User login
The Official Newspaper of the American Association for Thoracic Surgery
Young Faculty Hot Topics: How to find mentors
As someone less than 1 year into practice, I believe mentorship is one of the most critical essentials as a trainee and a junior attending. I have been privileged to have excellent mentors throughout my training and now, in my first job. A lot of this is luck, but I also have always put mentorship at the top of my list when looking for fellowships and jobs. In fact, part of the reason I took the job I currently have is because the contract clearly stated who my clinical and academic mentors would be. This showed the department’s dedication to grooming junior staff appropriately. Below is my take on how to find mentors.
Have multiple mentors
It’s good to have multiple mentors, each of whom can provide a different kind of mentorship. For junior faculty, key areas of mentorship include:
- Building clinical volume.
- Establishing your reputation as a safe and competent clinician/surgeon.
- Designing your academic/research career.
- Planning your overall career.
- Solving any political/administrative issues.
Currently, my division chief is my clinical/general mentor, from whom I seek clinical advice, political advice should I find myself in a tough situation as a junior attending, and personal advice, as well. We meet monthly to go over various things including clinical/research projects and any clinical issues. I have an academic mentor, who is a basic scientist; we review research ideas together. He reads over and critiques my grants, and he picks apart my presentations. I also have a very senior mentor, a retired thoracic surgeon, whom I seek when I have a challenging case; it is crucial to identify a senior surgeon who has an abundance of experience so you can pick his or her brain – a true resource. This is in addition to the mentors I have from my training, with whom I am still in contact. I think it is important to have mentors outside of your current work for certain situations.
Mentors do not have to be in your discipline
It’s useful to have mentors from different fields. As I stated above, my academic mentor is a basic scientist. I am a thoracic surgeon, but I consider my general surgery residency chair, who is an accomplished surgical oncologist, and my residency program director, a general surgeon, to be two of my important mentors. I think it’s a good idea to have someone outside of your discipline as your mentor, even someone in a nonsurgical discipline, as long as she or he provides what you need, such as general career decisions and research mentorship. Having people from different disciplines adds more perspective and depth. For women, female mentors may provide input on career decisions at different life stages.
Do your homework about your would-be mentors
When deciding among different jobs, I did as much homework as possible in researching my would-be clinical mentors, who in most cases are also your senior partners. This included speaking with other junior faculty members within the division, people who had worked with the person in the past, and current mentors who may know them. In my mind, I found the most valuable resources to be people who had worked in the past with potential new mentors or senior partners. They can provide unbiased, sometimes negative, opinions that others might be less willing to provide. In fact, I probably spent more time trying to understand to the negative comments, since this provided valuable information, too.
I always asked questions specific to the mentorship. Were they around to help you in the OR when needed, or was it more of a verbal “I’ll be around”? Were they good about giving the juniors clinical volume and sharing OR time? Did you feel like you grew under his or her mentorship?
In conclusion, my advice about mentorship is to have multiple mentors, each for different purposes. For those looking for fellowships and jobs, learning all you can about your would-be mentors goes a long way toward ensuring an ideal position.
Dr. Suzuki is a general thoracic surgeon at Boston Medical Center.
As someone less than 1 year into practice, I believe mentorship is one of the most critical essentials as a trainee and a junior attending. I have been privileged to have excellent mentors throughout my training and now, in my first job. A lot of this is luck, but I also have always put mentorship at the top of my list when looking for fellowships and jobs. In fact, part of the reason I took the job I currently have is because the contract clearly stated who my clinical and academic mentors would be. This showed the department’s dedication to grooming junior staff appropriately. Below is my take on how to find mentors.
Have multiple mentors
It’s good to have multiple mentors, each of whom can provide a different kind of mentorship. For junior faculty, key areas of mentorship include:
- Building clinical volume.
- Establishing your reputation as a safe and competent clinician/surgeon.
- Designing your academic/research career.
- Planning your overall career.
- Solving any political/administrative issues.
Currently, my division chief is my clinical/general mentor, from whom I seek clinical advice, political advice should I find myself in a tough situation as a junior attending, and personal advice, as well. We meet monthly to go over various things including clinical/research projects and any clinical issues. I have an academic mentor, who is a basic scientist; we review research ideas together. He reads over and critiques my grants, and he picks apart my presentations. I also have a very senior mentor, a retired thoracic surgeon, whom I seek when I have a challenging case; it is crucial to identify a senior surgeon who has an abundance of experience so you can pick his or her brain – a true resource. This is in addition to the mentors I have from my training, with whom I am still in contact. I think it is important to have mentors outside of your current work for certain situations.
Mentors do not have to be in your discipline
It’s useful to have mentors from different fields. As I stated above, my academic mentor is a basic scientist. I am a thoracic surgeon, but I consider my general surgery residency chair, who is an accomplished surgical oncologist, and my residency program director, a general surgeon, to be two of my important mentors. I think it’s a good idea to have someone outside of your discipline as your mentor, even someone in a nonsurgical discipline, as long as she or he provides what you need, such as general career decisions and research mentorship. Having people from different disciplines adds more perspective and depth. For women, female mentors may provide input on career decisions at different life stages.
Do your homework about your would-be mentors
When deciding among different jobs, I did as much homework as possible in researching my would-be clinical mentors, who in most cases are also your senior partners. This included speaking with other junior faculty members within the division, people who had worked with the person in the past, and current mentors who may know them. In my mind, I found the most valuable resources to be people who had worked in the past with potential new mentors or senior partners. They can provide unbiased, sometimes negative, opinions that others might be less willing to provide. In fact, I probably spent more time trying to understand to the negative comments, since this provided valuable information, too.
I always asked questions specific to the mentorship. Were they around to help you in the OR when needed, or was it more of a verbal “I’ll be around”? Were they good about giving the juniors clinical volume and sharing OR time? Did you feel like you grew under his or her mentorship?
In conclusion, my advice about mentorship is to have multiple mentors, each for different purposes. For those looking for fellowships and jobs, learning all you can about your would-be mentors goes a long way toward ensuring an ideal position.
Dr. Suzuki is a general thoracic surgeon at Boston Medical Center.
As someone less than 1 year into practice, I believe mentorship is one of the most critical essentials as a trainee and a junior attending. I have been privileged to have excellent mentors throughout my training and now, in my first job. A lot of this is luck, but I also have always put mentorship at the top of my list when looking for fellowships and jobs. In fact, part of the reason I took the job I currently have is because the contract clearly stated who my clinical and academic mentors would be. This showed the department’s dedication to grooming junior staff appropriately. Below is my take on how to find mentors.
Have multiple mentors
It’s good to have multiple mentors, each of whom can provide a different kind of mentorship. For junior faculty, key areas of mentorship include:
- Building clinical volume.
- Establishing your reputation as a safe and competent clinician/surgeon.
- Designing your academic/research career.
- Planning your overall career.
- Solving any political/administrative issues.
Currently, my division chief is my clinical/general mentor, from whom I seek clinical advice, political advice should I find myself in a tough situation as a junior attending, and personal advice, as well. We meet monthly to go over various things including clinical/research projects and any clinical issues. I have an academic mentor, who is a basic scientist; we review research ideas together. He reads over and critiques my grants, and he picks apart my presentations. I also have a very senior mentor, a retired thoracic surgeon, whom I seek when I have a challenging case; it is crucial to identify a senior surgeon who has an abundance of experience so you can pick his or her brain – a true resource. This is in addition to the mentors I have from my training, with whom I am still in contact. I think it is important to have mentors outside of your current work for certain situations.
Mentors do not have to be in your discipline
It’s useful to have mentors from different fields. As I stated above, my academic mentor is a basic scientist. I am a thoracic surgeon, but I consider my general surgery residency chair, who is an accomplished surgical oncologist, and my residency program director, a general surgeon, to be two of my important mentors. I think it’s a good idea to have someone outside of your discipline as your mentor, even someone in a nonsurgical discipline, as long as she or he provides what you need, such as general career decisions and research mentorship. Having people from different disciplines adds more perspective and depth. For women, female mentors may provide input on career decisions at different life stages.
Do your homework about your would-be mentors
When deciding among different jobs, I did as much homework as possible in researching my would-be clinical mentors, who in most cases are also your senior partners. This included speaking with other junior faculty members within the division, people who had worked with the person in the past, and current mentors who may know them. In my mind, I found the most valuable resources to be people who had worked in the past with potential new mentors or senior partners. They can provide unbiased, sometimes negative, opinions that others might be less willing to provide. In fact, I probably spent more time trying to understand to the negative comments, since this provided valuable information, too.
I always asked questions specific to the mentorship. Were they around to help you in the OR when needed, or was it more of a verbal “I’ll be around”? Were they good about giving the juniors clinical volume and sharing OR time? Did you feel like you grew under his or her mentorship?
In conclusion, my advice about mentorship is to have multiple mentors, each for different purposes. For those looking for fellowships and jobs, learning all you can about your would-be mentors goes a long way toward ensuring an ideal position.
Dr. Suzuki is a general thoracic surgeon at Boston Medical Center.
Young Faculty Hot Topics: Saying “yes” or saying “no”
The vast majority of us did not end up where we are today by saying “no” to opportunities throughout medical school, surgical training and now early in our clinical practice. In fact, many of us likely said “yes” to just about everything that came our way, and this was reasonable as the number of opportunities was manageable. As you move along your career as a cardiothoracic surgeon, the opportunities increase, especially if you consistently turn in a high performance.
A discussion of what to say “yes” or “no” to would be remiss without considering your individual career goals and time management. You’ve heard it before and here it is again: Write down your 5- and 10-year career plan. If you do not know where you are heading, you cannot plot the course. Then, based on those long-term career goals, drill down to your annual goals. Begin by identifying deadlines on the academic calendar each year and then work backward to determine what needs to be done in the months prior to those deadlines. Once you have a clear idea of what needs to be done on a month-by-month basis, on the Sunday of each week, create a list of daily goals. This method turns your long-term career goals into doable-size pieces of a larger puzzle that will keep you on trajectory.
Once you have charted your course using the above methods or some variation of them, you will have a clear idea of what opportunities are aligned with your long-term career plan. For example, if your goals are to build your clinical practice and become a program director, you may prioritize attending a course to introduce a new surgical technique into your practice and becoming the clerkship director for medical students instead of serving on hospital committees. Solicit advice from mentors and colleagues regarding certain opportunities if you are unsure whether these will help you achieve your career goals. Furthermore, identify senior cardiothoracic surgeons who have achieved the goals you are aiming for and ask them how they arrived at their position.
Oftentimes, it’s not about saying “yes” or “no,” but rather seeking out opportunities. Saying “yes” to opportunities that are pertinent to your career goals is critical, but there are other factors to consider when deciding whether to accept an opportunity. A major factor is the ratio of benefit to time commitment; clearly, the greater the benefit and the lower the time commitment, the better. However, there may be some opportunities that are beneficial and require a fair amount of time. Only you can decide whether the time necessary to commit to an opportunity is worth the benefit. Another factor to consider is what academic milestones are necessary for promotion at your institution; this may also vary by academic track within an institution. Be familiar with these requirements, and factor them into your goals as they are the foundation upon which you climb the academic ladder within your department.
Lastly, consider all the potential advantages of certain opportunities. For example, every year the STS solicits self-nominations for committees: Are there any committees that pertain to your career goals that will allow you to network with other cardiothoracic surgeons who may then become a mentor, sponsor, or collaborator?
I’m going to state the obvious: Only you know how you are spending every minute of every hour of each day. Why do I mention this? If you have said “yes” to too many things and are stretched too thin, you are at risk of underperforming and may begin to feel underappreciated; nobody else may realize how many hours you are working, but they will notice if your performance is subpar. Not only that, but you may be at risk of burnout. Unlike residency training, where we sprinted every day (and sometimes all night) and the light at the end of the tunnel was within view, we are now in an endurance race and need to pace ourselves for long, successful, and fulfilling careers. Ideally, we deliver what we promise, but if that balance is tipped, err on the side of underpromising and overdelivering. That scenario is much better than overpromising and underdelivering since the latter not only leads to a performance that might be less than your best but also could decrease your future opportunities.
When offered an opportunity, do not say “yes” immediately; collect some intel regarding the time commitment, determine whether it is aligned with your career goals and, if need be, discuss it with mentors and trusted colleagues before you say “yes.” Once you decide to say “yes,” jump in and hit the ground running! The beginning of your career is an exciting time with some flexibility in terms of choosing your own career adventures. Always be realistic about your goals and time to ensure a long, rewarding career.
Dr. Brown is a general thoracic surgeon at UC Davis Medical Center, Calif.
The vast majority of us did not end up where we are today by saying “no” to opportunities throughout medical school, surgical training and now early in our clinical practice. In fact, many of us likely said “yes” to just about everything that came our way, and this was reasonable as the number of opportunities was manageable. As you move along your career as a cardiothoracic surgeon, the opportunities increase, especially if you consistently turn in a high performance.
A discussion of what to say “yes” or “no” to would be remiss without considering your individual career goals and time management. You’ve heard it before and here it is again: Write down your 5- and 10-year career plan. If you do not know where you are heading, you cannot plot the course. Then, based on those long-term career goals, drill down to your annual goals. Begin by identifying deadlines on the academic calendar each year and then work backward to determine what needs to be done in the months prior to those deadlines. Once you have a clear idea of what needs to be done on a month-by-month basis, on the Sunday of each week, create a list of daily goals. This method turns your long-term career goals into doable-size pieces of a larger puzzle that will keep you on trajectory.
Once you have charted your course using the above methods or some variation of them, you will have a clear idea of what opportunities are aligned with your long-term career plan. For example, if your goals are to build your clinical practice and become a program director, you may prioritize attending a course to introduce a new surgical technique into your practice and becoming the clerkship director for medical students instead of serving on hospital committees. Solicit advice from mentors and colleagues regarding certain opportunities if you are unsure whether these will help you achieve your career goals. Furthermore, identify senior cardiothoracic surgeons who have achieved the goals you are aiming for and ask them how they arrived at their position.
Oftentimes, it’s not about saying “yes” or “no,” but rather seeking out opportunities. Saying “yes” to opportunities that are pertinent to your career goals is critical, but there are other factors to consider when deciding whether to accept an opportunity. A major factor is the ratio of benefit to time commitment; clearly, the greater the benefit and the lower the time commitment, the better. However, there may be some opportunities that are beneficial and require a fair amount of time. Only you can decide whether the time necessary to commit to an opportunity is worth the benefit. Another factor to consider is what academic milestones are necessary for promotion at your institution; this may also vary by academic track within an institution. Be familiar with these requirements, and factor them into your goals as they are the foundation upon which you climb the academic ladder within your department.
Lastly, consider all the potential advantages of certain opportunities. For example, every year the STS solicits self-nominations for committees: Are there any committees that pertain to your career goals that will allow you to network with other cardiothoracic surgeons who may then become a mentor, sponsor, or collaborator?
I’m going to state the obvious: Only you know how you are spending every minute of every hour of each day. Why do I mention this? If you have said “yes” to too many things and are stretched too thin, you are at risk of underperforming and may begin to feel underappreciated; nobody else may realize how many hours you are working, but they will notice if your performance is subpar. Not only that, but you may be at risk of burnout. Unlike residency training, where we sprinted every day (and sometimes all night) and the light at the end of the tunnel was within view, we are now in an endurance race and need to pace ourselves for long, successful, and fulfilling careers. Ideally, we deliver what we promise, but if that balance is tipped, err on the side of underpromising and overdelivering. That scenario is much better than overpromising and underdelivering since the latter not only leads to a performance that might be less than your best but also could decrease your future opportunities.
When offered an opportunity, do not say “yes” immediately; collect some intel regarding the time commitment, determine whether it is aligned with your career goals and, if need be, discuss it with mentors and trusted colleagues before you say “yes.” Once you decide to say “yes,” jump in and hit the ground running! The beginning of your career is an exciting time with some flexibility in terms of choosing your own career adventures. Always be realistic about your goals and time to ensure a long, rewarding career.
Dr. Brown is a general thoracic surgeon at UC Davis Medical Center, Calif.
The vast majority of us did not end up where we are today by saying “no” to opportunities throughout medical school, surgical training and now early in our clinical practice. In fact, many of us likely said “yes” to just about everything that came our way, and this was reasonable as the number of opportunities was manageable. As you move along your career as a cardiothoracic surgeon, the opportunities increase, especially if you consistently turn in a high performance.
A discussion of what to say “yes” or “no” to would be remiss without considering your individual career goals and time management. You’ve heard it before and here it is again: Write down your 5- and 10-year career plan. If you do not know where you are heading, you cannot plot the course. Then, based on those long-term career goals, drill down to your annual goals. Begin by identifying deadlines on the academic calendar each year and then work backward to determine what needs to be done in the months prior to those deadlines. Once you have a clear idea of what needs to be done on a month-by-month basis, on the Sunday of each week, create a list of daily goals. This method turns your long-term career goals into doable-size pieces of a larger puzzle that will keep you on trajectory.
Once you have charted your course using the above methods or some variation of them, you will have a clear idea of what opportunities are aligned with your long-term career plan. For example, if your goals are to build your clinical practice and become a program director, you may prioritize attending a course to introduce a new surgical technique into your practice and becoming the clerkship director for medical students instead of serving on hospital committees. Solicit advice from mentors and colleagues regarding certain opportunities if you are unsure whether these will help you achieve your career goals. Furthermore, identify senior cardiothoracic surgeons who have achieved the goals you are aiming for and ask them how they arrived at their position.
Oftentimes, it’s not about saying “yes” or “no,” but rather seeking out opportunities. Saying “yes” to opportunities that are pertinent to your career goals is critical, but there are other factors to consider when deciding whether to accept an opportunity. A major factor is the ratio of benefit to time commitment; clearly, the greater the benefit and the lower the time commitment, the better. However, there may be some opportunities that are beneficial and require a fair amount of time. Only you can decide whether the time necessary to commit to an opportunity is worth the benefit. Another factor to consider is what academic milestones are necessary for promotion at your institution; this may also vary by academic track within an institution. Be familiar with these requirements, and factor them into your goals as they are the foundation upon which you climb the academic ladder within your department.
Lastly, consider all the potential advantages of certain opportunities. For example, every year the STS solicits self-nominations for committees: Are there any committees that pertain to your career goals that will allow you to network with other cardiothoracic surgeons who may then become a mentor, sponsor, or collaborator?
I’m going to state the obvious: Only you know how you are spending every minute of every hour of each day. Why do I mention this? If you have said “yes” to too many things and are stretched too thin, you are at risk of underperforming and may begin to feel underappreciated; nobody else may realize how many hours you are working, but they will notice if your performance is subpar. Not only that, but you may be at risk of burnout. Unlike residency training, where we sprinted every day (and sometimes all night) and the light at the end of the tunnel was within view, we are now in an endurance race and need to pace ourselves for long, successful, and fulfilling careers. Ideally, we deliver what we promise, but if that balance is tipped, err on the side of underpromising and overdelivering. That scenario is much better than overpromising and underdelivering since the latter not only leads to a performance that might be less than your best but also could decrease your future opportunities.
When offered an opportunity, do not say “yes” immediately; collect some intel regarding the time commitment, determine whether it is aligned with your career goals and, if need be, discuss it with mentors and trusted colleagues before you say “yes.” Once you decide to say “yes,” jump in and hit the ground running! The beginning of your career is an exciting time with some flexibility in terms of choosing your own career adventures. Always be realistic about your goals and time to ensure a long, rewarding career.
Dr. Brown is a general thoracic surgeon at UC Davis Medical Center, Calif.
Readmission rates linked to hospital quality measures
Poorer-performing hospitals have higher readmission rates than better-performing hospitals for patients with similar diagnoses, a study shows.
Lead author Harlan M. Krumholz, MD, of Yale University, New Haven, Conn., and his colleagues analyzed Centers for Medicare and Medicaid Services hospital-wide readmission data and divided data from July 2014 through June 2015 into two random samples. Researchers used the first sample to calculate the risk-standardized readmission rate within 30 days for each hospital and classified hospitals into performance quartiles, with a lower readmission rate indicating better performance. The second study sample included patients who had two admissions for similar diagnoses at different hospitals that occurred more than 1 month and less than 1 year apart. Researchers compared the observed readmission rates among patients who had been admitted to hospitals in different performance quartiles. The analysis included all discharges occurring from July 1, 2014, through June 30, 2015, from short-term acute care or critical access hospitals in the United States involving Medicare patients who were aged 65 years or older.
Results found that among the patients hospitalized more than once for similar diagnoses at different hospitals, the readmission rate was significantly higher among patients admitted to the worst-performing quartile of hospitals than among those admitted to the best-performing quartile (absolute difference in readmission rate, 2.0 percentage points; 95% confidence interval, 0.4-3.5; P = .001) (N Engl J Med. 2017. doi: 10.1056/NEJMsa1702321). The differences in the comparisons of the other quartiles were smaller and not significant, according to the study. 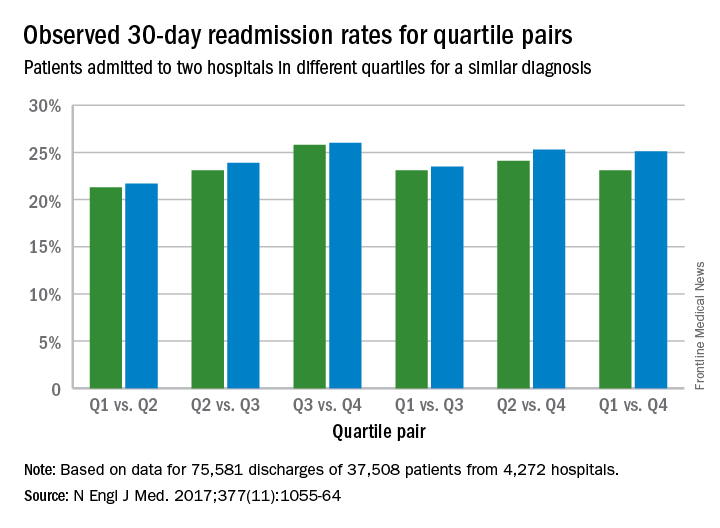
The findings suggest that hospital quality contributes at least in part to readmission rates, independent of patient factors, study authors concluded.
“This study addresses a persistent concern that national readmission measures may reflect differences in unmeasured factors rather than in hospital performance,” study authors noted in the study. “The findings suggest that hospital quality contributes at least in part to readmission rates, independent of patient factors. By studying patients who were admitted twice within 1 year with similar diagnoses to different hospitals, this study design was able to isolate hospital signals of performance while minimizing differences among the patients. In these cases, because the same patients had similar admissions at two hospitals, the characteristics of the patients, including their level of social disadvantage, level of education, or degree of underlying illness, were broadly the same. The alignment of the differences that we observed with the results of the CMS hospital-wide readmission measure also adds to evidence that the readmission measure classifies true differences in performance.”
Dr. Krumholz and seven coauthors reported receiving support from contracts with the Center for Medicare and Medicaid Services to develop and reevaluate performance measures that are used for public reporting.
[email protected]
On Twitter @legal_med
Poorer-performing hospitals have higher readmission rates than better-performing hospitals for patients with similar diagnoses, a study shows.
Lead author Harlan M. Krumholz, MD, of Yale University, New Haven, Conn., and his colleagues analyzed Centers for Medicare and Medicaid Services hospital-wide readmission data and divided data from July 2014 through June 2015 into two random samples. Researchers used the first sample to calculate the risk-standardized readmission rate within 30 days for each hospital and classified hospitals into performance quartiles, with a lower readmission rate indicating better performance. The second study sample included patients who had two admissions for similar diagnoses at different hospitals that occurred more than 1 month and less than 1 year apart. Researchers compared the observed readmission rates among patients who had been admitted to hospitals in different performance quartiles. The analysis included all discharges occurring from July 1, 2014, through June 30, 2015, from short-term acute care or critical access hospitals in the United States involving Medicare patients who were aged 65 years or older.
Results found that among the patients hospitalized more than once for similar diagnoses at different hospitals, the readmission rate was significantly higher among patients admitted to the worst-performing quartile of hospitals than among those admitted to the best-performing quartile (absolute difference in readmission rate, 2.0 percentage points; 95% confidence interval, 0.4-3.5; P = .001) (N Engl J Med. 2017. doi: 10.1056/NEJMsa1702321). The differences in the comparisons of the other quartiles were smaller and not significant, according to the study.
The findings suggest that hospital quality contributes at least in part to readmission rates, independent of patient factors, study authors concluded.
“This study addresses a persistent concern that national readmission measures may reflect differences in unmeasured factors rather than in hospital performance,” study authors noted in the study. “The findings suggest that hospital quality contributes at least in part to readmission rates, independent of patient factors. By studying patients who were admitted twice within 1 year with similar diagnoses to different hospitals, this study design was able to isolate hospital signals of performance while minimizing differences among the patients. In these cases, because the same patients had similar admissions at two hospitals, the characteristics of the patients, including their level of social disadvantage, level of education, or degree of underlying illness, were broadly the same. The alignment of the differences that we observed with the results of the CMS hospital-wide readmission measure also adds to evidence that the readmission measure classifies true differences in performance.”
Dr. Krumholz and seven coauthors reported receiving support from contracts with the Center for Medicare and Medicaid Services to develop and reevaluate performance measures that are used for public reporting.
[email protected]
On Twitter @legal_med
Poorer-performing hospitals have higher readmission rates than better-performing hospitals for patients with similar diagnoses, a study shows.
Lead author Harlan M. Krumholz, MD, of Yale University, New Haven, Conn., and his colleagues analyzed Centers for Medicare and Medicaid Services hospital-wide readmission data and divided data from July 2014 through June 2015 into two random samples. Researchers used the first sample to calculate the risk-standardized readmission rate within 30 days for each hospital and classified hospitals into performance quartiles, with a lower readmission rate indicating better performance. The second study sample included patients who had two admissions for similar diagnoses at different hospitals that occurred more than 1 month and less than 1 year apart. Researchers compared the observed readmission rates among patients who had been admitted to hospitals in different performance quartiles. The analysis included all discharges occurring from July 1, 2014, through June 30, 2015, from short-term acute care or critical access hospitals in the United States involving Medicare patients who were aged 65 years or older.
Results found that among the patients hospitalized more than once for similar diagnoses at different hospitals, the readmission rate was significantly higher among patients admitted to the worst-performing quartile of hospitals than among those admitted to the best-performing quartile (absolute difference in readmission rate, 2.0 percentage points; 95% confidence interval, 0.4-3.5; P = .001) (N Engl J Med. 2017. doi: 10.1056/NEJMsa1702321). The differences in the comparisons of the other quartiles were smaller and not significant, according to the study.
The findings suggest that hospital quality contributes at least in part to readmission rates, independent of patient factors, study authors concluded.
“This study addresses a persistent concern that national readmission measures may reflect differences in unmeasured factors rather than in hospital performance,” study authors noted in the study. “The findings suggest that hospital quality contributes at least in part to readmission rates, independent of patient factors. By studying patients who were admitted twice within 1 year with similar diagnoses to different hospitals, this study design was able to isolate hospital signals of performance while minimizing differences among the patients. In these cases, because the same patients had similar admissions at two hospitals, the characteristics of the patients, including their level of social disadvantage, level of education, or degree of underlying illness, were broadly the same. The alignment of the differences that we observed with the results of the CMS hospital-wide readmission measure also adds to evidence that the readmission measure classifies true differences in performance.”
Dr. Krumholz and seven coauthors reported receiving support from contracts with the Center for Medicare and Medicaid Services to develop and reevaluate performance measures that are used for public reporting.
[email protected]
On Twitter @legal_med
FROM NEJM
Key clinical point:
Major finding: The readmission rate was significantly higher among patients admitted to the worst-performing quartile of hospitals than among those admitted to the best-performing quartile (absolute difference in readmission rate, 2.0 percentage points).
Data source: Analysis of Centers for Medicare and Medicaid Services hospital-wide readmission data from July 2014 through June 2015.
Disclosures: Dr. Krumholz and seven coauthors reported receiving support from contracts with the Center for Medicare and Medicaid Services to develop and reevaluate performance measures that are used for public reporting.
CRP may predict survival after immunotherapy for lung cancer
CHICAGO – A baseline C-reactive protein (CRP) level above 50 mg/L independently predicted worse overall survival after immunotherapy in patients with advanced non–small cell lung cancer and small cell lung cancer in a retrospective study.
In 99 patients treated with nivolumab after a first-line platinum doublet, the median baseline CRP level was 22 mg/L. After a median follow-up of 8.5 months, 50% of patients were alive, and, based on univariate and multivariate analysis, both liver involvement and having a CRP level greater than 50 mg/L were significantly associated with inferior overall survival after immunotherapy.
The median overall survival after immunotherapy was 9.3 months versus 2.7 months with a CRP level of 50 mg/L or less versus above 50 mg/L, Abdul Rafeh Naqash, MD, of East Carolina University, Greenville, N.C., reported at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
Notably, significant increases in CRP level, compared with baseline, were seen at the time of grade 2 to grade 4 immune-related adverse events, which occurred in 38.4% of patients. This is a hypothesis-generating finding in that it suggests there is dysregulation of the immune system, in the context of immune checkpoint blockade, that leads to a more proinflammatory state, which ultimately leads to immune-related adverse events, Dr. Naqash said.
Study subjects were adults with a median age of 65 years who were treated during April 2015-March 2017. Most were white (64.7%), were male (64.6%), and had non–small cell lung cancer (88%). Most had stage IV disease (70.7%), and the most common site for metastases was the bones (35.4%) and the liver (24.2%). Patients’ CRP levels were measured at anti-PD-1–treatment initiation and serially with subsequent doses.
The findings are important because the identification of predictive biomarkers in patients treated with anti-PD-1 therapy could provide valuable insights into underlying mechanisms regulating patient responses, elucidate resistance mechanisms, and help with optimal selection of patients for treatment with and development of patient-tailored treatment, Dr. Naqash said, noting that identifying such biomarkers has thus far been a challenge.
However, this study is limited by its retrospective design and limited follow-up; the findings require validation in prospective lung cancer trials, he concluded.
Dr. Naqash reported having no disclosures.
CHICAGO – A baseline C-reactive protein (CRP) level above 50 mg/L independently predicted worse overall survival after immunotherapy in patients with advanced non–small cell lung cancer and small cell lung cancer in a retrospective study.
In 99 patients treated with nivolumab after a first-line platinum doublet, the median baseline CRP level was 22 mg/L. After a median follow-up of 8.5 months, 50% of patients were alive, and, based on univariate and multivariate analysis, both liver involvement and having a CRP level greater than 50 mg/L were significantly associated with inferior overall survival after immunotherapy.
The median overall survival after immunotherapy was 9.3 months versus 2.7 months with a CRP level of 50 mg/L or less versus above 50 mg/L, Abdul Rafeh Naqash, MD, of East Carolina University, Greenville, N.C., reported at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
Notably, significant increases in CRP level, compared with baseline, were seen at the time of grade 2 to grade 4 immune-related adverse events, which occurred in 38.4% of patients. This is a hypothesis-generating finding in that it suggests there is dysregulation of the immune system, in the context of immune checkpoint blockade, that leads to a more proinflammatory state, which ultimately leads to immune-related adverse events, Dr. Naqash said.
Study subjects were adults with a median age of 65 years who were treated during April 2015-March 2017. Most were white (64.7%), were male (64.6%), and had non–small cell lung cancer (88%). Most had stage IV disease (70.7%), and the most common site for metastases was the bones (35.4%) and the liver (24.2%). Patients’ CRP levels were measured at anti-PD-1–treatment initiation and serially with subsequent doses.
The findings are important because the identification of predictive biomarkers in patients treated with anti-PD-1 therapy could provide valuable insights into underlying mechanisms regulating patient responses, elucidate resistance mechanisms, and help with optimal selection of patients for treatment with and development of patient-tailored treatment, Dr. Naqash said, noting that identifying such biomarkers has thus far been a challenge.
However, this study is limited by its retrospective design and limited follow-up; the findings require validation in prospective lung cancer trials, he concluded.
Dr. Naqash reported having no disclosures.
CHICAGO – A baseline C-reactive protein (CRP) level above 50 mg/L independently predicted worse overall survival after immunotherapy in patients with advanced non–small cell lung cancer and small cell lung cancer in a retrospective study.
In 99 patients treated with nivolumab after a first-line platinum doublet, the median baseline CRP level was 22 mg/L. After a median follow-up of 8.5 months, 50% of patients were alive, and, based on univariate and multivariate analysis, both liver involvement and having a CRP level greater than 50 mg/L were significantly associated with inferior overall survival after immunotherapy.
The median overall survival after immunotherapy was 9.3 months versus 2.7 months with a CRP level of 50 mg/L or less versus above 50 mg/L, Abdul Rafeh Naqash, MD, of East Carolina University, Greenville, N.C., reported at the Chicago Multidisciplinary Symposium in Thoracic Oncology.
Notably, significant increases in CRP level, compared with baseline, were seen at the time of grade 2 to grade 4 immune-related adverse events, which occurred in 38.4% of patients. This is a hypothesis-generating finding in that it suggests there is dysregulation of the immune system, in the context of immune checkpoint blockade, that leads to a more proinflammatory state, which ultimately leads to immune-related adverse events, Dr. Naqash said.
Study subjects were adults with a median age of 65 years who were treated during April 2015-March 2017. Most were white (64.7%), were male (64.6%), and had non–small cell lung cancer (88%). Most had stage IV disease (70.7%), and the most common site for metastases was the bones (35.4%) and the liver (24.2%). Patients’ CRP levels were measured at anti-PD-1–treatment initiation and serially with subsequent doses.
The findings are important because the identification of predictive biomarkers in patients treated with anti-PD-1 therapy could provide valuable insights into underlying mechanisms regulating patient responses, elucidate resistance mechanisms, and help with optimal selection of patients for treatment with and development of patient-tailored treatment, Dr. Naqash said, noting that identifying such biomarkers has thus far been a challenge.
However, this study is limited by its retrospective design and limited follow-up; the findings require validation in prospective lung cancer trials, he concluded.
Dr. Naqash reported having no disclosures.
AT A SYMPOSIUM IN THORACIC ONCOLOGY
Key clinical point:
Major finding: Median overall survival after immunotherapy: 9.3 months vs. 2.7 months with CRP of 50 mg/L or less vs. above 50 mg/L.
Data source: A retrospective study of 99 patients.
Disclosures: Dr. Naqash reported having no disclosures.
While U.S. heart failure readmissions fall, deaths rise
DALLAS – U.S. hospitals have recently shown a consistent and disturbing disconnect between reductions in their heart failure hospital readmission rates and heart failure mortality. Readmissions have dropped while mortality has risen.
“Despite reductions in 30-day heart failure readmissions in 89% of U.S. hospitals” during 2009-2016, “30-day heart failure mortality rates increased at 73%* of these ‘successful’ hospitals” during the same period,” Ahmad A. Abdul-Aziz, MD, said at the annual scientific meeting of the Heart Failure Society of America.

These shifts in the outcomes of U.S. patients hospitalized for acute heart failure episodes are tied to the penalties that the Centers for Medicare & Medicaid Services began slapping on hospitals in 2013 for excess 30-day readmissions for heart failure patients and in 2014 for excess mortality. A problem with these two CMS programs is that the penalty on inferior readmissions performance is a lot stiffer than for excess mortality, Dr. Aziz noted: a 0.2% penalty on payments for high mortality, compared with a 3% penalty for excess readmissions, a disparity that can make hospitals focus more on the readmissions side, he suggested.
Dr. Aziz’s report isn’t the first to make this observation. Study results published earlier in 2017 used CMS Medicare data from 2008 to 2014 to show that during that period, heart failure 30-day mortality rates following hospital discharge rose by 1.3%, while 30-day readmissions fell by 2.1% (JAMA. 2017 July 18;318[3]:270-8). On the basis of these numbers, as many as 5,200 additional deaths to U.S. heart failure patients in 2014 “may be related to the Hospital Readmission Reduction Program” of CMS, Gregg C. Fonarow, MD, said during a separate talk at the meeting.

The analysis reported by Dr. Aziz included data from 3,265 U.S. hospitals for heart failure patients, and data from 1,621 hospitals that managed patients with acute MIs, another disease that the CMS has targeted for penalties based on 30-day readmissions and 30-day postdischarge mortality rates. During the 8-year period studied, heart failure 30-day readmissions fell by 2.2% while 30-day mortality rose by 1%. In contrast, among acute MI patients, readmissions fell by 3% and mortality also fell, by 2.2%, Dr. Abdul-Aziz reported.
Dr. Abdul-Aziz had no disclosures. Dr. Fonarow had been a consultant to Amgen, Janssen, Medtronic, Novartis, St. Jude, and ZS Pharma.
[email protected]
On Twitter @mitchelzoler
*This article was updated October 5, 2017
My colleagues and I have seen in results from recent trials a changing relationship between heart failure mortality and heart failure hospitalization. In the United States in particular, where penalties exist for high rates of hospital readmissions for heart failure, we are seeing more patients treated as outpatients and we see that these “outpatient” events are associated with the same risk for subsequent mortality as we had previously seen for heart failure hospitalization.
It may be that we are keeping patients out of the hospital to avoid a financial ding, but perhaps we are keeping out patients who really should be hospitalized.
What we have begun doing in trials is to look not just at hospitalizations but also consider the incidence of other heart failure events, such as patients treated for heart failure symptoms with an intravenous diuretic in the emergency department and patients who are kept in observation rooms and are not admitted. It’s not the same as a heart failure hospitalization, but some trials are now including these other heart failure events in their primary endpoint.

Scott D. Solomon, MD, professor of medicine at Harvard Medical School and director of noninvasive cardiology at Brigham and Women’s Hospital in Boston, made these comments as chair of the session where Dr. Aziz gave his report and in an interview. He has been a consultant to and/or received research support from Alnylam, Amgen, AstraZeneca, Bristol-Myers Squibb, Cytokinetics, GlaxoSmithKline, Ionis, Merck, Novartis, and Sanofi.
My colleagues and I have seen in results from recent trials a changing relationship between heart failure mortality and heart failure hospitalization. In the United States in particular, where penalties exist for high rates of hospital readmissions for heart failure, we are seeing more patients treated as outpatients and we see that these “outpatient” events are associated with the same risk for subsequent mortality as we had previously seen for heart failure hospitalization.
It may be that we are keeping patients out of the hospital to avoid a financial ding, but perhaps we are keeping out patients who really should be hospitalized.
What we have begun doing in trials is to look not just at hospitalizations but also consider the incidence of other heart failure events, such as patients treated for heart failure symptoms with an intravenous diuretic in the emergency department and patients who are kept in observation rooms and are not admitted. It’s not the same as a heart failure hospitalization, but some trials are now including these other heart failure events in their primary endpoint.
Scott D. Solomon, MD, professor of medicine at Harvard Medical School and director of noninvasive cardiology at Brigham and Women’s Hospital in Boston, made these comments as chair of the session where Dr. Aziz gave his report and in an interview. He has been a consultant to and/or received research support from Alnylam, Amgen, AstraZeneca, Bristol-Myers Squibb, Cytokinetics, GlaxoSmithKline, Ionis, Merck, Novartis, and Sanofi.
My colleagues and I have seen in results from recent trials a changing relationship between heart failure mortality and heart failure hospitalization. In the United States in particular, where penalties exist for high rates of hospital readmissions for heart failure, we are seeing more patients treated as outpatients and we see that these “outpatient” events are associated with the same risk for subsequent mortality as we had previously seen for heart failure hospitalization.
It may be that we are keeping patients out of the hospital to avoid a financial ding, but perhaps we are keeping out patients who really should be hospitalized.
What we have begun doing in trials is to look not just at hospitalizations but also consider the incidence of other heart failure events, such as patients treated for heart failure symptoms with an intravenous diuretic in the emergency department and patients who are kept in observation rooms and are not admitted. It’s not the same as a heart failure hospitalization, but some trials are now including these other heart failure events in their primary endpoint.
Scott D. Solomon, MD, professor of medicine at Harvard Medical School and director of noninvasive cardiology at Brigham and Women’s Hospital in Boston, made these comments as chair of the session where Dr. Aziz gave his report and in an interview. He has been a consultant to and/or received research support from Alnylam, Amgen, AstraZeneca, Bristol-Myers Squibb, Cytokinetics, GlaxoSmithKline, Ionis, Merck, Novartis, and Sanofi.
DALLAS – U.S. hospitals have recently shown a consistent and disturbing disconnect between reductions in their heart failure hospital readmission rates and heart failure mortality. Readmissions have dropped while mortality has risen.
“Despite reductions in 30-day heart failure readmissions in 89% of U.S. hospitals” during 2009-2016, “30-day heart failure mortality rates increased at 73%* of these ‘successful’ hospitals” during the same period,” Ahmad A. Abdul-Aziz, MD, said at the annual scientific meeting of the Heart Failure Society of America.
These shifts in the outcomes of U.S. patients hospitalized for acute heart failure episodes are tied to the penalties that the Centers for Medicare & Medicaid Services began slapping on hospitals in 2013 for excess 30-day readmissions for heart failure patients and in 2014 for excess mortality. A problem with these two CMS programs is that the penalty on inferior readmissions performance is a lot stiffer than for excess mortality, Dr. Aziz noted: a 0.2% penalty on payments for high mortality, compared with a 3% penalty for excess readmissions, a disparity that can make hospitals focus more on the readmissions side, he suggested.
Dr. Aziz’s report isn’t the first to make this observation. Study results published earlier in 2017 used CMS Medicare data from 2008 to 2014 to show that during that period, heart failure 30-day mortality rates following hospital discharge rose by 1.3%, while 30-day readmissions fell by 2.1% (JAMA. 2017 July 18;318[3]:270-8). On the basis of these numbers, as many as 5,200 additional deaths to U.S. heart failure patients in 2014 “may be related to the Hospital Readmission Reduction Program” of CMS, Gregg C. Fonarow, MD, said during a separate talk at the meeting.
The analysis reported by Dr. Aziz included data from 3,265 U.S. hospitals for heart failure patients, and data from 1,621 hospitals that managed patients with acute MIs, another disease that the CMS has targeted for penalties based on 30-day readmissions and 30-day postdischarge mortality rates. During the 8-year period studied, heart failure 30-day readmissions fell by 2.2% while 30-day mortality rose by 1%. In contrast, among acute MI patients, readmissions fell by 3% and mortality also fell, by 2.2%, Dr. Abdul-Aziz reported.
Dr. Abdul-Aziz had no disclosures. Dr. Fonarow had been a consultant to Amgen, Janssen, Medtronic, Novartis, St. Jude, and ZS Pharma.
[email protected]
On Twitter @mitchelzoler
*This article was updated October 5, 2017
DALLAS – U.S. hospitals have recently shown a consistent and disturbing disconnect between reductions in their heart failure hospital readmission rates and heart failure mortality. Readmissions have dropped while mortality has risen.
“Despite reductions in 30-day heart failure readmissions in 89% of U.S. hospitals” during 2009-2016, “30-day heart failure mortality rates increased at 73%* of these ‘successful’ hospitals” during the same period,” Ahmad A. Abdul-Aziz, MD, said at the annual scientific meeting of the Heart Failure Society of America.
These shifts in the outcomes of U.S. patients hospitalized for acute heart failure episodes are tied to the penalties that the Centers for Medicare & Medicaid Services began slapping on hospitals in 2013 for excess 30-day readmissions for heart failure patients and in 2014 for excess mortality. A problem with these two CMS programs is that the penalty on inferior readmissions performance is a lot stiffer than for excess mortality, Dr. Aziz noted: a 0.2% penalty on payments for high mortality, compared with a 3% penalty for excess readmissions, a disparity that can make hospitals focus more on the readmissions side, he suggested.
Dr. Aziz’s report isn’t the first to make this observation. Study results published earlier in 2017 used CMS Medicare data from 2008 to 2014 to show that during that period, heart failure 30-day mortality rates following hospital discharge rose by 1.3%, while 30-day readmissions fell by 2.1% (JAMA. 2017 July 18;318[3]:270-8). On the basis of these numbers, as many as 5,200 additional deaths to U.S. heart failure patients in 2014 “may be related to the Hospital Readmission Reduction Program” of CMS, Gregg C. Fonarow, MD, said during a separate talk at the meeting.
The analysis reported by Dr. Aziz included data from 3,265 U.S. hospitals for heart failure patients, and data from 1,621 hospitals that managed patients with acute MIs, another disease that the CMS has targeted for penalties based on 30-day readmissions and 30-day postdischarge mortality rates. During the 8-year period studied, heart failure 30-day readmissions fell by 2.2% while 30-day mortality rose by 1%. In contrast, among acute MI patients, readmissions fell by 3% and mortality also fell, by 2.2%, Dr. Abdul-Aziz reported.
Dr. Abdul-Aziz had no disclosures. Dr. Fonarow had been a consultant to Amgen, Janssen, Medtronic, Novartis, St. Jude, and ZS Pharma.
[email protected]
On Twitter @mitchelzoler
*This article was updated October 5, 2017
AT THE HFSA ANNUAL SCIENTIFIC MEETING
Key clinical point:
Major finding: From 2009 to 2016, U.S. 30-day heart failure readmissions fell by 2.2% while 30-day heart failure mortality rose by 1%.
Data source: Review of Medicare data for 3,265 U.S. hospitals managing heart failure patients.
Disclosures: Dr. Abdul-Aziz had no disclosures. Dr. Fonarow had been a consultant to Amgen, Janssen, Medtronic, Novartis, St. Jude, and ZS Pharma.
CMS alerts physicians of payment reductions for PQRS noncompliance
Doctors who did not adequately meet Physician Quality Reporting System (PQRS) requirements in 2016 will soon be receiving notification letters alerting them that their Medicare Part B physician fee schedule payments will be reduced by 2%.
Officials from the Centers for Medicare & Medicaid Services said in a statement that “the majority” of eligible professionals “successfully reported to PQRS and avoided the downward payment adjustment,” but did not state how many doctors are expected to receive letters.
The CMS noted that there are no hardship exemptions to avoid the payment reduction for 2018.
Doctors who did not adequately meet Physician Quality Reporting System (PQRS) requirements in 2016 will soon be receiving notification letters alerting them that their Medicare Part B physician fee schedule payments will be reduced by 2%.
Officials from the Centers for Medicare & Medicaid Services said in a statement that “the majority” of eligible professionals “successfully reported to PQRS and avoided the downward payment adjustment,” but did not state how many doctors are expected to receive letters.
The CMS noted that there are no hardship exemptions to avoid the payment reduction for 2018.
Doctors who did not adequately meet Physician Quality Reporting System (PQRS) requirements in 2016 will soon be receiving notification letters alerting them that their Medicare Part B physician fee schedule payments will be reduced by 2%.
Officials from the Centers for Medicare & Medicaid Services said in a statement that “the majority” of eligible professionals “successfully reported to PQRS and avoided the downward payment adjustment,” but did not state how many doctors are expected to receive letters.
The CMS noted that there are no hardship exemptions to avoid the payment reduction for 2018.
Statins linked to lower death rates in COPD
Receiving a statin prescription within a year after diagnosis of chronic obstructive pulmonary disease was associated with a 21% decrease in the subsequent risk of all-cause mortality and a 45% drop in risk of pulmonary mortality, according to the results of a large retrospective administrative database study.
The findings belie those of the recent Simvastatin in the Prevention of COPD Exacerbation (STATCOPE) trial, in which daily simvastatin (40 mg) did not affect exacerbation rates or time to first exacerbation in high-risk COPD patients, wrote Adam Raymakers, MSc, a doctoral candidate at the University of British Columbia, Vancouver, and his associates. Their study was observational, but the association between statin use and decreased mortality “persisted across several measures of statin exposure,” they wrote. “Our findings, in conjunction with previously reported evidence, suggests that there may be a specific subtype of COPD patients that may benefit from statin use.” The study appears in the September issue of Chest (2017;152;486-93).
To further explore the question, the researchers analyzed linked health databases from nearly 40,000 patients aged 50 years and older who had received at least three prescriptions for an anticholinergic or a short-acting beta agonist in 12 months some time between 1998 and 2007. The first prescription was considered the date of COPD “diagnosis.” The average age of the patients was 71 years; 55% were female.
A total of 7,775 patients (19.6%) who met this definition of incident COPD were prescribed a statin at least once during the subsequent year. These patients had a significantly reduced risk of subsequent all-cause mortality in univariate and multivariate analyses, with hazard ratios of 0.79 (95% confidence intervals, 0.68 to 0.91; P less than .002). Statins also showed a protective effect against pulmonary mortality, with univariate and multivariate hazard ratios of 0.52 (P = .01) and 0.55 (P = .03), respectively.
The protective effect of statins held up when the investigators narrowed the exposure period to 6 months after COPD diagnosis and when they expanded it to 18 months. Exposure to statins for 80% of the 1-year window after COPD diagnosis – a proxy for statin adherence – also led to a reduced risk of all-cause mortality, but the 95% confidence interval for the hazard ratio did not reach statistical significance (0.71 to 1.01; P = .06).
The most common prescription was for atorvastatin (49%), usually for 90 days (23%), 100 days (20%), or 30 days (15%), the researchers said. While the “possibility of the ‘healthy user’ or the ‘healthy adherer’ cannot be ignored,” they adjusted for other prescriptions, comorbidities, and income level, which should have helped eliminate this effect, they added. However, they lacked data on smoking and lung function assessments, both of which are “important confounders and contributors to mortality,” they acknowledged.
Canadian Institutes of Health Research supported the study. One coinvestigator disclosed consulting relationships with Teva, Pfizer, and Novartis. The others had no conflicts of interest.
Despite [its] limitations, the study results are intriguing and in line with findings from other retrospective cohorts. How then can we reconcile the apparent benefits observed in retrospective studies with the lack of clinical effect seen in prospective trials, particularly the Simvastatin in the Prevention of COPD Exacerbation (STATCOPE) study? Could it be that both negative and positive studies are “correct”? Prospective studies have thus far not been adequately powered for mortality as an endpoint. Perhaps the choice of the particular statin matters? While STATCOPE involved simvastatin, the majority of the cohort reported by Raymakers et al. received atorvastatin. [Or perhaps] the negative results of STATCOPE could be related to careful selection of study participants with a low burden of systemic inflammation.
This most recent study reinforces the idea that statins may play a beneficial role in COPD, but it isn’t clear which patients to target for therapy. It is unlikely that the findings by Raymakers et al. will reverse recent recommendations by the American College of Chest Physicians and Canadian Thoracic Society against the use of statins for the purpose of prevention of COPD exacerbations, but the suggestion of survival advantage related to statins certainly may breathe new life into an enthusiasm greatly tempered by STATCOPE.
Or Kalchiem-Dekel, MD, and Robert M. Reed, MD, are at the pulmonary and critical care medicine division, University of Maryland, Baltimore. Neither editorialist had conflicts of interest (Chest. 2017;152:456-7. doi: 10.1016/j.chest.2017.04.156).
Despite [its] limitations, the study results are intriguing and in line with findings from other retrospective cohorts. How then can we reconcile the apparent benefits observed in retrospective studies with the lack of clinical effect seen in prospective trials, particularly the Simvastatin in the Prevention of COPD Exacerbation (STATCOPE) study? Could it be that both negative and positive studies are “correct”? Prospective studies have thus far not been adequately powered for mortality as an endpoint. Perhaps the choice of the particular statin matters? While STATCOPE involved simvastatin, the majority of the cohort reported by Raymakers et al. received atorvastatin. [Or perhaps] the negative results of STATCOPE could be related to careful selection of study participants with a low burden of systemic inflammation.
This most recent study reinforces the idea that statins may play a beneficial role in COPD, but it isn’t clear which patients to target for therapy. It is unlikely that the findings by Raymakers et al. will reverse recent recommendations by the American College of Chest Physicians and Canadian Thoracic Society against the use of statins for the purpose of prevention of COPD exacerbations, but the suggestion of survival advantage related to statins certainly may breathe new life into an enthusiasm greatly tempered by STATCOPE.
Or Kalchiem-Dekel, MD, and Robert M. Reed, MD, are at the pulmonary and critical care medicine division, University of Maryland, Baltimore. Neither editorialist had conflicts of interest (Chest. 2017;152:456-7. doi: 10.1016/j.chest.2017.04.156).
Despite [its] limitations, the study results are intriguing and in line with findings from other retrospective cohorts. How then can we reconcile the apparent benefits observed in retrospective studies with the lack of clinical effect seen in prospective trials, particularly the Simvastatin in the Prevention of COPD Exacerbation (STATCOPE) study? Could it be that both negative and positive studies are “correct”? Prospective studies have thus far not been adequately powered for mortality as an endpoint. Perhaps the choice of the particular statin matters? While STATCOPE involved simvastatin, the majority of the cohort reported by Raymakers et al. received atorvastatin. [Or perhaps] the negative results of STATCOPE could be related to careful selection of study participants with a low burden of systemic inflammation.
This most recent study reinforces the idea that statins may play a beneficial role in COPD, but it isn’t clear which patients to target for therapy. It is unlikely that the findings by Raymakers et al. will reverse recent recommendations by the American College of Chest Physicians and Canadian Thoracic Society against the use of statins for the purpose of prevention of COPD exacerbations, but the suggestion of survival advantage related to statins certainly may breathe new life into an enthusiasm greatly tempered by STATCOPE.
Or Kalchiem-Dekel, MD, and Robert M. Reed, MD, are at the pulmonary and critical care medicine division, University of Maryland, Baltimore. Neither editorialist had conflicts of interest (Chest. 2017;152:456-7. doi: 10.1016/j.chest.2017.04.156).
Receiving a statin prescription within a year after diagnosis of chronic obstructive pulmonary disease was associated with a 21% decrease in the subsequent risk of all-cause mortality and a 45% drop in risk of pulmonary mortality, according to the results of a large retrospective administrative database study.
The findings belie those of the recent Simvastatin in the Prevention of COPD Exacerbation (STATCOPE) trial, in which daily simvastatin (40 mg) did not affect exacerbation rates or time to first exacerbation in high-risk COPD patients, wrote Adam Raymakers, MSc, a doctoral candidate at the University of British Columbia, Vancouver, and his associates. Their study was observational, but the association between statin use and decreased mortality “persisted across several measures of statin exposure,” they wrote. “Our findings, in conjunction with previously reported evidence, suggests that there may be a specific subtype of COPD patients that may benefit from statin use.” The study appears in the September issue of Chest (2017;152;486-93).
To further explore the question, the researchers analyzed linked health databases from nearly 40,000 patients aged 50 years and older who had received at least three prescriptions for an anticholinergic or a short-acting beta agonist in 12 months some time between 1998 and 2007. The first prescription was considered the date of COPD “diagnosis.” The average age of the patients was 71 years; 55% were female.
A total of 7,775 patients (19.6%) who met this definition of incident COPD were prescribed a statin at least once during the subsequent year. These patients had a significantly reduced risk of subsequent all-cause mortality in univariate and multivariate analyses, with hazard ratios of 0.79 (95% confidence intervals, 0.68 to 0.91; P less than .002). Statins also showed a protective effect against pulmonary mortality, with univariate and multivariate hazard ratios of 0.52 (P = .01) and 0.55 (P = .03), respectively.
The protective effect of statins held up when the investigators narrowed the exposure period to 6 months after COPD diagnosis and when they expanded it to 18 months. Exposure to statins for 80% of the 1-year window after COPD diagnosis – a proxy for statin adherence – also led to a reduced risk of all-cause mortality, but the 95% confidence interval for the hazard ratio did not reach statistical significance (0.71 to 1.01; P = .06).
The most common prescription was for atorvastatin (49%), usually for 90 days (23%), 100 days (20%), or 30 days (15%), the researchers said. While the “possibility of the ‘healthy user’ or the ‘healthy adherer’ cannot be ignored,” they adjusted for other prescriptions, comorbidities, and income level, which should have helped eliminate this effect, they added. However, they lacked data on smoking and lung function assessments, both of which are “important confounders and contributors to mortality,” they acknowledged.
Canadian Institutes of Health Research supported the study. One coinvestigator disclosed consulting relationships with Teva, Pfizer, and Novartis. The others had no conflicts of interest.
Receiving a statin prescription within a year after diagnosis of chronic obstructive pulmonary disease was associated with a 21% decrease in the subsequent risk of all-cause mortality and a 45% drop in risk of pulmonary mortality, according to the results of a large retrospective administrative database study.
The findings belie those of the recent Simvastatin in the Prevention of COPD Exacerbation (STATCOPE) trial, in which daily simvastatin (40 mg) did not affect exacerbation rates or time to first exacerbation in high-risk COPD patients, wrote Adam Raymakers, MSc, a doctoral candidate at the University of British Columbia, Vancouver, and his associates. Their study was observational, but the association between statin use and decreased mortality “persisted across several measures of statin exposure,” they wrote. “Our findings, in conjunction with previously reported evidence, suggests that there may be a specific subtype of COPD patients that may benefit from statin use.” The study appears in the September issue of Chest (2017;152;486-93).
To further explore the question, the researchers analyzed linked health databases from nearly 40,000 patients aged 50 years and older who had received at least three prescriptions for an anticholinergic or a short-acting beta agonist in 12 months some time between 1998 and 2007. The first prescription was considered the date of COPD “diagnosis.” The average age of the patients was 71 years; 55% were female.
A total of 7,775 patients (19.6%) who met this definition of incident COPD were prescribed a statin at least once during the subsequent year. These patients had a significantly reduced risk of subsequent all-cause mortality in univariate and multivariate analyses, with hazard ratios of 0.79 (95% confidence intervals, 0.68 to 0.91; P less than .002). Statins also showed a protective effect against pulmonary mortality, with univariate and multivariate hazard ratios of 0.52 (P = .01) and 0.55 (P = .03), respectively.
The protective effect of statins held up when the investigators narrowed the exposure period to 6 months after COPD diagnosis and when they expanded it to 18 months. Exposure to statins for 80% of the 1-year window after COPD diagnosis – a proxy for statin adherence – also led to a reduced risk of all-cause mortality, but the 95% confidence interval for the hazard ratio did not reach statistical significance (0.71 to 1.01; P = .06).
The most common prescription was for atorvastatin (49%), usually for 90 days (23%), 100 days (20%), or 30 days (15%), the researchers said. While the “possibility of the ‘healthy user’ or the ‘healthy adherer’ cannot be ignored,” they adjusted for other prescriptions, comorbidities, and income level, which should have helped eliminate this effect, they added. However, they lacked data on smoking and lung function assessments, both of which are “important confounders and contributors to mortality,” they acknowledged.
Canadian Institutes of Health Research supported the study. One coinvestigator disclosed consulting relationships with Teva, Pfizer, and Novartis. The others had no conflicts of interest.
FROM CHEST
Key clinical point: Statins might reduce the risk of death among patients with chronic obstructive pulmonary disease.
Major finding: Statin use was associated with a 21% decrease in risk of all-cause mortality and a 45% decrease in risk of pulmonary mortality.
Data source: A retrospective cohort study of 39,678 patients with COPD, including 7,775 prescribed statins.
Disclosures: Canadian Institutes of Health Research supported the study. One coinvestigator disclosed consulting relationships with Teva, Pfizer, and Novartis. The others had no conflicts of interest.
Hepatitis C falls as barrier to heart transplantation
DALLAS – The heart transplant team at Vanderbilt University has successfully placed hearts from deceased, hepatitis C virus–positive patients into recipients, and then eradicated the subsequent infection that appeared in most recipients using a standard regimen.
So far, five of nine heart transplant recipients who developed a posttransplant hepatitis C virus (HCV) infection had the infection eradicated using one of the highly effective HCV drug regimens, and an additional three patients from the series are nearing their 12th week without detectable virus following treatment that marks a sustained response, Kelly H. Schlendorf, MD, said at the annual scientific meeting of the Heart Failure Society of America. The ninth patient died after developing a pulmonary embolism during the 7th week on antiviral therapy.

The recipients have been patients in a marginal clinical state and facing a long projected wait on the heart-recipient queue of the United Network for Organ Sharing (UNOS), Dr. Schlendorf said in an interview.
These have been “patients with a morbidity and mortality risk from waiting that can be mitigated by expanding the donor pool.” She gave an example of a patient with a left ventricular assist device that required replacement by either a second device or transplant, “so getting the transplant quickly was a good thing,” said Dr. Schlendorf, a cardiologist at Vanderbilt in Nashville.
Based on her analysis of UNOS data, “upwards of 100” and perhaps as many as 300 additional donor hearts could be available annually for U.S. transplants if the organs weren’t excluded because of HCV infection.
The Vanderbilt team has so far approached 15 patients in their program wait-listed for hearts about the possibility of accepting an HCV-positive organ, and all 15 have given their consent, she said. “We spend a lot of time talking with patients and their caregivers about the risks and benefits and possible complications.”
The 13 recipients, starting in September 2016, included 12 patients who were HCV naive and 1 patient with a history of HCV exposure. All 13 received the program’s standard three-drug regimen for immunosuppression.
During close surveillance, 9 of the 13 developed an infection. Patients with genotype 1 HCV received 12 weeks of treatment with ledipasvir plus sofosbuvir. Those infected with genotype 3 received 12-24 weeks of treatment with sofosbuvir plus velpatasvir. Treatment with these direct-acting antivirals meant that patients had to adjust the time when they took their proton-pump inhibitors, and they needed to stop treatment with diltiazem and statins while on the antivirals.
“In the era of direct-acting antivirals, HCV-positive donors may provide a safe and effective way to expand the donor pool and reduce wait-list times,” Dr. Schlendorf said. She noted that in recent years an increased number of potential organ donors have been HCV positive. She also cautioned that so far follow-up has been relatively brief, with no patient yet followed as long as 1 year after transplant.
The direct-acting HCV antivirals are expensive, and some payers established clinical criteria that patients must meet to qualify for coverage of these regimens. “We have not encountered difficulties getting insurers to pay,” Dr. Schlendorf said. Despite the antivirals’ cost there are significant cost savings from fewer days in the ICU waiting for heart transplantation and a reduced need for mechanical support as a bridge to transplant, she noted.
[email protected]
On Twitter @mitchelzoler
DALLAS – The heart transplant team at Vanderbilt University has successfully placed hearts from deceased, hepatitis C virus–positive patients into recipients, and then eradicated the subsequent infection that appeared in most recipients using a standard regimen.
So far, five of nine heart transplant recipients who developed a posttransplant hepatitis C virus (HCV) infection had the infection eradicated using one of the highly effective HCV drug regimens, and an additional three patients from the series are nearing their 12th week without detectable virus following treatment that marks a sustained response, Kelly H. Schlendorf, MD, said at the annual scientific meeting of the Heart Failure Society of America. The ninth patient died after developing a pulmonary embolism during the 7th week on antiviral therapy.
The recipients have been patients in a marginal clinical state and facing a long projected wait on the heart-recipient queue of the United Network for Organ Sharing (UNOS), Dr. Schlendorf said in an interview.
These have been “patients with a morbidity and mortality risk from waiting that can be mitigated by expanding the donor pool.” She gave an example of a patient with a left ventricular assist device that required replacement by either a second device or transplant, “so getting the transplant quickly was a good thing,” said Dr. Schlendorf, a cardiologist at Vanderbilt in Nashville.
Based on her analysis of UNOS data, “upwards of 100” and perhaps as many as 300 additional donor hearts could be available annually for U.S. transplants if the organs weren’t excluded because of HCV infection.
The Vanderbilt team has so far approached 15 patients in their program wait-listed for hearts about the possibility of accepting an HCV-positive organ, and all 15 have given their consent, she said. “We spend a lot of time talking with patients and their caregivers about the risks and benefits and possible complications.”
The 13 recipients, starting in September 2016, included 12 patients who were HCV naive and 1 patient with a history of HCV exposure. All 13 received the program’s standard three-drug regimen for immunosuppression.
During close surveillance, 9 of the 13 developed an infection. Patients with genotype 1 HCV received 12 weeks of treatment with ledipasvir plus sofosbuvir. Those infected with genotype 3 received 12-24 weeks of treatment with sofosbuvir plus velpatasvir. Treatment with these direct-acting antivirals meant that patients had to adjust the time when they took their proton-pump inhibitors, and they needed to stop treatment with diltiazem and statins while on the antivirals.
“In the era of direct-acting antivirals, HCV-positive donors may provide a safe and effective way to expand the donor pool and reduce wait-list times,” Dr. Schlendorf said. She noted that in recent years an increased number of potential organ donors have been HCV positive. She also cautioned that so far follow-up has been relatively brief, with no patient yet followed as long as 1 year after transplant.
The direct-acting HCV antivirals are expensive, and some payers established clinical criteria that patients must meet to qualify for coverage of these regimens. “We have not encountered difficulties getting insurers to pay,” Dr. Schlendorf said. Despite the antivirals’ cost there are significant cost savings from fewer days in the ICU waiting for heart transplantation and a reduced need for mechanical support as a bridge to transplant, she noted.
[email protected]
On Twitter @mitchelzoler
DALLAS – The heart transplant team at Vanderbilt University has successfully placed hearts from deceased, hepatitis C virus–positive patients into recipients, and then eradicated the subsequent infection that appeared in most recipients using a standard regimen.
So far, five of nine heart transplant recipients who developed a posttransplant hepatitis C virus (HCV) infection had the infection eradicated using one of the highly effective HCV drug regimens, and an additional three patients from the series are nearing their 12th week without detectable virus following treatment that marks a sustained response, Kelly H. Schlendorf, MD, said at the annual scientific meeting of the Heart Failure Society of America. The ninth patient died after developing a pulmonary embolism during the 7th week on antiviral therapy.
The recipients have been patients in a marginal clinical state and facing a long projected wait on the heart-recipient queue of the United Network for Organ Sharing (UNOS), Dr. Schlendorf said in an interview.
These have been “patients with a morbidity and mortality risk from waiting that can be mitigated by expanding the donor pool.” She gave an example of a patient with a left ventricular assist device that required replacement by either a second device or transplant, “so getting the transplant quickly was a good thing,” said Dr. Schlendorf, a cardiologist at Vanderbilt in Nashville.
Based on her analysis of UNOS data, “upwards of 100” and perhaps as many as 300 additional donor hearts could be available annually for U.S. transplants if the organs weren’t excluded because of HCV infection.
The Vanderbilt team has so far approached 15 patients in their program wait-listed for hearts about the possibility of accepting an HCV-positive organ, and all 15 have given their consent, she said. “We spend a lot of time talking with patients and their caregivers about the risks and benefits and possible complications.”
The 13 recipients, starting in September 2016, included 12 patients who were HCV naive and 1 patient with a history of HCV exposure. All 13 received the program’s standard three-drug regimen for immunosuppression.
During close surveillance, 9 of the 13 developed an infection. Patients with genotype 1 HCV received 12 weeks of treatment with ledipasvir plus sofosbuvir. Those infected with genotype 3 received 12-24 weeks of treatment with sofosbuvir plus velpatasvir. Treatment with these direct-acting antivirals meant that patients had to adjust the time when they took their proton-pump inhibitors, and they needed to stop treatment with diltiazem and statins while on the antivirals.
“In the era of direct-acting antivirals, HCV-positive donors may provide a safe and effective way to expand the donor pool and reduce wait-list times,” Dr. Schlendorf said. She noted that in recent years an increased number of potential organ donors have been HCV positive. She also cautioned that so far follow-up has been relatively brief, with no patient yet followed as long as 1 year after transplant.
The direct-acting HCV antivirals are expensive, and some payers established clinical criteria that patients must meet to qualify for coverage of these regimens. “We have not encountered difficulties getting insurers to pay,” Dr. Schlendorf said. Despite the antivirals’ cost there are significant cost savings from fewer days in the ICU waiting for heart transplantation and a reduced need for mechanical support as a bridge to transplant, she noted.
[email protected]
On Twitter @mitchelzoler
AT THE HFSA ANNUAL SCIENTIFIC MEETING
Key clinical point:
Major finding: Eight of nine patients who developed HCV infection had it eradicated by a direct-acting antiviral regimen.
Data source: A series of 13 patients treated at one U.S. center.
Disclosures: Dr. Schlendorf had no disclosures.
Lobectomy shown safe after concurrent chemo and radiation
Lobectomy can be done safely after concurrent chemotherapy and high-dose radiation in patients with resectable N2-positive stage IIIA non–small cell lung cancer, according to study findings presented by Jessica S. Donington, MD.
Dr. Donington of New York University and her colleagues presented analysis of two prospective trials conducted by NRG Oncology, RTOG 0229 and RTOG 0839 at the AATS Annual Meeting. Both trials’ primary endpoints were mediastinal node sterilization after concurrent chemotherapy and full-dose radiation and those results were previously reported.
Dr. Donington and her fellow investigators specifically examined short-term surgical outcomes, given the significant controversy regarding the safety of resection after full-dose thoracic radiation. In both trials, patients received weekly carboplatin and paclitaxel. Those in the 0229 trial underwent 61.2 Gy of radiation in 34 fractions, while patients in the 0839 trial underwent 60 Gy in 30 fractions. In addition, patients in the 0839 trial were randomized 2:1 to receive weekly panitumumab, an EGFR monoclonal antibody, with their induction therapy.
Surgical expertise was considered essential to this treatment strategy. Therefore, all surgeons were certified by RTOG prior to enrolling patients, and all patients were surgically evaluated before beginning induction therapy to determine resectability and appropriateness for trimodality therapy. Of 125 eligible patients enrolled in the two trials, 93 patients (74%) underwent anatomic resection. A total of 77 patients underwent lobectomy, 8 underwent pneumonectomy, 6 underwent bilobectomy, and 2 patients had sleeve lobectomy.
Medical contraindication and persistent nodal disease found during post-induction invasive staging were the most common reasons patients didn’t undergo resection. Eighty-five of the 93 surgical patients had R0 resections (91%). Surgeons attempted 14 minimally invasive resections (15%), 2 of which uneventfully converted to open resection. Just over one-quarter (28%) of patients suffered greater than Grade 3 adverse events (AEs) related to surgery, the majority of which were pulmonary in nature.
The 30-day mortality rate was 4%, and all four deaths were linked to pulmonary adverse events, including acute respiratory distress syndrome, bronchopleural fistula, pulmonary artery hemorrhage, and respiratory failure. Multivariable analysis for mortality identified the addition of panitumumab and use of an extended resection to be associated with an increased risk for operative mortality.
In the patients undergoing lobectomy, rates for greater than Grade 3 adverse events and 30-day mortality were 26%, and 1.3%, respectively. Those are similar to rates reported for lobectomy without induction therapy in the National Inpatient Sample (NIS) and the STS General Thoracic Surgery Database over the same time period.
These two RTOG trials are the first to prospectively demonstrate that trimodality therapy with full-dose neoadjuvant radiation therapy is safe in a multi-institutional setting, Dr. Donington said.
As her conclusions, she listed that “we have demonstrated the safety of resection following full-dose concurrent CRT in a multi-insitutional setting, that EGFR-AB and T2/T3 stage was associated with decreased nonfatal morbidity, but that extended resection and EGFR-AB were associated with excessive surgical mortality.” Dr. Donington added that the morbidity and mortality for lobectomy compared favorably with large national databases.She pointed out several limitations of the study, which included the relatively small size, and the unexpected toxicity of the EGFR antibody, “which severely limited our ability to assess trimodality therapy.”
She added that “our short-term outcomes tell us nothing about the long-term oncologic benefit.
Dr. David R. Jones, chief of thoracic surgery at the Memorial Sloan-Kettering Cancer Center, New York, was the invited discussant of the paper. “Despite combining these [2] trials, there are still only 93 patients in the analysis and 77 of these had a lobectomy,” Dr. Jones stated. He pointed out that “there was a significant increase in 30- and 90-day mortality in the 16 patients who had more than a straightforward lobectomy,” and asked whether this increased mortality could be due to the use of radiation in the induction therapy.
Dr. Donington replied that there was a wide variation in causes of death, but that “the fact that these patients had induction therapy, be that radiation or chemo, and then went on to this bigger operation, it was overall a difficult thing for them to overcome.” Dr. Donington also agreed with a comment by Dr. Jones that it would be important to follow predicted postoperative diffusion capacity in these patients to potentially help determine the amount of lung to be taken and would be a valuable preoperative consideration.
Dr. Donington reported that two of her coauthors received grant support from NCI and AMGen for the work she was reporting, but that there were no other related disclosures. Dr. Jones reported that he had no disclosures.
Lobectomy can be done safely after concurrent chemotherapy and high-dose radiation in patients with resectable N2-positive stage IIIA non–small cell lung cancer, according to study findings presented by Jessica S. Donington, MD.
Dr. Donington of New York University and her colleagues presented analysis of two prospective trials conducted by NRG Oncology, RTOG 0229 and RTOG 0839 at the AATS Annual Meeting. Both trials’ primary endpoints were mediastinal node sterilization after concurrent chemotherapy and full-dose radiation and those results were previously reported.
Dr. Donington and her fellow investigators specifically examined short-term surgical outcomes, given the significant controversy regarding the safety of resection after full-dose thoracic radiation. In both trials, patients received weekly carboplatin and paclitaxel. Those in the 0229 trial underwent 61.2 Gy of radiation in 34 fractions, while patients in the 0839 trial underwent 60 Gy in 30 fractions. In addition, patients in the 0839 trial were randomized 2:1 to receive weekly panitumumab, an EGFR monoclonal antibody, with their induction therapy.
Surgical expertise was considered essential to this treatment strategy. Therefore, all surgeons were certified by RTOG prior to enrolling patients, and all patients were surgically evaluated before beginning induction therapy to determine resectability and appropriateness for trimodality therapy. Of 125 eligible patients enrolled in the two trials, 93 patients (74%) underwent anatomic resection. A total of 77 patients underwent lobectomy, 8 underwent pneumonectomy, 6 underwent bilobectomy, and 2 patients had sleeve lobectomy.
Medical contraindication and persistent nodal disease found during post-induction invasive staging were the most common reasons patients didn’t undergo resection. Eighty-five of the 93 surgical patients had R0 resections (91%). Surgeons attempted 14 minimally invasive resections (15%), 2 of which uneventfully converted to open resection. Just over one-quarter (28%) of patients suffered greater than Grade 3 adverse events (AEs) related to surgery, the majority of which were pulmonary in nature.
The 30-day mortality rate was 4%, and all four deaths were linked to pulmonary adverse events, including acute respiratory distress syndrome, bronchopleural fistula, pulmonary artery hemorrhage, and respiratory failure. Multivariable analysis for mortality identified the addition of panitumumab and use of an extended resection to be associated with an increased risk for operative mortality.
In the patients undergoing lobectomy, rates for greater than Grade 3 adverse events and 30-day mortality were 26%, and 1.3%, respectively. Those are similar to rates reported for lobectomy without induction therapy in the National Inpatient Sample (NIS) and the STS General Thoracic Surgery Database over the same time period.
These two RTOG trials are the first to prospectively demonstrate that trimodality therapy with full-dose neoadjuvant radiation therapy is safe in a multi-institutional setting, Dr. Donington said.
As her conclusions, she listed that “we have demonstrated the safety of resection following full-dose concurrent CRT in a multi-insitutional setting, that EGFR-AB and T2/T3 stage was associated with decreased nonfatal morbidity, but that extended resection and EGFR-AB were associated with excessive surgical mortality.” Dr. Donington added that the morbidity and mortality for lobectomy compared favorably with large national databases.She pointed out several limitations of the study, which included the relatively small size, and the unexpected toxicity of the EGFR antibody, “which severely limited our ability to assess trimodality therapy.”
She added that “our short-term outcomes tell us nothing about the long-term oncologic benefit.
Dr. David R. Jones, chief of thoracic surgery at the Memorial Sloan-Kettering Cancer Center, New York, was the invited discussant of the paper. “Despite combining these [2] trials, there are still only 93 patients in the analysis and 77 of these had a lobectomy,” Dr. Jones stated. He pointed out that “there was a significant increase in 30- and 90-day mortality in the 16 patients who had more than a straightforward lobectomy,” and asked whether this increased mortality could be due to the use of radiation in the induction therapy.
Dr. Donington replied that there was a wide variation in causes of death, but that “the fact that these patients had induction therapy, be that radiation or chemo, and then went on to this bigger operation, it was overall a difficult thing for them to overcome.” Dr. Donington also agreed with a comment by Dr. Jones that it would be important to follow predicted postoperative diffusion capacity in these patients to potentially help determine the amount of lung to be taken and would be a valuable preoperative consideration.
Dr. Donington reported that two of her coauthors received grant support from NCI and AMGen for the work she was reporting, but that there were no other related disclosures. Dr. Jones reported that he had no disclosures.
Lobectomy can be done safely after concurrent chemotherapy and high-dose radiation in patients with resectable N2-positive stage IIIA non–small cell lung cancer, according to study findings presented by Jessica S. Donington, MD.
Dr. Donington of New York University and her colleagues presented analysis of two prospective trials conducted by NRG Oncology, RTOG 0229 and RTOG 0839 at the AATS Annual Meeting. Both trials’ primary endpoints were mediastinal node sterilization after concurrent chemotherapy and full-dose radiation and those results were previously reported.
Dr. Donington and her fellow investigators specifically examined short-term surgical outcomes, given the significant controversy regarding the safety of resection after full-dose thoracic radiation. In both trials, patients received weekly carboplatin and paclitaxel. Those in the 0229 trial underwent 61.2 Gy of radiation in 34 fractions, while patients in the 0839 trial underwent 60 Gy in 30 fractions. In addition, patients in the 0839 trial were randomized 2:1 to receive weekly panitumumab, an EGFR monoclonal antibody, with their induction therapy.
Surgical expertise was considered essential to this treatment strategy. Therefore, all surgeons were certified by RTOG prior to enrolling patients, and all patients were surgically evaluated before beginning induction therapy to determine resectability and appropriateness for trimodality therapy. Of 125 eligible patients enrolled in the two trials, 93 patients (74%) underwent anatomic resection. A total of 77 patients underwent lobectomy, 8 underwent pneumonectomy, 6 underwent bilobectomy, and 2 patients had sleeve lobectomy.
Medical contraindication and persistent nodal disease found during post-induction invasive staging were the most common reasons patients didn’t undergo resection. Eighty-five of the 93 surgical patients had R0 resections (91%). Surgeons attempted 14 minimally invasive resections (15%), 2 of which uneventfully converted to open resection. Just over one-quarter (28%) of patients suffered greater than Grade 3 adverse events (AEs) related to surgery, the majority of which were pulmonary in nature.
The 30-day mortality rate was 4%, and all four deaths were linked to pulmonary adverse events, including acute respiratory distress syndrome, bronchopleural fistula, pulmonary artery hemorrhage, and respiratory failure. Multivariable analysis for mortality identified the addition of panitumumab and use of an extended resection to be associated with an increased risk for operative mortality.
In the patients undergoing lobectomy, rates for greater than Grade 3 adverse events and 30-day mortality were 26%, and 1.3%, respectively. Those are similar to rates reported for lobectomy without induction therapy in the National Inpatient Sample (NIS) and the STS General Thoracic Surgery Database over the same time period.
These two RTOG trials are the first to prospectively demonstrate that trimodality therapy with full-dose neoadjuvant radiation therapy is safe in a multi-institutional setting, Dr. Donington said.
As her conclusions, she listed that “we have demonstrated the safety of resection following full-dose concurrent CRT in a multi-insitutional setting, that EGFR-AB and T2/T3 stage was associated with decreased nonfatal morbidity, but that extended resection and EGFR-AB were associated with excessive surgical mortality.” Dr. Donington added that the morbidity and mortality for lobectomy compared favorably with large national databases.She pointed out several limitations of the study, which included the relatively small size, and the unexpected toxicity of the EGFR antibody, “which severely limited our ability to assess trimodality therapy.”
She added that “our short-term outcomes tell us nothing about the long-term oncologic benefit.
Dr. David R. Jones, chief of thoracic surgery at the Memorial Sloan-Kettering Cancer Center, New York, was the invited discussant of the paper. “Despite combining these [2] trials, there are still only 93 patients in the analysis and 77 of these had a lobectomy,” Dr. Jones stated. He pointed out that “there was a significant increase in 30- and 90-day mortality in the 16 patients who had more than a straightforward lobectomy,” and asked whether this increased mortality could be due to the use of radiation in the induction therapy.
Dr. Donington replied that there was a wide variation in causes of death, but that “the fact that these patients had induction therapy, be that radiation or chemo, and then went on to this bigger operation, it was overall a difficult thing for them to overcome.” Dr. Donington also agreed with a comment by Dr. Jones that it would be important to follow predicted postoperative diffusion capacity in these patients to potentially help determine the amount of lung to be taken and would be a valuable preoperative consideration.
Dr. Donington reported that two of her coauthors received grant support from NCI and AMGen for the work she was reporting, but that there were no other related disclosures. Dr. Jones reported that he had no disclosures.
FROM THE AMERICAN ASSOCIATION FOR THORACIC SURGERY ANNUAL MEETING
Doctors testify on health insurance stabilization
WASHINGTON – Physicians testifying before the Senate Health, Education, Labor & Pensions Committee offered recommendations that are generally in line with the narrow, focused legislation to stabilize the individual health insurance markets that Chairman Lamar Alexander (R-Tenn.) is hoping to introduce early in the week of Sept. 17.
Two key provisions of Chairman Alexander’s plan are extending the cost-sharing reduction (CSR) payments to insurers through the end of 2018 and providing additional flexibility to the process that allows states to come up with alternatives to the Affordable Care Act mandates.
Manny Sethi, MD, president of Healthy Tennessee, said he favored repealing and replacing the ACA but offered suggestions to fit the current legislative landscape.
“We must take three steps immediately,” Dr. Sethi, an orthopedic trauma surgeon, testified. “First, in order to stabilize the insurance markets, we must continue the cost-sharing reduction program. Premiums are rapidly rising as insurers fear they will be left bearing the cost. These soaring costs are forcing young members out, saturating the market with higher-need and higher-cost patients and further escalating prices in a troublesome cycle.
“Second, we must quickly create risk pools for those individuals with serious chronic conditions, allowing more affordable coverage options for young, healthy citizens,” Dr. Sethi continued. “Third, I believe a one-size-fits-all plan from Washington, D.C., doesn’t meet the needs of Tennesseans. Open the door for innovation, and allow more flexibility for states to create their own insurance products. For example, a catastrophic plan should be available regardless of age or income status, which is currently not the case.”
Opening the catastrophic plans to all would help bring people into the individual market, even if they don’t have access to any government subsidies, he said.
“Meeting with patients ... I do believe that creating a catastrophic plan open to all ages, all incomes, I think would bring younger folks, and people in general, into the insurance market because I think that’s the problem,” Dr. Sethi said. “You don’t want to pay more for your insurance than you do for your home mortgage. When you do that, something’s wrong.”
Susan Turney, MD, CEO of Marshfield (Wisc.) Clinic Health System, offered similar suggestions. She called for fully funding CSR payments for 2018 and beyond and also recommended creating a reinsurance program, establishing continuous coverage rules that encourage people to get and maintain coverage, enhancing risk adjustment for payments to carriers, and reinstating federal funding for outreach that was recently cut by the Trump administration.
But she also stressed a longer-term goal of how care is delivered, especially in rural areas.
“As we look at this short-term fix to a relatively small group of insured, we have to start thinking differently about how we provide care. The care delivery model needs to be above the payment system, and, once we figure out how to take care of our communities, we can then look differently at the way we support the practices who provide those services,” Dr. Turney said. “Most people don’t ask to get sick. We need to take care of them, and we need to figure out the best way to do that.”
Physicians’ organizations including the American Academy of Family Physicians, American Academy of Pediatrics, American College of Physicians, American Congress of Obstetricians and Gynecologists, American Osteopathic Association, and American Psychiatric Association, submitted a joint statement to the committee that advocated ensuring CSR funding through at least 2019, continuing reinsurance programs, continuing community outreach programs, and expanding public choice through a public option in all exchanges markets.
Chairman Alexander stressed that, in order for this narrowly focused bill to have a chance at passing, it will require a little compromise from both sides of the aisle.
“To get a result, Republicans will have to agree to something – additional funding through the Affordable Care Act – that some are reluctant to support,” he said. “And Democrats will have to agree to something – more flexibility for states – that some may be reluctant to support. I simply won’t be able to persuade the Republican majority in the Senate, the Republican majority in the House, and the Republican president to extend the cost-sharing payments without giving states meaningful flexibility.”
He stressed that the flexibility he is looking for in the 1332 waiver program will not alter consumer protections that are in place, including the ban on charging more for preexisting conditions, guaranteed issue, no annual or lifetime caps on benefits, and allowing those under 26 years of age to remain on their parent’s policy.
“Our goal is to see if we can come to a consensus by early next week so we can hand [Senate Majority Leader Mitch] McConnell and [Senate Minority Leader Chuck] Schumer an agreement that Congress can pass by the end of the month that would help limit premium increases for 18 million Americans next year and begin to lower premiums after that, and to prevent insurers from leaving the markets where those 18 million Americans buy insurance.”
WASHINGTON – Physicians testifying before the Senate Health, Education, Labor & Pensions Committee offered recommendations that are generally in line with the narrow, focused legislation to stabilize the individual health insurance markets that Chairman Lamar Alexander (R-Tenn.) is hoping to introduce early in the week of Sept. 17.
Two key provisions of Chairman Alexander’s plan are extending the cost-sharing reduction (CSR) payments to insurers through the end of 2018 and providing additional flexibility to the process that allows states to come up with alternatives to the Affordable Care Act mandates.
Manny Sethi, MD, president of Healthy Tennessee, said he favored repealing and replacing the ACA but offered suggestions to fit the current legislative landscape.
“We must take three steps immediately,” Dr. Sethi, an orthopedic trauma surgeon, testified. “First, in order to stabilize the insurance markets, we must continue the cost-sharing reduction program. Premiums are rapidly rising as insurers fear they will be left bearing the cost. These soaring costs are forcing young members out, saturating the market with higher-need and higher-cost patients and further escalating prices in a troublesome cycle.
“Second, we must quickly create risk pools for those individuals with serious chronic conditions, allowing more affordable coverage options for young, healthy citizens,” Dr. Sethi continued. “Third, I believe a one-size-fits-all plan from Washington, D.C., doesn’t meet the needs of Tennesseans. Open the door for innovation, and allow more flexibility for states to create their own insurance products. For example, a catastrophic plan should be available regardless of age or income status, which is currently not the case.”
Opening the catastrophic plans to all would help bring people into the individual market, even if they don’t have access to any government subsidies, he said.
“Meeting with patients ... I do believe that creating a catastrophic plan open to all ages, all incomes, I think would bring younger folks, and people in general, into the insurance market because I think that’s the problem,” Dr. Sethi said. “You don’t want to pay more for your insurance than you do for your home mortgage. When you do that, something’s wrong.”
Susan Turney, MD, CEO of Marshfield (Wisc.) Clinic Health System, offered similar suggestions. She called for fully funding CSR payments for 2018 and beyond and also recommended creating a reinsurance program, establishing continuous coverage rules that encourage people to get and maintain coverage, enhancing risk adjustment for payments to carriers, and reinstating federal funding for outreach that was recently cut by the Trump administration.
But she also stressed a longer-term goal of how care is delivered, especially in rural areas.
“As we look at this short-term fix to a relatively small group of insured, we have to start thinking differently about how we provide care. The care delivery model needs to be above the payment system, and, once we figure out how to take care of our communities, we can then look differently at the way we support the practices who provide those services,” Dr. Turney said. “Most people don’t ask to get sick. We need to take care of them, and we need to figure out the best way to do that.”
Physicians’ organizations including the American Academy of Family Physicians, American Academy of Pediatrics, American College of Physicians, American Congress of Obstetricians and Gynecologists, American Osteopathic Association, and American Psychiatric Association, submitted a joint statement to the committee that advocated ensuring CSR funding through at least 2019, continuing reinsurance programs, continuing community outreach programs, and expanding public choice through a public option in all exchanges markets.
Chairman Alexander stressed that, in order for this narrowly focused bill to have a chance at passing, it will require a little compromise from both sides of the aisle.
“To get a result, Republicans will have to agree to something – additional funding through the Affordable Care Act – that some are reluctant to support,” he said. “And Democrats will have to agree to something – more flexibility for states – that some may be reluctant to support. I simply won’t be able to persuade the Republican majority in the Senate, the Republican majority in the House, and the Republican president to extend the cost-sharing payments without giving states meaningful flexibility.”
He stressed that the flexibility he is looking for in the 1332 waiver program will not alter consumer protections that are in place, including the ban on charging more for preexisting conditions, guaranteed issue, no annual or lifetime caps on benefits, and allowing those under 26 years of age to remain on their parent’s policy.
“Our goal is to see if we can come to a consensus by early next week so we can hand [Senate Majority Leader Mitch] McConnell and [Senate Minority Leader Chuck] Schumer an agreement that Congress can pass by the end of the month that would help limit premium increases for 18 million Americans next year and begin to lower premiums after that, and to prevent insurers from leaving the markets where those 18 million Americans buy insurance.”
WASHINGTON – Physicians testifying before the Senate Health, Education, Labor & Pensions Committee offered recommendations that are generally in line with the narrow, focused legislation to stabilize the individual health insurance markets that Chairman Lamar Alexander (R-Tenn.) is hoping to introduce early in the week of Sept. 17.
Two key provisions of Chairman Alexander’s plan are extending the cost-sharing reduction (CSR) payments to insurers through the end of 2018 and providing additional flexibility to the process that allows states to come up with alternatives to the Affordable Care Act mandates.
Manny Sethi, MD, president of Healthy Tennessee, said he favored repealing and replacing the ACA but offered suggestions to fit the current legislative landscape.
“We must take three steps immediately,” Dr. Sethi, an orthopedic trauma surgeon, testified. “First, in order to stabilize the insurance markets, we must continue the cost-sharing reduction program. Premiums are rapidly rising as insurers fear they will be left bearing the cost. These soaring costs are forcing young members out, saturating the market with higher-need and higher-cost patients and further escalating prices in a troublesome cycle.
“Second, we must quickly create risk pools for those individuals with serious chronic conditions, allowing more affordable coverage options for young, healthy citizens,” Dr. Sethi continued. “Third, I believe a one-size-fits-all plan from Washington, D.C., doesn’t meet the needs of Tennesseans. Open the door for innovation, and allow more flexibility for states to create their own insurance products. For example, a catastrophic plan should be available regardless of age or income status, which is currently not the case.”
Opening the catastrophic plans to all would help bring people into the individual market, even if they don’t have access to any government subsidies, he said.
“Meeting with patients ... I do believe that creating a catastrophic plan open to all ages, all incomes, I think would bring younger folks, and people in general, into the insurance market because I think that’s the problem,” Dr. Sethi said. “You don’t want to pay more for your insurance than you do for your home mortgage. When you do that, something’s wrong.”
Susan Turney, MD, CEO of Marshfield (Wisc.) Clinic Health System, offered similar suggestions. She called for fully funding CSR payments for 2018 and beyond and also recommended creating a reinsurance program, establishing continuous coverage rules that encourage people to get and maintain coverage, enhancing risk adjustment for payments to carriers, and reinstating federal funding for outreach that was recently cut by the Trump administration.
But she also stressed a longer-term goal of how care is delivered, especially in rural areas.
“As we look at this short-term fix to a relatively small group of insured, we have to start thinking differently about how we provide care. The care delivery model needs to be above the payment system, and, once we figure out how to take care of our communities, we can then look differently at the way we support the practices who provide those services,” Dr. Turney said. “Most people don’t ask to get sick. We need to take care of them, and we need to figure out the best way to do that.”
Physicians’ organizations including the American Academy of Family Physicians, American Academy of Pediatrics, American College of Physicians, American Congress of Obstetricians and Gynecologists, American Osteopathic Association, and American Psychiatric Association, submitted a joint statement to the committee that advocated ensuring CSR funding through at least 2019, continuing reinsurance programs, continuing community outreach programs, and expanding public choice through a public option in all exchanges markets.
Chairman Alexander stressed that, in order for this narrowly focused bill to have a chance at passing, it will require a little compromise from both sides of the aisle.
“To get a result, Republicans will have to agree to something – additional funding through the Affordable Care Act – that some are reluctant to support,” he said. “And Democrats will have to agree to something – more flexibility for states – that some may be reluctant to support. I simply won’t be able to persuade the Republican majority in the Senate, the Republican majority in the House, and the Republican president to extend the cost-sharing payments without giving states meaningful flexibility.”
He stressed that the flexibility he is looking for in the 1332 waiver program will not alter consumer protections that are in place, including the ban on charging more for preexisting conditions, guaranteed issue, no annual or lifetime caps on benefits, and allowing those under 26 years of age to remain on their parent’s policy.
“Our goal is to see if we can come to a consensus by early next week so we can hand [Senate Majority Leader Mitch] McConnell and [Senate Minority Leader Chuck] Schumer an agreement that Congress can pass by the end of the month that would help limit premium increases for 18 million Americans next year and begin to lower premiums after that, and to prevent insurers from leaving the markets where those 18 million Americans buy insurance.”
AT A SENATE HELP COMMITTEE HEARING