User login
Is it safe to pair low-power fractional diode lasers with cosmetic injectables in a single session?
, results from a 6-year, single-center review showed.

“These treatments can be complementary in single-session treatments and can offer increased convenience for both patients and physicians,” primary study author Jordan V. Wang, MD, MBE, MBA, said during a virtual abstract session at the annual meeting of the American Society for Dermatologic Surgery.
To date, limited studies have demonstrated the safety of pairing botulinum neurotoxin type A and soft-tissue fillers with laser and other energy-based devices during the same treatment session on the same day, said Dr. Wang, medical research director at the Laser & Skin Surgery Center of New York. “Some concerns remain, though, regarding patient safety and efficacy,” he said. “Data on single-session treatment with low-power, low-density 1,927-nm and 1,440-nm fractional diode lasers and either botulinum neurotoxin or fillers are lacking.”
In a retrospective review of electronic medical records conducted from May 2015 to April 2021, Dr. Wang, Roy G. Geronemus, MD, and Carolyn Kushner, MD evaluated patients who received a single-session facial treatment with either BoNT-A or soft-tissue fillers and the low-power, low-density 1,927-nm and 1,440-nm fractional diode lasers (Clear+Brilliant Perméa and Original, Solta, Pleasanton, Calif.). Safety was assessed by documenting adverse events related to the spread of BoNT-A and fillers or laser treatment of filled areas within 4 weeks.
Adverse events they looked for related to botulinum neurotoxin use included eyelid ptosis; neck weakness or spasms; impairments in chewing, swallowing, speech, and respiration; and prescriptions of apraclonidine eye drops. Filler-related adverse events they looked for included product migration, unexpected loss of filler volume, vascular occlusion, acute pain, necrosis, blindness, and burn. “For both, we looked at hospital or emergency room transfers or admissions and referrals to ENT or ophthalmology,” Dr. Wang said.
During the 6-year study period, 525 patients had 1,562 single-session laser treatments with a mean 46.4 units of BoNT-A, and 398 patients had 1,237 single-session treatments with a mean 1.6 soft-tissue filler syringes. Among those who received BoNT-A, most (93%) were female, their mean age was 51 years, and 99% were treated with a 1,927-nm wavelength at a medium setting in 87% of cases. The top five injection sites were glabella (82%), forehead (69%), periorbital area (64%), neck (40%), and jawline and/or masseters (13%).
The researchers noted one case (0.06%) where apraclonidine eye drops were prescribed for ptosis. The patient had undergone eight other single-session treatments without issue. There were no other documented adverse events directly related to spread of BoNT-A. According to Dr. Wang, this rate of ptosis is lower than the incidence with BoNT-A alone in two landmark trials studying its effects on glabellar lines, which was reported as 5.4% and 1.0%.
Among the 398 patients who received soft-tissue fillers, most (94%) were female, their mean age was 54 years, and 99% were treated with a 1927nm wavelength at a medium setting in 97% of cases. The top five injection sites were cheeks and/or tear troughs (89%), perioral area and/or marionette lines (77%), lips (34%), nasolabial folds (19%), and temples (11%), and the mean number of filler syringes per treatment was 1.6. Slightly more than half (51%) had 1 session, while the remainder had 2 to greater than 10 sessions. The researchers observed no documented adverse events related to spread of fillers or laser treatment of filled areas.
“This laser is a low-powered device that creates small, superficial, and transient microchannels, which likely contributes to the safety of single-session treatments with cosmetic injectables,” Dr. Wang said. However, prospective studies are needed to further validate these results, he added.
“With this very mild laser, it is not surprising that combined treatment had no effect,” said Eric F. Bernstein, MD, MSE, director of the Main Line Center for Laser Surgery in Ardmore, Pa., who was asked to comment on the study results. “There have been numerous anecdotal reports of spreading of botulinum toxin effect to areas not in the target area for treatment following a variety of lasers, including the more powerful version of the laser used in this study. In addition, spread following vascular and other lasers has been reported,” he noted
The laser used in this study, Dr. Bernstein continued, “is low powered and emits a wavelength that is very superficially absorbed, resulting in injury to the stratum corneum, superficial epidermis, or possibly the very superficial dermis, and is often used by physician extenders and not physicians – although I suspect this is not the case in the current study. One can have a reasonable degree of confidence when combining this laser with injectables, but these results cannot be extrapolated to other devices.”
The abstract received the annual ASDS Carruthers Award during the meeting. Dr. Wang reported that he is a consultant or advisor to Allergan, Alastin, AVAVA, Cynosure, Lutronic, Novoxel, Sofwave, and Solta. Dr. Bernstein reported having received research funding from Cynosure, Candela, and Acclaro. He also has received consulting fees from Cynosure and holds ownership interest in Candela, Novoxel, OnSite, Joylux, and Acclaro and has served on the advisory board for Novoxel, Cynosure, and Acclaro.
, results from a 6-year, single-center review showed.
“These treatments can be complementary in single-session treatments and can offer increased convenience for both patients and physicians,” primary study author Jordan V. Wang, MD, MBE, MBA, said during a virtual abstract session at the annual meeting of the American Society for Dermatologic Surgery.
To date, limited studies have demonstrated the safety of pairing botulinum neurotoxin type A and soft-tissue fillers with laser and other energy-based devices during the same treatment session on the same day, said Dr. Wang, medical research director at the Laser & Skin Surgery Center of New York. “Some concerns remain, though, regarding patient safety and efficacy,” he said. “Data on single-session treatment with low-power, low-density 1,927-nm and 1,440-nm fractional diode lasers and either botulinum neurotoxin or fillers are lacking.”
In a retrospective review of electronic medical records conducted from May 2015 to April 2021, Dr. Wang, Roy G. Geronemus, MD, and Carolyn Kushner, MD evaluated patients who received a single-session facial treatment with either BoNT-A or soft-tissue fillers and the low-power, low-density 1,927-nm and 1,440-nm fractional diode lasers (Clear+Brilliant Perméa and Original, Solta, Pleasanton, Calif.). Safety was assessed by documenting adverse events related to the spread of BoNT-A and fillers or laser treatment of filled areas within 4 weeks.
Adverse events they looked for related to botulinum neurotoxin use included eyelid ptosis; neck weakness or spasms; impairments in chewing, swallowing, speech, and respiration; and prescriptions of apraclonidine eye drops. Filler-related adverse events they looked for included product migration, unexpected loss of filler volume, vascular occlusion, acute pain, necrosis, blindness, and burn. “For both, we looked at hospital or emergency room transfers or admissions and referrals to ENT or ophthalmology,” Dr. Wang said.
During the 6-year study period, 525 patients had 1,562 single-session laser treatments with a mean 46.4 units of BoNT-A, and 398 patients had 1,237 single-session treatments with a mean 1.6 soft-tissue filler syringes. Among those who received BoNT-A, most (93%) were female, their mean age was 51 years, and 99% were treated with a 1,927-nm wavelength at a medium setting in 87% of cases. The top five injection sites were glabella (82%), forehead (69%), periorbital area (64%), neck (40%), and jawline and/or masseters (13%).
The researchers noted one case (0.06%) where apraclonidine eye drops were prescribed for ptosis. The patient had undergone eight other single-session treatments without issue. There were no other documented adverse events directly related to spread of BoNT-A. According to Dr. Wang, this rate of ptosis is lower than the incidence with BoNT-A alone in two landmark trials studying its effects on glabellar lines, which was reported as 5.4% and 1.0%.
Among the 398 patients who received soft-tissue fillers, most (94%) were female, their mean age was 54 years, and 99% were treated with a 1927nm wavelength at a medium setting in 97% of cases. The top five injection sites were cheeks and/or tear troughs (89%), perioral area and/or marionette lines (77%), lips (34%), nasolabial folds (19%), and temples (11%), and the mean number of filler syringes per treatment was 1.6. Slightly more than half (51%) had 1 session, while the remainder had 2 to greater than 10 sessions. The researchers observed no documented adverse events related to spread of fillers or laser treatment of filled areas.
“This laser is a low-powered device that creates small, superficial, and transient microchannels, which likely contributes to the safety of single-session treatments with cosmetic injectables,” Dr. Wang said. However, prospective studies are needed to further validate these results, he added.
“With this very mild laser, it is not surprising that combined treatment had no effect,” said Eric F. Bernstein, MD, MSE, director of the Main Line Center for Laser Surgery in Ardmore, Pa., who was asked to comment on the study results. “There have been numerous anecdotal reports of spreading of botulinum toxin effect to areas not in the target area for treatment following a variety of lasers, including the more powerful version of the laser used in this study. In addition, spread following vascular and other lasers has been reported,” he noted
The laser used in this study, Dr. Bernstein continued, “is low powered and emits a wavelength that is very superficially absorbed, resulting in injury to the stratum corneum, superficial epidermis, or possibly the very superficial dermis, and is often used by physician extenders and not physicians – although I suspect this is not the case in the current study. One can have a reasonable degree of confidence when combining this laser with injectables, but these results cannot be extrapolated to other devices.”
The abstract received the annual ASDS Carruthers Award during the meeting. Dr. Wang reported that he is a consultant or advisor to Allergan, Alastin, AVAVA, Cynosure, Lutronic, Novoxel, Sofwave, and Solta. Dr. Bernstein reported having received research funding from Cynosure, Candela, and Acclaro. He also has received consulting fees from Cynosure and holds ownership interest in Candela, Novoxel, OnSite, Joylux, and Acclaro and has served on the advisory board for Novoxel, Cynosure, and Acclaro.
, results from a 6-year, single-center review showed.
“These treatments can be complementary in single-session treatments and can offer increased convenience for both patients and physicians,” primary study author Jordan V. Wang, MD, MBE, MBA, said during a virtual abstract session at the annual meeting of the American Society for Dermatologic Surgery.
To date, limited studies have demonstrated the safety of pairing botulinum neurotoxin type A and soft-tissue fillers with laser and other energy-based devices during the same treatment session on the same day, said Dr. Wang, medical research director at the Laser & Skin Surgery Center of New York. “Some concerns remain, though, regarding patient safety and efficacy,” he said. “Data on single-session treatment with low-power, low-density 1,927-nm and 1,440-nm fractional diode lasers and either botulinum neurotoxin or fillers are lacking.”
In a retrospective review of electronic medical records conducted from May 2015 to April 2021, Dr. Wang, Roy G. Geronemus, MD, and Carolyn Kushner, MD evaluated patients who received a single-session facial treatment with either BoNT-A or soft-tissue fillers and the low-power, low-density 1,927-nm and 1,440-nm fractional diode lasers (Clear+Brilliant Perméa and Original, Solta, Pleasanton, Calif.). Safety was assessed by documenting adverse events related to the spread of BoNT-A and fillers or laser treatment of filled areas within 4 weeks.
Adverse events they looked for related to botulinum neurotoxin use included eyelid ptosis; neck weakness or spasms; impairments in chewing, swallowing, speech, and respiration; and prescriptions of apraclonidine eye drops. Filler-related adverse events they looked for included product migration, unexpected loss of filler volume, vascular occlusion, acute pain, necrosis, blindness, and burn. “For both, we looked at hospital or emergency room transfers or admissions and referrals to ENT or ophthalmology,” Dr. Wang said.
During the 6-year study period, 525 patients had 1,562 single-session laser treatments with a mean 46.4 units of BoNT-A, and 398 patients had 1,237 single-session treatments with a mean 1.6 soft-tissue filler syringes. Among those who received BoNT-A, most (93%) were female, their mean age was 51 years, and 99% were treated with a 1,927-nm wavelength at a medium setting in 87% of cases. The top five injection sites were glabella (82%), forehead (69%), periorbital area (64%), neck (40%), and jawline and/or masseters (13%).
The researchers noted one case (0.06%) where apraclonidine eye drops were prescribed for ptosis. The patient had undergone eight other single-session treatments without issue. There were no other documented adverse events directly related to spread of BoNT-A. According to Dr. Wang, this rate of ptosis is lower than the incidence with BoNT-A alone in two landmark trials studying its effects on glabellar lines, which was reported as 5.4% and 1.0%.
Among the 398 patients who received soft-tissue fillers, most (94%) were female, their mean age was 54 years, and 99% were treated with a 1927nm wavelength at a medium setting in 97% of cases. The top five injection sites were cheeks and/or tear troughs (89%), perioral area and/or marionette lines (77%), lips (34%), nasolabial folds (19%), and temples (11%), and the mean number of filler syringes per treatment was 1.6. Slightly more than half (51%) had 1 session, while the remainder had 2 to greater than 10 sessions. The researchers observed no documented adverse events related to spread of fillers or laser treatment of filled areas.
“This laser is a low-powered device that creates small, superficial, and transient microchannels, which likely contributes to the safety of single-session treatments with cosmetic injectables,” Dr. Wang said. However, prospective studies are needed to further validate these results, he added.
“With this very mild laser, it is not surprising that combined treatment had no effect,” said Eric F. Bernstein, MD, MSE, director of the Main Line Center for Laser Surgery in Ardmore, Pa., who was asked to comment on the study results. “There have been numerous anecdotal reports of spreading of botulinum toxin effect to areas not in the target area for treatment following a variety of lasers, including the more powerful version of the laser used in this study. In addition, spread following vascular and other lasers has been reported,” he noted
The laser used in this study, Dr. Bernstein continued, “is low powered and emits a wavelength that is very superficially absorbed, resulting in injury to the stratum corneum, superficial epidermis, or possibly the very superficial dermis, and is often used by physician extenders and not physicians – although I suspect this is not the case in the current study. One can have a reasonable degree of confidence when combining this laser with injectables, but these results cannot be extrapolated to other devices.”
The abstract received the annual ASDS Carruthers Award during the meeting. Dr. Wang reported that he is a consultant or advisor to Allergan, Alastin, AVAVA, Cynosure, Lutronic, Novoxel, Sofwave, and Solta. Dr. Bernstein reported having received research funding from Cynosure, Candela, and Acclaro. He also has received consulting fees from Cynosure and holds ownership interest in Candela, Novoxel, OnSite, Joylux, and Acclaro and has served on the advisory board for Novoxel, Cynosure, and Acclaro.
FROM ASDS 2021
US Multi-Society Task Force lowers recommended CRC screening age
The U.S. Multi-Society Task Force on Colorectal Cancer (CRC) has lowered the recommended age to start CRC screening from 50 to 45 years of age for all average-risk individuals.
Although no studies have directly demonstrated the result of lowering the age of screening, lead author Swati G. Patel, MD, of University of Colorado Anschutz Medical Center, Aurora, and colleagues suggested that the increasing incidence of advanced CRC among younger individuals, coupled with the net benefit of screening, warrant a lower age threshold.
“Recent data ... show that CRC incidence rates in individuals ages 50 to 64 have increased by 1% annually between 2011 and 2016,” the authors wrote in Gastroenterology. “Similarly, CRC incidence and mortality rates in persons under age 50, termed early-age onset CRC (EAO-CRC), are also increasing.”
The task force of nine experts, representing the American Gastroenterological Association, the American College of Gastroenterology, and the American Society for Gastrointestinal Endoscopy, conducted a literature review and generated recommendations using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) criteria. In addition to recommending a lower age for initial screening, Dr. Patel and colleagues provided guidance for cessation of screening among older individuals.
Guidance for screening initiation
According to the authors, the present risk of CRC among younger individuals mirrors the historical risk for older individuals before screening was prevalent.
“The current CRC incidence rates in individuals ages 45 to 49 are similar to the incidence rates observed in 50-year-olds in 1992, before widespread CRC screening was performed,” they wrote.
Elevated rates among younger people have been disproportionately driven by rectal cancer, according to the authors. From 2006 to 2015, incidence of rectal cancer among Americans under 50 increased 1.7% per year, compared with 0.7% per year for colon cancer, based on data from the North American Association of Central Cancer Registries.
Associated mortality rates also increased, the authors noted. From 1999-2019, mortality from colon cancer among people 45-49 years increased from 6.4 to 6.6 deaths per 100,000 individuals, while deaths from rectal cancer increased from 1.3 to 1.7 per 100,000, according to the CDC. Concurrently, CRC-associated mortality rates among older individuals generally declined.
While these findings suggest a growing disease burden among the under-50-year age group, controlled data demonstrating the effects of earlier screening are lacking, Dr. Patel and colleagues noted. Still, they predicted that expanded screening would generate a net benefit.
“Although there are no CRC screening safety data for average-risk individuals [younger than] 50, there are ample data that colonoscopy for other indications (screening based on family history, symptom evaluation, etc.) is safer when comparing younger versus older individuals,” they wrote.
Supporting this claim, the authors cited three independently generated microsimulation models from the Agency for Healthcare Research and Quality that “showed a favorable balance of life-years gained compared with adverse events,” given 100% compliance.
Guidance for screening cessation
Like the situation with younger individuals, minimal data are available to determine the best time for screening cessation, according to the task force.
“There are no randomized or observational studies after 2017 that enrolled individuals over age 75 to inform the appropriate time to stop CRC screening,” the authors wrote. “In our search of 37 relevant articles, only one presented primary data for when to stop screening.”
This one available study showed that some individuals older than 74 do in fact gain benefit from screening,
“For example,” Dr. Patel and colleagues wrote, “women without a history of screening and no comorbidities benefitted from annual fecal immunochemical test (FIT) screening until age 90, whereas unscreened men with or without comorbidities benefited from annual FIT screening until age 88. Conversely, screening was not beneficial beyond age 66 in men or women with severe comorbidities.”
The task force therefore recommended personalized screening for individuals 76-85 years of age “based on the balance of benefits and harms and individual patient clinical factors and preferences.”
Screening for individuals 86 years and older, according to the task force, is unnecessary.
The authors disclosed relationships with Olympus America, Bayer Pharmaceuticals, Janssen Pharmaceuticals, and others.
This article was updated on Jan. 3, 2022.
The U.S. Multi-Society Task Force on Colorectal Cancer (CRC) has lowered the recommended age to start CRC screening from 50 to 45 years of age for all average-risk individuals.
Although no studies have directly demonstrated the result of lowering the age of screening, lead author Swati G. Patel, MD, of University of Colorado Anschutz Medical Center, Aurora, and colleagues suggested that the increasing incidence of advanced CRC among younger individuals, coupled with the net benefit of screening, warrant a lower age threshold.
“Recent data ... show that CRC incidence rates in individuals ages 50 to 64 have increased by 1% annually between 2011 and 2016,” the authors wrote in Gastroenterology. “Similarly, CRC incidence and mortality rates in persons under age 50, termed early-age onset CRC (EAO-CRC), are also increasing.”
The task force of nine experts, representing the American Gastroenterological Association, the American College of Gastroenterology, and the American Society for Gastrointestinal Endoscopy, conducted a literature review and generated recommendations using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) criteria. In addition to recommending a lower age for initial screening, Dr. Patel and colleagues provided guidance for cessation of screening among older individuals.
Guidance for screening initiation
According to the authors, the present risk of CRC among younger individuals mirrors the historical risk for older individuals before screening was prevalent.
“The current CRC incidence rates in individuals ages 45 to 49 are similar to the incidence rates observed in 50-year-olds in 1992, before widespread CRC screening was performed,” they wrote.
Elevated rates among younger people have been disproportionately driven by rectal cancer, according to the authors. From 2006 to 2015, incidence of rectal cancer among Americans under 50 increased 1.7% per year, compared with 0.7% per year for colon cancer, based on data from the North American Association of Central Cancer Registries.
Associated mortality rates also increased, the authors noted. From 1999-2019, mortality from colon cancer among people 45-49 years increased from 6.4 to 6.6 deaths per 100,000 individuals, while deaths from rectal cancer increased from 1.3 to 1.7 per 100,000, according to the CDC. Concurrently, CRC-associated mortality rates among older individuals generally declined.
While these findings suggest a growing disease burden among the under-50-year age group, controlled data demonstrating the effects of earlier screening are lacking, Dr. Patel and colleagues noted. Still, they predicted that expanded screening would generate a net benefit.
“Although there are no CRC screening safety data for average-risk individuals [younger than] 50, there are ample data that colonoscopy for other indications (screening based on family history, symptom evaluation, etc.) is safer when comparing younger versus older individuals,” they wrote.
Supporting this claim, the authors cited three independently generated microsimulation models from the Agency for Healthcare Research and Quality that “showed a favorable balance of life-years gained compared with adverse events,” given 100% compliance.
Guidance for screening cessation
Like the situation with younger individuals, minimal data are available to determine the best time for screening cessation, according to the task force.
“There are no randomized or observational studies after 2017 that enrolled individuals over age 75 to inform the appropriate time to stop CRC screening,” the authors wrote. “In our search of 37 relevant articles, only one presented primary data for when to stop screening.”
This one available study showed that some individuals older than 74 do in fact gain benefit from screening,
“For example,” Dr. Patel and colleagues wrote, “women without a history of screening and no comorbidities benefitted from annual fecal immunochemical test (FIT) screening until age 90, whereas unscreened men with or without comorbidities benefited from annual FIT screening until age 88. Conversely, screening was not beneficial beyond age 66 in men or women with severe comorbidities.”
The task force therefore recommended personalized screening for individuals 76-85 years of age “based on the balance of benefits and harms and individual patient clinical factors and preferences.”
Screening for individuals 86 years and older, according to the task force, is unnecessary.
The authors disclosed relationships with Olympus America, Bayer Pharmaceuticals, Janssen Pharmaceuticals, and others.
This article was updated on Jan. 3, 2022.
The U.S. Multi-Society Task Force on Colorectal Cancer (CRC) has lowered the recommended age to start CRC screening from 50 to 45 years of age for all average-risk individuals.
Although no studies have directly demonstrated the result of lowering the age of screening, lead author Swati G. Patel, MD, of University of Colorado Anschutz Medical Center, Aurora, and colleagues suggested that the increasing incidence of advanced CRC among younger individuals, coupled with the net benefit of screening, warrant a lower age threshold.
“Recent data ... show that CRC incidence rates in individuals ages 50 to 64 have increased by 1% annually between 2011 and 2016,” the authors wrote in Gastroenterology. “Similarly, CRC incidence and mortality rates in persons under age 50, termed early-age onset CRC (EAO-CRC), are also increasing.”
The task force of nine experts, representing the American Gastroenterological Association, the American College of Gastroenterology, and the American Society for Gastrointestinal Endoscopy, conducted a literature review and generated recommendations using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) criteria. In addition to recommending a lower age for initial screening, Dr. Patel and colleagues provided guidance for cessation of screening among older individuals.
Guidance for screening initiation
According to the authors, the present risk of CRC among younger individuals mirrors the historical risk for older individuals before screening was prevalent.
“The current CRC incidence rates in individuals ages 45 to 49 are similar to the incidence rates observed in 50-year-olds in 1992, before widespread CRC screening was performed,” they wrote.
Elevated rates among younger people have been disproportionately driven by rectal cancer, according to the authors. From 2006 to 2015, incidence of rectal cancer among Americans under 50 increased 1.7% per year, compared with 0.7% per year for colon cancer, based on data from the North American Association of Central Cancer Registries.
Associated mortality rates also increased, the authors noted. From 1999-2019, mortality from colon cancer among people 45-49 years increased from 6.4 to 6.6 deaths per 100,000 individuals, while deaths from rectal cancer increased from 1.3 to 1.7 per 100,000, according to the CDC. Concurrently, CRC-associated mortality rates among older individuals generally declined.
While these findings suggest a growing disease burden among the under-50-year age group, controlled data demonstrating the effects of earlier screening are lacking, Dr. Patel and colleagues noted. Still, they predicted that expanded screening would generate a net benefit.
“Although there are no CRC screening safety data for average-risk individuals [younger than] 50, there are ample data that colonoscopy for other indications (screening based on family history, symptom evaluation, etc.) is safer when comparing younger versus older individuals,” they wrote.
Supporting this claim, the authors cited three independently generated microsimulation models from the Agency for Healthcare Research and Quality that “showed a favorable balance of life-years gained compared with adverse events,” given 100% compliance.
Guidance for screening cessation
Like the situation with younger individuals, minimal data are available to determine the best time for screening cessation, according to the task force.
“There are no randomized or observational studies after 2017 that enrolled individuals over age 75 to inform the appropriate time to stop CRC screening,” the authors wrote. “In our search of 37 relevant articles, only one presented primary data for when to stop screening.”
This one available study showed that some individuals older than 74 do in fact gain benefit from screening,
“For example,” Dr. Patel and colleagues wrote, “women without a history of screening and no comorbidities benefitted from annual fecal immunochemical test (FIT) screening until age 90, whereas unscreened men with or without comorbidities benefited from annual FIT screening until age 88. Conversely, screening was not beneficial beyond age 66 in men or women with severe comorbidities.”
The task force therefore recommended personalized screening for individuals 76-85 years of age “based on the balance of benefits and harms and individual patient clinical factors and preferences.”
Screening for individuals 86 years and older, according to the task force, is unnecessary.
The authors disclosed relationships with Olympus America, Bayer Pharmaceuticals, Janssen Pharmaceuticals, and others.
This article was updated on Jan. 3, 2022.
FROM GASTROENTEROLOGY
RSV resurgence likely in wake of COVID-19
The impact of respiratory syncytial virus (RSV)will likely be greater in 2021 and 2022 in the United States than in previous years as a result of the ongoing COVID-19 pandemic, based on data from a simulation-modeling study involving approximately 19 million individuals.
Although RSV usually follows consistent patterns of timing and duration, the disease all but disappeared starting in March 2020 after the introduction of measures to mitigate the spread of COVID-19, Zhe Zheng, MBBS, of Yale University, New Haven, Conn., and colleagues wrote.
However, lifting of mitigation measures has resulted in emergence of RSV in various parts of the world in early 2021, and trends may be similar in the United States, but data are needed to plan for prophylaxis and hospital use, they noted.
In a study published in JAMA Network Open, the researchers developed a simulation model for epidemics of RSV based on historical data. They acquired inpatient records from New York during 2005-2014 and from California during 2003-2011. The primary clinical outcome was the estimated monthly hospitalizations for RSV.
The simulated study population was 19.45 million individuals. After evaluating several scenarios including continued low transmission associated with social distancing and other mitigation measures, the researchers focused on the likely scenario that introduction of RSV from other regions would likely spark RSV epidemics in the United States.
They determined that spring and summer 2021 would show an increase in hospitalizations for RSV. Overall, higher rates of virus introduction from other regions were associated with more intense spring and summer RSV epidemics, with the trade-off of smaller winter epidemics. In the model, the expected RSV epidemic in spring and summer 2021 in New York was small, with a peak incidence of 419 hospitalizations per 100,000 people in April; by contrast, for states with less seasonal variability, such as Florida, the model predicted a larger summer epidemic.
In the model, the mean age of hospitalization for children younger than 5 years for January 2022 was expected to be 1.17 years, compared with 0.84 years in January 2019, the researchers noted.
Across all age groups, the greatest relative increase in the incidence of RSV infection was predicted for children aged 1-4 years (ranging from 82% to 86%), as were lower respiratory infections (87%-101%) and hospitalization (99%-119%), compared with prepandemic levels.
Hospitalizations for children aged 1 year were predicted to double compared with prepandemic seasons; 707 per 100,000 children per year for 2021 and 2022 versus 355 per 100,000 children per year in a typical prepandemic season. However, the largest incidence of lower respiratory infections (30,075 per 100,000) was predicted for infants aged 3-5 months, and the largest incidence of hospitalizations (3,116 per 100,000) was predicted for infants younger than 3 months.
“Without virus importation, the risk of RSV infections across all age groups in the winter of 2021 and 2022 would be greater, as more susceptible individuals were spared from infections in the absence of summer epidemics,” the researchers noted.
The older mean hospitalization age seen in the model was similar to the reported median patient age in Australia both before the pandemic and during the reemergent RSV epidemic.
“This makes intuitive sense, since many children born in 2020 were spared from RSV infection due to the low virus activity; these children will be older when they get infected for the first time during the reemergent epidemics,” the researchers wrote. “Consequently, stakeholders should consider modifying prophylaxis guidelines to include high-risk infants less than 2 years of age for the 2021-2022 season.”
The study findings were limited by several factors including the lack of data on level of virus introduction or on the impact of lack of boosting on infants with only transplacentally acquired RSV antibodies, the researchers noted. Other limitations include the use of historical data and the lack of data on values outside those included in the model, as well as the inability to control for other factors that could influence RSV, such as vaccines or long-lasting antibodies.
However, the results suggest that the rate of imported infections is associated with RSV hospitalizations, and the model effectively captured the RSV epidemics in the United States in spring and summer 2021.
Models can guide clinical preparations
“Health care simulation modeling is a growing field, with very exciting implications,” Lenore Jarvis, MD, of George Washington University, Washington, said in an interview. The field has the potential ability to influence health care in a data-driven way, including, but not limited to, staffing and other hospital operations, as well as patient care decision-making. “In short, accurate modeling and predictions can help us to make informed health care decisions that can lead to increased quality of care, potential cost savings, and even to help save lives,” she said.
Although the details of transmission modeling were not mentioned in the study, the authors evaluated the performances of several models and scenarios. “Scenario 4, for example, was focused on in particular because it best captured the observed dynamics [for RSV] that emerged during the spring and summer of 2021,” Dr. Jarvis said.
“Pediatricians can speak to these trends firsthand. A decrease in expected RSV infections and hospitalizations in 2020, followed by an unprecedented and early increase in RSV infections and severity in 2021, and the factors that the authors account for make sense, such as reintroduction of RSV from other regions and low immunity in the population,” she said. “It also makes sense that, in these transmission modeling scenarios, the expected mean age of hospitalization because of RSV increased with a temporary (hopefully) increase in RSV hospitalizations in the 2021 season, and potentially the 2022 RSV season.”
As for additional research, Dr. Jarvis said she would like to see follow-up data on the RSV transmission modeling. “For example, with scenario 4, does this scenario continue to perform well in other time periods, such as the winter? If the modeling continues to be accurate during other periods of evaluation and reevaluation, this modeling could be very useful in helping pediatric clinics and hospitals to prepare for RSV care and hospital capacity management.”
The study was supported by grants to various researchers from the National Institute of Allergy and Infectious Diseases/National Institutes of Health, the National Center for Advancing Translational Science at the National Institutes of Health, and NIH Roadmap for Medical Research. Lead author Ms. Zheng had no financial conflicts to disclose. Her study coauthors disclosed relationships with companies including AbbVie, Merck, Pfizer, GlaxoSmithKline, MedImmune, and Janssen. Dr. Jarvis had no financial conflicts to disclose and serves on the Pediatric News editorial advisory board.
The impact of respiratory syncytial virus (RSV)will likely be greater in 2021 and 2022 in the United States than in previous years as a result of the ongoing COVID-19 pandemic, based on data from a simulation-modeling study involving approximately 19 million individuals.
Although RSV usually follows consistent patterns of timing and duration, the disease all but disappeared starting in March 2020 after the introduction of measures to mitigate the spread of COVID-19, Zhe Zheng, MBBS, of Yale University, New Haven, Conn., and colleagues wrote.
However, lifting of mitigation measures has resulted in emergence of RSV in various parts of the world in early 2021, and trends may be similar in the United States, but data are needed to plan for prophylaxis and hospital use, they noted.
In a study published in JAMA Network Open, the researchers developed a simulation model for epidemics of RSV based on historical data. They acquired inpatient records from New York during 2005-2014 and from California during 2003-2011. The primary clinical outcome was the estimated monthly hospitalizations for RSV.
The simulated study population was 19.45 million individuals. After evaluating several scenarios including continued low transmission associated with social distancing and other mitigation measures, the researchers focused on the likely scenario that introduction of RSV from other regions would likely spark RSV epidemics in the United States.
They determined that spring and summer 2021 would show an increase in hospitalizations for RSV. Overall, higher rates of virus introduction from other regions were associated with more intense spring and summer RSV epidemics, with the trade-off of smaller winter epidemics. In the model, the expected RSV epidemic in spring and summer 2021 in New York was small, with a peak incidence of 419 hospitalizations per 100,000 people in April; by contrast, for states with less seasonal variability, such as Florida, the model predicted a larger summer epidemic.
In the model, the mean age of hospitalization for children younger than 5 years for January 2022 was expected to be 1.17 years, compared with 0.84 years in January 2019, the researchers noted.
Across all age groups, the greatest relative increase in the incidence of RSV infection was predicted for children aged 1-4 years (ranging from 82% to 86%), as were lower respiratory infections (87%-101%) and hospitalization (99%-119%), compared with prepandemic levels.
Hospitalizations for children aged 1 year were predicted to double compared with prepandemic seasons; 707 per 100,000 children per year for 2021 and 2022 versus 355 per 100,000 children per year in a typical prepandemic season. However, the largest incidence of lower respiratory infections (30,075 per 100,000) was predicted for infants aged 3-5 months, and the largest incidence of hospitalizations (3,116 per 100,000) was predicted for infants younger than 3 months.
“Without virus importation, the risk of RSV infections across all age groups in the winter of 2021 and 2022 would be greater, as more susceptible individuals were spared from infections in the absence of summer epidemics,” the researchers noted.
The older mean hospitalization age seen in the model was similar to the reported median patient age in Australia both before the pandemic and during the reemergent RSV epidemic.
“This makes intuitive sense, since many children born in 2020 were spared from RSV infection due to the low virus activity; these children will be older when they get infected for the first time during the reemergent epidemics,” the researchers wrote. “Consequently, stakeholders should consider modifying prophylaxis guidelines to include high-risk infants less than 2 years of age for the 2021-2022 season.”
The study findings were limited by several factors including the lack of data on level of virus introduction or on the impact of lack of boosting on infants with only transplacentally acquired RSV antibodies, the researchers noted. Other limitations include the use of historical data and the lack of data on values outside those included in the model, as well as the inability to control for other factors that could influence RSV, such as vaccines or long-lasting antibodies.
However, the results suggest that the rate of imported infections is associated with RSV hospitalizations, and the model effectively captured the RSV epidemics in the United States in spring and summer 2021.
Models can guide clinical preparations
“Health care simulation modeling is a growing field, with very exciting implications,” Lenore Jarvis, MD, of George Washington University, Washington, said in an interview. The field has the potential ability to influence health care in a data-driven way, including, but not limited to, staffing and other hospital operations, as well as patient care decision-making. “In short, accurate modeling and predictions can help us to make informed health care decisions that can lead to increased quality of care, potential cost savings, and even to help save lives,” she said.
Although the details of transmission modeling were not mentioned in the study, the authors evaluated the performances of several models and scenarios. “Scenario 4, for example, was focused on in particular because it best captured the observed dynamics [for RSV] that emerged during the spring and summer of 2021,” Dr. Jarvis said.
“Pediatricians can speak to these trends firsthand. A decrease in expected RSV infections and hospitalizations in 2020, followed by an unprecedented and early increase in RSV infections and severity in 2021, and the factors that the authors account for make sense, such as reintroduction of RSV from other regions and low immunity in the population,” she said. “It also makes sense that, in these transmission modeling scenarios, the expected mean age of hospitalization because of RSV increased with a temporary (hopefully) increase in RSV hospitalizations in the 2021 season, and potentially the 2022 RSV season.”
As for additional research, Dr. Jarvis said she would like to see follow-up data on the RSV transmission modeling. “For example, with scenario 4, does this scenario continue to perform well in other time periods, such as the winter? If the modeling continues to be accurate during other periods of evaluation and reevaluation, this modeling could be very useful in helping pediatric clinics and hospitals to prepare for RSV care and hospital capacity management.”
The study was supported by grants to various researchers from the National Institute of Allergy and Infectious Diseases/National Institutes of Health, the National Center for Advancing Translational Science at the National Institutes of Health, and NIH Roadmap for Medical Research. Lead author Ms. Zheng had no financial conflicts to disclose. Her study coauthors disclosed relationships with companies including AbbVie, Merck, Pfizer, GlaxoSmithKline, MedImmune, and Janssen. Dr. Jarvis had no financial conflicts to disclose and serves on the Pediatric News editorial advisory board.
The impact of respiratory syncytial virus (RSV)will likely be greater in 2021 and 2022 in the United States than in previous years as a result of the ongoing COVID-19 pandemic, based on data from a simulation-modeling study involving approximately 19 million individuals.
Although RSV usually follows consistent patterns of timing and duration, the disease all but disappeared starting in March 2020 after the introduction of measures to mitigate the spread of COVID-19, Zhe Zheng, MBBS, of Yale University, New Haven, Conn., and colleagues wrote.
However, lifting of mitigation measures has resulted in emergence of RSV in various parts of the world in early 2021, and trends may be similar in the United States, but data are needed to plan for prophylaxis and hospital use, they noted.
In a study published in JAMA Network Open, the researchers developed a simulation model for epidemics of RSV based on historical data. They acquired inpatient records from New York during 2005-2014 and from California during 2003-2011. The primary clinical outcome was the estimated monthly hospitalizations for RSV.
The simulated study population was 19.45 million individuals. After evaluating several scenarios including continued low transmission associated with social distancing and other mitigation measures, the researchers focused on the likely scenario that introduction of RSV from other regions would likely spark RSV epidemics in the United States.
They determined that spring and summer 2021 would show an increase in hospitalizations for RSV. Overall, higher rates of virus introduction from other regions were associated with more intense spring and summer RSV epidemics, with the trade-off of smaller winter epidemics. In the model, the expected RSV epidemic in spring and summer 2021 in New York was small, with a peak incidence of 419 hospitalizations per 100,000 people in April; by contrast, for states with less seasonal variability, such as Florida, the model predicted a larger summer epidemic.
In the model, the mean age of hospitalization for children younger than 5 years for January 2022 was expected to be 1.17 years, compared with 0.84 years in January 2019, the researchers noted.
Across all age groups, the greatest relative increase in the incidence of RSV infection was predicted for children aged 1-4 years (ranging from 82% to 86%), as were lower respiratory infections (87%-101%) and hospitalization (99%-119%), compared with prepandemic levels.
Hospitalizations for children aged 1 year were predicted to double compared with prepandemic seasons; 707 per 100,000 children per year for 2021 and 2022 versus 355 per 100,000 children per year in a typical prepandemic season. However, the largest incidence of lower respiratory infections (30,075 per 100,000) was predicted for infants aged 3-5 months, and the largest incidence of hospitalizations (3,116 per 100,000) was predicted for infants younger than 3 months.
“Without virus importation, the risk of RSV infections across all age groups in the winter of 2021 and 2022 would be greater, as more susceptible individuals were spared from infections in the absence of summer epidemics,” the researchers noted.
The older mean hospitalization age seen in the model was similar to the reported median patient age in Australia both before the pandemic and during the reemergent RSV epidemic.
“This makes intuitive sense, since many children born in 2020 were spared from RSV infection due to the low virus activity; these children will be older when they get infected for the first time during the reemergent epidemics,” the researchers wrote. “Consequently, stakeholders should consider modifying prophylaxis guidelines to include high-risk infants less than 2 years of age for the 2021-2022 season.”
The study findings were limited by several factors including the lack of data on level of virus introduction or on the impact of lack of boosting on infants with only transplacentally acquired RSV antibodies, the researchers noted. Other limitations include the use of historical data and the lack of data on values outside those included in the model, as well as the inability to control for other factors that could influence RSV, such as vaccines or long-lasting antibodies.
However, the results suggest that the rate of imported infections is associated with RSV hospitalizations, and the model effectively captured the RSV epidemics in the United States in spring and summer 2021.
Models can guide clinical preparations
“Health care simulation modeling is a growing field, with very exciting implications,” Lenore Jarvis, MD, of George Washington University, Washington, said in an interview. The field has the potential ability to influence health care in a data-driven way, including, but not limited to, staffing and other hospital operations, as well as patient care decision-making. “In short, accurate modeling and predictions can help us to make informed health care decisions that can lead to increased quality of care, potential cost savings, and even to help save lives,” she said.
Although the details of transmission modeling were not mentioned in the study, the authors evaluated the performances of several models and scenarios. “Scenario 4, for example, was focused on in particular because it best captured the observed dynamics [for RSV] that emerged during the spring and summer of 2021,” Dr. Jarvis said.
“Pediatricians can speak to these trends firsthand. A decrease in expected RSV infections and hospitalizations in 2020, followed by an unprecedented and early increase in RSV infections and severity in 2021, and the factors that the authors account for make sense, such as reintroduction of RSV from other regions and low immunity in the population,” she said. “It also makes sense that, in these transmission modeling scenarios, the expected mean age of hospitalization because of RSV increased with a temporary (hopefully) increase in RSV hospitalizations in the 2021 season, and potentially the 2022 RSV season.”
As for additional research, Dr. Jarvis said she would like to see follow-up data on the RSV transmission modeling. “For example, with scenario 4, does this scenario continue to perform well in other time periods, such as the winter? If the modeling continues to be accurate during other periods of evaluation and reevaluation, this modeling could be very useful in helping pediatric clinics and hospitals to prepare for RSV care and hospital capacity management.”
The study was supported by grants to various researchers from the National Institute of Allergy and Infectious Diseases/National Institutes of Health, the National Center for Advancing Translational Science at the National Institutes of Health, and NIH Roadmap for Medical Research. Lead author Ms. Zheng had no financial conflicts to disclose. Her study coauthors disclosed relationships with companies including AbbVie, Merck, Pfizer, GlaxoSmithKline, MedImmune, and Janssen. Dr. Jarvis had no financial conflicts to disclose and serves on the Pediatric News editorial advisory board.
FROM JAMA NETWORK OPEN
FDA approves cabotegravir LA; New HIV PrEP option fills an important gap
SILVER SPRING, MD – .
The priority review approval was based on phase 2b-3 clinical trial data submitted to the agency this past August, after the study was stopped early due to encouraging efficacy results of the first pre-planned interim end-point analysis.
“Although TDF-FTC PrEP could be almost astoundingly effective in preventing HIV acquisition across populations and risk exposures, the adherence to the daily protocols was really challenging and difficult to attain initially and to maintain for some of our most vulnerable populations,” Raphael Landovitz, MD, MDC, lead study investigator and co-director of The Center for HIV Identification, Prevention, and Treatment Services at UCLA, Los Angeles, told this news organization.
Dr. Landovitz noted that population level benefits observed with PrEP were limited to people who were highly engaged in health care and well resourced, but the same benefits were not observed in the most vulnerable, highest-risk populations.
“The idea was, is there anything that we can do to improve ... choices for different options, some of which – like long-acting agents – would remove the obligation to adhere to daily prescribing or a post-coital and be more discreet,” he said.
Data demonstrated superiority versus TDF-FTC
Details of the prospective, phase 2b-3 randomized, double-blind, double-dummy, active-controlled trial among 4,566 cisgender MSM (men who have sex with men) and transgender women highlighted the superiority of CAB 600 mg intramuscularly versus placebo or active TDF-FTC (300 mg/200 mg), with CAB-LA reducing HIV infection risk by 66%. These results were published August 11 in the New England Journal of Medicine and previously reported by this news organization.
Investigators identified HIV infections in 57 participants (including 52 who acquired HIV infections after enrollment). The hazard ratio for incident HIV infection versus TDG-FTC was 0.34, P < .001. Notably, effects were consistent across prespecified subgroups and populations.
Additionally, integrase strand-transfer inhibitor (INSTI) resistance mutations were detected in 1 of 4 of baseline HIV infection cases among CAB participants, while 2 of 39 incident infections in TDF-FTC participants occurred despite drug concentrations indicating good PrEP adherence.
Adverse events, breakthrough infections, and other important considerations
Because the trial was halted early, long-term safety data were lacking, thereby prompting investigators to launch an ongoing, open-label extension. In the initial trial, injection site reactions were reported in 81.4% (1,724) of CAB participants, most beginning a median of 1 day (IQR 0-2 days) post-injection, mild to moderate in severity (60.8% pain, 23.7% tenderness), and lasting a median of 3 days (IQR 2-6 days). In comparison, injection site reactions were reported in 31.3% of TDF-FTC participants (who, incidentally, received at least one placebo injection).
Severe adverse events (grade 3 or higher) were similar between CAB and TDF-FTC groups, They consisted mostly of an increase in creatine kinase level (14.2% with CAB vs. 13.5% with TDF-FTC) and a decrease in creatinine clearance (7.0% with CAB vs. 8.3% with TDF-FTC).
Although weight gain was higher among CAB participants (1.23 kg/year vs. 0.37 kg/year, TDF-FTC participants), most of the differences were observed during the first 40 weeks and were driven by weight loss in the TDF-FDC group. Weight changes were similar (~1 kg/year) thereafter.
Importantly, study participants assigned CAB underwent an oral-tablet, 5-week lead-in phase, which might have contributed to eventual treatment failure.
In a companion piece published Nov. 1 in the Journal of Infectious Diseases, investigators noted that adherence to the oral lead-in was poor in roughly one-third of participants with incident, breakthrough infections. They wrote that the barriers to adherence with daily oral PrEP regimens coupled with the favorable CAB-LA safety profile suggested that “the oral phase before CAB-LA initiation might not be necessary or desirable.”
The question remains as to whether or not strategies entailing viral load or other RNA screening tests at follow-up clinic visits might be warranted.
“It’s one of the biggest sort of ‘what’s next’ questions that’s come out of this study,” Dr. Landovitz said. “We’re now testing the strategy of using viral load or RNA screening at every visit to see if, in fact, we can catch these breakthrough infections earlier and potentially avoid resistance,” he added.
Until more data are available, Dr. Landovitz said that “the guidance for the clinician would be that until you have resistance testing back on someone who breaks through cabotegravir PrEP to use a protease inhibitor-based treatment regimen, at least initially.”
Institutional changes to ensure delivery of injections, tracking, and follow-up to ensure optimal use of long-acting PrEP agents are likely to challenge already overburdened health care systems and may require additional strategies for implementation (for example, pharmacy or at-home administration). Despite these factors, CAB-LA approval is welcome news to clinicians and patients alike.
“We’re constantly searching for new drugs to expand our repertoire of what we can provide patients,” Lina Rosengren-Hovee, MD, MPH, assistant professor of medicine and infectious disease specialist at UNC Health, Chapel Hill, N.C., said in an interview. Dr. Rosengren-Hovee was not involved in the study.
“For folks under 30, the sexual and gender minority, Black, and Latino, they are the ones with the highest need for PrEP, that are in a position that places them at higher risk for HIV. Being able to offer an injectable option is ... a game changer,” she said.
Dr. Rosengren-Hovee reports no relevant financial relationships. Dr. Landovitz has consulting relationships with Gilead, Janssen, Roche, and Cepheus.
A version of this article first appeared on Medscape.com.
SILVER SPRING, MD – .
The priority review approval was based on phase 2b-3 clinical trial data submitted to the agency this past August, after the study was stopped early due to encouraging efficacy results of the first pre-planned interim end-point analysis.
“Although TDF-FTC PrEP could be almost astoundingly effective in preventing HIV acquisition across populations and risk exposures, the adherence to the daily protocols was really challenging and difficult to attain initially and to maintain for some of our most vulnerable populations,” Raphael Landovitz, MD, MDC, lead study investigator and co-director of The Center for HIV Identification, Prevention, and Treatment Services at UCLA, Los Angeles, told this news organization.
Dr. Landovitz noted that population level benefits observed with PrEP were limited to people who were highly engaged in health care and well resourced, but the same benefits were not observed in the most vulnerable, highest-risk populations.
“The idea was, is there anything that we can do to improve ... choices for different options, some of which – like long-acting agents – would remove the obligation to adhere to daily prescribing or a post-coital and be more discreet,” he said.
Data demonstrated superiority versus TDF-FTC
Details of the prospective, phase 2b-3 randomized, double-blind, double-dummy, active-controlled trial among 4,566 cisgender MSM (men who have sex with men) and transgender women highlighted the superiority of CAB 600 mg intramuscularly versus placebo or active TDF-FTC (300 mg/200 mg), with CAB-LA reducing HIV infection risk by 66%. These results were published August 11 in the New England Journal of Medicine and previously reported by this news organization.
Investigators identified HIV infections in 57 participants (including 52 who acquired HIV infections after enrollment). The hazard ratio for incident HIV infection versus TDG-FTC was 0.34, P < .001. Notably, effects were consistent across prespecified subgroups and populations.
Additionally, integrase strand-transfer inhibitor (INSTI) resistance mutations were detected in 1 of 4 of baseline HIV infection cases among CAB participants, while 2 of 39 incident infections in TDF-FTC participants occurred despite drug concentrations indicating good PrEP adherence.
Adverse events, breakthrough infections, and other important considerations
Because the trial was halted early, long-term safety data were lacking, thereby prompting investigators to launch an ongoing, open-label extension. In the initial trial, injection site reactions were reported in 81.4% (1,724) of CAB participants, most beginning a median of 1 day (IQR 0-2 days) post-injection, mild to moderate in severity (60.8% pain, 23.7% tenderness), and lasting a median of 3 days (IQR 2-6 days). In comparison, injection site reactions were reported in 31.3% of TDF-FTC participants (who, incidentally, received at least one placebo injection).
Severe adverse events (grade 3 or higher) were similar between CAB and TDF-FTC groups, They consisted mostly of an increase in creatine kinase level (14.2% with CAB vs. 13.5% with TDF-FTC) and a decrease in creatinine clearance (7.0% with CAB vs. 8.3% with TDF-FTC).
Although weight gain was higher among CAB participants (1.23 kg/year vs. 0.37 kg/year, TDF-FTC participants), most of the differences were observed during the first 40 weeks and were driven by weight loss in the TDF-FDC group. Weight changes were similar (~1 kg/year) thereafter.
Importantly, study participants assigned CAB underwent an oral-tablet, 5-week lead-in phase, which might have contributed to eventual treatment failure.
In a companion piece published Nov. 1 in the Journal of Infectious Diseases, investigators noted that adherence to the oral lead-in was poor in roughly one-third of participants with incident, breakthrough infections. They wrote that the barriers to adherence with daily oral PrEP regimens coupled with the favorable CAB-LA safety profile suggested that “the oral phase before CAB-LA initiation might not be necessary or desirable.”
The question remains as to whether or not strategies entailing viral load or other RNA screening tests at follow-up clinic visits might be warranted.
“It’s one of the biggest sort of ‘what’s next’ questions that’s come out of this study,” Dr. Landovitz said. “We’re now testing the strategy of using viral load or RNA screening at every visit to see if, in fact, we can catch these breakthrough infections earlier and potentially avoid resistance,” he added.
Until more data are available, Dr. Landovitz said that “the guidance for the clinician would be that until you have resistance testing back on someone who breaks through cabotegravir PrEP to use a protease inhibitor-based treatment regimen, at least initially.”
Institutional changes to ensure delivery of injections, tracking, and follow-up to ensure optimal use of long-acting PrEP agents are likely to challenge already overburdened health care systems and may require additional strategies for implementation (for example, pharmacy or at-home administration). Despite these factors, CAB-LA approval is welcome news to clinicians and patients alike.
“We’re constantly searching for new drugs to expand our repertoire of what we can provide patients,” Lina Rosengren-Hovee, MD, MPH, assistant professor of medicine and infectious disease specialist at UNC Health, Chapel Hill, N.C., said in an interview. Dr. Rosengren-Hovee was not involved in the study.
“For folks under 30, the sexual and gender minority, Black, and Latino, they are the ones with the highest need for PrEP, that are in a position that places them at higher risk for HIV. Being able to offer an injectable option is ... a game changer,” she said.
Dr. Rosengren-Hovee reports no relevant financial relationships. Dr. Landovitz has consulting relationships with Gilead, Janssen, Roche, and Cepheus.
A version of this article first appeared on Medscape.com.
SILVER SPRING, MD – .
The priority review approval was based on phase 2b-3 clinical trial data submitted to the agency this past August, after the study was stopped early due to encouraging efficacy results of the first pre-planned interim end-point analysis.
“Although TDF-FTC PrEP could be almost astoundingly effective in preventing HIV acquisition across populations and risk exposures, the adherence to the daily protocols was really challenging and difficult to attain initially and to maintain for some of our most vulnerable populations,” Raphael Landovitz, MD, MDC, lead study investigator and co-director of The Center for HIV Identification, Prevention, and Treatment Services at UCLA, Los Angeles, told this news organization.
Dr. Landovitz noted that population level benefits observed with PrEP were limited to people who were highly engaged in health care and well resourced, but the same benefits were not observed in the most vulnerable, highest-risk populations.
“The idea was, is there anything that we can do to improve ... choices for different options, some of which – like long-acting agents – would remove the obligation to adhere to daily prescribing or a post-coital and be more discreet,” he said.
Data demonstrated superiority versus TDF-FTC
Details of the prospective, phase 2b-3 randomized, double-blind, double-dummy, active-controlled trial among 4,566 cisgender MSM (men who have sex with men) and transgender women highlighted the superiority of CAB 600 mg intramuscularly versus placebo or active TDF-FTC (300 mg/200 mg), with CAB-LA reducing HIV infection risk by 66%. These results were published August 11 in the New England Journal of Medicine and previously reported by this news organization.
Investigators identified HIV infections in 57 participants (including 52 who acquired HIV infections after enrollment). The hazard ratio for incident HIV infection versus TDG-FTC was 0.34, P < .001. Notably, effects were consistent across prespecified subgroups and populations.
Additionally, integrase strand-transfer inhibitor (INSTI) resistance mutations were detected in 1 of 4 of baseline HIV infection cases among CAB participants, while 2 of 39 incident infections in TDF-FTC participants occurred despite drug concentrations indicating good PrEP adherence.
Adverse events, breakthrough infections, and other important considerations
Because the trial was halted early, long-term safety data were lacking, thereby prompting investigators to launch an ongoing, open-label extension. In the initial trial, injection site reactions were reported in 81.4% (1,724) of CAB participants, most beginning a median of 1 day (IQR 0-2 days) post-injection, mild to moderate in severity (60.8% pain, 23.7% tenderness), and lasting a median of 3 days (IQR 2-6 days). In comparison, injection site reactions were reported in 31.3% of TDF-FTC participants (who, incidentally, received at least one placebo injection).
Severe adverse events (grade 3 or higher) were similar between CAB and TDF-FTC groups, They consisted mostly of an increase in creatine kinase level (14.2% with CAB vs. 13.5% with TDF-FTC) and a decrease in creatinine clearance (7.0% with CAB vs. 8.3% with TDF-FTC).
Although weight gain was higher among CAB participants (1.23 kg/year vs. 0.37 kg/year, TDF-FTC participants), most of the differences were observed during the first 40 weeks and were driven by weight loss in the TDF-FDC group. Weight changes were similar (~1 kg/year) thereafter.
Importantly, study participants assigned CAB underwent an oral-tablet, 5-week lead-in phase, which might have contributed to eventual treatment failure.
In a companion piece published Nov. 1 in the Journal of Infectious Diseases, investigators noted that adherence to the oral lead-in was poor in roughly one-third of participants with incident, breakthrough infections. They wrote that the barriers to adherence with daily oral PrEP regimens coupled with the favorable CAB-LA safety profile suggested that “the oral phase before CAB-LA initiation might not be necessary or desirable.”
The question remains as to whether or not strategies entailing viral load or other RNA screening tests at follow-up clinic visits might be warranted.
“It’s one of the biggest sort of ‘what’s next’ questions that’s come out of this study,” Dr. Landovitz said. “We’re now testing the strategy of using viral load or RNA screening at every visit to see if, in fact, we can catch these breakthrough infections earlier and potentially avoid resistance,” he added.
Until more data are available, Dr. Landovitz said that “the guidance for the clinician would be that until you have resistance testing back on someone who breaks through cabotegravir PrEP to use a protease inhibitor-based treatment regimen, at least initially.”
Institutional changes to ensure delivery of injections, tracking, and follow-up to ensure optimal use of long-acting PrEP agents are likely to challenge already overburdened health care systems and may require additional strategies for implementation (for example, pharmacy or at-home administration). Despite these factors, CAB-LA approval is welcome news to clinicians and patients alike.
“We’re constantly searching for new drugs to expand our repertoire of what we can provide patients,” Lina Rosengren-Hovee, MD, MPH, assistant professor of medicine and infectious disease specialist at UNC Health, Chapel Hill, N.C., said in an interview. Dr. Rosengren-Hovee was not involved in the study.
“For folks under 30, the sexual and gender minority, Black, and Latino, they are the ones with the highest need for PrEP, that are in a position that places them at higher risk for HIV. Being able to offer an injectable option is ... a game changer,” she said.
Dr. Rosengren-Hovee reports no relevant financial relationships. Dr. Landovitz has consulting relationships with Gilead, Janssen, Roche, and Cepheus.
A version of this article first appeared on Medscape.com.
Ophthalmologist who developed medical botox dies at 89
his family confirmed to National Public Radio.
Four decades ago, Alan Brown Scott, MD, a native of Berkeley, Calif., turned the drug, once a deadly poison, into a revolutionary treatment for obscure eye diseases. It later became a well-known blockbuster treatment for reducing the appearance of wrinkles and treating hyperhidrosis (excessive sweating). Other approved medical uses include treatment of overactive bladder and urinary incontinence.
According to the American Society of Plastic Surgeons, its popularity for cosmetic use was boosted further during the pandemic and it was the No. 1 minimally invasive cosmetic procedure performed in 2020. Among the 13.3 million procedures, 4.4 million involved Botox.
According to Bloomberg Businessweek, Ed Schantz, who was working in the military’s biological weapons program, was the one to first send the toxin to Dr. Scott, who wanted to explore its properties for medical use.
The same Bloomberg article also noted that the original botulinum toxin itself “is so powerful that a tiny amount can suffocate a person by paralyzing the muscles used for breathing.”
Dr. Scott was looking for a way to help his patients avoid extensive surgeries.
“Specifically, he was aiming to treat people with strabismus, or cross-eyes, and blepharospasm, which is an uncontrollable closure of eyes. Today, it’s also used as a treatment to help with migraines, hair loss, and drooling,” NPR reported.
The New York Times once described Botox as “medicine’s answer to duct tape.”
Dr. Scott was the executive director of the Smith-Kettlewell Eye Research Institute in San Francisco when he did his pioneering research with botulinum toxin in the 1970s and 1980s, according to a 2002 article in SFGate.
In 1991, Dr. Scott sold the drug to Allergan, when it was called Oculinum. The next year, the name was officially changed to Botox.
In 2002, Dr. Scott told SFGate, when asked about the more popular use for the drug, “I think that’s a charming, slightly frivolous use,” adding, “but it’s not along the lines of what I was into, applications for serious disorders.”
According to Scientific American in 2016, Dr. Scott, then age 83, kept working on the noncosmetic benefits of botulism-toxin injections for eye-related disorders at the Strabismus Research Foundation,
He told Scientific American he was proud that his efforts “are directly helpful to people.”
“There are interesting and difficult problems still to be solved, and I’m a practicing physician and I see them every day,” he said.
Dr. Scott’s daughter, Ann Scott, told NPR: “He definitely loved his work and he was also a really great father.” She said her dad involved his children in his research and work.
She added, “He was a really calm, more of a quiet reserved person,” and said he was committed to teaching his students, many of them international students.
“That was what he really loved,” she said.
Dr. Scott, who died Dec. 16, was in intensive care for the last 10 days from an unspecified illness, his daughter told NPR.
A version of this article first appeared on Medscape.com.
his family confirmed to National Public Radio.
Four decades ago, Alan Brown Scott, MD, a native of Berkeley, Calif., turned the drug, once a deadly poison, into a revolutionary treatment for obscure eye diseases. It later became a well-known blockbuster treatment for reducing the appearance of wrinkles and treating hyperhidrosis (excessive sweating). Other approved medical uses include treatment of overactive bladder and urinary incontinence.
According to the American Society of Plastic Surgeons, its popularity for cosmetic use was boosted further during the pandemic and it was the No. 1 minimally invasive cosmetic procedure performed in 2020. Among the 13.3 million procedures, 4.4 million involved Botox.
According to Bloomberg Businessweek, Ed Schantz, who was working in the military’s biological weapons program, was the one to first send the toxin to Dr. Scott, who wanted to explore its properties for medical use.
The same Bloomberg article also noted that the original botulinum toxin itself “is so powerful that a tiny amount can suffocate a person by paralyzing the muscles used for breathing.”
Dr. Scott was looking for a way to help his patients avoid extensive surgeries.
“Specifically, he was aiming to treat people with strabismus, or cross-eyes, and blepharospasm, which is an uncontrollable closure of eyes. Today, it’s also used as a treatment to help with migraines, hair loss, and drooling,” NPR reported.
The New York Times once described Botox as “medicine’s answer to duct tape.”
Dr. Scott was the executive director of the Smith-Kettlewell Eye Research Institute in San Francisco when he did his pioneering research with botulinum toxin in the 1970s and 1980s, according to a 2002 article in SFGate.
In 1991, Dr. Scott sold the drug to Allergan, when it was called Oculinum. The next year, the name was officially changed to Botox.
In 2002, Dr. Scott told SFGate, when asked about the more popular use for the drug, “I think that’s a charming, slightly frivolous use,” adding, “but it’s not along the lines of what I was into, applications for serious disorders.”
According to Scientific American in 2016, Dr. Scott, then age 83, kept working on the noncosmetic benefits of botulism-toxin injections for eye-related disorders at the Strabismus Research Foundation,
He told Scientific American he was proud that his efforts “are directly helpful to people.”
“There are interesting and difficult problems still to be solved, and I’m a practicing physician and I see them every day,” he said.
Dr. Scott’s daughter, Ann Scott, told NPR: “He definitely loved his work and he was also a really great father.” She said her dad involved his children in his research and work.
She added, “He was a really calm, more of a quiet reserved person,” and said he was committed to teaching his students, many of them international students.
“That was what he really loved,” she said.
Dr. Scott, who died Dec. 16, was in intensive care for the last 10 days from an unspecified illness, his daughter told NPR.
A version of this article first appeared on Medscape.com.
his family confirmed to National Public Radio.
Four decades ago, Alan Brown Scott, MD, a native of Berkeley, Calif., turned the drug, once a deadly poison, into a revolutionary treatment for obscure eye diseases. It later became a well-known blockbuster treatment for reducing the appearance of wrinkles and treating hyperhidrosis (excessive sweating). Other approved medical uses include treatment of overactive bladder and urinary incontinence.
According to the American Society of Plastic Surgeons, its popularity for cosmetic use was boosted further during the pandemic and it was the No. 1 minimally invasive cosmetic procedure performed in 2020. Among the 13.3 million procedures, 4.4 million involved Botox.
According to Bloomberg Businessweek, Ed Schantz, who was working in the military’s biological weapons program, was the one to first send the toxin to Dr. Scott, who wanted to explore its properties for medical use.
The same Bloomberg article also noted that the original botulinum toxin itself “is so powerful that a tiny amount can suffocate a person by paralyzing the muscles used for breathing.”
Dr. Scott was looking for a way to help his patients avoid extensive surgeries.
“Specifically, he was aiming to treat people with strabismus, or cross-eyes, and blepharospasm, which is an uncontrollable closure of eyes. Today, it’s also used as a treatment to help with migraines, hair loss, and drooling,” NPR reported.
The New York Times once described Botox as “medicine’s answer to duct tape.”
Dr. Scott was the executive director of the Smith-Kettlewell Eye Research Institute in San Francisco when he did his pioneering research with botulinum toxin in the 1970s and 1980s, according to a 2002 article in SFGate.
In 1991, Dr. Scott sold the drug to Allergan, when it was called Oculinum. The next year, the name was officially changed to Botox.
In 2002, Dr. Scott told SFGate, when asked about the more popular use for the drug, “I think that’s a charming, slightly frivolous use,” adding, “but it’s not along the lines of what I was into, applications for serious disorders.”
According to Scientific American in 2016, Dr. Scott, then age 83, kept working on the noncosmetic benefits of botulism-toxin injections for eye-related disorders at the Strabismus Research Foundation,
He told Scientific American he was proud that his efforts “are directly helpful to people.”
“There are interesting and difficult problems still to be solved, and I’m a practicing physician and I see them every day,” he said.
Dr. Scott’s daughter, Ann Scott, told NPR: “He definitely loved his work and he was also a really great father.” She said her dad involved his children in his research and work.
She added, “He was a really calm, more of a quiet reserved person,” and said he was committed to teaching his students, many of them international students.
“That was what he really loved,” she said.
Dr. Scott, who died Dec. 16, was in intensive care for the last 10 days from an unspecified illness, his daughter told NPR.
A version of this article first appeared on Medscape.com.
Triple therapy for HER2-positive gastric cancer shrinks tumors for most in study
In HER2-positive gastric cancer, the addition of pembrolizumab (Keytruda, Merck) to trastuzumab (Herceptin, Roche) and platinum-based chemotherapy led to a significant improvement in overall response rate, according to results from the first interim analysis of the KEYNOTE-811 phase 3, randomized clinical trial.
The results of the trial, initially presented at the 2021 annual meeting of the American Society of Clinical Oncology and now published in Nature, were instrumental in the May 2021 FDA approval of pembrolizumab plus trastuzumab along with fluoropyrimidine- and platinum-containing chemotherapy for the first-line treatment locally advanced unresectable or metastatic HER2-positive gastric or gastroesophageal junction adenocarcinoma.
Pembrolizumab is an anti–programmed death–ligand 1 (PD-L1) antibody, which blocks a key immune escape mechanism employed by cancer cells. Trastuzumab causes an immune response that leads to HER2 internalization and cellular recycling, as well as stimulating HER2-specific T cells. Death of cancer cells from platinum-containing chemotherapy stimulates dendritic cells, which in turn promote tumor-specific T cells.
In her studies of immunotherapy and gastric cancer, lead author Yelena Janjigian, MD, chief of the gastrointestinal oncology service at Memorial Sloan Kettering Cancer Center, New York, noticed a trend in HER2-positive patients. “PD-L1 overexpression actually can occur and continue to increase while the patient is on trastuzumab as a mode of resistance,” Dr. Janjigian said in an interview.
That observation prompted the idea to combine a PD-L1 inhibitor in a phase 3 clinical trial. The results were striking. “I’ve never seen such depth of response. You could see responses as early as week 3 – after just one dose – and no one’s ever shown that before,” Dr. Janjigian said.
The new study randomized 264 patients to receive pembrolizumab or placebo in combination with trastuzumab plus fluoropyrimidine- and platinum-containing chemotherapy. In the intention-to-treat population, 81.3% of the population was male, and the primary tumor site was the stomach in 68.4%. The pembrolizumab group had a significantly higher objective response rate than the placebo group (74.4% vs. 51.9%; P = .00006).
The median decrease in lesion size was 65% in the pembrolizumab group and 49% in the placebo group. 32.3% of the pembrolizumab group had at least an 80% decrease in lesion size, versus 14.8% in the placebo group. The pembrolizumab group had more complete responses (11.3% vs. 3.1%).
The message from this is that biomarkers are critical, even if actionable ones are rare, Dr. Janjigian said. “Even though it feels like it’s only 10% or 5% of population, you start chipping away at it. How do we cure cancer? We cure it one percentage at a time through biomarker testing.”
Writing in a commentary published with the study, Myriam Chalabi, MD, a physician specializing in gastrointestinal oncology with the Netherlands Cancer Institute, Amsterdam, described the findings as “impressive in terms of the tumor responses.” But she was cautious saying data on progression-free survival and overall survival are needed to understand how well the proposed treatment would work long term.
“Given that PD-1 blockade seems to complement trastuzumab and chemotherapy for the treatment of HER2-positive gastric cancers, Janjigian and colleagues’ study has moved the field forward, and their findings could be the next, long-awaited development in the treatment of these cancers,” she wrote.
A key limitation is that the study looked at overall response rate, rather than the overall survival. The latter results should come within a year, Dr. Janjigian said.
The study was funded by Merck. Dr. Janjigian has received research funding from Merck, Rgenix, Bayer, Genentech/Roche, Bristol-Myers Squibb, and Eli Lilly, and has served on advisory boards for Rgenix, Merck Serono, Bristol-Myers Squibb, Eli Lilly, Pfizer, Bayer, Imugene, Merck Sharp & Dohme, Daiichi-Sankyo, Zymeworks, SeaGen, Basilea Pharmaceutical, and AstraZeneca. She has equity in Rgenix.
In HER2-positive gastric cancer, the addition of pembrolizumab (Keytruda, Merck) to trastuzumab (Herceptin, Roche) and platinum-based chemotherapy led to a significant improvement in overall response rate, according to results from the first interim analysis of the KEYNOTE-811 phase 3, randomized clinical trial.
The results of the trial, initially presented at the 2021 annual meeting of the American Society of Clinical Oncology and now published in Nature, were instrumental in the May 2021 FDA approval of pembrolizumab plus trastuzumab along with fluoropyrimidine- and platinum-containing chemotherapy for the first-line treatment locally advanced unresectable or metastatic HER2-positive gastric or gastroesophageal junction adenocarcinoma.
Pembrolizumab is an anti–programmed death–ligand 1 (PD-L1) antibody, which blocks a key immune escape mechanism employed by cancer cells. Trastuzumab causes an immune response that leads to HER2 internalization and cellular recycling, as well as stimulating HER2-specific T cells. Death of cancer cells from platinum-containing chemotherapy stimulates dendritic cells, which in turn promote tumor-specific T cells.
In her studies of immunotherapy and gastric cancer, lead author Yelena Janjigian, MD, chief of the gastrointestinal oncology service at Memorial Sloan Kettering Cancer Center, New York, noticed a trend in HER2-positive patients. “PD-L1 overexpression actually can occur and continue to increase while the patient is on trastuzumab as a mode of resistance,” Dr. Janjigian said in an interview.
That observation prompted the idea to combine a PD-L1 inhibitor in a phase 3 clinical trial. The results were striking. “I’ve never seen such depth of response. You could see responses as early as week 3 – after just one dose – and no one’s ever shown that before,” Dr. Janjigian said.
The new study randomized 264 patients to receive pembrolizumab or placebo in combination with trastuzumab plus fluoropyrimidine- and platinum-containing chemotherapy. In the intention-to-treat population, 81.3% of the population was male, and the primary tumor site was the stomach in 68.4%. The pembrolizumab group had a significantly higher objective response rate than the placebo group (74.4% vs. 51.9%; P = .00006).
The median decrease in lesion size was 65% in the pembrolizumab group and 49% in the placebo group. 32.3% of the pembrolizumab group had at least an 80% decrease in lesion size, versus 14.8% in the placebo group. The pembrolizumab group had more complete responses (11.3% vs. 3.1%).
The message from this is that biomarkers are critical, even if actionable ones are rare, Dr. Janjigian said. “Even though it feels like it’s only 10% or 5% of population, you start chipping away at it. How do we cure cancer? We cure it one percentage at a time through biomarker testing.”
Writing in a commentary published with the study, Myriam Chalabi, MD, a physician specializing in gastrointestinal oncology with the Netherlands Cancer Institute, Amsterdam, described the findings as “impressive in terms of the tumor responses.” But she was cautious saying data on progression-free survival and overall survival are needed to understand how well the proposed treatment would work long term.
“Given that PD-1 blockade seems to complement trastuzumab and chemotherapy for the treatment of HER2-positive gastric cancers, Janjigian and colleagues’ study has moved the field forward, and their findings could be the next, long-awaited development in the treatment of these cancers,” she wrote.
A key limitation is that the study looked at overall response rate, rather than the overall survival. The latter results should come within a year, Dr. Janjigian said.
The study was funded by Merck. Dr. Janjigian has received research funding from Merck, Rgenix, Bayer, Genentech/Roche, Bristol-Myers Squibb, and Eli Lilly, and has served on advisory boards for Rgenix, Merck Serono, Bristol-Myers Squibb, Eli Lilly, Pfizer, Bayer, Imugene, Merck Sharp & Dohme, Daiichi-Sankyo, Zymeworks, SeaGen, Basilea Pharmaceutical, and AstraZeneca. She has equity in Rgenix.
In HER2-positive gastric cancer, the addition of pembrolizumab (Keytruda, Merck) to trastuzumab (Herceptin, Roche) and platinum-based chemotherapy led to a significant improvement in overall response rate, according to results from the first interim analysis of the KEYNOTE-811 phase 3, randomized clinical trial.
The results of the trial, initially presented at the 2021 annual meeting of the American Society of Clinical Oncology and now published in Nature, were instrumental in the May 2021 FDA approval of pembrolizumab plus trastuzumab along with fluoropyrimidine- and platinum-containing chemotherapy for the first-line treatment locally advanced unresectable or metastatic HER2-positive gastric or gastroesophageal junction adenocarcinoma.
Pembrolizumab is an anti–programmed death–ligand 1 (PD-L1) antibody, which blocks a key immune escape mechanism employed by cancer cells. Trastuzumab causes an immune response that leads to HER2 internalization and cellular recycling, as well as stimulating HER2-specific T cells. Death of cancer cells from platinum-containing chemotherapy stimulates dendritic cells, which in turn promote tumor-specific T cells.
In her studies of immunotherapy and gastric cancer, lead author Yelena Janjigian, MD, chief of the gastrointestinal oncology service at Memorial Sloan Kettering Cancer Center, New York, noticed a trend in HER2-positive patients. “PD-L1 overexpression actually can occur and continue to increase while the patient is on trastuzumab as a mode of resistance,” Dr. Janjigian said in an interview.
That observation prompted the idea to combine a PD-L1 inhibitor in a phase 3 clinical trial. The results were striking. “I’ve never seen such depth of response. You could see responses as early as week 3 – after just one dose – and no one’s ever shown that before,” Dr. Janjigian said.
The new study randomized 264 patients to receive pembrolizumab or placebo in combination with trastuzumab plus fluoropyrimidine- and platinum-containing chemotherapy. In the intention-to-treat population, 81.3% of the population was male, and the primary tumor site was the stomach in 68.4%. The pembrolizumab group had a significantly higher objective response rate than the placebo group (74.4% vs. 51.9%; P = .00006).
The median decrease in lesion size was 65% in the pembrolizumab group and 49% in the placebo group. 32.3% of the pembrolizumab group had at least an 80% decrease in lesion size, versus 14.8% in the placebo group. The pembrolizumab group had more complete responses (11.3% vs. 3.1%).
The message from this is that biomarkers are critical, even if actionable ones are rare, Dr. Janjigian said. “Even though it feels like it’s only 10% or 5% of population, you start chipping away at it. How do we cure cancer? We cure it one percentage at a time through biomarker testing.”
Writing in a commentary published with the study, Myriam Chalabi, MD, a physician specializing in gastrointestinal oncology with the Netherlands Cancer Institute, Amsterdam, described the findings as “impressive in terms of the tumor responses.” But she was cautious saying data on progression-free survival and overall survival are needed to understand how well the proposed treatment would work long term.
“Given that PD-1 blockade seems to complement trastuzumab and chemotherapy for the treatment of HER2-positive gastric cancers, Janjigian and colleagues’ study has moved the field forward, and their findings could be the next, long-awaited development in the treatment of these cancers,” she wrote.
A key limitation is that the study looked at overall response rate, rather than the overall survival. The latter results should come within a year, Dr. Janjigian said.
The study was funded by Merck. Dr. Janjigian has received research funding from Merck, Rgenix, Bayer, Genentech/Roche, Bristol-Myers Squibb, and Eli Lilly, and has served on advisory boards for Rgenix, Merck Serono, Bristol-Myers Squibb, Eli Lilly, Pfizer, Bayer, Imugene, Merck Sharp & Dohme, Daiichi-Sankyo, Zymeworks, SeaGen, Basilea Pharmaceutical, and AstraZeneca. She has equity in Rgenix.
FROM NATURE
BMJ slams ‘incompetent’ Facebook fact-checking of vaccine article
According to an open letter written by outgoing BMJ editor-in-chief Fiona Godlee, MD, and incoming editor-in-chief Kamran Abbasi, MD, Facebook hired a third-party contractor to evaluate the article’s findings. This resulted in “inaccurate, incompetent, and irresponsible” conclusions that “should be of concern to anyone who values and relies on sources such as the BMJ for reliable medical information.”
The article in question investigated data integrity concerns at Pfizer vaccine clinical trial sites. In September 2020, the letter states, a former employee of the research group involved in Pfizer’s main vaccine trials, Ventavia, reached out to the BMJ and “began providing ... dozens of internal company documents, photos, audio recordings, and emails.” According to the company’s website, Ventavia “played a significant part in [COVID-19 clinical trial] recruitment” and “has received recognition by Pfizer for their contribution to vaccine trials.”
It was previously reported that the whistle-blower is a former regional director who was involved in Pfizer’s vaccine trials in Texas during the fall of 2020. She alleges “the company falsified data, unblinded patients, employed inadequately trained vaccinators, and was slow to follow up on adverse events reported in Pfizer’s pivotal phase 3 trial.”
The images provided to the BMJ “showed needles discarded in a plastic biohazard bag instead of a sharps container box” and another displayed “vaccine packaging materials with trial participants’ identification numbers written on them left out in the open, potentially unblinding participants.”
Despite informing Ventavia, the director’s concerns went unaddressed. She then filed a complaint with the Food and Drug Administration and was subsequently fired the same day. The FDA did not investigate the director’s allegations, said Dr. Godlee and Dr. Abbasi, even though the evidence “revealed a host of poor clinical trial research practices occurring at Ventavia that could impact data integrity and patient safety.”
Article labeled as ‘hoax,’ without pointing out errors
The BMJ hired an investigative reporter to follow up on the clinical trial claims. The findings were published in an article on Nov. 2, 2021, after the article “went through ... the usual high-level legal and editorial oversight and peer review,” according to the journal.
However, by Nov. 10, the journal began receiving complaints from readers unable to share the article on social media. Others had their posts flagged with warnings, such as “missing context ... independent fact-checkers say this information could mislead people.” Administrators of various Facebook groups were notified that posts containing the article were “partly false.”
Readers were informed that Facebook contractor Lead Stories performed the article’s “fact check.” Lead Stories is “an award-winning innovative fact checking and debunking website” and “an active part of Facebook’s partnership with third-party fact checkers” – with the latter granting them “access to listings of content that has been flagged as potentially false by Facebook’s systems or its users.” The company said they “decide independently if we want to fact check it or not.”
Lead Stories stated that they “can enter our fact checks into a tool provided by Facebook and Facebook then uses our data to help slow down the spread of false information on its platform.” Although the contractor is compensated, Lead Stories claims they have “no say or influence over what we fact check or what our conclusions are.”
Both editors question the validity of the fact check performed by Lead Stories, as it failed to provide any “assertions of fact” as to what the BMJ got wrong. Moreover, the editors take issue with Lead Stories referring to the journal as a “news blog” and using the phrase “hoax-alert” in the URL when publishing the story on its site.
The BMJ has reached out to Lead Stories and Facebook, said the letter, but Lead Stories refuses to “change anything about their article or actions that have led to Facebook flagging our article.” Requests for Facebook to remove the “fact-checking” label and allow “readers to freely share the article on [Facebook’s] platform” have been unfruitful.
Dr. Godlee and Dr. Abbasi expressed concern that other “high quality information provider[s] have been affected by the incompetence of Meta’s fact checking regime.” In November, Instagram censored Cochrane, an international provider of independent systematic medical reviews. Instagram, also owned by Meta, prohibited users from tagging Cochrane because the organization “repeatedly posted ... false content about COVID-19 or vaccines.” Cochrane refuted the allegations.
While “fact checking has been a staple of good journalism for decades,” said the editors, Meta has “apparently delegated responsibility to people incompetent in carrying out this crucial task.” They urged the company to reconsider its fact-checking strategy and review the issues that contributed to the error.
This news organization reached out to Meta for comment but did not receive a response at press time.
Lead Stories has posted a reply (Lead Stories’ Response To BMJ Open Letter Objecting To A Lead Stories Fact Check) to the BMJ’s complaint on its website.
A version of this article first appeared on Medscape.com.
According to an open letter written by outgoing BMJ editor-in-chief Fiona Godlee, MD, and incoming editor-in-chief Kamran Abbasi, MD, Facebook hired a third-party contractor to evaluate the article’s findings. This resulted in “inaccurate, incompetent, and irresponsible” conclusions that “should be of concern to anyone who values and relies on sources such as the BMJ for reliable medical information.”
The article in question investigated data integrity concerns at Pfizer vaccine clinical trial sites. In September 2020, the letter states, a former employee of the research group involved in Pfizer’s main vaccine trials, Ventavia, reached out to the BMJ and “began providing ... dozens of internal company documents, photos, audio recordings, and emails.” According to the company’s website, Ventavia “played a significant part in [COVID-19 clinical trial] recruitment” and “has received recognition by Pfizer for their contribution to vaccine trials.”
It was previously reported that the whistle-blower is a former regional director who was involved in Pfizer’s vaccine trials in Texas during the fall of 2020. She alleges “the company falsified data, unblinded patients, employed inadequately trained vaccinators, and was slow to follow up on adverse events reported in Pfizer’s pivotal phase 3 trial.”
The images provided to the BMJ “showed needles discarded in a plastic biohazard bag instead of a sharps container box” and another displayed “vaccine packaging materials with trial participants’ identification numbers written on them left out in the open, potentially unblinding participants.”
Despite informing Ventavia, the director’s concerns went unaddressed. She then filed a complaint with the Food and Drug Administration and was subsequently fired the same day. The FDA did not investigate the director’s allegations, said Dr. Godlee and Dr. Abbasi, even though the evidence “revealed a host of poor clinical trial research practices occurring at Ventavia that could impact data integrity and patient safety.”
Article labeled as ‘hoax,’ without pointing out errors
The BMJ hired an investigative reporter to follow up on the clinical trial claims. The findings were published in an article on Nov. 2, 2021, after the article “went through ... the usual high-level legal and editorial oversight and peer review,” according to the journal.
However, by Nov. 10, the journal began receiving complaints from readers unable to share the article on social media. Others had their posts flagged with warnings, such as “missing context ... independent fact-checkers say this information could mislead people.” Administrators of various Facebook groups were notified that posts containing the article were “partly false.”
Readers were informed that Facebook contractor Lead Stories performed the article’s “fact check.” Lead Stories is “an award-winning innovative fact checking and debunking website” and “an active part of Facebook’s partnership with third-party fact checkers” – with the latter granting them “access to listings of content that has been flagged as potentially false by Facebook’s systems or its users.” The company said they “decide independently if we want to fact check it or not.”
Lead Stories stated that they “can enter our fact checks into a tool provided by Facebook and Facebook then uses our data to help slow down the spread of false information on its platform.” Although the contractor is compensated, Lead Stories claims they have “no say or influence over what we fact check or what our conclusions are.”
Both editors question the validity of the fact check performed by Lead Stories, as it failed to provide any “assertions of fact” as to what the BMJ got wrong. Moreover, the editors take issue with Lead Stories referring to the journal as a “news blog” and using the phrase “hoax-alert” in the URL when publishing the story on its site.
The BMJ has reached out to Lead Stories and Facebook, said the letter, but Lead Stories refuses to “change anything about their article or actions that have led to Facebook flagging our article.” Requests for Facebook to remove the “fact-checking” label and allow “readers to freely share the article on [Facebook’s] platform” have been unfruitful.
Dr. Godlee and Dr. Abbasi expressed concern that other “high quality information provider[s] have been affected by the incompetence of Meta’s fact checking regime.” In November, Instagram censored Cochrane, an international provider of independent systematic medical reviews. Instagram, also owned by Meta, prohibited users from tagging Cochrane because the organization “repeatedly posted ... false content about COVID-19 or vaccines.” Cochrane refuted the allegations.
While “fact checking has been a staple of good journalism for decades,” said the editors, Meta has “apparently delegated responsibility to people incompetent in carrying out this crucial task.” They urged the company to reconsider its fact-checking strategy and review the issues that contributed to the error.
This news organization reached out to Meta for comment but did not receive a response at press time.
Lead Stories has posted a reply (Lead Stories’ Response To BMJ Open Letter Objecting To A Lead Stories Fact Check) to the BMJ’s complaint on its website.
A version of this article first appeared on Medscape.com.
According to an open letter written by outgoing BMJ editor-in-chief Fiona Godlee, MD, and incoming editor-in-chief Kamran Abbasi, MD, Facebook hired a third-party contractor to evaluate the article’s findings. This resulted in “inaccurate, incompetent, and irresponsible” conclusions that “should be of concern to anyone who values and relies on sources such as the BMJ for reliable medical information.”
The article in question investigated data integrity concerns at Pfizer vaccine clinical trial sites. In September 2020, the letter states, a former employee of the research group involved in Pfizer’s main vaccine trials, Ventavia, reached out to the BMJ and “began providing ... dozens of internal company documents, photos, audio recordings, and emails.” According to the company’s website, Ventavia “played a significant part in [COVID-19 clinical trial] recruitment” and “has received recognition by Pfizer for their contribution to vaccine trials.”
It was previously reported that the whistle-blower is a former regional director who was involved in Pfizer’s vaccine trials in Texas during the fall of 2020. She alleges “the company falsified data, unblinded patients, employed inadequately trained vaccinators, and was slow to follow up on adverse events reported in Pfizer’s pivotal phase 3 trial.”
The images provided to the BMJ “showed needles discarded in a plastic biohazard bag instead of a sharps container box” and another displayed “vaccine packaging materials with trial participants’ identification numbers written on them left out in the open, potentially unblinding participants.”
Despite informing Ventavia, the director’s concerns went unaddressed. She then filed a complaint with the Food and Drug Administration and was subsequently fired the same day. The FDA did not investigate the director’s allegations, said Dr. Godlee and Dr. Abbasi, even though the evidence “revealed a host of poor clinical trial research practices occurring at Ventavia that could impact data integrity and patient safety.”
Article labeled as ‘hoax,’ without pointing out errors
The BMJ hired an investigative reporter to follow up on the clinical trial claims. The findings were published in an article on Nov. 2, 2021, after the article “went through ... the usual high-level legal and editorial oversight and peer review,” according to the journal.
However, by Nov. 10, the journal began receiving complaints from readers unable to share the article on social media. Others had their posts flagged with warnings, such as “missing context ... independent fact-checkers say this information could mislead people.” Administrators of various Facebook groups were notified that posts containing the article were “partly false.”
Readers were informed that Facebook contractor Lead Stories performed the article’s “fact check.” Lead Stories is “an award-winning innovative fact checking and debunking website” and “an active part of Facebook’s partnership with third-party fact checkers” – with the latter granting them “access to listings of content that has been flagged as potentially false by Facebook’s systems or its users.” The company said they “decide independently if we want to fact check it or not.”
Lead Stories stated that they “can enter our fact checks into a tool provided by Facebook and Facebook then uses our data to help slow down the spread of false information on its platform.” Although the contractor is compensated, Lead Stories claims they have “no say or influence over what we fact check or what our conclusions are.”
Both editors question the validity of the fact check performed by Lead Stories, as it failed to provide any “assertions of fact” as to what the BMJ got wrong. Moreover, the editors take issue with Lead Stories referring to the journal as a “news blog” and using the phrase “hoax-alert” in the URL when publishing the story on its site.
The BMJ has reached out to Lead Stories and Facebook, said the letter, but Lead Stories refuses to “change anything about their article or actions that have led to Facebook flagging our article.” Requests for Facebook to remove the “fact-checking” label and allow “readers to freely share the article on [Facebook’s] platform” have been unfruitful.
Dr. Godlee and Dr. Abbasi expressed concern that other “high quality information provider[s] have been affected by the incompetence of Meta’s fact checking regime.” In November, Instagram censored Cochrane, an international provider of independent systematic medical reviews. Instagram, also owned by Meta, prohibited users from tagging Cochrane because the organization “repeatedly posted ... false content about COVID-19 or vaccines.” Cochrane refuted the allegations.
While “fact checking has been a staple of good journalism for decades,” said the editors, Meta has “apparently delegated responsibility to people incompetent in carrying out this crucial task.” They urged the company to reconsider its fact-checking strategy and review the issues that contributed to the error.
This news organization reached out to Meta for comment but did not receive a response at press time.
Lead Stories has posted a reply (Lead Stories’ Response To BMJ Open Letter Objecting To A Lead Stories Fact Check) to the BMJ’s complaint on its website.
A version of this article first appeared on Medscape.com.
Many clinicians feel ill-prepared for drug overdose deaths
new research suggests.
However, results from a survey study also showed that colleagues were an important source of support in the wake of this type of event.
“A patient overdose death can change clinical decision-making for providers experiencing high levels of stress related to the overdose death,” noted the investigators, led by Amy Yule, MD, director of adolescent addiction psychiatry, Boston Medical Center, and assistant professor of psychiatry at Boston University Medical Center.
The findings were presented by Dr. Yule at the annual meeting of the American Academy of Addiction Psychiatry.
All-time high
As reported by this news organization, there has recently been a record number of drug overdose deaths. And these deaths affect families, communities, and often providers, Dr. Yule told meeting attendees.
Previous research has looked at the impact of drug overdose deaths and the opioid epidemic on first responders and community health workers in the field of overdose prevention.
“But there’s less in the literature to my knowledge that describes the experience of providers and clinicians who are working in more formalized medical settings,” said Dr. Yule.
In December 2020, researchers sent an email to members of the Providers Clinical Support System (PCSS) inviting them to complete an anonymous survey. The PCSS program was created in response to the opioid overdose epidemic to train primary care clinicians in the prevention and treatment of opioid use disorders.
A total of 12,204 members received the email, 1,064 opened the survey link, and 523 completed the survey.
Participants were mostly White and female, with an average age of 52 years. Respondents had been practicing for an average of about 16 years.
The largest responder group was physicians (47%), followed by counselors (29%), nurse practitioners (17%), and nurses (7%).
Among physician respondents, 41% reported having received additional formal training in addiction.
Only 24% of the respondents indicated they received training in “postvention,” which refers to interventions after a suicide to support the bereaved. Such interventions “could be helpful in potentially preparing them for a drug overdose death in their practice,” said Dr. Yule.
Categories of preparedness
The survey inquired about three categories of preparedness: coping with a drug overdose death, providing support to a colleague, and talking with families who have lost a member to a drug overdose.
Overall, 59% said they felt somewhat or fairly well prepared for the first two categories and 55% for the third category.
“I think it’s notable that there is a higher percentage of people who felt not at all prepared to talk with family members (20.5%), compared to those who felt not at all prepared to cope with a drug overdose death (13.8%) or prepared to support a colleague (12%),” Dr. Yule said.
More than half of respondents (55%) indicated a drug overdose death had occurred in their own practice.
The survey also looked at frequency of consultations with colleagues, critical incident debriefing sessions, and interactions with a patient’s family.
Almost half (48%) of the sample said they consulted with a colleague after most patient overdose deaths. Only 24% said they had a critical incidence debriefing session after most of these events, and 20% said they interacted with the patient’s family.
Asked what resources they found helpful for coping with a recent patient drug overdose death, respondents flagged their colleagues and meetings with families.
The survey also examined provider trauma after a patient drug overdose death, using the Impact of Event Scale–R. “If the score is above a certain cutoff level, there is potential concern” for PTSD, Dr. Yule said.
Among the 141 respondents who had a patient drug overdose death in their practice during the previous year, 121 completed this trauma scale. Of these, 18% had “a very elevated” score, Dr. Yule reported.
Sources of support
Commenting on the survey study, Larissa Mooney, MD, associate professor and director of the addiction psychiatry division in the department of psychiatry and biobehavioral sciences at the University of California, Los Angeles, said it is not surprising that many providers do not feel adequately prepared to cope with an overdose death, or how to support a colleague after such an event.
“This is not routinely covered in training, and patient overdose may occur without warning signs,” said Dr. Mooney, who was not involved with the research.
However, these new findings suggest a range of potential sources of support for providers after a patient overdose death that may be helpful, “including colleagues, friends, therapy, supervision, and meeting with the patient’s family,” she said.
The study received funding from the PCSS. Dr. Yule disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
However, results from a survey study also showed that colleagues were an important source of support in the wake of this type of event.
“A patient overdose death can change clinical decision-making for providers experiencing high levels of stress related to the overdose death,” noted the investigators, led by Amy Yule, MD, director of adolescent addiction psychiatry, Boston Medical Center, and assistant professor of psychiatry at Boston University Medical Center.
The findings were presented by Dr. Yule at the annual meeting of the American Academy of Addiction Psychiatry.
All-time high
As reported by this news organization, there has recently been a record number of drug overdose deaths. And these deaths affect families, communities, and often providers, Dr. Yule told meeting attendees.
Previous research has looked at the impact of drug overdose deaths and the opioid epidemic on first responders and community health workers in the field of overdose prevention.
“But there’s less in the literature to my knowledge that describes the experience of providers and clinicians who are working in more formalized medical settings,” said Dr. Yule.
In December 2020, researchers sent an email to members of the Providers Clinical Support System (PCSS) inviting them to complete an anonymous survey. The PCSS program was created in response to the opioid overdose epidemic to train primary care clinicians in the prevention and treatment of opioid use disorders.
A total of 12,204 members received the email, 1,064 opened the survey link, and 523 completed the survey.
Participants were mostly White and female, with an average age of 52 years. Respondents had been practicing for an average of about 16 years.
The largest responder group was physicians (47%), followed by counselors (29%), nurse practitioners (17%), and nurses (7%).
Among physician respondents, 41% reported having received additional formal training in addiction.
Only 24% of the respondents indicated they received training in “postvention,” which refers to interventions after a suicide to support the bereaved. Such interventions “could be helpful in potentially preparing them for a drug overdose death in their practice,” said Dr. Yule.
Categories of preparedness
The survey inquired about three categories of preparedness: coping with a drug overdose death, providing support to a colleague, and talking with families who have lost a member to a drug overdose.
Overall, 59% said they felt somewhat or fairly well prepared for the first two categories and 55% for the third category.
“I think it’s notable that there is a higher percentage of people who felt not at all prepared to talk with family members (20.5%), compared to those who felt not at all prepared to cope with a drug overdose death (13.8%) or prepared to support a colleague (12%),” Dr. Yule said.
More than half of respondents (55%) indicated a drug overdose death had occurred in their own practice.
The survey also looked at frequency of consultations with colleagues, critical incident debriefing sessions, and interactions with a patient’s family.
Almost half (48%) of the sample said they consulted with a colleague after most patient overdose deaths. Only 24% said they had a critical incidence debriefing session after most of these events, and 20% said they interacted with the patient’s family.
Asked what resources they found helpful for coping with a recent patient drug overdose death, respondents flagged their colleagues and meetings with families.
The survey also examined provider trauma after a patient drug overdose death, using the Impact of Event Scale–R. “If the score is above a certain cutoff level, there is potential concern” for PTSD, Dr. Yule said.
Among the 141 respondents who had a patient drug overdose death in their practice during the previous year, 121 completed this trauma scale. Of these, 18% had “a very elevated” score, Dr. Yule reported.
Sources of support
Commenting on the survey study, Larissa Mooney, MD, associate professor and director of the addiction psychiatry division in the department of psychiatry and biobehavioral sciences at the University of California, Los Angeles, said it is not surprising that many providers do not feel adequately prepared to cope with an overdose death, or how to support a colleague after such an event.
“This is not routinely covered in training, and patient overdose may occur without warning signs,” said Dr. Mooney, who was not involved with the research.
However, these new findings suggest a range of potential sources of support for providers after a patient overdose death that may be helpful, “including colleagues, friends, therapy, supervision, and meeting with the patient’s family,” she said.
The study received funding from the PCSS. Dr. Yule disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
However, results from a survey study also showed that colleagues were an important source of support in the wake of this type of event.
“A patient overdose death can change clinical decision-making for providers experiencing high levels of stress related to the overdose death,” noted the investigators, led by Amy Yule, MD, director of adolescent addiction psychiatry, Boston Medical Center, and assistant professor of psychiatry at Boston University Medical Center.
The findings were presented by Dr. Yule at the annual meeting of the American Academy of Addiction Psychiatry.
All-time high
As reported by this news organization, there has recently been a record number of drug overdose deaths. And these deaths affect families, communities, and often providers, Dr. Yule told meeting attendees.
Previous research has looked at the impact of drug overdose deaths and the opioid epidemic on first responders and community health workers in the field of overdose prevention.
“But there’s less in the literature to my knowledge that describes the experience of providers and clinicians who are working in more formalized medical settings,” said Dr. Yule.
In December 2020, researchers sent an email to members of the Providers Clinical Support System (PCSS) inviting them to complete an anonymous survey. The PCSS program was created in response to the opioid overdose epidemic to train primary care clinicians in the prevention and treatment of opioid use disorders.
A total of 12,204 members received the email, 1,064 opened the survey link, and 523 completed the survey.
Participants were mostly White and female, with an average age of 52 years. Respondents had been practicing for an average of about 16 years.
The largest responder group was physicians (47%), followed by counselors (29%), nurse practitioners (17%), and nurses (7%).
Among physician respondents, 41% reported having received additional formal training in addiction.
Only 24% of the respondents indicated they received training in “postvention,” which refers to interventions after a suicide to support the bereaved. Such interventions “could be helpful in potentially preparing them for a drug overdose death in their practice,” said Dr. Yule.
Categories of preparedness
The survey inquired about three categories of preparedness: coping with a drug overdose death, providing support to a colleague, and talking with families who have lost a member to a drug overdose.
Overall, 59% said they felt somewhat or fairly well prepared for the first two categories and 55% for the third category.
“I think it’s notable that there is a higher percentage of people who felt not at all prepared to talk with family members (20.5%), compared to those who felt not at all prepared to cope with a drug overdose death (13.8%) or prepared to support a colleague (12%),” Dr. Yule said.
More than half of respondents (55%) indicated a drug overdose death had occurred in their own practice.
The survey also looked at frequency of consultations with colleagues, critical incident debriefing sessions, and interactions with a patient’s family.
Almost half (48%) of the sample said they consulted with a colleague after most patient overdose deaths. Only 24% said they had a critical incidence debriefing session after most of these events, and 20% said they interacted with the patient’s family.
Asked what resources they found helpful for coping with a recent patient drug overdose death, respondents flagged their colleagues and meetings with families.
The survey also examined provider trauma after a patient drug overdose death, using the Impact of Event Scale–R. “If the score is above a certain cutoff level, there is potential concern” for PTSD, Dr. Yule said.
Among the 141 respondents who had a patient drug overdose death in their practice during the previous year, 121 completed this trauma scale. Of these, 18% had “a very elevated” score, Dr. Yule reported.
Sources of support
Commenting on the survey study, Larissa Mooney, MD, associate professor and director of the addiction psychiatry division in the department of psychiatry and biobehavioral sciences at the University of California, Los Angeles, said it is not surprising that many providers do not feel adequately prepared to cope with an overdose death, or how to support a colleague after such an event.
“This is not routinely covered in training, and patient overdose may occur without warning signs,” said Dr. Mooney, who was not involved with the research.
However, these new findings suggest a range of potential sources of support for providers after a patient overdose death that may be helpful, “including colleagues, friends, therapy, supervision, and meeting with the patient’s family,” she said.
The study received funding from the PCSS. Dr. Yule disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAAP 2021
What is your diagnosis?
Answer: Infectious gastroparesis secondary to acute hepatitis A infection.
A computed tomography scan of the abdomen/pelvis demonstrated marked gastric distention without obvious obstructing mass and normal caliber small bowel and colon. Additional laboratory workup revealed a positive hepatitis A IgM antibody. Hepatitis B surface antigen and core IgM antibody were negative, as was the hepatitis C virus antibody. Human immunodeficiency virus antigen and antibody were negative. An esophagogastroduodenoscopy was performed that showed a large amount of food in a dilated and atonic stomach.
With conservative treatment, the patient’s liver enzymes trended down over the next 2 days to alanine aminotransferase 993 U/L, aspartate aminotransferase 244 U/L, and direct bilirubin 3.8 mg/dL. At the time of discharge, she was tolerating soft foods without any difficulty. She was educated on taking appropriate precautions to avoid transmitting the hepatitis A infection to others. Her risk factor for hepatitis A was recent incarceration.
Here we highlight a rare case of infectious gastroparesis secondary to hepatitis A infection. Hepatitis A virus is a small, nonenveloped, RNA-containing virus.1 It typically presents with a self-limited illness with liver failure occurring in rare cases. Common presenting symptoms including nausea, vomiting, jaundice, fever, diarrhea, and abdominal pain.Laboratory abnormalities include elevations in the serum aminotransferases, alkaline phosphatase, and total bilirubin.2 The diagnosis is confirmed with a positive hepatitis A IgM antibody. The most common route of transmission is the fecal-oral route such as through consumption of contaminated water and food or from person-to-person contact.1 Individuals can develop immunity to the virus either from prior infection or vaccination.
Gastroparesis refers to delayed emptying of gastric contents when mechanical obstruction has been ruled out. Common causes of gastroparesis include diabetes mellitus, medications, postoperative complications, and infections. Infectious gastroparesis may present acutely after a viral prodrome and symptoms may be severe and slow to resolve.3
References
1. Lemon SM. N Engl J Med. 1985 Oct 24;313(17):1059-67.
2. Tong MJ et al. J Infect Dis. 1995 Mar;171 Suppl 1:S15-8.
3. Bityutskiy LP. Am J Gastroenterol. 1997 Sep;92(9):1501-4.
Answer: Infectious gastroparesis secondary to acute hepatitis A infection.
A computed tomography scan of the abdomen/pelvis demonstrated marked gastric distention without obvious obstructing mass and normal caliber small bowel and colon. Additional laboratory workup revealed a positive hepatitis A IgM antibody. Hepatitis B surface antigen and core IgM antibody were negative, as was the hepatitis C virus antibody. Human immunodeficiency virus antigen and antibody were negative. An esophagogastroduodenoscopy was performed that showed a large amount of food in a dilated and atonic stomach.
With conservative treatment, the patient’s liver enzymes trended down over the next 2 days to alanine aminotransferase 993 U/L, aspartate aminotransferase 244 U/L, and direct bilirubin 3.8 mg/dL. At the time of discharge, she was tolerating soft foods without any difficulty. She was educated on taking appropriate precautions to avoid transmitting the hepatitis A infection to others. Her risk factor for hepatitis A was recent incarceration.
Here we highlight a rare case of infectious gastroparesis secondary to hepatitis A infection. Hepatitis A virus is a small, nonenveloped, RNA-containing virus.1 It typically presents with a self-limited illness with liver failure occurring in rare cases. Common presenting symptoms including nausea, vomiting, jaundice, fever, diarrhea, and abdominal pain.Laboratory abnormalities include elevations in the serum aminotransferases, alkaline phosphatase, and total bilirubin.2 The diagnosis is confirmed with a positive hepatitis A IgM antibody. The most common route of transmission is the fecal-oral route such as through consumption of contaminated water and food or from person-to-person contact.1 Individuals can develop immunity to the virus either from prior infection or vaccination.
Gastroparesis refers to delayed emptying of gastric contents when mechanical obstruction has been ruled out. Common causes of gastroparesis include diabetes mellitus, medications, postoperative complications, and infections. Infectious gastroparesis may present acutely after a viral prodrome and symptoms may be severe and slow to resolve.3
References
1. Lemon SM. N Engl J Med. 1985 Oct 24;313(17):1059-67.
2. Tong MJ et al. J Infect Dis. 1995 Mar;171 Suppl 1:S15-8.
3. Bityutskiy LP. Am J Gastroenterol. 1997 Sep;92(9):1501-4.
Answer: Infectious gastroparesis secondary to acute hepatitis A infection.
A computed tomography scan of the abdomen/pelvis demonstrated marked gastric distention without obvious obstructing mass and normal caliber small bowel and colon. Additional laboratory workup revealed a positive hepatitis A IgM antibody. Hepatitis B surface antigen and core IgM antibody were negative, as was the hepatitis C virus antibody. Human immunodeficiency virus antigen and antibody were negative. An esophagogastroduodenoscopy was performed that showed a large amount of food in a dilated and atonic stomach.
With conservative treatment, the patient’s liver enzymes trended down over the next 2 days to alanine aminotransferase 993 U/L, aspartate aminotransferase 244 U/L, and direct bilirubin 3.8 mg/dL. At the time of discharge, she was tolerating soft foods without any difficulty. She was educated on taking appropriate precautions to avoid transmitting the hepatitis A infection to others. Her risk factor for hepatitis A was recent incarceration.
Here we highlight a rare case of infectious gastroparesis secondary to hepatitis A infection. Hepatitis A virus is a small, nonenveloped, RNA-containing virus.1 It typically presents with a self-limited illness with liver failure occurring in rare cases. Common presenting symptoms including nausea, vomiting, jaundice, fever, diarrhea, and abdominal pain.Laboratory abnormalities include elevations in the serum aminotransferases, alkaline phosphatase, and total bilirubin.2 The diagnosis is confirmed with a positive hepatitis A IgM antibody. The most common route of transmission is the fecal-oral route such as through consumption of contaminated water and food or from person-to-person contact.1 Individuals can develop immunity to the virus either from prior infection or vaccination.
Gastroparesis refers to delayed emptying of gastric contents when mechanical obstruction has been ruled out. Common causes of gastroparesis include diabetes mellitus, medications, postoperative complications, and infections. Infectious gastroparesis may present acutely after a viral prodrome and symptoms may be severe and slow to resolve.3
References
1. Lemon SM. N Engl J Med. 1985 Oct 24;313(17):1059-67.
2. Tong MJ et al. J Infect Dis. 1995 Mar;171 Suppl 1:S15-8.
3. Bityutskiy LP. Am J Gastroenterol. 1997 Sep;92(9):1501-4.
A 33-year-old woman presented with a 10-day history of painless jaundice. During this time, she also noted decreased appetite, malaise, and pruritus. On occasion, she would have heartburn and belching that would improve with an antacid. She denied any right upper quadrant pain and weight loss. She was not currently taking any medications, including acetaminophen. She had a past medical history of methamphetamine use in recent remission. She had recently been incarcerated for about 1 month. 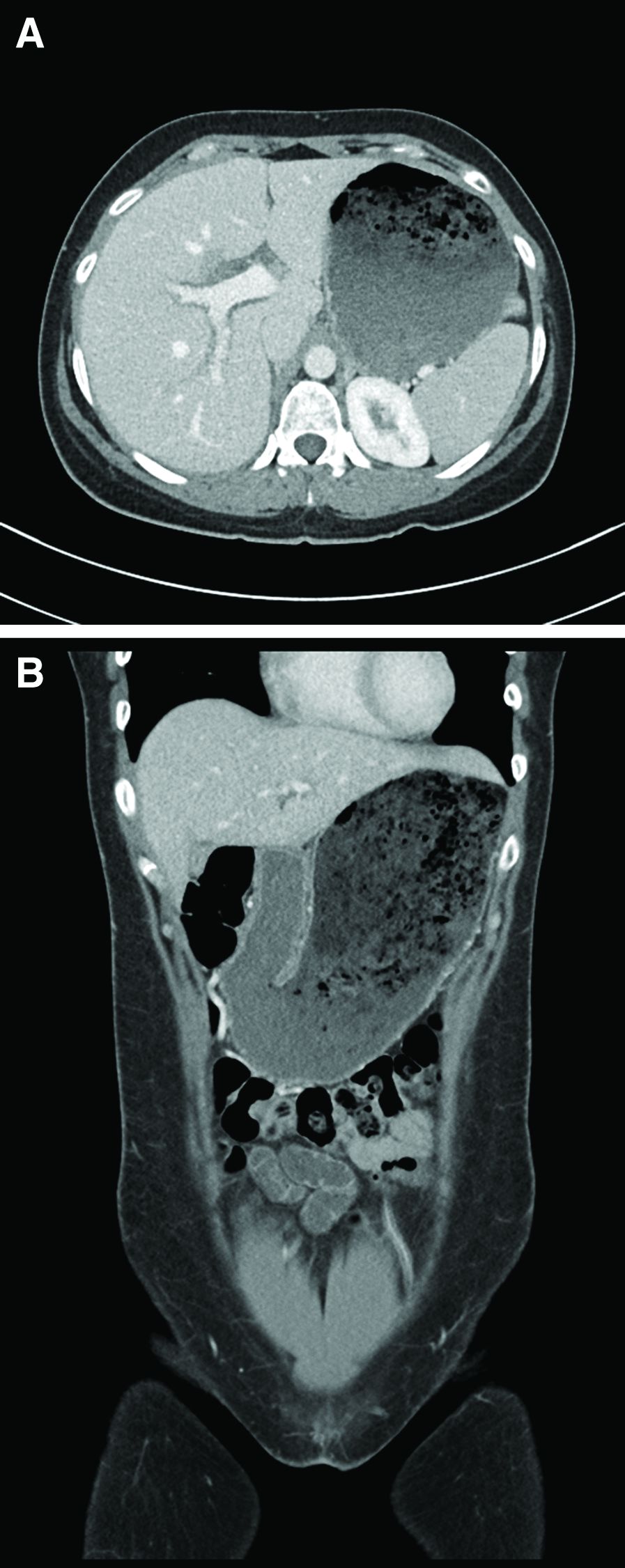
What is the most likely etiology of the patient's condition?
COVID-19 and coping with superimposed traumas
While 2022 is lurking around the corner, many of us still have 2020 on our minds. Social media posts are already emerging: “No new years resolutions. It is the circumstances turn to improve [sic],” one post declares. Others proclaim that it is difficult coming to terms with the idea that 2022 is actually pronounced “2020 too.” A critical difference exists between then and now – we have experienced months of living in limbo and rolling with the punches of pandemic life.

In some ways, it has become easy to think of the early pandemic days as a distant memory, yet respect that the impact of 2020 has been indelible for virtually all of us and feels palpable as if it were yesterday.
The year 2020 was marked by the beginning of the COVID-19 pandemic, which was accompanied by extreme uncertainty, loss of all kinds, and emotional turmoil. The early pandemic had a profound economic and social impact, with added stress tethered to political and race-related division in America that created divides among families and friends, and yielded ceaseless discourse related to divergent perspectives. This only exacerbated the stress that came with the pandemic, given that providing support and leaning on one another was more important than ever. All of this was compounded by natural disasters that have plagued the country.
So much was unprecedented. There was a collective sense of feeling “worn down,” and the burnout that was felt was quite profound. Enormous amounts of mental and physical effort were allocated to simply surviving, getting basic needs met, having enough food and supplies, and completing basic tasks. Ordinary relating felt taxing. At this stage of the pandemic, the COVID-19 experience can be conceived of as a traumatic stressor capable of eliciting a traumatic response and exacerbating other mental health symptoms. Our capacity to cope has been diminished. Anxiety rates have soared, as have rates of clinical depression. Those most affected have had lower household incomes, are unmarried, and have experienced pandemic-related stressors. The links between the impact of the pandemic on mental health have been clear.
The pandemic has forced the landscape of social support to dramatically change. Initially, we felt pulled to connect and we leaned into the use of virtual platforms to connect for all matters (simple social gatherings, big birthday events, family reunions, celebration of holidays, work duties, and academic work). However, “Zoom fatigue” began to set in, and our screen time was maxed out. There has been the added dynamic of frontline workers who did not have the option to work virtually or from home. This group largely has felt disconnected from others who didn’t understand the depth of their anxiety and loneliness of their experience. Health care workers have had to make challenging, life-and-death, patient-related decisions that called into question personal morals and ethics all while their own lives were at risk.
Fast-forward to the present, and support systems have either strengthened or worn down – which has yielded a unique dichotomy. Maintaining friendships has either felt of utmost importance given the impact of the disconnect and physical distance or has felt challenging given the mental energy expended from working and connecting virtually. Empathy burnout is also a real and important facet in the equation. We begin to ask the question: Are we checking in with others in the spirit of authentic relating, to cultivate real connection, or to check a box?
Impact of layered traumas
It is interesting to think about the pandemic’s traumatic impact being “superimposed” on top of the “ordinary traumas” experienced outside of the pandemic. We are essentially at the 2-year mark, in some ways have cultivated a sense of resilience and found ways to adapt, and in other ways at times feel right back where we were in early 2020. There were moments that felt hopeful, glimmers of normalcy, and setbacks that all ebbed and flowed – but even so, there have not been many “mental breaks,” only temporary and transient reprieves. Some got sick and died; some recovered; and others are still experiencing long-hauler syndrome and have lingering sequelae. Despite adaptation and resilience, one can’t help but wonder the impact of superimposed traumas on top of this collective trauma. Many of us have not even rebounded from the pandemic, and then are faced with loss, grief, challenges, illness, hard and big life decisions. We are challenged to answer the question: How do we endure in the face of this trauma inception?
It has been a challenging time for all, including those who are ordinarily happy-go-lucky, resilient, and see the glass half-full and are struggling with the idea of struggling. I am no “resilience expert” but gleaned much wisdom from responding to the Surfside, Fla., building collapse. This was a collective trauma that took place in the summer of 2021, and the wisdom of this event highlighted the value of collective healing and unification even in spite of the times. What happened in Surfside was a shock, and the loss was felt by those directly affected, the surrounding community, and those who were part of the disaster response efforts. All of those parties had been processing losses prior to this – loss of normalcy because of the pandemic, loss of people we loved as a result, other personal losses – and this community tragedy was yet another loss to disentangle on top of a period in U.S. history demarcated by a great lack of unity, divisiveness, anger, and hatred. The collapse highlighted the small size yet interconnectedness of the community and the power of connection and authentic relating. It was overwhelming in the moment but extremely heartening and beautiful to see the amount of willingness to drop everything and help. Despite feeling worn down from the pandemic, people drew upon their internal resources, natural goodness, and kindness “reserves” to provide support.
Responding to the collapse highlighted that resilience in the context of collective trauma requires flexibility, embracing uncertainty, cultivating unity, and paying attention to meeting basic needs/self-care. The role of kindness cannot be overemphasized. In the realm of reflecting on the notion of kindness, it is worth noting how much power there is to bearing witness to someone’s experience, especially when they are in pain. People often diminish the role or at the very least do not recognize the power of showing up for someone and just listening. Pandemic resilience, and coping with coalescing traumas, is likely composed of these same facets that were essential in the context of coping with the collapse.
It is not only the immediate impact of a trauma as much as the aftermath that needs to processed and worked through. In one sense, people feel that they should be adjusted to and accustomed to this new reality, and at the same time, one has to remember and reflect on how unnatural this experience has been. There is an impact of a cumulative onslaught of negative events, and it is hard to imagine not being phased, remaining unchanged, or not feeling affected. We may feel hardened and that there are limits to the compassion we have to offer others. We may be feel empathic. There can be desensitization and an apathy to others’ suffering when our patience is worn down and we have limited bandwidth. There are data to support the idea that a level of habituation occurs to individuals who experience multiple traumas, which yields a level of “sensitization” to the negative impact of subsequent events. It becomes easy to make comparisons of suffering. The challenge will be to rise above these and make a conscious effort to connect with who and how we were before we were worn down.
I am still in awe about how much I learned from the victims’ families, survivors, and my colleagues at Surfside – about pain, suffering, loss, resilience, coping, fortitude, and meaning making. We were all forced to think beyond ourselves, show up for others, and unify in a way that remedied this period of fragmentation. With respect to the pandemic and “where we are at now,” some elements of our lives are stabilizing; other aspects feel volatile from the fatigue of what we have been experiencing. This pandemic has not fully abated, but we can find some clarity in the value of setting boundaries and knowing our limits – but not overlooking the power of unity and kindness and the value of the reciprocating those qualities.
Dr. Feldman is a licensed clinical psychologist in private practice in Miami. She is an adjunct professor in the college of psychology at Nova Southeastern University, Fort Lauderdale, Fla., where she teaches clinical psychology doctoral students. She also serves on the board of directors of the Southeast Florida Association for Psychoanalytic Psychology. Dr. Feldman has no disclosures.
While 2022 is lurking around the corner, many of us still have 2020 on our minds. Social media posts are already emerging: “No new years resolutions. It is the circumstances turn to improve [sic],” one post declares. Others proclaim that it is difficult coming to terms with the idea that 2022 is actually pronounced “2020 too.” A critical difference exists between then and now – we have experienced months of living in limbo and rolling with the punches of pandemic life.
In some ways, it has become easy to think of the early pandemic days as a distant memory, yet respect that the impact of 2020 has been indelible for virtually all of us and feels palpable as if it were yesterday.
The year 2020 was marked by the beginning of the COVID-19 pandemic, which was accompanied by extreme uncertainty, loss of all kinds, and emotional turmoil. The early pandemic had a profound economic and social impact, with added stress tethered to political and race-related division in America that created divides among families and friends, and yielded ceaseless discourse related to divergent perspectives. This only exacerbated the stress that came with the pandemic, given that providing support and leaning on one another was more important than ever. All of this was compounded by natural disasters that have plagued the country.
So much was unprecedented. There was a collective sense of feeling “worn down,” and the burnout that was felt was quite profound. Enormous amounts of mental and physical effort were allocated to simply surviving, getting basic needs met, having enough food and supplies, and completing basic tasks. Ordinary relating felt taxing. At this stage of the pandemic, the COVID-19 experience can be conceived of as a traumatic stressor capable of eliciting a traumatic response and exacerbating other mental health symptoms. Our capacity to cope has been diminished. Anxiety rates have soared, as have rates of clinical depression. Those most affected have had lower household incomes, are unmarried, and have experienced pandemic-related stressors. The links between the impact of the pandemic on mental health have been clear.
The pandemic has forced the landscape of social support to dramatically change. Initially, we felt pulled to connect and we leaned into the use of virtual platforms to connect for all matters (simple social gatherings, big birthday events, family reunions, celebration of holidays, work duties, and academic work). However, “Zoom fatigue” began to set in, and our screen time was maxed out. There has been the added dynamic of frontline workers who did not have the option to work virtually or from home. This group largely has felt disconnected from others who didn’t understand the depth of their anxiety and loneliness of their experience. Health care workers have had to make challenging, life-and-death, patient-related decisions that called into question personal morals and ethics all while their own lives were at risk.
Fast-forward to the present, and support systems have either strengthened or worn down – which has yielded a unique dichotomy. Maintaining friendships has either felt of utmost importance given the impact of the disconnect and physical distance or has felt challenging given the mental energy expended from working and connecting virtually. Empathy burnout is also a real and important facet in the equation. We begin to ask the question: Are we checking in with others in the spirit of authentic relating, to cultivate real connection, or to check a box?
Impact of layered traumas
It is interesting to think about the pandemic’s traumatic impact being “superimposed” on top of the “ordinary traumas” experienced outside of the pandemic. We are essentially at the 2-year mark, in some ways have cultivated a sense of resilience and found ways to adapt, and in other ways at times feel right back where we were in early 2020. There were moments that felt hopeful, glimmers of normalcy, and setbacks that all ebbed and flowed – but even so, there have not been many “mental breaks,” only temporary and transient reprieves. Some got sick and died; some recovered; and others are still experiencing long-hauler syndrome and have lingering sequelae. Despite adaptation and resilience, one can’t help but wonder the impact of superimposed traumas on top of this collective trauma. Many of us have not even rebounded from the pandemic, and then are faced with loss, grief, challenges, illness, hard and big life decisions. We are challenged to answer the question: How do we endure in the face of this trauma inception?
It has been a challenging time for all, including those who are ordinarily happy-go-lucky, resilient, and see the glass half-full and are struggling with the idea of struggling. I am no “resilience expert” but gleaned much wisdom from responding to the Surfside, Fla., building collapse. This was a collective trauma that took place in the summer of 2021, and the wisdom of this event highlighted the value of collective healing and unification even in spite of the times. What happened in Surfside was a shock, and the loss was felt by those directly affected, the surrounding community, and those who were part of the disaster response efforts. All of those parties had been processing losses prior to this – loss of normalcy because of the pandemic, loss of people we loved as a result, other personal losses – and this community tragedy was yet another loss to disentangle on top of a period in U.S. history demarcated by a great lack of unity, divisiveness, anger, and hatred. The collapse highlighted the small size yet interconnectedness of the community and the power of connection and authentic relating. It was overwhelming in the moment but extremely heartening and beautiful to see the amount of willingness to drop everything and help. Despite feeling worn down from the pandemic, people drew upon their internal resources, natural goodness, and kindness “reserves” to provide support.
Responding to the collapse highlighted that resilience in the context of collective trauma requires flexibility, embracing uncertainty, cultivating unity, and paying attention to meeting basic needs/self-care. The role of kindness cannot be overemphasized. In the realm of reflecting on the notion of kindness, it is worth noting how much power there is to bearing witness to someone’s experience, especially when they are in pain. People often diminish the role or at the very least do not recognize the power of showing up for someone and just listening. Pandemic resilience, and coping with coalescing traumas, is likely composed of these same facets that were essential in the context of coping with the collapse.
It is not only the immediate impact of a trauma as much as the aftermath that needs to processed and worked through. In one sense, people feel that they should be adjusted to and accustomed to this new reality, and at the same time, one has to remember and reflect on how unnatural this experience has been. There is an impact of a cumulative onslaught of negative events, and it is hard to imagine not being phased, remaining unchanged, or not feeling affected. We may feel hardened and that there are limits to the compassion we have to offer others. We may be feel empathic. There can be desensitization and an apathy to others’ suffering when our patience is worn down and we have limited bandwidth. There are data to support the idea that a level of habituation occurs to individuals who experience multiple traumas, which yields a level of “sensitization” to the negative impact of subsequent events. It becomes easy to make comparisons of suffering. The challenge will be to rise above these and make a conscious effort to connect with who and how we were before we were worn down.
I am still in awe about how much I learned from the victims’ families, survivors, and my colleagues at Surfside – about pain, suffering, loss, resilience, coping, fortitude, and meaning making. We were all forced to think beyond ourselves, show up for others, and unify in a way that remedied this period of fragmentation. With respect to the pandemic and “where we are at now,” some elements of our lives are stabilizing; other aspects feel volatile from the fatigue of what we have been experiencing. This pandemic has not fully abated, but we can find some clarity in the value of setting boundaries and knowing our limits – but not overlooking the power of unity and kindness and the value of the reciprocating those qualities.
Dr. Feldman is a licensed clinical psychologist in private practice in Miami. She is an adjunct professor in the college of psychology at Nova Southeastern University, Fort Lauderdale, Fla., where she teaches clinical psychology doctoral students. She also serves on the board of directors of the Southeast Florida Association for Psychoanalytic Psychology. Dr. Feldman has no disclosures.
While 2022 is lurking around the corner, many of us still have 2020 on our minds. Social media posts are already emerging: “No new years resolutions. It is the circumstances turn to improve [sic],” one post declares. Others proclaim that it is difficult coming to terms with the idea that 2022 is actually pronounced “2020 too.” A critical difference exists between then and now – we have experienced months of living in limbo and rolling with the punches of pandemic life.
In some ways, it has become easy to think of the early pandemic days as a distant memory, yet respect that the impact of 2020 has been indelible for virtually all of us and feels palpable as if it were yesterday.
The year 2020 was marked by the beginning of the COVID-19 pandemic, which was accompanied by extreme uncertainty, loss of all kinds, and emotional turmoil. The early pandemic had a profound economic and social impact, with added stress tethered to political and race-related division in America that created divides among families and friends, and yielded ceaseless discourse related to divergent perspectives. This only exacerbated the stress that came with the pandemic, given that providing support and leaning on one another was more important than ever. All of this was compounded by natural disasters that have plagued the country.
So much was unprecedented. There was a collective sense of feeling “worn down,” and the burnout that was felt was quite profound. Enormous amounts of mental and physical effort were allocated to simply surviving, getting basic needs met, having enough food and supplies, and completing basic tasks. Ordinary relating felt taxing. At this stage of the pandemic, the COVID-19 experience can be conceived of as a traumatic stressor capable of eliciting a traumatic response and exacerbating other mental health symptoms. Our capacity to cope has been diminished. Anxiety rates have soared, as have rates of clinical depression. Those most affected have had lower household incomes, are unmarried, and have experienced pandemic-related stressors. The links between the impact of the pandemic on mental health have been clear.
The pandemic has forced the landscape of social support to dramatically change. Initially, we felt pulled to connect and we leaned into the use of virtual platforms to connect for all matters (simple social gatherings, big birthday events, family reunions, celebration of holidays, work duties, and academic work). However, “Zoom fatigue” began to set in, and our screen time was maxed out. There has been the added dynamic of frontline workers who did not have the option to work virtually or from home. This group largely has felt disconnected from others who didn’t understand the depth of their anxiety and loneliness of their experience. Health care workers have had to make challenging, life-and-death, patient-related decisions that called into question personal morals and ethics all while their own lives were at risk.
Fast-forward to the present, and support systems have either strengthened or worn down – which has yielded a unique dichotomy. Maintaining friendships has either felt of utmost importance given the impact of the disconnect and physical distance or has felt challenging given the mental energy expended from working and connecting virtually. Empathy burnout is also a real and important facet in the equation. We begin to ask the question: Are we checking in with others in the spirit of authentic relating, to cultivate real connection, or to check a box?
Impact of layered traumas
It is interesting to think about the pandemic’s traumatic impact being “superimposed” on top of the “ordinary traumas” experienced outside of the pandemic. We are essentially at the 2-year mark, in some ways have cultivated a sense of resilience and found ways to adapt, and in other ways at times feel right back where we were in early 2020. There were moments that felt hopeful, glimmers of normalcy, and setbacks that all ebbed and flowed – but even so, there have not been many “mental breaks,” only temporary and transient reprieves. Some got sick and died; some recovered; and others are still experiencing long-hauler syndrome and have lingering sequelae. Despite adaptation and resilience, one can’t help but wonder the impact of superimposed traumas on top of this collective trauma. Many of us have not even rebounded from the pandemic, and then are faced with loss, grief, challenges, illness, hard and big life decisions. We are challenged to answer the question: How do we endure in the face of this trauma inception?
It has been a challenging time for all, including those who are ordinarily happy-go-lucky, resilient, and see the glass half-full and are struggling with the idea of struggling. I am no “resilience expert” but gleaned much wisdom from responding to the Surfside, Fla., building collapse. This was a collective trauma that took place in the summer of 2021, and the wisdom of this event highlighted the value of collective healing and unification even in spite of the times. What happened in Surfside was a shock, and the loss was felt by those directly affected, the surrounding community, and those who were part of the disaster response efforts. All of those parties had been processing losses prior to this – loss of normalcy because of the pandemic, loss of people we loved as a result, other personal losses – and this community tragedy was yet another loss to disentangle on top of a period in U.S. history demarcated by a great lack of unity, divisiveness, anger, and hatred. The collapse highlighted the small size yet interconnectedness of the community and the power of connection and authentic relating. It was overwhelming in the moment but extremely heartening and beautiful to see the amount of willingness to drop everything and help. Despite feeling worn down from the pandemic, people drew upon their internal resources, natural goodness, and kindness “reserves” to provide support.
Responding to the collapse highlighted that resilience in the context of collective trauma requires flexibility, embracing uncertainty, cultivating unity, and paying attention to meeting basic needs/self-care. The role of kindness cannot be overemphasized. In the realm of reflecting on the notion of kindness, it is worth noting how much power there is to bearing witness to someone’s experience, especially when they are in pain. People often diminish the role or at the very least do not recognize the power of showing up for someone and just listening. Pandemic resilience, and coping with coalescing traumas, is likely composed of these same facets that were essential in the context of coping with the collapse.
It is not only the immediate impact of a trauma as much as the aftermath that needs to processed and worked through. In one sense, people feel that they should be adjusted to and accustomed to this new reality, and at the same time, one has to remember and reflect on how unnatural this experience has been. There is an impact of a cumulative onslaught of negative events, and it is hard to imagine not being phased, remaining unchanged, or not feeling affected. We may feel hardened and that there are limits to the compassion we have to offer others. We may be feel empathic. There can be desensitization and an apathy to others’ suffering when our patience is worn down and we have limited bandwidth. There are data to support the idea that a level of habituation occurs to individuals who experience multiple traumas, which yields a level of “sensitization” to the negative impact of subsequent events. It becomes easy to make comparisons of suffering. The challenge will be to rise above these and make a conscious effort to connect with who and how we were before we were worn down.
I am still in awe about how much I learned from the victims’ families, survivors, and my colleagues at Surfside – about pain, suffering, loss, resilience, coping, fortitude, and meaning making. We were all forced to think beyond ourselves, show up for others, and unify in a way that remedied this period of fragmentation. With respect to the pandemic and “where we are at now,” some elements of our lives are stabilizing; other aspects feel volatile from the fatigue of what we have been experiencing. This pandemic has not fully abated, but we can find some clarity in the value of setting boundaries and knowing our limits – but not overlooking the power of unity and kindness and the value of the reciprocating those qualities.
Dr. Feldman is a licensed clinical psychologist in private practice in Miami. She is an adjunct professor in the college of psychology at Nova Southeastern University, Fort Lauderdale, Fla., where she teaches clinical psychology doctoral students. She also serves on the board of directors of the Southeast Florida Association for Psychoanalytic Psychology. Dr. Feldman has no disclosures.