User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Divorce, custody, and parental consent for psychiatric treatment
Dear Dr. Mossman:
I treat children and adolescents in an acute inpatient setting. Sometimes a child of divorced parents—call him “Johnny”—is admitted to the hospital by one parent—for example the mother—but she doesn’t inform the father. Although the parents have joint custody, Mom doesn’t want me to contact Dad.
I tell Mom that I’d like to get clinical information and consent from Dad, but she refuses, saying, “This will make me look bad, and my ex-husband will try to take emergency custody of Johnny.” My hospital’s legal department says consent from both parents isn’t needed.
These scenarios always leave me feeling upset and confused. I’d appreciate clarification on how to handle these matters.—Submitted by “Dr. K”
Knowing the correct legal answer to a question often doesn’t supply the best clinical solution for your patient. Dr. K received a legally sound response from hospital administrators: a parent who has legal custody may authorize medical treatment for a minor child without first asking or informing the other parent. But Dr. K feels unsatisfied because the hospital didn’t provide what Dr. K sought: a clinically sound answer.
This article reviews custody arrangements and the legal rights they give divorced parents. Also, we will discuss the mother’s concerns and explain why—despite her fears—notifying and involving Johnny’s father can be important, even when it’s not legally required.
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online market-place of risk management publications and resources (www.prms.com).
Custody and urgent treatment
A minor—defined in most states as a person younger than age 18—legally cannot give consent for medical care except in limited circumstances, such as contraceptive care.1,2 When a minor undergoes psychiatric hospitalization, physicians usually must obtain consent from the minor’s legal custodian.
Married parents both have legal custody of their children. They also have equal rights to spend time with their children and make major decisions about their welfare, such as authorizing medical care. When parents divorce, these rights must be reassigned in a court-approved divorce decree. Table 1 explains some key terms used to describe custody arrangements after divorce.2,3
Several decades ago, children—especially those younger age 10—usually remained with their mothers, who received sole legal custody; fathers typically had visitation privileges.4 Now, however, most states’ statutes presume that divorced mothers and fathers will have joint legal custody.3
Joint legal custody lets both parents retain their individual legal authority to make decisions on behalf of minor children, although the children may spend most of their time in the physical custody of 1 parent. This means that when urgent medical care is needed—such as a psychiatric hospitalization—1 parent’s consent is sufficient legal authorization for treatment.1,2
What if a child’s parent claims to have legal custody, but the doctor isn’t sure? A doctor who in good faith relies on a parent’s statement can properly provide urgent treatment without delving into custody arrangements.2 In many states, noncustodial parents may authorize treatment in urgent situations—and even some nonurgent ones—if they happen to have physical control of the child when care is needed, such as during a visit.1
Table 1
Child custody: Key legal terms
| Term | Refers to |
|---|---|
| Custody arrangement | The specified times each parent will spend with a minor child and which parent(s) can make major decisions about a child’s welfare |
| Legal custody | A parent’s right to make major decisions about a child’s welfare, including medical care |
| Visitation | The child’s means of maintaining contact with a noncustodial parent |
| Physical custody | Who has physical possession of the child at a particular time, such as during visitation |
| Sole legal custody | A custody arrangement in which only one parent retains the right to make major decisions for the child |
| Joint legal custody | A custody arrangement in which both parents retain the right to make major decisions affecting the child |
| Modification of custody | A legal process in which a court changes a previous custody order |
| Source: Adapted from references 2,3 | |
Nonurgent treatment
After receiving urgent treatment, psychiatric patients typically need continuing, nonurgent care. Dr. K’s inquiry may be anticipating this scenario. In general, parents with joint custody have an equal right to authorize nonurgent care for their children, and Johnny’s treatment could proceed with only Mom’s consent.1 However, if Dr. K knows or has reason to think that Johnny’s father would refuse to give consent for ongoing, nonurgent psychiatric care, providing treatment over the father’s objection may be legally questionable. Under some joint legal custody agreements, both parents need to give consent for medical care and receive clinical information about their children.2
Moreover, trying to treat Johnny in the face of Dad’s explicit objection may be clinically unwise. Unfortunately, many couples’ conflicts are not resolved by divorce, and children can become pawns in ongoing postmarital battles. Such situations can exacerbate children’s emotional problems, which is the opposite of what Dr. K hopes to do for Johnny.
What can Dr. K do?
Address a parent’s fears. Few parents are at their levelheaded best when their children need psychiatric hospitalization. To help Mom and Johnny, Dr. K can point out these things:
- Many states, such as Ohio,5 give Dad the right to learn about Johnny’s treatment and access to treatment records.
- Sooner or later, Dad will find out about the hospitalization. The next time Johnny visits his father, he’ll probably tell Dad what happened. In a few weeks, Dad may receive insurance paperwork or a bill from the hospital.
- Dad may be far more upset and prone to retaliate if he finds out later and is excluded from Johnny’s treatment than if he is notified immediately and gets to participate in his son’s care.
- Realistically, Dad cannot take Johnny away because Mom has arranged for appropriate medical care. If hospitalization is indicated, Mom’s failure to get treatment for Johnny could be grounds for Dad to claim she’s an unfit parent.
Why both parents are needed
Johnny’s hospital care probably will benefit from Dad’s involvement for several reasons (Table 2).
More information. Child and adolescent psychiatrists agree that in most clinical situations it helps to obtain information from as many sources as possible.6-9 Johnny’s father might have crucial information relevant to diagnosis or treatment, such as family history details that Mom doesn’t know.
Debiasing. If Johnny spends time living with both parents, Dr. K should know how often symptoms appear in both environments. Dad’s perspective may be vital, but when postdivorce relationships are strained, what parents convey about each other can be biased. Getting information directly from both parents will give Dr. K a more realistic picture of the child’s environment and psychosocial stressors.7
Treatment planning. After a psychiatric hospitalization, both parents should be aware of Johnny’s diagnosis and treatment. Johnny may need careful supervision for recurrence of symptoms, such as suicidal or homicidal ideation, that can have life-threatening implications.
Medication management. If Johnny is taking medication, he’ll need to receive it regularly. Missing medication when Johnny is with Dad would reduce effectiveness and in some cases could be dangerous. Both parents also should know about possible side effects so they can provide good monitoring.
Psychotherapy. Often, family therapy is an important element of a child’s recovery and will achieve optimum results only if all family members participate. Also, children need consistency. If a behavioral plan is part of Johnny’s treatment, Mom and Dad will need to agree on the rules and implement them consistently at both homes.
Table 2
Why both parents’ input is valuable
| More information from different perspectives concerning behavior in a variety of contexts and settings |
| Less biased information |
| Better treatment planning |
| Better medication management |
| More effective therapy |
Work with parents
When one divorced parent is reluctant to inform the other about their child’s hospitalization, you can respond empathically to fears and concerns. Despite mental health professionals’ best efforts, psychiatric illness still generates feelings of stigma and shame. Divorced parents often feel guilty about the stress the divorce has brought to their children, and they may consciously or unconsciously blame themselves for their child’s illness. In the midst of an ongoing custody dispute, the parent initiating a psychiatric hospitalization may feel especially vulnerable and reluctant to inform the other parent about what’s happening.
Being attuned to these issues will help you address and normalize a parent’s fears. Parents should know that a court could support their seeking treatment for their children’s illness, and they could be contributing to medical neglect if they do not seek this treatment.
In rare instances, not informing the other parent may be the best clinical decision. In situations involving child abuse or extreme domestic violence, a parent’s learning about the hospitalization could create safety issues. In most instances, however, both Mom and Dad will see their child soon after hospitalization, so one parent cannot hope to conceal a hospitalization for very long. Involving both parents from the outset usually will give the child and his family the best shot at a positive outcome.
1. Berger JE. Consent by proxy for nonurgent pediatric care. Pediatrics 2003;112:1186-95.
2. Quinn KM, Weiner BA. Legal rights of children. In: Weiner BA, Wettstein RM, eds. Legal issues in mental health care. New York, NY: Plenum Press; 1993:309-47.
3. Kelly JB. The determination of child custody. Future Child 1994;4:121-242.
4. Melton GB, Petrila J, Poythress NG, Slobogin C. Psychological evaluations for the courts: a handbook for mental health professionals and lawyers. 3rd ed. New York, NY: Guilford Press; 2007.
5. Ohio Rev Code § 3109. 051(H).
6. American Academy of Child and Adolescent Psychiatry. Practice parameters for the psychiatric assessment of children and adolescents. J Am Acad Child Adolesc Psychiatry 1997;36(10 suppl):4S-20S.
7. American Academy of Child and Adolescent Psychiatry. Practice parameter for the assessment of the family. J Am Acad Child Adolesc Psychiatry 2007;46:922-37.
8. Bostic JQ, King RA. Clinical assessment of children and adolescents: content and structure. In: Martin A, Volkmar FR, eds. Lewis’s child and adolescent psychiatry: a comprehensive textbook. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:323-44.
9. Weston CG, Klykylo WM. The initial psychiatric evaluation of children and adolescents. In: Tasman A, Kay J, Lieberman J, eds. Psychiatry. 3rd ed. London, UK: John Wiley & Sons; 2008:546-54.

Douglas Mossman, MD
Christina G. Weston, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and volunteer professor of psychiatry and associate program director, Institute for Psychiatry and Law, University of Cincinnati College of Medicine. Dr. Weston is assistant professor and associate director, division of child and adolescent psychiatry, Wright State University Boonshoft School of Medicine, Dayton, OH.
Douglas Mossman, MD
Christina G. Weston, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and volunteer professor of psychiatry and associate program director, Institute for Psychiatry and Law, University of Cincinnati College of Medicine. Dr. Weston is assistant professor and associate director, division of child and adolescent psychiatry, Wright State University Boonshoft School of Medicine, Dayton, OH.
Douglas Mossman, MD
Christina G. Weston, MD
Dr. Mossman is director, Glenn M. Weaver Institute of Law and Psychiatry, University of Cincinnati College of Law, and volunteer professor of psychiatry and associate program director, Institute for Psychiatry and Law, University of Cincinnati College of Medicine. Dr. Weston is assistant professor and associate director, division of child and adolescent psychiatry, Wright State University Boonshoft School of Medicine, Dayton, OH.
Dear Dr. Mossman:
I treat children and adolescents in an acute inpatient setting. Sometimes a child of divorced parents—call him “Johnny”—is admitted to the hospital by one parent—for example the mother—but she doesn’t inform the father. Although the parents have joint custody, Mom doesn’t want me to contact Dad.
I tell Mom that I’d like to get clinical information and consent from Dad, but she refuses, saying, “This will make me look bad, and my ex-husband will try to take emergency custody of Johnny.” My hospital’s legal department says consent from both parents isn’t needed.
These scenarios always leave me feeling upset and confused. I’d appreciate clarification on how to handle these matters.—Submitted by “Dr. K”
Knowing the correct legal answer to a question often doesn’t supply the best clinical solution for your patient. Dr. K received a legally sound response from hospital administrators: a parent who has legal custody may authorize medical treatment for a minor child without first asking or informing the other parent. But Dr. K feels unsatisfied because the hospital didn’t provide what Dr. K sought: a clinically sound answer.
This article reviews custody arrangements and the legal rights they give divorced parents. Also, we will discuss the mother’s concerns and explain why—despite her fears—notifying and involving Johnny’s father can be important, even when it’s not legally required.
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online market-place of risk management publications and resources (www.prms.com).
Custody and urgent treatment
A minor—defined in most states as a person younger than age 18—legally cannot give consent for medical care except in limited circumstances, such as contraceptive care.1,2 When a minor undergoes psychiatric hospitalization, physicians usually must obtain consent from the minor’s legal custodian.
Married parents both have legal custody of their children. They also have equal rights to spend time with their children and make major decisions about their welfare, such as authorizing medical care. When parents divorce, these rights must be reassigned in a court-approved divorce decree. Table 1 explains some key terms used to describe custody arrangements after divorce.2,3
Several decades ago, children—especially those younger age 10—usually remained with their mothers, who received sole legal custody; fathers typically had visitation privileges.4 Now, however, most states’ statutes presume that divorced mothers and fathers will have joint legal custody.3
Joint legal custody lets both parents retain their individual legal authority to make decisions on behalf of minor children, although the children may spend most of their time in the physical custody of 1 parent. This means that when urgent medical care is needed—such as a psychiatric hospitalization—1 parent’s consent is sufficient legal authorization for treatment.1,2
What if a child’s parent claims to have legal custody, but the doctor isn’t sure? A doctor who in good faith relies on a parent’s statement can properly provide urgent treatment without delving into custody arrangements.2 In many states, noncustodial parents may authorize treatment in urgent situations—and even some nonurgent ones—if they happen to have physical control of the child when care is needed, such as during a visit.1
Table 1
Child custody: Key legal terms
| Term | Refers to |
|---|---|
| Custody arrangement | The specified times each parent will spend with a minor child and which parent(s) can make major decisions about a child’s welfare |
| Legal custody | A parent’s right to make major decisions about a child’s welfare, including medical care |
| Visitation | The child’s means of maintaining contact with a noncustodial parent |
| Physical custody | Who has physical possession of the child at a particular time, such as during visitation |
| Sole legal custody | A custody arrangement in which only one parent retains the right to make major decisions for the child |
| Joint legal custody | A custody arrangement in which both parents retain the right to make major decisions affecting the child |
| Modification of custody | A legal process in which a court changes a previous custody order |
| Source: Adapted from references 2,3 | |
Nonurgent treatment
After receiving urgent treatment, psychiatric patients typically need continuing, nonurgent care. Dr. K’s inquiry may be anticipating this scenario. In general, parents with joint custody have an equal right to authorize nonurgent care for their children, and Johnny’s treatment could proceed with only Mom’s consent.1 However, if Dr. K knows or has reason to think that Johnny’s father would refuse to give consent for ongoing, nonurgent psychiatric care, providing treatment over the father’s objection may be legally questionable. Under some joint legal custody agreements, both parents need to give consent for medical care and receive clinical information about their children.2
Moreover, trying to treat Johnny in the face of Dad’s explicit objection may be clinically unwise. Unfortunately, many couples’ conflicts are not resolved by divorce, and children can become pawns in ongoing postmarital battles. Such situations can exacerbate children’s emotional problems, which is the opposite of what Dr. K hopes to do for Johnny.
What can Dr. K do?
Address a parent’s fears. Few parents are at their levelheaded best when their children need psychiatric hospitalization. To help Mom and Johnny, Dr. K can point out these things:
- Many states, such as Ohio,5 give Dad the right to learn about Johnny’s treatment and access to treatment records.
- Sooner or later, Dad will find out about the hospitalization. The next time Johnny visits his father, he’ll probably tell Dad what happened. In a few weeks, Dad may receive insurance paperwork or a bill from the hospital.
- Dad may be far more upset and prone to retaliate if he finds out later and is excluded from Johnny’s treatment than if he is notified immediately and gets to participate in his son’s care.
- Realistically, Dad cannot take Johnny away because Mom has arranged for appropriate medical care. If hospitalization is indicated, Mom’s failure to get treatment for Johnny could be grounds for Dad to claim she’s an unfit parent.
Why both parents are needed
Johnny’s hospital care probably will benefit from Dad’s involvement for several reasons (Table 2).
More information. Child and adolescent psychiatrists agree that in most clinical situations it helps to obtain information from as many sources as possible.6-9 Johnny’s father might have crucial information relevant to diagnosis or treatment, such as family history details that Mom doesn’t know.
Debiasing. If Johnny spends time living with both parents, Dr. K should know how often symptoms appear in both environments. Dad’s perspective may be vital, but when postdivorce relationships are strained, what parents convey about each other can be biased. Getting information directly from both parents will give Dr. K a more realistic picture of the child’s environment and psychosocial stressors.7
Treatment planning. After a psychiatric hospitalization, both parents should be aware of Johnny’s diagnosis and treatment. Johnny may need careful supervision for recurrence of symptoms, such as suicidal or homicidal ideation, that can have life-threatening implications.
Medication management. If Johnny is taking medication, he’ll need to receive it regularly. Missing medication when Johnny is with Dad would reduce effectiveness and in some cases could be dangerous. Both parents also should know about possible side effects so they can provide good monitoring.
Psychotherapy. Often, family therapy is an important element of a child’s recovery and will achieve optimum results only if all family members participate. Also, children need consistency. If a behavioral plan is part of Johnny’s treatment, Mom and Dad will need to agree on the rules and implement them consistently at both homes.
Table 2
Why both parents’ input is valuable
| More information from different perspectives concerning behavior in a variety of contexts and settings |
| Less biased information |
| Better treatment planning |
| Better medication management |
| More effective therapy |
Work with parents
When one divorced parent is reluctant to inform the other about their child’s hospitalization, you can respond empathically to fears and concerns. Despite mental health professionals’ best efforts, psychiatric illness still generates feelings of stigma and shame. Divorced parents often feel guilty about the stress the divorce has brought to their children, and they may consciously or unconsciously blame themselves for their child’s illness. In the midst of an ongoing custody dispute, the parent initiating a psychiatric hospitalization may feel especially vulnerable and reluctant to inform the other parent about what’s happening.
Being attuned to these issues will help you address and normalize a parent’s fears. Parents should know that a court could support their seeking treatment for their children’s illness, and they could be contributing to medical neglect if they do not seek this treatment.
In rare instances, not informing the other parent may be the best clinical decision. In situations involving child abuse or extreme domestic violence, a parent’s learning about the hospitalization could create safety issues. In most instances, however, both Mom and Dad will see their child soon after hospitalization, so one parent cannot hope to conceal a hospitalization for very long. Involving both parents from the outset usually will give the child and his family the best shot at a positive outcome.
Dear Dr. Mossman:
I treat children and adolescents in an acute inpatient setting. Sometimes a child of divorced parents—call him “Johnny”—is admitted to the hospital by one parent—for example the mother—but she doesn’t inform the father. Although the parents have joint custody, Mom doesn’t want me to contact Dad.
I tell Mom that I’d like to get clinical information and consent from Dad, but she refuses, saying, “This will make me look bad, and my ex-husband will try to take emergency custody of Johnny.” My hospital’s legal department says consent from both parents isn’t needed.
These scenarios always leave me feeling upset and confused. I’d appreciate clarification on how to handle these matters.—Submitted by “Dr. K”
Knowing the correct legal answer to a question often doesn’t supply the best clinical solution for your patient. Dr. K received a legally sound response from hospital administrators: a parent who has legal custody may authorize medical treatment for a minor child without first asking or informing the other parent. But Dr. K feels unsatisfied because the hospital didn’t provide what Dr. K sought: a clinically sound answer.
This article reviews custody arrangements and the legal rights they give divorced parents. Also, we will discuss the mother’s concerns and explain why—despite her fears—notifying and involving Johnny’s father can be important, even when it’s not legally required.
- Submit your malpractice-related questions to Dr. Mossman at [email protected].
- Include your name, address, and practice location. If your question is chosen for publication, your name can be withheld by request.
- All readers who submit questions will be included in quarterly drawings for a $50 gift certificate for Professional Risk Management Services, Inc’s online market-place of risk management publications and resources (www.prms.com).
Custody and urgent treatment
A minor—defined in most states as a person younger than age 18—legally cannot give consent for medical care except in limited circumstances, such as contraceptive care.1,2 When a minor undergoes psychiatric hospitalization, physicians usually must obtain consent from the minor’s legal custodian.
Married parents both have legal custody of their children. They also have equal rights to spend time with their children and make major decisions about their welfare, such as authorizing medical care. When parents divorce, these rights must be reassigned in a court-approved divorce decree. Table 1 explains some key terms used to describe custody arrangements after divorce.2,3
Several decades ago, children—especially those younger age 10—usually remained with their mothers, who received sole legal custody; fathers typically had visitation privileges.4 Now, however, most states’ statutes presume that divorced mothers and fathers will have joint legal custody.3
Joint legal custody lets both parents retain their individual legal authority to make decisions on behalf of minor children, although the children may spend most of their time in the physical custody of 1 parent. This means that when urgent medical care is needed—such as a psychiatric hospitalization—1 parent’s consent is sufficient legal authorization for treatment.1,2
What if a child’s parent claims to have legal custody, but the doctor isn’t sure? A doctor who in good faith relies on a parent’s statement can properly provide urgent treatment without delving into custody arrangements.2 In many states, noncustodial parents may authorize treatment in urgent situations—and even some nonurgent ones—if they happen to have physical control of the child when care is needed, such as during a visit.1
Table 1
Child custody: Key legal terms
| Term | Refers to |
|---|---|
| Custody arrangement | The specified times each parent will spend with a minor child and which parent(s) can make major decisions about a child’s welfare |
| Legal custody | A parent’s right to make major decisions about a child’s welfare, including medical care |
| Visitation | The child’s means of maintaining contact with a noncustodial parent |
| Physical custody | Who has physical possession of the child at a particular time, such as during visitation |
| Sole legal custody | A custody arrangement in which only one parent retains the right to make major decisions for the child |
| Joint legal custody | A custody arrangement in which both parents retain the right to make major decisions affecting the child |
| Modification of custody | A legal process in which a court changes a previous custody order |
| Source: Adapted from references 2,3 | |
Nonurgent treatment
After receiving urgent treatment, psychiatric patients typically need continuing, nonurgent care. Dr. K’s inquiry may be anticipating this scenario. In general, parents with joint custody have an equal right to authorize nonurgent care for their children, and Johnny’s treatment could proceed with only Mom’s consent.1 However, if Dr. K knows or has reason to think that Johnny’s father would refuse to give consent for ongoing, nonurgent psychiatric care, providing treatment over the father’s objection may be legally questionable. Under some joint legal custody agreements, both parents need to give consent for medical care and receive clinical information about their children.2
Moreover, trying to treat Johnny in the face of Dad’s explicit objection may be clinically unwise. Unfortunately, many couples’ conflicts are not resolved by divorce, and children can become pawns in ongoing postmarital battles. Such situations can exacerbate children’s emotional problems, which is the opposite of what Dr. K hopes to do for Johnny.
What can Dr. K do?
Address a parent’s fears. Few parents are at their levelheaded best when their children need psychiatric hospitalization. To help Mom and Johnny, Dr. K can point out these things:
- Many states, such as Ohio,5 give Dad the right to learn about Johnny’s treatment and access to treatment records.
- Sooner or later, Dad will find out about the hospitalization. The next time Johnny visits his father, he’ll probably tell Dad what happened. In a few weeks, Dad may receive insurance paperwork or a bill from the hospital.
- Dad may be far more upset and prone to retaliate if he finds out later and is excluded from Johnny’s treatment than if he is notified immediately and gets to participate in his son’s care.
- Realistically, Dad cannot take Johnny away because Mom has arranged for appropriate medical care. If hospitalization is indicated, Mom’s failure to get treatment for Johnny could be grounds for Dad to claim she’s an unfit parent.
Why both parents are needed
Johnny’s hospital care probably will benefit from Dad’s involvement for several reasons (Table 2).
More information. Child and adolescent psychiatrists agree that in most clinical situations it helps to obtain information from as many sources as possible.6-9 Johnny’s father might have crucial information relevant to diagnosis or treatment, such as family history details that Mom doesn’t know.
Debiasing. If Johnny spends time living with both parents, Dr. K should know how often symptoms appear in both environments. Dad’s perspective may be vital, but when postdivorce relationships are strained, what parents convey about each other can be biased. Getting information directly from both parents will give Dr. K a more realistic picture of the child’s environment and psychosocial stressors.7
Treatment planning. After a psychiatric hospitalization, both parents should be aware of Johnny’s diagnosis and treatment. Johnny may need careful supervision for recurrence of symptoms, such as suicidal or homicidal ideation, that can have life-threatening implications.
Medication management. If Johnny is taking medication, he’ll need to receive it regularly. Missing medication when Johnny is with Dad would reduce effectiveness and in some cases could be dangerous. Both parents also should know about possible side effects so they can provide good monitoring.
Psychotherapy. Often, family therapy is an important element of a child’s recovery and will achieve optimum results only if all family members participate. Also, children need consistency. If a behavioral plan is part of Johnny’s treatment, Mom and Dad will need to agree on the rules and implement them consistently at both homes.
Table 2
Why both parents’ input is valuable
| More information from different perspectives concerning behavior in a variety of contexts and settings |
| Less biased information |
| Better treatment planning |
| Better medication management |
| More effective therapy |
Work with parents
When one divorced parent is reluctant to inform the other about their child’s hospitalization, you can respond empathically to fears and concerns. Despite mental health professionals’ best efforts, psychiatric illness still generates feelings of stigma and shame. Divorced parents often feel guilty about the stress the divorce has brought to their children, and they may consciously or unconsciously blame themselves for their child’s illness. In the midst of an ongoing custody dispute, the parent initiating a psychiatric hospitalization may feel especially vulnerable and reluctant to inform the other parent about what’s happening.
Being attuned to these issues will help you address and normalize a parent’s fears. Parents should know that a court could support their seeking treatment for their children’s illness, and they could be contributing to medical neglect if they do not seek this treatment.
In rare instances, not informing the other parent may be the best clinical decision. In situations involving child abuse or extreme domestic violence, a parent’s learning about the hospitalization could create safety issues. In most instances, however, both Mom and Dad will see their child soon after hospitalization, so one parent cannot hope to conceal a hospitalization for very long. Involving both parents from the outset usually will give the child and his family the best shot at a positive outcome.
1. Berger JE. Consent by proxy for nonurgent pediatric care. Pediatrics 2003;112:1186-95.
2. Quinn KM, Weiner BA. Legal rights of children. In: Weiner BA, Wettstein RM, eds. Legal issues in mental health care. New York, NY: Plenum Press; 1993:309-47.
3. Kelly JB. The determination of child custody. Future Child 1994;4:121-242.
4. Melton GB, Petrila J, Poythress NG, Slobogin C. Psychological evaluations for the courts: a handbook for mental health professionals and lawyers. 3rd ed. New York, NY: Guilford Press; 2007.
5. Ohio Rev Code § 3109. 051(H).
6. American Academy of Child and Adolescent Psychiatry. Practice parameters for the psychiatric assessment of children and adolescents. J Am Acad Child Adolesc Psychiatry 1997;36(10 suppl):4S-20S.
7. American Academy of Child and Adolescent Psychiatry. Practice parameter for the assessment of the family. J Am Acad Child Adolesc Psychiatry 2007;46:922-37.
8. Bostic JQ, King RA. Clinical assessment of children and adolescents: content and structure. In: Martin A, Volkmar FR, eds. Lewis’s child and adolescent psychiatry: a comprehensive textbook. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:323-44.
9. Weston CG, Klykylo WM. The initial psychiatric evaluation of children and adolescents. In: Tasman A, Kay J, Lieberman J, eds. Psychiatry. 3rd ed. London, UK: John Wiley & Sons; 2008:546-54.
1. Berger JE. Consent by proxy for nonurgent pediatric care. Pediatrics 2003;112:1186-95.
2. Quinn KM, Weiner BA. Legal rights of children. In: Weiner BA, Wettstein RM, eds. Legal issues in mental health care. New York, NY: Plenum Press; 1993:309-47.
3. Kelly JB. The determination of child custody. Future Child 1994;4:121-242.
4. Melton GB, Petrila J, Poythress NG, Slobogin C. Psychological evaluations for the courts: a handbook for mental health professionals and lawyers. 3rd ed. New York, NY: Guilford Press; 2007.
5. Ohio Rev Code § 3109. 051(H).
6. American Academy of Child and Adolescent Psychiatry. Practice parameters for the psychiatric assessment of children and adolescents. J Am Acad Child Adolesc Psychiatry 1997;36(10 suppl):4S-20S.
7. American Academy of Child and Adolescent Psychiatry. Practice parameter for the assessment of the family. J Am Acad Child Adolesc Psychiatry 2007;46:922-37.
8. Bostic JQ, King RA. Clinical assessment of children and adolescents: content and structure. In: Martin A, Volkmar FR, eds. Lewis’s child and adolescent psychiatry: a comprehensive textbook. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2007:323-44.
9. Weston CG, Klykylo WM. The initial psychiatric evaluation of children and adolescents. In: Tasman A, Kay J, Lieberman J, eds. Psychiatry. 3rd ed. London, UK: John Wiley & Sons; 2008:546-54.
Need to keep patients longer
I believe the ridiculously brief inpatient stays and restrictions on available medications are the worst part of psychiatric practice. Reports of patients going berserk fail to note the restrictions placed on physicians in maintaining long-term care.
In New Zealand, inpatient commitment laws—although complex—allow a patient to be involuntarily committed when it is foreseeable that the patient will decompensate without medications or other treatments. This policy permits much better long-term treatment.
Scott A. Joseph, MD
Clinical director
Bemidji Community Behavioral Health Hospital
Bemidji, MN
To comment on articles in this issue or other topics, send letters in care of Erica Vonderheid, Current Psychiatry, 110 Summit Avenue, Montvale, NJ 07645, [email protected] or click here.
I believe the ridiculously brief inpatient stays and restrictions on available medications are the worst part of psychiatric practice. Reports of patients going berserk fail to note the restrictions placed on physicians in maintaining long-term care.
In New Zealand, inpatient commitment laws—although complex—allow a patient to be involuntarily committed when it is foreseeable that the patient will decompensate without medications or other treatments. This policy permits much better long-term treatment.
Scott A. Joseph, MD
Clinical director
Bemidji Community Behavioral Health Hospital
Bemidji, MN
I believe the ridiculously brief inpatient stays and restrictions on available medications are the worst part of psychiatric practice. Reports of patients going berserk fail to note the restrictions placed on physicians in maintaining long-term care.
In New Zealand, inpatient commitment laws—although complex—allow a patient to be involuntarily committed when it is foreseeable that the patient will decompensate without medications or other treatments. This policy permits much better long-term treatment.
Scott A. Joseph, MD
Clinical director
Bemidji Community Behavioral Health Hospital
Bemidji, MN
To comment on articles in this issue or other topics, send letters in care of Erica Vonderheid, Current Psychiatry, 110 Summit Avenue, Montvale, NJ 07645, [email protected] or click here.
To comment on articles in this issue or other topics, send letters in care of Erica Vonderheid, Current Psychiatry, 110 Summit Avenue, Montvale, NJ 07645, [email protected] or click here.
Don’t abandon psychotherapy
I was surprised that I did not see my first choice of challenges to psychiatry on Dr. Nasrallah’s list: psychiatrists doing “med checks” and ignoring psychotherapy. This trend is bad for patients and psychiatrists.
Our relationship with patients is what allows healing to begin. Medications are fertilizer for the barren soil, and psychotherapy is the hard work of planting and tending the fields. We kid ourselves when we think medications are going to “fix” people.
Craig Heacock, MD
Fort Collins, CO
To comment on articles in this issue or other topics, send letters in care of Erica Vonderheid, Current Psychiatry, 110 Summit Avenue, Montvale, NJ 07645, [email protected] or click here.
I was surprised that I did not see my first choice of challenges to psychiatry on Dr. Nasrallah’s list: psychiatrists doing “med checks” and ignoring psychotherapy. This trend is bad for patients and psychiatrists.
Our relationship with patients is what allows healing to begin. Medications are fertilizer for the barren soil, and psychotherapy is the hard work of planting and tending the fields. We kid ourselves when we think medications are going to “fix” people.
Craig Heacock, MD
Fort Collins, CO
I was surprised that I did not see my first choice of challenges to psychiatry on Dr. Nasrallah’s list: psychiatrists doing “med checks” and ignoring psychotherapy. This trend is bad for patients and psychiatrists.
Our relationship with patients is what allows healing to begin. Medications are fertilizer for the barren soil, and psychotherapy is the hard work of planting and tending the fields. We kid ourselves when we think medications are going to “fix” people.
Craig Heacock, MD
Fort Collins, CO
To comment on articles in this issue or other topics, send letters in care of Erica Vonderheid, Current Psychiatry, 110 Summit Avenue, Montvale, NJ 07645, [email protected] or click here.
To comment on articles in this issue or other topics, send letters in care of Erica Vonderheid, Current Psychiatry, 110 Summit Avenue, Montvale, NJ 07645, [email protected] or click here.
More challenges to consider
I agree with Dr. Nasrallah’s observation that “As psychiatry’s promise grows, however, so do its frustrations.” In addition to Dr. Nasrallah’s list of 17 challenges to psychiatry, I propose adding the proliferation of industry-sponsored continuing medical education, unpublished unfavorable industry-sponsored research, and potential conflicts of interest when physicians are compensated by industry for conducting educational symposia.
Steven Singer, MD
Madison, WI
To comment on articles in this issue or other topics, send letters in care of Erica Vonderheid, Current Psychiatry, 110 Summit Avenue, Montvale, NJ 07645, [email protected] or click here.
I agree with Dr. Nasrallah’s observation that “As psychiatry’s promise grows, however, so do its frustrations.” In addition to Dr. Nasrallah’s list of 17 challenges to psychiatry, I propose adding the proliferation of industry-sponsored continuing medical education, unpublished unfavorable industry-sponsored research, and potential conflicts of interest when physicians are compensated by industry for conducting educational symposia.
Steven Singer, MD
Madison, WI
I agree with Dr. Nasrallah’s observation that “As psychiatry’s promise grows, however, so do its frustrations.” In addition to Dr. Nasrallah’s list of 17 challenges to psychiatry, I propose adding the proliferation of industry-sponsored continuing medical education, unpublished unfavorable industry-sponsored research, and potential conflicts of interest when physicians are compensated by industry for conducting educational symposia.
Steven Singer, MD
Madison, WI
To comment on articles in this issue or other topics, send letters in care of Erica Vonderheid, Current Psychiatry, 110 Summit Avenue, Montvale, NJ 07645, [email protected] or click here.
To comment on articles in this issue or other topics, send letters in care of Erica Vonderheid, Current Psychiatry, 110 Summit Avenue, Montvale, NJ 07645, [email protected] or click here.
‘What’s ailing psychiatry?’ Patient care is top concern
I thank my colleagues who responded to my survey about challenges facing psychiatry (“Your vote, please: What’s ailing psychiatry?” From the Editor, Current Psychiatry, June 2008).
Survey results indicate that psychiatrists care more about their patients than their pocketbooks. The 3 top-rated challenges address the “broken” public mental health system, lack of parity for mental illness, and the shortage of beds to hospitalize psychiatric patients. Close behind are inadequate philanthropy for psychiatric causes—such as education, research, and clinical programs—and dismal lack of adequate primary care for the seriously mentally ill. Unreimbursed time spent on paperwork, persistent stigma, and shrinking funds for research were tied, and low compensation for psychiatrists ranked after those ( Table ).
Among the lowest-ranked challenges, the high rate of off-label psychotropic use was considered least important, which makes sense given how many psychiatric disorders have no FDA-approved drugs. Similarly, the lack of evidence-based psychotherapy research may reflect the fact that a large portion of today’s psychiatric work is assessment, differential diagnosis, and medical management rather than psychotherapy. Other mental health professionals are doing the bulk of psychotherapeutic interventions.
Let me end by expressing my surprise that not one reader wrote about psychologists’ push for prescribing privileges as a threat to psychiatry—which I deliberately did not include on my list—even though it is a hot-button issue. This suggests to me that so many issues impact psychiatric practice that psychologists are under the radar. However, I expect this issue will reemerge in the future.
Henry A. Nasrallah, MD
Editor-in-Chief
To comment on articles in this issue or other topics, send letters in care of Erica Vonderheid, Current Psychiatry, 110 Summit Avenue, Montvale, NJ 07645, [email protected] or Click here.
I thank my colleagues who responded to my survey about challenges facing psychiatry (“Your vote, please: What’s ailing psychiatry?” From the Editor, Current Psychiatry, June 2008).
Survey results indicate that psychiatrists care more about their patients than their pocketbooks. The 3 top-rated challenges address the “broken” public mental health system, lack of parity for mental illness, and the shortage of beds to hospitalize psychiatric patients. Close behind are inadequate philanthropy for psychiatric causes—such as education, research, and clinical programs—and dismal lack of adequate primary care for the seriously mentally ill. Unreimbursed time spent on paperwork, persistent stigma, and shrinking funds for research were tied, and low compensation for psychiatrists ranked after those ( Table ).
Among the lowest-ranked challenges, the high rate of off-label psychotropic use was considered least important, which makes sense given how many psychiatric disorders have no FDA-approved drugs. Similarly, the lack of evidence-based psychotherapy research may reflect the fact that a large portion of today’s psychiatric work is assessment, differential diagnosis, and medical management rather than psychotherapy. Other mental health professionals are doing the bulk of psychotherapeutic interventions.
Let me end by expressing my surprise that not one reader wrote about psychologists’ push for prescribing privileges as a threat to psychiatry—which I deliberately did not include on my list—even though it is a hot-button issue. This suggests to me that so many issues impact psychiatric practice that psychologists are under the radar. However, I expect this issue will reemerge in the future.
Henry A. Nasrallah, MD
Editor-in-Chief
I thank my colleagues who responded to my survey about challenges facing psychiatry (“Your vote, please: What’s ailing psychiatry?” From the Editor, Current Psychiatry, June 2008).
Survey results indicate that psychiatrists care more about their patients than their pocketbooks. The 3 top-rated challenges address the “broken” public mental health system, lack of parity for mental illness, and the shortage of beds to hospitalize psychiatric patients. Close behind are inadequate philanthropy for psychiatric causes—such as education, research, and clinical programs—and dismal lack of adequate primary care for the seriously mentally ill. Unreimbursed time spent on paperwork, persistent stigma, and shrinking funds for research were tied, and low compensation for psychiatrists ranked after those ( Table ).
Among the lowest-ranked challenges, the high rate of off-label psychotropic use was considered least important, which makes sense given how many psychiatric disorders have no FDA-approved drugs. Similarly, the lack of evidence-based psychotherapy research may reflect the fact that a large portion of today’s psychiatric work is assessment, differential diagnosis, and medical management rather than psychotherapy. Other mental health professionals are doing the bulk of psychotherapeutic interventions.
Let me end by expressing my surprise that not one reader wrote about psychologists’ push for prescribing privileges as a threat to psychiatry—which I deliberately did not include on my list—even though it is a hot-button issue. This suggests to me that so many issues impact psychiatric practice that psychologists are under the radar. However, I expect this issue will reemerge in the future.
Henry A. Nasrallah, MD
Editor-in-Chief
To comment on articles in this issue or other topics, send letters in care of Erica Vonderheid, Current Psychiatry, 110 Summit Avenue, Montvale, NJ 07645, [email protected] or Click here.
To comment on articles in this issue or other topics, send letters in care of Erica Vonderheid, Current Psychiatry, 110 Summit Avenue, Montvale, NJ 07645, [email protected] or Click here.
Contrarian patients in clinical trials: Lessons from exceptions
The complex process by which psychiatric medications are discovered, developed, and tested culminates in “evidence-based medicine”—the backbone of psychopharmacology. Large controlled clinical trials are designed to demonstrate under highly controlled conditions that a newly synthesized molecule has sufficient efficacy and a reasonable side-effect profile to warrant FDA approval. Results are published, and the pharmaceutical company launches the approved medication in the community.
Not usually recognized is that a treasure trove of information may be buried in a preapproval clinical trial’s massive database. The pharmaceutical company might not “mine” this information without the likelihood of revenue enhancement, but the raw data may hold clinically useful revelations.
These may include clues about which patients are likely to respond (or not) or experience a serious side effect with the drug (or placebo). Some-times examining contrarian psychopharmacology—unexpected patterns of response or adverse effects—provides valuable insights with clinical applications. Here are some questions we could explore beyond the efficacy-safety-tolerability data published on atypical antipsychotics.
Drug efficacy
- What are the demographic, biologic, and clinical profiles of rapid responders vs delayed responders vs nonresponders?
- How do full responders differ from partial responders or complete nonresponders? Can we identify them in clinical settings?
- Can we predict who will respond or not to a particular antipsychotic? Why not report whether the nonresponders in a clinical trial responded to some other antipsychotic after the trial was completed? That information would be tremendously useful and cost-effective in clinical practice.
Placebo efficacy
- How do placebo responders differ from nonresponders?
- Are placebo nonresponders similar in some ways to drug nonresponders?
- Would placebo nonresponders respond to the active drug after the controlled trial is completed?
Side effects
Each atypical has common side effects, but we know little about patients who buck the trend. Consider the potentially useful insights from studying patients who:
- lose weight on olanzapine
- gain weight on ziprasidone
- get sedated with aripiprazole
- develop insomnia or extrapyramidal symptoms with quetiapine
- continue to menstruate regularly on risperidone.
Patients such as these are reported in clinical trials but not monitored or compared for their response rates.
Placebo
- What would we learn if we compared psychotic patients who developed sedation with those who developed insomnia while receiving placebo in a clinical trial? Would these 2 groups differ in their response to the antipsychotic?
- Some psychotic patients gain substantial weight (>7%) on placebo, whereas others lose quite a bit of weight. Do they differ in response rates or other traits?
Individualized therapy
Contrarian patients who develop unexpected responses (such as strong improvement on placebo or side effects the opposite of what is expected) represent missed opportunities for research to elucidate the heterogeneity of psychosis (as well as mania, depression, or anxiety). Understanding individual differences could enable practitioners to predict efficacy and tolerability and to match patients with the most suitable medications from the start. These insights could save time, reduce duration of illness, predict likely side effects, and ultimately reduce the costs of treatment.

Henry A. Nasrallah, MD
Editor-in-Chief
To comment on this editorial or other topics of interest, contact Dr. Nasrallah at [email protected] or click here
Henry A. Nasrallah, MD
Editor-in-Chief
To comment on this editorial or other topics of interest, contact Dr. Nasrallah at [email protected] or click here
Henry A. Nasrallah, MD
Editor-in-Chief
To comment on this editorial or other topics of interest, contact Dr. Nasrallah at [email protected] or click here
The complex process by which psychiatric medications are discovered, developed, and tested culminates in “evidence-based medicine”—the backbone of psychopharmacology. Large controlled clinical trials are designed to demonstrate under highly controlled conditions that a newly synthesized molecule has sufficient efficacy and a reasonable side-effect profile to warrant FDA approval. Results are published, and the pharmaceutical company launches the approved medication in the community.
Not usually recognized is that a treasure trove of information may be buried in a preapproval clinical trial’s massive database. The pharmaceutical company might not “mine” this information without the likelihood of revenue enhancement, but the raw data may hold clinically useful revelations.
These may include clues about which patients are likely to respond (or not) or experience a serious side effect with the drug (or placebo). Some-times examining contrarian psychopharmacology—unexpected patterns of response or adverse effects—provides valuable insights with clinical applications. Here are some questions we could explore beyond the efficacy-safety-tolerability data published on atypical antipsychotics.
Drug efficacy
- What are the demographic, biologic, and clinical profiles of rapid responders vs delayed responders vs nonresponders?
- How do full responders differ from partial responders or complete nonresponders? Can we identify them in clinical settings?
- Can we predict who will respond or not to a particular antipsychotic? Why not report whether the nonresponders in a clinical trial responded to some other antipsychotic after the trial was completed? That information would be tremendously useful and cost-effective in clinical practice.
Placebo efficacy
- How do placebo responders differ from nonresponders?
- Are placebo nonresponders similar in some ways to drug nonresponders?
- Would placebo nonresponders respond to the active drug after the controlled trial is completed?
Side effects
Each atypical has common side effects, but we know little about patients who buck the trend. Consider the potentially useful insights from studying patients who:
- lose weight on olanzapine
- gain weight on ziprasidone
- get sedated with aripiprazole
- develop insomnia or extrapyramidal symptoms with quetiapine
- continue to menstruate regularly on risperidone.
Patients such as these are reported in clinical trials but not monitored or compared for their response rates.
Placebo
- What would we learn if we compared psychotic patients who developed sedation with those who developed insomnia while receiving placebo in a clinical trial? Would these 2 groups differ in their response to the antipsychotic?
- Some psychotic patients gain substantial weight (>7%) on placebo, whereas others lose quite a bit of weight. Do they differ in response rates or other traits?
Individualized therapy
Contrarian patients who develop unexpected responses (such as strong improvement on placebo or side effects the opposite of what is expected) represent missed opportunities for research to elucidate the heterogeneity of psychosis (as well as mania, depression, or anxiety). Understanding individual differences could enable practitioners to predict efficacy and tolerability and to match patients with the most suitable medications from the start. These insights could save time, reduce duration of illness, predict likely side effects, and ultimately reduce the costs of treatment.
The complex process by which psychiatric medications are discovered, developed, and tested culminates in “evidence-based medicine”—the backbone of psychopharmacology. Large controlled clinical trials are designed to demonstrate under highly controlled conditions that a newly synthesized molecule has sufficient efficacy and a reasonable side-effect profile to warrant FDA approval. Results are published, and the pharmaceutical company launches the approved medication in the community.
Not usually recognized is that a treasure trove of information may be buried in a preapproval clinical trial’s massive database. The pharmaceutical company might not “mine” this information without the likelihood of revenue enhancement, but the raw data may hold clinically useful revelations.
These may include clues about which patients are likely to respond (or not) or experience a serious side effect with the drug (or placebo). Some-times examining contrarian psychopharmacology—unexpected patterns of response or adverse effects—provides valuable insights with clinical applications. Here are some questions we could explore beyond the efficacy-safety-tolerability data published on atypical antipsychotics.
Drug efficacy
- What are the demographic, biologic, and clinical profiles of rapid responders vs delayed responders vs nonresponders?
- How do full responders differ from partial responders or complete nonresponders? Can we identify them in clinical settings?
- Can we predict who will respond or not to a particular antipsychotic? Why not report whether the nonresponders in a clinical trial responded to some other antipsychotic after the trial was completed? That information would be tremendously useful and cost-effective in clinical practice.
Placebo efficacy
- How do placebo responders differ from nonresponders?
- Are placebo nonresponders similar in some ways to drug nonresponders?
- Would placebo nonresponders respond to the active drug after the controlled trial is completed?
Side effects
Each atypical has common side effects, but we know little about patients who buck the trend. Consider the potentially useful insights from studying patients who:
- lose weight on olanzapine
- gain weight on ziprasidone
- get sedated with aripiprazole
- develop insomnia or extrapyramidal symptoms with quetiapine
- continue to menstruate regularly on risperidone.
Patients such as these are reported in clinical trials but not monitored or compared for their response rates.
Placebo
- What would we learn if we compared psychotic patients who developed sedation with those who developed insomnia while receiving placebo in a clinical trial? Would these 2 groups differ in their response to the antipsychotic?
- Some psychotic patients gain substantial weight (>7%) on placebo, whereas others lose quite a bit of weight. Do they differ in response rates or other traits?
Individualized therapy
Contrarian patients who develop unexpected responses (such as strong improvement on placebo or side effects the opposite of what is expected) represent missed opportunities for research to elucidate the heterogeneity of psychosis (as well as mania, depression, or anxiety). Understanding individual differences could enable practitioners to predict efficacy and tolerability and to match patients with the most suitable medications from the start. These insights could save time, reduce duration of illness, predict likely side effects, and ultimately reduce the costs of treatment.
The wilting widow’s masquerading illness
CASE: Unexplained unresponsiveness
One month after being hospitalized with E coli sepsis—and just after completing a course of ciprofloxacin—Mrs. D, a 79-year-old widow, becomes withdrawn and has several days of worsening fatigue, weakness, and somnolence. Within 2 hours of being admitted to the hospital, she becomes flaccid and unresponsive, although she seems to be awake. She has decreased respirations and is intubated.
The neurology team finds her unresponsive to verbal and noxious stimuli, with some resistance to eye opening. Neurologic exam is nonfocal. Cranial nerve testing is intact, muscle strength and reflexes are normal and symmetrical, and sensory function is intact to light touch. MRI, ECG, chest radiography, and laboratory tests—including metabolic and infectious screenings—do not reveal acute pathology. Within hours, Mrs. D becomes much more responsive and is successfully extubated. Her rapid improvement rules out locked-in syndrome.
The next day, Mrs. D has another episode of reduced responsiveness that lasts several minutes and resolves quickly. The neurologist observes this episode—which occurred when Mrs. D’s daughter entered the room—and recommends a psychiatric consultation.
For the past 3 weeks Mrs. D has experienced depressed mood, low energy, poor sleep, memory complaints, and feeling as if her mind was “scattered.” She has stopped attending church, is isolating to her home, and has been hiding valuables because of an irrational fear that she would lose possessions from her estate. Her primary care physician noted markedly reduced speech during recent office visits and agrees with the family that Mrs. D seems depressed.
On psychiatric exam, Mrs. D’s speech is quiet and slow but coherent. Her mood is depressed with a flat affect. Her thought process is goal-directed, and her Mini-Mental State Examination (MMSE) score is 27/30, indicating her cognition is grossly intact.
Mrs. D develops a low-grade fever. Although the physician does not suspect an infection, he prescribes a prophylactic course of levofloxacin, 500 mg/d. After 2 days of monitoring and assessments, the psychiatrist attributes Mrs. D’s presentation to depression, prescribes bupropion, 100 mg/d, and zolpidem, 5 mg at bedtime, and refers her for psychiatric follow-up.
Six days after discharge, Mrs. D’s family brings her to the psychiatric emergency room. They report that since discharge she has remained fatigued and seems confused intermittently. Her depressive symptoms—decreased appetite, anhedonia, poor sleep, and agitation—persist, and her personal care has deteriorated.
The authors’ observations
The psychiatrist attributes Mrs. D’s declining functioning to a worsening mood disorder. Major depression with psychotic features can include:
- fearfulness
- suspiciousness
- delusions of poverty.
Mrs. D’s cognitive and behavioral status fluctuated during her initial medical hospitalization, and on 1 occasion she required intubation. Her confusion worsened after discharge. These aspects of her history, along with worsening psychosis, can indicate seizures.
Psychiatric manifestations of seizures have been recognized for centuries. Partial complex seizures—one of the most common seizure types—have been called “psychosensory” or “psychomotor” seizures because they often include psychiatric symptoms.1
Psychiatric symptoms most often occur with seizures involving the temporal lobe, and limbic system activation adds an affective dimension to perceptual data processed by the temporal neocortex.2 Frontal and parietal lobe seizure foci also are associated with behavior change.
Psychiatric manifestations of seizures can include:
- cognitive problems
- anxiety
- mood/affect, psychotic, and dissociative symptoms
- personality changes (Table 1).2-6
As many as 30% of patients with seizures experience prominent psychiatric symptoms.7 Approximately one-half have comorbid psychiatric syndromes.8
Table 1
Seizure-related psychiatric symptoms: What to look for
| Symptom type | Characteristic features with seizures |
|---|---|
| Cognitive: intellectual function, memory, orientation | Episodic, fluctuating course of changes Amnesia occurs with complex—but not simple—seizures |
| Anxiety | Occurs most often with temporal lobe seizures May appear as full-blown panic attack Agoraphobia is rare Associated seizure features may include disturbed consciousness, automatisms, and hallucinations |
| Mood and affect | Change in affect is often episodic and profound, without many other symptoms associated with major depression or mania |
| Psychotic | Usually manifests as a single symptom, often described as incongruous, fragmentary, or out of context2 Occurs most often with temporal lobe seizures3 Delusions (paranoid, grandiose), forced thinking Hallucinations: auditory, visual, olfactory, tactile, gustatory Negative symptoms (emotional withdrawal, blunted affect) may be more common in frontal lobe seizures4 |
| Dissociative: depersonalization, déjà vu, jamais vu | Symptoms tend to be less extreme than in patients with dissociative identity disorder or PTSD May occur more often in context of panic symptoms with temporal lobe seizures5 |
| Personality changes (in epilepsy) | May be due to underlying frontal or temporal lobe damage Includes anancastic personality, emotionally unstable personality, and Geschwind syndrome (hypergraphia, hyperreligiosity, hyposexuality, and viscous personality style—perseverative and difficult to disengage from conversation)6 |
| PTSD: posttraumatic stress disorder | |
EVALUATION: Continuing decline
The emergency room staff learns Mrs. D has a history of vague auditory hallucinations and has developed more overt paranoia, including thoughts that police may be out to harm her. She has difficulty responding to questions and can not offer details of her history; her speech is soft and her thought process appears slowed.
Mrs. D is admitted to the inpatient psychiatry service. Her family reports that she has episodes of disorientation, poor memory, staring, and paranoia about the police that last minutes to 1 hour.
On a subsequent examination 1 hour later, her speech difficulties are variable. She cannot speak fluently, has limited ability to repeat phrases, and cannot follow simple verbal commands. These symptoms persist only minutes. Mrs. D slowly becomes more conversant but appears tired. During the next few hours she is disoriented and tries to walk into the nursing station. Other repetitive activity includes putting on/taking offmultiple layers of clothing.
The authors’ observations
- A normal EEG does not guarantee the absence of recent seizures; a standard scalp EEG can miss epileptiform changes that may occur earlier in the ictal phase.9
- EEG abnormalities may occur in normal subjects.
- visual, olfactory, or tactile hallucinations
- mutism
- catatonia
- poor memory not due to inattention
- episodic aphasia, apraxia, or agnosia.
Mrs. D’s confusion level and speech abnormalities varied over time. Her speech arrest early in the admission appeared to be a Broca’s or expressive aphasia because she comprehended commands but was unable to speak. Later, her speech exhibited a mixed transcortical aphasia pattern—she was unable to speak or comprehend, but retained some ability to repeat. The changing aphasia patterns and the often abrupt starting and stopping of these symptoms were the clues that an active process was occurring, suggesting that seizures should be considered.
DIAGNOSIS: Irrefutable EEG evidence
Mrs. D receives another neurology consult. An EEG shows spike and wave discharges in both frontal lobes consistent with nonconvulsive status epilepticus (NCSE). During these bursts, the neurologist notes speech arrest and altered alertness. Phenytoin loading is administered as a single 800-mg oral dose followed by 100 mg twice daily, and Mrs. D is transferred to the neurology unit for further stabilization.
The authors’ observations
When evaluating whether a psychiatric presentation reflects an underlying general medical or neurologic disorder—including seizures—consider the clinical features outlined in Table 2.12
In Mrs. D’s case, several factors supported the diagnosis of depression. She had numerous depressive symptoms, including depressed mood, social withdrawal, low energy, poor sleep, and “scattered mind,” which the psychiatrist interpreted as poor concentration. Interestingly, she attributed her dramatic episode of mutism and unresponsiveness in the hospital to being depressed. Mrs. D also had a personal and family history of depression; she had experienced a possible major depressive episode in her late 20s but was never treated, and her brother had depression.
Several features of her presentation were atypical, however, and suggested a medical etiology. Her family described the onset of her symptoms as abrupt, and she declined rapidly. Mrs. D’s concern about her estate had no connection with reality, and she became more psychotic. The dramatic episode of decreased responsiveness that led to her intubation was both peculiar and brief.
Mrs. D’s symptoms had an episodic quality with sudden onset, were repeatedly associated with aphasia, and included some automatic behavior (including dressing and undressing) suggestive of seizures. Symptoms of depression should not be surprising in this context because depression may be the most common comorbid psychiatric condition in elderly persons with epilepsy.13 Indeed, Mrs. D’s ultimate diagnosis—NCSE—is characterized by great variability in presentation, ranging from mildly impaired attention and orientation to mood disturbance, speech disturbance, and psychosis. All of these symptoms are seen with seizures.
Further, NCSE can have gradual or sudden onset, varying intensity and duration of symptoms, and fluctuating responsiveness.14 At least 10% of patients presenting with NCSE have no history of seizures.15 Precipitating factors include infection and drug toxicity.14
OUTCOME: Dual treatment
During a one-week neurology hospitalization, Mrs. D continues to receive phenytoin. Long-term EEG monitoring reveals she is no longer in status epilepticus. The patient is prescribed citalopram, 10 mg/d, and olanzapine, 2.5 mg at bedtime, to resolve mild depressive symptoms and hallucinosis. Mrs. D is referred for both neurology and psychiatry outpatient follow-up.
Table 2
Is the patient’s disorder psychiatric or medical/neurologic?
| Are the symptoms typical of a psychiatric disorder, including the severity? |
| Are the onset and course of symptoms usual? |
| Does the patient have risk factors for psychiatric illness, such as a personal or family history of psychiatric illness? |
| Are psychiatric symptoms responding poorly to treatment? |
| Does the patient have a general medical or neurologic condition commonly associated with psychiatric symptoms? |
| Does the patient exhibit abnormal cognitive functioning, including memory impairment or altered level of consciousness? |
| Did the psychiatric symptoms emerge after an abrupt change in personality? |
| Source: Reference 12 |
- Ettinger AB, Kanner AM, eds. Psychiatric issues in epilepsy: a practical guide to diagnosis and treatment. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.
- Bupropion • Wellbutrin
- Ciprofloxacin • Cipro
- Citalopram • Celexa
- Levofloxacin • Levaquin
- Olanzapine • Zyprexa
- Phenytoin • Dilantin
- Zolpidem • Ambien
Dr. Saragoza reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Maixner receives research/grant support from Neuronetics Inc., and is a speaker for Pfizer Inc., Bristol-Meyers Squibb, Janssen LP, and AstraZeneca.
1. Taylor M. The fundamentals of clinical neuropsychiatry. New York, NY: Oxford University Press; 1999:298-324.
2. Gloor P. The role of the limbic system in experiential phenomena of temporal lobe epilepsy. Ann Neurol 1982;12(2):129-44.
3. Scheepers M. Epilepsy and behaviour. Curr Opin Neurol 2003;16:183-7.
4. Adachi N. Inter-ictal and post-ictal psychoses in frontal lobe epilepsy: a retrospective comparison with psychoses in temporal lobe epilepsy. Seizure 2000;9:328-35.
5. Toni C. Psychosensorial and related phenomena in panic disorder and in temporal lobe epilepsy. Compr Psychiatry 1996;37(2):125-33.
6. Tucker G. Seizure disorders presenting with psychiatric symptomatology. Psychiatr Clin North Am 1998;21(3):626-35.
7. Onuma T. Classification of psychiatric symptoms in patients with epilepsy. Epilepsia 2000;41(suppl 9):43-8.
8. Marsh L, Rao V. Psychiatric complications in patients with epilepsy: a review. Epilepsy Res 2002;49(1):11-33.
9. Stern T. ed. Massachusetts General Hospital handbook of general hospital psychiatry. 5th ed. St. Louis, MO: Mosby; 2004;457-62.
10. O’Sullivan S. The role of the standard EEG in clinical psychiatry. Human Psychopharmacol Clin Exp 2006;21:265-71.
11. Gelb D. Introduction to clinical neurology. 2nd ed. London, UK: Butterworth Heinemann; 2000;133-4.
12. Marsh CM. Psychiatric presentations of medical illness. Psychiatr Clin North Am 1997;20(1):181-2.
13. Cloyd J, Hauser W, Towne A, et al. Epidemiological and medical aspects of epilepsy in the elderly. Epilepsy Res 2006;68(suppl 1):S39-48.
14. Riggio S. Nonconvulsive status epilepticus: clinical features and diagnostic challenges. Psychiatr Clin North Am 2005;28:653-64.
15. Mehlhorn AJ, Brown DA. Safety concerns with fluoroquinolones. Ann Pharmacother 2007;41:1859-66.
CASE: Unexplained unresponsiveness
One month after being hospitalized with E coli sepsis—and just after completing a course of ciprofloxacin—Mrs. D, a 79-year-old widow, becomes withdrawn and has several days of worsening fatigue, weakness, and somnolence. Within 2 hours of being admitted to the hospital, she becomes flaccid and unresponsive, although she seems to be awake. She has decreased respirations and is intubated.
The neurology team finds her unresponsive to verbal and noxious stimuli, with some resistance to eye opening. Neurologic exam is nonfocal. Cranial nerve testing is intact, muscle strength and reflexes are normal and symmetrical, and sensory function is intact to light touch. MRI, ECG, chest radiography, and laboratory tests—including metabolic and infectious screenings—do not reveal acute pathology. Within hours, Mrs. D becomes much more responsive and is successfully extubated. Her rapid improvement rules out locked-in syndrome.
The next day, Mrs. D has another episode of reduced responsiveness that lasts several minutes and resolves quickly. The neurologist observes this episode—which occurred when Mrs. D’s daughter entered the room—and recommends a psychiatric consultation.
For the past 3 weeks Mrs. D has experienced depressed mood, low energy, poor sleep, memory complaints, and feeling as if her mind was “scattered.” She has stopped attending church, is isolating to her home, and has been hiding valuables because of an irrational fear that she would lose possessions from her estate. Her primary care physician noted markedly reduced speech during recent office visits and agrees with the family that Mrs. D seems depressed.
On psychiatric exam, Mrs. D’s speech is quiet and slow but coherent. Her mood is depressed with a flat affect. Her thought process is goal-directed, and her Mini-Mental State Examination (MMSE) score is 27/30, indicating her cognition is grossly intact.
Mrs. D develops a low-grade fever. Although the physician does not suspect an infection, he prescribes a prophylactic course of levofloxacin, 500 mg/d. After 2 days of monitoring and assessments, the psychiatrist attributes Mrs. D’s presentation to depression, prescribes bupropion, 100 mg/d, and zolpidem, 5 mg at bedtime, and refers her for psychiatric follow-up.
Six days after discharge, Mrs. D’s family brings her to the psychiatric emergency room. They report that since discharge she has remained fatigued and seems confused intermittently. Her depressive symptoms—decreased appetite, anhedonia, poor sleep, and agitation—persist, and her personal care has deteriorated.
The authors’ observations
The psychiatrist attributes Mrs. D’s declining functioning to a worsening mood disorder. Major depression with psychotic features can include:
- fearfulness
- suspiciousness
- delusions of poverty.
Mrs. D’s cognitive and behavioral status fluctuated during her initial medical hospitalization, and on 1 occasion she required intubation. Her confusion worsened after discharge. These aspects of her history, along with worsening psychosis, can indicate seizures.
Psychiatric manifestations of seizures have been recognized for centuries. Partial complex seizures—one of the most common seizure types—have been called “psychosensory” or “psychomotor” seizures because they often include psychiatric symptoms.1
Psychiatric symptoms most often occur with seizures involving the temporal lobe, and limbic system activation adds an affective dimension to perceptual data processed by the temporal neocortex.2 Frontal and parietal lobe seizure foci also are associated with behavior change.
Psychiatric manifestations of seizures can include:
- cognitive problems
- anxiety
- mood/affect, psychotic, and dissociative symptoms
- personality changes (Table 1).2-6
As many as 30% of patients with seizures experience prominent psychiatric symptoms.7 Approximately one-half have comorbid psychiatric syndromes.8
Table 1
Seizure-related psychiatric symptoms: What to look for
| Symptom type | Characteristic features with seizures |
|---|---|
| Cognitive: intellectual function, memory, orientation | Episodic, fluctuating course of changes Amnesia occurs with complex—but not simple—seizures |
| Anxiety | Occurs most often with temporal lobe seizures May appear as full-blown panic attack Agoraphobia is rare Associated seizure features may include disturbed consciousness, automatisms, and hallucinations |
| Mood and affect | Change in affect is often episodic and profound, without many other symptoms associated with major depression or mania |
| Psychotic | Usually manifests as a single symptom, often described as incongruous, fragmentary, or out of context2 Occurs most often with temporal lobe seizures3 Delusions (paranoid, grandiose), forced thinking Hallucinations: auditory, visual, olfactory, tactile, gustatory Negative symptoms (emotional withdrawal, blunted affect) may be more common in frontal lobe seizures4 |
| Dissociative: depersonalization, déjà vu, jamais vu | Symptoms tend to be less extreme than in patients with dissociative identity disorder or PTSD May occur more often in context of panic symptoms with temporal lobe seizures5 |
| Personality changes (in epilepsy) | May be due to underlying frontal or temporal lobe damage Includes anancastic personality, emotionally unstable personality, and Geschwind syndrome (hypergraphia, hyperreligiosity, hyposexuality, and viscous personality style—perseverative and difficult to disengage from conversation)6 |
| PTSD: posttraumatic stress disorder | |
EVALUATION: Continuing decline
The emergency room staff learns Mrs. D has a history of vague auditory hallucinations and has developed more overt paranoia, including thoughts that police may be out to harm her. She has difficulty responding to questions and can not offer details of her history; her speech is soft and her thought process appears slowed.
Mrs. D is admitted to the inpatient psychiatry service. Her family reports that she has episodes of disorientation, poor memory, staring, and paranoia about the police that last minutes to 1 hour.
On a subsequent examination 1 hour later, her speech difficulties are variable. She cannot speak fluently, has limited ability to repeat phrases, and cannot follow simple verbal commands. These symptoms persist only minutes. Mrs. D slowly becomes more conversant but appears tired. During the next few hours she is disoriented and tries to walk into the nursing station. Other repetitive activity includes putting on/taking offmultiple layers of clothing.
The authors’ observations
- A normal EEG does not guarantee the absence of recent seizures; a standard scalp EEG can miss epileptiform changes that may occur earlier in the ictal phase.9
- EEG abnormalities may occur in normal subjects.
- visual, olfactory, or tactile hallucinations
- mutism
- catatonia
- poor memory not due to inattention
- episodic aphasia, apraxia, or agnosia.
Mrs. D’s confusion level and speech abnormalities varied over time. Her speech arrest early in the admission appeared to be a Broca’s or expressive aphasia because she comprehended commands but was unable to speak. Later, her speech exhibited a mixed transcortical aphasia pattern—she was unable to speak or comprehend, but retained some ability to repeat. The changing aphasia patterns and the often abrupt starting and stopping of these symptoms were the clues that an active process was occurring, suggesting that seizures should be considered.
DIAGNOSIS: Irrefutable EEG evidence
Mrs. D receives another neurology consult. An EEG shows spike and wave discharges in both frontal lobes consistent with nonconvulsive status epilepticus (NCSE). During these bursts, the neurologist notes speech arrest and altered alertness. Phenytoin loading is administered as a single 800-mg oral dose followed by 100 mg twice daily, and Mrs. D is transferred to the neurology unit for further stabilization.
The authors’ observations
When evaluating whether a psychiatric presentation reflects an underlying general medical or neurologic disorder—including seizures—consider the clinical features outlined in Table 2.12
In Mrs. D’s case, several factors supported the diagnosis of depression. She had numerous depressive symptoms, including depressed mood, social withdrawal, low energy, poor sleep, and “scattered mind,” which the psychiatrist interpreted as poor concentration. Interestingly, she attributed her dramatic episode of mutism and unresponsiveness in the hospital to being depressed. Mrs. D also had a personal and family history of depression; she had experienced a possible major depressive episode in her late 20s but was never treated, and her brother had depression.
Several features of her presentation were atypical, however, and suggested a medical etiology. Her family described the onset of her symptoms as abrupt, and she declined rapidly. Mrs. D’s concern about her estate had no connection with reality, and she became more psychotic. The dramatic episode of decreased responsiveness that led to her intubation was both peculiar and brief.
Mrs. D’s symptoms had an episodic quality with sudden onset, were repeatedly associated with aphasia, and included some automatic behavior (including dressing and undressing) suggestive of seizures. Symptoms of depression should not be surprising in this context because depression may be the most common comorbid psychiatric condition in elderly persons with epilepsy.13 Indeed, Mrs. D’s ultimate diagnosis—NCSE—is characterized by great variability in presentation, ranging from mildly impaired attention and orientation to mood disturbance, speech disturbance, and psychosis. All of these symptoms are seen with seizures.
Further, NCSE can have gradual or sudden onset, varying intensity and duration of symptoms, and fluctuating responsiveness.14 At least 10% of patients presenting with NCSE have no history of seizures.15 Precipitating factors include infection and drug toxicity.14
OUTCOME: Dual treatment
During a one-week neurology hospitalization, Mrs. D continues to receive phenytoin. Long-term EEG monitoring reveals she is no longer in status epilepticus. The patient is prescribed citalopram, 10 mg/d, and olanzapine, 2.5 mg at bedtime, to resolve mild depressive symptoms and hallucinosis. Mrs. D is referred for both neurology and psychiatry outpatient follow-up.
Table 2
Is the patient’s disorder psychiatric or medical/neurologic?
| Are the symptoms typical of a psychiatric disorder, including the severity? |
| Are the onset and course of symptoms usual? |
| Does the patient have risk factors for psychiatric illness, such as a personal or family history of psychiatric illness? |
| Are psychiatric symptoms responding poorly to treatment? |
| Does the patient have a general medical or neurologic condition commonly associated with psychiatric symptoms? |
| Does the patient exhibit abnormal cognitive functioning, including memory impairment or altered level of consciousness? |
| Did the psychiatric symptoms emerge after an abrupt change in personality? |
| Source: Reference 12 |
- Ettinger AB, Kanner AM, eds. Psychiatric issues in epilepsy: a practical guide to diagnosis and treatment. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.
- Bupropion • Wellbutrin
- Ciprofloxacin • Cipro
- Citalopram • Celexa
- Levofloxacin • Levaquin
- Olanzapine • Zyprexa
- Phenytoin • Dilantin
- Zolpidem • Ambien
Dr. Saragoza reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Maixner receives research/grant support from Neuronetics Inc., and is a speaker for Pfizer Inc., Bristol-Meyers Squibb, Janssen LP, and AstraZeneca.
CASE: Unexplained unresponsiveness
One month after being hospitalized with E coli sepsis—and just after completing a course of ciprofloxacin—Mrs. D, a 79-year-old widow, becomes withdrawn and has several days of worsening fatigue, weakness, and somnolence. Within 2 hours of being admitted to the hospital, she becomes flaccid and unresponsive, although she seems to be awake. She has decreased respirations and is intubated.
The neurology team finds her unresponsive to verbal and noxious stimuli, with some resistance to eye opening. Neurologic exam is nonfocal. Cranial nerve testing is intact, muscle strength and reflexes are normal and symmetrical, and sensory function is intact to light touch. MRI, ECG, chest radiography, and laboratory tests—including metabolic and infectious screenings—do not reveal acute pathology. Within hours, Mrs. D becomes much more responsive and is successfully extubated. Her rapid improvement rules out locked-in syndrome.
The next day, Mrs. D has another episode of reduced responsiveness that lasts several minutes and resolves quickly. The neurologist observes this episode—which occurred when Mrs. D’s daughter entered the room—and recommends a psychiatric consultation.
For the past 3 weeks Mrs. D has experienced depressed mood, low energy, poor sleep, memory complaints, and feeling as if her mind was “scattered.” She has stopped attending church, is isolating to her home, and has been hiding valuables because of an irrational fear that she would lose possessions from her estate. Her primary care physician noted markedly reduced speech during recent office visits and agrees with the family that Mrs. D seems depressed.
On psychiatric exam, Mrs. D’s speech is quiet and slow but coherent. Her mood is depressed with a flat affect. Her thought process is goal-directed, and her Mini-Mental State Examination (MMSE) score is 27/30, indicating her cognition is grossly intact.
Mrs. D develops a low-grade fever. Although the physician does not suspect an infection, he prescribes a prophylactic course of levofloxacin, 500 mg/d. After 2 days of monitoring and assessments, the psychiatrist attributes Mrs. D’s presentation to depression, prescribes bupropion, 100 mg/d, and zolpidem, 5 mg at bedtime, and refers her for psychiatric follow-up.
Six days after discharge, Mrs. D’s family brings her to the psychiatric emergency room. They report that since discharge she has remained fatigued and seems confused intermittently. Her depressive symptoms—decreased appetite, anhedonia, poor sleep, and agitation—persist, and her personal care has deteriorated.
The authors’ observations
The psychiatrist attributes Mrs. D’s declining functioning to a worsening mood disorder. Major depression with psychotic features can include:
- fearfulness
- suspiciousness
- delusions of poverty.
Mrs. D’s cognitive and behavioral status fluctuated during her initial medical hospitalization, and on 1 occasion she required intubation. Her confusion worsened after discharge. These aspects of her history, along with worsening psychosis, can indicate seizures.
Psychiatric manifestations of seizures have been recognized for centuries. Partial complex seizures—one of the most common seizure types—have been called “psychosensory” or “psychomotor” seizures because they often include psychiatric symptoms.1
Psychiatric symptoms most often occur with seizures involving the temporal lobe, and limbic system activation adds an affective dimension to perceptual data processed by the temporal neocortex.2 Frontal and parietal lobe seizure foci also are associated with behavior change.
Psychiatric manifestations of seizures can include:
- cognitive problems
- anxiety
- mood/affect, psychotic, and dissociative symptoms
- personality changes (Table 1).2-6
As many as 30% of patients with seizures experience prominent psychiatric symptoms.7 Approximately one-half have comorbid psychiatric syndromes.8
Table 1
Seizure-related psychiatric symptoms: What to look for
| Symptom type | Characteristic features with seizures |
|---|---|
| Cognitive: intellectual function, memory, orientation | Episodic, fluctuating course of changes Amnesia occurs with complex—but not simple—seizures |
| Anxiety | Occurs most often with temporal lobe seizures May appear as full-blown panic attack Agoraphobia is rare Associated seizure features may include disturbed consciousness, automatisms, and hallucinations |
| Mood and affect | Change in affect is often episodic and profound, without many other symptoms associated with major depression or mania |
| Psychotic | Usually manifests as a single symptom, often described as incongruous, fragmentary, or out of context2 Occurs most often with temporal lobe seizures3 Delusions (paranoid, grandiose), forced thinking Hallucinations: auditory, visual, olfactory, tactile, gustatory Negative symptoms (emotional withdrawal, blunted affect) may be more common in frontal lobe seizures4 |
| Dissociative: depersonalization, déjà vu, jamais vu | Symptoms tend to be less extreme than in patients with dissociative identity disorder or PTSD May occur more often in context of panic symptoms with temporal lobe seizures5 |
| Personality changes (in epilepsy) | May be due to underlying frontal or temporal lobe damage Includes anancastic personality, emotionally unstable personality, and Geschwind syndrome (hypergraphia, hyperreligiosity, hyposexuality, and viscous personality style—perseverative and difficult to disengage from conversation)6 |
| PTSD: posttraumatic stress disorder | |
EVALUATION: Continuing decline
The emergency room staff learns Mrs. D has a history of vague auditory hallucinations and has developed more overt paranoia, including thoughts that police may be out to harm her. She has difficulty responding to questions and can not offer details of her history; her speech is soft and her thought process appears slowed.
Mrs. D is admitted to the inpatient psychiatry service. Her family reports that she has episodes of disorientation, poor memory, staring, and paranoia about the police that last minutes to 1 hour.
On a subsequent examination 1 hour later, her speech difficulties are variable. She cannot speak fluently, has limited ability to repeat phrases, and cannot follow simple verbal commands. These symptoms persist only minutes. Mrs. D slowly becomes more conversant but appears tired. During the next few hours she is disoriented and tries to walk into the nursing station. Other repetitive activity includes putting on/taking offmultiple layers of clothing.
The authors’ observations
- A normal EEG does not guarantee the absence of recent seizures; a standard scalp EEG can miss epileptiform changes that may occur earlier in the ictal phase.9
- EEG abnormalities may occur in normal subjects.
- visual, olfactory, or tactile hallucinations
- mutism
- catatonia
- poor memory not due to inattention
- episodic aphasia, apraxia, or agnosia.
Mrs. D’s confusion level and speech abnormalities varied over time. Her speech arrest early in the admission appeared to be a Broca’s or expressive aphasia because she comprehended commands but was unable to speak. Later, her speech exhibited a mixed transcortical aphasia pattern—she was unable to speak or comprehend, but retained some ability to repeat. The changing aphasia patterns and the often abrupt starting and stopping of these symptoms were the clues that an active process was occurring, suggesting that seizures should be considered.
DIAGNOSIS: Irrefutable EEG evidence
Mrs. D receives another neurology consult. An EEG shows spike and wave discharges in both frontal lobes consistent with nonconvulsive status epilepticus (NCSE). During these bursts, the neurologist notes speech arrest and altered alertness. Phenytoin loading is administered as a single 800-mg oral dose followed by 100 mg twice daily, and Mrs. D is transferred to the neurology unit for further stabilization.
The authors’ observations
When evaluating whether a psychiatric presentation reflects an underlying general medical or neurologic disorder—including seizures—consider the clinical features outlined in Table 2.12
In Mrs. D’s case, several factors supported the diagnosis of depression. She had numerous depressive symptoms, including depressed mood, social withdrawal, low energy, poor sleep, and “scattered mind,” which the psychiatrist interpreted as poor concentration. Interestingly, she attributed her dramatic episode of mutism and unresponsiveness in the hospital to being depressed. Mrs. D also had a personal and family history of depression; she had experienced a possible major depressive episode in her late 20s but was never treated, and her brother had depression.
Several features of her presentation were atypical, however, and suggested a medical etiology. Her family described the onset of her symptoms as abrupt, and she declined rapidly. Mrs. D’s concern about her estate had no connection with reality, and she became more psychotic. The dramatic episode of decreased responsiveness that led to her intubation was both peculiar and brief.
Mrs. D’s symptoms had an episodic quality with sudden onset, were repeatedly associated with aphasia, and included some automatic behavior (including dressing and undressing) suggestive of seizures. Symptoms of depression should not be surprising in this context because depression may be the most common comorbid psychiatric condition in elderly persons with epilepsy.13 Indeed, Mrs. D’s ultimate diagnosis—NCSE—is characterized by great variability in presentation, ranging from mildly impaired attention and orientation to mood disturbance, speech disturbance, and psychosis. All of these symptoms are seen with seizures.
Further, NCSE can have gradual or sudden onset, varying intensity and duration of symptoms, and fluctuating responsiveness.14 At least 10% of patients presenting with NCSE have no history of seizures.15 Precipitating factors include infection and drug toxicity.14
OUTCOME: Dual treatment
During a one-week neurology hospitalization, Mrs. D continues to receive phenytoin. Long-term EEG monitoring reveals she is no longer in status epilepticus. The patient is prescribed citalopram, 10 mg/d, and olanzapine, 2.5 mg at bedtime, to resolve mild depressive symptoms and hallucinosis. Mrs. D is referred for both neurology and psychiatry outpatient follow-up.
Table 2
Is the patient’s disorder psychiatric or medical/neurologic?
| Are the symptoms typical of a psychiatric disorder, including the severity? |
| Are the onset and course of symptoms usual? |
| Does the patient have risk factors for psychiatric illness, such as a personal or family history of psychiatric illness? |
| Are psychiatric symptoms responding poorly to treatment? |
| Does the patient have a general medical or neurologic condition commonly associated with psychiatric symptoms? |
| Does the patient exhibit abnormal cognitive functioning, including memory impairment or altered level of consciousness? |
| Did the psychiatric symptoms emerge after an abrupt change in personality? |
| Source: Reference 12 |
- Ettinger AB, Kanner AM, eds. Psychiatric issues in epilepsy: a practical guide to diagnosis and treatment. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.
- Bupropion • Wellbutrin
- Ciprofloxacin • Cipro
- Citalopram • Celexa
- Levofloxacin • Levaquin
- Olanzapine • Zyprexa
- Phenytoin • Dilantin
- Zolpidem • Ambien
Dr. Saragoza reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Maixner receives research/grant support from Neuronetics Inc., and is a speaker for Pfizer Inc., Bristol-Meyers Squibb, Janssen LP, and AstraZeneca.
1. Taylor M. The fundamentals of clinical neuropsychiatry. New York, NY: Oxford University Press; 1999:298-324.
2. Gloor P. The role of the limbic system in experiential phenomena of temporal lobe epilepsy. Ann Neurol 1982;12(2):129-44.
3. Scheepers M. Epilepsy and behaviour. Curr Opin Neurol 2003;16:183-7.
4. Adachi N. Inter-ictal and post-ictal psychoses in frontal lobe epilepsy: a retrospective comparison with psychoses in temporal lobe epilepsy. Seizure 2000;9:328-35.
5. Toni C. Psychosensorial and related phenomena in panic disorder and in temporal lobe epilepsy. Compr Psychiatry 1996;37(2):125-33.
6. Tucker G. Seizure disorders presenting with psychiatric symptomatology. Psychiatr Clin North Am 1998;21(3):626-35.
7. Onuma T. Classification of psychiatric symptoms in patients with epilepsy. Epilepsia 2000;41(suppl 9):43-8.
8. Marsh L, Rao V. Psychiatric complications in patients with epilepsy: a review. Epilepsy Res 2002;49(1):11-33.
9. Stern T. ed. Massachusetts General Hospital handbook of general hospital psychiatry. 5th ed. St. Louis, MO: Mosby; 2004;457-62.
10. O’Sullivan S. The role of the standard EEG in clinical psychiatry. Human Psychopharmacol Clin Exp 2006;21:265-71.
11. Gelb D. Introduction to clinical neurology. 2nd ed. London, UK: Butterworth Heinemann; 2000;133-4.
12. Marsh CM. Psychiatric presentations of medical illness. Psychiatr Clin North Am 1997;20(1):181-2.
13. Cloyd J, Hauser W, Towne A, et al. Epidemiological and medical aspects of epilepsy in the elderly. Epilepsy Res 2006;68(suppl 1):S39-48.
14. Riggio S. Nonconvulsive status epilepticus: clinical features and diagnostic challenges. Psychiatr Clin North Am 2005;28:653-64.
15. Mehlhorn AJ, Brown DA. Safety concerns with fluoroquinolones. Ann Pharmacother 2007;41:1859-66.
1. Taylor M. The fundamentals of clinical neuropsychiatry. New York, NY: Oxford University Press; 1999:298-324.
2. Gloor P. The role of the limbic system in experiential phenomena of temporal lobe epilepsy. Ann Neurol 1982;12(2):129-44.
3. Scheepers M. Epilepsy and behaviour. Curr Opin Neurol 2003;16:183-7.
4. Adachi N. Inter-ictal and post-ictal psychoses in frontal lobe epilepsy: a retrospective comparison with psychoses in temporal lobe epilepsy. Seizure 2000;9:328-35.
5. Toni C. Psychosensorial and related phenomena in panic disorder and in temporal lobe epilepsy. Compr Psychiatry 1996;37(2):125-33.
6. Tucker G. Seizure disorders presenting with psychiatric symptomatology. Psychiatr Clin North Am 1998;21(3):626-35.
7. Onuma T. Classification of psychiatric symptoms in patients with epilepsy. Epilepsia 2000;41(suppl 9):43-8.
8. Marsh L, Rao V. Psychiatric complications in patients with epilepsy: a review. Epilepsy Res 2002;49(1):11-33.
9. Stern T. ed. Massachusetts General Hospital handbook of general hospital psychiatry. 5th ed. St. Louis, MO: Mosby; 2004;457-62.
10. O’Sullivan S. The role of the standard EEG in clinical psychiatry. Human Psychopharmacol Clin Exp 2006;21:265-71.
11. Gelb D. Introduction to clinical neurology. 2nd ed. London, UK: Butterworth Heinemann; 2000;133-4.
12. Marsh CM. Psychiatric presentations of medical illness. Psychiatr Clin North Am 1997;20(1):181-2.
13. Cloyd J, Hauser W, Towne A, et al. Epidemiological and medical aspects of epilepsy in the elderly. Epilepsy Res 2006;68(suppl 1):S39-48.
14. Riggio S. Nonconvulsive status epilepticus: clinical features and diagnostic challenges. Psychiatr Clin North Am 2005;28:653-64.
15. Mehlhorn AJ, Brown DA. Safety concerns with fluoroquinolones. Ann Pharmacother 2007;41:1859-66.
Psychiatrist/patient boundaries: When it’s OK to stretch the line
Dr. M is facing financial challenges with his fledgling private practice and begins consulting at a weight loss clinic to supplement his income. He finds him-self attracted to Ms. Y, a weight-loss patient he is treating. They seem to click interpersonally, and he extends his office visits with her. Ms. Y clearly enjoys this extra attention, and Dr. M begins including personal disclosures in his conversations with her.
In his residency training, Dr. M was taught never to date a current or former patient, but he views this situation as different. Ms. Y is seeing him only for weight loss, and he rationalizes that he is providing her with medical care, not “psychiatric” care. On 2 occasions he gives her a limited quantity of benzodiazepines for mild anxiety, which he considers a transitory stress-related condition and not an “official” DSM-IV-TR disorder.
Eventually, Dr. M asks Ms. Y to dinner and she accepts. After they begin dating, he decides to transfer her to another clinic physician “just to be safe.”
Although many psychiatrists assume that psychiatrist/patient boundaries are well defined by ethical and legal standards, boundary issues are a complex and controversial aspect of clinical practice. Psychoanalysts initially defined psychiatrist/patient boundaries as a way of structuring the unique and intimate relationship that evolves during analysis.1,2 The introduction of other therapeutic techniques and changes in health care funding have combined to make psychiatrist/patient boundaries far more complex.
Boundary violations are about exploitation. Both the American Medical Association (AMA) and the Canadian Medical Association warn members to “scrupulously avoid using the physician/patient relationship to gratify their own emotional, financial, and sexual needs.”3
Boundaries represent the edge of appropriate behavior and serve 2 important purposes:
- They separate the therapeutic relationship from social, sexual, romantic, and business relationships and from relationships that transform into caretaking of the psychiatrist by the patient.
- They structure the professional relationship in ways that maintain the identity and roles of the patient and the professional.4
Psychiatry’s unique dilemmas
As are all physicians, psychiatrists are governed by the 9 biomedical ethics set forth in the AMA’s Principles of Medical Ethics. The American Psychiatric Association (APA), however, acknowledges that psychiatry has a “broader set of moral and ethical problems and dilemmas” that are unique to and magnified by the mental health setting.5 The APA has adopted 39 standards in addition to those set forth by the AMA. The first standard captures the unique responsibilities inherent in the psychiatrist/ patient relationship: A psychiatrist shall not gratify his or her own needs by exploiting the patient (Box).6
Sexual contact with patients is inherently harmful to patients, always unethical, and usually illegal.7 The rate of sexual misconduct among psychiatrists is unknown. National Practitioner Data Bank information is not available to the general public.8 Based on literature reviews and data from individual states9,10 and government agencies,11 an estimated 6% to10% of psychiatrists have had inappropriate sexual relations with patients.12 Estimates of sexual misconduct by psychiatrists:
All physicians are required to practice in accordance with the American Medical Association’s Principles of Medical Ethics. Because these guidelines can be difficult to interpret for psychiatry, the American Psychiatric Association provides further guidance with The Principles of Medical Ethics with Annotations Especially Applicable to Psychiatry. The following excerpts from annotations to the first 2 principles spell out the basic concepts underlying appropriate psychiatrist/patient boundaries:
‘A psychiatrist shall not gratify his or her own needs by exploiting the patient. The psychiatrist shall be ever vigilant about the impact that his or her conduct has upon the boundaries of the doctor/patient relationship, and thus upon the well-being of the patient. These requirements become particularly important because of the essentially private, highly personal, and sometimes intensely emotional nature of the relationship established with the psychiatrist.
‘The requirement that the physician conduct himself/herself with propriety in his or her profession and in all the actions of his or her life is especially important in the case of the psychiatrist because the patient tends to model his or her behavior after that of his or her psychiatrist by identification. Further, the necessary intensity of the treatment relationship may tend to activate sexual and other needs and fantasies on the part of both patient and psychiatrist, while weakening the objectivity necessary for control. Additionally, the inherent inequality in the doctor-patient relationship may lead to exploitation of the patient. Sexual activity with a current or former patient is unethical.’
Source: Reference 6
- increase if misconduct is based on patient complaints
- decrease if self-reports are used
- decrease even further if based on official investigations.4
American psychoanalyst Frieda Fromm-Reichman reportedly offered her colleagues a not-so-humorous admonition: “Don’t have sex with your patients; you will only disappoint them.”4
Nonsexual boundary violations—such as accepting gifts, entering into business arrangements, or trying to influence a patient’s political or religious beliefs or sexual orientation—occur more frequently than sexual misconduct.12 Although the impact of nonsexual violations generally is less serious, any relationship that coexists with the therapeutic relationship has the potential to impair your judgment and contaminate your ability to focus exclusively on your patient’s well-being.13 Be cautious about any decision that could affect the treatment relationship.14
Triangle relationships.Originally, this term referred to the patient/therapist/psychiatrist triad. The term now has a broader meaning that includes:
- encroachments into care by managed care companies and government regulatory agencies
- interactions with the patient’s family members
- providing psychiatric care in non-traditional settings such as schools or prisons
- serving as an expert witness.15
The framework of trust once considered a core feature of the psychiatrist/patient relationship is being undermined by a funding system that demands efficiency and economy.16 Recognizing that some settings sacrifice patients’ clinical needs to the interests of the organization, the APA’s Guidelines for Ethical Practice in Organized Settings stipulate that the psychiatrist must “strive to resolve these conflicts in a manner that is likely to be of greatest benefit to the patient” by (for example):
- informing a patient of financial incentives or penalties that limit your ability to provide appropriate treatment
- not with holding information the patient could use to make informed treatment decisions, including treatment options not provided by you.6
Psychiatrists who doubt that the system—such as a mental health clinic, hospital, or managed care contract provider or reviewer—upholds the standard of acceptable care have the “ethical responsibility” to improve the system.6
Another change in mental health care attempts to limit psychiatrists to “medication management” so that less expensive professionals can provide adjunctive therapies. The treating psychiatrist bears some responsibility, however, for the appropriateness of the patient’s therapeutic options.6 According to Reid,17 psychiatrists are responsible for knowing something about the care, treatment style, credentials, and even ethics of those with whom they share treatment or to whom they refer patients.
The American Academy of Child and Adolescent Psychiatry (AACAP) Code of Ethics addresses the unique challenges encountered when a patient’s opinions differ from those of parents and other authority figures, such as school staff. The AACAP standards consistently direct the psychiatrist to keep the child’s interest primary, explaining that “the child and adolescent psychiatrist may be called upon to participate in attempts to control or change the behavior of children or adolescents…[but] the child and adolescent psychiatrist will avoid acting solely as an agent of the parents, guardians, or agencies.”18
Another triangle can occur when a treating psychiatrist serves as an expert witness or other evaluator for forensic or disability purposes. The American Academy of Psychiatry and the Law (AAPL) recommends that psychiatrists avoid acting as expert witnesses for their patients or performing patient evaluations for legal purposes.19 While recognizing that certain situations may require a psychiatrist to serve a dual role, the AAPL stresses that sensitivity to differences between clinical and legal obligations remains important.
Avoid serving as an expert witness for your patient. The intrusion of another role into the doctor/patient relationship can alter the treatment process and permanently color future inter actions. Likewise, treating an individual whom you previously evaluated for forensic purposes raises similar concerns, including the possibility of a mercenary motivation. Even when no such motivation exists, these situations can create the appearance that you have conscripted a vulnerable individual into your practice.
Emerging trends
Crossings vs violations. Efforts to distinguish when an action is unethical or illegal have led some to differentiate boundary crossings from boundary violations. Unfortunately, the 2 terms continue to be used synonymously, which confuses rather than clarifies the issue:
- Boundary crossings are aimed at enhancing the therapist’s treatment efforts—such as a hug instead of a hand shake at the end of a particularly difficult treatment session.
- Boundary violations are invariably harmful and unethical because they serve the therapist’s needs rather than the patient’s needs or the therapeutic process.20
Rather than trying to differentiate between crossings and violations or to determine under what circumstances changing boundaries is acceptable, Sheets21 conceptualizes a boundary not as a line to cross, but as a continuum of behavior. Under-involvement is at one end, over-involvement at the other, and a “zone of helpfulness” is in the middle.
Glass uses a Venn diagram to illustrate that although most boundary crossings probably fall within the realm of ethical practice, gray areas alert therapists that they are approaching a violation (Figure).20 Five factors have been found to increase psychiatrists’ vulnerability to boundary violations (Table 1).22
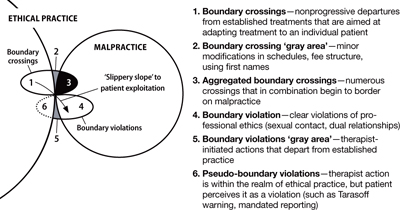
Figure Beware the ‘gray areas’ between boundary crossings, violations
Source: Glass L. The gray areas of boundary crossings and violations. Am J Psychother 2003;57(4):429-44. Republished with permission of the Association for the Advancement of PsychotherapyTable 1
Boundary violations: Factors that increase your vulnerability
| Life crises—effects of aging, career disappointments, unfulfilled hopes, or marital conflicts |
| Transitions—job changes or job loss |
| Medical illness |
| Arrogance—the belief that a boundary violation couldn’t happen to you and not recognizing the need for consultation |
| Stress points shared by the patient |
| Source: Reference 22 |
CASE CONTINUED: Board investigation
Dr. M’s relationship with Ms. Y grows intense, and he becomes increasingly concerned about her “clinginess.” After several months, Dr. M feels emotionally suffocated and ends the relationship. Despondent and suicidal, she seeks treatment in the local emergency room. Ms. Y tells the ER psychiatrist about her relationship with Dr. M and that she cannot go on without him in her life. The ER psychiatrist refers her to another psychiatrist for outpatient care, and, with Ms. Y’s permission, files a complaint about Dr. M with the state medical board and the district branch ethics committee.
The state medical board investigates Dr. M. He is contrite about his actions and their effect on Ms. Y. The state board refers Dr. M to an impaired physician’s program. He is required to attend a boundary violations course and undergo 1 year of practice supervision by a local psychiatrist. Several years later, Dr. M is doing well in his practice and has had no further complaints lodged against him.
Boundaries vs relationships. Using boundaries as a metaphor for maintaining the separation of therapist and patient was intended to serve the analytic process and to protect the patient’s welfare.2 Clearly, certain boundaries—such as sexual contact between psychiatrist and patient—must remain sacrosanct. Yet certain practices avoided in analysis may be appropriate for other therapeutic interventions. For example, whereas psychoanalysis has strict prohibitions against seeing patients anywhere except in the office, cognitive-behavioral therapists may find it useful to conduct sessions in public, or—under carefully arranged circumstances—even in a patient’s home. Other examples include accompanying a patient with agoraphobia to a public gathering or dining with a patient with anorexia.
Exercise caution when you decide to alter traditional boundaries. Even minor crossings that are not likely to progress to violations have the potential to contaminate the therapeutic relationship and place the psychiatrist on a “slippery slope” to patient exploitation.22,23 Some boundary issues are ambiguous, and extenuating circumstances can create a context that temporarily stretches a boundary beyond its normal limits,24 especially in small communities and rural settings where patients and treating psychiatrists are likely to know and encounter each other in social settings.25 Our recommendations for avoiding boundary violations appear in Table 2.
Except in clear cases of malfeasance, determining whether or not you have crossed a boundary is not a straightforward decision based on a single theoretical perspective or absolute standard.26 Regardless of whether a given boundary’s edge is well defined, 2 things are clear:
- unlike patients, psychiatrists have a professional code to honor27
- harm is determined by the meaning of the behavior to the patient and not the psychiatrist’s intentions.4
Table 2
Simple steps help avoid boundary violations
| Dos |
| Know your state’s statutes regarding medical ethics |
| Stay abreast of the American Psychiatric Association’s Principles of Medical Ethics |
| Consult with colleagues |
| Be aware of your weaknesses |
| Avoid ‘slippery slopes’ |
| Use objective documentation |
| Build a satisfying personal life |
| Don’ts |
| Don’t foster dependency |
| Don’t use patients for your own gratification |
| Don’t engage in extra-therapeutic contacts |
| Avoid physical contact |
| Don’t accept gifts or services |
Related Resources
- American Medical Association. Principles of medical ethics. www.ama-assn.org/ama/pub/category/2512.html.
- American Psychiatric Association. The principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association; 2008.
Disclosures
Drs. Marshall and Myers report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Teston is a speaker for Shire US, Inc.
1. Margison F. Boundary violations and psychotherapy. Curr Opin Psychiatry 1996;9(3):204-8.
2. Smith D, Fitzpatrick M. Patient-therapist boundary issues: an integrative review of theory and research. Prof Psychol Res Pr 1995;26(5):499-506.
3. Canadian Medical Association. Canadian Medical Association code of ethics. Ottawa, ON: Canadian Medical Association; 1996.
4. Sarkar S. Boundary violation and sexual exploitation in psychiatry and psychotherapy: a review. Advances in Psychiatric Treatment 2004;10:312-20.
5. Radeen J. The debate continues: unique ethics for psychiatry. Aust N Z J Psychiatry 2003;38:115-8.
6. American Psychiatric Association The principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association; 2008.
7. Zur O. To cross or not to cross: do boundaries in therapy protect or harm? The Psychotherapy Bulletin 2004;39(3):27-32.
8. Spickard W, Swiggart W, Manley G, et al. A continuing medical education approach to improve sexual boundaries of physicians. Bull Menninger Clin 2008;72(1):38-53.
9. Morrison J, Morrison T. Psychiatrists disciplined by a state medical board. Am J Psychiatry 2001;158:474-8.
10. Beecher L, Altchuler S. Sexual boundary violations. Minn Med 2005;88:42-4.
11. Dehlendorf C. Physicians disciplined for sex-related offenses. JAMA 1998;279(23):1883-8.
12. Garfinkel P, Dorian B, Sadavoy J, Bagby R. Boundary violations and departments of psychiatry. Can J Psychiatry 1997;42:764-70.
13. Gabbard G, Nadelson C. Professional boundaries in the physician-patient relationship. JAMA 1995;273(18):1445-9.
14. Nadelson C, Notman M. Boundaries in the doctor-patient relationship. Theor Med 2002;23:191-201.
15. Sarkar S, Adshead G. Ethics in forensic psychiatry. Curr Opin Psychiatry 2002;15:527-31.
16. Green S, Bloch S. Working in a flawed mental health care system: an ethical challenge. Am J Psychiatry 2001;158(9):1378-83.
17. Reid W. Treating clinicians and expert testimony. Journal of Practical Psychiatry and Behavioral Health 1998;4(2):121-4.
18. American Academy of Child and Adolescent Psychiatry. American Academy of Child and Adolescent Psychiatry code of ethics. Annotations to AACAP ethical code with special reference to evolving health care delivery and reimbursement systems. Washington, DC: American Academy of Child and Adolescent Psychiatry; 1995.
19. American Academy of Psychiatry and the Law. Ethics guidelines for the practice of forensic psychiatry. 2005. Available at: http://www.aapl.org/pdf/ETHICSGDLNS. pdf. Accessed June 3, 2008.
20. Glass L. The gray areas of boundary crossings and violations. Am J Psychother 2003;57(4):429-44.
21. Sheets V. Teach nurses how to maintain professional boundaries, recognize potential problems, and make better patient care decisions. Nurs Manage 2000;31(8):28-34.
22. Norris D, Gutheil T, Strasburger L. This couldn’t happen to me: boundary problems and sexual misconduct in the psychotherapy relationship. Psychiatr Serv 2003;54:517-22.
23. Galletly C. Crossing professional boundaries in medicine: the slippery slope to patient sexual exploitation. Med J Aust 2004;181(7):380-3.
24. Gutheil T, Gabbard G. Misuses and misunderstandings of boundary theory in clinical and regulatory settings. Am J Psychiatry 1998;155(3):409-14.
25. Simon R, Williams I. Maintaining treatment boundaries in small communities and rural areas. Psychiatr Serv 1999;50:1440-6.
26. Dvoskin J. Commentary: two sides to every story—the need for objectivity and evidence. J Am Acad Psychiatry Law 2005;33(4):482-3.
27. Gutheil T. Boundary issues and personality disorders. J Psychiatr Pract 2005;11(2):88-96.
Dr. M is facing financial challenges with his fledgling private practice and begins consulting at a weight loss clinic to supplement his income. He finds him-self attracted to Ms. Y, a weight-loss patient he is treating. They seem to click interpersonally, and he extends his office visits with her. Ms. Y clearly enjoys this extra attention, and Dr. M begins including personal disclosures in his conversations with her.
In his residency training, Dr. M was taught never to date a current or former patient, but he views this situation as different. Ms. Y is seeing him only for weight loss, and he rationalizes that he is providing her with medical care, not “psychiatric” care. On 2 occasions he gives her a limited quantity of benzodiazepines for mild anxiety, which he considers a transitory stress-related condition and not an “official” DSM-IV-TR disorder.
Eventually, Dr. M asks Ms. Y to dinner and she accepts. After they begin dating, he decides to transfer her to another clinic physician “just to be safe.”
Although many psychiatrists assume that psychiatrist/patient boundaries are well defined by ethical and legal standards, boundary issues are a complex and controversial aspect of clinical practice. Psychoanalysts initially defined psychiatrist/patient boundaries as a way of structuring the unique and intimate relationship that evolves during analysis.1,2 The introduction of other therapeutic techniques and changes in health care funding have combined to make psychiatrist/patient boundaries far more complex.
Boundary violations are about exploitation. Both the American Medical Association (AMA) and the Canadian Medical Association warn members to “scrupulously avoid using the physician/patient relationship to gratify their own emotional, financial, and sexual needs.”3
Boundaries represent the edge of appropriate behavior and serve 2 important purposes:
- They separate the therapeutic relationship from social, sexual, romantic, and business relationships and from relationships that transform into caretaking of the psychiatrist by the patient.
- They structure the professional relationship in ways that maintain the identity and roles of the patient and the professional.4
Psychiatry’s unique dilemmas
As are all physicians, psychiatrists are governed by the 9 biomedical ethics set forth in the AMA’s Principles of Medical Ethics. The American Psychiatric Association (APA), however, acknowledges that psychiatry has a “broader set of moral and ethical problems and dilemmas” that are unique to and magnified by the mental health setting.5 The APA has adopted 39 standards in addition to those set forth by the AMA. The first standard captures the unique responsibilities inherent in the psychiatrist/ patient relationship: A psychiatrist shall not gratify his or her own needs by exploiting the patient (Box).6
Sexual contact with patients is inherently harmful to patients, always unethical, and usually illegal.7 The rate of sexual misconduct among psychiatrists is unknown. National Practitioner Data Bank information is not available to the general public.8 Based on literature reviews and data from individual states9,10 and government agencies,11 an estimated 6% to10% of psychiatrists have had inappropriate sexual relations with patients.12 Estimates of sexual misconduct by psychiatrists:
All physicians are required to practice in accordance with the American Medical Association’s Principles of Medical Ethics. Because these guidelines can be difficult to interpret for psychiatry, the American Psychiatric Association provides further guidance with The Principles of Medical Ethics with Annotations Especially Applicable to Psychiatry. The following excerpts from annotations to the first 2 principles spell out the basic concepts underlying appropriate psychiatrist/patient boundaries:
‘A psychiatrist shall not gratify his or her own needs by exploiting the patient. The psychiatrist shall be ever vigilant about the impact that his or her conduct has upon the boundaries of the doctor/patient relationship, and thus upon the well-being of the patient. These requirements become particularly important because of the essentially private, highly personal, and sometimes intensely emotional nature of the relationship established with the psychiatrist.
‘The requirement that the physician conduct himself/herself with propriety in his or her profession and in all the actions of his or her life is especially important in the case of the psychiatrist because the patient tends to model his or her behavior after that of his or her psychiatrist by identification. Further, the necessary intensity of the treatment relationship may tend to activate sexual and other needs and fantasies on the part of both patient and psychiatrist, while weakening the objectivity necessary for control. Additionally, the inherent inequality in the doctor-patient relationship may lead to exploitation of the patient. Sexual activity with a current or former patient is unethical.’
Source: Reference 6
- increase if misconduct is based on patient complaints
- decrease if self-reports are used
- decrease even further if based on official investigations.4
American psychoanalyst Frieda Fromm-Reichman reportedly offered her colleagues a not-so-humorous admonition: “Don’t have sex with your patients; you will only disappoint them.”4
Nonsexual boundary violations—such as accepting gifts, entering into business arrangements, or trying to influence a patient’s political or religious beliefs or sexual orientation—occur more frequently than sexual misconduct.12 Although the impact of nonsexual violations generally is less serious, any relationship that coexists with the therapeutic relationship has the potential to impair your judgment and contaminate your ability to focus exclusively on your patient’s well-being.13 Be cautious about any decision that could affect the treatment relationship.14
Triangle relationships.Originally, this term referred to the patient/therapist/psychiatrist triad. The term now has a broader meaning that includes:
- encroachments into care by managed care companies and government regulatory agencies
- interactions with the patient’s family members
- providing psychiatric care in non-traditional settings such as schools or prisons
- serving as an expert witness.15
The framework of trust once considered a core feature of the psychiatrist/patient relationship is being undermined by a funding system that demands efficiency and economy.16 Recognizing that some settings sacrifice patients’ clinical needs to the interests of the organization, the APA’s Guidelines for Ethical Practice in Organized Settings stipulate that the psychiatrist must “strive to resolve these conflicts in a manner that is likely to be of greatest benefit to the patient” by (for example):
- informing a patient of financial incentives or penalties that limit your ability to provide appropriate treatment
- not with holding information the patient could use to make informed treatment decisions, including treatment options not provided by you.6
Psychiatrists who doubt that the system—such as a mental health clinic, hospital, or managed care contract provider or reviewer—upholds the standard of acceptable care have the “ethical responsibility” to improve the system.6
Another change in mental health care attempts to limit psychiatrists to “medication management” so that less expensive professionals can provide adjunctive therapies. The treating psychiatrist bears some responsibility, however, for the appropriateness of the patient’s therapeutic options.6 According to Reid,17 psychiatrists are responsible for knowing something about the care, treatment style, credentials, and even ethics of those with whom they share treatment or to whom they refer patients.
The American Academy of Child and Adolescent Psychiatry (AACAP) Code of Ethics addresses the unique challenges encountered when a patient’s opinions differ from those of parents and other authority figures, such as school staff. The AACAP standards consistently direct the psychiatrist to keep the child’s interest primary, explaining that “the child and adolescent psychiatrist may be called upon to participate in attempts to control or change the behavior of children or adolescents…[but] the child and adolescent psychiatrist will avoid acting solely as an agent of the parents, guardians, or agencies.”18
Another triangle can occur when a treating psychiatrist serves as an expert witness or other evaluator for forensic or disability purposes. The American Academy of Psychiatry and the Law (AAPL) recommends that psychiatrists avoid acting as expert witnesses for their patients or performing patient evaluations for legal purposes.19 While recognizing that certain situations may require a psychiatrist to serve a dual role, the AAPL stresses that sensitivity to differences between clinical and legal obligations remains important.
Avoid serving as an expert witness for your patient. The intrusion of another role into the doctor/patient relationship can alter the treatment process and permanently color future inter actions. Likewise, treating an individual whom you previously evaluated for forensic purposes raises similar concerns, including the possibility of a mercenary motivation. Even when no such motivation exists, these situations can create the appearance that you have conscripted a vulnerable individual into your practice.
Emerging trends
Crossings vs violations. Efforts to distinguish when an action is unethical or illegal have led some to differentiate boundary crossings from boundary violations. Unfortunately, the 2 terms continue to be used synonymously, which confuses rather than clarifies the issue:
- Boundary crossings are aimed at enhancing the therapist’s treatment efforts—such as a hug instead of a hand shake at the end of a particularly difficult treatment session.
- Boundary violations are invariably harmful and unethical because they serve the therapist’s needs rather than the patient’s needs or the therapeutic process.20
Rather than trying to differentiate between crossings and violations or to determine under what circumstances changing boundaries is acceptable, Sheets21 conceptualizes a boundary not as a line to cross, but as a continuum of behavior. Under-involvement is at one end, over-involvement at the other, and a “zone of helpfulness” is in the middle.
Glass uses a Venn diagram to illustrate that although most boundary crossings probably fall within the realm of ethical practice, gray areas alert therapists that they are approaching a violation (Figure).20 Five factors have been found to increase psychiatrists’ vulnerability to boundary violations (Table 1).22
Figure Beware the ‘gray areas’ between boundary crossings, violations
Source: Glass L. The gray areas of boundary crossings and violations. Am J Psychother 2003;57(4):429-44. Republished with permission of the Association for the Advancement of PsychotherapyTable 1
Boundary violations: Factors that increase your vulnerability
| Life crises—effects of aging, career disappointments, unfulfilled hopes, or marital conflicts |
| Transitions—job changes or job loss |
| Medical illness |
| Arrogance—the belief that a boundary violation couldn’t happen to you and not recognizing the need for consultation |
| Stress points shared by the patient |
| Source: Reference 22 |
CASE CONTINUED: Board investigation
Dr. M’s relationship with Ms. Y grows intense, and he becomes increasingly concerned about her “clinginess.” After several months, Dr. M feels emotionally suffocated and ends the relationship. Despondent and suicidal, she seeks treatment in the local emergency room. Ms. Y tells the ER psychiatrist about her relationship with Dr. M and that she cannot go on without him in her life. The ER psychiatrist refers her to another psychiatrist for outpatient care, and, with Ms. Y’s permission, files a complaint about Dr. M with the state medical board and the district branch ethics committee.
The state medical board investigates Dr. M. He is contrite about his actions and their effect on Ms. Y. The state board refers Dr. M to an impaired physician’s program. He is required to attend a boundary violations course and undergo 1 year of practice supervision by a local psychiatrist. Several years later, Dr. M is doing well in his practice and has had no further complaints lodged against him.
Boundaries vs relationships. Using boundaries as a metaphor for maintaining the separation of therapist and patient was intended to serve the analytic process and to protect the patient’s welfare.2 Clearly, certain boundaries—such as sexual contact between psychiatrist and patient—must remain sacrosanct. Yet certain practices avoided in analysis may be appropriate for other therapeutic interventions. For example, whereas psychoanalysis has strict prohibitions against seeing patients anywhere except in the office, cognitive-behavioral therapists may find it useful to conduct sessions in public, or—under carefully arranged circumstances—even in a patient’s home. Other examples include accompanying a patient with agoraphobia to a public gathering or dining with a patient with anorexia.
Exercise caution when you decide to alter traditional boundaries. Even minor crossings that are not likely to progress to violations have the potential to contaminate the therapeutic relationship and place the psychiatrist on a “slippery slope” to patient exploitation.22,23 Some boundary issues are ambiguous, and extenuating circumstances can create a context that temporarily stretches a boundary beyond its normal limits,24 especially in small communities and rural settings where patients and treating psychiatrists are likely to know and encounter each other in social settings.25 Our recommendations for avoiding boundary violations appear in Table 2.
Except in clear cases of malfeasance, determining whether or not you have crossed a boundary is not a straightforward decision based on a single theoretical perspective or absolute standard.26 Regardless of whether a given boundary’s edge is well defined, 2 things are clear:
- unlike patients, psychiatrists have a professional code to honor27
- harm is determined by the meaning of the behavior to the patient and not the psychiatrist’s intentions.4
Table 2
Simple steps help avoid boundary violations
| Dos |
| Know your state’s statutes regarding medical ethics |
| Stay abreast of the American Psychiatric Association’s Principles of Medical Ethics |
| Consult with colleagues |
| Be aware of your weaknesses |
| Avoid ‘slippery slopes’ |
| Use objective documentation |
| Build a satisfying personal life |
| Don’ts |
| Don’t foster dependency |
| Don’t use patients for your own gratification |
| Don’t engage in extra-therapeutic contacts |
| Avoid physical contact |
| Don’t accept gifts or services |
Related Resources
- American Medical Association. Principles of medical ethics. www.ama-assn.org/ama/pub/category/2512.html.
- American Psychiatric Association. The principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association; 2008.
Disclosures
Drs. Marshall and Myers report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Teston is a speaker for Shire US, Inc.
Dr. M is facing financial challenges with his fledgling private practice and begins consulting at a weight loss clinic to supplement his income. He finds him-self attracted to Ms. Y, a weight-loss patient he is treating. They seem to click interpersonally, and he extends his office visits with her. Ms. Y clearly enjoys this extra attention, and Dr. M begins including personal disclosures in his conversations with her.
In his residency training, Dr. M was taught never to date a current or former patient, but he views this situation as different. Ms. Y is seeing him only for weight loss, and he rationalizes that he is providing her with medical care, not “psychiatric” care. On 2 occasions he gives her a limited quantity of benzodiazepines for mild anxiety, which he considers a transitory stress-related condition and not an “official” DSM-IV-TR disorder.
Eventually, Dr. M asks Ms. Y to dinner and she accepts. After they begin dating, he decides to transfer her to another clinic physician “just to be safe.”
Although many psychiatrists assume that psychiatrist/patient boundaries are well defined by ethical and legal standards, boundary issues are a complex and controversial aspect of clinical practice. Psychoanalysts initially defined psychiatrist/patient boundaries as a way of structuring the unique and intimate relationship that evolves during analysis.1,2 The introduction of other therapeutic techniques and changes in health care funding have combined to make psychiatrist/patient boundaries far more complex.
Boundary violations are about exploitation. Both the American Medical Association (AMA) and the Canadian Medical Association warn members to “scrupulously avoid using the physician/patient relationship to gratify their own emotional, financial, and sexual needs.”3
Boundaries represent the edge of appropriate behavior and serve 2 important purposes:
- They separate the therapeutic relationship from social, sexual, romantic, and business relationships and from relationships that transform into caretaking of the psychiatrist by the patient.
- They structure the professional relationship in ways that maintain the identity and roles of the patient and the professional.4
Psychiatry’s unique dilemmas
As are all physicians, psychiatrists are governed by the 9 biomedical ethics set forth in the AMA’s Principles of Medical Ethics. The American Psychiatric Association (APA), however, acknowledges that psychiatry has a “broader set of moral and ethical problems and dilemmas” that are unique to and magnified by the mental health setting.5 The APA has adopted 39 standards in addition to those set forth by the AMA. The first standard captures the unique responsibilities inherent in the psychiatrist/ patient relationship: A psychiatrist shall not gratify his or her own needs by exploiting the patient (Box).6
Sexual contact with patients is inherently harmful to patients, always unethical, and usually illegal.7 The rate of sexual misconduct among psychiatrists is unknown. National Practitioner Data Bank information is not available to the general public.8 Based on literature reviews and data from individual states9,10 and government agencies,11 an estimated 6% to10% of psychiatrists have had inappropriate sexual relations with patients.12 Estimates of sexual misconduct by psychiatrists:
All physicians are required to practice in accordance with the American Medical Association’s Principles of Medical Ethics. Because these guidelines can be difficult to interpret for psychiatry, the American Psychiatric Association provides further guidance with The Principles of Medical Ethics with Annotations Especially Applicable to Psychiatry. The following excerpts from annotations to the first 2 principles spell out the basic concepts underlying appropriate psychiatrist/patient boundaries:
‘A psychiatrist shall not gratify his or her own needs by exploiting the patient. The psychiatrist shall be ever vigilant about the impact that his or her conduct has upon the boundaries of the doctor/patient relationship, and thus upon the well-being of the patient. These requirements become particularly important because of the essentially private, highly personal, and sometimes intensely emotional nature of the relationship established with the psychiatrist.
‘The requirement that the physician conduct himself/herself with propriety in his or her profession and in all the actions of his or her life is especially important in the case of the psychiatrist because the patient tends to model his or her behavior after that of his or her psychiatrist by identification. Further, the necessary intensity of the treatment relationship may tend to activate sexual and other needs and fantasies on the part of both patient and psychiatrist, while weakening the objectivity necessary for control. Additionally, the inherent inequality in the doctor-patient relationship may lead to exploitation of the patient. Sexual activity with a current or former patient is unethical.’
Source: Reference 6
- increase if misconduct is based on patient complaints
- decrease if self-reports are used
- decrease even further if based on official investigations.4
American psychoanalyst Frieda Fromm-Reichman reportedly offered her colleagues a not-so-humorous admonition: “Don’t have sex with your patients; you will only disappoint them.”4
Nonsexual boundary violations—such as accepting gifts, entering into business arrangements, or trying to influence a patient’s political or religious beliefs or sexual orientation—occur more frequently than sexual misconduct.12 Although the impact of nonsexual violations generally is less serious, any relationship that coexists with the therapeutic relationship has the potential to impair your judgment and contaminate your ability to focus exclusively on your patient’s well-being.13 Be cautious about any decision that could affect the treatment relationship.14
Triangle relationships.Originally, this term referred to the patient/therapist/psychiatrist triad. The term now has a broader meaning that includes:
- encroachments into care by managed care companies and government regulatory agencies
- interactions with the patient’s family members
- providing psychiatric care in non-traditional settings such as schools or prisons
- serving as an expert witness.15
The framework of trust once considered a core feature of the psychiatrist/patient relationship is being undermined by a funding system that demands efficiency and economy.16 Recognizing that some settings sacrifice patients’ clinical needs to the interests of the organization, the APA’s Guidelines for Ethical Practice in Organized Settings stipulate that the psychiatrist must “strive to resolve these conflicts in a manner that is likely to be of greatest benefit to the patient” by (for example):
- informing a patient of financial incentives or penalties that limit your ability to provide appropriate treatment
- not with holding information the patient could use to make informed treatment decisions, including treatment options not provided by you.6
Psychiatrists who doubt that the system—such as a mental health clinic, hospital, or managed care contract provider or reviewer—upholds the standard of acceptable care have the “ethical responsibility” to improve the system.6
Another change in mental health care attempts to limit psychiatrists to “medication management” so that less expensive professionals can provide adjunctive therapies. The treating psychiatrist bears some responsibility, however, for the appropriateness of the patient’s therapeutic options.6 According to Reid,17 psychiatrists are responsible for knowing something about the care, treatment style, credentials, and even ethics of those with whom they share treatment or to whom they refer patients.
The American Academy of Child and Adolescent Psychiatry (AACAP) Code of Ethics addresses the unique challenges encountered when a patient’s opinions differ from those of parents and other authority figures, such as school staff. The AACAP standards consistently direct the psychiatrist to keep the child’s interest primary, explaining that “the child and adolescent psychiatrist may be called upon to participate in attempts to control or change the behavior of children or adolescents…[but] the child and adolescent psychiatrist will avoid acting solely as an agent of the parents, guardians, or agencies.”18
Another triangle can occur when a treating psychiatrist serves as an expert witness or other evaluator for forensic or disability purposes. The American Academy of Psychiatry and the Law (AAPL) recommends that psychiatrists avoid acting as expert witnesses for their patients or performing patient evaluations for legal purposes.19 While recognizing that certain situations may require a psychiatrist to serve a dual role, the AAPL stresses that sensitivity to differences between clinical and legal obligations remains important.
Avoid serving as an expert witness for your patient. The intrusion of another role into the doctor/patient relationship can alter the treatment process and permanently color future inter actions. Likewise, treating an individual whom you previously evaluated for forensic purposes raises similar concerns, including the possibility of a mercenary motivation. Even when no such motivation exists, these situations can create the appearance that you have conscripted a vulnerable individual into your practice.
Emerging trends
Crossings vs violations. Efforts to distinguish when an action is unethical or illegal have led some to differentiate boundary crossings from boundary violations. Unfortunately, the 2 terms continue to be used synonymously, which confuses rather than clarifies the issue:
- Boundary crossings are aimed at enhancing the therapist’s treatment efforts—such as a hug instead of a hand shake at the end of a particularly difficult treatment session.
- Boundary violations are invariably harmful and unethical because they serve the therapist’s needs rather than the patient’s needs or the therapeutic process.20
Rather than trying to differentiate between crossings and violations or to determine under what circumstances changing boundaries is acceptable, Sheets21 conceptualizes a boundary not as a line to cross, but as a continuum of behavior. Under-involvement is at one end, over-involvement at the other, and a “zone of helpfulness” is in the middle.
Glass uses a Venn diagram to illustrate that although most boundary crossings probably fall within the realm of ethical practice, gray areas alert therapists that they are approaching a violation (Figure).20 Five factors have been found to increase psychiatrists’ vulnerability to boundary violations (Table 1).22
Figure Beware the ‘gray areas’ between boundary crossings, violations
Source: Glass L. The gray areas of boundary crossings and violations. Am J Psychother 2003;57(4):429-44. Republished with permission of the Association for the Advancement of PsychotherapyTable 1
Boundary violations: Factors that increase your vulnerability
| Life crises—effects of aging, career disappointments, unfulfilled hopes, or marital conflicts |
| Transitions—job changes or job loss |
| Medical illness |
| Arrogance—the belief that a boundary violation couldn’t happen to you and not recognizing the need for consultation |
| Stress points shared by the patient |
| Source: Reference 22 |
CASE CONTINUED: Board investigation
Dr. M’s relationship with Ms. Y grows intense, and he becomes increasingly concerned about her “clinginess.” After several months, Dr. M feels emotionally suffocated and ends the relationship. Despondent and suicidal, she seeks treatment in the local emergency room. Ms. Y tells the ER psychiatrist about her relationship with Dr. M and that she cannot go on without him in her life. The ER psychiatrist refers her to another psychiatrist for outpatient care, and, with Ms. Y’s permission, files a complaint about Dr. M with the state medical board and the district branch ethics committee.
The state medical board investigates Dr. M. He is contrite about his actions and their effect on Ms. Y. The state board refers Dr. M to an impaired physician’s program. He is required to attend a boundary violations course and undergo 1 year of practice supervision by a local psychiatrist. Several years later, Dr. M is doing well in his practice and has had no further complaints lodged against him.
Boundaries vs relationships. Using boundaries as a metaphor for maintaining the separation of therapist and patient was intended to serve the analytic process and to protect the patient’s welfare.2 Clearly, certain boundaries—such as sexual contact between psychiatrist and patient—must remain sacrosanct. Yet certain practices avoided in analysis may be appropriate for other therapeutic interventions. For example, whereas psychoanalysis has strict prohibitions against seeing patients anywhere except in the office, cognitive-behavioral therapists may find it useful to conduct sessions in public, or—under carefully arranged circumstances—even in a patient’s home. Other examples include accompanying a patient with agoraphobia to a public gathering or dining with a patient with anorexia.
Exercise caution when you decide to alter traditional boundaries. Even minor crossings that are not likely to progress to violations have the potential to contaminate the therapeutic relationship and place the psychiatrist on a “slippery slope” to patient exploitation.22,23 Some boundary issues are ambiguous, and extenuating circumstances can create a context that temporarily stretches a boundary beyond its normal limits,24 especially in small communities and rural settings where patients and treating psychiatrists are likely to know and encounter each other in social settings.25 Our recommendations for avoiding boundary violations appear in Table 2.
Except in clear cases of malfeasance, determining whether or not you have crossed a boundary is not a straightforward decision based on a single theoretical perspective or absolute standard.26 Regardless of whether a given boundary’s edge is well defined, 2 things are clear:
- unlike patients, psychiatrists have a professional code to honor27
- harm is determined by the meaning of the behavior to the patient and not the psychiatrist’s intentions.4
Table 2
Simple steps help avoid boundary violations
| Dos |
| Know your state’s statutes regarding medical ethics |
| Stay abreast of the American Psychiatric Association’s Principles of Medical Ethics |
| Consult with colleagues |
| Be aware of your weaknesses |
| Avoid ‘slippery slopes’ |
| Use objective documentation |
| Build a satisfying personal life |
| Don’ts |
| Don’t foster dependency |
| Don’t use patients for your own gratification |
| Don’t engage in extra-therapeutic contacts |
| Avoid physical contact |
| Don’t accept gifts or services |
Related Resources
- American Medical Association. Principles of medical ethics. www.ama-assn.org/ama/pub/category/2512.html.
- American Psychiatric Association. The principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association; 2008.
Disclosures
Drs. Marshall and Myers report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Teston is a speaker for Shire US, Inc.
1. Margison F. Boundary violations and psychotherapy. Curr Opin Psychiatry 1996;9(3):204-8.
2. Smith D, Fitzpatrick M. Patient-therapist boundary issues: an integrative review of theory and research. Prof Psychol Res Pr 1995;26(5):499-506.
3. Canadian Medical Association. Canadian Medical Association code of ethics. Ottawa, ON: Canadian Medical Association; 1996.
4. Sarkar S. Boundary violation and sexual exploitation in psychiatry and psychotherapy: a review. Advances in Psychiatric Treatment 2004;10:312-20.
5. Radeen J. The debate continues: unique ethics for psychiatry. Aust N Z J Psychiatry 2003;38:115-8.
6. American Psychiatric Association The principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association; 2008.
7. Zur O. To cross or not to cross: do boundaries in therapy protect or harm? The Psychotherapy Bulletin 2004;39(3):27-32.
8. Spickard W, Swiggart W, Manley G, et al. A continuing medical education approach to improve sexual boundaries of physicians. Bull Menninger Clin 2008;72(1):38-53.
9. Morrison J, Morrison T. Psychiatrists disciplined by a state medical board. Am J Psychiatry 2001;158:474-8.
10. Beecher L, Altchuler S. Sexual boundary violations. Minn Med 2005;88:42-4.
11. Dehlendorf C. Physicians disciplined for sex-related offenses. JAMA 1998;279(23):1883-8.
12. Garfinkel P, Dorian B, Sadavoy J, Bagby R. Boundary violations and departments of psychiatry. Can J Psychiatry 1997;42:764-70.
13. Gabbard G, Nadelson C. Professional boundaries in the physician-patient relationship. JAMA 1995;273(18):1445-9.
14. Nadelson C, Notman M. Boundaries in the doctor-patient relationship. Theor Med 2002;23:191-201.
15. Sarkar S, Adshead G. Ethics in forensic psychiatry. Curr Opin Psychiatry 2002;15:527-31.
16. Green S, Bloch S. Working in a flawed mental health care system: an ethical challenge. Am J Psychiatry 2001;158(9):1378-83.
17. Reid W. Treating clinicians and expert testimony. Journal of Practical Psychiatry and Behavioral Health 1998;4(2):121-4.
18. American Academy of Child and Adolescent Psychiatry. American Academy of Child and Adolescent Psychiatry code of ethics. Annotations to AACAP ethical code with special reference to evolving health care delivery and reimbursement systems. Washington, DC: American Academy of Child and Adolescent Psychiatry; 1995.
19. American Academy of Psychiatry and the Law. Ethics guidelines for the practice of forensic psychiatry. 2005. Available at: http://www.aapl.org/pdf/ETHICSGDLNS. pdf. Accessed June 3, 2008.
20. Glass L. The gray areas of boundary crossings and violations. Am J Psychother 2003;57(4):429-44.
21. Sheets V. Teach nurses how to maintain professional boundaries, recognize potential problems, and make better patient care decisions. Nurs Manage 2000;31(8):28-34.
22. Norris D, Gutheil T, Strasburger L. This couldn’t happen to me: boundary problems and sexual misconduct in the psychotherapy relationship. Psychiatr Serv 2003;54:517-22.
23. Galletly C. Crossing professional boundaries in medicine: the slippery slope to patient sexual exploitation. Med J Aust 2004;181(7):380-3.
24. Gutheil T, Gabbard G. Misuses and misunderstandings of boundary theory in clinical and regulatory settings. Am J Psychiatry 1998;155(3):409-14.
25. Simon R, Williams I. Maintaining treatment boundaries in small communities and rural areas. Psychiatr Serv 1999;50:1440-6.
26. Dvoskin J. Commentary: two sides to every story—the need for objectivity and evidence. J Am Acad Psychiatry Law 2005;33(4):482-3.
27. Gutheil T. Boundary issues and personality disorders. J Psychiatr Pract 2005;11(2):88-96.
1. Margison F. Boundary violations and psychotherapy. Curr Opin Psychiatry 1996;9(3):204-8.
2. Smith D, Fitzpatrick M. Patient-therapist boundary issues: an integrative review of theory and research. Prof Psychol Res Pr 1995;26(5):499-506.
3. Canadian Medical Association. Canadian Medical Association code of ethics. Ottawa, ON: Canadian Medical Association; 1996.
4. Sarkar S. Boundary violation and sexual exploitation in psychiatry and psychotherapy: a review. Advances in Psychiatric Treatment 2004;10:312-20.
5. Radeen J. The debate continues: unique ethics for psychiatry. Aust N Z J Psychiatry 2003;38:115-8.
6. American Psychiatric Association The principles of medical ethics with annotations especially applicable to psychiatry. Washington, DC: American Psychiatric Association; 2008.
7. Zur O. To cross or not to cross: do boundaries in therapy protect or harm? The Psychotherapy Bulletin 2004;39(3):27-32.
8. Spickard W, Swiggart W, Manley G, et al. A continuing medical education approach to improve sexual boundaries of physicians. Bull Menninger Clin 2008;72(1):38-53.
9. Morrison J, Morrison T. Psychiatrists disciplined by a state medical board. Am J Psychiatry 2001;158:474-8.
10. Beecher L, Altchuler S. Sexual boundary violations. Minn Med 2005;88:42-4.
11. Dehlendorf C. Physicians disciplined for sex-related offenses. JAMA 1998;279(23):1883-8.
12. Garfinkel P, Dorian B, Sadavoy J, Bagby R. Boundary violations and departments of psychiatry. Can J Psychiatry 1997;42:764-70.
13. Gabbard G, Nadelson C. Professional boundaries in the physician-patient relationship. JAMA 1995;273(18):1445-9.
14. Nadelson C, Notman M. Boundaries in the doctor-patient relationship. Theor Med 2002;23:191-201.
15. Sarkar S, Adshead G. Ethics in forensic psychiatry. Curr Opin Psychiatry 2002;15:527-31.
16. Green S, Bloch S. Working in a flawed mental health care system: an ethical challenge. Am J Psychiatry 2001;158(9):1378-83.
17. Reid W. Treating clinicians and expert testimony. Journal of Practical Psychiatry and Behavioral Health 1998;4(2):121-4.
18. American Academy of Child and Adolescent Psychiatry. American Academy of Child and Adolescent Psychiatry code of ethics. Annotations to AACAP ethical code with special reference to evolving health care delivery and reimbursement systems. Washington, DC: American Academy of Child and Adolescent Psychiatry; 1995.
19. American Academy of Psychiatry and the Law. Ethics guidelines for the practice of forensic psychiatry. 2005. Available at: http://www.aapl.org/pdf/ETHICSGDLNS. pdf. Accessed June 3, 2008.
20. Glass L. The gray areas of boundary crossings and violations. Am J Psychother 2003;57(4):429-44.
21. Sheets V. Teach nurses how to maintain professional boundaries, recognize potential problems, and make better patient care decisions. Nurs Manage 2000;31(8):28-34.
22. Norris D, Gutheil T, Strasburger L. This couldn’t happen to me: boundary problems and sexual misconduct in the psychotherapy relationship. Psychiatr Serv 2003;54:517-22.
23. Galletly C. Crossing professional boundaries in medicine: the slippery slope to patient sexual exploitation. Med J Aust 2004;181(7):380-3.
24. Gutheil T, Gabbard G. Misuses and misunderstandings of boundary theory in clinical and regulatory settings. Am J Psychiatry 1998;155(3):409-14.
25. Simon R, Williams I. Maintaining treatment boundaries in small communities and rural areas. Psychiatr Serv 1999;50:1440-6.
26. Dvoskin J. Commentary: two sides to every story—the need for objectivity and evidence. J Am Acad Psychiatry Law 2005;33(4):482-3.
27. Gutheil T. Boundary issues and personality disorders. J Psychiatr Pract 2005;11(2):88-96.
Subsyndromal depression
Mr. W, a 53-year-old divorced entrepreneur, presents to you for evaluation of poor concentration, decreased self-esteem, and difficulty making decisions that are interfering with his work. A longtime patient of another psychiatrist, Mr. W has a 26-year history of bipolar I disorder. He has not had a manic episode for 5 years but has had several depressive episodes.
During his last manic episode, Mr. W was hospitalized with expansive and irritable mood, racing thoughts, impulsive sexual behavior, psychomotor agitation, elevated self-esteem, marked distractibility, and paranoid ideas about his business partners. His discharge regimen included lithium titrated to 0.9 mEq/L and divalproex sodium, 1,500 mg/d, with lamotrigine, 200 mg/d, added to reduce depressive relapse risk. After several years of stable treatment, Mr. W complained of cognitive impairment. His psychiatrist discontinued lithium and added a low-dose stimulant—methylphenidate, 20 mg bid—to address Mr. W’s complaints of poor concentration.
Mr. W also is taking zolpidem, 10 mg as needed for onset insomnia, and receives weekly psychodynamic psychotherapy. His work performance problems persist despite these treatments, and his company is failing.
A poor course in bipolar disorder—as in Mr. W’s case—is frequently characterized by persistent or relapsing depression. Bipolar disorder is diagnosed by a manic, mixed, or hypomanic episode, but depression and depressive symptoms are most prominent in clinical practice. Likewise, major observational studies blame depression for most of the time spent ill in bipolar types I and II.1-8
A good deal of bipolar symptom burden is associated with subsyndromal depression—defined as having >2 but 5 and depressive symptoms are disproportionately responsible—compared with manic symptoms—for the impact of bipolar illness on patients and their families.9
This article offers clinically useful strategies to minimize subsyndromal depression in patients with bipolar disorder (Table 1). These strategies include an evidence-based approach to medication, the use of validated psychotherapies, regular sleep and socialization schedules, and careful monitoring of mood symptoms.
Table 1
How to minimize bipolar subsyndromal depression
| Monitor symptoms using validated clinician- and patient-rated tools at all visits |
| Use evidence-based treatments first |
| Eliminate ineffective medications |
| Use adequate doses of medications for different mood states |
| Monitor and treat adverse effects of successful treatments |
| Monitor and minimize medications that can worsen symptoms |
| Watch for the impact of medical conditions on mood |
| Be attentive to alcohol and substance use (including caffeine, nicotine, and energy drinks) |
| Monitor psychotherapies for symptom worsening |
| Address comorbid psychiatric conditions |
| Regularize social rhythms |
| Initiate validated psychosocial treatments |
| Engage the patient as a active participant in treatment |
Persistent depression
Randomized, controlled trials designed to obtain FDA approval of bipolar medications inadequately reflect the disabling, confounding nature of bipolar illness. Nearly all of these large studies of acute treatments for mood episodes are placebo-controlled trials with narrow inclusion and broad exclusion criteria. Eliminating subsyndromal symptoms is not their goal, and they are of little help in understanding how to manage residual symptoms.
A more realistic view of bipolar disorder comes from large observational studies that have examined its longitudinal course in outpatients under more or less ideal treatment conditions.10 These studies show that bipolar disorder is almost always recurrent and relapsing, but full recovery and functioning between episodes is not the norm. Most patients never achieve prolonged recovery, complete symptom relief, or return to full functioning.5,8,11
STEP-BD. Most patients in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) never recovered from a depressed episode during 2 years of prospective follow-up under optimal care. Only 58% of patients who entered the study during an episode of illness achieved 8 consecutive weeks of euthymia.5
Collaborative Depression study. Longitudinal data from the National Institute of Mental Health’s Collaborative Depression Study6,7 showed:
- patients with bipolar I disorder had depressive symptoms in approximately three-quarters of the weeks in which they reported significant symptoms
- patients with bipolar II disorder were depressed in nearly all sick weeks.
The Stanley Foundation Bipolar Network had similar findings, with bipolar disorder patients reporting 3 times as much time spent with depressed mood as with elevated mood.8 Poor social and occupational functioning predicted poor outcomes, suggesting an interplay between subsyndromal depression, poor functioning, and relapse.
Risk factors
Rapid cycling may be a marker for persistent, subsyndromal symptoms. Rapid cycling is defined clinically as 4 distinct mood episodes—switching to the opposite pole or 2 episodes of the same pole separated by ≥8 weeks of partial or full recovery—in the previous 12 months. Rapid cycling usually is diagnosed retrospectively—introducing patients’ recall bias—but may be more of a marker for symptom persistence than for defined episodes.
In STEP-BD, 32% of study entrants reported ≥4 mood episodes in the previous year, yet only 6% of that subgroup had ≥4 episodes after 1 year of prospective follow-up.12 This suggests:
- patients who retrospectively report rapid cycling may be chronically and persistently ill, rather than experiencing multiple discrete episodes
- rapid cycling is a marker for symptom persistence, subsyndromal depression, and lack of sustained remission.
- comorbid anxiety disorders (present in ≤50% of patients with bipolar I and II disorder)
- active and past substance use disorders (including nicotine dependence)
- early age of onset of the mood disorder.13-16
CASE CONTINUED: Restoring the cornerstone
You review Mr. W’s records. Recent lab values were essentially normal, with thyroid stimulating hormone 2.3 mIU/mL and stable renal function. He scores 11 on the Quick Inventory of Depressive Symptoms–self-rated version (QIDS-SR), indicating mild to moderate depressive symptom burden.
His mood chart and interview reveal that he has been depressed and anhedonic most of the day for 4 of the last 10 days. By systematically asking the depression questions in the DSM-IV-TR, you find that he does not meet criteria for depressed mood or anhedonia but has difficulty concentrating most of the day, persistent low self-esteem, and feeling “slowed.”
After you discuss lithium’s pros and cons with Mr. W, he agrees to try this mood stabilizer again. You explain the importance of preventing relapse to mania and of monitoring his cognitive performance at work.
Over time, you titrate lithium to a moderate serum level (0.5 to 0.7 mEq/L) and treat a resulting mild tremor with propranolol, 20 to 40 mg/d. Mr. W is tolerating lamotrigine well, so you continue this medication because of its potential to decrease the probability of relapse to depression. You also continue zolpidem, as needed, but discontinue methylphenidate because you think it may be contributing to sleep difficulties.
Managing medication
Nine drugs are FDA-approved for acute bipolar mania, but treatments for bipolar depression, maintenance treatment, and relapse prevention are far fewer, often partially effective, or effective for a limited number of patients. When depressive symptoms fail to resolve, a reasonable approach is to review patients’ medications and suggest alternatives with proven efficacy for bipolar disorder (Table 2). Patients can then accept or reject various options based on personal preference.
Combination strategies. Antimanic treatment is the cornerstone of treating bipolar I disorder, and preventing manic episodes should be a primary treatment goal. Thus, consider continuing treatments that have prevented mania for your patient—as lithium did in Mr. W’s case—while adding treatments aimed at depression. For example, adding lamotrigine to any antimanic agent is reasonable, especially if doing so does not add substantially to your patient’s side-effect burden.
Minimize antidepressants. Given the predominance and persistence of depressive symptoms in bipolar disorder, one can understand why clinicians and patients might try standard antidepressants without clear evidence supporting this practice. Antidepressants—especially venlafaxine and tricyclic antidepressants—are the most common and likely suspects when patients experience switching to mania, rapid cycling, and symptom persistence.17 Antidepressants’ negative effect has not been clearly defined, however, and may be patient-specific (related to patient factors rather than intrinsic to the compound).
In my clinical experience, minimizing antidepressant use in bipolar depression hastens rather than delays patients’ recovery. A prudent approach would be to use the minimum dose necessary and discontinue the antidepressant if possible. Also minimize medical pharmacotherapies—including corticosteroids and oral contraceptives—that may worsen mood symptoms, especially in patients with this history.
Avoid under-dosing. Inadequate dosing and duration often are overlooked as causes of treatment resistance in bipolar disorder and other illnesses.18 Bipolar disorder medications are hardly benign; every drug approved for any phase of bipolar disorder has a black-box warning. Understandably, clinicians and patients try to choose medications and dosages perceived to be most tolerable. Full-dose treatment trials may be warranted, however, given the high probability of incomplete recovery, impaired functioning, and risk of relapse with ineffective dosing.
Address iatrogenic causes. In addition, identify and eliminate medications and treatments that may be perpetuating patients’ bipolar symptoms. Stimulants such as methylphenidate and amphetamines may contribute to sleep disturbance and manic relapse and might be minimized or eliminated in a patient with continued symptoms and sleep disturbance.19
- Two trials of aripiprazole for bipolar depression failed to show benefit.20
- A trial that compared risperidone with lamotrigine and inositol for treatment-resistant bipolar depression suggested that risperidone may have hindered recovery.21
Table 2
Subsyndromal bipolar depression: Recommended medications*
| Medication | Initial and maximum dosages | Clinically important side effects |
|---|---|---|
| Quetiapine | Start at 50 mg and titrate to 300 mg within 4 to 7 days; maximum 600 mg | Sedation, somnolence, weight gain, gastrointestinal side effects, lipid abnormalities, increased fasting glucose, increased risk of diabetes |
| Olanzapine/fluoxetine | Start at 6 mg/25 mg; maximum 12 mg/50 mg | Weight gain, sedation, gastrointestinal side effects, lipid abnormalities, increased fasting glucose, increased risk of diabetes |
| Lamotrigine | Must be titrated per package labeling; start at 25 mg and titrate to 200 mg (12.5 mg titrated to 100 mg if patient is on valproate, 50 mg titrated to 400 mg if on carbamazepine or other enzyme inducer); maximum (per label) 500 mg | Rash, headache, balance difficulties, clumsiness; Stevens-Johnson syndrome or toxic epidermal necrolysis are rare but potentially fatal |
| Lithium | Start at 300 to 600 mg and use moderate blood levels (0.4 to 0.7 mEq/L); if no improvement in 4 to 8 weeks, titrate to 0.8 to 1.1 mEq/L | Tremor, nausea, diarrhea, increased thirst, increased urination, hair loss, thyroid abnormalities, weight gain, acne, worsening of psoriasis, diabetes insipidus, renal insufficiency |
| Divalproex | Start at 500 to 750 mg and increase to 15 to 20 mg/kg; usual target blood levels are >50 mg/dL | Nausea, abnormal liver function tests, weight gain, hair loss |
| Olanzapine | Start at 5 mg; maximum 30 mg | Weight gain, sedation, somnolence, lipid abnormalities, increased fasting glucose, increased risk of diabetes |
| Modafinil | Start at 50 to 100 mg and increase to 200 mg; higher dosages have not been systematically studied in bipolar disorder | Nervousness, insomnia |
| EPS: extrapyramidal symptoms | ||
| * Medications are listed in from most to least evidence supporting their use in treating bipolar depression | ||
CASE CONTINUED: Distressed by psychotherapy
You ask Mr. W about his psychodynamic psychotherapy, and he says that exploring his early life experiences and his work difficulty is increasing his anxiety. You recommend switching to cognitive-behavioral therapy (CBT) to work on delegating tasks that are not his strong areas and focusing on his marketing talents. You also encourage him to maintain regular sleep-wake cycles.
Some psychodynamic psychotherapies are thought to increase anxiety and mood instability in bipolar disorder patients. Examine the form and content of psychosocial approaches for their role in worsening your patients’ symptoms. As with medications, validated psychotherapeutic interventions—such as CBT for bipolar disorder, family-focused treatment, interpersonal social rhythm therapy, and long-term group psychotherapy23,24—are preferred over those not specifically studied in bipolar disorder.
- Establish a social rhythm that includes a regularized sleep-wake cycle and predictable daily schedules, with planned contact with people and organized activities.
- Decrease behaviors associated with mood fluctuation, such as substance use, irregular hours of sleep, conflicts in relationships and work, poor adherence to medications, and lack of regard for physical health.
CASE CONTINUED: Changes for the better
After several months of CBT and medication changes, Mr. W is continuing to work and shows some symptom improvement. His QIDS-SR scores have decreased to 6, indicating minimal to mild depressive symptom burden. He reports that most weeks he has no depressive symptoms, but he remains unable to focus on specific tasks for long periods. He continues to have difficulties when his work requires detailed, intensive activities.
Mr. W has developed a new relationship but gives high priority to keeping a regular schedule. Before going to sleep most nights, he records his mood in a diary to monitor his progress.
Mr. W may show additional improvement in work performance with continued daily mood monitoring and a regularized routine. The care of most patients with bipolar disorder must be systematically optimized over years, not weeks or months.26 Because medication adherence during well periods is essential, discuss and address adverse effects such as weight gain or urinary symptoms.
- minimize or eliminate ineffective and harmful treatments
- continue effective treatments, whether psychopharmacologic or psychosocial.
Tools for monitoring subsyndromal symptoms
| Encourage patient to keep a daily mood chart, including sleep-wake times |
Use standardized depression rating scales to monitor symptom changes:
|
| Use the Structured Clinical Interview for DSM-IV, Mood Module to verify whether or not the patient is in a mood episode |
| Use the Clinical Global Impression Severity Scale (BP version) as a measure of illness severity |
| Monitor use of caffeine, nicotine, alcohol, and other drugs of abuse by asking about the frequency and amounts used |
| Calculate body mass index at each visit to monitor for weight gain |
- Otto M, Reilly-Harrington N, Kogan JN, Henin A. Managing bipolar disorder: a cognitive behavior treatment program therapist guide (treatments that work). Oxford, UK: Oxford University Press; 2008.
- Inventory of Depressive Symptomatology (IDS) and Quick Inventory of Depressive Symptomatology (QIDS). Validity, reliability, administration, and scoring. www.ids-qids.org.
- Bipolar Clinic and Research Program, Massachusetts General Hospital. Resources for clinicians and patients, plus links to information on bipolar disorder. www.manicdepressive.org.
- Aripiprazole • Abilify
- Carbamazepine • Tegretol
- Divalproex • Depakote
- Lamotrigine • Lamictal
- Lithium • various
- Methylphenidate • various
- Modafinil • Provigil
- Olanzapine • Zyprexa
- Olanzapine/fluoxetine • Symbyax
- Propranolol • Inderal
- Quetiapine • Seroquel
- Valproate • Depacon
- Venlafaxine • Effexor
- Zolpidem • Ambien
Dr. Ostacher is a speaker for AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, GlaxoSmithKline, and Pfizer Inc.
1. Royal Australian and New Zealand College of Psychiatrists Clinical Practice Guidelines Team for Bipolar Disorder. Australian and New Zealand clinical practice guidelines for the treatment of bipolar disorder. Aust N Z J Psychiatry 2004;38:280-305.
2. Yatham LN, Kennedy SH, O’Donovan C, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) guidelines for the management of patients with bipolar disorder: consensus and controversies. Bipolar Disord 2005;7(suppl 3):5-69.
3. American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder. 2nd ed. Washington, DC: American Psychiatric Publishing, Inc; 2002.
4. Goodwin GM. And the Consensus Group of the British Association for Psychopharmacology. Evidence-based guidelines for treating bipolar disorder: recommendations from the British Association for Psychopharmacology. J Psychopharmacol 2003;17:149-73.
5. Perlis RH, Ostacher MJ, Patel J, et al. Predictors of recurrence in bipolar disorder: primary outcomes from the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Am J Psychiatry 2006;163:217-24.
6. Judd LL, Akiskal HS, Schettler PJ, et al. The long-term natural history of the weekly symptomatic status of bipolar I disorder. Arch Gen Psychiatry 2002;59:530-7.
7. Judd LL, Akiskal HS, Schettler PJ, et al. A prospective investigation of the natural history of the long-term weekly symptomatic status of bipolar II disorder. Arch Gen Psychiatry 2003;60:261-9.
8. Post RM, Denicoff KD, Leverich GS, et al. Morbidity in 258 bipolar outpatients followed for 1 year with daily prospective ratings on the NIMH life chart method. J Clin Psychiatry 2003;64:680-90.
9. Ostacher MJ, Nierenberg AA, Iosifescu D, et al. And the STEP-BD Family Experience Collaborative Study Group. Correlates of subjective and objective burden among caregivers of patients with bipolar disorder. Acta Psychiatr Scand 2008;118:49-56.
10. Sachs GS, Thase ME, Otto MW, et al. Rationale, design, and methods of the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Biol Psychiatry 2003;53:1028-42.
11. Tohen M, Zarate CA, Jr, Hennen J, et al. The McLean-Harvard First-Episode Mania Study: prediction of recovery and first recurrence. Am J Psychiatry 2003;160:2099-107.
12. Schneck C. What is the best treatment for rapid cycling? Presented at: Annual Meeting of the American Psychiatric Association; May 21-26, 2005; Atlanta, GA.
13. Perlis RH, Miyahara S, Marangell LB, et al. For the STEP-BD Investigators. Long-term implications of early onset in bipolar disorder: data from the first 1000 participants in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Biol Psychiatry 2004;55:875-81.
14. Weiss RD, Ostacher MJ, Otto MW, et al. For the STEP-BD Investigators. Does recovery from substance use disorder matter in patients with bipolar disorder? J Clin Psychiatry 2005;66:730-5.
15. Simon NM, Otto MW, Wisniewski SR, et al. Anxiety disorder comorbidity in bipolar disorder patients: data from the first 500 participants in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Am J Psychiatry 2004;161:2222-9.
16. Waxmonsky JA, Thomas MR, Miklowitz DJ, et al. Prevalence and correlates of tobacco use in bipolar disorder: data from the first 2000 participants in the Systematic Treatment Enhancement Program. Gen Hosp Psychiatry 2005;27:321-8.
17. Leverich GS, Altshuler LL, Frye MA, et al. Risk of switch in mood polarity to hypomania or mania in patients with bipolar depression during acute and continuation trials of venlafaxine, sertraline, and bupropion as adjuncts to mood stabilizers. Am J Psychiatry 2006;163:232-9.
18. Simon NM, Otto MW, Weiss RD, et al. Pharmacotherapy for bipolar disorder and comorbid conditions: baseline data from STEP-BD. J Clin Psychopharmacol 2004;24:512-20.
19. Ghaemi SN, Hsu DJ, Soldani F, Goodwin FK. Antidepressants in bipolar disorder: the case for caution. Bipolar Disord 2003;5:421-33.
20. Thase ME, Jonas A, Khan A, et al. Aripiprazole monotherapy in nonpsychotic bipolar I depression: results of 2 randomized, placebo-controlled studies. J Clin Psychopharmacol 2008;28:13-20.
21. Nierenberg AA, Ostacher MJ, Calabrese JR, et al. Treatment-resistant bipolar depression: a STEP-BD equipoise randomized effectiveness trial of antidepressant augmentation with lamotrigine, inositol, or risperidone. Am J Psychiatry 2006;163:210-6.
22. Frye MA, Grunze H, Suppes T, et al. A placebo-controlled evaluation of adjunctive modafinil in the treatment of bipolar depression. Am J Psychiatry 2007;164:1242-9.
23. Colom F, Vieta E, Martinez-Aran A, et al. A randomized trial on the efficacy of group psychoeducation in the prophylaxis of recurrences in bipolar patients whose disease is in remission. Arch Gen Psychiatry 2003;60:402-7.
24. Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression. N Engl J Med 2007;356:1711-22.
25. Frank E, Gonzalez JM, Fagiolini A. The importance of routine for preventing recurrence in bipolar disorder. Am J Psychiatry 2006;163:981-5.
26. Nierenberg AA, Ostacher MJ, Borrelli DJ, et al. The integration of measurement and management for the treatment of bipolar disorder: a STEP-BD model of collaborative care in psychiatry. J Clin Psychiatry 2006;67(suppl 11):3-7.
Mr. W, a 53-year-old divorced entrepreneur, presents to you for evaluation of poor concentration, decreased self-esteem, and difficulty making decisions that are interfering with his work. A longtime patient of another psychiatrist, Mr. W has a 26-year history of bipolar I disorder. He has not had a manic episode for 5 years but has had several depressive episodes.
During his last manic episode, Mr. W was hospitalized with expansive and irritable mood, racing thoughts, impulsive sexual behavior, psychomotor agitation, elevated self-esteem, marked distractibility, and paranoid ideas about his business partners. His discharge regimen included lithium titrated to 0.9 mEq/L and divalproex sodium, 1,500 mg/d, with lamotrigine, 200 mg/d, added to reduce depressive relapse risk. After several years of stable treatment, Mr. W complained of cognitive impairment. His psychiatrist discontinued lithium and added a low-dose stimulant—methylphenidate, 20 mg bid—to address Mr. W’s complaints of poor concentration.
Mr. W also is taking zolpidem, 10 mg as needed for onset insomnia, and receives weekly psychodynamic psychotherapy. His work performance problems persist despite these treatments, and his company is failing.
A poor course in bipolar disorder—as in Mr. W’s case—is frequently characterized by persistent or relapsing depression. Bipolar disorder is diagnosed by a manic, mixed, or hypomanic episode, but depression and depressive symptoms are most prominent in clinical practice. Likewise, major observational studies blame depression for most of the time spent ill in bipolar types I and II.1-8
A good deal of bipolar symptom burden is associated with subsyndromal depression—defined as having >2 but 5 and depressive symptoms are disproportionately responsible—compared with manic symptoms—for the impact of bipolar illness on patients and their families.9
This article offers clinically useful strategies to minimize subsyndromal depression in patients with bipolar disorder (Table 1). These strategies include an evidence-based approach to medication, the use of validated psychotherapies, regular sleep and socialization schedules, and careful monitoring of mood symptoms.
Table 1
How to minimize bipolar subsyndromal depression
| Monitor symptoms using validated clinician- and patient-rated tools at all visits |
| Use evidence-based treatments first |
| Eliminate ineffective medications |
| Use adequate doses of medications for different mood states |
| Monitor and treat adverse effects of successful treatments |
| Monitor and minimize medications that can worsen symptoms |
| Watch for the impact of medical conditions on mood |
| Be attentive to alcohol and substance use (including caffeine, nicotine, and energy drinks) |
| Monitor psychotherapies for symptom worsening |
| Address comorbid psychiatric conditions |
| Regularize social rhythms |
| Initiate validated psychosocial treatments |
| Engage the patient as a active participant in treatment |
Persistent depression
Randomized, controlled trials designed to obtain FDA approval of bipolar medications inadequately reflect the disabling, confounding nature of bipolar illness. Nearly all of these large studies of acute treatments for mood episodes are placebo-controlled trials with narrow inclusion and broad exclusion criteria. Eliminating subsyndromal symptoms is not their goal, and they are of little help in understanding how to manage residual symptoms.
A more realistic view of bipolar disorder comes from large observational studies that have examined its longitudinal course in outpatients under more or less ideal treatment conditions.10 These studies show that bipolar disorder is almost always recurrent and relapsing, but full recovery and functioning between episodes is not the norm. Most patients never achieve prolonged recovery, complete symptom relief, or return to full functioning.5,8,11
STEP-BD. Most patients in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) never recovered from a depressed episode during 2 years of prospective follow-up under optimal care. Only 58% of patients who entered the study during an episode of illness achieved 8 consecutive weeks of euthymia.5
Collaborative Depression study. Longitudinal data from the National Institute of Mental Health’s Collaborative Depression Study6,7 showed:
- patients with bipolar I disorder had depressive symptoms in approximately three-quarters of the weeks in which they reported significant symptoms
- patients with bipolar II disorder were depressed in nearly all sick weeks.
The Stanley Foundation Bipolar Network had similar findings, with bipolar disorder patients reporting 3 times as much time spent with depressed mood as with elevated mood.8 Poor social and occupational functioning predicted poor outcomes, suggesting an interplay between subsyndromal depression, poor functioning, and relapse.
Risk factors
Rapid cycling may be a marker for persistent, subsyndromal symptoms. Rapid cycling is defined clinically as 4 distinct mood episodes—switching to the opposite pole or 2 episodes of the same pole separated by ≥8 weeks of partial or full recovery—in the previous 12 months. Rapid cycling usually is diagnosed retrospectively—introducing patients’ recall bias—but may be more of a marker for symptom persistence than for defined episodes.
In STEP-BD, 32% of study entrants reported ≥4 mood episodes in the previous year, yet only 6% of that subgroup had ≥4 episodes after 1 year of prospective follow-up.12 This suggests:
- patients who retrospectively report rapid cycling may be chronically and persistently ill, rather than experiencing multiple discrete episodes
- rapid cycling is a marker for symptom persistence, subsyndromal depression, and lack of sustained remission.
- comorbid anxiety disorders (present in ≤50% of patients with bipolar I and II disorder)
- active and past substance use disorders (including nicotine dependence)
- early age of onset of the mood disorder.13-16
CASE CONTINUED: Restoring the cornerstone
You review Mr. W’s records. Recent lab values were essentially normal, with thyroid stimulating hormone 2.3 mIU/mL and stable renal function. He scores 11 on the Quick Inventory of Depressive Symptoms–self-rated version (QIDS-SR), indicating mild to moderate depressive symptom burden.
His mood chart and interview reveal that he has been depressed and anhedonic most of the day for 4 of the last 10 days. By systematically asking the depression questions in the DSM-IV-TR, you find that he does not meet criteria for depressed mood or anhedonia but has difficulty concentrating most of the day, persistent low self-esteem, and feeling “slowed.”
After you discuss lithium’s pros and cons with Mr. W, he agrees to try this mood stabilizer again. You explain the importance of preventing relapse to mania and of monitoring his cognitive performance at work.
Over time, you titrate lithium to a moderate serum level (0.5 to 0.7 mEq/L) and treat a resulting mild tremor with propranolol, 20 to 40 mg/d. Mr. W is tolerating lamotrigine well, so you continue this medication because of its potential to decrease the probability of relapse to depression. You also continue zolpidem, as needed, but discontinue methylphenidate because you think it may be contributing to sleep difficulties.
Managing medication
Nine drugs are FDA-approved for acute bipolar mania, but treatments for bipolar depression, maintenance treatment, and relapse prevention are far fewer, often partially effective, or effective for a limited number of patients. When depressive symptoms fail to resolve, a reasonable approach is to review patients’ medications and suggest alternatives with proven efficacy for bipolar disorder (Table 2). Patients can then accept or reject various options based on personal preference.
Combination strategies. Antimanic treatment is the cornerstone of treating bipolar I disorder, and preventing manic episodes should be a primary treatment goal. Thus, consider continuing treatments that have prevented mania for your patient—as lithium did in Mr. W’s case—while adding treatments aimed at depression. For example, adding lamotrigine to any antimanic agent is reasonable, especially if doing so does not add substantially to your patient’s side-effect burden.
Minimize antidepressants. Given the predominance and persistence of depressive symptoms in bipolar disorder, one can understand why clinicians and patients might try standard antidepressants without clear evidence supporting this practice. Antidepressants—especially venlafaxine and tricyclic antidepressants—are the most common and likely suspects when patients experience switching to mania, rapid cycling, and symptom persistence.17 Antidepressants’ negative effect has not been clearly defined, however, and may be patient-specific (related to patient factors rather than intrinsic to the compound).
In my clinical experience, minimizing antidepressant use in bipolar depression hastens rather than delays patients’ recovery. A prudent approach would be to use the minimum dose necessary and discontinue the antidepressant if possible. Also minimize medical pharmacotherapies—including corticosteroids and oral contraceptives—that may worsen mood symptoms, especially in patients with this history.
Avoid under-dosing. Inadequate dosing and duration often are overlooked as causes of treatment resistance in bipolar disorder and other illnesses.18 Bipolar disorder medications are hardly benign; every drug approved for any phase of bipolar disorder has a black-box warning. Understandably, clinicians and patients try to choose medications and dosages perceived to be most tolerable. Full-dose treatment trials may be warranted, however, given the high probability of incomplete recovery, impaired functioning, and risk of relapse with ineffective dosing.
Address iatrogenic causes. In addition, identify and eliminate medications and treatments that may be perpetuating patients’ bipolar symptoms. Stimulants such as methylphenidate and amphetamines may contribute to sleep disturbance and manic relapse and might be minimized or eliminated in a patient with continued symptoms and sleep disturbance.19
- Two trials of aripiprazole for bipolar depression failed to show benefit.20
- A trial that compared risperidone with lamotrigine and inositol for treatment-resistant bipolar depression suggested that risperidone may have hindered recovery.21
Table 2
Subsyndromal bipolar depression: Recommended medications*
| Medication | Initial and maximum dosages | Clinically important side effects |
|---|---|---|
| Quetiapine | Start at 50 mg and titrate to 300 mg within 4 to 7 days; maximum 600 mg | Sedation, somnolence, weight gain, gastrointestinal side effects, lipid abnormalities, increased fasting glucose, increased risk of diabetes |
| Olanzapine/fluoxetine | Start at 6 mg/25 mg; maximum 12 mg/50 mg | Weight gain, sedation, gastrointestinal side effects, lipid abnormalities, increased fasting glucose, increased risk of diabetes |
| Lamotrigine | Must be titrated per package labeling; start at 25 mg and titrate to 200 mg (12.5 mg titrated to 100 mg if patient is on valproate, 50 mg titrated to 400 mg if on carbamazepine or other enzyme inducer); maximum (per label) 500 mg | Rash, headache, balance difficulties, clumsiness; Stevens-Johnson syndrome or toxic epidermal necrolysis are rare but potentially fatal |
| Lithium | Start at 300 to 600 mg and use moderate blood levels (0.4 to 0.7 mEq/L); if no improvement in 4 to 8 weeks, titrate to 0.8 to 1.1 mEq/L | Tremor, nausea, diarrhea, increased thirst, increased urination, hair loss, thyroid abnormalities, weight gain, acne, worsening of psoriasis, diabetes insipidus, renal insufficiency |
| Divalproex | Start at 500 to 750 mg and increase to 15 to 20 mg/kg; usual target blood levels are >50 mg/dL | Nausea, abnormal liver function tests, weight gain, hair loss |
| Olanzapine | Start at 5 mg; maximum 30 mg | Weight gain, sedation, somnolence, lipid abnormalities, increased fasting glucose, increased risk of diabetes |
| Modafinil | Start at 50 to 100 mg and increase to 200 mg; higher dosages have not been systematically studied in bipolar disorder | Nervousness, insomnia |
| EPS: extrapyramidal symptoms | ||
| * Medications are listed in from most to least evidence supporting their use in treating bipolar depression | ||
CASE CONTINUED: Distressed by psychotherapy
You ask Mr. W about his psychodynamic psychotherapy, and he says that exploring his early life experiences and his work difficulty is increasing his anxiety. You recommend switching to cognitive-behavioral therapy (CBT) to work on delegating tasks that are not his strong areas and focusing on his marketing talents. You also encourage him to maintain regular sleep-wake cycles.
Some psychodynamic psychotherapies are thought to increase anxiety and mood instability in bipolar disorder patients. Examine the form and content of psychosocial approaches for their role in worsening your patients’ symptoms. As with medications, validated psychotherapeutic interventions—such as CBT for bipolar disorder, family-focused treatment, interpersonal social rhythm therapy, and long-term group psychotherapy23,24—are preferred over those not specifically studied in bipolar disorder.
- Establish a social rhythm that includes a regularized sleep-wake cycle and predictable daily schedules, with planned contact with people and organized activities.
- Decrease behaviors associated with mood fluctuation, such as substance use, irregular hours of sleep, conflicts in relationships and work, poor adherence to medications, and lack of regard for physical health.
CASE CONTINUED: Changes for the better
After several months of CBT and medication changes, Mr. W is continuing to work and shows some symptom improvement. His QIDS-SR scores have decreased to 6, indicating minimal to mild depressive symptom burden. He reports that most weeks he has no depressive symptoms, but he remains unable to focus on specific tasks for long periods. He continues to have difficulties when his work requires detailed, intensive activities.
Mr. W has developed a new relationship but gives high priority to keeping a regular schedule. Before going to sleep most nights, he records his mood in a diary to monitor his progress.
Mr. W may show additional improvement in work performance with continued daily mood monitoring and a regularized routine. The care of most patients with bipolar disorder must be systematically optimized over years, not weeks or months.26 Because medication adherence during well periods is essential, discuss and address adverse effects such as weight gain or urinary symptoms.
- minimize or eliminate ineffective and harmful treatments
- continue effective treatments, whether psychopharmacologic or psychosocial.
Tools for monitoring subsyndromal symptoms
| Encourage patient to keep a daily mood chart, including sleep-wake times |
Use standardized depression rating scales to monitor symptom changes:
|
| Use the Structured Clinical Interview for DSM-IV, Mood Module to verify whether or not the patient is in a mood episode |
| Use the Clinical Global Impression Severity Scale (BP version) as a measure of illness severity |
| Monitor use of caffeine, nicotine, alcohol, and other drugs of abuse by asking about the frequency and amounts used |
| Calculate body mass index at each visit to monitor for weight gain |
- Otto M, Reilly-Harrington N, Kogan JN, Henin A. Managing bipolar disorder: a cognitive behavior treatment program therapist guide (treatments that work). Oxford, UK: Oxford University Press; 2008.
- Inventory of Depressive Symptomatology (IDS) and Quick Inventory of Depressive Symptomatology (QIDS). Validity, reliability, administration, and scoring. www.ids-qids.org.
- Bipolar Clinic and Research Program, Massachusetts General Hospital. Resources for clinicians and patients, plus links to information on bipolar disorder. www.manicdepressive.org.
- Aripiprazole • Abilify
- Carbamazepine • Tegretol
- Divalproex • Depakote
- Lamotrigine • Lamictal
- Lithium • various
- Methylphenidate • various
- Modafinil • Provigil
- Olanzapine • Zyprexa
- Olanzapine/fluoxetine • Symbyax
- Propranolol • Inderal
- Quetiapine • Seroquel
- Valproate • Depacon
- Venlafaxine • Effexor
- Zolpidem • Ambien
Dr. Ostacher is a speaker for AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, GlaxoSmithKline, and Pfizer Inc.
Mr. W, a 53-year-old divorced entrepreneur, presents to you for evaluation of poor concentration, decreased self-esteem, and difficulty making decisions that are interfering with his work. A longtime patient of another psychiatrist, Mr. W has a 26-year history of bipolar I disorder. He has not had a manic episode for 5 years but has had several depressive episodes.
During his last manic episode, Mr. W was hospitalized with expansive and irritable mood, racing thoughts, impulsive sexual behavior, psychomotor agitation, elevated self-esteem, marked distractibility, and paranoid ideas about his business partners. His discharge regimen included lithium titrated to 0.9 mEq/L and divalproex sodium, 1,500 mg/d, with lamotrigine, 200 mg/d, added to reduce depressive relapse risk. After several years of stable treatment, Mr. W complained of cognitive impairment. His psychiatrist discontinued lithium and added a low-dose stimulant—methylphenidate, 20 mg bid—to address Mr. W’s complaints of poor concentration.
Mr. W also is taking zolpidem, 10 mg as needed for onset insomnia, and receives weekly psychodynamic psychotherapy. His work performance problems persist despite these treatments, and his company is failing.
A poor course in bipolar disorder—as in Mr. W’s case—is frequently characterized by persistent or relapsing depression. Bipolar disorder is diagnosed by a manic, mixed, or hypomanic episode, but depression and depressive symptoms are most prominent in clinical practice. Likewise, major observational studies blame depression for most of the time spent ill in bipolar types I and II.1-8
A good deal of bipolar symptom burden is associated with subsyndromal depression—defined as having >2 but 5 and depressive symptoms are disproportionately responsible—compared with manic symptoms—for the impact of bipolar illness on patients and their families.9
This article offers clinically useful strategies to minimize subsyndromal depression in patients with bipolar disorder (Table 1). These strategies include an evidence-based approach to medication, the use of validated psychotherapies, regular sleep and socialization schedules, and careful monitoring of mood symptoms.
Table 1
How to minimize bipolar subsyndromal depression
| Monitor symptoms using validated clinician- and patient-rated tools at all visits |
| Use evidence-based treatments first |
| Eliminate ineffective medications |
| Use adequate doses of medications for different mood states |
| Monitor and treat adverse effects of successful treatments |
| Monitor and minimize medications that can worsen symptoms |
| Watch for the impact of medical conditions on mood |
| Be attentive to alcohol and substance use (including caffeine, nicotine, and energy drinks) |
| Monitor psychotherapies for symptom worsening |
| Address comorbid psychiatric conditions |
| Regularize social rhythms |
| Initiate validated psychosocial treatments |
| Engage the patient as a active participant in treatment |
Persistent depression
Randomized, controlled trials designed to obtain FDA approval of bipolar medications inadequately reflect the disabling, confounding nature of bipolar illness. Nearly all of these large studies of acute treatments for mood episodes are placebo-controlled trials with narrow inclusion and broad exclusion criteria. Eliminating subsyndromal symptoms is not their goal, and they are of little help in understanding how to manage residual symptoms.
A more realistic view of bipolar disorder comes from large observational studies that have examined its longitudinal course in outpatients under more or less ideal treatment conditions.10 These studies show that bipolar disorder is almost always recurrent and relapsing, but full recovery and functioning between episodes is not the norm. Most patients never achieve prolonged recovery, complete symptom relief, or return to full functioning.5,8,11
STEP-BD. Most patients in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) never recovered from a depressed episode during 2 years of prospective follow-up under optimal care. Only 58% of patients who entered the study during an episode of illness achieved 8 consecutive weeks of euthymia.5
Collaborative Depression study. Longitudinal data from the National Institute of Mental Health’s Collaborative Depression Study6,7 showed:
- patients with bipolar I disorder had depressive symptoms in approximately three-quarters of the weeks in which they reported significant symptoms
- patients with bipolar II disorder were depressed in nearly all sick weeks.
The Stanley Foundation Bipolar Network had similar findings, with bipolar disorder patients reporting 3 times as much time spent with depressed mood as with elevated mood.8 Poor social and occupational functioning predicted poor outcomes, suggesting an interplay between subsyndromal depression, poor functioning, and relapse.
Risk factors
Rapid cycling may be a marker for persistent, subsyndromal symptoms. Rapid cycling is defined clinically as 4 distinct mood episodes—switching to the opposite pole or 2 episodes of the same pole separated by ≥8 weeks of partial or full recovery—in the previous 12 months. Rapid cycling usually is diagnosed retrospectively—introducing patients’ recall bias—but may be more of a marker for symptom persistence than for defined episodes.
In STEP-BD, 32% of study entrants reported ≥4 mood episodes in the previous year, yet only 6% of that subgroup had ≥4 episodes after 1 year of prospective follow-up.12 This suggests:
- patients who retrospectively report rapid cycling may be chronically and persistently ill, rather than experiencing multiple discrete episodes
- rapid cycling is a marker for symptom persistence, subsyndromal depression, and lack of sustained remission.
- comorbid anxiety disorders (present in ≤50% of patients with bipolar I and II disorder)
- active and past substance use disorders (including nicotine dependence)
- early age of onset of the mood disorder.13-16
CASE CONTINUED: Restoring the cornerstone
You review Mr. W’s records. Recent lab values were essentially normal, with thyroid stimulating hormone 2.3 mIU/mL and stable renal function. He scores 11 on the Quick Inventory of Depressive Symptoms–self-rated version (QIDS-SR), indicating mild to moderate depressive symptom burden.
His mood chart and interview reveal that he has been depressed and anhedonic most of the day for 4 of the last 10 days. By systematically asking the depression questions in the DSM-IV-TR, you find that he does not meet criteria for depressed mood or anhedonia but has difficulty concentrating most of the day, persistent low self-esteem, and feeling “slowed.”
After you discuss lithium’s pros and cons with Mr. W, he agrees to try this mood stabilizer again. You explain the importance of preventing relapse to mania and of monitoring his cognitive performance at work.
Over time, you titrate lithium to a moderate serum level (0.5 to 0.7 mEq/L) and treat a resulting mild tremor with propranolol, 20 to 40 mg/d. Mr. W is tolerating lamotrigine well, so you continue this medication because of its potential to decrease the probability of relapse to depression. You also continue zolpidem, as needed, but discontinue methylphenidate because you think it may be contributing to sleep difficulties.
Managing medication
Nine drugs are FDA-approved for acute bipolar mania, but treatments for bipolar depression, maintenance treatment, and relapse prevention are far fewer, often partially effective, or effective for a limited number of patients. When depressive symptoms fail to resolve, a reasonable approach is to review patients’ medications and suggest alternatives with proven efficacy for bipolar disorder (Table 2). Patients can then accept or reject various options based on personal preference.
Combination strategies. Antimanic treatment is the cornerstone of treating bipolar I disorder, and preventing manic episodes should be a primary treatment goal. Thus, consider continuing treatments that have prevented mania for your patient—as lithium did in Mr. W’s case—while adding treatments aimed at depression. For example, adding lamotrigine to any antimanic agent is reasonable, especially if doing so does not add substantially to your patient’s side-effect burden.
Minimize antidepressants. Given the predominance and persistence of depressive symptoms in bipolar disorder, one can understand why clinicians and patients might try standard antidepressants without clear evidence supporting this practice. Antidepressants—especially venlafaxine and tricyclic antidepressants—are the most common and likely suspects when patients experience switching to mania, rapid cycling, and symptom persistence.17 Antidepressants’ negative effect has not been clearly defined, however, and may be patient-specific (related to patient factors rather than intrinsic to the compound).
In my clinical experience, minimizing antidepressant use in bipolar depression hastens rather than delays patients’ recovery. A prudent approach would be to use the minimum dose necessary and discontinue the antidepressant if possible. Also minimize medical pharmacotherapies—including corticosteroids and oral contraceptives—that may worsen mood symptoms, especially in patients with this history.
Avoid under-dosing. Inadequate dosing and duration often are overlooked as causes of treatment resistance in bipolar disorder and other illnesses.18 Bipolar disorder medications are hardly benign; every drug approved for any phase of bipolar disorder has a black-box warning. Understandably, clinicians and patients try to choose medications and dosages perceived to be most tolerable. Full-dose treatment trials may be warranted, however, given the high probability of incomplete recovery, impaired functioning, and risk of relapse with ineffective dosing.
Address iatrogenic causes. In addition, identify and eliminate medications and treatments that may be perpetuating patients’ bipolar symptoms. Stimulants such as methylphenidate and amphetamines may contribute to sleep disturbance and manic relapse and might be minimized or eliminated in a patient with continued symptoms and sleep disturbance.19
- Two trials of aripiprazole for bipolar depression failed to show benefit.20
- A trial that compared risperidone with lamotrigine and inositol for treatment-resistant bipolar depression suggested that risperidone may have hindered recovery.21
Table 2
Subsyndromal bipolar depression: Recommended medications*
| Medication | Initial and maximum dosages | Clinically important side effects |
|---|---|---|
| Quetiapine | Start at 50 mg and titrate to 300 mg within 4 to 7 days; maximum 600 mg | Sedation, somnolence, weight gain, gastrointestinal side effects, lipid abnormalities, increased fasting glucose, increased risk of diabetes |
| Olanzapine/fluoxetine | Start at 6 mg/25 mg; maximum 12 mg/50 mg | Weight gain, sedation, gastrointestinal side effects, lipid abnormalities, increased fasting glucose, increased risk of diabetes |
| Lamotrigine | Must be titrated per package labeling; start at 25 mg and titrate to 200 mg (12.5 mg titrated to 100 mg if patient is on valproate, 50 mg titrated to 400 mg if on carbamazepine or other enzyme inducer); maximum (per label) 500 mg | Rash, headache, balance difficulties, clumsiness; Stevens-Johnson syndrome or toxic epidermal necrolysis are rare but potentially fatal |
| Lithium | Start at 300 to 600 mg and use moderate blood levels (0.4 to 0.7 mEq/L); if no improvement in 4 to 8 weeks, titrate to 0.8 to 1.1 mEq/L | Tremor, nausea, diarrhea, increased thirst, increased urination, hair loss, thyroid abnormalities, weight gain, acne, worsening of psoriasis, diabetes insipidus, renal insufficiency |
| Divalproex | Start at 500 to 750 mg and increase to 15 to 20 mg/kg; usual target blood levels are >50 mg/dL | Nausea, abnormal liver function tests, weight gain, hair loss |
| Olanzapine | Start at 5 mg; maximum 30 mg | Weight gain, sedation, somnolence, lipid abnormalities, increased fasting glucose, increased risk of diabetes |
| Modafinil | Start at 50 to 100 mg and increase to 200 mg; higher dosages have not been systematically studied in bipolar disorder | Nervousness, insomnia |
| EPS: extrapyramidal symptoms | ||
| * Medications are listed in from most to least evidence supporting their use in treating bipolar depression | ||
CASE CONTINUED: Distressed by psychotherapy
You ask Mr. W about his psychodynamic psychotherapy, and he says that exploring his early life experiences and his work difficulty is increasing his anxiety. You recommend switching to cognitive-behavioral therapy (CBT) to work on delegating tasks that are not his strong areas and focusing on his marketing talents. You also encourage him to maintain regular sleep-wake cycles.
Some psychodynamic psychotherapies are thought to increase anxiety and mood instability in bipolar disorder patients. Examine the form and content of psychosocial approaches for their role in worsening your patients’ symptoms. As with medications, validated psychotherapeutic interventions—such as CBT for bipolar disorder, family-focused treatment, interpersonal social rhythm therapy, and long-term group psychotherapy23,24—are preferred over those not specifically studied in bipolar disorder.
- Establish a social rhythm that includes a regularized sleep-wake cycle and predictable daily schedules, with planned contact with people and organized activities.
- Decrease behaviors associated with mood fluctuation, such as substance use, irregular hours of sleep, conflicts in relationships and work, poor adherence to medications, and lack of regard for physical health.
CASE CONTINUED: Changes for the better
After several months of CBT and medication changes, Mr. W is continuing to work and shows some symptom improvement. His QIDS-SR scores have decreased to 6, indicating minimal to mild depressive symptom burden. He reports that most weeks he has no depressive symptoms, but he remains unable to focus on specific tasks for long periods. He continues to have difficulties when his work requires detailed, intensive activities.
Mr. W has developed a new relationship but gives high priority to keeping a regular schedule. Before going to sleep most nights, he records his mood in a diary to monitor his progress.
Mr. W may show additional improvement in work performance with continued daily mood monitoring and a regularized routine. The care of most patients with bipolar disorder must be systematically optimized over years, not weeks or months.26 Because medication adherence during well periods is essential, discuss and address adverse effects such as weight gain or urinary symptoms.
- minimize or eliminate ineffective and harmful treatments
- continue effective treatments, whether psychopharmacologic or psychosocial.
Tools for monitoring subsyndromal symptoms
| Encourage patient to keep a daily mood chart, including sleep-wake times |
Use standardized depression rating scales to monitor symptom changes:
|
| Use the Structured Clinical Interview for DSM-IV, Mood Module to verify whether or not the patient is in a mood episode |
| Use the Clinical Global Impression Severity Scale (BP version) as a measure of illness severity |
| Monitor use of caffeine, nicotine, alcohol, and other drugs of abuse by asking about the frequency and amounts used |
| Calculate body mass index at each visit to monitor for weight gain |
- Otto M, Reilly-Harrington N, Kogan JN, Henin A. Managing bipolar disorder: a cognitive behavior treatment program therapist guide (treatments that work). Oxford, UK: Oxford University Press; 2008.
- Inventory of Depressive Symptomatology (IDS) and Quick Inventory of Depressive Symptomatology (QIDS). Validity, reliability, administration, and scoring. www.ids-qids.org.
- Bipolar Clinic and Research Program, Massachusetts General Hospital. Resources for clinicians and patients, plus links to information on bipolar disorder. www.manicdepressive.org.
- Aripiprazole • Abilify
- Carbamazepine • Tegretol
- Divalproex • Depakote
- Lamotrigine • Lamictal
- Lithium • various
- Methylphenidate • various
- Modafinil • Provigil
- Olanzapine • Zyprexa
- Olanzapine/fluoxetine • Symbyax
- Propranolol • Inderal
- Quetiapine • Seroquel
- Valproate • Depacon
- Venlafaxine • Effexor
- Zolpidem • Ambien
Dr. Ostacher is a speaker for AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, GlaxoSmithKline, and Pfizer Inc.
1. Royal Australian and New Zealand College of Psychiatrists Clinical Practice Guidelines Team for Bipolar Disorder. Australian and New Zealand clinical practice guidelines for the treatment of bipolar disorder. Aust N Z J Psychiatry 2004;38:280-305.
2. Yatham LN, Kennedy SH, O’Donovan C, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) guidelines for the management of patients with bipolar disorder: consensus and controversies. Bipolar Disord 2005;7(suppl 3):5-69.
3. American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder. 2nd ed. Washington, DC: American Psychiatric Publishing, Inc; 2002.
4. Goodwin GM. And the Consensus Group of the British Association for Psychopharmacology. Evidence-based guidelines for treating bipolar disorder: recommendations from the British Association for Psychopharmacology. J Psychopharmacol 2003;17:149-73.
5. Perlis RH, Ostacher MJ, Patel J, et al. Predictors of recurrence in bipolar disorder: primary outcomes from the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Am J Psychiatry 2006;163:217-24.
6. Judd LL, Akiskal HS, Schettler PJ, et al. The long-term natural history of the weekly symptomatic status of bipolar I disorder. Arch Gen Psychiatry 2002;59:530-7.
7. Judd LL, Akiskal HS, Schettler PJ, et al. A prospective investigation of the natural history of the long-term weekly symptomatic status of bipolar II disorder. Arch Gen Psychiatry 2003;60:261-9.
8. Post RM, Denicoff KD, Leverich GS, et al. Morbidity in 258 bipolar outpatients followed for 1 year with daily prospective ratings on the NIMH life chart method. J Clin Psychiatry 2003;64:680-90.
9. Ostacher MJ, Nierenberg AA, Iosifescu D, et al. And the STEP-BD Family Experience Collaborative Study Group. Correlates of subjective and objective burden among caregivers of patients with bipolar disorder. Acta Psychiatr Scand 2008;118:49-56.
10. Sachs GS, Thase ME, Otto MW, et al. Rationale, design, and methods of the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Biol Psychiatry 2003;53:1028-42.
11. Tohen M, Zarate CA, Jr, Hennen J, et al. The McLean-Harvard First-Episode Mania Study: prediction of recovery and first recurrence. Am J Psychiatry 2003;160:2099-107.
12. Schneck C. What is the best treatment for rapid cycling? Presented at: Annual Meeting of the American Psychiatric Association; May 21-26, 2005; Atlanta, GA.
13. Perlis RH, Miyahara S, Marangell LB, et al. For the STEP-BD Investigators. Long-term implications of early onset in bipolar disorder: data from the first 1000 participants in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Biol Psychiatry 2004;55:875-81.
14. Weiss RD, Ostacher MJ, Otto MW, et al. For the STEP-BD Investigators. Does recovery from substance use disorder matter in patients with bipolar disorder? J Clin Psychiatry 2005;66:730-5.
15. Simon NM, Otto MW, Wisniewski SR, et al. Anxiety disorder comorbidity in bipolar disorder patients: data from the first 500 participants in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Am J Psychiatry 2004;161:2222-9.
16. Waxmonsky JA, Thomas MR, Miklowitz DJ, et al. Prevalence and correlates of tobacco use in bipolar disorder: data from the first 2000 participants in the Systematic Treatment Enhancement Program. Gen Hosp Psychiatry 2005;27:321-8.
17. Leverich GS, Altshuler LL, Frye MA, et al. Risk of switch in mood polarity to hypomania or mania in patients with bipolar depression during acute and continuation trials of venlafaxine, sertraline, and bupropion as adjuncts to mood stabilizers. Am J Psychiatry 2006;163:232-9.
18. Simon NM, Otto MW, Weiss RD, et al. Pharmacotherapy for bipolar disorder and comorbid conditions: baseline data from STEP-BD. J Clin Psychopharmacol 2004;24:512-20.
19. Ghaemi SN, Hsu DJ, Soldani F, Goodwin FK. Antidepressants in bipolar disorder: the case for caution. Bipolar Disord 2003;5:421-33.
20. Thase ME, Jonas A, Khan A, et al. Aripiprazole monotherapy in nonpsychotic bipolar I depression: results of 2 randomized, placebo-controlled studies. J Clin Psychopharmacol 2008;28:13-20.
21. Nierenberg AA, Ostacher MJ, Calabrese JR, et al. Treatment-resistant bipolar depression: a STEP-BD equipoise randomized effectiveness trial of antidepressant augmentation with lamotrigine, inositol, or risperidone. Am J Psychiatry 2006;163:210-6.
22. Frye MA, Grunze H, Suppes T, et al. A placebo-controlled evaluation of adjunctive modafinil in the treatment of bipolar depression. Am J Psychiatry 2007;164:1242-9.
23. Colom F, Vieta E, Martinez-Aran A, et al. A randomized trial on the efficacy of group psychoeducation in the prophylaxis of recurrences in bipolar patients whose disease is in remission. Arch Gen Psychiatry 2003;60:402-7.
24. Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression. N Engl J Med 2007;356:1711-22.
25. Frank E, Gonzalez JM, Fagiolini A. The importance of routine for preventing recurrence in bipolar disorder. Am J Psychiatry 2006;163:981-5.
26. Nierenberg AA, Ostacher MJ, Borrelli DJ, et al. The integration of measurement and management for the treatment of bipolar disorder: a STEP-BD model of collaborative care in psychiatry. J Clin Psychiatry 2006;67(suppl 11):3-7.
1. Royal Australian and New Zealand College of Psychiatrists Clinical Practice Guidelines Team for Bipolar Disorder. Australian and New Zealand clinical practice guidelines for the treatment of bipolar disorder. Aust N Z J Psychiatry 2004;38:280-305.
2. Yatham LN, Kennedy SH, O’Donovan C, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) guidelines for the management of patients with bipolar disorder: consensus and controversies. Bipolar Disord 2005;7(suppl 3):5-69.
3. American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder. 2nd ed. Washington, DC: American Psychiatric Publishing, Inc; 2002.
4. Goodwin GM. And the Consensus Group of the British Association for Psychopharmacology. Evidence-based guidelines for treating bipolar disorder: recommendations from the British Association for Psychopharmacology. J Psychopharmacol 2003;17:149-73.
5. Perlis RH, Ostacher MJ, Patel J, et al. Predictors of recurrence in bipolar disorder: primary outcomes from the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Am J Psychiatry 2006;163:217-24.
6. Judd LL, Akiskal HS, Schettler PJ, et al. The long-term natural history of the weekly symptomatic status of bipolar I disorder. Arch Gen Psychiatry 2002;59:530-7.
7. Judd LL, Akiskal HS, Schettler PJ, et al. A prospective investigation of the natural history of the long-term weekly symptomatic status of bipolar II disorder. Arch Gen Psychiatry 2003;60:261-9.
8. Post RM, Denicoff KD, Leverich GS, et al. Morbidity in 258 bipolar outpatients followed for 1 year with daily prospective ratings on the NIMH life chart method. J Clin Psychiatry 2003;64:680-90.
9. Ostacher MJ, Nierenberg AA, Iosifescu D, et al. And the STEP-BD Family Experience Collaborative Study Group. Correlates of subjective and objective burden among caregivers of patients with bipolar disorder. Acta Psychiatr Scand 2008;118:49-56.
10. Sachs GS, Thase ME, Otto MW, et al. Rationale, design, and methods of the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Biol Psychiatry 2003;53:1028-42.
11. Tohen M, Zarate CA, Jr, Hennen J, et al. The McLean-Harvard First-Episode Mania Study: prediction of recovery and first recurrence. Am J Psychiatry 2003;160:2099-107.
12. Schneck C. What is the best treatment for rapid cycling? Presented at: Annual Meeting of the American Psychiatric Association; May 21-26, 2005; Atlanta, GA.
13. Perlis RH, Miyahara S, Marangell LB, et al. For the STEP-BD Investigators. Long-term implications of early onset in bipolar disorder: data from the first 1000 participants in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Biol Psychiatry 2004;55:875-81.
14. Weiss RD, Ostacher MJ, Otto MW, et al. For the STEP-BD Investigators. Does recovery from substance use disorder matter in patients with bipolar disorder? J Clin Psychiatry 2005;66:730-5.
15. Simon NM, Otto MW, Wisniewski SR, et al. Anxiety disorder comorbidity in bipolar disorder patients: data from the first 500 participants in the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Am J Psychiatry 2004;161:2222-9.
16. Waxmonsky JA, Thomas MR, Miklowitz DJ, et al. Prevalence and correlates of tobacco use in bipolar disorder: data from the first 2000 participants in the Systematic Treatment Enhancement Program. Gen Hosp Psychiatry 2005;27:321-8.
17. Leverich GS, Altshuler LL, Frye MA, et al. Risk of switch in mood polarity to hypomania or mania in patients with bipolar depression during acute and continuation trials of venlafaxine, sertraline, and bupropion as adjuncts to mood stabilizers. Am J Psychiatry 2006;163:232-9.
18. Simon NM, Otto MW, Weiss RD, et al. Pharmacotherapy for bipolar disorder and comorbid conditions: baseline data from STEP-BD. J Clin Psychopharmacol 2004;24:512-20.
19. Ghaemi SN, Hsu DJ, Soldani F, Goodwin FK. Antidepressants in bipolar disorder: the case for caution. Bipolar Disord 2003;5:421-33.
20. Thase ME, Jonas A, Khan A, et al. Aripiprazole monotherapy in nonpsychotic bipolar I depression: results of 2 randomized, placebo-controlled studies. J Clin Psychopharmacol 2008;28:13-20.
21. Nierenberg AA, Ostacher MJ, Calabrese JR, et al. Treatment-resistant bipolar depression: a STEP-BD equipoise randomized effectiveness trial of antidepressant augmentation with lamotrigine, inositol, or risperidone. Am J Psychiatry 2006;163:210-6.
22. Frye MA, Grunze H, Suppes T, et al. A placebo-controlled evaluation of adjunctive modafinil in the treatment of bipolar depression. Am J Psychiatry 2007;164:1242-9.
23. Colom F, Vieta E, Martinez-Aran A, et al. A randomized trial on the efficacy of group psychoeducation in the prophylaxis of recurrences in bipolar patients whose disease is in remission. Arch Gen Psychiatry 2003;60:402-7.
24. Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression. N Engl J Med 2007;356:1711-22.
25. Frank E, Gonzalez JM, Fagiolini A. The importance of routine for preventing recurrence in bipolar disorder. Am J Psychiatry 2006;163:981-5.
26. Nierenberg AA, Ostacher MJ, Borrelli DJ, et al. The integration of measurement and management for the treatment of bipolar disorder: a STEP-BD model of collaborative care in psychiatry. J Clin Psychiatry 2006;67(suppl 11):3-7.
Chronic nonmalignant pain: How to ‘turn down’ its physiologic triggers
Mrs. A, age 50, reports recurrent headaches and neck pain from a motor vehicle accident in 1999. At the time, MRI revealed degenerative changes at the C5-C6 vertebrae without bony stenosis or spinal injury. Treatment consisted of conservative measures and physical therapy; she was not a candidate for surgical intervention.
Although Mrs. A can manage activities of daily living, pain prevents her from pastimes she previously enjoyed, including painting and pottery, and is causing problems in her marriage.
Mrs. A’s pain became much worse approximately 1 year ago. In the past year, its severity has lead to multiple clinical presentations and consultations. She uses transdermal fentanyl, 75 mcg/hr every 72 hours, and acetaminophen/ hydrocodone, 5 mg/500 mg every 4 hours up to 6 times a day for breakthrough pain. Even so, she still rates her pain as 7 on a 10-point scale.
Pain is a complex perception with psychological and sensory components. It is the most common reason patients seek treatment at ambulatory medical settings.1 Most pain remits spontaneously or responds to simple treatment, but up to 25% of symptoms remain chronic.1
Chronic pain—defined as pain at ≥1 anatomic sites for ≥6 months—can substantially impair adaptation and vocational and interpersonal functioning. Treatments that focus solely on analgesics are shortsighted and often of limited benefit. Patients with chronic pain need a rehabilitative approach that incorporates psychiatric and psychological intervention.
Complex chronic pain
Most individuals with chronic pain can maintain basic functioning, work, relationships, and interests. They work with healthcare providers and obtain relief from medications or other interventions.
Some, however, are preoccupied with—and entirely debilitated by—their pain. For them, life revolves around the pain and perceived disability. Many if not all aspects of this patient’s life are contingent on pain and fears it might worsen.2 Preoccupation with pain can profoundly affect social activities and prevent employment. The patient may become dependent on others, and being a patient can become a primary psychosocial state. A chronic pain patient also may become increasingly preoccupied with medication use and possibly abuse.
- a general medical condition
- psychological factors
- both.
Pain disorder criteria often are perceived as insufficiently operationalized—there is no checklist of symptoms that collectively define the syndrome.5,6 The clinician must infer whether—and to what extent—psychological factors are involved in the pain.5 There are no guidelines to help psychiatrists ascertain whether psychological factors “have an important role” in pain (criteria C) or if pain is “not better accounted for” by a mood disorder (criteria E).6 This distinction can be indecipherable because of frequent comorbidity of mood disturbances with pain.7,8 Some clinicians have suggested that pain disorder be removed from the somato-form disorder classification and instead confined to Axis III.9
Table 1
DSM-IV-TR diagnostic criteria for pain disorder
| A. Pain in ≥1 anatomical sites |
| B. Produces distress or impairs social, occupational, or other functioning |
| C. Psychological factors have an important role in pain onset, severity, exacerbation, or maintenance |
| D. Not intentionally produced or feigned (as in factitious disorder or malingering) |
| E. Not better accounted for by a mood, anxiety, or psychotic disorder and does not meet criteria for dyspareunia |
| Subtypes |
| Pain disorder associated with psychological factors, which are judged to have the major role in pain onset, severity, exacerbation, or maintenance |
| Pain disorder associated with both psychological factors and a general medical condition, which are judged to have important roles in pain onset, severity, exacerbation, or maintenance |
| Pain disorder associated with a general medical condition.* If psychological factors are present, they do not have a major role in pain onset, severity, exacerbation, or maintenance |
| * Not considered a mental disorder (encoded on Axis III) Source: Adapted from Diagnostic and statistical manual of mental disorders. 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
What are the risk factors?
Psychological and social covariates play a substantial role in the chronic pain experience (Table 2). How patients experience chronic pain also is influenced by personality and premorbid, semi-dormant characteristics that become activated by the stress of unremitting pain.7
- mood
- thought patterns
- perceptions
- coping abilities
- personality.
Table 2
Patient factors that contribute to or perpetuate chronic pain
| Poor modulation of emotions (anger, depression, anxiety) |
| Somatization (using pain to avoid confl icts, express anger, or punish others) |
| Problematic cognitive styles (catastrophizing, perceived loss of control) |
| Poor coping skills |
| Psychiatric comorbidities |
Social/interpersonal variables:
|
Reinforcement for remaining sick and/or disabled:
|
| Source: Adapted from reference 3 |
CASE CONTINUED: Underlying causes
Psychological and psychosocial factors appear to play an important role in Mrs. A’s pain. After her husband’s job was restructured, the couple moved away from Mrs. A’s mother, which she found distressing. Additionally, Mrs. A reports that her son has incurred substantial gambling debt.
Mrs. A admits she has “a hard time” accepting these events, but she cannot acknowledge anger or frustration. She avoids questions about such feelings and focuses on her pain. She reports, “The pain is always there and ruins my entire life. Absolutely nothing gives me relief.”
She does not endorse depressive or psychotic symptoms. She sometimes has passive thoughts of death when she feels hopeless about her persistent pain, but she vehemently denies suicidal ideas, intent, or plans. She has smoked 1 pack of cigarettes per day for 12 years but denies alcohol abuse or use of illicit substances.
Biopsychosocial assessment
Assessing a chronic pain patient includes evaluating somatic, psychological, and social factors (Table 3).3 A biopsychosocial approach recognizes that the patient’s experience of pain, presentation, and response to treatment are determined by the interaction of:
- biological factors
- the patient’s psychological makeup
- psychological comorbidities
- the extent of social support
- extenuating environmental circumstances.3,10
A thorough psychiatric assessment may reveal psychiatric comorbidity and psychological conditions that mediate pain.8 Recognizing and treating coexisting psychiatric disorders often will enhance effective pain management.
Subsyndromal psychological factors—such as troubling affective states, problematic cognitive styles,14 and ineffective coping strategies and interpersonal skills—can accompany pain. If unattended, such factors can heighten the patient’s pain awareness and compromise rehabilitation.
For example, patients such as Mrs. A can aggravate pain by catastrophizing.15 Having a tendency to exaggerate pain and the significance of related life events interferes with their ability to attend to matters within their control and pursue productive activities.16 Catastrophizing is associated with increased pain and perceived disability, poor adjustment to pain, and marked emotional distress.17,18
How pain shapes beliefs. Pain can shape the manner with which patients make sense of events in their lives by altering the way they perceive themselves and the world. Problematic beliefs of the self (inadequacy and helplessness), of the world (dangerousness), and of the future (hopelessness) can produce significant distress. A patient with such beliefs may experience a loss of self-esteem, self-efficacy, and connections with others and may experience marked disappointment and disillusionment.
- substance abuse
- nonadherence with treatment
- withdrawal from support systems
- incapacitating emotional states, such as marked dysphoria, anger, or anxiety.
Table 3
Biopsychosocial assessment of chronic pain patients: 3 components
| Somatic factors |
| Determine pain onset/duration, location, quality, intensity, associated features, aggravating and alleviating factors |
| Single-dimension pain rating scales, such as Numeric Rating Scale or Visual Analog Scale |
| Review prescribed and over-the-counter analgesic use (adherence, excess use, impact on functional adaptation) |
| Psychological factors |
| Mood and affect, cognitive content and processes, coping skills |
| Psychiatric comorbidities (substance abuse/dependence; anxiety, sleep, and somatoform disorders; delirium; depression; sexual dysfunction) |
| Suicide risk assessment |
| Multidimensional pain rating scales, such as Coping Strategies Questionnaire or Multidimensional Pain Inventory |
| Social factors |
| Impact on relationships, including capacity for intimacy, mutuality, and sexuality |
| Impact on activities of daily living, vocational and recreational functioning |
| Determine functions patient can perform despite pain |
| Source: Adapted from reference 3 |
CASE CONTINUED: Multifaceted treatment
You prescribe amitriptyline, 20 mg at bed-time, for pain and refer Mrs. A for cognitive-behavioral therapy (CBT). The emphasis of therapy is to identify affective states and cognitive distortions that are temporally related to pain exacerbations, to develop coping skills to deal with stressors, and to effectively express her anger. Mrs. A learns relaxation techniques and self-hypnosis to reduce distress. These measures help reduce her pain severity ratings to 3 on a 10-point scale. She also participates in physical therapy and yoga classes, which increase her endurance.
Psychiatrists’ role in treatment
Many chronic nonmalignant pain syndromes—including arthritic conditions, back pain, and fibromyalgia—are tenacious and not easily cured. Treatment goals are to relieve pain and maximize the patient’s functioning and quality of life while minimizing risks of iatrogenic harm. As part of a biopsychosocial approach to care:
- diagnose and treat psychiatric comorbidities
- assess responses to treatment interventions
- refine treatment measures when patients do not achieve functional and adaptational goals
- initiate pharmacologic interventions for pain
- address subsyndromal emotional and cognitive impediments to functional restoration.
In initial CBT sessions, the goal is to elicit the patient’s:
- perception of pain
- life situations
- beliefs about his or her life, relationships, and the future
- coping measures.
Self-regulatory techniques—including relaxation training, biofeedback, and hypnosis—can facilitate relaxation and “turn down” the physiologic triggers that cause and perpetuate pain.25,26 Hypnosis can lead to dissociative states that modify how a patient experiences pain. There is modest evidence that self-regulatory techniques are effective for treating pain.27,28
Pharmacotherapy. Multiple pathophysiologic mechanisms—including ion channel up-regulation, spinal hyperexcitability, and descending neurotransmitter pathway impairment—play a role in chronic pain states. Several classes of psychoactive agents can mitigate pain (Table 4), and some psychotropics are FDA-approved for specific pain conditions (Table 5).
Individualize medication selection, considering:
- cost
- ease of use
- tolerability
- interactions with coadministered medications
- clinical comorbidities.
- opioid therapy fails
- patients become dependent on escalating doses of opioids.
Antidepressants influence pain by blocking monoamine reuptake. Those that influence noradrenergic and serotonergic transmission may have greater analgesic effects than those that affect serotonin or norepinephrine reuptake alone.31-33
Anticonvulsants mitigate pain by influencing sodium or calcium channel regulation, GABA activity, or combinations of the 3.
In randomized controlled trials that included patients with diabetic and postherpetic neuropathies:
- one-third of patients achieved ≥50% pain relief with tricyclic antidepressants (TCAs) or anticonvulsants
- adverse effects were slightly more common with TCAs.34,35
Because antidepressants and anticonvulsants have different presumed mechanisms of action for pain relief, anticonvulsants might be useful for patients whose pain persists despite optimal antidepressant dosing or for whom antidepressants are in-tolerable. Alternately, coadministering antidepressants and anticonvulsants might capitalize on complimentary mechanisms of action. With coadministration, lower doses may be sufficiently analgesic and avoid adverse effects.
Benzodiazepines have been used short-term to mitigate muscle spasm pain as in fibromyalgia, phantom limb pain, and restless legs syndrome.36,37 Long-term benzodiazepine use can lead to low activity levels, high use of ambulatory medical services, and high disability levels, however.38 if required for muscle spasm or restless legs syndrome, benzodiazepines may best be confined to short-term use.
Antipsychotics. Limited studies have evaluated antipsychotics’ efficacy for chronic pain.39,40 Some have been found to be useful in neuropathic pain.40 Antipsychotics are seldom used to treat pain because of limited efficacy data, potential side effects, and an abundance of alternate agents. Because risks—most notably extrapyramidal side effects and tardive dyskinesia—appear to outweigh analgesic efficacy, I would confine antipsychotics to pain patients with delirium or psychosis. Antipsychotics’ potential role in treating refractory pain might warrant further investigation.40
Stimulants may reduce sedation, dysphoria, and cognitive inefficiency that can accompany opioid use.
Table 4
Uses of psychotropics in patients with chronic pain
| Class/drug | Uses | Limitations |
|---|---|---|
| Antidepressants | Neuropathic pain, tension and migraine headache, FM, functional GI disorders, pain comorbid with depression/anxiety | NE/5-HT reuptake inhibitors are most effective for analgesia; side effects (TCAs may be least tolerable); drug interactions |
| Anticonvulsants | Neuropathic pain, migraine headache, central pain, phantom limb pain | Side effects (sedation, motor and GI effects, rash); drug interactions |
| Benzodiazepines | Muscle relaxation, restless legs syndrome, anxiety, insomnia | Abuse/dependence potential; sedation |
| Lithium | Cluster headache prophylaxis | Not effective for episodic cluster headache; risk of toxicity if dehydration occurs or with certain drug combinations |
| Stimulants | Opioid analgesia augmentation, opioid-induced fatigue and sedation | Abuse/dependence potential; overstimulation, anorexia, insomnia |
| Stimulants | Opioid analgesia augmentation, opioid-induced fatigue and sedation | Abuse/dependence potential; overstimulation, anorexia, insomnia |
| Antipsychotics | Neuropathic pain, migraine, cancer pain, delirium | Limited data; risks such as EPS and TD may outweigh benefi ts |
| EPS: extrapyramidal symptoms; FM: fibromyalgia; GI: gastrointestinal; NE: norepinephrine; 5-HT: serotonin; TCAs: tricyclic antidepressants; TD: tardive dyskinesia | ||
| Source: Adapted from reference 3 | ||
Table 5
Psychotropics approved for managing pain
| Drug | Indication |
|---|---|
| Carbamazepine | Trigeminal neuralgia |
| Divalproex | Migraine prophylaxis |
| Duloxetine | Diabetic neuropathy |
| Gabapentin | Postherpetic neuralgia |
| Pregabalin | Postherpetic neuralgia, diabetic neuropathy, fibromyalgia |
| Source: Adapted from reference 3 | |
- International Association for the Study of Pain. www.iasp-pain.org.
- Leo RJ. Clinical manual of pain management in psychiatry. Washington, DC: American Psychiatric Publishing; 2007.
- Loeser JD, Butler SH, Chapman CR, Turk DC. Bonica’s management of pain. 3rd ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2001.
- Acetaminophen/hydrocodone • Lortab, others
- Amitriptyline • Elavil, Endep
- Carbamazepine • Tegretol
- Divalproex • Depakote
- Duloxetine • Cymbalta
- Fentanyl transdermal • Duragesic
- Gabapentin • Neurontin
- Lithium • Eskalith, Lithobid
- Pregabalin • Lyrica
Dr. Leo reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Schappert SM. National Ambulatory Medical Care Survey: 1989 summary. Vital Health Stat 13 1992;(110):1-80.
2. Sternbach RA. Pain patients: traits and treatment. New York, NY: Academic Press; 1974.
3. Leo RJ. Clinical manual of pain management in psychiatry. Washington, DC: American Psychiatric Publishing; 2007.
4. Aigner M, Bach M. Clinical utility of DSM-IV pain disorder. Compr Psychiatry 1999;40(5):353-7.
5. Boland RJ. How could the validity of the DSM-IV pain disorder be improved in reference to the concept that it is supposed to identify? Curr Pain Headache Rep 2002;6(1):23-9.
6. Sullivan MD. DSM-IV pain disorder: a case against the diagnosis. Int Rev Psychiatry 2000;12:91-8.
7. Dersh J, Polatin PB, Gatchel RJ. Chronic pain and psychopathology: research findings and theoretical considerations. Psychosom Med 2002;64:773-86.
8. Fishbain DA. Approaches to treatment decisions for psychiatric comorbidity in the management of the chronic pain patient. Med Clin North Am 1999;83:737-60.
9. Mayou R, Kirmayer LJ, Simon G, et al. Somatoform disorders: time for a new approach in DSM-V. Am J Psychiatry 2005;162(5):847-55.
10. Gallagher RM. Treatment planning in pain medicine—integrating medical, physical, and behavioral therapies. Med Clin North Am 1999;83(3):823-49.
11. Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison of six methods. Pain 1986;27:117-26.
12. Rosenstiel AK, Keefe FJ. The use of coping strategies in chronic low back pain patients: relationship to patient characteristics and current adjustment. Pain 1983;17:33-44.
13. Kerns RD, Turk DC, Rudy TE. The West Haven-Yale multidimensional pain inventory (WHYMPI). Pain 1985;23:345-56.
14. Jensen MP, Turner JA, Romano JM, et al. Coping with chronic pain: a critical review. Pain 1991;47:249-83.
15. Sullivan MJL, Stanish W, Waite H, et al. Catastrophizing, pain, and disability in patients with soft-tissue injuries. Pain 1998;77:253-60.
16. Crombez G, Eccleston C, Baeyens F, et al. When somatic information threatens, catastrophic thinking enhances attentional interference. Pain 1998;75:187-98.
17. Hasenbring M, Hallner D, Klasen B. Psychological mechanisms in the transition from acute to chronic pain: over-or underrated? Schmerz. 2001;15:442-7.
18. Sullivan MJ, Thorn B, Haythornthwaite JA, et al. Theoretical perspectives on the relation between catastrophizing and pain. Clin J Pain 2001;17:52-64.
19. Arnstein P. The mediation of disability by self efficacy in different samples of chronic pain patients. Disabil Rehabil 2000;22(17):794-801.
20. Fishbain DA. The association of chronic pain and suicide. Semin Clin Neuropsychiatry 1999;4(3):221-7.
21. Astin JA, Beckner W, Soeken K, et al. Psychological interventions for rheumatoid arthritis: a meta-analysis of randomized controlled trials. Arthritis Rheum 2002;47:291-302.
22. Goldenberg DL, Burckhardt C, Crofford L. Management of fibromyalgia syndrome. JAMA 2004;292(19):2388-95.
23. Morley S, Eccleston C, Williams A. Systematic review and meta-analysis of randomized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache. Pain 1999;80:1-13.
24. Hoffman BM, Papas RK, Chatkoff DK, Kerns RD. Meta-analysis of psychological interventions for chronic low back pain. Health Psychol 2007;26(1):1-9.
25. Turner JA, Chapman CR. Psychological interventions for chronic pain: a critical review, II: operant conditioning, hypnosis, and cognitive-behavioral therapy. Pain 1982;12:23-46.
26. Turner JA, Chapman CR. Psychological interventions for chronic pain: a critical review, I: relaxation training and biofeedback. Pain 1982;12:1-21.
27. Carroll D, Seers K. Relaxation for the relief of chronic pain: a systematic review. J Adv Nurs 1998;27:476-87.
28. Keel PJ, Bodoky C, Gerhard U, et al. Comparison of integrated group therapy and group relaxation training for fibromyalgia. Clin J Pain 1998;14:232-8.
29. Eriksen J, Sjogren P, Bruera E, et al. Critical issues on opioids in chronic non-cancer pain: an epidemiological study. Pain 2006;125:172-9.
30. Ballantyne JC, Mao J. Opioid therapy for chronic pain. N Engl J Med 2003;349:1943-53.
31. Lynch ME. Antidepressants as analgesics: a review of randomized controlled trials. J Psychiatry Neurosci 2001;26(1):30-6.
32. McQuay HJ, Tramer M, Nye BA, et al. A systematic review of antidepressants in neuropathic pain. Pain 1996;68:217-27.
33. Sussman N. SNRI’s versus SSRI’s: mechanisms of action in treating depression and painful physical symptoms. Prim Care Companion J Clin Psychiatry 2003;5(suppl 7):19-26.
34. Collins SL, Moore RA, McQuay HJ, et al. Antidepressants and anticonvulsants for diabetic neuropathy and postherpetic neuralgia: a quantitative systematic review. J Pain Symptom Manage 2000;20:449-58.
35. McQuay HJ. Neuropathic pain: evidence matters. Eur J Pain 2002;6(suppl A):11-8.
36. Bartusch SL, Sanders BJ, D’Alessio JG, et al. Clonazepam for the treatment of lancinating phantom limb pain. Clin J Pain 1996;12:59-62.
37. Dellemijn PL, Fields HL. Do benzodiazepines have a role in chronic pain management? Pain 1994;57:137-52.
38. Ciccone DS, Just N, Bandilla EB, et al. Psychological correlates of opioid use in patients with chronic nonmalignant pain: a preliminary test of the downhill spiral hypothesis. J Pain Symptom Manage 2000;20:180-92.
39. Gomez-Perez FJ, Rull JA, Dies H, et al. Nortriptyline and fluphenazine in the symptomatic treatment of diabetic neuropathy: a double-blind cross-over study. Pain 1985;23:395-400.
40. Fishbain DA, Cutler RB, Lewis J, et al. Do the second-generation “atypical neuroleptics” have analgesic properties? A structured evidence-based review. Pain Med 2004;5:359-65.
Mrs. A, age 50, reports recurrent headaches and neck pain from a motor vehicle accident in 1999. At the time, MRI revealed degenerative changes at the C5-C6 vertebrae without bony stenosis or spinal injury. Treatment consisted of conservative measures and physical therapy; she was not a candidate for surgical intervention.
Although Mrs. A can manage activities of daily living, pain prevents her from pastimes she previously enjoyed, including painting and pottery, and is causing problems in her marriage.
Mrs. A’s pain became much worse approximately 1 year ago. In the past year, its severity has lead to multiple clinical presentations and consultations. She uses transdermal fentanyl, 75 mcg/hr every 72 hours, and acetaminophen/ hydrocodone, 5 mg/500 mg every 4 hours up to 6 times a day for breakthrough pain. Even so, she still rates her pain as 7 on a 10-point scale.
Pain is a complex perception with psychological and sensory components. It is the most common reason patients seek treatment at ambulatory medical settings.1 Most pain remits spontaneously or responds to simple treatment, but up to 25% of symptoms remain chronic.1
Chronic pain—defined as pain at ≥1 anatomic sites for ≥6 months—can substantially impair adaptation and vocational and interpersonal functioning. Treatments that focus solely on analgesics are shortsighted and often of limited benefit. Patients with chronic pain need a rehabilitative approach that incorporates psychiatric and psychological intervention.
Complex chronic pain
Most individuals with chronic pain can maintain basic functioning, work, relationships, and interests. They work with healthcare providers and obtain relief from medications or other interventions.
Some, however, are preoccupied with—and entirely debilitated by—their pain. For them, life revolves around the pain and perceived disability. Many if not all aspects of this patient’s life are contingent on pain and fears it might worsen.2 Preoccupation with pain can profoundly affect social activities and prevent employment. The patient may become dependent on others, and being a patient can become a primary psychosocial state. A chronic pain patient also may become increasingly preoccupied with medication use and possibly abuse.
- a general medical condition
- psychological factors
- both.
Pain disorder criteria often are perceived as insufficiently operationalized—there is no checklist of symptoms that collectively define the syndrome.5,6 The clinician must infer whether—and to what extent—psychological factors are involved in the pain.5 There are no guidelines to help psychiatrists ascertain whether psychological factors “have an important role” in pain (criteria C) or if pain is “not better accounted for” by a mood disorder (criteria E).6 This distinction can be indecipherable because of frequent comorbidity of mood disturbances with pain.7,8 Some clinicians have suggested that pain disorder be removed from the somato-form disorder classification and instead confined to Axis III.9
Table 1
DSM-IV-TR diagnostic criteria for pain disorder
| A. Pain in ≥1 anatomical sites |
| B. Produces distress or impairs social, occupational, or other functioning |
| C. Psychological factors have an important role in pain onset, severity, exacerbation, or maintenance |
| D. Not intentionally produced or feigned (as in factitious disorder or malingering) |
| E. Not better accounted for by a mood, anxiety, or psychotic disorder and does not meet criteria for dyspareunia |
| Subtypes |
| Pain disorder associated with psychological factors, which are judged to have the major role in pain onset, severity, exacerbation, or maintenance |
| Pain disorder associated with both psychological factors and a general medical condition, which are judged to have important roles in pain onset, severity, exacerbation, or maintenance |
| Pain disorder associated with a general medical condition.* If psychological factors are present, they do not have a major role in pain onset, severity, exacerbation, or maintenance |
| * Not considered a mental disorder (encoded on Axis III) Source: Adapted from Diagnostic and statistical manual of mental disorders. 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
What are the risk factors?
Psychological and social covariates play a substantial role in the chronic pain experience (Table 2). How patients experience chronic pain also is influenced by personality and premorbid, semi-dormant characteristics that become activated by the stress of unremitting pain.7
- mood
- thought patterns
- perceptions
- coping abilities
- personality.
Table 2
Patient factors that contribute to or perpetuate chronic pain
| Poor modulation of emotions (anger, depression, anxiety) |
| Somatization (using pain to avoid confl icts, express anger, or punish others) |
| Problematic cognitive styles (catastrophizing, perceived loss of control) |
| Poor coping skills |
| Psychiatric comorbidities |
Social/interpersonal variables:
|
Reinforcement for remaining sick and/or disabled:
|
| Source: Adapted from reference 3 |
CASE CONTINUED: Underlying causes
Psychological and psychosocial factors appear to play an important role in Mrs. A’s pain. After her husband’s job was restructured, the couple moved away from Mrs. A’s mother, which she found distressing. Additionally, Mrs. A reports that her son has incurred substantial gambling debt.
Mrs. A admits she has “a hard time” accepting these events, but she cannot acknowledge anger or frustration. She avoids questions about such feelings and focuses on her pain. She reports, “The pain is always there and ruins my entire life. Absolutely nothing gives me relief.”
She does not endorse depressive or psychotic symptoms. She sometimes has passive thoughts of death when she feels hopeless about her persistent pain, but she vehemently denies suicidal ideas, intent, or plans. She has smoked 1 pack of cigarettes per day for 12 years but denies alcohol abuse or use of illicit substances.
Biopsychosocial assessment
Assessing a chronic pain patient includes evaluating somatic, psychological, and social factors (Table 3).3 A biopsychosocial approach recognizes that the patient’s experience of pain, presentation, and response to treatment are determined by the interaction of:
- biological factors
- the patient’s psychological makeup
- psychological comorbidities
- the extent of social support
- extenuating environmental circumstances.3,10
A thorough psychiatric assessment may reveal psychiatric comorbidity and psychological conditions that mediate pain.8 Recognizing and treating coexisting psychiatric disorders often will enhance effective pain management.
Subsyndromal psychological factors—such as troubling affective states, problematic cognitive styles,14 and ineffective coping strategies and interpersonal skills—can accompany pain. If unattended, such factors can heighten the patient’s pain awareness and compromise rehabilitation.
For example, patients such as Mrs. A can aggravate pain by catastrophizing.15 Having a tendency to exaggerate pain and the significance of related life events interferes with their ability to attend to matters within their control and pursue productive activities.16 Catastrophizing is associated with increased pain and perceived disability, poor adjustment to pain, and marked emotional distress.17,18
How pain shapes beliefs. Pain can shape the manner with which patients make sense of events in their lives by altering the way they perceive themselves and the world. Problematic beliefs of the self (inadequacy and helplessness), of the world (dangerousness), and of the future (hopelessness) can produce significant distress. A patient with such beliefs may experience a loss of self-esteem, self-efficacy, and connections with others and may experience marked disappointment and disillusionment.
- substance abuse
- nonadherence with treatment
- withdrawal from support systems
- incapacitating emotional states, such as marked dysphoria, anger, or anxiety.
Table 3
Biopsychosocial assessment of chronic pain patients: 3 components
| Somatic factors |
| Determine pain onset/duration, location, quality, intensity, associated features, aggravating and alleviating factors |
| Single-dimension pain rating scales, such as Numeric Rating Scale or Visual Analog Scale |
| Review prescribed and over-the-counter analgesic use (adherence, excess use, impact on functional adaptation) |
| Psychological factors |
| Mood and affect, cognitive content and processes, coping skills |
| Psychiatric comorbidities (substance abuse/dependence; anxiety, sleep, and somatoform disorders; delirium; depression; sexual dysfunction) |
| Suicide risk assessment |
| Multidimensional pain rating scales, such as Coping Strategies Questionnaire or Multidimensional Pain Inventory |
| Social factors |
| Impact on relationships, including capacity for intimacy, mutuality, and sexuality |
| Impact on activities of daily living, vocational and recreational functioning |
| Determine functions patient can perform despite pain |
| Source: Adapted from reference 3 |
CASE CONTINUED: Multifaceted treatment
You prescribe amitriptyline, 20 mg at bed-time, for pain and refer Mrs. A for cognitive-behavioral therapy (CBT). The emphasis of therapy is to identify affective states and cognitive distortions that are temporally related to pain exacerbations, to develop coping skills to deal with stressors, and to effectively express her anger. Mrs. A learns relaxation techniques and self-hypnosis to reduce distress. These measures help reduce her pain severity ratings to 3 on a 10-point scale. She also participates in physical therapy and yoga classes, which increase her endurance.
Psychiatrists’ role in treatment
Many chronic nonmalignant pain syndromes—including arthritic conditions, back pain, and fibromyalgia—are tenacious and not easily cured. Treatment goals are to relieve pain and maximize the patient’s functioning and quality of life while minimizing risks of iatrogenic harm. As part of a biopsychosocial approach to care:
- diagnose and treat psychiatric comorbidities
- assess responses to treatment interventions
- refine treatment measures when patients do not achieve functional and adaptational goals
- initiate pharmacologic interventions for pain
- address subsyndromal emotional and cognitive impediments to functional restoration.
In initial CBT sessions, the goal is to elicit the patient’s:
- perception of pain
- life situations
- beliefs about his or her life, relationships, and the future
- coping measures.
Self-regulatory techniques—including relaxation training, biofeedback, and hypnosis—can facilitate relaxation and “turn down” the physiologic triggers that cause and perpetuate pain.25,26 Hypnosis can lead to dissociative states that modify how a patient experiences pain. There is modest evidence that self-regulatory techniques are effective for treating pain.27,28
Pharmacotherapy. Multiple pathophysiologic mechanisms—including ion channel up-regulation, spinal hyperexcitability, and descending neurotransmitter pathway impairment—play a role in chronic pain states. Several classes of psychoactive agents can mitigate pain (Table 4), and some psychotropics are FDA-approved for specific pain conditions (Table 5).
Individualize medication selection, considering:
- cost
- ease of use
- tolerability
- interactions with coadministered medications
- clinical comorbidities.
- opioid therapy fails
- patients become dependent on escalating doses of opioids.
Antidepressants influence pain by blocking monoamine reuptake. Those that influence noradrenergic and serotonergic transmission may have greater analgesic effects than those that affect serotonin or norepinephrine reuptake alone.31-33
Anticonvulsants mitigate pain by influencing sodium or calcium channel regulation, GABA activity, or combinations of the 3.
In randomized controlled trials that included patients with diabetic and postherpetic neuropathies:
- one-third of patients achieved ≥50% pain relief with tricyclic antidepressants (TCAs) or anticonvulsants
- adverse effects were slightly more common with TCAs.34,35
Because antidepressants and anticonvulsants have different presumed mechanisms of action for pain relief, anticonvulsants might be useful for patients whose pain persists despite optimal antidepressant dosing or for whom antidepressants are in-tolerable. Alternately, coadministering antidepressants and anticonvulsants might capitalize on complimentary mechanisms of action. With coadministration, lower doses may be sufficiently analgesic and avoid adverse effects.
Benzodiazepines have been used short-term to mitigate muscle spasm pain as in fibromyalgia, phantom limb pain, and restless legs syndrome.36,37 Long-term benzodiazepine use can lead to low activity levels, high use of ambulatory medical services, and high disability levels, however.38 if required for muscle spasm or restless legs syndrome, benzodiazepines may best be confined to short-term use.
Antipsychotics. Limited studies have evaluated antipsychotics’ efficacy for chronic pain.39,40 Some have been found to be useful in neuropathic pain.40 Antipsychotics are seldom used to treat pain because of limited efficacy data, potential side effects, and an abundance of alternate agents. Because risks—most notably extrapyramidal side effects and tardive dyskinesia—appear to outweigh analgesic efficacy, I would confine antipsychotics to pain patients with delirium or psychosis. Antipsychotics’ potential role in treating refractory pain might warrant further investigation.40
Stimulants may reduce sedation, dysphoria, and cognitive inefficiency that can accompany opioid use.
Table 4
Uses of psychotropics in patients with chronic pain
| Class/drug | Uses | Limitations |
|---|---|---|
| Antidepressants | Neuropathic pain, tension and migraine headache, FM, functional GI disorders, pain comorbid with depression/anxiety | NE/5-HT reuptake inhibitors are most effective for analgesia; side effects (TCAs may be least tolerable); drug interactions |
| Anticonvulsants | Neuropathic pain, migraine headache, central pain, phantom limb pain | Side effects (sedation, motor and GI effects, rash); drug interactions |
| Benzodiazepines | Muscle relaxation, restless legs syndrome, anxiety, insomnia | Abuse/dependence potential; sedation |
| Lithium | Cluster headache prophylaxis | Not effective for episodic cluster headache; risk of toxicity if dehydration occurs or with certain drug combinations |
| Stimulants | Opioid analgesia augmentation, opioid-induced fatigue and sedation | Abuse/dependence potential; overstimulation, anorexia, insomnia |
| Stimulants | Opioid analgesia augmentation, opioid-induced fatigue and sedation | Abuse/dependence potential; overstimulation, anorexia, insomnia |
| Antipsychotics | Neuropathic pain, migraine, cancer pain, delirium | Limited data; risks such as EPS and TD may outweigh benefi ts |
| EPS: extrapyramidal symptoms; FM: fibromyalgia; GI: gastrointestinal; NE: norepinephrine; 5-HT: serotonin; TCAs: tricyclic antidepressants; TD: tardive dyskinesia | ||
| Source: Adapted from reference 3 | ||
Table 5
Psychotropics approved for managing pain
| Drug | Indication |
|---|---|
| Carbamazepine | Trigeminal neuralgia |
| Divalproex | Migraine prophylaxis |
| Duloxetine | Diabetic neuropathy |
| Gabapentin | Postherpetic neuralgia |
| Pregabalin | Postherpetic neuralgia, diabetic neuropathy, fibromyalgia |
| Source: Adapted from reference 3 | |
- International Association for the Study of Pain. www.iasp-pain.org.
- Leo RJ. Clinical manual of pain management in psychiatry. Washington, DC: American Psychiatric Publishing; 2007.
- Loeser JD, Butler SH, Chapman CR, Turk DC. Bonica’s management of pain. 3rd ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2001.
- Acetaminophen/hydrocodone • Lortab, others
- Amitriptyline • Elavil, Endep
- Carbamazepine • Tegretol
- Divalproex • Depakote
- Duloxetine • Cymbalta
- Fentanyl transdermal • Duragesic
- Gabapentin • Neurontin
- Lithium • Eskalith, Lithobid
- Pregabalin • Lyrica
Dr. Leo reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Mrs. A, age 50, reports recurrent headaches and neck pain from a motor vehicle accident in 1999. At the time, MRI revealed degenerative changes at the C5-C6 vertebrae without bony stenosis or spinal injury. Treatment consisted of conservative measures and physical therapy; she was not a candidate for surgical intervention.
Although Mrs. A can manage activities of daily living, pain prevents her from pastimes she previously enjoyed, including painting and pottery, and is causing problems in her marriage.
Mrs. A’s pain became much worse approximately 1 year ago. In the past year, its severity has lead to multiple clinical presentations and consultations. She uses transdermal fentanyl, 75 mcg/hr every 72 hours, and acetaminophen/ hydrocodone, 5 mg/500 mg every 4 hours up to 6 times a day for breakthrough pain. Even so, she still rates her pain as 7 on a 10-point scale.
Pain is a complex perception with psychological and sensory components. It is the most common reason patients seek treatment at ambulatory medical settings.1 Most pain remits spontaneously or responds to simple treatment, but up to 25% of symptoms remain chronic.1
Chronic pain—defined as pain at ≥1 anatomic sites for ≥6 months—can substantially impair adaptation and vocational and interpersonal functioning. Treatments that focus solely on analgesics are shortsighted and often of limited benefit. Patients with chronic pain need a rehabilitative approach that incorporates psychiatric and psychological intervention.
Complex chronic pain
Most individuals with chronic pain can maintain basic functioning, work, relationships, and interests. They work with healthcare providers and obtain relief from medications or other interventions.
Some, however, are preoccupied with—and entirely debilitated by—their pain. For them, life revolves around the pain and perceived disability. Many if not all aspects of this patient’s life are contingent on pain and fears it might worsen.2 Preoccupation with pain can profoundly affect social activities and prevent employment. The patient may become dependent on others, and being a patient can become a primary psychosocial state. A chronic pain patient also may become increasingly preoccupied with medication use and possibly abuse.
- a general medical condition
- psychological factors
- both.
Pain disorder criteria often are perceived as insufficiently operationalized—there is no checklist of symptoms that collectively define the syndrome.5,6 The clinician must infer whether—and to what extent—psychological factors are involved in the pain.5 There are no guidelines to help psychiatrists ascertain whether psychological factors “have an important role” in pain (criteria C) or if pain is “not better accounted for” by a mood disorder (criteria E).6 This distinction can be indecipherable because of frequent comorbidity of mood disturbances with pain.7,8 Some clinicians have suggested that pain disorder be removed from the somato-form disorder classification and instead confined to Axis III.9
Table 1
DSM-IV-TR diagnostic criteria for pain disorder
| A. Pain in ≥1 anatomical sites |
| B. Produces distress or impairs social, occupational, or other functioning |
| C. Psychological factors have an important role in pain onset, severity, exacerbation, or maintenance |
| D. Not intentionally produced or feigned (as in factitious disorder or malingering) |
| E. Not better accounted for by a mood, anxiety, or psychotic disorder and does not meet criteria for dyspareunia |
| Subtypes |
| Pain disorder associated with psychological factors, which are judged to have the major role in pain onset, severity, exacerbation, or maintenance |
| Pain disorder associated with both psychological factors and a general medical condition, which are judged to have important roles in pain onset, severity, exacerbation, or maintenance |
| Pain disorder associated with a general medical condition.* If psychological factors are present, they do not have a major role in pain onset, severity, exacerbation, or maintenance |
| * Not considered a mental disorder (encoded on Axis III) Source: Adapted from Diagnostic and statistical manual of mental disorders. 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
What are the risk factors?
Psychological and social covariates play a substantial role in the chronic pain experience (Table 2). How patients experience chronic pain also is influenced by personality and premorbid, semi-dormant characteristics that become activated by the stress of unremitting pain.7
- mood
- thought patterns
- perceptions
- coping abilities
- personality.
Table 2
Patient factors that contribute to or perpetuate chronic pain
| Poor modulation of emotions (anger, depression, anxiety) |
| Somatization (using pain to avoid confl icts, express anger, or punish others) |
| Problematic cognitive styles (catastrophizing, perceived loss of control) |
| Poor coping skills |
| Psychiatric comorbidities |
Social/interpersonal variables:
|
Reinforcement for remaining sick and/or disabled:
|
| Source: Adapted from reference 3 |
CASE CONTINUED: Underlying causes
Psychological and psychosocial factors appear to play an important role in Mrs. A’s pain. After her husband’s job was restructured, the couple moved away from Mrs. A’s mother, which she found distressing. Additionally, Mrs. A reports that her son has incurred substantial gambling debt.
Mrs. A admits she has “a hard time” accepting these events, but she cannot acknowledge anger or frustration. She avoids questions about such feelings and focuses on her pain. She reports, “The pain is always there and ruins my entire life. Absolutely nothing gives me relief.”
She does not endorse depressive or psychotic symptoms. She sometimes has passive thoughts of death when she feels hopeless about her persistent pain, but she vehemently denies suicidal ideas, intent, or plans. She has smoked 1 pack of cigarettes per day for 12 years but denies alcohol abuse or use of illicit substances.
Biopsychosocial assessment
Assessing a chronic pain patient includes evaluating somatic, psychological, and social factors (Table 3).3 A biopsychosocial approach recognizes that the patient’s experience of pain, presentation, and response to treatment are determined by the interaction of:
- biological factors
- the patient’s psychological makeup
- psychological comorbidities
- the extent of social support
- extenuating environmental circumstances.3,10
A thorough psychiatric assessment may reveal psychiatric comorbidity and psychological conditions that mediate pain.8 Recognizing and treating coexisting psychiatric disorders often will enhance effective pain management.
Subsyndromal psychological factors—such as troubling affective states, problematic cognitive styles,14 and ineffective coping strategies and interpersonal skills—can accompany pain. If unattended, such factors can heighten the patient’s pain awareness and compromise rehabilitation.
For example, patients such as Mrs. A can aggravate pain by catastrophizing.15 Having a tendency to exaggerate pain and the significance of related life events interferes with their ability to attend to matters within their control and pursue productive activities.16 Catastrophizing is associated with increased pain and perceived disability, poor adjustment to pain, and marked emotional distress.17,18
How pain shapes beliefs. Pain can shape the manner with which patients make sense of events in their lives by altering the way they perceive themselves and the world. Problematic beliefs of the self (inadequacy and helplessness), of the world (dangerousness), and of the future (hopelessness) can produce significant distress. A patient with such beliefs may experience a loss of self-esteem, self-efficacy, and connections with others and may experience marked disappointment and disillusionment.
- substance abuse
- nonadherence with treatment
- withdrawal from support systems
- incapacitating emotional states, such as marked dysphoria, anger, or anxiety.
Table 3
Biopsychosocial assessment of chronic pain patients: 3 components
| Somatic factors |
| Determine pain onset/duration, location, quality, intensity, associated features, aggravating and alleviating factors |
| Single-dimension pain rating scales, such as Numeric Rating Scale or Visual Analog Scale |
| Review prescribed and over-the-counter analgesic use (adherence, excess use, impact on functional adaptation) |
| Psychological factors |
| Mood and affect, cognitive content and processes, coping skills |
| Psychiatric comorbidities (substance abuse/dependence; anxiety, sleep, and somatoform disorders; delirium; depression; sexual dysfunction) |
| Suicide risk assessment |
| Multidimensional pain rating scales, such as Coping Strategies Questionnaire or Multidimensional Pain Inventory |
| Social factors |
| Impact on relationships, including capacity for intimacy, mutuality, and sexuality |
| Impact on activities of daily living, vocational and recreational functioning |
| Determine functions patient can perform despite pain |
| Source: Adapted from reference 3 |
CASE CONTINUED: Multifaceted treatment
You prescribe amitriptyline, 20 mg at bed-time, for pain and refer Mrs. A for cognitive-behavioral therapy (CBT). The emphasis of therapy is to identify affective states and cognitive distortions that are temporally related to pain exacerbations, to develop coping skills to deal with stressors, and to effectively express her anger. Mrs. A learns relaxation techniques and self-hypnosis to reduce distress. These measures help reduce her pain severity ratings to 3 on a 10-point scale. She also participates in physical therapy and yoga classes, which increase her endurance.
Psychiatrists’ role in treatment
Many chronic nonmalignant pain syndromes—including arthritic conditions, back pain, and fibromyalgia—are tenacious and not easily cured. Treatment goals are to relieve pain and maximize the patient’s functioning and quality of life while minimizing risks of iatrogenic harm. As part of a biopsychosocial approach to care:
- diagnose and treat psychiatric comorbidities
- assess responses to treatment interventions
- refine treatment measures when patients do not achieve functional and adaptational goals
- initiate pharmacologic interventions for pain
- address subsyndromal emotional and cognitive impediments to functional restoration.
In initial CBT sessions, the goal is to elicit the patient’s:
- perception of pain
- life situations
- beliefs about his or her life, relationships, and the future
- coping measures.
Self-regulatory techniques—including relaxation training, biofeedback, and hypnosis—can facilitate relaxation and “turn down” the physiologic triggers that cause and perpetuate pain.25,26 Hypnosis can lead to dissociative states that modify how a patient experiences pain. There is modest evidence that self-regulatory techniques are effective for treating pain.27,28
Pharmacotherapy. Multiple pathophysiologic mechanisms—including ion channel up-regulation, spinal hyperexcitability, and descending neurotransmitter pathway impairment—play a role in chronic pain states. Several classes of psychoactive agents can mitigate pain (Table 4), and some psychotropics are FDA-approved for specific pain conditions (Table 5).
Individualize medication selection, considering:
- cost
- ease of use
- tolerability
- interactions with coadministered medications
- clinical comorbidities.
- opioid therapy fails
- patients become dependent on escalating doses of opioids.
Antidepressants influence pain by blocking monoamine reuptake. Those that influence noradrenergic and serotonergic transmission may have greater analgesic effects than those that affect serotonin or norepinephrine reuptake alone.31-33
Anticonvulsants mitigate pain by influencing sodium or calcium channel regulation, GABA activity, or combinations of the 3.
In randomized controlled trials that included patients with diabetic and postherpetic neuropathies:
- one-third of patients achieved ≥50% pain relief with tricyclic antidepressants (TCAs) or anticonvulsants
- adverse effects were slightly more common with TCAs.34,35
Because antidepressants and anticonvulsants have different presumed mechanisms of action for pain relief, anticonvulsants might be useful for patients whose pain persists despite optimal antidepressant dosing or for whom antidepressants are in-tolerable. Alternately, coadministering antidepressants and anticonvulsants might capitalize on complimentary mechanisms of action. With coadministration, lower doses may be sufficiently analgesic and avoid adverse effects.
Benzodiazepines have been used short-term to mitigate muscle spasm pain as in fibromyalgia, phantom limb pain, and restless legs syndrome.36,37 Long-term benzodiazepine use can lead to low activity levels, high use of ambulatory medical services, and high disability levels, however.38 if required for muscle spasm or restless legs syndrome, benzodiazepines may best be confined to short-term use.
Antipsychotics. Limited studies have evaluated antipsychotics’ efficacy for chronic pain.39,40 Some have been found to be useful in neuropathic pain.40 Antipsychotics are seldom used to treat pain because of limited efficacy data, potential side effects, and an abundance of alternate agents. Because risks—most notably extrapyramidal side effects and tardive dyskinesia—appear to outweigh analgesic efficacy, I would confine antipsychotics to pain patients with delirium or psychosis. Antipsychotics’ potential role in treating refractory pain might warrant further investigation.40
Stimulants may reduce sedation, dysphoria, and cognitive inefficiency that can accompany opioid use.
Table 4
Uses of psychotropics in patients with chronic pain
| Class/drug | Uses | Limitations |
|---|---|---|
| Antidepressants | Neuropathic pain, tension and migraine headache, FM, functional GI disorders, pain comorbid with depression/anxiety | NE/5-HT reuptake inhibitors are most effective for analgesia; side effects (TCAs may be least tolerable); drug interactions |
| Anticonvulsants | Neuropathic pain, migraine headache, central pain, phantom limb pain | Side effects (sedation, motor and GI effects, rash); drug interactions |
| Benzodiazepines | Muscle relaxation, restless legs syndrome, anxiety, insomnia | Abuse/dependence potential; sedation |
| Lithium | Cluster headache prophylaxis | Not effective for episodic cluster headache; risk of toxicity if dehydration occurs or with certain drug combinations |
| Stimulants | Opioid analgesia augmentation, opioid-induced fatigue and sedation | Abuse/dependence potential; overstimulation, anorexia, insomnia |
| Stimulants | Opioid analgesia augmentation, opioid-induced fatigue and sedation | Abuse/dependence potential; overstimulation, anorexia, insomnia |
| Antipsychotics | Neuropathic pain, migraine, cancer pain, delirium | Limited data; risks such as EPS and TD may outweigh benefi ts |
| EPS: extrapyramidal symptoms; FM: fibromyalgia; GI: gastrointestinal; NE: norepinephrine; 5-HT: serotonin; TCAs: tricyclic antidepressants; TD: tardive dyskinesia | ||
| Source: Adapted from reference 3 | ||
Table 5
Psychotropics approved for managing pain
| Drug | Indication |
|---|---|
| Carbamazepine | Trigeminal neuralgia |
| Divalproex | Migraine prophylaxis |
| Duloxetine | Diabetic neuropathy |
| Gabapentin | Postherpetic neuralgia |
| Pregabalin | Postherpetic neuralgia, diabetic neuropathy, fibromyalgia |
| Source: Adapted from reference 3 | |
- International Association for the Study of Pain. www.iasp-pain.org.
- Leo RJ. Clinical manual of pain management in psychiatry. Washington, DC: American Psychiatric Publishing; 2007.
- Loeser JD, Butler SH, Chapman CR, Turk DC. Bonica’s management of pain. 3rd ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2001.
- Acetaminophen/hydrocodone • Lortab, others
- Amitriptyline • Elavil, Endep
- Carbamazepine • Tegretol
- Divalproex • Depakote
- Duloxetine • Cymbalta
- Fentanyl transdermal • Duragesic
- Gabapentin • Neurontin
- Lithium • Eskalith, Lithobid
- Pregabalin • Lyrica
Dr. Leo reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Schappert SM. National Ambulatory Medical Care Survey: 1989 summary. Vital Health Stat 13 1992;(110):1-80.
2. Sternbach RA. Pain patients: traits and treatment. New York, NY: Academic Press; 1974.
3. Leo RJ. Clinical manual of pain management in psychiatry. Washington, DC: American Psychiatric Publishing; 2007.
4. Aigner M, Bach M. Clinical utility of DSM-IV pain disorder. Compr Psychiatry 1999;40(5):353-7.
5. Boland RJ. How could the validity of the DSM-IV pain disorder be improved in reference to the concept that it is supposed to identify? Curr Pain Headache Rep 2002;6(1):23-9.
6. Sullivan MD. DSM-IV pain disorder: a case against the diagnosis. Int Rev Psychiatry 2000;12:91-8.
7. Dersh J, Polatin PB, Gatchel RJ. Chronic pain and psychopathology: research findings and theoretical considerations. Psychosom Med 2002;64:773-86.
8. Fishbain DA. Approaches to treatment decisions for psychiatric comorbidity in the management of the chronic pain patient. Med Clin North Am 1999;83:737-60.
9. Mayou R, Kirmayer LJ, Simon G, et al. Somatoform disorders: time for a new approach in DSM-V. Am J Psychiatry 2005;162(5):847-55.
10. Gallagher RM. Treatment planning in pain medicine—integrating medical, physical, and behavioral therapies. Med Clin North Am 1999;83(3):823-49.
11. Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison of six methods. Pain 1986;27:117-26.
12. Rosenstiel AK, Keefe FJ. The use of coping strategies in chronic low back pain patients: relationship to patient characteristics and current adjustment. Pain 1983;17:33-44.
13. Kerns RD, Turk DC, Rudy TE. The West Haven-Yale multidimensional pain inventory (WHYMPI). Pain 1985;23:345-56.
14. Jensen MP, Turner JA, Romano JM, et al. Coping with chronic pain: a critical review. Pain 1991;47:249-83.
15. Sullivan MJL, Stanish W, Waite H, et al. Catastrophizing, pain, and disability in patients with soft-tissue injuries. Pain 1998;77:253-60.
16. Crombez G, Eccleston C, Baeyens F, et al. When somatic information threatens, catastrophic thinking enhances attentional interference. Pain 1998;75:187-98.
17. Hasenbring M, Hallner D, Klasen B. Psychological mechanisms in the transition from acute to chronic pain: over-or underrated? Schmerz. 2001;15:442-7.
18. Sullivan MJ, Thorn B, Haythornthwaite JA, et al. Theoretical perspectives on the relation between catastrophizing and pain. Clin J Pain 2001;17:52-64.
19. Arnstein P. The mediation of disability by self efficacy in different samples of chronic pain patients. Disabil Rehabil 2000;22(17):794-801.
20. Fishbain DA. The association of chronic pain and suicide. Semin Clin Neuropsychiatry 1999;4(3):221-7.
21. Astin JA, Beckner W, Soeken K, et al. Psychological interventions for rheumatoid arthritis: a meta-analysis of randomized controlled trials. Arthritis Rheum 2002;47:291-302.
22. Goldenberg DL, Burckhardt C, Crofford L. Management of fibromyalgia syndrome. JAMA 2004;292(19):2388-95.
23. Morley S, Eccleston C, Williams A. Systematic review and meta-analysis of randomized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache. Pain 1999;80:1-13.
24. Hoffman BM, Papas RK, Chatkoff DK, Kerns RD. Meta-analysis of psychological interventions for chronic low back pain. Health Psychol 2007;26(1):1-9.
25. Turner JA, Chapman CR. Psychological interventions for chronic pain: a critical review, II: operant conditioning, hypnosis, and cognitive-behavioral therapy. Pain 1982;12:23-46.
26. Turner JA, Chapman CR. Psychological interventions for chronic pain: a critical review, I: relaxation training and biofeedback. Pain 1982;12:1-21.
27. Carroll D, Seers K. Relaxation for the relief of chronic pain: a systematic review. J Adv Nurs 1998;27:476-87.
28. Keel PJ, Bodoky C, Gerhard U, et al. Comparison of integrated group therapy and group relaxation training for fibromyalgia. Clin J Pain 1998;14:232-8.
29. Eriksen J, Sjogren P, Bruera E, et al. Critical issues on opioids in chronic non-cancer pain: an epidemiological study. Pain 2006;125:172-9.
30. Ballantyne JC, Mao J. Opioid therapy for chronic pain. N Engl J Med 2003;349:1943-53.
31. Lynch ME. Antidepressants as analgesics: a review of randomized controlled trials. J Psychiatry Neurosci 2001;26(1):30-6.
32. McQuay HJ, Tramer M, Nye BA, et al. A systematic review of antidepressants in neuropathic pain. Pain 1996;68:217-27.
33. Sussman N. SNRI’s versus SSRI’s: mechanisms of action in treating depression and painful physical symptoms. Prim Care Companion J Clin Psychiatry 2003;5(suppl 7):19-26.
34. Collins SL, Moore RA, McQuay HJ, et al. Antidepressants and anticonvulsants for diabetic neuropathy and postherpetic neuralgia: a quantitative systematic review. J Pain Symptom Manage 2000;20:449-58.
35. McQuay HJ. Neuropathic pain: evidence matters. Eur J Pain 2002;6(suppl A):11-8.
36. Bartusch SL, Sanders BJ, D’Alessio JG, et al. Clonazepam for the treatment of lancinating phantom limb pain. Clin J Pain 1996;12:59-62.
37. Dellemijn PL, Fields HL. Do benzodiazepines have a role in chronic pain management? Pain 1994;57:137-52.
38. Ciccone DS, Just N, Bandilla EB, et al. Psychological correlates of opioid use in patients with chronic nonmalignant pain: a preliminary test of the downhill spiral hypothesis. J Pain Symptom Manage 2000;20:180-92.
39. Gomez-Perez FJ, Rull JA, Dies H, et al. Nortriptyline and fluphenazine in the symptomatic treatment of diabetic neuropathy: a double-blind cross-over study. Pain 1985;23:395-400.
40. Fishbain DA, Cutler RB, Lewis J, et al. Do the second-generation “atypical neuroleptics” have analgesic properties? A structured evidence-based review. Pain Med 2004;5:359-65.
1. Schappert SM. National Ambulatory Medical Care Survey: 1989 summary. Vital Health Stat 13 1992;(110):1-80.
2. Sternbach RA. Pain patients: traits and treatment. New York, NY: Academic Press; 1974.
3. Leo RJ. Clinical manual of pain management in psychiatry. Washington, DC: American Psychiatric Publishing; 2007.
4. Aigner M, Bach M. Clinical utility of DSM-IV pain disorder. Compr Psychiatry 1999;40(5):353-7.
5. Boland RJ. How could the validity of the DSM-IV pain disorder be improved in reference to the concept that it is supposed to identify? Curr Pain Headache Rep 2002;6(1):23-9.
6. Sullivan MD. DSM-IV pain disorder: a case against the diagnosis. Int Rev Psychiatry 2000;12:91-8.
7. Dersh J, Polatin PB, Gatchel RJ. Chronic pain and psychopathology: research findings and theoretical considerations. Psychosom Med 2002;64:773-86.
8. Fishbain DA. Approaches to treatment decisions for psychiatric comorbidity in the management of the chronic pain patient. Med Clin North Am 1999;83:737-60.
9. Mayou R, Kirmayer LJ, Simon G, et al. Somatoform disorders: time for a new approach in DSM-V. Am J Psychiatry 2005;162(5):847-55.
10. Gallagher RM. Treatment planning in pain medicine—integrating medical, physical, and behavioral therapies. Med Clin North Am 1999;83(3):823-49.
11. Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison of six methods. Pain 1986;27:117-26.
12. Rosenstiel AK, Keefe FJ. The use of coping strategies in chronic low back pain patients: relationship to patient characteristics and current adjustment. Pain 1983;17:33-44.
13. Kerns RD, Turk DC, Rudy TE. The West Haven-Yale multidimensional pain inventory (WHYMPI). Pain 1985;23:345-56.
14. Jensen MP, Turner JA, Romano JM, et al. Coping with chronic pain: a critical review. Pain 1991;47:249-83.
15. Sullivan MJL, Stanish W, Waite H, et al. Catastrophizing, pain, and disability in patients with soft-tissue injuries. Pain 1998;77:253-60.
16. Crombez G, Eccleston C, Baeyens F, et al. When somatic information threatens, catastrophic thinking enhances attentional interference. Pain 1998;75:187-98.
17. Hasenbring M, Hallner D, Klasen B. Psychological mechanisms in the transition from acute to chronic pain: over-or underrated? Schmerz. 2001;15:442-7.
18. Sullivan MJ, Thorn B, Haythornthwaite JA, et al. Theoretical perspectives on the relation between catastrophizing and pain. Clin J Pain 2001;17:52-64.
19. Arnstein P. The mediation of disability by self efficacy in different samples of chronic pain patients. Disabil Rehabil 2000;22(17):794-801.
20. Fishbain DA. The association of chronic pain and suicide. Semin Clin Neuropsychiatry 1999;4(3):221-7.
21. Astin JA, Beckner W, Soeken K, et al. Psychological interventions for rheumatoid arthritis: a meta-analysis of randomized controlled trials. Arthritis Rheum 2002;47:291-302.
22. Goldenberg DL, Burckhardt C, Crofford L. Management of fibromyalgia syndrome. JAMA 2004;292(19):2388-95.
23. Morley S, Eccleston C, Williams A. Systematic review and meta-analysis of randomized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache. Pain 1999;80:1-13.
24. Hoffman BM, Papas RK, Chatkoff DK, Kerns RD. Meta-analysis of psychological interventions for chronic low back pain. Health Psychol 2007;26(1):1-9.
25. Turner JA, Chapman CR. Psychological interventions for chronic pain: a critical review, II: operant conditioning, hypnosis, and cognitive-behavioral therapy. Pain 1982;12:23-46.
26. Turner JA, Chapman CR. Psychological interventions for chronic pain: a critical review, I: relaxation training and biofeedback. Pain 1982;12:1-21.
27. Carroll D, Seers K. Relaxation for the relief of chronic pain: a systematic review. J Adv Nurs 1998;27:476-87.
28. Keel PJ, Bodoky C, Gerhard U, et al. Comparison of integrated group therapy and group relaxation training for fibromyalgia. Clin J Pain 1998;14:232-8.
29. Eriksen J, Sjogren P, Bruera E, et al. Critical issues on opioids in chronic non-cancer pain: an epidemiological study. Pain 2006;125:172-9.
30. Ballantyne JC, Mao J. Opioid therapy for chronic pain. N Engl J Med 2003;349:1943-53.
31. Lynch ME. Antidepressants as analgesics: a review of randomized controlled trials. J Psychiatry Neurosci 2001;26(1):30-6.
32. McQuay HJ, Tramer M, Nye BA, et al. A systematic review of antidepressants in neuropathic pain. Pain 1996;68:217-27.
33. Sussman N. SNRI’s versus SSRI’s: mechanisms of action in treating depression and painful physical symptoms. Prim Care Companion J Clin Psychiatry 2003;5(suppl 7):19-26.
34. Collins SL, Moore RA, McQuay HJ, et al. Antidepressants and anticonvulsants for diabetic neuropathy and postherpetic neuralgia: a quantitative systematic review. J Pain Symptom Manage 2000;20:449-58.
35. McQuay HJ. Neuropathic pain: evidence matters. Eur J Pain 2002;6(suppl A):11-8.
36. Bartusch SL, Sanders BJ, D’Alessio JG, et al. Clonazepam for the treatment of lancinating phantom limb pain. Clin J Pain 1996;12:59-62.
37. Dellemijn PL, Fields HL. Do benzodiazepines have a role in chronic pain management? Pain 1994;57:137-52.
38. Ciccone DS, Just N, Bandilla EB, et al. Psychological correlates of opioid use in patients with chronic nonmalignant pain: a preliminary test of the downhill spiral hypothesis. J Pain Symptom Manage 2000;20:180-92.
39. Gomez-Perez FJ, Rull JA, Dies H, et al. Nortriptyline and fluphenazine in the symptomatic treatment of diabetic neuropathy: a double-blind cross-over study. Pain 1985;23:395-400.
40. Fishbain DA, Cutler RB, Lewis J, et al. Do the second-generation “atypical neuroleptics” have analgesic properties? A structured evidence-based review. Pain Med 2004;5:359-65.