User login
Zotarolimus Stent: Short-Term Dual Antiplatelet Therapy Is Safe
CHICAGO – A 3-month regimen of dual antiplatelet therapy may be a safe and effective alternative to the standard 12 months in selected recipients of the zotarolimus-eluting Endeavor stent.
This was the main finding of the 2,117-patient randomized, prospective RESET (Real Safety and Efficacy of 3-Month Dual Antiplatelet Therapy Following Zotarolimus-Eluting Stent Implantation) trial.

RESET was an open-label, randomized trial conducted at 26 South Korean centers. It was designed as a noninferiority study, meaning it was set up to evaluate the hypothesis that 3 months of dual antiplatelet therapy (DAPT) with clopidogrel and aspirin following implantation of the Endeavor drug-eluting stent doesn’t yield worse clinical outcomes than does the standard 12 months of DAPT.
Dr. Myeong-Ki Hong volunteered that an important study limitation in RESET was the exclusion of high-risk patients from participation. Among those ineligible were patients with a history of peripheral artery disease or cerebrovascular accident, those in cardiogenic shock or with a left ventricular ejection fraction less than 40%, and patients with severe renal or hepatic renal dysfunction. The lessons of RESET may not be applicable to such individuals.
Participants in RESET underwent percutaneous coronary intervention and implantation of a drug-eluting stent for unstable angina, acute MI, or stable angina. Half of RESET participants were randomized to receive the Endeavor stent with 3 months of DAPT before discontinuing clopidogrel and carrying on with aspirin monotherapy; the other half received various other drug-eluting stents accompanied by the standard, guideline-recommended 12 months of DAPT.
The primary study end point was the 12-month composite of cardiovascular death, acute MI, stent thrombosis, ischemia-driven target vessel revascularization, and TIMI (thrombolysis in myocardial infarction) major or minor bleeding. The combined end point occurred in exactly 4.7% of subjects in each study arm, Dr. Hong reported at the annual meeting of the American College of Cardiology.
The secondary end point (comprising all-cause mortality, stent thrombosis, or MI at 12 months of follow-up) occurred in 0.8% of patients assigned to 3 months of DAPT and 1.3% of controls, a nonsignificant difference, noted Dr. Hong, professor of medicine at Yonsei University, Seoul.
A key aim of DAPT, he pointed out, is the prevention of stent thrombosis. Two cases occurred in Endeavor stent recipients, both during their 3 months on DAPT; notably, no cases occurred in this group after discontinuation of clopidogrel. In contrast, three cases of stent thrombosis occurred in the control group on 12 months of DAPT, all during months 3-12.
Downsides of prolonged DAPT include increased risk of bleeding, financial cost, and poor patient adherence. Dr. Hong cited the following situations in which (based upon RESET) the placement of a zotarolimus-eluting stent and 3 months of DAPT might be useful:
• Patients at increased risk for bleeding complications.
• Patients with a high likelihood of noncardiac surgery or other invasive procedures in the coming year.
• Patients at low anatomical risk of stent thrombosis.
• Patients who are likely to be nonadherent to the prolonged DAPT regimen.
An impetus for the RESET trial was an earlier Korean registry that reported favorable long-term outcomes in 661 patients whose clopidogrel was discontinued 3 months after implantation of a zotarolimus-eluting stent (Circ. J. 2010;74:2314-21).
Audience member Dr. Antonio Colombo of Milan, who was honored as a "Legend of Cardiology" at the conference, rose to note that most studies from Korea and Japan report stent thrombosis rates that are half those seen in Europe and North America.
"I believe it’s not easy to translate these RESET conclusions to other populations. I think some genetic or other factors may play a role in these low thrombosis rates," he observed.
The study was sponsored by the South Korean Ministry of Health and Welfare, the Cardiovascular Research Center of Seoul, and Medtronic. Dr. Hong reported having no financial conflicts. Dr. Price reported serving as a consultant to Bristol-Myers Squibb, Sanofi, and more than a half-dozen other companies.
One of take-away lesson from this study is that in an anatomically low-risk population such as this, with a reference vessel diameter of 3.0 mm and an average of 1.3 treated lesions per patient, we’re getting very good with our drug-eluting stents. The expected 1-year event rate of about 10% was more than double what was actually observed.
Dr. Matthew J. Price |

These low event rates in both study arms underscore how difficult it’s going to be to ever definitively prove that short-duration DAPT is safe. RESET was a noninferiority study, and even with more than 2,100 randomized patients, the statistical noninferiority margins were broad enough that it’s theoretically possible for a safety signal to have gone undetected.
Matthew J. Price, M.D., is director of the cardiac catheterization laboratory at the Scripps Clinic in La Jolla, Calif. He was the study discussant at the meeting. Dr. Price reported serving as a consultant to Bristol-Myers Squibb, Sanofi, and more than a half-dozen other companies.
One of take-away lesson from this study is that in an anatomically low-risk population such as this, with a reference vessel diameter of 3.0 mm and an average of 1.3 treated lesions per patient, we’re getting very good with our drug-eluting stents. The expected 1-year event rate of about 10% was more than double what was actually observed.
Dr. Matthew J. Price |
These low event rates in both study arms underscore how difficult it’s going to be to ever definitively prove that short-duration DAPT is safe. RESET was a noninferiority study, and even with more than 2,100 randomized patients, the statistical noninferiority margins were broad enough that it’s theoretically possible for a safety signal to have gone undetected.
Matthew J. Price, M.D., is director of the cardiac catheterization laboratory at the Scripps Clinic in La Jolla, Calif. He was the study discussant at the meeting. Dr. Price reported serving as a consultant to Bristol-Myers Squibb, Sanofi, and more than a half-dozen other companies.
One of take-away lesson from this study is that in an anatomically low-risk population such as this, with a reference vessel diameter of 3.0 mm and an average of 1.3 treated lesions per patient, we’re getting very good with our drug-eluting stents. The expected 1-year event rate of about 10% was more than double what was actually observed.
Dr. Matthew J. Price |
These low event rates in both study arms underscore how difficult it’s going to be to ever definitively prove that short-duration DAPT is safe. RESET was a noninferiority study, and even with more than 2,100 randomized patients, the statistical noninferiority margins were broad enough that it’s theoretically possible for a safety signal to have gone undetected.
Matthew J. Price, M.D., is director of the cardiac catheterization laboratory at the Scripps Clinic in La Jolla, Calif. He was the study discussant at the meeting. Dr. Price reported serving as a consultant to Bristol-Myers Squibb, Sanofi, and more than a half-dozen other companies.
CHICAGO – A 3-month regimen of dual antiplatelet therapy may be a safe and effective alternative to the standard 12 months in selected recipients of the zotarolimus-eluting Endeavor stent.
This was the main finding of the 2,117-patient randomized, prospective RESET (Real Safety and Efficacy of 3-Month Dual Antiplatelet Therapy Following Zotarolimus-Eluting Stent Implantation) trial.
RESET was an open-label, randomized trial conducted at 26 South Korean centers. It was designed as a noninferiority study, meaning it was set up to evaluate the hypothesis that 3 months of dual antiplatelet therapy (DAPT) with clopidogrel and aspirin following implantation of the Endeavor drug-eluting stent doesn’t yield worse clinical outcomes than does the standard 12 months of DAPT.
Dr. Myeong-Ki Hong volunteered that an important study limitation in RESET was the exclusion of high-risk patients from participation. Among those ineligible were patients with a history of peripheral artery disease or cerebrovascular accident, those in cardiogenic shock or with a left ventricular ejection fraction less than 40%, and patients with severe renal or hepatic renal dysfunction. The lessons of RESET may not be applicable to such individuals.
Participants in RESET underwent percutaneous coronary intervention and implantation of a drug-eluting stent for unstable angina, acute MI, or stable angina. Half of RESET participants were randomized to receive the Endeavor stent with 3 months of DAPT before discontinuing clopidogrel and carrying on with aspirin monotherapy; the other half received various other drug-eluting stents accompanied by the standard, guideline-recommended 12 months of DAPT.
The primary study end point was the 12-month composite of cardiovascular death, acute MI, stent thrombosis, ischemia-driven target vessel revascularization, and TIMI (thrombolysis in myocardial infarction) major or minor bleeding. The combined end point occurred in exactly 4.7% of subjects in each study arm, Dr. Hong reported at the annual meeting of the American College of Cardiology.
The secondary end point (comprising all-cause mortality, stent thrombosis, or MI at 12 months of follow-up) occurred in 0.8% of patients assigned to 3 months of DAPT and 1.3% of controls, a nonsignificant difference, noted Dr. Hong, professor of medicine at Yonsei University, Seoul.
A key aim of DAPT, he pointed out, is the prevention of stent thrombosis. Two cases occurred in Endeavor stent recipients, both during their 3 months on DAPT; notably, no cases occurred in this group after discontinuation of clopidogrel. In contrast, three cases of stent thrombosis occurred in the control group on 12 months of DAPT, all during months 3-12.
Downsides of prolonged DAPT include increased risk of bleeding, financial cost, and poor patient adherence. Dr. Hong cited the following situations in which (based upon RESET) the placement of a zotarolimus-eluting stent and 3 months of DAPT might be useful:
• Patients at increased risk for bleeding complications.
• Patients with a high likelihood of noncardiac surgery or other invasive procedures in the coming year.
• Patients at low anatomical risk of stent thrombosis.
• Patients who are likely to be nonadherent to the prolonged DAPT regimen.
An impetus for the RESET trial was an earlier Korean registry that reported favorable long-term outcomes in 661 patients whose clopidogrel was discontinued 3 months after implantation of a zotarolimus-eluting stent (Circ. J. 2010;74:2314-21).
Audience member Dr. Antonio Colombo of Milan, who was honored as a "Legend of Cardiology" at the conference, rose to note that most studies from Korea and Japan report stent thrombosis rates that are half those seen in Europe and North America.
"I believe it’s not easy to translate these RESET conclusions to other populations. I think some genetic or other factors may play a role in these low thrombosis rates," he observed.
The study was sponsored by the South Korean Ministry of Health and Welfare, the Cardiovascular Research Center of Seoul, and Medtronic. Dr. Hong reported having no financial conflicts. Dr. Price reported serving as a consultant to Bristol-Myers Squibb, Sanofi, and more than a half-dozen other companies.
CHICAGO – A 3-month regimen of dual antiplatelet therapy may be a safe and effective alternative to the standard 12 months in selected recipients of the zotarolimus-eluting Endeavor stent.
This was the main finding of the 2,117-patient randomized, prospective RESET (Real Safety and Efficacy of 3-Month Dual Antiplatelet Therapy Following Zotarolimus-Eluting Stent Implantation) trial.
RESET was an open-label, randomized trial conducted at 26 South Korean centers. It was designed as a noninferiority study, meaning it was set up to evaluate the hypothesis that 3 months of dual antiplatelet therapy (DAPT) with clopidogrel and aspirin following implantation of the Endeavor drug-eluting stent doesn’t yield worse clinical outcomes than does the standard 12 months of DAPT.
Dr. Myeong-Ki Hong volunteered that an important study limitation in RESET was the exclusion of high-risk patients from participation. Among those ineligible were patients with a history of peripheral artery disease or cerebrovascular accident, those in cardiogenic shock or with a left ventricular ejection fraction less than 40%, and patients with severe renal or hepatic renal dysfunction. The lessons of RESET may not be applicable to such individuals.
Participants in RESET underwent percutaneous coronary intervention and implantation of a drug-eluting stent for unstable angina, acute MI, or stable angina. Half of RESET participants were randomized to receive the Endeavor stent with 3 months of DAPT before discontinuing clopidogrel and carrying on with aspirin monotherapy; the other half received various other drug-eluting stents accompanied by the standard, guideline-recommended 12 months of DAPT.
The primary study end point was the 12-month composite of cardiovascular death, acute MI, stent thrombosis, ischemia-driven target vessel revascularization, and TIMI (thrombolysis in myocardial infarction) major or minor bleeding. The combined end point occurred in exactly 4.7% of subjects in each study arm, Dr. Hong reported at the annual meeting of the American College of Cardiology.
The secondary end point (comprising all-cause mortality, stent thrombosis, or MI at 12 months of follow-up) occurred in 0.8% of patients assigned to 3 months of DAPT and 1.3% of controls, a nonsignificant difference, noted Dr. Hong, professor of medicine at Yonsei University, Seoul.
A key aim of DAPT, he pointed out, is the prevention of stent thrombosis. Two cases occurred in Endeavor stent recipients, both during their 3 months on DAPT; notably, no cases occurred in this group after discontinuation of clopidogrel. In contrast, three cases of stent thrombosis occurred in the control group on 12 months of DAPT, all during months 3-12.
Downsides of prolonged DAPT include increased risk of bleeding, financial cost, and poor patient adherence. Dr. Hong cited the following situations in which (based upon RESET) the placement of a zotarolimus-eluting stent and 3 months of DAPT might be useful:
• Patients at increased risk for bleeding complications.
• Patients with a high likelihood of noncardiac surgery or other invasive procedures in the coming year.
• Patients at low anatomical risk of stent thrombosis.
• Patients who are likely to be nonadherent to the prolonged DAPT regimen.
An impetus for the RESET trial was an earlier Korean registry that reported favorable long-term outcomes in 661 patients whose clopidogrel was discontinued 3 months after implantation of a zotarolimus-eluting stent (Circ. J. 2010;74:2314-21).
Audience member Dr. Antonio Colombo of Milan, who was honored as a "Legend of Cardiology" at the conference, rose to note that most studies from Korea and Japan report stent thrombosis rates that are half those seen in Europe and North America.
"I believe it’s not easy to translate these RESET conclusions to other populations. I think some genetic or other factors may play a role in these low thrombosis rates," he observed.
The study was sponsored by the South Korean Ministry of Health and Welfare, the Cardiovascular Research Center of Seoul, and Medtronic. Dr. Hong reported having no financial conflicts. Dr. Price reported serving as a consultant to Bristol-Myers Squibb, Sanofi, and more than a half-dozen other companies.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: Patients assigned to 3 months of dual antiplatelet therapy following implantation of a zotarolimus-eluting stent had a 1-year combined adverse event rate of 4.7%, identical to that in recipients of other drug-eluting stents plus the standard 12 months of dual antiplatelet therapy.
Data Source: An open-label, randomized trial including 2,117 patients who received a zotarolimus-eluting Endeavor stent and 3 months of dual antiplatelet therapy, or a different drug-eluting stent and the standard 12 months of dual antiplatelet therapy.
Disclosures: The study was sponsored by the South Korean Ministry of Health and Welfare, the Cardiovascular Research Center of Seoul, and Medtronic.
Acupuncture Improves Heart Rate Variability in CHD
CHICAGO – Traditional acupuncture improves heart rate variability, and it may prove to reduce the risk of sudden death for patients with established coronary heart disease, a pilot study suggests.
The blinded study with a sham-acupuncture control arm demonstrated that acupuncture accomplishes autonomic remodeling via sympathovagal modulation as reflected in increased heart rate variability (HRV), according to Dr. Puja K. Mehta of the Women's Heart Center at Cedars-Sinai Medical Center, Los Angeles. The clinically meaningful improvements in heart rate variability in this pilot study lay the groundwork for a future large outcome-based clinical trial of traditional acupuncture in patients with known CHD.
Diminished HRV in patients with CHD is accepted as a predictor of sudden cardiac death risk in clinical trials, Dr. Mehta noted at the annual meeting of the American College of Cardiology.
Sudden cardiac death accounts for roughly 150,000 deaths annually in Americans with established CHD. Traditional cardiovascular risk factors don’t fully account for the sudden cardiac death risk.
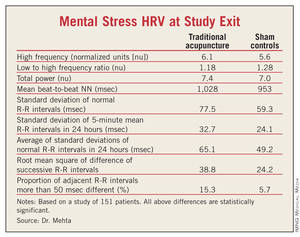
She reported on 151 patients with established CHD who were randomized to traditional acupuncture, sham acupuncture, or a wait-list control arm. The acupuncture, performed with stainless steel needles, was done three times per week for 12 weeks. Eight active CHD-specific traditional acupuncture sites were targeted. The sham-treatment group received a previously validated sham procedure at nonacupuncture sites. Patients were blinded as to whether they got real or sham acupuncture.
Heart rate variability was measured at baseline and after 12 weeks using 24-hour time and frequency domain measures and during a 5-minute mental arithmetic stress test and a 5-minute forehead cold pressor test.
Compared with the sham-treated controls, the traditional acupuncture recipients had 17% more high frequency HRV as determined by efferent vagal activity and 31% more heart rate variability on mental arithmetic stress testing at study’s end.
Dr. Mehta said that these results may actually underestimate the true clinical effect size of traditional acupuncture because sham acupuncture has previously been shown to have some mild therapeutic benefit compared with conventional placebos.
At study’s end, there were no differences between the acupuncture and sham control groups in blood pressure, serum lipids, insulin resistance, C-reactive protein, salivary cortisol, paroxysmal atrial tachyarrhythmia, or psychosocial variables, she noted.
The pilot study was supported by grants from the National Institutes of Health-National Center for Complementary and Alternative Medicine, the Barbara Streisand Women’s Cardiovascular Research and Education Program at Cedars-Sinai Medical Center, and foundation grants. Dr. Mehta reported having no financial conflicts.
CHICAGO – Traditional acupuncture improves heart rate variability, and it may prove to reduce the risk of sudden death for patients with established coronary heart disease, a pilot study suggests.
The blinded study with a sham-acupuncture control arm demonstrated that acupuncture accomplishes autonomic remodeling via sympathovagal modulation as reflected in increased heart rate variability (HRV), according to Dr. Puja K. Mehta of the Women's Heart Center at Cedars-Sinai Medical Center, Los Angeles. The clinically meaningful improvements in heart rate variability in this pilot study lay the groundwork for a future large outcome-based clinical trial of traditional acupuncture in patients with known CHD.
Diminished HRV in patients with CHD is accepted as a predictor of sudden cardiac death risk in clinical trials, Dr. Mehta noted at the annual meeting of the American College of Cardiology.
Sudden cardiac death accounts for roughly 150,000 deaths annually in Americans with established CHD. Traditional cardiovascular risk factors don’t fully account for the sudden cardiac death risk.
She reported on 151 patients with established CHD who were randomized to traditional acupuncture, sham acupuncture, or a wait-list control arm. The acupuncture, performed with stainless steel needles, was done three times per week for 12 weeks. Eight active CHD-specific traditional acupuncture sites were targeted. The sham-treatment group received a previously validated sham procedure at nonacupuncture sites. Patients were blinded as to whether they got real or sham acupuncture.
Heart rate variability was measured at baseline and after 12 weeks using 24-hour time and frequency domain measures and during a 5-minute mental arithmetic stress test and a 5-minute forehead cold pressor test.
Compared with the sham-treated controls, the traditional acupuncture recipients had 17% more high frequency HRV as determined by efferent vagal activity and 31% more heart rate variability on mental arithmetic stress testing at study’s end.
Dr. Mehta said that these results may actually underestimate the true clinical effect size of traditional acupuncture because sham acupuncture has previously been shown to have some mild therapeutic benefit compared with conventional placebos.
At study’s end, there were no differences between the acupuncture and sham control groups in blood pressure, serum lipids, insulin resistance, C-reactive protein, salivary cortisol, paroxysmal atrial tachyarrhythmia, or psychosocial variables, she noted.
The pilot study was supported by grants from the National Institutes of Health-National Center for Complementary and Alternative Medicine, the Barbara Streisand Women’s Cardiovascular Research and Education Program at Cedars-Sinai Medical Center, and foundation grants. Dr. Mehta reported having no financial conflicts.
CHICAGO – Traditional acupuncture improves heart rate variability, and it may prove to reduce the risk of sudden death for patients with established coronary heart disease, a pilot study suggests.
The blinded study with a sham-acupuncture control arm demonstrated that acupuncture accomplishes autonomic remodeling via sympathovagal modulation as reflected in increased heart rate variability (HRV), according to Dr. Puja K. Mehta of the Women's Heart Center at Cedars-Sinai Medical Center, Los Angeles. The clinically meaningful improvements in heart rate variability in this pilot study lay the groundwork for a future large outcome-based clinical trial of traditional acupuncture in patients with known CHD.
Diminished HRV in patients with CHD is accepted as a predictor of sudden cardiac death risk in clinical trials, Dr. Mehta noted at the annual meeting of the American College of Cardiology.
Sudden cardiac death accounts for roughly 150,000 deaths annually in Americans with established CHD. Traditional cardiovascular risk factors don’t fully account for the sudden cardiac death risk.
She reported on 151 patients with established CHD who were randomized to traditional acupuncture, sham acupuncture, or a wait-list control arm. The acupuncture, performed with stainless steel needles, was done three times per week for 12 weeks. Eight active CHD-specific traditional acupuncture sites were targeted. The sham-treatment group received a previously validated sham procedure at nonacupuncture sites. Patients were blinded as to whether they got real or sham acupuncture.
Heart rate variability was measured at baseline and after 12 weeks using 24-hour time and frequency domain measures and during a 5-minute mental arithmetic stress test and a 5-minute forehead cold pressor test.
Compared with the sham-treated controls, the traditional acupuncture recipients had 17% more high frequency HRV as determined by efferent vagal activity and 31% more heart rate variability on mental arithmetic stress testing at study’s end.
Dr. Mehta said that these results may actually underestimate the true clinical effect size of traditional acupuncture because sham acupuncture has previously been shown to have some mild therapeutic benefit compared with conventional placebos.
At study’s end, there were no differences between the acupuncture and sham control groups in blood pressure, serum lipids, insulin resistance, C-reactive protein, salivary cortisol, paroxysmal atrial tachyarrhythmia, or psychosocial variables, she noted.
The pilot study was supported by grants from the National Institutes of Health-National Center for Complementary and Alternative Medicine, the Barbara Streisand Women’s Cardiovascular Research and Education Program at Cedars-Sinai Medical Center, and foundation grants. Dr. Mehta reported having no financial conflicts.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: Compared with sham-treated controls, traditional acupuncture recipients had 17% more high frequency heart rate variability as determined by efferent vagal activity and 31% more heart rate variability on mental arithmetic stress testing at study’s end.
Data Source: The study included 151 patients with established CHD who were randomized to traditional acupuncture, sham acupuncture, or a wait-list control arm.
Disclosures: The pilot study was supported by grants from the National Institutes of Health-National Center for Complementary and Alternative Medicine, the Barbara Streisand Women’s Cardiovascular Research and Education Program at Cedars-Sinai Medical Center, and foundation grants. Dr. Mehta reported having no financial conflicts.
Ob.Gyn. Offices Ideal for Heart Risk Screening
CHICAGO – Cardiologists and ob.gyns. teamed up for a pilot project of the Women’s Cardiovascular Health Initiative aimed at improving primary cardiovascular prevention in middle-aged women.
An ob.gyn. is often the primary care physician for many middle-aged women, Dr. Jennifer Yu explained at the conference. The goal was to upgrade cardiovascular screening and education in ob.gyn. practices, without distracting ob.gyns. from their focus on reproductive health, and to direct at-risk women to specialized care as needed.
The project, sponsored by the nonprofit Cardiovascular Research Foundation, was implemented at 10 community-based ob.gyn. clinics around the country. Patients completed a one-page questionnaire addressing traditional and gestational cardiovascular risk factors and any current symptoms.
During a recent 2-year period, 2,234 middle-age women visiting these 10 clinics for routine ob.gyn. care completed the one-page survey and had their blood pressure measured. The payoff was substantial: 87% of the women turned out to have cardiovascular risk factors, and 42% had cardiovascular symptoms. In many cases, the women were unaware of their risk factors or the potential significance of their cardiovascular symptoms, according to Dr. Yu of Mount Sinai Medical Center, New York.
The project addresses the misconception that coronary artery disease is mainly a man’s disease, she said. Heart disease also is the No.1 cause of death in women, and cardiovascular mortality among women in the 35- to 44-year-old age group is rising by 1% annually.
The mean age of participants was 53 years; 56% were postmenopausal, and 27% of the postmenopausal women were on hormone replacement therapy.
The most prevalent cardiovascular symptoms included claudication in 10%, palpitations in 14%, exertional chest pain in 8%, resting chest pain in 10%, and shortness of breath in 35%.
Most of the women reported being sedentary; 14% had high blood pressure, 21% were hypercholesterolemic, and 7.5% had diabetes.
A history of gestational diabetes was reported by 8.8%, a history of gestational hypertension by 10%, and preeclampsia by 7.6%.
About 76% of the women had another primary care provider besides their ob.gyn. Those women were more likely to be aware that they had cardiovascular risk factors than were the 6% who indicated they had no primary care provider and the 18% who said their ob.gyn. is their primary care provider.
Among women with elevated blood pressure, 13% with a non–ob.gyn. primary care physician were unaware that they had high blood pressure, compared with 22% of hypertensive women with an ob.gyn. as their primary care physician and 27% of those with no primary care provider.
Similarly, 31% of women with a non–ob.gyn. primary care provider were unaware they were hypercholesterolemic, as were 38% of those whose ob.gyn. was their primary care physician and 51% of women with no primary care provider.
Of diabetic women with a non–ob.gyn. primary care provider, 18% didn’t know they had diabetes or were unaware of the associated cardiovascular risk. This was the case for 19% of diabetic women with an ob.gyn. primary care provider and 26% of women without a primary care provider.
One-quarter of the screened women were subsequently referred to another health care provider, typically a cardiologist, endocrinologist, or primary care physician.
The questionnaire was developed in consultation with leaders from the American College of Cardiology, the American Congress of Obstetricians and Gynecologists, and the Society of Cardiovascular Angiography and Interventions – Women in Innovations. The pilot screening was funded by Abbott Vascular. Dr. Yu reported having no financial conflicts.
CHICAGO – Cardiologists and ob.gyns. teamed up for a pilot project of the Women’s Cardiovascular Health Initiative aimed at improving primary cardiovascular prevention in middle-aged women.
An ob.gyn. is often the primary care physician for many middle-aged women, Dr. Jennifer Yu explained at the conference. The goal was to upgrade cardiovascular screening and education in ob.gyn. practices, without distracting ob.gyns. from their focus on reproductive health, and to direct at-risk women to specialized care as needed.
The project, sponsored by the nonprofit Cardiovascular Research Foundation, was implemented at 10 community-based ob.gyn. clinics around the country. Patients completed a one-page questionnaire addressing traditional and gestational cardiovascular risk factors and any current symptoms.
During a recent 2-year period, 2,234 middle-age women visiting these 10 clinics for routine ob.gyn. care completed the one-page survey and had their blood pressure measured. The payoff was substantial: 87% of the women turned out to have cardiovascular risk factors, and 42% had cardiovascular symptoms. In many cases, the women were unaware of their risk factors or the potential significance of their cardiovascular symptoms, according to Dr. Yu of Mount Sinai Medical Center, New York.
The project addresses the misconception that coronary artery disease is mainly a man’s disease, she said. Heart disease also is the No.1 cause of death in women, and cardiovascular mortality among women in the 35- to 44-year-old age group is rising by 1% annually.
The mean age of participants was 53 years; 56% were postmenopausal, and 27% of the postmenopausal women were on hormone replacement therapy.
The most prevalent cardiovascular symptoms included claudication in 10%, palpitations in 14%, exertional chest pain in 8%, resting chest pain in 10%, and shortness of breath in 35%.
Most of the women reported being sedentary; 14% had high blood pressure, 21% were hypercholesterolemic, and 7.5% had diabetes.
A history of gestational diabetes was reported by 8.8%, a history of gestational hypertension by 10%, and preeclampsia by 7.6%.
About 76% of the women had another primary care provider besides their ob.gyn. Those women were more likely to be aware that they had cardiovascular risk factors than were the 6% who indicated they had no primary care provider and the 18% who said their ob.gyn. is their primary care provider.
Among women with elevated blood pressure, 13% with a non–ob.gyn. primary care physician were unaware that they had high blood pressure, compared with 22% of hypertensive women with an ob.gyn. as their primary care physician and 27% of those with no primary care provider.
Similarly, 31% of women with a non–ob.gyn. primary care provider were unaware they were hypercholesterolemic, as were 38% of those whose ob.gyn. was their primary care physician and 51% of women with no primary care provider.
Of diabetic women with a non–ob.gyn. primary care provider, 18% didn’t know they had diabetes or were unaware of the associated cardiovascular risk. This was the case for 19% of diabetic women with an ob.gyn. primary care provider and 26% of women without a primary care provider.
One-quarter of the screened women were subsequently referred to another health care provider, typically a cardiologist, endocrinologist, or primary care physician.
The questionnaire was developed in consultation with leaders from the American College of Cardiology, the American Congress of Obstetricians and Gynecologists, and the Society of Cardiovascular Angiography and Interventions – Women in Innovations. The pilot screening was funded by Abbott Vascular. Dr. Yu reported having no financial conflicts.
CHICAGO – Cardiologists and ob.gyns. teamed up for a pilot project of the Women’s Cardiovascular Health Initiative aimed at improving primary cardiovascular prevention in middle-aged women.
An ob.gyn. is often the primary care physician for many middle-aged women, Dr. Jennifer Yu explained at the conference. The goal was to upgrade cardiovascular screening and education in ob.gyn. practices, without distracting ob.gyns. from their focus on reproductive health, and to direct at-risk women to specialized care as needed.
The project, sponsored by the nonprofit Cardiovascular Research Foundation, was implemented at 10 community-based ob.gyn. clinics around the country. Patients completed a one-page questionnaire addressing traditional and gestational cardiovascular risk factors and any current symptoms.
During a recent 2-year period, 2,234 middle-age women visiting these 10 clinics for routine ob.gyn. care completed the one-page survey and had their blood pressure measured. The payoff was substantial: 87% of the women turned out to have cardiovascular risk factors, and 42% had cardiovascular symptoms. In many cases, the women were unaware of their risk factors or the potential significance of their cardiovascular symptoms, according to Dr. Yu of Mount Sinai Medical Center, New York.
The project addresses the misconception that coronary artery disease is mainly a man’s disease, she said. Heart disease also is the No.1 cause of death in women, and cardiovascular mortality among women in the 35- to 44-year-old age group is rising by 1% annually.
The mean age of participants was 53 years; 56% were postmenopausal, and 27% of the postmenopausal women were on hormone replacement therapy.
The most prevalent cardiovascular symptoms included claudication in 10%, palpitations in 14%, exertional chest pain in 8%, resting chest pain in 10%, and shortness of breath in 35%.
Most of the women reported being sedentary; 14% had high blood pressure, 21% were hypercholesterolemic, and 7.5% had diabetes.
A history of gestational diabetes was reported by 8.8%, a history of gestational hypertension by 10%, and preeclampsia by 7.6%.
About 76% of the women had another primary care provider besides their ob.gyn. Those women were more likely to be aware that they had cardiovascular risk factors than were the 6% who indicated they had no primary care provider and the 18% who said their ob.gyn. is their primary care provider.
Among women with elevated blood pressure, 13% with a non–ob.gyn. primary care physician were unaware that they had high blood pressure, compared with 22% of hypertensive women with an ob.gyn. as their primary care physician and 27% of those with no primary care provider.
Similarly, 31% of women with a non–ob.gyn. primary care provider were unaware they were hypercholesterolemic, as were 38% of those whose ob.gyn. was their primary care physician and 51% of women with no primary care provider.
Of diabetic women with a non–ob.gyn. primary care provider, 18% didn’t know they had diabetes or were unaware of the associated cardiovascular risk. This was the case for 19% of diabetic women with an ob.gyn. primary care provider and 26% of women without a primary care provider.
One-quarter of the screened women were subsequently referred to another health care provider, typically a cardiologist, endocrinologist, or primary care physician.
The questionnaire was developed in consultation with leaders from the American College of Cardiology, the American Congress of Obstetricians and Gynecologists, and the Society of Cardiovascular Angiography and Interventions – Women in Innovations. The pilot screening was funded by Abbott Vascular. Dr. Yu reported having no financial conflicts.
FROM THE ANNUAL SCIENTIFIC SESSION OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: Of those screened, 87% of the women turned out to have cardiovascular risk factors and 42% had cardiovascular symptoms.
Data Source: During a 2-year period, 2,234 middle-age women were screened at 10 ob.gyn. practices and completed a one-page survey and blood pressure screening.
Disclosures: The questionnaire was developed in consultation with leaders from the American College of Cardiology, the American Congress of Obstetricians and Gynecologists, and the Society of Cardiovascular Angiography and Interventions – Women in Innovations. The pilot screening was funded by Abbott Vascular. Dr. Yu reported having no financial conflicts
Two Million Americans Estimated to Have Congenital Heart Disease
CHICAGO – Roughly 2 million American children and adults are living with a congenital heart disease.
The estimate is based on congenital heart disease rates in Quebec during 2000 and extrapolated to the 2010 U.S. population. The estimates project that roughly one million of these are American children, aged 17 years or younger, and 1 million are adults, and that about 12% of these patients have severe congenital heart disease, Dr. Ariane J. Marelli and her associates reported in a poster at the meeting. The estimates showed a slight preponderance of adults with congenital heart disease, compared with children, and also a slight preponderance of women and girls with congenital heart disease, compared with men and boys.
"The growing public health importance of congenital heart disease across the life span emphasizes the need for a public health surveillance infrastructure in the United States," wrote Dr. Marelli, a cardiologist and director of the Adult Unit for Congenital Heart Diseases at McGill University in Montreal, and her associates. "These estimates should inform future planning and organization to ensure a medical work force trained to provide optimal specialized care to individuals with congenital heart disease throughout childhood, adolescence, and mature adulthood."
Dr. Marelli and her associates created the Quebec Congenital Heart Disease database by combining data from three province-wide administrative data bases (Circulation 2007;115:163-72). They then applied the congenital heart disease prevalence numbers from Quebec in 2000 to the U.S. population in 2010 by making several extrapolations and adjustments and by using U.S. population statistics collected by the 2010 Census. The adjustments included projecting prevalence and severity levels from 2000 to 2010, and taking into account racial and ethnic differences between Quebec and the United States.
Dr. Marelli said that she had no disclosures.
CHICAGO – Roughly 2 million American children and adults are living with a congenital heart disease.
The estimate is based on congenital heart disease rates in Quebec during 2000 and extrapolated to the 2010 U.S. population. The estimates project that roughly one million of these are American children, aged 17 years or younger, and 1 million are adults, and that about 12% of these patients have severe congenital heart disease, Dr. Ariane J. Marelli and her associates reported in a poster at the meeting. The estimates showed a slight preponderance of adults with congenital heart disease, compared with children, and also a slight preponderance of women and girls with congenital heart disease, compared with men and boys.
"The growing public health importance of congenital heart disease across the life span emphasizes the need for a public health surveillance infrastructure in the United States," wrote Dr. Marelli, a cardiologist and director of the Adult Unit for Congenital Heart Diseases at McGill University in Montreal, and her associates. "These estimates should inform future planning and organization to ensure a medical work force trained to provide optimal specialized care to individuals with congenital heart disease throughout childhood, adolescence, and mature adulthood."
Dr. Marelli and her associates created the Quebec Congenital Heart Disease database by combining data from three province-wide administrative data bases (Circulation 2007;115:163-72). They then applied the congenital heart disease prevalence numbers from Quebec in 2000 to the U.S. population in 2010 by making several extrapolations and adjustments and by using U.S. population statistics collected by the 2010 Census. The adjustments included projecting prevalence and severity levels from 2000 to 2010, and taking into account racial and ethnic differences between Quebec and the United States.
Dr. Marelli said that she had no disclosures.
CHICAGO – Roughly 2 million American children and adults are living with a congenital heart disease.
The estimate is based on congenital heart disease rates in Quebec during 2000 and extrapolated to the 2010 U.S. population. The estimates project that roughly one million of these are American children, aged 17 years or younger, and 1 million are adults, and that about 12% of these patients have severe congenital heart disease, Dr. Ariane J. Marelli and her associates reported in a poster at the meeting. The estimates showed a slight preponderance of adults with congenital heart disease, compared with children, and also a slight preponderance of women and girls with congenital heart disease, compared with men and boys.
"The growing public health importance of congenital heart disease across the life span emphasizes the need for a public health surveillance infrastructure in the United States," wrote Dr. Marelli, a cardiologist and director of the Adult Unit for Congenital Heart Diseases at McGill University in Montreal, and her associates. "These estimates should inform future planning and organization to ensure a medical work force trained to provide optimal specialized care to individuals with congenital heart disease throughout childhood, adolescence, and mature adulthood."
Dr. Marelli and her associates created the Quebec Congenital Heart Disease database by combining data from three province-wide administrative data bases (Circulation 2007;115:163-72). They then applied the congenital heart disease prevalence numbers from Quebec in 2000 to the U.S. population in 2010 by making several extrapolations and adjustments and by using U.S. population statistics collected by the 2010 Census. The adjustments included projecting prevalence and severity levels from 2000 to 2010, and taking into account racial and ethnic differences between Quebec and the United States.
Dr. Marelli said that she had no disclosures.
FROM THE ANNUAL SCIENTIFC SESSION OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: About 2 million American adults and children were living with a congenital heart disease as of 2010.
Data Source: The estimate came from the observed prevalence of congenital heart diseases in Quebec in 2000 and extrapolating to U.S. data in the 2010 Census.
Disclosures: Dr. Marelli said that she had no disclosures.
Two More Clopidogrel Resistance Genes Found
CHICAGO – A novel genomic analysis technique known as exome analysis has pinpointed two previously unsuspected genes strongly related to platelet reactivity in patients on clopidogrel.
A hoped-for practical outcome from this finding is development of a rapid test for clopidogrel responsiveness. Before undergoing percutaneous coronary intervention, a swab could be run through a patient’s mouth and a quick analysis of the genetic sample would indicate whether clopidogrel would be an effective antiplatelet agent in that individual. Current assays require patients to already be on clopidogrel, which may or may not be providing them protection.

Dr. Matthew J. Price, director of the cardiac catheterization laboratory at the Scripps Clinic, La Jolla, Calif. presented the findings of the Genotype Information and Functional Testing Exome (GIFT EXOME) study, in which he and his coworkers performed whole exome analysis on genetic material obtained from 192 self-identified white participants in the earlier GRAVITAS (Gauging Responsiveness with A VerifyNow P2Y12 assay – Impact on Thrombosis And Safety) trial. That study, for which Dr. Price served as principal investigator, showed no benefit for double-dose clopidogrel in patients with high on-treatment platelet reactivity after percutaneous coronary intervention (JAMA 2011;305:1097-105).
In GIFT EXOME, three distinct genes were found to be associated with on-treatment platelet reactivity 12-24 hours post-PCI in patients taking clopidogrel. One of them, CYP2C18/9, was already known to be associated with platelet resistance to clopidogrel, although variants in this gene explain only a small portion of the overall variability in clopidogrel response. The finding of the other two genes, ATP2B2 and TIAM2, came as a surprise.
The ATP2B2 gene codes for a plasma membrane calcium transporting ATPase. It exports calcium ions out of the cell, so it plays a critical role in maintaining intracellular calcium homeostasis, thereby influencing platelet activation and aggregation, the cardiologist explained at the annual meeting of the American College of Cardiology.
TIAM2 (T-cell lymphoma invasion and metastasis 2) is the primary mediator of activation of a protein called Rac1, which is involved in platelet aggregation.
"These findings are preliminary, but identification of two genes critical to platelet function among the 21,000 genes we sequenced lends credibility to the validity of the result," Dr. Price observed.
The overall frequency of the ATP2B2 variant linked to platelet activity in the presence of clopidogrel is 27% in the white population, while for the key TIAM2 variant it’s about 13%, he said.
The next step in the GIFT EXOME project is to validate the results in more than 1,000 patients, an effort already underway.
As an aside, eight subjects in GIFT EXOME turned out to have genomes inconsistent with white race and were excluded from the study.
Whole exome analysis entails sequencing the entire protein-coding regions of the human genome. This high-powered technique identifies both single nucleotide polymorphisms and insertion/deletions. Exome analysis is far more likely to identify specific gene mutations that are causative of disease than is the older, widely utilized method of genome-wide association studies, which basically points investigators toward what Dr. Price calls "zip codes" of interest along the genome without zeroing in on specific culprit genes.
He said that the major challenge posed by whole exome analysis is the enormous computational muscle required. More than 400 days of serial supercomputer time went into analyzing the samples from 192 GIFT EXOME participants. In excess of 6.1 million single nucleotide polymorphisms and more than 500,000 insertion/deletions were detected. Computers are getting ever faster, though, and the reagents required for exome sequencing are getting more affordable, he noted.
The GIFT EXOME study was supported by Bristol-Myers Squibb/Sanofi. Dr. Price reported serving as a consultant to those companies and more than half a dozen others. He also holds an equity interest in Iverson Genetics.
CHICAGO – A novel genomic analysis technique known as exome analysis has pinpointed two previously unsuspected genes strongly related to platelet reactivity in patients on clopidogrel.
A hoped-for practical outcome from this finding is development of a rapid test for clopidogrel responsiveness. Before undergoing percutaneous coronary intervention, a swab could be run through a patient’s mouth and a quick analysis of the genetic sample would indicate whether clopidogrel would be an effective antiplatelet agent in that individual. Current assays require patients to already be on clopidogrel, which may or may not be providing them protection.
Dr. Matthew J. Price, director of the cardiac catheterization laboratory at the Scripps Clinic, La Jolla, Calif. presented the findings of the Genotype Information and Functional Testing Exome (GIFT EXOME) study, in which he and his coworkers performed whole exome analysis on genetic material obtained from 192 self-identified white participants in the earlier GRAVITAS (Gauging Responsiveness with A VerifyNow P2Y12 assay – Impact on Thrombosis And Safety) trial. That study, for which Dr. Price served as principal investigator, showed no benefit for double-dose clopidogrel in patients with high on-treatment platelet reactivity after percutaneous coronary intervention (JAMA 2011;305:1097-105).
In GIFT EXOME, three distinct genes were found to be associated with on-treatment platelet reactivity 12-24 hours post-PCI in patients taking clopidogrel. One of them, CYP2C18/9, was already known to be associated with platelet resistance to clopidogrel, although variants in this gene explain only a small portion of the overall variability in clopidogrel response. The finding of the other two genes, ATP2B2 and TIAM2, came as a surprise.
The ATP2B2 gene codes for a plasma membrane calcium transporting ATPase. It exports calcium ions out of the cell, so it plays a critical role in maintaining intracellular calcium homeostasis, thereby influencing platelet activation and aggregation, the cardiologist explained at the annual meeting of the American College of Cardiology.
TIAM2 (T-cell lymphoma invasion and metastasis 2) is the primary mediator of activation of a protein called Rac1, which is involved in platelet aggregation.
"These findings are preliminary, but identification of two genes critical to platelet function among the 21,000 genes we sequenced lends credibility to the validity of the result," Dr. Price observed.
The overall frequency of the ATP2B2 variant linked to platelet activity in the presence of clopidogrel is 27% in the white population, while for the key TIAM2 variant it’s about 13%, he said.
The next step in the GIFT EXOME project is to validate the results in more than 1,000 patients, an effort already underway.
As an aside, eight subjects in GIFT EXOME turned out to have genomes inconsistent with white race and were excluded from the study.
Whole exome analysis entails sequencing the entire protein-coding regions of the human genome. This high-powered technique identifies both single nucleotide polymorphisms and insertion/deletions. Exome analysis is far more likely to identify specific gene mutations that are causative of disease than is the older, widely utilized method of genome-wide association studies, which basically points investigators toward what Dr. Price calls "zip codes" of interest along the genome without zeroing in on specific culprit genes.
He said that the major challenge posed by whole exome analysis is the enormous computational muscle required. More than 400 days of serial supercomputer time went into analyzing the samples from 192 GIFT EXOME participants. In excess of 6.1 million single nucleotide polymorphisms and more than 500,000 insertion/deletions were detected. Computers are getting ever faster, though, and the reagents required for exome sequencing are getting more affordable, he noted.
The GIFT EXOME study was supported by Bristol-Myers Squibb/Sanofi. Dr. Price reported serving as a consultant to those companies and more than half a dozen others. He also holds an equity interest in Iverson Genetics.
CHICAGO – A novel genomic analysis technique known as exome analysis has pinpointed two previously unsuspected genes strongly related to platelet reactivity in patients on clopidogrel.
A hoped-for practical outcome from this finding is development of a rapid test for clopidogrel responsiveness. Before undergoing percutaneous coronary intervention, a swab could be run through a patient’s mouth and a quick analysis of the genetic sample would indicate whether clopidogrel would be an effective antiplatelet agent in that individual. Current assays require patients to already be on clopidogrel, which may or may not be providing them protection.
Dr. Matthew J. Price, director of the cardiac catheterization laboratory at the Scripps Clinic, La Jolla, Calif. presented the findings of the Genotype Information and Functional Testing Exome (GIFT EXOME) study, in which he and his coworkers performed whole exome analysis on genetic material obtained from 192 self-identified white participants in the earlier GRAVITAS (Gauging Responsiveness with A VerifyNow P2Y12 assay – Impact on Thrombosis And Safety) trial. That study, for which Dr. Price served as principal investigator, showed no benefit for double-dose clopidogrel in patients with high on-treatment platelet reactivity after percutaneous coronary intervention (JAMA 2011;305:1097-105).
In GIFT EXOME, three distinct genes were found to be associated with on-treatment platelet reactivity 12-24 hours post-PCI in patients taking clopidogrel. One of them, CYP2C18/9, was already known to be associated with platelet resistance to clopidogrel, although variants in this gene explain only a small portion of the overall variability in clopidogrel response. The finding of the other two genes, ATP2B2 and TIAM2, came as a surprise.
The ATP2B2 gene codes for a plasma membrane calcium transporting ATPase. It exports calcium ions out of the cell, so it plays a critical role in maintaining intracellular calcium homeostasis, thereby influencing platelet activation and aggregation, the cardiologist explained at the annual meeting of the American College of Cardiology.
TIAM2 (T-cell lymphoma invasion and metastasis 2) is the primary mediator of activation of a protein called Rac1, which is involved in platelet aggregation.
"These findings are preliminary, but identification of two genes critical to platelet function among the 21,000 genes we sequenced lends credibility to the validity of the result," Dr. Price observed.
The overall frequency of the ATP2B2 variant linked to platelet activity in the presence of clopidogrel is 27% in the white population, while for the key TIAM2 variant it’s about 13%, he said.
The next step in the GIFT EXOME project is to validate the results in more than 1,000 patients, an effort already underway.
As an aside, eight subjects in GIFT EXOME turned out to have genomes inconsistent with white race and were excluded from the study.
Whole exome analysis entails sequencing the entire protein-coding regions of the human genome. This high-powered technique identifies both single nucleotide polymorphisms and insertion/deletions. Exome analysis is far more likely to identify specific gene mutations that are causative of disease than is the older, widely utilized method of genome-wide association studies, which basically points investigators toward what Dr. Price calls "zip codes" of interest along the genome without zeroing in on specific culprit genes.
He said that the major challenge posed by whole exome analysis is the enormous computational muscle required. More than 400 days of serial supercomputer time went into analyzing the samples from 192 GIFT EXOME participants. In excess of 6.1 million single nucleotide polymorphisms and more than 500,000 insertion/deletions were detected. Computers are getting ever faster, though, and the reagents required for exome sequencing are getting more affordable, he noted.
The GIFT EXOME study was supported by Bristol-Myers Squibb/Sanofi. Dr. Price reported serving as a consultant to those companies and more than half a dozen others. He also holds an equity interest in Iverson Genetics.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: The overall frequency of the ATP2B2 variant linked to platelet activity in the presence of clopidogrel is 27% in the white population, while for the key TIAM2 variant it’s about 13%.
Data Source: Genetic material was obtained from 192 self-identified whites in the GRAVITAS trial to perform the Genotype Information and Functional Testing Exome (GIFT EXOME) study.
Disclosures: The GIFT EXOME study was supported by Bristol-Myers Squibb/Sanofi. Dr. Price reported serving as a consultant to those companies and more than half a dozen others. He also holds an equity interest in Iverson Genetics.
ISSUE-3: Pacemaker Prevents Neurally Mediated Fainting
CHICAGO – Implantation of a dual-chamber pacemaker effectively reduced fainting episodes in carefully selected patients with neurally mediated syncope, according to the findings of the International Study on Syncope of Uncertain Etiology-3.
"We think that after ISSUE-3, the efficacy of pacing is established and that no other randomized trials will be performed in this field to replicate the results," Dr. Michele Brignole, director of cardiology at Hospital del Tigullio in Lavagna, Italy, declared at the annual meeting of the American College of Cardiology.

ISSUE-3 was a randomized, double-blind, prospective clinical trial conducted in Europe and Canada. The study tested a specific management strategy for neurally mediated syncope (NMS) that relied upon placement of an implantable loop recorder (ILD) to document asystole as the cause of a syncopal event. Only patients with ILD documentation of a lengthy asystole were eligible to receive a pacemaker, and even then, only if they met additional clinical criteria.
Two prior clinical trials failed to show benefit for pacemaker implantation in patients with NMS. ISSUE-3 succeeded where the others failed for two reasons, in Dr. Brignole’s view: the strategy of documenting a syncopal episode with an ILD, and careful patient selection. The prior studies put pacemakers in unselected patients with NMS.
"I strongly recommend not putting in a pacemaker without documentation of the syncopal mechanism as asystole. If you don’t put in an ILD you’ll come back to the negative result of the other trials," the electrophysiologist said.
In ISSUE-3, 77 patients received a dual-chamber pacemaker and were randomized in double-blind fashion to pacemaker on or off. The primary endpoint was the occurrence of a first syncopal event during 2 years of follow-up. The rate was 25% in the pacemaker-on group, compared with 57% among those with the pacemaker off. The observed 32% absolute reduction in syncope and 57% relative reduction in syncope with pacemaker therapy were highly significant, he said.
The clinical criteria employed to define the population benefiting from pacemaker therapy included older age: Participants had to be more than 40 years old, since younger patients with NMS often experience a prodrome that enables them to head off fainting episodes through physical counter-pressure maneuvers. Indeed, the ISSUE-3 population averaged 63 years of age, with an 8-year history of NMS.
Study participants also had to have severe syncope that adversely affected their quality of life, with three or more episodes in the 2 years prior to enrollment. Most patients lacked premonitory symptoms, thus exposing them to a high risk of injury from falls. Other diseases, including carotid disease and aortic disease, were carefully ruled out.
During the screening phase of the study, 511 patients received an ILD. During up to 2 years of follow-up, an ECG-documented syncopal event occurred in 158 patients – 56% of the events were the result of asystole. Patients with syncope involving asystole lasting longer than 3 seconds or with nonsyncopal asystole for longer than 6 seconds were eligible for pacemaker implantation. The average length of asystole in study participants was 11 seconds.
Based upon this and earlier studies, Dr. Brignole estimated that 9% of patients with NMS meet the ISSUE-3 criteria for an ILD. Roughly 18% of ILD recipients would qualify for pacemaker therapy within 1 year, and 40% would qualify within 4 years.
In this select group, the number needed to treat with a pacemaker to avoid one syncopal episode in 2 years is three, he added.
Noting that one-quarter of ISSUE-3 participants experienced a syncopal event despite having their pacemaker turned on, Dr. Brignole said that the next step in the study will be a subgroup analysis to identify those patients most and least likely to benefit from this invasive device therapy.
The ISSUE-3 trial was funded by Medtronic. Dr. Brignole reported having no financial conflicts.
ISSUE-3 is an important study because it convincingly establishes pacemaker therapy in carefully selected patients as the first-ever treatment of proven effectiveness for neurally mediated syncope.
We’ve got a lot of people out there fainting three, four, five times a year. It’s a real problem, and I think the ISSUE-3 strategy is a very good one. It’s what I would do anyway as a clinician, but prior to this study I was doing so against the evidence of the previous randomized trials.
Dr. Rick A. Nishimura is ACC annual scientific session program committee cochair and professor of medicine at the Mayo Medical School in Rochester, Minn.
ISSUE-3 is an important study because it convincingly establishes pacemaker therapy in carefully selected patients as the first-ever treatment of proven effectiveness for neurally mediated syncope.
We’ve got a lot of people out there fainting three, four, five times a year. It’s a real problem, and I think the ISSUE-3 strategy is a very good one. It’s what I would do anyway as a clinician, but prior to this study I was doing so against the evidence of the previous randomized trials.
Dr. Rick A. Nishimura is ACC annual scientific session program committee cochair and professor of medicine at the Mayo Medical School in Rochester, Minn.
ISSUE-3 is an important study because it convincingly establishes pacemaker therapy in carefully selected patients as the first-ever treatment of proven effectiveness for neurally mediated syncope.
We’ve got a lot of people out there fainting three, four, five times a year. It’s a real problem, and I think the ISSUE-3 strategy is a very good one. It’s what I would do anyway as a clinician, but prior to this study I was doing so against the evidence of the previous randomized trials.
Dr. Rick A. Nishimura is ACC annual scientific session program committee cochair and professor of medicine at the Mayo Medical School in Rochester, Minn.
CHICAGO – Implantation of a dual-chamber pacemaker effectively reduced fainting episodes in carefully selected patients with neurally mediated syncope, according to the findings of the International Study on Syncope of Uncertain Etiology-3.
"We think that after ISSUE-3, the efficacy of pacing is established and that no other randomized trials will be performed in this field to replicate the results," Dr. Michele Brignole, director of cardiology at Hospital del Tigullio in Lavagna, Italy, declared at the annual meeting of the American College of Cardiology.
ISSUE-3 was a randomized, double-blind, prospective clinical trial conducted in Europe and Canada. The study tested a specific management strategy for neurally mediated syncope (NMS) that relied upon placement of an implantable loop recorder (ILD) to document asystole as the cause of a syncopal event. Only patients with ILD documentation of a lengthy asystole were eligible to receive a pacemaker, and even then, only if they met additional clinical criteria.
Two prior clinical trials failed to show benefit for pacemaker implantation in patients with NMS. ISSUE-3 succeeded where the others failed for two reasons, in Dr. Brignole’s view: the strategy of documenting a syncopal episode with an ILD, and careful patient selection. The prior studies put pacemakers in unselected patients with NMS.
"I strongly recommend not putting in a pacemaker without documentation of the syncopal mechanism as asystole. If you don’t put in an ILD you’ll come back to the negative result of the other trials," the electrophysiologist said.
In ISSUE-3, 77 patients received a dual-chamber pacemaker and were randomized in double-blind fashion to pacemaker on or off. The primary endpoint was the occurrence of a first syncopal event during 2 years of follow-up. The rate was 25% in the pacemaker-on group, compared with 57% among those with the pacemaker off. The observed 32% absolute reduction in syncope and 57% relative reduction in syncope with pacemaker therapy were highly significant, he said.
The clinical criteria employed to define the population benefiting from pacemaker therapy included older age: Participants had to be more than 40 years old, since younger patients with NMS often experience a prodrome that enables them to head off fainting episodes through physical counter-pressure maneuvers. Indeed, the ISSUE-3 population averaged 63 years of age, with an 8-year history of NMS.
Study participants also had to have severe syncope that adversely affected their quality of life, with three or more episodes in the 2 years prior to enrollment. Most patients lacked premonitory symptoms, thus exposing them to a high risk of injury from falls. Other diseases, including carotid disease and aortic disease, were carefully ruled out.
During the screening phase of the study, 511 patients received an ILD. During up to 2 years of follow-up, an ECG-documented syncopal event occurred in 158 patients – 56% of the events were the result of asystole. Patients with syncope involving asystole lasting longer than 3 seconds or with nonsyncopal asystole for longer than 6 seconds were eligible for pacemaker implantation. The average length of asystole in study participants was 11 seconds.
Based upon this and earlier studies, Dr. Brignole estimated that 9% of patients with NMS meet the ISSUE-3 criteria for an ILD. Roughly 18% of ILD recipients would qualify for pacemaker therapy within 1 year, and 40% would qualify within 4 years.
In this select group, the number needed to treat with a pacemaker to avoid one syncopal episode in 2 years is three, he added.
Noting that one-quarter of ISSUE-3 participants experienced a syncopal event despite having their pacemaker turned on, Dr. Brignole said that the next step in the study will be a subgroup analysis to identify those patients most and least likely to benefit from this invasive device therapy.
The ISSUE-3 trial was funded by Medtronic. Dr. Brignole reported having no financial conflicts.
CHICAGO – Implantation of a dual-chamber pacemaker effectively reduced fainting episodes in carefully selected patients with neurally mediated syncope, according to the findings of the International Study on Syncope of Uncertain Etiology-3.
"We think that after ISSUE-3, the efficacy of pacing is established and that no other randomized trials will be performed in this field to replicate the results," Dr. Michele Brignole, director of cardiology at Hospital del Tigullio in Lavagna, Italy, declared at the annual meeting of the American College of Cardiology.
ISSUE-3 was a randomized, double-blind, prospective clinical trial conducted in Europe and Canada. The study tested a specific management strategy for neurally mediated syncope (NMS) that relied upon placement of an implantable loop recorder (ILD) to document asystole as the cause of a syncopal event. Only patients with ILD documentation of a lengthy asystole were eligible to receive a pacemaker, and even then, only if they met additional clinical criteria.
Two prior clinical trials failed to show benefit for pacemaker implantation in patients with NMS. ISSUE-3 succeeded where the others failed for two reasons, in Dr. Brignole’s view: the strategy of documenting a syncopal episode with an ILD, and careful patient selection. The prior studies put pacemakers in unselected patients with NMS.
"I strongly recommend not putting in a pacemaker without documentation of the syncopal mechanism as asystole. If you don’t put in an ILD you’ll come back to the negative result of the other trials," the electrophysiologist said.
In ISSUE-3, 77 patients received a dual-chamber pacemaker and were randomized in double-blind fashion to pacemaker on or off. The primary endpoint was the occurrence of a first syncopal event during 2 years of follow-up. The rate was 25% in the pacemaker-on group, compared with 57% among those with the pacemaker off. The observed 32% absolute reduction in syncope and 57% relative reduction in syncope with pacemaker therapy were highly significant, he said.
The clinical criteria employed to define the population benefiting from pacemaker therapy included older age: Participants had to be more than 40 years old, since younger patients with NMS often experience a prodrome that enables them to head off fainting episodes through physical counter-pressure maneuvers. Indeed, the ISSUE-3 population averaged 63 years of age, with an 8-year history of NMS.
Study participants also had to have severe syncope that adversely affected their quality of life, with three or more episodes in the 2 years prior to enrollment. Most patients lacked premonitory symptoms, thus exposing them to a high risk of injury from falls. Other diseases, including carotid disease and aortic disease, were carefully ruled out.
During the screening phase of the study, 511 patients received an ILD. During up to 2 years of follow-up, an ECG-documented syncopal event occurred in 158 patients – 56% of the events were the result of asystole. Patients with syncope involving asystole lasting longer than 3 seconds or with nonsyncopal asystole for longer than 6 seconds were eligible for pacemaker implantation. The average length of asystole in study participants was 11 seconds.
Based upon this and earlier studies, Dr. Brignole estimated that 9% of patients with NMS meet the ISSUE-3 criteria for an ILD. Roughly 18% of ILD recipients would qualify for pacemaker therapy within 1 year, and 40% would qualify within 4 years.
In this select group, the number needed to treat with a pacemaker to avoid one syncopal episode in 2 years is three, he added.
Noting that one-quarter of ISSUE-3 participants experienced a syncopal event despite having their pacemaker turned on, Dr. Brignole said that the next step in the study will be a subgroup analysis to identify those patients most and least likely to benefit from this invasive device therapy.
The ISSUE-3 trial was funded by Medtronic. Dr. Brignole reported having no financial conflicts.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: Three carefully selected patients with neurally mediated syncope need to be treated with dual-chamber pacemaker therapy to prevent one syncopal episode in 2 years.
Data Source: In the randomized, double-blind, placebo-controlled, prospective, multicenter ISSUE-3 trial, 511 patients received an implantable loop recorder, 77 of whom received a dual-chamber pacemaker.
Disclosures: ISSUE-3 was supported by Medtronic. Dr. Brignole reported having no financial conflicts.
Renal Denervation Outcomes for Resistant Hypertension Persist at 3 Years
CHICAGO – Selective renal denervation for the treatment of resistant hypertension continues to rack up impressively large and durable blood pressure reductions and a solid safety profile 3 years post-procedure, according to the latest update from the Symplicity HTN-1 study, an open-label, uncontrolled investigation.
At baseline the 153 participants in the study conducted in Australia, the United States, and Europe had a mean office blood pressure of 175/98 mm Hg, despite being on an average of 5.1 antihypertensive medications. At 36 months post-denervation they maintained an average in-office blood pressure reduction of -33/-19 mm Hg, according to Dr. Paul A. Sobotka, professor of medicine at Ohio State University, Columbus.

The response rate rose over time. One month post-denervation, 31% of HTN-1 participants were nonresponders as defined by failure to reduce their office systolic blood pressure by at least 10 mm Hg compared to baseline. By 1 year follow-up, the nonresponder rate had fallen to 21%. At 2 years, it was 10%. And at 36 months it was zero.
In other words, the response rate climbed from 69% at 1 month to 100% at 3 years. Thus, it would be premature to repeat renal denervation or switch to alternative therapy because of blood pressure nonresponse at 6 months, the cardiologist said.
"The assumption had been that nonresponse represented inadequate treatment related either to the device or to the operator. That would not appear to be the case at this time. I assume that the nonresponder rate is primarily related to a patient-based characteristic. But so far, we can identify no patient characteristic or drug characteristic that predicts early nonresponse and later response. It’s a wonderful area to look into further," he continued.
The blood pressure reduction was similar regardless of patient age, diabetes status, or baseline renal function.
"What’s particularly gratifying to me is that elderly patients seem to have a significant reduction in systolic blood pressure and narrowing of pulse pressure. To the extent that [elevations of these parameters] are risk factors for the development of cerebrovascular disease, this therapy may have particular value in the elderly population," Dr. Sobotka noted.
With regard to long-term safety, there have been no hypotensive events requiring hospitalization and no change over time in mean electrolyte levels or estimated glomerular filtration rate.

"The absence of a significant reduction in eGFR in the presence of a 30 mm Hg decrease in systolic blood pressure is virtually unheralded in hypertension therapy. One would have expected that the reduction in blood pressure should have been accompanied by a significant reduction in eGFR, which was not seen. The eGFR looks to be stable over 3 years," Dr. Sobotka observed.
Bilateral selective renal denervation is a minimally invasive endovascular procedure targeting the sympathetic nerves running to and from the kidney. It is made possible by the fact that the renal afferent and efferent sympathetic nerves are located in the adventitia of the renal artery wall, well within reach of radiofrequency energy delivered by a special catheter.
Chronic activation of renal sympathetic outflow is a prominent feature in untreated essential hypertension. Animal studies have demonstrated that severing the renal sympathetic nerves reverses or prevents hypertension.
An estimated 15%-20% of patients diagnosed with hypertension are classified as having treatment-resistant hypertension as defined by a systolic blood pressure of at least 160 mm Hg despite three or more antihypertensive drugs.
The mean procedure time was 38 minutes, with an average of four radiofrequency ablations per artery delivered by the proprietary Medtronic Symplicity renal denervation system. Intravenous narcotics and sedatives were used for pain during ablation. Minor complications occurred in 4 of 153 patients. These consisted of three minor access site complications and one renal artery dissection that occurred prior to ablation and was stented with no further consequences.
In response to audience questions about the possibility of nerve sprouting eventually limiting the effectiveness of renal denervation, Dr. Sobotka said that studies in kidney transplant recipients indicate that while there is some regrowth of efferent fibers with partial neurologic activity, the outbound afferent fibers have little or no ability to reconnect.
"We haven’t reexamined neurologic function of the kidneys post-denervation. That needs to be looked at. But to give a pedestrian response, I’d say the blood pressure response is so significant that it’s hard to imagine that something at a neurologic level has regrown that has any clinical importance," the cardiologist explained.
The Symplicity HTN-1 study was an open-label and uncontrolled. In contrast, the Simplicity HTN-2 study features a randomized prospective crossover design. The 6-month results of HTN-2 have been published (Lancet 2010;376:1903-9). At the Chicago ACC meeting, HTN-2 chief investigator Dr. Murray Esler presented the 1-year findings, focusing on the 35 control subjects who crossed over to renal denervation after 6 months of usual care.
The control subjects had a baseline blood pressure of 178/98 mm Hg despite being on an average of five antihypertensive drugs. After 6 months of usual care, their blood pressure had increased to 190/100 mm Hg. But 6 months after undergoing the ablation procedure, their average office blood pressure was 166/92 mm Hg.
One patient was hospitalized for post-procedure hypotension. This individual was treated with intravenous fluids and a reduction in antihypertensive medication and was discharged without further incident. Such occurrences have been quite rare among the roughly 4,000 patients treated worldwide to date, according to Dr. Esler, associated director of the Baker IDI Heart and Diabetes Institute, Melbourne.
Two patients in the control arm had a total of three hypertensive episodes requiring hospitalization during the 6-month usual care phase prior to crossover to renal denervation.
"These patients, of course, ended up as very good treatment responders," he said.
These severe hypertensive episodes while on usual care, along with the natural tendency of blood pressure to rise from baseline to crossover in the control group despite medication, underscore the potential costs in delaying renal denervation, Dr. Esler commented.
A pivotal Phase-3 Symplicity HTN-3 trial is underway in the United States, where renal denervation remains investigational. The study, led by Dr. George Bakris, president of the American Society of Hypertension and professor of medicine at the University of Chicago, involves more than 500 patients with resistant hypertension. It features a blinded crossover study design. The Symplicity system is commercially available in Australia, Europe, and Asia.
Dr. Sobotka is a paid advisor to Medtronic. Dr. Esler has received research grants from and is a paid consultant to Medtronic and Ardian.
CHICAGO – Selective renal denervation for the treatment of resistant hypertension continues to rack up impressively large and durable blood pressure reductions and a solid safety profile 3 years post-procedure, according to the latest update from the Symplicity HTN-1 study, an open-label, uncontrolled investigation.
At baseline the 153 participants in the study conducted in Australia, the United States, and Europe had a mean office blood pressure of 175/98 mm Hg, despite being on an average of 5.1 antihypertensive medications. At 36 months post-denervation they maintained an average in-office blood pressure reduction of -33/-19 mm Hg, according to Dr. Paul A. Sobotka, professor of medicine at Ohio State University, Columbus.
The response rate rose over time. One month post-denervation, 31% of HTN-1 participants were nonresponders as defined by failure to reduce their office systolic blood pressure by at least 10 mm Hg compared to baseline. By 1 year follow-up, the nonresponder rate had fallen to 21%. At 2 years, it was 10%. And at 36 months it was zero.
In other words, the response rate climbed from 69% at 1 month to 100% at 3 years. Thus, it would be premature to repeat renal denervation or switch to alternative therapy because of blood pressure nonresponse at 6 months, the cardiologist said.
"The assumption had been that nonresponse represented inadequate treatment related either to the device or to the operator. That would not appear to be the case at this time. I assume that the nonresponder rate is primarily related to a patient-based characteristic. But so far, we can identify no patient characteristic or drug characteristic that predicts early nonresponse and later response. It’s a wonderful area to look into further," he continued.
The blood pressure reduction was similar regardless of patient age, diabetes status, or baseline renal function.
"What’s particularly gratifying to me is that elderly patients seem to have a significant reduction in systolic blood pressure and narrowing of pulse pressure. To the extent that [elevations of these parameters] are risk factors for the development of cerebrovascular disease, this therapy may have particular value in the elderly population," Dr. Sobotka noted.
With regard to long-term safety, there have been no hypotensive events requiring hospitalization and no change over time in mean electrolyte levels or estimated glomerular filtration rate.
"The absence of a significant reduction in eGFR in the presence of a 30 mm Hg decrease in systolic blood pressure is virtually unheralded in hypertension therapy. One would have expected that the reduction in blood pressure should have been accompanied by a significant reduction in eGFR, which was not seen. The eGFR looks to be stable over 3 years," Dr. Sobotka observed.
Bilateral selective renal denervation is a minimally invasive endovascular procedure targeting the sympathetic nerves running to and from the kidney. It is made possible by the fact that the renal afferent and efferent sympathetic nerves are located in the adventitia of the renal artery wall, well within reach of radiofrequency energy delivered by a special catheter.
Chronic activation of renal sympathetic outflow is a prominent feature in untreated essential hypertension. Animal studies have demonstrated that severing the renal sympathetic nerves reverses or prevents hypertension.
An estimated 15%-20% of patients diagnosed with hypertension are classified as having treatment-resistant hypertension as defined by a systolic blood pressure of at least 160 mm Hg despite three or more antihypertensive drugs.
The mean procedure time was 38 minutes, with an average of four radiofrequency ablations per artery delivered by the proprietary Medtronic Symplicity renal denervation system. Intravenous narcotics and sedatives were used for pain during ablation. Minor complications occurred in 4 of 153 patients. These consisted of three minor access site complications and one renal artery dissection that occurred prior to ablation and was stented with no further consequences.
In response to audience questions about the possibility of nerve sprouting eventually limiting the effectiveness of renal denervation, Dr. Sobotka said that studies in kidney transplant recipients indicate that while there is some regrowth of efferent fibers with partial neurologic activity, the outbound afferent fibers have little or no ability to reconnect.
"We haven’t reexamined neurologic function of the kidneys post-denervation. That needs to be looked at. But to give a pedestrian response, I’d say the blood pressure response is so significant that it’s hard to imagine that something at a neurologic level has regrown that has any clinical importance," the cardiologist explained.
The Symplicity HTN-1 study was an open-label and uncontrolled. In contrast, the Simplicity HTN-2 study features a randomized prospective crossover design. The 6-month results of HTN-2 have been published (Lancet 2010;376:1903-9). At the Chicago ACC meeting, HTN-2 chief investigator Dr. Murray Esler presented the 1-year findings, focusing on the 35 control subjects who crossed over to renal denervation after 6 months of usual care.
The control subjects had a baseline blood pressure of 178/98 mm Hg despite being on an average of five antihypertensive drugs. After 6 months of usual care, their blood pressure had increased to 190/100 mm Hg. But 6 months after undergoing the ablation procedure, their average office blood pressure was 166/92 mm Hg.
One patient was hospitalized for post-procedure hypotension. This individual was treated with intravenous fluids and a reduction in antihypertensive medication and was discharged without further incident. Such occurrences have been quite rare among the roughly 4,000 patients treated worldwide to date, according to Dr. Esler, associated director of the Baker IDI Heart and Diabetes Institute, Melbourne.
Two patients in the control arm had a total of three hypertensive episodes requiring hospitalization during the 6-month usual care phase prior to crossover to renal denervation.
"These patients, of course, ended up as very good treatment responders," he said.
These severe hypertensive episodes while on usual care, along with the natural tendency of blood pressure to rise from baseline to crossover in the control group despite medication, underscore the potential costs in delaying renal denervation, Dr. Esler commented.
A pivotal Phase-3 Symplicity HTN-3 trial is underway in the United States, where renal denervation remains investigational. The study, led by Dr. George Bakris, president of the American Society of Hypertension and professor of medicine at the University of Chicago, involves more than 500 patients with resistant hypertension. It features a blinded crossover study design. The Symplicity system is commercially available in Australia, Europe, and Asia.
Dr. Sobotka is a paid advisor to Medtronic. Dr. Esler has received research grants from and is a paid consultant to Medtronic and Ardian.
CHICAGO – Selective renal denervation for the treatment of resistant hypertension continues to rack up impressively large and durable blood pressure reductions and a solid safety profile 3 years post-procedure, according to the latest update from the Symplicity HTN-1 study, an open-label, uncontrolled investigation.
At baseline the 153 participants in the study conducted in Australia, the United States, and Europe had a mean office blood pressure of 175/98 mm Hg, despite being on an average of 5.1 antihypertensive medications. At 36 months post-denervation they maintained an average in-office blood pressure reduction of -33/-19 mm Hg, according to Dr. Paul A. Sobotka, professor of medicine at Ohio State University, Columbus.
The response rate rose over time. One month post-denervation, 31% of HTN-1 participants were nonresponders as defined by failure to reduce their office systolic blood pressure by at least 10 mm Hg compared to baseline. By 1 year follow-up, the nonresponder rate had fallen to 21%. At 2 years, it was 10%. And at 36 months it was zero.
In other words, the response rate climbed from 69% at 1 month to 100% at 3 years. Thus, it would be premature to repeat renal denervation or switch to alternative therapy because of blood pressure nonresponse at 6 months, the cardiologist said.
"The assumption had been that nonresponse represented inadequate treatment related either to the device or to the operator. That would not appear to be the case at this time. I assume that the nonresponder rate is primarily related to a patient-based characteristic. But so far, we can identify no patient characteristic or drug characteristic that predicts early nonresponse and later response. It’s a wonderful area to look into further," he continued.
The blood pressure reduction was similar regardless of patient age, diabetes status, or baseline renal function.
"What’s particularly gratifying to me is that elderly patients seem to have a significant reduction in systolic blood pressure and narrowing of pulse pressure. To the extent that [elevations of these parameters] are risk factors for the development of cerebrovascular disease, this therapy may have particular value in the elderly population," Dr. Sobotka noted.
With regard to long-term safety, there have been no hypotensive events requiring hospitalization and no change over time in mean electrolyte levels or estimated glomerular filtration rate.
"The absence of a significant reduction in eGFR in the presence of a 30 mm Hg decrease in systolic blood pressure is virtually unheralded in hypertension therapy. One would have expected that the reduction in blood pressure should have been accompanied by a significant reduction in eGFR, which was not seen. The eGFR looks to be stable over 3 years," Dr. Sobotka observed.
Bilateral selective renal denervation is a minimally invasive endovascular procedure targeting the sympathetic nerves running to and from the kidney. It is made possible by the fact that the renal afferent and efferent sympathetic nerves are located in the adventitia of the renal artery wall, well within reach of radiofrequency energy delivered by a special catheter.
Chronic activation of renal sympathetic outflow is a prominent feature in untreated essential hypertension. Animal studies have demonstrated that severing the renal sympathetic nerves reverses or prevents hypertension.
An estimated 15%-20% of patients diagnosed with hypertension are classified as having treatment-resistant hypertension as defined by a systolic blood pressure of at least 160 mm Hg despite three or more antihypertensive drugs.
The mean procedure time was 38 minutes, with an average of four radiofrequency ablations per artery delivered by the proprietary Medtronic Symplicity renal denervation system. Intravenous narcotics and sedatives were used for pain during ablation. Minor complications occurred in 4 of 153 patients. These consisted of three minor access site complications and one renal artery dissection that occurred prior to ablation and was stented with no further consequences.
In response to audience questions about the possibility of nerve sprouting eventually limiting the effectiveness of renal denervation, Dr. Sobotka said that studies in kidney transplant recipients indicate that while there is some regrowth of efferent fibers with partial neurologic activity, the outbound afferent fibers have little or no ability to reconnect.
"We haven’t reexamined neurologic function of the kidneys post-denervation. That needs to be looked at. But to give a pedestrian response, I’d say the blood pressure response is so significant that it’s hard to imagine that something at a neurologic level has regrown that has any clinical importance," the cardiologist explained.
The Symplicity HTN-1 study was an open-label and uncontrolled. In contrast, the Simplicity HTN-2 study features a randomized prospective crossover design. The 6-month results of HTN-2 have been published (Lancet 2010;376:1903-9). At the Chicago ACC meeting, HTN-2 chief investigator Dr. Murray Esler presented the 1-year findings, focusing on the 35 control subjects who crossed over to renal denervation after 6 months of usual care.
The control subjects had a baseline blood pressure of 178/98 mm Hg despite being on an average of five antihypertensive drugs. After 6 months of usual care, their blood pressure had increased to 190/100 mm Hg. But 6 months after undergoing the ablation procedure, their average office blood pressure was 166/92 mm Hg.
One patient was hospitalized for post-procedure hypotension. This individual was treated with intravenous fluids and a reduction in antihypertensive medication and was discharged without further incident. Such occurrences have been quite rare among the roughly 4,000 patients treated worldwide to date, according to Dr. Esler, associated director of the Baker IDI Heart and Diabetes Institute, Melbourne.
Two patients in the control arm had a total of three hypertensive episodes requiring hospitalization during the 6-month usual care phase prior to crossover to renal denervation.
"These patients, of course, ended up as very good treatment responders," he said.
These severe hypertensive episodes while on usual care, along with the natural tendency of blood pressure to rise from baseline to crossover in the control group despite medication, underscore the potential costs in delaying renal denervation, Dr. Esler commented.
A pivotal Phase-3 Symplicity HTN-3 trial is underway in the United States, where renal denervation remains investigational. The study, led by Dr. George Bakris, president of the American Society of Hypertension and professor of medicine at the University of Chicago, involves more than 500 patients with resistant hypertension. It features a blinded crossover study design. The Symplicity system is commercially available in Australia, Europe, and Asia.
Dr. Sobotka is a paid advisor to Medtronic. Dr. Esler has received research grants from and is a paid consultant to Medtronic and Ardian.
FROM THE ANNUAL SCIENTIFIC SESSION OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: At baseline the 153 participants had a mean office blood pressure of 175/98 mm Hg despite being on an average of 5.1 antihypertensive medications. At 36 months post-denervation they maintained an average in-office blood pressure reduction of -33/-19 mm Hg.
Data Source: Findings from Symplicity HTN-1 are based on an open-label, uncontrolled study. One-year data from a controlled, crossover study were also reported.
Disclosures: Dr. Sobotka is a paid advisor to Medtronic. Dr. Esler has received research grants from and is a paid consultant to Medtronic and Ardian.
Renal Disease Hypertension Goal Reset Below 140/90
CHICAGO – A U.S. foundation that makes recommendations for the management of patients with chronic kidney disease recently set a blood pressure goal of less than 140/90 mm Hg for these patients, upping the target from the 130/80 mm Hg level established in 2003 by the seventh report of the Joint National Committee on Prevention, Detection, and Evaluation, and Treatment of High Blood Pressure (JNC 7) (Hypertension 2003;42:1206-52).
The new goal, made by a panel assembled by the Kidney Disease: Improving Global Outcomes (KDIGO) foundation, will appear in a journal article within the next few weeks, Dr. George L. Bakris said at the meeting.

"We knew when we wrote JNC7 that a target systolic blood pressure of less than 130 mm Hg was not that defensible, but a number of us were concerned that if we set a higher target, most physicians would be content with 145 mm Hg; that’s what drove setting 130 mm Hg," said Dr. Bakris, a member of the JNC 7 writing group, as well as a member of the panel that wrote the new KDIGO guidelines.
Clear-cut, albeit limited, evidence from randomized, controlled trials addresses the appropriate target systolic blood pressure in patients with chronic kidney disease. Three controlled studies addressed the issue, none included patients with diabetic nephropathy, and all three enrolled patients with stage 3 chronic kidney disease, defined as a glomerular filtration rate of 30-59 mL/min per 1.73 m2.
For example, results from the REIN (Ramipril Efficacy in Nephropathy)-2 trial showed that intensive blood pressure lowering to less than 130/80 mm Hg was no more effective than was treatment to a conventional target, diastolic pressure less than 90 mm Hg, for preventing progression of patients to end-stage renal disease (Lancet 2005;365:939-46). And results from AASK (African-American Study of Kidney Disease and Hypertension) showed that intensive blood pressure reduction produced no improvement in the outcome of lost renal function, end-stage renal disease, or death compared with conventional blood pressure control (JAMA 2002;288:2421-31).
A recent observational study had similar findings. Results from the Kidney Early Evaluation Program showed that in more than 16,000 American adults with kidney disease, patients with a baseline systolic blood pressure of less than 130 mm Hg did no better than did patients with a baseline pressure of 130-139 mm Hg for progression to end-stage renal disease during 3 years of follow-up (Arch. Int. Med. 2012;172:41-7).
These results show that you "don’t need to get the [blood pressure] numbers down to the floor to get benefit," said Dr. Bakris, who is a professor of medicine and director of the hypertension center at the University of Chicago.
"A goal of less than 140/90 mm Hg is for everyone with chronic kidney disease, including patients with proteinuria. That may be a little surprising, but the evidence [supporting a lower goal in patients with proteinuria] is soft. This doesn’t mean that you can’t go lower than 130 mm Hg, but the evidence doesn’t really support it."
In addition, while ACE inhibitors and angiotensin-receptor blockers (ARBs) are "definitely indicated" as primary antihypertensive agents for patients with kidney disease, "there is no evidence that using these two classes in combination in patients with advanced kidney disease or in normotensive patients with kidney disease will change the natural history of the disease. The evidence that a combination of an ACE inhibitor and an ARB will reduce proteinuria is pretty good, but we don’t know whether that will lead to benefit in terms of slowing progression," Dr. Bakris said.
Dr. Bakris said that he has received research grants from Forest, Novartis, and Relypsa, that he has been a consultant to Takeda, Servier, Abbott, CVRx, Johnson & Johnson, and Eli Lilly, and that he has been a speaker for Takeda and Novartis.
CHICAGO – A U.S. foundation that makes recommendations for the management of patients with chronic kidney disease recently set a blood pressure goal of less than 140/90 mm Hg for these patients, upping the target from the 130/80 mm Hg level established in 2003 by the seventh report of the Joint National Committee on Prevention, Detection, and Evaluation, and Treatment of High Blood Pressure (JNC 7) (Hypertension 2003;42:1206-52).
The new goal, made by a panel assembled by the Kidney Disease: Improving Global Outcomes (KDIGO) foundation, will appear in a journal article within the next few weeks, Dr. George L. Bakris said at the meeting.
"We knew when we wrote JNC7 that a target systolic blood pressure of less than 130 mm Hg was not that defensible, but a number of us were concerned that if we set a higher target, most physicians would be content with 145 mm Hg; that’s what drove setting 130 mm Hg," said Dr. Bakris, a member of the JNC 7 writing group, as well as a member of the panel that wrote the new KDIGO guidelines.
Clear-cut, albeit limited, evidence from randomized, controlled trials addresses the appropriate target systolic blood pressure in patients with chronic kidney disease. Three controlled studies addressed the issue, none included patients with diabetic nephropathy, and all three enrolled patients with stage 3 chronic kidney disease, defined as a glomerular filtration rate of 30-59 mL/min per 1.73 m2.
For example, results from the REIN (Ramipril Efficacy in Nephropathy)-2 trial showed that intensive blood pressure lowering to less than 130/80 mm Hg was no more effective than was treatment to a conventional target, diastolic pressure less than 90 mm Hg, for preventing progression of patients to end-stage renal disease (Lancet 2005;365:939-46). And results from AASK (African-American Study of Kidney Disease and Hypertension) showed that intensive blood pressure reduction produced no improvement in the outcome of lost renal function, end-stage renal disease, or death compared with conventional blood pressure control (JAMA 2002;288:2421-31).
A recent observational study had similar findings. Results from the Kidney Early Evaluation Program showed that in more than 16,000 American adults with kidney disease, patients with a baseline systolic blood pressure of less than 130 mm Hg did no better than did patients with a baseline pressure of 130-139 mm Hg for progression to end-stage renal disease during 3 years of follow-up (Arch. Int. Med. 2012;172:41-7).
These results show that you "don’t need to get the [blood pressure] numbers down to the floor to get benefit," said Dr. Bakris, who is a professor of medicine and director of the hypertension center at the University of Chicago.
"A goal of less than 140/90 mm Hg is for everyone with chronic kidney disease, including patients with proteinuria. That may be a little surprising, but the evidence [supporting a lower goal in patients with proteinuria] is soft. This doesn’t mean that you can’t go lower than 130 mm Hg, but the evidence doesn’t really support it."
In addition, while ACE inhibitors and angiotensin-receptor blockers (ARBs) are "definitely indicated" as primary antihypertensive agents for patients with kidney disease, "there is no evidence that using these two classes in combination in patients with advanced kidney disease or in normotensive patients with kidney disease will change the natural history of the disease. The evidence that a combination of an ACE inhibitor and an ARB will reduce proteinuria is pretty good, but we don’t know whether that will lead to benefit in terms of slowing progression," Dr. Bakris said.
Dr. Bakris said that he has received research grants from Forest, Novartis, and Relypsa, that he has been a consultant to Takeda, Servier, Abbott, CVRx, Johnson & Johnson, and Eli Lilly, and that he has been a speaker for Takeda and Novartis.
CHICAGO – A U.S. foundation that makes recommendations for the management of patients with chronic kidney disease recently set a blood pressure goal of less than 140/90 mm Hg for these patients, upping the target from the 130/80 mm Hg level established in 2003 by the seventh report of the Joint National Committee on Prevention, Detection, and Evaluation, and Treatment of High Blood Pressure (JNC 7) (Hypertension 2003;42:1206-52).
The new goal, made by a panel assembled by the Kidney Disease: Improving Global Outcomes (KDIGO) foundation, will appear in a journal article within the next few weeks, Dr. George L. Bakris said at the meeting.
"We knew when we wrote JNC7 that a target systolic blood pressure of less than 130 mm Hg was not that defensible, but a number of us were concerned that if we set a higher target, most physicians would be content with 145 mm Hg; that’s what drove setting 130 mm Hg," said Dr. Bakris, a member of the JNC 7 writing group, as well as a member of the panel that wrote the new KDIGO guidelines.
Clear-cut, albeit limited, evidence from randomized, controlled trials addresses the appropriate target systolic blood pressure in patients with chronic kidney disease. Three controlled studies addressed the issue, none included patients with diabetic nephropathy, and all three enrolled patients with stage 3 chronic kidney disease, defined as a glomerular filtration rate of 30-59 mL/min per 1.73 m2.
For example, results from the REIN (Ramipril Efficacy in Nephropathy)-2 trial showed that intensive blood pressure lowering to less than 130/80 mm Hg was no more effective than was treatment to a conventional target, diastolic pressure less than 90 mm Hg, for preventing progression of patients to end-stage renal disease (Lancet 2005;365:939-46). And results from AASK (African-American Study of Kidney Disease and Hypertension) showed that intensive blood pressure reduction produced no improvement in the outcome of lost renal function, end-stage renal disease, or death compared with conventional blood pressure control (JAMA 2002;288:2421-31).
A recent observational study had similar findings. Results from the Kidney Early Evaluation Program showed that in more than 16,000 American adults with kidney disease, patients with a baseline systolic blood pressure of less than 130 mm Hg did no better than did patients with a baseline pressure of 130-139 mm Hg for progression to end-stage renal disease during 3 years of follow-up (Arch. Int. Med. 2012;172:41-7).
These results show that you "don’t need to get the [blood pressure] numbers down to the floor to get benefit," said Dr. Bakris, who is a professor of medicine and director of the hypertension center at the University of Chicago.
"A goal of less than 140/90 mm Hg is for everyone with chronic kidney disease, including patients with proteinuria. That may be a little surprising, but the evidence [supporting a lower goal in patients with proteinuria] is soft. This doesn’t mean that you can’t go lower than 130 mm Hg, but the evidence doesn’t really support it."
In addition, while ACE inhibitors and angiotensin-receptor blockers (ARBs) are "definitely indicated" as primary antihypertensive agents for patients with kidney disease, "there is no evidence that using these two classes in combination in patients with advanced kidney disease or in normotensive patients with kidney disease will change the natural history of the disease. The evidence that a combination of an ACE inhibitor and an ARB will reduce proteinuria is pretty good, but we don’t know whether that will lead to benefit in terms of slowing progression," Dr. Bakris said.
Dr. Bakris said that he has received research grants from Forest, Novartis, and Relypsa, that he has been a consultant to Takeda, Servier, Abbott, CVRx, Johnson & Johnson, and Eli Lilly, and that he has been a speaker for Takeda and Novartis.
EXPERT OPINION FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Rapid Rise in Systolic BP Midlife Predicts Greater LVMI
CHICAGO – The rate of increase in systolic blood pressure during an adult’s 30s, 40s, and 50s is a stronger predictor of later structural heart damage than is their absolute blood pressure.
This finding from the longest-running birth cohort study in the United Kingdom – now entering its 66th year of follow-up – has major implications for how high blood pressure is approached, according to Dr. Arjun K. Ghosh, a cardiologist at the National Heart and Lung Institute, Imperial College London.
"At the moment, if patients don’t reach that certain magic level of high blood pressure, they’re often not treated. They’re asked to come back, and a watch-and-wait policy is instituted," he noted at the annual meeting of the American College of Cardiology. "What we found in our study, in measuring people’s blood pressure from their 30s on, was that those with a faster rise in blood pressure had a heavier heart, or increased left ventricular mass, when they were 60-64 years of age. And this was true for any level of blood pressure, high or low. It actually wasn’t how high the blood pressure became as it was how quickly the blood pressure was rising."
A second key finding was that left ventricular hypertrophy was not reversed among hypertensive study participants whose blood pressure was normalized via medication. These patients had a significantly greater left ventricular mass indexed to body surface area (LVMI) as did their peers who had the same normal-range blood pressure but had never been treated for hypertension.
"This policy of watching and waiting for the blood pressure to cross a certain threshold before starting antihypertensive therapy may be waiting too long. The irreversible damage has already been done," Dr. Ghosh continued. "A new approach may be required. We need to identify those individuals whose blood pressure rises the fastest and target them with the most effective treatment."
His analysis involved 1,653 participants who were in the Medical Research Council National Survey of Health and Development and were born in Britain in a single week in March 1946. Subjects were followed serially, and underwent echocardiography and LVMI measurement at age 60-64.
The higher a subject’s systolic blood pressure at age 36, 43, 53, or 60-64, the greater the LVMI at age 60-64.
Moreover, individuals with well controlled blood pressure on antihypertensive therapy at age 60-64 had a mean LVMI that was 8.6 g/m2 greater than that of subjects not on treatment. Participants on antihypertensive therapy at age 53 had a mean LVMI that was 7.3 g/m2 higher than in those who weren’t, and individuals on treatment at age 43 had a mean LVMI at age 60-64 that was 11.5 g/m2 more than in those not on treatment at age 43.
A sharp increase in blood pressure between ages 43 and 53 was particularly detrimental for LV size at age 60-64. An increase of 1 standard deviation in systolic blood pressure during that time period was associated with a 4 g/m2 higher LVMI, whereas an increase of 1 standard deviation between ages 36 and 43 was associated with a 1 g/m2 increase.
As this was an observational study, a clinical trial needs to be conducted before the findings can be translated into a change in practice. This study would compare the watch-and-wait strategy of threshold-based antihypertensive therapy with this novel approach stressing early identification and treatment of patients with rapidly increased systolic blood pressure, Dr. Ghosh said. Such a study is eminently feasible and could yield results in about 5 years using as the end point change in left ventricular size, which is well-established as a key driver of heart failure.
This new concept that the trajectory at which blood pressure rises has an irreversible adverse impact on cardiac structure is quite plausible, according to Dr. Joanne Foody.
"I think the real kernel is there needs to be more ongoing monitoring, particularly in young adults, so we don’t miss that window," she said in an interview.
The challenge is that young people leave their pediatricians and, except for injuries or acute illnesses, may not see a physician again until they’re in their 40s, observed Dr. Foody, medical director of the cardiovascular wellness program at Brigham and Women’s Hospital, Boston.
"We need to do more for people and do it earlier. People don’t really start thinking about preventive health until they’re in their 40s and 50s," she said.
The study was sponsored by the U.K.’s Medical Research Council. Dr. Ghosh and Dr. Foody reported having no financial conflicts.
CHICAGO – The rate of increase in systolic blood pressure during an adult’s 30s, 40s, and 50s is a stronger predictor of later structural heart damage than is their absolute blood pressure.
This finding from the longest-running birth cohort study in the United Kingdom – now entering its 66th year of follow-up – has major implications for how high blood pressure is approached, according to Dr. Arjun K. Ghosh, a cardiologist at the National Heart and Lung Institute, Imperial College London.
"At the moment, if patients don’t reach that certain magic level of high blood pressure, they’re often not treated. They’re asked to come back, and a watch-and-wait policy is instituted," he noted at the annual meeting of the American College of Cardiology. "What we found in our study, in measuring people’s blood pressure from their 30s on, was that those with a faster rise in blood pressure had a heavier heart, or increased left ventricular mass, when they were 60-64 years of age. And this was true for any level of blood pressure, high or low. It actually wasn’t how high the blood pressure became as it was how quickly the blood pressure was rising."
A second key finding was that left ventricular hypertrophy was not reversed among hypertensive study participants whose blood pressure was normalized via medication. These patients had a significantly greater left ventricular mass indexed to body surface area (LVMI) as did their peers who had the same normal-range blood pressure but had never been treated for hypertension.
"This policy of watching and waiting for the blood pressure to cross a certain threshold before starting antihypertensive therapy may be waiting too long. The irreversible damage has already been done," Dr. Ghosh continued. "A new approach may be required. We need to identify those individuals whose blood pressure rises the fastest and target them with the most effective treatment."
His analysis involved 1,653 participants who were in the Medical Research Council National Survey of Health and Development and were born in Britain in a single week in March 1946. Subjects were followed serially, and underwent echocardiography and LVMI measurement at age 60-64.
The higher a subject’s systolic blood pressure at age 36, 43, 53, or 60-64, the greater the LVMI at age 60-64.
Moreover, individuals with well controlled blood pressure on antihypertensive therapy at age 60-64 had a mean LVMI that was 8.6 g/m2 greater than that of subjects not on treatment. Participants on antihypertensive therapy at age 53 had a mean LVMI that was 7.3 g/m2 higher than in those who weren’t, and individuals on treatment at age 43 had a mean LVMI at age 60-64 that was 11.5 g/m2 more than in those not on treatment at age 43.
A sharp increase in blood pressure between ages 43 and 53 was particularly detrimental for LV size at age 60-64. An increase of 1 standard deviation in systolic blood pressure during that time period was associated with a 4 g/m2 higher LVMI, whereas an increase of 1 standard deviation between ages 36 and 43 was associated with a 1 g/m2 increase.
As this was an observational study, a clinical trial needs to be conducted before the findings can be translated into a change in practice. This study would compare the watch-and-wait strategy of threshold-based antihypertensive therapy with this novel approach stressing early identification and treatment of patients with rapidly increased systolic blood pressure, Dr. Ghosh said. Such a study is eminently feasible and could yield results in about 5 years using as the end point change in left ventricular size, which is well-established as a key driver of heart failure.
This new concept that the trajectory at which blood pressure rises has an irreversible adverse impact on cardiac structure is quite plausible, according to Dr. Joanne Foody.
"I think the real kernel is there needs to be more ongoing monitoring, particularly in young adults, so we don’t miss that window," she said in an interview.
The challenge is that young people leave their pediatricians and, except for injuries or acute illnesses, may not see a physician again until they’re in their 40s, observed Dr. Foody, medical director of the cardiovascular wellness program at Brigham and Women’s Hospital, Boston.
"We need to do more for people and do it earlier. People don’t really start thinking about preventive health until they’re in their 40s and 50s," she said.
The study was sponsored by the U.K.’s Medical Research Council. Dr. Ghosh and Dr. Foody reported having no financial conflicts.
CHICAGO – The rate of increase in systolic blood pressure during an adult’s 30s, 40s, and 50s is a stronger predictor of later structural heart damage than is their absolute blood pressure.
This finding from the longest-running birth cohort study in the United Kingdom – now entering its 66th year of follow-up – has major implications for how high blood pressure is approached, according to Dr. Arjun K. Ghosh, a cardiologist at the National Heart and Lung Institute, Imperial College London.
"At the moment, if patients don’t reach that certain magic level of high blood pressure, they’re often not treated. They’re asked to come back, and a watch-and-wait policy is instituted," he noted at the annual meeting of the American College of Cardiology. "What we found in our study, in measuring people’s blood pressure from their 30s on, was that those with a faster rise in blood pressure had a heavier heart, or increased left ventricular mass, when they were 60-64 years of age. And this was true for any level of blood pressure, high or low. It actually wasn’t how high the blood pressure became as it was how quickly the blood pressure was rising."
A second key finding was that left ventricular hypertrophy was not reversed among hypertensive study participants whose blood pressure was normalized via medication. These patients had a significantly greater left ventricular mass indexed to body surface area (LVMI) as did their peers who had the same normal-range blood pressure but had never been treated for hypertension.
"This policy of watching and waiting for the blood pressure to cross a certain threshold before starting antihypertensive therapy may be waiting too long. The irreversible damage has already been done," Dr. Ghosh continued. "A new approach may be required. We need to identify those individuals whose blood pressure rises the fastest and target them with the most effective treatment."
His analysis involved 1,653 participants who were in the Medical Research Council National Survey of Health and Development and were born in Britain in a single week in March 1946. Subjects were followed serially, and underwent echocardiography and LVMI measurement at age 60-64.
The higher a subject’s systolic blood pressure at age 36, 43, 53, or 60-64, the greater the LVMI at age 60-64.
Moreover, individuals with well controlled blood pressure on antihypertensive therapy at age 60-64 had a mean LVMI that was 8.6 g/m2 greater than that of subjects not on treatment. Participants on antihypertensive therapy at age 53 had a mean LVMI that was 7.3 g/m2 higher than in those who weren’t, and individuals on treatment at age 43 had a mean LVMI at age 60-64 that was 11.5 g/m2 more than in those not on treatment at age 43.
A sharp increase in blood pressure between ages 43 and 53 was particularly detrimental for LV size at age 60-64. An increase of 1 standard deviation in systolic blood pressure during that time period was associated with a 4 g/m2 higher LVMI, whereas an increase of 1 standard deviation between ages 36 and 43 was associated with a 1 g/m2 increase.
As this was an observational study, a clinical trial needs to be conducted before the findings can be translated into a change in practice. This study would compare the watch-and-wait strategy of threshold-based antihypertensive therapy with this novel approach stressing early identification and treatment of patients with rapidly increased systolic blood pressure, Dr. Ghosh said. Such a study is eminently feasible and could yield results in about 5 years using as the end point change in left ventricular size, which is well-established as a key driver of heart failure.
This new concept that the trajectory at which blood pressure rises has an irreversible adverse impact on cardiac structure is quite plausible, according to Dr. Joanne Foody.
"I think the real kernel is there needs to be more ongoing monitoring, particularly in young adults, so we don’t miss that window," she said in an interview.
The challenge is that young people leave their pediatricians and, except for injuries or acute illnesses, may not see a physician again until they’re in their 40s, observed Dr. Foody, medical director of the cardiovascular wellness program at Brigham and Women’s Hospital, Boston.
"We need to do more for people and do it earlier. People don’t really start thinking about preventive health until they’re in their 40s and 50s," she said.
The study was sponsored by the U.K.’s Medical Research Council. Dr. Ghosh and Dr. Foody reported having no financial conflicts.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: The rate of increase in blood pressure in early midlife is a better predictor of increased left ventricular mass at age 60-64 than is the absolute level of blood pressure during those years.
Data Source: Data are from the Medical Research Council National Survey of Health and Development, a longitudinal observational study of a large cohort of people born in Britain during the same week in March 1946.
Disclosures: The study was sponsored by the U.K.’s Medical Research Council. Dr. Ghosh and Dr. Foody reported having no financial conflicts.
Showing Patients Their Coronary Calcium Scans Motivates Adherence
CHICAGO – Patients given a look at their coronary artery calcium CT scans are more likely to undertake cardiovascular risk reduction measures.
Further, the more abnormal the coronary artery calcium (CAC) score and its corresponding cardiac CT scan, the better the subsequent patient adherence with recommended risk reduction measures. So CAC scores are useful not only for risk stratification, but also for improving adherence to measures aimed at lowering risk, according to Dr. Nove Kalia of the University of Saskatchewan, Saskatoon.

He presented two related studies showing that patients who viewed their own CAC CT scan and had an elevated CAC score were more likely to lose weight and to adhere to prescribed statin therapy. He carried out both studies at Harbor-UCLA Medical Center in Torrance, Calif.
The weight loss study included 518 subjects followed for a mean of 3 years after their initial CAC CT scan. All participants were shown their scans and the significance of their CAC score was explained to them.
Any measurable weight loss at 3 years of follow up was present in 22% of subjects with a CAC score of 0, in 36% of those with a score of 1-99, in 32% of those with a score of 100-399, and in 38% of those with a score of 400 or above.
Compared to patients with a CAC score of 0, the likelihood of weight loss was 2.0-fold greater in patients with a CAC score of 1-99, 3.6-fold greater in those with a score of 100-399, and 3.3-fold greater in patients with a CAC score of 400 or above.
The higher the CAC score, the greater the average weight loss, ranging from 5 pounds in those with a score of 1-99 to 15 pounds with a score of 400 or greater.
"I think visualizing these coronary artery calcium images may be an important means of motivating patients even in an era of economic austerity," Dr. Kalia asserted. "The extra motivation you get from visualizing these images is helpful and probably translates into reduced long-term effects of coronary artery disease."
The statin adherence study involved 2,100 patients. At a mean follow up of 3 years, responses to a comprehensive patient questionnaire revealed that 36% of patients with a CAC score of 0 were compliant with their prescribed statin therapy, as compared to 52% of those with a CAC score of 1-99, 57% with a score of 100-399, and 59% with a CAC score of 400 or greater.
Compared to those with a CAC score of 0, adherence to statin therapy was 2.0-fold greater in patients with a score of 1-99, 2.4-fold greater with a score of 100-399, and 2.6-fold greater with a score of 400 or more.
Dr. Kalia reported having no financial conflicts.
CHICAGO – Patients given a look at their coronary artery calcium CT scans are more likely to undertake cardiovascular risk reduction measures.
Further, the more abnormal the coronary artery calcium (CAC) score and its corresponding cardiac CT scan, the better the subsequent patient adherence with recommended risk reduction measures. So CAC scores are useful not only for risk stratification, but also for improving adherence to measures aimed at lowering risk, according to Dr. Nove Kalia of the University of Saskatchewan, Saskatoon.
He presented two related studies showing that patients who viewed their own CAC CT scan and had an elevated CAC score were more likely to lose weight and to adhere to prescribed statin therapy. He carried out both studies at Harbor-UCLA Medical Center in Torrance, Calif.
The weight loss study included 518 subjects followed for a mean of 3 years after their initial CAC CT scan. All participants were shown their scans and the significance of their CAC score was explained to them.
Any measurable weight loss at 3 years of follow up was present in 22% of subjects with a CAC score of 0, in 36% of those with a score of 1-99, in 32% of those with a score of 100-399, and in 38% of those with a score of 400 or above.
Compared to patients with a CAC score of 0, the likelihood of weight loss was 2.0-fold greater in patients with a CAC score of 1-99, 3.6-fold greater in those with a score of 100-399, and 3.3-fold greater in patients with a CAC score of 400 or above.
The higher the CAC score, the greater the average weight loss, ranging from 5 pounds in those with a score of 1-99 to 15 pounds with a score of 400 or greater.
"I think visualizing these coronary artery calcium images may be an important means of motivating patients even in an era of economic austerity," Dr. Kalia asserted. "The extra motivation you get from visualizing these images is helpful and probably translates into reduced long-term effects of coronary artery disease."
The statin adherence study involved 2,100 patients. At a mean follow up of 3 years, responses to a comprehensive patient questionnaire revealed that 36% of patients with a CAC score of 0 were compliant with their prescribed statin therapy, as compared to 52% of those with a CAC score of 1-99, 57% with a score of 100-399, and 59% with a CAC score of 400 or greater.
Compared to those with a CAC score of 0, adherence to statin therapy was 2.0-fold greater in patients with a score of 1-99, 2.4-fold greater with a score of 100-399, and 2.6-fold greater with a score of 400 or more.
Dr. Kalia reported having no financial conflicts.
CHICAGO – Patients given a look at their coronary artery calcium CT scans are more likely to undertake cardiovascular risk reduction measures.
Further, the more abnormal the coronary artery calcium (CAC) score and its corresponding cardiac CT scan, the better the subsequent patient adherence with recommended risk reduction measures. So CAC scores are useful not only for risk stratification, but also for improving adherence to measures aimed at lowering risk, according to Dr. Nove Kalia of the University of Saskatchewan, Saskatoon.
He presented two related studies showing that patients who viewed their own CAC CT scan and had an elevated CAC score were more likely to lose weight and to adhere to prescribed statin therapy. He carried out both studies at Harbor-UCLA Medical Center in Torrance, Calif.
The weight loss study included 518 subjects followed for a mean of 3 years after their initial CAC CT scan. All participants were shown their scans and the significance of their CAC score was explained to them.
Any measurable weight loss at 3 years of follow up was present in 22% of subjects with a CAC score of 0, in 36% of those with a score of 1-99, in 32% of those with a score of 100-399, and in 38% of those with a score of 400 or above.
Compared to patients with a CAC score of 0, the likelihood of weight loss was 2.0-fold greater in patients with a CAC score of 1-99, 3.6-fold greater in those with a score of 100-399, and 3.3-fold greater in patients with a CAC score of 400 or above.
The higher the CAC score, the greater the average weight loss, ranging from 5 pounds in those with a score of 1-99 to 15 pounds with a score of 400 or greater.
"I think visualizing these coronary artery calcium images may be an important means of motivating patients even in an era of economic austerity," Dr. Kalia asserted. "The extra motivation you get from visualizing these images is helpful and probably translates into reduced long-term effects of coronary artery disease."
The statin adherence study involved 2,100 patients. At a mean follow up of 3 years, responses to a comprehensive patient questionnaire revealed that 36% of patients with a CAC score of 0 were compliant with their prescribed statin therapy, as compared to 52% of those with a CAC score of 1-99, 57% with a score of 100-399, and 59% with a CAC score of 400 or greater.
Compared to those with a CAC score of 0, adherence to statin therapy was 2.0-fold greater in patients with a score of 1-99, 2.4-fold greater with a score of 100-399, and 2.6-fold greater with a score of 400 or more.
Dr. Kalia reported having no financial conflicts.
FROM THE ANNUAL SCIENTIFIC SESSION OF THE AMERICAN COLLEGE OF CARDIOLOGY
Major Finding: Compared to patients with a CAC score of 0, adherence to statin therapy was 2.0-fold greater in patients with a CAC score of 1-99, 2.4-fold greater with a score of 100-399, and 2.6-fold greater with a score of 400 or more.
Data Source: Data were obtained from two single-center studies conducted at Harbor-UCLA Medical Center in Torrance, Calif.
Disclosures: Dr. Kalia reported having no financial conflicts.