User login
ID Practitioner is an independent news source that provides infectious disease specialists with timely and relevant news and commentary about clinical developments and the impact of health care policy on the infectious disease specialist’s practice. Specialty focus topics include antimicrobial resistance, emerging infections, global ID, hepatitis, HIV, hospital-acquired infections, immunizations and vaccines, influenza, mycoses, pediatric infections, and STIs. Infectious Diseases News is owned by Frontline Medical Communications.
sofosbuvir
ritonavir with dasabuvir
discount
support path
program
ritonavir
greedy
ledipasvir
assistance
viekira pak
vpak
advocacy
needy
protest
abbvie
paritaprevir
ombitasvir
direct-acting antivirals
dasabuvir
gilead
fake-ovir
support
v pak
oasis
harvoni
section[contains(@class, 'footer-nav-section-wrapper')]
div[contains(@class, 'pane-pub-article-idp')]
div[contains(@class, 'pane-medstat-latest-articles-articles-section')]
div[contains(@class, 'pane-pub-home-idp')]
div[contains(@class, 'pane-pub-topic-idp')]
Delta variant could drive herd immunity threshold over 80%
Because the Delta variant of SARS-CoV-2 spreads more easily than the original virus, the proportion of the population that needs to be vaccinated to reach herd immunity could be upward of 80% or more, experts say.
Also, it could be time to consider wearing an N95 mask in public indoor spaces regardless of vaccination status, according to a media briefing on Aug. 3 sponsored by the Infectious Diseases Society of America.
Furthermore, giving booster shots to the fully vaccinated is not the top public health priority now. Instead, third vaccinations should be reserved for more vulnerable populations – and efforts should focus on getting first vaccinations to unvaccinated people in the United States and around the world.
“The problem here is that the Delta variant is ... more transmissible than the original virus. That pushes the overall population herd immunity threshold much higher,” Ricardo Franco, MD, assistant professor of medicine at the University of Alabama at Birmingham, said during the briefing.
“For Delta, those threshold estimates go well over 80% and may be approaching 90%,” he said.
To put that figure in context, the original SARS-CoV-2 virus required an estimated 67% of the population to be vaccinated to achieve herd immunity. Also, measles has one of the highest herd immunity thresholds at 95%, Dr. Franco added.
Herd immunity is the point at which enough people are immunized that the entire population gains protection. And it’s already happening. “Unvaccinated people are actually benefiting from greater herd immunity protection in high-vaccination counties compared to low-vaccination ones,” he said.
Maximize mask protection
Unlike early in the COVID-19 pandemic with widespread shortages of personal protective equipment, face masks are now readily available. This includes N95 masks, which offer enhanced protection against SARS-CoV-2, Ezekiel J. Emanuel, MD, PhD, said during the briefing.
Following the July 27 CDC recommendation that most Americans wear masks indoors when in public places, “I do think we need to upgrade our masks,” said Dr. Emanuel, who is Diane v.S. Levy & Robert M. Levy professor at the University of Pennsylvania, Philadelphia.
“It’s not just any mask,” he added. “Good masks make a big difference and are very important.”
Mask protection is about blocking 0.3-mcm particles, “and I think we need to make sure that people have masks that can filter that out,” he said. Although surgical masks are very good, he added, “they’re not quite as good as N95s.” As their name implies, N95s filter out 95% of these particles.
Dr. Emanuel acknowledged that people are tired of COVID-19 and complying with public health measures but urged perseverance. “We’ve sacrificed a lot. We should not throw it away in just a few months because we are tired. We’re all tired, but we do have to do the little bit extra getting vaccinated, wearing masks indoors, and protecting ourselves, our families, and our communities.”
Dealing with a disconnect
In response to a reporter’s question about the possibility that the large crowd at the Lollapalooza music festival in Chicago could become a superspreader event, Dr. Emanuel said, “it is worrisome.”
“I would say that, if you’re going to go to a gathering like that, wearing an N95 mask is wise, and not spending too long at any one place is also wise,” he said.
On the plus side, the event was held outdoors with lots of air circulation, Dr. Emanuel said.
However, “this is the kind of thing where we’ve got a sort of disconnect between people’s desire to get back to normal ... and the fact that we’re in the middle of this upsurge.”
Another potential problem is the event brought people together from many different locations, so when they travel home, they could be “potentially seeding lots of other communities.”
Boosters for some, for now
Even though not officially recommended, some fully vaccinated Americans are seeking a third or booster vaccination on their own.
Asked for his opinion, Dr. Emanuel said: “We’re probably going to have to be giving boosters to immunocompromised people and people who are susceptible. That’s where we are going to start.”
More research is needed regarding booster shots, he said. “There are very small studies – and the ‘very small’ should be emphasized – given that we’ve given shots to over 160 million people.”
“But it does appear that the boosters increase the antibodies and protection,” he said.
Instead of boosters, it is more important for people who haven’t been vaccinated to get fully vaccinated.
“We need to put our priorities in the right places,” he said.
Emanuel noted that, except for people in rural areas that might have to travel long distances, access to vaccines is no longer an issue. “It’s very hard not to find a vaccine if you want it.”
A remaining hurdle is “battling a major disinformation initiative. I don’t think this is misinformation. I think there’s very clear evidence that it is disinformation – false facts about the vaccines being spread,” Dr. Emanuel said.
The breakthrough infection dilemma
Breakthrough cases “remain the vast minority of infections at this time ... that is reassuring,” Dr. Franco said.
Also, tracking symptomatic breakthrough infections remains easier than studying fully vaccinated people who become infected with SARS-CoV-2 but remain symptom free.
“We really don’t have a good handle on the frequency of asymptomatic cases,” Dr. Emanuel said. “If you’re missing breakthrough infections, a lot of them, you may be missing some [virus] evolution that would be very important for us to follow.” This missing information could include the emergence of new variants.
The asymptomatic breakthrough cases are the most worrisome group,” Dr. Emanuel said. “You get infected, you’re feeling fine. Maybe you’ve got a little sneeze or cough, but nothing unusual. And then you’re still able to transmit the Delta variant.”
The big picture
The upsurge in cases, hospitalizations, and deaths is a major challenge, Dr. Emanuel said. “We need to address that by getting many more people vaccinated right now with what are very good vaccines.”
“But it also means that we have to stop being U.S. focused alone.” He pointed out that Delta and other variants originated overseas, “so getting the world vaccinated ... has to be a top priority.”
“We are obviously all facing a challenge as we move into the fall,” Dr. Emanuel said. “With schools opening and employers bringing their employees back together, even if these groups are vaccinated, there are going to be major challenges for all of us.”
A version of this article first appeared on Medscape.com.
Because the Delta variant of SARS-CoV-2 spreads more easily than the original virus, the proportion of the population that needs to be vaccinated to reach herd immunity could be upward of 80% or more, experts say.
Also, it could be time to consider wearing an N95 mask in public indoor spaces regardless of vaccination status, according to a media briefing on Aug. 3 sponsored by the Infectious Diseases Society of America.
Furthermore, giving booster shots to the fully vaccinated is not the top public health priority now. Instead, third vaccinations should be reserved for more vulnerable populations – and efforts should focus on getting first vaccinations to unvaccinated people in the United States and around the world.
“The problem here is that the Delta variant is ... more transmissible than the original virus. That pushes the overall population herd immunity threshold much higher,” Ricardo Franco, MD, assistant professor of medicine at the University of Alabama at Birmingham, said during the briefing.
“For Delta, those threshold estimates go well over 80% and may be approaching 90%,” he said.
To put that figure in context, the original SARS-CoV-2 virus required an estimated 67% of the population to be vaccinated to achieve herd immunity. Also, measles has one of the highest herd immunity thresholds at 95%, Dr. Franco added.
Herd immunity is the point at which enough people are immunized that the entire population gains protection. And it’s already happening. “Unvaccinated people are actually benefiting from greater herd immunity protection in high-vaccination counties compared to low-vaccination ones,” he said.
Maximize mask protection
Unlike early in the COVID-19 pandemic with widespread shortages of personal protective equipment, face masks are now readily available. This includes N95 masks, which offer enhanced protection against SARS-CoV-2, Ezekiel J. Emanuel, MD, PhD, said during the briefing.
Following the July 27 CDC recommendation that most Americans wear masks indoors when in public places, “I do think we need to upgrade our masks,” said Dr. Emanuel, who is Diane v.S. Levy & Robert M. Levy professor at the University of Pennsylvania, Philadelphia.
“It’s not just any mask,” he added. “Good masks make a big difference and are very important.”
Mask protection is about blocking 0.3-mcm particles, “and I think we need to make sure that people have masks that can filter that out,” he said. Although surgical masks are very good, he added, “they’re not quite as good as N95s.” As their name implies, N95s filter out 95% of these particles.
Dr. Emanuel acknowledged that people are tired of COVID-19 and complying with public health measures but urged perseverance. “We’ve sacrificed a lot. We should not throw it away in just a few months because we are tired. We’re all tired, but we do have to do the little bit extra getting vaccinated, wearing masks indoors, and protecting ourselves, our families, and our communities.”
Dealing with a disconnect
In response to a reporter’s question about the possibility that the large crowd at the Lollapalooza music festival in Chicago could become a superspreader event, Dr. Emanuel said, “it is worrisome.”
“I would say that, if you’re going to go to a gathering like that, wearing an N95 mask is wise, and not spending too long at any one place is also wise,” he said.
On the plus side, the event was held outdoors with lots of air circulation, Dr. Emanuel said.
However, “this is the kind of thing where we’ve got a sort of disconnect between people’s desire to get back to normal ... and the fact that we’re in the middle of this upsurge.”
Another potential problem is the event brought people together from many different locations, so when they travel home, they could be “potentially seeding lots of other communities.”
Boosters for some, for now
Even though not officially recommended, some fully vaccinated Americans are seeking a third or booster vaccination on their own.
Asked for his opinion, Dr. Emanuel said: “We’re probably going to have to be giving boosters to immunocompromised people and people who are susceptible. That’s where we are going to start.”
More research is needed regarding booster shots, he said. “There are very small studies – and the ‘very small’ should be emphasized – given that we’ve given shots to over 160 million people.”
“But it does appear that the boosters increase the antibodies and protection,” he said.
Instead of boosters, it is more important for people who haven’t been vaccinated to get fully vaccinated.
“We need to put our priorities in the right places,” he said.
Emanuel noted that, except for people in rural areas that might have to travel long distances, access to vaccines is no longer an issue. “It’s very hard not to find a vaccine if you want it.”
A remaining hurdle is “battling a major disinformation initiative. I don’t think this is misinformation. I think there’s very clear evidence that it is disinformation – false facts about the vaccines being spread,” Dr. Emanuel said.
The breakthrough infection dilemma
Breakthrough cases “remain the vast minority of infections at this time ... that is reassuring,” Dr. Franco said.
Also, tracking symptomatic breakthrough infections remains easier than studying fully vaccinated people who become infected with SARS-CoV-2 but remain symptom free.
“We really don’t have a good handle on the frequency of asymptomatic cases,” Dr. Emanuel said. “If you’re missing breakthrough infections, a lot of them, you may be missing some [virus] evolution that would be very important for us to follow.” This missing information could include the emergence of new variants.
The asymptomatic breakthrough cases are the most worrisome group,” Dr. Emanuel said. “You get infected, you’re feeling fine. Maybe you’ve got a little sneeze or cough, but nothing unusual. And then you’re still able to transmit the Delta variant.”
The big picture
The upsurge in cases, hospitalizations, and deaths is a major challenge, Dr. Emanuel said. “We need to address that by getting many more people vaccinated right now with what are very good vaccines.”
“But it also means that we have to stop being U.S. focused alone.” He pointed out that Delta and other variants originated overseas, “so getting the world vaccinated ... has to be a top priority.”
“We are obviously all facing a challenge as we move into the fall,” Dr. Emanuel said. “With schools opening and employers bringing their employees back together, even if these groups are vaccinated, there are going to be major challenges for all of us.”
A version of this article first appeared on Medscape.com.
Because the Delta variant of SARS-CoV-2 spreads more easily than the original virus, the proportion of the population that needs to be vaccinated to reach herd immunity could be upward of 80% or more, experts say.
Also, it could be time to consider wearing an N95 mask in public indoor spaces regardless of vaccination status, according to a media briefing on Aug. 3 sponsored by the Infectious Diseases Society of America.
Furthermore, giving booster shots to the fully vaccinated is not the top public health priority now. Instead, third vaccinations should be reserved for more vulnerable populations – and efforts should focus on getting first vaccinations to unvaccinated people in the United States and around the world.
“The problem here is that the Delta variant is ... more transmissible than the original virus. That pushes the overall population herd immunity threshold much higher,” Ricardo Franco, MD, assistant professor of medicine at the University of Alabama at Birmingham, said during the briefing.
“For Delta, those threshold estimates go well over 80% and may be approaching 90%,” he said.
To put that figure in context, the original SARS-CoV-2 virus required an estimated 67% of the population to be vaccinated to achieve herd immunity. Also, measles has one of the highest herd immunity thresholds at 95%, Dr. Franco added.
Herd immunity is the point at which enough people are immunized that the entire population gains protection. And it’s already happening. “Unvaccinated people are actually benefiting from greater herd immunity protection in high-vaccination counties compared to low-vaccination ones,” he said.
Maximize mask protection
Unlike early in the COVID-19 pandemic with widespread shortages of personal protective equipment, face masks are now readily available. This includes N95 masks, which offer enhanced protection against SARS-CoV-2, Ezekiel J. Emanuel, MD, PhD, said during the briefing.
Following the July 27 CDC recommendation that most Americans wear masks indoors when in public places, “I do think we need to upgrade our masks,” said Dr. Emanuel, who is Diane v.S. Levy & Robert M. Levy professor at the University of Pennsylvania, Philadelphia.
“It’s not just any mask,” he added. “Good masks make a big difference and are very important.”
Mask protection is about blocking 0.3-mcm particles, “and I think we need to make sure that people have masks that can filter that out,” he said. Although surgical masks are very good, he added, “they’re not quite as good as N95s.” As their name implies, N95s filter out 95% of these particles.
Dr. Emanuel acknowledged that people are tired of COVID-19 and complying with public health measures but urged perseverance. “We’ve sacrificed a lot. We should not throw it away in just a few months because we are tired. We’re all tired, but we do have to do the little bit extra getting vaccinated, wearing masks indoors, and protecting ourselves, our families, and our communities.”
Dealing with a disconnect
In response to a reporter’s question about the possibility that the large crowd at the Lollapalooza music festival in Chicago could become a superspreader event, Dr. Emanuel said, “it is worrisome.”
“I would say that, if you’re going to go to a gathering like that, wearing an N95 mask is wise, and not spending too long at any one place is also wise,” he said.
On the plus side, the event was held outdoors with lots of air circulation, Dr. Emanuel said.
However, “this is the kind of thing where we’ve got a sort of disconnect between people’s desire to get back to normal ... and the fact that we’re in the middle of this upsurge.”
Another potential problem is the event brought people together from many different locations, so when they travel home, they could be “potentially seeding lots of other communities.”
Boosters for some, for now
Even though not officially recommended, some fully vaccinated Americans are seeking a third or booster vaccination on their own.
Asked for his opinion, Dr. Emanuel said: “We’re probably going to have to be giving boosters to immunocompromised people and people who are susceptible. That’s where we are going to start.”
More research is needed regarding booster shots, he said. “There are very small studies – and the ‘very small’ should be emphasized – given that we’ve given shots to over 160 million people.”
“But it does appear that the boosters increase the antibodies and protection,” he said.
Instead of boosters, it is more important for people who haven’t been vaccinated to get fully vaccinated.
“We need to put our priorities in the right places,” he said.
Emanuel noted that, except for people in rural areas that might have to travel long distances, access to vaccines is no longer an issue. “It’s very hard not to find a vaccine if you want it.”
A remaining hurdle is “battling a major disinformation initiative. I don’t think this is misinformation. I think there’s very clear evidence that it is disinformation – false facts about the vaccines being spread,” Dr. Emanuel said.
The breakthrough infection dilemma
Breakthrough cases “remain the vast minority of infections at this time ... that is reassuring,” Dr. Franco said.
Also, tracking symptomatic breakthrough infections remains easier than studying fully vaccinated people who become infected with SARS-CoV-2 but remain symptom free.
“We really don’t have a good handle on the frequency of asymptomatic cases,” Dr. Emanuel said. “If you’re missing breakthrough infections, a lot of them, you may be missing some [virus] evolution that would be very important for us to follow.” This missing information could include the emergence of new variants.
The asymptomatic breakthrough cases are the most worrisome group,” Dr. Emanuel said. “You get infected, you’re feeling fine. Maybe you’ve got a little sneeze or cough, but nothing unusual. And then you’re still able to transmit the Delta variant.”
The big picture
The upsurge in cases, hospitalizations, and deaths is a major challenge, Dr. Emanuel said. “We need to address that by getting many more people vaccinated right now with what are very good vaccines.”
“But it also means that we have to stop being U.S. focused alone.” He pointed out that Delta and other variants originated overseas, “so getting the world vaccinated ... has to be a top priority.”
“We are obviously all facing a challenge as we move into the fall,” Dr. Emanuel said. “With schools opening and employers bringing their employees back together, even if these groups are vaccinated, there are going to be major challenges for all of us.”
A version of this article first appeared on Medscape.com.
No higher risk of rheumatic and musculoskeletal disease flares seen after COVID-19 vaccination
Double-dose vaccination against SARS-CoV-2 in patients with rheumatic and musculoskeletal diseases (RMDs) doesn’t appear to boost the risk of flares, a new study shows. The risk of adverse effects after vaccination is high, just as it is in the general population, but no patients experienced allergic reactions.

“Our findings suggest that COVID-19 vaccines are safe in patients with rheumatic and musculoskeletal diseases. Overall, rates of flare are low and mild, while local and systemic reactions should be anticipated,” lead author Caoilfhionn Connolly, MD, MSc, a rheumatology fellow at Johns Hopkins University, Baltimore, said in an interview. “Many of our patients are at increased risk of severe infection and or complications from COVID-19. It has been shown that patients with RMDs are more willing to reconsider vaccination if it is recommended by a physician, and these data should help inform these critical discussions.”
The study appeared Aug. 4 in Arthritis & Rheumatology.
According to Dr. Connolly, the researchers launched their study to better understand the effect of two-dose SARS-CoV-2 messenger RNA vaccinations authorized for emergency use by the Food and Drug Administration (Pfizer and Moderna vaccines) on immunosuppressed patients. As she noted, patients with RMDs were largely excluded from vaccine trials, and “studies have shown that some patients with RMDs are hesitant about vaccination due to the lack of safety data.”
Some data about this patient population have started to appear. A study published July 21 in Lancet Rheumatology found that patients with systemic lupus erythematosus (SLE) reported few flares within a median of 3 days after receiving one or two doses of various COVID-19 vaccines. Side effects were common but were mainly mild or moderate.
For the new study, researchers surveyed 1,377 patients with RMDs who’d received two vaccination doses between December 2020 and April 2021. The patients had a median age of 47, 92% were female, and 10% were non-White. The patients had a variety of RMDs, including inflammatory arthritis (47%), SLE (20%), overlap connective tissue disease (20%), and Sjögren’s syndrome and myositis (each 5%).
A total of 11% said they’d experienced a flare that required treatment, but none were severe. In comparison, 56% of patients said they had experienced a flare of their RMD in the 6 months prior to their first vaccine dose. Several groups had a greater likelihood of flares, including those who’d had COVID-19 previously (adjusted incidence rate ratio [IRR], 2.09; P = .02). “COVID-19 can cause both acute and delayed inflammatory syndromes through activation of the immune system,” Dr. Connolly said. “Vaccination possibly triggered further activation of the immune system resulting in disease flare. This is an area that warrants further research.”
Patients who took combination immunomodulatory therapy were also more likely to flare after vaccination (IRR, 1.95; P < .001). And patients were more likely to report flares after vaccination if they experienced a flare in the 6 months preceding vaccination (IRR, 2.36; P < .001). “This may suggest more active disease at baseline,” Dr. Connolly said. “It is difficult to differentiate whether these patients would have experienced flare even without the vaccine.”
A number of factors didn’t appear to affect the likelihood of flares: gender, age, ethnicity, type of RMD, and type of vaccine.
Local and systemic side effects were frequently reported, including injection site pain (87% and 86% after first and second doses, respectively) and fatigue (60% and 80%, respectively). As is common among people receiving COVID-19 vaccines, side effects were more frequent after the second dose.
As for future research, “we are evaluating the long-term safety and efficacy of the COVID-19 vaccines in patients with RMDs,” study coauthor Julie J. Paik, MD, assistant professor of medicine at Johns Hopkins, said in an interview. “We are also evaluating the impact of changes in immunosuppression around vaccination.”
The study was funded by the Ben-Dov family and grants from several institutes of the National Institutes of Health. Dr. Connolly and Dr. Paik reported no relevant disclosures. Other study authors reported various financial relationships with pharmaceutical companies.
Double-dose vaccination against SARS-CoV-2 in patients with rheumatic and musculoskeletal diseases (RMDs) doesn’t appear to boost the risk of flares, a new study shows. The risk of adverse effects after vaccination is high, just as it is in the general population, but no patients experienced allergic reactions.
“Our findings suggest that COVID-19 vaccines are safe in patients with rheumatic and musculoskeletal diseases. Overall, rates of flare are low and mild, while local and systemic reactions should be anticipated,” lead author Caoilfhionn Connolly, MD, MSc, a rheumatology fellow at Johns Hopkins University, Baltimore, said in an interview. “Many of our patients are at increased risk of severe infection and or complications from COVID-19. It has been shown that patients with RMDs are more willing to reconsider vaccination if it is recommended by a physician, and these data should help inform these critical discussions.”
The study appeared Aug. 4 in Arthritis & Rheumatology.
According to Dr. Connolly, the researchers launched their study to better understand the effect of two-dose SARS-CoV-2 messenger RNA vaccinations authorized for emergency use by the Food and Drug Administration (Pfizer and Moderna vaccines) on immunosuppressed patients. As she noted, patients with RMDs were largely excluded from vaccine trials, and “studies have shown that some patients with RMDs are hesitant about vaccination due to the lack of safety data.”
Some data about this patient population have started to appear. A study published July 21 in Lancet Rheumatology found that patients with systemic lupus erythematosus (SLE) reported few flares within a median of 3 days after receiving one or two doses of various COVID-19 vaccines. Side effects were common but were mainly mild or moderate.
For the new study, researchers surveyed 1,377 patients with RMDs who’d received two vaccination doses between December 2020 and April 2021. The patients had a median age of 47, 92% were female, and 10% were non-White. The patients had a variety of RMDs, including inflammatory arthritis (47%), SLE (20%), overlap connective tissue disease (20%), and Sjögren’s syndrome and myositis (each 5%).
A total of 11% said they’d experienced a flare that required treatment, but none were severe. In comparison, 56% of patients said they had experienced a flare of their RMD in the 6 months prior to their first vaccine dose. Several groups had a greater likelihood of flares, including those who’d had COVID-19 previously (adjusted incidence rate ratio [IRR], 2.09; P = .02). “COVID-19 can cause both acute and delayed inflammatory syndromes through activation of the immune system,” Dr. Connolly said. “Vaccination possibly triggered further activation of the immune system resulting in disease flare. This is an area that warrants further research.”
Patients who took combination immunomodulatory therapy were also more likely to flare after vaccination (IRR, 1.95; P < .001). And patients were more likely to report flares after vaccination if they experienced a flare in the 6 months preceding vaccination (IRR, 2.36; P < .001). “This may suggest more active disease at baseline,” Dr. Connolly said. “It is difficult to differentiate whether these patients would have experienced flare even without the vaccine.”
A number of factors didn’t appear to affect the likelihood of flares: gender, age, ethnicity, type of RMD, and type of vaccine.
Local and systemic side effects were frequently reported, including injection site pain (87% and 86% after first and second doses, respectively) and fatigue (60% and 80%, respectively). As is common among people receiving COVID-19 vaccines, side effects were more frequent after the second dose.
As for future research, “we are evaluating the long-term safety and efficacy of the COVID-19 vaccines in patients with RMDs,” study coauthor Julie J. Paik, MD, assistant professor of medicine at Johns Hopkins, said in an interview. “We are also evaluating the impact of changes in immunosuppression around vaccination.”
The study was funded by the Ben-Dov family and grants from several institutes of the National Institutes of Health. Dr. Connolly and Dr. Paik reported no relevant disclosures. Other study authors reported various financial relationships with pharmaceutical companies.
Double-dose vaccination against SARS-CoV-2 in patients with rheumatic and musculoskeletal diseases (RMDs) doesn’t appear to boost the risk of flares, a new study shows. The risk of adverse effects after vaccination is high, just as it is in the general population, but no patients experienced allergic reactions.
“Our findings suggest that COVID-19 vaccines are safe in patients with rheumatic and musculoskeletal diseases. Overall, rates of flare are low and mild, while local and systemic reactions should be anticipated,” lead author Caoilfhionn Connolly, MD, MSc, a rheumatology fellow at Johns Hopkins University, Baltimore, said in an interview. “Many of our patients are at increased risk of severe infection and or complications from COVID-19. It has been shown that patients with RMDs are more willing to reconsider vaccination if it is recommended by a physician, and these data should help inform these critical discussions.”
The study appeared Aug. 4 in Arthritis & Rheumatology.
According to Dr. Connolly, the researchers launched their study to better understand the effect of two-dose SARS-CoV-2 messenger RNA vaccinations authorized for emergency use by the Food and Drug Administration (Pfizer and Moderna vaccines) on immunosuppressed patients. As she noted, patients with RMDs were largely excluded from vaccine trials, and “studies have shown that some patients with RMDs are hesitant about vaccination due to the lack of safety data.”
Some data about this patient population have started to appear. A study published July 21 in Lancet Rheumatology found that patients with systemic lupus erythematosus (SLE) reported few flares within a median of 3 days after receiving one or two doses of various COVID-19 vaccines. Side effects were common but were mainly mild or moderate.
For the new study, researchers surveyed 1,377 patients with RMDs who’d received two vaccination doses between December 2020 and April 2021. The patients had a median age of 47, 92% were female, and 10% were non-White. The patients had a variety of RMDs, including inflammatory arthritis (47%), SLE (20%), overlap connective tissue disease (20%), and Sjögren’s syndrome and myositis (each 5%).
A total of 11% said they’d experienced a flare that required treatment, but none were severe. In comparison, 56% of patients said they had experienced a flare of their RMD in the 6 months prior to their first vaccine dose. Several groups had a greater likelihood of flares, including those who’d had COVID-19 previously (adjusted incidence rate ratio [IRR], 2.09; P = .02). “COVID-19 can cause both acute and delayed inflammatory syndromes through activation of the immune system,” Dr. Connolly said. “Vaccination possibly triggered further activation of the immune system resulting in disease flare. This is an area that warrants further research.”
Patients who took combination immunomodulatory therapy were also more likely to flare after vaccination (IRR, 1.95; P < .001). And patients were more likely to report flares after vaccination if they experienced a flare in the 6 months preceding vaccination (IRR, 2.36; P < .001). “This may suggest more active disease at baseline,” Dr. Connolly said. “It is difficult to differentiate whether these patients would have experienced flare even without the vaccine.”
A number of factors didn’t appear to affect the likelihood of flares: gender, age, ethnicity, type of RMD, and type of vaccine.
Local and systemic side effects were frequently reported, including injection site pain (87% and 86% after first and second doses, respectively) and fatigue (60% and 80%, respectively). As is common among people receiving COVID-19 vaccines, side effects were more frequent after the second dose.
As for future research, “we are evaluating the long-term safety and efficacy of the COVID-19 vaccines in patients with RMDs,” study coauthor Julie J. Paik, MD, assistant professor of medicine at Johns Hopkins, said in an interview. “We are also evaluating the impact of changes in immunosuppression around vaccination.”
The study was funded by the Ben-Dov family and grants from several institutes of the National Institutes of Health. Dr. Connolly and Dr. Paik reported no relevant disclosures. Other study authors reported various financial relationships with pharmaceutical companies.
FROM ARTHRITIS & RHEUMATOLOGY
Shorter antibiotic course okay for UTIs in men with no fever
A week of antibiotics appears just as effective as 2 weeks in treating afebrile men with urinary tract infections (UTIs), researchers say.
Shortening the course of treatment could spare patients side effects from the medications and reduce the risk that bacteria will develop resistance to the drugs, said Dimitri Drekonja, MD, chief of infectious diseases at the Minneapolis VA Medical Center.
“You’d like to be on these drugs for as short [an] amount of time as gets the job done,” he told this news organization. The study was published online July 28 in JAMA.
Researchers have recently found that shorter courses of antimicrobials are effective in the treatment of other types of infection and for UTIs in women. However, UTIs in men are thought to be more complicated because the male urethra is longer.
To see whether reducing length of treatment could be effective in men as well, Dr. Drekonja and colleagues compared 7-day and 14-day regimens in men treated at U.S. Veterans Affairs medical centers in Minnesota and Texas.
They recruited 272 men who had symptoms of UTI and were willing to participate. All the men received trimethoprim/sulfamethoxazole or ciprofloxacin for 7 days. Half the men were randomly assigned to continue this treatment for an additional 7 days; the other half received placebo pills for an additional 7 days.
The average age of the men was 69 years. Urine samples were cultured from 87.9% of the men. In 60.7% of these samples, the researchers found more than 100,000 CFU/mL; in 16.3%, they found lower colony counts; and in 23.0%, they found no growth of bacteria. The most common organism they isolated was Escherchia coli.
Results for the two groups were similar. Symptoms resolved 14 days after completion of the course of treatment in 90.4% of those who received 14 days of antibiotics, versus 91.9% of those who received 7 days of antibiotics plus 7 days of placebo pills. At 1.5%, the difference between the two arms was within the predetermined boundary for noninferiority.
The percentage of those who experienced recurrence of symptoms within 28 days of stopping medication was also similar between the two groups. Among those who received 7 days of antibiotics, 10.3% experienced recurrence of symptoms, compared to 16.9% of those assigned to 14 days of antibiotics.
There was no significant difference in the resolution of UTI symptoms between the two groups by type of antibiotic, pretreatment bacteriuria count, or study site.
Adverse events were also similar in the two groups, occurring in 20.6% of the men who received 7 days of antibiotics, versus 24.3% of the men who received 14 days of treatment. In both groups, 8.8% of patients had diarrhea, which was the most common adverse event.
Clinicians should not worry that antibiotic resistance is more likely to develop or that symptoms will recur when patients don’t finish a prescribed course of treatment, Dr. Drekonja said. “That is an old piece of guidance that has persisted for such a long time,” he said. “And it makes all of us in the infectious disease field cringe.”
Rather, the current thinking is that the more antibiotics patients take, the more resistance bacteria will develop, he said.
The success of the 7-day regimen raises the question of whether an even shorter course would work equally well. It’s not clear how short a course of antibiotics will do the trick. Research in certain populations, such as patients with spinal cord injuries, has suggested that recurrences are more frequent with 3 days of antibiotics than with 14, “so there could be a floor that you do need to go beyond,” Dr. Drekonja said.
“We’re not really sure how much people need,” agreed Daniel Morgan, MD, a professor of epidemiology and public health and medicine at the University of Maryland, Baltimore, which is why this study is important. “It really defined that 1 week is better than 2 weeks,” he said in an interview.
Another way that clinicians can reduce the use of antibiotics by men with UTIs is to consider alternative diagnoses and to culture urine samples when UTI seems like the most likely cause of their symptoms, said Dr. Morgan, who co-authored an accompanying editorial.
He pointed out that the U.S. Food and Drug Administration has issued a black box warning on fluoroquinolones, including ciprofloxacin, because they increase the risk for tendinitis and tendon rupture. Nitrofurantoin and amoxicillin-clavulanate are better alternatives for UTIs, he said.
Even some men with fevers and UTIs may need no more than 7 days of antibiotics, said Dr. Morgan. Dr. Drekonja said he generally prescribes at least 10 days antibiotics for these men.
The study was funded by the VA Merit Review Program. Dr. Drekonja and Dr. Morgan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A week of antibiotics appears just as effective as 2 weeks in treating afebrile men with urinary tract infections (UTIs), researchers say.
Shortening the course of treatment could spare patients side effects from the medications and reduce the risk that bacteria will develop resistance to the drugs, said Dimitri Drekonja, MD, chief of infectious diseases at the Minneapolis VA Medical Center.
“You’d like to be on these drugs for as short [an] amount of time as gets the job done,” he told this news organization. The study was published online July 28 in JAMA.
Researchers have recently found that shorter courses of antimicrobials are effective in the treatment of other types of infection and for UTIs in women. However, UTIs in men are thought to be more complicated because the male urethra is longer.
To see whether reducing length of treatment could be effective in men as well, Dr. Drekonja and colleagues compared 7-day and 14-day regimens in men treated at U.S. Veterans Affairs medical centers in Minnesota and Texas.
They recruited 272 men who had symptoms of UTI and were willing to participate. All the men received trimethoprim/sulfamethoxazole or ciprofloxacin for 7 days. Half the men were randomly assigned to continue this treatment for an additional 7 days; the other half received placebo pills for an additional 7 days.
The average age of the men was 69 years. Urine samples were cultured from 87.9% of the men. In 60.7% of these samples, the researchers found more than 100,000 CFU/mL; in 16.3%, they found lower colony counts; and in 23.0%, they found no growth of bacteria. The most common organism they isolated was Escherchia coli.
Results for the two groups were similar. Symptoms resolved 14 days after completion of the course of treatment in 90.4% of those who received 14 days of antibiotics, versus 91.9% of those who received 7 days of antibiotics plus 7 days of placebo pills. At 1.5%, the difference between the two arms was within the predetermined boundary for noninferiority.
The percentage of those who experienced recurrence of symptoms within 28 days of stopping medication was also similar between the two groups. Among those who received 7 days of antibiotics, 10.3% experienced recurrence of symptoms, compared to 16.9% of those assigned to 14 days of antibiotics.
There was no significant difference in the resolution of UTI symptoms between the two groups by type of antibiotic, pretreatment bacteriuria count, or study site.
Adverse events were also similar in the two groups, occurring in 20.6% of the men who received 7 days of antibiotics, versus 24.3% of the men who received 14 days of treatment. In both groups, 8.8% of patients had diarrhea, which was the most common adverse event.
Clinicians should not worry that antibiotic resistance is more likely to develop or that symptoms will recur when patients don’t finish a prescribed course of treatment, Dr. Drekonja said. “That is an old piece of guidance that has persisted for such a long time,” he said. “And it makes all of us in the infectious disease field cringe.”
Rather, the current thinking is that the more antibiotics patients take, the more resistance bacteria will develop, he said.
The success of the 7-day regimen raises the question of whether an even shorter course would work equally well. It’s not clear how short a course of antibiotics will do the trick. Research in certain populations, such as patients with spinal cord injuries, has suggested that recurrences are more frequent with 3 days of antibiotics than with 14, “so there could be a floor that you do need to go beyond,” Dr. Drekonja said.
“We’re not really sure how much people need,” agreed Daniel Morgan, MD, a professor of epidemiology and public health and medicine at the University of Maryland, Baltimore, which is why this study is important. “It really defined that 1 week is better than 2 weeks,” he said in an interview.
Another way that clinicians can reduce the use of antibiotics by men with UTIs is to consider alternative diagnoses and to culture urine samples when UTI seems like the most likely cause of their symptoms, said Dr. Morgan, who co-authored an accompanying editorial.
He pointed out that the U.S. Food and Drug Administration has issued a black box warning on fluoroquinolones, including ciprofloxacin, because they increase the risk for tendinitis and tendon rupture. Nitrofurantoin and amoxicillin-clavulanate are better alternatives for UTIs, he said.
Even some men with fevers and UTIs may need no more than 7 days of antibiotics, said Dr. Morgan. Dr. Drekonja said he generally prescribes at least 10 days antibiotics for these men.
The study was funded by the VA Merit Review Program. Dr. Drekonja and Dr. Morgan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A week of antibiotics appears just as effective as 2 weeks in treating afebrile men with urinary tract infections (UTIs), researchers say.
Shortening the course of treatment could spare patients side effects from the medications and reduce the risk that bacteria will develop resistance to the drugs, said Dimitri Drekonja, MD, chief of infectious diseases at the Minneapolis VA Medical Center.
“You’d like to be on these drugs for as short [an] amount of time as gets the job done,” he told this news organization. The study was published online July 28 in JAMA.
Researchers have recently found that shorter courses of antimicrobials are effective in the treatment of other types of infection and for UTIs in women. However, UTIs in men are thought to be more complicated because the male urethra is longer.
To see whether reducing length of treatment could be effective in men as well, Dr. Drekonja and colleagues compared 7-day and 14-day regimens in men treated at U.S. Veterans Affairs medical centers in Minnesota and Texas.
They recruited 272 men who had symptoms of UTI and were willing to participate. All the men received trimethoprim/sulfamethoxazole or ciprofloxacin for 7 days. Half the men were randomly assigned to continue this treatment for an additional 7 days; the other half received placebo pills for an additional 7 days.
The average age of the men was 69 years. Urine samples were cultured from 87.9% of the men. In 60.7% of these samples, the researchers found more than 100,000 CFU/mL; in 16.3%, they found lower colony counts; and in 23.0%, they found no growth of bacteria. The most common organism they isolated was Escherchia coli.
Results for the two groups were similar. Symptoms resolved 14 days after completion of the course of treatment in 90.4% of those who received 14 days of antibiotics, versus 91.9% of those who received 7 days of antibiotics plus 7 days of placebo pills. At 1.5%, the difference between the two arms was within the predetermined boundary for noninferiority.
The percentage of those who experienced recurrence of symptoms within 28 days of stopping medication was also similar between the two groups. Among those who received 7 days of antibiotics, 10.3% experienced recurrence of symptoms, compared to 16.9% of those assigned to 14 days of antibiotics.
There was no significant difference in the resolution of UTI symptoms between the two groups by type of antibiotic, pretreatment bacteriuria count, or study site.
Adverse events were also similar in the two groups, occurring in 20.6% of the men who received 7 days of antibiotics, versus 24.3% of the men who received 14 days of treatment. In both groups, 8.8% of patients had diarrhea, which was the most common adverse event.
Clinicians should not worry that antibiotic resistance is more likely to develop or that symptoms will recur when patients don’t finish a prescribed course of treatment, Dr. Drekonja said. “That is an old piece of guidance that has persisted for such a long time,” he said. “And it makes all of us in the infectious disease field cringe.”
Rather, the current thinking is that the more antibiotics patients take, the more resistance bacteria will develop, he said.
The success of the 7-day regimen raises the question of whether an even shorter course would work equally well. It’s not clear how short a course of antibiotics will do the trick. Research in certain populations, such as patients with spinal cord injuries, has suggested that recurrences are more frequent with 3 days of antibiotics than with 14, “so there could be a floor that you do need to go beyond,” Dr. Drekonja said.
“We’re not really sure how much people need,” agreed Daniel Morgan, MD, a professor of epidemiology and public health and medicine at the University of Maryland, Baltimore, which is why this study is important. “It really defined that 1 week is better than 2 weeks,” he said in an interview.
Another way that clinicians can reduce the use of antibiotics by men with UTIs is to consider alternative diagnoses and to culture urine samples when UTI seems like the most likely cause of their symptoms, said Dr. Morgan, who co-authored an accompanying editorial.
He pointed out that the U.S. Food and Drug Administration has issued a black box warning on fluoroquinolones, including ciprofloxacin, because they increase the risk for tendinitis and tendon rupture. Nitrofurantoin and amoxicillin-clavulanate are better alternatives for UTIs, he said.
Even some men with fevers and UTIs may need no more than 7 days of antibiotics, said Dr. Morgan. Dr. Drekonja said he generally prescribes at least 10 days antibiotics for these men.
The study was funded by the VA Merit Review Program. Dr. Drekonja and Dr. Morgan have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Untreatable, drug-resistant fungus found in Texas and Washington, D.C.
The CDC has reported two clusters of Candida auris infections resistant to all antifungal medications in long-term care facilities in 2021. Because these panresistant infections occurred without any exposure to antifungal drugs, the cases are even more worrisome. These clusters are the first time such nosocomial transmission has been detected.
In the District of Columbia, three panresistant isolates were discovered through screening for skin colonization with resistant organisms at a long-term acute care facility (LTAC) that cares for patients who are seriously ill, often on mechanical ventilation.
In Texas, the resistant organisms were found both by screening and in specimens from ill patients at an LTAC and a short-term acute care hospital that share patients. Two were panresistant, and five others were resistant to fluconazole and echinocandins.
These clusters occurred simultaneously and independently of each other; there were no links between the two institutions.
Colonization of skin with C. auris can lead to invasive infections in 5%-10% of affected patients. Routine skin surveillance cultures are not commonly done for Candida, although perirectal cultures for vancomycin-resistant enterococci and nasal swabs for MRSA have been done for years. Some areas, like Los Angeles, have recommended screening for C. auris in high-risk patients – defined as those who were on a ventilator or had a tracheostomy admitted from an LTAC or skilled nursing facility in Los Angeles County, New York, New Jersey, or Illinois.
In the past, about 85% of C. auris isolates in the United States have been resistant to azoles (for example, fluconazole), 33% to amphotericin B, and 1% to echinocandins. Because of generally strong susceptibility, an echinocandin such as micafungin or caspofungin has been the drug of choice for an invasive Candida infection.
C. auris is particularly difficult to deal with for several reasons. First, it can continue to live in the environment, on both dry or moist surfaces, for up to 2 weeks. Outbreaks have occurred both from hand (person-to-person) transmission or via inanimate surfaces that have become contaminated. Equally troublesome is that people become colonized with the yeast indefinitely.
Meghan Lyman, MD, of the fungal diseases branch of the CDC’s National Center for Emerging and Zoonotic Infectious Diseases, said in an interview that facilities might be slow in recognizing the problem and in identifying the organism. “We encounter problems in noninvasive specimens, especially urine,” Dr. Lyman added.
“Sometimes ... they consider Candida [to represent] colonization so they will often not speciate it.” She emphasized the need for facilities that care for ventilated patients to consider screening. “Higher priority ... are places in areas where there’s a lot of C. auris transmission or in nearby areas that are likely to get introductions.” Even those that do speciate may have difficulty identifying C. auris.
Further, Dr. Lyman stressed “the importance of antifungal susceptibility testing and testing for resistance. Because that’s also something that’s not widely available at all hospitals and clinical labs ... you can send it to the [CDC’s] antimicrobial resistance lab network” for testing.
COVID-19 has brought particular challenges. Rodney E. Rohde, PhD, MS, professor and chair, clinical lab science program, Texas State University, San Marcos, said in an interview that he is worried about all the steroids and broad-spectrum antibiotics patients receive.
They’re “being given medical interventions, whether it’s ventilators or [extracorporeal membrane oxygenation] or IVs or central lines or catheters for UTIs and you’re creating highways, right for something that may be right there,” said Dr. Rohde, who was not involved in the CDC study. “It’s a perfect storm, not just for C. auris, but I worry about bacterial resistance agents, too, like MRSA and so forth, having kind of a spike in those types of infections with COVID. So, it’s kind of a doubly dangerous time, I think.”
Multiresistant bacteria are a major health problem, causing illnesses in 2.8 million people annually in the United States, and causing about 35,000 deaths.
Dr. Rohde raised another, rarely mentioned concern. “We’re in crisis mode. People are leaving our field more than they ever had before. The medical laboratory is being decimated because people have burned out after these past 14 months. And so I worry just about competent medical laboratory professionals that are on board to deal with these types of other crises that are popping up within hospitals and long-term care facilities. It kind of keeps me awake.”
Dr. Rohde and Dr. Lyman shared their concern that COVID caused a decrease in screening for other infections and drug-resistant organisms. Bare-bones staffing and shortages of personal protective equipment have likely fueled the spread of these infections as well.
In an outbreak of C. auris in a Florida hospital’s COVID unit in 2020, 35 of 67 patients became colonized, and 6 became ill. The epidemiologists investigating thought that contaminated gowns or gloves, computers, and other equipment were likely sources of transmission.
Low pay, especially in nursing homes, is another problem Dr. Rohde mentioned. It’s an additional problem in both acute and long-term care that “some of the lowest-paid people are the environmental services people, and so the turnover is crazy.” Yet, we rely on them to keep everyone safe. He added that, in addition to pay, he “tries to give them the appreciation and the recognition that they really deserve.”
There are a few specific measures that can be taken to protect patients. Dr. Lyman concluded. “The best way is identifying cases and really ensuring good infection control to prevent the spread.” It’s back to basics – limiting broad-spectrum antibiotics and invasive medical devices, and especially good handwashing and thorough cleaning.
Dr. Lyman and Dr. Rohde have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The CDC has reported two clusters of Candida auris infections resistant to all antifungal medications in long-term care facilities in 2021. Because these panresistant infections occurred without any exposure to antifungal drugs, the cases are even more worrisome. These clusters are the first time such nosocomial transmission has been detected.
In the District of Columbia, three panresistant isolates were discovered through screening for skin colonization with resistant organisms at a long-term acute care facility (LTAC) that cares for patients who are seriously ill, often on mechanical ventilation.
In Texas, the resistant organisms were found both by screening and in specimens from ill patients at an LTAC and a short-term acute care hospital that share patients. Two were panresistant, and five others were resistant to fluconazole and echinocandins.
These clusters occurred simultaneously and independently of each other; there were no links between the two institutions.
Colonization of skin with C. auris can lead to invasive infections in 5%-10% of affected patients. Routine skin surveillance cultures are not commonly done for Candida, although perirectal cultures for vancomycin-resistant enterococci and nasal swabs for MRSA have been done for years. Some areas, like Los Angeles, have recommended screening for C. auris in high-risk patients – defined as those who were on a ventilator or had a tracheostomy admitted from an LTAC or skilled nursing facility in Los Angeles County, New York, New Jersey, or Illinois.
In the past, about 85% of C. auris isolates in the United States have been resistant to azoles (for example, fluconazole), 33% to amphotericin B, and 1% to echinocandins. Because of generally strong susceptibility, an echinocandin such as micafungin or caspofungin has been the drug of choice for an invasive Candida infection.
C. auris is particularly difficult to deal with for several reasons. First, it can continue to live in the environment, on both dry or moist surfaces, for up to 2 weeks. Outbreaks have occurred both from hand (person-to-person) transmission or via inanimate surfaces that have become contaminated. Equally troublesome is that people become colonized with the yeast indefinitely.
Meghan Lyman, MD, of the fungal diseases branch of the CDC’s National Center for Emerging and Zoonotic Infectious Diseases, said in an interview that facilities might be slow in recognizing the problem and in identifying the organism. “We encounter problems in noninvasive specimens, especially urine,” Dr. Lyman added.
“Sometimes ... they consider Candida [to represent] colonization so they will often not speciate it.” She emphasized the need for facilities that care for ventilated patients to consider screening. “Higher priority ... are places in areas where there’s a lot of C. auris transmission or in nearby areas that are likely to get introductions.” Even those that do speciate may have difficulty identifying C. auris.
Further, Dr. Lyman stressed “the importance of antifungal susceptibility testing and testing for resistance. Because that’s also something that’s not widely available at all hospitals and clinical labs ... you can send it to the [CDC’s] antimicrobial resistance lab network” for testing.
COVID-19 has brought particular challenges. Rodney E. Rohde, PhD, MS, professor and chair, clinical lab science program, Texas State University, San Marcos, said in an interview that he is worried about all the steroids and broad-spectrum antibiotics patients receive.
They’re “being given medical interventions, whether it’s ventilators or [extracorporeal membrane oxygenation] or IVs or central lines or catheters for UTIs and you’re creating highways, right for something that may be right there,” said Dr. Rohde, who was not involved in the CDC study. “It’s a perfect storm, not just for C. auris, but I worry about bacterial resistance agents, too, like MRSA and so forth, having kind of a spike in those types of infections with COVID. So, it’s kind of a doubly dangerous time, I think.”
Multiresistant bacteria are a major health problem, causing illnesses in 2.8 million people annually in the United States, and causing about 35,000 deaths.
Dr. Rohde raised another, rarely mentioned concern. “We’re in crisis mode. People are leaving our field more than they ever had before. The medical laboratory is being decimated because people have burned out after these past 14 months. And so I worry just about competent medical laboratory professionals that are on board to deal with these types of other crises that are popping up within hospitals and long-term care facilities. It kind of keeps me awake.”
Dr. Rohde and Dr. Lyman shared their concern that COVID caused a decrease in screening for other infections and drug-resistant organisms. Bare-bones staffing and shortages of personal protective equipment have likely fueled the spread of these infections as well.
In an outbreak of C. auris in a Florida hospital’s COVID unit in 2020, 35 of 67 patients became colonized, and 6 became ill. The epidemiologists investigating thought that contaminated gowns or gloves, computers, and other equipment were likely sources of transmission.
Low pay, especially in nursing homes, is another problem Dr. Rohde mentioned. It’s an additional problem in both acute and long-term care that “some of the lowest-paid people are the environmental services people, and so the turnover is crazy.” Yet, we rely on them to keep everyone safe. He added that, in addition to pay, he “tries to give them the appreciation and the recognition that they really deserve.”
There are a few specific measures that can be taken to protect patients. Dr. Lyman concluded. “The best way is identifying cases and really ensuring good infection control to prevent the spread.” It’s back to basics – limiting broad-spectrum antibiotics and invasive medical devices, and especially good handwashing and thorough cleaning.
Dr. Lyman and Dr. Rohde have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The CDC has reported two clusters of Candida auris infections resistant to all antifungal medications in long-term care facilities in 2021. Because these panresistant infections occurred without any exposure to antifungal drugs, the cases are even more worrisome. These clusters are the first time such nosocomial transmission has been detected.
In the District of Columbia, three panresistant isolates were discovered through screening for skin colonization with resistant organisms at a long-term acute care facility (LTAC) that cares for patients who are seriously ill, often on mechanical ventilation.
In Texas, the resistant organisms were found both by screening and in specimens from ill patients at an LTAC and a short-term acute care hospital that share patients. Two were panresistant, and five others were resistant to fluconazole and echinocandins.
These clusters occurred simultaneously and independently of each other; there were no links between the two institutions.
Colonization of skin with C. auris can lead to invasive infections in 5%-10% of affected patients. Routine skin surveillance cultures are not commonly done for Candida, although perirectal cultures for vancomycin-resistant enterococci and nasal swabs for MRSA have been done for years. Some areas, like Los Angeles, have recommended screening for C. auris in high-risk patients – defined as those who were on a ventilator or had a tracheostomy admitted from an LTAC or skilled nursing facility in Los Angeles County, New York, New Jersey, or Illinois.
In the past, about 85% of C. auris isolates in the United States have been resistant to azoles (for example, fluconazole), 33% to amphotericin B, and 1% to echinocandins. Because of generally strong susceptibility, an echinocandin such as micafungin or caspofungin has been the drug of choice for an invasive Candida infection.
C. auris is particularly difficult to deal with for several reasons. First, it can continue to live in the environment, on both dry or moist surfaces, for up to 2 weeks. Outbreaks have occurred both from hand (person-to-person) transmission or via inanimate surfaces that have become contaminated. Equally troublesome is that people become colonized with the yeast indefinitely.
Meghan Lyman, MD, of the fungal diseases branch of the CDC’s National Center for Emerging and Zoonotic Infectious Diseases, said in an interview that facilities might be slow in recognizing the problem and in identifying the organism. “We encounter problems in noninvasive specimens, especially urine,” Dr. Lyman added.
“Sometimes ... they consider Candida [to represent] colonization so they will often not speciate it.” She emphasized the need for facilities that care for ventilated patients to consider screening. “Higher priority ... are places in areas where there’s a lot of C. auris transmission or in nearby areas that are likely to get introductions.” Even those that do speciate may have difficulty identifying C. auris.
Further, Dr. Lyman stressed “the importance of antifungal susceptibility testing and testing for resistance. Because that’s also something that’s not widely available at all hospitals and clinical labs ... you can send it to the [CDC’s] antimicrobial resistance lab network” for testing.
COVID-19 has brought particular challenges. Rodney E. Rohde, PhD, MS, professor and chair, clinical lab science program, Texas State University, San Marcos, said in an interview that he is worried about all the steroids and broad-spectrum antibiotics patients receive.
They’re “being given medical interventions, whether it’s ventilators or [extracorporeal membrane oxygenation] or IVs or central lines or catheters for UTIs and you’re creating highways, right for something that may be right there,” said Dr. Rohde, who was not involved in the CDC study. “It’s a perfect storm, not just for C. auris, but I worry about bacterial resistance agents, too, like MRSA and so forth, having kind of a spike in those types of infections with COVID. So, it’s kind of a doubly dangerous time, I think.”
Multiresistant bacteria are a major health problem, causing illnesses in 2.8 million people annually in the United States, and causing about 35,000 deaths.
Dr. Rohde raised another, rarely mentioned concern. “We’re in crisis mode. People are leaving our field more than they ever had before. The medical laboratory is being decimated because people have burned out after these past 14 months. And so I worry just about competent medical laboratory professionals that are on board to deal with these types of other crises that are popping up within hospitals and long-term care facilities. It kind of keeps me awake.”
Dr. Rohde and Dr. Lyman shared their concern that COVID caused a decrease in screening for other infections and drug-resistant organisms. Bare-bones staffing and shortages of personal protective equipment have likely fueled the spread of these infections as well.
In an outbreak of C. auris in a Florida hospital’s COVID unit in 2020, 35 of 67 patients became colonized, and 6 became ill. The epidemiologists investigating thought that contaminated gowns or gloves, computers, and other equipment were likely sources of transmission.
Low pay, especially in nursing homes, is another problem Dr. Rohde mentioned. It’s an additional problem in both acute and long-term care that “some of the lowest-paid people are the environmental services people, and so the turnover is crazy.” Yet, we rely on them to keep everyone safe. He added that, in addition to pay, he “tries to give them the appreciation and the recognition that they really deserve.”
There are a few specific measures that can be taken to protect patients. Dr. Lyman concluded. “The best way is identifying cases and really ensuring good infection control to prevent the spread.” It’s back to basics – limiting broad-spectrum antibiotics and invasive medical devices, and especially good handwashing and thorough cleaning.
Dr. Lyman and Dr. Rohde have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Increases in new COVID cases among children far outpace vaccinations
New COVID-19 cases in children soared by almost 86% over the course of just 1 week, while the number of 12- to 17-year-old children who have received at least one dose of vaccine rose by 5.4%, according to two separate sources.
Meanwhile, the increase over the past 2 weeks – from 23,551 new cases for July 16-22 to almost 72,000 – works out to almost 205%, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
Children represented 19.0% of the cases reported during the week of July 23-29, and they have made up 14.3% of all cases since the pandemic began, with the total number of cases in children now approaching 4.2 million, the AAP and CHA said in their weekly COVID report. About 22% of the U.S. population is under the age of 18 years.
As of Aug. 2, just over 9.8 million children aged 12-17 years had received at least one dose of the COVID vaccine, which was up by about 500,000, or 5.4%, from a week earlier, based on data from the Centers for Disease Control and Prevention.
Children aged 16-17 have reached a notable milestone on the journey that started with vaccine approval in December: 50.2% have gotten at least one dose and 40.3% are fully vaccinated. Among children aged 12-15 years, the proportion with at least one dose of vaccine is up to 39.5%, compared with 37.1% the previous week, while 29.0% are fully vaccinated (27.8% the week before), the CDC said on its COVID Data Tracker.
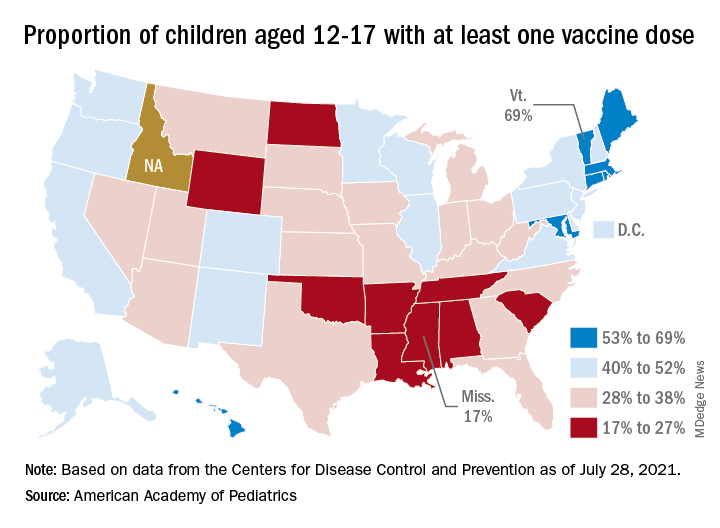
The national rates for child vaccination, however, tend to hide the disparities between states. There is a gap between Mississippi (lowest), where just 17% of children aged 12-17 years have gotten at least one dose, and Vermont (highest), which is up to 69%. Vermont also has the highest rate of vaccine completion (60%), while Alabama and Mississippi have the lowest (10%), according to a solo report from the AAP.
New COVID-19 cases in children soared by almost 86% over the course of just 1 week, while the number of 12- to 17-year-old children who have received at least one dose of vaccine rose by 5.4%, according to two separate sources.
Meanwhile, the increase over the past 2 weeks – from 23,551 new cases for July 16-22 to almost 72,000 – works out to almost 205%, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
Children represented 19.0% of the cases reported during the week of July 23-29, and they have made up 14.3% of all cases since the pandemic began, with the total number of cases in children now approaching 4.2 million, the AAP and CHA said in their weekly COVID report. About 22% of the U.S. population is under the age of 18 years.
As of Aug. 2, just over 9.8 million children aged 12-17 years had received at least one dose of the COVID vaccine, which was up by about 500,000, or 5.4%, from a week earlier, based on data from the Centers for Disease Control and Prevention.
Children aged 16-17 have reached a notable milestone on the journey that started with vaccine approval in December: 50.2% have gotten at least one dose and 40.3% are fully vaccinated. Among children aged 12-15 years, the proportion with at least one dose of vaccine is up to 39.5%, compared with 37.1% the previous week, while 29.0% are fully vaccinated (27.8% the week before), the CDC said on its COVID Data Tracker.
The national rates for child vaccination, however, tend to hide the disparities between states. There is a gap between Mississippi (lowest), where just 17% of children aged 12-17 years have gotten at least one dose, and Vermont (highest), which is up to 69%. Vermont also has the highest rate of vaccine completion (60%), while Alabama and Mississippi have the lowest (10%), according to a solo report from the AAP.
New COVID-19 cases in children soared by almost 86% over the course of just 1 week, while the number of 12- to 17-year-old children who have received at least one dose of vaccine rose by 5.4%, according to two separate sources.
Meanwhile, the increase over the past 2 weeks – from 23,551 new cases for July 16-22 to almost 72,000 – works out to almost 205%, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
Children represented 19.0% of the cases reported during the week of July 23-29, and they have made up 14.3% of all cases since the pandemic began, with the total number of cases in children now approaching 4.2 million, the AAP and CHA said in their weekly COVID report. About 22% of the U.S. population is under the age of 18 years.
As of Aug. 2, just over 9.8 million children aged 12-17 years had received at least one dose of the COVID vaccine, which was up by about 500,000, or 5.4%, from a week earlier, based on data from the Centers for Disease Control and Prevention.
Children aged 16-17 have reached a notable milestone on the journey that started with vaccine approval in December: 50.2% have gotten at least one dose and 40.3% are fully vaccinated. Among children aged 12-15 years, the proportion with at least one dose of vaccine is up to 39.5%, compared with 37.1% the previous week, while 29.0% are fully vaccinated (27.8% the week before), the CDC said on its COVID Data Tracker.
The national rates for child vaccination, however, tend to hide the disparities between states. There is a gap between Mississippi (lowest), where just 17% of children aged 12-17 years have gotten at least one dose, and Vermont (highest), which is up to 69%. Vermont also has the highest rate of vaccine completion (60%), while Alabama and Mississippi have the lowest (10%), according to a solo report from the AAP.
ACOG, SMFM urge all pregnant women to get COVID-19 vaccine
The American College of Obstetricians and Gynecologists (ACOG) and the Society for Maternal-Fetal Medicine (SMFM) strongly recommend that all pregnant women be vaccinated against COVID-19.
Only about 16% of pregnant people have received one or more doses of a COVID-19 vaccine, according to the Centers for Disease Control and Prevention, despite evidence that COVID-19 infection puts pregnant people at an increased risk of severe complications and death.
That CDC report in June also found that vaccination during pregnancy was lowest among Hispanic (11.9%) and non-Hispanic Black women (6%) and women aged 18-24 years (5.5%) and highest among non-Hispanic Asian women (24.7%) and women aged 35-49 years (22.7%).
Linda Eckert, MD, professor of obstetrics and gynecology at University of Washington, Seattle, and a member of ACOG’s immunization expert work group, said in an interview that previously, ACOG has said that pregnant women should have the opportunity to be vaccinated, should they choose it.
Now the urgency has increased, she said: “This is a strong recommendation.”
The recommendation comes after mounting evidence demonstrating that COVID-19 vaccines are safe during pregnancy “from tens of thousands of reporting individuals over the last several months, as well as the current low vaccination rates and concerning increase in cases,” ACOG and SMFM said in the statement.
Both organizations said the timing of the advisory comes amid growing concern about the Delta variant.

CDC Director Rochelle Walensky, MD, has called the variant “one of the most infectious respiratory viruses we know of.”
No evidence of maternal/fetal harm
There is no evidence that COVID-19 vaccines could cause maternal or fetal harm, ACOG stated.
“ACOG encourages its members to enthusiastically recommend vaccination to their patients. This means emphasizing the known safety of the vaccines and the increased risk of severe complications associated with COVID-19 infection, including death, during pregnancy,” said J. Martin Tucker, MD, FACOG, president of ACOG. “It is clear that pregnant people need to feel confident in the decision to choose vaccination, and a strong recommendation from their obstetrician-gynecologist could make a meaningful difference for many pregnant people.”
Pregnant women are considered high risk because of concerns about the effect of COVID-19 during and after pregnancy, and on their offspring.
As this news organization has reported, research published in The BMJ found that pregnant women with COVID-19 may be at higher risk of admission to a hospital intensive care unit.
Preterm birth rates also were found to be higher among pregnant women with COVID-19 than among pregnant women without the disease.
Dr. Eckert said several of her patients have declined the vaccine. Among the reasons are that they don’t want to take any medications while pregnant or that they have heard that effects of the vaccines were not studied in pregnant women.
“Sometimes as I review with them the ongoing data coming in from pregnant individuals and newborns, [these patients] may change their minds and get the vaccine,” Dr. Eckert said.
In some cases, a pregnant patient’s family has pressured the patient not to get the vaccine.
The ACOG/SMFM advice notes that pregnant women who have decided to wait until after delivery to be vaccinated “may be inadvertently exposing themselves to an increased risk of severe illness or death.”
The recommendation extends to those who have already given birth.
“Those who have recently delivered and were not vaccinated during pregnancy are also strongly encouraged to get vaccinated as soon as possible,” the statement reads.
ACOG has developed talking points about the safety and efficacy of COVID-19 vaccines for pregnant patients.
Dr. Eckert disclosed no relevant financial relationships.
The American College of Obstetricians and Gynecologists (ACOG) and the Society for Maternal-Fetal Medicine (SMFM) strongly recommend that all pregnant women be vaccinated against COVID-19.
Only about 16% of pregnant people have received one or more doses of a COVID-19 vaccine, according to the Centers for Disease Control and Prevention, despite evidence that COVID-19 infection puts pregnant people at an increased risk of severe complications and death.
That CDC report in June also found that vaccination during pregnancy was lowest among Hispanic (11.9%) and non-Hispanic Black women (6%) and women aged 18-24 years (5.5%) and highest among non-Hispanic Asian women (24.7%) and women aged 35-49 years (22.7%).
Linda Eckert, MD, professor of obstetrics and gynecology at University of Washington, Seattle, and a member of ACOG’s immunization expert work group, said in an interview that previously, ACOG has said that pregnant women should have the opportunity to be vaccinated, should they choose it.
Now the urgency has increased, she said: “This is a strong recommendation.”
The recommendation comes after mounting evidence demonstrating that COVID-19 vaccines are safe during pregnancy “from tens of thousands of reporting individuals over the last several months, as well as the current low vaccination rates and concerning increase in cases,” ACOG and SMFM said in the statement.
Both organizations said the timing of the advisory comes amid growing concern about the Delta variant.
CDC Director Rochelle Walensky, MD, has called the variant “one of the most infectious respiratory viruses we know of.”
No evidence of maternal/fetal harm
There is no evidence that COVID-19 vaccines could cause maternal or fetal harm, ACOG stated.
“ACOG encourages its members to enthusiastically recommend vaccination to their patients. This means emphasizing the known safety of the vaccines and the increased risk of severe complications associated with COVID-19 infection, including death, during pregnancy,” said J. Martin Tucker, MD, FACOG, president of ACOG. “It is clear that pregnant people need to feel confident in the decision to choose vaccination, and a strong recommendation from their obstetrician-gynecologist could make a meaningful difference for many pregnant people.”
Pregnant women are considered high risk because of concerns about the effect of COVID-19 during and after pregnancy, and on their offspring.
As this news organization has reported, research published in The BMJ found that pregnant women with COVID-19 may be at higher risk of admission to a hospital intensive care unit.
Preterm birth rates also were found to be higher among pregnant women with COVID-19 than among pregnant women without the disease.
Dr. Eckert said several of her patients have declined the vaccine. Among the reasons are that they don’t want to take any medications while pregnant or that they have heard that effects of the vaccines were not studied in pregnant women.
“Sometimes as I review with them the ongoing data coming in from pregnant individuals and newborns, [these patients] may change their minds and get the vaccine,” Dr. Eckert said.
In some cases, a pregnant patient’s family has pressured the patient not to get the vaccine.
The ACOG/SMFM advice notes that pregnant women who have decided to wait until after delivery to be vaccinated “may be inadvertently exposing themselves to an increased risk of severe illness or death.”
The recommendation extends to those who have already given birth.
“Those who have recently delivered and were not vaccinated during pregnancy are also strongly encouraged to get vaccinated as soon as possible,” the statement reads.
ACOG has developed talking points about the safety and efficacy of COVID-19 vaccines for pregnant patients.
Dr. Eckert disclosed no relevant financial relationships.
The American College of Obstetricians and Gynecologists (ACOG) and the Society for Maternal-Fetal Medicine (SMFM) strongly recommend that all pregnant women be vaccinated against COVID-19.
Only about 16% of pregnant people have received one or more doses of a COVID-19 vaccine, according to the Centers for Disease Control and Prevention, despite evidence that COVID-19 infection puts pregnant people at an increased risk of severe complications and death.
That CDC report in June also found that vaccination during pregnancy was lowest among Hispanic (11.9%) and non-Hispanic Black women (6%) and women aged 18-24 years (5.5%) and highest among non-Hispanic Asian women (24.7%) and women aged 35-49 years (22.7%).
Linda Eckert, MD, professor of obstetrics and gynecology at University of Washington, Seattle, and a member of ACOG’s immunization expert work group, said in an interview that previously, ACOG has said that pregnant women should have the opportunity to be vaccinated, should they choose it.
Now the urgency has increased, she said: “This is a strong recommendation.”
The recommendation comes after mounting evidence demonstrating that COVID-19 vaccines are safe during pregnancy “from tens of thousands of reporting individuals over the last several months, as well as the current low vaccination rates and concerning increase in cases,” ACOG and SMFM said in the statement.
Both organizations said the timing of the advisory comes amid growing concern about the Delta variant.
CDC Director Rochelle Walensky, MD, has called the variant “one of the most infectious respiratory viruses we know of.”
No evidence of maternal/fetal harm
There is no evidence that COVID-19 vaccines could cause maternal or fetal harm, ACOG stated.
“ACOG encourages its members to enthusiastically recommend vaccination to their patients. This means emphasizing the known safety of the vaccines and the increased risk of severe complications associated with COVID-19 infection, including death, during pregnancy,” said J. Martin Tucker, MD, FACOG, president of ACOG. “It is clear that pregnant people need to feel confident in the decision to choose vaccination, and a strong recommendation from their obstetrician-gynecologist could make a meaningful difference for many pregnant people.”
Pregnant women are considered high risk because of concerns about the effect of COVID-19 during and after pregnancy, and on their offspring.
As this news organization has reported, research published in The BMJ found that pregnant women with COVID-19 may be at higher risk of admission to a hospital intensive care unit.
Preterm birth rates also were found to be higher among pregnant women with COVID-19 than among pregnant women without the disease.
Dr. Eckert said several of her patients have declined the vaccine. Among the reasons are that they don’t want to take any medications while pregnant or that they have heard that effects of the vaccines were not studied in pregnant women.
“Sometimes as I review with them the ongoing data coming in from pregnant individuals and newborns, [these patients] may change their minds and get the vaccine,” Dr. Eckert said.
In some cases, a pregnant patient’s family has pressured the patient not to get the vaccine.
The ACOG/SMFM advice notes that pregnant women who have decided to wait until after delivery to be vaccinated “may be inadvertently exposing themselves to an increased risk of severe illness or death.”
The recommendation extends to those who have already given birth.
“Those who have recently delivered and were not vaccinated during pregnancy are also strongly encouraged to get vaccinated as soon as possible,” the statement reads.
ACOG has developed talking points about the safety and efficacy of COVID-19 vaccines for pregnant patients.
Dr. Eckert disclosed no relevant financial relationships.
Vaccination alone won’t counter rise of resistant variants: Study
Relaxation of nonpharmaceutical interventions once vaccination of the population has reached a tipping point short of herd immunity can increase the probability of the emergence of a resistant strain that natural selection then favors, according to new findings of a modeling study published online on July 30, 2021, in Scientific Reports.
Although vaccination is the best strategy for controlling viral spread, changes in our behavior and mindset will be increasingly required to stay ahead of vaccine-resistant strains, according to the authors of the report.
“We have become accustomed to thinking of the pandemic from the point of view of epidemiology, and advised to reduce transmission and the number of people getting sick and the death rate. As the pandemic spreads across years, there will be a new dimension to our thinking, both for policymakers and the public. And that’s the evolutionary perspective,” coauthor Fyodor Kondrashov, PhD, an evolutionary biologist at the Institute of Science and Technology, Klosterneuburg, Austria, said at a press briefing on July 299.
The coming “change of mentality” that Dr. Kondrashov foresees should reassure people that masking and social distancing even after being vaccinated aren’t futile. “It decreases the possibility that a vaccine-resistant strain is running around. We’re not just trying to prevent the spread, but the evolution of novel variants, which are so rare at this point that we haven’t yet identified them,” he said.
The study focused on evolution generically, rather than on specific variants. “We took the classical model used to study epidemiology of pandemics, the SIR [susceptible, infected, recovered] model, and we modified it to study the dynamics of rare mutations associated with emergence of a vaccine-resistant strain,” Simon A. Rella, the lead author of the study and a PhD student at the Institute of Science and Technology, explained at the briefing.
The researchers simulated the probability that a vaccine-resistant strain will emerge in a population of 10,000,000 individuals over 3 years, with vaccinations beginning after the first year. For eight scenarios, rates of infection, recovery, death, vaccination, and mutation and the percentage of individuals with resistant viral strains were factors in the model.
The model also simulated waves of low and high transmission, similar to the effects of large-scale interventions such as lockdowns.
Three factors
The study showed that a trio of factors increases the probability of a vaccine-resistant strain taking hold: slow rates of vaccination, high number of infected individuals, and faster mutation rate
These factors, Mr. Rella said, are obvious to some degree. “Every infected individual is like a mini-bioreactor, increasing the risk that mutations will appear that will endow the virus with the property of avoiding the immune system primed by a vaccine.”
Not as obvious, Mr. Rella added, is that, when most people are vaccinated, a vaccine-resistant strain has an advantage over the original strain and spreads faster.
But we can stop it, he said. “Our model shows that if at the time a vaccine campaign is close to finishing and nonpharmacological interventions are maintained, then there’s a chance to completely remove the vaccine-resistant mutations from the virus population.”
In scenarios in which a resistant strain became established, resistance initially emerged after about 60% of the population had been vaccinated. That makes nonpharmaceutical interventions such as masking and social distancing vitally important. Just under 50% of the U.S. population over the age of 12 has been fully vaccinated, according to the Centers for Disease Control and Prevention.
“Our results suggest that policymakers and individuals should consider maintaining nonpharmaceutical interventions and transmission-reducing behaviors throughout the entire vaccination period,” the investigators concluded.
A ‘powerful force’
“We hope for the best, that vaccine resistance has not developed, but caution that evolution is a very powerful force, and maintaining some precautions during vaccination may help to control that evolution,” said Dr. Kondrashov.
The investigators are relying on epidemiologists to determine which measures are most effective.
“It’s necessary to vaccinate as many people as fast as possible and as globally as possible and to maintain some level of nonpharmaceutical intervention to ensure rare variants have a chance to be suppressed instead of spread,” concluded Dr. Kondrashov.
He’s pessimistic because many countries are still having difficulty accessing vaccines, and vaccine efficacy wanes slightly over time. The authors warned that “the emergence of a partially or fully vaccine-resistant strain and its eventual establishment appears inevitable.”
The worst-case scenario is familiar to population biologists: rounds of “vaccine development playing catch up in the evolutionary arms race against novel strains,” the authors wrote.
Limitations of the study are that some parameters of the rate of evolution for vaccine-resistant strains aren’t known, and in creating the model, consideration was not given to effects of increased testing, rigorous contact tracing, rates of viral genome sequencing, and travel restrictions.
Rather, the model illustrates general principals by which vaccine resistance can evolve, Dr. Kondrashov said.
A version of this article first appeared on Medscape.com.
Relaxation of nonpharmaceutical interventions once vaccination of the population has reached a tipping point short of herd immunity can increase the probability of the emergence of a resistant strain that natural selection then favors, according to new findings of a modeling study published online on July 30, 2021, in Scientific Reports.
Although vaccination is the best strategy for controlling viral spread, changes in our behavior and mindset will be increasingly required to stay ahead of vaccine-resistant strains, according to the authors of the report.
“We have become accustomed to thinking of the pandemic from the point of view of epidemiology, and advised to reduce transmission and the number of people getting sick and the death rate. As the pandemic spreads across years, there will be a new dimension to our thinking, both for policymakers and the public. And that’s the evolutionary perspective,” coauthor Fyodor Kondrashov, PhD, an evolutionary biologist at the Institute of Science and Technology, Klosterneuburg, Austria, said at a press briefing on July 299.
The coming “change of mentality” that Dr. Kondrashov foresees should reassure people that masking and social distancing even after being vaccinated aren’t futile. “It decreases the possibility that a vaccine-resistant strain is running around. We’re not just trying to prevent the spread, but the evolution of novel variants, which are so rare at this point that we haven’t yet identified them,” he said.
The study focused on evolution generically, rather than on specific variants. “We took the classical model used to study epidemiology of pandemics, the SIR [susceptible, infected, recovered] model, and we modified it to study the dynamics of rare mutations associated with emergence of a vaccine-resistant strain,” Simon A. Rella, the lead author of the study and a PhD student at the Institute of Science and Technology, explained at the briefing.
The researchers simulated the probability that a vaccine-resistant strain will emerge in a population of 10,000,000 individuals over 3 years, with vaccinations beginning after the first year. For eight scenarios, rates of infection, recovery, death, vaccination, and mutation and the percentage of individuals with resistant viral strains were factors in the model.
The model also simulated waves of low and high transmission, similar to the effects of large-scale interventions such as lockdowns.
Three factors
The study showed that a trio of factors increases the probability of a vaccine-resistant strain taking hold: slow rates of vaccination, high number of infected individuals, and faster mutation rate
These factors, Mr. Rella said, are obvious to some degree. “Every infected individual is like a mini-bioreactor, increasing the risk that mutations will appear that will endow the virus with the property of avoiding the immune system primed by a vaccine.”
Not as obvious, Mr. Rella added, is that, when most people are vaccinated, a vaccine-resistant strain has an advantage over the original strain and spreads faster.
But we can stop it, he said. “Our model shows that if at the time a vaccine campaign is close to finishing and nonpharmacological interventions are maintained, then there’s a chance to completely remove the vaccine-resistant mutations from the virus population.”
In scenarios in which a resistant strain became established, resistance initially emerged after about 60% of the population had been vaccinated. That makes nonpharmaceutical interventions such as masking and social distancing vitally important. Just under 50% of the U.S. population over the age of 12 has been fully vaccinated, according to the Centers for Disease Control and Prevention.
“Our results suggest that policymakers and individuals should consider maintaining nonpharmaceutical interventions and transmission-reducing behaviors throughout the entire vaccination period,” the investigators concluded.
A ‘powerful force’
“We hope for the best, that vaccine resistance has not developed, but caution that evolution is a very powerful force, and maintaining some precautions during vaccination may help to control that evolution,” said Dr. Kondrashov.
The investigators are relying on epidemiologists to determine which measures are most effective.
“It’s necessary to vaccinate as many people as fast as possible and as globally as possible and to maintain some level of nonpharmaceutical intervention to ensure rare variants have a chance to be suppressed instead of spread,” concluded Dr. Kondrashov.
He’s pessimistic because many countries are still having difficulty accessing vaccines, and vaccine efficacy wanes slightly over time. The authors warned that “the emergence of a partially or fully vaccine-resistant strain and its eventual establishment appears inevitable.”
The worst-case scenario is familiar to population biologists: rounds of “vaccine development playing catch up in the evolutionary arms race against novel strains,” the authors wrote.
Limitations of the study are that some parameters of the rate of evolution for vaccine-resistant strains aren’t known, and in creating the model, consideration was not given to effects of increased testing, rigorous contact tracing, rates of viral genome sequencing, and travel restrictions.
Rather, the model illustrates general principals by which vaccine resistance can evolve, Dr. Kondrashov said.
A version of this article first appeared on Medscape.com.
Relaxation of nonpharmaceutical interventions once vaccination of the population has reached a tipping point short of herd immunity can increase the probability of the emergence of a resistant strain that natural selection then favors, according to new findings of a modeling study published online on July 30, 2021, in Scientific Reports.
Although vaccination is the best strategy for controlling viral spread, changes in our behavior and mindset will be increasingly required to stay ahead of vaccine-resistant strains, according to the authors of the report.
“We have become accustomed to thinking of the pandemic from the point of view of epidemiology, and advised to reduce transmission and the number of people getting sick and the death rate. As the pandemic spreads across years, there will be a new dimension to our thinking, both for policymakers and the public. And that’s the evolutionary perspective,” coauthor Fyodor Kondrashov, PhD, an evolutionary biologist at the Institute of Science and Technology, Klosterneuburg, Austria, said at a press briefing on July 299.
The coming “change of mentality” that Dr. Kondrashov foresees should reassure people that masking and social distancing even after being vaccinated aren’t futile. “It decreases the possibility that a vaccine-resistant strain is running around. We’re not just trying to prevent the spread, but the evolution of novel variants, which are so rare at this point that we haven’t yet identified them,” he said.
The study focused on evolution generically, rather than on specific variants. “We took the classical model used to study epidemiology of pandemics, the SIR [susceptible, infected, recovered] model, and we modified it to study the dynamics of rare mutations associated with emergence of a vaccine-resistant strain,” Simon A. Rella, the lead author of the study and a PhD student at the Institute of Science and Technology, explained at the briefing.
The researchers simulated the probability that a vaccine-resistant strain will emerge in a population of 10,000,000 individuals over 3 years, with vaccinations beginning after the first year. For eight scenarios, rates of infection, recovery, death, vaccination, and mutation and the percentage of individuals with resistant viral strains were factors in the model.
The model also simulated waves of low and high transmission, similar to the effects of large-scale interventions such as lockdowns.
Three factors
The study showed that a trio of factors increases the probability of a vaccine-resistant strain taking hold: slow rates of vaccination, high number of infected individuals, and faster mutation rate
These factors, Mr. Rella said, are obvious to some degree. “Every infected individual is like a mini-bioreactor, increasing the risk that mutations will appear that will endow the virus with the property of avoiding the immune system primed by a vaccine.”
Not as obvious, Mr. Rella added, is that, when most people are vaccinated, a vaccine-resistant strain has an advantage over the original strain and spreads faster.
But we can stop it, he said. “Our model shows that if at the time a vaccine campaign is close to finishing and nonpharmacological interventions are maintained, then there’s a chance to completely remove the vaccine-resistant mutations from the virus population.”
In scenarios in which a resistant strain became established, resistance initially emerged after about 60% of the population had been vaccinated. That makes nonpharmaceutical interventions such as masking and social distancing vitally important. Just under 50% of the U.S. population over the age of 12 has been fully vaccinated, according to the Centers for Disease Control and Prevention.
“Our results suggest that policymakers and individuals should consider maintaining nonpharmaceutical interventions and transmission-reducing behaviors throughout the entire vaccination period,” the investigators concluded.
A ‘powerful force’
“We hope for the best, that vaccine resistance has not developed, but caution that evolution is a very powerful force, and maintaining some precautions during vaccination may help to control that evolution,” said Dr. Kondrashov.
The investigators are relying on epidemiologists to determine which measures are most effective.
“It’s necessary to vaccinate as many people as fast as possible and as globally as possible and to maintain some level of nonpharmaceutical intervention to ensure rare variants have a chance to be suppressed instead of spread,” concluded Dr. Kondrashov.
He’s pessimistic because many countries are still having difficulty accessing vaccines, and vaccine efficacy wanes slightly over time. The authors warned that “the emergence of a partially or fully vaccine-resistant strain and its eventual establishment appears inevitable.”
The worst-case scenario is familiar to population biologists: rounds of “vaccine development playing catch up in the evolutionary arms race against novel strains,” the authors wrote.
Limitations of the study are that some parameters of the rate of evolution for vaccine-resistant strains aren’t known, and in creating the model, consideration was not given to effects of increased testing, rigorous contact tracing, rates of viral genome sequencing, and travel restrictions.
Rather, the model illustrates general principals by which vaccine resistance can evolve, Dr. Kondrashov said.
A version of this article first appeared on Medscape.com.
Indoor masking needed in almost 70% of U.S. counties: CDC data
In announcing new guidance on July 27, the CDC said vaccinated people should wear face masks in indoor public places with “high” or “substantial” community transmission rates of COVID-19.
Data from the CDC shows that designation covers 69.3% of all counties in the United States – 52.2% (1,680 counties) with high community transmission rates and 17.1% (551 counties) with substantial rates.
A county has “high transmission” if it reports 100 or more weekly cases per 100,000 residents or a 10% or higher test positivity rate in the last 7 days, the CDC said. “Substantial transmission” means a county reports 50-99 weekly cases per 100,000 residents or has a positivity rate between 8% and 9.9% in the last 7 days.
About 23% of U.S. counties had moderate rates of community transmission, and 7.67% had low rates.
To find out the transmission rate in your county, go to the CDC COVID data tracker.
Smithsonian requiring masks again
The Smithsonian now requires all visitors over age 2, regardless of vaccination status, to wear face masks indoors and in all museum spaces.
The Smithsonian said in a news release that fully vaccinated visitors won’t have to wear masks at the National Zoo or outdoor gardens for museums.
The new rule goes into effect Aug. 6. It reverses a rule that said fully vaccinated visitors didn’t have to wear masks indoors beginning June 28.
Indoor face masks will be required throughout the District of Columbia beginning July 31., D.C. Mayor Muriel Bowser.
House Republicans protest face mask policy
About 40 maskless Republican members of the U.S. House of Representatives filed onto the Senate floor on July 29 to protest a new rule requiring House members to wear face masks, the Hill reported.
Congress’s attending doctor said in a memo that the 435 members of the House, plus workers, must wear masks indoors, but not the 100 members of the Senate. The Senate is a smaller body and has had better mask compliance than the House.
Rep. Ronny Jackson (R-Tex.), told the Hill that Republicans wanted to show “what it was like on the floor of the Senate versus the floor of the House. Obviously, it’s vastly different.”
Among the group of Republicans who filed onto the Senate floor were Rep. Lauren Boebert of Colorado, Rep. Matt Gaetz and Rep. Byron Donalds of Florida, Rep. Marjorie Taylor Greene of Georgia, Rep. Chip Roy and Rep. Louie Gohmert of Texas, Rep. Madison Cawthorn of North Carolina, Rep. Warren Davidson of Ohio, and Rep. Andy Biggs of Arizona.
A version of this article first appeared on WebMD.com.
In announcing new guidance on July 27, the CDC said vaccinated people should wear face masks in indoor public places with “high” or “substantial” community transmission rates of COVID-19.
Data from the CDC shows that designation covers 69.3% of all counties in the United States – 52.2% (1,680 counties) with high community transmission rates and 17.1% (551 counties) with substantial rates.
A county has “high transmission” if it reports 100 or more weekly cases per 100,000 residents or a 10% or higher test positivity rate in the last 7 days, the CDC said. “Substantial transmission” means a county reports 50-99 weekly cases per 100,000 residents or has a positivity rate between 8% and 9.9% in the last 7 days.
About 23% of U.S. counties had moderate rates of community transmission, and 7.67% had low rates.
To find out the transmission rate in your county, go to the CDC COVID data tracker.
Smithsonian requiring masks again
The Smithsonian now requires all visitors over age 2, regardless of vaccination status, to wear face masks indoors and in all museum spaces.
The Smithsonian said in a news release that fully vaccinated visitors won’t have to wear masks at the National Zoo or outdoor gardens for museums.
The new rule goes into effect Aug. 6. It reverses a rule that said fully vaccinated visitors didn’t have to wear masks indoors beginning June 28.
Indoor face masks will be required throughout the District of Columbia beginning July 31., D.C. Mayor Muriel Bowser.
House Republicans protest face mask policy
About 40 maskless Republican members of the U.S. House of Representatives filed onto the Senate floor on July 29 to protest a new rule requiring House members to wear face masks, the Hill reported.
Congress’s attending doctor said in a memo that the 435 members of the House, plus workers, must wear masks indoors, but not the 100 members of the Senate. The Senate is a smaller body and has had better mask compliance than the House.
Rep. Ronny Jackson (R-Tex.), told the Hill that Republicans wanted to show “what it was like on the floor of the Senate versus the floor of the House. Obviously, it’s vastly different.”
Among the group of Republicans who filed onto the Senate floor were Rep. Lauren Boebert of Colorado, Rep. Matt Gaetz and Rep. Byron Donalds of Florida, Rep. Marjorie Taylor Greene of Georgia, Rep. Chip Roy and Rep. Louie Gohmert of Texas, Rep. Madison Cawthorn of North Carolina, Rep. Warren Davidson of Ohio, and Rep. Andy Biggs of Arizona.
A version of this article first appeared on WebMD.com.
In announcing new guidance on July 27, the CDC said vaccinated people should wear face masks in indoor public places with “high” or “substantial” community transmission rates of COVID-19.
Data from the CDC shows that designation covers 69.3% of all counties in the United States – 52.2% (1,680 counties) with high community transmission rates and 17.1% (551 counties) with substantial rates.
A county has “high transmission” if it reports 100 or more weekly cases per 100,000 residents or a 10% or higher test positivity rate in the last 7 days, the CDC said. “Substantial transmission” means a county reports 50-99 weekly cases per 100,000 residents or has a positivity rate between 8% and 9.9% in the last 7 days.
About 23% of U.S. counties had moderate rates of community transmission, and 7.67% had low rates.
To find out the transmission rate in your county, go to the CDC COVID data tracker.
Smithsonian requiring masks again
The Smithsonian now requires all visitors over age 2, regardless of vaccination status, to wear face masks indoors and in all museum spaces.
The Smithsonian said in a news release that fully vaccinated visitors won’t have to wear masks at the National Zoo or outdoor gardens for museums.
The new rule goes into effect Aug. 6. It reverses a rule that said fully vaccinated visitors didn’t have to wear masks indoors beginning June 28.
Indoor face masks will be required throughout the District of Columbia beginning July 31., D.C. Mayor Muriel Bowser.
House Republicans protest face mask policy
About 40 maskless Republican members of the U.S. House of Representatives filed onto the Senate floor on July 29 to protest a new rule requiring House members to wear face masks, the Hill reported.
Congress’s attending doctor said in a memo that the 435 members of the House, plus workers, must wear masks indoors, but not the 100 members of the Senate. The Senate is a smaller body and has had better mask compliance than the House.
Rep. Ronny Jackson (R-Tex.), told the Hill that Republicans wanted to show “what it was like on the floor of the Senate versus the floor of the House. Obviously, it’s vastly different.”
Among the group of Republicans who filed onto the Senate floor were Rep. Lauren Boebert of Colorado, Rep. Matt Gaetz and Rep. Byron Donalds of Florida, Rep. Marjorie Taylor Greene of Georgia, Rep. Chip Roy and Rep. Louie Gohmert of Texas, Rep. Madison Cawthorn of North Carolina, Rep. Warren Davidson of Ohio, and Rep. Andy Biggs of Arizona.
A version of this article first appeared on WebMD.com.
‘War has changed’: CDC says Delta as contagious as chicken pox
Internal Centers for Disease Control and Prevention documents support the high transmission rate of the Delta variant and put the risk in easier to understand terms.
In addition, the agency released a new study that shows that breakthrough infections in the vaccinated make people about as contagious as those who are unvaccinated. The new report, published July 30 in Morbidity and Mortality Weekly Report (MMWR), also reveals that the Delta variant likely causes more severe COVID-19 illness.
Given these recent findings, the internal CDC slide show advises that the agency should “acknowledge the war has changed.”
A ‘pivotal discovery’
CDC Director Rochelle Walensky, MD, MPH, said in a statement that the MMWR report demonstrates “that [D]elta infection resulted in similarly high SARS-CoV-2 viral loads in vaccinated and unvaccinated people.
“High viral loads suggest an increased risk of transmission and raised concern that, unlike with other variants, vaccinated people infected with [D]elta can transmit the virus,” she added. “This finding is concerning and was a pivotal discovery leading to CDC’s updated mask recommendation.”
The investigators analyzed 469 COVID-19 cases reported in Massachusetts residents July 3 through 17, 2021. The infections were associated with an outbreak following multiple events and large gatherings in Provincetown in that state’s easternmost Barnstable County, also known as Cape Cod.
Notably, 346 infections, or 74%, of the cases occurred in fully vaccinated individuals. This group had a median age of 42, and 87% were male. Also, 79% of the breakthrough infections were symptomatic.
Researchers also identified the Delta variant in 90% of 133 specimens collected for analysis. Furthermore, viral loads were about the same between samples taken from people who were fully vaccinated and those who were not.
Four of the five people hospitalized were fully vaccinated. No deaths were reported.
The publication of these results was highly anticipated following the CDC’s updated mask recommendations on July 27.
Outside the scope of the MMWR report is the total number of cases associated with the outbreak, including visitors from outside Massachusetts, which now approach 900 infections, NBC Boston reported.
‘Very sobering’ data
“The new information from the CDC around the [D]elta variant is very sobering,” David Hirschwerk, MD, infectious disease specialist at Northwell Health in New Hyde Park, N.Y., said in an interview.
“The CDC is trying to convey and present this uncertain situation clearly to the public based on new, accumulated data,” he said. For example, given the evidence for higher contagiousness of the Delta variant, Dr. Hirschwerk added, “there will be situations where vaccinated people get infected, because the amount of the virus overwhelms the immune protection.
“What is new that is concerning is that people who are vaccinated still have the potential to transmit the virus to the same degree,” he said.
The MMWR study “helps us better understand the question related to whether or not a person who has completed a COVID-19 series can spread the infection,” agreed Michelle Barron, MD, a professor in the division of infectious disease at the University of Colorado, Aurora.
“The message is that, because the [D]elta variant is much more contagious than the original strain, unvaccinated persons need to get vaccinated because it is nearly impossible to avoid the virus indefinitely,” Michael Lin, MD, MPH, infectious diseases specialist and epidemiologist at Rush University Medical Center, Chicago, said when asked to comment.
The new data highlight “that vaccinated persons, if they become sick, should still seek COVID-19 testing and should still isolate, as they are likely contagious,” Dr. Lin added.
More contagious than other infections
The internal CDC slide presentation also puts the new transmission risk in simple terms. Saying that the Delta variant is about as contagious as chicken pox, for example, immediately brings back vivid memories for some of staying indoors and away from friends during childhood or teenage outbreaks.
“A lot of people will remember getting chicken pox and then having their siblings get it shortly thereafter,” Dr. Barron said. “The only key thing to note is that this does not mean that the COVID-19 [D]elta variant mechanism of spread is the same as chicken pox and Ebola. The primary means of spread of COVID-19, even the Delta variant, is via droplets.”
This also means each person infected with the Delta variant could infect an average of eight or nine others.
In contrast, the original strain of the SARS-CoV-2 virus was about as infectious as the common cold. In other words, someone was likely to infect about two other people on average.
In addition to the cold, the CDC notes that the Delta variant is now more contagious than Ebola, the seasonal flu, or small pox.
These Delta variant comparisons are one tangible way of explaining why the CDC on July 27 recommended a return to masking in schools and other indoor spaces for people – vaccinated and unvaccinated – in about 70% of the counties across the United States.
In comparing the Delta variant with other infections, “I think the CDC is trying to help people understand a little bit better the situation we now face since the information is so new. We are in a very different position now than just a few weeks ago, and it is hard for people to accept this,” Dr. Hirschwerk said.
The Delta variant is so different that the CDC considers it almost acting like a new virus altogether.
The CDC’s internal documents were first released by The Washington Post on July 29. The slides cite communication challenges for the agency to continue promoting vaccination while also acknowledging that breakthrough cases are occurring and therefore the fully vaccinated, in some instances, are likely infecting others.
Moving back to science talk, the CDC used the recent outbreak in Barnstable County as an example. The cycle threshold, or Ct values, a measure of viral load, were about the same between 80 vaccinated people linked to the outbreak who had a mean Ct value of 21.9, compared with 65 other unvaccinated people with a Ct of 21.5.
Many experts are quick to note that vaccination remains essential, in part because a vaccinated person also walks around with a much lower risk for severe outcomes, hospitalization, and death. In the internal slide show, the CDC points out that vaccination reduces the risk for infection threefold.
“Even with this high amount of virus, [the Delta variant] did not necessarily make the vaccinated individuals as sick,” Dr. Barron said.
In her statement, Dr. Walensky credited collaboration with the Commonwealth of Massachusetts Department of Public Health and the CDC for the new data. She also thanked the residents of Barnstable County for participating in interviews done by contact tracers and their willingness to get tested and adhere to safety protocols after learning of their exposure.
Next moves by CDC?
The agency notes that next steps include consideration of prevention measures such as vaccine mandates for healthcare professionals to protect vulnerable populations, universal masking for source control and prevention, and reconsidering other community mitigation strategies.
Asked if this potential policy is appropriate and feasible, Dr. Lin said, “Yes, I believe that every person working in health care should be vaccinated for COVID-19, and it is feasible.”
Dr. Barron agreed as well. “We as health care providers choose to work in health care, and we should be doing everything feasible to ensure that we are protecting our patients and keeping our coworkers safe.”
“Whether you are a health care professional or not, I would urge everyone to get the COVID-19 vaccine, especially as cases across the country continue to rise,” Dr. Hirschwerk said. “Unequivocally vaccines protect you from the virus.”
A version of this article first appeared on Medscape.com.
Internal Centers for Disease Control and Prevention documents support the high transmission rate of the Delta variant and put the risk in easier to understand terms.
In addition, the agency released a new study that shows that breakthrough infections in the vaccinated make people about as contagious as those who are unvaccinated. The new report, published July 30 in Morbidity and Mortality Weekly Report (MMWR), also reveals that the Delta variant likely causes more severe COVID-19 illness.
Given these recent findings, the internal CDC slide show advises that the agency should “acknowledge the war has changed.”
A ‘pivotal discovery’
CDC Director Rochelle Walensky, MD, MPH, said in a statement that the MMWR report demonstrates “that [D]elta infection resulted in similarly high SARS-CoV-2 viral loads in vaccinated and unvaccinated people.
“High viral loads suggest an increased risk of transmission and raised concern that, unlike with other variants, vaccinated people infected with [D]elta can transmit the virus,” she added. “This finding is concerning and was a pivotal discovery leading to CDC’s updated mask recommendation.”
The investigators analyzed 469 COVID-19 cases reported in Massachusetts residents July 3 through 17, 2021. The infections were associated with an outbreak following multiple events and large gatherings in Provincetown in that state’s easternmost Barnstable County, also known as Cape Cod.
Notably, 346 infections, or 74%, of the cases occurred in fully vaccinated individuals. This group had a median age of 42, and 87% were male. Also, 79% of the breakthrough infections were symptomatic.
Researchers also identified the Delta variant in 90% of 133 specimens collected for analysis. Furthermore, viral loads were about the same between samples taken from people who were fully vaccinated and those who were not.
Four of the five people hospitalized were fully vaccinated. No deaths were reported.
The publication of these results was highly anticipated following the CDC’s updated mask recommendations on July 27.
Outside the scope of the MMWR report is the total number of cases associated with the outbreak, including visitors from outside Massachusetts, which now approach 900 infections, NBC Boston reported.
‘Very sobering’ data
“The new information from the CDC around the [D]elta variant is very sobering,” David Hirschwerk, MD, infectious disease specialist at Northwell Health in New Hyde Park, N.Y., said in an interview.
“The CDC is trying to convey and present this uncertain situation clearly to the public based on new, accumulated data,” he said. For example, given the evidence for higher contagiousness of the Delta variant, Dr. Hirschwerk added, “there will be situations where vaccinated people get infected, because the amount of the virus overwhelms the immune protection.
“What is new that is concerning is that people who are vaccinated still have the potential to transmit the virus to the same degree,” he said.
The MMWR study “helps us better understand the question related to whether or not a person who has completed a COVID-19 series can spread the infection,” agreed Michelle Barron, MD, a professor in the division of infectious disease at the University of Colorado, Aurora.
“The message is that, because the [D]elta variant is much more contagious than the original strain, unvaccinated persons need to get vaccinated because it is nearly impossible to avoid the virus indefinitely,” Michael Lin, MD, MPH, infectious diseases specialist and epidemiologist at Rush University Medical Center, Chicago, said when asked to comment.
The new data highlight “that vaccinated persons, if they become sick, should still seek COVID-19 testing and should still isolate, as they are likely contagious,” Dr. Lin added.
More contagious than other infections
The internal CDC slide presentation also puts the new transmission risk in simple terms. Saying that the Delta variant is about as contagious as chicken pox, for example, immediately brings back vivid memories for some of staying indoors and away from friends during childhood or teenage outbreaks.
“A lot of people will remember getting chicken pox and then having their siblings get it shortly thereafter,” Dr. Barron said. “The only key thing to note is that this does not mean that the COVID-19 [D]elta variant mechanism of spread is the same as chicken pox and Ebola. The primary means of spread of COVID-19, even the Delta variant, is via droplets.”
This also means each person infected with the Delta variant could infect an average of eight or nine others.
In contrast, the original strain of the SARS-CoV-2 virus was about as infectious as the common cold. In other words, someone was likely to infect about two other people on average.
In addition to the cold, the CDC notes that the Delta variant is now more contagious than Ebola, the seasonal flu, or small pox.
These Delta variant comparisons are one tangible way of explaining why the CDC on July 27 recommended a return to masking in schools and other indoor spaces for people – vaccinated and unvaccinated – in about 70% of the counties across the United States.
In comparing the Delta variant with other infections, “I think the CDC is trying to help people understand a little bit better the situation we now face since the information is so new. We are in a very different position now than just a few weeks ago, and it is hard for people to accept this,” Dr. Hirschwerk said.
The Delta variant is so different that the CDC considers it almost acting like a new virus altogether.
The CDC’s internal documents were first released by The Washington Post on July 29. The slides cite communication challenges for the agency to continue promoting vaccination while also acknowledging that breakthrough cases are occurring and therefore the fully vaccinated, in some instances, are likely infecting others.
Moving back to science talk, the CDC used the recent outbreak in Barnstable County as an example. The cycle threshold, or Ct values, a measure of viral load, were about the same between 80 vaccinated people linked to the outbreak who had a mean Ct value of 21.9, compared with 65 other unvaccinated people with a Ct of 21.5.
Many experts are quick to note that vaccination remains essential, in part because a vaccinated person also walks around with a much lower risk for severe outcomes, hospitalization, and death. In the internal slide show, the CDC points out that vaccination reduces the risk for infection threefold.
“Even with this high amount of virus, [the Delta variant] did not necessarily make the vaccinated individuals as sick,” Dr. Barron said.
In her statement, Dr. Walensky credited collaboration with the Commonwealth of Massachusetts Department of Public Health and the CDC for the new data. She also thanked the residents of Barnstable County for participating in interviews done by contact tracers and their willingness to get tested and adhere to safety protocols after learning of their exposure.
Next moves by CDC?
The agency notes that next steps include consideration of prevention measures such as vaccine mandates for healthcare professionals to protect vulnerable populations, universal masking for source control and prevention, and reconsidering other community mitigation strategies.
Asked if this potential policy is appropriate and feasible, Dr. Lin said, “Yes, I believe that every person working in health care should be vaccinated for COVID-19, and it is feasible.”
Dr. Barron agreed as well. “We as health care providers choose to work in health care, and we should be doing everything feasible to ensure that we are protecting our patients and keeping our coworkers safe.”
“Whether you are a health care professional or not, I would urge everyone to get the COVID-19 vaccine, especially as cases across the country continue to rise,” Dr. Hirschwerk said. “Unequivocally vaccines protect you from the virus.”
A version of this article first appeared on Medscape.com.
Internal Centers for Disease Control and Prevention documents support the high transmission rate of the Delta variant and put the risk in easier to understand terms.
In addition, the agency released a new study that shows that breakthrough infections in the vaccinated make people about as contagious as those who are unvaccinated. The new report, published July 30 in Morbidity and Mortality Weekly Report (MMWR), also reveals that the Delta variant likely causes more severe COVID-19 illness.
Given these recent findings, the internal CDC slide show advises that the agency should “acknowledge the war has changed.”
A ‘pivotal discovery’
CDC Director Rochelle Walensky, MD, MPH, said in a statement that the MMWR report demonstrates “that [D]elta infection resulted in similarly high SARS-CoV-2 viral loads in vaccinated and unvaccinated people.
“High viral loads suggest an increased risk of transmission and raised concern that, unlike with other variants, vaccinated people infected with [D]elta can transmit the virus,” she added. “This finding is concerning and was a pivotal discovery leading to CDC’s updated mask recommendation.”
The investigators analyzed 469 COVID-19 cases reported in Massachusetts residents July 3 through 17, 2021. The infections were associated with an outbreak following multiple events and large gatherings in Provincetown in that state’s easternmost Barnstable County, also known as Cape Cod.
Notably, 346 infections, or 74%, of the cases occurred in fully vaccinated individuals. This group had a median age of 42, and 87% were male. Also, 79% of the breakthrough infections were symptomatic.
Researchers also identified the Delta variant in 90% of 133 specimens collected for analysis. Furthermore, viral loads were about the same between samples taken from people who were fully vaccinated and those who were not.
Four of the five people hospitalized were fully vaccinated. No deaths were reported.
The publication of these results was highly anticipated following the CDC’s updated mask recommendations on July 27.
Outside the scope of the MMWR report is the total number of cases associated with the outbreak, including visitors from outside Massachusetts, which now approach 900 infections, NBC Boston reported.
‘Very sobering’ data
“The new information from the CDC around the [D]elta variant is very sobering,” David Hirschwerk, MD, infectious disease specialist at Northwell Health in New Hyde Park, N.Y., said in an interview.
“The CDC is trying to convey and present this uncertain situation clearly to the public based on new, accumulated data,” he said. For example, given the evidence for higher contagiousness of the Delta variant, Dr. Hirschwerk added, “there will be situations where vaccinated people get infected, because the amount of the virus overwhelms the immune protection.
“What is new that is concerning is that people who are vaccinated still have the potential to transmit the virus to the same degree,” he said.
The MMWR study “helps us better understand the question related to whether or not a person who has completed a COVID-19 series can spread the infection,” agreed Michelle Barron, MD, a professor in the division of infectious disease at the University of Colorado, Aurora.
“The message is that, because the [D]elta variant is much more contagious than the original strain, unvaccinated persons need to get vaccinated because it is nearly impossible to avoid the virus indefinitely,” Michael Lin, MD, MPH, infectious diseases specialist and epidemiologist at Rush University Medical Center, Chicago, said when asked to comment.
The new data highlight “that vaccinated persons, if they become sick, should still seek COVID-19 testing and should still isolate, as they are likely contagious,” Dr. Lin added.
More contagious than other infections
The internal CDC slide presentation also puts the new transmission risk in simple terms. Saying that the Delta variant is about as contagious as chicken pox, for example, immediately brings back vivid memories for some of staying indoors and away from friends during childhood or teenage outbreaks.
“A lot of people will remember getting chicken pox and then having their siblings get it shortly thereafter,” Dr. Barron said. “The only key thing to note is that this does not mean that the COVID-19 [D]elta variant mechanism of spread is the same as chicken pox and Ebola. The primary means of spread of COVID-19, even the Delta variant, is via droplets.”
This also means each person infected with the Delta variant could infect an average of eight or nine others.
In contrast, the original strain of the SARS-CoV-2 virus was about as infectious as the common cold. In other words, someone was likely to infect about two other people on average.
In addition to the cold, the CDC notes that the Delta variant is now more contagious than Ebola, the seasonal flu, or small pox.
These Delta variant comparisons are one tangible way of explaining why the CDC on July 27 recommended a return to masking in schools and other indoor spaces for people – vaccinated and unvaccinated – in about 70% of the counties across the United States.
In comparing the Delta variant with other infections, “I think the CDC is trying to help people understand a little bit better the situation we now face since the information is so new. We are in a very different position now than just a few weeks ago, and it is hard for people to accept this,” Dr. Hirschwerk said.
The Delta variant is so different that the CDC considers it almost acting like a new virus altogether.
The CDC’s internal documents were first released by The Washington Post on July 29. The slides cite communication challenges for the agency to continue promoting vaccination while also acknowledging that breakthrough cases are occurring and therefore the fully vaccinated, in some instances, are likely infecting others.
Moving back to science talk, the CDC used the recent outbreak in Barnstable County as an example. The cycle threshold, or Ct values, a measure of viral load, were about the same between 80 vaccinated people linked to the outbreak who had a mean Ct value of 21.9, compared with 65 other unvaccinated people with a Ct of 21.5.
Many experts are quick to note that vaccination remains essential, in part because a vaccinated person also walks around with a much lower risk for severe outcomes, hospitalization, and death. In the internal slide show, the CDC points out that vaccination reduces the risk for infection threefold.
“Even with this high amount of virus, [the Delta variant] did not necessarily make the vaccinated individuals as sick,” Dr. Barron said.
In her statement, Dr. Walensky credited collaboration with the Commonwealth of Massachusetts Department of Public Health and the CDC for the new data. She also thanked the residents of Barnstable County for participating in interviews done by contact tracers and their willingness to get tested and adhere to safety protocols after learning of their exposure.
Next moves by CDC?
The agency notes that next steps include consideration of prevention measures such as vaccine mandates for healthcare professionals to protect vulnerable populations, universal masking for source control and prevention, and reconsidering other community mitigation strategies.
Asked if this potential policy is appropriate and feasible, Dr. Lin said, “Yes, I believe that every person working in health care should be vaccinated for COVID-19, and it is feasible.”
Dr. Barron agreed as well. “We as health care providers choose to work in health care, and we should be doing everything feasible to ensure that we are protecting our patients and keeping our coworkers safe.”
“Whether you are a health care professional or not, I would urge everyone to get the COVID-19 vaccine, especially as cases across the country continue to rise,” Dr. Hirschwerk said. “Unequivocally vaccines protect you from the virus.”
A version of this article first appeared on Medscape.com.
COVID brings evolutionary virologists out of the shadows, into the fight
It has been a strange, exhausting year for many evolutionary virologists.
“Scientists are not used to having attention and are not used to being in the press and are not used to being attacked on Twitter,” Martha Nelson, PhD, a staff scientist who studies viral evolution at the National Institutes of Health, said in an interview.
Over the past year and a half, the theory of evolution has been thrust into the spotlight – more now than ever, perhaps, as the world is stalked by the Delta variant and fears arise of a mutation that’s even worse.
The origins of SARS-CoV-2 and the rise of the Delta variant have been debated, and vaccine efficacy and the possible need for booster shots have been speculated upon. In all these instances, consciously or not, there is engagement with the field of evolutionary virology.
It has been central to deepening the understanding of the ongoing pandemic, even as SARS-CoV-2 has exposed gaps in what we understand about how viruses behave and evolve.
Evolutionary virology experts believe that, after the pandemic, their expertise and tools could be applied to and integrated with clinical medicine to improve outcomes and understanding of disease.
“From our perspective, evolutionary biology has been a side dish and something that hasn’t been integrated into the core practice of medicine,” said Dr. Nelson. “I’m really curious to see how that changes over time.”
Pandemic evolution
Novel pathogens, antibiotic-resistant bacteria, and cancer cells are all products of ongoing evolution. “Just like cellular organisms, viruses have genomes, and all genomes evolve,” Eugene Koonin, PhD, evolutionary genomics group leader at the NIH, said in an interview.
Compared with cellular organisms, viruses evolve quite fast, he said.
A study published in the Proceedings of the National Academy of Sciences exemplifies evolutionary virology in action. In the study, Dr. Koonin and fellow researchers analyzed more than 300,000 genome sequences of SARS-CoV-2 variants that were publicly available as of January 2021 and mapped all the mutations in each sequence.
The researchers identified a small subset of mutations that arose independently more than once and that likely aided viral adaptation, said Nash Rochman, PhD, a research fellow at the NIH and coauthor of the PNAS study.
Many of these mutations were concentrated in two areas of the genome – the receptor binding domain of the spike protein, and a region of the nucleocapsid protein – and were often grouped together, possibly creating greater advantages for the virus than would have occurred individually, he said.
The researchers also found that, from the beginning of the pandemic, the SARS-CoV-2 genome has been evolving and diversifying in different regions around the world, allowing for the rise of new lineages and, possibly, even new species, Dr. Koonin said.
During the pandemic, researchers have used evolutionary virology tools to tackle many other questions. For example, Dr. Nelson tracked the spread of SARS-CoV-2 across Europe and North America. In a study that is currently undergoing peer review, the investigators found recently vaccinated individuals, who are only partially immune, are at the highest risk for incubating antibody-resistant variants.
C. Brandon Ogbunu, PhD, an evolutionary geneticist at Yale University, New Haven, Conn., whose work is focused on disease evolution, studied whether SARS-CoV-2 would evolve to become more transmissible, and if so, would it also become more or less virulent. His lab also investigated the transmission and spread of the virus.
“I think the last year, on one end, has been this opportunity to apply concepts and perspectives that we’ve been developing for the last several decades,” Dr. Ogbunu said in an interview. “At the same time, this pandemic has also been this wake-up call for many of us with regards to revealing the things we do not understand about the ways viruses infect, spread, and how evolution works within viruses.”
He emphasizes the need for evolutionary biology to partner with other fields – including information theory and biophysics – to help unlock viral mysteries: “We need to think very, very carefully about the way those fields intersect.”
Dr. Nelson also pointed to the need for better, more centralized data gathering in the United States.
The sheer volume of information scientists have collected about SARS-CoV-2 will aid in the study of virus evolution for years to come, said Dr. Koonin.
Evolution in medicine
Evolutionary virology and related research can be applied to medicine outside of the context of a global pandemic. “The principles and technical portions of evolutionary virology are very applicable to other diseases, including cancer,” Dr. Koonin said.
Viruses, bacteria, and cancer cells are all evolving systems. Viruses and bacteria are constantly evolving to thwart drugs and vaccines. How physicians and health care professionals practice medicine shapes the selection pressures driving how these pathogens evolve, Dr. Nelson said.
The rise of antibiotic-resistant bacteria is a particularly relevant example of how evolution affects the way physicians treat patients. Having an evolutionary perspective can help inform how to treat patients most effectively, both for individual patients as well as for broader public health, she said.
“For a long time, there’s been a lot of interest in pathogen evolution that hasn’t translated so much into clinical practice,” said Dr. Nelson. “There’s been kind of a gulf between the research side of evolutionary virology and pathogen emergence and actual practice of medicine.”
As genomic sequencing has become faster and cheaper, that gulf has started to narrow, she said. As this technology continues to prove itself by, for example, tracking the evolution of one virus in real time, Dr. Nelson hopes there will be a positive snowball effect, leading to more attention, investment, and improvements in genomic data and that its use in epidemiology and medicine will expand going forward.
Bringing viral evolution studies more into medicine will require a mindset shift, Dr. Ogbunu said. Clinical practice is, by design, very focused on the individual patient. Evolutionary biology, on the other hand, deals with populations and probabilities.
Being able to engage with evolutionary biology would help physicians better understand disease and explain it to their patients, he said.
To start, Dr. Nelson recommended requiring at least one course in evolutionary biology or evolutionary medicine in medical school and crafting continuing education in this area for physicians. (Presentations at conferences could be one way to do this.)
Dr. Nelson also recommended deeper engagement and collaboration between physicians who collect samples from patients and evolutionary biologists who analyze genetic data. This would improve the quality of the data, the analysis, and the eventual findings that could be relevant to patients and clinical practice.
Still, “my first and inevitable reaction is I would so much rather prefer to exist in relative obscurity,” said Dr. Koonin, noting that the tragedy of the pandemic outweighs the advancements in the field.
Although there’s no going back to prepandemic times, there is an enormous opportunity in the aftermath of COVID to increase dialogue between physicians and evolutionary virologists to improve medical practice as well as public health.
Dr. Nelson summed it up: “Everything we uncover about these pathogens may help us prevent something like this again.”
A version of this article first appeared on Medscape.com.
It has been a strange, exhausting year for many evolutionary virologists.
“Scientists are not used to having attention and are not used to being in the press and are not used to being attacked on Twitter,” Martha Nelson, PhD, a staff scientist who studies viral evolution at the National Institutes of Health, said in an interview.
Over the past year and a half, the theory of evolution has been thrust into the spotlight – more now than ever, perhaps, as the world is stalked by the Delta variant and fears arise of a mutation that’s even worse.
The origins of SARS-CoV-2 and the rise of the Delta variant have been debated, and vaccine efficacy and the possible need for booster shots have been speculated upon. In all these instances, consciously or not, there is engagement with the field of evolutionary virology.
It has been central to deepening the understanding of the ongoing pandemic, even as SARS-CoV-2 has exposed gaps in what we understand about how viruses behave and evolve.
Evolutionary virology experts believe that, after the pandemic, their expertise and tools could be applied to and integrated with clinical medicine to improve outcomes and understanding of disease.
“From our perspective, evolutionary biology has been a side dish and something that hasn’t been integrated into the core practice of medicine,” said Dr. Nelson. “I’m really curious to see how that changes over time.”
Pandemic evolution
Novel pathogens, antibiotic-resistant bacteria, and cancer cells are all products of ongoing evolution. “Just like cellular organisms, viruses have genomes, and all genomes evolve,” Eugene Koonin, PhD, evolutionary genomics group leader at the NIH, said in an interview.
Compared with cellular organisms, viruses evolve quite fast, he said.
A study published in the Proceedings of the National Academy of Sciences exemplifies evolutionary virology in action. In the study, Dr. Koonin and fellow researchers analyzed more than 300,000 genome sequences of SARS-CoV-2 variants that were publicly available as of January 2021 and mapped all the mutations in each sequence.
The researchers identified a small subset of mutations that arose independently more than once and that likely aided viral adaptation, said Nash Rochman, PhD, a research fellow at the NIH and coauthor of the PNAS study.
Many of these mutations were concentrated in two areas of the genome – the receptor binding domain of the spike protein, and a region of the nucleocapsid protein – and were often grouped together, possibly creating greater advantages for the virus than would have occurred individually, he said.
The researchers also found that, from the beginning of the pandemic, the SARS-CoV-2 genome has been evolving and diversifying in different regions around the world, allowing for the rise of new lineages and, possibly, even new species, Dr. Koonin said.
During the pandemic, researchers have used evolutionary virology tools to tackle many other questions. For example, Dr. Nelson tracked the spread of SARS-CoV-2 across Europe and North America. In a study that is currently undergoing peer review, the investigators found recently vaccinated individuals, who are only partially immune, are at the highest risk for incubating antibody-resistant variants.
C. Brandon Ogbunu, PhD, an evolutionary geneticist at Yale University, New Haven, Conn., whose work is focused on disease evolution, studied whether SARS-CoV-2 would evolve to become more transmissible, and if so, would it also become more or less virulent. His lab also investigated the transmission and spread of the virus.
“I think the last year, on one end, has been this opportunity to apply concepts and perspectives that we’ve been developing for the last several decades,” Dr. Ogbunu said in an interview. “At the same time, this pandemic has also been this wake-up call for many of us with regards to revealing the things we do not understand about the ways viruses infect, spread, and how evolution works within viruses.”
He emphasizes the need for evolutionary biology to partner with other fields – including information theory and biophysics – to help unlock viral mysteries: “We need to think very, very carefully about the way those fields intersect.”
Dr. Nelson also pointed to the need for better, more centralized data gathering in the United States.
The sheer volume of information scientists have collected about SARS-CoV-2 will aid in the study of virus evolution for years to come, said Dr. Koonin.
Evolution in medicine
Evolutionary virology and related research can be applied to medicine outside of the context of a global pandemic. “The principles and technical portions of evolutionary virology are very applicable to other diseases, including cancer,” Dr. Koonin said.
Viruses, bacteria, and cancer cells are all evolving systems. Viruses and bacteria are constantly evolving to thwart drugs and vaccines. How physicians and health care professionals practice medicine shapes the selection pressures driving how these pathogens evolve, Dr. Nelson said.
The rise of antibiotic-resistant bacteria is a particularly relevant example of how evolution affects the way physicians treat patients. Having an evolutionary perspective can help inform how to treat patients most effectively, both for individual patients as well as for broader public health, she said.
“For a long time, there’s been a lot of interest in pathogen evolution that hasn’t translated so much into clinical practice,” said Dr. Nelson. “There’s been kind of a gulf between the research side of evolutionary virology and pathogen emergence and actual practice of medicine.”
As genomic sequencing has become faster and cheaper, that gulf has started to narrow, she said. As this technology continues to prove itself by, for example, tracking the evolution of one virus in real time, Dr. Nelson hopes there will be a positive snowball effect, leading to more attention, investment, and improvements in genomic data and that its use in epidemiology and medicine will expand going forward.
Bringing viral evolution studies more into medicine will require a mindset shift, Dr. Ogbunu said. Clinical practice is, by design, very focused on the individual patient. Evolutionary biology, on the other hand, deals with populations and probabilities.
Being able to engage with evolutionary biology would help physicians better understand disease and explain it to their patients, he said.
To start, Dr. Nelson recommended requiring at least one course in evolutionary biology or evolutionary medicine in medical school and crafting continuing education in this area for physicians. (Presentations at conferences could be one way to do this.)
Dr. Nelson also recommended deeper engagement and collaboration between physicians who collect samples from patients and evolutionary biologists who analyze genetic data. This would improve the quality of the data, the analysis, and the eventual findings that could be relevant to patients and clinical practice.
Still, “my first and inevitable reaction is I would so much rather prefer to exist in relative obscurity,” said Dr. Koonin, noting that the tragedy of the pandemic outweighs the advancements in the field.
Although there’s no going back to prepandemic times, there is an enormous opportunity in the aftermath of COVID to increase dialogue between physicians and evolutionary virologists to improve medical practice as well as public health.
Dr. Nelson summed it up: “Everything we uncover about these pathogens may help us prevent something like this again.”
A version of this article first appeared on Medscape.com.
It has been a strange, exhausting year for many evolutionary virologists.
“Scientists are not used to having attention and are not used to being in the press and are not used to being attacked on Twitter,” Martha Nelson, PhD, a staff scientist who studies viral evolution at the National Institutes of Health, said in an interview.
Over the past year and a half, the theory of evolution has been thrust into the spotlight – more now than ever, perhaps, as the world is stalked by the Delta variant and fears arise of a mutation that’s even worse.
The origins of SARS-CoV-2 and the rise of the Delta variant have been debated, and vaccine efficacy and the possible need for booster shots have been speculated upon. In all these instances, consciously or not, there is engagement with the field of evolutionary virology.
It has been central to deepening the understanding of the ongoing pandemic, even as SARS-CoV-2 has exposed gaps in what we understand about how viruses behave and evolve.
Evolutionary virology experts believe that, after the pandemic, their expertise and tools could be applied to and integrated with clinical medicine to improve outcomes and understanding of disease.
“From our perspective, evolutionary biology has been a side dish and something that hasn’t been integrated into the core practice of medicine,” said Dr. Nelson. “I’m really curious to see how that changes over time.”
Pandemic evolution
Novel pathogens, antibiotic-resistant bacteria, and cancer cells are all products of ongoing evolution. “Just like cellular organisms, viruses have genomes, and all genomes evolve,” Eugene Koonin, PhD, evolutionary genomics group leader at the NIH, said in an interview.
Compared with cellular organisms, viruses evolve quite fast, he said.
A study published in the Proceedings of the National Academy of Sciences exemplifies evolutionary virology in action. In the study, Dr. Koonin and fellow researchers analyzed more than 300,000 genome sequences of SARS-CoV-2 variants that were publicly available as of January 2021 and mapped all the mutations in each sequence.
The researchers identified a small subset of mutations that arose independently more than once and that likely aided viral adaptation, said Nash Rochman, PhD, a research fellow at the NIH and coauthor of the PNAS study.
Many of these mutations were concentrated in two areas of the genome – the receptor binding domain of the spike protein, and a region of the nucleocapsid protein – and were often grouped together, possibly creating greater advantages for the virus than would have occurred individually, he said.
The researchers also found that, from the beginning of the pandemic, the SARS-CoV-2 genome has been evolving and diversifying in different regions around the world, allowing for the rise of new lineages and, possibly, even new species, Dr. Koonin said.
During the pandemic, researchers have used evolutionary virology tools to tackle many other questions. For example, Dr. Nelson tracked the spread of SARS-CoV-2 across Europe and North America. In a study that is currently undergoing peer review, the investigators found recently vaccinated individuals, who are only partially immune, are at the highest risk for incubating antibody-resistant variants.
C. Brandon Ogbunu, PhD, an evolutionary geneticist at Yale University, New Haven, Conn., whose work is focused on disease evolution, studied whether SARS-CoV-2 would evolve to become more transmissible, and if so, would it also become more or less virulent. His lab also investigated the transmission and spread of the virus.
“I think the last year, on one end, has been this opportunity to apply concepts and perspectives that we’ve been developing for the last several decades,” Dr. Ogbunu said in an interview. “At the same time, this pandemic has also been this wake-up call for many of us with regards to revealing the things we do not understand about the ways viruses infect, spread, and how evolution works within viruses.”
He emphasizes the need for evolutionary biology to partner with other fields – including information theory and biophysics – to help unlock viral mysteries: “We need to think very, very carefully about the way those fields intersect.”
Dr. Nelson also pointed to the need for better, more centralized data gathering in the United States.
The sheer volume of information scientists have collected about SARS-CoV-2 will aid in the study of virus evolution for years to come, said Dr. Koonin.
Evolution in medicine
Evolutionary virology and related research can be applied to medicine outside of the context of a global pandemic. “The principles and technical portions of evolutionary virology are very applicable to other diseases, including cancer,” Dr. Koonin said.
Viruses, bacteria, and cancer cells are all evolving systems. Viruses and bacteria are constantly evolving to thwart drugs and vaccines. How physicians and health care professionals practice medicine shapes the selection pressures driving how these pathogens evolve, Dr. Nelson said.
The rise of antibiotic-resistant bacteria is a particularly relevant example of how evolution affects the way physicians treat patients. Having an evolutionary perspective can help inform how to treat patients most effectively, both for individual patients as well as for broader public health, she said.
“For a long time, there’s been a lot of interest in pathogen evolution that hasn’t translated so much into clinical practice,” said Dr. Nelson. “There’s been kind of a gulf between the research side of evolutionary virology and pathogen emergence and actual practice of medicine.”
As genomic sequencing has become faster and cheaper, that gulf has started to narrow, she said. As this technology continues to prove itself by, for example, tracking the evolution of one virus in real time, Dr. Nelson hopes there will be a positive snowball effect, leading to more attention, investment, and improvements in genomic data and that its use in epidemiology and medicine will expand going forward.
Bringing viral evolution studies more into medicine will require a mindset shift, Dr. Ogbunu said. Clinical practice is, by design, very focused on the individual patient. Evolutionary biology, on the other hand, deals with populations and probabilities.
Being able to engage with evolutionary biology would help physicians better understand disease and explain it to their patients, he said.
To start, Dr. Nelson recommended requiring at least one course in evolutionary biology or evolutionary medicine in medical school and crafting continuing education in this area for physicians. (Presentations at conferences could be one way to do this.)
Dr. Nelson also recommended deeper engagement and collaboration between physicians who collect samples from patients and evolutionary biologists who analyze genetic data. This would improve the quality of the data, the analysis, and the eventual findings that could be relevant to patients and clinical practice.
Still, “my first and inevitable reaction is I would so much rather prefer to exist in relative obscurity,” said Dr. Koonin, noting that the tragedy of the pandemic outweighs the advancements in the field.
Although there’s no going back to prepandemic times, there is an enormous opportunity in the aftermath of COVID to increase dialogue between physicians and evolutionary virologists to improve medical practice as well as public health.
Dr. Nelson summed it up: “Everything we uncover about these pathogens may help us prevent something like this again.”
A version of this article first appeared on Medscape.com.