User login
Welcome to Current Psychiatry, a leading source of information, online and in print, for practitioners of psychiatry and its related subspecialties, including addiction psychiatry, child and adolescent psychiatry, and geriatric psychiatry. This Web site contains evidence-based reviews of the prevention, diagnosis, and treatment of mental illness and psychological disorders; case reports; updates on psychopharmacology; news about the specialty of psychiatry; pearls for practice; and other topics of interest and use to this audience.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-current-psychiatry')]
div[contains(@class, 'pane-pub-home-current-psychiatry')]
div[contains(@class, 'pane-pub-topic-current-psychiatry')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Bipolar depression and substance abuse
Lee S. Altman, MD, offers a cogent review of the risks and benefits associated with use of antidepressants to treat bipolar depression (Current Psychiatry, July 2005).
The article, however, did not address the role of comorbid substance abuse, which may increase morbidity in bipolar patients taking antidepressants. Substance abuse can increase the risk of acute switch to mania, but may easily be overlooked.
For example, a recent meta-analysis found no risk of manic switch when a mood stabilizer/antidepressant combination was used to treat bipolar depression. But like most clinical trials, all 12 studies reviewed in this meta-analysis excluded patients with substance abuse.1
By contrast, a study of bipolar patients that included substance abusers2 found that:
- more than one-half of patients with comorbid substance abuse had a history of antidepressant-induced mania or hypomania
- 29% experienced an antidepressant-induced switch even while receiving a concomitant mood stabilizer.
Approximately 60% of patients with bipolar type I disorder abuse substances at some point,3 so most bipolar patients will face this problem. This high prevalence, coupled with the fact that substance abuse comorbidity increases the risks associated with antidepressant use, reinforces the need for caution when treating bipolar depression.
Daniel Z. Lieberman, MD
Associate professor of psychiatry
and behavioral sciences
Director, Clinical Psychiatric Research Center
George Washington University
School of Medicine
Washington, DC
- Gijsman HJ, Geddes JR, Rendell JM, et al. Antidepressants for bipolar depression: a systematic review of randomized, controlled trials. Am J Psychiatry 2004;161:1537-47.
- Goldberg JF, Whiteside JE. The association between substance abuse and antidepressant-induced mania in bipolar disorder: a preliminary study. J Clin Psychiatry 2002;63:791-5.
- Regier DA, Farmer ME, Rae DS, et al. Comorbidity of mental disorders with alcohol and other drug abuse. Results from the Epidemiologic Catchment Area (ECA) Study. JAMA 1990; 264:2511-8.
Dr. Altman responds
Dr. Lieberman correctly highlights the important role of comorbid substance abuse with bipolar disorder. In fact, we both referenced the Goldberg-Whiteside study demonstrating the increased risk of antidepressant-induced mania among bipolar patients with comorbid substance abuse. This is one of many risk factors for switching mentioned in my article.1
Clearly, comorbid substance abuse is an important consideration when deciding whether to use antidepressants to treat bipolar depression.
Lee S. Altman, MD
Assistant professor of psychiatry
University of Colorado Health Sciences Center, Denver
- Goldberg JF, Truman CJ. Antidepressant-induced mania: an overview of current controversies. Bipolar Disorders 2003;5:407-20.
Lee S. Altman, MD, offers a cogent review of the risks and benefits associated with use of antidepressants to treat bipolar depression (Current Psychiatry, July 2005).
The article, however, did not address the role of comorbid substance abuse, which may increase morbidity in bipolar patients taking antidepressants. Substance abuse can increase the risk of acute switch to mania, but may easily be overlooked.
For example, a recent meta-analysis found no risk of manic switch when a mood stabilizer/antidepressant combination was used to treat bipolar depression. But like most clinical trials, all 12 studies reviewed in this meta-analysis excluded patients with substance abuse.1
By contrast, a study of bipolar patients that included substance abusers2 found that:
- more than one-half of patients with comorbid substance abuse had a history of antidepressant-induced mania or hypomania
- 29% experienced an antidepressant-induced switch even while receiving a concomitant mood stabilizer.
Approximately 60% of patients with bipolar type I disorder abuse substances at some point,3 so most bipolar patients will face this problem. This high prevalence, coupled with the fact that substance abuse comorbidity increases the risks associated with antidepressant use, reinforces the need for caution when treating bipolar depression.
Daniel Z. Lieberman, MD
Associate professor of psychiatry
and behavioral sciences
Director, Clinical Psychiatric Research Center
George Washington University
School of Medicine
Washington, DC
- Gijsman HJ, Geddes JR, Rendell JM, et al. Antidepressants for bipolar depression: a systematic review of randomized, controlled trials. Am J Psychiatry 2004;161:1537-47.
- Goldberg JF, Whiteside JE. The association between substance abuse and antidepressant-induced mania in bipolar disorder: a preliminary study. J Clin Psychiatry 2002;63:791-5.
- Regier DA, Farmer ME, Rae DS, et al. Comorbidity of mental disorders with alcohol and other drug abuse. Results from the Epidemiologic Catchment Area (ECA) Study. JAMA 1990; 264:2511-8.
Dr. Altman responds
Dr. Lieberman correctly highlights the important role of comorbid substance abuse with bipolar disorder. In fact, we both referenced the Goldberg-Whiteside study demonstrating the increased risk of antidepressant-induced mania among bipolar patients with comorbid substance abuse. This is one of many risk factors for switching mentioned in my article.1
Clearly, comorbid substance abuse is an important consideration when deciding whether to use antidepressants to treat bipolar depression.
Lee S. Altman, MD
Assistant professor of psychiatry
University of Colorado Health Sciences Center, Denver
- Goldberg JF, Truman CJ. Antidepressant-induced mania: an overview of current controversies. Bipolar Disorders 2003;5:407-20.
Lee S. Altman, MD, offers a cogent review of the risks and benefits associated with use of antidepressants to treat bipolar depression (Current Psychiatry, July 2005).
The article, however, did not address the role of comorbid substance abuse, which may increase morbidity in bipolar patients taking antidepressants. Substance abuse can increase the risk of acute switch to mania, but may easily be overlooked.
For example, a recent meta-analysis found no risk of manic switch when a mood stabilizer/antidepressant combination was used to treat bipolar depression. But like most clinical trials, all 12 studies reviewed in this meta-analysis excluded patients with substance abuse.1
By contrast, a study of bipolar patients that included substance abusers2 found that:
- more than one-half of patients with comorbid substance abuse had a history of antidepressant-induced mania or hypomania
- 29% experienced an antidepressant-induced switch even while receiving a concomitant mood stabilizer.
Approximately 60% of patients with bipolar type I disorder abuse substances at some point,3 so most bipolar patients will face this problem. This high prevalence, coupled with the fact that substance abuse comorbidity increases the risks associated with antidepressant use, reinforces the need for caution when treating bipolar depression.
Daniel Z. Lieberman, MD
Associate professor of psychiatry
and behavioral sciences
Director, Clinical Psychiatric Research Center
George Washington University
School of Medicine
Washington, DC
- Gijsman HJ, Geddes JR, Rendell JM, et al. Antidepressants for bipolar depression: a systematic review of randomized, controlled trials. Am J Psychiatry 2004;161:1537-47.
- Goldberg JF, Whiteside JE. The association between substance abuse and antidepressant-induced mania in bipolar disorder: a preliminary study. J Clin Psychiatry 2002;63:791-5.
- Regier DA, Farmer ME, Rae DS, et al. Comorbidity of mental disorders with alcohol and other drug abuse. Results from the Epidemiologic Catchment Area (ECA) Study. JAMA 1990; 264:2511-8.
Dr. Altman responds
Dr. Lieberman correctly highlights the important role of comorbid substance abuse with bipolar disorder. In fact, we both referenced the Goldberg-Whiteside study demonstrating the increased risk of antidepressant-induced mania among bipolar patients with comorbid substance abuse. This is one of many risk factors for switching mentioned in my article.1
Clearly, comorbid substance abuse is an important consideration when deciding whether to use antidepressants to treat bipolar depression.
Lee S. Altman, MD
Assistant professor of psychiatry
University of Colorado Health Sciences Center, Denver
- Goldberg JF, Truman CJ. Antidepressant-induced mania: an overview of current controversies. Bipolar Disorders 2003;5:407-20.
Raise the bar from response to recovery
Complete recovery must be our goal for each patient we treat. Richard Van Rhoads and Alan Gelenberg make this point in their article on treating major depressive illness to remission. Other Current Psychiatry authors who have emphasized recovery from psychiatric illness as a primary goal include:
- Pamela Wiegartz and Sonya Rasminsky on obsessive-compulsive disorder (April 2005)
- Lee Altman and Christopher Schneck on rapid-cycling bipolar disorder (November 2004)
- Willem Martens on schizophrenia (July 2004).
For years, psychiatry’s goal was symptom reduction, not recovery. The severely mentally ill were neglected at worst or warehoused in long-term institutional or custodial care. Treatment was limited to keeping patients from being an imminent risk to themselves or others.
Our options expanded gradually as safer medications were developed, effective psychotherapies were validated, and outpatient care brought a new focus on lifelong case management. Now we have tools to achieve much more-ambitious treatment goals.
Rather than being content with partial symptom remission, we need to vigorously promote recovery. Of course, some patients will still have residual symptoms and dysfunction, but let’s never give up too soon.

James Randolph Hillard, MD
James Randolph Hillard, MD
James Randolph Hillard, MD
Complete recovery must be our goal for each patient we treat. Richard Van Rhoads and Alan Gelenberg make this point in their article on treating major depressive illness to remission. Other Current Psychiatry authors who have emphasized recovery from psychiatric illness as a primary goal include:
- Pamela Wiegartz and Sonya Rasminsky on obsessive-compulsive disorder (April 2005)
- Lee Altman and Christopher Schneck on rapid-cycling bipolar disorder (November 2004)
- Willem Martens on schizophrenia (July 2004).
For years, psychiatry’s goal was symptom reduction, not recovery. The severely mentally ill were neglected at worst or warehoused in long-term institutional or custodial care. Treatment was limited to keeping patients from being an imminent risk to themselves or others.
Our options expanded gradually as safer medications were developed, effective psychotherapies were validated, and outpatient care brought a new focus on lifelong case management. Now we have tools to achieve much more-ambitious treatment goals.
Rather than being content with partial symptom remission, we need to vigorously promote recovery. Of course, some patients will still have residual symptoms and dysfunction, but let’s never give up too soon.
Complete recovery must be our goal for each patient we treat. Richard Van Rhoads and Alan Gelenberg make this point in their article on treating major depressive illness to remission. Other Current Psychiatry authors who have emphasized recovery from psychiatric illness as a primary goal include:
- Pamela Wiegartz and Sonya Rasminsky on obsessive-compulsive disorder (April 2005)
- Lee Altman and Christopher Schneck on rapid-cycling bipolar disorder (November 2004)
- Willem Martens on schizophrenia (July 2004).
For years, psychiatry’s goal was symptom reduction, not recovery. The severely mentally ill were neglected at worst or warehoused in long-term institutional or custodial care. Treatment was limited to keeping patients from being an imminent risk to themselves or others.
Our options expanded gradually as safer medications were developed, effective psychotherapies were validated, and outpatient care brought a new focus on lifelong case management. Now we have tools to achieve much more-ambitious treatment goals.
Rather than being content with partial symptom remission, we need to vigorously promote recovery. Of course, some patients will still have residual symptoms and dysfunction, but let’s never give up too soon.
The patient who got sick at sea
History: Depressed and dropping out
Ms. Q, age 23, presented 6 years ago with a profound anergic depression with suicidal thinking and social withdrawal. This caused her to drop out of high school for approximately 4 months. She also gained 30 lbs across 3 months, further diminishing her low self-image.
At the time, Ms. Q was diagnosed as having unipolar depression. Fluoxetine, 20 mg/d titrated to 40 mg/d, resolved her symptoms before she started college the following year.
Three years later, while continuing on fluoxetine at the same dosage, Ms. Q experienced dysphoric mania, with irritability, grandiosity, and impaired judgment. She was behaving promiscuously during this episode but was not using alcohol or other substances.
After a subsequent manic episode, she was diagnosed with bipolar type I affective disorder. Haloperidol, 10 mg/d for 2 weeks, resolved her mania. She was then maintained on fluoxetine, 50 mg/d, but was not given a mood stabilizer or antipsychotic.
Two years later, I was called in to consult on Ms. Q’s case. She was euthymic and stable at that time but 2 months earlier had experienced a euphoric manic episode characterized by 5 days of racing thoughts, lack of sleep, and manic motoric acceleration. She had stopped seeing her psychiatrist near college and admitted that she needed to work with someone more experienced than her primary care physician in addressing psychiatric symptoms.
When Ms. Q was age 4, her maternal aunt committed suicide via gas poisoning. Also, her paternal grandmother committed suicide before she was born, and her mother had been treated for dysthymia. She has no significant medical history.
Addressing Ms. Q’s bipolar affective disorder poses a clinical challenge. Controlling her mania is a priority but I also need to continue treating her depression, given her significant family history of affective disturbance.
Dr. Schneider’s observations
To address Ms. Q’s mania, I added controlled-release lithium, 900 mg/d, yielding a blood level of 0.9 mEq/L. Ms. Q was not rapid cycling, was taking her fluoxetine as prescribed, and was not abusing alcohol or drugs, so she seemed an appropriate candidate for lithium treatment.
To manage her depression, I cautiously continued fluoxetine, 40 mg/d. The antidepressant had not obviously destabilized her illness, and Ms. Q felt that it allowed her to work and maintain a social life.
Treatment: Cruising and cycling
After 8 months of stability, Ms. Q developed a sudden dysphoric hypomanic episode, with depressed mood, increased energy, racing thoughts, and inability to sleep. She had some insight into her condition and sought consultation with me.
Ms. Q’s parents reported that she had been taking lithium and fluoxetine as prescribed, was taking no other medications, was not using alcohol or drugs, and experienced no unusual stressors, change in diet, or other lifestyle changes. Having her symptoms re-emerge despite faithful medication adherence made Ms. Q extremely anxious and bewildered her and her parents.
Ms. Q later recalled that her parents had taken her on a coastal cruise to Mexico the week before her cycling episode, and that her symptoms emerged while on ship. She began to experience initial and mid-cycle insomnia and was unusually irritable over minor annoyances.
Having seen Ms. Q immediately after the cruise, I added olanzapine, 5 mg nightly for 5 days, to prevent a full-blown manic episode. About 6 days later, she said she was excessively tired, but her insomnia and irritability had ceased. I stopped olanzapine and returned Ms. Q to her previous regimen.
Dr. Schneider’s observations
Ms. Q appeared to have sustained an unexpected relapse into hypomania despite treatment adherence. At this point, I was concerned that:
- fluoxetine might have destabilized her illness
- her lithium level decreased without explanation
- or she had a “breakthrough” relapse while on medication.
Follow-up: A ‘sickening’ discovery
At follow up approximately 1 week later, Ms. Q reported that she had continuously worn scopolamine patches throughout the 8-day cruise to prevent motion sickness. She had forgotten to mention this, however, during our emergency consultation. She had experienced some mydriasis and dry mouth during the cruise but did not remove the patch for fear of seasickness.
On further questioning, Ms. Q said she knew the patch was designed to be used for 2 to 3 days maximum, but added she was responding well to its effects and foresaw no problems with extended use.
Dr. Schneider’s observations
This case illustrates the potentially destabilizing effects of a seemingly innocuous concomitant medication in patients with bipolar disorder.
Scopolamine, indicated for preventing nausea and vomiting associated with motion sickness, is a centrally acting belladonna alkaloid with primary anticholinergic activity. The agent is thought to block transmission from the vestibular nuclei to higher brain centers and from the reticular formation to the brain’s so-called “vomiting centers.”
The transdermal agent can cause drowsiness, dryness of secretory areas, and impaired motor function. It has no known direct pharmacokinetic interaction with lithium. Use for >5 consecutive days can cause anticholinergic delirium-like states, especially in older patients.
For Ms. Q, scopolamine’s direct anticholinergic action may have destabilized an affective disorder in remission. The putative mechanism of anticholinergic-induced psychosis, delirium, mania, and depression has not been well explained and may differ among these states. The serotonergic and cholinergic systems, however, are assumed to be in a type of balance. Cholinergic deficiencies—as seen in dementia or with medications that have anticholinergic potential—may increase sensitivity to serotonergic tone, thus contributing to Ms. Q’s switch to mania.1
Dr. Schneider’s observations
Ask the patient at each office visit if he or she is concomitantly using an over-the-counter (OTC) medication or a prescription agent from another physician. As with scopolamine, diet pills and oral contraceptives can also destabilize mood or cause depression. Often patients neglect to tell their psychiatrists they started taking an antibiotic, antihypertensive, or other medication since their last visit.
Undetected use of herbal supplements also is a burgeoning clinical problem. Most physicians do not routinely ask patients whether they are using a nonprescription medication, and some clinicians know little about these products’ side effects or interactions with other drugs. Adverse events associated with herbal agents (Table) are difficult to interpret because the purity and amounts of active compounds vary widely.
Table
Mood destabilization, other effects reported after herbal supplement use
| Herbal supplement | Common use(s) | Adverse effects in psychiatric patients |
|---|---|---|
| Dehydroepiandrosterone (DHEA) | Alzheimer’s dementia treatment, body muscle-fat ratio enhancement, stress relief, sexual enhancer | Acute mania when taken with other psychotropics;2 patients with history of affective disorder can exhibit mania when taking DHEA3 |
| Gingko biloba | Cognitive/memory enhancement | Nausea, diarrhea, bleeding in patients taking psychotropics4,5 |
| Massive purpura after concomitant gingko plus citalopram or venlafaxine (clinical experience) | ||
| Ginseng | Stimulant, also purportedly an aphrodisiac | Ginseng-induced mania in two patients with depressive disorders6,7 |
| Horny goat weed | Purported sexual enhancer for men | New-onset hypomania in 66-year-old man after ingesting compound for 2 weeks8 |
| St. John’s wort | Primary or secondary antidepressant | Multiple cases of mania induction, affective destabilization attributed to presumed cytotoxic effects9 |
Appetite suppressants have been reported to cause depression during use or withdrawal,10 but large epidemiologic studies have not determined which diet pills are most associated with depressive symptoms.
Oral contraceptives. Mood changes are an ongoing, noticeable side effect of oral contraceptives11 regardless of whether the patient is taking a psychotropic. Depression is a frequently cited reason for oral contraceptive discontinuation.12
The literature is mixed on how oral contraceptives stabilize or destabilize mood and affect. Hormone-induced mood changes may be caused by:
- estrogen-induced B6 deficiency and subsequent decrease in serotonin and gamma-aminobutyric acid (GABA) because of lower affinity for pyridoxal phosphatate13
- progesterone or estrogen-mediated augmentation of GABA-induced glutamate suppression
- progesterone-mediated increase in mono-amine oxidase activity, leading to lower serotonin concentrations.14
- Physicians’ Desk Reference supplements for over-the-counter medications and nutraceuticals. www.pdr.net/pdrnet/librarian (click on “PDRbookstore”).
- Farley D. How to get the most benefits with the fewest risks. Web MD. http://my.webmd.com/content/article/6/1680_51630.htm.
- Fluoxetine • Prozac
- Haloperdiol • Haldol
- Lithium • Eskalith, others
- Olanzapine • Zyprexa
- Scopolamine • Transderm Scop
Dr. Schneider is a consultant to and speaker for Bristol-Myers Squibb Co., Forest Pharmaceuticals, and Wyeth Pharmaceuticals. He holds research grants from the National Alliance for Research in Schizophrenia and Affective Disorders (NARSAD), the Stanley Medical Research Institute, and the Alzheimer’s Association (Ronald Reagan Research Award).
1. Cancelli I, Marcon G, Balestrieri M. Factors associated with complex visual hallucinations during antidepressant treatment. Hum Psychopharmacol 2004;19:577-84.
2. Vacheron-Trystram MN, Cheref S, Gauillard J, Plas J. A case report of mania precipitated by use of DHEA. Encephale 2002;28 (6 Pt 1):563-6.
3. Dean CE. Prasterone (DHEA) and mania. Ann Pharmacother 2000;34:1419-22.
4. Gilbert GJ. Gingko biloba. Neurology 1997;48:1137.-
5. Benjamin J, Muir T, Briggs K, Pentland B. A case of cerebral haemorrhage—can Gingko biloba be implicated? Postgrad Med J 2001;77:112-3.
6. Gonzalez-Seijo JC, Ramos YM, Lastra I. Manic episode and ginseng: report of a possible case. J Clin Psychopharmacol 1995;15:447-8.
7. Vazquez I, Aguera-Ortiz LF. Herbal products and serious side effects: a case of ginseng-induced manic episode. Acta Psychiatr Scand 2002;105:76-7.
8. Partin JF, Pushkin YR. Tachyarrhythmia and hypomania with horny goat weed. Psychosomatics 2004;45:536-7.
9. Moses EL, Mallinger AG. St. John’s wort: three cases of possible mania induction. J Clin Psychopharmacol 2000;20:115-7.
10. Patten SB. “Diet Pills” and major depression in the Canadian population. Can J Psychiatry 2001;46:438-40.
11. Oinonen KA, Mazmanian D. To what extent do oral contraceptives influence mood and affect? J Affect Disord 2002;70:229-40.
12. Goldzieher J. Hormonal contraception: pills, injections, and implants (3rd ed.) London, Ontario: Emis-Canada; 1994.
13. McCarty MF. High-dose pyridoxine as an ‘anti-stress’ strategy. Med Hypotheses 2000;54:803-7.
14. Sherwin B. Hormones, mood, and cognitive functioning in post-menopausal women. Obstet Gynecol 1996;87(suppl 2):20S-26S.
History: Depressed and dropping out
Ms. Q, age 23, presented 6 years ago with a profound anergic depression with suicidal thinking and social withdrawal. This caused her to drop out of high school for approximately 4 months. She also gained 30 lbs across 3 months, further diminishing her low self-image.
At the time, Ms. Q was diagnosed as having unipolar depression. Fluoxetine, 20 mg/d titrated to 40 mg/d, resolved her symptoms before she started college the following year.
Three years later, while continuing on fluoxetine at the same dosage, Ms. Q experienced dysphoric mania, with irritability, grandiosity, and impaired judgment. She was behaving promiscuously during this episode but was not using alcohol or other substances.
After a subsequent manic episode, she was diagnosed with bipolar type I affective disorder. Haloperidol, 10 mg/d for 2 weeks, resolved her mania. She was then maintained on fluoxetine, 50 mg/d, but was not given a mood stabilizer or antipsychotic.
Two years later, I was called in to consult on Ms. Q’s case. She was euthymic and stable at that time but 2 months earlier had experienced a euphoric manic episode characterized by 5 days of racing thoughts, lack of sleep, and manic motoric acceleration. She had stopped seeing her psychiatrist near college and admitted that she needed to work with someone more experienced than her primary care physician in addressing psychiatric symptoms.
When Ms. Q was age 4, her maternal aunt committed suicide via gas poisoning. Also, her paternal grandmother committed suicide before she was born, and her mother had been treated for dysthymia. She has no significant medical history.
Addressing Ms. Q’s bipolar affective disorder poses a clinical challenge. Controlling her mania is a priority but I also need to continue treating her depression, given her significant family history of affective disturbance.
Dr. Schneider’s observations
To address Ms. Q’s mania, I added controlled-release lithium, 900 mg/d, yielding a blood level of 0.9 mEq/L. Ms. Q was not rapid cycling, was taking her fluoxetine as prescribed, and was not abusing alcohol or drugs, so she seemed an appropriate candidate for lithium treatment.
To manage her depression, I cautiously continued fluoxetine, 40 mg/d. The antidepressant had not obviously destabilized her illness, and Ms. Q felt that it allowed her to work and maintain a social life.
Treatment: Cruising and cycling
After 8 months of stability, Ms. Q developed a sudden dysphoric hypomanic episode, with depressed mood, increased energy, racing thoughts, and inability to sleep. She had some insight into her condition and sought consultation with me.
Ms. Q’s parents reported that she had been taking lithium and fluoxetine as prescribed, was taking no other medications, was not using alcohol or drugs, and experienced no unusual stressors, change in diet, or other lifestyle changes. Having her symptoms re-emerge despite faithful medication adherence made Ms. Q extremely anxious and bewildered her and her parents.
Ms. Q later recalled that her parents had taken her on a coastal cruise to Mexico the week before her cycling episode, and that her symptoms emerged while on ship. She began to experience initial and mid-cycle insomnia and was unusually irritable over minor annoyances.
Having seen Ms. Q immediately after the cruise, I added olanzapine, 5 mg nightly for 5 days, to prevent a full-blown manic episode. About 6 days later, she said she was excessively tired, but her insomnia and irritability had ceased. I stopped olanzapine and returned Ms. Q to her previous regimen.
Dr. Schneider’s observations
Ms. Q appeared to have sustained an unexpected relapse into hypomania despite treatment adherence. At this point, I was concerned that:
- fluoxetine might have destabilized her illness
- her lithium level decreased without explanation
- or she had a “breakthrough” relapse while on medication.
Follow-up: A ‘sickening’ discovery
At follow up approximately 1 week later, Ms. Q reported that she had continuously worn scopolamine patches throughout the 8-day cruise to prevent motion sickness. She had forgotten to mention this, however, during our emergency consultation. She had experienced some mydriasis and dry mouth during the cruise but did not remove the patch for fear of seasickness.
On further questioning, Ms. Q said she knew the patch was designed to be used for 2 to 3 days maximum, but added she was responding well to its effects and foresaw no problems with extended use.
Dr. Schneider’s observations
This case illustrates the potentially destabilizing effects of a seemingly innocuous concomitant medication in patients with bipolar disorder.
Scopolamine, indicated for preventing nausea and vomiting associated with motion sickness, is a centrally acting belladonna alkaloid with primary anticholinergic activity. The agent is thought to block transmission from the vestibular nuclei to higher brain centers and from the reticular formation to the brain’s so-called “vomiting centers.”
The transdermal agent can cause drowsiness, dryness of secretory areas, and impaired motor function. It has no known direct pharmacokinetic interaction with lithium. Use for >5 consecutive days can cause anticholinergic delirium-like states, especially in older patients.
For Ms. Q, scopolamine’s direct anticholinergic action may have destabilized an affective disorder in remission. The putative mechanism of anticholinergic-induced psychosis, delirium, mania, and depression has not been well explained and may differ among these states. The serotonergic and cholinergic systems, however, are assumed to be in a type of balance. Cholinergic deficiencies—as seen in dementia or with medications that have anticholinergic potential—may increase sensitivity to serotonergic tone, thus contributing to Ms. Q’s switch to mania.1
Dr. Schneider’s observations
Ask the patient at each office visit if he or she is concomitantly using an over-the-counter (OTC) medication or a prescription agent from another physician. As with scopolamine, diet pills and oral contraceptives can also destabilize mood or cause depression. Often patients neglect to tell their psychiatrists they started taking an antibiotic, antihypertensive, or other medication since their last visit.
Undetected use of herbal supplements also is a burgeoning clinical problem. Most physicians do not routinely ask patients whether they are using a nonprescription medication, and some clinicians know little about these products’ side effects or interactions with other drugs. Adverse events associated with herbal agents (Table) are difficult to interpret because the purity and amounts of active compounds vary widely.
Table
Mood destabilization, other effects reported after herbal supplement use
| Herbal supplement | Common use(s) | Adverse effects in psychiatric patients |
|---|---|---|
| Dehydroepiandrosterone (DHEA) | Alzheimer’s dementia treatment, body muscle-fat ratio enhancement, stress relief, sexual enhancer | Acute mania when taken with other psychotropics;2 patients with history of affective disorder can exhibit mania when taking DHEA3 |
| Gingko biloba | Cognitive/memory enhancement | Nausea, diarrhea, bleeding in patients taking psychotropics4,5 |
| Massive purpura after concomitant gingko plus citalopram or venlafaxine (clinical experience) | ||
| Ginseng | Stimulant, also purportedly an aphrodisiac | Ginseng-induced mania in two patients with depressive disorders6,7 |
| Horny goat weed | Purported sexual enhancer for men | New-onset hypomania in 66-year-old man after ingesting compound for 2 weeks8 |
| St. John’s wort | Primary or secondary antidepressant | Multiple cases of mania induction, affective destabilization attributed to presumed cytotoxic effects9 |
Appetite suppressants have been reported to cause depression during use or withdrawal,10 but large epidemiologic studies have not determined which diet pills are most associated with depressive symptoms.
Oral contraceptives. Mood changes are an ongoing, noticeable side effect of oral contraceptives11 regardless of whether the patient is taking a psychotropic. Depression is a frequently cited reason for oral contraceptive discontinuation.12
The literature is mixed on how oral contraceptives stabilize or destabilize mood and affect. Hormone-induced mood changes may be caused by:
- estrogen-induced B6 deficiency and subsequent decrease in serotonin and gamma-aminobutyric acid (GABA) because of lower affinity for pyridoxal phosphatate13
- progesterone or estrogen-mediated augmentation of GABA-induced glutamate suppression
- progesterone-mediated increase in mono-amine oxidase activity, leading to lower serotonin concentrations.14
- Physicians’ Desk Reference supplements for over-the-counter medications and nutraceuticals. www.pdr.net/pdrnet/librarian (click on “PDRbookstore”).
- Farley D. How to get the most benefits with the fewest risks. Web MD. http://my.webmd.com/content/article/6/1680_51630.htm.
- Fluoxetine • Prozac
- Haloperdiol • Haldol
- Lithium • Eskalith, others
- Olanzapine • Zyprexa
- Scopolamine • Transderm Scop
Dr. Schneider is a consultant to and speaker for Bristol-Myers Squibb Co., Forest Pharmaceuticals, and Wyeth Pharmaceuticals. He holds research grants from the National Alliance for Research in Schizophrenia and Affective Disorders (NARSAD), the Stanley Medical Research Institute, and the Alzheimer’s Association (Ronald Reagan Research Award).
History: Depressed and dropping out
Ms. Q, age 23, presented 6 years ago with a profound anergic depression with suicidal thinking and social withdrawal. This caused her to drop out of high school for approximately 4 months. She also gained 30 lbs across 3 months, further diminishing her low self-image.
At the time, Ms. Q was diagnosed as having unipolar depression. Fluoxetine, 20 mg/d titrated to 40 mg/d, resolved her symptoms before she started college the following year.
Three years later, while continuing on fluoxetine at the same dosage, Ms. Q experienced dysphoric mania, with irritability, grandiosity, and impaired judgment. She was behaving promiscuously during this episode but was not using alcohol or other substances.
After a subsequent manic episode, she was diagnosed with bipolar type I affective disorder. Haloperidol, 10 mg/d for 2 weeks, resolved her mania. She was then maintained on fluoxetine, 50 mg/d, but was not given a mood stabilizer or antipsychotic.
Two years later, I was called in to consult on Ms. Q’s case. She was euthymic and stable at that time but 2 months earlier had experienced a euphoric manic episode characterized by 5 days of racing thoughts, lack of sleep, and manic motoric acceleration. She had stopped seeing her psychiatrist near college and admitted that she needed to work with someone more experienced than her primary care physician in addressing psychiatric symptoms.
When Ms. Q was age 4, her maternal aunt committed suicide via gas poisoning. Also, her paternal grandmother committed suicide before she was born, and her mother had been treated for dysthymia. She has no significant medical history.
Addressing Ms. Q’s bipolar affective disorder poses a clinical challenge. Controlling her mania is a priority but I also need to continue treating her depression, given her significant family history of affective disturbance.
Dr. Schneider’s observations
To address Ms. Q’s mania, I added controlled-release lithium, 900 mg/d, yielding a blood level of 0.9 mEq/L. Ms. Q was not rapid cycling, was taking her fluoxetine as prescribed, and was not abusing alcohol or drugs, so she seemed an appropriate candidate for lithium treatment.
To manage her depression, I cautiously continued fluoxetine, 40 mg/d. The antidepressant had not obviously destabilized her illness, and Ms. Q felt that it allowed her to work and maintain a social life.
Treatment: Cruising and cycling
After 8 months of stability, Ms. Q developed a sudden dysphoric hypomanic episode, with depressed mood, increased energy, racing thoughts, and inability to sleep. She had some insight into her condition and sought consultation with me.
Ms. Q’s parents reported that she had been taking lithium and fluoxetine as prescribed, was taking no other medications, was not using alcohol or drugs, and experienced no unusual stressors, change in diet, or other lifestyle changes. Having her symptoms re-emerge despite faithful medication adherence made Ms. Q extremely anxious and bewildered her and her parents.
Ms. Q later recalled that her parents had taken her on a coastal cruise to Mexico the week before her cycling episode, and that her symptoms emerged while on ship. She began to experience initial and mid-cycle insomnia and was unusually irritable over minor annoyances.
Having seen Ms. Q immediately after the cruise, I added olanzapine, 5 mg nightly for 5 days, to prevent a full-blown manic episode. About 6 days later, she said she was excessively tired, but her insomnia and irritability had ceased. I stopped olanzapine and returned Ms. Q to her previous regimen.
Dr. Schneider’s observations
Ms. Q appeared to have sustained an unexpected relapse into hypomania despite treatment adherence. At this point, I was concerned that:
- fluoxetine might have destabilized her illness
- her lithium level decreased without explanation
- or she had a “breakthrough” relapse while on medication.
Follow-up: A ‘sickening’ discovery
At follow up approximately 1 week later, Ms. Q reported that she had continuously worn scopolamine patches throughout the 8-day cruise to prevent motion sickness. She had forgotten to mention this, however, during our emergency consultation. She had experienced some mydriasis and dry mouth during the cruise but did not remove the patch for fear of seasickness.
On further questioning, Ms. Q said she knew the patch was designed to be used for 2 to 3 days maximum, but added she was responding well to its effects and foresaw no problems with extended use.
Dr. Schneider’s observations
This case illustrates the potentially destabilizing effects of a seemingly innocuous concomitant medication in patients with bipolar disorder.
Scopolamine, indicated for preventing nausea and vomiting associated with motion sickness, is a centrally acting belladonna alkaloid with primary anticholinergic activity. The agent is thought to block transmission from the vestibular nuclei to higher brain centers and from the reticular formation to the brain’s so-called “vomiting centers.”
The transdermal agent can cause drowsiness, dryness of secretory areas, and impaired motor function. It has no known direct pharmacokinetic interaction with lithium. Use for >5 consecutive days can cause anticholinergic delirium-like states, especially in older patients.
For Ms. Q, scopolamine’s direct anticholinergic action may have destabilized an affective disorder in remission. The putative mechanism of anticholinergic-induced psychosis, delirium, mania, and depression has not been well explained and may differ among these states. The serotonergic and cholinergic systems, however, are assumed to be in a type of balance. Cholinergic deficiencies—as seen in dementia or with medications that have anticholinergic potential—may increase sensitivity to serotonergic tone, thus contributing to Ms. Q’s switch to mania.1
Dr. Schneider’s observations
Ask the patient at each office visit if he or she is concomitantly using an over-the-counter (OTC) medication or a prescription agent from another physician. As with scopolamine, diet pills and oral contraceptives can also destabilize mood or cause depression. Often patients neglect to tell their psychiatrists they started taking an antibiotic, antihypertensive, or other medication since their last visit.
Undetected use of herbal supplements also is a burgeoning clinical problem. Most physicians do not routinely ask patients whether they are using a nonprescription medication, and some clinicians know little about these products’ side effects or interactions with other drugs. Adverse events associated with herbal agents (Table) are difficult to interpret because the purity and amounts of active compounds vary widely.
Table
Mood destabilization, other effects reported after herbal supplement use
| Herbal supplement | Common use(s) | Adverse effects in psychiatric patients |
|---|---|---|
| Dehydroepiandrosterone (DHEA) | Alzheimer’s dementia treatment, body muscle-fat ratio enhancement, stress relief, sexual enhancer | Acute mania when taken with other psychotropics;2 patients with history of affective disorder can exhibit mania when taking DHEA3 |
| Gingko biloba | Cognitive/memory enhancement | Nausea, diarrhea, bleeding in patients taking psychotropics4,5 |
| Massive purpura after concomitant gingko plus citalopram or venlafaxine (clinical experience) | ||
| Ginseng | Stimulant, also purportedly an aphrodisiac | Ginseng-induced mania in two patients with depressive disorders6,7 |
| Horny goat weed | Purported sexual enhancer for men | New-onset hypomania in 66-year-old man after ingesting compound for 2 weeks8 |
| St. John’s wort | Primary or secondary antidepressant | Multiple cases of mania induction, affective destabilization attributed to presumed cytotoxic effects9 |
Appetite suppressants have been reported to cause depression during use or withdrawal,10 but large epidemiologic studies have not determined which diet pills are most associated with depressive symptoms.
Oral contraceptives. Mood changes are an ongoing, noticeable side effect of oral contraceptives11 regardless of whether the patient is taking a psychotropic. Depression is a frequently cited reason for oral contraceptive discontinuation.12
The literature is mixed on how oral contraceptives stabilize or destabilize mood and affect. Hormone-induced mood changes may be caused by:
- estrogen-induced B6 deficiency and subsequent decrease in serotonin and gamma-aminobutyric acid (GABA) because of lower affinity for pyridoxal phosphatate13
- progesterone or estrogen-mediated augmentation of GABA-induced glutamate suppression
- progesterone-mediated increase in mono-amine oxidase activity, leading to lower serotonin concentrations.14
- Physicians’ Desk Reference supplements for over-the-counter medications and nutraceuticals. www.pdr.net/pdrnet/librarian (click on “PDRbookstore”).
- Farley D. How to get the most benefits with the fewest risks. Web MD. http://my.webmd.com/content/article/6/1680_51630.htm.
- Fluoxetine • Prozac
- Haloperdiol • Haldol
- Lithium • Eskalith, others
- Olanzapine • Zyprexa
- Scopolamine • Transderm Scop
Dr. Schneider is a consultant to and speaker for Bristol-Myers Squibb Co., Forest Pharmaceuticals, and Wyeth Pharmaceuticals. He holds research grants from the National Alliance for Research in Schizophrenia and Affective Disorders (NARSAD), the Stanley Medical Research Institute, and the Alzheimer’s Association (Ronald Reagan Research Award).
1. Cancelli I, Marcon G, Balestrieri M. Factors associated with complex visual hallucinations during antidepressant treatment. Hum Psychopharmacol 2004;19:577-84.
2. Vacheron-Trystram MN, Cheref S, Gauillard J, Plas J. A case report of mania precipitated by use of DHEA. Encephale 2002;28 (6 Pt 1):563-6.
3. Dean CE. Prasterone (DHEA) and mania. Ann Pharmacother 2000;34:1419-22.
4. Gilbert GJ. Gingko biloba. Neurology 1997;48:1137.-
5. Benjamin J, Muir T, Briggs K, Pentland B. A case of cerebral haemorrhage—can Gingko biloba be implicated? Postgrad Med J 2001;77:112-3.
6. Gonzalez-Seijo JC, Ramos YM, Lastra I. Manic episode and ginseng: report of a possible case. J Clin Psychopharmacol 1995;15:447-8.
7. Vazquez I, Aguera-Ortiz LF. Herbal products and serious side effects: a case of ginseng-induced manic episode. Acta Psychiatr Scand 2002;105:76-7.
8. Partin JF, Pushkin YR. Tachyarrhythmia and hypomania with horny goat weed. Psychosomatics 2004;45:536-7.
9. Moses EL, Mallinger AG. St. John’s wort: three cases of possible mania induction. J Clin Psychopharmacol 2000;20:115-7.
10. Patten SB. “Diet Pills” and major depression in the Canadian population. Can J Psychiatry 2001;46:438-40.
11. Oinonen KA, Mazmanian D. To what extent do oral contraceptives influence mood and affect? J Affect Disord 2002;70:229-40.
12. Goldzieher J. Hormonal contraception: pills, injections, and implants (3rd ed.) London, Ontario: Emis-Canada; 1994.
13. McCarty MF. High-dose pyridoxine as an ‘anti-stress’ strategy. Med Hypotheses 2000;54:803-7.
14. Sherwin B. Hormones, mood, and cognitive functioning in post-menopausal women. Obstet Gynecol 1996;87(suppl 2):20S-26S.
1. Cancelli I, Marcon G, Balestrieri M. Factors associated with complex visual hallucinations during antidepressant treatment. Hum Psychopharmacol 2004;19:577-84.
2. Vacheron-Trystram MN, Cheref S, Gauillard J, Plas J. A case report of mania precipitated by use of DHEA. Encephale 2002;28 (6 Pt 1):563-6.
3. Dean CE. Prasterone (DHEA) and mania. Ann Pharmacother 2000;34:1419-22.
4. Gilbert GJ. Gingko biloba. Neurology 1997;48:1137.-
5. Benjamin J, Muir T, Briggs K, Pentland B. A case of cerebral haemorrhage—can Gingko biloba be implicated? Postgrad Med J 2001;77:112-3.
6. Gonzalez-Seijo JC, Ramos YM, Lastra I. Manic episode and ginseng: report of a possible case. J Clin Psychopharmacol 1995;15:447-8.
7. Vazquez I, Aguera-Ortiz LF. Herbal products and serious side effects: a case of ginseng-induced manic episode. Acta Psychiatr Scand 2002;105:76-7.
8. Partin JF, Pushkin YR. Tachyarrhythmia and hypomania with horny goat weed. Psychosomatics 2004;45:536-7.
9. Moses EL, Mallinger AG. St. John’s wort: three cases of possible mania induction. J Clin Psychopharmacol 2000;20:115-7.
10. Patten SB. “Diet Pills” and major depression in the Canadian population. Can J Psychiatry 2001;46:438-40.
11. Oinonen KA, Mazmanian D. To what extent do oral contraceptives influence mood and affect? J Affect Disord 2002;70:229-40.
12. Goldzieher J. Hormonal contraception: pills, injections, and implants (3rd ed.) London, Ontario: Emis-Canada; 1994.
13. McCarty MF. High-dose pyridoxine as an ‘anti-stress’ strategy. Med Hypotheses 2000;54:803-7.
14. Sherwin B. Hormones, mood, and cognitive functioning in post-menopausal women. Obstet Gynecol 1996;87(suppl 2):20S-26S.
Tips to manage and prevent discontinuation syndromes
Abruptly stopping common psychotropics—particularly antidepressants, benzodiazepines, or atypical antipsychotics—can trigger a discontinuation syndrome, with:
- rebound or relapse of original symptoms
- uncomfortable new physical and psychological symptoms
- physiologic withdrawal at times.
To increase health professionals’ awareness of the risk of these adverse effects,1 this article describes discontinuation syndromes associated with various psychotropics and offers strategies to anticipate, recognize, and manage them.
Antidepressant Discontinuation Syndromes
Discontinuation syndromes can occur with tricyclic and tetracyclic antidepressants (TCAs), monoamine oxidase inhibitors (MAOIs), selective serotonin reuptake inhibitors (SSRIs), and other newer antidepressants. Symptoms usually start within a few days of stopping a drug—or less commonly, reducing its dosage—and are usually mild and self-limited. Serious outcomes have been reported.
Distinguishing antidepressant discontinuation symptoms from depression recurrence is important. Discontinuation symptoms emerge within 1 to 3 days, whereas depressive symptoms usually occur 2 to 3 weeks after an antidepressant is stopped. Discontinuation reactions remit within a few days, especially if the antidepressant is re-instituted.
TCAs block serotonin and norepinephrine reuptake, increasing the availability of these biogenic amines at receptor sites in the brain and other tissues. Abrupt discontinuation can cause physical symptoms—such as lethargy, headache, and tremor—and psychological symptoms including irritability, anxiety, agitation, and low mood (Table 1).2
Long-term use of TCAs with potent anticholinergic properties leads to upregulation of postsynaptic muscarinic receptors, creating a “supersensitive” state. Abrupt discontinuation can cause cholinergic rebound, with symptoms emerging as soon as 12 hours—but typically 24 to 48 hours—after the last dose.
Table 1
Discontinuation symptoms seen with TCAs
| Physical symptoms | Lethargy, headache, tremor, sweating, anorexia, insomnia, nausea, vomiting, diarrhea, akathisia (rare), parkinsonism (rare) |
| Psychological symptoms | Irritability, anxiety/agitation, low mood, excessive dreaming, nightmares, paradoxical activation resulting in manic/hypomanic symptoms (rare) |
| TCA: Tricyclic antidepressants | |
| Source: Reference 2 | |
MAOIs such as phenelzine and tranylcypromine inhibit the enzyme monoamine oxidase, which is responsible for monoamine degradation and increases synaptic monoamine concentrations. Discontinuation syndromes may include acute confusional states, paranoid delusions, hallucinations, or worsening of depressive symptoms.3 These problems rarely occur in clinical practice, however, because MAOIs’ serious side effects discourage doctors from prescribing them.
SSRIs and other agents. SSRIs block synaptic reuptake of serotonin. Serotonin-norepinephrine reuptake inhibitors (SNRIs) such as venlafaxine and duloxetine inhibit both serotonin and norepinephrine reuptake. Mirtazapine—an alpha2-adrenergic and heteroreceptor antagonist—increases serotonin and norepinephrine at the synapse. Bupropion increases dopamine and norepinephrine turnover in the CNS and also blocks serotonin.
Up to 30% of patients who stop taking SSRIs develop discontinuation symptoms.4 Six symptom clusters—disequilibrium, sensory symptoms, general somatic symptoms, sleep disturbance, GI symptoms, and affective symptoms—characterize the SSRI discontinuation syndrome (Table 2).5 The four most common symptoms—in decreasing order of frequency—are dizziness, nausea, lethargy, and headache.6 Ataxia, sensory abnormalities, and possibly aggressive and impulsive behavior differentiate this discontinuation syndrome from that of the TCAs.
Table 2
Discontinuation symptoms seen with SSRIs
| Type | Symptoms |
|---|---|
| Disequilibrium | Lightheadedness/dizziness, vertigo, ataxia |
| Sensory symptoms | Paraesthesia, numbness, electric shock-like sensations |
| General somatic symptoms | Lethargy, headache, tremor, sweating, anorexia |
| Sleep disturbance | Insomnia, nightmares, excessive dreaming |
| GI symptoms | Nausea, vomiting, diarrhea |
| Affective symptoms | Irritability, anxiety/agitation, low mood |
| SSRIs: Selective serotonin reuptake inhibitors | |
| Source: Reference 5 | |
Risk factors. Risk factors for SSRI discontinuation syndrome have been identified (Table 3).7 Symptoms usually begin 1 to 3 days after an SSRI is abruptly stopped and are usually mild. However, some patients report falls, inability to work, and difficulty walking and driving. Untreated symptoms are short-lived and remit within 1 to 2 weeks. They also remit if the original antidepressant is reintroduced or a pharmacologically similar agent is substituted.
Discontinuation syndrome risk among SSRIs is highest for paroxetine, intermediate for sertraline and fluvoxamine, and lowest for fluoxetine.4 Citalopram may cause a mild and transient discontinuation syndrome.8 Citalopram’s long elimination half-life (30 to 35 hours) and fewer and much less-potent active metabolites9 may explain its relatively low risk of discontinuation symptoms.
Discontinuation reactions have been reported to occur 100 times more frequently with paroxetine than with fluoxetine.10 Fluoxetine’s lower rate could be explained by its 2- to 3-day half-life, compared with half-lives of 33 hours or less for paroxetine, sertraline, citalopram, and fluvoxamine. A longer half-life might protect against a discontinuation syndrome.
Among other newer antidepressants:
- venlafaxine’s discontinuation syndrome is similar to the SSRI syndrome11
- no discontinuation symptoms have been reported with mirtazapine, bupropion, or duloxetine.
Table 3
SSRI discontinuation syndrome: The patient at risk…
| Is taking an SSRI with a relatively short half-life |
| Has received antidepressant treatment > 4 weeks |
| Has history of treatment-emergent anxiety, discontinuation symptoms, nonadherence |
| SSRI: Selective serotonin reuptake inhibitor |
| Source: Reference 7 |
Causes. Theories to explain SSRI discontinuation syndrome include cholinergic rebound,12 as described with TCAs, or a decrease in available synaptic serotonin coinciding with down-regulated serotonin receptors.13 Paroxetine’s pharmacologic properties—cholinergic effects, short halflife, and high potency of serotonin reuptake blockade—may explain its relatively high frequency of discontinuation symptoms.
Atypical Antipsychotic Discontinuation Syndromes
Except for aripiprazole—which is a partial dopamine receptor agonist—most atypical antipsychotics are serotonin-dopamine antagonists. Discontinuation syndrome occurs most commonly with clozapine.
Clozapine. Abruptly stopping clozapine can exacerbate psychosis or cause delirium, agitation, confusion, and diaphoresis. Less-common symptoms may include extrapyramidal effects, nausea, diarrhea, headache, or restlessness.14 Clozapine is a weak dopamine D2 antagonist and a potent antagonist at the serotonin 5HT2, alpha adrenergic, histaminergic, and anticholinergic receptors. Thus, rebound from cholinergic, serotonin, dopamine and/or adrenergic receptor supersensitivity is thought to cause its discontinuation syndrome.15
Other atypicals. Case reports describe tics and withdrawal-emergent dyskinesia with risperidone16 and supersensitivity psychosis and a cholinergic/serotonergic syndrome with olanzapine.17,18 Anecdotal reports suggest that abruptly discontinuing quetiapine can cause nausea, emesis, lightheadedness, diaphoresis, orthostasis, tachycardia, and nervousness.19,20 Although discontinuation syndromes have not been reported with ziprasidone or aripiprazole, tapering any atypical antipsychotic during discontinuation is prudent.
Benzodiazepine Discontinuation Syndromes
Benzodiazepines modulate the neurotransmitter activity of gamma-aminobutyric acid (GABA). They differ in their pharmacokinetic properties and have varying half-lives:
- chlordiazepoxide and diazepam have long half-lives (48 hours)
- clonazepam has an intermediate half-life (10 to 24 hours)
- alprazolam, lorazepam, and oxazepam have short half-lives (10 hours).
Abruptly discontinuing benzodiazepines can cause relapse or rebound of pretreatment symptoms. Rebound—with symptoms exceeding pretreatment levels—sometimes occurs after 4 weeks of therapy. The syndrome may last 1 to 3 weeks and is more common with agents having relatively short half-lives.21
Withdrawal. During benzodiazepine withdrawal, new symptoms emerge and pre-existing symptoms worsen. An autonomic component differentiates withdrawal from relapse or rebound. Prominent symptoms include excess sensitivity to light and sound, insomnia, tachycardia, mild systolic hypertension, anxiety, nausea, irritability, tremors, sweating, and abdominal distress. Less-common but serious symptoms include confusion, paranoid delusions, hallucinations, and seizures.22
Withdrawal symptoms are more likely to occur after 6 months of benzodiazepine therapy, when physical dependence also can develop. More-severe benzodiazepine discontinuation syndrome is associated with higher dosages, longer duration of therapy, shorter half-lives, and rapid tapers. Patient factors associated with withdrawal symptoms include:
- personality traits such as dependency and neuroticism
- high pretreatment anxious and depressive symptoms
- history of substance abuse or dependence.23
Preventing discontinuation syndromes
Antidepressants. For TCAs, no discontinuation protocols exist, although some experts suggest tapering regimens over 4 weeks to 3 months. For MAOIs, reducing dosages 10% per week has been suggested.24 The SSRI taper rate depends on the drug’s pharmacologic profile, how long the patient has been taking the SSRI, and the dosage.25
With paroxetine, for example, a gradual reduction of 10 mg/d per week is recommended, based on clinical trial experience. When you reach 20 mg/d, continue this dosage for 1 week before stopping treatment. If reducing a dosage or discontinuing paroxetine causes intolerable symptoms, consider resuming the previously prescribed dosage and then taper more gradually.26
Also gradually taper other SSRIs with short half-lives. Suggested taper regimens for sertraline and fluvoxamine call for weekly reductions of 50 mg/d until you reach 25 to 50 mg. It is not unusual for this final dosage to be lower than the starting dosage.25 Substituting fluoxetine—with its longer half-life—for other SSRIs at the end of treatment has been suggested to suppress withdrawal symptoms,27 although the safety and efficacy of this approach is unknown.5 With venlafaxine, taper over a minimum of 2 to 4 weeks.28
Antipsychotics. To prevent psychotic relapse when discontinuing clozapine, some experts advocate starting a new antipsychotic in a therapeutic dosage before stopping clozapine. When highdose clozapine must be withdrawn immediately, hospitalize the patient and consider using cholinergics to prevent cholinergic rebound.15
Data on managing discontinuation syndromes associated with risperidone, olanzapine, or quetiapine are limited. In some cases, reinstituting the original drug, gradually tapering the antipsychotic,18,19 or using prochlorperazine20 have been useful.
Benzodiazepines. Taper oral benzodiazepines if a patient has taken them >4 to 6 weeks. Also taper IV midazolam used >7 days to sedate a critically ill patient. For the elderly, an 8- to 10-week taper may be required to discontinue benzodiazepines used >3 months for insomnia.
The American Psychiatric Association practice guideline for patients with panic disorder29 recommends tapering benzodiazepines across 2 to 4 months, reducing dosages not more than 10% weekly. Another option is to reduce the daily dosage by 25% per week, but close monitoring and flexibility are required during this taper.
Outcomes when tapering benzodiazepines, according to Rickels et al,23 depend less on pharmacologic adjuvant treatment than on benzodiazepine dosage before the taper, initial psychopathology severity, and patient personality traits (such as passivity/dependency). Before tapering, those authors recommend that you:
- establish a stable patient-physician relationship
- aggressively treat clinically significant anxiety and depression symptoms with medication or other means while the patient continues the established benzodiazepine dosage.
When the taper is nearly complete, maintain the reduced benzodiazepine dosage several months before the final taper.23 Carbamazepine, imipramine, valproate, or trazodone may help alleviate benzodiazepine discontinuation symptoms in select patients.21
When discontinuation occurs
Medical comorbidity. Common medical conditions, including pregnancy or acute surgical procedures, may necessitate abrupt psychotropic discontinuation (Table 4).
Because up to 30% of medical patients have a psychiatric disorder,30 primary care physicians often start psychotropics to manage anxiety and depressive symptoms and may seek psychiatric advice when switching or stopping medications. Moreover, 10% to 15% of hospitalized medically ill patients require dosage reduction or discontinuation of psychotropics that are contributing to the clinical presentation.31
Table 4
Common conditions requiring abrupt psychotropic discontinuation
|
Switching. When switching psychotropics, effects from the first psychotropic may appear to be adverse effects of the new psychotropic. Thus, unrecognized discontinuation syndromes may lead to unnecessary treatment changes.
In our experience, a general rule is to cross-taper and decrease the psychotropic being discontinued by 10% every 1 to 2 weeks. Prescribe adequate dosages of the new psychotropic, closely monitor vital signs, and watch for emerging discontinuation symptoms.
Pregnancy. For women who become pregnant while taking psychotropics, consider the patient’s psychiatric stability, week of pregnancy, psychotropic agent, and treatment preferences when adjusting the treatment plan. In one study of 34 women who stopped psychotropics abruptly for fear of harming the fetus:
- 26 (70%) reported physical and psychological adverse effects
- 11 (30%) reported suicidal ideation, and 4 were hospitalized.32
Patient education. In the study described above, some of the pregnant women’s physicians were unaware of the risks associated with abrupt psychotropic discontinuation and others were aware but failed to inform their patients.32 Thus, patient and family/caregiver education is important. When stopping psychotropics, discuss their risks/benefits, address unrealistic expectations, and individualize therapy by tapering and providing adequate dosing. Watch for suicidality; a weekly telephone call might be useful.
Related resource
- Hardman JG, Limbird LE, Gilman AG. Goodman & Gilman’s the pharmacological basis of therapeutics (10th ed). New York: McGraw-Hill, 2001.
Drug Brand Names
- Alprazolam • Xanax
- Aripiprazole • Abilify
- Bupropion • Wellbutrin
- Carbamazepine • Equetro, Tegretol
- Chlordiazepoxide • Librium
- Citalopram • Celexa
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Diazepam • Valium
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Imipramine • Tofranil
- Lorazepam • Ativan
- Mirtazapine • Remeron
- Oxazepam • Serax
- Paroxetine • Paxil
- Phenelzine • Nardil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Tranylcypromine • Parnate
- Trazodone • Desyrel
- Sertraline • Zoloft
- Valproate • Depakene
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Young AH, Currie A. Physicians’ knowledge of antidepressant withdrawal effects: a survey. J Clin Psychiatry 1997;58(7):28-30.
2. Dilsaver SC, Greden JF, Snider RM. Antidepressant withdrawal syndromes: phenomenology and pathophysiology. Int Clin Psychopharmacol 1987;2(1):1-19.
3. Liskin B, Roose S, Walsh T. Acute psychosis following phenelzine discontinuation. J Clin Psychopharmacol 1985;5:46-7.
4. Coupland NJ, Bell CJ, Potokar JP. Serotonin reuptake inhibitor withdrawal. J Clin Psychopharmacol 1996;16(5):356-62.
5. Haddad PM. Antidepressant discontinuation syndromes. Drug Safety 2001;24(3):183-97.
6. Haddad P. The SSRI discontinuation syndrome. J Psychopharmacol 1998;2(3):305-13.
7. Schatzberg AF, Haddad P, Kaplan EM, et al. for the Discontinuation Consensus Panel Serotonin reuptake inhibitor discontinuation syndrome: a hypothetical definition. J Clin Psychiatry 1997;58(S7):5-10.
8. Markowitz JS, DeVane CL, Liston HL, et al. An assessment of selective serotonin reuptake inhibitor discontinuation symptoms with citalopram. Int Clin Psychopharmacol 2000;15(6):329-33.
9. Bezchlibnyk-Butler K, Aleksic I, Kennedy SH. Citalopram—a review of pharmacological and clinical effects. J Psychiatry Neurosci 2000;25(3):241-54.
10. Price JS, Waller PC, Wood SM, et al. A comparison of the post-marketing safety of four selective serotonin reuptake inhibitors, including the investigation of symptoms occurring on withdrawal. Br J Clin Pharmacol 1996;42:757-63.
11. Fava M, Mulroy R, Alpert J, et al. Emergence of adverse events following discontinuation of treatment with extended-release venlafaxine. Am J Psychiatry 1997;154(12):1760-2.
12. Barr LC, Goodman WK, Price LH. Physical symptoms associated with paroxetine discontinuation. Am J Psychiatry 1994;151(2):289.-
13. Schatzberg AF, Haddad P, Kaplan EM, et al. for the Discontinuation Consensus Panel Possible biological mechanisms of the serotonin reuptake inhibitor discontinuation syndrome. J Clin Psychiatry 1997;58(S7):23-7.
14. Shore D. Clinical implications of clozapine discontinuation: report of an NIMH workshop. Schizophr Bull 1995;21(2):333-8.
15. de Leon J, Stanilla JK, White AO, Simpson GM. Anticholinergics to treat clozapine withdrawal. J Clin Psychiatry 1994;55(3):119-20.
16. Rosebush PI, Kennedy K, Dalton B, Mazurek MF. Protracted akathisia after risperidone withdrawal. Am J Psychiatry 1997;154(3):437-8.
17. Llorca PM, Vaiva G, Lancon C. Supersensitivity psychosis in patients with schizophrenia after sudden olanzapine withdrawal. Can J Psychiatry 2001;46(1):87-8.
18. Nayudu SK, Scheftner WA. Case report of withdrawal syndrome after olanzapine discontinuation. J Clin Psychopharmacol 2000;20:489-90.
19. Thurstone CC, Alahi P. A possible case of quetiapine withdrawal syndrome. J Clin Psychiatry 2000;61:602-3.
20. Kim DR, Staab JP. Quetiapine discontinuation syndrome. Am J Psychiatry 2005 May;162(5):1020.-
21. McLean W, Ariano R. Benzodiazepine withdrawal schedule and symptoms In: Klasco RK (ed). DRUGDEX® System (vol. 124). Greenwood Village, CO: Thomson Micromedex, 2005.
22. Greenblatt DJ, Miller LG, Shader RI. Benzodiazepine discontinuation syndromes. J Psychiatr Res 1990;24(S2):73-9.
23. Rickels K, Schweizer E, Case WG, Greenblatt DJ. Long-term therapeutic use of benzodiazepines. I. Effects of abrupt discontinuation. Arch Gen Psychiatry 1990;47(10):899-907.
24. Lejoyeux M, Ades J, Mourad I, et al. Antidepressant withdrawal syndrome: recognition, prevalence and management. CNS Drugs 1996;5:278-92.
25. Rosenbaum JF, Zajecka J. Clinical management of antidepressant discontinuation. J Clin Psychiatry 1997;58(S7):37-40.
26. Paxil (paroxetine) package labeling GlaxoSmithKline, 2002.
27. Keuthen NJ, Cyr P, Ricciardi JA, et al. Medication withdrawal symptoms in obsessive-compulsive disorder patients treated with paroxetine. J Clin Psychopharmacol 1994;14(3):206-7.
28. Dallal A, Chouinard G. Withdrawal and rebound symptoms associated with abrupt discontinuation of venlafaxine. J Clin Psychopharmacol 1998;18(4):343-4.
29. American Psychiatric Association Work Group on Panic Disorder Practice guideline for the treatment of patients with panic disorder. Am J Psychiatry 1998;155(S5):1-34.
30. Spitzer RL, Williams JB, Kroenke K, et al. Utility of a new procedure for diagnosing mental disorders in primary care. The PRIME-MD 1000 study. JAMA 1994;272(22):1749-56.
31. Bronheim HE, Fulop G, Kunkel EJ, et al. The Academy of Psychosomatic Medicine practice guidelines for psychiatric consultation in the general medical setting. Psychosomatics 1998;39(4):S8-30.
32. Einarson A, Selby P, Koren G. Abrupt discontinuation of psychotropic drugs during pregnancy: fear of teratogenic risk and impact of counseling. J Psychiatry Neurosci 2001;26(1):44-8.
Abruptly stopping common psychotropics—particularly antidepressants, benzodiazepines, or atypical antipsychotics—can trigger a discontinuation syndrome, with:
- rebound or relapse of original symptoms
- uncomfortable new physical and psychological symptoms
- physiologic withdrawal at times.
To increase health professionals’ awareness of the risk of these adverse effects,1 this article describes discontinuation syndromes associated with various psychotropics and offers strategies to anticipate, recognize, and manage them.
Antidepressant Discontinuation Syndromes
Discontinuation syndromes can occur with tricyclic and tetracyclic antidepressants (TCAs), monoamine oxidase inhibitors (MAOIs), selective serotonin reuptake inhibitors (SSRIs), and other newer antidepressants. Symptoms usually start within a few days of stopping a drug—or less commonly, reducing its dosage—and are usually mild and self-limited. Serious outcomes have been reported.
Distinguishing antidepressant discontinuation symptoms from depression recurrence is important. Discontinuation symptoms emerge within 1 to 3 days, whereas depressive symptoms usually occur 2 to 3 weeks after an antidepressant is stopped. Discontinuation reactions remit within a few days, especially if the antidepressant is re-instituted.
TCAs block serotonin and norepinephrine reuptake, increasing the availability of these biogenic amines at receptor sites in the brain and other tissues. Abrupt discontinuation can cause physical symptoms—such as lethargy, headache, and tremor—and psychological symptoms including irritability, anxiety, agitation, and low mood (Table 1).2
Long-term use of TCAs with potent anticholinergic properties leads to upregulation of postsynaptic muscarinic receptors, creating a “supersensitive” state. Abrupt discontinuation can cause cholinergic rebound, with symptoms emerging as soon as 12 hours—but typically 24 to 48 hours—after the last dose.
Table 1
Discontinuation symptoms seen with TCAs
| Physical symptoms | Lethargy, headache, tremor, sweating, anorexia, insomnia, nausea, vomiting, diarrhea, akathisia (rare), parkinsonism (rare) |
| Psychological symptoms | Irritability, anxiety/agitation, low mood, excessive dreaming, nightmares, paradoxical activation resulting in manic/hypomanic symptoms (rare) |
| TCA: Tricyclic antidepressants | |
| Source: Reference 2 | |
MAOIs such as phenelzine and tranylcypromine inhibit the enzyme monoamine oxidase, which is responsible for monoamine degradation and increases synaptic monoamine concentrations. Discontinuation syndromes may include acute confusional states, paranoid delusions, hallucinations, or worsening of depressive symptoms.3 These problems rarely occur in clinical practice, however, because MAOIs’ serious side effects discourage doctors from prescribing them.
SSRIs and other agents. SSRIs block synaptic reuptake of serotonin. Serotonin-norepinephrine reuptake inhibitors (SNRIs) such as venlafaxine and duloxetine inhibit both serotonin and norepinephrine reuptake. Mirtazapine—an alpha2-adrenergic and heteroreceptor antagonist—increases serotonin and norepinephrine at the synapse. Bupropion increases dopamine and norepinephrine turnover in the CNS and also blocks serotonin.
Up to 30% of patients who stop taking SSRIs develop discontinuation symptoms.4 Six symptom clusters—disequilibrium, sensory symptoms, general somatic symptoms, sleep disturbance, GI symptoms, and affective symptoms—characterize the SSRI discontinuation syndrome (Table 2).5 The four most common symptoms—in decreasing order of frequency—are dizziness, nausea, lethargy, and headache.6 Ataxia, sensory abnormalities, and possibly aggressive and impulsive behavior differentiate this discontinuation syndrome from that of the TCAs.
Table 2
Discontinuation symptoms seen with SSRIs
| Type | Symptoms |
|---|---|
| Disequilibrium | Lightheadedness/dizziness, vertigo, ataxia |
| Sensory symptoms | Paraesthesia, numbness, electric shock-like sensations |
| General somatic symptoms | Lethargy, headache, tremor, sweating, anorexia |
| Sleep disturbance | Insomnia, nightmares, excessive dreaming |
| GI symptoms | Nausea, vomiting, diarrhea |
| Affective symptoms | Irritability, anxiety/agitation, low mood |
| SSRIs: Selective serotonin reuptake inhibitors | |
| Source: Reference 5 | |
Risk factors. Risk factors for SSRI discontinuation syndrome have been identified (Table 3).7 Symptoms usually begin 1 to 3 days after an SSRI is abruptly stopped and are usually mild. However, some patients report falls, inability to work, and difficulty walking and driving. Untreated symptoms are short-lived and remit within 1 to 2 weeks. They also remit if the original antidepressant is reintroduced or a pharmacologically similar agent is substituted.
Discontinuation syndrome risk among SSRIs is highest for paroxetine, intermediate for sertraline and fluvoxamine, and lowest for fluoxetine.4 Citalopram may cause a mild and transient discontinuation syndrome.8 Citalopram’s long elimination half-life (30 to 35 hours) and fewer and much less-potent active metabolites9 may explain its relatively low risk of discontinuation symptoms.
Discontinuation reactions have been reported to occur 100 times more frequently with paroxetine than with fluoxetine.10 Fluoxetine’s lower rate could be explained by its 2- to 3-day half-life, compared with half-lives of 33 hours or less for paroxetine, sertraline, citalopram, and fluvoxamine. A longer half-life might protect against a discontinuation syndrome.
Among other newer antidepressants:
- venlafaxine’s discontinuation syndrome is similar to the SSRI syndrome11
- no discontinuation symptoms have been reported with mirtazapine, bupropion, or duloxetine.
Table 3
SSRI discontinuation syndrome: The patient at risk…
| Is taking an SSRI with a relatively short half-life |
| Has received antidepressant treatment > 4 weeks |
| Has history of treatment-emergent anxiety, discontinuation symptoms, nonadherence |
| SSRI: Selective serotonin reuptake inhibitor |
| Source: Reference 7 |
Causes. Theories to explain SSRI discontinuation syndrome include cholinergic rebound,12 as described with TCAs, or a decrease in available synaptic serotonin coinciding with down-regulated serotonin receptors.13 Paroxetine’s pharmacologic properties—cholinergic effects, short halflife, and high potency of serotonin reuptake blockade—may explain its relatively high frequency of discontinuation symptoms.
Atypical Antipsychotic Discontinuation Syndromes
Except for aripiprazole—which is a partial dopamine receptor agonist—most atypical antipsychotics are serotonin-dopamine antagonists. Discontinuation syndrome occurs most commonly with clozapine.
Clozapine. Abruptly stopping clozapine can exacerbate psychosis or cause delirium, agitation, confusion, and diaphoresis. Less-common symptoms may include extrapyramidal effects, nausea, diarrhea, headache, or restlessness.14 Clozapine is a weak dopamine D2 antagonist and a potent antagonist at the serotonin 5HT2, alpha adrenergic, histaminergic, and anticholinergic receptors. Thus, rebound from cholinergic, serotonin, dopamine and/or adrenergic receptor supersensitivity is thought to cause its discontinuation syndrome.15
Other atypicals. Case reports describe tics and withdrawal-emergent dyskinesia with risperidone16 and supersensitivity psychosis and a cholinergic/serotonergic syndrome with olanzapine.17,18 Anecdotal reports suggest that abruptly discontinuing quetiapine can cause nausea, emesis, lightheadedness, diaphoresis, orthostasis, tachycardia, and nervousness.19,20 Although discontinuation syndromes have not been reported with ziprasidone or aripiprazole, tapering any atypical antipsychotic during discontinuation is prudent.
Benzodiazepine Discontinuation Syndromes
Benzodiazepines modulate the neurotransmitter activity of gamma-aminobutyric acid (GABA). They differ in their pharmacokinetic properties and have varying half-lives:
- chlordiazepoxide and diazepam have long half-lives (48 hours)
- clonazepam has an intermediate half-life (10 to 24 hours)
- alprazolam, lorazepam, and oxazepam have short half-lives (10 hours).
Abruptly discontinuing benzodiazepines can cause relapse or rebound of pretreatment symptoms. Rebound—with symptoms exceeding pretreatment levels—sometimes occurs after 4 weeks of therapy. The syndrome may last 1 to 3 weeks and is more common with agents having relatively short half-lives.21
Withdrawal. During benzodiazepine withdrawal, new symptoms emerge and pre-existing symptoms worsen. An autonomic component differentiates withdrawal from relapse or rebound. Prominent symptoms include excess sensitivity to light and sound, insomnia, tachycardia, mild systolic hypertension, anxiety, nausea, irritability, tremors, sweating, and abdominal distress. Less-common but serious symptoms include confusion, paranoid delusions, hallucinations, and seizures.22
Withdrawal symptoms are more likely to occur after 6 months of benzodiazepine therapy, when physical dependence also can develop. More-severe benzodiazepine discontinuation syndrome is associated with higher dosages, longer duration of therapy, shorter half-lives, and rapid tapers. Patient factors associated with withdrawal symptoms include:
- personality traits such as dependency and neuroticism
- high pretreatment anxious and depressive symptoms
- history of substance abuse or dependence.23
Preventing discontinuation syndromes
Antidepressants. For TCAs, no discontinuation protocols exist, although some experts suggest tapering regimens over 4 weeks to 3 months. For MAOIs, reducing dosages 10% per week has been suggested.24 The SSRI taper rate depends on the drug’s pharmacologic profile, how long the patient has been taking the SSRI, and the dosage.25
With paroxetine, for example, a gradual reduction of 10 mg/d per week is recommended, based on clinical trial experience. When you reach 20 mg/d, continue this dosage for 1 week before stopping treatment. If reducing a dosage or discontinuing paroxetine causes intolerable symptoms, consider resuming the previously prescribed dosage and then taper more gradually.26
Also gradually taper other SSRIs with short half-lives. Suggested taper regimens for sertraline and fluvoxamine call for weekly reductions of 50 mg/d until you reach 25 to 50 mg. It is not unusual for this final dosage to be lower than the starting dosage.25 Substituting fluoxetine—with its longer half-life—for other SSRIs at the end of treatment has been suggested to suppress withdrawal symptoms,27 although the safety and efficacy of this approach is unknown.5 With venlafaxine, taper over a minimum of 2 to 4 weeks.28
Antipsychotics. To prevent psychotic relapse when discontinuing clozapine, some experts advocate starting a new antipsychotic in a therapeutic dosage before stopping clozapine. When highdose clozapine must be withdrawn immediately, hospitalize the patient and consider using cholinergics to prevent cholinergic rebound.15
Data on managing discontinuation syndromes associated with risperidone, olanzapine, or quetiapine are limited. In some cases, reinstituting the original drug, gradually tapering the antipsychotic,18,19 or using prochlorperazine20 have been useful.
Benzodiazepines. Taper oral benzodiazepines if a patient has taken them >4 to 6 weeks. Also taper IV midazolam used >7 days to sedate a critically ill patient. For the elderly, an 8- to 10-week taper may be required to discontinue benzodiazepines used >3 months for insomnia.
The American Psychiatric Association practice guideline for patients with panic disorder29 recommends tapering benzodiazepines across 2 to 4 months, reducing dosages not more than 10% weekly. Another option is to reduce the daily dosage by 25% per week, but close monitoring and flexibility are required during this taper.
Outcomes when tapering benzodiazepines, according to Rickels et al,23 depend less on pharmacologic adjuvant treatment than on benzodiazepine dosage before the taper, initial psychopathology severity, and patient personality traits (such as passivity/dependency). Before tapering, those authors recommend that you:
- establish a stable patient-physician relationship
- aggressively treat clinically significant anxiety and depression symptoms with medication or other means while the patient continues the established benzodiazepine dosage.
When the taper is nearly complete, maintain the reduced benzodiazepine dosage several months before the final taper.23 Carbamazepine, imipramine, valproate, or trazodone may help alleviate benzodiazepine discontinuation symptoms in select patients.21
When discontinuation occurs
Medical comorbidity. Common medical conditions, including pregnancy or acute surgical procedures, may necessitate abrupt psychotropic discontinuation (Table 4).
Because up to 30% of medical patients have a psychiatric disorder,30 primary care physicians often start psychotropics to manage anxiety and depressive symptoms and may seek psychiatric advice when switching or stopping medications. Moreover, 10% to 15% of hospitalized medically ill patients require dosage reduction or discontinuation of psychotropics that are contributing to the clinical presentation.31
Table 4
Common conditions requiring abrupt psychotropic discontinuation
|
Switching. When switching psychotropics, effects from the first psychotropic may appear to be adverse effects of the new psychotropic. Thus, unrecognized discontinuation syndromes may lead to unnecessary treatment changes.
In our experience, a general rule is to cross-taper and decrease the psychotropic being discontinued by 10% every 1 to 2 weeks. Prescribe adequate dosages of the new psychotropic, closely monitor vital signs, and watch for emerging discontinuation symptoms.
Pregnancy. For women who become pregnant while taking psychotropics, consider the patient’s psychiatric stability, week of pregnancy, psychotropic agent, and treatment preferences when adjusting the treatment plan. In one study of 34 women who stopped psychotropics abruptly for fear of harming the fetus:
- 26 (70%) reported physical and psychological adverse effects
- 11 (30%) reported suicidal ideation, and 4 were hospitalized.32
Patient education. In the study described above, some of the pregnant women’s physicians were unaware of the risks associated with abrupt psychotropic discontinuation and others were aware but failed to inform their patients.32 Thus, patient and family/caregiver education is important. When stopping psychotropics, discuss their risks/benefits, address unrealistic expectations, and individualize therapy by tapering and providing adequate dosing. Watch for suicidality; a weekly telephone call might be useful.
Related resource
- Hardman JG, Limbird LE, Gilman AG. Goodman & Gilman’s the pharmacological basis of therapeutics (10th ed). New York: McGraw-Hill, 2001.
Drug Brand Names
- Alprazolam • Xanax
- Aripiprazole • Abilify
- Bupropion • Wellbutrin
- Carbamazepine • Equetro, Tegretol
- Chlordiazepoxide • Librium
- Citalopram • Celexa
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Diazepam • Valium
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Imipramine • Tofranil
- Lorazepam • Ativan
- Mirtazapine • Remeron
- Oxazepam • Serax
- Paroxetine • Paxil
- Phenelzine • Nardil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Tranylcypromine • Parnate
- Trazodone • Desyrel
- Sertraline • Zoloft
- Valproate • Depakene
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Abruptly stopping common psychotropics—particularly antidepressants, benzodiazepines, or atypical antipsychotics—can trigger a discontinuation syndrome, with:
- rebound or relapse of original symptoms
- uncomfortable new physical and psychological symptoms
- physiologic withdrawal at times.
To increase health professionals’ awareness of the risk of these adverse effects,1 this article describes discontinuation syndromes associated with various psychotropics and offers strategies to anticipate, recognize, and manage them.
Antidepressant Discontinuation Syndromes
Discontinuation syndromes can occur with tricyclic and tetracyclic antidepressants (TCAs), monoamine oxidase inhibitors (MAOIs), selective serotonin reuptake inhibitors (SSRIs), and other newer antidepressants. Symptoms usually start within a few days of stopping a drug—or less commonly, reducing its dosage—and are usually mild and self-limited. Serious outcomes have been reported.
Distinguishing antidepressant discontinuation symptoms from depression recurrence is important. Discontinuation symptoms emerge within 1 to 3 days, whereas depressive symptoms usually occur 2 to 3 weeks after an antidepressant is stopped. Discontinuation reactions remit within a few days, especially if the antidepressant is re-instituted.
TCAs block serotonin and norepinephrine reuptake, increasing the availability of these biogenic amines at receptor sites in the brain and other tissues. Abrupt discontinuation can cause physical symptoms—such as lethargy, headache, and tremor—and psychological symptoms including irritability, anxiety, agitation, and low mood (Table 1).2
Long-term use of TCAs with potent anticholinergic properties leads to upregulation of postsynaptic muscarinic receptors, creating a “supersensitive” state. Abrupt discontinuation can cause cholinergic rebound, with symptoms emerging as soon as 12 hours—but typically 24 to 48 hours—after the last dose.
Table 1
Discontinuation symptoms seen with TCAs
| Physical symptoms | Lethargy, headache, tremor, sweating, anorexia, insomnia, nausea, vomiting, diarrhea, akathisia (rare), parkinsonism (rare) |
| Psychological symptoms | Irritability, anxiety/agitation, low mood, excessive dreaming, nightmares, paradoxical activation resulting in manic/hypomanic symptoms (rare) |
| TCA: Tricyclic antidepressants | |
| Source: Reference 2 | |
MAOIs such as phenelzine and tranylcypromine inhibit the enzyme monoamine oxidase, which is responsible for monoamine degradation and increases synaptic monoamine concentrations. Discontinuation syndromes may include acute confusional states, paranoid delusions, hallucinations, or worsening of depressive symptoms.3 These problems rarely occur in clinical practice, however, because MAOIs’ serious side effects discourage doctors from prescribing them.
SSRIs and other agents. SSRIs block synaptic reuptake of serotonin. Serotonin-norepinephrine reuptake inhibitors (SNRIs) such as venlafaxine and duloxetine inhibit both serotonin and norepinephrine reuptake. Mirtazapine—an alpha2-adrenergic and heteroreceptor antagonist—increases serotonin and norepinephrine at the synapse. Bupropion increases dopamine and norepinephrine turnover in the CNS and also blocks serotonin.
Up to 30% of patients who stop taking SSRIs develop discontinuation symptoms.4 Six symptom clusters—disequilibrium, sensory symptoms, general somatic symptoms, sleep disturbance, GI symptoms, and affective symptoms—characterize the SSRI discontinuation syndrome (Table 2).5 The four most common symptoms—in decreasing order of frequency—are dizziness, nausea, lethargy, and headache.6 Ataxia, sensory abnormalities, and possibly aggressive and impulsive behavior differentiate this discontinuation syndrome from that of the TCAs.
Table 2
Discontinuation symptoms seen with SSRIs
| Type | Symptoms |
|---|---|
| Disequilibrium | Lightheadedness/dizziness, vertigo, ataxia |
| Sensory symptoms | Paraesthesia, numbness, electric shock-like sensations |
| General somatic symptoms | Lethargy, headache, tremor, sweating, anorexia |
| Sleep disturbance | Insomnia, nightmares, excessive dreaming |
| GI symptoms | Nausea, vomiting, diarrhea |
| Affective symptoms | Irritability, anxiety/agitation, low mood |
| SSRIs: Selective serotonin reuptake inhibitors | |
| Source: Reference 5 | |
Risk factors. Risk factors for SSRI discontinuation syndrome have been identified (Table 3).7 Symptoms usually begin 1 to 3 days after an SSRI is abruptly stopped and are usually mild. However, some patients report falls, inability to work, and difficulty walking and driving. Untreated symptoms are short-lived and remit within 1 to 2 weeks. They also remit if the original antidepressant is reintroduced or a pharmacologically similar agent is substituted.
Discontinuation syndrome risk among SSRIs is highest for paroxetine, intermediate for sertraline and fluvoxamine, and lowest for fluoxetine.4 Citalopram may cause a mild and transient discontinuation syndrome.8 Citalopram’s long elimination half-life (30 to 35 hours) and fewer and much less-potent active metabolites9 may explain its relatively low risk of discontinuation symptoms.
Discontinuation reactions have been reported to occur 100 times more frequently with paroxetine than with fluoxetine.10 Fluoxetine’s lower rate could be explained by its 2- to 3-day half-life, compared with half-lives of 33 hours or less for paroxetine, sertraline, citalopram, and fluvoxamine. A longer half-life might protect against a discontinuation syndrome.
Among other newer antidepressants:
- venlafaxine’s discontinuation syndrome is similar to the SSRI syndrome11
- no discontinuation symptoms have been reported with mirtazapine, bupropion, or duloxetine.
Table 3
SSRI discontinuation syndrome: The patient at risk…
| Is taking an SSRI with a relatively short half-life |
| Has received antidepressant treatment > 4 weeks |
| Has history of treatment-emergent anxiety, discontinuation symptoms, nonadherence |
| SSRI: Selective serotonin reuptake inhibitor |
| Source: Reference 7 |
Causes. Theories to explain SSRI discontinuation syndrome include cholinergic rebound,12 as described with TCAs, or a decrease in available synaptic serotonin coinciding with down-regulated serotonin receptors.13 Paroxetine’s pharmacologic properties—cholinergic effects, short halflife, and high potency of serotonin reuptake blockade—may explain its relatively high frequency of discontinuation symptoms.
Atypical Antipsychotic Discontinuation Syndromes
Except for aripiprazole—which is a partial dopamine receptor agonist—most atypical antipsychotics are serotonin-dopamine antagonists. Discontinuation syndrome occurs most commonly with clozapine.
Clozapine. Abruptly stopping clozapine can exacerbate psychosis or cause delirium, agitation, confusion, and diaphoresis. Less-common symptoms may include extrapyramidal effects, nausea, diarrhea, headache, or restlessness.14 Clozapine is a weak dopamine D2 antagonist and a potent antagonist at the serotonin 5HT2, alpha adrenergic, histaminergic, and anticholinergic receptors. Thus, rebound from cholinergic, serotonin, dopamine and/or adrenergic receptor supersensitivity is thought to cause its discontinuation syndrome.15
Other atypicals. Case reports describe tics and withdrawal-emergent dyskinesia with risperidone16 and supersensitivity psychosis and a cholinergic/serotonergic syndrome with olanzapine.17,18 Anecdotal reports suggest that abruptly discontinuing quetiapine can cause nausea, emesis, lightheadedness, diaphoresis, orthostasis, tachycardia, and nervousness.19,20 Although discontinuation syndromes have not been reported with ziprasidone or aripiprazole, tapering any atypical antipsychotic during discontinuation is prudent.
Benzodiazepine Discontinuation Syndromes
Benzodiazepines modulate the neurotransmitter activity of gamma-aminobutyric acid (GABA). They differ in their pharmacokinetic properties and have varying half-lives:
- chlordiazepoxide and diazepam have long half-lives (48 hours)
- clonazepam has an intermediate half-life (10 to 24 hours)
- alprazolam, lorazepam, and oxazepam have short half-lives (10 hours).
Abruptly discontinuing benzodiazepines can cause relapse or rebound of pretreatment symptoms. Rebound—with symptoms exceeding pretreatment levels—sometimes occurs after 4 weeks of therapy. The syndrome may last 1 to 3 weeks and is more common with agents having relatively short half-lives.21
Withdrawal. During benzodiazepine withdrawal, new symptoms emerge and pre-existing symptoms worsen. An autonomic component differentiates withdrawal from relapse or rebound. Prominent symptoms include excess sensitivity to light and sound, insomnia, tachycardia, mild systolic hypertension, anxiety, nausea, irritability, tremors, sweating, and abdominal distress. Less-common but serious symptoms include confusion, paranoid delusions, hallucinations, and seizures.22
Withdrawal symptoms are more likely to occur after 6 months of benzodiazepine therapy, when physical dependence also can develop. More-severe benzodiazepine discontinuation syndrome is associated with higher dosages, longer duration of therapy, shorter half-lives, and rapid tapers. Patient factors associated with withdrawal symptoms include:
- personality traits such as dependency and neuroticism
- high pretreatment anxious and depressive symptoms
- history of substance abuse or dependence.23
Preventing discontinuation syndromes
Antidepressants. For TCAs, no discontinuation protocols exist, although some experts suggest tapering regimens over 4 weeks to 3 months. For MAOIs, reducing dosages 10% per week has been suggested.24 The SSRI taper rate depends on the drug’s pharmacologic profile, how long the patient has been taking the SSRI, and the dosage.25
With paroxetine, for example, a gradual reduction of 10 mg/d per week is recommended, based on clinical trial experience. When you reach 20 mg/d, continue this dosage for 1 week before stopping treatment. If reducing a dosage or discontinuing paroxetine causes intolerable symptoms, consider resuming the previously prescribed dosage and then taper more gradually.26
Also gradually taper other SSRIs with short half-lives. Suggested taper regimens for sertraline and fluvoxamine call for weekly reductions of 50 mg/d until you reach 25 to 50 mg. It is not unusual for this final dosage to be lower than the starting dosage.25 Substituting fluoxetine—with its longer half-life—for other SSRIs at the end of treatment has been suggested to suppress withdrawal symptoms,27 although the safety and efficacy of this approach is unknown.5 With venlafaxine, taper over a minimum of 2 to 4 weeks.28
Antipsychotics. To prevent psychotic relapse when discontinuing clozapine, some experts advocate starting a new antipsychotic in a therapeutic dosage before stopping clozapine. When highdose clozapine must be withdrawn immediately, hospitalize the patient and consider using cholinergics to prevent cholinergic rebound.15
Data on managing discontinuation syndromes associated with risperidone, olanzapine, or quetiapine are limited. In some cases, reinstituting the original drug, gradually tapering the antipsychotic,18,19 or using prochlorperazine20 have been useful.
Benzodiazepines. Taper oral benzodiazepines if a patient has taken them >4 to 6 weeks. Also taper IV midazolam used >7 days to sedate a critically ill patient. For the elderly, an 8- to 10-week taper may be required to discontinue benzodiazepines used >3 months for insomnia.
The American Psychiatric Association practice guideline for patients with panic disorder29 recommends tapering benzodiazepines across 2 to 4 months, reducing dosages not more than 10% weekly. Another option is to reduce the daily dosage by 25% per week, but close monitoring and flexibility are required during this taper.
Outcomes when tapering benzodiazepines, according to Rickels et al,23 depend less on pharmacologic adjuvant treatment than on benzodiazepine dosage before the taper, initial psychopathology severity, and patient personality traits (such as passivity/dependency). Before tapering, those authors recommend that you:
- establish a stable patient-physician relationship
- aggressively treat clinically significant anxiety and depression symptoms with medication or other means while the patient continues the established benzodiazepine dosage.
When the taper is nearly complete, maintain the reduced benzodiazepine dosage several months before the final taper.23 Carbamazepine, imipramine, valproate, or trazodone may help alleviate benzodiazepine discontinuation symptoms in select patients.21
When discontinuation occurs
Medical comorbidity. Common medical conditions, including pregnancy or acute surgical procedures, may necessitate abrupt psychotropic discontinuation (Table 4).
Because up to 30% of medical patients have a psychiatric disorder,30 primary care physicians often start psychotropics to manage anxiety and depressive symptoms and may seek psychiatric advice when switching or stopping medications. Moreover, 10% to 15% of hospitalized medically ill patients require dosage reduction or discontinuation of psychotropics that are contributing to the clinical presentation.31
Table 4
Common conditions requiring abrupt psychotropic discontinuation
|
Switching. When switching psychotropics, effects from the first psychotropic may appear to be adverse effects of the new psychotropic. Thus, unrecognized discontinuation syndromes may lead to unnecessary treatment changes.
In our experience, a general rule is to cross-taper and decrease the psychotropic being discontinued by 10% every 1 to 2 weeks. Prescribe adequate dosages of the new psychotropic, closely monitor vital signs, and watch for emerging discontinuation symptoms.
Pregnancy. For women who become pregnant while taking psychotropics, consider the patient’s psychiatric stability, week of pregnancy, psychotropic agent, and treatment preferences when adjusting the treatment plan. In one study of 34 women who stopped psychotropics abruptly for fear of harming the fetus:
- 26 (70%) reported physical and psychological adverse effects
- 11 (30%) reported suicidal ideation, and 4 were hospitalized.32
Patient education. In the study described above, some of the pregnant women’s physicians were unaware of the risks associated with abrupt psychotropic discontinuation and others were aware but failed to inform their patients.32 Thus, patient and family/caregiver education is important. When stopping psychotropics, discuss their risks/benefits, address unrealistic expectations, and individualize therapy by tapering and providing adequate dosing. Watch for suicidality; a weekly telephone call might be useful.
Related resource
- Hardman JG, Limbird LE, Gilman AG. Goodman & Gilman’s the pharmacological basis of therapeutics (10th ed). New York: McGraw-Hill, 2001.
Drug Brand Names
- Alprazolam • Xanax
- Aripiprazole • Abilify
- Bupropion • Wellbutrin
- Carbamazepine • Equetro, Tegretol
- Chlordiazepoxide • Librium
- Citalopram • Celexa
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Diazepam • Valium
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Imipramine • Tofranil
- Lorazepam • Ativan
- Mirtazapine • Remeron
- Oxazepam • Serax
- Paroxetine • Paxil
- Phenelzine • Nardil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Tranylcypromine • Parnate
- Trazodone • Desyrel
- Sertraline • Zoloft
- Valproate • Depakene
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Young AH, Currie A. Physicians’ knowledge of antidepressant withdrawal effects: a survey. J Clin Psychiatry 1997;58(7):28-30.
2. Dilsaver SC, Greden JF, Snider RM. Antidepressant withdrawal syndromes: phenomenology and pathophysiology. Int Clin Psychopharmacol 1987;2(1):1-19.
3. Liskin B, Roose S, Walsh T. Acute psychosis following phenelzine discontinuation. J Clin Psychopharmacol 1985;5:46-7.
4. Coupland NJ, Bell CJ, Potokar JP. Serotonin reuptake inhibitor withdrawal. J Clin Psychopharmacol 1996;16(5):356-62.
5. Haddad PM. Antidepressant discontinuation syndromes. Drug Safety 2001;24(3):183-97.
6. Haddad P. The SSRI discontinuation syndrome. J Psychopharmacol 1998;2(3):305-13.
7. Schatzberg AF, Haddad P, Kaplan EM, et al. for the Discontinuation Consensus Panel Serotonin reuptake inhibitor discontinuation syndrome: a hypothetical definition. J Clin Psychiatry 1997;58(S7):5-10.
8. Markowitz JS, DeVane CL, Liston HL, et al. An assessment of selective serotonin reuptake inhibitor discontinuation symptoms with citalopram. Int Clin Psychopharmacol 2000;15(6):329-33.
9. Bezchlibnyk-Butler K, Aleksic I, Kennedy SH. Citalopram—a review of pharmacological and clinical effects. J Psychiatry Neurosci 2000;25(3):241-54.
10. Price JS, Waller PC, Wood SM, et al. A comparison of the post-marketing safety of four selective serotonin reuptake inhibitors, including the investigation of symptoms occurring on withdrawal. Br J Clin Pharmacol 1996;42:757-63.
11. Fava M, Mulroy R, Alpert J, et al. Emergence of adverse events following discontinuation of treatment with extended-release venlafaxine. Am J Psychiatry 1997;154(12):1760-2.
12. Barr LC, Goodman WK, Price LH. Physical symptoms associated with paroxetine discontinuation. Am J Psychiatry 1994;151(2):289.-
13. Schatzberg AF, Haddad P, Kaplan EM, et al. for the Discontinuation Consensus Panel Possible biological mechanisms of the serotonin reuptake inhibitor discontinuation syndrome. J Clin Psychiatry 1997;58(S7):23-7.
14. Shore D. Clinical implications of clozapine discontinuation: report of an NIMH workshop. Schizophr Bull 1995;21(2):333-8.
15. de Leon J, Stanilla JK, White AO, Simpson GM. Anticholinergics to treat clozapine withdrawal. J Clin Psychiatry 1994;55(3):119-20.
16. Rosebush PI, Kennedy K, Dalton B, Mazurek MF. Protracted akathisia after risperidone withdrawal. Am J Psychiatry 1997;154(3):437-8.
17. Llorca PM, Vaiva G, Lancon C. Supersensitivity psychosis in patients with schizophrenia after sudden olanzapine withdrawal. Can J Psychiatry 2001;46(1):87-8.
18. Nayudu SK, Scheftner WA. Case report of withdrawal syndrome after olanzapine discontinuation. J Clin Psychopharmacol 2000;20:489-90.
19. Thurstone CC, Alahi P. A possible case of quetiapine withdrawal syndrome. J Clin Psychiatry 2000;61:602-3.
20. Kim DR, Staab JP. Quetiapine discontinuation syndrome. Am J Psychiatry 2005 May;162(5):1020.-
21. McLean W, Ariano R. Benzodiazepine withdrawal schedule and symptoms In: Klasco RK (ed). DRUGDEX® System (vol. 124). Greenwood Village, CO: Thomson Micromedex, 2005.
22. Greenblatt DJ, Miller LG, Shader RI. Benzodiazepine discontinuation syndromes. J Psychiatr Res 1990;24(S2):73-9.
23. Rickels K, Schweizer E, Case WG, Greenblatt DJ. Long-term therapeutic use of benzodiazepines. I. Effects of abrupt discontinuation. Arch Gen Psychiatry 1990;47(10):899-907.
24. Lejoyeux M, Ades J, Mourad I, et al. Antidepressant withdrawal syndrome: recognition, prevalence and management. CNS Drugs 1996;5:278-92.
25. Rosenbaum JF, Zajecka J. Clinical management of antidepressant discontinuation. J Clin Psychiatry 1997;58(S7):37-40.
26. Paxil (paroxetine) package labeling GlaxoSmithKline, 2002.
27. Keuthen NJ, Cyr P, Ricciardi JA, et al. Medication withdrawal symptoms in obsessive-compulsive disorder patients treated with paroxetine. J Clin Psychopharmacol 1994;14(3):206-7.
28. Dallal A, Chouinard G. Withdrawal and rebound symptoms associated with abrupt discontinuation of venlafaxine. J Clin Psychopharmacol 1998;18(4):343-4.
29. American Psychiatric Association Work Group on Panic Disorder Practice guideline for the treatment of patients with panic disorder. Am J Psychiatry 1998;155(S5):1-34.
30. Spitzer RL, Williams JB, Kroenke K, et al. Utility of a new procedure for diagnosing mental disorders in primary care. The PRIME-MD 1000 study. JAMA 1994;272(22):1749-56.
31. Bronheim HE, Fulop G, Kunkel EJ, et al. The Academy of Psychosomatic Medicine practice guidelines for psychiatric consultation in the general medical setting. Psychosomatics 1998;39(4):S8-30.
32. Einarson A, Selby P, Koren G. Abrupt discontinuation of psychotropic drugs during pregnancy: fear of teratogenic risk and impact of counseling. J Psychiatry Neurosci 2001;26(1):44-8.
1. Young AH, Currie A. Physicians’ knowledge of antidepressant withdrawal effects: a survey. J Clin Psychiatry 1997;58(7):28-30.
2. Dilsaver SC, Greden JF, Snider RM. Antidepressant withdrawal syndromes: phenomenology and pathophysiology. Int Clin Psychopharmacol 1987;2(1):1-19.
3. Liskin B, Roose S, Walsh T. Acute psychosis following phenelzine discontinuation. J Clin Psychopharmacol 1985;5:46-7.
4. Coupland NJ, Bell CJ, Potokar JP. Serotonin reuptake inhibitor withdrawal. J Clin Psychopharmacol 1996;16(5):356-62.
5. Haddad PM. Antidepressant discontinuation syndromes. Drug Safety 2001;24(3):183-97.
6. Haddad P. The SSRI discontinuation syndrome. J Psychopharmacol 1998;2(3):305-13.
7. Schatzberg AF, Haddad P, Kaplan EM, et al. for the Discontinuation Consensus Panel Serotonin reuptake inhibitor discontinuation syndrome: a hypothetical definition. J Clin Psychiatry 1997;58(S7):5-10.
8. Markowitz JS, DeVane CL, Liston HL, et al. An assessment of selective serotonin reuptake inhibitor discontinuation symptoms with citalopram. Int Clin Psychopharmacol 2000;15(6):329-33.
9. Bezchlibnyk-Butler K, Aleksic I, Kennedy SH. Citalopram—a review of pharmacological and clinical effects. J Psychiatry Neurosci 2000;25(3):241-54.
10. Price JS, Waller PC, Wood SM, et al. A comparison of the post-marketing safety of four selective serotonin reuptake inhibitors, including the investigation of symptoms occurring on withdrawal. Br J Clin Pharmacol 1996;42:757-63.
11. Fava M, Mulroy R, Alpert J, et al. Emergence of adverse events following discontinuation of treatment with extended-release venlafaxine. Am J Psychiatry 1997;154(12):1760-2.
12. Barr LC, Goodman WK, Price LH. Physical symptoms associated with paroxetine discontinuation. Am J Psychiatry 1994;151(2):289.-
13. Schatzberg AF, Haddad P, Kaplan EM, et al. for the Discontinuation Consensus Panel Possible biological mechanisms of the serotonin reuptake inhibitor discontinuation syndrome. J Clin Psychiatry 1997;58(S7):23-7.
14. Shore D. Clinical implications of clozapine discontinuation: report of an NIMH workshop. Schizophr Bull 1995;21(2):333-8.
15. de Leon J, Stanilla JK, White AO, Simpson GM. Anticholinergics to treat clozapine withdrawal. J Clin Psychiatry 1994;55(3):119-20.
16. Rosebush PI, Kennedy K, Dalton B, Mazurek MF. Protracted akathisia after risperidone withdrawal. Am J Psychiatry 1997;154(3):437-8.
17. Llorca PM, Vaiva G, Lancon C. Supersensitivity psychosis in patients with schizophrenia after sudden olanzapine withdrawal. Can J Psychiatry 2001;46(1):87-8.
18. Nayudu SK, Scheftner WA. Case report of withdrawal syndrome after olanzapine discontinuation. J Clin Psychopharmacol 2000;20:489-90.
19. Thurstone CC, Alahi P. A possible case of quetiapine withdrawal syndrome. J Clin Psychiatry 2000;61:602-3.
20. Kim DR, Staab JP. Quetiapine discontinuation syndrome. Am J Psychiatry 2005 May;162(5):1020.-
21. McLean W, Ariano R. Benzodiazepine withdrawal schedule and symptoms In: Klasco RK (ed). DRUGDEX® System (vol. 124). Greenwood Village, CO: Thomson Micromedex, 2005.
22. Greenblatt DJ, Miller LG, Shader RI. Benzodiazepine discontinuation syndromes. J Psychiatr Res 1990;24(S2):73-9.
23. Rickels K, Schweizer E, Case WG, Greenblatt DJ. Long-term therapeutic use of benzodiazepines. I. Effects of abrupt discontinuation. Arch Gen Psychiatry 1990;47(10):899-907.
24. Lejoyeux M, Ades J, Mourad I, et al. Antidepressant withdrawal syndrome: recognition, prevalence and management. CNS Drugs 1996;5:278-92.
25. Rosenbaum JF, Zajecka J. Clinical management of antidepressant discontinuation. J Clin Psychiatry 1997;58(S7):37-40.
26. Paxil (paroxetine) package labeling GlaxoSmithKline, 2002.
27. Keuthen NJ, Cyr P, Ricciardi JA, et al. Medication withdrawal symptoms in obsessive-compulsive disorder patients treated with paroxetine. J Clin Psychopharmacol 1994;14(3):206-7.
28. Dallal A, Chouinard G. Withdrawal and rebound symptoms associated with abrupt discontinuation of venlafaxine. J Clin Psychopharmacol 1998;18(4):343-4.
29. American Psychiatric Association Work Group on Panic Disorder Practice guideline for the treatment of patients with panic disorder. Am J Psychiatry 1998;155(S5):1-34.
30. Spitzer RL, Williams JB, Kroenke K, et al. Utility of a new procedure for diagnosing mental disorders in primary care. The PRIME-MD 1000 study. JAMA 1994;272(22):1749-56.
31. Bronheim HE, Fulop G, Kunkel EJ, et al. The Academy of Psychosomatic Medicine practice guidelines for psychiatric consultation in the general medical setting. Psychosomatics 1998;39(4):S8-30.
32. Einarson A, Selby P, Koren G. Abrupt discontinuation of psychotropic drugs during pregnancy: fear of teratogenic risk and impact of counseling. J Psychiatry Neurosci 2001;26(1):44-8.
Treating depression to remission: Target recovery, and give patients back their lives
Remission is considered the standard of treatment for major depression,1-4 but many patients fall short of this goal:
- 25% to 50% of those who respond to treatment have residual symptoms5
- 60% to 70% respond to treatment, but only 20% to 40% achieve remission.6
We offer practical, evidence-based suggestions and resources to help you take more of your patients beyond response to remission and then to recovery (Table 1).7,8
Table 1
Outcomes in depression: Defining the 4 ‘R’s
| Outcome | Definition | Comment |
|---|---|---|
| Response | Clinically significant reduction of symptoms | 50% reduction in symptoms on psychometric scales may leave severely depressed patients with disabling symptoms |
| Remission | Depression resolves completely or nearly completely, with return to baseline function | Score of ≤7 on the HRSD used in many studies; ACNP Task Force defines remission by 9 core depression symptoms in DSM-IV-TR |
| Recovery | Remission lasts for extended time; signifies end of a major depressive episode | ACNP Task Force defines recovery as 4 months of remission |
| Relapse | Return to full symptoms during remission but before recovery; signifies re-emergence of current depressive episode | Residual symptoms during response or remission greatly increase chances of relapse |
| HRSD: Hamilton Rating Scale for Depression | ||
| ACNP: American College of Neuropsychopharmacology | ||
| DSM-IV-TR: Diagnostic and statistical manual of mental disorders, 4th ed., text rev. | ||
| Source: References 7, 8 | ||
Case report: missing the target
Ms. M, age 32, develops depressive symptoms after taking on several new projects in her work as an accountant. At first she notices difficulty falling asleep at night and that she seems tired all day. Typically efficient and neat, she finds herself absently staring at her computer screen while a messy pile of unfinished paperwork accumulates on her desk.
She begins chastising herself for falling behind, yet she feels she will never catch up. When she unexpectedly bursts out sobbing in a board meeting, she knows she needs help.
Ms. M reports that she has been taking fluoxetine, 20 mg/d, for 4 weeks as her primary care physician prescribed, with no improvement. She has no history of depression or other psychiatric illness, is taking no other medication, and has no medical illnesses. Her brother has a history of bipolar disorder.
Initial diagnostic workup includes laboratory tests such as thyroid stimulating hormone, vitamin B12, and folate. All values are within normal limits. Her Hamilton Rating Scale for Depression (HRSD) score is 17, indicating moderate depression.
The psychiatrist increases fluoxetine to 40 mg/d, and after about 3 weeks Ms. M starts feeling better. Her hopelessness lifts, she is more engaged, and her sleep improves, yet she continues to feel sluggish and dazed. Her financial reports contain uncharacteristic errors, and her pace is noticeably slow. Twice her supervisor approaches her about substandard work, then a week later warns that she will lose her job unless she improves.
Barriers to remission. Patient, provider, and health care system barriers prevent patients with major depression from achieving remission (Table 2).3 Patients may feel better with antidepressant therapy but do not recognize and report residual depressive symptoms, such as Ms. M’s fatigue and substandard job performance.
Clinicians also play a role in depression undertreatment. For example, in a study of 239 patients with ≥ 5 depression symptoms,9 28% did not receive treatment consistent with depression management guidelines.
Fava et al10 suggested the following reasons for depression undertreatment: “… clinicians have partial therapeutic targets, neglect residual symptoms, and equate therapeutic response with full remission.” Others have found that physicians may underdose medications or fail to plan treatment in clear phases.11
Table 2
Barriers to remission during depression treatment
| Who and what | Behavior and system problems |
|---|---|
| Patients | Nonadherence to treatment, underreporting of symptoms, satisfaction with suboptimal outcomes, failure to recognize depressive symptoms, underestimating depression severity, limited access to care, reluctance to see a mental health specialist |
| Providers | Medication under-dosing, inadequate treatment duration, inaccurate diagnosis, failure to recognize residual symptoms, limited training in interpersonal skills, inadequate time to evaluate and treat depression, failure to consider psychotherapeutic approaches |
| Health care systems | Limited therapeutic choices, limited number of mental health care visits, restricted access to providers |
| Source: Reference 3 | |
Relapse risk
Increased risk of relapse is perhaps the greatest cost of undertreated major depression. Patients with residual subsyndromal depressive symptoms relapse five times faster than patients in full remission.12
Residual symptoms may be a more powerful relapse predictor than number of past depressive episodes:13
- Chronic mood symptoms for ≥ 2 years double the relapse risk.14
- 50% to 80% of patients in partial remission relapse.15
In a study of patients in recovery from a major depressive episode, 76% (13 of 17) with residual symptoms relapsed within 15 months, compared with 25% (10 of 40) who completely recovered.16
Illness course. After a first major depressive episode, 26 patients with residual subsyndromal symptoms showed a more-severe, chronic illness compared with 70 asymptomatic patients:
- those with residual symptoms had more depression recurrences, with faster relapse and shorter intervals when they felt well
- subsequent depressive episodes occurred >3 times sooner
- well intervals between depressive episodes were 7 times shorter.17
The authors noted that “patients recovering from major depressive episodes with residual subsyndromal depression experience very rapid episode relapse and have strikingly more chronic future courses of illness that are characterized by early and more frequent episode relapses and recurrences.”18 Each major depression recurrence increases the risk of a successive episode.13,19,20
Treatment resistance. Over time, incomplete remission may contribute to treatment resistance,21 although this theory remains untested.
Social health costs
Residual depressive symptoms and impaired psychosocial, interpersonal, and occupational functioning are strongly correlated. In a study of patients who recovered from a major depressive episode, those with residual symptoms scored significantly worse on markers of social performance, relationships, and occupational functioning.6
Psychosocial costs. Compared with the general population, persons with subsyndromal depression have poorer health status and job functioning (as did Ms. M), and greater familial discord, financial strain, irritability, restricted activity, and number of days in bed.22 In 635 patients with chronic depression treated for 12 weeks with imipramine or sertraline:
- nonresponders scored lowest in psychosocial functioning
- responders scored in a mid-range
- remitters scored highest—as well or nearly as well as healthy controls did.23
Occupational costs. Depression leads to workplace absenteeism—twice the rate of nondepressed workers—and less effectiveness. Depressed persons are seven times more likely to be unemployed, employed part-time, or in jobs below their education levels, compared with community samples.24
Medical costs of depressed persons average twice those of the nondepressed,25 and depressed persons use three times as many health care services.26 Depression may increase the risk of:
- cardiac morbidity and mortality
- poor glycemic control in diabetic patients
- HIV progression
- cerebrovascular events
- and overall mortality.
Depression is associated with worse outcomes after myocardial infarction and among nursing home patients, stroke patients, and those with cancer or HIV infection.21
How to improve remission rates
To improve remission rates, we recommend that you follow a rational treatment progression and observe established guidelines, as described in the follow-up report on Ms. M:
Case continued: Part way there. Back at the psychiatrist’s office for 30-day medication monitoring, Ms. M reports that increasing her antidepressant has worked—no more crying in meetings or feeling down on herself. She even sleeps better. Her HRSD score is now 10, indicating improvement, though with some residual symptoms.
When the psychiatrist asks about her job performance, Ms. M is surprised to learn that her fatigue and disorganized thoughts might be lingering features of depression. She said she thought she just wasn’t trying hard enough.
Following practice guidelines,27 the psychiatrist increases fluoxetine to 60 mg/d. This higher dosage remains less than the maximum recommended 80 mg/d, and Ms. M has shown partial improvement with fluoxetine.
Patients being treated for depression need adequate follow-up to ensure they are improving. As with Ms. M, encourage patients to describe residual symptoms and functional domains that remain suboptimal. Educate them about the importance of taking antidepressants as prescribed ( Box). If poor response continues, address possible nonadherence.
Use objective assessments. Global, haphazard, or subjective assessments of patient progress can miss important ongoing depressive symptoms. We recommend using patient- or clinician-rated symptom scales to rapidly identify and monitor residual symptoms ( Table 3).
You may wish to design your own questionnaires to elicit easily missed data or symptoms particular to a certain treatment—such as common side effects of the medication a patient is taking. Nurses or other providers in a busy practice can help assess patients between or before doctor visits.
Keep in mind that the common practice of defining treatment response as a 50% reduction in HRSD scores7,8 leaves many patients with residual depressive symptoms. For example, an HRSD score reduction from 32 to 16 would signify treatment response, but this patient would remain quite depressed.
- Full remission from depression is the treatment goal, and any lesser outcome requires further attention
- Finding the proper medication may require trial and error, and several weeks may pass before a drug’s therapeutic effect occurs
- Continuing to take the medication as prescribed is important to achieving remission
- Medication may have predictable side effects
Table 3
Useful scales to identify and monitor depressive symptoms
| Scale | Administration | Features |
|---|---|---|
| Hamilton Rating Scale for Depression (21- or 17-item HRSD versions) | 15 to 20 minutes, clinician-rated | Focuses on somatic symptoms, excellent reliability, often used to evaluate response to medications |
| Beck Depression Inventory (BDI versions I or II) | 5 to 10 minutes, self-administered | Focuses on behavioral and cognitive elements (somatic symptoms added to BDI-II), good for measuring depression severity, not for depression screening |
| Zung Self-Rating Depression Scale | 5 to 10 minutes, self-administered | Good for screening, not studied as extensively as Hamilton and Beck scales |
| Montgomery-Asberg Depression Rating Scale | 5 to 10 minutes, clinician-rated | 10 items, often used in research |
A Stepwise approach
An expert panel recommends a stepwise approach for patients who respond inadequately to initial antidepressant therapy (Algorithm).27
Re-evaluate the diagnosis. Patients with bipolar disorder or comorbid medical or psychiatric disorders may need medications other than antidepressants. Address concomitant substance abuse, which may interfere with depression treatment. Also exclude or appropriately treat depressive symptoms associated with general medical conditions, such as hypothyroidism.
Optimize dosages. Consider increasing medication dosages as needed until limited by side effects or the drug’s safety profile. Before exceeding an FDA-recommended dosage (Table 4), obtain the patient’s informed consent and document this discussion in the chart.
Consider augmenting or switching. For patients who continue to show partial response, consider combining the initial medication with another antidepressant or augment with another agent, such as lithium, stimulants, thyroid hormone, or even atypical antipsychotics. For patients with no response to optimal dosages of the initial medication after 3 to 4 weeks, try switching to another antidepressant—not necessarily in a different class. One switch within the same class is reasonable.
Some authors emphasize the choice of antidepressant in attaining remission. Although no antidepressant is clearly more efficacious than another, those with fewer side effects (such as selective serotonin reuptake inhibitors vs. tricyclics) may improve adherence.
Numerous trials have shown higher remission rates with serotonin/norepinephrine reuptake inhibitors such as venlafaxine or duloxetine than with other antidepressants.28-30 This evidence is not universally accepted, however.31 Depressive illness probably has a heterogeneous biology, and with greater understanding we may eventually tailor treatment to individual patients’ needs.
Consider psychotherapy or ECT. Patients who do not achieve remission with medication may be candidates for combined treatment with psychotherapy or electroconvulsive therapy (ECT). Life issues—such as family or work stressors—may need to be addressed along with depressive symptoms.
Algorithm A stepwise approach to remission when antidepressant therapy falls short
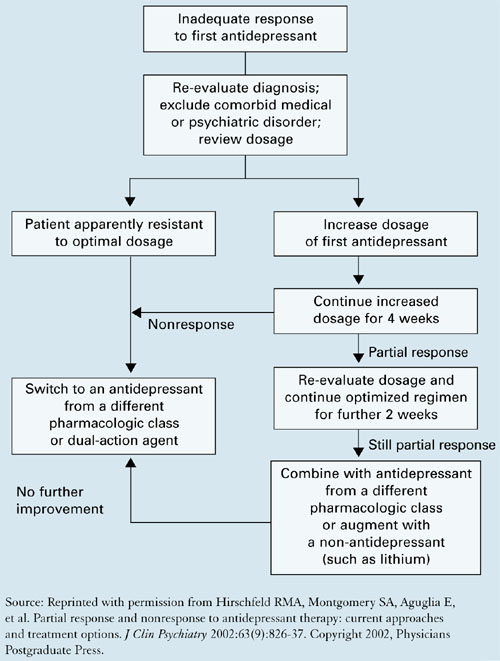
Table 4
Using common antidepressants for adults with major depression
| FDA-approved maximum dosage* | |||
|---|---|---|---|
| Antidepressant mg/d | mg/d | (mg/kg/d) | Common side effects at maximum dosage* |
| SSRIs | |||
| Citalopram | 80 | (1.0) | Nausea, dry mouth, somnolence |
| Escitalopram | 20 | Nausea, delayed ejaculation, insomnia | |
| Fluoxetine | 80 | (1.33) | Nausea, headache, insomnia |
| Paroxetine | 50 | (0.83) | Nausea, somnolence, headache |
| Sertraline | 200 | (3.33) | Nausea, headache, insomnia |
| SNRIs | |||
| Duloxetine | 120 | Nausea, dry mouth, fatigue | |
| Venlafaxine | 375 | (6.25) | Nausea, somnolence, dry mouth |
| Tricyclics | |||
| Amitriptyline | 300 | (5.0) | Drowsiness, dry mouth, dizziness |
| Desipramine | 300 | (5.0) | Same as above |
| Imipramine | 300 | Same as above | |
| Nortriptyline | 200 | (1.67) | Same as above |
| Others | |||
| Bupropion | 450 | (7.5) | Insomnia, dry mouth, headache |
| Mirtazapine | 45 | (0.75) | Somnolence, dry mouth, increased appetite |
| SSRIs: selective serotonin reuptake inhibitors | |||
| SNRIs: serotonin-norepinephrine reuptake inhibitors | |||
| * Informed consent discussion and documentation is recommended for dosages that exceed FDA-approved maximums. | |||
| Sources: Food and Drug Administration, and Kaplan HI, Sadock B. Kaplan & Sadock’s synopsis of psychiatry (9th ed). Philadelphia: Lippincott Williams & Wilkins, 2002. | |||
Case: monitoring after remission
Ms. M feels back to normal 2 weeks after starting fluoxetine at 60 mg/d. She experienced some transient nausea and headache at this dosage but did not stop the medication because her psychiatrist had told her these side effects might occur.
Ms. M also agrees to short-term psychotherapy to address self-esteem issues that may have contributed to her depressive episode. She soon files the mountain of papers on her desk and corrects erroneous financial statements she has made. Her supervisor is relieved—and so is she.
The psychiatrist schedules monthly medication monitoring and plans to gradually reduce the fluoxetine dosage if depressive symptoms remain in remission for 6 months. Because Ms. M had no past depressive episodes, the medication trial may not need to be extended past 6 months.
Related resources
- McManamy J. McMan’s Depression and Bipolar Web. Treating to remission. http://www.mcmanweb.com/article-181.htm.
- American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder (2nd ed.). http://www.psych.org/psych_pract/treatg/pg/Depression2e.book.cfm.
- Stahl S. Essential psychopharmacology: Neuroscientific basis and practical applications (2nd ed.). Cambridge, UK: Cambridge University Presss, 2004, chapters 5-7.
Drug brand names
- Amitriptyline • Elavil, Endep
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Desipramine • Norpramin
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Imipramine • Tofranil
- Mirtazapine • Remeron
- Nortriptyline • Pamelor
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosures
Dr. Van Rhoads reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Gelenberg receives research grants from Pfizer Inc. and Novartis Pharmaceuticals Corp. He is a consultant or a speaker for Eli Lilly and Co., Pfizer Inc., Bristol-Myers Squibb Co., AstraZeneca Pharmaceuticals, Wyeth, GlaxoSmithKline, and Cyberonics.
1. Agency for Health Care Policy and Research. Clinical practice guideline, number 5: Depression in primary care: vol. 2. Treatment of major depression. AHCPR publication 93-0551. Rockville, MD: US Department of Health and Human Services, 1993.
2. American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder. Am J Psychiatry 2000;157(suppl 4):1-45.
3. Hirschfeld RM, Keller MB, Panico BS, et al. The National Depressive and Manic-Depressive Association consensus statement on the undertreatment of depression. JAMA 1997;277:333-40.
4. Crismon ML, Trivedi M, Pigott TA, et al. The Texas Medication Algorithm Project: Report of the Texas Consensus Conference Panel on medication treatment of major depressive disorder. J Clin Psychiatry 1999;60:142-56.
5. Nierenberg AA, Keefe BR, Leslie VA, et al. Residual symptoms in depressed patients who respond acutely to fluoxetine. J Clin Psychiatry 1999;60:221-5.
6. Kennedy N, Paykel ES. Residual symptoms at remission from depression: impact on long-term outcome. J Affect Disord 2004;80(2-3):135-44.
7. Rush AJ, Kraemer HC, Sackeim HA, et al. Report by the ACNP Task Force on Response and Remission in Major Depressive Disorder. Submitted for publication.
8. Keller M. Past, present, and future directions for defining optimal treatment outcome in depression: remission and beyond. JAMA 2003;289(23):3152-60.
9. Nutting P, Rost K, Diceinson M, et al. Barriers to initiating depression treatment in primary care practice. J Gen Intern Med 2002;17:103-11.
10. Fava GA, Rafanelli C, Grandi S, et al. Letter to the editor. Arch Gen Psychiatry 1999;56:765.-
11. Ramana R, Paykel ES, Cooper Z, et al. Remission and relapse in major depression: a two year prospective follow-up study. Psychol Med 1995;25(6):1171-80.
12. Judd LL, Akiskal HS, Maser JD, et al. Major depressive disorder: a prospective study of residual subthreshold depressive symptoms as a predictor of rapid relapse. J Affect Disord 1999;50:97-108.
13. Pintor L, Gastó G, Navarro V, et al. Relapse of major depression after complete and partial remission during a 2-year follow-up. J Affect Disord 2003;73:237-44.
14. Lin E, Katon W, Von Korff M, et al. Relapse of depression in primary care: rate and clinical predictors. Arch Fam Med 1998;7(5):443-9.
15. Cornwall P, Scott J. Partial remission in depressive disorders. Acta Psychiatr Scand 1997;95(4):265-71.
16. Paykel ES, Ramana R, Cooper Z, et al. Residual symptoms after partial remission: an important outcome in depression. Psychol Med 1995;25(6):1171-80.
17. Judd LL, Paulus MJ, Schettler PJ, et al. Does incomplete recovery from first lifetime major depressive episode herald a chronic course of illness? Am J Psychiatry 2000;157(9):1501-4.
18. Judd LL, Paulus MP, Zeller P. The role of residual subthreshold depressive symptoms in early episode relapse in unipolar major depressive disorder. Arch Gen Psychiatry 1999;56(8):764-5.
19. Solomon DA, Keller MB, Leon AC, et al. Multiple recurrences of major depressive disorder. Am J Psychiatry 2000;157(2):229-33.
20. Kennedy N, Paykel ES. Residual symptoms at remission from depression: impact on long-term outcome. J Affect Disord 2004;80(2-3):135-44.
21. Zajecka JM. Treating depression to remission. J Clin Psychiatry 2003;64(suppl 15):7-12.
22. Judd LL, Paulus MP, Wells KB, Rapaport MH. Socioeconomic burden of subsyndromal depressive symptoms and major depressionin a sample of the general population. Am J Psychiatry 1996;153(11):1411-7.
23. Miller IW, Keitner GI, Schatzberg AF, et al. The treatment of chronic depression, part 3: psychosocial functioning before and after treatment with sertraline or imipramine. J Clin Psychiatry 1998;59(11):608-19.
24. Druss B, Schlesinger M, Allen H. Depressive symptoms, satisfaction with health care, and 2-year work outcomes in an employed population. Am J Psychiatry 2001;158(5):731-4.
25. Simon G, Ormel J, VonKorff M, et al. Health care costs associated with depressive and anxiety disorders in primary care. Am J Psychiatry 1995;152(3):352-7.
26. Katon W, Schulberg H. Epidemiology of depression in primary care. Gen Hosp Psychiatry 1992;14(4):237-47.
27. Hirschfeld RMA, Montgomery SA, Aguglia E, et al. Partial response and nonresponse to antidepressant therapy: current approaches and treatment options. J Clin Psychiatry 2002;63(9):826-37.
28. Thase ME, Entsuah AR, Rudolph RL. Remission rates during treatment with venlafaxine or selective serotonin reuptake inhibitors. Br J Psychiatry 2001;178:234-41.
29. Kelsey J, Entsuah R. Venlafaxine offers significant therapeutic benefits over existing SSRI treatments irrespective of the patient’s depressive duration (poster presentation). Montreal: Collegium Internationale Neuropsychopharmacologicum, June 2002.
30. Thase ME. Effectiveness of antidepressants: comparative remission rates. J Clin Psychiatry 2003;64(suppl 2):3-7.
31. Shelton C. Long-term management of major depressive disorder: are differences among antidepressant treatments meaningful? J Clin Psychiatry 2004;65(suppl 17):29-33.
Remission is considered the standard of treatment for major depression,1-4 but many patients fall short of this goal:
- 25% to 50% of those who respond to treatment have residual symptoms5
- 60% to 70% respond to treatment, but only 20% to 40% achieve remission.6
We offer practical, evidence-based suggestions and resources to help you take more of your patients beyond response to remission and then to recovery (Table 1).7,8
Table 1
Outcomes in depression: Defining the 4 ‘R’s
| Outcome | Definition | Comment |
|---|---|---|
| Response | Clinically significant reduction of symptoms | 50% reduction in symptoms on psychometric scales may leave severely depressed patients with disabling symptoms |
| Remission | Depression resolves completely or nearly completely, with return to baseline function | Score of ≤7 on the HRSD used in many studies; ACNP Task Force defines remission by 9 core depression symptoms in DSM-IV-TR |
| Recovery | Remission lasts for extended time; signifies end of a major depressive episode | ACNP Task Force defines recovery as 4 months of remission |
| Relapse | Return to full symptoms during remission but before recovery; signifies re-emergence of current depressive episode | Residual symptoms during response or remission greatly increase chances of relapse |
| HRSD: Hamilton Rating Scale for Depression | ||
| ACNP: American College of Neuropsychopharmacology | ||
| DSM-IV-TR: Diagnostic and statistical manual of mental disorders, 4th ed., text rev. | ||
| Source: References 7, 8 | ||
Case report: missing the target
Ms. M, age 32, develops depressive symptoms after taking on several new projects in her work as an accountant. At first she notices difficulty falling asleep at night and that she seems tired all day. Typically efficient and neat, she finds herself absently staring at her computer screen while a messy pile of unfinished paperwork accumulates on her desk.
She begins chastising herself for falling behind, yet she feels she will never catch up. When she unexpectedly bursts out sobbing in a board meeting, she knows she needs help.
Ms. M reports that she has been taking fluoxetine, 20 mg/d, for 4 weeks as her primary care physician prescribed, with no improvement. She has no history of depression or other psychiatric illness, is taking no other medication, and has no medical illnesses. Her brother has a history of bipolar disorder.
Initial diagnostic workup includes laboratory tests such as thyroid stimulating hormone, vitamin B12, and folate. All values are within normal limits. Her Hamilton Rating Scale for Depression (HRSD) score is 17, indicating moderate depression.
The psychiatrist increases fluoxetine to 40 mg/d, and after about 3 weeks Ms. M starts feeling better. Her hopelessness lifts, she is more engaged, and her sleep improves, yet she continues to feel sluggish and dazed. Her financial reports contain uncharacteristic errors, and her pace is noticeably slow. Twice her supervisor approaches her about substandard work, then a week later warns that she will lose her job unless she improves.
Barriers to remission. Patient, provider, and health care system barriers prevent patients with major depression from achieving remission (Table 2).3 Patients may feel better with antidepressant therapy but do not recognize and report residual depressive symptoms, such as Ms. M’s fatigue and substandard job performance.
Clinicians also play a role in depression undertreatment. For example, in a study of 239 patients with ≥ 5 depression symptoms,9 28% did not receive treatment consistent with depression management guidelines.
Fava et al10 suggested the following reasons for depression undertreatment: “… clinicians have partial therapeutic targets, neglect residual symptoms, and equate therapeutic response with full remission.” Others have found that physicians may underdose medications or fail to plan treatment in clear phases.11
Table 2
Barriers to remission during depression treatment
| Who and what | Behavior and system problems |
|---|---|
| Patients | Nonadherence to treatment, underreporting of symptoms, satisfaction with suboptimal outcomes, failure to recognize depressive symptoms, underestimating depression severity, limited access to care, reluctance to see a mental health specialist |
| Providers | Medication under-dosing, inadequate treatment duration, inaccurate diagnosis, failure to recognize residual symptoms, limited training in interpersonal skills, inadequate time to evaluate and treat depression, failure to consider psychotherapeutic approaches |
| Health care systems | Limited therapeutic choices, limited number of mental health care visits, restricted access to providers |
| Source: Reference 3 | |
Relapse risk
Increased risk of relapse is perhaps the greatest cost of undertreated major depression. Patients with residual subsyndromal depressive symptoms relapse five times faster than patients in full remission.12
Residual symptoms may be a more powerful relapse predictor than number of past depressive episodes:13
- Chronic mood symptoms for ≥ 2 years double the relapse risk.14
- 50% to 80% of patients in partial remission relapse.15
In a study of patients in recovery from a major depressive episode, 76% (13 of 17) with residual symptoms relapsed within 15 months, compared with 25% (10 of 40) who completely recovered.16
Illness course. After a first major depressive episode, 26 patients with residual subsyndromal symptoms showed a more-severe, chronic illness compared with 70 asymptomatic patients:
- those with residual symptoms had more depression recurrences, with faster relapse and shorter intervals when they felt well
- subsequent depressive episodes occurred >3 times sooner
- well intervals between depressive episodes were 7 times shorter.17
The authors noted that “patients recovering from major depressive episodes with residual subsyndromal depression experience very rapid episode relapse and have strikingly more chronic future courses of illness that are characterized by early and more frequent episode relapses and recurrences.”18 Each major depression recurrence increases the risk of a successive episode.13,19,20
Treatment resistance. Over time, incomplete remission may contribute to treatment resistance,21 although this theory remains untested.
Social health costs
Residual depressive symptoms and impaired psychosocial, interpersonal, and occupational functioning are strongly correlated. In a study of patients who recovered from a major depressive episode, those with residual symptoms scored significantly worse on markers of social performance, relationships, and occupational functioning.6
Psychosocial costs. Compared with the general population, persons with subsyndromal depression have poorer health status and job functioning (as did Ms. M), and greater familial discord, financial strain, irritability, restricted activity, and number of days in bed.22 In 635 patients with chronic depression treated for 12 weeks with imipramine or sertraline:
- nonresponders scored lowest in psychosocial functioning
- responders scored in a mid-range
- remitters scored highest—as well or nearly as well as healthy controls did.23
Occupational costs. Depression leads to workplace absenteeism—twice the rate of nondepressed workers—and less effectiveness. Depressed persons are seven times more likely to be unemployed, employed part-time, or in jobs below their education levels, compared with community samples.24
Medical costs of depressed persons average twice those of the nondepressed,25 and depressed persons use three times as many health care services.26 Depression may increase the risk of:
- cardiac morbidity and mortality
- poor glycemic control in diabetic patients
- HIV progression
- cerebrovascular events
- and overall mortality.
Depression is associated with worse outcomes after myocardial infarction and among nursing home patients, stroke patients, and those with cancer or HIV infection.21
How to improve remission rates
To improve remission rates, we recommend that you follow a rational treatment progression and observe established guidelines, as described in the follow-up report on Ms. M:
Case continued: Part way there. Back at the psychiatrist’s office for 30-day medication monitoring, Ms. M reports that increasing her antidepressant has worked—no more crying in meetings or feeling down on herself. She even sleeps better. Her HRSD score is now 10, indicating improvement, though with some residual symptoms.
When the psychiatrist asks about her job performance, Ms. M is surprised to learn that her fatigue and disorganized thoughts might be lingering features of depression. She said she thought she just wasn’t trying hard enough.
Following practice guidelines,27 the psychiatrist increases fluoxetine to 60 mg/d. This higher dosage remains less than the maximum recommended 80 mg/d, and Ms. M has shown partial improvement with fluoxetine.
Patients being treated for depression need adequate follow-up to ensure they are improving. As with Ms. M, encourage patients to describe residual symptoms and functional domains that remain suboptimal. Educate them about the importance of taking antidepressants as prescribed ( Box). If poor response continues, address possible nonadherence.
Use objective assessments. Global, haphazard, or subjective assessments of patient progress can miss important ongoing depressive symptoms. We recommend using patient- or clinician-rated symptom scales to rapidly identify and monitor residual symptoms ( Table 3).
You may wish to design your own questionnaires to elicit easily missed data or symptoms particular to a certain treatment—such as common side effects of the medication a patient is taking. Nurses or other providers in a busy practice can help assess patients between or before doctor visits.
Keep in mind that the common practice of defining treatment response as a 50% reduction in HRSD scores7,8 leaves many patients with residual depressive symptoms. For example, an HRSD score reduction from 32 to 16 would signify treatment response, but this patient would remain quite depressed.
- Full remission from depression is the treatment goal, and any lesser outcome requires further attention
- Finding the proper medication may require trial and error, and several weeks may pass before a drug’s therapeutic effect occurs
- Continuing to take the medication as prescribed is important to achieving remission
- Medication may have predictable side effects
Table 3
Useful scales to identify and monitor depressive symptoms
| Scale | Administration | Features |
|---|---|---|
| Hamilton Rating Scale for Depression (21- or 17-item HRSD versions) | 15 to 20 minutes, clinician-rated | Focuses on somatic symptoms, excellent reliability, often used to evaluate response to medications |
| Beck Depression Inventory (BDI versions I or II) | 5 to 10 minutes, self-administered | Focuses on behavioral and cognitive elements (somatic symptoms added to BDI-II), good for measuring depression severity, not for depression screening |
| Zung Self-Rating Depression Scale | 5 to 10 minutes, self-administered | Good for screening, not studied as extensively as Hamilton and Beck scales |
| Montgomery-Asberg Depression Rating Scale | 5 to 10 minutes, clinician-rated | 10 items, often used in research |
A Stepwise approach
An expert panel recommends a stepwise approach for patients who respond inadequately to initial antidepressant therapy (Algorithm).27
Re-evaluate the diagnosis. Patients with bipolar disorder or comorbid medical or psychiatric disorders may need medications other than antidepressants. Address concomitant substance abuse, which may interfere with depression treatment. Also exclude or appropriately treat depressive symptoms associated with general medical conditions, such as hypothyroidism.
Optimize dosages. Consider increasing medication dosages as needed until limited by side effects or the drug’s safety profile. Before exceeding an FDA-recommended dosage (Table 4), obtain the patient’s informed consent and document this discussion in the chart.
Consider augmenting or switching. For patients who continue to show partial response, consider combining the initial medication with another antidepressant or augment with another agent, such as lithium, stimulants, thyroid hormone, or even atypical antipsychotics. For patients with no response to optimal dosages of the initial medication after 3 to 4 weeks, try switching to another antidepressant—not necessarily in a different class. One switch within the same class is reasonable.
Some authors emphasize the choice of antidepressant in attaining remission. Although no antidepressant is clearly more efficacious than another, those with fewer side effects (such as selective serotonin reuptake inhibitors vs. tricyclics) may improve adherence.
Numerous trials have shown higher remission rates with serotonin/norepinephrine reuptake inhibitors such as venlafaxine or duloxetine than with other antidepressants.28-30 This evidence is not universally accepted, however.31 Depressive illness probably has a heterogeneous biology, and with greater understanding we may eventually tailor treatment to individual patients’ needs.
Consider psychotherapy or ECT. Patients who do not achieve remission with medication may be candidates for combined treatment with psychotherapy or electroconvulsive therapy (ECT). Life issues—such as family or work stressors—may need to be addressed along with depressive symptoms.
Algorithm A stepwise approach to remission when antidepressant therapy falls short
Table 4
Using common antidepressants for adults with major depression
| FDA-approved maximum dosage* | |||
|---|---|---|---|
| Antidepressant mg/d | mg/d | (mg/kg/d) | Common side effects at maximum dosage* |
| SSRIs | |||
| Citalopram | 80 | (1.0) | Nausea, dry mouth, somnolence |
| Escitalopram | 20 | Nausea, delayed ejaculation, insomnia | |
| Fluoxetine | 80 | (1.33) | Nausea, headache, insomnia |
| Paroxetine | 50 | (0.83) | Nausea, somnolence, headache |
| Sertraline | 200 | (3.33) | Nausea, headache, insomnia |
| SNRIs | |||
| Duloxetine | 120 | Nausea, dry mouth, fatigue | |
| Venlafaxine | 375 | (6.25) | Nausea, somnolence, dry mouth |
| Tricyclics | |||
| Amitriptyline | 300 | (5.0) | Drowsiness, dry mouth, dizziness |
| Desipramine | 300 | (5.0) | Same as above |
| Imipramine | 300 | Same as above | |
| Nortriptyline | 200 | (1.67) | Same as above |
| Others | |||
| Bupropion | 450 | (7.5) | Insomnia, dry mouth, headache |
| Mirtazapine | 45 | (0.75) | Somnolence, dry mouth, increased appetite |
| SSRIs: selective serotonin reuptake inhibitors | |||
| SNRIs: serotonin-norepinephrine reuptake inhibitors | |||
| * Informed consent discussion and documentation is recommended for dosages that exceed FDA-approved maximums. | |||
| Sources: Food and Drug Administration, and Kaplan HI, Sadock B. Kaplan & Sadock’s synopsis of psychiatry (9th ed). Philadelphia: Lippincott Williams & Wilkins, 2002. | |||
Case: monitoring after remission
Ms. M feels back to normal 2 weeks after starting fluoxetine at 60 mg/d. She experienced some transient nausea and headache at this dosage but did not stop the medication because her psychiatrist had told her these side effects might occur.
Ms. M also agrees to short-term psychotherapy to address self-esteem issues that may have contributed to her depressive episode. She soon files the mountain of papers on her desk and corrects erroneous financial statements she has made. Her supervisor is relieved—and so is she.
The psychiatrist schedules monthly medication monitoring and plans to gradually reduce the fluoxetine dosage if depressive symptoms remain in remission for 6 months. Because Ms. M had no past depressive episodes, the medication trial may not need to be extended past 6 months.
Related resources
- McManamy J. McMan’s Depression and Bipolar Web. Treating to remission. http://www.mcmanweb.com/article-181.htm.
- American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder (2nd ed.). http://www.psych.org/psych_pract/treatg/pg/Depression2e.book.cfm.
- Stahl S. Essential psychopharmacology: Neuroscientific basis and practical applications (2nd ed.). Cambridge, UK: Cambridge University Presss, 2004, chapters 5-7.
Drug brand names
- Amitriptyline • Elavil, Endep
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Desipramine • Norpramin
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Imipramine • Tofranil
- Mirtazapine • Remeron
- Nortriptyline • Pamelor
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosures
Dr. Van Rhoads reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Gelenberg receives research grants from Pfizer Inc. and Novartis Pharmaceuticals Corp. He is a consultant or a speaker for Eli Lilly and Co., Pfizer Inc., Bristol-Myers Squibb Co., AstraZeneca Pharmaceuticals, Wyeth, GlaxoSmithKline, and Cyberonics.
Remission is considered the standard of treatment for major depression,1-4 but many patients fall short of this goal:
- 25% to 50% of those who respond to treatment have residual symptoms5
- 60% to 70% respond to treatment, but only 20% to 40% achieve remission.6
We offer practical, evidence-based suggestions and resources to help you take more of your patients beyond response to remission and then to recovery (Table 1).7,8
Table 1
Outcomes in depression: Defining the 4 ‘R’s
| Outcome | Definition | Comment |
|---|---|---|
| Response | Clinically significant reduction of symptoms | 50% reduction in symptoms on psychometric scales may leave severely depressed patients with disabling symptoms |
| Remission | Depression resolves completely or nearly completely, with return to baseline function | Score of ≤7 on the HRSD used in many studies; ACNP Task Force defines remission by 9 core depression symptoms in DSM-IV-TR |
| Recovery | Remission lasts for extended time; signifies end of a major depressive episode | ACNP Task Force defines recovery as 4 months of remission |
| Relapse | Return to full symptoms during remission but before recovery; signifies re-emergence of current depressive episode | Residual symptoms during response or remission greatly increase chances of relapse |
| HRSD: Hamilton Rating Scale for Depression | ||
| ACNP: American College of Neuropsychopharmacology | ||
| DSM-IV-TR: Diagnostic and statistical manual of mental disorders, 4th ed., text rev. | ||
| Source: References 7, 8 | ||
Case report: missing the target
Ms. M, age 32, develops depressive symptoms after taking on several new projects in her work as an accountant. At first she notices difficulty falling asleep at night and that she seems tired all day. Typically efficient and neat, she finds herself absently staring at her computer screen while a messy pile of unfinished paperwork accumulates on her desk.
She begins chastising herself for falling behind, yet she feels she will never catch up. When she unexpectedly bursts out sobbing in a board meeting, she knows she needs help.
Ms. M reports that she has been taking fluoxetine, 20 mg/d, for 4 weeks as her primary care physician prescribed, with no improvement. She has no history of depression or other psychiatric illness, is taking no other medication, and has no medical illnesses. Her brother has a history of bipolar disorder.
Initial diagnostic workup includes laboratory tests such as thyroid stimulating hormone, vitamin B12, and folate. All values are within normal limits. Her Hamilton Rating Scale for Depression (HRSD) score is 17, indicating moderate depression.
The psychiatrist increases fluoxetine to 40 mg/d, and after about 3 weeks Ms. M starts feeling better. Her hopelessness lifts, she is more engaged, and her sleep improves, yet she continues to feel sluggish and dazed. Her financial reports contain uncharacteristic errors, and her pace is noticeably slow. Twice her supervisor approaches her about substandard work, then a week later warns that she will lose her job unless she improves.
Barriers to remission. Patient, provider, and health care system barriers prevent patients with major depression from achieving remission (Table 2).3 Patients may feel better with antidepressant therapy but do not recognize and report residual depressive symptoms, such as Ms. M’s fatigue and substandard job performance.
Clinicians also play a role in depression undertreatment. For example, in a study of 239 patients with ≥ 5 depression symptoms,9 28% did not receive treatment consistent with depression management guidelines.
Fava et al10 suggested the following reasons for depression undertreatment: “… clinicians have partial therapeutic targets, neglect residual symptoms, and equate therapeutic response with full remission.” Others have found that physicians may underdose medications or fail to plan treatment in clear phases.11
Table 2
Barriers to remission during depression treatment
| Who and what | Behavior and system problems |
|---|---|
| Patients | Nonadherence to treatment, underreporting of symptoms, satisfaction with suboptimal outcomes, failure to recognize depressive symptoms, underestimating depression severity, limited access to care, reluctance to see a mental health specialist |
| Providers | Medication under-dosing, inadequate treatment duration, inaccurate diagnosis, failure to recognize residual symptoms, limited training in interpersonal skills, inadequate time to evaluate and treat depression, failure to consider psychotherapeutic approaches |
| Health care systems | Limited therapeutic choices, limited number of mental health care visits, restricted access to providers |
| Source: Reference 3 | |
Relapse risk
Increased risk of relapse is perhaps the greatest cost of undertreated major depression. Patients with residual subsyndromal depressive symptoms relapse five times faster than patients in full remission.12
Residual symptoms may be a more powerful relapse predictor than number of past depressive episodes:13
- Chronic mood symptoms for ≥ 2 years double the relapse risk.14
- 50% to 80% of patients in partial remission relapse.15
In a study of patients in recovery from a major depressive episode, 76% (13 of 17) with residual symptoms relapsed within 15 months, compared with 25% (10 of 40) who completely recovered.16
Illness course. After a first major depressive episode, 26 patients with residual subsyndromal symptoms showed a more-severe, chronic illness compared with 70 asymptomatic patients:
- those with residual symptoms had more depression recurrences, with faster relapse and shorter intervals when they felt well
- subsequent depressive episodes occurred >3 times sooner
- well intervals between depressive episodes were 7 times shorter.17
The authors noted that “patients recovering from major depressive episodes with residual subsyndromal depression experience very rapid episode relapse and have strikingly more chronic future courses of illness that are characterized by early and more frequent episode relapses and recurrences.”18 Each major depression recurrence increases the risk of a successive episode.13,19,20
Treatment resistance. Over time, incomplete remission may contribute to treatment resistance,21 although this theory remains untested.
Social health costs
Residual depressive symptoms and impaired psychosocial, interpersonal, and occupational functioning are strongly correlated. In a study of patients who recovered from a major depressive episode, those with residual symptoms scored significantly worse on markers of social performance, relationships, and occupational functioning.6
Psychosocial costs. Compared with the general population, persons with subsyndromal depression have poorer health status and job functioning (as did Ms. M), and greater familial discord, financial strain, irritability, restricted activity, and number of days in bed.22 In 635 patients with chronic depression treated for 12 weeks with imipramine or sertraline:
- nonresponders scored lowest in psychosocial functioning
- responders scored in a mid-range
- remitters scored highest—as well or nearly as well as healthy controls did.23
Occupational costs. Depression leads to workplace absenteeism—twice the rate of nondepressed workers—and less effectiveness. Depressed persons are seven times more likely to be unemployed, employed part-time, or in jobs below their education levels, compared with community samples.24
Medical costs of depressed persons average twice those of the nondepressed,25 and depressed persons use three times as many health care services.26 Depression may increase the risk of:
- cardiac morbidity and mortality
- poor glycemic control in diabetic patients
- HIV progression
- cerebrovascular events
- and overall mortality.
Depression is associated with worse outcomes after myocardial infarction and among nursing home patients, stroke patients, and those with cancer or HIV infection.21
How to improve remission rates
To improve remission rates, we recommend that you follow a rational treatment progression and observe established guidelines, as described in the follow-up report on Ms. M:
Case continued: Part way there. Back at the psychiatrist’s office for 30-day medication monitoring, Ms. M reports that increasing her antidepressant has worked—no more crying in meetings or feeling down on herself. She even sleeps better. Her HRSD score is now 10, indicating improvement, though with some residual symptoms.
When the psychiatrist asks about her job performance, Ms. M is surprised to learn that her fatigue and disorganized thoughts might be lingering features of depression. She said she thought she just wasn’t trying hard enough.
Following practice guidelines,27 the psychiatrist increases fluoxetine to 60 mg/d. This higher dosage remains less than the maximum recommended 80 mg/d, and Ms. M has shown partial improvement with fluoxetine.
Patients being treated for depression need adequate follow-up to ensure they are improving. As with Ms. M, encourage patients to describe residual symptoms and functional domains that remain suboptimal. Educate them about the importance of taking antidepressants as prescribed ( Box). If poor response continues, address possible nonadherence.
Use objective assessments. Global, haphazard, or subjective assessments of patient progress can miss important ongoing depressive symptoms. We recommend using patient- or clinician-rated symptom scales to rapidly identify and monitor residual symptoms ( Table 3).
You may wish to design your own questionnaires to elicit easily missed data or symptoms particular to a certain treatment—such as common side effects of the medication a patient is taking. Nurses or other providers in a busy practice can help assess patients between or before doctor visits.
Keep in mind that the common practice of defining treatment response as a 50% reduction in HRSD scores7,8 leaves many patients with residual depressive symptoms. For example, an HRSD score reduction from 32 to 16 would signify treatment response, but this patient would remain quite depressed.
- Full remission from depression is the treatment goal, and any lesser outcome requires further attention
- Finding the proper medication may require trial and error, and several weeks may pass before a drug’s therapeutic effect occurs
- Continuing to take the medication as prescribed is important to achieving remission
- Medication may have predictable side effects
Table 3
Useful scales to identify and monitor depressive symptoms
| Scale | Administration | Features |
|---|---|---|
| Hamilton Rating Scale for Depression (21- or 17-item HRSD versions) | 15 to 20 minutes, clinician-rated | Focuses on somatic symptoms, excellent reliability, often used to evaluate response to medications |
| Beck Depression Inventory (BDI versions I or II) | 5 to 10 minutes, self-administered | Focuses on behavioral and cognitive elements (somatic symptoms added to BDI-II), good for measuring depression severity, not for depression screening |
| Zung Self-Rating Depression Scale | 5 to 10 minutes, self-administered | Good for screening, not studied as extensively as Hamilton and Beck scales |
| Montgomery-Asberg Depression Rating Scale | 5 to 10 minutes, clinician-rated | 10 items, often used in research |
A Stepwise approach
An expert panel recommends a stepwise approach for patients who respond inadequately to initial antidepressant therapy (Algorithm).27
Re-evaluate the diagnosis. Patients with bipolar disorder or comorbid medical or psychiatric disorders may need medications other than antidepressants. Address concomitant substance abuse, which may interfere with depression treatment. Also exclude or appropriately treat depressive symptoms associated with general medical conditions, such as hypothyroidism.
Optimize dosages. Consider increasing medication dosages as needed until limited by side effects or the drug’s safety profile. Before exceeding an FDA-recommended dosage (Table 4), obtain the patient’s informed consent and document this discussion in the chart.
Consider augmenting or switching. For patients who continue to show partial response, consider combining the initial medication with another antidepressant or augment with another agent, such as lithium, stimulants, thyroid hormone, or even atypical antipsychotics. For patients with no response to optimal dosages of the initial medication after 3 to 4 weeks, try switching to another antidepressant—not necessarily in a different class. One switch within the same class is reasonable.
Some authors emphasize the choice of antidepressant in attaining remission. Although no antidepressant is clearly more efficacious than another, those with fewer side effects (such as selective serotonin reuptake inhibitors vs. tricyclics) may improve adherence.
Numerous trials have shown higher remission rates with serotonin/norepinephrine reuptake inhibitors such as venlafaxine or duloxetine than with other antidepressants.28-30 This evidence is not universally accepted, however.31 Depressive illness probably has a heterogeneous biology, and with greater understanding we may eventually tailor treatment to individual patients’ needs.
Consider psychotherapy or ECT. Patients who do not achieve remission with medication may be candidates for combined treatment with psychotherapy or electroconvulsive therapy (ECT). Life issues—such as family or work stressors—may need to be addressed along with depressive symptoms.
Algorithm A stepwise approach to remission when antidepressant therapy falls short
Table 4
Using common antidepressants for adults with major depression
| FDA-approved maximum dosage* | |||
|---|---|---|---|
| Antidepressant mg/d | mg/d | (mg/kg/d) | Common side effects at maximum dosage* |
| SSRIs | |||
| Citalopram | 80 | (1.0) | Nausea, dry mouth, somnolence |
| Escitalopram | 20 | Nausea, delayed ejaculation, insomnia | |
| Fluoxetine | 80 | (1.33) | Nausea, headache, insomnia |
| Paroxetine | 50 | (0.83) | Nausea, somnolence, headache |
| Sertraline | 200 | (3.33) | Nausea, headache, insomnia |
| SNRIs | |||
| Duloxetine | 120 | Nausea, dry mouth, fatigue | |
| Venlafaxine | 375 | (6.25) | Nausea, somnolence, dry mouth |
| Tricyclics | |||
| Amitriptyline | 300 | (5.0) | Drowsiness, dry mouth, dizziness |
| Desipramine | 300 | (5.0) | Same as above |
| Imipramine | 300 | Same as above | |
| Nortriptyline | 200 | (1.67) | Same as above |
| Others | |||
| Bupropion | 450 | (7.5) | Insomnia, dry mouth, headache |
| Mirtazapine | 45 | (0.75) | Somnolence, dry mouth, increased appetite |
| SSRIs: selective serotonin reuptake inhibitors | |||
| SNRIs: serotonin-norepinephrine reuptake inhibitors | |||
| * Informed consent discussion and documentation is recommended for dosages that exceed FDA-approved maximums. | |||
| Sources: Food and Drug Administration, and Kaplan HI, Sadock B. Kaplan & Sadock’s synopsis of psychiatry (9th ed). Philadelphia: Lippincott Williams & Wilkins, 2002. | |||
Case: monitoring after remission
Ms. M feels back to normal 2 weeks after starting fluoxetine at 60 mg/d. She experienced some transient nausea and headache at this dosage but did not stop the medication because her psychiatrist had told her these side effects might occur.
Ms. M also agrees to short-term psychotherapy to address self-esteem issues that may have contributed to her depressive episode. She soon files the mountain of papers on her desk and corrects erroneous financial statements she has made. Her supervisor is relieved—and so is she.
The psychiatrist schedules monthly medication monitoring and plans to gradually reduce the fluoxetine dosage if depressive symptoms remain in remission for 6 months. Because Ms. M had no past depressive episodes, the medication trial may not need to be extended past 6 months.
Related resources
- McManamy J. McMan’s Depression and Bipolar Web. Treating to remission. http://www.mcmanweb.com/article-181.htm.
- American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder (2nd ed.). http://www.psych.org/psych_pract/treatg/pg/Depression2e.book.cfm.
- Stahl S. Essential psychopharmacology: Neuroscientific basis and practical applications (2nd ed.). Cambridge, UK: Cambridge University Presss, 2004, chapters 5-7.
Drug brand names
- Amitriptyline • Elavil, Endep
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Desipramine • Norpramin
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Imipramine • Tofranil
- Mirtazapine • Remeron
- Nortriptyline • Pamelor
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosures
Dr. Van Rhoads reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Gelenberg receives research grants from Pfizer Inc. and Novartis Pharmaceuticals Corp. He is a consultant or a speaker for Eli Lilly and Co., Pfizer Inc., Bristol-Myers Squibb Co., AstraZeneca Pharmaceuticals, Wyeth, GlaxoSmithKline, and Cyberonics.
1. Agency for Health Care Policy and Research. Clinical practice guideline, number 5: Depression in primary care: vol. 2. Treatment of major depression. AHCPR publication 93-0551. Rockville, MD: US Department of Health and Human Services, 1993.
2. American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder. Am J Psychiatry 2000;157(suppl 4):1-45.
3. Hirschfeld RM, Keller MB, Panico BS, et al. The National Depressive and Manic-Depressive Association consensus statement on the undertreatment of depression. JAMA 1997;277:333-40.
4. Crismon ML, Trivedi M, Pigott TA, et al. The Texas Medication Algorithm Project: Report of the Texas Consensus Conference Panel on medication treatment of major depressive disorder. J Clin Psychiatry 1999;60:142-56.
5. Nierenberg AA, Keefe BR, Leslie VA, et al. Residual symptoms in depressed patients who respond acutely to fluoxetine. J Clin Psychiatry 1999;60:221-5.
6. Kennedy N, Paykel ES. Residual symptoms at remission from depression: impact on long-term outcome. J Affect Disord 2004;80(2-3):135-44.
7. Rush AJ, Kraemer HC, Sackeim HA, et al. Report by the ACNP Task Force on Response and Remission in Major Depressive Disorder. Submitted for publication.
8. Keller M. Past, present, and future directions for defining optimal treatment outcome in depression: remission and beyond. JAMA 2003;289(23):3152-60.
9. Nutting P, Rost K, Diceinson M, et al. Barriers to initiating depression treatment in primary care practice. J Gen Intern Med 2002;17:103-11.
10. Fava GA, Rafanelli C, Grandi S, et al. Letter to the editor. Arch Gen Psychiatry 1999;56:765.-
11. Ramana R, Paykel ES, Cooper Z, et al. Remission and relapse in major depression: a two year prospective follow-up study. Psychol Med 1995;25(6):1171-80.
12. Judd LL, Akiskal HS, Maser JD, et al. Major depressive disorder: a prospective study of residual subthreshold depressive symptoms as a predictor of rapid relapse. J Affect Disord 1999;50:97-108.
13. Pintor L, Gastó G, Navarro V, et al. Relapse of major depression after complete and partial remission during a 2-year follow-up. J Affect Disord 2003;73:237-44.
14. Lin E, Katon W, Von Korff M, et al. Relapse of depression in primary care: rate and clinical predictors. Arch Fam Med 1998;7(5):443-9.
15. Cornwall P, Scott J. Partial remission in depressive disorders. Acta Psychiatr Scand 1997;95(4):265-71.
16. Paykel ES, Ramana R, Cooper Z, et al. Residual symptoms after partial remission: an important outcome in depression. Psychol Med 1995;25(6):1171-80.
17. Judd LL, Paulus MJ, Schettler PJ, et al. Does incomplete recovery from first lifetime major depressive episode herald a chronic course of illness? Am J Psychiatry 2000;157(9):1501-4.
18. Judd LL, Paulus MP, Zeller P. The role of residual subthreshold depressive symptoms in early episode relapse in unipolar major depressive disorder. Arch Gen Psychiatry 1999;56(8):764-5.
19. Solomon DA, Keller MB, Leon AC, et al. Multiple recurrences of major depressive disorder. Am J Psychiatry 2000;157(2):229-33.
20. Kennedy N, Paykel ES. Residual symptoms at remission from depression: impact on long-term outcome. J Affect Disord 2004;80(2-3):135-44.
21. Zajecka JM. Treating depression to remission. J Clin Psychiatry 2003;64(suppl 15):7-12.
22. Judd LL, Paulus MP, Wells KB, Rapaport MH. Socioeconomic burden of subsyndromal depressive symptoms and major depressionin a sample of the general population. Am J Psychiatry 1996;153(11):1411-7.
23. Miller IW, Keitner GI, Schatzberg AF, et al. The treatment of chronic depression, part 3: psychosocial functioning before and after treatment with sertraline or imipramine. J Clin Psychiatry 1998;59(11):608-19.
24. Druss B, Schlesinger M, Allen H. Depressive symptoms, satisfaction with health care, and 2-year work outcomes in an employed population. Am J Psychiatry 2001;158(5):731-4.
25. Simon G, Ormel J, VonKorff M, et al. Health care costs associated with depressive and anxiety disorders in primary care. Am J Psychiatry 1995;152(3):352-7.
26. Katon W, Schulberg H. Epidemiology of depression in primary care. Gen Hosp Psychiatry 1992;14(4):237-47.
27. Hirschfeld RMA, Montgomery SA, Aguglia E, et al. Partial response and nonresponse to antidepressant therapy: current approaches and treatment options. J Clin Psychiatry 2002;63(9):826-37.
28. Thase ME, Entsuah AR, Rudolph RL. Remission rates during treatment with venlafaxine or selective serotonin reuptake inhibitors. Br J Psychiatry 2001;178:234-41.
29. Kelsey J, Entsuah R. Venlafaxine offers significant therapeutic benefits over existing SSRI treatments irrespective of the patient’s depressive duration (poster presentation). Montreal: Collegium Internationale Neuropsychopharmacologicum, June 2002.
30. Thase ME. Effectiveness of antidepressants: comparative remission rates. J Clin Psychiatry 2003;64(suppl 2):3-7.
31. Shelton C. Long-term management of major depressive disorder: are differences among antidepressant treatments meaningful? J Clin Psychiatry 2004;65(suppl 17):29-33.
1. Agency for Health Care Policy and Research. Clinical practice guideline, number 5: Depression in primary care: vol. 2. Treatment of major depression. AHCPR publication 93-0551. Rockville, MD: US Department of Health and Human Services, 1993.
2. American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder. Am J Psychiatry 2000;157(suppl 4):1-45.
3. Hirschfeld RM, Keller MB, Panico BS, et al. The National Depressive and Manic-Depressive Association consensus statement on the undertreatment of depression. JAMA 1997;277:333-40.
4. Crismon ML, Trivedi M, Pigott TA, et al. The Texas Medication Algorithm Project: Report of the Texas Consensus Conference Panel on medication treatment of major depressive disorder. J Clin Psychiatry 1999;60:142-56.
5. Nierenberg AA, Keefe BR, Leslie VA, et al. Residual symptoms in depressed patients who respond acutely to fluoxetine. J Clin Psychiatry 1999;60:221-5.
6. Kennedy N, Paykel ES. Residual symptoms at remission from depression: impact on long-term outcome. J Affect Disord 2004;80(2-3):135-44.
7. Rush AJ, Kraemer HC, Sackeim HA, et al. Report by the ACNP Task Force on Response and Remission in Major Depressive Disorder. Submitted for publication.
8. Keller M. Past, present, and future directions for defining optimal treatment outcome in depression: remission and beyond. JAMA 2003;289(23):3152-60.
9. Nutting P, Rost K, Diceinson M, et al. Barriers to initiating depression treatment in primary care practice. J Gen Intern Med 2002;17:103-11.
10. Fava GA, Rafanelli C, Grandi S, et al. Letter to the editor. Arch Gen Psychiatry 1999;56:765.-
11. Ramana R, Paykel ES, Cooper Z, et al. Remission and relapse in major depression: a two year prospective follow-up study. Psychol Med 1995;25(6):1171-80.
12. Judd LL, Akiskal HS, Maser JD, et al. Major depressive disorder: a prospective study of residual subthreshold depressive symptoms as a predictor of rapid relapse. J Affect Disord 1999;50:97-108.
13. Pintor L, Gastó G, Navarro V, et al. Relapse of major depression after complete and partial remission during a 2-year follow-up. J Affect Disord 2003;73:237-44.
14. Lin E, Katon W, Von Korff M, et al. Relapse of depression in primary care: rate and clinical predictors. Arch Fam Med 1998;7(5):443-9.
15. Cornwall P, Scott J. Partial remission in depressive disorders. Acta Psychiatr Scand 1997;95(4):265-71.
16. Paykel ES, Ramana R, Cooper Z, et al. Residual symptoms after partial remission: an important outcome in depression. Psychol Med 1995;25(6):1171-80.
17. Judd LL, Paulus MJ, Schettler PJ, et al. Does incomplete recovery from first lifetime major depressive episode herald a chronic course of illness? Am J Psychiatry 2000;157(9):1501-4.
18. Judd LL, Paulus MP, Zeller P. The role of residual subthreshold depressive symptoms in early episode relapse in unipolar major depressive disorder. Arch Gen Psychiatry 1999;56(8):764-5.
19. Solomon DA, Keller MB, Leon AC, et al. Multiple recurrences of major depressive disorder. Am J Psychiatry 2000;157(2):229-33.
20. Kennedy N, Paykel ES. Residual symptoms at remission from depression: impact on long-term outcome. J Affect Disord 2004;80(2-3):135-44.
21. Zajecka JM. Treating depression to remission. J Clin Psychiatry 2003;64(suppl 15):7-12.
22. Judd LL, Paulus MP, Wells KB, Rapaport MH. Socioeconomic burden of subsyndromal depressive symptoms and major depressionin a sample of the general population. Am J Psychiatry 1996;153(11):1411-7.
23. Miller IW, Keitner GI, Schatzberg AF, et al. The treatment of chronic depression, part 3: psychosocial functioning before and after treatment with sertraline or imipramine. J Clin Psychiatry 1998;59(11):608-19.
24. Druss B, Schlesinger M, Allen H. Depressive symptoms, satisfaction with health care, and 2-year work outcomes in an employed population. Am J Psychiatry 2001;158(5):731-4.
25. Simon G, Ormel J, VonKorff M, et al. Health care costs associated with depressive and anxiety disorders in primary care. Am J Psychiatry 1995;152(3):352-7.
26. Katon W, Schulberg H. Epidemiology of depression in primary care. Gen Hosp Psychiatry 1992;14(4):237-47.
27. Hirschfeld RMA, Montgomery SA, Aguglia E, et al. Partial response and nonresponse to antidepressant therapy: current approaches and treatment options. J Clin Psychiatry 2002;63(9):826-37.
28. Thase ME, Entsuah AR, Rudolph RL. Remission rates during treatment with venlafaxine or selective serotonin reuptake inhibitors. Br J Psychiatry 2001;178:234-41.
29. Kelsey J, Entsuah R. Venlafaxine offers significant therapeutic benefits over existing SSRI treatments irrespective of the patient’s depressive duration (poster presentation). Montreal: Collegium Internationale Neuropsychopharmacologicum, June 2002.
30. Thase ME. Effectiveness of antidepressants: comparative remission rates. J Clin Psychiatry 2003;64(suppl 2):3-7.
31. Shelton C. Long-term management of major depressive disorder: are differences among antidepressant treatments meaningful? J Clin Psychiatry 2004;65(suppl 17):29-33.
A prescription to improve drug regimens?
One day we may be able to consistently choose medications that offer optimal benefit and minimal adverse events—without subjecting our patients to unsuccessful trials. Thanks to quantitative EEG (OEEG) testing and pharmacogenetic testing, that day may be coming closer.
How quantitative eeg works
QEEG adds modern computer and statistical analyses to traditional EEG recordings. The computer creates a graphic display on a schematic map of the head. The procedure is often called brain electrical activity mapping (BEAM) or simply “mapping.” New tool: Genotyping makes prescribing safer, more effective, Current Psychiatry, September 2004.) Physicians can order any combination of gene tests, which cost about $150 to $200 each, or all available tests for a discounted price of approximately $600.
Genelex and Signature Genetics can create individualized CYP-450 function reports to facilitate prescribing and customized reports that take into account the patient’s medication and diet regimen. Genelex also offers an Internet-based software tool, GeneMedRx, which allows doctors to customize medication regimens based on both potential drug-drug interactions and genomic information.
Signature Genetics offers a prospective assessment of drugs based on genetic test results. This assessment provides a comprehensive report of which medications are affected by the test results.
Genetic profiling can help psychiatrists improve the likelihood of treatment success and minimize potential drug-drug interactions and adverse reactions. Patients will be more satisfied, knowing that their medications fit their individual needs. Also, as more is learned about genetic analysis, genetic testing could one day reveal susceptibility to Alzheimer’s disease, heart attack risk, or other medical problems.
As with quantitative EEG, however, few insurance companies cover genetic testing. Also, patients found to have a higher likelihood of developing certain diseases could potentially be charged higher health insurance premiums.
Related resources
Indiana University School of Medicine. Drug interactions table. http://medicine.iupui.edu/flockhart/clinlist.htm
Luo J. Psyber Psychiatry. Prescribing Information: scroll with the changes (online, handheld resources on drug-drug interaction, medications’ effect on CYP-450 system. Current Psychiatry 2003;2(8 online edition). http://www.currentpsychiatry.com/article_pages.asp?AID=666&UID=8877
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
(accessed July 27, 2005)
1. Children’s Hospital Boston. Child Health A to Z. What is qEEG? Available at: http://www.childrenshospital.org/cfapps/A2ZtopicDisplay.cfm?Topic=Quan titative%20EEG
2. UCLA Quantitative EEG Laboratory. QEEG Cordance. Available at: http://www.qeeg.npi.ucla.edu/cordance/
3. Cook IA, Leuchter AF, Witte E, et al. Neurophysiologic predictors of treatment response to fluoxetine in major depression. Psychiatry Res 1999;85:263-73.
4. Cook IA, Leuchter AF, Morgan M, et al. Early changes in prefrontal activity characterize clinical responders to antidepressants. Neuropsychopharmacology 2002;27:120-31.
5. Song DH, Shin DW, Jon DI, Ha EH. Effects of methylphenidate on quantitative EEG of boys with attention-deficit hyperactivity disorder in continuous performance test. Yonsei Med J 2005;46:34-41.
6. Nuwer M. Assessment of digital EEG, quantitative EEG, and EEG brain mapping: report of the American Academy of Neurology and the American Clinical Neurophysiology Society. Neurology 1997;49:277-92.
One day we may be able to consistently choose medications that offer optimal benefit and minimal adverse events—without subjecting our patients to unsuccessful trials. Thanks to quantitative EEG (OEEG) testing and pharmacogenetic testing, that day may be coming closer.
How quantitative eeg works
QEEG adds modern computer and statistical analyses to traditional EEG recordings. The computer creates a graphic display on a schematic map of the head. The procedure is often called brain electrical activity mapping (BEAM) or simply “mapping.” New tool: Genotyping makes prescribing safer, more effective, Current Psychiatry, September 2004.) Physicians can order any combination of gene tests, which cost about $150 to $200 each, or all available tests for a discounted price of approximately $600.
Genelex and Signature Genetics can create individualized CYP-450 function reports to facilitate prescribing and customized reports that take into account the patient’s medication and diet regimen. Genelex also offers an Internet-based software tool, GeneMedRx, which allows doctors to customize medication regimens based on both potential drug-drug interactions and genomic information.
Signature Genetics offers a prospective assessment of drugs based on genetic test results. This assessment provides a comprehensive report of which medications are affected by the test results.
Genetic profiling can help psychiatrists improve the likelihood of treatment success and minimize potential drug-drug interactions and adverse reactions. Patients will be more satisfied, knowing that their medications fit their individual needs. Also, as more is learned about genetic analysis, genetic testing could one day reveal susceptibility to Alzheimer’s disease, heart attack risk, or other medical problems.
As with quantitative EEG, however, few insurance companies cover genetic testing. Also, patients found to have a higher likelihood of developing certain diseases could potentially be charged higher health insurance premiums.
Related resources
Indiana University School of Medicine. Drug interactions table. http://medicine.iupui.edu/flockhart/clinlist.htm
Luo J. Psyber Psychiatry. Prescribing Information: scroll with the changes (online, handheld resources on drug-drug interaction, medications’ effect on CYP-450 system. Current Psychiatry 2003;2(8 online edition). http://www.currentpsychiatry.com/article_pages.asp?AID=666&UID=8877
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
One day we may be able to consistently choose medications that offer optimal benefit and minimal adverse events—without subjecting our patients to unsuccessful trials. Thanks to quantitative EEG (OEEG) testing and pharmacogenetic testing, that day may be coming closer.
How quantitative eeg works
QEEG adds modern computer and statistical analyses to traditional EEG recordings. The computer creates a graphic display on a schematic map of the head. The procedure is often called brain electrical activity mapping (BEAM) or simply “mapping.” New tool: Genotyping makes prescribing safer, more effective, Current Psychiatry, September 2004.) Physicians can order any combination of gene tests, which cost about $150 to $200 each, or all available tests for a discounted price of approximately $600.
Genelex and Signature Genetics can create individualized CYP-450 function reports to facilitate prescribing and customized reports that take into account the patient’s medication and diet regimen. Genelex also offers an Internet-based software tool, GeneMedRx, which allows doctors to customize medication regimens based on both potential drug-drug interactions and genomic information.
Signature Genetics offers a prospective assessment of drugs based on genetic test results. This assessment provides a comprehensive report of which medications are affected by the test results.
Genetic profiling can help psychiatrists improve the likelihood of treatment success and minimize potential drug-drug interactions and adverse reactions. Patients will be more satisfied, knowing that their medications fit their individual needs. Also, as more is learned about genetic analysis, genetic testing could one day reveal susceptibility to Alzheimer’s disease, heart attack risk, or other medical problems.
As with quantitative EEG, however, few insurance companies cover genetic testing. Also, patients found to have a higher likelihood of developing certain diseases could potentially be charged higher health insurance premiums.
Related resources
Indiana University School of Medicine. Drug interactions table. http://medicine.iupui.edu/flockhart/clinlist.htm
Luo J. Psyber Psychiatry. Prescribing Information: scroll with the changes (online, handheld resources on drug-drug interaction, medications’ effect on CYP-450 system. Current Psychiatry 2003;2(8 online edition). http://www.currentpsychiatry.com/article_pages.asp?AID=666&UID=8877
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
(accessed July 27, 2005)
1. Children’s Hospital Boston. Child Health A to Z. What is qEEG? Available at: http://www.childrenshospital.org/cfapps/A2ZtopicDisplay.cfm?Topic=Quan titative%20EEG
2. UCLA Quantitative EEG Laboratory. QEEG Cordance. Available at: http://www.qeeg.npi.ucla.edu/cordance/
3. Cook IA, Leuchter AF, Witte E, et al. Neurophysiologic predictors of treatment response to fluoxetine in major depression. Psychiatry Res 1999;85:263-73.
4. Cook IA, Leuchter AF, Morgan M, et al. Early changes in prefrontal activity characterize clinical responders to antidepressants. Neuropsychopharmacology 2002;27:120-31.
5. Song DH, Shin DW, Jon DI, Ha EH. Effects of methylphenidate on quantitative EEG of boys with attention-deficit hyperactivity disorder in continuous performance test. Yonsei Med J 2005;46:34-41.
6. Nuwer M. Assessment of digital EEG, quantitative EEG, and EEG brain mapping: report of the American Academy of Neurology and the American Clinical Neurophysiology Society. Neurology 1997;49:277-92.
(accessed July 27, 2005)
1. Children’s Hospital Boston. Child Health A to Z. What is qEEG? Available at: http://www.childrenshospital.org/cfapps/A2ZtopicDisplay.cfm?Topic=Quan titative%20EEG
2. UCLA Quantitative EEG Laboratory. QEEG Cordance. Available at: http://www.qeeg.npi.ucla.edu/cordance/
3. Cook IA, Leuchter AF, Witte E, et al. Neurophysiologic predictors of treatment response to fluoxetine in major depression. Psychiatry Res 1999;85:263-73.
4. Cook IA, Leuchter AF, Morgan M, et al. Early changes in prefrontal activity characterize clinical responders to antidepressants. Neuropsychopharmacology 2002;27:120-31.
5. Song DH, Shin DW, Jon DI, Ha EH. Effects of methylphenidate on quantitative EEG of boys with attention-deficit hyperactivity disorder in continuous performance test. Yonsei Med J 2005;46:34-41.
6. Nuwer M. Assessment of digital EEG, quantitative EEG, and EEG brain mapping: report of the American Academy of Neurology and the American Clinical Neurophysiology Society. Neurology 1997;49:277-92.
Promote medication adherence, one stage at a time
Almost one-half of patients prescribed psychotropics do not take recommended dosages, but interrogating them can make them defensive and compromise your therapeutic alliance. When a patient resists starting a psychotropic, targeted interventions tied to a medication-specific transtheoretical approach can help.
Stages of change
Willey et al1 validated Prochaska and DiClemente’s stages of change2 for patients prescribed medications. Their modification provides quick assessment of how ready a patient is to commit to taking medication.
If your patient does not start a psychotropic, acknowledge that some find it difficult to take medication as directed. After you determine the patient’s stage of change, I suggest that you tailor interventions to match that level (Table), then work toward the action stage: commitment to adherence.
With stage-specific interventions, patients feel empowered to make their own decisions, rather than coerced or pressured to take medications.
Table
Assessing readiness to start medication
| Stage of change2 | Patient statement | Suggested interventions |
|---|---|---|
| Precontemplation | I do not intend to take the medication as directed |
|
| Contemplation | I intend to take the medication as directed, but not right now |
|
| Preparation | I plan to take the medication as directed in the near future |
|
| Action | I am ready to take the medication as directed |
|
1. Willey C, Redding C, Stafford J, et al. Stages of change for adherence with medication regimens for chronic disease: development and validation of a measure. Clin Ther 2000;22(7):858-71.
2. Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: toward and integrative model of change. J Cosult Clin Psychol 1983;51:390-5.
Deborah S. Finnell, is a board-certified nurse practitioner in psychiatric mental health nursing and addictions nursing at Canandaigua VA Medical Center and assistant professor of nursing, State University of New York, Buffalo.
Almost one-half of patients prescribed psychotropics do not take recommended dosages, but interrogating them can make them defensive and compromise your therapeutic alliance. When a patient resists starting a psychotropic, targeted interventions tied to a medication-specific transtheoretical approach can help.
Stages of change
Willey et al1 validated Prochaska and DiClemente’s stages of change2 for patients prescribed medications. Their modification provides quick assessment of how ready a patient is to commit to taking medication.
If your patient does not start a psychotropic, acknowledge that some find it difficult to take medication as directed. After you determine the patient’s stage of change, I suggest that you tailor interventions to match that level (Table), then work toward the action stage: commitment to adherence.
With stage-specific interventions, patients feel empowered to make their own decisions, rather than coerced or pressured to take medications.
Table
Assessing readiness to start medication
| Stage of change2 | Patient statement | Suggested interventions |
|---|---|---|
| Precontemplation | I do not intend to take the medication as directed |
|
| Contemplation | I intend to take the medication as directed, but not right now |
|
| Preparation | I plan to take the medication as directed in the near future |
|
| Action | I am ready to take the medication as directed |
|
Almost one-half of patients prescribed psychotropics do not take recommended dosages, but interrogating them can make them defensive and compromise your therapeutic alliance. When a patient resists starting a psychotropic, targeted interventions tied to a medication-specific transtheoretical approach can help.
Stages of change
Willey et al1 validated Prochaska and DiClemente’s stages of change2 for patients prescribed medications. Their modification provides quick assessment of how ready a patient is to commit to taking medication.
If your patient does not start a psychotropic, acknowledge that some find it difficult to take medication as directed. After you determine the patient’s stage of change, I suggest that you tailor interventions to match that level (Table), then work toward the action stage: commitment to adherence.
With stage-specific interventions, patients feel empowered to make their own decisions, rather than coerced or pressured to take medications.
Table
Assessing readiness to start medication
| Stage of change2 | Patient statement | Suggested interventions |
|---|---|---|
| Precontemplation | I do not intend to take the medication as directed |
|
| Contemplation | I intend to take the medication as directed, but not right now |
|
| Preparation | I plan to take the medication as directed in the near future |
|
| Action | I am ready to take the medication as directed |
|
1. Willey C, Redding C, Stafford J, et al. Stages of change for adherence with medication regimens for chronic disease: development and validation of a measure. Clin Ther 2000;22(7):858-71.
2. Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: toward and integrative model of change. J Cosult Clin Psychol 1983;51:390-5.
Deborah S. Finnell, is a board-certified nurse practitioner in psychiatric mental health nursing and addictions nursing at Canandaigua VA Medical Center and assistant professor of nursing, State University of New York, Buffalo.
1. Willey C, Redding C, Stafford J, et al. Stages of change for adherence with medication regimens for chronic disease: development and validation of a measure. Clin Ther 2000;22(7):858-71.
2. Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: toward and integrative model of change. J Cosult Clin Psychol 1983;51:390-5.
Deborah S. Finnell, is a board-certified nurse practitioner in psychiatric mental health nursing and addictions nursing at Canandaigua VA Medical Center and assistant professor of nursing, State University of New York, Buffalo.
In-session anxiety: 5 steps to help patients relax
Patients with anxiety disorders often struggle with in-session anxiety. Five simple steps can help you reduce their anxiety and teach them how to manage their fear within minutes.
Step 1: During a session, encourage patients to rate their current anxiety on a scale from 0 to 100 with 100 being the most intense.
Step 2: Ask patients to identify the score at which anxiety is too distressing or impairs functioning. Because patient perception distinguishes grades of anxiety, this activity helps differentiate between mild anxiety they can manage, moderate anxiety that needs immediate, non-pharmacologic intervention, and extreme anxiety that may require medication.
Step 3: Have patients identify which anxiety symptoms are most distressing:
- physiologic symptoms such as palpitations, tremors, and tachypnea
- affective symptoms (unpleasant feelings, anxious affect)
- cognitive symptoms (racing thoughts, impaired concentration, thoughts of impending doom, loss of control).
Knowing which symptoms are most bothersome helps you tailor your intervention. Patients also see how anxiety symptoms are not equally distressing.
Step 4: Choose one of two interventions depending on which symptoms predominate, and tell the patient you are teaching him or her a coping skill.
For cognitive symptoms, ask the patient to look around the room and describe in detail what he sees over the next 3 minutes. If time remains, ask him how he would make the room more presentable. Avoid eye contact during this time so that the patient stays focused on observing the room.
For physiologic and affective symptoms, try the “safe-place technique.” Ask the patient to close his eyes and recall a time when he felt safe and content. During the next 3 minutes, have him describe the situation, people, and positive feelings involved. Don’t let the patient get sidetracked by negative thoughts or attention to the present. Ask him to slowly open his eyes when finished.
Step 5: Ask the patient to rate anxiety symptoms again on the same 0-to-100 scale. This second score often is significantly reduced (usually between 10 and 60 points). If one technique is not effective, try the other if time permits.
These interventions also show patients that they can control their anxiousness. Encourage patients to try other anxiety- or stress-management techniques and rate their effectiveness using the 0-to-100 scale.1 Have them record effective methods in a notebook so they can develop a personalized repertoire of calming activities and techniques.
1. Copeland ME. Wellness Recovery Action Plan. West Dummerston, VT: Peach Press; 2002;62-71.
Dr. Pinninti is associate professor of psychiatry, School of Osteopathic Medicine, University of Medicine and Dentistry of New Jersey, and medical director, Steininger Behavioral Care Services, Camden, NJ.
Dr. Mago is assistant professor of psychiatry, Thomas Jefferson University, Philadelphia, PA.
Patients with anxiety disorders often struggle with in-session anxiety. Five simple steps can help you reduce their anxiety and teach them how to manage their fear within minutes.
Step 1: During a session, encourage patients to rate their current anxiety on a scale from 0 to 100 with 100 being the most intense.
Step 2: Ask patients to identify the score at which anxiety is too distressing or impairs functioning. Because patient perception distinguishes grades of anxiety, this activity helps differentiate between mild anxiety they can manage, moderate anxiety that needs immediate, non-pharmacologic intervention, and extreme anxiety that may require medication.
Step 3: Have patients identify which anxiety symptoms are most distressing:
- physiologic symptoms such as palpitations, tremors, and tachypnea
- affective symptoms (unpleasant feelings, anxious affect)
- cognitive symptoms (racing thoughts, impaired concentration, thoughts of impending doom, loss of control).
Knowing which symptoms are most bothersome helps you tailor your intervention. Patients also see how anxiety symptoms are not equally distressing.
Step 4: Choose one of two interventions depending on which symptoms predominate, and tell the patient you are teaching him or her a coping skill.
For cognitive symptoms, ask the patient to look around the room and describe in detail what he sees over the next 3 minutes. If time remains, ask him how he would make the room more presentable. Avoid eye contact during this time so that the patient stays focused on observing the room.
For physiologic and affective symptoms, try the “safe-place technique.” Ask the patient to close his eyes and recall a time when he felt safe and content. During the next 3 minutes, have him describe the situation, people, and positive feelings involved. Don’t let the patient get sidetracked by negative thoughts or attention to the present. Ask him to slowly open his eyes when finished.
Step 5: Ask the patient to rate anxiety symptoms again on the same 0-to-100 scale. This second score often is significantly reduced (usually between 10 and 60 points). If one technique is not effective, try the other if time permits.
These interventions also show patients that they can control their anxiousness. Encourage patients to try other anxiety- or stress-management techniques and rate their effectiveness using the 0-to-100 scale.1 Have them record effective methods in a notebook so they can develop a personalized repertoire of calming activities and techniques.
Patients with anxiety disorders often struggle with in-session anxiety. Five simple steps can help you reduce their anxiety and teach them how to manage their fear within minutes.
Step 1: During a session, encourage patients to rate their current anxiety on a scale from 0 to 100 with 100 being the most intense.
Step 2: Ask patients to identify the score at which anxiety is too distressing or impairs functioning. Because patient perception distinguishes grades of anxiety, this activity helps differentiate between mild anxiety they can manage, moderate anxiety that needs immediate, non-pharmacologic intervention, and extreme anxiety that may require medication.
Step 3: Have patients identify which anxiety symptoms are most distressing:
- physiologic symptoms such as palpitations, tremors, and tachypnea
- affective symptoms (unpleasant feelings, anxious affect)
- cognitive symptoms (racing thoughts, impaired concentration, thoughts of impending doom, loss of control).
Knowing which symptoms are most bothersome helps you tailor your intervention. Patients also see how anxiety symptoms are not equally distressing.
Step 4: Choose one of two interventions depending on which symptoms predominate, and tell the patient you are teaching him or her a coping skill.
For cognitive symptoms, ask the patient to look around the room and describe in detail what he sees over the next 3 minutes. If time remains, ask him how he would make the room more presentable. Avoid eye contact during this time so that the patient stays focused on observing the room.
For physiologic and affective symptoms, try the “safe-place technique.” Ask the patient to close his eyes and recall a time when he felt safe and content. During the next 3 minutes, have him describe the situation, people, and positive feelings involved. Don’t let the patient get sidetracked by negative thoughts or attention to the present. Ask him to slowly open his eyes when finished.
Step 5: Ask the patient to rate anxiety symptoms again on the same 0-to-100 scale. This second score often is significantly reduced (usually between 10 and 60 points). If one technique is not effective, try the other if time permits.
These interventions also show patients that they can control their anxiousness. Encourage patients to try other anxiety- or stress-management techniques and rate their effectiveness using the 0-to-100 scale.1 Have them record effective methods in a notebook so they can develop a personalized repertoire of calming activities and techniques.
1. Copeland ME. Wellness Recovery Action Plan. West Dummerston, VT: Peach Press; 2002;62-71.
Dr. Pinninti is associate professor of psychiatry, School of Osteopathic Medicine, University of Medicine and Dentistry of New Jersey, and medical director, Steininger Behavioral Care Services, Camden, NJ.
Dr. Mago is assistant professor of psychiatry, Thomas Jefferson University, Philadelphia, PA.
1. Copeland ME. Wellness Recovery Action Plan. West Dummerston, VT: Peach Press; 2002;62-71.
Dr. Pinninti is associate professor of psychiatry, School of Osteopathic Medicine, University of Medicine and Dentistry of New Jersey, and medical director, Steininger Behavioral Care Services, Camden, NJ.
Dr. Mago is assistant professor of psychiatry, Thomas Jefferson University, Philadelphia, PA.
Advances in detecting alcohol abuse
The article on carbohydrate-deficient transferrin percentage testing (%CDT) by Drs. Peter Miller and Raymond Anton with Cynthia Dominick was informative and relevant (Out of the Pipeline, Current Psychiatry, June 2005).
The benefits and drawbacks of %CDT testing were mentioned, including factors that affect %CDT values. The %CDT test mentioned in the article—which used an exchange column separation followed by turbidimetric measurement—was the first %CDT test approved by the FDA a couple years ago. Early this year, a second %CDT test received FDA approval.
A recent article1 indicated that this new %CDT test, which quantifies CDT as a percentage of total transferrin using capillary electrophoresis, was reported to provide better precision of its assay, and had a inter-day variation of
According to the article, this new test is an automated “walk-away” system that requires little technician involvement. Thus, it can prevent increased labor costs.
Adegboyega Oyemade, MD
Chief resident, department of psychiatry
Albany Medical Center
Albany, NY
Minesh Patel, MD
Fellow in child and adolescent psychiatry,
New York Medical College
Westchester Medical Center, Valhalla, NY
Reference
1. Bean P. New advances in CDT testing provide simultaneous detection and confirmation of alcohol abuse. On the Risk 2005;21:58-61.
The article on carbohydrate-deficient transferrin percentage testing (%CDT) by Drs. Peter Miller and Raymond Anton with Cynthia Dominick was informative and relevant (Out of the Pipeline, Current Psychiatry, June 2005).
The benefits and drawbacks of %CDT testing were mentioned, including factors that affect %CDT values. The %CDT test mentioned in the article—which used an exchange column separation followed by turbidimetric measurement—was the first %CDT test approved by the FDA a couple years ago. Early this year, a second %CDT test received FDA approval.
A recent article1 indicated that this new %CDT test, which quantifies CDT as a percentage of total transferrin using capillary electrophoresis, was reported to provide better precision of its assay, and had a inter-day variation of
According to the article, this new test is an automated “walk-away” system that requires little technician involvement. Thus, it can prevent increased labor costs.
Adegboyega Oyemade, MD
Chief resident, department of psychiatry
Albany Medical Center
Albany, NY
Minesh Patel, MD
Fellow in child and adolescent psychiatry,
New York Medical College
Westchester Medical Center, Valhalla, NY
The article on carbohydrate-deficient transferrin percentage testing (%CDT) by Drs. Peter Miller and Raymond Anton with Cynthia Dominick was informative and relevant (Out of the Pipeline, Current Psychiatry, June 2005).
The benefits and drawbacks of %CDT testing were mentioned, including factors that affect %CDT values. The %CDT test mentioned in the article—which used an exchange column separation followed by turbidimetric measurement—was the first %CDT test approved by the FDA a couple years ago. Early this year, a second %CDT test received FDA approval.
A recent article1 indicated that this new %CDT test, which quantifies CDT as a percentage of total transferrin using capillary electrophoresis, was reported to provide better precision of its assay, and had a inter-day variation of
According to the article, this new test is an automated “walk-away” system that requires little technician involvement. Thus, it can prevent increased labor costs.
Adegboyega Oyemade, MD
Chief resident, department of psychiatry
Albany Medical Center
Albany, NY
Minesh Patel, MD
Fellow in child and adolescent psychiatry,
New York Medical College
Westchester Medical Center, Valhalla, NY
Reference
1. Bean P. New advances in CDT testing provide simultaneous detection and confirmation of alcohol abuse. On the Risk 2005;21:58-61.
Reference
1. Bean P. New advances in CDT testing provide simultaneous detection and confirmation of alcohol abuse. On the Risk 2005;21:58-61.
Why troubled youths don’t ‘connect’
“Adolescent violence: What school shooters feel, and how psychiatrists can help” (Current Psychiatry, June 2005) is a good article but falls short. Youths do need “connection, connection, connection,” but this observation is too general.
I am a Bowen Family Systems Theory (BFST) coach and BFST emphasizes the family or system in which the patient finds himself. If a positive child/family relationship were as simple as just connecting, the family or system would already have done so. If it has not, it probably cannot for many reasons.
BFST explores family generational information, stressors within the family, and the anxieties these youngsters are being asked to lug around with them. All treatment, especially with children, needs to include looking at family patterns, helping “identified patients” see where they are in the system and to whom they are reacting, and helping them change their behavior so that they can differentiate themselves from others. The universal rule of change is that a person can only change himself. Working to change others is counterproductive and ineffective.
Armed with at least a preliminary understanding of these concepts, patients can march forward on their own. No one gets blamed and there is no polarization. Instead, the youth can stay neutral in the face of problems and stand for his or her beliefs. Kids with these skills need not resort to violence. They have many other choices.
M. Cybil Britton, APRN, BC
Omni House, Inc. (community mental health clinic)
Glen Burnie, MD
“Adolescent violence: What school shooters feel, and how psychiatrists can help” (Current Psychiatry, June 2005) is a good article but falls short. Youths do need “connection, connection, connection,” but this observation is too general.
I am a Bowen Family Systems Theory (BFST) coach and BFST emphasizes the family or system in which the patient finds himself. If a positive child/family relationship were as simple as just connecting, the family or system would already have done so. If it has not, it probably cannot for many reasons.
BFST explores family generational information, stressors within the family, and the anxieties these youngsters are being asked to lug around with them. All treatment, especially with children, needs to include looking at family patterns, helping “identified patients” see where they are in the system and to whom they are reacting, and helping them change their behavior so that they can differentiate themselves from others. The universal rule of change is that a person can only change himself. Working to change others is counterproductive and ineffective.
Armed with at least a preliminary understanding of these concepts, patients can march forward on their own. No one gets blamed and there is no polarization. Instead, the youth can stay neutral in the face of problems and stand for his or her beliefs. Kids with these skills need not resort to violence. They have many other choices.
M. Cybil Britton, APRN, BC
Omni House, Inc. (community mental health clinic)
Glen Burnie, MD
“Adolescent violence: What school shooters feel, and how psychiatrists can help” (Current Psychiatry, June 2005) is a good article but falls short. Youths do need “connection, connection, connection,” but this observation is too general.
I am a Bowen Family Systems Theory (BFST) coach and BFST emphasizes the family or system in which the patient finds himself. If a positive child/family relationship were as simple as just connecting, the family or system would already have done so. If it has not, it probably cannot for many reasons.
BFST explores family generational information, stressors within the family, and the anxieties these youngsters are being asked to lug around with them. All treatment, especially with children, needs to include looking at family patterns, helping “identified patients” see where they are in the system and to whom they are reacting, and helping them change their behavior so that they can differentiate themselves from others. The universal rule of change is that a person can only change himself. Working to change others is counterproductive and ineffective.
Armed with at least a preliminary understanding of these concepts, patients can march forward on their own. No one gets blamed and there is no polarization. Instead, the youth can stay neutral in the face of problems and stand for his or her beliefs. Kids with these skills need not resort to violence. They have many other choices.
M. Cybil Britton, APRN, BC
Omni House, Inc. (community mental health clinic)
Glen Burnie, MD