User login
Endocrine Society: Annual Meeting (ENDO 2013)
Control of congenital adrenal hyperplasia improves with more frequent steroid dosing
SAN FRANCISCO – Administering daily hydrocortisone prescriptions in four divided doses, instead of three, can improve control of congenital adrenal hyperplasia and obviate the need for additional steroids, British researchers found in a retrospective cross-sectional study.
A decade ago, it was assumed that children with poorly controlled moderate-to-severe disease "needed higher doses rather than more frequent dosing; if patients were not controlled on three-times-a-day dosing, we’d increase the dose. Now, we go four times a day, and don’t necessarily have to increase the dose. We see better control with QID dosing," said lead investigator Dr. Anbezhil Subbarayan, a pediatric endocrinologist at Great Ormond Street Hospital for Children in London.

His team compared 107 children under treatment there with a similar cohort treated a decade ago and found that the approach led to a reduction in mean daily hydrocortisone doses from 17.5 mg/m2 to 13.3 mg/m2 and a drop in mean daily doses of 9 alpha-fludrocortisone, administered in one or two divided doses, from 112 mcg/m2 to 102 mcg/m2.
That led to a corresponding drop in the prevalence of steroid-induced systolic hypertension from 58% of patients to 21%; a drop in diastolic hypertension prevalence from 24% to 9%; and improvement in mean body mass index standard deviation scores (BMI-SDS) from 1.57 to 0.98. The results were also published online(Clin. Endocrinol [Oxf] 2013 [doi:10.1111/cen.12265]).
"Our message" is that "patients under poor control should [try] four-times-a-day" hydrocortisone dosing. With a half-life of just 4-6 hours, spacing out hydrocortisone administration "should improve control in patients with moderate-to-severe disease without increasing the need for steroids, which can worsen cardiovascular risk factors," Dr. Subbarayan said at the Endocrine Society’s annual meeting.
"Ideally, the first hydrocortisone dose should be given at 4:00 a.m. Some parents are motivated" to do that; for those who find it impractical, "we try to encourage giving hydrocortisone first thing in the morning, maybe at 6:00 a.m." For children with mild disease, divided doses three times a day might be enough, he said.
Despite reduced steroid doses and cardiovascular risk factors, obesity and systolic hypertension remain problematic in kids with congenital adrenal hyperplasia.
The team found that 24% of their children were obese (BMI-SDS greater than 2), and that BMI-SD scores were significantly higher, compared with British children overall. The mean systolic blood pressure of 108 mm Hg (SD 13.5) was higher, as well. Differences in diastolic pressure did not reach statistical significance.
The values were assessed during annual reviews when the children were admitted to the hospital for 24 hours for serial monitoring of cortisol levels and clinical parameters, and dose adjustments. The median age in the study was 9.2 years; 64% were girls.
The authors said they have no disclosures.
SAN FRANCISCO – Administering daily hydrocortisone prescriptions in four divided doses, instead of three, can improve control of congenital adrenal hyperplasia and obviate the need for additional steroids, British researchers found in a retrospective cross-sectional study.
A decade ago, it was assumed that children with poorly controlled moderate-to-severe disease "needed higher doses rather than more frequent dosing; if patients were not controlled on three-times-a-day dosing, we’d increase the dose. Now, we go four times a day, and don’t necessarily have to increase the dose. We see better control with QID dosing," said lead investigator Dr. Anbezhil Subbarayan, a pediatric endocrinologist at Great Ormond Street Hospital for Children in London.
His team compared 107 children under treatment there with a similar cohort treated a decade ago and found that the approach led to a reduction in mean daily hydrocortisone doses from 17.5 mg/m2 to 13.3 mg/m2 and a drop in mean daily doses of 9 alpha-fludrocortisone, administered in one or two divided doses, from 112 mcg/m2 to 102 mcg/m2.
That led to a corresponding drop in the prevalence of steroid-induced systolic hypertension from 58% of patients to 21%; a drop in diastolic hypertension prevalence from 24% to 9%; and improvement in mean body mass index standard deviation scores (BMI-SDS) from 1.57 to 0.98. The results were also published online(Clin. Endocrinol [Oxf] 2013 [doi:10.1111/cen.12265]).
"Our message" is that "patients under poor control should [try] four-times-a-day" hydrocortisone dosing. With a half-life of just 4-6 hours, spacing out hydrocortisone administration "should improve control in patients with moderate-to-severe disease without increasing the need for steroids, which can worsen cardiovascular risk factors," Dr. Subbarayan said at the Endocrine Society’s annual meeting.
"Ideally, the first hydrocortisone dose should be given at 4:00 a.m. Some parents are motivated" to do that; for those who find it impractical, "we try to encourage giving hydrocortisone first thing in the morning, maybe at 6:00 a.m." For children with mild disease, divided doses three times a day might be enough, he said.
Despite reduced steroid doses and cardiovascular risk factors, obesity and systolic hypertension remain problematic in kids with congenital adrenal hyperplasia.
The team found that 24% of their children were obese (BMI-SDS greater than 2), and that BMI-SD scores were significantly higher, compared with British children overall. The mean systolic blood pressure of 108 mm Hg (SD 13.5) was higher, as well. Differences in diastolic pressure did not reach statistical significance.
The values were assessed during annual reviews when the children were admitted to the hospital for 24 hours for serial monitoring of cortisol levels and clinical parameters, and dose adjustments. The median age in the study was 9.2 years; 64% were girls.
The authors said they have no disclosures.
SAN FRANCISCO – Administering daily hydrocortisone prescriptions in four divided doses, instead of three, can improve control of congenital adrenal hyperplasia and obviate the need for additional steroids, British researchers found in a retrospective cross-sectional study.
A decade ago, it was assumed that children with poorly controlled moderate-to-severe disease "needed higher doses rather than more frequent dosing; if patients were not controlled on three-times-a-day dosing, we’d increase the dose. Now, we go four times a day, and don’t necessarily have to increase the dose. We see better control with QID dosing," said lead investigator Dr. Anbezhil Subbarayan, a pediatric endocrinologist at Great Ormond Street Hospital for Children in London.
His team compared 107 children under treatment there with a similar cohort treated a decade ago and found that the approach led to a reduction in mean daily hydrocortisone doses from 17.5 mg/m2 to 13.3 mg/m2 and a drop in mean daily doses of 9 alpha-fludrocortisone, administered in one or two divided doses, from 112 mcg/m2 to 102 mcg/m2.
That led to a corresponding drop in the prevalence of steroid-induced systolic hypertension from 58% of patients to 21%; a drop in diastolic hypertension prevalence from 24% to 9%; and improvement in mean body mass index standard deviation scores (BMI-SDS) from 1.57 to 0.98. The results were also published online(Clin. Endocrinol [Oxf] 2013 [doi:10.1111/cen.12265]).
"Our message" is that "patients under poor control should [try] four-times-a-day" hydrocortisone dosing. With a half-life of just 4-6 hours, spacing out hydrocortisone administration "should improve control in patients with moderate-to-severe disease without increasing the need for steroids, which can worsen cardiovascular risk factors," Dr. Subbarayan said at the Endocrine Society’s annual meeting.
"Ideally, the first hydrocortisone dose should be given at 4:00 a.m. Some parents are motivated" to do that; for those who find it impractical, "we try to encourage giving hydrocortisone first thing in the morning, maybe at 6:00 a.m." For children with mild disease, divided doses three times a day might be enough, he said.
Despite reduced steroid doses and cardiovascular risk factors, obesity and systolic hypertension remain problematic in kids with congenital adrenal hyperplasia.
The team found that 24% of their children were obese (BMI-SDS greater than 2), and that BMI-SD scores were significantly higher, compared with British children overall. The mean systolic blood pressure of 108 mm Hg (SD 13.5) was higher, as well. Differences in diastolic pressure did not reach statistical significance.
The values were assessed during annual reviews when the children were admitted to the hospital for 24 hours for serial monitoring of cortisol levels and clinical parameters, and dose adjustments. The median age in the study was 9.2 years; 64% were girls.
The authors said they have no disclosures.
AT ENDO 2013
Major finding: Administering daily hydrocortisone in four divided doses, instead of increasing the prescription and sticking with three divided doses, reduced the prevalence of steroid-induced systolic hypertension in children with congenital adrenal hyperplasia from 58% to 21%.
Data source: Retrospective, cross-sectional study of 107 patients.
Disclosures: The authors said they have no disclosures.

Slight cognition benefit found for testosterone gel after menopause
SAN FRANCISCO – Postmenopausal women showed a modest improvement in verbal learning and memory after being on testosterone gel for 6 months, according to researchers from Monash University in Melbourne.
Ninety healthy, cognitively normal women aged 55-65 years were randomized in the trial to 0.22 g transdermal testosterone gel (LibiGel) daily, or to placebo.
At the end of 26 weeks, women on testosterone scored 1.6 points better on the 48-point International Shopping List Task, meaning that they recalled a total of 1.6 more words while being read three lists containing 16 words each. The placebo group improved a bit from the mean baseline score of 33.7 words, as well, but not quite as much. There were no other significant differences in well-being and cognitive function.

Lead investigator Susan Davis, chair of Women’s Health at Monash, said the finding, and a few similar ones from previous work, provide "evidence for the conduct of large-scale clinical studies" to see if testosterone can help preserve cognition as women age. "Possibly, there’s a beneficial effect, but it does need to be explored."
"Women complain of loss of memory after menopause. ... We hypothesize that women after menopause are not operating in their optimum cognitive range." That could have something to do with naturally declining levels of testosterone; supplementation could be more about "optimizing normality rather than treating a disease," she said at the Endocrine Society’s annual meeting.
There’s evidence, mostly from trials in men, that the hormone has "an important role in brain function," she said.
Mean serum total testosterone was at the lower limit of normal in both groups at baseline; it increased a mean of 1.9 nmol/L in the treated group and remained largely unchanged in the placebo group. Women on systemic hormone therapy were excluded from the study.
Dr. Davis did not mention any adverse events but noted that the literature on testosterone therapy in women "has not shown anything sinister" with physiologic doses.
She was the lead investigator in a trial of 814 women that found a modest benefit for testosterone patches on libido. Breast cancer was diagnosed in four women treated for up to 2 years in the study, but none in the placebo group; vaginal bleeding was more common in the treated group, as well (N. Engl. J. Med. 2008;359:2005-17).
Dr. Davis is the principal investigator and a scientific board member for BioSante Pharmaceuticals, makers of the testosterone gel used in the study. She is also an investigator for and consultant to Trimel, maker of an intranasal testosterone gel. The work was supported by BioSante.
BioSante Pharmaceuticals,
SAN FRANCISCO – Postmenopausal women showed a modest improvement in verbal learning and memory after being on testosterone gel for 6 months, according to researchers from Monash University in Melbourne.
Ninety healthy, cognitively normal women aged 55-65 years were randomized in the trial to 0.22 g transdermal testosterone gel (LibiGel) daily, or to placebo.
At the end of 26 weeks, women on testosterone scored 1.6 points better on the 48-point International Shopping List Task, meaning that they recalled a total of 1.6 more words while being read three lists containing 16 words each. The placebo group improved a bit from the mean baseline score of 33.7 words, as well, but not quite as much. There were no other significant differences in well-being and cognitive function.
Lead investigator Susan Davis, chair of Women’s Health at Monash, said the finding, and a few similar ones from previous work, provide "evidence for the conduct of large-scale clinical studies" to see if testosterone can help preserve cognition as women age. "Possibly, there’s a beneficial effect, but it does need to be explored."
"Women complain of loss of memory after menopause. ... We hypothesize that women after menopause are not operating in their optimum cognitive range." That could have something to do with naturally declining levels of testosterone; supplementation could be more about "optimizing normality rather than treating a disease," she said at the Endocrine Society’s annual meeting.
There’s evidence, mostly from trials in men, that the hormone has "an important role in brain function," she said.
Mean serum total testosterone was at the lower limit of normal in both groups at baseline; it increased a mean of 1.9 nmol/L in the treated group and remained largely unchanged in the placebo group. Women on systemic hormone therapy were excluded from the study.
Dr. Davis did not mention any adverse events but noted that the literature on testosterone therapy in women "has not shown anything sinister" with physiologic doses.
She was the lead investigator in a trial of 814 women that found a modest benefit for testosterone patches on libido. Breast cancer was diagnosed in four women treated for up to 2 years in the study, but none in the placebo group; vaginal bleeding was more common in the treated group, as well (N. Engl. J. Med. 2008;359:2005-17).
Dr. Davis is the principal investigator and a scientific board member for BioSante Pharmaceuticals, makers of the testosterone gel used in the study. She is also an investigator for and consultant to Trimel, maker of an intranasal testosterone gel. The work was supported by BioSante.
SAN FRANCISCO – Postmenopausal women showed a modest improvement in verbal learning and memory after being on testosterone gel for 6 months, according to researchers from Monash University in Melbourne.
Ninety healthy, cognitively normal women aged 55-65 years were randomized in the trial to 0.22 g transdermal testosterone gel (LibiGel) daily, or to placebo.
At the end of 26 weeks, women on testosterone scored 1.6 points better on the 48-point International Shopping List Task, meaning that they recalled a total of 1.6 more words while being read three lists containing 16 words each. The placebo group improved a bit from the mean baseline score of 33.7 words, as well, but not quite as much. There were no other significant differences in well-being and cognitive function.
Lead investigator Susan Davis, chair of Women’s Health at Monash, said the finding, and a few similar ones from previous work, provide "evidence for the conduct of large-scale clinical studies" to see if testosterone can help preserve cognition as women age. "Possibly, there’s a beneficial effect, but it does need to be explored."
"Women complain of loss of memory after menopause. ... We hypothesize that women after menopause are not operating in their optimum cognitive range." That could have something to do with naturally declining levels of testosterone; supplementation could be more about "optimizing normality rather than treating a disease," she said at the Endocrine Society’s annual meeting.
There’s evidence, mostly from trials in men, that the hormone has "an important role in brain function," she said.
Mean serum total testosterone was at the lower limit of normal in both groups at baseline; it increased a mean of 1.9 nmol/L in the treated group and remained largely unchanged in the placebo group. Women on systemic hormone therapy were excluded from the study.
Dr. Davis did not mention any adverse events but noted that the literature on testosterone therapy in women "has not shown anything sinister" with physiologic doses.
She was the lead investigator in a trial of 814 women that found a modest benefit for testosterone patches on libido. Breast cancer was diagnosed in four women treated for up to 2 years in the study, but none in the placebo group; vaginal bleeding was more common in the treated group, as well (N. Engl. J. Med. 2008;359:2005-17).
Dr. Davis is the principal investigator and a scientific board member for BioSante Pharmaceuticals, makers of the testosterone gel used in the study. She is also an investigator for and consultant to Trimel, maker of an intranasal testosterone gel. The work was supported by BioSante.
BioSante Pharmaceuticals,
BioSante Pharmaceuticals,
AT ENDO 2013
Major finding: After 6 months of daily testosterone gel, women scored 1.57 points better on the 48-point International Shopping List Task test.
Data Source: A randomized, placebo-controlled trial in 90 postmenopausal women.
Disclosures: The lead investigator is the principal investigator and a scientific board member for BioSante Pharmaceuticals, makers of the testosterone gel used in the study. She is also an investigator for and consultant to Trimel, maker of an intranasal testosterone gel.

Pituitary tumor size not definitive for Cushing's
SAN FRANCISCO – The size of a pituitary tumor on magnetic resonance imaging in a patient with ACTH-dependent Cushing’s syndrome can’t differentiate between etiologies, but combining that information with biochemical test results could help avoid costly and difficult inferior petrosal sinus sampling in some patients, a study of 131 cases suggests.
If MRI shows a pituitary tumor larger than 6 mm in size, the finding is 40% sensitive and 96% specific for a diagnosis of Cushing’s disease as the cause of adrenocorticotropic hormone (ACTH)-dependent Cushing’s syndrome, and additional information from biochemical testing may help further differentiate this from ectopic ACTH secretion, Dr. Divya Yogi-Morren and her associates reported at the Endocrine Society’s Annual Meeting.

Pituitary tumors were seen on MRI in 6 of 26 patients with ectopic ACTH secretion (23%) and 73 of 105 patients with Cushing’s disease (69%), with mean measurements of 4.5 mm in the ectopic ACTH secretion group and 8 mm in the Cushing’s disease group. All but one tumor in the ectopic ACTH secretion group were 6 mm or smaller in diameter, but one was 14 mm.
Because pituitary "incidentalomas" as large as 14 mm can be seen in patients with ectopic ACTH secretion, the presence of a pituitary tumor can’t definitively discriminate between ectopic ACTH secretion and Cushing’s disease, said Dr. Yogi-Morren, a fellow at the Cleveland Clinic.
That finding contradicts part of a 2003 consensus statement that said the presence of a focal pituitary lesion larger than 6 mm on MRI could provide a definitive diagnosis of Cushing’s disease, with no further evaluation needed in patients who have a classic clinical presentation and dynamic biochemical testing results that are compatible with a pituitary etiology (J. Clin. Endocrinol. Metab. 2003;88:5593-602). The 6-mm cutoff, said Dr. Yogi-Morren, came from an earlier study reporting that 10% of 100 normal, healthy adults had focal pituitary abnormalities on MRI ranging from 3 to 6 mm in diameter that were consistent with a diagnosis of asymptomatic pituitary adenomas (Ann. Intern. Med. 1994;120:817-20).
A traditional workup of a patient with ACTH-dependent Cushing’s syndrome might include a clinical history, biochemical testing, neuroimaging, and an inferior petrosal sinus sampling (IPSS). Biochemical testing typically includes tests for hypokalemia, measurement of cortisol and ACTH levels, a high-dose dexamethasone suppression test, and a corticotropin-releasing hormone (CRH) stimulation test. Although IPSS is the gold standard for differentiating between the two etiologies, it is expensive and technically difficult, especially in institutions that don’t regularly do the procedure, so it would be desirable to avoid IPSS if it’s not needed in a subset of patients, Dr. Yogi-Morren said.
The investigators reviewed charts from two centers (the Cleveland Clinic and the M.D. Anderson Cancer Center, Houston) for patients with ACTH-dependent Cushing’s syndrome seen during 2000-2012.
ACTH levels were significantly different between groups, averaging 162 pg/mL (range, 58-671 pg/mL) in patients with ectopic ACTH secretion, compared with a mean 71 pg/mL in patients with Cushing’s disease (range, 16-209 pg/mL), she reported. Although there was some overlap between groups in the range of ACTH levels, all patients with an ACTH level higher than 210 pg/mL had ectopic ACTH secretion.
Median serum potassium levels at baseline were 2.9 mmol/L in the ectopic ACTH secretion group and 3.8 mmol/L in the Cushing’s disease group, a significant difference. Again, there was some overlap between groups in the range of potassium levels, but all patients with a baseline potassium level lower than 2.7 mmol/L had ectopic ACTH secretion, she said.
Among patients who underwent a high-dose dexamethasone suppression test, cortisol levels decreased by less than 50% in 88% of patients with ectopic ACTH secretion and in 26% of patients with Cushing’s disease.
Most patients did not undergo a standardized, formal CRH stimulation test, so investigators extracted the ACTH response to CRH in peripheral plasma during the IPSS test. As expected, they found a significantly higher percent increase in ACTH in response to CRH during IPSS in the Cushing’s disease group, ranging up to more than a 1,000% increase. In the ectopic ACTH secretion group, 40% of patients did have an ACTH increase greater than 50%, ranging as high as a 200%-300% increase in ACTH in a couple of patients.
"Although there was some overlap in the biochemical testing, it is possible that it provides some additional proof to differentiate between ectopic ACTH secretion and Cushing’s disease," Dr. Yogi-Morren said.
In the ectopic ACTH secretion group, the source of the secretion remained occult in seven patients. The most common identifiable cause was a bronchial carcinoid tumor, in six patients. Three patients each had small cell lung cancer, a thymic carcinoid tumor, or a pancreatic neuroendocrine tumor. One patient each had a bladder neuroendocrine tumor, ovarian endometrioid cancer, medullary thyroid cancer, or a metastatic neuroendocrine tumor from an unknown primary cancer.
The ectopic ACTH secretion group had a median age of 41 years and was 63% female. The Cushing’s disease group had a median age of 46 years and was 76% female.
Dr. Yogi-Morren reported having no financial disclosures.
[email protected]
On Twitter @sherryboschert
SAN FRANCISCO – The size of a pituitary tumor on magnetic resonance imaging in a patient with ACTH-dependent Cushing’s syndrome can’t differentiate between etiologies, but combining that information with biochemical test results could help avoid costly and difficult inferior petrosal sinus sampling in some patients, a study of 131 cases suggests.
If MRI shows a pituitary tumor larger than 6 mm in size, the finding is 40% sensitive and 96% specific for a diagnosis of Cushing’s disease as the cause of adrenocorticotropic hormone (ACTH)-dependent Cushing’s syndrome, and additional information from biochemical testing may help further differentiate this from ectopic ACTH secretion, Dr. Divya Yogi-Morren and her associates reported at the Endocrine Society’s Annual Meeting.
Pituitary tumors were seen on MRI in 6 of 26 patients with ectopic ACTH secretion (23%) and 73 of 105 patients with Cushing’s disease (69%), with mean measurements of 4.5 mm in the ectopic ACTH secretion group and 8 mm in the Cushing’s disease group. All but one tumor in the ectopic ACTH secretion group were 6 mm or smaller in diameter, but one was 14 mm.
Because pituitary "incidentalomas" as large as 14 mm can be seen in patients with ectopic ACTH secretion, the presence of a pituitary tumor can’t definitively discriminate between ectopic ACTH secretion and Cushing’s disease, said Dr. Yogi-Morren, a fellow at the Cleveland Clinic.
That finding contradicts part of a 2003 consensus statement that said the presence of a focal pituitary lesion larger than 6 mm on MRI could provide a definitive diagnosis of Cushing’s disease, with no further evaluation needed in patients who have a classic clinical presentation and dynamic biochemical testing results that are compatible with a pituitary etiology (J. Clin. Endocrinol. Metab. 2003;88:5593-602). The 6-mm cutoff, said Dr. Yogi-Morren, came from an earlier study reporting that 10% of 100 normal, healthy adults had focal pituitary abnormalities on MRI ranging from 3 to 6 mm in diameter that were consistent with a diagnosis of asymptomatic pituitary adenomas (Ann. Intern. Med. 1994;120:817-20).
A traditional workup of a patient with ACTH-dependent Cushing’s syndrome might include a clinical history, biochemical testing, neuroimaging, and an inferior petrosal sinus sampling (IPSS). Biochemical testing typically includes tests for hypokalemia, measurement of cortisol and ACTH levels, a high-dose dexamethasone suppression test, and a corticotropin-releasing hormone (CRH) stimulation test. Although IPSS is the gold standard for differentiating between the two etiologies, it is expensive and technically difficult, especially in institutions that don’t regularly do the procedure, so it would be desirable to avoid IPSS if it’s not needed in a subset of patients, Dr. Yogi-Morren said.
The investigators reviewed charts from two centers (the Cleveland Clinic and the M.D. Anderson Cancer Center, Houston) for patients with ACTH-dependent Cushing’s syndrome seen during 2000-2012.
ACTH levels were significantly different between groups, averaging 162 pg/mL (range, 58-671 pg/mL) in patients with ectopic ACTH secretion, compared with a mean 71 pg/mL in patients with Cushing’s disease (range, 16-209 pg/mL), she reported. Although there was some overlap between groups in the range of ACTH levels, all patients with an ACTH level higher than 210 pg/mL had ectopic ACTH secretion.
Median serum potassium levels at baseline were 2.9 mmol/L in the ectopic ACTH secretion group and 3.8 mmol/L in the Cushing’s disease group, a significant difference. Again, there was some overlap between groups in the range of potassium levels, but all patients with a baseline potassium level lower than 2.7 mmol/L had ectopic ACTH secretion, she said.
Among patients who underwent a high-dose dexamethasone suppression test, cortisol levels decreased by less than 50% in 88% of patients with ectopic ACTH secretion and in 26% of patients with Cushing’s disease.
Most patients did not undergo a standardized, formal CRH stimulation test, so investigators extracted the ACTH response to CRH in peripheral plasma during the IPSS test. As expected, they found a significantly higher percent increase in ACTH in response to CRH during IPSS in the Cushing’s disease group, ranging up to more than a 1,000% increase. In the ectopic ACTH secretion group, 40% of patients did have an ACTH increase greater than 50%, ranging as high as a 200%-300% increase in ACTH in a couple of patients.
"Although there was some overlap in the biochemical testing, it is possible that it provides some additional proof to differentiate between ectopic ACTH secretion and Cushing’s disease," Dr. Yogi-Morren said.
In the ectopic ACTH secretion group, the source of the secretion remained occult in seven patients. The most common identifiable cause was a bronchial carcinoid tumor, in six patients. Three patients each had small cell lung cancer, a thymic carcinoid tumor, or a pancreatic neuroendocrine tumor. One patient each had a bladder neuroendocrine tumor, ovarian endometrioid cancer, medullary thyroid cancer, or a metastatic neuroendocrine tumor from an unknown primary cancer.
The ectopic ACTH secretion group had a median age of 41 years and was 63% female. The Cushing’s disease group had a median age of 46 years and was 76% female.
Dr. Yogi-Morren reported having no financial disclosures.
[email protected]
On Twitter @sherryboschert
SAN FRANCISCO – The size of a pituitary tumor on magnetic resonance imaging in a patient with ACTH-dependent Cushing’s syndrome can’t differentiate between etiologies, but combining that information with biochemical test results could help avoid costly and difficult inferior petrosal sinus sampling in some patients, a study of 131 cases suggests.
If MRI shows a pituitary tumor larger than 6 mm in size, the finding is 40% sensitive and 96% specific for a diagnosis of Cushing’s disease as the cause of adrenocorticotropic hormone (ACTH)-dependent Cushing’s syndrome, and additional information from biochemical testing may help further differentiate this from ectopic ACTH secretion, Dr. Divya Yogi-Morren and her associates reported at the Endocrine Society’s Annual Meeting.
Pituitary tumors were seen on MRI in 6 of 26 patients with ectopic ACTH secretion (23%) and 73 of 105 patients with Cushing’s disease (69%), with mean measurements of 4.5 mm in the ectopic ACTH secretion group and 8 mm in the Cushing’s disease group. All but one tumor in the ectopic ACTH secretion group were 6 mm or smaller in diameter, but one was 14 mm.
Because pituitary "incidentalomas" as large as 14 mm can be seen in patients with ectopic ACTH secretion, the presence of a pituitary tumor can’t definitively discriminate between ectopic ACTH secretion and Cushing’s disease, said Dr. Yogi-Morren, a fellow at the Cleveland Clinic.
That finding contradicts part of a 2003 consensus statement that said the presence of a focal pituitary lesion larger than 6 mm on MRI could provide a definitive diagnosis of Cushing’s disease, with no further evaluation needed in patients who have a classic clinical presentation and dynamic biochemical testing results that are compatible with a pituitary etiology (J. Clin. Endocrinol. Metab. 2003;88:5593-602). The 6-mm cutoff, said Dr. Yogi-Morren, came from an earlier study reporting that 10% of 100 normal, healthy adults had focal pituitary abnormalities on MRI ranging from 3 to 6 mm in diameter that were consistent with a diagnosis of asymptomatic pituitary adenomas (Ann. Intern. Med. 1994;120:817-20).
A traditional workup of a patient with ACTH-dependent Cushing’s syndrome might include a clinical history, biochemical testing, neuroimaging, and an inferior petrosal sinus sampling (IPSS). Biochemical testing typically includes tests for hypokalemia, measurement of cortisol and ACTH levels, a high-dose dexamethasone suppression test, and a corticotropin-releasing hormone (CRH) stimulation test. Although IPSS is the gold standard for differentiating between the two etiologies, it is expensive and technically difficult, especially in institutions that don’t regularly do the procedure, so it would be desirable to avoid IPSS if it’s not needed in a subset of patients, Dr. Yogi-Morren said.
The investigators reviewed charts from two centers (the Cleveland Clinic and the M.D. Anderson Cancer Center, Houston) for patients with ACTH-dependent Cushing’s syndrome seen during 2000-2012.
ACTH levels were significantly different between groups, averaging 162 pg/mL (range, 58-671 pg/mL) in patients with ectopic ACTH secretion, compared with a mean 71 pg/mL in patients with Cushing’s disease (range, 16-209 pg/mL), she reported. Although there was some overlap between groups in the range of ACTH levels, all patients with an ACTH level higher than 210 pg/mL had ectopic ACTH secretion.
Median serum potassium levels at baseline were 2.9 mmol/L in the ectopic ACTH secretion group and 3.8 mmol/L in the Cushing’s disease group, a significant difference. Again, there was some overlap between groups in the range of potassium levels, but all patients with a baseline potassium level lower than 2.7 mmol/L had ectopic ACTH secretion, she said.
Among patients who underwent a high-dose dexamethasone suppression test, cortisol levels decreased by less than 50% in 88% of patients with ectopic ACTH secretion and in 26% of patients with Cushing’s disease.
Most patients did not undergo a standardized, formal CRH stimulation test, so investigators extracted the ACTH response to CRH in peripheral plasma during the IPSS test. As expected, they found a significantly higher percent increase in ACTH in response to CRH during IPSS in the Cushing’s disease group, ranging up to more than a 1,000% increase. In the ectopic ACTH secretion group, 40% of patients did have an ACTH increase greater than 50%, ranging as high as a 200%-300% increase in ACTH in a couple of patients.
"Although there was some overlap in the biochemical testing, it is possible that it provides some additional proof to differentiate between ectopic ACTH secretion and Cushing’s disease," Dr. Yogi-Morren said.
In the ectopic ACTH secretion group, the source of the secretion remained occult in seven patients. The most common identifiable cause was a bronchial carcinoid tumor, in six patients. Three patients each had small cell lung cancer, a thymic carcinoid tumor, or a pancreatic neuroendocrine tumor. One patient each had a bladder neuroendocrine tumor, ovarian endometrioid cancer, medullary thyroid cancer, or a metastatic neuroendocrine tumor from an unknown primary cancer.
The ectopic ACTH secretion group had a median age of 41 years and was 63% female. The Cushing’s disease group had a median age of 46 years and was 76% female.
Dr. Yogi-Morren reported having no financial disclosures.
[email protected]
On Twitter @sherryboschert
AT ENDO 2013
Major finding: A pituitary tumor larger than 6 mm on MRI was 40% sensitive and 96% specific for a diagnosis of Cushing’s disease as the cause of ACTH-dependent Cushing’s syndrome.
Data source: Retrospective study of 131 patients with ACTH-dependent Cushing’s syndrome, 26 from ectopic ACTH secretion and 105 from Cushing’s disease.
Disclosures: Dr. Yogi-Morren reported having no financial disclosures.

Tight glycemic control normalized thyroid function after pediatric heart surgery
SAN FRANCISCO – Tight glycemic control helps normalize thyroid hormone concentrations following cardiac surgery in children, according to results from a randomized trial presented at the Endocrine Society’s annual meeting.
That could be important because "it’s well known that cardiac surgical procedures can induce nonthyroidal illness in children" – a brief free-hormone surge followed by low T3 (triiodothyronine) and T4 (thyroxine) and increased rT3 (reverse triiodothyronine). It’s associated with longer recoveries, said lead investigator Dr. Carmen Soto-Rivera, an endocrinologist at Boston Children’s Hospital.
But it’s difficult to say what the clinical implications of her team’s findings are, she noted, because "we still don’t know if nonthyroidal illness is adaptive or maladaptive."
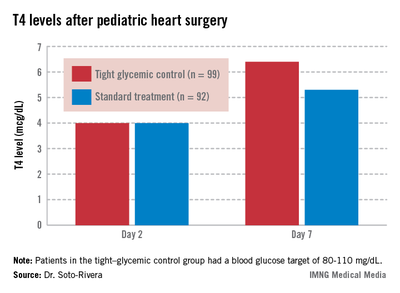
The study involved 191 children who underwent cardiac surgery with cardiopulmonary bypass. After surgery, her team randomized 99 children who were 0-36 months old to tight glycemic control, with a blood glucose target of 80-110 mg/dL; and 92 others to the standard treatment, permissive hyperglycemia; their median blood glucose hovered around 120 mg/dL.
Two days after surgery, 98% of the children had T4 and T3 levels below age-specific normal ranges, consistent with nonthyroidal illness. The thyroid hormone binding ratio (THBR) was normal in most of the patients, so it did not explain the drop in T4 and T3.
The groups had begun to separate by day 7. Tight-control patients had a higher median T4 than did patients on standard treatment (6.4 vs. 5.3 mcg/dL; P = .02) and a greater median T4 change from day 2 (2.4 vs. 1.3 mcg/dL, P = .02).
The trend continued among children still in the hospital on day 14. The 30 tight-control patients, compared with 37 on standard treatment, had a higher median T3 (104.5 vs. 74 ng/dL; P = .02) and a greater change from day 2 (26 vs. 5 ng/dL; P = .02). They had a higher T4 on day 14 too, but the difference was not significant.
"Interestingly, we found that [tight glucose control] resulted in lower [C-reactive protein] levels by day 7," about 3 mg/L, versus about 4 mg/L in the standard-treatment arm (P = .01). Perhaps "the faster increase in thyroid hormone levels may be mediated by decreased inhibition of deiodinases due to lowered inflammation," Dr. Soto-Rivera said.
The findings differ from previous reports of tight glucose control increasing peripheral inactivation of thyroid hormone, she said. "We believe that because our glucose targets were higher and we had [a low] rate of hypoglycemia in both arms, we potentially prevented a fasting response in these children," leading to decreased inhibition of the thyroid axis, she added.
"We believe that almost no one was treated with thyroid replacement during [the study], but we are in the process of confirming this," she said.
The project was a subgroup analysis of a larger trial that found no significant benefit for tight glycemic control on infection rates, mortality, length of stay, and organ failure following pediatric heart surgery (N. Engl. J. Med. 2012;367:1208-1219).
Dr. Soto-Rivera said she had no disclosures. The National Institutes of Health funded the project.
SAN FRANCISCO – Tight glycemic control helps normalize thyroid hormone concentrations following cardiac surgery in children, according to results from a randomized trial presented at the Endocrine Society’s annual meeting.
That could be important because "it’s well known that cardiac surgical procedures can induce nonthyroidal illness in children" – a brief free-hormone surge followed by low T3 (triiodothyronine) and T4 (thyroxine) and increased rT3 (reverse triiodothyronine). It’s associated with longer recoveries, said lead investigator Dr. Carmen Soto-Rivera, an endocrinologist at Boston Children’s Hospital.
But it’s difficult to say what the clinical implications of her team’s findings are, she noted, because "we still don’t know if nonthyroidal illness is adaptive or maladaptive."
The study involved 191 children who underwent cardiac surgery with cardiopulmonary bypass. After surgery, her team randomized 99 children who were 0-36 months old to tight glycemic control, with a blood glucose target of 80-110 mg/dL; and 92 others to the standard treatment, permissive hyperglycemia; their median blood glucose hovered around 120 mg/dL.
Two days after surgery, 98% of the children had T4 and T3 levels below age-specific normal ranges, consistent with nonthyroidal illness. The thyroid hormone binding ratio (THBR) was normal in most of the patients, so it did not explain the drop in T4 and T3.
The groups had begun to separate by day 7. Tight-control patients had a higher median T4 than did patients on standard treatment (6.4 vs. 5.3 mcg/dL; P = .02) and a greater median T4 change from day 2 (2.4 vs. 1.3 mcg/dL, P = .02).
The trend continued among children still in the hospital on day 14. The 30 tight-control patients, compared with 37 on standard treatment, had a higher median T3 (104.5 vs. 74 ng/dL; P = .02) and a greater change from day 2 (26 vs. 5 ng/dL; P = .02). They had a higher T4 on day 14 too, but the difference was not significant.
"Interestingly, we found that [tight glucose control] resulted in lower [C-reactive protein] levels by day 7," about 3 mg/L, versus about 4 mg/L in the standard-treatment arm (P = .01). Perhaps "the faster increase in thyroid hormone levels may be mediated by decreased inhibition of deiodinases due to lowered inflammation," Dr. Soto-Rivera said.
The findings differ from previous reports of tight glucose control increasing peripheral inactivation of thyroid hormone, she said. "We believe that because our glucose targets were higher and we had [a low] rate of hypoglycemia in both arms, we potentially prevented a fasting response in these children," leading to decreased inhibition of the thyroid axis, she added.
"We believe that almost no one was treated with thyroid replacement during [the study], but we are in the process of confirming this," she said.
The project was a subgroup analysis of a larger trial that found no significant benefit for tight glycemic control on infection rates, mortality, length of stay, and organ failure following pediatric heart surgery (N. Engl. J. Med. 2012;367:1208-1219).
Dr. Soto-Rivera said she had no disclosures. The National Institutes of Health funded the project.
SAN FRANCISCO – Tight glycemic control helps normalize thyroid hormone concentrations following cardiac surgery in children, according to results from a randomized trial presented at the Endocrine Society’s annual meeting.
That could be important because "it’s well known that cardiac surgical procedures can induce nonthyroidal illness in children" – a brief free-hormone surge followed by low T3 (triiodothyronine) and T4 (thyroxine) and increased rT3 (reverse triiodothyronine). It’s associated with longer recoveries, said lead investigator Dr. Carmen Soto-Rivera, an endocrinologist at Boston Children’s Hospital.
But it’s difficult to say what the clinical implications of her team’s findings are, she noted, because "we still don’t know if nonthyroidal illness is adaptive or maladaptive."
The study involved 191 children who underwent cardiac surgery with cardiopulmonary bypass. After surgery, her team randomized 99 children who were 0-36 months old to tight glycemic control, with a blood glucose target of 80-110 mg/dL; and 92 others to the standard treatment, permissive hyperglycemia; their median blood glucose hovered around 120 mg/dL.
Two days after surgery, 98% of the children had T4 and T3 levels below age-specific normal ranges, consistent with nonthyroidal illness. The thyroid hormone binding ratio (THBR) was normal in most of the patients, so it did not explain the drop in T4 and T3.
The groups had begun to separate by day 7. Tight-control patients had a higher median T4 than did patients on standard treatment (6.4 vs. 5.3 mcg/dL; P = .02) and a greater median T4 change from day 2 (2.4 vs. 1.3 mcg/dL, P = .02).
The trend continued among children still in the hospital on day 14. The 30 tight-control patients, compared with 37 on standard treatment, had a higher median T3 (104.5 vs. 74 ng/dL; P = .02) and a greater change from day 2 (26 vs. 5 ng/dL; P = .02). They had a higher T4 on day 14 too, but the difference was not significant.
"Interestingly, we found that [tight glucose control] resulted in lower [C-reactive protein] levels by day 7," about 3 mg/L, versus about 4 mg/L in the standard-treatment arm (P = .01). Perhaps "the faster increase in thyroid hormone levels may be mediated by decreased inhibition of deiodinases due to lowered inflammation," Dr. Soto-Rivera said.
The findings differ from previous reports of tight glucose control increasing peripheral inactivation of thyroid hormone, she said. "We believe that because our glucose targets were higher and we had [a low] rate of hypoglycemia in both arms, we potentially prevented a fasting response in these children," leading to decreased inhibition of the thyroid axis, she added.
"We believe that almost no one was treated with thyroid replacement during [the study], but we are in the process of confirming this," she said.
The project was a subgroup analysis of a larger trial that found no significant benefit for tight glycemic control on infection rates, mortality, length of stay, and organ failure following pediatric heart surgery (N. Engl. J. Med. 2012;367:1208-1219).
Dr. Soto-Rivera said she had no disclosures. The National Institutes of Health funded the project.
AT ENDO 2013
Major finding: Seven days after heart surgery, children on tight glycemic control had significantly higher median T4 levels than did children on standard treatment (6.4 vs. 5.3 mcg/dL).
Data source: Randomized trial of 191 children following heart surgery.
Disclosures: Dr. Soto-Rivera said she has no disclosures. The National Institutes of Health funded the project.
Copeptin helped differential diagnosis of hyponatremia
SAN FRANCISCO – Measuring plasma copeptin levels may provide an accurate and easier way to identify the cause of severe hyponatremia, compared with measuring arginine vasopressin levels, preliminary data on 175 patients suggested.
A plasma copeptin level greater than 70 pmol/L correlated with a diagnosis of hypovolemic or diuretic-induced hyponatremia requiring saline infusion with 91% specificity. A copeptin/urinary sodium ratio greater than 1.84 identified patients who clearly needed saline infusion with a specificity of 90%, Dr. Nicole Nigro reported at the annual meeting of the Endocrine Society.
"The differential diagnosis of hyponatremia is not easy to make" and often relies on detecting adequate or inadequate plasma levels of arginine vasopressin (AVP), she said in an interview. Blood samples for AVP measurements must be kept on ice, making handling and transportation to the lab more difficult. AVP mostly attaches to platelets, it clears rapidly, and AVP levels are known to be very unstable.

Copeptin, on the other hand, is very stable in plasma, easy to measure, and released by the body in an equimolar ratio with AVP, said Dr. Nigro of University Hospital, Basel, Switzerland.
She presented data on the first 175 patients in an ongoing study that has enrolled 290 of an expected 300 consecutive patients who present with severe hypo-osmolar hyponatremia at the emergency departments of two Swiss tertiary referral centers. All patients had a sodium level below 125 mmol/L. Three experts who were blinded to patients’ copeptin levels made the final diagnoses based on a clinical algorithm, a chart review, and response to therapy.
The median plasma copeptin level was 2.8 pmol/L in 17 patients diagnosed with primary polydipsia, 13.2 pmol/L in 45 patients with diuretic-induced hyponatremia, 13 pmol/L in 56 patients with syndrome of inappropriate antidiuretic hormone, 28 pmol/L in 25 patients with hypervolemic hyponatremia, and 55 pmol/L in 32 patients with hypovolemic hyponatremia, Dr. Nigro reported in an oral presentation and a featured poster at the meeting.
The 77 patients who required saline infusion had significantly higher copeptin levels (27 pmol/L), than patients who did not need saline (12 pmol/L).
Dr. Nigro’s hospital routinely measures copeptin levels but is not yet using them to guide the differential diagnosis of hyponatremia. If the current study produces clear findings when it’s finished, the investigators next may conduct a study that uses copeptin levels to guide treatment of patients with severe hyponatremia.
Ultimately, "copeptin may help us to guide the therapy and management of these patients with severe hyponatremia," she suggested.
Some of Dr. Nigro’s associates in the study have been speakers for B.R.A.H.M.S./Thermo Fisher Scientific. She reported having no other relevant financial disclosures.
On Twitter @sherryboschert
SAN FRANCISCO – Measuring plasma copeptin levels may provide an accurate and easier way to identify the cause of severe hyponatremia, compared with measuring arginine vasopressin levels, preliminary data on 175 patients suggested.
A plasma copeptin level greater than 70 pmol/L correlated with a diagnosis of hypovolemic or diuretic-induced hyponatremia requiring saline infusion with 91% specificity. A copeptin/urinary sodium ratio greater than 1.84 identified patients who clearly needed saline infusion with a specificity of 90%, Dr. Nicole Nigro reported at the annual meeting of the Endocrine Society.
"The differential diagnosis of hyponatremia is not easy to make" and often relies on detecting adequate or inadequate plasma levels of arginine vasopressin (AVP), she said in an interview. Blood samples for AVP measurements must be kept on ice, making handling and transportation to the lab more difficult. AVP mostly attaches to platelets, it clears rapidly, and AVP levels are known to be very unstable.
Copeptin, on the other hand, is very stable in plasma, easy to measure, and released by the body in an equimolar ratio with AVP, said Dr. Nigro of University Hospital, Basel, Switzerland.
She presented data on the first 175 patients in an ongoing study that has enrolled 290 of an expected 300 consecutive patients who present with severe hypo-osmolar hyponatremia at the emergency departments of two Swiss tertiary referral centers. All patients had a sodium level below 125 mmol/L. Three experts who were blinded to patients’ copeptin levels made the final diagnoses based on a clinical algorithm, a chart review, and response to therapy.
The median plasma copeptin level was 2.8 pmol/L in 17 patients diagnosed with primary polydipsia, 13.2 pmol/L in 45 patients with diuretic-induced hyponatremia, 13 pmol/L in 56 patients with syndrome of inappropriate antidiuretic hormone, 28 pmol/L in 25 patients with hypervolemic hyponatremia, and 55 pmol/L in 32 patients with hypovolemic hyponatremia, Dr. Nigro reported in an oral presentation and a featured poster at the meeting.
The 77 patients who required saline infusion had significantly higher copeptin levels (27 pmol/L), than patients who did not need saline (12 pmol/L).
Dr. Nigro’s hospital routinely measures copeptin levels but is not yet using them to guide the differential diagnosis of hyponatremia. If the current study produces clear findings when it’s finished, the investigators next may conduct a study that uses copeptin levels to guide treatment of patients with severe hyponatremia.
Ultimately, "copeptin may help us to guide the therapy and management of these patients with severe hyponatremia," she suggested.
Some of Dr. Nigro’s associates in the study have been speakers for B.R.A.H.M.S./Thermo Fisher Scientific. She reported having no other relevant financial disclosures.
On Twitter @sherryboschert
SAN FRANCISCO – Measuring plasma copeptin levels may provide an accurate and easier way to identify the cause of severe hyponatremia, compared with measuring arginine vasopressin levels, preliminary data on 175 patients suggested.
A plasma copeptin level greater than 70 pmol/L correlated with a diagnosis of hypovolemic or diuretic-induced hyponatremia requiring saline infusion with 91% specificity. A copeptin/urinary sodium ratio greater than 1.84 identified patients who clearly needed saline infusion with a specificity of 90%, Dr. Nicole Nigro reported at the annual meeting of the Endocrine Society.
"The differential diagnosis of hyponatremia is not easy to make" and often relies on detecting adequate or inadequate plasma levels of arginine vasopressin (AVP), she said in an interview. Blood samples for AVP measurements must be kept on ice, making handling and transportation to the lab more difficult. AVP mostly attaches to platelets, it clears rapidly, and AVP levels are known to be very unstable.
Copeptin, on the other hand, is very stable in plasma, easy to measure, and released by the body in an equimolar ratio with AVP, said Dr. Nigro of University Hospital, Basel, Switzerland.
She presented data on the first 175 patients in an ongoing study that has enrolled 290 of an expected 300 consecutive patients who present with severe hypo-osmolar hyponatremia at the emergency departments of two Swiss tertiary referral centers. All patients had a sodium level below 125 mmol/L. Three experts who were blinded to patients’ copeptin levels made the final diagnoses based on a clinical algorithm, a chart review, and response to therapy.
The median plasma copeptin level was 2.8 pmol/L in 17 patients diagnosed with primary polydipsia, 13.2 pmol/L in 45 patients with diuretic-induced hyponatremia, 13 pmol/L in 56 patients with syndrome of inappropriate antidiuretic hormone, 28 pmol/L in 25 patients with hypervolemic hyponatremia, and 55 pmol/L in 32 patients with hypovolemic hyponatremia, Dr. Nigro reported in an oral presentation and a featured poster at the meeting.
The 77 patients who required saline infusion had significantly higher copeptin levels (27 pmol/L), than patients who did not need saline (12 pmol/L).
Dr. Nigro’s hospital routinely measures copeptin levels but is not yet using them to guide the differential diagnosis of hyponatremia. If the current study produces clear findings when it’s finished, the investigators next may conduct a study that uses copeptin levels to guide treatment of patients with severe hyponatremia.
Ultimately, "copeptin may help us to guide the therapy and management of these patients with severe hyponatremia," she suggested.
Some of Dr. Nigro’s associates in the study have been speakers for B.R.A.H.M.S./Thermo Fisher Scientific. She reported having no other relevant financial disclosures.
On Twitter @sherryboschert
AT ENDO 2013
Major finding: A plasma copeptin level greater than 70 pmol/L in patients presenting with severe hypo-osmolar hyponatremia correlated with a diagnosis of hypovolemic or diuretic-induced hyponatremia requiring saline infusion with 91% specificity.
Data source: A prospective, multicenter observational study of 175 consecutive patients presenting to emergency departments at two Swiss tertiary referral centers.
Disclosures: Some of Dr. Nigro’s associates in the study have been speakers for B.R.A.H.M.S./Thermo Fisher Scientific. She reported having no other relevant financial disclosures.

Testosterone gel's pain relief modest in opioid-induced androgen deficiency
SAN FRANCISCO – Men with opioid-induced androgen deficiency had a modest improvement in two laboratory measures of pain tolerance after 14 weeks of testosterone gel treatment but no significant improvements in subjective measures of pain perception, findings from a randomized trial showed.
Thirty-six men in the study received daily 5-g applications of 1% testosterone gel, while 29 others received a placebo gel. The patients were about 50 years old on average and had been taking opioids for at least a month, mostly for back pain.

There was no statistically significant difference in overall subjective Brief Pain Inventory scores at week 14, but there was a nonsignificant trend for less pain interference with daily life among treated men and a trend on the Short Form (SF)–36 for fewer emotional problems.
In the lab, testosterone subjects had about a 5-W improvement in their toleration of a blunted pressure pin applied to their forearms, from a baseline tolerance of 27 W. Men in the placebo group had a tolerance reduction of about 5 W, from a baseline score of 19 W. That difference, and a modest improvement in thumb-pressure tolerance in the treated group, were both significant. Other trends toward greater pain tolerance in the testosterone group were not.
"Objective pain perception showed improvement in the testosterone arm," said lead investigator Dr. Shehzad Basaria, director of Boston University’s androgen clinical research unit. But that improvement trend was not seen with subjective pain perception, he noted, and the magnitude of the change was "small."
Nonetheless, "when you start an analgesic drug, laboratory pain improves before a person says he is subjectively better," Dr. Basaria said at the Endocrine Society’s annual meeting. "We need to do a larger and longer-term study to see if [the lab findings] translate into improvements in subjective" perceptions.
For now, he noted, "I would initiate testosterone replacement only for [current] indications. I would not initiate it for pain control. If pain improves, that’s a bonus."
Testosterone did not affect opioid requirements; there was no significant difference in opioid use between the two groups at the end of the study. At baseline, patients had a mean total testosterone concentration of 228 ng/dL and a mean free testosterone concentration of 44 pg/mL; dosing was adjusted in the testosterone arm at 2 weeks to achieve total serum concentrations of 500-1,000 ng/dL.
Dr. Basaria said he had no relevant financial disclosures. The study was funded by AbbVie Pharmaceuticals, makers of the AndroGel testosterone gel used in the study.
SAN FRANCISCO – Men with opioid-induced androgen deficiency had a modest improvement in two laboratory measures of pain tolerance after 14 weeks of testosterone gel treatment but no significant improvements in subjective measures of pain perception, findings from a randomized trial showed.
Thirty-six men in the study received daily 5-g applications of 1% testosterone gel, while 29 others received a placebo gel. The patients were about 50 years old on average and had been taking opioids for at least a month, mostly for back pain.
There was no statistically significant difference in overall subjective Brief Pain Inventory scores at week 14, but there was a nonsignificant trend for less pain interference with daily life among treated men and a trend on the Short Form (SF)–36 for fewer emotional problems.
In the lab, testosterone subjects had about a 5-W improvement in their toleration of a blunted pressure pin applied to their forearms, from a baseline tolerance of 27 W. Men in the placebo group had a tolerance reduction of about 5 W, from a baseline score of 19 W. That difference, and a modest improvement in thumb-pressure tolerance in the treated group, were both significant. Other trends toward greater pain tolerance in the testosterone group were not.
"Objective pain perception showed improvement in the testosterone arm," said lead investigator Dr. Shehzad Basaria, director of Boston University’s androgen clinical research unit. But that improvement trend was not seen with subjective pain perception, he noted, and the magnitude of the change was "small."
Nonetheless, "when you start an analgesic drug, laboratory pain improves before a person says he is subjectively better," Dr. Basaria said at the Endocrine Society’s annual meeting. "We need to do a larger and longer-term study to see if [the lab findings] translate into improvements in subjective" perceptions.
For now, he noted, "I would initiate testosterone replacement only for [current] indications. I would not initiate it for pain control. If pain improves, that’s a bonus."
Testosterone did not affect opioid requirements; there was no significant difference in opioid use between the two groups at the end of the study. At baseline, patients had a mean total testosterone concentration of 228 ng/dL and a mean free testosterone concentration of 44 pg/mL; dosing was adjusted in the testosterone arm at 2 weeks to achieve total serum concentrations of 500-1,000 ng/dL.
Dr. Basaria said he had no relevant financial disclosures. The study was funded by AbbVie Pharmaceuticals, makers of the AndroGel testosterone gel used in the study.
SAN FRANCISCO – Men with opioid-induced androgen deficiency had a modest improvement in two laboratory measures of pain tolerance after 14 weeks of testosterone gel treatment but no significant improvements in subjective measures of pain perception, findings from a randomized trial showed.
Thirty-six men in the study received daily 5-g applications of 1% testosterone gel, while 29 others received a placebo gel. The patients were about 50 years old on average and had been taking opioids for at least a month, mostly for back pain.
There was no statistically significant difference in overall subjective Brief Pain Inventory scores at week 14, but there was a nonsignificant trend for less pain interference with daily life among treated men and a trend on the Short Form (SF)–36 for fewer emotional problems.
In the lab, testosterone subjects had about a 5-W improvement in their toleration of a blunted pressure pin applied to their forearms, from a baseline tolerance of 27 W. Men in the placebo group had a tolerance reduction of about 5 W, from a baseline score of 19 W. That difference, and a modest improvement in thumb-pressure tolerance in the treated group, were both significant. Other trends toward greater pain tolerance in the testosterone group were not.
"Objective pain perception showed improvement in the testosterone arm," said lead investigator Dr. Shehzad Basaria, director of Boston University’s androgen clinical research unit. But that improvement trend was not seen with subjective pain perception, he noted, and the magnitude of the change was "small."
Nonetheless, "when you start an analgesic drug, laboratory pain improves before a person says he is subjectively better," Dr. Basaria said at the Endocrine Society’s annual meeting. "We need to do a larger and longer-term study to see if [the lab findings] translate into improvements in subjective" perceptions.
For now, he noted, "I would initiate testosterone replacement only for [current] indications. I would not initiate it for pain control. If pain improves, that’s a bonus."
Testosterone did not affect opioid requirements; there was no significant difference in opioid use between the two groups at the end of the study. At baseline, patients had a mean total testosterone concentration of 228 ng/dL and a mean free testosterone concentration of 44 pg/mL; dosing was adjusted in the testosterone arm at 2 weeks to achieve total serum concentrations of 500-1,000 ng/dL.
Dr. Basaria said he had no relevant financial disclosures. The study was funded by AbbVie Pharmaceuticals, makers of the AndroGel testosterone gel used in the study.
AT ENDO 2013
Major finding: Men treated with testosterone gel for 14 weeks had about a 5-W improvement in their toleration of a blunted pressure pin applied to their forearms; men on placebo lost about 5 W of tolerance.
Data Source: A randomized, blinded controlled trial of testosterone gel in 65 men with opioid-induced androgen deficiency.
Disclosures: The lead investigator said he had no relevant financial disclosures. The study was funded by AbbVie Pharmaceuticals, makers of the AndroGel testosterone gel used in the study.

When prescribed by mail, vitamin D compliance is low
SAN FRANCISCO – Only one-quarter of patients who were informed by mail to take vitamin D because of insufficient levels found in a blood test met their target of at least 30 ng/mL 6 months later, according to a chart review.
This less-than-ideal compliance among 338 osteopenic patients in a University of Toronto osteoporosis program may be partly attributable to the fact that the importance of the treatment wasn’t adequately addressed while the patients were in the clinic.

After blood tests there, 265 patients (78%) were mailed a form letter telling them that they had insufficient vitamin D levels, defined as 20-29 ng/mL, and to take 4,000 IU/day for 3 months and then 2,000 IU/day thereafter.
Meanwhile, 73 (22%) received a letter telling them they were deficient, with levels of less than 20 ng/mL, and to take one 50,000 IU pill per week and 2,000 IU/day for 3 months, then switch to 2,000 IU/day.
"We were recommending fairly high doses of vitamin D, and that may have been intimidating," especially for a largely asymptomatic condition. "There was no chance really for them to discuss face-to-face with a clinician what their vitamin D status meant, and what treatment entailed," lead investigator Dr. Vithika Sivabalasundaram, an internal medicine resident at the university, said at the Endocrine Society’s annual meeting.
Perhaps not surprisingly, only half (169) of the patients followed through with repeat blood tests after 6 months, as instructed. Of those, just 56% (95) met the target of at least 30 ng/mL. The others (74) were largely unchanged or actually lost ground.
The lesson is probably that "we need to inform our patients of the benefits of vitamin D on bone health, and that there’s fairly low toxicity associated with taking vitamin D," Dr. Sivabalasundaram said.
To that end, when patients get their blood drawn in the clinic, they’re now "informed that they might be placed on this vitamin D protocol, so when they receive the letter, they are not surprised by it and they understand what it means. That wasn’t done before. We are [also] having a nurse phone [patients] to discuss their vitamin D status and answer their questions. We are developing an information pamphlet" as well, and plan to translate the letter into other languages, she said, adding that "right now, we are just sending [it] out in English," which may be a problem for the clinic’s multicultural population.
The only predictor of hitting the 30 ng/mL mark in the study was how soon after 6 months patients got their blood checked, which was probably a surrogate for how seriously they took the protocol, Dr. Sivabalasundaram said.
Baseline vitamin D status and use of glucocorticoids didn’t predict success, nor did past osteoporotic fractures. "We thought that would motivate patients, but we didn’t see that," she said.
Patients with malabsorption syndrome were less likely to hit the mark, as were obese patients, "which makes sense because vitamin D is sequestered into fat cells," she said.
Patients were about 60 years old on average, mostly women, and mostly white.
Dr. Sivabalasundaram said that she had no conflicts to disclose. One of her coinvestigators has been a speaker and advisory group member for several pharmaceutical companies.
SAN FRANCISCO – Only one-quarter of patients who were informed by mail to take vitamin D because of insufficient levels found in a blood test met their target of at least 30 ng/mL 6 months later, according to a chart review.
This less-than-ideal compliance among 338 osteopenic patients in a University of Toronto osteoporosis program may be partly attributable to the fact that the importance of the treatment wasn’t adequately addressed while the patients were in the clinic.
After blood tests there, 265 patients (78%) were mailed a form letter telling them that they had insufficient vitamin D levels, defined as 20-29 ng/mL, and to take 4,000 IU/day for 3 months and then 2,000 IU/day thereafter.
Meanwhile, 73 (22%) received a letter telling them they were deficient, with levels of less than 20 ng/mL, and to take one 50,000 IU pill per week and 2,000 IU/day for 3 months, then switch to 2,000 IU/day.
"We were recommending fairly high doses of vitamin D, and that may have been intimidating," especially for a largely asymptomatic condition. "There was no chance really for them to discuss face-to-face with a clinician what their vitamin D status meant, and what treatment entailed," lead investigator Dr. Vithika Sivabalasundaram, an internal medicine resident at the university, said at the Endocrine Society’s annual meeting.
Perhaps not surprisingly, only half (169) of the patients followed through with repeat blood tests after 6 months, as instructed. Of those, just 56% (95) met the target of at least 30 ng/mL. The others (74) were largely unchanged or actually lost ground.
The lesson is probably that "we need to inform our patients of the benefits of vitamin D on bone health, and that there’s fairly low toxicity associated with taking vitamin D," Dr. Sivabalasundaram said.
To that end, when patients get their blood drawn in the clinic, they’re now "informed that they might be placed on this vitamin D protocol, so when they receive the letter, they are not surprised by it and they understand what it means. That wasn’t done before. We are [also] having a nurse phone [patients] to discuss their vitamin D status and answer their questions. We are developing an information pamphlet" as well, and plan to translate the letter into other languages, she said, adding that "right now, we are just sending [it] out in English," which may be a problem for the clinic’s multicultural population.
The only predictor of hitting the 30 ng/mL mark in the study was how soon after 6 months patients got their blood checked, which was probably a surrogate for how seriously they took the protocol, Dr. Sivabalasundaram said.
Baseline vitamin D status and use of glucocorticoids didn’t predict success, nor did past osteoporotic fractures. "We thought that would motivate patients, but we didn’t see that," she said.
Patients with malabsorption syndrome were less likely to hit the mark, as were obese patients, "which makes sense because vitamin D is sequestered into fat cells," she said.
Patients were about 60 years old on average, mostly women, and mostly white.
Dr. Sivabalasundaram said that she had no conflicts to disclose. One of her coinvestigators has been a speaker and advisory group member for several pharmaceutical companies.
SAN FRANCISCO – Only one-quarter of patients who were informed by mail to take vitamin D because of insufficient levels found in a blood test met their target of at least 30 ng/mL 6 months later, according to a chart review.
This less-than-ideal compliance among 338 osteopenic patients in a University of Toronto osteoporosis program may be partly attributable to the fact that the importance of the treatment wasn’t adequately addressed while the patients were in the clinic.
After blood tests there, 265 patients (78%) were mailed a form letter telling them that they had insufficient vitamin D levels, defined as 20-29 ng/mL, and to take 4,000 IU/day for 3 months and then 2,000 IU/day thereafter.
Meanwhile, 73 (22%) received a letter telling them they were deficient, with levels of less than 20 ng/mL, and to take one 50,000 IU pill per week and 2,000 IU/day for 3 months, then switch to 2,000 IU/day.
"We were recommending fairly high doses of vitamin D, and that may have been intimidating," especially for a largely asymptomatic condition. "There was no chance really for them to discuss face-to-face with a clinician what their vitamin D status meant, and what treatment entailed," lead investigator Dr. Vithika Sivabalasundaram, an internal medicine resident at the university, said at the Endocrine Society’s annual meeting.
Perhaps not surprisingly, only half (169) of the patients followed through with repeat blood tests after 6 months, as instructed. Of those, just 56% (95) met the target of at least 30 ng/mL. The others (74) were largely unchanged or actually lost ground.
The lesson is probably that "we need to inform our patients of the benefits of vitamin D on bone health, and that there’s fairly low toxicity associated with taking vitamin D," Dr. Sivabalasundaram said.
To that end, when patients get their blood drawn in the clinic, they’re now "informed that they might be placed on this vitamin D protocol, so when they receive the letter, they are not surprised by it and they understand what it means. That wasn’t done before. We are [also] having a nurse phone [patients] to discuss their vitamin D status and answer their questions. We are developing an information pamphlet" as well, and plan to translate the letter into other languages, she said, adding that "right now, we are just sending [it] out in English," which may be a problem for the clinic’s multicultural population.
The only predictor of hitting the 30 ng/mL mark in the study was how soon after 6 months patients got their blood checked, which was probably a surrogate for how seriously they took the protocol, Dr. Sivabalasundaram said.
Baseline vitamin D status and use of glucocorticoids didn’t predict success, nor did past osteoporotic fractures. "We thought that would motivate patients, but we didn’t see that," she said.
Patients with malabsorption syndrome were less likely to hit the mark, as were obese patients, "which makes sense because vitamin D is sequestered into fat cells," she said.
Patients were about 60 years old on average, mostly women, and mostly white.
Dr. Sivabalasundaram said that she had no conflicts to disclose. One of her coinvestigators has been a speaker and advisory group member for several pharmaceutical companies.
AT ENDO 2013
Major finding: Roughly half of 338 osteopenic women completed a 6-month vitamin D protocol, and just over half of those who did hit the target of 30 ng/mL.
Data Source: Chart review.
Disclosures: Dr. Sivabalasundaram said that she had no disclosures. One of her coinvestigators has been a speaker and advisory group member for several pharmaceutical companies.

Anti-Müllerian hormone identified PCOS in small study
SAN FRANCISCO – An anti-Müllerian hormone level of 3.4 ng/mL or greater identified polycystic ovary syndrome in a study of 31 nonobese adolescents.
That cutoff was determined to best discriminate between PCOS and controls, with a positive predictive value of 75% and a negative predictive value of 61% in a study of 15 nonobese adolescents with PCOS aged 13-21 years, and 16 controls, reported Dr. Aviva Sopher at the Endocrine Society’s Annual Meeting.
The goal of the study wasn’t to define a definitive anti-Müllerian hormone (AMH) cutoff; that may come later as Dr. Sopher’s group and others continue to investigate the matter. Instead, the project was a preliminary proof-of-concept effort to gauge the utility of AMH in adolescent PCOS diagnosis.

For now, because there was "overlap in AMH values between PCOS and controls" and "a normal adolescent girl with polyfollicular ovaries and no other symptoms can have an AMH in the range that we think of [as signifying] PCOS, I wouldn’t use AMH on its own. I am suggesting the use of AMH in conjunction with clinical presentation and lab work," said Dr. Sopher, a pediatric endocrinologist at Columbia University in New York.
The hope, however, is that AMH will eventually replace the need for ultrasound; the transabdominal approach is "suboptimal" in adolescents, and transvaginal ultrasound is "overly invasive in this age group," she said.
The hormone is produced by growing follicles and is a marker of their number. Blood levels were assessed in the study by enzyme-linked immunosorbent assay (ELISA). PCOS was diagnosed by National Institutes of Health criteria (Fertil. Steril. 2010; 93:1938-41).
AMH was significantly higher in subjects with PCOS (4.4 ng/mL) than in controls (2.4 ng/mL), and correlated significantly with average ovarian size, the appearance of polycystic ovaries, free testosterone, and androstenedione.
The PCOS participants were 1.5-fold more likely to have an AMH level of more that 3.4 ng/mL than were the healthy controls, and that cutoff had a positive predictive value for PCOS of 75% and a negative predictive value of non-PCOS of 61%.
Mean ovarian size was similar in both groups (7.1 cc in subjects with PCOS versus 6.7 cc in controls), as were body mass index z-scores (0.45 vs. 0.19) and percent body fat (36.6% vs. 34.2%). The differences were not significant.
The subjects were at least 2 years post menarche. Exclusion criteria included premature birth; other potential causes of hirsutism and irregular menses; and birth control pill use within 3 months of enrollment. Normal-weight girls were selected "to exclude the confounding factor of obesity," Dr. Sopher said.
AMH is a useful adjunct to diagnose adolescent PCOS, and it has the potential to replace ultrasound as a marker of follicle count, she concluded.
The authors said they had nothing to disclose. The study was funded by the National Institutes of Health.
"I think AMH will diagnose women with an increased number of follicles, irrespective of their androgens. If in addition they have elevated androgen levels, they will be most probably have PCOS," said Dr. Rodolfo Rey.
But the value proposed in this study "is quite low. Many apparently normal girls have values over 3.4 ng/mL. The range of AMH is quite large" in teenagers and young women – perhaps up to 6-7 ng/mL. "This study needs more controls [to capture] the whole range of normal," he said.
Several investigators have proposed replacing ultrasound with AMH to diagnose PCOS in adult women, but "the problem is always the cutoff level. I haven’t seen studies that give cutoff values that could replace ultrasound. We don’t have enough data," he said.
Also, not all PCOS patients have polycystic ovaries. "AMH is reflecting the number of follicles rather than the levels of androgens." By relying on it too heavily, it’s possible to miss hyperandrogenism without polycystic ovaries.
Dr. Rey is a pediatric endocrinologist at Children’s Hospital in Buenos Aires, Argentina. He has received honoraria from Beckman Coulter for his work on AMH assays.
"I think AMH will diagnose women with an increased number of follicles, irrespective of their androgens. If in addition they have elevated androgen levels, they will be most probably have PCOS," said Dr. Rodolfo Rey.
But the value proposed in this study "is quite low. Many apparently normal girls have values over 3.4 ng/mL. The range of AMH is quite large" in teenagers and young women – perhaps up to 6-7 ng/mL. "This study needs more controls [to capture] the whole range of normal," he said.
Several investigators have proposed replacing ultrasound with AMH to diagnose PCOS in adult women, but "the problem is always the cutoff level. I haven’t seen studies that give cutoff values that could replace ultrasound. We don’t have enough data," he said.
Also, not all PCOS patients have polycystic ovaries. "AMH is reflecting the number of follicles rather than the levels of androgens." By relying on it too heavily, it’s possible to miss hyperandrogenism without polycystic ovaries.
Dr. Rey is a pediatric endocrinologist at Children’s Hospital in Buenos Aires, Argentina. He has received honoraria from Beckman Coulter for his work on AMH assays.
"I think AMH will diagnose women with an increased number of follicles, irrespective of their androgens. If in addition they have elevated androgen levels, they will be most probably have PCOS," said Dr. Rodolfo Rey.
But the value proposed in this study "is quite low. Many apparently normal girls have values over 3.4 ng/mL. The range of AMH is quite large" in teenagers and young women – perhaps up to 6-7 ng/mL. "This study needs more controls [to capture] the whole range of normal," he said.
Several investigators have proposed replacing ultrasound with AMH to diagnose PCOS in adult women, but "the problem is always the cutoff level. I haven’t seen studies that give cutoff values that could replace ultrasound. We don’t have enough data," he said.
Also, not all PCOS patients have polycystic ovaries. "AMH is reflecting the number of follicles rather than the levels of androgens." By relying on it too heavily, it’s possible to miss hyperandrogenism without polycystic ovaries.
Dr. Rey is a pediatric endocrinologist at Children’s Hospital in Buenos Aires, Argentina. He has received honoraria from Beckman Coulter for his work on AMH assays.
SAN FRANCISCO – An anti-Müllerian hormone level of 3.4 ng/mL or greater identified polycystic ovary syndrome in a study of 31 nonobese adolescents.
That cutoff was determined to best discriminate between PCOS and controls, with a positive predictive value of 75% and a negative predictive value of 61% in a study of 15 nonobese adolescents with PCOS aged 13-21 years, and 16 controls, reported Dr. Aviva Sopher at the Endocrine Society’s Annual Meeting.
The goal of the study wasn’t to define a definitive anti-Müllerian hormone (AMH) cutoff; that may come later as Dr. Sopher’s group and others continue to investigate the matter. Instead, the project was a preliminary proof-of-concept effort to gauge the utility of AMH in adolescent PCOS diagnosis.
For now, because there was "overlap in AMH values between PCOS and controls" and "a normal adolescent girl with polyfollicular ovaries and no other symptoms can have an AMH in the range that we think of [as signifying] PCOS, I wouldn’t use AMH on its own. I am suggesting the use of AMH in conjunction with clinical presentation and lab work," said Dr. Sopher, a pediatric endocrinologist at Columbia University in New York.
The hope, however, is that AMH will eventually replace the need for ultrasound; the transabdominal approach is "suboptimal" in adolescents, and transvaginal ultrasound is "overly invasive in this age group," she said.
The hormone is produced by growing follicles and is a marker of their number. Blood levels were assessed in the study by enzyme-linked immunosorbent assay (ELISA). PCOS was diagnosed by National Institutes of Health criteria (Fertil. Steril. 2010; 93:1938-41).
AMH was significantly higher in subjects with PCOS (4.4 ng/mL) than in controls (2.4 ng/mL), and correlated significantly with average ovarian size, the appearance of polycystic ovaries, free testosterone, and androstenedione.
The PCOS participants were 1.5-fold more likely to have an AMH level of more that 3.4 ng/mL than were the healthy controls, and that cutoff had a positive predictive value for PCOS of 75% and a negative predictive value of non-PCOS of 61%.
Mean ovarian size was similar in both groups (7.1 cc in subjects with PCOS versus 6.7 cc in controls), as were body mass index z-scores (0.45 vs. 0.19) and percent body fat (36.6% vs. 34.2%). The differences were not significant.
The subjects were at least 2 years post menarche. Exclusion criteria included premature birth; other potential causes of hirsutism and irregular menses; and birth control pill use within 3 months of enrollment. Normal-weight girls were selected "to exclude the confounding factor of obesity," Dr. Sopher said.
AMH is a useful adjunct to diagnose adolescent PCOS, and it has the potential to replace ultrasound as a marker of follicle count, she concluded.
The authors said they had nothing to disclose. The study was funded by the National Institutes of Health.
SAN FRANCISCO – An anti-Müllerian hormone level of 3.4 ng/mL or greater identified polycystic ovary syndrome in a study of 31 nonobese adolescents.
That cutoff was determined to best discriminate between PCOS and controls, with a positive predictive value of 75% and a negative predictive value of 61% in a study of 15 nonobese adolescents with PCOS aged 13-21 years, and 16 controls, reported Dr. Aviva Sopher at the Endocrine Society’s Annual Meeting.
The goal of the study wasn’t to define a definitive anti-Müllerian hormone (AMH) cutoff; that may come later as Dr. Sopher’s group and others continue to investigate the matter. Instead, the project was a preliminary proof-of-concept effort to gauge the utility of AMH in adolescent PCOS diagnosis.
For now, because there was "overlap in AMH values between PCOS and controls" and "a normal adolescent girl with polyfollicular ovaries and no other symptoms can have an AMH in the range that we think of [as signifying] PCOS, I wouldn’t use AMH on its own. I am suggesting the use of AMH in conjunction with clinical presentation and lab work," said Dr. Sopher, a pediatric endocrinologist at Columbia University in New York.
The hope, however, is that AMH will eventually replace the need for ultrasound; the transabdominal approach is "suboptimal" in adolescents, and transvaginal ultrasound is "overly invasive in this age group," she said.
The hormone is produced by growing follicles and is a marker of their number. Blood levels were assessed in the study by enzyme-linked immunosorbent assay (ELISA). PCOS was diagnosed by National Institutes of Health criteria (Fertil. Steril. 2010; 93:1938-41).
AMH was significantly higher in subjects with PCOS (4.4 ng/mL) than in controls (2.4 ng/mL), and correlated significantly with average ovarian size, the appearance of polycystic ovaries, free testosterone, and androstenedione.
The PCOS participants were 1.5-fold more likely to have an AMH level of more that 3.4 ng/mL than were the healthy controls, and that cutoff had a positive predictive value for PCOS of 75% and a negative predictive value of non-PCOS of 61%.
Mean ovarian size was similar in both groups (7.1 cc in subjects with PCOS versus 6.7 cc in controls), as were body mass index z-scores (0.45 vs. 0.19) and percent body fat (36.6% vs. 34.2%). The differences were not significant.
The subjects were at least 2 years post menarche. Exclusion criteria included premature birth; other potential causes of hirsutism and irregular menses; and birth control pill use within 3 months of enrollment. Normal-weight girls were selected "to exclude the confounding factor of obesity," Dr. Sopher said.
AMH is a useful adjunct to diagnose adolescent PCOS, and it has the potential to replace ultrasound as a marker of follicle count, she concluded.
The authors said they had nothing to disclose. The study was funded by the National Institutes of Health.
AT ENDO 2013
Major finding: An anti-Müllerian hormone cutoff level of 3.4 ng/mL discriminated between PCOS patients and controls.
Data source: Prospective, case-control trial with 31 subjects.
Disclosures: The investigators said they had nothing to disclose. The study was funded by the National Institutes of Health.

Androgens helped even young boys with Klinefelter's
SAN FRANCISCO – Boys with Klinefelter’s syndrome felt better about themselves and had a better quality of life after 2 years of low-dose androgen therapy, in a randomized placebo-controlled trial.
At the end of 2 years, treated boys scored about 10 points better on questionnaires measuring aspects of anxiety, depression, and behavioral problems. "A standard deviation is about 15 points, so a difference of 10 points represents a moderate effect size. Families noticed quite dramatic improvements in social function, depression symptoms, and anxiety symptoms," said lead investigator Dr. Judith Ross, a pediatric endocrinologist at the duPont Hospital for Children in Wilmington, Del.
Although "it’s important that the findings are replicated with longer-term studies, gradual, age-appropriate androgen replacement should be considered to optimize self-image and quality of life in childhood," she said at the Endocrine Society annual meeting.
Androgen replacement is already standard practice in adolescents and adults with the condition, but not in boys. To see if it would make a difference, investigators from the duPont Hospital for Children randomized 39 boys aged 4-12 years old to 0.06 mg/kg per day of oxandrolone, and 41 to placebo capsules.
Her team monitored oxandrolone patients carefully for undue bone age advancement, lipid-level changes, liver function elevations, blood pressure increases, pubertal changes before age 8, and other possible complications. The only significant problem they found was a drop in six boys of HDL cholesterol below 20 mg/dL, which led to dose reductions.
Doses were dropped a bit in other subjects, too; by the end of the study, placebo patients were receiving an average of about 0.045 mg/kg per day and oxandrolone patients were taking an average of about 0.042 mg/kg per day. "Dose individualization is key to avoid side effects and to optimize positive outcomes. I can’t overemphasize how important this is. Physician consultation and dose adjustment are very important in managing the use of oxandrolone in boys with Klinefelter’s syndrome," Dr. Ross said.
Scores on the self-reported Revised Children's Manifest Anxiety Scale improved among oxandrolone boys about 10 points from the upper 90s at baseline, with 100 as the population mean. Boys on placebo stayed in the mid-90s throughout the trial. The results were similar for worry scores.
On the Children's Depression Inventory, also a self-reported questionnaire with 100 as the population mean, the scores of treated boys improved more than 10 points from the mid-90s on measures of success in interpersonal relationships, with smaller gains in measurements of self-like and confidence in the future. Boys on placebo started with similar scores, but made no significant gains.
Treated boys remained in the mid-80s on the parent-reported Child Behavior Checklist's measures of social problems such as getting teased, acting too young, and being disliked. Boys on placebo dropped about 5 points; 100 again represented the population mean.
The differences were statistically significant, and the groups well matched for karyotype, socioeconomic status, and race, Dr. Ross. The oxandrolone group was about 1.3 years younger on average, which was taken into account in the statistical analysis. Neurocognitive outcomes are currently under analysis.
The authors said they had no relevant financial disclosures. The National Institutes of Health funded the work.
SAN FRANCISCO – Boys with Klinefelter’s syndrome felt better about themselves and had a better quality of life after 2 years of low-dose androgen therapy, in a randomized placebo-controlled trial.
At the end of 2 years, treated boys scored about 10 points better on questionnaires measuring aspects of anxiety, depression, and behavioral problems. "A standard deviation is about 15 points, so a difference of 10 points represents a moderate effect size. Families noticed quite dramatic improvements in social function, depression symptoms, and anxiety symptoms," said lead investigator Dr. Judith Ross, a pediatric endocrinologist at the duPont Hospital for Children in Wilmington, Del.
Although "it’s important that the findings are replicated with longer-term studies, gradual, age-appropriate androgen replacement should be considered to optimize self-image and quality of life in childhood," she said at the Endocrine Society annual meeting.
Androgen replacement is already standard practice in adolescents and adults with the condition, but not in boys. To see if it would make a difference, investigators from the duPont Hospital for Children randomized 39 boys aged 4-12 years old to 0.06 mg/kg per day of oxandrolone, and 41 to placebo capsules.
Her team monitored oxandrolone patients carefully for undue bone age advancement, lipid-level changes, liver function elevations, blood pressure increases, pubertal changes before age 8, and other possible complications. The only significant problem they found was a drop in six boys of HDL cholesterol below 20 mg/dL, which led to dose reductions.
Doses were dropped a bit in other subjects, too; by the end of the study, placebo patients were receiving an average of about 0.045 mg/kg per day and oxandrolone patients were taking an average of about 0.042 mg/kg per day. "Dose individualization is key to avoid side effects and to optimize positive outcomes. I can’t overemphasize how important this is. Physician consultation and dose adjustment are very important in managing the use of oxandrolone in boys with Klinefelter’s syndrome," Dr. Ross said.
Scores on the self-reported Revised Children's Manifest Anxiety Scale improved among oxandrolone boys about 10 points from the upper 90s at baseline, with 100 as the population mean. Boys on placebo stayed in the mid-90s throughout the trial. The results were similar for worry scores.
On the Children's Depression Inventory, also a self-reported questionnaire with 100 as the population mean, the scores of treated boys improved more than 10 points from the mid-90s on measures of success in interpersonal relationships, with smaller gains in measurements of self-like and confidence in the future. Boys on placebo started with similar scores, but made no significant gains.
Treated boys remained in the mid-80s on the parent-reported Child Behavior Checklist's measures of social problems such as getting teased, acting too young, and being disliked. Boys on placebo dropped about 5 points; 100 again represented the population mean.
The differences were statistically significant, and the groups well matched for karyotype, socioeconomic status, and race, Dr. Ross. The oxandrolone group was about 1.3 years younger on average, which was taken into account in the statistical analysis. Neurocognitive outcomes are currently under analysis.
The authors said they had no relevant financial disclosures. The National Institutes of Health funded the work.
SAN FRANCISCO – Boys with Klinefelter’s syndrome felt better about themselves and had a better quality of life after 2 years of low-dose androgen therapy, in a randomized placebo-controlled trial.
At the end of 2 years, treated boys scored about 10 points better on questionnaires measuring aspects of anxiety, depression, and behavioral problems. "A standard deviation is about 15 points, so a difference of 10 points represents a moderate effect size. Families noticed quite dramatic improvements in social function, depression symptoms, and anxiety symptoms," said lead investigator Dr. Judith Ross, a pediatric endocrinologist at the duPont Hospital for Children in Wilmington, Del.
Although "it’s important that the findings are replicated with longer-term studies, gradual, age-appropriate androgen replacement should be considered to optimize self-image and quality of life in childhood," she said at the Endocrine Society annual meeting.
Androgen replacement is already standard practice in adolescents and adults with the condition, but not in boys. To see if it would make a difference, investigators from the duPont Hospital for Children randomized 39 boys aged 4-12 years old to 0.06 mg/kg per day of oxandrolone, and 41 to placebo capsules.
Her team monitored oxandrolone patients carefully for undue bone age advancement, lipid-level changes, liver function elevations, blood pressure increases, pubertal changes before age 8, and other possible complications. The only significant problem they found was a drop in six boys of HDL cholesterol below 20 mg/dL, which led to dose reductions.
Doses were dropped a bit in other subjects, too; by the end of the study, placebo patients were receiving an average of about 0.045 mg/kg per day and oxandrolone patients were taking an average of about 0.042 mg/kg per day. "Dose individualization is key to avoid side effects and to optimize positive outcomes. I can’t overemphasize how important this is. Physician consultation and dose adjustment are very important in managing the use of oxandrolone in boys with Klinefelter’s syndrome," Dr. Ross said.
Scores on the self-reported Revised Children's Manifest Anxiety Scale improved among oxandrolone boys about 10 points from the upper 90s at baseline, with 100 as the population mean. Boys on placebo stayed in the mid-90s throughout the trial. The results were similar for worry scores.
On the Children's Depression Inventory, also a self-reported questionnaire with 100 as the population mean, the scores of treated boys improved more than 10 points from the mid-90s on measures of success in interpersonal relationships, with smaller gains in measurements of self-like and confidence in the future. Boys on placebo started with similar scores, but made no significant gains.
Treated boys remained in the mid-80s on the parent-reported Child Behavior Checklist's measures of social problems such as getting teased, acting too young, and being disliked. Boys on placebo dropped about 5 points; 100 again represented the population mean.
The differences were statistically significant, and the groups well matched for karyotype, socioeconomic status, and race, Dr. Ross. The oxandrolone group was about 1.3 years younger on average, which was taken into account in the statistical analysis. Neurocognitive outcomes are currently under analysis.
The authors said they had no relevant financial disclosures. The National Institutes of Health funded the work.
AT ENDO 2013
Major finding: Klinefelter’s patients had a moderate improvement in various social adjustment scores after 2 years of low-dose androgen therapy.
Data Source: A randomized controlled trial in 80 boys with Klinefelter’s syndrome aged 4-12 years.
Disclosures: The authors said they had no relevant financial disclosures. The National Institutes of Health funded the work.
Obesity: It's the endocannabinoids, man
There’s a growing recognition that inadequate sleep may contribute to overeating and, thus, to our massive obesity epidemic. Now there’s a prime suspect to help explain why that may be so.
It’s the endocannabinoids, man.

You’ve heard of them. They’re like the cannabinoids in marijuana that make eating so pleasurable and trigger the "munchies," except these are natural appetite stimulants in the body that control the pleasurable aspects of eating. A study presented at the annual meeting of the Endocrine Society showed that nine healthy, lean, young adults had higher blood levels of the endocannabinoid molecule 2-arachidonoylglycerol (2-AG) after only 4.5 hours of sleep compared with a normal night’s sleep when they got 8.5 hours in bed.
Researchers controlled what the participants ate and did during 6 nights in a sleep lab, testing their blood levels every hour for 24 hours after the second night of sleep.
They randomized participants to the normal-sleep or partial-sleep-restriction groups and had them return a month later in a crossover design to spend another 6 nights in the sleep lab experiencing whichever sleep pattern they hadn’t been randomized to initially.
The results showed a circadian rhythm to endocannabinoid levels, with 2-AG peaking in the early afternoon in both groups but being significantly higher in the sleep-restriction group, reported Erin C. Hanlon, Ph.D. and her associates.
Previous studies of the relationship between sleep and endocannabinoids had looked at only single time points or narrower time intervals, she said. The current results extend findings from at least a dozen previous studies in the last 5 years on related topics. In three studies, researchers reported an association between shortened sleep duration and increased eating of snacks and high-energy foods, such as in this study: Am. J. Clin. Nutr. 2012;95:818-24. Two other studies showed that decreased sleep was associated with increased risk for obesity. And seven other carefully controlled laboratory studies found that sleep restriction impaired glucose metabolism, altered peripherally secreted hormones that modulate feeding behavior, and increased participants’ ratings of appetite and hunger, said Dr. Hanlon of the University of Chicago.
Is lack of sleep the only cause of the obesity epidemic? Of course not. But a quick look at national data suggests that it could be a major factor, if these preliminary studies are on to something.
According to the Centers for Disease Control and Prevention, 35% of nearly 75,000 U.S. adults in 12 states reported in 2009 that they get less than 7 hours of sleep in a typical 24-hour period. Want to guess how many Americans reported being overweight in 2012? That would be 36%, according to a Gallup poll, with another 26% saying that they’re obese.
And are endocannabinoids the only endogenous players that affect overeating? Unlikely. But the endocannabinoid system is a target for development of potential pharmaceutical treatments for obesity, Dr. Hanlon said. Someday soon, I suppose, you may be able to buy a pill to counteract the munchie effects of excessive endocannabinoids. Or, we could all just get a good night’s sleep.
Dr. Hanlon reported having no financial disclosures. Her research was funded by the National Institutes of Health, the Department of Defense, and the Medical College of Wisconsin.
On Twitter @sherryboschert
There’s a growing recognition that inadequate sleep may contribute to overeating and, thus, to our massive obesity epidemic. Now there’s a prime suspect to help explain why that may be so.
It’s the endocannabinoids, man.
You’ve heard of them. They’re like the cannabinoids in marijuana that make eating so pleasurable and trigger the "munchies," except these are natural appetite stimulants in the body that control the pleasurable aspects of eating. A study presented at the annual meeting of the Endocrine Society showed that nine healthy, lean, young adults had higher blood levels of the endocannabinoid molecule 2-arachidonoylglycerol (2-AG) after only 4.5 hours of sleep compared with a normal night’s sleep when they got 8.5 hours in bed.
Researchers controlled what the participants ate and did during 6 nights in a sleep lab, testing their blood levels every hour for 24 hours after the second night of sleep.
They randomized participants to the normal-sleep or partial-sleep-restriction groups and had them return a month later in a crossover design to spend another 6 nights in the sleep lab experiencing whichever sleep pattern they hadn’t been randomized to initially.
The results showed a circadian rhythm to endocannabinoid levels, with 2-AG peaking in the early afternoon in both groups but being significantly higher in the sleep-restriction group, reported Erin C. Hanlon, Ph.D. and her associates.
Previous studies of the relationship between sleep and endocannabinoids had looked at only single time points or narrower time intervals, she said. The current results extend findings from at least a dozen previous studies in the last 5 years on related topics. In three studies, researchers reported an association between shortened sleep duration and increased eating of snacks and high-energy foods, such as in this study: Am. J. Clin. Nutr. 2012;95:818-24. Two other studies showed that decreased sleep was associated with increased risk for obesity. And seven other carefully controlled laboratory studies found that sleep restriction impaired glucose metabolism, altered peripherally secreted hormones that modulate feeding behavior, and increased participants’ ratings of appetite and hunger, said Dr. Hanlon of the University of Chicago.
Is lack of sleep the only cause of the obesity epidemic? Of course not. But a quick look at national data suggests that it could be a major factor, if these preliminary studies are on to something.
According to the Centers for Disease Control and Prevention, 35% of nearly 75,000 U.S. adults in 12 states reported in 2009 that they get less than 7 hours of sleep in a typical 24-hour period. Want to guess how many Americans reported being overweight in 2012? That would be 36%, according to a Gallup poll, with another 26% saying that they’re obese.
And are endocannabinoids the only endogenous players that affect overeating? Unlikely. But the endocannabinoid system is a target for development of potential pharmaceutical treatments for obesity, Dr. Hanlon said. Someday soon, I suppose, you may be able to buy a pill to counteract the munchie effects of excessive endocannabinoids. Or, we could all just get a good night’s sleep.
Dr. Hanlon reported having no financial disclosures. Her research was funded by the National Institutes of Health, the Department of Defense, and the Medical College of Wisconsin.
On Twitter @sherryboschert
There’s a growing recognition that inadequate sleep may contribute to overeating and, thus, to our massive obesity epidemic. Now there’s a prime suspect to help explain why that may be so.
It’s the endocannabinoids, man.
You’ve heard of them. They’re like the cannabinoids in marijuana that make eating so pleasurable and trigger the "munchies," except these are natural appetite stimulants in the body that control the pleasurable aspects of eating. A study presented at the annual meeting of the Endocrine Society showed that nine healthy, lean, young adults had higher blood levels of the endocannabinoid molecule 2-arachidonoylglycerol (2-AG) after only 4.5 hours of sleep compared with a normal night’s sleep when they got 8.5 hours in bed.
Researchers controlled what the participants ate and did during 6 nights in a sleep lab, testing their blood levels every hour for 24 hours after the second night of sleep.
They randomized participants to the normal-sleep or partial-sleep-restriction groups and had them return a month later in a crossover design to spend another 6 nights in the sleep lab experiencing whichever sleep pattern they hadn’t been randomized to initially.
The results showed a circadian rhythm to endocannabinoid levels, with 2-AG peaking in the early afternoon in both groups but being significantly higher in the sleep-restriction group, reported Erin C. Hanlon, Ph.D. and her associates.
Previous studies of the relationship between sleep and endocannabinoids had looked at only single time points or narrower time intervals, she said. The current results extend findings from at least a dozen previous studies in the last 5 years on related topics. In three studies, researchers reported an association between shortened sleep duration and increased eating of snacks and high-energy foods, such as in this study: Am. J. Clin. Nutr. 2012;95:818-24. Two other studies showed that decreased sleep was associated with increased risk for obesity. And seven other carefully controlled laboratory studies found that sleep restriction impaired glucose metabolism, altered peripherally secreted hormones that modulate feeding behavior, and increased participants’ ratings of appetite and hunger, said Dr. Hanlon of the University of Chicago.
Is lack of sleep the only cause of the obesity epidemic? Of course not. But a quick look at national data suggests that it could be a major factor, if these preliminary studies are on to something.
According to the Centers for Disease Control and Prevention, 35% of nearly 75,000 U.S. adults in 12 states reported in 2009 that they get less than 7 hours of sleep in a typical 24-hour period. Want to guess how many Americans reported being overweight in 2012? That would be 36%, according to a Gallup poll, with another 26% saying that they’re obese.
And are endocannabinoids the only endogenous players that affect overeating? Unlikely. But the endocannabinoid system is a target for development of potential pharmaceutical treatments for obesity, Dr. Hanlon said. Someday soon, I suppose, you may be able to buy a pill to counteract the munchie effects of excessive endocannabinoids. Or, we could all just get a good night’s sleep.
Dr. Hanlon reported having no financial disclosures. Her research was funded by the National Institutes of Health, the Department of Defense, and the Medical College of Wisconsin.
On Twitter @sherryboschert
