User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Resistant somatoform symptoms: Try CBT and antidepressants
Treatment-resistant somatoform disorders are chronic (duration >1 year), can cause significant functional impairment, and respond poorly to routine care.
In the somatoform category, DSM-IV-TR includes diverse diagnoses such as conversion disorder, hypochondriasis, pain disorder, and body dysmorphic disorder. But like mismatched shoes, these disorders do not fit together well—one reason they are often misdiagnosed and ineffectively treated. This article describes:
- debate about how to categorize somatoform disorders—as psychological or physiologic
- evidence supporting psychotherapy and antidepressants to help patients with treatment-resistant somatoform disorders.
Psychobiologic causes of somatoform disorders are poorly understood. In a recent review, Rief and Barsky1 emphasized that somatoform symptoms such as abdominal pain, headaches, or dizziness “are not strictly mental events, but are associated with a diversity of biological processes.” They propose that the following factors might contribute to somatoform disorders.
Autonomic physiologic arousal may lead patients to misperceive the meaning of normal bodily symptoms, but most studies have been equivocal or correlate closely with changes in the cardiovascular system. For example, patients with somatoform spectrum disorders who performed mentally distressing tasks did not have the same decrease in heart rate after completing the task as normal controls did, suggesting a deficit in autonomic reactivity.
Hypothalamic-pituitary-adrenal (HPA) axis studies also have been equivocal. Some have found low cortisol in patients with somatoform disorders—suggesting commonalities with conditions such as posttraumatic stress disorder—but other studies have found normal or even elevated cortisol. Although a relationship between the HPA axis and somatoform disorders is likely, its nature remains unclear or may be indirect.
Serotonin is known to alter pain perception in major depressive disorder, so this neurotransmitter also probably plays a role in somatoform disorders. Low serotonin—mediated in part by alterations in branched-chain amino acid concentration—may be linked to increased pain perception.
Perception and filtering of body signals. A signal-filtering model of somatoform symptoms proposes that physical sensations enter consciousness influenced by numerous factors. These signals are then sent to a filter system, which itself is subject to factors that may decrease its activity. Cortical perception of distress may occur and symptoms begin to manifest if enough factors come into play.
Which category?
Somatoform disorders are common in primary care. A medical utilization survey of 1,500 primary care patients found somatization symptoms in >20%.3 Controlling for comorbid psychiatric or medical illness did not change the study’s findings, which suggests that somatization is a distinct entity and not a symptom of another underlying disorder.
Little is known about somatoform disorders’ pathophysiology (Box 1),1 but their unifying theme is that psychological factors contribute to, amplify, or alter the presentation of physical illness. Not only do these disorders not form a coherent DSM category, but—as described by Mayou et al2—the lack of clearly defined thresholds between normal and pathologic behaviors is one of numerous problems that complicate diagnosis and treatment (Box 2).
Psychosomatic diad. Despite DSM-IV’s claims to etiologic neutrality, the origin of somatoform disorders’ physical symptoms clearly is meant to be psychological. As Lipowski4 said, somatization is “a tendency to experience and express somatic distress and symptoms unaccounted for by pathological findings, to attribute them to physical illness, and to seek medical help for them. It is often assumed that somatization becomes manifest in response to psychosocial stress brought about by life events that are personally stressful to the individual.”
Kroenke and others,5,6 however, have pointed out 2 shortcomings of this definition:
- the difficulty in knowing when a physical symptom truly is unexplained, especially in patients with comorbid medical illness5
- the instability of somatoform diagnoses (in a cohort examined with the same questionnaire 12 months apart, 43% of “lifetime somatic symptoms” patients reported at the first screening were not reported at the second).6
Similarly, Mayou et al2 contend that because most patients with somatoform disorders are treated by primary care physicians, having their disorders understood as psychiatric does not serve them well.
Psychiatric component. Conversely, patients with somatization disorder often have psychological symptoms, and many have personality disorders. The number of somatic symptoms with unexplained cause may be a normally distributed trait, with somatization disorders at the extreme end of the spectrum. Thus:
- Hypochondriasis could be reconsidered as health anxiety disorder because it features anxiety about potential illness.2
- Conversion disorders might be regrouped with other disorders focused on dissociation.2
- Body dysmorphic disorder might be regrouped with obsessive-compulsive disorder.7
These changes would shift focus away from the disorders’ physiologic presentations, emphasize the psychiatric disorders to which they likely are related, and provide insight into treatments and clinical investigations.
Pain disorder could be removed from DSM because of persistent concerns about the validity of this diagnostic category. Tyrer8 reviewed his clinical experience and reported shifting from a view that people with excessive pain had a psychiatric disorder to the view that living with chronic pain produces a profile similar to that of a person with a psychiatric disorder.
- Somatoform disorders lack clearly defined thresholds that establish a difference between normal and pathologic behaviors
- Somatoform disorders do not form a coherent category, and exclusion criteria are ambiguous
- By existing, the category suggests that some disorders are physical and others are mental, leaving little room for intermediate or mixed conditions
- Patients reject the term “somatoform” because it conveys doubt about the reality of their conditions
- Somatoform disorders are incompatible with some cultures’ views of mental illness (for example, the DSM translation used in China does not include the somatoform category)
- Nonspecific somatoform illness subcategories cannot achieve established reliability standards in studies examining diagnoses
- Medical-legal cases and insurance entitlements are complicated by unclear descriptions of somatoform disorders
- Carefully evaluate for mood, anxiety, and substance use disorders
- Assess over-the-counter, prescription, and illicit drugs the patient may be using to control pain and other physical symptoms
- Review medical and psychiatric records, laboratory and radiographic findings
- Discuss the patient’s case with his or her primary care physician, and provide formal feedback or a consultation letter
- Treat comorbid psychiatric disorders with medications such as selective serotonin reuptake inhibitors or venlafaxine, which have improved somatoform symptoms in randomized, controlled trials
- Offer the patient cognitive-behavioral therapy (10 to 20 sessions) that focuses on reducing somatoform symptoms, and advise the primary care provider to schedule monthly follow-up intervals
New treatment approaches
As the categorization debate continues, a treatment approach is developing that includes cognitive-behavioral therapy (CBT) and antidepressants to address the psychological and physiologic effects of resistant somatoform disorders (Box 3).
Consultation letters. Sending a consultation letter to the patient’s primary care physician is considered the standard of care (Box 4).11 In the study that introduced the consultation letter,12 patients with somatization disorder were randomly assigned to treatment (a consultation letter) or control (treatment as usual). Health care utilization costs declined approximately 50%—largely because of decreased hospitalization—when patients’ physicians received consultation letters, compared with no change for usual treatment.
Consultation letters may reduce health care spending but are less effective in improving symptoms. Evidence is changing treatment as psychotherapies have been found to help patients with somatoform disorders.
Group psychotherapy. In a controlled trial, primary care patients with somatization disorder received short-term group CBT or treatment as usual, with follow-up 6 months later. Those in the CBT group—who had received patient education and relaxation training—showed moderate but significant improvement in physical illness and somatic preoccupation, hypochondriasis, and medication use. Usual-care patients did not improve.13
CBT vs relaxation. A group of 191 inpatients described as “highly impaired” by somatization syndrome—≥8 DSM-IV somatoform symptoms—was evaluated for psychopathology, subjective health status, and life satisfaction. They then were randomly assigned to somatization-focused CBT (“soma”) or relaxation training and compared with 34 control patients. At 1-year follow-up, doctor visits had declined significantly in patients who received CBT (“soma”), and their somatoform symptoms were reduced compared with controls’.11
Psychotherapy vs listening. In a randomized, controlled trial, 102 patients with chronic refractory irritable bowel syndrome were assigned to receive exploratory psychotherapy or supportive listening. After 12 weeks, psychotherapy was more effective in improving physical and psychological symptoms, although the difference was statistically significant only in women. After 1 year, patients who received psychotherapy remained well and control patients who declined psychotherapy had relapsed.14
CBT vs usual treatment. In a randomized controlled trial, 84 patients with somatization disorder received 10 CBT sessions or treatment as usual. CBT’s goals were to:
- reduce physiologic arousal though relaxation techniques
- enhance activity regulation through increasing exercise and meaningful pleasurable activities and pacing activities
- increase awareness of emotions
- modify dysfunctional beliefs
- enhance communication of thoughts and emotions
- reduce spousal reinforcement of illness behavior.
Psychotherapy’s success in these and other studies supports the idea that somatoform spectrum disorders resemble other conditions—such as mood and anxiety disorders—that respond to psychological treatment.
Antidepressant therapy
Controlled trials also have shown that some antidepressants are more effective than placebo in improving somatoform symptoms.
St. John’s wort. In a randomized, placebo-controlled, double-blind trial, 184 patients with somatoform disorders but not major depression received St. John’s wort extract, 300 mg bid, or placebo. After 6 weeks, 45% of patients responded to St. John’s wort, compared with 21% for placebo (P=0.0006). Six measures determined response; St. John’s wort and placebo were equally well tolerated.16
Describe somatoform disorder, its relapsing course, and low morbidity and mortality rates
Encourage the primary care physician to:
- serve as the patient’s primary doctor and avoid fragmented care from numerous sources
- schedule regular appointments with the patient
- perform physical exams at each visit
- eliminate unnecessary tests or hospitalizations
- avoid statements such as “it’s all in your head” when medical tests are negative
Primary outcome was change in the 15-item Patient Health Questionnaire (PHQ-15) somatic symptom severity score. After 12 weeks, PHQ-15 scores declined significantly (P P=0.097). Among secondary measures, venlafaxine ER was more effective than placebo in improving bodily pain (P=0.03), physical symptoms (P=0.02), and anxiety (P=0.02).17
Citalopram. In an 8-week trial, investigators compared the efficacy of a selective serotonin reuptake inhibitor (SSRI) and a selective noradrenaline reuptake inhibitor (SNRI) on pain symptoms in 35 patients with somatoform pain disorder. Patients were randomly assigned to double-blind treatment with the SSRI citalopram, 40 mg/d (n=17), or the SNRI reboxetine, 8 mg/d (n=18).
In patients receiving citalopram, scores decreased significantly from baseline on the Present Pain Intensity scale (3.5 vs 2.8, P=0.045) and Total Pain Rating Index of the McGill Pain Questionnaire (41.9 vs 30, P=0.004), but these scores did not change significantly in patients receiving reboxetine. Depression symptoms, as measured by the Zung Self-Rating Depression Scale, did not change significantly in either group.
The authors concluded that citalopram was moderately effective for somatoform pain disorder in this small trial. Although antidepressants’ efficacy for somatoform symptoms may be mediated through changes in comorbid mood and anxiety disorders, these authors observed that citalopram’s analgesic effect appeared to be independent of how patients rated their depressive symptoms.18
Treatment recommendations
Based on the evidence and our experience, we recommend offering CBT to patients with recent symptom onset and insight into their comorbid mood and anxiety disorders. If the patient does not improve after 8 to 12 sessions, consider adding an antidepressant such as:
- citalopram, 20 to 60 mg/d
- venlafaxine XR, 150 to 375 mg/d.
Side effects are a frequent concern in this patient population, so titrate dosages slowly. Aim for the target antidepressant dosages used to treat major depression, and avoid declaring a treatment failure without first completing adequate trials. Once the patient is stable on medication, continue for a least 1 somatization-free year.
Allow patients to discuss their physical concerns, and attempt to support them in their suffering. At the same time, help them focus on attaining realistic goals for occupational and social functioning.
Work closely with the primary care provider in treatment planning to avoid sending the patient mixed messages. Communicating in the spirit of respect and collaboration with primary care colleagues can help prevent “splitting,” in which the patient may come to idealize one practitioner and devalue the other.
Remember that patients with somatization can become medically ill. Remind their primary care providers to perform expected evaluations as dictated by objective findings.
Related resources
- VHA/DoD clinical practice guideline for the management of medically unexplained symptoms: chronic pain and fatigue (brief summary). www.guideline.gov/summary/summary.aspx?doc_id=3415.
- Abbey SE. Somatization and somatoform disorders. In: Levenson JL, ed. The American Psychiatric Publishing textbook of psychosomatic medicine. Washington, DC: American Psychiatric Publishing; 2005:271-96.
Drug brand names
- Citalopram • Celexa
- Venlafaxine extended-release • Effexor XR
Dr. Marcangelo reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Wise is a consultant to or speaker for Eli Lilly and Co., GlaxoSmithKline, and Pfizer.
1. Rief W, Barsky AJ. Psychobiological perspectives on somatoform disorders. Psychoneuroendocrinology 2005;30(10):996-1002.
2. Mayou R, Kirmayer LJ, Simon G, et al. Somatoform disorders: time for a new approach in DSM-V. Am J Psychiatry 2005;162(5):847-55.
3. Barsky AJ, Orav EJ, Bates DW. Somatization increases medical utilization and costs independent of psychiatric and medical comorbidity. Arch Gen Psychiatry 2005;62(8):903-10.
4. Lipowski ZJ. Somatization: the experience and communication of psychological distress as somatic symptoms. Psychother Psychosom 1987;47(3-4):160-7.
5. Kroenke K. Physical symptom disorder: a simpler diagnostic category for somatization-spectrum conditions. J Psychosom Res 2006;60(4):335-9.
6. Simon GE, Gureje O. Stability of somatization disorder and somatization symptoms among primary care patients. Arch Gen Psychiatry 1999;56(1):90-5.
7. Phillips KA, McElroy SL, Hudson JI, Pope HG, Jr. Body dysmorphic disorder: an obsessive-compulsive spectrum disorder, a form of affective spectrum disorder, or both? J Clin Psychiatry 1995;56(suppl 4):41-51.
8. Tyrer S. Psychosomatic pain. Br J Psychiatry 2006;188:91-3.
9. Starcevic V. Somatoform disorders and DSM-V: conceptual and political issues in the debate. Psychosomatics 2006;47(4):277-81.
10. Hiller W, Rief W. Why DSM-III was right to introduce the concept of somatoform disorders. Psychosomatics 2005;46(2):105-8.
11. Bleichhardt G, Timmer B, Rief W. Cognitive-behavioural therapy for patients with multiple somatoform symptoms—a randomised controlled trial in tertiary care. J Psychosom Res 2004;56(4):449-54.
12. Smith GR, Jr, Monson RA, Ray DC. Psychiatric consultation in somatization disorder. A randomized controlled study. N Engl J Med 1986;314(22):1407-13.
13. Lidbeck J. Group therapy for somatization disorders in general practice: effectiveness of a short cognitive-behavioural treatment model. Acta Psychiatr Scand 1997;96(1):14-24.
14. Guthrie E, Creed F, Dawson D, Tomenson B. A randomised controlled trial of psychotherapy in patients with refractory irritable bowel syndrome. Br J Psychiatry 1993;163:315-21.
15. Allen LA, Woolfolk RL, Escobar JI, et al. Cognitive-behavioral therapy for somatization disorder: a randomized controlled trial. Arch Intern Med 2006;166(14):1512-8.
16. Muller T, Mannel M, Murck H, Rahlfs VW. Treatment of somatoform disorders with St. John’s wort: a randomized, double-blind and placebo-controlled trial. Psychosom Med 2004;66(4):538-47.
17. Kroenke K, Messina N, 3rd, Benattia I, et al. Venlafaxine extended release in the short-term treatment of depressed and anxious primary care patients with multisomatoform disorder. J Clin Psychiatry 2006;67(1):72-80.
18. Aragona M, Bancheri L, Perinelli D, et al. Randomized double-blind comparison of serotonergic (citalopram) versus noradrenergic (reboxetine) reuptake inhibitors in outpatients with somatoform, DSM-IV-TR pain disorder. Eur J Pain 2005;9(1):33-8.
Treatment-resistant somatoform disorders are chronic (duration >1 year), can cause significant functional impairment, and respond poorly to routine care.
In the somatoform category, DSM-IV-TR includes diverse diagnoses such as conversion disorder, hypochondriasis, pain disorder, and body dysmorphic disorder. But like mismatched shoes, these disorders do not fit together well—one reason they are often misdiagnosed and ineffectively treated. This article describes:
- debate about how to categorize somatoform disorders—as psychological or physiologic
- evidence supporting psychotherapy and antidepressants to help patients with treatment-resistant somatoform disorders.
Psychobiologic causes of somatoform disorders are poorly understood. In a recent review, Rief and Barsky1 emphasized that somatoform symptoms such as abdominal pain, headaches, or dizziness “are not strictly mental events, but are associated with a diversity of biological processes.” They propose that the following factors might contribute to somatoform disorders.
Autonomic physiologic arousal may lead patients to misperceive the meaning of normal bodily symptoms, but most studies have been equivocal or correlate closely with changes in the cardiovascular system. For example, patients with somatoform spectrum disorders who performed mentally distressing tasks did not have the same decrease in heart rate after completing the task as normal controls did, suggesting a deficit in autonomic reactivity.
Hypothalamic-pituitary-adrenal (HPA) axis studies also have been equivocal. Some have found low cortisol in patients with somatoform disorders—suggesting commonalities with conditions such as posttraumatic stress disorder—but other studies have found normal or even elevated cortisol. Although a relationship between the HPA axis and somatoform disorders is likely, its nature remains unclear or may be indirect.
Serotonin is known to alter pain perception in major depressive disorder, so this neurotransmitter also probably plays a role in somatoform disorders. Low serotonin—mediated in part by alterations in branched-chain amino acid concentration—may be linked to increased pain perception.
Perception and filtering of body signals. A signal-filtering model of somatoform symptoms proposes that physical sensations enter consciousness influenced by numerous factors. These signals are then sent to a filter system, which itself is subject to factors that may decrease its activity. Cortical perception of distress may occur and symptoms begin to manifest if enough factors come into play.
Which category?
Somatoform disorders are common in primary care. A medical utilization survey of 1,500 primary care patients found somatization symptoms in >20%.3 Controlling for comorbid psychiatric or medical illness did not change the study’s findings, which suggests that somatization is a distinct entity and not a symptom of another underlying disorder.
Little is known about somatoform disorders’ pathophysiology (Box 1),1 but their unifying theme is that psychological factors contribute to, amplify, or alter the presentation of physical illness. Not only do these disorders not form a coherent DSM category, but—as described by Mayou et al2—the lack of clearly defined thresholds between normal and pathologic behaviors is one of numerous problems that complicate diagnosis and treatment (Box 2).
Psychosomatic diad. Despite DSM-IV’s claims to etiologic neutrality, the origin of somatoform disorders’ physical symptoms clearly is meant to be psychological. As Lipowski4 said, somatization is “a tendency to experience and express somatic distress and symptoms unaccounted for by pathological findings, to attribute them to physical illness, and to seek medical help for them. It is often assumed that somatization becomes manifest in response to psychosocial stress brought about by life events that are personally stressful to the individual.”
Kroenke and others,5,6 however, have pointed out 2 shortcomings of this definition:
- the difficulty in knowing when a physical symptom truly is unexplained, especially in patients with comorbid medical illness5
- the instability of somatoform diagnoses (in a cohort examined with the same questionnaire 12 months apart, 43% of “lifetime somatic symptoms” patients reported at the first screening were not reported at the second).6
Similarly, Mayou et al2 contend that because most patients with somatoform disorders are treated by primary care physicians, having their disorders understood as psychiatric does not serve them well.
Psychiatric component. Conversely, patients with somatization disorder often have psychological symptoms, and many have personality disorders. The number of somatic symptoms with unexplained cause may be a normally distributed trait, with somatization disorders at the extreme end of the spectrum. Thus:
- Hypochondriasis could be reconsidered as health anxiety disorder because it features anxiety about potential illness.2
- Conversion disorders might be regrouped with other disorders focused on dissociation.2
- Body dysmorphic disorder might be regrouped with obsessive-compulsive disorder.7
These changes would shift focus away from the disorders’ physiologic presentations, emphasize the psychiatric disorders to which they likely are related, and provide insight into treatments and clinical investigations.
Pain disorder could be removed from DSM because of persistent concerns about the validity of this diagnostic category. Tyrer8 reviewed his clinical experience and reported shifting from a view that people with excessive pain had a psychiatric disorder to the view that living with chronic pain produces a profile similar to that of a person with a psychiatric disorder.
- Somatoform disorders lack clearly defined thresholds that establish a difference between normal and pathologic behaviors
- Somatoform disorders do not form a coherent category, and exclusion criteria are ambiguous
- By existing, the category suggests that some disorders are physical and others are mental, leaving little room for intermediate or mixed conditions
- Patients reject the term “somatoform” because it conveys doubt about the reality of their conditions
- Somatoform disorders are incompatible with some cultures’ views of mental illness (for example, the DSM translation used in China does not include the somatoform category)
- Nonspecific somatoform illness subcategories cannot achieve established reliability standards in studies examining diagnoses
- Medical-legal cases and insurance entitlements are complicated by unclear descriptions of somatoform disorders
- Carefully evaluate for mood, anxiety, and substance use disorders
- Assess over-the-counter, prescription, and illicit drugs the patient may be using to control pain and other physical symptoms
- Review medical and psychiatric records, laboratory and radiographic findings
- Discuss the patient’s case with his or her primary care physician, and provide formal feedback or a consultation letter
- Treat comorbid psychiatric disorders with medications such as selective serotonin reuptake inhibitors or venlafaxine, which have improved somatoform symptoms in randomized, controlled trials
- Offer the patient cognitive-behavioral therapy (10 to 20 sessions) that focuses on reducing somatoform symptoms, and advise the primary care provider to schedule monthly follow-up intervals
New treatment approaches
As the categorization debate continues, a treatment approach is developing that includes cognitive-behavioral therapy (CBT) and antidepressants to address the psychological and physiologic effects of resistant somatoform disorders (Box 3).
Consultation letters. Sending a consultation letter to the patient’s primary care physician is considered the standard of care (Box 4).11 In the study that introduced the consultation letter,12 patients with somatization disorder were randomly assigned to treatment (a consultation letter) or control (treatment as usual). Health care utilization costs declined approximately 50%—largely because of decreased hospitalization—when patients’ physicians received consultation letters, compared with no change for usual treatment.
Consultation letters may reduce health care spending but are less effective in improving symptoms. Evidence is changing treatment as psychotherapies have been found to help patients with somatoform disorders.
Group psychotherapy. In a controlled trial, primary care patients with somatization disorder received short-term group CBT or treatment as usual, with follow-up 6 months later. Those in the CBT group—who had received patient education and relaxation training—showed moderate but significant improvement in physical illness and somatic preoccupation, hypochondriasis, and medication use. Usual-care patients did not improve.13
CBT vs relaxation. A group of 191 inpatients described as “highly impaired” by somatization syndrome—≥8 DSM-IV somatoform symptoms—was evaluated for psychopathology, subjective health status, and life satisfaction. They then were randomly assigned to somatization-focused CBT (“soma”) or relaxation training and compared with 34 control patients. At 1-year follow-up, doctor visits had declined significantly in patients who received CBT (“soma”), and their somatoform symptoms were reduced compared with controls’.11
Psychotherapy vs listening. In a randomized, controlled trial, 102 patients with chronic refractory irritable bowel syndrome were assigned to receive exploratory psychotherapy or supportive listening. After 12 weeks, psychotherapy was more effective in improving physical and psychological symptoms, although the difference was statistically significant only in women. After 1 year, patients who received psychotherapy remained well and control patients who declined psychotherapy had relapsed.14
CBT vs usual treatment. In a randomized controlled trial, 84 patients with somatization disorder received 10 CBT sessions or treatment as usual. CBT’s goals were to:
- reduce physiologic arousal though relaxation techniques
- enhance activity regulation through increasing exercise and meaningful pleasurable activities and pacing activities
- increase awareness of emotions
- modify dysfunctional beliefs
- enhance communication of thoughts and emotions
- reduce spousal reinforcement of illness behavior.
Psychotherapy’s success in these and other studies supports the idea that somatoform spectrum disorders resemble other conditions—such as mood and anxiety disorders—that respond to psychological treatment.
Antidepressant therapy
Controlled trials also have shown that some antidepressants are more effective than placebo in improving somatoform symptoms.
St. John’s wort. In a randomized, placebo-controlled, double-blind trial, 184 patients with somatoform disorders but not major depression received St. John’s wort extract, 300 mg bid, or placebo. After 6 weeks, 45% of patients responded to St. John’s wort, compared with 21% for placebo (P=0.0006). Six measures determined response; St. John’s wort and placebo were equally well tolerated.16
Describe somatoform disorder, its relapsing course, and low morbidity and mortality rates
Encourage the primary care physician to:
- serve as the patient’s primary doctor and avoid fragmented care from numerous sources
- schedule regular appointments with the patient
- perform physical exams at each visit
- eliminate unnecessary tests or hospitalizations
- avoid statements such as “it’s all in your head” when medical tests are negative
Primary outcome was change in the 15-item Patient Health Questionnaire (PHQ-15) somatic symptom severity score. After 12 weeks, PHQ-15 scores declined significantly (P P=0.097). Among secondary measures, venlafaxine ER was more effective than placebo in improving bodily pain (P=0.03), physical symptoms (P=0.02), and anxiety (P=0.02).17
Citalopram. In an 8-week trial, investigators compared the efficacy of a selective serotonin reuptake inhibitor (SSRI) and a selective noradrenaline reuptake inhibitor (SNRI) on pain symptoms in 35 patients with somatoform pain disorder. Patients were randomly assigned to double-blind treatment with the SSRI citalopram, 40 mg/d (n=17), or the SNRI reboxetine, 8 mg/d (n=18).
In patients receiving citalopram, scores decreased significantly from baseline on the Present Pain Intensity scale (3.5 vs 2.8, P=0.045) and Total Pain Rating Index of the McGill Pain Questionnaire (41.9 vs 30, P=0.004), but these scores did not change significantly in patients receiving reboxetine. Depression symptoms, as measured by the Zung Self-Rating Depression Scale, did not change significantly in either group.
The authors concluded that citalopram was moderately effective for somatoform pain disorder in this small trial. Although antidepressants’ efficacy for somatoform symptoms may be mediated through changes in comorbid mood and anxiety disorders, these authors observed that citalopram’s analgesic effect appeared to be independent of how patients rated their depressive symptoms.18
Treatment recommendations
Based on the evidence and our experience, we recommend offering CBT to patients with recent symptom onset and insight into their comorbid mood and anxiety disorders. If the patient does not improve after 8 to 12 sessions, consider adding an antidepressant such as:
- citalopram, 20 to 60 mg/d
- venlafaxine XR, 150 to 375 mg/d.
Side effects are a frequent concern in this patient population, so titrate dosages slowly. Aim for the target antidepressant dosages used to treat major depression, and avoid declaring a treatment failure without first completing adequate trials. Once the patient is stable on medication, continue for a least 1 somatization-free year.
Allow patients to discuss their physical concerns, and attempt to support them in their suffering. At the same time, help them focus on attaining realistic goals for occupational and social functioning.
Work closely with the primary care provider in treatment planning to avoid sending the patient mixed messages. Communicating in the spirit of respect and collaboration with primary care colleagues can help prevent “splitting,” in which the patient may come to idealize one practitioner and devalue the other.
Remember that patients with somatization can become medically ill. Remind their primary care providers to perform expected evaluations as dictated by objective findings.
Related resources
- VHA/DoD clinical practice guideline for the management of medically unexplained symptoms: chronic pain and fatigue (brief summary). www.guideline.gov/summary/summary.aspx?doc_id=3415.
- Abbey SE. Somatization and somatoform disorders. In: Levenson JL, ed. The American Psychiatric Publishing textbook of psychosomatic medicine. Washington, DC: American Psychiatric Publishing; 2005:271-96.
Drug brand names
- Citalopram • Celexa
- Venlafaxine extended-release • Effexor XR
Dr. Marcangelo reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Wise is a consultant to or speaker for Eli Lilly and Co., GlaxoSmithKline, and Pfizer.
Treatment-resistant somatoform disorders are chronic (duration >1 year), can cause significant functional impairment, and respond poorly to routine care.
In the somatoform category, DSM-IV-TR includes diverse diagnoses such as conversion disorder, hypochondriasis, pain disorder, and body dysmorphic disorder. But like mismatched shoes, these disorders do not fit together well—one reason they are often misdiagnosed and ineffectively treated. This article describes:
- debate about how to categorize somatoform disorders—as psychological or physiologic
- evidence supporting psychotherapy and antidepressants to help patients with treatment-resistant somatoform disorders.
Psychobiologic causes of somatoform disorders are poorly understood. In a recent review, Rief and Barsky1 emphasized that somatoform symptoms such as abdominal pain, headaches, or dizziness “are not strictly mental events, but are associated with a diversity of biological processes.” They propose that the following factors might contribute to somatoform disorders.
Autonomic physiologic arousal may lead patients to misperceive the meaning of normal bodily symptoms, but most studies have been equivocal or correlate closely with changes in the cardiovascular system. For example, patients with somatoform spectrum disorders who performed mentally distressing tasks did not have the same decrease in heart rate after completing the task as normal controls did, suggesting a deficit in autonomic reactivity.
Hypothalamic-pituitary-adrenal (HPA) axis studies also have been equivocal. Some have found low cortisol in patients with somatoform disorders—suggesting commonalities with conditions such as posttraumatic stress disorder—but other studies have found normal or even elevated cortisol. Although a relationship between the HPA axis and somatoform disorders is likely, its nature remains unclear or may be indirect.
Serotonin is known to alter pain perception in major depressive disorder, so this neurotransmitter also probably plays a role in somatoform disorders. Low serotonin—mediated in part by alterations in branched-chain amino acid concentration—may be linked to increased pain perception.
Perception and filtering of body signals. A signal-filtering model of somatoform symptoms proposes that physical sensations enter consciousness influenced by numerous factors. These signals are then sent to a filter system, which itself is subject to factors that may decrease its activity. Cortical perception of distress may occur and symptoms begin to manifest if enough factors come into play.
Which category?
Somatoform disorders are common in primary care. A medical utilization survey of 1,500 primary care patients found somatization symptoms in >20%.3 Controlling for comorbid psychiatric or medical illness did not change the study’s findings, which suggests that somatization is a distinct entity and not a symptom of another underlying disorder.
Little is known about somatoform disorders’ pathophysiology (Box 1),1 but their unifying theme is that psychological factors contribute to, amplify, or alter the presentation of physical illness. Not only do these disorders not form a coherent DSM category, but—as described by Mayou et al2—the lack of clearly defined thresholds between normal and pathologic behaviors is one of numerous problems that complicate diagnosis and treatment (Box 2).
Psychosomatic diad. Despite DSM-IV’s claims to etiologic neutrality, the origin of somatoform disorders’ physical symptoms clearly is meant to be psychological. As Lipowski4 said, somatization is “a tendency to experience and express somatic distress and symptoms unaccounted for by pathological findings, to attribute them to physical illness, and to seek medical help for them. It is often assumed that somatization becomes manifest in response to psychosocial stress brought about by life events that are personally stressful to the individual.”
Kroenke and others,5,6 however, have pointed out 2 shortcomings of this definition:
- the difficulty in knowing when a physical symptom truly is unexplained, especially in patients with comorbid medical illness5
- the instability of somatoform diagnoses (in a cohort examined with the same questionnaire 12 months apart, 43% of “lifetime somatic symptoms” patients reported at the first screening were not reported at the second).6
Similarly, Mayou et al2 contend that because most patients with somatoform disorders are treated by primary care physicians, having their disorders understood as psychiatric does not serve them well.
Psychiatric component. Conversely, patients with somatization disorder often have psychological symptoms, and many have personality disorders. The number of somatic symptoms with unexplained cause may be a normally distributed trait, with somatization disorders at the extreme end of the spectrum. Thus:
- Hypochondriasis could be reconsidered as health anxiety disorder because it features anxiety about potential illness.2
- Conversion disorders might be regrouped with other disorders focused on dissociation.2
- Body dysmorphic disorder might be regrouped with obsessive-compulsive disorder.7
These changes would shift focus away from the disorders’ physiologic presentations, emphasize the psychiatric disorders to which they likely are related, and provide insight into treatments and clinical investigations.
Pain disorder could be removed from DSM because of persistent concerns about the validity of this diagnostic category. Tyrer8 reviewed his clinical experience and reported shifting from a view that people with excessive pain had a psychiatric disorder to the view that living with chronic pain produces a profile similar to that of a person with a psychiatric disorder.
- Somatoform disorders lack clearly defined thresholds that establish a difference between normal and pathologic behaviors
- Somatoform disorders do not form a coherent category, and exclusion criteria are ambiguous
- By existing, the category suggests that some disorders are physical and others are mental, leaving little room for intermediate or mixed conditions
- Patients reject the term “somatoform” because it conveys doubt about the reality of their conditions
- Somatoform disorders are incompatible with some cultures’ views of mental illness (for example, the DSM translation used in China does not include the somatoform category)
- Nonspecific somatoform illness subcategories cannot achieve established reliability standards in studies examining diagnoses
- Medical-legal cases and insurance entitlements are complicated by unclear descriptions of somatoform disorders
- Carefully evaluate for mood, anxiety, and substance use disorders
- Assess over-the-counter, prescription, and illicit drugs the patient may be using to control pain and other physical symptoms
- Review medical and psychiatric records, laboratory and radiographic findings
- Discuss the patient’s case with his or her primary care physician, and provide formal feedback or a consultation letter
- Treat comorbid psychiatric disorders with medications such as selective serotonin reuptake inhibitors or venlafaxine, which have improved somatoform symptoms in randomized, controlled trials
- Offer the patient cognitive-behavioral therapy (10 to 20 sessions) that focuses on reducing somatoform symptoms, and advise the primary care provider to schedule monthly follow-up intervals
New treatment approaches
As the categorization debate continues, a treatment approach is developing that includes cognitive-behavioral therapy (CBT) and antidepressants to address the psychological and physiologic effects of resistant somatoform disorders (Box 3).
Consultation letters. Sending a consultation letter to the patient’s primary care physician is considered the standard of care (Box 4).11 In the study that introduced the consultation letter,12 patients with somatization disorder were randomly assigned to treatment (a consultation letter) or control (treatment as usual). Health care utilization costs declined approximately 50%—largely because of decreased hospitalization—when patients’ physicians received consultation letters, compared with no change for usual treatment.
Consultation letters may reduce health care spending but are less effective in improving symptoms. Evidence is changing treatment as psychotherapies have been found to help patients with somatoform disorders.
Group psychotherapy. In a controlled trial, primary care patients with somatization disorder received short-term group CBT or treatment as usual, with follow-up 6 months later. Those in the CBT group—who had received patient education and relaxation training—showed moderate but significant improvement in physical illness and somatic preoccupation, hypochondriasis, and medication use. Usual-care patients did not improve.13
CBT vs relaxation. A group of 191 inpatients described as “highly impaired” by somatization syndrome—≥8 DSM-IV somatoform symptoms—was evaluated for psychopathology, subjective health status, and life satisfaction. They then were randomly assigned to somatization-focused CBT (“soma”) or relaxation training and compared with 34 control patients. At 1-year follow-up, doctor visits had declined significantly in patients who received CBT (“soma”), and their somatoform symptoms were reduced compared with controls’.11
Psychotherapy vs listening. In a randomized, controlled trial, 102 patients with chronic refractory irritable bowel syndrome were assigned to receive exploratory psychotherapy or supportive listening. After 12 weeks, psychotherapy was more effective in improving physical and psychological symptoms, although the difference was statistically significant only in women. After 1 year, patients who received psychotherapy remained well and control patients who declined psychotherapy had relapsed.14
CBT vs usual treatment. In a randomized controlled trial, 84 patients with somatization disorder received 10 CBT sessions or treatment as usual. CBT’s goals were to:
- reduce physiologic arousal though relaxation techniques
- enhance activity regulation through increasing exercise and meaningful pleasurable activities and pacing activities
- increase awareness of emotions
- modify dysfunctional beliefs
- enhance communication of thoughts and emotions
- reduce spousal reinforcement of illness behavior.
Psychotherapy’s success in these and other studies supports the idea that somatoform spectrum disorders resemble other conditions—such as mood and anxiety disorders—that respond to psychological treatment.
Antidepressant therapy
Controlled trials also have shown that some antidepressants are more effective than placebo in improving somatoform symptoms.
St. John’s wort. In a randomized, placebo-controlled, double-blind trial, 184 patients with somatoform disorders but not major depression received St. John’s wort extract, 300 mg bid, or placebo. After 6 weeks, 45% of patients responded to St. John’s wort, compared with 21% for placebo (P=0.0006). Six measures determined response; St. John’s wort and placebo were equally well tolerated.16
Describe somatoform disorder, its relapsing course, and low morbidity and mortality rates
Encourage the primary care physician to:
- serve as the patient’s primary doctor and avoid fragmented care from numerous sources
- schedule regular appointments with the patient
- perform physical exams at each visit
- eliminate unnecessary tests or hospitalizations
- avoid statements such as “it’s all in your head” when medical tests are negative
Primary outcome was change in the 15-item Patient Health Questionnaire (PHQ-15) somatic symptom severity score. After 12 weeks, PHQ-15 scores declined significantly (P P=0.097). Among secondary measures, venlafaxine ER was more effective than placebo in improving bodily pain (P=0.03), physical symptoms (P=0.02), and anxiety (P=0.02).17
Citalopram. In an 8-week trial, investigators compared the efficacy of a selective serotonin reuptake inhibitor (SSRI) and a selective noradrenaline reuptake inhibitor (SNRI) on pain symptoms in 35 patients with somatoform pain disorder. Patients were randomly assigned to double-blind treatment with the SSRI citalopram, 40 mg/d (n=17), or the SNRI reboxetine, 8 mg/d (n=18).
In patients receiving citalopram, scores decreased significantly from baseline on the Present Pain Intensity scale (3.5 vs 2.8, P=0.045) and Total Pain Rating Index of the McGill Pain Questionnaire (41.9 vs 30, P=0.004), but these scores did not change significantly in patients receiving reboxetine. Depression symptoms, as measured by the Zung Self-Rating Depression Scale, did not change significantly in either group.
The authors concluded that citalopram was moderately effective for somatoform pain disorder in this small trial. Although antidepressants’ efficacy for somatoform symptoms may be mediated through changes in comorbid mood and anxiety disorders, these authors observed that citalopram’s analgesic effect appeared to be independent of how patients rated their depressive symptoms.18
Treatment recommendations
Based on the evidence and our experience, we recommend offering CBT to patients with recent symptom onset and insight into their comorbid mood and anxiety disorders. If the patient does not improve after 8 to 12 sessions, consider adding an antidepressant such as:
- citalopram, 20 to 60 mg/d
- venlafaxine XR, 150 to 375 mg/d.
Side effects are a frequent concern in this patient population, so titrate dosages slowly. Aim for the target antidepressant dosages used to treat major depression, and avoid declaring a treatment failure without first completing adequate trials. Once the patient is stable on medication, continue for a least 1 somatization-free year.
Allow patients to discuss their physical concerns, and attempt to support them in their suffering. At the same time, help them focus on attaining realistic goals for occupational and social functioning.
Work closely with the primary care provider in treatment planning to avoid sending the patient mixed messages. Communicating in the spirit of respect and collaboration with primary care colleagues can help prevent “splitting,” in which the patient may come to idealize one practitioner and devalue the other.
Remember that patients with somatization can become medically ill. Remind their primary care providers to perform expected evaluations as dictated by objective findings.
Related resources
- VHA/DoD clinical practice guideline for the management of medically unexplained symptoms: chronic pain and fatigue (brief summary). www.guideline.gov/summary/summary.aspx?doc_id=3415.
- Abbey SE. Somatization and somatoform disorders. In: Levenson JL, ed. The American Psychiatric Publishing textbook of psychosomatic medicine. Washington, DC: American Psychiatric Publishing; 2005:271-96.
Drug brand names
- Citalopram • Celexa
- Venlafaxine extended-release • Effexor XR
Dr. Marcangelo reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Wise is a consultant to or speaker for Eli Lilly and Co., GlaxoSmithKline, and Pfizer.
1. Rief W, Barsky AJ. Psychobiological perspectives on somatoform disorders. Psychoneuroendocrinology 2005;30(10):996-1002.
2. Mayou R, Kirmayer LJ, Simon G, et al. Somatoform disorders: time for a new approach in DSM-V. Am J Psychiatry 2005;162(5):847-55.
3. Barsky AJ, Orav EJ, Bates DW. Somatization increases medical utilization and costs independent of psychiatric and medical comorbidity. Arch Gen Psychiatry 2005;62(8):903-10.
4. Lipowski ZJ. Somatization: the experience and communication of psychological distress as somatic symptoms. Psychother Psychosom 1987;47(3-4):160-7.
5. Kroenke K. Physical symptom disorder: a simpler diagnostic category for somatization-spectrum conditions. J Psychosom Res 2006;60(4):335-9.
6. Simon GE, Gureje O. Stability of somatization disorder and somatization symptoms among primary care patients. Arch Gen Psychiatry 1999;56(1):90-5.
7. Phillips KA, McElroy SL, Hudson JI, Pope HG, Jr. Body dysmorphic disorder: an obsessive-compulsive spectrum disorder, a form of affective spectrum disorder, or both? J Clin Psychiatry 1995;56(suppl 4):41-51.
8. Tyrer S. Psychosomatic pain. Br J Psychiatry 2006;188:91-3.
9. Starcevic V. Somatoform disorders and DSM-V: conceptual and political issues in the debate. Psychosomatics 2006;47(4):277-81.
10. Hiller W, Rief W. Why DSM-III was right to introduce the concept of somatoform disorders. Psychosomatics 2005;46(2):105-8.
11. Bleichhardt G, Timmer B, Rief W. Cognitive-behavioural therapy for patients with multiple somatoform symptoms—a randomised controlled trial in tertiary care. J Psychosom Res 2004;56(4):449-54.
12. Smith GR, Jr, Monson RA, Ray DC. Psychiatric consultation in somatization disorder. A randomized controlled study. N Engl J Med 1986;314(22):1407-13.
13. Lidbeck J. Group therapy for somatization disorders in general practice: effectiveness of a short cognitive-behavioural treatment model. Acta Psychiatr Scand 1997;96(1):14-24.
14. Guthrie E, Creed F, Dawson D, Tomenson B. A randomised controlled trial of psychotherapy in patients with refractory irritable bowel syndrome. Br J Psychiatry 1993;163:315-21.
15. Allen LA, Woolfolk RL, Escobar JI, et al. Cognitive-behavioral therapy for somatization disorder: a randomized controlled trial. Arch Intern Med 2006;166(14):1512-8.
16. Muller T, Mannel M, Murck H, Rahlfs VW. Treatment of somatoform disorders with St. John’s wort: a randomized, double-blind and placebo-controlled trial. Psychosom Med 2004;66(4):538-47.
17. Kroenke K, Messina N, 3rd, Benattia I, et al. Venlafaxine extended release in the short-term treatment of depressed and anxious primary care patients with multisomatoform disorder. J Clin Psychiatry 2006;67(1):72-80.
18. Aragona M, Bancheri L, Perinelli D, et al. Randomized double-blind comparison of serotonergic (citalopram) versus noradrenergic (reboxetine) reuptake inhibitors in outpatients with somatoform, DSM-IV-TR pain disorder. Eur J Pain 2005;9(1):33-8.
1. Rief W, Barsky AJ. Psychobiological perspectives on somatoform disorders. Psychoneuroendocrinology 2005;30(10):996-1002.
2. Mayou R, Kirmayer LJ, Simon G, et al. Somatoform disorders: time for a new approach in DSM-V. Am J Psychiatry 2005;162(5):847-55.
3. Barsky AJ, Orav EJ, Bates DW. Somatization increases medical utilization and costs independent of psychiatric and medical comorbidity. Arch Gen Psychiatry 2005;62(8):903-10.
4. Lipowski ZJ. Somatization: the experience and communication of psychological distress as somatic symptoms. Psychother Psychosom 1987;47(3-4):160-7.
5. Kroenke K. Physical symptom disorder: a simpler diagnostic category for somatization-spectrum conditions. J Psychosom Res 2006;60(4):335-9.
6. Simon GE, Gureje O. Stability of somatization disorder and somatization symptoms among primary care patients. Arch Gen Psychiatry 1999;56(1):90-5.
7. Phillips KA, McElroy SL, Hudson JI, Pope HG, Jr. Body dysmorphic disorder: an obsessive-compulsive spectrum disorder, a form of affective spectrum disorder, or both? J Clin Psychiatry 1995;56(suppl 4):41-51.
8. Tyrer S. Psychosomatic pain. Br J Psychiatry 2006;188:91-3.
9. Starcevic V. Somatoform disorders and DSM-V: conceptual and political issues in the debate. Psychosomatics 2006;47(4):277-81.
10. Hiller W, Rief W. Why DSM-III was right to introduce the concept of somatoform disorders. Psychosomatics 2005;46(2):105-8.
11. Bleichhardt G, Timmer B, Rief W. Cognitive-behavioural therapy for patients with multiple somatoform symptoms—a randomised controlled trial in tertiary care. J Psychosom Res 2004;56(4):449-54.
12. Smith GR, Jr, Monson RA, Ray DC. Psychiatric consultation in somatization disorder. A randomized controlled study. N Engl J Med 1986;314(22):1407-13.
13. Lidbeck J. Group therapy for somatization disorders in general practice: effectiveness of a short cognitive-behavioural treatment model. Acta Psychiatr Scand 1997;96(1):14-24.
14. Guthrie E, Creed F, Dawson D, Tomenson B. A randomised controlled trial of psychotherapy in patients with refractory irritable bowel syndrome. Br J Psychiatry 1993;163:315-21.
15. Allen LA, Woolfolk RL, Escobar JI, et al. Cognitive-behavioral therapy for somatization disorder: a randomized controlled trial. Arch Intern Med 2006;166(14):1512-8.
16. Muller T, Mannel M, Murck H, Rahlfs VW. Treatment of somatoform disorders with St. John’s wort: a randomized, double-blind and placebo-controlled trial. Psychosom Med 2004;66(4):538-47.
17. Kroenke K, Messina N, 3rd, Benattia I, et al. Venlafaxine extended release in the short-term treatment of depressed and anxious primary care patients with multisomatoform disorder. J Clin Psychiatry 2006;67(1):72-80.
18. Aragona M, Bancheri L, Perinelli D, et al. Randomized double-blind comparison of serotonergic (citalopram) versus noradrenergic (reboxetine) reuptake inhibitors in outpatients with somatoform, DSM-IV-TR pain disorder. Eur J Pain 2005;9(1):33-8.
Transsexualism: Clinical guide to gender identity disorder
Adults with gender identity disorder (GID)—commonly termed transsexualism—may seek psychiatric assessment and treatment for a variety of reasons. Some—but not all—might be candidates for hormone replacement therapies or sex reassignment surgery (SRS). For those with gender dysphoria, psychological assessment and psychotherapy are suggested and sometimes required.
Your role in the GID patient’s gender exploration and transition must be tailored to his or her gender identity and individual circumstances. For patients who are not candidates for surgery or cannot afford it, you may assist in exploring options for living with one’s gender identity.
WHAT IS GID?
Gender identity disorder is a rare, complex condition in which individuals of unambiguous genotype and phenotype identify with the opposite gender. One in 54,000 individuals are estimated to have GID:
- 75% are biologic males desiring reassignment to female gender (MTF)
- 25% are females desiring to be male (FTM).1
Table 1
DSM-IV-TR criteria for gender identity disorder
| Criterion A | A strong and persistent cross-gender identification defined as the desire to be or the insistence that one is of the other sex (must not be merely a desire for any perceived cultural advantages of being the other sex) |
| Criterion B | Persistent discomfort with one’s assigned sex or a sense of inappropriateness in the gender role of that sex |
| Criterion C | The disturbance is not concurrent with a physical intersex condition (such as partial androgen insensitivity syndrome or congenital adrenal hyperplasia) |
| Criterion D | The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning |
| Source: Reference 2 | |
ICD-10 diagnoses for gender identity disorder in adults
| Diagnosis | Criteria |
|---|---|
| Transsexualism |
|
| Dual-role transvestism |
|
| Other gender identity disorders | No specific criteria; could be used for persons with an intersexed condition |
| Gender identify disorder, unspecified | No specific criteria; could be used for persons with an intersexed condition |
| Source: Adapted from International Classification of Diseases, 10th ed. (ICD-10) | |
Epidemiologic studies of GID are rare, but in a survey by Rachlin et al4 of 23 MTFs and 70 FTMs:
- most underwent hormone therapy (64% of MTFs, 80% of FTMs) and/or name change (45% of MTFs, 72% of FTMs)
- none of the MTFs had breast augmentation, whereas 52% of FTMs had undergone mastectomy and reconstruction and another 33% were actively planning it
- 3% of FTMs had genital surgery, 16% were planning it, and 29% had decided definitely not to have it
- 9% of MTFs decided definitely not to have genital surgery; 23% had undergone genital surgery, and another 35% were actively planning it.
Biologic basis. GID’s cause remains unknown. Organic differences in brain anatomy have been identified in patients with GID. Zhou et al6 showed that the volume of the central subdivision of the bed nucleus of the stria terminalis (BSTc)—a brain area essential for sexual behavior—is larger in men than in women. A female-sized BSTc was found in MTF GID patients.
Research, mainly on biologic boys, indicates that GIDs are usually associated with behavioral difficulties, relationship problems with peers and parents, and—most notably—separation anxiety disorder.7 An audit of the files of 124 children and adolescents with GID showed that 42% experienced loss of one or both parents, mainly through separation.8
Psychiatric comorbidity. Studies using standardized diagnostic instruments to assess psychiatric comorbidity in GID are rare. A study of 31 patients with GID found that many met diagnostic criteria for lifetime psychiatric comorbidity, including:
- 71% for Axis I disorders (primarily mood and anxiety disorders)
- 42% for comorbid personality disorders, primarily a cluster B diagnosis
- 45% for substance-related disorders
- 6.5% for psychotic disorders
- 3.2% for eating disorders.9
TREATING PATIENTS WITH GID
Psychotherapy. GID treatment decisions are made without clear prospective data. Standards of care are determined by the World Professional Association for Transgender Health (WPATH).12 Psychotherapy is often given before SRS but is not required. The therapist is left to determine the treatment terms and goals.
Your role in treating patients with GID goes beyond making an accurate diagnosis, identifying comorbid psychopathology, and instituting a treatment plan. Other tasks include:
- counseling the patient about the range of treatment options and their implications
- engaging in psychotherapy
- ascertaining eligibility and readiness for hormones and surgical therapy
- making formal recommendations to medical and surgical colleagues
- documenting the patient’s relevant history in a letter of recommendation
- educating support systems
- being available for follow-up.
Candidates for triadic therapy. For appropriately screened adults with severe GID, the therapeutic approach relies on triadic therapy:
- a 3-phase approach centered around real-life experience in the desired role
- hormones of the desired gender
- and surgery to change the genitalia and secondary sex characteristics.
HORMONE THERAPY
WPATH has established eligibility and readiness criteria for HRT in patients with GID (Table 3). Administering cross-sex hormones (testosterone in women; estrogens in men) brings about important physical changes as well as psychological relief. The prescribing physician need not be an endocrinologist but should become well-versed in relevant data.
Table 3
WPATH criteria for hormone replacement therapy*
| Eligibility criteria 3 criteria exist |
|
| Readiness criteria All 3 must exist |
|
| Source: World Professional Association for Transgender Health (WPATH) | |
Table 4
Sample hormonal regimens for transsexual patients*
| Medication | Starting dose | Subsequent dose | When to change doses | |
|---|---|---|---|---|
| Female to male | Testosterone enanthanate or testosterone cypionate | 200 mg IM every 2 weeks | 100 to 150 mg IM every 2 weeks | After masculinization complete and/or oophorectomy/hysterectomy |
| Transdermal testosterone | 5 mg to skin every day | Usually stays the same | Little data exist on efficacy; effective for maintenance, and may be less efficacious during transition | |
| Male to female | Conjugated estrogens | 1.25 mg/d (or 0.625 mg/d for smokers) | 2.5 mg/d (Do not increase in smokers) | To obtain best clinical results, or if testosterone is not suppressed After sexual reassignment surgery, dose may be decreased without losing secondary sexual characteristics |
| OR oral estradiol | 1 mg/d | 2 mg/d | ||
| OR transdermal estradiol | 0.1 mg patch/week | Two 0.1 mg patches/week | ||
| Spironolactone | 200 mg/d | May discontinue | After sexual assignment surgery | |
| Medroxyprogesterone† | 10 mg/d | May increase to 20 to 40 mg/d (usually not needed) | If testosterone is not suppressed and patient/doctor does not want to increase estrogen | |
| OR micronized progesterone | 100 mg bid | May discontinue after breast development is complete | Micronized progesterone is more costly but may lessen side effects of anxiety, as compared with medroxyprogesterone | |
| * Professional consensus does not exist regarding the most efficacious and safest dosing regimens for gender transition. This table reflects reasonable starting and maintenance doses that are supported in the (admittedly less than optimal) medical literature, and reflect the author’s opinion and practice. This table is not meant to include all possible hormone regimens, only several of the most commonly used medications. | ||||
| † Professional consensus does not exist regarding progesterone’s role in MTF transition. | ||||
| Adapted and reprinted with permission from Table VII in Oriel KA. Medical care of transsexual patients. J Gay Lesbian Med Asso 2000;4(4):193. | ||||
Transdermal testosterone is an option for biologic females who are leery of injections.13 Patches result in stable testosterone levels in the male range but may cause skin irritation in >50% of patients. Use transdermal estrogen in males with clotting abnormalities or who are age >40.
Medical workup. Basic medical monitoring includes serial physical examinations, vital signs, weight measurements, laboratory assessment, and screening for pelvic malignancies.
For biologic males receiving estrogen, pretreatment laboratory assessment includes free testosterone, fasting glucose, liver function tests, and complete blood count, with reassessment at 6 and 12 months and annually thereafter. Obtain pretreatment prolactin levels and repeat annually. If hyperprolactinemia fails to develop within 3 years, no further measurements are necessary. Monitor for breast and prostate cancer, and instruct patients to perform self-breast exams. Following orchiectomy, estrogen doses can be reduced by one-third to one-half.
For biologic women receiving androgen, obtain pretreatment liver function tests and complete blood count, then reassess at 6 months, 12 months, and annually thereafter. Do yearly liver palpation examinations.
Physiologic changes. Biologic males treated with estrogens can expect breast growth, redistribution of fat in keeping with female habitus, decreased upper body strength, decreased body hair, retardation of male pattern balding, diminished testicular size, and decrease in erection firmness and frequency. MTF transsexuals require electrolysis to remove facial hair, as HRT does not do this.
Biologic females treated with testosterone can expect deepening of the voice, clitoral enlargement, mild breast atrophy, increased facial and body hair and male-pattern baldness, increased upper body strength, weight gain, and decreased hip fat.
With effective and continuous dosages, most changes begin in 2 to 4 months, start becoming irreversible in 6 to 12 months, start to level off in 2 years, and are mostly complete in 5 years. Men with insufficient breast growth following HRT may pursue breast augmentation surgery.
Voice changes. Hormone therapy generally is presumed to “masculinize” the voice of FTM transsexuals. In one series, after initiation of hormone therapy, 12 of 16 (75%) FTM transsexuals believed they had a voice that always would be considered masculine.14,15
For MTF transsexuals, no surgical technique of pitch elevation is satisfactorily safe and effective. The most widely used—cricothyroid approximation—may not be long-lasting and can decrease range, loudness, and vocal quality.13
HRT COMPLICATIONS
Medical complications. Biologic males treated with estrogens and progestins may be at increased risk for blood clotting, benign pituitary prolactinomas, infertility, weight gain, liver disease, gallstones, somnolence, hypertension, and diabetes mellitus.
Biologic females treated with testosterone may be at increased risk for acne, cardiovascular disease from shifts of lipid profiles to male patterns, benign and malignant liver tumors, and hepatic dysfunction.
Psychiatric issues. Physical masculinization occurs much more rapidly and results in a more convincing opposite sex appearance in FTMs than feminization does in MTFs.16,17 Behaving masculine may be more socially acceptable for women and therefore easier than it is for men to behave convincingly feminine without being characterized.
Cross-sex hormones contribute to the expression of sex-dimorphic behaviors in adulthood.18,19 Estrogen appears to influence affect intensity, whereas androgens influence aggression and sexual motivation. Earlier studies established that untreated MTFs and FTMs do not differ in sex hormone levels from their biologic counterparts.20,21
After 3 months of HRT, transsexuals’ sex hormones are in the range of their identified sex. FTMs treated with androgens become more prone to aggression and exhibit increased sexual motivation and arousability associated with an overall dampened affect. MTFs treated with estrogen show decreased irritability and sexual arousability.22
SEX REASSIGNMENT SURGERY
The cost of SRS often is prohibitive. Patients may turn to the Internet or foreign venues for hormone therapy and surgical procedures. Thailand is a popular overseas destination, where the average cost for MTF surgery is approximately $6,000 to $9,000. In the United States the cost of counseling, hormones, electrolysis, and surgeries is typically $30,000 to $40,000.23
Surgical options are not limited to genital reassignment but include mammoplasty (breast augmentation for MTF), chest reduction surgery (FTM), trachea shave surgery, forehead/brow ridge contouring, chin and jaw contouring, scalp advancement surgery, cheek implant surgery, alarplasty (nasal base resection to narrow a nose), and chin contouring.
Some insurance companies assert that transsexual procedures are not medically necessary and are declining coverage. WPATH contends that sex reassignment is effective and medically indicated in severe GID.
Postsurgical outcomes. Patients who are emotionally healthy, have adequate social support, and attain reasonable cosmetic results are most satisfied with life after SRS.24 In studies of GID patients, the best predictor of postoperative psychopathology was poor surgical results.25
FTMs are transformed through the use of hormones and generally are not perceived as visibly different from other men. Genital surgery is often seen as a final step in completing the transition to the identified gender.
FTMs may elect to have their female reproductive organs removed, along with construction of male external genitalia through phalloplasty or metoidioplasty. The decision to pursue surgery and the type of procedure depend on peer influence.26 Although a phalloplasty does not provide a fully functioning and completely authentic-appearing penis, most FTMs report being satisfied with life after surgery and have few regrets.27-31
Long-term postoperative follow-up by the surgeon and mental health professional is associated with good psychosocial outcome.
Legal considerations. An individual’s new surgically created gender can cause legal complications in jurisdictions that do not recognize the new gender. Some states are amending laws to make allowances for these advances in medical science.32
- World Professional Association For Transgender Health. (formerly the Harry Benjamin International Gender Dysphoria Association [HBIGDA]). www.hbigda.org. Includes a directory of transgender organizations.
- North American gender programs and service centers
CAMH Gender Identity Clinic. Toronto, Ontario, Canada
Gender Identity Project, New York, NY
Gendercare Gender Clinic (Web clinic for gender variance). www.gendercare.com.
Ingersoll Gender Center, Seattle, Washington
Johns Hopkins Center for Sexual Health & Medicine, Baltimore, Maryland
Program in Human Sexuality, Transgender Services at the University of Minnesota - Sexology organizations and information
American Association of Sex Educators, Counselors, and Therapists. www.aasect.org.
Kinsey Institute at Indiana University. www.indiana.edu/%7Ekinsey.
Sexuality Information and Education Council of the United States. www.siecus.org.
Social Science Research Council. www.ssrc.org.
Society for the Scientific Study of Sexuality. www.sexscience.org.
- Conjugated equine estrogens • Premarin
- Estradiol (oral) • Estrace
- Estradiol (transdermal) • Climara
- Medroxyprogesterone (oral) • Provera
- Medroxyprogesterone (IM) • Depo-Provera
- Micronized progesterone • Prometrium
- Spironolactone • Aldactone
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Laden M, Walinder J, Lundstrom B. Prevalence, incidence and sex ratio of transsexualism. Acta Psychiatr Scand 1996;93(4):221-3.
2. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
3. World Health Organization (WHO). The ICD-10 classification of mental and behavioural disorders: diagnostic criteria for research. Geneva; 1993.
4. Rachlin K. Transgender individuals’ experiences of psychotherapy. Int J Transgender 2002;6-1.
5. Pfäfflin F, Junge A. Thirty years of international follow-up studies after sex reassignment surgery: a comprehensive review, 1961-1991. Dusseldorf: Symposium Publishing; 1998.
6. Zhou JN, Hofman MA, Gooren LJ, Swaab DF. A sex difference in the human brain and its relation to transsexuality. Nature 1995;378(6552):68-70.
7. Coates S, Pearson ES. Extreme boyhood femininity: isolated behavior or pervasive disorder? J Am Acad Child Psychiatry 1985;24(6):702-9.
8. Zucker KJ. Associated psychopathology in children with gender identity disorders. In: DiCeglie D, Freedman D, eds. A stranger in my own body: atypical gender identity development and mental health. London: Karnac Books; 1998.
9. Hepp U, Kramer B, Schnyder U, et al. Psychiatric comorbidity in gender identity disorder. J Psychosom Res 2005;58(3):259-61.
10. Cole S, Denny D, Eyler A, Samons S. Issues in transgender. In: Szuchman L, Muscarella F, eds. Psychological perspective on human sexuality. New York: John Wiley; 2000.
11. Jones B, Hill M. Mental health issues in lesbian, gay, bisexual, and transgender communities. Rev Psychol 2002;21:15-31.
12. Harry Benjamin international gender association standards of care for gender identity disorders, 6th version. Minneapolis, MN: The Harry Benjamin International Gender Dysphoria Association; 2001.
13. Assecheman J, Gooren LJG. Hormone treatment in transsexuals: interdisciplinary approaches in clinical management. J Psychol Human Sex 1992;5(4):39-54.
14. Van Borsel J, De Cuypere G, Van den Berghe H. Physical appearance and voice in male-to-female transsexuals. J Voice 2001;15(4):570-5.
15. Van Borsel J, De Cuypere G, Rubens R, Destaerke B. Voice problems in female-to-male transsexuals. Int J Lang Commun Disord 2000;35(3):427-42.
16. Spiegel J, Jalisi S. Contemporary diagnosis and management of head and neck cancer. Otolaryngol Clin North Am 2005;38(1):xiii-xiv.
17. Meyer WJ, 3rd, Webb A, Stuart CA, et al. Physical and hormonal evaluation of transsexual patients: a longitudinal study. Arch Sex Behav 1986;15(2):121-38.
18. Archer J. The influence of testosterone on human aggression. Br J Psychol 1991;82(Pt 1):1-28.
19. Van de Poll ME, Van Goozen SHM. Hypothalamic involvement in sexuality and hostility: comparative psychologic aspects. In: Swaab DF, Mirmiran M, Ravid R, Van Leeuwen FW, eds. The human hypothalamus in health and disease, progress in research. Amsterdam: Elsevier; 1992;343-61.
20. Spijkstra JJ, Spinder T, Gooren LJ. Short-term patterns of pulsatile luteinizing hormone secretion do not differ between male-to-female transsexuals and heterosexual men. Psychoneuroendocrinology 1988;13(3):279-83.
21. Spinder J, Spijkstra JJ, Gooren LJ, Burger CW. Pulsatile luteinizing hormone release and ovarian steroid levels in female-to-male transsexuals compared to heterosexual women. Psychoneuroendocrinology 1989;14(1-2):97-102.
22. Slabbekoorn D, Van Goozen S, Gooren L, Cohen-Kettenis P. Effects of cross-sex hormone treatment on emotionality in transsexuals. Int J Transgender [serial online] 2001;5(3). Available at: http://www.symposion.com/ijt/ijtvo05no03_02.htm. Accessed January 11, 2007.
23. Conway L. Vaginoplasty: male to female sex reassignment surgery: historical notes, descriptions, photos, and links. Available at: http://ai.eecs.umich.edu/people/conway/TS/SRS.html. Accessed January 12, 2007.
24. Bodlund O, Kullgren G. Transsexualism-general outcome and prognostic factors: a five-year follow-up study of nineteen transsexuals in the process of changing sex. Arch Sex Behav 1996;25(3):303-16.
25. Ross MW, Need JA. Effects of adequacy of gender reassignment surgery on psychologic adjustment: a followup of fourteen male-to-female patients. Arch Sex Behav 1989;18(2):145-53.
26. Rachlin K. Factors which influence individual’s decisions when considering female-to-male genital reconstructive surgery. Int J Transgender [serial online];1999;3(3). Available at: http://www.symposion.com/ijt/ijt990302.htm. Accessed January 11, 2007.
27. Lundstrom B, Pauly I, Walinder J. Outcome of sex reassignment surgery. Acta Psychiatr Scand 1984;70(4):289-94.
28. Kuiper B, Cohen-Kettenis P. Sex reassignment surgery: a study of 141 Dutch transsexuals. Arch Sex Behav 1988;17(5):439-57.
29. Green R, Fleming D. Transsexual surgery followup: status in the 1990s. Ann Rev Sex Res 1990;7:351-69.
30. Tsoi WF. Follow-up study of transsexuals after sex-reassignment surgery. Singapore Med J 1993;34(6):515-7.
31. Tsoi WF. Male to female transsexuals: a comparison. Singapore Med J 1992;33(2):182-5.
32. Harish D, Sharma BR. Medical advances in transsexualism and the legal implications. Am J Forensic Med Pathol 2003;24(1):100-5.
Adults with gender identity disorder (GID)—commonly termed transsexualism—may seek psychiatric assessment and treatment for a variety of reasons. Some—but not all—might be candidates for hormone replacement therapies or sex reassignment surgery (SRS). For those with gender dysphoria, psychological assessment and psychotherapy are suggested and sometimes required.
Your role in the GID patient’s gender exploration and transition must be tailored to his or her gender identity and individual circumstances. For patients who are not candidates for surgery or cannot afford it, you may assist in exploring options for living with one’s gender identity.
WHAT IS GID?
Gender identity disorder is a rare, complex condition in which individuals of unambiguous genotype and phenotype identify with the opposite gender. One in 54,000 individuals are estimated to have GID:
- 75% are biologic males desiring reassignment to female gender (MTF)
- 25% are females desiring to be male (FTM).1
Table 1
DSM-IV-TR criteria for gender identity disorder
| Criterion A | A strong and persistent cross-gender identification defined as the desire to be or the insistence that one is of the other sex (must not be merely a desire for any perceived cultural advantages of being the other sex) |
| Criterion B | Persistent discomfort with one’s assigned sex or a sense of inappropriateness in the gender role of that sex |
| Criterion C | The disturbance is not concurrent with a physical intersex condition (such as partial androgen insensitivity syndrome or congenital adrenal hyperplasia) |
| Criterion D | The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning |
| Source: Reference 2 | |
ICD-10 diagnoses for gender identity disorder in adults
| Diagnosis | Criteria |
|---|---|
| Transsexualism |
|
| Dual-role transvestism |
|
| Other gender identity disorders | No specific criteria; could be used for persons with an intersexed condition |
| Gender identify disorder, unspecified | No specific criteria; could be used for persons with an intersexed condition |
| Source: Adapted from International Classification of Diseases, 10th ed. (ICD-10) | |
Epidemiologic studies of GID are rare, but in a survey by Rachlin et al4 of 23 MTFs and 70 FTMs:
- most underwent hormone therapy (64% of MTFs, 80% of FTMs) and/or name change (45% of MTFs, 72% of FTMs)
- none of the MTFs had breast augmentation, whereas 52% of FTMs had undergone mastectomy and reconstruction and another 33% were actively planning it
- 3% of FTMs had genital surgery, 16% were planning it, and 29% had decided definitely not to have it
- 9% of MTFs decided definitely not to have genital surgery; 23% had undergone genital surgery, and another 35% were actively planning it.
Biologic basis. GID’s cause remains unknown. Organic differences in brain anatomy have been identified in patients with GID. Zhou et al6 showed that the volume of the central subdivision of the bed nucleus of the stria terminalis (BSTc)—a brain area essential for sexual behavior—is larger in men than in women. A female-sized BSTc was found in MTF GID patients.
Research, mainly on biologic boys, indicates that GIDs are usually associated with behavioral difficulties, relationship problems with peers and parents, and—most notably—separation anxiety disorder.7 An audit of the files of 124 children and adolescents with GID showed that 42% experienced loss of one or both parents, mainly through separation.8
Psychiatric comorbidity. Studies using standardized diagnostic instruments to assess psychiatric comorbidity in GID are rare. A study of 31 patients with GID found that many met diagnostic criteria for lifetime psychiatric comorbidity, including:
- 71% for Axis I disorders (primarily mood and anxiety disorders)
- 42% for comorbid personality disorders, primarily a cluster B diagnosis
- 45% for substance-related disorders
- 6.5% for psychotic disorders
- 3.2% for eating disorders.9
TREATING PATIENTS WITH GID
Psychotherapy. GID treatment decisions are made without clear prospective data. Standards of care are determined by the World Professional Association for Transgender Health (WPATH).12 Psychotherapy is often given before SRS but is not required. The therapist is left to determine the treatment terms and goals.
Your role in treating patients with GID goes beyond making an accurate diagnosis, identifying comorbid psychopathology, and instituting a treatment plan. Other tasks include:
- counseling the patient about the range of treatment options and their implications
- engaging in psychotherapy
- ascertaining eligibility and readiness for hormones and surgical therapy
- making formal recommendations to medical and surgical colleagues
- documenting the patient’s relevant history in a letter of recommendation
- educating support systems
- being available for follow-up.
Candidates for triadic therapy. For appropriately screened adults with severe GID, the therapeutic approach relies on triadic therapy:
- a 3-phase approach centered around real-life experience in the desired role
- hormones of the desired gender
- and surgery to change the genitalia and secondary sex characteristics.
HORMONE THERAPY
WPATH has established eligibility and readiness criteria for HRT in patients with GID (Table 3). Administering cross-sex hormones (testosterone in women; estrogens in men) brings about important physical changes as well as psychological relief. The prescribing physician need not be an endocrinologist but should become well-versed in relevant data.
Table 3
WPATH criteria for hormone replacement therapy*
| Eligibility criteria 3 criteria exist |
|
| Readiness criteria All 3 must exist |
|
| Source: World Professional Association for Transgender Health (WPATH) | |
Table 4
Sample hormonal regimens for transsexual patients*
| Medication | Starting dose | Subsequent dose | When to change doses | |
|---|---|---|---|---|
| Female to male | Testosterone enanthanate or testosterone cypionate | 200 mg IM every 2 weeks | 100 to 150 mg IM every 2 weeks | After masculinization complete and/or oophorectomy/hysterectomy |
| Transdermal testosterone | 5 mg to skin every day | Usually stays the same | Little data exist on efficacy; effective for maintenance, and may be less efficacious during transition | |
| Male to female | Conjugated estrogens | 1.25 mg/d (or 0.625 mg/d for smokers) | 2.5 mg/d (Do not increase in smokers) | To obtain best clinical results, or if testosterone is not suppressed After sexual reassignment surgery, dose may be decreased without losing secondary sexual characteristics |
| OR oral estradiol | 1 mg/d | 2 mg/d | ||
| OR transdermal estradiol | 0.1 mg patch/week | Two 0.1 mg patches/week | ||
| Spironolactone | 200 mg/d | May discontinue | After sexual assignment surgery | |
| Medroxyprogesterone† | 10 mg/d | May increase to 20 to 40 mg/d (usually not needed) | If testosterone is not suppressed and patient/doctor does not want to increase estrogen | |
| OR micronized progesterone | 100 mg bid | May discontinue after breast development is complete | Micronized progesterone is more costly but may lessen side effects of anxiety, as compared with medroxyprogesterone | |
| * Professional consensus does not exist regarding the most efficacious and safest dosing regimens for gender transition. This table reflects reasonable starting and maintenance doses that are supported in the (admittedly less than optimal) medical literature, and reflect the author’s opinion and practice. This table is not meant to include all possible hormone regimens, only several of the most commonly used medications. | ||||
| † Professional consensus does not exist regarding progesterone’s role in MTF transition. | ||||
| Adapted and reprinted with permission from Table VII in Oriel KA. Medical care of transsexual patients. J Gay Lesbian Med Asso 2000;4(4):193. | ||||
Transdermal testosterone is an option for biologic females who are leery of injections.13 Patches result in stable testosterone levels in the male range but may cause skin irritation in >50% of patients. Use transdermal estrogen in males with clotting abnormalities or who are age >40.
Medical workup. Basic medical monitoring includes serial physical examinations, vital signs, weight measurements, laboratory assessment, and screening for pelvic malignancies.
For biologic males receiving estrogen, pretreatment laboratory assessment includes free testosterone, fasting glucose, liver function tests, and complete blood count, with reassessment at 6 and 12 months and annually thereafter. Obtain pretreatment prolactin levels and repeat annually. If hyperprolactinemia fails to develop within 3 years, no further measurements are necessary. Monitor for breast and prostate cancer, and instruct patients to perform self-breast exams. Following orchiectomy, estrogen doses can be reduced by one-third to one-half.
For biologic women receiving androgen, obtain pretreatment liver function tests and complete blood count, then reassess at 6 months, 12 months, and annually thereafter. Do yearly liver palpation examinations.
Physiologic changes. Biologic males treated with estrogens can expect breast growth, redistribution of fat in keeping with female habitus, decreased upper body strength, decreased body hair, retardation of male pattern balding, diminished testicular size, and decrease in erection firmness and frequency. MTF transsexuals require electrolysis to remove facial hair, as HRT does not do this.
Biologic females treated with testosterone can expect deepening of the voice, clitoral enlargement, mild breast atrophy, increased facial and body hair and male-pattern baldness, increased upper body strength, weight gain, and decreased hip fat.
With effective and continuous dosages, most changes begin in 2 to 4 months, start becoming irreversible in 6 to 12 months, start to level off in 2 years, and are mostly complete in 5 years. Men with insufficient breast growth following HRT may pursue breast augmentation surgery.
Voice changes. Hormone therapy generally is presumed to “masculinize” the voice of FTM transsexuals. In one series, after initiation of hormone therapy, 12 of 16 (75%) FTM transsexuals believed they had a voice that always would be considered masculine.14,15
For MTF transsexuals, no surgical technique of pitch elevation is satisfactorily safe and effective. The most widely used—cricothyroid approximation—may not be long-lasting and can decrease range, loudness, and vocal quality.13
HRT COMPLICATIONS
Medical complications. Biologic males treated with estrogens and progestins may be at increased risk for blood clotting, benign pituitary prolactinomas, infertility, weight gain, liver disease, gallstones, somnolence, hypertension, and diabetes mellitus.
Biologic females treated with testosterone may be at increased risk for acne, cardiovascular disease from shifts of lipid profiles to male patterns, benign and malignant liver tumors, and hepatic dysfunction.
Psychiatric issues. Physical masculinization occurs much more rapidly and results in a more convincing opposite sex appearance in FTMs than feminization does in MTFs.16,17 Behaving masculine may be more socially acceptable for women and therefore easier than it is for men to behave convincingly feminine without being characterized.
Cross-sex hormones contribute to the expression of sex-dimorphic behaviors in adulthood.18,19 Estrogen appears to influence affect intensity, whereas androgens influence aggression and sexual motivation. Earlier studies established that untreated MTFs and FTMs do not differ in sex hormone levels from their biologic counterparts.20,21
After 3 months of HRT, transsexuals’ sex hormones are in the range of their identified sex. FTMs treated with androgens become more prone to aggression and exhibit increased sexual motivation and arousability associated with an overall dampened affect. MTFs treated with estrogen show decreased irritability and sexual arousability.22
SEX REASSIGNMENT SURGERY
The cost of SRS often is prohibitive. Patients may turn to the Internet or foreign venues for hormone therapy and surgical procedures. Thailand is a popular overseas destination, where the average cost for MTF surgery is approximately $6,000 to $9,000. In the United States the cost of counseling, hormones, electrolysis, and surgeries is typically $30,000 to $40,000.23
Surgical options are not limited to genital reassignment but include mammoplasty (breast augmentation for MTF), chest reduction surgery (FTM), trachea shave surgery, forehead/brow ridge contouring, chin and jaw contouring, scalp advancement surgery, cheek implant surgery, alarplasty (nasal base resection to narrow a nose), and chin contouring.
Some insurance companies assert that transsexual procedures are not medically necessary and are declining coverage. WPATH contends that sex reassignment is effective and medically indicated in severe GID.
Postsurgical outcomes. Patients who are emotionally healthy, have adequate social support, and attain reasonable cosmetic results are most satisfied with life after SRS.24 In studies of GID patients, the best predictor of postoperative psychopathology was poor surgical results.25
FTMs are transformed through the use of hormones and generally are not perceived as visibly different from other men. Genital surgery is often seen as a final step in completing the transition to the identified gender.
FTMs may elect to have their female reproductive organs removed, along with construction of male external genitalia through phalloplasty or metoidioplasty. The decision to pursue surgery and the type of procedure depend on peer influence.26 Although a phalloplasty does not provide a fully functioning and completely authentic-appearing penis, most FTMs report being satisfied with life after surgery and have few regrets.27-31
Long-term postoperative follow-up by the surgeon and mental health professional is associated with good psychosocial outcome.
Legal considerations. An individual’s new surgically created gender can cause legal complications in jurisdictions that do not recognize the new gender. Some states are amending laws to make allowances for these advances in medical science.32
- World Professional Association For Transgender Health. (formerly the Harry Benjamin International Gender Dysphoria Association [HBIGDA]). www.hbigda.org. Includes a directory of transgender organizations.
- North American gender programs and service centers
CAMH Gender Identity Clinic. Toronto, Ontario, Canada
Gender Identity Project, New York, NY
Gendercare Gender Clinic (Web clinic for gender variance). www.gendercare.com.
Ingersoll Gender Center, Seattle, Washington
Johns Hopkins Center for Sexual Health & Medicine, Baltimore, Maryland
Program in Human Sexuality, Transgender Services at the University of Minnesota - Sexology organizations and information
American Association of Sex Educators, Counselors, and Therapists. www.aasect.org.
Kinsey Institute at Indiana University. www.indiana.edu/%7Ekinsey.
Sexuality Information and Education Council of the United States. www.siecus.org.
Social Science Research Council. www.ssrc.org.
Society for the Scientific Study of Sexuality. www.sexscience.org.
- Conjugated equine estrogens • Premarin
- Estradiol (oral) • Estrace
- Estradiol (transdermal) • Climara
- Medroxyprogesterone (oral) • Provera
- Medroxyprogesterone (IM) • Depo-Provera
- Micronized progesterone • Prometrium
- Spironolactone • Aldactone
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Adults with gender identity disorder (GID)—commonly termed transsexualism—may seek psychiatric assessment and treatment for a variety of reasons. Some—but not all—might be candidates for hormone replacement therapies or sex reassignment surgery (SRS). For those with gender dysphoria, psychological assessment and psychotherapy are suggested and sometimes required.
Your role in the GID patient’s gender exploration and transition must be tailored to his or her gender identity and individual circumstances. For patients who are not candidates for surgery or cannot afford it, you may assist in exploring options for living with one’s gender identity.
WHAT IS GID?
Gender identity disorder is a rare, complex condition in which individuals of unambiguous genotype and phenotype identify with the opposite gender. One in 54,000 individuals are estimated to have GID:
- 75% are biologic males desiring reassignment to female gender (MTF)
- 25% are females desiring to be male (FTM).1
Table 1
DSM-IV-TR criteria for gender identity disorder
| Criterion A | A strong and persistent cross-gender identification defined as the desire to be or the insistence that one is of the other sex (must not be merely a desire for any perceived cultural advantages of being the other sex) |
| Criterion B | Persistent discomfort with one’s assigned sex or a sense of inappropriateness in the gender role of that sex |
| Criterion C | The disturbance is not concurrent with a physical intersex condition (such as partial androgen insensitivity syndrome or congenital adrenal hyperplasia) |
| Criterion D | The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning |
| Source: Reference 2 | |
ICD-10 diagnoses for gender identity disorder in adults
| Diagnosis | Criteria |
|---|---|
| Transsexualism |
|
| Dual-role transvestism |
|
| Other gender identity disorders | No specific criteria; could be used for persons with an intersexed condition |
| Gender identify disorder, unspecified | No specific criteria; could be used for persons with an intersexed condition |
| Source: Adapted from International Classification of Diseases, 10th ed. (ICD-10) | |
Epidemiologic studies of GID are rare, but in a survey by Rachlin et al4 of 23 MTFs and 70 FTMs:
- most underwent hormone therapy (64% of MTFs, 80% of FTMs) and/or name change (45% of MTFs, 72% of FTMs)
- none of the MTFs had breast augmentation, whereas 52% of FTMs had undergone mastectomy and reconstruction and another 33% were actively planning it
- 3% of FTMs had genital surgery, 16% were planning it, and 29% had decided definitely not to have it
- 9% of MTFs decided definitely not to have genital surgery; 23% had undergone genital surgery, and another 35% were actively planning it.
Biologic basis. GID’s cause remains unknown. Organic differences in brain anatomy have been identified in patients with GID. Zhou et al6 showed that the volume of the central subdivision of the bed nucleus of the stria terminalis (BSTc)—a brain area essential for sexual behavior—is larger in men than in women. A female-sized BSTc was found in MTF GID patients.
Research, mainly on biologic boys, indicates that GIDs are usually associated with behavioral difficulties, relationship problems with peers and parents, and—most notably—separation anxiety disorder.7 An audit of the files of 124 children and adolescents with GID showed that 42% experienced loss of one or both parents, mainly through separation.8
Psychiatric comorbidity. Studies using standardized diagnostic instruments to assess psychiatric comorbidity in GID are rare. A study of 31 patients with GID found that many met diagnostic criteria for lifetime psychiatric comorbidity, including:
- 71% for Axis I disorders (primarily mood and anxiety disorders)
- 42% for comorbid personality disorders, primarily a cluster B diagnosis
- 45% for substance-related disorders
- 6.5% for psychotic disorders
- 3.2% for eating disorders.9
TREATING PATIENTS WITH GID
Psychotherapy. GID treatment decisions are made without clear prospective data. Standards of care are determined by the World Professional Association for Transgender Health (WPATH).12 Psychotherapy is often given before SRS but is not required. The therapist is left to determine the treatment terms and goals.
Your role in treating patients with GID goes beyond making an accurate diagnosis, identifying comorbid psychopathology, and instituting a treatment plan. Other tasks include:
- counseling the patient about the range of treatment options and their implications
- engaging in psychotherapy
- ascertaining eligibility and readiness for hormones and surgical therapy
- making formal recommendations to medical and surgical colleagues
- documenting the patient’s relevant history in a letter of recommendation
- educating support systems
- being available for follow-up.
Candidates for triadic therapy. For appropriately screened adults with severe GID, the therapeutic approach relies on triadic therapy:
- a 3-phase approach centered around real-life experience in the desired role
- hormones of the desired gender
- and surgery to change the genitalia and secondary sex characteristics.
HORMONE THERAPY
WPATH has established eligibility and readiness criteria for HRT in patients with GID (Table 3). Administering cross-sex hormones (testosterone in women; estrogens in men) brings about important physical changes as well as psychological relief. The prescribing physician need not be an endocrinologist but should become well-versed in relevant data.
Table 3
WPATH criteria for hormone replacement therapy*
| Eligibility criteria 3 criteria exist |
|
| Readiness criteria All 3 must exist |
|
| Source: World Professional Association for Transgender Health (WPATH) | |
Table 4
Sample hormonal regimens for transsexual patients*
| Medication | Starting dose | Subsequent dose | When to change doses | |
|---|---|---|---|---|
| Female to male | Testosterone enanthanate or testosterone cypionate | 200 mg IM every 2 weeks | 100 to 150 mg IM every 2 weeks | After masculinization complete and/or oophorectomy/hysterectomy |
| Transdermal testosterone | 5 mg to skin every day | Usually stays the same | Little data exist on efficacy; effective for maintenance, and may be less efficacious during transition | |
| Male to female | Conjugated estrogens | 1.25 mg/d (or 0.625 mg/d for smokers) | 2.5 mg/d (Do not increase in smokers) | To obtain best clinical results, or if testosterone is not suppressed After sexual reassignment surgery, dose may be decreased without losing secondary sexual characteristics |
| OR oral estradiol | 1 mg/d | 2 mg/d | ||
| OR transdermal estradiol | 0.1 mg patch/week | Two 0.1 mg patches/week | ||
| Spironolactone | 200 mg/d | May discontinue | After sexual assignment surgery | |
| Medroxyprogesterone† | 10 mg/d | May increase to 20 to 40 mg/d (usually not needed) | If testosterone is not suppressed and patient/doctor does not want to increase estrogen | |
| OR micronized progesterone | 100 mg bid | May discontinue after breast development is complete | Micronized progesterone is more costly but may lessen side effects of anxiety, as compared with medroxyprogesterone | |
| * Professional consensus does not exist regarding the most efficacious and safest dosing regimens for gender transition. This table reflects reasonable starting and maintenance doses that are supported in the (admittedly less than optimal) medical literature, and reflect the author’s opinion and practice. This table is not meant to include all possible hormone regimens, only several of the most commonly used medications. | ||||
| † Professional consensus does not exist regarding progesterone’s role in MTF transition. | ||||
| Adapted and reprinted with permission from Table VII in Oriel KA. Medical care of transsexual patients. J Gay Lesbian Med Asso 2000;4(4):193. | ||||
Transdermal testosterone is an option for biologic females who are leery of injections.13 Patches result in stable testosterone levels in the male range but may cause skin irritation in >50% of patients. Use transdermal estrogen in males with clotting abnormalities or who are age >40.
Medical workup. Basic medical monitoring includes serial physical examinations, vital signs, weight measurements, laboratory assessment, and screening for pelvic malignancies.
For biologic males receiving estrogen, pretreatment laboratory assessment includes free testosterone, fasting glucose, liver function tests, and complete blood count, with reassessment at 6 and 12 months and annually thereafter. Obtain pretreatment prolactin levels and repeat annually. If hyperprolactinemia fails to develop within 3 years, no further measurements are necessary. Monitor for breast and prostate cancer, and instruct patients to perform self-breast exams. Following orchiectomy, estrogen doses can be reduced by one-third to one-half.
For biologic women receiving androgen, obtain pretreatment liver function tests and complete blood count, then reassess at 6 months, 12 months, and annually thereafter. Do yearly liver palpation examinations.
Physiologic changes. Biologic males treated with estrogens can expect breast growth, redistribution of fat in keeping with female habitus, decreased upper body strength, decreased body hair, retardation of male pattern balding, diminished testicular size, and decrease in erection firmness and frequency. MTF transsexuals require electrolysis to remove facial hair, as HRT does not do this.
Biologic females treated with testosterone can expect deepening of the voice, clitoral enlargement, mild breast atrophy, increased facial and body hair and male-pattern baldness, increased upper body strength, weight gain, and decreased hip fat.
With effective and continuous dosages, most changes begin in 2 to 4 months, start becoming irreversible in 6 to 12 months, start to level off in 2 years, and are mostly complete in 5 years. Men with insufficient breast growth following HRT may pursue breast augmentation surgery.
Voice changes. Hormone therapy generally is presumed to “masculinize” the voice of FTM transsexuals. In one series, after initiation of hormone therapy, 12 of 16 (75%) FTM transsexuals believed they had a voice that always would be considered masculine.14,15
For MTF transsexuals, no surgical technique of pitch elevation is satisfactorily safe and effective. The most widely used—cricothyroid approximation—may not be long-lasting and can decrease range, loudness, and vocal quality.13
HRT COMPLICATIONS
Medical complications. Biologic males treated with estrogens and progestins may be at increased risk for blood clotting, benign pituitary prolactinomas, infertility, weight gain, liver disease, gallstones, somnolence, hypertension, and diabetes mellitus.
Biologic females treated with testosterone may be at increased risk for acne, cardiovascular disease from shifts of lipid profiles to male patterns, benign and malignant liver tumors, and hepatic dysfunction.
Psychiatric issues. Physical masculinization occurs much more rapidly and results in a more convincing opposite sex appearance in FTMs than feminization does in MTFs.16,17 Behaving masculine may be more socially acceptable for women and therefore easier than it is for men to behave convincingly feminine without being characterized.
Cross-sex hormones contribute to the expression of sex-dimorphic behaviors in adulthood.18,19 Estrogen appears to influence affect intensity, whereas androgens influence aggression and sexual motivation. Earlier studies established that untreated MTFs and FTMs do not differ in sex hormone levels from their biologic counterparts.20,21
After 3 months of HRT, transsexuals’ sex hormones are in the range of their identified sex. FTMs treated with androgens become more prone to aggression and exhibit increased sexual motivation and arousability associated with an overall dampened affect. MTFs treated with estrogen show decreased irritability and sexual arousability.22
SEX REASSIGNMENT SURGERY
The cost of SRS often is prohibitive. Patients may turn to the Internet or foreign venues for hormone therapy and surgical procedures. Thailand is a popular overseas destination, where the average cost for MTF surgery is approximately $6,000 to $9,000. In the United States the cost of counseling, hormones, electrolysis, and surgeries is typically $30,000 to $40,000.23
Surgical options are not limited to genital reassignment but include mammoplasty (breast augmentation for MTF), chest reduction surgery (FTM), trachea shave surgery, forehead/brow ridge contouring, chin and jaw contouring, scalp advancement surgery, cheek implant surgery, alarplasty (nasal base resection to narrow a nose), and chin contouring.
Some insurance companies assert that transsexual procedures are not medically necessary and are declining coverage. WPATH contends that sex reassignment is effective and medically indicated in severe GID.
Postsurgical outcomes. Patients who are emotionally healthy, have adequate social support, and attain reasonable cosmetic results are most satisfied with life after SRS.24 In studies of GID patients, the best predictor of postoperative psychopathology was poor surgical results.25
FTMs are transformed through the use of hormones and generally are not perceived as visibly different from other men. Genital surgery is often seen as a final step in completing the transition to the identified gender.
FTMs may elect to have their female reproductive organs removed, along with construction of male external genitalia through phalloplasty or metoidioplasty. The decision to pursue surgery and the type of procedure depend on peer influence.26 Although a phalloplasty does not provide a fully functioning and completely authentic-appearing penis, most FTMs report being satisfied with life after surgery and have few regrets.27-31
Long-term postoperative follow-up by the surgeon and mental health professional is associated with good psychosocial outcome.
Legal considerations. An individual’s new surgically created gender can cause legal complications in jurisdictions that do not recognize the new gender. Some states are amending laws to make allowances for these advances in medical science.32
- World Professional Association For Transgender Health. (formerly the Harry Benjamin International Gender Dysphoria Association [HBIGDA]). www.hbigda.org. Includes a directory of transgender organizations.
- North American gender programs and service centers
CAMH Gender Identity Clinic. Toronto, Ontario, Canada
Gender Identity Project, New York, NY
Gendercare Gender Clinic (Web clinic for gender variance). www.gendercare.com.
Ingersoll Gender Center, Seattle, Washington
Johns Hopkins Center for Sexual Health & Medicine, Baltimore, Maryland
Program in Human Sexuality, Transgender Services at the University of Minnesota - Sexology organizations and information
American Association of Sex Educators, Counselors, and Therapists. www.aasect.org.
Kinsey Institute at Indiana University. www.indiana.edu/%7Ekinsey.
Sexuality Information and Education Council of the United States. www.siecus.org.
Social Science Research Council. www.ssrc.org.
Society for the Scientific Study of Sexuality. www.sexscience.org.
- Conjugated equine estrogens • Premarin
- Estradiol (oral) • Estrace
- Estradiol (transdermal) • Climara
- Medroxyprogesterone (oral) • Provera
- Medroxyprogesterone (IM) • Depo-Provera
- Micronized progesterone • Prometrium
- Spironolactone • Aldactone
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Laden M, Walinder J, Lundstrom B. Prevalence, incidence and sex ratio of transsexualism. Acta Psychiatr Scand 1996;93(4):221-3.
2. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
3. World Health Organization (WHO). The ICD-10 classification of mental and behavioural disorders: diagnostic criteria for research. Geneva; 1993.
4. Rachlin K. Transgender individuals’ experiences of psychotherapy. Int J Transgender 2002;6-1.
5. Pfäfflin F, Junge A. Thirty years of international follow-up studies after sex reassignment surgery: a comprehensive review, 1961-1991. Dusseldorf: Symposium Publishing; 1998.
6. Zhou JN, Hofman MA, Gooren LJ, Swaab DF. A sex difference in the human brain and its relation to transsexuality. Nature 1995;378(6552):68-70.
7. Coates S, Pearson ES. Extreme boyhood femininity: isolated behavior or pervasive disorder? J Am Acad Child Psychiatry 1985;24(6):702-9.
8. Zucker KJ. Associated psychopathology in children with gender identity disorders. In: DiCeglie D, Freedman D, eds. A stranger in my own body: atypical gender identity development and mental health. London: Karnac Books; 1998.
9. Hepp U, Kramer B, Schnyder U, et al. Psychiatric comorbidity in gender identity disorder. J Psychosom Res 2005;58(3):259-61.
10. Cole S, Denny D, Eyler A, Samons S. Issues in transgender. In: Szuchman L, Muscarella F, eds. Psychological perspective on human sexuality. New York: John Wiley; 2000.
11. Jones B, Hill M. Mental health issues in lesbian, gay, bisexual, and transgender communities. Rev Psychol 2002;21:15-31.
12. Harry Benjamin international gender association standards of care for gender identity disorders, 6th version. Minneapolis, MN: The Harry Benjamin International Gender Dysphoria Association; 2001.
13. Assecheman J, Gooren LJG. Hormone treatment in transsexuals: interdisciplinary approaches in clinical management. J Psychol Human Sex 1992;5(4):39-54.
14. Van Borsel J, De Cuypere G, Van den Berghe H. Physical appearance and voice in male-to-female transsexuals. J Voice 2001;15(4):570-5.
15. Van Borsel J, De Cuypere G, Rubens R, Destaerke B. Voice problems in female-to-male transsexuals. Int J Lang Commun Disord 2000;35(3):427-42.
16. Spiegel J, Jalisi S. Contemporary diagnosis and management of head and neck cancer. Otolaryngol Clin North Am 2005;38(1):xiii-xiv.
17. Meyer WJ, 3rd, Webb A, Stuart CA, et al. Physical and hormonal evaluation of transsexual patients: a longitudinal study. Arch Sex Behav 1986;15(2):121-38.
18. Archer J. The influence of testosterone on human aggression. Br J Psychol 1991;82(Pt 1):1-28.
19. Van de Poll ME, Van Goozen SHM. Hypothalamic involvement in sexuality and hostility: comparative psychologic aspects. In: Swaab DF, Mirmiran M, Ravid R, Van Leeuwen FW, eds. The human hypothalamus in health and disease, progress in research. Amsterdam: Elsevier; 1992;343-61.
20. Spijkstra JJ, Spinder T, Gooren LJ. Short-term patterns of pulsatile luteinizing hormone secretion do not differ between male-to-female transsexuals and heterosexual men. Psychoneuroendocrinology 1988;13(3):279-83.
21. Spinder J, Spijkstra JJ, Gooren LJ, Burger CW. Pulsatile luteinizing hormone release and ovarian steroid levels in female-to-male transsexuals compared to heterosexual women. Psychoneuroendocrinology 1989;14(1-2):97-102.
22. Slabbekoorn D, Van Goozen S, Gooren L, Cohen-Kettenis P. Effects of cross-sex hormone treatment on emotionality in transsexuals. Int J Transgender [serial online] 2001;5(3). Available at: http://www.symposion.com/ijt/ijtvo05no03_02.htm. Accessed January 11, 2007.
23. Conway L. Vaginoplasty: male to female sex reassignment surgery: historical notes, descriptions, photos, and links. Available at: http://ai.eecs.umich.edu/people/conway/TS/SRS.html. Accessed January 12, 2007.
24. Bodlund O, Kullgren G. Transsexualism-general outcome and prognostic factors: a five-year follow-up study of nineteen transsexuals in the process of changing sex. Arch Sex Behav 1996;25(3):303-16.
25. Ross MW, Need JA. Effects of adequacy of gender reassignment surgery on psychologic adjustment: a followup of fourteen male-to-female patients. Arch Sex Behav 1989;18(2):145-53.
26. Rachlin K. Factors which influence individual’s decisions when considering female-to-male genital reconstructive surgery. Int J Transgender [serial online];1999;3(3). Available at: http://www.symposion.com/ijt/ijt990302.htm. Accessed January 11, 2007.
27. Lundstrom B, Pauly I, Walinder J. Outcome of sex reassignment surgery. Acta Psychiatr Scand 1984;70(4):289-94.
28. Kuiper B, Cohen-Kettenis P. Sex reassignment surgery: a study of 141 Dutch transsexuals. Arch Sex Behav 1988;17(5):439-57.
29. Green R, Fleming D. Transsexual surgery followup: status in the 1990s. Ann Rev Sex Res 1990;7:351-69.
30. Tsoi WF. Follow-up study of transsexuals after sex-reassignment surgery. Singapore Med J 1993;34(6):515-7.
31. Tsoi WF. Male to female transsexuals: a comparison. Singapore Med J 1992;33(2):182-5.
32. Harish D, Sharma BR. Medical advances in transsexualism and the legal implications. Am J Forensic Med Pathol 2003;24(1):100-5.
1. Laden M, Walinder J, Lundstrom B. Prevalence, incidence and sex ratio of transsexualism. Acta Psychiatr Scand 1996;93(4):221-3.
2. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
3. World Health Organization (WHO). The ICD-10 classification of mental and behavioural disorders: diagnostic criteria for research. Geneva; 1993.
4. Rachlin K. Transgender individuals’ experiences of psychotherapy. Int J Transgender 2002;6-1.
5. Pfäfflin F, Junge A. Thirty years of international follow-up studies after sex reassignment surgery: a comprehensive review, 1961-1991. Dusseldorf: Symposium Publishing; 1998.
6. Zhou JN, Hofman MA, Gooren LJ, Swaab DF. A sex difference in the human brain and its relation to transsexuality. Nature 1995;378(6552):68-70.
7. Coates S, Pearson ES. Extreme boyhood femininity: isolated behavior or pervasive disorder? J Am Acad Child Psychiatry 1985;24(6):702-9.
8. Zucker KJ. Associated psychopathology in children with gender identity disorders. In: DiCeglie D, Freedman D, eds. A stranger in my own body: atypical gender identity development and mental health. London: Karnac Books; 1998.
9. Hepp U, Kramer B, Schnyder U, et al. Psychiatric comorbidity in gender identity disorder. J Psychosom Res 2005;58(3):259-61.
10. Cole S, Denny D, Eyler A, Samons S. Issues in transgender. In: Szuchman L, Muscarella F, eds. Psychological perspective on human sexuality. New York: John Wiley; 2000.
11. Jones B, Hill M. Mental health issues in lesbian, gay, bisexual, and transgender communities. Rev Psychol 2002;21:15-31.
12. Harry Benjamin international gender association standards of care for gender identity disorders, 6th version. Minneapolis, MN: The Harry Benjamin International Gender Dysphoria Association; 2001.
13. Assecheman J, Gooren LJG. Hormone treatment in transsexuals: interdisciplinary approaches in clinical management. J Psychol Human Sex 1992;5(4):39-54.
14. Van Borsel J, De Cuypere G, Van den Berghe H. Physical appearance and voice in male-to-female transsexuals. J Voice 2001;15(4):570-5.
15. Van Borsel J, De Cuypere G, Rubens R, Destaerke B. Voice problems in female-to-male transsexuals. Int J Lang Commun Disord 2000;35(3):427-42.
16. Spiegel J, Jalisi S. Contemporary diagnosis and management of head and neck cancer. Otolaryngol Clin North Am 2005;38(1):xiii-xiv.
17. Meyer WJ, 3rd, Webb A, Stuart CA, et al. Physical and hormonal evaluation of transsexual patients: a longitudinal study. Arch Sex Behav 1986;15(2):121-38.
18. Archer J. The influence of testosterone on human aggression. Br J Psychol 1991;82(Pt 1):1-28.
19. Van de Poll ME, Van Goozen SHM. Hypothalamic involvement in sexuality and hostility: comparative psychologic aspects. In: Swaab DF, Mirmiran M, Ravid R, Van Leeuwen FW, eds. The human hypothalamus in health and disease, progress in research. Amsterdam: Elsevier; 1992;343-61.
20. Spijkstra JJ, Spinder T, Gooren LJ. Short-term patterns of pulsatile luteinizing hormone secretion do not differ between male-to-female transsexuals and heterosexual men. Psychoneuroendocrinology 1988;13(3):279-83.
21. Spinder J, Spijkstra JJ, Gooren LJ, Burger CW. Pulsatile luteinizing hormone release and ovarian steroid levels in female-to-male transsexuals compared to heterosexual women. Psychoneuroendocrinology 1989;14(1-2):97-102.
22. Slabbekoorn D, Van Goozen S, Gooren L, Cohen-Kettenis P. Effects of cross-sex hormone treatment on emotionality in transsexuals. Int J Transgender [serial online] 2001;5(3). Available at: http://www.symposion.com/ijt/ijtvo05no03_02.htm. Accessed January 11, 2007.
23. Conway L. Vaginoplasty: male to female sex reassignment surgery: historical notes, descriptions, photos, and links. Available at: http://ai.eecs.umich.edu/people/conway/TS/SRS.html. Accessed January 12, 2007.
24. Bodlund O, Kullgren G. Transsexualism-general outcome and prognostic factors: a five-year follow-up study of nineteen transsexuals in the process of changing sex. Arch Sex Behav 1996;25(3):303-16.
25. Ross MW, Need JA. Effects of adequacy of gender reassignment surgery on psychologic adjustment: a followup of fourteen male-to-female patients. Arch Sex Behav 1989;18(2):145-53.
26. Rachlin K. Factors which influence individual’s decisions when considering female-to-male genital reconstructive surgery. Int J Transgender [serial online];1999;3(3). Available at: http://www.symposion.com/ijt/ijt990302.htm. Accessed January 11, 2007.
27. Lundstrom B, Pauly I, Walinder J. Outcome of sex reassignment surgery. Acta Psychiatr Scand 1984;70(4):289-94.
28. Kuiper B, Cohen-Kettenis P. Sex reassignment surgery: a study of 141 Dutch transsexuals. Arch Sex Behav 1988;17(5):439-57.
29. Green R, Fleming D. Transsexual surgery followup: status in the 1990s. Ann Rev Sex Res 1990;7:351-69.
30. Tsoi WF. Follow-up study of transsexuals after sex-reassignment surgery. Singapore Med J 1993;34(6):515-7.
31. Tsoi WF. Male to female transsexuals: a comparison. Singapore Med J 1992;33(2):182-5.
32. Harish D, Sharma BR. Medical advances in transsexualism and the legal implications. Am J Forensic Med Pathol 2003;24(1):100-5.
Antipsychotics equivalent? CUtLASS renews the debate
When treating chronic psychotic disorders, U.S. psychiatrists generally prefer second-generation antipsychotics (SGAs) to first-generation antipsychotics (FGAs) because of widely held views1,2 that SGAs:
- are more effective for negative and cognitive symptoms
- produce fewer troublesome side effects
- help patients realize a better quality of life.
These beliefs have been challenged by two large-scale, government-supported studies: the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) in the United States3-6 and more recently the Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study (CUtLASS) from the United Kingdom.7,8
CATIE and CUtLASS data suggest that the SGA advantage has been exaggerated, if in fact such an advantage exists. Other Current Psychiatry articles for the clinical practitioner have discussed the CATIE findings.9-11 This article addresses the CUtLASS results in the context of the trial’s methodology, using information from the primary publications7,8 and technical report.12
Cutlass study
Design. CUtLASS included 2 “bands” (Table 1):
- Band 1 compared the clinical usefulness and cost effectiveness of FGAs and SGAs in treating schizophrenia7
- Band 2 compared the effectiveness of clozapine versus other SGAs in treating refractory schizophrenia.8
CUtLASS Band 1 was not as extensive in scope as CATIE, and its design had some important differences (Table 2). Patients were referred for participation because their psychiatrists were considering a change in antipsychotic medication to address adverse effects or inadequate response. Fewer patients were recruited than expected—40% of the planned sample during 30 months of recruitment—but researchers considered the size sufficient to compare the effectiveness of FGAs and SGAs.
Patients were randomly assigned to treatment with an antipsychotic class, either:
- an FGA (1 of 11 options—including 5 depot formulations—chosen by the treating clinician)
- or an SGA (risperidone, olanzapine, quetiapine, or amisulpride, also chosen by the clinician).
Physicians and patients were not blinded to the medications used. They could choose medications within patients’ assigned classes and switch as needed in ways that mimicked clinical practice. Trained assessors, who were blinded to the medications being used, evaluated the patients after 12, 26, and 52 weeks.
Quality of life was the primary outcome measure.13 Secondary measures included symptoms, side effects, patient satisfaction, and cost of care.
Band 1 results. Patients assigned to the SGA or FGA classes showed no significant differences in quality of life measures or schizophrenia symptoms. If anything, the findings slightly favored the FGAs.
Patient satisfaction and overall cost of care were similar, and rates of extrapyramidal symptoms (EPS), tardive dyskinesia, and akathisia did not differ significantly.
Clozapine comparison. In CUtLASS band 2, a different sample of 136 schizophrenia patients who had responded poorly to ≥2 antipsychotics was randomly assigned to clozapine or one of the above four SGAs. During the 1-year comparison trial, clozapine:
- was found to be significantly more effective (P=0.01) in managing patients’ symptoms, as measured by total Positive and Negative Syndrome Scale (PANSS) score
- showed a trend (P=0.08) towards providing these treatment-resistant patients with a better quality of life.8
Table 1
Summary of CUtLASS trial design and results
Band 1
|
Band 2
|
| CUtLASS: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study |
| FGA: First-generation antipsychotic |
| PANSS: Positive and Negative Syndrome Scale |
| SGA: Second-generation antipsychotic |
Table 2
Comparing designs of the CUtLASS and CATIE schizophrenia trials
| CUtLASS | CATIE | |
|---|---|---|
| Trial duration | 12 months | 18 months |
| Clinical sites | 14 (United Kingdom) | 57 (United States) |
| Number of Subjects | 227 | 1,460 |
| Gender and age | 68% male; mean age 41 | 74% male; mean age 41 |
| Mental illness duration (mean) | 14 years | 16 years |
| Diagnosis | 75% schizophrenia | 100% schizophrenia |
| First-episode patients included? | Yes (13% of sample) | No |
| % of patients receiving antipsychotics at enrollment | 99% | 74% |
| Baseline PANSS score (mean) | 82% FGAs; 40% depot | 15% FGAs; <5% depot |
| Baseline PANSS score | 72.2 | 75.7 |
| Baseline EPS scores | Low | Low |
| Antipsychotic options in randomization | 2 classes (SGA or FGA) (50% of subjects assigned to an FGA) | 4 SGAs, 1 FGA (20% of subjects assigned to an FGA) |
| % of subjects given sulpiride | 49% | 0% |
| Administration methodology | Medication blinded to raters but not to patients and physicians | Medication blinded to patients and physicians |
| Primary outcome | Quality of life | Discontinuation of medication |
| Long-acting antipsychotic option? | Yes | No |
| Antipsychotic switching | All patients switched agents; 49% changed antipsychotic class | 15% stayed on some agent |
| CATIE: Clinical Antipsychotic Trials of Intervention Effectiveness | ||
| CUtLASS: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study | ||
| EPS: Extrapyramidal symptom | ||
| FGA: First-generation antipsychotic | ||
| PANSS: Positive and Negative Syndrome Scale | ||
| SGA: Second-generation antipsychotic | ||
Comparing catie, cutlass data
The CUtLASS findings are not identical to those of CATIE phase 114 but are remarkably similar: no differences in effectiveness were seen between FGAs and SGA when treating patients with chronic schizophrenia.15,16
CUtLASS investigators concluded that “in people with schizophrenia whose medication is changed for clinical reasons, there is no disadvantage across 1 year in terms of quality of life, symptoms, or associated costs of care in using FGAs rather than nonclozapine SGAs.”7
By confirming CATIE’s results, is CUtLASS the final word on antipsychotic treatment of chronic schizophrenia? Or is it just another piece of the puzzle? CATIE and CUtLASS add much to our knowledge, but methodologic “flies in the ointment” plague all clinical trials. We must consider potential biases and confounding factors to properly interpret and apply their findings.
Although the CUtLASS trial was well-constructed and executed, its conclusions—like those of CATIE—merit careful scrutiny. Its patient recruitment methods and study design involved choices and compromises that are appropriate to evaluate17,18 as we weigh CUtLASS’ contribution to the SGA/FGA debate (Table 3).
Table 3
‘Flies in the ointment’ of the CUtLASS trial design
| Who was studied |
|
| What was compared |
|
| Other Issues |
|
| CUtLASS: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study | |
| EPS: Extrapyramidal symptom | |
| FGA: First-generation antipsychotic | |
| SGA: Second-generation antipsychotic | |
Who was studied?
Selection questions. CUtLASS researchers had problems recruiting patients for their study, in part because clinicians were reluctant to expose their patients to a 50% probability of being assigned to an FGA. Only 40% of the targeted sample was recruited, and participating clinicians referred only 20% to 37% of their eligible patients to the study.12 Thus, one could ask:
- Were enrolled subjects truly representative of the population from which they were drawn?
- Or did selection bias result in a disproportionate inclusion of individuals with certain characteristics?
Is it possible, for example, that clinicians preferentially referred medication-noncompliant patients to CUtLASS because they believed the benefits of depot FGAs—such as more assured adherence—would compensate for the potential benefits of SGAs—better efficacy/tolerability?19
Treatment resistance. Although patients were randomly assigned to FGAs or SGAs, a significantly greater proportion of those whose antipsychotics were being changed because of treatment resistance were assigned to receive SGAs. Treatment resistance was one reason that 88% of subjects in the SGA arm were referred to the trial, compared with 70% of subjects in the FGA arm (P<0.01).12 The extent to which this differential assignment may have biased results against SGAs is unclear.
EPS risk. CUtLASS-1 patients had been ill a mean of 14 years and had low baseline EPS rates despite receiving long-term antipsychotics (primarily FGAs). Even so, FGAs and SGAs showed similar rates of akathisia and other EPS. Thus—as with the CATIE results—the extent to which CUtLASS-1 findings may apply beyond chronic schizophrenia patients at relatively low risk for EPS is unclear.11,17
Impact of switching. Although patients were referred to CUtLASS because of adverse effects or inadequate response to one or more antipsychotics, they were only moderately ill (mean PANSS total score 72)20 and probably were deriving some benefit from their baseline antipsychotics. Before randomization, 82% of patients were receiving an FGA and 19% an SGA. Consequently, a far larger percentage of patients in the SGA group had to switch to a different medication class as the trial began.
As observed in CATIE, switching antipsychotics often has short-term negative consequences for patients,21 although switching classes (as in CUtLASS) may have had a different impact than switching individual antipsychotics (as in CATIE). If unequal antipsychotic switching rates in the two arms differentially affected patients’ quality of life, we would expect to see this effect emerge at the 12-week assessment, which is precisely where the greatest difference in Quality of Life Scale (QLS)13 scores appeared.
The mean QLS score for patients in the SGA arm was 2.6 points lower than in the FGA group at 12 weeks. This difference disappeared and, in fact, reversed at 26 weeks, but this 12-week effect had a strong impact on results of the 52-week intent-to-treat analysis. CUtLASS—like CATIE—might exemplify the risks of switching patients from treatment with partially effective antipsychotics.22
What was compared?
Classes vs individual drugs. The decision in CUtLASS-1 to compare antipsychotic classes rather than individual agents makes it difficult to interpret its findings. Antipsychotics are not homogeneous; clear differences exist within both the SGA and FGA classes in terms of individual agents’ efficacy and tolerability, and each SGA has a reasonably well-established and different side-effect profile.23
Sulpiride was the most commonly used FGA in CUtLASS-1 (by 49% of FGA patients). Sulpiride has some unusual attributes—such as lower EPS liability—and is not available in the United States. Thus, including this agent might have affected how applicable CUtLASS findings are to clinical practice in the United States.
Oral vs depot delivery. Individuals assigned to an FGA could receive either oral or long-acting depot medication, whereas those assigned to an SGA could receive only oral medication. At baseline, 84 of 227 CUtLASS-1 participants were receiving a depot antipsychotic, which was discontinued during randomization in 72 patients. During the 1-year study, the number of patients receiving a depot antipsychotic tripled from 12 to 35, suggesting the usefulness of long-acting agents in this population.19
Cross-class switching. Although participating physicians and their patients were urged to stay within assigned antipsychotic classes at least for the first 12 weeks and ideally for 1 year, a high rate of cross-class switching occurred (Figure). At the 52-week assessment, 51 of 118 patients (43%) in the intent-to-treat FGA group were receiving SGAs instead.
The CUtLASS authors’ assert that the trial refutes the hypothesis that using SGAs is superior to using FGAs in improving quality of life. This conclusion is difficult to justify when so many patients assigned to the FGA class actually were receiving SGAs. The conclusion is further weakened if differential switching rates put SGAs at a disadvantage in the first 12 weeks of the trial.
A more accurate conclusion of the intent-to-treat comparison appears in the technical report: “There was no statistically significant difference in terms of quality of life or symptoms over 1 year in commencing [italics added] conventional antipsychotic drugs rather than new atypical drugs.”12
Figure CUtLASS-1: Did switching rate affect trial outcome?
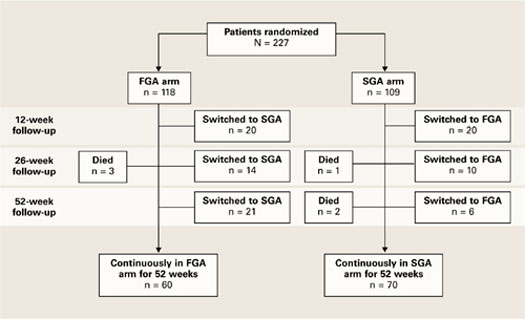
The high rate of cross-class medication switching in CUtLASS-1 may have weakened the study’s conclusion that virtually no difference in effectiveness exists between first- and second-generation antipsychotics. At the 52-week assessment, 51 of 118 patients (43%) in the intent-to-treat FGA group were receiving SGAs instead. Not shown in the figure is that 4 of the total 55 patients who switched from FGAs to SGAs had switched back to FGAs by the 52-week assessment.
CUtLASS: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study
FGA: First-generation antipsychotic
SGA: Second-generation antipsychotic
Source: Adapted from reference 7, Figure 1
Clinical implications
Notwithstanding these cautionary notes, CUtLASS-1 findings add to the questions raised by CATIE about the relative effectiveness of SGAs and FGAs. At a minimum, the data indicate that the SGA advantage has been overstated or oversimplified and that FGAs may be suitable options for meeting the needs of some patients with psychosis (particularly those at low risk for EPS).
Depot antipsychotics. CUtLASS also suggests a wider role for long-acting antipsychotics in chronic psychotic disorders, beyond treating patients with severe nonadherence.19,23 The number of patients receiving long-acting agents tripled over the 1-year study.12
Clozapine. Both CATIE and CUtLASS-2 confirmed clozapine’s superior efficacy for patients with treatment-resistant psychotic illness (Table 4). CUtLASS-2 also reaffirmed the challenges of clozapine’s metabolic and other side effects, such as sedation, hypotension, and hypersalivation.
All-cause discontinuation was significantly higher (P<0.05) in patients taking clozapine (73%) than in those taking other SGAs (52%). Even so, clozapine-group patients achieved significantly greater symptom reduction and tended toward a higher quality of life than other SGA-group patients.
Table 4
Clinical ‘pearls’ from the CUtLASS trial data
|
| CUtLASS: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study |
| EPS: Extrapyramidal symptom |
| FGA: First-generation antipsychotic |
| SGA: Second-generation antipsychotic |
Overview. In conclusion, one can reasonably conclude from analyzing the CATIE and CUtLASS data that:
- FGA-SGA differences are not as great as previously thought.
- Substantial differences exist among agents within both antipsychotic classes, particularly in side effect profiles.
- Neither study disproves the following presumed benefit of SGAs: that compared with FGAs, SGAs provide an equivalent antipsychotic effect and pose a lower risk of problems related to unmitigated dopamine blockade—such as EPS, dysphoria, bradyphrenia, neuroleptic-induced deficit syndrome, and tardive dyskinesia.11
- To use antipsychotics effectively and optimize individual treatment, consider the CATIE and CUtLASS trials in the contexts of their designs and the results of other studies of patients with chronic schizophrenia.
Related resources
- Heres S, Davis J, Maino K, et al. Why olanzapine beats risperidone, risperidone beats quetiapine, and quetiapine beats olanzapine: An exploratory analysis of head-head comparison studies of second-generation antipsychotics. Am J Psychiatry 2006;163:185-94.
Drug brand names
- Clozapine • Clozaril
- Quetiapine • Seroquel
- Olanzapine • Zyprexa
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Kane JM, Leucht S, Carpenter D, et al. Expert consensus guideline series: optimizing pharmacologic treatment of psychotic disorders. J Clin Psychiatry 2003;64(suppl 12):1-100.
2. Tandon R, Fleischhacker WW. Comparative efficacy of antipsychotics in the treatment of schizophrenia: a critical assessment. Schizophr Res 2005;79:145-55.
3. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med 2005;353:1209-23.
4. McEvoy JP, Lieberman JA, Stroup TS, et al. Effectiveness of clozapine versus olanzapine, quetiapine, and risperidone in patients with chronic schizophrenia who did not respond to prior antipsychotic treatment. Am J Psychiatry 2006;163:600-10.
5. Stroup TS, Lieberman JA, McEvoy JP, et al. Effectiveness of olanzapine, quetiapine, risperidone, and ziprasidone in patients with chronic schizophrenia following discontinuation of a previous atypical antipsychotic. Am J Psychiatry 2006;163:611-22.
6. Rosenheck RA, Leslie DL, Sindelar J, et al. Cost-effectiveness of second-generation antipsychotics and perphenazine in a randomized trial of treatment for chronic schizophrenia. Am J Psychiatry 2006;163:2080-9.
7. Jones PB, Barnes T, Davies L, et al. Randomized controlled trial of the effect on quality of life of second- vs first-generation antipsychotic drugs in schizophrenia: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study (CUtLASS). Arch Gen Psychiatry 2006;63:1079-87.
8. Lewis SW, Barnes TRE, Davies L, et al. Randomised controlled trial of effect of prescription of clozapine versus other second-generation antipsychotic drugs in resistant schizophrenia. Schizophr Bull 2006;32:715-23.
9. Nasrallah HA. CATIE’s surprises: in antipsychotics’ square-off, were there winners or losers? Current Psychiatry 2006;5(2):49-65.
10. Buckley PF. Which antipsychotic do I choose next? CATIE phase 2 offers insights on efficacy and tolerability. Current Psychiatry 2006;5(9):27-43.
11. Tandon R, Constantine R. Avoiding EPS is key to realizing ‘atypical’ benefits. Current Psychiatry 2006;5(11):35-45.
12. Lewis SW, Davies L, Jones PB, et al. Randomised controlled trials of conventional antipsychotic versus new atypical drugs, and new atypical drugs versus clozapine, in people with schizophrenia responding poorly to, or intolerant of, current drug treatment. Health Technology Assessment 2006;10(#17):1-182.Available at http://www.hta.ac.uk/project/1078.asp. Accessed January 3, 2007.
13. Heinrichs DW, Hanlon TE, Carpenter WT. The Quality of Life Scale: an instrument for assessing the schizophrenic deficit syndrome. Schizophr Bull 1984;10:388-98.
14. Tandon R, Davis JM, Carpenter WT. CATIE, CUtLASS, and the FGA-SGA debate (letter). Arch Gen Psychiatry 2007 (in press).
15. Lieberman J. Comparative effectiveness of antipsychotic drugs: a commentary on the Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study and Clinical Antipsychotic Trials of Intervention Effectiveness. Arch Gen Psychiatry 2006;63:1069-72.
16. Rosenheck RA. Outcomes, costs, and policy caution: a commentary on the Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study. Arch Gen Psychiatry 2006;63:1074-6.
17. Tandon R. Comparative effectiveness of antipsychotics in the treatment of schizophrenia: what CATIE tells us—Parts 1 and 2. International Drug Therapy Newsletter 2006;41(7,9):51-8,67-74.
18. Meltzer HY, Bobo WV. Interpreting the efficacy findings in the CATIE study: what clinicians should know. CNS Spectrums 2006;11(suppl 7):14-24.
19. Kane JM. Review of treatments that can ameliorate nonadherence in patients with schizophrenia. J Clin Psychiatry 2006;67(suppl 5):9-14.
20. Leucht S, Kane JM, Kissling W, et al. What does the PANSS mean? Schizophr Res 2006;79:231-8.
21. Essock SM, Covell NH, Davis SM, et al. Effectiveness of switching antipsychotic medications. Am J Psychiatry 2006;163:2090-5.
22. Davis JM, Marder S, Tamminga CA. Switch or stay? Am J Psychiatry 2006;163:2032-3.
23. Tandon R, Targum SD, Nasrallah HA, et al. Strategies for maximizing clinical effectiveness in the treatment of schizophrenia. Journal of Psychiatric Practice 2006;12:348-63.
When treating chronic psychotic disorders, U.S. psychiatrists generally prefer second-generation antipsychotics (SGAs) to first-generation antipsychotics (FGAs) because of widely held views1,2 that SGAs:
- are more effective for negative and cognitive symptoms
- produce fewer troublesome side effects
- help patients realize a better quality of life.
These beliefs have been challenged by two large-scale, government-supported studies: the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) in the United States3-6 and more recently the Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study (CUtLASS) from the United Kingdom.7,8
CATIE and CUtLASS data suggest that the SGA advantage has been exaggerated, if in fact such an advantage exists. Other Current Psychiatry articles for the clinical practitioner have discussed the CATIE findings.9-11 This article addresses the CUtLASS results in the context of the trial’s methodology, using information from the primary publications7,8 and technical report.12
Cutlass study
Design. CUtLASS included 2 “bands” (Table 1):
- Band 1 compared the clinical usefulness and cost effectiveness of FGAs and SGAs in treating schizophrenia7
- Band 2 compared the effectiveness of clozapine versus other SGAs in treating refractory schizophrenia.8
CUtLASS Band 1 was not as extensive in scope as CATIE, and its design had some important differences (Table 2). Patients were referred for participation because their psychiatrists were considering a change in antipsychotic medication to address adverse effects or inadequate response. Fewer patients were recruited than expected—40% of the planned sample during 30 months of recruitment—but researchers considered the size sufficient to compare the effectiveness of FGAs and SGAs.
Patients were randomly assigned to treatment with an antipsychotic class, either:
- an FGA (1 of 11 options—including 5 depot formulations—chosen by the treating clinician)
- or an SGA (risperidone, olanzapine, quetiapine, or amisulpride, also chosen by the clinician).
Physicians and patients were not blinded to the medications used. They could choose medications within patients’ assigned classes and switch as needed in ways that mimicked clinical practice. Trained assessors, who were blinded to the medications being used, evaluated the patients after 12, 26, and 52 weeks.
Quality of life was the primary outcome measure.13 Secondary measures included symptoms, side effects, patient satisfaction, and cost of care.
Band 1 results. Patients assigned to the SGA or FGA classes showed no significant differences in quality of life measures or schizophrenia symptoms. If anything, the findings slightly favored the FGAs.
Patient satisfaction and overall cost of care were similar, and rates of extrapyramidal symptoms (EPS), tardive dyskinesia, and akathisia did not differ significantly.
Clozapine comparison. In CUtLASS band 2, a different sample of 136 schizophrenia patients who had responded poorly to ≥2 antipsychotics was randomly assigned to clozapine or one of the above four SGAs. During the 1-year comparison trial, clozapine:
- was found to be significantly more effective (P=0.01) in managing patients’ symptoms, as measured by total Positive and Negative Syndrome Scale (PANSS) score
- showed a trend (P=0.08) towards providing these treatment-resistant patients with a better quality of life.8
Table 1
Summary of CUtLASS trial design and results
Band 1
|
Band 2
|
| CUtLASS: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study |
| FGA: First-generation antipsychotic |
| PANSS: Positive and Negative Syndrome Scale |
| SGA: Second-generation antipsychotic |
Table 2
Comparing designs of the CUtLASS and CATIE schizophrenia trials
| CUtLASS | CATIE | |
|---|---|---|
| Trial duration | 12 months | 18 months |
| Clinical sites | 14 (United Kingdom) | 57 (United States) |
| Number of Subjects | 227 | 1,460 |
| Gender and age | 68% male; mean age 41 | 74% male; mean age 41 |
| Mental illness duration (mean) | 14 years | 16 years |
| Diagnosis | 75% schizophrenia | 100% schizophrenia |
| First-episode patients included? | Yes (13% of sample) | No |
| % of patients receiving antipsychotics at enrollment | 99% | 74% |
| Baseline PANSS score (mean) | 82% FGAs; 40% depot | 15% FGAs; <5% depot |
| Baseline PANSS score | 72.2 | 75.7 |
| Baseline EPS scores | Low | Low |
| Antipsychotic options in randomization | 2 classes (SGA or FGA) (50% of subjects assigned to an FGA) | 4 SGAs, 1 FGA (20% of subjects assigned to an FGA) |
| % of subjects given sulpiride | 49% | 0% |
| Administration methodology | Medication blinded to raters but not to patients and physicians | Medication blinded to patients and physicians |
| Primary outcome | Quality of life | Discontinuation of medication |
| Long-acting antipsychotic option? | Yes | No |
| Antipsychotic switching | All patients switched agents; 49% changed antipsychotic class | 15% stayed on some agent |
| CATIE: Clinical Antipsychotic Trials of Intervention Effectiveness | ||
| CUtLASS: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study | ||
| EPS: Extrapyramidal symptom | ||
| FGA: First-generation antipsychotic | ||
| PANSS: Positive and Negative Syndrome Scale | ||
| SGA: Second-generation antipsychotic | ||
Comparing catie, cutlass data
The CUtLASS findings are not identical to those of CATIE phase 114 but are remarkably similar: no differences in effectiveness were seen between FGAs and SGA when treating patients with chronic schizophrenia.15,16
CUtLASS investigators concluded that “in people with schizophrenia whose medication is changed for clinical reasons, there is no disadvantage across 1 year in terms of quality of life, symptoms, or associated costs of care in using FGAs rather than nonclozapine SGAs.”7
By confirming CATIE’s results, is CUtLASS the final word on antipsychotic treatment of chronic schizophrenia? Or is it just another piece of the puzzle? CATIE and CUtLASS add much to our knowledge, but methodologic “flies in the ointment” plague all clinical trials. We must consider potential biases and confounding factors to properly interpret and apply their findings.
Although the CUtLASS trial was well-constructed and executed, its conclusions—like those of CATIE—merit careful scrutiny. Its patient recruitment methods and study design involved choices and compromises that are appropriate to evaluate17,18 as we weigh CUtLASS’ contribution to the SGA/FGA debate (Table 3).
Table 3
‘Flies in the ointment’ of the CUtLASS trial design
| Who was studied |
|
| What was compared |
|
| Other Issues |
|
| CUtLASS: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study | |
| EPS: Extrapyramidal symptom | |
| FGA: First-generation antipsychotic | |
| SGA: Second-generation antipsychotic | |
Who was studied?
Selection questions. CUtLASS researchers had problems recruiting patients for their study, in part because clinicians were reluctant to expose their patients to a 50% probability of being assigned to an FGA. Only 40% of the targeted sample was recruited, and participating clinicians referred only 20% to 37% of their eligible patients to the study.12 Thus, one could ask:
- Were enrolled subjects truly representative of the population from which they were drawn?
- Or did selection bias result in a disproportionate inclusion of individuals with certain characteristics?
Is it possible, for example, that clinicians preferentially referred medication-noncompliant patients to CUtLASS because they believed the benefits of depot FGAs—such as more assured adherence—would compensate for the potential benefits of SGAs—better efficacy/tolerability?19
Treatment resistance. Although patients were randomly assigned to FGAs or SGAs, a significantly greater proportion of those whose antipsychotics were being changed because of treatment resistance were assigned to receive SGAs. Treatment resistance was one reason that 88% of subjects in the SGA arm were referred to the trial, compared with 70% of subjects in the FGA arm (P<0.01).12 The extent to which this differential assignment may have biased results against SGAs is unclear.
EPS risk. CUtLASS-1 patients had been ill a mean of 14 years and had low baseline EPS rates despite receiving long-term antipsychotics (primarily FGAs). Even so, FGAs and SGAs showed similar rates of akathisia and other EPS. Thus—as with the CATIE results—the extent to which CUtLASS-1 findings may apply beyond chronic schizophrenia patients at relatively low risk for EPS is unclear.11,17
Impact of switching. Although patients were referred to CUtLASS because of adverse effects or inadequate response to one or more antipsychotics, they were only moderately ill (mean PANSS total score 72)20 and probably were deriving some benefit from their baseline antipsychotics. Before randomization, 82% of patients were receiving an FGA and 19% an SGA. Consequently, a far larger percentage of patients in the SGA group had to switch to a different medication class as the trial began.
As observed in CATIE, switching antipsychotics often has short-term negative consequences for patients,21 although switching classes (as in CUtLASS) may have had a different impact than switching individual antipsychotics (as in CATIE). If unequal antipsychotic switching rates in the two arms differentially affected patients’ quality of life, we would expect to see this effect emerge at the 12-week assessment, which is precisely where the greatest difference in Quality of Life Scale (QLS)13 scores appeared.
The mean QLS score for patients in the SGA arm was 2.6 points lower than in the FGA group at 12 weeks. This difference disappeared and, in fact, reversed at 26 weeks, but this 12-week effect had a strong impact on results of the 52-week intent-to-treat analysis. CUtLASS—like CATIE—might exemplify the risks of switching patients from treatment with partially effective antipsychotics.22
What was compared?
Classes vs individual drugs. The decision in CUtLASS-1 to compare antipsychotic classes rather than individual agents makes it difficult to interpret its findings. Antipsychotics are not homogeneous; clear differences exist within both the SGA and FGA classes in terms of individual agents’ efficacy and tolerability, and each SGA has a reasonably well-established and different side-effect profile.23
Sulpiride was the most commonly used FGA in CUtLASS-1 (by 49% of FGA patients). Sulpiride has some unusual attributes—such as lower EPS liability—and is not available in the United States. Thus, including this agent might have affected how applicable CUtLASS findings are to clinical practice in the United States.
Oral vs depot delivery. Individuals assigned to an FGA could receive either oral or long-acting depot medication, whereas those assigned to an SGA could receive only oral medication. At baseline, 84 of 227 CUtLASS-1 participants were receiving a depot antipsychotic, which was discontinued during randomization in 72 patients. During the 1-year study, the number of patients receiving a depot antipsychotic tripled from 12 to 35, suggesting the usefulness of long-acting agents in this population.19
Cross-class switching. Although participating physicians and their patients were urged to stay within assigned antipsychotic classes at least for the first 12 weeks and ideally for 1 year, a high rate of cross-class switching occurred (Figure). At the 52-week assessment, 51 of 118 patients (43%) in the intent-to-treat FGA group were receiving SGAs instead.
The CUtLASS authors’ assert that the trial refutes the hypothesis that using SGAs is superior to using FGAs in improving quality of life. This conclusion is difficult to justify when so many patients assigned to the FGA class actually were receiving SGAs. The conclusion is further weakened if differential switching rates put SGAs at a disadvantage in the first 12 weeks of the trial.
A more accurate conclusion of the intent-to-treat comparison appears in the technical report: “There was no statistically significant difference in terms of quality of life or symptoms over 1 year in commencing [italics added] conventional antipsychotic drugs rather than new atypical drugs.”12
Figure CUtLASS-1: Did switching rate affect trial outcome?
The high rate of cross-class medication switching in CUtLASS-1 may have weakened the study’s conclusion that virtually no difference in effectiveness exists between first- and second-generation antipsychotics. At the 52-week assessment, 51 of 118 patients (43%) in the intent-to-treat FGA group were receiving SGAs instead. Not shown in the figure is that 4 of the total 55 patients who switched from FGAs to SGAs had switched back to FGAs by the 52-week assessment.
CUtLASS: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study
FGA: First-generation antipsychotic
SGA: Second-generation antipsychotic
Source: Adapted from reference 7, Figure 1
Clinical implications
Notwithstanding these cautionary notes, CUtLASS-1 findings add to the questions raised by CATIE about the relative effectiveness of SGAs and FGAs. At a minimum, the data indicate that the SGA advantage has been overstated or oversimplified and that FGAs may be suitable options for meeting the needs of some patients with psychosis (particularly those at low risk for EPS).
Depot antipsychotics. CUtLASS also suggests a wider role for long-acting antipsychotics in chronic psychotic disorders, beyond treating patients with severe nonadherence.19,23 The number of patients receiving long-acting agents tripled over the 1-year study.12
Clozapine. Both CATIE and CUtLASS-2 confirmed clozapine’s superior efficacy for patients with treatment-resistant psychotic illness (Table 4). CUtLASS-2 also reaffirmed the challenges of clozapine’s metabolic and other side effects, such as sedation, hypotension, and hypersalivation.
All-cause discontinuation was significantly higher (P<0.05) in patients taking clozapine (73%) than in those taking other SGAs (52%). Even so, clozapine-group patients achieved significantly greater symptom reduction and tended toward a higher quality of life than other SGA-group patients.
Table 4
Clinical ‘pearls’ from the CUtLASS trial data
|
| CUtLASS: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study |
| EPS: Extrapyramidal symptom |
| FGA: First-generation antipsychotic |
| SGA: Second-generation antipsychotic |
Overview. In conclusion, one can reasonably conclude from analyzing the CATIE and CUtLASS data that:
- FGA-SGA differences are not as great as previously thought.
- Substantial differences exist among agents within both antipsychotic classes, particularly in side effect profiles.
- Neither study disproves the following presumed benefit of SGAs: that compared with FGAs, SGAs provide an equivalent antipsychotic effect and pose a lower risk of problems related to unmitigated dopamine blockade—such as EPS, dysphoria, bradyphrenia, neuroleptic-induced deficit syndrome, and tardive dyskinesia.11
- To use antipsychotics effectively and optimize individual treatment, consider the CATIE and CUtLASS trials in the contexts of their designs and the results of other studies of patients with chronic schizophrenia.
Related resources
- Heres S, Davis J, Maino K, et al. Why olanzapine beats risperidone, risperidone beats quetiapine, and quetiapine beats olanzapine: An exploratory analysis of head-head comparison studies of second-generation antipsychotics. Am J Psychiatry 2006;163:185-94.
Drug brand names
- Clozapine • Clozaril
- Quetiapine • Seroquel
- Olanzapine • Zyprexa
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
When treating chronic psychotic disorders, U.S. psychiatrists generally prefer second-generation antipsychotics (SGAs) to first-generation antipsychotics (FGAs) because of widely held views1,2 that SGAs:
- are more effective for negative and cognitive symptoms
- produce fewer troublesome side effects
- help patients realize a better quality of life.
These beliefs have been challenged by two large-scale, government-supported studies: the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) in the United States3-6 and more recently the Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study (CUtLASS) from the United Kingdom.7,8
CATIE and CUtLASS data suggest that the SGA advantage has been exaggerated, if in fact such an advantage exists. Other Current Psychiatry articles for the clinical practitioner have discussed the CATIE findings.9-11 This article addresses the CUtLASS results in the context of the trial’s methodology, using information from the primary publications7,8 and technical report.12
Cutlass study
Design. CUtLASS included 2 “bands” (Table 1):
- Band 1 compared the clinical usefulness and cost effectiveness of FGAs and SGAs in treating schizophrenia7
- Band 2 compared the effectiveness of clozapine versus other SGAs in treating refractory schizophrenia.8
CUtLASS Band 1 was not as extensive in scope as CATIE, and its design had some important differences (Table 2). Patients were referred for participation because their psychiatrists were considering a change in antipsychotic medication to address adverse effects or inadequate response. Fewer patients were recruited than expected—40% of the planned sample during 30 months of recruitment—but researchers considered the size sufficient to compare the effectiveness of FGAs and SGAs.
Patients were randomly assigned to treatment with an antipsychotic class, either:
- an FGA (1 of 11 options—including 5 depot formulations—chosen by the treating clinician)
- or an SGA (risperidone, olanzapine, quetiapine, or amisulpride, also chosen by the clinician).
Physicians and patients were not blinded to the medications used. They could choose medications within patients’ assigned classes and switch as needed in ways that mimicked clinical practice. Trained assessors, who were blinded to the medications being used, evaluated the patients after 12, 26, and 52 weeks.
Quality of life was the primary outcome measure.13 Secondary measures included symptoms, side effects, patient satisfaction, and cost of care.
Band 1 results. Patients assigned to the SGA or FGA classes showed no significant differences in quality of life measures or schizophrenia symptoms. If anything, the findings slightly favored the FGAs.
Patient satisfaction and overall cost of care were similar, and rates of extrapyramidal symptoms (EPS), tardive dyskinesia, and akathisia did not differ significantly.
Clozapine comparison. In CUtLASS band 2, a different sample of 136 schizophrenia patients who had responded poorly to ≥2 antipsychotics was randomly assigned to clozapine or one of the above four SGAs. During the 1-year comparison trial, clozapine:
- was found to be significantly more effective (P=0.01) in managing patients’ symptoms, as measured by total Positive and Negative Syndrome Scale (PANSS) score
- showed a trend (P=0.08) towards providing these treatment-resistant patients with a better quality of life.8
Table 1
Summary of CUtLASS trial design and results
Band 1
|
Band 2
|
| CUtLASS: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study |
| FGA: First-generation antipsychotic |
| PANSS: Positive and Negative Syndrome Scale |
| SGA: Second-generation antipsychotic |
Table 2
Comparing designs of the CUtLASS and CATIE schizophrenia trials
| CUtLASS | CATIE | |
|---|---|---|
| Trial duration | 12 months | 18 months |
| Clinical sites | 14 (United Kingdom) | 57 (United States) |
| Number of Subjects | 227 | 1,460 |
| Gender and age | 68% male; mean age 41 | 74% male; mean age 41 |
| Mental illness duration (mean) | 14 years | 16 years |
| Diagnosis | 75% schizophrenia | 100% schizophrenia |
| First-episode patients included? | Yes (13% of sample) | No |
| % of patients receiving antipsychotics at enrollment | 99% | 74% |
| Baseline PANSS score (mean) | 82% FGAs; 40% depot | 15% FGAs; <5% depot |
| Baseline PANSS score | 72.2 | 75.7 |
| Baseline EPS scores | Low | Low |
| Antipsychotic options in randomization | 2 classes (SGA or FGA) (50% of subjects assigned to an FGA) | 4 SGAs, 1 FGA (20% of subjects assigned to an FGA) |
| % of subjects given sulpiride | 49% | 0% |
| Administration methodology | Medication blinded to raters but not to patients and physicians | Medication blinded to patients and physicians |
| Primary outcome | Quality of life | Discontinuation of medication |
| Long-acting antipsychotic option? | Yes | No |
| Antipsychotic switching | All patients switched agents; 49% changed antipsychotic class | 15% stayed on some agent |
| CATIE: Clinical Antipsychotic Trials of Intervention Effectiveness | ||
| CUtLASS: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study | ||
| EPS: Extrapyramidal symptom | ||
| FGA: First-generation antipsychotic | ||
| PANSS: Positive and Negative Syndrome Scale | ||
| SGA: Second-generation antipsychotic | ||
Comparing catie, cutlass data
The CUtLASS findings are not identical to those of CATIE phase 114 but are remarkably similar: no differences in effectiveness were seen between FGAs and SGA when treating patients with chronic schizophrenia.15,16
CUtLASS investigators concluded that “in people with schizophrenia whose medication is changed for clinical reasons, there is no disadvantage across 1 year in terms of quality of life, symptoms, or associated costs of care in using FGAs rather than nonclozapine SGAs.”7
By confirming CATIE’s results, is CUtLASS the final word on antipsychotic treatment of chronic schizophrenia? Or is it just another piece of the puzzle? CATIE and CUtLASS add much to our knowledge, but methodologic “flies in the ointment” plague all clinical trials. We must consider potential biases and confounding factors to properly interpret and apply their findings.
Although the CUtLASS trial was well-constructed and executed, its conclusions—like those of CATIE—merit careful scrutiny. Its patient recruitment methods and study design involved choices and compromises that are appropriate to evaluate17,18 as we weigh CUtLASS’ contribution to the SGA/FGA debate (Table 3).
Table 3
‘Flies in the ointment’ of the CUtLASS trial design
| Who was studied |
|
| What was compared |
|
| Other Issues |
|
| CUtLASS: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study | |
| EPS: Extrapyramidal symptom | |
| FGA: First-generation antipsychotic | |
| SGA: Second-generation antipsychotic | |
Who was studied?
Selection questions. CUtLASS researchers had problems recruiting patients for their study, in part because clinicians were reluctant to expose their patients to a 50% probability of being assigned to an FGA. Only 40% of the targeted sample was recruited, and participating clinicians referred only 20% to 37% of their eligible patients to the study.12 Thus, one could ask:
- Were enrolled subjects truly representative of the population from which they were drawn?
- Or did selection bias result in a disproportionate inclusion of individuals with certain characteristics?
Is it possible, for example, that clinicians preferentially referred medication-noncompliant patients to CUtLASS because they believed the benefits of depot FGAs—such as more assured adherence—would compensate for the potential benefits of SGAs—better efficacy/tolerability?19
Treatment resistance. Although patients were randomly assigned to FGAs or SGAs, a significantly greater proportion of those whose antipsychotics were being changed because of treatment resistance were assigned to receive SGAs. Treatment resistance was one reason that 88% of subjects in the SGA arm were referred to the trial, compared with 70% of subjects in the FGA arm (P<0.01).12 The extent to which this differential assignment may have biased results against SGAs is unclear.
EPS risk. CUtLASS-1 patients had been ill a mean of 14 years and had low baseline EPS rates despite receiving long-term antipsychotics (primarily FGAs). Even so, FGAs and SGAs showed similar rates of akathisia and other EPS. Thus—as with the CATIE results—the extent to which CUtLASS-1 findings may apply beyond chronic schizophrenia patients at relatively low risk for EPS is unclear.11,17
Impact of switching. Although patients were referred to CUtLASS because of adverse effects or inadequate response to one or more antipsychotics, they were only moderately ill (mean PANSS total score 72)20 and probably were deriving some benefit from their baseline antipsychotics. Before randomization, 82% of patients were receiving an FGA and 19% an SGA. Consequently, a far larger percentage of patients in the SGA group had to switch to a different medication class as the trial began.
As observed in CATIE, switching antipsychotics often has short-term negative consequences for patients,21 although switching classes (as in CUtLASS) may have had a different impact than switching individual antipsychotics (as in CATIE). If unequal antipsychotic switching rates in the two arms differentially affected patients’ quality of life, we would expect to see this effect emerge at the 12-week assessment, which is precisely where the greatest difference in Quality of Life Scale (QLS)13 scores appeared.
The mean QLS score for patients in the SGA arm was 2.6 points lower than in the FGA group at 12 weeks. This difference disappeared and, in fact, reversed at 26 weeks, but this 12-week effect had a strong impact on results of the 52-week intent-to-treat analysis. CUtLASS—like CATIE—might exemplify the risks of switching patients from treatment with partially effective antipsychotics.22
What was compared?
Classes vs individual drugs. The decision in CUtLASS-1 to compare antipsychotic classes rather than individual agents makes it difficult to interpret its findings. Antipsychotics are not homogeneous; clear differences exist within both the SGA and FGA classes in terms of individual agents’ efficacy and tolerability, and each SGA has a reasonably well-established and different side-effect profile.23
Sulpiride was the most commonly used FGA in CUtLASS-1 (by 49% of FGA patients). Sulpiride has some unusual attributes—such as lower EPS liability—and is not available in the United States. Thus, including this agent might have affected how applicable CUtLASS findings are to clinical practice in the United States.
Oral vs depot delivery. Individuals assigned to an FGA could receive either oral or long-acting depot medication, whereas those assigned to an SGA could receive only oral medication. At baseline, 84 of 227 CUtLASS-1 participants were receiving a depot antipsychotic, which was discontinued during randomization in 72 patients. During the 1-year study, the number of patients receiving a depot antipsychotic tripled from 12 to 35, suggesting the usefulness of long-acting agents in this population.19
Cross-class switching. Although participating physicians and their patients were urged to stay within assigned antipsychotic classes at least for the first 12 weeks and ideally for 1 year, a high rate of cross-class switching occurred (Figure). At the 52-week assessment, 51 of 118 patients (43%) in the intent-to-treat FGA group were receiving SGAs instead.
The CUtLASS authors’ assert that the trial refutes the hypothesis that using SGAs is superior to using FGAs in improving quality of life. This conclusion is difficult to justify when so many patients assigned to the FGA class actually were receiving SGAs. The conclusion is further weakened if differential switching rates put SGAs at a disadvantage in the first 12 weeks of the trial.
A more accurate conclusion of the intent-to-treat comparison appears in the technical report: “There was no statistically significant difference in terms of quality of life or symptoms over 1 year in commencing [italics added] conventional antipsychotic drugs rather than new atypical drugs.”12
Figure CUtLASS-1: Did switching rate affect trial outcome?
The high rate of cross-class medication switching in CUtLASS-1 may have weakened the study’s conclusion that virtually no difference in effectiveness exists between first- and second-generation antipsychotics. At the 52-week assessment, 51 of 118 patients (43%) in the intent-to-treat FGA group were receiving SGAs instead. Not shown in the figure is that 4 of the total 55 patients who switched from FGAs to SGAs had switched back to FGAs by the 52-week assessment.
CUtLASS: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study
FGA: First-generation antipsychotic
SGA: Second-generation antipsychotic
Source: Adapted from reference 7, Figure 1
Clinical implications
Notwithstanding these cautionary notes, CUtLASS-1 findings add to the questions raised by CATIE about the relative effectiveness of SGAs and FGAs. At a minimum, the data indicate that the SGA advantage has been overstated or oversimplified and that FGAs may be suitable options for meeting the needs of some patients with psychosis (particularly those at low risk for EPS).
Depot antipsychotics. CUtLASS also suggests a wider role for long-acting antipsychotics in chronic psychotic disorders, beyond treating patients with severe nonadherence.19,23 The number of patients receiving long-acting agents tripled over the 1-year study.12
Clozapine. Both CATIE and CUtLASS-2 confirmed clozapine’s superior efficacy for patients with treatment-resistant psychotic illness (Table 4). CUtLASS-2 also reaffirmed the challenges of clozapine’s metabolic and other side effects, such as sedation, hypotension, and hypersalivation.
All-cause discontinuation was significantly higher (P<0.05) in patients taking clozapine (73%) than in those taking other SGAs (52%). Even so, clozapine-group patients achieved significantly greater symptom reduction and tended toward a higher quality of life than other SGA-group patients.
Table 4
Clinical ‘pearls’ from the CUtLASS trial data
|
| CUtLASS: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study |
| EPS: Extrapyramidal symptom |
| FGA: First-generation antipsychotic |
| SGA: Second-generation antipsychotic |
Overview. In conclusion, one can reasonably conclude from analyzing the CATIE and CUtLASS data that:
- FGA-SGA differences are not as great as previously thought.
- Substantial differences exist among agents within both antipsychotic classes, particularly in side effect profiles.
- Neither study disproves the following presumed benefit of SGAs: that compared with FGAs, SGAs provide an equivalent antipsychotic effect and pose a lower risk of problems related to unmitigated dopamine blockade—such as EPS, dysphoria, bradyphrenia, neuroleptic-induced deficit syndrome, and tardive dyskinesia.11
- To use antipsychotics effectively and optimize individual treatment, consider the CATIE and CUtLASS trials in the contexts of their designs and the results of other studies of patients with chronic schizophrenia.
Related resources
- Heres S, Davis J, Maino K, et al. Why olanzapine beats risperidone, risperidone beats quetiapine, and quetiapine beats olanzapine: An exploratory analysis of head-head comparison studies of second-generation antipsychotics. Am J Psychiatry 2006;163:185-94.
Drug brand names
- Clozapine • Clozaril
- Quetiapine • Seroquel
- Olanzapine • Zyprexa
- Risperidone • Risperdal
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Kane JM, Leucht S, Carpenter D, et al. Expert consensus guideline series: optimizing pharmacologic treatment of psychotic disorders. J Clin Psychiatry 2003;64(suppl 12):1-100.
2. Tandon R, Fleischhacker WW. Comparative efficacy of antipsychotics in the treatment of schizophrenia: a critical assessment. Schizophr Res 2005;79:145-55.
3. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med 2005;353:1209-23.
4. McEvoy JP, Lieberman JA, Stroup TS, et al. Effectiveness of clozapine versus olanzapine, quetiapine, and risperidone in patients with chronic schizophrenia who did not respond to prior antipsychotic treatment. Am J Psychiatry 2006;163:600-10.
5. Stroup TS, Lieberman JA, McEvoy JP, et al. Effectiveness of olanzapine, quetiapine, risperidone, and ziprasidone in patients with chronic schizophrenia following discontinuation of a previous atypical antipsychotic. Am J Psychiatry 2006;163:611-22.
6. Rosenheck RA, Leslie DL, Sindelar J, et al. Cost-effectiveness of second-generation antipsychotics and perphenazine in a randomized trial of treatment for chronic schizophrenia. Am J Psychiatry 2006;163:2080-9.
7. Jones PB, Barnes T, Davies L, et al. Randomized controlled trial of the effect on quality of life of second- vs first-generation antipsychotic drugs in schizophrenia: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study (CUtLASS). Arch Gen Psychiatry 2006;63:1079-87.
8. Lewis SW, Barnes TRE, Davies L, et al. Randomised controlled trial of effect of prescription of clozapine versus other second-generation antipsychotic drugs in resistant schizophrenia. Schizophr Bull 2006;32:715-23.
9. Nasrallah HA. CATIE’s surprises: in antipsychotics’ square-off, were there winners or losers? Current Psychiatry 2006;5(2):49-65.
10. Buckley PF. Which antipsychotic do I choose next? CATIE phase 2 offers insights on efficacy and tolerability. Current Psychiatry 2006;5(9):27-43.
11. Tandon R, Constantine R. Avoiding EPS is key to realizing ‘atypical’ benefits. Current Psychiatry 2006;5(11):35-45.
12. Lewis SW, Davies L, Jones PB, et al. Randomised controlled trials of conventional antipsychotic versus new atypical drugs, and new atypical drugs versus clozapine, in people with schizophrenia responding poorly to, or intolerant of, current drug treatment. Health Technology Assessment 2006;10(#17):1-182.Available at http://www.hta.ac.uk/project/1078.asp. Accessed January 3, 2007.
13. Heinrichs DW, Hanlon TE, Carpenter WT. The Quality of Life Scale: an instrument for assessing the schizophrenic deficit syndrome. Schizophr Bull 1984;10:388-98.
14. Tandon R, Davis JM, Carpenter WT. CATIE, CUtLASS, and the FGA-SGA debate (letter). Arch Gen Psychiatry 2007 (in press).
15. Lieberman J. Comparative effectiveness of antipsychotic drugs: a commentary on the Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study and Clinical Antipsychotic Trials of Intervention Effectiveness. Arch Gen Psychiatry 2006;63:1069-72.
16. Rosenheck RA. Outcomes, costs, and policy caution: a commentary on the Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study. Arch Gen Psychiatry 2006;63:1074-6.
17. Tandon R. Comparative effectiveness of antipsychotics in the treatment of schizophrenia: what CATIE tells us—Parts 1 and 2. International Drug Therapy Newsletter 2006;41(7,9):51-8,67-74.
18. Meltzer HY, Bobo WV. Interpreting the efficacy findings in the CATIE study: what clinicians should know. CNS Spectrums 2006;11(suppl 7):14-24.
19. Kane JM. Review of treatments that can ameliorate nonadherence in patients with schizophrenia. J Clin Psychiatry 2006;67(suppl 5):9-14.
20. Leucht S, Kane JM, Kissling W, et al. What does the PANSS mean? Schizophr Res 2006;79:231-8.
21. Essock SM, Covell NH, Davis SM, et al. Effectiveness of switching antipsychotic medications. Am J Psychiatry 2006;163:2090-5.
22. Davis JM, Marder S, Tamminga CA. Switch or stay? Am J Psychiatry 2006;163:2032-3.
23. Tandon R, Targum SD, Nasrallah HA, et al. Strategies for maximizing clinical effectiveness in the treatment of schizophrenia. Journal of Psychiatric Practice 2006;12:348-63.
1. Kane JM, Leucht S, Carpenter D, et al. Expert consensus guideline series: optimizing pharmacologic treatment of psychotic disorders. J Clin Psychiatry 2003;64(suppl 12):1-100.
2. Tandon R, Fleischhacker WW. Comparative efficacy of antipsychotics in the treatment of schizophrenia: a critical assessment. Schizophr Res 2005;79:145-55.
3. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med 2005;353:1209-23.
4. McEvoy JP, Lieberman JA, Stroup TS, et al. Effectiveness of clozapine versus olanzapine, quetiapine, and risperidone in patients with chronic schizophrenia who did not respond to prior antipsychotic treatment. Am J Psychiatry 2006;163:600-10.
5. Stroup TS, Lieberman JA, McEvoy JP, et al. Effectiveness of olanzapine, quetiapine, risperidone, and ziprasidone in patients with chronic schizophrenia following discontinuation of a previous atypical antipsychotic. Am J Psychiatry 2006;163:611-22.
6. Rosenheck RA, Leslie DL, Sindelar J, et al. Cost-effectiveness of second-generation antipsychotics and perphenazine in a randomized trial of treatment for chronic schizophrenia. Am J Psychiatry 2006;163:2080-9.
7. Jones PB, Barnes T, Davies L, et al. Randomized controlled trial of the effect on quality of life of second- vs first-generation antipsychotic drugs in schizophrenia: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study (CUtLASS). Arch Gen Psychiatry 2006;63:1079-87.
8. Lewis SW, Barnes TRE, Davies L, et al. Randomised controlled trial of effect of prescription of clozapine versus other second-generation antipsychotic drugs in resistant schizophrenia. Schizophr Bull 2006;32:715-23.
9. Nasrallah HA. CATIE’s surprises: in antipsychotics’ square-off, were there winners or losers? Current Psychiatry 2006;5(2):49-65.
10. Buckley PF. Which antipsychotic do I choose next? CATIE phase 2 offers insights on efficacy and tolerability. Current Psychiatry 2006;5(9):27-43.
11. Tandon R, Constantine R. Avoiding EPS is key to realizing ‘atypical’ benefits. Current Psychiatry 2006;5(11):35-45.
12. Lewis SW, Davies L, Jones PB, et al. Randomised controlled trials of conventional antipsychotic versus new atypical drugs, and new atypical drugs versus clozapine, in people with schizophrenia responding poorly to, or intolerant of, current drug treatment. Health Technology Assessment 2006;10(#17):1-182.Available at http://www.hta.ac.uk/project/1078.asp. Accessed January 3, 2007.
13. Heinrichs DW, Hanlon TE, Carpenter WT. The Quality of Life Scale: an instrument for assessing the schizophrenic deficit syndrome. Schizophr Bull 1984;10:388-98.
14. Tandon R, Davis JM, Carpenter WT. CATIE, CUtLASS, and the FGA-SGA debate (letter). Arch Gen Psychiatry 2007 (in press).
15. Lieberman J. Comparative effectiveness of antipsychotic drugs: a commentary on the Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study and Clinical Antipsychotic Trials of Intervention Effectiveness. Arch Gen Psychiatry 2006;63:1069-72.
16. Rosenheck RA. Outcomes, costs, and policy caution: a commentary on the Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study. Arch Gen Psychiatry 2006;63:1074-6.
17. Tandon R. Comparative effectiveness of antipsychotics in the treatment of schizophrenia: what CATIE tells us—Parts 1 and 2. International Drug Therapy Newsletter 2006;41(7,9):51-8,67-74.
18. Meltzer HY, Bobo WV. Interpreting the efficacy findings in the CATIE study: what clinicians should know. CNS Spectrums 2006;11(suppl 7):14-24.
19. Kane JM. Review of treatments that can ameliorate nonadherence in patients with schizophrenia. J Clin Psychiatry 2006;67(suppl 5):9-14.
20. Leucht S, Kane JM, Kissling W, et al. What does the PANSS mean? Schizophr Res 2006;79:231-8.
21. Essock SM, Covell NH, Davis SM, et al. Effectiveness of switching antipsychotic medications. Am J Psychiatry 2006;163:2090-5.
22. Davis JM, Marder S, Tamminga CA. Switch or stay? Am J Psychiatry 2006;163:2032-3.
23. Tandon R, Targum SD, Nasrallah HA, et al. Strategies for maximizing clinical effectiveness in the treatment of schizophrenia. Journal of Psychiatric Practice 2006;12:348-63.
Does marijuana contribute to psychotic illness?
Evidence grows that marijuana use can cause acute psychosis, bring forward in time a first schizophrenia episode, and worsen the prognosis of patients with psychotic disorders.
Roger, age 16, had been smoking marijuana on and off for about 2 years. His parents knew but believed this was a stage and not dangerous; they had tried marijuana in their youth without harm. Roger’s smoking had increased to several joints daily since he started a relationship with an older girl, who shared and encouraged his habit.
His parents became worried when Roger began making unusual comments, saying that food did not taste “right” and he thought someone was poisoning him. They brought Roger for psychiatric consultation at the recommendation of their family physician.
History and examination revealed that Roger had experienced vague persecutory ideas for several weeks but no systematized delusions or hallucinations. I told Roger and his parents he probably had a drug-induced psychosis and that symptoms would likely disappear without recurrence if he stopped using marijuana. At 2-weeks’ follow-up, he described no more psychotic experiences and said he now realized the danger for him of smoking marijuana. A review 1 month later showed Roger was doing well, and I discharged him after reinforcing the importance of abstinence. But his case didn’t end there.
The dopaminergic effect of cannabinoid receptors (such as CB1) may be one biologic mechanism, according to preliminary evidence. But the dopaminergic pathway might not be the most relevant mechanism, because the primary psychoactive constituent of marijuana—delta-9-tetrahydrocannabinol (delta-9-THC)—causes or increases psychotic symptoms in patients with schizophrenia despite treatment with dopamine receptor antagonists.2
Gene-environment interactions also appear to be relevant. A functional polymorphism in the catechol-O-methyltransferase (COMT) gene (COMT Val158 Met) moderates the influence of cannabis use on developing psychosis, according to a birth cohort study of 803 New Zealanders. COMT valine158 allele carriers were most likely to exhibit psychotic symptoms and develop schizophreniform disorder if they used cannabis during adolescence. This association did not apply to adult-onset cannabis use.3
Results were similar in a study in which 30 patients with a psychotic disorder, 12 relatives of patients with a psychotic disorder, and 32 healthy controls received delta-9-THC or placebo.4
Two years later, I received a request for information about Roger’s episode from an acute inpatient facility. Roger had been admitted after an incident at the local mall in which he screamed at people and accused bystanders of trying to harm him. Despite using marijuana only occasionally, his behavior had been deteriorating and was becoming increasingly bizarre. The attending psychiatrist believed Roger had schizophrenia.
Clinicians regularly deal with patients such as Roger who suffer from a psychotic disorder and use marijuana. This is hardly surprising because marijuana is the most widely used illicit drug. In 2006, 5% of 12th graders in the United States reported using marijuana daily during the previous month, and 42% had tried it at least once.1
Is psychotic patients’ use of marijuana a coincidence? Self-medication? Or could cannabis cause psychotic illness? This debate elicits strong views among community and professional groups. To help you provide up-to-date advice to patients and families, this review:
- describes the growing body of evidence on the mental health consequences of marijuana use
- seeks to help you detect and deal with the effects of marijuana use in clinical practice.
Marijuana and psychosis
Although the neurobiologic association is unclear (Box 1),2-4 up to 15% of users report psychotic phenomena after consuming marijuana.5 Naturalistic and experimental studies have confirmed that marijuana can induce short-lived psychotic experiences.
In two parallel trials, 22 healthy individuals6 and 13 stable, antipsychotic-treated schizophrenia patients7 were given 2.5 mg and 5 mg intravenously of delta-9-tetrahydrocannabinol (delta-9-THC)—the primary psychoactive constituent of marijuana. Both groups developed dose-related, transient, schizophrenia-like symptoms and altered perceptions:
- Healthy volunteers showed the full range of psychotic symptoms. One individual said, “I thought you were giving me THC through the blood pressure machine and the sheets.”2
- Schizophrenia patients tended to report increases in the symptoms of their specific conditions. Those with paranoid illnesses, for example, reported an escalation in persecutory ideas.
Transient psychotic phenomena are not equivalent to a psychotic illness, however. To meet diagnostic criteria for a psychotic disorder, symptoms must be persistent and impair psychosocial functioning.
Early reports. Anecdotal clinical reports that marijuana use could cause psychosis emerged in the 1960s but were largely ignored. Many clinicians assumed that psychotic individuals used marijuana to relieve troubling symptoms (self-medication).
A 15-year, longitudinal study examined the incidence of schizophrenia in >50,000 Swedish conscripts and concluded that marijuana use during adolescence increased the risk of schizophrenia.8 Skeptics questioned the validity of the diagnosis and the etiologic role of other drugs in this study and suggested that prodromal symptoms might have led to marijuana use, rather than marijuana triggering the psychosis.
Recent evidence. Better-designed studies have shown that marijuana use increases the risk of psychosis later in life.
Adolescents who used marijuana by age 15 were more likely to develop a schizophreniform disorder by age 26 than nonusers, according to data from 759 New Zealanders who took part in a prospective, longitudinal, general population study. Marijuana use by age 15 was associated with a higher risk than later use (by age 18).9
A 3-year, longitudinal, population-based study from the Netherlands found marijuana use associated with increased risk of psychosis in 4,045 previously psychosis-free individuals. More than 50% of psychosis diagnoses could be attributed to marijuana use.10
Data from the 21-year longitudinal Christchurch Health and Development Study in New Zealand showed elevated rates of psychotic symptoms in young people with cannabis dependence at ages 18 and 21. The associations remained even after adjustments were made for previous psychotic symptoms and other confounding factors.11
Follow-up analysis of data from the Swedish military conscripts study8 showed that the use of other psychoactive drugs or prodromal cases in the cohort did not explain the association between self-reported marijuana use and hospital admissions for schizophrenia and other psychoses.12
- Starting marijuana use in adolescence
- Using cannabis often (weekly or daily) or for long periods
- Unusual, psychotic-like experiences (such as fleeting persecutory ideas or ideas of reference) or displaying high “psychoticism” on the self-report Symptom Checklist-90-R
- Family history of psychosis
- Prior cannabis-induced psychotic episode
- Cannabis use increases the risk of developing psychosis and is estimated to double the risk for later schizophrenia (5 to 10 new cases per 10,000 person-years)
- The association is not an artifact of confounding factors such as prodromal symptoms or concurrent use of other substances (including amphetamines)
- The risk increases with the frequency and length of use (a dose-effect relationship)
- Self-medication is not the connection between cannabis use and schizophrenia, according to empiric evidence
Researchers in Israel cross-linked a cohort of 9,724 youths aged 16 to 17 screened by the Israeli Draft Board with a national registry of psychiatric hospital admissions for schizophrenia in the following 4 to 15 years. Self-reported drug abuse (mostly marijuana) was higher in adolescents who were later hospitalized for schizophrenia (12.4%) than in those not hospitalized (5.9%).13
Is the diagnosis worthwhile? Acute-phase cannabis-induced psychosis and schizophrenia have similar presentations, making differential diagnosis difficult. If their treatment also is similar, is it clinically meaningful to distinguish whether marijuana use or schizophrenia triggered psychotic symptoms? The answer is yes, because:
- schizophrenia has a worse course and prognosis
- many patients with cannabis-induced psychosis do not develop schizophrenia.
Diagnostic clues. Some clinicians believe cannabis-induced psychosis is more likely than schizophrenia to feature:
- expansive mood
- derealization or depersonalization experiences
- visual hallucinations
- less overall severity.
Consider the course. The only way to differentiate the two disorders is to consider the illness course. Cannabis-induced psychotic episodes occur during periods of intoxication or withdrawal, tend to be short-lived, and usually respond well to treatment if the person abstains.
Up to one-half of patients with a cannabis-induced psychosis develop a schizophrenia-spectrum disorder. Monitoring them (such as at 6-month intervals) is important, therefore, because schizophrenia onset often occurs >12 months after the cannabis-induced psychosis.
Summary. A review of these 5 studies concluded that evidence supports the hypothesis that marijuana use acts as a risk factor in schizophrenia onset.14 Although marijuana use is not a “necessary” causal factor in psychotic illness—most users do not develop the disorder, and many persons with schizophrenia do not use marijuana—strong evidence indicates that it is one of many factors that can cause a psychotic illness (Box 2).9-14
Who is at risk?
Can marijuana cause psychosis in any person or specifically in those at increased risk of psychosis? If the latter, then marijuana—rather than causing new, unanticipated cases—might bring forward schizophrenia onset in individuals who would have developed it later. This explanation is consistent with data showing that persons born in more-recent cohorts seem to have an earlier age of schizophrenia onset.15
Vulnerability for psychosis. Evidence strongly suggests that marijuana-induced psychotic symptoms are more prevalent among vulnerable or psychosis-prone individuals.
- When given 2.5 mg of delta-9-THC, 80% of 13 patients with well-controlled schizophrenia experienced high Positive and Negative Syndrome Scale scores, compared with 35% of 22 healthy controls.2
- Unusual perceptions or thought influence were more common following marijuana use in all participants in a naturalistic experiment, but much more so in “at risk” individuals who had previously described isolated psychotic symptoms.16
- Adolescents and young adults ages 14 to 24 who used marijuana and displayed high “psychoticism” scores at baseline had more than twice the risk of a psychosis outcome 4 years later than did those without high scores.17
Schizophrenia onset. Marijuana users who suffer a drug-induced psychosis are at very high risk of developing a psychotic illness later on. A ≥3-year follow-up study18 of 535 patients who had not been treated for psychotic problems before being diagnosed with marijuana-induced psychotic symptoms found that:
- marijuana-induced psychotic episodes often remitted quickly with minimal treatment
- about one-half of patients were diagnosed with a schizophrenia-spectrum disorder (mostly paranoid schizophrenia) at follow up
- the gap between the marijuana-induced episode and diagnosis of a schizophrenia-spectrum disorder was >1 year in 47% of cases.
- the first episode of schizophrenia in these patients occurred several years earlier than in schizophrenia patients without marijuana-induced psychosis.
Although these findings require replication, they challenge the belief that marijuana-induced psychosis is benign (Box 3).
Implications for treatment
Most psychiatric practitioners treat patients who have psychotic illness and use marijuana (Box 4). Compared with nonusers, these patients tend to have:
- earlier age of schizophrenia onset
- more psychotic symptoms
- worse prognosis because of poorer treatment adherence
- increased symptom severity and persistence
- higher relapse rates.19
Therefore, ask patients with psychotic disorders about their marijuana use, and treat both the marijuana use and the psychosis. Evidence to guide treatment is scarce, however. Nicotine, marijuana, and alcohol use are often intertwined. This suggests that treatments that target a variety of substances may be more efficient than targeted ones, even if the generic interventions are brief.20
A study of marijuana users with early psychosis showed, for example, that marijuana-focused treatment was not more effective than psychoeducation, although both resulted in reduced use.21 In nonpsychotic individuals, giving 90 adult patients incentive vouchers to exchange for retail items each time they provided a marijuana-negative urine specimen resulted in increased abstinence rates over a 12-month period (Box 5).22,23 Cognitive-behavioral therapy helped to sustain the vouchers’ positive effect on abstinence after the initial 14-week treatment.23
Efficacy. In voucher-based reinforcement therapy, patients receive vouchers or monetary incentives redeemable for goods and services, contingent on satisfying predetermined therapeutic goals. A meta-analysis22 showed this therapy model can produce better outcomes in substance use disorders, compared with control treatment.
Marijuana abstinence. A 12-month study of 90 cannabis-dependent adults23 found that voucher-based reinforcement therapy could extend marijuana abstinence. During the 14 weeks of active treatment, participants could redeem vouchers for goods or services—such as movie passes, sports/hobby equipment, work materials, or vocational classes.
- Participants earned a voucher worth $1.50 for the first negative specimen.
- Voucher values increased by $1.50 for each consecutive negative specimen.
- Two consecutive negative specimens earned a $10 bonus.
- Voucher values dropped back to $1.50 if participants provided a cannabinoid-positive specimen or failed to submit a scheduled specimen. Values then could re-escalate according to the same schedule.
Treatment with first-generation antipsychotics does not appear to decrease substance use. Several studies suggest that clozapine decreases the use of nicotine, alcohol, or other substances among patients with schizophrenia,24 though this does not necessarily apply to other second-generation antipsychotics (Box 6).
- Ask about marijuana use when evaluating all patients, particularly young ones
- Educate patients and, if appropriate, families about the risks of marijuana use. One way to do this without sounding judgmental or confrontational is to follow the principles of motivational interviewing
- Treat both the psychosis and the substance use
- Generic interventions that target drug use might be more effective than those specific to cannabis use because psychotic patients often abuse a variety of substances
- Psychoeducation might be as effective as cannabis-specific treatments
- Abstinence-based vouchers are a simple intervention with some evidence of effectiveness
- Clozapine, which seems to reduce relapse of substance use in these patients, might be the antipsychotic of choice
Implications for prevention
Psychiatric practitioners can play an important role in making young people aware of the mental health risks of using marijuana. Marijuana use fluctuates population-wide, depending in part on public perception of its harmfulness. Its use may diminish, therefore, as information on its mental health hazards percolates into high schools and the community at large. We also have the duty to make policy makers and legislators aware of this information.25
Related resources
- National Institute on Drug Abuse. https://www.drugabuse.gov/drugs-abuse/marijuana.
- Cannabis dependence. www.mentalhealth.com/dis/p20-sb03.html.
- Castle D, Murray R, eds. Marijuana and madness: psychiatry and neurobiology. Cambridge, UK: Cambridge University Press; 2004.
- Hall W, Pacula RL. Cannabis use and dependence: public health and public policy. Cambridge, UK: Cambridge University Press; 2003.
Drug brand names
- Clozapine • Clozaril
Disclosure
Dr. Rey reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Teen drug use continues down in 2006, particularly among older teens; but use of prescription-type drugs remains high. Ann Arbor, MI: University of Michigan News and Information Services; Dec. 21, 2006. Available at: http://monitoringthefuture.org. Accessed January 2, 2007.
2. D’Souza DC, Cho HS, Perry EB, Krystal JH. Cannabinoid ’model’ psychosis, dopamine-cannabinoid interactions and implications for schizophrenia. In: Castle D, Murray R, eds. Marijuana and madness: psychiatry and neurobiology. Cambridge, UK: Cambridge University Press; 2004:142-65.
3. Caspi A, Moffitt TE, Cannon M, et al. Moderation of the effect of adolescent-onset cannabis use on adult psychosis by a functional polymorphism in the catechol-O-methyltransferase gene: longitudinal evidence of a gene X environment interaction. Biol Psychiatry 2005;57(10):1117-27.
4. Henquet C, Rosa A, Krabbendam L, et al. An experimental study of catechol-O-methyltransferase Val158 Met moderation of Δ-9-tetrahydrocannabinol-induced effects on psychosis and cognition. Neuropsychopharmacol 2006;31:2748-57.
5. Thomas H. A community survey of adverse effects of cannabis use. Drug Alcohol Depend 1996;42(3):201-7.
6. D’Souza DC, Perry E, MacDougall L, et al. The psychotomimetic effects of intravenous delta-9-tetrahydrocannabinol in healthy individuals: implications for psychosis. Neuropsychopharmacology 2004;29:1558-72.
7. D’Souza DC, Abi-Saab WM, Madonick S, et al. Delta-9-tetrahydrocannabinol effects in schizophrenia: implications for cognition, psychosis, and addiction. Biol Psychiatry 2005;57:594-608.
8. Andreasson S, Allebeck P, Engstrom A, Rydberg U. Cannabis and schizophrenia. A longitudinal study of Swedish conscripts. Lancet 1987;2(8574):1483-6.
9. Arseneault L, Cannon M, Poulton R, et al. Cannabis use in adolescence and risk for adult psychosis: longitudinal prospective study. BMJ 2002;325(7374):1212-3.
10. van Os J, Bak M, Hanssen M, et al. Cannabis use and psychosis: a longitudinal population-based study. Am J Epidemiol 2002;156(4):319-27.
11. Fergusson DM, Horwood LJ, Swain-Campbell NR. Cannabis dependence and psychotic symptoms in young people. Psychol Med 2003;33(1):15-21.
12. Zammit S, Allebeck P, Andreasson S, et al. Self reported cannabis use as a risk factor for schizophrenia in Swedish conscripts of 1969: historical cohort study. BMJ 2002;325(7374):1199-201.
13. Weiser M, Knobler HY, Noy S, Kaplan Z. Clinical characteristics of adolescents later hospitalized for schizophrenia. Am J Med Genet 2002;114:949-55.
14. Smit F, Bolier L, Cuijpers P. Cannabis use and the risk of later schizophrenia: a review. Addiction 2004;99(4):425-30.
15. Di Maggio C, Martinez M, Menard JF, et al. Evidence of a cohort effect for age at onset of schizophrenia. Am J Psychiatry 2001;158(3):489-92.
16. Verdoux H, Gindre C, Sorbara F, et al. Effects of cannabis and psychosis vulnerability in daily life: an experience sampling test study. Psychol Med 2003;33(1):23-32.
17. Henquet C, Krabbendam L, Spauwen J, et al. Prospective cohort study of cannabis use, predisposition for psychosis, and psychotic symptoms in young people. BMJ 2005;330(7481):11-4.
18. Arendt M, Rosenberg R, Foldager L, et al. Cannabis-induced psychosis and subsequent schizophrenia-spectrum disorders: follow-up study of 535 incident cases. Br J Psychiatry 2005;187:510-5.
19. Pencer A, Addington J, Addington D. Outcome of a first episode of psychosis in adolescence: a 2-year follow-up. Psychiatry Res 2005;133(1):35-43.
20. McCambridge J, Strang J. The efficacy of single-session motivational interviewing in reducing drug consumption and perceptions of drug-related risk and harm among young people: results from a multi-site cluster randomized trial. Addiction 2004;99(1):39-52.
21. Edwards J, Elkins K, Hinton M, et al. Randomized controlled trial of a cannabis-focused intervention for young people with first-episode psychosis. Acta Psychiatr Scand 2006;114(2):109-17.
22. Lussier JP, Heil SH, Mongeon JA, et al. A meta-analysis of voucher-based reinforcement therapy for substance use disorders. Addiction 2006;101:192-203.
23. Budney AJ, Moore BA, Rocha HL, Higgins ST. Clinical trial of abstinence-based vouchers and cognitive-behavioral therapy for cannabis dependence. J Consult Clin Psychol 2006;74(2):307-16.
24. Brunette MF, Drake RE, Xie H, et al. Clozapine use and relapses of substance use disorder among patients with co-occurring schizophrenia and substance use disorders. Schizophr Bull 2006;32(4):637-43.
25. Hall W, Degenhardt L. What are the policy implications of the evidence on cannabis and psychosis? Can J Psychiatry 2006;51(9):566-74.
Evidence grows that marijuana use can cause acute psychosis, bring forward in time a first schizophrenia episode, and worsen the prognosis of patients with psychotic disorders.
Roger, age 16, had been smoking marijuana on and off for about 2 years. His parents knew but believed this was a stage and not dangerous; they had tried marijuana in their youth without harm. Roger’s smoking had increased to several joints daily since he started a relationship with an older girl, who shared and encouraged his habit.
His parents became worried when Roger began making unusual comments, saying that food did not taste “right” and he thought someone was poisoning him. They brought Roger for psychiatric consultation at the recommendation of their family physician.
History and examination revealed that Roger had experienced vague persecutory ideas for several weeks but no systematized delusions or hallucinations. I told Roger and his parents he probably had a drug-induced psychosis and that symptoms would likely disappear without recurrence if he stopped using marijuana. At 2-weeks’ follow-up, he described no more psychotic experiences and said he now realized the danger for him of smoking marijuana. A review 1 month later showed Roger was doing well, and I discharged him after reinforcing the importance of abstinence. But his case didn’t end there.
The dopaminergic effect of cannabinoid receptors (such as CB1) may be one biologic mechanism, according to preliminary evidence. But the dopaminergic pathway might not be the most relevant mechanism, because the primary psychoactive constituent of marijuana—delta-9-tetrahydrocannabinol (delta-9-THC)—causes or increases psychotic symptoms in patients with schizophrenia despite treatment with dopamine receptor antagonists.2
Gene-environment interactions also appear to be relevant. A functional polymorphism in the catechol-O-methyltransferase (COMT) gene (COMT Val158 Met) moderates the influence of cannabis use on developing psychosis, according to a birth cohort study of 803 New Zealanders. COMT valine158 allele carriers were most likely to exhibit psychotic symptoms and develop schizophreniform disorder if they used cannabis during adolescence. This association did not apply to adult-onset cannabis use.3
Results were similar in a study in which 30 patients with a psychotic disorder, 12 relatives of patients with a psychotic disorder, and 32 healthy controls received delta-9-THC or placebo.4
Two years later, I received a request for information about Roger’s episode from an acute inpatient facility. Roger had been admitted after an incident at the local mall in which he screamed at people and accused bystanders of trying to harm him. Despite using marijuana only occasionally, his behavior had been deteriorating and was becoming increasingly bizarre. The attending psychiatrist believed Roger had schizophrenia.
Clinicians regularly deal with patients such as Roger who suffer from a psychotic disorder and use marijuana. This is hardly surprising because marijuana is the most widely used illicit drug. In 2006, 5% of 12th graders in the United States reported using marijuana daily during the previous month, and 42% had tried it at least once.1
Is psychotic patients’ use of marijuana a coincidence? Self-medication? Or could cannabis cause psychotic illness? This debate elicits strong views among community and professional groups. To help you provide up-to-date advice to patients and families, this review:
- describes the growing body of evidence on the mental health consequences of marijuana use
- seeks to help you detect and deal with the effects of marijuana use in clinical practice.
Marijuana and psychosis
Although the neurobiologic association is unclear (Box 1),2-4 up to 15% of users report psychotic phenomena after consuming marijuana.5 Naturalistic and experimental studies have confirmed that marijuana can induce short-lived psychotic experiences.
In two parallel trials, 22 healthy individuals6 and 13 stable, antipsychotic-treated schizophrenia patients7 were given 2.5 mg and 5 mg intravenously of delta-9-tetrahydrocannabinol (delta-9-THC)—the primary psychoactive constituent of marijuana. Both groups developed dose-related, transient, schizophrenia-like symptoms and altered perceptions:
- Healthy volunteers showed the full range of psychotic symptoms. One individual said, “I thought you were giving me THC through the blood pressure machine and the sheets.”2
- Schizophrenia patients tended to report increases in the symptoms of their specific conditions. Those with paranoid illnesses, for example, reported an escalation in persecutory ideas.
Transient psychotic phenomena are not equivalent to a psychotic illness, however. To meet diagnostic criteria for a psychotic disorder, symptoms must be persistent and impair psychosocial functioning.
Early reports. Anecdotal clinical reports that marijuana use could cause psychosis emerged in the 1960s but were largely ignored. Many clinicians assumed that psychotic individuals used marijuana to relieve troubling symptoms (self-medication).
A 15-year, longitudinal study examined the incidence of schizophrenia in >50,000 Swedish conscripts and concluded that marijuana use during adolescence increased the risk of schizophrenia.8 Skeptics questioned the validity of the diagnosis and the etiologic role of other drugs in this study and suggested that prodromal symptoms might have led to marijuana use, rather than marijuana triggering the psychosis.
Recent evidence. Better-designed studies have shown that marijuana use increases the risk of psychosis later in life.
Adolescents who used marijuana by age 15 were more likely to develop a schizophreniform disorder by age 26 than nonusers, according to data from 759 New Zealanders who took part in a prospective, longitudinal, general population study. Marijuana use by age 15 was associated with a higher risk than later use (by age 18).9
A 3-year, longitudinal, population-based study from the Netherlands found marijuana use associated with increased risk of psychosis in 4,045 previously psychosis-free individuals. More than 50% of psychosis diagnoses could be attributed to marijuana use.10
Data from the 21-year longitudinal Christchurch Health and Development Study in New Zealand showed elevated rates of psychotic symptoms in young people with cannabis dependence at ages 18 and 21. The associations remained even after adjustments were made for previous psychotic symptoms and other confounding factors.11
Follow-up analysis of data from the Swedish military conscripts study8 showed that the use of other psychoactive drugs or prodromal cases in the cohort did not explain the association between self-reported marijuana use and hospital admissions for schizophrenia and other psychoses.12
- Starting marijuana use in adolescence
- Using cannabis often (weekly or daily) or for long periods
- Unusual, psychotic-like experiences (such as fleeting persecutory ideas or ideas of reference) or displaying high “psychoticism” on the self-report Symptom Checklist-90-R
- Family history of psychosis
- Prior cannabis-induced psychotic episode
- Cannabis use increases the risk of developing psychosis and is estimated to double the risk for later schizophrenia (5 to 10 new cases per 10,000 person-years)
- The association is not an artifact of confounding factors such as prodromal symptoms or concurrent use of other substances (including amphetamines)
- The risk increases with the frequency and length of use (a dose-effect relationship)
- Self-medication is not the connection between cannabis use and schizophrenia, according to empiric evidence
Researchers in Israel cross-linked a cohort of 9,724 youths aged 16 to 17 screened by the Israeli Draft Board with a national registry of psychiatric hospital admissions for schizophrenia in the following 4 to 15 years. Self-reported drug abuse (mostly marijuana) was higher in adolescents who were later hospitalized for schizophrenia (12.4%) than in those not hospitalized (5.9%).13
Is the diagnosis worthwhile? Acute-phase cannabis-induced psychosis and schizophrenia have similar presentations, making differential diagnosis difficult. If their treatment also is similar, is it clinically meaningful to distinguish whether marijuana use or schizophrenia triggered psychotic symptoms? The answer is yes, because:
- schizophrenia has a worse course and prognosis
- many patients with cannabis-induced psychosis do not develop schizophrenia.
Diagnostic clues. Some clinicians believe cannabis-induced psychosis is more likely than schizophrenia to feature:
- expansive mood
- derealization or depersonalization experiences
- visual hallucinations
- less overall severity.
Consider the course. The only way to differentiate the two disorders is to consider the illness course. Cannabis-induced psychotic episodes occur during periods of intoxication or withdrawal, tend to be short-lived, and usually respond well to treatment if the person abstains.
Up to one-half of patients with a cannabis-induced psychosis develop a schizophrenia-spectrum disorder. Monitoring them (such as at 6-month intervals) is important, therefore, because schizophrenia onset often occurs >12 months after the cannabis-induced psychosis.
Summary. A review of these 5 studies concluded that evidence supports the hypothesis that marijuana use acts as a risk factor in schizophrenia onset.14 Although marijuana use is not a “necessary” causal factor in psychotic illness—most users do not develop the disorder, and many persons with schizophrenia do not use marijuana—strong evidence indicates that it is one of many factors that can cause a psychotic illness (Box 2).9-14
Who is at risk?
Can marijuana cause psychosis in any person or specifically in those at increased risk of psychosis? If the latter, then marijuana—rather than causing new, unanticipated cases—might bring forward schizophrenia onset in individuals who would have developed it later. This explanation is consistent with data showing that persons born in more-recent cohorts seem to have an earlier age of schizophrenia onset.15
Vulnerability for psychosis. Evidence strongly suggests that marijuana-induced psychotic symptoms are more prevalent among vulnerable or psychosis-prone individuals.
- When given 2.5 mg of delta-9-THC, 80% of 13 patients with well-controlled schizophrenia experienced high Positive and Negative Syndrome Scale scores, compared with 35% of 22 healthy controls.2
- Unusual perceptions or thought influence were more common following marijuana use in all participants in a naturalistic experiment, but much more so in “at risk” individuals who had previously described isolated psychotic symptoms.16
- Adolescents and young adults ages 14 to 24 who used marijuana and displayed high “psychoticism” scores at baseline had more than twice the risk of a psychosis outcome 4 years later than did those without high scores.17
Schizophrenia onset. Marijuana users who suffer a drug-induced psychosis are at very high risk of developing a psychotic illness later on. A ≥3-year follow-up study18 of 535 patients who had not been treated for psychotic problems before being diagnosed with marijuana-induced psychotic symptoms found that:
- marijuana-induced psychotic episodes often remitted quickly with minimal treatment
- about one-half of patients were diagnosed with a schizophrenia-spectrum disorder (mostly paranoid schizophrenia) at follow up
- the gap between the marijuana-induced episode and diagnosis of a schizophrenia-spectrum disorder was >1 year in 47% of cases.
- the first episode of schizophrenia in these patients occurred several years earlier than in schizophrenia patients without marijuana-induced psychosis.
Although these findings require replication, they challenge the belief that marijuana-induced psychosis is benign (Box 3).
Implications for treatment
Most psychiatric practitioners treat patients who have psychotic illness and use marijuana (Box 4). Compared with nonusers, these patients tend to have:
- earlier age of schizophrenia onset
- more psychotic symptoms
- worse prognosis because of poorer treatment adherence
- increased symptom severity and persistence
- higher relapse rates.19
Therefore, ask patients with psychotic disorders about their marijuana use, and treat both the marijuana use and the psychosis. Evidence to guide treatment is scarce, however. Nicotine, marijuana, and alcohol use are often intertwined. This suggests that treatments that target a variety of substances may be more efficient than targeted ones, even if the generic interventions are brief.20
A study of marijuana users with early psychosis showed, for example, that marijuana-focused treatment was not more effective than psychoeducation, although both resulted in reduced use.21 In nonpsychotic individuals, giving 90 adult patients incentive vouchers to exchange for retail items each time they provided a marijuana-negative urine specimen resulted in increased abstinence rates over a 12-month period (Box 5).22,23 Cognitive-behavioral therapy helped to sustain the vouchers’ positive effect on abstinence after the initial 14-week treatment.23
Efficacy. In voucher-based reinforcement therapy, patients receive vouchers or monetary incentives redeemable for goods and services, contingent on satisfying predetermined therapeutic goals. A meta-analysis22 showed this therapy model can produce better outcomes in substance use disorders, compared with control treatment.
Marijuana abstinence. A 12-month study of 90 cannabis-dependent adults23 found that voucher-based reinforcement therapy could extend marijuana abstinence. During the 14 weeks of active treatment, participants could redeem vouchers for goods or services—such as movie passes, sports/hobby equipment, work materials, or vocational classes.
- Participants earned a voucher worth $1.50 for the first negative specimen.
- Voucher values increased by $1.50 for each consecutive negative specimen.
- Two consecutive negative specimens earned a $10 bonus.
- Voucher values dropped back to $1.50 if participants provided a cannabinoid-positive specimen or failed to submit a scheduled specimen. Values then could re-escalate according to the same schedule.
Treatment with first-generation antipsychotics does not appear to decrease substance use. Several studies suggest that clozapine decreases the use of nicotine, alcohol, or other substances among patients with schizophrenia,24 though this does not necessarily apply to other second-generation antipsychotics (Box 6).
- Ask about marijuana use when evaluating all patients, particularly young ones
- Educate patients and, if appropriate, families about the risks of marijuana use. One way to do this without sounding judgmental or confrontational is to follow the principles of motivational interviewing
- Treat both the psychosis and the substance use
- Generic interventions that target drug use might be more effective than those specific to cannabis use because psychotic patients often abuse a variety of substances
- Psychoeducation might be as effective as cannabis-specific treatments
- Abstinence-based vouchers are a simple intervention with some evidence of effectiveness
- Clozapine, which seems to reduce relapse of substance use in these patients, might be the antipsychotic of choice
Implications for prevention
Psychiatric practitioners can play an important role in making young people aware of the mental health risks of using marijuana. Marijuana use fluctuates population-wide, depending in part on public perception of its harmfulness. Its use may diminish, therefore, as information on its mental health hazards percolates into high schools and the community at large. We also have the duty to make policy makers and legislators aware of this information.25
Related resources
- National Institute on Drug Abuse. https://www.drugabuse.gov/drugs-abuse/marijuana.
- Cannabis dependence. www.mentalhealth.com/dis/p20-sb03.html.
- Castle D, Murray R, eds. Marijuana and madness: psychiatry and neurobiology. Cambridge, UK: Cambridge University Press; 2004.
- Hall W, Pacula RL. Cannabis use and dependence: public health and public policy. Cambridge, UK: Cambridge University Press; 2003.
Drug brand names
- Clozapine • Clozaril
Disclosure
Dr. Rey reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Evidence grows that marijuana use can cause acute psychosis, bring forward in time a first schizophrenia episode, and worsen the prognosis of patients with psychotic disorders.
Roger, age 16, had been smoking marijuana on and off for about 2 years. His parents knew but believed this was a stage and not dangerous; they had tried marijuana in their youth without harm. Roger’s smoking had increased to several joints daily since he started a relationship with an older girl, who shared and encouraged his habit.
His parents became worried when Roger began making unusual comments, saying that food did not taste “right” and he thought someone was poisoning him. They brought Roger for psychiatric consultation at the recommendation of their family physician.
History and examination revealed that Roger had experienced vague persecutory ideas for several weeks but no systematized delusions or hallucinations. I told Roger and his parents he probably had a drug-induced psychosis and that symptoms would likely disappear without recurrence if he stopped using marijuana. At 2-weeks’ follow-up, he described no more psychotic experiences and said he now realized the danger for him of smoking marijuana. A review 1 month later showed Roger was doing well, and I discharged him after reinforcing the importance of abstinence. But his case didn’t end there.
The dopaminergic effect of cannabinoid receptors (such as CB1) may be one biologic mechanism, according to preliminary evidence. But the dopaminergic pathway might not be the most relevant mechanism, because the primary psychoactive constituent of marijuana—delta-9-tetrahydrocannabinol (delta-9-THC)—causes or increases psychotic symptoms in patients with schizophrenia despite treatment with dopamine receptor antagonists.2
Gene-environment interactions also appear to be relevant. A functional polymorphism in the catechol-O-methyltransferase (COMT) gene (COMT Val158 Met) moderates the influence of cannabis use on developing psychosis, according to a birth cohort study of 803 New Zealanders. COMT valine158 allele carriers were most likely to exhibit psychotic symptoms and develop schizophreniform disorder if they used cannabis during adolescence. This association did not apply to adult-onset cannabis use.3
Results were similar in a study in which 30 patients with a psychotic disorder, 12 relatives of patients with a psychotic disorder, and 32 healthy controls received delta-9-THC or placebo.4
Two years later, I received a request for information about Roger’s episode from an acute inpatient facility. Roger had been admitted after an incident at the local mall in which he screamed at people and accused bystanders of trying to harm him. Despite using marijuana only occasionally, his behavior had been deteriorating and was becoming increasingly bizarre. The attending psychiatrist believed Roger had schizophrenia.
Clinicians regularly deal with patients such as Roger who suffer from a psychotic disorder and use marijuana. This is hardly surprising because marijuana is the most widely used illicit drug. In 2006, 5% of 12th graders in the United States reported using marijuana daily during the previous month, and 42% had tried it at least once.1
Is psychotic patients’ use of marijuana a coincidence? Self-medication? Or could cannabis cause psychotic illness? This debate elicits strong views among community and professional groups. To help you provide up-to-date advice to patients and families, this review:
- describes the growing body of evidence on the mental health consequences of marijuana use
- seeks to help you detect and deal with the effects of marijuana use in clinical practice.
Marijuana and psychosis
Although the neurobiologic association is unclear (Box 1),2-4 up to 15% of users report psychotic phenomena after consuming marijuana.5 Naturalistic and experimental studies have confirmed that marijuana can induce short-lived psychotic experiences.
In two parallel trials, 22 healthy individuals6 and 13 stable, antipsychotic-treated schizophrenia patients7 were given 2.5 mg and 5 mg intravenously of delta-9-tetrahydrocannabinol (delta-9-THC)—the primary psychoactive constituent of marijuana. Both groups developed dose-related, transient, schizophrenia-like symptoms and altered perceptions:
- Healthy volunteers showed the full range of psychotic symptoms. One individual said, “I thought you were giving me THC through the blood pressure machine and the sheets.”2
- Schizophrenia patients tended to report increases in the symptoms of their specific conditions. Those with paranoid illnesses, for example, reported an escalation in persecutory ideas.
Transient psychotic phenomena are not equivalent to a psychotic illness, however. To meet diagnostic criteria for a psychotic disorder, symptoms must be persistent and impair psychosocial functioning.
Early reports. Anecdotal clinical reports that marijuana use could cause psychosis emerged in the 1960s but were largely ignored. Many clinicians assumed that psychotic individuals used marijuana to relieve troubling symptoms (self-medication).
A 15-year, longitudinal study examined the incidence of schizophrenia in >50,000 Swedish conscripts and concluded that marijuana use during adolescence increased the risk of schizophrenia.8 Skeptics questioned the validity of the diagnosis and the etiologic role of other drugs in this study and suggested that prodromal symptoms might have led to marijuana use, rather than marijuana triggering the psychosis.
Recent evidence. Better-designed studies have shown that marijuana use increases the risk of psychosis later in life.
Adolescents who used marijuana by age 15 were more likely to develop a schizophreniform disorder by age 26 than nonusers, according to data from 759 New Zealanders who took part in a prospective, longitudinal, general population study. Marijuana use by age 15 was associated with a higher risk than later use (by age 18).9
A 3-year, longitudinal, population-based study from the Netherlands found marijuana use associated with increased risk of psychosis in 4,045 previously psychosis-free individuals. More than 50% of psychosis diagnoses could be attributed to marijuana use.10
Data from the 21-year longitudinal Christchurch Health and Development Study in New Zealand showed elevated rates of psychotic symptoms in young people with cannabis dependence at ages 18 and 21. The associations remained even after adjustments were made for previous psychotic symptoms and other confounding factors.11
Follow-up analysis of data from the Swedish military conscripts study8 showed that the use of other psychoactive drugs or prodromal cases in the cohort did not explain the association between self-reported marijuana use and hospital admissions for schizophrenia and other psychoses.12
- Starting marijuana use in adolescence
- Using cannabis often (weekly or daily) or for long periods
- Unusual, psychotic-like experiences (such as fleeting persecutory ideas or ideas of reference) or displaying high “psychoticism” on the self-report Symptom Checklist-90-R
- Family history of psychosis
- Prior cannabis-induced psychotic episode
- Cannabis use increases the risk of developing psychosis and is estimated to double the risk for later schizophrenia (5 to 10 new cases per 10,000 person-years)
- The association is not an artifact of confounding factors such as prodromal symptoms or concurrent use of other substances (including amphetamines)
- The risk increases with the frequency and length of use (a dose-effect relationship)
- Self-medication is not the connection between cannabis use and schizophrenia, according to empiric evidence
Researchers in Israel cross-linked a cohort of 9,724 youths aged 16 to 17 screened by the Israeli Draft Board with a national registry of psychiatric hospital admissions for schizophrenia in the following 4 to 15 years. Self-reported drug abuse (mostly marijuana) was higher in adolescents who were later hospitalized for schizophrenia (12.4%) than in those not hospitalized (5.9%).13
Is the diagnosis worthwhile? Acute-phase cannabis-induced psychosis and schizophrenia have similar presentations, making differential diagnosis difficult. If their treatment also is similar, is it clinically meaningful to distinguish whether marijuana use or schizophrenia triggered psychotic symptoms? The answer is yes, because:
- schizophrenia has a worse course and prognosis
- many patients with cannabis-induced psychosis do not develop schizophrenia.
Diagnostic clues. Some clinicians believe cannabis-induced psychosis is more likely than schizophrenia to feature:
- expansive mood
- derealization or depersonalization experiences
- visual hallucinations
- less overall severity.
Consider the course. The only way to differentiate the two disorders is to consider the illness course. Cannabis-induced psychotic episodes occur during periods of intoxication or withdrawal, tend to be short-lived, and usually respond well to treatment if the person abstains.
Up to one-half of patients with a cannabis-induced psychosis develop a schizophrenia-spectrum disorder. Monitoring them (such as at 6-month intervals) is important, therefore, because schizophrenia onset often occurs >12 months after the cannabis-induced psychosis.
Summary. A review of these 5 studies concluded that evidence supports the hypothesis that marijuana use acts as a risk factor in schizophrenia onset.14 Although marijuana use is not a “necessary” causal factor in psychotic illness—most users do not develop the disorder, and many persons with schizophrenia do not use marijuana—strong evidence indicates that it is one of many factors that can cause a psychotic illness (Box 2).9-14
Who is at risk?
Can marijuana cause psychosis in any person or specifically in those at increased risk of psychosis? If the latter, then marijuana—rather than causing new, unanticipated cases—might bring forward schizophrenia onset in individuals who would have developed it later. This explanation is consistent with data showing that persons born in more-recent cohorts seem to have an earlier age of schizophrenia onset.15
Vulnerability for psychosis. Evidence strongly suggests that marijuana-induced psychotic symptoms are more prevalent among vulnerable or psychosis-prone individuals.
- When given 2.5 mg of delta-9-THC, 80% of 13 patients with well-controlled schizophrenia experienced high Positive and Negative Syndrome Scale scores, compared with 35% of 22 healthy controls.2
- Unusual perceptions or thought influence were more common following marijuana use in all participants in a naturalistic experiment, but much more so in “at risk” individuals who had previously described isolated psychotic symptoms.16
- Adolescents and young adults ages 14 to 24 who used marijuana and displayed high “psychoticism” scores at baseline had more than twice the risk of a psychosis outcome 4 years later than did those without high scores.17
Schizophrenia onset. Marijuana users who suffer a drug-induced psychosis are at very high risk of developing a psychotic illness later on. A ≥3-year follow-up study18 of 535 patients who had not been treated for psychotic problems before being diagnosed with marijuana-induced psychotic symptoms found that:
- marijuana-induced psychotic episodes often remitted quickly with minimal treatment
- about one-half of patients were diagnosed with a schizophrenia-spectrum disorder (mostly paranoid schizophrenia) at follow up
- the gap between the marijuana-induced episode and diagnosis of a schizophrenia-spectrum disorder was >1 year in 47% of cases.
- the first episode of schizophrenia in these patients occurred several years earlier than in schizophrenia patients without marijuana-induced psychosis.
Although these findings require replication, they challenge the belief that marijuana-induced psychosis is benign (Box 3).
Implications for treatment
Most psychiatric practitioners treat patients who have psychotic illness and use marijuana (Box 4). Compared with nonusers, these patients tend to have:
- earlier age of schizophrenia onset
- more psychotic symptoms
- worse prognosis because of poorer treatment adherence
- increased symptom severity and persistence
- higher relapse rates.19
Therefore, ask patients with psychotic disorders about their marijuana use, and treat both the marijuana use and the psychosis. Evidence to guide treatment is scarce, however. Nicotine, marijuana, and alcohol use are often intertwined. This suggests that treatments that target a variety of substances may be more efficient than targeted ones, even if the generic interventions are brief.20
A study of marijuana users with early psychosis showed, for example, that marijuana-focused treatment was not more effective than psychoeducation, although both resulted in reduced use.21 In nonpsychotic individuals, giving 90 adult patients incentive vouchers to exchange for retail items each time they provided a marijuana-negative urine specimen resulted in increased abstinence rates over a 12-month period (Box 5).22,23 Cognitive-behavioral therapy helped to sustain the vouchers’ positive effect on abstinence after the initial 14-week treatment.23
Efficacy. In voucher-based reinforcement therapy, patients receive vouchers or monetary incentives redeemable for goods and services, contingent on satisfying predetermined therapeutic goals. A meta-analysis22 showed this therapy model can produce better outcomes in substance use disorders, compared with control treatment.
Marijuana abstinence. A 12-month study of 90 cannabis-dependent adults23 found that voucher-based reinforcement therapy could extend marijuana abstinence. During the 14 weeks of active treatment, participants could redeem vouchers for goods or services—such as movie passes, sports/hobby equipment, work materials, or vocational classes.
- Participants earned a voucher worth $1.50 for the first negative specimen.
- Voucher values increased by $1.50 for each consecutive negative specimen.
- Two consecutive negative specimens earned a $10 bonus.
- Voucher values dropped back to $1.50 if participants provided a cannabinoid-positive specimen or failed to submit a scheduled specimen. Values then could re-escalate according to the same schedule.
Treatment with first-generation antipsychotics does not appear to decrease substance use. Several studies suggest that clozapine decreases the use of nicotine, alcohol, or other substances among patients with schizophrenia,24 though this does not necessarily apply to other second-generation antipsychotics (Box 6).
- Ask about marijuana use when evaluating all patients, particularly young ones
- Educate patients and, if appropriate, families about the risks of marijuana use. One way to do this without sounding judgmental or confrontational is to follow the principles of motivational interviewing
- Treat both the psychosis and the substance use
- Generic interventions that target drug use might be more effective than those specific to cannabis use because psychotic patients often abuse a variety of substances
- Psychoeducation might be as effective as cannabis-specific treatments
- Abstinence-based vouchers are a simple intervention with some evidence of effectiveness
- Clozapine, which seems to reduce relapse of substance use in these patients, might be the antipsychotic of choice
Implications for prevention
Psychiatric practitioners can play an important role in making young people aware of the mental health risks of using marijuana. Marijuana use fluctuates population-wide, depending in part on public perception of its harmfulness. Its use may diminish, therefore, as information on its mental health hazards percolates into high schools and the community at large. We also have the duty to make policy makers and legislators aware of this information.25
Related resources
- National Institute on Drug Abuse. https://www.drugabuse.gov/drugs-abuse/marijuana.
- Cannabis dependence. www.mentalhealth.com/dis/p20-sb03.html.
- Castle D, Murray R, eds. Marijuana and madness: psychiatry and neurobiology. Cambridge, UK: Cambridge University Press; 2004.
- Hall W, Pacula RL. Cannabis use and dependence: public health and public policy. Cambridge, UK: Cambridge University Press; 2003.
Drug brand names
- Clozapine • Clozaril
Disclosure
Dr. Rey reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Teen drug use continues down in 2006, particularly among older teens; but use of prescription-type drugs remains high. Ann Arbor, MI: University of Michigan News and Information Services; Dec. 21, 2006. Available at: http://monitoringthefuture.org. Accessed January 2, 2007.
2. D’Souza DC, Cho HS, Perry EB, Krystal JH. Cannabinoid ’model’ psychosis, dopamine-cannabinoid interactions and implications for schizophrenia. In: Castle D, Murray R, eds. Marijuana and madness: psychiatry and neurobiology. Cambridge, UK: Cambridge University Press; 2004:142-65.
3. Caspi A, Moffitt TE, Cannon M, et al. Moderation of the effect of adolescent-onset cannabis use on adult psychosis by a functional polymorphism in the catechol-O-methyltransferase gene: longitudinal evidence of a gene X environment interaction. Biol Psychiatry 2005;57(10):1117-27.
4. Henquet C, Rosa A, Krabbendam L, et al. An experimental study of catechol-O-methyltransferase Val158 Met moderation of Δ-9-tetrahydrocannabinol-induced effects on psychosis and cognition. Neuropsychopharmacol 2006;31:2748-57.
5. Thomas H. A community survey of adverse effects of cannabis use. Drug Alcohol Depend 1996;42(3):201-7.
6. D’Souza DC, Perry E, MacDougall L, et al. The psychotomimetic effects of intravenous delta-9-tetrahydrocannabinol in healthy individuals: implications for psychosis. Neuropsychopharmacology 2004;29:1558-72.
7. D’Souza DC, Abi-Saab WM, Madonick S, et al. Delta-9-tetrahydrocannabinol effects in schizophrenia: implications for cognition, psychosis, and addiction. Biol Psychiatry 2005;57:594-608.
8. Andreasson S, Allebeck P, Engstrom A, Rydberg U. Cannabis and schizophrenia. A longitudinal study of Swedish conscripts. Lancet 1987;2(8574):1483-6.
9. Arseneault L, Cannon M, Poulton R, et al. Cannabis use in adolescence and risk for adult psychosis: longitudinal prospective study. BMJ 2002;325(7374):1212-3.
10. van Os J, Bak M, Hanssen M, et al. Cannabis use and psychosis: a longitudinal population-based study. Am J Epidemiol 2002;156(4):319-27.
11. Fergusson DM, Horwood LJ, Swain-Campbell NR. Cannabis dependence and psychotic symptoms in young people. Psychol Med 2003;33(1):15-21.
12. Zammit S, Allebeck P, Andreasson S, et al. Self reported cannabis use as a risk factor for schizophrenia in Swedish conscripts of 1969: historical cohort study. BMJ 2002;325(7374):1199-201.
13. Weiser M, Knobler HY, Noy S, Kaplan Z. Clinical characteristics of adolescents later hospitalized for schizophrenia. Am J Med Genet 2002;114:949-55.
14. Smit F, Bolier L, Cuijpers P. Cannabis use and the risk of later schizophrenia: a review. Addiction 2004;99(4):425-30.
15. Di Maggio C, Martinez M, Menard JF, et al. Evidence of a cohort effect for age at onset of schizophrenia. Am J Psychiatry 2001;158(3):489-92.
16. Verdoux H, Gindre C, Sorbara F, et al. Effects of cannabis and psychosis vulnerability in daily life: an experience sampling test study. Psychol Med 2003;33(1):23-32.
17. Henquet C, Krabbendam L, Spauwen J, et al. Prospective cohort study of cannabis use, predisposition for psychosis, and psychotic symptoms in young people. BMJ 2005;330(7481):11-4.
18. Arendt M, Rosenberg R, Foldager L, et al. Cannabis-induced psychosis and subsequent schizophrenia-spectrum disorders: follow-up study of 535 incident cases. Br J Psychiatry 2005;187:510-5.
19. Pencer A, Addington J, Addington D. Outcome of a first episode of psychosis in adolescence: a 2-year follow-up. Psychiatry Res 2005;133(1):35-43.
20. McCambridge J, Strang J. The efficacy of single-session motivational interviewing in reducing drug consumption and perceptions of drug-related risk and harm among young people: results from a multi-site cluster randomized trial. Addiction 2004;99(1):39-52.
21. Edwards J, Elkins K, Hinton M, et al. Randomized controlled trial of a cannabis-focused intervention for young people with first-episode psychosis. Acta Psychiatr Scand 2006;114(2):109-17.
22. Lussier JP, Heil SH, Mongeon JA, et al. A meta-analysis of voucher-based reinforcement therapy for substance use disorders. Addiction 2006;101:192-203.
23. Budney AJ, Moore BA, Rocha HL, Higgins ST. Clinical trial of abstinence-based vouchers and cognitive-behavioral therapy for cannabis dependence. J Consult Clin Psychol 2006;74(2):307-16.
24. Brunette MF, Drake RE, Xie H, et al. Clozapine use and relapses of substance use disorder among patients with co-occurring schizophrenia and substance use disorders. Schizophr Bull 2006;32(4):637-43.
25. Hall W, Degenhardt L. What are the policy implications of the evidence on cannabis and psychosis? Can J Psychiatry 2006;51(9):566-74.
1. Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Teen drug use continues down in 2006, particularly among older teens; but use of prescription-type drugs remains high. Ann Arbor, MI: University of Michigan News and Information Services; Dec. 21, 2006. Available at: http://monitoringthefuture.org. Accessed January 2, 2007.
2. D’Souza DC, Cho HS, Perry EB, Krystal JH. Cannabinoid ’model’ psychosis, dopamine-cannabinoid interactions and implications for schizophrenia. In: Castle D, Murray R, eds. Marijuana and madness: psychiatry and neurobiology. Cambridge, UK: Cambridge University Press; 2004:142-65.
3. Caspi A, Moffitt TE, Cannon M, et al. Moderation of the effect of adolescent-onset cannabis use on adult psychosis by a functional polymorphism in the catechol-O-methyltransferase gene: longitudinal evidence of a gene X environment interaction. Biol Psychiatry 2005;57(10):1117-27.
4. Henquet C, Rosa A, Krabbendam L, et al. An experimental study of catechol-O-methyltransferase Val158 Met moderation of Δ-9-tetrahydrocannabinol-induced effects on psychosis and cognition. Neuropsychopharmacol 2006;31:2748-57.
5. Thomas H. A community survey of adverse effects of cannabis use. Drug Alcohol Depend 1996;42(3):201-7.
6. D’Souza DC, Perry E, MacDougall L, et al. The psychotomimetic effects of intravenous delta-9-tetrahydrocannabinol in healthy individuals: implications for psychosis. Neuropsychopharmacology 2004;29:1558-72.
7. D’Souza DC, Abi-Saab WM, Madonick S, et al. Delta-9-tetrahydrocannabinol effects in schizophrenia: implications for cognition, psychosis, and addiction. Biol Psychiatry 2005;57:594-608.
8. Andreasson S, Allebeck P, Engstrom A, Rydberg U. Cannabis and schizophrenia. A longitudinal study of Swedish conscripts. Lancet 1987;2(8574):1483-6.
9. Arseneault L, Cannon M, Poulton R, et al. Cannabis use in adolescence and risk for adult psychosis: longitudinal prospective study. BMJ 2002;325(7374):1212-3.
10. van Os J, Bak M, Hanssen M, et al. Cannabis use and psychosis: a longitudinal population-based study. Am J Epidemiol 2002;156(4):319-27.
11. Fergusson DM, Horwood LJ, Swain-Campbell NR. Cannabis dependence and psychotic symptoms in young people. Psychol Med 2003;33(1):15-21.
12. Zammit S, Allebeck P, Andreasson S, et al. Self reported cannabis use as a risk factor for schizophrenia in Swedish conscripts of 1969: historical cohort study. BMJ 2002;325(7374):1199-201.
13. Weiser M, Knobler HY, Noy S, Kaplan Z. Clinical characteristics of adolescents later hospitalized for schizophrenia. Am J Med Genet 2002;114:949-55.
14. Smit F, Bolier L, Cuijpers P. Cannabis use and the risk of later schizophrenia: a review. Addiction 2004;99(4):425-30.
15. Di Maggio C, Martinez M, Menard JF, et al. Evidence of a cohort effect for age at onset of schizophrenia. Am J Psychiatry 2001;158(3):489-92.
16. Verdoux H, Gindre C, Sorbara F, et al. Effects of cannabis and psychosis vulnerability in daily life: an experience sampling test study. Psychol Med 2003;33(1):23-32.
17. Henquet C, Krabbendam L, Spauwen J, et al. Prospective cohort study of cannabis use, predisposition for psychosis, and psychotic symptoms in young people. BMJ 2005;330(7481):11-4.
18. Arendt M, Rosenberg R, Foldager L, et al. Cannabis-induced psychosis and subsequent schizophrenia-spectrum disorders: follow-up study of 535 incident cases. Br J Psychiatry 2005;187:510-5.
19. Pencer A, Addington J, Addington D. Outcome of a first episode of psychosis in adolescence: a 2-year follow-up. Psychiatry Res 2005;133(1):35-43.
20. McCambridge J, Strang J. The efficacy of single-session motivational interviewing in reducing drug consumption and perceptions of drug-related risk and harm among young people: results from a multi-site cluster randomized trial. Addiction 2004;99(1):39-52.
21. Edwards J, Elkins K, Hinton M, et al. Randomized controlled trial of a cannabis-focused intervention for young people with first-episode psychosis. Acta Psychiatr Scand 2006;114(2):109-17.
22. Lussier JP, Heil SH, Mongeon JA, et al. A meta-analysis of voucher-based reinforcement therapy for substance use disorders. Addiction 2006;101:192-203.
23. Budney AJ, Moore BA, Rocha HL, Higgins ST. Clinical trial of abstinence-based vouchers and cognitive-behavioral therapy for cannabis dependence. J Consult Clin Psychol 2006;74(2):307-16.
24. Brunette MF, Drake RE, Xie H, et al. Clozapine use and relapses of substance use disorder among patients with co-occurring schizophrenia and substance use disorders. Schizophr Bull 2006;32(4):637-43.
25. Hall W, Degenhardt L. What are the policy implications of the evidence on cannabis and psychosis? Can J Psychiatry 2006;51(9):566-74.
Malpractice distress: Help yourself and others survive
‘Immediately after the event I was a wreck. I vaguely remember talking to the family; I don’t know if I was much use to them. … That night I got drunk. It was the only way I could sleep. A sensitive colleague came and sat with me.”1
Besides being targets of malpractice suits, psychiatrists also serve as resources for colleagues who are sued. Specific actions can help you and those you counsel deal with the stress of an adverse event before and during litigation. Remember that:
- anticipation is the best defense
- knowledge is power
- action counters passivity
- a supportive environment is essential.
ANTICIPATING LITIGATION
What is the risk? No nationwide reporting system tracks the incidence of medical malpractice claims, but industry experts suggest a claim is leveled against 7% of psychiatrists each year.2 The risk is higher for other medical specialists: a recent survey by the American College of Obstetricians and Gynecologists found that 89% of practicing ObGyns had been sued at least once in their careers.3 Because a claim usually takes several years to resolve, a substantial number of physicians—including psychiatrists—are involved in litigation at any one time.
Successfully anticipating litigation begins with being familiar with your state’s statute of limitations—usually 2 to 3 years after discovery of the incident, with exceptions for children, the disabled, and designated special circumstances. If a plaintiff’s case is not filed within this time, a disputed outcome can never be the subject of a malpractice claim.
Adverse events. The severity of the outcome, the nature of your relationship with the patient, and the degree of your responsibility for an adverse event contribute to the intensity of your initial emotional response. If a mistake caused the event, your reaction may be even more severe.4-6 Whatever the event’s specifics, you may ruminate about your role and degree of responsibility (Table 1).
Table 1
Nagging questions after a ‘bad’ patient outcome
|
Expect that your view of the circumstances will generate a complex array of feelings: shock, anxiety, depression, shame, guilt, self-blame, disbelief, self-doubt and inadequacy, anger, and even relief from not having to work with a difficult patient anymore.
Patient suicide. More than one-half of psychiatrists and up to one-third of psychiatric residents experience a patient suicide.7-10 The Joint Commission on Accreditation of Healthcare Organizations reports that suicide is the most frequent sentinel event, representing 501 (13.1%) of the total 3,811 sentinel events reviewed since 1995.11 Professional Risk Management Services, a major medical malpractice insurer of psychiatrists, reports that suicide and attempted suicide are the most frequently identifiable causes of liability payments (Figure).
Figure 1 Psychiatric claims by cause of loss in the United States, 1998 to 2005
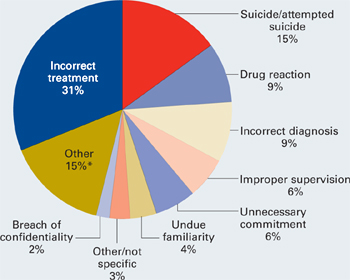
Almost all lawsuits assert multiple allegations of negligence, and “cause of loss” represents the main allegation made in the claim or lawsuit. Thus, the category of “incorrect treatment” may be alleged in a lawsuit based on a patient suicide, but the main or chief allegation/complaint is stated as “incorrect treatment.” The most frequent identifiable cause of loss is suicide and attempted suicide.
* “Other” includes administrative issues, abandonment, premises liability, Tarasoff, third parties (such as parents), retained object, libel/slander, boundary violation, deleted duplicate file, Fen-phen, lack of informed consent, forensic issues, and miscellaneous.
Source: Prepared by Professional Risk Management Services, Inc. Reprinted with permission.
Psychiatrists’ feelings of distress after a patient suicide mirror the personal sense of failure and inadequacy most physicians feel when they are unable to prevent a patient’s death or serious injury. At the same time, we must:
- deal with the event’s medical complications, with relevant notifications and disclosures (Table 2)
- address the emotional pain of the injured patient or family
- participate in mandated reviews
- recognize and manage our emotional disruption (Table 3).
Table 2
Recommended medical steps, notifications,
and disclosures after an adverse event
| MEDICAL STEPS Take necessary actions to limit further injury or disability Obtain appropriate consultations Review the medical record; anticipate the patient’s follow-up needs and make recommendations for further treatment |
| NOTIFICATIONS Follow the health care system’s and insurer’s guidelines for notifying the patient/family Inform the institution’s risk manager and your professional liability carrier as soon as possible Write a description of the event for the record and a narrative for your personal file (and your lawyer’s) in case a suit is filed later Do not talk with the media |
| DISCLOSURES Acknowledge your ethical obligation to be truthful Follow your institution’s and insurer’s disclosure guidelines Expect to feel intimidated and uneasy in discussing your role in the event Expect the patient/family to be angry and disappointed in you Convey an interest in the patient’s/family’s emotional state; express sorrow for their loss Tell the patient/family what you know for sure; don’t speculate about what is not known, and don’t make false promises or false reassurances Don’t hurry; give the patient/family time to ask questions Expect to feel better after a truthful exchange |
Table 3
Managing your emotions before and during litigation
| Anticipate having repeated thoughts and preoccupations about the event; work toward a realistic view of it |
| Recognize your feelings and work to understand their source |
| Talk with a trusted confidant (your spouse, colleague, etc.) about your feelings |
| Monitor your emotional and physical status and, if indicated, seek appropriate consultation |
| Avoid situations that generate anxiety and increase stress |
| Monitor and address changes in relationships with family, patients, colleagues, and staff |
| Be understanding of yourself and others; develop a realistic view of yourself as a ‘good doctor’ |
| Engage in active sports and take regular vacations unrelated to professional activities |
| Control what can be controlled |
Self-evaluation. To cope with distress when a patient dies, you could attend the funeral. If the death was by suicide, consider consulting with a therapist about your reactions or review the case with your supervisor. You also might:
- make changes in your practice that alert you to problem patients
- introduce a more structured approach to patients with particular clinical conditions, using practice guidelines as a resource12,13
- become more alert to patients who may benefit from consultation or referral.
Balance the time you devote to work and personal life. Schedule regular time for recreation and active sports, which can help you prepare for the prolonged stress that follows being sued. Engage a personal physician to monitor your physical and emotional health and to recommend appropriate referrals when indicated.
KNOWLEDGE IS POWER
What can I expect? A lawsuit generates a mixture of common emotions and exacerbates those felt at the time of the bad outcome: shock, outrage, anxiety, anguish, dread, depression, helplessness, hopelessness, feelings of being misunderstood, and the anger and vulnerability associated with a narcissistic injury. As one ObGyn stated, learning that a lawsuit was filed “just prolonged my misery.”14
Each of us reacts in our own way to a lawsuit—and differently to each lawsuit if we are sued more than once—because of:
- our personality traits and personal circumstances
- the specifics of each case
- our relationship with the patient
- the public nature of a lawsuit
- a range of other variables that makes each case unique.
Suddenly, we who perceive ourselves as caring, beneficent, well-meaning, and devoted to our patients are publicly accused of being careless and incompetent, of harming the patient by failing to meet our minimal obligations. Psychiatrists Richard Ferrell and Trevor Price15 capture the impact of these allegations:
"Here are the sense of assault and violation, the feelings of outrage and fear. Most painfully, here is the narcissistic injury, the astonishing wound to our understanding of ourselves as admirable, well-meaning people."
Litigation is a lengthy process with defined stages (Table 4). We have little control over a slow-paced process that involves an array of participants (lawyers, judges, jury, and experts) whose behavior is not predictable. This makes us feel dependent, vulnerable, and impotent.
Table 4
Stages of litigation: What happens in court
| Stage | Definitions |
|---|---|
| Summons | Notification that a suit has been filed |
| Complaint | The nature of the allegation in legal terms |
| Pleadings | The attorney begins to communicate with the court by filing motions, a request that the court do something |
| Discovery | A process designed to obtain information about the case:
|
| Summary judgment | A motion asking the court, after the facts have been established by discovery, to decide the validity of the case; if granted, the case is resolved without a trial by jury |
| Settlement | An agreement between parties that resolves their legal dispute |
| Trial | Case is presented to the judge or a judge and jury to determine culpability |
| Verdict | Decision reached by the deciding body |
| Post-trial | If the defendant receives an unfavorable verdict, motions may be offered to the court to void or appeal the verdict |
BE ACTIVE, NOT PASSIVE
What you can do. Contact your insurer and risk manager immediately. Inquire about the average length of litigation in your jurisdiction (might be 1 to 5 or more years, depending on locality, type of case, and severity of injury). Ask your lawyer to describe the steps in the process and your role as the case proceeds.
Take whatever steps are necessary to cover your clinical duties. If your initial emotional reaction is disruptive, obtain coverage or rearrange your schedule. Expect to change or limit your schedule before depositions and during trial to allow adequate time for preparation.
Accept the fact that you must play by rules far different from those of medical care. Litigation is time-consuming and frustrating. Delays and “continuances” are common in legal proceedings, so expect them. Consider adapting to your own situation strategies that other sued physicians have found useful in regaining control over their lives and work (Table 5).
Table 5
Regaining control: Managing your practice during litigation
| Learn as much as you can about the legal process |
| Introduce good risk management strategies, such as efficient record-keeping, into your practice |
| Clarify the responsibilities of office personnel and coverage responsibilities with associates |
| Rearrange office schedules during periods of increased stress |
| Re-evaluate your time commitments to work and family |
| Participate in relevant continuing education |
| Make sure your financial and estate planning is current |
| Cooperate with legal counsel |
| Devote sufficient time to deposition preparation and other demands of the case |
| Carefully evaluate the advice of legal and insurance counsel regarding a settlement |
| Do not try to “fit patients in” while on trial; trial is a full-time job |
GET NEEDED SUPPORT
Talking about the case. Sharing with responsible confidants your emotional reactions to being sued is healthy for you and others affected. Lawyers, however, may caution you not to “talk to anybody” about the case. They don’t want you to say anything that would suggest liability or jeopardize their defense of the case.
As psychiatrists, we know this is not good psychological advice. The support of others is a natural help during major life events that cause enormous stress and disruption.16 You can resolve this dilemma by accepting the discipline of talking about your feelings regarding the case without discussing the specifics of the case.
In addition to lawyers and claims representatives, you may talk with your spouse or another trusted person or colleague about your feelings. When other physicians or psychiatrists formally consult with you about their litigation experiences, you are protected by the confidentiality inherent in the doctor-patient relationship.
Trust issues. Trust lies at the core of psychotherapeutic work. After being sued, you may find it difficult to re-establish trusting and comfortable relationships with patients, especially those who are seriously ill.
Well-trained, competent physicians who keep current with standards of care and have good relationships with patients do not expect to be sued. Psychiatrists often feel unrealistically immune to litigation because we believe our training helps us understand our own psychology and relationships with others. A charge of negligence exposes our vulnerabilities and leaves us feeling hurt and betrayed. As one psychiatrist ruefully observed, “I lost my innocence.”14
Countertransference feelings may emerge. Most physicians acknowledge that after being sued their relationships with patients change17,18—a particularly distressing outcome for psychiatrists. We may feel uncomfortable and threatened when we need to “stretch the patient-doctor relationship in a paternalistic direction,” such as when a psychotic patient needs involuntary commitment.15
Feelings that you must change the way you practice and chronic anxiety about your work are barriers to good practice. You may contemplate changing practice circumstances or retiring early. Personal therapy may help if you remain uneasy or cannot resolve life choices that overshadow your work with patients.
Medical or psychiatric care. Be alert to the point at which you or others involved in litigation need a referral for medical or psychiatric consultation. Sued physicians, their families, or colleagues often experience diagnosable psychiatric conditions or other behavioral problems, such as:
- major depression
- adjustment disorders
- posttraumatic stress disorder
- worsening of a previously diagnosed psychiatric illness
- physical symptoms that require diagnosis and treatment
- alcohol and drug misuse or abuse
- anxiety and distress that interfere with work
- self-medication, especially for insomnia
- disturbances and dysfunctional behaviors that affect marital and family life.19,20
SUPPORT YOUR COLLEAGUES
When consulting with other physicians, be aware of litigation factors that may influence treatment.
Become familiar with the climate of litigation in the jurisdiction where the case was filed, including the incidence and outcome of cases. For example, does an attempted suicide case usually result in settlement or—if it goes to trial—take 2 to 5 or more years to resolve? More than 70% of cases filed nationwide result in no payment (no settlement) for the plaintiff. If cases go to trial, physicians win 80% of the time.21
Recognize that the source of the physician’s distress may be the trauma associated with the initial bad outcome, rather than the malpractice suit itself. As the case progresses and facts emerge, you may play a large role in helping your physician patient correct previous distortions of the event. Certain periods—during trial, for example—might require more-frequent visits, medication, and expressions of support.
You may harbor a bias about the case, but withhold judgment until it is resolved.
Related resources
- American College of Obstetricians and Gynecologists. From exam room to court room: navigating litigation and coping with stress (CD-ROM) http://sales.acog.com/acb/stores/1/product1.cfm?SID=1&Product_ID=589).
- Charles SC, Frisch PR. Adverse events, stress and litigation: a physician’s guide. New York: Oxford University Press; 2005.
- Physician Litigation Stress Resource Center. www.physicianlitigationstress.org.
Disclosure
Dr. Charles reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Anonymous. Looking back… BMJ 2000;320(7237):812.-
2. Martin G, Tracy JD. President and CEO, Professional Risk Management Services. Personal communication. October 20, 2006.
3. American College of Obstetricians and Gynecologists. ACOG 2006 Professional Liability Survey. Washington, DC; 2006. Available at: http://www.acog.org/departments/dept_notice.cfm?recno=4&bulletin=3963. Accessed January 16, 2007.
4. Christensen JF, Levinson W, Dunn PM. The heart of darkness: the impact of perceived mistakes on physicians. J Gen Intern Med 1992;7(4):424-31.
5. Wu AW. Medical error: the second victim. The doctor who makes the mistake needs help too. BMJ 2000;320(7237):726-7.
6. Aasland OG, Forde R. Impact of feeling responsible for adverse events on doctors’ personal and professional lives: the importance of being open to criticism from colleagues. Quality & Safety in Health Care 2005;14:13-7.
7. Alexander DA, Klein S, Grey NM, et al. Suicide by patients: questionnaire study of its effect on consultant psychiatrists. BMJ 2000;320:1571-4.
8. Chemtob CM, Hamada RS, Bauer G, et al. Patients’ suicides: frequency and impact on psychiatrists. Am J Psychiatry 1988;145:224-8.
9. Brown HN. The impact of suicide on therapists in training. Compr Psychiatry 1987;28:101-12.
10. Ellis TE, Dickey TO, Jones EC. Patient suicide in psychiatric residency programs: a national survey of training and postvention practices. Academic Psychiatry 1998;22:181-9.
11. Joint Commission on Accreditation of Healthcare Organizations. Sentinel event statistics. Available at: http://www.jointcommission.org/NR/rdonlyres/74540565-4D0F-4992-863E-8F9E949E6B56/0/se_stats_6_30_06.pdf. Accessed November 27, 2006.
12. Hendin H, Lipschitz A, Maltsberger JT, et al. Therapists’ reactions to patients’ suicides. Am J Psychiatry 2000;157(12):2022-7.
13. Practice guidelines for the treatment of psychiatric disorders (compendium 2006) Arlington, VA: American Psychiatric Publishing; 2006.
14. Charles SC, Frisch PR. Adverse events, stress and litigation: a physician’s guide. New York: Oxford University Press; 2005:94,120.
15. Ferrell RB, Price TRP. Effects of malpractice suits on physicians. In: Gold JH, Nemiah JC, eds. Beyond transference. Washington, DC: American Psychiatric Press; 1993:141-58.
16. Watson PJ, Friedman MJ, Gibson LE, et al. Early intervention in trauma-related problems. In: Ursano R, Norwood AE, eds. Trauma and disaster: responses and management. Review of psychiatry vol. 22. Washington, DC: American Psychiatric Press; 2003:100-1.
17. Charles SC, Psykoty CE, Nelson A. Physicians on trial—self-reported reactions to malpractice trials. West J Med 1988;148:358-60.
18. Charles SC. The doctor-patient relationship and medical malpractice litigation. Bull Menninger Clin 1993;57(2):195-207.
19. Charles SC, Wilbert JR, Franke KJ. Sued and non-sued physicians’ self-reported reactions to malpractice litigation. Am J Psychiatry 1985;142:437-40.
20. Martin CA, Wilson JA, Fiebelman ND, et al. Physicians’ psychologic reactions to malpractice litigation. South Med J 1991;84:1300-4.
21. Outcome of closed medical malpractice claims. National data (1985-2005). Physician Insurers Association of America (PIAA). Rockville, MD; 2006.
‘Immediately after the event I was a wreck. I vaguely remember talking to the family; I don’t know if I was much use to them. … That night I got drunk. It was the only way I could sleep. A sensitive colleague came and sat with me.”1
Besides being targets of malpractice suits, psychiatrists also serve as resources for colleagues who are sued. Specific actions can help you and those you counsel deal with the stress of an adverse event before and during litigation. Remember that:
- anticipation is the best defense
- knowledge is power
- action counters passivity
- a supportive environment is essential.
ANTICIPATING LITIGATION
What is the risk? No nationwide reporting system tracks the incidence of medical malpractice claims, but industry experts suggest a claim is leveled against 7% of psychiatrists each year.2 The risk is higher for other medical specialists: a recent survey by the American College of Obstetricians and Gynecologists found that 89% of practicing ObGyns had been sued at least once in their careers.3 Because a claim usually takes several years to resolve, a substantial number of physicians—including psychiatrists—are involved in litigation at any one time.
Successfully anticipating litigation begins with being familiar with your state’s statute of limitations—usually 2 to 3 years after discovery of the incident, with exceptions for children, the disabled, and designated special circumstances. If a plaintiff’s case is not filed within this time, a disputed outcome can never be the subject of a malpractice claim.
Adverse events. The severity of the outcome, the nature of your relationship with the patient, and the degree of your responsibility for an adverse event contribute to the intensity of your initial emotional response. If a mistake caused the event, your reaction may be even more severe.4-6 Whatever the event’s specifics, you may ruminate about your role and degree of responsibility (Table 1).
Table 1
Nagging questions after a ‘bad’ patient outcome
|
Expect that your view of the circumstances will generate a complex array of feelings: shock, anxiety, depression, shame, guilt, self-blame, disbelief, self-doubt and inadequacy, anger, and even relief from not having to work with a difficult patient anymore.
Patient suicide. More than one-half of psychiatrists and up to one-third of psychiatric residents experience a patient suicide.7-10 The Joint Commission on Accreditation of Healthcare Organizations reports that suicide is the most frequent sentinel event, representing 501 (13.1%) of the total 3,811 sentinel events reviewed since 1995.11 Professional Risk Management Services, a major medical malpractice insurer of psychiatrists, reports that suicide and attempted suicide are the most frequently identifiable causes of liability payments (Figure).
Figure 1 Psychiatric claims by cause of loss in the United States, 1998 to 2005
Almost all lawsuits assert multiple allegations of negligence, and “cause of loss” represents the main allegation made in the claim or lawsuit. Thus, the category of “incorrect treatment” may be alleged in a lawsuit based on a patient suicide, but the main or chief allegation/complaint is stated as “incorrect treatment.” The most frequent identifiable cause of loss is suicide and attempted suicide.
* “Other” includes administrative issues, abandonment, premises liability, Tarasoff, third parties (such as parents), retained object, libel/slander, boundary violation, deleted duplicate file, Fen-phen, lack of informed consent, forensic issues, and miscellaneous.
Source: Prepared by Professional Risk Management Services, Inc. Reprinted with permission.
Psychiatrists’ feelings of distress after a patient suicide mirror the personal sense of failure and inadequacy most physicians feel when they are unable to prevent a patient’s death or serious injury. At the same time, we must:
- deal with the event’s medical complications, with relevant notifications and disclosures (Table 2)
- address the emotional pain of the injured patient or family
- participate in mandated reviews
- recognize and manage our emotional disruption (Table 3).
Table 2
Recommended medical steps, notifications,
and disclosures after an adverse event
| MEDICAL STEPS Take necessary actions to limit further injury or disability Obtain appropriate consultations Review the medical record; anticipate the patient’s follow-up needs and make recommendations for further treatment |
| NOTIFICATIONS Follow the health care system’s and insurer’s guidelines for notifying the patient/family Inform the institution’s risk manager and your professional liability carrier as soon as possible Write a description of the event for the record and a narrative for your personal file (and your lawyer’s) in case a suit is filed later Do not talk with the media |
| DISCLOSURES Acknowledge your ethical obligation to be truthful Follow your institution’s and insurer’s disclosure guidelines Expect to feel intimidated and uneasy in discussing your role in the event Expect the patient/family to be angry and disappointed in you Convey an interest in the patient’s/family’s emotional state; express sorrow for their loss Tell the patient/family what you know for sure; don’t speculate about what is not known, and don’t make false promises or false reassurances Don’t hurry; give the patient/family time to ask questions Expect to feel better after a truthful exchange |
Table 3
Managing your emotions before and during litigation
| Anticipate having repeated thoughts and preoccupations about the event; work toward a realistic view of it |
| Recognize your feelings and work to understand their source |
| Talk with a trusted confidant (your spouse, colleague, etc.) about your feelings |
| Monitor your emotional and physical status and, if indicated, seek appropriate consultation |
| Avoid situations that generate anxiety and increase stress |
| Monitor and address changes in relationships with family, patients, colleagues, and staff |
| Be understanding of yourself and others; develop a realistic view of yourself as a ‘good doctor’ |
| Engage in active sports and take regular vacations unrelated to professional activities |
| Control what can be controlled |
Self-evaluation. To cope with distress when a patient dies, you could attend the funeral. If the death was by suicide, consider consulting with a therapist about your reactions or review the case with your supervisor. You also might:
- make changes in your practice that alert you to problem patients
- introduce a more structured approach to patients with particular clinical conditions, using practice guidelines as a resource12,13
- become more alert to patients who may benefit from consultation or referral.
Balance the time you devote to work and personal life. Schedule regular time for recreation and active sports, which can help you prepare for the prolonged stress that follows being sued. Engage a personal physician to monitor your physical and emotional health and to recommend appropriate referrals when indicated.
KNOWLEDGE IS POWER
What can I expect? A lawsuit generates a mixture of common emotions and exacerbates those felt at the time of the bad outcome: shock, outrage, anxiety, anguish, dread, depression, helplessness, hopelessness, feelings of being misunderstood, and the anger and vulnerability associated with a narcissistic injury. As one ObGyn stated, learning that a lawsuit was filed “just prolonged my misery.”14
Each of us reacts in our own way to a lawsuit—and differently to each lawsuit if we are sued more than once—because of:
- our personality traits and personal circumstances
- the specifics of each case
- our relationship with the patient
- the public nature of a lawsuit
- a range of other variables that makes each case unique.
Suddenly, we who perceive ourselves as caring, beneficent, well-meaning, and devoted to our patients are publicly accused of being careless and incompetent, of harming the patient by failing to meet our minimal obligations. Psychiatrists Richard Ferrell and Trevor Price15 capture the impact of these allegations:
"Here are the sense of assault and violation, the feelings of outrage and fear. Most painfully, here is the narcissistic injury, the astonishing wound to our understanding of ourselves as admirable, well-meaning people."
Litigation is a lengthy process with defined stages (Table 4). We have little control over a slow-paced process that involves an array of participants (lawyers, judges, jury, and experts) whose behavior is not predictable. This makes us feel dependent, vulnerable, and impotent.
Table 4
Stages of litigation: What happens in court
| Stage | Definitions |
|---|---|
| Summons | Notification that a suit has been filed |
| Complaint | The nature of the allegation in legal terms |
| Pleadings | The attorney begins to communicate with the court by filing motions, a request that the court do something |
| Discovery | A process designed to obtain information about the case:
|
| Summary judgment | A motion asking the court, after the facts have been established by discovery, to decide the validity of the case; if granted, the case is resolved without a trial by jury |
| Settlement | An agreement between parties that resolves their legal dispute |
| Trial | Case is presented to the judge or a judge and jury to determine culpability |
| Verdict | Decision reached by the deciding body |
| Post-trial | If the defendant receives an unfavorable verdict, motions may be offered to the court to void or appeal the verdict |
BE ACTIVE, NOT PASSIVE
What you can do. Contact your insurer and risk manager immediately. Inquire about the average length of litigation in your jurisdiction (might be 1 to 5 or more years, depending on locality, type of case, and severity of injury). Ask your lawyer to describe the steps in the process and your role as the case proceeds.
Take whatever steps are necessary to cover your clinical duties. If your initial emotional reaction is disruptive, obtain coverage or rearrange your schedule. Expect to change or limit your schedule before depositions and during trial to allow adequate time for preparation.
Accept the fact that you must play by rules far different from those of medical care. Litigation is time-consuming and frustrating. Delays and “continuances” are common in legal proceedings, so expect them. Consider adapting to your own situation strategies that other sued physicians have found useful in regaining control over their lives and work (Table 5).
Table 5
Regaining control: Managing your practice during litigation
| Learn as much as you can about the legal process |
| Introduce good risk management strategies, such as efficient record-keeping, into your practice |
| Clarify the responsibilities of office personnel and coverage responsibilities with associates |
| Rearrange office schedules during periods of increased stress |
| Re-evaluate your time commitments to work and family |
| Participate in relevant continuing education |
| Make sure your financial and estate planning is current |
| Cooperate with legal counsel |
| Devote sufficient time to deposition preparation and other demands of the case |
| Carefully evaluate the advice of legal and insurance counsel regarding a settlement |
| Do not try to “fit patients in” while on trial; trial is a full-time job |
GET NEEDED SUPPORT
Talking about the case. Sharing with responsible confidants your emotional reactions to being sued is healthy for you and others affected. Lawyers, however, may caution you not to “talk to anybody” about the case. They don’t want you to say anything that would suggest liability or jeopardize their defense of the case.
As psychiatrists, we know this is not good psychological advice. The support of others is a natural help during major life events that cause enormous stress and disruption.16 You can resolve this dilemma by accepting the discipline of talking about your feelings regarding the case without discussing the specifics of the case.
In addition to lawyers and claims representatives, you may talk with your spouse or another trusted person or colleague about your feelings. When other physicians or psychiatrists formally consult with you about their litigation experiences, you are protected by the confidentiality inherent in the doctor-patient relationship.
Trust issues. Trust lies at the core of psychotherapeutic work. After being sued, you may find it difficult to re-establish trusting and comfortable relationships with patients, especially those who are seriously ill.
Well-trained, competent physicians who keep current with standards of care and have good relationships with patients do not expect to be sued. Psychiatrists often feel unrealistically immune to litigation because we believe our training helps us understand our own psychology and relationships with others. A charge of negligence exposes our vulnerabilities and leaves us feeling hurt and betrayed. As one psychiatrist ruefully observed, “I lost my innocence.”14
Countertransference feelings may emerge. Most physicians acknowledge that after being sued their relationships with patients change17,18—a particularly distressing outcome for psychiatrists. We may feel uncomfortable and threatened when we need to “stretch the patient-doctor relationship in a paternalistic direction,” such as when a psychotic patient needs involuntary commitment.15
Feelings that you must change the way you practice and chronic anxiety about your work are barriers to good practice. You may contemplate changing practice circumstances or retiring early. Personal therapy may help if you remain uneasy or cannot resolve life choices that overshadow your work with patients.
Medical or psychiatric care. Be alert to the point at which you or others involved in litigation need a referral for medical or psychiatric consultation. Sued physicians, their families, or colleagues often experience diagnosable psychiatric conditions or other behavioral problems, such as:
- major depression
- adjustment disorders
- posttraumatic stress disorder
- worsening of a previously diagnosed psychiatric illness
- physical symptoms that require diagnosis and treatment
- alcohol and drug misuse or abuse
- anxiety and distress that interfere with work
- self-medication, especially for insomnia
- disturbances and dysfunctional behaviors that affect marital and family life.19,20
SUPPORT YOUR COLLEAGUES
When consulting with other physicians, be aware of litigation factors that may influence treatment.
Become familiar with the climate of litigation in the jurisdiction where the case was filed, including the incidence and outcome of cases. For example, does an attempted suicide case usually result in settlement or—if it goes to trial—take 2 to 5 or more years to resolve? More than 70% of cases filed nationwide result in no payment (no settlement) for the plaintiff. If cases go to trial, physicians win 80% of the time.21
Recognize that the source of the physician’s distress may be the trauma associated with the initial bad outcome, rather than the malpractice suit itself. As the case progresses and facts emerge, you may play a large role in helping your physician patient correct previous distortions of the event. Certain periods—during trial, for example—might require more-frequent visits, medication, and expressions of support.
You may harbor a bias about the case, but withhold judgment until it is resolved.
Related resources
- American College of Obstetricians and Gynecologists. From exam room to court room: navigating litigation and coping with stress (CD-ROM) http://sales.acog.com/acb/stores/1/product1.cfm?SID=1&Product_ID=589).
- Charles SC, Frisch PR. Adverse events, stress and litigation: a physician’s guide. New York: Oxford University Press; 2005.
- Physician Litigation Stress Resource Center. www.physicianlitigationstress.org.
Disclosure
Dr. Charles reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
‘Immediately after the event I was a wreck. I vaguely remember talking to the family; I don’t know if I was much use to them. … That night I got drunk. It was the only way I could sleep. A sensitive colleague came and sat with me.”1
Besides being targets of malpractice suits, psychiatrists also serve as resources for colleagues who are sued. Specific actions can help you and those you counsel deal with the stress of an adverse event before and during litigation. Remember that:
- anticipation is the best defense
- knowledge is power
- action counters passivity
- a supportive environment is essential.
ANTICIPATING LITIGATION
What is the risk? No nationwide reporting system tracks the incidence of medical malpractice claims, but industry experts suggest a claim is leveled against 7% of psychiatrists each year.2 The risk is higher for other medical specialists: a recent survey by the American College of Obstetricians and Gynecologists found that 89% of practicing ObGyns had been sued at least once in their careers.3 Because a claim usually takes several years to resolve, a substantial number of physicians—including psychiatrists—are involved in litigation at any one time.
Successfully anticipating litigation begins with being familiar with your state’s statute of limitations—usually 2 to 3 years after discovery of the incident, with exceptions for children, the disabled, and designated special circumstances. If a plaintiff’s case is not filed within this time, a disputed outcome can never be the subject of a malpractice claim.
Adverse events. The severity of the outcome, the nature of your relationship with the patient, and the degree of your responsibility for an adverse event contribute to the intensity of your initial emotional response. If a mistake caused the event, your reaction may be even more severe.4-6 Whatever the event’s specifics, you may ruminate about your role and degree of responsibility (Table 1).
Table 1
Nagging questions after a ‘bad’ patient outcome
|
Expect that your view of the circumstances will generate a complex array of feelings: shock, anxiety, depression, shame, guilt, self-blame, disbelief, self-doubt and inadequacy, anger, and even relief from not having to work with a difficult patient anymore.
Patient suicide. More than one-half of psychiatrists and up to one-third of psychiatric residents experience a patient suicide.7-10 The Joint Commission on Accreditation of Healthcare Organizations reports that suicide is the most frequent sentinel event, representing 501 (13.1%) of the total 3,811 sentinel events reviewed since 1995.11 Professional Risk Management Services, a major medical malpractice insurer of psychiatrists, reports that suicide and attempted suicide are the most frequently identifiable causes of liability payments (Figure).
Figure 1 Psychiatric claims by cause of loss in the United States, 1998 to 2005
Almost all lawsuits assert multiple allegations of negligence, and “cause of loss” represents the main allegation made in the claim or lawsuit. Thus, the category of “incorrect treatment” may be alleged in a lawsuit based on a patient suicide, but the main or chief allegation/complaint is stated as “incorrect treatment.” The most frequent identifiable cause of loss is suicide and attempted suicide.
* “Other” includes administrative issues, abandonment, premises liability, Tarasoff, third parties (such as parents), retained object, libel/slander, boundary violation, deleted duplicate file, Fen-phen, lack of informed consent, forensic issues, and miscellaneous.
Source: Prepared by Professional Risk Management Services, Inc. Reprinted with permission.
Psychiatrists’ feelings of distress after a patient suicide mirror the personal sense of failure and inadequacy most physicians feel when they are unable to prevent a patient’s death or serious injury. At the same time, we must:
- deal with the event’s medical complications, with relevant notifications and disclosures (Table 2)
- address the emotional pain of the injured patient or family
- participate in mandated reviews
- recognize and manage our emotional disruption (Table 3).
Table 2
Recommended medical steps, notifications,
and disclosures after an adverse event
| MEDICAL STEPS Take necessary actions to limit further injury or disability Obtain appropriate consultations Review the medical record; anticipate the patient’s follow-up needs and make recommendations for further treatment |
| NOTIFICATIONS Follow the health care system’s and insurer’s guidelines for notifying the patient/family Inform the institution’s risk manager and your professional liability carrier as soon as possible Write a description of the event for the record and a narrative for your personal file (and your lawyer’s) in case a suit is filed later Do not talk with the media |
| DISCLOSURES Acknowledge your ethical obligation to be truthful Follow your institution’s and insurer’s disclosure guidelines Expect to feel intimidated and uneasy in discussing your role in the event Expect the patient/family to be angry and disappointed in you Convey an interest in the patient’s/family’s emotional state; express sorrow for their loss Tell the patient/family what you know for sure; don’t speculate about what is not known, and don’t make false promises or false reassurances Don’t hurry; give the patient/family time to ask questions Expect to feel better after a truthful exchange |
Table 3
Managing your emotions before and during litigation
| Anticipate having repeated thoughts and preoccupations about the event; work toward a realistic view of it |
| Recognize your feelings and work to understand their source |
| Talk with a trusted confidant (your spouse, colleague, etc.) about your feelings |
| Monitor your emotional and physical status and, if indicated, seek appropriate consultation |
| Avoid situations that generate anxiety and increase stress |
| Monitor and address changes in relationships with family, patients, colleagues, and staff |
| Be understanding of yourself and others; develop a realistic view of yourself as a ‘good doctor’ |
| Engage in active sports and take regular vacations unrelated to professional activities |
| Control what can be controlled |
Self-evaluation. To cope with distress when a patient dies, you could attend the funeral. If the death was by suicide, consider consulting with a therapist about your reactions or review the case with your supervisor. You also might:
- make changes in your practice that alert you to problem patients
- introduce a more structured approach to patients with particular clinical conditions, using practice guidelines as a resource12,13
- become more alert to patients who may benefit from consultation or referral.
Balance the time you devote to work and personal life. Schedule regular time for recreation and active sports, which can help you prepare for the prolonged stress that follows being sued. Engage a personal physician to monitor your physical and emotional health and to recommend appropriate referrals when indicated.
KNOWLEDGE IS POWER
What can I expect? A lawsuit generates a mixture of common emotions and exacerbates those felt at the time of the bad outcome: shock, outrage, anxiety, anguish, dread, depression, helplessness, hopelessness, feelings of being misunderstood, and the anger and vulnerability associated with a narcissistic injury. As one ObGyn stated, learning that a lawsuit was filed “just prolonged my misery.”14
Each of us reacts in our own way to a lawsuit—and differently to each lawsuit if we are sued more than once—because of:
- our personality traits and personal circumstances
- the specifics of each case
- our relationship with the patient
- the public nature of a lawsuit
- a range of other variables that makes each case unique.
Suddenly, we who perceive ourselves as caring, beneficent, well-meaning, and devoted to our patients are publicly accused of being careless and incompetent, of harming the patient by failing to meet our minimal obligations. Psychiatrists Richard Ferrell and Trevor Price15 capture the impact of these allegations:
"Here are the sense of assault and violation, the feelings of outrage and fear. Most painfully, here is the narcissistic injury, the astonishing wound to our understanding of ourselves as admirable, well-meaning people."
Litigation is a lengthy process with defined stages (Table 4). We have little control over a slow-paced process that involves an array of participants (lawyers, judges, jury, and experts) whose behavior is not predictable. This makes us feel dependent, vulnerable, and impotent.
Table 4
Stages of litigation: What happens in court
| Stage | Definitions |
|---|---|
| Summons | Notification that a suit has been filed |
| Complaint | The nature of the allegation in legal terms |
| Pleadings | The attorney begins to communicate with the court by filing motions, a request that the court do something |
| Discovery | A process designed to obtain information about the case:
|
| Summary judgment | A motion asking the court, after the facts have been established by discovery, to decide the validity of the case; if granted, the case is resolved without a trial by jury |
| Settlement | An agreement between parties that resolves their legal dispute |
| Trial | Case is presented to the judge or a judge and jury to determine culpability |
| Verdict | Decision reached by the deciding body |
| Post-trial | If the defendant receives an unfavorable verdict, motions may be offered to the court to void or appeal the verdict |
BE ACTIVE, NOT PASSIVE
What you can do. Contact your insurer and risk manager immediately. Inquire about the average length of litigation in your jurisdiction (might be 1 to 5 or more years, depending on locality, type of case, and severity of injury). Ask your lawyer to describe the steps in the process and your role as the case proceeds.
Take whatever steps are necessary to cover your clinical duties. If your initial emotional reaction is disruptive, obtain coverage or rearrange your schedule. Expect to change or limit your schedule before depositions and during trial to allow adequate time for preparation.
Accept the fact that you must play by rules far different from those of medical care. Litigation is time-consuming and frustrating. Delays and “continuances” are common in legal proceedings, so expect them. Consider adapting to your own situation strategies that other sued physicians have found useful in regaining control over their lives and work (Table 5).
Table 5
Regaining control: Managing your practice during litigation
| Learn as much as you can about the legal process |
| Introduce good risk management strategies, such as efficient record-keeping, into your practice |
| Clarify the responsibilities of office personnel and coverage responsibilities with associates |
| Rearrange office schedules during periods of increased stress |
| Re-evaluate your time commitments to work and family |
| Participate in relevant continuing education |
| Make sure your financial and estate planning is current |
| Cooperate with legal counsel |
| Devote sufficient time to deposition preparation and other demands of the case |
| Carefully evaluate the advice of legal and insurance counsel regarding a settlement |
| Do not try to “fit patients in” while on trial; trial is a full-time job |
GET NEEDED SUPPORT
Talking about the case. Sharing with responsible confidants your emotional reactions to being sued is healthy for you and others affected. Lawyers, however, may caution you not to “talk to anybody” about the case. They don’t want you to say anything that would suggest liability or jeopardize their defense of the case.
As psychiatrists, we know this is not good psychological advice. The support of others is a natural help during major life events that cause enormous stress and disruption.16 You can resolve this dilemma by accepting the discipline of talking about your feelings regarding the case without discussing the specifics of the case.
In addition to lawyers and claims representatives, you may talk with your spouse or another trusted person or colleague about your feelings. When other physicians or psychiatrists formally consult with you about their litigation experiences, you are protected by the confidentiality inherent in the doctor-patient relationship.
Trust issues. Trust lies at the core of psychotherapeutic work. After being sued, you may find it difficult to re-establish trusting and comfortable relationships with patients, especially those who are seriously ill.
Well-trained, competent physicians who keep current with standards of care and have good relationships with patients do not expect to be sued. Psychiatrists often feel unrealistically immune to litigation because we believe our training helps us understand our own psychology and relationships with others. A charge of negligence exposes our vulnerabilities and leaves us feeling hurt and betrayed. As one psychiatrist ruefully observed, “I lost my innocence.”14
Countertransference feelings may emerge. Most physicians acknowledge that after being sued their relationships with patients change17,18—a particularly distressing outcome for psychiatrists. We may feel uncomfortable and threatened when we need to “stretch the patient-doctor relationship in a paternalistic direction,” such as when a psychotic patient needs involuntary commitment.15
Feelings that you must change the way you practice and chronic anxiety about your work are barriers to good practice. You may contemplate changing practice circumstances or retiring early. Personal therapy may help if you remain uneasy or cannot resolve life choices that overshadow your work with patients.
Medical or psychiatric care. Be alert to the point at which you or others involved in litigation need a referral for medical or psychiatric consultation. Sued physicians, their families, or colleagues often experience diagnosable psychiatric conditions or other behavioral problems, such as:
- major depression
- adjustment disorders
- posttraumatic stress disorder
- worsening of a previously diagnosed psychiatric illness
- physical symptoms that require diagnosis and treatment
- alcohol and drug misuse or abuse
- anxiety and distress that interfere with work
- self-medication, especially for insomnia
- disturbances and dysfunctional behaviors that affect marital and family life.19,20
SUPPORT YOUR COLLEAGUES
When consulting with other physicians, be aware of litigation factors that may influence treatment.
Become familiar with the climate of litigation in the jurisdiction where the case was filed, including the incidence and outcome of cases. For example, does an attempted suicide case usually result in settlement or—if it goes to trial—take 2 to 5 or more years to resolve? More than 70% of cases filed nationwide result in no payment (no settlement) for the plaintiff. If cases go to trial, physicians win 80% of the time.21
Recognize that the source of the physician’s distress may be the trauma associated with the initial bad outcome, rather than the malpractice suit itself. As the case progresses and facts emerge, you may play a large role in helping your physician patient correct previous distortions of the event. Certain periods—during trial, for example—might require more-frequent visits, medication, and expressions of support.
You may harbor a bias about the case, but withhold judgment until it is resolved.
Related resources
- American College of Obstetricians and Gynecologists. From exam room to court room: navigating litigation and coping with stress (CD-ROM) http://sales.acog.com/acb/stores/1/product1.cfm?SID=1&Product_ID=589).
- Charles SC, Frisch PR. Adverse events, stress and litigation: a physician’s guide. New York: Oxford University Press; 2005.
- Physician Litigation Stress Resource Center. www.physicianlitigationstress.org.
Disclosure
Dr. Charles reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Anonymous. Looking back… BMJ 2000;320(7237):812.-
2. Martin G, Tracy JD. President and CEO, Professional Risk Management Services. Personal communication. October 20, 2006.
3. American College of Obstetricians and Gynecologists. ACOG 2006 Professional Liability Survey. Washington, DC; 2006. Available at: http://www.acog.org/departments/dept_notice.cfm?recno=4&bulletin=3963. Accessed January 16, 2007.
4. Christensen JF, Levinson W, Dunn PM. The heart of darkness: the impact of perceived mistakes on physicians. J Gen Intern Med 1992;7(4):424-31.
5. Wu AW. Medical error: the second victim. The doctor who makes the mistake needs help too. BMJ 2000;320(7237):726-7.
6. Aasland OG, Forde R. Impact of feeling responsible for adverse events on doctors’ personal and professional lives: the importance of being open to criticism from colleagues. Quality & Safety in Health Care 2005;14:13-7.
7. Alexander DA, Klein S, Grey NM, et al. Suicide by patients: questionnaire study of its effect on consultant psychiatrists. BMJ 2000;320:1571-4.
8. Chemtob CM, Hamada RS, Bauer G, et al. Patients’ suicides: frequency and impact on psychiatrists. Am J Psychiatry 1988;145:224-8.
9. Brown HN. The impact of suicide on therapists in training. Compr Psychiatry 1987;28:101-12.
10. Ellis TE, Dickey TO, Jones EC. Patient suicide in psychiatric residency programs: a national survey of training and postvention practices. Academic Psychiatry 1998;22:181-9.
11. Joint Commission on Accreditation of Healthcare Organizations. Sentinel event statistics. Available at: http://www.jointcommission.org/NR/rdonlyres/74540565-4D0F-4992-863E-8F9E949E6B56/0/se_stats_6_30_06.pdf. Accessed November 27, 2006.
12. Hendin H, Lipschitz A, Maltsberger JT, et al. Therapists’ reactions to patients’ suicides. Am J Psychiatry 2000;157(12):2022-7.
13. Practice guidelines for the treatment of psychiatric disorders (compendium 2006) Arlington, VA: American Psychiatric Publishing; 2006.
14. Charles SC, Frisch PR. Adverse events, stress and litigation: a physician’s guide. New York: Oxford University Press; 2005:94,120.
15. Ferrell RB, Price TRP. Effects of malpractice suits on physicians. In: Gold JH, Nemiah JC, eds. Beyond transference. Washington, DC: American Psychiatric Press; 1993:141-58.
16. Watson PJ, Friedman MJ, Gibson LE, et al. Early intervention in trauma-related problems. In: Ursano R, Norwood AE, eds. Trauma and disaster: responses and management. Review of psychiatry vol. 22. Washington, DC: American Psychiatric Press; 2003:100-1.
17. Charles SC, Psykoty CE, Nelson A. Physicians on trial—self-reported reactions to malpractice trials. West J Med 1988;148:358-60.
18. Charles SC. The doctor-patient relationship and medical malpractice litigation. Bull Menninger Clin 1993;57(2):195-207.
19. Charles SC, Wilbert JR, Franke KJ. Sued and non-sued physicians’ self-reported reactions to malpractice litigation. Am J Psychiatry 1985;142:437-40.
20. Martin CA, Wilson JA, Fiebelman ND, et al. Physicians’ psychologic reactions to malpractice litigation. South Med J 1991;84:1300-4.
21. Outcome of closed medical malpractice claims. National data (1985-2005). Physician Insurers Association of America (PIAA). Rockville, MD; 2006.
1. Anonymous. Looking back… BMJ 2000;320(7237):812.-
2. Martin G, Tracy JD. President and CEO, Professional Risk Management Services. Personal communication. October 20, 2006.
3. American College of Obstetricians and Gynecologists. ACOG 2006 Professional Liability Survey. Washington, DC; 2006. Available at: http://www.acog.org/departments/dept_notice.cfm?recno=4&bulletin=3963. Accessed January 16, 2007.
4. Christensen JF, Levinson W, Dunn PM. The heart of darkness: the impact of perceived mistakes on physicians. J Gen Intern Med 1992;7(4):424-31.
5. Wu AW. Medical error: the second victim. The doctor who makes the mistake needs help too. BMJ 2000;320(7237):726-7.
6. Aasland OG, Forde R. Impact of feeling responsible for adverse events on doctors’ personal and professional lives: the importance of being open to criticism from colleagues. Quality & Safety in Health Care 2005;14:13-7.
7. Alexander DA, Klein S, Grey NM, et al. Suicide by patients: questionnaire study of its effect on consultant psychiatrists. BMJ 2000;320:1571-4.
8. Chemtob CM, Hamada RS, Bauer G, et al. Patients’ suicides: frequency and impact on psychiatrists. Am J Psychiatry 1988;145:224-8.
9. Brown HN. The impact of suicide on therapists in training. Compr Psychiatry 1987;28:101-12.
10. Ellis TE, Dickey TO, Jones EC. Patient suicide in psychiatric residency programs: a national survey of training and postvention practices. Academic Psychiatry 1998;22:181-9.
11. Joint Commission on Accreditation of Healthcare Organizations. Sentinel event statistics. Available at: http://www.jointcommission.org/NR/rdonlyres/74540565-4D0F-4992-863E-8F9E949E6B56/0/se_stats_6_30_06.pdf. Accessed November 27, 2006.
12. Hendin H, Lipschitz A, Maltsberger JT, et al. Therapists’ reactions to patients’ suicides. Am J Psychiatry 2000;157(12):2022-7.
13. Practice guidelines for the treatment of psychiatric disorders (compendium 2006) Arlington, VA: American Psychiatric Publishing; 2006.
14. Charles SC, Frisch PR. Adverse events, stress and litigation: a physician’s guide. New York: Oxford University Press; 2005:94,120.
15. Ferrell RB, Price TRP. Effects of malpractice suits on physicians. In: Gold JH, Nemiah JC, eds. Beyond transference. Washington, DC: American Psychiatric Press; 1993:141-58.
16. Watson PJ, Friedman MJ, Gibson LE, et al. Early intervention in trauma-related problems. In: Ursano R, Norwood AE, eds. Trauma and disaster: responses and management. Review of psychiatry vol. 22. Washington, DC: American Psychiatric Press; 2003:100-1.
17. Charles SC, Psykoty CE, Nelson A. Physicians on trial—self-reported reactions to malpractice trials. West J Med 1988;148:358-60.
18. Charles SC. The doctor-patient relationship and medical malpractice litigation. Bull Menninger Clin 1993;57(2):195-207.
19. Charles SC, Wilbert JR, Franke KJ. Sued and non-sued physicians’ self-reported reactions to malpractice litigation. Am J Psychiatry 1985;142:437-40.
20. Martin CA, Wilson JA, Fiebelman ND, et al. Physicians’ psychologic reactions to malpractice litigation. South Med J 1991;84:1300-4.
21. Outcome of closed medical malpractice claims. National data (1985-2005). Physician Insurers Association of America (PIAA). Rockville, MD; 2006.
PowerPoint: 6 presentation peeves
Effective use of Microsoft PowerPoint can enhance a presentation. Too often, however, speakers obfuscate information by adding fancy effects or showing indecipherable slides, or are ill-prepared or overly dependent on the slides to deliver their message.
PowerPoint is not just for professional lecturers; psychiatrists often are asked to address community or professional organizations and patient advocacy groups. Your ability to clearly explain complicated concepts to lay audiences can help market yourself as a desirable referral source.
This article describes 6 common PowerPoint presentation pitfalls, why they occur, and how to avoid them. Resources to help you create better PowerPoint presentations also are listed (see Related resources).
1 The speaker is in the dark
We’ve all seen it: As soon as the speaker starts a PowerPoint presentation, a helpful audience member turns down the lights. Fearing the projection will not be discernible, the speaker elects to make him/herself less visible in deference to the slides.
This misses the point. The audience came to hear you, so the slides should enhance your talk and not compete with you. To overvalue the slides is to ignore years of pedagogic research showing that learning flourishes when teacher and student are actively engaged.
Most modern LCD projectors are powerful enough to use in ambient light. If a slide is difficult to read, it’s often because of bad slide design, such as poorly contrasting colors or small type sizes (see peeve number 4).
Dimming the lights during a video presentation is acceptable because video usually is more visible in the dark and is the presentation’s focus when running. After the video is finished, restore the lights and return the focus to the speaker.
2 Too many bullets
The bulleted list in the PowerPoint default template is not always the best way to display information. Many speakers are reluctant to stray from this style, however, because they doubt their ability to cover all the points or worry that the audience will miss the information on the screen.
Don’t worry: Audiences are more likely to remember an effective presentation than perfectly complete slides.
3 He’s reading, not speaking
Speakers sometimes read from bulleted lists because they are not sufficiently familiar with their talk. They either turn away from the audience to read off the projected slides or—more commonly—face the audience but look down to read from a computer monitor.
Watching someone read aloud is boring. The audience will disengage if you appear unprepared and uninterested in them.
There is no substitute for planning and practicing your talk in advance. You don’t have to memorize it, but be familiar enough with your talk to require only occasional glances at the monitor. Even talented extemporaneous speakers can improve their performances with planning and practice.
4 ‘I know you can’t read this… ’
Seemingly every PowerPoint presentation includes at least one slide filled with tiny text and graphics. The speaker will laugh, saying, “I apologize, I know you can’t read this, but the point I’m trying to make is…”
This is the worst of many variations of difficult-to-read slides. Speakers also commonly scan material from textbooks into a slide rather than create it anew.
Projecting an indecipherable slide is the inexcusable result of poor planning or laziness. Breaking down a complex idea into understandable chunks of information is hard work, but that is what effective teachers do. Albert Einstein said, “If you can’t explain something simply, you don’t understand it well.” When audiences see difficult-to-read slides, they will suspect you don’t know what you’re talking about.
5 ‘Windows’ dressing
PowerPoint has many bells and whistles to enhance a presentation. Avoid them.
Transitions. PowerPoint offers more than 50 ways to transition from one slide to the next. But despite a century of film innovation, Steven Spielberg still relies on the same three transitions D.W. Griffith used in his silent films: the direct cut, the dissolve, and the wipe. All other transitions are rare in professional film; likewise, they have no place in your presentation.
Animations can be useful. For example, a slide with several bullet points is less distracting if the points are introduced one at a time. As with transitions, simple animations are best; watching words fly around a slide before settling in place has lost its novelty.
Graphics. Other built-in PowerPoint functions—such as prepackaged clip art and sound effects—are of little use. The clip art in particular looks lame and outmoded.
If your presentation calls for graphics, use high-quality photographs. PowerPoint supports numerous image formats including BMP, PCX, PNG, JPEG, and GIF (see Related resources for a comparison of each format’s advantages and disadvantages).
Most images from scanners or digital cameras are at higher resolutions than needed; computer monitors generally cannot display detail beyond 96 dots per inch (DPI), and photographs should be resampled accordingly to reduce file sizes. Resizing the image within PowerPoint does not change the resolution; you need a photo-editing program such as Adobe Photoshop, Corel Paint Shop, or Macromedia Fireworks (while there, be sure to crop out unnecessary parts of the photo).
Humor and comics. Including comic strips in a presentation has become somewhat hackneyed and overused. Use comics minimally and only when they help illustrate an important point.
6 ‘Do you have a handout?’
When audience members request printouts of slide presentations, speakers usually respond with straight printouts of the PowerPoint slides.
This makes little sense. Seeing the slides minus the speaker is like watching a documentary with the narration turned off. The more effective slides are as speaking aids, the less appropriate they are for stand-alone information.
Instead, create annotated slide printouts for distribution. Your best bet is to export the presentation to Microsoft Word, which creates a document containing pictures of the slides with adjacent notes. You could print out your slides using the PowerPoint notes function, but this only lets you print slides or notes on separate documents.
- TechRepublic.com. 10 slide design tips for producing powerful and effective presentations. http://articles.techrepublic.com.com/5100-10881-6117178.html.
- Microsoft guidelines for selecting a picture format in an Office XP program. http://support.microsoft.com/kb/320314.
- Tufte ER. The cognitive style of PowerPoint: pitching out corrupts within. Cheshire CT: Graphics Press; 2006. (Edward Tufte, professor emeritus at Yale University, is an authority on presenting graphic information).
- Presentation Zen, a blog maintained by Garr Reynolds, former program manager for worldwide user group relations at Apple. www.presentationzen.com.
- PowerPoint does rocket science. Tufte’s analysis shows the mismanagement resulting from NASA’s insistence on using PowerPoint to present technical analyses, ultimately leading to the Columbia shuttle disaster. www.edwardtufte.com/bboard/q-and-a-fetch-msg?msg_id=0001yB&topic_id=1.
- Peter Norvig’s PowerPoint version of the Gettysburg Address, an intriguing example of “death by PowerPoint.” www.norvig.com/Gettysburg.
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Effective use of Microsoft PowerPoint can enhance a presentation. Too often, however, speakers obfuscate information by adding fancy effects or showing indecipherable slides, or are ill-prepared or overly dependent on the slides to deliver their message.
PowerPoint is not just for professional lecturers; psychiatrists often are asked to address community or professional organizations and patient advocacy groups. Your ability to clearly explain complicated concepts to lay audiences can help market yourself as a desirable referral source.
This article describes 6 common PowerPoint presentation pitfalls, why they occur, and how to avoid them. Resources to help you create better PowerPoint presentations also are listed (see Related resources).
1 The speaker is in the dark
We’ve all seen it: As soon as the speaker starts a PowerPoint presentation, a helpful audience member turns down the lights. Fearing the projection will not be discernible, the speaker elects to make him/herself less visible in deference to the slides.
This misses the point. The audience came to hear you, so the slides should enhance your talk and not compete with you. To overvalue the slides is to ignore years of pedagogic research showing that learning flourishes when teacher and student are actively engaged.
Most modern LCD projectors are powerful enough to use in ambient light. If a slide is difficult to read, it’s often because of bad slide design, such as poorly contrasting colors or small type sizes (see peeve number 4).
Dimming the lights during a video presentation is acceptable because video usually is more visible in the dark and is the presentation’s focus when running. After the video is finished, restore the lights and return the focus to the speaker.
2 Too many bullets
The bulleted list in the PowerPoint default template is not always the best way to display information. Many speakers are reluctant to stray from this style, however, because they doubt their ability to cover all the points or worry that the audience will miss the information on the screen.
Don’t worry: Audiences are more likely to remember an effective presentation than perfectly complete slides.
3 He’s reading, not speaking
Speakers sometimes read from bulleted lists because they are not sufficiently familiar with their talk. They either turn away from the audience to read off the projected slides or—more commonly—face the audience but look down to read from a computer monitor.
Watching someone read aloud is boring. The audience will disengage if you appear unprepared and uninterested in them.
There is no substitute for planning and practicing your talk in advance. You don’t have to memorize it, but be familiar enough with your talk to require only occasional glances at the monitor. Even talented extemporaneous speakers can improve their performances with planning and practice.
4 ‘I know you can’t read this… ’
Seemingly every PowerPoint presentation includes at least one slide filled with tiny text and graphics. The speaker will laugh, saying, “I apologize, I know you can’t read this, but the point I’m trying to make is…”
This is the worst of many variations of difficult-to-read slides. Speakers also commonly scan material from textbooks into a slide rather than create it anew.
Projecting an indecipherable slide is the inexcusable result of poor planning or laziness. Breaking down a complex idea into understandable chunks of information is hard work, but that is what effective teachers do. Albert Einstein said, “If you can’t explain something simply, you don’t understand it well.” When audiences see difficult-to-read slides, they will suspect you don’t know what you’re talking about.
5 ‘Windows’ dressing
PowerPoint has many bells and whistles to enhance a presentation. Avoid them.
Transitions. PowerPoint offers more than 50 ways to transition from one slide to the next. But despite a century of film innovation, Steven Spielberg still relies on the same three transitions D.W. Griffith used in his silent films: the direct cut, the dissolve, and the wipe. All other transitions are rare in professional film; likewise, they have no place in your presentation.
Animations can be useful. For example, a slide with several bullet points is less distracting if the points are introduced one at a time. As with transitions, simple animations are best; watching words fly around a slide before settling in place has lost its novelty.
Graphics. Other built-in PowerPoint functions—such as prepackaged clip art and sound effects—are of little use. The clip art in particular looks lame and outmoded.
If your presentation calls for graphics, use high-quality photographs. PowerPoint supports numerous image formats including BMP, PCX, PNG, JPEG, and GIF (see Related resources for a comparison of each format’s advantages and disadvantages).
Most images from scanners or digital cameras are at higher resolutions than needed; computer monitors generally cannot display detail beyond 96 dots per inch (DPI), and photographs should be resampled accordingly to reduce file sizes. Resizing the image within PowerPoint does not change the resolution; you need a photo-editing program such as Adobe Photoshop, Corel Paint Shop, or Macromedia Fireworks (while there, be sure to crop out unnecessary parts of the photo).
Humor and comics. Including comic strips in a presentation has become somewhat hackneyed and overused. Use comics minimally and only when they help illustrate an important point.
6 ‘Do you have a handout?’
When audience members request printouts of slide presentations, speakers usually respond with straight printouts of the PowerPoint slides.
This makes little sense. Seeing the slides minus the speaker is like watching a documentary with the narration turned off. The more effective slides are as speaking aids, the less appropriate they are for stand-alone information.
Instead, create annotated slide printouts for distribution. Your best bet is to export the presentation to Microsoft Word, which creates a document containing pictures of the slides with adjacent notes. You could print out your slides using the PowerPoint notes function, but this only lets you print slides or notes on separate documents.
- TechRepublic.com. 10 slide design tips for producing powerful and effective presentations. http://articles.techrepublic.com.com/5100-10881-6117178.html.
- Microsoft guidelines for selecting a picture format in an Office XP program. http://support.microsoft.com/kb/320314.
- Tufte ER. The cognitive style of PowerPoint: pitching out corrupts within. Cheshire CT: Graphics Press; 2006. (Edward Tufte, professor emeritus at Yale University, is an authority on presenting graphic information).
- Presentation Zen, a blog maintained by Garr Reynolds, former program manager for worldwide user group relations at Apple. www.presentationzen.com.
- PowerPoint does rocket science. Tufte’s analysis shows the mismanagement resulting from NASA’s insistence on using PowerPoint to present technical analyses, ultimately leading to the Columbia shuttle disaster. www.edwardtufte.com/bboard/q-and-a-fetch-msg?msg_id=0001yB&topic_id=1.
- Peter Norvig’s PowerPoint version of the Gettysburg Address, an intriguing example of “death by PowerPoint.” www.norvig.com/Gettysburg.
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Effective use of Microsoft PowerPoint can enhance a presentation. Too often, however, speakers obfuscate information by adding fancy effects or showing indecipherable slides, or are ill-prepared or overly dependent on the slides to deliver their message.
PowerPoint is not just for professional lecturers; psychiatrists often are asked to address community or professional organizations and patient advocacy groups. Your ability to clearly explain complicated concepts to lay audiences can help market yourself as a desirable referral source.
This article describes 6 common PowerPoint presentation pitfalls, why they occur, and how to avoid them. Resources to help you create better PowerPoint presentations also are listed (see Related resources).
1 The speaker is in the dark
We’ve all seen it: As soon as the speaker starts a PowerPoint presentation, a helpful audience member turns down the lights. Fearing the projection will not be discernible, the speaker elects to make him/herself less visible in deference to the slides.
This misses the point. The audience came to hear you, so the slides should enhance your talk and not compete with you. To overvalue the slides is to ignore years of pedagogic research showing that learning flourishes when teacher and student are actively engaged.
Most modern LCD projectors are powerful enough to use in ambient light. If a slide is difficult to read, it’s often because of bad slide design, such as poorly contrasting colors or small type sizes (see peeve number 4).
Dimming the lights during a video presentation is acceptable because video usually is more visible in the dark and is the presentation’s focus when running. After the video is finished, restore the lights and return the focus to the speaker.
2 Too many bullets
The bulleted list in the PowerPoint default template is not always the best way to display information. Many speakers are reluctant to stray from this style, however, because they doubt their ability to cover all the points or worry that the audience will miss the information on the screen.
Don’t worry: Audiences are more likely to remember an effective presentation than perfectly complete slides.
3 He’s reading, not speaking
Speakers sometimes read from bulleted lists because they are not sufficiently familiar with their talk. They either turn away from the audience to read off the projected slides or—more commonly—face the audience but look down to read from a computer monitor.
Watching someone read aloud is boring. The audience will disengage if you appear unprepared and uninterested in them.
There is no substitute for planning and practicing your talk in advance. You don’t have to memorize it, but be familiar enough with your talk to require only occasional glances at the monitor. Even talented extemporaneous speakers can improve their performances with planning and practice.
4 ‘I know you can’t read this… ’
Seemingly every PowerPoint presentation includes at least one slide filled with tiny text and graphics. The speaker will laugh, saying, “I apologize, I know you can’t read this, but the point I’m trying to make is…”
This is the worst of many variations of difficult-to-read slides. Speakers also commonly scan material from textbooks into a slide rather than create it anew.
Projecting an indecipherable slide is the inexcusable result of poor planning or laziness. Breaking down a complex idea into understandable chunks of information is hard work, but that is what effective teachers do. Albert Einstein said, “If you can’t explain something simply, you don’t understand it well.” When audiences see difficult-to-read slides, they will suspect you don’t know what you’re talking about.
5 ‘Windows’ dressing
PowerPoint has many bells and whistles to enhance a presentation. Avoid them.
Transitions. PowerPoint offers more than 50 ways to transition from one slide to the next. But despite a century of film innovation, Steven Spielberg still relies on the same three transitions D.W. Griffith used in his silent films: the direct cut, the dissolve, and the wipe. All other transitions are rare in professional film; likewise, they have no place in your presentation.
Animations can be useful. For example, a slide with several bullet points is less distracting if the points are introduced one at a time. As with transitions, simple animations are best; watching words fly around a slide before settling in place has lost its novelty.
Graphics. Other built-in PowerPoint functions—such as prepackaged clip art and sound effects—are of little use. The clip art in particular looks lame and outmoded.
If your presentation calls for graphics, use high-quality photographs. PowerPoint supports numerous image formats including BMP, PCX, PNG, JPEG, and GIF (see Related resources for a comparison of each format’s advantages and disadvantages).
Most images from scanners or digital cameras are at higher resolutions than needed; computer monitors generally cannot display detail beyond 96 dots per inch (DPI), and photographs should be resampled accordingly to reduce file sizes. Resizing the image within PowerPoint does not change the resolution; you need a photo-editing program such as Adobe Photoshop, Corel Paint Shop, or Macromedia Fireworks (while there, be sure to crop out unnecessary parts of the photo).
Humor and comics. Including comic strips in a presentation has become somewhat hackneyed and overused. Use comics minimally and only when they help illustrate an important point.
6 ‘Do you have a handout?’
When audience members request printouts of slide presentations, speakers usually respond with straight printouts of the PowerPoint slides.
This makes little sense. Seeing the slides minus the speaker is like watching a documentary with the narration turned off. The more effective slides are as speaking aids, the less appropriate they are for stand-alone information.
Instead, create annotated slide printouts for distribution. Your best bet is to export the presentation to Microsoft Word, which creates a document containing pictures of the slides with adjacent notes. You could print out your slides using the PowerPoint notes function, but this only lets you print slides or notes on separate documents.
- TechRepublic.com. 10 slide design tips for producing powerful and effective presentations. http://articles.techrepublic.com.com/5100-10881-6117178.html.
- Microsoft guidelines for selecting a picture format in an Office XP program. http://support.microsoft.com/kb/320314.
- Tufte ER. The cognitive style of PowerPoint: pitching out corrupts within. Cheshire CT: Graphics Press; 2006. (Edward Tufte, professor emeritus at Yale University, is an authority on presenting graphic information).
- Presentation Zen, a blog maintained by Garr Reynolds, former program manager for worldwide user group relations at Apple. www.presentationzen.com.
- PowerPoint does rocket science. Tufte’s analysis shows the mismanagement resulting from NASA’s insistence on using PowerPoint to present technical analyses, ultimately leading to the Columbia shuttle disaster. www.edwardtufte.com/bboard/q-and-a-fetch-msg?msg_id=0001yB&topic_id=1.
- Peter Norvig’s PowerPoint version of the Gettysburg Address, an intriguing example of “death by PowerPoint.” www.norvig.com/Gettysburg.
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Varenicline
Varenicline tartrate—the first nicotine-free medication FDA-approved for smoking cessation in nearly a decade (Table 1)—has helped patients stop smoking and remain smoke-free for up to 1 year in clinical trials. Its selective action on the receptor subtype that makes tobacco enjoyable offers a novel approach to antismoking therapy.
Table 1
Varenicline: Fast facts
| Brand name: Chantix |
| Class: Partial nicotinic acetylcholine receptor agonist |
| Indication: Tobacco dependence |
| Approval date: May 10, 2006 |
| Manufacturer: Pfizer |
| Dosing forms: 0.5- and 1-mg tablets |
| Recommended dosage: 0.5 mg/d for 3 days, 0.5 mg bid for next 4 days, then 1 mg bid for 11 weeks. Patients who quit successfully should receive an additional 12-week course to reduce relapse risk. |
How it works
Unlike other FDA-approved smoking cessation treatments such as nicotine replacement therapy and sustained-release bupropion, varenicline selectively targets the α4β2 nicotinic acetylcholine receptor (nAChR),1 which helps mediate nicotine’s reinforcing effects.2-4 By targeting this receptor subtype, varenicline ultimately diminishes these effects in the mesocorticolimbic dopamine system—the brain’s “reward center.”
As a partial α4β2 nAChR agonist, varenicline offers a two-pronged approach to smoking cessation:1
- During abstinence, varenicline stimulates low-level dopamine release by binding to α4β2 receptors located on dopamine neurons. This action, which compensates for loss of exogenous nicotine after quitting, can help counteract craving and other signs and symptoms of nicotine withdrawal caused by dopamine depletion.
- If the patient resumes smoking, varenicline makes tobacco less pleasurable by competitively binding at the α4β2 receptor.1,5
Pharmacokinetics
Varenicline is rapidly absorbed across the gut mucosa and reaches maximum concentration in approximately 4 hours. After repeated dosing, the drug reaches steady-state concentrations within 4 days, and its elimination half-life is 17 to 24 hours.
Because varenicline’s simple benzazepine structure lacks bulky moieties that would promote hepatic biotransformation,5 90% of the drug is excreted through the kidneys. To date, no clinically relevant drug-drug interactions have been reported.6
Efficacy
Varenicline showed a dose-dependent effect in phase-2 clinical trials,7,8 with 1 mg bid providing optimal efficacy and tolerability. Compared with placebo, varenicline was significantly more effective in initiating:
- continuous abstinence for ≥4 weeks during active treatment, confirmed by measuring carbon monoxide (CO) in exhaled breath
- long-term abstinence, evidenced by self-report and exhaled CO ≤10 ppm at 24 and 52 weeks.7,8
Odds ratios calculated for patients who stayed smoke-free for ≥4 weeks during 7 to 12 weeks of active treatment suggest that smokers who use varenicline, 1 mg bid, are approximately 4 to 8 times more likely to achieve short-term abstinence during this active treatment period than those who received placebo.7,8
In phase-3 trials,9-11 patients were also followed for up to 1 year and received brief, standardized counseling along with medication or placebo—as recommended in the U.S. Department of Health and Human Services Clinical Practice Guideline, Treating Tobacco Use and Dependence.12
12-week treatment trials.9,10 A total of 2,052 adults in two randomized, double-blind trials received varenicline, sustained-release (SR) bupropion, or placebo for 12 weeks. Based on phase-2 trial results—which showed that varenicline was better tolerated after a 1-week dosage titration period—varenicline was given at:
- 0.5 mg/d for days 1 through 3
- 0.5 mg bid for days 4 through 7
- 1 mg bid through week 12.
Bupropion SR was given at 150 mg/d for days 1 through 3, then 150 mg bid through week 12.
Patients were then followed for up to 40 weeks after drug discontinuation. Patients had been smoking ≥10 cigarettes/day at baseline and were motivated to stop smoking.
Overall, varenicline was associated with higher short- and long-term abstinence rates compared with bupropion SR or placebo (Table 2), although the comparison with bupropion SR was not statistically significant (P=0.057) for weeks 9 through 52 in one study.9 As in the phase-2 studies, abstinence was confirmed by measuring CO in exhaled breath.
Compared with placebo, varenicline also reduced cravings and other signs and symptoms of tobacco withdrawal as measured with the Brief Questionnaire of Smoking Urges and Minnesota Nicotine Withdrawal Scale.9,10
Relapse prevention study. Tonstad et al11 investigated whether extended varenicline treatment prolongs smoking abstinence. A total of 1,210 patients who quit smoking after 12 weeks of open-label varenicline treatment continued taking varenicline at 1 mg bid or were switched to placebo during a 3-month, double-blind phase.
Compared with placebo, rates of continuous smoking abstinence were significantly higher among the varenicline group during the double-blind active treatment phase (70.5% vs. 49.6%) and for 6 months after drug discontinuation (43.6% vs. 36.9%).11 These data suggest that an extended varenicline regimen might promote long-term abstinence.6,13
Table 2
Smoking abstinence* rates among patients
during varenicline phase-3 clinical trials
| 4 weeks of continued abstinence, weeks 9 through 12 | Continued abstinence, weeks 9 through 24 | Continued abstinence, weeks 9 through 52 | |
|---|---|---|---|
| Gonzales et al 20069 | |||
| Varenicline, 1 mg bid | 44% | 29.5% | 21.9% |
| Bupropion SR, 150 mg bid | 29.5% | 20.7% | 16.1% |
| Placebo | 17.7% | 10.5% | 8.4% |
| Jorenby et al 200610 | |||
| Varenicline, 1 mg bid | 43.9% | 29.7% | 23% |
| Bupropion SR, 150 mg bid | 29.8% | 20.2% | 14.6% |
| Placebo | 17.6% | 13.2% | 10.3% |
| * Confirmed by self-report and exhaled carbon monoxide ≤10 ppm. | |||
Tolerability
Overall, varenicline was safe and well tolerated in clinical trials.
Nausea was the most commonly reported adverse event in fixed-dose, placebo-controlled studies.6 Although approximately 3% of patients stopped varenicline prematurely because of upset stomach,6 most rated their nausea as mild to moderate and reported reduced nausea with continued varenicline use. For patients with intolerable nausea, consider reducing the dosage.
Sleep disturbance, constipation, flatulence, and vomiting were twice as prevalent among the varenicline groups compared with placebo.6 Overall treatment discontinuation rates were similar with varenicline, 1 mg bid, and placebo (12% vs. 10%) in 12-week phase-2 and phase-3 clinical trials.6
To improve tolerability, the FDA recommends splitting varenicline into twice-daily doses.6,13
Dosing
Start varenicline at 0.5 mg/d for 3 days, 0.5 mg bid for the next 4 days, then 1 mg bid through week 12. To improve tolerability, advise patients to take varenicline after eating and with a full glass of water.
Setting a target quit date (TQD) is a critical element of smoking cessation treatment. Schedule the TQD for the same day the patient begins 1 mg bid varenicline dosing so that the medication is approaching maximal steady-state concentrations during the quit attempt to help counter withdrawal. Allow patients to continue smoking during the 1-week titration period, but stress the importance of trying to quit on the TQD.
Because varenicline is primarily eliminated through the kidneys, limit dosages to 0.5 mg bid in patients with severe renal impairment (estimated creatinine clearance 6,13
Varenicline has not been studied in patients with substance use and other psychiatric disorders—patients who account for most of a psychiatrist’s caseload and whose nicotine dependence is difficult to treat. Even so, the medication’s lack of discernible drug-drug interactions and selectivity of α4β2 nAChR action make varenicline worth considering for these patients.
Varenicline also has not been tested or approved for use in adolescent or pregnant smokers; research is needed on how the medication works in these patients.
Role of behavioral treatment
The Clinical Practice Guideline, Treating Tobacco Use and Dependence12 suggests combining antismoking pharmacotherapy with counseling to maximize outcome. To that end, varenicline’s manufacturer has developed a personalized behavioral support program for patients taking the medication.14 Adjunctive therapy via the Internet, telephone, or direct mail can complement other extra-treatment supports—such as toll-free quit lines and classes offered through health organizations—and more-formal, intensive behavioral interventions.
Related resources
- Varenicline Web site. www.chantix.com.
- World Health Organization. Causes of death. In: Epidemiology and burden of disease. Geneva: World Health Organization, 2003.
- Fiore MC, Bailey WC, Cohen SJ, et al. Clinical practice guideline. Treating tobacco use and dependence. Rockville, MD: U.S. Department of Health and Human Services, 2000. www.surgeongeneral.gov/tobacco/treating_tobacco_use.pdf.
Drug brand names
- Bupropion SR • Wellbutrin, Zyban
- Varenicline • Chantix
Disclosures
Dr. Anthenelli is a consultant for Alkermes and Cephalon and a speaker and consultant for Pfizer and sanofi-aventis.
The Tri-State Tobacco and Alcohol Research Center receives research grants from Addex, Ortho-McNeil Neurologics, and sanofi-aventis.
Dr. Anthenelli and the Tri-State Tobacco and Alcohol Research Center were members of the Varenicline Study Group.
Acknowledgments
The writing of this article was supported in part by National Institutes of Health Grant Awards Nos. AA013957 and AA013307.
The author thanks Reene Cantwell for her technical assistance in preparing this article.
1. Coe JW, Brooks PR, Vetelino MG, et al. Varenicline: an alpha4beta2 nicotinic receptor partial agonist for smoking cessation. J Med Chem 2005;48:3474-7.
2. Marubio LM, Gardier AM, Durier S, et al. Effects of nicotine in the dopaminergic system of mice lacking the alpha4 subunit of neuronal nicotinic acetylcholine receptors. Eur J Neurosci 2003;17:1329-37.
3. Picciotto MR, Zoli M, Rimondini R, et al. Acetylcholine receptors containing the beta2 subunit are involved in the reinforcing properties of nicotine. Nature 1998;391:173-7.
4. Tapper AR, McKinney SL, Nashmi R, et al. Nicotine activation of α4* receptors: sufficient for reward, tolerance, and sensitization. Science 2004;306:1029-32.
5. Obach RS, Reed-Hagen AE, Krueger SS, et al. Metabolism and disposition of varenicline, a selective alpha4beta2 acetylcholine receptor partial agonist, in vivo and in vitro. Drug Metab Dispos 2006;34:121-30.
6. Chantix (varenicline) package insert. Available at: http://www.pfizer.com/pfizer/download/uspi_chantix.pdf. Accessed November 28, 2006.
7. Oncken C, Gonzales D, Nides M, et al. Efficacy and safety of the novel selective nicotinic acetylcholine receptor partial agonist, varenicline, for smoking cessation. Arch Intern Med 2006;166:1571-7.
8. Nides M, Oncken C, Gonzales D, et al. Smoking cessation with varenicline, a selective alpha4beta2 nicotinic receptor partial agonist: results from a 7-week, randomized, placebo- and bupropion-controlled trial with 1-year follow-up. Arch Intern Med 2006;166:1561-8.
9. Gonzales D, Rennard SI, Nides M, et al. Varenicline Phase 3 Study Group. Varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs sustained-release bupropion and placebo for smoking cessation: a randomized controlled trial. JAMA 2006;296:47-55.
10. Jorenby DE, Hays JT, Rigotti NA, et al. Varenicline Phase 3 Study Group. Efficacy of varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs placebo or sustained-release bupropion for smoking cessation: a randomized controlled trial. JAMA 2006;296:56-63.
11. Tonstad S, Tonnesen P, Hajek P, et al. Effect of maintenance therapy with varenicline on smoking cessation: a randomized controlled trial. JAMA 2006;296:64-71.
12. Fiore MC, Bailey WC, Cohen SJ, et al. Clinical practice guideline. Treating tobacco use and dependence. Rockville, MD: U.S. Department of Health and Human Services, 2000. Available at: http://www.surgeongeneral.gov/tobacco/treating_tobacco_use.pdf. Accessed November 30, 2006.
13. Varenicline (Chantix) for tobacco dependence. Med Lett Drugs Ther 2006;48:66-8.
14. Varenicline. Web site. Available at: http://www.chantix.com. Accessed November 30, 2006.
Varenicline tartrate—the first nicotine-free medication FDA-approved for smoking cessation in nearly a decade (Table 1)—has helped patients stop smoking and remain smoke-free for up to 1 year in clinical trials. Its selective action on the receptor subtype that makes tobacco enjoyable offers a novel approach to antismoking therapy.
Table 1
Varenicline: Fast facts
| Brand name: Chantix |
| Class: Partial nicotinic acetylcholine receptor agonist |
| Indication: Tobacco dependence |
| Approval date: May 10, 2006 |
| Manufacturer: Pfizer |
| Dosing forms: 0.5- and 1-mg tablets |
| Recommended dosage: 0.5 mg/d for 3 days, 0.5 mg bid for next 4 days, then 1 mg bid for 11 weeks. Patients who quit successfully should receive an additional 12-week course to reduce relapse risk. |
How it works
Unlike other FDA-approved smoking cessation treatments such as nicotine replacement therapy and sustained-release bupropion, varenicline selectively targets the α4β2 nicotinic acetylcholine receptor (nAChR),1 which helps mediate nicotine’s reinforcing effects.2-4 By targeting this receptor subtype, varenicline ultimately diminishes these effects in the mesocorticolimbic dopamine system—the brain’s “reward center.”
As a partial α4β2 nAChR agonist, varenicline offers a two-pronged approach to smoking cessation:1
- During abstinence, varenicline stimulates low-level dopamine release by binding to α4β2 receptors located on dopamine neurons. This action, which compensates for loss of exogenous nicotine after quitting, can help counteract craving and other signs and symptoms of nicotine withdrawal caused by dopamine depletion.
- If the patient resumes smoking, varenicline makes tobacco less pleasurable by competitively binding at the α4β2 receptor.1,5
Pharmacokinetics
Varenicline is rapidly absorbed across the gut mucosa and reaches maximum concentration in approximately 4 hours. After repeated dosing, the drug reaches steady-state concentrations within 4 days, and its elimination half-life is 17 to 24 hours.
Because varenicline’s simple benzazepine structure lacks bulky moieties that would promote hepatic biotransformation,5 90% of the drug is excreted through the kidneys. To date, no clinically relevant drug-drug interactions have been reported.6
Efficacy
Varenicline showed a dose-dependent effect in phase-2 clinical trials,7,8 with 1 mg bid providing optimal efficacy and tolerability. Compared with placebo, varenicline was significantly more effective in initiating:
- continuous abstinence for ≥4 weeks during active treatment, confirmed by measuring carbon monoxide (CO) in exhaled breath
- long-term abstinence, evidenced by self-report and exhaled CO ≤10 ppm at 24 and 52 weeks.7,8
Odds ratios calculated for patients who stayed smoke-free for ≥4 weeks during 7 to 12 weeks of active treatment suggest that smokers who use varenicline, 1 mg bid, are approximately 4 to 8 times more likely to achieve short-term abstinence during this active treatment period than those who received placebo.7,8
In phase-3 trials,9-11 patients were also followed for up to 1 year and received brief, standardized counseling along with medication or placebo—as recommended in the U.S. Department of Health and Human Services Clinical Practice Guideline, Treating Tobacco Use and Dependence.12
12-week treatment trials.9,10 A total of 2,052 adults in two randomized, double-blind trials received varenicline, sustained-release (SR) bupropion, or placebo for 12 weeks. Based on phase-2 trial results—which showed that varenicline was better tolerated after a 1-week dosage titration period—varenicline was given at:
- 0.5 mg/d for days 1 through 3
- 0.5 mg bid for days 4 through 7
- 1 mg bid through week 12.
Bupropion SR was given at 150 mg/d for days 1 through 3, then 150 mg bid through week 12.
Patients were then followed for up to 40 weeks after drug discontinuation. Patients had been smoking ≥10 cigarettes/day at baseline and were motivated to stop smoking.
Overall, varenicline was associated with higher short- and long-term abstinence rates compared with bupropion SR or placebo (Table 2), although the comparison with bupropion SR was not statistically significant (P=0.057) for weeks 9 through 52 in one study.9 As in the phase-2 studies, abstinence was confirmed by measuring CO in exhaled breath.
Compared with placebo, varenicline also reduced cravings and other signs and symptoms of tobacco withdrawal as measured with the Brief Questionnaire of Smoking Urges and Minnesota Nicotine Withdrawal Scale.9,10
Relapse prevention study. Tonstad et al11 investigated whether extended varenicline treatment prolongs smoking abstinence. A total of 1,210 patients who quit smoking after 12 weeks of open-label varenicline treatment continued taking varenicline at 1 mg bid or were switched to placebo during a 3-month, double-blind phase.
Compared with placebo, rates of continuous smoking abstinence were significantly higher among the varenicline group during the double-blind active treatment phase (70.5% vs. 49.6%) and for 6 months after drug discontinuation (43.6% vs. 36.9%).11 These data suggest that an extended varenicline regimen might promote long-term abstinence.6,13
Table 2
Smoking abstinence* rates among patients
during varenicline phase-3 clinical trials
| 4 weeks of continued abstinence, weeks 9 through 12 | Continued abstinence, weeks 9 through 24 | Continued abstinence, weeks 9 through 52 | |
|---|---|---|---|
| Gonzales et al 20069 | |||
| Varenicline, 1 mg bid | 44% | 29.5% | 21.9% |
| Bupropion SR, 150 mg bid | 29.5% | 20.7% | 16.1% |
| Placebo | 17.7% | 10.5% | 8.4% |
| Jorenby et al 200610 | |||
| Varenicline, 1 mg bid | 43.9% | 29.7% | 23% |
| Bupropion SR, 150 mg bid | 29.8% | 20.2% | 14.6% |
| Placebo | 17.6% | 13.2% | 10.3% |
| * Confirmed by self-report and exhaled carbon monoxide ≤10 ppm. | |||
Tolerability
Overall, varenicline was safe and well tolerated in clinical trials.
Nausea was the most commonly reported adverse event in fixed-dose, placebo-controlled studies.6 Although approximately 3% of patients stopped varenicline prematurely because of upset stomach,6 most rated their nausea as mild to moderate and reported reduced nausea with continued varenicline use. For patients with intolerable nausea, consider reducing the dosage.
Sleep disturbance, constipation, flatulence, and vomiting were twice as prevalent among the varenicline groups compared with placebo.6 Overall treatment discontinuation rates were similar with varenicline, 1 mg bid, and placebo (12% vs. 10%) in 12-week phase-2 and phase-3 clinical trials.6
To improve tolerability, the FDA recommends splitting varenicline into twice-daily doses.6,13
Dosing
Start varenicline at 0.5 mg/d for 3 days, 0.5 mg bid for the next 4 days, then 1 mg bid through week 12. To improve tolerability, advise patients to take varenicline after eating and with a full glass of water.
Setting a target quit date (TQD) is a critical element of smoking cessation treatment. Schedule the TQD for the same day the patient begins 1 mg bid varenicline dosing so that the medication is approaching maximal steady-state concentrations during the quit attempt to help counter withdrawal. Allow patients to continue smoking during the 1-week titration period, but stress the importance of trying to quit on the TQD.
Because varenicline is primarily eliminated through the kidneys, limit dosages to 0.5 mg bid in patients with severe renal impairment (estimated creatinine clearance 6,13
Varenicline has not been studied in patients with substance use and other psychiatric disorders—patients who account for most of a psychiatrist’s caseload and whose nicotine dependence is difficult to treat. Even so, the medication’s lack of discernible drug-drug interactions and selectivity of α4β2 nAChR action make varenicline worth considering for these patients.
Varenicline also has not been tested or approved for use in adolescent or pregnant smokers; research is needed on how the medication works in these patients.
Role of behavioral treatment
The Clinical Practice Guideline, Treating Tobacco Use and Dependence12 suggests combining antismoking pharmacotherapy with counseling to maximize outcome. To that end, varenicline’s manufacturer has developed a personalized behavioral support program for patients taking the medication.14 Adjunctive therapy via the Internet, telephone, or direct mail can complement other extra-treatment supports—such as toll-free quit lines and classes offered through health organizations—and more-formal, intensive behavioral interventions.
Related resources
- Varenicline Web site. www.chantix.com.
- World Health Organization. Causes of death. In: Epidemiology and burden of disease. Geneva: World Health Organization, 2003.
- Fiore MC, Bailey WC, Cohen SJ, et al. Clinical practice guideline. Treating tobacco use and dependence. Rockville, MD: U.S. Department of Health and Human Services, 2000. www.surgeongeneral.gov/tobacco/treating_tobacco_use.pdf.
Drug brand names
- Bupropion SR • Wellbutrin, Zyban
- Varenicline • Chantix
Disclosures
Dr. Anthenelli is a consultant for Alkermes and Cephalon and a speaker and consultant for Pfizer and sanofi-aventis.
The Tri-State Tobacco and Alcohol Research Center receives research grants from Addex, Ortho-McNeil Neurologics, and sanofi-aventis.
Dr. Anthenelli and the Tri-State Tobacco and Alcohol Research Center were members of the Varenicline Study Group.
Acknowledgments
The writing of this article was supported in part by National Institutes of Health Grant Awards Nos. AA013957 and AA013307.
The author thanks Reene Cantwell for her technical assistance in preparing this article.
Varenicline tartrate—the first nicotine-free medication FDA-approved for smoking cessation in nearly a decade (Table 1)—has helped patients stop smoking and remain smoke-free for up to 1 year in clinical trials. Its selective action on the receptor subtype that makes tobacco enjoyable offers a novel approach to antismoking therapy.
Table 1
Varenicline: Fast facts
| Brand name: Chantix |
| Class: Partial nicotinic acetylcholine receptor agonist |
| Indication: Tobacco dependence |
| Approval date: May 10, 2006 |
| Manufacturer: Pfizer |
| Dosing forms: 0.5- and 1-mg tablets |
| Recommended dosage: 0.5 mg/d for 3 days, 0.5 mg bid for next 4 days, then 1 mg bid for 11 weeks. Patients who quit successfully should receive an additional 12-week course to reduce relapse risk. |
How it works
Unlike other FDA-approved smoking cessation treatments such as nicotine replacement therapy and sustained-release bupropion, varenicline selectively targets the α4β2 nicotinic acetylcholine receptor (nAChR),1 which helps mediate nicotine’s reinforcing effects.2-4 By targeting this receptor subtype, varenicline ultimately diminishes these effects in the mesocorticolimbic dopamine system—the brain’s “reward center.”
As a partial α4β2 nAChR agonist, varenicline offers a two-pronged approach to smoking cessation:1
- During abstinence, varenicline stimulates low-level dopamine release by binding to α4β2 receptors located on dopamine neurons. This action, which compensates for loss of exogenous nicotine after quitting, can help counteract craving and other signs and symptoms of nicotine withdrawal caused by dopamine depletion.
- If the patient resumes smoking, varenicline makes tobacco less pleasurable by competitively binding at the α4β2 receptor.1,5
Pharmacokinetics
Varenicline is rapidly absorbed across the gut mucosa and reaches maximum concentration in approximately 4 hours. After repeated dosing, the drug reaches steady-state concentrations within 4 days, and its elimination half-life is 17 to 24 hours.
Because varenicline’s simple benzazepine structure lacks bulky moieties that would promote hepatic biotransformation,5 90% of the drug is excreted through the kidneys. To date, no clinically relevant drug-drug interactions have been reported.6
Efficacy
Varenicline showed a dose-dependent effect in phase-2 clinical trials,7,8 with 1 mg bid providing optimal efficacy and tolerability. Compared with placebo, varenicline was significantly more effective in initiating:
- continuous abstinence for ≥4 weeks during active treatment, confirmed by measuring carbon monoxide (CO) in exhaled breath
- long-term abstinence, evidenced by self-report and exhaled CO ≤10 ppm at 24 and 52 weeks.7,8
Odds ratios calculated for patients who stayed smoke-free for ≥4 weeks during 7 to 12 weeks of active treatment suggest that smokers who use varenicline, 1 mg bid, are approximately 4 to 8 times more likely to achieve short-term abstinence during this active treatment period than those who received placebo.7,8
In phase-3 trials,9-11 patients were also followed for up to 1 year and received brief, standardized counseling along with medication or placebo—as recommended in the U.S. Department of Health and Human Services Clinical Practice Guideline, Treating Tobacco Use and Dependence.12
12-week treatment trials.9,10 A total of 2,052 adults in two randomized, double-blind trials received varenicline, sustained-release (SR) bupropion, or placebo for 12 weeks. Based on phase-2 trial results—which showed that varenicline was better tolerated after a 1-week dosage titration period—varenicline was given at:
- 0.5 mg/d for days 1 through 3
- 0.5 mg bid for days 4 through 7
- 1 mg bid through week 12.
Bupropion SR was given at 150 mg/d for days 1 through 3, then 150 mg bid through week 12.
Patients were then followed for up to 40 weeks after drug discontinuation. Patients had been smoking ≥10 cigarettes/day at baseline and were motivated to stop smoking.
Overall, varenicline was associated with higher short- and long-term abstinence rates compared with bupropion SR or placebo (Table 2), although the comparison with bupropion SR was not statistically significant (P=0.057) for weeks 9 through 52 in one study.9 As in the phase-2 studies, abstinence was confirmed by measuring CO in exhaled breath.
Compared with placebo, varenicline also reduced cravings and other signs and symptoms of tobacco withdrawal as measured with the Brief Questionnaire of Smoking Urges and Minnesota Nicotine Withdrawal Scale.9,10
Relapse prevention study. Tonstad et al11 investigated whether extended varenicline treatment prolongs smoking abstinence. A total of 1,210 patients who quit smoking after 12 weeks of open-label varenicline treatment continued taking varenicline at 1 mg bid or were switched to placebo during a 3-month, double-blind phase.
Compared with placebo, rates of continuous smoking abstinence were significantly higher among the varenicline group during the double-blind active treatment phase (70.5% vs. 49.6%) and for 6 months after drug discontinuation (43.6% vs. 36.9%).11 These data suggest that an extended varenicline regimen might promote long-term abstinence.6,13
Table 2
Smoking abstinence* rates among patients
during varenicline phase-3 clinical trials
| 4 weeks of continued abstinence, weeks 9 through 12 | Continued abstinence, weeks 9 through 24 | Continued abstinence, weeks 9 through 52 | |
|---|---|---|---|
| Gonzales et al 20069 | |||
| Varenicline, 1 mg bid | 44% | 29.5% | 21.9% |
| Bupropion SR, 150 mg bid | 29.5% | 20.7% | 16.1% |
| Placebo | 17.7% | 10.5% | 8.4% |
| Jorenby et al 200610 | |||
| Varenicline, 1 mg bid | 43.9% | 29.7% | 23% |
| Bupropion SR, 150 mg bid | 29.8% | 20.2% | 14.6% |
| Placebo | 17.6% | 13.2% | 10.3% |
| * Confirmed by self-report and exhaled carbon monoxide ≤10 ppm. | |||
Tolerability
Overall, varenicline was safe and well tolerated in clinical trials.
Nausea was the most commonly reported adverse event in fixed-dose, placebo-controlled studies.6 Although approximately 3% of patients stopped varenicline prematurely because of upset stomach,6 most rated their nausea as mild to moderate and reported reduced nausea with continued varenicline use. For patients with intolerable nausea, consider reducing the dosage.
Sleep disturbance, constipation, flatulence, and vomiting were twice as prevalent among the varenicline groups compared with placebo.6 Overall treatment discontinuation rates were similar with varenicline, 1 mg bid, and placebo (12% vs. 10%) in 12-week phase-2 and phase-3 clinical trials.6
To improve tolerability, the FDA recommends splitting varenicline into twice-daily doses.6,13
Dosing
Start varenicline at 0.5 mg/d for 3 days, 0.5 mg bid for the next 4 days, then 1 mg bid through week 12. To improve tolerability, advise patients to take varenicline after eating and with a full glass of water.
Setting a target quit date (TQD) is a critical element of smoking cessation treatment. Schedule the TQD for the same day the patient begins 1 mg bid varenicline dosing so that the medication is approaching maximal steady-state concentrations during the quit attempt to help counter withdrawal. Allow patients to continue smoking during the 1-week titration period, but stress the importance of trying to quit on the TQD.
Because varenicline is primarily eliminated through the kidneys, limit dosages to 0.5 mg bid in patients with severe renal impairment (estimated creatinine clearance 6,13
Varenicline has not been studied in patients with substance use and other psychiatric disorders—patients who account for most of a psychiatrist’s caseload and whose nicotine dependence is difficult to treat. Even so, the medication’s lack of discernible drug-drug interactions and selectivity of α4β2 nAChR action make varenicline worth considering for these patients.
Varenicline also has not been tested or approved for use in adolescent or pregnant smokers; research is needed on how the medication works in these patients.
Role of behavioral treatment
The Clinical Practice Guideline, Treating Tobacco Use and Dependence12 suggests combining antismoking pharmacotherapy with counseling to maximize outcome. To that end, varenicline’s manufacturer has developed a personalized behavioral support program for patients taking the medication.14 Adjunctive therapy via the Internet, telephone, or direct mail can complement other extra-treatment supports—such as toll-free quit lines and classes offered through health organizations—and more-formal, intensive behavioral interventions.
Related resources
- Varenicline Web site. www.chantix.com.
- World Health Organization. Causes of death. In: Epidemiology and burden of disease. Geneva: World Health Organization, 2003.
- Fiore MC, Bailey WC, Cohen SJ, et al. Clinical practice guideline. Treating tobacco use and dependence. Rockville, MD: U.S. Department of Health and Human Services, 2000. www.surgeongeneral.gov/tobacco/treating_tobacco_use.pdf.
Drug brand names
- Bupropion SR • Wellbutrin, Zyban
- Varenicline • Chantix
Disclosures
Dr. Anthenelli is a consultant for Alkermes and Cephalon and a speaker and consultant for Pfizer and sanofi-aventis.
The Tri-State Tobacco and Alcohol Research Center receives research grants from Addex, Ortho-McNeil Neurologics, and sanofi-aventis.
Dr. Anthenelli and the Tri-State Tobacco and Alcohol Research Center were members of the Varenicline Study Group.
Acknowledgments
The writing of this article was supported in part by National Institutes of Health Grant Awards Nos. AA013957 and AA013307.
The author thanks Reene Cantwell for her technical assistance in preparing this article.
1. Coe JW, Brooks PR, Vetelino MG, et al. Varenicline: an alpha4beta2 nicotinic receptor partial agonist for smoking cessation. J Med Chem 2005;48:3474-7.
2. Marubio LM, Gardier AM, Durier S, et al. Effects of nicotine in the dopaminergic system of mice lacking the alpha4 subunit of neuronal nicotinic acetylcholine receptors. Eur J Neurosci 2003;17:1329-37.
3. Picciotto MR, Zoli M, Rimondini R, et al. Acetylcholine receptors containing the beta2 subunit are involved in the reinforcing properties of nicotine. Nature 1998;391:173-7.
4. Tapper AR, McKinney SL, Nashmi R, et al. Nicotine activation of α4* receptors: sufficient for reward, tolerance, and sensitization. Science 2004;306:1029-32.
5. Obach RS, Reed-Hagen AE, Krueger SS, et al. Metabolism and disposition of varenicline, a selective alpha4beta2 acetylcholine receptor partial agonist, in vivo and in vitro. Drug Metab Dispos 2006;34:121-30.
6. Chantix (varenicline) package insert. Available at: http://www.pfizer.com/pfizer/download/uspi_chantix.pdf. Accessed November 28, 2006.
7. Oncken C, Gonzales D, Nides M, et al. Efficacy and safety of the novel selective nicotinic acetylcholine receptor partial agonist, varenicline, for smoking cessation. Arch Intern Med 2006;166:1571-7.
8. Nides M, Oncken C, Gonzales D, et al. Smoking cessation with varenicline, a selective alpha4beta2 nicotinic receptor partial agonist: results from a 7-week, randomized, placebo- and bupropion-controlled trial with 1-year follow-up. Arch Intern Med 2006;166:1561-8.
9. Gonzales D, Rennard SI, Nides M, et al. Varenicline Phase 3 Study Group. Varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs sustained-release bupropion and placebo for smoking cessation: a randomized controlled trial. JAMA 2006;296:47-55.
10. Jorenby DE, Hays JT, Rigotti NA, et al. Varenicline Phase 3 Study Group. Efficacy of varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs placebo or sustained-release bupropion for smoking cessation: a randomized controlled trial. JAMA 2006;296:56-63.
11. Tonstad S, Tonnesen P, Hajek P, et al. Effect of maintenance therapy with varenicline on smoking cessation: a randomized controlled trial. JAMA 2006;296:64-71.
12. Fiore MC, Bailey WC, Cohen SJ, et al. Clinical practice guideline. Treating tobacco use and dependence. Rockville, MD: U.S. Department of Health and Human Services, 2000. Available at: http://www.surgeongeneral.gov/tobacco/treating_tobacco_use.pdf. Accessed November 30, 2006.
13. Varenicline (Chantix) for tobacco dependence. Med Lett Drugs Ther 2006;48:66-8.
14. Varenicline. Web site. Available at: http://www.chantix.com. Accessed November 30, 2006.
1. Coe JW, Brooks PR, Vetelino MG, et al. Varenicline: an alpha4beta2 nicotinic receptor partial agonist for smoking cessation. J Med Chem 2005;48:3474-7.
2. Marubio LM, Gardier AM, Durier S, et al. Effects of nicotine in the dopaminergic system of mice lacking the alpha4 subunit of neuronal nicotinic acetylcholine receptors. Eur J Neurosci 2003;17:1329-37.
3. Picciotto MR, Zoli M, Rimondini R, et al. Acetylcholine receptors containing the beta2 subunit are involved in the reinforcing properties of nicotine. Nature 1998;391:173-7.
4. Tapper AR, McKinney SL, Nashmi R, et al. Nicotine activation of α4* receptors: sufficient for reward, tolerance, and sensitization. Science 2004;306:1029-32.
5. Obach RS, Reed-Hagen AE, Krueger SS, et al. Metabolism and disposition of varenicline, a selective alpha4beta2 acetylcholine receptor partial agonist, in vivo and in vitro. Drug Metab Dispos 2006;34:121-30.
6. Chantix (varenicline) package insert. Available at: http://www.pfizer.com/pfizer/download/uspi_chantix.pdf. Accessed November 28, 2006.
7. Oncken C, Gonzales D, Nides M, et al. Efficacy and safety of the novel selective nicotinic acetylcholine receptor partial agonist, varenicline, for smoking cessation. Arch Intern Med 2006;166:1571-7.
8. Nides M, Oncken C, Gonzales D, et al. Smoking cessation with varenicline, a selective alpha4beta2 nicotinic receptor partial agonist: results from a 7-week, randomized, placebo- and bupropion-controlled trial with 1-year follow-up. Arch Intern Med 2006;166:1561-8.
9. Gonzales D, Rennard SI, Nides M, et al. Varenicline Phase 3 Study Group. Varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs sustained-release bupropion and placebo for smoking cessation: a randomized controlled trial. JAMA 2006;296:47-55.
10. Jorenby DE, Hays JT, Rigotti NA, et al. Varenicline Phase 3 Study Group. Efficacy of varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs placebo or sustained-release bupropion for smoking cessation: a randomized controlled trial. JAMA 2006;296:56-63.
11. Tonstad S, Tonnesen P, Hajek P, et al. Effect of maintenance therapy with varenicline on smoking cessation: a randomized controlled trial. JAMA 2006;296:64-71.
12. Fiore MC, Bailey WC, Cohen SJ, et al. Clinical practice guideline. Treating tobacco use and dependence. Rockville, MD: U.S. Department of Health and Human Services, 2000. Available at: http://www.surgeongeneral.gov/tobacco/treating_tobacco_use.pdf. Accessed November 30, 2006.
13. Varenicline (Chantix) for tobacco dependence. Med Lett Drugs Ther 2006;48:66-8.
14. Varenicline. Web site. Available at: http://www.chantix.com. Accessed November 30, 2006.
Supportive questions help assess suicide risk
Assessing suicide risk is a fundamental skill for all psychiatrists. Early in training we are taught to look for prior attempts, family history of suicide, related psychiatric diagnoses (such as depression, psychosis, or substance abuse), symptomatology, and medical comorbidities, as well as demographic risk factors such as age, race, marital status, and religion.
This tendency to focus on data, document risks factors, and differentiate between ideation, intent, and plan may cause us to overlook why a patient wants to commit suicide, however. And rapid-fire questioning—particularly about suicide—can compromise rapport and leave the patient feeling alienated.
Positive inquiry
I always end the suicide risk assessment component of the interview by asking, “What keeps you from killing yourself?” Patients’ responses to this question often reveal compelling reasons why they do not want to harm themselves, including meaningful relationships or religious beliefs.
Examining these so-called protective factors—or the lack thereof—in conjunction with the overall clinical picture often can help clarify the patient’s risk of suicide. When patients identify factors that prevent them from committing suicide, such as a relationship with a loving spouse or a religious conviction, I am inclined to use a more liberal treatment plan, such as immediate outpatient follow-up, rather than a more conservative approach, such as inpatient hospitalization.
Asking a supportive question helps to end difficult discussions on a positive note. After talking about ways a patient has thought about ending his or her life, for example, I can use a protective factor as the endpoint to the suicide risk evaluation before segueing into other questions.
Supportive interviewing embodies a framework of inquiry in which mental health clinicians can gather valuable information and at the same time build up the patient’s psychological defenses. This line of questioning does not guarantee a successful suicide-risk assessment. However, focusing on protective factors ensures that these difficult conversations—often undertaken when patients are under extreme stress—accomplish more than simply gathering data.
Dr. Neimark is an attending psychiatrist, Mercy Hospital of Philadelphia.
Assessing suicide risk is a fundamental skill for all psychiatrists. Early in training we are taught to look for prior attempts, family history of suicide, related psychiatric diagnoses (such as depression, psychosis, or substance abuse), symptomatology, and medical comorbidities, as well as demographic risk factors such as age, race, marital status, and religion.
This tendency to focus on data, document risks factors, and differentiate between ideation, intent, and plan may cause us to overlook why a patient wants to commit suicide, however. And rapid-fire questioning—particularly about suicide—can compromise rapport and leave the patient feeling alienated.
Positive inquiry
I always end the suicide risk assessment component of the interview by asking, “What keeps you from killing yourself?” Patients’ responses to this question often reveal compelling reasons why they do not want to harm themselves, including meaningful relationships or religious beliefs.
Examining these so-called protective factors—or the lack thereof—in conjunction with the overall clinical picture often can help clarify the patient’s risk of suicide. When patients identify factors that prevent them from committing suicide, such as a relationship with a loving spouse or a religious conviction, I am inclined to use a more liberal treatment plan, such as immediate outpatient follow-up, rather than a more conservative approach, such as inpatient hospitalization.
Asking a supportive question helps to end difficult discussions on a positive note. After talking about ways a patient has thought about ending his or her life, for example, I can use a protective factor as the endpoint to the suicide risk evaluation before segueing into other questions.
Supportive interviewing embodies a framework of inquiry in which mental health clinicians can gather valuable information and at the same time build up the patient’s psychological defenses. This line of questioning does not guarantee a successful suicide-risk assessment. However, focusing on protective factors ensures that these difficult conversations—often undertaken when patients are under extreme stress—accomplish more than simply gathering data.
Assessing suicide risk is a fundamental skill for all psychiatrists. Early in training we are taught to look for prior attempts, family history of suicide, related psychiatric diagnoses (such as depression, psychosis, or substance abuse), symptomatology, and medical comorbidities, as well as demographic risk factors such as age, race, marital status, and religion.
This tendency to focus on data, document risks factors, and differentiate between ideation, intent, and plan may cause us to overlook why a patient wants to commit suicide, however. And rapid-fire questioning—particularly about suicide—can compromise rapport and leave the patient feeling alienated.
Positive inquiry
I always end the suicide risk assessment component of the interview by asking, “What keeps you from killing yourself?” Patients’ responses to this question often reveal compelling reasons why they do not want to harm themselves, including meaningful relationships or religious beliefs.
Examining these so-called protective factors—or the lack thereof—in conjunction with the overall clinical picture often can help clarify the patient’s risk of suicide. When patients identify factors that prevent them from committing suicide, such as a relationship with a loving spouse or a religious conviction, I am inclined to use a more liberal treatment plan, such as immediate outpatient follow-up, rather than a more conservative approach, such as inpatient hospitalization.
Asking a supportive question helps to end difficult discussions on a positive note. After talking about ways a patient has thought about ending his or her life, for example, I can use a protective factor as the endpoint to the suicide risk evaluation before segueing into other questions.
Supportive interviewing embodies a framework of inquiry in which mental health clinicians can gather valuable information and at the same time build up the patient’s psychological defenses. This line of questioning does not guarantee a successful suicide-risk assessment. However, focusing on protective factors ensures that these difficult conversations—often undertaken when patients are under extreme stress—accomplish more than simply gathering data.
Dr. Neimark is an attending psychiatrist, Mercy Hospital of Philadelphia.
Dr. Neimark is an attending psychiatrist, Mercy Hospital of Philadelphia.
Jump-starting depression treatment
The serendipitous discovery of medications that can improve mood transformed depression treatment more than 50 years ago.1 Most antidepressants produced since then could be called “me-too” medications because they all work by affecting the release of monoamines—serotonin, norepinephrine, and dopamine—which, in turn, modulate the activity of neurons that release glutamate.
Weeks may pass before antidepressants’ effect on monoamine-releasing neurons produces a therapeutic benefit, however, leaving many patients impaired or even suicidal. This delayed onset of action might be explained by antidepressants’ indirect blockade of glutamate. The route to more rapid results, therefore, might be to cut out the monoamine middlemen.
Glutamate clues
Glutamate, instead of monoamines, might offer a more direct means to affect mood and could be a new target for antidepressant treatment:2
- Positron-emission tomography of neuron function in depressed patients shows abnormal activity in neurons that release glutamate—so-called glutamate neurons.
- Approximately 60 % of neurons are glutamate neurons, the largest network of neurons in the brain.
- Increased glutamate activity is seen in depressed patients.
- Animal studies have shown that blocking the N-methyl-D-aspartate (NMDA) receptor—1 of 3 types of glutamate receptors—decreases depressive behavior.
- Chronic administration of antidepressant medication reduces the expression of NMDA receptors.
Rapid glutamate blockade
Prompted by evidence that glutamate may be involved in mood disorders, researchers at the National Institute of Mental Health designed a study to determine if blocking the NMDA receptor can produce a rapid antidepressant effect.3 They chose the agent ketamine for this study because of its potent affinity for the NMDA receptor.
Ketamine was developed in the 1960s as a general anaesthetic, and its use in the United States is limited almost exclusively to veterinary medicine. The drug’s propensity to induce perceptual disturbances limits its clinical use but enhances its illicit use.
Eighteen patients with treatment-resistant depression were enrolled in a randomized, placebo-controlled, double-blind, crossover study. After 2 weeks without medication, they received a single infusion of IV ketamine or placebo. One week later they received the alternate intervention. Changes in Hamilton Rating Scale for Depression scores were assessed after each infusion.
Figure Decrease in depressive symptoms with IV ketamine
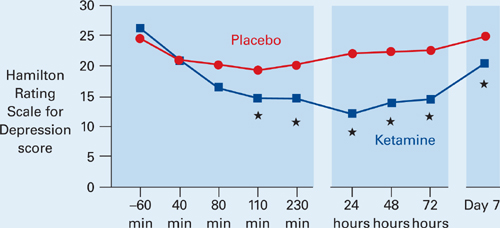
* = P <0.05
Patients who received ketamine (blue) showed a marked reduction of depressive symptoms within 2 hours compared with those who received placebo (red).
Source: Reference 3Patients receiving ketamine showed a robust and sustained reduction in depressive symptoms compared with placebo within 110 minutes (Figure). “To our knowledge,” the authors wrote, “there has never been a report of any other drug or somatic treatment—such as sleep deprivation, thyrotropin-releasing hormone, antidepressant, dexamethasone, or electroconvulsive therapy—that results in such a dramatic rapid and prolonged response with a single administration.”
Seventy-one percent of patients responded to IV ketamine within 24 hours, which is comparable to reported response rates after 8 weeks with oral antidepressants such as bupropion (62%), selective serotonin reuptake inhibitors (63%), and venlafaxine (65%).4,5
Caution and caveats
Despite these “dramatic” results, we must be cautious about extrapolating too much from this small study. Glutamate blockers such as ketamine can have serious adverse effects—including psychosis—and patients may not tolerate long-term interventions. Likewise, oral administration of memantine—another NMDA blocker—in a double-blind study did not effectively treat depression.6 Finally, subjects in the ketamine trial had chronic, treatment-resistant depression, and the results might not apply to other forms of depression.
The results suggest the possibility of a new option for depression treatment, however. Specifically, this option could expedite response and “jump-start” treatment through a novel mechanism so that persons with depression can get back on their feet more rapidly.
Drug brand names
- Bupropion • Wellbutrin
- Ketamine • Ketalar
- Memantine • Namenda
- Venlafaxine • Effexor
1. Higgins ES, George MS. Neuroscientific foundations of clinical psychiatry. Philadelphia, PA: Lippincott Williams and Wilkins; 2007. In press.
2. Kugaya A, Sanacora G. Beyond monoamines: glutamatergic function in mood disorders. CNS Spectrums 2005;10(10):808-19.
3. Zarate CA, Jr, Singh JB, Carlson PJ, et al. A randomized trial of an N-methyl-D-aspartate antagonist in treatment-resistant major depression. Arch Gen Psychiatry 2006;63(8):856-64.
4. Thase ME, Haight BR, Richard N, et al. Remission rates following antidepressant therapy with bupropion or selective serotonin reuptake inhibitors: a meta-analysis of original data from 7 randomized controlled trials. J Clin Psychiatry 2005;66(8):974-81.
5. Entsuah AR, Huang H, Thase ME. Response and remission rates in different subpopulations with major depressive disorder administered venlafaxine, selective serotonin reuptake inhibitors, or placebo. J Clin Psychiatry 2001;62(11):869-77.
6. Zarate CA, Jr, Singh JB, Quiroz JA, et al. A double-blind, placebo-controlled study of memantine in the treatment of major depression. Am J Psychiatry 2006;163(1):153-5.
The serendipitous discovery of medications that can improve mood transformed depression treatment more than 50 years ago.1 Most antidepressants produced since then could be called “me-too” medications because they all work by affecting the release of monoamines—serotonin, norepinephrine, and dopamine—which, in turn, modulate the activity of neurons that release glutamate.
Weeks may pass before antidepressants’ effect on monoamine-releasing neurons produces a therapeutic benefit, however, leaving many patients impaired or even suicidal. This delayed onset of action might be explained by antidepressants’ indirect blockade of glutamate. The route to more rapid results, therefore, might be to cut out the monoamine middlemen.
Glutamate clues
Glutamate, instead of monoamines, might offer a more direct means to affect mood and could be a new target for antidepressant treatment:2
- Positron-emission tomography of neuron function in depressed patients shows abnormal activity in neurons that release glutamate—so-called glutamate neurons.
- Approximately 60 % of neurons are glutamate neurons, the largest network of neurons in the brain.
- Increased glutamate activity is seen in depressed patients.
- Animal studies have shown that blocking the N-methyl-D-aspartate (NMDA) receptor—1 of 3 types of glutamate receptors—decreases depressive behavior.
- Chronic administration of antidepressant medication reduces the expression of NMDA receptors.
Rapid glutamate blockade
Prompted by evidence that glutamate may be involved in mood disorders, researchers at the National Institute of Mental Health designed a study to determine if blocking the NMDA receptor can produce a rapid antidepressant effect.3 They chose the agent ketamine for this study because of its potent affinity for the NMDA receptor.
Ketamine was developed in the 1960s as a general anaesthetic, and its use in the United States is limited almost exclusively to veterinary medicine. The drug’s propensity to induce perceptual disturbances limits its clinical use but enhances its illicit use.
Eighteen patients with treatment-resistant depression were enrolled in a randomized, placebo-controlled, double-blind, crossover study. After 2 weeks without medication, they received a single infusion of IV ketamine or placebo. One week later they received the alternate intervention. Changes in Hamilton Rating Scale for Depression scores were assessed after each infusion.
Figure Decrease in depressive symptoms with IV ketamine
* = P <0.05
Patients who received ketamine (blue) showed a marked reduction of depressive symptoms within 2 hours compared with those who received placebo (red).
Source: Reference 3Patients receiving ketamine showed a robust and sustained reduction in depressive symptoms compared with placebo within 110 minutes (Figure). “To our knowledge,” the authors wrote, “there has never been a report of any other drug or somatic treatment—such as sleep deprivation, thyrotropin-releasing hormone, antidepressant, dexamethasone, or electroconvulsive therapy—that results in such a dramatic rapid and prolonged response with a single administration.”
Seventy-one percent of patients responded to IV ketamine within 24 hours, which is comparable to reported response rates after 8 weeks with oral antidepressants such as bupropion (62%), selective serotonin reuptake inhibitors (63%), and venlafaxine (65%).4,5
Caution and caveats
Despite these “dramatic” results, we must be cautious about extrapolating too much from this small study. Glutamate blockers such as ketamine can have serious adverse effects—including psychosis—and patients may not tolerate long-term interventions. Likewise, oral administration of memantine—another NMDA blocker—in a double-blind study did not effectively treat depression.6 Finally, subjects in the ketamine trial had chronic, treatment-resistant depression, and the results might not apply to other forms of depression.
The results suggest the possibility of a new option for depression treatment, however. Specifically, this option could expedite response and “jump-start” treatment through a novel mechanism so that persons with depression can get back on their feet more rapidly.
Drug brand names
- Bupropion • Wellbutrin
- Ketamine • Ketalar
- Memantine • Namenda
- Venlafaxine • Effexor
The serendipitous discovery of medications that can improve mood transformed depression treatment more than 50 years ago.1 Most antidepressants produced since then could be called “me-too” medications because they all work by affecting the release of monoamines—serotonin, norepinephrine, and dopamine—which, in turn, modulate the activity of neurons that release glutamate.
Weeks may pass before antidepressants’ effect on monoamine-releasing neurons produces a therapeutic benefit, however, leaving many patients impaired or even suicidal. This delayed onset of action might be explained by antidepressants’ indirect blockade of glutamate. The route to more rapid results, therefore, might be to cut out the monoamine middlemen.
Glutamate clues
Glutamate, instead of monoamines, might offer a more direct means to affect mood and could be a new target for antidepressant treatment:2
- Positron-emission tomography of neuron function in depressed patients shows abnormal activity in neurons that release glutamate—so-called glutamate neurons.
- Approximately 60 % of neurons are glutamate neurons, the largest network of neurons in the brain.
- Increased glutamate activity is seen in depressed patients.
- Animal studies have shown that blocking the N-methyl-D-aspartate (NMDA) receptor—1 of 3 types of glutamate receptors—decreases depressive behavior.
- Chronic administration of antidepressant medication reduces the expression of NMDA receptors.
Rapid glutamate blockade
Prompted by evidence that glutamate may be involved in mood disorders, researchers at the National Institute of Mental Health designed a study to determine if blocking the NMDA receptor can produce a rapid antidepressant effect.3 They chose the agent ketamine for this study because of its potent affinity for the NMDA receptor.
Ketamine was developed in the 1960s as a general anaesthetic, and its use in the United States is limited almost exclusively to veterinary medicine. The drug’s propensity to induce perceptual disturbances limits its clinical use but enhances its illicit use.
Eighteen patients with treatment-resistant depression were enrolled in a randomized, placebo-controlled, double-blind, crossover study. After 2 weeks without medication, they received a single infusion of IV ketamine or placebo. One week later they received the alternate intervention. Changes in Hamilton Rating Scale for Depression scores were assessed after each infusion.
Figure Decrease in depressive symptoms with IV ketamine
* = P <0.05
Patients who received ketamine (blue) showed a marked reduction of depressive symptoms within 2 hours compared with those who received placebo (red).
Source: Reference 3Patients receiving ketamine showed a robust and sustained reduction in depressive symptoms compared with placebo within 110 minutes (Figure). “To our knowledge,” the authors wrote, “there has never been a report of any other drug or somatic treatment—such as sleep deprivation, thyrotropin-releasing hormone, antidepressant, dexamethasone, or electroconvulsive therapy—that results in such a dramatic rapid and prolonged response with a single administration.”
Seventy-one percent of patients responded to IV ketamine within 24 hours, which is comparable to reported response rates after 8 weeks with oral antidepressants such as bupropion (62%), selective serotonin reuptake inhibitors (63%), and venlafaxine (65%).4,5
Caution and caveats
Despite these “dramatic” results, we must be cautious about extrapolating too much from this small study. Glutamate blockers such as ketamine can have serious adverse effects—including psychosis—and patients may not tolerate long-term interventions. Likewise, oral administration of memantine—another NMDA blocker—in a double-blind study did not effectively treat depression.6 Finally, subjects in the ketamine trial had chronic, treatment-resistant depression, and the results might not apply to other forms of depression.
The results suggest the possibility of a new option for depression treatment, however. Specifically, this option could expedite response and “jump-start” treatment through a novel mechanism so that persons with depression can get back on their feet more rapidly.
Drug brand names
- Bupropion • Wellbutrin
- Ketamine • Ketalar
- Memantine • Namenda
- Venlafaxine • Effexor
1. Higgins ES, George MS. Neuroscientific foundations of clinical psychiatry. Philadelphia, PA: Lippincott Williams and Wilkins; 2007. In press.
2. Kugaya A, Sanacora G. Beyond monoamines: glutamatergic function in mood disorders. CNS Spectrums 2005;10(10):808-19.
3. Zarate CA, Jr, Singh JB, Carlson PJ, et al. A randomized trial of an N-methyl-D-aspartate antagonist in treatment-resistant major depression. Arch Gen Psychiatry 2006;63(8):856-64.
4. Thase ME, Haight BR, Richard N, et al. Remission rates following antidepressant therapy with bupropion or selective serotonin reuptake inhibitors: a meta-analysis of original data from 7 randomized controlled trials. J Clin Psychiatry 2005;66(8):974-81.
5. Entsuah AR, Huang H, Thase ME. Response and remission rates in different subpopulations with major depressive disorder administered venlafaxine, selective serotonin reuptake inhibitors, or placebo. J Clin Psychiatry 2001;62(11):869-77.
6. Zarate CA, Jr, Singh JB, Quiroz JA, et al. A double-blind, placebo-controlled study of memantine in the treatment of major depression. Am J Psychiatry 2006;163(1):153-5.
1. Higgins ES, George MS. Neuroscientific foundations of clinical psychiatry. Philadelphia, PA: Lippincott Williams and Wilkins; 2007. In press.
2. Kugaya A, Sanacora G. Beyond monoamines: glutamatergic function in mood disorders. CNS Spectrums 2005;10(10):808-19.
3. Zarate CA, Jr, Singh JB, Carlson PJ, et al. A randomized trial of an N-methyl-D-aspartate antagonist in treatment-resistant major depression. Arch Gen Psychiatry 2006;63(8):856-64.
4. Thase ME, Haight BR, Richard N, et al. Remission rates following antidepressant therapy with bupropion or selective serotonin reuptake inhibitors: a meta-analysis of original data from 7 randomized controlled trials. J Clin Psychiatry 2005;66(8):974-81.
5. Entsuah AR, Huang H, Thase ME. Response and remission rates in different subpopulations with major depressive disorder administered venlafaxine, selective serotonin reuptake inhibitors, or placebo. J Clin Psychiatry 2001;62(11):869-77.
6. Zarate CA, Jr, Singh JB, Quiroz JA, et al. A double-blind, placebo-controlled study of memantine in the treatment of major depression. Am J Psychiatry 2006;163(1):153-5.
Looking at the big picture
Thank you for Dr. Henry Nasrallah’s editorial, “Our mission: To meet your needs,” which questions mental health professionals’ role and suggests new ways of looking at our clients (Current Psychiatry, September 2006). Finally, someone is questioning the DSM-IV-TR, the woeful lack of breakthroughs in many disorders, the interface between medicine and psychiatry, and the disparity of payment for mental health treatment.
Psychiatry could be leading thinking on a wider basis. With proper focus, emotional health could be a primary factor in physical medicine rather than the other way around. People who are mentally healthy are less likely to be physically ill, but there is no research to prove this.
Consider taking the focus off the individual patient and looking at larger systems such as the family, church, and community. Psychotherapy will not be able to heal and help people to have successful and productive lives if it stays mired in the individual. Looking at systems allows psychiatry to lead rather than follow and engage in wellness activities such as consulting for schools, families, and political systems. But the profession must look at itself first.
M. Cybil Britton, APRN, BC
Severna Park, MD
Thank you for Dr. Henry Nasrallah’s editorial, “Our mission: To meet your needs,” which questions mental health professionals’ role and suggests new ways of looking at our clients (Current Psychiatry, September 2006). Finally, someone is questioning the DSM-IV-TR, the woeful lack of breakthroughs in many disorders, the interface between medicine and psychiatry, and the disparity of payment for mental health treatment.
Psychiatry could be leading thinking on a wider basis. With proper focus, emotional health could be a primary factor in physical medicine rather than the other way around. People who are mentally healthy are less likely to be physically ill, but there is no research to prove this.
Consider taking the focus off the individual patient and looking at larger systems such as the family, church, and community. Psychotherapy will not be able to heal and help people to have successful and productive lives if it stays mired in the individual. Looking at systems allows psychiatry to lead rather than follow and engage in wellness activities such as consulting for schools, families, and political systems. But the profession must look at itself first.
M. Cybil Britton, APRN, BC
Severna Park, MD
Thank you for Dr. Henry Nasrallah’s editorial, “Our mission: To meet your needs,” which questions mental health professionals’ role and suggests new ways of looking at our clients (Current Psychiatry, September 2006). Finally, someone is questioning the DSM-IV-TR, the woeful lack of breakthroughs in many disorders, the interface between medicine and psychiatry, and the disparity of payment for mental health treatment.
Psychiatry could be leading thinking on a wider basis. With proper focus, emotional health could be a primary factor in physical medicine rather than the other way around. People who are mentally healthy are less likely to be physically ill, but there is no research to prove this.
Consider taking the focus off the individual patient and looking at larger systems such as the family, church, and community. Psychotherapy will not be able to heal and help people to have successful and productive lives if it stays mired in the individual. Looking at systems allows psychiatry to lead rather than follow and engage in wellness activities such as consulting for schools, families, and political systems. But the profession must look at itself first.
M. Cybil Britton, APRN, BC
Severna Park, MD