User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
A perplexing case of altered mental status
Discuss this article at www.facebook.com/CurrentPsychiatry
CASE: Agitated and paranoid
Mr. E, age 55, presents to the emergency department (ED) with a 2-week history of altered mental status (AMS). His wife reports, “He was normal one day and the next day he was not.” Mr. E also presents with sleep disturbance, decreased appetite and speech, and a 20-lb weight loss. His family reports no recent stressors or head trauma. Mr. E is agitated in the ED and receives a single dose of IV haloperidol, 5 mg. He exhibits paranoia and is afraid to get a CT scan. The medical team attempts a lumbar puncture (LP), but Mr. E does not cooperate.
His laboratory values are: potassium, 3.0 mEq/L; creatinine, 1.60 mg/dL; calcium, 10.6 mg/dL; thyroid-stimulating hormone, 0.177 IU/L; vitamin B12, >1500 pg/mL; folate, >20 ng/mL; and creatine kinase, 281 U/L. Urine drug screen is positive for benzodiazepines and opiates, neither of which was prescribed, and blood alcohol is negative.
Mr. E is admitted for further workup of AMS. His daughter-in-law states that Mr. E is an alcoholic and she is concerned that he may have mixed drugs and alcohol. The medical service starts Mr. E on empiric antimicrobials—vancomycin, ceftriaxone, and acyclovir—because of his AMS, and performs an LP to rule out intracranial pathology. His LP results are unremarkable.
Mr. E appears to be confused during psychiatric evaluation. He requests to be “hypnotized on a helicopter to find out what is wrong with me.” His wife states that Mr. E drank vodka daily but decreased his alcohol consumption after surgery 5 months ago. Before his current admission, he was drinking approximately half a glass of vodka every few days, according to his wife. Mr. E says he has no prior psychiatric admissions. During the mental status exam, his eye contact is poor, with latency of response to questions, thought blocking, and psychomotor retardation. He is alert, oriented to time, place, and person, and cooperative. He cannot concentrate or focus during the interview. He denies suicidal or homicidal ideation.
The authors’ observations
Mr. E appeared to be delirious, as evidenced by the sudden onset of waxing and waning changes in consciousness, attention deficits, and cognition. He also had a history of daily alcohol use and decreased his alcohol intake after a surgery 5 months ago, which puts him at risk for Wernicke’s encephalopathy.1-3 The type of surgery and whether he received adequate thiamine supplementation at that time was unclear. Because Mr. E is older, he has a higher risk of mortality and morbidity from delirium.4,5 We started Mr. E on quetiapine, 50 mg/d, for delirium and an IV lorazepam taper, starting at 2 mg every 8 hours, because the extent of his alcohol and benzodiazepine use was unclear—we weren’t sure how forthcoming he was about his alcohol use. He received IV thiamine supplementation followed by oral thiamine, 100 mg/d.
The authors’ recommendations
We requested a neurology consult, EEG, CSF cultures, and brain MRI (Table 1).6 EEG, chest radiography, thyroid scan, and CT scan were normal and MRI showed no acute intracranial process. However, there was a redemonstration of increased T1 signal seen within the bilateral basal ganglia and relative diminutive appearance to the bilateral mamillary bodies, which suggests possible liver disease and/or alcohol abuse. These findings were unchanged from an MRI Mr. E received 10 years ago, were consistent with his history of alcohol abuse, and may indicate an underlying predisposition to delirium. A CT scan of the abdomen showed hepatic cirrhosis with prominent, tortuous vessels of the upper abdomen, subtle ill-defined hypodensity of the anterior aspect of the liver, and an enlarged spleen.
Mr. E’s mental functioning did not improve with quetiapine and lorazepam. Further evaluation revealed a negative human immunodeficiency virus test and normal heavy metals, ammonia, ceruloplasmin, and thiamine. We suspected limbic encephalitis because of Mr. E’s memory problems and behavioral and psychiatric manifestations,7 but CSF was unremarkable and limbic encephalitis workup of CSF and paraneoplastic antibody panel were negative.
Mr. E’s primary care physician stated that at an appointment 1 month ago, Mr. E was alert, oriented, and conversational with normal thought processing. At that time he had presented with rectal bleeding, occult blood in his stool, and an unintentional 25-lb weight loss over 2 months. It was not clear if his weight loss was caused by poor nutrition—which is common among chronic alcoholics—or an occult disease process.
After 10 days, Mr. E was discharged home from the medicine service with no clear cause of his AMS.
Table 1
Suggested workup for altered mental status
| Complete blood count, basic metabolic profile, creatine kinase |
| Thyroid-stimulating hormone, thyroid scan |
| Vitamin B12, folate, thiamine |
| Blood alcohol, urine drug screen |
| Urine analysis and cultures |
| Lumbar puncture—CSF staining and cultures |
| Chest radiography |
| CT and MRI scan of brain |
| Electroencephalography |
| Neuropsychiatric testing |
| CSF: cerebrospinal fluid Source: Reference 6 |
EVALUATION: Worsening behavior
One week later, Mr. E presents to the ED with continued AMS and worsening behavior at home. Two days ago, he attempted to strangle his dog and cut himself with a knife. His paranoia was worsening and his oral intake continued to decrease. In the ED, Mr. E does not want a chest radiograph because, “I don’t like radiation contaminating my body”; his family stated that he had been suspicious of radiography all of his life. He receives empiric ceftriaxone because of a possible urinary tract infection. Urine culture is positive for Pseudomonas aeruginosa and he is switched to ciprofloxacin. Mr. E is admitted for further workup.
Mr. E’s mother states, “I think this change in behavior is related to my son drinking alcohol for 20 years. This is exactly how he acted when he was on drugs. I think he is having a flashback.” She also reports her son purchased multiple chemicals—the details of which are unclear—that he left lying around the house.
His wife says that after discharge a week ago, Mr. E was stable for 1 or 2 days and then “he started going downhill.” He became more paranoid and he started talking about cameras watching him in his house. Mr. E took quetiapine, 50 mg/d, for a few days, then refused because he thought there was something in the medication. Mr. E’s family feels that at times he is responding to internal stimuli. He makes statements about his DNA being changed and reports that he has 2 wives and the wife in the room was not the real one, which suggests Capgras syndrome. His wife provides a home medication list that includes vitamin B complex, vitamins B12, E, and C, a multivitamin, zinc, magnesium, fish oil, garlic, calcium, glucosamine, chondroitin, herbal supplements, and gingko. The psychiatry team recommends switching from quetiapine to olanzapine, 15 mg/d, because Mr. E was paranoid about taking quetiapine.
We determine that Mr. E does not have medical decision-making capacity.
Because his symptoms do not improve, Mr. E is transferred to the psychiatric intensive care unit. His mental status shows little change while there. Neuropsychiatric testing shows only “cognitive deficits.” He shows signs consistent with neurologic dysfunction in terms of stimulus-bound responding and perseveration, which is compatible with the bilateral basal ganglia lesion seen on MRI. However, some of his behaviors suggest psychiatric and motivationally driven or manipulative etiology. During this testing he was difficult to evaluate and needed to be convinced to engage. At times he was illogical and at other times he showed good focus and recall. It is difficult to draw more definitive conclusions and Mr. E is discharged home with minor improvement in his symptoms. He didn’t attend follow-up appointments. During a courtesy call a few months after his admission, his wife revealed that Mr. E had died after shooting himself. It is unclear if it was an accident or suicide.
The authors’ observations
Mr. E’s diagnosis remains unclear (for a summary of his clinical course, see Table 2). Although his initial presentation was consistent with delirium, the lack of an identifiable medical cause, prolonged time course, and lack of improvement with dopamine blocking agents suggest additional diagnoses such as Wernicke-Korsakoff syndrome, rapidly progressive dementia, or a substance-induced disorder. He displayed paranoia and bizarre delusions, which would suggest a thought disorder. However, he also had a history of substance use. A few months after we saw Mr. E, “bath salt” (methylenedioxypyrovalerone) abuse gained national attention. Patients with bath salt intoxication present with confusion, paranoia, and behavioral disturbances as well as a prolonged course.8
Mr. E’s CT and MRI scans, history of alcohol use, and cirrhosis also point to Wernicke-Korsakoff syndrome as an underlying diagnosis. It is unclear whether Mr. E experienced alcohol withdrawal and IV glucose without adequate thiamine replacement during a prior surgery. However, MRI findings were unchanged from a previous study 10 years ago.
It is puzzling whether Mr. E’s AMS was a first psychotic break, a result of drug and alcohol use, rapidly progressing dementia, or another neurologic problem that we have not identified. Our tentative diagnosis was Wernicke-Korsakoff syndrome because of his history of alcohol use and imaging findings.
Although we used a multidisciplinary team approach that included psychiatry, internal medicine, neurology, neuropsychology, and an aggressive and thorough workup, we could not establish a definitive diagnosis. Unsolved cases such as this can leave patients and clinicians frustrated and may lead to unfavorable outcomes. Additional resources such as a telephone call after the first missed appointment may have been warranted.
Table 2
Mr. E’s clinical course
| Symptoms | Treatment | |
|---|---|---|
| First ED visit | Agitation Confusion Sleep disturbance Decreased appetite and speech 20-lb weight loss | Empiric antimicrobials for possible meningitis Haloperidol for agitation Quetiapine for delirium Lorazepam taper Thiamine supplementation |
| Second ED visit | Violent behavior Worsening paranoia Responding to internal stimuli Mr. E believes he has 2 wives, but the wife in the room is not the real one, which suggests possible Capgras syndrome Cognitive deficits on mental status exam | Switch from ceftriaxone to ciprofloxacin for Pseudomonas aeruginosa Switch from quetiapine to olanzapine |
| ED: emergency department | ||
Related Resources
- Kaufman DM. Clinical neurology for psychiatrists. 6th ed. Philadelphia, PA: Saunders Elsevier; 2007.
- Sidhu KS, Balon R, Ajluni V, et al. Standard EEG and the difficult-to-assess mental status. Ann Clin Psychiatry. 2009;21(2):103-108.
Drug Brand Names
- Acyclovir • Zovirax
- Ceftriaxone • Rocephin
- Ciprofloxacin • Cipro
- Haloperidol • Haldol
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Thiamine • Betaxin
- Vancomycin • Vancocin
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Jiang W, Gagliardi JP, Raj YP, et al. Acute psychotic disorder after gastric bypass surgery: differential diagnosis and treatment. Am J Psychiatry. 2006;163(1):15-19.
2. Harrison RA, Vu T, Hunter AJ. Wernicke’s encephalopathy in a patient with schizophrenia. J Gen Intern Med. 2006;21(12):C8-C11.
3. Sechi GP, Serra A. Wernicke’s encephalopathy: new clinical settings and recent advances in diagnosis and treatment. Lancet Neurol. 2007;6(5):442-455.
4. American Psychiatric Association. Practice guidelines for the treatment of patients with delirium. Am J Psychiatry. 1999;156(5 suppl):1-20.
5. Sharon KI, Fearing MA, Marcantonio RA. Delirium. In: Halter JB Ouslander JG, Tinetti ME, et al, eds. Hazzard’s geriatric medicine and gerontology. 6th ed. New York, NY: McGraw-Hill Medical; 2009:647–658.
6. Sadock BJ, Sadock VA. Delirium dementia, and amnestic and other cognitive disorders. In: Sadock BJ, Kaplan HI, Sadock VA. Kaplan and Sadock’s synopsis of psychiatry: behavioral sciences/clinical psychiatry. Philadelphia, PA: Lippincott Williams and Wilkins; 2007:319–372.
7. Ahmad SA, Archer HA, Rice CM, et al. Seronegative limbic encephalitis: case report, literature review and proposed treatment algorithm. Pract Neurol. 2011;11(6):355-361.
8. Ross EA, Watson M, Goldberger B. “Bath salts” intoxication. N Engl J Med. 2011;365(10):967-968.
Discuss this article at www.facebook.com/CurrentPsychiatry
CASE: Agitated and paranoid
Mr. E, age 55, presents to the emergency department (ED) with a 2-week history of altered mental status (AMS). His wife reports, “He was normal one day and the next day he was not.” Mr. E also presents with sleep disturbance, decreased appetite and speech, and a 20-lb weight loss. His family reports no recent stressors or head trauma. Mr. E is agitated in the ED and receives a single dose of IV haloperidol, 5 mg. He exhibits paranoia and is afraid to get a CT scan. The medical team attempts a lumbar puncture (LP), but Mr. E does not cooperate.
His laboratory values are: potassium, 3.0 mEq/L; creatinine, 1.60 mg/dL; calcium, 10.6 mg/dL; thyroid-stimulating hormone, 0.177 IU/L; vitamin B12, >1500 pg/mL; folate, >20 ng/mL; and creatine kinase, 281 U/L. Urine drug screen is positive for benzodiazepines and opiates, neither of which was prescribed, and blood alcohol is negative.
Mr. E is admitted for further workup of AMS. His daughter-in-law states that Mr. E is an alcoholic and she is concerned that he may have mixed drugs and alcohol. The medical service starts Mr. E on empiric antimicrobials—vancomycin, ceftriaxone, and acyclovir—because of his AMS, and performs an LP to rule out intracranial pathology. His LP results are unremarkable.
Mr. E appears to be confused during psychiatric evaluation. He requests to be “hypnotized on a helicopter to find out what is wrong with me.” His wife states that Mr. E drank vodka daily but decreased his alcohol consumption after surgery 5 months ago. Before his current admission, he was drinking approximately half a glass of vodka every few days, according to his wife. Mr. E says he has no prior psychiatric admissions. During the mental status exam, his eye contact is poor, with latency of response to questions, thought blocking, and psychomotor retardation. He is alert, oriented to time, place, and person, and cooperative. He cannot concentrate or focus during the interview. He denies suicidal or homicidal ideation.
The authors’ observations
Mr. E appeared to be delirious, as evidenced by the sudden onset of waxing and waning changes in consciousness, attention deficits, and cognition. He also had a history of daily alcohol use and decreased his alcohol intake after a surgery 5 months ago, which puts him at risk for Wernicke’s encephalopathy.1-3 The type of surgery and whether he received adequate thiamine supplementation at that time was unclear. Because Mr. E is older, he has a higher risk of mortality and morbidity from delirium.4,5 We started Mr. E on quetiapine, 50 mg/d, for delirium and an IV lorazepam taper, starting at 2 mg every 8 hours, because the extent of his alcohol and benzodiazepine use was unclear—we weren’t sure how forthcoming he was about his alcohol use. He received IV thiamine supplementation followed by oral thiamine, 100 mg/d.
The authors’ recommendations
We requested a neurology consult, EEG, CSF cultures, and brain MRI (Table 1).6 EEG, chest radiography, thyroid scan, and CT scan were normal and MRI showed no acute intracranial process. However, there was a redemonstration of increased T1 signal seen within the bilateral basal ganglia and relative diminutive appearance to the bilateral mamillary bodies, which suggests possible liver disease and/or alcohol abuse. These findings were unchanged from an MRI Mr. E received 10 years ago, were consistent with his history of alcohol abuse, and may indicate an underlying predisposition to delirium. A CT scan of the abdomen showed hepatic cirrhosis with prominent, tortuous vessels of the upper abdomen, subtle ill-defined hypodensity of the anterior aspect of the liver, and an enlarged spleen.
Mr. E’s mental functioning did not improve with quetiapine and lorazepam. Further evaluation revealed a negative human immunodeficiency virus test and normal heavy metals, ammonia, ceruloplasmin, and thiamine. We suspected limbic encephalitis because of Mr. E’s memory problems and behavioral and psychiatric manifestations,7 but CSF was unremarkable and limbic encephalitis workup of CSF and paraneoplastic antibody panel were negative.
Mr. E’s primary care physician stated that at an appointment 1 month ago, Mr. E was alert, oriented, and conversational with normal thought processing. At that time he had presented with rectal bleeding, occult blood in his stool, and an unintentional 25-lb weight loss over 2 months. It was not clear if his weight loss was caused by poor nutrition—which is common among chronic alcoholics—or an occult disease process.
After 10 days, Mr. E was discharged home from the medicine service with no clear cause of his AMS.
Table 1
Suggested workup for altered mental status
| Complete blood count, basic metabolic profile, creatine kinase |
| Thyroid-stimulating hormone, thyroid scan |
| Vitamin B12, folate, thiamine |
| Blood alcohol, urine drug screen |
| Urine analysis and cultures |
| Lumbar puncture—CSF staining and cultures |
| Chest radiography |
| CT and MRI scan of brain |
| Electroencephalography |
| Neuropsychiatric testing |
| CSF: cerebrospinal fluid Source: Reference 6 |
EVALUATION: Worsening behavior
One week later, Mr. E presents to the ED with continued AMS and worsening behavior at home. Two days ago, he attempted to strangle his dog and cut himself with a knife. His paranoia was worsening and his oral intake continued to decrease. In the ED, Mr. E does not want a chest radiograph because, “I don’t like radiation contaminating my body”; his family stated that he had been suspicious of radiography all of his life. He receives empiric ceftriaxone because of a possible urinary tract infection. Urine culture is positive for Pseudomonas aeruginosa and he is switched to ciprofloxacin. Mr. E is admitted for further workup.
Mr. E’s mother states, “I think this change in behavior is related to my son drinking alcohol for 20 years. This is exactly how he acted when he was on drugs. I think he is having a flashback.” She also reports her son purchased multiple chemicals—the details of which are unclear—that he left lying around the house.
His wife says that after discharge a week ago, Mr. E was stable for 1 or 2 days and then “he started going downhill.” He became more paranoid and he started talking about cameras watching him in his house. Mr. E took quetiapine, 50 mg/d, for a few days, then refused because he thought there was something in the medication. Mr. E’s family feels that at times he is responding to internal stimuli. He makes statements about his DNA being changed and reports that he has 2 wives and the wife in the room was not the real one, which suggests Capgras syndrome. His wife provides a home medication list that includes vitamin B complex, vitamins B12, E, and C, a multivitamin, zinc, magnesium, fish oil, garlic, calcium, glucosamine, chondroitin, herbal supplements, and gingko. The psychiatry team recommends switching from quetiapine to olanzapine, 15 mg/d, because Mr. E was paranoid about taking quetiapine.
We determine that Mr. E does not have medical decision-making capacity.
Because his symptoms do not improve, Mr. E is transferred to the psychiatric intensive care unit. His mental status shows little change while there. Neuropsychiatric testing shows only “cognitive deficits.” He shows signs consistent with neurologic dysfunction in terms of stimulus-bound responding and perseveration, which is compatible with the bilateral basal ganglia lesion seen on MRI. However, some of his behaviors suggest psychiatric and motivationally driven or manipulative etiology. During this testing he was difficult to evaluate and needed to be convinced to engage. At times he was illogical and at other times he showed good focus and recall. It is difficult to draw more definitive conclusions and Mr. E is discharged home with minor improvement in his symptoms. He didn’t attend follow-up appointments. During a courtesy call a few months after his admission, his wife revealed that Mr. E had died after shooting himself. It is unclear if it was an accident or suicide.
The authors’ observations
Mr. E’s diagnosis remains unclear (for a summary of his clinical course, see Table 2). Although his initial presentation was consistent with delirium, the lack of an identifiable medical cause, prolonged time course, and lack of improvement with dopamine blocking agents suggest additional diagnoses such as Wernicke-Korsakoff syndrome, rapidly progressive dementia, or a substance-induced disorder. He displayed paranoia and bizarre delusions, which would suggest a thought disorder. However, he also had a history of substance use. A few months after we saw Mr. E, “bath salt” (methylenedioxypyrovalerone) abuse gained national attention. Patients with bath salt intoxication present with confusion, paranoia, and behavioral disturbances as well as a prolonged course.8
Mr. E’s CT and MRI scans, history of alcohol use, and cirrhosis also point to Wernicke-Korsakoff syndrome as an underlying diagnosis. It is unclear whether Mr. E experienced alcohol withdrawal and IV glucose without adequate thiamine replacement during a prior surgery. However, MRI findings were unchanged from a previous study 10 years ago.
It is puzzling whether Mr. E’s AMS was a first psychotic break, a result of drug and alcohol use, rapidly progressing dementia, or another neurologic problem that we have not identified. Our tentative diagnosis was Wernicke-Korsakoff syndrome because of his history of alcohol use and imaging findings.
Although we used a multidisciplinary team approach that included psychiatry, internal medicine, neurology, neuropsychology, and an aggressive and thorough workup, we could not establish a definitive diagnosis. Unsolved cases such as this can leave patients and clinicians frustrated and may lead to unfavorable outcomes. Additional resources such as a telephone call after the first missed appointment may have been warranted.
Table 2
Mr. E’s clinical course
| Symptoms | Treatment | |
|---|---|---|
| First ED visit | Agitation Confusion Sleep disturbance Decreased appetite and speech 20-lb weight loss | Empiric antimicrobials for possible meningitis Haloperidol for agitation Quetiapine for delirium Lorazepam taper Thiamine supplementation |
| Second ED visit | Violent behavior Worsening paranoia Responding to internal stimuli Mr. E believes he has 2 wives, but the wife in the room is not the real one, which suggests possible Capgras syndrome Cognitive deficits on mental status exam | Switch from ceftriaxone to ciprofloxacin for Pseudomonas aeruginosa Switch from quetiapine to olanzapine |
| ED: emergency department | ||
Related Resources
- Kaufman DM. Clinical neurology for psychiatrists. 6th ed. Philadelphia, PA: Saunders Elsevier; 2007.
- Sidhu KS, Balon R, Ajluni V, et al. Standard EEG and the difficult-to-assess mental status. Ann Clin Psychiatry. 2009;21(2):103-108.
Drug Brand Names
- Acyclovir • Zovirax
- Ceftriaxone • Rocephin
- Ciprofloxacin • Cipro
- Haloperidol • Haldol
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Thiamine • Betaxin
- Vancomycin • Vancocin
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at www.facebook.com/CurrentPsychiatry
CASE: Agitated and paranoid
Mr. E, age 55, presents to the emergency department (ED) with a 2-week history of altered mental status (AMS). His wife reports, “He was normal one day and the next day he was not.” Mr. E also presents with sleep disturbance, decreased appetite and speech, and a 20-lb weight loss. His family reports no recent stressors or head trauma. Mr. E is agitated in the ED and receives a single dose of IV haloperidol, 5 mg. He exhibits paranoia and is afraid to get a CT scan. The medical team attempts a lumbar puncture (LP), but Mr. E does not cooperate.
His laboratory values are: potassium, 3.0 mEq/L; creatinine, 1.60 mg/dL; calcium, 10.6 mg/dL; thyroid-stimulating hormone, 0.177 IU/L; vitamin B12, >1500 pg/mL; folate, >20 ng/mL; and creatine kinase, 281 U/L. Urine drug screen is positive for benzodiazepines and opiates, neither of which was prescribed, and blood alcohol is negative.
Mr. E is admitted for further workup of AMS. His daughter-in-law states that Mr. E is an alcoholic and she is concerned that he may have mixed drugs and alcohol. The medical service starts Mr. E on empiric antimicrobials—vancomycin, ceftriaxone, and acyclovir—because of his AMS, and performs an LP to rule out intracranial pathology. His LP results are unremarkable.
Mr. E appears to be confused during psychiatric evaluation. He requests to be “hypnotized on a helicopter to find out what is wrong with me.” His wife states that Mr. E drank vodka daily but decreased his alcohol consumption after surgery 5 months ago. Before his current admission, he was drinking approximately half a glass of vodka every few days, according to his wife. Mr. E says he has no prior psychiatric admissions. During the mental status exam, his eye contact is poor, with latency of response to questions, thought blocking, and psychomotor retardation. He is alert, oriented to time, place, and person, and cooperative. He cannot concentrate or focus during the interview. He denies suicidal or homicidal ideation.
The authors’ observations
Mr. E appeared to be delirious, as evidenced by the sudden onset of waxing and waning changes in consciousness, attention deficits, and cognition. He also had a history of daily alcohol use and decreased his alcohol intake after a surgery 5 months ago, which puts him at risk for Wernicke’s encephalopathy.1-3 The type of surgery and whether he received adequate thiamine supplementation at that time was unclear. Because Mr. E is older, he has a higher risk of mortality and morbidity from delirium.4,5 We started Mr. E on quetiapine, 50 mg/d, for delirium and an IV lorazepam taper, starting at 2 mg every 8 hours, because the extent of his alcohol and benzodiazepine use was unclear—we weren’t sure how forthcoming he was about his alcohol use. He received IV thiamine supplementation followed by oral thiamine, 100 mg/d.
The authors’ recommendations
We requested a neurology consult, EEG, CSF cultures, and brain MRI (Table 1).6 EEG, chest radiography, thyroid scan, and CT scan were normal and MRI showed no acute intracranial process. However, there was a redemonstration of increased T1 signal seen within the bilateral basal ganglia and relative diminutive appearance to the bilateral mamillary bodies, which suggests possible liver disease and/or alcohol abuse. These findings were unchanged from an MRI Mr. E received 10 years ago, were consistent with his history of alcohol abuse, and may indicate an underlying predisposition to delirium. A CT scan of the abdomen showed hepatic cirrhosis with prominent, tortuous vessels of the upper abdomen, subtle ill-defined hypodensity of the anterior aspect of the liver, and an enlarged spleen.
Mr. E’s mental functioning did not improve with quetiapine and lorazepam. Further evaluation revealed a negative human immunodeficiency virus test and normal heavy metals, ammonia, ceruloplasmin, and thiamine. We suspected limbic encephalitis because of Mr. E’s memory problems and behavioral and psychiatric manifestations,7 but CSF was unremarkable and limbic encephalitis workup of CSF and paraneoplastic antibody panel were negative.
Mr. E’s primary care physician stated that at an appointment 1 month ago, Mr. E was alert, oriented, and conversational with normal thought processing. At that time he had presented with rectal bleeding, occult blood in his stool, and an unintentional 25-lb weight loss over 2 months. It was not clear if his weight loss was caused by poor nutrition—which is common among chronic alcoholics—or an occult disease process.
After 10 days, Mr. E was discharged home from the medicine service with no clear cause of his AMS.
Table 1
Suggested workup for altered mental status
| Complete blood count, basic metabolic profile, creatine kinase |
| Thyroid-stimulating hormone, thyroid scan |
| Vitamin B12, folate, thiamine |
| Blood alcohol, urine drug screen |
| Urine analysis and cultures |
| Lumbar puncture—CSF staining and cultures |
| Chest radiography |
| CT and MRI scan of brain |
| Electroencephalography |
| Neuropsychiatric testing |
| CSF: cerebrospinal fluid Source: Reference 6 |
EVALUATION: Worsening behavior
One week later, Mr. E presents to the ED with continued AMS and worsening behavior at home. Two days ago, he attempted to strangle his dog and cut himself with a knife. His paranoia was worsening and his oral intake continued to decrease. In the ED, Mr. E does not want a chest radiograph because, “I don’t like radiation contaminating my body”; his family stated that he had been suspicious of radiography all of his life. He receives empiric ceftriaxone because of a possible urinary tract infection. Urine culture is positive for Pseudomonas aeruginosa and he is switched to ciprofloxacin. Mr. E is admitted for further workup.
Mr. E’s mother states, “I think this change in behavior is related to my son drinking alcohol for 20 years. This is exactly how he acted when he was on drugs. I think he is having a flashback.” She also reports her son purchased multiple chemicals—the details of which are unclear—that he left lying around the house.
His wife says that after discharge a week ago, Mr. E was stable for 1 or 2 days and then “he started going downhill.” He became more paranoid and he started talking about cameras watching him in his house. Mr. E took quetiapine, 50 mg/d, for a few days, then refused because he thought there was something in the medication. Mr. E’s family feels that at times he is responding to internal stimuli. He makes statements about his DNA being changed and reports that he has 2 wives and the wife in the room was not the real one, which suggests Capgras syndrome. His wife provides a home medication list that includes vitamin B complex, vitamins B12, E, and C, a multivitamin, zinc, magnesium, fish oil, garlic, calcium, glucosamine, chondroitin, herbal supplements, and gingko. The psychiatry team recommends switching from quetiapine to olanzapine, 15 mg/d, because Mr. E was paranoid about taking quetiapine.
We determine that Mr. E does not have medical decision-making capacity.
Because his symptoms do not improve, Mr. E is transferred to the psychiatric intensive care unit. His mental status shows little change while there. Neuropsychiatric testing shows only “cognitive deficits.” He shows signs consistent with neurologic dysfunction in terms of stimulus-bound responding and perseveration, which is compatible with the bilateral basal ganglia lesion seen on MRI. However, some of his behaviors suggest psychiatric and motivationally driven or manipulative etiology. During this testing he was difficult to evaluate and needed to be convinced to engage. At times he was illogical and at other times he showed good focus and recall. It is difficult to draw more definitive conclusions and Mr. E is discharged home with minor improvement in his symptoms. He didn’t attend follow-up appointments. During a courtesy call a few months after his admission, his wife revealed that Mr. E had died after shooting himself. It is unclear if it was an accident or suicide.
The authors’ observations
Mr. E’s diagnosis remains unclear (for a summary of his clinical course, see Table 2). Although his initial presentation was consistent with delirium, the lack of an identifiable medical cause, prolonged time course, and lack of improvement with dopamine blocking agents suggest additional diagnoses such as Wernicke-Korsakoff syndrome, rapidly progressive dementia, or a substance-induced disorder. He displayed paranoia and bizarre delusions, which would suggest a thought disorder. However, he also had a history of substance use. A few months after we saw Mr. E, “bath salt” (methylenedioxypyrovalerone) abuse gained national attention. Patients with bath salt intoxication present with confusion, paranoia, and behavioral disturbances as well as a prolonged course.8
Mr. E’s CT and MRI scans, history of alcohol use, and cirrhosis also point to Wernicke-Korsakoff syndrome as an underlying diagnosis. It is unclear whether Mr. E experienced alcohol withdrawal and IV glucose without adequate thiamine replacement during a prior surgery. However, MRI findings were unchanged from a previous study 10 years ago.
It is puzzling whether Mr. E’s AMS was a first psychotic break, a result of drug and alcohol use, rapidly progressing dementia, or another neurologic problem that we have not identified. Our tentative diagnosis was Wernicke-Korsakoff syndrome because of his history of alcohol use and imaging findings.
Although we used a multidisciplinary team approach that included psychiatry, internal medicine, neurology, neuropsychology, and an aggressive and thorough workup, we could not establish a definitive diagnosis. Unsolved cases such as this can leave patients and clinicians frustrated and may lead to unfavorable outcomes. Additional resources such as a telephone call after the first missed appointment may have been warranted.
Table 2
Mr. E’s clinical course
| Symptoms | Treatment | |
|---|---|---|
| First ED visit | Agitation Confusion Sleep disturbance Decreased appetite and speech 20-lb weight loss | Empiric antimicrobials for possible meningitis Haloperidol for agitation Quetiapine for delirium Lorazepam taper Thiamine supplementation |
| Second ED visit | Violent behavior Worsening paranoia Responding to internal stimuli Mr. E believes he has 2 wives, but the wife in the room is not the real one, which suggests possible Capgras syndrome Cognitive deficits on mental status exam | Switch from ceftriaxone to ciprofloxacin for Pseudomonas aeruginosa Switch from quetiapine to olanzapine |
| ED: emergency department | ||
Related Resources
- Kaufman DM. Clinical neurology for psychiatrists. 6th ed. Philadelphia, PA: Saunders Elsevier; 2007.
- Sidhu KS, Balon R, Ajluni V, et al. Standard EEG and the difficult-to-assess mental status. Ann Clin Psychiatry. 2009;21(2):103-108.
Drug Brand Names
- Acyclovir • Zovirax
- Ceftriaxone • Rocephin
- Ciprofloxacin • Cipro
- Haloperidol • Haldol
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Thiamine • Betaxin
- Vancomycin • Vancocin
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Jiang W, Gagliardi JP, Raj YP, et al. Acute psychotic disorder after gastric bypass surgery: differential diagnosis and treatment. Am J Psychiatry. 2006;163(1):15-19.
2. Harrison RA, Vu T, Hunter AJ. Wernicke’s encephalopathy in a patient with schizophrenia. J Gen Intern Med. 2006;21(12):C8-C11.
3. Sechi GP, Serra A. Wernicke’s encephalopathy: new clinical settings and recent advances in diagnosis and treatment. Lancet Neurol. 2007;6(5):442-455.
4. American Psychiatric Association. Practice guidelines for the treatment of patients with delirium. Am J Psychiatry. 1999;156(5 suppl):1-20.
5. Sharon KI, Fearing MA, Marcantonio RA. Delirium. In: Halter JB Ouslander JG, Tinetti ME, et al, eds. Hazzard’s geriatric medicine and gerontology. 6th ed. New York, NY: McGraw-Hill Medical; 2009:647–658.
6. Sadock BJ, Sadock VA. Delirium dementia, and amnestic and other cognitive disorders. In: Sadock BJ, Kaplan HI, Sadock VA. Kaplan and Sadock’s synopsis of psychiatry: behavioral sciences/clinical psychiatry. Philadelphia, PA: Lippincott Williams and Wilkins; 2007:319–372.
7. Ahmad SA, Archer HA, Rice CM, et al. Seronegative limbic encephalitis: case report, literature review and proposed treatment algorithm. Pract Neurol. 2011;11(6):355-361.
8. Ross EA, Watson M, Goldberger B. “Bath salts” intoxication. N Engl J Med. 2011;365(10):967-968.
1. Jiang W, Gagliardi JP, Raj YP, et al. Acute psychotic disorder after gastric bypass surgery: differential diagnosis and treatment. Am J Psychiatry. 2006;163(1):15-19.
2. Harrison RA, Vu T, Hunter AJ. Wernicke’s encephalopathy in a patient with schizophrenia. J Gen Intern Med. 2006;21(12):C8-C11.
3. Sechi GP, Serra A. Wernicke’s encephalopathy: new clinical settings and recent advances in diagnosis and treatment. Lancet Neurol. 2007;6(5):442-455.
4. American Psychiatric Association. Practice guidelines for the treatment of patients with delirium. Am J Psychiatry. 1999;156(5 suppl):1-20.
5. Sharon KI, Fearing MA, Marcantonio RA. Delirium. In: Halter JB Ouslander JG, Tinetti ME, et al, eds. Hazzard’s geriatric medicine and gerontology. 6th ed. New York, NY: McGraw-Hill Medical; 2009:647–658.
6. Sadock BJ, Sadock VA. Delirium dementia, and amnestic and other cognitive disorders. In: Sadock BJ, Kaplan HI, Sadock VA. Kaplan and Sadock’s synopsis of psychiatry: behavioral sciences/clinical psychiatry. Philadelphia, PA: Lippincott Williams and Wilkins; 2007:319–372.
7. Ahmad SA, Archer HA, Rice CM, et al. Seronegative limbic encephalitis: case report, literature review and proposed treatment algorithm. Pract Neurol. 2011;11(6):355-361.
8. Ross EA, Watson M, Goldberger B. “Bath salts” intoxication. N Engl J Med. 2011;365(10):967-968.
Clarification on melatonin
Although I was impressed by Drs. Scott R. Beach and Shamim H. Nejad’s Pearl (“Using melatonin to reset the clock of hospitalized older patients” Current Psychiatry, April 2012, p. 38; http://bit.ly/1GCrHB8), their recommended melatonin dosage (3 to 9 mg) seems high. Zhdanova et al recommended a much lower dose that can decrease time it takes to fall asleep, and said higher doses may cause daytime sleepiness and confusion. "How to lower suicide risk in depressed children and adolescents,” (Current Psychiatry, May 2012, p. 21-31; http://bit.ly/1FCwZR3), the diagnosis of mood disorders is challenged by the need to discern the difference between fear and unhappiness and mood disorders such as anxiety and depression. Fear and unhappiness are part of life, whereas a mood disorder is an illness. Ambivalent outcomes from studies of antidepressants in children and adolescents come from the inability to know when a child’s unhappiness stems from environmental factors rather than biological mood problems.
As a child and adolescent psychiatrist, I feel it is important to not “medicalize” a child’s experience because doing so may discourage a thorough inventory of sources of stress and unhappiness. Sometimes it is difficult to know what is going on in a child’s life. All self-reports are distorted, especially from children.
An important source of childhood stress may be medically undertreated. Failure in school often plays a part and predates the onset of “depression.” School failure is not an incidental issue because school is the most important area of a child’s life outside of family; failing is painful and demoralizing. A child who is failing often is very unhappy. I have known children who have committed suicide after failing “again.” Often, a child fails his or her classes because of untreated attention-deficit/hyperactivity disorder (ADHD). Diagnosing and treating ADHD can make a real difference in a child’s life. The best antidepressant is success.
In my experience, the risk of suicide can be lessened by the positive mood response to success. When we “medicalize” a child’s unhappiness rather than address the causes, we might be worsening his or her sense of alienation, which may drive suicidality.
Rodney Vivian, MD
Private Practice
Cincinnati, OH
Although I was impressed by Drs. Scott R. Beach and Shamim H. Nejad’s Pearl (“Using melatonin to reset the clock of hospitalized older patients” Current Psychiatry, April 2012, p. 38; http://bit.ly/1GCrHB8), their recommended melatonin dosage (3 to 9 mg) seems high. Zhdanova et al recommended a much lower dose that can decrease time it takes to fall asleep, and said higher doses may cause daytime sleepiness and confusion. "How to lower suicide risk in depressed children and adolescents,” (Current Psychiatry, May 2012, p. 21-31; http://bit.ly/1FCwZR3), the diagnosis of mood disorders is challenged by the need to discern the difference between fear and unhappiness and mood disorders such as anxiety and depression. Fear and unhappiness are part of life, whereas a mood disorder is an illness. Ambivalent outcomes from studies of antidepressants in children and adolescents come from the inability to know when a child’s unhappiness stems from environmental factors rather than biological mood problems.
As a child and adolescent psychiatrist, I feel it is important to not “medicalize” a child’s experience because doing so may discourage a thorough inventory of sources of stress and unhappiness. Sometimes it is difficult to know what is going on in a child’s life. All self-reports are distorted, especially from children.
An important source of childhood stress may be medically undertreated. Failure in school often plays a part and predates the onset of “depression.” School failure is not an incidental issue because school is the most important area of a child’s life outside of family; failing is painful and demoralizing. A child who is failing often is very unhappy. I have known children who have committed suicide after failing “again.” Often, a child fails his or her classes because of untreated attention-deficit/hyperactivity disorder (ADHD). Diagnosing and treating ADHD can make a real difference in a child’s life. The best antidepressant is success.
In my experience, the risk of suicide can be lessened by the positive mood response to success. When we “medicalize” a child’s unhappiness rather than address the causes, we might be worsening his or her sense of alienation, which may drive suicidality.
Rodney Vivian, MD
Private Practice
Cincinnati, OH
Although I was impressed by Drs. Scott R. Beach and Shamim H. Nejad’s Pearl (“Using melatonin to reset the clock of hospitalized older patients” Current Psychiatry, April 2012, p. 38; http://bit.ly/1GCrHB8), their recommended melatonin dosage (3 to 9 mg) seems high. Zhdanova et al recommended a much lower dose that can decrease time it takes to fall asleep, and said higher doses may cause daytime sleepiness and confusion. "How to lower suicide risk in depressed children and adolescents,” (Current Psychiatry, May 2012, p. 21-31; http://bit.ly/1FCwZR3), the diagnosis of mood disorders is challenged by the need to discern the difference between fear and unhappiness and mood disorders such as anxiety and depression. Fear and unhappiness are part of life, whereas a mood disorder is an illness. Ambivalent outcomes from studies of antidepressants in children and adolescents come from the inability to know when a child’s unhappiness stems from environmental factors rather than biological mood problems.
As a child and adolescent psychiatrist, I feel it is important to not “medicalize” a child’s experience because doing so may discourage a thorough inventory of sources of stress and unhappiness. Sometimes it is difficult to know what is going on in a child’s life. All self-reports are distorted, especially from children.
An important source of childhood stress may be medically undertreated. Failure in school often plays a part and predates the onset of “depression.” School failure is not an incidental issue because school is the most important area of a child’s life outside of family; failing is painful and demoralizing. A child who is failing often is very unhappy. I have known children who have committed suicide after failing “again.” Often, a child fails his or her classes because of untreated attention-deficit/hyperactivity disorder (ADHD). Diagnosing and treating ADHD can make a real difference in a child’s life. The best antidepressant is success.
In my experience, the risk of suicide can be lessened by the positive mood response to success. When we “medicalize” a child’s unhappiness rather than address the causes, we might be worsening his or her sense of alienation, which may drive suicidality.
Rodney Vivian, MD
Private Practice
Cincinnati, OH
Suicide rehearsals: A high-risk psychiatric emergency
A suicide rehearsal is a behavioral enactment of a suicide method, usually as part of a suicide plan. A mental suicide rehearsal is a process that evolves over time into a plan. Patients who are intent on attempting suicide usually do not reveal their plans. However, behavioral rehearsals display specific clinical characteristics that speak louder than the guarded patient’s denials, revealing the patient’s suicide plan (Table).
Suicide rehearsals may precede suicide attempts or suicide completions. The percentage of patients who stage suicide rehearsals before attempting or completing suicide is unknown; however, in my experience, suicide rehearsals are relatively common. This article describes suicide rehearsals, and offers 4 cases that illustrate what clinicians can learn from rehearsals to improve their patients’ safety.
Table
Clinical characteristics of suicide rehearsals
| Guarded patient |
| Behavioral enactment of a suicide method |
| Lethal means |
| Presumptive acute, high risk of suicide |
| Severe mental illness |
| Suicide attempt often within hours or days |
| Rehearsal usually covert |
| Rehearsal event or multiple events |
The psychology behind suicide rehearsals
Rehearsing suicidal behavior can lower the barrier to a suicide plan, thereby increasing a patient’s resolve and risk. Joiner1 notes that engaging in behavioral or mental suicide rehearsals increases the risk of suicide. Moreover, rehearsals diminish the prohibition against suicidal behavior and the fear of pain and dying. Examples of rehearsal psychology include:
- overcoming ambivalence about dying
- desensitizing anxiety about performing the suicide act
- testing or “perfecting” the method of a planned suicide
- firming one’s resolve to complete suicide.
Other non-lethal motivations include “a cry for help” and self-injurious behaviors motivated by external gains. Patients who do not intend to attempt suicide may openly rehearse low-risk methods, such as superficial cutting.
Rehearsal characteristics
Suicide rehearsals can be confused with aborted, interrupted, or failed suicide attempts. Suicide rehearsals usually are associated with severe psychiatric illness and high-risk lethal methods of attempting suicide. My experience is that suicide attempts or suicide completions often follow a rehearsal within a few hours or days. However, no short-term suicide risk factors—within hours, days, or weeks—can predict when or if a rehearsed suicide will proceed to a suicide attempt.2
A suicide rehearsal is presumptive evidence that the patient is at acute, high risk for suicide and immediate clinical intervention is necessary. A rehearsal allows the clinician to explore the various methods of suicide that the patient has considered, including prior rehearsals. Knowledge of prior rehearsals can inform the clinician’s management of the current suicide rehearsal.
Suicide rehearsals often are conducted covertly. On inpatient psychiatric units, the rehearsal usually is discovered by staff members or reported by other patients. In outpatient settings, the patient or a significant other may report a rehearsal.
The suicide method displayed in a rehearsal may change. A patient who is rehearsing a hanging may attempt suicide by overdose or a firearm. In a systematic review of prior suicide attempts (N = 1,397), Isometsä et al3 found that 82% of patients used 2 or more different methods in suicide attempts, including the completed suicide. However, in a cohort study of 48,649 individuals admitted to a hospital after an attempted suicide, Runeson et al4 found that patients who attempt suicide often used the same method in completed suicide (ie, >90% by hanging for both men and women). Therefore, when taking measures to restrict the patient’s access to lethal means, safety efforts should not be limited to the method used in the suicide rehearsal. Patients can always substitute methods.
Making overall preparations for suicide—for example, making a will, giving away valuable possessions, or putting financial affairs in order—could be confused with a suicide rehearsal, which displays the lethal method to be used in a suicide attempt, often after preparations are made. Suicide rehearsals tend to occur much closer in time to the suicide attempt than preparations for suicide. Similarly, a patient’s plan to hoard drugs for a suicide attempt is not the same as ingesting a sub-lethal dose of a drug to test his or her resolve to die.
By definition, impulsive suicide attempts are not rehearsed. However, an individual’s suicide rehearsal can impulsively segue into a suicide attempt. In a case control study (N = 153) Simon et al5 found that 24% of patients spent 6 found that 26% of individuals with lifetime suicide ideation transitioned from suicide ideation to an unplanned suicide attempt. In my experience, a suicide rehearsal before a suicide completion is presumptive evidence against an impulsive suicide.
Patients contemplating suicide may visit Web sites with instructions on “how to suicide,” providing “virtual” opportunities to rehearse suicide.7 Patients who are at risk for suicide should be asked if they have searched the Internet for suicide methodology.
What we can learn from rehearsals
Although the following case examples are fictional, they illustrate suicide rehearsals encountered in my clinical and forensic practice.
CASE 1: Looking for a location
Ms. B, a 28-year-old divorced mother of 2, is observed tarrying at the high point of a bridge on successive days. When police arrive and question her, she becomes agitated and distraught. Ms. B admits to “scoping out” the bridge and is taken to a hospital emergency room (ER). In the ER, Ms. B discloses, “I was looking for a good spot to jump.” She tells the triage nurse that she is very depressed but, “I couldn’t do it to my children.” Ms. B is placed in an unlocked room while she waits to be assessed by a psychiatrist. She leaves the ER, runs to a nearby parking garage, and jumps from the top level to her death.
Comment: A patient’s denial of suicide intent following a suicide rehearsal cannot be relied upon. Ms. B’s rehearsal revealed a plan with high-risk suicide intent and a lethal suicide method. Systematic suicide assessment that informs immediate clinical intervention is required.
CASE 2: Changing lethal means
Mr. N, a 43-year-old chief executive officer of a large company, is observed by an assistant loading and unloading a revolver at his desk. Alarmed, the assistant calls the company physician. Mr. N refuses psychiatric treatment, saying, “I’ll be all right; this is just a passing thing.” His wife tells the physician that her husband has a history of bipolar disorder but no prior suicide attempts. Guns and ammunition are removed from the home. One week later, Mr. N is found hanging in his garage. A loaded pistol is discovered in the glove compartment of his car.
Comment: There is no certainty that a subsequent suicide attempt will replicate the rehearsed method. A psychological autopsy was conducted, but no explanation was found for why Mr. N chose hanging after having rehearsed suicide with a loaded handgun. His wife thought that her husband, a very tidy person, did not want to leave a mess.
CASE 3: Grieving and depressed
Mr. O, age 67, is depressed after recently losing his wife. He considers a number of suicide methods. Mr. O decides to use a plastic bag to suffocate himself because he believes that this method will allow him to change his mind. Mr. O practices tying the bag tight around his neck. During this rehearsal, he realizes that he does not want to die. Instead, he pursues grief counseling.
Comment: For some patients, the act of rehearsing suicide can help them resolve ambivalent feelings about wanting to die in favor of wanting to live.
CASE 4: Suicide method and the Internet
Ms. S, a 22-year-old college student, is undergoing outpatient treatment for depression. She is accumulating prescription drugs to take as an overdose. Ms. S also searches the Internet for information about other suicide methods. Because she wants a “sure” method of suicide, she persuades an acquaintance to purchase a handgun. In private, Ms. S places the unloaded gun to her head and plays “Russian roulette,” pulling the trigger several times. Her mother discovers the gun and confronts her daughter. Ms. S is hospitalized on a closed psychiatric unit and tells a staff member, “I was practicing suicide with the gun.” Before Ms. S is discharged from the hospital, her parents are advised to watch for suicidal behaviors, especially the recurrence of rehearsals that indicate an acute, high suicide risk. Ms. S’s Internet use is restricted and monitored.
Comment: Suicide rehearsal with a gun reinforces the belief that a firearm death is quick and easy.8 Reaching for a loaded gun takes less time than most other methods of suicide. Patients who rehearse suicide with a gun should be prevented from having access to any firearms, weapons, or other highly lethal means of suicide.
Recognition and intervention
A guarded psychiatric inpatient who is intent on attempting suicide is unmasked when the discovery of a suicidal rehearsal reveals a suicide plan. This creates an opportunity for clinicians to intervene. The patient may attempt to cover up suicidal intent by stating, “I was just playing around” or “I just wanted to get attention.” Recognizing the emergency posed by a suicide rehearsal informs treatment. Safety measures—including 1-to-1 supervision—may be necessary during a period of acute, high suicide risk. The patient’s diagnosis, severity of illness, and treatment require reevaluation.
An outpatient who performs a suicide rehearsal should be considered at acute, high risk for suicide, and immediate psychiatric hospitalization may be necessary. Whether as an inpatient or outpatient, the patient’s suicide intent and plan require careful exploration. The information gained will guide treatment and management decisions. Continuing systematic suicide risk assessment is essential.
Related Resources
- American Association of Suicidology. www.suicidology.org.
- Joiner T. Why people die by suicide. Cambridge, MA: Harvard University Press; 2007.
- American Psychiatric Association. Practice guideline for the assessment and treatment of patients with suicidal behaviors. Washington, DC: American Psychiatric Publishing, Inc. 2003.
- Simon RI. Preventing patient suicide: clinical assessment and management. Arlington, VA: American Psychiatric Publishing, Inc.; 2011.
Disclosure
Dr. Simon reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Joiner TE, Jr. The trajectory of suicidal behavior over time. Suicide Life Threat Behav. 2002;32(1):33-41.
2. Simon RI. Imminent suicide: the illusion of short-term prediction. Suicide Life Threat Behav. 2006;36(3):296-301.
3. Isometsä ET, Lönnqvist JK. Suicide attempts preceding completed suicide. Br J Psychiatry. 1998;173:531-535.
4. Runeson B, Tidemalm D, Dahlin M, et al. Method of attempted suicide as a predictor of subsequent successful suicide: national long-term cohort study. BMJ. 2010;341:c3222. doi:10.1136/bmj.63222.
5. Simon TR, Swann AC, Powell KE, et al. Characteristics of impulsive suicide attempts and attempters. Suicide Life Threat Behav. 2001;32(suppl):49-59.
6. Kessler RC, Borges G, Walters EE. Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Study. Arch Gen Psychiatry. 1999;56(7):617-626.
7. Recupero PR. Suicide and the Internet. In: Simon RI Hales RE, eds. The American Psychiatric Publishing textbook of suicide assessment and management. 2nd ed. Arlington, VA: American Psychiatric Publishing, Inc.; 2012:515–538.
8. Simon RI. Gun safety management with patients at risk for suicide. Suicide Life Threat Behav. 2007;37(5):518-526.
A suicide rehearsal is a behavioral enactment of a suicide method, usually as part of a suicide plan. A mental suicide rehearsal is a process that evolves over time into a plan. Patients who are intent on attempting suicide usually do not reveal their plans. However, behavioral rehearsals display specific clinical characteristics that speak louder than the guarded patient’s denials, revealing the patient’s suicide plan (Table).
Suicide rehearsals may precede suicide attempts or suicide completions. The percentage of patients who stage suicide rehearsals before attempting or completing suicide is unknown; however, in my experience, suicide rehearsals are relatively common. This article describes suicide rehearsals, and offers 4 cases that illustrate what clinicians can learn from rehearsals to improve their patients’ safety.
Table
Clinical characteristics of suicide rehearsals
| Guarded patient |
| Behavioral enactment of a suicide method |
| Lethal means |
| Presumptive acute, high risk of suicide |
| Severe mental illness |
| Suicide attempt often within hours or days |
| Rehearsal usually covert |
| Rehearsal event or multiple events |
The psychology behind suicide rehearsals
Rehearsing suicidal behavior can lower the barrier to a suicide plan, thereby increasing a patient’s resolve and risk. Joiner1 notes that engaging in behavioral or mental suicide rehearsals increases the risk of suicide. Moreover, rehearsals diminish the prohibition against suicidal behavior and the fear of pain and dying. Examples of rehearsal psychology include:
- overcoming ambivalence about dying
- desensitizing anxiety about performing the suicide act
- testing or “perfecting” the method of a planned suicide
- firming one’s resolve to complete suicide.
Other non-lethal motivations include “a cry for help” and self-injurious behaviors motivated by external gains. Patients who do not intend to attempt suicide may openly rehearse low-risk methods, such as superficial cutting.
Rehearsal characteristics
Suicide rehearsals can be confused with aborted, interrupted, or failed suicide attempts. Suicide rehearsals usually are associated with severe psychiatric illness and high-risk lethal methods of attempting suicide. My experience is that suicide attempts or suicide completions often follow a rehearsal within a few hours or days. However, no short-term suicide risk factors—within hours, days, or weeks—can predict when or if a rehearsed suicide will proceed to a suicide attempt.2
A suicide rehearsal is presumptive evidence that the patient is at acute, high risk for suicide and immediate clinical intervention is necessary. A rehearsal allows the clinician to explore the various methods of suicide that the patient has considered, including prior rehearsals. Knowledge of prior rehearsals can inform the clinician’s management of the current suicide rehearsal.
Suicide rehearsals often are conducted covertly. On inpatient psychiatric units, the rehearsal usually is discovered by staff members or reported by other patients. In outpatient settings, the patient or a significant other may report a rehearsal.
The suicide method displayed in a rehearsal may change. A patient who is rehearsing a hanging may attempt suicide by overdose or a firearm. In a systematic review of prior suicide attempts (N = 1,397), Isometsä et al3 found that 82% of patients used 2 or more different methods in suicide attempts, including the completed suicide. However, in a cohort study of 48,649 individuals admitted to a hospital after an attempted suicide, Runeson et al4 found that patients who attempt suicide often used the same method in completed suicide (ie, >90% by hanging for both men and women). Therefore, when taking measures to restrict the patient’s access to lethal means, safety efforts should not be limited to the method used in the suicide rehearsal. Patients can always substitute methods.
Making overall preparations for suicide—for example, making a will, giving away valuable possessions, or putting financial affairs in order—could be confused with a suicide rehearsal, which displays the lethal method to be used in a suicide attempt, often after preparations are made. Suicide rehearsals tend to occur much closer in time to the suicide attempt than preparations for suicide. Similarly, a patient’s plan to hoard drugs for a suicide attempt is not the same as ingesting a sub-lethal dose of a drug to test his or her resolve to die.
By definition, impulsive suicide attempts are not rehearsed. However, an individual’s suicide rehearsal can impulsively segue into a suicide attempt. In a case control study (N = 153) Simon et al5 found that 24% of patients spent 6 found that 26% of individuals with lifetime suicide ideation transitioned from suicide ideation to an unplanned suicide attempt. In my experience, a suicide rehearsal before a suicide completion is presumptive evidence against an impulsive suicide.
Patients contemplating suicide may visit Web sites with instructions on “how to suicide,” providing “virtual” opportunities to rehearse suicide.7 Patients who are at risk for suicide should be asked if they have searched the Internet for suicide methodology.
What we can learn from rehearsals
Although the following case examples are fictional, they illustrate suicide rehearsals encountered in my clinical and forensic practice.
CASE 1: Looking for a location
Ms. B, a 28-year-old divorced mother of 2, is observed tarrying at the high point of a bridge on successive days. When police arrive and question her, she becomes agitated and distraught. Ms. B admits to “scoping out” the bridge and is taken to a hospital emergency room (ER). In the ER, Ms. B discloses, “I was looking for a good spot to jump.” She tells the triage nurse that she is very depressed but, “I couldn’t do it to my children.” Ms. B is placed in an unlocked room while she waits to be assessed by a psychiatrist. She leaves the ER, runs to a nearby parking garage, and jumps from the top level to her death.
Comment: A patient’s denial of suicide intent following a suicide rehearsal cannot be relied upon. Ms. B’s rehearsal revealed a plan with high-risk suicide intent and a lethal suicide method. Systematic suicide assessment that informs immediate clinical intervention is required.
CASE 2: Changing lethal means
Mr. N, a 43-year-old chief executive officer of a large company, is observed by an assistant loading and unloading a revolver at his desk. Alarmed, the assistant calls the company physician. Mr. N refuses psychiatric treatment, saying, “I’ll be all right; this is just a passing thing.” His wife tells the physician that her husband has a history of bipolar disorder but no prior suicide attempts. Guns and ammunition are removed from the home. One week later, Mr. N is found hanging in his garage. A loaded pistol is discovered in the glove compartment of his car.
Comment: There is no certainty that a subsequent suicide attempt will replicate the rehearsed method. A psychological autopsy was conducted, but no explanation was found for why Mr. N chose hanging after having rehearsed suicide with a loaded handgun. His wife thought that her husband, a very tidy person, did not want to leave a mess.
CASE 3: Grieving and depressed
Mr. O, age 67, is depressed after recently losing his wife. He considers a number of suicide methods. Mr. O decides to use a plastic bag to suffocate himself because he believes that this method will allow him to change his mind. Mr. O practices tying the bag tight around his neck. During this rehearsal, he realizes that he does not want to die. Instead, he pursues grief counseling.
Comment: For some patients, the act of rehearsing suicide can help them resolve ambivalent feelings about wanting to die in favor of wanting to live.
CASE 4: Suicide method and the Internet
Ms. S, a 22-year-old college student, is undergoing outpatient treatment for depression. She is accumulating prescription drugs to take as an overdose. Ms. S also searches the Internet for information about other suicide methods. Because she wants a “sure” method of suicide, she persuades an acquaintance to purchase a handgun. In private, Ms. S places the unloaded gun to her head and plays “Russian roulette,” pulling the trigger several times. Her mother discovers the gun and confronts her daughter. Ms. S is hospitalized on a closed psychiatric unit and tells a staff member, “I was practicing suicide with the gun.” Before Ms. S is discharged from the hospital, her parents are advised to watch for suicidal behaviors, especially the recurrence of rehearsals that indicate an acute, high suicide risk. Ms. S’s Internet use is restricted and monitored.
Comment: Suicide rehearsal with a gun reinforces the belief that a firearm death is quick and easy.8 Reaching for a loaded gun takes less time than most other methods of suicide. Patients who rehearse suicide with a gun should be prevented from having access to any firearms, weapons, or other highly lethal means of suicide.
Recognition and intervention
A guarded psychiatric inpatient who is intent on attempting suicide is unmasked when the discovery of a suicidal rehearsal reveals a suicide plan. This creates an opportunity for clinicians to intervene. The patient may attempt to cover up suicidal intent by stating, “I was just playing around” or “I just wanted to get attention.” Recognizing the emergency posed by a suicide rehearsal informs treatment. Safety measures—including 1-to-1 supervision—may be necessary during a period of acute, high suicide risk. The patient’s diagnosis, severity of illness, and treatment require reevaluation.
An outpatient who performs a suicide rehearsal should be considered at acute, high risk for suicide, and immediate psychiatric hospitalization may be necessary. Whether as an inpatient or outpatient, the patient’s suicide intent and plan require careful exploration. The information gained will guide treatment and management decisions. Continuing systematic suicide risk assessment is essential.
Related Resources
- American Association of Suicidology. www.suicidology.org.
- Joiner T. Why people die by suicide. Cambridge, MA: Harvard University Press; 2007.
- American Psychiatric Association. Practice guideline for the assessment and treatment of patients with suicidal behaviors. Washington, DC: American Psychiatric Publishing, Inc. 2003.
- Simon RI. Preventing patient suicide: clinical assessment and management. Arlington, VA: American Psychiatric Publishing, Inc.; 2011.
Disclosure
Dr. Simon reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
A suicide rehearsal is a behavioral enactment of a suicide method, usually as part of a suicide plan. A mental suicide rehearsal is a process that evolves over time into a plan. Patients who are intent on attempting suicide usually do not reveal their plans. However, behavioral rehearsals display specific clinical characteristics that speak louder than the guarded patient’s denials, revealing the patient’s suicide plan (Table).
Suicide rehearsals may precede suicide attempts or suicide completions. The percentage of patients who stage suicide rehearsals before attempting or completing suicide is unknown; however, in my experience, suicide rehearsals are relatively common. This article describes suicide rehearsals, and offers 4 cases that illustrate what clinicians can learn from rehearsals to improve their patients’ safety.
Table
Clinical characteristics of suicide rehearsals
| Guarded patient |
| Behavioral enactment of a suicide method |
| Lethal means |
| Presumptive acute, high risk of suicide |
| Severe mental illness |
| Suicide attempt often within hours or days |
| Rehearsal usually covert |
| Rehearsal event or multiple events |
The psychology behind suicide rehearsals
Rehearsing suicidal behavior can lower the barrier to a suicide plan, thereby increasing a patient’s resolve and risk. Joiner1 notes that engaging in behavioral or mental suicide rehearsals increases the risk of suicide. Moreover, rehearsals diminish the prohibition against suicidal behavior and the fear of pain and dying. Examples of rehearsal psychology include:
- overcoming ambivalence about dying
- desensitizing anxiety about performing the suicide act
- testing or “perfecting” the method of a planned suicide
- firming one’s resolve to complete suicide.
Other non-lethal motivations include “a cry for help” and self-injurious behaviors motivated by external gains. Patients who do not intend to attempt suicide may openly rehearse low-risk methods, such as superficial cutting.
Rehearsal characteristics
Suicide rehearsals can be confused with aborted, interrupted, or failed suicide attempts. Suicide rehearsals usually are associated with severe psychiatric illness and high-risk lethal methods of attempting suicide. My experience is that suicide attempts or suicide completions often follow a rehearsal within a few hours or days. However, no short-term suicide risk factors—within hours, days, or weeks—can predict when or if a rehearsed suicide will proceed to a suicide attempt.2
A suicide rehearsal is presumptive evidence that the patient is at acute, high risk for suicide and immediate clinical intervention is necessary. A rehearsal allows the clinician to explore the various methods of suicide that the patient has considered, including prior rehearsals. Knowledge of prior rehearsals can inform the clinician’s management of the current suicide rehearsal.
Suicide rehearsals often are conducted covertly. On inpatient psychiatric units, the rehearsal usually is discovered by staff members or reported by other patients. In outpatient settings, the patient or a significant other may report a rehearsal.
The suicide method displayed in a rehearsal may change. A patient who is rehearsing a hanging may attempt suicide by overdose or a firearm. In a systematic review of prior suicide attempts (N = 1,397), Isometsä et al3 found that 82% of patients used 2 or more different methods in suicide attempts, including the completed suicide. However, in a cohort study of 48,649 individuals admitted to a hospital after an attempted suicide, Runeson et al4 found that patients who attempt suicide often used the same method in completed suicide (ie, >90% by hanging for both men and women). Therefore, when taking measures to restrict the patient’s access to lethal means, safety efforts should not be limited to the method used in the suicide rehearsal. Patients can always substitute methods.
Making overall preparations for suicide—for example, making a will, giving away valuable possessions, or putting financial affairs in order—could be confused with a suicide rehearsal, which displays the lethal method to be used in a suicide attempt, often after preparations are made. Suicide rehearsals tend to occur much closer in time to the suicide attempt than preparations for suicide. Similarly, a patient’s plan to hoard drugs for a suicide attempt is not the same as ingesting a sub-lethal dose of a drug to test his or her resolve to die.
By definition, impulsive suicide attempts are not rehearsed. However, an individual’s suicide rehearsal can impulsively segue into a suicide attempt. In a case control study (N = 153) Simon et al5 found that 24% of patients spent 6 found that 26% of individuals with lifetime suicide ideation transitioned from suicide ideation to an unplanned suicide attempt. In my experience, a suicide rehearsal before a suicide completion is presumptive evidence against an impulsive suicide.
Patients contemplating suicide may visit Web sites with instructions on “how to suicide,” providing “virtual” opportunities to rehearse suicide.7 Patients who are at risk for suicide should be asked if they have searched the Internet for suicide methodology.
What we can learn from rehearsals
Although the following case examples are fictional, they illustrate suicide rehearsals encountered in my clinical and forensic practice.
CASE 1: Looking for a location
Ms. B, a 28-year-old divorced mother of 2, is observed tarrying at the high point of a bridge on successive days. When police arrive and question her, she becomes agitated and distraught. Ms. B admits to “scoping out” the bridge and is taken to a hospital emergency room (ER). In the ER, Ms. B discloses, “I was looking for a good spot to jump.” She tells the triage nurse that she is very depressed but, “I couldn’t do it to my children.” Ms. B is placed in an unlocked room while she waits to be assessed by a psychiatrist. She leaves the ER, runs to a nearby parking garage, and jumps from the top level to her death.
Comment: A patient’s denial of suicide intent following a suicide rehearsal cannot be relied upon. Ms. B’s rehearsal revealed a plan with high-risk suicide intent and a lethal suicide method. Systematic suicide assessment that informs immediate clinical intervention is required.
CASE 2: Changing lethal means
Mr. N, a 43-year-old chief executive officer of a large company, is observed by an assistant loading and unloading a revolver at his desk. Alarmed, the assistant calls the company physician. Mr. N refuses psychiatric treatment, saying, “I’ll be all right; this is just a passing thing.” His wife tells the physician that her husband has a history of bipolar disorder but no prior suicide attempts. Guns and ammunition are removed from the home. One week later, Mr. N is found hanging in his garage. A loaded pistol is discovered in the glove compartment of his car.
Comment: There is no certainty that a subsequent suicide attempt will replicate the rehearsed method. A psychological autopsy was conducted, but no explanation was found for why Mr. N chose hanging after having rehearsed suicide with a loaded handgun. His wife thought that her husband, a very tidy person, did not want to leave a mess.
CASE 3: Grieving and depressed
Mr. O, age 67, is depressed after recently losing his wife. He considers a number of suicide methods. Mr. O decides to use a plastic bag to suffocate himself because he believes that this method will allow him to change his mind. Mr. O practices tying the bag tight around his neck. During this rehearsal, he realizes that he does not want to die. Instead, he pursues grief counseling.
Comment: For some patients, the act of rehearsing suicide can help them resolve ambivalent feelings about wanting to die in favor of wanting to live.
CASE 4: Suicide method and the Internet
Ms. S, a 22-year-old college student, is undergoing outpatient treatment for depression. She is accumulating prescription drugs to take as an overdose. Ms. S also searches the Internet for information about other suicide methods. Because she wants a “sure” method of suicide, she persuades an acquaintance to purchase a handgun. In private, Ms. S places the unloaded gun to her head and plays “Russian roulette,” pulling the trigger several times. Her mother discovers the gun and confronts her daughter. Ms. S is hospitalized on a closed psychiatric unit and tells a staff member, “I was practicing suicide with the gun.” Before Ms. S is discharged from the hospital, her parents are advised to watch for suicidal behaviors, especially the recurrence of rehearsals that indicate an acute, high suicide risk. Ms. S’s Internet use is restricted and monitored.
Comment: Suicide rehearsal with a gun reinforces the belief that a firearm death is quick and easy.8 Reaching for a loaded gun takes less time than most other methods of suicide. Patients who rehearse suicide with a gun should be prevented from having access to any firearms, weapons, or other highly lethal means of suicide.
Recognition and intervention
A guarded psychiatric inpatient who is intent on attempting suicide is unmasked when the discovery of a suicidal rehearsal reveals a suicide plan. This creates an opportunity for clinicians to intervene. The patient may attempt to cover up suicidal intent by stating, “I was just playing around” or “I just wanted to get attention.” Recognizing the emergency posed by a suicide rehearsal informs treatment. Safety measures—including 1-to-1 supervision—may be necessary during a period of acute, high suicide risk. The patient’s diagnosis, severity of illness, and treatment require reevaluation.
An outpatient who performs a suicide rehearsal should be considered at acute, high risk for suicide, and immediate psychiatric hospitalization may be necessary. Whether as an inpatient or outpatient, the patient’s suicide intent and plan require careful exploration. The information gained will guide treatment and management decisions. Continuing systematic suicide risk assessment is essential.
Related Resources
- American Association of Suicidology. www.suicidology.org.
- Joiner T. Why people die by suicide. Cambridge, MA: Harvard University Press; 2007.
- American Psychiatric Association. Practice guideline for the assessment and treatment of patients with suicidal behaviors. Washington, DC: American Psychiatric Publishing, Inc. 2003.
- Simon RI. Preventing patient suicide: clinical assessment and management. Arlington, VA: American Psychiatric Publishing, Inc.; 2011.
Disclosure
Dr. Simon reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Joiner TE, Jr. The trajectory of suicidal behavior over time. Suicide Life Threat Behav. 2002;32(1):33-41.
2. Simon RI. Imminent suicide: the illusion of short-term prediction. Suicide Life Threat Behav. 2006;36(3):296-301.
3. Isometsä ET, Lönnqvist JK. Suicide attempts preceding completed suicide. Br J Psychiatry. 1998;173:531-535.
4. Runeson B, Tidemalm D, Dahlin M, et al. Method of attempted suicide as a predictor of subsequent successful suicide: national long-term cohort study. BMJ. 2010;341:c3222. doi:10.1136/bmj.63222.
5. Simon TR, Swann AC, Powell KE, et al. Characteristics of impulsive suicide attempts and attempters. Suicide Life Threat Behav. 2001;32(suppl):49-59.
6. Kessler RC, Borges G, Walters EE. Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Study. Arch Gen Psychiatry. 1999;56(7):617-626.
7. Recupero PR. Suicide and the Internet. In: Simon RI Hales RE, eds. The American Psychiatric Publishing textbook of suicide assessment and management. 2nd ed. Arlington, VA: American Psychiatric Publishing, Inc.; 2012:515–538.
8. Simon RI. Gun safety management with patients at risk for suicide. Suicide Life Threat Behav. 2007;37(5):518-526.
1. Joiner TE, Jr. The trajectory of suicidal behavior over time. Suicide Life Threat Behav. 2002;32(1):33-41.
2. Simon RI. Imminent suicide: the illusion of short-term prediction. Suicide Life Threat Behav. 2006;36(3):296-301.
3. Isometsä ET, Lönnqvist JK. Suicide attempts preceding completed suicide. Br J Psychiatry. 1998;173:531-535.
4. Runeson B, Tidemalm D, Dahlin M, et al. Method of attempted suicide as a predictor of subsequent successful suicide: national long-term cohort study. BMJ. 2010;341:c3222. doi:10.1136/bmj.63222.
5. Simon TR, Swann AC, Powell KE, et al. Characteristics of impulsive suicide attempts and attempters. Suicide Life Threat Behav. 2001;32(suppl):49-59.
6. Kessler RC, Borges G, Walters EE. Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Study. Arch Gen Psychiatry. 1999;56(7):617-626.
7. Recupero PR. Suicide and the Internet. In: Simon RI Hales RE, eds. The American Psychiatric Publishing textbook of suicide assessment and management. 2nd ed. Arlington, VA: American Psychiatric Publishing, Inc.; 2012:515–538.
8. Simon RI. Gun safety management with patients at risk for suicide. Suicide Life Threat Behav. 2007;37(5):518-526.
Trichotillomania: Targeting the root of the disorder
An estimated 1% of Americans have trichotillomania (TTM), an impulse-control disorder in which patients experience pleasure or gratification from recurrently pulling out their own hair, resulting in noticeable hair loss.1,2 This disorder is more commonly diagnosed in women, likely reflecting treatment-seeking bias; women may be more likely to seek care for TTM because of social stigma associated with hair loss.2 Avulsion of hair usually occurs at the scalp, but also can be seen in multiple sites, including eyebrows, eyelashes, beards, and pubic regions; the number of sites typically increases with the patient’s age.3
The lifetime prevalence of comorbid axis I disorders in patients with TTM is 82%.3 Because of this, TTM often is first encountered in a psychiatric setting. Psychiatrists should have knowledge of TTM diagnosis and treatment because they may be the only point of care for TTM patients. When considering a TTM diagnosis, be aware that in some cultures rending hair is a mourning ritual or a rite of passage.3
Evidence for cognitive therapies
Behavioral models suggest TTM behaviors are learned and maintained by both classical and operant conditioning. Therapies that target the cognitive processes that trigger urges to pull, the avulsion of hair, and recognizing the consequences have the best empirical support.3
Habit reversal training (HRT) is considered the most effective treatment for TTM.3 One trial found a single 2-hour HRT intervention resulted in greater reductions in hair pulling episodes and higher remission rates compared with placebo.3 HRT trains patients to create a competing response, such as fist clenching, that is incompatible and blocks the undesired response.
Other therapeutic approaches to TTM include acceptance and commitment therapy, cognitive-behavioral therapy (CBT), and dialectical behavioral therapy-enhanced HRT. Evidence is most robust for CBT-HRT; randomized controlled trials found a statistically significant reduction in TTM in patients receiving CBT-HRT.3 One review suggests CBT-HRT should be considered first-line therapy for TTM.3
Pharmacologic options
Although no medications are FDA-approved for treating TTM, options include clomipramine, olanzapine, fluoxetine, pimozide, inositol, naltrexone, and N-acetylcysteine.2,3 The most robust trials of pharmacotherapy monotherapy were for N-acetylcysteine and naltrexone; both medications had significantly greater reduction in hair-pulling symptoms compared with placebo.3 Some evidence suggests combined pharmacotherapy and psychotherapy might be an effective approach.2,3
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
2. Woods DW, Flessner C, Franklin ME, et al. Understanding and treating trichotillomania: what we know and what we don’t know. Psychiatr Clin North Am. 2006;29(2):487-501, ix.
3. Duke DC, Keeley ML, Geffken GR, et al. Trichotillomania: a current review. Clin Psychol Rev. 2010;30(2):181-193.
An estimated 1% of Americans have trichotillomania (TTM), an impulse-control disorder in which patients experience pleasure or gratification from recurrently pulling out their own hair, resulting in noticeable hair loss.1,2 This disorder is more commonly diagnosed in women, likely reflecting treatment-seeking bias; women may be more likely to seek care for TTM because of social stigma associated with hair loss.2 Avulsion of hair usually occurs at the scalp, but also can be seen in multiple sites, including eyebrows, eyelashes, beards, and pubic regions; the number of sites typically increases with the patient’s age.3
The lifetime prevalence of comorbid axis I disorders in patients with TTM is 82%.3 Because of this, TTM often is first encountered in a psychiatric setting. Psychiatrists should have knowledge of TTM diagnosis and treatment because they may be the only point of care for TTM patients. When considering a TTM diagnosis, be aware that in some cultures rending hair is a mourning ritual or a rite of passage.3
Evidence for cognitive therapies
Behavioral models suggest TTM behaviors are learned and maintained by both classical and operant conditioning. Therapies that target the cognitive processes that trigger urges to pull, the avulsion of hair, and recognizing the consequences have the best empirical support.3
Habit reversal training (HRT) is considered the most effective treatment for TTM.3 One trial found a single 2-hour HRT intervention resulted in greater reductions in hair pulling episodes and higher remission rates compared with placebo.3 HRT trains patients to create a competing response, such as fist clenching, that is incompatible and blocks the undesired response.
Other therapeutic approaches to TTM include acceptance and commitment therapy, cognitive-behavioral therapy (CBT), and dialectical behavioral therapy-enhanced HRT. Evidence is most robust for CBT-HRT; randomized controlled trials found a statistically significant reduction in TTM in patients receiving CBT-HRT.3 One review suggests CBT-HRT should be considered first-line therapy for TTM.3
Pharmacologic options
Although no medications are FDA-approved for treating TTM, options include clomipramine, olanzapine, fluoxetine, pimozide, inositol, naltrexone, and N-acetylcysteine.2,3 The most robust trials of pharmacotherapy monotherapy were for N-acetylcysteine and naltrexone; both medications had significantly greater reduction in hair-pulling symptoms compared with placebo.3 Some evidence suggests combined pharmacotherapy and psychotherapy might be an effective approach.2,3
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
An estimated 1% of Americans have trichotillomania (TTM), an impulse-control disorder in which patients experience pleasure or gratification from recurrently pulling out their own hair, resulting in noticeable hair loss.1,2 This disorder is more commonly diagnosed in women, likely reflecting treatment-seeking bias; women may be more likely to seek care for TTM because of social stigma associated with hair loss.2 Avulsion of hair usually occurs at the scalp, but also can be seen in multiple sites, including eyebrows, eyelashes, beards, and pubic regions; the number of sites typically increases with the patient’s age.3
The lifetime prevalence of comorbid axis I disorders in patients with TTM is 82%.3 Because of this, TTM often is first encountered in a psychiatric setting. Psychiatrists should have knowledge of TTM diagnosis and treatment because they may be the only point of care for TTM patients. When considering a TTM diagnosis, be aware that in some cultures rending hair is a mourning ritual or a rite of passage.3
Evidence for cognitive therapies
Behavioral models suggest TTM behaviors are learned and maintained by both classical and operant conditioning. Therapies that target the cognitive processes that trigger urges to pull, the avulsion of hair, and recognizing the consequences have the best empirical support.3
Habit reversal training (HRT) is considered the most effective treatment for TTM.3 One trial found a single 2-hour HRT intervention resulted in greater reductions in hair pulling episodes and higher remission rates compared with placebo.3 HRT trains patients to create a competing response, such as fist clenching, that is incompatible and blocks the undesired response.
Other therapeutic approaches to TTM include acceptance and commitment therapy, cognitive-behavioral therapy (CBT), and dialectical behavioral therapy-enhanced HRT. Evidence is most robust for CBT-HRT; randomized controlled trials found a statistically significant reduction in TTM in patients receiving CBT-HRT.3 One review suggests CBT-HRT should be considered first-line therapy for TTM.3
Pharmacologic options
Although no medications are FDA-approved for treating TTM, options include clomipramine, olanzapine, fluoxetine, pimozide, inositol, naltrexone, and N-acetylcysteine.2,3 The most robust trials of pharmacotherapy monotherapy were for N-acetylcysteine and naltrexone; both medications had significantly greater reduction in hair-pulling symptoms compared with placebo.3 Some evidence suggests combined pharmacotherapy and psychotherapy might be an effective approach.2,3
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
2. Woods DW, Flessner C, Franklin ME, et al. Understanding and treating trichotillomania: what we know and what we don’t know. Psychiatr Clin North Am. 2006;29(2):487-501, ix.
3. Duke DC, Keeley ML, Geffken GR, et al. Trichotillomania: a current review. Clin Psychol Rev. 2010;30(2):181-193.
1. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
2. Woods DW, Flessner C, Franklin ME, et al. Understanding and treating trichotillomania: what we know and what we don’t know. Psychiatr Clin North Am. 2006;29(2):487-501, ix.
3. Duke DC, Keeley ML, Geffken GR, et al. Trichotillomania: a current review. Clin Psychol Rev. 2010;30(2):181-193.
‘Bugs in my skin’: What you should know about delusional infestation
Patients with delusional infestation (DI) falsely believe that they are infested with tiny infectious agents—typically vermin, insects, or small animals—that crawl on, in, or under their skin, leaving marks and building nests.1 Patients often describe the pathogens on the skin of hands, arms, feet, lower legs, scalp, or genital areas. They state the pathogen is difficult to diagnose and usually is contracted by human contact. Most patients with DI engage in intensive, repetitive, and often dangerous self-cleansing to get rid of the pathogens, which results in skin lesions.1 Less often, patients believe they are infested with bacteria or viruses.1
The typical DI patient is a middle age or older female with few social contacts, no psychiatric history, and normal cognitive and social function.1 Geriatric patients with dementia and vision or hearing impairment who live in a nursing home may develop DI; it also may be seen in geriatric patients with vascular encephalopathy.
What to consider
First rule out a genuine infestation by referring your patient for dermatologic and microbiologic testing. Order basic laboratory tests to assess inflammation markers—complete blood cell count, erythrocyte sedimentation rate, C-reactive protein, electrolytes, liver function, thyroid-stimulating hormone, and fasting glucose.1 Suggest a cranial MRI to rule out a brain disorder. Also, perform a urinalysis for cocaine, amphetamines, or cannabinoids, which can cause DI.1 Rule out medical conditions that are associated with pruritus and psychiatric symptoms, including endocrine, renal, hepatic, rheumatoid, and nutritional conditions.
Treating DI patients
Collaborate with a dermatologist, microbiologist, and primary care physician because these clinicians can deliver medical interventions, such as treating skin lesions and prescribing non-sedating antihistamines to alleviate pruritus. The Table1 offers other suggestions for managing DI patients.
Pharmacotherapy. Although high-quality evidence supporting antipsychotics for treating DI is lacking, olanzapine and risperidone are considered first-line agents; haloperidol and perphenazine also are recommended.1 Response and remission rates are similar with typical and atypical antipsychotics and the median onset of efficacy with antipsychotics is approximately 1.5 weeks.1,2 Antidepressants—including escitalopram, sertraline, mirtazapine, and venlafaxine—have been shown to effectively treat DI.3 In treatment-resistant cases, pimozide and electroconvulsive therapy have been used.1
Psychotherapy is effective for only 10% of DI patients.4
Table
Treating patients with DI: What to do and what to avoid
| Do’s | Don’t |
|---|---|
| Do acknowledge and empathize with your patient’s concerns | Don’t try to convince your patient he or she is wrong about the self-diagnosis |
| Do perform a thorough physical exam and diagnostic investigation | Don’t use words such as “delusional” or “psychotic” |
| Do paraphrase symptoms as “sensations” or “crawling” instead of reinforcing or questioning them | Don’t start psychopharmacology until you establish rapport with your patient |
| Do indicate that symptoms could be secondary to overactivity of the nervous system or “unexplained dermopathy” | |
| Do suggest that antipsychotics may help reduce your patient’s distress and itching | |
| DI: delusional infestation Source: Adapted from reference 1 | |
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Freudenmann RW, Lepping P. Delusional infestation. Clin Microbiol Rev. 2009;22(4):690-732.
2. Freudenmann RW, Lepping P. Second-generation antipsychotics in primary and secondary delusional parasitosis: outcome and efficacy. J Clin Psychopharmacol. 2008;28(5):500-508.
3. Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 12 new-generation antidepressants: a multiple-treatments meta-analysis. Lancet. 2009;373(9665):746-758.
4. Wykoff RF. Delusions of parasitosis: a review. Rev Infect Dis. 1987;9(3):433-437.
Patients with delusional infestation (DI) falsely believe that they are infested with tiny infectious agents—typically vermin, insects, or small animals—that crawl on, in, or under their skin, leaving marks and building nests.1 Patients often describe the pathogens on the skin of hands, arms, feet, lower legs, scalp, or genital areas. They state the pathogen is difficult to diagnose and usually is contracted by human contact. Most patients with DI engage in intensive, repetitive, and often dangerous self-cleansing to get rid of the pathogens, which results in skin lesions.1 Less often, patients believe they are infested with bacteria or viruses.1
The typical DI patient is a middle age or older female with few social contacts, no psychiatric history, and normal cognitive and social function.1 Geriatric patients with dementia and vision or hearing impairment who live in a nursing home may develop DI; it also may be seen in geriatric patients with vascular encephalopathy.
What to consider
First rule out a genuine infestation by referring your patient for dermatologic and microbiologic testing. Order basic laboratory tests to assess inflammation markers—complete blood cell count, erythrocyte sedimentation rate, C-reactive protein, electrolytes, liver function, thyroid-stimulating hormone, and fasting glucose.1 Suggest a cranial MRI to rule out a brain disorder. Also, perform a urinalysis for cocaine, amphetamines, or cannabinoids, which can cause DI.1 Rule out medical conditions that are associated with pruritus and psychiatric symptoms, including endocrine, renal, hepatic, rheumatoid, and nutritional conditions.
Treating DI patients
Collaborate with a dermatologist, microbiologist, and primary care physician because these clinicians can deliver medical interventions, such as treating skin lesions and prescribing non-sedating antihistamines to alleviate pruritus. The Table1 offers other suggestions for managing DI patients.
Pharmacotherapy. Although high-quality evidence supporting antipsychotics for treating DI is lacking, olanzapine and risperidone are considered first-line agents; haloperidol and perphenazine also are recommended.1 Response and remission rates are similar with typical and atypical antipsychotics and the median onset of efficacy with antipsychotics is approximately 1.5 weeks.1,2 Antidepressants—including escitalopram, sertraline, mirtazapine, and venlafaxine—have been shown to effectively treat DI.3 In treatment-resistant cases, pimozide and electroconvulsive therapy have been used.1
Psychotherapy is effective for only 10% of DI patients.4
Table
Treating patients with DI: What to do and what to avoid
| Do’s | Don’t |
|---|---|
| Do acknowledge and empathize with your patient’s concerns | Don’t try to convince your patient he or she is wrong about the self-diagnosis |
| Do perform a thorough physical exam and diagnostic investigation | Don’t use words such as “delusional” or “psychotic” |
| Do paraphrase symptoms as “sensations” or “crawling” instead of reinforcing or questioning them | Don’t start psychopharmacology until you establish rapport with your patient |
| Do indicate that symptoms could be secondary to overactivity of the nervous system or “unexplained dermopathy” | |
| Do suggest that antipsychotics may help reduce your patient’s distress and itching | |
| DI: delusional infestation Source: Adapted from reference 1 | |
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Patients with delusional infestation (DI) falsely believe that they are infested with tiny infectious agents—typically vermin, insects, or small animals—that crawl on, in, or under their skin, leaving marks and building nests.1 Patients often describe the pathogens on the skin of hands, arms, feet, lower legs, scalp, or genital areas. They state the pathogen is difficult to diagnose and usually is contracted by human contact. Most patients with DI engage in intensive, repetitive, and often dangerous self-cleansing to get rid of the pathogens, which results in skin lesions.1 Less often, patients believe they are infested with bacteria or viruses.1
The typical DI patient is a middle age or older female with few social contacts, no psychiatric history, and normal cognitive and social function.1 Geriatric patients with dementia and vision or hearing impairment who live in a nursing home may develop DI; it also may be seen in geriatric patients with vascular encephalopathy.
What to consider
First rule out a genuine infestation by referring your patient for dermatologic and microbiologic testing. Order basic laboratory tests to assess inflammation markers—complete blood cell count, erythrocyte sedimentation rate, C-reactive protein, electrolytes, liver function, thyroid-stimulating hormone, and fasting glucose.1 Suggest a cranial MRI to rule out a brain disorder. Also, perform a urinalysis for cocaine, amphetamines, or cannabinoids, which can cause DI.1 Rule out medical conditions that are associated with pruritus and psychiatric symptoms, including endocrine, renal, hepatic, rheumatoid, and nutritional conditions.
Treating DI patients
Collaborate with a dermatologist, microbiologist, and primary care physician because these clinicians can deliver medical interventions, such as treating skin lesions and prescribing non-sedating antihistamines to alleviate pruritus. The Table1 offers other suggestions for managing DI patients.
Pharmacotherapy. Although high-quality evidence supporting antipsychotics for treating DI is lacking, olanzapine and risperidone are considered first-line agents; haloperidol and perphenazine also are recommended.1 Response and remission rates are similar with typical and atypical antipsychotics and the median onset of efficacy with antipsychotics is approximately 1.5 weeks.1,2 Antidepressants—including escitalopram, sertraline, mirtazapine, and venlafaxine—have been shown to effectively treat DI.3 In treatment-resistant cases, pimozide and electroconvulsive therapy have been used.1
Psychotherapy is effective for only 10% of DI patients.4
Table
Treating patients with DI: What to do and what to avoid
| Do’s | Don’t |
|---|---|
| Do acknowledge and empathize with your patient’s concerns | Don’t try to convince your patient he or she is wrong about the self-diagnosis |
| Do perform a thorough physical exam and diagnostic investigation | Don’t use words such as “delusional” or “psychotic” |
| Do paraphrase symptoms as “sensations” or “crawling” instead of reinforcing or questioning them | Don’t start psychopharmacology until you establish rapport with your patient |
| Do indicate that symptoms could be secondary to overactivity of the nervous system or “unexplained dermopathy” | |
| Do suggest that antipsychotics may help reduce your patient’s distress and itching | |
| DI: delusional infestation Source: Adapted from reference 1 | |
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Freudenmann RW, Lepping P. Delusional infestation. Clin Microbiol Rev. 2009;22(4):690-732.
2. Freudenmann RW, Lepping P. Second-generation antipsychotics in primary and secondary delusional parasitosis: outcome and efficacy. J Clin Psychopharmacol. 2008;28(5):500-508.
3. Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 12 new-generation antidepressants: a multiple-treatments meta-analysis. Lancet. 2009;373(9665):746-758.
4. Wykoff RF. Delusions of parasitosis: a review. Rev Infect Dis. 1987;9(3):433-437.
1. Freudenmann RW, Lepping P. Delusional infestation. Clin Microbiol Rev. 2009;22(4):690-732.
2. Freudenmann RW, Lepping P. Second-generation antipsychotics in primary and secondary delusional parasitosis: outcome and efficacy. J Clin Psychopharmacol. 2008;28(5):500-508.
3. Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 12 new-generation antidepressants: a multiple-treatments meta-analysis. Lancet. 2009;373(9665):746-758.
4. Wykoff RF. Delusions of parasitosis: a review. Rev Infect Dis. 1987;9(3):433-437.
Playing through the pain: Psychiatric risks among athletes
Discuss this article at www.facebook.com/CurrentPsychiatry

Suck it up. Tough it out. There is no “I” in team. These are a few of the messages athletes receive from coaches, teammates, and fans. There are norms, values, and expectations in every culture, including sports, that affect behavior and emotional expression. When taking a patient’s history, clinicians may ask about participation in sports because it provides health and lifestyle information. However, many clinicians fail to consider the extent to which sport participation can influence a person’s explanatory style, experience of injury, and attitude toward medications. Whether your patient is an elite athlete or someone who participates in sports solely for exercise, the extent to which he or she identifies as an athlete is worth exploring.
Research on athletes has focused on physical aspects of injury, but this may be just a small component of an athlete’s devastation after serious injury. In this article, we discuss athletes’:
- psychiatric risks after injury
- expression of pain
- risks of having an identity driven solely by sports
- distress tolerance.
We also provide tips for making a differential diagnosis and providing treatment. This information is based on our experience treating athletes, supplemented by relevant literature.
Psychiatric risks after injury
Research has explored eating disorders and substance use among athletes, but clinicians generally are less aware of the prevalence of mood and anxiety disorders in this population. Although participating in sports can protect against emotional distress, athletes who sustain an injury are at risk for major depressive disorder, posttraumatic stress disorder (PTSD), or an adjustment disorder.1 Only about 10% of injured athletes have severe, long-term psychological consequences,2 but the prevalence of anger and depression after an injury is well documented.3,4 Researchers have found that injured athletes experience clinically significant depression 6 times as often as non-injured athletes.5 Injured athletes also exhibit significantly greater anxiety and lower self-esteem than non-injured controls immediately after injury and at 2-month follow-up; those with more severe injuries are more likely to become depressed.6 Non-injured athletes seem to experience depression at the same rate as the general population.7
Injury and expression of pain
Psychiatric illnesses often are underreported and undertreated in athletes.8 This may be because athletes feel that admitting they have a psychiatric illness or symptoms could threaten their status with their team. One professional figure skater we treated failed to seek recommended treatment for a psychiatric disorder because she feared she would be asked to leave her skating company. Her symptoms dangerously escalated before she was hospitalized.
Based on our clinical experience, many athletes feel acute pressure to play through psychological and physical pain. Some athletes continue to play with an injury to hold on to a paycheck or scholarship. Some continue to play even though they no longer enjoy the sport to prevent letting down parents or coaches; others know no other way but to “tough it out.” Supporters such as coaches, parents, or teammates may encourage athletes to play with injury, and sometimes provide medication to do so.
Mostly, however, the pressure to continue to play despite injury comes from athletes themselves. The culture of sport may lead athletes to minimize pain, fear, and self doubt.9 Athletes who fuse the culture of sport with their own being may underreport physical and psychiatric symptoms. In a survey of National Collegiate Athletic Association Division I athletes, Nixon9 found that 70% of respondents reported having been injured at least once, and more than one-half felt pressure to play while injured. Feeling pressure to perform with injury was affected by “starter” status, and whites and men scored highest on pressure scales, although women showed a roughly equal probability of playing through injury. Students who received an athletic scholarship experienced more injuries that required surgery. There was no difference in pain expression between players of contact and non-contact sports. Finally, athletes may be less likely to seek pharmacologic treatments because of cultural messages that emphasize ideas such as “the body is a temple.”
Loss of identity
An athlete’s injury should be analyzed for meaning; what may seem insignificant to one person may be quite different for another. When injury makes athletic activity impossible, an athlete may suffer more distress than someone who does not exercise regularly. Understanding the significance of the experience for an athlete is crucial to achieving recovery.10 For example, to a non-athlete a fractured wrist may be an annoyance, but it may be disastrous to a collegiate pitcher who is forced to be inactive when scouts for Major League Baseball teams search for prospects.
To an athlete, injury can mean loss of identity. Whereas most people become competent in many aspects of life, and develop support systems across multiple contexts, an athlete—particularly an extraordinarily talented one—may have focused only on his or her sport. Although athletics can help young people develop confidence, participation also can be a trap. Individuals with strong athletic identities are less likely to explore other career, educational, and lifestyle options.11 In the context of team sports, an athlete may feel less emotionally supported if an injury results in the loss of his or her central role with the team. Helping athletes form an identity that is not based solely on sports is ideal because subsequent injuries could lead to recurrent struggles with loss of identity.
Athletes who achieve higher levels of success have higher levels of depression and higher suicidal ideation after injury.12 An athlete may attempt or complete suicide, particularly those who are injured (Box).13-16
Student athletes. When working with student athletes, it is crucial to understand the lifestyle that promotes forming a single-factor identity. Student athletes may be required to train 2 or 3 times a day, rarely spend their school breaks in tropical locations, often miss social events, and may forgo commencement ceremonies. When an injury suddenly makes these perpetual sacrifices seem to be in vain, the risk of psychiatric illness may increase.
Suicides by several high-profile athletes have called attention to the severity of psychiatric risks among athletes. In June 2002, 20-year-old Nathan Eisert died of a self-inflicted gunshot wound 5 weeks after being released from the Western Kentucky University basketball team for academic reasons; the year before, he had suffered a serious ankle injury.13 Former National Football League (NFL) player Kenny McKinley committed suicide in September 2010, after a knee injury sidelined him.14 In May 2012, former NFL star Junior Seau, who had retired in 2011, fatally shot himself.15
For some athletes, career-ending injuries lead to suicidal behaviors. A study of 5 athletes who attempted suicide after sustaining an injury found 5 common characteristics:
- all were successful in their sport before getting injured
- all sustained an injury severe enough to warrant surgery
- all endured a lengthy rehabilitation
- all were not as successful at their sport when they returned to play
- all were replaced by a teammate.16
Tolerating distress
Athletes often use their sport as an outlet for emotional expression. When an injury removes that outlet, an athlete may develop anxiety and disappointment. Left alone to manage these emotions, an athlete may become irritable, passive, socially isolated, depressed, or suicidal.17 Trying but failing to find socially acceptable ways to express these feelings may intensify depression or anger. Difficult life issues, such as avoided losses, relationship issues, or various insecurities, may come to the surface when an athlete’s primary coping skill is lost. In addition, without the support of the athletic “family” (eg, teammates, coaches, staff) many athletes turn to alcohol or drugs unless they have alternate coping strategies and social supports.18
Overtraining and stress
The differential diagnosis for athletes who present with psychiatric symptoms includes several mood and anxiety disorders and other conditions (Table). When evaluating athletes who have depressive symptoms, it is essential to rule out overtraining syndrome (OTS). A common phenomenon among athletes, OTS is characterized by athletic “staleness” and chronic fatigue.19 Although there are no official OTS diagnostic criteria, characteristic symptoms include decreased physical performance or stamina, fatigue, insomnia, change in appetite, irritability, restlessness, excitability, anxiety, weight loss, loss of motivation, and poor concentration.19 The primary distinction between OTS and depression is that OTS results from athletic endeavors and can be reversed by reducing activity.
Experiencing an injury—or even a near-miss—can be terrifying to a person who derives his or her identity from a fully functioning body and feels that a perfectly working body is essential to an acceptable life. Such athletes may develop acute stress disorder or PTSD.20,21 We treated a hockey player who just missed being involved in a serious incident on the ice. “I watched my whole athletic career up to that point flash before my eyes.… I keep getting flashes of that,” he said. After the incident, he experienced hypervigilance, avoidance, and anxiety—both on and off the ice—and was diagnosed with acute stress disorder. Similarly, we cared for a young running back whose physical symptoms had abated after experiencing a concussion. He developed an irrational fear that he would become injured again. Neither athlete had a history of psychiatric illness or serious injury, and both were paralyzed by the idea of returning to play. One of these athletes successfully engaged in exposure therapy, and the other experienced severe avoidance, hopelessness, depression, nightmares, and flashbacks before seeking treatment.
Table
Differential diagnosis of conditions associated with athletic injury
| Acute stress disorder |
| Adjustment disorder |
| Anxiety disorder NOS |
| Depressive disorder NOS |
| Major depressive disorder |
| Overtraining syndrome |
| Postconcussion syndrome |
| Posttraumatic stress disorder |
| NOS: Not otherwise specified |
Substance use: Common and risky
Anecdotal and clinical evidence suggests that athletes in different sports engage in different substance abuse patterns. Studies show that college athletes use alcohol at higher rates than non-athletes.22,23 In 2000, the American College of Sports Medicine reported that athletes’ abuse of recreational drugs far surpasses their abuse of performance-enhancing drugs.24 Some athletes may use prescription pain medications recreationally or to self-medicate emotional pain as a result of injury. Athletes may not understand the risks of recreational use of prescription medications or illicit substances—such as cocaine’s deleterious cardiovascular effects—and may hesitate to discuss their self-medicating with physicians.
Some athletes abuse performance-enhancing drugs, such as anabolic steroids, androstenedione, stimulants, diuretics, and creatine.25 Side effects of these substances include liver disease, brain hemorrhage, weight loss, and depression.25
Our recommendations
Working with athletes—particularly injured athletes who have internalized sports culture—requires informed clinical effort, whether your patient is a student athlete, elite athlete, leisure athlete, or former athlete. Successful diagnosis and treatment requires understanding the meaning of athletics in your patient’s life and the extent to which he or she has “back-up” stress relievers and support systems, and assessing for cognitive dysfunction that may contribute to mood or anxiety symptoms. During evaluation, take a careful history to distinguish major depression or adjustment disorders from OTS, and assess for PTSD symptoms. When treating an injured athlete, help the patient determine whether he or she can find another outlet—preferably more than one—to replace athletics.
For an athlete who has depressive symptoms, we recommend determining whether the patient’s symptoms remit after a brief period of rest before initiating pharmacotherapy. For patients who exhibit minimal neurovegetative features, we recommend psychotherapy as a first-line treatment. Many athletes are reluctant to take medication and would be more likely to follow through with cognitive-behavioral and biofeedback interventions.
If a patient requires pharmacotherapy, ask about his or her feelings toward medications that may impact adherence. For example, is a gymnast worried about weight gain? Is a sprinter concerned with lethargy? When prescribing, be aware of the prevalence of drug and alcohol problems among athletes, understand how habits and temptations differ among sports cultures, and provide patients with psychoeducation about substance abuse when appropriate.
Related Resources
- International Society for Sports Psychiatry. http://sportspsychiatry.org.
- Sabo D, Miller KE, Melnick MJ, et al. High school athletic participation and adolescent suicide: a nationwide U.S. study. Int Rev Sociol Sport. 2005;40(1):5-23. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2563797. Accessed June 7, 2012.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Brewer BW, Linder DE, Phelps CM. Situational correlates of emotional adjustment to athletic injury. Clin J Sport Med. 1995;5(4):241-245.
2. Brewer BW, Petrie TA. Psychopathology in sport and exercise. In: Van Raalte JL Brewer BW, eds. Exploring sport and exercise psychology. Washington, DC: American Psychological Association; 1996:257–274.
3. May J, Sieb G. Athletic injuries: psychosocial factors in the onset sequelae, rehabilitation and prevention. In: May JR, Asken MJ, eds. Sport psychology: the psychological health of the athlete. New York, NY: PMA Publishing; 1987: 157–185.
4. Quackenbush N, Crossman J. Injured athletes: a study of emotional responses. J Sport Behav. 1994;17:178-187.
5. Perna F, Roh J, Newcomer R, et al. Clinical depression among injured athletes: an empirical assessment. Presented at: Association for the Advancement of Applied Sport Psychology annual convention; September 1998; Hyannis, MA.
6. Leddy MH, Lambert MJ, Ogles BM. Psychological consequences of athletic injury among high-level competitors. Res Q Exerc Sport. 1994;65(4):347-354.
7. Schwenk TL. The stigmatisation and denial of mental illness in athletes. Br J Sports Med. 2000;34(1):4-5.
8. Rotella RJ, Heyman SR. Stress injury, and the psychological rehabilitation of athletes. In: Williams HR, ed. Applied sports psychology: personal growth to peak performance. 2nd ed. Mountain View, CA: Mayfield Publishing; 1993: 338–355.
9. Nixon HL, II. Explaining pain and injury attitudes and experiences in sport in terms of gender race, and sports status factors. Journal of Sport Social Issues. 1996;20(1):33-44.
10. Harris LL. Integrating and analyzing psychosocial and stage theories to challenge the development of the injured collegiate athlete. J Athl Train. 2003;38(1):75-82.
11. Brown C, Hartley DL. Athletic identity and career maturation of male college student athletes. International Journal of Sport Psychology. 1998;29(1):17-26.
12. Baum AL. Suicide in athletes: a review and commentary. Clin Sports Med. 2005;24(4):853-859, ix.
13. Ho J. Suicide on campus. CBS News. http://www.cbsnews.com/2100-500195_162-654130.html. Published February 11 2009. Accessed June 7, 2012.
14. Bunch J, Jones LH. Broncos WR Kenny McKinley found dead in apparent suicide. Denver Post. http://www.denverpost.com/sports/ci_16127852. Published September 20 2010. Accessed June 7, 2012.
15. Saraceno J. Junior Seau’s death came with ‘zero warning.’ USA Today. http://www.usatoday.com/sports/football/nfl/story/2012-05-02/junior-seau-dead-gunshot/54712488/1. Published May 3 2012. Accessed June 7, 2012.
16. Smith AM, Milliner EK. Injured athletes and the risk of suicide. J Athl Train. 1994;29(4):337-341.
17. Putukian M, Wilfert M. National Collegiate Athletic Association. Student-athletes also face dangers from depression. http://fs.ncaa.org/Docs/NCAANewsArchive/2004/Association-Wide/student-athletes+also+face+dangers+from+depression+-+4-12-04.html. Published April 12 2004. Accessed June 6, 2012.
18. Perna FM, Antoni MH, Baum A, et al. Cognitive behavioral stress management effects on injury and illness among competitive athletes: a randomized clinical trial. Ann Behav Med. 2003;25(1):66-73.
19. Armstrong LE, VanHeest JL. The unknown mechanism of the overtraining syndrome: clues from depression and psychoneuroimmunology. Sports Med. 2002;32(3):185-209.
20. Newcomer RR, Perna FM. Features of posttraumatic distress among adolescent athletes. J Athl Train. 2003;38(2):163-166.
21. Newcomer R, Roh J, Perna F, et al. Injury as a traumatic experience: Intrusive thoughts and avoidance behavior associated with injury among college student-athletes. J Appl Sport Psychol. 1998;10(suppl):S54.
22. Hildebrand KM, Johnson DJ, Bogle K. Comparison of patterns of alcohol use between high school and college athletes and non-athletes. College Student Journal. 2001;35:358-365.
23. Wilson GS, Pritchard ME, Schaffer J. Athletic status and drinking behavior in college students: the influence of gender and coping styles. J Am Coll Health. 2004;52(6):269-273.
24. Wadler GI. American College of Sports Medicine. Cocaine abuse in sports. http://www.acsm.org/docs/current-comments/cocainabuse.pdf. Accessed June 6, 2012.
25. Mayo Clinic. Performance-enhancing drugs: know the risks. http://www.mayoclinic.com/health/performance-enhancing-drugs/hq01105. Published December 23, 2010.
Discuss this article at www.facebook.com/CurrentPsychiatry
Suck it up. Tough it out. There is no “I” in team. These are a few of the messages athletes receive from coaches, teammates, and fans. There are norms, values, and expectations in every culture, including sports, that affect behavior and emotional expression. When taking a patient’s history, clinicians may ask about participation in sports because it provides health and lifestyle information. However, many clinicians fail to consider the extent to which sport participation can influence a person’s explanatory style, experience of injury, and attitude toward medications. Whether your patient is an elite athlete or someone who participates in sports solely for exercise, the extent to which he or she identifies as an athlete is worth exploring.
Research on athletes has focused on physical aspects of injury, but this may be just a small component of an athlete’s devastation after serious injury. In this article, we discuss athletes’:
- psychiatric risks after injury
- expression of pain
- risks of having an identity driven solely by sports
- distress tolerance.
We also provide tips for making a differential diagnosis and providing treatment. This information is based on our experience treating athletes, supplemented by relevant literature.
Psychiatric risks after injury
Research has explored eating disorders and substance use among athletes, but clinicians generally are less aware of the prevalence of mood and anxiety disorders in this population. Although participating in sports can protect against emotional distress, athletes who sustain an injury are at risk for major depressive disorder, posttraumatic stress disorder (PTSD), or an adjustment disorder.1 Only about 10% of injured athletes have severe, long-term psychological consequences,2 but the prevalence of anger and depression after an injury is well documented.3,4 Researchers have found that injured athletes experience clinically significant depression 6 times as often as non-injured athletes.5 Injured athletes also exhibit significantly greater anxiety and lower self-esteem than non-injured controls immediately after injury and at 2-month follow-up; those with more severe injuries are more likely to become depressed.6 Non-injured athletes seem to experience depression at the same rate as the general population.7
Injury and expression of pain
Psychiatric illnesses often are underreported and undertreated in athletes.8 This may be because athletes feel that admitting they have a psychiatric illness or symptoms could threaten their status with their team. One professional figure skater we treated failed to seek recommended treatment for a psychiatric disorder because she feared she would be asked to leave her skating company. Her symptoms dangerously escalated before she was hospitalized.
Based on our clinical experience, many athletes feel acute pressure to play through psychological and physical pain. Some athletes continue to play with an injury to hold on to a paycheck or scholarship. Some continue to play even though they no longer enjoy the sport to prevent letting down parents or coaches; others know no other way but to “tough it out.” Supporters such as coaches, parents, or teammates may encourage athletes to play with injury, and sometimes provide medication to do so.
Mostly, however, the pressure to continue to play despite injury comes from athletes themselves. The culture of sport may lead athletes to minimize pain, fear, and self doubt.9 Athletes who fuse the culture of sport with their own being may underreport physical and psychiatric symptoms. In a survey of National Collegiate Athletic Association Division I athletes, Nixon9 found that 70% of respondents reported having been injured at least once, and more than one-half felt pressure to play while injured. Feeling pressure to perform with injury was affected by “starter” status, and whites and men scored highest on pressure scales, although women showed a roughly equal probability of playing through injury. Students who received an athletic scholarship experienced more injuries that required surgery. There was no difference in pain expression between players of contact and non-contact sports. Finally, athletes may be less likely to seek pharmacologic treatments because of cultural messages that emphasize ideas such as “the body is a temple.”
Loss of identity
An athlete’s injury should be analyzed for meaning; what may seem insignificant to one person may be quite different for another. When injury makes athletic activity impossible, an athlete may suffer more distress than someone who does not exercise regularly. Understanding the significance of the experience for an athlete is crucial to achieving recovery.10 For example, to a non-athlete a fractured wrist may be an annoyance, but it may be disastrous to a collegiate pitcher who is forced to be inactive when scouts for Major League Baseball teams search for prospects.
To an athlete, injury can mean loss of identity. Whereas most people become competent in many aspects of life, and develop support systems across multiple contexts, an athlete—particularly an extraordinarily talented one—may have focused only on his or her sport. Although athletics can help young people develop confidence, participation also can be a trap. Individuals with strong athletic identities are less likely to explore other career, educational, and lifestyle options.11 In the context of team sports, an athlete may feel less emotionally supported if an injury results in the loss of his or her central role with the team. Helping athletes form an identity that is not based solely on sports is ideal because subsequent injuries could lead to recurrent struggles with loss of identity.
Athletes who achieve higher levels of success have higher levels of depression and higher suicidal ideation after injury.12 An athlete may attempt or complete suicide, particularly those who are injured (Box).13-16
Student athletes. When working with student athletes, it is crucial to understand the lifestyle that promotes forming a single-factor identity. Student athletes may be required to train 2 or 3 times a day, rarely spend their school breaks in tropical locations, often miss social events, and may forgo commencement ceremonies. When an injury suddenly makes these perpetual sacrifices seem to be in vain, the risk of psychiatric illness may increase.
Suicides by several high-profile athletes have called attention to the severity of psychiatric risks among athletes. In June 2002, 20-year-old Nathan Eisert died of a self-inflicted gunshot wound 5 weeks after being released from the Western Kentucky University basketball team for academic reasons; the year before, he had suffered a serious ankle injury.13 Former National Football League (NFL) player Kenny McKinley committed suicide in September 2010, after a knee injury sidelined him.14 In May 2012, former NFL star Junior Seau, who had retired in 2011, fatally shot himself.15
For some athletes, career-ending injuries lead to suicidal behaviors. A study of 5 athletes who attempted suicide after sustaining an injury found 5 common characteristics:
- all were successful in their sport before getting injured
- all sustained an injury severe enough to warrant surgery
- all endured a lengthy rehabilitation
- all were not as successful at their sport when they returned to play
- all were replaced by a teammate.16
Tolerating distress
Athletes often use their sport as an outlet for emotional expression. When an injury removes that outlet, an athlete may develop anxiety and disappointment. Left alone to manage these emotions, an athlete may become irritable, passive, socially isolated, depressed, or suicidal.17 Trying but failing to find socially acceptable ways to express these feelings may intensify depression or anger. Difficult life issues, such as avoided losses, relationship issues, or various insecurities, may come to the surface when an athlete’s primary coping skill is lost. In addition, without the support of the athletic “family” (eg, teammates, coaches, staff) many athletes turn to alcohol or drugs unless they have alternate coping strategies and social supports.18
Overtraining and stress
The differential diagnosis for athletes who present with psychiatric symptoms includes several mood and anxiety disorders and other conditions (Table). When evaluating athletes who have depressive symptoms, it is essential to rule out overtraining syndrome (OTS). A common phenomenon among athletes, OTS is characterized by athletic “staleness” and chronic fatigue.19 Although there are no official OTS diagnostic criteria, characteristic symptoms include decreased physical performance or stamina, fatigue, insomnia, change in appetite, irritability, restlessness, excitability, anxiety, weight loss, loss of motivation, and poor concentration.19 The primary distinction between OTS and depression is that OTS results from athletic endeavors and can be reversed by reducing activity.
Experiencing an injury—or even a near-miss—can be terrifying to a person who derives his or her identity from a fully functioning body and feels that a perfectly working body is essential to an acceptable life. Such athletes may develop acute stress disorder or PTSD.20,21 We treated a hockey player who just missed being involved in a serious incident on the ice. “I watched my whole athletic career up to that point flash before my eyes.… I keep getting flashes of that,” he said. After the incident, he experienced hypervigilance, avoidance, and anxiety—both on and off the ice—and was diagnosed with acute stress disorder. Similarly, we cared for a young running back whose physical symptoms had abated after experiencing a concussion. He developed an irrational fear that he would become injured again. Neither athlete had a history of psychiatric illness or serious injury, and both were paralyzed by the idea of returning to play. One of these athletes successfully engaged in exposure therapy, and the other experienced severe avoidance, hopelessness, depression, nightmares, and flashbacks before seeking treatment.
Table
Differential diagnosis of conditions associated with athletic injury
| Acute stress disorder |
| Adjustment disorder |
| Anxiety disorder NOS |
| Depressive disorder NOS |
| Major depressive disorder |
| Overtraining syndrome |
| Postconcussion syndrome |
| Posttraumatic stress disorder |
| NOS: Not otherwise specified |
Substance use: Common and risky
Anecdotal and clinical evidence suggests that athletes in different sports engage in different substance abuse patterns. Studies show that college athletes use alcohol at higher rates than non-athletes.22,23 In 2000, the American College of Sports Medicine reported that athletes’ abuse of recreational drugs far surpasses their abuse of performance-enhancing drugs.24 Some athletes may use prescription pain medications recreationally or to self-medicate emotional pain as a result of injury. Athletes may not understand the risks of recreational use of prescription medications or illicit substances—such as cocaine’s deleterious cardiovascular effects—and may hesitate to discuss their self-medicating with physicians.
Some athletes abuse performance-enhancing drugs, such as anabolic steroids, androstenedione, stimulants, diuretics, and creatine.25 Side effects of these substances include liver disease, brain hemorrhage, weight loss, and depression.25
Our recommendations
Working with athletes—particularly injured athletes who have internalized sports culture—requires informed clinical effort, whether your patient is a student athlete, elite athlete, leisure athlete, or former athlete. Successful diagnosis and treatment requires understanding the meaning of athletics in your patient’s life and the extent to which he or she has “back-up” stress relievers and support systems, and assessing for cognitive dysfunction that may contribute to mood or anxiety symptoms. During evaluation, take a careful history to distinguish major depression or adjustment disorders from OTS, and assess for PTSD symptoms. When treating an injured athlete, help the patient determine whether he or she can find another outlet—preferably more than one—to replace athletics.
For an athlete who has depressive symptoms, we recommend determining whether the patient’s symptoms remit after a brief period of rest before initiating pharmacotherapy. For patients who exhibit minimal neurovegetative features, we recommend psychotherapy as a first-line treatment. Many athletes are reluctant to take medication and would be more likely to follow through with cognitive-behavioral and biofeedback interventions.
If a patient requires pharmacotherapy, ask about his or her feelings toward medications that may impact adherence. For example, is a gymnast worried about weight gain? Is a sprinter concerned with lethargy? When prescribing, be aware of the prevalence of drug and alcohol problems among athletes, understand how habits and temptations differ among sports cultures, and provide patients with psychoeducation about substance abuse when appropriate.
Related Resources
- International Society for Sports Psychiatry. http://sportspsychiatry.org.
- Sabo D, Miller KE, Melnick MJ, et al. High school athletic participation and adolescent suicide: a nationwide U.S. study. Int Rev Sociol Sport. 2005;40(1):5-23. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2563797. Accessed June 7, 2012.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at www.facebook.com/CurrentPsychiatry
Suck it up. Tough it out. There is no “I” in team. These are a few of the messages athletes receive from coaches, teammates, and fans. There are norms, values, and expectations in every culture, including sports, that affect behavior and emotional expression. When taking a patient’s history, clinicians may ask about participation in sports because it provides health and lifestyle information. However, many clinicians fail to consider the extent to which sport participation can influence a person’s explanatory style, experience of injury, and attitude toward medications. Whether your patient is an elite athlete or someone who participates in sports solely for exercise, the extent to which he or she identifies as an athlete is worth exploring.
Research on athletes has focused on physical aspects of injury, but this may be just a small component of an athlete’s devastation after serious injury. In this article, we discuss athletes’:
- psychiatric risks after injury
- expression of pain
- risks of having an identity driven solely by sports
- distress tolerance.
We also provide tips for making a differential diagnosis and providing treatment. This information is based on our experience treating athletes, supplemented by relevant literature.
Psychiatric risks after injury
Research has explored eating disorders and substance use among athletes, but clinicians generally are less aware of the prevalence of mood and anxiety disorders in this population. Although participating in sports can protect against emotional distress, athletes who sustain an injury are at risk for major depressive disorder, posttraumatic stress disorder (PTSD), or an adjustment disorder.1 Only about 10% of injured athletes have severe, long-term psychological consequences,2 but the prevalence of anger and depression after an injury is well documented.3,4 Researchers have found that injured athletes experience clinically significant depression 6 times as often as non-injured athletes.5 Injured athletes also exhibit significantly greater anxiety and lower self-esteem than non-injured controls immediately after injury and at 2-month follow-up; those with more severe injuries are more likely to become depressed.6 Non-injured athletes seem to experience depression at the same rate as the general population.7
Injury and expression of pain
Psychiatric illnesses often are underreported and undertreated in athletes.8 This may be because athletes feel that admitting they have a psychiatric illness or symptoms could threaten their status with their team. One professional figure skater we treated failed to seek recommended treatment for a psychiatric disorder because she feared she would be asked to leave her skating company. Her symptoms dangerously escalated before she was hospitalized.
Based on our clinical experience, many athletes feel acute pressure to play through psychological and physical pain. Some athletes continue to play with an injury to hold on to a paycheck or scholarship. Some continue to play even though they no longer enjoy the sport to prevent letting down parents or coaches; others know no other way but to “tough it out.” Supporters such as coaches, parents, or teammates may encourage athletes to play with injury, and sometimes provide medication to do so.
Mostly, however, the pressure to continue to play despite injury comes from athletes themselves. The culture of sport may lead athletes to minimize pain, fear, and self doubt.9 Athletes who fuse the culture of sport with their own being may underreport physical and psychiatric symptoms. In a survey of National Collegiate Athletic Association Division I athletes, Nixon9 found that 70% of respondents reported having been injured at least once, and more than one-half felt pressure to play while injured. Feeling pressure to perform with injury was affected by “starter” status, and whites and men scored highest on pressure scales, although women showed a roughly equal probability of playing through injury. Students who received an athletic scholarship experienced more injuries that required surgery. There was no difference in pain expression between players of contact and non-contact sports. Finally, athletes may be less likely to seek pharmacologic treatments because of cultural messages that emphasize ideas such as “the body is a temple.”
Loss of identity
An athlete’s injury should be analyzed for meaning; what may seem insignificant to one person may be quite different for another. When injury makes athletic activity impossible, an athlete may suffer more distress than someone who does not exercise regularly. Understanding the significance of the experience for an athlete is crucial to achieving recovery.10 For example, to a non-athlete a fractured wrist may be an annoyance, but it may be disastrous to a collegiate pitcher who is forced to be inactive when scouts for Major League Baseball teams search for prospects.
To an athlete, injury can mean loss of identity. Whereas most people become competent in many aspects of life, and develop support systems across multiple contexts, an athlete—particularly an extraordinarily talented one—may have focused only on his or her sport. Although athletics can help young people develop confidence, participation also can be a trap. Individuals with strong athletic identities are less likely to explore other career, educational, and lifestyle options.11 In the context of team sports, an athlete may feel less emotionally supported if an injury results in the loss of his or her central role with the team. Helping athletes form an identity that is not based solely on sports is ideal because subsequent injuries could lead to recurrent struggles with loss of identity.
Athletes who achieve higher levels of success have higher levels of depression and higher suicidal ideation after injury.12 An athlete may attempt or complete suicide, particularly those who are injured (Box).13-16
Student athletes. When working with student athletes, it is crucial to understand the lifestyle that promotes forming a single-factor identity. Student athletes may be required to train 2 or 3 times a day, rarely spend their school breaks in tropical locations, often miss social events, and may forgo commencement ceremonies. When an injury suddenly makes these perpetual sacrifices seem to be in vain, the risk of psychiatric illness may increase.
Suicides by several high-profile athletes have called attention to the severity of psychiatric risks among athletes. In June 2002, 20-year-old Nathan Eisert died of a self-inflicted gunshot wound 5 weeks after being released from the Western Kentucky University basketball team for academic reasons; the year before, he had suffered a serious ankle injury.13 Former National Football League (NFL) player Kenny McKinley committed suicide in September 2010, after a knee injury sidelined him.14 In May 2012, former NFL star Junior Seau, who had retired in 2011, fatally shot himself.15
For some athletes, career-ending injuries lead to suicidal behaviors. A study of 5 athletes who attempted suicide after sustaining an injury found 5 common characteristics:
- all were successful in their sport before getting injured
- all sustained an injury severe enough to warrant surgery
- all endured a lengthy rehabilitation
- all were not as successful at their sport when they returned to play
- all were replaced by a teammate.16
Tolerating distress
Athletes often use their sport as an outlet for emotional expression. When an injury removes that outlet, an athlete may develop anxiety and disappointment. Left alone to manage these emotions, an athlete may become irritable, passive, socially isolated, depressed, or suicidal.17 Trying but failing to find socially acceptable ways to express these feelings may intensify depression or anger. Difficult life issues, such as avoided losses, relationship issues, or various insecurities, may come to the surface when an athlete’s primary coping skill is lost. In addition, without the support of the athletic “family” (eg, teammates, coaches, staff) many athletes turn to alcohol or drugs unless they have alternate coping strategies and social supports.18
Overtraining and stress
The differential diagnosis for athletes who present with psychiatric symptoms includes several mood and anxiety disorders and other conditions (Table). When evaluating athletes who have depressive symptoms, it is essential to rule out overtraining syndrome (OTS). A common phenomenon among athletes, OTS is characterized by athletic “staleness” and chronic fatigue.19 Although there are no official OTS diagnostic criteria, characteristic symptoms include decreased physical performance or stamina, fatigue, insomnia, change in appetite, irritability, restlessness, excitability, anxiety, weight loss, loss of motivation, and poor concentration.19 The primary distinction between OTS and depression is that OTS results from athletic endeavors and can be reversed by reducing activity.
Experiencing an injury—or even a near-miss—can be terrifying to a person who derives his or her identity from a fully functioning body and feels that a perfectly working body is essential to an acceptable life. Such athletes may develop acute stress disorder or PTSD.20,21 We treated a hockey player who just missed being involved in a serious incident on the ice. “I watched my whole athletic career up to that point flash before my eyes.… I keep getting flashes of that,” he said. After the incident, he experienced hypervigilance, avoidance, and anxiety—both on and off the ice—and was diagnosed with acute stress disorder. Similarly, we cared for a young running back whose physical symptoms had abated after experiencing a concussion. He developed an irrational fear that he would become injured again. Neither athlete had a history of psychiatric illness or serious injury, and both were paralyzed by the idea of returning to play. One of these athletes successfully engaged in exposure therapy, and the other experienced severe avoidance, hopelessness, depression, nightmares, and flashbacks before seeking treatment.
Table
Differential diagnosis of conditions associated with athletic injury
| Acute stress disorder |
| Adjustment disorder |
| Anxiety disorder NOS |
| Depressive disorder NOS |
| Major depressive disorder |
| Overtraining syndrome |
| Postconcussion syndrome |
| Posttraumatic stress disorder |
| NOS: Not otherwise specified |
Substance use: Common and risky
Anecdotal and clinical evidence suggests that athletes in different sports engage in different substance abuse patterns. Studies show that college athletes use alcohol at higher rates than non-athletes.22,23 In 2000, the American College of Sports Medicine reported that athletes’ abuse of recreational drugs far surpasses their abuse of performance-enhancing drugs.24 Some athletes may use prescription pain medications recreationally or to self-medicate emotional pain as a result of injury. Athletes may not understand the risks of recreational use of prescription medications or illicit substances—such as cocaine’s deleterious cardiovascular effects—and may hesitate to discuss their self-medicating with physicians.
Some athletes abuse performance-enhancing drugs, such as anabolic steroids, androstenedione, stimulants, diuretics, and creatine.25 Side effects of these substances include liver disease, brain hemorrhage, weight loss, and depression.25
Our recommendations
Working with athletes—particularly injured athletes who have internalized sports culture—requires informed clinical effort, whether your patient is a student athlete, elite athlete, leisure athlete, or former athlete. Successful diagnosis and treatment requires understanding the meaning of athletics in your patient’s life and the extent to which he or she has “back-up” stress relievers and support systems, and assessing for cognitive dysfunction that may contribute to mood or anxiety symptoms. During evaluation, take a careful history to distinguish major depression or adjustment disorders from OTS, and assess for PTSD symptoms. When treating an injured athlete, help the patient determine whether he or she can find another outlet—preferably more than one—to replace athletics.
For an athlete who has depressive symptoms, we recommend determining whether the patient’s symptoms remit after a brief period of rest before initiating pharmacotherapy. For patients who exhibit minimal neurovegetative features, we recommend psychotherapy as a first-line treatment. Many athletes are reluctant to take medication and would be more likely to follow through with cognitive-behavioral and biofeedback interventions.
If a patient requires pharmacotherapy, ask about his or her feelings toward medications that may impact adherence. For example, is a gymnast worried about weight gain? Is a sprinter concerned with lethargy? When prescribing, be aware of the prevalence of drug and alcohol problems among athletes, understand how habits and temptations differ among sports cultures, and provide patients with psychoeducation about substance abuse when appropriate.
Related Resources
- International Society for Sports Psychiatry. http://sportspsychiatry.org.
- Sabo D, Miller KE, Melnick MJ, et al. High school athletic participation and adolescent suicide: a nationwide U.S. study. Int Rev Sociol Sport. 2005;40(1):5-23. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2563797. Accessed June 7, 2012.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Brewer BW, Linder DE, Phelps CM. Situational correlates of emotional adjustment to athletic injury. Clin J Sport Med. 1995;5(4):241-245.
2. Brewer BW, Petrie TA. Psychopathology in sport and exercise. In: Van Raalte JL Brewer BW, eds. Exploring sport and exercise psychology. Washington, DC: American Psychological Association; 1996:257–274.
3. May J, Sieb G. Athletic injuries: psychosocial factors in the onset sequelae, rehabilitation and prevention. In: May JR, Asken MJ, eds. Sport psychology: the psychological health of the athlete. New York, NY: PMA Publishing; 1987: 157–185.
4. Quackenbush N, Crossman J. Injured athletes: a study of emotional responses. J Sport Behav. 1994;17:178-187.
5. Perna F, Roh J, Newcomer R, et al. Clinical depression among injured athletes: an empirical assessment. Presented at: Association for the Advancement of Applied Sport Psychology annual convention; September 1998; Hyannis, MA.
6. Leddy MH, Lambert MJ, Ogles BM. Psychological consequences of athletic injury among high-level competitors. Res Q Exerc Sport. 1994;65(4):347-354.
7. Schwenk TL. The stigmatisation and denial of mental illness in athletes. Br J Sports Med. 2000;34(1):4-5.
8. Rotella RJ, Heyman SR. Stress injury, and the psychological rehabilitation of athletes. In: Williams HR, ed. Applied sports psychology: personal growth to peak performance. 2nd ed. Mountain View, CA: Mayfield Publishing; 1993: 338–355.
9. Nixon HL, II. Explaining pain and injury attitudes and experiences in sport in terms of gender race, and sports status factors. Journal of Sport Social Issues. 1996;20(1):33-44.
10. Harris LL. Integrating and analyzing psychosocial and stage theories to challenge the development of the injured collegiate athlete. J Athl Train. 2003;38(1):75-82.
11. Brown C, Hartley DL. Athletic identity and career maturation of male college student athletes. International Journal of Sport Psychology. 1998;29(1):17-26.
12. Baum AL. Suicide in athletes: a review and commentary. Clin Sports Med. 2005;24(4):853-859, ix.
13. Ho J. Suicide on campus. CBS News. http://www.cbsnews.com/2100-500195_162-654130.html. Published February 11 2009. Accessed June 7, 2012.
14. Bunch J, Jones LH. Broncos WR Kenny McKinley found dead in apparent suicide. Denver Post. http://www.denverpost.com/sports/ci_16127852. Published September 20 2010. Accessed June 7, 2012.
15. Saraceno J. Junior Seau’s death came with ‘zero warning.’ USA Today. http://www.usatoday.com/sports/football/nfl/story/2012-05-02/junior-seau-dead-gunshot/54712488/1. Published May 3 2012. Accessed June 7, 2012.
16. Smith AM, Milliner EK. Injured athletes and the risk of suicide. J Athl Train. 1994;29(4):337-341.
17. Putukian M, Wilfert M. National Collegiate Athletic Association. Student-athletes also face dangers from depression. http://fs.ncaa.org/Docs/NCAANewsArchive/2004/Association-Wide/student-athletes+also+face+dangers+from+depression+-+4-12-04.html. Published April 12 2004. Accessed June 6, 2012.
18. Perna FM, Antoni MH, Baum A, et al. Cognitive behavioral stress management effects on injury and illness among competitive athletes: a randomized clinical trial. Ann Behav Med. 2003;25(1):66-73.
19. Armstrong LE, VanHeest JL. The unknown mechanism of the overtraining syndrome: clues from depression and psychoneuroimmunology. Sports Med. 2002;32(3):185-209.
20. Newcomer RR, Perna FM. Features of posttraumatic distress among adolescent athletes. J Athl Train. 2003;38(2):163-166.
21. Newcomer R, Roh J, Perna F, et al. Injury as a traumatic experience: Intrusive thoughts and avoidance behavior associated with injury among college student-athletes. J Appl Sport Psychol. 1998;10(suppl):S54.
22. Hildebrand KM, Johnson DJ, Bogle K. Comparison of patterns of alcohol use between high school and college athletes and non-athletes. College Student Journal. 2001;35:358-365.
23. Wilson GS, Pritchard ME, Schaffer J. Athletic status and drinking behavior in college students: the influence of gender and coping styles. J Am Coll Health. 2004;52(6):269-273.
24. Wadler GI. American College of Sports Medicine. Cocaine abuse in sports. http://www.acsm.org/docs/current-comments/cocainabuse.pdf. Accessed June 6, 2012.
25. Mayo Clinic. Performance-enhancing drugs: know the risks. http://www.mayoclinic.com/health/performance-enhancing-drugs/hq01105. Published December 23, 2010.
1. Brewer BW, Linder DE, Phelps CM. Situational correlates of emotional adjustment to athletic injury. Clin J Sport Med. 1995;5(4):241-245.
2. Brewer BW, Petrie TA. Psychopathology in sport and exercise. In: Van Raalte JL Brewer BW, eds. Exploring sport and exercise psychology. Washington, DC: American Psychological Association; 1996:257–274.
3. May J, Sieb G. Athletic injuries: psychosocial factors in the onset sequelae, rehabilitation and prevention. In: May JR, Asken MJ, eds. Sport psychology: the psychological health of the athlete. New York, NY: PMA Publishing; 1987: 157–185.
4. Quackenbush N, Crossman J. Injured athletes: a study of emotional responses. J Sport Behav. 1994;17:178-187.
5. Perna F, Roh J, Newcomer R, et al. Clinical depression among injured athletes: an empirical assessment. Presented at: Association for the Advancement of Applied Sport Psychology annual convention; September 1998; Hyannis, MA.
6. Leddy MH, Lambert MJ, Ogles BM. Psychological consequences of athletic injury among high-level competitors. Res Q Exerc Sport. 1994;65(4):347-354.
7. Schwenk TL. The stigmatisation and denial of mental illness in athletes. Br J Sports Med. 2000;34(1):4-5.
8. Rotella RJ, Heyman SR. Stress injury, and the psychological rehabilitation of athletes. In: Williams HR, ed. Applied sports psychology: personal growth to peak performance. 2nd ed. Mountain View, CA: Mayfield Publishing; 1993: 338–355.
9. Nixon HL, II. Explaining pain and injury attitudes and experiences in sport in terms of gender race, and sports status factors. Journal of Sport Social Issues. 1996;20(1):33-44.
10. Harris LL. Integrating and analyzing psychosocial and stage theories to challenge the development of the injured collegiate athlete. J Athl Train. 2003;38(1):75-82.
11. Brown C, Hartley DL. Athletic identity and career maturation of male college student athletes. International Journal of Sport Psychology. 1998;29(1):17-26.
12. Baum AL. Suicide in athletes: a review and commentary. Clin Sports Med. 2005;24(4):853-859, ix.
13. Ho J. Suicide on campus. CBS News. http://www.cbsnews.com/2100-500195_162-654130.html. Published February 11 2009. Accessed June 7, 2012.
14. Bunch J, Jones LH. Broncos WR Kenny McKinley found dead in apparent suicide. Denver Post. http://www.denverpost.com/sports/ci_16127852. Published September 20 2010. Accessed June 7, 2012.
15. Saraceno J. Junior Seau’s death came with ‘zero warning.’ USA Today. http://www.usatoday.com/sports/football/nfl/story/2012-05-02/junior-seau-dead-gunshot/54712488/1. Published May 3 2012. Accessed June 7, 2012.
16. Smith AM, Milliner EK. Injured athletes and the risk of suicide. J Athl Train. 1994;29(4):337-341.
17. Putukian M, Wilfert M. National Collegiate Athletic Association. Student-athletes also face dangers from depression. http://fs.ncaa.org/Docs/NCAANewsArchive/2004/Association-Wide/student-athletes+also+face+dangers+from+depression+-+4-12-04.html. Published April 12 2004. Accessed June 6, 2012.
18. Perna FM, Antoni MH, Baum A, et al. Cognitive behavioral stress management effects on injury and illness among competitive athletes: a randomized clinical trial. Ann Behav Med. 2003;25(1):66-73.
19. Armstrong LE, VanHeest JL. The unknown mechanism of the overtraining syndrome: clues from depression and psychoneuroimmunology. Sports Med. 2002;32(3):185-209.
20. Newcomer RR, Perna FM. Features of posttraumatic distress among adolescent athletes. J Athl Train. 2003;38(2):163-166.
21. Newcomer R, Roh J, Perna F, et al. Injury as a traumatic experience: Intrusive thoughts and avoidance behavior associated with injury among college student-athletes. J Appl Sport Psychol. 1998;10(suppl):S54.
22. Hildebrand KM, Johnson DJ, Bogle K. Comparison of patterns of alcohol use between high school and college athletes and non-athletes. College Student Journal. 2001;35:358-365.
23. Wilson GS, Pritchard ME, Schaffer J. Athletic status and drinking behavior in college students: the influence of gender and coping styles. J Am Coll Health. 2004;52(6):269-273.
24. Wadler GI. American College of Sports Medicine. Cocaine abuse in sports. http://www.acsm.org/docs/current-comments/cocainabuse.pdf. Accessed June 6, 2012.
25. Mayo Clinic. Performance-enhancing drugs: know the risks. http://www.mayoclinic.com/health/performance-enhancing-drugs/hq01105. Published December 23, 2010.
Strategies for managing patients with chronic subjective dizziness
Discuss this article at www.facebook.com/CurrentPsychiatry
Chronic subjective dizziness (CSD) is characterized by persistent (>3 months) dizziness, lightheadedness, or unsteadiness, without vertigo or ataxia. Symptoms often are worse in highly stimulating visual environments (eg, busy malls or grocery stores) or settings with indistinct visual orientation cues (eg, large open areas, heavy fog). Neuro-otologic examination and laboratory testing reveal no active vestibular deficits.1
CSD is not a psychiatric illness, but exists at the interface of psychiatry and neuro-otology. For example, anxiety and depressive disorders often accompany CSD, but are not an integral part of it. Treatment outcomes are good and prognosis for full function is high.
Conditions that cause dizziness
Vertigo—a sensation of rotation or linear movement of self or surroundings—occurs in discrete attacks that typically have an acute onset and are caused by neuro-otologic conditions.2 Symptoms may last for seconds (benign paroxysmal positional vertigo [BPPV]), hours (Meniere’s disease), minutes to days (vestibular migraine), or weeks (vestibular neuronitis). Unsteadiness, a swaying or rocking sensation, dizziness, and a disturbed sense of spatial orientation without illusory movement may be acute, subacute, or chronic. These symptoms may accompany vertigo or occur independently.2 Psychiatric disorders (panic), dysautonomias (vasovagal spells), and cardiovascular conditions (dysrhythmias) may cause episodic unsteadiness and dizziness, but not vertigo. Several illnesses can cause persistent unsteadiness and dizziness, including bilateral peripheral vestibular deficits, central vestibular lesions (strokes), proprioceptive or visual loss (neuropathies), and generalized anxiety disorder.
Up to 30% of patients who experience episodic balance problems develop persistent unsteadiness or dizziness (ie, CSD).3 Clinical history, exam, and laboratory tests may be normal or identify previous triggering events (eg, past vestibular insults), but transient conditions cannot explain patients’ persistent symptoms. Often, patients describe a transition from episodic vertigo and ataxia to chronic, often daily unsteadiness and dizziness. In this situation, the illness that started the problem often is not the one that continues to be distressing. Rather, patients develop hypersensitivity to motion stimuli (visual, vestibular, and proprioceptive inputs) and hypervigilance about motion environments that last long after the trigger event has resolved. These CSD features are thought to arise from threat-related failure of postural control systems to return to normal functioning after shifting into high-risk strategies during the acute events that disrupted balance.
5 strategies for managing CSD
1. Develop a common language among other clinicians you work with. The concept of CSD will be new to most patients and their referring clinicians, so they will need to hear about it more than once. From a neuro-otologic standpoint, make a point of separating past and present problems (ie, not the vestibular neuronitis, BPPV, etc., that the patient previously had, but the CSD they presently have). From a psychological standpoint, talk in behavioral terms—hypersensitivity to motion, hypervigilance about motion environments, use of safety maneuvers (eg, touching a wall when walking), and avoiding situations that provoke dizziness. These are reflexive, fear-driven symptoms, but patients understand them better in terms of dizziness and unsteadiness.
2. Keep in mind that dizziness is the chief complaint. As patients go from primary care to otolaryngology, audiology, vestibular rehabilitation, and psychiatry, the problem is dizziness. You may find anxiety or depression along the way, but dizziness comes first for these patients.
3. Educate patients and referring physicians. Give patients and their referring physicians materials that define CSD and its differential diagnosis.3 Check off patients’ symptoms in the diagnostic list and circle their medical comorbidities, if present. For psychiatrists, this is a good point to start discussing behavioral morbidity and treatment.
4. Screen for coexisting medical-psychiatric diagnoses (eg, Meniere’s disease, panic disorder) or primarily psychiatric problems (conversion disorder). In addition to the otologic exam for vestibular diseases, patients should be screened for migraine, traumatic brain injury, dysautonomia, and dysrhythmias. Ask patients to complete symptom self-reports, including the Patient Health Questionnaire-9 (for depression) and Generalized Anxiety Disorder-7 (for anxiety).
5. Treat the patient’s primary problem (eg, CSD, vertigo, ataxia, or headache) first. If headache and balance symptoms are intertwined, use venlafaxine or combine a selective serotonin reuptake inhibitor (SSRI) with a separate migraine prophylactic agent.
Treatment options
Pharmacotherapy. Five open-label studies found SSRIs are effective for CSD even for patients without psychiatric comorbidity.3 Use a “start low, go slow” strategy to avoid aggravating symptoms. Final doses usually are in the lower half of the therapeutic range. Full treatment response may take 8 to 12 weeks. Vestibular suppressants such as meclizine work reasonably well for acute vertigo, but have no role in treating CSD.
Vestibular and balance rehabilitation therapy (VBRT) is an exercise program performed at home by patients but overseen by specially trained physical therapists. It is an excellent habituation/desensitization program that can be integrated with medication and psychotherapy. All patients with CSD should undergo VBRT.
Cognitive-behavioral therapy may be helpful for treating psychiatric morbidity (anxiety, depression, phobic avoidance) in patients with CSD, but it appears to be less effective for physical symptoms of dizziness.3
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Staab JP, Ruckenstein MJ. Expanding the differential diagnosis of chronic dizziness. Arch Otolaryngol Head Neck Surg. 2007;133(2):170-176.
2. Bisdorff A, Von Brevern M, Lempert T, et al. Classification of vestibular symptoms: towards an international classification of vestibular disorders. J Vestib Res. 2009;19(1-2):1-13.
3. Staab JP. Psychological aspects of vestibular disorders. In: Eggers SD Zee DS, eds Vertigo and imbalance: clinical neurophysiology of the vestibular system. Boston, MA: Elsevier. 2010;502-522.
Discuss this article at www.facebook.com/CurrentPsychiatry
Chronic subjective dizziness (CSD) is characterized by persistent (>3 months) dizziness, lightheadedness, or unsteadiness, without vertigo or ataxia. Symptoms often are worse in highly stimulating visual environments (eg, busy malls or grocery stores) or settings with indistinct visual orientation cues (eg, large open areas, heavy fog). Neuro-otologic examination and laboratory testing reveal no active vestibular deficits.1
CSD is not a psychiatric illness, but exists at the interface of psychiatry and neuro-otology. For example, anxiety and depressive disorders often accompany CSD, but are not an integral part of it. Treatment outcomes are good and prognosis for full function is high.
Conditions that cause dizziness
Vertigo—a sensation of rotation or linear movement of self or surroundings—occurs in discrete attacks that typically have an acute onset and are caused by neuro-otologic conditions.2 Symptoms may last for seconds (benign paroxysmal positional vertigo [BPPV]), hours (Meniere’s disease), minutes to days (vestibular migraine), or weeks (vestibular neuronitis). Unsteadiness, a swaying or rocking sensation, dizziness, and a disturbed sense of spatial orientation without illusory movement may be acute, subacute, or chronic. These symptoms may accompany vertigo or occur independently.2 Psychiatric disorders (panic), dysautonomias (vasovagal spells), and cardiovascular conditions (dysrhythmias) may cause episodic unsteadiness and dizziness, but not vertigo. Several illnesses can cause persistent unsteadiness and dizziness, including bilateral peripheral vestibular deficits, central vestibular lesions (strokes), proprioceptive or visual loss (neuropathies), and generalized anxiety disorder.
Up to 30% of patients who experience episodic balance problems develop persistent unsteadiness or dizziness (ie, CSD).3 Clinical history, exam, and laboratory tests may be normal or identify previous triggering events (eg, past vestibular insults), but transient conditions cannot explain patients’ persistent symptoms. Often, patients describe a transition from episodic vertigo and ataxia to chronic, often daily unsteadiness and dizziness. In this situation, the illness that started the problem often is not the one that continues to be distressing. Rather, patients develop hypersensitivity to motion stimuli (visual, vestibular, and proprioceptive inputs) and hypervigilance about motion environments that last long after the trigger event has resolved. These CSD features are thought to arise from threat-related failure of postural control systems to return to normal functioning after shifting into high-risk strategies during the acute events that disrupted balance.
5 strategies for managing CSD
1. Develop a common language among other clinicians you work with. The concept of CSD will be new to most patients and their referring clinicians, so they will need to hear about it more than once. From a neuro-otologic standpoint, make a point of separating past and present problems (ie, not the vestibular neuronitis, BPPV, etc., that the patient previously had, but the CSD they presently have). From a psychological standpoint, talk in behavioral terms—hypersensitivity to motion, hypervigilance about motion environments, use of safety maneuvers (eg, touching a wall when walking), and avoiding situations that provoke dizziness. These are reflexive, fear-driven symptoms, but patients understand them better in terms of dizziness and unsteadiness.
2. Keep in mind that dizziness is the chief complaint. As patients go from primary care to otolaryngology, audiology, vestibular rehabilitation, and psychiatry, the problem is dizziness. You may find anxiety or depression along the way, but dizziness comes first for these patients.
3. Educate patients and referring physicians. Give patients and their referring physicians materials that define CSD and its differential diagnosis.3 Check off patients’ symptoms in the diagnostic list and circle their medical comorbidities, if present. For psychiatrists, this is a good point to start discussing behavioral morbidity and treatment.
4. Screen for coexisting medical-psychiatric diagnoses (eg, Meniere’s disease, panic disorder) or primarily psychiatric problems (conversion disorder). In addition to the otologic exam for vestibular diseases, patients should be screened for migraine, traumatic brain injury, dysautonomia, and dysrhythmias. Ask patients to complete symptom self-reports, including the Patient Health Questionnaire-9 (for depression) and Generalized Anxiety Disorder-7 (for anxiety).
5. Treat the patient’s primary problem (eg, CSD, vertigo, ataxia, or headache) first. If headache and balance symptoms are intertwined, use venlafaxine or combine a selective serotonin reuptake inhibitor (SSRI) with a separate migraine prophylactic agent.
Treatment options
Pharmacotherapy. Five open-label studies found SSRIs are effective for CSD even for patients without psychiatric comorbidity.3 Use a “start low, go slow” strategy to avoid aggravating symptoms. Final doses usually are in the lower half of the therapeutic range. Full treatment response may take 8 to 12 weeks. Vestibular suppressants such as meclizine work reasonably well for acute vertigo, but have no role in treating CSD.
Vestibular and balance rehabilitation therapy (VBRT) is an exercise program performed at home by patients but overseen by specially trained physical therapists. It is an excellent habituation/desensitization program that can be integrated with medication and psychotherapy. All patients with CSD should undergo VBRT.
Cognitive-behavioral therapy may be helpful for treating psychiatric morbidity (anxiety, depression, phobic avoidance) in patients with CSD, but it appears to be less effective for physical symptoms of dizziness.3
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at www.facebook.com/CurrentPsychiatry
Chronic subjective dizziness (CSD) is characterized by persistent (>3 months) dizziness, lightheadedness, or unsteadiness, without vertigo or ataxia. Symptoms often are worse in highly stimulating visual environments (eg, busy malls or grocery stores) or settings with indistinct visual orientation cues (eg, large open areas, heavy fog). Neuro-otologic examination and laboratory testing reveal no active vestibular deficits.1
CSD is not a psychiatric illness, but exists at the interface of psychiatry and neuro-otology. For example, anxiety and depressive disorders often accompany CSD, but are not an integral part of it. Treatment outcomes are good and prognosis for full function is high.
Conditions that cause dizziness
Vertigo—a sensation of rotation or linear movement of self or surroundings—occurs in discrete attacks that typically have an acute onset and are caused by neuro-otologic conditions.2 Symptoms may last for seconds (benign paroxysmal positional vertigo [BPPV]), hours (Meniere’s disease), minutes to days (vestibular migraine), or weeks (vestibular neuronitis). Unsteadiness, a swaying or rocking sensation, dizziness, and a disturbed sense of spatial orientation without illusory movement may be acute, subacute, or chronic. These symptoms may accompany vertigo or occur independently.2 Psychiatric disorders (panic), dysautonomias (vasovagal spells), and cardiovascular conditions (dysrhythmias) may cause episodic unsteadiness and dizziness, but not vertigo. Several illnesses can cause persistent unsteadiness and dizziness, including bilateral peripheral vestibular deficits, central vestibular lesions (strokes), proprioceptive or visual loss (neuropathies), and generalized anxiety disorder.
Up to 30% of patients who experience episodic balance problems develop persistent unsteadiness or dizziness (ie, CSD).3 Clinical history, exam, and laboratory tests may be normal or identify previous triggering events (eg, past vestibular insults), but transient conditions cannot explain patients’ persistent symptoms. Often, patients describe a transition from episodic vertigo and ataxia to chronic, often daily unsteadiness and dizziness. In this situation, the illness that started the problem often is not the one that continues to be distressing. Rather, patients develop hypersensitivity to motion stimuli (visual, vestibular, and proprioceptive inputs) and hypervigilance about motion environments that last long after the trigger event has resolved. These CSD features are thought to arise from threat-related failure of postural control systems to return to normal functioning after shifting into high-risk strategies during the acute events that disrupted balance.
5 strategies for managing CSD
1. Develop a common language among other clinicians you work with. The concept of CSD will be new to most patients and their referring clinicians, so they will need to hear about it more than once. From a neuro-otologic standpoint, make a point of separating past and present problems (ie, not the vestibular neuronitis, BPPV, etc., that the patient previously had, but the CSD they presently have). From a psychological standpoint, talk in behavioral terms—hypersensitivity to motion, hypervigilance about motion environments, use of safety maneuvers (eg, touching a wall when walking), and avoiding situations that provoke dizziness. These are reflexive, fear-driven symptoms, but patients understand them better in terms of dizziness and unsteadiness.
2. Keep in mind that dizziness is the chief complaint. As patients go from primary care to otolaryngology, audiology, vestibular rehabilitation, and psychiatry, the problem is dizziness. You may find anxiety or depression along the way, but dizziness comes first for these patients.
3. Educate patients and referring physicians. Give patients and their referring physicians materials that define CSD and its differential diagnosis.3 Check off patients’ symptoms in the diagnostic list and circle their medical comorbidities, if present. For psychiatrists, this is a good point to start discussing behavioral morbidity and treatment.
4. Screen for coexisting medical-psychiatric diagnoses (eg, Meniere’s disease, panic disorder) or primarily psychiatric problems (conversion disorder). In addition to the otologic exam for vestibular diseases, patients should be screened for migraine, traumatic brain injury, dysautonomia, and dysrhythmias. Ask patients to complete symptom self-reports, including the Patient Health Questionnaire-9 (for depression) and Generalized Anxiety Disorder-7 (for anxiety).
5. Treat the patient’s primary problem (eg, CSD, vertigo, ataxia, or headache) first. If headache and balance symptoms are intertwined, use venlafaxine or combine a selective serotonin reuptake inhibitor (SSRI) with a separate migraine prophylactic agent.
Treatment options
Pharmacotherapy. Five open-label studies found SSRIs are effective for CSD even for patients without psychiatric comorbidity.3 Use a “start low, go slow” strategy to avoid aggravating symptoms. Final doses usually are in the lower half of the therapeutic range. Full treatment response may take 8 to 12 weeks. Vestibular suppressants such as meclizine work reasonably well for acute vertigo, but have no role in treating CSD.
Vestibular and balance rehabilitation therapy (VBRT) is an exercise program performed at home by patients but overseen by specially trained physical therapists. It is an excellent habituation/desensitization program that can be integrated with medication and psychotherapy. All patients with CSD should undergo VBRT.
Cognitive-behavioral therapy may be helpful for treating psychiatric morbidity (anxiety, depression, phobic avoidance) in patients with CSD, but it appears to be less effective for physical symptoms of dizziness.3
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Staab JP, Ruckenstein MJ. Expanding the differential diagnosis of chronic dizziness. Arch Otolaryngol Head Neck Surg. 2007;133(2):170-176.
2. Bisdorff A, Von Brevern M, Lempert T, et al. Classification of vestibular symptoms: towards an international classification of vestibular disorders. J Vestib Res. 2009;19(1-2):1-13.
3. Staab JP. Psychological aspects of vestibular disorders. In: Eggers SD Zee DS, eds Vertigo and imbalance: clinical neurophysiology of the vestibular system. Boston, MA: Elsevier. 2010;502-522.
1. Staab JP, Ruckenstein MJ. Expanding the differential diagnosis of chronic dizziness. Arch Otolaryngol Head Neck Surg. 2007;133(2):170-176.
2. Bisdorff A, Von Brevern M, Lempert T, et al. Classification of vestibular symptoms: towards an international classification of vestibular disorders. J Vestib Res. 2009;19(1-2):1-13.
3. Staab JP. Psychological aspects of vestibular disorders. In: Eggers SD Zee DS, eds Vertigo and imbalance: clinical neurophysiology of the vestibular system. Boston, MA: Elsevier. 2010;502-522.
The hazards of serendipity
For many scientists and clinicians, serendipity is a welcome blessing. It can result in the fortuitous discovery of a new treatment for a previously untreatable illness. In psychiatry, there are several examples, including chlorpromazine for psychosis and monoamine oxidase inhibitors and tricyclics for depression. But serendipity also can have a downside. It can skew and misdirect research efforts into one direction to the exclusion of others, which can be a curse in the pursuit of scientific truth.
For example, consider major depressive disorder (MDD), which is a major public health challenge with enormous direct and indirect costs to society. MDD is the most disabling medical disorder not just in psychiatry, but in the entire field of medicine (psychiatry claims 3 other disorders in the top 5: schizophrenia, bipolar disorder, and alcohol abuse).1 In the United States, 8% to 10% of the population—children, adolescents, adults, and geriatric patients—suffer from depression at some point in their lives, and many will attempt suicide or die from self-inflicted injury if their depression is left untreated.2 In the United States, 34,000 persons die each year from suicide3; most of them have MDD.4
Despite the gravity of depression’s disabling effects, MDD treatment barely has budged from the entrenched model constructed around increasing the availability of ≥1 monoamines—serotonin, norepinephrine, and dopamine—in the brain. For the past 5 decades, researchers have not deviated from the therapeutic dogma spawned by serendipity. Yet the efficacy of antidepressants from tricyclics to selective serotonin reuptake inhibitors to serotonin-norepinephrine reuptake inhibitors has been less than stellar, with remission in a few patients, partial response in others, and treatment resistance in many.
This is not surprising given that depression is a diverse syndrome, a heterogeneous gamut of disorders with variable pathogenesis but a shared clinical phenotype. So why did the pharmaceutical industry continue to develop drugs that inhibit the reuptake of one monoamine or another instead of innovating and developing novel agents with diverse mechanisms of action? Powerful inertia of the serendipitously discovered older antidepressants has persisted, without the benefit of new, “out-of-the-monoamine-box” innovative discovery based on emerging pathophysiologic research in mood disorders.
Things finally may be changing. Basic neuroscience and animal models have generated a wealth of new mechanisms and pathways that seem to work in animal models of depression, such as learned helplessness and social defeat.5 The old mold of monoamine reuptake inhibition soon may be replaced by a plethora of alternatives that may transform the landscape of depression treatment.
Emerging therapeutic targets
Consider the following novel mechanisms that may become the basis for creating entirely new antidepressants in the foreseeable future, by design, not by serendipity:
- corticotropin-releasing factor (CRF) and glucocorticoids
- neurokinin system
- brain derived neurotropic factor (BDNF) and other neurotropins, such as fibroblast growth factor (FGF) or vascular endothelial growth factor (VEGF)
- phosphodiesterase inhibitors
- glutamate pathway modulators
- hypothalamic feeding peptides
- circadian gene products
- other evolving antidepressants
It is heartening to psychiatrists and their chronically depressed patients that many novel mechanisms and therapeutic targets have emerged, thanks to intensive research, not serendipity and happenstance. Although that’s uplifting news, the sobering downside is the lack of sufficient resources to expedite translational research. We need far more funding than what is available, and several pharmaceutical companies have dismantled their psychiatry research infrastructure and laid off thousands of scientists. This may be the time when strong philanthropic support may have to come to the rescue of this worthy cause, similar to how the Bill & Melinda Gates Foundation has focused on eradicating malaria. If only a multi-billionaire would adopt depression research as his or her pet charity with the goal of discovering several effective new treatments for the most disabling medical disorder in the world. What a fantastic legacy that would be.
Serendipity is out, intensive (and expensive!) brain research is in! Calling all enlightened billionaires…
1. World Health Organization. The world health report 2001—mental health: new understanding new hope. 2001. http://www.who.int/whr/2001/en. Accessed June 12, 2012.
2. Robins LN, Regier DA. Psychiatric disorders in America. New York NY: The Free Press; 1991.
3. Centers for Disease Control and Prevention. WISQARS leading causes of death reports 1999-2007. http://webappa.cdc.gov/sasweb/ncipc/leadcaus10.html. Accessed June 11, 2012.
4. Ghosh TB, Victor BS. Suicide. In: Hales RE Yudofsky SC, Talbott JA, eds. The American Psychiatric Publishing textbook of psychiatry. 3rd ed. Arlington, VA: American Psychiatric Publishing; 1999.
5. Berton O, Nestler EJ. New approaches to antidepressant drug discovery: beyond monoamines. Nat Rev Neurosci. 2006;7(2):137-151.

Henry A. Nasrallah, MD
Editor-in-Chief
To comment on this editorial or other topics of interest, visit http://www.facebook.com/CurrentPsychiatry or click on the “Send Letters” link.
Henry A. Nasrallah, MD
Editor-in-Chief
To comment on this editorial or other topics of interest, visit http://www.facebook.com/CurrentPsychiatry or click on the “Send Letters” link.
Henry A. Nasrallah, MD
Editor-in-Chief
To comment on this editorial or other topics of interest, visit http://www.facebook.com/CurrentPsychiatry or click on the “Send Letters” link.
For many scientists and clinicians, serendipity is a welcome blessing. It can result in the fortuitous discovery of a new treatment for a previously untreatable illness. In psychiatry, there are several examples, including chlorpromazine for psychosis and monoamine oxidase inhibitors and tricyclics for depression. But serendipity also can have a downside. It can skew and misdirect research efforts into one direction to the exclusion of others, which can be a curse in the pursuit of scientific truth.
For example, consider major depressive disorder (MDD), which is a major public health challenge with enormous direct and indirect costs to society. MDD is the most disabling medical disorder not just in psychiatry, but in the entire field of medicine (psychiatry claims 3 other disorders in the top 5: schizophrenia, bipolar disorder, and alcohol abuse).1 In the United States, 8% to 10% of the population—children, adolescents, adults, and geriatric patients—suffer from depression at some point in their lives, and many will attempt suicide or die from self-inflicted injury if their depression is left untreated.2 In the United States, 34,000 persons die each year from suicide3; most of them have MDD.4
Despite the gravity of depression’s disabling effects, MDD treatment barely has budged from the entrenched model constructed around increasing the availability of ≥1 monoamines—serotonin, norepinephrine, and dopamine—in the brain. For the past 5 decades, researchers have not deviated from the therapeutic dogma spawned by serendipity. Yet the efficacy of antidepressants from tricyclics to selective serotonin reuptake inhibitors to serotonin-norepinephrine reuptake inhibitors has been less than stellar, with remission in a few patients, partial response in others, and treatment resistance in many.
This is not surprising given that depression is a diverse syndrome, a heterogeneous gamut of disorders with variable pathogenesis but a shared clinical phenotype. So why did the pharmaceutical industry continue to develop drugs that inhibit the reuptake of one monoamine or another instead of innovating and developing novel agents with diverse mechanisms of action? Powerful inertia of the serendipitously discovered older antidepressants has persisted, without the benefit of new, “out-of-the-monoamine-box” innovative discovery based on emerging pathophysiologic research in mood disorders.
Things finally may be changing. Basic neuroscience and animal models have generated a wealth of new mechanisms and pathways that seem to work in animal models of depression, such as learned helplessness and social defeat.5 The old mold of monoamine reuptake inhibition soon may be replaced by a plethora of alternatives that may transform the landscape of depression treatment.
Emerging therapeutic targets
Consider the following novel mechanisms that may become the basis for creating entirely new antidepressants in the foreseeable future, by design, not by serendipity:
- corticotropin-releasing factor (CRF) and glucocorticoids
- neurokinin system
- brain derived neurotropic factor (BDNF) and other neurotropins, such as fibroblast growth factor (FGF) or vascular endothelial growth factor (VEGF)
- phosphodiesterase inhibitors
- glutamate pathway modulators
- hypothalamic feeding peptides
- circadian gene products
- other evolving antidepressants
It is heartening to psychiatrists and their chronically depressed patients that many novel mechanisms and therapeutic targets have emerged, thanks to intensive research, not serendipity and happenstance. Although that’s uplifting news, the sobering downside is the lack of sufficient resources to expedite translational research. We need far more funding than what is available, and several pharmaceutical companies have dismantled their psychiatry research infrastructure and laid off thousands of scientists. This may be the time when strong philanthropic support may have to come to the rescue of this worthy cause, similar to how the Bill & Melinda Gates Foundation has focused on eradicating malaria. If only a multi-billionaire would adopt depression research as his or her pet charity with the goal of discovering several effective new treatments for the most disabling medical disorder in the world. What a fantastic legacy that would be.
Serendipity is out, intensive (and expensive!) brain research is in! Calling all enlightened billionaires…
For many scientists and clinicians, serendipity is a welcome blessing. It can result in the fortuitous discovery of a new treatment for a previously untreatable illness. In psychiatry, there are several examples, including chlorpromazine for psychosis and monoamine oxidase inhibitors and tricyclics for depression. But serendipity also can have a downside. It can skew and misdirect research efforts into one direction to the exclusion of others, which can be a curse in the pursuit of scientific truth.
For example, consider major depressive disorder (MDD), which is a major public health challenge with enormous direct and indirect costs to society. MDD is the most disabling medical disorder not just in psychiatry, but in the entire field of medicine (psychiatry claims 3 other disorders in the top 5: schizophrenia, bipolar disorder, and alcohol abuse).1 In the United States, 8% to 10% of the population—children, adolescents, adults, and geriatric patients—suffer from depression at some point in their lives, and many will attempt suicide or die from self-inflicted injury if their depression is left untreated.2 In the United States, 34,000 persons die each year from suicide3; most of them have MDD.4
Despite the gravity of depression’s disabling effects, MDD treatment barely has budged from the entrenched model constructed around increasing the availability of ≥1 monoamines—serotonin, norepinephrine, and dopamine—in the brain. For the past 5 decades, researchers have not deviated from the therapeutic dogma spawned by serendipity. Yet the efficacy of antidepressants from tricyclics to selective serotonin reuptake inhibitors to serotonin-norepinephrine reuptake inhibitors has been less than stellar, with remission in a few patients, partial response in others, and treatment resistance in many.
This is not surprising given that depression is a diverse syndrome, a heterogeneous gamut of disorders with variable pathogenesis but a shared clinical phenotype. So why did the pharmaceutical industry continue to develop drugs that inhibit the reuptake of one monoamine or another instead of innovating and developing novel agents with diverse mechanisms of action? Powerful inertia of the serendipitously discovered older antidepressants has persisted, without the benefit of new, “out-of-the-monoamine-box” innovative discovery based on emerging pathophysiologic research in mood disorders.
Things finally may be changing. Basic neuroscience and animal models have generated a wealth of new mechanisms and pathways that seem to work in animal models of depression, such as learned helplessness and social defeat.5 The old mold of monoamine reuptake inhibition soon may be replaced by a plethora of alternatives that may transform the landscape of depression treatment.
Emerging therapeutic targets
Consider the following novel mechanisms that may become the basis for creating entirely new antidepressants in the foreseeable future, by design, not by serendipity:
- corticotropin-releasing factor (CRF) and glucocorticoids
- neurokinin system
- brain derived neurotropic factor (BDNF) and other neurotropins, such as fibroblast growth factor (FGF) or vascular endothelial growth factor (VEGF)
- phosphodiesterase inhibitors
- glutamate pathway modulators
- hypothalamic feeding peptides
- circadian gene products
- other evolving antidepressants
It is heartening to psychiatrists and their chronically depressed patients that many novel mechanisms and therapeutic targets have emerged, thanks to intensive research, not serendipity and happenstance. Although that’s uplifting news, the sobering downside is the lack of sufficient resources to expedite translational research. We need far more funding than what is available, and several pharmaceutical companies have dismantled their psychiatry research infrastructure and laid off thousands of scientists. This may be the time when strong philanthropic support may have to come to the rescue of this worthy cause, similar to how the Bill & Melinda Gates Foundation has focused on eradicating malaria. If only a multi-billionaire would adopt depression research as his or her pet charity with the goal of discovering several effective new treatments for the most disabling medical disorder in the world. What a fantastic legacy that would be.
Serendipity is out, intensive (and expensive!) brain research is in! Calling all enlightened billionaires…
1. World Health Organization. The world health report 2001—mental health: new understanding new hope. 2001. http://www.who.int/whr/2001/en. Accessed June 12, 2012.
2. Robins LN, Regier DA. Psychiatric disorders in America. New York NY: The Free Press; 1991.
3. Centers for Disease Control and Prevention. WISQARS leading causes of death reports 1999-2007. http://webappa.cdc.gov/sasweb/ncipc/leadcaus10.html. Accessed June 11, 2012.
4. Ghosh TB, Victor BS. Suicide. In: Hales RE Yudofsky SC, Talbott JA, eds. The American Psychiatric Publishing textbook of psychiatry. 3rd ed. Arlington, VA: American Psychiatric Publishing; 1999.
5. Berton O, Nestler EJ. New approaches to antidepressant drug discovery: beyond monoamines. Nat Rev Neurosci. 2006;7(2):137-151.
1. World Health Organization. The world health report 2001—mental health: new understanding new hope. 2001. http://www.who.int/whr/2001/en. Accessed June 12, 2012.
2. Robins LN, Regier DA. Psychiatric disorders in America. New York NY: The Free Press; 1991.
3. Centers for Disease Control and Prevention. WISQARS leading causes of death reports 1999-2007. http://webappa.cdc.gov/sasweb/ncipc/leadcaus10.html. Accessed June 11, 2012.
4. Ghosh TB, Victor BS. Suicide. In: Hales RE Yudofsky SC, Talbott JA, eds. The American Psychiatric Publishing textbook of psychiatry. 3rd ed. Arlington, VA: American Psychiatric Publishing; 1999.
5. Berton O, Nestler EJ. New approaches to antidepressant drug discovery: beyond monoamines. Nat Rev Neurosci. 2006;7(2):137-151.
When is off-label prescribing appropriate?
Discuss this article at www.facebook.com/CurrentPsychiatry
Off-label prescribing (OLP)—prescribing a medication in a manner different from that approved by the FDA—is common and can be clinically beneficial. A survey of 200 British psychiatrists found that 65% had prescribed a medication off-label within the previous month.1 However, OLP often is not supported by strong evidence and carries clinical risks, such as adverse effects and unproven efficacy. A 2006 study found that only 4% of off-label prescriptions of psychiatric medications were supported by strong scientific evidence.2
OLP may become unavoidable for several reasons, including:
- lack of data from quality trials on a specific indication or patient population
- patients seen in clinical practice vary from those evaluated in clinical trials (Figure 1)
- the need to treat patients who do not respond to first-line therapies or have treatment-resistant conditions.
At times, OLP may be a psychiatrist’s only option: >80% of DSM-IV-TR diagnoses have no FDA-approved medication.3
No practice guidelines are available to help clinicians decide when OLP is appropriate. Psychiatrists must rely on multiple, sometimes-conflicting sources to determine whether evidence is sufficient to support off-label use in a specific clinical scenario. This article looks at types of OLP and offers suggestions for clinicians who are considering prescribing a medication outside of its approved use.
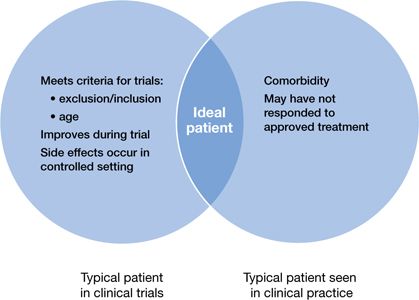
Figure 1: Clinical trial patients vs ‘real world’ patients
The FDA’s role
Once the FDA approves a medication for a specific indication, physicians legally are permitted to prescribe that drug for indications, patient populations, or dosages not included on the FDA-approved label.2,4 The FDA oversees and regulates pharmaceutical companies, not physicians.4 Currently, pharmaceutical companies cannot market a drug for an indication not included on the label, but physicians are free to use the drug for any condition or disease.5
When is OLP used?
According to Baldwin et al,6 prescribing that is considered off-label generally falls into 1 of the following 4 categories:
Indication. This type of OLP is prescribing a medication for an indication other than those included on the FDA-approved label. The off-label indication may be a logical extension of an approved indication. For example, a medication approved for treating erectile dysfunction might be prescribed to a patient who is experiencing antidepressant-induced sexual dysfunction.
If a pharmaceutical company wishes to expand the indications of a medication they must seek supplemental approval from the FDA. This is a long, expensive process. In certain situations, it may be in the patient’s best interest to prescribe a medication off-label until that indication becomes approved. When clinicians identify new uses for existing medications while they care for patients, it is considered field discovery, and this innovative process may occur years before such indications receive FDA approval.
Dosage. The most common example of this type of OLP in psychiatry is prescribing higher-than-approved dosages of antidepressants or antipsychotics for patients who do not respond to the maximum approved dosages. The effectiveness of this strategy is unknown.6
Duration. This typically entails prescribing a medication for a period of time longer than specified on the label. For example, many antidepressants are approved only for treating depressive illness. Therefore, continuing an antidepressant as maintenance therapy for a patient who is in remission could be considered off-label. Benzodiazepines are approved primarily for short-term management of anxiety, but commonly are prescribed for patients with chronic, disabling anxiety disorders who do not respond to other medications.6
Patient age. The FDA approves medications for use in patients within a specified age range based on patients evaluated in clinical trials, and most trials of psychotropics include patients age 18 to 65. However, it is highly unlikely that a 17-year-old patient’s drug metabolism changes substantially when he or she reaches age 18, or when a 65-year-old turns 66. Research has demonstrated that medications can be effective outside of strict age ranges. For example, randomized controlled trials (RCTs) have shown that antidepressants are efficacious in treating depression in geriatric patients, and selective serotonin reuptake inhibitors are efficacious in treating obsessive-compulsive disorder (OCD) in children and adolescents.6
Few medications have been approved for treating geriatric patients with psychiatric illness. For example, no drugs are approved for treating psychotic, behavioral, and mood symptoms that may accompany dementia. For this reason, clinicians often prescribe psychotropics off-label to these patients.
The rate of psychotropic prescriptions to children and adolescents—particularly antidepressants and antipsychotics—has been increasing.7-9 The British Association for Psychopharmacology suggested that it may be reasonable to apply what we know regarding adults’ responses to drug treatment to children and adolescents with schizophrenia or OCD, but more caution is required in young patients with mood or anxiety disorders.10
Combination therapy is another type of OLP. Often a disease state consists of multiple underlying syndromes, and treating individual syndromes is a common strategy. For example, in addition to depressed mood, a patient with major depressive disorder also may have insomnia and poor concentration. A medication approved for treating depressed mood may not improve insomnia or poor concentration. Therefore, combination therapy may be necessary, but likely would be off-label. Combination therapy also may be tried when a patient does not respond to monotherapy. For example, although the evidence supporting the practice is inconclusive, clinicians commonly prescribe >1 antipsychotic to patients with schizophrenia or other psychotic disorders.
Help for making OLP decisions
Position statements/policies. The American Psychiatric Association (APA) and the American Medical Association support OLP when the practice is based on sound scientific evidence and medical opinion.11 The APA position statement encourages clinicians to use various compendia, including the American Hospital Formulary Service (AHFS) Drug Information, in conjunction with peer-reviewed literature to determine the medical acceptability of off-label uses.11
Evidence-based medicine includes a hierarchy of scientific and clinical evidence that can justify medical decisions. At the top of this hierarchy are large RCTs and smaller RCTs; cohort studies, case-control studies, poorly controlled or uncontrolled studies, case reports, and expert opinion are less valuable (Figure 2).4
Searching through all available resources for evidence supporting a specific off-label use is a cumbersome, time-consuming process. For this reason, clinicians may refer to compendia that evaluate and rate the available evidence supporting off-label use of medication, such as the AHFS Drug Information and DrugDex. Other resources include peer-reviewed medical journals. Physicians can contribute to knowledge of off-label uses by sharing their experiences, both good and bad, with their colleagues via presentations, publications, and/or initiating a study.
Other resources. Gazarian et al12 delineated 3 situations where OLP might be considered appropriate: use justified by high-quality evidence, use in research trials, and exceptional use justified by individual clinical circumstances. Exceptional use would require all of the following:
- the patient has a serious disease or condition
- evidence supports a potential beneficial effect of the off-label treatment
- potential benefits outweigh potential risks
- standard therapy has failed or is inappropriate
- an institutional drug committee approved the off-label use
- the patient provides written informed consent.12
Other authors13,14 have offered recommendations for psychiatrists considering OLP:
- Study available literature and assess whether sufficient evidence supports the proposed off-label use.
- If evidence is lacking, learn about the medication and its potential risks (interactions, adverse effects, and FDA “black-box” warnings). Also consult other resources for additional information and research, including peers and experts in the field.
- Consider and document risks and benefits of the proposed off-label use. Explain these, as well as uncertainties and potential costs, to patients and/or their families, and obtain and document informed consent.
- Cautiously initiate the off-label therapy, monitor patients closely, and meticulously document efficacy and tolerance.
Prescribing medications on-label does not guarantee safety or efficacy. Likewise, OLP does not imply a safety hazard or lack of efficacy. OLP may be in the best interest of the patient. Nonetheless, the practice must be carried out responsibly with utmost caution and consideration of acute and long-term burdens to patients, along with an assessment of the risk vs benefit of the proposed therapy.
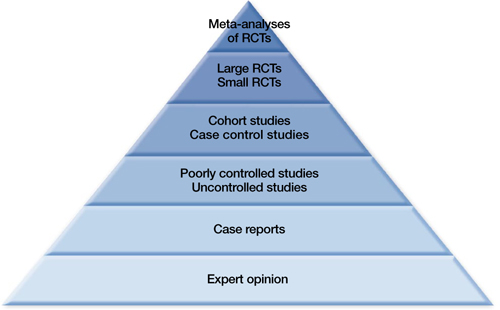
Figure 2: The hierarchy of sources for evidence-based medicine
RCTs: randomized controlled trials
Source: Reference 4Related Resource
- Mossman D. Why off-label isn’t off base. Current Psychiatry. 2009;8(2):19-22.
Disclosures
Dr. Ali receives research/grant support from Cyberonics and is a speaker for Merck.
Dr Ajmal reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Lowe-Ponsford F, Baldwin D. Off-label prescribing by psychiatrists. Psychiatric Bulletin. 2000;24:415-417.
2. Radley DC, Finkelstein SN, Stafford RS. Off-label prescribing among office-based physicians. Arch Intern Med. 2006;166(9):1021-1026.
3. Devulapalli K, Nasrallah HA. An analysis of the high psychotropic off-label use in psychiatric disorders: the majority of psychiatric diagnoses have no approved drug. Asian Journal of Psychiatry. 2009;2(1):29-36.
4. Dresser R, Frader J. Off-label prescribing: a call for heightened professional and government oversight. J Law Med Ethics. 2009;37(3):476-486, 396.
5. Food, Drug, and Cosmetic Act, 21 USC §396 (2010).
6. Baldwin DS, Kosky N. Off-label prescribing in psychiatric practice. Advances in Psychiatric Treatment. 2007;13:414-422.
7. Zito JM, Safer DJ, dosReis S, et al. Trends in the prescribing of psychotropic medications to preschoolers. JAMA. 2000;283(8):1025-1030.
8. Tournier M, Greenfield B, Galbaud du Fort G, et al. Patterns of antidepressant use in Quebec children and adolescents: trends and predictors. Psychiatry Res. 2010;179(1):57-63.
9. Cooper WO, Arbogast PG, Ding H, et al. Trends in prescribing of antipsychotic medications for US children. Ambul Pediatr. 2006;6(2):79-83.
10. Child and learning disability psychopharmacology. J Psychopharmacol. 1997;11(4):291-294.
11. American Psychiatric Association. Position statement on patient access to treatments prescribed by their physicians. 2007. http://www.psychiatry.org/advocacy—newsroom/position-statements/apa-position-statements. Accessed May 24 2012.
12. Gazarian M, Kelly M, McPhee JR, et al. Off-label use of medicines: consensus recommendations for evaluating appropriateness. Med J Aust. 2006;185(10):544-548.
13. Kramer SI, McCall WV. Off-label prescribing: 7 steps for safer more effective prescribing. Current Psychiatry. 2006;5(4):14-28.
14. Royal College of Psychiatrists. Use of licensed medicines for unlicensed applications in psychiatric practice. College report CR142. http://www.rcpsych.ac.uk/files/pdfversion/cr142.pdf. Accessed May 24 2012.
Discuss this article at www.facebook.com/CurrentPsychiatry
Off-label prescribing (OLP)—prescribing a medication in a manner different from that approved by the FDA—is common and can be clinically beneficial. A survey of 200 British psychiatrists found that 65% had prescribed a medication off-label within the previous month.1 However, OLP often is not supported by strong evidence and carries clinical risks, such as adverse effects and unproven efficacy. A 2006 study found that only 4% of off-label prescriptions of psychiatric medications were supported by strong scientific evidence.2
OLP may become unavoidable for several reasons, including:
- lack of data from quality trials on a specific indication or patient population
- patients seen in clinical practice vary from those evaluated in clinical trials (Figure 1)
- the need to treat patients who do not respond to first-line therapies or have treatment-resistant conditions.
At times, OLP may be a psychiatrist’s only option: >80% of DSM-IV-TR diagnoses have no FDA-approved medication.3
No practice guidelines are available to help clinicians decide when OLP is appropriate. Psychiatrists must rely on multiple, sometimes-conflicting sources to determine whether evidence is sufficient to support off-label use in a specific clinical scenario. This article looks at types of OLP and offers suggestions for clinicians who are considering prescribing a medication outside of its approved use.
Figure 1: Clinical trial patients vs ‘real world’ patients
The FDA’s role
Once the FDA approves a medication for a specific indication, physicians legally are permitted to prescribe that drug for indications, patient populations, or dosages not included on the FDA-approved label.2,4 The FDA oversees and regulates pharmaceutical companies, not physicians.4 Currently, pharmaceutical companies cannot market a drug for an indication not included on the label, but physicians are free to use the drug for any condition or disease.5
When is OLP used?
According to Baldwin et al,6 prescribing that is considered off-label generally falls into 1 of the following 4 categories:
Indication. This type of OLP is prescribing a medication for an indication other than those included on the FDA-approved label. The off-label indication may be a logical extension of an approved indication. For example, a medication approved for treating erectile dysfunction might be prescribed to a patient who is experiencing antidepressant-induced sexual dysfunction.
If a pharmaceutical company wishes to expand the indications of a medication they must seek supplemental approval from the FDA. This is a long, expensive process. In certain situations, it may be in the patient’s best interest to prescribe a medication off-label until that indication becomes approved. When clinicians identify new uses for existing medications while they care for patients, it is considered field discovery, and this innovative process may occur years before such indications receive FDA approval.
Dosage. The most common example of this type of OLP in psychiatry is prescribing higher-than-approved dosages of antidepressants or antipsychotics for patients who do not respond to the maximum approved dosages. The effectiveness of this strategy is unknown.6
Duration. This typically entails prescribing a medication for a period of time longer than specified on the label. For example, many antidepressants are approved only for treating depressive illness. Therefore, continuing an antidepressant as maintenance therapy for a patient who is in remission could be considered off-label. Benzodiazepines are approved primarily for short-term management of anxiety, but commonly are prescribed for patients with chronic, disabling anxiety disorders who do not respond to other medications.6
Patient age. The FDA approves medications for use in patients within a specified age range based on patients evaluated in clinical trials, and most trials of psychotropics include patients age 18 to 65. However, it is highly unlikely that a 17-year-old patient’s drug metabolism changes substantially when he or she reaches age 18, or when a 65-year-old turns 66. Research has demonstrated that medications can be effective outside of strict age ranges. For example, randomized controlled trials (RCTs) have shown that antidepressants are efficacious in treating depression in geriatric patients, and selective serotonin reuptake inhibitors are efficacious in treating obsessive-compulsive disorder (OCD) in children and adolescents.6
Few medications have been approved for treating geriatric patients with psychiatric illness. For example, no drugs are approved for treating psychotic, behavioral, and mood symptoms that may accompany dementia. For this reason, clinicians often prescribe psychotropics off-label to these patients.
The rate of psychotropic prescriptions to children and adolescents—particularly antidepressants and antipsychotics—has been increasing.7-9 The British Association for Psychopharmacology suggested that it may be reasonable to apply what we know regarding adults’ responses to drug treatment to children and adolescents with schizophrenia or OCD, but more caution is required in young patients with mood or anxiety disorders.10
Combination therapy is another type of OLP. Often a disease state consists of multiple underlying syndromes, and treating individual syndromes is a common strategy. For example, in addition to depressed mood, a patient with major depressive disorder also may have insomnia and poor concentration. A medication approved for treating depressed mood may not improve insomnia or poor concentration. Therefore, combination therapy may be necessary, but likely would be off-label. Combination therapy also may be tried when a patient does not respond to monotherapy. For example, although the evidence supporting the practice is inconclusive, clinicians commonly prescribe >1 antipsychotic to patients with schizophrenia or other psychotic disorders.
Help for making OLP decisions
Position statements/policies. The American Psychiatric Association (APA) and the American Medical Association support OLP when the practice is based on sound scientific evidence and medical opinion.11 The APA position statement encourages clinicians to use various compendia, including the American Hospital Formulary Service (AHFS) Drug Information, in conjunction with peer-reviewed literature to determine the medical acceptability of off-label uses.11
Evidence-based medicine includes a hierarchy of scientific and clinical evidence that can justify medical decisions. At the top of this hierarchy are large RCTs and smaller RCTs; cohort studies, case-control studies, poorly controlled or uncontrolled studies, case reports, and expert opinion are less valuable (Figure 2).4
Searching through all available resources for evidence supporting a specific off-label use is a cumbersome, time-consuming process. For this reason, clinicians may refer to compendia that evaluate and rate the available evidence supporting off-label use of medication, such as the AHFS Drug Information and DrugDex. Other resources include peer-reviewed medical journals. Physicians can contribute to knowledge of off-label uses by sharing their experiences, both good and bad, with their colleagues via presentations, publications, and/or initiating a study.
Other resources. Gazarian et al12 delineated 3 situations where OLP might be considered appropriate: use justified by high-quality evidence, use in research trials, and exceptional use justified by individual clinical circumstances. Exceptional use would require all of the following:
- the patient has a serious disease or condition
- evidence supports a potential beneficial effect of the off-label treatment
- potential benefits outweigh potential risks
- standard therapy has failed or is inappropriate
- an institutional drug committee approved the off-label use
- the patient provides written informed consent.12
Other authors13,14 have offered recommendations for psychiatrists considering OLP:
- Study available literature and assess whether sufficient evidence supports the proposed off-label use.
- If evidence is lacking, learn about the medication and its potential risks (interactions, adverse effects, and FDA “black-box” warnings). Also consult other resources for additional information and research, including peers and experts in the field.
- Consider and document risks and benefits of the proposed off-label use. Explain these, as well as uncertainties and potential costs, to patients and/or their families, and obtain and document informed consent.
- Cautiously initiate the off-label therapy, monitor patients closely, and meticulously document efficacy and tolerance.
Prescribing medications on-label does not guarantee safety or efficacy. Likewise, OLP does not imply a safety hazard or lack of efficacy. OLP may be in the best interest of the patient. Nonetheless, the practice must be carried out responsibly with utmost caution and consideration of acute and long-term burdens to patients, along with an assessment of the risk vs benefit of the proposed therapy.
Figure 2: The hierarchy of sources for evidence-based medicine
RCTs: randomized controlled trials
Source: Reference 4Related Resource
- Mossman D. Why off-label isn’t off base. Current Psychiatry. 2009;8(2):19-22.
Disclosures
Dr. Ali receives research/grant support from Cyberonics and is a speaker for Merck.
Dr Ajmal reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at www.facebook.com/CurrentPsychiatry
Off-label prescribing (OLP)—prescribing a medication in a manner different from that approved by the FDA—is common and can be clinically beneficial. A survey of 200 British psychiatrists found that 65% had prescribed a medication off-label within the previous month.1 However, OLP often is not supported by strong evidence and carries clinical risks, such as adverse effects and unproven efficacy. A 2006 study found that only 4% of off-label prescriptions of psychiatric medications were supported by strong scientific evidence.2
OLP may become unavoidable for several reasons, including:
- lack of data from quality trials on a specific indication or patient population
- patients seen in clinical practice vary from those evaluated in clinical trials (Figure 1)
- the need to treat patients who do not respond to first-line therapies or have treatment-resistant conditions.
At times, OLP may be a psychiatrist’s only option: >80% of DSM-IV-TR diagnoses have no FDA-approved medication.3
No practice guidelines are available to help clinicians decide when OLP is appropriate. Psychiatrists must rely on multiple, sometimes-conflicting sources to determine whether evidence is sufficient to support off-label use in a specific clinical scenario. This article looks at types of OLP and offers suggestions for clinicians who are considering prescribing a medication outside of its approved use.
Figure 1: Clinical trial patients vs ‘real world’ patients
The FDA’s role
Once the FDA approves a medication for a specific indication, physicians legally are permitted to prescribe that drug for indications, patient populations, or dosages not included on the FDA-approved label.2,4 The FDA oversees and regulates pharmaceutical companies, not physicians.4 Currently, pharmaceutical companies cannot market a drug for an indication not included on the label, but physicians are free to use the drug for any condition or disease.5
When is OLP used?
According to Baldwin et al,6 prescribing that is considered off-label generally falls into 1 of the following 4 categories:
Indication. This type of OLP is prescribing a medication for an indication other than those included on the FDA-approved label. The off-label indication may be a logical extension of an approved indication. For example, a medication approved for treating erectile dysfunction might be prescribed to a patient who is experiencing antidepressant-induced sexual dysfunction.
If a pharmaceutical company wishes to expand the indications of a medication they must seek supplemental approval from the FDA. This is a long, expensive process. In certain situations, it may be in the patient’s best interest to prescribe a medication off-label until that indication becomes approved. When clinicians identify new uses for existing medications while they care for patients, it is considered field discovery, and this innovative process may occur years before such indications receive FDA approval.
Dosage. The most common example of this type of OLP in psychiatry is prescribing higher-than-approved dosages of antidepressants or antipsychotics for patients who do not respond to the maximum approved dosages. The effectiveness of this strategy is unknown.6
Duration. This typically entails prescribing a medication for a period of time longer than specified on the label. For example, many antidepressants are approved only for treating depressive illness. Therefore, continuing an antidepressant as maintenance therapy for a patient who is in remission could be considered off-label. Benzodiazepines are approved primarily for short-term management of anxiety, but commonly are prescribed for patients with chronic, disabling anxiety disorders who do not respond to other medications.6
Patient age. The FDA approves medications for use in patients within a specified age range based on patients evaluated in clinical trials, and most trials of psychotropics include patients age 18 to 65. However, it is highly unlikely that a 17-year-old patient’s drug metabolism changes substantially when he or she reaches age 18, or when a 65-year-old turns 66. Research has demonstrated that medications can be effective outside of strict age ranges. For example, randomized controlled trials (RCTs) have shown that antidepressants are efficacious in treating depression in geriatric patients, and selective serotonin reuptake inhibitors are efficacious in treating obsessive-compulsive disorder (OCD) in children and adolescents.6
Few medications have been approved for treating geriatric patients with psychiatric illness. For example, no drugs are approved for treating psychotic, behavioral, and mood symptoms that may accompany dementia. For this reason, clinicians often prescribe psychotropics off-label to these patients.
The rate of psychotropic prescriptions to children and adolescents—particularly antidepressants and antipsychotics—has been increasing.7-9 The British Association for Psychopharmacology suggested that it may be reasonable to apply what we know regarding adults’ responses to drug treatment to children and adolescents with schizophrenia or OCD, but more caution is required in young patients with mood or anxiety disorders.10
Combination therapy is another type of OLP. Often a disease state consists of multiple underlying syndromes, and treating individual syndromes is a common strategy. For example, in addition to depressed mood, a patient with major depressive disorder also may have insomnia and poor concentration. A medication approved for treating depressed mood may not improve insomnia or poor concentration. Therefore, combination therapy may be necessary, but likely would be off-label. Combination therapy also may be tried when a patient does not respond to monotherapy. For example, although the evidence supporting the practice is inconclusive, clinicians commonly prescribe >1 antipsychotic to patients with schizophrenia or other psychotic disorders.
Help for making OLP decisions
Position statements/policies. The American Psychiatric Association (APA) and the American Medical Association support OLP when the practice is based on sound scientific evidence and medical opinion.11 The APA position statement encourages clinicians to use various compendia, including the American Hospital Formulary Service (AHFS) Drug Information, in conjunction with peer-reviewed literature to determine the medical acceptability of off-label uses.11
Evidence-based medicine includes a hierarchy of scientific and clinical evidence that can justify medical decisions. At the top of this hierarchy are large RCTs and smaller RCTs; cohort studies, case-control studies, poorly controlled or uncontrolled studies, case reports, and expert opinion are less valuable (Figure 2).4
Searching through all available resources for evidence supporting a specific off-label use is a cumbersome, time-consuming process. For this reason, clinicians may refer to compendia that evaluate and rate the available evidence supporting off-label use of medication, such as the AHFS Drug Information and DrugDex. Other resources include peer-reviewed medical journals. Physicians can contribute to knowledge of off-label uses by sharing their experiences, both good and bad, with their colleagues via presentations, publications, and/or initiating a study.
Other resources. Gazarian et al12 delineated 3 situations where OLP might be considered appropriate: use justified by high-quality evidence, use in research trials, and exceptional use justified by individual clinical circumstances. Exceptional use would require all of the following:
- the patient has a serious disease or condition
- evidence supports a potential beneficial effect of the off-label treatment
- potential benefits outweigh potential risks
- standard therapy has failed or is inappropriate
- an institutional drug committee approved the off-label use
- the patient provides written informed consent.12
Other authors13,14 have offered recommendations for psychiatrists considering OLP:
- Study available literature and assess whether sufficient evidence supports the proposed off-label use.
- If evidence is lacking, learn about the medication and its potential risks (interactions, adverse effects, and FDA “black-box” warnings). Also consult other resources for additional information and research, including peers and experts in the field.
- Consider and document risks and benefits of the proposed off-label use. Explain these, as well as uncertainties and potential costs, to patients and/or their families, and obtain and document informed consent.
- Cautiously initiate the off-label therapy, monitor patients closely, and meticulously document efficacy and tolerance.
Prescribing medications on-label does not guarantee safety or efficacy. Likewise, OLP does not imply a safety hazard or lack of efficacy. OLP may be in the best interest of the patient. Nonetheless, the practice must be carried out responsibly with utmost caution and consideration of acute and long-term burdens to patients, along with an assessment of the risk vs benefit of the proposed therapy.
Figure 2: The hierarchy of sources for evidence-based medicine
RCTs: randomized controlled trials
Source: Reference 4Related Resource
- Mossman D. Why off-label isn’t off base. Current Psychiatry. 2009;8(2):19-22.
Disclosures
Dr. Ali receives research/grant support from Cyberonics and is a speaker for Merck.
Dr Ajmal reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Lowe-Ponsford F, Baldwin D. Off-label prescribing by psychiatrists. Psychiatric Bulletin. 2000;24:415-417.
2. Radley DC, Finkelstein SN, Stafford RS. Off-label prescribing among office-based physicians. Arch Intern Med. 2006;166(9):1021-1026.
3. Devulapalli K, Nasrallah HA. An analysis of the high psychotropic off-label use in psychiatric disorders: the majority of psychiatric diagnoses have no approved drug. Asian Journal of Psychiatry. 2009;2(1):29-36.
4. Dresser R, Frader J. Off-label prescribing: a call for heightened professional and government oversight. J Law Med Ethics. 2009;37(3):476-486, 396.
5. Food, Drug, and Cosmetic Act, 21 USC §396 (2010).
6. Baldwin DS, Kosky N. Off-label prescribing in psychiatric practice. Advances in Psychiatric Treatment. 2007;13:414-422.
7. Zito JM, Safer DJ, dosReis S, et al. Trends in the prescribing of psychotropic medications to preschoolers. JAMA. 2000;283(8):1025-1030.
8. Tournier M, Greenfield B, Galbaud du Fort G, et al. Patterns of antidepressant use in Quebec children and adolescents: trends and predictors. Psychiatry Res. 2010;179(1):57-63.
9. Cooper WO, Arbogast PG, Ding H, et al. Trends in prescribing of antipsychotic medications for US children. Ambul Pediatr. 2006;6(2):79-83.
10. Child and learning disability psychopharmacology. J Psychopharmacol. 1997;11(4):291-294.
11. American Psychiatric Association. Position statement on patient access to treatments prescribed by their physicians. 2007. http://www.psychiatry.org/advocacy—newsroom/position-statements/apa-position-statements. Accessed May 24 2012.
12. Gazarian M, Kelly M, McPhee JR, et al. Off-label use of medicines: consensus recommendations for evaluating appropriateness. Med J Aust. 2006;185(10):544-548.
13. Kramer SI, McCall WV. Off-label prescribing: 7 steps for safer more effective prescribing. Current Psychiatry. 2006;5(4):14-28.
14. Royal College of Psychiatrists. Use of licensed medicines for unlicensed applications in psychiatric practice. College report CR142. http://www.rcpsych.ac.uk/files/pdfversion/cr142.pdf. Accessed May 24 2012.
1. Lowe-Ponsford F, Baldwin D. Off-label prescribing by psychiatrists. Psychiatric Bulletin. 2000;24:415-417.
2. Radley DC, Finkelstein SN, Stafford RS. Off-label prescribing among office-based physicians. Arch Intern Med. 2006;166(9):1021-1026.
3. Devulapalli K, Nasrallah HA. An analysis of the high psychotropic off-label use in psychiatric disorders: the majority of psychiatric diagnoses have no approved drug. Asian Journal of Psychiatry. 2009;2(1):29-36.
4. Dresser R, Frader J. Off-label prescribing: a call for heightened professional and government oversight. J Law Med Ethics. 2009;37(3):476-486, 396.
5. Food, Drug, and Cosmetic Act, 21 USC §396 (2010).
6. Baldwin DS, Kosky N. Off-label prescribing in psychiatric practice. Advances in Psychiatric Treatment. 2007;13:414-422.
7. Zito JM, Safer DJ, dosReis S, et al. Trends in the prescribing of psychotropic medications to preschoolers. JAMA. 2000;283(8):1025-1030.
8. Tournier M, Greenfield B, Galbaud du Fort G, et al. Patterns of antidepressant use in Quebec children and adolescents: trends and predictors. Psychiatry Res. 2010;179(1):57-63.
9. Cooper WO, Arbogast PG, Ding H, et al. Trends in prescribing of antipsychotic medications for US children. Ambul Pediatr. 2006;6(2):79-83.
10. Child and learning disability psychopharmacology. J Psychopharmacol. 1997;11(4):291-294.
11. American Psychiatric Association. Position statement on patient access to treatments prescribed by their physicians. 2007. http://www.psychiatry.org/advocacy—newsroom/position-statements/apa-position-statements. Accessed May 24 2012.
12. Gazarian M, Kelly M, McPhee JR, et al. Off-label use of medicines: consensus recommendations for evaluating appropriateness. Med J Aust. 2006;185(10):544-548.
13. Kramer SI, McCall WV. Off-label prescribing: 7 steps for safer more effective prescribing. Current Psychiatry. 2006;5(4):14-28.
14. Royal College of Psychiatrists. Use of licensed medicines for unlicensed applications in psychiatric practice. College report CR142. http://www.rcpsych.ac.uk/files/pdfversion/cr142.pdf. Accessed May 24 2012.
Treating resistant depression
We read “Personalizing depression treatment: 2 clinical tools” (Current Psychiatry , March 2012, p. 26-33; http://bit.ly/1nZQCXY) with interest. With lack of response or partial response to major depressive disorder (MDD) treatment, the authors’ reminder to not assume treatment resistance without systematic review of the patient’s clinical status—using the SAFER Interview—and adequacy of medication trials—using the Antidepressant Treatment Response Questionnaire (ATRQ)—is well taken.
The authors noted that the ATRQ considers only pharmacotherapy and electroconvulsive therapy (ECT), and that comprehensive assessment of treatment-resistant depression (TRD) requires asking about depression-specific, evidence-based psychotherapies. We would add that assessment should consider transcranial magnetic stimulation (TMS), which is FDA-approved for TRD and is included in the American Psychiatric Association’s treatment guidelines for MDD. The U.S. Department of Health and Human Services’ Agency for Healthcare Research and Quality characterizes TMS as having “high strength of evidence” for efficacy from well-controlled randomized controlled trials.Transcranial magnetic stimulation for major depressive disorder,” noted “The disappointing remission rates (approximately 25% to 30%) achieved in both the first and second phases of STAR*D [Sequenced Treatment Alternatives to Relieve Depression], coupled with the substantial drop off in both the subsequent chances of remission and attenuated durability of effect, argue for an earlier consideration of SGA [second-generation antipsychotics] augmentation or TMS.”Is psychiatry ripe for creative destruction?” From the Editor, Current Psychiatry , April 2012, p. 20-21; http://bit.ly/KsXAE3), psychiatrists make diagnoses by speaking with and listening to their patients, the same way we have done for decades.
Dr. Nasrallah writes, “Numerous lab data have been developed for psychiatric disorders, but extensive heterogeneity has prevented diagnostic or commercial use of those tests…” This is another way of saying that these tests essentially are useless for the practicing clinician. Diagnosis aside, any clinically based psychiatrist knows that our medications work unpredictably and inconsistently, practical psychopharmacology is a matter of trial and error, and the “gold standard” of current knowledge, the randomized placebo-controlled study, has limited applications when treating an individual patient. The sort of “creative destruction” that Dr. Nasrallah writes about cannot correct the shortcomings of current psychiatric practice.
It is wishful thinking that giving the specialty a new name or pretending to have knowledge we do not possess would “lead to a quantum leap toward a brilliant future anchored in cutting-edge neuroscience.” Until new, clinically relevant knowledge is acquired, the call for creative destruction is premature.
Boris Vatel, MD
Lecturer, Department of Psychology
University of Evansville
Evansville, IN
We read “Personalizing depression treatment: 2 clinical tools” (Current Psychiatry , March 2012, p. 26-33; http://bit.ly/1nZQCXY) with interest. With lack of response or partial response to major depressive disorder (MDD) treatment, the authors’ reminder to not assume treatment resistance without systematic review of the patient’s clinical status—using the SAFER Interview—and adequacy of medication trials—using the Antidepressant Treatment Response Questionnaire (ATRQ)—is well taken.
The authors noted that the ATRQ considers only pharmacotherapy and electroconvulsive therapy (ECT), and that comprehensive assessment of treatment-resistant depression (TRD) requires asking about depression-specific, evidence-based psychotherapies. We would add that assessment should consider transcranial magnetic stimulation (TMS), which is FDA-approved for TRD and is included in the American Psychiatric Association’s treatment guidelines for MDD. The U.S. Department of Health and Human Services’ Agency for Healthcare Research and Quality characterizes TMS as having “high strength of evidence” for efficacy from well-controlled randomized controlled trials.Transcranial magnetic stimulation for major depressive disorder,” noted “The disappointing remission rates (approximately 25% to 30%) achieved in both the first and second phases of STAR*D [Sequenced Treatment Alternatives to Relieve Depression], coupled with the substantial drop off in both the subsequent chances of remission and attenuated durability of effect, argue for an earlier consideration of SGA [second-generation antipsychotics] augmentation or TMS.”Is psychiatry ripe for creative destruction?” From the Editor, Current Psychiatry , April 2012, p. 20-21; http://bit.ly/KsXAE3), psychiatrists make diagnoses by speaking with and listening to their patients, the same way we have done for decades.
Dr. Nasrallah writes, “Numerous lab data have been developed for psychiatric disorders, but extensive heterogeneity has prevented diagnostic or commercial use of those tests…” This is another way of saying that these tests essentially are useless for the practicing clinician. Diagnosis aside, any clinically based psychiatrist knows that our medications work unpredictably and inconsistently, practical psychopharmacology is a matter of trial and error, and the “gold standard” of current knowledge, the randomized placebo-controlled study, has limited applications when treating an individual patient. The sort of “creative destruction” that Dr. Nasrallah writes about cannot correct the shortcomings of current psychiatric practice.
It is wishful thinking that giving the specialty a new name or pretending to have knowledge we do not possess would “lead to a quantum leap toward a brilliant future anchored in cutting-edge neuroscience.” Until new, clinically relevant knowledge is acquired, the call for creative destruction is premature.
Boris Vatel, MD
Lecturer, Department of Psychology
University of Evansville
Evansville, IN
We read “Personalizing depression treatment: 2 clinical tools” (Current Psychiatry , March 2012, p. 26-33; http://bit.ly/1nZQCXY) with interest. With lack of response or partial response to major depressive disorder (MDD) treatment, the authors’ reminder to not assume treatment resistance without systematic review of the patient’s clinical status—using the SAFER Interview—and adequacy of medication trials—using the Antidepressant Treatment Response Questionnaire (ATRQ)—is well taken.
The authors noted that the ATRQ considers only pharmacotherapy and electroconvulsive therapy (ECT), and that comprehensive assessment of treatment-resistant depression (TRD) requires asking about depression-specific, evidence-based psychotherapies. We would add that assessment should consider transcranial magnetic stimulation (TMS), which is FDA-approved for TRD and is included in the American Psychiatric Association’s treatment guidelines for MDD. The U.S. Department of Health and Human Services’ Agency for Healthcare Research and Quality characterizes TMS as having “high strength of evidence” for efficacy from well-controlled randomized controlled trials.Transcranial magnetic stimulation for major depressive disorder,” noted “The disappointing remission rates (approximately 25% to 30%) achieved in both the first and second phases of STAR*D [Sequenced Treatment Alternatives to Relieve Depression], coupled with the substantial drop off in both the subsequent chances of remission and attenuated durability of effect, argue for an earlier consideration of SGA [second-generation antipsychotics] augmentation or TMS.”Is psychiatry ripe for creative destruction?” From the Editor, Current Psychiatry , April 2012, p. 20-21; http://bit.ly/KsXAE3), psychiatrists make diagnoses by speaking with and listening to their patients, the same way we have done for decades.
Dr. Nasrallah writes, “Numerous lab data have been developed for psychiatric disorders, but extensive heterogeneity has prevented diagnostic or commercial use of those tests…” This is another way of saying that these tests essentially are useless for the practicing clinician. Diagnosis aside, any clinically based psychiatrist knows that our medications work unpredictably and inconsistently, practical psychopharmacology is a matter of trial and error, and the “gold standard” of current knowledge, the randomized placebo-controlled study, has limited applications when treating an individual patient. The sort of “creative destruction” that Dr. Nasrallah writes about cannot correct the shortcomings of current psychiatric practice.
It is wishful thinking that giving the specialty a new name or pretending to have knowledge we do not possess would “lead to a quantum leap toward a brilliant future anchored in cutting-edge neuroscience.” Until new, clinically relevant knowledge is acquired, the call for creative destruction is premature.
Boris Vatel, MD
Lecturer, Department of Psychology
University of Evansville
Evansville, IN