User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Benzodiazepines and stimulants for patients with substance use disorders
Although benzodiazepines and stimulants have well-documented efficacy for numerous psychiatric disorders, psychiatrists hesitate to prescribe these medications to patients with substance use disorders (SUDs)—even to those with a comorbid condition that likely would respond to a benzodiazepine or stimulant—because of risk of abuse or dependence. Conventional practice typically has focused on treating active substance use first rather than using simultaneous treatments. Prejudice, fear, and misinformation can influence this decision.
We believe these cases lie on a continuum. At one extreme, ignoring a past or present SUD may lead a remitted patient toward relapse, or further delay recovery for an active user. At the other end, psychiatrists who overreact to a remote history of substance use may deprive patients of legitimate pharmacologic symptom relief. Most cases lie somewhere in the middle.
A literature review does not support the assertion that the use of these medications leads to future substance use or worsens active use, especially for stimulants. In fact, stepwise—as opposed to concurrent—treatment for both conditions actually may delay recovery and increase patients’ risk for morbidity.
We outline issues involved in these complex clinical situations, point out controversies, review relevant research data, and offer guidelines for treatment.
CASE 1 Panic disorder in sobriety
Since he was a teen, Mr. A, age 51, drank heavily, which cost him jobs and relationships. After being convicted for driving under the influence, he was court-ordered to attend a rehabilitation facility, where, as he describes it, he “finally turned [his] life around.” He followed up residential treatment with regular attendance at Alcoholics Anonymous meetings.
After 1 year of sobriety, Mr. A develops increasingly frequent episodes of intense anxiety with sweating, nausea, chest pain, and hyperventilation and is diagnosed with panic disorder. His internist prescribes alprazolam, 0.5 mg 3 times a day, which provides some symptom relief, and refers him for follow-up psychiatric care. At his first visit, Mr. A confides to his psychiatrist that he is taking much more than the prescribed dosage of alprazolam, even when he is not experiencing anxiety, and is contemplating “buying it on the street” if his dosage is not raised to “at least 3 mg 3 times a day.”
CASE 2 Anxiety in controlled psychosis
Ms. B, age 40, had her first psychotic break at age 18 and was diagnosed with schizophrenia. Since then, she has had multiple psychiatric hospitalizations, usually presenting with auditory hallucinations and a recurring delusion that the person who calls herself Ms. B’s mother is really an actress “playing” her mother. At times this delusion has led Ms. B to attack her “imposter” mother. Over several years Ms. B began to drink heavily, but recently achieved a few months of sobriety by attending dual-diagnosis groups at her local community mental health center and individual psychotherapy sessions with her case manager. Fortunately, Ms. B’s psychosis has been stabilized with risperidone long-acting injection, 25 mg every 2 weeks, which she tolerates well.
When her beloved calico cat passes away, Ms. B experiences intense anxiety. Ms. B’s friend tells her she “needs some Valium,” but her psychiatrist, case manager, and the other patients in her dual-diagnosis group are not sure this is a good idea.
Benzodiazepines
Pros. There are multiple legitimate uses of benzodiazepines in general medicine and psychiatric practice, based upon their considerable sedative/hypnotic, anxiolytic, anticonvulsant, and muscle-relaxant properties (Table 1).1
Recommendations regarding benzodiazepine use for anxious patients with a history of SUD are not clear-cut. First, it often is difficult to determine whether the patient truly has an anxiety disorder or is suffering anxiety symptoms secondary to substance use and/or withdrawal. In addition, even if a diagnosis of a separate anxiety disorder is established, psychiatrists debate how to treat such patients. Some clinicians maintain that benzodiazepines should be used only for acute detoxification, and that ongoing benzodiazepine use will lead to relapse or benzodiazepine dependence. However, in a prospective study of 545 alcohol use disorder (AUD) patients receiving benzodiazepines for anxiety disorders, Mueller et al2 found no association—at 12 months or at 12 years—between benzodiazepine use and AUD recurrence. Furthermore, there was no difference in benzodiazepine usage when comparing patients with and without an AUD.3
Table 1
Clinical uses of benzodiazepines
| Insomnia |
| Anxiety disorders (eg, generalized anxiety disorder, panic disorder, posttraumatic stress disorder, social phobia, and obsessive-compulsive disorder) |
| Side effects of other psychiatric medications (eg, akathisia with antipsychotics or tremor with lithium) |
| Alcohol or benzodiazepine withdrawal |
| Acute agitation states, either as monotherapy or as adjuncts to antipsychotics or mood stabilizers |
| Catatonia |
| Source: Reference 1 |
Cons. Although widely prescribed—and despite their efficacy in numerous conditions— both acute or long-term benzodiazepine use frequently causes adverse effects.4 Patients may develop tolerance, which can lead to escalating dosages and/or to withdrawal symptoms when patients attempt to cut back. Benzodiazepines eventually become ineffective for sleep, and continued use can cause rebound insomnia. Also, with many patients taking benzodiazepines long-term, clinicians struggle to differentiate between “real” anxiety symptoms and subtle states of withdrawal from fluctuating benzodiazepine blood levels.5
Geriatric patients who take benzodiazepines are at risk for falls and hip fractures.4 Although older dementia patients are at particular risk for cognitive problems— including frank delirium—secondary to benzodiazepine use, patients of all ages are susceptible to these medications’ deleterious neurocognitive effects.
Benzodiazepines can lead to excessive sedation, thereby impairing performance at work or school, and have been implicated as a cause of motor vehicle accidents.6 Finally, a serious drawback to benzodiazepine use is possible lethality in overdose, especially when combined with alcohol.
Benzodiazepine prescribing should not be taken lightly. Always analyze the difference between benzodiazepines’ well-documented efficacy and their adverse effect profile. This risk-benefit analysis becomes much more complex for patients with SUDs.
Special considerations. Patients at higher risk for benzodiazepine abuse include those with:
- severe alcohol dependence (ie, long-term use, drinking since a young age [“Type II”])
- intravenous drug use
- comorbid alcoholism and antisocial personality disorder.7,8
Exercise special caution when considering benzodiazepines for patients with severe psychiatric illness such as schizophrenia-spectrum disorders, bipolar disorder, or severe depression. Patients with schizophrenia have high rates of alcohol, cocaine, cannabis, and benzodiazepine abuse.9,10 Bipolar disorder patients show similar vulnerability—up to 56% of patients screen positive for substance abuse or dependence.11 Vulnerability to addiction in severely ill psychiatric patients is thought to be related to several factors, including:
- use of drugs as self-medication
- genetic predisposition
- environment/lifestyle that supports substance abuse
- neurobiologic deficits that lead to lack of inhibition of reward-seeking behaviors.11
Bipolar disorder patients in particular score high on measures of sensation seeking, which leaves them vulnerable to abusing all classes of substances.12
In a 6-year study of 203 patients with severe psychiatric illnesses and SUDs, Brunette et al13 found that these patients were 2.5 times more likely than patients with severe psychiatric illness alone to abuse prescribed benzodiazepines. In an analysis of Medicaid records, Clark et al14 found similar vulnerability in patients with major depressive disorder (MDD) and SUD. Not only did these patients show a higher rate of benzodiazepine use than patients with MDD without SUD, but the dual-diagnosis group also gravitated toward more addictive high-potency/fast-acting benzodiazepines, such as alprazolam, estazolam, or triazolam.
Case discussion/suggestions. Initially, Mr. A may seem to be an appropriate candidate for closely monitored benzodiazepine use. However, he shows a pattern of misuse, likely related to his history of severe alcohol dependence and alprazolam use. This benzodiazepine is fast-acting and has a short half-life, and thus is highly reinforcing.
Similarly, Ms. B might benefit from benzodiazepine treatment. However, her history of schizophrenia and alcohol abuse makes her a risky candidate, and alternative treatments for anxiety symptoms should be considered. If prescribed at all, a benzodiazepine should be used only short-term (eg, 1 to 2 weeks).
In general, avoid prescribing benzodiazepines to most patients who have an ongoing or past SUD.15 Consider making an exception for SUD patients with comorbid anxiety disorders, with close monitoring of their benzodiazepine use. Clonazepam, chlordiazepoxide, clorazepate, and oxazepam may be less reinforcing for SUD patients than diazepam, lorazepam, alprazolam, estazolam, or triazolam.7,16 The drawbacks of benzodiazepines, especially in the situations described above, point to the need to find alternative treatments (Table 2).17 Keep in mind nonpharmacologic options, which completely avoid the risks of medication misuse and diversion. Cognitive-behavioral therapy (CBT), for instance, has well-documented efficacy in treating insomnia and anxiety disorders.18,19
Table 2
Alternatives to benzodiazepines for anxiety and/or insomnia
| Treatment option | Comments |
|---|---|
| CBT, relaxation techniques, sleep hygiene counseling | Many advantages to nonpharmacologic interventions (eg, fewer side effects, no risk of substance dependence) |
| Antihistamines (eg, diphenhydramine, 25 to 50 mg at bedtime* for sleep, or 2 to 3 times a day for anxiety) | Can be used for anxiety or insomnia; can cause confusion in older patients |
| Atypical antipsychotics | Off-label use; many agents in this class have metabolic side effects |
| SSRIs/SNRIs | First-line for many anxiety disorders, including panic disorder, GAD; possible weight gain and sexual side effects |
| Mirtazapine (7.5 to 30 mg at bedtime*) | Sedation side effect helps with sleep; weight gain and oversedation limit use |
| Trazodone (25 to 100 mg at bedtime*) | Commonly used off-label as a sleep aid |
| Monoamine oxidase inhibitors | May be useful for social phobia; dietary restrictions and side effects limit use |
| Doxepin (3 to 6 mg at bedtime) | Minimal anticholinergic and alpha-blockade side effects at this dose; FDA-approved for insomnia |
| Gabapentin (300 to 2,000 mg/d* in divided doses) | Off-label use, mild anxiolytic and sedative properties, relatively weight neutral |
| Beta blockers (eg, propranolol, 20 to 80 mg twice a day*) | Useful for peripheral manifestations of anxiety; may be effective for social phobias |
| Pregabalin (50 to 200 mg 3 times a day*) | Off-label use; industry-sponsored studies show comparable to SNRIs for anxiety |
| Non-benzodiazepine GABAA receptor modulators | Short-term option for primary insomnia, some abuse potential |
| Melatonin (1 to 3 mg at bedtime*) | Mild and ‘natural’ but not always an effective sleep aid |
| *Off-label approximate doses based on the authors’ clinical experience and consensus of the literature; agents listed may require slow titration and close monitoring for adverse effects CBT: cognitive-behavioral therapy; GABA: gamma-aminobutyric acid; GAD: generalized anxiety disorder; SNRI: serotoninnorepinephrine reuptake inhibitor; SSRI: selective serotonin reuptake inhibitor Source: Reference 17 | |
CASE 3 Adult ADHD and marijuana use
Mr. C, age 30, presents to a psychiatrist with ongoing complaints of inattention, fatigue, and difficulty staying organized. A self-report screen yields symptoms consistent with adult attention-deficit/hyperactivity disorder (ADHD). Mr. C’s school and job history and collateral history from his wife appear to corroborate his assertion that his symptoms have been lifelong. He later admits to regular marijuana use. After further discussion and full evaluation of his substance use, Mr. C is started on bupropion, titrated to 300 mg/d. After 2 months, despite faithful attendance at appointments and openness about his continued marijuana use, Mr. C’s symptoms remain unchanged. He asks about atomoxetine.
Stimulants
Pros. Despite many clinicians’ hesitance to prescribe controlled substances to patients with SUDs, psychostimulants should be considered in a variety of scenarios. Although nonstimulant options are available, stimulants consistently have demonstrated superior efficacy over other treatments and remain first-line agents for adult ADHD.20 Methylphenidate, mixed amphetamine salts, lisdexamfetamine, and atomoxetine are FDA-approved for adult ADHD. Both stimulant classes (methylphenidate and amphetamine-based products) are equally effective for ADHD. In addition, stimulants are used to treat narcolepsy, cognitive disorders such as traumatic brain injury, and as augmentation to antidepressants for MDD.
ADHD affects 5% to 12% of children, and >60% of patients remain symptomatic into adulthood and require continued treatment.21 In particular, problematic inattention may persist throughout adulthood. ADHD does not appear to be an independent risk factor for SUDs in children and adolescents.22 However, substance use increases sharply as ADHD patients enter late adolescence and adulthood, and eventually becomes a problem for 20% of adolescents and adults with ADHD. Conversely, 17% to 50% of patients with alcohol, cocaine, or opioid dependence have co-occurring ADHD.23
Withholding ADHD treatment based on concerns about future or increased current substance abuse is unfounded. A meta-analysis of 6 studies that included 674 medicated and 360 unmedicated patients with ADHD who were followed at least 4 years demonstrated that childhood treatment of ADHD with stimulants reduces the risk of developing alcohol and other drug disorders in adulthood.24 Regarding the effect stimulants have on active substance use, a 12-week, double-blind, randomized controlled trial of 48 cocaine-dependent adults with ADHD showed methylphenidate did not change cocaine abuse or craving, but did improve ADHD symptoms.25
Clinicians also must assess whether untreated ADHD symptoms impair patients’ work or other activities. Driving is a particular concern because ADHD is associated with risky driving habits, motor vehicle accidents, traffic violations, and driving license suspensions.26 In a study that administered cognitive tests to 27 adults with ADHD, methylphenidate treatment improved cognitive performance related to driving (eg, better visual-motor coordination under high-stress conditions, improved visual orientation, and sustained visual attention).27 It is likely this effect could be generalized to other activities where safety is important. Finally, appropriate stimulant treatment may improve participation in rehabilitative programs.
Cons. Despite their positive effects, stimulants can have adverse effects and consequences.28 In routinely prescribed dosages, methylphenidate and amphetamines can cause symptoms related to sympathetic activation, including anxiety, tics, anorexia/ weight loss, and sleep disturbance. A 5-year study of 79 school-age children prescribed methylphenidate, dextroamphetamine, or pemoline, which is no longer available in the United States, showed a significant association between adherence to stimulants and persistence of physiological (eg, headaches, insomnia, anorexia) and mood-related (eg, irritability, dysphoria) side effects.29 Stimulants’ sympathomimetic properties also can lead to dangerous drug-drug interactions with monoamine oxidase inhibitors. For both methylphenidate and amphetamines, overdose can lead to seizures, cardiac toxicity, dysrhythmias, and hyperthermia. All stimulants carry an FDA “black-box” warning that lists increased risk of cardiac complications, sudden death, and psychiatric complications such as psychosis or mania.30
Special considerations. All stimulants have potential for diversion or abuse. Pay close attention to these issues, especially in vulnerable populations and situations where rates of abuse and diversion are elevated. Among college students, white patients, fraternity/sorority members, and individuals with lower grade point averages may be at higher risk for nonmedical stimulant use.31 Adults who misuse or divert stimulants commonly have a history of substance abuse and conduct disorder.32 Short-acting stimulants are abused 4 times more often than extended-release preparations.33
If your ADHD patient has active substance use, be clear that continued substance use is likely to limit stimulants’ effectiveness. In patients who are actively using substances, it will be difficult to disentangle apparent nonresponse to stimulants from the negative cognitive effects of substance use.
Case discussion/suggestions. As Mr. C’s case illustrates, there are alternatives to stimulants for ADHD. For example, atomoxetine, a selective norepinephrine reuptake inhibitor, may be considered a first-line agent in patients with mostly inattentive ADHD symptoms and comorbid stimulant abuse, or for those in whom stimulants cause adverse effects such as mood lability or tics.34 Other alternatives to stimulants are listed in Table 3.35
Because Mr. C did not respond to bupropion, which presumably was tried first because of his ongoing substance use, he asked about atomoxetine. This agent is not addictive and there is no evidence that it leads to or exacerbates substance use. Depending on Mr. C’s symptom profile, atomoxetine might be a good choice. Continued monitoring of his marijuana use and frequent assessment of his motivation to quit are necessary. Psychoeducation about the cognitive effects of marijuana, including inattention and poor concentration, is important.
If Mr. C does not respond to atomoxetine, his psychiatrist will face a difficult decision. Setting Mr. C’s marijuana use aside, symptoms that do not respond to atomoxetine or a second-line agent are likely to respond to a stimulant. However, several issues must be addressed. If Mr. C’s motivation to stop using marijuana is low, how motivated is he to improve his ADHD symptoms? Next, would marijuana’s depressive/blunting effects counteract the anticipated benefit of a stimulant? Also, what is the risk that Mr. C might sell or exchange his stimulants to obtain marijuana? Assessing these complicated questions is key. Another important factor in Mr. C’s case is his wife’s involvement. Does she monitor his marijuana use? Would she be willing to supervise Mr. C’s stimulant use, and would he allow it?
Past or present SUDs are not an absolute contraindication to stimulant use. You should affirm the diagnosis and identify target symptoms. Consider nonstimulant alternatives if appropriate.
Table 3
Alternatives to stimulants for ADHD
| Treatment option | Comments |
|---|---|
| Atomoxetine | Effectiveness may be limited to inattentive type |
| Modafinil | Well-tolerated but expensive, limited evidence, no FDA indication; may be a consideration in ADHD + SUD |
| α2-adrenergic agonist (eg, clonidine or guanfacine) | Useful when hyperactivity/impulsivity symptoms predominate, or when stimulant-induced insomnia occurs |
| Bupropion | Some evidence of mild efficacy, especially useful if nicotine dependence also is a target for treatment |
| Psychotherapy | Can be useful as adjunctive treatment, but as monotherapy it is of little benefit in ADHD |
| ADHD: attention-deficit/hyperactivity disorder; SUD: substance abuse disorder Source: Reference 35 | |
Legal liabilities
Being aware of the medicolegal issues of benzodiazepine and/or stimulant prescribing is crucial because a court may find a psychiatrist liable for negative outcomes (eg, suicide) when controlled substances are prescribed to a patient with a history of addiction.36 The most prudent course is to weigh the pros and cons for each patient individually, taking into consideration the factors described above.8 This is consistent with guidelines from the American Psychiatric Association and the British Association for Psychopharmacology,37 both of which call for extreme caution in these cases.
Educate patients and caregivers about the risks of taking a controlled substance, including misuse, diversion, and theft. Provide and document explicit instructions that the patient will receive stimulants from only a single provider. Remind patients that state and federal authorities closely track controlled medications. Finally, a “stimulant contract” or “benzodiazepine contract,” similar to a pain or narcotic contact, may be useful to formally document discussions about appropriate medication use.
Related Resources
- National Institute on Drug Abuse. Prescription drugs: abuse and addiction. Research Report Series, 2005. http://drugabuse.gov/ResearchReports/Prescription/Prescription.html.
- Galanter M, Kleber HD. The American Psychiatric Publishing textbook of substance abuse treatment. 4th ed. Arlington, VA: American Psychiatric Publishing, Inc; 2008.
Drug Brand Names
- Alprazolam • Xanax
- Atomoxetine • Strattera
- Bupropion • Wellbutrin, others
- Chlordiazepoxide • Librium
- Clonazepam • Klonopin
- Clonidine • Catapres
- Clorazepate • Tranxene
- Dextroamphetamine • Dexedrine
- Diazepam • Valium
- Diphenhydramine • Benadryl, others
- Doxepin • Silenor
- Estazolam • ProSom
- Gabapentin • Neurontin
- Guanfacine • Tenex, Intuniv
- Lisdexamfetamine • Vyvanse
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Methylphenidate • Ritalin, Concerta, others
- Mirtazapine • Remeron
- Mixed amphetamine salts • Adderall
- Modafinil • Provigil
- Oxazepam • Serax
- Pemoline • Cylert
- Propranolol • Inderal
- Trazodone • Desyrel, Oleptro
- Triazolam • Halcion
Disclosures
Dr. Casher is a speaker for AstraZeneca and Pfizer Inc.
Drs. Gih and Bess report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Ashton H. Guidelines for the rational use of benzodiazepines. When and what to use. Drugs. 1994;48(1):25.-
2. Mueller TI, Pagano ME, Rodriguez BF, et al. Long-term use of benzodiazepines in participants with comorbid anxiety and alcohol use disorders. Alcohol Clin Exp Res. 2005;29(8):1411-1418.
3. Mueller TI, Goldenberg IM, Gordon AL, et al. Benzodiazepine use in anxiety disordered patients with and without a history of alcoholism. J Clin Psychiatry. 1996;57(2):83-89.
4. Ashton H. The diagnosis and management of benzodiazepine dependence. Curr Opin Psychiatry. 2005;(18):249-255.
5. Back SE, Brady KT. Anxiety disorders with comorbid substance use disorders: diagnostic and treatment considerations. Psychiatric Annals. 2008;38(11):724-729.
6. Walsh JM, Flegel R, Cangianelli LA, et al. Epidemiology of alcohol and other drug use among motor vehicle crash victims admitted to a trauma center. Traffic Inj Prev. 2004;5(3):254-260.
7. Ciraulo DA, Nace EP. Benzodiazepine treatment of anxiety or insomnia in substance abuse patients. Am J Addict. 2000;9(4):276-279;discussion 280–284.
8. Sattar S, Bhatia S. Benzodiazepines for substance abusers. Current Psychiatry. 2003;2(5):25-34.
9. Regier DA, Farmer ME, Rae DS, et al. Comorbidity of mental disorders with alcohol and other drug abuse. Results from the Epidemiologic Catchment Area (ECA) Study. JAMA. 1990;264(19):2511-2518.
10. Kendler KS, Gallagher TJ, Abelson JM, et al. Lifetime prevalence, demographic risk factors, and diagnostic validity of nonaffective psychosis as assessed in a US community sample. The National Comorbidity Survey. Arch Gen Psychiatry. 1996;53(11):1022-1031
11. Buckley PF. Prevalence and consequences of the dual diagnosis of substance abuse and severe mental illness. J Clin Psychiatry. 2006;67(suppl 7):5-9.
12. Bizzarri JV, Sbrana A, Rucci P, et al. The spectrum of substance abuse in bipolar disorder: reasons for use, sensation seeking and substance sensitivity. Bipolar Disord. 2007;9(3):213-220.
13. Brunette MF, Noordsy DL, Xie H, et al. Benzodiazepine use and abuse among patients with severe mental illness and co-occurring substance use disorders. Psychiatr Serv. 2003;54(10):1395-1401.
14. Clark RE, Xie H, Brunette MF, et al. Benzodiazepine prescription practices and substance abuse in persons with severe mental illness. J Clin Psychiatry. 2004;65(2):151-155.
15. Longo LP. Addiction: part I. Benzodiazepines—side effects abuse risk and alternatives. Am Fam Physician. 2000;61(7):2121-2128.
16. Ciraulo DA, Barnhill JG, Ciraulo AM, et al. Alterations in pharmacodynamics of anxiolytics in abstinent alcoholic men: subjective responses, abuse liability, and electroencephalographic effects of alprazolam, diazepam, and buspirone. J Clin Pharmacol. 1997;37(1):64-73.
17. Casher MI, Bess JD. Manual of inpatient psychiatry. Cambridge United Kingdom: Cambridge University Press; 2010.
18. Hofmann S, Smits JA. Cognitive-behavioral therapy for adult anxiety disorders: a meta-analysis of randomized placebo-controlled trials. J Clin Psychiatry. 2008;69(4):621-632.
19. Morgenthaler T, Kramer M, Alessi C, et al. Practice parameters for the psychological and behavioral treatment of insomnia: an update. An American Academy of Sleep Medicine report. Sleep. 2006;29(11):1415-1419.
20. Wilens TE. Drug therapy for adults with attention-deficit hyperactivity disorder. Drugs. 2003;63(22):2395-2411.
21. Faraone SV, Biederman J, Mick E. The age-dependent decline of attention deficit hyperactivity disorder: a meta-analysis of follow-up studies. Psychol Med. 2006;36(2):159-165.
22. Biederman J, Wilens T, Mick E, et al. Is ADHD a risk factor for psychoactive substance use disorders? Findings from a four-year prospective follow-up study. J Am Acad Child Adolesc Psychiatry. 1997;36(1):21-29.
23. Waid L, Johnson D, Anton R. Attention-deficit hyperactivity disorder and substance abuse. In: Kranzler HR Rounsaville BJ, eds. Dual diagnosis and treatment: substance abuse and comorbid medical and psychiatric disorders. vol 8. New York, NY: Marcel Dekker; 1998:393–425.
24. Wilens TE, Faraone SV, Biederman J, et al. Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics. 2003;111(1):179-185.
25. Schubiner H, Saules KK, Arfken CL, et al. Double-blind placebo-controlled trial of methylphenidate in the treatment of adult ADHD patients with comorbid cocaine dependence. Exp Clin Psychopharmacol. 2002;10(3):286-294.
26. Barkley RA, Murphy KR, Kwasnik D. Motor vehicle driving competencies and risks in teens and young adults with attention deficit hyperactivity disorder. Pediatrics. 1996;98(6 Pt 1):1089-1095.
27. Sobanski E, Sabljic D, Alm B, et al. Driving-related risks and impact of methylphenidate treatment on driving in adults with attention-deficit/hyperactivity disorder (ADHD). J Neural Transm. 2008;115(2):347-356.
28. Leonard BE, McCartan D, White J, et al. Methylphenidate: a review of its neuropharmacological, neuropsychological and adverse clinical effects. Hum Psychopharmacol. 2004;19(3):151-180.
29. Charach A, Ickowicz A, Schachar R. Stimulant treatment over five years: adherence effectiveness, and adverse effects. J Am Acad Child Adolesc Psychiatry. 2004;43(5):559-567.
30. Schatzberg AF, Nemeroff CB. The American Psychiatric Publishing textbook of psychopharmacology. 4th ed. Arlington VA: American Psychiatric Publishing, Inc; 2009.
31. Wilens TE, Adler LA, Adams J, et al. Misuse and diversion of stimulants prescribed for ADHD: a systematic review of the literature. J Am Acad Child Adolesc Psychiatry. 2008;47(1):21-31.
32. Wilens TE, Gignac M, Swezey A, et al. Characteristics of adolescents and young adults with ADHD who divert or misuse their prescribed medications. J Am Acad Child Adolesc Psychiatry. 2006;45(4):408-414.
33. Bright GM. Abuse of medications employed for the treatment of ADHD: results from a large-scale community survey. Medscape J Med. 2008;10(5):111.-
34. Biederman J, Spencer T, Wilens T. Evidence-based pharmacotherapy for attention-deficit hyperactivity disorder. Int J Neuropsychopharmacol. 2004;7(1):77-97.
35. Mann N, Bitsios P. Modafinil treatment of amphetamine abuse in adult ADHD. J Psychopharmacol. 2009;23(4):468-471.
36. Grant JE. Prudent prescribing for patients with addictions. Current Psychiatry. 2006;5(10):99-102.
37. Lingford-Hughes AR, Welch S, Nutt DJ. and the British Association for Psychopharmacology. Evidence-based guidelines for the pharmacological management of substance misuse addiction and comorbidity: recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2004;18(3):293-335.
Although benzodiazepines and stimulants have well-documented efficacy for numerous psychiatric disorders, psychiatrists hesitate to prescribe these medications to patients with substance use disorders (SUDs)—even to those with a comorbid condition that likely would respond to a benzodiazepine or stimulant—because of risk of abuse or dependence. Conventional practice typically has focused on treating active substance use first rather than using simultaneous treatments. Prejudice, fear, and misinformation can influence this decision.
We believe these cases lie on a continuum. At one extreme, ignoring a past or present SUD may lead a remitted patient toward relapse, or further delay recovery for an active user. At the other end, psychiatrists who overreact to a remote history of substance use may deprive patients of legitimate pharmacologic symptom relief. Most cases lie somewhere in the middle.
A literature review does not support the assertion that the use of these medications leads to future substance use or worsens active use, especially for stimulants. In fact, stepwise—as opposed to concurrent—treatment for both conditions actually may delay recovery and increase patients’ risk for morbidity.
We outline issues involved in these complex clinical situations, point out controversies, review relevant research data, and offer guidelines for treatment.
CASE 1 Panic disorder in sobriety
Since he was a teen, Mr. A, age 51, drank heavily, which cost him jobs and relationships. After being convicted for driving under the influence, he was court-ordered to attend a rehabilitation facility, where, as he describes it, he “finally turned [his] life around.” He followed up residential treatment with regular attendance at Alcoholics Anonymous meetings.
After 1 year of sobriety, Mr. A develops increasingly frequent episodes of intense anxiety with sweating, nausea, chest pain, and hyperventilation and is diagnosed with panic disorder. His internist prescribes alprazolam, 0.5 mg 3 times a day, which provides some symptom relief, and refers him for follow-up psychiatric care. At his first visit, Mr. A confides to his psychiatrist that he is taking much more than the prescribed dosage of alprazolam, even when he is not experiencing anxiety, and is contemplating “buying it on the street” if his dosage is not raised to “at least 3 mg 3 times a day.”
CASE 2 Anxiety in controlled psychosis
Ms. B, age 40, had her first psychotic break at age 18 and was diagnosed with schizophrenia. Since then, she has had multiple psychiatric hospitalizations, usually presenting with auditory hallucinations and a recurring delusion that the person who calls herself Ms. B’s mother is really an actress “playing” her mother. At times this delusion has led Ms. B to attack her “imposter” mother. Over several years Ms. B began to drink heavily, but recently achieved a few months of sobriety by attending dual-diagnosis groups at her local community mental health center and individual psychotherapy sessions with her case manager. Fortunately, Ms. B’s psychosis has been stabilized with risperidone long-acting injection, 25 mg every 2 weeks, which she tolerates well.
When her beloved calico cat passes away, Ms. B experiences intense anxiety. Ms. B’s friend tells her she “needs some Valium,” but her psychiatrist, case manager, and the other patients in her dual-diagnosis group are not sure this is a good idea.
Benzodiazepines
Pros. There are multiple legitimate uses of benzodiazepines in general medicine and psychiatric practice, based upon their considerable sedative/hypnotic, anxiolytic, anticonvulsant, and muscle-relaxant properties (Table 1).1
Recommendations regarding benzodiazepine use for anxious patients with a history of SUD are not clear-cut. First, it often is difficult to determine whether the patient truly has an anxiety disorder or is suffering anxiety symptoms secondary to substance use and/or withdrawal. In addition, even if a diagnosis of a separate anxiety disorder is established, psychiatrists debate how to treat such patients. Some clinicians maintain that benzodiazepines should be used only for acute detoxification, and that ongoing benzodiazepine use will lead to relapse or benzodiazepine dependence. However, in a prospective study of 545 alcohol use disorder (AUD) patients receiving benzodiazepines for anxiety disorders, Mueller et al2 found no association—at 12 months or at 12 years—between benzodiazepine use and AUD recurrence. Furthermore, there was no difference in benzodiazepine usage when comparing patients with and without an AUD.3
Table 1
Clinical uses of benzodiazepines
| Insomnia |
| Anxiety disorders (eg, generalized anxiety disorder, panic disorder, posttraumatic stress disorder, social phobia, and obsessive-compulsive disorder) |
| Side effects of other psychiatric medications (eg, akathisia with antipsychotics or tremor with lithium) |
| Alcohol or benzodiazepine withdrawal |
| Acute agitation states, either as monotherapy or as adjuncts to antipsychotics or mood stabilizers |
| Catatonia |
| Source: Reference 1 |
Cons. Although widely prescribed—and despite their efficacy in numerous conditions— both acute or long-term benzodiazepine use frequently causes adverse effects.4 Patients may develop tolerance, which can lead to escalating dosages and/or to withdrawal symptoms when patients attempt to cut back. Benzodiazepines eventually become ineffective for sleep, and continued use can cause rebound insomnia. Also, with many patients taking benzodiazepines long-term, clinicians struggle to differentiate between “real” anxiety symptoms and subtle states of withdrawal from fluctuating benzodiazepine blood levels.5
Geriatric patients who take benzodiazepines are at risk for falls and hip fractures.4 Although older dementia patients are at particular risk for cognitive problems— including frank delirium—secondary to benzodiazepine use, patients of all ages are susceptible to these medications’ deleterious neurocognitive effects.
Benzodiazepines can lead to excessive sedation, thereby impairing performance at work or school, and have been implicated as a cause of motor vehicle accidents.6 Finally, a serious drawback to benzodiazepine use is possible lethality in overdose, especially when combined with alcohol.
Benzodiazepine prescribing should not be taken lightly. Always analyze the difference between benzodiazepines’ well-documented efficacy and their adverse effect profile. This risk-benefit analysis becomes much more complex for patients with SUDs.
Special considerations. Patients at higher risk for benzodiazepine abuse include those with:
- severe alcohol dependence (ie, long-term use, drinking since a young age [“Type II”])
- intravenous drug use
- comorbid alcoholism and antisocial personality disorder.7,8
Exercise special caution when considering benzodiazepines for patients with severe psychiatric illness such as schizophrenia-spectrum disorders, bipolar disorder, or severe depression. Patients with schizophrenia have high rates of alcohol, cocaine, cannabis, and benzodiazepine abuse.9,10 Bipolar disorder patients show similar vulnerability—up to 56% of patients screen positive for substance abuse or dependence.11 Vulnerability to addiction in severely ill psychiatric patients is thought to be related to several factors, including:
- use of drugs as self-medication
- genetic predisposition
- environment/lifestyle that supports substance abuse
- neurobiologic deficits that lead to lack of inhibition of reward-seeking behaviors.11
Bipolar disorder patients in particular score high on measures of sensation seeking, which leaves them vulnerable to abusing all classes of substances.12
In a 6-year study of 203 patients with severe psychiatric illnesses and SUDs, Brunette et al13 found that these patients were 2.5 times more likely than patients with severe psychiatric illness alone to abuse prescribed benzodiazepines. In an analysis of Medicaid records, Clark et al14 found similar vulnerability in patients with major depressive disorder (MDD) and SUD. Not only did these patients show a higher rate of benzodiazepine use than patients with MDD without SUD, but the dual-diagnosis group also gravitated toward more addictive high-potency/fast-acting benzodiazepines, such as alprazolam, estazolam, or triazolam.
Case discussion/suggestions. Initially, Mr. A may seem to be an appropriate candidate for closely monitored benzodiazepine use. However, he shows a pattern of misuse, likely related to his history of severe alcohol dependence and alprazolam use. This benzodiazepine is fast-acting and has a short half-life, and thus is highly reinforcing.
Similarly, Ms. B might benefit from benzodiazepine treatment. However, her history of schizophrenia and alcohol abuse makes her a risky candidate, and alternative treatments for anxiety symptoms should be considered. If prescribed at all, a benzodiazepine should be used only short-term (eg, 1 to 2 weeks).
In general, avoid prescribing benzodiazepines to most patients who have an ongoing or past SUD.15 Consider making an exception for SUD patients with comorbid anxiety disorders, with close monitoring of their benzodiazepine use. Clonazepam, chlordiazepoxide, clorazepate, and oxazepam may be less reinforcing for SUD patients than diazepam, lorazepam, alprazolam, estazolam, or triazolam.7,16 The drawbacks of benzodiazepines, especially in the situations described above, point to the need to find alternative treatments (Table 2).17 Keep in mind nonpharmacologic options, which completely avoid the risks of medication misuse and diversion. Cognitive-behavioral therapy (CBT), for instance, has well-documented efficacy in treating insomnia and anxiety disorders.18,19
Table 2
Alternatives to benzodiazepines for anxiety and/or insomnia
| Treatment option | Comments |
|---|---|
| CBT, relaxation techniques, sleep hygiene counseling | Many advantages to nonpharmacologic interventions (eg, fewer side effects, no risk of substance dependence) |
| Antihistamines (eg, diphenhydramine, 25 to 50 mg at bedtime* for sleep, or 2 to 3 times a day for anxiety) | Can be used for anxiety or insomnia; can cause confusion in older patients |
| Atypical antipsychotics | Off-label use; many agents in this class have metabolic side effects |
| SSRIs/SNRIs | First-line for many anxiety disorders, including panic disorder, GAD; possible weight gain and sexual side effects |
| Mirtazapine (7.5 to 30 mg at bedtime*) | Sedation side effect helps with sleep; weight gain and oversedation limit use |
| Trazodone (25 to 100 mg at bedtime*) | Commonly used off-label as a sleep aid |
| Monoamine oxidase inhibitors | May be useful for social phobia; dietary restrictions and side effects limit use |
| Doxepin (3 to 6 mg at bedtime) | Minimal anticholinergic and alpha-blockade side effects at this dose; FDA-approved for insomnia |
| Gabapentin (300 to 2,000 mg/d* in divided doses) | Off-label use, mild anxiolytic and sedative properties, relatively weight neutral |
| Beta blockers (eg, propranolol, 20 to 80 mg twice a day*) | Useful for peripheral manifestations of anxiety; may be effective for social phobias |
| Pregabalin (50 to 200 mg 3 times a day*) | Off-label use; industry-sponsored studies show comparable to SNRIs for anxiety |
| Non-benzodiazepine GABAA receptor modulators | Short-term option for primary insomnia, some abuse potential |
| Melatonin (1 to 3 mg at bedtime*) | Mild and ‘natural’ but not always an effective sleep aid |
| *Off-label approximate doses based on the authors’ clinical experience and consensus of the literature; agents listed may require slow titration and close monitoring for adverse effects CBT: cognitive-behavioral therapy; GABA: gamma-aminobutyric acid; GAD: generalized anxiety disorder; SNRI: serotoninnorepinephrine reuptake inhibitor; SSRI: selective serotonin reuptake inhibitor Source: Reference 17 | |
CASE 3 Adult ADHD and marijuana use
Mr. C, age 30, presents to a psychiatrist with ongoing complaints of inattention, fatigue, and difficulty staying organized. A self-report screen yields symptoms consistent with adult attention-deficit/hyperactivity disorder (ADHD). Mr. C’s school and job history and collateral history from his wife appear to corroborate his assertion that his symptoms have been lifelong. He later admits to regular marijuana use. After further discussion and full evaluation of his substance use, Mr. C is started on bupropion, titrated to 300 mg/d. After 2 months, despite faithful attendance at appointments and openness about his continued marijuana use, Mr. C’s symptoms remain unchanged. He asks about atomoxetine.
Stimulants
Pros. Despite many clinicians’ hesitance to prescribe controlled substances to patients with SUDs, psychostimulants should be considered in a variety of scenarios. Although nonstimulant options are available, stimulants consistently have demonstrated superior efficacy over other treatments and remain first-line agents for adult ADHD.20 Methylphenidate, mixed amphetamine salts, lisdexamfetamine, and atomoxetine are FDA-approved for adult ADHD. Both stimulant classes (methylphenidate and amphetamine-based products) are equally effective for ADHD. In addition, stimulants are used to treat narcolepsy, cognitive disorders such as traumatic brain injury, and as augmentation to antidepressants for MDD.
ADHD affects 5% to 12% of children, and >60% of patients remain symptomatic into adulthood and require continued treatment.21 In particular, problematic inattention may persist throughout adulthood. ADHD does not appear to be an independent risk factor for SUDs in children and adolescents.22 However, substance use increases sharply as ADHD patients enter late adolescence and adulthood, and eventually becomes a problem for 20% of adolescents and adults with ADHD. Conversely, 17% to 50% of patients with alcohol, cocaine, or opioid dependence have co-occurring ADHD.23
Withholding ADHD treatment based on concerns about future or increased current substance abuse is unfounded. A meta-analysis of 6 studies that included 674 medicated and 360 unmedicated patients with ADHD who were followed at least 4 years demonstrated that childhood treatment of ADHD with stimulants reduces the risk of developing alcohol and other drug disorders in adulthood.24 Regarding the effect stimulants have on active substance use, a 12-week, double-blind, randomized controlled trial of 48 cocaine-dependent adults with ADHD showed methylphenidate did not change cocaine abuse or craving, but did improve ADHD symptoms.25
Clinicians also must assess whether untreated ADHD symptoms impair patients’ work or other activities. Driving is a particular concern because ADHD is associated with risky driving habits, motor vehicle accidents, traffic violations, and driving license suspensions.26 In a study that administered cognitive tests to 27 adults with ADHD, methylphenidate treatment improved cognitive performance related to driving (eg, better visual-motor coordination under high-stress conditions, improved visual orientation, and sustained visual attention).27 It is likely this effect could be generalized to other activities where safety is important. Finally, appropriate stimulant treatment may improve participation in rehabilitative programs.
Cons. Despite their positive effects, stimulants can have adverse effects and consequences.28 In routinely prescribed dosages, methylphenidate and amphetamines can cause symptoms related to sympathetic activation, including anxiety, tics, anorexia/ weight loss, and sleep disturbance. A 5-year study of 79 school-age children prescribed methylphenidate, dextroamphetamine, or pemoline, which is no longer available in the United States, showed a significant association between adherence to stimulants and persistence of physiological (eg, headaches, insomnia, anorexia) and mood-related (eg, irritability, dysphoria) side effects.29 Stimulants’ sympathomimetic properties also can lead to dangerous drug-drug interactions with monoamine oxidase inhibitors. For both methylphenidate and amphetamines, overdose can lead to seizures, cardiac toxicity, dysrhythmias, and hyperthermia. All stimulants carry an FDA “black-box” warning that lists increased risk of cardiac complications, sudden death, and psychiatric complications such as psychosis or mania.30
Special considerations. All stimulants have potential for diversion or abuse. Pay close attention to these issues, especially in vulnerable populations and situations where rates of abuse and diversion are elevated. Among college students, white patients, fraternity/sorority members, and individuals with lower grade point averages may be at higher risk for nonmedical stimulant use.31 Adults who misuse or divert stimulants commonly have a history of substance abuse and conduct disorder.32 Short-acting stimulants are abused 4 times more often than extended-release preparations.33
If your ADHD patient has active substance use, be clear that continued substance use is likely to limit stimulants’ effectiveness. In patients who are actively using substances, it will be difficult to disentangle apparent nonresponse to stimulants from the negative cognitive effects of substance use.
Case discussion/suggestions. As Mr. C’s case illustrates, there are alternatives to stimulants for ADHD. For example, atomoxetine, a selective norepinephrine reuptake inhibitor, may be considered a first-line agent in patients with mostly inattentive ADHD symptoms and comorbid stimulant abuse, or for those in whom stimulants cause adverse effects such as mood lability or tics.34 Other alternatives to stimulants are listed in Table 3.35
Because Mr. C did not respond to bupropion, which presumably was tried first because of his ongoing substance use, he asked about atomoxetine. This agent is not addictive and there is no evidence that it leads to or exacerbates substance use. Depending on Mr. C’s symptom profile, atomoxetine might be a good choice. Continued monitoring of his marijuana use and frequent assessment of his motivation to quit are necessary. Psychoeducation about the cognitive effects of marijuana, including inattention and poor concentration, is important.
If Mr. C does not respond to atomoxetine, his psychiatrist will face a difficult decision. Setting Mr. C’s marijuana use aside, symptoms that do not respond to atomoxetine or a second-line agent are likely to respond to a stimulant. However, several issues must be addressed. If Mr. C’s motivation to stop using marijuana is low, how motivated is he to improve his ADHD symptoms? Next, would marijuana’s depressive/blunting effects counteract the anticipated benefit of a stimulant? Also, what is the risk that Mr. C might sell or exchange his stimulants to obtain marijuana? Assessing these complicated questions is key. Another important factor in Mr. C’s case is his wife’s involvement. Does she monitor his marijuana use? Would she be willing to supervise Mr. C’s stimulant use, and would he allow it?
Past or present SUDs are not an absolute contraindication to stimulant use. You should affirm the diagnosis and identify target symptoms. Consider nonstimulant alternatives if appropriate.
Table 3
Alternatives to stimulants for ADHD
| Treatment option | Comments |
|---|---|
| Atomoxetine | Effectiveness may be limited to inattentive type |
| Modafinil | Well-tolerated but expensive, limited evidence, no FDA indication; may be a consideration in ADHD + SUD |
| α2-adrenergic agonist (eg, clonidine or guanfacine) | Useful when hyperactivity/impulsivity symptoms predominate, or when stimulant-induced insomnia occurs |
| Bupropion | Some evidence of mild efficacy, especially useful if nicotine dependence also is a target for treatment |
| Psychotherapy | Can be useful as adjunctive treatment, but as monotherapy it is of little benefit in ADHD |
| ADHD: attention-deficit/hyperactivity disorder; SUD: substance abuse disorder Source: Reference 35 | |
Legal liabilities
Being aware of the medicolegal issues of benzodiazepine and/or stimulant prescribing is crucial because a court may find a psychiatrist liable for negative outcomes (eg, suicide) when controlled substances are prescribed to a patient with a history of addiction.36 The most prudent course is to weigh the pros and cons for each patient individually, taking into consideration the factors described above.8 This is consistent with guidelines from the American Psychiatric Association and the British Association for Psychopharmacology,37 both of which call for extreme caution in these cases.
Educate patients and caregivers about the risks of taking a controlled substance, including misuse, diversion, and theft. Provide and document explicit instructions that the patient will receive stimulants from only a single provider. Remind patients that state and federal authorities closely track controlled medications. Finally, a “stimulant contract” or “benzodiazepine contract,” similar to a pain or narcotic contact, may be useful to formally document discussions about appropriate medication use.
Related Resources
- National Institute on Drug Abuse. Prescription drugs: abuse and addiction. Research Report Series, 2005. http://drugabuse.gov/ResearchReports/Prescription/Prescription.html.
- Galanter M, Kleber HD. The American Psychiatric Publishing textbook of substance abuse treatment. 4th ed. Arlington, VA: American Psychiatric Publishing, Inc; 2008.
Drug Brand Names
- Alprazolam • Xanax
- Atomoxetine • Strattera
- Bupropion • Wellbutrin, others
- Chlordiazepoxide • Librium
- Clonazepam • Klonopin
- Clonidine • Catapres
- Clorazepate • Tranxene
- Dextroamphetamine • Dexedrine
- Diazepam • Valium
- Diphenhydramine • Benadryl, others
- Doxepin • Silenor
- Estazolam • ProSom
- Gabapentin • Neurontin
- Guanfacine • Tenex, Intuniv
- Lisdexamfetamine • Vyvanse
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Methylphenidate • Ritalin, Concerta, others
- Mirtazapine • Remeron
- Mixed amphetamine salts • Adderall
- Modafinil • Provigil
- Oxazepam • Serax
- Pemoline • Cylert
- Propranolol • Inderal
- Trazodone • Desyrel, Oleptro
- Triazolam • Halcion
Disclosures
Dr. Casher is a speaker for AstraZeneca and Pfizer Inc.
Drs. Gih and Bess report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Although benzodiazepines and stimulants have well-documented efficacy for numerous psychiatric disorders, psychiatrists hesitate to prescribe these medications to patients with substance use disorders (SUDs)—even to those with a comorbid condition that likely would respond to a benzodiazepine or stimulant—because of risk of abuse or dependence. Conventional practice typically has focused on treating active substance use first rather than using simultaneous treatments. Prejudice, fear, and misinformation can influence this decision.
We believe these cases lie on a continuum. At one extreme, ignoring a past or present SUD may lead a remitted patient toward relapse, or further delay recovery for an active user. At the other end, psychiatrists who overreact to a remote history of substance use may deprive patients of legitimate pharmacologic symptom relief. Most cases lie somewhere in the middle.
A literature review does not support the assertion that the use of these medications leads to future substance use or worsens active use, especially for stimulants. In fact, stepwise—as opposed to concurrent—treatment for both conditions actually may delay recovery and increase patients’ risk for morbidity.
We outline issues involved in these complex clinical situations, point out controversies, review relevant research data, and offer guidelines for treatment.
CASE 1 Panic disorder in sobriety
Since he was a teen, Mr. A, age 51, drank heavily, which cost him jobs and relationships. After being convicted for driving under the influence, he was court-ordered to attend a rehabilitation facility, where, as he describes it, he “finally turned [his] life around.” He followed up residential treatment with regular attendance at Alcoholics Anonymous meetings.
After 1 year of sobriety, Mr. A develops increasingly frequent episodes of intense anxiety with sweating, nausea, chest pain, and hyperventilation and is diagnosed with panic disorder. His internist prescribes alprazolam, 0.5 mg 3 times a day, which provides some symptom relief, and refers him for follow-up psychiatric care. At his first visit, Mr. A confides to his psychiatrist that he is taking much more than the prescribed dosage of alprazolam, even when he is not experiencing anxiety, and is contemplating “buying it on the street” if his dosage is not raised to “at least 3 mg 3 times a day.”
CASE 2 Anxiety in controlled psychosis
Ms. B, age 40, had her first psychotic break at age 18 and was diagnosed with schizophrenia. Since then, she has had multiple psychiatric hospitalizations, usually presenting with auditory hallucinations and a recurring delusion that the person who calls herself Ms. B’s mother is really an actress “playing” her mother. At times this delusion has led Ms. B to attack her “imposter” mother. Over several years Ms. B began to drink heavily, but recently achieved a few months of sobriety by attending dual-diagnosis groups at her local community mental health center and individual psychotherapy sessions with her case manager. Fortunately, Ms. B’s psychosis has been stabilized with risperidone long-acting injection, 25 mg every 2 weeks, which she tolerates well.
When her beloved calico cat passes away, Ms. B experiences intense anxiety. Ms. B’s friend tells her she “needs some Valium,” but her psychiatrist, case manager, and the other patients in her dual-diagnosis group are not sure this is a good idea.
Benzodiazepines
Pros. There are multiple legitimate uses of benzodiazepines in general medicine and psychiatric practice, based upon their considerable sedative/hypnotic, anxiolytic, anticonvulsant, and muscle-relaxant properties (Table 1).1
Recommendations regarding benzodiazepine use for anxious patients with a history of SUD are not clear-cut. First, it often is difficult to determine whether the patient truly has an anxiety disorder or is suffering anxiety symptoms secondary to substance use and/or withdrawal. In addition, even if a diagnosis of a separate anxiety disorder is established, psychiatrists debate how to treat such patients. Some clinicians maintain that benzodiazepines should be used only for acute detoxification, and that ongoing benzodiazepine use will lead to relapse or benzodiazepine dependence. However, in a prospective study of 545 alcohol use disorder (AUD) patients receiving benzodiazepines for anxiety disorders, Mueller et al2 found no association—at 12 months or at 12 years—between benzodiazepine use and AUD recurrence. Furthermore, there was no difference in benzodiazepine usage when comparing patients with and without an AUD.3
Table 1
Clinical uses of benzodiazepines
| Insomnia |
| Anxiety disorders (eg, generalized anxiety disorder, panic disorder, posttraumatic stress disorder, social phobia, and obsessive-compulsive disorder) |
| Side effects of other psychiatric medications (eg, akathisia with antipsychotics or tremor with lithium) |
| Alcohol or benzodiazepine withdrawal |
| Acute agitation states, either as monotherapy or as adjuncts to antipsychotics or mood stabilizers |
| Catatonia |
| Source: Reference 1 |
Cons. Although widely prescribed—and despite their efficacy in numerous conditions— both acute or long-term benzodiazepine use frequently causes adverse effects.4 Patients may develop tolerance, which can lead to escalating dosages and/or to withdrawal symptoms when patients attempt to cut back. Benzodiazepines eventually become ineffective for sleep, and continued use can cause rebound insomnia. Also, with many patients taking benzodiazepines long-term, clinicians struggle to differentiate between “real” anxiety symptoms and subtle states of withdrawal from fluctuating benzodiazepine blood levels.5
Geriatric patients who take benzodiazepines are at risk for falls and hip fractures.4 Although older dementia patients are at particular risk for cognitive problems— including frank delirium—secondary to benzodiazepine use, patients of all ages are susceptible to these medications’ deleterious neurocognitive effects.
Benzodiazepines can lead to excessive sedation, thereby impairing performance at work or school, and have been implicated as a cause of motor vehicle accidents.6 Finally, a serious drawback to benzodiazepine use is possible lethality in overdose, especially when combined with alcohol.
Benzodiazepine prescribing should not be taken lightly. Always analyze the difference between benzodiazepines’ well-documented efficacy and their adverse effect profile. This risk-benefit analysis becomes much more complex for patients with SUDs.
Special considerations. Patients at higher risk for benzodiazepine abuse include those with:
- severe alcohol dependence (ie, long-term use, drinking since a young age [“Type II”])
- intravenous drug use
- comorbid alcoholism and antisocial personality disorder.7,8
Exercise special caution when considering benzodiazepines for patients with severe psychiatric illness such as schizophrenia-spectrum disorders, bipolar disorder, or severe depression. Patients with schizophrenia have high rates of alcohol, cocaine, cannabis, and benzodiazepine abuse.9,10 Bipolar disorder patients show similar vulnerability—up to 56% of patients screen positive for substance abuse or dependence.11 Vulnerability to addiction in severely ill psychiatric patients is thought to be related to several factors, including:
- use of drugs as self-medication
- genetic predisposition
- environment/lifestyle that supports substance abuse
- neurobiologic deficits that lead to lack of inhibition of reward-seeking behaviors.11
Bipolar disorder patients in particular score high on measures of sensation seeking, which leaves them vulnerable to abusing all classes of substances.12
In a 6-year study of 203 patients with severe psychiatric illnesses and SUDs, Brunette et al13 found that these patients were 2.5 times more likely than patients with severe psychiatric illness alone to abuse prescribed benzodiazepines. In an analysis of Medicaid records, Clark et al14 found similar vulnerability in patients with major depressive disorder (MDD) and SUD. Not only did these patients show a higher rate of benzodiazepine use than patients with MDD without SUD, but the dual-diagnosis group also gravitated toward more addictive high-potency/fast-acting benzodiazepines, such as alprazolam, estazolam, or triazolam.
Case discussion/suggestions. Initially, Mr. A may seem to be an appropriate candidate for closely monitored benzodiazepine use. However, he shows a pattern of misuse, likely related to his history of severe alcohol dependence and alprazolam use. This benzodiazepine is fast-acting and has a short half-life, and thus is highly reinforcing.
Similarly, Ms. B might benefit from benzodiazepine treatment. However, her history of schizophrenia and alcohol abuse makes her a risky candidate, and alternative treatments for anxiety symptoms should be considered. If prescribed at all, a benzodiazepine should be used only short-term (eg, 1 to 2 weeks).
In general, avoid prescribing benzodiazepines to most patients who have an ongoing or past SUD.15 Consider making an exception for SUD patients with comorbid anxiety disorders, with close monitoring of their benzodiazepine use. Clonazepam, chlordiazepoxide, clorazepate, and oxazepam may be less reinforcing for SUD patients than diazepam, lorazepam, alprazolam, estazolam, or triazolam.7,16 The drawbacks of benzodiazepines, especially in the situations described above, point to the need to find alternative treatments (Table 2).17 Keep in mind nonpharmacologic options, which completely avoid the risks of medication misuse and diversion. Cognitive-behavioral therapy (CBT), for instance, has well-documented efficacy in treating insomnia and anxiety disorders.18,19
Table 2
Alternatives to benzodiazepines for anxiety and/or insomnia
| Treatment option | Comments |
|---|---|
| CBT, relaxation techniques, sleep hygiene counseling | Many advantages to nonpharmacologic interventions (eg, fewer side effects, no risk of substance dependence) |
| Antihistamines (eg, diphenhydramine, 25 to 50 mg at bedtime* for sleep, or 2 to 3 times a day for anxiety) | Can be used for anxiety or insomnia; can cause confusion in older patients |
| Atypical antipsychotics | Off-label use; many agents in this class have metabolic side effects |
| SSRIs/SNRIs | First-line for many anxiety disorders, including panic disorder, GAD; possible weight gain and sexual side effects |
| Mirtazapine (7.5 to 30 mg at bedtime*) | Sedation side effect helps with sleep; weight gain and oversedation limit use |
| Trazodone (25 to 100 mg at bedtime*) | Commonly used off-label as a sleep aid |
| Monoamine oxidase inhibitors | May be useful for social phobia; dietary restrictions and side effects limit use |
| Doxepin (3 to 6 mg at bedtime) | Minimal anticholinergic and alpha-blockade side effects at this dose; FDA-approved for insomnia |
| Gabapentin (300 to 2,000 mg/d* in divided doses) | Off-label use, mild anxiolytic and sedative properties, relatively weight neutral |
| Beta blockers (eg, propranolol, 20 to 80 mg twice a day*) | Useful for peripheral manifestations of anxiety; may be effective for social phobias |
| Pregabalin (50 to 200 mg 3 times a day*) | Off-label use; industry-sponsored studies show comparable to SNRIs for anxiety |
| Non-benzodiazepine GABAA receptor modulators | Short-term option for primary insomnia, some abuse potential |
| Melatonin (1 to 3 mg at bedtime*) | Mild and ‘natural’ but not always an effective sleep aid |
| *Off-label approximate doses based on the authors’ clinical experience and consensus of the literature; agents listed may require slow titration and close monitoring for adverse effects CBT: cognitive-behavioral therapy; GABA: gamma-aminobutyric acid; GAD: generalized anxiety disorder; SNRI: serotoninnorepinephrine reuptake inhibitor; SSRI: selective serotonin reuptake inhibitor Source: Reference 17 | |
CASE 3 Adult ADHD and marijuana use
Mr. C, age 30, presents to a psychiatrist with ongoing complaints of inattention, fatigue, and difficulty staying organized. A self-report screen yields symptoms consistent with adult attention-deficit/hyperactivity disorder (ADHD). Mr. C’s school and job history and collateral history from his wife appear to corroborate his assertion that his symptoms have been lifelong. He later admits to regular marijuana use. After further discussion and full evaluation of his substance use, Mr. C is started on bupropion, titrated to 300 mg/d. After 2 months, despite faithful attendance at appointments and openness about his continued marijuana use, Mr. C’s symptoms remain unchanged. He asks about atomoxetine.
Stimulants
Pros. Despite many clinicians’ hesitance to prescribe controlled substances to patients with SUDs, psychostimulants should be considered in a variety of scenarios. Although nonstimulant options are available, stimulants consistently have demonstrated superior efficacy over other treatments and remain first-line agents for adult ADHD.20 Methylphenidate, mixed amphetamine salts, lisdexamfetamine, and atomoxetine are FDA-approved for adult ADHD. Both stimulant classes (methylphenidate and amphetamine-based products) are equally effective for ADHD. In addition, stimulants are used to treat narcolepsy, cognitive disorders such as traumatic brain injury, and as augmentation to antidepressants for MDD.
ADHD affects 5% to 12% of children, and >60% of patients remain symptomatic into adulthood and require continued treatment.21 In particular, problematic inattention may persist throughout adulthood. ADHD does not appear to be an independent risk factor for SUDs in children and adolescents.22 However, substance use increases sharply as ADHD patients enter late adolescence and adulthood, and eventually becomes a problem for 20% of adolescents and adults with ADHD. Conversely, 17% to 50% of patients with alcohol, cocaine, or opioid dependence have co-occurring ADHD.23
Withholding ADHD treatment based on concerns about future or increased current substance abuse is unfounded. A meta-analysis of 6 studies that included 674 medicated and 360 unmedicated patients with ADHD who were followed at least 4 years demonstrated that childhood treatment of ADHD with stimulants reduces the risk of developing alcohol and other drug disorders in adulthood.24 Regarding the effect stimulants have on active substance use, a 12-week, double-blind, randomized controlled trial of 48 cocaine-dependent adults with ADHD showed methylphenidate did not change cocaine abuse or craving, but did improve ADHD symptoms.25
Clinicians also must assess whether untreated ADHD symptoms impair patients’ work or other activities. Driving is a particular concern because ADHD is associated with risky driving habits, motor vehicle accidents, traffic violations, and driving license suspensions.26 In a study that administered cognitive tests to 27 adults with ADHD, methylphenidate treatment improved cognitive performance related to driving (eg, better visual-motor coordination under high-stress conditions, improved visual orientation, and sustained visual attention).27 It is likely this effect could be generalized to other activities where safety is important. Finally, appropriate stimulant treatment may improve participation in rehabilitative programs.
Cons. Despite their positive effects, stimulants can have adverse effects and consequences.28 In routinely prescribed dosages, methylphenidate and amphetamines can cause symptoms related to sympathetic activation, including anxiety, tics, anorexia/ weight loss, and sleep disturbance. A 5-year study of 79 school-age children prescribed methylphenidate, dextroamphetamine, or pemoline, which is no longer available in the United States, showed a significant association between adherence to stimulants and persistence of physiological (eg, headaches, insomnia, anorexia) and mood-related (eg, irritability, dysphoria) side effects.29 Stimulants’ sympathomimetic properties also can lead to dangerous drug-drug interactions with monoamine oxidase inhibitors. For both methylphenidate and amphetamines, overdose can lead to seizures, cardiac toxicity, dysrhythmias, and hyperthermia. All stimulants carry an FDA “black-box” warning that lists increased risk of cardiac complications, sudden death, and psychiatric complications such as psychosis or mania.30
Special considerations. All stimulants have potential for diversion or abuse. Pay close attention to these issues, especially in vulnerable populations and situations where rates of abuse and diversion are elevated. Among college students, white patients, fraternity/sorority members, and individuals with lower grade point averages may be at higher risk for nonmedical stimulant use.31 Adults who misuse or divert stimulants commonly have a history of substance abuse and conduct disorder.32 Short-acting stimulants are abused 4 times more often than extended-release preparations.33
If your ADHD patient has active substance use, be clear that continued substance use is likely to limit stimulants’ effectiveness. In patients who are actively using substances, it will be difficult to disentangle apparent nonresponse to stimulants from the negative cognitive effects of substance use.
Case discussion/suggestions. As Mr. C’s case illustrates, there are alternatives to stimulants for ADHD. For example, atomoxetine, a selective norepinephrine reuptake inhibitor, may be considered a first-line agent in patients with mostly inattentive ADHD symptoms and comorbid stimulant abuse, or for those in whom stimulants cause adverse effects such as mood lability or tics.34 Other alternatives to stimulants are listed in Table 3.35
Because Mr. C did not respond to bupropion, which presumably was tried first because of his ongoing substance use, he asked about atomoxetine. This agent is not addictive and there is no evidence that it leads to or exacerbates substance use. Depending on Mr. C’s symptom profile, atomoxetine might be a good choice. Continued monitoring of his marijuana use and frequent assessment of his motivation to quit are necessary. Psychoeducation about the cognitive effects of marijuana, including inattention and poor concentration, is important.
If Mr. C does not respond to atomoxetine, his psychiatrist will face a difficult decision. Setting Mr. C’s marijuana use aside, symptoms that do not respond to atomoxetine or a second-line agent are likely to respond to a stimulant. However, several issues must be addressed. If Mr. C’s motivation to stop using marijuana is low, how motivated is he to improve his ADHD symptoms? Next, would marijuana’s depressive/blunting effects counteract the anticipated benefit of a stimulant? Also, what is the risk that Mr. C might sell or exchange his stimulants to obtain marijuana? Assessing these complicated questions is key. Another important factor in Mr. C’s case is his wife’s involvement. Does she monitor his marijuana use? Would she be willing to supervise Mr. C’s stimulant use, and would he allow it?
Past or present SUDs are not an absolute contraindication to stimulant use. You should affirm the diagnosis and identify target symptoms. Consider nonstimulant alternatives if appropriate.
Table 3
Alternatives to stimulants for ADHD
| Treatment option | Comments |
|---|---|
| Atomoxetine | Effectiveness may be limited to inattentive type |
| Modafinil | Well-tolerated but expensive, limited evidence, no FDA indication; may be a consideration in ADHD + SUD |
| α2-adrenergic agonist (eg, clonidine or guanfacine) | Useful when hyperactivity/impulsivity symptoms predominate, or when stimulant-induced insomnia occurs |
| Bupropion | Some evidence of mild efficacy, especially useful if nicotine dependence also is a target for treatment |
| Psychotherapy | Can be useful as adjunctive treatment, but as monotherapy it is of little benefit in ADHD |
| ADHD: attention-deficit/hyperactivity disorder; SUD: substance abuse disorder Source: Reference 35 | |
Legal liabilities
Being aware of the medicolegal issues of benzodiazepine and/or stimulant prescribing is crucial because a court may find a psychiatrist liable for negative outcomes (eg, suicide) when controlled substances are prescribed to a patient with a history of addiction.36 The most prudent course is to weigh the pros and cons for each patient individually, taking into consideration the factors described above.8 This is consistent with guidelines from the American Psychiatric Association and the British Association for Psychopharmacology,37 both of which call for extreme caution in these cases.
Educate patients and caregivers about the risks of taking a controlled substance, including misuse, diversion, and theft. Provide and document explicit instructions that the patient will receive stimulants from only a single provider. Remind patients that state and federal authorities closely track controlled medications. Finally, a “stimulant contract” or “benzodiazepine contract,” similar to a pain or narcotic contact, may be useful to formally document discussions about appropriate medication use.
Related Resources
- National Institute on Drug Abuse. Prescription drugs: abuse and addiction. Research Report Series, 2005. http://drugabuse.gov/ResearchReports/Prescription/Prescription.html.
- Galanter M, Kleber HD. The American Psychiatric Publishing textbook of substance abuse treatment. 4th ed. Arlington, VA: American Psychiatric Publishing, Inc; 2008.
Drug Brand Names
- Alprazolam • Xanax
- Atomoxetine • Strattera
- Bupropion • Wellbutrin, others
- Chlordiazepoxide • Librium
- Clonazepam • Klonopin
- Clonidine • Catapres
- Clorazepate • Tranxene
- Dextroamphetamine • Dexedrine
- Diazepam • Valium
- Diphenhydramine • Benadryl, others
- Doxepin • Silenor
- Estazolam • ProSom
- Gabapentin • Neurontin
- Guanfacine • Tenex, Intuniv
- Lisdexamfetamine • Vyvanse
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Methylphenidate • Ritalin, Concerta, others
- Mirtazapine • Remeron
- Mixed amphetamine salts • Adderall
- Modafinil • Provigil
- Oxazepam • Serax
- Pemoline • Cylert
- Propranolol • Inderal
- Trazodone • Desyrel, Oleptro
- Triazolam • Halcion
Disclosures
Dr. Casher is a speaker for AstraZeneca and Pfizer Inc.
Drs. Gih and Bess report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Ashton H. Guidelines for the rational use of benzodiazepines. When and what to use. Drugs. 1994;48(1):25.-
2. Mueller TI, Pagano ME, Rodriguez BF, et al. Long-term use of benzodiazepines in participants with comorbid anxiety and alcohol use disorders. Alcohol Clin Exp Res. 2005;29(8):1411-1418.
3. Mueller TI, Goldenberg IM, Gordon AL, et al. Benzodiazepine use in anxiety disordered patients with and without a history of alcoholism. J Clin Psychiatry. 1996;57(2):83-89.
4. Ashton H. The diagnosis and management of benzodiazepine dependence. Curr Opin Psychiatry. 2005;(18):249-255.
5. Back SE, Brady KT. Anxiety disorders with comorbid substance use disorders: diagnostic and treatment considerations. Psychiatric Annals. 2008;38(11):724-729.
6. Walsh JM, Flegel R, Cangianelli LA, et al. Epidemiology of alcohol and other drug use among motor vehicle crash victims admitted to a trauma center. Traffic Inj Prev. 2004;5(3):254-260.
7. Ciraulo DA, Nace EP. Benzodiazepine treatment of anxiety or insomnia in substance abuse patients. Am J Addict. 2000;9(4):276-279;discussion 280–284.
8. Sattar S, Bhatia S. Benzodiazepines for substance abusers. Current Psychiatry. 2003;2(5):25-34.
9. Regier DA, Farmer ME, Rae DS, et al. Comorbidity of mental disorders with alcohol and other drug abuse. Results from the Epidemiologic Catchment Area (ECA) Study. JAMA. 1990;264(19):2511-2518.
10. Kendler KS, Gallagher TJ, Abelson JM, et al. Lifetime prevalence, demographic risk factors, and diagnostic validity of nonaffective psychosis as assessed in a US community sample. The National Comorbidity Survey. Arch Gen Psychiatry. 1996;53(11):1022-1031
11. Buckley PF. Prevalence and consequences of the dual diagnosis of substance abuse and severe mental illness. J Clin Psychiatry. 2006;67(suppl 7):5-9.
12. Bizzarri JV, Sbrana A, Rucci P, et al. The spectrum of substance abuse in bipolar disorder: reasons for use, sensation seeking and substance sensitivity. Bipolar Disord. 2007;9(3):213-220.
13. Brunette MF, Noordsy DL, Xie H, et al. Benzodiazepine use and abuse among patients with severe mental illness and co-occurring substance use disorders. Psychiatr Serv. 2003;54(10):1395-1401.
14. Clark RE, Xie H, Brunette MF, et al. Benzodiazepine prescription practices and substance abuse in persons with severe mental illness. J Clin Psychiatry. 2004;65(2):151-155.
15. Longo LP. Addiction: part I. Benzodiazepines—side effects abuse risk and alternatives. Am Fam Physician. 2000;61(7):2121-2128.
16. Ciraulo DA, Barnhill JG, Ciraulo AM, et al. Alterations in pharmacodynamics of anxiolytics in abstinent alcoholic men: subjective responses, abuse liability, and electroencephalographic effects of alprazolam, diazepam, and buspirone. J Clin Pharmacol. 1997;37(1):64-73.
17. Casher MI, Bess JD. Manual of inpatient psychiatry. Cambridge United Kingdom: Cambridge University Press; 2010.
18. Hofmann S, Smits JA. Cognitive-behavioral therapy for adult anxiety disorders: a meta-analysis of randomized placebo-controlled trials. J Clin Psychiatry. 2008;69(4):621-632.
19. Morgenthaler T, Kramer M, Alessi C, et al. Practice parameters for the psychological and behavioral treatment of insomnia: an update. An American Academy of Sleep Medicine report. Sleep. 2006;29(11):1415-1419.
20. Wilens TE. Drug therapy for adults with attention-deficit hyperactivity disorder. Drugs. 2003;63(22):2395-2411.
21. Faraone SV, Biederman J, Mick E. The age-dependent decline of attention deficit hyperactivity disorder: a meta-analysis of follow-up studies. Psychol Med. 2006;36(2):159-165.
22. Biederman J, Wilens T, Mick E, et al. Is ADHD a risk factor for psychoactive substance use disorders? Findings from a four-year prospective follow-up study. J Am Acad Child Adolesc Psychiatry. 1997;36(1):21-29.
23. Waid L, Johnson D, Anton R. Attention-deficit hyperactivity disorder and substance abuse. In: Kranzler HR Rounsaville BJ, eds. Dual diagnosis and treatment: substance abuse and comorbid medical and psychiatric disorders. vol 8. New York, NY: Marcel Dekker; 1998:393–425.
24. Wilens TE, Faraone SV, Biederman J, et al. Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics. 2003;111(1):179-185.
25. Schubiner H, Saules KK, Arfken CL, et al. Double-blind placebo-controlled trial of methylphenidate in the treatment of adult ADHD patients with comorbid cocaine dependence. Exp Clin Psychopharmacol. 2002;10(3):286-294.
26. Barkley RA, Murphy KR, Kwasnik D. Motor vehicle driving competencies and risks in teens and young adults with attention deficit hyperactivity disorder. Pediatrics. 1996;98(6 Pt 1):1089-1095.
27. Sobanski E, Sabljic D, Alm B, et al. Driving-related risks and impact of methylphenidate treatment on driving in adults with attention-deficit/hyperactivity disorder (ADHD). J Neural Transm. 2008;115(2):347-356.
28. Leonard BE, McCartan D, White J, et al. Methylphenidate: a review of its neuropharmacological, neuropsychological and adverse clinical effects. Hum Psychopharmacol. 2004;19(3):151-180.
29. Charach A, Ickowicz A, Schachar R. Stimulant treatment over five years: adherence effectiveness, and adverse effects. J Am Acad Child Adolesc Psychiatry. 2004;43(5):559-567.
30. Schatzberg AF, Nemeroff CB. The American Psychiatric Publishing textbook of psychopharmacology. 4th ed. Arlington VA: American Psychiatric Publishing, Inc; 2009.
31. Wilens TE, Adler LA, Adams J, et al. Misuse and diversion of stimulants prescribed for ADHD: a systematic review of the literature. J Am Acad Child Adolesc Psychiatry. 2008;47(1):21-31.
32. Wilens TE, Gignac M, Swezey A, et al. Characteristics of adolescents and young adults with ADHD who divert or misuse their prescribed medications. J Am Acad Child Adolesc Psychiatry. 2006;45(4):408-414.
33. Bright GM. Abuse of medications employed for the treatment of ADHD: results from a large-scale community survey. Medscape J Med. 2008;10(5):111.-
34. Biederman J, Spencer T, Wilens T. Evidence-based pharmacotherapy for attention-deficit hyperactivity disorder. Int J Neuropsychopharmacol. 2004;7(1):77-97.
35. Mann N, Bitsios P. Modafinil treatment of amphetamine abuse in adult ADHD. J Psychopharmacol. 2009;23(4):468-471.
36. Grant JE. Prudent prescribing for patients with addictions. Current Psychiatry. 2006;5(10):99-102.
37. Lingford-Hughes AR, Welch S, Nutt DJ. and the British Association for Psychopharmacology. Evidence-based guidelines for the pharmacological management of substance misuse addiction and comorbidity: recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2004;18(3):293-335.
1. Ashton H. Guidelines for the rational use of benzodiazepines. When and what to use. Drugs. 1994;48(1):25.-
2. Mueller TI, Pagano ME, Rodriguez BF, et al. Long-term use of benzodiazepines in participants with comorbid anxiety and alcohol use disorders. Alcohol Clin Exp Res. 2005;29(8):1411-1418.
3. Mueller TI, Goldenberg IM, Gordon AL, et al. Benzodiazepine use in anxiety disordered patients with and without a history of alcoholism. J Clin Psychiatry. 1996;57(2):83-89.
4. Ashton H. The diagnosis and management of benzodiazepine dependence. Curr Opin Psychiatry. 2005;(18):249-255.
5. Back SE, Brady KT. Anxiety disorders with comorbid substance use disorders: diagnostic and treatment considerations. Psychiatric Annals. 2008;38(11):724-729.
6. Walsh JM, Flegel R, Cangianelli LA, et al. Epidemiology of alcohol and other drug use among motor vehicle crash victims admitted to a trauma center. Traffic Inj Prev. 2004;5(3):254-260.
7. Ciraulo DA, Nace EP. Benzodiazepine treatment of anxiety or insomnia in substance abuse patients. Am J Addict. 2000;9(4):276-279;discussion 280–284.
8. Sattar S, Bhatia S. Benzodiazepines for substance abusers. Current Psychiatry. 2003;2(5):25-34.
9. Regier DA, Farmer ME, Rae DS, et al. Comorbidity of mental disorders with alcohol and other drug abuse. Results from the Epidemiologic Catchment Area (ECA) Study. JAMA. 1990;264(19):2511-2518.
10. Kendler KS, Gallagher TJ, Abelson JM, et al. Lifetime prevalence, demographic risk factors, and diagnostic validity of nonaffective psychosis as assessed in a US community sample. The National Comorbidity Survey. Arch Gen Psychiatry. 1996;53(11):1022-1031
11. Buckley PF. Prevalence and consequences of the dual diagnosis of substance abuse and severe mental illness. J Clin Psychiatry. 2006;67(suppl 7):5-9.
12. Bizzarri JV, Sbrana A, Rucci P, et al. The spectrum of substance abuse in bipolar disorder: reasons for use, sensation seeking and substance sensitivity. Bipolar Disord. 2007;9(3):213-220.
13. Brunette MF, Noordsy DL, Xie H, et al. Benzodiazepine use and abuse among patients with severe mental illness and co-occurring substance use disorders. Psychiatr Serv. 2003;54(10):1395-1401.
14. Clark RE, Xie H, Brunette MF, et al. Benzodiazepine prescription practices and substance abuse in persons with severe mental illness. J Clin Psychiatry. 2004;65(2):151-155.
15. Longo LP. Addiction: part I. Benzodiazepines—side effects abuse risk and alternatives. Am Fam Physician. 2000;61(7):2121-2128.
16. Ciraulo DA, Barnhill JG, Ciraulo AM, et al. Alterations in pharmacodynamics of anxiolytics in abstinent alcoholic men: subjective responses, abuse liability, and electroencephalographic effects of alprazolam, diazepam, and buspirone. J Clin Pharmacol. 1997;37(1):64-73.
17. Casher MI, Bess JD. Manual of inpatient psychiatry. Cambridge United Kingdom: Cambridge University Press; 2010.
18. Hofmann S, Smits JA. Cognitive-behavioral therapy for adult anxiety disorders: a meta-analysis of randomized placebo-controlled trials. J Clin Psychiatry. 2008;69(4):621-632.
19. Morgenthaler T, Kramer M, Alessi C, et al. Practice parameters for the psychological and behavioral treatment of insomnia: an update. An American Academy of Sleep Medicine report. Sleep. 2006;29(11):1415-1419.
20. Wilens TE. Drug therapy for adults with attention-deficit hyperactivity disorder. Drugs. 2003;63(22):2395-2411.
21. Faraone SV, Biederman J, Mick E. The age-dependent decline of attention deficit hyperactivity disorder: a meta-analysis of follow-up studies. Psychol Med. 2006;36(2):159-165.
22. Biederman J, Wilens T, Mick E, et al. Is ADHD a risk factor for psychoactive substance use disorders? Findings from a four-year prospective follow-up study. J Am Acad Child Adolesc Psychiatry. 1997;36(1):21-29.
23. Waid L, Johnson D, Anton R. Attention-deficit hyperactivity disorder and substance abuse. In: Kranzler HR Rounsaville BJ, eds. Dual diagnosis and treatment: substance abuse and comorbid medical and psychiatric disorders. vol 8. New York, NY: Marcel Dekker; 1998:393–425.
24. Wilens TE, Faraone SV, Biederman J, et al. Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics. 2003;111(1):179-185.
25. Schubiner H, Saules KK, Arfken CL, et al. Double-blind placebo-controlled trial of methylphenidate in the treatment of adult ADHD patients with comorbid cocaine dependence. Exp Clin Psychopharmacol. 2002;10(3):286-294.
26. Barkley RA, Murphy KR, Kwasnik D. Motor vehicle driving competencies and risks in teens and young adults with attention deficit hyperactivity disorder. Pediatrics. 1996;98(6 Pt 1):1089-1095.
27. Sobanski E, Sabljic D, Alm B, et al. Driving-related risks and impact of methylphenidate treatment on driving in adults with attention-deficit/hyperactivity disorder (ADHD). J Neural Transm. 2008;115(2):347-356.
28. Leonard BE, McCartan D, White J, et al. Methylphenidate: a review of its neuropharmacological, neuropsychological and adverse clinical effects. Hum Psychopharmacol. 2004;19(3):151-180.
29. Charach A, Ickowicz A, Schachar R. Stimulant treatment over five years: adherence effectiveness, and adverse effects. J Am Acad Child Adolesc Psychiatry. 2004;43(5):559-567.
30. Schatzberg AF, Nemeroff CB. The American Psychiatric Publishing textbook of psychopharmacology. 4th ed. Arlington VA: American Psychiatric Publishing, Inc; 2009.
31. Wilens TE, Adler LA, Adams J, et al. Misuse and diversion of stimulants prescribed for ADHD: a systematic review of the literature. J Am Acad Child Adolesc Psychiatry. 2008;47(1):21-31.
32. Wilens TE, Gignac M, Swezey A, et al. Characteristics of adolescents and young adults with ADHD who divert or misuse their prescribed medications. J Am Acad Child Adolesc Psychiatry. 2006;45(4):408-414.
33. Bright GM. Abuse of medications employed for the treatment of ADHD: results from a large-scale community survey. Medscape J Med. 2008;10(5):111.-
34. Biederman J, Spencer T, Wilens T. Evidence-based pharmacotherapy for attention-deficit hyperactivity disorder. Int J Neuropsychopharmacol. 2004;7(1):77-97.
35. Mann N, Bitsios P. Modafinil treatment of amphetamine abuse in adult ADHD. J Psychopharmacol. 2009;23(4):468-471.
36. Grant JE. Prudent prescribing for patients with addictions. Current Psychiatry. 2006;5(10):99-102.
37. Lingford-Hughes AR, Welch S, Nutt DJ. and the British Association for Psychopharmacology. Evidence-based guidelines for the pharmacological management of substance misuse addiction and comorbidity: recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2004;18(3):293-335.
Emerging research on biomarkers that may help clarify diagnosis
Diabetic and depressed
CASE: Worsening depression
Mr. N, age 64, is a disabled factory worker with a complicated medical history. He has poorly controlled type II diabetes mellitus; obesity (body mass index 40 kg/m2); complicated cryptogenic cirrhosis with prior esophageal varices, portal gastropathy, splenomegaly, and no encephalopathy; surgically treated colon adenocarcinoma; and bilateral thalamic and right occipital infarcts with residual left homonymous hemianopsia and vertical gaze paresis. Mr. N sustained a perioperative stroke 18 months ago while undergoing a colectomy procedure for colon adenocarcinoma; an MRI done at that time showed the bilateral thalamic and right occipital infarcts. While in the internal medicine consultation clinic, Mr. N expresses suicidal and homicidal thoughts, which prompted the internal medicine team to refer him to the emergency department (ED). The team deems Mr. N’s medical problems stable except for diabetic dyscontrol.
In the ED, Mr. N says he feels sad, worthless, and “tired” of his complex family issues and multiple medical conditions. He says he’s had these feeling for at least a year, but his depression has worsened in the last few days. Mr. N is tearful while explaining his discouragement with following a diet for diabetes; earlier that day he ate an entire chocolate cake. He says all 3 of his children have ongoing substance abuse and relationship problems, but he is particularly focused on his youngest daughter, who is involved with a man who is addicted to drugs and physically abuses her and her children. Mr. N describes a detailed plan to shoot him and then commit suicide. This disclosure prompts the ED physician to admit Mr. N to ensure his safety and stabilize his mood.
Mr. N’s temperature is 36. 4°C (97. 5°F), blood pressure is 123/60 mm Hg, pulse is 81 beats per minute, respiratory rate is 24 breaths per minute, and oxygen saturation is 96% on ambient air. His physical exam is notable only for dysphoria and mild gynecomastia. He shows no evidence of acute cardiopulmonary, gastrointestinal, or other neurologic changes. His serum glucose is 650 mg/dL, and his recent hemoglobin A1c (HbA1c) is 10. 9%. His other laboratory tests include a hemoglobin of 11. 7 g/dL; white cell count, 3500/mm3; platelet count, 41, 000/mm3; sodium, 129 mEq/L; potassium, 5. 0 mEq/L; alkaline phosphatase, 90 U/L; aspartate aminotransferase, 23 U/L; alanine aminotransferase, 21 U/L; total bilirubin, 1. 8 mg/dL; creatinine, 1. 2 mg/dL; prothrombin time, 10. 4 sec; and arterial ammonia, <50 ?g/dL. Arterial blood gases are normal.
A year ago, his primary care physician prescribed fluoxetine, 20 mg/d, for fatigue and chronic back pain and neuropathic pain related to diabetes. We continue Mr. N’s outpatient prescription of fluoxetine, 20 mg/d, and low-dose acetaminophen as needed for pain. Furosemide, 40 mg/d, spironolactone, 100 mg/d, and propranolol sustained release, 60 mg/d, are maintained for complications of cirrhosis. Insulin aspart, 22 units with breakfast, 24 units with lunch, and 24 units with supper, also are administered routinely.
We consult with the internal medicine, ophthalmology, neurology, endocrinology, and diabetes services to assist in evaluating and managing Mr. N’s multiple medical conditions.
The authors’ observations
Depression and other forms of psychopathology may be underrecognized in geriatric patients because older adults may not report psychiatric symptoms that are secondary to physical conditions. Cognitive impairment in some older adults also may lead to underreporting of symptoms. Mr. N denies a history of depression, which we confirmed with his wife, daughter, and primary care physician. The late onset of his initial presentation prompted close investigation for a potential medical etiology (Table 1).1,2
We considered post-stroke depression because shortly after Mr. N’s stroke, his neurologist described emotional lability and frustration related to his poor vision. Depression occurs in one-third of chronic stroke survivors and is prevalent among patients referred for neurologic rehabilitation.1 Premorbid neuroticism3 and a history of mental illness are predictors of post-stroke depression. Stroke laterality is not related to risk of post-stroke depressive symptoms,3 but women have a higher risk of developing post-stroke depression.3
Table 1
When to consider medical causes of depressive symptoms
| Late onset of initial depressive presentation |
| Known underlying medical condition, such as cancer, diabetes, or stroke |
| Atypical symptoms and signs of depression, such as hypersomnia, hyperphagia, or agitation |
| Absence of personal or family history of psychiatric illnesses |
| Illicit substance use |
| Medication use (eg, opioids, reserpine, methyldopa, chemotherapy agents, steroids, and oral contraceptives) |
| Treatment resistance or unusual response to treatment |
| Sudden onset of mental symptoms (eg, sudden episode of uncontrollable crying) |
| Source: References 1,2 |
Diabetes and depression
Up to 30% of patients with type 2 diabetes mellitus report a lifetime history of major depression.2 Depression increases the risk of hyperglycemia and accompanying long-term metabolic complications.4,5 Few studies have explored the effects of poor glycemic control on depressive symptoms among diabetic patients.6-9 A literature review revealed no large-scale study investigating worsened depressive symptoms in patients with poor glycemic control.10,11
The cross-sectional difference between a single episode of major depression and adjustment disorder can be subtle. DSM-IV-TR describes the latter as a maladaptive reaction to an identifiable psychosocial stressor, or stressors, that occurs within 3 months of onset of that stressor (Table 2).12 Because we did not deem Mr. N’s depressive symptoms, which were evident only when he was hyperglycemic, to be grossly disproportionate to his stressors, we diagnose him with major depression rather than adjustment disorder.
Table 2
DSM-IV-TR diagnostic criteria for adjustment disorder
| A. The development of emotional or behavioral symptoms in response to an identifiable stressor(s) that occurs within 3 months of the onset of the stressor(s) |
B. These symptoms or behaviors are clinically significant, as evidenced by either of the following:
|
| C. The stress-related disturbance does not meet criteria for another specific axis I disorder and is not merely an exacerbation of a pre-existing axis I or axis II disorder |
| D. The symptoms do not represent bereavement |
| E. Once the stressor (or its consequences) has terminated, the symptoms do not persist for more than an additional 6 months |
Specify whether the condition is acute or chronic, as follows:
|
| Source: Reference 12 |
EVALUATION: No psychiatric history
On admission, Mr. N is overwhelmed, tearful, and dysphoric when describing his situation. He displays no evidence of psychosis, but his judgment and insight are impaired. He shows no change in consciousness or ability to stay awake. Mr. N acknowledges hypersomnolence, anhedonia, anergia, and decreased concentration and continues to express suicidal and homicidal thoughts. He repeatedly denies any personal or family psychiatric history or personal substance abuse, including alcohol and nicotine.
TREATMENT: Glycemic control
Mr. N receives 1 L of saline in the ED and is encouraged to drink more water during hospitalization. With appropriate insulin dosing, Mr. N’s serum glucose levels improve from 650 to 426 mg/dL by the next morning. On his third hospital day, Mr. N’s glucose level is 155 mg/dL in the morning. With tighter glycemic control, his dysphoria improves. He is future-oriented, markedly less dysphoric, and denies homicidal or suicidal ideation. Mr. N is interested in participating in group therapy, and his insight and judgment regarding his homicidal and suicidal thoughts improve. He still doesn’t fully understand the importance of diabetic control, and he struggles with his diet.
On the fourth hospital day, Mr. N’s glucose level rises to 325 mg/dL in the early evening. Subsequently, his mood deteriorates; he becomes increasingly withdrawn and somnolent. With appropriate attention to his dietary intake and supplemental insulin, his serum glucose improves to the 100 to 200 mg/dL range overnight, and his mood improves. When the glucose is controlled, he attends group therapy, tends to his hygiene, denies feeling hopeless, and offers several ideas about how to manage his family situation. After his glucose rises, Mr. N becomes isolative, hopeless, and unable to cope with stressors. With considerable education about the importance of glycemic control, Mr. N is hopeful and future-oriented when he is discharged after 9 days of hospitalization. At outpatient evaluation, he continues to report euthymia with adequate glycemic control.
The authors’ observations
Patients with hyperglycemia may experience symptoms secondary to volume depletion and hyperosmolality. The severity of these symptoms generally is proportional to the extent and duration of the hyperosmolar state. Initially, most patients complain of polyuria and polydipsia, but in more severe cases, mental status changes may evolve and include lethargy, twitching, cloudiness, motor or sensory defects, seizures, and coma. Some evidence shows that hyperglycemic patients with hyperosmolality are symptomatic only if hypernatremia is present.13 Mr. N was hyponatremic, which resolved with aggressive hydration and insulin administration.
Traditionally, depression has been observed to worsen glycemic control in diabetic patients; discussion of increased glucose levels leading to worsened depression rarely has been reported. In a meta-analysis, Lustman et al7 revealed that depression is significantly associated with hyperglycemia. A review by Li et al14 demonstrated that depression is much more common in patients with diabetes compared with general population and 45% of diabetes patients with depression were undiagnosed. Calhoun et al15 showed that for every 1-unit increase in HbA1c the odds of depressive symptoms increase by 22%. Researchers also found a positive relationship between depression and glycemic control in American Indians.15
Mr. N’s case is further evidence that the relationship between diabetes and depression is bidirectional and diagnosis and treatment of each illness impacts the other. Although this case does not confirm causality, it highlights the importance of aggressive approaches to screening and treatment of depression in patients with diabetes, and vice versa.
Related Resources
- Katon W, Russo J, Lin EH, et al. Depression and diabetes: factors associated with major depression at five-year follow-up. Psychosomatics. 2009; 50(6): 570-579.
- Biessels GJ, Luchsinger JA. Diabetes and the brain. New York, NY: Humana Press; 2009.
Drug Brand Names
- Fluoxetine • Prozac
- Furosemide • Lasix
- Insulin aspart • NovoLog
- Insulin glargine • Lantus
- Methyldopa • Aldomet
- Propranolol • Inderal
- Reserpine • Serpasil
- Spironolactone • Aldactone
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Srivastava A, Taly AB, Gupta A, et al. Post-stroke depression: prevalence and relationship with disability in chronic stroke survivors. Ann Indian Acad Neurol. 2010;13(2):123-127.
2. Marcus MD, Wing RR, Guare J, et al. Lifetime prevalence of major depression and its effect on treatment outcome in obese type II diabetic patients. Diabetes Care. 1992;15(2):253-255.
3. Storor DL, Byrne GJ. Pre-morbid personality and depression following stroke. Int Psychogeriatr. 2006;18(3):457-469.
4. Songar A, Kocabasoglu N, Balcioglu I, et al. The relationship between diabetics’ metabolic control levels and psychiatric symptomatology. Integrative Psychiatry. 1993;9:34-40.
5. Von Dras DD, Lichty W. Correlates of depression in diabetic adults. Behav Health Aging. 1990;1:79-84.
6. Lustman PJ, Clouse RE. Depression in diabetic patients: the relationship between mood and glycemic control. J Diabetes Complications. 2005;19(2):113-122.
7. Lustman PJ, Anderson RJ, Freedland KE, et al. Depression and poor glycemic control: a meta-analytic review of the literature. Diabetes Care. 2000;23(7):934-942.
8. Lustman PJ, Griffith LS, Clouse RE. Depression in adults with diabetes: results of a 5-yr follow-up study. Diabetes Care. 1988;11:605-612.
9. Van der Does FE, De Neeling JN, Snoek FJ, et al. Symptoms and well-being in relation to glycemic control in type II diabetes. Diabetes Care. 1996;19:204-210.
10. Genuth S. A case for blood glucose control. Adv Intern Med. 1995;40:573-623.
11. Wrigley M, Mayou R. Psychological factors and admission for poor glycaemic control: a study of psychological and social factors in poorly controlled insulin dependent diabetic patients. J Psychosom Res. 1991;35:335-343.
12. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
13. Magee MF, Bhatt BA. Management of decompensated diabetes. Diabetic ketoacidosis and hyperglycemic hyperosmolar syndrome. Crit Care Clin. 2001;17(1):75-106.
14. Li C, Ford ES, Zhao G, et al. Prevalence and correlates of undiagnosed depression among U.S. adults with diabetes: the Behavioral Risk Factor Surveillance System, 2006. Diabetes Res Clin Pract. 2009;83(2):268-279.
15. Calhoun D, Beals J, Carter EA, et al. Relationship between glycemic control and depression among American Indians in the Strong Heart Study. J Diabetes Complications. 2010;24:217-222.
CASE: Worsening depression
Mr. N, age 64, is a disabled factory worker with a complicated medical history. He has poorly controlled type II diabetes mellitus; obesity (body mass index 40 kg/m2); complicated cryptogenic cirrhosis with prior esophageal varices, portal gastropathy, splenomegaly, and no encephalopathy; surgically treated colon adenocarcinoma; and bilateral thalamic and right occipital infarcts with residual left homonymous hemianopsia and vertical gaze paresis. Mr. N sustained a perioperative stroke 18 months ago while undergoing a colectomy procedure for colon adenocarcinoma; an MRI done at that time showed the bilateral thalamic and right occipital infarcts. While in the internal medicine consultation clinic, Mr. N expresses suicidal and homicidal thoughts, which prompted the internal medicine team to refer him to the emergency department (ED). The team deems Mr. N’s medical problems stable except for diabetic dyscontrol.
In the ED, Mr. N says he feels sad, worthless, and “tired” of his complex family issues and multiple medical conditions. He says he’s had these feeling for at least a year, but his depression has worsened in the last few days. Mr. N is tearful while explaining his discouragement with following a diet for diabetes; earlier that day he ate an entire chocolate cake. He says all 3 of his children have ongoing substance abuse and relationship problems, but he is particularly focused on his youngest daughter, who is involved with a man who is addicted to drugs and physically abuses her and her children. Mr. N describes a detailed plan to shoot him and then commit suicide. This disclosure prompts the ED physician to admit Mr. N to ensure his safety and stabilize his mood.
Mr. N’s temperature is 36. 4°C (97. 5°F), blood pressure is 123/60 mm Hg, pulse is 81 beats per minute, respiratory rate is 24 breaths per minute, and oxygen saturation is 96% on ambient air. His physical exam is notable only for dysphoria and mild gynecomastia. He shows no evidence of acute cardiopulmonary, gastrointestinal, or other neurologic changes. His serum glucose is 650 mg/dL, and his recent hemoglobin A1c (HbA1c) is 10. 9%. His other laboratory tests include a hemoglobin of 11. 7 g/dL; white cell count, 3500/mm3; platelet count, 41, 000/mm3; sodium, 129 mEq/L; potassium, 5. 0 mEq/L; alkaline phosphatase, 90 U/L; aspartate aminotransferase, 23 U/L; alanine aminotransferase, 21 U/L; total bilirubin, 1. 8 mg/dL; creatinine, 1. 2 mg/dL; prothrombin time, 10. 4 sec; and arterial ammonia, <50 ?g/dL. Arterial blood gases are normal.
A year ago, his primary care physician prescribed fluoxetine, 20 mg/d, for fatigue and chronic back pain and neuropathic pain related to diabetes. We continue Mr. N’s outpatient prescription of fluoxetine, 20 mg/d, and low-dose acetaminophen as needed for pain. Furosemide, 40 mg/d, spironolactone, 100 mg/d, and propranolol sustained release, 60 mg/d, are maintained for complications of cirrhosis. Insulin aspart, 22 units with breakfast, 24 units with lunch, and 24 units with supper, also are administered routinely.
We consult with the internal medicine, ophthalmology, neurology, endocrinology, and diabetes services to assist in evaluating and managing Mr. N’s multiple medical conditions.
The authors’ observations
Depression and other forms of psychopathology may be underrecognized in geriatric patients because older adults may not report psychiatric symptoms that are secondary to physical conditions. Cognitive impairment in some older adults also may lead to underreporting of symptoms. Mr. N denies a history of depression, which we confirmed with his wife, daughter, and primary care physician. The late onset of his initial presentation prompted close investigation for a potential medical etiology (Table 1).1,2
We considered post-stroke depression because shortly after Mr. N’s stroke, his neurologist described emotional lability and frustration related to his poor vision. Depression occurs in one-third of chronic stroke survivors and is prevalent among patients referred for neurologic rehabilitation.1 Premorbid neuroticism3 and a history of mental illness are predictors of post-stroke depression. Stroke laterality is not related to risk of post-stroke depressive symptoms,3 but women have a higher risk of developing post-stroke depression.3
Table 1
When to consider medical causes of depressive symptoms
| Late onset of initial depressive presentation |
| Known underlying medical condition, such as cancer, diabetes, or stroke |
| Atypical symptoms and signs of depression, such as hypersomnia, hyperphagia, or agitation |
| Absence of personal or family history of psychiatric illnesses |
| Illicit substance use |
| Medication use (eg, opioids, reserpine, methyldopa, chemotherapy agents, steroids, and oral contraceptives) |
| Treatment resistance or unusual response to treatment |
| Sudden onset of mental symptoms (eg, sudden episode of uncontrollable crying) |
| Source: References 1,2 |
Diabetes and depression
Up to 30% of patients with type 2 diabetes mellitus report a lifetime history of major depression.2 Depression increases the risk of hyperglycemia and accompanying long-term metabolic complications.4,5 Few studies have explored the effects of poor glycemic control on depressive symptoms among diabetic patients.6-9 A literature review revealed no large-scale study investigating worsened depressive symptoms in patients with poor glycemic control.10,11
The cross-sectional difference between a single episode of major depression and adjustment disorder can be subtle. DSM-IV-TR describes the latter as a maladaptive reaction to an identifiable psychosocial stressor, or stressors, that occurs within 3 months of onset of that stressor (Table 2).12 Because we did not deem Mr. N’s depressive symptoms, which were evident only when he was hyperglycemic, to be grossly disproportionate to his stressors, we diagnose him with major depression rather than adjustment disorder.
Table 2
DSM-IV-TR diagnostic criteria for adjustment disorder
| A. The development of emotional or behavioral symptoms in response to an identifiable stressor(s) that occurs within 3 months of the onset of the stressor(s) |
B. These symptoms or behaviors are clinically significant, as evidenced by either of the following:
|
| C. The stress-related disturbance does not meet criteria for another specific axis I disorder and is not merely an exacerbation of a pre-existing axis I or axis II disorder |
| D. The symptoms do not represent bereavement |
| E. Once the stressor (or its consequences) has terminated, the symptoms do not persist for more than an additional 6 months |
Specify whether the condition is acute or chronic, as follows:
|
| Source: Reference 12 |
EVALUATION: No psychiatric history
On admission, Mr. N is overwhelmed, tearful, and dysphoric when describing his situation. He displays no evidence of psychosis, but his judgment and insight are impaired. He shows no change in consciousness or ability to stay awake. Mr. N acknowledges hypersomnolence, anhedonia, anergia, and decreased concentration and continues to express suicidal and homicidal thoughts. He repeatedly denies any personal or family psychiatric history or personal substance abuse, including alcohol and nicotine.
TREATMENT: Glycemic control
Mr. N receives 1 L of saline in the ED and is encouraged to drink more water during hospitalization. With appropriate insulin dosing, Mr. N’s serum glucose levels improve from 650 to 426 mg/dL by the next morning. On his third hospital day, Mr. N’s glucose level is 155 mg/dL in the morning. With tighter glycemic control, his dysphoria improves. He is future-oriented, markedly less dysphoric, and denies homicidal or suicidal ideation. Mr. N is interested in participating in group therapy, and his insight and judgment regarding his homicidal and suicidal thoughts improve. He still doesn’t fully understand the importance of diabetic control, and he struggles with his diet.
On the fourth hospital day, Mr. N’s glucose level rises to 325 mg/dL in the early evening. Subsequently, his mood deteriorates; he becomes increasingly withdrawn and somnolent. With appropriate attention to his dietary intake and supplemental insulin, his serum glucose improves to the 100 to 200 mg/dL range overnight, and his mood improves. When the glucose is controlled, he attends group therapy, tends to his hygiene, denies feeling hopeless, and offers several ideas about how to manage his family situation. After his glucose rises, Mr. N becomes isolative, hopeless, and unable to cope with stressors. With considerable education about the importance of glycemic control, Mr. N is hopeful and future-oriented when he is discharged after 9 days of hospitalization. At outpatient evaluation, he continues to report euthymia with adequate glycemic control.
The authors’ observations
Patients with hyperglycemia may experience symptoms secondary to volume depletion and hyperosmolality. The severity of these symptoms generally is proportional to the extent and duration of the hyperosmolar state. Initially, most patients complain of polyuria and polydipsia, but in more severe cases, mental status changes may evolve and include lethargy, twitching, cloudiness, motor or sensory defects, seizures, and coma. Some evidence shows that hyperglycemic patients with hyperosmolality are symptomatic only if hypernatremia is present.13 Mr. N was hyponatremic, which resolved with aggressive hydration and insulin administration.
Traditionally, depression has been observed to worsen glycemic control in diabetic patients; discussion of increased glucose levels leading to worsened depression rarely has been reported. In a meta-analysis, Lustman et al7 revealed that depression is significantly associated with hyperglycemia. A review by Li et al14 demonstrated that depression is much more common in patients with diabetes compared with general population and 45% of diabetes patients with depression were undiagnosed. Calhoun et al15 showed that for every 1-unit increase in HbA1c the odds of depressive symptoms increase by 22%. Researchers also found a positive relationship between depression and glycemic control in American Indians.15
Mr. N’s case is further evidence that the relationship between diabetes and depression is bidirectional and diagnosis and treatment of each illness impacts the other. Although this case does not confirm causality, it highlights the importance of aggressive approaches to screening and treatment of depression in patients with diabetes, and vice versa.
Related Resources
- Katon W, Russo J, Lin EH, et al. Depression and diabetes: factors associated with major depression at five-year follow-up. Psychosomatics. 2009; 50(6): 570-579.
- Biessels GJ, Luchsinger JA. Diabetes and the brain. New York, NY: Humana Press; 2009.
Drug Brand Names
- Fluoxetine • Prozac
- Furosemide • Lasix
- Insulin aspart • NovoLog
- Insulin glargine • Lantus
- Methyldopa • Aldomet
- Propranolol • Inderal
- Reserpine • Serpasil
- Spironolactone • Aldactone
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Worsening depression
Mr. N, age 64, is a disabled factory worker with a complicated medical history. He has poorly controlled type II diabetes mellitus; obesity (body mass index 40 kg/m2); complicated cryptogenic cirrhosis with prior esophageal varices, portal gastropathy, splenomegaly, and no encephalopathy; surgically treated colon adenocarcinoma; and bilateral thalamic and right occipital infarcts with residual left homonymous hemianopsia and vertical gaze paresis. Mr. N sustained a perioperative stroke 18 months ago while undergoing a colectomy procedure for colon adenocarcinoma; an MRI done at that time showed the bilateral thalamic and right occipital infarcts. While in the internal medicine consultation clinic, Mr. N expresses suicidal and homicidal thoughts, which prompted the internal medicine team to refer him to the emergency department (ED). The team deems Mr. N’s medical problems stable except for diabetic dyscontrol.
In the ED, Mr. N says he feels sad, worthless, and “tired” of his complex family issues and multiple medical conditions. He says he’s had these feeling for at least a year, but his depression has worsened in the last few days. Mr. N is tearful while explaining his discouragement with following a diet for diabetes; earlier that day he ate an entire chocolate cake. He says all 3 of his children have ongoing substance abuse and relationship problems, but he is particularly focused on his youngest daughter, who is involved with a man who is addicted to drugs and physically abuses her and her children. Mr. N describes a detailed plan to shoot him and then commit suicide. This disclosure prompts the ED physician to admit Mr. N to ensure his safety and stabilize his mood.
Mr. N’s temperature is 36. 4°C (97. 5°F), blood pressure is 123/60 mm Hg, pulse is 81 beats per minute, respiratory rate is 24 breaths per minute, and oxygen saturation is 96% on ambient air. His physical exam is notable only for dysphoria and mild gynecomastia. He shows no evidence of acute cardiopulmonary, gastrointestinal, or other neurologic changes. His serum glucose is 650 mg/dL, and his recent hemoglobin A1c (HbA1c) is 10. 9%. His other laboratory tests include a hemoglobin of 11. 7 g/dL; white cell count, 3500/mm3; platelet count, 41, 000/mm3; sodium, 129 mEq/L; potassium, 5. 0 mEq/L; alkaline phosphatase, 90 U/L; aspartate aminotransferase, 23 U/L; alanine aminotransferase, 21 U/L; total bilirubin, 1. 8 mg/dL; creatinine, 1. 2 mg/dL; prothrombin time, 10. 4 sec; and arterial ammonia, <50 ?g/dL. Arterial blood gases are normal.
A year ago, his primary care physician prescribed fluoxetine, 20 mg/d, for fatigue and chronic back pain and neuropathic pain related to diabetes. We continue Mr. N’s outpatient prescription of fluoxetine, 20 mg/d, and low-dose acetaminophen as needed for pain. Furosemide, 40 mg/d, spironolactone, 100 mg/d, and propranolol sustained release, 60 mg/d, are maintained for complications of cirrhosis. Insulin aspart, 22 units with breakfast, 24 units with lunch, and 24 units with supper, also are administered routinely.
We consult with the internal medicine, ophthalmology, neurology, endocrinology, and diabetes services to assist in evaluating and managing Mr. N’s multiple medical conditions.
The authors’ observations
Depression and other forms of psychopathology may be underrecognized in geriatric patients because older adults may not report psychiatric symptoms that are secondary to physical conditions. Cognitive impairment in some older adults also may lead to underreporting of symptoms. Mr. N denies a history of depression, which we confirmed with his wife, daughter, and primary care physician. The late onset of his initial presentation prompted close investigation for a potential medical etiology (Table 1).1,2
We considered post-stroke depression because shortly after Mr. N’s stroke, his neurologist described emotional lability and frustration related to his poor vision. Depression occurs in one-third of chronic stroke survivors and is prevalent among patients referred for neurologic rehabilitation.1 Premorbid neuroticism3 and a history of mental illness are predictors of post-stroke depression. Stroke laterality is not related to risk of post-stroke depressive symptoms,3 but women have a higher risk of developing post-stroke depression.3
Table 1
When to consider medical causes of depressive symptoms
| Late onset of initial depressive presentation |
| Known underlying medical condition, such as cancer, diabetes, or stroke |
| Atypical symptoms and signs of depression, such as hypersomnia, hyperphagia, or agitation |
| Absence of personal or family history of psychiatric illnesses |
| Illicit substance use |
| Medication use (eg, opioids, reserpine, methyldopa, chemotherapy agents, steroids, and oral contraceptives) |
| Treatment resistance or unusual response to treatment |
| Sudden onset of mental symptoms (eg, sudden episode of uncontrollable crying) |
| Source: References 1,2 |
Diabetes and depression
Up to 30% of patients with type 2 diabetes mellitus report a lifetime history of major depression.2 Depression increases the risk of hyperglycemia and accompanying long-term metabolic complications.4,5 Few studies have explored the effects of poor glycemic control on depressive symptoms among diabetic patients.6-9 A literature review revealed no large-scale study investigating worsened depressive symptoms in patients with poor glycemic control.10,11
The cross-sectional difference between a single episode of major depression and adjustment disorder can be subtle. DSM-IV-TR describes the latter as a maladaptive reaction to an identifiable psychosocial stressor, or stressors, that occurs within 3 months of onset of that stressor (Table 2).12 Because we did not deem Mr. N’s depressive symptoms, which were evident only when he was hyperglycemic, to be grossly disproportionate to his stressors, we diagnose him with major depression rather than adjustment disorder.
Table 2
DSM-IV-TR diagnostic criteria for adjustment disorder
| A. The development of emotional or behavioral symptoms in response to an identifiable stressor(s) that occurs within 3 months of the onset of the stressor(s) |
B. These symptoms or behaviors are clinically significant, as evidenced by either of the following:
|
| C. The stress-related disturbance does not meet criteria for another specific axis I disorder and is not merely an exacerbation of a pre-existing axis I or axis II disorder |
| D. The symptoms do not represent bereavement |
| E. Once the stressor (or its consequences) has terminated, the symptoms do not persist for more than an additional 6 months |
Specify whether the condition is acute or chronic, as follows:
|
| Source: Reference 12 |
EVALUATION: No psychiatric history
On admission, Mr. N is overwhelmed, tearful, and dysphoric when describing his situation. He displays no evidence of psychosis, but his judgment and insight are impaired. He shows no change in consciousness or ability to stay awake. Mr. N acknowledges hypersomnolence, anhedonia, anergia, and decreased concentration and continues to express suicidal and homicidal thoughts. He repeatedly denies any personal or family psychiatric history or personal substance abuse, including alcohol and nicotine.
TREATMENT: Glycemic control
Mr. N receives 1 L of saline in the ED and is encouraged to drink more water during hospitalization. With appropriate insulin dosing, Mr. N’s serum glucose levels improve from 650 to 426 mg/dL by the next morning. On his third hospital day, Mr. N’s glucose level is 155 mg/dL in the morning. With tighter glycemic control, his dysphoria improves. He is future-oriented, markedly less dysphoric, and denies homicidal or suicidal ideation. Mr. N is interested in participating in group therapy, and his insight and judgment regarding his homicidal and suicidal thoughts improve. He still doesn’t fully understand the importance of diabetic control, and he struggles with his diet.
On the fourth hospital day, Mr. N’s glucose level rises to 325 mg/dL in the early evening. Subsequently, his mood deteriorates; he becomes increasingly withdrawn and somnolent. With appropriate attention to his dietary intake and supplemental insulin, his serum glucose improves to the 100 to 200 mg/dL range overnight, and his mood improves. When the glucose is controlled, he attends group therapy, tends to his hygiene, denies feeling hopeless, and offers several ideas about how to manage his family situation. After his glucose rises, Mr. N becomes isolative, hopeless, and unable to cope with stressors. With considerable education about the importance of glycemic control, Mr. N is hopeful and future-oriented when he is discharged after 9 days of hospitalization. At outpatient evaluation, he continues to report euthymia with adequate glycemic control.
The authors’ observations
Patients with hyperglycemia may experience symptoms secondary to volume depletion and hyperosmolality. The severity of these symptoms generally is proportional to the extent and duration of the hyperosmolar state. Initially, most patients complain of polyuria and polydipsia, but in more severe cases, mental status changes may evolve and include lethargy, twitching, cloudiness, motor or sensory defects, seizures, and coma. Some evidence shows that hyperglycemic patients with hyperosmolality are symptomatic only if hypernatremia is present.13 Mr. N was hyponatremic, which resolved with aggressive hydration and insulin administration.
Traditionally, depression has been observed to worsen glycemic control in diabetic patients; discussion of increased glucose levels leading to worsened depression rarely has been reported. In a meta-analysis, Lustman et al7 revealed that depression is significantly associated with hyperglycemia. A review by Li et al14 demonstrated that depression is much more common in patients with diabetes compared with general population and 45% of diabetes patients with depression were undiagnosed. Calhoun et al15 showed that for every 1-unit increase in HbA1c the odds of depressive symptoms increase by 22%. Researchers also found a positive relationship between depression and glycemic control in American Indians.15
Mr. N’s case is further evidence that the relationship between diabetes and depression is bidirectional and diagnosis and treatment of each illness impacts the other. Although this case does not confirm causality, it highlights the importance of aggressive approaches to screening and treatment of depression in patients with diabetes, and vice versa.
Related Resources
- Katon W, Russo J, Lin EH, et al. Depression and diabetes: factors associated with major depression at five-year follow-up. Psychosomatics. 2009; 50(6): 570-579.
- Biessels GJ, Luchsinger JA. Diabetes and the brain. New York, NY: Humana Press; 2009.
Drug Brand Names
- Fluoxetine • Prozac
- Furosemide • Lasix
- Insulin aspart • NovoLog
- Insulin glargine • Lantus
- Methyldopa • Aldomet
- Propranolol • Inderal
- Reserpine • Serpasil
- Spironolactone • Aldactone
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Srivastava A, Taly AB, Gupta A, et al. Post-stroke depression: prevalence and relationship with disability in chronic stroke survivors. Ann Indian Acad Neurol. 2010;13(2):123-127.
2. Marcus MD, Wing RR, Guare J, et al. Lifetime prevalence of major depression and its effect on treatment outcome in obese type II diabetic patients. Diabetes Care. 1992;15(2):253-255.
3. Storor DL, Byrne GJ. Pre-morbid personality and depression following stroke. Int Psychogeriatr. 2006;18(3):457-469.
4. Songar A, Kocabasoglu N, Balcioglu I, et al. The relationship between diabetics’ metabolic control levels and psychiatric symptomatology. Integrative Psychiatry. 1993;9:34-40.
5. Von Dras DD, Lichty W. Correlates of depression in diabetic adults. Behav Health Aging. 1990;1:79-84.
6. Lustman PJ, Clouse RE. Depression in diabetic patients: the relationship between mood and glycemic control. J Diabetes Complications. 2005;19(2):113-122.
7. Lustman PJ, Anderson RJ, Freedland KE, et al. Depression and poor glycemic control: a meta-analytic review of the literature. Diabetes Care. 2000;23(7):934-942.
8. Lustman PJ, Griffith LS, Clouse RE. Depression in adults with diabetes: results of a 5-yr follow-up study. Diabetes Care. 1988;11:605-612.
9. Van der Does FE, De Neeling JN, Snoek FJ, et al. Symptoms and well-being in relation to glycemic control in type II diabetes. Diabetes Care. 1996;19:204-210.
10. Genuth S. A case for blood glucose control. Adv Intern Med. 1995;40:573-623.
11. Wrigley M, Mayou R. Psychological factors and admission for poor glycaemic control: a study of psychological and social factors in poorly controlled insulin dependent diabetic patients. J Psychosom Res. 1991;35:335-343.
12. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
13. Magee MF, Bhatt BA. Management of decompensated diabetes. Diabetic ketoacidosis and hyperglycemic hyperosmolar syndrome. Crit Care Clin. 2001;17(1):75-106.
14. Li C, Ford ES, Zhao G, et al. Prevalence and correlates of undiagnosed depression among U.S. adults with diabetes: the Behavioral Risk Factor Surveillance System, 2006. Diabetes Res Clin Pract. 2009;83(2):268-279.
15. Calhoun D, Beals J, Carter EA, et al. Relationship between glycemic control and depression among American Indians in the Strong Heart Study. J Diabetes Complications. 2010;24:217-222.
1. Srivastava A, Taly AB, Gupta A, et al. Post-stroke depression: prevalence and relationship with disability in chronic stroke survivors. Ann Indian Acad Neurol. 2010;13(2):123-127.
2. Marcus MD, Wing RR, Guare J, et al. Lifetime prevalence of major depression and its effect on treatment outcome in obese type II diabetic patients. Diabetes Care. 1992;15(2):253-255.
3. Storor DL, Byrne GJ. Pre-morbid personality and depression following stroke. Int Psychogeriatr. 2006;18(3):457-469.
4. Songar A, Kocabasoglu N, Balcioglu I, et al. The relationship between diabetics’ metabolic control levels and psychiatric symptomatology. Integrative Psychiatry. 1993;9:34-40.
5. Von Dras DD, Lichty W. Correlates of depression in diabetic adults. Behav Health Aging. 1990;1:79-84.
6. Lustman PJ, Clouse RE. Depression in diabetic patients: the relationship between mood and glycemic control. J Diabetes Complications. 2005;19(2):113-122.
7. Lustman PJ, Anderson RJ, Freedland KE, et al. Depression and poor glycemic control: a meta-analytic review of the literature. Diabetes Care. 2000;23(7):934-942.
8. Lustman PJ, Griffith LS, Clouse RE. Depression in adults with diabetes: results of a 5-yr follow-up study. Diabetes Care. 1988;11:605-612.
9. Van der Does FE, De Neeling JN, Snoek FJ, et al. Symptoms and well-being in relation to glycemic control in type II diabetes. Diabetes Care. 1996;19:204-210.
10. Genuth S. A case for blood glucose control. Adv Intern Med. 1995;40:573-623.
11. Wrigley M, Mayou R. Psychological factors and admission for poor glycaemic control: a study of psychological and social factors in poorly controlled insulin dependent diabetic patients. J Psychosom Res. 1991;35:335-343.
12. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
13. Magee MF, Bhatt BA. Management of decompensated diabetes. Diabetic ketoacidosis and hyperglycemic hyperosmolar syndrome. Crit Care Clin. 2001;17(1):75-106.
14. Li C, Ford ES, Zhao G, et al. Prevalence and correlates of undiagnosed depression among U.S. adults with diabetes: the Behavioral Risk Factor Surveillance System, 2006. Diabetes Res Clin Pract. 2009;83(2):268-279.
15. Calhoun D, Beals J, Carter EA, et al. Relationship between glycemic control and depression among American Indians in the Strong Heart Study. J Diabetes Complications. 2010;24:217-222.
Vilazodone for major depressive disorder
In January 2011, the FDA approved vilazodone for the treatment of major depressive disorder (MDD) (Table 1).
Vilazodone was discovered by Merck KGaA in Germany.1 In February 2001, Merck KGaA licensed vilazodone to GlaxoSmithKline. In April 2003, GlaxoSmithKline returned all rights to Merck KGaA because phase IIb clinical data did not support progression to phase III clinical trials. In September 2004, Genaissance Pharmaceuticals Inc. acquired an exclusive worldwide license from Merck KGaA to develop and commercialize vilazodone for depression treatment.2 Subsequently, Clinical Data Inc. acquired Genaissance Pharmaceuticals Inc., including vilazodone, and proceeded with 2 phase III trials and a large safety trial resulting in FDA approval. In February 2011, Forest Laboratories Inc. acquired Clinical Data Inc. and will launch vilazodone in second quarter of 2011.
Table 1
Vilazodone: Fast facts
| Brand name: Viibryd |
| Class: Serotonin reuptake inhibitor and 5-HT1A receptor partial agonist |
| Indication: Major depressive disorder |
| Approval date: January 24, 2011 |
| Availability date: Second quarter of 2011 |
| Manufacturer: Forest Laboratories Inc. |
| Dosage forms: 10 mg, 20 mg, and 40 mg tablets |
| Starting dose: 10 mg/d |
| Target dose: 40 mg/d |
How it works
Similar to all antidepressants, vilazodone’s mechanism of action is not fully understood, but is thought to be related to its inhibition of serotonin (ie, 5-HT) reuptake and partial agonism of 5-HT1A receptors.3 Vilazodone technically is not a selective serotonin reuptake inhibitor (SSRI) because it has greater affinity for the 5-HT1A receptor (0.2nM) than it does for the 5-HT reuptake pump (0.5nM).4
Vilazodone was developed based on the theory that inhibition of 5-HT1A autoreceptor inhibition was responsible for SSRIs’ delayed (approximately 2 weeks) onset of antidepressant efficacy. Briefly, this theory is as follows: In humans, 5-HT1A receptors are primarily presynaptic in the raphe nuclei and postsynaptic 5-HT1A receptors predominate in the neocortex and limbic regions of the brain.5 Presynaptically, 5-HT1A are autoreceptors, ie, serotonin stimulation of these receptors results in inhibition of firing of 5-HT neurons, while postsynaptically they may be involved in downstream serotonergic effects such as sexual function.5 SSRIs are thought to work as antidepressants by increasing 5-HT concentration in the synapse but their initial effect is to turn off 5-HT neuronal firing as a result of increased concentration of 5-HT at the presynaptic 5-HT1A autoreceptor. Subsequently, these 5-HT1A autoreceptors subsensitize such that 5-HT neuronal firing rate returns to normal. The time course for this subsensitization parallels the onset of SSRI antidepressant efficacy. For several years, efforts have been made to antagonize the 5-HT1A presynaptic autoreceptors as a means of potentially shortening SSRIs’ onset of efficacy.6-8
Pharmacokinetics
Vilazodone is absorbed in the gastrointestinal tract and reaches peak concentration at a median of 4 to 5 hours. Its bioavailability increases when taken with food such that Cmax (maximum concentration) is increased by 147% to 160%, and area under the curve is increased by 64% to 85%. Its absolute bioavailability in the presence of food is 72%.4 In systemic circulation, the drug is 96% to 99% protein-bound.3 Vilazodone is eliminated primarily through cytochrome P450 (CYP) 3A4 metabolism in the liver.3
Terminal half-life of vilazodone is 25 hours. In general, steady state is achieved in 4 to 5 times the half-life at a stable dose. However, dosing guidelines for vilazodone recommend titration over 2 weeks to achieve a target of 40 mg/d. Thus, steady state will not be achieved until the patient has been on the stable target dose for approximately 2.5 weeks.3
Efficacy
Vilazodone’ efficacy for MDD treatment was established in 2 pivotal 8-week, randomized, double-blind, placebo-controlled, but not active-controlled, trials (Table 2).9-11 Study participants were outpatients age 18 to 65 who met DSM-IV-TR criteria for MDD. Patients were required to have a 17-item Hamilton Rating Scale for Depression (HAM-D-17) score >22 and a HAM-D-17 item 1 (depressed mood) score >2.
In the first clinical trial, 410 patients were randomly assigned to vilazodone or placebo. In the vilazodone group, patients were started on 10 mg/d for 1 week, titrated to 20 mg/d for a second week, and then 40 mg/d for the remainder of the study. At week 8, the mean change from baseline on the Montgomery-Åsberg Depression Rating Scale (MADRS), HAM-D-17, Clinical Global Impression-Improvement scale (CGI-I), Clinical Global Impression-Severity scale (CGI-S), and Hamilton Anxiety scale (HAM-A) was statistically greater with vilazodone than placebo (P <.05).9 Compared with placebo, vilazodone-treated patients showed a statistically significant (P <. 05) improvement in MADRS and HAM-D-17 scores at week 1. Approximately 12% more vilazodone-treated patients achieved response (defined as ≥50% decrease in total score at end of treatment) on the primary efficacy measure, which was MADRS (40.4% vs 28.1%, P=.007), and the 2 secondary efficacy measures, which were HAM-D-17 (44.4% vs 32.7%, P =.011) and CGI-I (48.0 vs 32.7, P =.001). Remission rates (MADRS <10) were not reported in this study, but the authors stated that there was no statistical difference in remission rates between the vilazodone and placebo groups.9
In a second trial, which featured design and titration schedule identical to that of the first study, 481 patients were randomized to vilazodone or placebo.10 At week 8, the vilazodone-treated patients had significantly greater improvement in MADRS, HAM-D-17, HAM-A, CGI-S, and CGI-I score compared with the placebo group (P <.05). Approximately 14% more patients in the vilazodone group were MADRS responders compared with placebo (44% vs 30%, P =.002). Remission rates were not statistically different between patients taking vilazodone vs placebo (27% vs 20% respectively).10 Demonstrating a statistically significant difference between a 27% vs 20% remission rate would require a much larger number of patients than were included in this study.
Table 2
Efficacy of vilazodone in phase III clinical trials
| Trial | Drug response rate | Placebo response rate | Drug-specific response rate* | NNT† | Average reduction in MADRS change (drug minus placebo) (mean) | Average reduction in HAM-D change (drug minus placebo) (mean) |
|---|---|---|---|---|---|---|
| Rickels et al9 | 40% | 28% | 12% | 100/12=8 | 12.9 to 9.6 (3.3) | 10.4 to 8.6 (1.8) |
| Khan et al10 | 44% | 30% | 14% | 100/14=7 | 13.3 to 10.8 (2.5) | 10.7 to 9.1 (1.6) |
| HAM-D: Hamilton Rating Scale for Depression; MADRS: Montgomery-Åsburg Depression Rating Scale; NNT: number needed to treat *Difference in response rate between the drug and placebo groups. This rate is what the drug added to the treatment effects seen as a result of time and clinical management provided in the trial †The number of patients who need to be treated to benefit (ie, achieve response) one additional patient compared with placebo Source: Reference 11. Table reproduced with permission from Sheldon H. Preskorn, MD | ||||||
Tolerability
Vilazodone’s safety was evaluated in 2, 177 patients (age 18 to 70) diagnosed with MDD who participated in clinical studies, including the two 8-week, randomized, doubleblind, placebo-controlled studies (N=891) and a 52-week, open-label study of 599 patients.12 Overall, 7.1% of patients who received vilazodone discontinued treatment because of an adverse reaction, compared with 3.2% of placebo-treated patients in the double-blind studies.3 Diarrhea, nausea, and headache were the most commonly reported adverse events; the incidence of headache was similar to that in the placebo group (13.2% vs 14.2%).10 These adverse events are consistent with serotonin agonism, mild to moderate intensity, and occurred mainly during the first week of treatment.3
Doses up to 80 mg/d have not been associated with clinically significant changes in ECG parameters or laboratory parameters in serum chemistry hematology and urine analysis.9,10 The drug had no effect on weight as measured by mean change from baseline.9,10
In one 8-week trial, there were no substantial differences between vilazodone and placebo in Arizona Sexual Experience Scale (ASEX) scores at treatment end for either sex.9 ASEX is a 5-item scale used to assess sexual dysfunction; a score >18 indicates clinically significant sexual dysfunction. At baseline, mean ASEX scores among men were 15.8 in the placebo group and 16.5 in the vilazodone group. Among women, the mean ASEX score was 21.2 in both groups.9 Overall sexual function for men and women was similar for vilazodone and placebo, as measured by the Changes in Sexual Function Questionnaire.10 The most commonly reported sexual adverse effect was decreased libido.10
Contraindications
Vilazodone is contraindicated for concomitant use with monoamine oxidase inhibitors (MAOIs) or within 14 days of stopping or starting an MAOI. Vilazodone is contraindicated in patients taking strong CYP3A4 inhibitors (eg, ketoconazole) because of increased vilazodone concentrations and resulting concentration-dependent adverse effects.3 Concomitant administration of strong CYP3A4 inducers (eg, rifampin) might result in a reduction in vilazodone levels leading to lack or loss of efficacy.13
As with other antidepressants, vilazodone carries a black-box warning about increased risk of suicidal thinking and behavior in children, adolescents, and young adults taking antidepressants for MDD and other psychiatric disorders.3 Vilazodone showed evidence of developmental toxicity in rats, but was not teratogenic in rats or rabbits. There are no adequate, well-controlled studies of vilazodone in pregnant women and no human data regarding vilazodone concentrations in breast milk.3 Women taking vilazodone are advised to breastfeed only if the potential benefits outweigh the risks. Vilazodone is not recommended for use in pediatric patients.3
Similar to other antidepressants, vilazodone labeling carries warnings about serotonin syndrome, seizures, abnormal bleeding, activation of mania/hypomania, and hyponatremia.4
Dosing
Vilazodone is available as 10 mg, 20 mg, and 40 mg tablets. The recommended target dose for vilazodone is 40 mg/d, with a starting dose of 10 mg/d for 7 days, followed by 20 mg/d for 7 days, then 40 mg/d.3 The drug should be taken with food, but unlike other psychotropics, the manufacturer does not recommended a specific calorie amount.3 Dose tapering is recommended when the drug is discontinued.3
Dose should be reduced to 20 mg/d when vilazodone is coadministered with strong CYP3A4 inhibitors, such as azole antifungals, macrolides, protease inhibitors, and verapamil.13 No dosage adjustment is recommended based on age, mild or moderate liver impairment, or renal impairment of any severity.3 Vilazodone has not been studied in patients with severe hepatic impairment.3
How does vilazodone compare?
Ideally, it would be good to know how vilazodone compares with other marketed antidepressants. Unfortunately, there are no published head-to-head comparison data to address this matter. The number needed to treat with vilazodone is between 7 and 8 based on the data from the 2 phase III trials (Table 2).9-11 This is comparable to other antidepressants. One phase III study showed a statistically greater reduction in depressive symptomatology in vilazodone-treated patients after 1 week, 9 but that was not replicated in the second trial.10
Related Resources
- Khan A. Vilazodone, a novel dual-acting serotonergic antidepressant for managing major depression. Expert Opin Investig Drugs. 2009;18(11):1753-1764.
Drug Brand Names
- Ketoconazole • Nizoral
- Rifampin • Rifadin
- Verapamil • Isoptin
- Vilazodone • Viibryd
Disclosures
Drs. Kalia and Mittal report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Since January 2010, Dr. Preskorn has received grant/research support from Abbott Laboratories, Bristol-Myers Squibb, Eli Lilly and Company, Ipsen, Link Medicine, Pfizer Inc, Sunovion, Takeda, and Targacept. He has been a consultant to Abbott Laboratories, Allergan, Biovail, Boehringer Ingelheim, Eisai, Eli Lilly and Company, Evotec Johnson and Johnson, Labopharm, Merck, NovaDel Pharma, Orexigen, Prexa, Psylin Neurosciences Inc., and Sunovion. He is on the speakers bureau of Eisai, Pfizer Inc., and Sunovion.
1. Bartoszyk GD, Hegenbart R, Ziegler H. EMD 68843 a serotonin reuptake inhibitor with selective presynaptic 5-HT1A receptor agonistic properties. Eur J Pharmacol. 1997;322(2-3):147-153.
2. de Paulis T. Drug evaluation: vilazodone—a combined SSRI and 5-HT1A partial agonist for the treatment of depression. IDrugs 2007;10(3):193-201.
3. Viibryd [package insert]. New Haven CT: Trovis Pharmaceuticals, LLC; 2011.
4. Heinrich T, Böttcher H, Schiemann K, et al. Dual 5-HT1A agonists and 5-HT re-uptake inhibitors by combination of indole-butyl-amine and chromenonyl-piperazine structural elements in a single molecular entity. Bioorg Med Chem. 2004;12(18):4843-4852.
5. Blier P, Ward NM. Is there a role for 5-HT1A agonists in the treatment of depression? Biol Psychiatry. 2003;53:193-203.
6. Bielski RJ, Cunningham L, Horrigan JP, et al. Gepirone extended-release in the treatment of adult outpatients with major depressive disorder: a double-blind, randomized, placebo-controlled, parallel-group study. J Clin Psychiatry. 2008;69:571-577.
7. Gammans RE, Stringfellow JC, Hvizdos AJ, et al. Use of buspirone in patients with generalized anxiety disorder and coexisting depressive symptoms. A meta-analysis of eight randomized, controlled studies. Neuropsychobiology. 1992;25:193-201.
8. Robinson DS, Rickels K, Feighner J, et al. Clinical effects of the 5-HT1A partial agonists in depression: a composite analysis of buspirone in the treatment of depression. J Clin Psychopharmacol. 1990;10(3 suppl):67S-76S.
9. Rickels K, Athanasiou M, Robinson DS, et al. Evidence for efficacy and tolerability of vilazodone in the treatment of major depressive disorder: a randomized, double-blind, placebo-controlled trial. J Clin Psychiatry. 2009;70(3):326-333.
10. Khan A, Cutler AJ, Kajdasz DK, et al. Efficacy and tolerability of vilazodone, a dual-acting serotonergic antidepressant, in the treatment of patients with MDD. Poster presented at: American Psychiatric Association Annual Meeting; New Orleans, LA; May 25, 2010.
11. Mittal MS, Kalia R, Preskorn SH. Vilazodone a 5-HT1A receptor partial agonist and serotonin reuptake pump inhibitor: what can be gleaned from its history and its clinical data? J Psychiatr Pract. In press.
12. Robinson D, Kajdasz D, Gallipoli S, et al. A one-year open-label study assessing the safety and tolerability of vilazodone in patients with MDD. Poster presented at: American Psychiatric Association Annual Meeting: New Orleans, LA; May 25, 2010.
13. Preskorn SH, Flockhart D. 2010 guide to psychiatric drug interactions. Primary Psychiatry. 2009;16(12):45-74.
In January 2011, the FDA approved vilazodone for the treatment of major depressive disorder (MDD) (Table 1).
Vilazodone was discovered by Merck KGaA in Germany.1 In February 2001, Merck KGaA licensed vilazodone to GlaxoSmithKline. In April 2003, GlaxoSmithKline returned all rights to Merck KGaA because phase IIb clinical data did not support progression to phase III clinical trials. In September 2004, Genaissance Pharmaceuticals Inc. acquired an exclusive worldwide license from Merck KGaA to develop and commercialize vilazodone for depression treatment.2 Subsequently, Clinical Data Inc. acquired Genaissance Pharmaceuticals Inc., including vilazodone, and proceeded with 2 phase III trials and a large safety trial resulting in FDA approval. In February 2011, Forest Laboratories Inc. acquired Clinical Data Inc. and will launch vilazodone in second quarter of 2011.
Table 1
Vilazodone: Fast facts
| Brand name: Viibryd |
| Class: Serotonin reuptake inhibitor and 5-HT1A receptor partial agonist |
| Indication: Major depressive disorder |
| Approval date: January 24, 2011 |
| Availability date: Second quarter of 2011 |
| Manufacturer: Forest Laboratories Inc. |
| Dosage forms: 10 mg, 20 mg, and 40 mg tablets |
| Starting dose: 10 mg/d |
| Target dose: 40 mg/d |
How it works
Similar to all antidepressants, vilazodone’s mechanism of action is not fully understood, but is thought to be related to its inhibition of serotonin (ie, 5-HT) reuptake and partial agonism of 5-HT1A receptors.3 Vilazodone technically is not a selective serotonin reuptake inhibitor (SSRI) because it has greater affinity for the 5-HT1A receptor (0.2nM) than it does for the 5-HT reuptake pump (0.5nM).4
Vilazodone was developed based on the theory that inhibition of 5-HT1A autoreceptor inhibition was responsible for SSRIs’ delayed (approximately 2 weeks) onset of antidepressant efficacy. Briefly, this theory is as follows: In humans, 5-HT1A receptors are primarily presynaptic in the raphe nuclei and postsynaptic 5-HT1A receptors predominate in the neocortex and limbic regions of the brain.5 Presynaptically, 5-HT1A are autoreceptors, ie, serotonin stimulation of these receptors results in inhibition of firing of 5-HT neurons, while postsynaptically they may be involved in downstream serotonergic effects such as sexual function.5 SSRIs are thought to work as antidepressants by increasing 5-HT concentration in the synapse but their initial effect is to turn off 5-HT neuronal firing as a result of increased concentration of 5-HT at the presynaptic 5-HT1A autoreceptor. Subsequently, these 5-HT1A autoreceptors subsensitize such that 5-HT neuronal firing rate returns to normal. The time course for this subsensitization parallels the onset of SSRI antidepressant efficacy. For several years, efforts have been made to antagonize the 5-HT1A presynaptic autoreceptors as a means of potentially shortening SSRIs’ onset of efficacy.6-8
Pharmacokinetics
Vilazodone is absorbed in the gastrointestinal tract and reaches peak concentration at a median of 4 to 5 hours. Its bioavailability increases when taken with food such that Cmax (maximum concentration) is increased by 147% to 160%, and area under the curve is increased by 64% to 85%. Its absolute bioavailability in the presence of food is 72%.4 In systemic circulation, the drug is 96% to 99% protein-bound.3 Vilazodone is eliminated primarily through cytochrome P450 (CYP) 3A4 metabolism in the liver.3
Terminal half-life of vilazodone is 25 hours. In general, steady state is achieved in 4 to 5 times the half-life at a stable dose. However, dosing guidelines for vilazodone recommend titration over 2 weeks to achieve a target of 40 mg/d. Thus, steady state will not be achieved until the patient has been on the stable target dose for approximately 2.5 weeks.3
Efficacy
Vilazodone’ efficacy for MDD treatment was established in 2 pivotal 8-week, randomized, double-blind, placebo-controlled, but not active-controlled, trials (Table 2).9-11 Study participants were outpatients age 18 to 65 who met DSM-IV-TR criteria for MDD. Patients were required to have a 17-item Hamilton Rating Scale for Depression (HAM-D-17) score >22 and a HAM-D-17 item 1 (depressed mood) score >2.
In the first clinical trial, 410 patients were randomly assigned to vilazodone or placebo. In the vilazodone group, patients were started on 10 mg/d for 1 week, titrated to 20 mg/d for a second week, and then 40 mg/d for the remainder of the study. At week 8, the mean change from baseline on the Montgomery-Åsberg Depression Rating Scale (MADRS), HAM-D-17, Clinical Global Impression-Improvement scale (CGI-I), Clinical Global Impression-Severity scale (CGI-S), and Hamilton Anxiety scale (HAM-A) was statistically greater with vilazodone than placebo (P <.05).9 Compared with placebo, vilazodone-treated patients showed a statistically significant (P <. 05) improvement in MADRS and HAM-D-17 scores at week 1. Approximately 12% more vilazodone-treated patients achieved response (defined as ≥50% decrease in total score at end of treatment) on the primary efficacy measure, which was MADRS (40.4% vs 28.1%, P=.007), and the 2 secondary efficacy measures, which were HAM-D-17 (44.4% vs 32.7%, P =.011) and CGI-I (48.0 vs 32.7, P =.001). Remission rates (MADRS <10) were not reported in this study, but the authors stated that there was no statistical difference in remission rates between the vilazodone and placebo groups.9
In a second trial, which featured design and titration schedule identical to that of the first study, 481 patients were randomized to vilazodone or placebo.10 At week 8, the vilazodone-treated patients had significantly greater improvement in MADRS, HAM-D-17, HAM-A, CGI-S, and CGI-I score compared with the placebo group (P <.05). Approximately 14% more patients in the vilazodone group were MADRS responders compared with placebo (44% vs 30%, P =.002). Remission rates were not statistically different between patients taking vilazodone vs placebo (27% vs 20% respectively).10 Demonstrating a statistically significant difference between a 27% vs 20% remission rate would require a much larger number of patients than were included in this study.
Table 2
Efficacy of vilazodone in phase III clinical trials
| Trial | Drug response rate | Placebo response rate | Drug-specific response rate* | NNT† | Average reduction in MADRS change (drug minus placebo) (mean) | Average reduction in HAM-D change (drug minus placebo) (mean) |
|---|---|---|---|---|---|---|
| Rickels et al9 | 40% | 28% | 12% | 100/12=8 | 12.9 to 9.6 (3.3) | 10.4 to 8.6 (1.8) |
| Khan et al10 | 44% | 30% | 14% | 100/14=7 | 13.3 to 10.8 (2.5) | 10.7 to 9.1 (1.6) |
| HAM-D: Hamilton Rating Scale for Depression; MADRS: Montgomery-Åsburg Depression Rating Scale; NNT: number needed to treat *Difference in response rate between the drug and placebo groups. This rate is what the drug added to the treatment effects seen as a result of time and clinical management provided in the trial †The number of patients who need to be treated to benefit (ie, achieve response) one additional patient compared with placebo Source: Reference 11. Table reproduced with permission from Sheldon H. Preskorn, MD | ||||||
Tolerability
Vilazodone’s safety was evaluated in 2, 177 patients (age 18 to 70) diagnosed with MDD who participated in clinical studies, including the two 8-week, randomized, doubleblind, placebo-controlled studies (N=891) and a 52-week, open-label study of 599 patients.12 Overall, 7.1% of patients who received vilazodone discontinued treatment because of an adverse reaction, compared with 3.2% of placebo-treated patients in the double-blind studies.3 Diarrhea, nausea, and headache were the most commonly reported adverse events; the incidence of headache was similar to that in the placebo group (13.2% vs 14.2%).10 These adverse events are consistent with serotonin agonism, mild to moderate intensity, and occurred mainly during the first week of treatment.3
Doses up to 80 mg/d have not been associated with clinically significant changes in ECG parameters or laboratory parameters in serum chemistry hematology and urine analysis.9,10 The drug had no effect on weight as measured by mean change from baseline.9,10
In one 8-week trial, there were no substantial differences between vilazodone and placebo in Arizona Sexual Experience Scale (ASEX) scores at treatment end for either sex.9 ASEX is a 5-item scale used to assess sexual dysfunction; a score >18 indicates clinically significant sexual dysfunction. At baseline, mean ASEX scores among men were 15.8 in the placebo group and 16.5 in the vilazodone group. Among women, the mean ASEX score was 21.2 in both groups.9 Overall sexual function for men and women was similar for vilazodone and placebo, as measured by the Changes in Sexual Function Questionnaire.10 The most commonly reported sexual adverse effect was decreased libido.10
Contraindications
Vilazodone is contraindicated for concomitant use with monoamine oxidase inhibitors (MAOIs) or within 14 days of stopping or starting an MAOI. Vilazodone is contraindicated in patients taking strong CYP3A4 inhibitors (eg, ketoconazole) because of increased vilazodone concentrations and resulting concentration-dependent adverse effects.3 Concomitant administration of strong CYP3A4 inducers (eg, rifampin) might result in a reduction in vilazodone levels leading to lack or loss of efficacy.13
As with other antidepressants, vilazodone carries a black-box warning about increased risk of suicidal thinking and behavior in children, adolescents, and young adults taking antidepressants for MDD and other psychiatric disorders.3 Vilazodone showed evidence of developmental toxicity in rats, but was not teratogenic in rats or rabbits. There are no adequate, well-controlled studies of vilazodone in pregnant women and no human data regarding vilazodone concentrations in breast milk.3 Women taking vilazodone are advised to breastfeed only if the potential benefits outweigh the risks. Vilazodone is not recommended for use in pediatric patients.3
Similar to other antidepressants, vilazodone labeling carries warnings about serotonin syndrome, seizures, abnormal bleeding, activation of mania/hypomania, and hyponatremia.4
Dosing
Vilazodone is available as 10 mg, 20 mg, and 40 mg tablets. The recommended target dose for vilazodone is 40 mg/d, with a starting dose of 10 mg/d for 7 days, followed by 20 mg/d for 7 days, then 40 mg/d.3 The drug should be taken with food, but unlike other psychotropics, the manufacturer does not recommended a specific calorie amount.3 Dose tapering is recommended when the drug is discontinued.3
Dose should be reduced to 20 mg/d when vilazodone is coadministered with strong CYP3A4 inhibitors, such as azole antifungals, macrolides, protease inhibitors, and verapamil.13 No dosage adjustment is recommended based on age, mild or moderate liver impairment, or renal impairment of any severity.3 Vilazodone has not been studied in patients with severe hepatic impairment.3
How does vilazodone compare?
Ideally, it would be good to know how vilazodone compares with other marketed antidepressants. Unfortunately, there are no published head-to-head comparison data to address this matter. The number needed to treat with vilazodone is between 7 and 8 based on the data from the 2 phase III trials (Table 2).9-11 This is comparable to other antidepressants. One phase III study showed a statistically greater reduction in depressive symptomatology in vilazodone-treated patients after 1 week, 9 but that was not replicated in the second trial.10
Related Resources
- Khan A. Vilazodone, a novel dual-acting serotonergic antidepressant for managing major depression. Expert Opin Investig Drugs. 2009;18(11):1753-1764.
Drug Brand Names
- Ketoconazole • Nizoral
- Rifampin • Rifadin
- Verapamil • Isoptin
- Vilazodone • Viibryd
Disclosures
Drs. Kalia and Mittal report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Since January 2010, Dr. Preskorn has received grant/research support from Abbott Laboratories, Bristol-Myers Squibb, Eli Lilly and Company, Ipsen, Link Medicine, Pfizer Inc, Sunovion, Takeda, and Targacept. He has been a consultant to Abbott Laboratories, Allergan, Biovail, Boehringer Ingelheim, Eisai, Eli Lilly and Company, Evotec Johnson and Johnson, Labopharm, Merck, NovaDel Pharma, Orexigen, Prexa, Psylin Neurosciences Inc., and Sunovion. He is on the speakers bureau of Eisai, Pfizer Inc., and Sunovion.
In January 2011, the FDA approved vilazodone for the treatment of major depressive disorder (MDD) (Table 1).
Vilazodone was discovered by Merck KGaA in Germany.1 In February 2001, Merck KGaA licensed vilazodone to GlaxoSmithKline. In April 2003, GlaxoSmithKline returned all rights to Merck KGaA because phase IIb clinical data did not support progression to phase III clinical trials. In September 2004, Genaissance Pharmaceuticals Inc. acquired an exclusive worldwide license from Merck KGaA to develop and commercialize vilazodone for depression treatment.2 Subsequently, Clinical Data Inc. acquired Genaissance Pharmaceuticals Inc., including vilazodone, and proceeded with 2 phase III trials and a large safety trial resulting in FDA approval. In February 2011, Forest Laboratories Inc. acquired Clinical Data Inc. and will launch vilazodone in second quarter of 2011.
Table 1
Vilazodone: Fast facts
| Brand name: Viibryd |
| Class: Serotonin reuptake inhibitor and 5-HT1A receptor partial agonist |
| Indication: Major depressive disorder |
| Approval date: January 24, 2011 |
| Availability date: Second quarter of 2011 |
| Manufacturer: Forest Laboratories Inc. |
| Dosage forms: 10 mg, 20 mg, and 40 mg tablets |
| Starting dose: 10 mg/d |
| Target dose: 40 mg/d |
How it works
Similar to all antidepressants, vilazodone’s mechanism of action is not fully understood, but is thought to be related to its inhibition of serotonin (ie, 5-HT) reuptake and partial agonism of 5-HT1A receptors.3 Vilazodone technically is not a selective serotonin reuptake inhibitor (SSRI) because it has greater affinity for the 5-HT1A receptor (0.2nM) than it does for the 5-HT reuptake pump (0.5nM).4
Vilazodone was developed based on the theory that inhibition of 5-HT1A autoreceptor inhibition was responsible for SSRIs’ delayed (approximately 2 weeks) onset of antidepressant efficacy. Briefly, this theory is as follows: In humans, 5-HT1A receptors are primarily presynaptic in the raphe nuclei and postsynaptic 5-HT1A receptors predominate in the neocortex and limbic regions of the brain.5 Presynaptically, 5-HT1A are autoreceptors, ie, serotonin stimulation of these receptors results in inhibition of firing of 5-HT neurons, while postsynaptically they may be involved in downstream serotonergic effects such as sexual function.5 SSRIs are thought to work as antidepressants by increasing 5-HT concentration in the synapse but their initial effect is to turn off 5-HT neuronal firing as a result of increased concentration of 5-HT at the presynaptic 5-HT1A autoreceptor. Subsequently, these 5-HT1A autoreceptors subsensitize such that 5-HT neuronal firing rate returns to normal. The time course for this subsensitization parallels the onset of SSRI antidepressant efficacy. For several years, efforts have been made to antagonize the 5-HT1A presynaptic autoreceptors as a means of potentially shortening SSRIs’ onset of efficacy.6-8
Pharmacokinetics
Vilazodone is absorbed in the gastrointestinal tract and reaches peak concentration at a median of 4 to 5 hours. Its bioavailability increases when taken with food such that Cmax (maximum concentration) is increased by 147% to 160%, and area under the curve is increased by 64% to 85%. Its absolute bioavailability in the presence of food is 72%.4 In systemic circulation, the drug is 96% to 99% protein-bound.3 Vilazodone is eliminated primarily through cytochrome P450 (CYP) 3A4 metabolism in the liver.3
Terminal half-life of vilazodone is 25 hours. In general, steady state is achieved in 4 to 5 times the half-life at a stable dose. However, dosing guidelines for vilazodone recommend titration over 2 weeks to achieve a target of 40 mg/d. Thus, steady state will not be achieved until the patient has been on the stable target dose for approximately 2.5 weeks.3
Efficacy
Vilazodone’ efficacy for MDD treatment was established in 2 pivotal 8-week, randomized, double-blind, placebo-controlled, but not active-controlled, trials (Table 2).9-11 Study participants were outpatients age 18 to 65 who met DSM-IV-TR criteria for MDD. Patients were required to have a 17-item Hamilton Rating Scale for Depression (HAM-D-17) score >22 and a HAM-D-17 item 1 (depressed mood) score >2.
In the first clinical trial, 410 patients were randomly assigned to vilazodone or placebo. In the vilazodone group, patients were started on 10 mg/d for 1 week, titrated to 20 mg/d for a second week, and then 40 mg/d for the remainder of the study. At week 8, the mean change from baseline on the Montgomery-Åsberg Depression Rating Scale (MADRS), HAM-D-17, Clinical Global Impression-Improvement scale (CGI-I), Clinical Global Impression-Severity scale (CGI-S), and Hamilton Anxiety scale (HAM-A) was statistically greater with vilazodone than placebo (P <.05).9 Compared with placebo, vilazodone-treated patients showed a statistically significant (P <. 05) improvement in MADRS and HAM-D-17 scores at week 1. Approximately 12% more vilazodone-treated patients achieved response (defined as ≥50% decrease in total score at end of treatment) on the primary efficacy measure, which was MADRS (40.4% vs 28.1%, P=.007), and the 2 secondary efficacy measures, which were HAM-D-17 (44.4% vs 32.7%, P =.011) and CGI-I (48.0 vs 32.7, P =.001). Remission rates (MADRS <10) were not reported in this study, but the authors stated that there was no statistical difference in remission rates between the vilazodone and placebo groups.9
In a second trial, which featured design and titration schedule identical to that of the first study, 481 patients were randomized to vilazodone or placebo.10 At week 8, the vilazodone-treated patients had significantly greater improvement in MADRS, HAM-D-17, HAM-A, CGI-S, and CGI-I score compared with the placebo group (P <.05). Approximately 14% more patients in the vilazodone group were MADRS responders compared with placebo (44% vs 30%, P =.002). Remission rates were not statistically different between patients taking vilazodone vs placebo (27% vs 20% respectively).10 Demonstrating a statistically significant difference between a 27% vs 20% remission rate would require a much larger number of patients than were included in this study.
Table 2
Efficacy of vilazodone in phase III clinical trials
| Trial | Drug response rate | Placebo response rate | Drug-specific response rate* | NNT† | Average reduction in MADRS change (drug minus placebo) (mean) | Average reduction in HAM-D change (drug minus placebo) (mean) |
|---|---|---|---|---|---|---|
| Rickels et al9 | 40% | 28% | 12% | 100/12=8 | 12.9 to 9.6 (3.3) | 10.4 to 8.6 (1.8) |
| Khan et al10 | 44% | 30% | 14% | 100/14=7 | 13.3 to 10.8 (2.5) | 10.7 to 9.1 (1.6) |
| HAM-D: Hamilton Rating Scale for Depression; MADRS: Montgomery-Åsburg Depression Rating Scale; NNT: number needed to treat *Difference in response rate between the drug and placebo groups. This rate is what the drug added to the treatment effects seen as a result of time and clinical management provided in the trial †The number of patients who need to be treated to benefit (ie, achieve response) one additional patient compared with placebo Source: Reference 11. Table reproduced with permission from Sheldon H. Preskorn, MD | ||||||
Tolerability
Vilazodone’s safety was evaluated in 2, 177 patients (age 18 to 70) diagnosed with MDD who participated in clinical studies, including the two 8-week, randomized, doubleblind, placebo-controlled studies (N=891) and a 52-week, open-label study of 599 patients.12 Overall, 7.1% of patients who received vilazodone discontinued treatment because of an adverse reaction, compared with 3.2% of placebo-treated patients in the double-blind studies.3 Diarrhea, nausea, and headache were the most commonly reported adverse events; the incidence of headache was similar to that in the placebo group (13.2% vs 14.2%).10 These adverse events are consistent with serotonin agonism, mild to moderate intensity, and occurred mainly during the first week of treatment.3
Doses up to 80 mg/d have not been associated with clinically significant changes in ECG parameters or laboratory parameters in serum chemistry hematology and urine analysis.9,10 The drug had no effect on weight as measured by mean change from baseline.9,10
In one 8-week trial, there were no substantial differences between vilazodone and placebo in Arizona Sexual Experience Scale (ASEX) scores at treatment end for either sex.9 ASEX is a 5-item scale used to assess sexual dysfunction; a score >18 indicates clinically significant sexual dysfunction. At baseline, mean ASEX scores among men were 15.8 in the placebo group and 16.5 in the vilazodone group. Among women, the mean ASEX score was 21.2 in both groups.9 Overall sexual function for men and women was similar for vilazodone and placebo, as measured by the Changes in Sexual Function Questionnaire.10 The most commonly reported sexual adverse effect was decreased libido.10
Contraindications
Vilazodone is contraindicated for concomitant use with monoamine oxidase inhibitors (MAOIs) or within 14 days of stopping or starting an MAOI. Vilazodone is contraindicated in patients taking strong CYP3A4 inhibitors (eg, ketoconazole) because of increased vilazodone concentrations and resulting concentration-dependent adverse effects.3 Concomitant administration of strong CYP3A4 inducers (eg, rifampin) might result in a reduction in vilazodone levels leading to lack or loss of efficacy.13
As with other antidepressants, vilazodone carries a black-box warning about increased risk of suicidal thinking and behavior in children, adolescents, and young adults taking antidepressants for MDD and other psychiatric disorders.3 Vilazodone showed evidence of developmental toxicity in rats, but was not teratogenic in rats or rabbits. There are no adequate, well-controlled studies of vilazodone in pregnant women and no human data regarding vilazodone concentrations in breast milk.3 Women taking vilazodone are advised to breastfeed only if the potential benefits outweigh the risks. Vilazodone is not recommended for use in pediatric patients.3
Similar to other antidepressants, vilazodone labeling carries warnings about serotonin syndrome, seizures, abnormal bleeding, activation of mania/hypomania, and hyponatremia.4
Dosing
Vilazodone is available as 10 mg, 20 mg, and 40 mg tablets. The recommended target dose for vilazodone is 40 mg/d, with a starting dose of 10 mg/d for 7 days, followed by 20 mg/d for 7 days, then 40 mg/d.3 The drug should be taken with food, but unlike other psychotropics, the manufacturer does not recommended a specific calorie amount.3 Dose tapering is recommended when the drug is discontinued.3
Dose should be reduced to 20 mg/d when vilazodone is coadministered with strong CYP3A4 inhibitors, such as azole antifungals, macrolides, protease inhibitors, and verapamil.13 No dosage adjustment is recommended based on age, mild or moderate liver impairment, or renal impairment of any severity.3 Vilazodone has not been studied in patients with severe hepatic impairment.3
How does vilazodone compare?
Ideally, it would be good to know how vilazodone compares with other marketed antidepressants. Unfortunately, there are no published head-to-head comparison data to address this matter. The number needed to treat with vilazodone is between 7 and 8 based on the data from the 2 phase III trials (Table 2).9-11 This is comparable to other antidepressants. One phase III study showed a statistically greater reduction in depressive symptomatology in vilazodone-treated patients after 1 week, 9 but that was not replicated in the second trial.10
Related Resources
- Khan A. Vilazodone, a novel dual-acting serotonergic antidepressant for managing major depression. Expert Opin Investig Drugs. 2009;18(11):1753-1764.
Drug Brand Names
- Ketoconazole • Nizoral
- Rifampin • Rifadin
- Verapamil • Isoptin
- Vilazodone • Viibryd
Disclosures
Drs. Kalia and Mittal report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Since January 2010, Dr. Preskorn has received grant/research support from Abbott Laboratories, Bristol-Myers Squibb, Eli Lilly and Company, Ipsen, Link Medicine, Pfizer Inc, Sunovion, Takeda, and Targacept. He has been a consultant to Abbott Laboratories, Allergan, Biovail, Boehringer Ingelheim, Eisai, Eli Lilly and Company, Evotec Johnson and Johnson, Labopharm, Merck, NovaDel Pharma, Orexigen, Prexa, Psylin Neurosciences Inc., and Sunovion. He is on the speakers bureau of Eisai, Pfizer Inc., and Sunovion.
1. Bartoszyk GD, Hegenbart R, Ziegler H. EMD 68843 a serotonin reuptake inhibitor with selective presynaptic 5-HT1A receptor agonistic properties. Eur J Pharmacol. 1997;322(2-3):147-153.
2. de Paulis T. Drug evaluation: vilazodone—a combined SSRI and 5-HT1A partial agonist for the treatment of depression. IDrugs 2007;10(3):193-201.
3. Viibryd [package insert]. New Haven CT: Trovis Pharmaceuticals, LLC; 2011.
4. Heinrich T, Böttcher H, Schiemann K, et al. Dual 5-HT1A agonists and 5-HT re-uptake inhibitors by combination of indole-butyl-amine and chromenonyl-piperazine structural elements in a single molecular entity. Bioorg Med Chem. 2004;12(18):4843-4852.
5. Blier P, Ward NM. Is there a role for 5-HT1A agonists in the treatment of depression? Biol Psychiatry. 2003;53:193-203.
6. Bielski RJ, Cunningham L, Horrigan JP, et al. Gepirone extended-release in the treatment of adult outpatients with major depressive disorder: a double-blind, randomized, placebo-controlled, parallel-group study. J Clin Psychiatry. 2008;69:571-577.
7. Gammans RE, Stringfellow JC, Hvizdos AJ, et al. Use of buspirone in patients with generalized anxiety disorder and coexisting depressive symptoms. A meta-analysis of eight randomized, controlled studies. Neuropsychobiology. 1992;25:193-201.
8. Robinson DS, Rickels K, Feighner J, et al. Clinical effects of the 5-HT1A partial agonists in depression: a composite analysis of buspirone in the treatment of depression. J Clin Psychopharmacol. 1990;10(3 suppl):67S-76S.
9. Rickels K, Athanasiou M, Robinson DS, et al. Evidence for efficacy and tolerability of vilazodone in the treatment of major depressive disorder: a randomized, double-blind, placebo-controlled trial. J Clin Psychiatry. 2009;70(3):326-333.
10. Khan A, Cutler AJ, Kajdasz DK, et al. Efficacy and tolerability of vilazodone, a dual-acting serotonergic antidepressant, in the treatment of patients with MDD. Poster presented at: American Psychiatric Association Annual Meeting; New Orleans, LA; May 25, 2010.
11. Mittal MS, Kalia R, Preskorn SH. Vilazodone a 5-HT1A receptor partial agonist and serotonin reuptake pump inhibitor: what can be gleaned from its history and its clinical data? J Psychiatr Pract. In press.
12. Robinson D, Kajdasz D, Gallipoli S, et al. A one-year open-label study assessing the safety and tolerability of vilazodone in patients with MDD. Poster presented at: American Psychiatric Association Annual Meeting: New Orleans, LA; May 25, 2010.
13. Preskorn SH, Flockhart D. 2010 guide to psychiatric drug interactions. Primary Psychiatry. 2009;16(12):45-74.
1. Bartoszyk GD, Hegenbart R, Ziegler H. EMD 68843 a serotonin reuptake inhibitor with selective presynaptic 5-HT1A receptor agonistic properties. Eur J Pharmacol. 1997;322(2-3):147-153.
2. de Paulis T. Drug evaluation: vilazodone—a combined SSRI and 5-HT1A partial agonist for the treatment of depression. IDrugs 2007;10(3):193-201.
3. Viibryd [package insert]. New Haven CT: Trovis Pharmaceuticals, LLC; 2011.
4. Heinrich T, Böttcher H, Schiemann K, et al. Dual 5-HT1A agonists and 5-HT re-uptake inhibitors by combination of indole-butyl-amine and chromenonyl-piperazine structural elements in a single molecular entity. Bioorg Med Chem. 2004;12(18):4843-4852.
5. Blier P, Ward NM. Is there a role for 5-HT1A agonists in the treatment of depression? Biol Psychiatry. 2003;53:193-203.
6. Bielski RJ, Cunningham L, Horrigan JP, et al. Gepirone extended-release in the treatment of adult outpatients with major depressive disorder: a double-blind, randomized, placebo-controlled, parallel-group study. J Clin Psychiatry. 2008;69:571-577.
7. Gammans RE, Stringfellow JC, Hvizdos AJ, et al. Use of buspirone in patients with generalized anxiety disorder and coexisting depressive symptoms. A meta-analysis of eight randomized, controlled studies. Neuropsychobiology. 1992;25:193-201.
8. Robinson DS, Rickels K, Feighner J, et al. Clinical effects of the 5-HT1A partial agonists in depression: a composite analysis of buspirone in the treatment of depression. J Clin Psychopharmacol. 1990;10(3 suppl):67S-76S.
9. Rickels K, Athanasiou M, Robinson DS, et al. Evidence for efficacy and tolerability of vilazodone in the treatment of major depressive disorder: a randomized, double-blind, placebo-controlled trial. J Clin Psychiatry. 2009;70(3):326-333.
10. Khan A, Cutler AJ, Kajdasz DK, et al. Efficacy and tolerability of vilazodone, a dual-acting serotonergic antidepressant, in the treatment of patients with MDD. Poster presented at: American Psychiatric Association Annual Meeting; New Orleans, LA; May 25, 2010.
11. Mittal MS, Kalia R, Preskorn SH. Vilazodone a 5-HT1A receptor partial agonist and serotonin reuptake pump inhibitor: what can be gleaned from its history and its clinical data? J Psychiatr Pract. In press.
12. Robinson D, Kajdasz D, Gallipoli S, et al. A one-year open-label study assessing the safety and tolerability of vilazodone in patients with MDD. Poster presented at: American Psychiatric Association Annual Meeting: New Orleans, LA; May 25, 2010.
13. Preskorn SH, Flockhart D. 2010 guide to psychiatric drug interactions. Primary Psychiatry. 2009;16(12):45-74.
New-onset psychosis: Consider epilepsy
Interictal psychosis of epilepsy (IPE) is schizophrenia-like psychosis associated with epilepsy that cannot be directly linked to an ictus. IPE often is indistinguishable from primary schizophrenia. This phenomenon commonly occurs in patients with a history of temporal lobe epilepsy (TLE); in those with frequent seizures; and in patients with a long history of epilepsy (>10 years).1 Interictal psychosis rarely precedes seizure activity2 and few cases have been reported. The epidemiology and clinical characteristics of IPE are poorly defined.3 We recently treated a patient with suspected IPE.
Mr. R, age 18, presented to our emergency department with his mother, who stated that her son was behaving strangely and had slow speech for 4 days. He had decreased social interaction, reduced appetite, poor hygiene, decreased sleep, and auditory hallucinations. Mr. R demonstrated hypervigilance and paranoia. He repeatedly checked rooms in his house for intruders. Mr. R also expressed suicidal ideation and exhibited cognitive decline of memory, attention, and fund of knowledge. His physical exam, routine laboratory investigations, CT, and MRI were within normal limits. Urine drug screen was positive for marijuana. We made a clinical diagnosis of acute psychosis.
Mr. R was admitted and started on ziprasidone, titrated to 160 mg/d; however, he could not tolerate this medication because of orthostatic hypotension. We discontinued ziprasidone and started risperidone, titrated to 4 mg/d. By day 4 Mr. R remained psychotic and marijuana intoxication was ruled out. EEG demonstrated rare intermittent left temporal sharp slow wave discharges and sharply contoured slow waves. This suggested an underlying seizure disorder, although Mr. R had no history of seizure.
The psychosis resolved 3 weeks later with risperidone, 2 mg/d, risperidone long-acting injection, 25 mg every 2 weeks, and carbamazepine, 400 mg/d. Mr. R was discharged home on these medications. He was noncompliant with treatment and continued to smoke marijuana. Four months later, Mr. R was rehospitalized for strange behavior. When seen in the outpatient clinic for follow-up, Mr. R admitted that he had his first witnessed seizure before his last hospitalization. Mr. R was restarted on risperidone, 4 mg/d, and risperidone long-acting injection, 25 mg every 2 weeks. To increase compliance, we switched carbamazepine to divalproex sodium extended-release, 500 mg/d. He remains stable, but continues to smoke marijuana.
Our case illustrates that IPE may be a presenting feature of TLE. Because IPE may occur in patients who do not have a history of TLE, EEG monitoring should be considered in the workup of new-onset psychosis.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Elliott B, Joyce E, Shorvon S. Delusions, illusions and hallucinations in epilepsy: 2. complex phenomena and psychosis. Epilepsy Res. 2009;85(2-3):172-186.
2. Norton A, Massano J, Timóteo S, et al. "Full moon fits": focal temporal epilepsy presenting as first episode psychosis. Euro Psychiatry. 2009;24(suppl 1):1180.-
3. Cascella NG, Schretlen DJ, Sawa A. Schizophrenia and epilepsy: is there a shared susceptibility? Neurosci Res. 2009;63(4):227-235.
Interictal psychosis of epilepsy (IPE) is schizophrenia-like psychosis associated with epilepsy that cannot be directly linked to an ictus. IPE often is indistinguishable from primary schizophrenia. This phenomenon commonly occurs in patients with a history of temporal lobe epilepsy (TLE); in those with frequent seizures; and in patients with a long history of epilepsy (>10 years).1 Interictal psychosis rarely precedes seizure activity2 and few cases have been reported. The epidemiology and clinical characteristics of IPE are poorly defined.3 We recently treated a patient with suspected IPE.
Mr. R, age 18, presented to our emergency department with his mother, who stated that her son was behaving strangely and had slow speech for 4 days. He had decreased social interaction, reduced appetite, poor hygiene, decreased sleep, and auditory hallucinations. Mr. R demonstrated hypervigilance and paranoia. He repeatedly checked rooms in his house for intruders. Mr. R also expressed suicidal ideation and exhibited cognitive decline of memory, attention, and fund of knowledge. His physical exam, routine laboratory investigations, CT, and MRI were within normal limits. Urine drug screen was positive for marijuana. We made a clinical diagnosis of acute psychosis.
Mr. R was admitted and started on ziprasidone, titrated to 160 mg/d; however, he could not tolerate this medication because of orthostatic hypotension. We discontinued ziprasidone and started risperidone, titrated to 4 mg/d. By day 4 Mr. R remained psychotic and marijuana intoxication was ruled out. EEG demonstrated rare intermittent left temporal sharp slow wave discharges and sharply contoured slow waves. This suggested an underlying seizure disorder, although Mr. R had no history of seizure.
The psychosis resolved 3 weeks later with risperidone, 2 mg/d, risperidone long-acting injection, 25 mg every 2 weeks, and carbamazepine, 400 mg/d. Mr. R was discharged home on these medications. He was noncompliant with treatment and continued to smoke marijuana. Four months later, Mr. R was rehospitalized for strange behavior. When seen in the outpatient clinic for follow-up, Mr. R admitted that he had his first witnessed seizure before his last hospitalization. Mr. R was restarted on risperidone, 4 mg/d, and risperidone long-acting injection, 25 mg every 2 weeks. To increase compliance, we switched carbamazepine to divalproex sodium extended-release, 500 mg/d. He remains stable, but continues to smoke marijuana.
Our case illustrates that IPE may be a presenting feature of TLE. Because IPE may occur in patients who do not have a history of TLE, EEG monitoring should be considered in the workup of new-onset psychosis.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Interictal psychosis of epilepsy (IPE) is schizophrenia-like psychosis associated with epilepsy that cannot be directly linked to an ictus. IPE often is indistinguishable from primary schizophrenia. This phenomenon commonly occurs in patients with a history of temporal lobe epilepsy (TLE); in those with frequent seizures; and in patients with a long history of epilepsy (>10 years).1 Interictal psychosis rarely precedes seizure activity2 and few cases have been reported. The epidemiology and clinical characteristics of IPE are poorly defined.3 We recently treated a patient with suspected IPE.
Mr. R, age 18, presented to our emergency department with his mother, who stated that her son was behaving strangely and had slow speech for 4 days. He had decreased social interaction, reduced appetite, poor hygiene, decreased sleep, and auditory hallucinations. Mr. R demonstrated hypervigilance and paranoia. He repeatedly checked rooms in his house for intruders. Mr. R also expressed suicidal ideation and exhibited cognitive decline of memory, attention, and fund of knowledge. His physical exam, routine laboratory investigations, CT, and MRI were within normal limits. Urine drug screen was positive for marijuana. We made a clinical diagnosis of acute psychosis.
Mr. R was admitted and started on ziprasidone, titrated to 160 mg/d; however, he could not tolerate this medication because of orthostatic hypotension. We discontinued ziprasidone and started risperidone, titrated to 4 mg/d. By day 4 Mr. R remained psychotic and marijuana intoxication was ruled out. EEG demonstrated rare intermittent left temporal sharp slow wave discharges and sharply contoured slow waves. This suggested an underlying seizure disorder, although Mr. R had no history of seizure.
The psychosis resolved 3 weeks later with risperidone, 2 mg/d, risperidone long-acting injection, 25 mg every 2 weeks, and carbamazepine, 400 mg/d. Mr. R was discharged home on these medications. He was noncompliant with treatment and continued to smoke marijuana. Four months later, Mr. R was rehospitalized for strange behavior. When seen in the outpatient clinic for follow-up, Mr. R admitted that he had his first witnessed seizure before his last hospitalization. Mr. R was restarted on risperidone, 4 mg/d, and risperidone long-acting injection, 25 mg every 2 weeks. To increase compliance, we switched carbamazepine to divalproex sodium extended-release, 500 mg/d. He remains stable, but continues to smoke marijuana.
Our case illustrates that IPE may be a presenting feature of TLE. Because IPE may occur in patients who do not have a history of TLE, EEG monitoring should be considered in the workup of new-onset psychosis.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Elliott B, Joyce E, Shorvon S. Delusions, illusions and hallucinations in epilepsy: 2. complex phenomena and psychosis. Epilepsy Res. 2009;85(2-3):172-186.
2. Norton A, Massano J, Timóteo S, et al. "Full moon fits": focal temporal epilepsy presenting as first episode psychosis. Euro Psychiatry. 2009;24(suppl 1):1180.-
3. Cascella NG, Schretlen DJ, Sawa A. Schizophrenia and epilepsy: is there a shared susceptibility? Neurosci Res. 2009;63(4):227-235.
1. Elliott B, Joyce E, Shorvon S. Delusions, illusions and hallucinations in epilepsy: 2. complex phenomena and psychosis. Epilepsy Res. 2009;85(2-3):172-186.
2. Norton A, Massano J, Timóteo S, et al. "Full moon fits": focal temporal epilepsy presenting as first episode psychosis. Euro Psychiatry. 2009;24(suppl 1):1180.-
3. Cascella NG, Schretlen DJ, Sawa A. Schizophrenia and epilepsy: is there a shared susceptibility? Neurosci Res. 2009;63(4):227-235.
Treating depression in medical residents
Residents in psychiatry and other specialties experience depressive illness at rates similar to or higher than the general population. Residency training is a major psychosocial stressor.1 Having to master a large body of medical knowledge while facing feared inadequacy or failure creates a demanding emotional climate for physicians in training. When added to other mood disorder risk factors, such as genetic vulnerability and fatigue, continuous performance demands can lead to the onset of a major depressive episode. Assisting the newest members of our profession by providing needed mental health treatment can be challenging but rewarding.
Are residents ‘special’ patients?
Some residents who realize they are depressed are tempted to self-diagnose and self-prescribe or obtain informal consultation from peers or family members who are physicians. The best treatment for depressed residents is to provide the same meticulous, excellent, and thoughtful care that you provide for your nonphysician patients. Many depressed residents who seek psychiatric treatment are relieved to share their symptoms and stresses with a professional who is there to treat, not teach, them.2
Residents from nonpsychiatric specialties may be assessed and treated by psychiatry faculty at their home institutions or by providers in the community. For psychiatrists who supervise residents, establishing liaisons with private practice clinicians who can offer rapid treatment access for physicians in training can be effective. To avoid conflicts of interest, it is crucial that psychiatry residents are treated by providers other than their own faculty.
Factors that may lead residents to avoid seeking treatment include:
- The culture of medicine reinforces the stereotype that physicians are “strong” and “tough,” implying that the need for depression treatment is a weakness.
- Fear of stigma can extend to fear of receiving negative evaluations by supervisors if depression is acknowledged.
- Residents have logistic difficulties participating in treatment—a busy and inflexible schedule makes it hard to attend appointments.
- Altruism can hinder some residents from obtaining self-care. These residents may perceive a “good doctor” as one who is self-sacrificing for his or her patients.
Treatment
The same collaborative approach to establishing a healthy therapeutic relationship with nonphysician patients is equally effective with physicians in training. Residents usually are open to using evidence-based combined modalities, eg, pharmacotherapy and specific structured psychotherapies such as cognitive-behavioral therapy or interpersonal psychotherapy.
Occasionally a resident will lobby for special treatment. For example, a resident may insist that the psychiatrist rearrange other patients’ appointments to accommodate the resident’s schedule. Also, residents may be unwilling or unable to see themselves in the patient role. They may attempt to define their treatment in singular and distinctive ways, setting themselves apart from nonphysician patients. These barriers can be overcome by setting appropriate boundaries with patients early in treatment. It is the psychiatrist’s responsibility to gently but firmly set limits with residents so that treatment can be effective.
Disclosure
Dr. Gay reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Residents in psychiatry and other specialties experience depressive illness at rates similar to or higher than the general population. Residency training is a major psychosocial stressor.1 Having to master a large body of medical knowledge while facing feared inadequacy or failure creates a demanding emotional climate for physicians in training. When added to other mood disorder risk factors, such as genetic vulnerability and fatigue, continuous performance demands can lead to the onset of a major depressive episode. Assisting the newest members of our profession by providing needed mental health treatment can be challenging but rewarding.
Are residents ‘special’ patients?
Some residents who realize they are depressed are tempted to self-diagnose and self-prescribe or obtain informal consultation from peers or family members who are physicians. The best treatment for depressed residents is to provide the same meticulous, excellent, and thoughtful care that you provide for your nonphysician patients. Many depressed residents who seek psychiatric treatment are relieved to share their symptoms and stresses with a professional who is there to treat, not teach, them.2
Residents from nonpsychiatric specialties may be assessed and treated by psychiatry faculty at their home institutions or by providers in the community. For psychiatrists who supervise residents, establishing liaisons with private practice clinicians who can offer rapid treatment access for physicians in training can be effective. To avoid conflicts of interest, it is crucial that psychiatry residents are treated by providers other than their own faculty.
Factors that may lead residents to avoid seeking treatment include:
- The culture of medicine reinforces the stereotype that physicians are “strong” and “tough,” implying that the need for depression treatment is a weakness.
- Fear of stigma can extend to fear of receiving negative evaluations by supervisors if depression is acknowledged.
- Residents have logistic difficulties participating in treatment—a busy and inflexible schedule makes it hard to attend appointments.
- Altruism can hinder some residents from obtaining self-care. These residents may perceive a “good doctor” as one who is self-sacrificing for his or her patients.
Treatment
The same collaborative approach to establishing a healthy therapeutic relationship with nonphysician patients is equally effective with physicians in training. Residents usually are open to using evidence-based combined modalities, eg, pharmacotherapy and specific structured psychotherapies such as cognitive-behavioral therapy or interpersonal psychotherapy.
Occasionally a resident will lobby for special treatment. For example, a resident may insist that the psychiatrist rearrange other patients’ appointments to accommodate the resident’s schedule. Also, residents may be unwilling or unable to see themselves in the patient role. They may attempt to define their treatment in singular and distinctive ways, setting themselves apart from nonphysician patients. These barriers can be overcome by setting appropriate boundaries with patients early in treatment. It is the psychiatrist’s responsibility to gently but firmly set limits with residents so that treatment can be effective.
Disclosure
Dr. Gay reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Residents in psychiatry and other specialties experience depressive illness at rates similar to or higher than the general population. Residency training is a major psychosocial stressor.1 Having to master a large body of medical knowledge while facing feared inadequacy or failure creates a demanding emotional climate for physicians in training. When added to other mood disorder risk factors, such as genetic vulnerability and fatigue, continuous performance demands can lead to the onset of a major depressive episode. Assisting the newest members of our profession by providing needed mental health treatment can be challenging but rewarding.
Are residents ‘special’ patients?
Some residents who realize they are depressed are tempted to self-diagnose and self-prescribe or obtain informal consultation from peers or family members who are physicians. The best treatment for depressed residents is to provide the same meticulous, excellent, and thoughtful care that you provide for your nonphysician patients. Many depressed residents who seek psychiatric treatment are relieved to share their symptoms and stresses with a professional who is there to treat, not teach, them.2
Residents from nonpsychiatric specialties may be assessed and treated by psychiatry faculty at their home institutions or by providers in the community. For psychiatrists who supervise residents, establishing liaisons with private practice clinicians who can offer rapid treatment access for physicians in training can be effective. To avoid conflicts of interest, it is crucial that psychiatry residents are treated by providers other than their own faculty.
Factors that may lead residents to avoid seeking treatment include:
- The culture of medicine reinforces the stereotype that physicians are “strong” and “tough,” implying that the need for depression treatment is a weakness.
- Fear of stigma can extend to fear of receiving negative evaluations by supervisors if depression is acknowledged.
- Residents have logistic difficulties participating in treatment—a busy and inflexible schedule makes it hard to attend appointments.
- Altruism can hinder some residents from obtaining self-care. These residents may perceive a “good doctor” as one who is self-sacrificing for his or her patients.
Treatment
The same collaborative approach to establishing a healthy therapeutic relationship with nonphysician patients is equally effective with physicians in training. Residents usually are open to using evidence-based combined modalities, eg, pharmacotherapy and specific structured psychotherapies such as cognitive-behavioral therapy or interpersonal psychotherapy.
Occasionally a resident will lobby for special treatment. For example, a resident may insist that the psychiatrist rearrange other patients’ appointments to accommodate the resident’s schedule. Also, residents may be unwilling or unable to see themselves in the patient role. They may attempt to define their treatment in singular and distinctive ways, setting themselves apart from nonphysician patients. These barriers can be overcome by setting appropriate boundaries with patients early in treatment. It is the psychiatrist’s responsibility to gently but firmly set limits with residents so that treatment can be effective.
Disclosure
Dr. Gay reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Temporary tattoos: Alternative to adolescent self-harm?
Although self-harm behaviors such as burning or cutting are common among adolescents, they are a source of concern for parents and friends, and challenging to treat. Treatments have focused on distracting stimuli such as ice or the sting of a rubber band snapped on the wrist. Tattooing may be an alternative somatic strategy that can decrease self-harm and counter negative body image.1,2
In a study of 423 individuals with body modification (tattoos and piercings), 27% admitted to cutting themselves during childhood.3 This study’s authors concluded that these practices became a substitute for self-harm, helped patients overcome traumatic experiences, and improved satisfaction with body image.
In line with these observations, we decided to offer temporary tattooing to residents in our 60-bed child and adolescent treatment center. Patients were age 6 to 20 and 70% were female. We received consent from all patients’ guardians after explaining the temporary, nontoxic nature of the ink or decals.
Our first trials were with adolescent females with a history of cutting, but we offered temporary tattooing to all patients within a few months. Overall, 7 females and 3 males, all of whom had an axis I mood disorder, participated in temporary tattooing as an alternative to self-harm. We noted borderline personality traits in female patients who engaged in severe self-harm. Patients either drew on themselves or, with therapist supervision, “tattooed” other patients using self-selected designs.
One older teenage girl used cutting to manage flashbacks of sexual abuse from a family member. She had multiple scars from the cutting despite outpatient, hospital, and residential treatment over several years without symptom improvement. After 1 year of tattooing, her cutting episodes decreased from several times per month to once every 3 months. She also reported an improvement in positive perception of her body image from 0 on a 1-to-10 scale on admission to 5 at 1 year.
A younger teenage female without visible scars used cutting to manage feelings of being ugly associated with memories of sexual abuse. She reported that over 3 months, drawing tattoos improved her feelings about her body from 0/10 to 4/10, and she no longer reported thoughts of cutting or self-harm. Over 3 months, a male teenager without scars who cut himself when distressed about female relationships instead used tattoos to draw his conflicted feelings on his arm.
Tattoo designs included:
- flowers, vines, and roses
- patients’ psychological issues
- 2 faces for a patient dealing with internal and external relationship conflicts
- 2 flags to represent melding different cultures
- 2 hearts fused to represent issues with the intensities of love
- foreign words to indicate secrecy and alienation
- fantasy daydreams reflected as unicorns and dolphins.
Patients’ conversations with their therapists about the tattoos enabled detailed discussions about abuse, body image, and relationships.
Parents and some of our staff initially were concerned that temporary tattoos would increase self-harm or high-risk behaviors. This did not occur, perhaps because patients felt the designs helped them visually express feelings and conflicts.
Our clinical experience indicates that temporary tattooing may be a method of discussing and altering self-harm behaviors and negative body image in adolescent inpatients. Further evaluation of this strategy is warranted.
Disclosure
Dr. Masters reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Muehlenkamp JJ, Swanson DJ, Brausch AM. Self-objectification risk taking and self-harm in college women. Psychology of Women Quarterly. 2005;29:24-32.
2. Carroll L, Anderson R. Body piercing tattooing, self-esteem, and body investment in adolescent girls. Adolescence. 2002;37:627-637.
3. Stirm A, Hinz A. Tattoos body piercings, and self injury: is there a connection? Investigations on a core group of participants practicing body modification. Psychother Res. 2008;18:326-333.
Although self-harm behaviors such as burning or cutting are common among adolescents, they are a source of concern for parents and friends, and challenging to treat. Treatments have focused on distracting stimuli such as ice or the sting of a rubber band snapped on the wrist. Tattooing may be an alternative somatic strategy that can decrease self-harm and counter negative body image.1,2
In a study of 423 individuals with body modification (tattoos and piercings), 27% admitted to cutting themselves during childhood.3 This study’s authors concluded that these practices became a substitute for self-harm, helped patients overcome traumatic experiences, and improved satisfaction with body image.
In line with these observations, we decided to offer temporary tattooing to residents in our 60-bed child and adolescent treatment center. Patients were age 6 to 20 and 70% were female. We received consent from all patients’ guardians after explaining the temporary, nontoxic nature of the ink or decals.
Our first trials were with adolescent females with a history of cutting, but we offered temporary tattooing to all patients within a few months. Overall, 7 females and 3 males, all of whom had an axis I mood disorder, participated in temporary tattooing as an alternative to self-harm. We noted borderline personality traits in female patients who engaged in severe self-harm. Patients either drew on themselves or, with therapist supervision, “tattooed” other patients using self-selected designs.
One older teenage girl used cutting to manage flashbacks of sexual abuse from a family member. She had multiple scars from the cutting despite outpatient, hospital, and residential treatment over several years without symptom improvement. After 1 year of tattooing, her cutting episodes decreased from several times per month to once every 3 months. She also reported an improvement in positive perception of her body image from 0 on a 1-to-10 scale on admission to 5 at 1 year.
A younger teenage female without visible scars used cutting to manage feelings of being ugly associated with memories of sexual abuse. She reported that over 3 months, drawing tattoos improved her feelings about her body from 0/10 to 4/10, and she no longer reported thoughts of cutting or self-harm. Over 3 months, a male teenager without scars who cut himself when distressed about female relationships instead used tattoos to draw his conflicted feelings on his arm.
Tattoo designs included:
- flowers, vines, and roses
- patients’ psychological issues
- 2 faces for a patient dealing with internal and external relationship conflicts
- 2 flags to represent melding different cultures
- 2 hearts fused to represent issues with the intensities of love
- foreign words to indicate secrecy and alienation
- fantasy daydreams reflected as unicorns and dolphins.
Patients’ conversations with their therapists about the tattoos enabled detailed discussions about abuse, body image, and relationships.
Parents and some of our staff initially were concerned that temporary tattoos would increase self-harm or high-risk behaviors. This did not occur, perhaps because patients felt the designs helped them visually express feelings and conflicts.
Our clinical experience indicates that temporary tattooing may be a method of discussing and altering self-harm behaviors and negative body image in adolescent inpatients. Further evaluation of this strategy is warranted.
Disclosure
Dr. Masters reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Although self-harm behaviors such as burning or cutting are common among adolescents, they are a source of concern for parents and friends, and challenging to treat. Treatments have focused on distracting stimuli such as ice or the sting of a rubber band snapped on the wrist. Tattooing may be an alternative somatic strategy that can decrease self-harm and counter negative body image.1,2
In a study of 423 individuals with body modification (tattoos and piercings), 27% admitted to cutting themselves during childhood.3 This study’s authors concluded that these practices became a substitute for self-harm, helped patients overcome traumatic experiences, and improved satisfaction with body image.
In line with these observations, we decided to offer temporary tattooing to residents in our 60-bed child and adolescent treatment center. Patients were age 6 to 20 and 70% were female. We received consent from all patients’ guardians after explaining the temporary, nontoxic nature of the ink or decals.
Our first trials were with adolescent females with a history of cutting, but we offered temporary tattooing to all patients within a few months. Overall, 7 females and 3 males, all of whom had an axis I mood disorder, participated in temporary tattooing as an alternative to self-harm. We noted borderline personality traits in female patients who engaged in severe self-harm. Patients either drew on themselves or, with therapist supervision, “tattooed” other patients using self-selected designs.
One older teenage girl used cutting to manage flashbacks of sexual abuse from a family member. She had multiple scars from the cutting despite outpatient, hospital, and residential treatment over several years without symptom improvement. After 1 year of tattooing, her cutting episodes decreased from several times per month to once every 3 months. She also reported an improvement in positive perception of her body image from 0 on a 1-to-10 scale on admission to 5 at 1 year.
A younger teenage female without visible scars used cutting to manage feelings of being ugly associated with memories of sexual abuse. She reported that over 3 months, drawing tattoos improved her feelings about her body from 0/10 to 4/10, and she no longer reported thoughts of cutting or self-harm. Over 3 months, a male teenager without scars who cut himself when distressed about female relationships instead used tattoos to draw his conflicted feelings on his arm.
Tattoo designs included:
- flowers, vines, and roses
- patients’ psychological issues
- 2 faces for a patient dealing with internal and external relationship conflicts
- 2 flags to represent melding different cultures
- 2 hearts fused to represent issues with the intensities of love
- foreign words to indicate secrecy and alienation
- fantasy daydreams reflected as unicorns and dolphins.
Patients’ conversations with their therapists about the tattoos enabled detailed discussions about abuse, body image, and relationships.
Parents and some of our staff initially were concerned that temporary tattoos would increase self-harm or high-risk behaviors. This did not occur, perhaps because patients felt the designs helped them visually express feelings and conflicts.
Our clinical experience indicates that temporary tattooing may be a method of discussing and altering self-harm behaviors and negative body image in adolescent inpatients. Further evaluation of this strategy is warranted.
Disclosure
Dr. Masters reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Muehlenkamp JJ, Swanson DJ, Brausch AM. Self-objectification risk taking and self-harm in college women. Psychology of Women Quarterly. 2005;29:24-32.
2. Carroll L, Anderson R. Body piercing tattooing, self-esteem, and body investment in adolescent girls. Adolescence. 2002;37:627-637.
3. Stirm A, Hinz A. Tattoos body piercings, and self injury: is there a connection? Investigations on a core group of participants practicing body modification. Psychother Res. 2008;18:326-333.
1. Muehlenkamp JJ, Swanson DJ, Brausch AM. Self-objectification risk taking and self-harm in college women. Psychology of Women Quarterly. 2005;29:24-32.
2. Carroll L, Anderson R. Body piercing tattooing, self-esteem, and body investment in adolescent girls. Adolescence. 2002;37:627-637.
3. Stirm A, Hinz A. Tattoos body piercings, and self injury: is there a connection? Investigations on a core group of participants practicing body modification. Psychother Res. 2008;18:326-333.
HIV screening: Latest testing guidelines
• Patients with mental illness are at elevated risk for HIV infection.
• Fourth-generation (p24) HIV testing allows accurate, office-based screening during the period of highest infectivity.
• Psychiatrists may be uniquely able to discuss and alter patients’ high-risk behaviors related to HIV transmission and treatment.
Substance use and high-risk sexual behaviors are common among persons with severe mental illness and make them vulnerable to human immunodeficiency virus (HIV) infection.1-3 The prevalence of HIV is 3 times higher among these patients compared with individuals who are not mentally ill. This article reviews risk factors for HIV transmission, HIV screening recommendations, and current testing options, including the fourth-generation HIV test.
According to the World Health Organization, in 2009:
- 33 million people were infected with HIV
- there were 2.6 million new infections
- 1.8 million people died from causes related to acquired immune deficiency syndrome (AIDS).4
In the United States, approximately 1 million people are living with HIV; 55, 000 new cases were diagnosed in North America in 2009.5 The demographics of those infected with HIV in the United States have changed substantially. Most newly infected individuals are African American, and younger adults have higher rates of new infections.6 With the introduction of standardized antiviral medication combinations and federal programs to provide universal access to medications in the mid 1990s, the number of AIDS cases and mortality dropped, but there have not been similar gains in the past decade.6
In countries With access to antiviral medications, medical advances in HIV treatment have transformed an infection with a high mortality rate into a chronic illness. However, the rate of new cases has not changed significantly in the past 10 years. Early detection and treatment initiation reduces high-risk behavior and subsequent transmission in patients with HIV. Evidence suggests that detecting HIV in the acute phase of the illness, when the viral load is high, reduces HIV transmission.1,5,6
HIV screening
HIV screening should be part of routine psychiatric practice, especially in community and forensic settings. We recommend that all psychiatrists understand HIV screening guidelines from the Centers for Disease Control and Prevention (CDC)7 and the American College of Physicians (ACP).8 The CDC (2006)7 and ACP (2009)8 guidelines recommend HIV screening for:
- all patients age 13 to 64, unless the prevalence of undiagnosed HIV infection in your patients has been documented to be <0. 1%7
- all patients seeking treatment for sexually transmitted diseases, including each visit for a new complaint7
- all pregnant women7
- any patient who received a blood transfusion between 1978 and 1985.8
Rescreening frequency is determined on an individual basis, taking into consideration the patient’s risk of contracting HIV. The ACP guidelines recommend using rapid tests when available.8 Although the false positive rates are higher with rapid tests, the benefits of early detection and reducing transmission outweigh the cost of confirming positive tests.8
The fourth-generation test
The gold standard for HIV screening is the enzyme-linked immunosorbent assay antibody test followed by a western blot.8 This has a high sensitivity and specificity but there is a window of time between infection and detectable antibodies in serum during which patients have high virus levels (Figure).9 The combined antibody and antigen p24 test is a fourth-generation screening tool that detects HIV in the acute phase of the illness without requiring expensive ribonucleic acid viral tests.10 The fourth-generation test’s capacity to detect infection during the antibody-negative window when infectivity is highest may help decrease HIV transmission.11
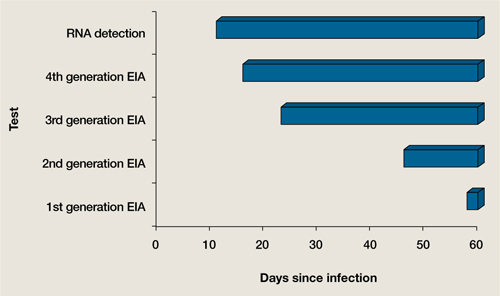
Figure When can HIV tests detect the virus?
EIA: enzyme immunoassay; HIV: human immunodeficiency virus; RNA: ribonucleic acid
Source: Adapted from reference 9
Psychiatrists’ role
Because psychiatrists routinely interact with patients who have an increased risk of HIV, they may be uniquely qualified to help these individuals. Psychiatrists often are comfortable discussing patients’ sexual and substance use history, which allows them to uncover and effectively address high-risk behaviors with appropriate testing and counseling. If testing confirms HIV infection, psychiatrists also can discuss altering high-risk behaviors (Table),1,2 which has significant implications not only for patients, but also for public health.
Table
HIV transmission risk factors
| Intravenous drug use |
| Nonintravenous cocaine use |
| Sex without barrier protection, especially in patients with multiple partners |
| Sex trade or sex work |
| HIV: human immunodeficiency virus |
| Source: References 1,2 |
Related Resource
- Centers for Disease Control and Prevention. HIV/AIDS. www.cdc.gov/hiv.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Rosenberg SD, Goodman LA, Osher FC, et al. Prevalence of HIV, hepatitis B, and hepatitis C in people with severe mental illness. Am J Health. 2001;91:31-37.
2. Quinn TC, Glasser D, Cannon RO, et al. Human immunodeficiency virus infection among patients attending clinics for sexually transmitted diseases. N Eng J Med. 1988;318:197-203.
3. Erickson B, Wasserheit JN, Rompalo AM, et al. Routine voluntary HIV screening in STD clinic clients: characterization of infected clients. Sex Transm Dis. 1990;17:194-199.
4. World Health Organization. Global summary of the AIDS epidemic. Available at: http://www.who.int/hiv/data/2009_global_summary.png. Accessed February 10 2011.
5. Hall HI, Song R, Rhodes P, et al. Estimation of HIV incidence in the United States. JAMA. 2008;300:520-529.
6. Glynn MK, Lee LM, McKenna MT. The status of national HIV case surveillance United States 2006. Public Health Rep. 2007;122(suppl 1):63-71.
7. Branson BM, Handsfield HH, Lampe MA, et al. and the Centers for Disease Control and Prevention. Revised recommendations for HIV testing of adults adolescents, and pregnant women in health-care settings. MMWR Recomm Rep. 2006;55(RR-14):1-17; quiz CE1-CE4.
8. Qaseem A, Snow V, Shekelle P, et al. and the Clinical Efficacy Assessment Subcommittee American College of Physicians. Screening for HIV in health care settings: a guidance statement from the American College of Physicians and HIV Medicine Association. Ann Intern Med. 2009;150:125-131.
9. Branson BM. The future of HIV testing. J Acquir Immune Defic Syndr. 2010;55:S102-S105.
10. Eshleman S, Khaki L, Laeyendecker O, et al. Detection of individuals with acute HIV-1 infection using the ARCHITECT HIV Ag/Ab combo assay. J Acquir Immune Defic Syndr. 2009;52:121-124.
11. Pandori MW, Hackett J, Jr, Louie B, et al. Assessment of the ability of a fourth-generation immunoassay for human immunodeficiency virus (HIV) antibody and p24 antigen to detect both acute and recent HIV infections in a high-risk setting. J Clin Microbiol. 2009;47:2639-2642.
John Onate, MD
Dr. Onate is Health Sciences Assistant Clinical Professor, Department of Psychiatry and Behavioral Sciences
Travis Fisher, MD
Dr. Fisher is Fellow, Department of Psychosomatic Medicine, University of California Davis Medical Center, Sacramento, CA.
Robert M. McCarron, DO
Series Editor
John Onate, MD
Dr. Onate is Health Sciences Assistant Clinical Professor, Department of Psychiatry and Behavioral Sciences
Travis Fisher, MD
Dr. Fisher is Fellow, Department of Psychosomatic Medicine, University of California Davis Medical Center, Sacramento, CA.
Robert M. McCarron, DO
Series Editor
John Onate, MD
Dr. Onate is Health Sciences Assistant Clinical Professor, Department of Psychiatry and Behavioral Sciences
Travis Fisher, MD
Dr. Fisher is Fellow, Department of Psychosomatic Medicine, University of California Davis Medical Center, Sacramento, CA.
Robert M. McCarron, DO
Series Editor
• Patients with mental illness are at elevated risk for HIV infection.
• Fourth-generation (p24) HIV testing allows accurate, office-based screening during the period of highest infectivity.
• Psychiatrists may be uniquely able to discuss and alter patients’ high-risk behaviors related to HIV transmission and treatment.
Substance use and high-risk sexual behaviors are common among persons with severe mental illness and make them vulnerable to human immunodeficiency virus (HIV) infection.1-3 The prevalence of HIV is 3 times higher among these patients compared with individuals who are not mentally ill. This article reviews risk factors for HIV transmission, HIV screening recommendations, and current testing options, including the fourth-generation HIV test.
According to the World Health Organization, in 2009:
- 33 million people were infected with HIV
- there were 2.6 million new infections
- 1.8 million people died from causes related to acquired immune deficiency syndrome (AIDS).4
In the United States, approximately 1 million people are living with HIV; 55, 000 new cases were diagnosed in North America in 2009.5 The demographics of those infected with HIV in the United States have changed substantially. Most newly infected individuals are African American, and younger adults have higher rates of new infections.6 With the introduction of standardized antiviral medication combinations and federal programs to provide universal access to medications in the mid 1990s, the number of AIDS cases and mortality dropped, but there have not been similar gains in the past decade.6
In countries With access to antiviral medications, medical advances in HIV treatment have transformed an infection with a high mortality rate into a chronic illness. However, the rate of new cases has not changed significantly in the past 10 years. Early detection and treatment initiation reduces high-risk behavior and subsequent transmission in patients with HIV. Evidence suggests that detecting HIV in the acute phase of the illness, when the viral load is high, reduces HIV transmission.1,5,6
HIV screening
HIV screening should be part of routine psychiatric practice, especially in community and forensic settings. We recommend that all psychiatrists understand HIV screening guidelines from the Centers for Disease Control and Prevention (CDC)7 and the American College of Physicians (ACP).8 The CDC (2006)7 and ACP (2009)8 guidelines recommend HIV screening for:
- all patients age 13 to 64, unless the prevalence of undiagnosed HIV infection in your patients has been documented to be <0. 1%7
- all patients seeking treatment for sexually transmitted diseases, including each visit for a new complaint7
- all pregnant women7
- any patient who received a blood transfusion between 1978 and 1985.8
Rescreening frequency is determined on an individual basis, taking into consideration the patient’s risk of contracting HIV. The ACP guidelines recommend using rapid tests when available.8 Although the false positive rates are higher with rapid tests, the benefits of early detection and reducing transmission outweigh the cost of confirming positive tests.8
The fourth-generation test
The gold standard for HIV screening is the enzyme-linked immunosorbent assay antibody test followed by a western blot.8 This has a high sensitivity and specificity but there is a window of time between infection and detectable antibodies in serum during which patients have high virus levels (Figure).9 The combined antibody and antigen p24 test is a fourth-generation screening tool that detects HIV in the acute phase of the illness without requiring expensive ribonucleic acid viral tests.10 The fourth-generation test’s capacity to detect infection during the antibody-negative window when infectivity is highest may help decrease HIV transmission.11
Figure When can HIV tests detect the virus?
EIA: enzyme immunoassay; HIV: human immunodeficiency virus; RNA: ribonucleic acid
Source: Adapted from reference 9
Psychiatrists’ role
Because psychiatrists routinely interact with patients who have an increased risk of HIV, they may be uniquely qualified to help these individuals. Psychiatrists often are comfortable discussing patients’ sexual and substance use history, which allows them to uncover and effectively address high-risk behaviors with appropriate testing and counseling. If testing confirms HIV infection, psychiatrists also can discuss altering high-risk behaviors (Table),1,2 which has significant implications not only for patients, but also for public health.
Table
HIV transmission risk factors
| Intravenous drug use |
| Nonintravenous cocaine use |
| Sex without barrier protection, especially in patients with multiple partners |
| Sex trade or sex work |
| HIV: human immunodeficiency virus |
| Source: References 1,2 |
Related Resource
- Centers for Disease Control and Prevention. HIV/AIDS. www.cdc.gov/hiv.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
• Patients with mental illness are at elevated risk for HIV infection.
• Fourth-generation (p24) HIV testing allows accurate, office-based screening during the period of highest infectivity.
• Psychiatrists may be uniquely able to discuss and alter patients’ high-risk behaviors related to HIV transmission and treatment.
Substance use and high-risk sexual behaviors are common among persons with severe mental illness and make them vulnerable to human immunodeficiency virus (HIV) infection.1-3 The prevalence of HIV is 3 times higher among these patients compared with individuals who are not mentally ill. This article reviews risk factors for HIV transmission, HIV screening recommendations, and current testing options, including the fourth-generation HIV test.
According to the World Health Organization, in 2009:
- 33 million people were infected with HIV
- there were 2.6 million new infections
- 1.8 million people died from causes related to acquired immune deficiency syndrome (AIDS).4
In the United States, approximately 1 million people are living with HIV; 55, 000 new cases were diagnosed in North America in 2009.5 The demographics of those infected with HIV in the United States have changed substantially. Most newly infected individuals are African American, and younger adults have higher rates of new infections.6 With the introduction of standardized antiviral medication combinations and federal programs to provide universal access to medications in the mid 1990s, the number of AIDS cases and mortality dropped, but there have not been similar gains in the past decade.6
In countries With access to antiviral medications, medical advances in HIV treatment have transformed an infection with a high mortality rate into a chronic illness. However, the rate of new cases has not changed significantly in the past 10 years. Early detection and treatment initiation reduces high-risk behavior and subsequent transmission in patients with HIV. Evidence suggests that detecting HIV in the acute phase of the illness, when the viral load is high, reduces HIV transmission.1,5,6
HIV screening
HIV screening should be part of routine psychiatric practice, especially in community and forensic settings. We recommend that all psychiatrists understand HIV screening guidelines from the Centers for Disease Control and Prevention (CDC)7 and the American College of Physicians (ACP).8 The CDC (2006)7 and ACP (2009)8 guidelines recommend HIV screening for:
- all patients age 13 to 64, unless the prevalence of undiagnosed HIV infection in your patients has been documented to be <0. 1%7
- all patients seeking treatment for sexually transmitted diseases, including each visit for a new complaint7
- all pregnant women7
- any patient who received a blood transfusion between 1978 and 1985.8
Rescreening frequency is determined on an individual basis, taking into consideration the patient’s risk of contracting HIV. The ACP guidelines recommend using rapid tests when available.8 Although the false positive rates are higher with rapid tests, the benefits of early detection and reducing transmission outweigh the cost of confirming positive tests.8
The fourth-generation test
The gold standard for HIV screening is the enzyme-linked immunosorbent assay antibody test followed by a western blot.8 This has a high sensitivity and specificity but there is a window of time between infection and detectable antibodies in serum during which patients have high virus levels (Figure).9 The combined antibody and antigen p24 test is a fourth-generation screening tool that detects HIV in the acute phase of the illness without requiring expensive ribonucleic acid viral tests.10 The fourth-generation test’s capacity to detect infection during the antibody-negative window when infectivity is highest may help decrease HIV transmission.11
Figure When can HIV tests detect the virus?
EIA: enzyme immunoassay; HIV: human immunodeficiency virus; RNA: ribonucleic acid
Source: Adapted from reference 9
Psychiatrists’ role
Because psychiatrists routinely interact with patients who have an increased risk of HIV, they may be uniquely qualified to help these individuals. Psychiatrists often are comfortable discussing patients’ sexual and substance use history, which allows them to uncover and effectively address high-risk behaviors with appropriate testing and counseling. If testing confirms HIV infection, psychiatrists also can discuss altering high-risk behaviors (Table),1,2 which has significant implications not only for patients, but also for public health.
Table
HIV transmission risk factors
| Intravenous drug use |
| Nonintravenous cocaine use |
| Sex without barrier protection, especially in patients with multiple partners |
| Sex trade or sex work |
| HIV: human immunodeficiency virus |
| Source: References 1,2 |
Related Resource
- Centers for Disease Control and Prevention. HIV/AIDS. www.cdc.gov/hiv.
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Rosenberg SD, Goodman LA, Osher FC, et al. Prevalence of HIV, hepatitis B, and hepatitis C in people with severe mental illness. Am J Health. 2001;91:31-37.
2. Quinn TC, Glasser D, Cannon RO, et al. Human immunodeficiency virus infection among patients attending clinics for sexually transmitted diseases. N Eng J Med. 1988;318:197-203.
3. Erickson B, Wasserheit JN, Rompalo AM, et al. Routine voluntary HIV screening in STD clinic clients: characterization of infected clients. Sex Transm Dis. 1990;17:194-199.
4. World Health Organization. Global summary of the AIDS epidemic. Available at: http://www.who.int/hiv/data/2009_global_summary.png. Accessed February 10 2011.
5. Hall HI, Song R, Rhodes P, et al. Estimation of HIV incidence in the United States. JAMA. 2008;300:520-529.
6. Glynn MK, Lee LM, McKenna MT. The status of national HIV case surveillance United States 2006. Public Health Rep. 2007;122(suppl 1):63-71.
7. Branson BM, Handsfield HH, Lampe MA, et al. and the Centers for Disease Control and Prevention. Revised recommendations for HIV testing of adults adolescents, and pregnant women in health-care settings. MMWR Recomm Rep. 2006;55(RR-14):1-17; quiz CE1-CE4.
8. Qaseem A, Snow V, Shekelle P, et al. and the Clinical Efficacy Assessment Subcommittee American College of Physicians. Screening for HIV in health care settings: a guidance statement from the American College of Physicians and HIV Medicine Association. Ann Intern Med. 2009;150:125-131.
9. Branson BM. The future of HIV testing. J Acquir Immune Defic Syndr. 2010;55:S102-S105.
10. Eshleman S, Khaki L, Laeyendecker O, et al. Detection of individuals with acute HIV-1 infection using the ARCHITECT HIV Ag/Ab combo assay. J Acquir Immune Defic Syndr. 2009;52:121-124.
11. Pandori MW, Hackett J, Jr, Louie B, et al. Assessment of the ability of a fourth-generation immunoassay for human immunodeficiency virus (HIV) antibody and p24 antigen to detect both acute and recent HIV infections in a high-risk setting. J Clin Microbiol. 2009;47:2639-2642.
1. Rosenberg SD, Goodman LA, Osher FC, et al. Prevalence of HIV, hepatitis B, and hepatitis C in people with severe mental illness. Am J Health. 2001;91:31-37.
2. Quinn TC, Glasser D, Cannon RO, et al. Human immunodeficiency virus infection among patients attending clinics for sexually transmitted diseases. N Eng J Med. 1988;318:197-203.
3. Erickson B, Wasserheit JN, Rompalo AM, et al. Routine voluntary HIV screening in STD clinic clients: characterization of infected clients. Sex Transm Dis. 1990;17:194-199.
4. World Health Organization. Global summary of the AIDS epidemic. Available at: http://www.who.int/hiv/data/2009_global_summary.png. Accessed February 10 2011.
5. Hall HI, Song R, Rhodes P, et al. Estimation of HIV incidence in the United States. JAMA. 2008;300:520-529.
6. Glynn MK, Lee LM, McKenna MT. The status of national HIV case surveillance United States 2006. Public Health Rep. 2007;122(suppl 1):63-71.
7. Branson BM, Handsfield HH, Lampe MA, et al. and the Centers for Disease Control and Prevention. Revised recommendations for HIV testing of adults adolescents, and pregnant women in health-care settings. MMWR Recomm Rep. 2006;55(RR-14):1-17; quiz CE1-CE4.
8. Qaseem A, Snow V, Shekelle P, et al. and the Clinical Efficacy Assessment Subcommittee American College of Physicians. Screening for HIV in health care settings: a guidance statement from the American College of Physicians and HIV Medicine Association. Ann Intern Med. 2009;150:125-131.
9. Branson BM. The future of HIV testing. J Acquir Immune Defic Syndr. 2010;55:S102-S105.
10. Eshleman S, Khaki L, Laeyendecker O, et al. Detection of individuals with acute HIV-1 infection using the ARCHITECT HIV Ag/Ab combo assay. J Acquir Immune Defic Syndr. 2009;52:121-124.
11. Pandori MW, Hackett J, Jr, Louie B, et al. Assessment of the ability of a fourth-generation immunoassay for human immunodeficiency virus (HIV) antibody and p24 antigen to detect both acute and recent HIV infections in a high-risk setting. J Clin Microbiol. 2009;47:2639-2642.
Mood swings and ODD
I needed an intellectual oasis to deal with the anguish and frustration triggered by the monumental amount of misleading information that was included in the well-written article “Not all mood swings are bipolar disorder” (Current Psychiatry, February 2011, p. 38-52). Fortunately, a commentary by Dr. Irene Abramovich (“Breaking the box,” Comments & Controversies, Current Psychiatry, February 2011, p. 59) appeared as a therapeutic elixir. I believe that the “mood swings” article is filled with examples of how dangerous “cookbook” medicine can be.
Dr. Kowatch and colleagues use an expression that can be applied to the so-called diagnoses oppositional defiant disorder (ODD) and conduct disorder (CD): “Mood swings are analogous to a fever in pediatrics—they indicate something potentially is wrong with the patient, but they are not diagnostic as an isolated symptom. “ A similar concept was my position in a debate titled “Childhood conduct disorder and oppositional-defiant disorders are common manifestations of bipolar disorder” in which I argued that ODD and CD are behavioral expressions of genuine diagnoses.1 Besides bipolar disorder, I also have seen obsessive-compulsive disorder, social anxiety disorder, and even sexual abuse labeled as “ODD” because the child refuses to be around people (such as a classroom) or is distracted by intrusive thoughts or flashbacks and turns hostile when reproached in front of the class.
In my view, Dr. Kowatch and colleagues give undeserved credit to the behavioral scales (the “cookbooks” of psychiatry) to make diagnoses and seem to miss warning signs in patients’ family history, ie, “history of depression and anxiety” (many times this translates as agitated/dysphoric mania) and “drinking problems, “ which frequently is found in undiagnosed bipolar spectrum patients who use alcohol to “shoot down” racing thoughts that interfere with normal sleep.
From January 2010 to February 2011, I reviewed charts and interviewed patients and families of 1, 654 patients with diagnoses of attention-deficit/hyperactivity disorder co-morbid with ODD, bipolar disorder, generalized anxiety disorder, and even 2 diagnoses that are not allowed by DSM rules: autism and mental retardation. The data from this study, which covers 12 counties that represent the 5 geographical areas of Florida, are being analyzed. In the meantime, I refer readers to my poster presentation from the 2010 U. S. Psychiatric and Mental Health Congress “Extinction of oppositional-defiant symptoms following treatment with mood stabilizers. “2 In this study 44 patients were followed for at least 5 years (10 patients were observed for 7 years and a similar number for 6) and none had “oppositional” behavior after the diagnoses were treated. One caveat is that I placed antipsychotics in the same category as conventional mood stabilizers because 5 patients considered to be “inattentive” and “oppositional” actually had schizophrenia.
I oppose the authors’ assertion that “it can be difficult to differentiate the mood swings and symptoms of ODD from those of pediatric BD. “ My experience is that it is simple if we consider all diagnostic possibilities and obtain a thorough family history, which usually includes alcoholism, cannabis abuse, moodiness, suicide completion, unstable lifestyle, etc.
Manuel Mota-Castillo, MD
Assistant Clinical Professor
St. Matthews University
Voluntary Faculty
University of Central Florida
Lake Mary, FL
References
1. Mota-Castillo M, Steiner H. Childhood conduct disorder and oppositional-defiant disorder are common manifestations of bipolar disorder pro and con. Journal of Bipolar Disorders: Reviews and Commentaries. 2005;3:3,15-17.
2. Mota-Castillo M. Extinction of oppositional-defiant symptoms following treatment with mood stabilizers. Poster presented at: 23rd Annual U.S. Psychiatric and Mental Health Congress; November 20 2010; Orlando, FL.
The authors respond
We never suggested that clinicians use “cookbook medicine. “ The “behavioral scales” we recommended in our article are well-validated and reliable tools that allow a clinician to effectively elicit a great deal of useful information from patients and their parents about presenting problems and symptoms. This information can be used with other clinical information to make an accurate diagnosis and subsequent treatment plan.
The purpose of our article was to share our experiences in the differential diagnosis of mood swings in children and adolescents and to suggest that there are other diagnoses that cause mood swings besides bipolar disorder. Although a family history of mood disorders is important, it is also important to recognize that a recent, state-of-the-art study by Birmaher et al1 reported that 10% of children of parents with bipolar disorder had a bipolar spectrum disorder. That means that 90% did not have bipolar disorder. It is important to remember this when evaluating children of parents with bipolar disorder. Although these children’s risk for developing bipolar disorder is increased compared with the general population, it is more likely that they will not develop bipolar disorder.
Robert A. Kowatch, MD, PhD
Professor of Psychiatry and Pediatrics
Erin Monroe, CNS
Clinical Nurse Specialist
Division of Psychiatry
Sergio V. Delgado, MD
Associate Professor of Psychiatry
and Pediatrics
Cincinnati Children’s Hospital Medical Center
Cincinnati, OH
1. Birmaher B, Axelson D, Monk K, et al. Lifetime psychiatric disorders in school-aged offspring of parents with bipolar disorder: the Pittsburgh Bipolar Offspring study. Arch Gen Psychiatry. 2009;66(3):287-296.
I needed an intellectual oasis to deal with the anguish and frustration triggered by the monumental amount of misleading information that was included in the well-written article “Not all mood swings are bipolar disorder” (Current Psychiatry, February 2011, p. 38-52). Fortunately, a commentary by Dr. Irene Abramovich (“Breaking the box,” Comments & Controversies, Current Psychiatry, February 2011, p. 59) appeared as a therapeutic elixir. I believe that the “mood swings” article is filled with examples of how dangerous “cookbook” medicine can be.
Dr. Kowatch and colleagues use an expression that can be applied to the so-called diagnoses oppositional defiant disorder (ODD) and conduct disorder (CD): “Mood swings are analogous to a fever in pediatrics—they indicate something potentially is wrong with the patient, but they are not diagnostic as an isolated symptom. “ A similar concept was my position in a debate titled “Childhood conduct disorder and oppositional-defiant disorders are common manifestations of bipolar disorder” in which I argued that ODD and CD are behavioral expressions of genuine diagnoses.1 Besides bipolar disorder, I also have seen obsessive-compulsive disorder, social anxiety disorder, and even sexual abuse labeled as “ODD” because the child refuses to be around people (such as a classroom) or is distracted by intrusive thoughts or flashbacks and turns hostile when reproached in front of the class.
In my view, Dr. Kowatch and colleagues give undeserved credit to the behavioral scales (the “cookbooks” of psychiatry) to make diagnoses and seem to miss warning signs in patients’ family history, ie, “history of depression and anxiety” (many times this translates as agitated/dysphoric mania) and “drinking problems, “ which frequently is found in undiagnosed bipolar spectrum patients who use alcohol to “shoot down” racing thoughts that interfere with normal sleep.
From January 2010 to February 2011, I reviewed charts and interviewed patients and families of 1, 654 patients with diagnoses of attention-deficit/hyperactivity disorder co-morbid with ODD, bipolar disorder, generalized anxiety disorder, and even 2 diagnoses that are not allowed by DSM rules: autism and mental retardation. The data from this study, which covers 12 counties that represent the 5 geographical areas of Florida, are being analyzed. In the meantime, I refer readers to my poster presentation from the 2010 U. S. Psychiatric and Mental Health Congress “Extinction of oppositional-defiant symptoms following treatment with mood stabilizers. “2 In this study 44 patients were followed for at least 5 years (10 patients were observed for 7 years and a similar number for 6) and none had “oppositional” behavior after the diagnoses were treated. One caveat is that I placed antipsychotics in the same category as conventional mood stabilizers because 5 patients considered to be “inattentive” and “oppositional” actually had schizophrenia.
I oppose the authors’ assertion that “it can be difficult to differentiate the mood swings and symptoms of ODD from those of pediatric BD. “ My experience is that it is simple if we consider all diagnostic possibilities and obtain a thorough family history, which usually includes alcoholism, cannabis abuse, moodiness, suicide completion, unstable lifestyle, etc.
Manuel Mota-Castillo, MD
Assistant Clinical Professor
St. Matthews University
Voluntary Faculty
University of Central Florida
Lake Mary, FL
References
1. Mota-Castillo M, Steiner H. Childhood conduct disorder and oppositional-defiant disorder are common manifestations of bipolar disorder pro and con. Journal of Bipolar Disorders: Reviews and Commentaries. 2005;3:3,15-17.
2. Mota-Castillo M. Extinction of oppositional-defiant symptoms following treatment with mood stabilizers. Poster presented at: 23rd Annual U.S. Psychiatric and Mental Health Congress; November 20 2010; Orlando, FL.
The authors respond
We never suggested that clinicians use “cookbook medicine. “ The “behavioral scales” we recommended in our article are well-validated and reliable tools that allow a clinician to effectively elicit a great deal of useful information from patients and their parents about presenting problems and symptoms. This information can be used with other clinical information to make an accurate diagnosis and subsequent treatment plan.
The purpose of our article was to share our experiences in the differential diagnosis of mood swings in children and adolescents and to suggest that there are other diagnoses that cause mood swings besides bipolar disorder. Although a family history of mood disorders is important, it is also important to recognize that a recent, state-of-the-art study by Birmaher et al1 reported that 10% of children of parents with bipolar disorder had a bipolar spectrum disorder. That means that 90% did not have bipolar disorder. It is important to remember this when evaluating children of parents with bipolar disorder. Although these children’s risk for developing bipolar disorder is increased compared with the general population, it is more likely that they will not develop bipolar disorder.
Robert A. Kowatch, MD, PhD
Professor of Psychiatry and Pediatrics
Erin Monroe, CNS
Clinical Nurse Specialist
Division of Psychiatry
Sergio V. Delgado, MD
Associate Professor of Psychiatry
and Pediatrics
Cincinnati Children’s Hospital Medical Center
Cincinnati, OH
I needed an intellectual oasis to deal with the anguish and frustration triggered by the monumental amount of misleading information that was included in the well-written article “Not all mood swings are bipolar disorder” (Current Psychiatry, February 2011, p. 38-52). Fortunately, a commentary by Dr. Irene Abramovich (“Breaking the box,” Comments & Controversies, Current Psychiatry, February 2011, p. 59) appeared as a therapeutic elixir. I believe that the “mood swings” article is filled with examples of how dangerous “cookbook” medicine can be.
Dr. Kowatch and colleagues use an expression that can be applied to the so-called diagnoses oppositional defiant disorder (ODD) and conduct disorder (CD): “Mood swings are analogous to a fever in pediatrics—they indicate something potentially is wrong with the patient, but they are not diagnostic as an isolated symptom. “ A similar concept was my position in a debate titled “Childhood conduct disorder and oppositional-defiant disorders are common manifestations of bipolar disorder” in which I argued that ODD and CD are behavioral expressions of genuine diagnoses.1 Besides bipolar disorder, I also have seen obsessive-compulsive disorder, social anxiety disorder, and even sexual abuse labeled as “ODD” because the child refuses to be around people (such as a classroom) or is distracted by intrusive thoughts or flashbacks and turns hostile when reproached in front of the class.
In my view, Dr. Kowatch and colleagues give undeserved credit to the behavioral scales (the “cookbooks” of psychiatry) to make diagnoses and seem to miss warning signs in patients’ family history, ie, “history of depression and anxiety” (many times this translates as agitated/dysphoric mania) and “drinking problems, “ which frequently is found in undiagnosed bipolar spectrum patients who use alcohol to “shoot down” racing thoughts that interfere with normal sleep.
From January 2010 to February 2011, I reviewed charts and interviewed patients and families of 1, 654 patients with diagnoses of attention-deficit/hyperactivity disorder co-morbid with ODD, bipolar disorder, generalized anxiety disorder, and even 2 diagnoses that are not allowed by DSM rules: autism and mental retardation. The data from this study, which covers 12 counties that represent the 5 geographical areas of Florida, are being analyzed. In the meantime, I refer readers to my poster presentation from the 2010 U. S. Psychiatric and Mental Health Congress “Extinction of oppositional-defiant symptoms following treatment with mood stabilizers. “2 In this study 44 patients were followed for at least 5 years (10 patients were observed for 7 years and a similar number for 6) and none had “oppositional” behavior after the diagnoses were treated. One caveat is that I placed antipsychotics in the same category as conventional mood stabilizers because 5 patients considered to be “inattentive” and “oppositional” actually had schizophrenia.
I oppose the authors’ assertion that “it can be difficult to differentiate the mood swings and symptoms of ODD from those of pediatric BD. “ My experience is that it is simple if we consider all diagnostic possibilities and obtain a thorough family history, which usually includes alcoholism, cannabis abuse, moodiness, suicide completion, unstable lifestyle, etc.
Manuel Mota-Castillo, MD
Assistant Clinical Professor
St. Matthews University
Voluntary Faculty
University of Central Florida
Lake Mary, FL
References
1. Mota-Castillo M, Steiner H. Childhood conduct disorder and oppositional-defiant disorder are common manifestations of bipolar disorder pro and con. Journal of Bipolar Disorders: Reviews and Commentaries. 2005;3:3,15-17.
2. Mota-Castillo M. Extinction of oppositional-defiant symptoms following treatment with mood stabilizers. Poster presented at: 23rd Annual U.S. Psychiatric and Mental Health Congress; November 20 2010; Orlando, FL.
The authors respond
We never suggested that clinicians use “cookbook medicine. “ The “behavioral scales” we recommended in our article are well-validated and reliable tools that allow a clinician to effectively elicit a great deal of useful information from patients and their parents about presenting problems and symptoms. This information can be used with other clinical information to make an accurate diagnosis and subsequent treatment plan.
The purpose of our article was to share our experiences in the differential diagnosis of mood swings in children and adolescents and to suggest that there are other diagnoses that cause mood swings besides bipolar disorder. Although a family history of mood disorders is important, it is also important to recognize that a recent, state-of-the-art study by Birmaher et al1 reported that 10% of children of parents with bipolar disorder had a bipolar spectrum disorder. That means that 90% did not have bipolar disorder. It is important to remember this when evaluating children of parents with bipolar disorder. Although these children’s risk for developing bipolar disorder is increased compared with the general population, it is more likely that they will not develop bipolar disorder.
Robert A. Kowatch, MD, PhD
Professor of Psychiatry and Pediatrics
Erin Monroe, CNS
Clinical Nurse Specialist
Division of Psychiatry
Sergio V. Delgado, MD
Associate Professor of Psychiatry
and Pediatrics
Cincinnati Children’s Hospital Medical Center
Cincinnati, OH
1. Birmaher B, Axelson D, Monk K, et al. Lifetime psychiatric disorders in school-aged offspring of parents with bipolar disorder: the Pittsburgh Bipolar Offspring study. Arch Gen Psychiatry. 2009;66(3):287-296.
1. Birmaher B, Axelson D, Monk K, et al. Lifetime psychiatric disorders in school-aged offspring of parents with bipolar disorder: the Pittsburgh Bipolar Offspring study. Arch Gen Psychiatry. 2009;66(3):287-296.
Mood swings and BPD
I thought Dr. Kowatch and colleagues took an important first step in pointing out that not all mood swings in children and adolescents are symptoms of bipolar disorder (“Not all mood swings are bipolar disorder,“ Current Psychiatry, February 2011, p. 38-52). They reviewed some of the other psychiatric conditions known to cause labile moods. One glaring omission is borderline personality disorder (BPD).
I am the medical director of a specialized unit that uses dialectical behavioral therapy (DBT) to treat children and adolescents with BPD. We have treated approximately 300 young women on the residential unit and many present similarly: multiple hospitalizations, multiple robust yet failed medication trials, severe and recurrent self-injury, suicide attempts, and a large degree of hopelessness. Most arrive with previous diagnoses of mood disorder not otherwise specified, bipolar disorder, oppositional defiant disorder, attention-deficit/hyperactivity disorder, and others. It is when their outpatient psychiatrists and mental health teams have grown frustrated at the lack of enduring progress and are faced with the treatment demands of the borderline patient that a BPD diagnosis is considered. Even though research suggests that BPD—or at least some of its symptoms—begins in the late latency period of childhood,1 treatment typically is not sought until late adolescence. This is the case despite the fact that BPD has a better prognosis than other serious mental illnesses, such as bipolar disorder.2,3 Adult BPD patients almost universally recognize that their inability to regulate their mood started in late childhood and early adolescence. Structural and functional neuroimaging has revealed a dysfunctional network of brain regions that seem to mediate important aspects of BPD symptomatology.4-6
These children have marked mood swings and great difficulty regulating their moods. The mood swings of BPD are not responsive to current medication unless there is comorbid bipolar disorder, in which case treatment with mood stabilizers helps improve vegetative symptoms such as sleep and energy, and reduce racing thoughts, pressured speech, and irritability. What these medications do not treat is the “reactive” mood swings that are characteristic of BPD. The mood reactivity often is triggered by interpersonal or intrapersonal conflict and rarely is long-lived.
Many children and adolescents are moody and most do not have a major psychiatric disorder. Of those who do, it is a great risk to patients’ health to not consider BPD, especially given new and empirically validated treatments, such as DBT. Astute clinicians should keep this diagnosis in mind when treating adolescents with moodiness, particularly when the mood is predominantly reactive to life’s stressors, when other features of the presentation do not fit neatly into a bipolar picture, and when multiple medications fail. On our unit, we have seen that the cognitive-behavioral strategies of DBT help patients even when BPD is not the diagnosis.
I would like to thank Dr. Kowatch and colleagues for expanding our thinking on mood swings and encourage readers to go one step further.
Blaise Aguirre, MD
Medical Director
Adolescent DBT Residential Program
McLean Hospital
Belmont, MA
Instructor in Psychiatry
Harvard Medical School
Boston, MA
References
1. Zanarini MC, Frankenburg FR, Khera GS, et al. Treatment histories of borderline inpatients. Compr Psychiatry. 2001;42:144-150.
2. Tohen M, Hennen J, Zarate CM Jr, et al. Two-year syndromal and functional recovery in 219 cases of first-episode major affective disorder with psychotic features. Am J Psychiatry. 2000;157:220-228.
3. Coryell W, Endicott J, Maser JD, et al. The likelihood of recurrence in bipolar affective disorder: the importance of episode recency. J Affect Disord. 1995;33:201-206.
4. De La Fuente JM, Goldman S, Stanus E, et al. Brain glucose metabolism in borderline personality disorder. J Psychiatr Res. 1997;31:531-541.
5. Soloff PH, Meltzer CC, Becker C, et al. Impulsivity and prefrontal hypometabolism in borderline personality disorder. Psychiatry Res. 2003;123:153-163.
6. Juengling FD, Schmahl C, Hesslinger B, et al. Positron emission tomography in female patients with borderline personality disorder. J Psychiatr Res. 2003;37:109-115.
The authors respond
We welcome comments about the importance of a thorough diagnostic evaluation to tease out possible etiologies of “mood swings, “ including psychosocial factors, as in personality disorders. Nevertheless, the debate about diagnosing personality disorders in children and adolescents is not settled. Developmentally, children and adolescents have continuous changes in biology and brain function. There is significantly more empirical evidence of reactive attachment disorders in childhood and adolescence that integrate the affective changes seen in children who live in chaotic environments. DSM defines BPD as a pervasive pattern of instability of interpersonal relationships that begins by early adulthood.1 Many children with diagnoses of posttraumatic stress disorder, mood disorder, bipolar disorder, oppositional defiant disorder, attention-deficit/hyperactivity disorder, etc. also can have difficulties in relating to others caused by their neurobiologic deficits, which also may limit response to medication. Furthermore, children with learning disorders also can misperceive motives of others and thus have pervasive patterns of relational instability.
The research Dr. Aguirre suggested is based on treatment histories and not rigorous study methodology. Most empirical evidence of personality disorders is strongly influenced by psychoanalytic literature regarding object relations, which is in flux because of emerging attention to attachment theory and progress in neurologic studies in the evaluation of temperamental variations related to the influence of mirror neurons.2
We also take issue with the comment that “BPD has a better prognosis than other serious men tal illn esses, such as bipolar disorder” There have been significant efforts in studying the role family can have in the outcomes of mood disorder treatment.3
Finally, there is evidence that in adults medication can be beneficial in treating the affective deregulation of patients with BPD who do not have comorbid disorders.4
Robert A. Kowatch, MD, PhD
Professor of Psychiatry and Pediatrics
Erin Monroe, CNS
Clinical Nurse Specialist
Division of Psychiatry
Sergio V. Delgado, MD
Associate Professor of Psychiatry
and Pediatrics
Cincinnati Children’s Hospital Medical Center
Cincinnati, OH
1. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
2. Zald DH, Cowan RL, Riccardi P, et al. Midbrain dopamine receptor availability is inversely associated with novelty-seeking traits in humans. J Neurosci. 2008;28(53):14372-14378.
3. Miklowitz DJ, Axelson DA, Birmaher B, et al. Family-focused treatment for adolescents with bipolar disorder: results of a 2-year randomized trial. Arch Gen Psychiatry. 2008;65(9):1053-1061.
4. Stoffers J, VÖllum BA, RÜcker G, et al. Pharmacological interventions for borderline personality disorder. Cochrane Database Syst Rev. 2010;16:CD005653.-
I thought Dr. Kowatch and colleagues took an important first step in pointing out that not all mood swings in children and adolescents are symptoms of bipolar disorder (“Not all mood swings are bipolar disorder,“ Current Psychiatry, February 2011, p. 38-52). They reviewed some of the other psychiatric conditions known to cause labile moods. One glaring omission is borderline personality disorder (BPD).
I am the medical director of a specialized unit that uses dialectical behavioral therapy (DBT) to treat children and adolescents with BPD. We have treated approximately 300 young women on the residential unit and many present similarly: multiple hospitalizations, multiple robust yet failed medication trials, severe and recurrent self-injury, suicide attempts, and a large degree of hopelessness. Most arrive with previous diagnoses of mood disorder not otherwise specified, bipolar disorder, oppositional defiant disorder, attention-deficit/hyperactivity disorder, and others. It is when their outpatient psychiatrists and mental health teams have grown frustrated at the lack of enduring progress and are faced with the treatment demands of the borderline patient that a BPD diagnosis is considered. Even though research suggests that BPD—or at least some of its symptoms—begins in the late latency period of childhood,1 treatment typically is not sought until late adolescence. This is the case despite the fact that BPD has a better prognosis than other serious mental illnesses, such as bipolar disorder.2,3 Adult BPD patients almost universally recognize that their inability to regulate their mood started in late childhood and early adolescence. Structural and functional neuroimaging has revealed a dysfunctional network of brain regions that seem to mediate important aspects of BPD symptomatology.4-6
These children have marked mood swings and great difficulty regulating their moods. The mood swings of BPD are not responsive to current medication unless there is comorbid bipolar disorder, in which case treatment with mood stabilizers helps improve vegetative symptoms such as sleep and energy, and reduce racing thoughts, pressured speech, and irritability. What these medications do not treat is the “reactive” mood swings that are characteristic of BPD. The mood reactivity often is triggered by interpersonal or intrapersonal conflict and rarely is long-lived.
Many children and adolescents are moody and most do not have a major psychiatric disorder. Of those who do, it is a great risk to patients’ health to not consider BPD, especially given new and empirically validated treatments, such as DBT. Astute clinicians should keep this diagnosis in mind when treating adolescents with moodiness, particularly when the mood is predominantly reactive to life’s stressors, when other features of the presentation do not fit neatly into a bipolar picture, and when multiple medications fail. On our unit, we have seen that the cognitive-behavioral strategies of DBT help patients even when BPD is not the diagnosis.
I would like to thank Dr. Kowatch and colleagues for expanding our thinking on mood swings and encourage readers to go one step further.
Blaise Aguirre, MD
Medical Director
Adolescent DBT Residential Program
McLean Hospital
Belmont, MA
Instructor in Psychiatry
Harvard Medical School
Boston, MA
References
1. Zanarini MC, Frankenburg FR, Khera GS, et al. Treatment histories of borderline inpatients. Compr Psychiatry. 2001;42:144-150.
2. Tohen M, Hennen J, Zarate CM Jr, et al. Two-year syndromal and functional recovery in 219 cases of first-episode major affective disorder with psychotic features. Am J Psychiatry. 2000;157:220-228.
3. Coryell W, Endicott J, Maser JD, et al. The likelihood of recurrence in bipolar affective disorder: the importance of episode recency. J Affect Disord. 1995;33:201-206.
4. De La Fuente JM, Goldman S, Stanus E, et al. Brain glucose metabolism in borderline personality disorder. J Psychiatr Res. 1997;31:531-541.
5. Soloff PH, Meltzer CC, Becker C, et al. Impulsivity and prefrontal hypometabolism in borderline personality disorder. Psychiatry Res. 2003;123:153-163.
6. Juengling FD, Schmahl C, Hesslinger B, et al. Positron emission tomography in female patients with borderline personality disorder. J Psychiatr Res. 2003;37:109-115.
The authors respond
We welcome comments about the importance of a thorough diagnostic evaluation to tease out possible etiologies of “mood swings, “ including psychosocial factors, as in personality disorders. Nevertheless, the debate about diagnosing personality disorders in children and adolescents is not settled. Developmentally, children and adolescents have continuous changes in biology and brain function. There is significantly more empirical evidence of reactive attachment disorders in childhood and adolescence that integrate the affective changes seen in children who live in chaotic environments. DSM defines BPD as a pervasive pattern of instability of interpersonal relationships that begins by early adulthood.1 Many children with diagnoses of posttraumatic stress disorder, mood disorder, bipolar disorder, oppositional defiant disorder, attention-deficit/hyperactivity disorder, etc. also can have difficulties in relating to others caused by their neurobiologic deficits, which also may limit response to medication. Furthermore, children with learning disorders also can misperceive motives of others and thus have pervasive patterns of relational instability.
The research Dr. Aguirre suggested is based on treatment histories and not rigorous study methodology. Most empirical evidence of personality disorders is strongly influenced by psychoanalytic literature regarding object relations, which is in flux because of emerging attention to attachment theory and progress in neurologic studies in the evaluation of temperamental variations related to the influence of mirror neurons.2
We also take issue with the comment that “BPD has a better prognosis than other serious men tal illn esses, such as bipolar disorder” There have been significant efforts in studying the role family can have in the outcomes of mood disorder treatment.3
Finally, there is evidence that in adults medication can be beneficial in treating the affective deregulation of patients with BPD who do not have comorbid disorders.4
Robert A. Kowatch, MD, PhD
Professor of Psychiatry and Pediatrics
Erin Monroe, CNS
Clinical Nurse Specialist
Division of Psychiatry
Sergio V. Delgado, MD
Associate Professor of Psychiatry
and Pediatrics
Cincinnati Children’s Hospital Medical Center
Cincinnati, OH
I thought Dr. Kowatch and colleagues took an important first step in pointing out that not all mood swings in children and adolescents are symptoms of bipolar disorder (“Not all mood swings are bipolar disorder,“ Current Psychiatry, February 2011, p. 38-52). They reviewed some of the other psychiatric conditions known to cause labile moods. One glaring omission is borderline personality disorder (BPD).
I am the medical director of a specialized unit that uses dialectical behavioral therapy (DBT) to treat children and adolescents with BPD. We have treated approximately 300 young women on the residential unit and many present similarly: multiple hospitalizations, multiple robust yet failed medication trials, severe and recurrent self-injury, suicide attempts, and a large degree of hopelessness. Most arrive with previous diagnoses of mood disorder not otherwise specified, bipolar disorder, oppositional defiant disorder, attention-deficit/hyperactivity disorder, and others. It is when their outpatient psychiatrists and mental health teams have grown frustrated at the lack of enduring progress and are faced with the treatment demands of the borderline patient that a BPD diagnosis is considered. Even though research suggests that BPD—or at least some of its symptoms—begins in the late latency period of childhood,1 treatment typically is not sought until late adolescence. This is the case despite the fact that BPD has a better prognosis than other serious mental illnesses, such as bipolar disorder.2,3 Adult BPD patients almost universally recognize that their inability to regulate their mood started in late childhood and early adolescence. Structural and functional neuroimaging has revealed a dysfunctional network of brain regions that seem to mediate important aspects of BPD symptomatology.4-6
These children have marked mood swings and great difficulty regulating their moods. The mood swings of BPD are not responsive to current medication unless there is comorbid bipolar disorder, in which case treatment with mood stabilizers helps improve vegetative symptoms such as sleep and energy, and reduce racing thoughts, pressured speech, and irritability. What these medications do not treat is the “reactive” mood swings that are characteristic of BPD. The mood reactivity often is triggered by interpersonal or intrapersonal conflict and rarely is long-lived.
Many children and adolescents are moody and most do not have a major psychiatric disorder. Of those who do, it is a great risk to patients’ health to not consider BPD, especially given new and empirically validated treatments, such as DBT. Astute clinicians should keep this diagnosis in mind when treating adolescents with moodiness, particularly when the mood is predominantly reactive to life’s stressors, when other features of the presentation do not fit neatly into a bipolar picture, and when multiple medications fail. On our unit, we have seen that the cognitive-behavioral strategies of DBT help patients even when BPD is not the diagnosis.
I would like to thank Dr. Kowatch and colleagues for expanding our thinking on mood swings and encourage readers to go one step further.
Blaise Aguirre, MD
Medical Director
Adolescent DBT Residential Program
McLean Hospital
Belmont, MA
Instructor in Psychiatry
Harvard Medical School
Boston, MA
References
1. Zanarini MC, Frankenburg FR, Khera GS, et al. Treatment histories of borderline inpatients. Compr Psychiatry. 2001;42:144-150.
2. Tohen M, Hennen J, Zarate CM Jr, et al. Two-year syndromal and functional recovery in 219 cases of first-episode major affective disorder with psychotic features. Am J Psychiatry. 2000;157:220-228.
3. Coryell W, Endicott J, Maser JD, et al. The likelihood of recurrence in bipolar affective disorder: the importance of episode recency. J Affect Disord. 1995;33:201-206.
4. De La Fuente JM, Goldman S, Stanus E, et al. Brain glucose metabolism in borderline personality disorder. J Psychiatr Res. 1997;31:531-541.
5. Soloff PH, Meltzer CC, Becker C, et al. Impulsivity and prefrontal hypometabolism in borderline personality disorder. Psychiatry Res. 2003;123:153-163.
6. Juengling FD, Schmahl C, Hesslinger B, et al. Positron emission tomography in female patients with borderline personality disorder. J Psychiatr Res. 2003;37:109-115.
The authors respond
We welcome comments about the importance of a thorough diagnostic evaluation to tease out possible etiologies of “mood swings, “ including psychosocial factors, as in personality disorders. Nevertheless, the debate about diagnosing personality disorders in children and adolescents is not settled. Developmentally, children and adolescents have continuous changes in biology and brain function. There is significantly more empirical evidence of reactive attachment disorders in childhood and adolescence that integrate the affective changes seen in children who live in chaotic environments. DSM defines BPD as a pervasive pattern of instability of interpersonal relationships that begins by early adulthood.1 Many children with diagnoses of posttraumatic stress disorder, mood disorder, bipolar disorder, oppositional defiant disorder, attention-deficit/hyperactivity disorder, etc. also can have difficulties in relating to others caused by their neurobiologic deficits, which also may limit response to medication. Furthermore, children with learning disorders also can misperceive motives of others and thus have pervasive patterns of relational instability.
The research Dr. Aguirre suggested is based on treatment histories and not rigorous study methodology. Most empirical evidence of personality disorders is strongly influenced by psychoanalytic literature regarding object relations, which is in flux because of emerging attention to attachment theory and progress in neurologic studies in the evaluation of temperamental variations related to the influence of mirror neurons.2
We also take issue with the comment that “BPD has a better prognosis than other serious men tal illn esses, such as bipolar disorder” There have been significant efforts in studying the role family can have in the outcomes of mood disorder treatment.3
Finally, there is evidence that in adults medication can be beneficial in treating the affective deregulation of patients with BPD who do not have comorbid disorders.4
Robert A. Kowatch, MD, PhD
Professor of Psychiatry and Pediatrics
Erin Monroe, CNS
Clinical Nurse Specialist
Division of Psychiatry
Sergio V. Delgado, MD
Associate Professor of Psychiatry
and Pediatrics
Cincinnati Children’s Hospital Medical Center
Cincinnati, OH
1. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
2. Zald DH, Cowan RL, Riccardi P, et al. Midbrain dopamine receptor availability is inversely associated with novelty-seeking traits in humans. J Neurosci. 2008;28(53):14372-14378.
3. Miklowitz DJ, Axelson DA, Birmaher B, et al. Family-focused treatment for adolescents with bipolar disorder: results of a 2-year randomized trial. Arch Gen Psychiatry. 2008;65(9):1053-1061.
4. Stoffers J, VÖllum BA, RÜcker G, et al. Pharmacological interventions for borderline personality disorder. Cochrane Database Syst Rev. 2010;16:CD005653.-
1. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
2. Zald DH, Cowan RL, Riccardi P, et al. Midbrain dopamine receptor availability is inversely associated with novelty-seeking traits in humans. J Neurosci. 2008;28(53):14372-14378.
3. Miklowitz DJ, Axelson DA, Birmaher B, et al. Family-focused treatment for adolescents with bipolar disorder: results of a 2-year randomized trial. Arch Gen Psychiatry. 2008;65(9):1053-1061.
4. Stoffers J, VÖllum BA, RÜcker G, et al. Pharmacological interventions for borderline personality disorder. Cochrane Database Syst Rev. 2010;16:CD005653.-