User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
First Hike of Medicare Funding for Residencies in 25 Years Aims to Help Shortages
Residency programs across the country may have a few more slots for incoming residents due to a recent bump in Medicare funding.
Case in point: The University of Alabama at Birmingham (UAB). The state has one of the top stroke rates in the country, and yet UAB has the only hospital in the state training future doctors to help stroke patients recover. “Our hospital cares for Alabama’s sickest patients, many who need rehabilitation services,” said Craig Hoesley, MD, senior associate dean for medical education, who oversees graduate medical education (GME) or residency programs.
After decades of stagnant support, a recent bump in Medicare funding will allow UAB to add two more physical medicine and rehabilitation residents to the four residencies already receiving such funding.
Medicare also awarded UAB more funding last year to add an addiction medicine fellowship, one of two such training programs in the state for the specialty that helps treat patients fighting addiction.
UAB is among healthcare systems and hospitals nationwide benefiting from a recent hike in Medicare funding for residency programs after some 25 years at the same level of federal support. Medicare is the largest funder of training positions. Otherwise, hospitals finance training through means such as state support.
The latest round of funding, which went into effect in July, adds 200 positions to the doctor pipeline, creating more openings for residents seeking positions after medical school.
In the next few months, the Centers for Medicare & Medicaid Services (CMS) will notify teaching hospitals whether they’ll receive the next round of Medicare funding for more residency positions. At that time, CMS will have awarded nearly half of the 1200 residency training slots Congress approved in the past few years. In 2020 — for the first time since 1996 — Congress approved adding 1000 residency slots at teaching hospitals nationwide. CMS awards the money for 200 slots each year for 5 years.
More than half of the initial round of funding focused on training primary care specialists, with other slots designated for mental health specialists. Last year, Congress also approved a separate allocation of 200 more Medicare-funded residency positions, with at least half designated for psychiatry and related subspecialty residencies to help meet the growing need for more mental health specialists. On August 1, CMS announced it would distribute the funds next year, effective in 2026.
The additional Medicare funding attempts to address the shortage of healthcare providers and ensure future access to care, including in rural and underserved communities. The Association of American Medical Colleges (AAMC) estimates the nation will face a shortage of up to 86,000 physicians by 2036, including primary care doctors and specialists.
In addition, more than 100 million Americans, nearly a third of the nation, don’t have access to primary care due to the physician shortages in their communities, according to the National Association of Community Health Centers.
Major medical organizations, medical schools, and hospital groups have been pushing for years for increased Medicare funding to train new doctors to keep up with the demand for healthcare services and offset the physician shortage. As a cost-saving measure, Medicare set its cap in 1996 for how much it will reimburse each hospital offering GME training. However, according to the medical groups that continue to advocate to Congress for more funding, the funding hasn’t kept pace with the growing healthcare needs or rising medical school enrollment.
Adding Residency Spots
In April, Dr. Hoesley of UAB spoke at a Congressional briefing among health systems and hospitals that benefited from the additional funding. He told Congressional leaders how the increased number of GME positions affects UAB Medicine and its ability to care for rural areas.
“We have entire counties in Alabama that don’t have physicians. One way to address the physician shortage is to grow the GME programs. The funding we received will help us grow these programs and care for residents in our state.”
Still, the Medicare funding is only a drop in the bucket, Dr. Hoesley said. “We rely on Medicare funding alongside other funding partners to train residents and expand our care across the state.” He said many UAB residency programs are over their Medicare funding cap and would like to grow, but they can’t without more funding.
Mount Sinai Health System in New York City also will be able to expand its residency program after receiving Medicare support in the latest round of funding. The health system will use the federal funds to train an additional vascular surgeon. Mount Sinai currently receives CMS funding to train three residents in the specialty.
Over a 5-year program, that means CMS funding will help train 20 residents in the specialty that treats blood vessel blockages and diseases of the veins and arteries generally associated with aging.
“The funding is amazing,” said Peter L. Faries, MD, a surgery professor and system chief of vascular surgery at the Icahn School of Medicine at Mount Sinai, New York City, who directs the residency program.
“We don’t have the capacity to provide an individual training program without the funding. It’s not economically feasible.”
The need for more vascular surgeons increases as the population continues to age, he said. Mount Sinai treats patients throughout New York, including underserved areas in Harlem, the Bronx, Washington Heights, Brooklyn, and Queens. “These individuals might not receive an appropriate level of vascular care if we don’t have clinicians to treat them.”
Of the recent funding, Dr. Faries said it’s taken the residency program 15 years of advocacy to increase by two slots. “It’s a long process to get funding.” Vascular training programs can remain very selective with Medicare funding, typically receiving two applicants for every position,” said Dr. Faries.
Pushing for More Funds
Nearly 98,000 students enrolled in medical school this year, according to the National Resident Matching Program. A total of 44,853 applicants vied for the 38,494 first-year residency positions and 3009 second-year slots, leaving 3350 medical school graduates without a match.
“There are not enough spots to meet the growing demand,” said Jesse M. Ehrenfeld, MD, MPH, immediate past president of the American Medical Association. “Graduate medical education funding has not kept up.”
Despite the increase in medical school graduates over the past two decades, Medicare-supported training opportunities remained frozen at the 1996 level. A limited number of training positions meant residency programs couldn’t expand the physician pipeline to offset an aging workforce, contributing to the shortage. “The way to solve this is to expand GME,” Dr. Ehrenfeld said. “We continue to advocate to remove the cap.”
Dr. Ehrenfeld also told this news organization that he doesn’t mind that Congress recently designated GME funding to certain specialties, such as psychiatry, because he believes the need is great for residency spots across the board. “The good news is people recognize it’s challenging to get much through Congress.” He’s optimistic, though, about recent legislative efforts to increase funding.
AAMC, representing about a third of the nation’s 1100 teaching hospitals and health systems, feels the same. Congress “acknowledges and continues to recognize that the shortage is not getting better, and one way to address it is to increase Medicare-supported GME positions,” said Leonard Marquez, senior director of government relations and legislative advocacy.
Still, he said that the Medicare funding bump is only making a small dent in the need. AAMC estimates the average cost to train residents is $23 billion annually, and Medicare only funds 20% of that, or $5 billion. “Our members are at the point where they say: We already can’t add new training positions,” Mr. Marquez said. He added that without increasing residency slots, patient care will suffer. “We have to do anything possible we can to increase access to care.”
Mr. Marquez also believes Medicare funding should increase residency positions across the specialty spectrum, not just for psychiatry and primary care. He said that the targeted funding may prevent some teaching hospitals from applying for residency positions if they need other types of specialists based on their community’s needs.
Among the current proposals before Congress, the Resident Physician Shortage Reduction Act of 2023 would add 14,000 Medicare-supported residency slots over 7 years. Mr. Marquez said it may be more realistic to expect fewer new slots. A decision on potential legislation is expected at the end of the year. He said that if the medical groups aren’t pleased with the decision, they’ll advocate again in 2025.
A version of this article first appeared on Medscape.com.
Residency programs across the country may have a few more slots for incoming residents due to a recent bump in Medicare funding.
Case in point: The University of Alabama at Birmingham (UAB). The state has one of the top stroke rates in the country, and yet UAB has the only hospital in the state training future doctors to help stroke patients recover. “Our hospital cares for Alabama’s sickest patients, many who need rehabilitation services,” said Craig Hoesley, MD, senior associate dean for medical education, who oversees graduate medical education (GME) or residency programs.
After decades of stagnant support, a recent bump in Medicare funding will allow UAB to add two more physical medicine and rehabilitation residents to the four residencies already receiving such funding.
Medicare also awarded UAB more funding last year to add an addiction medicine fellowship, one of two such training programs in the state for the specialty that helps treat patients fighting addiction.
UAB is among healthcare systems and hospitals nationwide benefiting from a recent hike in Medicare funding for residency programs after some 25 years at the same level of federal support. Medicare is the largest funder of training positions. Otherwise, hospitals finance training through means such as state support.
The latest round of funding, which went into effect in July, adds 200 positions to the doctor pipeline, creating more openings for residents seeking positions after medical school.
In the next few months, the Centers for Medicare & Medicaid Services (CMS) will notify teaching hospitals whether they’ll receive the next round of Medicare funding for more residency positions. At that time, CMS will have awarded nearly half of the 1200 residency training slots Congress approved in the past few years. In 2020 — for the first time since 1996 — Congress approved adding 1000 residency slots at teaching hospitals nationwide. CMS awards the money for 200 slots each year for 5 years.
More than half of the initial round of funding focused on training primary care specialists, with other slots designated for mental health specialists. Last year, Congress also approved a separate allocation of 200 more Medicare-funded residency positions, with at least half designated for psychiatry and related subspecialty residencies to help meet the growing need for more mental health specialists. On August 1, CMS announced it would distribute the funds next year, effective in 2026.
The additional Medicare funding attempts to address the shortage of healthcare providers and ensure future access to care, including in rural and underserved communities. The Association of American Medical Colleges (AAMC) estimates the nation will face a shortage of up to 86,000 physicians by 2036, including primary care doctors and specialists.
In addition, more than 100 million Americans, nearly a third of the nation, don’t have access to primary care due to the physician shortages in their communities, according to the National Association of Community Health Centers.
Major medical organizations, medical schools, and hospital groups have been pushing for years for increased Medicare funding to train new doctors to keep up with the demand for healthcare services and offset the physician shortage. As a cost-saving measure, Medicare set its cap in 1996 for how much it will reimburse each hospital offering GME training. However, according to the medical groups that continue to advocate to Congress for more funding, the funding hasn’t kept pace with the growing healthcare needs or rising medical school enrollment.
Adding Residency Spots
In April, Dr. Hoesley of UAB spoke at a Congressional briefing among health systems and hospitals that benefited from the additional funding. He told Congressional leaders how the increased number of GME positions affects UAB Medicine and its ability to care for rural areas.
“We have entire counties in Alabama that don’t have physicians. One way to address the physician shortage is to grow the GME programs. The funding we received will help us grow these programs and care for residents in our state.”
Still, the Medicare funding is only a drop in the bucket, Dr. Hoesley said. “We rely on Medicare funding alongside other funding partners to train residents and expand our care across the state.” He said many UAB residency programs are over their Medicare funding cap and would like to grow, but they can’t without more funding.
Mount Sinai Health System in New York City also will be able to expand its residency program after receiving Medicare support in the latest round of funding. The health system will use the federal funds to train an additional vascular surgeon. Mount Sinai currently receives CMS funding to train three residents in the specialty.
Over a 5-year program, that means CMS funding will help train 20 residents in the specialty that treats blood vessel blockages and diseases of the veins and arteries generally associated with aging.
“The funding is amazing,” said Peter L. Faries, MD, a surgery professor and system chief of vascular surgery at the Icahn School of Medicine at Mount Sinai, New York City, who directs the residency program.
“We don’t have the capacity to provide an individual training program without the funding. It’s not economically feasible.”
The need for more vascular surgeons increases as the population continues to age, he said. Mount Sinai treats patients throughout New York, including underserved areas in Harlem, the Bronx, Washington Heights, Brooklyn, and Queens. “These individuals might not receive an appropriate level of vascular care if we don’t have clinicians to treat them.”
Of the recent funding, Dr. Faries said it’s taken the residency program 15 years of advocacy to increase by two slots. “It’s a long process to get funding.” Vascular training programs can remain very selective with Medicare funding, typically receiving two applicants for every position,” said Dr. Faries.
Pushing for More Funds
Nearly 98,000 students enrolled in medical school this year, according to the National Resident Matching Program. A total of 44,853 applicants vied for the 38,494 first-year residency positions and 3009 second-year slots, leaving 3350 medical school graduates without a match.
“There are not enough spots to meet the growing demand,” said Jesse M. Ehrenfeld, MD, MPH, immediate past president of the American Medical Association. “Graduate medical education funding has not kept up.”
Despite the increase in medical school graduates over the past two decades, Medicare-supported training opportunities remained frozen at the 1996 level. A limited number of training positions meant residency programs couldn’t expand the physician pipeline to offset an aging workforce, contributing to the shortage. “The way to solve this is to expand GME,” Dr. Ehrenfeld said. “We continue to advocate to remove the cap.”
Dr. Ehrenfeld also told this news organization that he doesn’t mind that Congress recently designated GME funding to certain specialties, such as psychiatry, because he believes the need is great for residency spots across the board. “The good news is people recognize it’s challenging to get much through Congress.” He’s optimistic, though, about recent legislative efforts to increase funding.
AAMC, representing about a third of the nation’s 1100 teaching hospitals and health systems, feels the same. Congress “acknowledges and continues to recognize that the shortage is not getting better, and one way to address it is to increase Medicare-supported GME positions,” said Leonard Marquez, senior director of government relations and legislative advocacy.
Still, he said that the Medicare funding bump is only making a small dent in the need. AAMC estimates the average cost to train residents is $23 billion annually, and Medicare only funds 20% of that, or $5 billion. “Our members are at the point where they say: We already can’t add new training positions,” Mr. Marquez said. He added that without increasing residency slots, patient care will suffer. “We have to do anything possible we can to increase access to care.”
Mr. Marquez also believes Medicare funding should increase residency positions across the specialty spectrum, not just for psychiatry and primary care. He said that the targeted funding may prevent some teaching hospitals from applying for residency positions if they need other types of specialists based on their community’s needs.
Among the current proposals before Congress, the Resident Physician Shortage Reduction Act of 2023 would add 14,000 Medicare-supported residency slots over 7 years. Mr. Marquez said it may be more realistic to expect fewer new slots. A decision on potential legislation is expected at the end of the year. He said that if the medical groups aren’t pleased with the decision, they’ll advocate again in 2025.
A version of this article first appeared on Medscape.com.
Residency programs across the country may have a few more slots for incoming residents due to a recent bump in Medicare funding.
Case in point: The University of Alabama at Birmingham (UAB). The state has one of the top stroke rates in the country, and yet UAB has the only hospital in the state training future doctors to help stroke patients recover. “Our hospital cares for Alabama’s sickest patients, many who need rehabilitation services,” said Craig Hoesley, MD, senior associate dean for medical education, who oversees graduate medical education (GME) or residency programs.
After decades of stagnant support, a recent bump in Medicare funding will allow UAB to add two more physical medicine and rehabilitation residents to the four residencies already receiving such funding.
Medicare also awarded UAB more funding last year to add an addiction medicine fellowship, one of two such training programs in the state for the specialty that helps treat patients fighting addiction.
UAB is among healthcare systems and hospitals nationwide benefiting from a recent hike in Medicare funding for residency programs after some 25 years at the same level of federal support. Medicare is the largest funder of training positions. Otherwise, hospitals finance training through means such as state support.
The latest round of funding, which went into effect in July, adds 200 positions to the doctor pipeline, creating more openings for residents seeking positions after medical school.
In the next few months, the Centers for Medicare & Medicaid Services (CMS) will notify teaching hospitals whether they’ll receive the next round of Medicare funding for more residency positions. At that time, CMS will have awarded nearly half of the 1200 residency training slots Congress approved in the past few years. In 2020 — for the first time since 1996 — Congress approved adding 1000 residency slots at teaching hospitals nationwide. CMS awards the money for 200 slots each year for 5 years.
More than half of the initial round of funding focused on training primary care specialists, with other slots designated for mental health specialists. Last year, Congress also approved a separate allocation of 200 more Medicare-funded residency positions, with at least half designated for psychiatry and related subspecialty residencies to help meet the growing need for more mental health specialists. On August 1, CMS announced it would distribute the funds next year, effective in 2026.
The additional Medicare funding attempts to address the shortage of healthcare providers and ensure future access to care, including in rural and underserved communities. The Association of American Medical Colleges (AAMC) estimates the nation will face a shortage of up to 86,000 physicians by 2036, including primary care doctors and specialists.
In addition, more than 100 million Americans, nearly a third of the nation, don’t have access to primary care due to the physician shortages in their communities, according to the National Association of Community Health Centers.
Major medical organizations, medical schools, and hospital groups have been pushing for years for increased Medicare funding to train new doctors to keep up with the demand for healthcare services and offset the physician shortage. As a cost-saving measure, Medicare set its cap in 1996 for how much it will reimburse each hospital offering GME training. However, according to the medical groups that continue to advocate to Congress for more funding, the funding hasn’t kept pace with the growing healthcare needs or rising medical school enrollment.
Adding Residency Spots
In April, Dr. Hoesley of UAB spoke at a Congressional briefing among health systems and hospitals that benefited from the additional funding. He told Congressional leaders how the increased number of GME positions affects UAB Medicine and its ability to care for rural areas.
“We have entire counties in Alabama that don’t have physicians. One way to address the physician shortage is to grow the GME programs. The funding we received will help us grow these programs and care for residents in our state.”
Still, the Medicare funding is only a drop in the bucket, Dr. Hoesley said. “We rely on Medicare funding alongside other funding partners to train residents and expand our care across the state.” He said many UAB residency programs are over their Medicare funding cap and would like to grow, but they can’t without more funding.
Mount Sinai Health System in New York City also will be able to expand its residency program after receiving Medicare support in the latest round of funding. The health system will use the federal funds to train an additional vascular surgeon. Mount Sinai currently receives CMS funding to train three residents in the specialty.
Over a 5-year program, that means CMS funding will help train 20 residents in the specialty that treats blood vessel blockages and diseases of the veins and arteries generally associated with aging.
“The funding is amazing,” said Peter L. Faries, MD, a surgery professor and system chief of vascular surgery at the Icahn School of Medicine at Mount Sinai, New York City, who directs the residency program.
“We don’t have the capacity to provide an individual training program without the funding. It’s not economically feasible.”
The need for more vascular surgeons increases as the population continues to age, he said. Mount Sinai treats patients throughout New York, including underserved areas in Harlem, the Bronx, Washington Heights, Brooklyn, and Queens. “These individuals might not receive an appropriate level of vascular care if we don’t have clinicians to treat them.”
Of the recent funding, Dr. Faries said it’s taken the residency program 15 years of advocacy to increase by two slots. “It’s a long process to get funding.” Vascular training programs can remain very selective with Medicare funding, typically receiving two applicants for every position,” said Dr. Faries.
Pushing for More Funds
Nearly 98,000 students enrolled in medical school this year, according to the National Resident Matching Program. A total of 44,853 applicants vied for the 38,494 first-year residency positions and 3009 second-year slots, leaving 3350 medical school graduates without a match.
“There are not enough spots to meet the growing demand,” said Jesse M. Ehrenfeld, MD, MPH, immediate past president of the American Medical Association. “Graduate medical education funding has not kept up.”
Despite the increase in medical school graduates over the past two decades, Medicare-supported training opportunities remained frozen at the 1996 level. A limited number of training positions meant residency programs couldn’t expand the physician pipeline to offset an aging workforce, contributing to the shortage. “The way to solve this is to expand GME,” Dr. Ehrenfeld said. “We continue to advocate to remove the cap.”
Dr. Ehrenfeld also told this news organization that he doesn’t mind that Congress recently designated GME funding to certain specialties, such as psychiatry, because he believes the need is great for residency spots across the board. “The good news is people recognize it’s challenging to get much through Congress.” He’s optimistic, though, about recent legislative efforts to increase funding.
AAMC, representing about a third of the nation’s 1100 teaching hospitals and health systems, feels the same. Congress “acknowledges and continues to recognize that the shortage is not getting better, and one way to address it is to increase Medicare-supported GME positions,” said Leonard Marquez, senior director of government relations and legislative advocacy.
Still, he said that the Medicare funding bump is only making a small dent in the need. AAMC estimates the average cost to train residents is $23 billion annually, and Medicare only funds 20% of that, or $5 billion. “Our members are at the point where they say: We already can’t add new training positions,” Mr. Marquez said. He added that without increasing residency slots, patient care will suffer. “We have to do anything possible we can to increase access to care.”
Mr. Marquez also believes Medicare funding should increase residency positions across the specialty spectrum, not just for psychiatry and primary care. He said that the targeted funding may prevent some teaching hospitals from applying for residency positions if they need other types of specialists based on their community’s needs.
Among the current proposals before Congress, the Resident Physician Shortage Reduction Act of 2023 would add 14,000 Medicare-supported residency slots over 7 years. Mr. Marquez said it may be more realistic to expect fewer new slots. A decision on potential legislation is expected at the end of the year. He said that if the medical groups aren’t pleased with the decision, they’ll advocate again in 2025.
A version of this article first appeared on Medscape.com.
Beyond the Title: How PAs Handle the Burden of MD-Level Responsibilities
Within the physician assistant (PA) community, many PAs have expressed the heavy weight of their job expectation and their subsequent feelings of discontent.
Mirela Bruza-Augatis, PhD, MS, PA-C, a researcher at the National Commission on Certification of Physician Assistants, said the sentiment is similar to what she’s heard from colleagues, as well as seen in her own research examining PA work-life balance.
“Unfortunately, part of this is just the culture of medicine — and other healthcare workers report similar experiences. The patient comes first, and you are secondary,” she said. “You have to make do with the resources you have, and that’s not always enough.”
Yet, despite the challenges of working as a PA in today’s healthcare industry, many are finding ways not just to survive but to thrive. Brian McCambley, DHSc, PA-C, who works as both an emergency medicine PA and a system wellness officer at Nuvance Health, has been looking at ways to improve morale (and, consequently, lower turnover rates), especially among new PA recruits.
He said that the first step is finding the right practice environment. He encourages even experienced PAs to take the time to understand the culture of any practice they consider joining — and ask a lot of questions about what kind of support is available.
“Ask the right questions from the very beginning. What does the job truly entail? What is the culture within the group that you’ll be joining? Talk to the entire team to get a real sense of what’s going on there day to day,” he said. “One benefit of being a PA is that most of us are trained as generalists. We have a lot of mobility between specialties. If the work hours, culture, or fit doesn’t work, it is possible to morph and try something different.”
See How Other PAs Are Managing
Dr. Bruza-Augatis added that finding peer support is also beneficial. She said being able to discuss your experiences with other PAs, both within your workplace and outside of it, offers more than just the benefit of knowing you are not alone.
“When you talk to other colleagues who have had similar experiences, they may have found solutions to help,” she said. “The solution that works for one person may not work for everyone. But it can at least offer some ideas and help you focus on the things you may be able to control and change.”
Raquelle Akavan, DMSc, PA-C, founder of the popular PA Moms® group, agreed on both points. She said that finding both institutional and personal support is remarkably helpful in dealing with the stressors most PAs face both at work and home. With that kind of support in place, you can start to set the appropriate boundaries to help ensure you aren’t feeling overwhelmed by all the expectations placed on you.
“This is crucial to finding good work-life integration,” she said. “You can set boundaries with both your patients and your managers. You can carve out time for your family and let your job know that you won’t be taking calls between 5:00 pm and 9:00 pm. You can go to your manager and let them know what you need to do your job well — whether it’s a scribe, continuing medical education, or help managing the workload.”
Speak Up
Advocating for yourself is key, said Hope Cook, PA-C, who works as both a PA in a dermatology practice and as a licensed life coach. She said that taking the time to be self-aware of the work stressors that negatively affect you allows you to “give yourself permission” to do something about them.
“Like any profession, you have to know your limits,” she said. “If you need more collaboration from your team, you need to figure out how to get that. You need to ask for it. If you feel like you have insufficient training to deal with the complexity of the patients who are coming to see you, you need to talk to the practice about how to fix that. It’s important to let people know what support you need. And, if they aren’t going to help provide it, understand that it may be time to go elsewhere.”
None of these things are necessarily easy, said Dr. McCambley. But replacing a PA costs a practice significant time and money. So, finding ways to promote growth and resilience early on in your career will help protect you from later burnout, and save the healthcare organization in the long run, too. He believes Nuvance has had great success in their efforts to support clinician wellness across the board by having PAs contribute to leadership discussions and decisions.
“When you can get with like-minded folks and sit with hospital administration to talk about the best ways to get PAs intermixed with the medical staff and how to support them in their roles, you can make a difference,” he told this news organization. “I’ve been at my healthcare institution for 26 years. We PAs didn’t really have a big voice at the beginning. But, little by little, by having important discussions with our leadership, we’ve been able to show our medical staff that PAs bring something really important to the table — and that it benefits everyone when we support them.”
A version of this article first appeared on Medscape.com.
Within the physician assistant (PA) community, many PAs have expressed the heavy weight of their job expectation and their subsequent feelings of discontent.
Mirela Bruza-Augatis, PhD, MS, PA-C, a researcher at the National Commission on Certification of Physician Assistants, said the sentiment is similar to what she’s heard from colleagues, as well as seen in her own research examining PA work-life balance.
“Unfortunately, part of this is just the culture of medicine — and other healthcare workers report similar experiences. The patient comes first, and you are secondary,” she said. “You have to make do with the resources you have, and that’s not always enough.”
Yet, despite the challenges of working as a PA in today’s healthcare industry, many are finding ways not just to survive but to thrive. Brian McCambley, DHSc, PA-C, who works as both an emergency medicine PA and a system wellness officer at Nuvance Health, has been looking at ways to improve morale (and, consequently, lower turnover rates), especially among new PA recruits.
He said that the first step is finding the right practice environment. He encourages even experienced PAs to take the time to understand the culture of any practice they consider joining — and ask a lot of questions about what kind of support is available.
“Ask the right questions from the very beginning. What does the job truly entail? What is the culture within the group that you’ll be joining? Talk to the entire team to get a real sense of what’s going on there day to day,” he said. “One benefit of being a PA is that most of us are trained as generalists. We have a lot of mobility between specialties. If the work hours, culture, or fit doesn’t work, it is possible to morph and try something different.”
See How Other PAs Are Managing
Dr. Bruza-Augatis added that finding peer support is also beneficial. She said being able to discuss your experiences with other PAs, both within your workplace and outside of it, offers more than just the benefit of knowing you are not alone.
“When you talk to other colleagues who have had similar experiences, they may have found solutions to help,” she said. “The solution that works for one person may not work for everyone. But it can at least offer some ideas and help you focus on the things you may be able to control and change.”
Raquelle Akavan, DMSc, PA-C, founder of the popular PA Moms® group, agreed on both points. She said that finding both institutional and personal support is remarkably helpful in dealing with the stressors most PAs face both at work and home. With that kind of support in place, you can start to set the appropriate boundaries to help ensure you aren’t feeling overwhelmed by all the expectations placed on you.
“This is crucial to finding good work-life integration,” she said. “You can set boundaries with both your patients and your managers. You can carve out time for your family and let your job know that you won’t be taking calls between 5:00 pm and 9:00 pm. You can go to your manager and let them know what you need to do your job well — whether it’s a scribe, continuing medical education, or help managing the workload.”
Speak Up
Advocating for yourself is key, said Hope Cook, PA-C, who works as both a PA in a dermatology practice and as a licensed life coach. She said that taking the time to be self-aware of the work stressors that negatively affect you allows you to “give yourself permission” to do something about them.
“Like any profession, you have to know your limits,” she said. “If you need more collaboration from your team, you need to figure out how to get that. You need to ask for it. If you feel like you have insufficient training to deal with the complexity of the patients who are coming to see you, you need to talk to the practice about how to fix that. It’s important to let people know what support you need. And, if they aren’t going to help provide it, understand that it may be time to go elsewhere.”
None of these things are necessarily easy, said Dr. McCambley. But replacing a PA costs a practice significant time and money. So, finding ways to promote growth and resilience early on in your career will help protect you from later burnout, and save the healthcare organization in the long run, too. He believes Nuvance has had great success in their efforts to support clinician wellness across the board by having PAs contribute to leadership discussions and decisions.
“When you can get with like-minded folks and sit with hospital administration to talk about the best ways to get PAs intermixed with the medical staff and how to support them in their roles, you can make a difference,” he told this news organization. “I’ve been at my healthcare institution for 26 years. We PAs didn’t really have a big voice at the beginning. But, little by little, by having important discussions with our leadership, we’ve been able to show our medical staff that PAs bring something really important to the table — and that it benefits everyone when we support them.”
A version of this article first appeared on Medscape.com.
Within the physician assistant (PA) community, many PAs have expressed the heavy weight of their job expectation and their subsequent feelings of discontent.
Mirela Bruza-Augatis, PhD, MS, PA-C, a researcher at the National Commission on Certification of Physician Assistants, said the sentiment is similar to what she’s heard from colleagues, as well as seen in her own research examining PA work-life balance.
“Unfortunately, part of this is just the culture of medicine — and other healthcare workers report similar experiences. The patient comes first, and you are secondary,” she said. “You have to make do with the resources you have, and that’s not always enough.”
Yet, despite the challenges of working as a PA in today’s healthcare industry, many are finding ways not just to survive but to thrive. Brian McCambley, DHSc, PA-C, who works as both an emergency medicine PA and a system wellness officer at Nuvance Health, has been looking at ways to improve morale (and, consequently, lower turnover rates), especially among new PA recruits.
He said that the first step is finding the right practice environment. He encourages even experienced PAs to take the time to understand the culture of any practice they consider joining — and ask a lot of questions about what kind of support is available.
“Ask the right questions from the very beginning. What does the job truly entail? What is the culture within the group that you’ll be joining? Talk to the entire team to get a real sense of what’s going on there day to day,” he said. “One benefit of being a PA is that most of us are trained as generalists. We have a lot of mobility between specialties. If the work hours, culture, or fit doesn’t work, it is possible to morph and try something different.”
See How Other PAs Are Managing
Dr. Bruza-Augatis added that finding peer support is also beneficial. She said being able to discuss your experiences with other PAs, both within your workplace and outside of it, offers more than just the benefit of knowing you are not alone.
“When you talk to other colleagues who have had similar experiences, they may have found solutions to help,” she said. “The solution that works for one person may not work for everyone. But it can at least offer some ideas and help you focus on the things you may be able to control and change.”
Raquelle Akavan, DMSc, PA-C, founder of the popular PA Moms® group, agreed on both points. She said that finding both institutional and personal support is remarkably helpful in dealing with the stressors most PAs face both at work and home. With that kind of support in place, you can start to set the appropriate boundaries to help ensure you aren’t feeling overwhelmed by all the expectations placed on you.
“This is crucial to finding good work-life integration,” she said. “You can set boundaries with both your patients and your managers. You can carve out time for your family and let your job know that you won’t be taking calls between 5:00 pm and 9:00 pm. You can go to your manager and let them know what you need to do your job well — whether it’s a scribe, continuing medical education, or help managing the workload.”
Speak Up
Advocating for yourself is key, said Hope Cook, PA-C, who works as both a PA in a dermatology practice and as a licensed life coach. She said that taking the time to be self-aware of the work stressors that negatively affect you allows you to “give yourself permission” to do something about them.
“Like any profession, you have to know your limits,” she said. “If you need more collaboration from your team, you need to figure out how to get that. You need to ask for it. If you feel like you have insufficient training to deal with the complexity of the patients who are coming to see you, you need to talk to the practice about how to fix that. It’s important to let people know what support you need. And, if they aren’t going to help provide it, understand that it may be time to go elsewhere.”
None of these things are necessarily easy, said Dr. McCambley. But replacing a PA costs a practice significant time and money. So, finding ways to promote growth and resilience early on in your career will help protect you from later burnout, and save the healthcare organization in the long run, too. He believes Nuvance has had great success in their efforts to support clinician wellness across the board by having PAs contribute to leadership discussions and decisions.
“When you can get with like-minded folks and sit with hospital administration to talk about the best ways to get PAs intermixed with the medical staff and how to support them in their roles, you can make a difference,” he told this news organization. “I’ve been at my healthcare institution for 26 years. We PAs didn’t really have a big voice at the beginning. But, little by little, by having important discussions with our leadership, we’ve been able to show our medical staff that PAs bring something really important to the table — and that it benefits everyone when we support them.”
A version of this article first appeared on Medscape.com.
FDA’s Stricter Regulation of Lab-Developed Tests Faces Lawsuits and Lingering Concerns
The Food and Drug Administration (FDA) plans to scrutinize the safety and efficacy of lab-developed tests — those designed, manufactured, and used in a single laboratory — far more thoroughly in the future.
Under a rule finalized in April, the FDA will treat facilities that develop and use lab tests as manufacturers and regulate tests as medical devices. That means that most lab tests will need an FDA review before going on sale.
The FDA will also impose new quality standards, requiring test manufacturers to report adverse events and create a registry of lab tests under the new rule, which will be phased in over 4 years.
FDA officials have been concerned for years about the reliability of commercial lab tests, which have ballooned into a multibillion-dollar industry.
Consumer groups have long urged the FDA to regulate lab tests more strictly, arguing that the lack of scrutiny allows doctors and patients to be exploited by bad actors such as Theranos, which falsely claimed that its tests could diagnose multiple diseases with a single drop of blood.
“When it comes to some of these tests that doctors are recommending for patients, many doctors are just crossing their fingers and relying on the representation of the company because nobody is checking” to verify a manufacturer’s claims, said Joshua Sharfstein, MD, vice dean for public health practice and community engagement at the Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland.
Nearly 12,000 Labs Making Medical Tests
Although the FDA estimates there are nearly 12,000 labs manufacturing medical tests, agency officials said they don’t know how many tests are being marketed. The FDA already requires that home test kits marketed directly to consumers, such as those used to detect COVID-19, get clearance from the agency before being sold.
“There’s plenty of time for industry to get its act together to develop the data that it might need to make a premarket application,” said Peter Lurie, MD, PhD, a former associate commissioner at the FDA. In 2015, Dr. Lurie led a report outlining some of the dangers of unregulated lab tests.
For the average physician who orders lab tests, nothing is going to immediately change because of the final rule, said Dr. Lurie, now president of the Center for Science in the Public Interest, a nonprofit consumer watchdog.
“Tomorrow, this will look just the same as it does today,” Dr. Lurie said. “For the next 3 years, the companies will be scurrying behind the scenes to comply with the early stages of implementation. But most of that will be invisible to the average practitioner.”
Dr. Lurie predicted the FDA will focus its scrutiny on tests that pose the greatest potential risk to patients, such as ones used to diagnose serious diseases or guide treatment for life-threatening conditions. “The least significant tests will likely get very limited, if any, scrutiny,” said Dr. Lurie, adding that the FDA will likely issue guidance about how it plans to define low- and high-risk tests. “My suspicion is that it will be probably a small minority of products that are subject to full premarket approval.”
Lab Industry Groups Push Back
But imposing new rules with the potential to affect an industry’s bottom line is no easy task.
The American Clinical Laboratory Association, which represents the lab industry, said in a statement that the FDA rule will “limit access to scores of critical tests, increase healthcare costs, and undermine innovation in new diagnostics.” Another industry group, the Association for Molecular Pathology, has warned of “significant and harmful disruption to laboratory medicine.”
The two associations have filed separate lawsuits, charging that the FDA overstepped the authority granted by Congress. In their lawsuits, groups claim that lab tests are professional services, not manufactured products. The groups noted that the Centers for Medicare & Medicaid Services (CMS) already inspects lab facilities. CMS does not assess the tests’ quality or reliability.
A recent Supreme Court decision could make those lawsuits more likely to succeed, said David Simon, JD, LLM, PhD, an assistant professor of law at the Northeastern University School of Law, Boston, Massachusetts.
In the case of Loper Bright Enterprises v. Raimondo, decided in June, justices overturned a long-standing precedent known as Chevron deference, which required courts to defer to federal agencies when interpreting ambiguous laws. That means that courts no longer have to accept the FDA’s definition of a device, Dr. Simon said.
“Because judges may have more active roles in defining agency authority, federal agencies may have correspondingly less robust roles in policymaking,” Dr. Simon wrote in an editorial coauthored with Michael J. Young, MD, MPhil, of Harvard Medical School, Boston.
The Supreme Court ruling could pressure Congress to more clearly define FDA’s ruling in regulating lab tests, Dr. Simon and Dr. Young wrote.
Members of Congress first introduced a bill to clarify the FDA’s role in regulating lab tests, called the VALID Act, in 2020. The bill stalled and, despite efforts to revive it, still hasn’t passed.
FDA officials have said they remain “open to working with Congress,” noting that any future legislation about lab-developed tests would supersede their current policy.
In an interview, Dr. Simon noted the FDA significantly narrowed the scope of the final rule in response to comments from critics who objected to an earlier version of the policy proposed in 2023. The final rule carves out several categories of tests that won’t need to apply for “premarket review.”
Notably, a “grandfather clause” will allow some lab tests already on the market to continue being sold without undergoing FDA’s premarket review process. In explaining the exemption, FDA officials said they did not want doctors and patients to lose access to tests on which they rely. But Dr. Lurie noted that because the FDA views all these tests as under its jurisdiction, the agency could opt to take a closer look “at a very old device that is causing a problem today.”
The FDA also will exempt tests approved by New York State’s Clinical Laboratory Evaluation Program, which conducts its own stringent reviews. And the FDA will continue to allow hospitals to develop tests for patients within their healthcare system without going through the FDA approval process, if no FDA-approved tests are available.
Hospital-based tests play a critical role in treating infectious diseases, said Amesh Adalja, MD, an infectious diseases specialist and senior scholar at the Johns Hopkins Center for Health Security. For example, a large research hospital treating a patient with cytomegalovirus may need to develop its own test to determine whether the infection is resistant to antiviral drugs, Dr. Adalja said.
“With novel infectious disease outbreaks, researchers are able to move quickly to make diagnostic tests months and months before commercial laboratories are able to get through regulatory processes,” Dr. Adalja said.
To help scientists respond quickly to emergencies, the FDA published special guidance for labs that develop unauthorized lab tests for disease outbreaks.
Medical groups such as the American Hospital Association and Infectious Diseases Society of America remain concerned about the burden of complying with new regulations.
“Many vital tests developed in hospitals and health systems may be subjected to unnecessary and costly paperwork,” said Stacey Hughes, executive vice president of the American Hospital Association, in a statement.
Other groups, such as the American Society of Clinical Oncology, praised the new FDA policy. In comments submitted to the FDA in 2023, the cancer group said it “emphatically supports” requiring lab tests to undergo FDA review.
“We appreciate FDA action to modernize oversight of these tests and are hopeful this rule will increase focus on the need to balance rapid diagnostic innovation with patient safety and access” Everett Vokes, MD, the group’s board chair, said in a statement released after the FDA’s final rule was published.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration (FDA) plans to scrutinize the safety and efficacy of lab-developed tests — those designed, manufactured, and used in a single laboratory — far more thoroughly in the future.
Under a rule finalized in April, the FDA will treat facilities that develop and use lab tests as manufacturers and regulate tests as medical devices. That means that most lab tests will need an FDA review before going on sale.
The FDA will also impose new quality standards, requiring test manufacturers to report adverse events and create a registry of lab tests under the new rule, which will be phased in over 4 years.
FDA officials have been concerned for years about the reliability of commercial lab tests, which have ballooned into a multibillion-dollar industry.
Consumer groups have long urged the FDA to regulate lab tests more strictly, arguing that the lack of scrutiny allows doctors and patients to be exploited by bad actors such as Theranos, which falsely claimed that its tests could diagnose multiple diseases with a single drop of blood.
“When it comes to some of these tests that doctors are recommending for patients, many doctors are just crossing their fingers and relying on the representation of the company because nobody is checking” to verify a manufacturer’s claims, said Joshua Sharfstein, MD, vice dean for public health practice and community engagement at the Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland.
Nearly 12,000 Labs Making Medical Tests
Although the FDA estimates there are nearly 12,000 labs manufacturing medical tests, agency officials said they don’t know how many tests are being marketed. The FDA already requires that home test kits marketed directly to consumers, such as those used to detect COVID-19, get clearance from the agency before being sold.
“There’s plenty of time for industry to get its act together to develop the data that it might need to make a premarket application,” said Peter Lurie, MD, PhD, a former associate commissioner at the FDA. In 2015, Dr. Lurie led a report outlining some of the dangers of unregulated lab tests.
For the average physician who orders lab tests, nothing is going to immediately change because of the final rule, said Dr. Lurie, now president of the Center for Science in the Public Interest, a nonprofit consumer watchdog.
“Tomorrow, this will look just the same as it does today,” Dr. Lurie said. “For the next 3 years, the companies will be scurrying behind the scenes to comply with the early stages of implementation. But most of that will be invisible to the average practitioner.”
Dr. Lurie predicted the FDA will focus its scrutiny on tests that pose the greatest potential risk to patients, such as ones used to diagnose serious diseases or guide treatment for life-threatening conditions. “The least significant tests will likely get very limited, if any, scrutiny,” said Dr. Lurie, adding that the FDA will likely issue guidance about how it plans to define low- and high-risk tests. “My suspicion is that it will be probably a small minority of products that are subject to full premarket approval.”
Lab Industry Groups Push Back
But imposing new rules with the potential to affect an industry’s bottom line is no easy task.
The American Clinical Laboratory Association, which represents the lab industry, said in a statement that the FDA rule will “limit access to scores of critical tests, increase healthcare costs, and undermine innovation in new diagnostics.” Another industry group, the Association for Molecular Pathology, has warned of “significant and harmful disruption to laboratory medicine.”
The two associations have filed separate lawsuits, charging that the FDA overstepped the authority granted by Congress. In their lawsuits, groups claim that lab tests are professional services, not manufactured products. The groups noted that the Centers for Medicare & Medicaid Services (CMS) already inspects lab facilities. CMS does not assess the tests’ quality or reliability.
A recent Supreme Court decision could make those lawsuits more likely to succeed, said David Simon, JD, LLM, PhD, an assistant professor of law at the Northeastern University School of Law, Boston, Massachusetts.
In the case of Loper Bright Enterprises v. Raimondo, decided in June, justices overturned a long-standing precedent known as Chevron deference, which required courts to defer to federal agencies when interpreting ambiguous laws. That means that courts no longer have to accept the FDA’s definition of a device, Dr. Simon said.
“Because judges may have more active roles in defining agency authority, federal agencies may have correspondingly less robust roles in policymaking,” Dr. Simon wrote in an editorial coauthored with Michael J. Young, MD, MPhil, of Harvard Medical School, Boston.
The Supreme Court ruling could pressure Congress to more clearly define FDA’s ruling in regulating lab tests, Dr. Simon and Dr. Young wrote.
Members of Congress first introduced a bill to clarify the FDA’s role in regulating lab tests, called the VALID Act, in 2020. The bill stalled and, despite efforts to revive it, still hasn’t passed.
FDA officials have said they remain “open to working with Congress,” noting that any future legislation about lab-developed tests would supersede their current policy.
In an interview, Dr. Simon noted the FDA significantly narrowed the scope of the final rule in response to comments from critics who objected to an earlier version of the policy proposed in 2023. The final rule carves out several categories of tests that won’t need to apply for “premarket review.”
Notably, a “grandfather clause” will allow some lab tests already on the market to continue being sold without undergoing FDA’s premarket review process. In explaining the exemption, FDA officials said they did not want doctors and patients to lose access to tests on which they rely. But Dr. Lurie noted that because the FDA views all these tests as under its jurisdiction, the agency could opt to take a closer look “at a very old device that is causing a problem today.”
The FDA also will exempt tests approved by New York State’s Clinical Laboratory Evaluation Program, which conducts its own stringent reviews. And the FDA will continue to allow hospitals to develop tests for patients within their healthcare system without going through the FDA approval process, if no FDA-approved tests are available.
Hospital-based tests play a critical role in treating infectious diseases, said Amesh Adalja, MD, an infectious diseases specialist and senior scholar at the Johns Hopkins Center for Health Security. For example, a large research hospital treating a patient with cytomegalovirus may need to develop its own test to determine whether the infection is resistant to antiviral drugs, Dr. Adalja said.
“With novel infectious disease outbreaks, researchers are able to move quickly to make diagnostic tests months and months before commercial laboratories are able to get through regulatory processes,” Dr. Adalja said.
To help scientists respond quickly to emergencies, the FDA published special guidance for labs that develop unauthorized lab tests for disease outbreaks.
Medical groups such as the American Hospital Association and Infectious Diseases Society of America remain concerned about the burden of complying with new regulations.
“Many vital tests developed in hospitals and health systems may be subjected to unnecessary and costly paperwork,” said Stacey Hughes, executive vice president of the American Hospital Association, in a statement.
Other groups, such as the American Society of Clinical Oncology, praised the new FDA policy. In comments submitted to the FDA in 2023, the cancer group said it “emphatically supports” requiring lab tests to undergo FDA review.
“We appreciate FDA action to modernize oversight of these tests and are hopeful this rule will increase focus on the need to balance rapid diagnostic innovation with patient safety and access” Everett Vokes, MD, the group’s board chair, said in a statement released after the FDA’s final rule was published.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration (FDA) plans to scrutinize the safety and efficacy of lab-developed tests — those designed, manufactured, and used in a single laboratory — far more thoroughly in the future.
Under a rule finalized in April, the FDA will treat facilities that develop and use lab tests as manufacturers and regulate tests as medical devices. That means that most lab tests will need an FDA review before going on sale.
The FDA will also impose new quality standards, requiring test manufacturers to report adverse events and create a registry of lab tests under the new rule, which will be phased in over 4 years.
FDA officials have been concerned for years about the reliability of commercial lab tests, which have ballooned into a multibillion-dollar industry.
Consumer groups have long urged the FDA to regulate lab tests more strictly, arguing that the lack of scrutiny allows doctors and patients to be exploited by bad actors such as Theranos, which falsely claimed that its tests could diagnose multiple diseases with a single drop of blood.
“When it comes to some of these tests that doctors are recommending for patients, many doctors are just crossing their fingers and relying on the representation of the company because nobody is checking” to verify a manufacturer’s claims, said Joshua Sharfstein, MD, vice dean for public health practice and community engagement at the Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland.
Nearly 12,000 Labs Making Medical Tests
Although the FDA estimates there are nearly 12,000 labs manufacturing medical tests, agency officials said they don’t know how many tests are being marketed. The FDA already requires that home test kits marketed directly to consumers, such as those used to detect COVID-19, get clearance from the agency before being sold.
“There’s plenty of time for industry to get its act together to develop the data that it might need to make a premarket application,” said Peter Lurie, MD, PhD, a former associate commissioner at the FDA. In 2015, Dr. Lurie led a report outlining some of the dangers of unregulated lab tests.
For the average physician who orders lab tests, nothing is going to immediately change because of the final rule, said Dr. Lurie, now president of the Center for Science in the Public Interest, a nonprofit consumer watchdog.
“Tomorrow, this will look just the same as it does today,” Dr. Lurie said. “For the next 3 years, the companies will be scurrying behind the scenes to comply with the early stages of implementation. But most of that will be invisible to the average practitioner.”
Dr. Lurie predicted the FDA will focus its scrutiny on tests that pose the greatest potential risk to patients, such as ones used to diagnose serious diseases or guide treatment for life-threatening conditions. “The least significant tests will likely get very limited, if any, scrutiny,” said Dr. Lurie, adding that the FDA will likely issue guidance about how it plans to define low- and high-risk tests. “My suspicion is that it will be probably a small minority of products that are subject to full premarket approval.”
Lab Industry Groups Push Back
But imposing new rules with the potential to affect an industry’s bottom line is no easy task.
The American Clinical Laboratory Association, which represents the lab industry, said in a statement that the FDA rule will “limit access to scores of critical tests, increase healthcare costs, and undermine innovation in new diagnostics.” Another industry group, the Association for Molecular Pathology, has warned of “significant and harmful disruption to laboratory medicine.”
The two associations have filed separate lawsuits, charging that the FDA overstepped the authority granted by Congress. In their lawsuits, groups claim that lab tests are professional services, not manufactured products. The groups noted that the Centers for Medicare & Medicaid Services (CMS) already inspects lab facilities. CMS does not assess the tests’ quality or reliability.
A recent Supreme Court decision could make those lawsuits more likely to succeed, said David Simon, JD, LLM, PhD, an assistant professor of law at the Northeastern University School of Law, Boston, Massachusetts.
In the case of Loper Bright Enterprises v. Raimondo, decided in June, justices overturned a long-standing precedent known as Chevron deference, which required courts to defer to federal agencies when interpreting ambiguous laws. That means that courts no longer have to accept the FDA’s definition of a device, Dr. Simon said.
“Because judges may have more active roles in defining agency authority, federal agencies may have correspondingly less robust roles in policymaking,” Dr. Simon wrote in an editorial coauthored with Michael J. Young, MD, MPhil, of Harvard Medical School, Boston.
The Supreme Court ruling could pressure Congress to more clearly define FDA’s ruling in regulating lab tests, Dr. Simon and Dr. Young wrote.
Members of Congress first introduced a bill to clarify the FDA’s role in regulating lab tests, called the VALID Act, in 2020. The bill stalled and, despite efforts to revive it, still hasn’t passed.
FDA officials have said they remain “open to working with Congress,” noting that any future legislation about lab-developed tests would supersede their current policy.
In an interview, Dr. Simon noted the FDA significantly narrowed the scope of the final rule in response to comments from critics who objected to an earlier version of the policy proposed in 2023. The final rule carves out several categories of tests that won’t need to apply for “premarket review.”
Notably, a “grandfather clause” will allow some lab tests already on the market to continue being sold without undergoing FDA’s premarket review process. In explaining the exemption, FDA officials said they did not want doctors and patients to lose access to tests on which they rely. But Dr. Lurie noted that because the FDA views all these tests as under its jurisdiction, the agency could opt to take a closer look “at a very old device that is causing a problem today.”
The FDA also will exempt tests approved by New York State’s Clinical Laboratory Evaluation Program, which conducts its own stringent reviews. And the FDA will continue to allow hospitals to develop tests for patients within their healthcare system without going through the FDA approval process, if no FDA-approved tests are available.
Hospital-based tests play a critical role in treating infectious diseases, said Amesh Adalja, MD, an infectious diseases specialist and senior scholar at the Johns Hopkins Center for Health Security. For example, a large research hospital treating a patient with cytomegalovirus may need to develop its own test to determine whether the infection is resistant to antiviral drugs, Dr. Adalja said.
“With novel infectious disease outbreaks, researchers are able to move quickly to make diagnostic tests months and months before commercial laboratories are able to get through regulatory processes,” Dr. Adalja said.
To help scientists respond quickly to emergencies, the FDA published special guidance for labs that develop unauthorized lab tests for disease outbreaks.
Medical groups such as the American Hospital Association and Infectious Diseases Society of America remain concerned about the burden of complying with new regulations.
“Many vital tests developed in hospitals and health systems may be subjected to unnecessary and costly paperwork,” said Stacey Hughes, executive vice president of the American Hospital Association, in a statement.
Other groups, such as the American Society of Clinical Oncology, praised the new FDA policy. In comments submitted to the FDA in 2023, the cancer group said it “emphatically supports” requiring lab tests to undergo FDA review.
“We appreciate FDA action to modernize oversight of these tests and are hopeful this rule will increase focus on the need to balance rapid diagnostic innovation with patient safety and access” Everett Vokes, MD, the group’s board chair, said in a statement released after the FDA’s final rule was published.
A version of this article first appeared on Medscape.com.
When You and Your Malpractice Insurer Disagree on Your Case
You’ve been sued for medical malpractice. If you are a physician in the United States, that is not an unlikely scenario.
An analysis by the American Medical Association shows that almost half of all physicians are sued by the time they reach 54. In some specialties, such as ob.gyn., one is almost guaranteed to be sued at some point.
But that’s what medical malpractice insurance is for, right? Your medical malpractice insurer will assign an attorney to take care of you and help you through this situation. Won’t they?
Maybe so, but the attorney and the claims representative your insurer assigns to your case may have a different idea about how to proceed than you do. Though the defense attorney assigned to you represents you, he or she gets paid by the insurance carrier.
This can create a conflict when your defense counsel and your insurance claims representative aim to take your case in a direction you don’t like.
Disagreements might include:
- Choice of expert witnesses
- Tactical decisions related to trial strategy
- Public relations considerations
- Admissions of liability
- Allocation of resources
To Settle or Not?
One of the most challenging — and common — disagreements is whether to settle the case.
Sometimes a malpractice insurer wants to settle the case against the defendant doctor’s wishes. Or the doctor wants to settle but is pushed into going to trial. In the following case, one doctor had to face the consequences of a decision he didn’t even make.
The Underlying Medical Malpractice Case
Dr. D was sued by a patient who had allegedly called Dr. D’s office six times in 2 days complaining of intermittent chest pain.
Dr. D had been swamped with patients and couldn’t squeeze this patient in for an office visit, but he did call back. The patient later claimed that during the call he told the doctor he was suffering from chest pain. The doctor recalled that the patient had complained of abdominal discomfort that began after he had exercised.
The physician wrote a prescription for an ECG at the local hospital and called to ensure that the patient could just walk in. The ECG was allegedly abnormal but was not read as representing an impending or current heart attack. Later that evening, however, the patient went to the emergency department of another hospital where it was confirmed that he had suffered a heart attack. The patient underwent cardiac catheterization and stent placement to address a blockage in his left anterior descending artery.
The patient subsequently sued Dr. D and the hospital where he had the original ECG. Dr. D contacted his medical malpractice insurance company. The insurance company assigned an attorney to represent Dr. D. Discovery in the case began.
The plaintiff’s own medical expert testified in a deposition that there was no way for the heart attack to have been prevented and that the treatment would have been the same either way. But Dr. D could not find a record of the phone calls with the patient, and he had not noted his conversation the patient in their medical records.
Dr. D held a policy for $1 million, and his state had a fund that would kick in an additional $1 million. But the plaintiffs demanded $4 million to settle.
A month before trial, the plaintiff’s attorney sent a threatening letter to Dr. D’s attorney warning him that Dr. D was underinsured and suggesting that it would be in the physician’s best interests to settle.
“I want to stress to you that it is not my desire to harm your client’s reputation or to destroy his business,” wrote the plaintiff’s attorney. “However, now is the time to avoid consequences such as these by making a good faith effort to get this case resolved.”
The letter went on to note that the defense attorney should give Dr. D a copy of the letter so that everyone would be aware of the potential consequences of an award against Dr. D in excess of his limits of insurance coverage. The plaintiff’s attorney even suggested that Dr. D should retain personal counsel.
Dr. D’s defense attorney downplayed the letter and assured him that there was no reason to worry.
Meanwhile the case inched closer to trial.
The codefendant hospital settled with the plaintiff on the night before jury selection, leaving Dr. D in the uncomfortable position of being the only defendant in the case. At this point, Dr. D decided he would like to settle, and he sent his attorney an email telling him so. But the attorney instead referred him to an insurance company claims.
Just days before the trial was to start, Dr. D repeatedly told the claims representative assigned to his claim that he did not want to go to trial but rather wanted to settle. The representative told Dr. D that he had no choice in whether the action settled.
A committee at the insurance company had decided to proceed with the trial rather than settle.
The trial proved a painful debacle for Dr. D. His attorney’s idea of showing a “gotcha” video of the allegedly permanently injured plaintiff carrying a large, heavy box backfired when the jury was shown by the plaintiff that the box actually contained ice cream cones and weighed very little.
Prior to trial, the plaintiff offered to settle for $1 million. On the first day of trial, they lowered that amount to $750,000, yet the defense attorney did not settle the case, and it proceeded to a jury verdict. The jury awarded the plaintiff over $4 million — well in excess of Dr. D’s policy limits.
The Follow-up
Dr. D was horrified, but the insurance company claims representative said the insurer would promptly offer $2 million in available insurance coverage to settle the case post verdict. This did not happen. Instead, the insurer chose to appeal the verdict against Dr. D’s wishes.
Ultimately, Dr. D was forced to hire his own lawyer. He ultimately sued the insurance company for breach of contract and bad faith.
The insurance company eventually attempted to settle with the plaintiffs’ counsel, but the plaintiff refused to accept the available insurance coverage. The insurance carrier still has not posted the entire appeal bond. The case is still pending.
Protecting Yourself
The lesson from Dr. D’s experience: Understand that the insurance company is not your friend. It’s a business looking out for its own interests.
The plaintiff’s attorney was absolutely correct in suggesting that Dr. D retain his own attorney to represent his own interests. You should hire your own lawyer when:
- You disagree with your insurer on how to proceed in a case.
- You receive a demand that exceeds your available insurance coverage or for damages that may not be covered by your policy, such as punitive damages.
- Your insurance carrier attempts to deny insurance coverage for your claim or sends you a letter stating that it is “reserving its rights” not to cover or to limit coverage for your claim.
Retaining independent counsel protects your interests, not those of your insurance company.
Independent counsel can give you a second opinion on the strengths and weaknesses of your claim, help you prepare for your deposition, and attend court dates with you to ensure that you are completely protected.
Independent counsel can challenge your insurance company’s decision to deny or limit your insurance coverage and ensure that you receive all of the benefits to which you are entitled under your insurance policy. Some policies may include an independent lawyer to be paid for by your insurance carrier in case of a conflicts.
The most important takeaway? Your medical malpractice insurance carrier is not your friend, so act accordingly in times of conflict.
A version of this article first appeared on Medscape.com.
You’ve been sued for medical malpractice. If you are a physician in the United States, that is not an unlikely scenario.
An analysis by the American Medical Association shows that almost half of all physicians are sued by the time they reach 54. In some specialties, such as ob.gyn., one is almost guaranteed to be sued at some point.
But that’s what medical malpractice insurance is for, right? Your medical malpractice insurer will assign an attorney to take care of you and help you through this situation. Won’t they?
Maybe so, but the attorney and the claims representative your insurer assigns to your case may have a different idea about how to proceed than you do. Though the defense attorney assigned to you represents you, he or she gets paid by the insurance carrier.
This can create a conflict when your defense counsel and your insurance claims representative aim to take your case in a direction you don’t like.
Disagreements might include:
- Choice of expert witnesses
- Tactical decisions related to trial strategy
- Public relations considerations
- Admissions of liability
- Allocation of resources
To Settle or Not?
One of the most challenging — and common — disagreements is whether to settle the case.
Sometimes a malpractice insurer wants to settle the case against the defendant doctor’s wishes. Or the doctor wants to settle but is pushed into going to trial. In the following case, one doctor had to face the consequences of a decision he didn’t even make.
The Underlying Medical Malpractice Case
Dr. D was sued by a patient who had allegedly called Dr. D’s office six times in 2 days complaining of intermittent chest pain.
Dr. D had been swamped with patients and couldn’t squeeze this patient in for an office visit, but he did call back. The patient later claimed that during the call he told the doctor he was suffering from chest pain. The doctor recalled that the patient had complained of abdominal discomfort that began after he had exercised.
The physician wrote a prescription for an ECG at the local hospital and called to ensure that the patient could just walk in. The ECG was allegedly abnormal but was not read as representing an impending or current heart attack. Later that evening, however, the patient went to the emergency department of another hospital where it was confirmed that he had suffered a heart attack. The patient underwent cardiac catheterization and stent placement to address a blockage in his left anterior descending artery.
The patient subsequently sued Dr. D and the hospital where he had the original ECG. Dr. D contacted his medical malpractice insurance company. The insurance company assigned an attorney to represent Dr. D. Discovery in the case began.
The plaintiff’s own medical expert testified in a deposition that there was no way for the heart attack to have been prevented and that the treatment would have been the same either way. But Dr. D could not find a record of the phone calls with the patient, and he had not noted his conversation the patient in their medical records.
Dr. D held a policy for $1 million, and his state had a fund that would kick in an additional $1 million. But the plaintiffs demanded $4 million to settle.
A month before trial, the plaintiff’s attorney sent a threatening letter to Dr. D’s attorney warning him that Dr. D was underinsured and suggesting that it would be in the physician’s best interests to settle.
“I want to stress to you that it is not my desire to harm your client’s reputation or to destroy his business,” wrote the plaintiff’s attorney. “However, now is the time to avoid consequences such as these by making a good faith effort to get this case resolved.”
The letter went on to note that the defense attorney should give Dr. D a copy of the letter so that everyone would be aware of the potential consequences of an award against Dr. D in excess of his limits of insurance coverage. The plaintiff’s attorney even suggested that Dr. D should retain personal counsel.
Dr. D’s defense attorney downplayed the letter and assured him that there was no reason to worry.
Meanwhile the case inched closer to trial.
The codefendant hospital settled with the plaintiff on the night before jury selection, leaving Dr. D in the uncomfortable position of being the only defendant in the case. At this point, Dr. D decided he would like to settle, and he sent his attorney an email telling him so. But the attorney instead referred him to an insurance company claims.
Just days before the trial was to start, Dr. D repeatedly told the claims representative assigned to his claim that he did not want to go to trial but rather wanted to settle. The representative told Dr. D that he had no choice in whether the action settled.
A committee at the insurance company had decided to proceed with the trial rather than settle.
The trial proved a painful debacle for Dr. D. His attorney’s idea of showing a “gotcha” video of the allegedly permanently injured plaintiff carrying a large, heavy box backfired when the jury was shown by the plaintiff that the box actually contained ice cream cones and weighed very little.
Prior to trial, the plaintiff offered to settle for $1 million. On the first day of trial, they lowered that amount to $750,000, yet the defense attorney did not settle the case, and it proceeded to a jury verdict. The jury awarded the plaintiff over $4 million — well in excess of Dr. D’s policy limits.
The Follow-up
Dr. D was horrified, but the insurance company claims representative said the insurer would promptly offer $2 million in available insurance coverage to settle the case post verdict. This did not happen. Instead, the insurer chose to appeal the verdict against Dr. D’s wishes.
Ultimately, Dr. D was forced to hire his own lawyer. He ultimately sued the insurance company for breach of contract and bad faith.
The insurance company eventually attempted to settle with the plaintiffs’ counsel, but the plaintiff refused to accept the available insurance coverage. The insurance carrier still has not posted the entire appeal bond. The case is still pending.
Protecting Yourself
The lesson from Dr. D’s experience: Understand that the insurance company is not your friend. It’s a business looking out for its own interests.
The plaintiff’s attorney was absolutely correct in suggesting that Dr. D retain his own attorney to represent his own interests. You should hire your own lawyer when:
- You disagree with your insurer on how to proceed in a case.
- You receive a demand that exceeds your available insurance coverage or for damages that may not be covered by your policy, such as punitive damages.
- Your insurance carrier attempts to deny insurance coverage for your claim or sends you a letter stating that it is “reserving its rights” not to cover or to limit coverage for your claim.
Retaining independent counsel protects your interests, not those of your insurance company.
Independent counsel can give you a second opinion on the strengths and weaknesses of your claim, help you prepare for your deposition, and attend court dates with you to ensure that you are completely protected.
Independent counsel can challenge your insurance company’s decision to deny or limit your insurance coverage and ensure that you receive all of the benefits to which you are entitled under your insurance policy. Some policies may include an independent lawyer to be paid for by your insurance carrier in case of a conflicts.
The most important takeaway? Your medical malpractice insurance carrier is not your friend, so act accordingly in times of conflict.
A version of this article first appeared on Medscape.com.
You’ve been sued for medical malpractice. If you are a physician in the United States, that is not an unlikely scenario.
An analysis by the American Medical Association shows that almost half of all physicians are sued by the time they reach 54. In some specialties, such as ob.gyn., one is almost guaranteed to be sued at some point.
But that’s what medical malpractice insurance is for, right? Your medical malpractice insurer will assign an attorney to take care of you and help you through this situation. Won’t they?
Maybe so, but the attorney and the claims representative your insurer assigns to your case may have a different idea about how to proceed than you do. Though the defense attorney assigned to you represents you, he or she gets paid by the insurance carrier.
This can create a conflict when your defense counsel and your insurance claims representative aim to take your case in a direction you don’t like.
Disagreements might include:
- Choice of expert witnesses
- Tactical decisions related to trial strategy
- Public relations considerations
- Admissions of liability
- Allocation of resources
To Settle or Not?
One of the most challenging — and common — disagreements is whether to settle the case.
Sometimes a malpractice insurer wants to settle the case against the defendant doctor’s wishes. Or the doctor wants to settle but is pushed into going to trial. In the following case, one doctor had to face the consequences of a decision he didn’t even make.
The Underlying Medical Malpractice Case
Dr. D was sued by a patient who had allegedly called Dr. D’s office six times in 2 days complaining of intermittent chest pain.
Dr. D had been swamped with patients and couldn’t squeeze this patient in for an office visit, but he did call back. The patient later claimed that during the call he told the doctor he was suffering from chest pain. The doctor recalled that the patient had complained of abdominal discomfort that began after he had exercised.
The physician wrote a prescription for an ECG at the local hospital and called to ensure that the patient could just walk in. The ECG was allegedly abnormal but was not read as representing an impending or current heart attack. Later that evening, however, the patient went to the emergency department of another hospital where it was confirmed that he had suffered a heart attack. The patient underwent cardiac catheterization and stent placement to address a blockage in his left anterior descending artery.
The patient subsequently sued Dr. D and the hospital where he had the original ECG. Dr. D contacted his medical malpractice insurance company. The insurance company assigned an attorney to represent Dr. D. Discovery in the case began.
The plaintiff’s own medical expert testified in a deposition that there was no way for the heart attack to have been prevented and that the treatment would have been the same either way. But Dr. D could not find a record of the phone calls with the patient, and he had not noted his conversation the patient in their medical records.
Dr. D held a policy for $1 million, and his state had a fund that would kick in an additional $1 million. But the plaintiffs demanded $4 million to settle.
A month before trial, the plaintiff’s attorney sent a threatening letter to Dr. D’s attorney warning him that Dr. D was underinsured and suggesting that it would be in the physician’s best interests to settle.
“I want to stress to you that it is not my desire to harm your client’s reputation or to destroy his business,” wrote the plaintiff’s attorney. “However, now is the time to avoid consequences such as these by making a good faith effort to get this case resolved.”
The letter went on to note that the defense attorney should give Dr. D a copy of the letter so that everyone would be aware of the potential consequences of an award against Dr. D in excess of his limits of insurance coverage. The plaintiff’s attorney even suggested that Dr. D should retain personal counsel.
Dr. D’s defense attorney downplayed the letter and assured him that there was no reason to worry.
Meanwhile the case inched closer to trial.
The codefendant hospital settled with the plaintiff on the night before jury selection, leaving Dr. D in the uncomfortable position of being the only defendant in the case. At this point, Dr. D decided he would like to settle, and he sent his attorney an email telling him so. But the attorney instead referred him to an insurance company claims.
Just days before the trial was to start, Dr. D repeatedly told the claims representative assigned to his claim that he did not want to go to trial but rather wanted to settle. The representative told Dr. D that he had no choice in whether the action settled.
A committee at the insurance company had decided to proceed with the trial rather than settle.
The trial proved a painful debacle for Dr. D. His attorney’s idea of showing a “gotcha” video of the allegedly permanently injured plaintiff carrying a large, heavy box backfired when the jury was shown by the plaintiff that the box actually contained ice cream cones and weighed very little.
Prior to trial, the plaintiff offered to settle for $1 million. On the first day of trial, they lowered that amount to $750,000, yet the defense attorney did not settle the case, and it proceeded to a jury verdict. The jury awarded the plaintiff over $4 million — well in excess of Dr. D’s policy limits.
The Follow-up
Dr. D was horrified, but the insurance company claims representative said the insurer would promptly offer $2 million in available insurance coverage to settle the case post verdict. This did not happen. Instead, the insurer chose to appeal the verdict against Dr. D’s wishes.
Ultimately, Dr. D was forced to hire his own lawyer. He ultimately sued the insurance company for breach of contract and bad faith.
The insurance company eventually attempted to settle with the plaintiffs’ counsel, but the plaintiff refused to accept the available insurance coverage. The insurance carrier still has not posted the entire appeal bond. The case is still pending.
Protecting Yourself
The lesson from Dr. D’s experience: Understand that the insurance company is not your friend. It’s a business looking out for its own interests.
The plaintiff’s attorney was absolutely correct in suggesting that Dr. D retain his own attorney to represent his own interests. You should hire your own lawyer when:
- You disagree with your insurer on how to proceed in a case.
- You receive a demand that exceeds your available insurance coverage or for damages that may not be covered by your policy, such as punitive damages.
- Your insurance carrier attempts to deny insurance coverage for your claim or sends you a letter stating that it is “reserving its rights” not to cover or to limit coverage for your claim.
Retaining independent counsel protects your interests, not those of your insurance company.
Independent counsel can give you a second opinion on the strengths and weaknesses of your claim, help you prepare for your deposition, and attend court dates with you to ensure that you are completely protected.
Independent counsel can challenge your insurance company’s decision to deny or limit your insurance coverage and ensure that you receive all of the benefits to which you are entitled under your insurance policy. Some policies may include an independent lawyer to be paid for by your insurance carrier in case of a conflicts.
The most important takeaway? Your medical malpractice insurance carrier is not your friend, so act accordingly in times of conflict.
A version of this article first appeared on Medscape.com.
Coffee’s ‘Sweet Spot’: Daily Consumption and Cardiometabolic Risk
Each and every day, 1 billion people on this planet ingest a particular psychoactive substance. This chemical has fairly profound physiologic effects. It increases levels of nitric oxide in the blood, leads to vasodilation, and, of course, makes you feel more awake. The substance comes in many forms but almost always in a liquid medium. Do you have it yet? That’s right. The substance is caffeine, quite possibly the healthiest recreational drug that has ever been discovered.
This might be my New England upbringing speaking, but when it comes to lifestyle and health, one of the rules I’ve internalized is that things that are pleasurable are generally bad for you. I know, I know — some of you love to exercise. Some of you love doing crosswords. But you know what I mean. I’m talking French fries, smoked meats, drugs, smoking, alcohol, binge-watching Firefly. You’d be suspicious if a study came out suggesting that eating ice cream in bed reduces your risk for heart attack, and so would I. So I’m always on the lookout for those unicorns of lifestyle factors, those rare things that you want to do and are also good for you.
So far, the data are strong for three things: sleeping, (safe) sexual activity, and coffee. You’ll have to stay tuned for articles about the first two. Today, we’re brewing up some deeper insights about the power of java.
I was inspired to write this article because of a paper, “Habitual Coffee, Tea, and Caffeine Consumption, Circulating Metabolites, and the Risk of Cardiometabolic Multimorbidity,” appearing September 17 in The Journal of Clinical Endocrinology and Metabolism (JCEM).
This is not the first study to suggest that coffee intake may be beneficial. A 2013 meta-analysis summarized the results of 36 studies with more than a million participants and found a U-shaped relationship between coffee intake and cardiovascular risk. The sweet spot was at three to five cups a day; people drinking that much coffee had about a 15% reduced risk for cardiovascular disease compared with nondrinkers.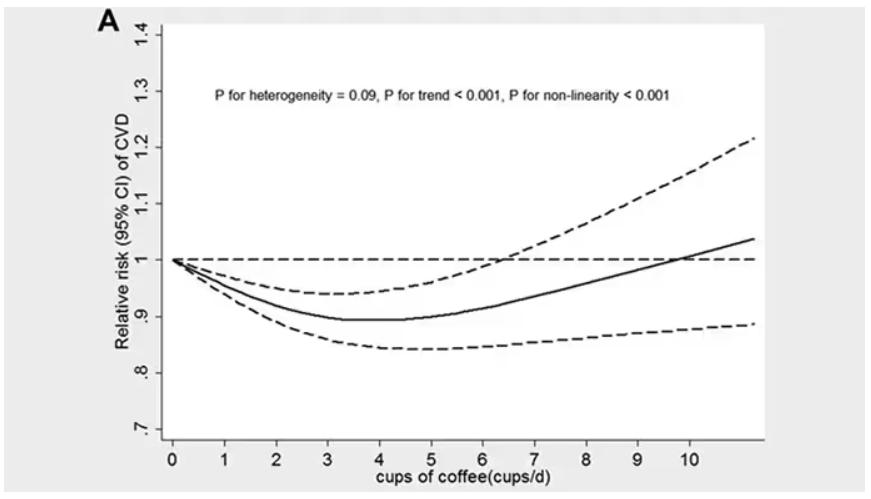
But here’s the thing. Coffee contains caffeine, but it is much more than that. It is a heady brew of various chemicals and compounds, phenols, and chlorogenic acids. And, of course, you can get caffeine from stuff that isn’t coffee — natural things like tea — and decidedly unnatural things like energy drinks. How do you figure out where the benefit really lies?
The JCEM study leveraged the impressive UK Biobank dataset to figure this out. The Biobank recruited more than half a million people from the UK between 2006 and 2010 and collected a wealth of data from each of them: surveys, blood samples, biometrics, medical imaging — the works. And then they followed what would happen to those people medically over time. It’s a pretty amazing resource.
But for the purposes of this study, what you need to know is that just under 200,000 of those participants met the key criteria for this study: being free from cardiovascular disease at baseline; having completed a detailed survey about their coffee, tea, and other caffeinated beverage intake; and having adequate follow-up. A subset of that number, just under 100,000, had metabolomic data — which is where this study really gets interesting.
We’ll dive into the metabolome in a moment, but first let’s just talk about the main finding, the relationship between coffee, tea, or caffeine and cardiovascular disease. But to do that, we need to acknowledge that people who drink a lot of coffee are different from people who don’t, and it might be those differences, not the coffee itself, that are beneficial.
What were those differences? People who drank more coffee tended to be a bit older, were less likely to be female, and were slightly more likely to engage in physical activity. They ate less processed meat but also fewer vegetables. Some of those factors, like being female, are generally protective against cardiovascular disease; but some, like age, are definitely not. The authors adjusted for these and multiple other factors, including alcohol intake, BMI, kidney function, and many others to try to disentangle the effect of being the type of person who drinks a lot of coffee from the drinking a lot of coffee itself.
These are the results of the fully adjusted model. Compared with nonconsumers, you can see that people in the higher range of coffee, tea, or just caffeine intake have almost a 40% reduction in cardiovascular disease in follow-up.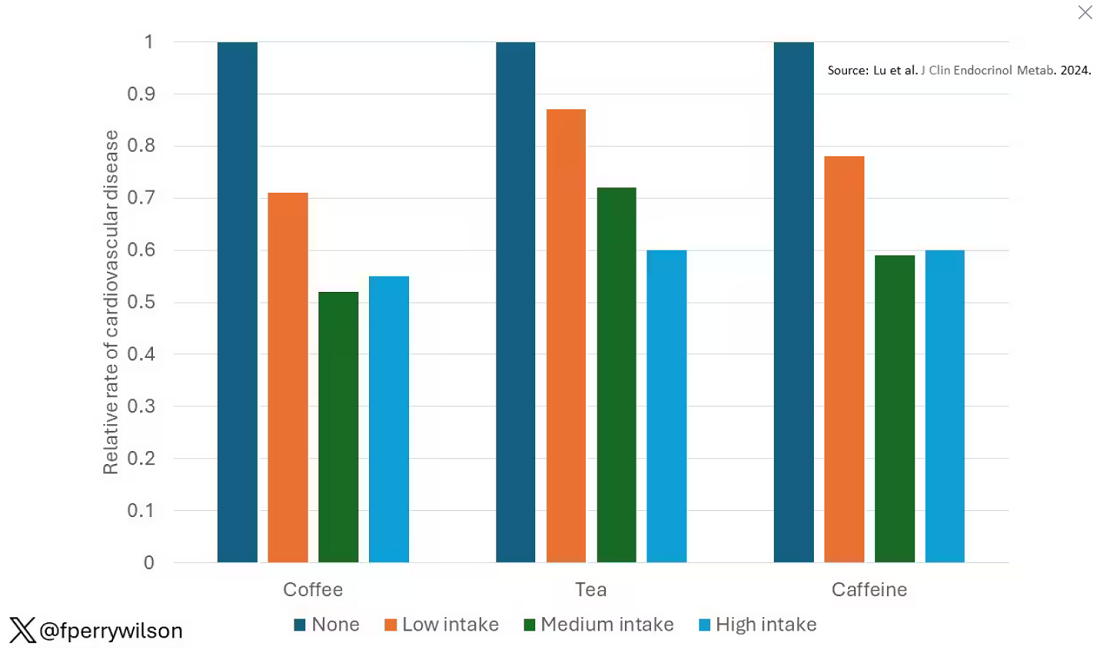
Looking at the benefit across the spectrum of intake, you again see that U-shaped curve, suggesting that a sweet spot for daily consumption can be found around 3 cups of coffee or tea (or 250 mg of caffeine). A standard energy drink contains about 120 mg of caffeine. 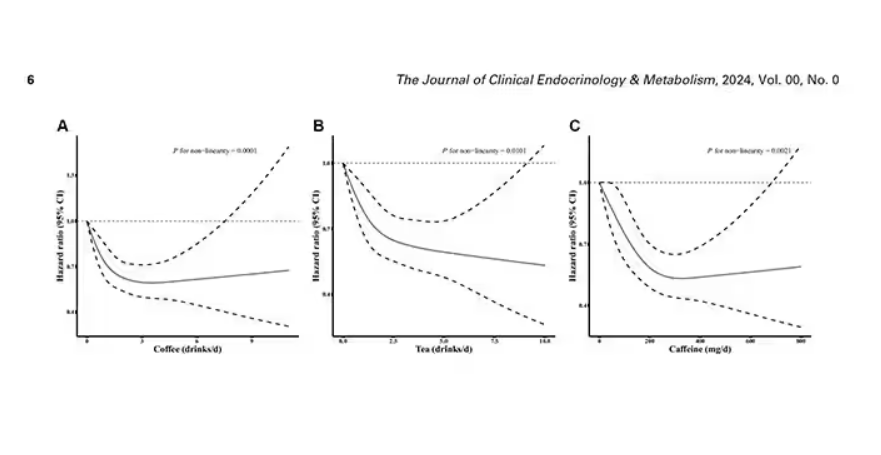
But if this is true, it would be good to know why. To figure that out, the authors turned to the metabolome. The idea here is that your body is constantly breaking stuff down, taking all these proteins and chemicals and compounds that we ingest and turning them into metabolites. Using advanced measurement techniques, researchers can measure hundreds or even thousands of metabolites from a single blood sample. They provide information, obviously, about the food you eat and the drinks you drink, but what is really intriguing is that some metabolites are associated with better health and some with worse
In this study, researchers measured 168 individual metabolites. Eighty of them, nearly half, were significantly altered in people who drank more coffee.
This figure summarizes the findings, and yes, this is way too complicated. 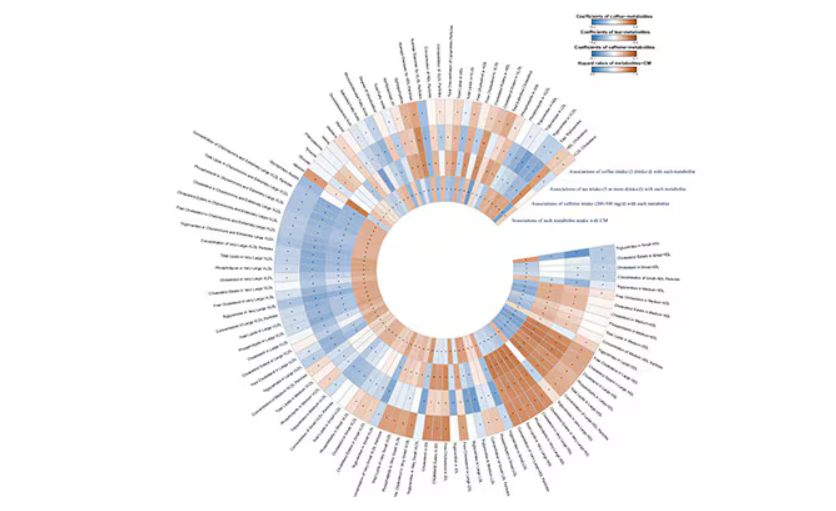
But here’s how to interpret it. The inner ring shows you how certain metabolites are associated with cardiovascular disease. The outer rings show you how those metabolites are associated with coffee, tea, or caffeine. The interesting part is that the sections of the ring (outer rings and inner rings) are very different colors.
Like here.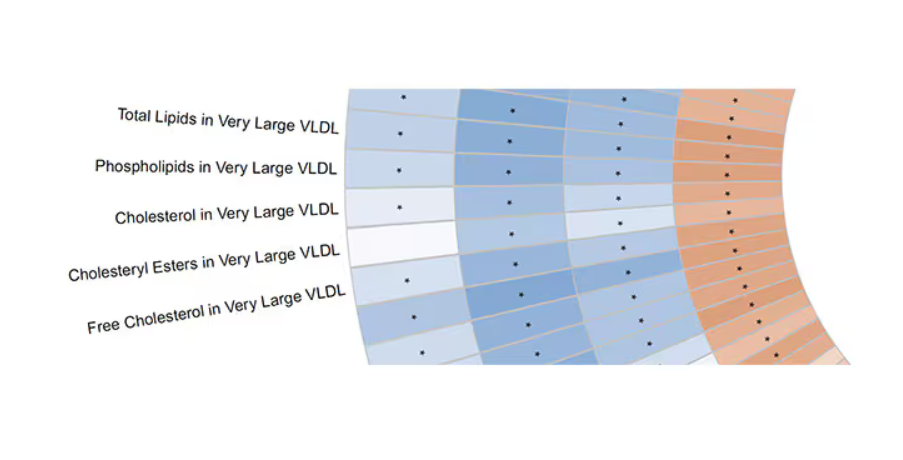
What you see here is a fairly profound effect that coffee, tea, or caffeine intake has on metabolites of VLDL — bad cholesterol. The beverages lower it, and, of course, higher levels lead to cardiovascular disease. This means that this is a potential causal pathway from coffee intake to heart protection.
And that’s not the only one.
You see a similar relationship for saturated fatty acids. Higher levels lead to cardiovascular disease, and coffee intake lowers levels. The reverse works too: Lower levels of histidine (an amino acid) increase cardiovascular risk, and coffee seems to raise those levels.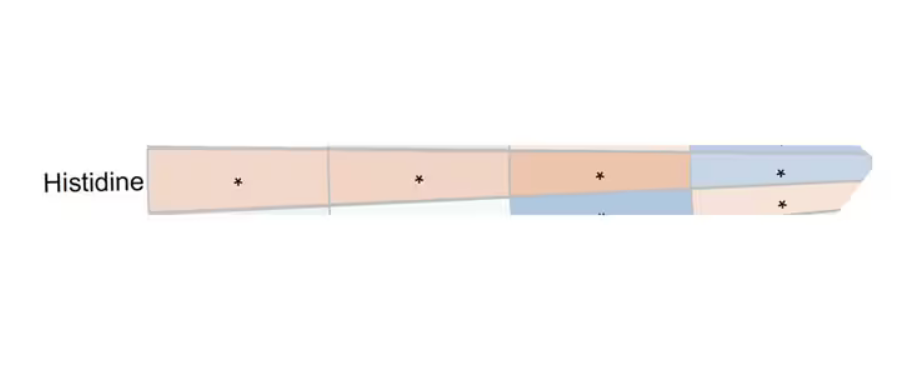
Is this all too good to be true? It’s hard to say. The data on coffee’s benefits have been remarkably consistent. Still, I wouldn’t be a good doctor if I didn’t mention that clearly there is a difference between a cup of black coffee and a venti caramel Frappuccino.
Nevertheless, coffee remains firmly in my holy trinity of enjoyable things that are, for whatever reason, still good for you. So, when you’re having that second, or third, or maybe fourth cup of the day, you can take that to heart.
Dr. Wilson, associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator, reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Each and every day, 1 billion people on this planet ingest a particular psychoactive substance. This chemical has fairly profound physiologic effects. It increases levels of nitric oxide in the blood, leads to vasodilation, and, of course, makes you feel more awake. The substance comes in many forms but almost always in a liquid medium. Do you have it yet? That’s right. The substance is caffeine, quite possibly the healthiest recreational drug that has ever been discovered.
This might be my New England upbringing speaking, but when it comes to lifestyle and health, one of the rules I’ve internalized is that things that are pleasurable are generally bad for you. I know, I know — some of you love to exercise. Some of you love doing crosswords. But you know what I mean. I’m talking French fries, smoked meats, drugs, smoking, alcohol, binge-watching Firefly. You’d be suspicious if a study came out suggesting that eating ice cream in bed reduces your risk for heart attack, and so would I. So I’m always on the lookout for those unicorns of lifestyle factors, those rare things that you want to do and are also good for you.
So far, the data are strong for three things: sleeping, (safe) sexual activity, and coffee. You’ll have to stay tuned for articles about the first two. Today, we’re brewing up some deeper insights about the power of java.
I was inspired to write this article because of a paper, “Habitual Coffee, Tea, and Caffeine Consumption, Circulating Metabolites, and the Risk of Cardiometabolic Multimorbidity,” appearing September 17 in The Journal of Clinical Endocrinology and Metabolism (JCEM).
This is not the first study to suggest that coffee intake may be beneficial. A 2013 meta-analysis summarized the results of 36 studies with more than a million participants and found a U-shaped relationship between coffee intake and cardiovascular risk. The sweet spot was at three to five cups a day; people drinking that much coffee had about a 15% reduced risk for cardiovascular disease compared with nondrinkers.
But here’s the thing. Coffee contains caffeine, but it is much more than that. It is a heady brew of various chemicals and compounds, phenols, and chlorogenic acids. And, of course, you can get caffeine from stuff that isn’t coffee — natural things like tea — and decidedly unnatural things like energy drinks. How do you figure out where the benefit really lies?
The JCEM study leveraged the impressive UK Biobank dataset to figure this out. The Biobank recruited more than half a million people from the UK between 2006 and 2010 and collected a wealth of data from each of them: surveys, blood samples, biometrics, medical imaging — the works. And then they followed what would happen to those people medically over time. It’s a pretty amazing resource.
But for the purposes of this study, what you need to know is that just under 200,000 of those participants met the key criteria for this study: being free from cardiovascular disease at baseline; having completed a detailed survey about their coffee, tea, and other caffeinated beverage intake; and having adequate follow-up. A subset of that number, just under 100,000, had metabolomic data — which is where this study really gets interesting.
We’ll dive into the metabolome in a moment, but first let’s just talk about the main finding, the relationship between coffee, tea, or caffeine and cardiovascular disease. But to do that, we need to acknowledge that people who drink a lot of coffee are different from people who don’t, and it might be those differences, not the coffee itself, that are beneficial.
What were those differences? People who drank more coffee tended to be a bit older, were less likely to be female, and were slightly more likely to engage in physical activity. They ate less processed meat but also fewer vegetables. Some of those factors, like being female, are generally protective against cardiovascular disease; but some, like age, are definitely not. The authors adjusted for these and multiple other factors, including alcohol intake, BMI, kidney function, and many others to try to disentangle the effect of being the type of person who drinks a lot of coffee from the drinking a lot of coffee itself.
These are the results of the fully adjusted model. Compared with nonconsumers, you can see that people in the higher range of coffee, tea, or just caffeine intake have almost a 40% reduction in cardiovascular disease in follow-up.
Looking at the benefit across the spectrum of intake, you again see that U-shaped curve, suggesting that a sweet spot for daily consumption can be found around 3 cups of coffee or tea (or 250 mg of caffeine). A standard energy drink contains about 120 mg of caffeine.
But if this is true, it would be good to know why. To figure that out, the authors turned to the metabolome. The idea here is that your body is constantly breaking stuff down, taking all these proteins and chemicals and compounds that we ingest and turning them into metabolites. Using advanced measurement techniques, researchers can measure hundreds or even thousands of metabolites from a single blood sample. They provide information, obviously, about the food you eat and the drinks you drink, but what is really intriguing is that some metabolites are associated with better health and some with worse
In this study, researchers measured 168 individual metabolites. Eighty of them, nearly half, were significantly altered in people who drank more coffee.
This figure summarizes the findings, and yes, this is way too complicated.
But here’s how to interpret it. The inner ring shows you how certain metabolites are associated with cardiovascular disease. The outer rings show you how those metabolites are associated with coffee, tea, or caffeine. The interesting part is that the sections of the ring (outer rings and inner rings) are very different colors.
Like here.
What you see here is a fairly profound effect that coffee, tea, or caffeine intake has on metabolites of VLDL — bad cholesterol. The beverages lower it, and, of course, higher levels lead to cardiovascular disease. This means that this is a potential causal pathway from coffee intake to heart protection.
And that’s not the only one.
You see a similar relationship for saturated fatty acids. Higher levels lead to cardiovascular disease, and coffee intake lowers levels. The reverse works too: Lower levels of histidine (an amino acid) increase cardiovascular risk, and coffee seems to raise those levels.
Is this all too good to be true? It’s hard to say. The data on coffee’s benefits have been remarkably consistent. Still, I wouldn’t be a good doctor if I didn’t mention that clearly there is a difference between a cup of black coffee and a venti caramel Frappuccino.
Nevertheless, coffee remains firmly in my holy trinity of enjoyable things that are, for whatever reason, still good for you. So, when you’re having that second, or third, or maybe fourth cup of the day, you can take that to heart.
Dr. Wilson, associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator, reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Each and every day, 1 billion people on this planet ingest a particular psychoactive substance. This chemical has fairly profound physiologic effects. It increases levels of nitric oxide in the blood, leads to vasodilation, and, of course, makes you feel more awake. The substance comes in many forms but almost always in a liquid medium. Do you have it yet? That’s right. The substance is caffeine, quite possibly the healthiest recreational drug that has ever been discovered.
This might be my New England upbringing speaking, but when it comes to lifestyle and health, one of the rules I’ve internalized is that things that are pleasurable are generally bad for you. I know, I know — some of you love to exercise. Some of you love doing crosswords. But you know what I mean. I’m talking French fries, smoked meats, drugs, smoking, alcohol, binge-watching Firefly. You’d be suspicious if a study came out suggesting that eating ice cream in bed reduces your risk for heart attack, and so would I. So I’m always on the lookout for those unicorns of lifestyle factors, those rare things that you want to do and are also good for you.
So far, the data are strong for three things: sleeping, (safe) sexual activity, and coffee. You’ll have to stay tuned for articles about the first two. Today, we’re brewing up some deeper insights about the power of java.
I was inspired to write this article because of a paper, “Habitual Coffee, Tea, and Caffeine Consumption, Circulating Metabolites, and the Risk of Cardiometabolic Multimorbidity,” appearing September 17 in The Journal of Clinical Endocrinology and Metabolism (JCEM).
This is not the first study to suggest that coffee intake may be beneficial. A 2013 meta-analysis summarized the results of 36 studies with more than a million participants and found a U-shaped relationship between coffee intake and cardiovascular risk. The sweet spot was at three to five cups a day; people drinking that much coffee had about a 15% reduced risk for cardiovascular disease compared with nondrinkers.
But here’s the thing. Coffee contains caffeine, but it is much more than that. It is a heady brew of various chemicals and compounds, phenols, and chlorogenic acids. And, of course, you can get caffeine from stuff that isn’t coffee — natural things like tea — and decidedly unnatural things like energy drinks. How do you figure out where the benefit really lies?
The JCEM study leveraged the impressive UK Biobank dataset to figure this out. The Biobank recruited more than half a million people from the UK between 2006 and 2010 and collected a wealth of data from each of them: surveys, blood samples, biometrics, medical imaging — the works. And then they followed what would happen to those people medically over time. It’s a pretty amazing resource.
But for the purposes of this study, what you need to know is that just under 200,000 of those participants met the key criteria for this study: being free from cardiovascular disease at baseline; having completed a detailed survey about their coffee, tea, and other caffeinated beverage intake; and having adequate follow-up. A subset of that number, just under 100,000, had metabolomic data — which is where this study really gets interesting.
We’ll dive into the metabolome in a moment, but first let’s just talk about the main finding, the relationship between coffee, tea, or caffeine and cardiovascular disease. But to do that, we need to acknowledge that people who drink a lot of coffee are different from people who don’t, and it might be those differences, not the coffee itself, that are beneficial.
What were those differences? People who drank more coffee tended to be a bit older, were less likely to be female, and were slightly more likely to engage in physical activity. They ate less processed meat but also fewer vegetables. Some of those factors, like being female, are generally protective against cardiovascular disease; but some, like age, are definitely not. The authors adjusted for these and multiple other factors, including alcohol intake, BMI, kidney function, and many others to try to disentangle the effect of being the type of person who drinks a lot of coffee from the drinking a lot of coffee itself.
These are the results of the fully adjusted model. Compared with nonconsumers, you can see that people in the higher range of coffee, tea, or just caffeine intake have almost a 40% reduction in cardiovascular disease in follow-up.
Looking at the benefit across the spectrum of intake, you again see that U-shaped curve, suggesting that a sweet spot for daily consumption can be found around 3 cups of coffee or tea (or 250 mg of caffeine). A standard energy drink contains about 120 mg of caffeine.
But if this is true, it would be good to know why. To figure that out, the authors turned to the metabolome. The idea here is that your body is constantly breaking stuff down, taking all these proteins and chemicals and compounds that we ingest and turning them into metabolites. Using advanced measurement techniques, researchers can measure hundreds or even thousands of metabolites from a single blood sample. They provide information, obviously, about the food you eat and the drinks you drink, but what is really intriguing is that some metabolites are associated with better health and some with worse
In this study, researchers measured 168 individual metabolites. Eighty of them, nearly half, were significantly altered in people who drank more coffee.
This figure summarizes the findings, and yes, this is way too complicated.
But here’s how to interpret it. The inner ring shows you how certain metabolites are associated with cardiovascular disease. The outer rings show you how those metabolites are associated with coffee, tea, or caffeine. The interesting part is that the sections of the ring (outer rings and inner rings) are very different colors.
Like here.
What you see here is a fairly profound effect that coffee, tea, or caffeine intake has on metabolites of VLDL — bad cholesterol. The beverages lower it, and, of course, higher levels lead to cardiovascular disease. This means that this is a potential causal pathway from coffee intake to heart protection.
And that’s not the only one.
You see a similar relationship for saturated fatty acids. Higher levels lead to cardiovascular disease, and coffee intake lowers levels. The reverse works too: Lower levels of histidine (an amino acid) increase cardiovascular risk, and coffee seems to raise those levels.
Is this all too good to be true? It’s hard to say. The data on coffee’s benefits have been remarkably consistent. Still, I wouldn’t be a good doctor if I didn’t mention that clearly there is a difference between a cup of black coffee and a venti caramel Frappuccino.
Nevertheless, coffee remains firmly in my holy trinity of enjoyable things that are, for whatever reason, still good for you. So, when you’re having that second, or third, or maybe fourth cup of the day, you can take that to heart.
Dr. Wilson, associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator, reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Why More Doctors Are Joining Unions
With huge shifts over the past decade in the way doctors are employed — half of all doctors now work for a health system or large medical group — the idea of unionizing is not only being explored but gaining traction within the profession. In fact, 8% of the physician workforce (or 70,000 physicians) belong to a union, according to statistics gathered in 2022.
Exact numbers are hard to come by, and, interestingly, although the American Medical Association (AMA) “ supports the right of physicians to engage in collective bargaining,” the organization doesn’t track union membership among physicians, according to an AMA spokesperson.
Forming a Union
One challenge is that forming a union is not only time-consuming but also difficult, owing to several barriers. For starters, the laws dictating unionization differ by state, and the rules governing unionization vary if a hospital is public or private. If there’s enough momentum from doctors leading unionization efforts, approval from hospital leaders is required before an official election can be requested from the National Labor Relations Board.
That said, for doctors who are in a union — the two most popular are the Union of American Physicians and Dentists and the Doctors Council branch of the Service Employees International Union (SEIU)—the benefits are immense, especially because union members can focus on what matters, such as providing the best patient care possible.
, reported WBUR in Boston.
Belonging Matters
“When you build a relationship with your patients, it’s special, and that connection isn’t replaceable,” said Nicholas VenOsdel, MD, a pediatrician at Allina Health Primary Care in Hastings, Minnesota, and a union member of the Doctors Council. “However, a lot of us have felt like that hasn’t been respected as the climate of healthcare has changed so fast.”
In fact, autonomy over how much time doctors spend with patients is driving a lot of interest in unionization.
“We don’t necessarily have that autonomy now,” said Amber Higgins, MD, an emergency physician and an obstetrician at ChristianaCare, a hospital network in Newark, Delaware, and a member of the Doctors Council. “There are so many other demands, whether it’s billing, patient documentation, or other demands from the employer, and all of that takes time away from patient care.”
Another primary driver of physician unionization is the physician burnout epidemic. Physicians collectively complain that they spend more time on electronic health record documentation and bureaucratic administration. Yet if unions can improve these working conditions, the benefit to physicians and their patients would be a welcome change.
Union members are bullish and believe that having a cohesive voice will make a difference.
“We need to use our collective voices to get back to focusing on patient care instead of staring at a computer screen for 80% of the day,” Dr. Higgins told this news organization. “So much of medicine involves getting to the correct diagnosis, listening to patients, observing them, and building a relationship with them. We need time to build that.”
With corporate consolidation and a profit-driven mandate by healthcare systems, doctors are increasingly frustrated and feel that their voices haven’t been heard enough when it comes to issues like workplace safety, working hours, and benefits, said Stuart Bussey, MD, JD, a family practice physician and president of the Union of American Physicians and Dentists in Sacramento, California.
However, he adds that urging doctors to join together to fight for a better working environment hasn’t been easy.
“Doctors are individualists, and they don’t know how to work in packs like hospital administrators do,” said Dr. Bussey. “They’re hard to organize, but I want them to understand that unless they join hands, sign petitions, and speak as one voice, they’re going to lose out on an amazing opportunity.”
Overcoming Misperceptions About Unions
One barrier to doctors getting involved is the sentiment that unions might do the opposite of what’s intended — that is, they might further reduce a doctor’s autonomy and work flexibility. Or there may be a perception that the drive to join a union is predicated on making more money.
Though he’s now in a union, Dr. VenOsdel, who has been in a hospital-based practice for 7 years, admits that he initially felt very differently about unions than he does today.
“Even though I have family members in healthcare unions, I had a neutral to even slightly negative view of unions,” said Dr. VenOsdel. “It took me working directly with the Minnesota Nurses Association and the Doctors Council to learn the other side of the story.”
Armed with more information, he began lobbying for stricter rules about how his state’s large healthcare systems were closing hospitals and ending much-needed community services.
“I remember standing at the Capitol in Minnesota and telling one of the members that I once felt negatively about unions,” he added. “I realized then that I only knew what employers were telling me via such things as emails about strikes — that information was all being shared from the employers’ perspective.”
The other misperception is that unions only exist to argue against management, including against colleagues who are also part of the management structure, said Dr. Higgins.
“Some doctors perceive being in a union as ‘how can those same leaders also be in a union,’” she said. She feels that they currently don’t have leadership representing them that can help with such things as restructuring their support teams or getting them help with certain tasks. “That’s another way unions can help.”
Social Justice Plays a Role
For Dr. VenOsdel, being part of a union has helped him return to what he calls the “art” of medicine.
“Philosophically, the union gave me an option for change in what felt like a hopeless situation,” he said. “It wasn’t just that I was tossing the keys to someone else and saying, ‘I can’t fix this.’ Instead, we’re taking the reins back and fixing things ourselves.”
Bussey argues that as the uneven balance between administrators and providers in many healthcare organizations grows, the time to consider forming a union is now.
“We’re in a $4 trillion medical industrial revolution,” he said. “Administrators and bureaucrats are multiplying 30-fold times vs providers, and most of that $4 trillion supports things that don’t contribute to the doctor-patient relationship.”
Furthermore, union proponents say that where a one-on-one relationship between doctor and patient once existed, that has now been “triangulated” to include administrators.
“We’ve lost power in every way,” Dr. Bussey said. “We have the degrees, the liability, and the knowledge — we should have more power to make our workplaces safer and better.”
Ultimately, for some unionized doctors, the very holding of a union card is rooted in supporting social justice issues.
“When doctors realize how powerful a tool a union can be for social justice and change, this will alter perceptions of unions within our profession,” Dr. VenOsdel said. “Our union helps give us a voice to stand up for other staff who aren’t unionized and, most importantly, to stand up for the patients who need us.”
A version of this article first appeared on Medscape.com.
With huge shifts over the past decade in the way doctors are employed — half of all doctors now work for a health system or large medical group — the idea of unionizing is not only being explored but gaining traction within the profession. In fact, 8% of the physician workforce (or 70,000 physicians) belong to a union, according to statistics gathered in 2022.
Exact numbers are hard to come by, and, interestingly, although the American Medical Association (AMA) “ supports the right of physicians to engage in collective bargaining,” the organization doesn’t track union membership among physicians, according to an AMA spokesperson.
Forming a Union
One challenge is that forming a union is not only time-consuming but also difficult, owing to several barriers. For starters, the laws dictating unionization differ by state, and the rules governing unionization vary if a hospital is public or private. If there’s enough momentum from doctors leading unionization efforts, approval from hospital leaders is required before an official election can be requested from the National Labor Relations Board.
That said, for doctors who are in a union — the two most popular are the Union of American Physicians and Dentists and the Doctors Council branch of the Service Employees International Union (SEIU)—the benefits are immense, especially because union members can focus on what matters, such as providing the best patient care possible.
, reported WBUR in Boston.
Belonging Matters
“When you build a relationship with your patients, it’s special, and that connection isn’t replaceable,” said Nicholas VenOsdel, MD, a pediatrician at Allina Health Primary Care in Hastings, Minnesota, and a union member of the Doctors Council. “However, a lot of us have felt like that hasn’t been respected as the climate of healthcare has changed so fast.”
In fact, autonomy over how much time doctors spend with patients is driving a lot of interest in unionization.
“We don’t necessarily have that autonomy now,” said Amber Higgins, MD, an emergency physician and an obstetrician at ChristianaCare, a hospital network in Newark, Delaware, and a member of the Doctors Council. “There are so many other demands, whether it’s billing, patient documentation, or other demands from the employer, and all of that takes time away from patient care.”
Another primary driver of physician unionization is the physician burnout epidemic. Physicians collectively complain that they spend more time on electronic health record documentation and bureaucratic administration. Yet if unions can improve these working conditions, the benefit to physicians and their patients would be a welcome change.
Union members are bullish and believe that having a cohesive voice will make a difference.
“We need to use our collective voices to get back to focusing on patient care instead of staring at a computer screen for 80% of the day,” Dr. Higgins told this news organization. “So much of medicine involves getting to the correct diagnosis, listening to patients, observing them, and building a relationship with them. We need time to build that.”
With corporate consolidation and a profit-driven mandate by healthcare systems, doctors are increasingly frustrated and feel that their voices haven’t been heard enough when it comes to issues like workplace safety, working hours, and benefits, said Stuart Bussey, MD, JD, a family practice physician and president of the Union of American Physicians and Dentists in Sacramento, California.
However, he adds that urging doctors to join together to fight for a better working environment hasn’t been easy.
“Doctors are individualists, and they don’t know how to work in packs like hospital administrators do,” said Dr. Bussey. “They’re hard to organize, but I want them to understand that unless they join hands, sign petitions, and speak as one voice, they’re going to lose out on an amazing opportunity.”
Overcoming Misperceptions About Unions
One barrier to doctors getting involved is the sentiment that unions might do the opposite of what’s intended — that is, they might further reduce a doctor’s autonomy and work flexibility. Or there may be a perception that the drive to join a union is predicated on making more money.
Though he’s now in a union, Dr. VenOsdel, who has been in a hospital-based practice for 7 years, admits that he initially felt very differently about unions than he does today.
“Even though I have family members in healthcare unions, I had a neutral to even slightly negative view of unions,” said Dr. VenOsdel. “It took me working directly with the Minnesota Nurses Association and the Doctors Council to learn the other side of the story.”
Armed with more information, he began lobbying for stricter rules about how his state’s large healthcare systems were closing hospitals and ending much-needed community services.
“I remember standing at the Capitol in Minnesota and telling one of the members that I once felt negatively about unions,” he added. “I realized then that I only knew what employers were telling me via such things as emails about strikes — that information was all being shared from the employers’ perspective.”
The other misperception is that unions only exist to argue against management, including against colleagues who are also part of the management structure, said Dr. Higgins.
“Some doctors perceive being in a union as ‘how can those same leaders also be in a union,’” she said. She feels that they currently don’t have leadership representing them that can help with such things as restructuring their support teams or getting them help with certain tasks. “That’s another way unions can help.”
Social Justice Plays a Role
For Dr. VenOsdel, being part of a union has helped him return to what he calls the “art” of medicine.
“Philosophically, the union gave me an option for change in what felt like a hopeless situation,” he said. “It wasn’t just that I was tossing the keys to someone else and saying, ‘I can’t fix this.’ Instead, we’re taking the reins back and fixing things ourselves.”
Bussey argues that as the uneven balance between administrators and providers in many healthcare organizations grows, the time to consider forming a union is now.
“We’re in a $4 trillion medical industrial revolution,” he said. “Administrators and bureaucrats are multiplying 30-fold times vs providers, and most of that $4 trillion supports things that don’t contribute to the doctor-patient relationship.”
Furthermore, union proponents say that where a one-on-one relationship between doctor and patient once existed, that has now been “triangulated” to include administrators.
“We’ve lost power in every way,” Dr. Bussey said. “We have the degrees, the liability, and the knowledge — we should have more power to make our workplaces safer and better.”
Ultimately, for some unionized doctors, the very holding of a union card is rooted in supporting social justice issues.
“When doctors realize how powerful a tool a union can be for social justice and change, this will alter perceptions of unions within our profession,” Dr. VenOsdel said. “Our union helps give us a voice to stand up for other staff who aren’t unionized and, most importantly, to stand up for the patients who need us.”
A version of this article first appeared on Medscape.com.
With huge shifts over the past decade in the way doctors are employed — half of all doctors now work for a health system or large medical group — the idea of unionizing is not only being explored but gaining traction within the profession. In fact, 8% of the physician workforce (or 70,000 physicians) belong to a union, according to statistics gathered in 2022.
Exact numbers are hard to come by, and, interestingly, although the American Medical Association (AMA) “ supports the right of physicians to engage in collective bargaining,” the organization doesn’t track union membership among physicians, according to an AMA spokesperson.
Forming a Union
One challenge is that forming a union is not only time-consuming but also difficult, owing to several barriers. For starters, the laws dictating unionization differ by state, and the rules governing unionization vary if a hospital is public or private. If there’s enough momentum from doctors leading unionization efforts, approval from hospital leaders is required before an official election can be requested from the National Labor Relations Board.
That said, for doctors who are in a union — the two most popular are the Union of American Physicians and Dentists and the Doctors Council branch of the Service Employees International Union (SEIU)—the benefits are immense, especially because union members can focus on what matters, such as providing the best patient care possible.
, reported WBUR in Boston.
Belonging Matters
“When you build a relationship with your patients, it’s special, and that connection isn’t replaceable,” said Nicholas VenOsdel, MD, a pediatrician at Allina Health Primary Care in Hastings, Minnesota, and a union member of the Doctors Council. “However, a lot of us have felt like that hasn’t been respected as the climate of healthcare has changed so fast.”
In fact, autonomy over how much time doctors spend with patients is driving a lot of interest in unionization.
“We don’t necessarily have that autonomy now,” said Amber Higgins, MD, an emergency physician and an obstetrician at ChristianaCare, a hospital network in Newark, Delaware, and a member of the Doctors Council. “There are so many other demands, whether it’s billing, patient documentation, or other demands from the employer, and all of that takes time away from patient care.”
Another primary driver of physician unionization is the physician burnout epidemic. Physicians collectively complain that they spend more time on electronic health record documentation and bureaucratic administration. Yet if unions can improve these working conditions, the benefit to physicians and their patients would be a welcome change.
Union members are bullish and believe that having a cohesive voice will make a difference.
“We need to use our collective voices to get back to focusing on patient care instead of staring at a computer screen for 80% of the day,” Dr. Higgins told this news organization. “So much of medicine involves getting to the correct diagnosis, listening to patients, observing them, and building a relationship with them. We need time to build that.”
With corporate consolidation and a profit-driven mandate by healthcare systems, doctors are increasingly frustrated and feel that their voices haven’t been heard enough when it comes to issues like workplace safety, working hours, and benefits, said Stuart Bussey, MD, JD, a family practice physician and president of the Union of American Physicians and Dentists in Sacramento, California.
However, he adds that urging doctors to join together to fight for a better working environment hasn’t been easy.
“Doctors are individualists, and they don’t know how to work in packs like hospital administrators do,” said Dr. Bussey. “They’re hard to organize, but I want them to understand that unless they join hands, sign petitions, and speak as one voice, they’re going to lose out on an amazing opportunity.”
Overcoming Misperceptions About Unions
One barrier to doctors getting involved is the sentiment that unions might do the opposite of what’s intended — that is, they might further reduce a doctor’s autonomy and work flexibility. Or there may be a perception that the drive to join a union is predicated on making more money.
Though he’s now in a union, Dr. VenOsdel, who has been in a hospital-based practice for 7 years, admits that he initially felt very differently about unions than he does today.
“Even though I have family members in healthcare unions, I had a neutral to even slightly negative view of unions,” said Dr. VenOsdel. “It took me working directly with the Minnesota Nurses Association and the Doctors Council to learn the other side of the story.”
Armed with more information, he began lobbying for stricter rules about how his state’s large healthcare systems were closing hospitals and ending much-needed community services.
“I remember standing at the Capitol in Minnesota and telling one of the members that I once felt negatively about unions,” he added. “I realized then that I only knew what employers were telling me via such things as emails about strikes — that information was all being shared from the employers’ perspective.”
The other misperception is that unions only exist to argue against management, including against colleagues who are also part of the management structure, said Dr. Higgins.
“Some doctors perceive being in a union as ‘how can those same leaders also be in a union,’” she said. She feels that they currently don’t have leadership representing them that can help with such things as restructuring their support teams or getting them help with certain tasks. “That’s another way unions can help.”
Social Justice Plays a Role
For Dr. VenOsdel, being part of a union has helped him return to what he calls the “art” of medicine.
“Philosophically, the union gave me an option for change in what felt like a hopeless situation,” he said. “It wasn’t just that I was tossing the keys to someone else and saying, ‘I can’t fix this.’ Instead, we’re taking the reins back and fixing things ourselves.”
Bussey argues that as the uneven balance between administrators and providers in many healthcare organizations grows, the time to consider forming a union is now.
“We’re in a $4 trillion medical industrial revolution,” he said. “Administrators and bureaucrats are multiplying 30-fold times vs providers, and most of that $4 trillion supports things that don’t contribute to the doctor-patient relationship.”
Furthermore, union proponents say that where a one-on-one relationship between doctor and patient once existed, that has now been “triangulated” to include administrators.
“We’ve lost power in every way,” Dr. Bussey said. “We have the degrees, the liability, and the knowledge — we should have more power to make our workplaces safer and better.”
Ultimately, for some unionized doctors, the very holding of a union card is rooted in supporting social justice issues.
“When doctors realize how powerful a tool a union can be for social justice and change, this will alter perceptions of unions within our profession,” Dr. VenOsdel said. “Our union helps give us a voice to stand up for other staff who aren’t unionized and, most importantly, to stand up for the patients who need us.”
A version of this article first appeared on Medscape.com.
Vacationing Doctors Intervene After Shark Attack
Ryan Forbess, MD: I live at the beach in Orange Beach, Alabama. I’ve lived in Hawaii, the Caymans, and other beach areas for years. I’ve seen a lot of sharks but never a shark attack. Not until now.
Mohammad Ali, MD: Ryan and I have been friends for 20 years. Every year, my family goes to 30A in Florida (a popular resort stretch of highway) to celebrate my wife’s birthday, and the Forbesses always meet us there. This year we had a group of about 18 people.
On Friday, it was beautiful, and we decided to make it a beach day. We had nine kids with us. So by the time we rounded them up and got there, it was noon, and there was nowhere to sit. We almost turned around and went to the pool. But my wife finally found a spot for an umbrella.
Dr. Forbess: We were in the water boogie boarding. I was with my 8-year-old son, and Mo was with his daughter who is the same age. Suddenly, we noticed a lot of commotion just to the left of us. My first thought was: Someone saw a shark, not an attack. They’re so rare. But seeing one would scare people.
We grabbed our kids and started running out of the water. As we got closer to the shore,
Dr. Ali: It was mass panic. People were screaming and running out of the water. Other people were running in and grabbing their kids. Everyone just looked frantic.
We saw two men dragging this poor girl out of the water. It was surreal. The majority of her right leg was severed, her femur bone visible and stark white; it didn’t look real. I kept telling myself I was in a dream and now I’d wake up.
A young EMT who was there had put an informal tourniquet on her leg, but she was still bleeding. So I compressed the femoral artery as hard as I could, something I’m very familiar with doing.
Dr. Forbess: People asked me later what we used for a tourniquet. I said, “Mo’s big hands.” I tease him because most doctors play golf or go fishing; Mo lives in the gym. He was just holding pressure.
The girl’s left hand was also severed off at the wrist. There were two nurses there, and they helped with holding tourniquets on her arm.
Lulu (the girl’s name) was 15 years old. She was in and out of consciousness. At one point, her face started getting really pale, so we tried to lift her extremities up to keep the blood flow to the heart. With such severe blood loss, I thought she might go into cardiovascular shock, and we would have to start compressions. But she had a pulse, and she was breathing.
Dr. Ali: The beach was very crowded, and a lot of people had gathered around. Everyone was emotional, shocked, really shaken up. But they gave us space to work.
Dr. Forbess: People were handing us things — towels, a ratchet strap to use as a tourniquet. There was even an anesthesiologist there who said, “If you need an airway, let me know.” It was like we had a trauma team.
Dr. Ali: Lulu’s mom had been having lunch with friends. When she saw all the commotion, she ran down to the beach to look for her daughter. It was heartbreaking to hear her screams when she saw Lulu. But I was able to tune it out because we had to just concentrate on decreasing the loss of blood.
Dr. Forbess: Another girl came over and said, “That’s my sister.” Lulu has a twin. So she sat there holding Lulu’s hand and being with her the whole time.
Waiting for the EMTs to get there, the seconds were like hours. It seemed like it took forever. Finally, they came, and we were able to get the real tourniquets on, get her boarded and off the beach.
After that, they closed the beach. We got all our stuff and got on the little trolley that would take us back to the house. The lady who was driving asked us, “Did y’all hear about the shark attack?” My wife said, “Yeah, we were there.” And she said, “No, there was one an hour and a half ago.”
Dr. Ali: What we didn’t know was there had been two other attacks that day. Around the same time, one of Lulu’s friends was bitten and got a flesh wound on her heel. And before that, about 4 miles away, there was a serious injury: A lady in her 40s lost her hand and forearm and was bitten in the pelvis.
Dr. Forbess: At that point, my wife leaned back to me and said, “You know we’re never going to the beach again, right? We’re never ever going to the beach.”
If we had known about those attacks, we definitely wouldn’t have been in the water.
Dr. Ali: My wife has never liked going in the water. The evening before, we had debated about taking our daughters in the ocean because she was worried about sharks. I had given her this condescending speech about waist-deep water and the statistical probabilities of ever witnessing a shark attack. I was in trouble.
Dr. Forbess: We didn’t know if Lulu would make it. I’ve done rural family medicine in Oklahoma, so I’ve seen my fair share of injuries — guys on oil rigs, this and that. But I had never seen anything like this kind of trauma and blood loss.
Later that day, I called my office manager to catch up with her and told her what happened. She was actually in Pensacola having dinner across the street from Sacred Heart Hospital where they had taken Lulu. She went over to the emergency room to try to find out Lulu’s status — she was alive.
My office manager was able to go upstairs and talk to Lulu’s mom. Then she called, and we talked to her mom on the phone. She just said, “Thank you for helping my daughter.” It was an emotional moment.
Dr. Ali: It was such a relief. We had no idea how things would turn out. Even if Lulu did survive, was she going to be neurologically sound? But thank God she was. We were so relieved to hear her mom say that it was looking good. We still didn’t know for sure. But at least she was alive and seemed to be functioning.
Dr. Forbess: A few days later, my wife and I went to go visit her at the hospital. Her mom and her grandma were there. They were giving us hugs. We FaceTimed Mo because he was back in Jackson. It was really amazing.
What are the odds? The chances of a shark attack are about one in 12 million. And to have two physicians trained in trauma, a trauma nurse, another nurse, and an anesthesiologist less than 20 yards away when it happened? It’s crazy to think about.
Dr. Ali: And we almost weren’t there. We could have turned away.
Dr. Forbess: Humans are on top of the food chain. Or we think we are. But water really isn’t our element. Against a 12-foot bull shark, we don’t stand a chance. Lulu is here though. It’s unbelievable.
Her mom told me that when Lulu woke up, she just said, “I made it!” That girl is meant to be here. She is a tough girl with a great personality. She has these new prosthetics now that she can move with her mind; it’s like Star Wars. She says she wants to be a physician someday. So she’ll probably cure cancer.
Dr. Forbess is a family medicine physician at Orange Beach Family Medicine in Orange Beach, Alabama. Dr. Ali is an interventional radiologist with Baptist Memorial Health in Jackson, Mississippi.
A version of this article first appeared on Medscape.com.
Ryan Forbess, MD: I live at the beach in Orange Beach, Alabama. I’ve lived in Hawaii, the Caymans, and other beach areas for years. I’ve seen a lot of sharks but never a shark attack. Not until now.
Mohammad Ali, MD: Ryan and I have been friends for 20 years. Every year, my family goes to 30A in Florida (a popular resort stretch of highway) to celebrate my wife’s birthday, and the Forbesses always meet us there. This year we had a group of about 18 people.
On Friday, it was beautiful, and we decided to make it a beach day. We had nine kids with us. So by the time we rounded them up and got there, it was noon, and there was nowhere to sit. We almost turned around and went to the pool. But my wife finally found a spot for an umbrella.
Dr. Forbess: We were in the water boogie boarding. I was with my 8-year-old son, and Mo was with his daughter who is the same age. Suddenly, we noticed a lot of commotion just to the left of us. My first thought was: Someone saw a shark, not an attack. They’re so rare. But seeing one would scare people.
We grabbed our kids and started running out of the water. As we got closer to the shore,
Dr. Ali: It was mass panic. People were screaming and running out of the water. Other people were running in and grabbing their kids. Everyone just looked frantic.
We saw two men dragging this poor girl out of the water. It was surreal. The majority of her right leg was severed, her femur bone visible and stark white; it didn’t look real. I kept telling myself I was in a dream and now I’d wake up.
A young EMT who was there had put an informal tourniquet on her leg, but she was still bleeding. So I compressed the femoral artery as hard as I could, something I’m very familiar with doing.
Dr. Forbess: People asked me later what we used for a tourniquet. I said, “Mo’s big hands.” I tease him because most doctors play golf or go fishing; Mo lives in the gym. He was just holding pressure.
The girl’s left hand was also severed off at the wrist. There were two nurses there, and they helped with holding tourniquets on her arm.
Lulu (the girl’s name) was 15 years old. She was in and out of consciousness. At one point, her face started getting really pale, so we tried to lift her extremities up to keep the blood flow to the heart. With such severe blood loss, I thought she might go into cardiovascular shock, and we would have to start compressions. But she had a pulse, and she was breathing.
Dr. Ali: The beach was very crowded, and a lot of people had gathered around. Everyone was emotional, shocked, really shaken up. But they gave us space to work.
Dr. Forbess: People were handing us things — towels, a ratchet strap to use as a tourniquet. There was even an anesthesiologist there who said, “If you need an airway, let me know.” It was like we had a trauma team.
Dr. Ali: Lulu’s mom had been having lunch with friends. When she saw all the commotion, she ran down to the beach to look for her daughter. It was heartbreaking to hear her screams when she saw Lulu. But I was able to tune it out because we had to just concentrate on decreasing the loss of blood.
Dr. Forbess: Another girl came over and said, “That’s my sister.” Lulu has a twin. So she sat there holding Lulu’s hand and being with her the whole time.
Waiting for the EMTs to get there, the seconds were like hours. It seemed like it took forever. Finally, they came, and we were able to get the real tourniquets on, get her boarded and off the beach.
After that, they closed the beach. We got all our stuff and got on the little trolley that would take us back to the house. The lady who was driving asked us, “Did y’all hear about the shark attack?” My wife said, “Yeah, we were there.” And she said, “No, there was one an hour and a half ago.”
Dr. Ali: What we didn’t know was there had been two other attacks that day. Around the same time, one of Lulu’s friends was bitten and got a flesh wound on her heel. And before that, about 4 miles away, there was a serious injury: A lady in her 40s lost her hand and forearm and was bitten in the pelvis.
Dr. Forbess: At that point, my wife leaned back to me and said, “You know we’re never going to the beach again, right? We’re never ever going to the beach.”
If we had known about those attacks, we definitely wouldn’t have been in the water.
Dr. Ali: My wife has never liked going in the water. The evening before, we had debated about taking our daughters in the ocean because she was worried about sharks. I had given her this condescending speech about waist-deep water and the statistical probabilities of ever witnessing a shark attack. I was in trouble.
Dr. Forbess: We didn’t know if Lulu would make it. I’ve done rural family medicine in Oklahoma, so I’ve seen my fair share of injuries — guys on oil rigs, this and that. But I had never seen anything like this kind of trauma and blood loss.
Later that day, I called my office manager to catch up with her and told her what happened. She was actually in Pensacola having dinner across the street from Sacred Heart Hospital where they had taken Lulu. She went over to the emergency room to try to find out Lulu’s status — she was alive.
My office manager was able to go upstairs and talk to Lulu’s mom. Then she called, and we talked to her mom on the phone. She just said, “Thank you for helping my daughter.” It was an emotional moment.
Dr. Ali: It was such a relief. We had no idea how things would turn out. Even if Lulu did survive, was she going to be neurologically sound? But thank God she was. We were so relieved to hear her mom say that it was looking good. We still didn’t know for sure. But at least she was alive and seemed to be functioning.
Dr. Forbess: A few days later, my wife and I went to go visit her at the hospital. Her mom and her grandma were there. They were giving us hugs. We FaceTimed Mo because he was back in Jackson. It was really amazing.
What are the odds? The chances of a shark attack are about one in 12 million. And to have two physicians trained in trauma, a trauma nurse, another nurse, and an anesthesiologist less than 20 yards away when it happened? It’s crazy to think about.
Dr. Ali: And we almost weren’t there. We could have turned away.
Dr. Forbess: Humans are on top of the food chain. Or we think we are. But water really isn’t our element. Against a 12-foot bull shark, we don’t stand a chance. Lulu is here though. It’s unbelievable.
Her mom told me that when Lulu woke up, she just said, “I made it!” That girl is meant to be here. She is a tough girl with a great personality. She has these new prosthetics now that she can move with her mind; it’s like Star Wars. She says she wants to be a physician someday. So she’ll probably cure cancer.
Dr. Forbess is a family medicine physician at Orange Beach Family Medicine in Orange Beach, Alabama. Dr. Ali is an interventional radiologist with Baptist Memorial Health in Jackson, Mississippi.
A version of this article first appeared on Medscape.com.
Ryan Forbess, MD: I live at the beach in Orange Beach, Alabama. I’ve lived in Hawaii, the Caymans, and other beach areas for years. I’ve seen a lot of sharks but never a shark attack. Not until now.
Mohammad Ali, MD: Ryan and I have been friends for 20 years. Every year, my family goes to 30A in Florida (a popular resort stretch of highway) to celebrate my wife’s birthday, and the Forbesses always meet us there. This year we had a group of about 18 people.
On Friday, it was beautiful, and we decided to make it a beach day. We had nine kids with us. So by the time we rounded them up and got there, it was noon, and there was nowhere to sit. We almost turned around and went to the pool. But my wife finally found a spot for an umbrella.
Dr. Forbess: We were in the water boogie boarding. I was with my 8-year-old son, and Mo was with his daughter who is the same age. Suddenly, we noticed a lot of commotion just to the left of us. My first thought was: Someone saw a shark, not an attack. They’re so rare. But seeing one would scare people.
We grabbed our kids and started running out of the water. As we got closer to the shore,
Dr. Ali: It was mass panic. People were screaming and running out of the water. Other people were running in and grabbing their kids. Everyone just looked frantic.
We saw two men dragging this poor girl out of the water. It was surreal. The majority of her right leg was severed, her femur bone visible and stark white; it didn’t look real. I kept telling myself I was in a dream and now I’d wake up.
A young EMT who was there had put an informal tourniquet on her leg, but she was still bleeding. So I compressed the femoral artery as hard as I could, something I’m very familiar with doing.
Dr. Forbess: People asked me later what we used for a tourniquet. I said, “Mo’s big hands.” I tease him because most doctors play golf or go fishing; Mo lives in the gym. He was just holding pressure.
The girl’s left hand was also severed off at the wrist. There were two nurses there, and they helped with holding tourniquets on her arm.
Lulu (the girl’s name) was 15 years old. She was in and out of consciousness. At one point, her face started getting really pale, so we tried to lift her extremities up to keep the blood flow to the heart. With such severe blood loss, I thought she might go into cardiovascular shock, and we would have to start compressions. But she had a pulse, and she was breathing.
Dr. Ali: The beach was very crowded, and a lot of people had gathered around. Everyone was emotional, shocked, really shaken up. But they gave us space to work.
Dr. Forbess: People were handing us things — towels, a ratchet strap to use as a tourniquet. There was even an anesthesiologist there who said, “If you need an airway, let me know.” It was like we had a trauma team.
Dr. Ali: Lulu’s mom had been having lunch with friends. When she saw all the commotion, she ran down to the beach to look for her daughter. It was heartbreaking to hear her screams when she saw Lulu. But I was able to tune it out because we had to just concentrate on decreasing the loss of blood.
Dr. Forbess: Another girl came over and said, “That’s my sister.” Lulu has a twin. So she sat there holding Lulu’s hand and being with her the whole time.
Waiting for the EMTs to get there, the seconds were like hours. It seemed like it took forever. Finally, they came, and we were able to get the real tourniquets on, get her boarded and off the beach.
After that, they closed the beach. We got all our stuff and got on the little trolley that would take us back to the house. The lady who was driving asked us, “Did y’all hear about the shark attack?” My wife said, “Yeah, we were there.” And she said, “No, there was one an hour and a half ago.”
Dr. Ali: What we didn’t know was there had been two other attacks that day. Around the same time, one of Lulu’s friends was bitten and got a flesh wound on her heel. And before that, about 4 miles away, there was a serious injury: A lady in her 40s lost her hand and forearm and was bitten in the pelvis.
Dr. Forbess: At that point, my wife leaned back to me and said, “You know we’re never going to the beach again, right? We’re never ever going to the beach.”
If we had known about those attacks, we definitely wouldn’t have been in the water.
Dr. Ali: My wife has never liked going in the water. The evening before, we had debated about taking our daughters in the ocean because she was worried about sharks. I had given her this condescending speech about waist-deep water and the statistical probabilities of ever witnessing a shark attack. I was in trouble.
Dr. Forbess: We didn’t know if Lulu would make it. I’ve done rural family medicine in Oklahoma, so I’ve seen my fair share of injuries — guys on oil rigs, this and that. But I had never seen anything like this kind of trauma and blood loss.
Later that day, I called my office manager to catch up with her and told her what happened. She was actually in Pensacola having dinner across the street from Sacred Heart Hospital where they had taken Lulu. She went over to the emergency room to try to find out Lulu’s status — she was alive.
My office manager was able to go upstairs and talk to Lulu’s mom. Then she called, and we talked to her mom on the phone. She just said, “Thank you for helping my daughter.” It was an emotional moment.
Dr. Ali: It was such a relief. We had no idea how things would turn out. Even if Lulu did survive, was she going to be neurologically sound? But thank God she was. We were so relieved to hear her mom say that it was looking good. We still didn’t know for sure. But at least she was alive and seemed to be functioning.
Dr. Forbess: A few days later, my wife and I went to go visit her at the hospital. Her mom and her grandma were there. They were giving us hugs. We FaceTimed Mo because he was back in Jackson. It was really amazing.
What are the odds? The chances of a shark attack are about one in 12 million. And to have two physicians trained in trauma, a trauma nurse, another nurse, and an anesthesiologist less than 20 yards away when it happened? It’s crazy to think about.
Dr. Ali: And we almost weren’t there. We could have turned away.
Dr. Forbess: Humans are on top of the food chain. Or we think we are. But water really isn’t our element. Against a 12-foot bull shark, we don’t stand a chance. Lulu is here though. It’s unbelievable.
Her mom told me that when Lulu woke up, she just said, “I made it!” That girl is meant to be here. She is a tough girl with a great personality. She has these new prosthetics now that she can move with her mind; it’s like Star Wars. She says she wants to be a physician someday. So she’ll probably cure cancer.
Dr. Forbess is a family medicine physician at Orange Beach Family Medicine in Orange Beach, Alabama. Dr. Ali is an interventional radiologist with Baptist Memorial Health in Jackson, Mississippi.
A version of this article first appeared on Medscape.com.
Delayed Bleeding: The Silent Risk for Seniors
This discussion was recorded on August 2, 2024. This transcript has been edited for clarity.
Robert D. Glatter, MD: Today, we’ll be discussing the results of a new study published in The Journal of Emergency Medicine, looking at the incidence of delayed intracranial hemorrhage among older patients taking preinjury anticoagulants who present to the emergency department (ED) with blunt head trauma.
Joining me today is the lead author of the study, Dr. Richard Shih, professor of emergency medicine at Florida Atlantic University. Also joining me is Dr. Christina Shenvi, associate professor of emergency medicine at the University of North Carolina (UNC) Chapel Hill, with fellowship training in geriatric emergency medicine.
Welcome to both of you.
Richard D. Shih, MD: Thanks, Rob.
Christina L. Shenvi, MD, PhD, MBA: Thanks. Pleasure to be here.
ICH Study Methodology
Dr. Glatter: It’s a pleasure to have you. Rich, this is a great study and targeted toward a population we see daily in the emergency department. I want you to describe your methodology, patient selection, and how you went about organizing your study to look at this important finding of delayed intracranial hemorrhage, especially in those on anticoagulants.
Dr. Shih: This all started for our research team when we first read the 2012 Annals of Emergency Medicine paper. The first author was Vincenzo Menditto, and he looked at a group of patients that had minor head injury, were anticoagulated, and had negative initial head CTs.
There were about 100 patients, of which about 10 of them did not consent, but they hospitalized all these patients. These were anticoagulated, negative-first head CTs. They hospitalized the patients and then did a routine second CT at about 24 hours. They also followed them for a week, and it turned out a little over 7% of them had delayed head CT.
We were wondering how many delayed intracranial hemorrhages we had missed because current practice for us was that, if patients had a good physical exam, their head CT was normal, and everything looked good, we would send them home.
Because of that, a number of people across the country wanted to verify those findings from the Menditto study. We tried to design a good study to answer that question. We happen to have a very large geriatric population in Florida, and our ED census is very high for age over 65, at nearly 60%.
There are two Level I trauma centers in Palm Beach County. We included a second multicenter hospital, and we prospectively enrolled patients. We know the current state of practice is not to routinely do second CTs, so we followed these patients over time and followed their medical records to try to identify delayed bleeding. That’s how we set up our methodology.
Is It Safe to Discharge Patients With Trauma After 24 Hours?
Dr. Glatter: For the bulk of these patients with negative head CTs, it’s been my practice that when they’re stable and they look fine and there’s no other apparent, distracting painful trauma, injuries and so forth, they’re safe to discharge.
The secondary outcome in your study is interesting: the need for neurosurgical intervention in terms of those with delayed intracranial hemorrhage.
Dr. Shih: I do believe that it’s certainly not the problem that Menditto described, which is 7%. There are two other prospective studies that have looked at this issue with delayed bleeding on anticoagulants. Both of these also showed a relatively low rate of delayed bleeding, which is between like 0.2% and 1.0%. In our study, it was 0.4%.
The difference in the studies is that Menditto and colleagues routinely did 24-hour head CTs. They admitted everybody. For these other studies, routine head CT was not part of it. My bet is that there is a rate of delayed bleeding somewhere in between that seen in the Menditto study and that in all the other studies.
However, talking about significant intracranial hemorrhage, ones that perhaps need neurosurgery, I believe most of them are not significant. There’s some number that do occur, but the vast majority of those probably don’t need neurosurgery. We had 14 delayed bleeds out of 6000 patients with head trauma. One of them ended up requiring neurosurgery, so the answer is not zero, but I don’t think it’s 7% either.
Dr. Glatter: Dr. Shenvi, I want to bring you into the conversation to talk about your experience at UNC, and how you run things in terms of older patients with blunt head trauma on preinjury anticoagulants.
Dr. Shenvi: Thanks, Rob. I remember when this paper came out showing this 7% rate of delayed bleeding and the question was, “Should we be admitting all these people?” Partly just from an overwhelming need for capacity that that would bring, it just wasn’t practical to say, “We’re going to admit every patient with a negative head CT to the hospital and rescan them.” That would be hundreds or thousands of patients each year in any given facility.
The other thing is that delayed bleeds don’t always happen just in the first 24 hours. It’s not even a matter of bringing patients into observation for 24 hours, watching them, and rescanning them if they have symptoms. It can occur several days out. That never, in almost any institution that I know of, became standard practice.
The way that it did change my care was to give good return precautions to patients, to make sure they have somebody with them to say, “Hey, sometimes you can have bleeding several days out after a fall, even though your CT scan here today looks perfect,” and to alert them that if they start having severe headaches, vomiting, or other symptoms of intracranial hemorrhage, that they should come back.
I don’t think it ever became standard practice, and for good reason, because that was one study. The subsequent studies that Richard mentioned, pretty quickly on the heels of that initial one, showed a much lower rate of delayed ICH with the caveats that the methodology was different.
Shift in Anticoagulants
Dr. Shenvi: One other big change from that original study, and now to Richard’s study, is the shift in anticoagulants. Back in the initial study you mentioned, it was all warfarin. We know from other studies looking at warfarin vs the direct oral anticoagulants (DOACs) that DOACs have lower rates of ICH after a head injury, lower rates of need for neurosurgical intervention, and lower rates of discharge to a skilled nursing facility after an intracranial hemorrhage.
Across the board, we know that the DOACs tend to do better. It’s difficult to compare newer studies because it’s a different medication. It did inform my practice to have an awareness of delayed intracranial hemorrhage so that I warn patients more proactively.
Dr. Glatter: I haven’t seen a patient on warfarin in years. I don’t know if either of you have, but it’s all DOACs now unless there’s some other reason. That shift is quite apparent.
Dr. Shih: The problem with looking at delayed bleeding for DOACs vs warfarin is the numbers were so low. I think we had 13 people, and seven were in the no-anticoagulant group. The numbers are even lower, so it’s hard to say.
I just wanted to comment on something that Dr. Shenvi said, and I pretty much agree with everything that she said. Anticoagulants and warfarin, and that Menditto study, have a carryover effect. People group DOACs with warfarin similarly. When a patient is brought in, the first thing they talk about with head trauma is, “Oh, they’re on an anticoagulant” or “They’re not on an anticoagulant.” It’s so ingrained.
I believe that, in emergency medicine, we’re pressed for space and time and we’re not as affected by that 24-hour observation. Maybe many of our surgeons will automatically admit those patients.
I haven’t seen a guideline from the United States, but there are two international guidelines. One is from Austria from 2019, and one is from Scandinavia. Both recommended 24-hour observation if you’re on an anticoagulant.
There is a bit of controversy left over with that. Hopefully, as more and more of information, like in our study, comes out, people will be a little bit more clear about it. I don’t think there’s a need to routinely admit them.
I do want to mention that the Menditto study had such a massive impact on everybody. They pointed out one subgroup (and it’s such a small number of patients). They had seven cases of delayed bleeding; four or five of them were within that 24 hours, and a couple were diagnosed later over the next couple days.
Of those seven people, four of them had international normalized ratios (INRs) greater than 3. Of those four patients, I’ve heard people talk about this and recommend, “Okay, that’s the subgroup I would admit.” There’s a toss-up with what to do with DOAC because it’s very hard to tell whether there’s an issue, whether there are problems with their dosing, and whatever.
We actually recently looked at that. We have a much larger sample than four: close to 300 patients who were on warfarin. We looked at patients who had INRs below 3 and above 3, and we didn’t show a difference. We still don’t believe that warfarin is a big issue with delayed bleeding.
Should We Be Asking: ‘Are They on Blood Thinners?’
Dr. Shenvi: One of the interesting trends related to warfarin and the DOACs vs no anticoagulant is that as you mentioned, Dr Shih, the first question out of people’s mouths or the first piece of information emergency medical services gives you when they come in with a patient who’s had a head injury is, “Are they on blood thinners or not?”
Yet, the paradigm is shifting to say it’s not actually the blood thinners themselves that are giving older patients the higher risk for bleeding; it’s age and other comorbidities.
Certainly, if you’re on an anticoagulant and you start to bleed, your prognosis is much worse because the bleeding doesn’t stop. In terms of who has a bleeding event, there’s much less impact of anticoagulation than we used to think. That, in part, may be due to the change from warfarin to other medications.
Some of the experts I’ve talked to who have done the research on this have said, “Well, actually, warfarin was more of a marker for being much older and more frail, because it was primarily prescribed to older patients who have significant heart disease, atrial fibrillation, and so on.” It was more a marker for somebody who is at risk for an intracranial hemorrhage. There are many changes that have happened in the past 10 years with medications and also our understanding.
Challenges in Patient Follow-up
Dr. Glatter: That’s a great point. One thing, Rich, I want to ask you about is in terms of your proxy outcome assessment. When you use that at 14 and 60 days with telephone follow-up and then chart review at 60 and 90 days (because, obviously, everyone can’t get another head CT or it’s difficult to follow patients up), did you find that worked out well in your prospective cohort study, in terms of using that as a proxy, so to speak?
Dr. Shih: I would say to a certain extent. Unfortunately, we don’t have access to the patients to come back to follow up all of them, and there was obviously a large number of patients in our study.
The next best thing was that we had dedicated research assistants calling all of the patients at 14 days and 60 days. I’ve certainly read research studies where, when they call them, they get 80%-90% follow-up, but we did not achieve that.
I don’t know if people are more inundated with spam phone calls now, or the older people are just afraid of picking up their phone sometimes with all the scams and so forth. I totally understand, but in all honesty, we only had about a 30%-35% follow-up using that follow-up pathway.
Then the proxy pathway was to look at their charts at 60 and 90 days. Also, we looked at the Florida death registry, which is pretty good, and then finally, we had both Level I trauma centers in the county that we were in participating. It’s standard practice that if you have an intracranial hemorrhage at a non–Level I trauma center, you would be transferred to a Level I trauma center. That’s the protocol. I know that’s not followed 100% of the time, but that’s part of the proxy follow-up. You could criticize the study for not having closer to 90% actual contact, but that’s the best we could do.
Dr. Glatter: I think that’s admirable. Using that paradigm of what you described certainly allows the reader to understand the difficulty in assessing patients that don’t get follow-up head CT, and hardly anyone does that, as we know.
To your point of having both Level I trauma centers in the county, that makes it pretty secure. If we’re going to do a study encompassing a similar type of regional aspect, it would be similar.
Dr. Shenvi: I think your proxies, to your credit, were as good as you can get. You can never get a 100% follow-up, but you really looked at all the different avenues by which patients might present, either in the death registry or a Level I center. Well done on that aspect.
Determining When to Admit Patients for Observation
Dr. Glatter: In terms of admissions: You admit a patient, then you hear back that this patient should not have been admitted because they had a negative head CT, but you put them in anyway in the sense of delayed bleeding happening or not happening.
It’s interesting. Maybe the insurers will start looking at this in some capacity, based on your study, that because it’s so infrequent that you see delayed bleeding, that admitting someone for any reason whatsoever would be declined. Do you see that being an issue? In other words, [do you see] this leading to a pattern in terms of the payers?
Dr. Shih: Certainly, you could interpret it that way, and that would be unfortunate. The [incidence of] delayed bleeding is definitely not zero. That’s the first thing.
The second thing is that when you’re dealing with an older population, having some sense that they’re not doing well is an important contributor to trying to fully assess what’s going on — whether or not they have a bleed or whether they’re at risk for falling again and then hitting their head and causing a second bleed, and making sure they can do the activities of daily life. There really should be some room for a physician to say, “They just got here, and we don’t know him that well. There’s something that bothers me about this person” and have the ability to watch them for at least another 24 hours. That’s how I feel.
Dr. Shenvi: In my location, it would be difficult to try to admit somebody purely for observation for delayed bleeding. I think we would get a lot of pushback on that. The reasons I might admit a patient after a fall with a negative head CT, though, are all the things that, Rob, you alluded to earlier — which are, what made them fall in the first place and were they unable to get up?
I had this happen just this week. A patient who fell couldn’t get off the ground for 12 hours, and so now she’s dehydrated and delirious with slight rhabdomyolysis. Then you’re admitting them either for the sequelae of the fall that are not related to the intracranial hemorrhage, or the fact that they are so debilitated and deconditioned that they cannot take care of themselves. They need physical therapy. Often, we will have physical and occupational therapists come see them in the ED during business hours and help make an assessment of whether they are safe to go home or whether they fall again. That can give more evidence for the need for admission.
Dr. Glatter: To bring artificial intelligence into this discussion, algorithms that are out there that say, “Push a button and the patient’s safe for discharge.” Well, this argues for a clinical gestalt and a human being to make an assessment because you can use these predictive models, which are coming and they’re going to be here soon, and they already are in some sense. Again, we have to use clinical human judgment.
Dr. Shih: I agree.
Advice for Primary Care Physicians
Dr. Glatter: What return precautions do you discuss with patients who’ve had blunt head trauma that maybe had a head CT, or even didn’t? What are the main things we’re looking for?
Dr. Shenvi: What I usually tell people is if you start to have a worse headache, nausea or vomiting, any weakness in one area of your body, or vision changes, and if there’s a family member or friend there, I’ll say, “If you notice that they’re acting differently or seem confused, come back.”
Dr. Shih: I agree with what she said, and I’m also going to add one thing. The most important part is they are trying to prevent a subsequent fall. We know that when they’ve fallen and they present to the ED, they’re at even higher risk for falling and reinjuring themselves, and that’s a population that’s already at risk.
One of the secondary studies that we published out of this project was looking at follow-up with their primary care physicians, and there were two things that we wanted to address. The first was, how often did they do it? Then, when they did do it, did their primary care physicians try to address and prevent subsequent falls?
Both the answers are actually bad. Amazingly, just over like 60% followed up.
In some of our subsequent research, because we’re in the midst of a randomized, controlled trial where we do a home visit, when we initially see these individuals that have fallen, they’ll schedule a home visit for us. Then a week or two later, when we schedule the home visit, many of them cancel because they think, Oh, that was a one-off and it’s not going to happen again. Part of the problem is the patients, because many of them believe that they just slipped and fell and it’s not going to happen again, or they’re not prone to it.
The second issue was when patients did go to a primary care physician, we have found that some primary care physicians believe that falling and injuring themselves is just part of the normal aging process. A percentage of them don’t go over assessment for fall risk or even initiate fall prevention treatments or programs.
I try to take that time to tell them that this is very common in their age group, and believe it or not, a fall from standing is the way people really injure themselves, and there may be ways to prevent subsequent falls and injuries.
Dr. Glatter: Absolutely. Do you find that their medications are a contributor in some sense? Say they’re antihypertensive, have issues of orthostasis, or a new medication was added in the last week.
Dr. Shenvi: It’s all of the above. Sometimes it’s one thing, like they just started tamsulosin for their kidney stone, they stood up, they felt lightheaded, and they fell. Usually, it’s multifactorial with some changes in their gait, vision, balance, reflex time, and strength, plus the medications or the need for assistive devices. Maybe they can’t take care of their home as well as they used to and there are things on the floor. It’s really all of the above.
‘Harder to Unlearn Something Than to Learn It’
Dr. Glatter: Would either of you like to add any additional points to the discussion or add a few pearls?
Dr. Shenvi: This just highlights the challenge of how it’s harder to unlearn something than to learn it, where one study that maybe wasn’t quite looking at what we needed to, or practice and prescribing patterns have changed, so it’s no longer really relevant.
The things that we learned from that, or the fears that we instilled in our minds of, Uh oh, they could go home and have delayed bleeding, are much harder to unlearn, and it takes more studies to unlearn that idea than it did to actually put it into place.
I’m glad that your team has done this much larger, prospective study and hopefully will reduce the concern about this entity.
Dr. Shih: I appreciate that segue. It is amazing that, for paramedics and medical students, the first thing out of their mouth is, “Are they on an anticoagulant?”
In terms of the risk of developing an intracranial hemorrhage, I think it’s much less than the weight we’ve put on it before. However, I believe if they have a bleed, the bleeds are worse. It’s kind of a double-edged sword. It’s still an important factor, but it doesn’t come with the Oh my gosh, they’re on an anticoagulant that everybody thinks about.
No. 1 Cause of Traumatic Injury Is a Fall from Standing
Dr. Glatter: These are obviously ground-level falls in most patients and not motor vehicle crashes. That’s an important part in the population that you looked at that should be mentioned clearly.
Dr. Shih: It’s astonishing. I’ve been a program director for over 20 years, and geriatrics is not well taught in the curriculum. It’s astonishing for many of our trainees and emergency physicians in general that the number-one cause for traumatic injury is a fall from standing.
Certainly, we get patients coming in the trauma center like a 95-year-old person who’s on a ladder putting up his Christmas lights. I’m like, oh my God.
For the vast majority, it’s closer to 90%, but in our study, for the patients we looked at, it was 80% that fall from standing. That’s the mechanism that causes these bleeds and these major injuries.
Dr. Shenvi: That’s reflective of what we see, so it’s good that that’s what you looked at also.
Dr. Glatter: Absolutely. Well, thank you both. This has been a very informative discussion. I appreciate your time, and our readers will certainly benefit from your knowledge and expertise. Thank you again.
Dr. Glatter, assistant professor of emergency medicine at Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York, is a medical adviser for this news organization. He disclosed having no relevant financial conflicts. Dr. Shih is professor of emergency medicine at the Charles E. Schmidt College of Medicine at Florida Atlantic University, Boca Raton. His current grant funding and area of research interest involves geriatric emergency department patients with head injury and fall-related injury. He disclosed receiving a research grant from The Florida Medical Malpractice Joint Underwriting Association Grant for Safety of Health Care Services). Dr. Shenvi, associate professor of emergency medicine at the University of North Carolina at Chapel Hill, disclosed ties with the American College of Emergency Physicians, Institute for Healthcare Improvement, AstraZeneca, and CurvaFix.
A version of this article appeared on Medscape.com.
This discussion was recorded on August 2, 2024. This transcript has been edited for clarity.
Robert D. Glatter, MD: Today, we’ll be discussing the results of a new study published in The Journal of Emergency Medicine, looking at the incidence of delayed intracranial hemorrhage among older patients taking preinjury anticoagulants who present to the emergency department (ED) with blunt head trauma.
Joining me today is the lead author of the study, Dr. Richard Shih, professor of emergency medicine at Florida Atlantic University. Also joining me is Dr. Christina Shenvi, associate professor of emergency medicine at the University of North Carolina (UNC) Chapel Hill, with fellowship training in geriatric emergency medicine.
Welcome to both of you.
Richard D. Shih, MD: Thanks, Rob.
Christina L. Shenvi, MD, PhD, MBA: Thanks. Pleasure to be here.
ICH Study Methodology
Dr. Glatter: It’s a pleasure to have you. Rich, this is a great study and targeted toward a population we see daily in the emergency department. I want you to describe your methodology, patient selection, and how you went about organizing your study to look at this important finding of delayed intracranial hemorrhage, especially in those on anticoagulants.
Dr. Shih: This all started for our research team when we first read the 2012 Annals of Emergency Medicine paper. The first author was Vincenzo Menditto, and he looked at a group of patients that had minor head injury, were anticoagulated, and had negative initial head CTs.
There were about 100 patients, of which about 10 of them did not consent, but they hospitalized all these patients. These were anticoagulated, negative-first head CTs. They hospitalized the patients and then did a routine second CT at about 24 hours. They also followed them for a week, and it turned out a little over 7% of them had delayed head CT.
We were wondering how many delayed intracranial hemorrhages we had missed because current practice for us was that, if patients had a good physical exam, their head CT was normal, and everything looked good, we would send them home.
Because of that, a number of people across the country wanted to verify those findings from the Menditto study. We tried to design a good study to answer that question. We happen to have a very large geriatric population in Florida, and our ED census is very high for age over 65, at nearly 60%.
There are two Level I trauma centers in Palm Beach County. We included a second multicenter hospital, and we prospectively enrolled patients. We know the current state of practice is not to routinely do second CTs, so we followed these patients over time and followed their medical records to try to identify delayed bleeding. That’s how we set up our methodology.
Is It Safe to Discharge Patients With Trauma After 24 Hours?
Dr. Glatter: For the bulk of these patients with negative head CTs, it’s been my practice that when they’re stable and they look fine and there’s no other apparent, distracting painful trauma, injuries and so forth, they’re safe to discharge.
The secondary outcome in your study is interesting: the need for neurosurgical intervention in terms of those with delayed intracranial hemorrhage.
Dr. Shih: I do believe that it’s certainly not the problem that Menditto described, which is 7%. There are two other prospective studies that have looked at this issue with delayed bleeding on anticoagulants. Both of these also showed a relatively low rate of delayed bleeding, which is between like 0.2% and 1.0%. In our study, it was 0.4%.
The difference in the studies is that Menditto and colleagues routinely did 24-hour head CTs. They admitted everybody. For these other studies, routine head CT was not part of it. My bet is that there is a rate of delayed bleeding somewhere in between that seen in the Menditto study and that in all the other studies.
However, talking about significant intracranial hemorrhage, ones that perhaps need neurosurgery, I believe most of them are not significant. There’s some number that do occur, but the vast majority of those probably don’t need neurosurgery. We had 14 delayed bleeds out of 6000 patients with head trauma. One of them ended up requiring neurosurgery, so the answer is not zero, but I don’t think it’s 7% either.
Dr. Glatter: Dr. Shenvi, I want to bring you into the conversation to talk about your experience at UNC, and how you run things in terms of older patients with blunt head trauma on preinjury anticoagulants.
Dr. Shenvi: Thanks, Rob. I remember when this paper came out showing this 7% rate of delayed bleeding and the question was, “Should we be admitting all these people?” Partly just from an overwhelming need for capacity that that would bring, it just wasn’t practical to say, “We’re going to admit every patient with a negative head CT to the hospital and rescan them.” That would be hundreds or thousands of patients each year in any given facility.
The other thing is that delayed bleeds don’t always happen just in the first 24 hours. It’s not even a matter of bringing patients into observation for 24 hours, watching them, and rescanning them if they have symptoms. It can occur several days out. That never, in almost any institution that I know of, became standard practice.
The way that it did change my care was to give good return precautions to patients, to make sure they have somebody with them to say, “Hey, sometimes you can have bleeding several days out after a fall, even though your CT scan here today looks perfect,” and to alert them that if they start having severe headaches, vomiting, or other symptoms of intracranial hemorrhage, that they should come back.
I don’t think it ever became standard practice, and for good reason, because that was one study. The subsequent studies that Richard mentioned, pretty quickly on the heels of that initial one, showed a much lower rate of delayed ICH with the caveats that the methodology was different.
Shift in Anticoagulants
Dr. Shenvi: One other big change from that original study, and now to Richard’s study, is the shift in anticoagulants. Back in the initial study you mentioned, it was all warfarin. We know from other studies looking at warfarin vs the direct oral anticoagulants (DOACs) that DOACs have lower rates of ICH after a head injury, lower rates of need for neurosurgical intervention, and lower rates of discharge to a skilled nursing facility after an intracranial hemorrhage.
Across the board, we know that the DOACs tend to do better. It’s difficult to compare newer studies because it’s a different medication. It did inform my practice to have an awareness of delayed intracranial hemorrhage so that I warn patients more proactively.
Dr. Glatter: I haven’t seen a patient on warfarin in years. I don’t know if either of you have, but it’s all DOACs now unless there’s some other reason. That shift is quite apparent.
Dr. Shih: The problem with looking at delayed bleeding for DOACs vs warfarin is the numbers were so low. I think we had 13 people, and seven were in the no-anticoagulant group. The numbers are even lower, so it’s hard to say.
I just wanted to comment on something that Dr. Shenvi said, and I pretty much agree with everything that she said. Anticoagulants and warfarin, and that Menditto study, have a carryover effect. People group DOACs with warfarin similarly. When a patient is brought in, the first thing they talk about with head trauma is, “Oh, they’re on an anticoagulant” or “They’re not on an anticoagulant.” It’s so ingrained.
I believe that, in emergency medicine, we’re pressed for space and time and we’re not as affected by that 24-hour observation. Maybe many of our surgeons will automatically admit those patients.
I haven’t seen a guideline from the United States, but there are two international guidelines. One is from Austria from 2019, and one is from Scandinavia. Both recommended 24-hour observation if you’re on an anticoagulant.
There is a bit of controversy left over with that. Hopefully, as more and more of information, like in our study, comes out, people will be a little bit more clear about it. I don’t think there’s a need to routinely admit them.
I do want to mention that the Menditto study had such a massive impact on everybody. They pointed out one subgroup (and it’s such a small number of patients). They had seven cases of delayed bleeding; four or five of them were within that 24 hours, and a couple were diagnosed later over the next couple days.
Of those seven people, four of them had international normalized ratios (INRs) greater than 3. Of those four patients, I’ve heard people talk about this and recommend, “Okay, that’s the subgroup I would admit.” There’s a toss-up with what to do with DOAC because it’s very hard to tell whether there’s an issue, whether there are problems with their dosing, and whatever.
We actually recently looked at that. We have a much larger sample than four: close to 300 patients who were on warfarin. We looked at patients who had INRs below 3 and above 3, and we didn’t show a difference. We still don’t believe that warfarin is a big issue with delayed bleeding.
Should We Be Asking: ‘Are They on Blood Thinners?’
Dr. Shenvi: One of the interesting trends related to warfarin and the DOACs vs no anticoagulant is that as you mentioned, Dr Shih, the first question out of people’s mouths or the first piece of information emergency medical services gives you when they come in with a patient who’s had a head injury is, “Are they on blood thinners or not?”
Yet, the paradigm is shifting to say it’s not actually the blood thinners themselves that are giving older patients the higher risk for bleeding; it’s age and other comorbidities.
Certainly, if you’re on an anticoagulant and you start to bleed, your prognosis is much worse because the bleeding doesn’t stop. In terms of who has a bleeding event, there’s much less impact of anticoagulation than we used to think. That, in part, may be due to the change from warfarin to other medications.
Some of the experts I’ve talked to who have done the research on this have said, “Well, actually, warfarin was more of a marker for being much older and more frail, because it was primarily prescribed to older patients who have significant heart disease, atrial fibrillation, and so on.” It was more a marker for somebody who is at risk for an intracranial hemorrhage. There are many changes that have happened in the past 10 years with medications and also our understanding.
Challenges in Patient Follow-up
Dr. Glatter: That’s a great point. One thing, Rich, I want to ask you about is in terms of your proxy outcome assessment. When you use that at 14 and 60 days with telephone follow-up and then chart review at 60 and 90 days (because, obviously, everyone can’t get another head CT or it’s difficult to follow patients up), did you find that worked out well in your prospective cohort study, in terms of using that as a proxy, so to speak?
Dr. Shih: I would say to a certain extent. Unfortunately, we don’t have access to the patients to come back to follow up all of them, and there was obviously a large number of patients in our study.
The next best thing was that we had dedicated research assistants calling all of the patients at 14 days and 60 days. I’ve certainly read research studies where, when they call them, they get 80%-90% follow-up, but we did not achieve that.
I don’t know if people are more inundated with spam phone calls now, or the older people are just afraid of picking up their phone sometimes with all the scams and so forth. I totally understand, but in all honesty, we only had about a 30%-35% follow-up using that follow-up pathway.
Then the proxy pathway was to look at their charts at 60 and 90 days. Also, we looked at the Florida death registry, which is pretty good, and then finally, we had both Level I trauma centers in the county that we were in participating. It’s standard practice that if you have an intracranial hemorrhage at a non–Level I trauma center, you would be transferred to a Level I trauma center. That’s the protocol. I know that’s not followed 100% of the time, but that’s part of the proxy follow-up. You could criticize the study for not having closer to 90% actual contact, but that’s the best we could do.
Dr. Glatter: I think that’s admirable. Using that paradigm of what you described certainly allows the reader to understand the difficulty in assessing patients that don’t get follow-up head CT, and hardly anyone does that, as we know.
To your point of having both Level I trauma centers in the county, that makes it pretty secure. If we’re going to do a study encompassing a similar type of regional aspect, it would be similar.
Dr. Shenvi: I think your proxies, to your credit, were as good as you can get. You can never get a 100% follow-up, but you really looked at all the different avenues by which patients might present, either in the death registry or a Level I center. Well done on that aspect.
Determining When to Admit Patients for Observation
Dr. Glatter: In terms of admissions: You admit a patient, then you hear back that this patient should not have been admitted because they had a negative head CT, but you put them in anyway in the sense of delayed bleeding happening or not happening.
It’s interesting. Maybe the insurers will start looking at this in some capacity, based on your study, that because it’s so infrequent that you see delayed bleeding, that admitting someone for any reason whatsoever would be declined. Do you see that being an issue? In other words, [do you see] this leading to a pattern in terms of the payers?
Dr. Shih: Certainly, you could interpret it that way, and that would be unfortunate. The [incidence of] delayed bleeding is definitely not zero. That’s the first thing.
The second thing is that when you’re dealing with an older population, having some sense that they’re not doing well is an important contributor to trying to fully assess what’s going on — whether or not they have a bleed or whether they’re at risk for falling again and then hitting their head and causing a second bleed, and making sure they can do the activities of daily life. There really should be some room for a physician to say, “They just got here, and we don’t know him that well. There’s something that bothers me about this person” and have the ability to watch them for at least another 24 hours. That’s how I feel.
Dr. Shenvi: In my location, it would be difficult to try to admit somebody purely for observation for delayed bleeding. I think we would get a lot of pushback on that. The reasons I might admit a patient after a fall with a negative head CT, though, are all the things that, Rob, you alluded to earlier — which are, what made them fall in the first place and were they unable to get up?
I had this happen just this week. A patient who fell couldn’t get off the ground for 12 hours, and so now she’s dehydrated and delirious with slight rhabdomyolysis. Then you’re admitting them either for the sequelae of the fall that are not related to the intracranial hemorrhage, or the fact that they are so debilitated and deconditioned that they cannot take care of themselves. They need physical therapy. Often, we will have physical and occupational therapists come see them in the ED during business hours and help make an assessment of whether they are safe to go home or whether they fall again. That can give more evidence for the need for admission.
Dr. Glatter: To bring artificial intelligence into this discussion, algorithms that are out there that say, “Push a button and the patient’s safe for discharge.” Well, this argues for a clinical gestalt and a human being to make an assessment because you can use these predictive models, which are coming and they’re going to be here soon, and they already are in some sense. Again, we have to use clinical human judgment.
Dr. Shih: I agree.
Advice for Primary Care Physicians
Dr. Glatter: What return precautions do you discuss with patients who’ve had blunt head trauma that maybe had a head CT, or even didn’t? What are the main things we’re looking for?
Dr. Shenvi: What I usually tell people is if you start to have a worse headache, nausea or vomiting, any weakness in one area of your body, or vision changes, and if there’s a family member or friend there, I’ll say, “If you notice that they’re acting differently or seem confused, come back.”
Dr. Shih: I agree with what she said, and I’m also going to add one thing. The most important part is they are trying to prevent a subsequent fall. We know that when they’ve fallen and they present to the ED, they’re at even higher risk for falling and reinjuring themselves, and that’s a population that’s already at risk.
One of the secondary studies that we published out of this project was looking at follow-up with their primary care physicians, and there were two things that we wanted to address. The first was, how often did they do it? Then, when they did do it, did their primary care physicians try to address and prevent subsequent falls?
Both the answers are actually bad. Amazingly, just over like 60% followed up.
In some of our subsequent research, because we’re in the midst of a randomized, controlled trial where we do a home visit, when we initially see these individuals that have fallen, they’ll schedule a home visit for us. Then a week or two later, when we schedule the home visit, many of them cancel because they think, Oh, that was a one-off and it’s not going to happen again. Part of the problem is the patients, because many of them believe that they just slipped and fell and it’s not going to happen again, or they’re not prone to it.
The second issue was when patients did go to a primary care physician, we have found that some primary care physicians believe that falling and injuring themselves is just part of the normal aging process. A percentage of them don’t go over assessment for fall risk or even initiate fall prevention treatments or programs.
I try to take that time to tell them that this is very common in their age group, and believe it or not, a fall from standing is the way people really injure themselves, and there may be ways to prevent subsequent falls and injuries.
Dr. Glatter: Absolutely. Do you find that their medications are a contributor in some sense? Say they’re antihypertensive, have issues of orthostasis, or a new medication was added in the last week.
Dr. Shenvi: It’s all of the above. Sometimes it’s one thing, like they just started tamsulosin for their kidney stone, they stood up, they felt lightheaded, and they fell. Usually, it’s multifactorial with some changes in their gait, vision, balance, reflex time, and strength, plus the medications or the need for assistive devices. Maybe they can’t take care of their home as well as they used to and there are things on the floor. It’s really all of the above.
‘Harder to Unlearn Something Than to Learn It’
Dr. Glatter: Would either of you like to add any additional points to the discussion or add a few pearls?
Dr. Shenvi: This just highlights the challenge of how it’s harder to unlearn something than to learn it, where one study that maybe wasn’t quite looking at what we needed to, or practice and prescribing patterns have changed, so it’s no longer really relevant.
The things that we learned from that, or the fears that we instilled in our minds of, Uh oh, they could go home and have delayed bleeding, are much harder to unlearn, and it takes more studies to unlearn that idea than it did to actually put it into place.
I’m glad that your team has done this much larger, prospective study and hopefully will reduce the concern about this entity.
Dr. Shih: I appreciate that segue. It is amazing that, for paramedics and medical students, the first thing out of their mouth is, “Are they on an anticoagulant?”
In terms of the risk of developing an intracranial hemorrhage, I think it’s much less than the weight we’ve put on it before. However, I believe if they have a bleed, the bleeds are worse. It’s kind of a double-edged sword. It’s still an important factor, but it doesn’t come with the Oh my gosh, they’re on an anticoagulant that everybody thinks about.
No. 1 Cause of Traumatic Injury Is a Fall from Standing
Dr. Glatter: These are obviously ground-level falls in most patients and not motor vehicle crashes. That’s an important part in the population that you looked at that should be mentioned clearly.
Dr. Shih: It’s astonishing. I’ve been a program director for over 20 years, and geriatrics is not well taught in the curriculum. It’s astonishing for many of our trainees and emergency physicians in general that the number-one cause for traumatic injury is a fall from standing.
Certainly, we get patients coming in the trauma center like a 95-year-old person who’s on a ladder putting up his Christmas lights. I’m like, oh my God.
For the vast majority, it’s closer to 90%, but in our study, for the patients we looked at, it was 80% that fall from standing. That’s the mechanism that causes these bleeds and these major injuries.
Dr. Shenvi: That’s reflective of what we see, so it’s good that that’s what you looked at also.
Dr. Glatter: Absolutely. Well, thank you both. This has been a very informative discussion. I appreciate your time, and our readers will certainly benefit from your knowledge and expertise. Thank you again.
Dr. Glatter, assistant professor of emergency medicine at Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York, is a medical adviser for this news organization. He disclosed having no relevant financial conflicts. Dr. Shih is professor of emergency medicine at the Charles E. Schmidt College of Medicine at Florida Atlantic University, Boca Raton. His current grant funding and area of research interest involves geriatric emergency department patients with head injury and fall-related injury. He disclosed receiving a research grant from The Florida Medical Malpractice Joint Underwriting Association Grant for Safety of Health Care Services). Dr. Shenvi, associate professor of emergency medicine at the University of North Carolina at Chapel Hill, disclosed ties with the American College of Emergency Physicians, Institute for Healthcare Improvement, AstraZeneca, and CurvaFix.
A version of this article appeared on Medscape.com.
This discussion was recorded on August 2, 2024. This transcript has been edited for clarity.
Robert D. Glatter, MD: Today, we’ll be discussing the results of a new study published in The Journal of Emergency Medicine, looking at the incidence of delayed intracranial hemorrhage among older patients taking preinjury anticoagulants who present to the emergency department (ED) with blunt head trauma.
Joining me today is the lead author of the study, Dr. Richard Shih, professor of emergency medicine at Florida Atlantic University. Also joining me is Dr. Christina Shenvi, associate professor of emergency medicine at the University of North Carolina (UNC) Chapel Hill, with fellowship training in geriatric emergency medicine.
Welcome to both of you.
Richard D. Shih, MD: Thanks, Rob.
Christina L. Shenvi, MD, PhD, MBA: Thanks. Pleasure to be here.
ICH Study Methodology
Dr. Glatter: It’s a pleasure to have you. Rich, this is a great study and targeted toward a population we see daily in the emergency department. I want you to describe your methodology, patient selection, and how you went about organizing your study to look at this important finding of delayed intracranial hemorrhage, especially in those on anticoagulants.
Dr. Shih: This all started for our research team when we first read the 2012 Annals of Emergency Medicine paper. The first author was Vincenzo Menditto, and he looked at a group of patients that had minor head injury, were anticoagulated, and had negative initial head CTs.
There were about 100 patients, of which about 10 of them did not consent, but they hospitalized all these patients. These were anticoagulated, negative-first head CTs. They hospitalized the patients and then did a routine second CT at about 24 hours. They also followed them for a week, and it turned out a little over 7% of them had delayed head CT.
We were wondering how many delayed intracranial hemorrhages we had missed because current practice for us was that, if patients had a good physical exam, their head CT was normal, and everything looked good, we would send them home.
Because of that, a number of people across the country wanted to verify those findings from the Menditto study. We tried to design a good study to answer that question. We happen to have a very large geriatric population in Florida, and our ED census is very high for age over 65, at nearly 60%.
There are two Level I trauma centers in Palm Beach County. We included a second multicenter hospital, and we prospectively enrolled patients. We know the current state of practice is not to routinely do second CTs, so we followed these patients over time and followed their medical records to try to identify delayed bleeding. That’s how we set up our methodology.
Is It Safe to Discharge Patients With Trauma After 24 Hours?
Dr. Glatter: For the bulk of these patients with negative head CTs, it’s been my practice that when they’re stable and they look fine and there’s no other apparent, distracting painful trauma, injuries and so forth, they’re safe to discharge.
The secondary outcome in your study is interesting: the need for neurosurgical intervention in terms of those with delayed intracranial hemorrhage.
Dr. Shih: I do believe that it’s certainly not the problem that Menditto described, which is 7%. There are two other prospective studies that have looked at this issue with delayed bleeding on anticoagulants. Both of these also showed a relatively low rate of delayed bleeding, which is between like 0.2% and 1.0%. In our study, it was 0.4%.
The difference in the studies is that Menditto and colleagues routinely did 24-hour head CTs. They admitted everybody. For these other studies, routine head CT was not part of it. My bet is that there is a rate of delayed bleeding somewhere in between that seen in the Menditto study and that in all the other studies.
However, talking about significant intracranial hemorrhage, ones that perhaps need neurosurgery, I believe most of them are not significant. There’s some number that do occur, but the vast majority of those probably don’t need neurosurgery. We had 14 delayed bleeds out of 6000 patients with head trauma. One of them ended up requiring neurosurgery, so the answer is not zero, but I don’t think it’s 7% either.
Dr. Glatter: Dr. Shenvi, I want to bring you into the conversation to talk about your experience at UNC, and how you run things in terms of older patients with blunt head trauma on preinjury anticoagulants.
Dr. Shenvi: Thanks, Rob. I remember when this paper came out showing this 7% rate of delayed bleeding and the question was, “Should we be admitting all these people?” Partly just from an overwhelming need for capacity that that would bring, it just wasn’t practical to say, “We’re going to admit every patient with a negative head CT to the hospital and rescan them.” That would be hundreds or thousands of patients each year in any given facility.
The other thing is that delayed bleeds don’t always happen just in the first 24 hours. It’s not even a matter of bringing patients into observation for 24 hours, watching them, and rescanning them if they have symptoms. It can occur several days out. That never, in almost any institution that I know of, became standard practice.
The way that it did change my care was to give good return precautions to patients, to make sure they have somebody with them to say, “Hey, sometimes you can have bleeding several days out after a fall, even though your CT scan here today looks perfect,” and to alert them that if they start having severe headaches, vomiting, or other symptoms of intracranial hemorrhage, that they should come back.
I don’t think it ever became standard practice, and for good reason, because that was one study. The subsequent studies that Richard mentioned, pretty quickly on the heels of that initial one, showed a much lower rate of delayed ICH with the caveats that the methodology was different.
Shift in Anticoagulants
Dr. Shenvi: One other big change from that original study, and now to Richard’s study, is the shift in anticoagulants. Back in the initial study you mentioned, it was all warfarin. We know from other studies looking at warfarin vs the direct oral anticoagulants (DOACs) that DOACs have lower rates of ICH after a head injury, lower rates of need for neurosurgical intervention, and lower rates of discharge to a skilled nursing facility after an intracranial hemorrhage.
Across the board, we know that the DOACs tend to do better. It’s difficult to compare newer studies because it’s a different medication. It did inform my practice to have an awareness of delayed intracranial hemorrhage so that I warn patients more proactively.
Dr. Glatter: I haven’t seen a patient on warfarin in years. I don’t know if either of you have, but it’s all DOACs now unless there’s some other reason. That shift is quite apparent.
Dr. Shih: The problem with looking at delayed bleeding for DOACs vs warfarin is the numbers were so low. I think we had 13 people, and seven were in the no-anticoagulant group. The numbers are even lower, so it’s hard to say.
I just wanted to comment on something that Dr. Shenvi said, and I pretty much agree with everything that she said. Anticoagulants and warfarin, and that Menditto study, have a carryover effect. People group DOACs with warfarin similarly. When a patient is brought in, the first thing they talk about with head trauma is, “Oh, they’re on an anticoagulant” or “They’re not on an anticoagulant.” It’s so ingrained.
I believe that, in emergency medicine, we’re pressed for space and time and we’re not as affected by that 24-hour observation. Maybe many of our surgeons will automatically admit those patients.
I haven’t seen a guideline from the United States, but there are two international guidelines. One is from Austria from 2019, and one is from Scandinavia. Both recommended 24-hour observation if you’re on an anticoagulant.
There is a bit of controversy left over with that. Hopefully, as more and more of information, like in our study, comes out, people will be a little bit more clear about it. I don’t think there’s a need to routinely admit them.
I do want to mention that the Menditto study had such a massive impact on everybody. They pointed out one subgroup (and it’s such a small number of patients). They had seven cases of delayed bleeding; four or five of them were within that 24 hours, and a couple were diagnosed later over the next couple days.
Of those seven people, four of them had international normalized ratios (INRs) greater than 3. Of those four patients, I’ve heard people talk about this and recommend, “Okay, that’s the subgroup I would admit.” There’s a toss-up with what to do with DOAC because it’s very hard to tell whether there’s an issue, whether there are problems with their dosing, and whatever.
We actually recently looked at that. We have a much larger sample than four: close to 300 patients who were on warfarin. We looked at patients who had INRs below 3 and above 3, and we didn’t show a difference. We still don’t believe that warfarin is a big issue with delayed bleeding.
Should We Be Asking: ‘Are They on Blood Thinners?’
Dr. Shenvi: One of the interesting trends related to warfarin and the DOACs vs no anticoagulant is that as you mentioned, Dr Shih, the first question out of people’s mouths or the first piece of information emergency medical services gives you when they come in with a patient who’s had a head injury is, “Are they on blood thinners or not?”
Yet, the paradigm is shifting to say it’s not actually the blood thinners themselves that are giving older patients the higher risk for bleeding; it’s age and other comorbidities.
Certainly, if you’re on an anticoagulant and you start to bleed, your prognosis is much worse because the bleeding doesn’t stop. In terms of who has a bleeding event, there’s much less impact of anticoagulation than we used to think. That, in part, may be due to the change from warfarin to other medications.
Some of the experts I’ve talked to who have done the research on this have said, “Well, actually, warfarin was more of a marker for being much older and more frail, because it was primarily prescribed to older patients who have significant heart disease, atrial fibrillation, and so on.” It was more a marker for somebody who is at risk for an intracranial hemorrhage. There are many changes that have happened in the past 10 years with medications and also our understanding.
Challenges in Patient Follow-up
Dr. Glatter: That’s a great point. One thing, Rich, I want to ask you about is in terms of your proxy outcome assessment. When you use that at 14 and 60 days with telephone follow-up and then chart review at 60 and 90 days (because, obviously, everyone can’t get another head CT or it’s difficult to follow patients up), did you find that worked out well in your prospective cohort study, in terms of using that as a proxy, so to speak?
Dr. Shih: I would say to a certain extent. Unfortunately, we don’t have access to the patients to come back to follow up all of them, and there was obviously a large number of patients in our study.
The next best thing was that we had dedicated research assistants calling all of the patients at 14 days and 60 days. I’ve certainly read research studies where, when they call them, they get 80%-90% follow-up, but we did not achieve that.
I don’t know if people are more inundated with spam phone calls now, or the older people are just afraid of picking up their phone sometimes with all the scams and so forth. I totally understand, but in all honesty, we only had about a 30%-35% follow-up using that follow-up pathway.
Then the proxy pathway was to look at their charts at 60 and 90 days. Also, we looked at the Florida death registry, which is pretty good, and then finally, we had both Level I trauma centers in the county that we were in participating. It’s standard practice that if you have an intracranial hemorrhage at a non–Level I trauma center, you would be transferred to a Level I trauma center. That’s the protocol. I know that’s not followed 100% of the time, but that’s part of the proxy follow-up. You could criticize the study for not having closer to 90% actual contact, but that’s the best we could do.
Dr. Glatter: I think that’s admirable. Using that paradigm of what you described certainly allows the reader to understand the difficulty in assessing patients that don’t get follow-up head CT, and hardly anyone does that, as we know.
To your point of having both Level I trauma centers in the county, that makes it pretty secure. If we’re going to do a study encompassing a similar type of regional aspect, it would be similar.
Dr. Shenvi: I think your proxies, to your credit, were as good as you can get. You can never get a 100% follow-up, but you really looked at all the different avenues by which patients might present, either in the death registry or a Level I center. Well done on that aspect.
Determining When to Admit Patients for Observation
Dr. Glatter: In terms of admissions: You admit a patient, then you hear back that this patient should not have been admitted because they had a negative head CT, but you put them in anyway in the sense of delayed bleeding happening or not happening.
It’s interesting. Maybe the insurers will start looking at this in some capacity, based on your study, that because it’s so infrequent that you see delayed bleeding, that admitting someone for any reason whatsoever would be declined. Do you see that being an issue? In other words, [do you see] this leading to a pattern in terms of the payers?
Dr. Shih: Certainly, you could interpret it that way, and that would be unfortunate. The [incidence of] delayed bleeding is definitely not zero. That’s the first thing.
The second thing is that when you’re dealing with an older population, having some sense that they’re not doing well is an important contributor to trying to fully assess what’s going on — whether or not they have a bleed or whether they’re at risk for falling again and then hitting their head and causing a second bleed, and making sure they can do the activities of daily life. There really should be some room for a physician to say, “They just got here, and we don’t know him that well. There’s something that bothers me about this person” and have the ability to watch them for at least another 24 hours. That’s how I feel.
Dr. Shenvi: In my location, it would be difficult to try to admit somebody purely for observation for delayed bleeding. I think we would get a lot of pushback on that. The reasons I might admit a patient after a fall with a negative head CT, though, are all the things that, Rob, you alluded to earlier — which are, what made them fall in the first place and were they unable to get up?
I had this happen just this week. A patient who fell couldn’t get off the ground for 12 hours, and so now she’s dehydrated and delirious with slight rhabdomyolysis. Then you’re admitting them either for the sequelae of the fall that are not related to the intracranial hemorrhage, or the fact that they are so debilitated and deconditioned that they cannot take care of themselves. They need physical therapy. Often, we will have physical and occupational therapists come see them in the ED during business hours and help make an assessment of whether they are safe to go home or whether they fall again. That can give more evidence for the need for admission.
Dr. Glatter: To bring artificial intelligence into this discussion, algorithms that are out there that say, “Push a button and the patient’s safe for discharge.” Well, this argues for a clinical gestalt and a human being to make an assessment because you can use these predictive models, which are coming and they’re going to be here soon, and they already are in some sense. Again, we have to use clinical human judgment.
Dr. Shih: I agree.
Advice for Primary Care Physicians
Dr. Glatter: What return precautions do you discuss with patients who’ve had blunt head trauma that maybe had a head CT, or even didn’t? What are the main things we’re looking for?
Dr. Shenvi: What I usually tell people is if you start to have a worse headache, nausea or vomiting, any weakness in one area of your body, or vision changes, and if there’s a family member or friend there, I’ll say, “If you notice that they’re acting differently or seem confused, come back.”
Dr. Shih: I agree with what she said, and I’m also going to add one thing. The most important part is they are trying to prevent a subsequent fall. We know that when they’ve fallen and they present to the ED, they’re at even higher risk for falling and reinjuring themselves, and that’s a population that’s already at risk.
One of the secondary studies that we published out of this project was looking at follow-up with their primary care physicians, and there were two things that we wanted to address. The first was, how often did they do it? Then, when they did do it, did their primary care physicians try to address and prevent subsequent falls?
Both the answers are actually bad. Amazingly, just over like 60% followed up.
In some of our subsequent research, because we’re in the midst of a randomized, controlled trial where we do a home visit, when we initially see these individuals that have fallen, they’ll schedule a home visit for us. Then a week or two later, when we schedule the home visit, many of them cancel because they think, Oh, that was a one-off and it’s not going to happen again. Part of the problem is the patients, because many of them believe that they just slipped and fell and it’s not going to happen again, or they’re not prone to it.
The second issue was when patients did go to a primary care physician, we have found that some primary care physicians believe that falling and injuring themselves is just part of the normal aging process. A percentage of them don’t go over assessment for fall risk or even initiate fall prevention treatments or programs.
I try to take that time to tell them that this is very common in their age group, and believe it or not, a fall from standing is the way people really injure themselves, and there may be ways to prevent subsequent falls and injuries.
Dr. Glatter: Absolutely. Do you find that their medications are a contributor in some sense? Say they’re antihypertensive, have issues of orthostasis, or a new medication was added in the last week.
Dr. Shenvi: It’s all of the above. Sometimes it’s one thing, like they just started tamsulosin for their kidney stone, they stood up, they felt lightheaded, and they fell. Usually, it’s multifactorial with some changes in their gait, vision, balance, reflex time, and strength, plus the medications or the need for assistive devices. Maybe they can’t take care of their home as well as they used to and there are things on the floor. It’s really all of the above.
‘Harder to Unlearn Something Than to Learn It’
Dr. Glatter: Would either of you like to add any additional points to the discussion or add a few pearls?
Dr. Shenvi: This just highlights the challenge of how it’s harder to unlearn something than to learn it, where one study that maybe wasn’t quite looking at what we needed to, or practice and prescribing patterns have changed, so it’s no longer really relevant.
The things that we learned from that, or the fears that we instilled in our minds of, Uh oh, they could go home and have delayed bleeding, are much harder to unlearn, and it takes more studies to unlearn that idea than it did to actually put it into place.
I’m glad that your team has done this much larger, prospective study and hopefully will reduce the concern about this entity.
Dr. Shih: I appreciate that segue. It is amazing that, for paramedics and medical students, the first thing out of their mouth is, “Are they on an anticoagulant?”
In terms of the risk of developing an intracranial hemorrhage, I think it’s much less than the weight we’ve put on it before. However, I believe if they have a bleed, the bleeds are worse. It’s kind of a double-edged sword. It’s still an important factor, but it doesn’t come with the Oh my gosh, they’re on an anticoagulant that everybody thinks about.
No. 1 Cause of Traumatic Injury Is a Fall from Standing
Dr. Glatter: These are obviously ground-level falls in most patients and not motor vehicle crashes. That’s an important part in the population that you looked at that should be mentioned clearly.
Dr. Shih: It’s astonishing. I’ve been a program director for over 20 years, and geriatrics is not well taught in the curriculum. It’s astonishing for many of our trainees and emergency physicians in general that the number-one cause for traumatic injury is a fall from standing.
Certainly, we get patients coming in the trauma center like a 95-year-old person who’s on a ladder putting up his Christmas lights. I’m like, oh my God.
For the vast majority, it’s closer to 90%, but in our study, for the patients we looked at, it was 80% that fall from standing. That’s the mechanism that causes these bleeds and these major injuries.
Dr. Shenvi: That’s reflective of what we see, so it’s good that that’s what you looked at also.
Dr. Glatter: Absolutely. Well, thank you both. This has been a very informative discussion. I appreciate your time, and our readers will certainly benefit from your knowledge and expertise. Thank you again.
Dr. Glatter, assistant professor of emergency medicine at Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York, is a medical adviser for this news organization. He disclosed having no relevant financial conflicts. Dr. Shih is professor of emergency medicine at the Charles E. Schmidt College of Medicine at Florida Atlantic University, Boca Raton. His current grant funding and area of research interest involves geriatric emergency department patients with head injury and fall-related injury. He disclosed receiving a research grant from The Florida Medical Malpractice Joint Underwriting Association Grant for Safety of Health Care Services). Dr. Shenvi, associate professor of emergency medicine at the University of North Carolina at Chapel Hill, disclosed ties with the American College of Emergency Physicians, Institute for Healthcare Improvement, AstraZeneca, and CurvaFix.
A version of this article appeared on Medscape.com.
Gram Stain Doesn’t Improve UTI Diagnosis in the ED
TOPLINE:
Compared with other urine analysis methods, urine Gram stain has a moderate predictive value for detecting gram-negative bacteria in urine culture but does not significantly improve urinary tract infection (UTI) diagnosis in the emergency department (ED).
METHODOLOGY:
- Researchers conducted an observational cohort study at the University Medical Center Groningen in the Netherlands, encompassing 1358 episodes across 1136 patients suspected of having a UTI.
- The study included the following predefined subgroups: patients using urinary catheters and patients with leukopenia (< 4.0×10⁹ leucocytes/L). Urine dipstick nitrite, automated urinalysis, Gram stain, and urine cultures were performed on urine samples collected from patients presenting at the ED.
- The sensitivity and specificity of Gram stain for “many” bacteria (quantified as > 15/high power field) were compared with those of urine dipstick nitrite and automated bacterial counting in urinalysis.
TAKEAWAY:
- The sensitivity and specificity of Gram stain for “many” bacteria were 51.3% and 91.0%, respectively, with an accuracy of 76.8%.
- Gram stain showed a positive predictive value (PPV) of 84.7% for gram-negative rods in urine culture; however, the PPV was only 38.4% for gram-positive cocci.
- In the catheter subgroup, the presence of monomorphic bacteria quantified as “many” had a higher PPV for diagnosing a UTI than the presence of polymorphic bacteria with the same quantification.
- The overall performance of Gram stain in diagnosing a UTI in the ED was comparable to that of automated bacterial counting in urinalysis but better than that of urine dipstick nitrite.
IN PRACTICE:
“With the exception of a moderate prediction of gram-negative bacteria in the UC [urine culture], urine GS [Gram stain] does not improve UTI diagnosis at the ED compared to other urine parameters,” the authors wrote.
SOURCE:
The study was led by Stephanie J.M. Middelkoop, University of Groningen, University Medical Center Groningen, the Netherlands. It was published online on August 16, 2024, in Infectious Diseases.
LIMITATIONS:
The study’s limitations included a small sample size within the leukopenia subgroup, which may have affected the generalizability of the findings. Additionally, the potential influence of refrigeration of urine samples on bacterial growth could have affected the results. In this study, indwelling catheters were not replaced before urine sample collection, which may have affected the accuracy of UTI diagnosis in patients using catheters.
DISCLOSURES:
No conflicts of interest were disclosed by the authors.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Compared with other urine analysis methods, urine Gram stain has a moderate predictive value for detecting gram-negative bacteria in urine culture but does not significantly improve urinary tract infection (UTI) diagnosis in the emergency department (ED).
METHODOLOGY:
- Researchers conducted an observational cohort study at the University Medical Center Groningen in the Netherlands, encompassing 1358 episodes across 1136 patients suspected of having a UTI.
- The study included the following predefined subgroups: patients using urinary catheters and patients with leukopenia (< 4.0×10⁹ leucocytes/L). Urine dipstick nitrite, automated urinalysis, Gram stain, and urine cultures were performed on urine samples collected from patients presenting at the ED.
- The sensitivity and specificity of Gram stain for “many” bacteria (quantified as > 15/high power field) were compared with those of urine dipstick nitrite and automated bacterial counting in urinalysis.
TAKEAWAY:
- The sensitivity and specificity of Gram stain for “many” bacteria were 51.3% and 91.0%, respectively, with an accuracy of 76.8%.
- Gram stain showed a positive predictive value (PPV) of 84.7% for gram-negative rods in urine culture; however, the PPV was only 38.4% for gram-positive cocci.
- In the catheter subgroup, the presence of monomorphic bacteria quantified as “many” had a higher PPV for diagnosing a UTI than the presence of polymorphic bacteria with the same quantification.
- The overall performance of Gram stain in diagnosing a UTI in the ED was comparable to that of automated bacterial counting in urinalysis but better than that of urine dipstick nitrite.
IN PRACTICE:
“With the exception of a moderate prediction of gram-negative bacteria in the UC [urine culture], urine GS [Gram stain] does not improve UTI diagnosis at the ED compared to other urine parameters,” the authors wrote.
SOURCE:
The study was led by Stephanie J.M. Middelkoop, University of Groningen, University Medical Center Groningen, the Netherlands. It was published online on August 16, 2024, in Infectious Diseases.
LIMITATIONS:
The study’s limitations included a small sample size within the leukopenia subgroup, which may have affected the generalizability of the findings. Additionally, the potential influence of refrigeration of urine samples on bacterial growth could have affected the results. In this study, indwelling catheters were not replaced before urine sample collection, which may have affected the accuracy of UTI diagnosis in patients using catheters.
DISCLOSURES:
No conflicts of interest were disclosed by the authors.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Compared with other urine analysis methods, urine Gram stain has a moderate predictive value for detecting gram-negative bacteria in urine culture but does not significantly improve urinary tract infection (UTI) diagnosis in the emergency department (ED).
METHODOLOGY:
- Researchers conducted an observational cohort study at the University Medical Center Groningen in the Netherlands, encompassing 1358 episodes across 1136 patients suspected of having a UTI.
- The study included the following predefined subgroups: patients using urinary catheters and patients with leukopenia (< 4.0×10⁹ leucocytes/L). Urine dipstick nitrite, automated urinalysis, Gram stain, and urine cultures were performed on urine samples collected from patients presenting at the ED.
- The sensitivity and specificity of Gram stain for “many” bacteria (quantified as > 15/high power field) were compared with those of urine dipstick nitrite and automated bacterial counting in urinalysis.
TAKEAWAY:
- The sensitivity and specificity of Gram stain for “many” bacteria were 51.3% and 91.0%, respectively, with an accuracy of 76.8%.
- Gram stain showed a positive predictive value (PPV) of 84.7% for gram-negative rods in urine culture; however, the PPV was only 38.4% for gram-positive cocci.
- In the catheter subgroup, the presence of monomorphic bacteria quantified as “many” had a higher PPV for diagnosing a UTI than the presence of polymorphic bacteria with the same quantification.
- The overall performance of Gram stain in diagnosing a UTI in the ED was comparable to that of automated bacterial counting in urinalysis but better than that of urine dipstick nitrite.
IN PRACTICE:
“With the exception of a moderate prediction of gram-negative bacteria in the UC [urine culture], urine GS [Gram stain] does not improve UTI diagnosis at the ED compared to other urine parameters,” the authors wrote.
SOURCE:
The study was led by Stephanie J.M. Middelkoop, University of Groningen, University Medical Center Groningen, the Netherlands. It was published online on August 16, 2024, in Infectious Diseases.
LIMITATIONS:
The study’s limitations included a small sample size within the leukopenia subgroup, which may have affected the generalizability of the findings. Additionally, the potential influence of refrigeration of urine samples on bacterial growth could have affected the results. In this study, indwelling catheters were not replaced before urine sample collection, which may have affected the accuracy of UTI diagnosis in patients using catheters.
DISCLOSURES:
No conflicts of interest were disclosed by the authors.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
More Than the Paycheck: Top Non-Salary Perks for Doctors
Holly Wyatt, MD, had spent 20 years in UCHealth with no plans to leave. Her home, support system, and lifestyle were all rooted in Denver. But in 2020, The University of Alabama at Birmingham (UAB) made the endocrinologist an offer she couldn’t resist.
The pay increase and a bump to full professorship weren’t enough to lure her across the country. But then UAB sweetened the deal with fewer clinic hours and paid time to create. “I didn’t have to fit into the typical ‘see patients 5 days a week, bill this many dollars,’ ” she said.
With no minimum billable hours, she could spend her time on clinical trials, designing programs, and recording podcasts. “When they offered that, I said, ‘Ooh, that’s enticing.’ ”
After a couple of visits to the campus, she began the job transition.
Doctors are looking for more than base pay. For many physicians, like Dr. Wyatt, non-salary incentives carry a lot of weight in the recruitment and job-hunting process.
“Some of the usual suspects are CME [continuing medical education] budget, signing bonuses, relocation assistance, loan repayment programs, and housing allowances,” said Jake Jorgovan, partner at Alpha Apex Group, a physician recruiting firm in Denver.
Post pandemic, doctors are vying for other benefits, perks that support their interests, work-life balance, and financial stability. “We’ve come across offers like sabbatical opportunities, paid time for research or personal projects, and even concierge services that handle things like grocery shopping or pet care,” said Mr. Jorgovan.
Amid physician shortages, doctors have more bargaining power than ever.
Money Still Talks
Financial perks are still the premiere portion of a benefits package, according to Marc Adam, physician recruiter at MASC Medical, a medical recruitment firm in Fort Lauderdale, Florida.
New data from the medical staffing company AMN Healthcare reported that the average signing bonus for physicians is $31,103. The average relocation allowance is $11,000, and the average CME allowance is $4000.
“CME budget and loan repayment programs are big because they directly impact career advancement and financial well-being,” Mr. Jorgovan said. Employers have historically been hesitant to offer these kinds of long-term benefits because of the financial commitment and planning involved, but that’s changing.
Mr. Adam said that short-term financial perks, like relocation assistance and signing bonuses, tend to be more important for younger doctors. They’re not yet financially established, so the relocation support and bonus funds have more impact as they take on a new role, he said.
Mid- and late-career doctors, on the other hand, are less beholden to these types of bonuses. Mr. Adam has recruited established doctors from across the country to Florida, and he said that the relocation allowance and singing bonus didn’t even rank in their top five priorities. Similarly, in Birmingham, Dr. Wyatt recently reread her offer letter from UAB and was surprised to find a relocation stipend that she never used. “I had no idea,” she said.
Vying for Time
Mid- and late-career doctors who have a better financial safety net tend to seek benefits that boost their quality of life.
One of Mr. Adam’s recent job-searching clients was unwilling to compromise on priorities like specific location and a 4-day workweek.
Four-day workweeks, flexible scheduling, and options for remote work are increasingly popular, especially since the pandemic. Some physicians, like those in primary care, are looking for dedicated charting hours — paid days or half-days set aside for updating the electronic medical records. Other doctors are negotiating multistate telehealth licensing paid by their employer and work-from-home telehealth hours.
“Work life has been slowly increasing over the 14 years I’ve been doing this. And post COVID, the employer’s willingness to be flexible with those types of accommodations increased,” said Mr. Adam.
Priya Jaisinghani, MD, an endocrinologist and obesity medicine specialist in her second year of practice, NYU Langone Health, New York City, said work-life balance can be a priority for young doctors, too. After training in New York during the pandemic, Dr. Jaisinghani was all too aware of the risk for burnout. So she negotiated a 4-day workweek when she took her first job out of fellowship in 2022. “I was able to prioritize work-life balance from the start,” she said.
Support for the Career You Want
When Dr. Jaisinghani signed her first contract in 2022 with NYU, her move from New Jersey to New York wasn’t far enough to warrant a relocation allowance. “There was a signing bonus, sure,” she said. But what really grabbed her attention were perks like mentorship, access to trainees, and autonomy.
Perks that support long-term growth — like CME allowance, teaching opportunities, or access to leadership tracks — are especially important to young doctors. “After dedicating so many years to medical training, you want to look for some degree of autonomy in building your practice,” she said. NYU offered her that kind of freedom and support.
On top of personal growth, young physicians are looking for perks that will allow them to build the practice they want for their patients,Dr. Jaisinghani told this news organization. A lot of young doctors don’t know that they can negotiate for schedule preferences, office space, their own exam room, and dedicated support staff. However, they can and should because these factors influence their daily work life and patient experience.
Experienced doctors are also looking for perks that support the career they want. Recruitment experts say that doctors tend to look for opportunities that accommodate their interests. One of Mr. Jorgovan’s recent clients took a position because it offered a generous CME budget and dedicated research hours. Similarly, Dr. Wyatt at UAB moved because her contract included paid time to create.
“It really comes down to the need for balance — being able to keep learning while also having time for personal life and family,” Mr. Jorgovan said.
Making and Meeting Demand
Thanks to the rising demand, doctors have more power than ever to negotiate the perks they want and need.
The existing physician shortage — driven by retiring doctors and an aging patient population — was only exacerbated by the pandemic. Now, a number of new market entries are further increasing competition for talent, according to AMN Healthcare’s report. Retail clinics, urgent care, telehealth companies, and private equity firms compete for the same doctors, driving up salaries and doctor bargaining power.
“Physicians were always in the driver’s seat, and their bargaining power has only increased,” Mr. Adam said. Healthcare systems, once reticent about flexible working arrangements or loan repayment, are reconsidering.
Even young doctors have more negotiating power than they realize, but they might need help. “It’s underrated to get a contracts lawyer as a young doctor, but I think it’s smart,” Dr. Jaisinghani said. They’re often more familiar with salaries in the area, flexibility options, and potential benefits, none of which doctors are taught in training, she said.
Mr. Adam said that the pandemic opened employers’ eyes to the fact that doctors have the bargaining power. There’s a stark need for their talent and a lot of public support for their service. So hiring managers are listening and are ready to offer “creative benefits to accommodate the market demand,” he said.
In her new position at UAB, Dr. Wyatt said that money will always matter. “When your salary is low, bumping that salary will make you happier.” But after a certain point, she said, other things become more important — like your time, the work you do, and the people you work with. Her perks at UAB offer more than money can. “I get up in the morning, and I’m excited — [the work] excites me,” she said.
A version of this article first appeared on Medscape.com.
Holly Wyatt, MD, had spent 20 years in UCHealth with no plans to leave. Her home, support system, and lifestyle were all rooted in Denver. But in 2020, The University of Alabama at Birmingham (UAB) made the endocrinologist an offer she couldn’t resist.
The pay increase and a bump to full professorship weren’t enough to lure her across the country. But then UAB sweetened the deal with fewer clinic hours and paid time to create. “I didn’t have to fit into the typical ‘see patients 5 days a week, bill this many dollars,’ ” she said.
With no minimum billable hours, she could spend her time on clinical trials, designing programs, and recording podcasts. “When they offered that, I said, ‘Ooh, that’s enticing.’ ”
After a couple of visits to the campus, she began the job transition.
Doctors are looking for more than base pay. For many physicians, like Dr. Wyatt, non-salary incentives carry a lot of weight in the recruitment and job-hunting process.
“Some of the usual suspects are CME [continuing medical education] budget, signing bonuses, relocation assistance, loan repayment programs, and housing allowances,” said Jake Jorgovan, partner at Alpha Apex Group, a physician recruiting firm in Denver.
Post pandemic, doctors are vying for other benefits, perks that support their interests, work-life balance, and financial stability. “We’ve come across offers like sabbatical opportunities, paid time for research or personal projects, and even concierge services that handle things like grocery shopping or pet care,” said Mr. Jorgovan.
Amid physician shortages, doctors have more bargaining power than ever.
Money Still Talks
Financial perks are still the premiere portion of a benefits package, according to Marc Adam, physician recruiter at MASC Medical, a medical recruitment firm in Fort Lauderdale, Florida.
New data from the medical staffing company AMN Healthcare reported that the average signing bonus for physicians is $31,103. The average relocation allowance is $11,000, and the average CME allowance is $4000.
“CME budget and loan repayment programs are big because they directly impact career advancement and financial well-being,” Mr. Jorgovan said. Employers have historically been hesitant to offer these kinds of long-term benefits because of the financial commitment and planning involved, but that’s changing.
Mr. Adam said that short-term financial perks, like relocation assistance and signing bonuses, tend to be more important for younger doctors. They’re not yet financially established, so the relocation support and bonus funds have more impact as they take on a new role, he said.
Mid- and late-career doctors, on the other hand, are less beholden to these types of bonuses. Mr. Adam has recruited established doctors from across the country to Florida, and he said that the relocation allowance and singing bonus didn’t even rank in their top five priorities. Similarly, in Birmingham, Dr. Wyatt recently reread her offer letter from UAB and was surprised to find a relocation stipend that she never used. “I had no idea,” she said.
Vying for Time
Mid- and late-career doctors who have a better financial safety net tend to seek benefits that boost their quality of life.
One of Mr. Adam’s recent job-searching clients was unwilling to compromise on priorities like specific location and a 4-day workweek.
Four-day workweeks, flexible scheduling, and options for remote work are increasingly popular, especially since the pandemic. Some physicians, like those in primary care, are looking for dedicated charting hours — paid days or half-days set aside for updating the electronic medical records. Other doctors are negotiating multistate telehealth licensing paid by their employer and work-from-home telehealth hours.
“Work life has been slowly increasing over the 14 years I’ve been doing this. And post COVID, the employer’s willingness to be flexible with those types of accommodations increased,” said Mr. Adam.
Priya Jaisinghani, MD, an endocrinologist and obesity medicine specialist in her second year of practice, NYU Langone Health, New York City, said work-life balance can be a priority for young doctors, too. After training in New York during the pandemic, Dr. Jaisinghani was all too aware of the risk for burnout. So she negotiated a 4-day workweek when she took her first job out of fellowship in 2022. “I was able to prioritize work-life balance from the start,” she said.
Support for the Career You Want
When Dr. Jaisinghani signed her first contract in 2022 with NYU, her move from New Jersey to New York wasn’t far enough to warrant a relocation allowance. “There was a signing bonus, sure,” she said. But what really grabbed her attention were perks like mentorship, access to trainees, and autonomy.
Perks that support long-term growth — like CME allowance, teaching opportunities, or access to leadership tracks — are especially important to young doctors. “After dedicating so many years to medical training, you want to look for some degree of autonomy in building your practice,” she said. NYU offered her that kind of freedom and support.
On top of personal growth, young physicians are looking for perks that will allow them to build the practice they want for their patients,Dr. Jaisinghani told this news organization. A lot of young doctors don’t know that they can negotiate for schedule preferences, office space, their own exam room, and dedicated support staff. However, they can and should because these factors influence their daily work life and patient experience.
Experienced doctors are also looking for perks that support the career they want. Recruitment experts say that doctors tend to look for opportunities that accommodate their interests. One of Mr. Jorgovan’s recent clients took a position because it offered a generous CME budget and dedicated research hours. Similarly, Dr. Wyatt at UAB moved because her contract included paid time to create.
“It really comes down to the need for balance — being able to keep learning while also having time for personal life and family,” Mr. Jorgovan said.
Making and Meeting Demand
Thanks to the rising demand, doctors have more power than ever to negotiate the perks they want and need.
The existing physician shortage — driven by retiring doctors and an aging patient population — was only exacerbated by the pandemic. Now, a number of new market entries are further increasing competition for talent, according to AMN Healthcare’s report. Retail clinics, urgent care, telehealth companies, and private equity firms compete for the same doctors, driving up salaries and doctor bargaining power.
“Physicians were always in the driver’s seat, and their bargaining power has only increased,” Mr. Adam said. Healthcare systems, once reticent about flexible working arrangements or loan repayment, are reconsidering.
Even young doctors have more negotiating power than they realize, but they might need help. “It’s underrated to get a contracts lawyer as a young doctor, but I think it’s smart,” Dr. Jaisinghani said. They’re often more familiar with salaries in the area, flexibility options, and potential benefits, none of which doctors are taught in training, she said.
Mr. Adam said that the pandemic opened employers’ eyes to the fact that doctors have the bargaining power. There’s a stark need for their talent and a lot of public support for their service. So hiring managers are listening and are ready to offer “creative benefits to accommodate the market demand,” he said.
In her new position at UAB, Dr. Wyatt said that money will always matter. “When your salary is low, bumping that salary will make you happier.” But after a certain point, she said, other things become more important — like your time, the work you do, and the people you work with. Her perks at UAB offer more than money can. “I get up in the morning, and I’m excited — [the work] excites me,” she said.
A version of this article first appeared on Medscape.com.
Holly Wyatt, MD, had spent 20 years in UCHealth with no plans to leave. Her home, support system, and lifestyle were all rooted in Denver. But in 2020, The University of Alabama at Birmingham (UAB) made the endocrinologist an offer she couldn’t resist.
The pay increase and a bump to full professorship weren’t enough to lure her across the country. But then UAB sweetened the deal with fewer clinic hours and paid time to create. “I didn’t have to fit into the typical ‘see patients 5 days a week, bill this many dollars,’ ” she said.
With no minimum billable hours, she could spend her time on clinical trials, designing programs, and recording podcasts. “When they offered that, I said, ‘Ooh, that’s enticing.’ ”
After a couple of visits to the campus, she began the job transition.
Doctors are looking for more than base pay. For many physicians, like Dr. Wyatt, non-salary incentives carry a lot of weight in the recruitment and job-hunting process.
“Some of the usual suspects are CME [continuing medical education] budget, signing bonuses, relocation assistance, loan repayment programs, and housing allowances,” said Jake Jorgovan, partner at Alpha Apex Group, a physician recruiting firm in Denver.
Post pandemic, doctors are vying for other benefits, perks that support their interests, work-life balance, and financial stability. “We’ve come across offers like sabbatical opportunities, paid time for research or personal projects, and even concierge services that handle things like grocery shopping or pet care,” said Mr. Jorgovan.
Amid physician shortages, doctors have more bargaining power than ever.
Money Still Talks
Financial perks are still the premiere portion of a benefits package, according to Marc Adam, physician recruiter at MASC Medical, a medical recruitment firm in Fort Lauderdale, Florida.
New data from the medical staffing company AMN Healthcare reported that the average signing bonus for physicians is $31,103. The average relocation allowance is $11,000, and the average CME allowance is $4000.
“CME budget and loan repayment programs are big because they directly impact career advancement and financial well-being,” Mr. Jorgovan said. Employers have historically been hesitant to offer these kinds of long-term benefits because of the financial commitment and planning involved, but that’s changing.
Mr. Adam said that short-term financial perks, like relocation assistance and signing bonuses, tend to be more important for younger doctors. They’re not yet financially established, so the relocation support and bonus funds have more impact as they take on a new role, he said.
Mid- and late-career doctors, on the other hand, are less beholden to these types of bonuses. Mr. Adam has recruited established doctors from across the country to Florida, and he said that the relocation allowance and singing bonus didn’t even rank in their top five priorities. Similarly, in Birmingham, Dr. Wyatt recently reread her offer letter from UAB and was surprised to find a relocation stipend that she never used. “I had no idea,” she said.
Vying for Time
Mid- and late-career doctors who have a better financial safety net tend to seek benefits that boost their quality of life.
One of Mr. Adam’s recent job-searching clients was unwilling to compromise on priorities like specific location and a 4-day workweek.
Four-day workweeks, flexible scheduling, and options for remote work are increasingly popular, especially since the pandemic. Some physicians, like those in primary care, are looking for dedicated charting hours — paid days or half-days set aside for updating the electronic medical records. Other doctors are negotiating multistate telehealth licensing paid by their employer and work-from-home telehealth hours.
“Work life has been slowly increasing over the 14 years I’ve been doing this. And post COVID, the employer’s willingness to be flexible with those types of accommodations increased,” said Mr. Adam.
Priya Jaisinghani, MD, an endocrinologist and obesity medicine specialist in her second year of practice, NYU Langone Health, New York City, said work-life balance can be a priority for young doctors, too. After training in New York during the pandemic, Dr. Jaisinghani was all too aware of the risk for burnout. So she negotiated a 4-day workweek when she took her first job out of fellowship in 2022. “I was able to prioritize work-life balance from the start,” she said.
Support for the Career You Want
When Dr. Jaisinghani signed her first contract in 2022 with NYU, her move from New Jersey to New York wasn’t far enough to warrant a relocation allowance. “There was a signing bonus, sure,” she said. But what really grabbed her attention were perks like mentorship, access to trainees, and autonomy.
Perks that support long-term growth — like CME allowance, teaching opportunities, or access to leadership tracks — are especially important to young doctors. “After dedicating so many years to medical training, you want to look for some degree of autonomy in building your practice,” she said. NYU offered her that kind of freedom and support.
On top of personal growth, young physicians are looking for perks that will allow them to build the practice they want for their patients,Dr. Jaisinghani told this news organization. A lot of young doctors don’t know that they can negotiate for schedule preferences, office space, their own exam room, and dedicated support staff. However, they can and should because these factors influence their daily work life and patient experience.
Experienced doctors are also looking for perks that support the career they want. Recruitment experts say that doctors tend to look for opportunities that accommodate their interests. One of Mr. Jorgovan’s recent clients took a position because it offered a generous CME budget and dedicated research hours. Similarly, Dr. Wyatt at UAB moved because her contract included paid time to create.
“It really comes down to the need for balance — being able to keep learning while also having time for personal life and family,” Mr. Jorgovan said.
Making and Meeting Demand
Thanks to the rising demand, doctors have more power than ever to negotiate the perks they want and need.
The existing physician shortage — driven by retiring doctors and an aging patient population — was only exacerbated by the pandemic. Now, a number of new market entries are further increasing competition for talent, according to AMN Healthcare’s report. Retail clinics, urgent care, telehealth companies, and private equity firms compete for the same doctors, driving up salaries and doctor bargaining power.
“Physicians were always in the driver’s seat, and their bargaining power has only increased,” Mr. Adam said. Healthcare systems, once reticent about flexible working arrangements or loan repayment, are reconsidering.
Even young doctors have more negotiating power than they realize, but they might need help. “It’s underrated to get a contracts lawyer as a young doctor, but I think it’s smart,” Dr. Jaisinghani said. They’re often more familiar with salaries in the area, flexibility options, and potential benefits, none of which doctors are taught in training, she said.
Mr. Adam said that the pandemic opened employers’ eyes to the fact that doctors have the bargaining power. There’s a stark need for their talent and a lot of public support for their service. So hiring managers are listening and are ready to offer “creative benefits to accommodate the market demand,” he said.
In her new position at UAB, Dr. Wyatt said that money will always matter. “When your salary is low, bumping that salary will make you happier.” But after a certain point, she said, other things become more important — like your time, the work you do, and the people you work with. Her perks at UAB offer more than money can. “I get up in the morning, and I’m excited — [the work] excites me,” she said.
A version of this article first appeared on Medscape.com.