User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
L-methylfolate: Another weapon against depression
Discuss this article at www.facebook.com/CurrentPsychiatry
Combination therapies for major depressive disorder (MDD) may enhance antidepressant efficacy and long-term results by working synergistically to regulate monoamines availability. Low levels of serum and red blood cell folate are linked to severe symptoms of depression and some patients are less likely to respond to antidepressants.1 Even in patients with normal serum or red blood cell folate levels, CNS folate levels may be suboptimal.1
L-methylfolate is the centrally active derivative of folate that regulates synthesis of trimonoamines serotonin, dopamine, and norepinephrine and is a key regulator of the cofactor tetrahydrobiopterin (BH4). BH4 is required by tryptophan hydroxylase for serotonin synthesis and by tyrosine hydroxylase for dopamine and norepinephrine synthesis.2
Evidence suggests adding L-methylfolate to selective serotonin reuptake inhibitors (SSRIs) or serotonin–norepinephrine reuptake inhibitors (SNRIs) when starting pharmacotherapy leads to greater reduction of depressive symptoms in a shorter time compared with SSRI or SNRI monotherapy.1 In a study of patients with MDD who partially responded or did not respond to SSRIs, adjunctive L-methylfolate, 15 mg/d, produced greater response rates compared with SSRIs plus placebo.3 L-methylfolate also was well tolerated in combination with SSRI or SNRI therapy. The rates of adverse effects were not significantly different in patients taking L-methylfolate plus an SSRI or SNRI compared with those taking SSRI or SNRI monotherapy.1
MDD patients who may benefit from L-methylfolate include those with low levels of folate and its active metabolites—such as L-methylfolate—and inadequate response to antidepressants. Patients who have an alcohol use disorder, eating disorders, genetic C677-T polymorphism (present in half of the general population), or gastrointestinal disorders are at risk for low folate levels, as well as those who are pregnant.2
Folic acid needs to be converted to L-methylfolate to cross the blood-brain barrier, whereas L-methylfolate can be used directly by the brain.2 Therefore, patients who take medications that can interfere with the conversion of folate to L-methylfolate might benefit from adjunctive L-methylfolate. These medications include lamotrigine, valproate, oral contraceptives, metformin, warfarin, fenofibrates, and certain retinoids.1 Patients with C677-T polymorphism and patients from Hispanic or Mediterranean populations have shown impaired ability to convert folic acid to L-methylfolate.2
Disclosure
Dr. Fluitt reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Ginsberg LD, Oubre AY, Daoud YA. L-methylfolate plus SSRI or SNRI from treatment initiation compared to SSRI or SNRI monotherapy in a major depressive episode. Innov Clin Neurosci. 2011;8(1):19-28.
2. Stahl SM. L-methylfolate: a vitamin for your monoamines. J Clin Psychiatry. 2008;69(9):1352-1353.
3. Papkostas G, Shelton RC, Zajecka JM, et al. L-methylfolate as adjunctive therapy for selective serotonin reuptake inhibitor-resistant major depressive disorder: results of two randomized, double-blind, parallel-sequential trials. Poster presented at: European Congress of Psychiatry; March 12-15, 2011; Vienna, Austria.
Discuss this article at www.facebook.com/CurrentPsychiatry
Combination therapies for major depressive disorder (MDD) may enhance antidepressant efficacy and long-term results by working synergistically to regulate monoamines availability. Low levels of serum and red blood cell folate are linked to severe symptoms of depression and some patients are less likely to respond to antidepressants.1 Even in patients with normal serum or red blood cell folate levels, CNS folate levels may be suboptimal.1
L-methylfolate is the centrally active derivative of folate that regulates synthesis of trimonoamines serotonin, dopamine, and norepinephrine and is a key regulator of the cofactor tetrahydrobiopterin (BH4). BH4 is required by tryptophan hydroxylase for serotonin synthesis and by tyrosine hydroxylase for dopamine and norepinephrine synthesis.2
Evidence suggests adding L-methylfolate to selective serotonin reuptake inhibitors (SSRIs) or serotonin–norepinephrine reuptake inhibitors (SNRIs) when starting pharmacotherapy leads to greater reduction of depressive symptoms in a shorter time compared with SSRI or SNRI monotherapy.1 In a study of patients with MDD who partially responded or did not respond to SSRIs, adjunctive L-methylfolate, 15 mg/d, produced greater response rates compared with SSRIs plus placebo.3 L-methylfolate also was well tolerated in combination with SSRI or SNRI therapy. The rates of adverse effects were not significantly different in patients taking L-methylfolate plus an SSRI or SNRI compared with those taking SSRI or SNRI monotherapy.1
MDD patients who may benefit from L-methylfolate include those with low levels of folate and its active metabolites—such as L-methylfolate—and inadequate response to antidepressants. Patients who have an alcohol use disorder, eating disorders, genetic C677-T polymorphism (present in half of the general population), or gastrointestinal disorders are at risk for low folate levels, as well as those who are pregnant.2
Folic acid needs to be converted to L-methylfolate to cross the blood-brain barrier, whereas L-methylfolate can be used directly by the brain.2 Therefore, patients who take medications that can interfere with the conversion of folate to L-methylfolate might benefit from adjunctive L-methylfolate. These medications include lamotrigine, valproate, oral contraceptives, metformin, warfarin, fenofibrates, and certain retinoids.1 Patients with C677-T polymorphism and patients from Hispanic or Mediterranean populations have shown impaired ability to convert folic acid to L-methylfolate.2
Disclosure
Dr. Fluitt reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at www.facebook.com/CurrentPsychiatry
Combination therapies for major depressive disorder (MDD) may enhance antidepressant efficacy and long-term results by working synergistically to regulate monoamines availability. Low levels of serum and red blood cell folate are linked to severe symptoms of depression and some patients are less likely to respond to antidepressants.1 Even in patients with normal serum or red blood cell folate levels, CNS folate levels may be suboptimal.1
L-methylfolate is the centrally active derivative of folate that regulates synthesis of trimonoamines serotonin, dopamine, and norepinephrine and is a key regulator of the cofactor tetrahydrobiopterin (BH4). BH4 is required by tryptophan hydroxylase for serotonin synthesis and by tyrosine hydroxylase for dopamine and norepinephrine synthesis.2
Evidence suggests adding L-methylfolate to selective serotonin reuptake inhibitors (SSRIs) or serotonin–norepinephrine reuptake inhibitors (SNRIs) when starting pharmacotherapy leads to greater reduction of depressive symptoms in a shorter time compared with SSRI or SNRI monotherapy.1 In a study of patients with MDD who partially responded or did not respond to SSRIs, adjunctive L-methylfolate, 15 mg/d, produced greater response rates compared with SSRIs plus placebo.3 L-methylfolate also was well tolerated in combination with SSRI or SNRI therapy. The rates of adverse effects were not significantly different in patients taking L-methylfolate plus an SSRI or SNRI compared with those taking SSRI or SNRI monotherapy.1
MDD patients who may benefit from L-methylfolate include those with low levels of folate and its active metabolites—such as L-methylfolate—and inadequate response to antidepressants. Patients who have an alcohol use disorder, eating disorders, genetic C677-T polymorphism (present in half of the general population), or gastrointestinal disorders are at risk for low folate levels, as well as those who are pregnant.2
Folic acid needs to be converted to L-methylfolate to cross the blood-brain barrier, whereas L-methylfolate can be used directly by the brain.2 Therefore, patients who take medications that can interfere with the conversion of folate to L-methylfolate might benefit from adjunctive L-methylfolate. These medications include lamotrigine, valproate, oral contraceptives, metformin, warfarin, fenofibrates, and certain retinoids.1 Patients with C677-T polymorphism and patients from Hispanic or Mediterranean populations have shown impaired ability to convert folic acid to L-methylfolate.2
Disclosure
Dr. Fluitt reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Ginsberg LD, Oubre AY, Daoud YA. L-methylfolate plus SSRI or SNRI from treatment initiation compared to SSRI or SNRI monotherapy in a major depressive episode. Innov Clin Neurosci. 2011;8(1):19-28.
2. Stahl SM. L-methylfolate: a vitamin for your monoamines. J Clin Psychiatry. 2008;69(9):1352-1353.
3. Papkostas G, Shelton RC, Zajecka JM, et al. L-methylfolate as adjunctive therapy for selective serotonin reuptake inhibitor-resistant major depressive disorder: results of two randomized, double-blind, parallel-sequential trials. Poster presented at: European Congress of Psychiatry; March 12-15, 2011; Vienna, Austria.
1. Ginsberg LD, Oubre AY, Daoud YA. L-methylfolate plus SSRI or SNRI from treatment initiation compared to SSRI or SNRI monotherapy in a major depressive episode. Innov Clin Neurosci. 2011;8(1):19-28.
2. Stahl SM. L-methylfolate: a vitamin for your monoamines. J Clin Psychiatry. 2008;69(9):1352-1353.
3. Papkostas G, Shelton RC, Zajecka JM, et al. L-methylfolate as adjunctive therapy for selective serotonin reuptake inhibitor-resistant major depressive disorder: results of two randomized, double-blind, parallel-sequential trials. Poster presented at: European Congress of Psychiatry; March 12-15, 2011; Vienna, Austria.
Suicide assessment: Targeting acute risk factors
At his wife’s urging, Mr. L, age 34, presents to the local emergency room (ER). Approximately 1 week ago, he woke up in the middle of the night and told her he was afraid he would die because he had heart palpitations, a choking sensation, dizziness, and shortness of breath.
The ER physician rules out an acute medical illness and requests a psychiatric consultation. Mr. L is reluctant to talk to the psychiatrist, saying he has just had a difficult couple of weeks because of problems at work. With Mr. L’s permission, the psychiatrist speaks with his wife and learns that for several weeks Mr. L has been having problems falling asleep and has been waking up early. Mrs. L noticed her husband is unable to sit still, not enjoying his favorite television shows, and drinking more alcohol at night.
The clinical picture became clearer after Mr. L tells the psychiatrist that approximately 1 month ago, he lost his appetite, had low energy and concentration, and began to feel depressed. He denies having suicidal thoughts or plans, but says his suffering is increasing and he doesn’t know what to do.
Suicide is our worst outcome; at times it can seem like we are helpless to change its frequency or evaluate its likelihood. As clinicians, we are not expected to predict who will commit suicide, but are expected to perform an adequate suicide risk assessment and determine who is at high risk. We need to clearly document a patient’s suicide risk level in his or her chart, and our subsequent actions need to be consistent with that assessment. For instance, arranging for additional supports—including psychiatric hospitalization when necessary—for a patient deemed to be at high risk for suicide is considered the standard of care. In this article, I:
- discuss demographic factors related to suicide
- explore the importance of time-related suicide risk factors and the few treatments shown to reduce suicide risk
- review protective and preventive factors.
Sobering statistics
Over the past decade, suicide rates in the United States have remained fixed at slightly more than 30,000 per year. In 2009—the most recent year for which statistics are available from the Centers for Disease Control and Prevention—there were 36,547 suicides in the United States, making it the 10th leading cause of death.1 The rates of suicide completions and attempts vary by sex and age. Males complete suicide 4 times more often than females, whereas females attempt suicide 3 times more often. Among individuals age 15 to 24, 86% of those who completed suicide were male; in older persons (age >65), 85% were male.2 Although rates of completed suicide are highest among older adults, rates of suicide attempts are greatest among young persons. The ratio of attempted-to-completed suicide is 100 to 200:1 in individuals age 15 to 24 but 4:1 in those age >65.2
Whites and Native Americans have the highest suicide rates (12.3 and 12.9 per 100,000, respectively).2 Guns are the most common method of completed suicide in all age groups in the United States: they are used in 53% of all suicides and 76% of those among persons age >70.3 In >90% of completed suicides, the decedent had been diagnosed with ≥1 psychiatric disorder.3 By far, the most common psychiatric illness is major depressive disorder, present in 75% of those who commit suicide.3
Understanding intent
Many physicians believe that patients will tell them if they are feeling worse and are starting to think more seriously about suicide. There is no better example of this than the “contract for safety” or “no-harm contract,” in which a patient signs a paper agreeing to notify a clinician if he begins to develop more intense suicidal feelings. Studies have shown that these “no-harm contracts” do not prevent suicide; this makes sense because if a patient decides to kill himself, telling a clinician puts up an obstacle.4-6
Patients who commit suicide often communicate their suicidal intent, but usually tell family members rather than clinicians. In 1 study, 78% of patients who committed suicide on an inpatient unit denied suicidal ideation at their last communication with staff; although 60% told their spouse and 50% told other relatives, only 18% told their physician.7 In this study, precautions provided a false sense of security: 51% of patients were receiving 15-minute suicide checks or 1-to-1 observation at the time of suicide.7
Who is at risk?
The most recent American Psychiatric Association Task Force Report on Suicide identified 57 risk factors for suicide.8,9 This has led to confusion among clinicians and may have led some clinicians to repeatedly ask patients about suicidal ideation rather than conduct a suicide risk assessment.
Although a history of suicide attempts and a family history of suicide are well-established risk factors,9 these are not acute factors. It is important to differentiate between suicide attempts and suicide completions. Although many suicide attempts are accurate substitutes for actual suicides, there is a spectrum of intent in suicide attempts that differentiates them in terms of lethality.10 Clinicians need a more thorough understanding of who is at acute risk for suicide, which will help them make decisions about patients’ imminent risk to themselves.
In the only study that examined time-related predictors of suicide, Fawcett et al11 used the Schedule for Affective Disorders and Schizophrenia (SADS) to evaluate 954 patients with major affective disorders over 10 years. Raters were blinded to treatment, and clinicians could use any combination of psychotherapy or pharmacotherapy. These researchers found that acute risk factors—those associated with suicide within 1 year—were psychic anxiety, anhedonia, diminished concentration, insomnia, panic attacks, and active alcohol abuse (Table 1).11 These factors were present in the context of an underlying depressive disorder. Hopelessness, suicidal ideation, and a history of suicide attempts were linked to suicide between 2 and 10 years.
Busch et al12 performed a retrospective study on an inpatient unit using the SADS to evaluate symptoms present the week before patients’ suicides. They found that 79% of patients had extreme psychic anxiety, agitation, or both, and that 54% had active psychosis. The same authors studied an additional 12 cases of inpatient suicide and found 9 patients had severe anxiety, agitation, or both, and insomnia. The median time to suicide from admission was 3.5 days and none of the 12 patients had been started on an antidepressant, antipsychotic, or anxiolytic. This underscores the need to initiate symptomatic treatment quickly, even before reaching a definitive diagnosis.
The Columbia Suicide Severity Rating Scale (C-SSRS), which evaluates suicide ideation and behavior in the past week and lifetime, has predictive validity in determining those at highest risk for making a suicide attempt within up to 24 weeks of follow-up.13 A limitation of the C-SSRS is that it has predictive validity for suicide attempts only, and not suicide completions.
Table 1
Acute suicide risk factors: 3 A’s + 3 P’s
| Alcohol abuse |
| Attention (or concentration) impairment |
| Awake (insomnia) |
| Panic attacks |
| Pleasure (diminished) |
| Psychic anxiety |
| Source: Reference 11 |
Treatments to lower risk
Although identifying risk factors such as older age, being unmarried, male sex, experiencing a recent loss, a family history of completed suicide, and being white or Native American are helpful in evaluating a patient’s suicide risk, they are not time-sensitive or modifiable, which limits their value.
In contrast, most of the acute risk factors identified by Fawcett et al potentially are treatable. Psychic anxiety, insomnia, and panic attacks can be treated with benzodiazepines or other anxiolytics and sedative/hypnotics. Active psychosis, which Busch et al identified as a risk factor for inpatient suicide, may respond to antipsychotics.
Other medications have been identified as modifying suicide risk (Table 2).14-20 Among patients with major affective disorders, lithium has been shown to reduce suicidal acts by 93%, suicide attempts by 93%, and suicide completions by 82%.14 Lithium produces the largest suicide risk reduction in unipolar depression, at 100%, followed by bipolar II disorder (82%) and bipolar I disorder (67%).15 Several studies have demonstrated that lithium can reduce the mortality rate from suicide for patients with affective disorders, and that this effect persists.16,17
Clozapine has been associated with reduced rates of suicide attempts and completed suicides in patients with chronic psychosis. In a meta-analysis, long-term clozapine treatment was associated with an approximately 3-fold overall reduction of risk of suicidal behaviors,18 although a prospective study found no reduction in risk of completed suicide in patients with schizophrenia treated with clozapine.19
In one study, electroconvulsive therapy (ECT) reduced suicidal thoughts and acts by 38% after 1 week and 80% overall.20 There have been reports of amelioration of suicidal thoughts after just 1 ECT treatment.21 There are no published studies that show a reduction in suicide completions with ECT; however, this may be due to the relatively small number of patients who receive ECT and the infrequency of completed suicides.
Protective factors. The balance between protective factors and risk factors determines appropriate clinical decision making when attempting to evaluate a patient’s suicide risk. Perhaps the best measure of protective factors is the Reasons for Living Inventory, developed by Linehan et al,22 which has been validated in some populations, including adolescents and young adults.23 This inventory delineates protective factors against suicidal ideation and behavior rather than completed suicides.
Similar to suicide protection, suicide prevention focuses on factors that can serve as obstacles to a patient’s desire or ability to commit suicide. A large systematic literature review by Mann et al24 found that only primary care physician education and restricting access to lethal means prevented suicide. When working to remove lethal means from a suicidal patient’s home, it is critical to verify that this has been done rather than merely making a suggestion to a family member. It is necessary to follow up with a phone call and document the completion of this task.
When a patient commits suicide, it is common for psychiatrists to feel like there must have been something they could have done to prevent such a tragedy. Although typically that is not the case, there is more we can do to improve our suicide risk assessment skills. Focusing on acute, modifiable suicide risk factors may help us lower a patient’s risk. Also, shortening the time frame now considered acute (within 1 year) to hours and days and looking for additional risk factors may improve mental health professionals’ ability to accurately assess acute suicide risk.
Table 2
Treatments to lower suicide risk
| Acute |
| Benzodiazepines—to diminish panic, anxiety, insomnia |
| Antipsychotics—if acute psychosis is present |
| Trazodone (or non-benzodiazepine hypnotics)—if insomnia is present without daytime anxiety |
| Diagnosis–specific |
| Clozapine—for patients with schizophrenia and high suicide risk |
| Lithium—for patients with bipolar disorder (if not contraindicated); consider for patients with refractory unipolar depression at high suicide risk |
| Electroconvulsive therapy—for patients with severe depression and high suicide risk |
| Source: References 14-20 |
CASE CONTINUED: Hospitalization and improvement
The psychiatrist determines Mr. L is at high risk for suicide and recommends psychiatric hospitalization. She starts him on citalopram, 10 mg/d, and clonazepam, 0.5 mg twice daily and 1 mg at bedtime, to help with anxiety and insomnia. After 3 days, Mr. L tolerates the medications, sleeps better, and feels more hopeful about the future. The psychiatrist increases citalopram to 20 mg/d.
Four days later, Mr. L is eating better, can concentrate, and denies further episodes of dizziness or anxiety. The inpatient psychiatrist assesses his acute suicide risk as low and discharges him to a week-long partial hospitalization program.
Related Resources
- American Association of Suicidology. www.suicidology.org.
- Harvard School of Public Health. Means Matter. www.hsph.harvard.edu/means-matter.
- Simon RI. Preventing patient suicide: clinical assessment and management. Arlington, VA: American Psychiatric Publishing; 2011.
Drug Brand Names
- Citalopram • Celexa
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Lithium • Eskalith, Lithobid
- Trazodone • Desyrel, Oleptro
Disclosure
Dr. Freeman reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Centers for Disease Control and Prevention. US death rate falls for 10th straight year. http://www.cdc.gov/media/releases/2011/p0316_deathrate.html. Published March 16 2011. Accessed November 22, 2011.
2. Centers for Disease Control and Prevention. Suicide: facts at a glance. http://www.cdc.gov/violenceprevention/suicide. Published Summer 2010. Accessed November 17 2011.
3. Karch DL, Dahlberg LL, Patel N. Surveillance for violent deaths—National Violent Death Reporting System 16 states, 2007. MMWR Surveill Summ. 2010;59(4):1-50.
4. Resnick PJ. Recognizing that the suicidal patient views you as an ‘adversary.’ Current Psychiatry. 2002;1(1):8.-
5. Stanford EJ, Goetz RR, Bloom JD. The No Harm Contract in the emergency assessment of suicidal risk. J Clin Psychiatry. 1994;55(8):344-348.
6. Edwards SJ, Sachmann MD. No-suicide contracts no-suicide agreements, and no-suicide assurances: a study of their nature, utilization, perceived effectiveness, and potential to cause harm. Crisis. 2010;31(6):290-302.
7. Busch KA, Fawcett J, Jacobs DG. Clinical correlates of inpatient suicide. J Clin Psychiatry. 2003;64(1):14-19.
8. American Psychiatric Association. Practice guideline for the assessment and treatment of patients with suicidal behaviors. http://psychiatryonline.org/content.aspx?bookid=28§ionid=1673332#56008. Published November 2003. Accessed November 22 2011.
9. Jacobs DG, Brewer ML. Application of the APA practice guidelines on suicide to clinical practice. CNS Spectr. 2006;11(6):447-454.
10. Nasser EH, Overholser JC. Assessing varying degrees of lethality in depressed adolescent suicide attempters. Acta Psychiatr Scand. 1999;99(6):423-431.
11. Fawcett J, Scheftner WA, Fogg L, et al. Time-related predictors of suicide in major affective disorder. Am J Psychiatry. 1990;147(9):1189-1194.
12. Busch KA, Fawcett J. A fine-grained study of patients who commit suicide. Psychiatric Ann. 2004;34(5):357-364.
13. Posner K, Brown GK, Stanley B, et al. The Columbia-Suicide Severity Rating Scale (C-SSRS): initial validity and internal consistency findings from three multi-site studies with adolescents and adults. Am J Psychiatry. 2011;168:1266-1277.
14. Müller-Oerlinghausen B, Berghöfer A, Ahrens B. The antisuicidal and mortality-reducing effect of lithium prophylaxis: consequences for guidelines in clinical psychiatry. Can J Psychiatry. 2003;48(7):433-439.
15. Tondo L, Hennen J, Baldessarini RJ. Lower suicide risk with long-term lithium treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand. 2001;104(3):163-172.
16. Kessing LV, Søndergård L, Kvist K, et al. Suicide risk in patients treated with lithium. Arch Gen Psychiatry. 2005;62(8):860-866.
17. Baldessarini RJ, Tondo L, Hennen J. Lithium treatment and suicide risk in major affective disorders: update and new findings. J Clin Psychiatry. 2003;64(suppl 5):44-52.
18. Hennen J, Baldessarini RJ. Suicidal risk during treatment with clozapine: a meta-analysis. Schizophr Res. 2005;73(2-3):139-145.
19. Kuo CJ, Tsai SY, Lo CH, et al. Risk factors for completed suicide in schizophrenia. J Clin Psychiatry. 2005;66(5):579-585.
20. Kobeissi J, Aloysi A, Tobias K, et al. Resolution of severe suicidality with a single electroconvulsive therapy. J ECT. 2011;27(1):86-88.
21. Kellner CH, Fink M, Knapp R, et al. Relief of expressed suicidal intent by ECT: a consortium for research in ECT study. Am J Psychiatry. 2005;162(5):977-982.
22. Linehan MM, Goodstein JL, Nielsen SL, et al. Reasons for staying alive when you are thinking of killing yourself: the reasons for living inventory. J Consult Clin Psychol. 1983;51(2):276-286.
23. Cole DA. Validation of the reasons for living inventory in general and delinquent adolescent samples. J Abnorm Child Psychol. 1989;17(1):13-27.
24. Mann JJ, Apter A, Bertolote J, et al. Suicide prevention strategies: a systematic review. JAMA. 2005;294(16):2064-2074.
At his wife’s urging, Mr. L, age 34, presents to the local emergency room (ER). Approximately 1 week ago, he woke up in the middle of the night and told her he was afraid he would die because he had heart palpitations, a choking sensation, dizziness, and shortness of breath.
The ER physician rules out an acute medical illness and requests a psychiatric consultation. Mr. L is reluctant to talk to the psychiatrist, saying he has just had a difficult couple of weeks because of problems at work. With Mr. L’s permission, the psychiatrist speaks with his wife and learns that for several weeks Mr. L has been having problems falling asleep and has been waking up early. Mrs. L noticed her husband is unable to sit still, not enjoying his favorite television shows, and drinking more alcohol at night.
The clinical picture became clearer after Mr. L tells the psychiatrist that approximately 1 month ago, he lost his appetite, had low energy and concentration, and began to feel depressed. He denies having suicidal thoughts or plans, but says his suffering is increasing and he doesn’t know what to do.
Suicide is our worst outcome; at times it can seem like we are helpless to change its frequency or evaluate its likelihood. As clinicians, we are not expected to predict who will commit suicide, but are expected to perform an adequate suicide risk assessment and determine who is at high risk. We need to clearly document a patient’s suicide risk level in his or her chart, and our subsequent actions need to be consistent with that assessment. For instance, arranging for additional supports—including psychiatric hospitalization when necessary—for a patient deemed to be at high risk for suicide is considered the standard of care. In this article, I:
- discuss demographic factors related to suicide
- explore the importance of time-related suicide risk factors and the few treatments shown to reduce suicide risk
- review protective and preventive factors.
Sobering statistics
Over the past decade, suicide rates in the United States have remained fixed at slightly more than 30,000 per year. In 2009—the most recent year for which statistics are available from the Centers for Disease Control and Prevention—there were 36,547 suicides in the United States, making it the 10th leading cause of death.1 The rates of suicide completions and attempts vary by sex and age. Males complete suicide 4 times more often than females, whereas females attempt suicide 3 times more often. Among individuals age 15 to 24, 86% of those who completed suicide were male; in older persons (age >65), 85% were male.2 Although rates of completed suicide are highest among older adults, rates of suicide attempts are greatest among young persons. The ratio of attempted-to-completed suicide is 100 to 200:1 in individuals age 15 to 24 but 4:1 in those age >65.2
Whites and Native Americans have the highest suicide rates (12.3 and 12.9 per 100,000, respectively).2 Guns are the most common method of completed suicide in all age groups in the United States: they are used in 53% of all suicides and 76% of those among persons age >70.3 In >90% of completed suicides, the decedent had been diagnosed with ≥1 psychiatric disorder.3 By far, the most common psychiatric illness is major depressive disorder, present in 75% of those who commit suicide.3
Understanding intent
Many physicians believe that patients will tell them if they are feeling worse and are starting to think more seriously about suicide. There is no better example of this than the “contract for safety” or “no-harm contract,” in which a patient signs a paper agreeing to notify a clinician if he begins to develop more intense suicidal feelings. Studies have shown that these “no-harm contracts” do not prevent suicide; this makes sense because if a patient decides to kill himself, telling a clinician puts up an obstacle.4-6
Patients who commit suicide often communicate their suicidal intent, but usually tell family members rather than clinicians. In 1 study, 78% of patients who committed suicide on an inpatient unit denied suicidal ideation at their last communication with staff; although 60% told their spouse and 50% told other relatives, only 18% told their physician.7 In this study, precautions provided a false sense of security: 51% of patients were receiving 15-minute suicide checks or 1-to-1 observation at the time of suicide.7
Who is at risk?
The most recent American Psychiatric Association Task Force Report on Suicide identified 57 risk factors for suicide.8,9 This has led to confusion among clinicians and may have led some clinicians to repeatedly ask patients about suicidal ideation rather than conduct a suicide risk assessment.
Although a history of suicide attempts and a family history of suicide are well-established risk factors,9 these are not acute factors. It is important to differentiate between suicide attempts and suicide completions. Although many suicide attempts are accurate substitutes for actual suicides, there is a spectrum of intent in suicide attempts that differentiates them in terms of lethality.10 Clinicians need a more thorough understanding of who is at acute risk for suicide, which will help them make decisions about patients’ imminent risk to themselves.
In the only study that examined time-related predictors of suicide, Fawcett et al11 used the Schedule for Affective Disorders and Schizophrenia (SADS) to evaluate 954 patients with major affective disorders over 10 years. Raters were blinded to treatment, and clinicians could use any combination of psychotherapy or pharmacotherapy. These researchers found that acute risk factors—those associated with suicide within 1 year—were psychic anxiety, anhedonia, diminished concentration, insomnia, panic attacks, and active alcohol abuse (Table 1).11 These factors were present in the context of an underlying depressive disorder. Hopelessness, suicidal ideation, and a history of suicide attempts were linked to suicide between 2 and 10 years.
Busch et al12 performed a retrospective study on an inpatient unit using the SADS to evaluate symptoms present the week before patients’ suicides. They found that 79% of patients had extreme psychic anxiety, agitation, or both, and that 54% had active psychosis. The same authors studied an additional 12 cases of inpatient suicide and found 9 patients had severe anxiety, agitation, or both, and insomnia. The median time to suicide from admission was 3.5 days and none of the 12 patients had been started on an antidepressant, antipsychotic, or anxiolytic. This underscores the need to initiate symptomatic treatment quickly, even before reaching a definitive diagnosis.
The Columbia Suicide Severity Rating Scale (C-SSRS), which evaluates suicide ideation and behavior in the past week and lifetime, has predictive validity in determining those at highest risk for making a suicide attempt within up to 24 weeks of follow-up.13 A limitation of the C-SSRS is that it has predictive validity for suicide attempts only, and not suicide completions.
Table 1
Acute suicide risk factors: 3 A’s + 3 P’s
| Alcohol abuse |
| Attention (or concentration) impairment |
| Awake (insomnia) |
| Panic attacks |
| Pleasure (diminished) |
| Psychic anxiety |
| Source: Reference 11 |
Treatments to lower risk
Although identifying risk factors such as older age, being unmarried, male sex, experiencing a recent loss, a family history of completed suicide, and being white or Native American are helpful in evaluating a patient’s suicide risk, they are not time-sensitive or modifiable, which limits their value.
In contrast, most of the acute risk factors identified by Fawcett et al potentially are treatable. Psychic anxiety, insomnia, and panic attacks can be treated with benzodiazepines or other anxiolytics and sedative/hypnotics. Active psychosis, which Busch et al identified as a risk factor for inpatient suicide, may respond to antipsychotics.
Other medications have been identified as modifying suicide risk (Table 2).14-20 Among patients with major affective disorders, lithium has been shown to reduce suicidal acts by 93%, suicide attempts by 93%, and suicide completions by 82%.14 Lithium produces the largest suicide risk reduction in unipolar depression, at 100%, followed by bipolar II disorder (82%) and bipolar I disorder (67%).15 Several studies have demonstrated that lithium can reduce the mortality rate from suicide for patients with affective disorders, and that this effect persists.16,17
Clozapine has been associated with reduced rates of suicide attempts and completed suicides in patients with chronic psychosis. In a meta-analysis, long-term clozapine treatment was associated with an approximately 3-fold overall reduction of risk of suicidal behaviors,18 although a prospective study found no reduction in risk of completed suicide in patients with schizophrenia treated with clozapine.19
In one study, electroconvulsive therapy (ECT) reduced suicidal thoughts and acts by 38% after 1 week and 80% overall.20 There have been reports of amelioration of suicidal thoughts after just 1 ECT treatment.21 There are no published studies that show a reduction in suicide completions with ECT; however, this may be due to the relatively small number of patients who receive ECT and the infrequency of completed suicides.
Protective factors. The balance between protective factors and risk factors determines appropriate clinical decision making when attempting to evaluate a patient’s suicide risk. Perhaps the best measure of protective factors is the Reasons for Living Inventory, developed by Linehan et al,22 which has been validated in some populations, including adolescents and young adults.23 This inventory delineates protective factors against suicidal ideation and behavior rather than completed suicides.
Similar to suicide protection, suicide prevention focuses on factors that can serve as obstacles to a patient’s desire or ability to commit suicide. A large systematic literature review by Mann et al24 found that only primary care physician education and restricting access to lethal means prevented suicide. When working to remove lethal means from a suicidal patient’s home, it is critical to verify that this has been done rather than merely making a suggestion to a family member. It is necessary to follow up with a phone call and document the completion of this task.
When a patient commits suicide, it is common for psychiatrists to feel like there must have been something they could have done to prevent such a tragedy. Although typically that is not the case, there is more we can do to improve our suicide risk assessment skills. Focusing on acute, modifiable suicide risk factors may help us lower a patient’s risk. Also, shortening the time frame now considered acute (within 1 year) to hours and days and looking for additional risk factors may improve mental health professionals’ ability to accurately assess acute suicide risk.
Table 2
Treatments to lower suicide risk
| Acute |
| Benzodiazepines—to diminish panic, anxiety, insomnia |
| Antipsychotics—if acute psychosis is present |
| Trazodone (or non-benzodiazepine hypnotics)—if insomnia is present without daytime anxiety |
| Diagnosis–specific |
| Clozapine—for patients with schizophrenia and high suicide risk |
| Lithium—for patients with bipolar disorder (if not contraindicated); consider for patients with refractory unipolar depression at high suicide risk |
| Electroconvulsive therapy—for patients with severe depression and high suicide risk |
| Source: References 14-20 |
CASE CONTINUED: Hospitalization and improvement
The psychiatrist determines Mr. L is at high risk for suicide and recommends psychiatric hospitalization. She starts him on citalopram, 10 mg/d, and clonazepam, 0.5 mg twice daily and 1 mg at bedtime, to help with anxiety and insomnia. After 3 days, Mr. L tolerates the medications, sleeps better, and feels more hopeful about the future. The psychiatrist increases citalopram to 20 mg/d.
Four days later, Mr. L is eating better, can concentrate, and denies further episodes of dizziness or anxiety. The inpatient psychiatrist assesses his acute suicide risk as low and discharges him to a week-long partial hospitalization program.
Related Resources
- American Association of Suicidology. www.suicidology.org.
- Harvard School of Public Health. Means Matter. www.hsph.harvard.edu/means-matter.
- Simon RI. Preventing patient suicide: clinical assessment and management. Arlington, VA: American Psychiatric Publishing; 2011.
Drug Brand Names
- Citalopram • Celexa
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Lithium • Eskalith, Lithobid
- Trazodone • Desyrel, Oleptro
Disclosure
Dr. Freeman reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
At his wife’s urging, Mr. L, age 34, presents to the local emergency room (ER). Approximately 1 week ago, he woke up in the middle of the night and told her he was afraid he would die because he had heart palpitations, a choking sensation, dizziness, and shortness of breath.
The ER physician rules out an acute medical illness and requests a psychiatric consultation. Mr. L is reluctant to talk to the psychiatrist, saying he has just had a difficult couple of weeks because of problems at work. With Mr. L’s permission, the psychiatrist speaks with his wife and learns that for several weeks Mr. L has been having problems falling asleep and has been waking up early. Mrs. L noticed her husband is unable to sit still, not enjoying his favorite television shows, and drinking more alcohol at night.
The clinical picture became clearer after Mr. L tells the psychiatrist that approximately 1 month ago, he lost his appetite, had low energy and concentration, and began to feel depressed. He denies having suicidal thoughts or plans, but says his suffering is increasing and he doesn’t know what to do.
Suicide is our worst outcome; at times it can seem like we are helpless to change its frequency or evaluate its likelihood. As clinicians, we are not expected to predict who will commit suicide, but are expected to perform an adequate suicide risk assessment and determine who is at high risk. We need to clearly document a patient’s suicide risk level in his or her chart, and our subsequent actions need to be consistent with that assessment. For instance, arranging for additional supports—including psychiatric hospitalization when necessary—for a patient deemed to be at high risk for suicide is considered the standard of care. In this article, I:
- discuss demographic factors related to suicide
- explore the importance of time-related suicide risk factors and the few treatments shown to reduce suicide risk
- review protective and preventive factors.
Sobering statistics
Over the past decade, suicide rates in the United States have remained fixed at slightly more than 30,000 per year. In 2009—the most recent year for which statistics are available from the Centers for Disease Control and Prevention—there were 36,547 suicides in the United States, making it the 10th leading cause of death.1 The rates of suicide completions and attempts vary by sex and age. Males complete suicide 4 times more often than females, whereas females attempt suicide 3 times more often. Among individuals age 15 to 24, 86% of those who completed suicide were male; in older persons (age >65), 85% were male.2 Although rates of completed suicide are highest among older adults, rates of suicide attempts are greatest among young persons. The ratio of attempted-to-completed suicide is 100 to 200:1 in individuals age 15 to 24 but 4:1 in those age >65.2
Whites and Native Americans have the highest suicide rates (12.3 and 12.9 per 100,000, respectively).2 Guns are the most common method of completed suicide in all age groups in the United States: they are used in 53% of all suicides and 76% of those among persons age >70.3 In >90% of completed suicides, the decedent had been diagnosed with ≥1 psychiatric disorder.3 By far, the most common psychiatric illness is major depressive disorder, present in 75% of those who commit suicide.3
Understanding intent
Many physicians believe that patients will tell them if they are feeling worse and are starting to think more seriously about suicide. There is no better example of this than the “contract for safety” or “no-harm contract,” in which a patient signs a paper agreeing to notify a clinician if he begins to develop more intense suicidal feelings. Studies have shown that these “no-harm contracts” do not prevent suicide; this makes sense because if a patient decides to kill himself, telling a clinician puts up an obstacle.4-6
Patients who commit suicide often communicate their suicidal intent, but usually tell family members rather than clinicians. In 1 study, 78% of patients who committed suicide on an inpatient unit denied suicidal ideation at their last communication with staff; although 60% told their spouse and 50% told other relatives, only 18% told their physician.7 In this study, precautions provided a false sense of security: 51% of patients were receiving 15-minute suicide checks or 1-to-1 observation at the time of suicide.7
Who is at risk?
The most recent American Psychiatric Association Task Force Report on Suicide identified 57 risk factors for suicide.8,9 This has led to confusion among clinicians and may have led some clinicians to repeatedly ask patients about suicidal ideation rather than conduct a suicide risk assessment.
Although a history of suicide attempts and a family history of suicide are well-established risk factors,9 these are not acute factors. It is important to differentiate between suicide attempts and suicide completions. Although many suicide attempts are accurate substitutes for actual suicides, there is a spectrum of intent in suicide attempts that differentiates them in terms of lethality.10 Clinicians need a more thorough understanding of who is at acute risk for suicide, which will help them make decisions about patients’ imminent risk to themselves.
In the only study that examined time-related predictors of suicide, Fawcett et al11 used the Schedule for Affective Disorders and Schizophrenia (SADS) to evaluate 954 patients with major affective disorders over 10 years. Raters were blinded to treatment, and clinicians could use any combination of psychotherapy or pharmacotherapy. These researchers found that acute risk factors—those associated with suicide within 1 year—were psychic anxiety, anhedonia, diminished concentration, insomnia, panic attacks, and active alcohol abuse (Table 1).11 These factors were present in the context of an underlying depressive disorder. Hopelessness, suicidal ideation, and a history of suicide attempts were linked to suicide between 2 and 10 years.
Busch et al12 performed a retrospective study on an inpatient unit using the SADS to evaluate symptoms present the week before patients’ suicides. They found that 79% of patients had extreme psychic anxiety, agitation, or both, and that 54% had active psychosis. The same authors studied an additional 12 cases of inpatient suicide and found 9 patients had severe anxiety, agitation, or both, and insomnia. The median time to suicide from admission was 3.5 days and none of the 12 patients had been started on an antidepressant, antipsychotic, or anxiolytic. This underscores the need to initiate symptomatic treatment quickly, even before reaching a definitive diagnosis.
The Columbia Suicide Severity Rating Scale (C-SSRS), which evaluates suicide ideation and behavior in the past week and lifetime, has predictive validity in determining those at highest risk for making a suicide attempt within up to 24 weeks of follow-up.13 A limitation of the C-SSRS is that it has predictive validity for suicide attempts only, and not suicide completions.
Table 1
Acute suicide risk factors: 3 A’s + 3 P’s
| Alcohol abuse |
| Attention (or concentration) impairment |
| Awake (insomnia) |
| Panic attacks |
| Pleasure (diminished) |
| Psychic anxiety |
| Source: Reference 11 |
Treatments to lower risk
Although identifying risk factors such as older age, being unmarried, male sex, experiencing a recent loss, a family history of completed suicide, and being white or Native American are helpful in evaluating a patient’s suicide risk, they are not time-sensitive or modifiable, which limits their value.
In contrast, most of the acute risk factors identified by Fawcett et al potentially are treatable. Psychic anxiety, insomnia, and panic attacks can be treated with benzodiazepines or other anxiolytics and sedative/hypnotics. Active psychosis, which Busch et al identified as a risk factor for inpatient suicide, may respond to antipsychotics.
Other medications have been identified as modifying suicide risk (Table 2).14-20 Among patients with major affective disorders, lithium has been shown to reduce suicidal acts by 93%, suicide attempts by 93%, and suicide completions by 82%.14 Lithium produces the largest suicide risk reduction in unipolar depression, at 100%, followed by bipolar II disorder (82%) and bipolar I disorder (67%).15 Several studies have demonstrated that lithium can reduce the mortality rate from suicide for patients with affective disorders, and that this effect persists.16,17
Clozapine has been associated with reduced rates of suicide attempts and completed suicides in patients with chronic psychosis. In a meta-analysis, long-term clozapine treatment was associated with an approximately 3-fold overall reduction of risk of suicidal behaviors,18 although a prospective study found no reduction in risk of completed suicide in patients with schizophrenia treated with clozapine.19
In one study, electroconvulsive therapy (ECT) reduced suicidal thoughts and acts by 38% after 1 week and 80% overall.20 There have been reports of amelioration of suicidal thoughts after just 1 ECT treatment.21 There are no published studies that show a reduction in suicide completions with ECT; however, this may be due to the relatively small number of patients who receive ECT and the infrequency of completed suicides.
Protective factors. The balance between protective factors and risk factors determines appropriate clinical decision making when attempting to evaluate a patient’s suicide risk. Perhaps the best measure of protective factors is the Reasons for Living Inventory, developed by Linehan et al,22 which has been validated in some populations, including adolescents and young adults.23 This inventory delineates protective factors against suicidal ideation and behavior rather than completed suicides.
Similar to suicide protection, suicide prevention focuses on factors that can serve as obstacles to a patient’s desire or ability to commit suicide. A large systematic literature review by Mann et al24 found that only primary care physician education and restricting access to lethal means prevented suicide. When working to remove lethal means from a suicidal patient’s home, it is critical to verify that this has been done rather than merely making a suggestion to a family member. It is necessary to follow up with a phone call and document the completion of this task.
When a patient commits suicide, it is common for psychiatrists to feel like there must have been something they could have done to prevent such a tragedy. Although typically that is not the case, there is more we can do to improve our suicide risk assessment skills. Focusing on acute, modifiable suicide risk factors may help us lower a patient’s risk. Also, shortening the time frame now considered acute (within 1 year) to hours and days and looking for additional risk factors may improve mental health professionals’ ability to accurately assess acute suicide risk.
Table 2
Treatments to lower suicide risk
| Acute |
| Benzodiazepines—to diminish panic, anxiety, insomnia |
| Antipsychotics—if acute psychosis is present |
| Trazodone (or non-benzodiazepine hypnotics)—if insomnia is present without daytime anxiety |
| Diagnosis–specific |
| Clozapine—for patients with schizophrenia and high suicide risk |
| Lithium—for patients with bipolar disorder (if not contraindicated); consider for patients with refractory unipolar depression at high suicide risk |
| Electroconvulsive therapy—for patients with severe depression and high suicide risk |
| Source: References 14-20 |
CASE CONTINUED: Hospitalization and improvement
The psychiatrist determines Mr. L is at high risk for suicide and recommends psychiatric hospitalization. She starts him on citalopram, 10 mg/d, and clonazepam, 0.5 mg twice daily and 1 mg at bedtime, to help with anxiety and insomnia. After 3 days, Mr. L tolerates the medications, sleeps better, and feels more hopeful about the future. The psychiatrist increases citalopram to 20 mg/d.
Four days later, Mr. L is eating better, can concentrate, and denies further episodes of dizziness or anxiety. The inpatient psychiatrist assesses his acute suicide risk as low and discharges him to a week-long partial hospitalization program.
Related Resources
- American Association of Suicidology. www.suicidology.org.
- Harvard School of Public Health. Means Matter. www.hsph.harvard.edu/means-matter.
- Simon RI. Preventing patient suicide: clinical assessment and management. Arlington, VA: American Psychiatric Publishing; 2011.
Drug Brand Names
- Citalopram • Celexa
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Lithium • Eskalith, Lithobid
- Trazodone • Desyrel, Oleptro
Disclosure
Dr. Freeman reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Centers for Disease Control and Prevention. US death rate falls for 10th straight year. http://www.cdc.gov/media/releases/2011/p0316_deathrate.html. Published March 16 2011. Accessed November 22, 2011.
2. Centers for Disease Control and Prevention. Suicide: facts at a glance. http://www.cdc.gov/violenceprevention/suicide. Published Summer 2010. Accessed November 17 2011.
3. Karch DL, Dahlberg LL, Patel N. Surveillance for violent deaths—National Violent Death Reporting System 16 states, 2007. MMWR Surveill Summ. 2010;59(4):1-50.
4. Resnick PJ. Recognizing that the suicidal patient views you as an ‘adversary.’ Current Psychiatry. 2002;1(1):8.-
5. Stanford EJ, Goetz RR, Bloom JD. The No Harm Contract in the emergency assessment of suicidal risk. J Clin Psychiatry. 1994;55(8):344-348.
6. Edwards SJ, Sachmann MD. No-suicide contracts no-suicide agreements, and no-suicide assurances: a study of their nature, utilization, perceived effectiveness, and potential to cause harm. Crisis. 2010;31(6):290-302.
7. Busch KA, Fawcett J, Jacobs DG. Clinical correlates of inpatient suicide. J Clin Psychiatry. 2003;64(1):14-19.
8. American Psychiatric Association. Practice guideline for the assessment and treatment of patients with suicidal behaviors. http://psychiatryonline.org/content.aspx?bookid=28§ionid=1673332#56008. Published November 2003. Accessed November 22 2011.
9. Jacobs DG, Brewer ML. Application of the APA practice guidelines on suicide to clinical practice. CNS Spectr. 2006;11(6):447-454.
10. Nasser EH, Overholser JC. Assessing varying degrees of lethality in depressed adolescent suicide attempters. Acta Psychiatr Scand. 1999;99(6):423-431.
11. Fawcett J, Scheftner WA, Fogg L, et al. Time-related predictors of suicide in major affective disorder. Am J Psychiatry. 1990;147(9):1189-1194.
12. Busch KA, Fawcett J. A fine-grained study of patients who commit suicide. Psychiatric Ann. 2004;34(5):357-364.
13. Posner K, Brown GK, Stanley B, et al. The Columbia-Suicide Severity Rating Scale (C-SSRS): initial validity and internal consistency findings from three multi-site studies with adolescents and adults. Am J Psychiatry. 2011;168:1266-1277.
14. Müller-Oerlinghausen B, Berghöfer A, Ahrens B. The antisuicidal and mortality-reducing effect of lithium prophylaxis: consequences for guidelines in clinical psychiatry. Can J Psychiatry. 2003;48(7):433-439.
15. Tondo L, Hennen J, Baldessarini RJ. Lower suicide risk with long-term lithium treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand. 2001;104(3):163-172.
16. Kessing LV, Søndergård L, Kvist K, et al. Suicide risk in patients treated with lithium. Arch Gen Psychiatry. 2005;62(8):860-866.
17. Baldessarini RJ, Tondo L, Hennen J. Lithium treatment and suicide risk in major affective disorders: update and new findings. J Clin Psychiatry. 2003;64(suppl 5):44-52.
18. Hennen J, Baldessarini RJ. Suicidal risk during treatment with clozapine: a meta-analysis. Schizophr Res. 2005;73(2-3):139-145.
19. Kuo CJ, Tsai SY, Lo CH, et al. Risk factors for completed suicide in schizophrenia. J Clin Psychiatry. 2005;66(5):579-585.
20. Kobeissi J, Aloysi A, Tobias K, et al. Resolution of severe suicidality with a single electroconvulsive therapy. J ECT. 2011;27(1):86-88.
21. Kellner CH, Fink M, Knapp R, et al. Relief of expressed suicidal intent by ECT: a consortium for research in ECT study. Am J Psychiatry. 2005;162(5):977-982.
22. Linehan MM, Goodstein JL, Nielsen SL, et al. Reasons for staying alive when you are thinking of killing yourself: the reasons for living inventory. J Consult Clin Psychol. 1983;51(2):276-286.
23. Cole DA. Validation of the reasons for living inventory in general and delinquent adolescent samples. J Abnorm Child Psychol. 1989;17(1):13-27.
24. Mann JJ, Apter A, Bertolote J, et al. Suicide prevention strategies: a systematic review. JAMA. 2005;294(16):2064-2074.
1. Centers for Disease Control and Prevention. US death rate falls for 10th straight year. http://www.cdc.gov/media/releases/2011/p0316_deathrate.html. Published March 16 2011. Accessed November 22, 2011.
2. Centers for Disease Control and Prevention. Suicide: facts at a glance. http://www.cdc.gov/violenceprevention/suicide. Published Summer 2010. Accessed November 17 2011.
3. Karch DL, Dahlberg LL, Patel N. Surveillance for violent deaths—National Violent Death Reporting System 16 states, 2007. MMWR Surveill Summ. 2010;59(4):1-50.
4. Resnick PJ. Recognizing that the suicidal patient views you as an ‘adversary.’ Current Psychiatry. 2002;1(1):8.-
5. Stanford EJ, Goetz RR, Bloom JD. The No Harm Contract in the emergency assessment of suicidal risk. J Clin Psychiatry. 1994;55(8):344-348.
6. Edwards SJ, Sachmann MD. No-suicide contracts no-suicide agreements, and no-suicide assurances: a study of their nature, utilization, perceived effectiveness, and potential to cause harm. Crisis. 2010;31(6):290-302.
7. Busch KA, Fawcett J, Jacobs DG. Clinical correlates of inpatient suicide. J Clin Psychiatry. 2003;64(1):14-19.
8. American Psychiatric Association. Practice guideline for the assessment and treatment of patients with suicidal behaviors. http://psychiatryonline.org/content.aspx?bookid=28§ionid=1673332#56008. Published November 2003. Accessed November 22 2011.
9. Jacobs DG, Brewer ML. Application of the APA practice guidelines on suicide to clinical practice. CNS Spectr. 2006;11(6):447-454.
10. Nasser EH, Overholser JC. Assessing varying degrees of lethality in depressed adolescent suicide attempters. Acta Psychiatr Scand. 1999;99(6):423-431.
11. Fawcett J, Scheftner WA, Fogg L, et al. Time-related predictors of suicide in major affective disorder. Am J Psychiatry. 1990;147(9):1189-1194.
12. Busch KA, Fawcett J. A fine-grained study of patients who commit suicide. Psychiatric Ann. 2004;34(5):357-364.
13. Posner K, Brown GK, Stanley B, et al. The Columbia-Suicide Severity Rating Scale (C-SSRS): initial validity and internal consistency findings from three multi-site studies with adolescents and adults. Am J Psychiatry. 2011;168:1266-1277.
14. Müller-Oerlinghausen B, Berghöfer A, Ahrens B. The antisuicidal and mortality-reducing effect of lithium prophylaxis: consequences for guidelines in clinical psychiatry. Can J Psychiatry. 2003;48(7):433-439.
15. Tondo L, Hennen J, Baldessarini RJ. Lower suicide risk with long-term lithium treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand. 2001;104(3):163-172.
16. Kessing LV, Søndergård L, Kvist K, et al. Suicide risk in patients treated with lithium. Arch Gen Psychiatry. 2005;62(8):860-866.
17. Baldessarini RJ, Tondo L, Hennen J. Lithium treatment and suicide risk in major affective disorders: update and new findings. J Clin Psychiatry. 2003;64(suppl 5):44-52.
18. Hennen J, Baldessarini RJ. Suicidal risk during treatment with clozapine: a meta-analysis. Schizophr Res. 2005;73(2-3):139-145.
19. Kuo CJ, Tsai SY, Lo CH, et al. Risk factors for completed suicide in schizophrenia. J Clin Psychiatry. 2005;66(5):579-585.
20. Kobeissi J, Aloysi A, Tobias K, et al. Resolution of severe suicidality with a single electroconvulsive therapy. J ECT. 2011;27(1):86-88.
21. Kellner CH, Fink M, Knapp R, et al. Relief of expressed suicidal intent by ECT: a consortium for research in ECT study. Am J Psychiatry. 2005;162(5):977-982.
22. Linehan MM, Goodstein JL, Nielsen SL, et al. Reasons for staying alive when you are thinking of killing yourself: the reasons for living inventory. J Consult Clin Psychol. 1983;51(2):276-286.
23. Cole DA. Validation of the reasons for living inventory in general and delinquent adolescent samples. J Abnorm Child Psychol. 1989;17(1):13-27.
24. Mann JJ, Apter A, Bertolote J, et al. Suicide prevention strategies: a systematic review. JAMA. 2005;294(16):2064-2074.
Psychostimulants for older adults
Discuss this article at www.facebook.com/CurrentPsychiatry
Psychostimulants are recognized for their role in managing attention-deficit/hyperactivity disorder (ADHD), but also have found a treatment niche in conditions such as apathy, fatigue, and depression.1 Psychostimulants—methylphenidate, amphetamines, and their respective isomers—are known to promote wakefulness, increase energy, and help improve attention. Although these medications can provide much-needed relief to many older patients, clinicians need to be mindful of possible side effects and safety concerns when prescribing psychostimulants for geriatric patients.
Most psychostimulant research has evaluated children and younger adults; however, geriatric patients (age >65) deserve special consideration. Although these patients’ changing physiology often presents treatment challenges and may predispose individuals to adverse events, emerging evidence suggests that psychostimulants are valuable in treating motivational and attentional symptoms that do not respond to other treatments. Older adults’ diminished treatment response to antidepressants, fatigue, and comorbid medical illness make stimulants an attractive treatment option. However, there is a paucity of research addressing psychostimulant use in geriatric patients. Moreover, psychostimulants should be used in older patients only after carefully considering potential side effects and general medical safety.
This article will focus on clinical scenarios in late life—such as apathy, ADHD, and depression in medically ill patients—when treatment with psychostimulants may be useful. Psychostimulants are FDA-approved primarily for use in ADHD and other uses are considered off-label. We will highlight research in this population and use case vignettes as examples to present a sensible approach to treating geriatric patients with psychostimulants (Table).
Table
Using psychostimulants in older adults
| Category | Comment(s) |
|---|---|
| Clinical utility | Apathy, ADHD, fatigue, depression in medically ill patients |
| Starting dosage | Methylphenidate: 10 mg/d (typical dose is 20 mg/d) Consider a 5 mg/d starting dosage for frail patients Give the second dose mid-afternoon to avoid insomnia Dextroamphetamine: 10 mg/d (typical dose is 20 mg/d) Consider a 5 mg/d starting dosage for frail patients Give the second dose mid-afternoon to avoid insomnia |
| Comorbid medical conditions that warrant concern | Cardiac or glaucoma history |
| Possible drug-drug interactions | MAOIs: Serotonin syndrome, hypertensive crisis TCAs: Increased antidepressant levels Warfarin: Increased warfarin levels |
| Safety monitoring | Heart rate, blood pressure, weight |
| ADHD: attention-deficit/hyperactivity disorder; MAOIs: monoamine oxidase inhibitors; TCAs: tricyclic antidepressants | |
Stimulants and apathy
Apathy is a loss of motivation, interest, or initiative that is not attributable to cognitive impairment, diminished consciousness, or emotional suffering.2 Considered a distinct entity from depression, apathy is common late in life, particularly in persons with dementia of the Alzheimer’s type (DAT); 70% to 90% of patients may experience apathy at some stage of dementia.3 Apathy is linked to impairment in activities of daily living and needing more assistance from caregivers, which increases caregiver burden. Treating apathetic symptoms may improve quality of life for the patient and caregivers. For a case study of an older patient with apathy treated with a psychostimulant, see Box 1.
Apathy has been treated successfully with a variety of stimulant medications. In an open-label study, patients with DAT who received methylphenidate, 10 to 20 mg/d, showed significant improvement in Apathy Evaluation Scale (AES) scores.4 Similarly, Herrmann et al5 also demonstrated improvements in AES scores in DAT patients taking methylphenidate, 20 mg/d, compared with placebo. Although methylphenidate appears to have the strongest evidence for treating apathy, dextroamphetamine also has been shown to produce modest improvements in apathy scale measures.6 A double-blind, placebo-controlled crossover study showed that dextroamphetamine, 20 mg/d, significantly improved scores on neuropsychiatric inventory scales that were driven by apathy subscales.6 However, this trial was small (N = 8).
Preliminary evidence indicates that psychostimulants may improve apathetic symptoms in patients with dementia. In Mr. A’s case (Box 1), he experienced apathy symptoms that affected his quality of life and that of those around him. He showed a clear lack of interest and motivation and indifference. This scenario is common among geriatric patients and may be misinterpreted as depression. Although the overlap may be considerable, screening for apathy may help determine a treatment course with psychostimulants instead of antidepressants, thus avoiding unnecessary medication trials.
Mr. A, age 76, has dementia of the Alzheimer’s type. His family brings him to a psychiatrist because Mr. A exhibits a generalized loss of interest. His history reveals a gradual onset of memory problems with steady decline. Current deficits include problems with forgetfulness, misplacing items, increasing difficulty with names, occasional repetitiveness, and mild word finding difficulty. His family complains that Mr. A does not take care of himself, sits all day long, is not interested in his favorite TV shows, is indifferent to his physical health, is not interested in catching up with friends, and has been doing very little from day to day. He does not seek food but cleans his plate when served. His family became concerned when Mr. A showed no excitement in going to his grandson’s baseball game, which he had previously enjoyed. Mr. A denies any concerns and scores a 3 out of 15 on the Geriatric Depression Scale. Mr. A’s family rated him 4 on the same scale.
On the Apathy Evaluation Scale (AES), he scores 46 (moderate severity). We start methylphenidate, 5 mg administered in the morning and early evening (5 pm). Subsequent conversations 2 weeks later with Mr. A’s family revealed Mr. A’s interest levels have improved and reported no side effects. We increase methylphenidate to 10 mg twice a day. Mr. A has remarkably improved hygiene 1 month later and is more engaged in the interview. He scored a 32 (mild severity) on the AES and the family notes that he is interested in watching his grandson play baseball. During this treatment, we did not change Mr. A’s other medications—donepezil, 10 mg/d, and bupropion, 150 mg/d.
Stimulants for ADHD
ADHD is a neurobehavioral disorder that is identified in approximately 8% of children and persists in 4% of adults.7 ADHD is characterized by impulsivity, motor restlessness, and inattention; the latter feature generally is more prominent with advancing age.8 If left untreated, ADHD has societal burdens, such as educational and occupational impairments.9 There is little data on ADHD in older adults and no placebo-controlled trials. For a case study of an older patient with ADHD treated with stimulants, see Box 2.10
Psychostimulants are considered the mainstay of ADHD treatment. First-line treatments include methylphenidate and amphetamines. A meta-analysis found a significant improvement in ADHD symptoms in adult patients taking psychostimulants compared with placebo, with no difference between immediate-release and long-acting formulations.11 Although these findings were reported in younger adults, they may be relevant for older persons as well. Wetzel and Burke12 described how ADHD presents in older adults and argued that the benefits of treating ADHD in this age group often outweigh the risks associated with psychostimulants, which can be diminished through careful screening.
Individuals who present with ADHD symptoms in late life often appear to be high functioning. Some may describe achieving academic and professional success, but may report chronic problems associated with inefficient learning and distraction compared with their peers because of untreated inattention symptoms. Faraone et al13 argue that similar to other illnesses, ADHD is represented by a spectrum of disease, which may be diagnosed in late life or as subthreshold ADHD. Individuals who did not meet diagnostic criteria in childhood or were not evaluated or treated may experience unremitting symptoms that contribute to functional impairment, persistent discouragement, and distress. Frustrations with distractibility, disorganization, and incompletion of tasks may have a psychological impact reflected by low self-esteem and irritability, and be a chronic source of occupational and relationship dysfunction. Diagnosing and treating ADHD in late life can improve longstanding functional impairments and overall quality of life.
Mr. J, age 66, is an attorney who presents for evaluation after he identified common features in friends who have attention-deficit/hyperactivity disorder (ADHD). In grade school, Mr. J’s teachers told him that he employed very little effort and was not meeting his potential, although he performed exceptionally well. He reports similar experiences throughout his education and says he was careful to select classes that were interesting, but did not require demanding projects or burdensome homework. In law school, he felt academically challenged for the first time but realized he had limited study skills. Mr. J graduated in the top 26th percentile of his class using “an unbelievable amount of effort compared with other students.”
Mr. J describes significant impairment in organizational skills and ability to keep track of time, procrastination, incompletion of tasks, and substantial distractibility during conferences. He says he has difficulty reading briefs depending on his emotional connection to the subject matter. Family history revealed that his mother likely had undiagnosed ADHD. He recently married and his wife encouraged him to seek treatment for “forgetfulness.” Mr. J maintains a busy, successful law practice but has become increasingly frustrated by his inability to follow through on simple tasks that could help grow the practice and generate revenue.
Mr. J has an elevated score on the Adult ADHD Symptom Rating Scale.10 He is referred to his primary care physician to evaluate his general health before beginning medication. At follow-up, Mr. J was started on lisdexamfetamine, 20 mg/d, titrated to 40 mg/d. On subsequent visits he reports improved symptoms without side effects. His vital signs are normal and he reports feeling more productive in his work and achieving significant improvement in the day-to-day operations of his practice.
Other uses
Depression. Although not a first-line treatment, psychostimulants have shown benefit for treating depressive disorders, particularly when patients require immediate improvement. These scenarios are common among medically ill patients, such as those with cancer, stroke, or human immunodeficiency virus (HIV), when it is urgent for patients to participate in their treatment plan. A double-blind, placebo-controlled, randomized study that looked at older depressed patients with medical comorbidities found that methylphenidate was well tolerated, worked quickly, and effectively treated depression.14 However, these results must be interpreted cautiously because the entire study was conducted in 8 days, which included a crossover design that administered methylphenidate 10 mg/d and 20 mg/d for 2 days each. A review of stimulant effectiveness in patients whose depression was associated with HIV, stroke, or cancer and in medically ill patients argued that although benefits have been reported, they must be interpreted tentatively because of a lack of randomized trials.15 However, limited evidence supports an effect of stimulants in treating fatigue, anorexia, pain, and sedation in these populations.15
Stimulants’ immediate onset of action may be particularly useful in terminally ill patients who suffer from fatigue or depression. A double-blind, placebo-controlled, randomized study demonstrated that augmenting citalopram, 20 to 40 mg/d, with methylphenidate, mean dose 15 mg/d, for 3 weeks in older depressed patients significantly improved treatment response and accelerated time to remission compared with citalopram and placebo.16 However, a recent Cochrane review did not show clear efficacy for psychostimulants to treat depression.17
Fatigue. Along with depression, fatigue frequently is seen in older patients with medical illnesses. Mood disorders, medical comorbidities, and sleep disturbances are linked to fatigue. Underlying medical causes such as hypothyroidism, anemia, and electrolyte imbalances should be ruled out before starting a psychostimulant. A review by Minton et al18 that looked at cancer-related fatigue suggested that methylphenidate can be beneficial, although the evidence is mixed.
Interferon-alpha treatment for hepatitis C can cause depression and fatigue, and psychostimulants may help treat fatigue-related side effects.19 Fatigue may present as an isolated symptom in interferon-alpha treatment and psychostimulant use may prevent patients from taking an additional medication, therefore decreasing the risk of further side effects.
Fall risk. Some evidence supports using psychostimulants to lower the risk of falling and hypoactive delirium. A recent review by Elie et al20 concluded that stimulants could improve cognitive function in end-of-life hypoactive delirium. Additionally, a randomized, placebo-controlled, double-blind study that evaluated fall risk concluded that methylphenidate, 20 mg/d, might improve some aspects of executive function and gait stability in older adults.21 The authors hypothesized that improved cognition associated with psychostimulant use may play a role in improving fall risk.
Safety concerns
Clinicians should be aware of safety considerations and possible side effects when prescribing psychostimulants. Psychostimulants are controlled substances and are subject to restrictions (Box 3).22 In 2007, the FDA issued warnings regarding an association between psychostimulant use and sudden death, myocardial infarction, and stroke in patients with preexisting cardiac abnormalities or heart problems.23 Also, some evidence indicates that psychostimulants can increase heart rate and systolic blood pressure. These parameters should be monitored during treatment. Reducing or stopping psychostimulants generally reverses cardiovascular effects. Although the evidence to support these events appears sparse, perform a thorough history before beginning a stimulant and make appropriate referrals as indicated. In November 2011, the FDA reported that psychostimulant use in children and young adults is not associated with adverse cardiovascular events, including stroke, heart attack, and sudden cardiac death.24
Less common side effects reported with psychostimulants include anxiety, insomnia, hallucinations, anorexia, delirium, palpitations, and headache. A meta-analysis of studies of adults with ADHD found that adverse events related to psychostimulants were relatively rare; the most common side effects were diminished appetite and difficulty sleeping.25 Sleep-related side effects can be avoided by dosing these medications earlier in the day, typically before 5 pm. Herrmann et al5 reported 2 cases of apparent delirium and 1 with irregular heartbeat in patients with DAT taking methylphenidate vs placebo. However, most patients in this study experienced mild or no adverse events.
Other safety concerns involve using methylphenidate in patients with glaucoma. In theory, stimulants could exacerbate an acute attack of glaucoma in patients with narrow-angle glaucoma. Patients at risk should be referred to an ophthalmologist for an assessment.
Review other medications the patient is taking and assess for possible drug-drug interactions. Combining monoamine oxidase inhibitors (MAOIs) and methylphenidate warrants caution because of the risk of serotonin syndrome and hypertensive crisis. However, there are case reports of successful MAOI/methylphenidate therapy.26 Additionally, methylphenidate increases levels of warfarin and tricyclic antidepressants when taken with these agents.27 Psychostimulants generally are well tolerated by most individuals and taking a careful history may help prevent adverse events.
As schedule II controlled substances, psychostimulants are subject to prescribing limitations. The current Drug Enforcement Administration (DEA) policy on schedule II controlled substances allows for the equivalent of a 90-day supply of medication to be written with multiple prescriptions. DEA requirements for multiple prescriptions include:
- Each prescription issued is for a legitimate medical purpose by an individual practitioner acting in the usual course of his/her professional practice
- The individual practitioner must provide written instructions on each prescription indicating the earliest date on which a pharmacy may fill each prescription
- The issuance of multiple prescriptions is permissible under applicable state laws
- The individual practitioner fully complies with all other applicable requirements under the Controlled Substances Act and implementing regulations, as well as any additional requirements under state law.22
Related Resources
- Kessler RC, Adler L, Ames M, et al. The World Health Organization Adult ADHD Self-Report Scale (ASRS): a short screening scale for use in the general population. Psychol Med. 2005;35(2):245-256.
- Alexopoulos GS, Salzman C. Treatment of depression with heterocyclic antidepressants, monoamine oxidase inhibitors, and psychomotor stimulants. In: Salzman C, ed. Clinical geriatric psychopharmacology. Baltimore, MD: Williams and Wilkins; 1998:184-244.
Drug Brand Names
- Bupropion • Wellbutrin, Zyban
- Citalopram • Celexa
- Dexmethylphenidate • Focalin
- Dextroamphetamine • Dexedrine
- Donepezil • Aricept
- Lisdexamfetamine • Vyvanse
- Methamphetamine • Desoxyn
- Methylphenidate • Ritalin, Concerta
- Mixed amphetamine salts • Adderall
- Warfarin • Coumadin
Disclosures
Dr. Padala receives research funding from the Department of Veterans Health Administration and the Alzheimer’s Association.
Drs. Franzen, Wetzel, and Burke report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Ballas C, Evans D, Dinges D. Psychostimulants and wakefulness promoting agents. In: Schatzberg A Nemeroff C, eds. The American Psychiatric Publishing textbook of psychopharmacology. 4th ed. Arlington, VA: American Psychiatric Publishing, Inc.; 2010: 843-860.
2. Marin RS. Apathy: a neuropsychiatric syndrome. J Neuropsychiatry Clin Neurosci. 1991;3(3):243-254.
3. Dolder CR, Davis LN, McKinsey J. Use of psychostimulants in patients with dementia. Ann Pharmacother. 2010;44(10):1624-1632.
4. Padala PR, Burke WJ, Shostrom VK, et al. Methylphenidate for apathy and functional status in dementia of the Alzheimer type. Am J Geriatr Psychiatry. 2010;18(4):371-374.
5. Herrmann N, Rothenburg LS, Black SE, et al. Methylphenidate for the treatment of apathy in Alzheimer disease: prediction of response using dextroamphetamine challenge. J Clin Psychopharmacol. 2008;28(3):296-301.
6. Huey ED, Garcia C, Wassermann EM, et al. Stimulant treatment of frontotemporal dementia in 8 patients. J Clin Psychiatry. 2008;69(12):1981-1982.
7. Centers for Disease Control and Prevention (CDC). Mental health in the United States: prevalence of diagnosis and medication treatment for attention-deficit/hyperactivity disorder—United States 2003. MMWR Morb Wkly Rep. 2005;54(34):842-847.
8. Biederman J, Mick E, Faraone SV. Age-dependent decline of attention deficit hyperactivity disorder: impact of remission definition and symptom type. Am J Psychiatry. 2000;157(5):816-818.
9. Biederman J, Faraone SV. The effects of attention-deficit/hyperactivity disorder on employment and household income. Med Gen Med. 2006;8(13):12.-
10. Adult ADHD Self-Report Scale (ASRS-v1. 1) symptom checklist instructions. http://www.hcp.med.harvard.edu/ncs/ftpdir/adhd/18%20Question%20ADHD-ASRS-v1-1.pdf. Accessed November 15 2011.
11. Faraone SV, Glatt SJ. A comparison of the efficacy of medications for adult attention-deficit/hyperactivity disorder using meta-analysis of effect sizes. J Clin Psychiatry. 2010;71(6):754-763.
12. Wetzel MW, Burke WJ. Addressing attention-deficit/hyperactivity disorder in late adulthood. Clinical Geriatrics. 2008;16(11):33-39.
13. Faraone SV, Kunwar A, Adamson J, et al. Personality traits among ADHD adults: implications of late-onset and subthreshold diagnoses. Psychol Med. 2009;39(4):685-693.
14. Wallace AE, Kofoed LL, West AN. Double-blind placebo-controlled trial of methylphenidate in older, depressed, medically ill patients. Am J Psychiatry. 1995;152(6):929-931.
15. Orr K, Taylor D. Psychostimulants in the treatment of depression: a review of the evidence. CNS Drugs. 2007;21(3):239-257.
16. Lavretsky H, Park S, Siddarth P, et al. Methylphenidate-enhanced antidepressant response to citalopram in the elderly: a double-blind, placebo-controlled pilot trial. Am J Geriatr Psychiatry. 2006;14(2):181-185.
17. Candy M, Jones L, Williams R, et al. Psychostimulants for depression. Cochrane Database Syst Rev. 2008;16(2):CD006722.-
18. Minton O, Richardson A, Sharpe M, et al. Psychostimulants for the management of cancer-related fatigue: a systematic review and meta-analysis. J Pain Symptom Manage. 2011;41(4):761-767.
19. Raison CL, Demetrashvili M, Capuron L, et al. Neuropsychiatric adverse events of interferon-α: recognition and management. CNS Drugs. 2005;19(2):105-123.
20. Elie D, Gagnon P, Gagnon B, et al. Using psychostimulants in end-of-life patients with hypoactive delirium and cognitive disorders: a literature review [in French]. Can J Psychiatry. 2010;55:386-393.
21. Ben-Itzhak R, Giladi N, Gruendlinger L, et al. Can methylphenidate reduce fall risk in community-living older adults? A double-blind, single-dose cross-over study. J Am Geriatr Soc. 2008;56(4):695-700.
22. U.S. Department of Justice Drug Enforcement Administration. Issuance of multiple prescriptions for Schedule II controlled substances. http://www.deadiversion.usdoj.gov/faq/mult_rx_faq.htm. Accessed November 1, 2011.
23. U.S. Food and Drug Administration. FDA directs ADHD drug manufacturers to notify patients about cardiovascular adverse events and psychiatric adverse events. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2007/ucm108849.htm. Accessed November 1, 2011.
24. U.S. Food and Drug Administration. FDA Drug Safety Communication: safety review update of medications used to treat attention-deficit/hyperactivity disorder (ADHD) in children and young adults. http://www.fda.gov/Drugs/DrugSafety/ucm277770.htm. Accessed November 2, 2011.
25. Peterson K, McDonagh MS, Fu R. Comparative benefits and harms of competing medications for adults with attention-deficit hyperactivity disorder: a systematic review and indirect comparison meta-analysis. Psychopharmacology (Berl). 2008;197(1):1-11.
26. Leonard BE, McCartan D, White J, et al. Methylphenidate: a review of its neuropharmacological, neuropsychological and adverse effects. Hum Psychopharmacol. 2004;19(3):151-180.
27. Howard P, Shuster J, Twycross R, et al. Psychostimulants. J Pain Symptom Manage. 2010;40(5):789-795.
Discuss this article at www.facebook.com/CurrentPsychiatry
Psychostimulants are recognized for their role in managing attention-deficit/hyperactivity disorder (ADHD), but also have found a treatment niche in conditions such as apathy, fatigue, and depression.1 Psychostimulants—methylphenidate, amphetamines, and their respective isomers—are known to promote wakefulness, increase energy, and help improve attention. Although these medications can provide much-needed relief to many older patients, clinicians need to be mindful of possible side effects and safety concerns when prescribing psychostimulants for geriatric patients.
Most psychostimulant research has evaluated children and younger adults; however, geriatric patients (age >65) deserve special consideration. Although these patients’ changing physiology often presents treatment challenges and may predispose individuals to adverse events, emerging evidence suggests that psychostimulants are valuable in treating motivational and attentional symptoms that do not respond to other treatments. Older adults’ diminished treatment response to antidepressants, fatigue, and comorbid medical illness make stimulants an attractive treatment option. However, there is a paucity of research addressing psychostimulant use in geriatric patients. Moreover, psychostimulants should be used in older patients only after carefully considering potential side effects and general medical safety.
This article will focus on clinical scenarios in late life—such as apathy, ADHD, and depression in medically ill patients—when treatment with psychostimulants may be useful. Psychostimulants are FDA-approved primarily for use in ADHD and other uses are considered off-label. We will highlight research in this population and use case vignettes as examples to present a sensible approach to treating geriatric patients with psychostimulants (Table).
Table
Using psychostimulants in older adults
| Category | Comment(s) |
|---|---|
| Clinical utility | Apathy, ADHD, fatigue, depression in medically ill patients |
| Starting dosage | Methylphenidate: 10 mg/d (typical dose is 20 mg/d) Consider a 5 mg/d starting dosage for frail patients Give the second dose mid-afternoon to avoid insomnia Dextroamphetamine: 10 mg/d (typical dose is 20 mg/d) Consider a 5 mg/d starting dosage for frail patients Give the second dose mid-afternoon to avoid insomnia |
| Comorbid medical conditions that warrant concern | Cardiac or glaucoma history |
| Possible drug-drug interactions | MAOIs: Serotonin syndrome, hypertensive crisis TCAs: Increased antidepressant levels Warfarin: Increased warfarin levels |
| Safety monitoring | Heart rate, blood pressure, weight |
| ADHD: attention-deficit/hyperactivity disorder; MAOIs: monoamine oxidase inhibitors; TCAs: tricyclic antidepressants | |
Stimulants and apathy
Apathy is a loss of motivation, interest, or initiative that is not attributable to cognitive impairment, diminished consciousness, or emotional suffering.2 Considered a distinct entity from depression, apathy is common late in life, particularly in persons with dementia of the Alzheimer’s type (DAT); 70% to 90% of patients may experience apathy at some stage of dementia.3 Apathy is linked to impairment in activities of daily living and needing more assistance from caregivers, which increases caregiver burden. Treating apathetic symptoms may improve quality of life for the patient and caregivers. For a case study of an older patient with apathy treated with a psychostimulant, see Box 1.
Apathy has been treated successfully with a variety of stimulant medications. In an open-label study, patients with DAT who received methylphenidate, 10 to 20 mg/d, showed significant improvement in Apathy Evaluation Scale (AES) scores.4 Similarly, Herrmann et al5 also demonstrated improvements in AES scores in DAT patients taking methylphenidate, 20 mg/d, compared with placebo. Although methylphenidate appears to have the strongest evidence for treating apathy, dextroamphetamine also has been shown to produce modest improvements in apathy scale measures.6 A double-blind, placebo-controlled crossover study showed that dextroamphetamine, 20 mg/d, significantly improved scores on neuropsychiatric inventory scales that were driven by apathy subscales.6 However, this trial was small (N = 8).
Preliminary evidence indicates that psychostimulants may improve apathetic symptoms in patients with dementia. In Mr. A’s case (Box 1), he experienced apathy symptoms that affected his quality of life and that of those around him. He showed a clear lack of interest and motivation and indifference. This scenario is common among geriatric patients and may be misinterpreted as depression. Although the overlap may be considerable, screening for apathy may help determine a treatment course with psychostimulants instead of antidepressants, thus avoiding unnecessary medication trials.
Mr. A, age 76, has dementia of the Alzheimer’s type. His family brings him to a psychiatrist because Mr. A exhibits a generalized loss of interest. His history reveals a gradual onset of memory problems with steady decline. Current deficits include problems with forgetfulness, misplacing items, increasing difficulty with names, occasional repetitiveness, and mild word finding difficulty. His family complains that Mr. A does not take care of himself, sits all day long, is not interested in his favorite TV shows, is indifferent to his physical health, is not interested in catching up with friends, and has been doing very little from day to day. He does not seek food but cleans his plate when served. His family became concerned when Mr. A showed no excitement in going to his grandson’s baseball game, which he had previously enjoyed. Mr. A denies any concerns and scores a 3 out of 15 on the Geriatric Depression Scale. Mr. A’s family rated him 4 on the same scale.
On the Apathy Evaluation Scale (AES), he scores 46 (moderate severity). We start methylphenidate, 5 mg administered in the morning and early evening (5 pm). Subsequent conversations 2 weeks later with Mr. A’s family revealed Mr. A’s interest levels have improved and reported no side effects. We increase methylphenidate to 10 mg twice a day. Mr. A has remarkably improved hygiene 1 month later and is more engaged in the interview. He scored a 32 (mild severity) on the AES and the family notes that he is interested in watching his grandson play baseball. During this treatment, we did not change Mr. A’s other medications—donepezil, 10 mg/d, and bupropion, 150 mg/d.
Stimulants for ADHD
ADHD is a neurobehavioral disorder that is identified in approximately 8% of children and persists in 4% of adults.7 ADHD is characterized by impulsivity, motor restlessness, and inattention; the latter feature generally is more prominent with advancing age.8 If left untreated, ADHD has societal burdens, such as educational and occupational impairments.9 There is little data on ADHD in older adults and no placebo-controlled trials. For a case study of an older patient with ADHD treated with stimulants, see Box 2.10
Psychostimulants are considered the mainstay of ADHD treatment. First-line treatments include methylphenidate and amphetamines. A meta-analysis found a significant improvement in ADHD symptoms in adult patients taking psychostimulants compared with placebo, with no difference between immediate-release and long-acting formulations.11 Although these findings were reported in younger adults, they may be relevant for older persons as well. Wetzel and Burke12 described how ADHD presents in older adults and argued that the benefits of treating ADHD in this age group often outweigh the risks associated with psychostimulants, which can be diminished through careful screening.
Individuals who present with ADHD symptoms in late life often appear to be high functioning. Some may describe achieving academic and professional success, but may report chronic problems associated with inefficient learning and distraction compared with their peers because of untreated inattention symptoms. Faraone et al13 argue that similar to other illnesses, ADHD is represented by a spectrum of disease, which may be diagnosed in late life or as subthreshold ADHD. Individuals who did not meet diagnostic criteria in childhood or were not evaluated or treated may experience unremitting symptoms that contribute to functional impairment, persistent discouragement, and distress. Frustrations with distractibility, disorganization, and incompletion of tasks may have a psychological impact reflected by low self-esteem and irritability, and be a chronic source of occupational and relationship dysfunction. Diagnosing and treating ADHD in late life can improve longstanding functional impairments and overall quality of life.
Mr. J, age 66, is an attorney who presents for evaluation after he identified common features in friends who have attention-deficit/hyperactivity disorder (ADHD). In grade school, Mr. J’s teachers told him that he employed very little effort and was not meeting his potential, although he performed exceptionally well. He reports similar experiences throughout his education and says he was careful to select classes that were interesting, but did not require demanding projects or burdensome homework. In law school, he felt academically challenged for the first time but realized he had limited study skills. Mr. J graduated in the top 26th percentile of his class using “an unbelievable amount of effort compared with other students.”
Mr. J describes significant impairment in organizational skills and ability to keep track of time, procrastination, incompletion of tasks, and substantial distractibility during conferences. He says he has difficulty reading briefs depending on his emotional connection to the subject matter. Family history revealed that his mother likely had undiagnosed ADHD. He recently married and his wife encouraged him to seek treatment for “forgetfulness.” Mr. J maintains a busy, successful law practice but has become increasingly frustrated by his inability to follow through on simple tasks that could help grow the practice and generate revenue.
Mr. J has an elevated score on the Adult ADHD Symptom Rating Scale.10 He is referred to his primary care physician to evaluate his general health before beginning medication. At follow-up, Mr. J was started on lisdexamfetamine, 20 mg/d, titrated to 40 mg/d. On subsequent visits he reports improved symptoms without side effects. His vital signs are normal and he reports feeling more productive in his work and achieving significant improvement in the day-to-day operations of his practice.
Other uses
Depression. Although not a first-line treatment, psychostimulants have shown benefit for treating depressive disorders, particularly when patients require immediate improvement. These scenarios are common among medically ill patients, such as those with cancer, stroke, or human immunodeficiency virus (HIV), when it is urgent for patients to participate in their treatment plan. A double-blind, placebo-controlled, randomized study that looked at older depressed patients with medical comorbidities found that methylphenidate was well tolerated, worked quickly, and effectively treated depression.14 However, these results must be interpreted cautiously because the entire study was conducted in 8 days, which included a crossover design that administered methylphenidate 10 mg/d and 20 mg/d for 2 days each. A review of stimulant effectiveness in patients whose depression was associated with HIV, stroke, or cancer and in medically ill patients argued that although benefits have been reported, they must be interpreted tentatively because of a lack of randomized trials.15 However, limited evidence supports an effect of stimulants in treating fatigue, anorexia, pain, and sedation in these populations.15
Stimulants’ immediate onset of action may be particularly useful in terminally ill patients who suffer from fatigue or depression. A double-blind, placebo-controlled, randomized study demonstrated that augmenting citalopram, 20 to 40 mg/d, with methylphenidate, mean dose 15 mg/d, for 3 weeks in older depressed patients significantly improved treatment response and accelerated time to remission compared with citalopram and placebo.16 However, a recent Cochrane review did not show clear efficacy for psychostimulants to treat depression.17
Fatigue. Along with depression, fatigue frequently is seen in older patients with medical illnesses. Mood disorders, medical comorbidities, and sleep disturbances are linked to fatigue. Underlying medical causes such as hypothyroidism, anemia, and electrolyte imbalances should be ruled out before starting a psychostimulant. A review by Minton et al18 that looked at cancer-related fatigue suggested that methylphenidate can be beneficial, although the evidence is mixed.
Interferon-alpha treatment for hepatitis C can cause depression and fatigue, and psychostimulants may help treat fatigue-related side effects.19 Fatigue may present as an isolated symptom in interferon-alpha treatment and psychostimulant use may prevent patients from taking an additional medication, therefore decreasing the risk of further side effects.
Fall risk. Some evidence supports using psychostimulants to lower the risk of falling and hypoactive delirium. A recent review by Elie et al20 concluded that stimulants could improve cognitive function in end-of-life hypoactive delirium. Additionally, a randomized, placebo-controlled, double-blind study that evaluated fall risk concluded that methylphenidate, 20 mg/d, might improve some aspects of executive function and gait stability in older adults.21 The authors hypothesized that improved cognition associated with psychostimulant use may play a role in improving fall risk.
Safety concerns
Clinicians should be aware of safety considerations and possible side effects when prescribing psychostimulants. Psychostimulants are controlled substances and are subject to restrictions (Box 3).22 In 2007, the FDA issued warnings regarding an association between psychostimulant use and sudden death, myocardial infarction, and stroke in patients with preexisting cardiac abnormalities or heart problems.23 Also, some evidence indicates that psychostimulants can increase heart rate and systolic blood pressure. These parameters should be monitored during treatment. Reducing or stopping psychostimulants generally reverses cardiovascular effects. Although the evidence to support these events appears sparse, perform a thorough history before beginning a stimulant and make appropriate referrals as indicated. In November 2011, the FDA reported that psychostimulant use in children and young adults is not associated with adverse cardiovascular events, including stroke, heart attack, and sudden cardiac death.24
Less common side effects reported with psychostimulants include anxiety, insomnia, hallucinations, anorexia, delirium, palpitations, and headache. A meta-analysis of studies of adults with ADHD found that adverse events related to psychostimulants were relatively rare; the most common side effects were diminished appetite and difficulty sleeping.25 Sleep-related side effects can be avoided by dosing these medications earlier in the day, typically before 5 pm. Herrmann et al5 reported 2 cases of apparent delirium and 1 with irregular heartbeat in patients with DAT taking methylphenidate vs placebo. However, most patients in this study experienced mild or no adverse events.
Other safety concerns involve using methylphenidate in patients with glaucoma. In theory, stimulants could exacerbate an acute attack of glaucoma in patients with narrow-angle glaucoma. Patients at risk should be referred to an ophthalmologist for an assessment.
Review other medications the patient is taking and assess for possible drug-drug interactions. Combining monoamine oxidase inhibitors (MAOIs) and methylphenidate warrants caution because of the risk of serotonin syndrome and hypertensive crisis. However, there are case reports of successful MAOI/methylphenidate therapy.26 Additionally, methylphenidate increases levels of warfarin and tricyclic antidepressants when taken with these agents.27 Psychostimulants generally are well tolerated by most individuals and taking a careful history may help prevent adverse events.
As schedule II controlled substances, psychostimulants are subject to prescribing limitations. The current Drug Enforcement Administration (DEA) policy on schedule II controlled substances allows for the equivalent of a 90-day supply of medication to be written with multiple prescriptions. DEA requirements for multiple prescriptions include:
- Each prescription issued is for a legitimate medical purpose by an individual practitioner acting in the usual course of his/her professional practice
- The individual practitioner must provide written instructions on each prescription indicating the earliest date on which a pharmacy may fill each prescription
- The issuance of multiple prescriptions is permissible under applicable state laws
- The individual practitioner fully complies with all other applicable requirements under the Controlled Substances Act and implementing regulations, as well as any additional requirements under state law.22
Related Resources
- Kessler RC, Adler L, Ames M, et al. The World Health Organization Adult ADHD Self-Report Scale (ASRS): a short screening scale for use in the general population. Psychol Med. 2005;35(2):245-256.
- Alexopoulos GS, Salzman C. Treatment of depression with heterocyclic antidepressants, monoamine oxidase inhibitors, and psychomotor stimulants. In: Salzman C, ed. Clinical geriatric psychopharmacology. Baltimore, MD: Williams and Wilkins; 1998:184-244.
Drug Brand Names
- Bupropion • Wellbutrin, Zyban
- Citalopram • Celexa
- Dexmethylphenidate • Focalin
- Dextroamphetamine • Dexedrine
- Donepezil • Aricept
- Lisdexamfetamine • Vyvanse
- Methamphetamine • Desoxyn
- Methylphenidate • Ritalin, Concerta
- Mixed amphetamine salts • Adderall
- Warfarin • Coumadin
Disclosures
Dr. Padala receives research funding from the Department of Veterans Health Administration and the Alzheimer’s Association.
Drs. Franzen, Wetzel, and Burke report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at www.facebook.com/CurrentPsychiatry
Psychostimulants are recognized for their role in managing attention-deficit/hyperactivity disorder (ADHD), but also have found a treatment niche in conditions such as apathy, fatigue, and depression.1 Psychostimulants—methylphenidate, amphetamines, and their respective isomers—are known to promote wakefulness, increase energy, and help improve attention. Although these medications can provide much-needed relief to many older patients, clinicians need to be mindful of possible side effects and safety concerns when prescribing psychostimulants for geriatric patients.
Most psychostimulant research has evaluated children and younger adults; however, geriatric patients (age >65) deserve special consideration. Although these patients’ changing physiology often presents treatment challenges and may predispose individuals to adverse events, emerging evidence suggests that psychostimulants are valuable in treating motivational and attentional symptoms that do not respond to other treatments. Older adults’ diminished treatment response to antidepressants, fatigue, and comorbid medical illness make stimulants an attractive treatment option. However, there is a paucity of research addressing psychostimulant use in geriatric patients. Moreover, psychostimulants should be used in older patients only after carefully considering potential side effects and general medical safety.
This article will focus on clinical scenarios in late life—such as apathy, ADHD, and depression in medically ill patients—when treatment with psychostimulants may be useful. Psychostimulants are FDA-approved primarily for use in ADHD and other uses are considered off-label. We will highlight research in this population and use case vignettes as examples to present a sensible approach to treating geriatric patients with psychostimulants (Table).
Table
Using psychostimulants in older adults
| Category | Comment(s) |
|---|---|
| Clinical utility | Apathy, ADHD, fatigue, depression in medically ill patients |
| Starting dosage | Methylphenidate: 10 mg/d (typical dose is 20 mg/d) Consider a 5 mg/d starting dosage for frail patients Give the second dose mid-afternoon to avoid insomnia Dextroamphetamine: 10 mg/d (typical dose is 20 mg/d) Consider a 5 mg/d starting dosage for frail patients Give the second dose mid-afternoon to avoid insomnia |
| Comorbid medical conditions that warrant concern | Cardiac or glaucoma history |
| Possible drug-drug interactions | MAOIs: Serotonin syndrome, hypertensive crisis TCAs: Increased antidepressant levels Warfarin: Increased warfarin levels |
| Safety monitoring | Heart rate, blood pressure, weight |
| ADHD: attention-deficit/hyperactivity disorder; MAOIs: monoamine oxidase inhibitors; TCAs: tricyclic antidepressants | |
Stimulants and apathy
Apathy is a loss of motivation, interest, or initiative that is not attributable to cognitive impairment, diminished consciousness, or emotional suffering.2 Considered a distinct entity from depression, apathy is common late in life, particularly in persons with dementia of the Alzheimer’s type (DAT); 70% to 90% of patients may experience apathy at some stage of dementia.3 Apathy is linked to impairment in activities of daily living and needing more assistance from caregivers, which increases caregiver burden. Treating apathetic symptoms may improve quality of life for the patient and caregivers. For a case study of an older patient with apathy treated with a psychostimulant, see Box 1.
Apathy has been treated successfully with a variety of stimulant medications. In an open-label study, patients with DAT who received methylphenidate, 10 to 20 mg/d, showed significant improvement in Apathy Evaluation Scale (AES) scores.4 Similarly, Herrmann et al5 also demonstrated improvements in AES scores in DAT patients taking methylphenidate, 20 mg/d, compared with placebo. Although methylphenidate appears to have the strongest evidence for treating apathy, dextroamphetamine also has been shown to produce modest improvements in apathy scale measures.6 A double-blind, placebo-controlled crossover study showed that dextroamphetamine, 20 mg/d, significantly improved scores on neuropsychiatric inventory scales that were driven by apathy subscales.6 However, this trial was small (N = 8).
Preliminary evidence indicates that psychostimulants may improve apathetic symptoms in patients with dementia. In Mr. A’s case (Box 1), he experienced apathy symptoms that affected his quality of life and that of those around him. He showed a clear lack of interest and motivation and indifference. This scenario is common among geriatric patients and may be misinterpreted as depression. Although the overlap may be considerable, screening for apathy may help determine a treatment course with psychostimulants instead of antidepressants, thus avoiding unnecessary medication trials.
Mr. A, age 76, has dementia of the Alzheimer’s type. His family brings him to a psychiatrist because Mr. A exhibits a generalized loss of interest. His history reveals a gradual onset of memory problems with steady decline. Current deficits include problems with forgetfulness, misplacing items, increasing difficulty with names, occasional repetitiveness, and mild word finding difficulty. His family complains that Mr. A does not take care of himself, sits all day long, is not interested in his favorite TV shows, is indifferent to his physical health, is not interested in catching up with friends, and has been doing very little from day to day. He does not seek food but cleans his plate when served. His family became concerned when Mr. A showed no excitement in going to his grandson’s baseball game, which he had previously enjoyed. Mr. A denies any concerns and scores a 3 out of 15 on the Geriatric Depression Scale. Mr. A’s family rated him 4 on the same scale.
On the Apathy Evaluation Scale (AES), he scores 46 (moderate severity). We start methylphenidate, 5 mg administered in the morning and early evening (5 pm). Subsequent conversations 2 weeks later with Mr. A’s family revealed Mr. A’s interest levels have improved and reported no side effects. We increase methylphenidate to 10 mg twice a day. Mr. A has remarkably improved hygiene 1 month later and is more engaged in the interview. He scored a 32 (mild severity) on the AES and the family notes that he is interested in watching his grandson play baseball. During this treatment, we did not change Mr. A’s other medications—donepezil, 10 mg/d, and bupropion, 150 mg/d.
Stimulants for ADHD
ADHD is a neurobehavioral disorder that is identified in approximately 8% of children and persists in 4% of adults.7 ADHD is characterized by impulsivity, motor restlessness, and inattention; the latter feature generally is more prominent with advancing age.8 If left untreated, ADHD has societal burdens, such as educational and occupational impairments.9 There is little data on ADHD in older adults and no placebo-controlled trials. For a case study of an older patient with ADHD treated with stimulants, see Box 2.10
Psychostimulants are considered the mainstay of ADHD treatment. First-line treatments include methylphenidate and amphetamines. A meta-analysis found a significant improvement in ADHD symptoms in adult patients taking psychostimulants compared with placebo, with no difference between immediate-release and long-acting formulations.11 Although these findings were reported in younger adults, they may be relevant for older persons as well. Wetzel and Burke12 described how ADHD presents in older adults and argued that the benefits of treating ADHD in this age group often outweigh the risks associated with psychostimulants, which can be diminished through careful screening.
Individuals who present with ADHD symptoms in late life often appear to be high functioning. Some may describe achieving academic and professional success, but may report chronic problems associated with inefficient learning and distraction compared with their peers because of untreated inattention symptoms. Faraone et al13 argue that similar to other illnesses, ADHD is represented by a spectrum of disease, which may be diagnosed in late life or as subthreshold ADHD. Individuals who did not meet diagnostic criteria in childhood or were not evaluated or treated may experience unremitting symptoms that contribute to functional impairment, persistent discouragement, and distress. Frustrations with distractibility, disorganization, and incompletion of tasks may have a psychological impact reflected by low self-esteem and irritability, and be a chronic source of occupational and relationship dysfunction. Diagnosing and treating ADHD in late life can improve longstanding functional impairments and overall quality of life.
Mr. J, age 66, is an attorney who presents for evaluation after he identified common features in friends who have attention-deficit/hyperactivity disorder (ADHD). In grade school, Mr. J’s teachers told him that he employed very little effort and was not meeting his potential, although he performed exceptionally well. He reports similar experiences throughout his education and says he was careful to select classes that were interesting, but did not require demanding projects or burdensome homework. In law school, he felt academically challenged for the first time but realized he had limited study skills. Mr. J graduated in the top 26th percentile of his class using “an unbelievable amount of effort compared with other students.”
Mr. J describes significant impairment in organizational skills and ability to keep track of time, procrastination, incompletion of tasks, and substantial distractibility during conferences. He says he has difficulty reading briefs depending on his emotional connection to the subject matter. Family history revealed that his mother likely had undiagnosed ADHD. He recently married and his wife encouraged him to seek treatment for “forgetfulness.” Mr. J maintains a busy, successful law practice but has become increasingly frustrated by his inability to follow through on simple tasks that could help grow the practice and generate revenue.
Mr. J has an elevated score on the Adult ADHD Symptom Rating Scale.10 He is referred to his primary care physician to evaluate his general health before beginning medication. At follow-up, Mr. J was started on lisdexamfetamine, 20 mg/d, titrated to 40 mg/d. On subsequent visits he reports improved symptoms without side effects. His vital signs are normal and he reports feeling more productive in his work and achieving significant improvement in the day-to-day operations of his practice.
Other uses
Depression. Although not a first-line treatment, psychostimulants have shown benefit for treating depressive disorders, particularly when patients require immediate improvement. These scenarios are common among medically ill patients, such as those with cancer, stroke, or human immunodeficiency virus (HIV), when it is urgent for patients to participate in their treatment plan. A double-blind, placebo-controlled, randomized study that looked at older depressed patients with medical comorbidities found that methylphenidate was well tolerated, worked quickly, and effectively treated depression.14 However, these results must be interpreted cautiously because the entire study was conducted in 8 days, which included a crossover design that administered methylphenidate 10 mg/d and 20 mg/d for 2 days each. A review of stimulant effectiveness in patients whose depression was associated with HIV, stroke, or cancer and in medically ill patients argued that although benefits have been reported, they must be interpreted tentatively because of a lack of randomized trials.15 However, limited evidence supports an effect of stimulants in treating fatigue, anorexia, pain, and sedation in these populations.15
Stimulants’ immediate onset of action may be particularly useful in terminally ill patients who suffer from fatigue or depression. A double-blind, placebo-controlled, randomized study demonstrated that augmenting citalopram, 20 to 40 mg/d, with methylphenidate, mean dose 15 mg/d, for 3 weeks in older depressed patients significantly improved treatment response and accelerated time to remission compared with citalopram and placebo.16 However, a recent Cochrane review did not show clear efficacy for psychostimulants to treat depression.17
Fatigue. Along with depression, fatigue frequently is seen in older patients with medical illnesses. Mood disorders, medical comorbidities, and sleep disturbances are linked to fatigue. Underlying medical causes such as hypothyroidism, anemia, and electrolyte imbalances should be ruled out before starting a psychostimulant. A review by Minton et al18 that looked at cancer-related fatigue suggested that methylphenidate can be beneficial, although the evidence is mixed.
Interferon-alpha treatment for hepatitis C can cause depression and fatigue, and psychostimulants may help treat fatigue-related side effects.19 Fatigue may present as an isolated symptom in interferon-alpha treatment and psychostimulant use may prevent patients from taking an additional medication, therefore decreasing the risk of further side effects.
Fall risk. Some evidence supports using psychostimulants to lower the risk of falling and hypoactive delirium. A recent review by Elie et al20 concluded that stimulants could improve cognitive function in end-of-life hypoactive delirium. Additionally, a randomized, placebo-controlled, double-blind study that evaluated fall risk concluded that methylphenidate, 20 mg/d, might improve some aspects of executive function and gait stability in older adults.21 The authors hypothesized that improved cognition associated with psychostimulant use may play a role in improving fall risk.
Safety concerns
Clinicians should be aware of safety considerations and possible side effects when prescribing psychostimulants. Psychostimulants are controlled substances and are subject to restrictions (Box 3).22 In 2007, the FDA issued warnings regarding an association between psychostimulant use and sudden death, myocardial infarction, and stroke in patients with preexisting cardiac abnormalities or heart problems.23 Also, some evidence indicates that psychostimulants can increase heart rate and systolic blood pressure. These parameters should be monitored during treatment. Reducing or stopping psychostimulants generally reverses cardiovascular effects. Although the evidence to support these events appears sparse, perform a thorough history before beginning a stimulant and make appropriate referrals as indicated. In November 2011, the FDA reported that psychostimulant use in children and young adults is not associated with adverse cardiovascular events, including stroke, heart attack, and sudden cardiac death.24
Less common side effects reported with psychostimulants include anxiety, insomnia, hallucinations, anorexia, delirium, palpitations, and headache. A meta-analysis of studies of adults with ADHD found that adverse events related to psychostimulants were relatively rare; the most common side effects were diminished appetite and difficulty sleeping.25 Sleep-related side effects can be avoided by dosing these medications earlier in the day, typically before 5 pm. Herrmann et al5 reported 2 cases of apparent delirium and 1 with irregular heartbeat in patients with DAT taking methylphenidate vs placebo. However, most patients in this study experienced mild or no adverse events.
Other safety concerns involve using methylphenidate in patients with glaucoma. In theory, stimulants could exacerbate an acute attack of glaucoma in patients with narrow-angle glaucoma. Patients at risk should be referred to an ophthalmologist for an assessment.
Review other medications the patient is taking and assess for possible drug-drug interactions. Combining monoamine oxidase inhibitors (MAOIs) and methylphenidate warrants caution because of the risk of serotonin syndrome and hypertensive crisis. However, there are case reports of successful MAOI/methylphenidate therapy.26 Additionally, methylphenidate increases levels of warfarin and tricyclic antidepressants when taken with these agents.27 Psychostimulants generally are well tolerated by most individuals and taking a careful history may help prevent adverse events.
As schedule II controlled substances, psychostimulants are subject to prescribing limitations. The current Drug Enforcement Administration (DEA) policy on schedule II controlled substances allows for the equivalent of a 90-day supply of medication to be written with multiple prescriptions. DEA requirements for multiple prescriptions include:
- Each prescription issued is for a legitimate medical purpose by an individual practitioner acting in the usual course of his/her professional practice
- The individual practitioner must provide written instructions on each prescription indicating the earliest date on which a pharmacy may fill each prescription
- The issuance of multiple prescriptions is permissible under applicable state laws
- The individual practitioner fully complies with all other applicable requirements under the Controlled Substances Act and implementing regulations, as well as any additional requirements under state law.22
Related Resources
- Kessler RC, Adler L, Ames M, et al. The World Health Organization Adult ADHD Self-Report Scale (ASRS): a short screening scale for use in the general population. Psychol Med. 2005;35(2):245-256.
- Alexopoulos GS, Salzman C. Treatment of depression with heterocyclic antidepressants, monoamine oxidase inhibitors, and psychomotor stimulants. In: Salzman C, ed. Clinical geriatric psychopharmacology. Baltimore, MD: Williams and Wilkins; 1998:184-244.
Drug Brand Names
- Bupropion • Wellbutrin, Zyban
- Citalopram • Celexa
- Dexmethylphenidate • Focalin
- Dextroamphetamine • Dexedrine
- Donepezil • Aricept
- Lisdexamfetamine • Vyvanse
- Methamphetamine • Desoxyn
- Methylphenidate • Ritalin, Concerta
- Mixed amphetamine salts • Adderall
- Warfarin • Coumadin
Disclosures
Dr. Padala receives research funding from the Department of Veterans Health Administration and the Alzheimer’s Association.
Drs. Franzen, Wetzel, and Burke report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Ballas C, Evans D, Dinges D. Psychostimulants and wakefulness promoting agents. In: Schatzberg A Nemeroff C, eds. The American Psychiatric Publishing textbook of psychopharmacology. 4th ed. Arlington, VA: American Psychiatric Publishing, Inc.; 2010: 843-860.
2. Marin RS. Apathy: a neuropsychiatric syndrome. J Neuropsychiatry Clin Neurosci. 1991;3(3):243-254.
3. Dolder CR, Davis LN, McKinsey J. Use of psychostimulants in patients with dementia. Ann Pharmacother. 2010;44(10):1624-1632.
4. Padala PR, Burke WJ, Shostrom VK, et al. Methylphenidate for apathy and functional status in dementia of the Alzheimer type. Am J Geriatr Psychiatry. 2010;18(4):371-374.
5. Herrmann N, Rothenburg LS, Black SE, et al. Methylphenidate for the treatment of apathy in Alzheimer disease: prediction of response using dextroamphetamine challenge. J Clin Psychopharmacol. 2008;28(3):296-301.
6. Huey ED, Garcia C, Wassermann EM, et al. Stimulant treatment of frontotemporal dementia in 8 patients. J Clin Psychiatry. 2008;69(12):1981-1982.
7. Centers for Disease Control and Prevention (CDC). Mental health in the United States: prevalence of diagnosis and medication treatment for attention-deficit/hyperactivity disorder—United States 2003. MMWR Morb Wkly Rep. 2005;54(34):842-847.
8. Biederman J, Mick E, Faraone SV. Age-dependent decline of attention deficit hyperactivity disorder: impact of remission definition and symptom type. Am J Psychiatry. 2000;157(5):816-818.
9. Biederman J, Faraone SV. The effects of attention-deficit/hyperactivity disorder on employment and household income. Med Gen Med. 2006;8(13):12.-
10. Adult ADHD Self-Report Scale (ASRS-v1. 1) symptom checklist instructions. http://www.hcp.med.harvard.edu/ncs/ftpdir/adhd/18%20Question%20ADHD-ASRS-v1-1.pdf. Accessed November 15 2011.
11. Faraone SV, Glatt SJ. A comparison of the efficacy of medications for adult attention-deficit/hyperactivity disorder using meta-analysis of effect sizes. J Clin Psychiatry. 2010;71(6):754-763.
12. Wetzel MW, Burke WJ. Addressing attention-deficit/hyperactivity disorder in late adulthood. Clinical Geriatrics. 2008;16(11):33-39.
13. Faraone SV, Kunwar A, Adamson J, et al. Personality traits among ADHD adults: implications of late-onset and subthreshold diagnoses. Psychol Med. 2009;39(4):685-693.
14. Wallace AE, Kofoed LL, West AN. Double-blind placebo-controlled trial of methylphenidate in older, depressed, medically ill patients. Am J Psychiatry. 1995;152(6):929-931.
15. Orr K, Taylor D. Psychostimulants in the treatment of depression: a review of the evidence. CNS Drugs. 2007;21(3):239-257.
16. Lavretsky H, Park S, Siddarth P, et al. Methylphenidate-enhanced antidepressant response to citalopram in the elderly: a double-blind, placebo-controlled pilot trial. Am J Geriatr Psychiatry. 2006;14(2):181-185.
17. Candy M, Jones L, Williams R, et al. Psychostimulants for depression. Cochrane Database Syst Rev. 2008;16(2):CD006722.-
18. Minton O, Richardson A, Sharpe M, et al. Psychostimulants for the management of cancer-related fatigue: a systematic review and meta-analysis. J Pain Symptom Manage. 2011;41(4):761-767.
19. Raison CL, Demetrashvili M, Capuron L, et al. Neuropsychiatric adverse events of interferon-α: recognition and management. CNS Drugs. 2005;19(2):105-123.
20. Elie D, Gagnon P, Gagnon B, et al. Using psychostimulants in end-of-life patients with hypoactive delirium and cognitive disorders: a literature review [in French]. Can J Psychiatry. 2010;55:386-393.
21. Ben-Itzhak R, Giladi N, Gruendlinger L, et al. Can methylphenidate reduce fall risk in community-living older adults? A double-blind, single-dose cross-over study. J Am Geriatr Soc. 2008;56(4):695-700.
22. U.S. Department of Justice Drug Enforcement Administration. Issuance of multiple prescriptions for Schedule II controlled substances. http://www.deadiversion.usdoj.gov/faq/mult_rx_faq.htm. Accessed November 1, 2011.
23. U.S. Food and Drug Administration. FDA directs ADHD drug manufacturers to notify patients about cardiovascular adverse events and psychiatric adverse events. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2007/ucm108849.htm. Accessed November 1, 2011.
24. U.S. Food and Drug Administration. FDA Drug Safety Communication: safety review update of medications used to treat attention-deficit/hyperactivity disorder (ADHD) in children and young adults. http://www.fda.gov/Drugs/DrugSafety/ucm277770.htm. Accessed November 2, 2011.
25. Peterson K, McDonagh MS, Fu R. Comparative benefits and harms of competing medications for adults with attention-deficit hyperactivity disorder: a systematic review and indirect comparison meta-analysis. Psychopharmacology (Berl). 2008;197(1):1-11.
26. Leonard BE, McCartan D, White J, et al. Methylphenidate: a review of its neuropharmacological, neuropsychological and adverse effects. Hum Psychopharmacol. 2004;19(3):151-180.
27. Howard P, Shuster J, Twycross R, et al. Psychostimulants. J Pain Symptom Manage. 2010;40(5):789-795.
1. Ballas C, Evans D, Dinges D. Psychostimulants and wakefulness promoting agents. In: Schatzberg A Nemeroff C, eds. The American Psychiatric Publishing textbook of psychopharmacology. 4th ed. Arlington, VA: American Psychiatric Publishing, Inc.; 2010: 843-860.
2. Marin RS. Apathy: a neuropsychiatric syndrome. J Neuropsychiatry Clin Neurosci. 1991;3(3):243-254.
3. Dolder CR, Davis LN, McKinsey J. Use of psychostimulants in patients with dementia. Ann Pharmacother. 2010;44(10):1624-1632.
4. Padala PR, Burke WJ, Shostrom VK, et al. Methylphenidate for apathy and functional status in dementia of the Alzheimer type. Am J Geriatr Psychiatry. 2010;18(4):371-374.
5. Herrmann N, Rothenburg LS, Black SE, et al. Methylphenidate for the treatment of apathy in Alzheimer disease: prediction of response using dextroamphetamine challenge. J Clin Psychopharmacol. 2008;28(3):296-301.
6. Huey ED, Garcia C, Wassermann EM, et al. Stimulant treatment of frontotemporal dementia in 8 patients. J Clin Psychiatry. 2008;69(12):1981-1982.
7. Centers for Disease Control and Prevention (CDC). Mental health in the United States: prevalence of diagnosis and medication treatment for attention-deficit/hyperactivity disorder—United States 2003. MMWR Morb Wkly Rep. 2005;54(34):842-847.
8. Biederman J, Mick E, Faraone SV. Age-dependent decline of attention deficit hyperactivity disorder: impact of remission definition and symptom type. Am J Psychiatry. 2000;157(5):816-818.
9. Biederman J, Faraone SV. The effects of attention-deficit/hyperactivity disorder on employment and household income. Med Gen Med. 2006;8(13):12.-
10. Adult ADHD Self-Report Scale (ASRS-v1. 1) symptom checklist instructions. http://www.hcp.med.harvard.edu/ncs/ftpdir/adhd/18%20Question%20ADHD-ASRS-v1-1.pdf. Accessed November 15 2011.
11. Faraone SV, Glatt SJ. A comparison of the efficacy of medications for adult attention-deficit/hyperactivity disorder using meta-analysis of effect sizes. J Clin Psychiatry. 2010;71(6):754-763.
12. Wetzel MW, Burke WJ. Addressing attention-deficit/hyperactivity disorder in late adulthood. Clinical Geriatrics. 2008;16(11):33-39.
13. Faraone SV, Kunwar A, Adamson J, et al. Personality traits among ADHD adults: implications of late-onset and subthreshold diagnoses. Psychol Med. 2009;39(4):685-693.
14. Wallace AE, Kofoed LL, West AN. Double-blind placebo-controlled trial of methylphenidate in older, depressed, medically ill patients. Am J Psychiatry. 1995;152(6):929-931.
15. Orr K, Taylor D. Psychostimulants in the treatment of depression: a review of the evidence. CNS Drugs. 2007;21(3):239-257.
16. Lavretsky H, Park S, Siddarth P, et al. Methylphenidate-enhanced antidepressant response to citalopram in the elderly: a double-blind, placebo-controlled pilot trial. Am J Geriatr Psychiatry. 2006;14(2):181-185.
17. Candy M, Jones L, Williams R, et al. Psychostimulants for depression. Cochrane Database Syst Rev. 2008;16(2):CD006722.-
18. Minton O, Richardson A, Sharpe M, et al. Psychostimulants for the management of cancer-related fatigue: a systematic review and meta-analysis. J Pain Symptom Manage. 2011;41(4):761-767.
19. Raison CL, Demetrashvili M, Capuron L, et al. Neuropsychiatric adverse events of interferon-α: recognition and management. CNS Drugs. 2005;19(2):105-123.
20. Elie D, Gagnon P, Gagnon B, et al. Using psychostimulants in end-of-life patients with hypoactive delirium and cognitive disorders: a literature review [in French]. Can J Psychiatry. 2010;55:386-393.
21. Ben-Itzhak R, Giladi N, Gruendlinger L, et al. Can methylphenidate reduce fall risk in community-living older adults? A double-blind, single-dose cross-over study. J Am Geriatr Soc. 2008;56(4):695-700.
22. U.S. Department of Justice Drug Enforcement Administration. Issuance of multiple prescriptions for Schedule II controlled substances. http://www.deadiversion.usdoj.gov/faq/mult_rx_faq.htm. Accessed November 1, 2011.
23. U.S. Food and Drug Administration. FDA directs ADHD drug manufacturers to notify patients about cardiovascular adverse events and psychiatric adverse events. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2007/ucm108849.htm. Accessed November 1, 2011.
24. U.S. Food and Drug Administration. FDA Drug Safety Communication: safety review update of medications used to treat attention-deficit/hyperactivity disorder (ADHD) in children and young adults. http://www.fda.gov/Drugs/DrugSafety/ucm277770.htm. Accessed November 2, 2011.
25. Peterson K, McDonagh MS, Fu R. Comparative benefits and harms of competing medications for adults with attention-deficit hyperactivity disorder: a systematic review and indirect comparison meta-analysis. Psychopharmacology (Berl). 2008;197(1):1-11.
26. Leonard BE, McCartan D, White J, et al. Methylphenidate: a review of its neuropharmacological, neuropsychological and adverse effects. Hum Psychopharmacol. 2004;19(3):151-180.
27. Howard P, Shuster J, Twycross R, et al. Psychostimulants. J Pain Symptom Manage. 2010;40(5):789-795.
How to care for patients who have delusions with religious content
Discuss this article at www.facebook.com/CurrentPsychiatry
Mr. D, a 72-year-old Christian with a long history of schizophrenia, presents to the emergency room with concerns about evil spirits in his home who have poisoned him. He has called for police assistance on numerous occasions and has tried to kill the evil spirits with his rifle, but states “they are bulletproof.” He is unable to sleep and is “fearful for my life every night because that is when the demons come out.” Mr. D also believes that God is “more powerful than the evil spirits.” Two elders at his church have prayed with him and encouraged him to go to the hospital.
Delusions with religious content (DRC) are associated with poorer clinical outcomes and dangerousness.1-6 Most mental health professionals will encounter patients with DRC because this type of delusion is relatively common in patients with symptoms of mania or psychosis. For example, in a study of 193 inpatients with schizophrenia, 24% had religious delusions.1 The prevalence of DRC varies considerably among populations and can be influenced by the local religion and culture.7-9 This article reviews clinical challenges and assessment and management strategies for patients with DRC.
A challenging course
In a UK study of 193 inpatients with schizophrenia, compared with patients with other types of delusions, those with DRC:
- had higher Positive and Negative Syndrome Scale scores and lower Global Assessment of Functioning scores
- waited longer before reengaging in treatment
- were prescribed more medications.1
In addition, compared with patients with other types of delusions, patients with DRC often hold these delusions with greater conviction,1,2 making them more challenging to treat.
Dangerousness in patients with DRC can manifest as self-harm or harm to others. Extreme examples include self-inflicted enucleation of the eye and autocastration. In a review of 9 cases of severe ocular self-injury, 4 patients had DRC.3 Genital self-mutilation associated with DRC is rare, but several cases of psychotic men who performed autocastration based on a literal, erroneous interpretation of a passage in the Bible (Matthew 19:12) have been reported.4,5 Patients with DRC have committed rape and murder because they believed they were the antichrist.6
In this article we use the phrase “delusions with religious content” instead of “religious delusions” because this distinction highlights that many subtypes of delusions can have a religious theme. Categories of delusions with religious themes include:
- persecutory (often involving Satan)
- grandiose (messianic delusions)
- guilt delusions.
Categorizing DRC is important because some are associated with more distress or dangerousness than others. For example, case studies of self-inflicted eye injuries found that most patients had guilt delusions with religious themes that referenced punishing transgressions, controlling unacceptable sexual impulses, and attaining prescience by destroying vision.3,10 In our example, Mr. D is experiencing a persecutory DRC. Also, using the label “religious delusion” can inadvertently pathologize religious experiences.
Tips for effective evaluation
DSM-IV-TR offers no specific guidelines for assessing DRC vs nondelusional religious beliefs.11 There is risk of pathologizing religious beliefs when listening to content alone.11-15 Instead, focus on the conviction, pervasiveness,2 uniqueness or bizarreness, and associated emotional distress of the delusion to the patient (Table 1).2,12,16-18
In the context of the patient’s spiritual history, deviations from conventional religious beliefs and practices are important factors in determining whether a religious belief is authentic or delusional. Involving family members and/or spiritual care professionals (eg, chaplains and clergy) can be especially helpful when making this differentiation.16,17 In the hospital, chaplains often are familiar with a variety of faith traditions and may provide important insight into the patient’s beliefs. In the community, clergy members from the patient’s faith also may provide valuable perspective.
Similar to how having a basic familiarity with a patient’s culture can improve care, a better understanding of a patient’s spiritual or religious beliefs and practices can build rapport and the therapeutic alliance.16,17 This is particularly important with patients with DRC because these individuals often have a poor therapeutic alliance and engagement with providers.19 Because many psychiatrists have limited time and may not be familiar with every patient’s spiritual or religious background, consultation with spiritual care professionals may be helpful.
Assess whether your patient has reservations about psychiatric treatment. Some may believe that seeking care from a doctor is evidence of weak faith, whereas others may feel that psychiatric treatment is forbidden or incompatible with their religious beliefs.19-22 Mental health clinicians need to consider their own religious biases that may cause them to minimize or pathologize a patient’s religiosity.20,23 Working collaboratively with spiritual care professionals may help reduce clinician biases or assumptions.24
Table 1
Assessing patients with DRC
| Use caution when making a diagnosis to decrease risk of pathologizing religious beliefs |
| Do not focus solely on the content of the delusion; instead look at conviction, pervasiveness, bizarreness, and associated distress |
| Look at the spiritual/religious context and deviations from conventional religious beliefs of the patient’s culture |
| Establish an open dialogue with the patient, the family, and individuals from the patient’s faith community to understand the psychosocial issues and any reservations about psychiatric care |
| Be aware of the categories of delusions, especially those associated with harm (eg, grandiose antichrist delusions, guilt delusions, and some persecutory delusions) |
| Perform a thorough safety assessment that includes previous self-harm, drug use, and severity of mental illness |
| Be vigilant for patients who are actively seeking evidence to support their misguided/dangerous beliefs |
| DRC: delusions with religious content Source: References 2,12,16-18 |
Evaluating safety
When constructing a differential diagnosis and evaluating patients for safety, remember that DRC are a feature of many psychiatric disorders (eg, persecutory DRC in schizophrenia, grandiose DRC in mania). Consider the course and severity of the patient’s illness, and determine if he or she has a history or evidence of self-injury or substance abuse. Be cognizant of the categories of delusions in the context of the diagnosis. For example, grandiose delusions that involve the antichrist can be associated with harm toward others.6 Patients who express extreme feelings of guilt or shame (as seen in psychotic depression) and the need to be physically punished may be at risk for self-harm. Finally, patients seeking evidence to support misguided and dangerous beliefs—for example, obsessing over a religious text regarding self-injury while in a delusional state—may be at high risk for self-harm.18
Researchers have suggested clinicians question patients to determine if they trust their delusions.25 Patients who trust their delusions may appear calm if they already have decided to act on their thoughts.25 Preventive measures for patients at risk of self-harm include close observation, hospitalization, and pharmacotherapy.
Pharmacotherapy for DRC
There are no clear recommendations on specific psychotropics or dosages for treating patients with DRC. When a patient with DRC is at high risk of self-harm or harming others, using antipsychotics, anxiolytics, hypnotics, or a combination of these agents sometimes is needed to quell agitation, along with close observation and restraints when necessary (Table 2).5,18,25,26 Mr. D benefited from risperidone, 3 mg at bedtime, and zolpidem, 10 mg as needed for insomnia.
Table 2
Treating patients with DRC
| If a patient is at risk for self-harm or harming others, take preventive measures such as hospitalization or close observation |
| Rapid tranquilization may be necessary to reduce risk of harm |
| Encourage positive religious coping and spiritual practices, when appropriate |
| DRC: delusions with religious content Source: References 5,18,25,26 |
Using spirituality to cope
Many persistently mentally ill patients identify themselves as religious and use religious activities or beliefs to cope with their illness.27,28 In a study of 1,824 seriously mentally ill patients, self-reports of religiousness were positively associated with psychological well-being and diminished psychiatric symptoms.29 Longitudinal research has shown that some aspects of spirituality and religion are associated with positive mental and physical health effects, whereas other aspects can worsen symptoms.30 Specifically, positive religious coping such as benevolent religious reappraisals (eg, “Jesus is my shield and savior”), collaborative religious coping, and spiritual support are associated with positive mental health.31 However, negative religious coping, such as punishing God reappraisals and reappraisals of God’s power (eg, “my illness is punishment for my sins”), are associated with distress and personal loss.32
For patients with psychotic disorders—and with schizophrenia in particular—religious beliefs can be a source of meaning, hope, strength, and recovery. In a study of 115 outpatients with psychosis, 71% used positive religious coping, compared with 14% who used negative religious coping.33 Among 38 patients with DRC, 45% used spirituality and religion to help cope with their illness, even though they received less support from religious communities than patients with other types of delusions.19 In this study, the authors suggest that positive religious coping among patients with DRC may alleviate delusion severity by decreasing levels of conviction and fear and preventing maladjusted behaviors.19 Religious beliefs and activities are associated with fewer hospitalizations among patients with persistent mental illness28 and are a significant protective factor against suicide in patients with psychotic disorders.34,35 However, some studies have found that intense, obsessive participation in spiritual activities can worsen psychiatric symptoms and undermine recovery.1,36,37
Addressing religion in treatment.
Although many studies have emphasized the importance of religion to patients with psychosis, evidence-based guidelines on how best to address religion/spirituality in the clinical setting in patients with psychosis have yet to be established. In a 2011 study, a spiritual assessment was well tolerated by 40 patients with psychotic disorders and improved patients’ appointment attendance compared with a control group who received traditional care only.26
Many mental health providers feel ill-equipped or are uncomfortable exploring spiritual or religious issues with patients. Enlisting the help of spiritual care professionals when assessing patients with DRC may improve evaluation and care (Table 3). Spiritual care professionals typically are experienced in exploring subjects associated with DRC, such as guilt, morality, conscience, repentance, and confession.24 Spiritual care professionals also may be able to assist patients with religious coping and provide comfort and support.
Finally, spiritual care professionals can help patients connect or reconnect to a spiritual or religious community. In Mr. D’s case, the hospital chaplain deterred him from focusing on the reason the evil spirits were trying to punish him and guided him toward positive religious coping. Mr. D felt we were listening to him on a deeper level and understanding his spiritual struggles. The chaplain’s involvement also enhanced Mr. D’s relationship with the psychiatrist.
Table 3
When to elicit help from spiritual care professionals
| To better understand the patient’s religious background |
| To reduce biases when the clinician comes from a different religious background or no religious background |
| To help identify positive and negative religious coping, and to reinforce positive coping |
| To connect or reconnect patients to members of their faith community or to help them find a religious community |
Related Resources
- Mohr S, Borras L, Betrisey C, et al. Delusions with religious content in patients with psychosis: how they interact with spiritual coping. Psychiatry. 2010;73(2):158-172.
- Huguelet P, Mohr S, Betrisey C, et al. A randomized trial of spiritual assessment of outpatients with schizophrenia: patients’ and clinicians’ experience. Psychiatr Serv. 2011;62(1):79-86.
Drug Brand Names
- Risperidone • Risperdal
- Zolpidem • Ambien
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgements
The authors acknowledge the support and guidance of Rev. Sean Doll O’Mahoney, Rev. Julie Hanada, Rev. Stephen King, PhD, Rev. George Fitchett, PhD, Patricia Murphy, PhD, LCPC, and Kevin Flannelly, PhD.
1. Siddle R, Haddock G, Tarrier N, et al. Religious delusions in patients admitted to hospital with schizophrenia. Soc Psychiatry Psychiatr Epidemiol. 2002;37(3):130-138.
2. Appelbaum PS, Robbins PC, Roth LH. Dimensional approach to delusions: comparison across types and diagnoses. Am J Psychiatry. 1999;156(12):1938-1943.
3. Field HL, Waldfogel S. Severe ocular self-injury. Gen Hosp Psychiatry. 1995;17(3):224-227.
4. Kushner AW. Two cases of auto-castration due to religious delusions. Br J Med Psychol. 1967;40(3):293-298.
5. Waugh AC. Autocastration and biblical delusions in schizophrenia. Br J Psychiatry. 1986;149:656-658.
6. Silva JA, Leong GB, Weinstock R. Violent behaviors associated with the antichrist delusion. J Forensic Sci. 1997;42(6):1058-1061.
7. Atallah SF, El-Dosoky AR, Coker EM, et al. A 22-year retrospective analysis of the changing frequency and patterns of religious symptoms among inpatients with psychotic illness in Egypt. Soc Psychiatry Psychiatr Epidemiol. 2001;36(8):407-415.
8. Bhavsar V, Bhugra D. Religious delusions: finding meanings in psychosis. Psychopathology. 2008;41(3):165-172.
9. Kim K, Hwu H, Zhang LD, et al. Schizophrenic delusions in Seoul, Shanghai and Taipei: a transcultural study. J Korean Med Sci. 2001;16(1):88-94.
10. Kennedy BL, Feldmann TB. Self-inflicted eye injuries: case presentations and a literature review. Hosp Community Psychiatry. 1994;45(5):470-474.
11. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
12. Sanderson S, Vandenberg B, Paese P. Authentic religious experience or insanity? J Clin Psychol. 1999;55(5):607-616.
13. O’Connor S, Vandenberg B. Psychosis of faith? Clinicians’ assessment of religious beliefs. J Consult Clin Psychol. 2005;73(4):610-616.
14. Spitzer M. On defining delusions. Compr Psychiatry. 1990;31(5):377-397.
15. Pierre JM. Faith or delusion? At the crossroads of religion and psychosis. J Psychiatr Pract. 2001;7(3):163-172.
16. Blass DM. A pragmatic approach to teaching psychiatry residents the assessment and treatment of religious patients. Acad Psychiatry. 2007;31(1):25-31.
17. Westermeyer J. Cultural factors in clinical assessment. J Consult Clin Psychol. 1987;55(4):471-478.
18. Clark RA. Self-mutilation accompanying religious delusions: a case report and review. J Clin Psychiatry. 1981;42(6):243-245.
19. Mohr S, Borras L, Betrisey C, et al. Delusions with religious content in patients with psychosis: how they interact with spiritual coping. Psychiatry. 2010;73(2):158-172.
20. Greenberg D, Witztum E. Problems in the treatment of religious patients. Am J Psychother. 1991;45(4):554-565.
21. Peteet JR. Issues in the treatment of religious patients. Am J Psychother. 1981;35(4):559-564.
22. Borras L, Mohr S, Brandt PY, et al. Religious beliefs in schizophrenia: their relevance for adherence to treatment. Schizophr Bull. 2007;33(5):1238-1246.
23. Ng F. The interface between religion and psychosis. Australas Psychiatry. 2007;15(1):62-66.
24. Sacks JM. Religious issues in psychotherapy. J Relig Health. 1985;24(1):26-30.
25. Shore D, Anderson DJ, Cutler NR. Prediction of self-mutilation in hospitalized schizophrenics. Am J Psychiatry. 1978;135(11):1406-1407.
26. Huguelet P, Mohr S, Betrisey C, et al. A randomized trial of spiritual assessment of outpatients with schizophrenia: patients’ and clinicians’ experience. Psychiatr Serv. 2011;62(1):79-86.
27. Kroll J, Sheehan W. Religious beliefs and practices among 52 psychiatric inpatients in Minnesota. Am J Psychiatry. 1989;146(1):67-72.
28. Tepper L, Rogers SA, Coleman EM, et al. The prevalence of religious coping among persons with persistent mental illness. Psychiatr Serv. 2001;52(5):660-665.
29. Corrigan P, McCorkle B, Schell B, et al. Religion and spirituality in the lives of people with serious mental illness. Community Ment Health J. 2003;39(6):487-499.
30. Koenig HG, McCullough ME, Larson DB. Handbook of religion and health. New York NY: Oxford University Press; 2001.
31. Pargament KI, Koenig HG, Perez LM. The many methods of religious coping: development and initial validation of the RCOPE. J Clin Psychol. 2000;56(4):519-543.
32. Phillips RE, III, Stein CH. God’s will God’s punishment, or God’s limitations? Religious coping strategies reported by young adults living with serious mental illness. J Clin Psychol. 2007;63(6):529-540.
33. Mohr S, Brandt PY, Borras L, et al. Toward an integration of spirituality and religiousness into the psychosocial dimension of schizophrenia. Am J Psychiatry. 2006;163(11):1952-1959.
34. Breier A, Astrachan BM. Characterization of schizophrenic patients who commit suicide. Am J Psychiatry. 1984;141(2):206-209.
35. Jarbin H, Von Knorring AL. Suicide and suicide attempts in adolescent-onset psychotic disorders. Nord J Psychiatry. 2004;58(2):115-123.
36. Brewerton TD. Hyperreligiosity in psychotic disorders. J Nerv Ment Dis. 1994;182(5):302-304.
37. Getz GE, Fleck DE, Strakowski SM. Frequency and severity of religious delusions in Christian patients with psychosis. Psychiatry Res. 2001;103(1):87-91.
Discuss this article at www.facebook.com/CurrentPsychiatry
Mr. D, a 72-year-old Christian with a long history of schizophrenia, presents to the emergency room with concerns about evil spirits in his home who have poisoned him. He has called for police assistance on numerous occasions and has tried to kill the evil spirits with his rifle, but states “they are bulletproof.” He is unable to sleep and is “fearful for my life every night because that is when the demons come out.” Mr. D also believes that God is “more powerful than the evil spirits.” Two elders at his church have prayed with him and encouraged him to go to the hospital.
Delusions with religious content (DRC) are associated with poorer clinical outcomes and dangerousness.1-6 Most mental health professionals will encounter patients with DRC because this type of delusion is relatively common in patients with symptoms of mania or psychosis. For example, in a study of 193 inpatients with schizophrenia, 24% had religious delusions.1 The prevalence of DRC varies considerably among populations and can be influenced by the local religion and culture.7-9 This article reviews clinical challenges and assessment and management strategies for patients with DRC.
A challenging course
In a UK study of 193 inpatients with schizophrenia, compared with patients with other types of delusions, those with DRC:
- had higher Positive and Negative Syndrome Scale scores and lower Global Assessment of Functioning scores
- waited longer before reengaging in treatment
- were prescribed more medications.1
In addition, compared with patients with other types of delusions, patients with DRC often hold these delusions with greater conviction,1,2 making them more challenging to treat.
Dangerousness in patients with DRC can manifest as self-harm or harm to others. Extreme examples include self-inflicted enucleation of the eye and autocastration. In a review of 9 cases of severe ocular self-injury, 4 patients had DRC.3 Genital self-mutilation associated with DRC is rare, but several cases of psychotic men who performed autocastration based on a literal, erroneous interpretation of a passage in the Bible (Matthew 19:12) have been reported.4,5 Patients with DRC have committed rape and murder because they believed they were the antichrist.6
In this article we use the phrase “delusions with religious content” instead of “religious delusions” because this distinction highlights that many subtypes of delusions can have a religious theme. Categories of delusions with religious themes include:
- persecutory (often involving Satan)
- grandiose (messianic delusions)
- guilt delusions.
Categorizing DRC is important because some are associated with more distress or dangerousness than others. For example, case studies of self-inflicted eye injuries found that most patients had guilt delusions with religious themes that referenced punishing transgressions, controlling unacceptable sexual impulses, and attaining prescience by destroying vision.3,10 In our example, Mr. D is experiencing a persecutory DRC. Also, using the label “religious delusion” can inadvertently pathologize religious experiences.
Tips for effective evaluation
DSM-IV-TR offers no specific guidelines for assessing DRC vs nondelusional religious beliefs.11 There is risk of pathologizing religious beliefs when listening to content alone.11-15 Instead, focus on the conviction, pervasiveness,2 uniqueness or bizarreness, and associated emotional distress of the delusion to the patient (Table 1).2,12,16-18
In the context of the patient’s spiritual history, deviations from conventional religious beliefs and practices are important factors in determining whether a religious belief is authentic or delusional. Involving family members and/or spiritual care professionals (eg, chaplains and clergy) can be especially helpful when making this differentiation.16,17 In the hospital, chaplains often are familiar with a variety of faith traditions and may provide important insight into the patient’s beliefs. In the community, clergy members from the patient’s faith also may provide valuable perspective.
Similar to how having a basic familiarity with a patient’s culture can improve care, a better understanding of a patient’s spiritual or religious beliefs and practices can build rapport and the therapeutic alliance.16,17 This is particularly important with patients with DRC because these individuals often have a poor therapeutic alliance and engagement with providers.19 Because many psychiatrists have limited time and may not be familiar with every patient’s spiritual or religious background, consultation with spiritual care professionals may be helpful.
Assess whether your patient has reservations about psychiatric treatment. Some may believe that seeking care from a doctor is evidence of weak faith, whereas others may feel that psychiatric treatment is forbidden or incompatible with their religious beliefs.19-22 Mental health clinicians need to consider their own religious biases that may cause them to minimize or pathologize a patient’s religiosity.20,23 Working collaboratively with spiritual care professionals may help reduce clinician biases or assumptions.24
Table 1
Assessing patients with DRC
| Use caution when making a diagnosis to decrease risk of pathologizing religious beliefs |
| Do not focus solely on the content of the delusion; instead look at conviction, pervasiveness, bizarreness, and associated distress |
| Look at the spiritual/religious context and deviations from conventional religious beliefs of the patient’s culture |
| Establish an open dialogue with the patient, the family, and individuals from the patient’s faith community to understand the psychosocial issues and any reservations about psychiatric care |
| Be aware of the categories of delusions, especially those associated with harm (eg, grandiose antichrist delusions, guilt delusions, and some persecutory delusions) |
| Perform a thorough safety assessment that includes previous self-harm, drug use, and severity of mental illness |
| Be vigilant for patients who are actively seeking evidence to support their misguided/dangerous beliefs |
| DRC: delusions with religious content Source: References 2,12,16-18 |
Evaluating safety
When constructing a differential diagnosis and evaluating patients for safety, remember that DRC are a feature of many psychiatric disorders (eg, persecutory DRC in schizophrenia, grandiose DRC in mania). Consider the course and severity of the patient’s illness, and determine if he or she has a history or evidence of self-injury or substance abuse. Be cognizant of the categories of delusions in the context of the diagnosis. For example, grandiose delusions that involve the antichrist can be associated with harm toward others.6 Patients who express extreme feelings of guilt or shame (as seen in psychotic depression) and the need to be physically punished may be at risk for self-harm. Finally, patients seeking evidence to support misguided and dangerous beliefs—for example, obsessing over a religious text regarding self-injury while in a delusional state—may be at high risk for self-harm.18
Researchers have suggested clinicians question patients to determine if they trust their delusions.25 Patients who trust their delusions may appear calm if they already have decided to act on their thoughts.25 Preventive measures for patients at risk of self-harm include close observation, hospitalization, and pharmacotherapy.
Pharmacotherapy for DRC
There are no clear recommendations on specific psychotropics or dosages for treating patients with DRC. When a patient with DRC is at high risk of self-harm or harming others, using antipsychotics, anxiolytics, hypnotics, or a combination of these agents sometimes is needed to quell agitation, along with close observation and restraints when necessary (Table 2).5,18,25,26 Mr. D benefited from risperidone, 3 mg at bedtime, and zolpidem, 10 mg as needed for insomnia.
Table 2
Treating patients with DRC
| If a patient is at risk for self-harm or harming others, take preventive measures such as hospitalization or close observation |
| Rapid tranquilization may be necessary to reduce risk of harm |
| Encourage positive religious coping and spiritual practices, when appropriate |
| DRC: delusions with religious content Source: References 5,18,25,26 |
Using spirituality to cope
Many persistently mentally ill patients identify themselves as religious and use religious activities or beliefs to cope with their illness.27,28 In a study of 1,824 seriously mentally ill patients, self-reports of religiousness were positively associated with psychological well-being and diminished psychiatric symptoms.29 Longitudinal research has shown that some aspects of spirituality and religion are associated with positive mental and physical health effects, whereas other aspects can worsen symptoms.30 Specifically, positive religious coping such as benevolent religious reappraisals (eg, “Jesus is my shield and savior”), collaborative religious coping, and spiritual support are associated with positive mental health.31 However, negative religious coping, such as punishing God reappraisals and reappraisals of God’s power (eg, “my illness is punishment for my sins”), are associated with distress and personal loss.32
For patients with psychotic disorders—and with schizophrenia in particular—religious beliefs can be a source of meaning, hope, strength, and recovery. In a study of 115 outpatients with psychosis, 71% used positive religious coping, compared with 14% who used negative religious coping.33 Among 38 patients with DRC, 45% used spirituality and religion to help cope with their illness, even though they received less support from religious communities than patients with other types of delusions.19 In this study, the authors suggest that positive religious coping among patients with DRC may alleviate delusion severity by decreasing levels of conviction and fear and preventing maladjusted behaviors.19 Religious beliefs and activities are associated with fewer hospitalizations among patients with persistent mental illness28 and are a significant protective factor against suicide in patients with psychotic disorders.34,35 However, some studies have found that intense, obsessive participation in spiritual activities can worsen psychiatric symptoms and undermine recovery.1,36,37
Addressing religion in treatment.
Although many studies have emphasized the importance of religion to patients with psychosis, evidence-based guidelines on how best to address religion/spirituality in the clinical setting in patients with psychosis have yet to be established. In a 2011 study, a spiritual assessment was well tolerated by 40 patients with psychotic disorders and improved patients’ appointment attendance compared with a control group who received traditional care only.26
Many mental health providers feel ill-equipped or are uncomfortable exploring spiritual or religious issues with patients. Enlisting the help of spiritual care professionals when assessing patients with DRC may improve evaluation and care (Table 3). Spiritual care professionals typically are experienced in exploring subjects associated with DRC, such as guilt, morality, conscience, repentance, and confession.24 Spiritual care professionals also may be able to assist patients with religious coping and provide comfort and support.
Finally, spiritual care professionals can help patients connect or reconnect to a spiritual or religious community. In Mr. D’s case, the hospital chaplain deterred him from focusing on the reason the evil spirits were trying to punish him and guided him toward positive religious coping. Mr. D felt we were listening to him on a deeper level and understanding his spiritual struggles. The chaplain’s involvement also enhanced Mr. D’s relationship with the psychiatrist.
Table 3
When to elicit help from spiritual care professionals
| To better understand the patient’s religious background |
| To reduce biases when the clinician comes from a different religious background or no religious background |
| To help identify positive and negative religious coping, and to reinforce positive coping |
| To connect or reconnect patients to members of their faith community or to help them find a religious community |
Related Resources
- Mohr S, Borras L, Betrisey C, et al. Delusions with religious content in patients with psychosis: how they interact with spiritual coping. Psychiatry. 2010;73(2):158-172.
- Huguelet P, Mohr S, Betrisey C, et al. A randomized trial of spiritual assessment of outpatients with schizophrenia: patients’ and clinicians’ experience. Psychiatr Serv. 2011;62(1):79-86.
Drug Brand Names
- Risperidone • Risperdal
- Zolpidem • Ambien
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgements
The authors acknowledge the support and guidance of Rev. Sean Doll O’Mahoney, Rev. Julie Hanada, Rev. Stephen King, PhD, Rev. George Fitchett, PhD, Patricia Murphy, PhD, LCPC, and Kevin Flannelly, PhD.
Discuss this article at www.facebook.com/CurrentPsychiatry
Mr. D, a 72-year-old Christian with a long history of schizophrenia, presents to the emergency room with concerns about evil spirits in his home who have poisoned him. He has called for police assistance on numerous occasions and has tried to kill the evil spirits with his rifle, but states “they are bulletproof.” He is unable to sleep and is “fearful for my life every night because that is when the demons come out.” Mr. D also believes that God is “more powerful than the evil spirits.” Two elders at his church have prayed with him and encouraged him to go to the hospital.
Delusions with religious content (DRC) are associated with poorer clinical outcomes and dangerousness.1-6 Most mental health professionals will encounter patients with DRC because this type of delusion is relatively common in patients with symptoms of mania or psychosis. For example, in a study of 193 inpatients with schizophrenia, 24% had religious delusions.1 The prevalence of DRC varies considerably among populations and can be influenced by the local religion and culture.7-9 This article reviews clinical challenges and assessment and management strategies for patients with DRC.
A challenging course
In a UK study of 193 inpatients with schizophrenia, compared with patients with other types of delusions, those with DRC:
- had higher Positive and Negative Syndrome Scale scores and lower Global Assessment of Functioning scores
- waited longer before reengaging in treatment
- were prescribed more medications.1
In addition, compared with patients with other types of delusions, patients with DRC often hold these delusions with greater conviction,1,2 making them more challenging to treat.
Dangerousness in patients with DRC can manifest as self-harm or harm to others. Extreme examples include self-inflicted enucleation of the eye and autocastration. In a review of 9 cases of severe ocular self-injury, 4 patients had DRC.3 Genital self-mutilation associated with DRC is rare, but several cases of psychotic men who performed autocastration based on a literal, erroneous interpretation of a passage in the Bible (Matthew 19:12) have been reported.4,5 Patients with DRC have committed rape and murder because they believed they were the antichrist.6
In this article we use the phrase “delusions with religious content” instead of “religious delusions” because this distinction highlights that many subtypes of delusions can have a religious theme. Categories of delusions with religious themes include:
- persecutory (often involving Satan)
- grandiose (messianic delusions)
- guilt delusions.
Categorizing DRC is important because some are associated with more distress or dangerousness than others. For example, case studies of self-inflicted eye injuries found that most patients had guilt delusions with religious themes that referenced punishing transgressions, controlling unacceptable sexual impulses, and attaining prescience by destroying vision.3,10 In our example, Mr. D is experiencing a persecutory DRC. Also, using the label “religious delusion” can inadvertently pathologize religious experiences.
Tips for effective evaluation
DSM-IV-TR offers no specific guidelines for assessing DRC vs nondelusional religious beliefs.11 There is risk of pathologizing religious beliefs when listening to content alone.11-15 Instead, focus on the conviction, pervasiveness,2 uniqueness or bizarreness, and associated emotional distress of the delusion to the patient (Table 1).2,12,16-18
In the context of the patient’s spiritual history, deviations from conventional religious beliefs and practices are important factors in determining whether a religious belief is authentic or delusional. Involving family members and/or spiritual care professionals (eg, chaplains and clergy) can be especially helpful when making this differentiation.16,17 In the hospital, chaplains often are familiar with a variety of faith traditions and may provide important insight into the patient’s beliefs. In the community, clergy members from the patient’s faith also may provide valuable perspective.
Similar to how having a basic familiarity with a patient’s culture can improve care, a better understanding of a patient’s spiritual or religious beliefs and practices can build rapport and the therapeutic alliance.16,17 This is particularly important with patients with DRC because these individuals often have a poor therapeutic alliance and engagement with providers.19 Because many psychiatrists have limited time and may not be familiar with every patient’s spiritual or religious background, consultation with spiritual care professionals may be helpful.
Assess whether your patient has reservations about psychiatric treatment. Some may believe that seeking care from a doctor is evidence of weak faith, whereas others may feel that psychiatric treatment is forbidden or incompatible with their religious beliefs.19-22 Mental health clinicians need to consider their own religious biases that may cause them to minimize or pathologize a patient’s religiosity.20,23 Working collaboratively with spiritual care professionals may help reduce clinician biases or assumptions.24
Table 1
Assessing patients with DRC
| Use caution when making a diagnosis to decrease risk of pathologizing religious beliefs |
| Do not focus solely on the content of the delusion; instead look at conviction, pervasiveness, bizarreness, and associated distress |
| Look at the spiritual/religious context and deviations from conventional religious beliefs of the patient’s culture |
| Establish an open dialogue with the patient, the family, and individuals from the patient’s faith community to understand the psychosocial issues and any reservations about psychiatric care |
| Be aware of the categories of delusions, especially those associated with harm (eg, grandiose antichrist delusions, guilt delusions, and some persecutory delusions) |
| Perform a thorough safety assessment that includes previous self-harm, drug use, and severity of mental illness |
| Be vigilant for patients who are actively seeking evidence to support their misguided/dangerous beliefs |
| DRC: delusions with religious content Source: References 2,12,16-18 |
Evaluating safety
When constructing a differential diagnosis and evaluating patients for safety, remember that DRC are a feature of many psychiatric disorders (eg, persecutory DRC in schizophrenia, grandiose DRC in mania). Consider the course and severity of the patient’s illness, and determine if he or she has a history or evidence of self-injury or substance abuse. Be cognizant of the categories of delusions in the context of the diagnosis. For example, grandiose delusions that involve the antichrist can be associated with harm toward others.6 Patients who express extreme feelings of guilt or shame (as seen in psychotic depression) and the need to be physically punished may be at risk for self-harm. Finally, patients seeking evidence to support misguided and dangerous beliefs—for example, obsessing over a religious text regarding self-injury while in a delusional state—may be at high risk for self-harm.18
Researchers have suggested clinicians question patients to determine if they trust their delusions.25 Patients who trust their delusions may appear calm if they already have decided to act on their thoughts.25 Preventive measures for patients at risk of self-harm include close observation, hospitalization, and pharmacotherapy.
Pharmacotherapy for DRC
There are no clear recommendations on specific psychotropics or dosages for treating patients with DRC. When a patient with DRC is at high risk of self-harm or harming others, using antipsychotics, anxiolytics, hypnotics, or a combination of these agents sometimes is needed to quell agitation, along with close observation and restraints when necessary (Table 2).5,18,25,26 Mr. D benefited from risperidone, 3 mg at bedtime, and zolpidem, 10 mg as needed for insomnia.
Table 2
Treating patients with DRC
| If a patient is at risk for self-harm or harming others, take preventive measures such as hospitalization or close observation |
| Rapid tranquilization may be necessary to reduce risk of harm |
| Encourage positive religious coping and spiritual practices, when appropriate |
| DRC: delusions with religious content Source: References 5,18,25,26 |
Using spirituality to cope
Many persistently mentally ill patients identify themselves as religious and use religious activities or beliefs to cope with their illness.27,28 In a study of 1,824 seriously mentally ill patients, self-reports of religiousness were positively associated with psychological well-being and diminished psychiatric symptoms.29 Longitudinal research has shown that some aspects of spirituality and religion are associated with positive mental and physical health effects, whereas other aspects can worsen symptoms.30 Specifically, positive religious coping such as benevolent religious reappraisals (eg, “Jesus is my shield and savior”), collaborative religious coping, and spiritual support are associated with positive mental health.31 However, negative religious coping, such as punishing God reappraisals and reappraisals of God’s power (eg, “my illness is punishment for my sins”), are associated with distress and personal loss.32
For patients with psychotic disorders—and with schizophrenia in particular—religious beliefs can be a source of meaning, hope, strength, and recovery. In a study of 115 outpatients with psychosis, 71% used positive religious coping, compared with 14% who used negative religious coping.33 Among 38 patients with DRC, 45% used spirituality and religion to help cope with their illness, even though they received less support from religious communities than patients with other types of delusions.19 In this study, the authors suggest that positive religious coping among patients with DRC may alleviate delusion severity by decreasing levels of conviction and fear and preventing maladjusted behaviors.19 Religious beliefs and activities are associated with fewer hospitalizations among patients with persistent mental illness28 and are a significant protective factor against suicide in patients with psychotic disorders.34,35 However, some studies have found that intense, obsessive participation in spiritual activities can worsen psychiatric symptoms and undermine recovery.1,36,37
Addressing religion in treatment.
Although many studies have emphasized the importance of religion to patients with psychosis, evidence-based guidelines on how best to address religion/spirituality in the clinical setting in patients with psychosis have yet to be established. In a 2011 study, a spiritual assessment was well tolerated by 40 patients with psychotic disorders and improved patients’ appointment attendance compared with a control group who received traditional care only.26
Many mental health providers feel ill-equipped or are uncomfortable exploring spiritual or religious issues with patients. Enlisting the help of spiritual care professionals when assessing patients with DRC may improve evaluation and care (Table 3). Spiritual care professionals typically are experienced in exploring subjects associated with DRC, such as guilt, morality, conscience, repentance, and confession.24 Spiritual care professionals also may be able to assist patients with religious coping and provide comfort and support.
Finally, spiritual care professionals can help patients connect or reconnect to a spiritual or religious community. In Mr. D’s case, the hospital chaplain deterred him from focusing on the reason the evil spirits were trying to punish him and guided him toward positive religious coping. Mr. D felt we were listening to him on a deeper level and understanding his spiritual struggles. The chaplain’s involvement also enhanced Mr. D’s relationship with the psychiatrist.
Table 3
When to elicit help from spiritual care professionals
| To better understand the patient’s religious background |
| To reduce biases when the clinician comes from a different religious background or no religious background |
| To help identify positive and negative religious coping, and to reinforce positive coping |
| To connect or reconnect patients to members of their faith community or to help them find a religious community |
Related Resources
- Mohr S, Borras L, Betrisey C, et al. Delusions with religious content in patients with psychosis: how they interact with spiritual coping. Psychiatry. 2010;73(2):158-172.
- Huguelet P, Mohr S, Betrisey C, et al. A randomized trial of spiritual assessment of outpatients with schizophrenia: patients’ and clinicians’ experience. Psychiatr Serv. 2011;62(1):79-86.
Drug Brand Names
- Risperidone • Risperdal
- Zolpidem • Ambien
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgements
The authors acknowledge the support and guidance of Rev. Sean Doll O’Mahoney, Rev. Julie Hanada, Rev. Stephen King, PhD, Rev. George Fitchett, PhD, Patricia Murphy, PhD, LCPC, and Kevin Flannelly, PhD.
1. Siddle R, Haddock G, Tarrier N, et al. Religious delusions in patients admitted to hospital with schizophrenia. Soc Psychiatry Psychiatr Epidemiol. 2002;37(3):130-138.
2. Appelbaum PS, Robbins PC, Roth LH. Dimensional approach to delusions: comparison across types and diagnoses. Am J Psychiatry. 1999;156(12):1938-1943.
3. Field HL, Waldfogel S. Severe ocular self-injury. Gen Hosp Psychiatry. 1995;17(3):224-227.
4. Kushner AW. Two cases of auto-castration due to religious delusions. Br J Med Psychol. 1967;40(3):293-298.
5. Waugh AC. Autocastration and biblical delusions in schizophrenia. Br J Psychiatry. 1986;149:656-658.
6. Silva JA, Leong GB, Weinstock R. Violent behaviors associated with the antichrist delusion. J Forensic Sci. 1997;42(6):1058-1061.
7. Atallah SF, El-Dosoky AR, Coker EM, et al. A 22-year retrospective analysis of the changing frequency and patterns of religious symptoms among inpatients with psychotic illness in Egypt. Soc Psychiatry Psychiatr Epidemiol. 2001;36(8):407-415.
8. Bhavsar V, Bhugra D. Religious delusions: finding meanings in psychosis. Psychopathology. 2008;41(3):165-172.
9. Kim K, Hwu H, Zhang LD, et al. Schizophrenic delusions in Seoul, Shanghai and Taipei: a transcultural study. J Korean Med Sci. 2001;16(1):88-94.
10. Kennedy BL, Feldmann TB. Self-inflicted eye injuries: case presentations and a literature review. Hosp Community Psychiatry. 1994;45(5):470-474.
11. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
12. Sanderson S, Vandenberg B, Paese P. Authentic religious experience or insanity? J Clin Psychol. 1999;55(5):607-616.
13. O’Connor S, Vandenberg B. Psychosis of faith? Clinicians’ assessment of religious beliefs. J Consult Clin Psychol. 2005;73(4):610-616.
14. Spitzer M. On defining delusions. Compr Psychiatry. 1990;31(5):377-397.
15. Pierre JM. Faith or delusion? At the crossroads of religion and psychosis. J Psychiatr Pract. 2001;7(3):163-172.
16. Blass DM. A pragmatic approach to teaching psychiatry residents the assessment and treatment of religious patients. Acad Psychiatry. 2007;31(1):25-31.
17. Westermeyer J. Cultural factors in clinical assessment. J Consult Clin Psychol. 1987;55(4):471-478.
18. Clark RA. Self-mutilation accompanying religious delusions: a case report and review. J Clin Psychiatry. 1981;42(6):243-245.
19. Mohr S, Borras L, Betrisey C, et al. Delusions with religious content in patients with psychosis: how they interact with spiritual coping. Psychiatry. 2010;73(2):158-172.
20. Greenberg D, Witztum E. Problems in the treatment of religious patients. Am J Psychother. 1991;45(4):554-565.
21. Peteet JR. Issues in the treatment of religious patients. Am J Psychother. 1981;35(4):559-564.
22. Borras L, Mohr S, Brandt PY, et al. Religious beliefs in schizophrenia: their relevance for adherence to treatment. Schizophr Bull. 2007;33(5):1238-1246.
23. Ng F. The interface between religion and psychosis. Australas Psychiatry. 2007;15(1):62-66.
24. Sacks JM. Religious issues in psychotherapy. J Relig Health. 1985;24(1):26-30.
25. Shore D, Anderson DJ, Cutler NR. Prediction of self-mutilation in hospitalized schizophrenics. Am J Psychiatry. 1978;135(11):1406-1407.
26. Huguelet P, Mohr S, Betrisey C, et al. A randomized trial of spiritual assessment of outpatients with schizophrenia: patients’ and clinicians’ experience. Psychiatr Serv. 2011;62(1):79-86.
27. Kroll J, Sheehan W. Religious beliefs and practices among 52 psychiatric inpatients in Minnesota. Am J Psychiatry. 1989;146(1):67-72.
28. Tepper L, Rogers SA, Coleman EM, et al. The prevalence of religious coping among persons with persistent mental illness. Psychiatr Serv. 2001;52(5):660-665.
29. Corrigan P, McCorkle B, Schell B, et al. Religion and spirituality in the lives of people with serious mental illness. Community Ment Health J. 2003;39(6):487-499.
30. Koenig HG, McCullough ME, Larson DB. Handbook of religion and health. New York NY: Oxford University Press; 2001.
31. Pargament KI, Koenig HG, Perez LM. The many methods of religious coping: development and initial validation of the RCOPE. J Clin Psychol. 2000;56(4):519-543.
32. Phillips RE, III, Stein CH. God’s will God’s punishment, or God’s limitations? Religious coping strategies reported by young adults living with serious mental illness. J Clin Psychol. 2007;63(6):529-540.
33. Mohr S, Brandt PY, Borras L, et al. Toward an integration of spirituality and religiousness into the psychosocial dimension of schizophrenia. Am J Psychiatry. 2006;163(11):1952-1959.
34. Breier A, Astrachan BM. Characterization of schizophrenic patients who commit suicide. Am J Psychiatry. 1984;141(2):206-209.
35. Jarbin H, Von Knorring AL. Suicide and suicide attempts in adolescent-onset psychotic disorders. Nord J Psychiatry. 2004;58(2):115-123.
36. Brewerton TD. Hyperreligiosity in psychotic disorders. J Nerv Ment Dis. 1994;182(5):302-304.
37. Getz GE, Fleck DE, Strakowski SM. Frequency and severity of religious delusions in Christian patients with psychosis. Psychiatry Res. 2001;103(1):87-91.
1. Siddle R, Haddock G, Tarrier N, et al. Religious delusions in patients admitted to hospital with schizophrenia. Soc Psychiatry Psychiatr Epidemiol. 2002;37(3):130-138.
2. Appelbaum PS, Robbins PC, Roth LH. Dimensional approach to delusions: comparison across types and diagnoses. Am J Psychiatry. 1999;156(12):1938-1943.
3. Field HL, Waldfogel S. Severe ocular self-injury. Gen Hosp Psychiatry. 1995;17(3):224-227.
4. Kushner AW. Two cases of auto-castration due to religious delusions. Br J Med Psychol. 1967;40(3):293-298.
5. Waugh AC. Autocastration and biblical delusions in schizophrenia. Br J Psychiatry. 1986;149:656-658.
6. Silva JA, Leong GB, Weinstock R. Violent behaviors associated with the antichrist delusion. J Forensic Sci. 1997;42(6):1058-1061.
7. Atallah SF, El-Dosoky AR, Coker EM, et al. A 22-year retrospective analysis of the changing frequency and patterns of religious symptoms among inpatients with psychotic illness in Egypt. Soc Psychiatry Psychiatr Epidemiol. 2001;36(8):407-415.
8. Bhavsar V, Bhugra D. Religious delusions: finding meanings in psychosis. Psychopathology. 2008;41(3):165-172.
9. Kim K, Hwu H, Zhang LD, et al. Schizophrenic delusions in Seoul, Shanghai and Taipei: a transcultural study. J Korean Med Sci. 2001;16(1):88-94.
10. Kennedy BL, Feldmann TB. Self-inflicted eye injuries: case presentations and a literature review. Hosp Community Psychiatry. 1994;45(5):470-474.
11. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
12. Sanderson S, Vandenberg B, Paese P. Authentic religious experience or insanity? J Clin Psychol. 1999;55(5):607-616.
13. O’Connor S, Vandenberg B. Psychosis of faith? Clinicians’ assessment of religious beliefs. J Consult Clin Psychol. 2005;73(4):610-616.
14. Spitzer M. On defining delusions. Compr Psychiatry. 1990;31(5):377-397.
15. Pierre JM. Faith or delusion? At the crossroads of religion and psychosis. J Psychiatr Pract. 2001;7(3):163-172.
16. Blass DM. A pragmatic approach to teaching psychiatry residents the assessment and treatment of religious patients. Acad Psychiatry. 2007;31(1):25-31.
17. Westermeyer J. Cultural factors in clinical assessment. J Consult Clin Psychol. 1987;55(4):471-478.
18. Clark RA. Self-mutilation accompanying religious delusions: a case report and review. J Clin Psychiatry. 1981;42(6):243-245.
19. Mohr S, Borras L, Betrisey C, et al. Delusions with religious content in patients with psychosis: how they interact with spiritual coping. Psychiatry. 2010;73(2):158-172.
20. Greenberg D, Witztum E. Problems in the treatment of religious patients. Am J Psychother. 1991;45(4):554-565.
21. Peteet JR. Issues in the treatment of religious patients. Am J Psychother. 1981;35(4):559-564.
22. Borras L, Mohr S, Brandt PY, et al. Religious beliefs in schizophrenia: their relevance for adherence to treatment. Schizophr Bull. 2007;33(5):1238-1246.
23. Ng F. The interface between religion and psychosis. Australas Psychiatry. 2007;15(1):62-66.
24. Sacks JM. Religious issues in psychotherapy. J Relig Health. 1985;24(1):26-30.
25. Shore D, Anderson DJ, Cutler NR. Prediction of self-mutilation in hospitalized schizophrenics. Am J Psychiatry. 1978;135(11):1406-1407.
26. Huguelet P, Mohr S, Betrisey C, et al. A randomized trial of spiritual assessment of outpatients with schizophrenia: patients’ and clinicians’ experience. Psychiatr Serv. 2011;62(1):79-86.
27. Kroll J, Sheehan W. Religious beliefs and practices among 52 psychiatric inpatients in Minnesota. Am J Psychiatry. 1989;146(1):67-72.
28. Tepper L, Rogers SA, Coleman EM, et al. The prevalence of religious coping among persons with persistent mental illness. Psychiatr Serv. 2001;52(5):660-665.
29. Corrigan P, McCorkle B, Schell B, et al. Religion and spirituality in the lives of people with serious mental illness. Community Ment Health J. 2003;39(6):487-499.
30. Koenig HG, McCullough ME, Larson DB. Handbook of religion and health. New York NY: Oxford University Press; 2001.
31. Pargament KI, Koenig HG, Perez LM. The many methods of religious coping: development and initial validation of the RCOPE. J Clin Psychol. 2000;56(4):519-543.
32. Phillips RE, III, Stein CH. God’s will God’s punishment, or God’s limitations? Religious coping strategies reported by young adults living with serious mental illness. J Clin Psychol. 2007;63(6):529-540.
33. Mohr S, Brandt PY, Borras L, et al. Toward an integration of spirituality and religiousness into the psychosocial dimension of schizophrenia. Am J Psychiatry. 2006;163(11):1952-1959.
34. Breier A, Astrachan BM. Characterization of schizophrenic patients who commit suicide. Am J Psychiatry. 1984;141(2):206-209.
35. Jarbin H, Von Knorring AL. Suicide and suicide attempts in adolescent-onset psychotic disorders. Nord J Psychiatry. 2004;58(2):115-123.
36. Brewerton TD. Hyperreligiosity in psychotic disorders. J Nerv Ment Dis. 1994;182(5):302-304.
37. Getz GE, Fleck DE, Strakowski SM. Frequency and severity of religious delusions in Christian patients with psychosis. Psychiatry Res. 2001;103(1):87-91.
Treating patients with suspected ultra-rapid cycling bipolar disorder
Ultra-rapid cycling bipolar disorder: A critical look
Ultra-rapid cycling (URC) entered the psychiatric lexicon in the 1990s as a proposed descriptor for manic/hypomanic, mixed, or depressed episodes of bipolar disorder (BD) that occur every few days or weeks. DSM-IV-TR incorporates rapid cycling (RC)—but not URC—as a course specifier that occurs in 10% to 15% of patients with BD who have ≥4 distinct affective episodes per year, each fulfilling duration criteria and separated by identifiable recovery periods (unless an episode directly changes polarity). Since then, the terms RC and URC have seemingly metamorphosed into imprecise, popular colloquialisms meant to loosely describe frequent mood changes rather than distinct episodes over extended time periods, with little regard for the associated signs that define manic or hypomanic episodes.
This article examines the meaning and validity of URC in BD, its relevance and differentiation from rapid mood shifts in patients without BD, and concepts relevant to treatment extrapolated from studies of RC BD.
Imprecise nomenclature
Post et al1 coined the terms “ultra-rapid cycling” and “ultra-ultra-rapid cycling” (also called “ultradian cycling”) to describe mood episodes that occur monthly (URC) or over the course of as little as 1 day (ultradian cycling). These constructs are controversial because they lack demonstrated content validity and discriminant validity relative to other disorders. (“Content validity” refers to whether the features thought to comprise an entity of interest accurately and meaningfully do so; “discriminant validity” tells researchers and clinicians whether the proposed description of a clinical entity uniquely differentiates it from other disorders—avoiding “false-positive” suspected cases.) Clinicians therefore must pay careful attention to non-bipolar psychiatric problems that can present with rapid mood changes but without the psychomotor and related signs that define bipolar mood episodes. In their looser, nontechnical meanings, “rapid cycling” or “ultra-rapid cycling” may be synonymous with affective lability. RC is neither a diagnosis in itself nor a criterion for diagnosing BD. Rather, it is a course specifier to describe episode frequency in patients with past unambiguous manic or hypomanic episodes.
In children and adolescents, whose presentations often are atypical and can be hard to differentiate from other forms of behavioral or temperamental dysregulation, severe non-episodic mood dysregulation without signs of mania or hypomania may indicate a phenomenon separate from BD.2 Geller and colleagues3 proposed using the term “episodes” to frame the duration of a DSM-IV-defined syndrome of mania/hypomania or depression, while reserving the term “cycling” to connote patterns of mood alternation within a given episode. It is not clear whether this concept of “cycling” differs qualitatively from mood lability that arises during a mood episode in children or adults, and notably, this perspective does not account for changes in psychomotor signs in conjunction with changes in mood.
Clinicians also sometimes blur the concept of “mixed episodes” with RC or URC. DSM-IV-TR defines mixed episodes within bipolar I disorder (BD I) based on criteria for a simultaneous manic and depressive episode, rather than on frequent oscillations between affective poles. These and other differential diagnostic considerations for suspected URC are summarized in Table 1.4
A further concern regarding nomenclature involves the distinction between cyclicity (ie, successive episodes regardless of pole direction) and changes in polarity (ie, switches from depression to mania/hypomania or vice versa). Some mood disorder patients may have rapid oscillations from euthymia to depression while never changing polarity to mania/hypomania and may be best described as having recurrent brief depression.
Table 1
Differential diagnosis in suspected URC
| Phenomenon | Considerations for assessment |
|---|---|
| Mixed episodes in bipolar I disorder, or mixed depressive episodes in bipolar II disorder | DSM-IV-TR mixed episodes entail the co-occurrence of manic and depressive symptoms during the same episode without an intervening period of recovery. ICD-10 includes “rapid alternation of manic, hypomanic or depressive symptoms…from day to day or even hour to hour” in its definition of a mixed episode |
| Distress responses to acute environmental adversities (eg, adjustment disorders with mixed disturbance of emotions and conduct) | One would expect an absence of corresponding sleep-wake cycle changes or speech-language and psychomotor disturbances |
| Intoxication/withdrawal from psychoactive substances or drug-induced mental status changes (eg, corticosteroids, amphetamine, cocaine); a history of substance abuse also may be associated with development of URC in BD patients4 | Substance-induced mood fluctuations caused by intoxication/withdrawal can mimic affective cycling |
| Disinhibition states and frontal lobe syndromes as seen in traumatic brain injury and other CNS disorders, such as multiple sclerosis | Assess for signs of perseveration and history of head trauma or neurologic damage from cumulative toxic-metabolic insults (eg, chronic alcoholism) |
| Autonomic hyperarousal, emotional volatility, and hyperreactivity to environmental stresses, suggestive of PTSD | Determine the presence of a trauma history and review whether DSM-IV-TR symptoms and associated features of PTSD exist, including re-experiencing/reliving and avoidance, as well as paranoid thinking, dissociation, and nightmares |
| Recurrent mood shifts related to premenstrual dysphoric disorder may mimic URC. Other endocrine dysfunctions also may present with URC (eg, thyroid or ovarian malignancies) | Affirm the independent presence of BD before inferring its manifestations solely from premenstrual mood changes |
| Trait affective instability associated with borderline personality disorder | Trait mood instability is more chronic and enduring than episodic, and would not be expected to occur in tandem with signs of psychomotor activation that define mania/hypomania |
| BD: bipolar disorder; ICD-10: International Statistical Classification of Diseases and Related Health Problems, 10th revision; PTSD: posttraumatic stress disorder; URC: ultra-rapid cycling | |
Duration criteria
Clinicians and researchers have debated the minimum duration criteria for identifying manic or hypomanic episodes, and the extent to which suspected hypomanic periods of short duration constitute distinct illness phases. Although DSM-IV-TR designates 4 days as a minimum time for classifying an episode of hypomania, empirical studies suggest that mood symptoms lasting as few as 2 days may comprise a valid and reliably distinct entity relevant to RC.5 More limited data (mainly case observations) identify “affective oscillations” and “mood shifts” occurring faster than once per 24 hours in BD patients without comorbid personality disorders.6 Phenomenologic studies that have focused on 24- to 48-hour switch cycles have described new-onset URC arising spontaneously or following closed head injuries.7 In children and younger adolescents, reports have identified long index manic episodes (mean durations as long as 80 weeks)8 that involve continual (ultradian) mood cycling in as many as 80% of cases.9
Is URC a valid construct?
A central controversy surrounding the validity and meaningfulness of URC as a BD subtype involves its sole focus on mood variation rather than the fuller constellation of associated signs and symptoms that define episodes of mania/hypomania or depression. Abrupt, sudden, drastic, or dramatic mood shifts from one moment to the next are nowhere to be found in the DSM-IV-TR definition of BD, and the construct of mood lability or affective instability is neither a cardinal nor defining element of BD. Although individuals with BD I or bipolar II disorder (BD II) may have periods of affective lability, rapid shifts in mood are neither necessary nor sufficient for a BD diagnosis, and may indicate other types of psychopathology when affective instability occurs in the absence of a history of discernible manic or hypomanic episodes.
Studies by our group10 and others11 have shown that overattention to mood variation without considering associated cognitive, speech-language, chronobiologic, and motor signs of mania/hypomania accounts for substantial overdiagnosis of BD in patients with non-specific mood disturbances, particularly in those with active substance abuse or borderline personality disorder (BPD). Whereas the construct of RC BD attempts to account for changes in energy and psychomotor function as part of recurrent syndromes of mania/hypomania, existing literature on URC does not. Assessing mood changes in <24 hours also precludes assessing associated phenomena that occur over longer periods, such as changes in the sleep-wake cycle.
A rigorous, systematic approach to differential diagnosis for patients with affective instability is essential.
Borderline personality disorder
A common diagnostic debate regarding URC involves how to differentiate it from the chronic mood instability and reactivity inherent to BPD. Although some authors have suggested that RC BD and affective instability in BPD may be the same entity,12 others object to unifying the 2 conditions without considering their phenomenologic and other clinical differences. For example, affective instability arising from borderline character organization is thought to reflect a patient’s impaired capacity to self-regulate his or her internal state and emotional responses to interpersonal and other environmental stresses, or difficulty managing impulses. By contrast, manic or depressive phases of BD tend not to be “triggered” by interpersonal conflicts or frustrations. Furthermore, reframing intense mood reactions to the environment as bipolar variants carries several pitfalls: doing so wrongly accords patients a passive role in their reactions to life events, inaccurately reinforces a sense of victimization in response to stress, and diverts inquiry away from a patient’s active role in life decisions and circumstances that may be unsatisfying, self-defeating, or volatile.
Two key considerations may be helpful in discriminating rapid mood changes in BD vs BPD. First, some longitudinal studies indicate that RC often is a transient, rather than enduring, phenomenon in BD,13 in contrast to the nonvarying, trait feature of affective instability in persons with BPD. It is unknown whether URC is more enduring than transient. Notably, whereas bipolar mood episodes constitute deviations from a baseline state, affective instability in BPD is a baseline characteristic, rather than a deviation from it. Second, by definition, a BPD diagnosis hinges on additional elements unrelated to mood disturbances, such as interpersonal styles or defense mechanisms that involve splitting, projection, and projective identification, feelings of numbness, boredom, or emptiness, identity diffusion, fears of abandonment, and proclivities toward self-mutilation or other self-injurious behaviors as a means to alleviate tension and stress. These characteristics do not overlap with the core elements of BD.
Affective lability in patients with BPD entails prominent oscillations between anger and anxiety, or depression and anxiety, but not depression and elation14; by contrast, affective instability in BD has been linked with greater oscillations between euthymia and depression, and euthymia and elation, but not euthymia and anger.15 Moreover, daily mood fluctuations in patients with BD appear to occur in a relatively random fashion,16 whereas in BPD mood fluctuations are reactions that appear intimately linked to distressing interpersonal experiences.
See the table below, entitled “Rapid cycling and ultra-rapid cycling BD: A comparison,” comparing the phenomenology of RC and URC and a discussion of studies that explored genetic markers or family patterns that may be related to RC or URC.
Treatment considerations
No systematic studies exist for treating URC. Because most clinical trials of BD focus on treatment or prevention of a single episode rather than changes of mood over time, it is difficult to draw inferences about the ability of any treatment to attenuate marked, day-to-day mood variations. Some antimanic drugs, such as carbamazepine, have been suggested to offer better prophylactic efficacy compared with lithium for “non-classical” BD presentations, although the efficacy of carbamazepine has not been studied in URC.
Broadly speaking, treatment for URC, similar to RC, pragmatically involves:
- identifying and eliminating sources of mood destabilization (eg, substance abuse, erratic sleep patterns)
- treating medical comorbidities such as hypothyroidism
- optimizing treatment with mood stabilizing agents
- exercising caution when using antidepressants (see below).
Interestingly, despite frequent allusion to certain medications as “mood stabilizers,” no controlled study has examined mood instability on a day-to-day basis as a primary outcome measure in BD treatment, which limits the ability to surmise that any drug could be expected to diminish mood oscillations that occur over the course of days, or within a single day. However, a post hoc analysis by our group17 compared randomized treatment with lamotrigine or placebo over 6 months in RC BD I or BD II. Using prospective life charting, we found patients who received lamotrigine were almost twice as likely as those receiving placebo to achieve euthymia from one week to the next, which suggests the possibility that lamotrigine may offer benefit for affective instability in BD I or BD II patients, in addition to preventing discrete mood episodes.
Antidepressant controversy. Concerns that antidepressants might acutely induce mania or accelerate cycling frequency over long time periods have led to a contentious, long-standing debate within psychopharmacology. As noted in the box below, several long-term naturalistic follow-up studies have reported RC as a perceived consequence of antidepressants in most RC patients, although efforts to differentiate cycle acceleration caused by antidepressants (or other iatrogenic factors) from the natural course of illness remains exceedingly difficult without prospective randomized trials. (Antidepressants might cause more affective recurrences, but having multiple episodes may also cause more antidepressant prescriptions.) Some researchers (eg, Schneck et al18) have reported more frequent episodes among patients taking antidepressants but did not consider that patients with multiple episodes may be more likely to receive antidepressants, which fail to ameliorate acute or recurrent affective episodes. Importantly, a recent multi-site randomized trial by Ghaemi et al19 found that after a favorable acute response to antidepressants plus mood stabilizers, patients with preexisting RC who were randomized to continue antidepressants for up to 1 year had a 3-fold increased likelihood of developing a new depressive episode, which affirms suggestions that antidepressants do not help—but may exacerbate—cycling in patients with RC. No studies in BD have examined whether URC is more likely to arise as a consequence of antidepressant use.
Mood stabilizers and other biologic therapies. A small body of literature specifically addresses pharmacotherapy of URC in patients with BD (Table 2).19-26 A limitation of most existing literature is its focus on case reports, small open trials, or anecdotal observations rather than large, randomized controlled trials using systematic outcome measures. Extrapolation from reports focusing on patients with DSM-IV-TR RC is limited because it is uncertain whether URC differs fundamentally from RC and studies of DSM-IV-TR RC typically examine acute response during an index episode or time until relapse during maintenance therapy, rather than impact on mood changes over time.
Psychotherapy. A limited database on the efficacy of adjunctive cognitive-behavioral therapy (CBT) in RC BD describes improvement in depressive symptoms over short-term follow-up.27 No long-term studies of CBT or other structured psychotherapies have focused on RC or URC. Intuitively, one might expect that psychoeducation targeting sleep hygiene, substance use, stress management and coping skills, medication adherence, and prodrome recognition would be of value to patients with BD who experience frequent mood episodes, especially in those who may be unaware of or unfamiliar with basic concepts related to BD. In addition, relevant concepts from dialectical behavior therapy may be beneficial for BD patients with possible URC, such as skills to enhance emotional regulation, distress tolerance, mindfulness, and interpersonal effectiveness.
Table 2
Evidence-based treatments for ultra-rapid cycling BD
| Intervention | Strength of evidence | Comment |
|---|---|---|
| Antidepressant elimination | Cycling frequency may lengthen during antidepressant-free periods among patients with RC20; long-term (up to 1 year) antidepressant use in RC patients may increase the likelihood of depressive recurrences19 | Findings based mostly on small sample sizes; no controlled trials of antidepressant cessation as an intervention specifically for URC |
| Lithium | Single case report of ECT-induced URC resolved by lithium augmentation during continued ECT22 | No large-scale or randomized trials |
| Carbamazepine | No controlled trials or case reports | Possible anti-cycling benefits relevant for URC could be inferred from post hoc studies among patients with RC |
| Divalproex | Single case report describing resolution of a 48-hour cycle after augmentation of lithium with divalproex23 | No large-scale or randomized trials |
| Lamotrigine | Single case report of 100 mg/d lamotrigine augmentation to divalproex yielded 8 months of remission in a 25-year-old man with BD II and a long-standing pattern of 3 days of hypomania followed by 5 days of depression24 | No large-scale or randomized trials |
| Topiramate | Single case report in URC describing reduction of cycling frequency over 3 years25 | Multiple large scale placebo-controlled studies in bipolar mania have been negative |
| Second-generation antipsychotics | No controlled trials or case reports | Possible anti-cycling benefits relevant for URC could be inferred from post hoc studies in RC |
| Combinations of ≥2 mood stabilizing drugs | No controlled trials or case reports | Combining multiple anti-cycling agents is intuitively logical but largely unstudied |
| Nimodipine | 1 unipolar and 11 BD patients treated in randomized, off-on-off-on fashion (begun at 90 mg/d, increased up to 720 mg/d, mean duration of 12 weeks on active drug)26 | Response in 5 of 9 completers. Findings await replication with larger sample sizes |
| Hypermetabolic thyroid hormone (levothyroxine) | Findings from a small (N = 11) study of adjunctive high-dose levothyroxine (0.15 to 0.4 mg/d, with dosages increased by 0.05 to 0.1 mg/d every 1 to 2 weeks); an unspecified subgroup had “a very rapid cycling pattern” (reviewed by Bauer et al21) | 10 of 11 RC patients had reductions in depressive symptoms, 5 of 7 had improvement from baseline manic symptoms (observation period >60 days) |
| ECT | Case reports of improvement with ECT in refractory RC that was presumed secondary to tricyclic antidepressants | Reports of induction of URC by ECT22; whether or not ECT would more likely improve or exacerbate cyclicity for a given patient may require empirical determination |
| BD: bipolar disorder; BD II: bipolar II disorder; ECT: electroconvulsive therapy; RC: rapid cycling; URC: ultra-rapid cycling | ||
Treatment monitoring. Prospective life charting allows patients to systematically record manic/hypomanic and depressive symptoms day-to-day and week-to-week, thus creating a measure that may be particularly relevant for patients whose moods change rapidly. Simple mood charts (see Related Resources) typically take into account the severity of symptoms of either polarity with ratings of mild, moderate, or severe. Such visual records permit simple calculations over the course of a given interval (eg, week-by-week or across months) of several important parameters, including:
- number of days euthymic
- number of days with depression
- number of days with abnormal mood elevation
- number of occasions in which moods of both polarities occur on the same day.
Tracking these parameters during a treatment allows clinicians to make quantitative comparisons over time as a method of determining whether or not meaningful changes are occurring in cyclicity. See the figure below for an example of a completed mood chart and its interpretation.
Additional recommendations for assessing and managing cyclicity in BD are summarized in Table 3.
Table 3
Tips for managing suspected ultra-rapid cycling BD
| Do’s | Don’ts |
|---|---|
| Ascertain a history of ≥1 lifetime manic or hypomanic episode to diagnose BD | Diagnose BD solely on the presence of rapid mood fluctuations |
| Determine the presence of changes in sleep, energy, speech-language, and related behavior as correlates of mood to differentiate syndromes from isolated variation in mood | Ignore constellations of associated signs and symptoms of mania/hypomania |
| Obtain patient history to assess for head trauma or other medical and neurologic events that could have affective or other psychiatric manifestations | Disregard possible medical etiologies for new-onset affective dysregulation |
| Ascertain the resolution of 1 episode before counting the resurgence of symptoms as constituting a new episode; a waxing and waning course may reflect illness chronicity with incomplete recovery rather than true cyclicity | Misidentify incomplete recovery from an existing episode as the occurrence of new multiple episodes, which would inflate false-positive cases of RC or URC |
| Advise patients to refrain from alcohol or illicit substances that could destabilize mood | Assume that comorbid alcohol or illicit substance abuse will remit only after mood stabilization has been achieved, rather than the reverse |
| Monitor changes in sleep-wake cycles and the effects of erratic sleep or sleep deprivation on mood | Ignore the effects of poor sleep hygiene on mood |
| Minimize antidepressant exposure in patients with RC or URC | Continue long-term antidepressant maintenance therapy in patients with manic or mixed features or ongoing oscillations between mania/hypomania and depression |
| Assure euthyroid status and consider the potential utility of hypermetabolic levothyroxine | Assume that RC or URC will resolve solely by normalizing or optimizing thyroid function |
| Use rational, pharmacodynamically nonredundant anti-cycling drugs | Ignore the cumulative burden of adverse effects of multiple drugs |
| Consider the potential role for ECT as a strategy to arrest URC during any phase of BD | Assume ECT has value only during acute depressive phases of BD |
| Use prospective mood charting to document the evolution of mood changes over time, particularly when gauging treatment efficacy | Rely solely on impressionistic recall of mood states or polarity changes as reflecting distinct phasic changes |
| BD: bipolar disorder; ECT: electroconvulsive therapy; RC: rapid cycling; URC: ultra-rapid cycling | |
Table
Rapid cycling and ultra-rapid cycling BD: A comparison
| Construct | Rapid cycling | Ultra-rapid cycling |
|---|---|---|
| Bipolar I vs II | Predominantly BD IIa | No systematic data |
| Sex | Predominantly women | No systematic data |
| Longitudinal course | May be a transient phenomenon that can occur at any timeb or an enduring phenomenon that may persist for yearsc | Ultradian patterns may be more common across the first several episodes among pediatric BD patientsd |
| Age at onset | Associated with younger age at onsete | May be more evident in prepubescent onset mood disordersd; ultradian cycling more likely when onset occurs before age 13 than in adulthoode |
| Diurnal variation in mood | Morning-to-evening mood switches usually involve depression to mania/hypomania, with the opposite typifying evening-to-morning mood switchesf | Not reported |
| Relationship to environmental stresses | Life stresses may precede initial affective episodes but may be less important as subsequent episodes arise with increasing automaticity | No systematic data |
| Relationship to menstrual cycle | Despite case reports and self-reported links between RC and menstrual mood exacerbations, prospective data do not identify associations between RC and menstrual patternsg,h | No systematic data |
| Subclinical hypothyroidism | Bauer and Whybrow identified hypothyroidism independent of lithium use in 60% of 30 rapidly cycling BD patients, with evidence of improvement in a separate study of 11 RC patients given suprametabolic levothyroxine (reviewed by Bauer et ali) | No systematic data |
| Relationship to psychosis | Nonea | No systematic data |
| Relationship to antidepressant use | Naturalistic observations suggest RC may occur later in the illness course as a result of antidepressant use.c Small open case series data suggest shorter intermorbid intervals on antidepressants with longer intervals off antidepressants.j RC patients often receive antidepressants, but causal relationships are not well-documented.k Some case-control data dispute links between antidepressant use and RCl | No specific published cases |
| Considerations for suicide risk | RC linked with more serious suicide attemptsl | Suicide attempts may be associated with cycling within an episodem or rapid shifting in moodn |
| Time course for judging treatment efficacy | Efforts to diminish acute affective instability may be measured over the course of days to weeks | By definition, treatment of RC involves relapse prevention over the course of 1 year |
| BD: bipolar disorder; RC: rapid cycling | ||
| References a. Schneck CD, Miklowitz DJ, Calabrese JR, et al. Phenomenology of rapid-cycling bipolar disorder: data from the first 500 participants in the Systematic Treatment Enhancement Program. Am J Psychiatry. 2004;161(10):1902-1908. b. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics, diagnosis, family history, and course. Arch Gen Psychiatry. 1992;49(2):126-131. c. Koukopoulos A, Sani G, Koukopoulos AE, et al. Duration and stability of the rapid-cycling course: a long-term personal follow-up of 109 patients. J Affect Disord. 2003;73(1-2):75-85. d. Geller B, Tillman R, Bolhofner K, et al. Child bipolar I disorder: prospective continuity with adult bipolar I disorder; characteristics of second and third episodes; predictors of 8-year outcome. Arch Gen Psychiatry. 2008;65(10):1125-1133. e. Post RM, Leverich GS, Kupka RW, et al. Early-onset bipolar disorder and treatment delay are risk factors for poor outcome in adulthood. J Clin Psychiatry. 2010;71(7):864-872. f. Feldman-Naim S, Turner EH, Leibenluft E. Diurnal variation in the direction of mood switches in patients with rapid-cycling bipolar disorder. J Clin Psychiatry. 1997;58(2):79-84. g. Leibenluft E, Ashman SB, Feldman-Naim S, et al. Lack of relationship between menstrual cycle phase and mood in a sample of women with rapid cycling bipolar disorder. Biol Psychiatry. 1999;46(4):577-580. h. Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry. 1988;145(2):179-184. i. Bauer M, Beaulieu S, Dunner DL, et al. Rapid cycling bipolar disorder—diagnostic concepts. Bipolar Disord. 2008;10(1 Pt 2):153-162. j. Wehr TA, Goodwin FK. Can antidepressants cause mania and worsen the course of affective illness? Am J Psychiatry. 1987;144(11):1403-1411. k. Schneck CD, Miklowitz DJ, Miyahara S, et al. The prospective course of rapid-cycling bipolar disorder: findings from the STEP-BD. Am J Psychiatry. 2008;165(3):370-377. l. Coryell W, Solomon D, Turvey C, et al. The long-term course of rapid-cycling bipolar disorder. Arch Gen Psychiatry. 2003;60(9):914-920. m. Fawcett J, Scheftner W, Clark D, et al. Clinical predictors of suicide in patients with major affective disorders: a controlled prospective study. Am J Psychiatry. 1987;144(1):35-40. n. MacKinnon DF, Potash JB, McMahon FJ, et al. Rapid mood switching and suicidality in familial bipolar disorder. Bipolar Disord. 2005;7(5):441-448. | ||
From a biologic perspective, a handful of preliminary studies have examined genetic markers or familial patterns that might be related to rapid cycling (RC) or ultra-rapid cycling (URC). These include a reported link between URC and the low activity variant of the catechol-o-methyltransferase gene polymorphism in a small group of patients with velo-cardio-facial syndrome,a although this finding was not replicated in a larger sample.a Other preliminary reports on RC have implicated both the long (l) and short (s) allelic variants of the serotonin transporter gene (SLC6A4), the val66met variant of the brain-derived neurotrophic factor gene, and the circadian cryptochrome 2 (CRY2) gene (reviewed by Bauer et alb). These candidate loci have been examined in RC but not URC.
URC has not been examined as a familial entity, although in the National Institute of Mental Health Collaborative Depression Study, DSM-IV-TR RC did not occur with elevated frequency in bipolar pedigrees.c Rapid mood switches—abrupt rather than gradual transitions from one affective pole to another—appear to be only slightly, nonsignificantly more common in first-degree bipolar relatives of BD patients who themselves have rapid rather than gradual transitions from one affective pole to the other.d
Neuroimaging studies in BD seldom focus on subpopulations with RC or URC, and have been confined mainly to case reports that have yielded limited, non-generalizable observations, such as state-dependent variations in prefrontal activity during tasks of facial recognition (reviewed by Bauer et alb).
References
a. Papolos DF, Veit S, Faedda GL, et al. Ultra-ultra rapid cycling bipolar disorder is associated with the low activity catecholamine-O-methyltransferase allele. Mol Psychiatry. 1998;3(4):346-349.
b. Bauer M, Beaulieu S, Dunner DL, et al. Rapid cycling bipolar disorder—diagnostic concepts. Bipolar Disord. 2008;10(1 Pt 2):153-162.
c. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics, diagnosis, family history, and course. Arch Gen Psychiatry. 1992;49(2):126-131.
d. MacKinnon DF, Potash JB, McMahon FJ, et al. Rapid mood switching and suicidality in familial bipolar disorder. Bipolar Disord. 2005;7(5):441-448.
Figure: Example of prospective mood charting to document changes in manic/hypomanic and depressive symptoms across time
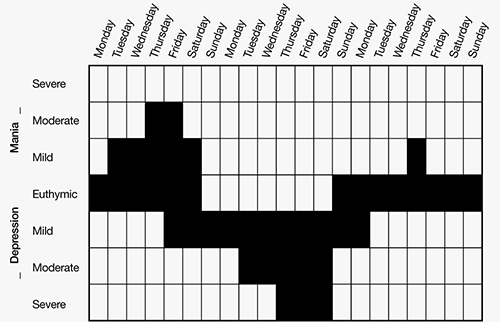
In the above example, the prevalence and severity of mood symptoms are identified over 21 days. Note the distinctly separate phases of mood elevation followed by depression, whereas euthymia was present only 6 of 21 days (29% of the time). Symptoms of at least moderate severity were more prominently depressive (5 of 21 days, or 24% of the time) than manic/hypomanic (2 of 21 days, or approximately 10% of the time). Mood charting does not capture associate DSM-IV-TR criteria for a mood episode but instead focuses solely on longitudinal changes in mood elevation or depression
Related Resources
- American Psychiatric Association practice guideline for the treatment of patients with bipolar disorder (revision). Am J Psychiatry. 2002;159(4 suppl):1-50.
- Massachusetts General Hospital Bipolar Clinic and Research Program. Sample mood chart (downloadable). www.manicdepressive.org/moodchart.html.
Drug Brand Names
- Carbamazepine • Equetro, Tegretol
- Divalproex • Depakote
- Lamotrigine • Lamictal
- Levothyroxine • Synthroid
- Lithium • Lithobid
- Nimodipine • Nimotop
- Topiramate • Topamax
Disclosures
Dr. Goldberg is on the speakers’ bureaus for AstraZeneca, Dey Pharmaceuticals, Eli Lilly and Company, Merck, and Sunovion and is a consultant for Axon Advisors, Dey Pharmaceuticals, Eli Lilly and Company, and Grünenthal Group.
Acknowledgment
The author wishes to thank David L. Dunner, MD, for his helpful comments regarding this article.
1. Kramlinger KG, Post RM. Ultra-rapid and ultradian cycling in bipolar affective illness. Br J Psychiatry. 1996;168(3):314-323.
2. Leibenluft E. Severe mood dysregulation irritability, and the diagnostic boundaries of bipolar disorder in youths. Am J Psychiatry. 2011;168(2):129-142.
3. Geller B, Tillman R, Bolhofner K. Proposed definitions of bipolar I disorder episodes and daily rapid cycling phenomena in preschoolers school-aged children, adolescents, and adults. J Child Adolesc Psychopharmacol. 2007;17(2):217-222.
4. Feinman JA, Dunner DL. The effect of alcohol and substance abuse on the course of bipolar affective disorder. J Affect Disord. 1996;37(1):43-49.
5. Maj M, Pirozzi R, Formicola AM, et al. Reliability and validity of four alternative definitions of rapid-cycling bipolar disorder. Am J Psychiatry. 1999;156(9):1421-1424.
6. Jenner FA, Gjessing LR, Cox JR, et al. A manic depressive psychotic with a persistent forty-eight hour cycle. Br J Psychiatry. 1967;113(501):895-910.
7. Zwil AS, McAllister TW, Cohen I, et al. Ultra-rapid cycling bipolar affective disorder following a closed-head injury. Brain Inj. 1993;7(2):147-152.
8. Geller B, Tillman R, Craney JL, et al. Four-year prospective outcome and natural history of mania in children with a prepubertal and early adolescent bipolar disorder phenotype. Arch Gen Psychiatry. 2004;61(5):459-467.
9. Geller B, Sun K, Zimerman B, et al. Complex and rapid-cycling in bipolar children and adolescents: a preliminary study. J Affect Disord. 1995;34(4):259-268.
10. Goldberg JF, Garno JL, Callahan AM, et al. Overdiagnosis of bipolar disorder among substance use disorder inpatients with mood instability. J Clin Psychiatry. 2008;69(11):1751-1757.
11. Zimmerman M, Ruggero CJ, Chelminski I, et al. Psychiatric diagnoses in patients previously overdiagnosed with bipolar disorder. J Clin Psychiatry. 2010;71(1):26-31.
12. MacKinnon DF, Pies R. Affective instability as rapid cycling: theoretical and clinical implications for borderline personality and bipolar spectrum disorders. Bipolar Disord. 2006;8(1):1-14.
13. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics diagnosis, family history, and course. Arch Gen Psychiatry. 1992;49(2):126-131.
14. Koenigsberg HW, Harvey PD, Mitropoulou V, et al. Characterizing affective instability in borderline personality disorder. Am J Psychiatry. 2002;159(5):784-788.
15. Henry C, Mitropoulou V, New AS, et al. Affective instability and impulsivity in borderline personality and bipolar II disorders: similarities and differences. J Psychiatr Res. 2001;35(6):307-312.
16. Gottschalk A, Bauer MS, Whybrow PC. Evidence of chaotic mood variation in bipolar disorder. Arch Gen Psychiatry. 1995;52(11):947-959.
17. Goldberg JF, Bowden CL, Calabrese JR, et al. Six-month prospective life charting of mood symptoms with lamotrigine monotherapy versus placebo in rapid cycling bipolar disorder. Biol Psychiatry. 2008;63(1):125-130.
18. Schneck CD, Miklowitz DJ, Miyahara S, et al. The prospective course of rapid-cycling bipolar disorder: findings from the STEP-BD. Am J Psychiatry. 2008;165(3):370-377.
19. Ghaemi SN, Ostacher MM, El-Mallakh RS, et al. Antidepressant discontinuation in bipolar depression: a Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) randomized clinical trial of long-term effectiveness and safety. J Clin Psychiatry. 2010;71(4):372-380.
20. Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry. 1988;145(2):179-184.
21. Bauer M, Beaulieu S, Dunner DL, et al. Rapid cycling bipolar disorder—diagnostic concepts. Bipolar Disord. 2008;10(1 Pt 2):153-162.
22. Zavorotnyy M, Diemer J, Patzelt J, et al. Occurrence of ultra-rapid cycling during electroconvulsive therapy in bipolar depression. World J Biol Psychiatry. 2009;10(4 Pt 3):987-990.
23. Lepkifker E, Iancu I, Dannon P, et al. Valproic acid in ultra-rapid cycling: a case report. Clin Neuropharmacol. 1995;18(1):72-75.
24. Woo YS, Chae JH, Jun TY, et al. Lamotrigine added to valproate successfully treated a case of ultra-rapid cycling bipolar disorder. Psychiatry Clin Neurosci. 2007;61(1):130-131.
25. Karama S, Lal S. Adjunctive topiramate in ultradian cycling bipolar disorder: case report with 3-year follow-up. Eur Psychiatry. 2006;21(4):280-281.
26. Pazzaglia PJ, Post RM, Ketter TA, et al. Preliminary controlled trial of nimodipine in ultra-rapid cycling affective dysregulation. Psychiatry Res. 1993;49(3):257-272.
27. Reilly-Harrington NA, Deckersbach T, Knauz R, et al. Cognitive behavioral therapy for rapid-cycling bipolar disorder: a pilot study. J Psychiatr Pract. 2007;13(5):291-297.
Ultra-rapid cycling (URC) entered the psychiatric lexicon in the 1990s as a proposed descriptor for manic/hypomanic, mixed, or depressed episodes of bipolar disorder (BD) that occur every few days or weeks. DSM-IV-TR incorporates rapid cycling (RC)—but not URC—as a course specifier that occurs in 10% to 15% of patients with BD who have ≥4 distinct affective episodes per year, each fulfilling duration criteria and separated by identifiable recovery periods (unless an episode directly changes polarity). Since then, the terms RC and URC have seemingly metamorphosed into imprecise, popular colloquialisms meant to loosely describe frequent mood changes rather than distinct episodes over extended time periods, with little regard for the associated signs that define manic or hypomanic episodes.
This article examines the meaning and validity of URC in BD, its relevance and differentiation from rapid mood shifts in patients without BD, and concepts relevant to treatment extrapolated from studies of RC BD.
Imprecise nomenclature
Post et al1 coined the terms “ultra-rapid cycling” and “ultra-ultra-rapid cycling” (also called “ultradian cycling”) to describe mood episodes that occur monthly (URC) or over the course of as little as 1 day (ultradian cycling). These constructs are controversial because they lack demonstrated content validity and discriminant validity relative to other disorders. (“Content validity” refers to whether the features thought to comprise an entity of interest accurately and meaningfully do so; “discriminant validity” tells researchers and clinicians whether the proposed description of a clinical entity uniquely differentiates it from other disorders—avoiding “false-positive” suspected cases.) Clinicians therefore must pay careful attention to non-bipolar psychiatric problems that can present with rapid mood changes but without the psychomotor and related signs that define bipolar mood episodes. In their looser, nontechnical meanings, “rapid cycling” or “ultra-rapid cycling” may be synonymous with affective lability. RC is neither a diagnosis in itself nor a criterion for diagnosing BD. Rather, it is a course specifier to describe episode frequency in patients with past unambiguous manic or hypomanic episodes.
In children and adolescents, whose presentations often are atypical and can be hard to differentiate from other forms of behavioral or temperamental dysregulation, severe non-episodic mood dysregulation without signs of mania or hypomania may indicate a phenomenon separate from BD.2 Geller and colleagues3 proposed using the term “episodes” to frame the duration of a DSM-IV-defined syndrome of mania/hypomania or depression, while reserving the term “cycling” to connote patterns of mood alternation within a given episode. It is not clear whether this concept of “cycling” differs qualitatively from mood lability that arises during a mood episode in children or adults, and notably, this perspective does not account for changes in psychomotor signs in conjunction with changes in mood.
Clinicians also sometimes blur the concept of “mixed episodes” with RC or URC. DSM-IV-TR defines mixed episodes within bipolar I disorder (BD I) based on criteria for a simultaneous manic and depressive episode, rather than on frequent oscillations between affective poles. These and other differential diagnostic considerations for suspected URC are summarized in Table 1.4
A further concern regarding nomenclature involves the distinction between cyclicity (ie, successive episodes regardless of pole direction) and changes in polarity (ie, switches from depression to mania/hypomania or vice versa). Some mood disorder patients may have rapid oscillations from euthymia to depression while never changing polarity to mania/hypomania and may be best described as having recurrent brief depression.
Table 1
Differential diagnosis in suspected URC
| Phenomenon | Considerations for assessment |
|---|---|
| Mixed episodes in bipolar I disorder, or mixed depressive episodes in bipolar II disorder | DSM-IV-TR mixed episodes entail the co-occurrence of manic and depressive symptoms during the same episode without an intervening period of recovery. ICD-10 includes “rapid alternation of manic, hypomanic or depressive symptoms…from day to day or even hour to hour” in its definition of a mixed episode |
| Distress responses to acute environmental adversities (eg, adjustment disorders with mixed disturbance of emotions and conduct) | One would expect an absence of corresponding sleep-wake cycle changes or speech-language and psychomotor disturbances |
| Intoxication/withdrawal from psychoactive substances or drug-induced mental status changes (eg, corticosteroids, amphetamine, cocaine); a history of substance abuse also may be associated with development of URC in BD patients4 | Substance-induced mood fluctuations caused by intoxication/withdrawal can mimic affective cycling |
| Disinhibition states and frontal lobe syndromes as seen in traumatic brain injury and other CNS disorders, such as multiple sclerosis | Assess for signs of perseveration and history of head trauma or neurologic damage from cumulative toxic-metabolic insults (eg, chronic alcoholism) |
| Autonomic hyperarousal, emotional volatility, and hyperreactivity to environmental stresses, suggestive of PTSD | Determine the presence of a trauma history and review whether DSM-IV-TR symptoms and associated features of PTSD exist, including re-experiencing/reliving and avoidance, as well as paranoid thinking, dissociation, and nightmares |
| Recurrent mood shifts related to premenstrual dysphoric disorder may mimic URC. Other endocrine dysfunctions also may present with URC (eg, thyroid or ovarian malignancies) | Affirm the independent presence of BD before inferring its manifestations solely from premenstrual mood changes |
| Trait affective instability associated with borderline personality disorder | Trait mood instability is more chronic and enduring than episodic, and would not be expected to occur in tandem with signs of psychomotor activation that define mania/hypomania |
| BD: bipolar disorder; ICD-10: International Statistical Classification of Diseases and Related Health Problems, 10th revision; PTSD: posttraumatic stress disorder; URC: ultra-rapid cycling | |
Duration criteria
Clinicians and researchers have debated the minimum duration criteria for identifying manic or hypomanic episodes, and the extent to which suspected hypomanic periods of short duration constitute distinct illness phases. Although DSM-IV-TR designates 4 days as a minimum time for classifying an episode of hypomania, empirical studies suggest that mood symptoms lasting as few as 2 days may comprise a valid and reliably distinct entity relevant to RC.5 More limited data (mainly case observations) identify “affective oscillations” and “mood shifts” occurring faster than once per 24 hours in BD patients without comorbid personality disorders.6 Phenomenologic studies that have focused on 24- to 48-hour switch cycles have described new-onset URC arising spontaneously or following closed head injuries.7 In children and younger adolescents, reports have identified long index manic episodes (mean durations as long as 80 weeks)8 that involve continual (ultradian) mood cycling in as many as 80% of cases.9
Is URC a valid construct?
A central controversy surrounding the validity and meaningfulness of URC as a BD subtype involves its sole focus on mood variation rather than the fuller constellation of associated signs and symptoms that define episodes of mania/hypomania or depression. Abrupt, sudden, drastic, or dramatic mood shifts from one moment to the next are nowhere to be found in the DSM-IV-TR definition of BD, and the construct of mood lability or affective instability is neither a cardinal nor defining element of BD. Although individuals with BD I or bipolar II disorder (BD II) may have periods of affective lability, rapid shifts in mood are neither necessary nor sufficient for a BD diagnosis, and may indicate other types of psychopathology when affective instability occurs in the absence of a history of discernible manic or hypomanic episodes.
Studies by our group10 and others11 have shown that overattention to mood variation without considering associated cognitive, speech-language, chronobiologic, and motor signs of mania/hypomania accounts for substantial overdiagnosis of BD in patients with non-specific mood disturbances, particularly in those with active substance abuse or borderline personality disorder (BPD). Whereas the construct of RC BD attempts to account for changes in energy and psychomotor function as part of recurrent syndromes of mania/hypomania, existing literature on URC does not. Assessing mood changes in <24 hours also precludes assessing associated phenomena that occur over longer periods, such as changes in the sleep-wake cycle.
A rigorous, systematic approach to differential diagnosis for patients with affective instability is essential.
Borderline personality disorder
A common diagnostic debate regarding URC involves how to differentiate it from the chronic mood instability and reactivity inherent to BPD. Although some authors have suggested that RC BD and affective instability in BPD may be the same entity,12 others object to unifying the 2 conditions without considering their phenomenologic and other clinical differences. For example, affective instability arising from borderline character organization is thought to reflect a patient’s impaired capacity to self-regulate his or her internal state and emotional responses to interpersonal and other environmental stresses, or difficulty managing impulses. By contrast, manic or depressive phases of BD tend not to be “triggered” by interpersonal conflicts or frustrations. Furthermore, reframing intense mood reactions to the environment as bipolar variants carries several pitfalls: doing so wrongly accords patients a passive role in their reactions to life events, inaccurately reinforces a sense of victimization in response to stress, and diverts inquiry away from a patient’s active role in life decisions and circumstances that may be unsatisfying, self-defeating, or volatile.
Two key considerations may be helpful in discriminating rapid mood changes in BD vs BPD. First, some longitudinal studies indicate that RC often is a transient, rather than enduring, phenomenon in BD,13 in contrast to the nonvarying, trait feature of affective instability in persons with BPD. It is unknown whether URC is more enduring than transient. Notably, whereas bipolar mood episodes constitute deviations from a baseline state, affective instability in BPD is a baseline characteristic, rather than a deviation from it. Second, by definition, a BPD diagnosis hinges on additional elements unrelated to mood disturbances, such as interpersonal styles or defense mechanisms that involve splitting, projection, and projective identification, feelings of numbness, boredom, or emptiness, identity diffusion, fears of abandonment, and proclivities toward self-mutilation or other self-injurious behaviors as a means to alleviate tension and stress. These characteristics do not overlap with the core elements of BD.
Affective lability in patients with BPD entails prominent oscillations between anger and anxiety, or depression and anxiety, but not depression and elation14; by contrast, affective instability in BD has been linked with greater oscillations between euthymia and depression, and euthymia and elation, but not euthymia and anger.15 Moreover, daily mood fluctuations in patients with BD appear to occur in a relatively random fashion,16 whereas in BPD mood fluctuations are reactions that appear intimately linked to distressing interpersonal experiences.
See the table below, entitled “Rapid cycling and ultra-rapid cycling BD: A comparison,” comparing the phenomenology of RC and URC and a discussion of studies that explored genetic markers or family patterns that may be related to RC or URC.
Treatment considerations
No systematic studies exist for treating URC. Because most clinical trials of BD focus on treatment or prevention of a single episode rather than changes of mood over time, it is difficult to draw inferences about the ability of any treatment to attenuate marked, day-to-day mood variations. Some antimanic drugs, such as carbamazepine, have been suggested to offer better prophylactic efficacy compared with lithium for “non-classical” BD presentations, although the efficacy of carbamazepine has not been studied in URC.
Broadly speaking, treatment for URC, similar to RC, pragmatically involves:
- identifying and eliminating sources of mood destabilization (eg, substance abuse, erratic sleep patterns)
- treating medical comorbidities such as hypothyroidism
- optimizing treatment with mood stabilizing agents
- exercising caution when using antidepressants (see below).
Interestingly, despite frequent allusion to certain medications as “mood stabilizers,” no controlled study has examined mood instability on a day-to-day basis as a primary outcome measure in BD treatment, which limits the ability to surmise that any drug could be expected to diminish mood oscillations that occur over the course of days, or within a single day. However, a post hoc analysis by our group17 compared randomized treatment with lamotrigine or placebo over 6 months in RC BD I or BD II. Using prospective life charting, we found patients who received lamotrigine were almost twice as likely as those receiving placebo to achieve euthymia from one week to the next, which suggests the possibility that lamotrigine may offer benefit for affective instability in BD I or BD II patients, in addition to preventing discrete mood episodes.
Antidepressant controversy. Concerns that antidepressants might acutely induce mania or accelerate cycling frequency over long time periods have led to a contentious, long-standing debate within psychopharmacology. As noted in the box below, several long-term naturalistic follow-up studies have reported RC as a perceived consequence of antidepressants in most RC patients, although efforts to differentiate cycle acceleration caused by antidepressants (or other iatrogenic factors) from the natural course of illness remains exceedingly difficult without prospective randomized trials. (Antidepressants might cause more affective recurrences, but having multiple episodes may also cause more antidepressant prescriptions.) Some researchers (eg, Schneck et al18) have reported more frequent episodes among patients taking antidepressants but did not consider that patients with multiple episodes may be more likely to receive antidepressants, which fail to ameliorate acute or recurrent affective episodes. Importantly, a recent multi-site randomized trial by Ghaemi et al19 found that after a favorable acute response to antidepressants plus mood stabilizers, patients with preexisting RC who were randomized to continue antidepressants for up to 1 year had a 3-fold increased likelihood of developing a new depressive episode, which affirms suggestions that antidepressants do not help—but may exacerbate—cycling in patients with RC. No studies in BD have examined whether URC is more likely to arise as a consequence of antidepressant use.
Mood stabilizers and other biologic therapies. A small body of literature specifically addresses pharmacotherapy of URC in patients with BD (Table 2).19-26 A limitation of most existing literature is its focus on case reports, small open trials, or anecdotal observations rather than large, randomized controlled trials using systematic outcome measures. Extrapolation from reports focusing on patients with DSM-IV-TR RC is limited because it is uncertain whether URC differs fundamentally from RC and studies of DSM-IV-TR RC typically examine acute response during an index episode or time until relapse during maintenance therapy, rather than impact on mood changes over time.
Psychotherapy. A limited database on the efficacy of adjunctive cognitive-behavioral therapy (CBT) in RC BD describes improvement in depressive symptoms over short-term follow-up.27 No long-term studies of CBT or other structured psychotherapies have focused on RC or URC. Intuitively, one might expect that psychoeducation targeting sleep hygiene, substance use, stress management and coping skills, medication adherence, and prodrome recognition would be of value to patients with BD who experience frequent mood episodes, especially in those who may be unaware of or unfamiliar with basic concepts related to BD. In addition, relevant concepts from dialectical behavior therapy may be beneficial for BD patients with possible URC, such as skills to enhance emotional regulation, distress tolerance, mindfulness, and interpersonal effectiveness.
Table 2
Evidence-based treatments for ultra-rapid cycling BD
| Intervention | Strength of evidence | Comment |
|---|---|---|
| Antidepressant elimination | Cycling frequency may lengthen during antidepressant-free periods among patients with RC20; long-term (up to 1 year) antidepressant use in RC patients may increase the likelihood of depressive recurrences19 | Findings based mostly on small sample sizes; no controlled trials of antidepressant cessation as an intervention specifically for URC |
| Lithium | Single case report of ECT-induced URC resolved by lithium augmentation during continued ECT22 | No large-scale or randomized trials |
| Carbamazepine | No controlled trials or case reports | Possible anti-cycling benefits relevant for URC could be inferred from post hoc studies among patients with RC |
| Divalproex | Single case report describing resolution of a 48-hour cycle after augmentation of lithium with divalproex23 | No large-scale or randomized trials |
| Lamotrigine | Single case report of 100 mg/d lamotrigine augmentation to divalproex yielded 8 months of remission in a 25-year-old man with BD II and a long-standing pattern of 3 days of hypomania followed by 5 days of depression24 | No large-scale or randomized trials |
| Topiramate | Single case report in URC describing reduction of cycling frequency over 3 years25 | Multiple large scale placebo-controlled studies in bipolar mania have been negative |
| Second-generation antipsychotics | No controlled trials or case reports | Possible anti-cycling benefits relevant for URC could be inferred from post hoc studies in RC |
| Combinations of ≥2 mood stabilizing drugs | No controlled trials or case reports | Combining multiple anti-cycling agents is intuitively logical but largely unstudied |
| Nimodipine | 1 unipolar and 11 BD patients treated in randomized, off-on-off-on fashion (begun at 90 mg/d, increased up to 720 mg/d, mean duration of 12 weeks on active drug)26 | Response in 5 of 9 completers. Findings await replication with larger sample sizes |
| Hypermetabolic thyroid hormone (levothyroxine) | Findings from a small (N = 11) study of adjunctive high-dose levothyroxine (0.15 to 0.4 mg/d, with dosages increased by 0.05 to 0.1 mg/d every 1 to 2 weeks); an unspecified subgroup had “a very rapid cycling pattern” (reviewed by Bauer et al21) | 10 of 11 RC patients had reductions in depressive symptoms, 5 of 7 had improvement from baseline manic symptoms (observation period >60 days) |
| ECT | Case reports of improvement with ECT in refractory RC that was presumed secondary to tricyclic antidepressants | Reports of induction of URC by ECT22; whether or not ECT would more likely improve or exacerbate cyclicity for a given patient may require empirical determination |
| BD: bipolar disorder; BD II: bipolar II disorder; ECT: electroconvulsive therapy; RC: rapid cycling; URC: ultra-rapid cycling | ||
Treatment monitoring. Prospective life charting allows patients to systematically record manic/hypomanic and depressive symptoms day-to-day and week-to-week, thus creating a measure that may be particularly relevant for patients whose moods change rapidly. Simple mood charts (see Related Resources) typically take into account the severity of symptoms of either polarity with ratings of mild, moderate, or severe. Such visual records permit simple calculations over the course of a given interval (eg, week-by-week or across months) of several important parameters, including:
- number of days euthymic
- number of days with depression
- number of days with abnormal mood elevation
- number of occasions in which moods of both polarities occur on the same day.
Tracking these parameters during a treatment allows clinicians to make quantitative comparisons over time as a method of determining whether or not meaningful changes are occurring in cyclicity. See the figure below for an example of a completed mood chart and its interpretation.
Additional recommendations for assessing and managing cyclicity in BD are summarized in Table 3.
Table 3
Tips for managing suspected ultra-rapid cycling BD
| Do’s | Don’ts |
|---|---|
| Ascertain a history of ≥1 lifetime manic or hypomanic episode to diagnose BD | Diagnose BD solely on the presence of rapid mood fluctuations |
| Determine the presence of changes in sleep, energy, speech-language, and related behavior as correlates of mood to differentiate syndromes from isolated variation in mood | Ignore constellations of associated signs and symptoms of mania/hypomania |
| Obtain patient history to assess for head trauma or other medical and neurologic events that could have affective or other psychiatric manifestations | Disregard possible medical etiologies for new-onset affective dysregulation |
| Ascertain the resolution of 1 episode before counting the resurgence of symptoms as constituting a new episode; a waxing and waning course may reflect illness chronicity with incomplete recovery rather than true cyclicity | Misidentify incomplete recovery from an existing episode as the occurrence of new multiple episodes, which would inflate false-positive cases of RC or URC |
| Advise patients to refrain from alcohol or illicit substances that could destabilize mood | Assume that comorbid alcohol or illicit substance abuse will remit only after mood stabilization has been achieved, rather than the reverse |
| Monitor changes in sleep-wake cycles and the effects of erratic sleep or sleep deprivation on mood | Ignore the effects of poor sleep hygiene on mood |
| Minimize antidepressant exposure in patients with RC or URC | Continue long-term antidepressant maintenance therapy in patients with manic or mixed features or ongoing oscillations between mania/hypomania and depression |
| Assure euthyroid status and consider the potential utility of hypermetabolic levothyroxine | Assume that RC or URC will resolve solely by normalizing or optimizing thyroid function |
| Use rational, pharmacodynamically nonredundant anti-cycling drugs | Ignore the cumulative burden of adverse effects of multiple drugs |
| Consider the potential role for ECT as a strategy to arrest URC during any phase of BD | Assume ECT has value only during acute depressive phases of BD |
| Use prospective mood charting to document the evolution of mood changes over time, particularly when gauging treatment efficacy | Rely solely on impressionistic recall of mood states or polarity changes as reflecting distinct phasic changes |
| BD: bipolar disorder; ECT: electroconvulsive therapy; RC: rapid cycling; URC: ultra-rapid cycling | |
Table
Rapid cycling and ultra-rapid cycling BD: A comparison
| Construct | Rapid cycling | Ultra-rapid cycling |
|---|---|---|
| Bipolar I vs II | Predominantly BD IIa | No systematic data |
| Sex | Predominantly women | No systematic data |
| Longitudinal course | May be a transient phenomenon that can occur at any timeb or an enduring phenomenon that may persist for yearsc | Ultradian patterns may be more common across the first several episodes among pediatric BD patientsd |
| Age at onset | Associated with younger age at onsete | May be more evident in prepubescent onset mood disordersd; ultradian cycling more likely when onset occurs before age 13 than in adulthoode |
| Diurnal variation in mood | Morning-to-evening mood switches usually involve depression to mania/hypomania, with the opposite typifying evening-to-morning mood switchesf | Not reported |
| Relationship to environmental stresses | Life stresses may precede initial affective episodes but may be less important as subsequent episodes arise with increasing automaticity | No systematic data |
| Relationship to menstrual cycle | Despite case reports and self-reported links between RC and menstrual mood exacerbations, prospective data do not identify associations between RC and menstrual patternsg,h | No systematic data |
| Subclinical hypothyroidism | Bauer and Whybrow identified hypothyroidism independent of lithium use in 60% of 30 rapidly cycling BD patients, with evidence of improvement in a separate study of 11 RC patients given suprametabolic levothyroxine (reviewed by Bauer et ali) | No systematic data |
| Relationship to psychosis | Nonea | No systematic data |
| Relationship to antidepressant use | Naturalistic observations suggest RC may occur later in the illness course as a result of antidepressant use.c Small open case series data suggest shorter intermorbid intervals on antidepressants with longer intervals off antidepressants.j RC patients often receive antidepressants, but causal relationships are not well-documented.k Some case-control data dispute links between antidepressant use and RCl | No specific published cases |
| Considerations for suicide risk | RC linked with more serious suicide attemptsl | Suicide attempts may be associated with cycling within an episodem or rapid shifting in moodn |
| Time course for judging treatment efficacy | Efforts to diminish acute affective instability may be measured over the course of days to weeks | By definition, treatment of RC involves relapse prevention over the course of 1 year |
| BD: bipolar disorder; RC: rapid cycling | ||
| References a. Schneck CD, Miklowitz DJ, Calabrese JR, et al. Phenomenology of rapid-cycling bipolar disorder: data from the first 500 participants in the Systematic Treatment Enhancement Program. Am J Psychiatry. 2004;161(10):1902-1908. b. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics, diagnosis, family history, and course. Arch Gen Psychiatry. 1992;49(2):126-131. c. Koukopoulos A, Sani G, Koukopoulos AE, et al. Duration and stability of the rapid-cycling course: a long-term personal follow-up of 109 patients. J Affect Disord. 2003;73(1-2):75-85. d. Geller B, Tillman R, Bolhofner K, et al. Child bipolar I disorder: prospective continuity with adult bipolar I disorder; characteristics of second and third episodes; predictors of 8-year outcome. Arch Gen Psychiatry. 2008;65(10):1125-1133. e. Post RM, Leverich GS, Kupka RW, et al. Early-onset bipolar disorder and treatment delay are risk factors for poor outcome in adulthood. J Clin Psychiatry. 2010;71(7):864-872. f. Feldman-Naim S, Turner EH, Leibenluft E. Diurnal variation in the direction of mood switches in patients with rapid-cycling bipolar disorder. J Clin Psychiatry. 1997;58(2):79-84. g. Leibenluft E, Ashman SB, Feldman-Naim S, et al. Lack of relationship between menstrual cycle phase and mood in a sample of women with rapid cycling bipolar disorder. Biol Psychiatry. 1999;46(4):577-580. h. Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry. 1988;145(2):179-184. i. Bauer M, Beaulieu S, Dunner DL, et al. Rapid cycling bipolar disorder—diagnostic concepts. Bipolar Disord. 2008;10(1 Pt 2):153-162. j. Wehr TA, Goodwin FK. Can antidepressants cause mania and worsen the course of affective illness? Am J Psychiatry. 1987;144(11):1403-1411. k. Schneck CD, Miklowitz DJ, Miyahara S, et al. The prospective course of rapid-cycling bipolar disorder: findings from the STEP-BD. Am J Psychiatry. 2008;165(3):370-377. l. Coryell W, Solomon D, Turvey C, et al. The long-term course of rapid-cycling bipolar disorder. Arch Gen Psychiatry. 2003;60(9):914-920. m. Fawcett J, Scheftner W, Clark D, et al. Clinical predictors of suicide in patients with major affective disorders: a controlled prospective study. Am J Psychiatry. 1987;144(1):35-40. n. MacKinnon DF, Potash JB, McMahon FJ, et al. Rapid mood switching and suicidality in familial bipolar disorder. Bipolar Disord. 2005;7(5):441-448. | ||
From a biologic perspective, a handful of preliminary studies have examined genetic markers or familial patterns that might be related to rapid cycling (RC) or ultra-rapid cycling (URC). These include a reported link between URC and the low activity variant of the catechol-o-methyltransferase gene polymorphism in a small group of patients with velo-cardio-facial syndrome,a although this finding was not replicated in a larger sample.a Other preliminary reports on RC have implicated both the long (l) and short (s) allelic variants of the serotonin transporter gene (SLC6A4), the val66met variant of the brain-derived neurotrophic factor gene, and the circadian cryptochrome 2 (CRY2) gene (reviewed by Bauer et alb). These candidate loci have been examined in RC but not URC.
URC has not been examined as a familial entity, although in the National Institute of Mental Health Collaborative Depression Study, DSM-IV-TR RC did not occur with elevated frequency in bipolar pedigrees.c Rapid mood switches—abrupt rather than gradual transitions from one affective pole to another—appear to be only slightly, nonsignificantly more common in first-degree bipolar relatives of BD patients who themselves have rapid rather than gradual transitions from one affective pole to the other.d
Neuroimaging studies in BD seldom focus on subpopulations with RC or URC, and have been confined mainly to case reports that have yielded limited, non-generalizable observations, such as state-dependent variations in prefrontal activity during tasks of facial recognition (reviewed by Bauer et alb).
References
a. Papolos DF, Veit S, Faedda GL, et al. Ultra-ultra rapid cycling bipolar disorder is associated with the low activity catecholamine-O-methyltransferase allele. Mol Psychiatry. 1998;3(4):346-349.
b. Bauer M, Beaulieu S, Dunner DL, et al. Rapid cycling bipolar disorder—diagnostic concepts. Bipolar Disord. 2008;10(1 Pt 2):153-162.
c. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics, diagnosis, family history, and course. Arch Gen Psychiatry. 1992;49(2):126-131.
d. MacKinnon DF, Potash JB, McMahon FJ, et al. Rapid mood switching and suicidality in familial bipolar disorder. Bipolar Disord. 2005;7(5):441-448.
Figure: Example of prospective mood charting to document changes in manic/hypomanic and depressive symptoms across time
In the above example, the prevalence and severity of mood symptoms are identified over 21 days. Note the distinctly separate phases of mood elevation followed by depression, whereas euthymia was present only 6 of 21 days (29% of the time). Symptoms of at least moderate severity were more prominently depressive (5 of 21 days, or 24% of the time) than manic/hypomanic (2 of 21 days, or approximately 10% of the time). Mood charting does not capture associate DSM-IV-TR criteria for a mood episode but instead focuses solely on longitudinal changes in mood elevation or depression
Related Resources
- American Psychiatric Association practice guideline for the treatment of patients with bipolar disorder (revision). Am J Psychiatry. 2002;159(4 suppl):1-50.
- Massachusetts General Hospital Bipolar Clinic and Research Program. Sample mood chart (downloadable). www.manicdepressive.org/moodchart.html.
Drug Brand Names
- Carbamazepine • Equetro, Tegretol
- Divalproex • Depakote
- Lamotrigine • Lamictal
- Levothyroxine • Synthroid
- Lithium • Lithobid
- Nimodipine • Nimotop
- Topiramate • Topamax
Disclosures
Dr. Goldberg is on the speakers’ bureaus for AstraZeneca, Dey Pharmaceuticals, Eli Lilly and Company, Merck, and Sunovion and is a consultant for Axon Advisors, Dey Pharmaceuticals, Eli Lilly and Company, and Grünenthal Group.
Acknowledgment
The author wishes to thank David L. Dunner, MD, for his helpful comments regarding this article.
Ultra-rapid cycling (URC) entered the psychiatric lexicon in the 1990s as a proposed descriptor for manic/hypomanic, mixed, or depressed episodes of bipolar disorder (BD) that occur every few days or weeks. DSM-IV-TR incorporates rapid cycling (RC)—but not URC—as a course specifier that occurs in 10% to 15% of patients with BD who have ≥4 distinct affective episodes per year, each fulfilling duration criteria and separated by identifiable recovery periods (unless an episode directly changes polarity). Since then, the terms RC and URC have seemingly metamorphosed into imprecise, popular colloquialisms meant to loosely describe frequent mood changes rather than distinct episodes over extended time periods, with little regard for the associated signs that define manic or hypomanic episodes.
This article examines the meaning and validity of URC in BD, its relevance and differentiation from rapid mood shifts in patients without BD, and concepts relevant to treatment extrapolated from studies of RC BD.
Imprecise nomenclature
Post et al1 coined the terms “ultra-rapid cycling” and “ultra-ultra-rapid cycling” (also called “ultradian cycling”) to describe mood episodes that occur monthly (URC) or over the course of as little as 1 day (ultradian cycling). These constructs are controversial because they lack demonstrated content validity and discriminant validity relative to other disorders. (“Content validity” refers to whether the features thought to comprise an entity of interest accurately and meaningfully do so; “discriminant validity” tells researchers and clinicians whether the proposed description of a clinical entity uniquely differentiates it from other disorders—avoiding “false-positive” suspected cases.) Clinicians therefore must pay careful attention to non-bipolar psychiatric problems that can present with rapid mood changes but without the psychomotor and related signs that define bipolar mood episodes. In their looser, nontechnical meanings, “rapid cycling” or “ultra-rapid cycling” may be synonymous with affective lability. RC is neither a diagnosis in itself nor a criterion for diagnosing BD. Rather, it is a course specifier to describe episode frequency in patients with past unambiguous manic or hypomanic episodes.
In children and adolescents, whose presentations often are atypical and can be hard to differentiate from other forms of behavioral or temperamental dysregulation, severe non-episodic mood dysregulation without signs of mania or hypomania may indicate a phenomenon separate from BD.2 Geller and colleagues3 proposed using the term “episodes” to frame the duration of a DSM-IV-defined syndrome of mania/hypomania or depression, while reserving the term “cycling” to connote patterns of mood alternation within a given episode. It is not clear whether this concept of “cycling” differs qualitatively from mood lability that arises during a mood episode in children or adults, and notably, this perspective does not account for changes in psychomotor signs in conjunction with changes in mood.
Clinicians also sometimes blur the concept of “mixed episodes” with RC or URC. DSM-IV-TR defines mixed episodes within bipolar I disorder (BD I) based on criteria for a simultaneous manic and depressive episode, rather than on frequent oscillations between affective poles. These and other differential diagnostic considerations for suspected URC are summarized in Table 1.4
A further concern regarding nomenclature involves the distinction between cyclicity (ie, successive episodes regardless of pole direction) and changes in polarity (ie, switches from depression to mania/hypomania or vice versa). Some mood disorder patients may have rapid oscillations from euthymia to depression while never changing polarity to mania/hypomania and may be best described as having recurrent brief depression.
Table 1
Differential diagnosis in suspected URC
| Phenomenon | Considerations for assessment |
|---|---|
| Mixed episodes in bipolar I disorder, or mixed depressive episodes in bipolar II disorder | DSM-IV-TR mixed episodes entail the co-occurrence of manic and depressive symptoms during the same episode without an intervening period of recovery. ICD-10 includes “rapid alternation of manic, hypomanic or depressive symptoms…from day to day or even hour to hour” in its definition of a mixed episode |
| Distress responses to acute environmental adversities (eg, adjustment disorders with mixed disturbance of emotions and conduct) | One would expect an absence of corresponding sleep-wake cycle changes or speech-language and psychomotor disturbances |
| Intoxication/withdrawal from psychoactive substances or drug-induced mental status changes (eg, corticosteroids, amphetamine, cocaine); a history of substance abuse also may be associated with development of URC in BD patients4 | Substance-induced mood fluctuations caused by intoxication/withdrawal can mimic affective cycling |
| Disinhibition states and frontal lobe syndromes as seen in traumatic brain injury and other CNS disorders, such as multiple sclerosis | Assess for signs of perseveration and history of head trauma or neurologic damage from cumulative toxic-metabolic insults (eg, chronic alcoholism) |
| Autonomic hyperarousal, emotional volatility, and hyperreactivity to environmental stresses, suggestive of PTSD | Determine the presence of a trauma history and review whether DSM-IV-TR symptoms and associated features of PTSD exist, including re-experiencing/reliving and avoidance, as well as paranoid thinking, dissociation, and nightmares |
| Recurrent mood shifts related to premenstrual dysphoric disorder may mimic URC. Other endocrine dysfunctions also may present with URC (eg, thyroid or ovarian malignancies) | Affirm the independent presence of BD before inferring its manifestations solely from premenstrual mood changes |
| Trait affective instability associated with borderline personality disorder | Trait mood instability is more chronic and enduring than episodic, and would not be expected to occur in tandem with signs of psychomotor activation that define mania/hypomania |
| BD: bipolar disorder; ICD-10: International Statistical Classification of Diseases and Related Health Problems, 10th revision; PTSD: posttraumatic stress disorder; URC: ultra-rapid cycling | |
Duration criteria
Clinicians and researchers have debated the minimum duration criteria for identifying manic or hypomanic episodes, and the extent to which suspected hypomanic periods of short duration constitute distinct illness phases. Although DSM-IV-TR designates 4 days as a minimum time for classifying an episode of hypomania, empirical studies suggest that mood symptoms lasting as few as 2 days may comprise a valid and reliably distinct entity relevant to RC.5 More limited data (mainly case observations) identify “affective oscillations” and “mood shifts” occurring faster than once per 24 hours in BD patients without comorbid personality disorders.6 Phenomenologic studies that have focused on 24- to 48-hour switch cycles have described new-onset URC arising spontaneously or following closed head injuries.7 In children and younger adolescents, reports have identified long index manic episodes (mean durations as long as 80 weeks)8 that involve continual (ultradian) mood cycling in as many as 80% of cases.9
Is URC a valid construct?
A central controversy surrounding the validity and meaningfulness of URC as a BD subtype involves its sole focus on mood variation rather than the fuller constellation of associated signs and symptoms that define episodes of mania/hypomania or depression. Abrupt, sudden, drastic, or dramatic mood shifts from one moment to the next are nowhere to be found in the DSM-IV-TR definition of BD, and the construct of mood lability or affective instability is neither a cardinal nor defining element of BD. Although individuals with BD I or bipolar II disorder (BD II) may have periods of affective lability, rapid shifts in mood are neither necessary nor sufficient for a BD diagnosis, and may indicate other types of psychopathology when affective instability occurs in the absence of a history of discernible manic or hypomanic episodes.
Studies by our group10 and others11 have shown that overattention to mood variation without considering associated cognitive, speech-language, chronobiologic, and motor signs of mania/hypomania accounts for substantial overdiagnosis of BD in patients with non-specific mood disturbances, particularly in those with active substance abuse or borderline personality disorder (BPD). Whereas the construct of RC BD attempts to account for changes in energy and psychomotor function as part of recurrent syndromes of mania/hypomania, existing literature on URC does not. Assessing mood changes in <24 hours also precludes assessing associated phenomena that occur over longer periods, such as changes in the sleep-wake cycle.
A rigorous, systematic approach to differential diagnosis for patients with affective instability is essential.
Borderline personality disorder
A common diagnostic debate regarding URC involves how to differentiate it from the chronic mood instability and reactivity inherent to BPD. Although some authors have suggested that RC BD and affective instability in BPD may be the same entity,12 others object to unifying the 2 conditions without considering their phenomenologic and other clinical differences. For example, affective instability arising from borderline character organization is thought to reflect a patient’s impaired capacity to self-regulate his or her internal state and emotional responses to interpersonal and other environmental stresses, or difficulty managing impulses. By contrast, manic or depressive phases of BD tend not to be “triggered” by interpersonal conflicts or frustrations. Furthermore, reframing intense mood reactions to the environment as bipolar variants carries several pitfalls: doing so wrongly accords patients a passive role in their reactions to life events, inaccurately reinforces a sense of victimization in response to stress, and diverts inquiry away from a patient’s active role in life decisions and circumstances that may be unsatisfying, self-defeating, or volatile.
Two key considerations may be helpful in discriminating rapid mood changes in BD vs BPD. First, some longitudinal studies indicate that RC often is a transient, rather than enduring, phenomenon in BD,13 in contrast to the nonvarying, trait feature of affective instability in persons with BPD. It is unknown whether URC is more enduring than transient. Notably, whereas bipolar mood episodes constitute deviations from a baseline state, affective instability in BPD is a baseline characteristic, rather than a deviation from it. Second, by definition, a BPD diagnosis hinges on additional elements unrelated to mood disturbances, such as interpersonal styles or defense mechanisms that involve splitting, projection, and projective identification, feelings of numbness, boredom, or emptiness, identity diffusion, fears of abandonment, and proclivities toward self-mutilation or other self-injurious behaviors as a means to alleviate tension and stress. These characteristics do not overlap with the core elements of BD.
Affective lability in patients with BPD entails prominent oscillations between anger and anxiety, or depression and anxiety, but not depression and elation14; by contrast, affective instability in BD has been linked with greater oscillations between euthymia and depression, and euthymia and elation, but not euthymia and anger.15 Moreover, daily mood fluctuations in patients with BD appear to occur in a relatively random fashion,16 whereas in BPD mood fluctuations are reactions that appear intimately linked to distressing interpersonal experiences.
See the table below, entitled “Rapid cycling and ultra-rapid cycling BD: A comparison,” comparing the phenomenology of RC and URC and a discussion of studies that explored genetic markers or family patterns that may be related to RC or URC.
Treatment considerations
No systematic studies exist for treating URC. Because most clinical trials of BD focus on treatment or prevention of a single episode rather than changes of mood over time, it is difficult to draw inferences about the ability of any treatment to attenuate marked, day-to-day mood variations. Some antimanic drugs, such as carbamazepine, have been suggested to offer better prophylactic efficacy compared with lithium for “non-classical” BD presentations, although the efficacy of carbamazepine has not been studied in URC.
Broadly speaking, treatment for URC, similar to RC, pragmatically involves:
- identifying and eliminating sources of mood destabilization (eg, substance abuse, erratic sleep patterns)
- treating medical comorbidities such as hypothyroidism
- optimizing treatment with mood stabilizing agents
- exercising caution when using antidepressants (see below).
Interestingly, despite frequent allusion to certain medications as “mood stabilizers,” no controlled study has examined mood instability on a day-to-day basis as a primary outcome measure in BD treatment, which limits the ability to surmise that any drug could be expected to diminish mood oscillations that occur over the course of days, or within a single day. However, a post hoc analysis by our group17 compared randomized treatment with lamotrigine or placebo over 6 months in RC BD I or BD II. Using prospective life charting, we found patients who received lamotrigine were almost twice as likely as those receiving placebo to achieve euthymia from one week to the next, which suggests the possibility that lamotrigine may offer benefit for affective instability in BD I or BD II patients, in addition to preventing discrete mood episodes.
Antidepressant controversy. Concerns that antidepressants might acutely induce mania or accelerate cycling frequency over long time periods have led to a contentious, long-standing debate within psychopharmacology. As noted in the box below, several long-term naturalistic follow-up studies have reported RC as a perceived consequence of antidepressants in most RC patients, although efforts to differentiate cycle acceleration caused by antidepressants (or other iatrogenic factors) from the natural course of illness remains exceedingly difficult without prospective randomized trials. (Antidepressants might cause more affective recurrences, but having multiple episodes may also cause more antidepressant prescriptions.) Some researchers (eg, Schneck et al18) have reported more frequent episodes among patients taking antidepressants but did not consider that patients with multiple episodes may be more likely to receive antidepressants, which fail to ameliorate acute or recurrent affective episodes. Importantly, a recent multi-site randomized trial by Ghaemi et al19 found that after a favorable acute response to antidepressants plus mood stabilizers, patients with preexisting RC who were randomized to continue antidepressants for up to 1 year had a 3-fold increased likelihood of developing a new depressive episode, which affirms suggestions that antidepressants do not help—but may exacerbate—cycling in patients with RC. No studies in BD have examined whether URC is more likely to arise as a consequence of antidepressant use.
Mood stabilizers and other biologic therapies. A small body of literature specifically addresses pharmacotherapy of URC in patients with BD (Table 2).19-26 A limitation of most existing literature is its focus on case reports, small open trials, or anecdotal observations rather than large, randomized controlled trials using systematic outcome measures. Extrapolation from reports focusing on patients with DSM-IV-TR RC is limited because it is uncertain whether URC differs fundamentally from RC and studies of DSM-IV-TR RC typically examine acute response during an index episode or time until relapse during maintenance therapy, rather than impact on mood changes over time.
Psychotherapy. A limited database on the efficacy of adjunctive cognitive-behavioral therapy (CBT) in RC BD describes improvement in depressive symptoms over short-term follow-up.27 No long-term studies of CBT or other structured psychotherapies have focused on RC or URC. Intuitively, one might expect that psychoeducation targeting sleep hygiene, substance use, stress management and coping skills, medication adherence, and prodrome recognition would be of value to patients with BD who experience frequent mood episodes, especially in those who may be unaware of or unfamiliar with basic concepts related to BD. In addition, relevant concepts from dialectical behavior therapy may be beneficial for BD patients with possible URC, such as skills to enhance emotional regulation, distress tolerance, mindfulness, and interpersonal effectiveness.
Table 2
Evidence-based treatments for ultra-rapid cycling BD
| Intervention | Strength of evidence | Comment |
|---|---|---|
| Antidepressant elimination | Cycling frequency may lengthen during antidepressant-free periods among patients with RC20; long-term (up to 1 year) antidepressant use in RC patients may increase the likelihood of depressive recurrences19 | Findings based mostly on small sample sizes; no controlled trials of antidepressant cessation as an intervention specifically for URC |
| Lithium | Single case report of ECT-induced URC resolved by lithium augmentation during continued ECT22 | No large-scale or randomized trials |
| Carbamazepine | No controlled trials or case reports | Possible anti-cycling benefits relevant for URC could be inferred from post hoc studies among patients with RC |
| Divalproex | Single case report describing resolution of a 48-hour cycle after augmentation of lithium with divalproex23 | No large-scale or randomized trials |
| Lamotrigine | Single case report of 100 mg/d lamotrigine augmentation to divalproex yielded 8 months of remission in a 25-year-old man with BD II and a long-standing pattern of 3 days of hypomania followed by 5 days of depression24 | No large-scale or randomized trials |
| Topiramate | Single case report in URC describing reduction of cycling frequency over 3 years25 | Multiple large scale placebo-controlled studies in bipolar mania have been negative |
| Second-generation antipsychotics | No controlled trials or case reports | Possible anti-cycling benefits relevant for URC could be inferred from post hoc studies in RC |
| Combinations of ≥2 mood stabilizing drugs | No controlled trials or case reports | Combining multiple anti-cycling agents is intuitively logical but largely unstudied |
| Nimodipine | 1 unipolar and 11 BD patients treated in randomized, off-on-off-on fashion (begun at 90 mg/d, increased up to 720 mg/d, mean duration of 12 weeks on active drug)26 | Response in 5 of 9 completers. Findings await replication with larger sample sizes |
| Hypermetabolic thyroid hormone (levothyroxine) | Findings from a small (N = 11) study of adjunctive high-dose levothyroxine (0.15 to 0.4 mg/d, with dosages increased by 0.05 to 0.1 mg/d every 1 to 2 weeks); an unspecified subgroup had “a very rapid cycling pattern” (reviewed by Bauer et al21) | 10 of 11 RC patients had reductions in depressive symptoms, 5 of 7 had improvement from baseline manic symptoms (observation period >60 days) |
| ECT | Case reports of improvement with ECT in refractory RC that was presumed secondary to tricyclic antidepressants | Reports of induction of URC by ECT22; whether or not ECT would more likely improve or exacerbate cyclicity for a given patient may require empirical determination |
| BD: bipolar disorder; BD II: bipolar II disorder; ECT: electroconvulsive therapy; RC: rapid cycling; URC: ultra-rapid cycling | ||
Treatment monitoring. Prospective life charting allows patients to systematically record manic/hypomanic and depressive symptoms day-to-day and week-to-week, thus creating a measure that may be particularly relevant for patients whose moods change rapidly. Simple mood charts (see Related Resources) typically take into account the severity of symptoms of either polarity with ratings of mild, moderate, or severe. Such visual records permit simple calculations over the course of a given interval (eg, week-by-week or across months) of several important parameters, including:
- number of days euthymic
- number of days with depression
- number of days with abnormal mood elevation
- number of occasions in which moods of both polarities occur on the same day.
Tracking these parameters during a treatment allows clinicians to make quantitative comparisons over time as a method of determining whether or not meaningful changes are occurring in cyclicity. See the figure below for an example of a completed mood chart and its interpretation.
Additional recommendations for assessing and managing cyclicity in BD are summarized in Table 3.
Table 3
Tips for managing suspected ultra-rapid cycling BD
| Do’s | Don’ts |
|---|---|
| Ascertain a history of ≥1 lifetime manic or hypomanic episode to diagnose BD | Diagnose BD solely on the presence of rapid mood fluctuations |
| Determine the presence of changes in sleep, energy, speech-language, and related behavior as correlates of mood to differentiate syndromes from isolated variation in mood | Ignore constellations of associated signs and symptoms of mania/hypomania |
| Obtain patient history to assess for head trauma or other medical and neurologic events that could have affective or other psychiatric manifestations | Disregard possible medical etiologies for new-onset affective dysregulation |
| Ascertain the resolution of 1 episode before counting the resurgence of symptoms as constituting a new episode; a waxing and waning course may reflect illness chronicity with incomplete recovery rather than true cyclicity | Misidentify incomplete recovery from an existing episode as the occurrence of new multiple episodes, which would inflate false-positive cases of RC or URC |
| Advise patients to refrain from alcohol or illicit substances that could destabilize mood | Assume that comorbid alcohol or illicit substance abuse will remit only after mood stabilization has been achieved, rather than the reverse |
| Monitor changes in sleep-wake cycles and the effects of erratic sleep or sleep deprivation on mood | Ignore the effects of poor sleep hygiene on mood |
| Minimize antidepressant exposure in patients with RC or URC | Continue long-term antidepressant maintenance therapy in patients with manic or mixed features or ongoing oscillations between mania/hypomania and depression |
| Assure euthyroid status and consider the potential utility of hypermetabolic levothyroxine | Assume that RC or URC will resolve solely by normalizing or optimizing thyroid function |
| Use rational, pharmacodynamically nonredundant anti-cycling drugs | Ignore the cumulative burden of adverse effects of multiple drugs |
| Consider the potential role for ECT as a strategy to arrest URC during any phase of BD | Assume ECT has value only during acute depressive phases of BD |
| Use prospective mood charting to document the evolution of mood changes over time, particularly when gauging treatment efficacy | Rely solely on impressionistic recall of mood states or polarity changes as reflecting distinct phasic changes |
| BD: bipolar disorder; ECT: electroconvulsive therapy; RC: rapid cycling; URC: ultra-rapid cycling | |
Table
Rapid cycling and ultra-rapid cycling BD: A comparison
| Construct | Rapid cycling | Ultra-rapid cycling |
|---|---|---|
| Bipolar I vs II | Predominantly BD IIa | No systematic data |
| Sex | Predominantly women | No systematic data |
| Longitudinal course | May be a transient phenomenon that can occur at any timeb or an enduring phenomenon that may persist for yearsc | Ultradian patterns may be more common across the first several episodes among pediatric BD patientsd |
| Age at onset | Associated with younger age at onsete | May be more evident in prepubescent onset mood disordersd; ultradian cycling more likely when onset occurs before age 13 than in adulthoode |
| Diurnal variation in mood | Morning-to-evening mood switches usually involve depression to mania/hypomania, with the opposite typifying evening-to-morning mood switchesf | Not reported |
| Relationship to environmental stresses | Life stresses may precede initial affective episodes but may be less important as subsequent episodes arise with increasing automaticity | No systematic data |
| Relationship to menstrual cycle | Despite case reports and self-reported links between RC and menstrual mood exacerbations, prospective data do not identify associations between RC and menstrual patternsg,h | No systematic data |
| Subclinical hypothyroidism | Bauer and Whybrow identified hypothyroidism independent of lithium use in 60% of 30 rapidly cycling BD patients, with evidence of improvement in a separate study of 11 RC patients given suprametabolic levothyroxine (reviewed by Bauer et ali) | No systematic data |
| Relationship to psychosis | Nonea | No systematic data |
| Relationship to antidepressant use | Naturalistic observations suggest RC may occur later in the illness course as a result of antidepressant use.c Small open case series data suggest shorter intermorbid intervals on antidepressants with longer intervals off antidepressants.j RC patients often receive antidepressants, but causal relationships are not well-documented.k Some case-control data dispute links between antidepressant use and RCl | No specific published cases |
| Considerations for suicide risk | RC linked with more serious suicide attemptsl | Suicide attempts may be associated with cycling within an episodem or rapid shifting in moodn |
| Time course for judging treatment efficacy | Efforts to diminish acute affective instability may be measured over the course of days to weeks | By definition, treatment of RC involves relapse prevention over the course of 1 year |
| BD: bipolar disorder; RC: rapid cycling | ||
| References a. Schneck CD, Miklowitz DJ, Calabrese JR, et al. Phenomenology of rapid-cycling bipolar disorder: data from the first 500 participants in the Systematic Treatment Enhancement Program. Am J Psychiatry. 2004;161(10):1902-1908. b. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics, diagnosis, family history, and course. Arch Gen Psychiatry. 1992;49(2):126-131. c. Koukopoulos A, Sani G, Koukopoulos AE, et al. Duration and stability of the rapid-cycling course: a long-term personal follow-up of 109 patients. J Affect Disord. 2003;73(1-2):75-85. d. Geller B, Tillman R, Bolhofner K, et al. Child bipolar I disorder: prospective continuity with adult bipolar I disorder; characteristics of second and third episodes; predictors of 8-year outcome. Arch Gen Psychiatry. 2008;65(10):1125-1133. e. Post RM, Leverich GS, Kupka RW, et al. Early-onset bipolar disorder and treatment delay are risk factors for poor outcome in adulthood. J Clin Psychiatry. 2010;71(7):864-872. f. Feldman-Naim S, Turner EH, Leibenluft E. Diurnal variation in the direction of mood switches in patients with rapid-cycling bipolar disorder. J Clin Psychiatry. 1997;58(2):79-84. g. Leibenluft E, Ashman SB, Feldman-Naim S, et al. Lack of relationship between menstrual cycle phase and mood in a sample of women with rapid cycling bipolar disorder. Biol Psychiatry. 1999;46(4):577-580. h. Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry. 1988;145(2):179-184. i. Bauer M, Beaulieu S, Dunner DL, et al. Rapid cycling bipolar disorder—diagnostic concepts. Bipolar Disord. 2008;10(1 Pt 2):153-162. j. Wehr TA, Goodwin FK. Can antidepressants cause mania and worsen the course of affective illness? Am J Psychiatry. 1987;144(11):1403-1411. k. Schneck CD, Miklowitz DJ, Miyahara S, et al. The prospective course of rapid-cycling bipolar disorder: findings from the STEP-BD. Am J Psychiatry. 2008;165(3):370-377. l. Coryell W, Solomon D, Turvey C, et al. The long-term course of rapid-cycling bipolar disorder. Arch Gen Psychiatry. 2003;60(9):914-920. m. Fawcett J, Scheftner W, Clark D, et al. Clinical predictors of suicide in patients with major affective disorders: a controlled prospective study. Am J Psychiatry. 1987;144(1):35-40. n. MacKinnon DF, Potash JB, McMahon FJ, et al. Rapid mood switching and suicidality in familial bipolar disorder. Bipolar Disord. 2005;7(5):441-448. | ||
From a biologic perspective, a handful of preliminary studies have examined genetic markers or familial patterns that might be related to rapid cycling (RC) or ultra-rapid cycling (URC). These include a reported link between URC and the low activity variant of the catechol-o-methyltransferase gene polymorphism in a small group of patients with velo-cardio-facial syndrome,a although this finding was not replicated in a larger sample.a Other preliminary reports on RC have implicated both the long (l) and short (s) allelic variants of the serotonin transporter gene (SLC6A4), the val66met variant of the brain-derived neurotrophic factor gene, and the circadian cryptochrome 2 (CRY2) gene (reviewed by Bauer et alb). These candidate loci have been examined in RC but not URC.
URC has not been examined as a familial entity, although in the National Institute of Mental Health Collaborative Depression Study, DSM-IV-TR RC did not occur with elevated frequency in bipolar pedigrees.c Rapid mood switches—abrupt rather than gradual transitions from one affective pole to another—appear to be only slightly, nonsignificantly more common in first-degree bipolar relatives of BD patients who themselves have rapid rather than gradual transitions from one affective pole to the other.d
Neuroimaging studies in BD seldom focus on subpopulations with RC or URC, and have been confined mainly to case reports that have yielded limited, non-generalizable observations, such as state-dependent variations in prefrontal activity during tasks of facial recognition (reviewed by Bauer et alb).
References
a. Papolos DF, Veit S, Faedda GL, et al. Ultra-ultra rapid cycling bipolar disorder is associated with the low activity catecholamine-O-methyltransferase allele. Mol Psychiatry. 1998;3(4):346-349.
b. Bauer M, Beaulieu S, Dunner DL, et al. Rapid cycling bipolar disorder—diagnostic concepts. Bipolar Disord. 2008;10(1 Pt 2):153-162.
c. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics, diagnosis, family history, and course. Arch Gen Psychiatry. 1992;49(2):126-131.
d. MacKinnon DF, Potash JB, McMahon FJ, et al. Rapid mood switching and suicidality in familial bipolar disorder. Bipolar Disord. 2005;7(5):441-448.
Figure: Example of prospective mood charting to document changes in manic/hypomanic and depressive symptoms across time
In the above example, the prevalence and severity of mood symptoms are identified over 21 days. Note the distinctly separate phases of mood elevation followed by depression, whereas euthymia was present only 6 of 21 days (29% of the time). Symptoms of at least moderate severity were more prominently depressive (5 of 21 days, or 24% of the time) than manic/hypomanic (2 of 21 days, or approximately 10% of the time). Mood charting does not capture associate DSM-IV-TR criteria for a mood episode but instead focuses solely on longitudinal changes in mood elevation or depression
Related Resources
- American Psychiatric Association practice guideline for the treatment of patients with bipolar disorder (revision). Am J Psychiatry. 2002;159(4 suppl):1-50.
- Massachusetts General Hospital Bipolar Clinic and Research Program. Sample mood chart (downloadable). www.manicdepressive.org/moodchart.html.
Drug Brand Names
- Carbamazepine • Equetro, Tegretol
- Divalproex • Depakote
- Lamotrigine • Lamictal
- Levothyroxine • Synthroid
- Lithium • Lithobid
- Nimodipine • Nimotop
- Topiramate • Topamax
Disclosures
Dr. Goldberg is on the speakers’ bureaus for AstraZeneca, Dey Pharmaceuticals, Eli Lilly and Company, Merck, and Sunovion and is a consultant for Axon Advisors, Dey Pharmaceuticals, Eli Lilly and Company, and Grünenthal Group.
Acknowledgment
The author wishes to thank David L. Dunner, MD, for his helpful comments regarding this article.
1. Kramlinger KG, Post RM. Ultra-rapid and ultradian cycling in bipolar affective illness. Br J Psychiatry. 1996;168(3):314-323.
2. Leibenluft E. Severe mood dysregulation irritability, and the diagnostic boundaries of bipolar disorder in youths. Am J Psychiatry. 2011;168(2):129-142.
3. Geller B, Tillman R, Bolhofner K. Proposed definitions of bipolar I disorder episodes and daily rapid cycling phenomena in preschoolers school-aged children, adolescents, and adults. J Child Adolesc Psychopharmacol. 2007;17(2):217-222.
4. Feinman JA, Dunner DL. The effect of alcohol and substance abuse on the course of bipolar affective disorder. J Affect Disord. 1996;37(1):43-49.
5. Maj M, Pirozzi R, Formicola AM, et al. Reliability and validity of four alternative definitions of rapid-cycling bipolar disorder. Am J Psychiatry. 1999;156(9):1421-1424.
6. Jenner FA, Gjessing LR, Cox JR, et al. A manic depressive psychotic with a persistent forty-eight hour cycle. Br J Psychiatry. 1967;113(501):895-910.
7. Zwil AS, McAllister TW, Cohen I, et al. Ultra-rapid cycling bipolar affective disorder following a closed-head injury. Brain Inj. 1993;7(2):147-152.
8. Geller B, Tillman R, Craney JL, et al. Four-year prospective outcome and natural history of mania in children with a prepubertal and early adolescent bipolar disorder phenotype. Arch Gen Psychiatry. 2004;61(5):459-467.
9. Geller B, Sun K, Zimerman B, et al. Complex and rapid-cycling in bipolar children and adolescents: a preliminary study. J Affect Disord. 1995;34(4):259-268.
10. Goldberg JF, Garno JL, Callahan AM, et al. Overdiagnosis of bipolar disorder among substance use disorder inpatients with mood instability. J Clin Psychiatry. 2008;69(11):1751-1757.
11. Zimmerman M, Ruggero CJ, Chelminski I, et al. Psychiatric diagnoses in patients previously overdiagnosed with bipolar disorder. J Clin Psychiatry. 2010;71(1):26-31.
12. MacKinnon DF, Pies R. Affective instability as rapid cycling: theoretical and clinical implications for borderline personality and bipolar spectrum disorders. Bipolar Disord. 2006;8(1):1-14.
13. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics diagnosis, family history, and course. Arch Gen Psychiatry. 1992;49(2):126-131.
14. Koenigsberg HW, Harvey PD, Mitropoulou V, et al. Characterizing affective instability in borderline personality disorder. Am J Psychiatry. 2002;159(5):784-788.
15. Henry C, Mitropoulou V, New AS, et al. Affective instability and impulsivity in borderline personality and bipolar II disorders: similarities and differences. J Psychiatr Res. 2001;35(6):307-312.
16. Gottschalk A, Bauer MS, Whybrow PC. Evidence of chaotic mood variation in bipolar disorder. Arch Gen Psychiatry. 1995;52(11):947-959.
17. Goldberg JF, Bowden CL, Calabrese JR, et al. Six-month prospective life charting of mood symptoms with lamotrigine monotherapy versus placebo in rapid cycling bipolar disorder. Biol Psychiatry. 2008;63(1):125-130.
18. Schneck CD, Miklowitz DJ, Miyahara S, et al. The prospective course of rapid-cycling bipolar disorder: findings from the STEP-BD. Am J Psychiatry. 2008;165(3):370-377.
19. Ghaemi SN, Ostacher MM, El-Mallakh RS, et al. Antidepressant discontinuation in bipolar depression: a Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) randomized clinical trial of long-term effectiveness and safety. J Clin Psychiatry. 2010;71(4):372-380.
20. Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry. 1988;145(2):179-184.
21. Bauer M, Beaulieu S, Dunner DL, et al. Rapid cycling bipolar disorder—diagnostic concepts. Bipolar Disord. 2008;10(1 Pt 2):153-162.
22. Zavorotnyy M, Diemer J, Patzelt J, et al. Occurrence of ultra-rapid cycling during electroconvulsive therapy in bipolar depression. World J Biol Psychiatry. 2009;10(4 Pt 3):987-990.
23. Lepkifker E, Iancu I, Dannon P, et al. Valproic acid in ultra-rapid cycling: a case report. Clin Neuropharmacol. 1995;18(1):72-75.
24. Woo YS, Chae JH, Jun TY, et al. Lamotrigine added to valproate successfully treated a case of ultra-rapid cycling bipolar disorder. Psychiatry Clin Neurosci. 2007;61(1):130-131.
25. Karama S, Lal S. Adjunctive topiramate in ultradian cycling bipolar disorder: case report with 3-year follow-up. Eur Psychiatry. 2006;21(4):280-281.
26. Pazzaglia PJ, Post RM, Ketter TA, et al. Preliminary controlled trial of nimodipine in ultra-rapid cycling affective dysregulation. Psychiatry Res. 1993;49(3):257-272.
27. Reilly-Harrington NA, Deckersbach T, Knauz R, et al. Cognitive behavioral therapy for rapid-cycling bipolar disorder: a pilot study. J Psychiatr Pract. 2007;13(5):291-297.
1. Kramlinger KG, Post RM. Ultra-rapid and ultradian cycling in bipolar affective illness. Br J Psychiatry. 1996;168(3):314-323.
2. Leibenluft E. Severe mood dysregulation irritability, and the diagnostic boundaries of bipolar disorder in youths. Am J Psychiatry. 2011;168(2):129-142.
3. Geller B, Tillman R, Bolhofner K. Proposed definitions of bipolar I disorder episodes and daily rapid cycling phenomena in preschoolers school-aged children, adolescents, and adults. J Child Adolesc Psychopharmacol. 2007;17(2):217-222.
4. Feinman JA, Dunner DL. The effect of alcohol and substance abuse on the course of bipolar affective disorder. J Affect Disord. 1996;37(1):43-49.
5. Maj M, Pirozzi R, Formicola AM, et al. Reliability and validity of four alternative definitions of rapid-cycling bipolar disorder. Am J Psychiatry. 1999;156(9):1421-1424.
6. Jenner FA, Gjessing LR, Cox JR, et al. A manic depressive psychotic with a persistent forty-eight hour cycle. Br J Psychiatry. 1967;113(501):895-910.
7. Zwil AS, McAllister TW, Cohen I, et al. Ultra-rapid cycling bipolar affective disorder following a closed-head injury. Brain Inj. 1993;7(2):147-152.
8. Geller B, Tillman R, Craney JL, et al. Four-year prospective outcome and natural history of mania in children with a prepubertal and early adolescent bipolar disorder phenotype. Arch Gen Psychiatry. 2004;61(5):459-467.
9. Geller B, Sun K, Zimerman B, et al. Complex and rapid-cycling in bipolar children and adolescents: a preliminary study. J Affect Disord. 1995;34(4):259-268.
10. Goldberg JF, Garno JL, Callahan AM, et al. Overdiagnosis of bipolar disorder among substance use disorder inpatients with mood instability. J Clin Psychiatry. 2008;69(11):1751-1757.
11. Zimmerman M, Ruggero CJ, Chelminski I, et al. Psychiatric diagnoses in patients previously overdiagnosed with bipolar disorder. J Clin Psychiatry. 2010;71(1):26-31.
12. MacKinnon DF, Pies R. Affective instability as rapid cycling: theoretical and clinical implications for borderline personality and bipolar spectrum disorders. Bipolar Disord. 2006;8(1):1-14.
13. Coryell W, Endicott J, Keller M. Rapidly cycling affective disorder. Demographics diagnosis, family history, and course. Arch Gen Psychiatry. 1992;49(2):126-131.
14. Koenigsberg HW, Harvey PD, Mitropoulou V, et al. Characterizing affective instability in borderline personality disorder. Am J Psychiatry. 2002;159(5):784-788.
15. Henry C, Mitropoulou V, New AS, et al. Affective instability and impulsivity in borderline personality and bipolar II disorders: similarities and differences. J Psychiatr Res. 2001;35(6):307-312.
16. Gottschalk A, Bauer MS, Whybrow PC. Evidence of chaotic mood variation in bipolar disorder. Arch Gen Psychiatry. 1995;52(11):947-959.
17. Goldberg JF, Bowden CL, Calabrese JR, et al. Six-month prospective life charting of mood symptoms with lamotrigine monotherapy versus placebo in rapid cycling bipolar disorder. Biol Psychiatry. 2008;63(1):125-130.
18. Schneck CD, Miklowitz DJ, Miyahara S, et al. The prospective course of rapid-cycling bipolar disorder: findings from the STEP-BD. Am J Psychiatry. 2008;165(3):370-377.
19. Ghaemi SN, Ostacher MM, El-Mallakh RS, et al. Antidepressant discontinuation in bipolar depression: a Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) randomized clinical trial of long-term effectiveness and safety. J Clin Psychiatry. 2010;71(4):372-380.
20. Wehr TA, Sack DA, Rosenthal NE, et al. Rapid cycling affective disorder: contributing factors and treatment responses in 51 patients. Am J Psychiatry. 1988;145(2):179-184.
21. Bauer M, Beaulieu S, Dunner DL, et al. Rapid cycling bipolar disorder—diagnostic concepts. Bipolar Disord. 2008;10(1 Pt 2):153-162.
22. Zavorotnyy M, Diemer J, Patzelt J, et al. Occurrence of ultra-rapid cycling during electroconvulsive therapy in bipolar depression. World J Biol Psychiatry. 2009;10(4 Pt 3):987-990.
23. Lepkifker E, Iancu I, Dannon P, et al. Valproic acid in ultra-rapid cycling: a case report. Clin Neuropharmacol. 1995;18(1):72-75.
24. Woo YS, Chae JH, Jun TY, et al. Lamotrigine added to valproate successfully treated a case of ultra-rapid cycling bipolar disorder. Psychiatry Clin Neurosci. 2007;61(1):130-131.
25. Karama S, Lal S. Adjunctive topiramate in ultradian cycling bipolar disorder: case report with 3-year follow-up. Eur Psychiatry. 2006;21(4):280-281.
26. Pazzaglia PJ, Post RM, Ketter TA, et al. Preliminary controlled trial of nimodipine in ultra-rapid cycling affective dysregulation. Psychiatry Res. 1993;49(3):257-272.
27. Reilly-Harrington NA, Deckersbach T, Knauz R, et al. Cognitive behavioral therapy for rapid-cycling bipolar disorder: a pilot study. J Psychiatr Pract. 2007;13(5):291-297.
Disoriented and forgetful
CASE: Disoriented and delusional
Ms. P, a 53-year-old registered nurse, is admitted to the inpatient psychiatric unit with confusion, markedly disorganized thought processes, delayed verbal responsiveness, mood lability, and persecutory delusions. Shortly before hospitalization, Ms. P traveled approximately 360 miles from her daughter’s home with a male companion. Noting changes in her mental status, the man brought Ms. P to the local hospital. She was then transferred to our facility.
At admission, Ms. P is not oriented to time. She denies auditory or visual hallucinations and does not display psychomotor agitation or retardation. She reports her mood as sad and her affect is mildly labile. Insight and judgment are considered poor.
Five years ago, Ms. P and her mother were diagnosed with Fabry’s disease (FD) based on genetic analysis. Both women are carriers for the mutations and Ms. P’s mother was found to have almost absent galactosidase activity.
The authors’ observations
FD is an X-linked recessive glycolipid storage disease caused by deficient activity of the lysosomal storage enzyme α-galactosidase A. The disorder affects both men and women and leads to progressive intracellular accumulation of globotriaosylceramide and other related glycosphingolipids.1,2 The earliest FD symptoms—burning pain and acroparesthesias—typically appear in childhood (Table 1).2 FD often is misdiagnosed in women because women tend to display neurologic symptoms later than men, with typical symptom onset in the teenage years.3,4 Often, these symptoms are confused with psychiatric disorders or vague neurologic or pain syndromes.5 In patients with no family history of FD, accurate diagnosis may not be made until adulthood.
Laboratory, dermatologic, and genetic tests can accurately determine the presence of FD.1 However, because multiple organ systems are involved, initially attributing symptoms to FD is challenging, particularly in women.1,3,5 For men, diagnosis can be established by measuring plasma or urinary globotriaosylceramide or plasma α-galactosidase A in addition to genetic analysis. In women, genetic analysis is a better diagnosis strategy because elevations in globotriaosylceramide or α-galactosidase A may not be prominent. An algorithm for diagnosing and assessing patients with FD has been proposed.2
Table 1
Typical signs and symptoms of Fabry’s disease
| Typical time at onset | Signs/symptoms |
|---|---|
| Childhood and adolescence (age ≤16) | Neuropathic pain Ophthalmologic abnormalities (cornea verticillata and tortuous retinal blood vessels) Hearing impairment Dyshidrosis (hypohidrosis and hyperhidrosis) Hypersensitivity to heat and cold Gastrointestinal disturbances and abdominal pain Lethargy and tiredness Angiokeratomas Onset of renal and cardiac signs (eg, microalbuminuria, proteinuria, abnormal heart rate variability) |
| Early adulthood (age 17 to 30) | Extension of any of the above Proteinuria and progressive renal failure Cardiomyopathy Transient ischemic attacks, strokes Facial dysmorphism |
| Later adulthood (age >30) | Worsening of any of the above Heart disease (eg, left ventricular hypertrophy, angina, arrhythmia, and dyspnea) Transient ischemic attacks, strokes Osteopenia and osteoporosis |
| Source: Mehta A, Beck M, Eyskens F, et al. Fabry disease: a review of current management strategies. QJM. 2010;103(9):641-659, by permission of Oxford University Press | |
HISTORY: Cognitive deterioration
Ms. P has had psychiatric symptoms such as depression and anxiety since childhood. However, 3 years ago she started to experience psychological and cognitive deterioration. Medical records indicate that Ms. P described memory and concentration problems over the previous few years. She also reported pain, weakness, and numbness in her left leg after surgery for a work-related back injury, for which she received a financial settlement through workers’ compensation. Shortly thereafter, Ms. P separated from her third husband, moved in with her parents, and found work as a psychiatric nurse. She was dismissed after 6 weeks because she could not learn the electronic medical record system and had difficulty with memory and attention. Her performance on the Mini-Mental State Exam6 at that time was 28 out of 30, which was within normal limits.
After her parents died 3 years ago, Ms. P lived with her daughter, who became her primary caregiver and legal guardian. Ms. P’s daughter notes that her mother’s impulsive and risky behaviors grew more pronounced. Ms. P went on shopping sprees and became sexually promiscuous.
Ms. P’s psychiatric history includes childhood sexual abuse, hospitalization for a suicide attempt at age 19, and courses of psychotherapy and pharmacotherapy. In addition to FD, Ms. P’s medical history consists of coronary artery disease, type 2 diabetes mellitus, hypercholesterolemia, obesity, arthritis, back pain, fibromyalgia, and gastroesophageal reflux disease. Her family history is notable for alcohol abuse (both parents and a brother), lung cancer (mother), myocardial infarction (father), and Alzheimer’s disease (father).
The authors’ observations
Because α-galactosidase A is ubiquitous throughout the body, in addition to neurologic symptoms, FD involves multiple organ systems, with possible dermatologic, renal, gastrointestinal, cardiac, and cerebrovascular dysfunction. Despite growth in FD research, including the Fabry Outcomes Survey,3 the psychosocial and neuropsychiatric implications of the disease remain unclear.7 Behavioral presentations are idiosyncratic and unstable over time, depending on the structures impacted by progressive glycosphingolipid accumulation. Premature cardiovascular events (onset between age 30 and 40 for women), greater incidence of ischemic stroke or transient ischemic attack (7% to 30%), and frequent evidence of white matter lesions put FD patients at greater risk for developing presenile vascular dementia.1,3 Nearly all male FD patients with dementia show some evidence of stroke or transient ischemic attack; cognitive functioning has not been well explored in female patients.4 In a heterogeneous sample of 15 FD patients age 7 to 61, Segal et al8 noted deficits in attention, processing speed, and executive function .75 to 1.95 standard deviations below normative means. No patients in this study had a history of stroke or transient ischemic attack; neuroimaging studies were not reported. Kolodny and Pastores9 suggested multiple mechanisms for cognitive disruption, suggesting that mild dementia late in the disease course could be secondary to diffuse leukomalacia, multiple strokes, or possibly to lipid storage in hippocampal and frontal lobe neurons.
Psychiatric comorbidity
Psychiatric illness, such as depression or a personality disorder, may be comorbid with FD, although pathologic mechanisms remain unclear.7,10,11 Hypothesized mechanisms include:
- psychosocial stress from chronic disease
- white matter changes
- disruption of impaired L-arginine-nitric oxide pathways.7,12
Crosbie et al13 noted that FD patients presented with greater psychological distress as measured by the Minnesota Multiphasic Personality Inventory-2 than patients with Gaucher disease or chronic heart disease. However, no significant differences were found between patients with FD and those diagnosed with a pain disorder. In the Segal et al study, out of 11 adult FD patients, 4 were diagnosed with major depressive disorder, 1 with schizophrenia, 2 with schizotypal personality disorder, and 1 with borderline personality disorder.8
EVALUATION: Brain abnormalities
Head CT scans (conducted 2 years ago and 6 months ago) revealed prominent cortical sulci likely caused by underlying volume loss, especially in bifrontal areas. A brain MRI performed 2 months ago indicated a moderate degree of subcortical atrophy in bilateral frontal and parietal regions. These radiology findings suggest mild to moderate frontal atrophy, mild degree of white matter changes, and slightly enlarged ventricles. An EEG showed background slowing and lack of an alpha rhythm, indicative of cerebral cortical dysfunction.
Ms. P’s α-galactosidase A level was within normal limits; however, normal enzyme levels frequently are reported in symptomatic and asymptomatic female FD patients.14 A dermatology consult confirmed the presence of skin findings characteristic of FD (ie, multiple cherry red papules extensively distributed throughout Ms. P’s chest, abdomen, and back, as well as upper and lower extremities).
Ms. P completed 2 neuropsychological assessments separated by 5 months. For a summary of the results of these tests, see the table titled “Ms. P’s neuropsychological assessment results”. Both assessments revealed grossly impaired intellectual capacity, memory, processing speed, and motor functioning. During the assessment, Ms. P could understand all directions with minimal changes from standardized protocols. Ms. P became insistent that she would not be able to complete memory tasks successfully. She gave up prematurely on tasks, saying they were too difficult. She admitted to guessing on several items because she did not want to continue the task.
Ms. P’s performance on tasks measuring effort and validity of a person’s neuropsychological presentation was consistent with someone exaggerating neurologic symptoms. A person with true dementia may perform as poorly as Ms. P did. However, Ms. P’s scores likely underestimated her level of functioning, even if she was experiencing dementia. Ms. P could not complete tasks individuals with severe dementia complete successfully, such as simple addition and subtraction and digit repetition. Ms. P recalled several recent and remote events, such as her breakfast menu and location of her first assessment, but could not recall words practiced multiple times. Although Ms. P’s scores on a complex card-sorting task were in the impaired range, a detailed review of her pattern indicated that although Ms. P could not generate any correct sorting categories, she made few repetitive responses and errors. This pattern is consistent with someone who understands task requirements, but deliberately avoids answering correctly. This suggests that she retained some ability for hypotheses generation and problem solving; however, because she exaggerated her symptoms, specific deficits could not be determined.
The authors’ observations
Ms. P presented with an interesting manifestation of neuropsychiatric symptoms in the context of FD; however, common cardiac and cerebrovascular features of the disease were not fully developed. Ms. P experienced progressive cognitive and behavioral changes for 2 years before her admission (Table 2), which may represent a prodromal period leading up to what appeared to be a frontally mediated dementia syndrome. Müller et al15 described a patient with FD who displayed a behavioral profile similar to Ms. P’s that included increasingly unstable mood for at least 3 years, borderline personality disorder features, and rapidly fluctuating mood. A case study reported that risperidone, 1 mg/d, used to treat psychosis in a male FD patient caused extrapyramidal symptoms.16
Ms. P presented with no evidence of stroke or transient ischemic attacks, which is atypical for FD patients with cognitive impairment. However, neuroimaging did reveal frontal atrophy that may be associated with her impulse control deficits, risk-taking behavior, emotional instability, and poor judgment. Her cognitive testing was notable for impairment and exaggeration of symptoms consistent with personality disorder symptoms. Possible reasons for exaggeration include a desire to maintain the sick role or secondary gain related to obtaining disability income.
Ms. P’s behavior pattern could be caused by dementia with frontal features, possibly secondary to FD, in combination with personality and psychiatric pathology.
The mainstay of FD treatment is enzyme replacement therapy (ERT), which addresses the underlying enzyme deficiency. Available research indicates that ERT may reduce symptom severity and slow disease progression; however, further studies are needed to determine if it will reduce outcomes such as stroke, ischemic heart disease, or renal disease.2
Table 2
Symptoms that preceded Ms. P’s admission
| Time frame | Symptoms |
|---|---|
| 24 months before admission | Depressed mood Decreased ability to manage independent activities of daily living (eg, finances, cooking) Minimal objective cognitive impairment |
| 12 months before admission | Increased depression Mild to moderate decline in cognitive functioning Visual and auditory hallucinations Impulsivity/poor impulse control Irrational decision-making Increased risky behavior |
| 6 months before admission | Severe cognitive decline with cognitive symptom exaggeration Psychiatric symptom exaggeration Disorganized thinking Continued risky behavior and poor decision-making |
TREATMENT: Persistent deficits
Ms. P is started on risperidone rapidly titrated to 4 mg/d for delusional thinking and behavioral disturbance. After initially improving, she develops delirium when risperidone is increased to 4 mg/d. She has visual hallucinations, marked confusion with disorientation, worsened short-term memory, and an unsteady, shuffling gait. Risperidone is tapered and discontinued and Ms. P’s motor symptoms resolve within 2 days; however, she remains confused and delusional. We start her on quetiapine, 25 mg/d titrated to 50 mg/d, and her agitation and delusional thinking progressively decline. Memantine, titrated to 20 mg/d, and rivastigmine, started at 3 mg/d titrated to 9 mg/d, are added to address her cognitive symptoms.
Over several weeks, Ms. P’s mental status slowly improves and her drug-induced delirium completely resolves. However, she has persistent cognitive impairment characterized by compromised short-term memory and poor insight into her medical and psychological condition. She maintains unrealistic expectations about her ability to live independently and return to the workforce. The treatment team recommends that Ms. P’s daughter pursue guardianship and that she receive around-the-clock supervision after discharge from the hospital.
Table
Ms. P’s neuropsychological assessment results
| June | November | |
|---|---|---|
| Intellectual functioning | ||
| Wechsler Adult Intelligence Scale-III | ||
| FSIQ | 60 | |
| VIQ | 68 | |
| PIQ | 56 | |
| Ravens Colored Progressive Matrices | 70 | |
| Premorbid intellectual functioning estimates | ||
| Peabody Picture Vocabulary Test-2 | 89 | |
| Barona Demographic Estimate | 104 | 104 |
| North American Adult Reading Test | 99 | |
| Memory functioning | ||
| Wechsler Memory Scale-III | ||
| Immediate memory | 45 | |
| General delay memory | 47 | |
| Auditory recognition delay | 55 | |
| California Verbal Learning Test-II | ||
| Trial 1 (immediate recall) | <60 (raw = 3) | |
| Trial 5 | <60 (raw = 3) | |
| Total Words Learned | <60 (raw = 15) | |
| Short Delay Free Recall | <60 (raw = 2) | |
| Long Delay Free Recall | <60 (raw = 4) | |
| Executive functioning | ||
| Trail Making Test A | 88 | 88 |
| Trail Making Test B | failed to understand | failed to understand |
| Wisconsin Card Sort-64 | ||
| Number of categories | <60 (raw = 0) | |
| Errors | 81 | |
| Percent conceptual level responses | 74 | |
| Perseverative responses | 107 | |
| Perseverative errors | 108 | |
| COWAT FAS | 65 | 69 |
| Category exemplar | 69 | 80 |
| Motor functioning | ||
| Finger Tapping Dominant Hand | 68 | |
| Finger Tapping Non-Dominant Hand | 62 | |
| Invalidity/effort | ||
| TOMM | ||
| Trial 1 | raw = 34 | raw = 37 |
| Trial 2 | raw = 42 | raw = 45 |
| Recognition | raw = 44 | |
| MSVT verbal | fail | |
| MSVT nonverbal | fail | |
| Scores provided are standardized (mean = 100; SD = 15). Raw scores are also provided when indicated. COWAT: Controlled oral word association test; FSIQ: Full Scale IQ; MSVT: Medical Symptom Validity Test; PIQ: Performance IQ; TOMM: Test of Memory Malingering; VIQ: Verbal IQ | ||
Related Resources
- National Institute of Neurological Disorders and Stroke. Fabry disease information page. www.ninds.nih.gov/disorders/fabrys/fabrys.htm.
- National Fabry Disease Foundation. www.thenfdf.org.
- Rozenfeld P, Neumann PM. Treatment of Fabry disease: current and emerging strategies. Curr Pharm Biotechnol. 2011;12(6):916-922.
Drug Brand Names
- Donepezil • Aricept
- Memantine • Namenda
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Rivastigmine • Exelon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Eng CM, Germain DP, Banikazemi M, et al. Fabry disease: guidelines for the evaluation and management of multi-organ system involvement. Genet Med. 2006;8(9):539-548.
2. Mehta A, Beck M, Eyskens F, et al. Fabry disease: a review of current management strategies. QJM. 2010;103(9):641-659.
3. Deegan PB, Baehner AF, Barba Romero MA, et al. Natural history of Fabry disease in females in the Fabry Outcome Survey. J Med Genet. 2006;43(4):347-352.
4. Fellgiebel A, Müller MJ, Ginsberg L. CNS manifestations of Fabry’s disease. Lancet Neurol. 2006;5(9):791-795.
5. Møller AT, Jensen TS. Neurological manifestations in Fabry’s disease. Nat Clin Pract Neurol. 2007;3(2):95-106.
6. Folstein MF, Folstein SE, McHugh PR. Mini-mental state: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189-198.
7. Müller MJ. Neuropsychiatric and psychosocial aspects of Fabry disease. In: Mehta A Beck M, Sunder-Plassman G, eds. Fabry disease: perspectives from 5 years of FOS. Oxford, United Kingdom: Oxford PharmaGenesis Ltd; 2006. http://www.ncbi.nlm.nih.gov/books/nbk11618. Accessed October 31, 2011.
8. Segal P, Kohn Y, Pollak Y, et al. Psychiatric and cognitive profile in Anderson-Fabry patients: a preliminary study. J Inherit Metab Dis. 2010;33(4):429-436.
9. Kolodny EH, Pastores GM. Anderson-Fabry disease: Extrarenal neurologic manifestations. J Am Soc Nephrol. 2002;13(suppl 2):S150-153.
10. Grewal RP. Psychiatric disorders in patients with Fabry disease. Int J Psychiatry Med. 1993;23(3):307-312.
11. Müller MJ, Müller KM, Dascalescu A, et al. Psychiatric and neuropsychological signs and symptoms in patients with Fabry disease: literature review [in German]. Fortschr Neurol Psychiatr. 2005;73(11):687-693.
12. Segal P, Raas-Rothschild A. Neuropsychiatric manifestations of AFD. In: Elstein D Altarescu G, Beck M, eds. Fabry disease. New York, NY: Springer; 2010:321–324.
13. Crosbie TW, Packman W, Packman S. Psychological aspects of patients with Fabry disease. J Inherit Metab Dis. 2009;32(6):745-753.
14. Linthorst GE, Poorthuis BJ, Hollak CE. Enzyme activity for determination of presence of Fabry disease in women results in 40% false-negative results. J Am Coll Cardiol. 2008;51(21):2082.-
15. Müller MJ, Fellgiebel A, Scheurich A, et al. Recurrent brief depression in female patient with Fabry disease. Bipolar Disord. 2006;8(4):418-419.
16. Shen YC, Haw-Ming L, Lin CC, et al. Psychosis in a patient with Fabry’s disease and treatment with aripiprazole. Prog Neuropsychopharmacol Biol Psychiatry. 2007;31(3):779-780.
CASE: Disoriented and delusional
Ms. P, a 53-year-old registered nurse, is admitted to the inpatient psychiatric unit with confusion, markedly disorganized thought processes, delayed verbal responsiveness, mood lability, and persecutory delusions. Shortly before hospitalization, Ms. P traveled approximately 360 miles from her daughter’s home with a male companion. Noting changes in her mental status, the man brought Ms. P to the local hospital. She was then transferred to our facility.
At admission, Ms. P is not oriented to time. She denies auditory or visual hallucinations and does not display psychomotor agitation or retardation. She reports her mood as sad and her affect is mildly labile. Insight and judgment are considered poor.
Five years ago, Ms. P and her mother were diagnosed with Fabry’s disease (FD) based on genetic analysis. Both women are carriers for the mutations and Ms. P’s mother was found to have almost absent galactosidase activity.
The authors’ observations
FD is an X-linked recessive glycolipid storage disease caused by deficient activity of the lysosomal storage enzyme α-galactosidase A. The disorder affects both men and women and leads to progressive intracellular accumulation of globotriaosylceramide and other related glycosphingolipids.1,2 The earliest FD symptoms—burning pain and acroparesthesias—typically appear in childhood (Table 1).2 FD often is misdiagnosed in women because women tend to display neurologic symptoms later than men, with typical symptom onset in the teenage years.3,4 Often, these symptoms are confused with psychiatric disorders or vague neurologic or pain syndromes.5 In patients with no family history of FD, accurate diagnosis may not be made until adulthood.
Laboratory, dermatologic, and genetic tests can accurately determine the presence of FD.1 However, because multiple organ systems are involved, initially attributing symptoms to FD is challenging, particularly in women.1,3,5 For men, diagnosis can be established by measuring plasma or urinary globotriaosylceramide or plasma α-galactosidase A in addition to genetic analysis. In women, genetic analysis is a better diagnosis strategy because elevations in globotriaosylceramide or α-galactosidase A may not be prominent. An algorithm for diagnosing and assessing patients with FD has been proposed.2
Table 1
Typical signs and symptoms of Fabry’s disease
| Typical time at onset | Signs/symptoms |
|---|---|
| Childhood and adolescence (age ≤16) | Neuropathic pain Ophthalmologic abnormalities (cornea verticillata and tortuous retinal blood vessels) Hearing impairment Dyshidrosis (hypohidrosis and hyperhidrosis) Hypersensitivity to heat and cold Gastrointestinal disturbances and abdominal pain Lethargy and tiredness Angiokeratomas Onset of renal and cardiac signs (eg, microalbuminuria, proteinuria, abnormal heart rate variability) |
| Early adulthood (age 17 to 30) | Extension of any of the above Proteinuria and progressive renal failure Cardiomyopathy Transient ischemic attacks, strokes Facial dysmorphism |
| Later adulthood (age >30) | Worsening of any of the above Heart disease (eg, left ventricular hypertrophy, angina, arrhythmia, and dyspnea) Transient ischemic attacks, strokes Osteopenia and osteoporosis |
| Source: Mehta A, Beck M, Eyskens F, et al. Fabry disease: a review of current management strategies. QJM. 2010;103(9):641-659, by permission of Oxford University Press | |
HISTORY: Cognitive deterioration
Ms. P has had psychiatric symptoms such as depression and anxiety since childhood. However, 3 years ago she started to experience psychological and cognitive deterioration. Medical records indicate that Ms. P described memory and concentration problems over the previous few years. She also reported pain, weakness, and numbness in her left leg after surgery for a work-related back injury, for which she received a financial settlement through workers’ compensation. Shortly thereafter, Ms. P separated from her third husband, moved in with her parents, and found work as a psychiatric nurse. She was dismissed after 6 weeks because she could not learn the electronic medical record system and had difficulty with memory and attention. Her performance on the Mini-Mental State Exam6 at that time was 28 out of 30, which was within normal limits.
After her parents died 3 years ago, Ms. P lived with her daughter, who became her primary caregiver and legal guardian. Ms. P’s daughter notes that her mother’s impulsive and risky behaviors grew more pronounced. Ms. P went on shopping sprees and became sexually promiscuous.
Ms. P’s psychiatric history includes childhood sexual abuse, hospitalization for a suicide attempt at age 19, and courses of psychotherapy and pharmacotherapy. In addition to FD, Ms. P’s medical history consists of coronary artery disease, type 2 diabetes mellitus, hypercholesterolemia, obesity, arthritis, back pain, fibromyalgia, and gastroesophageal reflux disease. Her family history is notable for alcohol abuse (both parents and a brother), lung cancer (mother), myocardial infarction (father), and Alzheimer’s disease (father).
The authors’ observations
Because α-galactosidase A is ubiquitous throughout the body, in addition to neurologic symptoms, FD involves multiple organ systems, with possible dermatologic, renal, gastrointestinal, cardiac, and cerebrovascular dysfunction. Despite growth in FD research, including the Fabry Outcomes Survey,3 the psychosocial and neuropsychiatric implications of the disease remain unclear.7 Behavioral presentations are idiosyncratic and unstable over time, depending on the structures impacted by progressive glycosphingolipid accumulation. Premature cardiovascular events (onset between age 30 and 40 for women), greater incidence of ischemic stroke or transient ischemic attack (7% to 30%), and frequent evidence of white matter lesions put FD patients at greater risk for developing presenile vascular dementia.1,3 Nearly all male FD patients with dementia show some evidence of stroke or transient ischemic attack; cognitive functioning has not been well explored in female patients.4 In a heterogeneous sample of 15 FD patients age 7 to 61, Segal et al8 noted deficits in attention, processing speed, and executive function .75 to 1.95 standard deviations below normative means. No patients in this study had a history of stroke or transient ischemic attack; neuroimaging studies were not reported. Kolodny and Pastores9 suggested multiple mechanisms for cognitive disruption, suggesting that mild dementia late in the disease course could be secondary to diffuse leukomalacia, multiple strokes, or possibly to lipid storage in hippocampal and frontal lobe neurons.
Psychiatric comorbidity
Psychiatric illness, such as depression or a personality disorder, may be comorbid with FD, although pathologic mechanisms remain unclear.7,10,11 Hypothesized mechanisms include:
- psychosocial stress from chronic disease
- white matter changes
- disruption of impaired L-arginine-nitric oxide pathways.7,12
Crosbie et al13 noted that FD patients presented with greater psychological distress as measured by the Minnesota Multiphasic Personality Inventory-2 than patients with Gaucher disease or chronic heart disease. However, no significant differences were found between patients with FD and those diagnosed with a pain disorder. In the Segal et al study, out of 11 adult FD patients, 4 were diagnosed with major depressive disorder, 1 with schizophrenia, 2 with schizotypal personality disorder, and 1 with borderline personality disorder.8
EVALUATION: Brain abnormalities
Head CT scans (conducted 2 years ago and 6 months ago) revealed prominent cortical sulci likely caused by underlying volume loss, especially in bifrontal areas. A brain MRI performed 2 months ago indicated a moderate degree of subcortical atrophy in bilateral frontal and parietal regions. These radiology findings suggest mild to moderate frontal atrophy, mild degree of white matter changes, and slightly enlarged ventricles. An EEG showed background slowing and lack of an alpha rhythm, indicative of cerebral cortical dysfunction.
Ms. P’s α-galactosidase A level was within normal limits; however, normal enzyme levels frequently are reported in symptomatic and asymptomatic female FD patients.14 A dermatology consult confirmed the presence of skin findings characteristic of FD (ie, multiple cherry red papules extensively distributed throughout Ms. P’s chest, abdomen, and back, as well as upper and lower extremities).
Ms. P completed 2 neuropsychological assessments separated by 5 months. For a summary of the results of these tests, see the table titled “Ms. P’s neuropsychological assessment results”. Both assessments revealed grossly impaired intellectual capacity, memory, processing speed, and motor functioning. During the assessment, Ms. P could understand all directions with minimal changes from standardized protocols. Ms. P became insistent that she would not be able to complete memory tasks successfully. She gave up prematurely on tasks, saying they were too difficult. She admitted to guessing on several items because she did not want to continue the task.
Ms. P’s performance on tasks measuring effort and validity of a person’s neuropsychological presentation was consistent with someone exaggerating neurologic symptoms. A person with true dementia may perform as poorly as Ms. P did. However, Ms. P’s scores likely underestimated her level of functioning, even if she was experiencing dementia. Ms. P could not complete tasks individuals with severe dementia complete successfully, such as simple addition and subtraction and digit repetition. Ms. P recalled several recent and remote events, such as her breakfast menu and location of her first assessment, but could not recall words practiced multiple times. Although Ms. P’s scores on a complex card-sorting task were in the impaired range, a detailed review of her pattern indicated that although Ms. P could not generate any correct sorting categories, she made few repetitive responses and errors. This pattern is consistent with someone who understands task requirements, but deliberately avoids answering correctly. This suggests that she retained some ability for hypotheses generation and problem solving; however, because she exaggerated her symptoms, specific deficits could not be determined.
The authors’ observations
Ms. P presented with an interesting manifestation of neuropsychiatric symptoms in the context of FD; however, common cardiac and cerebrovascular features of the disease were not fully developed. Ms. P experienced progressive cognitive and behavioral changes for 2 years before her admission (Table 2), which may represent a prodromal period leading up to what appeared to be a frontally mediated dementia syndrome. Müller et al15 described a patient with FD who displayed a behavioral profile similar to Ms. P’s that included increasingly unstable mood for at least 3 years, borderline personality disorder features, and rapidly fluctuating mood. A case study reported that risperidone, 1 mg/d, used to treat psychosis in a male FD patient caused extrapyramidal symptoms.16
Ms. P presented with no evidence of stroke or transient ischemic attacks, which is atypical for FD patients with cognitive impairment. However, neuroimaging did reveal frontal atrophy that may be associated with her impulse control deficits, risk-taking behavior, emotional instability, and poor judgment. Her cognitive testing was notable for impairment and exaggeration of symptoms consistent with personality disorder symptoms. Possible reasons for exaggeration include a desire to maintain the sick role or secondary gain related to obtaining disability income.
Ms. P’s behavior pattern could be caused by dementia with frontal features, possibly secondary to FD, in combination with personality and psychiatric pathology.
The mainstay of FD treatment is enzyme replacement therapy (ERT), which addresses the underlying enzyme deficiency. Available research indicates that ERT may reduce symptom severity and slow disease progression; however, further studies are needed to determine if it will reduce outcomes such as stroke, ischemic heart disease, or renal disease.2
Table 2
Symptoms that preceded Ms. P’s admission
| Time frame | Symptoms |
|---|---|
| 24 months before admission | Depressed mood Decreased ability to manage independent activities of daily living (eg, finances, cooking) Minimal objective cognitive impairment |
| 12 months before admission | Increased depression Mild to moderate decline in cognitive functioning Visual and auditory hallucinations Impulsivity/poor impulse control Irrational decision-making Increased risky behavior |
| 6 months before admission | Severe cognitive decline with cognitive symptom exaggeration Psychiatric symptom exaggeration Disorganized thinking Continued risky behavior and poor decision-making |
TREATMENT: Persistent deficits
Ms. P is started on risperidone rapidly titrated to 4 mg/d for delusional thinking and behavioral disturbance. After initially improving, she develops delirium when risperidone is increased to 4 mg/d. She has visual hallucinations, marked confusion with disorientation, worsened short-term memory, and an unsteady, shuffling gait. Risperidone is tapered and discontinued and Ms. P’s motor symptoms resolve within 2 days; however, she remains confused and delusional. We start her on quetiapine, 25 mg/d titrated to 50 mg/d, and her agitation and delusional thinking progressively decline. Memantine, titrated to 20 mg/d, and rivastigmine, started at 3 mg/d titrated to 9 mg/d, are added to address her cognitive symptoms.
Over several weeks, Ms. P’s mental status slowly improves and her drug-induced delirium completely resolves. However, she has persistent cognitive impairment characterized by compromised short-term memory and poor insight into her medical and psychological condition. She maintains unrealistic expectations about her ability to live independently and return to the workforce. The treatment team recommends that Ms. P’s daughter pursue guardianship and that she receive around-the-clock supervision after discharge from the hospital.
Table
Ms. P’s neuropsychological assessment results
| June | November | |
|---|---|---|
| Intellectual functioning | ||
| Wechsler Adult Intelligence Scale-III | ||
| FSIQ | 60 | |
| VIQ | 68 | |
| PIQ | 56 | |
| Ravens Colored Progressive Matrices | 70 | |
| Premorbid intellectual functioning estimates | ||
| Peabody Picture Vocabulary Test-2 | 89 | |
| Barona Demographic Estimate | 104 | 104 |
| North American Adult Reading Test | 99 | |
| Memory functioning | ||
| Wechsler Memory Scale-III | ||
| Immediate memory | 45 | |
| General delay memory | 47 | |
| Auditory recognition delay | 55 | |
| California Verbal Learning Test-II | ||
| Trial 1 (immediate recall) | <60 (raw = 3) | |
| Trial 5 | <60 (raw = 3) | |
| Total Words Learned | <60 (raw = 15) | |
| Short Delay Free Recall | <60 (raw = 2) | |
| Long Delay Free Recall | <60 (raw = 4) | |
| Executive functioning | ||
| Trail Making Test A | 88 | 88 |
| Trail Making Test B | failed to understand | failed to understand |
| Wisconsin Card Sort-64 | ||
| Number of categories | <60 (raw = 0) | |
| Errors | 81 | |
| Percent conceptual level responses | 74 | |
| Perseverative responses | 107 | |
| Perseverative errors | 108 | |
| COWAT FAS | 65 | 69 |
| Category exemplar | 69 | 80 |
| Motor functioning | ||
| Finger Tapping Dominant Hand | 68 | |
| Finger Tapping Non-Dominant Hand | 62 | |
| Invalidity/effort | ||
| TOMM | ||
| Trial 1 | raw = 34 | raw = 37 |
| Trial 2 | raw = 42 | raw = 45 |
| Recognition | raw = 44 | |
| MSVT verbal | fail | |
| MSVT nonverbal | fail | |
| Scores provided are standardized (mean = 100; SD = 15). Raw scores are also provided when indicated. COWAT: Controlled oral word association test; FSIQ: Full Scale IQ; MSVT: Medical Symptom Validity Test; PIQ: Performance IQ; TOMM: Test of Memory Malingering; VIQ: Verbal IQ | ||
Related Resources
- National Institute of Neurological Disorders and Stroke. Fabry disease information page. www.ninds.nih.gov/disorders/fabrys/fabrys.htm.
- National Fabry Disease Foundation. www.thenfdf.org.
- Rozenfeld P, Neumann PM. Treatment of Fabry disease: current and emerging strategies. Curr Pharm Biotechnol. 2011;12(6):916-922.
Drug Brand Names
- Donepezil • Aricept
- Memantine • Namenda
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Rivastigmine • Exelon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Disoriented and delusional
Ms. P, a 53-year-old registered nurse, is admitted to the inpatient psychiatric unit with confusion, markedly disorganized thought processes, delayed verbal responsiveness, mood lability, and persecutory delusions. Shortly before hospitalization, Ms. P traveled approximately 360 miles from her daughter’s home with a male companion. Noting changes in her mental status, the man brought Ms. P to the local hospital. She was then transferred to our facility.
At admission, Ms. P is not oriented to time. She denies auditory or visual hallucinations and does not display psychomotor agitation or retardation. She reports her mood as sad and her affect is mildly labile. Insight and judgment are considered poor.
Five years ago, Ms. P and her mother were diagnosed with Fabry’s disease (FD) based on genetic analysis. Both women are carriers for the mutations and Ms. P’s mother was found to have almost absent galactosidase activity.
The authors’ observations
FD is an X-linked recessive glycolipid storage disease caused by deficient activity of the lysosomal storage enzyme α-galactosidase A. The disorder affects both men and women and leads to progressive intracellular accumulation of globotriaosylceramide and other related glycosphingolipids.1,2 The earliest FD symptoms—burning pain and acroparesthesias—typically appear in childhood (Table 1).2 FD often is misdiagnosed in women because women tend to display neurologic symptoms later than men, with typical symptom onset in the teenage years.3,4 Often, these symptoms are confused with psychiatric disorders or vague neurologic or pain syndromes.5 In patients with no family history of FD, accurate diagnosis may not be made until adulthood.
Laboratory, dermatologic, and genetic tests can accurately determine the presence of FD.1 However, because multiple organ systems are involved, initially attributing symptoms to FD is challenging, particularly in women.1,3,5 For men, diagnosis can be established by measuring plasma or urinary globotriaosylceramide or plasma α-galactosidase A in addition to genetic analysis. In women, genetic analysis is a better diagnosis strategy because elevations in globotriaosylceramide or α-galactosidase A may not be prominent. An algorithm for diagnosing and assessing patients with FD has been proposed.2
Table 1
Typical signs and symptoms of Fabry’s disease
| Typical time at onset | Signs/symptoms |
|---|---|
| Childhood and adolescence (age ≤16) | Neuropathic pain Ophthalmologic abnormalities (cornea verticillata and tortuous retinal blood vessels) Hearing impairment Dyshidrosis (hypohidrosis and hyperhidrosis) Hypersensitivity to heat and cold Gastrointestinal disturbances and abdominal pain Lethargy and tiredness Angiokeratomas Onset of renal and cardiac signs (eg, microalbuminuria, proteinuria, abnormal heart rate variability) |
| Early adulthood (age 17 to 30) | Extension of any of the above Proteinuria and progressive renal failure Cardiomyopathy Transient ischemic attacks, strokes Facial dysmorphism |
| Later adulthood (age >30) | Worsening of any of the above Heart disease (eg, left ventricular hypertrophy, angina, arrhythmia, and dyspnea) Transient ischemic attacks, strokes Osteopenia and osteoporosis |
| Source: Mehta A, Beck M, Eyskens F, et al. Fabry disease: a review of current management strategies. QJM. 2010;103(9):641-659, by permission of Oxford University Press | |
HISTORY: Cognitive deterioration
Ms. P has had psychiatric symptoms such as depression and anxiety since childhood. However, 3 years ago she started to experience psychological and cognitive deterioration. Medical records indicate that Ms. P described memory and concentration problems over the previous few years. She also reported pain, weakness, and numbness in her left leg after surgery for a work-related back injury, for which she received a financial settlement through workers’ compensation. Shortly thereafter, Ms. P separated from her third husband, moved in with her parents, and found work as a psychiatric nurse. She was dismissed after 6 weeks because she could not learn the electronic medical record system and had difficulty with memory and attention. Her performance on the Mini-Mental State Exam6 at that time was 28 out of 30, which was within normal limits.
After her parents died 3 years ago, Ms. P lived with her daughter, who became her primary caregiver and legal guardian. Ms. P’s daughter notes that her mother’s impulsive and risky behaviors grew more pronounced. Ms. P went on shopping sprees and became sexually promiscuous.
Ms. P’s psychiatric history includes childhood sexual abuse, hospitalization for a suicide attempt at age 19, and courses of psychotherapy and pharmacotherapy. In addition to FD, Ms. P’s medical history consists of coronary artery disease, type 2 diabetes mellitus, hypercholesterolemia, obesity, arthritis, back pain, fibromyalgia, and gastroesophageal reflux disease. Her family history is notable for alcohol abuse (both parents and a brother), lung cancer (mother), myocardial infarction (father), and Alzheimer’s disease (father).
The authors’ observations
Because α-galactosidase A is ubiquitous throughout the body, in addition to neurologic symptoms, FD involves multiple organ systems, with possible dermatologic, renal, gastrointestinal, cardiac, and cerebrovascular dysfunction. Despite growth in FD research, including the Fabry Outcomes Survey,3 the psychosocial and neuropsychiatric implications of the disease remain unclear.7 Behavioral presentations are idiosyncratic and unstable over time, depending on the structures impacted by progressive glycosphingolipid accumulation. Premature cardiovascular events (onset between age 30 and 40 for women), greater incidence of ischemic stroke or transient ischemic attack (7% to 30%), and frequent evidence of white matter lesions put FD patients at greater risk for developing presenile vascular dementia.1,3 Nearly all male FD patients with dementia show some evidence of stroke or transient ischemic attack; cognitive functioning has not been well explored in female patients.4 In a heterogeneous sample of 15 FD patients age 7 to 61, Segal et al8 noted deficits in attention, processing speed, and executive function .75 to 1.95 standard deviations below normative means. No patients in this study had a history of stroke or transient ischemic attack; neuroimaging studies were not reported. Kolodny and Pastores9 suggested multiple mechanisms for cognitive disruption, suggesting that mild dementia late in the disease course could be secondary to diffuse leukomalacia, multiple strokes, or possibly to lipid storage in hippocampal and frontal lobe neurons.
Psychiatric comorbidity
Psychiatric illness, such as depression or a personality disorder, may be comorbid with FD, although pathologic mechanisms remain unclear.7,10,11 Hypothesized mechanisms include:
- psychosocial stress from chronic disease
- white matter changes
- disruption of impaired L-arginine-nitric oxide pathways.7,12
Crosbie et al13 noted that FD patients presented with greater psychological distress as measured by the Minnesota Multiphasic Personality Inventory-2 than patients with Gaucher disease or chronic heart disease. However, no significant differences were found between patients with FD and those diagnosed with a pain disorder. In the Segal et al study, out of 11 adult FD patients, 4 were diagnosed with major depressive disorder, 1 with schizophrenia, 2 with schizotypal personality disorder, and 1 with borderline personality disorder.8
EVALUATION: Brain abnormalities
Head CT scans (conducted 2 years ago and 6 months ago) revealed prominent cortical sulci likely caused by underlying volume loss, especially in bifrontal areas. A brain MRI performed 2 months ago indicated a moderate degree of subcortical atrophy in bilateral frontal and parietal regions. These radiology findings suggest mild to moderate frontal atrophy, mild degree of white matter changes, and slightly enlarged ventricles. An EEG showed background slowing and lack of an alpha rhythm, indicative of cerebral cortical dysfunction.
Ms. P’s α-galactosidase A level was within normal limits; however, normal enzyme levels frequently are reported in symptomatic and asymptomatic female FD patients.14 A dermatology consult confirmed the presence of skin findings characteristic of FD (ie, multiple cherry red papules extensively distributed throughout Ms. P’s chest, abdomen, and back, as well as upper and lower extremities).
Ms. P completed 2 neuropsychological assessments separated by 5 months. For a summary of the results of these tests, see the table titled “Ms. P’s neuropsychological assessment results”. Both assessments revealed grossly impaired intellectual capacity, memory, processing speed, and motor functioning. During the assessment, Ms. P could understand all directions with minimal changes from standardized protocols. Ms. P became insistent that she would not be able to complete memory tasks successfully. She gave up prematurely on tasks, saying they were too difficult. She admitted to guessing on several items because she did not want to continue the task.
Ms. P’s performance on tasks measuring effort and validity of a person’s neuropsychological presentation was consistent with someone exaggerating neurologic symptoms. A person with true dementia may perform as poorly as Ms. P did. However, Ms. P’s scores likely underestimated her level of functioning, even if she was experiencing dementia. Ms. P could not complete tasks individuals with severe dementia complete successfully, such as simple addition and subtraction and digit repetition. Ms. P recalled several recent and remote events, such as her breakfast menu and location of her first assessment, but could not recall words practiced multiple times. Although Ms. P’s scores on a complex card-sorting task were in the impaired range, a detailed review of her pattern indicated that although Ms. P could not generate any correct sorting categories, she made few repetitive responses and errors. This pattern is consistent with someone who understands task requirements, but deliberately avoids answering correctly. This suggests that she retained some ability for hypotheses generation and problem solving; however, because she exaggerated her symptoms, specific deficits could not be determined.
The authors’ observations
Ms. P presented with an interesting manifestation of neuropsychiatric symptoms in the context of FD; however, common cardiac and cerebrovascular features of the disease were not fully developed. Ms. P experienced progressive cognitive and behavioral changes for 2 years before her admission (Table 2), which may represent a prodromal period leading up to what appeared to be a frontally mediated dementia syndrome. Müller et al15 described a patient with FD who displayed a behavioral profile similar to Ms. P’s that included increasingly unstable mood for at least 3 years, borderline personality disorder features, and rapidly fluctuating mood. A case study reported that risperidone, 1 mg/d, used to treat psychosis in a male FD patient caused extrapyramidal symptoms.16
Ms. P presented with no evidence of stroke or transient ischemic attacks, which is atypical for FD patients with cognitive impairment. However, neuroimaging did reveal frontal atrophy that may be associated with her impulse control deficits, risk-taking behavior, emotional instability, and poor judgment. Her cognitive testing was notable for impairment and exaggeration of symptoms consistent with personality disorder symptoms. Possible reasons for exaggeration include a desire to maintain the sick role or secondary gain related to obtaining disability income.
Ms. P’s behavior pattern could be caused by dementia with frontal features, possibly secondary to FD, in combination with personality and psychiatric pathology.
The mainstay of FD treatment is enzyme replacement therapy (ERT), which addresses the underlying enzyme deficiency. Available research indicates that ERT may reduce symptom severity and slow disease progression; however, further studies are needed to determine if it will reduce outcomes such as stroke, ischemic heart disease, or renal disease.2
Table 2
Symptoms that preceded Ms. P’s admission
| Time frame | Symptoms |
|---|---|
| 24 months before admission | Depressed mood Decreased ability to manage independent activities of daily living (eg, finances, cooking) Minimal objective cognitive impairment |
| 12 months before admission | Increased depression Mild to moderate decline in cognitive functioning Visual and auditory hallucinations Impulsivity/poor impulse control Irrational decision-making Increased risky behavior |
| 6 months before admission | Severe cognitive decline with cognitive symptom exaggeration Psychiatric symptom exaggeration Disorganized thinking Continued risky behavior and poor decision-making |
TREATMENT: Persistent deficits
Ms. P is started on risperidone rapidly titrated to 4 mg/d for delusional thinking and behavioral disturbance. After initially improving, she develops delirium when risperidone is increased to 4 mg/d. She has visual hallucinations, marked confusion with disorientation, worsened short-term memory, and an unsteady, shuffling gait. Risperidone is tapered and discontinued and Ms. P’s motor symptoms resolve within 2 days; however, she remains confused and delusional. We start her on quetiapine, 25 mg/d titrated to 50 mg/d, and her agitation and delusional thinking progressively decline. Memantine, titrated to 20 mg/d, and rivastigmine, started at 3 mg/d titrated to 9 mg/d, are added to address her cognitive symptoms.
Over several weeks, Ms. P’s mental status slowly improves and her drug-induced delirium completely resolves. However, she has persistent cognitive impairment characterized by compromised short-term memory and poor insight into her medical and psychological condition. She maintains unrealistic expectations about her ability to live independently and return to the workforce. The treatment team recommends that Ms. P’s daughter pursue guardianship and that she receive around-the-clock supervision after discharge from the hospital.
Table
Ms. P’s neuropsychological assessment results
| June | November | |
|---|---|---|
| Intellectual functioning | ||
| Wechsler Adult Intelligence Scale-III | ||
| FSIQ | 60 | |
| VIQ | 68 | |
| PIQ | 56 | |
| Ravens Colored Progressive Matrices | 70 | |
| Premorbid intellectual functioning estimates | ||
| Peabody Picture Vocabulary Test-2 | 89 | |
| Barona Demographic Estimate | 104 | 104 |
| North American Adult Reading Test | 99 | |
| Memory functioning | ||
| Wechsler Memory Scale-III | ||
| Immediate memory | 45 | |
| General delay memory | 47 | |
| Auditory recognition delay | 55 | |
| California Verbal Learning Test-II | ||
| Trial 1 (immediate recall) | <60 (raw = 3) | |
| Trial 5 | <60 (raw = 3) | |
| Total Words Learned | <60 (raw = 15) | |
| Short Delay Free Recall | <60 (raw = 2) | |
| Long Delay Free Recall | <60 (raw = 4) | |
| Executive functioning | ||
| Trail Making Test A | 88 | 88 |
| Trail Making Test B | failed to understand | failed to understand |
| Wisconsin Card Sort-64 | ||
| Number of categories | <60 (raw = 0) | |
| Errors | 81 | |
| Percent conceptual level responses | 74 | |
| Perseverative responses | 107 | |
| Perseverative errors | 108 | |
| COWAT FAS | 65 | 69 |
| Category exemplar | 69 | 80 |
| Motor functioning | ||
| Finger Tapping Dominant Hand | 68 | |
| Finger Tapping Non-Dominant Hand | 62 | |
| Invalidity/effort | ||
| TOMM | ||
| Trial 1 | raw = 34 | raw = 37 |
| Trial 2 | raw = 42 | raw = 45 |
| Recognition | raw = 44 | |
| MSVT verbal | fail | |
| MSVT nonverbal | fail | |
| Scores provided are standardized (mean = 100; SD = 15). Raw scores are also provided when indicated. COWAT: Controlled oral word association test; FSIQ: Full Scale IQ; MSVT: Medical Symptom Validity Test; PIQ: Performance IQ; TOMM: Test of Memory Malingering; VIQ: Verbal IQ | ||
Related Resources
- National Institute of Neurological Disorders and Stroke. Fabry disease information page. www.ninds.nih.gov/disorders/fabrys/fabrys.htm.
- National Fabry Disease Foundation. www.thenfdf.org.
- Rozenfeld P, Neumann PM. Treatment of Fabry disease: current and emerging strategies. Curr Pharm Biotechnol. 2011;12(6):916-922.
Drug Brand Names
- Donepezil • Aricept
- Memantine • Namenda
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Rivastigmine • Exelon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Eng CM, Germain DP, Banikazemi M, et al. Fabry disease: guidelines for the evaluation and management of multi-organ system involvement. Genet Med. 2006;8(9):539-548.
2. Mehta A, Beck M, Eyskens F, et al. Fabry disease: a review of current management strategies. QJM. 2010;103(9):641-659.
3. Deegan PB, Baehner AF, Barba Romero MA, et al. Natural history of Fabry disease in females in the Fabry Outcome Survey. J Med Genet. 2006;43(4):347-352.
4. Fellgiebel A, Müller MJ, Ginsberg L. CNS manifestations of Fabry’s disease. Lancet Neurol. 2006;5(9):791-795.
5. Møller AT, Jensen TS. Neurological manifestations in Fabry’s disease. Nat Clin Pract Neurol. 2007;3(2):95-106.
6. Folstein MF, Folstein SE, McHugh PR. Mini-mental state: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189-198.
7. Müller MJ. Neuropsychiatric and psychosocial aspects of Fabry disease. In: Mehta A Beck M, Sunder-Plassman G, eds. Fabry disease: perspectives from 5 years of FOS. Oxford, United Kingdom: Oxford PharmaGenesis Ltd; 2006. http://www.ncbi.nlm.nih.gov/books/nbk11618. Accessed October 31, 2011.
8. Segal P, Kohn Y, Pollak Y, et al. Psychiatric and cognitive profile in Anderson-Fabry patients: a preliminary study. J Inherit Metab Dis. 2010;33(4):429-436.
9. Kolodny EH, Pastores GM. Anderson-Fabry disease: Extrarenal neurologic manifestations. J Am Soc Nephrol. 2002;13(suppl 2):S150-153.
10. Grewal RP. Psychiatric disorders in patients with Fabry disease. Int J Psychiatry Med. 1993;23(3):307-312.
11. Müller MJ, Müller KM, Dascalescu A, et al. Psychiatric and neuropsychological signs and symptoms in patients with Fabry disease: literature review [in German]. Fortschr Neurol Psychiatr. 2005;73(11):687-693.
12. Segal P, Raas-Rothschild A. Neuropsychiatric manifestations of AFD. In: Elstein D Altarescu G, Beck M, eds. Fabry disease. New York, NY: Springer; 2010:321–324.
13. Crosbie TW, Packman W, Packman S. Psychological aspects of patients with Fabry disease. J Inherit Metab Dis. 2009;32(6):745-753.
14. Linthorst GE, Poorthuis BJ, Hollak CE. Enzyme activity for determination of presence of Fabry disease in women results in 40% false-negative results. J Am Coll Cardiol. 2008;51(21):2082.-
15. Müller MJ, Fellgiebel A, Scheurich A, et al. Recurrent brief depression in female patient with Fabry disease. Bipolar Disord. 2006;8(4):418-419.
16. Shen YC, Haw-Ming L, Lin CC, et al. Psychosis in a patient with Fabry’s disease and treatment with aripiprazole. Prog Neuropsychopharmacol Biol Psychiatry. 2007;31(3):779-780.
1. Eng CM, Germain DP, Banikazemi M, et al. Fabry disease: guidelines for the evaluation and management of multi-organ system involvement. Genet Med. 2006;8(9):539-548.
2. Mehta A, Beck M, Eyskens F, et al. Fabry disease: a review of current management strategies. QJM. 2010;103(9):641-659.
3. Deegan PB, Baehner AF, Barba Romero MA, et al. Natural history of Fabry disease in females in the Fabry Outcome Survey. J Med Genet. 2006;43(4):347-352.
4. Fellgiebel A, Müller MJ, Ginsberg L. CNS manifestations of Fabry’s disease. Lancet Neurol. 2006;5(9):791-795.
5. Møller AT, Jensen TS. Neurological manifestations in Fabry’s disease. Nat Clin Pract Neurol. 2007;3(2):95-106.
6. Folstein MF, Folstein SE, McHugh PR. Mini-mental state: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189-198.
7. Müller MJ. Neuropsychiatric and psychosocial aspects of Fabry disease. In: Mehta A Beck M, Sunder-Plassman G, eds. Fabry disease: perspectives from 5 years of FOS. Oxford, United Kingdom: Oxford PharmaGenesis Ltd; 2006. http://www.ncbi.nlm.nih.gov/books/nbk11618. Accessed October 31, 2011.
8. Segal P, Kohn Y, Pollak Y, et al. Psychiatric and cognitive profile in Anderson-Fabry patients: a preliminary study. J Inherit Metab Dis. 2010;33(4):429-436.
9. Kolodny EH, Pastores GM. Anderson-Fabry disease: Extrarenal neurologic manifestations. J Am Soc Nephrol. 2002;13(suppl 2):S150-153.
10. Grewal RP. Psychiatric disorders in patients with Fabry disease. Int J Psychiatry Med. 1993;23(3):307-312.
11. Müller MJ, Müller KM, Dascalescu A, et al. Psychiatric and neuropsychological signs and symptoms in patients with Fabry disease: literature review [in German]. Fortschr Neurol Psychiatr. 2005;73(11):687-693.
12. Segal P, Raas-Rothschild A. Neuropsychiatric manifestations of AFD. In: Elstein D Altarescu G, Beck M, eds. Fabry disease. New York, NY: Springer; 2010:321–324.
13. Crosbie TW, Packman W, Packman S. Psychological aspects of patients with Fabry disease. J Inherit Metab Dis. 2009;32(6):745-753.
14. Linthorst GE, Poorthuis BJ, Hollak CE. Enzyme activity for determination of presence of Fabry disease in women results in 40% false-negative results. J Am Coll Cardiol. 2008;51(21):2082.-
15. Müller MJ, Fellgiebel A, Scheurich A, et al. Recurrent brief depression in female patient with Fabry disease. Bipolar Disord. 2006;8(4):418-419.
16. Shen YC, Haw-Ming L, Lin CC, et al. Psychosis in a patient with Fabry’s disease and treatment with aripiprazole. Prog Neuropsychopharmacol Biol Psychiatry. 2007;31(3):779-780.
College mental health: How to provide care for students in need
Each year thousands of college students seek treatment at their school’s mental health service, but few psychiatrists are delivering this care. Most of the 4,500 degree-granting institutions of higher education (IHEs) in the United States1 provide some type of psychological or mental health counseling support to their students, and approximately 10% of the student body seeks care annually.2 In 2010, nearly 24% of students who visited their college counseling service were taking psychiatric medications at the time of their visit, up from 9% in 1994.2
Nevertheless, for various historical and practical reasons, psychiatrists have played—and continue to play—a somewhat peripheral role in college mental health systems. Although interest in psychiatric care at IHEs has been increasing (Box 1),3 until recently, most college counseling services had no direct access to psychiatric services and currently <1% of college services are directed by psychiatrists.2
This article examines some of the unique challenges faced by psychiatrists who work in a college mental health service, including how this setting may affect assessment, medication management, and crisis counseling. I use the terms “counseling services” and “mental health services” interchangeably because schools differ in the name they use for this office.
In recent years, the psychiatric community has begun to take steps to recognize college mental health as a specific practice area.3 In 2004, as president of the American Psychiatric Association (APA), Current Psychiatry Section Editor Michelle B. Riba, MD, MS convened a task force on college mental health. Subsequently, the APA added a section on college mental health to its public information Web site “Healthy Minds. Healthy Lives” (www.healthyminds.org).
The University of Michigan has taken a national leadership role in college psychiatry and college mental health. Since 2003, the University of Michigan Depression Center has hosted a yearly Depression on College Campuses national conference. Content from past conferences is available at www.depressioncenter.org/docc.
Organizations dedicated to college mental health and suicide prevention also have taken a role in disseminating information. Chief among them are the Jed Foundation, Active Minds on Campus, the Suicide Prevention Resource Center, Penn State’s Center for Collegiate Mental Health, and the National Research Consortium of Counseling Centers in Higher Education. More needs to be done to expand efforts related to college mental health and educate the psychiatric community and community at large about these vital concerns.
Managing medications and crises
Most college mental health services are directed by psychologists because of how IHEs historically structured these services (Box 2).4 Although counseling center staffing generally includes relatively few psychiatrists, those who do serve in this setting typically serve 2 primary roles: medication managers and crisis clinicians.
Medication management. Counseling centers are seeing more students who are either already taking psychotropics or need assessment and medication management. In the United States, 14% of students seen at college counseling centers are referred for psychiatric evaluation; however, on average, schools provide 2 hours of psychiatric services per week for every 1,000 students.2
Managing medications for college students poses several challenges. For most students, interaction with their college’s health and/or mental health system may be the first time they receive care not under the direct oversight of their family. Families and their feelings about psychiatric medication can play a major role in planning, executing, and managing psychiatric care, even for students who are legal adults. Family attitudes toward psychiatry and patients’ fears of disappointing parents who may feel distraught because their child has a psychiatric illness may impact a young person’s decision to accept medication or comply with treatment. Students often are insured by their family, and parents might receive an Explanation of Benefits and will learn of the student’s pharmacotherapy even if the student does not want them to know. College psychiatrists and students always need to consider decisions about how and when to include parents in discussions about medications.
College psychiatrists also must be sensitive to the unique vicissitudes of the school calendar and the developmental trajectory of college life. Decisions about when to start a medication or even which medication to prescribe might depend on how close a students is to exams or summer break. For example, a student experiencing severe anxiety a week before exams probably is better treated with a short-term benzodiazepine prescribed on an as-needed basis than a selective serotonin reuptake inhibitor, which in the first few weeks might only disrupt the student’s ability to function academically and not improve symptoms.5
Assessment also must consider the context of the academic year. For example, students may be “homesick” when they first enter college. Although such students may present with prominent and seemingly severe symptoms of anxiety or depression, more often than not the condition is self-limiting and resolves with support and watchful waiting. For example, many years ago a student presented to my institution’s counseling office in severe acute panic at the beginning of his first year at college. He had never been away from home, had not yet received his dorm phone, and did not know how to use a pay phone. His anxiety resolved as soon as I let him use my office phone to call his family. He ultimately made an excellent adjustment to college life.
Because most counseling services are set up primarily to provide talk therapy, most students who receive psychiatric medication also are engaged in psychotherapy. In these situations, psychiatrists must manage the same challenges in communication and coordination of care that occur in any split treatment agreement. These problems may be more easily addressed when the psychotherapist and prescriber both work in the college counseling center. Unfortunately, at some institutions, the psychiatrist or prescribing physician assistant or nurse practitioner may be based at the college’s health service,6 which can make coordination of care more challenging.
Crisis management. College counseling centers often manage students in crisis. Each year, approximately 6% of college students report suicidal ideation and 1% to 2% report suicide attempts.7 In 2010 there were 14 psychiatric hospitalizations for every 10,000 students on college campuses.2 Because psychiatrists are trained to manage patients with severe pathology and have emergency room training, college counseling psychiatrists often are looked to for assessment and consultation for students in crisis. In many cases, a student in crisis also will need psychopharmacologic intervention. In the event of a suicide or death on campus, the college psychiatrist often is called upon to address postvention planning and management of the clinical and community response.
Psychiatrists who manage student crises need to be cognizant of the unique elements of college life: Does the student live in a dormitory or with family? Could a relative who lives nearby help supervise an anxious patient who is cutting herself? Is the student in treatment with a therapist “back home” who could provide history or intervene? A crisis that occurs early in the school year, when a new student is less likely to have a network of friends or other supports, may need to be managed differently from one that occurs later, when the student might have people who could provide some comfort for a short time. The psychiatrist should know what level of support and supervision is available in the residence halls.
Although it is helpful for college counseling centers to maintain ongoing communication and coordination of services with local clinics and/or university medical centers, it is especially important for those who manage crises to have strong communication with local emergency rooms (ERs) and community crisis services. Because these services likely are managed by physicians, the campus psychiatrist is well placed to consult and coordinate care with local ERs because during a crisis, physician-to-physician communication often is more effective than campus counselor-to-ER physician communication. Ideally, college psychiatrists should have regular communication with ER physicians to discuss campus trends—such as particular drugs being used with unusual frequency or suicides on campus that might raise concerns of suicide contagion—and educate ER clinicians about services and programs the college offers.8
Barreira and Snider4 described the early development of college counseling services as flowing from 2 separate streams. Counseling services at colleges began to appear in the middle of the 20th century and grew out of academic and career advising offices. These programs typically had a “developmental”—as opposed to a clinical—orientation. Most of these services were and continue to be directed by counseling psychologists.
At the same time, some larger institutions—particularly the “Ivys”—hired psychiatrists to provide mental health care. Sometimes these clinicians were based at the school health service, while other institutions had parallel systems of counseling and mental health services. Today most colleges have integrated these programs into a single service.
An opportunity for training
Psychiatrists’ training may make them well-suited to address clinical issues that typically arise among college students. For example, students who have difficulty in college often struggle with issues at the border of physical and emotional health. Many students experience significant levels of stress, and many struggle with poor or inconsistent eating and nutrition and inadequate sleep. In fact, severely sleep-deprived students may present with symptoms that mimic depression.5 Psychiatrists have credibility in addressing these issues with individual students and the campus community. Psychiatrists also have training and experience in diagnosing and managing patients with substance abuse and can educate students, parents, faculty, and university administrators about these disorders.
College mental health services can be valuable training venues for senior psychiatric residents and child and adolescent fellows.9 College students can provide exposure to a broad array of problems—such as anxiety disorders, obsessive-compulsive disorder, dysthymic disorder, adjustment disorders, and panic disorder—that psychiatric trainees may not confront in a hospital clinic. Students are particularly responsive to short-term talk therapies with or without medication management, and working with this population can be a strong antidote to the “therapeutic nihilism”—the unfortunate sense that talk therapies are of limited effectiveness and that only pharmacotherapy can help psychiatric problems—often experienced by psychiatric trainees who spend much of their time working with patients with serious, chronic illnesses. Psychiatric residents can be particularly helpful in managing student patients who require combined medication and talk therapy.
College-based psychiatrists are well suited for educating residents about developmental issues of “emerging adulthood,” including:
- exploration of and anxieties about relationships and sexuality
- balancing connectedness to family with increasing sense of autonomy and independence
- establishing personal life goals and values and career choices and goals.10
College counseling services also are an excellent setting for residents to learn principles of community mental health and medico-legal concepts related to confidentiality, duty to warn, and disability law.11
Treatment outside college
Because college students have high rates of substance abuse12 and other psychiatric disorders, it is important for psychiatrists who treat these patients in private practice or community-based clinics to develop a basic awareness of and competency in relevant developmental and clinical issues. Psychiatrists who work in emergency services in areas with high concentrations of college students need to be particularly attuned to issues related to college mental health, substance abuse, and life on campus.8
Related Resources
- The Jed Foundation. www.jedfoundation.org.
- National Research Consortium of Counseling Centers in Higher Education. www.cmhc.utexas.edu/researchconsortium.html.
Disclosure
Dr. Schwartz reports no financial relationship with any companies whose products are mentioned in this article or with manufacturers of competing products.
1. US Department of Education National Center for Education Statistics. Degree-granting institutions by control and type of institution: Selected years, 1949-50 through 2009-10. http://nces.ed.gov/programs/digest/d10/tables/dt10_275.asp. Accessed August 22, 2011.
2. Gallagher RP. National survey of counseling center directors 2010. International Association of Counseling Services. http://www.iacsinc.org. Accessed August 22 2011.
3. Schwartz V, Kay J. The crisis in college and university mental health. Psychiatric Times. July 27 2009.
4. Barreira P, Snider M. History of college counseling and mental health services and role of the community mental health model. In: Kay J Schwartz V, eds. Mental health care in the college community. Hoboken, NJ: Wiley and Sons; 2010:21–31.
5. Schwartz V. Medications. In: Grayson PA Meilman PW, eds. College mental health practice. New York, NY: Routledge; 2006:59–78.
6. Barr V, Rando R, Krylowicz B, et al. The Association for University and College Counseling Centers Directors Annual Survey. 2010. http://aucccd.org/img/pdfs/aucccd_directors_survey_monograph_2010.pdf. Accessed September 1, 2011.
7. American College Health Association. National college health assessment II: reference group executive summary Fall 2010. Linthicum MD: American College Health Association; 2011.
8. Glick RL, Schwartz V. Assessment and management: special considerations for college students in psychiatric crisis. Psychiatric Issues in Emergency Care Settings. 2007;6(4):7-13.
9. Kay J, Schwartz V. Psychiatry residency training in college mental health services. In: Kay J Schwartz V, eds. Mental health care in the college community. Hoboken, NJ: Wiley and Sons; 2010.
10. Arnett JJ. Emerging adulthood: the winding road from the late teens through the twenties. New York NY: Oxford University Press; 2004.
11. Bower K, Schwartz V. Legal and ethical issues in college mental health. In: Kay J Schwartz V, eds. Mental health care in the college community. Hoboken, NJ: Wiley and Sons; 2010.
12. Hingson R, White A. Magnitude and prevention of college alcohol and drug misuse. In: Kay J Schwartz V, eds. Mental health care in the college community. Hoboken, NJ: Wiley and Sons; 2010.
Each year thousands of college students seek treatment at their school’s mental health service, but few psychiatrists are delivering this care. Most of the 4,500 degree-granting institutions of higher education (IHEs) in the United States1 provide some type of psychological or mental health counseling support to their students, and approximately 10% of the student body seeks care annually.2 In 2010, nearly 24% of students who visited their college counseling service were taking psychiatric medications at the time of their visit, up from 9% in 1994.2
Nevertheless, for various historical and practical reasons, psychiatrists have played—and continue to play—a somewhat peripheral role in college mental health systems. Although interest in psychiatric care at IHEs has been increasing (Box 1),3 until recently, most college counseling services had no direct access to psychiatric services and currently <1% of college services are directed by psychiatrists.2
This article examines some of the unique challenges faced by psychiatrists who work in a college mental health service, including how this setting may affect assessment, medication management, and crisis counseling. I use the terms “counseling services” and “mental health services” interchangeably because schools differ in the name they use for this office.
In recent years, the psychiatric community has begun to take steps to recognize college mental health as a specific practice area.3 In 2004, as president of the American Psychiatric Association (APA), Current Psychiatry Section Editor Michelle B. Riba, MD, MS convened a task force on college mental health. Subsequently, the APA added a section on college mental health to its public information Web site “Healthy Minds. Healthy Lives” (www.healthyminds.org).
The University of Michigan has taken a national leadership role in college psychiatry and college mental health. Since 2003, the University of Michigan Depression Center has hosted a yearly Depression on College Campuses national conference. Content from past conferences is available at www.depressioncenter.org/docc.
Organizations dedicated to college mental health and suicide prevention also have taken a role in disseminating information. Chief among them are the Jed Foundation, Active Minds on Campus, the Suicide Prevention Resource Center, Penn State’s Center for Collegiate Mental Health, and the National Research Consortium of Counseling Centers in Higher Education. More needs to be done to expand efforts related to college mental health and educate the psychiatric community and community at large about these vital concerns.
Managing medications and crises
Most college mental health services are directed by psychologists because of how IHEs historically structured these services (Box 2).4 Although counseling center staffing generally includes relatively few psychiatrists, those who do serve in this setting typically serve 2 primary roles: medication managers and crisis clinicians.
Medication management. Counseling centers are seeing more students who are either already taking psychotropics or need assessment and medication management. In the United States, 14% of students seen at college counseling centers are referred for psychiatric evaluation; however, on average, schools provide 2 hours of psychiatric services per week for every 1,000 students.2
Managing medications for college students poses several challenges. For most students, interaction with their college’s health and/or mental health system may be the first time they receive care not under the direct oversight of their family. Families and their feelings about psychiatric medication can play a major role in planning, executing, and managing psychiatric care, even for students who are legal adults. Family attitudes toward psychiatry and patients’ fears of disappointing parents who may feel distraught because their child has a psychiatric illness may impact a young person’s decision to accept medication or comply with treatment. Students often are insured by their family, and parents might receive an Explanation of Benefits and will learn of the student’s pharmacotherapy even if the student does not want them to know. College psychiatrists and students always need to consider decisions about how and when to include parents in discussions about medications.
College psychiatrists also must be sensitive to the unique vicissitudes of the school calendar and the developmental trajectory of college life. Decisions about when to start a medication or even which medication to prescribe might depend on how close a students is to exams or summer break. For example, a student experiencing severe anxiety a week before exams probably is better treated with a short-term benzodiazepine prescribed on an as-needed basis than a selective serotonin reuptake inhibitor, which in the first few weeks might only disrupt the student’s ability to function academically and not improve symptoms.5
Assessment also must consider the context of the academic year. For example, students may be “homesick” when they first enter college. Although such students may present with prominent and seemingly severe symptoms of anxiety or depression, more often than not the condition is self-limiting and resolves with support and watchful waiting. For example, many years ago a student presented to my institution’s counseling office in severe acute panic at the beginning of his first year at college. He had never been away from home, had not yet received his dorm phone, and did not know how to use a pay phone. His anxiety resolved as soon as I let him use my office phone to call his family. He ultimately made an excellent adjustment to college life.
Because most counseling services are set up primarily to provide talk therapy, most students who receive psychiatric medication also are engaged in psychotherapy. In these situations, psychiatrists must manage the same challenges in communication and coordination of care that occur in any split treatment agreement. These problems may be more easily addressed when the psychotherapist and prescriber both work in the college counseling center. Unfortunately, at some institutions, the psychiatrist or prescribing physician assistant or nurse practitioner may be based at the college’s health service,6 which can make coordination of care more challenging.
Crisis management. College counseling centers often manage students in crisis. Each year, approximately 6% of college students report suicidal ideation and 1% to 2% report suicide attempts.7 In 2010 there were 14 psychiatric hospitalizations for every 10,000 students on college campuses.2 Because psychiatrists are trained to manage patients with severe pathology and have emergency room training, college counseling psychiatrists often are looked to for assessment and consultation for students in crisis. In many cases, a student in crisis also will need psychopharmacologic intervention. In the event of a suicide or death on campus, the college psychiatrist often is called upon to address postvention planning and management of the clinical and community response.
Psychiatrists who manage student crises need to be cognizant of the unique elements of college life: Does the student live in a dormitory or with family? Could a relative who lives nearby help supervise an anxious patient who is cutting herself? Is the student in treatment with a therapist “back home” who could provide history or intervene? A crisis that occurs early in the school year, when a new student is less likely to have a network of friends or other supports, may need to be managed differently from one that occurs later, when the student might have people who could provide some comfort for a short time. The psychiatrist should know what level of support and supervision is available in the residence halls.
Although it is helpful for college counseling centers to maintain ongoing communication and coordination of services with local clinics and/or university medical centers, it is especially important for those who manage crises to have strong communication with local emergency rooms (ERs) and community crisis services. Because these services likely are managed by physicians, the campus psychiatrist is well placed to consult and coordinate care with local ERs because during a crisis, physician-to-physician communication often is more effective than campus counselor-to-ER physician communication. Ideally, college psychiatrists should have regular communication with ER physicians to discuss campus trends—such as particular drugs being used with unusual frequency or suicides on campus that might raise concerns of suicide contagion—and educate ER clinicians about services and programs the college offers.8
Barreira and Snider4 described the early development of college counseling services as flowing from 2 separate streams. Counseling services at colleges began to appear in the middle of the 20th century and grew out of academic and career advising offices. These programs typically had a “developmental”—as opposed to a clinical—orientation. Most of these services were and continue to be directed by counseling psychologists.
At the same time, some larger institutions—particularly the “Ivys”—hired psychiatrists to provide mental health care. Sometimes these clinicians were based at the school health service, while other institutions had parallel systems of counseling and mental health services. Today most colleges have integrated these programs into a single service.
An opportunity for training
Psychiatrists’ training may make them well-suited to address clinical issues that typically arise among college students. For example, students who have difficulty in college often struggle with issues at the border of physical and emotional health. Many students experience significant levels of stress, and many struggle with poor or inconsistent eating and nutrition and inadequate sleep. In fact, severely sleep-deprived students may present with symptoms that mimic depression.5 Psychiatrists have credibility in addressing these issues with individual students and the campus community. Psychiatrists also have training and experience in diagnosing and managing patients with substance abuse and can educate students, parents, faculty, and university administrators about these disorders.
College mental health services can be valuable training venues for senior psychiatric residents and child and adolescent fellows.9 College students can provide exposure to a broad array of problems—such as anxiety disorders, obsessive-compulsive disorder, dysthymic disorder, adjustment disorders, and panic disorder—that psychiatric trainees may not confront in a hospital clinic. Students are particularly responsive to short-term talk therapies with or without medication management, and working with this population can be a strong antidote to the “therapeutic nihilism”—the unfortunate sense that talk therapies are of limited effectiveness and that only pharmacotherapy can help psychiatric problems—often experienced by psychiatric trainees who spend much of their time working with patients with serious, chronic illnesses. Psychiatric residents can be particularly helpful in managing student patients who require combined medication and talk therapy.
College-based psychiatrists are well suited for educating residents about developmental issues of “emerging adulthood,” including:
- exploration of and anxieties about relationships and sexuality
- balancing connectedness to family with increasing sense of autonomy and independence
- establishing personal life goals and values and career choices and goals.10
College counseling services also are an excellent setting for residents to learn principles of community mental health and medico-legal concepts related to confidentiality, duty to warn, and disability law.11
Treatment outside college
Because college students have high rates of substance abuse12 and other psychiatric disorders, it is important for psychiatrists who treat these patients in private practice or community-based clinics to develop a basic awareness of and competency in relevant developmental and clinical issues. Psychiatrists who work in emergency services in areas with high concentrations of college students need to be particularly attuned to issues related to college mental health, substance abuse, and life on campus.8
Related Resources
- The Jed Foundation. www.jedfoundation.org.
- National Research Consortium of Counseling Centers in Higher Education. www.cmhc.utexas.edu/researchconsortium.html.
Disclosure
Dr. Schwartz reports no financial relationship with any companies whose products are mentioned in this article or with manufacturers of competing products.
Each year thousands of college students seek treatment at their school’s mental health service, but few psychiatrists are delivering this care. Most of the 4,500 degree-granting institutions of higher education (IHEs) in the United States1 provide some type of psychological or mental health counseling support to their students, and approximately 10% of the student body seeks care annually.2 In 2010, nearly 24% of students who visited their college counseling service were taking psychiatric medications at the time of their visit, up from 9% in 1994.2
Nevertheless, for various historical and practical reasons, psychiatrists have played—and continue to play—a somewhat peripheral role in college mental health systems. Although interest in psychiatric care at IHEs has been increasing (Box 1),3 until recently, most college counseling services had no direct access to psychiatric services and currently <1% of college services are directed by psychiatrists.2
This article examines some of the unique challenges faced by psychiatrists who work in a college mental health service, including how this setting may affect assessment, medication management, and crisis counseling. I use the terms “counseling services” and “mental health services” interchangeably because schools differ in the name they use for this office.
In recent years, the psychiatric community has begun to take steps to recognize college mental health as a specific practice area.3 In 2004, as president of the American Psychiatric Association (APA), Current Psychiatry Section Editor Michelle B. Riba, MD, MS convened a task force on college mental health. Subsequently, the APA added a section on college mental health to its public information Web site “Healthy Minds. Healthy Lives” (www.healthyminds.org).
The University of Michigan has taken a national leadership role in college psychiatry and college mental health. Since 2003, the University of Michigan Depression Center has hosted a yearly Depression on College Campuses national conference. Content from past conferences is available at www.depressioncenter.org/docc.
Organizations dedicated to college mental health and suicide prevention also have taken a role in disseminating information. Chief among them are the Jed Foundation, Active Minds on Campus, the Suicide Prevention Resource Center, Penn State’s Center for Collegiate Mental Health, and the National Research Consortium of Counseling Centers in Higher Education. More needs to be done to expand efforts related to college mental health and educate the psychiatric community and community at large about these vital concerns.
Managing medications and crises
Most college mental health services are directed by psychologists because of how IHEs historically structured these services (Box 2).4 Although counseling center staffing generally includes relatively few psychiatrists, those who do serve in this setting typically serve 2 primary roles: medication managers and crisis clinicians.
Medication management. Counseling centers are seeing more students who are either already taking psychotropics or need assessment and medication management. In the United States, 14% of students seen at college counseling centers are referred for psychiatric evaluation; however, on average, schools provide 2 hours of psychiatric services per week for every 1,000 students.2
Managing medications for college students poses several challenges. For most students, interaction with their college’s health and/or mental health system may be the first time they receive care not under the direct oversight of their family. Families and their feelings about psychiatric medication can play a major role in planning, executing, and managing psychiatric care, even for students who are legal adults. Family attitudes toward psychiatry and patients’ fears of disappointing parents who may feel distraught because their child has a psychiatric illness may impact a young person’s decision to accept medication or comply with treatment. Students often are insured by their family, and parents might receive an Explanation of Benefits and will learn of the student’s pharmacotherapy even if the student does not want them to know. College psychiatrists and students always need to consider decisions about how and when to include parents in discussions about medications.
College psychiatrists also must be sensitive to the unique vicissitudes of the school calendar and the developmental trajectory of college life. Decisions about when to start a medication or even which medication to prescribe might depend on how close a students is to exams or summer break. For example, a student experiencing severe anxiety a week before exams probably is better treated with a short-term benzodiazepine prescribed on an as-needed basis than a selective serotonin reuptake inhibitor, which in the first few weeks might only disrupt the student’s ability to function academically and not improve symptoms.5
Assessment also must consider the context of the academic year. For example, students may be “homesick” when they first enter college. Although such students may present with prominent and seemingly severe symptoms of anxiety or depression, more often than not the condition is self-limiting and resolves with support and watchful waiting. For example, many years ago a student presented to my institution’s counseling office in severe acute panic at the beginning of his first year at college. He had never been away from home, had not yet received his dorm phone, and did not know how to use a pay phone. His anxiety resolved as soon as I let him use my office phone to call his family. He ultimately made an excellent adjustment to college life.
Because most counseling services are set up primarily to provide talk therapy, most students who receive psychiatric medication also are engaged in psychotherapy. In these situations, psychiatrists must manage the same challenges in communication and coordination of care that occur in any split treatment agreement. These problems may be more easily addressed when the psychotherapist and prescriber both work in the college counseling center. Unfortunately, at some institutions, the psychiatrist or prescribing physician assistant or nurse practitioner may be based at the college’s health service,6 which can make coordination of care more challenging.
Crisis management. College counseling centers often manage students in crisis. Each year, approximately 6% of college students report suicidal ideation and 1% to 2% report suicide attempts.7 In 2010 there were 14 psychiatric hospitalizations for every 10,000 students on college campuses.2 Because psychiatrists are trained to manage patients with severe pathology and have emergency room training, college counseling psychiatrists often are looked to for assessment and consultation for students in crisis. In many cases, a student in crisis also will need psychopharmacologic intervention. In the event of a suicide or death on campus, the college psychiatrist often is called upon to address postvention planning and management of the clinical and community response.
Psychiatrists who manage student crises need to be cognizant of the unique elements of college life: Does the student live in a dormitory or with family? Could a relative who lives nearby help supervise an anxious patient who is cutting herself? Is the student in treatment with a therapist “back home” who could provide history or intervene? A crisis that occurs early in the school year, when a new student is less likely to have a network of friends or other supports, may need to be managed differently from one that occurs later, when the student might have people who could provide some comfort for a short time. The psychiatrist should know what level of support and supervision is available in the residence halls.
Although it is helpful for college counseling centers to maintain ongoing communication and coordination of services with local clinics and/or university medical centers, it is especially important for those who manage crises to have strong communication with local emergency rooms (ERs) and community crisis services. Because these services likely are managed by physicians, the campus psychiatrist is well placed to consult and coordinate care with local ERs because during a crisis, physician-to-physician communication often is more effective than campus counselor-to-ER physician communication. Ideally, college psychiatrists should have regular communication with ER physicians to discuss campus trends—such as particular drugs being used with unusual frequency or suicides on campus that might raise concerns of suicide contagion—and educate ER clinicians about services and programs the college offers.8
Barreira and Snider4 described the early development of college counseling services as flowing from 2 separate streams. Counseling services at colleges began to appear in the middle of the 20th century and grew out of academic and career advising offices. These programs typically had a “developmental”—as opposed to a clinical—orientation. Most of these services were and continue to be directed by counseling psychologists.
At the same time, some larger institutions—particularly the “Ivys”—hired psychiatrists to provide mental health care. Sometimes these clinicians were based at the school health service, while other institutions had parallel systems of counseling and mental health services. Today most colleges have integrated these programs into a single service.
An opportunity for training
Psychiatrists’ training may make them well-suited to address clinical issues that typically arise among college students. For example, students who have difficulty in college often struggle with issues at the border of physical and emotional health. Many students experience significant levels of stress, and many struggle with poor or inconsistent eating and nutrition and inadequate sleep. In fact, severely sleep-deprived students may present with symptoms that mimic depression.5 Psychiatrists have credibility in addressing these issues with individual students and the campus community. Psychiatrists also have training and experience in diagnosing and managing patients with substance abuse and can educate students, parents, faculty, and university administrators about these disorders.
College mental health services can be valuable training venues for senior psychiatric residents and child and adolescent fellows.9 College students can provide exposure to a broad array of problems—such as anxiety disorders, obsessive-compulsive disorder, dysthymic disorder, adjustment disorders, and panic disorder—that psychiatric trainees may not confront in a hospital clinic. Students are particularly responsive to short-term talk therapies with or without medication management, and working with this population can be a strong antidote to the “therapeutic nihilism”—the unfortunate sense that talk therapies are of limited effectiveness and that only pharmacotherapy can help psychiatric problems—often experienced by psychiatric trainees who spend much of their time working with patients with serious, chronic illnesses. Psychiatric residents can be particularly helpful in managing student patients who require combined medication and talk therapy.
College-based psychiatrists are well suited for educating residents about developmental issues of “emerging adulthood,” including:
- exploration of and anxieties about relationships and sexuality
- balancing connectedness to family with increasing sense of autonomy and independence
- establishing personal life goals and values and career choices and goals.10
College counseling services also are an excellent setting for residents to learn principles of community mental health and medico-legal concepts related to confidentiality, duty to warn, and disability law.11
Treatment outside college
Because college students have high rates of substance abuse12 and other psychiatric disorders, it is important for psychiatrists who treat these patients in private practice or community-based clinics to develop a basic awareness of and competency in relevant developmental and clinical issues. Psychiatrists who work in emergency services in areas with high concentrations of college students need to be particularly attuned to issues related to college mental health, substance abuse, and life on campus.8
Related Resources
- The Jed Foundation. www.jedfoundation.org.
- National Research Consortium of Counseling Centers in Higher Education. www.cmhc.utexas.edu/researchconsortium.html.
Disclosure
Dr. Schwartz reports no financial relationship with any companies whose products are mentioned in this article or with manufacturers of competing products.
1. US Department of Education National Center for Education Statistics. Degree-granting institutions by control and type of institution: Selected years, 1949-50 through 2009-10. http://nces.ed.gov/programs/digest/d10/tables/dt10_275.asp. Accessed August 22, 2011.
2. Gallagher RP. National survey of counseling center directors 2010. International Association of Counseling Services. http://www.iacsinc.org. Accessed August 22 2011.
3. Schwartz V, Kay J. The crisis in college and university mental health. Psychiatric Times. July 27 2009.
4. Barreira P, Snider M. History of college counseling and mental health services and role of the community mental health model. In: Kay J Schwartz V, eds. Mental health care in the college community. Hoboken, NJ: Wiley and Sons; 2010:21–31.
5. Schwartz V. Medications. In: Grayson PA Meilman PW, eds. College mental health practice. New York, NY: Routledge; 2006:59–78.
6. Barr V, Rando R, Krylowicz B, et al. The Association for University and College Counseling Centers Directors Annual Survey. 2010. http://aucccd.org/img/pdfs/aucccd_directors_survey_monograph_2010.pdf. Accessed September 1, 2011.
7. American College Health Association. National college health assessment II: reference group executive summary Fall 2010. Linthicum MD: American College Health Association; 2011.
8. Glick RL, Schwartz V. Assessment and management: special considerations for college students in psychiatric crisis. Psychiatric Issues in Emergency Care Settings. 2007;6(4):7-13.
9. Kay J, Schwartz V. Psychiatry residency training in college mental health services. In: Kay J Schwartz V, eds. Mental health care in the college community. Hoboken, NJ: Wiley and Sons; 2010.
10. Arnett JJ. Emerging adulthood: the winding road from the late teens through the twenties. New York NY: Oxford University Press; 2004.
11. Bower K, Schwartz V. Legal and ethical issues in college mental health. In: Kay J Schwartz V, eds. Mental health care in the college community. Hoboken, NJ: Wiley and Sons; 2010.
12. Hingson R, White A. Magnitude and prevention of college alcohol and drug misuse. In: Kay J Schwartz V, eds. Mental health care in the college community. Hoboken, NJ: Wiley and Sons; 2010.
1. US Department of Education National Center for Education Statistics. Degree-granting institutions by control and type of institution: Selected years, 1949-50 through 2009-10. http://nces.ed.gov/programs/digest/d10/tables/dt10_275.asp. Accessed August 22, 2011.
2. Gallagher RP. National survey of counseling center directors 2010. International Association of Counseling Services. http://www.iacsinc.org. Accessed August 22 2011.
3. Schwartz V, Kay J. The crisis in college and university mental health. Psychiatric Times. July 27 2009.
4. Barreira P, Snider M. History of college counseling and mental health services and role of the community mental health model. In: Kay J Schwartz V, eds. Mental health care in the college community. Hoboken, NJ: Wiley and Sons; 2010:21–31.
5. Schwartz V. Medications. In: Grayson PA Meilman PW, eds. College mental health practice. New York, NY: Routledge; 2006:59–78.
6. Barr V, Rando R, Krylowicz B, et al. The Association for University and College Counseling Centers Directors Annual Survey. 2010. http://aucccd.org/img/pdfs/aucccd_directors_survey_monograph_2010.pdf. Accessed September 1, 2011.
7. American College Health Association. National college health assessment II: reference group executive summary Fall 2010. Linthicum MD: American College Health Association; 2011.
8. Glick RL, Schwartz V. Assessment and management: special considerations for college students in psychiatric crisis. Psychiatric Issues in Emergency Care Settings. 2007;6(4):7-13.
9. Kay J, Schwartz V. Psychiatry residency training in college mental health services. In: Kay J Schwartz V, eds. Mental health care in the college community. Hoboken, NJ: Wiley and Sons; 2010.
10. Arnett JJ. Emerging adulthood: the winding road from the late teens through the twenties. New York NY: Oxford University Press; 2004.
11. Bower K, Schwartz V. Legal and ethical issues in college mental health. In: Kay J Schwartz V, eds. Mental health care in the college community. Hoboken, NJ: Wiley and Sons; 2010.
12. Hingson R, White A. Magnitude and prevention of college alcohol and drug misuse. In: Kay J Schwartz V, eds. Mental health care in the college community. Hoboken, NJ: Wiley and Sons; 2010.
Bullying HURTs! Assessing and managing the bullied child
Technological developments—most notably, the increasing popularity of social networking sites such as Facebook—have led to a resurgence in the prevalence of bullying.1,2 The unlimited reach and anonymity of “cyber” bullying has introduced new challenges for pediatricians and child psychiatrists. Traditional bullying—defined as a specific form of aggression that is intentional, repeated, and involves a disparity of power between the victim and perpetrators—remains more common, with 54% of middle school students reporting verbal bullying, compared with 14% reporting at least 1 episode of electronic bullying over 2 months.2 Compared with students who weren’t bullied, middle and high school students who were bullied were 3 times more likely to report seriously considering suicide, engaging in intentional self-harm, being physically hurt by a family member, and witnessing violence in their families.3
Although bullying occurs frequently and is closely associated with several psychiatric conditions, including attention-deficit/hyperactivity disorder,4 depression,1 and anxiety,1 clinicians often don’t thoroughly assess patients to determine if they’ve been bullied and rarely intervene. The mnemonic HURT may aid in the clinical assessment and management of bullied children.
Help empower the child who is being bullied by encouraging him or her to find appropriate help from teachers, school counselors, or other resources, which may decrease the likelihood of psychological and physical consequences.
Understand the risk factors for being bullied, including less parental support,2 violent family encounters,3 and obesity,3 that may contribute to a child’s emotional experiences or behavior in ways that make him or her an easy target for bullying.2
Recognize a child who is at risk for being bullied and ask about his or her peer relations at school and use of online social networks. At-risk children warrant further evaluation for depression, anxiety, loneliness, and low self-esteem.
Teach the child why others engage in bullying so he or she may avoid actions and words that instigate or provoke a bully, and discuss techniques for dealing with confrontations.
Disclosures
Dr. Madaan is a consultant for The NOW Coalition for Bipolar Disorder and Avanir Pharmaceuticals and has pending research support from Merck and Otsuka.
Ms. Kepple reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgement
The authors would like to thank Sara Kepple for her assistance with this article.
1. Kowalski RM. Cyber bullying: recognizing and treating victim and aggressor. Psychiatric Times. October 1, 2008.
2. Wang J, Iannotti RJ, Nansel TR. School bullying among adolescents in the United States: physical, verbal, relational, and cyber. J Adolesc Health. 2009;45(4):368-375.
3. Centers for Disease Control and Prevention. Bullying among middle school and high school students—Massachusetts, 2009. MMWR Morb Mortal Wkly Rep. 2011;60(15):465-471.
4. Holmberg K. The association of bullying and health complaints in children with attention-deficit/hyperactivity disorder. Postgrad Med. 2010;122(5):62-68.
Technological developments—most notably, the increasing popularity of social networking sites such as Facebook—have led to a resurgence in the prevalence of bullying.1,2 The unlimited reach and anonymity of “cyber” bullying has introduced new challenges for pediatricians and child psychiatrists. Traditional bullying—defined as a specific form of aggression that is intentional, repeated, and involves a disparity of power between the victim and perpetrators—remains more common, with 54% of middle school students reporting verbal bullying, compared with 14% reporting at least 1 episode of electronic bullying over 2 months.2 Compared with students who weren’t bullied, middle and high school students who were bullied were 3 times more likely to report seriously considering suicide, engaging in intentional self-harm, being physically hurt by a family member, and witnessing violence in their families.3
Although bullying occurs frequently and is closely associated with several psychiatric conditions, including attention-deficit/hyperactivity disorder,4 depression,1 and anxiety,1 clinicians often don’t thoroughly assess patients to determine if they’ve been bullied and rarely intervene. The mnemonic HURT may aid in the clinical assessment and management of bullied children.
Help empower the child who is being bullied by encouraging him or her to find appropriate help from teachers, school counselors, or other resources, which may decrease the likelihood of psychological and physical consequences.
Understand the risk factors for being bullied, including less parental support,2 violent family encounters,3 and obesity,3 that may contribute to a child’s emotional experiences or behavior in ways that make him or her an easy target for bullying.2
Recognize a child who is at risk for being bullied and ask about his or her peer relations at school and use of online social networks. At-risk children warrant further evaluation for depression, anxiety, loneliness, and low self-esteem.
Teach the child why others engage in bullying so he or she may avoid actions and words that instigate or provoke a bully, and discuss techniques for dealing with confrontations.
Disclosures
Dr. Madaan is a consultant for The NOW Coalition for Bipolar Disorder and Avanir Pharmaceuticals and has pending research support from Merck and Otsuka.
Ms. Kepple reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgement
The authors would like to thank Sara Kepple for her assistance with this article.
Technological developments—most notably, the increasing popularity of social networking sites such as Facebook—have led to a resurgence in the prevalence of bullying.1,2 The unlimited reach and anonymity of “cyber” bullying has introduced new challenges for pediatricians and child psychiatrists. Traditional bullying—defined as a specific form of aggression that is intentional, repeated, and involves a disparity of power between the victim and perpetrators—remains more common, with 54% of middle school students reporting verbal bullying, compared with 14% reporting at least 1 episode of electronic bullying over 2 months.2 Compared with students who weren’t bullied, middle and high school students who were bullied were 3 times more likely to report seriously considering suicide, engaging in intentional self-harm, being physically hurt by a family member, and witnessing violence in their families.3
Although bullying occurs frequently and is closely associated with several psychiatric conditions, including attention-deficit/hyperactivity disorder,4 depression,1 and anxiety,1 clinicians often don’t thoroughly assess patients to determine if they’ve been bullied and rarely intervene. The mnemonic HURT may aid in the clinical assessment and management of bullied children.
Help empower the child who is being bullied by encouraging him or her to find appropriate help from teachers, school counselors, or other resources, which may decrease the likelihood of psychological and physical consequences.
Understand the risk factors for being bullied, including less parental support,2 violent family encounters,3 and obesity,3 that may contribute to a child’s emotional experiences or behavior in ways that make him or her an easy target for bullying.2
Recognize a child who is at risk for being bullied and ask about his or her peer relations at school and use of online social networks. At-risk children warrant further evaluation for depression, anxiety, loneliness, and low self-esteem.
Teach the child why others engage in bullying so he or she may avoid actions and words that instigate or provoke a bully, and discuss techniques for dealing with confrontations.
Disclosures
Dr. Madaan is a consultant for The NOW Coalition for Bipolar Disorder and Avanir Pharmaceuticals and has pending research support from Merck and Otsuka.
Ms. Kepple reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgement
The authors would like to thank Sara Kepple for her assistance with this article.
1. Kowalski RM. Cyber bullying: recognizing and treating victim and aggressor. Psychiatric Times. October 1, 2008.
2. Wang J, Iannotti RJ, Nansel TR. School bullying among adolescents in the United States: physical, verbal, relational, and cyber. J Adolesc Health. 2009;45(4):368-375.
3. Centers for Disease Control and Prevention. Bullying among middle school and high school students—Massachusetts, 2009. MMWR Morb Mortal Wkly Rep. 2011;60(15):465-471.
4. Holmberg K. The association of bullying and health complaints in children with attention-deficit/hyperactivity disorder. Postgrad Med. 2010;122(5):62-68.
1. Kowalski RM. Cyber bullying: recognizing and treating victim and aggressor. Psychiatric Times. October 1, 2008.
2. Wang J, Iannotti RJ, Nansel TR. School bullying among adolescents in the United States: physical, verbal, relational, and cyber. J Adolesc Health. 2009;45(4):368-375.
3. Centers for Disease Control and Prevention. Bullying among middle school and high school students—Massachusetts, 2009. MMWR Morb Mortal Wkly Rep. 2011;60(15):465-471.
4. Holmberg K. The association of bullying and health complaints in children with attention-deficit/hyperactivity disorder. Postgrad Med. 2010;122(5):62-68.
Psychotropic-induced dry mouth: Don’t overlook this potentially serious side effect
Discuss this article at www.facebook.com/CurrentPsychiatry
Xerostomia, commonly known as “dry mouth,” is a reported side effect of >1,800 drugs from >80 classes.1 This condition often goes unrecognized and untreated, but it can significantly affect patients’ quality of life and cause oral and medical health problems.2,3 Although psychotropic medications are not the only offenders, they comprise a large portion of the agents that can cause dry mouth. Antidepressants, anticonvulsants, anxiolytics, antipsychotics, anticholinergics, and alpha agonists can cause xerostomia.4 The risk of salivary hypofunction increases with polypharmacy and may be especially likely when ≥3 drugs are taken per day.5
Among all reported side effects of antidepressants and antipsychotics, dry mouth often is the most prevalent complaint. For example, in a study of 5 antidepressants 35% to 46% of patients reported dry mouth.6 Rates are similar in users of various antipsychotics. Patients with severe, persistent mental illness often cite side effects as the primary reason for psychotropic noncompliance.7-9
Few psychiatrists routinely screen patients for xerostomia, and if a patient reports this side effect, they may be unlikely to address it or understand its implications because of more pressing concerns such as psychosis or risk of suicide. Historically, education in general medical training about the effects of oral health on a patient’s overall health has been limited. It is crucial for psychiatrists to be aware of potential problems related to dry mouth and the impact it can have on their patients. In this article, we:
- describe how dry mouth can impact a patient’s oral, medical, and psychiatric health
- provide psychiatrists with an understanding of pathology related to xerostomia
- explain how psychiatrists can screen for xerostomia
- discuss the benefits patients may receive when psychiatrists collaborate with dental clinicians to manage this condition.
Implications of xerostomia
Saliva provides a protective function. It is an antimicrobial, buffering, and lubricating agent that aids cleansing and removal of food debris within the mouth. It also helps maintain oral mucosa and remineralizing of tooth structure.10
Psychotropics can affect the amount of saliva secreted and may alter the composition of saliva via their receptor affects on the dual sympathetic and parasympathetic innervations of the salivary glands.11 When the protective environment produced by saliva is altered, patients may start to develop oral problems before experiencing dryness. A 50% reduction in saliva flow may occur before they become aware of the problem.12,13
Patients may not taste food properly, experience cracked lips, or have trouble eating, oral pain, or dentures that no longer fit well.14 Additionally, oral diseases such as dental decay and periodontal disease (Photos 1 and 2), inflamed soft tissue, and candidiasis (Photo 3) also may occur.10,15 Patients may begin to notice dry mouth when they wake at night, which could disrupt sleep. Patients with xerostomia can accumulate excessive amounts of plaque on their teeth and the dorsum of the tongue. The increased bacterial count and release of volatile sulfide gases that occur with dry mouth may explain some cases of halitosis.16,17 Patients also may have difficulty swallowing or speaking and be unaware of the oral health destruction occurring as a result of reduced saliva. Some experts report oral bacteria levels can skyrocket as much as 10-fold in people who take medications that cause dry mouth.18
Infections of the mouth can create havoc elsewhere in the body. The evidence base that establishes an association between periodontal disease and other chronic inflammatory conditions such as diabetes, cardiovascular disease, cancer, and rheumatoid arthritis is steadily growing.19-22 Periodontal disease also is a risk factor for preeclampsia and other illnesses that can negatively affect neonatal health.23,24
Failure to recognize xerostomia caused by psychotropic medications may lead to an increase in cavities, periodontal disease, and chronic systemic inflammatory conditions that can shorten a patient’s life span. Recognizing and treating causes of xerostomia is vital because doing so may halt this chain of events.

Photo 1
This patient complained of dry mouth and exhibits decay (a) and evidence of periodontal disease. Plaque and calculus is present (b), along with gingival recession from the loss of attachment and bone (c). This patient was taking venlafaxine, zolpidem, and alprazolam
Photo 2
Dental cavities were restored with tooth-colored restorations (arrows) on this patient, who has xerostomia. Every effort must be made to manage this patient’s dry mouth or the restorations may fail due to recurrent decay
Photo 3
This partial denture wearer, who complained of dry mouth, has evidence of palatal irritation and sores as a result of xerostomia and use of a partial denture. This patient was taking bupropion, esomeprazole, and tolterodine
Psychiatric patients’ oral health
Psychiatric patients’ oral health status often is poor. Several studies found that compared with the general population, patients who have severe, persistent mental illness are at higher risk to be missing teeth, schedule fewer visits to the dentist, and neglect oral hygiene.25-28 Periodontal disease also could be a problem in these patients.29 Although some evidence suggests mental illness may make patients less likely to go to the dentist, psychotropic medications also may contribute to their dental difficulties.
Screening for xerostomia
Simply advising patients of the problems related to xerostomia and asking several questions may help prevent pain and deterioration in function within the oral cavity (Table 1).14,30
You can perform a simple in-office assessment of the oral cavity by visual inspection and by placing a dry tongue blade against the inside of the cheek mucosa. If the blade sticks to the mucosa and a gentle tug is needed to lift it away, xerostomia may be present.30 Conversely, a healthy mouth will have a collection of saliva on the floor of the oral cavity, and pulling a tongue blade away from the inside of the cheek will not require any effort (Photos 4 and 5).
Table 1
Screening questions for xerostomia
| Does the amount of saliva in your mouth seem to have decreased? |
| Do you have any trouble swallowing, speaking, or eating dry foods? |
| Do you sip liquids more often to help you swallow? |
| Do you notice any dryness or cracking of your lips? |
| Do you have mouth sores or a burning feeling in the mouth? |
| When was the last time you saw your dentist? (Patients with xerostomia may need to see their dentist more frequently) |
| Are you aware of any halitosis (ie, mouth odor)? |
| Source: Reference 14 |

Photo 4
The arrow shows the normal appearance of saliva collecting on the floor of the mouth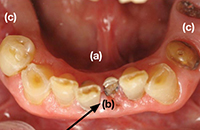
Photo 5
This patient complained of dry mouth. Note the floor of the mouth is free of saliva (a). Decay is present (b), and the patient is missing posterior teeth (c). This patient was taking clonidine, metoprolol, hydrochlorothiazide, amlodipine, and irbesartan
Treatment options
Patients who have reduced salivary flow as a result of a medication may become so affected by dryness that their drug regimen may need to be changed. However, the greatest concern is for deteriorating oral health among patients who may be unaware xerostomia is occurring.31
Counsel patients who take medications that can affect their salivary function about the importance of seeing a dentist regularly, and provide referrals when appropriate. Depending upon the patient’s oral health, dentists recommend patients with xerostomia have their teeth cleaned/examined 3 or 4 times per year, rather than the 2 times per year allowed by third-party payers (ie, insurance companies). Also advise patients to be diligent in their oral hygiene practices, including flossing and brushing the teeth and tongue, and to avoid foods that are sticky and/or have high sucrose content (Table 2). Recommend using a toothpaste containing fluoride—preferably one free of sodium lauryl sulfate, which could contribute to mouth sores14—and drinking fluoridated water. Explain to patients that their dentist may recommend in-office high-fluoride applications, high-fluoride prescription toothpaste, and/or “mouth trays” that contain high fluoride gel. Tell patients to avoid cigarettes and caffeinated beverages, which can increase dryness. Alcohol use should be minimized and mouth rinses containing alcohol should not be used.
Many over-the-counter products are available to address xerostomia, including toothpastes, mouth rinses, and gels. Salivary substitutes—which are available as sprays, liquids, tablets, and swab sticks—imitate saliva and may provide a temporary reprieve from dryness. Although none of these products will cure dry mouth, they may help manage the condition. Advise patients to eat foods that stimulate saliva production, such as carrots, apples, and celery, and to chew sugarless gum and candies, which also will stimulate salivary flow.
The FDA has approved 2 prescription drugs for treating xerostomia: cevimeline and pilocarpine. Cevimeline is approved for treating dry mouth associated with Sjögren’s syndrome and pilocarpine is approved for treating dry mouth caused by head and neck radiation therapy; however, these medications’ role in treating dry mouth in psychiatric patients has not been investigated. Both agents are contraindicated in patients with narrow-angle glaucoma, uncontrolled asthma, or liver disease, and should be prescribed with caution for patients with cardiovascular disease, chronic respiratory conditions, or kidney disease.32
Acupuncture and electrostimulation are being studied as a treatment for xerostomia. Trials have found acupuncture improves symptoms of xerostomia,33,34 and 1 study found electrostimulation improved xerostomia in patients with Sjögren’s syndrome.35 Both approaches require more study to confirm their effectiveness.33-35
Table 2
Managing dry mouth: What to tell patients
| Oral hygiene. Tell patients to be diligent in their oral hygiene practices, including brushing and flossing. They should use a toothpaste containing fluoride—preferably one free of sodium lauryl sulfate—and schedule regular dental visits, where they can receive high-fluoride applications or be prescribed high-fluoride prescription toothpastes |
| Diet. Advise patients to avoid foods high in sucrose content, rinse their mouth with water soon after eating, and drink fluoridated water regularly. Tell them that they may be able to stimulate saliva flow with sugarless gum, candies, and foods such as celery and carrots |
| Drying agents. Instruct patients to avoid cigarettes, caffeinated beverages, and mouth rinses that contain alcohol. Explain that some patients may benefit from sleeping in a room with a cool air humidifier |
| Over-the-counter products. Suggest patients try salivary substitutes, which are dispensed in spray bottles, rinses, swish bottles, or oral swab sticks. In addition, products such as dry-mouth toothpaste and moisturizing gels also may help relieve their symptoms |
- Persson K, Axtelius B, Söderfeldt B, et al. Monitoring oral health and dental attendance in an outpatient psychiatric population. J Psychiatr Ment Health Nurs. 2009;16(3):263-271.
- Keene JJ Jr, Galasko GT, Land MF. Antidepressant use in psychiatry and medicine: importance for dental practice. J Am Dent Assoc. 2003;134(1):71-79.
Drug Brand Names
- Alprazolam • Xanax
- Amlodipine • Norvasc
- Bupropion • Wellbutrin, Zyban
- Cevimeline • Evoxac
- Clonidine • Catapres, Kapvay, others
- Esomeprazole • Nexium
- Irbesartan • Avapro
- Metoprolol • Lopressor, Toprol
- Pilocarpine • Salagen
- Tolterodine • Detrol
- Venlafaxine • Effexor
- Zolpidem • Ambien
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Drymouth.info. Overview of drugs and dry mouth. http://drymouth.info/practitioner/overview.asp. Accessed September 2, 2011.
2. Stewart CM, Berg KM, Cha S, et al. Salivary dysfunction and quality of life in Sjögren syndrome: a critical oral-systemic connection. J Am Dent Assoc. 2008;139(3):291-299.
3. Friedman PK. Xerostomia: The invisible oral health condition. http://www.dentistryiq.com/index/display/article-display/295922/articles/woman-dentist-journal/health/xerostomia-the-invisible-oral-health-condition.html. Accessed September 6, 2011.
4. Physician Desk Reference. Montvale NJ: PDR Network LLC.; 2011.
5. Bardow A, Lagerlof F, Nauntofte B, et al. The role of saliva. In: Fejerskov O, Kidd E, eds. Dental caries: the disease and its clinical management. Oxford, United Kingdom: Blackwell Munksgaard; 2008:195.
6. Vanderkooy JD, Kennedy SH, Bagby RM. Antidepressant side effects in depression patients treated in a naturalistic setting: a study of bupropion moclobemide, paroxetine, sertraline, and venlafaxine. Can J Psychiatry. 2002;47(2):174-180.
7. Löffler W, Kilian R, Toumi M, et al. Schizophrenic patients’ subjective reasons for compliance and noncompliance with neuroleptic treatment. Pharmacopsychiatry. 2003;36(3):105-112.
8. Lambert M, Conus P, Eide P, et al. Impact of present and past antipsychotic side effects on attitude toward typical antipsychotic treatment and adherence. Eur Psychiatry. 2004;19(7):415-422.
9. Rettenbacher MA, Hofer A, Eder U, et al. Compliance in schizophrenia: psychopathology, side effects, and patients’ attitudes toward the illness and medication. J Clin Psychiatry. 2004;65(9):1211-1218.
10. Bulkacz J, Carranza FA. Defense mechanisms of the gingiva. In: Newman MG, Takei HH, Klokkevold PR, et al, eds. Carranza’s clinical periodontology. St. Louis, MO: Elsevier Saunders; 2011:69–70.
11. Szabadi E, Tavernor S. Hypo-and hyper-salivation induced by psychoactive drugs. CNS Drugs. 1999;11(6):449-466.
12. Guggenheimer J, Moore PA. Xerostomia: etiology recognition and treatment. J Am Dent Assoc. 2003;134(1):61-69.
13. Dawes C. Physiological factors affecting salivary flow rate oral sugar clearance, and the sensation of dry mouth in man. J Dent Res. 1987;66:648-653.
14. Bartels CL. Xerostomia information for dentists. http://www.homesteadschools.com/dental/courses/Xerostomia/Course.htm. Accessed August 15, 2011.
15. Sitheeque MA, Samaranayake LP. Chronic hyperplastic candidosis/candidiasis (candidal leukoplakia). Crit Rev Oral Biol Med. 2003;14(4):253-267.
16. Porter SR, Scully C. Oral malodour (halitosis). BMJ. 2006;333(7569):632-635.
17. Quirynen M, Van den Veide S, Vanderkerckhove B, et al. Oral malodor. In: Newman MG, Takei HH, Klokkevold PR, et al, eds. Carranza’s clinical periodontology. St. Louis, MO: Elsevier Saunders; 2011:333.
18. Papas A. Dry mouth from drugs: more than just an annoying side effect. Tufts University Heath and Nutrition Letter. 2000;3.-
19. American Academy of Periodontology. Gum disease information from the American Academy of Periodontology http://perio.org. Accessed August 12, 2011.
20. Geismar K, Stoltze K, Sigurd B, et al. Periodontal disease and coronary heart disease. J Periodontol. 2006;77(9):1547-1554.
21. Lee HJ, Garcia RI, Janket SJ, et al. The association between cumulative periodontal disease and stroke history in older adults. J Periodontol. 2006;77(10):1744-1754.
22. Friedewald VE, Kornman KS, Beck JD, et al. The American Journal of Cardiology and Journal of Periodontology editors’ consensus: periodontitis and atherosclerotic cardiovascular disease. J Periodontol. 2009;80(7):1021-1032.
23. Contreras A, Herrera JA, Soto JE, et al. Periodontitis is associated with preeclampsia in pregnant women. J Periodontol. 2006;77(2):182-188.
24. Dasanayake AP, Li Y, Wiener H, et al. Salivary Actinomyces naeslundii genospecies 2 and Lactobacillus casei levels predict pregnancy outcomes. J Periodontol. 2005;76(2):171-177.
25. McCreadie RG, Stevens H, Henderson J, et al. The dental health of people with schizophrenia. Acta Psychiatr Scand. 2004;110(4):306-310.
26. Anttila S, Knuuttila M, Ylöstalo P, et al. Symptoms of depression and anxiety in relation to dental health behavior and self-perceived dental treatment need. Eur J Oral Sci. 2006;114(2):109-114.
27. Sjögren R, Nordström G. Oral health status of psychiatric patients. J Clin Nurs. 2000;9(4):632-638.
28. Ramon T, Grinshpoon A, Zusman SP, et al. Oral health and treatment needs of institutionalized chronic psychiatric patients in Israel. Eur Psychiatry. 2003;18(3):101-105.
29. Portilla MI, Mafla AC, Arteaga JJ. Periodontal status in female psychiatric patients. Colomb Med. 2009;40(2):167-176.
30. Navazesh M. ADA Council on Scientific Affairs and Division of Science. How can oral health care providers determine if patients have dry mouth? J Am Dent Assoc. 2003;134(5):613-620.
31. Mignogna MD, Fedele S, Lo Russo L, et al. Sjögren’s syndrome: the diagnostic potential of early oral manifestations preceding hyposalivation/xerostomia. J Oral Pathol Med. 2005;34(1):1-6.
32. Spolarich AE. Managing the side effects of medications. J Dent Hyg. 2000;74(1):57-69.
33. Johnstone PA, Niemtzow RC, Riffenburgh RH. Acupuncture for xerostomia: clinical update. Cancer. 2002;94(4):1151-1156.
34. Garcia MK, Chiang JS, Cohen L, et al. Acupuncture for radiation-induced xerostomia in patients with cancer: a pilot study. Head Neck. 2009;31(10):1360-1368.
35. Strietzel FP, Lafaurie GI, Mendoza GR, et al. Efficacy and safety of an intraoral electrostimulation device for xerostomia relief: a multicenter, randomized trial. Arthritis Rheum. 2011;63(1):180-190.
Discuss this article at www.facebook.com/CurrentPsychiatry
Xerostomia, commonly known as “dry mouth,” is a reported side effect of >1,800 drugs from >80 classes.1 This condition often goes unrecognized and untreated, but it can significantly affect patients’ quality of life and cause oral and medical health problems.2,3 Although psychotropic medications are not the only offenders, they comprise a large portion of the agents that can cause dry mouth. Antidepressants, anticonvulsants, anxiolytics, antipsychotics, anticholinergics, and alpha agonists can cause xerostomia.4 The risk of salivary hypofunction increases with polypharmacy and may be especially likely when ≥3 drugs are taken per day.5
Among all reported side effects of antidepressants and antipsychotics, dry mouth often is the most prevalent complaint. For example, in a study of 5 antidepressants 35% to 46% of patients reported dry mouth.6 Rates are similar in users of various antipsychotics. Patients with severe, persistent mental illness often cite side effects as the primary reason for psychotropic noncompliance.7-9
Few psychiatrists routinely screen patients for xerostomia, and if a patient reports this side effect, they may be unlikely to address it or understand its implications because of more pressing concerns such as psychosis or risk of suicide. Historically, education in general medical training about the effects of oral health on a patient’s overall health has been limited. It is crucial for psychiatrists to be aware of potential problems related to dry mouth and the impact it can have on their patients. In this article, we:
- describe how dry mouth can impact a patient’s oral, medical, and psychiatric health
- provide psychiatrists with an understanding of pathology related to xerostomia
- explain how psychiatrists can screen for xerostomia
- discuss the benefits patients may receive when psychiatrists collaborate with dental clinicians to manage this condition.
Implications of xerostomia
Saliva provides a protective function. It is an antimicrobial, buffering, and lubricating agent that aids cleansing and removal of food debris within the mouth. It also helps maintain oral mucosa and remineralizing of tooth structure.10
Psychotropics can affect the amount of saliva secreted and may alter the composition of saliva via their receptor affects on the dual sympathetic and parasympathetic innervations of the salivary glands.11 When the protective environment produced by saliva is altered, patients may start to develop oral problems before experiencing dryness. A 50% reduction in saliva flow may occur before they become aware of the problem.12,13
Patients may not taste food properly, experience cracked lips, or have trouble eating, oral pain, or dentures that no longer fit well.14 Additionally, oral diseases such as dental decay and periodontal disease (Photos 1 and 2), inflamed soft tissue, and candidiasis (Photo 3) also may occur.10,15 Patients may begin to notice dry mouth when they wake at night, which could disrupt sleep. Patients with xerostomia can accumulate excessive amounts of plaque on their teeth and the dorsum of the tongue. The increased bacterial count and release of volatile sulfide gases that occur with dry mouth may explain some cases of halitosis.16,17 Patients also may have difficulty swallowing or speaking and be unaware of the oral health destruction occurring as a result of reduced saliva. Some experts report oral bacteria levels can skyrocket as much as 10-fold in people who take medications that cause dry mouth.18
Infections of the mouth can create havoc elsewhere in the body. The evidence base that establishes an association between periodontal disease and other chronic inflammatory conditions such as diabetes, cardiovascular disease, cancer, and rheumatoid arthritis is steadily growing.19-22 Periodontal disease also is a risk factor for preeclampsia and other illnesses that can negatively affect neonatal health.23,24
Failure to recognize xerostomia caused by psychotropic medications may lead to an increase in cavities, periodontal disease, and chronic systemic inflammatory conditions that can shorten a patient’s life span. Recognizing and treating causes of xerostomia is vital because doing so may halt this chain of events.
Photo 1
This patient complained of dry mouth and exhibits decay (a) and evidence of periodontal disease. Plaque and calculus is present (b), along with gingival recession from the loss of attachment and bone (c). This patient was taking venlafaxine, zolpidem, and alprazolam
Photo 2
Dental cavities were restored with tooth-colored restorations (arrows) on this patient, who has xerostomia. Every effort must be made to manage this patient’s dry mouth or the restorations may fail due to recurrent decay
Photo 3
This partial denture wearer, who complained of dry mouth, has evidence of palatal irritation and sores as a result of xerostomia and use of a partial denture. This patient was taking bupropion, esomeprazole, and tolterodine
Psychiatric patients’ oral health
Psychiatric patients’ oral health status often is poor. Several studies found that compared with the general population, patients who have severe, persistent mental illness are at higher risk to be missing teeth, schedule fewer visits to the dentist, and neglect oral hygiene.25-28 Periodontal disease also could be a problem in these patients.29 Although some evidence suggests mental illness may make patients less likely to go to the dentist, psychotropic medications also may contribute to their dental difficulties.
Screening for xerostomia
Simply advising patients of the problems related to xerostomia and asking several questions may help prevent pain and deterioration in function within the oral cavity (Table 1).14,30
You can perform a simple in-office assessment of the oral cavity by visual inspection and by placing a dry tongue blade against the inside of the cheek mucosa. If the blade sticks to the mucosa and a gentle tug is needed to lift it away, xerostomia may be present.30 Conversely, a healthy mouth will have a collection of saliva on the floor of the oral cavity, and pulling a tongue blade away from the inside of the cheek will not require any effort (Photos 4 and 5).
Table 1
Screening questions for xerostomia
| Does the amount of saliva in your mouth seem to have decreased? |
| Do you have any trouble swallowing, speaking, or eating dry foods? |
| Do you sip liquids more often to help you swallow? |
| Do you notice any dryness or cracking of your lips? |
| Do you have mouth sores or a burning feeling in the mouth? |
| When was the last time you saw your dentist? (Patients with xerostomia may need to see their dentist more frequently) |
| Are you aware of any halitosis (ie, mouth odor)? |
| Source: Reference 14 |
Photo 4
The arrow shows the normal appearance of saliva collecting on the floor of the mouth
Photo 5
This patient complained of dry mouth. Note the floor of the mouth is free of saliva (a). Decay is present (b), and the patient is missing posterior teeth (c). This patient was taking clonidine, metoprolol, hydrochlorothiazide, amlodipine, and irbesartan
Treatment options
Patients who have reduced salivary flow as a result of a medication may become so affected by dryness that their drug regimen may need to be changed. However, the greatest concern is for deteriorating oral health among patients who may be unaware xerostomia is occurring.31
Counsel patients who take medications that can affect their salivary function about the importance of seeing a dentist regularly, and provide referrals when appropriate. Depending upon the patient’s oral health, dentists recommend patients with xerostomia have their teeth cleaned/examined 3 or 4 times per year, rather than the 2 times per year allowed by third-party payers (ie, insurance companies). Also advise patients to be diligent in their oral hygiene practices, including flossing and brushing the teeth and tongue, and to avoid foods that are sticky and/or have high sucrose content (Table 2). Recommend using a toothpaste containing fluoride—preferably one free of sodium lauryl sulfate, which could contribute to mouth sores14—and drinking fluoridated water. Explain to patients that their dentist may recommend in-office high-fluoride applications, high-fluoride prescription toothpaste, and/or “mouth trays” that contain high fluoride gel. Tell patients to avoid cigarettes and caffeinated beverages, which can increase dryness. Alcohol use should be minimized and mouth rinses containing alcohol should not be used.
Many over-the-counter products are available to address xerostomia, including toothpastes, mouth rinses, and gels. Salivary substitutes—which are available as sprays, liquids, tablets, and swab sticks—imitate saliva and may provide a temporary reprieve from dryness. Although none of these products will cure dry mouth, they may help manage the condition. Advise patients to eat foods that stimulate saliva production, such as carrots, apples, and celery, and to chew sugarless gum and candies, which also will stimulate salivary flow.
The FDA has approved 2 prescription drugs for treating xerostomia: cevimeline and pilocarpine. Cevimeline is approved for treating dry mouth associated with Sjögren’s syndrome and pilocarpine is approved for treating dry mouth caused by head and neck radiation therapy; however, these medications’ role in treating dry mouth in psychiatric patients has not been investigated. Both agents are contraindicated in patients with narrow-angle glaucoma, uncontrolled asthma, or liver disease, and should be prescribed with caution for patients with cardiovascular disease, chronic respiratory conditions, or kidney disease.32
Acupuncture and electrostimulation are being studied as a treatment for xerostomia. Trials have found acupuncture improves symptoms of xerostomia,33,34 and 1 study found electrostimulation improved xerostomia in patients with Sjögren’s syndrome.35 Both approaches require more study to confirm their effectiveness.33-35
Table 2
Managing dry mouth: What to tell patients
| Oral hygiene. Tell patients to be diligent in their oral hygiene practices, including brushing and flossing. They should use a toothpaste containing fluoride—preferably one free of sodium lauryl sulfate—and schedule regular dental visits, where they can receive high-fluoride applications or be prescribed high-fluoride prescription toothpastes |
| Diet. Advise patients to avoid foods high in sucrose content, rinse their mouth with water soon after eating, and drink fluoridated water regularly. Tell them that they may be able to stimulate saliva flow with sugarless gum, candies, and foods such as celery and carrots |
| Drying agents. Instruct patients to avoid cigarettes, caffeinated beverages, and mouth rinses that contain alcohol. Explain that some patients may benefit from sleeping in a room with a cool air humidifier |
| Over-the-counter products. Suggest patients try salivary substitutes, which are dispensed in spray bottles, rinses, swish bottles, or oral swab sticks. In addition, products such as dry-mouth toothpaste and moisturizing gels also may help relieve their symptoms |
- Persson K, Axtelius B, Söderfeldt B, et al. Monitoring oral health and dental attendance in an outpatient psychiatric population. J Psychiatr Ment Health Nurs. 2009;16(3):263-271.
- Keene JJ Jr, Galasko GT, Land MF. Antidepressant use in psychiatry and medicine: importance for dental practice. J Am Dent Assoc. 2003;134(1):71-79.
Drug Brand Names
- Alprazolam • Xanax
- Amlodipine • Norvasc
- Bupropion • Wellbutrin, Zyban
- Cevimeline • Evoxac
- Clonidine • Catapres, Kapvay, others
- Esomeprazole • Nexium
- Irbesartan • Avapro
- Metoprolol • Lopressor, Toprol
- Pilocarpine • Salagen
- Tolterodine • Detrol
- Venlafaxine • Effexor
- Zolpidem • Ambien
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at www.facebook.com/CurrentPsychiatry
Xerostomia, commonly known as “dry mouth,” is a reported side effect of >1,800 drugs from >80 classes.1 This condition often goes unrecognized and untreated, but it can significantly affect patients’ quality of life and cause oral and medical health problems.2,3 Although psychotropic medications are not the only offenders, they comprise a large portion of the agents that can cause dry mouth. Antidepressants, anticonvulsants, anxiolytics, antipsychotics, anticholinergics, and alpha agonists can cause xerostomia.4 The risk of salivary hypofunction increases with polypharmacy and may be especially likely when ≥3 drugs are taken per day.5
Among all reported side effects of antidepressants and antipsychotics, dry mouth often is the most prevalent complaint. For example, in a study of 5 antidepressants 35% to 46% of patients reported dry mouth.6 Rates are similar in users of various antipsychotics. Patients with severe, persistent mental illness often cite side effects as the primary reason for psychotropic noncompliance.7-9
Few psychiatrists routinely screen patients for xerostomia, and if a patient reports this side effect, they may be unlikely to address it or understand its implications because of more pressing concerns such as psychosis or risk of suicide. Historically, education in general medical training about the effects of oral health on a patient’s overall health has been limited. It is crucial for psychiatrists to be aware of potential problems related to dry mouth and the impact it can have on their patients. In this article, we:
- describe how dry mouth can impact a patient’s oral, medical, and psychiatric health
- provide psychiatrists with an understanding of pathology related to xerostomia
- explain how psychiatrists can screen for xerostomia
- discuss the benefits patients may receive when psychiatrists collaborate with dental clinicians to manage this condition.
Implications of xerostomia
Saliva provides a protective function. It is an antimicrobial, buffering, and lubricating agent that aids cleansing and removal of food debris within the mouth. It also helps maintain oral mucosa and remineralizing of tooth structure.10
Psychotropics can affect the amount of saliva secreted and may alter the composition of saliva via their receptor affects on the dual sympathetic and parasympathetic innervations of the salivary glands.11 When the protective environment produced by saliva is altered, patients may start to develop oral problems before experiencing dryness. A 50% reduction in saliva flow may occur before they become aware of the problem.12,13
Patients may not taste food properly, experience cracked lips, or have trouble eating, oral pain, or dentures that no longer fit well.14 Additionally, oral diseases such as dental decay and periodontal disease (Photos 1 and 2), inflamed soft tissue, and candidiasis (Photo 3) also may occur.10,15 Patients may begin to notice dry mouth when they wake at night, which could disrupt sleep. Patients with xerostomia can accumulate excessive amounts of plaque on their teeth and the dorsum of the tongue. The increased bacterial count and release of volatile sulfide gases that occur with dry mouth may explain some cases of halitosis.16,17 Patients also may have difficulty swallowing or speaking and be unaware of the oral health destruction occurring as a result of reduced saliva. Some experts report oral bacteria levels can skyrocket as much as 10-fold in people who take medications that cause dry mouth.18
Infections of the mouth can create havoc elsewhere in the body. The evidence base that establishes an association between periodontal disease and other chronic inflammatory conditions such as diabetes, cardiovascular disease, cancer, and rheumatoid arthritis is steadily growing.19-22 Periodontal disease also is a risk factor for preeclampsia and other illnesses that can negatively affect neonatal health.23,24
Failure to recognize xerostomia caused by psychotropic medications may lead to an increase in cavities, periodontal disease, and chronic systemic inflammatory conditions that can shorten a patient’s life span. Recognizing and treating causes of xerostomia is vital because doing so may halt this chain of events.
Photo 1
This patient complained of dry mouth and exhibits decay (a) and evidence of periodontal disease. Plaque and calculus is present (b), along with gingival recession from the loss of attachment and bone (c). This patient was taking venlafaxine, zolpidem, and alprazolam
Photo 2
Dental cavities were restored with tooth-colored restorations (arrows) on this patient, who has xerostomia. Every effort must be made to manage this patient’s dry mouth or the restorations may fail due to recurrent decay
Photo 3
This partial denture wearer, who complained of dry mouth, has evidence of palatal irritation and sores as a result of xerostomia and use of a partial denture. This patient was taking bupropion, esomeprazole, and tolterodine
Psychiatric patients’ oral health
Psychiatric patients’ oral health status often is poor. Several studies found that compared with the general population, patients who have severe, persistent mental illness are at higher risk to be missing teeth, schedule fewer visits to the dentist, and neglect oral hygiene.25-28 Periodontal disease also could be a problem in these patients.29 Although some evidence suggests mental illness may make patients less likely to go to the dentist, psychotropic medications also may contribute to their dental difficulties.
Screening for xerostomia
Simply advising patients of the problems related to xerostomia and asking several questions may help prevent pain and deterioration in function within the oral cavity (Table 1).14,30
You can perform a simple in-office assessment of the oral cavity by visual inspection and by placing a dry tongue blade against the inside of the cheek mucosa. If the blade sticks to the mucosa and a gentle tug is needed to lift it away, xerostomia may be present.30 Conversely, a healthy mouth will have a collection of saliva on the floor of the oral cavity, and pulling a tongue blade away from the inside of the cheek will not require any effort (Photos 4 and 5).
Table 1
Screening questions for xerostomia
| Does the amount of saliva in your mouth seem to have decreased? |
| Do you have any trouble swallowing, speaking, or eating dry foods? |
| Do you sip liquids more often to help you swallow? |
| Do you notice any dryness or cracking of your lips? |
| Do you have mouth sores or a burning feeling in the mouth? |
| When was the last time you saw your dentist? (Patients with xerostomia may need to see their dentist more frequently) |
| Are you aware of any halitosis (ie, mouth odor)? |
| Source: Reference 14 |
Photo 4
The arrow shows the normal appearance of saliva collecting on the floor of the mouth
Photo 5
This patient complained of dry mouth. Note the floor of the mouth is free of saliva (a). Decay is present (b), and the patient is missing posterior teeth (c). This patient was taking clonidine, metoprolol, hydrochlorothiazide, amlodipine, and irbesartan
Treatment options
Patients who have reduced salivary flow as a result of a medication may become so affected by dryness that their drug regimen may need to be changed. However, the greatest concern is for deteriorating oral health among patients who may be unaware xerostomia is occurring.31
Counsel patients who take medications that can affect their salivary function about the importance of seeing a dentist regularly, and provide referrals when appropriate. Depending upon the patient’s oral health, dentists recommend patients with xerostomia have their teeth cleaned/examined 3 or 4 times per year, rather than the 2 times per year allowed by third-party payers (ie, insurance companies). Also advise patients to be diligent in their oral hygiene practices, including flossing and brushing the teeth and tongue, and to avoid foods that are sticky and/or have high sucrose content (Table 2). Recommend using a toothpaste containing fluoride—preferably one free of sodium lauryl sulfate, which could contribute to mouth sores14—and drinking fluoridated water. Explain to patients that their dentist may recommend in-office high-fluoride applications, high-fluoride prescription toothpaste, and/or “mouth trays” that contain high fluoride gel. Tell patients to avoid cigarettes and caffeinated beverages, which can increase dryness. Alcohol use should be minimized and mouth rinses containing alcohol should not be used.
Many over-the-counter products are available to address xerostomia, including toothpastes, mouth rinses, and gels. Salivary substitutes—which are available as sprays, liquids, tablets, and swab sticks—imitate saliva and may provide a temporary reprieve from dryness. Although none of these products will cure dry mouth, they may help manage the condition. Advise patients to eat foods that stimulate saliva production, such as carrots, apples, and celery, and to chew sugarless gum and candies, which also will stimulate salivary flow.
The FDA has approved 2 prescription drugs for treating xerostomia: cevimeline and pilocarpine. Cevimeline is approved for treating dry mouth associated with Sjögren’s syndrome and pilocarpine is approved for treating dry mouth caused by head and neck radiation therapy; however, these medications’ role in treating dry mouth in psychiatric patients has not been investigated. Both agents are contraindicated in patients with narrow-angle glaucoma, uncontrolled asthma, or liver disease, and should be prescribed with caution for patients with cardiovascular disease, chronic respiratory conditions, or kidney disease.32
Acupuncture and electrostimulation are being studied as a treatment for xerostomia. Trials have found acupuncture improves symptoms of xerostomia,33,34 and 1 study found electrostimulation improved xerostomia in patients with Sjögren’s syndrome.35 Both approaches require more study to confirm their effectiveness.33-35
Table 2
Managing dry mouth: What to tell patients
| Oral hygiene. Tell patients to be diligent in their oral hygiene practices, including brushing and flossing. They should use a toothpaste containing fluoride—preferably one free of sodium lauryl sulfate—and schedule regular dental visits, where they can receive high-fluoride applications or be prescribed high-fluoride prescription toothpastes |
| Diet. Advise patients to avoid foods high in sucrose content, rinse their mouth with water soon after eating, and drink fluoridated water regularly. Tell them that they may be able to stimulate saliva flow with sugarless gum, candies, and foods such as celery and carrots |
| Drying agents. Instruct patients to avoid cigarettes, caffeinated beverages, and mouth rinses that contain alcohol. Explain that some patients may benefit from sleeping in a room with a cool air humidifier |
| Over-the-counter products. Suggest patients try salivary substitutes, which are dispensed in spray bottles, rinses, swish bottles, or oral swab sticks. In addition, products such as dry-mouth toothpaste and moisturizing gels also may help relieve their symptoms |
- Persson K, Axtelius B, Söderfeldt B, et al. Monitoring oral health and dental attendance in an outpatient psychiatric population. J Psychiatr Ment Health Nurs. 2009;16(3):263-271.
- Keene JJ Jr, Galasko GT, Land MF. Antidepressant use in psychiatry and medicine: importance for dental practice. J Am Dent Assoc. 2003;134(1):71-79.
Drug Brand Names
- Alprazolam • Xanax
- Amlodipine • Norvasc
- Bupropion • Wellbutrin, Zyban
- Cevimeline • Evoxac
- Clonidine • Catapres, Kapvay, others
- Esomeprazole • Nexium
- Irbesartan • Avapro
- Metoprolol • Lopressor, Toprol
- Pilocarpine • Salagen
- Tolterodine • Detrol
- Venlafaxine • Effexor
- Zolpidem • Ambien
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Drymouth.info. Overview of drugs and dry mouth. http://drymouth.info/practitioner/overview.asp. Accessed September 2, 2011.
2. Stewart CM, Berg KM, Cha S, et al. Salivary dysfunction and quality of life in Sjögren syndrome: a critical oral-systemic connection. J Am Dent Assoc. 2008;139(3):291-299.
3. Friedman PK. Xerostomia: The invisible oral health condition. http://www.dentistryiq.com/index/display/article-display/295922/articles/woman-dentist-journal/health/xerostomia-the-invisible-oral-health-condition.html. Accessed September 6, 2011.
4. Physician Desk Reference. Montvale NJ: PDR Network LLC.; 2011.
5. Bardow A, Lagerlof F, Nauntofte B, et al. The role of saliva. In: Fejerskov O, Kidd E, eds. Dental caries: the disease and its clinical management. Oxford, United Kingdom: Blackwell Munksgaard; 2008:195.
6. Vanderkooy JD, Kennedy SH, Bagby RM. Antidepressant side effects in depression patients treated in a naturalistic setting: a study of bupropion moclobemide, paroxetine, sertraline, and venlafaxine. Can J Psychiatry. 2002;47(2):174-180.
7. Löffler W, Kilian R, Toumi M, et al. Schizophrenic patients’ subjective reasons for compliance and noncompliance with neuroleptic treatment. Pharmacopsychiatry. 2003;36(3):105-112.
8. Lambert M, Conus P, Eide P, et al. Impact of present and past antipsychotic side effects on attitude toward typical antipsychotic treatment and adherence. Eur Psychiatry. 2004;19(7):415-422.
9. Rettenbacher MA, Hofer A, Eder U, et al. Compliance in schizophrenia: psychopathology, side effects, and patients’ attitudes toward the illness and medication. J Clin Psychiatry. 2004;65(9):1211-1218.
10. Bulkacz J, Carranza FA. Defense mechanisms of the gingiva. In: Newman MG, Takei HH, Klokkevold PR, et al, eds. Carranza’s clinical periodontology. St. Louis, MO: Elsevier Saunders; 2011:69–70.
11. Szabadi E, Tavernor S. Hypo-and hyper-salivation induced by psychoactive drugs. CNS Drugs. 1999;11(6):449-466.
12. Guggenheimer J, Moore PA. Xerostomia: etiology recognition and treatment. J Am Dent Assoc. 2003;134(1):61-69.
13. Dawes C. Physiological factors affecting salivary flow rate oral sugar clearance, and the sensation of dry mouth in man. J Dent Res. 1987;66:648-653.
14. Bartels CL. Xerostomia information for dentists. http://www.homesteadschools.com/dental/courses/Xerostomia/Course.htm. Accessed August 15, 2011.
15. Sitheeque MA, Samaranayake LP. Chronic hyperplastic candidosis/candidiasis (candidal leukoplakia). Crit Rev Oral Biol Med. 2003;14(4):253-267.
16. Porter SR, Scully C. Oral malodour (halitosis). BMJ. 2006;333(7569):632-635.
17. Quirynen M, Van den Veide S, Vanderkerckhove B, et al. Oral malodor. In: Newman MG, Takei HH, Klokkevold PR, et al, eds. Carranza’s clinical periodontology. St. Louis, MO: Elsevier Saunders; 2011:333.
18. Papas A. Dry mouth from drugs: more than just an annoying side effect. Tufts University Heath and Nutrition Letter. 2000;3.-
19. American Academy of Periodontology. Gum disease information from the American Academy of Periodontology http://perio.org. Accessed August 12, 2011.
20. Geismar K, Stoltze K, Sigurd B, et al. Periodontal disease and coronary heart disease. J Periodontol. 2006;77(9):1547-1554.
21. Lee HJ, Garcia RI, Janket SJ, et al. The association between cumulative periodontal disease and stroke history in older adults. J Periodontol. 2006;77(10):1744-1754.
22. Friedewald VE, Kornman KS, Beck JD, et al. The American Journal of Cardiology and Journal of Periodontology editors’ consensus: periodontitis and atherosclerotic cardiovascular disease. J Periodontol. 2009;80(7):1021-1032.
23. Contreras A, Herrera JA, Soto JE, et al. Periodontitis is associated with preeclampsia in pregnant women. J Periodontol. 2006;77(2):182-188.
24. Dasanayake AP, Li Y, Wiener H, et al. Salivary Actinomyces naeslundii genospecies 2 and Lactobacillus casei levels predict pregnancy outcomes. J Periodontol. 2005;76(2):171-177.
25. McCreadie RG, Stevens H, Henderson J, et al. The dental health of people with schizophrenia. Acta Psychiatr Scand. 2004;110(4):306-310.
26. Anttila S, Knuuttila M, Ylöstalo P, et al. Symptoms of depression and anxiety in relation to dental health behavior and self-perceived dental treatment need. Eur J Oral Sci. 2006;114(2):109-114.
27. Sjögren R, Nordström G. Oral health status of psychiatric patients. J Clin Nurs. 2000;9(4):632-638.
28. Ramon T, Grinshpoon A, Zusman SP, et al. Oral health and treatment needs of institutionalized chronic psychiatric patients in Israel. Eur Psychiatry. 2003;18(3):101-105.
29. Portilla MI, Mafla AC, Arteaga JJ. Periodontal status in female psychiatric patients. Colomb Med. 2009;40(2):167-176.
30. Navazesh M. ADA Council on Scientific Affairs and Division of Science. How can oral health care providers determine if patients have dry mouth? J Am Dent Assoc. 2003;134(5):613-620.
31. Mignogna MD, Fedele S, Lo Russo L, et al. Sjögren’s syndrome: the diagnostic potential of early oral manifestations preceding hyposalivation/xerostomia. J Oral Pathol Med. 2005;34(1):1-6.
32. Spolarich AE. Managing the side effects of medications. J Dent Hyg. 2000;74(1):57-69.
33. Johnstone PA, Niemtzow RC, Riffenburgh RH. Acupuncture for xerostomia: clinical update. Cancer. 2002;94(4):1151-1156.
34. Garcia MK, Chiang JS, Cohen L, et al. Acupuncture for radiation-induced xerostomia in patients with cancer: a pilot study. Head Neck. 2009;31(10):1360-1368.
35. Strietzel FP, Lafaurie GI, Mendoza GR, et al. Efficacy and safety of an intraoral electrostimulation device for xerostomia relief: a multicenter, randomized trial. Arthritis Rheum. 2011;63(1):180-190.
1. Drymouth.info. Overview of drugs and dry mouth. http://drymouth.info/practitioner/overview.asp. Accessed September 2, 2011.
2. Stewart CM, Berg KM, Cha S, et al. Salivary dysfunction and quality of life in Sjögren syndrome: a critical oral-systemic connection. J Am Dent Assoc. 2008;139(3):291-299.
3. Friedman PK. Xerostomia: The invisible oral health condition. http://www.dentistryiq.com/index/display/article-display/295922/articles/woman-dentist-journal/health/xerostomia-the-invisible-oral-health-condition.html. Accessed September 6, 2011.
4. Physician Desk Reference. Montvale NJ: PDR Network LLC.; 2011.
5. Bardow A, Lagerlof F, Nauntofte B, et al. The role of saliva. In: Fejerskov O, Kidd E, eds. Dental caries: the disease and its clinical management. Oxford, United Kingdom: Blackwell Munksgaard; 2008:195.
6. Vanderkooy JD, Kennedy SH, Bagby RM. Antidepressant side effects in depression patients treated in a naturalistic setting: a study of bupropion moclobemide, paroxetine, sertraline, and venlafaxine. Can J Psychiatry. 2002;47(2):174-180.
7. Löffler W, Kilian R, Toumi M, et al. Schizophrenic patients’ subjective reasons for compliance and noncompliance with neuroleptic treatment. Pharmacopsychiatry. 2003;36(3):105-112.
8. Lambert M, Conus P, Eide P, et al. Impact of present and past antipsychotic side effects on attitude toward typical antipsychotic treatment and adherence. Eur Psychiatry. 2004;19(7):415-422.
9. Rettenbacher MA, Hofer A, Eder U, et al. Compliance in schizophrenia: psychopathology, side effects, and patients’ attitudes toward the illness and medication. J Clin Psychiatry. 2004;65(9):1211-1218.
10. Bulkacz J, Carranza FA. Defense mechanisms of the gingiva. In: Newman MG, Takei HH, Klokkevold PR, et al, eds. Carranza’s clinical periodontology. St. Louis, MO: Elsevier Saunders; 2011:69–70.
11. Szabadi E, Tavernor S. Hypo-and hyper-salivation induced by psychoactive drugs. CNS Drugs. 1999;11(6):449-466.
12. Guggenheimer J, Moore PA. Xerostomia: etiology recognition and treatment. J Am Dent Assoc. 2003;134(1):61-69.
13. Dawes C. Physiological factors affecting salivary flow rate oral sugar clearance, and the sensation of dry mouth in man. J Dent Res. 1987;66:648-653.
14. Bartels CL. Xerostomia information for dentists. http://www.homesteadschools.com/dental/courses/Xerostomia/Course.htm. Accessed August 15, 2011.
15. Sitheeque MA, Samaranayake LP. Chronic hyperplastic candidosis/candidiasis (candidal leukoplakia). Crit Rev Oral Biol Med. 2003;14(4):253-267.
16. Porter SR, Scully C. Oral malodour (halitosis). BMJ. 2006;333(7569):632-635.
17. Quirynen M, Van den Veide S, Vanderkerckhove B, et al. Oral malodor. In: Newman MG, Takei HH, Klokkevold PR, et al, eds. Carranza’s clinical periodontology. St. Louis, MO: Elsevier Saunders; 2011:333.
18. Papas A. Dry mouth from drugs: more than just an annoying side effect. Tufts University Heath and Nutrition Letter. 2000;3.-
19. American Academy of Periodontology. Gum disease information from the American Academy of Periodontology http://perio.org. Accessed August 12, 2011.
20. Geismar K, Stoltze K, Sigurd B, et al. Periodontal disease and coronary heart disease. J Periodontol. 2006;77(9):1547-1554.
21. Lee HJ, Garcia RI, Janket SJ, et al. The association between cumulative periodontal disease and stroke history in older adults. J Periodontol. 2006;77(10):1744-1754.
22. Friedewald VE, Kornman KS, Beck JD, et al. The American Journal of Cardiology and Journal of Periodontology editors’ consensus: periodontitis and atherosclerotic cardiovascular disease. J Periodontol. 2009;80(7):1021-1032.
23. Contreras A, Herrera JA, Soto JE, et al. Periodontitis is associated with preeclampsia in pregnant women. J Periodontol. 2006;77(2):182-188.
24. Dasanayake AP, Li Y, Wiener H, et al. Salivary Actinomyces naeslundii genospecies 2 and Lactobacillus casei levels predict pregnancy outcomes. J Periodontol. 2005;76(2):171-177.
25. McCreadie RG, Stevens H, Henderson J, et al. The dental health of people with schizophrenia. Acta Psychiatr Scand. 2004;110(4):306-310.
26. Anttila S, Knuuttila M, Ylöstalo P, et al. Symptoms of depression and anxiety in relation to dental health behavior and self-perceived dental treatment need. Eur J Oral Sci. 2006;114(2):109-114.
27. Sjögren R, Nordström G. Oral health status of psychiatric patients. J Clin Nurs. 2000;9(4):632-638.
28. Ramon T, Grinshpoon A, Zusman SP, et al. Oral health and treatment needs of institutionalized chronic psychiatric patients in Israel. Eur Psychiatry. 2003;18(3):101-105.
29. Portilla MI, Mafla AC, Arteaga JJ. Periodontal status in female psychiatric patients. Colomb Med. 2009;40(2):167-176.
30. Navazesh M. ADA Council on Scientific Affairs and Division of Science. How can oral health care providers determine if patients have dry mouth? J Am Dent Assoc. 2003;134(5):613-620.
31. Mignogna MD, Fedele S, Lo Russo L, et al. Sjögren’s syndrome: the diagnostic potential of early oral manifestations preceding hyposalivation/xerostomia. J Oral Pathol Med. 2005;34(1):1-6.
32. Spolarich AE. Managing the side effects of medications. J Dent Hyg. 2000;74(1):57-69.
33. Johnstone PA, Niemtzow RC, Riffenburgh RH. Acupuncture for xerostomia: clinical update. Cancer. 2002;94(4):1151-1156.
34. Garcia MK, Chiang JS, Cohen L, et al. Acupuncture for radiation-induced xerostomia in patients with cancer: a pilot study. Head Neck. 2009;31(10):1360-1368.
35. Strietzel FP, Lafaurie GI, Mendoza GR, et al. Efficacy and safety of an intraoral electrostimulation device for xerostomia relief: a multicenter, randomized trial. Arthritis Rheum. 2011;63(1):180-190.