User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Practicing psychiatry via Skype: Medicolegal considerations
Dear Dr. Mossman:
I practice in a region with few psychiatrists and very little public transportation. For many patients, coming to my office is inconvenient, expensive, or time-consuming. Sometimes, their emotional problems make it hard for them to travel, and sometimes, bad weather makes travel difficult. I am considering providing remote treatment via Skype. Is this a reasonable idea? What are the risks of using this technology in my practice? — Submitted by “Dr. A”
Diagnosing and treating patients without a face-to-face encounter is not new. Doctors have provided “remote treatment” since shortly after telephones were invented.1 Until recently, however, forensic psychiatrists advised colleagues not to diagnose patients or start treatment based on phone contact alone.2
The Internet has revolutionized our attitudes about many things. Communication technologies that seemed miraculous a generation ago have become commonplace and have transformed standards for ordinary and “acceptable” human contact. A quick Internet search of “telephone psychotherapy” turns up hundreds of mental health professionals who offer remote treatment services to patients via computers and Web cams.
Physicians in many specialties practice telemedicine, often with the support and encouragement of state governments and third-party payers. To decide whether to include telepsychiatry in your psychiatric practice, you should know:
- what “telemedicine” means and includes
- the possible advantages of offering remote health care
- potential risks and ambiguity about legal matters.
Defining telemedicine
Studies of remote, closed-circuit “telediagnosis” extend back more than 4 decades, closely following mid-20th century advancements in audio and video relay technologies that made space broadcasts possible.3 Then as now, “telemedicine” simply means conveying health-related information from 1 site to another for diagnostic or treatment purposes.4 It’s an adaptation of available technology to deliver care more easily, with the goal of improving patients’ access to care and health status.
Telemedicine usage accelerated as the Internet and related technologies developed. Telemedicine programs in the United States increased by 1,500% from 1993 to 1998.4 Telemedicine use has grown 10% annually in recent years and has become a $4 billion per year industry in the United States.5 Recently enacted federal legislation is likely to extend health care coverage to 36 million Americans and require coverage of pre-existing conditions. To make these changes affordable, health care delivery will need to exploit new, efficiency-enhancing technologies.6
Advantages of telemedicine
State governments and some third-party payers have recognized that telemedicine can overcome geographic and cost barriers to health services and patient education.5,7-9 Although closed-circuit video transmission has served this purpose for some time, Skype—free software that allows individuals to make video phone calls over the Internet using their computers—is an option that doctors are using to treat patients.10-12
Research suggests that telepsychiatry may provide huge benefits to medically underserved areas while reducing health care costs.4 Telepsychiatry can reduce travel time and expenses for professionals and patients, and it also may lower wait times and “no-show” rates (Table 1).4 Telepsychiatry lets patients see caregivers when winter weather makes roads unsafe. It may allow geriatric patients who can no longer drive to access psychiatric care and it lowers health care’s “carbon footprint,” making it “eco-friendly.”13
Social media strategies are playing an expanding role in medical education,14,15 and this probably will help practitioners feel more at ease about incorporating the underlying technologies into work with patients. Increased use of laptops and mobile phones lends itself well to telepsychiatry applications,13 and studies have examined the feasibility of psychotherapies delivered via remote communication devices.16 Smartphone apps are being designed to assist mental health professionals17 and consumers.18
Table 1
Potential benefits of telemedicine
| Category | Benefit(s) |
|---|---|
| Access | Patients can see specialists more readily Addresses regional doctor shortages Reduces health care disparities between urban and rural areas |
| Urgent care | Facilitates information transfer for rapid interventions |
| Productivity | Provides a conduit for clinicians to share skills and expertise Facilitates remote monitoring and home care |
| Cost | No travel costs Alternative revenue stream for health care organizations that offer more broadly delivered medical services |
| Patient-centric care | Care is taken to the patient Translator services are more readily available |
| Source: Reference 4 | |
Potential pitfalls and drawbacks
Although convenience, access, cost, and fossil fuel savings may favor video-chat doctor visits, telemedicine has downsides, some of which apply specifically to psychiatry. First, no current technology provides psychiatrists with “the rich multidimensional aspects of a person-to-person encounter,”19 and remote communication may change what patients tell us, how they feel when they tell us things, and how they feel when we respond. Often, an inherent awkwardness affects many forms of Internet communication.20
Also uncertain is whether Skype is compliant with the Health Insurance Portability and Accountability Act and protects doctor-patient privacy well enough to satisfy ethical standards—although it probably is far better than e-mail in this regard. Third-party payers often will not reimburse for telephone calls and may balk at paying for Skype-based therapy, even in states that require insurers to reimburse for telemedicine.
Psychiatrists typically have limited physical contact with patients, but we often check weight and vital signs when we prescribe certain psychotropic medications. Results from home- and drugstore-based blood pressure monitors may not be accurate enough for treatment purposes. Remote communication also reduces the quality of visual information,20 which can be crucial—for example, when good lighting and visual resolution is needed to decide whether a skin rash might be drug-induced.
Telemedicine raises concerns about licensure and meeting adequate standards of care. Medical care usually is deemed to have occurred in the state where the patient is located. For example, only physicians licensed to practice medicine in California are legally permitted to treat patients in California. As is the case with any treatment, care delivered via telemedicine must include appropriate patient examination and diagnosis.21
Help and guidance
Despite these potential drawbacks, many state agencies recognize the promise of telemedicine, and have developed networks to promote it (Table 2).7-9,22,23 These networks have various goals but share a common pattern of establishing infrastructure, policies, and organized results. In the future, states may adopt laws or regulations that address conflicts in malpractice standards and liability coverage, licensing, accreditation, reimbursement, privacy, and data protection policies that now may impede or inhibit use of telepsychiatric services across jurisdictional boundaries. Last year, Ohio produced regulations to guide psychiatrists in prescribing medication remotely without an in-person examination. The University of Hawaii suggested steps that its state legislature might take to help providers predict the potential legal ramifications of telemedicine.6
Further help for telepsychiatry practitioners may be found in practice standards and guidelines developed by the American Telemedicine Association.24,25 These documents gave guidance and support for the practice of telemedicine and for providing appropriate telepsychiatry health services.
Table 2
Telemedicine services available in different states
| State/Network | Description |
|---|---|
| Arizona www.narbha.org7 | The Northern Arizona Regional Behavioral Health Authority manages a comprehensive telemental health network (NARBHAnet) that uses 2-way videoconferencing to connect mental health experts and patients. It has provided >50,000 clinical psychiatric sessions |
| Kansas www.kumc.edu8 | The University of Kansas Medical Center provides specialty services (including telepsychiatry) through 14 clinical sites in rural Kansas. Cost-sharing helps the telepsychiatric application be successful |
| Montana www.emtn.org9 | Eastern Montana Telemedicine Network is a consortium of not-for-profit facilities that link health care providers and their patients in Montana and Wyoming. This telemental health network includes shared sites for all physicians practicing in the network and has yielded large out-of-pocket savings for patients |
| Oregon www.ortelehealth.org22 | The Telehealth Alliance of Oregon, which began in 2001 as a committee of the Oregon Telecommunications Coordinating Council, was created by the legislature and has served as advisors to the governor and the legislature regarding telecommunications in Oregon |
| Texas www.jsahealthmd.com23 | The Burke Center provides services to people in 12 counties in East Texas. It uses telepsychiatry services to conduct emergency evaluations, therefore keeping people in mental health crises out of emergency rooms |
What should Dr. A do?
In answer to Dr. A’s question, many factors favor including telepsychiatry in her practice. Yet we know little about the accuracy and reliability of psychiatric assessments made solely via Skype or other remote video technology in ordinary practice. Legislation and legal rules about acceptable practices are ambiguous, although in the absence of clear guidance, psychiatrists should assume that all usual professional standards and expectations about adequate care apply to treatment via Skype or other remote communication methods.
Related Resources
- Skype. www.skype.com.
- American Telemedicine Association. www.americantelemed.org.
1. Lipman M. The doctor will Skype you now. Consum Rep. 2011;76(8):12.-
2. Simon RI. Clinical psychiatry and the law. 2nd ed. Washington DC: American Psychiatric Press; 1992.
3. Murphy RL, Jr, Bird KT. Telediagnosis: a new community health resource. Observations on the feasibility of telediagnosis based on 1000 patient transactions. Am J Public Health. 1974;64(2):113-119.
4. Hilty DM, Yellowlees PM, Cobb HC, et al. Models of telepsychiatric consultation—liaison service to rural primary care. Psychosomatics. 2006;47(2):152-157.
5. Freudenheim M. The doctor will see you now. Please log on. New York Times. May 29 2010:BU1.
6. University of Hawai’i. Report to the 2009 legislature: preliminary report by the John A. Burns School of Medicine on the current practices of Hawai’i telemedicine system for 2009. http://www.hawaii.edu/offices/eaur/govrel/reports/2009. Published November 2008. Accessed September 27 2011.
7. Northern Arizona Regional Behavioral Health Authority. http://www.narbha.org. Accessed September 27 2011.
8. University of Kansas Medical Center. http://www.kumc.edu. Accessed September 27 2011.
9. Eastern Montana Telemedicine Network. http://www.emtn.org. Accessed September 27 2011.
10. Ciccia AH, Whitford B, Krumm M, et al. Improving the access of young urban children to speech, language and hearing screening via telehealth. J Telemed Telecare. 2011;17(5):240-244.
11. Hori M, Kubota M, Ando K, et al. The effect of videophone communication (with skype and webcam) for elderly patients with dementia and their caregivers [in Japanese]. Gan To Kagaku Ryoho. 2009;36(suppl 1):36-38.
12. Klock C, Gomes Rde P. Web conferencing systems: Skype and MSN in telepathology. Diagn Pathol. 2008;3(suppl 1):S13.-
13. Luo J. VoIP: The right call for your practice? Current Psychiatry. 2005;4(10):24-27.
14. George DR, Dellasega C. Use of social media in graduate-level medical humanities education: two pilot studies from Penn State College of Medicine. Med Teach. 2011;33(8):e429-434.
15. Lillis S, Gibbons V, Lawrenson R. The experience of final year medical students undertaking a general practice run with a distance education component. Rural Remote Health. 2010;10(1):1268.-
16. Bee PE, Bower P, Lovell K, et al. Psychotherapy mediated by remote communication technologies: a meta-analytic review. BMC Psychiatry. 2008;8:60.-
17. Maheu MM. iPhone app reviews for psychologists and mental health professionals. http://telehealth.net/blog/554. Accessed September 27 2011.
18. Maheu MM. iPhone apps reviews for mental health psychology and personal growth consumers. http://telehealth.net/blog/557. Accessed September 27, 2011.
19. Eckardt MH. The use of the telephone to extend our therapeutic availability. J Am Acad Psychoanal Dyn Psychiatry. 2011;39(1):151-153.
20. Hoffman J. When your therapist is only a click away. New York Times. September 23 2011:ST1.
21. Medical Board of California. Practicing medicine through telemedicine technology. http://www.mbc.ca.gov/licensee/telemedicine.html. Accessed September 27 2011.
22. Telehealth Alliance of Oregon. http://www.ortelehealth.org. Accessed October 31 2011.
23. JSA Health Telepsychiatry. http://jsahealthmd.com. Accessed September 27 2011.
24. American Telemedicine Association. Telemental standards and guidelines. http://www.americantelemed.org/i4a/pages/index.cfm?pageID=3311. Accessed September 27 2011.
25. American Telemedicine Association. Evidence-based practice for telemental health. http://www.americantelemed.org/i4a/forms/form.cfm?id=25&pageid=3718&showTitle=1. Accessed September 27 2011.
Helen M. Farrell, MD
Dr. Farrell is an instructor at Harvard Medical School and a staff psychiatrist at Beth Israel Deaconess Medical Center, Boston, MA
Douglas Mossman, MD
Dr. Mossman is administrative director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and Adjunct Professor of Clinical Psychiatry and Training Director for the University of Cincinnati Forensic Psychiatry Fellowship, Cincinnati, OH
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Helen M. Farrell, MD
Dr. Farrell is an instructor at Harvard Medical School and a staff psychiatrist at Beth Israel Deaconess Medical Center, Boston, MA
Douglas Mossman, MD
Dr. Mossman is administrative director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and Adjunct Professor of Clinical Psychiatry and Training Director for the University of Cincinnati Forensic Psychiatry Fellowship, Cincinnati, OH
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Helen M. Farrell, MD
Dr. Farrell is an instructor at Harvard Medical School and a staff psychiatrist at Beth Israel Deaconess Medical Center, Boston, MA
Douglas Mossman, MD
Dr. Mossman is administrative director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and Adjunct Professor of Clinical Psychiatry and Training Director for the University of Cincinnati Forensic Psychiatry Fellowship, Cincinnati, OH
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dear Dr. Mossman:
I practice in a region with few psychiatrists and very little public transportation. For many patients, coming to my office is inconvenient, expensive, or time-consuming. Sometimes, their emotional problems make it hard for them to travel, and sometimes, bad weather makes travel difficult. I am considering providing remote treatment via Skype. Is this a reasonable idea? What are the risks of using this technology in my practice? — Submitted by “Dr. A”
Diagnosing and treating patients without a face-to-face encounter is not new. Doctors have provided “remote treatment” since shortly after telephones were invented.1 Until recently, however, forensic psychiatrists advised colleagues not to diagnose patients or start treatment based on phone contact alone.2
The Internet has revolutionized our attitudes about many things. Communication technologies that seemed miraculous a generation ago have become commonplace and have transformed standards for ordinary and “acceptable” human contact. A quick Internet search of “telephone psychotherapy” turns up hundreds of mental health professionals who offer remote treatment services to patients via computers and Web cams.
Physicians in many specialties practice telemedicine, often with the support and encouragement of state governments and third-party payers. To decide whether to include telepsychiatry in your psychiatric practice, you should know:
- what “telemedicine” means and includes
- the possible advantages of offering remote health care
- potential risks and ambiguity about legal matters.
Defining telemedicine
Studies of remote, closed-circuit “telediagnosis” extend back more than 4 decades, closely following mid-20th century advancements in audio and video relay technologies that made space broadcasts possible.3 Then as now, “telemedicine” simply means conveying health-related information from 1 site to another for diagnostic or treatment purposes.4 It’s an adaptation of available technology to deliver care more easily, with the goal of improving patients’ access to care and health status.
Telemedicine usage accelerated as the Internet and related technologies developed. Telemedicine programs in the United States increased by 1,500% from 1993 to 1998.4 Telemedicine use has grown 10% annually in recent years and has become a $4 billion per year industry in the United States.5 Recently enacted federal legislation is likely to extend health care coverage to 36 million Americans and require coverage of pre-existing conditions. To make these changes affordable, health care delivery will need to exploit new, efficiency-enhancing technologies.6
Advantages of telemedicine
State governments and some third-party payers have recognized that telemedicine can overcome geographic and cost barriers to health services and patient education.5,7-9 Although closed-circuit video transmission has served this purpose for some time, Skype—free software that allows individuals to make video phone calls over the Internet using their computers—is an option that doctors are using to treat patients.10-12
Research suggests that telepsychiatry may provide huge benefits to medically underserved areas while reducing health care costs.4 Telepsychiatry can reduce travel time and expenses for professionals and patients, and it also may lower wait times and “no-show” rates (Table 1).4 Telepsychiatry lets patients see caregivers when winter weather makes roads unsafe. It may allow geriatric patients who can no longer drive to access psychiatric care and it lowers health care’s “carbon footprint,” making it “eco-friendly.”13
Social media strategies are playing an expanding role in medical education,14,15 and this probably will help practitioners feel more at ease about incorporating the underlying technologies into work with patients. Increased use of laptops and mobile phones lends itself well to telepsychiatry applications,13 and studies have examined the feasibility of psychotherapies delivered via remote communication devices.16 Smartphone apps are being designed to assist mental health professionals17 and consumers.18
Table 1
Potential benefits of telemedicine
| Category | Benefit(s) |
|---|---|
| Access | Patients can see specialists more readily Addresses regional doctor shortages Reduces health care disparities between urban and rural areas |
| Urgent care | Facilitates information transfer for rapid interventions |
| Productivity | Provides a conduit for clinicians to share skills and expertise Facilitates remote monitoring and home care |
| Cost | No travel costs Alternative revenue stream for health care organizations that offer more broadly delivered medical services |
| Patient-centric care | Care is taken to the patient Translator services are more readily available |
| Source: Reference 4 | |
Potential pitfalls and drawbacks
Although convenience, access, cost, and fossil fuel savings may favor video-chat doctor visits, telemedicine has downsides, some of which apply specifically to psychiatry. First, no current technology provides psychiatrists with “the rich multidimensional aspects of a person-to-person encounter,”19 and remote communication may change what patients tell us, how they feel when they tell us things, and how they feel when we respond. Often, an inherent awkwardness affects many forms of Internet communication.20
Also uncertain is whether Skype is compliant with the Health Insurance Portability and Accountability Act and protects doctor-patient privacy well enough to satisfy ethical standards—although it probably is far better than e-mail in this regard. Third-party payers often will not reimburse for telephone calls and may balk at paying for Skype-based therapy, even in states that require insurers to reimburse for telemedicine.
Psychiatrists typically have limited physical contact with patients, but we often check weight and vital signs when we prescribe certain psychotropic medications. Results from home- and drugstore-based blood pressure monitors may not be accurate enough for treatment purposes. Remote communication also reduces the quality of visual information,20 which can be crucial—for example, when good lighting and visual resolution is needed to decide whether a skin rash might be drug-induced.
Telemedicine raises concerns about licensure and meeting adequate standards of care. Medical care usually is deemed to have occurred in the state where the patient is located. For example, only physicians licensed to practice medicine in California are legally permitted to treat patients in California. As is the case with any treatment, care delivered via telemedicine must include appropriate patient examination and diagnosis.21
Help and guidance
Despite these potential drawbacks, many state agencies recognize the promise of telemedicine, and have developed networks to promote it (Table 2).7-9,22,23 These networks have various goals but share a common pattern of establishing infrastructure, policies, and organized results. In the future, states may adopt laws or regulations that address conflicts in malpractice standards and liability coverage, licensing, accreditation, reimbursement, privacy, and data protection policies that now may impede or inhibit use of telepsychiatric services across jurisdictional boundaries. Last year, Ohio produced regulations to guide psychiatrists in prescribing medication remotely without an in-person examination. The University of Hawaii suggested steps that its state legislature might take to help providers predict the potential legal ramifications of telemedicine.6
Further help for telepsychiatry practitioners may be found in practice standards and guidelines developed by the American Telemedicine Association.24,25 These documents gave guidance and support for the practice of telemedicine and for providing appropriate telepsychiatry health services.
Table 2
Telemedicine services available in different states
| State/Network | Description |
|---|---|
| Arizona www.narbha.org7 | The Northern Arizona Regional Behavioral Health Authority manages a comprehensive telemental health network (NARBHAnet) that uses 2-way videoconferencing to connect mental health experts and patients. It has provided >50,000 clinical psychiatric sessions |
| Kansas www.kumc.edu8 | The University of Kansas Medical Center provides specialty services (including telepsychiatry) through 14 clinical sites in rural Kansas. Cost-sharing helps the telepsychiatric application be successful |
| Montana www.emtn.org9 | Eastern Montana Telemedicine Network is a consortium of not-for-profit facilities that link health care providers and their patients in Montana and Wyoming. This telemental health network includes shared sites for all physicians practicing in the network and has yielded large out-of-pocket savings for patients |
| Oregon www.ortelehealth.org22 | The Telehealth Alliance of Oregon, which began in 2001 as a committee of the Oregon Telecommunications Coordinating Council, was created by the legislature and has served as advisors to the governor and the legislature regarding telecommunications in Oregon |
| Texas www.jsahealthmd.com23 | The Burke Center provides services to people in 12 counties in East Texas. It uses telepsychiatry services to conduct emergency evaluations, therefore keeping people in mental health crises out of emergency rooms |
What should Dr. A do?
In answer to Dr. A’s question, many factors favor including telepsychiatry in her practice. Yet we know little about the accuracy and reliability of psychiatric assessments made solely via Skype or other remote video technology in ordinary practice. Legislation and legal rules about acceptable practices are ambiguous, although in the absence of clear guidance, psychiatrists should assume that all usual professional standards and expectations about adequate care apply to treatment via Skype or other remote communication methods.
Related Resources
- Skype. www.skype.com.
- American Telemedicine Association. www.americantelemed.org.
Dear Dr. Mossman:
I practice in a region with few psychiatrists and very little public transportation. For many patients, coming to my office is inconvenient, expensive, or time-consuming. Sometimes, their emotional problems make it hard for them to travel, and sometimes, bad weather makes travel difficult. I am considering providing remote treatment via Skype. Is this a reasonable idea? What are the risks of using this technology in my practice? — Submitted by “Dr. A”
Diagnosing and treating patients without a face-to-face encounter is not new. Doctors have provided “remote treatment” since shortly after telephones were invented.1 Until recently, however, forensic psychiatrists advised colleagues not to diagnose patients or start treatment based on phone contact alone.2
The Internet has revolutionized our attitudes about many things. Communication technologies that seemed miraculous a generation ago have become commonplace and have transformed standards for ordinary and “acceptable” human contact. A quick Internet search of “telephone psychotherapy” turns up hundreds of mental health professionals who offer remote treatment services to patients via computers and Web cams.
Physicians in many specialties practice telemedicine, often with the support and encouragement of state governments and third-party payers. To decide whether to include telepsychiatry in your psychiatric practice, you should know:
- what “telemedicine” means and includes
- the possible advantages of offering remote health care
- potential risks and ambiguity about legal matters.
Defining telemedicine
Studies of remote, closed-circuit “telediagnosis” extend back more than 4 decades, closely following mid-20th century advancements in audio and video relay technologies that made space broadcasts possible.3 Then as now, “telemedicine” simply means conveying health-related information from 1 site to another for diagnostic or treatment purposes.4 It’s an adaptation of available technology to deliver care more easily, with the goal of improving patients’ access to care and health status.
Telemedicine usage accelerated as the Internet and related technologies developed. Telemedicine programs in the United States increased by 1,500% from 1993 to 1998.4 Telemedicine use has grown 10% annually in recent years and has become a $4 billion per year industry in the United States.5 Recently enacted federal legislation is likely to extend health care coverage to 36 million Americans and require coverage of pre-existing conditions. To make these changes affordable, health care delivery will need to exploit new, efficiency-enhancing technologies.6
Advantages of telemedicine
State governments and some third-party payers have recognized that telemedicine can overcome geographic and cost barriers to health services and patient education.5,7-9 Although closed-circuit video transmission has served this purpose for some time, Skype—free software that allows individuals to make video phone calls over the Internet using their computers—is an option that doctors are using to treat patients.10-12
Research suggests that telepsychiatry may provide huge benefits to medically underserved areas while reducing health care costs.4 Telepsychiatry can reduce travel time and expenses for professionals and patients, and it also may lower wait times and “no-show” rates (Table 1).4 Telepsychiatry lets patients see caregivers when winter weather makes roads unsafe. It may allow geriatric patients who can no longer drive to access psychiatric care and it lowers health care’s “carbon footprint,” making it “eco-friendly.”13
Social media strategies are playing an expanding role in medical education,14,15 and this probably will help practitioners feel more at ease about incorporating the underlying technologies into work with patients. Increased use of laptops and mobile phones lends itself well to telepsychiatry applications,13 and studies have examined the feasibility of psychotherapies delivered via remote communication devices.16 Smartphone apps are being designed to assist mental health professionals17 and consumers.18
Table 1
Potential benefits of telemedicine
| Category | Benefit(s) |
|---|---|
| Access | Patients can see specialists more readily Addresses regional doctor shortages Reduces health care disparities between urban and rural areas |
| Urgent care | Facilitates information transfer for rapid interventions |
| Productivity | Provides a conduit for clinicians to share skills and expertise Facilitates remote monitoring and home care |
| Cost | No travel costs Alternative revenue stream for health care organizations that offer more broadly delivered medical services |
| Patient-centric care | Care is taken to the patient Translator services are more readily available |
| Source: Reference 4 | |
Potential pitfalls and drawbacks
Although convenience, access, cost, and fossil fuel savings may favor video-chat doctor visits, telemedicine has downsides, some of which apply specifically to psychiatry. First, no current technology provides psychiatrists with “the rich multidimensional aspects of a person-to-person encounter,”19 and remote communication may change what patients tell us, how they feel when they tell us things, and how they feel when we respond. Often, an inherent awkwardness affects many forms of Internet communication.20
Also uncertain is whether Skype is compliant with the Health Insurance Portability and Accountability Act and protects doctor-patient privacy well enough to satisfy ethical standards—although it probably is far better than e-mail in this regard. Third-party payers often will not reimburse for telephone calls and may balk at paying for Skype-based therapy, even in states that require insurers to reimburse for telemedicine.
Psychiatrists typically have limited physical contact with patients, but we often check weight and vital signs when we prescribe certain psychotropic medications. Results from home- and drugstore-based blood pressure monitors may not be accurate enough for treatment purposes. Remote communication also reduces the quality of visual information,20 which can be crucial—for example, when good lighting and visual resolution is needed to decide whether a skin rash might be drug-induced.
Telemedicine raises concerns about licensure and meeting adequate standards of care. Medical care usually is deemed to have occurred in the state where the patient is located. For example, only physicians licensed to practice medicine in California are legally permitted to treat patients in California. As is the case with any treatment, care delivered via telemedicine must include appropriate patient examination and diagnosis.21
Help and guidance
Despite these potential drawbacks, many state agencies recognize the promise of telemedicine, and have developed networks to promote it (Table 2).7-9,22,23 These networks have various goals but share a common pattern of establishing infrastructure, policies, and organized results. In the future, states may adopt laws or regulations that address conflicts in malpractice standards and liability coverage, licensing, accreditation, reimbursement, privacy, and data protection policies that now may impede or inhibit use of telepsychiatric services across jurisdictional boundaries. Last year, Ohio produced regulations to guide psychiatrists in prescribing medication remotely without an in-person examination. The University of Hawaii suggested steps that its state legislature might take to help providers predict the potential legal ramifications of telemedicine.6
Further help for telepsychiatry practitioners may be found in practice standards and guidelines developed by the American Telemedicine Association.24,25 These documents gave guidance and support for the practice of telemedicine and for providing appropriate telepsychiatry health services.
Table 2
Telemedicine services available in different states
| State/Network | Description |
|---|---|
| Arizona www.narbha.org7 | The Northern Arizona Regional Behavioral Health Authority manages a comprehensive telemental health network (NARBHAnet) that uses 2-way videoconferencing to connect mental health experts and patients. It has provided >50,000 clinical psychiatric sessions |
| Kansas www.kumc.edu8 | The University of Kansas Medical Center provides specialty services (including telepsychiatry) through 14 clinical sites in rural Kansas. Cost-sharing helps the telepsychiatric application be successful |
| Montana www.emtn.org9 | Eastern Montana Telemedicine Network is a consortium of not-for-profit facilities that link health care providers and their patients in Montana and Wyoming. This telemental health network includes shared sites for all physicians practicing in the network and has yielded large out-of-pocket savings for patients |
| Oregon www.ortelehealth.org22 | The Telehealth Alliance of Oregon, which began in 2001 as a committee of the Oregon Telecommunications Coordinating Council, was created by the legislature and has served as advisors to the governor and the legislature regarding telecommunications in Oregon |
| Texas www.jsahealthmd.com23 | The Burke Center provides services to people in 12 counties in East Texas. It uses telepsychiatry services to conduct emergency evaluations, therefore keeping people in mental health crises out of emergency rooms |
What should Dr. A do?
In answer to Dr. A’s question, many factors favor including telepsychiatry in her practice. Yet we know little about the accuracy and reliability of psychiatric assessments made solely via Skype or other remote video technology in ordinary practice. Legislation and legal rules about acceptable practices are ambiguous, although in the absence of clear guidance, psychiatrists should assume that all usual professional standards and expectations about adequate care apply to treatment via Skype or other remote communication methods.
Related Resources
- Skype. www.skype.com.
- American Telemedicine Association. www.americantelemed.org.
1. Lipman M. The doctor will Skype you now. Consum Rep. 2011;76(8):12.-
2. Simon RI. Clinical psychiatry and the law. 2nd ed. Washington DC: American Psychiatric Press; 1992.
3. Murphy RL, Jr, Bird KT. Telediagnosis: a new community health resource. Observations on the feasibility of telediagnosis based on 1000 patient transactions. Am J Public Health. 1974;64(2):113-119.
4. Hilty DM, Yellowlees PM, Cobb HC, et al. Models of telepsychiatric consultation—liaison service to rural primary care. Psychosomatics. 2006;47(2):152-157.
5. Freudenheim M. The doctor will see you now. Please log on. New York Times. May 29 2010:BU1.
6. University of Hawai’i. Report to the 2009 legislature: preliminary report by the John A. Burns School of Medicine on the current practices of Hawai’i telemedicine system for 2009. http://www.hawaii.edu/offices/eaur/govrel/reports/2009. Published November 2008. Accessed September 27 2011.
7. Northern Arizona Regional Behavioral Health Authority. http://www.narbha.org. Accessed September 27 2011.
8. University of Kansas Medical Center. http://www.kumc.edu. Accessed September 27 2011.
9. Eastern Montana Telemedicine Network. http://www.emtn.org. Accessed September 27 2011.
10. Ciccia AH, Whitford B, Krumm M, et al. Improving the access of young urban children to speech, language and hearing screening via telehealth. J Telemed Telecare. 2011;17(5):240-244.
11. Hori M, Kubota M, Ando K, et al. The effect of videophone communication (with skype and webcam) for elderly patients with dementia and their caregivers [in Japanese]. Gan To Kagaku Ryoho. 2009;36(suppl 1):36-38.
12. Klock C, Gomes Rde P. Web conferencing systems: Skype and MSN in telepathology. Diagn Pathol. 2008;3(suppl 1):S13.-
13. Luo J. VoIP: The right call for your practice? Current Psychiatry. 2005;4(10):24-27.
14. George DR, Dellasega C. Use of social media in graduate-level medical humanities education: two pilot studies from Penn State College of Medicine. Med Teach. 2011;33(8):e429-434.
15. Lillis S, Gibbons V, Lawrenson R. The experience of final year medical students undertaking a general practice run with a distance education component. Rural Remote Health. 2010;10(1):1268.-
16. Bee PE, Bower P, Lovell K, et al. Psychotherapy mediated by remote communication technologies: a meta-analytic review. BMC Psychiatry. 2008;8:60.-
17. Maheu MM. iPhone app reviews for psychologists and mental health professionals. http://telehealth.net/blog/554. Accessed September 27 2011.
18. Maheu MM. iPhone apps reviews for mental health psychology and personal growth consumers. http://telehealth.net/blog/557. Accessed September 27, 2011.
19. Eckardt MH. The use of the telephone to extend our therapeutic availability. J Am Acad Psychoanal Dyn Psychiatry. 2011;39(1):151-153.
20. Hoffman J. When your therapist is only a click away. New York Times. September 23 2011:ST1.
21. Medical Board of California. Practicing medicine through telemedicine technology. http://www.mbc.ca.gov/licensee/telemedicine.html. Accessed September 27 2011.
22. Telehealth Alliance of Oregon. http://www.ortelehealth.org. Accessed October 31 2011.
23. JSA Health Telepsychiatry. http://jsahealthmd.com. Accessed September 27 2011.
24. American Telemedicine Association. Telemental standards and guidelines. http://www.americantelemed.org/i4a/pages/index.cfm?pageID=3311. Accessed September 27 2011.
25. American Telemedicine Association. Evidence-based practice for telemental health. http://www.americantelemed.org/i4a/forms/form.cfm?id=25&pageid=3718&showTitle=1. Accessed September 27 2011.
1. Lipman M. The doctor will Skype you now. Consum Rep. 2011;76(8):12.-
2. Simon RI. Clinical psychiatry and the law. 2nd ed. Washington DC: American Psychiatric Press; 1992.
3. Murphy RL, Jr, Bird KT. Telediagnosis: a new community health resource. Observations on the feasibility of telediagnosis based on 1000 patient transactions. Am J Public Health. 1974;64(2):113-119.
4. Hilty DM, Yellowlees PM, Cobb HC, et al. Models of telepsychiatric consultation—liaison service to rural primary care. Psychosomatics. 2006;47(2):152-157.
5. Freudenheim M. The doctor will see you now. Please log on. New York Times. May 29 2010:BU1.
6. University of Hawai’i. Report to the 2009 legislature: preliminary report by the John A. Burns School of Medicine on the current practices of Hawai’i telemedicine system for 2009. http://www.hawaii.edu/offices/eaur/govrel/reports/2009. Published November 2008. Accessed September 27 2011.
7. Northern Arizona Regional Behavioral Health Authority. http://www.narbha.org. Accessed September 27 2011.
8. University of Kansas Medical Center. http://www.kumc.edu. Accessed September 27 2011.
9. Eastern Montana Telemedicine Network. http://www.emtn.org. Accessed September 27 2011.
10. Ciccia AH, Whitford B, Krumm M, et al. Improving the access of young urban children to speech, language and hearing screening via telehealth. J Telemed Telecare. 2011;17(5):240-244.
11. Hori M, Kubota M, Ando K, et al. The effect of videophone communication (with skype and webcam) for elderly patients with dementia and their caregivers [in Japanese]. Gan To Kagaku Ryoho. 2009;36(suppl 1):36-38.
12. Klock C, Gomes Rde P. Web conferencing systems: Skype and MSN in telepathology. Diagn Pathol. 2008;3(suppl 1):S13.-
13. Luo J. VoIP: The right call for your practice? Current Psychiatry. 2005;4(10):24-27.
14. George DR, Dellasega C. Use of social media in graduate-level medical humanities education: two pilot studies from Penn State College of Medicine. Med Teach. 2011;33(8):e429-434.
15. Lillis S, Gibbons V, Lawrenson R. The experience of final year medical students undertaking a general practice run with a distance education component. Rural Remote Health. 2010;10(1):1268.-
16. Bee PE, Bower P, Lovell K, et al. Psychotherapy mediated by remote communication technologies: a meta-analytic review. BMC Psychiatry. 2008;8:60.-
17. Maheu MM. iPhone app reviews for psychologists and mental health professionals. http://telehealth.net/blog/554. Accessed September 27 2011.
18. Maheu MM. iPhone apps reviews for mental health psychology and personal growth consumers. http://telehealth.net/blog/557. Accessed September 27, 2011.
19. Eckardt MH. The use of the telephone to extend our therapeutic availability. J Am Acad Psychoanal Dyn Psychiatry. 2011;39(1):151-153.
20. Hoffman J. When your therapist is only a click away. New York Times. September 23 2011:ST1.
21. Medical Board of California. Practicing medicine through telemedicine technology. http://www.mbc.ca.gov/licensee/telemedicine.html. Accessed September 27 2011.
22. Telehealth Alliance of Oregon. http://www.ortelehealth.org. Accessed October 31 2011.
23. JSA Health Telepsychiatry. http://jsahealthmd.com. Accessed September 27 2011.
24. American Telemedicine Association. Telemental standards and guidelines. http://www.americantelemed.org/i4a/pages/index.cfm?pageID=3311. Accessed September 27 2011.
25. American Telemedicine Association. Evidence-based practice for telemental health. http://www.americantelemed.org/i4a/forms/form.cfm?id=25&pageid=3718&showTitle=1. Accessed September 27 2011.
The antipsychiatry movement: Who and why
Psychiatry is the only medical specialty with a longtime nemesis; it’s called “antipsychiatry,” and it has been active for almost 2 centuries. Although psychiatry has evolved into a major scientific and medical discipline, the century-old primitive stage of psychiatric treatments instigated an antagonism toward psychiatry that persists to the present day.
A recent flurry of books critical of psychiatry is evidence of how the antipsychiatry movement is being propagated by journalists and critics whose views of psychiatry are unflattering despite the abundance of scientific advances that are gradually elucidating the causes and treatments of serious mental disorders.
What are the “wrongdoings” of psychiatry that generate the long-standing protests and assaults? The original “sin” of psychiatry appears to be locking up and “abusing” mentally ill patients in asylums, which 2 centuries ago was considered a humane advance to save seriously disabled patients from homelessness, persecution, neglect, victimization, or imprisonment. The deteriorating conditions of “lunatic” asylums in the 19th and 20th centuries were blamed on psychiatry, not the poor funding of such institutions in an era of almost complete ignorance about the medical basis of mental illness. Other perceived misdeeds of psychiatry include:
- Medicalizing madness (contradicting the archaic notion that psychosis is a type of behavior, not an illness)
- Drastic measures to control severe mental illness in the pre-pharmacotherapy era, including excessive use of electroconvulsive therapy (ECT), performing lobotomies, or resecting various body parts
- Use of physical and/or chemical restraints for violent or actively suicidal patients
- Serious or intolerable side effects of some antipsychotic medications
- Labeling slaves’ healthy desire to escape from their masters in the 19th century as an illness (“drapetomania”)
- Regarding psychoanalysis as unscientific and even harmful
- Labeling homosexuality as a mental disorder until American Psychiatric Association members voted it out of DSM-II in 1973
- The arbitrariness of psychiatric diagnoses based on committee-consensus criteria rather than valid and objective scientific evidence and the lack of biomarkers (this is a legitimate complaint but many physiological tests are being developed)
- Psychoactive drugs allegedly are used to control children (antipsychiatry tends to minimize the existence of serious mental illness among children, although childhood physical diseases are readily accepted)
- Psychiatry is a pseudoscience that pathologizes normal variations of human behaviors, thoughts, or emotions
- Psychiatrists are complicit with drug companies and employ drugs of dubious efficacy (eg, antidepressants) or safety (eg, antipsychotics).
Most of the above reasons are exaggerations or attributed to psychiatry during an era of primitive understanding of psychiatric brain disorders. Harmful interventions such as frontal lobotomy—for which its neurosurgeon inventor received the 1949 Nobel Prize in Medicine—were a product of a desperate time when no effective and safe treatments were available. Although regarded as an effective treatment for mood disorders, ECT certainly was abused many decades ago when it was used (without anesthesia) in patients who were unlikely to benefit from it.
David Cooper1 coined the term “antipsychiatry” in 1967. Years before him, Michel Foucault propagated a paradigm shift that regarded delusions not as madness or illness, but as a behavioral variant or an “anomaly of judgment.”2 That antimedicalization movement was supported by the First Church of Christ, Scientist, the legal system, and even the then-new specialty of neurology, plus social workers and “reformers” who criticized mental hospitals for failing to conduct scientific investigations.3
Formerly institutionalized patients such as Clifford Beers4 demanded improvements in shabby state hospital conditions more than a century ago and generated antipsychiatry sentiments in other formerly institutionalized persons. Such antipathy was exacerbated by bizarre psychiatrists such as Henry Cotton at Trenton State Hospital in New Jersey, who advocated that removing various body parts (killing or disfiguring patients) improved mental health.5
Other ardent antipsychiatrists included French playwright and former asylum patient Antonin Artaud in the 1920s and psychoanalysts Jacques Lacan and Erich Fromm, who authored antipsychiatry writings from a “secular-humanistic” viewpoint. ECT use in the 1930s and frontal leucotomy in the 1940s understandably intensified fear toward psychiatric therapies. When antipsychotic medications were discovered in the 1950s (eventually helping to shut down most asylums), these medications’ neurologic side effects (dystonia, akathisia, parkinsonism, and tardive dyskinesia) prompted another outcry by antipsychiatry groups, although there was no better alternative to control psychosis.
In the 1950s, a right-wing antipsychiatry movement regarded psychiatry as “subversive, left-wing, anti-American, and communist” because it deprived individuals of their rights. Psychologist Hans Eysenck rejected psychiatric medical approaches in favor of errors in learning as a cause of mental illness (as if learning is not a neurobiologic event).
The 1960s witnessed a surge of antipsychiatry activities by various groups, including prominent psychiatrists such as R.D. Laing, Theodore Lidz, and Silvano Arieti, all of whom argued that psychosis is “understandable” as a method of coping with a “sick society” or due to “schizophrenogenic parents” who inflict damage on their offspring. Thomas Szasz is a prominent psychiatrist who proclaimed mental illness is a myth.6 I recall shuddering when he spoke at the University of Rochester during my residency, declaring schizophrenia a myth when I had admitted 3 patients with severe, disabling psychosis earlier that day. I summoned the chutzpah to tell him that in my experience haloperidol surely reduced the symptoms of the so-called “myth”! Szasz collaborated with the Church of Scientology to form the Citizens Commission on Human Rights. Interestingly, Christian Scientists and some fundamental Protestants3 agreed with Szasz’s contention that insanity is a moral, not a medical, issue.
A major impact of the antipsychiatry movement is evident in Italy due to the efforts of Franco Basaglia, an influential “psychiatrist-reformer.” Basaglia was so outraged with the dilapidated and prison-like conditions of mental institutions that he convinced the Italian Parliament to pass a law in 19787 that abruptly dismantled and closed all mental hospitals in Italy. Because of uncontrolled psychosis or mania, many patients who were released ended up in prisons, which had similar or worse repressive conditions as the dismantled asylums. Many chronically hospitalized patients died because of self-neglect or victimization within a few months of their abrupt discharge.
Finally, the antipsychiatry movement aggressively criticizes the pharmaceutical industry’s research, tactics, and influence on psychiatry. Also included in the attacks are academic psychiatrists who conduct FDA clinical trials for new drugs and educate practitioners about the efficacy/safety and indications of new FDA-approved drugs. Although industry research grants are deposited at the investigators’ universities, critics mistakenly assume these psychiatrists personally benefit. The content of all educational programs about psychiatric drugs is strictly restricted to the FDA-approved product label, but critics assume that expert speakers, who are compensated for their time and effort, are promoting the drug rather than educating practitioners about the efficacy, safety, tolerability, and proper use of new medications. Part of the motive for attacking this collaboration is the tenet held by many in the antipsychiatry movement that medications are ineffective, unnecessary, or even dangerous. I wish antipsychiatrists would spend a week on an acute psychiatric unit to witness the need for and benefit from psychotropic medications for psychotic, manic, or depressed patients. Although psychiatric patients experience side effects, they are no worse than those experienced by cancer, arthritis, or diabetes patients.
The antipsychiatry movement is regarded by some as “intellectual halitosis” and by others as a thorn in the side of mainstream psychiatry; most believe that many of its claims are unfair exaggerations based on events and primitive conditions of more than a century ago. However, although irritating and often unfair, antipsychiatry helps keep us honest and rigorous about what we do, motivating us to relentlessly seek better diagnostic models and treatment paradigms. Psychiatry is far more scientific today than it was a century ago, but misperceptions about psychiatry continue to be driven by abuses of the past. The best antidote for antipsychiatry allegations is a combination of personal integrity, scientific progress, and sound evidence-based clinical care.
1. Cooper DG. Psychiatry and antipsychiatry. London, United Kingdom: Tavistock Publications; 1967.
2. Rabinow P, ed. Psychiatric power. In: Foucault M. Ethics, subjectivity, and truth. New York, NY: The New Press; 1997.
3. Dain N. Critics and dissenters: reflection on “anti-psychiatry” in the United States. J Hist Behav Sci. 1989;25(1):3-25.
4. Beers CW. A mind that found itself. Pittsburgh, PA: University of Pittsburgh Press; 1981.
5. Freckelton I. Madhouse: a tragic tale of megalomania and modern medicine (Book review). Psychiatry, Psychology, and Law. 2005;12:435-438.
6. Szasz T. The myth of mental illness. American Psychologist. 1960;15:113-118.
7. Palermo GB. The 1978 Italian mental health law—a personal evaluation: a review. J R Soc Med. 1991;84(2):99-102.

Henry A. Nasrallah, MD
Editor-in-Chief
To comment on this editorial or other topics of interest, visit http://www.facebook.com/CurrentPsychiatry, or click on the “Send Letters” link.
Henry A. Nasrallah, MD
Editor-in-Chief
To comment on this editorial or other topics of interest, visit http://www.facebook.com/CurrentPsychiatry, or click on the “Send Letters” link.
Henry A. Nasrallah, MD
Editor-in-Chief
To comment on this editorial or other topics of interest, visit http://www.facebook.com/CurrentPsychiatry, or click on the “Send Letters” link.
Psychiatry is the only medical specialty with a longtime nemesis; it’s called “antipsychiatry,” and it has been active for almost 2 centuries. Although psychiatry has evolved into a major scientific and medical discipline, the century-old primitive stage of psychiatric treatments instigated an antagonism toward psychiatry that persists to the present day.
A recent flurry of books critical of psychiatry is evidence of how the antipsychiatry movement is being propagated by journalists and critics whose views of psychiatry are unflattering despite the abundance of scientific advances that are gradually elucidating the causes and treatments of serious mental disorders.
What are the “wrongdoings” of psychiatry that generate the long-standing protests and assaults? The original “sin” of psychiatry appears to be locking up and “abusing” mentally ill patients in asylums, which 2 centuries ago was considered a humane advance to save seriously disabled patients from homelessness, persecution, neglect, victimization, or imprisonment. The deteriorating conditions of “lunatic” asylums in the 19th and 20th centuries were blamed on psychiatry, not the poor funding of such institutions in an era of almost complete ignorance about the medical basis of mental illness. Other perceived misdeeds of psychiatry include:
- Medicalizing madness (contradicting the archaic notion that psychosis is a type of behavior, not an illness)
- Drastic measures to control severe mental illness in the pre-pharmacotherapy era, including excessive use of electroconvulsive therapy (ECT), performing lobotomies, or resecting various body parts
- Use of physical and/or chemical restraints for violent or actively suicidal patients
- Serious or intolerable side effects of some antipsychotic medications
- Labeling slaves’ healthy desire to escape from their masters in the 19th century as an illness (“drapetomania”)
- Regarding psychoanalysis as unscientific and even harmful
- Labeling homosexuality as a mental disorder until American Psychiatric Association members voted it out of DSM-II in 1973
- The arbitrariness of psychiatric diagnoses based on committee-consensus criteria rather than valid and objective scientific evidence and the lack of biomarkers (this is a legitimate complaint but many physiological tests are being developed)
- Psychoactive drugs allegedly are used to control children (antipsychiatry tends to minimize the existence of serious mental illness among children, although childhood physical diseases are readily accepted)
- Psychiatry is a pseudoscience that pathologizes normal variations of human behaviors, thoughts, or emotions
- Psychiatrists are complicit with drug companies and employ drugs of dubious efficacy (eg, antidepressants) or safety (eg, antipsychotics).
Most of the above reasons are exaggerations or attributed to psychiatry during an era of primitive understanding of psychiatric brain disorders. Harmful interventions such as frontal lobotomy—for which its neurosurgeon inventor received the 1949 Nobel Prize in Medicine—were a product of a desperate time when no effective and safe treatments were available. Although regarded as an effective treatment for mood disorders, ECT certainly was abused many decades ago when it was used (without anesthesia) in patients who were unlikely to benefit from it.
David Cooper1 coined the term “antipsychiatry” in 1967. Years before him, Michel Foucault propagated a paradigm shift that regarded delusions not as madness or illness, but as a behavioral variant or an “anomaly of judgment.”2 That antimedicalization movement was supported by the First Church of Christ, Scientist, the legal system, and even the then-new specialty of neurology, plus social workers and “reformers” who criticized mental hospitals for failing to conduct scientific investigations.3
Formerly institutionalized patients such as Clifford Beers4 demanded improvements in shabby state hospital conditions more than a century ago and generated antipsychiatry sentiments in other formerly institutionalized persons. Such antipathy was exacerbated by bizarre psychiatrists such as Henry Cotton at Trenton State Hospital in New Jersey, who advocated that removing various body parts (killing or disfiguring patients) improved mental health.5
Other ardent antipsychiatrists included French playwright and former asylum patient Antonin Artaud in the 1920s and psychoanalysts Jacques Lacan and Erich Fromm, who authored antipsychiatry writings from a “secular-humanistic” viewpoint. ECT use in the 1930s and frontal leucotomy in the 1940s understandably intensified fear toward psychiatric therapies. When antipsychotic medications were discovered in the 1950s (eventually helping to shut down most asylums), these medications’ neurologic side effects (dystonia, akathisia, parkinsonism, and tardive dyskinesia) prompted another outcry by antipsychiatry groups, although there was no better alternative to control psychosis.
In the 1950s, a right-wing antipsychiatry movement regarded psychiatry as “subversive, left-wing, anti-American, and communist” because it deprived individuals of their rights. Psychologist Hans Eysenck rejected psychiatric medical approaches in favor of errors in learning as a cause of mental illness (as if learning is not a neurobiologic event).
The 1960s witnessed a surge of antipsychiatry activities by various groups, including prominent psychiatrists such as R.D. Laing, Theodore Lidz, and Silvano Arieti, all of whom argued that psychosis is “understandable” as a method of coping with a “sick society” or due to “schizophrenogenic parents” who inflict damage on their offspring. Thomas Szasz is a prominent psychiatrist who proclaimed mental illness is a myth.6 I recall shuddering when he spoke at the University of Rochester during my residency, declaring schizophrenia a myth when I had admitted 3 patients with severe, disabling psychosis earlier that day. I summoned the chutzpah to tell him that in my experience haloperidol surely reduced the symptoms of the so-called “myth”! Szasz collaborated with the Church of Scientology to form the Citizens Commission on Human Rights. Interestingly, Christian Scientists and some fundamental Protestants3 agreed with Szasz’s contention that insanity is a moral, not a medical, issue.
A major impact of the antipsychiatry movement is evident in Italy due to the efforts of Franco Basaglia, an influential “psychiatrist-reformer.” Basaglia was so outraged with the dilapidated and prison-like conditions of mental institutions that he convinced the Italian Parliament to pass a law in 19787 that abruptly dismantled and closed all mental hospitals in Italy. Because of uncontrolled psychosis or mania, many patients who were released ended up in prisons, which had similar or worse repressive conditions as the dismantled asylums. Many chronically hospitalized patients died because of self-neglect or victimization within a few months of their abrupt discharge.
Finally, the antipsychiatry movement aggressively criticizes the pharmaceutical industry’s research, tactics, and influence on psychiatry. Also included in the attacks are academic psychiatrists who conduct FDA clinical trials for new drugs and educate practitioners about the efficacy/safety and indications of new FDA-approved drugs. Although industry research grants are deposited at the investigators’ universities, critics mistakenly assume these psychiatrists personally benefit. The content of all educational programs about psychiatric drugs is strictly restricted to the FDA-approved product label, but critics assume that expert speakers, who are compensated for their time and effort, are promoting the drug rather than educating practitioners about the efficacy, safety, tolerability, and proper use of new medications. Part of the motive for attacking this collaboration is the tenet held by many in the antipsychiatry movement that medications are ineffective, unnecessary, or even dangerous. I wish antipsychiatrists would spend a week on an acute psychiatric unit to witness the need for and benefit from psychotropic medications for psychotic, manic, or depressed patients. Although psychiatric patients experience side effects, they are no worse than those experienced by cancer, arthritis, or diabetes patients.
The antipsychiatry movement is regarded by some as “intellectual halitosis” and by others as a thorn in the side of mainstream psychiatry; most believe that many of its claims are unfair exaggerations based on events and primitive conditions of more than a century ago. However, although irritating and often unfair, antipsychiatry helps keep us honest and rigorous about what we do, motivating us to relentlessly seek better diagnostic models and treatment paradigms. Psychiatry is far more scientific today than it was a century ago, but misperceptions about psychiatry continue to be driven by abuses of the past. The best antidote for antipsychiatry allegations is a combination of personal integrity, scientific progress, and sound evidence-based clinical care.
Psychiatry is the only medical specialty with a longtime nemesis; it’s called “antipsychiatry,” and it has been active for almost 2 centuries. Although psychiatry has evolved into a major scientific and medical discipline, the century-old primitive stage of psychiatric treatments instigated an antagonism toward psychiatry that persists to the present day.
A recent flurry of books critical of psychiatry is evidence of how the antipsychiatry movement is being propagated by journalists and critics whose views of psychiatry are unflattering despite the abundance of scientific advances that are gradually elucidating the causes and treatments of serious mental disorders.
What are the “wrongdoings” of psychiatry that generate the long-standing protests and assaults? The original “sin” of psychiatry appears to be locking up and “abusing” mentally ill patients in asylums, which 2 centuries ago was considered a humane advance to save seriously disabled patients from homelessness, persecution, neglect, victimization, or imprisonment. The deteriorating conditions of “lunatic” asylums in the 19th and 20th centuries were blamed on psychiatry, not the poor funding of such institutions in an era of almost complete ignorance about the medical basis of mental illness. Other perceived misdeeds of psychiatry include:
- Medicalizing madness (contradicting the archaic notion that psychosis is a type of behavior, not an illness)
- Drastic measures to control severe mental illness in the pre-pharmacotherapy era, including excessive use of electroconvulsive therapy (ECT), performing lobotomies, or resecting various body parts
- Use of physical and/or chemical restraints for violent or actively suicidal patients
- Serious or intolerable side effects of some antipsychotic medications
- Labeling slaves’ healthy desire to escape from their masters in the 19th century as an illness (“drapetomania”)
- Regarding psychoanalysis as unscientific and even harmful
- Labeling homosexuality as a mental disorder until American Psychiatric Association members voted it out of DSM-II in 1973
- The arbitrariness of psychiatric diagnoses based on committee-consensus criteria rather than valid and objective scientific evidence and the lack of biomarkers (this is a legitimate complaint but many physiological tests are being developed)
- Psychoactive drugs allegedly are used to control children (antipsychiatry tends to minimize the existence of serious mental illness among children, although childhood physical diseases are readily accepted)
- Psychiatry is a pseudoscience that pathologizes normal variations of human behaviors, thoughts, or emotions
- Psychiatrists are complicit with drug companies and employ drugs of dubious efficacy (eg, antidepressants) or safety (eg, antipsychotics).
Most of the above reasons are exaggerations or attributed to psychiatry during an era of primitive understanding of psychiatric brain disorders. Harmful interventions such as frontal lobotomy—for which its neurosurgeon inventor received the 1949 Nobel Prize in Medicine—were a product of a desperate time when no effective and safe treatments were available. Although regarded as an effective treatment for mood disorders, ECT certainly was abused many decades ago when it was used (without anesthesia) in patients who were unlikely to benefit from it.
David Cooper1 coined the term “antipsychiatry” in 1967. Years before him, Michel Foucault propagated a paradigm shift that regarded delusions not as madness or illness, but as a behavioral variant or an “anomaly of judgment.”2 That antimedicalization movement was supported by the First Church of Christ, Scientist, the legal system, and even the then-new specialty of neurology, plus social workers and “reformers” who criticized mental hospitals for failing to conduct scientific investigations.3
Formerly institutionalized patients such as Clifford Beers4 demanded improvements in shabby state hospital conditions more than a century ago and generated antipsychiatry sentiments in other formerly institutionalized persons. Such antipathy was exacerbated by bizarre psychiatrists such as Henry Cotton at Trenton State Hospital in New Jersey, who advocated that removing various body parts (killing or disfiguring patients) improved mental health.5
Other ardent antipsychiatrists included French playwright and former asylum patient Antonin Artaud in the 1920s and psychoanalysts Jacques Lacan and Erich Fromm, who authored antipsychiatry writings from a “secular-humanistic” viewpoint. ECT use in the 1930s and frontal leucotomy in the 1940s understandably intensified fear toward psychiatric therapies. When antipsychotic medications were discovered in the 1950s (eventually helping to shut down most asylums), these medications’ neurologic side effects (dystonia, akathisia, parkinsonism, and tardive dyskinesia) prompted another outcry by antipsychiatry groups, although there was no better alternative to control psychosis.
In the 1950s, a right-wing antipsychiatry movement regarded psychiatry as “subversive, left-wing, anti-American, and communist” because it deprived individuals of their rights. Psychologist Hans Eysenck rejected psychiatric medical approaches in favor of errors in learning as a cause of mental illness (as if learning is not a neurobiologic event).
The 1960s witnessed a surge of antipsychiatry activities by various groups, including prominent psychiatrists such as R.D. Laing, Theodore Lidz, and Silvano Arieti, all of whom argued that psychosis is “understandable” as a method of coping with a “sick society” or due to “schizophrenogenic parents” who inflict damage on their offspring. Thomas Szasz is a prominent psychiatrist who proclaimed mental illness is a myth.6 I recall shuddering when he spoke at the University of Rochester during my residency, declaring schizophrenia a myth when I had admitted 3 patients with severe, disabling psychosis earlier that day. I summoned the chutzpah to tell him that in my experience haloperidol surely reduced the symptoms of the so-called “myth”! Szasz collaborated with the Church of Scientology to form the Citizens Commission on Human Rights. Interestingly, Christian Scientists and some fundamental Protestants3 agreed with Szasz’s contention that insanity is a moral, not a medical, issue.
A major impact of the antipsychiatry movement is evident in Italy due to the efforts of Franco Basaglia, an influential “psychiatrist-reformer.” Basaglia was so outraged with the dilapidated and prison-like conditions of mental institutions that he convinced the Italian Parliament to pass a law in 19787 that abruptly dismantled and closed all mental hospitals in Italy. Because of uncontrolled psychosis or mania, many patients who were released ended up in prisons, which had similar or worse repressive conditions as the dismantled asylums. Many chronically hospitalized patients died because of self-neglect or victimization within a few months of their abrupt discharge.
Finally, the antipsychiatry movement aggressively criticizes the pharmaceutical industry’s research, tactics, and influence on psychiatry. Also included in the attacks are academic psychiatrists who conduct FDA clinical trials for new drugs and educate practitioners about the efficacy/safety and indications of new FDA-approved drugs. Although industry research grants are deposited at the investigators’ universities, critics mistakenly assume these psychiatrists personally benefit. The content of all educational programs about psychiatric drugs is strictly restricted to the FDA-approved product label, but critics assume that expert speakers, who are compensated for their time and effort, are promoting the drug rather than educating practitioners about the efficacy, safety, tolerability, and proper use of new medications. Part of the motive for attacking this collaboration is the tenet held by many in the antipsychiatry movement that medications are ineffective, unnecessary, or even dangerous. I wish antipsychiatrists would spend a week on an acute psychiatric unit to witness the need for and benefit from psychotropic medications for psychotic, manic, or depressed patients. Although psychiatric patients experience side effects, they are no worse than those experienced by cancer, arthritis, or diabetes patients.
The antipsychiatry movement is regarded by some as “intellectual halitosis” and by others as a thorn in the side of mainstream psychiatry; most believe that many of its claims are unfair exaggerations based on events and primitive conditions of more than a century ago. However, although irritating and often unfair, antipsychiatry helps keep us honest and rigorous about what we do, motivating us to relentlessly seek better diagnostic models and treatment paradigms. Psychiatry is far more scientific today than it was a century ago, but misperceptions about psychiatry continue to be driven by abuses of the past. The best antidote for antipsychiatry allegations is a combination of personal integrity, scientific progress, and sound evidence-based clinical care.
1. Cooper DG. Psychiatry and antipsychiatry. London, United Kingdom: Tavistock Publications; 1967.
2. Rabinow P, ed. Psychiatric power. In: Foucault M. Ethics, subjectivity, and truth. New York, NY: The New Press; 1997.
3. Dain N. Critics and dissenters: reflection on “anti-psychiatry” in the United States. J Hist Behav Sci. 1989;25(1):3-25.
4. Beers CW. A mind that found itself. Pittsburgh, PA: University of Pittsburgh Press; 1981.
5. Freckelton I. Madhouse: a tragic tale of megalomania and modern medicine (Book review). Psychiatry, Psychology, and Law. 2005;12:435-438.
6. Szasz T. The myth of mental illness. American Psychologist. 1960;15:113-118.
7. Palermo GB. The 1978 Italian mental health law—a personal evaluation: a review. J R Soc Med. 1991;84(2):99-102.
1. Cooper DG. Psychiatry and antipsychiatry. London, United Kingdom: Tavistock Publications; 1967.
2. Rabinow P, ed. Psychiatric power. In: Foucault M. Ethics, subjectivity, and truth. New York, NY: The New Press; 1997.
3. Dain N. Critics and dissenters: reflection on “anti-psychiatry” in the United States. J Hist Behav Sci. 1989;25(1):3-25.
4. Beers CW. A mind that found itself. Pittsburgh, PA: University of Pittsburgh Press; 1981.
5. Freckelton I. Madhouse: a tragic tale of megalomania and modern medicine (Book review). Psychiatry, Psychology, and Law. 2005;12:435-438.
6. Szasz T. The myth of mental illness. American Psychologist. 1960;15:113-118.
7. Palermo GB. The 1978 Italian mental health law—a personal evaluation: a review. J R Soc Med. 1991;84(2):99-102.
Diagnostic dilemmas with OCD and other anxiety disorders
A questionable diagnosis
CASE: Space traveler
Mr. O, age 69, is a patient at a long-term psychiatric hospital. He has a 56-year psychiatric history, a current diagnosis of schizoaffective disorder, and suffered a torn rotator cuff approximately 5 years ago. His medication regimen is haloperidol decanoate, 100 mg IM every month, duloxetine, 60 mg/d, and naproxen, as needed for chronic pain.
He frequently lies on the floor. Attendants urge him to get up and join groups or sit with other patients but he complains of pain and soon finds another spot on the floor to use as a bed.
Eight months earlier, a homeless shelter sent Mr. O to the emergency room (ER) because he tried to eat a dollar bill and a sock. In the ER he was inattentive, with loose associations and bizarre delusions; he believed he was on a spaceship. Mr. O was admitted to the hospital, where clinicians noted that his behavior remained bizarre and he complained of insomnia. They also noted a history of setting fires, which complicated discharge planning and contributed to their decision to transfer him to our psychiatric facility for longer-term care.
During our initial interview, Mr. O readily picks himself off the floor. His responses are logical and direct but abrupt and unelaborated. His first and most vehement complaint is pain. Zolpidem, he says, is the only treatment that helps.
He says he began using zolpidem approximately 5 years ago because pain from a shoulder injury kept him awake at night. When he could not obtain the drug by prescription, he bought it on the street. One day when living in the homeless shelter, he took 30 or 40 mg of zolpidem, then “blacked out” and awoke in the ER.
His first experience with psychiatric treatment was the result of problems getting along with his single mother because of “petty things” such as shooting off a BB gun in their apartment, he says. As a teenager he was sent to a boarding school; as a young adult, to a psychiatric hospital. After his release he returned to his mother’s apartment. He worked steadily for 20 years before he obtained Social Security benefits, and then worked intermittently “off the books” until approximately 15 years ago. Mr. O lived with his mother until her death 17 years earlier, and then in her apartment alone until a fire, which he set accidentally by smoking in bed after taking zolpidem, forced him to leave 3 years ago. He says, “My whole life was in that place.” He was admitted to a psychiatric hospital for an unknown reason, which was his first psychiatric admission in 40 years. After he was released from the hospital, Mr. O lived in various homeless shelters and adult homes until his current hospitalization.
The author’s observations
An effective and well-tolerated drug with a reputation for rarely being abused, zolpidem is widely prescribed as a hypnotic. Zolpidem and benzodiazepines have different chemical structures but both act at the GABAA receptor and have comparable behavioral effects.1 The reported incidence of zolpidem abuse is much lower than the reported rate of benzodiazepine abuse when used for sleep2; however, abuse, dependence, and withdrawal have been reported.2-4 Zolpidem abuse seems to be more common among patients with a history of abusing other substances or a history of psychiatric illness.2 A French study4 found that abusers fell into 2 groups. The younger group (median age 35) used higher doses—a median of 300 mg/d—and took zolpidem in the daytime to achieve euphoria. A second, older group (median age 42) used lower doses—a median of 200 mg/d—at nighttime to sleep.
There are few reports of delirium and symptoms such as visual hallucinations and distortions associated with zolpidem use.5,6 These reactions have occurred in persons without a history of psychosis. They usually are associated with doses ≥10 mg.
In the ER Mr. O showed a disturbance in consciousness with inability to focus attention and a perceptual disturbance (he believed he was in a spaceship) that developed over hours to days. He met criteria for delirium, possibly caused by zolpidem, but his presentation also could have been attributable to an underlying psychiatric disorder.
ER and inpatient psychiatrists noted Mr. O was intoxicated with zolpidem when the shelter brought him to the ER, but both groups diagnosed schizoaffective disorder and treated him with antipsychotics. They saw his >50-year psychiatric history as evidence of an underlying, long-standing condition such as schizoaffective illness.
However, features of Mr. O’s illness are not typical of a chronic psychotic illness. He recalls psychiatric hospitalizations in his youth and recently, but not for the 40 years in between. Mr. O says he has never experienced auditory hallucinations. For these reasons, our treatment team obtains old medical records to investigate his early history (Table).
Table
Mr. O’s clinical course
| Age | Symptoms/behaviors | Diagnosis |
|---|---|---|
| 17 | Temper tantrums and destructive behaviors. No delusions or hallucinations but a flat affect and hostile attitude | Primary behavior disorder, simple adult maladjustment |
| 22 | Returned to the psychiatric hospital when his welfare payments stopped; “psychopathic” symptoms; described as defiant and resented authority and regular work | Primary behavior disorder |
| 24 | His mother complained that he stole from her and carried a weapon; while hospitalized, described as manageable and without overt psychotic symptoms | Primary behavior disorder |
| 26 | Arrested for causing property damage while intoxicated on alcohol; silly laugh, loose associations, irrelevant and incoherent speech, and believed hospital staff were against him | Psychosis with psychopathic personality |
| 66 | A fire that he set accidentally while smoking in bed after taking zolpidem destroyed his home | Diagnosis unknown |
| 68 | Transferred from a homeless shelter to the ER after he took 30 to 40 mg of zolpidem and exhibited bizarre behaviors | Schizoaffective disorder |
| 69 | More spontaneous, remains logical and relevant after haloperidol is discontinued; no delusions or hallucinations, still complains of pain | Substance use disorder and personality disorder |
| ER: emergency room | ||
HISTORY: Destructive and defiant
Mr. O’s mother reported that he had been a nervous, restless child who would scream and yell at the slightest provocation. At age 10 he became wantonly destructive. His mother bought him an expensive toy that he destroyed after a short time; he asked for another toy, which he also destroyed. When such behavior became more frequent, she took him to a city hospital, where he was treated for 6 weeks and released at age 13. He was sent to a boarding school but soon was expelled for drinking and selling beer.
Mr. O was admitted to long-term psychiatric facilities 6 times in the next 10 years, from the late 1950s to the late 1960s. He was first admitted at age 17 for temper tantrums during which he fired an air rifle and smashed windows in the home he shared with his mother. During examination he had no delusions or hallucinations but did have flat affect and a hostile attitude. Doctors documented that almost all his tantrums were as a result of interactions with his mother.
Records from this psychiatric admission state that Mr. O showed no unusual distractibility, “psychotic trends,” or paranoid thinking. After approximately 6 months in the hospital he was discharged home with the diagnosis of primary behavior disorder, simple adult maladjustment. Mr. O, who was age 18 at the time, and his mother were eager for him to complete high school and learn auto mechanics.
Nine months later, he returned to the psychiatric facility because of excessive drinking and inability to secure employment, according to his records. In the hospital, he was productive and reliable. When he was discharged home 3 months later, doctors wrote that his determination to stop drinking was firmly fixed. They encouraged Mr. O to complete high school as a night student and find employment during the day. His mother was delighted with his improvement.
A third admission, less than 2 months later, occurred after he broke a window during an argument with his mother. He had a job but quit. After 5 months he was discharged with the same diagnosis of primary behavior disorder, but his mother would not let him back in her home. He was referred to the social service department to be placed on welfare.
A year later, Mr. O had trouble managing his welfare allotment and moved repeatedly. He said he returned to the psychiatric hospital because his welfare payments had been discontinued. During this admission, doctors noted “psychopathic” symptoms; Mr. O was defiant and resented authority and regular work. Mr. O eloped from the hospital several times and brought beer into the building. After 18 months he was discharged with the same diagnosis, with plans to apply for welfare. He was not prescribed medication.
Mr. O’s fifth admission came nearly 2 years later after his mother complained that he stole from her home and carried a weapon. In the hospital he was described as manageable and without overt psychotic symptoms. When he was discharged a little more than a year after being admitted, doctors wrote that he was a psychopath who had a history of drinking, stealing, and delinquent tendencies as a teenager. His diagnosis remained primary behavior disorder.
A year after this discharge, Mr. O was arrested for causing serious property damage when he was intoxicated on alcohol. Subsequently he was readmitted.
After a few months in the hospital, Mr. O changed. He developed a silly laugh, loose associations, irrelevant and incoherent speech, and a belief that hospital staff were against him. Although Mr. O denied auditory hallucinations, a psychiatrist wrote that he seemed to be experiencing hallucinations and prescribed chlorpromazine. The next day Mr. O slashed his arms and legs in several places, requiring many sutures. His diagnosis was changed to psychosis with psychopathic personality. However, within a few months, psychiatrists determined that Mr. O had recovered, so they stopped chlorpromazine. Months later, clinicians wrote that Mr. O was idle most of the time, neat, clean, and not involved in arguments with other patients. He was discharged after 1 month in the hospital.
Over the years, psychiatrists had differing opinions about Mr. O’s diagnosis. One noted that his mental illness was characterized by emotional instability and poor judgment. He had impulsive reactions without regard for others, rapid mood swings, irritability, and depression with transient paranoia. Another clinician detected evidence of schizoid personality disorder because Mr. O did not experience hallucinations or a gross thought disorder, but did have rambling, circumstantial, autistic (unrealistic), and ambivalent thought content. Another psychiatrist wrote Mr. O best fit in the category of psychosis with psychopathic personality, which was his diagnosis at discharge from his sixth hospitalization.
The author’s observations
Mr. O’s old medical records revealed the diagnostic thinking and treatment practices of a past era. They did not demonstrate that Mr. O met current criteria for schizophrenia or schizoaffective disorder, although he may have had a brief psychotic episode. Because there was little support for a diagnosis of schizoaffective illness and haloperidol use, we stopped the drug but continued duloxetine for chronic pain. It was clear that he has a substance use disorder and perhaps met criteria for antisocial personality disorder.
OUTCOME: Further explanations
Approximately 2 months after stopping haloperidol, Mr. O is more spontaneous, logical, and relevant. He does not have delusions or hallucinations. Despite further attempts at pain management with physical therapy and increased doses of duloxetine, he still complains of pain. We do not prescribe zolpidem.
Mr. O is unwilling to discuss the incident more than 40 years ago when he cut his arms and legs except to say, “That’s the past. My life wasn’t so good at that time.” When we ask why he had been a client of Adult Protective Services 5 years before he was burned out of his apartment, he admitted that he was 21 months in arrears in his rent. “I used to do this thing called crack,” he explains. He was discharged to an adult home with a prescription for duloxetine after he promised to never smoke in his room again.
Related Resource
- Aggarwal A, Sharma DD. Zolpidem withdrawal delirium: a case report. J Neuropsychiatry Clin Neurosci. 2010;22(4):451.
Drug Brand Names
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Duloxetine • Cymbalta
- Haloperidol decanoate • Haloperidol decanoate
- Haloperidol • Haldol
- Naproxen • Naproxyn, Aleve, others
- Zolpidem • Ambien
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Rush CR. Behavioral pharmacology of zolpidem relative to benzodiazepines: a review. Pharmacol Biochem Behav. 1998;61(3):253-269.
2. Hajak G, Müller WE, Wittchen HU, et al. Abuse and dependence potential for the non-benzodiazepine hypnotics zolpidem and zopiclone: a review of case reports and epidemiological data. Addiction. 2003;98(10):1371-1378.
3. Madrak LN, Rosenberg M. Zolpidem abuse. Am J Psychiatry. 2001;158(8):1330-1331.
4. Victorri-Vigneau C, Dailly E, Veyrac G, et al. Evidence of zolpidem abuse and dependence: results of the French Centre for Evaluation and Information on Pharmacodepencence (CEIP) network survey. Br J Clin Pharmacol. 2007;64(2):198-209.
5. Markowitz JS, Brewerton TD. Zolpidem-induced psychosis. Ann Clin Psychiatry. 1996;8(2):89-91.
6. Tsai MJ, Huang YB, Wu PC. A novel clinical pattern of visual hallucination after zolpidem use. J Toxicol Clin Toxicol. 2003;41(6):869-872.
CASE: Space traveler
Mr. O, age 69, is a patient at a long-term psychiatric hospital. He has a 56-year psychiatric history, a current diagnosis of schizoaffective disorder, and suffered a torn rotator cuff approximately 5 years ago. His medication regimen is haloperidol decanoate, 100 mg IM every month, duloxetine, 60 mg/d, and naproxen, as needed for chronic pain.
He frequently lies on the floor. Attendants urge him to get up and join groups or sit with other patients but he complains of pain and soon finds another spot on the floor to use as a bed.
Eight months earlier, a homeless shelter sent Mr. O to the emergency room (ER) because he tried to eat a dollar bill and a sock. In the ER he was inattentive, with loose associations and bizarre delusions; he believed he was on a spaceship. Mr. O was admitted to the hospital, where clinicians noted that his behavior remained bizarre and he complained of insomnia. They also noted a history of setting fires, which complicated discharge planning and contributed to their decision to transfer him to our psychiatric facility for longer-term care.
During our initial interview, Mr. O readily picks himself off the floor. His responses are logical and direct but abrupt and unelaborated. His first and most vehement complaint is pain. Zolpidem, he says, is the only treatment that helps.
He says he began using zolpidem approximately 5 years ago because pain from a shoulder injury kept him awake at night. When he could not obtain the drug by prescription, he bought it on the street. One day when living in the homeless shelter, he took 30 or 40 mg of zolpidem, then “blacked out” and awoke in the ER.
His first experience with psychiatric treatment was the result of problems getting along with his single mother because of “petty things” such as shooting off a BB gun in their apartment, he says. As a teenager he was sent to a boarding school; as a young adult, to a psychiatric hospital. After his release he returned to his mother’s apartment. He worked steadily for 20 years before he obtained Social Security benefits, and then worked intermittently “off the books” until approximately 15 years ago. Mr. O lived with his mother until her death 17 years earlier, and then in her apartment alone until a fire, which he set accidentally by smoking in bed after taking zolpidem, forced him to leave 3 years ago. He says, “My whole life was in that place.” He was admitted to a psychiatric hospital for an unknown reason, which was his first psychiatric admission in 40 years. After he was released from the hospital, Mr. O lived in various homeless shelters and adult homes until his current hospitalization.
The author’s observations
An effective and well-tolerated drug with a reputation for rarely being abused, zolpidem is widely prescribed as a hypnotic. Zolpidem and benzodiazepines have different chemical structures but both act at the GABAA receptor and have comparable behavioral effects.1 The reported incidence of zolpidem abuse is much lower than the reported rate of benzodiazepine abuse when used for sleep2; however, abuse, dependence, and withdrawal have been reported.2-4 Zolpidem abuse seems to be more common among patients with a history of abusing other substances or a history of psychiatric illness.2 A French study4 found that abusers fell into 2 groups. The younger group (median age 35) used higher doses—a median of 300 mg/d—and took zolpidem in the daytime to achieve euphoria. A second, older group (median age 42) used lower doses—a median of 200 mg/d—at nighttime to sleep.
There are few reports of delirium and symptoms such as visual hallucinations and distortions associated with zolpidem use.5,6 These reactions have occurred in persons without a history of psychosis. They usually are associated with doses ≥10 mg.
In the ER Mr. O showed a disturbance in consciousness with inability to focus attention and a perceptual disturbance (he believed he was in a spaceship) that developed over hours to days. He met criteria for delirium, possibly caused by zolpidem, but his presentation also could have been attributable to an underlying psychiatric disorder.
ER and inpatient psychiatrists noted Mr. O was intoxicated with zolpidem when the shelter brought him to the ER, but both groups diagnosed schizoaffective disorder and treated him with antipsychotics. They saw his >50-year psychiatric history as evidence of an underlying, long-standing condition such as schizoaffective illness.
However, features of Mr. O’s illness are not typical of a chronic psychotic illness. He recalls psychiatric hospitalizations in his youth and recently, but not for the 40 years in between. Mr. O says he has never experienced auditory hallucinations. For these reasons, our treatment team obtains old medical records to investigate his early history (Table).
Table
Mr. O’s clinical course
| Age | Symptoms/behaviors | Diagnosis |
|---|---|---|
| 17 | Temper tantrums and destructive behaviors. No delusions or hallucinations but a flat affect and hostile attitude | Primary behavior disorder, simple adult maladjustment |
| 22 | Returned to the psychiatric hospital when his welfare payments stopped; “psychopathic” symptoms; described as defiant and resented authority and regular work | Primary behavior disorder |
| 24 | His mother complained that he stole from her and carried a weapon; while hospitalized, described as manageable and without overt psychotic symptoms | Primary behavior disorder |
| 26 | Arrested for causing property damage while intoxicated on alcohol; silly laugh, loose associations, irrelevant and incoherent speech, and believed hospital staff were against him | Psychosis with psychopathic personality |
| 66 | A fire that he set accidentally while smoking in bed after taking zolpidem destroyed his home | Diagnosis unknown |
| 68 | Transferred from a homeless shelter to the ER after he took 30 to 40 mg of zolpidem and exhibited bizarre behaviors | Schizoaffective disorder |
| 69 | More spontaneous, remains logical and relevant after haloperidol is discontinued; no delusions or hallucinations, still complains of pain | Substance use disorder and personality disorder |
| ER: emergency room | ||
HISTORY: Destructive and defiant
Mr. O’s mother reported that he had been a nervous, restless child who would scream and yell at the slightest provocation. At age 10 he became wantonly destructive. His mother bought him an expensive toy that he destroyed after a short time; he asked for another toy, which he also destroyed. When such behavior became more frequent, she took him to a city hospital, where he was treated for 6 weeks and released at age 13. He was sent to a boarding school but soon was expelled for drinking and selling beer.
Mr. O was admitted to long-term psychiatric facilities 6 times in the next 10 years, from the late 1950s to the late 1960s. He was first admitted at age 17 for temper tantrums during which he fired an air rifle and smashed windows in the home he shared with his mother. During examination he had no delusions or hallucinations but did have flat affect and a hostile attitude. Doctors documented that almost all his tantrums were as a result of interactions with his mother.
Records from this psychiatric admission state that Mr. O showed no unusual distractibility, “psychotic trends,” or paranoid thinking. After approximately 6 months in the hospital he was discharged home with the diagnosis of primary behavior disorder, simple adult maladjustment. Mr. O, who was age 18 at the time, and his mother were eager for him to complete high school and learn auto mechanics.
Nine months later, he returned to the psychiatric facility because of excessive drinking and inability to secure employment, according to his records. In the hospital, he was productive and reliable. When he was discharged home 3 months later, doctors wrote that his determination to stop drinking was firmly fixed. They encouraged Mr. O to complete high school as a night student and find employment during the day. His mother was delighted with his improvement.
A third admission, less than 2 months later, occurred after he broke a window during an argument with his mother. He had a job but quit. After 5 months he was discharged with the same diagnosis of primary behavior disorder, but his mother would not let him back in her home. He was referred to the social service department to be placed on welfare.
A year later, Mr. O had trouble managing his welfare allotment and moved repeatedly. He said he returned to the psychiatric hospital because his welfare payments had been discontinued. During this admission, doctors noted “psychopathic” symptoms; Mr. O was defiant and resented authority and regular work. Mr. O eloped from the hospital several times and brought beer into the building. After 18 months he was discharged with the same diagnosis, with plans to apply for welfare. He was not prescribed medication.
Mr. O’s fifth admission came nearly 2 years later after his mother complained that he stole from her home and carried a weapon. In the hospital he was described as manageable and without overt psychotic symptoms. When he was discharged a little more than a year after being admitted, doctors wrote that he was a psychopath who had a history of drinking, stealing, and delinquent tendencies as a teenager. His diagnosis remained primary behavior disorder.
A year after this discharge, Mr. O was arrested for causing serious property damage when he was intoxicated on alcohol. Subsequently he was readmitted.
After a few months in the hospital, Mr. O changed. He developed a silly laugh, loose associations, irrelevant and incoherent speech, and a belief that hospital staff were against him. Although Mr. O denied auditory hallucinations, a psychiatrist wrote that he seemed to be experiencing hallucinations and prescribed chlorpromazine. The next day Mr. O slashed his arms and legs in several places, requiring many sutures. His diagnosis was changed to psychosis with psychopathic personality. However, within a few months, psychiatrists determined that Mr. O had recovered, so they stopped chlorpromazine. Months later, clinicians wrote that Mr. O was idle most of the time, neat, clean, and not involved in arguments with other patients. He was discharged after 1 month in the hospital.
Over the years, psychiatrists had differing opinions about Mr. O’s diagnosis. One noted that his mental illness was characterized by emotional instability and poor judgment. He had impulsive reactions without regard for others, rapid mood swings, irritability, and depression with transient paranoia. Another clinician detected evidence of schizoid personality disorder because Mr. O did not experience hallucinations or a gross thought disorder, but did have rambling, circumstantial, autistic (unrealistic), and ambivalent thought content. Another psychiatrist wrote Mr. O best fit in the category of psychosis with psychopathic personality, which was his diagnosis at discharge from his sixth hospitalization.
The author’s observations
Mr. O’s old medical records revealed the diagnostic thinking and treatment practices of a past era. They did not demonstrate that Mr. O met current criteria for schizophrenia or schizoaffective disorder, although he may have had a brief psychotic episode. Because there was little support for a diagnosis of schizoaffective illness and haloperidol use, we stopped the drug but continued duloxetine for chronic pain. It was clear that he has a substance use disorder and perhaps met criteria for antisocial personality disorder.
OUTCOME: Further explanations
Approximately 2 months after stopping haloperidol, Mr. O is more spontaneous, logical, and relevant. He does not have delusions or hallucinations. Despite further attempts at pain management with physical therapy and increased doses of duloxetine, he still complains of pain. We do not prescribe zolpidem.
Mr. O is unwilling to discuss the incident more than 40 years ago when he cut his arms and legs except to say, “That’s the past. My life wasn’t so good at that time.” When we ask why he had been a client of Adult Protective Services 5 years before he was burned out of his apartment, he admitted that he was 21 months in arrears in his rent. “I used to do this thing called crack,” he explains. He was discharged to an adult home with a prescription for duloxetine after he promised to never smoke in his room again.
Related Resource
- Aggarwal A, Sharma DD. Zolpidem withdrawal delirium: a case report. J Neuropsychiatry Clin Neurosci. 2010;22(4):451.
Drug Brand Names
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Duloxetine • Cymbalta
- Haloperidol decanoate • Haloperidol decanoate
- Haloperidol • Haldol
- Naproxen • Naproxyn, Aleve, others
- Zolpidem • Ambien
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Space traveler
Mr. O, age 69, is a patient at a long-term psychiatric hospital. He has a 56-year psychiatric history, a current diagnosis of schizoaffective disorder, and suffered a torn rotator cuff approximately 5 years ago. His medication regimen is haloperidol decanoate, 100 mg IM every month, duloxetine, 60 mg/d, and naproxen, as needed for chronic pain.
He frequently lies on the floor. Attendants urge him to get up and join groups or sit with other patients but he complains of pain and soon finds another spot on the floor to use as a bed.
Eight months earlier, a homeless shelter sent Mr. O to the emergency room (ER) because he tried to eat a dollar bill and a sock. In the ER he was inattentive, with loose associations and bizarre delusions; he believed he was on a spaceship. Mr. O was admitted to the hospital, where clinicians noted that his behavior remained bizarre and he complained of insomnia. They also noted a history of setting fires, which complicated discharge planning and contributed to their decision to transfer him to our psychiatric facility for longer-term care.
During our initial interview, Mr. O readily picks himself off the floor. His responses are logical and direct but abrupt and unelaborated. His first and most vehement complaint is pain. Zolpidem, he says, is the only treatment that helps.
He says he began using zolpidem approximately 5 years ago because pain from a shoulder injury kept him awake at night. When he could not obtain the drug by prescription, he bought it on the street. One day when living in the homeless shelter, he took 30 or 40 mg of zolpidem, then “blacked out” and awoke in the ER.
His first experience with psychiatric treatment was the result of problems getting along with his single mother because of “petty things” such as shooting off a BB gun in their apartment, he says. As a teenager he was sent to a boarding school; as a young adult, to a psychiatric hospital. After his release he returned to his mother’s apartment. He worked steadily for 20 years before he obtained Social Security benefits, and then worked intermittently “off the books” until approximately 15 years ago. Mr. O lived with his mother until her death 17 years earlier, and then in her apartment alone until a fire, which he set accidentally by smoking in bed after taking zolpidem, forced him to leave 3 years ago. He says, “My whole life was in that place.” He was admitted to a psychiatric hospital for an unknown reason, which was his first psychiatric admission in 40 years. After he was released from the hospital, Mr. O lived in various homeless shelters and adult homes until his current hospitalization.
The author’s observations
An effective and well-tolerated drug with a reputation for rarely being abused, zolpidem is widely prescribed as a hypnotic. Zolpidem and benzodiazepines have different chemical structures but both act at the GABAA receptor and have comparable behavioral effects.1 The reported incidence of zolpidem abuse is much lower than the reported rate of benzodiazepine abuse when used for sleep2; however, abuse, dependence, and withdrawal have been reported.2-4 Zolpidem abuse seems to be more common among patients with a history of abusing other substances or a history of psychiatric illness.2 A French study4 found that abusers fell into 2 groups. The younger group (median age 35) used higher doses—a median of 300 mg/d—and took zolpidem in the daytime to achieve euphoria. A second, older group (median age 42) used lower doses—a median of 200 mg/d—at nighttime to sleep.
There are few reports of delirium and symptoms such as visual hallucinations and distortions associated with zolpidem use.5,6 These reactions have occurred in persons without a history of psychosis. They usually are associated with doses ≥10 mg.
In the ER Mr. O showed a disturbance in consciousness with inability to focus attention and a perceptual disturbance (he believed he was in a spaceship) that developed over hours to days. He met criteria for delirium, possibly caused by zolpidem, but his presentation also could have been attributable to an underlying psychiatric disorder.
ER and inpatient psychiatrists noted Mr. O was intoxicated with zolpidem when the shelter brought him to the ER, but both groups diagnosed schizoaffective disorder and treated him with antipsychotics. They saw his >50-year psychiatric history as evidence of an underlying, long-standing condition such as schizoaffective illness.
However, features of Mr. O’s illness are not typical of a chronic psychotic illness. He recalls psychiatric hospitalizations in his youth and recently, but not for the 40 years in between. Mr. O says he has never experienced auditory hallucinations. For these reasons, our treatment team obtains old medical records to investigate his early history (Table).
Table
Mr. O’s clinical course
| Age | Symptoms/behaviors | Diagnosis |
|---|---|---|
| 17 | Temper tantrums and destructive behaviors. No delusions or hallucinations but a flat affect and hostile attitude | Primary behavior disorder, simple adult maladjustment |
| 22 | Returned to the psychiatric hospital when his welfare payments stopped; “psychopathic” symptoms; described as defiant and resented authority and regular work | Primary behavior disorder |
| 24 | His mother complained that he stole from her and carried a weapon; while hospitalized, described as manageable and without overt psychotic symptoms | Primary behavior disorder |
| 26 | Arrested for causing property damage while intoxicated on alcohol; silly laugh, loose associations, irrelevant and incoherent speech, and believed hospital staff were against him | Psychosis with psychopathic personality |
| 66 | A fire that he set accidentally while smoking in bed after taking zolpidem destroyed his home | Diagnosis unknown |
| 68 | Transferred from a homeless shelter to the ER after he took 30 to 40 mg of zolpidem and exhibited bizarre behaviors | Schizoaffective disorder |
| 69 | More spontaneous, remains logical and relevant after haloperidol is discontinued; no delusions or hallucinations, still complains of pain | Substance use disorder and personality disorder |
| ER: emergency room | ||
HISTORY: Destructive and defiant
Mr. O’s mother reported that he had been a nervous, restless child who would scream and yell at the slightest provocation. At age 10 he became wantonly destructive. His mother bought him an expensive toy that he destroyed after a short time; he asked for another toy, which he also destroyed. When such behavior became more frequent, she took him to a city hospital, where he was treated for 6 weeks and released at age 13. He was sent to a boarding school but soon was expelled for drinking and selling beer.
Mr. O was admitted to long-term psychiatric facilities 6 times in the next 10 years, from the late 1950s to the late 1960s. He was first admitted at age 17 for temper tantrums during which he fired an air rifle and smashed windows in the home he shared with his mother. During examination he had no delusions or hallucinations but did have flat affect and a hostile attitude. Doctors documented that almost all his tantrums were as a result of interactions with his mother.
Records from this psychiatric admission state that Mr. O showed no unusual distractibility, “psychotic trends,” or paranoid thinking. After approximately 6 months in the hospital he was discharged home with the diagnosis of primary behavior disorder, simple adult maladjustment. Mr. O, who was age 18 at the time, and his mother were eager for him to complete high school and learn auto mechanics.
Nine months later, he returned to the psychiatric facility because of excessive drinking and inability to secure employment, according to his records. In the hospital, he was productive and reliable. When he was discharged home 3 months later, doctors wrote that his determination to stop drinking was firmly fixed. They encouraged Mr. O to complete high school as a night student and find employment during the day. His mother was delighted with his improvement.
A third admission, less than 2 months later, occurred after he broke a window during an argument with his mother. He had a job but quit. After 5 months he was discharged with the same diagnosis of primary behavior disorder, but his mother would not let him back in her home. He was referred to the social service department to be placed on welfare.
A year later, Mr. O had trouble managing his welfare allotment and moved repeatedly. He said he returned to the psychiatric hospital because his welfare payments had been discontinued. During this admission, doctors noted “psychopathic” symptoms; Mr. O was defiant and resented authority and regular work. Mr. O eloped from the hospital several times and brought beer into the building. After 18 months he was discharged with the same diagnosis, with plans to apply for welfare. He was not prescribed medication.
Mr. O’s fifth admission came nearly 2 years later after his mother complained that he stole from her home and carried a weapon. In the hospital he was described as manageable and without overt psychotic symptoms. When he was discharged a little more than a year after being admitted, doctors wrote that he was a psychopath who had a history of drinking, stealing, and delinquent tendencies as a teenager. His diagnosis remained primary behavior disorder.
A year after this discharge, Mr. O was arrested for causing serious property damage when he was intoxicated on alcohol. Subsequently he was readmitted.
After a few months in the hospital, Mr. O changed. He developed a silly laugh, loose associations, irrelevant and incoherent speech, and a belief that hospital staff were against him. Although Mr. O denied auditory hallucinations, a psychiatrist wrote that he seemed to be experiencing hallucinations and prescribed chlorpromazine. The next day Mr. O slashed his arms and legs in several places, requiring many sutures. His diagnosis was changed to psychosis with psychopathic personality. However, within a few months, psychiatrists determined that Mr. O had recovered, so they stopped chlorpromazine. Months later, clinicians wrote that Mr. O was idle most of the time, neat, clean, and not involved in arguments with other patients. He was discharged after 1 month in the hospital.
Over the years, psychiatrists had differing opinions about Mr. O’s diagnosis. One noted that his mental illness was characterized by emotional instability and poor judgment. He had impulsive reactions without regard for others, rapid mood swings, irritability, and depression with transient paranoia. Another clinician detected evidence of schizoid personality disorder because Mr. O did not experience hallucinations or a gross thought disorder, but did have rambling, circumstantial, autistic (unrealistic), and ambivalent thought content. Another psychiatrist wrote Mr. O best fit in the category of psychosis with psychopathic personality, which was his diagnosis at discharge from his sixth hospitalization.
The author’s observations
Mr. O’s old medical records revealed the diagnostic thinking and treatment practices of a past era. They did not demonstrate that Mr. O met current criteria for schizophrenia or schizoaffective disorder, although he may have had a brief psychotic episode. Because there was little support for a diagnosis of schizoaffective illness and haloperidol use, we stopped the drug but continued duloxetine for chronic pain. It was clear that he has a substance use disorder and perhaps met criteria for antisocial personality disorder.
OUTCOME: Further explanations
Approximately 2 months after stopping haloperidol, Mr. O is more spontaneous, logical, and relevant. He does not have delusions or hallucinations. Despite further attempts at pain management with physical therapy and increased doses of duloxetine, he still complains of pain. We do not prescribe zolpidem.
Mr. O is unwilling to discuss the incident more than 40 years ago when he cut his arms and legs except to say, “That’s the past. My life wasn’t so good at that time.” When we ask why he had been a client of Adult Protective Services 5 years before he was burned out of his apartment, he admitted that he was 21 months in arrears in his rent. “I used to do this thing called crack,” he explains. He was discharged to an adult home with a prescription for duloxetine after he promised to never smoke in his room again.
Related Resource
- Aggarwal A, Sharma DD. Zolpidem withdrawal delirium: a case report. J Neuropsychiatry Clin Neurosci. 2010;22(4):451.
Drug Brand Names
- Chlorpromazine • Thorazine
- Clozapine • Clozaril
- Duloxetine • Cymbalta
- Haloperidol decanoate • Haloperidol decanoate
- Haloperidol • Haldol
- Naproxen • Naproxyn, Aleve, others
- Zolpidem • Ambien
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Rush CR. Behavioral pharmacology of zolpidem relative to benzodiazepines: a review. Pharmacol Biochem Behav. 1998;61(3):253-269.
2. Hajak G, Müller WE, Wittchen HU, et al. Abuse and dependence potential for the non-benzodiazepine hypnotics zolpidem and zopiclone: a review of case reports and epidemiological data. Addiction. 2003;98(10):1371-1378.
3. Madrak LN, Rosenberg M. Zolpidem abuse. Am J Psychiatry. 2001;158(8):1330-1331.
4. Victorri-Vigneau C, Dailly E, Veyrac G, et al. Evidence of zolpidem abuse and dependence: results of the French Centre for Evaluation and Information on Pharmacodepencence (CEIP) network survey. Br J Clin Pharmacol. 2007;64(2):198-209.
5. Markowitz JS, Brewerton TD. Zolpidem-induced psychosis. Ann Clin Psychiatry. 1996;8(2):89-91.
6. Tsai MJ, Huang YB, Wu PC. A novel clinical pattern of visual hallucination after zolpidem use. J Toxicol Clin Toxicol. 2003;41(6):869-872.
1. Rush CR. Behavioral pharmacology of zolpidem relative to benzodiazepines: a review. Pharmacol Biochem Behav. 1998;61(3):253-269.
2. Hajak G, Müller WE, Wittchen HU, et al. Abuse and dependence potential for the non-benzodiazepine hypnotics zolpidem and zopiclone: a review of case reports and epidemiological data. Addiction. 2003;98(10):1371-1378.
3. Madrak LN, Rosenberg M. Zolpidem abuse. Am J Psychiatry. 2001;158(8):1330-1331.
4. Victorri-Vigneau C, Dailly E, Veyrac G, et al. Evidence of zolpidem abuse and dependence: results of the French Centre for Evaluation and Information on Pharmacodepencence (CEIP) network survey. Br J Clin Pharmacol. 2007;64(2):198-209.
5. Markowitz JS, Brewerton TD. Zolpidem-induced psychosis. Ann Clin Psychiatry. 1996;8(2):89-91.
6. Tsai MJ, Huang YB, Wu PC. A novel clinical pattern of visual hallucination after zolpidem use. J Toxicol Clin Toxicol. 2003;41(6):869-872.
New-onset psychosis: Check caffeine use
Caffeine belongs to the xanthine chemical group and its stimulant effects are the result of its competitive antagonism on adenosine receptors A1 and A2A in the CNS. Caffeine also slows the rate of dopamine reuptake and increases glutamate release, which theoretically could cause neuropsychiatric symptoms.1,2 Toxicity ranges have been recorded at 150 to 200 mg/kg. Increased psychotic features in schizophrenia patients have been reported at doses as low as 10 mg/kg.1 Earlier studies of caffeine use in patients with psychotic disorders reveal induction in thought disorders, social withdrawal, and euphoric activation3; however, these results have been variable.1
The American Association of Poison Control Centers reported 4,600 caffeine-related calls in 2005; one-half of which involved patients age <19.4 For a list of the caffeine content of 20 popular drinks, see the Table.
TABLE
Caffeine content of 20 popular drinksa
| Drink | Caffeine concentration (mg/oz) |
|---|---|
| Energy Citrus Vitamin Water | 2.5 |
| Coca-Cola Classic | 2.9 |
| Pepsi Cola | 3.2 |
| Dr. Pepper | 3.4 |
| Mountain Dew | 4.5 |
| Amp | 8.9 |
| Full Throttle | 9 |
| Tab Energy | 9.1 |
| SoBe Adrenaline Rush | 9.5 |
| Red Bull | 9.6 |
| Monster | 10 |
| Rockstar | 10 |
| No Fear | 10.9 |
| Jolt Cola | 11.9 |
| NOS | 16.3 |
| Wired X344 | 21.5 |
| Fuel Cell | 90 |
| Powershot | 100 |
| RedLine Power Rush | 140 |
| Ammo | 171 |
| aFor comparison, the caffeine concentration of McDonald’s coffee is 9.1 mg/oz Source: Reissig CJ, Strain EC, Griffiths RR. Caffeinated energy drinks—a growing problem. Drug Alcohol Depend. 2009;99(1-3):1-10. | |
Caffeine-induced psychosis?
My team recently treated a woman with prodromal psychotic symptoms for whom ingesting a high dose of caffeine precipitated a psychotic break.
Ms. P, age 19, presented to our Naval outpatient psychiatry clinic reporting a decline in her ability to organize her thoughts over the past 6 months. She said at times she experienced visual hallucinations and feeling that she was being followed but no one was there. Ms. P also stated she felt other people were talking about her and described ideas of reference. She described her prodrome as an unrelenting and existential interest in the number 33.
The patient drank 4 cups of coffee each day, plus an additional 3 to 4 cups of coffee and 2 to 3 Monster energy drinks on days she was on duty. Ms. P was ingesting approximately 21 to 22 mg/kg/d of caffeine. Basic lab and radiographic work were unremarkable. We asked her to reduce or discontinue her use of caffeinated beverages and return for follow-up in 1 to 2 weeks.
When Ms. P returned 2 weeks later, she said she had reduced her caffeine intake to a periodic cup of coffee or Monster drink. She reported improved sleep quality and quantity; moreover, she experienced a substantial decline in thought disruptions and paranoid thought patterns. However, over the next 4 weeks Ms. P’s reality testing gradually deteriorated, so we prescribed ziprasidone, 20 mg/d, which dissipated her perceptual disturbances. Ms. P tolerated the low-dose antipsychotic and medically retired from military service.
Disclosure
Dr. Whiting reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products. The views expressed in this article are those of the author and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the United States Government.
1. Cerimele JM, Stern AP, Jutras-Aswad D. Psychosis following excessive ingestion of energy drinks in a patient with schizophrenia. Am J Psychiatry. 2010;167(3):353.-
2. Lucas PB, Pickar D, Kelsoe, et al. Effects of the acute administration of caffeine in patients with schizophrenia. Biol Psychiatry. 1990;28(1):35-40.
3. De Freitas B, Schwartz G. Effects of caffeine in chronic psychiatric patients. Am J Psychiatry. 1979;136(10):1337-1338.
4. Lai MW, Klein-Schwartz W, Rodgers GC, et al. 2005 annual report of the American Association of Point Control Centers’ national poisoning and exposure database. Clin Toxicology (Phila). 2006;44:803-932.
Caffeine belongs to the xanthine chemical group and its stimulant effects are the result of its competitive antagonism on adenosine receptors A1 and A2A in the CNS. Caffeine also slows the rate of dopamine reuptake and increases glutamate release, which theoretically could cause neuropsychiatric symptoms.1,2 Toxicity ranges have been recorded at 150 to 200 mg/kg. Increased psychotic features in schizophrenia patients have been reported at doses as low as 10 mg/kg.1 Earlier studies of caffeine use in patients with psychotic disorders reveal induction in thought disorders, social withdrawal, and euphoric activation3; however, these results have been variable.1
The American Association of Poison Control Centers reported 4,600 caffeine-related calls in 2005; one-half of which involved patients age <19.4 For a list of the caffeine content of 20 popular drinks, see the Table.
TABLE
Caffeine content of 20 popular drinksa
| Drink | Caffeine concentration (mg/oz) |
|---|---|
| Energy Citrus Vitamin Water | 2.5 |
| Coca-Cola Classic | 2.9 |
| Pepsi Cola | 3.2 |
| Dr. Pepper | 3.4 |
| Mountain Dew | 4.5 |
| Amp | 8.9 |
| Full Throttle | 9 |
| Tab Energy | 9.1 |
| SoBe Adrenaline Rush | 9.5 |
| Red Bull | 9.6 |
| Monster | 10 |
| Rockstar | 10 |
| No Fear | 10.9 |
| Jolt Cola | 11.9 |
| NOS | 16.3 |
| Wired X344 | 21.5 |
| Fuel Cell | 90 |
| Powershot | 100 |
| RedLine Power Rush | 140 |
| Ammo | 171 |
| aFor comparison, the caffeine concentration of McDonald’s coffee is 9.1 mg/oz Source: Reissig CJ, Strain EC, Griffiths RR. Caffeinated energy drinks—a growing problem. Drug Alcohol Depend. 2009;99(1-3):1-10. | |
Caffeine-induced psychosis?
My team recently treated a woman with prodromal psychotic symptoms for whom ingesting a high dose of caffeine precipitated a psychotic break.
Ms. P, age 19, presented to our Naval outpatient psychiatry clinic reporting a decline in her ability to organize her thoughts over the past 6 months. She said at times she experienced visual hallucinations and feeling that she was being followed but no one was there. Ms. P also stated she felt other people were talking about her and described ideas of reference. She described her prodrome as an unrelenting and existential interest in the number 33.
The patient drank 4 cups of coffee each day, plus an additional 3 to 4 cups of coffee and 2 to 3 Monster energy drinks on days she was on duty. Ms. P was ingesting approximately 21 to 22 mg/kg/d of caffeine. Basic lab and radiographic work were unremarkable. We asked her to reduce or discontinue her use of caffeinated beverages and return for follow-up in 1 to 2 weeks.
When Ms. P returned 2 weeks later, she said she had reduced her caffeine intake to a periodic cup of coffee or Monster drink. She reported improved sleep quality and quantity; moreover, she experienced a substantial decline in thought disruptions and paranoid thought patterns. However, over the next 4 weeks Ms. P’s reality testing gradually deteriorated, so we prescribed ziprasidone, 20 mg/d, which dissipated her perceptual disturbances. Ms. P tolerated the low-dose antipsychotic and medically retired from military service.
Disclosure
Dr. Whiting reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products. The views expressed in this article are those of the author and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the United States Government.
Caffeine belongs to the xanthine chemical group and its stimulant effects are the result of its competitive antagonism on adenosine receptors A1 and A2A in the CNS. Caffeine also slows the rate of dopamine reuptake and increases glutamate release, which theoretically could cause neuropsychiatric symptoms.1,2 Toxicity ranges have been recorded at 150 to 200 mg/kg. Increased psychotic features in schizophrenia patients have been reported at doses as low as 10 mg/kg.1 Earlier studies of caffeine use in patients with psychotic disorders reveal induction in thought disorders, social withdrawal, and euphoric activation3; however, these results have been variable.1
The American Association of Poison Control Centers reported 4,600 caffeine-related calls in 2005; one-half of which involved patients age <19.4 For a list of the caffeine content of 20 popular drinks, see the Table.
TABLE
Caffeine content of 20 popular drinksa
| Drink | Caffeine concentration (mg/oz) |
|---|---|
| Energy Citrus Vitamin Water | 2.5 |
| Coca-Cola Classic | 2.9 |
| Pepsi Cola | 3.2 |
| Dr. Pepper | 3.4 |
| Mountain Dew | 4.5 |
| Amp | 8.9 |
| Full Throttle | 9 |
| Tab Energy | 9.1 |
| SoBe Adrenaline Rush | 9.5 |
| Red Bull | 9.6 |
| Monster | 10 |
| Rockstar | 10 |
| No Fear | 10.9 |
| Jolt Cola | 11.9 |
| NOS | 16.3 |
| Wired X344 | 21.5 |
| Fuel Cell | 90 |
| Powershot | 100 |
| RedLine Power Rush | 140 |
| Ammo | 171 |
| aFor comparison, the caffeine concentration of McDonald’s coffee is 9.1 mg/oz Source: Reissig CJ, Strain EC, Griffiths RR. Caffeinated energy drinks—a growing problem. Drug Alcohol Depend. 2009;99(1-3):1-10. | |
Caffeine-induced psychosis?
My team recently treated a woman with prodromal psychotic symptoms for whom ingesting a high dose of caffeine precipitated a psychotic break.
Ms. P, age 19, presented to our Naval outpatient psychiatry clinic reporting a decline in her ability to organize her thoughts over the past 6 months. She said at times she experienced visual hallucinations and feeling that she was being followed but no one was there. Ms. P also stated she felt other people were talking about her and described ideas of reference. She described her prodrome as an unrelenting and existential interest in the number 33.
The patient drank 4 cups of coffee each day, plus an additional 3 to 4 cups of coffee and 2 to 3 Monster energy drinks on days she was on duty. Ms. P was ingesting approximately 21 to 22 mg/kg/d of caffeine. Basic lab and radiographic work were unremarkable. We asked her to reduce or discontinue her use of caffeinated beverages and return for follow-up in 1 to 2 weeks.
When Ms. P returned 2 weeks later, she said she had reduced her caffeine intake to a periodic cup of coffee or Monster drink. She reported improved sleep quality and quantity; moreover, she experienced a substantial decline in thought disruptions and paranoid thought patterns. However, over the next 4 weeks Ms. P’s reality testing gradually deteriorated, so we prescribed ziprasidone, 20 mg/d, which dissipated her perceptual disturbances. Ms. P tolerated the low-dose antipsychotic and medically retired from military service.
Disclosure
Dr. Whiting reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products. The views expressed in this article are those of the author and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the United States Government.
1. Cerimele JM, Stern AP, Jutras-Aswad D. Psychosis following excessive ingestion of energy drinks in a patient with schizophrenia. Am J Psychiatry. 2010;167(3):353.-
2. Lucas PB, Pickar D, Kelsoe, et al. Effects of the acute administration of caffeine in patients with schizophrenia. Biol Psychiatry. 1990;28(1):35-40.
3. De Freitas B, Schwartz G. Effects of caffeine in chronic psychiatric patients. Am J Psychiatry. 1979;136(10):1337-1338.
4. Lai MW, Klein-Schwartz W, Rodgers GC, et al. 2005 annual report of the American Association of Point Control Centers’ national poisoning and exposure database. Clin Toxicology (Phila). 2006;44:803-932.
1. Cerimele JM, Stern AP, Jutras-Aswad D. Psychosis following excessive ingestion of energy drinks in a patient with schizophrenia. Am J Psychiatry. 2010;167(3):353.-
2. Lucas PB, Pickar D, Kelsoe, et al. Effects of the acute administration of caffeine in patients with schizophrenia. Biol Psychiatry. 1990;28(1):35-40.
3. De Freitas B, Schwartz G. Effects of caffeine in chronic psychiatric patients. Am J Psychiatry. 1979;136(10):1337-1338.
4. Lai MW, Klein-Schwartz W, Rodgers GC, et al. 2005 annual report of the American Association of Point Control Centers’ national poisoning and exposure database. Clin Toxicology (Phila). 2006;44:803-932.
Valproate-induced hair loss: What to tell patients
Ms. B, age 29, has bipolar disorder that is stabilized by valproate, 1,250 mg/d. After 1 month of treatment, she shows scalp hair loss. She takes no other medications and is distressed because she had never experienced such copious hair loss. Ms. B’s blood valproate level is at a therapeutic level. She wants to know if the hair loss will be permanent and what she can do to stop it.
Up to 28% of patients who take valproate suffer temporary alopecia.1,2 In most cases, hair loss is associated with long-term valproate pharmacotherapy. Hair loss appears to be dose-related2 and may be more common in women than in men. Usually patients will report gradual but steady hair loss, commonly beginning 2 to 6 months after initiating treatment.3 Complete hair loss is rare and new hair growth typically begins approximately 2 to 3 months after alopecia onset.
Valproate can cause telogen effluvium, a non-scarring form of alopecia that occurs by precipitating the follicles into a premature rest phase. Other medications that may cause this type of hair loss include desipramine, imipramine, selective serotonin reuptake inhibitors, dopaminergics, anticoagulants, beta blockers, angiotensin-converting enzyme inhibitors, and cimetidine, as well as withdrawal from minoxidil, oral contraceptives, sulfasalazine, and antithyroid medicines.3
Advising patients
In addition to reducing a patient’s valproate dosage when clinically feasible, you can suggest pharmacologic and lifestyle changes to help patients minimize hair loss:
1. Recommend a biotin supplement. Valproate can cause biotin deficiency and may lead to low serum and liver tissue biotinidase enzyme4; a major clinical manifestation of biotin deficiency is alopecia.
2. Tell patients to avoid taking valproate during meals to prevent its chelating effect on food. The chelating effect of valproate makes metals that facilitate hair growth, such as zinc and selenium, unavailable for absorption.5
3. Recommend zinc and selenium supplements, which can help stop further hair loss and regenerate hair.5
4. Suggest practical advice for hair care, including using soft brushes and mild shampoos and avoiding dyes, heated curlers, and hair dryers.
5. Consider minoxidil therapy. However, this is an expensive option and there are no cases documenting its use for alopecia caused by mood stabilizers.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Castro-Gago M, Gómez-Lado C, Eirís-Puñal J, et al. Serum biotinidase activity in children treated with valproic acid and carbamazepine. J Child Neurol. 2010;25(1):32-35.
2. Patrizi A, Savoia F, Negosanti F, et al. Telogen effluvium caused by magnesium valproate and lamotrigine. Acta Derm Venereol. 2005;85(1):77-78.
3. Mercke Y, Sheng H, Khan T, et al. Hair loss in psychopharmacology. Ann Clin Psychiatry. 2000;12(1):35-42.
4. Yilmaz Y, Tasdemir HA, Paksu MS. The influence of valproic acid treatment on hair and serum zinc levels and serum biotinidase activity. Eur J Paediatr Neurol. 2009;13(5):439-443.
4. Fatemi SH, Calabrese JR. Treatment of valproate-induced alopecia. Ann Pharmacother. 1995;29(12):1302.-
Ms. B, age 29, has bipolar disorder that is stabilized by valproate, 1,250 mg/d. After 1 month of treatment, she shows scalp hair loss. She takes no other medications and is distressed because she had never experienced such copious hair loss. Ms. B’s blood valproate level is at a therapeutic level. She wants to know if the hair loss will be permanent and what she can do to stop it.
Up to 28% of patients who take valproate suffer temporary alopecia.1,2 In most cases, hair loss is associated with long-term valproate pharmacotherapy. Hair loss appears to be dose-related2 and may be more common in women than in men. Usually patients will report gradual but steady hair loss, commonly beginning 2 to 6 months after initiating treatment.3 Complete hair loss is rare and new hair growth typically begins approximately 2 to 3 months after alopecia onset.
Valproate can cause telogen effluvium, a non-scarring form of alopecia that occurs by precipitating the follicles into a premature rest phase. Other medications that may cause this type of hair loss include desipramine, imipramine, selective serotonin reuptake inhibitors, dopaminergics, anticoagulants, beta blockers, angiotensin-converting enzyme inhibitors, and cimetidine, as well as withdrawal from minoxidil, oral contraceptives, sulfasalazine, and antithyroid medicines.3
Advising patients
In addition to reducing a patient’s valproate dosage when clinically feasible, you can suggest pharmacologic and lifestyle changes to help patients minimize hair loss:
1. Recommend a biotin supplement. Valproate can cause biotin deficiency and may lead to low serum and liver tissue biotinidase enzyme4; a major clinical manifestation of biotin deficiency is alopecia.
2. Tell patients to avoid taking valproate during meals to prevent its chelating effect on food. The chelating effect of valproate makes metals that facilitate hair growth, such as zinc and selenium, unavailable for absorption.5
3. Recommend zinc and selenium supplements, which can help stop further hair loss and regenerate hair.5
4. Suggest practical advice for hair care, including using soft brushes and mild shampoos and avoiding dyes, heated curlers, and hair dryers.
5. Consider minoxidil therapy. However, this is an expensive option and there are no cases documenting its use for alopecia caused by mood stabilizers.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Ms. B, age 29, has bipolar disorder that is stabilized by valproate, 1,250 mg/d. After 1 month of treatment, she shows scalp hair loss. She takes no other medications and is distressed because she had never experienced such copious hair loss. Ms. B’s blood valproate level is at a therapeutic level. She wants to know if the hair loss will be permanent and what she can do to stop it.
Up to 28% of patients who take valproate suffer temporary alopecia.1,2 In most cases, hair loss is associated with long-term valproate pharmacotherapy. Hair loss appears to be dose-related2 and may be more common in women than in men. Usually patients will report gradual but steady hair loss, commonly beginning 2 to 6 months after initiating treatment.3 Complete hair loss is rare and new hair growth typically begins approximately 2 to 3 months after alopecia onset.
Valproate can cause telogen effluvium, a non-scarring form of alopecia that occurs by precipitating the follicles into a premature rest phase. Other medications that may cause this type of hair loss include desipramine, imipramine, selective serotonin reuptake inhibitors, dopaminergics, anticoagulants, beta blockers, angiotensin-converting enzyme inhibitors, and cimetidine, as well as withdrawal from minoxidil, oral contraceptives, sulfasalazine, and antithyroid medicines.3
Advising patients
In addition to reducing a patient’s valproate dosage when clinically feasible, you can suggest pharmacologic and lifestyle changes to help patients minimize hair loss:
1. Recommend a biotin supplement. Valproate can cause biotin deficiency and may lead to low serum and liver tissue biotinidase enzyme4; a major clinical manifestation of biotin deficiency is alopecia.
2. Tell patients to avoid taking valproate during meals to prevent its chelating effect on food. The chelating effect of valproate makes metals that facilitate hair growth, such as zinc and selenium, unavailable for absorption.5
3. Recommend zinc and selenium supplements, which can help stop further hair loss and regenerate hair.5
4. Suggest practical advice for hair care, including using soft brushes and mild shampoos and avoiding dyes, heated curlers, and hair dryers.
5. Consider minoxidil therapy. However, this is an expensive option and there are no cases documenting its use for alopecia caused by mood stabilizers.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Castro-Gago M, Gómez-Lado C, Eirís-Puñal J, et al. Serum biotinidase activity in children treated with valproic acid and carbamazepine. J Child Neurol. 2010;25(1):32-35.
2. Patrizi A, Savoia F, Negosanti F, et al. Telogen effluvium caused by magnesium valproate and lamotrigine. Acta Derm Venereol. 2005;85(1):77-78.
3. Mercke Y, Sheng H, Khan T, et al. Hair loss in psychopharmacology. Ann Clin Psychiatry. 2000;12(1):35-42.
4. Yilmaz Y, Tasdemir HA, Paksu MS. The influence of valproic acid treatment on hair and serum zinc levels and serum biotinidase activity. Eur J Paediatr Neurol. 2009;13(5):439-443.
4. Fatemi SH, Calabrese JR. Treatment of valproate-induced alopecia. Ann Pharmacother. 1995;29(12):1302.-
1. Castro-Gago M, Gómez-Lado C, Eirís-Puñal J, et al. Serum biotinidase activity in children treated with valproic acid and carbamazepine. J Child Neurol. 2010;25(1):32-35.
2. Patrizi A, Savoia F, Negosanti F, et al. Telogen effluvium caused by magnesium valproate and lamotrigine. Acta Derm Venereol. 2005;85(1):77-78.
3. Mercke Y, Sheng H, Khan T, et al. Hair loss in psychopharmacology. Ann Clin Psychiatry. 2000;12(1):35-42.
4. Yilmaz Y, Tasdemir HA, Paksu MS. The influence of valproic acid treatment on hair and serum zinc levels and serum biotinidase activity. Eur J Paediatr Neurol. 2009;13(5):439-443.
4. Fatemi SH, Calabrese JR. Treatment of valproate-induced alopecia. Ann Pharmacother. 1995;29(12):1302.-
Negative symptoms
I read and enjoyed Dr. Nasrallah’s excellent summary of schizophrenia symptoms in “The primary and secondary symptoms of schizophrenia: Current and future management” (Current Psychiatry, supplement to September 2011, p. S5-S9).
I have a suggestion to add to the list of secondary negative symptoms based only on my observations: demoralization caused by repeated failures in all dimensions—self, interpersonal, social, and industrial. I have seen demoralization in schizophrenia patients manifest as low self-esteem, hopelessness, apathy, and self reproach.
Robert A. Williams, MD
Biological Psychiatry Institute, Ltd.
Phoenix, AZ
I read and enjoyed Dr. Nasrallah’s excellent summary of schizophrenia symptoms in “The primary and secondary symptoms of schizophrenia: Current and future management” (Current Psychiatry, supplement to September 2011, p. S5-S9).
I have a suggestion to add to the list of secondary negative symptoms based only on my observations: demoralization caused by repeated failures in all dimensions—self, interpersonal, social, and industrial. I have seen demoralization in schizophrenia patients manifest as low self-esteem, hopelessness, apathy, and self reproach.
Robert A. Williams, MD
Biological Psychiatry Institute, Ltd.
Phoenix, AZ
I read and enjoyed Dr. Nasrallah’s excellent summary of schizophrenia symptoms in “The primary and secondary symptoms of schizophrenia: Current and future management” (Current Psychiatry, supplement to September 2011, p. S5-S9).
I have a suggestion to add to the list of secondary negative symptoms based only on my observations: demoralization caused by repeated failures in all dimensions—self, interpersonal, social, and industrial. I have seen demoralization in schizophrenia patients manifest as low self-esteem, hopelessness, apathy, and self reproach.
Robert A. Williams, MD
Biological Psychiatry Institute, Ltd.
Phoenix, AZ
Assessing capacity
We agree with Drs. Meraj and Poje in “Capacity assessment: A fundamental skill” (Current Psychiatry, September 2011, p. 72-73) that clinical judgment often is used in addition to or in lieu of quantitative scales when evaluating medical decision-making capacity. We further agree that the formulation by Appelbaum1 is invaluable in such cases.
However, we disagree with the authors’ emphasis on “ability to retain information” as 1 of 4 criteria for decision-making, because long-term declarative memory is irrelevant to a patient’s ability to reason from stable values and preferences.
We use the mnemonic CURA to recall Appelbaum’s criteria: the patient must Communicate a choice; Understand relevant facts; Reason about information; and, importantly, Appreciate the consequences.
We add that the stringency for demonstrating decision-making capacity should increase with greater consequences of the patient’s choice. A clinician may judge a patient to have capacity to consent to low-risk diagnostics, and then the same clinician might appropriately judge that patient lacks capacity to refuse life-saving treatment. A useful model is a “sliding scale” of capacity evaluation,2 wherein the threshold for a given decision is proportional to the likely outcome at stake.
Timothy Kreider, MD, PhD
Psychiatry Resident
University of Pennsylvania
Philadelphia, PA
Rashi Aggarwal, MD
Assistant Professor
Department of Psychiatry
New Jersey Medical School
Newark, NJ
References
1. Appelbaum PS. Clinical practice. Assessment of patients’ competence to consent to treatment. N Engl J Med. 2007;357(18):1834-1840.
2. Drane JF. Competency to give an informed consent. A model for making clinical assessments. JAMA. 1984;252(7):925-927.
The authors respond
Thank you for your letter. We emphasize that memory deficits should be implicated in any condition that negatively affects capacity (eg, delirium, dementia). Memory would be beneficial to a patient undergoing capacity evaluation.
For example, consider a 70-year-old male with a history of dementia who is admitted to the neurology service with delirium and refuses a procedure in the evening despite frequent reassurance. The next morning the same patient doesn’t remember seeing you and denies refusing the procedure. His decision-making is greatly affected by fluctuating cognition and memory.
Another scenario would be a patient with such a significant impairment in short-term memory that she is unable to follow the basis of the argument. How could a patient unable to recall the basis of an argument be entrusted to make an intelligent decision?
We argue that memory should be taken in account in these evaluations. Although we agree in principle with the comments made by Drs. Kreider and Aggarwal, it is important to make capacity evaluations on a case-by-case basis and our article presents basic principles to help guide a typical clinician making those assessments.
Adeel Meraj, MD
Third-Year Psychiatry Resident
University of Kansas Medical Center
Kansas City, KS
Albert Poje, PhD
Assistant Professor of Psychology
Department of Psychiatry and Behavioral Sciences
University of Kansas Medical Center
Kansas City, KS
We agree with Drs. Meraj and Poje in “Capacity assessment: A fundamental skill” (Current Psychiatry, September 2011, p. 72-73) that clinical judgment often is used in addition to or in lieu of quantitative scales when evaluating medical decision-making capacity. We further agree that the formulation by Appelbaum1 is invaluable in such cases.
However, we disagree with the authors’ emphasis on “ability to retain information” as 1 of 4 criteria for decision-making, because long-term declarative memory is irrelevant to a patient’s ability to reason from stable values and preferences.
We use the mnemonic CURA to recall Appelbaum’s criteria: the patient must Communicate a choice; Understand relevant facts; Reason about information; and, importantly, Appreciate the consequences.
We add that the stringency for demonstrating decision-making capacity should increase with greater consequences of the patient’s choice. A clinician may judge a patient to have capacity to consent to low-risk diagnostics, and then the same clinician might appropriately judge that patient lacks capacity to refuse life-saving treatment. A useful model is a “sliding scale” of capacity evaluation,2 wherein the threshold for a given decision is proportional to the likely outcome at stake.
Timothy Kreider, MD, PhD
Psychiatry Resident
University of Pennsylvania
Philadelphia, PA
Rashi Aggarwal, MD
Assistant Professor
Department of Psychiatry
New Jersey Medical School
Newark, NJ
References
1. Appelbaum PS. Clinical practice. Assessment of patients’ competence to consent to treatment. N Engl J Med. 2007;357(18):1834-1840.
2. Drane JF. Competency to give an informed consent. A model for making clinical assessments. JAMA. 1984;252(7):925-927.
The authors respond
Thank you for your letter. We emphasize that memory deficits should be implicated in any condition that negatively affects capacity (eg, delirium, dementia). Memory would be beneficial to a patient undergoing capacity evaluation.
For example, consider a 70-year-old male with a history of dementia who is admitted to the neurology service with delirium and refuses a procedure in the evening despite frequent reassurance. The next morning the same patient doesn’t remember seeing you and denies refusing the procedure. His decision-making is greatly affected by fluctuating cognition and memory.
Another scenario would be a patient with such a significant impairment in short-term memory that she is unable to follow the basis of the argument. How could a patient unable to recall the basis of an argument be entrusted to make an intelligent decision?
We argue that memory should be taken in account in these evaluations. Although we agree in principle with the comments made by Drs. Kreider and Aggarwal, it is important to make capacity evaluations on a case-by-case basis and our article presents basic principles to help guide a typical clinician making those assessments.
Adeel Meraj, MD
Third-Year Psychiatry Resident
University of Kansas Medical Center
Kansas City, KS
Albert Poje, PhD
Assistant Professor of Psychology
Department of Psychiatry and Behavioral Sciences
University of Kansas Medical Center
Kansas City, KS
We agree with Drs. Meraj and Poje in “Capacity assessment: A fundamental skill” (Current Psychiatry, September 2011, p. 72-73) that clinical judgment often is used in addition to or in lieu of quantitative scales when evaluating medical decision-making capacity. We further agree that the formulation by Appelbaum1 is invaluable in such cases.
However, we disagree with the authors’ emphasis on “ability to retain information” as 1 of 4 criteria for decision-making, because long-term declarative memory is irrelevant to a patient’s ability to reason from stable values and preferences.
We use the mnemonic CURA to recall Appelbaum’s criteria: the patient must Communicate a choice; Understand relevant facts; Reason about information; and, importantly, Appreciate the consequences.
We add that the stringency for demonstrating decision-making capacity should increase with greater consequences of the patient’s choice. A clinician may judge a patient to have capacity to consent to low-risk diagnostics, and then the same clinician might appropriately judge that patient lacks capacity to refuse life-saving treatment. A useful model is a “sliding scale” of capacity evaluation,2 wherein the threshold for a given decision is proportional to the likely outcome at stake.
Timothy Kreider, MD, PhD
Psychiatry Resident
University of Pennsylvania
Philadelphia, PA
Rashi Aggarwal, MD
Assistant Professor
Department of Psychiatry
New Jersey Medical School
Newark, NJ
References
1. Appelbaum PS. Clinical practice. Assessment of patients’ competence to consent to treatment. N Engl J Med. 2007;357(18):1834-1840.
2. Drane JF. Competency to give an informed consent. A model for making clinical assessments. JAMA. 1984;252(7):925-927.
The authors respond
Thank you for your letter. We emphasize that memory deficits should be implicated in any condition that negatively affects capacity (eg, delirium, dementia). Memory would be beneficial to a patient undergoing capacity evaluation.
For example, consider a 70-year-old male with a history of dementia who is admitted to the neurology service with delirium and refuses a procedure in the evening despite frequent reassurance. The next morning the same patient doesn’t remember seeing you and denies refusing the procedure. His decision-making is greatly affected by fluctuating cognition and memory.
Another scenario would be a patient with such a significant impairment in short-term memory that she is unable to follow the basis of the argument. How could a patient unable to recall the basis of an argument be entrusted to make an intelligent decision?
We argue that memory should be taken in account in these evaluations. Although we agree in principle with the comments made by Drs. Kreider and Aggarwal, it is important to make capacity evaluations on a case-by-case basis and our article presents basic principles to help guide a typical clinician making those assessments.
Adeel Meraj, MD
Third-Year Psychiatry Resident
University of Kansas Medical Center
Kansas City, KS
Albert Poje, PhD
Assistant Professor of Psychology
Department of Psychiatry and Behavioral Sciences
University of Kansas Medical Center
Kansas City, KS
Comments & Controversies
Discuss this article at www.facebook.com/CurrentPsychiatry
Assessing capacity
We agree with Drs. Meraj and Poje in “Capacity assessment: A fundamental skill” (Current Psychiatry, September 2011, p. 72-73) that clinical judgment often is used in addition to or in lieu of quantitative scales when evaluating medical decision-making capacity. We further agree that the formulation by AppelbaumThe primary and secondary symptoms of schizophrenia: Current and future management” (Current Psychiatry, supplement to September 2011, p. S5-S9).
I have a suggestion to add to the list of secondary negative symptoms based only on my observations: demoralization caused by repeated failures in all dimensions—self, interpersonal, social, and industrial. I have seen demoralization in schizophrenia patients manifest as low self-esteem, hopelessness, apathy, and self reproach.
Robert A. Williams, MD
Biological Psychiatry Institute, Ltd.
Phoenix, AZ
Discuss this article at www.facebook.com/CurrentPsychiatry
Assessing capacity
We agree with Drs. Meraj and Poje in “Capacity assessment: A fundamental skill” (Current Psychiatry, September 2011, p. 72-73) that clinical judgment often is used in addition to or in lieu of quantitative scales when evaluating medical decision-making capacity. We further agree that the formulation by AppelbaumThe primary and secondary symptoms of schizophrenia: Current and future management” (Current Psychiatry, supplement to September 2011, p. S5-S9).
I have a suggestion to add to the list of secondary negative symptoms based only on my observations: demoralization caused by repeated failures in all dimensions—self, interpersonal, social, and industrial. I have seen demoralization in schizophrenia patients manifest as low self-esteem, hopelessness, apathy, and self reproach.
Robert A. Williams, MD
Biological Psychiatry Institute, Ltd.
Phoenix, AZ
Discuss this article at www.facebook.com/CurrentPsychiatry
Assessing capacity
We agree with Drs. Meraj and Poje in “Capacity assessment: A fundamental skill” (Current Psychiatry, September 2011, p. 72-73) that clinical judgment often is used in addition to or in lieu of quantitative scales when evaluating medical decision-making capacity. We further agree that the formulation by AppelbaumThe primary and secondary symptoms of schizophrenia: Current and future management” (Current Psychiatry, supplement to September 2011, p. S5-S9).
I have a suggestion to add to the list of secondary negative symptoms based only on my observations: demoralization caused by repeated failures in all dimensions—self, interpersonal, social, and industrial. I have seen demoralization in schizophrenia patients manifest as low self-esteem, hopelessness, apathy, and self reproach.
Robert A. Williams, MD
Biological Psychiatry Institute, Ltd.
Phoenix, AZ
Strategies to reduce alcohol use in problem drinkers
Alcohol dependence is not an acute illness. Progression from alcohol use to dependence typically takes years, and alcohol dependence is a chronic illness with symptom severity that increases over time.1,2 As the level of alcohol intake increases, the probability of developing an alcohol use disorder, cirrhosis, seizures, cancer, hypertension, stroke, and injuries significantly increases.3,4 Most alcohol-related harm occurs in high-risk drinkers who do not meet DSM-IV-TR criteria for an alcohol use disorder.5,6
Clinicians therefore have an opportunity to intervene at early stages of alcohol use to help prevent progression to dependence and reduce harm. The concept of a continuum from low-to high-risk alcohol use is replacing the disease-oriented model that focuses on identifying and treating individuals who meet DSM-IV-TR criteria for alcohol use disorders (Figure 1).4,7 Efforts to provide screening and intervention earlier in the disease course have:
- mainly been carried out in the primary care setting
- been aimed at nontreatment-seeking, nondependent individuals
- led to recommendations for safe alcohol consumption limits.8-10
One of the largest outreach efforts is a federally funded screening, brief intervention, referral to treatment (SBIRT) program established in 17 states that targets hospital emergency rooms, community health centers, and trauma centers.11
Although research on the use of brief interventions for problem drinking in psychiatric settings is limited,12-15 psychiatrists can employ these strategies, even during a brief medication management visit.
Figure 1: Recommended treatment based on type of alcohol use
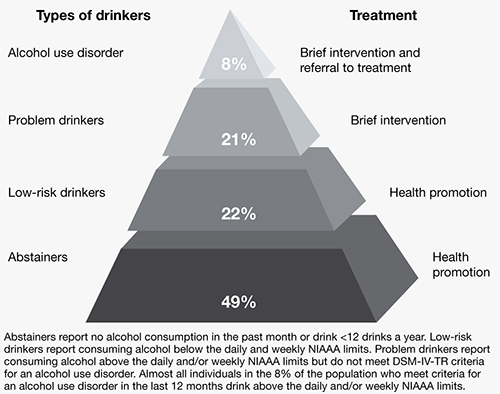
NIAAA: National Institute on Alcohol Abuse and Alcoholism
Source: References 7,16
How much is too much?
The National Institute on Alcohol Abuse and Alcoholism (NIAAA) recommends men age <65 drink no more than 4 drinks/day and no more than 14 drinks/week and women of any age and men age ≥65 drink no more than 3 drinks/day and no more than 7 drinks/week.16 A standard drink is defined as 14 grams of absolute ethanol (12 ounces of beer, 5 ounces of wine, or 1.5 ounces of distilled spirits). Drinking above these levels is likely to result in harm and is defined as hazardous or at-risk use.10,17,18 Harmful use is alcohol consumption that has resulted in adverse mental or physical effects.10,17,18 We use “problem drinking” to describe both at-risk and harmful use as alcohol intake that exceeds NIAAA-recommended limits but does not meet DSM-IV-TR criteria for an alcohol use disorder.
In the United States, approximately 20% of the population exceeds NIAAA recommended alcohol intake guidelines without meeting criteria for an alcohol use disorder.18 Problem drinkers have an increased risk of developing an alcohol use disorder, nicotine dependence, liver disease, financial problems, marital disruptions, injuries, and driver’s license suspensions.4-6,19
Problem drinking is common in psychiatric populations and may lead to difficulties beyond those experienced in the general population.20,21 For example, problem drinking in individuals with bipolar disorder is associated with reduced medication compliance, greater functional impairment, and possibly more suicide attempts.22,23 Even moderate alcohol use below the NIAAA-recommend levels may increase symptom severity in patients with bipolar disorder.22,23
Interviewing techniques
Interventions to identify and treat problem drinkers have focused on the primary care setting because these physicians often are the only medical professionals problem drinkers encounter.8-10 The style of counseling is based on motivational interviewing. Providers use therapeutic empathy, describe risk, deal with ambivalence and resistance, assess motivation to change, emphasize patient responsibility and self-efficacy, and provide a menu of specific strategies to reduce alcohol use. However, unlike standard motivational interviewing, in brief interventions, providers use clear, directive advice to reduce alcohol consumption in the context of the medical provider role. Brief interventions also draw on cognitive-behavioral therapy and general education strategies utilizing contracting, goal setting, and written materials such as self-help manuals.24
Clinicians’ time demands have driven an effort to make interventions for problem drinkers efficient and time-limited. A single short intervention (5 to 15 minutes) can be effective, but 2 to 4 sessions of 5 to 15 minutes each seems to be more effective.8,10 The emphasis is on increasing a patient’s insight and awareness of risk to prompt him or her to establish and manage a goal to reduce alcohol intake. As opposed to abstinence, which is commonly recommended for patients with alcohol use disorders, reducing intake typically is encouraged for problem drinkers.9,10,16,18 For patients who use alcohol over the recommended limits and also meet criteria for an alcohol use disorder, clinicians can deliver a brief intervention, but should recommend abstinence from drinking and provide referral for further treatment.9,10,16,18
Compared with controls, problem drinkers who receive a brief intervention are twice as likely to moderate their drinking at 6 to 12 months25 and significantly reduce alcohol intake by approximately 4 drinks per week at follow-ups of 12 months or more.8,10,26 In addition, providing brief interventions significantly decreases the proportion of individuals whose alcohol intake exceeds recommended levels.10 A meta-analysis and a systemic review indicate brief interventions for problem drinkers reduce morbidity and mortality resulting from motor vehicle crashes, falls, suicide attempts, domestic violence, assaults, and child abuse.5,27
A brief intervention
Screening and brief intervention guidelines suggest a standard approach for assessing and managing problem drinking and alcohol use disorders.7,16 This approach can be described by the “5 As of intervention” (Table 1),10 which is one way to summarize the different brief intervention strategies described in the literature.7,9,10,16-18,28-30
Ask. Asking a question about any alcohol use is a simple way to initiate a conversation about the topic (“Do you sometimes drink beer, wine, or other alcoholic beverages?”). Incorporating questions about alcohol consumption into inquiries about other health habits (eg, smoking, exercise) may decrease patients’ defensiveness. If your patient reports using alcohol, follow up by screening for ≥5 drinks a day for men or ≥4 drinks a day for women (“In the past year, how many times have you had 5 or more drinks a day?”). Use at this level ≥1 times a year indicates a positive screen that provides good sensitivity and specificity for detecting problem drinking and alcohol use disorders.18 Then ask about weekly alcohol intake (“On average, how many days a week do you have an alcoholic drink?” “On a typical drinking day how many drinks do you have?”). Presenting a chart that describes what constitutes a standard drink—available from the NIAAA (see Related Resources)—may be helpful.
You also can use additional questions from the CAGE screening test (Table 2).31 In clinics with a more formal screening protocol, patients may be asked to complete a written self-report such as the Alcohol Use Disorders Identification Test (AUDIT). This 10-question survey covers domains of alcohol consumption, drinking behavior, and alcohol-related problems.17,18 If your patient is a problem drinker, further assessment could determine if he or she has an alcohol use disorder.
Advise. Provide feedback about your patient’s drinking and its consequences along with clear recommendations in an empathic, nonconfrontational manner (“You’re drinking more than is medically safe; I strongly recommend you cut down”). Comparing your patient’s drinking pattern to population norms may be helpful (“Less than 20% of people drink a much as you”).7,16 When possible, tie the consequences of the patient’s drinking to his or her current physical, mental, family, social, and legal concerns. Convey your concerns empathically, as a medical provider providing health recommendations (“As your doctor, I am concerned about how much you drink and how it is affecting your health”). However, to respect patient autonomy, give a medical recommendation, rather than a directive (“As your doctor, I feel I should tell you” rather than “You should”). Finally, express a clear message of your willingness to help.
Assess your patient’s readiness to change (“Given what we’ve talked about, are you willing to consider making changes in your drinking?”). Showing the links between alcohol use and personal consequences may improve patient engagement (“If you keep drinking at your current levels, do you think your goal of improving your grades will be easier, harder, or no different?”).28 If your patient is willing to make a change, negotiate a patient-specific goal, such as reducing drinking to within the recommended limits, using alcohol only a few days a week instead of every day, or abstaining for a defined period. If the patient is not willing to change, restate your concern regarding his or her health-related consequences and your willingness to help.
Assist. After you’ve negotiated a goal with your patient, discuss a treatment plan to help the patient achieve the goal. This should include steps the patient will take to reduce or quit drinking. Consider offering handouts on standard drink sizes, alcohol-associated harms, and strategies for cutting down or abstaining (eg, pacing use, spacing drinks by including nonalcoholic beverages, plans to handle urges, using alcohol money for other items), and calendars for tracking drinking (ie, a drinking diary). Help your patient identify situations where he or she is likely to have difficulty achieving the goal and strategies for avoiding or managing such situations. Ask patients to identify a family member or friend who can help them. Refer patients who have an alcohol use disorder to addiction treatment.
For patients who are not willing to change, discuss the perceived benefits of continued drinking vs reducing or stopping drinking to encourage them to reflect on their alcohol use patterns. Discuss any potential barriers to change. Keep in mind ambivalence and reluctance to change drinking patterns are common and many patients are unaware of the risks of their alcohol use. This discussion may lead patients to contemplate change later.
Arrange. Schedule a follow-up appointment to reinforce the treatment plan with further support, feedback, and assistance in setting, achieving, and maintaining realistic goals. Consider a follow-up phone call 2 weeks after the brief intervention to check on progress and a follow-up appointment in 1 month. Clinical staff may have the opportunity to e-mail or text message patients to check on progress between face-to-face visits. At the follow-up appointment, ask if your patient was able to meet and sustain the drinking goal. If so, support continued adherence, renegotiate drinking goals if indicated, and encourage follow-up with at least annual rescreening. When patients are unable to meet their treatment goals, acknowledge that change is difficult, encourage any positive changes, and address barriers to reaching the goal. Reemphasize your willingness to help, reevaluate the diagnosis, treatment plan, and goals, and schedule close follow-up. Consider engaging significant others in the treatment process.
Table 1
Brief interventions: ‘5As’ to address alcohol use
Ask: Screen for use
|
Advise: Provide strong direct personal advice to change
|
Assess: Determine willingness to change
|
Assist: Help the patient make a change if he or she is ready
|
Arrange: Reinforce change effort with follow-up
|
| Source: Reference 10 |
Table 2
CAGE questionnaire to detect alcohol use disorders
| Cut down | ‘Have you ever felt you ought to cut down on your drinking?’ |
| Annoyed | ‘Have people annoyed you by criticizing your drinking?’ |
| Guilt | ‘Have you ever felt bad or guilty about your drinking?’ |
| Eye-opener | ‘Have you ever had a drink first thing in the morning to steady your nerves or get rid of a hangover?’ |
| Source: Reference 31 | |
Use in psychiatric practice
Problem drinking may not be adequately addressed in psychiatric settings. In a survey of problem drinkers identified in the general population, only 64% discussed their drinking during a mental health visit and only 40% received counseling about their alcohol use from their mental health provider.32 In a study of 200 psychiatric inpatients, 49% exhibited problem drinking as measured by AUDIT, but only 27% of patients had alcohol use recorded in their medical record.33 In addition, routine use of screening tools such as CAGE or AUDIT appears to be low in many psychiatric settings even though research has shown that tools such as AUDIT or computerized screening may be effective for identifying problem drinking in psychiatric outpatient settings.20,21,34
Several small studies support the efficacy of brief interventions for problem drinking in psychiatric settings. A study in a psychiatric emergency service found patients with either schizophrenia/bipolar disorder or depression/anxiety decreased their drinking by about 7 drinks a week over 6 months after a brief intervention.15 This study was small and the decrease in alcohol intake was not significant within the 2 population groups (P = .10 for schizophrenia/bipolar disorder, n = 34, P = .05 for depression/anxiety, n = 53); however, there was a significant decrease for all patients with follow-up (P = .0096, N = 55).15 In another study, psychiatric inpatients with problem drinking who received a brief motivational intervention demonstrated a statistically significant reduction in alcohol consumption at 6 months compared with patients who received only an information packet,13 but health-related outcomes at 5 years did not differ between the 2 groups.14 Finally, in a study of 344 nonpsychotic psychiatric outpatients with problem drinking, one-half of those who received a brief telephone intervention reduced their drinking to non-hazardous levels at a 6-month follow-up (intervention 43.8%, control 27.7%).12
- National Institute on Alcohol Abuse and Alcoholism. www.niaaa.nih.gov.
- Saunders JB, Aasland OG, Babor TF, et al. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption—II. Addiction. 1993;88(6):791-804.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Schuckit MA, Anthenelli RM, Bucholz KK, et al. The time course of development of alcohol-related problems in men and women. J Stud Alcohol. 1995;56(2):218-225.
2. Wagner FA, Anthony JC. From first drug use to drug dependence; developmental periods of risk for dependence upon marijuana cocaine, and alcohol. Neuropsychopharmacology. 2002;26(4):479-488.
3. Rehm J, Room R, Graham K, et al. The relationship of average volume of alcohol consumption and patterns of drinking to burden of disease: an overview. Addiction. 2003;98(9):1209-1228.
4. Dawson DA, Li TK, Grant BF. A prospective study of risk drinking: at risk for what? Drug Alcohol Depend. 2008;95(1-2):62-72.
5. Dinh-Zarr T, Goss C, Heitman E, et al. Interventions for preventing injuries in problem drinkers. Cochrane Database Syst Rev. 2004;(3):CD001857.-
6. Bradley KA, Donovan DM, Larson EB. How much is too much? Advising patients about safe levels of alcohol consumption. Arch Intern Med. 1993;153(24):2734-2740.
7. Babor TF, Higgins-Biddle JC. Brief intervention for hazardous and harmful drinking: a manual for use in primary care. World Health Organization. http://whqlibdoc.who.int/hq/2001/WHO_MSD_MSB_01.6b.pdf. Accessed August 18 2011.
8. Kaner EF, Dickinson HO, Beyer F, et al. The effectiveness of brief alcohol interventions in primary care settings: a systematic review. Drug Alcohol Rev. 2009;28(3):301-323.
9. Fleming M, Manwell LB. Brief intervention in primary care settings. A primary treatment method for at-risk problem, and dependent drinkers. Alcohol Res Health. 1999;23(2):128-137.
10. Whitlock EP, Polen MR, Green CA, et al. Behavioral counseling interventions in primary care to reduce risky/harmful alcohol use by adults: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2004;140(7):557-568.
11. Madras BK, Compton WM, Avula D, et al. Screening, brief interventions, referral to treatment (SBIRT) for illicit drug and alcohol use at multiple healthcare sites: comparison at intake and 6 months later. Drug Alcohol Depend. 2009;99(1-3):280-295.
12. Eberhard S, Nordström G, Höglund P, et al. Secondary prevention of hazardous alcohol consumption in psychiatric out-patients: a randomised controlled study. Soc Psychiatry Psychiatr Epidemiol. 2009;44(12):1013-1021.
13. Hulse GK, Tait RJ. Six-month outcomes associated with a brief alcohol intervention for adult in-patients with psychiatric disorders. Drug Alcohol Rev. 2002;21(2):105-112.
14. Hulse GK, Tait RJ. Five-year outcomes of a brief alcohol intervention for adult in-patients with psychiatric disorders. Addiction. 2003;98(8):1061-1068.
15. Milner KK, Barry KL, Blow FC, et al. Brief interventions for patients presenting to the Psychiatric Emergency Service (PES) with major mental illnesses and at-risk drinking. Community Ment Health J. 2010;46(2):149-155.
16. U.S. Department of Health and Human Services. Helping patients who drink too much: a clinician’s guide. http://pubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/guide.pdf. Updated 2005. Accessed August 18, 2011.
17. Fiellin DA, Reid MC, O’Connor PG. Outpatient management of patients with alcohol problems. Ann Intern Med. 2000;133(10):815-827.
18. Willenbring ML, Massey SH, Gardner MB. Helping patients who drink too much: an evidence-based guide for primary care clinicians. Am Fam Physician. 2009;80(1):44-50.
19. Batty GD, Lewars H, Emslie C, et al. Internationally recognized guidelines for ‘sensible’ alcohol consumption: is exceeding them actually detrimental to health and social circumstances? Evidence from a population-based cohort study. J Public Health (Oxf). 2009;31(3):360-365.
20. Barry KL, Milner K, Blow FC, et al. Screening psychiatric emergency department patients with major mental illnesses for at-risk drinking. Psychiatr Serv. 2006;57(7):1039-1042.
21. Satre D, Wolfe W, Eisendrath S, et al. Computerized screening for alcohol and drug use among adults seeking outpatient psychiatric services. Psychiatr Serv. 2008;59(4):441-444.
22. Goldstein BI, Velyvis VP, Parikh SV. The association between moderate alcohol use and illness severity in bipolar disorder: a preliminary report. J Clin Psychiatry. 2006;67(1):102-106.
23. Lagerberg TV, Andreassen OA, Ringen PA, et al. Excessive substance use in bipolar disorder is associated with impaired functioning rather than clinical characteristics, a descriptive study. BMC Psychiatry. 2010;10:9.-
24. Fleming MF, Balousek SL, Grossberg PM, et al. Brief physician advice for heavy drinking college students: a randomized controlled trial in college health clinics. J Stud Alcohol Drugs. 2010;71(1):23-31.
25. Wilk AI, Jensen NM, Havighurst TC. Meta-analysis of randomized control trials addressing brief interventions in heavy alcohol drinkers. J Gen Intern Med. 1997;12(5):274-283.
26. Bertholet N, Daeppen JB, Wietlisbach V, et al. Reduction of alcohol consumption by brief alcohol intervention in primary care: systematic review and meta-analysis. Arch Intern Med. 2005;165(9):986-995.
27. Cuijpers P, Riper H, Lemmers L. The effects on mortality of brief interventions for problem drinking: a meta-analysis. Addiction. 2004;99(7):839-845.
28. Grossberg P, Halperin A, Mackenzie S, et al. Inside the physician’s black bag: critical ingredients of brief alcohol interventions. Subst Abus. 2010;31(4):240-250.
29. D’Onofrio G, Pantalon MV, Degutis LC, et al. Development and implementation of an emergency practitioner-performed brief intervention for hazardous and harmful drinkers in the emergency department. Acad Emerg Med. 2005;12(3):249-256.
30. Moyer A, Finney JW, Swearingen CE, et al. Brief interventions for alcohol problems: a meta-analytic review of controlled investigations in treatment-seeking and non-treatment-seeking populations. Addiction. 2002;97(3):279-292.
31. Ewing JA. Detecting alcoholism: the CAGE questionnaire. JAMA. 1984;252(14):1905-1907.
32. Weisner C, Matzger H. Missed opportunities in addressing drinking behavior in medical and mental health services. Alcohol Clin Exp Res. 2003;27(7):1132-1141.
33. Barnaby B, Drummond C, McCloud A, et al. Substance misuse in psychiatric inpatients: comparison of a screening questionnaire survey with case notes. BMJ. 2003;327(7418):783-784.
34. Freimuth M. Another missed opportunity? Recognition of alcohol use problems by mental health providers. Psychotherapy: Theory Research, Practice, Training. 2008;45(3):405-409.
Alcohol dependence is not an acute illness. Progression from alcohol use to dependence typically takes years, and alcohol dependence is a chronic illness with symptom severity that increases over time.1,2 As the level of alcohol intake increases, the probability of developing an alcohol use disorder, cirrhosis, seizures, cancer, hypertension, stroke, and injuries significantly increases.3,4 Most alcohol-related harm occurs in high-risk drinkers who do not meet DSM-IV-TR criteria for an alcohol use disorder.5,6
Clinicians therefore have an opportunity to intervene at early stages of alcohol use to help prevent progression to dependence and reduce harm. The concept of a continuum from low-to high-risk alcohol use is replacing the disease-oriented model that focuses on identifying and treating individuals who meet DSM-IV-TR criteria for alcohol use disorders (Figure 1).4,7 Efforts to provide screening and intervention earlier in the disease course have:
- mainly been carried out in the primary care setting
- been aimed at nontreatment-seeking, nondependent individuals
- led to recommendations for safe alcohol consumption limits.8-10
One of the largest outreach efforts is a federally funded screening, brief intervention, referral to treatment (SBIRT) program established in 17 states that targets hospital emergency rooms, community health centers, and trauma centers.11
Although research on the use of brief interventions for problem drinking in psychiatric settings is limited,12-15 psychiatrists can employ these strategies, even during a brief medication management visit.
Figure 1: Recommended treatment based on type of alcohol use
NIAAA: National Institute on Alcohol Abuse and Alcoholism
Source: References 7,16
How much is too much?
The National Institute on Alcohol Abuse and Alcoholism (NIAAA) recommends men age <65 drink no more than 4 drinks/day and no more than 14 drinks/week and women of any age and men age ≥65 drink no more than 3 drinks/day and no more than 7 drinks/week.16 A standard drink is defined as 14 grams of absolute ethanol (12 ounces of beer, 5 ounces of wine, or 1.5 ounces of distilled spirits). Drinking above these levels is likely to result in harm and is defined as hazardous or at-risk use.10,17,18 Harmful use is alcohol consumption that has resulted in adverse mental or physical effects.10,17,18 We use “problem drinking” to describe both at-risk and harmful use as alcohol intake that exceeds NIAAA-recommended limits but does not meet DSM-IV-TR criteria for an alcohol use disorder.
In the United States, approximately 20% of the population exceeds NIAAA recommended alcohol intake guidelines without meeting criteria for an alcohol use disorder.18 Problem drinkers have an increased risk of developing an alcohol use disorder, nicotine dependence, liver disease, financial problems, marital disruptions, injuries, and driver’s license suspensions.4-6,19
Problem drinking is common in psychiatric populations and may lead to difficulties beyond those experienced in the general population.20,21 For example, problem drinking in individuals with bipolar disorder is associated with reduced medication compliance, greater functional impairment, and possibly more suicide attempts.22,23 Even moderate alcohol use below the NIAAA-recommend levels may increase symptom severity in patients with bipolar disorder.22,23
Interviewing techniques
Interventions to identify and treat problem drinkers have focused on the primary care setting because these physicians often are the only medical professionals problem drinkers encounter.8-10 The style of counseling is based on motivational interviewing. Providers use therapeutic empathy, describe risk, deal with ambivalence and resistance, assess motivation to change, emphasize patient responsibility and self-efficacy, and provide a menu of specific strategies to reduce alcohol use. However, unlike standard motivational interviewing, in brief interventions, providers use clear, directive advice to reduce alcohol consumption in the context of the medical provider role. Brief interventions also draw on cognitive-behavioral therapy and general education strategies utilizing contracting, goal setting, and written materials such as self-help manuals.24
Clinicians’ time demands have driven an effort to make interventions for problem drinkers efficient and time-limited. A single short intervention (5 to 15 minutes) can be effective, but 2 to 4 sessions of 5 to 15 minutes each seems to be more effective.8,10 The emphasis is on increasing a patient’s insight and awareness of risk to prompt him or her to establish and manage a goal to reduce alcohol intake. As opposed to abstinence, which is commonly recommended for patients with alcohol use disorders, reducing intake typically is encouraged for problem drinkers.9,10,16,18 For patients who use alcohol over the recommended limits and also meet criteria for an alcohol use disorder, clinicians can deliver a brief intervention, but should recommend abstinence from drinking and provide referral for further treatment.9,10,16,18
Compared with controls, problem drinkers who receive a brief intervention are twice as likely to moderate their drinking at 6 to 12 months25 and significantly reduce alcohol intake by approximately 4 drinks per week at follow-ups of 12 months or more.8,10,26 In addition, providing brief interventions significantly decreases the proportion of individuals whose alcohol intake exceeds recommended levels.10 A meta-analysis and a systemic review indicate brief interventions for problem drinkers reduce morbidity and mortality resulting from motor vehicle crashes, falls, suicide attempts, domestic violence, assaults, and child abuse.5,27
A brief intervention
Screening and brief intervention guidelines suggest a standard approach for assessing and managing problem drinking and alcohol use disorders.7,16 This approach can be described by the “5 As of intervention” (Table 1),10 which is one way to summarize the different brief intervention strategies described in the literature.7,9,10,16-18,28-30
Ask. Asking a question about any alcohol use is a simple way to initiate a conversation about the topic (“Do you sometimes drink beer, wine, or other alcoholic beverages?”). Incorporating questions about alcohol consumption into inquiries about other health habits (eg, smoking, exercise) may decrease patients’ defensiveness. If your patient reports using alcohol, follow up by screening for ≥5 drinks a day for men or ≥4 drinks a day for women (“In the past year, how many times have you had 5 or more drinks a day?”). Use at this level ≥1 times a year indicates a positive screen that provides good sensitivity and specificity for detecting problem drinking and alcohol use disorders.18 Then ask about weekly alcohol intake (“On average, how many days a week do you have an alcoholic drink?” “On a typical drinking day how many drinks do you have?”). Presenting a chart that describes what constitutes a standard drink—available from the NIAAA (see Related Resources)—may be helpful.
You also can use additional questions from the CAGE screening test (Table 2).31 In clinics with a more formal screening protocol, patients may be asked to complete a written self-report such as the Alcohol Use Disorders Identification Test (AUDIT). This 10-question survey covers domains of alcohol consumption, drinking behavior, and alcohol-related problems.17,18 If your patient is a problem drinker, further assessment could determine if he or she has an alcohol use disorder.
Advise. Provide feedback about your patient’s drinking and its consequences along with clear recommendations in an empathic, nonconfrontational manner (“You’re drinking more than is medically safe; I strongly recommend you cut down”). Comparing your patient’s drinking pattern to population norms may be helpful (“Less than 20% of people drink a much as you”).7,16 When possible, tie the consequences of the patient’s drinking to his or her current physical, mental, family, social, and legal concerns. Convey your concerns empathically, as a medical provider providing health recommendations (“As your doctor, I am concerned about how much you drink and how it is affecting your health”). However, to respect patient autonomy, give a medical recommendation, rather than a directive (“As your doctor, I feel I should tell you” rather than “You should”). Finally, express a clear message of your willingness to help.
Assess your patient’s readiness to change (“Given what we’ve talked about, are you willing to consider making changes in your drinking?”). Showing the links between alcohol use and personal consequences may improve patient engagement (“If you keep drinking at your current levels, do you think your goal of improving your grades will be easier, harder, or no different?”).28 If your patient is willing to make a change, negotiate a patient-specific goal, such as reducing drinking to within the recommended limits, using alcohol only a few days a week instead of every day, or abstaining for a defined period. If the patient is not willing to change, restate your concern regarding his or her health-related consequences and your willingness to help.
Assist. After you’ve negotiated a goal with your patient, discuss a treatment plan to help the patient achieve the goal. This should include steps the patient will take to reduce or quit drinking. Consider offering handouts on standard drink sizes, alcohol-associated harms, and strategies for cutting down or abstaining (eg, pacing use, spacing drinks by including nonalcoholic beverages, plans to handle urges, using alcohol money for other items), and calendars for tracking drinking (ie, a drinking diary). Help your patient identify situations where he or she is likely to have difficulty achieving the goal and strategies for avoiding or managing such situations. Ask patients to identify a family member or friend who can help them. Refer patients who have an alcohol use disorder to addiction treatment.
For patients who are not willing to change, discuss the perceived benefits of continued drinking vs reducing or stopping drinking to encourage them to reflect on their alcohol use patterns. Discuss any potential barriers to change. Keep in mind ambivalence and reluctance to change drinking patterns are common and many patients are unaware of the risks of their alcohol use. This discussion may lead patients to contemplate change later.
Arrange. Schedule a follow-up appointment to reinforce the treatment plan with further support, feedback, and assistance in setting, achieving, and maintaining realistic goals. Consider a follow-up phone call 2 weeks after the brief intervention to check on progress and a follow-up appointment in 1 month. Clinical staff may have the opportunity to e-mail or text message patients to check on progress between face-to-face visits. At the follow-up appointment, ask if your patient was able to meet and sustain the drinking goal. If so, support continued adherence, renegotiate drinking goals if indicated, and encourage follow-up with at least annual rescreening. When patients are unable to meet their treatment goals, acknowledge that change is difficult, encourage any positive changes, and address barriers to reaching the goal. Reemphasize your willingness to help, reevaluate the diagnosis, treatment plan, and goals, and schedule close follow-up. Consider engaging significant others in the treatment process.
Table 1
Brief interventions: ‘5As’ to address alcohol use
Ask: Screen for use
|
Advise: Provide strong direct personal advice to change
|
Assess: Determine willingness to change
|
Assist: Help the patient make a change if he or she is ready
|
Arrange: Reinforce change effort with follow-up
|
| Source: Reference 10 |
Table 2
CAGE questionnaire to detect alcohol use disorders
| Cut down | ‘Have you ever felt you ought to cut down on your drinking?’ |
| Annoyed | ‘Have people annoyed you by criticizing your drinking?’ |
| Guilt | ‘Have you ever felt bad or guilty about your drinking?’ |
| Eye-opener | ‘Have you ever had a drink first thing in the morning to steady your nerves or get rid of a hangover?’ |
| Source: Reference 31 | |
Use in psychiatric practice
Problem drinking may not be adequately addressed in psychiatric settings. In a survey of problem drinkers identified in the general population, only 64% discussed their drinking during a mental health visit and only 40% received counseling about their alcohol use from their mental health provider.32 In a study of 200 psychiatric inpatients, 49% exhibited problem drinking as measured by AUDIT, but only 27% of patients had alcohol use recorded in their medical record.33 In addition, routine use of screening tools such as CAGE or AUDIT appears to be low in many psychiatric settings even though research has shown that tools such as AUDIT or computerized screening may be effective for identifying problem drinking in psychiatric outpatient settings.20,21,34
Several small studies support the efficacy of brief interventions for problem drinking in psychiatric settings. A study in a psychiatric emergency service found patients with either schizophrenia/bipolar disorder or depression/anxiety decreased their drinking by about 7 drinks a week over 6 months after a brief intervention.15 This study was small and the decrease in alcohol intake was not significant within the 2 population groups (P = .10 for schizophrenia/bipolar disorder, n = 34, P = .05 for depression/anxiety, n = 53); however, there was a significant decrease for all patients with follow-up (P = .0096, N = 55).15 In another study, psychiatric inpatients with problem drinking who received a brief motivational intervention demonstrated a statistically significant reduction in alcohol consumption at 6 months compared with patients who received only an information packet,13 but health-related outcomes at 5 years did not differ between the 2 groups.14 Finally, in a study of 344 nonpsychotic psychiatric outpatients with problem drinking, one-half of those who received a brief telephone intervention reduced their drinking to non-hazardous levels at a 6-month follow-up (intervention 43.8%, control 27.7%).12
- National Institute on Alcohol Abuse and Alcoholism. www.niaaa.nih.gov.
- Saunders JB, Aasland OG, Babor TF, et al. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption—II. Addiction. 1993;88(6):791-804.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Alcohol dependence is not an acute illness. Progression from alcohol use to dependence typically takes years, and alcohol dependence is a chronic illness with symptom severity that increases over time.1,2 As the level of alcohol intake increases, the probability of developing an alcohol use disorder, cirrhosis, seizures, cancer, hypertension, stroke, and injuries significantly increases.3,4 Most alcohol-related harm occurs in high-risk drinkers who do not meet DSM-IV-TR criteria for an alcohol use disorder.5,6
Clinicians therefore have an opportunity to intervene at early stages of alcohol use to help prevent progression to dependence and reduce harm. The concept of a continuum from low-to high-risk alcohol use is replacing the disease-oriented model that focuses on identifying and treating individuals who meet DSM-IV-TR criteria for alcohol use disorders (Figure 1).4,7 Efforts to provide screening and intervention earlier in the disease course have:
- mainly been carried out in the primary care setting
- been aimed at nontreatment-seeking, nondependent individuals
- led to recommendations for safe alcohol consumption limits.8-10
One of the largest outreach efforts is a federally funded screening, brief intervention, referral to treatment (SBIRT) program established in 17 states that targets hospital emergency rooms, community health centers, and trauma centers.11
Although research on the use of brief interventions for problem drinking in psychiatric settings is limited,12-15 psychiatrists can employ these strategies, even during a brief medication management visit.
Figure 1: Recommended treatment based on type of alcohol use
NIAAA: National Institute on Alcohol Abuse and Alcoholism
Source: References 7,16
How much is too much?
The National Institute on Alcohol Abuse and Alcoholism (NIAAA) recommends men age <65 drink no more than 4 drinks/day and no more than 14 drinks/week and women of any age and men age ≥65 drink no more than 3 drinks/day and no more than 7 drinks/week.16 A standard drink is defined as 14 grams of absolute ethanol (12 ounces of beer, 5 ounces of wine, or 1.5 ounces of distilled spirits). Drinking above these levels is likely to result in harm and is defined as hazardous or at-risk use.10,17,18 Harmful use is alcohol consumption that has resulted in adverse mental or physical effects.10,17,18 We use “problem drinking” to describe both at-risk and harmful use as alcohol intake that exceeds NIAAA-recommended limits but does not meet DSM-IV-TR criteria for an alcohol use disorder.
In the United States, approximately 20% of the population exceeds NIAAA recommended alcohol intake guidelines without meeting criteria for an alcohol use disorder.18 Problem drinkers have an increased risk of developing an alcohol use disorder, nicotine dependence, liver disease, financial problems, marital disruptions, injuries, and driver’s license suspensions.4-6,19
Problem drinking is common in psychiatric populations and may lead to difficulties beyond those experienced in the general population.20,21 For example, problem drinking in individuals with bipolar disorder is associated with reduced medication compliance, greater functional impairment, and possibly more suicide attempts.22,23 Even moderate alcohol use below the NIAAA-recommend levels may increase symptom severity in patients with bipolar disorder.22,23
Interviewing techniques
Interventions to identify and treat problem drinkers have focused on the primary care setting because these physicians often are the only medical professionals problem drinkers encounter.8-10 The style of counseling is based on motivational interviewing. Providers use therapeutic empathy, describe risk, deal with ambivalence and resistance, assess motivation to change, emphasize patient responsibility and self-efficacy, and provide a menu of specific strategies to reduce alcohol use. However, unlike standard motivational interviewing, in brief interventions, providers use clear, directive advice to reduce alcohol consumption in the context of the medical provider role. Brief interventions also draw on cognitive-behavioral therapy and general education strategies utilizing contracting, goal setting, and written materials such as self-help manuals.24
Clinicians’ time demands have driven an effort to make interventions for problem drinkers efficient and time-limited. A single short intervention (5 to 15 minutes) can be effective, but 2 to 4 sessions of 5 to 15 minutes each seems to be more effective.8,10 The emphasis is on increasing a patient’s insight and awareness of risk to prompt him or her to establish and manage a goal to reduce alcohol intake. As opposed to abstinence, which is commonly recommended for patients with alcohol use disorders, reducing intake typically is encouraged for problem drinkers.9,10,16,18 For patients who use alcohol over the recommended limits and also meet criteria for an alcohol use disorder, clinicians can deliver a brief intervention, but should recommend abstinence from drinking and provide referral for further treatment.9,10,16,18
Compared with controls, problem drinkers who receive a brief intervention are twice as likely to moderate their drinking at 6 to 12 months25 and significantly reduce alcohol intake by approximately 4 drinks per week at follow-ups of 12 months or more.8,10,26 In addition, providing brief interventions significantly decreases the proportion of individuals whose alcohol intake exceeds recommended levels.10 A meta-analysis and a systemic review indicate brief interventions for problem drinkers reduce morbidity and mortality resulting from motor vehicle crashes, falls, suicide attempts, domestic violence, assaults, and child abuse.5,27
A brief intervention
Screening and brief intervention guidelines suggest a standard approach for assessing and managing problem drinking and alcohol use disorders.7,16 This approach can be described by the “5 As of intervention” (Table 1),10 which is one way to summarize the different brief intervention strategies described in the literature.7,9,10,16-18,28-30
Ask. Asking a question about any alcohol use is a simple way to initiate a conversation about the topic (“Do you sometimes drink beer, wine, or other alcoholic beverages?”). Incorporating questions about alcohol consumption into inquiries about other health habits (eg, smoking, exercise) may decrease patients’ defensiveness. If your patient reports using alcohol, follow up by screening for ≥5 drinks a day for men or ≥4 drinks a day for women (“In the past year, how many times have you had 5 or more drinks a day?”). Use at this level ≥1 times a year indicates a positive screen that provides good sensitivity and specificity for detecting problem drinking and alcohol use disorders.18 Then ask about weekly alcohol intake (“On average, how many days a week do you have an alcoholic drink?” “On a typical drinking day how many drinks do you have?”). Presenting a chart that describes what constitutes a standard drink—available from the NIAAA (see Related Resources)—may be helpful.
You also can use additional questions from the CAGE screening test (Table 2).31 In clinics with a more formal screening protocol, patients may be asked to complete a written self-report such as the Alcohol Use Disorders Identification Test (AUDIT). This 10-question survey covers domains of alcohol consumption, drinking behavior, and alcohol-related problems.17,18 If your patient is a problem drinker, further assessment could determine if he or she has an alcohol use disorder.
Advise. Provide feedback about your patient’s drinking and its consequences along with clear recommendations in an empathic, nonconfrontational manner (“You’re drinking more than is medically safe; I strongly recommend you cut down”). Comparing your patient’s drinking pattern to population norms may be helpful (“Less than 20% of people drink a much as you”).7,16 When possible, tie the consequences of the patient’s drinking to his or her current physical, mental, family, social, and legal concerns. Convey your concerns empathically, as a medical provider providing health recommendations (“As your doctor, I am concerned about how much you drink and how it is affecting your health”). However, to respect patient autonomy, give a medical recommendation, rather than a directive (“As your doctor, I feel I should tell you” rather than “You should”). Finally, express a clear message of your willingness to help.
Assess your patient’s readiness to change (“Given what we’ve talked about, are you willing to consider making changes in your drinking?”). Showing the links between alcohol use and personal consequences may improve patient engagement (“If you keep drinking at your current levels, do you think your goal of improving your grades will be easier, harder, or no different?”).28 If your patient is willing to make a change, negotiate a patient-specific goal, such as reducing drinking to within the recommended limits, using alcohol only a few days a week instead of every day, or abstaining for a defined period. If the patient is not willing to change, restate your concern regarding his or her health-related consequences and your willingness to help.
Assist. After you’ve negotiated a goal with your patient, discuss a treatment plan to help the patient achieve the goal. This should include steps the patient will take to reduce or quit drinking. Consider offering handouts on standard drink sizes, alcohol-associated harms, and strategies for cutting down or abstaining (eg, pacing use, spacing drinks by including nonalcoholic beverages, plans to handle urges, using alcohol money for other items), and calendars for tracking drinking (ie, a drinking diary). Help your patient identify situations where he or she is likely to have difficulty achieving the goal and strategies for avoiding or managing such situations. Ask patients to identify a family member or friend who can help them. Refer patients who have an alcohol use disorder to addiction treatment.
For patients who are not willing to change, discuss the perceived benefits of continued drinking vs reducing or stopping drinking to encourage them to reflect on their alcohol use patterns. Discuss any potential barriers to change. Keep in mind ambivalence and reluctance to change drinking patterns are common and many patients are unaware of the risks of their alcohol use. This discussion may lead patients to contemplate change later.
Arrange. Schedule a follow-up appointment to reinforce the treatment plan with further support, feedback, and assistance in setting, achieving, and maintaining realistic goals. Consider a follow-up phone call 2 weeks after the brief intervention to check on progress and a follow-up appointment in 1 month. Clinical staff may have the opportunity to e-mail or text message patients to check on progress between face-to-face visits. At the follow-up appointment, ask if your patient was able to meet and sustain the drinking goal. If so, support continued adherence, renegotiate drinking goals if indicated, and encourage follow-up with at least annual rescreening. When patients are unable to meet their treatment goals, acknowledge that change is difficult, encourage any positive changes, and address barriers to reaching the goal. Reemphasize your willingness to help, reevaluate the diagnosis, treatment plan, and goals, and schedule close follow-up. Consider engaging significant others in the treatment process.
Table 1
Brief interventions: ‘5As’ to address alcohol use
Ask: Screen for use
|
Advise: Provide strong direct personal advice to change
|
Assess: Determine willingness to change
|
Assist: Help the patient make a change if he or she is ready
|
Arrange: Reinforce change effort with follow-up
|
| Source: Reference 10 |
Table 2
CAGE questionnaire to detect alcohol use disorders
| Cut down | ‘Have you ever felt you ought to cut down on your drinking?’ |
| Annoyed | ‘Have people annoyed you by criticizing your drinking?’ |
| Guilt | ‘Have you ever felt bad or guilty about your drinking?’ |
| Eye-opener | ‘Have you ever had a drink first thing in the morning to steady your nerves or get rid of a hangover?’ |
| Source: Reference 31 | |
Use in psychiatric practice
Problem drinking may not be adequately addressed in psychiatric settings. In a survey of problem drinkers identified in the general population, only 64% discussed their drinking during a mental health visit and only 40% received counseling about their alcohol use from their mental health provider.32 In a study of 200 psychiatric inpatients, 49% exhibited problem drinking as measured by AUDIT, but only 27% of patients had alcohol use recorded in their medical record.33 In addition, routine use of screening tools such as CAGE or AUDIT appears to be low in many psychiatric settings even though research has shown that tools such as AUDIT or computerized screening may be effective for identifying problem drinking in psychiatric outpatient settings.20,21,34
Several small studies support the efficacy of brief interventions for problem drinking in psychiatric settings. A study in a psychiatric emergency service found patients with either schizophrenia/bipolar disorder or depression/anxiety decreased their drinking by about 7 drinks a week over 6 months after a brief intervention.15 This study was small and the decrease in alcohol intake was not significant within the 2 population groups (P = .10 for schizophrenia/bipolar disorder, n = 34, P = .05 for depression/anxiety, n = 53); however, there was a significant decrease for all patients with follow-up (P = .0096, N = 55).15 In another study, psychiatric inpatients with problem drinking who received a brief motivational intervention demonstrated a statistically significant reduction in alcohol consumption at 6 months compared with patients who received only an information packet,13 but health-related outcomes at 5 years did not differ between the 2 groups.14 Finally, in a study of 344 nonpsychotic psychiatric outpatients with problem drinking, one-half of those who received a brief telephone intervention reduced their drinking to non-hazardous levels at a 6-month follow-up (intervention 43.8%, control 27.7%).12
- National Institute on Alcohol Abuse and Alcoholism. www.niaaa.nih.gov.
- Saunders JB, Aasland OG, Babor TF, et al. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption—II. Addiction. 1993;88(6):791-804.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Schuckit MA, Anthenelli RM, Bucholz KK, et al. The time course of development of alcohol-related problems in men and women. J Stud Alcohol. 1995;56(2):218-225.
2. Wagner FA, Anthony JC. From first drug use to drug dependence; developmental periods of risk for dependence upon marijuana cocaine, and alcohol. Neuropsychopharmacology. 2002;26(4):479-488.
3. Rehm J, Room R, Graham K, et al. The relationship of average volume of alcohol consumption and patterns of drinking to burden of disease: an overview. Addiction. 2003;98(9):1209-1228.
4. Dawson DA, Li TK, Grant BF. A prospective study of risk drinking: at risk for what? Drug Alcohol Depend. 2008;95(1-2):62-72.
5. Dinh-Zarr T, Goss C, Heitman E, et al. Interventions for preventing injuries in problem drinkers. Cochrane Database Syst Rev. 2004;(3):CD001857.-
6. Bradley KA, Donovan DM, Larson EB. How much is too much? Advising patients about safe levels of alcohol consumption. Arch Intern Med. 1993;153(24):2734-2740.
7. Babor TF, Higgins-Biddle JC. Brief intervention for hazardous and harmful drinking: a manual for use in primary care. World Health Organization. http://whqlibdoc.who.int/hq/2001/WHO_MSD_MSB_01.6b.pdf. Accessed August 18 2011.
8. Kaner EF, Dickinson HO, Beyer F, et al. The effectiveness of brief alcohol interventions in primary care settings: a systematic review. Drug Alcohol Rev. 2009;28(3):301-323.
9. Fleming M, Manwell LB. Brief intervention in primary care settings. A primary treatment method for at-risk problem, and dependent drinkers. Alcohol Res Health. 1999;23(2):128-137.
10. Whitlock EP, Polen MR, Green CA, et al. Behavioral counseling interventions in primary care to reduce risky/harmful alcohol use by adults: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2004;140(7):557-568.
11. Madras BK, Compton WM, Avula D, et al. Screening, brief interventions, referral to treatment (SBIRT) for illicit drug and alcohol use at multiple healthcare sites: comparison at intake and 6 months later. Drug Alcohol Depend. 2009;99(1-3):280-295.
12. Eberhard S, Nordström G, Höglund P, et al. Secondary prevention of hazardous alcohol consumption in psychiatric out-patients: a randomised controlled study. Soc Psychiatry Psychiatr Epidemiol. 2009;44(12):1013-1021.
13. Hulse GK, Tait RJ. Six-month outcomes associated with a brief alcohol intervention for adult in-patients with psychiatric disorders. Drug Alcohol Rev. 2002;21(2):105-112.
14. Hulse GK, Tait RJ. Five-year outcomes of a brief alcohol intervention for adult in-patients with psychiatric disorders. Addiction. 2003;98(8):1061-1068.
15. Milner KK, Barry KL, Blow FC, et al. Brief interventions for patients presenting to the Psychiatric Emergency Service (PES) with major mental illnesses and at-risk drinking. Community Ment Health J. 2010;46(2):149-155.
16. U.S. Department of Health and Human Services. Helping patients who drink too much: a clinician’s guide. http://pubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/guide.pdf. Updated 2005. Accessed August 18, 2011.
17. Fiellin DA, Reid MC, O’Connor PG. Outpatient management of patients with alcohol problems. Ann Intern Med. 2000;133(10):815-827.
18. Willenbring ML, Massey SH, Gardner MB. Helping patients who drink too much: an evidence-based guide for primary care clinicians. Am Fam Physician. 2009;80(1):44-50.
19. Batty GD, Lewars H, Emslie C, et al. Internationally recognized guidelines for ‘sensible’ alcohol consumption: is exceeding them actually detrimental to health and social circumstances? Evidence from a population-based cohort study. J Public Health (Oxf). 2009;31(3):360-365.
20. Barry KL, Milner K, Blow FC, et al. Screening psychiatric emergency department patients with major mental illnesses for at-risk drinking. Psychiatr Serv. 2006;57(7):1039-1042.
21. Satre D, Wolfe W, Eisendrath S, et al. Computerized screening for alcohol and drug use among adults seeking outpatient psychiatric services. Psychiatr Serv. 2008;59(4):441-444.
22. Goldstein BI, Velyvis VP, Parikh SV. The association between moderate alcohol use and illness severity in bipolar disorder: a preliminary report. J Clin Psychiatry. 2006;67(1):102-106.
23. Lagerberg TV, Andreassen OA, Ringen PA, et al. Excessive substance use in bipolar disorder is associated with impaired functioning rather than clinical characteristics, a descriptive study. BMC Psychiatry. 2010;10:9.-
24. Fleming MF, Balousek SL, Grossberg PM, et al. Brief physician advice for heavy drinking college students: a randomized controlled trial in college health clinics. J Stud Alcohol Drugs. 2010;71(1):23-31.
25. Wilk AI, Jensen NM, Havighurst TC. Meta-analysis of randomized control trials addressing brief interventions in heavy alcohol drinkers. J Gen Intern Med. 1997;12(5):274-283.
26. Bertholet N, Daeppen JB, Wietlisbach V, et al. Reduction of alcohol consumption by brief alcohol intervention in primary care: systematic review and meta-analysis. Arch Intern Med. 2005;165(9):986-995.
27. Cuijpers P, Riper H, Lemmers L. The effects on mortality of brief interventions for problem drinking: a meta-analysis. Addiction. 2004;99(7):839-845.
28. Grossberg P, Halperin A, Mackenzie S, et al. Inside the physician’s black bag: critical ingredients of brief alcohol interventions. Subst Abus. 2010;31(4):240-250.
29. D’Onofrio G, Pantalon MV, Degutis LC, et al. Development and implementation of an emergency practitioner-performed brief intervention for hazardous and harmful drinkers in the emergency department. Acad Emerg Med. 2005;12(3):249-256.
30. Moyer A, Finney JW, Swearingen CE, et al. Brief interventions for alcohol problems: a meta-analytic review of controlled investigations in treatment-seeking and non-treatment-seeking populations. Addiction. 2002;97(3):279-292.
31. Ewing JA. Detecting alcoholism: the CAGE questionnaire. JAMA. 1984;252(14):1905-1907.
32. Weisner C, Matzger H. Missed opportunities in addressing drinking behavior in medical and mental health services. Alcohol Clin Exp Res. 2003;27(7):1132-1141.
33. Barnaby B, Drummond C, McCloud A, et al. Substance misuse in psychiatric inpatients: comparison of a screening questionnaire survey with case notes. BMJ. 2003;327(7418):783-784.
34. Freimuth M. Another missed opportunity? Recognition of alcohol use problems by mental health providers. Psychotherapy: Theory Research, Practice, Training. 2008;45(3):405-409.
1. Schuckit MA, Anthenelli RM, Bucholz KK, et al. The time course of development of alcohol-related problems in men and women. J Stud Alcohol. 1995;56(2):218-225.
2. Wagner FA, Anthony JC. From first drug use to drug dependence; developmental periods of risk for dependence upon marijuana cocaine, and alcohol. Neuropsychopharmacology. 2002;26(4):479-488.
3. Rehm J, Room R, Graham K, et al. The relationship of average volume of alcohol consumption and patterns of drinking to burden of disease: an overview. Addiction. 2003;98(9):1209-1228.
4. Dawson DA, Li TK, Grant BF. A prospective study of risk drinking: at risk for what? Drug Alcohol Depend. 2008;95(1-2):62-72.
5. Dinh-Zarr T, Goss C, Heitman E, et al. Interventions for preventing injuries in problem drinkers. Cochrane Database Syst Rev. 2004;(3):CD001857.-
6. Bradley KA, Donovan DM, Larson EB. How much is too much? Advising patients about safe levels of alcohol consumption. Arch Intern Med. 1993;153(24):2734-2740.
7. Babor TF, Higgins-Biddle JC. Brief intervention for hazardous and harmful drinking: a manual for use in primary care. World Health Organization. http://whqlibdoc.who.int/hq/2001/WHO_MSD_MSB_01.6b.pdf. Accessed August 18 2011.
8. Kaner EF, Dickinson HO, Beyer F, et al. The effectiveness of brief alcohol interventions in primary care settings: a systematic review. Drug Alcohol Rev. 2009;28(3):301-323.
9. Fleming M, Manwell LB. Brief intervention in primary care settings. A primary treatment method for at-risk problem, and dependent drinkers. Alcohol Res Health. 1999;23(2):128-137.
10. Whitlock EP, Polen MR, Green CA, et al. Behavioral counseling interventions in primary care to reduce risky/harmful alcohol use by adults: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2004;140(7):557-568.
11. Madras BK, Compton WM, Avula D, et al. Screening, brief interventions, referral to treatment (SBIRT) for illicit drug and alcohol use at multiple healthcare sites: comparison at intake and 6 months later. Drug Alcohol Depend. 2009;99(1-3):280-295.
12. Eberhard S, Nordström G, Höglund P, et al. Secondary prevention of hazardous alcohol consumption in psychiatric out-patients: a randomised controlled study. Soc Psychiatry Psychiatr Epidemiol. 2009;44(12):1013-1021.
13. Hulse GK, Tait RJ. Six-month outcomes associated with a brief alcohol intervention for adult in-patients with psychiatric disorders. Drug Alcohol Rev. 2002;21(2):105-112.
14. Hulse GK, Tait RJ. Five-year outcomes of a brief alcohol intervention for adult in-patients with psychiatric disorders. Addiction. 2003;98(8):1061-1068.
15. Milner KK, Barry KL, Blow FC, et al. Brief interventions for patients presenting to the Psychiatric Emergency Service (PES) with major mental illnesses and at-risk drinking. Community Ment Health J. 2010;46(2):149-155.
16. U.S. Department of Health and Human Services. Helping patients who drink too much: a clinician’s guide. http://pubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/guide.pdf. Updated 2005. Accessed August 18, 2011.
17. Fiellin DA, Reid MC, O’Connor PG. Outpatient management of patients with alcohol problems. Ann Intern Med. 2000;133(10):815-827.
18. Willenbring ML, Massey SH, Gardner MB. Helping patients who drink too much: an evidence-based guide for primary care clinicians. Am Fam Physician. 2009;80(1):44-50.
19. Batty GD, Lewars H, Emslie C, et al. Internationally recognized guidelines for ‘sensible’ alcohol consumption: is exceeding them actually detrimental to health and social circumstances? Evidence from a population-based cohort study. J Public Health (Oxf). 2009;31(3):360-365.
20. Barry KL, Milner K, Blow FC, et al. Screening psychiatric emergency department patients with major mental illnesses for at-risk drinking. Psychiatr Serv. 2006;57(7):1039-1042.
21. Satre D, Wolfe W, Eisendrath S, et al. Computerized screening for alcohol and drug use among adults seeking outpatient psychiatric services. Psychiatr Serv. 2008;59(4):441-444.
22. Goldstein BI, Velyvis VP, Parikh SV. The association between moderate alcohol use and illness severity in bipolar disorder: a preliminary report. J Clin Psychiatry. 2006;67(1):102-106.
23. Lagerberg TV, Andreassen OA, Ringen PA, et al. Excessive substance use in bipolar disorder is associated with impaired functioning rather than clinical characteristics, a descriptive study. BMC Psychiatry. 2010;10:9.-
24. Fleming MF, Balousek SL, Grossberg PM, et al. Brief physician advice for heavy drinking college students: a randomized controlled trial in college health clinics. J Stud Alcohol Drugs. 2010;71(1):23-31.
25. Wilk AI, Jensen NM, Havighurst TC. Meta-analysis of randomized control trials addressing brief interventions in heavy alcohol drinkers. J Gen Intern Med. 1997;12(5):274-283.
26. Bertholet N, Daeppen JB, Wietlisbach V, et al. Reduction of alcohol consumption by brief alcohol intervention in primary care: systematic review and meta-analysis. Arch Intern Med. 2005;165(9):986-995.
27. Cuijpers P, Riper H, Lemmers L. The effects on mortality of brief interventions for problem drinking: a meta-analysis. Addiction. 2004;99(7):839-845.
28. Grossberg P, Halperin A, Mackenzie S, et al. Inside the physician’s black bag: critical ingredients of brief alcohol interventions. Subst Abus. 2010;31(4):240-250.
29. D’Onofrio G, Pantalon MV, Degutis LC, et al. Development and implementation of an emergency practitioner-performed brief intervention for hazardous and harmful drinkers in the emergency department. Acad Emerg Med. 2005;12(3):249-256.
30. Moyer A, Finney JW, Swearingen CE, et al. Brief interventions for alcohol problems: a meta-analytic review of controlled investigations in treatment-seeking and non-treatment-seeking populations. Addiction. 2002;97(3):279-292.
31. Ewing JA. Detecting alcoholism: the CAGE questionnaire. JAMA. 1984;252(14):1905-1907.
32. Weisner C, Matzger H. Missed opportunities in addressing drinking behavior in medical and mental health services. Alcohol Clin Exp Res. 2003;27(7):1132-1141.
33. Barnaby B, Drummond C, McCloud A, et al. Substance misuse in psychiatric inpatients: comparison of a screening questionnaire survey with case notes. BMJ. 2003;327(7418):783-784.
34. Freimuth M. Another missed opportunity? Recognition of alcohol use problems by mental health providers. Psychotherapy: Theory Research, Practice, Training. 2008;45(3):405-409.