazole, 500 mg orally 3 times daily for 10 days |
| First episode, allergy, or intolerance to metronidazole, pregnant, breast feeding, or age <10 years (SOR: A; SOR: C for preference over metronidazole) | Vancomycin, 125 mg orally 4 times daily for 10 days |
| Unable to take oral medication (SOR: C) | Metronidazole 500 mg IV 4 times daily |
| First recurrence (SOR: C) | As for first episode or Option #1 below |
| Second or greater recurrence: | |
| Option #1 (SOR: B, single RCT) | Metronidazole or vancomycin, plus S boulardii. (500 mg twice daily [3 x 1010 CFUs]) |
| Option #2 (SOR: C) | Vancomycin or metronidazole plus rifampin 300 mg oral twice daily for 10 days |
| Option #3 (SOR: C) | Vancomycin tapered dose: |
| 125 mg orally 4 times daily for 7 days | |
| 125 mg orally twice daily for 7 days | |
| 125 mg orally once daily for 7 days | |
| 125 mg orally every other day for 7 days | |
| 125 mg orally every 3 days for 14 days | |
| Option #4 (SOR: C) | Vancomycin plus cholestyramine 4 g twice daily for 10 days |
Recommendations from others
The American College of Gastroenterology and the American College of Physicians treatment guidelines for CDAD both call for treatment with oral metronidazole 250 mg 4 times daily or 500 mg 3 times daily.7,8 The American College of Gastroenterology recommends vancomycin (125 mg orally 4 times daily) when there is an intolerance or confirmed resistance to metronidazole, failure of response, when the patient is pregnant, breast feeding, or under 10 years of age, critically ill from colitis, or when the diarrhea could be related to Staphylococcus aureus.. In milder cases, treatment may involve only discontinuation of antibiotics and supportive therapy with observation. Opiates and antispasmodics should be avoided. These guidelines do not recommend any treatment over another for therapy of multiple recurrences.
Discontinue the offending antibiotic and treat the infection; prevent outbreaks via patient-to-patient transmission
Joe Tribuna, MD
Kimdary Chek, MD, MDH
Most cases of Clostridium difficile–.associated diarrhea are caused by antibiotic use; it is therefore one of the most common nosocomial infections. In addition to discontinuing use of the offending antibiotic and treating the infection, it is also important to prevent further outbreaks via patient-to-patient transmission. In our hospital, once a patient is diagnosed with C difficile., contact precautions are instituted. If the patient is incontinent, isolation in a single room is required. If the patient is continent
1. Teasley DG, Gerding DN, Olson MM, et al. Prospective randomised trial of metronidazole versus vancomycin for Clostridium-difficile-associated diarrhoea and colitis. Lancet 1983;2:1043-1046.
2. Wenisch C, Parschalk B, Hasenhundl M, Hirschl AM, Graninger W. Comparison of vancomycin, teicoplanin, metronidazole, and fusidic acid for the treatment of Clostridium difficile-associated diarrhea. Clin Infect Dis 1996;22:813-818.
3. Fekety R, Silva J, Kauffman C, Buggy B, Deery HG. Treatment of antibiotic-associated Clostridium difficile colitis with oral vancomycin: comparison of two dosage regimens. Am J Med 1989;86:15-19.
4. Bolton RP, Culshaw MA. Faecal metronidazole concentrations during oral and intravenous therapy for antibiotic associated colitis due to Clostridium difficile. Gut 1986;27:1169-1172.
5. Bartlett JG, Tedesco FJ, Shull S, Lowe B, Chang T. Symptomatic relapse after oral vancomycin therapy of antibiotic-associated pseudomembranous colitis. Gastroenterology 1980;78:431-434.
6. McFarland LV, Surawicz CM, Greenberg RN, Fekety R, Elmer GW, Moyer KA, et al. A randomized placebo-controlled trial of Saccharomyces boulardii in combination with standard antibiotics for Clostridium difficile disease. JAMA 1994;271:1913-1918.
7. Fekety R. Guidelines for the diagnosis and management of Clostridium difficile-associated diarrhea and colitis. American College of Gastroenterology, Practice Parameters Committee. Am J Gastroenterol 1997;92:739-750.
8. Hurley B.W., Nguyen C. C. Drug therapy: use of antimicrobial agents as first-line drug therapy for CDAD. PIER: Clinical Guidance from ACP, 2004. Available at: pier.acponline.org/physicians/diseases/d320/d320.html. Accessed on July 14, 2004.
1. Teasley DG, Gerding DN, Olson MM, et al. Prospective randomised trial of metronidazole versus vancomycin for Clostridium-difficile-associated diarrhoea and colitis. Lancet 1983;2:1043-1046.
2. Wenisch C, Parschalk B, Hasenhundl M, Hirschl AM, Graninger W. Comparison of vancomycin, teicoplanin, metronidazole, and fusidic acid for the treatment of Clostridium difficile-associated diarrhea. Clin Infect Dis 1996;22:813-818.
3. Fekety R, Silva J, Kauffman C, Buggy B, Deery HG. Treatment of antibiotic-associated Clostridium difficile colitis with oral vancomycin: comparison of two dosage regimens. Am J Med 1989;86:15-19.
4. Bolton RP, Culshaw MA. Faecal metronidazole concentrations during oral and intravenous therapy for antibiotic associated colitis due to Clostridium difficile. Gut 1986;27:1169-1172.
5. Bartlett JG, Tedesco FJ, Shull S, Lowe B, Chang T. Symptomatic relapse after oral vancomycin therapy of antibiotic-associated pseudomembranous colitis. Gastroenterology 1980;78:431-434.
6. McFarland LV, Surawicz CM, Greenberg RN, Fekety R, Elmer GW, Moyer KA, et al. A randomized placebo-controlled trial of Saccharomyces boulardii in combination with standard antibiotics for Clostridium difficile disease. JAMA 1994;271:1913-1918.
7. Fekety R. Guidelines for the diagnosis and management of Clostridium difficile-associated diarrhea and colitis. American College of Gastroenterology, Practice Parameters Committee. Am J Gastroenterol 1997;92:739-750.
8. Hurley B.W., Nguyen C. C. Drug therapy: use of antimicrobial agents as first-line drug therapy for CDAD. PIER: Clinical Guidance from ACP, 2004. Available at: pier.acponline.org/physicians/diseases/d320/d320.html. Accessed on July 14, 2004.
Evidence-based answers from the Family Physicians Inquiries Network
Does neonatal circumcision decrease morbidity?
Evidence suggests that neonatal circumcision decreases the incidence of childhood urinary tract infections, phimosis, paraphimosis, balanitis and other genital dermatoses, invasive penile cancer, and the sexually transmitted diseases human papilloma virus (HPV) and HIV (strength of recommendation [SOR]: B, based on case control and cohort studies). The benefits of decreased incidence of HPV and HIV infections go beyond the index patient and have public health implications on the transmission of these diseases (SOR: B). Further, a decrease in HPV incidence and transmission may lead to a lower incidence of cervical cancer (SOR: B).
While there appears to be some evidence for reduced morbidity with routine circumcision, decisions regarding routine neonatal circumcision requires balancing risks and benefits of the procedure with the alternatives in the context of social, familial, and religious beliefs.
Evidence summary
Observational studies have shown at least a 10- to 12-fold increase in urinary tract infections (UTIs) in uncircumcised male infants compared with their circumcised counterparts.1 The number of male infants that need to be circumcised to prevent 1 UTI is estimated to be between 44 and 100.2,3 The only randomized controlled trial of circumcision for UTI prevention was not during the neonatal period (average age was 30 months) and focused on secondary prevention.4 It demonstrated a statistically significant decrease in the rate of bacteriuria. The long-term effect on UTI incidence, renal scarring, and subsequent complications such as hypertension and end-stage renal disease is unknown.
Evidence from case series supports the protective effect of circumcision on the rates of penile cancer. A review of 592 cases of penile cancer revealed that none of those affected had been circumcised in infancy.5 In another series of 89 men with penile cancer, only 2 had been circumcised in infancy, while 87 were uncircumcised.6 Since HPV is thought to be a major etiologic agent in both penile cancer and cervical cancer, investigators studied the link between circumcision status and cervical cancer. In a meta-analysis of 7 case-control studies, penile HPV was detected 2.7 times more often in uncircumcised men after controlling for confounders.7 In this same meta-analysis, monogamous female partners of high-risk circumcised men (men with more than 6 lifetime partners) had a lower risk of cervical cancer than women whose high-risk partner was uncircumcised (adjusted odds ratio=0.42; 95% confidence interval [CI], 0.23–0.79).7
The evidence that circumcision prevents most sexually transmitted diseases is not very strong, with the exception of HIV and genital ulcer disease. Most of these studies are from sub-Saharan Africa, where rates of HIV infection are extremely high. A meta-analysis of 15 observational studies in Africa, with adjustment for potential confounding factors, found that circumcision decreased the risk of acquiring HIV by more than half (relative risk [RR]=0.42; 95% CI, 0.34–0.54).8 A more recent prospective study from India showed a strong protective effect of circumcision against HIV infection (RR=0.15; 95% CI, 0.04–0.62).9 This study found no protective effect of circumcision against herpes, syphilis, or gonorrhea, suggesting a biological rather than a behavioral explanation for the protective effect of circumcision against HIV.
A conservative estimate of the post-neonatal childhood circumcision rate for purely medical reasons is 2% to 5%; estimates go as high as 7% to 10%.10 The most common medical indication for circumcision is phimosis, followed by recurrent balanitis and paraphimosis. Circumcision may also be protective against genital dermatoses; a case-control study found an age-adjusted odds ratio of 3.2 (95% CI, 2.3–4.6) for penile skin diseases in uncircumcised men compared with circumcised men.11
Recommendations from others
Circumcision rates vary widely worldwide, with strong cultural and religious preferences. Most major organizations have cautiously neutral opinions on circumcision, stating that medical benefits are not large enough to justify routine neonatal circumcision. The American Academy of Pediatrics Task Force on Circumcision recommends parents “should be given accurate and unbiased information” and that “parents should determine what is in the best interest of the child.”12 The American Medical Association, American College of Obstetrics and Gynecology, and the American Academy of Family Physicians all use similar statements.13-15
Explain risks and benefits of circumcision to parents so they make informed decisions
A dilemma exists in the practice of recommending circumcision to parents of newborn males. Although the evidence shows that morbidity is decreased in circumcised males, the occurrence of complications (such as UTI or balanitis) is believed to be preventable through good hygiene, and the incidence of the preventable disease (such as penile cancer) is so low in the general population as to not justify the procedure. The challenge is there because the procedure is not without pain or risk of complications.
This is the basis for the American Academy of Pediatrics not recommending routine neonatal circumcision. The consensus was that the evidence was not sufficient to support it. Since then, many studies have been published on HPV and HIV transmission, the incidence of phimosis and paraphimosis, UTI, and balanitis, and how circumcision reduces the incidence of these diseases. Again, these are believed to be preventable through hygiene and condom use. In practice, it is difficult to persuade parents because these complications usually occur much later in life. Most patients made their decisions on circumcision based on religious or cultural experiences.
1. Wiswell TE. The prepuce, urinary tract infections, and the consequences. Pediatrics 2000;105:860-862.
2. Sethi N, Schwierling K, Kim J, et al. Newborn circumcision and urinary tract infections. Pediatrics 2001;107:212.-
3. Christakis DA, Harvey E, Zerr DM, Feudtner C, Wright JA, Connell FA. A trade off analysis of routine newborn circumcision. Pediatrics 2000;105:246-249.
4. Nayir A. Circumcision for the prevention of significant bacteriuria in boys. Pediatr Nephrol 2001;16:1129-1134.Erratum in: Pediatr Nephrol. 2002; 17: 307.
5. Lerman SE, Liao JC. Neonatal circumcision. Pediatr Clin North Am 2001;48:1539-557.
6. Mallon E, Hawkins D, Dinneen M, et al. Circumcision and genital dermatoses. Arch Dermatol 2000;136:350-354.
7. Schoen EJ. The relationship between circumcision and cancer of the penis. CA Cancer J Clin 1991;41:306-309.
8. Schoen EJ, Oehrli M, Colby C, Machin G. The highly protective effect of newborn circumcision against invasive penile cancer. Pediatrics 2000;105:E36.-
9. Castellsague X, Bosch FX, Munoz N, et al. Male circumcision, penile human papillomavirus infection, and cervical cancer in female partners. N Engl J Med 2002;346:1105-1112.
10. Weiss HA, Quigley MA, Hayes RJ. Male circumcision and risk of HIV infection in sub-Saharan Africa: a systematic review and meta-analysis. AIDS 2000;14:2361-2370.
11. Reynolds SJ, Shepherd ME, Risbud AR, et al. Male circumcision and risk of HIV-1 and other sexually transmitted infections in India. Lancet 2004;363:1039-1040.
12. American Academy of Pediatrics. Task Force on Circumcision. Circumcision policy statement. Pediatrics 1999;103:686-693.
13. American Medical Association. Report 10 of the Council on Scientific Affairs (I-99) Neonatal Circumcision. Available at: www.ama-assn.org/ama/pub/category/ 13585.html. Accessed on December 8, 2004.
14. American College of Obstetricians and Gynecologists. ACOG Committee Opinion Number 260: Circumcision. Obstet Gynecol 2001;98:707-708.
15. American Academy of Family Physicians. Position Paper on Neonatal Circumcision. Available at: www.aafp.org/ x1462.xml. Accessed on December 8, 2004.
Evidence suggests that neonatal circumcision decreases the incidence of childhood urinary tract infections, phimosis, paraphimosis, balanitis and other genital dermatoses, invasive penile cancer, and the sexually transmitted diseases human papilloma virus (HPV) and HIV (strength of recommendation [SOR]: B, based on case control and cohort studies). The benefits of decreased incidence of HPV and HIV infections go beyond the index patient and have public health implications on the transmission of these diseases (SOR: B). Further, a decrease in HPV incidence and transmission may lead to a lower incidence of cervical cancer (SOR: B).
While there appears to be some evidence for reduced morbidity with routine circumcision, decisions regarding routine neonatal circumcision requires balancing risks and benefits of the procedure with the alternatives in the context of social, familial, and religious beliefs.
Evidence summary
Observational studies have shown at least a 10- to 12-fold increase in urinary tract infections (UTIs) in uncircumcised male infants compared with their circumcised counterparts.1 The number of male infants that need to be circumcised to prevent 1 UTI is estimated to be between 44 and 100.2,3 The only randomized controlled trial of circumcision for UTI prevention was not during the neonatal period (average age was 30 months) and focused on secondary prevention.4 It demonstrated a statistically significant decrease in the rate of bacteriuria. The long-term effect on UTI incidence, renal scarring, and subsequent complications such as hypertension and end-stage renal disease is unknown.
Evidence from case series supports the protective effect of circumcision on the rates of penile cancer. A review of 592 cases of penile cancer revealed that none of those affected had been circumcised in infancy.5 In another series of 89 men with penile cancer, only 2 had been circumcised in infancy, while 87 were uncircumcised.6 Since HPV is thought to be a major etiologic agent in both penile cancer and cervical cancer, investigators studied the link between circumcision status and cervical cancer. In a meta-analysis of 7 case-control studies, penile HPV was detected 2.7 times more often in uncircumcised men after controlling for confounders.7 In this same meta-analysis, monogamous female partners of high-risk circumcised men (men with more than 6 lifetime partners) had a lower risk of cervical cancer than women whose high-risk partner was uncircumcised (adjusted odds ratio=0.42; 95% confidence interval [CI], 0.23–0.79).7
The evidence that circumcision prevents most sexually transmitted diseases is not very strong, with the exception of HIV and genital ulcer disease. Most of these studies are from sub-Saharan Africa, where rates of HIV infection are extremely high. A meta-analysis of 15 observational studies in Africa, with adjustment for potential confounding factors, found that circumcision decreased the risk of acquiring HIV by more than half (relative risk [RR]=0.42; 95% CI, 0.34–0.54).8 A more recent prospective study from India showed a strong protective effect of circumcision against HIV infection (RR=0.15; 95% CI, 0.04–0.62).9 This study found no protective effect of circumcision against herpes, syphilis, or gonorrhea, suggesting a biological rather than a behavioral explanation for the protective effect of circumcision against HIV.
A conservative estimate of the post-neonatal childhood circumcision rate for purely medical reasons is 2% to 5%; estimates go as high as 7% to 10%.10 The most common medical indication for circumcision is phimosis, followed by recurrent balanitis and paraphimosis. Circumcision may also be protective against genital dermatoses; a case-control study found an age-adjusted odds ratio of 3.2 (95% CI, 2.3–4.6) for penile skin diseases in uncircumcised men compared with circumcised men.11
Recommendations from others
Circumcision rates vary widely worldwide, with strong cultural and religious preferences. Most major organizations have cautiously neutral opinions on circumcision, stating that medical benefits are not large enough to justify routine neonatal circumcision. The American Academy of Pediatrics Task Force on Circumcision recommends parents “should be given accurate and unbiased information” and that “parents should determine what is in the best interest of the child.”12 The American Medical Association, American College of Obstetrics and Gynecology, and the American Academy of Family Physicians all use similar statements.13-15
Explain risks and benefits of circumcision to parents so they make informed decisions
A dilemma exists in the practice of recommending circumcision to parents of newborn males. Although the evidence shows that morbidity is decreased in circumcised males, the occurrence of complications (such as UTI or balanitis) is believed to be preventable through good hygiene, and the incidence of the preventable disease (such as penile cancer) is so low in the general population as to not justify the procedure. The challenge is there because the procedure is not without pain or risk of complications.
This is the basis for the American Academy of Pediatrics not recommending routine neonatal circumcision. The consensus was that the evidence was not sufficient to support it. Since then, many studies have been published on HPV and HIV transmission, the incidence of phimosis and paraphimosis, UTI, and balanitis, and how circumcision reduces the incidence of these diseases. Again, these are believed to be preventable through hygiene and condom use. In practice, it is difficult to persuade parents because these complications usually occur much later in life. Most patients made their decisions on circumcision based on religious or cultural experiences.
Evidence suggests that neonatal circumcision decreases the incidence of childhood urinary tract infections, phimosis, paraphimosis, balanitis and other genital dermatoses, invasive penile cancer, and the sexually transmitted diseases human papilloma virus (HPV) and HIV (strength of recommendation [SOR]: B, based on case control and cohort studies). The benefits of decreased incidence of HPV and HIV infections go beyond the index patient and have public health implications on the transmission of these diseases (SOR: B). Further, a decrease in HPV incidence and transmission may lead to a lower incidence of cervical cancer (SOR: B).
While there appears to be some evidence for reduced morbidity with routine circumcision, decisions regarding routine neonatal circumcision requires balancing risks and benefits of the procedure with the alternatives in the context of social, familial, and religious beliefs.
Evidence summary
Observational studies have shown at least a 10- to 12-fold increase in urinary tract infections (UTIs) in uncircumcised male infants compared with their circumcised counterparts.1 The number of male infants that need to be circumcised to prevent 1 UTI is estimated to be between 44 and 100.2,3 The only randomized controlled trial of circumcision for UTI prevention was not during the neonatal period (average age was 30 months) and focused on secondary prevention.4 It demonstrated a statistically significant decrease in the rate of bacteriuria. The long-term effect on UTI incidence, renal scarring, and subsequent complications such as hypertension and end-stage renal disease is unknown.
Evidence from case series supports the protective effect of circumcision on the rates of penile cancer. A review of 592 cases of penile cancer revealed that none of those affected had been circumcised in infancy.5 In another series of 89 men with penile cancer, only 2 had been circumcised in infancy, while 87 were uncircumcised.6 Since HPV is thought to be a major etiologic agent in both penile cancer and cervical cancer, investigators studied the link between circumcision status and cervical cancer. In a meta-analysis of 7 case-control studies, penile HPV was detected 2.7 times more often in uncircumcised men after controlling for confounders.7 In this same meta-analysis, monogamous female partners of high-risk circumcised men (men with more than 6 lifetime partners) had a lower risk of cervical cancer than women whose high-risk partner was uncircumcised (adjusted odds ratio=0.42; 95% confidence interval [CI], 0.23–0.79).7
The evidence that circumcision prevents most sexually transmitted diseases is not very strong, with the exception of HIV and genital ulcer disease. Most of these studies are from sub-Saharan Africa, where rates of HIV infection are extremely high. A meta-analysis of 15 observational studies in Africa, with adjustment for potential confounding factors, found that circumcision decreased the risk of acquiring HIV by more than half (relative risk [RR]=0.42; 95% CI, 0.34–0.54).8 A more recent prospective study from India showed a strong protective effect of circumcision against HIV infection (RR=0.15; 95% CI, 0.04–0.62).9 This study found no protective effect of circumcision against herpes, syphilis, or gonorrhea, suggesting a biological rather than a behavioral explanation for the protective effect of circumcision against HIV.
A conservative estimate of the post-neonatal childhood circumcision rate for purely medical reasons is 2% to 5%; estimates go as high as 7% to 10%.10 The most common medical indication for circumcision is phimosis, followed by recurrent balanitis and paraphimosis. Circumcision may also be protective against genital dermatoses; a case-control study found an age-adjusted odds ratio of 3.2 (95% CI, 2.3–4.6) for penile skin diseases in uncircumcised men compared with circumcised men.11
Recommendations from others
Circumcision rates vary widely worldwide, with strong cultural and religious preferences. Most major organizations have cautiously neutral opinions on circumcision, stating that medical benefits are not large enough to justify routine neonatal circumcision. The American Academy of Pediatrics Task Force on Circumcision recommends parents “should be given accurate and unbiased information” and that “parents should determine what is in the best interest of the child.”12 The American Medical Association, American College of Obstetrics and Gynecology, and the American Academy of Family Physicians all use similar statements.13-15
Explain risks and benefits of circumcision to parents so they make informed decisions
A dilemma exists in the practice of recommending circumcision to parents of newborn males. Although the evidence shows that morbidity is decreased in circumcised males, the occurrence of complications (such as UTI or balanitis) is believed to be preventable through good hygiene, and the incidence of the preventable disease (such as penile cancer) is so low in the general population as to not justify the procedure. The challenge is there because the procedure is not without pain or risk of complications.
This is the basis for the American Academy of Pediatrics not recommending routine neonatal circumcision. The consensus was that the evidence was not sufficient to support it. Since then, many studies have been published on HPV and HIV transmission, the incidence of phimosis and paraphimosis, UTI, and balanitis, and how circumcision reduces the incidence of these diseases. Again, these are believed to be preventable through hygiene and condom use. In practice, it is difficult to persuade parents because these complications usually occur much later in life. Most patients made their decisions on circumcision based on religious or cultural experiences.
1. Wiswell TE. The prepuce, urinary tract infections, and the consequences. Pediatrics 2000;105:860-862.
2. Sethi N, Schwierling K, Kim J, et al. Newborn circumcision and urinary tract infections. Pediatrics 2001;107:212.-
3. Christakis DA, Harvey E, Zerr DM, Feudtner C, Wright JA, Connell FA. A trade off analysis of routine newborn circumcision. Pediatrics 2000;105:246-249.
4. Nayir A. Circumcision for the prevention of significant bacteriuria in boys. Pediatr Nephrol 2001;16:1129-1134.Erratum in: Pediatr Nephrol. 2002; 17: 307.
5. Lerman SE, Liao JC. Neonatal circumcision. Pediatr Clin North Am 2001;48:1539-557.
6. Mallon E, Hawkins D, Dinneen M, et al. Circumcision and genital dermatoses. Arch Dermatol 2000;136:350-354.
7. Schoen EJ. The relationship between circumcision and cancer of the penis. CA Cancer J Clin 1991;41:306-309.
8. Schoen EJ, Oehrli M, Colby C, Machin G. The highly protective effect of newborn circumcision against invasive penile cancer. Pediatrics 2000;105:E36.-
9. Castellsague X, Bosch FX, Munoz N, et al. Male circumcision, penile human papillomavirus infection, and cervical cancer in female partners. N Engl J Med 2002;346:1105-1112.
10. Weiss HA, Quigley MA, Hayes RJ. Male circumcision and risk of HIV infection in sub-Saharan Africa: a systematic review and meta-analysis. AIDS 2000;14:2361-2370.
11. Reynolds SJ, Shepherd ME, Risbud AR, et al. Male circumcision and risk of HIV-1 and other sexually transmitted infections in India. Lancet 2004;363:1039-1040.
12. American Academy of Pediatrics. Task Force on Circumcision. Circumcision policy statement. Pediatrics 1999;103:686-693.
13. American Medical Association. Report 10 of the Council on Scientific Affairs (I-99) Neonatal Circumcision. Available at: www.ama-assn.org/ama/pub/category/ 13585.html. Accessed on December 8, 2004.
14. American College of Obstetricians and Gynecologists. ACOG Committee Opinion Number 260: Circumcision. Obstet Gynecol 2001;98:707-708.
15. American Academy of Family Physicians. Position Paper on Neonatal Circumcision. Available at: www.aafp.org/ x1462.xml. Accessed on December 8, 2004.
1. Wiswell TE. The prepuce, urinary tract infections, and the consequences. Pediatrics 2000;105:860-862.
2. Sethi N, Schwierling K, Kim J, et al. Newborn circumcision and urinary tract infections. Pediatrics 2001;107:212.-
3. Christakis DA, Harvey E, Zerr DM, Feudtner C, Wright JA, Connell FA. A trade off analysis of routine newborn circumcision. Pediatrics 2000;105:246-249.
4. Nayir A. Circumcision for the prevention of significant bacteriuria in boys. Pediatr Nephrol 2001;16:1129-1134.Erratum in: Pediatr Nephrol. 2002; 17: 307.
5. Lerman SE, Liao JC. Neonatal circumcision. Pediatr Clin North Am 2001;48:1539-557.
6. Mallon E, Hawkins D, Dinneen M, et al. Circumcision and genital dermatoses. Arch Dermatol 2000;136:350-354.
7. Schoen EJ. The relationship between circumcision and cancer of the penis. CA Cancer J Clin 1991;41:306-309.
8. Schoen EJ, Oehrli M, Colby C, Machin G. The highly protective effect of newborn circumcision against invasive penile cancer. Pediatrics 2000;105:E36.-
9. Castellsague X, Bosch FX, Munoz N, et al. Male circumcision, penile human papillomavirus infection, and cervical cancer in female partners. N Engl J Med 2002;346:1105-1112.
10. Weiss HA, Quigley MA, Hayes RJ. Male circumcision and risk of HIV infection in sub-Saharan Africa: a systematic review and meta-analysis. AIDS 2000;14:2361-2370.
11. Reynolds SJ, Shepherd ME, Risbud AR, et al. Male circumcision and risk of HIV-1 and other sexually transmitted infections in India. Lancet 2004;363:1039-1040.
12. American Academy of Pediatrics. Task Force on Circumcision. Circumcision policy statement. Pediatrics 1999;103:686-693.
13. American Medical Association. Report 10 of the Council on Scientific Affairs (I-99) Neonatal Circumcision. Available at: www.ama-assn.org/ama/pub/category/ 13585.html. Accessed on December 8, 2004.
14. American College of Obstetricians and Gynecologists. ACOG Committee Opinion Number 260: Circumcision. Obstet Gynecol 2001;98:707-708.
15. American Academy of Family Physicians. Position Paper on Neonatal Circumcision. Available at: www.aafp.org/ x1462.xml. Accessed on December 8, 2004.
Evidence-based answers from the Family Physicians Inquiries Network
Does acyclovir help herpes simplex virus cold sores if treatment is delayed?
When herpes simplex virus (HSV) type 1 lesions are in the papule or vesicle stage, there is no benefit to starting oral acyclovir (strength of recommendation [SOR]: C, based on expert opinion). However, topical acyclovir 5% cream applied 5 times a day decreases pain and the duration of hard crust (SOR: B, extrapolated from randomized controlled trials [RCTs]).
If started at the onset of symptoms (during the prodrome stage), acyclovir (400 mg 5 times daily for 5 days) decreases pain and healing time to loss of crust and valacyclovir (2 g twice daily for 1 day) reduces the lesion duration and time to healing and may prevent lesion development (SOR: A, based on RCTs).
Evidence summary
Cold sores, or herpes labialis, are caused by HSV. Recurrent lesions progress quickly through several stages (prodrome, erythema, papule, vesicle, ulcer, crust, residual swelling, healed).1 Because of the rapid development of the vesicle stage (<12 hours) and the rapid decrease in detectable virus after 48 hours, studies of antiviral therapy empirically require early treatment within the first several hours of signs or symptoms of a recurrence. For this reason, there are no controlled trials of oral medications given later than 12 hours after the onset of recurrent symptoms.
Although limited, the clearest indication of appropriate timing for HSV 1 treatment with acyclovir comes from a well-designed, double-blinded RCT of 174 adults with a history of culture confirmed HSV labialis who initiated self-treatment with acyclovir 400 mg or placebo 5 times a day for 5 days. Patients were asked to defer treatment until the next episode if they awoke with the lesion or first noticed them in the vesicle or ulcer stage. Ninety-seven percent of the patients started treatment within 1 hour of signs/symptoms of a recurrence. Of the 174 patients, 90 had lesions in the prodrome or erythema stage at the start of treatment and 84 had lesions in the papule or vesicle stage.
Overall, acyclovir did not effect lesion progression, size, or healing time to loss of hard crust or normal skin. However, the mean duration of pain for all patients significantly decreased (2.5 days vs 3.8 days for placebo, P=.01). For the subgroup of patients who started acyclovir treatment in the prodrome or erythema stage, the mean duration of pain significantly decreased (2.5 days vs 3.9 days for placebo, P=.02), as did healing time to loss of crust (5.8 days vs 7.9 days for placebo, P=.03). Among those who started acyclovir in the papular stage, the trend was toward drug benefit, but this was not statistically significant (mean pain duration: 2.5 vs. 3.6, P=.36; mean healing time to loss of crust: 8.0 vs. 7.2, P=.52).2 This evidence supports early (prodrome or erythema stage) but not late (macule, papule, vesicle, or crusted stage) treatment of HSV 1 with oral acyclovir.
Topical application of 5% acyclovir cream significantly decreases clinician-assessed duration of the episode and duration of patient-reported pain, based on 2 double-blind, multicenter RCTs that used a vehicle control. In these trials, 686 and 699 patients self-initiated treatment 5 times a day for 4 days beginning within 1 hour of the onset of a recurrent lesion. In the first study, the mean clinician-assessed duration of the episode with topical acyclovir was 4.3 vs 4.8 days for placebo (hazard ratio [HR]=1.23; 95% confidence interval [CI], 1.06–1.44), and the mean duration of patient-assessed pain was 2.9 vs 3.2 days (HR=1.20; 95% CI, 1.03–1.40). The second study showed a mean clinician-assessed duration with topical acyclovir of 4.6 vs 5.2 days for control (HR=1.24; 95% CI, 1.06–1.44), and the mean duration of patient-assessed pain was 3.1 vs 3.5 days (HR=1.21; 95% CI, 1.04–1.40). Benefits were seen regardless of whether treatment was initiated early (prodrome or erythema stage) or late (macule, papule, vesicle or crusted stage).3
Recent studies of valacyclovir (the L-valine ester of acyclovir, which has 3 to 5 times greater bioavailability) offer the most promise for effective self-initiated treatment of recurrent herpes labialis. In a report of 2 well-designed, multicenter RCTs, valacyclovir at the FDA-approved dosage of 2 g twice daily for 1 day at the onset of symptoms (before visible signs of a cold sore) significantly decreased the mean duration of the lesion and time to lesion healing. In the first study (n=603), episode duration was decreased by 1.1 days (5.0 days vs 6.1 days for placebo; 95% CI, –1.6 to –0.6) and in the second study (n=605) by 1.0 day (5.3 vs 6.3 days for placebo; 95% CI, –1.0 to –0.5). In the first study, the time to lesion healing was decreased by 1.3 days (4.8 vs 6.1 days for placebo; 95% CI, –1.9 to –0.7) and in the second study by 1.2 days (5.1 vs. 6.4 days; 95% CI, –1.8 to –0.7). There also was a trend towards preventing the development of lesions, but this was not statistically significant.4
Recommendations from others
The BMJ Clinical Evidence Guideline reiterates that no trials compare early vs late treatment, so no firm conclusions about the efficacy of delayed treatment can be drawn.5 UpToDate reports that HSV 1 studies take into account that acyclovir acts only during active viral replication, which largely precedes symptoms, and thus suggest that it has little effect if begun after the appearance of lesions.6
For late presenters, review local care and hygiene; for all patients, review management of recurrences
Owen McCormack, DO
Baylor College of Medicine, Houston, TX
Patients seek treatment for herpes labialis due to bothersome physical symptoms and psychosocial implications. Many patients can identify prodromal symptoms such as localized itching, burning, irritation, or pain. Diagnosis of the initial episode is frequently delayed as patients are evaluated after the time period when studies have shown the most benefit from antivirals. For the late presenters, I review local care and hygiene, and for all patients I review management of recurrences.
Patient-initiated treatment is effective for those who can recognize the earliest signs and symptoms and start treatment immediately with either a topical or systemic antiviral. Both formulations decrease the lesion time to healing and pain if started at the first onset of symptoms.
Cost is an important consideration when selecting a particular formulation. Approximate price for the regimens presented here are $12 for 5 days of oral acyclovir, $27 for 1 day of oral valacyclovir, and $37 for a 2-g tube of acyclovir cream, which can be used for more than 1 episode.7 Other factors to consider are pill burden, duration of treatment, patient preference, and lifestyle. Patients can keep a refill or medicine on-hand to manage recurrences with the advice to begin immediately with onset of signs or symptoms.
1. Spruance S, Overall J, Kern E, Krueger G, Pliam V, Miller W. The natural history of recurrent herpes simplex labialis. JAMA 1977;297:69-75.
2. Spruance S, Stewart J, Rowe N, McKoeugh M, Wenerstrom G, Freeman D. Treatment of recurrent herpes simplex labialis with oral acyclovir. J Infect Dis 1990;161:181-190.
3. Spruance S, Nett R, Marbury T, Wolff R, Johnson J, Spaulding T. Acyclovir cream for treatment of herpes simplex labialis: results of two randomized, double-blind, vehicle-controlled multicenter clinical trials. Antimicrobial Agents Chemother 2002;46:2238-2243.
4. Spruance S, Jones T, Blatter M, et al. High-dose, short-duration, early valacyclovir therapy for episodic treatment of cold sores: results of two randomized, placebo-controlled, multicenter studies. Antimicrobial Agents Chemother 2003;47:1072-1080.
5. Clin Evid [online] Issue 10 2003. London: BMJ Publishing Group, last updated December 2002. Available at: http://clinicalevidence.com. Accessed on May 19, 2004.
6. Klein R. Treatment and prevention of herpes simplex virus type 1 infection. UpToDate version 12.2, last updated February 25, 2004. Available at: UpToDate.com. Accessed on July 14, 2004.
7. Availableat: www. drugstore.com. Accessed on August 18, 2004.
When herpes simplex virus (HSV) type 1 lesions are in the papule or vesicle stage, there is no benefit to starting oral acyclovir (strength of recommendation [SOR]: C, based on expert opinion). However, topical acyclovir 5% cream applied 5 times a day decreases pain and the duration of hard crust (SOR: B, extrapolated from randomized controlled trials [RCTs]).
If started at the onset of symptoms (during the prodrome stage), acyclovir (400 mg 5 times daily for 5 days) decreases pain and healing time to loss of crust and valacyclovir (2 g twice daily for 1 day) reduces the lesion duration and time to healing and may prevent lesion development (SOR: A, based on RCTs).
Evidence summary
Cold sores, or herpes labialis, are caused by HSV. Recurrent lesions progress quickly through several stages (prodrome, erythema, papule, vesicle, ulcer, crust, residual swelling, healed).1 Because of the rapid development of the vesicle stage (<12 hours) and the rapid decrease in detectable virus after 48 hours, studies of antiviral therapy empirically require early treatment within the first several hours of signs or symptoms of a recurrence. For this reason, there are no controlled trials of oral medications given later than 12 hours after the onset of recurrent symptoms.
Although limited, the clearest indication of appropriate timing for HSV 1 treatment with acyclovir comes from a well-designed, double-blinded RCT of 174 adults with a history of culture confirmed HSV labialis who initiated self-treatment with acyclovir 400 mg or placebo 5 times a day for 5 days. Patients were asked to defer treatment until the next episode if they awoke with the lesion or first noticed them in the vesicle or ulcer stage. Ninety-seven percent of the patients started treatment within 1 hour of signs/symptoms of a recurrence. Of the 174 patients, 90 had lesions in the prodrome or erythema stage at the start of treatment and 84 had lesions in the papule or vesicle stage.
Overall, acyclovir did not effect lesion progression, size, or healing time to loss of hard crust or normal skin. However, the mean duration of pain for all patients significantly decreased (2.5 days vs 3.8 days for placebo, P=.01). For the subgroup of patients who started acyclovir treatment in the prodrome or erythema stage, the mean duration of pain significantly decreased (2.5 days vs 3.9 days for placebo, P=.02), as did healing time to loss of crust (5.8 days vs 7.9 days for placebo, P=.03). Among those who started acyclovir in the papular stage, the trend was toward drug benefit, but this was not statistically significant (mean pain duration: 2.5 vs. 3.6, P=.36; mean healing time to loss of crust: 8.0 vs. 7.2, P=.52).2 This evidence supports early (prodrome or erythema stage) but not late (macule, papule, vesicle, or crusted stage) treatment of HSV 1 with oral acyclovir.
Topical application of 5% acyclovir cream significantly decreases clinician-assessed duration of the episode and duration of patient-reported pain, based on 2 double-blind, multicenter RCTs that used a vehicle control. In these trials, 686 and 699 patients self-initiated treatment 5 times a day for 4 days beginning within 1 hour of the onset of a recurrent lesion. In the first study, the mean clinician-assessed duration of the episode with topical acyclovir was 4.3 vs 4.8 days for placebo (hazard ratio [HR]=1.23; 95% confidence interval [CI], 1.06–1.44), and the mean duration of patient-assessed pain was 2.9 vs 3.2 days (HR=1.20; 95% CI, 1.03–1.40). The second study showed a mean clinician-assessed duration with topical acyclovir of 4.6 vs 5.2 days for control (HR=1.24; 95% CI, 1.06–1.44), and the mean duration of patient-assessed pain was 3.1 vs 3.5 days (HR=1.21; 95% CI, 1.04–1.40). Benefits were seen regardless of whether treatment was initiated early (prodrome or erythema stage) or late (macule, papule, vesicle or crusted stage).3
Recent studies of valacyclovir (the L-valine ester of acyclovir, which has 3 to 5 times greater bioavailability) offer the most promise for effective self-initiated treatment of recurrent herpes labialis. In a report of 2 well-designed, multicenter RCTs, valacyclovir at the FDA-approved dosage of 2 g twice daily for 1 day at the onset of symptoms (before visible signs of a cold sore) significantly decreased the mean duration of the lesion and time to lesion healing. In the first study (n=603), episode duration was decreased by 1.1 days (5.0 days vs 6.1 days for placebo; 95% CI, –1.6 to –0.6) and in the second study (n=605) by 1.0 day (5.3 vs 6.3 days for placebo; 95% CI, –1.0 to –0.5). In the first study, the time to lesion healing was decreased by 1.3 days (4.8 vs 6.1 days for placebo; 95% CI, –1.9 to –0.7) and in the second study by 1.2 days (5.1 vs. 6.4 days; 95% CI, –1.8 to –0.7). There also was a trend towards preventing the development of lesions, but this was not statistically significant.4
Recommendations from others
The BMJ Clinical Evidence Guideline reiterates that no trials compare early vs late treatment, so no firm conclusions about the efficacy of delayed treatment can be drawn.5 UpToDate reports that HSV 1 studies take into account that acyclovir acts only during active viral replication, which largely precedes symptoms, and thus suggest that it has little effect if begun after the appearance of lesions.6
For late presenters, review local care and hygiene; for all patients, review management of recurrences
Owen McCormack, DO
Baylor College of Medicine, Houston, TX
Patients seek treatment for herpes labialis due to bothersome physical symptoms and psychosocial implications. Many patients can identify prodromal symptoms such as localized itching, burning, irritation, or pain. Diagnosis of the initial episode is frequently delayed as patients are evaluated after the time period when studies have shown the most benefit from antivirals. For the late presenters, I review local care and hygiene, and for all patients I review management of recurrences.
Patient-initiated treatment is effective for those who can recognize the earliest signs and symptoms and start treatment immediately with either a topical or systemic antiviral. Both formulations decrease the lesion time to healing and pain if started at the first onset of symptoms.
Cost is an important consideration when selecting a particular formulation. Approximate price for the regimens presented here are $12 for 5 days of oral acyclovir, $27 for 1 day of oral valacyclovir, and $37 for a 2-g tube of acyclovir cream, which can be used for more than 1 episode.7 Other factors to consider are pill burden, duration of treatment, patient preference, and lifestyle. Patients can keep a refill or medicine on-hand to manage recurrences with the advice to begin immediately with onset of signs or symptoms.
When herpes simplex virus (HSV) type 1 lesions are in the papule or vesicle stage, there is no benefit to starting oral acyclovir (strength of recommendation [SOR]: C, based on expert opinion). However, topical acyclovir 5% cream applied 5 times a day decreases pain and the duration of hard crust (SOR: B, extrapolated from randomized controlled trials [RCTs]).
If started at the onset of symptoms (during the prodrome stage), acyclovir (400 mg 5 times daily for 5 days) decreases pain and healing time to loss of crust and valacyclovir (2 g twice daily for 1 day) reduces the lesion duration and time to healing and may prevent lesion development (SOR: A, based on RCTs).
Evidence summary
Cold sores, or herpes labialis, are caused by HSV. Recurrent lesions progress quickly through several stages (prodrome, erythema, papule, vesicle, ulcer, crust, residual swelling, healed).1 Because of the rapid development of the vesicle stage (<12 hours) and the rapid decrease in detectable virus after 48 hours, studies of antiviral therapy empirically require early treatment within the first several hours of signs or symptoms of a recurrence. For this reason, there are no controlled trials of oral medications given later than 12 hours after the onset of recurrent symptoms.
Although limited, the clearest indication of appropriate timing for HSV 1 treatment with acyclovir comes from a well-designed, double-blinded RCT of 174 adults with a history of culture confirmed HSV labialis who initiated self-treatment with acyclovir 400 mg or placebo 5 times a day for 5 days. Patients were asked to defer treatment until the next episode if they awoke with the lesion or first noticed them in the vesicle or ulcer stage. Ninety-seven percent of the patients started treatment within 1 hour of signs/symptoms of a recurrence. Of the 174 patients, 90 had lesions in the prodrome or erythema stage at the start of treatment and 84 had lesions in the papule or vesicle stage.
Overall, acyclovir did not effect lesion progression, size, or healing time to loss of hard crust or normal skin. However, the mean duration of pain for all patients significantly decreased (2.5 days vs 3.8 days for placebo, P=.01). For the subgroup of patients who started acyclovir treatment in the prodrome or erythema stage, the mean duration of pain significantly decreased (2.5 days vs 3.9 days for placebo, P=.02), as did healing time to loss of crust (5.8 days vs 7.9 days for placebo, P=.03). Among those who started acyclovir in the papular stage, the trend was toward drug benefit, but this was not statistically significant (mean pain duration: 2.5 vs. 3.6, P=.36; mean healing time to loss of crust: 8.0 vs. 7.2, P=.52).2 This evidence supports early (prodrome or erythema stage) but not late (macule, papule, vesicle, or crusted stage) treatment of HSV 1 with oral acyclovir.
Topical application of 5% acyclovir cream significantly decreases clinician-assessed duration of the episode and duration of patient-reported pain, based on 2 double-blind, multicenter RCTs that used a vehicle control. In these trials, 686 and 699 patients self-initiated treatment 5 times a day for 4 days beginning within 1 hour of the onset of a recurrent lesion. In the first study, the mean clinician-assessed duration of the episode with topical acyclovir was 4.3 vs 4.8 days for placebo (hazard ratio [HR]=1.23; 95% confidence interval [CI], 1.06–1.44), and the mean duration of patient-assessed pain was 2.9 vs 3.2 days (HR=1.20; 95% CI, 1.03–1.40). The second study showed a mean clinician-assessed duration with topical acyclovir of 4.6 vs 5.2 days for control (HR=1.24; 95% CI, 1.06–1.44), and the mean duration of patient-assessed pain was 3.1 vs 3.5 days (HR=1.21; 95% CI, 1.04–1.40). Benefits were seen regardless of whether treatment was initiated early (prodrome or erythema stage) or late (macule, papule, vesicle or crusted stage).3
Recent studies of valacyclovir (the L-valine ester of acyclovir, which has 3 to 5 times greater bioavailability) offer the most promise for effective self-initiated treatment of recurrent herpes labialis. In a report of 2 well-designed, multicenter RCTs, valacyclovir at the FDA-approved dosage of 2 g twice daily for 1 day at the onset of symptoms (before visible signs of a cold sore) significantly decreased the mean duration of the lesion and time to lesion healing. In the first study (n=603), episode duration was decreased by 1.1 days (5.0 days vs 6.1 days for placebo; 95% CI, –1.6 to –0.6) and in the second study (n=605) by 1.0 day (5.3 vs 6.3 days for placebo; 95% CI, –1.0 to –0.5). In the first study, the time to lesion healing was decreased by 1.3 days (4.8 vs 6.1 days for placebo; 95% CI, –1.9 to –0.7) and in the second study by 1.2 days (5.1 vs. 6.4 days; 95% CI, –1.8 to –0.7). There also was a trend towards preventing the development of lesions, but this was not statistically significant.4
Recommendations from others
The BMJ Clinical Evidence Guideline reiterates that no trials compare early vs late treatment, so no firm conclusions about the efficacy of delayed treatment can be drawn.5 UpToDate reports that HSV 1 studies take into account that acyclovir acts only during active viral replication, which largely precedes symptoms, and thus suggest that it has little effect if begun after the appearance of lesions.6
For late presenters, review local care and hygiene; for all patients, review management of recurrences
Owen McCormack, DO
Baylor College of Medicine, Houston, TX
Patients seek treatment for herpes labialis due to bothersome physical symptoms and psychosocial implications. Many patients can identify prodromal symptoms such as localized itching, burning, irritation, or pain. Diagnosis of the initial episode is frequently delayed as patients are evaluated after the time period when studies have shown the most benefit from antivirals. For the late presenters, I review local care and hygiene, and for all patients I review management of recurrences.
Patient-initiated treatment is effective for those who can recognize the earliest signs and symptoms and start treatment immediately with either a topical or systemic antiviral. Both formulations decrease the lesion time to healing and pain if started at the first onset of symptoms.
Cost is an important consideration when selecting a particular formulation. Approximate price for the regimens presented here are $12 for 5 days of oral acyclovir, $27 for 1 day of oral valacyclovir, and $37 for a 2-g tube of acyclovir cream, which can be used for more than 1 episode.7 Other factors to consider are pill burden, duration of treatment, patient preference, and lifestyle. Patients can keep a refill or medicine on-hand to manage recurrences with the advice to begin immediately with onset of signs or symptoms.
1. Spruance S, Overall J, Kern E, Krueger G, Pliam V, Miller W. The natural history of recurrent herpes simplex labialis. JAMA 1977;297:69-75.
2. Spruance S, Stewart J, Rowe N, McKoeugh M, Wenerstrom G, Freeman D. Treatment of recurrent herpes simplex labialis with oral acyclovir. J Infect Dis 1990;161:181-190.
3. Spruance S, Nett R, Marbury T, Wolff R, Johnson J, Spaulding T. Acyclovir cream for treatment of herpes simplex labialis: results of two randomized, double-blind, vehicle-controlled multicenter clinical trials. Antimicrobial Agents Chemother 2002;46:2238-2243.
4. Spruance S, Jones T, Blatter M, et al. High-dose, short-duration, early valacyclovir therapy for episodic treatment of cold sores: results of two randomized, placebo-controlled, multicenter studies. Antimicrobial Agents Chemother 2003;47:1072-1080.
5. Clin Evid [online] Issue 10 2003. London: BMJ Publishing Group, last updated December 2002. Available at: http://clinicalevidence.com. Accessed on May 19, 2004.
6. Klein R. Treatment and prevention of herpes simplex virus type 1 infection. UpToDate version 12.2, last updated February 25, 2004. Available at: UpToDate.com. Accessed on July 14, 2004.
7. Availableat: www. drugstore.com. Accessed on August 18, 2004.
1. Spruance S, Overall J, Kern E, Krueger G, Pliam V, Miller W. The natural history of recurrent herpes simplex labialis. JAMA 1977;297:69-75.
2. Spruance S, Stewart J, Rowe N, McKoeugh M, Wenerstrom G, Freeman D. Treatment of recurrent herpes simplex labialis with oral acyclovir. J Infect Dis 1990;161:181-190.
3. Spruance S, Nett R, Marbury T, Wolff R, Johnson J, Spaulding T. Acyclovir cream for treatment of herpes simplex labialis: results of two randomized, double-blind, vehicle-controlled multicenter clinical trials. Antimicrobial Agents Chemother 2002;46:2238-2243.
4. Spruance S, Jones T, Blatter M, et al. High-dose, short-duration, early valacyclovir therapy for episodic treatment of cold sores: results of two randomized, placebo-controlled, multicenter studies. Antimicrobial Agents Chemother 2003;47:1072-1080.
5. Clin Evid [online] Issue 10 2003. London: BMJ Publishing Group, last updated December 2002. Available at: http://clinicalevidence.com. Accessed on May 19, 2004.
6. Klein R. Treatment and prevention of herpes simplex virus type 1 infection. UpToDate version 12.2, last updated February 25, 2004. Available at: UpToDate.com. Accessed on July 14, 2004.
7. Availableat: www. drugstore.com. Accessed on August 18, 2004.
Evidence-based answers from the Family Physicians Inquiries Network
For knee pain, how predictive is physical examination for meniscal injury?
No single clinical examination element, or combination of such elements, reliably detects meniscal injury. The McMurray test is best for ruling in meniscal pathology. Assuming a 9% prevalence of meniscal tears among all knee injuries (a rate reflecting national primary care data), the posttest probability that a patient with McMurray’s sign has a meniscal injury ranges from <30% to 63% (strength of recommendation [SOR]: B). In contrast, the absence of any positive physical examination findings effectively rules out meniscal pathology, yielding a posttest probability of 0.8% for lateral meniscus injury, 1.0% for medial meniscus injury, and 3.8% for any meniscal injury among primary care populations (SOR: B).
Evidence summary
The accuracy of physical examination findings for meniscal injury varies widely among meta-analyses. In a meta-analysis of 13 studies, no physical examination test—including assessment for joint effusion, McMurray test, joint line tenderness, or the Apley compression test—yielded clinically significant positive or negative likelihood ratios for a meniscal tear ( Table ). The McMurray test performed best, but at 9% to 11% pretest probability of JFP_1104_CI.final 10/18/04 11:06 AM Page 918 meniscal lesions, based on prevalence estimates among primary care/specialist populations,2 the posttest probability of a positive exam is still <30%.
A meta-analysis of 4 studies by Jackson compared the utility of the McMurray test and joint line tenderness.3 For detecting meniscal tears, the McMurray test had a clinically and statistically significant positive likelihood ratio of 17.33, corresponding to a posttest probability of nearly 61%. Negative likelihood ratios for the McMurray test and joint line tenderness (0.5 and 0.8) were not clinically significant, indicating that absence of the McMurray sign or joint line tenderness alone is of little benefit in ruling out meniscal injury.
In another meta-analysis including 9 studies of meniscal injury diagnosis,4 individual tests for joint line tenderness, joint effusion, the medial-lateral grind test, and the McMurray test failed to yield statistically significant likelihood ratios for the presence or absence of meniscal tears ( Table footnotes). Positive and negative likelihood ratios for aggregate physical examination were 2.7 (95% confidence interval [CI], 1.4–5.1) and 0.4 (95% CI, 0.2–0.7), which are statistically, but not clinically, significant values for ruling meniscal lesions in or out.
Jackson’s meta-analysis also calculated the posttest probability of injury for a composite meniscal examination. Based on the positive likelihood ratio of 3.1 (95% CI, 0.54–5.7) and negative likelihood ratio of 0.19 (95% CI, 0.11–0.77), the posttest probability of a medial meniscal tear was 17% in the setting of composite physical exam findings and 1% in the absence of physical exam findings. For a lateral meniscal tear, based on the positive likelihood ratio of 11 (95% CI, 1.8–20.2), and negative likelihood ratio of 0.13 (95% CI, 0.0–0.25), the posttest probability of injury with a positive exam was 41% and with a negative exam 0.8%.
Authors of all meta-analyses noted the lack of standardization in physical examination maneuvers (especially the McMurray test)5 and, in some cases, no specification of how physical examination tests were performed. Authors analyzed the utility of the aggregate and composite knee examinations without specifying what constituted such an exam. No study included in the meta-analyses used control subjects without meniscal pathology, and few studies were blinded. Lack of blinding may have introduced verification bias; use of specialty patients in all studies made referral bias likely. Studies were heterogeneous and results were associated with wide confidence intervals, introducing an element of random error into the processes of combining and interpreting data.
TABLE
Physical exams for meniscal tear
| Summary characteristics | Solomon et al 4 | Scholten et al 1 | Jackson et al 3 |
| 9 studies 1018 patients Specialist population Specialist examiners | 13 studies 2231 patients Specialist population Specialist examiners | 4 studies 424 patients Specialist population Specialist examiners | |
| McMurray | Positive likelihood ratio (95% CI) | ||
| 1.3 (0.9–1.7) | 1.5–9.5 | 17.3 (2.7–68) | |
| Joint line tenderness | 0.9 (0.8–1.0) | 0.8–14.9 | 1.1 (0.7–1.6) |
| Aggregate exam | 2.7 (1.4–5.1) | — | — |
| Aggregate exam, medial meniscus tears | — | — | 3.1 (0.54–5.7) |
| Aggregate exam, lateral meniscus tears | — | — | 11 (1.8–20.2) |
| McMurray | Negative likelihood ratio (95% CI) | ||
| 0.8 (0.6–1.1) | 0.4–0.9 | 0.5 (0.3–0.8) | |
| Joint line tenderness | 1.1 (1.0–1.3) | 0.2–2.1 | 0.8 (0.3–3.5) |
| Aggregate exam | 0.4 (0.2–0.7) | — | — |
| Aggregate exam, medial meniscus tears | — | — | 0.19 (0.11–0.77) |
| Aggregate exam, lateral meniscus tears | — | — | 0.13 (0–0.25) |
| Note: The results are presented as likelihood ratios, which represent the change in the odds of a diagnosis, based on the outcome of the test. For example, given a positive likelihood ratio of 2, if a test result is positive, the odds of the disease being present is doubled. A positive likelihood ratio >10 provides strong evidence that the disorder is present. A negative likelihood ratio <0.1 provides strong evidence that the disorder is not present. Scores between 0.5 and 2.0 are neutral. In Scholten’s meta-analysis, likelihood ratios are given in ranges (no composite value given). | |||
Recommendations from others
The American Academy of Orthopaedic Surgeons’ clinical guideline on the evaluation and treatment of knee injuries lists the following findings as associated with a meniscal tear: delayed swelling of the knee, twisting injury, painful popping and catching, effusion, joint line tenderness, positive McMurray’s test, and negative radiography.6 The guideline fails to list the strength and type of supporting evidence for these associations.
The American College of Radiology’s Appropriateness Criteria for Acute Trauma to the Knee states that decision rules for meniscal tears and other soft tissue injuries to the knee are being investigated, but it fails to mention specific evaluation strategies for meniscal tears.7
Meniscus injury likely with suggestive history, joint line tenderness, and an inability to squat because of pain
Roy Henderson, MD
Director, Sports Medicine Fellowship, MacNeal Family Practice Residency Program, Chicago, Ill
I often suspect meniscal injuries as a cause of knee pain but am rarely certain based on physical examination alone. I look for a history of joint line pain, locking, or popping with movement. If the patient lacks joint line tenderness, a meniscal injury is unlikely. The McMurray test is usually negative. In the absence of another explanation for the patient’s symptoms, a meniscus injury is high on my list in the presence of a suggestive history, joint line tenderness, and an inability to squat because of pain. When my suspicion is high I usually resort to an MRI.
1. Scholten RJ, Deville WL, Opstelten W, Bijl D, van der Plas CG, Bouter LM. The accuracy of physical diagnostic tests for assessing meniscal lesions of the knee: a meta-analysis. J Fam Pract 2001;50:938-944.
2. National Ambulatory Medical Care Survey 1996. Available at: ftp://ftp.cdc.gov/pub/Health-Statistics/NCHS/Datasets/NAMCS/. Accessed on August 18, 2004.
3. Jackson JL, O’Malley PG, Kroenke K. Evaluation of acute knee pain in primary care. Ann Intern Med 2003;139:575-588.
4. Solomon DH, Simel DL, Bates DW, Katz JN, Schaffer JL. The rational clinical examination. Does this patient have a torn meniscus or ligament of the knee?. JAMA 2001;286:1610-1620.
5. Stratford PW, Binkley J. A review of the McMurray test: definition, interpretation, and clinical usefulness. J Orthop Sports Phys Ther 1995;22:116-120.
6. American Academy of Orthopaedic Surgeons. AAOS Clinical Guideline on Knee Injury: Support Document. Last updated February 26, 2002. Rosemont, Ill: American Academy of Orthopaedic Surgeons; 2001. Available at: http://www.guidelines.gov. Accessed on September 30, 2004.
7. American College of Radiology (ACR) Expert. Panel on Musculoskeletal Imaging ACR Appropriateness Criteria for Acute Trauma to the Knee. Updated October 1, 2002. Reston, Va: American College of Radiology; 2001. Available at: http://www.acr.org/cgi-bin/fr?tmpl:appcrit,pdf:0365374_acute_trauma_to_knee.ac.p df. Accessed on September 30, 2004.
No single clinical examination element, or combination of such elements, reliably detects meniscal injury. The McMurray test is best for ruling in meniscal pathology. Assuming a 9% prevalence of meniscal tears among all knee injuries (a rate reflecting national primary care data), the posttest probability that a patient with McMurray’s sign has a meniscal injury ranges from <30% to 63% (strength of recommendation [SOR]: B). In contrast, the absence of any positive physical examination findings effectively rules out meniscal pathology, yielding a posttest probability of 0.8% for lateral meniscus injury, 1.0% for medial meniscus injury, and 3.8% for any meniscal injury among primary care populations (SOR: B).
Evidence summary
The accuracy of physical examination findings for meniscal injury varies widely among meta-analyses. In a meta-analysis of 13 studies, no physical examination test—including assessment for joint effusion, McMurray test, joint line tenderness, or the Apley compression test—yielded clinically significant positive or negative likelihood ratios for a meniscal tear ( Table ). The McMurray test performed best, but at 9% to 11% pretest probability of JFP_1104_CI.final 10/18/04 11:06 AM Page 918 meniscal lesions, based on prevalence estimates among primary care/specialist populations,2 the posttest probability of a positive exam is still <30%.
A meta-analysis of 4 studies by Jackson compared the utility of the McMurray test and joint line tenderness.3 For detecting meniscal tears, the McMurray test had a clinically and statistically significant positive likelihood ratio of 17.33, corresponding to a posttest probability of nearly 61%. Negative likelihood ratios for the McMurray test and joint line tenderness (0.5 and 0.8) were not clinically significant, indicating that absence of the McMurray sign or joint line tenderness alone is of little benefit in ruling out meniscal injury.
In another meta-analysis including 9 studies of meniscal injury diagnosis,4 individual tests for joint line tenderness, joint effusion, the medial-lateral grind test, and the McMurray test failed to yield statistically significant likelihood ratios for the presence or absence of meniscal tears ( Table footnotes). Positive and negative likelihood ratios for aggregate physical examination were 2.7 (95% confidence interval [CI], 1.4–5.1) and 0.4 (95% CI, 0.2–0.7), which are statistically, but not clinically, significant values for ruling meniscal lesions in or out.
Jackson’s meta-analysis also calculated the posttest probability of injury for a composite meniscal examination. Based on the positive likelihood ratio of 3.1 (95% CI, 0.54–5.7) and negative likelihood ratio of 0.19 (95% CI, 0.11–0.77), the posttest probability of a medial meniscal tear was 17% in the setting of composite physical exam findings and 1% in the absence of physical exam findings. For a lateral meniscal tear, based on the positive likelihood ratio of 11 (95% CI, 1.8–20.2), and negative likelihood ratio of 0.13 (95% CI, 0.0–0.25), the posttest probability of injury with a positive exam was 41% and with a negative exam 0.8%.
Authors of all meta-analyses noted the lack of standardization in physical examination maneuvers (especially the McMurray test)5 and, in some cases, no specification of how physical examination tests were performed. Authors analyzed the utility of the aggregate and composite knee examinations without specifying what constituted such an exam. No study included in the meta-analyses used control subjects without meniscal pathology, and few studies were blinded. Lack of blinding may have introduced verification bias; use of specialty patients in all studies made referral bias likely. Studies were heterogeneous and results were associated with wide confidence intervals, introducing an element of random error into the processes of combining and interpreting data.
TABLE
Physical exams for meniscal tear
| Summary characteristics | Solomon et al 4 | Scholten et al 1 | Jackson et al 3 |
| 9 studies 1018 patients Specialist population Specialist examiners | 13 studies 2231 patients Specialist population Specialist examiners | 4 studies 424 patients Specialist population Specialist examiners | |
| McMurray | Positive likelihood ratio (95% CI) | ||
| 1.3 (0.9–1.7) | 1.5–9.5 | 17.3 (2.7–68) | |
| Joint line tenderness | 0.9 (0.8–1.0) | 0.8–14.9 | 1.1 (0.7–1.6) |
| Aggregate exam | 2.7 (1.4–5.1) | — | — |
| Aggregate exam, medial meniscus tears | — | — | 3.1 (0.54–5.7) |
| Aggregate exam, lateral meniscus tears | — | — | 11 (1.8–20.2) |
| McMurray | Negative likelihood ratio (95% CI) | ||
| 0.8 (0.6–1.1) | 0.4–0.9 | 0.5 (0.3–0.8) | |
| Joint line tenderness | 1.1 (1.0–1.3) | 0.2–2.1 | 0.8 (0.3–3.5) |
| Aggregate exam | 0.4 (0.2–0.7) | — | — |
| Aggregate exam, medial meniscus tears | — | — | 0.19 (0.11–0.77) |
| Aggregate exam, lateral meniscus tears | — | — | 0.13 (0–0.25) |
| Note: The results are presented as likelihood ratios, which represent the change in the odds of a diagnosis, based on the outcome of the test. For example, given a positive likelihood ratio of 2, if a test result is positive, the odds of the disease being present is doubled. A positive likelihood ratio >10 provides strong evidence that the disorder is present. A negative likelihood ratio <0.1 provides strong evidence that the disorder is not present. Scores between 0.5 and 2.0 are neutral. In Scholten’s meta-analysis, likelihood ratios are given in ranges (no composite value given). | |||
Recommendations from others
The American Academy of Orthopaedic Surgeons’ clinical guideline on the evaluation and treatment of knee injuries lists the following findings as associated with a meniscal tear: delayed swelling of the knee, twisting injury, painful popping and catching, effusion, joint line tenderness, positive McMurray’s test, and negative radiography.6 The guideline fails to list the strength and type of supporting evidence for these associations.
The American College of Radiology’s Appropriateness Criteria for Acute Trauma to the Knee states that decision rules for meniscal tears and other soft tissue injuries to the knee are being investigated, but it fails to mention specific evaluation strategies for meniscal tears.7
Meniscus injury likely with suggestive history, joint line tenderness, and an inability to squat because of pain
Roy Henderson, MD
Director, Sports Medicine Fellowship, MacNeal Family Practice Residency Program, Chicago, Ill
I often suspect meniscal injuries as a cause of knee pain but am rarely certain based on physical examination alone. I look for a history of joint line pain, locking, or popping with movement. If the patient lacks joint line tenderness, a meniscal injury is unlikely. The McMurray test is usually negative. In the absence of another explanation for the patient’s symptoms, a meniscus injury is high on my list in the presence of a suggestive history, joint line tenderness, and an inability to squat because of pain. When my suspicion is high I usually resort to an MRI.
No single clinical examination element, or combination of such elements, reliably detects meniscal injury. The McMurray test is best for ruling in meniscal pathology. Assuming a 9% prevalence of meniscal tears among all knee injuries (a rate reflecting national primary care data), the posttest probability that a patient with McMurray’s sign has a meniscal injury ranges from <30% to 63% (strength of recommendation [SOR]: B). In contrast, the absence of any positive physical examination findings effectively rules out meniscal pathology, yielding a posttest probability of 0.8% for lateral meniscus injury, 1.0% for medial meniscus injury, and 3.8% for any meniscal injury among primary care populations (SOR: B).
Evidence summary
The accuracy of physical examination findings for meniscal injury varies widely among meta-analyses. In a meta-analysis of 13 studies, no physical examination test—including assessment for joint effusion, McMurray test, joint line tenderness, or the Apley compression test—yielded clinically significant positive or negative likelihood ratios for a meniscal tear ( Table ). The McMurray test performed best, but at 9% to 11% pretest probability of JFP_1104_CI.final 10/18/04 11:06 AM Page 918 meniscal lesions, based on prevalence estimates among primary care/specialist populations,2 the posttest probability of a positive exam is still <30%.
A meta-analysis of 4 studies by Jackson compared the utility of the McMurray test and joint line tenderness.3 For detecting meniscal tears, the McMurray test had a clinically and statistically significant positive likelihood ratio of 17.33, corresponding to a posttest probability of nearly 61%. Negative likelihood ratios for the McMurray test and joint line tenderness (0.5 and 0.8) were not clinically significant, indicating that absence of the McMurray sign or joint line tenderness alone is of little benefit in ruling out meniscal injury.
In another meta-analysis including 9 studies of meniscal injury diagnosis,4 individual tests for joint line tenderness, joint effusion, the medial-lateral grind test, and the McMurray test failed to yield statistically significant likelihood ratios for the presence or absence of meniscal tears ( Table footnotes). Positive and negative likelihood ratios for aggregate physical examination were 2.7 (95% confidence interval [CI], 1.4–5.1) and 0.4 (95% CI, 0.2–0.7), which are statistically, but not clinically, significant values for ruling meniscal lesions in or out.
Jackson’s meta-analysis also calculated the posttest probability of injury for a composite meniscal examination. Based on the positive likelihood ratio of 3.1 (95% CI, 0.54–5.7) and negative likelihood ratio of 0.19 (95% CI, 0.11–0.77), the posttest probability of a medial meniscal tear was 17% in the setting of composite physical exam findings and 1% in the absence of physical exam findings. For a lateral meniscal tear, based on the positive likelihood ratio of 11 (95% CI, 1.8–20.2), and negative likelihood ratio of 0.13 (95% CI, 0.0–0.25), the posttest probability of injury with a positive exam was 41% and with a negative exam 0.8%.
Authors of all meta-analyses noted the lack of standardization in physical examination maneuvers (especially the McMurray test)5 and, in some cases, no specification of how physical examination tests were performed. Authors analyzed the utility of the aggregate and composite knee examinations without specifying what constituted such an exam. No study included in the meta-analyses used control subjects without meniscal pathology, and few studies were blinded. Lack of blinding may have introduced verification bias; use of specialty patients in all studies made referral bias likely. Studies were heterogeneous and results were associated with wide confidence intervals, introducing an element of random error into the processes of combining and interpreting data.
TABLE
Physical exams for meniscal tear
| Summary characteristics | Solomon et al 4 | Scholten et al 1 | Jackson et al 3 |
| 9 studies 1018 patients Specialist population Specialist examiners | 13 studies 2231 patients Specialist population Specialist examiners | 4 studies 424 patients Specialist population Specialist examiners | |
| McMurray | Positive likelihood ratio (95% CI) | ||
| 1.3 (0.9–1.7) | 1.5–9.5 | 17.3 (2.7–68) | |
| Joint line tenderness | 0.9 (0.8–1.0) | 0.8–14.9 | 1.1 (0.7–1.6) |
| Aggregate exam | 2.7 (1.4–5.1) | — | — |
| Aggregate exam, medial meniscus tears | — | — | 3.1 (0.54–5.7) |
| Aggregate exam, lateral meniscus tears | — | — | 11 (1.8–20.2) |
| McMurray | Negative likelihood ratio (95% CI) | ||
| 0.8 (0.6–1.1) | 0.4–0.9 | 0.5 (0.3–0.8) | |
| Joint line tenderness | 1.1 (1.0–1.3) | 0.2–2.1 | 0.8 (0.3–3.5) |
| Aggregate exam | 0.4 (0.2–0.7) | — | — |
| Aggregate exam, medial meniscus tears | — | — | 0.19 (0.11–0.77) |
| Aggregate exam, lateral meniscus tears | — | — | 0.13 (0–0.25) |
| Note: The results are presented as likelihood ratios, which represent the change in the odds of a diagnosis, based on the outcome of the test. For example, given a positive likelihood ratio of 2, if a test result is positive, the odds of the disease being present is doubled. A positive likelihood ratio >10 provides strong evidence that the disorder is present. A negative likelihood ratio <0.1 provides strong evidence that the disorder is not present. Scores between 0.5 and 2.0 are neutral. In Scholten’s meta-analysis, likelihood ratios are given in ranges (no composite value given). | |||
Recommendations from others
The American Academy of Orthopaedic Surgeons’ clinical guideline on the evaluation and treatment of knee injuries lists the following findings as associated with a meniscal tear: delayed swelling of the knee, twisting injury, painful popping and catching, effusion, joint line tenderness, positive McMurray’s test, and negative radiography.6 The guideline fails to list the strength and type of supporting evidence for these associations.
The American College of Radiology’s Appropriateness Criteria for Acute Trauma to the Knee states that decision rules for meniscal tears and other soft tissue injuries to the knee are being investigated, but it fails to mention specific evaluation strategies for meniscal tears.7
Meniscus injury likely with suggestive history, joint line tenderness, and an inability to squat because of pain
Roy Henderson, MD
Director, Sports Medicine Fellowship, MacNeal Family Practice Residency Program, Chicago, Ill
I often suspect meniscal injuries as a cause of knee pain but am rarely certain based on physical examination alone. I look for a history of joint line pain, locking, or popping with movement. If the patient lacks joint line tenderness, a meniscal injury is unlikely. The McMurray test is usually negative. In the absence of another explanation for the patient’s symptoms, a meniscus injury is high on my list in the presence of a suggestive history, joint line tenderness, and an inability to squat because of pain. When my suspicion is high I usually resort to an MRI.
1. Scholten RJ, Deville WL, Opstelten W, Bijl D, van der Plas CG, Bouter LM. The accuracy of physical diagnostic tests for assessing meniscal lesions of the knee: a meta-analysis. J Fam Pract 2001;50:938-944.
2. National Ambulatory Medical Care Survey 1996. Available at: ftp://ftp.cdc.gov/pub/Health-Statistics/NCHS/Datasets/NAMCS/. Accessed on August 18, 2004.
3. Jackson JL, O’Malley PG, Kroenke K. Evaluation of acute knee pain in primary care. Ann Intern Med 2003;139:575-588.
4. Solomon DH, Simel DL, Bates DW, Katz JN, Schaffer JL. The rational clinical examination. Does this patient have a torn meniscus or ligament of the knee?. JAMA 2001;286:1610-1620.
5. Stratford PW, Binkley J. A review of the McMurray test: definition, interpretation, and clinical usefulness. J Orthop Sports Phys Ther 1995;22:116-120.
6. American Academy of Orthopaedic Surgeons. AAOS Clinical Guideline on Knee Injury: Support Document. Last updated February 26, 2002. Rosemont, Ill: American Academy of Orthopaedic Surgeons; 2001. Available at: http://www.guidelines.gov. Accessed on September 30, 2004.
7. American College of Radiology (ACR) Expert. Panel on Musculoskeletal Imaging ACR Appropriateness Criteria for Acute Trauma to the Knee. Updated October 1, 2002. Reston, Va: American College of Radiology; 2001. Available at: http://www.acr.org/cgi-bin/fr?tmpl:appcrit,pdf:0365374_acute_trauma_to_knee.ac.p df. Accessed on September 30, 2004.
1. Scholten RJ, Deville WL, Opstelten W, Bijl D, van der Plas CG, Bouter LM. The accuracy of physical diagnostic tests for assessing meniscal lesions of the knee: a meta-analysis. J Fam Pract 2001;50:938-944.
2. National Ambulatory Medical Care Survey 1996. Available at: ftp://ftp.cdc.gov/pub/Health-Statistics/NCHS/Datasets/NAMCS/. Accessed on August 18, 2004.
3. Jackson JL, O’Malley PG, Kroenke K. Evaluation of acute knee pain in primary care. Ann Intern Med 2003;139:575-588.
4. Solomon DH, Simel DL, Bates DW, Katz JN, Schaffer JL. The rational clinical examination. Does this patient have a torn meniscus or ligament of the knee?. JAMA 2001;286:1610-1620.
5. Stratford PW, Binkley J. A review of the McMurray test: definition, interpretation, and clinical usefulness. J Orthop Sports Phys Ther 1995;22:116-120.
6. American Academy of Orthopaedic Surgeons. AAOS Clinical Guideline on Knee Injury: Support Document. Last updated February 26, 2002. Rosemont, Ill: American Academy of Orthopaedic Surgeons; 2001. Available at: http://www.guidelines.gov. Accessed on September 30, 2004.
7. American College of Radiology (ACR) Expert. Panel on Musculoskeletal Imaging ACR Appropriateness Criteria for Acute Trauma to the Knee. Updated October 1, 2002. Reston, Va: American College of Radiology; 2001. Available at: http://www.acr.org/cgi-bin/fr?tmpl:appcrit,pdf:0365374_acute_trauma_to_knee.ac.p df. Accessed on September 30, 2004.
Evidence-based answers from the Family Physicians Inquiries Network
Do acetaminophen and an NSAID combined relieve osteoarthritis pain better than either alone?
Combining nonsteroidal anti-inflammatory drugs (NSAIDs) and acetaminophen for short courses provides more relief of pain in osteoarthritis with-out an increase in side effects (strength of recommendation [SOR]=B). Combining acetaminophen at 4 g/d with an NSAID can also decrease the daily dose of NSAID required for pain relief, thus reducing the potential risk from higher-dose NSAID therapy (SOR=B).
Over the long term, however, this combination may increase the risk of upper gastrointestinal (GI) bleeding more than that conferred by the NSAID alone (SOR=B). If combination therapy is necessary, limiting the dose of acetaminophen to 2 g/d minimizes gastrointestinal toxicity. Acetaminophen alone at the lowest dose to provide pain relief is the safest pharmacologic choice for patients with osteoarthritis.
Evidence summary
Clinical guidelines for osteoarthritis recommend acetaminophen as first-line therapy followed by an NSAID or cyclooxygenase-2 (COX-2) inhibitor, and many patients are treated with combination therapy.
Several small randomized controlled trials have compared the individual efficacy of NSAIDs and acetaminophen in osteoarthritis and have found that both provide more pain relief than placebo.1-3There is a trend toward improved pain relief with NSAIDs compared with acetaminophen in the initial treatment period; however, few long-term studies of efficacy have been reported. One randomized controlled trial comparing 750 mg/d naproxen (Aleve, Naprosyn) with 2600 mg/d acetaminophen for 2 years found similar pain relief for both medications and a dropout rate of 65% in both groups.2 Similar numbers of persons taking acetaminophen or naproxen dropped out because of adverse effects (20%) or lack of efficacy (19%), and no difference was seen in functional improvement between the 2 groups.
A 6-week randomized double-blind crossover trial of 227 patients comparing 75 mg diclofenac and 200 mg misoprostol (Arthrotec) with acetaminophen 4 g/d found the diclofenac-misoprostol combination provided more pain control than acetaminophen alone. Adverse events were slightly more common in the diclofenac group (54% vs 46%; P=.046).4
The COX-2 inhibitors rofecoxib (Vioxx) and celecoxib (Celebrex) have been shown to provide equal pain relief compared with naproxen for patients with osteoarthritis.5 One industry-sponsored randomized trial found rofecoxib superior to celecoxib, and both superior to acetaminophen in treatment of osteoarthritis pain.6 There was no difference in the incidence of side effects among the 3 medications. Thirty percent of patients taking 4 g/d acetaminophen discontinued the study because of lack of efficacy, compared with 20% of those taking either celecoxib or rofecoxib.6
Few studies have evaluated the safety or efficacy of the combination of NSAIDs and acetaminophen in osteoarthritis. One double-blind, double-dummy crossover trial of 18 patients with osteoarthritis of the hip compared naproxen at doses of 500 mg and 1000 mg, with and without 4 g/d of acetaminophen, and 1500 mg/d of naproxen alone over 5 one-week trial periods.7Adding acetaminophen improved patient-reported pain scores compared with naproxen alone. Higher doses of naproxen alone provided less pain relief than a lower dose of naproxen combined with acetaminophen. GI side effects increased with the increase in naproxen dose, but were unaffected by the addition of acetaminophen. Functional ability was not affected during this short study. A similar study by the same researchers of patients with rheumatoid arthritis found similar results.7
One randomized, double-blind, crossover trial compared single doses of tolmetin (Tolectin, 100, 150, 200 mg) and acetaminophen (400 mg) alone and in combination with placebo in the control of experimentally induced pain (thermal and electrical stimulation). Acetaminophen alone did not differ from placebo in pain control; however, the combinations of acetaminophen with tolmetin provided similar pain relief to higher doses of tolmetin alone.8 No studies have evaluated the efficacy or safety of acetaminophen combined with rofecoxib or celecoxib.
Regarding the risks of combining acetaminophen with NSAIDs, 1 nested case-control study based on the entire enrollment panel of the British National Health Service characterized the risk of upper GI side effects among persons taking NSAIDs or acetaminophen alone or in combination. The study evaluated medications in use at the time of an upper GI bleed, controlling for age, sex, and concomitant medications (corticosteroids, H2 receptor antagonists, omeprazole, anticoagulants, and others) and excluding patients with varices, alcohol-related disorders, liver disease, and cancer; no attempt was made to control other comorbidities. The relative risk of upper GI perforation or bleeding for patients taking 2g/d acetaminophen or high-dose NSAIDs was 2.4 (95% confidence interval [CI], 1.7–3.5) and 3.6 (95% CI, 2.9–4.3), respectively. Concomitant use of an NSAID with 2 g/d of acetaminophen showed a relative risk of upper GI perforation or bleed of 16.6 (95% CI, 11.0–24.9). Acetaminophen doses <2 g/d conferred no additional risk for serious upper GI side effects.9
A systematic review of selective COX-2 inhibitors vs naproxen found fewer endoscopically detected ulcers in patients taking celecoxib but no difference in serious gastrointestinal bleeds.5 A meta-analysis of randomized controlled trials found a higher incidence of serious thrombotic cardiovascular events among patients taking COX-2 inhibitors compared with naprosyn.10 The safety profile of rofecoxib and celecoxib in the long-term treatment of pain is not fully understood at this time.
Recommendations from others
The American College of Rheumatology (ACR) recommends acetaminophen up to 4 g/d as a first-line pharmacologic treatment for osteoarthritis of the hip and knee, and advises NSAIDs be used at the lowest effective dose if they are necessary for pain control.11 The ACR does not specifically comment on combining NSAID and acetaminophen use. The American Academy of Orthopaedic Surgeons recommends initial use of an NSAID or acetaminophen, but does not comment on the combination of NSAIDs and acetaminophen.12
Adding acetaminophen may be more desirable than switching NSAIDs
Joseph Saseen, PharmD, FCCP, BCPS
University of Colorado Health Sciences Center, Denver
Compared with NSAIDs, acetaminophen has a complementary analgesic mechanism of action and can be safely used in many patients. Additive effects of acetaminophen have not been well described with all NSAIDs (eg, COX-2 inhibitors); however, this combination is inexpensive and overall appears to effectively augment analgesia when combined with NSAIDs. Although observational data demonstrate an increased risk of upper GI bleeding with this combination, selection bias (higher-risk patients being on combination therapy) could reasonably explain this association. Adding acetaminophen may be more desirable than switching NSAIDs for patients with osteoarthritis that have a partial response to their current NSAID therapy.
- Amoxicillin • Amoxil, Biomox, Polymox, Trimox, Wymox
- Cephalexin • Biocef, Keflex
- Celecoxib • Celebrex
- Diclofenac/Misoprostol • Arthrotec
- Ipratropium • Atrovent
- Labetalol • Trandate
- Methyldopa • Aldomet
- Naproxen • Aleve, Anaprox, Naprosyn
- Nitrofurantoin • Furadantin, Macrobid, Macrodantin
- Rofecoxib • Vioxx
- Tiotropium • Spiriva
- Tolmetin • Tolectin
- Triamcinalone • Aristocort, Atolone, Kenacort
- Sulfamethoxazole/Trimethoprim • Bactrim,Cotrim,
- Septra, Sulfatrim
- Sulfisoxazole • Gantrisin
1. Amadio P Jr, Cummings DM. Evaluation of acetaminophen in the management of osteoarthritis of the knee. Curr Ther Res 1983;34:59-66.
2. Williams HJ, Ward JR, Egger MJ, et al. Comparison of naproxen and acetaminophen in a two-year study of treatment of osteoarthritis of the knee. Arthritis Rheum 1993;36:1196-1206.
3. Bradley JD, Brandt KD, Katz BP, Kalasinski LA, Ryan SI. Treatment of knee osteoarthritis: relationship of clinical features of joint inflammation to the response to a nonsteroidal antiinflammatory drug or pure analgesic. J Rheumatol 1992;19:1950-1954.
4. Pincus T, Koch GG, Sokka T, et al. A randomized, double-blind, crossover clinical trial of diclofenac plus misoprostol versus acetaminophen for patients with osteoarthritis of the hip or knee. Arthritis Rheum 2001;44:1587-1598.
5. Deeks JJ, Smith LA, Bradley MD. Efficacy, tolerability, and upper gastrointestinal safety of celecoxib for treatment of osteoarthritis and rheumatoid arthritis: systematic review of randomised controlled trials. BMJ 2002;325:619.-
6. Geba GP, Weaver AL, Polis AB, Dixon ME, Schnitzer TJ. Vioxx. Acetaminophen Celecoxib Trial (VACT) Group. Efficacy of rofecoxib, celecoxib, and acetaminophen in osteoarthritis of the knee: a randomized trial. JAMA 2002;287:64-71.
7. Seideman P, Samuelson P, Neander G. Naproxen and paracetamol compared with naproxen only in coxarthrosis. Increased effect of the combination in 18 patients. Acta Orthop Scand 1993;64:285-288.
8. Stacher G, Bauer P, Ehn I, Schreiber E. Effects of tolmetin, paracetamol, and of two combinations of tolmetin and paracetamol as compared to placebo on experimentally induced pain. A double blind study. Int J Clin Pharmacol Biopharm 1979;17:250-255.
9. Garcia Rodriguez LA, Hernandez-Diaz S. The risk of upper gastrointestinal complications associated with nonsteroidal anti-inflammatory drugs, glucocorticoids, acetaminophen, and combinations of these agents. Arthritis Res 2001;3:98-101.
10. Mukherjee D, Nissen SE, Topol EJ. Risk of cardiovascular events associated with selective COX-2 inhibitors. JAMA 2001;286:954-959.
11. Recommendations for the medical management of osteoarthritis of the hip and knee: 2000 update. American College of Rheumatology Subcommittee on Osteoarthritis Guidelines. Arthritis Rheum 2000;43:1905-1915.
12. AAOS Clinical Guideline on Osteoarthritis of the Knee. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2003. Available at: www.aaos.org/wordhtml/pdfs_r/guidelin/suprt_oakn.pdf. Accessed on May 11, 2004.
Combining nonsteroidal anti-inflammatory drugs (NSAIDs) and acetaminophen for short courses provides more relief of pain in osteoarthritis with-out an increase in side effects (strength of recommendation [SOR]=B). Combining acetaminophen at 4 g/d with an NSAID can also decrease the daily dose of NSAID required for pain relief, thus reducing the potential risk from higher-dose NSAID therapy (SOR=B).
Over the long term, however, this combination may increase the risk of upper gastrointestinal (GI) bleeding more than that conferred by the NSAID alone (SOR=B). If combination therapy is necessary, limiting the dose of acetaminophen to 2 g/d minimizes gastrointestinal toxicity. Acetaminophen alone at the lowest dose to provide pain relief is the safest pharmacologic choice for patients with osteoarthritis.
Evidence summary
Clinical guidelines for osteoarthritis recommend acetaminophen as first-line therapy followed by an NSAID or cyclooxygenase-2 (COX-2) inhibitor, and many patients are treated with combination therapy.
Several small randomized controlled trials have compared the individual efficacy of NSAIDs and acetaminophen in osteoarthritis and have found that both provide more pain relief than placebo.1-3There is a trend toward improved pain relief with NSAIDs compared with acetaminophen in the initial treatment period; however, few long-term studies of efficacy have been reported. One randomized controlled trial comparing 750 mg/d naproxen (Aleve, Naprosyn) with 2600 mg/d acetaminophen for 2 years found similar pain relief for both medications and a dropout rate of 65% in both groups.2 Similar numbers of persons taking acetaminophen or naproxen dropped out because of adverse effects (20%) or lack of efficacy (19%), and no difference was seen in functional improvement between the 2 groups.
A 6-week randomized double-blind crossover trial of 227 patients comparing 75 mg diclofenac and 200 mg misoprostol (Arthrotec) with acetaminophen 4 g/d found the diclofenac-misoprostol combination provided more pain control than acetaminophen alone. Adverse events were slightly more common in the diclofenac group (54% vs 46%; P=.046).4
The COX-2 inhibitors rofecoxib (Vioxx) and celecoxib (Celebrex) have been shown to provide equal pain relief compared with naproxen for patients with osteoarthritis.5 One industry-sponsored randomized trial found rofecoxib superior to celecoxib, and both superior to acetaminophen in treatment of osteoarthritis pain.6 There was no difference in the incidence of side effects among the 3 medications. Thirty percent of patients taking 4 g/d acetaminophen discontinued the study because of lack of efficacy, compared with 20% of those taking either celecoxib or rofecoxib.6
Few studies have evaluated the safety or efficacy of the combination of NSAIDs and acetaminophen in osteoarthritis. One double-blind, double-dummy crossover trial of 18 patients with osteoarthritis of the hip compared naproxen at doses of 500 mg and 1000 mg, with and without 4 g/d of acetaminophen, and 1500 mg/d of naproxen alone over 5 one-week trial periods.7Adding acetaminophen improved patient-reported pain scores compared with naproxen alone. Higher doses of naproxen alone provided less pain relief than a lower dose of naproxen combined with acetaminophen. GI side effects increased with the increase in naproxen dose, but were unaffected by the addition of acetaminophen. Functional ability was not affected during this short study. A similar study by the same researchers of patients with rheumatoid arthritis found similar results.7
One randomized, double-blind, crossover trial compared single doses of tolmetin (Tolectin, 100, 150, 200 mg) and acetaminophen (400 mg) alone and in combination with placebo in the control of experimentally induced pain (thermal and electrical stimulation). Acetaminophen alone did not differ from placebo in pain control; however, the combinations of acetaminophen with tolmetin provided similar pain relief to higher doses of tolmetin alone.8 No studies have evaluated the efficacy or safety of acetaminophen combined with rofecoxib or celecoxib.
Regarding the risks of combining acetaminophen with NSAIDs, 1 nested case-control study based on the entire enrollment panel of the British National Health Service characterized the risk of upper GI side effects among persons taking NSAIDs or acetaminophen alone or in combination. The study evaluated medications in use at the time of an upper GI bleed, controlling for age, sex, and concomitant medications (corticosteroids, H2 receptor antagonists, omeprazole, anticoagulants, and others) and excluding patients with varices, alcohol-related disorders, liver disease, and cancer; no attempt was made to control other comorbidities. The relative risk of upper GI perforation or bleeding for patients taking 2g/d acetaminophen or high-dose NSAIDs was 2.4 (95% confidence interval [CI], 1.7–3.5) and 3.6 (95% CI, 2.9–4.3), respectively. Concomitant use of an NSAID with 2 g/d of acetaminophen showed a relative risk of upper GI perforation or bleed of 16.6 (95% CI, 11.0–24.9). Acetaminophen doses <2 g/d conferred no additional risk for serious upper GI side effects.9
A systematic review of selective COX-2 inhibitors vs naproxen found fewer endoscopically detected ulcers in patients taking celecoxib but no difference in serious gastrointestinal bleeds.5 A meta-analysis of randomized controlled trials found a higher incidence of serious thrombotic cardiovascular events among patients taking COX-2 inhibitors compared with naprosyn.10 The safety profile of rofecoxib and celecoxib in the long-term treatment of pain is not fully understood at this time.
Recommendations from others
The American College of Rheumatology (ACR) recommends acetaminophen up to 4 g/d as a first-line pharmacologic treatment for osteoarthritis of the hip and knee, and advises NSAIDs be used at the lowest effective dose if they are necessary for pain control.11 The ACR does not specifically comment on combining NSAID and acetaminophen use. The American Academy of Orthopaedic Surgeons recommends initial use of an NSAID or acetaminophen, but does not comment on the combination of NSAIDs and acetaminophen.12
Adding acetaminophen may be more desirable than switching NSAIDs
Joseph Saseen, PharmD, FCCP, BCPS
University of Colorado Health Sciences Center, Denver
Compared with NSAIDs, acetaminophen has a complementary analgesic mechanism of action and can be safely used in many patients. Additive effects of acetaminophen have not been well described with all NSAIDs (eg, COX-2 inhibitors); however, this combination is inexpensive and overall appears to effectively augment analgesia when combined with NSAIDs. Although observational data demonstrate an increased risk of upper GI bleeding with this combination, selection bias (higher-risk patients being on combination therapy) could reasonably explain this association. Adding acetaminophen may be more desirable than switching NSAIDs for patients with osteoarthritis that have a partial response to their current NSAID therapy.
- Amoxicillin • Amoxil, Biomox, Polymox, Trimox, Wymox
- Cephalexin • Biocef, Keflex
- Celecoxib • Celebrex
- Diclofenac/Misoprostol • Arthrotec
- Ipratropium • Atrovent
- Labetalol • Trandate
- Methyldopa • Aldomet
- Naproxen • Aleve, Anaprox, Naprosyn
- Nitrofurantoin • Furadantin, Macrobid, Macrodantin
- Rofecoxib • Vioxx
- Tiotropium • Spiriva
- Tolmetin • Tolectin
- Triamcinalone • Aristocort, Atolone, Kenacort
- Sulfamethoxazole/Trimethoprim • Bactrim,Cotrim,
- Septra, Sulfatrim
- Sulfisoxazole • Gantrisin
Combining nonsteroidal anti-inflammatory drugs (NSAIDs) and acetaminophen for short courses provides more relief of pain in osteoarthritis with-out an increase in side effects (strength of recommendation [SOR]=B). Combining acetaminophen at 4 g/d with an NSAID can also decrease the daily dose of NSAID required for pain relief, thus reducing the potential risk from higher-dose NSAID therapy (SOR=B).
Over the long term, however, this combination may increase the risk of upper gastrointestinal (GI) bleeding more than that conferred by the NSAID alone (SOR=B). If combination therapy is necessary, limiting the dose of acetaminophen to 2 g/d minimizes gastrointestinal toxicity. Acetaminophen alone at the lowest dose to provide pain relief is the safest pharmacologic choice for patients with osteoarthritis.
Evidence summary
Clinical guidelines for osteoarthritis recommend acetaminophen as first-line therapy followed by an NSAID or cyclooxygenase-2 (COX-2) inhibitor, and many patients are treated with combination therapy.
Several small randomized controlled trials have compared the individual efficacy of NSAIDs and acetaminophen in osteoarthritis and have found that both provide more pain relief than placebo.1-3There is a trend toward improved pain relief with NSAIDs compared with acetaminophen in the initial treatment period; however, few long-term studies of efficacy have been reported. One randomized controlled trial comparing 750 mg/d naproxen (Aleve, Naprosyn) with 2600 mg/d acetaminophen for 2 years found similar pain relief for both medications and a dropout rate of 65% in both groups.2 Similar numbers of persons taking acetaminophen or naproxen dropped out because of adverse effects (20%) or lack of efficacy (19%), and no difference was seen in functional improvement between the 2 groups.
A 6-week randomized double-blind crossover trial of 227 patients comparing 75 mg diclofenac and 200 mg misoprostol (Arthrotec) with acetaminophen 4 g/d found the diclofenac-misoprostol combination provided more pain control than acetaminophen alone. Adverse events were slightly more common in the diclofenac group (54% vs 46%; P=.046).4
The COX-2 inhibitors rofecoxib (Vioxx) and celecoxib (Celebrex) have been shown to provide equal pain relief compared with naproxen for patients with osteoarthritis.5 One industry-sponsored randomized trial found rofecoxib superior to celecoxib, and both superior to acetaminophen in treatment of osteoarthritis pain.6 There was no difference in the incidence of side effects among the 3 medications. Thirty percent of patients taking 4 g/d acetaminophen discontinued the study because of lack of efficacy, compared with 20% of those taking either celecoxib or rofecoxib.6
Few studies have evaluated the safety or efficacy of the combination of NSAIDs and acetaminophen in osteoarthritis. One double-blind, double-dummy crossover trial of 18 patients with osteoarthritis of the hip compared naproxen at doses of 500 mg and 1000 mg, with and without 4 g/d of acetaminophen, and 1500 mg/d of naproxen alone over 5 one-week trial periods.7Adding acetaminophen improved patient-reported pain scores compared with naproxen alone. Higher doses of naproxen alone provided less pain relief than a lower dose of naproxen combined with acetaminophen. GI side effects increased with the increase in naproxen dose, but were unaffected by the addition of acetaminophen. Functional ability was not affected during this short study. A similar study by the same researchers of patients with rheumatoid arthritis found similar results.7
One randomized, double-blind, crossover trial compared single doses of tolmetin (Tolectin, 100, 150, 200 mg) and acetaminophen (400 mg) alone and in combination with placebo in the control of experimentally induced pain (thermal and electrical stimulation). Acetaminophen alone did not differ from placebo in pain control; however, the combinations of acetaminophen with tolmetin provided similar pain relief to higher doses of tolmetin alone.8 No studies have evaluated the efficacy or safety of acetaminophen combined with rofecoxib or celecoxib.
Regarding the risks of combining acetaminophen with NSAIDs, 1 nested case-control study based on the entire enrollment panel of the British National Health Service characterized the risk of upper GI side effects among persons taking NSAIDs or acetaminophen alone or in combination. The study evaluated medications in use at the time of an upper GI bleed, controlling for age, sex, and concomitant medications (corticosteroids, H2 receptor antagonists, omeprazole, anticoagulants, and others) and excluding patients with varices, alcohol-related disorders, liver disease, and cancer; no attempt was made to control other comorbidities. The relative risk of upper GI perforation or bleeding for patients taking 2g/d acetaminophen or high-dose NSAIDs was 2.4 (95% confidence interval [CI], 1.7–3.5) and 3.6 (95% CI, 2.9–4.3), respectively. Concomitant use of an NSAID with 2 g/d of acetaminophen showed a relative risk of upper GI perforation or bleed of 16.6 (95% CI, 11.0–24.9). Acetaminophen doses <2 g/d conferred no additional risk for serious upper GI side effects.9
A systematic review of selective COX-2 inhibitors vs naproxen found fewer endoscopically detected ulcers in patients taking celecoxib but no difference in serious gastrointestinal bleeds.5 A meta-analysis of randomized controlled trials found a higher incidence of serious thrombotic cardiovascular events among patients taking COX-2 inhibitors compared with naprosyn.10 The safety profile of rofecoxib and celecoxib in the long-term treatment of pain is not fully understood at this time.
Recommendations from others
The American College of Rheumatology (ACR) recommends acetaminophen up to 4 g/d as a first-line pharmacologic treatment for osteoarthritis of the hip and knee, and advises NSAIDs be used at the lowest effective dose if they are necessary for pain control.11 The ACR does not specifically comment on combining NSAID and acetaminophen use. The American Academy of Orthopaedic Surgeons recommends initial use of an NSAID or acetaminophen, but does not comment on the combination of NSAIDs and acetaminophen.12
Adding acetaminophen may be more desirable than switching NSAIDs
Joseph Saseen, PharmD, FCCP, BCPS
University of Colorado Health Sciences Center, Denver
Compared with NSAIDs, acetaminophen has a complementary analgesic mechanism of action and can be safely used in many patients. Additive effects of acetaminophen have not been well described with all NSAIDs (eg, COX-2 inhibitors); however, this combination is inexpensive and overall appears to effectively augment analgesia when combined with NSAIDs. Although observational data demonstrate an increased risk of upper GI bleeding with this combination, selection bias (higher-risk patients being on combination therapy) could reasonably explain this association. Adding acetaminophen may be more desirable than switching NSAIDs for patients with osteoarthritis that have a partial response to their current NSAID therapy.
- Amoxicillin • Amoxil, Biomox, Polymox, Trimox, Wymox
- Cephalexin • Biocef, Keflex
- Celecoxib • Celebrex
- Diclofenac/Misoprostol • Arthrotec
- Ipratropium • Atrovent
- Labetalol • Trandate
- Methyldopa • Aldomet
- Naproxen • Aleve, Anaprox, Naprosyn
- Nitrofurantoin • Furadantin, Macrobid, Macrodantin
- Rofecoxib • Vioxx
- Tiotropium • Spiriva
- Tolmetin • Tolectin
- Triamcinalone • Aristocort, Atolone, Kenacort
- Sulfamethoxazole/Trimethoprim • Bactrim,Cotrim,
- Septra, Sulfatrim
- Sulfisoxazole • Gantrisin
1. Amadio P Jr, Cummings DM. Evaluation of acetaminophen in the management of osteoarthritis of the knee. Curr Ther Res 1983;34:59-66.
2. Williams HJ, Ward JR, Egger MJ, et al. Comparison of naproxen and acetaminophen in a two-year study of treatment of osteoarthritis of the knee. Arthritis Rheum 1993;36:1196-1206.
3. Bradley JD, Brandt KD, Katz BP, Kalasinski LA, Ryan SI. Treatment of knee osteoarthritis: relationship of clinical features of joint inflammation to the response to a nonsteroidal antiinflammatory drug or pure analgesic. J Rheumatol 1992;19:1950-1954.
4. Pincus T, Koch GG, Sokka T, et al. A randomized, double-blind, crossover clinical trial of diclofenac plus misoprostol versus acetaminophen for patients with osteoarthritis of the hip or knee. Arthritis Rheum 2001;44:1587-1598.
5. Deeks JJ, Smith LA, Bradley MD. Efficacy, tolerability, and upper gastrointestinal safety of celecoxib for treatment of osteoarthritis and rheumatoid arthritis: systematic review of randomised controlled trials. BMJ 2002;325:619.-
6. Geba GP, Weaver AL, Polis AB, Dixon ME, Schnitzer TJ. Vioxx. Acetaminophen Celecoxib Trial (VACT) Group. Efficacy of rofecoxib, celecoxib, and acetaminophen in osteoarthritis of the knee: a randomized trial. JAMA 2002;287:64-71.
7. Seideman P, Samuelson P, Neander G. Naproxen and paracetamol compared with naproxen only in coxarthrosis. Increased effect of the combination in 18 patients. Acta Orthop Scand 1993;64:285-288.
8. Stacher G, Bauer P, Ehn I, Schreiber E. Effects of tolmetin, paracetamol, and of two combinations of tolmetin and paracetamol as compared to placebo on experimentally induced pain. A double blind study. Int J Clin Pharmacol Biopharm 1979;17:250-255.
9. Garcia Rodriguez LA, Hernandez-Diaz S. The risk of upper gastrointestinal complications associated with nonsteroidal anti-inflammatory drugs, glucocorticoids, acetaminophen, and combinations of these agents. Arthritis Res 2001;3:98-101.
10. Mukherjee D, Nissen SE, Topol EJ. Risk of cardiovascular events associated with selective COX-2 inhibitors. JAMA 2001;286:954-959.
11. Recommendations for the medical management of osteoarthritis of the hip and knee: 2000 update. American College of Rheumatology Subcommittee on Osteoarthritis Guidelines. Arthritis Rheum 2000;43:1905-1915.
12. AAOS Clinical Guideline on Osteoarthritis of the Knee. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2003. Available at: www.aaos.org/wordhtml/pdfs_r/guidelin/suprt_oakn.pdf. Accessed on May 11, 2004.
1. Amadio P Jr, Cummings DM. Evaluation of acetaminophen in the management of osteoarthritis of the knee. Curr Ther Res 1983;34:59-66.
2. Williams HJ, Ward JR, Egger MJ, et al. Comparison of naproxen and acetaminophen in a two-year study of treatment of osteoarthritis of the knee. Arthritis Rheum 1993;36:1196-1206.
3. Bradley JD, Brandt KD, Katz BP, Kalasinski LA, Ryan SI. Treatment of knee osteoarthritis: relationship of clinical features of joint inflammation to the response to a nonsteroidal antiinflammatory drug or pure analgesic. J Rheumatol 1992;19:1950-1954.
4. Pincus T, Koch GG, Sokka T, et al. A randomized, double-blind, crossover clinical trial of diclofenac plus misoprostol versus acetaminophen for patients with osteoarthritis of the hip or knee. Arthritis Rheum 2001;44:1587-1598.
5. Deeks JJ, Smith LA, Bradley MD. Efficacy, tolerability, and upper gastrointestinal safety of celecoxib for treatment of osteoarthritis and rheumatoid arthritis: systematic review of randomised controlled trials. BMJ 2002;325:619.-
6. Geba GP, Weaver AL, Polis AB, Dixon ME, Schnitzer TJ. Vioxx. Acetaminophen Celecoxib Trial (VACT) Group. Efficacy of rofecoxib, celecoxib, and acetaminophen in osteoarthritis of the knee: a randomized trial. JAMA 2002;287:64-71.
7. Seideman P, Samuelson P, Neander G. Naproxen and paracetamol compared with naproxen only in coxarthrosis. Increased effect of the combination in 18 patients. Acta Orthop Scand 1993;64:285-288.
8. Stacher G, Bauer P, Ehn I, Schreiber E. Effects of tolmetin, paracetamol, and of two combinations of tolmetin and paracetamol as compared to placebo on experimentally induced pain. A double blind study. Int J Clin Pharmacol Biopharm 1979;17:250-255.
9. Garcia Rodriguez LA, Hernandez-Diaz S. The risk of upper gastrointestinal complications associated with nonsteroidal anti-inflammatory drugs, glucocorticoids, acetaminophen, and combinations of these agents. Arthritis Res 2001;3:98-101.
10. Mukherjee D, Nissen SE, Topol EJ. Risk of cardiovascular events associated with selective COX-2 inhibitors. JAMA 2001;286:954-959.
11. Recommendations for the medical management of osteoarthritis of the hip and knee: 2000 update. American College of Rheumatology Subcommittee on Osteoarthritis Guidelines. Arthritis Rheum 2000;43:1905-1915.
12. AAOS Clinical Guideline on Osteoarthritis of the Knee. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2003. Available at: www.aaos.org/wordhtml/pdfs_r/guidelin/suprt_oakn.pdf. Accessed on May 11, 2004.
Evidence-based answers from the Family Physicians Inquiries Network
Should home apnea monitoring be recommended to prevent SIDS?
While home apnea monitoring may find an increased incidence of apnea and bradycardia in preterm infants compared with term infants, no association links these events with sudden infant death syndrome (SIDS). Apnea of prematurity is not a proven risk factor for SIDS. Since apnea of prematurity has not been shown to be a precursor to SIDS, home apnea monitoring for the purpose of preventing SIDS cannot be recommended (strength of recommendation [SOR]: B, based on a single prospective cohort study and multiple case-control studies). Neonates with significant neurologic or pulmonary disease may benefit from apnea monitoring (SOR: C, expert opinion).
Evidence summary
Multiple case-control studies have identified risk factors for SIDS, which are presented along (with odds ratios) in Table 1.1-6 None of these case-control studies found apnea of prematurity to be a risk factor for SIDS.
A prospective cohort study of 1079 infants monitored for cardiorespiratory events, the Collaborative Home Infant Monitor Evaluation (CHIME) study, demonstrated that prior to 43 weeks postconceptional age, preterm infants had a statistically significant greater risk of extreme events (apnea or bradycardia longer than 30 seconds) compared with healthy term infants (Table 2). After 43 weeks postconceptional age, there were no differences in incidence of apnea or bradycardia, comparing preterm and term infants. Neither preterm infants nor infants with apnea, bradycardia, or apparent life-threatening events had increased incidences of SIDS.7
Significant financial costs are associated with home monitoring. The average monthly cost is $300 to $400, not including physician fees. This would lead to an estimated annual cost of $24 million dollars if every infant <1500 grams in the United States were monitored.8
The psychological costs of home apnea monitoring have also been studied. One hundred and four parents of monitored and unmonitored infants were enrolled in a questionnaire study to determine emotional distress and family functioning. As is common among families in the postpartum period, all experienced increased stress. But parents of monitored infants, compared with parents of unmonitored infants, had an increased incidence of subjective depression (number needed to harm [NNH]=7) and hostility (NNH=12) at 2 weeks postpartum. Interestingly, at 1-year follow-up interviews, 83% of parents who had consistently used the monitor reported feeling more secure for having used it and 69% believed that monitor use had been helpful.9
Recommendations from others
The American Academy of Pediatrics (AAP) acknowledges that no established predictive or precursor relationship exists between prolonged apnea and SIDS, stating that the “prevention of SIDS is not an acceptable indication for home cardiorespiratory monitoring.” They issue a weak recommendation that home cardiorespiratory monitoring may be necessary for recurrent apnea, recurrent bradycardia, hypoxemia, chronic lung disease, and technology-dependent infants. Finally, they state that monitoring should be discontinued at 43 weeks postconceptional age or after cessation of extreme cardiorespiratory events, whichever occurs last. The AAP recommends proven practices such as supine sleeping position, a safe sleeping environment, and elimination of prenatal and postnatal exposure to tobacco smoke to decrease the risk of SIDS.8
TABLE 1
Risk factors for SIDS
| Risk factor | Odds ratio (95% CI) |
|---|---|
| Maternal factors | |
| Transport problems for prenatal care1 | 11.8 (2.7–52.7) |
| Education 12 years1 | 4.2 (1.1–15.5) |
| Prenatal smoke exposure3 | 3.7 (2.9–4.6) |
| <7 prenatal visits1 | 3.3 (1.1–9.8) |
| Unmarried3 | 2.0 (1.6–2.5) |
| Paternal factors | |
| Education≤ 12 years1 | 8.8 (1.1–70.8) |
| Parental factors | |
| Parental smoking4 | 5.19 (2.26–11.91) |
| Passive smoke | |
| exposure—all sources5 | 3.50 (1.81–6.75) |
| Maternal consumption of alcohol | |
| First trimester1 | 6.7 (2.2–20.1) |
| Any trimester1 | 3.4 (1.4–10.9) |
| Binge drinking—first trimester1 | 6.3 (1.8–22.8) |
| Binge drinking—any trimester1 | 3.9 (1.4–10.9) |
| Infant care | |
| <3 well-child visits1 | 13.8 (1.7–109.9) |
| Sleeping prone4 | 6.96 (1.51–31.97) |
| ≥2 layers of clothing1 | 3.9 (1.4–10.9) |
| Routine use of reused mattress2 | 3.1 (1.5–6.2) |
| Drug treatment in previous week4 | 2.33 (1.10–4.54) |
| Infant demographics | |
| Low birth weight (2500 g)3 | 3.6 (2.4–5.2) |
| Black3 | 2.5 (1.6–3.9) |
| Male gender6 | 1.47 (1.26–1.70) |
| Table adapted from multiple case-control studies. | |
Apnea monitors are not the answer
Matthew Gannons, MD
Department of Family and Community Medicine and Orthopaedic Surgery, Medical College of Wisconsin
An episode of SIDS is devastating to parents and leaves physicians questioning what more could have been done to prevent the tragedy. Apnea monitors, however, are not the answer. There are clearly downsides to apnea monitors and the added stress they place on parents. I do not think anyone would argue this would be a small price to pay if they helped to prevent SIDS; unfortunately, this is not the case.
I find it interesting that although apnea monitors add stress to parents, most would use them again and many felt they were helpful. This highlights the importance of education and clear communication with parents about SIDS and its prevention. Anecdotally, I have yet to have parents who did not stop using apnea monitor early because of the constant false alarms.
1. Iyasu S, Randall LL, Welty TK, et al. Risk factors for sudden infant death syndrome among northern plains Indians. JAMA 2002;288:2717-2723.
2. Tappin D, Brooke H, Ecob R, Gibson A. Used infant mat-tresses and sudden infant death syndrome in Scotland: case-control study. BMJ 2002;325:1007.-
3. Paris CA, Remler R, Daling JR. Risk factors for sudden infant death syndrome: changes associated with sleep position recommendations. J Pediatr 2001;139:771-777.
4. Brooke H, Gibson A, Tappin D, Brown H. Case-control study of sudden infant death syndrome in Scotland, 1992–1995. BMJ 1997;314:1516-1520.
5. Klonoff-Cohen HS, Edelstein SL, Lefkowitz ES, et al. The effect of passive smoking and tobacco exposure through breast milk on sudden infant death syndrome. JAMA 1995;273:795-798.
6. Millar WJ, Hill GB. Prevalence of and risk factors for sudden infant death syndrome in Canada. CMAJ 1993;149:629-635.
7. Ramanathan, R, Corwin MJ, Hunt CE, et al. Cardiorespiratory events recorded on home monitors: Comparison of healthy infants with those at increased risk for SIDS. JAMA 2001;285:2199-2207.
8. Committee on Fetus and Newborn. American Academy of Pediatrics. Apnea, sudden infant death syndrome, and home monitoring. Pediatrics 2003;111:914-917.
9. Abendroth D, Moser DK, Dracup K, Doering LV. Do apnea monitors decrease emotional distress in parents of infants at high risk for cardiopulmonary arrest? J Pediatr Health Care 1999;13:50-57.
While home apnea monitoring may find an increased incidence of apnea and bradycardia in preterm infants compared with term infants, no association links these events with sudden infant death syndrome (SIDS). Apnea of prematurity is not a proven risk factor for SIDS. Since apnea of prematurity has not been shown to be a precursor to SIDS, home apnea monitoring for the purpose of preventing SIDS cannot be recommended (strength of recommendation [SOR]: B, based on a single prospective cohort study and multiple case-control studies). Neonates with significant neurologic or pulmonary disease may benefit from apnea monitoring (SOR: C, expert opinion).
Evidence summary
Multiple case-control studies have identified risk factors for SIDS, which are presented along (with odds ratios) in Table 1.1-6 None of these case-control studies found apnea of prematurity to be a risk factor for SIDS.
A prospective cohort study of 1079 infants monitored for cardiorespiratory events, the Collaborative Home Infant Monitor Evaluation (CHIME) study, demonstrated that prior to 43 weeks postconceptional age, preterm infants had a statistically significant greater risk of extreme events (apnea or bradycardia longer than 30 seconds) compared with healthy term infants (Table 2). After 43 weeks postconceptional age, there were no differences in incidence of apnea or bradycardia, comparing preterm and term infants. Neither preterm infants nor infants with apnea, bradycardia, or apparent life-threatening events had increased incidences of SIDS.7
Significant financial costs are associated with home monitoring. The average monthly cost is $300 to $400, not including physician fees. This would lead to an estimated annual cost of $24 million dollars if every infant <1500 grams in the United States were monitored.8
The psychological costs of home apnea monitoring have also been studied. One hundred and four parents of monitored and unmonitored infants were enrolled in a questionnaire study to determine emotional distress and family functioning. As is common among families in the postpartum period, all experienced increased stress. But parents of monitored infants, compared with parents of unmonitored infants, had an increased incidence of subjective depression (number needed to harm [NNH]=7) and hostility (NNH=12) at 2 weeks postpartum. Interestingly, at 1-year follow-up interviews, 83% of parents who had consistently used the monitor reported feeling more secure for having used it and 69% believed that monitor use had been helpful.9
Recommendations from others
The American Academy of Pediatrics (AAP) acknowledges that no established predictive or precursor relationship exists between prolonged apnea and SIDS, stating that the “prevention of SIDS is not an acceptable indication for home cardiorespiratory monitoring.” They issue a weak recommendation that home cardiorespiratory monitoring may be necessary for recurrent apnea, recurrent bradycardia, hypoxemia, chronic lung disease, and technology-dependent infants. Finally, they state that monitoring should be discontinued at 43 weeks postconceptional age or after cessation of extreme cardiorespiratory events, whichever occurs last. The AAP recommends proven practices such as supine sleeping position, a safe sleeping environment, and elimination of prenatal and postnatal exposure to tobacco smoke to decrease the risk of SIDS.8
TABLE 1
Risk factors for SIDS
| Risk factor | Odds ratio (95% CI) |
|---|---|
| Maternal factors | |
| Transport problems for prenatal care1 | 11.8 (2.7–52.7) |
| Education 12 years1 | 4.2 (1.1–15.5) |
| Prenatal smoke exposure3 | 3.7 (2.9–4.6) |
| <7 prenatal visits1 | 3.3 (1.1–9.8) |
| Unmarried3 | 2.0 (1.6–2.5) |
| Paternal factors | |
| Education≤ 12 years1 | 8.8 (1.1–70.8) |
| Parental factors | |
| Parental smoking4 | 5.19 (2.26–11.91) |
| Passive smoke | |
| exposure—all sources5 | 3.50 (1.81–6.75) |
| Maternal consumption of alcohol | |
| First trimester1 | 6.7 (2.2–20.1) |
| Any trimester1 | 3.4 (1.4–10.9) |
| Binge drinking—first trimester1 | 6.3 (1.8–22.8) |
| Binge drinking—any trimester1 | 3.9 (1.4–10.9) |
| Infant care | |
| <3 well-child visits1 | 13.8 (1.7–109.9) |
| Sleeping prone4 | 6.96 (1.51–31.97) |
| ≥2 layers of clothing1 | 3.9 (1.4–10.9) |
| Routine use of reused mattress2 | 3.1 (1.5–6.2) |
| Drug treatment in previous week4 | 2.33 (1.10–4.54) |
| Infant demographics | |
| Low birth weight (2500 g)3 | 3.6 (2.4–5.2) |
| Black3 | 2.5 (1.6–3.9) |
| Male gender6 | 1.47 (1.26–1.70) |
| Table adapted from multiple case-control studies. | |
Apnea monitors are not the answer
Matthew Gannons, MD
Department of Family and Community Medicine and Orthopaedic Surgery, Medical College of Wisconsin
An episode of SIDS is devastating to parents and leaves physicians questioning what more could have been done to prevent the tragedy. Apnea monitors, however, are not the answer. There are clearly downsides to apnea monitors and the added stress they place on parents. I do not think anyone would argue this would be a small price to pay if they helped to prevent SIDS; unfortunately, this is not the case.
I find it interesting that although apnea monitors add stress to parents, most would use them again and many felt they were helpful. This highlights the importance of education and clear communication with parents about SIDS and its prevention. Anecdotally, I have yet to have parents who did not stop using apnea monitor early because of the constant false alarms.
While home apnea monitoring may find an increased incidence of apnea and bradycardia in preterm infants compared with term infants, no association links these events with sudden infant death syndrome (SIDS). Apnea of prematurity is not a proven risk factor for SIDS. Since apnea of prematurity has not been shown to be a precursor to SIDS, home apnea monitoring for the purpose of preventing SIDS cannot be recommended (strength of recommendation [SOR]: B, based on a single prospective cohort study and multiple case-control studies). Neonates with significant neurologic or pulmonary disease may benefit from apnea monitoring (SOR: C, expert opinion).
Evidence summary
Multiple case-control studies have identified risk factors for SIDS, which are presented along (with odds ratios) in Table 1.1-6 None of these case-control studies found apnea of prematurity to be a risk factor for SIDS.
A prospective cohort study of 1079 infants monitored for cardiorespiratory events, the Collaborative Home Infant Monitor Evaluation (CHIME) study, demonstrated that prior to 43 weeks postconceptional age, preterm infants had a statistically significant greater risk of extreme events (apnea or bradycardia longer than 30 seconds) compared with healthy term infants (Table 2). After 43 weeks postconceptional age, there were no differences in incidence of apnea or bradycardia, comparing preterm and term infants. Neither preterm infants nor infants with apnea, bradycardia, or apparent life-threatening events had increased incidences of SIDS.7
Significant financial costs are associated with home monitoring. The average monthly cost is $300 to $400, not including physician fees. This would lead to an estimated annual cost of $24 million dollars if every infant <1500 grams in the United States were monitored.8
The psychological costs of home apnea monitoring have also been studied. One hundred and four parents of monitored and unmonitored infants were enrolled in a questionnaire study to determine emotional distress and family functioning. As is common among families in the postpartum period, all experienced increased stress. But parents of monitored infants, compared with parents of unmonitored infants, had an increased incidence of subjective depression (number needed to harm [NNH]=7) and hostility (NNH=12) at 2 weeks postpartum. Interestingly, at 1-year follow-up interviews, 83% of parents who had consistently used the monitor reported feeling more secure for having used it and 69% believed that monitor use had been helpful.9
Recommendations from others
The American Academy of Pediatrics (AAP) acknowledges that no established predictive or precursor relationship exists between prolonged apnea and SIDS, stating that the “prevention of SIDS is not an acceptable indication for home cardiorespiratory monitoring.” They issue a weak recommendation that home cardiorespiratory monitoring may be necessary for recurrent apnea, recurrent bradycardia, hypoxemia, chronic lung disease, and technology-dependent infants. Finally, they state that monitoring should be discontinued at 43 weeks postconceptional age or after cessation of extreme cardiorespiratory events, whichever occurs last. The AAP recommends proven practices such as supine sleeping position, a safe sleeping environment, and elimination of prenatal and postnatal exposure to tobacco smoke to decrease the risk of SIDS.8
TABLE 1
Risk factors for SIDS
| Risk factor | Odds ratio (95% CI) |
|---|---|
| Maternal factors | |
| Transport problems for prenatal care1 | 11.8 (2.7–52.7) |
| Education 12 years1 | 4.2 (1.1–15.5) |
| Prenatal smoke exposure3 | 3.7 (2.9–4.6) |
| <7 prenatal visits1 | 3.3 (1.1–9.8) |
| Unmarried3 | 2.0 (1.6–2.5) |
| Paternal factors | |
| Education≤ 12 years1 | 8.8 (1.1–70.8) |
| Parental factors | |
| Parental smoking4 | 5.19 (2.26–11.91) |
| Passive smoke | |
| exposure—all sources5 | 3.50 (1.81–6.75) |
| Maternal consumption of alcohol | |
| First trimester1 | 6.7 (2.2–20.1) |
| Any trimester1 | 3.4 (1.4–10.9) |
| Binge drinking—first trimester1 | 6.3 (1.8–22.8) |
| Binge drinking—any trimester1 | 3.9 (1.4–10.9) |
| Infant care | |
| <3 well-child visits1 | 13.8 (1.7–109.9) |
| Sleeping prone4 | 6.96 (1.51–31.97) |
| ≥2 layers of clothing1 | 3.9 (1.4–10.9) |
| Routine use of reused mattress2 | 3.1 (1.5–6.2) |
| Drug treatment in previous week4 | 2.33 (1.10–4.54) |
| Infant demographics | |
| Low birth weight (2500 g)3 | 3.6 (2.4–5.2) |
| Black3 | 2.5 (1.6–3.9) |
| Male gender6 | 1.47 (1.26–1.70) |
| Table adapted from multiple case-control studies. | |
Apnea monitors are not the answer
Matthew Gannons, MD
Department of Family and Community Medicine and Orthopaedic Surgery, Medical College of Wisconsin
An episode of SIDS is devastating to parents and leaves physicians questioning what more could have been done to prevent the tragedy. Apnea monitors, however, are not the answer. There are clearly downsides to apnea monitors and the added stress they place on parents. I do not think anyone would argue this would be a small price to pay if they helped to prevent SIDS; unfortunately, this is not the case.
I find it interesting that although apnea monitors add stress to parents, most would use them again and many felt they were helpful. This highlights the importance of education and clear communication with parents about SIDS and its prevention. Anecdotally, I have yet to have parents who did not stop using apnea monitor early because of the constant false alarms.
1. Iyasu S, Randall LL, Welty TK, et al. Risk factors for sudden infant death syndrome among northern plains Indians. JAMA 2002;288:2717-2723.
2. Tappin D, Brooke H, Ecob R, Gibson A. Used infant mat-tresses and sudden infant death syndrome in Scotland: case-control study. BMJ 2002;325:1007.-
3. Paris CA, Remler R, Daling JR. Risk factors for sudden infant death syndrome: changes associated with sleep position recommendations. J Pediatr 2001;139:771-777.
4. Brooke H, Gibson A, Tappin D, Brown H. Case-control study of sudden infant death syndrome in Scotland, 1992–1995. BMJ 1997;314:1516-1520.
5. Klonoff-Cohen HS, Edelstein SL, Lefkowitz ES, et al. The effect of passive smoking and tobacco exposure through breast milk on sudden infant death syndrome. JAMA 1995;273:795-798.
6. Millar WJ, Hill GB. Prevalence of and risk factors for sudden infant death syndrome in Canada. CMAJ 1993;149:629-635.
7. Ramanathan, R, Corwin MJ, Hunt CE, et al. Cardiorespiratory events recorded on home monitors: Comparison of healthy infants with those at increased risk for SIDS. JAMA 2001;285:2199-2207.
8. Committee on Fetus and Newborn. American Academy of Pediatrics. Apnea, sudden infant death syndrome, and home monitoring. Pediatrics 2003;111:914-917.
9. Abendroth D, Moser DK, Dracup K, Doering LV. Do apnea monitors decrease emotional distress in parents of infants at high risk for cardiopulmonary arrest? J Pediatr Health Care 1999;13:50-57.
1. Iyasu S, Randall LL, Welty TK, et al. Risk factors for sudden infant death syndrome among northern plains Indians. JAMA 2002;288:2717-2723.
2. Tappin D, Brooke H, Ecob R, Gibson A. Used infant mat-tresses and sudden infant death syndrome in Scotland: case-control study. BMJ 2002;325:1007.-
3. Paris CA, Remler R, Daling JR. Risk factors for sudden infant death syndrome: changes associated with sleep position recommendations. J Pediatr 2001;139:771-777.
4. Brooke H, Gibson A, Tappin D, Brown H. Case-control study of sudden infant death syndrome in Scotland, 1992–1995. BMJ 1997;314:1516-1520.
5. Klonoff-Cohen HS, Edelstein SL, Lefkowitz ES, et al. The effect of passive smoking and tobacco exposure through breast milk on sudden infant death syndrome. JAMA 1995;273:795-798.
6. Millar WJ, Hill GB. Prevalence of and risk factors for sudden infant death syndrome in Canada. CMAJ 1993;149:629-635.
7. Ramanathan, R, Corwin MJ, Hunt CE, et al. Cardiorespiratory events recorded on home monitors: Comparison of healthy infants with those at increased risk for SIDS. JAMA 2001;285:2199-2207.
8. Committee on Fetus and Newborn. American Academy of Pediatrics. Apnea, sudden infant death syndrome, and home monitoring. Pediatrics 2003;111:914-917.
9. Abendroth D, Moser DK, Dracup K, Doering LV. Do apnea monitors decrease emotional distress in parents of infants at high risk for cardiopulmonary arrest? J Pediatr Health Care 1999;13:50-57.
Evidence-based answers from the Family Physicians Inquiries Network
What is the prognosis of postherpetic neuralgia?
Postherpetic neuralgia occurs rarely among patients aged <50 years with herpes zoster. The incidence, duration, and severity of post-herpetic neuralgia increases with age, but older patients usually have only mild pain. Most cases resolve spontaneously within 3 months.1,2
Even in the highest-risk group, people aged >70 years, 25% had some pain at 3 months, but only 10% had pain at 1 year, and none had severe pain. Only a few patients have pain that persists for years (strength of recommendation: A, based on a well-done prospective cohort study).
Evidence summary
Postherpetic neuralgia is defined as pain that persists more than 1 month following onset of herpes zoster. The annual incidence of herpes zoster in population-based studies ranges from 1/1000 to 2/1000.1,3 Among adults aged >60 years, the annual incidence increases to 3.6/1000 for men and 5.6/1000 for women.1
In a prospective study performed in a primary care setting in Iceland, all cases of herpes zoster and postherpetic neuralgia occurring over 4.5 years in a population of 100,000 were identified, and all cases of postherpetic neuralgia were followed for up to 7.6 years. Few patients (4%) received antiviral medication.
In this study, postherpetic neuralgia followed herpes zoster in 2% of patients under age 40, 21% between the ages of 40 and 60, and in 40% of those over age 60.1,2 Subjects self-described pain as none, mild, moderate, or severe. Patients aged >60 years had the worst prognosis: 18% still had mild pain at 3 months and 6% had moderate or severe pain. At 1 year, 8% had mild pain and 2% had moderate pain. No patients had severe pain after 12 months.1,2
Among the 14 patients with pain persisting >12 months, 7 had complete resolution of pain, 5 had persisting pain that either improved or remained mild, 1 had ongoing moderate pain at 7 years, and 1 was lost to follow-up.2 (See Table.) Although postherpetic neuralgia can recur after resolution,4 no recurrence of pain was found among 183 randomly selected patients who had had resolution by 1 year.2
These results are similar to those found in an analysis of a retrospective cohort drawn from a large general practice network database,5 as well as other population-based studies.6,7 The prognosis is better than that reported in the placebo arms of trials of acute herpes zoster treatment.4 Patients in such trials are more likely to have severe disease than those seen in primary care settings.
TABLE
Risk of postherpetic neuralgia by age
| Age (y) | Pain at 3 mo | Pain at 1 y |
|---|---|---|
| >50 | 3% mild | 0% |
| 50–59 | 4% mild | 4% mild |
| 60–69 | 9% mild | 3% mild |
| 4% moderate to severe | 1% moderate | |
| ≥70 | 18% mild | 8% mild |
| 6% moderate to severe | 2% moderate |
Recommendations from others
A British guideline states that 5% of herpes zoster patients have postherpetic neuralgia 1 year after shingles.8 A review in the New England Journal of Medicine states that 48% of herpes zoster patients aged >70 years have postherpetic neuralgia at 1 year.9 This prevalence comes from a retrospective cohort study that combined patients presenting to a referral center with herpes zoster or postherpetic neuralgia into a single cohort, thus overestimating the prevalence of postherpetic neuralgia and providing a less reliable prognosis.10
Larry Halverson, MD
Cox Health Systems Family Practice Residency Program, Springfield, Missouri
Knowing the overall good prognosis for postherpetic neuralgia is helpful as I encounter patients with shingles. This answer is consistent with my experience. Fear of potential interminable pain and anecdotal experience with prolonged patient suffering has seduced me to start medications to “prevent” this problem. In some cases, my unnecessary (and unproven) “preventive” medications have produced new problems. Future research should focus on effective pain treatment options instead of prevention of a condition that usually resolves with time.
1. Helgason S, Sigurdsson JA, Gudmundsson S. The clinical course of herpes zoster: a prospective study in primary care. Eur J Gen Pract 1996;2:12-16.
2. Helgason S, Peturrson G, Gudmundsson S, Sigurdsson JA. Prevalence of postherpetic neuralgia after a single episode of herpes zoster: prospective study with long term follow up. BMJ 2000;321:1-4.
3. MacDonald BK, Cockerell OC, Sander JW, Shorvon SD. The incidence and lifetime prevalence of neurological disorders in a prospective community-based study in the UK. Brain 2000;123:665-676.
4. Alper BS, Lewis PR. Does treatment of acute herpes zoster prevent or shorten postherpetic neuralgia? J Fam Pract 2000;49:255-264.
5. Opstelten W, Mauritz J, de Wit N, van Wijck A, Stalman W. Herpes zoster and postherpetic neuralgia: incidence and risk indicators using a general practice research database. Fam Pract 2002;19:471-475.
6. Ragozzino MW, Melton LJ, Kurland LT, Chu CP, Perry HO. Population-based study of herpes zoster and its sequelae. Medicine (Baltimore) 1982;61:310-316.
7. Choo PW, Galil K, Donahue JG, Walker AM, Spiegelman D, Platt R. Risk factors for postherpetic neuralgia. Arch Intern Med 1997;157:1217-1224.
8. Guidelines for the management of shingles. Report of a working group of the British Society for the Study of Infection (BSSI). J Infect 1995;30:193-200.
9. Wood AJJ. Postherpetic neuralgia—pathogenesis, treatment and prevention. N Engl J Med 1996;335:32-41.
10. Morgas JM, Kierland RR. The outcome of patients with herpes zoster. Arch Dermatol 1957;75:193-196.
Postherpetic neuralgia occurs rarely among patients aged <50 years with herpes zoster. The incidence, duration, and severity of post-herpetic neuralgia increases with age, but older patients usually have only mild pain. Most cases resolve spontaneously within 3 months.1,2
Even in the highest-risk group, people aged >70 years, 25% had some pain at 3 months, but only 10% had pain at 1 year, and none had severe pain. Only a few patients have pain that persists for years (strength of recommendation: A, based on a well-done prospective cohort study).
Evidence summary
Postherpetic neuralgia is defined as pain that persists more than 1 month following onset of herpes zoster. The annual incidence of herpes zoster in population-based studies ranges from 1/1000 to 2/1000.1,3 Among adults aged >60 years, the annual incidence increases to 3.6/1000 for men and 5.6/1000 for women.1
In a prospective study performed in a primary care setting in Iceland, all cases of herpes zoster and postherpetic neuralgia occurring over 4.5 years in a population of 100,000 were identified, and all cases of postherpetic neuralgia were followed for up to 7.6 years. Few patients (4%) received antiviral medication.
In this study, postherpetic neuralgia followed herpes zoster in 2% of patients under age 40, 21% between the ages of 40 and 60, and in 40% of those over age 60.1,2 Subjects self-described pain as none, mild, moderate, or severe. Patients aged >60 years had the worst prognosis: 18% still had mild pain at 3 months and 6% had moderate or severe pain. At 1 year, 8% had mild pain and 2% had moderate pain. No patients had severe pain after 12 months.1,2
Among the 14 patients with pain persisting >12 months, 7 had complete resolution of pain, 5 had persisting pain that either improved or remained mild, 1 had ongoing moderate pain at 7 years, and 1 was lost to follow-up.2 (See Table.) Although postherpetic neuralgia can recur after resolution,4 no recurrence of pain was found among 183 randomly selected patients who had had resolution by 1 year.2
These results are similar to those found in an analysis of a retrospective cohort drawn from a large general practice network database,5 as well as other population-based studies.6,7 The prognosis is better than that reported in the placebo arms of trials of acute herpes zoster treatment.4 Patients in such trials are more likely to have severe disease than those seen in primary care settings.
TABLE
Risk of postherpetic neuralgia by age
| Age (y) | Pain at 3 mo | Pain at 1 y |
|---|---|---|
| >50 | 3% mild | 0% |
| 50–59 | 4% mild | 4% mild |
| 60–69 | 9% mild | 3% mild |
| 4% moderate to severe | 1% moderate | |
| ≥70 | 18% mild | 8% mild |
| 6% moderate to severe | 2% moderate |
Recommendations from others
A British guideline states that 5% of herpes zoster patients have postherpetic neuralgia 1 year after shingles.8 A review in the New England Journal of Medicine states that 48% of herpes zoster patients aged >70 years have postherpetic neuralgia at 1 year.9 This prevalence comes from a retrospective cohort study that combined patients presenting to a referral center with herpes zoster or postherpetic neuralgia into a single cohort, thus overestimating the prevalence of postherpetic neuralgia and providing a less reliable prognosis.10
Larry Halverson, MD
Cox Health Systems Family Practice Residency Program, Springfield, Missouri
Knowing the overall good prognosis for postherpetic neuralgia is helpful as I encounter patients with shingles. This answer is consistent with my experience. Fear of potential interminable pain and anecdotal experience with prolonged patient suffering has seduced me to start medications to “prevent” this problem. In some cases, my unnecessary (and unproven) “preventive” medications have produced new problems. Future research should focus on effective pain treatment options instead of prevention of a condition that usually resolves with time.
Postherpetic neuralgia occurs rarely among patients aged <50 years with herpes zoster. The incidence, duration, and severity of post-herpetic neuralgia increases with age, but older patients usually have only mild pain. Most cases resolve spontaneously within 3 months.1,2
Even in the highest-risk group, people aged >70 years, 25% had some pain at 3 months, but only 10% had pain at 1 year, and none had severe pain. Only a few patients have pain that persists for years (strength of recommendation: A, based on a well-done prospective cohort study).
Evidence summary
Postherpetic neuralgia is defined as pain that persists more than 1 month following onset of herpes zoster. The annual incidence of herpes zoster in population-based studies ranges from 1/1000 to 2/1000.1,3 Among adults aged >60 years, the annual incidence increases to 3.6/1000 for men and 5.6/1000 for women.1
In a prospective study performed in a primary care setting in Iceland, all cases of herpes zoster and postherpetic neuralgia occurring over 4.5 years in a population of 100,000 were identified, and all cases of postherpetic neuralgia were followed for up to 7.6 years. Few patients (4%) received antiviral medication.
In this study, postherpetic neuralgia followed herpes zoster in 2% of patients under age 40, 21% between the ages of 40 and 60, and in 40% of those over age 60.1,2 Subjects self-described pain as none, mild, moderate, or severe. Patients aged >60 years had the worst prognosis: 18% still had mild pain at 3 months and 6% had moderate or severe pain. At 1 year, 8% had mild pain and 2% had moderate pain. No patients had severe pain after 12 months.1,2
Among the 14 patients with pain persisting >12 months, 7 had complete resolution of pain, 5 had persisting pain that either improved or remained mild, 1 had ongoing moderate pain at 7 years, and 1 was lost to follow-up.2 (See Table.) Although postherpetic neuralgia can recur after resolution,4 no recurrence of pain was found among 183 randomly selected patients who had had resolution by 1 year.2
These results are similar to those found in an analysis of a retrospective cohort drawn from a large general practice network database,5 as well as other population-based studies.6,7 The prognosis is better than that reported in the placebo arms of trials of acute herpes zoster treatment.4 Patients in such trials are more likely to have severe disease than those seen in primary care settings.
TABLE
Risk of postherpetic neuralgia by age
| Age (y) | Pain at 3 mo | Pain at 1 y |
|---|---|---|
| >50 | 3% mild | 0% |
| 50–59 | 4% mild | 4% mild |
| 60–69 | 9% mild | 3% mild |
| 4% moderate to severe | 1% moderate | |
| ≥70 | 18% mild | 8% mild |
| 6% moderate to severe | 2% moderate |
Recommendations from others
A British guideline states that 5% of herpes zoster patients have postherpetic neuralgia 1 year after shingles.8 A review in the New England Journal of Medicine states that 48% of herpes zoster patients aged >70 years have postherpetic neuralgia at 1 year.9 This prevalence comes from a retrospective cohort study that combined patients presenting to a referral center with herpes zoster or postherpetic neuralgia into a single cohort, thus overestimating the prevalence of postherpetic neuralgia and providing a less reliable prognosis.10
Larry Halverson, MD
Cox Health Systems Family Practice Residency Program, Springfield, Missouri
Knowing the overall good prognosis for postherpetic neuralgia is helpful as I encounter patients with shingles. This answer is consistent with my experience. Fear of potential interminable pain and anecdotal experience with prolonged patient suffering has seduced me to start medications to “prevent” this problem. In some cases, my unnecessary (and unproven) “preventive” medications have produced new problems. Future research should focus on effective pain treatment options instead of prevention of a condition that usually resolves with time.
1. Helgason S, Sigurdsson JA, Gudmundsson S. The clinical course of herpes zoster: a prospective study in primary care. Eur J Gen Pract 1996;2:12-16.
2. Helgason S, Peturrson G, Gudmundsson S, Sigurdsson JA. Prevalence of postherpetic neuralgia after a single episode of herpes zoster: prospective study with long term follow up. BMJ 2000;321:1-4.
3. MacDonald BK, Cockerell OC, Sander JW, Shorvon SD. The incidence and lifetime prevalence of neurological disorders in a prospective community-based study in the UK. Brain 2000;123:665-676.
4. Alper BS, Lewis PR. Does treatment of acute herpes zoster prevent or shorten postherpetic neuralgia? J Fam Pract 2000;49:255-264.
5. Opstelten W, Mauritz J, de Wit N, van Wijck A, Stalman W. Herpes zoster and postherpetic neuralgia: incidence and risk indicators using a general practice research database. Fam Pract 2002;19:471-475.
6. Ragozzino MW, Melton LJ, Kurland LT, Chu CP, Perry HO. Population-based study of herpes zoster and its sequelae. Medicine (Baltimore) 1982;61:310-316.
7. Choo PW, Galil K, Donahue JG, Walker AM, Spiegelman D, Platt R. Risk factors for postherpetic neuralgia. Arch Intern Med 1997;157:1217-1224.
8. Guidelines for the management of shingles. Report of a working group of the British Society for the Study of Infection (BSSI). J Infect 1995;30:193-200.
9. Wood AJJ. Postherpetic neuralgia—pathogenesis, treatment and prevention. N Engl J Med 1996;335:32-41.
10. Morgas JM, Kierland RR. The outcome of patients with herpes zoster. Arch Dermatol 1957;75:193-196.
1. Helgason S, Sigurdsson JA, Gudmundsson S. The clinical course of herpes zoster: a prospective study in primary care. Eur J Gen Pract 1996;2:12-16.
2. Helgason S, Peturrson G, Gudmundsson S, Sigurdsson JA. Prevalence of postherpetic neuralgia after a single episode of herpes zoster: prospective study with long term follow up. BMJ 2000;321:1-4.
3. MacDonald BK, Cockerell OC, Sander JW, Shorvon SD. The incidence and lifetime prevalence of neurological disorders in a prospective community-based study in the UK. Brain 2000;123:665-676.
4. Alper BS, Lewis PR. Does treatment of acute herpes zoster prevent or shorten postherpetic neuralgia? J Fam Pract 2000;49:255-264.
5. Opstelten W, Mauritz J, de Wit N, van Wijck A, Stalman W. Herpes zoster and postherpetic neuralgia: incidence and risk indicators using a general practice research database. Fam Pract 2002;19:471-475.
6. Ragozzino MW, Melton LJ, Kurland LT, Chu CP, Perry HO. Population-based study of herpes zoster and its sequelae. Medicine (Baltimore) 1982;61:310-316.
7. Choo PW, Galil K, Donahue JG, Walker AM, Spiegelman D, Platt R. Risk factors for postherpetic neuralgia. Arch Intern Med 1997;157:1217-1224.
8. Guidelines for the management of shingles. Report of a working group of the British Society for the Study of Infection (BSSI). J Infect 1995;30:193-200.
9. Wood AJJ. Postherpetic neuralgia—pathogenesis, treatment and prevention. N Engl J Med 1996;335:32-41.
10. Morgas JM, Kierland RR. The outcome of patients with herpes zoster. Arch Dermatol 1957;75:193-196.
Evidence-based answers from the Family Physicians Inquiries Network
Are drug therapies effective in treating Bell’s palsy?
Early use of corticosteroid therapy results in less autonomic synkinesis and possibly improved rates of recovery in adults (strength of recommendation: C); there is no proven benefit in children (SOR: B).
Adding acyclovir (Zovirax) to prednisone therapy may improve recovery rates compared with prednisone alone (SOR: C).
The results of 1 nonblinded study indicate that intramuscular methylcobalamin (vitamin B12) used alone or in combination with prednisone may shorten time to recovery (SOR: C).
See the Patient Information at the end of this article.
Evidence summary
Bell’s palsy is a lower motor neuron disease of the facial nerve characterized by a transient paralysis. Healing is occasionally incomplete, resulting in residual nerve dysfunction, including partial palsy and motor synkinesis (involuntary movement accompanying a voluntary one) and autonomic synkinesis (involuntary lacrimation after a voluntary muscle movement). Bell’s palsy is associated with significant edema and ischemia of the facial nerve as it passes through its bony canal.
Herpes simplex reactivation has been shown to be associated with a large proportion of cases.
Corticosteroids are the most studied form of therapy for Bell’s palsy (Table). Early work in England culminated in 1971 with a well-performed study demonstrating lower rates of incomplete recovery with prednisolone compared with corticotrophin.1 A potentially definitive randomized controlled trial in 1970 was stopped prematurely because of investigators’ subjective impression that prednisone markedly reduced postauricular pain.2 Subsequently, the highest-quality study had few patients (n=51) and reported no difference in outcomes between patients receiving 10 days of oral prednisone plus vitamins and those receiving vitamins alone.3
One open randomized controlled trial demonstrated shorter mean recovery times with intramuscular methylcobalamin (1.95 weeks) and methylcobalamin plus prednisone (2.0 weeks) compared with prednisone alone (9.6 weeks).4 Another trial of 239 patients showed improved rates of autonomic synkinesis after treatment with 16 days of prednisone compared with placebo.5
A randomized, controlled trial of children 2 to 6 years of age found no significant differences in short-term recovery after treatment with methylprednisolone compared with untreated controls.6 Eventually, all these children recovered normal facial nerve function within 12 months.
Two randomized controlled trials have assessed the efficacy of acyclovir for treatment of Bell’s palsy. One trial compared prednisone with acyclovir and found patients treated with prednisone had better complete recovery rates, 93.6% versus 77.7% (absolute risk reduction [ARR]=15.9%, 95% confidence interval [CI]=2.8%–29%], number needed to treat [NNT]=7).7
Another study demonstrated that the combination of prednisone and acyclovir had greater complete recovery rates compared with prednisone alone (92% vs. 76%, ARR=16%, 95% CI=1.7%–30.3%, NNT=7).8
Overall, the data suggest corticosteroid therapy may provide a small clinical benefit in adult patients with Bell’s palsy. In many of these studies, patients who had contraindications to steroid therapy (peptic ulcer disease, uncontrolled diabetes, hypertension, or immunosuppression) were excluded.
If no contraindications to steroids exist, it is resonable to initiate treatment with corticosteroids for an adult patient with new-onset Bell’s palsy. Most studies have started patients on steroids within 10 days of onset of symptoms.
TABLE
Therapies for Bell’s palsy
| Drug | Dosage | SOR |
|---|---|---|
| Prednisone (adults only) | Total from 410 mg over 10 days, to 760 mg over 16 days (tapering doses) | C |
| Acyclovir | 400 mg 5x/d for 10 days | C |
| Methylcobalamin | 500 (g IM 3x/wk until full recovery, or for 8 weeks | C |
| SOR, Strength of recommendation | ||
Recommendations from others
A practice parameter from the American Academy of Neurology states that steroids are safe and probably effective (SOR: B), whereas acyclovir is safe and possibly effective (SOR: C).9 Systematic reviews from the Cochrane Database report that available evidence from randomized controlled trials does not show significant benefit from treating Bell’s palsy with corticosteroids and that clinical trials on acyclovir are inconclusive and therefore cannot be used to make recommendations regarding its use.10,11
Steven H. Horowitz, MD
University of Vermont College of Medicine, Burlington
My practice of neurology began before the era of corticosteroid treatment for Bell’s palsy. Despite the lack of convincing evidenced-based data, it is my clinical impression that there are far fewer patients today with incompletely resolved Bell’s palsy than before the widespread use of steroids. Permanent facial deformities seemed more common back then. Therefore, in the absence of harmful effects, I will continue treating with steroids.
PATIENT INFORMATION
What is Bell’s palsy?
Weakness and slumping on one side of the face are common features of this condition in which the nerve controlling the face has been injured. Other symptoms are:
- Inability to move affected side of the face
- Drooping mouth, unblinking eye
- Numbness
- Twitching of facial muscles
- Taste disturbance
- Increased sensitivity to sound.
Symptoms usually start suddenly. Pain behind the ear may be felt hours to days before other symptoms appear. People between ages 30 and 60 years are most likely to be affected, but this disorder can happen at any age.
Any sudden weakness of the face also suggests the possibility of stroke—a serious emergency. You should contact your physician immediately.
Possible causes
The most common cause of Bell’s palsy is an infection of the facial nerve by the herpes simplex virus. Your doctor will also ask about possible recent trauma to the face and will check for swelling of facial tissues or a mass pressing on the facial nerve.
What to expect
In many cases, the symptoms of Bell’s palsy go away in about 3 weeks without treatment, and the face regains its normal appearance. A good sign that this will happen is if the weakness or other symptoms begin to resolve after 1 week.
In other cases, symptoms may take several months to disappear. Lasting effects are possible, though rare.
Treatments your doctor may prescribe
If a viral infection is the likely cause of your symptoms, your doctor may have you take acyclovir (Zovirax), famciclovir (Famvir), or another antiviral medication to speed your recovery. These antiviral medications are taken as pills, usually a few times a day for 10 days.
A steroid (prednisone, for example) may also help to reduce swelling that could be pressing on the facial nerve. This medication is also administered as a pill over 1 to 2 weeks.
If you cannot blink, and dryness of the eye is one of your symptoms, your doctor will ask you to use moisturizing eye drops to protect the eye from damage while you recover.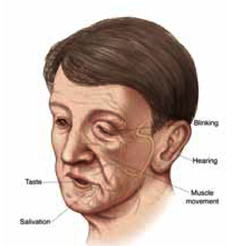
The variety of different symptoms you are experiencing is due to the fact the facial nerve controls normal functions from your forehead to your chin—including tearing, taste, muscle movement, and blinking.
1. Taverner D, Cohen SB, Hutchinson BC. Comparison of corticotrophin and prednisolone in treatment of idiopathic facial paralysis (Bell’s palsy). Br Med J 1971;4:20-2.
2. Adour KK, Wingerd J, Bell DN, Manning JJ, Hurley JP. Prednisone treatment for idiopathic facial paralysis (Bell’s palsy). N Engl J Med 1972;287:1268-72.
3. May M, Wette R, Hardin WB, Jr, Sullivan J. The use of steroids in Bell’s palsy: a prospective controlled study. Laryngoscope 1976;86:1111-22.
4. Jalaludin MA. Methylcobalamin treatment of Bell’s palsy. Methods Find Exp Clin Pharmacol 1995;17:539-44.
5. Wolf SM, Wagner JH, Davidson S, Forsythe A. Treatment of Bell palsy with prednisone: a prospective, randomized study. Neurology 1978;28:158-61.
6. Unuvar E, Oguz F, Sidal M, Kilic A. Corticosteroid treatment of childhood Bell’s palsy. Pediatr Neurol 1999;21:814-6.
7. De Diego JI, Prim MP, De Sarria MJ, Madero R, Gavilan J. Idiopathic facial paralysis: a randomized, prospective, and controlled study using single-dose prednisone versus acyclovir three times daily. Laryngoscope 1998;108:573-5.
8. Adour KK, Rubayaines JM, Von Doersten PG, Byl FM, Trent CS, Quesenberry CP, Jr, et al. Bell’s palsy treatment with acyclovir and prednisone compared with prednisone alone: a double-blind, randomized, controlled trial. Ann Otol Rhinol Laryngol 1996;105:371-8.
9. Grogan PM, Gronseth GS. Practice parameter: Steroids, acyclovir, and surgery for Bell’s palsy (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2001;56:830-6.
10. Salinas RA, Alvarez G, Alvarez MI, Ferreira J. Corticosteroids for Bell’s palsy (idiopathic facial paralysis) (Cochrane Review). In: The Cochrane Library, Issue 2, 2002. Oxford: Update Software. Updated quarterly.
11. Sipe J, Dunn L. Aciclovir for Bell’s palsy (idiopathic facial paralysis) (Cochrane Review). In: The Cochrane Library, Issue 2, 2002. Oxford: Update Software. Updated quarterly.
Early use of corticosteroid therapy results in less autonomic synkinesis and possibly improved rates of recovery in adults (strength of recommendation: C); there is no proven benefit in children (SOR: B).
Adding acyclovir (Zovirax) to prednisone therapy may improve recovery rates compared with prednisone alone (SOR: C).
The results of 1 nonblinded study indicate that intramuscular methylcobalamin (vitamin B12) used alone or in combination with prednisone may shorten time to recovery (SOR: C).
See the Patient Information at the end of this article.
Evidence summary
Bell’s palsy is a lower motor neuron disease of the facial nerve characterized by a transient paralysis. Healing is occasionally incomplete, resulting in residual nerve dysfunction, including partial palsy and motor synkinesis (involuntary movement accompanying a voluntary one) and autonomic synkinesis (involuntary lacrimation after a voluntary muscle movement). Bell’s palsy is associated with significant edema and ischemia of the facial nerve as it passes through its bony canal.
Herpes simplex reactivation has been shown to be associated with a large proportion of cases.
Corticosteroids are the most studied form of therapy for Bell’s palsy (Table). Early work in England culminated in 1971 with a well-performed study demonstrating lower rates of incomplete recovery with prednisolone compared with corticotrophin.1 A potentially definitive randomized controlled trial in 1970 was stopped prematurely because of investigators’ subjective impression that prednisone markedly reduced postauricular pain.2 Subsequently, the highest-quality study had few patients (n=51) and reported no difference in outcomes between patients receiving 10 days of oral prednisone plus vitamins and those receiving vitamins alone.3
One open randomized controlled trial demonstrated shorter mean recovery times with intramuscular methylcobalamin (1.95 weeks) and methylcobalamin plus prednisone (2.0 weeks) compared with prednisone alone (9.6 weeks).4 Another trial of 239 patients showed improved rates of autonomic synkinesis after treatment with 16 days of prednisone compared with placebo.5
A randomized, controlled trial of children 2 to 6 years of age found no significant differences in short-term recovery after treatment with methylprednisolone compared with untreated controls.6 Eventually, all these children recovered normal facial nerve function within 12 months.
Two randomized controlled trials have assessed the efficacy of acyclovir for treatment of Bell’s palsy. One trial compared prednisone with acyclovir and found patients treated with prednisone had better complete recovery rates, 93.6% versus 77.7% (absolute risk reduction [ARR]=15.9%, 95% confidence interval [CI]=2.8%–29%], number needed to treat [NNT]=7).7
Another study demonstrated that the combination of prednisone and acyclovir had greater complete recovery rates compared with prednisone alone (92% vs. 76%, ARR=16%, 95% CI=1.7%–30.3%, NNT=7).8
Overall, the data suggest corticosteroid therapy may provide a small clinical benefit in adult patients with Bell’s palsy. In many of these studies, patients who had contraindications to steroid therapy (peptic ulcer disease, uncontrolled diabetes, hypertension, or immunosuppression) were excluded.
If no contraindications to steroids exist, it is resonable to initiate treatment with corticosteroids for an adult patient with new-onset Bell’s palsy. Most studies have started patients on steroids within 10 days of onset of symptoms.
TABLE
Therapies for Bell’s palsy
| Drug | Dosage | SOR |
|---|---|---|
| Prednisone (adults only) | Total from 410 mg over 10 days, to 760 mg over 16 days (tapering doses) | C |
| Acyclovir | 400 mg 5x/d for 10 days | C |
| Methylcobalamin | 500 (g IM 3x/wk until full recovery, or for 8 weeks | C |
| SOR, Strength of recommendation | ||
Recommendations from others
A practice parameter from the American Academy of Neurology states that steroids are safe and probably effective (SOR: B), whereas acyclovir is safe and possibly effective (SOR: C).9 Systematic reviews from the Cochrane Database report that available evidence from randomized controlled trials does not show significant benefit from treating Bell’s palsy with corticosteroids and that clinical trials on acyclovir are inconclusive and therefore cannot be used to make recommendations regarding its use.10,11
Steven H. Horowitz, MD
University of Vermont College of Medicine, Burlington
My practice of neurology began before the era of corticosteroid treatment for Bell’s palsy. Despite the lack of convincing evidenced-based data, it is my clinical impression that there are far fewer patients today with incompletely resolved Bell’s palsy than before the widespread use of steroids. Permanent facial deformities seemed more common back then. Therefore, in the absence of harmful effects, I will continue treating with steroids.
PATIENT INFORMATION
What is Bell’s palsy?
Weakness and slumping on one side of the face are common features of this condition in which the nerve controlling the face has been injured. Other symptoms are:
- Inability to move affected side of the face
- Drooping mouth, unblinking eye
- Numbness
- Twitching of facial muscles
- Taste disturbance
- Increased sensitivity to sound.
Symptoms usually start suddenly. Pain behind the ear may be felt hours to days before other symptoms appear. People between ages 30 and 60 years are most likely to be affected, but this disorder can happen at any age.
Any sudden weakness of the face also suggests the possibility of stroke—a serious emergency. You should contact your physician immediately.
Possible causes
The most common cause of Bell’s palsy is an infection of the facial nerve by the herpes simplex virus. Your doctor will also ask about possible recent trauma to the face and will check for swelling of facial tissues or a mass pressing on the facial nerve.
What to expect
In many cases, the symptoms of Bell’s palsy go away in about 3 weeks without treatment, and the face regains its normal appearance. A good sign that this will happen is if the weakness or other symptoms begin to resolve after 1 week.
In other cases, symptoms may take several months to disappear. Lasting effects are possible, though rare.
Treatments your doctor may prescribe
If a viral infection is the likely cause of your symptoms, your doctor may have you take acyclovir (Zovirax), famciclovir (Famvir), or another antiviral medication to speed your recovery. These antiviral medications are taken as pills, usually a few times a day for 10 days.
A steroid (prednisone, for example) may also help to reduce swelling that could be pressing on the facial nerve. This medication is also administered as a pill over 1 to 2 weeks.
If you cannot blink, and dryness of the eye is one of your symptoms, your doctor will ask you to use moisturizing eye drops to protect the eye from damage while you recover.
The variety of different symptoms you are experiencing is due to the fact the facial nerve controls normal functions from your forehead to your chin—including tearing, taste, muscle movement, and blinking.
Early use of corticosteroid therapy results in less autonomic synkinesis and possibly improved rates of recovery in adults (strength of recommendation: C); there is no proven benefit in children (SOR: B).
Adding acyclovir (Zovirax) to prednisone therapy may improve recovery rates compared with prednisone alone (SOR: C).
The results of 1 nonblinded study indicate that intramuscular methylcobalamin (vitamin B12) used alone or in combination with prednisone may shorten time to recovery (SOR: C).
See the Patient Information at the end of this article.
Evidence summary
Bell’s palsy is a lower motor neuron disease of the facial nerve characterized by a transient paralysis. Healing is occasionally incomplete, resulting in residual nerve dysfunction, including partial palsy and motor synkinesis (involuntary movement accompanying a voluntary one) and autonomic synkinesis (involuntary lacrimation after a voluntary muscle movement). Bell’s palsy is associated with significant edema and ischemia of the facial nerve as it passes through its bony canal.
Herpes simplex reactivation has been shown to be associated with a large proportion of cases.
Corticosteroids are the most studied form of therapy for Bell’s palsy (Table). Early work in England culminated in 1971 with a well-performed study demonstrating lower rates of incomplete recovery with prednisolone compared with corticotrophin.1 A potentially definitive randomized controlled trial in 1970 was stopped prematurely because of investigators’ subjective impression that prednisone markedly reduced postauricular pain.2 Subsequently, the highest-quality study had few patients (n=51) and reported no difference in outcomes between patients receiving 10 days of oral prednisone plus vitamins and those receiving vitamins alone.3
One open randomized controlled trial demonstrated shorter mean recovery times with intramuscular methylcobalamin (1.95 weeks) and methylcobalamin plus prednisone (2.0 weeks) compared with prednisone alone (9.6 weeks).4 Another trial of 239 patients showed improved rates of autonomic synkinesis after treatment with 16 days of prednisone compared with placebo.5
A randomized, controlled trial of children 2 to 6 years of age found no significant differences in short-term recovery after treatment with methylprednisolone compared with untreated controls.6 Eventually, all these children recovered normal facial nerve function within 12 months.
Two randomized controlled trials have assessed the efficacy of acyclovir for treatment of Bell’s palsy. One trial compared prednisone with acyclovir and found patients treated with prednisone had better complete recovery rates, 93.6% versus 77.7% (absolute risk reduction [ARR]=15.9%, 95% confidence interval [CI]=2.8%–29%], number needed to treat [NNT]=7).7
Another study demonstrated that the combination of prednisone and acyclovir had greater complete recovery rates compared with prednisone alone (92% vs. 76%, ARR=16%, 95% CI=1.7%–30.3%, NNT=7).8
Overall, the data suggest corticosteroid therapy may provide a small clinical benefit in adult patients with Bell’s palsy. In many of these studies, patients who had contraindications to steroid therapy (peptic ulcer disease, uncontrolled diabetes, hypertension, or immunosuppression) were excluded.
If no contraindications to steroids exist, it is resonable to initiate treatment with corticosteroids for an adult patient with new-onset Bell’s palsy. Most studies have started patients on steroids within 10 days of onset of symptoms.
TABLE
Therapies for Bell’s palsy
| Drug | Dosage | SOR |
|---|---|---|
| Prednisone (adults only) | Total from 410 mg over 10 days, to 760 mg over 16 days (tapering doses) | C |
| Acyclovir | 400 mg 5x/d for 10 days | C |
| Methylcobalamin | 500 (g IM 3x/wk until full recovery, or for 8 weeks | C |
| SOR, Strength of recommendation | ||
Recommendations from others
A practice parameter from the American Academy of Neurology states that steroids are safe and probably effective (SOR: B), whereas acyclovir is safe and possibly effective (SOR: C).9 Systematic reviews from the Cochrane Database report that available evidence from randomized controlled trials does not show significant benefit from treating Bell’s palsy with corticosteroids and that clinical trials on acyclovir are inconclusive and therefore cannot be used to make recommendations regarding its use.10,11
Steven H. Horowitz, MD
University of Vermont College of Medicine, Burlington
My practice of neurology began before the era of corticosteroid treatment for Bell’s palsy. Despite the lack of convincing evidenced-based data, it is my clinical impression that there are far fewer patients today with incompletely resolved Bell’s palsy than before the widespread use of steroids. Permanent facial deformities seemed more common back then. Therefore, in the absence of harmful effects, I will continue treating with steroids.
PATIENT INFORMATION
What is Bell’s palsy?
Weakness and slumping on one side of the face are common features of this condition in which the nerve controlling the face has been injured. Other symptoms are:
- Inability to move affected side of the face
- Drooping mouth, unblinking eye
- Numbness
- Twitching of facial muscles
- Taste disturbance
- Increased sensitivity to sound.
Symptoms usually start suddenly. Pain behind the ear may be felt hours to days before other symptoms appear. People between ages 30 and 60 years are most likely to be affected, but this disorder can happen at any age.
Any sudden weakness of the face also suggests the possibility of stroke—a serious emergency. You should contact your physician immediately.
Possible causes
The most common cause of Bell’s palsy is an infection of the facial nerve by the herpes simplex virus. Your doctor will also ask about possible recent trauma to the face and will check for swelling of facial tissues or a mass pressing on the facial nerve.
What to expect
In many cases, the symptoms of Bell’s palsy go away in about 3 weeks without treatment, and the face regains its normal appearance. A good sign that this will happen is if the weakness or other symptoms begin to resolve after 1 week.
In other cases, symptoms may take several months to disappear. Lasting effects are possible, though rare.
Treatments your doctor may prescribe
If a viral infection is the likely cause of your symptoms, your doctor may have you take acyclovir (Zovirax), famciclovir (Famvir), or another antiviral medication to speed your recovery. These antiviral medications are taken as pills, usually a few times a day for 10 days.
A steroid (prednisone, for example) may also help to reduce swelling that could be pressing on the facial nerve. This medication is also administered as a pill over 1 to 2 weeks.
If you cannot blink, and dryness of the eye is one of your symptoms, your doctor will ask you to use moisturizing eye drops to protect the eye from damage while you recover.
The variety of different symptoms you are experiencing is due to the fact the facial nerve controls normal functions from your forehead to your chin—including tearing, taste, muscle movement, and blinking.
1. Taverner D, Cohen SB, Hutchinson BC. Comparison of corticotrophin and prednisolone in treatment of idiopathic facial paralysis (Bell’s palsy). Br Med J 1971;4:20-2.
2. Adour KK, Wingerd J, Bell DN, Manning JJ, Hurley JP. Prednisone treatment for idiopathic facial paralysis (Bell’s palsy). N Engl J Med 1972;287:1268-72.
3. May M, Wette R, Hardin WB, Jr, Sullivan J. The use of steroids in Bell’s palsy: a prospective controlled study. Laryngoscope 1976;86:1111-22.
4. Jalaludin MA. Methylcobalamin treatment of Bell’s palsy. Methods Find Exp Clin Pharmacol 1995;17:539-44.
5. Wolf SM, Wagner JH, Davidson S, Forsythe A. Treatment of Bell palsy with prednisone: a prospective, randomized study. Neurology 1978;28:158-61.
6. Unuvar E, Oguz F, Sidal M, Kilic A. Corticosteroid treatment of childhood Bell’s palsy. Pediatr Neurol 1999;21:814-6.
7. De Diego JI, Prim MP, De Sarria MJ, Madero R, Gavilan J. Idiopathic facial paralysis: a randomized, prospective, and controlled study using single-dose prednisone versus acyclovir three times daily. Laryngoscope 1998;108:573-5.
8. Adour KK, Rubayaines JM, Von Doersten PG, Byl FM, Trent CS, Quesenberry CP, Jr, et al. Bell’s palsy treatment with acyclovir and prednisone compared with prednisone alone: a double-blind, randomized, controlled trial. Ann Otol Rhinol Laryngol 1996;105:371-8.
9. Grogan PM, Gronseth GS. Practice parameter: Steroids, acyclovir, and surgery for Bell’s palsy (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2001;56:830-6.
10. Salinas RA, Alvarez G, Alvarez MI, Ferreira J. Corticosteroids for Bell’s palsy (idiopathic facial paralysis) (Cochrane Review). In: The Cochrane Library, Issue 2, 2002. Oxford: Update Software. Updated quarterly.
11. Sipe J, Dunn L. Aciclovir for Bell’s palsy (idiopathic facial paralysis) (Cochrane Review). In: The Cochrane Library, Issue 2, 2002. Oxford: Update Software. Updated quarterly.
1. Taverner D, Cohen SB, Hutchinson BC. Comparison of corticotrophin and prednisolone in treatment of idiopathic facial paralysis (Bell’s palsy). Br Med J 1971;4:20-2.
2. Adour KK, Wingerd J, Bell DN, Manning JJ, Hurley JP. Prednisone treatment for idiopathic facial paralysis (Bell’s palsy). N Engl J Med 1972;287:1268-72.
3. May M, Wette R, Hardin WB, Jr, Sullivan J. The use of steroids in Bell’s palsy: a prospective controlled study. Laryngoscope 1976;86:1111-22.
4. Jalaludin MA. Methylcobalamin treatment of Bell’s palsy. Methods Find Exp Clin Pharmacol 1995;17:539-44.
5. Wolf SM, Wagner JH, Davidson S, Forsythe A. Treatment of Bell palsy with prednisone: a prospective, randomized study. Neurology 1978;28:158-61.
6. Unuvar E, Oguz F, Sidal M, Kilic A. Corticosteroid treatment of childhood Bell’s palsy. Pediatr Neurol 1999;21:814-6.
7. De Diego JI, Prim MP, De Sarria MJ, Madero R, Gavilan J. Idiopathic facial paralysis: a randomized, prospective, and controlled study using single-dose prednisone versus acyclovir three times daily. Laryngoscope 1998;108:573-5.
8. Adour KK, Rubayaines JM, Von Doersten PG, Byl FM, Trent CS, Quesenberry CP, Jr, et al. Bell’s palsy treatment with acyclovir and prednisone compared with prednisone alone: a double-blind, randomized, controlled trial. Ann Otol Rhinol Laryngol 1996;105:371-8.
9. Grogan PM, Gronseth GS. Practice parameter: Steroids, acyclovir, and surgery for Bell’s palsy (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2001;56:830-6.
10. Salinas RA, Alvarez G, Alvarez MI, Ferreira J. Corticosteroids for Bell’s palsy (idiopathic facial paralysis) (Cochrane Review). In: The Cochrane Library, Issue 2, 2002. Oxford: Update Software. Updated quarterly.
11. Sipe J, Dunn L. Aciclovir for Bell’s palsy (idiopathic facial paralysis) (Cochrane Review). In: The Cochrane Library, Issue 2, 2002. Oxford: Update Software. Updated quarterly.
Evidence-based answers from the Family Physicians Inquiries Network