User login
Few U.S. Stroke Patients Get Clot-Busting Treatment
(Reuters Health) - Not all U.S. stroke patients eligible for thrombolytic therapy actually receive it - and the odds of getting this therapy may depend on where they live, a large study finds.
Dr. James Burke of the University of Michigan and the VA Ann Arbor Health System and colleagues examined 844,241 hospital admissions for ischemic stroke from 2007 to 2010 among U.S. patients insured by Medicare.
They sorted patients into 3,436 different hospital service areas based on home postal code to assess regional variation in thrombolysis treatment rates.
Patients were 78 years old on average. About 57% were women, and most were white. The majority had hypertension and many also had diabetes, high cholesterol or arrhythmia.
Overall, just 3.9% of these patients received thrombolysis, the researchers report online June 2 in the journal Stroke. The treatment wasn't given at all in 20% of regions, and it was more likely to occur in places with higher population density.
In the 20 regions with the highest rates of thrombolysis, roughly 10% to 14% of patients received the treatment.
After accounting for the number of strokes in each region, the proportion of patients receiving thrombolysis ranged from 2.2% in the bottom fifth of regions to 5.9% in the top fifth.
Older patients, women and minorities were less likely to receive the treatment. Regions with the lowest proportion of college graduates also had a smaller percentage of people treated with thrombolysis.
Not every patient with stroke should receive thrombolysis. One study in Cincinnati estimated that about 6% of stroke patients would be eligible, but the new findings of higher rates in the highest-performing regions suggest that more patients could benefit if they could be transported more quickly to hospitals where thrombolysis is available, the authors say.
By boosting use of the treatment in regions where it's least likely to happen up to the level in places where the therapy is most common, researchers estimated that an additional 92,847 stroke patients might get thrombolysis, averting disability for 8,078 of them.
"Prompt recognition and reaction to warning signs and effective emergency service systems can minimize delays in pre-hospital dispatch, assessment and transport, and ultimately increase the number of stroke patients reaching the hospital and being prepared for thrombolytic therapy within the 4.5-hour time window," Dr. Maurizio Paciaroni, a stroke specialist at the University of Perugia in Italy who wasn't involved in the study, said by email.
"For a variety of reasons, only a minority of patients get to the hospital within the first couple hours of a stroke," Burke said by email. Patients might not recognize symptoms or call 911 soon enough, and even when they do seek help quickly they might not end up at a hospital that's equipped to provide thrombolysis, he added.
The best outcomes are for patients who receive thrombolysis within the first hour after the blood vessel becomes blocked, said Dr. Brian Silver, director of the Comprehensive Stroke Center at Rhode Island Hospital and researcher at Brown University.
"When patients don't receive this treatment, they are up to 50% less likely to have a better outcome," Silver, who wasn't involved with the study, said by email. "This means, for some, residual speech difficulties, paralysis, vision loss, cognitive impairment and depression."
Globally, 15 million people suffer strokes each year; five million of them die and another five million are left permanently disabled, according to the World Health Organization.
(Reuters Health) - Not all U.S. stroke patients eligible for thrombolytic therapy actually receive it - and the odds of getting this therapy may depend on where they live, a large study finds.
Dr. James Burke of the University of Michigan and the VA Ann Arbor Health System and colleagues examined 844,241 hospital admissions for ischemic stroke from 2007 to 2010 among U.S. patients insured by Medicare.
They sorted patients into 3,436 different hospital service areas based on home postal code to assess regional variation in thrombolysis treatment rates.
Patients were 78 years old on average. About 57% were women, and most were white. The majority had hypertension and many also had diabetes, high cholesterol or arrhythmia.
Overall, just 3.9% of these patients received thrombolysis, the researchers report online June 2 in the journal Stroke. The treatment wasn't given at all in 20% of regions, and it was more likely to occur in places with higher population density.
In the 20 regions with the highest rates of thrombolysis, roughly 10% to 14% of patients received the treatment.
After accounting for the number of strokes in each region, the proportion of patients receiving thrombolysis ranged from 2.2% in the bottom fifth of regions to 5.9% in the top fifth.
Older patients, women and minorities were less likely to receive the treatment. Regions with the lowest proportion of college graduates also had a smaller percentage of people treated with thrombolysis.
Not every patient with stroke should receive thrombolysis. One study in Cincinnati estimated that about 6% of stroke patients would be eligible, but the new findings of higher rates in the highest-performing regions suggest that more patients could benefit if they could be transported more quickly to hospitals where thrombolysis is available, the authors say.
By boosting use of the treatment in regions where it's least likely to happen up to the level in places where the therapy is most common, researchers estimated that an additional 92,847 stroke patients might get thrombolysis, averting disability for 8,078 of them.
"Prompt recognition and reaction to warning signs and effective emergency service systems can minimize delays in pre-hospital dispatch, assessment and transport, and ultimately increase the number of stroke patients reaching the hospital and being prepared for thrombolytic therapy within the 4.5-hour time window," Dr. Maurizio Paciaroni, a stroke specialist at the University of Perugia in Italy who wasn't involved in the study, said by email.
"For a variety of reasons, only a minority of patients get to the hospital within the first couple hours of a stroke," Burke said by email. Patients might not recognize symptoms or call 911 soon enough, and even when they do seek help quickly they might not end up at a hospital that's equipped to provide thrombolysis, he added.
The best outcomes are for patients who receive thrombolysis within the first hour after the blood vessel becomes blocked, said Dr. Brian Silver, director of the Comprehensive Stroke Center at Rhode Island Hospital and researcher at Brown University.
"When patients don't receive this treatment, they are up to 50% less likely to have a better outcome," Silver, who wasn't involved with the study, said by email. "This means, for some, residual speech difficulties, paralysis, vision loss, cognitive impairment and depression."
Globally, 15 million people suffer strokes each year; five million of them die and another five million are left permanently disabled, according to the World Health Organization.
(Reuters Health) - Not all U.S. stroke patients eligible for thrombolytic therapy actually receive it - and the odds of getting this therapy may depend on where they live, a large study finds.
Dr. James Burke of the University of Michigan and the VA Ann Arbor Health System and colleagues examined 844,241 hospital admissions for ischemic stroke from 2007 to 2010 among U.S. patients insured by Medicare.
They sorted patients into 3,436 different hospital service areas based on home postal code to assess regional variation in thrombolysis treatment rates.
Patients were 78 years old on average. About 57% were women, and most were white. The majority had hypertension and many also had diabetes, high cholesterol or arrhythmia.
Overall, just 3.9% of these patients received thrombolysis, the researchers report online June 2 in the journal Stroke. The treatment wasn't given at all in 20% of regions, and it was more likely to occur in places with higher population density.
In the 20 regions with the highest rates of thrombolysis, roughly 10% to 14% of patients received the treatment.
After accounting for the number of strokes in each region, the proportion of patients receiving thrombolysis ranged from 2.2% in the bottom fifth of regions to 5.9% in the top fifth.
Older patients, women and minorities were less likely to receive the treatment. Regions with the lowest proportion of college graduates also had a smaller percentage of people treated with thrombolysis.
Not every patient with stroke should receive thrombolysis. One study in Cincinnati estimated that about 6% of stroke patients would be eligible, but the new findings of higher rates in the highest-performing regions suggest that more patients could benefit if they could be transported more quickly to hospitals where thrombolysis is available, the authors say.
By boosting use of the treatment in regions where it's least likely to happen up to the level in places where the therapy is most common, researchers estimated that an additional 92,847 stroke patients might get thrombolysis, averting disability for 8,078 of them.
"Prompt recognition and reaction to warning signs and effective emergency service systems can minimize delays in pre-hospital dispatch, assessment and transport, and ultimately increase the number of stroke patients reaching the hospital and being prepared for thrombolytic therapy within the 4.5-hour time window," Dr. Maurizio Paciaroni, a stroke specialist at the University of Perugia in Italy who wasn't involved in the study, said by email.
"For a variety of reasons, only a minority of patients get to the hospital within the first couple hours of a stroke," Burke said by email. Patients might not recognize symptoms or call 911 soon enough, and even when they do seek help quickly they might not end up at a hospital that's equipped to provide thrombolysis, he added.
The best outcomes are for patients who receive thrombolysis within the first hour after the blood vessel becomes blocked, said Dr. Brian Silver, director of the Comprehensive Stroke Center at Rhode Island Hospital and researcher at Brown University.
"When patients don't receive this treatment, they are up to 50% less likely to have a better outcome," Silver, who wasn't involved with the study, said by email. "This means, for some, residual speech difficulties, paralysis, vision loss, cognitive impairment and depression."
Globally, 15 million people suffer strokes each year; five million of them die and another five million are left permanently disabled, according to the World Health Organization.
HSCT outcomes ‘encouraging’ in JAKi responders
![]()
Photo by Chad McNeeley
VIENNA—Outcomes of hematopoietic stem cell transplant (HSCT) are encouraging in myelofibrosis (MF) patients who respond well to JAK inhibitors, according to researchers.
The group found that patients with the best response to JAK inhibition had a 2-year survival probability of 91% after HSCT, compared to 32% for patients with
leukemic transformation while on a JAK inhibitor.
In addition, receiving a JAK inhibitor until HSCT could prevent the return of MF-related symptoms.
Mohamed Shanavas, MD, of Princess Margaret Cancer Centre in Toronto, Ontario, Canada, presented these findings at the 20th Congress of the European Hematology Association (abstract S450*).
The decision to undergo HSCT is a complex one in MF, particularly for those patients who are responding to JAK inhibitors. So Dr Shanavas and his colleagues undertook a retrospective, multicenter analysis to determine if there is an association between response to JAK inhibition and HSCT outcome.
The investigators analyzed the outcomes of 100 patients who had a first HSCT for primary MF, post-essential thrombocythemia MF, or post-polycythemia vera MF. Patients had to have exposure to a JAK inhibitor but no history of leukemic transformation prior to taking a JAK inhibitor.
Response criteria
The researchers stratified patients’ JAK1/2 response according to the following criteria:
- Group A: Clinical improvement: Fifty percent or greater reduction in palpable spleen length for spleen palpable by ≥ 10 cm, or complete resolution of splenomegaly for spleen < 10 cm
- Group B: Stable disease: Spleen response not meeting the criteria of clinical improvement
- Group C: A 10% to 19% increase in blasts, new onset of anemia requiring transfusions, or intolerance to treatment due to side effects
- Group D: Progressive disease: New splenomegaly > 5 cm, 100% increase in spleen 5-10 cm, or 50% increase in spleen > 10 cm
- Group E: Leukemic transformation: Bone marrow or circulating blasts ≥ 20%.
Patient and treatment characteristics
Patients were a median age of 59 (range, 32–72). Fifty-seven had primary MF, 21 had post-essential thrombocythemia MF, and 22 had post-polycythemia vera MF. Sixty-two patients had JAK2V617F-mutated disease, 37 were wild-type, and 1 had unknown JAK status.
The majority of patients had intermediate-2 or high-risk disease according to their DIPSS scores, and 42 had a transplant comorbidity index score of 3 or greater.
Most patients (n=91) had ruxolitinib as their JAK inhibitor, 6 had momelotinib, and 3 had another inhibitor.
The median duration of JAK inhibitor therapy was 5 months (range, 1–36), and 66 patients were on treatment at the time of transplant. Thirty patients had previously discontinued JAK therapy, and the status of 4 was unknown.
In terms of their response to JAK inhibitors, 23 patients were in group A (clinical improvement), 31 in group B (stable disease), 15 in group C (increased blasts/transfusion need/intolerance), 18 in group D (progressive disease), and 13 in group E (leukemic transformation).
Fifty patients received a matched unrelated donor transplant, 36 had a matched sibling donor, and 14 had either a mismatched unrelated donor or a haploidentical transplant.
Fifty-six patients had a reduced-intensity conditioning regimen, and 44 had full intensity. Fifty percent of patients had T-cell depletion prior to transplant.
Outcomes
Patients who stopped JAK inhibitor therapy 6 or more days prior to transplant (n=20) experienced more “withdrawal symptoms”—the return of MF-related symptoms—than patients in whom the interval was less than 6 days (n=46). For the most part, withdrawal symptoms were non-severe in nature.
Two patients had fatal HSCT-related toxicity of venoocclusive disease, 4 had primary graft failure, and 4 had secondary graft failure. Forty-three percent of cytomegalovirus-seropositive patients had reactivation, 6 patients had Epstein-Barr virus reactivation, 6 had adenovirus or human polyomavirus BK infections, and 7 had invasive fungal infections.
Grade 2-4 acute graft-vs-host disease (GVHD) occurred in 37% of patients at day 100, and grade 3-4 occurred in 16%. Chronic GVHD of all grades occurred in 48% of patients, and extensive chronic GVHD occurred in 23%.
The cumulative incidence of relapse at 2 years was 17%, and non-relapse mortality was 28%. Overall survival (OS) was 61%.
“We analyzed this outcome based upon the response to JAK inhibitors,” Dr Shanavas said. “Patients who were deriving clinical improvement, group A, had a superior outcome, with a probability of survival of 91% at 2 years. Patients who had leukemic transformation, group E, had an inferior OS of 32% at 2 years.”
He noted that the outcomes appeared similar in the other 3 groups, so the researchers combined them for further analysis.
“As expected,” he said, “patients who had leukemic transformation had a significantly higher relapse rate than the other groups.”
The researchers then performed a multivariate analysis and found that response to JAK inhibitors, DIPSS score prior to JAK therapy, and donor type had a significant effect on OS.
The team concluded that prior exposure to JAK inhibitors does not have a negative effect on early HSCT outcomes. And actually, patients who undergo HSCT while responding to JAK inhibitors have encouraging outcomes. ![]()
*Information in the abstract differs from that presented at the meeting.
![]()
Photo by Chad McNeeley
VIENNA—Outcomes of hematopoietic stem cell transplant (HSCT) are encouraging in myelofibrosis (MF) patients who respond well to JAK inhibitors, according to researchers.
The group found that patients with the best response to JAK inhibition had a 2-year survival probability of 91% after HSCT, compared to 32% for patients with
leukemic transformation while on a JAK inhibitor.
In addition, receiving a JAK inhibitor until HSCT could prevent the return of MF-related symptoms.
Mohamed Shanavas, MD, of Princess Margaret Cancer Centre in Toronto, Ontario, Canada, presented these findings at the 20th Congress of the European Hematology Association (abstract S450*).
The decision to undergo HSCT is a complex one in MF, particularly for those patients who are responding to JAK inhibitors. So Dr Shanavas and his colleagues undertook a retrospective, multicenter analysis to determine if there is an association between response to JAK inhibition and HSCT outcome.
The investigators analyzed the outcomes of 100 patients who had a first HSCT for primary MF, post-essential thrombocythemia MF, or post-polycythemia vera MF. Patients had to have exposure to a JAK inhibitor but no history of leukemic transformation prior to taking a JAK inhibitor.
Response criteria
The researchers stratified patients’ JAK1/2 response according to the following criteria:
- Group A: Clinical improvement: Fifty percent or greater reduction in palpable spleen length for spleen palpable by ≥ 10 cm, or complete resolution of splenomegaly for spleen < 10 cm
- Group B: Stable disease: Spleen response not meeting the criteria of clinical improvement
- Group C: A 10% to 19% increase in blasts, new onset of anemia requiring transfusions, or intolerance to treatment due to side effects
- Group D: Progressive disease: New splenomegaly > 5 cm, 100% increase in spleen 5-10 cm, or 50% increase in spleen > 10 cm
- Group E: Leukemic transformation: Bone marrow or circulating blasts ≥ 20%.
Patient and treatment characteristics
Patients were a median age of 59 (range, 32–72). Fifty-seven had primary MF, 21 had post-essential thrombocythemia MF, and 22 had post-polycythemia vera MF. Sixty-two patients had JAK2V617F-mutated disease, 37 were wild-type, and 1 had unknown JAK status.
The majority of patients had intermediate-2 or high-risk disease according to their DIPSS scores, and 42 had a transplant comorbidity index score of 3 or greater.
Most patients (n=91) had ruxolitinib as their JAK inhibitor, 6 had momelotinib, and 3 had another inhibitor.
The median duration of JAK inhibitor therapy was 5 months (range, 1–36), and 66 patients were on treatment at the time of transplant. Thirty patients had previously discontinued JAK therapy, and the status of 4 was unknown.
In terms of their response to JAK inhibitors, 23 patients were in group A (clinical improvement), 31 in group B (stable disease), 15 in group C (increased blasts/transfusion need/intolerance), 18 in group D (progressive disease), and 13 in group E (leukemic transformation).
Fifty patients received a matched unrelated donor transplant, 36 had a matched sibling donor, and 14 had either a mismatched unrelated donor or a haploidentical transplant.
Fifty-six patients had a reduced-intensity conditioning regimen, and 44 had full intensity. Fifty percent of patients had T-cell depletion prior to transplant.
Outcomes
Patients who stopped JAK inhibitor therapy 6 or more days prior to transplant (n=20) experienced more “withdrawal symptoms”—the return of MF-related symptoms—than patients in whom the interval was less than 6 days (n=46). For the most part, withdrawal symptoms were non-severe in nature.
Two patients had fatal HSCT-related toxicity of venoocclusive disease, 4 had primary graft failure, and 4 had secondary graft failure. Forty-three percent of cytomegalovirus-seropositive patients had reactivation, 6 patients had Epstein-Barr virus reactivation, 6 had adenovirus or human polyomavirus BK infections, and 7 had invasive fungal infections.
Grade 2-4 acute graft-vs-host disease (GVHD) occurred in 37% of patients at day 100, and grade 3-4 occurred in 16%. Chronic GVHD of all grades occurred in 48% of patients, and extensive chronic GVHD occurred in 23%.
The cumulative incidence of relapse at 2 years was 17%, and non-relapse mortality was 28%. Overall survival (OS) was 61%.
“We analyzed this outcome based upon the response to JAK inhibitors,” Dr Shanavas said. “Patients who were deriving clinical improvement, group A, had a superior outcome, with a probability of survival of 91% at 2 years. Patients who had leukemic transformation, group E, had an inferior OS of 32% at 2 years.”
He noted that the outcomes appeared similar in the other 3 groups, so the researchers combined them for further analysis.
“As expected,” he said, “patients who had leukemic transformation had a significantly higher relapse rate than the other groups.”
The researchers then performed a multivariate analysis and found that response to JAK inhibitors, DIPSS score prior to JAK therapy, and donor type had a significant effect on OS.
The team concluded that prior exposure to JAK inhibitors does not have a negative effect on early HSCT outcomes. And actually, patients who undergo HSCT while responding to JAK inhibitors have encouraging outcomes. ![]()
*Information in the abstract differs from that presented at the meeting.
![]()
Photo by Chad McNeeley
VIENNA—Outcomes of hematopoietic stem cell transplant (HSCT) are encouraging in myelofibrosis (MF) patients who respond well to JAK inhibitors, according to researchers.
The group found that patients with the best response to JAK inhibition had a 2-year survival probability of 91% after HSCT, compared to 32% for patients with
leukemic transformation while on a JAK inhibitor.
In addition, receiving a JAK inhibitor until HSCT could prevent the return of MF-related symptoms.
Mohamed Shanavas, MD, of Princess Margaret Cancer Centre in Toronto, Ontario, Canada, presented these findings at the 20th Congress of the European Hematology Association (abstract S450*).
The decision to undergo HSCT is a complex one in MF, particularly for those patients who are responding to JAK inhibitors. So Dr Shanavas and his colleagues undertook a retrospective, multicenter analysis to determine if there is an association between response to JAK inhibition and HSCT outcome.
The investigators analyzed the outcomes of 100 patients who had a first HSCT for primary MF, post-essential thrombocythemia MF, or post-polycythemia vera MF. Patients had to have exposure to a JAK inhibitor but no history of leukemic transformation prior to taking a JAK inhibitor.
Response criteria
The researchers stratified patients’ JAK1/2 response according to the following criteria:
- Group A: Clinical improvement: Fifty percent or greater reduction in palpable spleen length for spleen palpable by ≥ 10 cm, or complete resolution of splenomegaly for spleen < 10 cm
- Group B: Stable disease: Spleen response not meeting the criteria of clinical improvement
- Group C: A 10% to 19% increase in blasts, new onset of anemia requiring transfusions, or intolerance to treatment due to side effects
- Group D: Progressive disease: New splenomegaly > 5 cm, 100% increase in spleen 5-10 cm, or 50% increase in spleen > 10 cm
- Group E: Leukemic transformation: Bone marrow or circulating blasts ≥ 20%.
Patient and treatment characteristics
Patients were a median age of 59 (range, 32–72). Fifty-seven had primary MF, 21 had post-essential thrombocythemia MF, and 22 had post-polycythemia vera MF. Sixty-two patients had JAK2V617F-mutated disease, 37 were wild-type, and 1 had unknown JAK status.
The majority of patients had intermediate-2 or high-risk disease according to their DIPSS scores, and 42 had a transplant comorbidity index score of 3 or greater.
Most patients (n=91) had ruxolitinib as their JAK inhibitor, 6 had momelotinib, and 3 had another inhibitor.
The median duration of JAK inhibitor therapy was 5 months (range, 1–36), and 66 patients were on treatment at the time of transplant. Thirty patients had previously discontinued JAK therapy, and the status of 4 was unknown.
In terms of their response to JAK inhibitors, 23 patients were in group A (clinical improvement), 31 in group B (stable disease), 15 in group C (increased blasts/transfusion need/intolerance), 18 in group D (progressive disease), and 13 in group E (leukemic transformation).
Fifty patients received a matched unrelated donor transplant, 36 had a matched sibling donor, and 14 had either a mismatched unrelated donor or a haploidentical transplant.
Fifty-six patients had a reduced-intensity conditioning regimen, and 44 had full intensity. Fifty percent of patients had T-cell depletion prior to transplant.
Outcomes
Patients who stopped JAK inhibitor therapy 6 or more days prior to transplant (n=20) experienced more “withdrawal symptoms”—the return of MF-related symptoms—than patients in whom the interval was less than 6 days (n=46). For the most part, withdrawal symptoms were non-severe in nature.
Two patients had fatal HSCT-related toxicity of venoocclusive disease, 4 had primary graft failure, and 4 had secondary graft failure. Forty-three percent of cytomegalovirus-seropositive patients had reactivation, 6 patients had Epstein-Barr virus reactivation, 6 had adenovirus or human polyomavirus BK infections, and 7 had invasive fungal infections.
Grade 2-4 acute graft-vs-host disease (GVHD) occurred in 37% of patients at day 100, and grade 3-4 occurred in 16%. Chronic GVHD of all grades occurred in 48% of patients, and extensive chronic GVHD occurred in 23%.
The cumulative incidence of relapse at 2 years was 17%, and non-relapse mortality was 28%. Overall survival (OS) was 61%.
“We analyzed this outcome based upon the response to JAK inhibitors,” Dr Shanavas said. “Patients who were deriving clinical improvement, group A, had a superior outcome, with a probability of survival of 91% at 2 years. Patients who had leukemic transformation, group E, had an inferior OS of 32% at 2 years.”
He noted that the outcomes appeared similar in the other 3 groups, so the researchers combined them for further analysis.
“As expected,” he said, “patients who had leukemic transformation had a significantly higher relapse rate than the other groups.”
The researchers then performed a multivariate analysis and found that response to JAK inhibitors, DIPSS score prior to JAK therapy, and donor type had a significant effect on OS.
The team concluded that prior exposure to JAK inhibitors does not have a negative effect on early HSCT outcomes. And actually, patients who undergo HSCT while responding to JAK inhibitors have encouraging outcomes. ![]()
*Information in the abstract differs from that presented at the meeting.
Pain problems prevalent in adults with hemophilia

TORONTO—A survey of adult hemophilia patients suggests there is room for improvement in assessing and managing disease-related pain.
Roughly 85% of patients surveyed for this study, known as P-FiQ, said they had experienced acute and/or chronic pain in the past 6 months.
Although most patients had no trouble caring for themselves, the pain often had an impact on their daily lives, especially with regard to physical activity and overall mobility.
“Pain and discomfort are significant challenges for people with hemophilia,” said study investigator Michael Recht, MD, PhD, of Oregon Health Sciences University in Portland.
“These results emphasize the importance of providing comprehensive care and support beyond traditional therapy to people living with bleeding disorders.”
Dr Recht and his colleagues presented results of the P-FiQ study in 3 posters at the ISTH 2015 Congress (abstracts PO277-MON, PO297-WED, and PO298-WED).
The study included adult males with mild to severe hemophilia who had a history of joint pain or bleeding. Subjects were asked to assess pain and functional impairment using patient-reported outcome instruments.
During routine visits over the course of a year, 164 participants completed a pain history and 5 questionnaires: the EQ-5D-5L; Brief Pain Inventory Short Form, version 2; International Physical Activity Questionnaire; SF-36v2; and Hemophilia Activities List.
The patients had a median age of 34. More patients had hemophilia A (n=122) than hemophilia B (n=42), and few (n=10) had inhibitors. Sixty-one percent of patients had self-reported arthritis, bone, or joint problems.
Current patient-reported treatment regimens (n=163) were prophylaxis (42%), on-demand treatment (39%), or mostly on-demand treatment (19%). Twenty-five of the 31 patients using on-demand treatment reported using infusions ahead of activity.
Pain prevalence and management
Most participants (85.2%) said they had experienced acute and/or chronic pain over the past 6 months. Twenty-nine percent said they had experienced acute and chronic pain, 32.7% had chronic pain only, 23.5% had acute pain only, and 14.8% reported no pain.
Acute pain was most frequently described as sharp, aching, shooting, and throbbing. Chronic pain was often described as aching, nagging, throbbing, and sharp.
The most common analgesics used for acute or chronic pain were acetaminophen (69.4% and 58%, respectively), NSAIDs (40% and 52%, respectively), and hydrocodone-acetaminophen (29.4% and 33%, respectively).
The most common nonanalgesic strategies used for acute or chronic pain were ice (72.9% and 37%, respectively), rest (48.2% and 34%, respectively), factor VIII/IX or bypassing agent (48.2% and 24%, respectively), elevation (34.1% and 28%, respectively), relaxation (30.6% and 23.0%, respectively), compression (27.1% and 21%, respectively), and heat (24.7% and 15%, respectively).
Impact of pain on daily life
When completing the EQ-5D-5L questionnaire, most patients reported problems with mobility, performing usual activities, and pain or discomfort. However, most patients said they had no problems with self-care (78%) or anxiety/depression (58.5%).
A similar proportion of patients reported slight and moderate pain and discomfort (29.9% and 31.1%, respectively). Pain and discomfort was severe for 11% of patients and extreme for 1.2%, but 26.8% of patients reported no pain or discomfort.
When it came to mobility, patients reported slight (32.3%), moderate (19.5%), and severe (8.5%) problems, and 1.2% of patients said they were unable to get around. However, 38.4% of patients reported having no such problems.
About 44% of patients reported no problems performing usual activities, but 37.2% had slight problems, 14.6% had moderate problems, and 1.8% of patients each had severe problems or were unable to perform usual activities.
For the Brief Pain Inventory, pain severity and interference with daily activities were rated on a scale of 0 to 10, with 0 being no pain/no interference and 10 being pain as bad as you can imagine/pain that completely interferes with daily life.
The overall median pain severity and pain interference were 3.0 (range, 1.3-4.8) and 2.9 (range, 0.7-5.2), respectively. The median worst pain was 6.0, least pain 2.0, average pain 3.0, and current pain 2.0. Ankles were the most frequently reported site of pain.
When completing the International Physical Activity Questionnaire, 49.3% of patients (73/148) reported no activity in the prior week.
The median SF-36v2 scores were lower for physical health domains than mental health domains, and the overall median health score was 3.0 (range, 2.0-3.0).
The median score on the Hemophilia Activities List was 76.1 (range, 59.2-95.1). And patients said hemophilia had a greater impact on their lower extremities than upper extremities.
Dr Recht and his colleagues said these results substantiate the high prevalence of pain in adults with hemophilia. And the study highlights opportunities to improve the assessment and management of pain in these patients.
Study investigators have received funding/consulting fees from—or are employees/shareholders of—Novo Nordisk, Baxter, Biogen, Bayer, OctaPharma, Pfizer, CSL Behring, Kendrion, Alexion, Grifols, OPKO Health, Sanofi, Merck, and ProMeticLife Sciences. ![]()
TORONTO—A survey of adult hemophilia patients suggests there is room for improvement in assessing and managing disease-related pain.
Roughly 85% of patients surveyed for this study, known as P-FiQ, said they had experienced acute and/or chronic pain in the past 6 months.
Although most patients had no trouble caring for themselves, the pain often had an impact on their daily lives, especially with regard to physical activity and overall mobility.
“Pain and discomfort are significant challenges for people with hemophilia,” said study investigator Michael Recht, MD, PhD, of Oregon Health Sciences University in Portland.
“These results emphasize the importance of providing comprehensive care and support beyond traditional therapy to people living with bleeding disorders.”
Dr Recht and his colleagues presented results of the P-FiQ study in 3 posters at the ISTH 2015 Congress (abstracts PO277-MON, PO297-WED, and PO298-WED).
The study included adult males with mild to severe hemophilia who had a history of joint pain or bleeding. Subjects were asked to assess pain and functional impairment using patient-reported outcome instruments.
During routine visits over the course of a year, 164 participants completed a pain history and 5 questionnaires: the EQ-5D-5L; Brief Pain Inventory Short Form, version 2; International Physical Activity Questionnaire; SF-36v2; and Hemophilia Activities List.
The patients had a median age of 34. More patients had hemophilia A (n=122) than hemophilia B (n=42), and few (n=10) had inhibitors. Sixty-one percent of patients had self-reported arthritis, bone, or joint problems.
Current patient-reported treatment regimens (n=163) were prophylaxis (42%), on-demand treatment (39%), or mostly on-demand treatment (19%). Twenty-five of the 31 patients using on-demand treatment reported using infusions ahead of activity.
Pain prevalence and management
Most participants (85.2%) said they had experienced acute and/or chronic pain over the past 6 months. Twenty-nine percent said they had experienced acute and chronic pain, 32.7% had chronic pain only, 23.5% had acute pain only, and 14.8% reported no pain.
Acute pain was most frequently described as sharp, aching, shooting, and throbbing. Chronic pain was often described as aching, nagging, throbbing, and sharp.
The most common analgesics used for acute or chronic pain were acetaminophen (69.4% and 58%, respectively), NSAIDs (40% and 52%, respectively), and hydrocodone-acetaminophen (29.4% and 33%, respectively).
The most common nonanalgesic strategies used for acute or chronic pain were ice (72.9% and 37%, respectively), rest (48.2% and 34%, respectively), factor VIII/IX or bypassing agent (48.2% and 24%, respectively), elevation (34.1% and 28%, respectively), relaxation (30.6% and 23.0%, respectively), compression (27.1% and 21%, respectively), and heat (24.7% and 15%, respectively).
Impact of pain on daily life
When completing the EQ-5D-5L questionnaire, most patients reported problems with mobility, performing usual activities, and pain or discomfort. However, most patients said they had no problems with self-care (78%) or anxiety/depression (58.5%).
A similar proportion of patients reported slight and moderate pain and discomfort (29.9% and 31.1%, respectively). Pain and discomfort was severe for 11% of patients and extreme for 1.2%, but 26.8% of patients reported no pain or discomfort.
When it came to mobility, patients reported slight (32.3%), moderate (19.5%), and severe (8.5%) problems, and 1.2% of patients said they were unable to get around. However, 38.4% of patients reported having no such problems.
About 44% of patients reported no problems performing usual activities, but 37.2% had slight problems, 14.6% had moderate problems, and 1.8% of patients each had severe problems or were unable to perform usual activities.
For the Brief Pain Inventory, pain severity and interference with daily activities were rated on a scale of 0 to 10, with 0 being no pain/no interference and 10 being pain as bad as you can imagine/pain that completely interferes with daily life.
The overall median pain severity and pain interference were 3.0 (range, 1.3-4.8) and 2.9 (range, 0.7-5.2), respectively. The median worst pain was 6.0, least pain 2.0, average pain 3.0, and current pain 2.0. Ankles were the most frequently reported site of pain.
When completing the International Physical Activity Questionnaire, 49.3% of patients (73/148) reported no activity in the prior week.
The median SF-36v2 scores were lower for physical health domains than mental health domains, and the overall median health score was 3.0 (range, 2.0-3.0).
The median score on the Hemophilia Activities List was 76.1 (range, 59.2-95.1). And patients said hemophilia had a greater impact on their lower extremities than upper extremities.
Dr Recht and his colleagues said these results substantiate the high prevalence of pain in adults with hemophilia. And the study highlights opportunities to improve the assessment and management of pain in these patients.
Study investigators have received funding/consulting fees from—or are employees/shareholders of—Novo Nordisk, Baxter, Biogen, Bayer, OctaPharma, Pfizer, CSL Behring, Kendrion, Alexion, Grifols, OPKO Health, Sanofi, Merck, and ProMeticLife Sciences. ![]()
TORONTO—A survey of adult hemophilia patients suggests there is room for improvement in assessing and managing disease-related pain.
Roughly 85% of patients surveyed for this study, known as P-FiQ, said they had experienced acute and/or chronic pain in the past 6 months.
Although most patients had no trouble caring for themselves, the pain often had an impact on their daily lives, especially with regard to physical activity and overall mobility.
“Pain and discomfort are significant challenges for people with hemophilia,” said study investigator Michael Recht, MD, PhD, of Oregon Health Sciences University in Portland.
“These results emphasize the importance of providing comprehensive care and support beyond traditional therapy to people living with bleeding disorders.”
Dr Recht and his colleagues presented results of the P-FiQ study in 3 posters at the ISTH 2015 Congress (abstracts PO277-MON, PO297-WED, and PO298-WED).
The study included adult males with mild to severe hemophilia who had a history of joint pain or bleeding. Subjects were asked to assess pain and functional impairment using patient-reported outcome instruments.
During routine visits over the course of a year, 164 participants completed a pain history and 5 questionnaires: the EQ-5D-5L; Brief Pain Inventory Short Form, version 2; International Physical Activity Questionnaire; SF-36v2; and Hemophilia Activities List.
The patients had a median age of 34. More patients had hemophilia A (n=122) than hemophilia B (n=42), and few (n=10) had inhibitors. Sixty-one percent of patients had self-reported arthritis, bone, or joint problems.
Current patient-reported treatment regimens (n=163) were prophylaxis (42%), on-demand treatment (39%), or mostly on-demand treatment (19%). Twenty-five of the 31 patients using on-demand treatment reported using infusions ahead of activity.
Pain prevalence and management
Most participants (85.2%) said they had experienced acute and/or chronic pain over the past 6 months. Twenty-nine percent said they had experienced acute and chronic pain, 32.7% had chronic pain only, 23.5% had acute pain only, and 14.8% reported no pain.
Acute pain was most frequently described as sharp, aching, shooting, and throbbing. Chronic pain was often described as aching, nagging, throbbing, and sharp.
The most common analgesics used for acute or chronic pain were acetaminophen (69.4% and 58%, respectively), NSAIDs (40% and 52%, respectively), and hydrocodone-acetaminophen (29.4% and 33%, respectively).
The most common nonanalgesic strategies used for acute or chronic pain were ice (72.9% and 37%, respectively), rest (48.2% and 34%, respectively), factor VIII/IX or bypassing agent (48.2% and 24%, respectively), elevation (34.1% and 28%, respectively), relaxation (30.6% and 23.0%, respectively), compression (27.1% and 21%, respectively), and heat (24.7% and 15%, respectively).
Impact of pain on daily life
When completing the EQ-5D-5L questionnaire, most patients reported problems with mobility, performing usual activities, and pain or discomfort. However, most patients said they had no problems with self-care (78%) or anxiety/depression (58.5%).
A similar proportion of patients reported slight and moderate pain and discomfort (29.9% and 31.1%, respectively). Pain and discomfort was severe for 11% of patients and extreme for 1.2%, but 26.8% of patients reported no pain or discomfort.
When it came to mobility, patients reported slight (32.3%), moderate (19.5%), and severe (8.5%) problems, and 1.2% of patients said they were unable to get around. However, 38.4% of patients reported having no such problems.
About 44% of patients reported no problems performing usual activities, but 37.2% had slight problems, 14.6% had moderate problems, and 1.8% of patients each had severe problems or were unable to perform usual activities.
For the Brief Pain Inventory, pain severity and interference with daily activities were rated on a scale of 0 to 10, with 0 being no pain/no interference and 10 being pain as bad as you can imagine/pain that completely interferes with daily life.
The overall median pain severity and pain interference were 3.0 (range, 1.3-4.8) and 2.9 (range, 0.7-5.2), respectively. The median worst pain was 6.0, least pain 2.0, average pain 3.0, and current pain 2.0. Ankles were the most frequently reported site of pain.
When completing the International Physical Activity Questionnaire, 49.3% of patients (73/148) reported no activity in the prior week.
The median SF-36v2 scores were lower for physical health domains than mental health domains, and the overall median health score was 3.0 (range, 2.0-3.0).
The median score on the Hemophilia Activities List was 76.1 (range, 59.2-95.1). And patients said hemophilia had a greater impact on their lower extremities than upper extremities.
Dr Recht and his colleagues said these results substantiate the high prevalence of pain in adults with hemophilia. And the study highlights opportunities to improve the assessment and management of pain in these patients.
Study investigators have received funding/consulting fees from—or are employees/shareholders of—Novo Nordisk, Baxter, Biogen, Bayer, OctaPharma, Pfizer, CSL Behring, Kendrion, Alexion, Grifols, OPKO Health, Sanofi, Merck, and ProMeticLife Sciences. ![]()
PI3Kδ/γ inhibitor generates rapid responses in CLL

VIENNA—New research indicates that duvelisib, a dual inhibitor of PI3Kδ and PI3Kγ, can generate rapid partial responses in treatment-naïve patients with chronic lymphocytic leukemia (CLL).
The 18 patients in the expansion cohort of a phase 1 study of duvelisib had a median time to response of 3.7 months, according to iwCLL response criteria.
And 47% of the responses occurred by the first assessment on day 1 of cycle 3.
“One thing that does seem to be different with this drug is that you’re getting your [partial responses] a bit faster than you see with some of the other drugs,” said Susan O’Brien, MD, of UC Irvine Health in Orange, California.
“[W]hat that means in the long run is not completely clear, but there’s no question that the responses are very rapid.”
Dr O’Brien presented these findings at the 20th Congress of the European Hematology Association (abstract S434*). The research was funded by Infinity Pharmaceuticals, Inc., the company developing duvelisib.
Older CLL patients with comorbidities and patients with high-risk genomic alterations, such as 17p deletion and TP53 mutations, often don’t fare well on the standard chemoimmunotherapy. Duvelisib is being developed as a potential alternative for these patients and others with hematologic malignancies.
In the dose-escalation portion of this phase 1 study, duvelisib at 25 mg twice daily was well-tolerated and exhibited clinical activity in relapsed/refractory CLL, even in those patients with TP53 mutations and 17p deletion.
So investigators conducted the expansion cohort with 18 patients who received duvelisib at the same dose in 28-day cycles. Duvelisib is given continuously until patients have an adverse event or lose their response.
Patient demographics
Dr O’Brien said there was nothing unusual about the demographics of the study population, except the risk factors: 83% of the patients were over 65, “which is very different from what you would see in a chemoimmunotherapy trial.”
She noted that the patients’ median age was 74, and 56% of patients had either a 17p deletion or TP53 mutation.
“And that’s very unusual because . . . the percentage of patients with that abnormality in frontline CLL is about 5% to 10%,” she added.
Patients were a median of 3 years (range, 0–9) from their initial diagnosis, 47% had Rai stage 3 or greater disease, 44% had splenomegaly, and 11% had grade 4 cytopenia.
Response
Patients stayed on treatment for a median of 14 months (range, 1–20). Eight (44%) discontinued treatment—6 (33%) due to an adverse event, 1 withdrew consent, and 1 discontinued for other reasons.
The best overall response rate was 88%, which consisted of 15 partial responses. Two patients (12%) had stable disease, and there were no complete responses or cases of progressive disease.
One patient with a TP53 mutation/17p deletion withdrew consent prior to the first efficacy assessment.
“There’s no upfront progression,” Dr O’Brien said, “and the response rate was identical for patients with high-risk disease or 17p deletion.”
The median progression-free survival was not yet reached, and the rate was 92% at 18 months. One patient progressed at cycle 13.
The median overall survival was also not reached, with a 94% survival rate at 18 months. One patient died of progressive disease approximately 5 months after the last dose.
Adverse events
The most frequent adverse events (AEs) occurring in more than 25% of patients were, in order of frequency, diarrhea, rash, cough, neutropenia, peripheral edema, fatigue, nausea, pyrexia, ALT/AST increase, anemia, and dizziness.
Grade 3 AEs included diarrhea (22%), ALT/AST increase (17%), rash (11%), neutropenia (6%), fatigue (6%), and anemia (6%). The only grade 4 AE was neutropenia (28%).
Serious AEs in more than 1 patient included diarrhea (n=3), colitis (n=2), dehydration (n=2), pneumonia (n=2), and pneumonitis (n=2).
The AEs leading to treatment discontinuation were increased ALT/AST, dehydration, and spinal stenosis (all in 1 patient), as well as arthritis, pneumonitis, colitis, diarrhea, and stomatitis.
“We tend to see the transaminitis and the pneumonitis earlier, and then the late toxicity tends to be the diarrhea and colitis,” Dr O’ Brien said. “The one toxicity where I would not be inclined to try and re-treat a patient is pneumonitis, but I do think colitis can be successfully re-treated.”
Pharmacodynamic studies show very rapid inhibition of phosphorylated AKT following treatment, which is sustained throughout the whole first cycle. And following 1 cycle of duvelisib, there is near-complete inhibition of CLL proliferation, as evidenced by the reduction in Ki67.
Given these data, the investigators recommended further development of duvelisib in treatment-naïve CLL. ![]()
*Information in the abstract differs from that presented at the meeting.
VIENNA—New research indicates that duvelisib, a dual inhibitor of PI3Kδ and PI3Kγ, can generate rapid partial responses in treatment-naïve patients with chronic lymphocytic leukemia (CLL).
The 18 patients in the expansion cohort of a phase 1 study of duvelisib had a median time to response of 3.7 months, according to iwCLL response criteria.
And 47% of the responses occurred by the first assessment on day 1 of cycle 3.
“One thing that does seem to be different with this drug is that you’re getting your [partial responses] a bit faster than you see with some of the other drugs,” said Susan O’Brien, MD, of UC Irvine Health in Orange, California.
“[W]hat that means in the long run is not completely clear, but there’s no question that the responses are very rapid.”
Dr O’Brien presented these findings at the 20th Congress of the European Hematology Association (abstract S434*). The research was funded by Infinity Pharmaceuticals, Inc., the company developing duvelisib.
Older CLL patients with comorbidities and patients with high-risk genomic alterations, such as 17p deletion and TP53 mutations, often don’t fare well on the standard chemoimmunotherapy. Duvelisib is being developed as a potential alternative for these patients and others with hematologic malignancies.
In the dose-escalation portion of this phase 1 study, duvelisib at 25 mg twice daily was well-tolerated and exhibited clinical activity in relapsed/refractory CLL, even in those patients with TP53 mutations and 17p deletion.
So investigators conducted the expansion cohort with 18 patients who received duvelisib at the same dose in 28-day cycles. Duvelisib is given continuously until patients have an adverse event or lose their response.
Patient demographics
Dr O’Brien said there was nothing unusual about the demographics of the study population, except the risk factors: 83% of the patients were over 65, “which is very different from what you would see in a chemoimmunotherapy trial.”
She noted that the patients’ median age was 74, and 56% of patients had either a 17p deletion or TP53 mutation.
“And that’s very unusual because . . . the percentage of patients with that abnormality in frontline CLL is about 5% to 10%,” she added.
Patients were a median of 3 years (range, 0–9) from their initial diagnosis, 47% had Rai stage 3 or greater disease, 44% had splenomegaly, and 11% had grade 4 cytopenia.
Response
Patients stayed on treatment for a median of 14 months (range, 1–20). Eight (44%) discontinued treatment—6 (33%) due to an adverse event, 1 withdrew consent, and 1 discontinued for other reasons.
The best overall response rate was 88%, which consisted of 15 partial responses. Two patients (12%) had stable disease, and there were no complete responses or cases of progressive disease.
One patient with a TP53 mutation/17p deletion withdrew consent prior to the first efficacy assessment.
“There’s no upfront progression,” Dr O’Brien said, “and the response rate was identical for patients with high-risk disease or 17p deletion.”
The median progression-free survival was not yet reached, and the rate was 92% at 18 months. One patient progressed at cycle 13.
The median overall survival was also not reached, with a 94% survival rate at 18 months. One patient died of progressive disease approximately 5 months after the last dose.
Adverse events
The most frequent adverse events (AEs) occurring in more than 25% of patients were, in order of frequency, diarrhea, rash, cough, neutropenia, peripheral edema, fatigue, nausea, pyrexia, ALT/AST increase, anemia, and dizziness.
Grade 3 AEs included diarrhea (22%), ALT/AST increase (17%), rash (11%), neutropenia (6%), fatigue (6%), and anemia (6%). The only grade 4 AE was neutropenia (28%).
Serious AEs in more than 1 patient included diarrhea (n=3), colitis (n=2), dehydration (n=2), pneumonia (n=2), and pneumonitis (n=2).
The AEs leading to treatment discontinuation were increased ALT/AST, dehydration, and spinal stenosis (all in 1 patient), as well as arthritis, pneumonitis, colitis, diarrhea, and stomatitis.
“We tend to see the transaminitis and the pneumonitis earlier, and then the late toxicity tends to be the diarrhea and colitis,” Dr O’ Brien said. “The one toxicity where I would not be inclined to try and re-treat a patient is pneumonitis, but I do think colitis can be successfully re-treated.”
Pharmacodynamic studies show very rapid inhibition of phosphorylated AKT following treatment, which is sustained throughout the whole first cycle. And following 1 cycle of duvelisib, there is near-complete inhibition of CLL proliferation, as evidenced by the reduction in Ki67.
Given these data, the investigators recommended further development of duvelisib in treatment-naïve CLL. ![]()
*Information in the abstract differs from that presented at the meeting.
VIENNA—New research indicates that duvelisib, a dual inhibitor of PI3Kδ and PI3Kγ, can generate rapid partial responses in treatment-naïve patients with chronic lymphocytic leukemia (CLL).
The 18 patients in the expansion cohort of a phase 1 study of duvelisib had a median time to response of 3.7 months, according to iwCLL response criteria.
And 47% of the responses occurred by the first assessment on day 1 of cycle 3.
“One thing that does seem to be different with this drug is that you’re getting your [partial responses] a bit faster than you see with some of the other drugs,” said Susan O’Brien, MD, of UC Irvine Health in Orange, California.
“[W]hat that means in the long run is not completely clear, but there’s no question that the responses are very rapid.”
Dr O’Brien presented these findings at the 20th Congress of the European Hematology Association (abstract S434*). The research was funded by Infinity Pharmaceuticals, Inc., the company developing duvelisib.
Older CLL patients with comorbidities and patients with high-risk genomic alterations, such as 17p deletion and TP53 mutations, often don’t fare well on the standard chemoimmunotherapy. Duvelisib is being developed as a potential alternative for these patients and others with hematologic malignancies.
In the dose-escalation portion of this phase 1 study, duvelisib at 25 mg twice daily was well-tolerated and exhibited clinical activity in relapsed/refractory CLL, even in those patients with TP53 mutations and 17p deletion.
So investigators conducted the expansion cohort with 18 patients who received duvelisib at the same dose in 28-day cycles. Duvelisib is given continuously until patients have an adverse event or lose their response.
Patient demographics
Dr O’Brien said there was nothing unusual about the demographics of the study population, except the risk factors: 83% of the patients were over 65, “which is very different from what you would see in a chemoimmunotherapy trial.”
She noted that the patients’ median age was 74, and 56% of patients had either a 17p deletion or TP53 mutation.
“And that’s very unusual because . . . the percentage of patients with that abnormality in frontline CLL is about 5% to 10%,” she added.
Patients were a median of 3 years (range, 0–9) from their initial diagnosis, 47% had Rai stage 3 or greater disease, 44% had splenomegaly, and 11% had grade 4 cytopenia.
Response
Patients stayed on treatment for a median of 14 months (range, 1–20). Eight (44%) discontinued treatment—6 (33%) due to an adverse event, 1 withdrew consent, and 1 discontinued for other reasons.
The best overall response rate was 88%, which consisted of 15 partial responses. Two patients (12%) had stable disease, and there were no complete responses or cases of progressive disease.
One patient with a TP53 mutation/17p deletion withdrew consent prior to the first efficacy assessment.
“There’s no upfront progression,” Dr O’Brien said, “and the response rate was identical for patients with high-risk disease or 17p deletion.”
The median progression-free survival was not yet reached, and the rate was 92% at 18 months. One patient progressed at cycle 13.
The median overall survival was also not reached, with a 94% survival rate at 18 months. One patient died of progressive disease approximately 5 months after the last dose.
Adverse events
The most frequent adverse events (AEs) occurring in more than 25% of patients were, in order of frequency, diarrhea, rash, cough, neutropenia, peripheral edema, fatigue, nausea, pyrexia, ALT/AST increase, anemia, and dizziness.
Grade 3 AEs included diarrhea (22%), ALT/AST increase (17%), rash (11%), neutropenia (6%), fatigue (6%), and anemia (6%). The only grade 4 AE was neutropenia (28%).
Serious AEs in more than 1 patient included diarrhea (n=3), colitis (n=2), dehydration (n=2), pneumonia (n=2), and pneumonitis (n=2).
The AEs leading to treatment discontinuation were increased ALT/AST, dehydration, and spinal stenosis (all in 1 patient), as well as arthritis, pneumonitis, colitis, diarrhea, and stomatitis.
“We tend to see the transaminitis and the pneumonitis earlier, and then the late toxicity tends to be the diarrhea and colitis,” Dr O’ Brien said. “The one toxicity where I would not be inclined to try and re-treat a patient is pneumonitis, but I do think colitis can be successfully re-treated.”
Pharmacodynamic studies show very rapid inhibition of phosphorylated AKT following treatment, which is sustained throughout the whole first cycle. And following 1 cycle of duvelisib, there is near-complete inhibition of CLL proliferation, as evidenced by the reduction in Ki67.
Given these data, the investigators recommended further development of duvelisib in treatment-naïve CLL. ![]()
*Information in the abstract differs from that presented at the meeting.
Mutations linked to response, survival in aplastic anemia

Photo by Graham Colm
Scientists have identified genetic mutations that appear to be associated with treatment outcomes in patients with aplastic anemia.
When compared to unmutated patients, individuals with mutations in PIGA, BCOR, and BCORL1 tended to have better responses to immunosuppressive therapy and superior survival rates.
Other mutations—such as DNMT3A, ASXL1, and RUNX1—were associated with inferior response and survival rates.
Still, the investigators noted that clonal dynamics were “highly variable” in the patient samples they analyzed and might not necessarily have predicted outcomes.
Neal S. Young, MD, of the National Heart, Lung, and Blood Institute in Bethesda, Maryland, and his colleagues described this research in NEJM.
The team used next-generation DNA sequencing and array-based karyotyping to analyze 668 blood samples from 439 patients, including serial samples from 82 patients.
The investigators identified 249 somatic mutations in 156 patients (36%). The most common mutations occurred in the BCOR (9.3%), BCORL1 (9.3%), DNMT3A (8.4%), PIGA (7.5%), and ASXL1 (6.2%) genes.
Thirty-six percent of patients had multiple mutations. And some patients had multiple mutations in
the same genes, including PIGA, BCOR, DNMT3A, ASXL1, RUNX1, and ZRSR2.
The investigators identified clonal hematopoiesis in 47% of patients, most frequently as acquired mutations.
The team also found that, largely, the presence and number of mutations a patient had was positively correlated with the patient’s age. The exceptions were PIGA, BCOR, and BCORL1 mutations.
Patients with mutations in PIGA, BCOR, or BCORL1 had better responses to immunosuppressive therapy and better overall and progression-free survival than unmutated patients.
Other mutations were associated with worse outcomes. Patients with mutations in ASXL1, DNMT3A, TP53, RUNX1, JAK2, JAK3, or CSMD1 did not respond as well as unmutated patients to immunosuppressive therapy.
Mutations in ASXL1, DNMT3A, TP53, RUNX1, and CSMD1 were associated with worse overall survival, and mutations in ASXL1, DNMT3A, RUNX1, JAK2, and JAK3 were associated with worse progression-free survival.
The investigators also observed an increase in the size of clones with DNMT3A, ASXL1, RUNX1, or U2AF1 mutations. But the size of clones with PIGA, BCOR, or BCORL1 mutations remained stable or decreased with time. ![]()
Photo by Graham Colm
Scientists have identified genetic mutations that appear to be associated with treatment outcomes in patients with aplastic anemia.
When compared to unmutated patients, individuals with mutations in PIGA, BCOR, and BCORL1 tended to have better responses to immunosuppressive therapy and superior survival rates.
Other mutations—such as DNMT3A, ASXL1, and RUNX1—were associated with inferior response and survival rates.
Still, the investigators noted that clonal dynamics were “highly variable” in the patient samples they analyzed and might not necessarily have predicted outcomes.
Neal S. Young, MD, of the National Heart, Lung, and Blood Institute in Bethesda, Maryland, and his colleagues described this research in NEJM.
The team used next-generation DNA sequencing and array-based karyotyping to analyze 668 blood samples from 439 patients, including serial samples from 82 patients.
The investigators identified 249 somatic mutations in 156 patients (36%). The most common mutations occurred in the BCOR (9.3%), BCORL1 (9.3%), DNMT3A (8.4%), PIGA (7.5%), and ASXL1 (6.2%) genes.
Thirty-six percent of patients had multiple mutations. And some patients had multiple mutations in
the same genes, including PIGA, BCOR, DNMT3A, ASXL1, RUNX1, and ZRSR2.
The investigators identified clonal hematopoiesis in 47% of patients, most frequently as acquired mutations.
The team also found that, largely, the presence and number of mutations a patient had was positively correlated with the patient’s age. The exceptions were PIGA, BCOR, and BCORL1 mutations.
Patients with mutations in PIGA, BCOR, or BCORL1 had better responses to immunosuppressive therapy and better overall and progression-free survival than unmutated patients.
Other mutations were associated with worse outcomes. Patients with mutations in ASXL1, DNMT3A, TP53, RUNX1, JAK2, JAK3, or CSMD1 did not respond as well as unmutated patients to immunosuppressive therapy.
Mutations in ASXL1, DNMT3A, TP53, RUNX1, and CSMD1 were associated with worse overall survival, and mutations in ASXL1, DNMT3A, RUNX1, JAK2, and JAK3 were associated with worse progression-free survival.
The investigators also observed an increase in the size of clones with DNMT3A, ASXL1, RUNX1, or U2AF1 mutations. But the size of clones with PIGA, BCOR, or BCORL1 mutations remained stable or decreased with time. ![]()
Photo by Graham Colm
Scientists have identified genetic mutations that appear to be associated with treatment outcomes in patients with aplastic anemia.
When compared to unmutated patients, individuals with mutations in PIGA, BCOR, and BCORL1 tended to have better responses to immunosuppressive therapy and superior survival rates.
Other mutations—such as DNMT3A, ASXL1, and RUNX1—were associated with inferior response and survival rates.
Still, the investigators noted that clonal dynamics were “highly variable” in the patient samples they analyzed and might not necessarily have predicted outcomes.
Neal S. Young, MD, of the National Heart, Lung, and Blood Institute in Bethesda, Maryland, and his colleagues described this research in NEJM.
The team used next-generation DNA sequencing and array-based karyotyping to analyze 668 blood samples from 439 patients, including serial samples from 82 patients.
The investigators identified 249 somatic mutations in 156 patients (36%). The most common mutations occurred in the BCOR (9.3%), BCORL1 (9.3%), DNMT3A (8.4%), PIGA (7.5%), and ASXL1 (6.2%) genes.
Thirty-six percent of patients had multiple mutations. And some patients had multiple mutations in
the same genes, including PIGA, BCOR, DNMT3A, ASXL1, RUNX1, and ZRSR2.
The investigators identified clonal hematopoiesis in 47% of patients, most frequently as acquired mutations.
The team also found that, largely, the presence and number of mutations a patient had was positively correlated with the patient’s age. The exceptions were PIGA, BCOR, and BCORL1 mutations.
Patients with mutations in PIGA, BCOR, or BCORL1 had better responses to immunosuppressive therapy and better overall and progression-free survival than unmutated patients.
Other mutations were associated with worse outcomes. Patients with mutations in ASXL1, DNMT3A, TP53, RUNX1, JAK2, JAK3, or CSMD1 did not respond as well as unmutated patients to immunosuppressive therapy.
Mutations in ASXL1, DNMT3A, TP53, RUNX1, and CSMD1 were associated with worse overall survival, and mutations in ASXL1, DNMT3A, RUNX1, JAK2, and JAK3 were associated with worse progression-free survival.
The investigators also observed an increase in the size of clones with DNMT3A, ASXL1, RUNX1, or U2AF1 mutations. But the size of clones with PIGA, BCOR, or BCORL1 mutations remained stable or decreased with time. ![]()
LISTEN NOW: Gastroenterologist, John Pandolfino, MD, on Best Practices for Colonoscopies, Treating C. diff Infections
John Pandolfino, MD, chief of gastroenterology and hepatology at Northwestern University’s Feinberg School of Medicine in Chicago, talks about best practices for colonoscopies and treating C. diff infections.
John Pandolfino, MD, chief of gastroenterology and hepatology at Northwestern University’s Feinberg School of Medicine in Chicago, talks about best practices for colonoscopies and treating C. diff infections.
John Pandolfino, MD, chief of gastroenterology and hepatology at Northwestern University’s Feinberg School of Medicine in Chicago, talks about best practices for colonoscopies and treating C. diff infections.
LISTEN NOW: Hospitalist Lisa Shieh on Choosing Wisely
Excerpt of our interviews with Choosing Wisely, Lisa Shieh, MD, PhD, of Stanford University School of Medicine, discusses an example of a Choosing Wisely program.
Excerpt of our interviews with Choosing Wisely, Lisa Shieh, MD, PhD, of Stanford University School of Medicine, discusses an example of a Choosing Wisely program.
Excerpt of our interviews with Choosing Wisely, Lisa Shieh, MD, PhD, of Stanford University School of Medicine, discusses an example of a Choosing Wisely program.
LISTEN NOW: Gregory Seymann, MD, on Choosing Wisely
Gregory Seymann, MD, discusses a Choosing Wisely program.
Gregory Seymann, MD, discusses a Choosing Wisely program.
Gregory Seymann, MD, discusses a Choosing Wisely program.
Perceptions of Current Note Quality
The electronic health record (EHR) has revolutionized the practice of medicine. As part of the economic stimulus package in 2009, Congress enacted the Health Information Technology for Economic and Clinical Health Act, which included incentives for physicians and hospitals to adopt an EHR by 2015. In the setting of more limited duty hours and demands for increased clinical productivity, EHRs have functions that may improve the quality and efficiency of clinical documentation.[1, 2, 3, 4, 5]
The process of note writing and the use of notes for clinical care have changed substantially with EHR implementation. Use of efficiency tools (ie, copy forward functions and autopopulation of data) may increase the speed of documentation.[5] Notes in an EHR are more legible and accessible and may be able to organize data to improve clinical care.[6]
Yet, many have commented on the negative consequences of documentation in an EHR. In a New England Journal of Medicine Perspective article, Drs. Hartzband and Groopman wrote, we have observed the electronic medical record become a powerful vehicle for perpetuating erroneous information, leading to diagnostic errors that gain momentum when passed on electronically.[7] As a result, the copy forward and autopopulation functions have come under significant scrutiny.[8, 9, 10] A survey conducted at 2 academic institutions found that 71% of residents and attendings believed that the copy forward function led to inconsistencies and outdated information.[11] Autopopulation has been criticized for creating lengthy notes full of trivial or redundant data, a phenomenon termed note bloat. Bloated notes may be less effective as a communication tool.[12] Additionally, the process of composing a note often stimulates critical thinking and may lead to changes in care. The act of copying forward a previous note and autopopulating data bypasses that process and in effect may suppress critical thinking.[13] Previous studies have raised numerous concerns regarding copy forward and autopopulation functionality in the EHR. Many have described the duplication of outdated data and the possibility of the introduction and perpetuation of errors.[14, 15, 16] The Veterans Affairs (VA) Puget Sound Health system evaluated 6322 copy events and found that 1 in 10 electronic patient charts contained an instance of high‐risk copying.[17] In a survey of faculty and residents at a single academic medical center, the majority of users of copy and paste functionality recognized the hazards; they responded that their notes may contain more outdated (66%) and more inconsistent information (69%). Yet, most felt copy forwarding improved the documentation of the entire hospital course (87%), overall physician documentation (69%), and should definitely be continued (91%).[11] Others have complained about the impact of copy forward on the expression of clinical reasoning.[7, 9, 18]
Previous discussions on the topic of overall note quality following EHR implementation have been limited to perspectives or opinion pieces of individual attending providers.[18] We conducted a survey across 4 academic institutions to analyze both housestaff and attendings perceptions of the quality of notes since the implementation of an EHR to better inform the discussion of the impact of an EHR on note quality.
METHODS
Participants
Surveys were administered via email to interns, residents (second‐, third‐, or fourth‐year residents, hereafter referred to as residents) and attendings at 4 academic hospitals that use the Epic EHR (Epic Corp., Madison, WI). The 4 institutions each adopted the Epic EHR, with mandatory faculty and resident training, between 1 and 5 years prior to the survey. Three of the institutions previously used systems with electronic notes, whereas the fourth institution previously used a system with handwritten notes. The study participation emails included a link to an online survey in REDCap.[19] We included interns and residents from the following types of residency programs: internal medicine categorical or primary care, medicine‐pediatrics, or medicine‐psychiatry. For housestaff (the combination of both interns and residents), exclusion criteria included preliminary or transitional year interns, or any interns or residents from other specialties who rotate on the medicine service. For attendings, participants included hospitalists, general internal medicine attendings, chief residents, and subspecialty medicine attendings, each of whom had worked for any amount of time on the inpatient medicine teaching service in the prior 12 months.
Design
We developed 3 unique surveys for interns, residents, and attendings to assess their perception of inpatient progress notes (see Supporting Information, Appendix, in the online version of this article). The surveys incorporated questions from 2 previously published sources, the 9‐item Physician Documentation Quality Instrument (PDQI‐9) (see online Appendix), a validated note‐scoring tool, and the Accreditation Council for Graduate Medical Education note‐writing competency checklists.[20] Additionally, faculty at the participating institutions developed questions to address practices and attitudes toward autopopulation, copy forward, and the purposes of a progress note. Responses were based on a 5‐point Likert scale. The intern and resident surveys asked for self‐evaluation of their own progress notes and those of their peers, whereas the attending surveys asked for assessment of housestaff notes.
The survey was left open for a total of 55 days and participants were sent reminder emails. The study received a waiver from the institutional review board at all 4 institutions.
Data Analysis
Study data were collected and managed using REDCap electronic data capture tools hosted at the University of California, San Francisco (UCSF).[19] The survey data were analyzed and the figures were created using Microsoft Excel 2008 (Microsoft Corp., Redmond, WA). Mean values for each survey question were calculated. Differences between the means among the groups were assessed using 2‐sample t tests. P values <0.05 were considered statistically significant.
RESULTS
Demographics
We received 99 completed surveys from interns, 155 completed surveys from residents, and 153 completed surveys from attendings across the 4 institutions. The overall response rate for interns was 68%, ranging from 59% at the University of California, San Diego (UCSD) to 74% at the University of Iowa. The overall response rate for residents was 49%, ranging from 38% at UCSF to 66% at the University of California, Los Angeles. The overall response rate for attendings was 70%, ranging from 53% at UCSD to 74% at UCSF.
A total of 78% of interns and 72% of residents had used an EHR at a prior institution. Of the residents, 90 were second‐year residents, 64 were third‐year residents, and 2 were fourth‐year residents. A total of 76% of attendings self‐identified as hospitalists.
Overall Assessment of Note Quality
Participants were asked to rate the quality of progress notes on a 5‐point scale (poor, fair, good, very good, excellent). Half of interns and residents rated their own progress notes as very good or excellent. A total of 44% percent of interns and 24% of residents rated their peers notes as very good or excellent, whereas only 15% of attending physicians rated housestaff notes as very good or excellent.
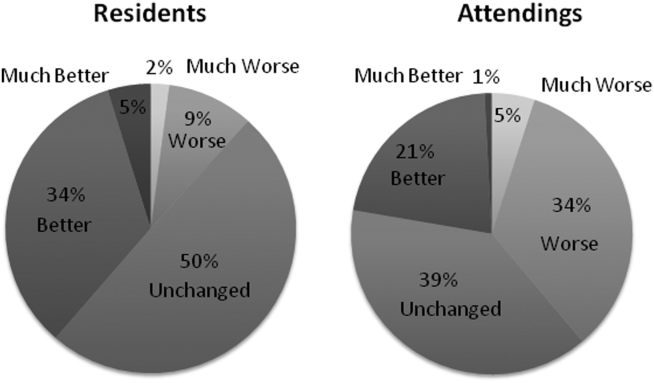
When asked to rate the change in progress note quality since their hospital had adopted the EHR, the majority of residents answered unchanged or better, and the majority of attendings answered unchanged or worse (Figure 1).
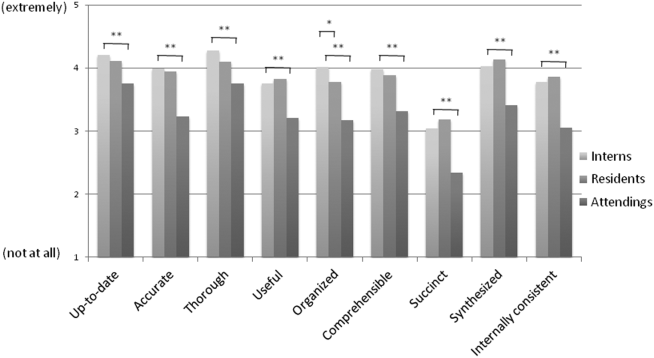
PDQI‐9 Framework
Participants answered each PDQI‐9 question on a 5‐point Likert scale ranging from not at all (1) to extremely (5). In 8 of the 9 PDQI‐9 domains, there were no significant differences between interns and residents. Across each domain, attending perceptions of housestaff notes were significantly lower than housestaff perceptions of their own notes (P<0.001) (Figure 2). Both housestaff and attendings gave the highest ratings to thorough, up to date, and synthesized and the lowest rating to succinct.
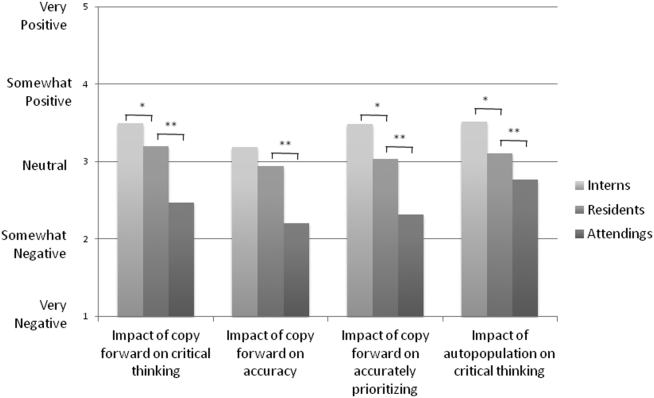
Copy Forward and Autopopulation
Overall, the effect of copy forward and autopopulation on critical thinking, note accuracy, and prioritizing the problem list was thought to be neutral or somewhat positive by interns, neutral by residents, and neutral or somewhat negative by attendings (P<0.001) (Figure 3). In all, 16% of interns, 22% of residents, and 55% of attendings reported that copy forward had a somewhat negative or very negative impact on critical thinking (P<0.001). In all, 16% of interns, 29% of residents and 39% of attendings thought that autopopulation had a somewhat negative or very negative impact on critical thinking (P<0.001).
Purpose of Progress Notes
Participants were provided with 7 possible purposes of a progress note and asked to rate the importance of each stated purpose. There was nearly perfect agreement between interns, residents, and attendings in the rank order of the importance of each purpose of a progress note (Table 1). Attendings and housestaff ranked communication with other providers and documenting important events and the plan for the day as the 2 most important purposes of a progress note, and billing and quality improvement as less important.
| Interns | Residents | Attendings | |
|---|---|---|---|
| Communication with other providers | 1 | 1 | 2 |
| Documenting important events and the plan for the day | 2 | 2 | 1 |
| Prioritizing issues going forward in the patient's care | 3 | 3 | 3 |
| Medicolegal | 4 | 4 | 4 |
| Stimulate critical thinking | 5 | 5 | 5 |
| Billing | 6 | 6 | 6 |
| Quality improvement | 7 | 7 | 7 |
DISCUSSION
This is the first large multicenter analysis of both attendings and housestaff perceptions of note quality in the EHR era. The findings provide insight into important differences and similarities in the perceptions of the 2 groups. Most striking is the difference in opinion of overall note quality, with only a small minority of faculty rating current housestaff notes as very good or excellent, whereas a much larger proportion of housestaff rated their own notes and those of their peers to be of high quality. Though participants were not specifically asked why note quality in general was suboptimal, housestaff and faculty rankings of specific domains from the PDQI‐9 may yield an important clue. Specifically, all groups expressed that the weakest attribute of current progress notes is succinct. This finding is consistent with the note bloat phenomenon, which has been maligned as a consequence of EHR implementation.[7, 14, 18, 21, 22]
One interesting finding was that only 5% of interns rated the notes of other housestaff as fair or poor. One possible explanation for this may be the tendency for an individual to enhance or augment the status or performance of the group to which he or she belongs as a mechanism to increase self‐image, known as the social identity theory.[23] Thus, housestaff may not criticize their peers to allow for identification with a group that is not deficient in note writing.
The more positive assessment of overall note quality among housestaff could be related to the different roles of housestaff and attendings on a teaching service. On a teaching service, housestaff are typically the writer, whereas attendings are almost exclusively the reader of progress notes. Housestaff may reap benefits, including efficiency, beyond the finished product. A perception of higher quality may reflect the process of note writing, data gathering, and critical thinking required to build an assessment and plan. The scores on the PDQI‐9 support this notion, as housestaff rated all 9 domains significantly higher than attendings.
Housestaff and attendings held greater differences of opinion with respect to the EHR's impact on note quality. Generally, housestaff perceived the EHR to have improved progress note quality, whereas attendings perceived the opposite. One explanation could be that these results reflect changing stages of development of physicians well described through the RIME framework (reporter, interpreter, manager, educator). Attendings may expect notes to reflect synthesis and analysis, whereas trainees may be satisfied with the data gathering that an EHR facilitates. In our survey, the trend of answers from intern to resident to attending suggests an evolving process of attitudes toward note quality.
The above reasons may also explain why housestaff were generally more positive than attendings about the effect of copy forward and autopopulation functions on critical thinking. Perhaps, as these functions can potentially increase efficiency and decrease time spent at the computer, although data are mixed on this finding, housestaff may have more time to spend with patients or develop a thorough plan and thus rate these functions positively.
Notably, housestaff and attendings had excellent agreement on the purposes of a progress note. They agreed that the 2 most important purposes were communication with other providers and documenting important events and the plan for the day. These are the 2 listed purposes that are most directly related to patient care. If future interventions to improve note quality require housestaff and attendings to significantly change their behavior, a focus on the impact on patient care might yield the best results.
There were several limitations in our study. Any study based on self‐assessment is subject to bias. A previous meta‐analysis and review described poor to moderate correlations between self‐assessed and external measures of performance.[24, 25] The survey data were aggregated from 4 institutions despite somewhat different, though relatively high, response rates between the institutions. There could be a response bias; those who did not respond may have systematically different perceptions of note quality. It should be noted that the general demographics of the respondents reflected those of the housestaff and attendings at 4 academic centers. All 4 of the participating institutions adopted the Epic EHR within the last several years of the survey being administered, and perceptions of note quality may be biased depending on the prior system used (ie, change from handwritten to electronic vs electronic to other electronic system). In addition, the survey results reflect experience with only 1 EHR, and our results may not apply to other EHR vendors or institutions like the VA, which have a long‐standing system in place. Last, we did not explore the impact of perceived note quality on the measured or perceived quality of care. One previous study found no direct correlation between note quality and clinical quality.[26]
There are several future directions for research based on our findings. First, potential differences between housestaff and attending perceptions of note quality could be further teased apart by studying the perceptions of attendings on a nonteaching service who write their own daily progress notes. Second, housestaff perceptions on why copy forward and autopopulation may increase critical thinking could be explored further with more direct questioning. Finally, although our study captured only perceptions of note quality, validated tools could be used to objectively measure note quality; these measurements could then be compared to perception of note quality as well as clinical outcomes.
Given the prevalence and the apparent belief that the benefits of an EHR outweigh the hazards, institutions should embrace these innovations but take steps to mitigate the potential errors and problems associated with copy forward and autopopulation. The results of our study should help inform future interventions.
Acknowledgements
The authors acknowledge the contributions of Russell Leslie from the University of Iowa.
Disclosure: Nothing to report.
- , , , et al. Systematic review: impact of health information technology on quality, efficiency, and costs of medical care. Ann Intern Med. 2006;144(10):742–752.
- , , , , . Clinical information technologies and inpatient outcomes: a multiple hospital study. Arch Intern Med. 2009;169(2):108–114.
- , , , et al. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. JAMA. 1998;280(15):1311–1316.
- , , , . Electronic health records and quality of diabetes care. N Engl J Med. 2011;365(9):825–833.
- , , , et al. The impact of a clinical information system in an intensive care unit. J Clin Monit Comput. 2008;22(1):31–36.
- , . Can electronic clinical documentation help prevent diagnostic errors? N Engl J Med. 2010;362(12):1066–1069.
- , . Off the record—avoiding the pitfalls of going electronic. N Eng J Med. 2008;358(16):1656–1658.
- , , . Copying and pasting of examinations within the electronic medical record. Int J Med Inform. 2007;76(suppl 1):S122–S128.
- , . Copy and paste: a remediable hazard of electronic health records. Am J Med. 2009;122(6):495–496.
- , , . The role of copy‐and‐paste in the hospital electronic health record. JAMA Intern Med. 2014;174(8):1217–1218.
- , , , , , . Physicians’ attitudes towards copy and pasting in electronic note writing. J Gen Intern Med. 2009;24(1):63–68.
- , , , , . Medical education in the electronic medical record (EMR) era: benefits, challenges, and future directions. Acad Med. 2013;88(6):748–752.
- , . Educational impact of the electronic medical record. J Surg Educ. 2012;69(1):105–112.
- , , , , , . Direct text entry in electronic progress notes. An evaluation of input errors. Methods Inf Med. 2003;42(1):61–67.
- . The clinical record: a 200‐year‐old 21st‐century challenge. Ann Intern Med. 2010;153(10):682–683.
- . Sloppy and paste. Morbidity and Mortality Rounds on the Web. Available at: http://www.webmm.ahrq.gov/case.aspx?caseID=274. Published July 2012. Accessed September 26, 2014.
- , , , . Are electronic medical records trustworthy? Observations on copying, pasting and duplication. AMIA Annu Symp Proc. 2003:269–273.
- . A piece of my mind. John Lennon's elbow. JAMA. 2012;308(5):463–464.
- , , , , , . Research electronic data capture (REDCap)—a metadata‐driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381.
- , , . ACGME competency note checklist. Available at: http://www.im.org/p/cm/ld/fid=831. Accessed August 8, 2013.
- , , , . Assessing electronic note quality using the Physician Documentation Quality Instrument (PDQI‐9). Appl Clin Inform. 2012;3(2):164–174.
- , , , . Quantifying clinical narrative redundancy in an electronic health record. J Am Med Inform Assoc. 2010;17(1):49–53.
- , . The social identity theory of intergroup behavior. In: Psychology of Intergroup Relations. 2nd ed. Chicago, IL: Nelson‐Hall Publishers; 1986:7–24.
- , . Student self‐assessment in higher education: a meta‐analysis. Rev Educ Res. 1989;59:395–430.
- . A review of the validity and accuracy of self‐assessments in health professions training. Acad Med. 1991;66:762–769.
- , , , , . Association of note quality and quality of care: a cross‐sectional study. BMJ Qual Saf. 2014;23(5):406–413.
The electronic health record (EHR) has revolutionized the practice of medicine. As part of the economic stimulus package in 2009, Congress enacted the Health Information Technology for Economic and Clinical Health Act, which included incentives for physicians and hospitals to adopt an EHR by 2015. In the setting of more limited duty hours and demands for increased clinical productivity, EHRs have functions that may improve the quality and efficiency of clinical documentation.[1, 2, 3, 4, 5]
The process of note writing and the use of notes for clinical care have changed substantially with EHR implementation. Use of efficiency tools (ie, copy forward functions and autopopulation of data) may increase the speed of documentation.[5] Notes in an EHR are more legible and accessible and may be able to organize data to improve clinical care.[6]
Yet, many have commented on the negative consequences of documentation in an EHR. In a New England Journal of Medicine Perspective article, Drs. Hartzband and Groopman wrote, we have observed the electronic medical record become a powerful vehicle for perpetuating erroneous information, leading to diagnostic errors that gain momentum when passed on electronically.[7] As a result, the copy forward and autopopulation functions have come under significant scrutiny.[8, 9, 10] A survey conducted at 2 academic institutions found that 71% of residents and attendings believed that the copy forward function led to inconsistencies and outdated information.[11] Autopopulation has been criticized for creating lengthy notes full of trivial or redundant data, a phenomenon termed note bloat. Bloated notes may be less effective as a communication tool.[12] Additionally, the process of composing a note often stimulates critical thinking and may lead to changes in care. The act of copying forward a previous note and autopopulating data bypasses that process and in effect may suppress critical thinking.[13] Previous studies have raised numerous concerns regarding copy forward and autopopulation functionality in the EHR. Many have described the duplication of outdated data and the possibility of the introduction and perpetuation of errors.[14, 15, 16] The Veterans Affairs (VA) Puget Sound Health system evaluated 6322 copy events and found that 1 in 10 electronic patient charts contained an instance of high‐risk copying.[17] In a survey of faculty and residents at a single academic medical center, the majority of users of copy and paste functionality recognized the hazards; they responded that their notes may contain more outdated (66%) and more inconsistent information (69%). Yet, most felt copy forwarding improved the documentation of the entire hospital course (87%), overall physician documentation (69%), and should definitely be continued (91%).[11] Others have complained about the impact of copy forward on the expression of clinical reasoning.[7, 9, 18]
Previous discussions on the topic of overall note quality following EHR implementation have been limited to perspectives or opinion pieces of individual attending providers.[18] We conducted a survey across 4 academic institutions to analyze both housestaff and attendings perceptions of the quality of notes since the implementation of an EHR to better inform the discussion of the impact of an EHR on note quality.
METHODS
Participants
Surveys were administered via email to interns, residents (second‐, third‐, or fourth‐year residents, hereafter referred to as residents) and attendings at 4 academic hospitals that use the Epic EHR (Epic Corp., Madison, WI). The 4 institutions each adopted the Epic EHR, with mandatory faculty and resident training, between 1 and 5 years prior to the survey. Three of the institutions previously used systems with electronic notes, whereas the fourth institution previously used a system with handwritten notes. The study participation emails included a link to an online survey in REDCap.[19] We included interns and residents from the following types of residency programs: internal medicine categorical or primary care, medicine‐pediatrics, or medicine‐psychiatry. For housestaff (the combination of both interns and residents), exclusion criteria included preliminary or transitional year interns, or any interns or residents from other specialties who rotate on the medicine service. For attendings, participants included hospitalists, general internal medicine attendings, chief residents, and subspecialty medicine attendings, each of whom had worked for any amount of time on the inpatient medicine teaching service in the prior 12 months.
Design
We developed 3 unique surveys for interns, residents, and attendings to assess their perception of inpatient progress notes (see Supporting Information, Appendix, in the online version of this article). The surveys incorporated questions from 2 previously published sources, the 9‐item Physician Documentation Quality Instrument (PDQI‐9) (see online Appendix), a validated note‐scoring tool, and the Accreditation Council for Graduate Medical Education note‐writing competency checklists.[20] Additionally, faculty at the participating institutions developed questions to address practices and attitudes toward autopopulation, copy forward, and the purposes of a progress note. Responses were based on a 5‐point Likert scale. The intern and resident surveys asked for self‐evaluation of their own progress notes and those of their peers, whereas the attending surveys asked for assessment of housestaff notes.
The survey was left open for a total of 55 days and participants were sent reminder emails. The study received a waiver from the institutional review board at all 4 institutions.
Data Analysis
Study data were collected and managed using REDCap electronic data capture tools hosted at the University of California, San Francisco (UCSF).[19] The survey data were analyzed and the figures were created using Microsoft Excel 2008 (Microsoft Corp., Redmond, WA). Mean values for each survey question were calculated. Differences between the means among the groups were assessed using 2‐sample t tests. P values <0.05 were considered statistically significant.
RESULTS
Demographics
We received 99 completed surveys from interns, 155 completed surveys from residents, and 153 completed surveys from attendings across the 4 institutions. The overall response rate for interns was 68%, ranging from 59% at the University of California, San Diego (UCSD) to 74% at the University of Iowa. The overall response rate for residents was 49%, ranging from 38% at UCSF to 66% at the University of California, Los Angeles. The overall response rate for attendings was 70%, ranging from 53% at UCSD to 74% at UCSF.
A total of 78% of interns and 72% of residents had used an EHR at a prior institution. Of the residents, 90 were second‐year residents, 64 were third‐year residents, and 2 were fourth‐year residents. A total of 76% of attendings self‐identified as hospitalists.
Overall Assessment of Note Quality
Participants were asked to rate the quality of progress notes on a 5‐point scale (poor, fair, good, very good, excellent). Half of interns and residents rated their own progress notes as very good or excellent. A total of 44% percent of interns and 24% of residents rated their peers notes as very good or excellent, whereas only 15% of attending physicians rated housestaff notes as very good or excellent.
When asked to rate the change in progress note quality since their hospital had adopted the EHR, the majority of residents answered unchanged or better, and the majority of attendings answered unchanged or worse (Figure 1).
PDQI‐9 Framework
Participants answered each PDQI‐9 question on a 5‐point Likert scale ranging from not at all (1) to extremely (5). In 8 of the 9 PDQI‐9 domains, there were no significant differences between interns and residents. Across each domain, attending perceptions of housestaff notes were significantly lower than housestaff perceptions of their own notes (P<0.001) (Figure 2). Both housestaff and attendings gave the highest ratings to thorough, up to date, and synthesized and the lowest rating to succinct.
Copy Forward and Autopopulation
Overall, the effect of copy forward and autopopulation on critical thinking, note accuracy, and prioritizing the problem list was thought to be neutral or somewhat positive by interns, neutral by residents, and neutral or somewhat negative by attendings (P<0.001) (Figure 3). In all, 16% of interns, 22% of residents, and 55% of attendings reported that copy forward had a somewhat negative or very negative impact on critical thinking (P<0.001). In all, 16% of interns, 29% of residents and 39% of attendings thought that autopopulation had a somewhat negative or very negative impact on critical thinking (P<0.001).
Purpose of Progress Notes
Participants were provided with 7 possible purposes of a progress note and asked to rate the importance of each stated purpose. There was nearly perfect agreement between interns, residents, and attendings in the rank order of the importance of each purpose of a progress note (Table 1). Attendings and housestaff ranked communication with other providers and documenting important events and the plan for the day as the 2 most important purposes of a progress note, and billing and quality improvement as less important.
| Interns | Residents | Attendings | |
|---|---|---|---|
| Communication with other providers | 1 | 1 | 2 |
| Documenting important events and the plan for the day | 2 | 2 | 1 |
| Prioritizing issues going forward in the patient's care | 3 | 3 | 3 |
| Medicolegal | 4 | 4 | 4 |
| Stimulate critical thinking | 5 | 5 | 5 |
| Billing | 6 | 6 | 6 |
| Quality improvement | 7 | 7 | 7 |
DISCUSSION
This is the first large multicenter analysis of both attendings and housestaff perceptions of note quality in the EHR era. The findings provide insight into important differences and similarities in the perceptions of the 2 groups. Most striking is the difference in opinion of overall note quality, with only a small minority of faculty rating current housestaff notes as very good or excellent, whereas a much larger proportion of housestaff rated their own notes and those of their peers to be of high quality. Though participants were not specifically asked why note quality in general was suboptimal, housestaff and faculty rankings of specific domains from the PDQI‐9 may yield an important clue. Specifically, all groups expressed that the weakest attribute of current progress notes is succinct. This finding is consistent with the note bloat phenomenon, which has been maligned as a consequence of EHR implementation.[7, 14, 18, 21, 22]
One interesting finding was that only 5% of interns rated the notes of other housestaff as fair or poor. One possible explanation for this may be the tendency for an individual to enhance or augment the status or performance of the group to which he or she belongs as a mechanism to increase self‐image, known as the social identity theory.[23] Thus, housestaff may not criticize their peers to allow for identification with a group that is not deficient in note writing.
The more positive assessment of overall note quality among housestaff could be related to the different roles of housestaff and attendings on a teaching service. On a teaching service, housestaff are typically the writer, whereas attendings are almost exclusively the reader of progress notes. Housestaff may reap benefits, including efficiency, beyond the finished product. A perception of higher quality may reflect the process of note writing, data gathering, and critical thinking required to build an assessment and plan. The scores on the PDQI‐9 support this notion, as housestaff rated all 9 domains significantly higher than attendings.
Housestaff and attendings held greater differences of opinion with respect to the EHR's impact on note quality. Generally, housestaff perceived the EHR to have improved progress note quality, whereas attendings perceived the opposite. One explanation could be that these results reflect changing stages of development of physicians well described through the RIME framework (reporter, interpreter, manager, educator). Attendings may expect notes to reflect synthesis and analysis, whereas trainees may be satisfied with the data gathering that an EHR facilitates. In our survey, the trend of answers from intern to resident to attending suggests an evolving process of attitudes toward note quality.
The above reasons may also explain why housestaff were generally more positive than attendings about the effect of copy forward and autopopulation functions on critical thinking. Perhaps, as these functions can potentially increase efficiency and decrease time spent at the computer, although data are mixed on this finding, housestaff may have more time to spend with patients or develop a thorough plan and thus rate these functions positively.
Notably, housestaff and attendings had excellent agreement on the purposes of a progress note. They agreed that the 2 most important purposes were communication with other providers and documenting important events and the plan for the day. These are the 2 listed purposes that are most directly related to patient care. If future interventions to improve note quality require housestaff and attendings to significantly change their behavior, a focus on the impact on patient care might yield the best results.
There were several limitations in our study. Any study based on self‐assessment is subject to bias. A previous meta‐analysis and review described poor to moderate correlations between self‐assessed and external measures of performance.[24, 25] The survey data were aggregated from 4 institutions despite somewhat different, though relatively high, response rates between the institutions. There could be a response bias; those who did not respond may have systematically different perceptions of note quality. It should be noted that the general demographics of the respondents reflected those of the housestaff and attendings at 4 academic centers. All 4 of the participating institutions adopted the Epic EHR within the last several years of the survey being administered, and perceptions of note quality may be biased depending on the prior system used (ie, change from handwritten to electronic vs electronic to other electronic system). In addition, the survey results reflect experience with only 1 EHR, and our results may not apply to other EHR vendors or institutions like the VA, which have a long‐standing system in place. Last, we did not explore the impact of perceived note quality on the measured or perceived quality of care. One previous study found no direct correlation between note quality and clinical quality.[26]
There are several future directions for research based on our findings. First, potential differences between housestaff and attending perceptions of note quality could be further teased apart by studying the perceptions of attendings on a nonteaching service who write their own daily progress notes. Second, housestaff perceptions on why copy forward and autopopulation may increase critical thinking could be explored further with more direct questioning. Finally, although our study captured only perceptions of note quality, validated tools could be used to objectively measure note quality; these measurements could then be compared to perception of note quality as well as clinical outcomes.
Given the prevalence and the apparent belief that the benefits of an EHR outweigh the hazards, institutions should embrace these innovations but take steps to mitigate the potential errors and problems associated with copy forward and autopopulation. The results of our study should help inform future interventions.
Acknowledgements
The authors acknowledge the contributions of Russell Leslie from the University of Iowa.
Disclosure: Nothing to report.
The electronic health record (EHR) has revolutionized the practice of medicine. As part of the economic stimulus package in 2009, Congress enacted the Health Information Technology for Economic and Clinical Health Act, which included incentives for physicians and hospitals to adopt an EHR by 2015. In the setting of more limited duty hours and demands for increased clinical productivity, EHRs have functions that may improve the quality and efficiency of clinical documentation.[1, 2, 3, 4, 5]
The process of note writing and the use of notes for clinical care have changed substantially with EHR implementation. Use of efficiency tools (ie, copy forward functions and autopopulation of data) may increase the speed of documentation.[5] Notes in an EHR are more legible and accessible and may be able to organize data to improve clinical care.[6]
Yet, many have commented on the negative consequences of documentation in an EHR. In a New England Journal of Medicine Perspective article, Drs. Hartzband and Groopman wrote, we have observed the electronic medical record become a powerful vehicle for perpetuating erroneous information, leading to diagnostic errors that gain momentum when passed on electronically.[7] As a result, the copy forward and autopopulation functions have come under significant scrutiny.[8, 9, 10] A survey conducted at 2 academic institutions found that 71% of residents and attendings believed that the copy forward function led to inconsistencies and outdated information.[11] Autopopulation has been criticized for creating lengthy notes full of trivial or redundant data, a phenomenon termed note bloat. Bloated notes may be less effective as a communication tool.[12] Additionally, the process of composing a note often stimulates critical thinking and may lead to changes in care. The act of copying forward a previous note and autopopulating data bypasses that process and in effect may suppress critical thinking.[13] Previous studies have raised numerous concerns regarding copy forward and autopopulation functionality in the EHR. Many have described the duplication of outdated data and the possibility of the introduction and perpetuation of errors.[14, 15, 16] The Veterans Affairs (VA) Puget Sound Health system evaluated 6322 copy events and found that 1 in 10 electronic patient charts contained an instance of high‐risk copying.[17] In a survey of faculty and residents at a single academic medical center, the majority of users of copy and paste functionality recognized the hazards; they responded that their notes may contain more outdated (66%) and more inconsistent information (69%). Yet, most felt copy forwarding improved the documentation of the entire hospital course (87%), overall physician documentation (69%), and should definitely be continued (91%).[11] Others have complained about the impact of copy forward on the expression of clinical reasoning.[7, 9, 18]
Previous discussions on the topic of overall note quality following EHR implementation have been limited to perspectives or opinion pieces of individual attending providers.[18] We conducted a survey across 4 academic institutions to analyze both housestaff and attendings perceptions of the quality of notes since the implementation of an EHR to better inform the discussion of the impact of an EHR on note quality.
METHODS
Participants
Surveys were administered via email to interns, residents (second‐, third‐, or fourth‐year residents, hereafter referred to as residents) and attendings at 4 academic hospitals that use the Epic EHR (Epic Corp., Madison, WI). The 4 institutions each adopted the Epic EHR, with mandatory faculty and resident training, between 1 and 5 years prior to the survey. Three of the institutions previously used systems with electronic notes, whereas the fourth institution previously used a system with handwritten notes. The study participation emails included a link to an online survey in REDCap.[19] We included interns and residents from the following types of residency programs: internal medicine categorical or primary care, medicine‐pediatrics, or medicine‐psychiatry. For housestaff (the combination of both interns and residents), exclusion criteria included preliminary or transitional year interns, or any interns or residents from other specialties who rotate on the medicine service. For attendings, participants included hospitalists, general internal medicine attendings, chief residents, and subspecialty medicine attendings, each of whom had worked for any amount of time on the inpatient medicine teaching service in the prior 12 months.
Design
We developed 3 unique surveys for interns, residents, and attendings to assess their perception of inpatient progress notes (see Supporting Information, Appendix, in the online version of this article). The surveys incorporated questions from 2 previously published sources, the 9‐item Physician Documentation Quality Instrument (PDQI‐9) (see online Appendix), a validated note‐scoring tool, and the Accreditation Council for Graduate Medical Education note‐writing competency checklists.[20] Additionally, faculty at the participating institutions developed questions to address practices and attitudes toward autopopulation, copy forward, and the purposes of a progress note. Responses were based on a 5‐point Likert scale. The intern and resident surveys asked for self‐evaluation of their own progress notes and those of their peers, whereas the attending surveys asked for assessment of housestaff notes.
The survey was left open for a total of 55 days and participants were sent reminder emails. The study received a waiver from the institutional review board at all 4 institutions.
Data Analysis
Study data were collected and managed using REDCap electronic data capture tools hosted at the University of California, San Francisco (UCSF).[19] The survey data were analyzed and the figures were created using Microsoft Excel 2008 (Microsoft Corp., Redmond, WA). Mean values for each survey question were calculated. Differences between the means among the groups were assessed using 2‐sample t tests. P values <0.05 were considered statistically significant.
RESULTS
Demographics
We received 99 completed surveys from interns, 155 completed surveys from residents, and 153 completed surveys from attendings across the 4 institutions. The overall response rate for interns was 68%, ranging from 59% at the University of California, San Diego (UCSD) to 74% at the University of Iowa. The overall response rate for residents was 49%, ranging from 38% at UCSF to 66% at the University of California, Los Angeles. The overall response rate for attendings was 70%, ranging from 53% at UCSD to 74% at UCSF.
A total of 78% of interns and 72% of residents had used an EHR at a prior institution. Of the residents, 90 were second‐year residents, 64 were third‐year residents, and 2 were fourth‐year residents. A total of 76% of attendings self‐identified as hospitalists.
Overall Assessment of Note Quality
Participants were asked to rate the quality of progress notes on a 5‐point scale (poor, fair, good, very good, excellent). Half of interns and residents rated their own progress notes as very good or excellent. A total of 44% percent of interns and 24% of residents rated their peers notes as very good or excellent, whereas only 15% of attending physicians rated housestaff notes as very good or excellent.
When asked to rate the change in progress note quality since their hospital had adopted the EHR, the majority of residents answered unchanged or better, and the majority of attendings answered unchanged or worse (Figure 1).
PDQI‐9 Framework
Participants answered each PDQI‐9 question on a 5‐point Likert scale ranging from not at all (1) to extremely (5). In 8 of the 9 PDQI‐9 domains, there were no significant differences between interns and residents. Across each domain, attending perceptions of housestaff notes were significantly lower than housestaff perceptions of their own notes (P<0.001) (Figure 2). Both housestaff and attendings gave the highest ratings to thorough, up to date, and synthesized and the lowest rating to succinct.
Copy Forward and Autopopulation
Overall, the effect of copy forward and autopopulation on critical thinking, note accuracy, and prioritizing the problem list was thought to be neutral or somewhat positive by interns, neutral by residents, and neutral or somewhat negative by attendings (P<0.001) (Figure 3). In all, 16% of interns, 22% of residents, and 55% of attendings reported that copy forward had a somewhat negative or very negative impact on critical thinking (P<0.001). In all, 16% of interns, 29% of residents and 39% of attendings thought that autopopulation had a somewhat negative or very negative impact on critical thinking (P<0.001).
Purpose of Progress Notes
Participants were provided with 7 possible purposes of a progress note and asked to rate the importance of each stated purpose. There was nearly perfect agreement between interns, residents, and attendings in the rank order of the importance of each purpose of a progress note (Table 1). Attendings and housestaff ranked communication with other providers and documenting important events and the plan for the day as the 2 most important purposes of a progress note, and billing and quality improvement as less important.
| Interns | Residents | Attendings | |
|---|---|---|---|
| Communication with other providers | 1 | 1 | 2 |
| Documenting important events and the plan for the day | 2 | 2 | 1 |
| Prioritizing issues going forward in the patient's care | 3 | 3 | 3 |
| Medicolegal | 4 | 4 | 4 |
| Stimulate critical thinking | 5 | 5 | 5 |
| Billing | 6 | 6 | 6 |
| Quality improvement | 7 | 7 | 7 |
DISCUSSION
This is the first large multicenter analysis of both attendings and housestaff perceptions of note quality in the EHR era. The findings provide insight into important differences and similarities in the perceptions of the 2 groups. Most striking is the difference in opinion of overall note quality, with only a small minority of faculty rating current housestaff notes as very good or excellent, whereas a much larger proportion of housestaff rated their own notes and those of their peers to be of high quality. Though participants were not specifically asked why note quality in general was suboptimal, housestaff and faculty rankings of specific domains from the PDQI‐9 may yield an important clue. Specifically, all groups expressed that the weakest attribute of current progress notes is succinct. This finding is consistent with the note bloat phenomenon, which has been maligned as a consequence of EHR implementation.[7, 14, 18, 21, 22]
One interesting finding was that only 5% of interns rated the notes of other housestaff as fair or poor. One possible explanation for this may be the tendency for an individual to enhance or augment the status or performance of the group to which he or she belongs as a mechanism to increase self‐image, known as the social identity theory.[23] Thus, housestaff may not criticize their peers to allow for identification with a group that is not deficient in note writing.
The more positive assessment of overall note quality among housestaff could be related to the different roles of housestaff and attendings on a teaching service. On a teaching service, housestaff are typically the writer, whereas attendings are almost exclusively the reader of progress notes. Housestaff may reap benefits, including efficiency, beyond the finished product. A perception of higher quality may reflect the process of note writing, data gathering, and critical thinking required to build an assessment and plan. The scores on the PDQI‐9 support this notion, as housestaff rated all 9 domains significantly higher than attendings.
Housestaff and attendings held greater differences of opinion with respect to the EHR's impact on note quality. Generally, housestaff perceived the EHR to have improved progress note quality, whereas attendings perceived the opposite. One explanation could be that these results reflect changing stages of development of physicians well described through the RIME framework (reporter, interpreter, manager, educator). Attendings may expect notes to reflect synthesis and analysis, whereas trainees may be satisfied with the data gathering that an EHR facilitates. In our survey, the trend of answers from intern to resident to attending suggests an evolving process of attitudes toward note quality.
The above reasons may also explain why housestaff were generally more positive than attendings about the effect of copy forward and autopopulation functions on critical thinking. Perhaps, as these functions can potentially increase efficiency and decrease time spent at the computer, although data are mixed on this finding, housestaff may have more time to spend with patients or develop a thorough plan and thus rate these functions positively.
Notably, housestaff and attendings had excellent agreement on the purposes of a progress note. They agreed that the 2 most important purposes were communication with other providers and documenting important events and the plan for the day. These are the 2 listed purposes that are most directly related to patient care. If future interventions to improve note quality require housestaff and attendings to significantly change their behavior, a focus on the impact on patient care might yield the best results.
There were several limitations in our study. Any study based on self‐assessment is subject to bias. A previous meta‐analysis and review described poor to moderate correlations between self‐assessed and external measures of performance.[24, 25] The survey data were aggregated from 4 institutions despite somewhat different, though relatively high, response rates between the institutions. There could be a response bias; those who did not respond may have systematically different perceptions of note quality. It should be noted that the general demographics of the respondents reflected those of the housestaff and attendings at 4 academic centers. All 4 of the participating institutions adopted the Epic EHR within the last several years of the survey being administered, and perceptions of note quality may be biased depending on the prior system used (ie, change from handwritten to electronic vs electronic to other electronic system). In addition, the survey results reflect experience with only 1 EHR, and our results may not apply to other EHR vendors or institutions like the VA, which have a long‐standing system in place. Last, we did not explore the impact of perceived note quality on the measured or perceived quality of care. One previous study found no direct correlation between note quality and clinical quality.[26]
There are several future directions for research based on our findings. First, potential differences between housestaff and attending perceptions of note quality could be further teased apart by studying the perceptions of attendings on a nonteaching service who write their own daily progress notes. Second, housestaff perceptions on why copy forward and autopopulation may increase critical thinking could be explored further with more direct questioning. Finally, although our study captured only perceptions of note quality, validated tools could be used to objectively measure note quality; these measurements could then be compared to perception of note quality as well as clinical outcomes.
Given the prevalence and the apparent belief that the benefits of an EHR outweigh the hazards, institutions should embrace these innovations but take steps to mitigate the potential errors and problems associated with copy forward and autopopulation. The results of our study should help inform future interventions.
Acknowledgements
The authors acknowledge the contributions of Russell Leslie from the University of Iowa.
Disclosure: Nothing to report.
- , , , et al. Systematic review: impact of health information technology on quality, efficiency, and costs of medical care. Ann Intern Med. 2006;144(10):742–752.
- , , , , . Clinical information technologies and inpatient outcomes: a multiple hospital study. Arch Intern Med. 2009;169(2):108–114.
- , , , et al. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. JAMA. 1998;280(15):1311–1316.
- , , , . Electronic health records and quality of diabetes care. N Engl J Med. 2011;365(9):825–833.
- , , , et al. The impact of a clinical information system in an intensive care unit. J Clin Monit Comput. 2008;22(1):31–36.
- , . Can electronic clinical documentation help prevent diagnostic errors? N Engl J Med. 2010;362(12):1066–1069.
- , . Off the record—avoiding the pitfalls of going electronic. N Eng J Med. 2008;358(16):1656–1658.
- , , . Copying and pasting of examinations within the electronic medical record. Int J Med Inform. 2007;76(suppl 1):S122–S128.
- , . Copy and paste: a remediable hazard of electronic health records. Am J Med. 2009;122(6):495–496.
- , , . The role of copy‐and‐paste in the hospital electronic health record. JAMA Intern Med. 2014;174(8):1217–1218.
- , , , , , . Physicians’ attitudes towards copy and pasting in electronic note writing. J Gen Intern Med. 2009;24(1):63–68.
- , , , , . Medical education in the electronic medical record (EMR) era: benefits, challenges, and future directions. Acad Med. 2013;88(6):748–752.
- , . Educational impact of the electronic medical record. J Surg Educ. 2012;69(1):105–112.
- , , , , , . Direct text entry in electronic progress notes. An evaluation of input errors. Methods Inf Med. 2003;42(1):61–67.
- . The clinical record: a 200‐year‐old 21st‐century challenge. Ann Intern Med. 2010;153(10):682–683.
- . Sloppy and paste. Morbidity and Mortality Rounds on the Web. Available at: http://www.webmm.ahrq.gov/case.aspx?caseID=274. Published July 2012. Accessed September 26, 2014.
- , , , . Are electronic medical records trustworthy? Observations on copying, pasting and duplication. AMIA Annu Symp Proc. 2003:269–273.
- . A piece of my mind. John Lennon's elbow. JAMA. 2012;308(5):463–464.
- , , , , , . Research electronic data capture (REDCap)—a metadata‐driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381.
- , , . ACGME competency note checklist. Available at: http://www.im.org/p/cm/ld/fid=831. Accessed August 8, 2013.
- , , , . Assessing electronic note quality using the Physician Documentation Quality Instrument (PDQI‐9). Appl Clin Inform. 2012;3(2):164–174.
- , , , . Quantifying clinical narrative redundancy in an electronic health record. J Am Med Inform Assoc. 2010;17(1):49–53.
- , . The social identity theory of intergroup behavior. In: Psychology of Intergroup Relations. 2nd ed. Chicago, IL: Nelson‐Hall Publishers; 1986:7–24.
- , . Student self‐assessment in higher education: a meta‐analysis. Rev Educ Res. 1989;59:395–430.
- . A review of the validity and accuracy of self‐assessments in health professions training. Acad Med. 1991;66:762–769.
- , , , , . Association of note quality and quality of care: a cross‐sectional study. BMJ Qual Saf. 2014;23(5):406–413.
- , , , et al. Systematic review: impact of health information technology on quality, efficiency, and costs of medical care. Ann Intern Med. 2006;144(10):742–752.
- , , , , . Clinical information technologies and inpatient outcomes: a multiple hospital study. Arch Intern Med. 2009;169(2):108–114.
- , , , et al. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. JAMA. 1998;280(15):1311–1316.
- , , , . Electronic health records and quality of diabetes care. N Engl J Med. 2011;365(9):825–833.
- , , , et al. The impact of a clinical information system in an intensive care unit. J Clin Monit Comput. 2008;22(1):31–36.
- , . Can electronic clinical documentation help prevent diagnostic errors? N Engl J Med. 2010;362(12):1066–1069.
- , . Off the record—avoiding the pitfalls of going electronic. N Eng J Med. 2008;358(16):1656–1658.
- , , . Copying and pasting of examinations within the electronic medical record. Int J Med Inform. 2007;76(suppl 1):S122–S128.
- , . Copy and paste: a remediable hazard of electronic health records. Am J Med. 2009;122(6):495–496.
- , , . The role of copy‐and‐paste in the hospital electronic health record. JAMA Intern Med. 2014;174(8):1217–1218.
- , , , , , . Physicians’ attitudes towards copy and pasting in electronic note writing. J Gen Intern Med. 2009;24(1):63–68.
- , , , , . Medical education in the electronic medical record (EMR) era: benefits, challenges, and future directions. Acad Med. 2013;88(6):748–752.
- , . Educational impact of the electronic medical record. J Surg Educ. 2012;69(1):105–112.
- , , , , , . Direct text entry in electronic progress notes. An evaluation of input errors. Methods Inf Med. 2003;42(1):61–67.
- . The clinical record: a 200‐year‐old 21st‐century challenge. Ann Intern Med. 2010;153(10):682–683.
- . Sloppy and paste. Morbidity and Mortality Rounds on the Web. Available at: http://www.webmm.ahrq.gov/case.aspx?caseID=274. Published July 2012. Accessed September 26, 2014.
- , , , . Are electronic medical records trustworthy? Observations on copying, pasting and duplication. AMIA Annu Symp Proc. 2003:269–273.
- . A piece of my mind. John Lennon's elbow. JAMA. 2012;308(5):463–464.
- , , , , , . Research electronic data capture (REDCap)—a metadata‐driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381.
- , , . ACGME competency note checklist. Available at: http://www.im.org/p/cm/ld/fid=831. Accessed August 8, 2013.
- , , , . Assessing electronic note quality using the Physician Documentation Quality Instrument (PDQI‐9). Appl Clin Inform. 2012;3(2):164–174.
- , , , . Quantifying clinical narrative redundancy in an electronic health record. J Am Med Inform Assoc. 2010;17(1):49–53.
- , . The social identity theory of intergroup behavior. In: Psychology of Intergroup Relations. 2nd ed. Chicago, IL: Nelson‐Hall Publishers; 1986:7–24.
- , . Student self‐assessment in higher education: a meta‐analysis. Rev Educ Res. 1989;59:395–430.
- . A review of the validity and accuracy of self‐assessments in health professions training. Acad Med. 1991;66:762–769.
- , , , , . Association of note quality and quality of care: a cross‐sectional study. BMJ Qual Saf. 2014;23(5):406–413.
© 2015 Society of Hospital Medicine
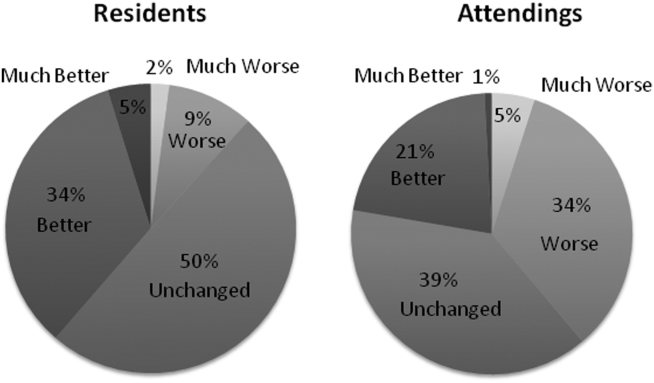
Clonal hematopoiesis explored in aplastic anemia
Clonal hematopoiesis was detected in DNA samples from approximately half of 439 patients with aplastic anemia, and a third of the study population carried mutations in candidate genes that correlated with clinical outcomes, according to a report published online July 2 in the New England Journal of Medicine.
Most patients with aplastic anemia respond to immunosuppressive therapy or bone marrow transplantation, but about 15% later develop myelodysplastic syndromes, acute myeloid leukemia (AML), or both. Historically, this has been attributed to “clonal evolution,” but a more accurate term is clonal hematopoiesis. However, not all patients with clonal hematopoiesis go on to develop late myelodysplastic syndromes or AML, said Dr. Tetsuichi Yoshizato of the department of pathology and tumor biology at Kyoto (Japan) University and associates.
To clarify the role of clonal hematopoiesis in aplastic anemia, the investigators analyzed DNA in blood, bone marrow, and buccal samples from 439 patients with bone marrow failure who were treated at three specialized centers in the United States and Japan.
Targeted sequencing of a panel of genes that are recurrently mutated in myeloid cancers was performed; 249 mutations were detected in candidate genes for myelodysplastic syndromes/AML in 36% of the study population. And about one-third of patients whose DNA harbored mutations had multiple (as many as 7) mutations. The most frequently mutated genes were BCOR and BCORL1 (in 9.3% of patients), PIGA (7.5%), DNMT3A (8.4%), and ASXL1 (6.2%), which together accounted for 77% of all mutation-positive patients, the investigators reported.
In addition, 47% of patients had expanded hematopoietic cell clones. Clones carrying certain mutations were associated with a better response to immunosuppressive treatment, while clones carrying several other mutations were associated with a poor treatment response, lower survival, and progression to myelodysplastic syndromes/AML. Mutations in PIGA and BCOR and BCORL1 correlated with a better response to immunosuppressive therapy and better overall and progression-free survival; mutations in a subgroup of genes that included DNMT3A and ASXL1 were associated with worse outcomes.
The pattern of mutations in individual patients, however, varied markedly over time and was often unpredictable. “It should be underscored that the complex dynamics of clonal hematopoiesis are highly variable and not necessarily determinative,” Dr. Yoshizato and associates said (N. Engl. J. Med. 2015 July 2 [doi:10.1056/NEJMoa1414799]).
Although further genetic research is needed before these findings can be applied clinically to guide prognosis and treatment, they already “have implications for bone marrow failure, for early events in leukemogenesis, and for normal aging,” the investigators added.
Clonal hematopoiesis was detected in DNA samples from approximately half of 439 patients with aplastic anemia, and a third of the study population carried mutations in candidate genes that correlated with clinical outcomes, according to a report published online July 2 in the New England Journal of Medicine.
Most patients with aplastic anemia respond to immunosuppressive therapy or bone marrow transplantation, but about 15% later develop myelodysplastic syndromes, acute myeloid leukemia (AML), or both. Historically, this has been attributed to “clonal evolution,” but a more accurate term is clonal hematopoiesis. However, not all patients with clonal hematopoiesis go on to develop late myelodysplastic syndromes or AML, said Dr. Tetsuichi Yoshizato of the department of pathology and tumor biology at Kyoto (Japan) University and associates.
To clarify the role of clonal hematopoiesis in aplastic anemia, the investigators analyzed DNA in blood, bone marrow, and buccal samples from 439 patients with bone marrow failure who were treated at three specialized centers in the United States and Japan.
Targeted sequencing of a panel of genes that are recurrently mutated in myeloid cancers was performed; 249 mutations were detected in candidate genes for myelodysplastic syndromes/AML in 36% of the study population. And about one-third of patients whose DNA harbored mutations had multiple (as many as 7) mutations. The most frequently mutated genes were BCOR and BCORL1 (in 9.3% of patients), PIGA (7.5%), DNMT3A (8.4%), and ASXL1 (6.2%), which together accounted for 77% of all mutation-positive patients, the investigators reported.
In addition, 47% of patients had expanded hematopoietic cell clones. Clones carrying certain mutations were associated with a better response to immunosuppressive treatment, while clones carrying several other mutations were associated with a poor treatment response, lower survival, and progression to myelodysplastic syndromes/AML. Mutations in PIGA and BCOR and BCORL1 correlated with a better response to immunosuppressive therapy and better overall and progression-free survival; mutations in a subgroup of genes that included DNMT3A and ASXL1 were associated with worse outcomes.
The pattern of mutations in individual patients, however, varied markedly over time and was often unpredictable. “It should be underscored that the complex dynamics of clonal hematopoiesis are highly variable and not necessarily determinative,” Dr. Yoshizato and associates said (N. Engl. J. Med. 2015 July 2 [doi:10.1056/NEJMoa1414799]).
Although further genetic research is needed before these findings can be applied clinically to guide prognosis and treatment, they already “have implications for bone marrow failure, for early events in leukemogenesis, and for normal aging,” the investigators added.
Clonal hematopoiesis was detected in DNA samples from approximately half of 439 patients with aplastic anemia, and a third of the study population carried mutations in candidate genes that correlated with clinical outcomes, according to a report published online July 2 in the New England Journal of Medicine.
Most patients with aplastic anemia respond to immunosuppressive therapy or bone marrow transplantation, but about 15% later develop myelodysplastic syndromes, acute myeloid leukemia (AML), or both. Historically, this has been attributed to “clonal evolution,” but a more accurate term is clonal hematopoiesis. However, not all patients with clonal hematopoiesis go on to develop late myelodysplastic syndromes or AML, said Dr. Tetsuichi Yoshizato of the department of pathology and tumor biology at Kyoto (Japan) University and associates.
To clarify the role of clonal hematopoiesis in aplastic anemia, the investigators analyzed DNA in blood, bone marrow, and buccal samples from 439 patients with bone marrow failure who were treated at three specialized centers in the United States and Japan.
Targeted sequencing of a panel of genes that are recurrently mutated in myeloid cancers was performed; 249 mutations were detected in candidate genes for myelodysplastic syndromes/AML in 36% of the study population. And about one-third of patients whose DNA harbored mutations had multiple (as many as 7) mutations. The most frequently mutated genes were BCOR and BCORL1 (in 9.3% of patients), PIGA (7.5%), DNMT3A (8.4%), and ASXL1 (6.2%), which together accounted for 77% of all mutation-positive patients, the investigators reported.
In addition, 47% of patients had expanded hematopoietic cell clones. Clones carrying certain mutations were associated with a better response to immunosuppressive treatment, while clones carrying several other mutations were associated with a poor treatment response, lower survival, and progression to myelodysplastic syndromes/AML. Mutations in PIGA and BCOR and BCORL1 correlated with a better response to immunosuppressive therapy and better overall and progression-free survival; mutations in a subgroup of genes that included DNMT3A and ASXL1 were associated with worse outcomes.
The pattern of mutations in individual patients, however, varied markedly over time and was often unpredictable. “It should be underscored that the complex dynamics of clonal hematopoiesis are highly variable and not necessarily determinative,” Dr. Yoshizato and associates said (N. Engl. J. Med. 2015 July 2 [doi:10.1056/NEJMoa1414799]).
Although further genetic research is needed before these findings can be applied clinically to guide prognosis and treatment, they already “have implications for bone marrow failure, for early events in leukemogenesis, and for normal aging,” the investigators added.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Clonal hematopoiesis was detected in 47% of 439 patients with aplastic anemia, and some of the mutations were related to clinical outcomes.
Major finding: The most frequently mutated genes were BCOR and BCORL1 (in 9.3% of patients), PIGA (7.5%), DNMT3A (8.4%), and ASXL1 (6.2%), which together accounted for 77% of all mutation-positive patients.
Data source: DNA analysis of blood, bone marrow, and buccal samples from 439 patients with aplastic anemia treated at three medical centers in the United States and Japan.
Disclosures: This work was supported by the Ministry of Health, Labor, and Welfare of Japan; the Japan Society for the Promotion of Science; the National Heart, Lung, and Blood Institute; the Aplastic Anemia and MDS International Foundation; and the Scott Hamilton Cancer Alliance for Research, Education, and Survivorship Foundation. Dr. Yoshizato reported having no relevant financial disclosures; an associate reported receiving a grant from Daiichi-Sankyo unrelated to this work.