User login
Who is going to make the wise choice?
Failure of academic medicine to improve value will undermine professionalism and threaten autonomy because outside forces, such as insurers and regulators, will surely impose change if academic leaders and physicians fail. [1]
The verdict is indoctors order too many tests. This problem is most prominent in academic health centers (AHCs), where the use of testing resources is higher than in community hospitals.[2] Most prior attempts to improve the value of care at AHCs have been driven by faculty and hospital administration in a top‐down fashion with only transient success.[3] We believe that successful and sustainable change should start with the housestaff, who are training in a system afflicted by wasteful overuse of healthcare resources. Therefore, we created a housestaff‐led initiative called the Vanderbilt Choosing Wisely Steering Committee to change the culture of academic medicine. If AHCs are going to start choosing wisely, housestaff must be part of the engine behind the change.
FORMING THE VANDERBILT CHOOSING WISELY STEERING COMMITTEE
The idea for the Vanderbilt Choosing Wisely Steering Committee (VCWSC) was born in December 2013 during a monthly Graduate Medical Education Committee meeting involving housestaff and faculty representatives from multiple subspecialties. At that time, the national Choosing Wisely campaign was in full stride, with more than 50 organizations having proposed top 5 lists of tests and procedures that should be questioned.[4] Several participants at the meeting decided to create a steering committee to integrate these proposals into daily practice at Vanderbilt University Medical Center.
Housestaff have formed the core of the VCWSC from the beginning. The initial members were residents on the Graduate Medical Education Committee, including a fifth‐year radiology resident and a second‐year internal medicine resident who served as the first co‐chairs. More housestaff were recruited by email and word‐of‐mouth. Currently, the committee is composed of residents from the departments of internal medicine, radiology, pediatrics, neurology, anesthesiology, pathology, and general surgery. These residents perform all of the committee's vital functions, including organizing biweekly meetings, brainstorming and carrying out high‐value care initiatives, and recruiting new members. Of course, this committee would not have the authority to create real change without the guidance of numerous faculty supporters, including the designated institutional official and the associate vice chancellor for health affairs. However, we firmly believe that the primary reason this committee has been successful is that it is led by housestaff.
THE IMPORTANCE OF HOUSESTAFF LEADERSHIP
Residents are at the front line of care delivery at academic health centers (AHCs). Innumerable tests and procedures at these institutions are ordered and performed by housestaff. Therefore, culture change in academic medicine will not occur without housestaff culture change. Unfortunately, residents have been shown to have a lower level of competency with regard to high‐value care than more experienced providers.[5] The housestaff‐led VCWSC is uniquely positioned to address this problem by using personal experience and peer‐to‐peer communication to address the fears, biases, and knowledge gaps that cause trainees to waste healthcare resources. Resident members of the VCWSC wrestle daily with the temptation to overtest to avoid missing something or make a rare diagnosis. They are familiar with the systems that encourage overutilization, like shortcuts in ordering software that allow automatically recurring orders. Perhaps most importantly, they are able to discuss high‐value care with other trainees as equals, instead of trying to enforce compliance with a set of restrictions put in place by supervisors.
A SYSTEMATIC STRATEGY FOR EFFECTING CHANGE
To successfully implement high‐value care initiatives, the VCWSC follows a strategy proposed by John Kotter for effecting change in large organizations.[6] According to Kotter, it is critical to create a vision for change, communicate the vision effectively, and empower others to act on the vision. The VCWSC's vision for change is to encourage optimal medical practice by implementing Choosing Wisely top 5 recommendations. To communicate this vision, the VCWSC follows the rhetorical style of the national Choosing Wisely campaign. The American Board of Internal Medicine Foundation researched this rhetoric extensively in the years leading up to the development of the top 5 lists. They found that simply asking providers to judiciously distribute healthcare resources often created a feeling of patient abandonment. Instead, providers are much more likely to respond to messages that encourage wise choices that enhance professional fulfillment, patient well‐being, and the overall quality of care.[4] Therefore, the VCWSC emphasizes these same values in its e‐mails, fliers, and presentations. Importantly, the VCWSC does not directly limit providers abilities to order tests or perform procedures. Instead, the VCWSC uses education and data to empower others to act on the Choosing Wisely vision for high‐value care.
After communicating the vision for change, Kotter recommends sustaining the vision by creating short‐term wins.[6] To demonstrate these wins, the VCWSC collects data on the effects of its initiatives and celebrates the success of individuals and teams through regular widely distributed emails. Initially this involved manually counting the number of tests ordered by many providers. Fortunately, experts from the Department of Bioinformatics partnered with the VCWSC to create an automated data collection system that is much more efficient, enabling the committee to quickly collect and analyze data on tests and procedures at Vanderbilt University Medical Center. These data are fed back to participants in various initiatives, and they are used to demonstrate the efficacy of these initiatives to others throughout the medical center, thus garnering trust and encouraging others to participate in VCWSC projects. With enough short‐term wins, the VCWSC hopes to achieve Kotter's ultimate goal, which is to consolidate and institutionalize changes to have a lasting impact.[6]
REDUCING DAILY LABSAN EARLY SUCCESS OF THE VCWSC
One example of the committee's early success is the reduction of routine complete blood counts (CBCs) and basic metabolic panels (BMPs) on internal medicine services, as recommended in the Choosing Wisely top 5 list proposed by the Society of Hospital Medicine. Prior studies on reducing routine labs required interventions like displaying charges at the time of test ordering,[7, 8] using financial incentives,[2, 9] and eliminating the ability to order recurring daily labs.[10] Instead of replicating these efforts, the VCWSC decided to use an educational campaign and real‐time data feedback to focus on the root of the problema culture of overtesting. After obtaining the support of the internal medicine residency program leadership, the VCWSC distributed an evidence‐based flier (see Supporting Information in the online version of this article) summarizing the harms of and misconceptions surrounding excessive lab testing. These data were also presented at housestaff conferences.
Following this initial educational intervention, the VCWSC began tracking the labs ordered for patients on housestaff internal medicine teams to see what proportion have a BMP or CBC drawn each day of their hospitalization. Each week, the teams are sent an email with their lab rate compared to the lab rates of analogous teams. At the end of each month, all internal medicine housestaff and faculty are notified which teams had the lowest lab rate for the month. The VCWSC does not attempt to define an unnecessary lab or offer incentives; the teams are simply reminded that ordering fewer labs can be good for patient care. Since the initiative began, the teams have succeeded in reducing the percentage of patients receiving a CBC and BMP each day from an average of 90% to below 70%.
FUTURE DIRECTIONS
Moving forward, the VCWSC hopes to further engrain the culture of Choosing Wisely into daily practice at Vanderbilt University Medical Center. The labs initiative has expanded to many services including surgery, neurology, and the medical intensive care unit. Other initiatives are focusing on excessive telemetry monitoring and daily chest radiographs in intensive care units. In addition, the VCWSC is collaborating with other AHCs to help them implement their own Choosing Wisely projects.
A CALL FOR MORE HOUSESTAFF CHOOSING WISELY INITIATIVES
Housestaff are perfectly positioned to lead a change in the culture of academic medicine toward high‐value care. The VCWSC has already seen promising results, and we hope that similar initiatives will be created at AHCs across the country. By following John Kotter's recommendations for implementing change and using the Choosing Wisely top 5 lists as a guide, housestaff‐run committees like the VCWSC have the potential to change the culture of medicine at every AHC. If we do not want outside regulators to decide the future of academic medicine, we must find a way to cut down on wasteful spending and unnecessary testing. Residents everywhere, let us choose wisely together.
Acknowledgements
The authors of this study acknowledge the faculty, residents, and medical students who have supported the efforts of the Vanderbilt University Choosing Wisely Steering Committee.
Disclosures: Dr. Brady serves on the board of the ACGME but receives no financial payment other than compensation for travel expenses to board meetings. He also was Chair of the Board for the American Academy on Communication in Healthcare in 2014.
- , , Teaching value in academic environments. Shifting the ivory tower. JAMA. 2013;310(16):1671–1672.
- , , , , A trial of two strategies to modify the test‐ordering behavior of medical residents. N Engl J Med. 1980;303(23):1330–1336.
- , , , Techniques to improve physicians' use of diagnostic tests: a new conceptual framework. JAMA. 1998;280(23):2020–2027.
- , , Engaging physicians and consumers in conversations about treatment overuse and waste: a short history of the Choosing Wisely campaign. Acad Med. 2014;89(7):990–995.
- , , , , , “Choosing Wisely” in an academic department of medicine [published online June 26, 2014]. Am J Med Qual. doi:10.1177/1062860614540982.
- Leading change; why transformation efforts fail. Harv Bus Rev. 1995;March‐April:57–67.
- , , , et al. Impact of providing fee data on laboratory test ordering: a controlled clinical trial. JAMA Intern Med. 2013;173(10):903–908.
- , , The effect on test ordering of informing physicians of the charges for outpatient diagnostic tests. N Engl J Med. 1990;322(21):1499–1504.
- , , , et al. Targeted reduction in neurosurgical laboratory utilization: resident‐led effort at a single academic institution. J Neurosurg. 2014;120(1):173–177.
- , , , et al. The impact of peer management on test‐ordering behavior. Ann Intern Med. 2004;141(3):196–204.
Failure of academic medicine to improve value will undermine professionalism and threaten autonomy because outside forces, such as insurers and regulators, will surely impose change if academic leaders and physicians fail. [1]
The verdict is indoctors order too many tests. This problem is most prominent in academic health centers (AHCs), where the use of testing resources is higher than in community hospitals.[2] Most prior attempts to improve the value of care at AHCs have been driven by faculty and hospital administration in a top‐down fashion with only transient success.[3] We believe that successful and sustainable change should start with the housestaff, who are training in a system afflicted by wasteful overuse of healthcare resources. Therefore, we created a housestaff‐led initiative called the Vanderbilt Choosing Wisely Steering Committee to change the culture of academic medicine. If AHCs are going to start choosing wisely, housestaff must be part of the engine behind the change.
FORMING THE VANDERBILT CHOOSING WISELY STEERING COMMITTEE
The idea for the Vanderbilt Choosing Wisely Steering Committee (VCWSC) was born in December 2013 during a monthly Graduate Medical Education Committee meeting involving housestaff and faculty representatives from multiple subspecialties. At that time, the national Choosing Wisely campaign was in full stride, with more than 50 organizations having proposed top 5 lists of tests and procedures that should be questioned.[4] Several participants at the meeting decided to create a steering committee to integrate these proposals into daily practice at Vanderbilt University Medical Center.
Housestaff have formed the core of the VCWSC from the beginning. The initial members were residents on the Graduate Medical Education Committee, including a fifth‐year radiology resident and a second‐year internal medicine resident who served as the first co‐chairs. More housestaff were recruited by email and word‐of‐mouth. Currently, the committee is composed of residents from the departments of internal medicine, radiology, pediatrics, neurology, anesthesiology, pathology, and general surgery. These residents perform all of the committee's vital functions, including organizing biweekly meetings, brainstorming and carrying out high‐value care initiatives, and recruiting new members. Of course, this committee would not have the authority to create real change without the guidance of numerous faculty supporters, including the designated institutional official and the associate vice chancellor for health affairs. However, we firmly believe that the primary reason this committee has been successful is that it is led by housestaff.
THE IMPORTANCE OF HOUSESTAFF LEADERSHIP
Residents are at the front line of care delivery at academic health centers (AHCs). Innumerable tests and procedures at these institutions are ordered and performed by housestaff. Therefore, culture change in academic medicine will not occur without housestaff culture change. Unfortunately, residents have been shown to have a lower level of competency with regard to high‐value care than more experienced providers.[5] The housestaff‐led VCWSC is uniquely positioned to address this problem by using personal experience and peer‐to‐peer communication to address the fears, biases, and knowledge gaps that cause trainees to waste healthcare resources. Resident members of the VCWSC wrestle daily with the temptation to overtest to avoid missing something or make a rare diagnosis. They are familiar with the systems that encourage overutilization, like shortcuts in ordering software that allow automatically recurring orders. Perhaps most importantly, they are able to discuss high‐value care with other trainees as equals, instead of trying to enforce compliance with a set of restrictions put in place by supervisors.
A SYSTEMATIC STRATEGY FOR EFFECTING CHANGE
To successfully implement high‐value care initiatives, the VCWSC follows a strategy proposed by John Kotter for effecting change in large organizations.[6] According to Kotter, it is critical to create a vision for change, communicate the vision effectively, and empower others to act on the vision. The VCWSC's vision for change is to encourage optimal medical practice by implementing Choosing Wisely top 5 recommendations. To communicate this vision, the VCWSC follows the rhetorical style of the national Choosing Wisely campaign. The American Board of Internal Medicine Foundation researched this rhetoric extensively in the years leading up to the development of the top 5 lists. They found that simply asking providers to judiciously distribute healthcare resources often created a feeling of patient abandonment. Instead, providers are much more likely to respond to messages that encourage wise choices that enhance professional fulfillment, patient well‐being, and the overall quality of care.[4] Therefore, the VCWSC emphasizes these same values in its e‐mails, fliers, and presentations. Importantly, the VCWSC does not directly limit providers abilities to order tests or perform procedures. Instead, the VCWSC uses education and data to empower others to act on the Choosing Wisely vision for high‐value care.
After communicating the vision for change, Kotter recommends sustaining the vision by creating short‐term wins.[6] To demonstrate these wins, the VCWSC collects data on the effects of its initiatives and celebrates the success of individuals and teams through regular widely distributed emails. Initially this involved manually counting the number of tests ordered by many providers. Fortunately, experts from the Department of Bioinformatics partnered with the VCWSC to create an automated data collection system that is much more efficient, enabling the committee to quickly collect and analyze data on tests and procedures at Vanderbilt University Medical Center. These data are fed back to participants in various initiatives, and they are used to demonstrate the efficacy of these initiatives to others throughout the medical center, thus garnering trust and encouraging others to participate in VCWSC projects. With enough short‐term wins, the VCWSC hopes to achieve Kotter's ultimate goal, which is to consolidate and institutionalize changes to have a lasting impact.[6]
REDUCING DAILY LABSAN EARLY SUCCESS OF THE VCWSC
One example of the committee's early success is the reduction of routine complete blood counts (CBCs) and basic metabolic panels (BMPs) on internal medicine services, as recommended in the Choosing Wisely top 5 list proposed by the Society of Hospital Medicine. Prior studies on reducing routine labs required interventions like displaying charges at the time of test ordering,[7, 8] using financial incentives,[2, 9] and eliminating the ability to order recurring daily labs.[10] Instead of replicating these efforts, the VCWSC decided to use an educational campaign and real‐time data feedback to focus on the root of the problema culture of overtesting. After obtaining the support of the internal medicine residency program leadership, the VCWSC distributed an evidence‐based flier (see Supporting Information in the online version of this article) summarizing the harms of and misconceptions surrounding excessive lab testing. These data were also presented at housestaff conferences.
Following this initial educational intervention, the VCWSC began tracking the labs ordered for patients on housestaff internal medicine teams to see what proportion have a BMP or CBC drawn each day of their hospitalization. Each week, the teams are sent an email with their lab rate compared to the lab rates of analogous teams. At the end of each month, all internal medicine housestaff and faculty are notified which teams had the lowest lab rate for the month. The VCWSC does not attempt to define an unnecessary lab or offer incentives; the teams are simply reminded that ordering fewer labs can be good for patient care. Since the initiative began, the teams have succeeded in reducing the percentage of patients receiving a CBC and BMP each day from an average of 90% to below 70%.
FUTURE DIRECTIONS
Moving forward, the VCWSC hopes to further engrain the culture of Choosing Wisely into daily practice at Vanderbilt University Medical Center. The labs initiative has expanded to many services including surgery, neurology, and the medical intensive care unit. Other initiatives are focusing on excessive telemetry monitoring and daily chest radiographs in intensive care units. In addition, the VCWSC is collaborating with other AHCs to help them implement their own Choosing Wisely projects.
A CALL FOR MORE HOUSESTAFF CHOOSING WISELY INITIATIVES
Housestaff are perfectly positioned to lead a change in the culture of academic medicine toward high‐value care. The VCWSC has already seen promising results, and we hope that similar initiatives will be created at AHCs across the country. By following John Kotter's recommendations for implementing change and using the Choosing Wisely top 5 lists as a guide, housestaff‐run committees like the VCWSC have the potential to change the culture of medicine at every AHC. If we do not want outside regulators to decide the future of academic medicine, we must find a way to cut down on wasteful spending and unnecessary testing. Residents everywhere, let us choose wisely together.
Acknowledgements
The authors of this study acknowledge the faculty, residents, and medical students who have supported the efforts of the Vanderbilt University Choosing Wisely Steering Committee.
Disclosures: Dr. Brady serves on the board of the ACGME but receives no financial payment other than compensation for travel expenses to board meetings. He also was Chair of the Board for the American Academy on Communication in Healthcare in 2014.
Failure of academic medicine to improve value will undermine professionalism and threaten autonomy because outside forces, such as insurers and regulators, will surely impose change if academic leaders and physicians fail. [1]
The verdict is indoctors order too many tests. This problem is most prominent in academic health centers (AHCs), where the use of testing resources is higher than in community hospitals.[2] Most prior attempts to improve the value of care at AHCs have been driven by faculty and hospital administration in a top‐down fashion with only transient success.[3] We believe that successful and sustainable change should start with the housestaff, who are training in a system afflicted by wasteful overuse of healthcare resources. Therefore, we created a housestaff‐led initiative called the Vanderbilt Choosing Wisely Steering Committee to change the culture of academic medicine. If AHCs are going to start choosing wisely, housestaff must be part of the engine behind the change.
FORMING THE VANDERBILT CHOOSING WISELY STEERING COMMITTEE
The idea for the Vanderbilt Choosing Wisely Steering Committee (VCWSC) was born in December 2013 during a monthly Graduate Medical Education Committee meeting involving housestaff and faculty representatives from multiple subspecialties. At that time, the national Choosing Wisely campaign was in full stride, with more than 50 organizations having proposed top 5 lists of tests and procedures that should be questioned.[4] Several participants at the meeting decided to create a steering committee to integrate these proposals into daily practice at Vanderbilt University Medical Center.
Housestaff have formed the core of the VCWSC from the beginning. The initial members were residents on the Graduate Medical Education Committee, including a fifth‐year radiology resident and a second‐year internal medicine resident who served as the first co‐chairs. More housestaff were recruited by email and word‐of‐mouth. Currently, the committee is composed of residents from the departments of internal medicine, radiology, pediatrics, neurology, anesthesiology, pathology, and general surgery. These residents perform all of the committee's vital functions, including organizing biweekly meetings, brainstorming and carrying out high‐value care initiatives, and recruiting new members. Of course, this committee would not have the authority to create real change without the guidance of numerous faculty supporters, including the designated institutional official and the associate vice chancellor for health affairs. However, we firmly believe that the primary reason this committee has been successful is that it is led by housestaff.
THE IMPORTANCE OF HOUSESTAFF LEADERSHIP
Residents are at the front line of care delivery at academic health centers (AHCs). Innumerable tests and procedures at these institutions are ordered and performed by housestaff. Therefore, culture change in academic medicine will not occur without housestaff culture change. Unfortunately, residents have been shown to have a lower level of competency with regard to high‐value care than more experienced providers.[5] The housestaff‐led VCWSC is uniquely positioned to address this problem by using personal experience and peer‐to‐peer communication to address the fears, biases, and knowledge gaps that cause trainees to waste healthcare resources. Resident members of the VCWSC wrestle daily with the temptation to overtest to avoid missing something or make a rare diagnosis. They are familiar with the systems that encourage overutilization, like shortcuts in ordering software that allow automatically recurring orders. Perhaps most importantly, they are able to discuss high‐value care with other trainees as equals, instead of trying to enforce compliance with a set of restrictions put in place by supervisors.
A SYSTEMATIC STRATEGY FOR EFFECTING CHANGE
To successfully implement high‐value care initiatives, the VCWSC follows a strategy proposed by John Kotter for effecting change in large organizations.[6] According to Kotter, it is critical to create a vision for change, communicate the vision effectively, and empower others to act on the vision. The VCWSC's vision for change is to encourage optimal medical practice by implementing Choosing Wisely top 5 recommendations. To communicate this vision, the VCWSC follows the rhetorical style of the national Choosing Wisely campaign. The American Board of Internal Medicine Foundation researched this rhetoric extensively in the years leading up to the development of the top 5 lists. They found that simply asking providers to judiciously distribute healthcare resources often created a feeling of patient abandonment. Instead, providers are much more likely to respond to messages that encourage wise choices that enhance professional fulfillment, patient well‐being, and the overall quality of care.[4] Therefore, the VCWSC emphasizes these same values in its e‐mails, fliers, and presentations. Importantly, the VCWSC does not directly limit providers abilities to order tests or perform procedures. Instead, the VCWSC uses education and data to empower others to act on the Choosing Wisely vision for high‐value care.
After communicating the vision for change, Kotter recommends sustaining the vision by creating short‐term wins.[6] To demonstrate these wins, the VCWSC collects data on the effects of its initiatives and celebrates the success of individuals and teams through regular widely distributed emails. Initially this involved manually counting the number of tests ordered by many providers. Fortunately, experts from the Department of Bioinformatics partnered with the VCWSC to create an automated data collection system that is much more efficient, enabling the committee to quickly collect and analyze data on tests and procedures at Vanderbilt University Medical Center. These data are fed back to participants in various initiatives, and they are used to demonstrate the efficacy of these initiatives to others throughout the medical center, thus garnering trust and encouraging others to participate in VCWSC projects. With enough short‐term wins, the VCWSC hopes to achieve Kotter's ultimate goal, which is to consolidate and institutionalize changes to have a lasting impact.[6]
REDUCING DAILY LABSAN EARLY SUCCESS OF THE VCWSC
One example of the committee's early success is the reduction of routine complete blood counts (CBCs) and basic metabolic panels (BMPs) on internal medicine services, as recommended in the Choosing Wisely top 5 list proposed by the Society of Hospital Medicine. Prior studies on reducing routine labs required interventions like displaying charges at the time of test ordering,[7, 8] using financial incentives,[2, 9] and eliminating the ability to order recurring daily labs.[10] Instead of replicating these efforts, the VCWSC decided to use an educational campaign and real‐time data feedback to focus on the root of the problema culture of overtesting. After obtaining the support of the internal medicine residency program leadership, the VCWSC distributed an evidence‐based flier (see Supporting Information in the online version of this article) summarizing the harms of and misconceptions surrounding excessive lab testing. These data were also presented at housestaff conferences.
Following this initial educational intervention, the VCWSC began tracking the labs ordered for patients on housestaff internal medicine teams to see what proportion have a BMP or CBC drawn each day of their hospitalization. Each week, the teams are sent an email with their lab rate compared to the lab rates of analogous teams. At the end of each month, all internal medicine housestaff and faculty are notified which teams had the lowest lab rate for the month. The VCWSC does not attempt to define an unnecessary lab or offer incentives; the teams are simply reminded that ordering fewer labs can be good for patient care. Since the initiative began, the teams have succeeded in reducing the percentage of patients receiving a CBC and BMP each day from an average of 90% to below 70%.
FUTURE DIRECTIONS
Moving forward, the VCWSC hopes to further engrain the culture of Choosing Wisely into daily practice at Vanderbilt University Medical Center. The labs initiative has expanded to many services including surgery, neurology, and the medical intensive care unit. Other initiatives are focusing on excessive telemetry monitoring and daily chest radiographs in intensive care units. In addition, the VCWSC is collaborating with other AHCs to help them implement their own Choosing Wisely projects.
A CALL FOR MORE HOUSESTAFF CHOOSING WISELY INITIATIVES
Housestaff are perfectly positioned to lead a change in the culture of academic medicine toward high‐value care. The VCWSC has already seen promising results, and we hope that similar initiatives will be created at AHCs across the country. By following John Kotter's recommendations for implementing change and using the Choosing Wisely top 5 lists as a guide, housestaff‐run committees like the VCWSC have the potential to change the culture of medicine at every AHC. If we do not want outside regulators to decide the future of academic medicine, we must find a way to cut down on wasteful spending and unnecessary testing. Residents everywhere, let us choose wisely together.
Acknowledgements
The authors of this study acknowledge the faculty, residents, and medical students who have supported the efforts of the Vanderbilt University Choosing Wisely Steering Committee.
Disclosures: Dr. Brady serves on the board of the ACGME but receives no financial payment other than compensation for travel expenses to board meetings. He also was Chair of the Board for the American Academy on Communication in Healthcare in 2014.
- , , Teaching value in academic environments. Shifting the ivory tower. JAMA. 2013;310(16):1671–1672.
- , , , , A trial of two strategies to modify the test‐ordering behavior of medical residents. N Engl J Med. 1980;303(23):1330–1336.
- , , , Techniques to improve physicians' use of diagnostic tests: a new conceptual framework. JAMA. 1998;280(23):2020–2027.
- , , Engaging physicians and consumers in conversations about treatment overuse and waste: a short history of the Choosing Wisely campaign. Acad Med. 2014;89(7):990–995.
- , , , , , “Choosing Wisely” in an academic department of medicine [published online June 26, 2014]. Am J Med Qual. doi:10.1177/1062860614540982.
- Leading change; why transformation efforts fail. Harv Bus Rev. 1995;March‐April:57–67.
- , , , et al. Impact of providing fee data on laboratory test ordering: a controlled clinical trial. JAMA Intern Med. 2013;173(10):903–908.
- , , The effect on test ordering of informing physicians of the charges for outpatient diagnostic tests. N Engl J Med. 1990;322(21):1499–1504.
- , , , et al. Targeted reduction in neurosurgical laboratory utilization: resident‐led effort at a single academic institution. J Neurosurg. 2014;120(1):173–177.
- , , , et al. The impact of peer management on test‐ordering behavior. Ann Intern Med. 2004;141(3):196–204.
- , , Teaching value in academic environments. Shifting the ivory tower. JAMA. 2013;310(16):1671–1672.
- , , , , A trial of two strategies to modify the test‐ordering behavior of medical residents. N Engl J Med. 1980;303(23):1330–1336.
- , , , Techniques to improve physicians' use of diagnostic tests: a new conceptual framework. JAMA. 1998;280(23):2020–2027.
- , , Engaging physicians and consumers in conversations about treatment overuse and waste: a short history of the Choosing Wisely campaign. Acad Med. 2014;89(7):990–995.
- , , , , , “Choosing Wisely” in an academic department of medicine [published online June 26, 2014]. Am J Med Qual. doi:10.1177/1062860614540982.
- Leading change; why transformation efforts fail. Harv Bus Rev. 1995;March‐April:57–67.
- , , , et al. Impact of providing fee data on laboratory test ordering: a controlled clinical trial. JAMA Intern Med. 2013;173(10):903–908.
- , , The effect on test ordering of informing physicians of the charges for outpatient diagnostic tests. N Engl J Med. 1990;322(21):1499–1504.
- , , , et al. Targeted reduction in neurosurgical laboratory utilization: resident‐led effort at a single academic institution. J Neurosurg. 2014;120(1):173–177.
- , , , et al. The impact of peer management on test‐ordering behavior. Ann Intern Med. 2004;141(3):196–204.
After Great Recession, women at higher risk of anxiety
Women in the United States were more likely to be diagnosed with anxiety after the Great Recession than during or before the recession, according to Rada K. Dagher, Ph.D., and her associates.
During the recession, the odds ratio for an anxiety diagnosis in women was slightly higher than it was before the downturn, but not by a significant amount. Afterward, the OR nationwide was 1.17. Women living in the Northeast and Midwest were at a significantly higher risk than were women living in the other regions of the country, with ORs of 1.43 and 1.53, respectively. Women who were unemployed or whose household income stood at less than 100% of the federal poverty level also were at a higher risk.
In contrast, depression was less likely during and after the recession in both men and women. Men had a lower risk of an anxiety diagnosis and lower Kessler 6 scores post recession as well. In addition, a low household income and unemployment had little to no effect on mental illness risk, although men living in the Northeast were more likely to suffer from depression post recession, with an OR of 1.17.
“In general, past studies suggest higher vulnerability of men to the negative mental health consequences of economic recessions. However, this may not be the case anymore given the increasingly high labor force participation rate of women and work becoming an important part of the self-identity of the majority of women,” the investigators noted.
Future studies should investigate why depression diagnoses were lower, and whether those findings can be attributed to fewer visits to mental health providers, higher levels of social support, or “more time for exercise and leisure activities,” they wrote.
Find the full study in PLoS ONE (doi: 10.1371/journal.pone.0124103).
Women in the United States were more likely to be diagnosed with anxiety after the Great Recession than during or before the recession, according to Rada K. Dagher, Ph.D., and her associates.
During the recession, the odds ratio for an anxiety diagnosis in women was slightly higher than it was before the downturn, but not by a significant amount. Afterward, the OR nationwide was 1.17. Women living in the Northeast and Midwest were at a significantly higher risk than were women living in the other regions of the country, with ORs of 1.43 and 1.53, respectively. Women who were unemployed or whose household income stood at less than 100% of the federal poverty level also were at a higher risk.
In contrast, depression was less likely during and after the recession in both men and women. Men had a lower risk of an anxiety diagnosis and lower Kessler 6 scores post recession as well. In addition, a low household income and unemployment had little to no effect on mental illness risk, although men living in the Northeast were more likely to suffer from depression post recession, with an OR of 1.17.
“In general, past studies suggest higher vulnerability of men to the negative mental health consequences of economic recessions. However, this may not be the case anymore given the increasingly high labor force participation rate of women and work becoming an important part of the self-identity of the majority of women,” the investigators noted.
Future studies should investigate why depression diagnoses were lower, and whether those findings can be attributed to fewer visits to mental health providers, higher levels of social support, or “more time for exercise and leisure activities,” they wrote.
Find the full study in PLoS ONE (doi: 10.1371/journal.pone.0124103).
Women in the United States were more likely to be diagnosed with anxiety after the Great Recession than during or before the recession, according to Rada K. Dagher, Ph.D., and her associates.
During the recession, the odds ratio for an anxiety diagnosis in women was slightly higher than it was before the downturn, but not by a significant amount. Afterward, the OR nationwide was 1.17. Women living in the Northeast and Midwest were at a significantly higher risk than were women living in the other regions of the country, with ORs of 1.43 and 1.53, respectively. Women who were unemployed or whose household income stood at less than 100% of the federal poverty level also were at a higher risk.
In contrast, depression was less likely during and after the recession in both men and women. Men had a lower risk of an anxiety diagnosis and lower Kessler 6 scores post recession as well. In addition, a low household income and unemployment had little to no effect on mental illness risk, although men living in the Northeast were more likely to suffer from depression post recession, with an OR of 1.17.
“In general, past studies suggest higher vulnerability of men to the negative mental health consequences of economic recessions. However, this may not be the case anymore given the increasingly high labor force participation rate of women and work becoming an important part of the self-identity of the majority of women,” the investigators noted.
Future studies should investigate why depression diagnoses were lower, and whether those findings can be attributed to fewer visits to mental health providers, higher levels of social support, or “more time for exercise and leisure activities,” they wrote.
Find the full study in PLoS ONE (doi: 10.1371/journal.pone.0124103).
Oral cancer survival lower with positive margins, public insurance
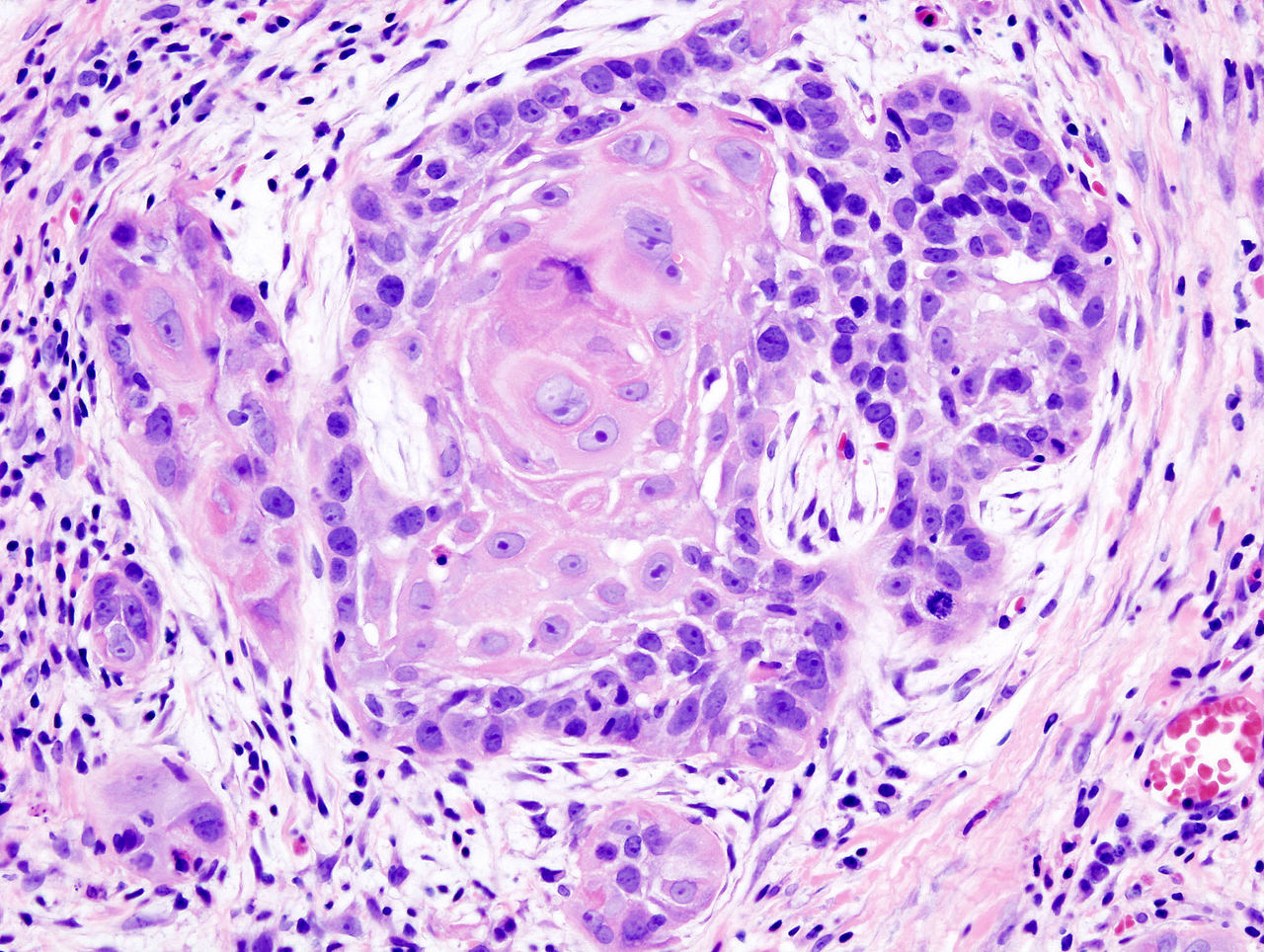
In patients who underwent surgical treatment for stage I or II oral cavity squamous cell cancer, positive tumor margin, the use of radiation or chemotherapy, treatment in a nonacademic facility, and having public health insurance were significantly associated with lower 5-year survival rates, according to a retrospective analysis published online in the JAMA Otolaryngology–Head & Neck Surgery.
The findings suggest that some factors associated with lower 5-year survival rates “may be targets for quality improvement efforts,” wrote Alexander L. Luryi of Yale University, New Haven, Conn., and colleagues.
Seventy percent of 6,830 patients who underwent surgery for stage I or II oral cavity squamous cell cancer (OCSCC) from 2003 to 2006 survived 5 years, according to information from the National Cancer Data Base.
Multivariate analysis showed higher survival rates were significantly associated with neck dissection (hazard ratio, 0.85; P = .003). Lower survival rates were significantly associated with radiation therapy (HR, 1.31; P < .001), chemotherapy (HR, 1.34; P = .03), nonprivate insurance (HR Medicaid, 1.96; HR Medicare, 1.45; P < .001), and nonacademic treatment facility (HR, 1.13; P = .03).
Care at academic centers compared with nonacademic centers was associated with improved survival, possibly due to health care provider expertise, the study authors noted (JAMA Otolaryngol. Head Neck Surg. 2015 May 14 [doi:10.1001/jamaoto.2015.0719]).
Survival rates were lower in patients treated at nonacademic cancer centers, but multivariate analysis showed no association between facility-based case volume and survival. Patients insured through Medicaid and Medicare had significantly lower 5-year survival rates (P < .001 for both). That finding may be the result of inconsistent treatment and follow-up, the investigators said, or worse baseline health among that patient population.
Controversy exists over the relationship between positive margins and outcomes, and the implications for aggressiveness of surgery. The study found positive margins were significantly associated with poorer outcomes, the researchers noted, which supports the use of aggressive surgery in early OCSCC to achieve negative margins.
Radiation and chemotherapy were linked to worse outcomes, and those therapies were possibly indicators of less aggressive resection in localized disease. The analysis could not adjust for potential confounding effects of perineural and lymphovascular invasion, because the information was not recorded in the National Cancer Data Base.
The study indicated a positive impact by neck dissection on survival. Patients with occult neck disease who underwent neck dissection likely would have been restaged to stage III or higher and removed from the early stage sample, the authors explained, which would account for higher survival rates for those remaining. Prospective trials are needed to determine the role of elective neck dissection in early OCSCC, the researchers added.
The William U. Gardner Memorial Research Fund at Yale University supported the study. Dr. Luryi and coauthors reported having no disclosures.
In patients who underwent surgical treatment for stage I or II oral cavity squamous cell cancer, positive tumor margin, the use of radiation or chemotherapy, treatment in a nonacademic facility, and having public health insurance were significantly associated with lower 5-year survival rates, according to a retrospective analysis published online in the JAMA Otolaryngology–Head & Neck Surgery.
The findings suggest that some factors associated with lower 5-year survival rates “may be targets for quality improvement efforts,” wrote Alexander L. Luryi of Yale University, New Haven, Conn., and colleagues.
Seventy percent of 6,830 patients who underwent surgery for stage I or II oral cavity squamous cell cancer (OCSCC) from 2003 to 2006 survived 5 years, according to information from the National Cancer Data Base.
Multivariate analysis showed higher survival rates were significantly associated with neck dissection (hazard ratio, 0.85; P = .003). Lower survival rates were significantly associated with radiation therapy (HR, 1.31; P < .001), chemotherapy (HR, 1.34; P = .03), nonprivate insurance (HR Medicaid, 1.96; HR Medicare, 1.45; P < .001), and nonacademic treatment facility (HR, 1.13; P = .03).
Care at academic centers compared with nonacademic centers was associated with improved survival, possibly due to health care provider expertise, the study authors noted (JAMA Otolaryngol. Head Neck Surg. 2015 May 14 [doi:10.1001/jamaoto.2015.0719]).
Survival rates were lower in patients treated at nonacademic cancer centers, but multivariate analysis showed no association between facility-based case volume and survival. Patients insured through Medicaid and Medicare had significantly lower 5-year survival rates (P < .001 for both). That finding may be the result of inconsistent treatment and follow-up, the investigators said, or worse baseline health among that patient population.
Controversy exists over the relationship between positive margins and outcomes, and the implications for aggressiveness of surgery. The study found positive margins were significantly associated with poorer outcomes, the researchers noted, which supports the use of aggressive surgery in early OCSCC to achieve negative margins.
Radiation and chemotherapy were linked to worse outcomes, and those therapies were possibly indicators of less aggressive resection in localized disease. The analysis could not adjust for potential confounding effects of perineural and lymphovascular invasion, because the information was not recorded in the National Cancer Data Base.
The study indicated a positive impact by neck dissection on survival. Patients with occult neck disease who underwent neck dissection likely would have been restaged to stage III or higher and removed from the early stage sample, the authors explained, which would account for higher survival rates for those remaining. Prospective trials are needed to determine the role of elective neck dissection in early OCSCC, the researchers added.
The William U. Gardner Memorial Research Fund at Yale University supported the study. Dr. Luryi and coauthors reported having no disclosures.
In patients who underwent surgical treatment for stage I or II oral cavity squamous cell cancer, positive tumor margin, the use of radiation or chemotherapy, treatment in a nonacademic facility, and having public health insurance were significantly associated with lower 5-year survival rates, according to a retrospective analysis published online in the JAMA Otolaryngology–Head & Neck Surgery.
The findings suggest that some factors associated with lower 5-year survival rates “may be targets for quality improvement efforts,” wrote Alexander L. Luryi of Yale University, New Haven, Conn., and colleagues.
Seventy percent of 6,830 patients who underwent surgery for stage I or II oral cavity squamous cell cancer (OCSCC) from 2003 to 2006 survived 5 years, according to information from the National Cancer Data Base.
Multivariate analysis showed higher survival rates were significantly associated with neck dissection (hazard ratio, 0.85; P = .003). Lower survival rates were significantly associated with radiation therapy (HR, 1.31; P < .001), chemotherapy (HR, 1.34; P = .03), nonprivate insurance (HR Medicaid, 1.96; HR Medicare, 1.45; P < .001), and nonacademic treatment facility (HR, 1.13; P = .03).
Care at academic centers compared with nonacademic centers was associated with improved survival, possibly due to health care provider expertise, the study authors noted (JAMA Otolaryngol. Head Neck Surg. 2015 May 14 [doi:10.1001/jamaoto.2015.0719]).
Survival rates were lower in patients treated at nonacademic cancer centers, but multivariate analysis showed no association between facility-based case volume and survival. Patients insured through Medicaid and Medicare had significantly lower 5-year survival rates (P < .001 for both). That finding may be the result of inconsistent treatment and follow-up, the investigators said, or worse baseline health among that patient population.
Controversy exists over the relationship between positive margins and outcomes, and the implications for aggressiveness of surgery. The study found positive margins were significantly associated with poorer outcomes, the researchers noted, which supports the use of aggressive surgery in early OCSCC to achieve negative margins.
Radiation and chemotherapy were linked to worse outcomes, and those therapies were possibly indicators of less aggressive resection in localized disease. The analysis could not adjust for potential confounding effects of perineural and lymphovascular invasion, because the information was not recorded in the National Cancer Data Base.
The study indicated a positive impact by neck dissection on survival. Patients with occult neck disease who underwent neck dissection likely would have been restaged to stage III or higher and removed from the early stage sample, the authors explained, which would account for higher survival rates for those remaining. Prospective trials are needed to determine the role of elective neck dissection in early OCSCC, the researchers added.
The William U. Gardner Memorial Research Fund at Yale University supported the study. Dr. Luryi and coauthors reported having no disclosures.
FROM JAMA OTOLARYNGOLOGY–HEAD & NECK SURGERY
Key clinical point: Treatment factors such as neck dissection, tumor margins, type of insurance, and health care facility impact 5-year survival after surgery for early stage oral cavity cancer.
Major finding: Radiation, chemotherapy, positive tumor margin, nonacademic facility, and nonprivate insurance were significantly associated with lower 5-year survival.
Data source: Retrospective study of 6,830 patients in National Cancer Data Base who underwent surgery to treat stage I or II oral cavity squamous cell cancer.
Disclosures: The William U. Gardner Memorial Research Fund at Yale University supported the study. Dr. Luryi and coauthors reported having no disclosures.
Focus on Seizures
Seizure Safety Tips
Nicotinamide cuts rate of nonmelanoma skin cancer in those at high risk
Nicotinamide, an inexpensive, over-the-counter form of vitamin B3, is safe and efficacious for the chemoprevention of nonmelanoma skin cancer in patients at high risk, according to data from the Australian Oral Nicotinamide to Reduce Actinic Cancer (ONTRAC) Study.
Results reported in a press briefing held before the annual meeting of the American Society of Clinical Oncology showed that patients taking nicotinamide were about one-fourth less likely than peers taking a placebo to develop new basal cell and squamous cell skin cancers. They also had a smaller reduction in new actinic keratoses.
“Nicotinamide, vitamin B3, significantly reduced nonmelanoma skin cancers and keratoses in just 12 months in a group of pretty high-risk patients. It’s safe, it’s almost obscenely inexpensive, and it’s already widely commercially available, so this one’s ready to go straight into the clinic,” commented senior investigator Dr. Diona Damian, professor of dermatology at the University of Sydney.
She cautioned that the results apply only to the population studied: adults who had experienced two or more nonmelanoma skin cancers in the past 5 years.
“These are the people we’d be recommending it for – people who have already got a skin cancer track record. It’s not something that we’d recommend at this stage for the general population,” she said. Likewise, the findings do not speak to patients at the other end of the spectrum who are in treatment for advanced or metastatic skin cancer, as they also were excluded.
That said, the researchers are planning additional studies in other populations, such patients who are at high risk because they have immunosuppression, according to Dr. Damian.
“We still need the overall skin cancer prevention strategies of sun-safe behavior, sunscreen, and regular skin surveillance,” she stressed, “but we now have an additional exciting opportunity for affordable skin cancer chemoprevention which we can instantly translate into clinical practice.”
Dr. Peter Paul Yu, ASCO President and a medical oncologist and hematologist who is director of cancer research at the Palo Alto Medical Foundation, Sunnyvale, Calif., commented, “This is a very exciting prevention trial. We all know that we clamor for preventing rather than treating diseases, and this is a major advance for us.”
Exposure to ultraviolet light packs a one-two punch to the skin, both damaging cellular DNA and suppressing the skin’s immune response, according to Dr. Damian. The investigators opted to test nicotinamide as it counters both of these events.
The 386 patients in ONTRAC had heavily sun damaged skin, with a mean of 8 nonmelanoma skin cancers in the past 5 years and 50 keratoses at baseline. They were randomized evenly to receive nicotinamide (500 mg twice daily) or placebo for 12 months.
Results showed that the average number of new nonmelanoma skin cancers per patient during the treatment period was 1.77 in the nicotinamide group and 2.42 in the placebo group. The difference translated to a 23% lower rate of new cancers with the vitamin.
“There were comparable reductions seen for both basal and squamous cell carcinomas,” Dr. Damian noted. “Interestingly, this reduction in skin cancers seemed to start as early as the first 3-month visit. And then when people stopped taking their tablets after 12 months, the benefit was no longer seen. In other words, you need to continue taking the tablets in order for them to be effective.”
The nicotinamide group also had a roughly 15% lower rate of new actinic keratoses, compared with the placebo group.
“Nicotinamide was very well tolerated. There was no difference in adverse events, blood parameters, or blood pressure in the two arms” of the study, reported Dr. Damian. She stressed that it is critically important to distinguish nicotinamide from niacin (nicotinic acid), another form of vitamin B3 that has a host of side effects such as headache and flushing.
“One of the great things about [nicotinamide] is that it really has hardly any drug interactions, which means that elderly patients who may be taking a whole cocktail of medications for their heart disease and their hypertension, and whatever else, the nicotinamide won’t interact with those,” she added.
Some evidence also has shown nonsteroidal anti-inflammatory drugs to reduce the risk of skin cancer. “The advantage of nicotinamide is that it doesn’t have the potential gastrointestinal bleeding or renal side effects of nonsteroidals, so it may be suitable for a group of people who aren’t suitable for taking nonsteroidals,” she said. “In our ONTRAC study, we didn’t find synergy or additional benefit in people who were coincidentally taking nonsteroidals for other indications.”
The trial’s results should be generalizable to similar high-risk patients in less sunny parts of the world, Dr. Damian said. “If their skin has shown that degree of damage to get skin cancer, then we suspect nicotinamide would offer benefits to them as well.”
Dr. Damian disclosed no relevant conflicts of interest. The study was funded by the National Health & Medical Research Council.
Nicotinamide, an inexpensive, over-the-counter form of vitamin B3, is safe and efficacious for the chemoprevention of nonmelanoma skin cancer in patients at high risk, according to data from the Australian Oral Nicotinamide to Reduce Actinic Cancer (ONTRAC) Study.
Results reported in a press briefing held before the annual meeting of the American Society of Clinical Oncology showed that patients taking nicotinamide were about one-fourth less likely than peers taking a placebo to develop new basal cell and squamous cell skin cancers. They also had a smaller reduction in new actinic keratoses.
“Nicotinamide, vitamin B3, significantly reduced nonmelanoma skin cancers and keratoses in just 12 months in a group of pretty high-risk patients. It’s safe, it’s almost obscenely inexpensive, and it’s already widely commercially available, so this one’s ready to go straight into the clinic,” commented senior investigator Dr. Diona Damian, professor of dermatology at the University of Sydney.
She cautioned that the results apply only to the population studied: adults who had experienced two or more nonmelanoma skin cancers in the past 5 years.
“These are the people we’d be recommending it for – people who have already got a skin cancer track record. It’s not something that we’d recommend at this stage for the general population,” she said. Likewise, the findings do not speak to patients at the other end of the spectrum who are in treatment for advanced or metastatic skin cancer, as they also were excluded.
That said, the researchers are planning additional studies in other populations, such patients who are at high risk because they have immunosuppression, according to Dr. Damian.
“We still need the overall skin cancer prevention strategies of sun-safe behavior, sunscreen, and regular skin surveillance,” she stressed, “but we now have an additional exciting opportunity for affordable skin cancer chemoprevention which we can instantly translate into clinical practice.”
Dr. Peter Paul Yu, ASCO President and a medical oncologist and hematologist who is director of cancer research at the Palo Alto Medical Foundation, Sunnyvale, Calif., commented, “This is a very exciting prevention trial. We all know that we clamor for preventing rather than treating diseases, and this is a major advance for us.”
Exposure to ultraviolet light packs a one-two punch to the skin, both damaging cellular DNA and suppressing the skin’s immune response, according to Dr. Damian. The investigators opted to test nicotinamide as it counters both of these events.
The 386 patients in ONTRAC had heavily sun damaged skin, with a mean of 8 nonmelanoma skin cancers in the past 5 years and 50 keratoses at baseline. They were randomized evenly to receive nicotinamide (500 mg twice daily) or placebo for 12 months.
Results showed that the average number of new nonmelanoma skin cancers per patient during the treatment period was 1.77 in the nicotinamide group and 2.42 in the placebo group. The difference translated to a 23% lower rate of new cancers with the vitamin.
“There were comparable reductions seen for both basal and squamous cell carcinomas,” Dr. Damian noted. “Interestingly, this reduction in skin cancers seemed to start as early as the first 3-month visit. And then when people stopped taking their tablets after 12 months, the benefit was no longer seen. In other words, you need to continue taking the tablets in order for them to be effective.”
The nicotinamide group also had a roughly 15% lower rate of new actinic keratoses, compared with the placebo group.
“Nicotinamide was very well tolerated. There was no difference in adverse events, blood parameters, or blood pressure in the two arms” of the study, reported Dr. Damian. She stressed that it is critically important to distinguish nicotinamide from niacin (nicotinic acid), another form of vitamin B3 that has a host of side effects such as headache and flushing.
“One of the great things about [nicotinamide] is that it really has hardly any drug interactions, which means that elderly patients who may be taking a whole cocktail of medications for their heart disease and their hypertension, and whatever else, the nicotinamide won’t interact with those,” she added.
Some evidence also has shown nonsteroidal anti-inflammatory drugs to reduce the risk of skin cancer. “The advantage of nicotinamide is that it doesn’t have the potential gastrointestinal bleeding or renal side effects of nonsteroidals, so it may be suitable for a group of people who aren’t suitable for taking nonsteroidals,” she said. “In our ONTRAC study, we didn’t find synergy or additional benefit in people who were coincidentally taking nonsteroidals for other indications.”
The trial’s results should be generalizable to similar high-risk patients in less sunny parts of the world, Dr. Damian said. “If their skin has shown that degree of damage to get skin cancer, then we suspect nicotinamide would offer benefits to them as well.”
Dr. Damian disclosed no relevant conflicts of interest. The study was funded by the National Health & Medical Research Council.
Nicotinamide, an inexpensive, over-the-counter form of vitamin B3, is safe and efficacious for the chemoprevention of nonmelanoma skin cancer in patients at high risk, according to data from the Australian Oral Nicotinamide to Reduce Actinic Cancer (ONTRAC) Study.
Results reported in a press briefing held before the annual meeting of the American Society of Clinical Oncology showed that patients taking nicotinamide were about one-fourth less likely than peers taking a placebo to develop new basal cell and squamous cell skin cancers. They also had a smaller reduction in new actinic keratoses.
“Nicotinamide, vitamin B3, significantly reduced nonmelanoma skin cancers and keratoses in just 12 months in a group of pretty high-risk patients. It’s safe, it’s almost obscenely inexpensive, and it’s already widely commercially available, so this one’s ready to go straight into the clinic,” commented senior investigator Dr. Diona Damian, professor of dermatology at the University of Sydney.
She cautioned that the results apply only to the population studied: adults who had experienced two or more nonmelanoma skin cancers in the past 5 years.
“These are the people we’d be recommending it for – people who have already got a skin cancer track record. It’s not something that we’d recommend at this stage for the general population,” she said. Likewise, the findings do not speak to patients at the other end of the spectrum who are in treatment for advanced or metastatic skin cancer, as they also were excluded.
That said, the researchers are planning additional studies in other populations, such patients who are at high risk because they have immunosuppression, according to Dr. Damian.
“We still need the overall skin cancer prevention strategies of sun-safe behavior, sunscreen, and regular skin surveillance,” she stressed, “but we now have an additional exciting opportunity for affordable skin cancer chemoprevention which we can instantly translate into clinical practice.”
Dr. Peter Paul Yu, ASCO President and a medical oncologist and hematologist who is director of cancer research at the Palo Alto Medical Foundation, Sunnyvale, Calif., commented, “This is a very exciting prevention trial. We all know that we clamor for preventing rather than treating diseases, and this is a major advance for us.”
Exposure to ultraviolet light packs a one-two punch to the skin, both damaging cellular DNA and suppressing the skin’s immune response, according to Dr. Damian. The investigators opted to test nicotinamide as it counters both of these events.
The 386 patients in ONTRAC had heavily sun damaged skin, with a mean of 8 nonmelanoma skin cancers in the past 5 years and 50 keratoses at baseline. They were randomized evenly to receive nicotinamide (500 mg twice daily) or placebo for 12 months.
Results showed that the average number of new nonmelanoma skin cancers per patient during the treatment period was 1.77 in the nicotinamide group and 2.42 in the placebo group. The difference translated to a 23% lower rate of new cancers with the vitamin.
“There were comparable reductions seen for both basal and squamous cell carcinomas,” Dr. Damian noted. “Interestingly, this reduction in skin cancers seemed to start as early as the first 3-month visit. And then when people stopped taking their tablets after 12 months, the benefit was no longer seen. In other words, you need to continue taking the tablets in order for them to be effective.”
The nicotinamide group also had a roughly 15% lower rate of new actinic keratoses, compared with the placebo group.
“Nicotinamide was very well tolerated. There was no difference in adverse events, blood parameters, or blood pressure in the two arms” of the study, reported Dr. Damian. She stressed that it is critically important to distinguish nicotinamide from niacin (nicotinic acid), another form of vitamin B3 that has a host of side effects such as headache and flushing.
“One of the great things about [nicotinamide] is that it really has hardly any drug interactions, which means that elderly patients who may be taking a whole cocktail of medications for their heart disease and their hypertension, and whatever else, the nicotinamide won’t interact with those,” she added.
Some evidence also has shown nonsteroidal anti-inflammatory drugs to reduce the risk of skin cancer. “The advantage of nicotinamide is that it doesn’t have the potential gastrointestinal bleeding or renal side effects of nonsteroidals, so it may be suitable for a group of people who aren’t suitable for taking nonsteroidals,” she said. “In our ONTRAC study, we didn’t find synergy or additional benefit in people who were coincidentally taking nonsteroidals for other indications.”
The trial’s results should be generalizable to similar high-risk patients in less sunny parts of the world, Dr. Damian said. “If their skin has shown that degree of damage to get skin cancer, then we suspect nicotinamide would offer benefits to them as well.”
Dr. Damian disclosed no relevant conflicts of interest. The study was funded by the National Health & Medical Research Council.
FROM THE ASCO 2015 PRESSCAST
Key clinical point: Nicotinamide, an inexpensive oral vitamin, protects against nonmelanoma skin cancer in patients at high risk.
Major finding: Patients taking nicotinamide had a 23% lower rate of new basal cell and squamous cell carcinomas.
Data source: A randomized, placebo-controlled phase III trial among 386 patients with past nonmelanoma skin cancers.
Disclosures: Dr. Damian disclosed no relevant conflicts of interest. The study was funded by the National Health & Medical Research Council.
Managing open wounds in ob.gyn.
Negative pressure wound therapy is a wound management system for chronic open subcutaneous or intra-abdominal wounds. Some popular commercial systems include V.A.C. therapy (KCI, San Antonio) and the Chariker-Jeter wound-sealing kit (Smith and Nephew, London). Within ob.gyn. and gynecologic oncology, they have use in the management of postoperative superficial wound dehiscence from routine surgery and in the management of the open abdomen.
The primary benefit of negative pressure wound therapy (NPWT) is the acceleration of wound healing. Postoperative superficial wound dehiscence can occur as a result of surgical factors such as wound infection and subcutaneous seroma/hematoma or systematic factors such as poor nutrition and wound ischemia.
Acceleration of wound healing results from the design of the NPWT systems. They consist of semipermeable dressings (foam), sealed with an adhesive sheet that is connected to a portable pump. By the application of –50 to –175 mm Hg of continuous or intermittent suction, the edges of the wound are drawn together, and this deforming process promotes tissue remodeling at the cellular level. Other potential benefits of negative pressure are increased blood flow, a decrease in mediators of inflammation, and an increase in collagen organization via changes in wound biochemistry.

An alternative to NPWT would be traditional gauze dressings, which can also be applied in the case of superficial wound dehiscence. These are changed up to three times a day, however, and this can result in significant patient discomfort, caregiver difficulties, and prolonged healing of weeks to months. In contrast, NPWT dressings are changed once every 2-3 days. They are also versatile and can be fit to traditionally shaped abdominal wounds, as well as difficult to dress vulvar and groin wounds (J. Obstet. Gynaecol. Can. 2011;33:1031-7).
In a series of 27 gynecologic oncology patients in whom NPWT was employed after primary wound–healing failure, there was a 96% reduction in the size of the wounds with a median number of therapy days of 32 (range, 3-88). The majority of these patients were also managed as outpatients without complication (Gynecol. Oncol. 2004;92:586-91).
There are some contraindications to NPWT that should be considered. The major, and perhaps most common, is an ongoing wound infection.
A wound that needs to be evaluated at least daily to assess the response to antibiotic therapy or need for debridement should not be managed with NPWT until the wound is deemed stable. There should be no devitalized tissue present in the wound upon application of the NPWT. If any necrotic tissue is present, then wound debridement is warranted until only well-vascularized tissue remains.
Another contraindication is the presence of malignant tissue in the wound. Negative pressure can promote this tissue growth and lead to chronic nonhealing. Other considerations would include adhesive allergies and fragile skin due to chronic steroid use or collagen vascular disorders, as NPWT can lead to skin necrosis.

Finally, the involvement of vital organs, such as exposed bowel, is a contraindication to the NPWT systems, as constant suction can promote fistula formation or hemorrhage. However, in the setting of an open abdomen after trauma surgery, there has been the development of intra-abdominal wound management systems that may be appropriate.
Although rare in obstetrics, gynecology, and gynecologic oncology, delayed abdominal closure may be necessary. This can occur after reoperation for bowel injury, in cases where bowel wall edema and increased intra-abdominal pressure preclude closure, or in cases of massive hemorrhage (for example, ruptured ectopic pregnancy) where patient instability necessitates rapid termination of the surgical case. These wounds can be managed with temporary abdominal closure techniques such as retention sutures, a Bogota bag, or loose packing (World. J. Surg. 2015; 39: 912-25).
The negative pressure systems developed for these instances are the V.A.C. abdominal dressing (KCI), Renasys NPWT (Smith and Nephew), and ABThera open abdomen negative pressure therapy (KCI). They consist of a perforated plastic sheet with foam attachments that is placed directly in the abdomen to cover the intestine. This is then covered with an adhesive dressing that is cut to accommodate the suction attachment for the negative pressure pump. This setup is easily applied and taken down, and therefore facilitates frequent abdominal washouts until true facial closure can be achieved.
There are many benefits to NPWT for the management of superficial and deep wound dehiscence in the ob.gyn. or gynecologic oncology patient. NPWT should be considered primarily with any surgical wound healing by secondary intention.
Dr. Doll is a third-year fellow in gynecologic oncology at the University of North Carolina at Chapel Hill. Dr. Gehrig is professor and director of gynecologic oncology at the university. The authors reported having no relevant financial disclosures.
Negative pressure wound therapy is a wound management system for chronic open subcutaneous or intra-abdominal wounds. Some popular commercial systems include V.A.C. therapy (KCI, San Antonio) and the Chariker-Jeter wound-sealing kit (Smith and Nephew, London). Within ob.gyn. and gynecologic oncology, they have use in the management of postoperative superficial wound dehiscence from routine surgery and in the management of the open abdomen.
The primary benefit of negative pressure wound therapy (NPWT) is the acceleration of wound healing. Postoperative superficial wound dehiscence can occur as a result of surgical factors such as wound infection and subcutaneous seroma/hematoma or systematic factors such as poor nutrition and wound ischemia.
Acceleration of wound healing results from the design of the NPWT systems. They consist of semipermeable dressings (foam), sealed with an adhesive sheet that is connected to a portable pump. By the application of –50 to –175 mm Hg of continuous or intermittent suction, the edges of the wound are drawn together, and this deforming process promotes tissue remodeling at the cellular level. Other potential benefits of negative pressure are increased blood flow, a decrease in mediators of inflammation, and an increase in collagen organization via changes in wound biochemistry.
An alternative to NPWT would be traditional gauze dressings, which can also be applied in the case of superficial wound dehiscence. These are changed up to three times a day, however, and this can result in significant patient discomfort, caregiver difficulties, and prolonged healing of weeks to months. In contrast, NPWT dressings are changed once every 2-3 days. They are also versatile and can be fit to traditionally shaped abdominal wounds, as well as difficult to dress vulvar and groin wounds (J. Obstet. Gynaecol. Can. 2011;33:1031-7).
In a series of 27 gynecologic oncology patients in whom NPWT was employed after primary wound–healing failure, there was a 96% reduction in the size of the wounds with a median number of therapy days of 32 (range, 3-88). The majority of these patients were also managed as outpatients without complication (Gynecol. Oncol. 2004;92:586-91).
There are some contraindications to NPWT that should be considered. The major, and perhaps most common, is an ongoing wound infection.
A wound that needs to be evaluated at least daily to assess the response to antibiotic therapy or need for debridement should not be managed with NPWT until the wound is deemed stable. There should be no devitalized tissue present in the wound upon application of the NPWT. If any necrotic tissue is present, then wound debridement is warranted until only well-vascularized tissue remains.
Another contraindication is the presence of malignant tissue in the wound. Negative pressure can promote this tissue growth and lead to chronic nonhealing. Other considerations would include adhesive allergies and fragile skin due to chronic steroid use or collagen vascular disorders, as NPWT can lead to skin necrosis.
Finally, the involvement of vital organs, such as exposed bowel, is a contraindication to the NPWT systems, as constant suction can promote fistula formation or hemorrhage. However, in the setting of an open abdomen after trauma surgery, there has been the development of intra-abdominal wound management systems that may be appropriate.
Although rare in obstetrics, gynecology, and gynecologic oncology, delayed abdominal closure may be necessary. This can occur after reoperation for bowel injury, in cases where bowel wall edema and increased intra-abdominal pressure preclude closure, or in cases of massive hemorrhage (for example, ruptured ectopic pregnancy) where patient instability necessitates rapid termination of the surgical case. These wounds can be managed with temporary abdominal closure techniques such as retention sutures, a Bogota bag, or loose packing (World. J. Surg. 2015; 39: 912-25).
The negative pressure systems developed for these instances are the V.A.C. abdominal dressing (KCI), Renasys NPWT (Smith and Nephew), and ABThera open abdomen negative pressure therapy (KCI). They consist of a perforated plastic sheet with foam attachments that is placed directly in the abdomen to cover the intestine. This is then covered with an adhesive dressing that is cut to accommodate the suction attachment for the negative pressure pump. This setup is easily applied and taken down, and therefore facilitates frequent abdominal washouts until true facial closure can be achieved.
There are many benefits to NPWT for the management of superficial and deep wound dehiscence in the ob.gyn. or gynecologic oncology patient. NPWT should be considered primarily with any surgical wound healing by secondary intention.
Dr. Doll is a third-year fellow in gynecologic oncology at the University of North Carolina at Chapel Hill. Dr. Gehrig is professor and director of gynecologic oncology at the university. The authors reported having no relevant financial disclosures.
Negative pressure wound therapy is a wound management system for chronic open subcutaneous or intra-abdominal wounds. Some popular commercial systems include V.A.C. therapy (KCI, San Antonio) and the Chariker-Jeter wound-sealing kit (Smith and Nephew, London). Within ob.gyn. and gynecologic oncology, they have use in the management of postoperative superficial wound dehiscence from routine surgery and in the management of the open abdomen.
The primary benefit of negative pressure wound therapy (NPWT) is the acceleration of wound healing. Postoperative superficial wound dehiscence can occur as a result of surgical factors such as wound infection and subcutaneous seroma/hematoma or systematic factors such as poor nutrition and wound ischemia.
Acceleration of wound healing results from the design of the NPWT systems. They consist of semipermeable dressings (foam), sealed with an adhesive sheet that is connected to a portable pump. By the application of –50 to –175 mm Hg of continuous or intermittent suction, the edges of the wound are drawn together, and this deforming process promotes tissue remodeling at the cellular level. Other potential benefits of negative pressure are increased blood flow, a decrease in mediators of inflammation, and an increase in collagen organization via changes in wound biochemistry.
An alternative to NPWT would be traditional gauze dressings, which can also be applied in the case of superficial wound dehiscence. These are changed up to three times a day, however, and this can result in significant patient discomfort, caregiver difficulties, and prolonged healing of weeks to months. In contrast, NPWT dressings are changed once every 2-3 days. They are also versatile and can be fit to traditionally shaped abdominal wounds, as well as difficult to dress vulvar and groin wounds (J. Obstet. Gynaecol. Can. 2011;33:1031-7).
In a series of 27 gynecologic oncology patients in whom NPWT was employed after primary wound–healing failure, there was a 96% reduction in the size of the wounds with a median number of therapy days of 32 (range, 3-88). The majority of these patients were also managed as outpatients without complication (Gynecol. Oncol. 2004;92:586-91).
There are some contraindications to NPWT that should be considered. The major, and perhaps most common, is an ongoing wound infection.
A wound that needs to be evaluated at least daily to assess the response to antibiotic therapy or need for debridement should not be managed with NPWT until the wound is deemed stable. There should be no devitalized tissue present in the wound upon application of the NPWT. If any necrotic tissue is present, then wound debridement is warranted until only well-vascularized tissue remains.
Another contraindication is the presence of malignant tissue in the wound. Negative pressure can promote this tissue growth and lead to chronic nonhealing. Other considerations would include adhesive allergies and fragile skin due to chronic steroid use or collagen vascular disorders, as NPWT can lead to skin necrosis.
Finally, the involvement of vital organs, such as exposed bowel, is a contraindication to the NPWT systems, as constant suction can promote fistula formation or hemorrhage. However, in the setting of an open abdomen after trauma surgery, there has been the development of intra-abdominal wound management systems that may be appropriate.
Although rare in obstetrics, gynecology, and gynecologic oncology, delayed abdominal closure may be necessary. This can occur after reoperation for bowel injury, in cases where bowel wall edema and increased intra-abdominal pressure preclude closure, or in cases of massive hemorrhage (for example, ruptured ectopic pregnancy) where patient instability necessitates rapid termination of the surgical case. These wounds can be managed with temporary abdominal closure techniques such as retention sutures, a Bogota bag, or loose packing (World. J. Surg. 2015; 39: 912-25).
The negative pressure systems developed for these instances are the V.A.C. abdominal dressing (KCI), Renasys NPWT (Smith and Nephew), and ABThera open abdomen negative pressure therapy (KCI). They consist of a perforated plastic sheet with foam attachments that is placed directly in the abdomen to cover the intestine. This is then covered with an adhesive dressing that is cut to accommodate the suction attachment for the negative pressure pump. This setup is easily applied and taken down, and therefore facilitates frequent abdominal washouts until true facial closure can be achieved.
There are many benefits to NPWT for the management of superficial and deep wound dehiscence in the ob.gyn. or gynecologic oncology patient. NPWT should be considered primarily with any surgical wound healing by secondary intention.
Dr. Doll is a third-year fellow in gynecologic oncology at the University of North Carolina at Chapel Hill. Dr. Gehrig is professor and director of gynecologic oncology at the university. The authors reported having no relevant financial disclosures.

Adding mAb to treatment extends PFS in MM

Photo by Linda Bartlett
The monoclonal antibody (mAb) elotuzumab may be a useful addition to the multiple myeloma (MM) arsenal, according to investigators involved in the phase 3 ELOQUENT-2 trial.
The trial showed that adding elotuzumab to treatment with lenalidomide and dexamethasone extended progression-free survival (PFS) in relapsed MM patients by about 5 months, on average, when compared to treatment with just lenalidomide and dexamethasone.
“It appears that, for patients with relapsed multiple myeloma who would otherwise be offered lenalidomide and dexamethasone, addition of this new targeted drug makes the outcomes even better,” said study investigator Sagar Lonial, MD, of Emory University in Atlanta, Georgia.
Dr Lonial presented data from ELOQUENT-2 at a presscast in advance of the 2015 ASCO Annual Meeting. Full data from the study will be presented at the meeting on June 2 as abstract 8508.
The study was funded by Bristol-Myers Squibb and AbbVie, the companies developing elotuzumab.
Dr Lonial explained that elotuzumab attaches to the cell surface protein SLAMF7, which is found on MM cells and natural killer (NK) cells. Scientists believe that elotuzumab mounts a 2-pronged attack on MM by targeting myeloma cells directly and by enhancing NK cells’ ability to kill myeloma cells.
In ELOQUENT-2, 646 patients with recurrent MM were randomized to receive elotuzumab plus lenalidomide and dexamethasone or only lenalidomide and dexamethasone (control).
The patients’ median age was 66. They had failed 1 to 3 prior treatments, and 35% of them were refractory to their last therapy. Thirty-two percent of patients had del(17p), and 9% had t[4;14].
At a median follow-up of 24 months, elotuzumab had reduced the risk of MM progression and death by 30%. Patients in the elotuzumab arm had significantly longer PFS than patients in the control arm—a median of 19.4 months and 14.9 months, respectively (P=0.0004).
The 1-year PFS was 68% in the elotuzumab arm and 57% in the control arm. The 2-year PFS was 41% and 27%, respectively. Dr Lonial pointed out that, unlike some other therapies, elotuzumab continued to improve PFS over time.
“[T]he idea of the maintenance of benefit over time really speaks to the power of an immune-based approach when we treat cancer,” he said.
“Patients who received elotuzumab had a longer duration of remission [and] a higher overall response rate, and this improvement in clinical parameters occurred without a significant increase in adverse events or toxicity. In fact, there was no reduction in quality of life for [patients in the] 3-drug arm.”
Mild infusion reactions occurred after the first few doses in 10% of patients who received elotuzumab. Most of these reactions were grade 1 or 2.
Common grade 3-4 adverse events (occurring in ≥ 15% of patients) in both the elotuzumab and control arms were neutropenia (25% and 33%, respectively) and anemia (15% and 16%, respectively).
In all, 210 patients died, 94 in the elotuzumab arm and 116 in the control arm.
“Based on this randomized, phase 3 trial, we hope that we will soon have a new treatment option for patients with relapsed or refractory myeloma . . . ,” Dr Lonial said.
The US Food and Drug Administration has already granted elotuzumab breakthrough therapy designation to treat MM patients who have received at least 1 prior therapy. ![]()
Photo by Linda Bartlett
The monoclonal antibody (mAb) elotuzumab may be a useful addition to the multiple myeloma (MM) arsenal, according to investigators involved in the phase 3 ELOQUENT-2 trial.
The trial showed that adding elotuzumab to treatment with lenalidomide and dexamethasone extended progression-free survival (PFS) in relapsed MM patients by about 5 months, on average, when compared to treatment with just lenalidomide and dexamethasone.
“It appears that, for patients with relapsed multiple myeloma who would otherwise be offered lenalidomide and dexamethasone, addition of this new targeted drug makes the outcomes even better,” said study investigator Sagar Lonial, MD, of Emory University in Atlanta, Georgia.
Dr Lonial presented data from ELOQUENT-2 at a presscast in advance of the 2015 ASCO Annual Meeting. Full data from the study will be presented at the meeting on June 2 as abstract 8508.
The study was funded by Bristol-Myers Squibb and AbbVie, the companies developing elotuzumab.
Dr Lonial explained that elotuzumab attaches to the cell surface protein SLAMF7, which is found on MM cells and natural killer (NK) cells. Scientists believe that elotuzumab mounts a 2-pronged attack on MM by targeting myeloma cells directly and by enhancing NK cells’ ability to kill myeloma cells.
In ELOQUENT-2, 646 patients with recurrent MM were randomized to receive elotuzumab plus lenalidomide and dexamethasone or only lenalidomide and dexamethasone (control).
The patients’ median age was 66. They had failed 1 to 3 prior treatments, and 35% of them were refractory to their last therapy. Thirty-two percent of patients had del(17p), and 9% had t[4;14].
At a median follow-up of 24 months, elotuzumab had reduced the risk of MM progression and death by 30%. Patients in the elotuzumab arm had significantly longer PFS than patients in the control arm—a median of 19.4 months and 14.9 months, respectively (P=0.0004).
The 1-year PFS was 68% in the elotuzumab arm and 57% in the control arm. The 2-year PFS was 41% and 27%, respectively. Dr Lonial pointed out that, unlike some other therapies, elotuzumab continued to improve PFS over time.
“[T]he idea of the maintenance of benefit over time really speaks to the power of an immune-based approach when we treat cancer,” he said.
“Patients who received elotuzumab had a longer duration of remission [and] a higher overall response rate, and this improvement in clinical parameters occurred without a significant increase in adverse events or toxicity. In fact, there was no reduction in quality of life for [patients in the] 3-drug arm.”
Mild infusion reactions occurred after the first few doses in 10% of patients who received elotuzumab. Most of these reactions were grade 1 or 2.
Common grade 3-4 adverse events (occurring in ≥ 15% of patients) in both the elotuzumab and control arms were neutropenia (25% and 33%, respectively) and anemia (15% and 16%, respectively).
In all, 210 patients died, 94 in the elotuzumab arm and 116 in the control arm.
“Based on this randomized, phase 3 trial, we hope that we will soon have a new treatment option for patients with relapsed or refractory myeloma . . . ,” Dr Lonial said.
The US Food and Drug Administration has already granted elotuzumab breakthrough therapy designation to treat MM patients who have received at least 1 prior therapy. ![]()
Photo by Linda Bartlett
The monoclonal antibody (mAb) elotuzumab may be a useful addition to the multiple myeloma (MM) arsenal, according to investigators involved in the phase 3 ELOQUENT-2 trial.
The trial showed that adding elotuzumab to treatment with lenalidomide and dexamethasone extended progression-free survival (PFS) in relapsed MM patients by about 5 months, on average, when compared to treatment with just lenalidomide and dexamethasone.
“It appears that, for patients with relapsed multiple myeloma who would otherwise be offered lenalidomide and dexamethasone, addition of this new targeted drug makes the outcomes even better,” said study investigator Sagar Lonial, MD, of Emory University in Atlanta, Georgia.
Dr Lonial presented data from ELOQUENT-2 at a presscast in advance of the 2015 ASCO Annual Meeting. Full data from the study will be presented at the meeting on June 2 as abstract 8508.
The study was funded by Bristol-Myers Squibb and AbbVie, the companies developing elotuzumab.
Dr Lonial explained that elotuzumab attaches to the cell surface protein SLAMF7, which is found on MM cells and natural killer (NK) cells. Scientists believe that elotuzumab mounts a 2-pronged attack on MM by targeting myeloma cells directly and by enhancing NK cells’ ability to kill myeloma cells.
In ELOQUENT-2, 646 patients with recurrent MM were randomized to receive elotuzumab plus lenalidomide and dexamethasone or only lenalidomide and dexamethasone (control).
The patients’ median age was 66. They had failed 1 to 3 prior treatments, and 35% of them were refractory to their last therapy. Thirty-two percent of patients had del(17p), and 9% had t[4;14].
At a median follow-up of 24 months, elotuzumab had reduced the risk of MM progression and death by 30%. Patients in the elotuzumab arm had significantly longer PFS than patients in the control arm—a median of 19.4 months and 14.9 months, respectively (P=0.0004).
The 1-year PFS was 68% in the elotuzumab arm and 57% in the control arm. The 2-year PFS was 41% and 27%, respectively. Dr Lonial pointed out that, unlike some other therapies, elotuzumab continued to improve PFS over time.
“[T]he idea of the maintenance of benefit over time really speaks to the power of an immune-based approach when we treat cancer,” he said.
“Patients who received elotuzumab had a longer duration of remission [and] a higher overall response rate, and this improvement in clinical parameters occurred without a significant increase in adverse events or toxicity. In fact, there was no reduction in quality of life for [patients in the] 3-drug arm.”
Mild infusion reactions occurred after the first few doses in 10% of patients who received elotuzumab. Most of these reactions were grade 1 or 2.
Common grade 3-4 adverse events (occurring in ≥ 15% of patients) in both the elotuzumab and control arms were neutropenia (25% and 33%, respectively) and anemia (15% and 16%, respectively).
In all, 210 patients died, 94 in the elotuzumab arm and 116 in the control arm.
“Based on this randomized, phase 3 trial, we hope that we will soon have a new treatment option for patients with relapsed or refractory myeloma . . . ,” Dr Lonial said.
The US Food and Drug Administration has already granted elotuzumab breakthrough therapy designation to treat MM patients who have received at least 1 prior therapy. ![]()
Modified T cells may treat GVHD
Image from PLOS ONE
A T-cell therapy designed to mitigate graft-vs-host disease (GVHD) is both feasible and safe, according to results of a pilot study published in Molecular Therapy.
To create this therapy, researchers transduced donor T cells with γ-retroviruses carrying a CD34-TK75 fusion gene.
The team said this allows them to track the cells via PET/CT and induce apoptosis by administering the antiviral drug ganciclovir if patients begin showing signs of GVHD.
“If donor T cells expand and cause severe graft-vs-host disease, we can give the patient ganciclovir, and it should kill the T cells and stop the process,” said study author John F. DiPersio, MD, PhD, of the Washington University School of Medicine in St Louis, Missouri.
Dr DiPersio and his colleagues tested the CD34-TK75-enriched T cells in 8 patients—4 with acute myeloid leukemia and 4 with myelodysplastic syndromes—who relapsed after allogeneic transplant. Six patients underwent [18F]FHBG PET/CT to track the T cells at several time points after infusion.
Patients received T-cell infusions ranging from 0.1 × 106 cells/kg to 1.3 × 106 cells/kg. Seven of the 8 patients received chemotherapy before T-cell infusion.
Four patients achieved a complete remission, 1 had progressive disease, and 3 patients died before the researchers could evaluate them for response.
Two patients developed GVHD—1 before T-cell infusion and 1 after. The patient who developed GVHD before infusion had grade 2 liver GVHD that resolved after an increased dose of steroids. The patient ultimately died of relapsed leukemia.
The patient who developed GVHD after T-cell infusion did not respond to chemotherapy or T-cell infusion. At 64 days after infusion, he exhibited symptoms consistent with grade 4 liver GVHD. He was treated with high-dose steroids and ganciclovir but did not respond. His primary cause of death was relapsed/progressive disease.
The mean overall survival after T-cell infusion was 165 days, 4 patients were still alive at 6 months, and 1 patient lived 408 days. All of the patients ultimately died.
The researchers said they did not detect any replication competent retrovirus or any antibodies against CD34-TK in any of the patients. The team also said there were no toxicities related to the CD34-TK75-enriched T cells.
Among patients who underwent imaging, there was no clear distinction between the [18F]FHBG biodistribution at baseline and later time points. And there was no difference between images in the patient who developed GVHD after infusion and patients who did not.
Past work from Dr DiPersio’s lab showed that leukemic mice that receive donor T cells and go on to develop GVHD show a characteristic migration pattern of the T cells through the body. When the cells gather early in the thymus, the mice develop GVHD. When T cells don’t migrate to the thymus, GVHD doesn’t occur.
In the current study, the patients received a relatively small number of CD34-TK75-enriched T cells, so the researchers were not able to show whether the migration patterns in mice were similar in humans.
However, based on the results of this study, Dr DiPersio and his colleagues are participating in a larger trial in partnership with a company based in Italy. The researchers are planning to include patients from multiple medical centers, and each participant should receive about 50 times more of the CD34-TK75-enriched T cells than were administered in this trial.
Washington University is the only center in the new trial that will be able to perform the imaging studies examining migration patterns of the T cells. ![]()
Image from PLOS ONE
A T-cell therapy designed to mitigate graft-vs-host disease (GVHD) is both feasible and safe, according to results of a pilot study published in Molecular Therapy.
To create this therapy, researchers transduced donor T cells with γ-retroviruses carrying a CD34-TK75 fusion gene.
The team said this allows them to track the cells via PET/CT and induce apoptosis by administering the antiviral drug ganciclovir if patients begin showing signs of GVHD.
“If donor T cells expand and cause severe graft-vs-host disease, we can give the patient ganciclovir, and it should kill the T cells and stop the process,” said study author John F. DiPersio, MD, PhD, of the Washington University School of Medicine in St Louis, Missouri.
Dr DiPersio and his colleagues tested the CD34-TK75-enriched T cells in 8 patients—4 with acute myeloid leukemia and 4 with myelodysplastic syndromes—who relapsed after allogeneic transplant. Six patients underwent [18F]FHBG PET/CT to track the T cells at several time points after infusion.
Patients received T-cell infusions ranging from 0.1 × 106 cells/kg to 1.3 × 106 cells/kg. Seven of the 8 patients received chemotherapy before T-cell infusion.
Four patients achieved a complete remission, 1 had progressive disease, and 3 patients died before the researchers could evaluate them for response.
Two patients developed GVHD—1 before T-cell infusion and 1 after. The patient who developed GVHD before infusion had grade 2 liver GVHD that resolved after an increased dose of steroids. The patient ultimately died of relapsed leukemia.
The patient who developed GVHD after T-cell infusion did not respond to chemotherapy or T-cell infusion. At 64 days after infusion, he exhibited symptoms consistent with grade 4 liver GVHD. He was treated with high-dose steroids and ganciclovir but did not respond. His primary cause of death was relapsed/progressive disease.
The mean overall survival after T-cell infusion was 165 days, 4 patients were still alive at 6 months, and 1 patient lived 408 days. All of the patients ultimately died.
The researchers said they did not detect any replication competent retrovirus or any antibodies against CD34-TK in any of the patients. The team also said there were no toxicities related to the CD34-TK75-enriched T cells.
Among patients who underwent imaging, there was no clear distinction between the [18F]FHBG biodistribution at baseline and later time points. And there was no difference between images in the patient who developed GVHD after infusion and patients who did not.
Past work from Dr DiPersio’s lab showed that leukemic mice that receive donor T cells and go on to develop GVHD show a characteristic migration pattern of the T cells through the body. When the cells gather early in the thymus, the mice develop GVHD. When T cells don’t migrate to the thymus, GVHD doesn’t occur.
In the current study, the patients received a relatively small number of CD34-TK75-enriched T cells, so the researchers were not able to show whether the migration patterns in mice were similar in humans.
However, based on the results of this study, Dr DiPersio and his colleagues are participating in a larger trial in partnership with a company based in Italy. The researchers are planning to include patients from multiple medical centers, and each participant should receive about 50 times more of the CD34-TK75-enriched T cells than were administered in this trial.
Washington University is the only center in the new trial that will be able to perform the imaging studies examining migration patterns of the T cells. ![]()
Image from PLOS ONE
A T-cell therapy designed to mitigate graft-vs-host disease (GVHD) is both feasible and safe, according to results of a pilot study published in Molecular Therapy.
To create this therapy, researchers transduced donor T cells with γ-retroviruses carrying a CD34-TK75 fusion gene.
The team said this allows them to track the cells via PET/CT and induce apoptosis by administering the antiviral drug ganciclovir if patients begin showing signs of GVHD.
“If donor T cells expand and cause severe graft-vs-host disease, we can give the patient ganciclovir, and it should kill the T cells and stop the process,” said study author John F. DiPersio, MD, PhD, of the Washington University School of Medicine in St Louis, Missouri.
Dr DiPersio and his colleagues tested the CD34-TK75-enriched T cells in 8 patients—4 with acute myeloid leukemia and 4 with myelodysplastic syndromes—who relapsed after allogeneic transplant. Six patients underwent [18F]FHBG PET/CT to track the T cells at several time points after infusion.
Patients received T-cell infusions ranging from 0.1 × 106 cells/kg to 1.3 × 106 cells/kg. Seven of the 8 patients received chemotherapy before T-cell infusion.
Four patients achieved a complete remission, 1 had progressive disease, and 3 patients died before the researchers could evaluate them for response.
Two patients developed GVHD—1 before T-cell infusion and 1 after. The patient who developed GVHD before infusion had grade 2 liver GVHD that resolved after an increased dose of steroids. The patient ultimately died of relapsed leukemia.
The patient who developed GVHD after T-cell infusion did not respond to chemotherapy or T-cell infusion. At 64 days after infusion, he exhibited symptoms consistent with grade 4 liver GVHD. He was treated with high-dose steroids and ganciclovir but did not respond. His primary cause of death was relapsed/progressive disease.
The mean overall survival after T-cell infusion was 165 days, 4 patients were still alive at 6 months, and 1 patient lived 408 days. All of the patients ultimately died.
The researchers said they did not detect any replication competent retrovirus or any antibodies against CD34-TK in any of the patients. The team also said there were no toxicities related to the CD34-TK75-enriched T cells.
Among patients who underwent imaging, there was no clear distinction between the [18F]FHBG biodistribution at baseline and later time points. And there was no difference between images in the patient who developed GVHD after infusion and patients who did not.
Past work from Dr DiPersio’s lab showed that leukemic mice that receive donor T cells and go on to develop GVHD show a characteristic migration pattern of the T cells through the body. When the cells gather early in the thymus, the mice develop GVHD. When T cells don’t migrate to the thymus, GVHD doesn’t occur.
In the current study, the patients received a relatively small number of CD34-TK75-enriched T cells, so the researchers were not able to show whether the migration patterns in mice were similar in humans.
However, based on the results of this study, Dr DiPersio and his colleagues are participating in a larger trial in partnership with a company based in Italy. The researchers are planning to include patients from multiple medical centers, and each participant should receive about 50 times more of the CD34-TK75-enriched T cells than were administered in this trial.
Washington University is the only center in the new trial that will be able to perform the imaging studies examining migration patterns of the T cells. ![]()
Company stops phase 3 PTCL trial

for use in a clinical trial
Photo by Esther Dyson
Takeda Pharmaceutical Company Limited has announced its decision to discontinue its phase 3 trial of the aurora A kinase inhibitor alisertib (MLN8237) in patients with relapsed or refractory peripheral T-cell lymphoma (PTCL).
Results of a pre-specified interim analysis indicated that alisertib was unlikely to meet the study’s primary endpoint: providing superior progression-free survival over the standard of care for PTCL.
Takeda said patients enrolled in the trial may continue to receive alisertib if they are thought to be benefitting from it and no safety concerns are present.
The company is encouraging patients to consult their study investigators to address any questions and before making any changes to their medication.
Takeda is working with trial investigators and local regulatory authorities to ensure that PTCL patients who participated in the study receive appropriate care.
The company is still investigating alisertib for use in small-cell lung cancer.
“While we are disappointed that alisertib will not be further investigated for relapsed or refractory peripheral T-cell lymphoma, we are optimistic about alisertib’s clinical development program in small-cell lung cancer,” said Michael Vasconcelles, MD, global head of the Takeda Oncology Therapeutic Unit.
“The randomized, phase 2 study of alisertib in small-cell lung cancer will continue as planned and is currently underway. Takeda also continues to support investigator-initiated research with alisertib and will evaluate its potential use in other oncology indications going forward.” ![]()
for use in a clinical trial
Photo by Esther Dyson
Takeda Pharmaceutical Company Limited has announced its decision to discontinue its phase 3 trial of the aurora A kinase inhibitor alisertib (MLN8237) in patients with relapsed or refractory peripheral T-cell lymphoma (PTCL).
Results of a pre-specified interim analysis indicated that alisertib was unlikely to meet the study’s primary endpoint: providing superior progression-free survival over the standard of care for PTCL.
Takeda said patients enrolled in the trial may continue to receive alisertib if they are thought to be benefitting from it and no safety concerns are present.
The company is encouraging patients to consult their study investigators to address any questions and before making any changes to their medication.
Takeda is working with trial investigators and local regulatory authorities to ensure that PTCL patients who participated in the study receive appropriate care.
The company is still investigating alisertib for use in small-cell lung cancer.
“While we are disappointed that alisertib will not be further investigated for relapsed or refractory peripheral T-cell lymphoma, we are optimistic about alisertib’s clinical development program in small-cell lung cancer,” said Michael Vasconcelles, MD, global head of the Takeda Oncology Therapeutic Unit.
“The randomized, phase 2 study of alisertib in small-cell lung cancer will continue as planned and is currently underway. Takeda also continues to support investigator-initiated research with alisertib and will evaluate its potential use in other oncology indications going forward.” ![]()
for use in a clinical trial
Photo by Esther Dyson
Takeda Pharmaceutical Company Limited has announced its decision to discontinue its phase 3 trial of the aurora A kinase inhibitor alisertib (MLN8237) in patients with relapsed or refractory peripheral T-cell lymphoma (PTCL).
Results of a pre-specified interim analysis indicated that alisertib was unlikely to meet the study’s primary endpoint: providing superior progression-free survival over the standard of care for PTCL.
Takeda said patients enrolled in the trial may continue to receive alisertib if they are thought to be benefitting from it and no safety concerns are present.
The company is encouraging patients to consult their study investigators to address any questions and before making any changes to their medication.
Takeda is working with trial investigators and local regulatory authorities to ensure that PTCL patients who participated in the study receive appropriate care.
The company is still investigating alisertib for use in small-cell lung cancer.
“While we are disappointed that alisertib will not be further investigated for relapsed or refractory peripheral T-cell lymphoma, we are optimistic about alisertib’s clinical development program in small-cell lung cancer,” said Michael Vasconcelles, MD, global head of the Takeda Oncology Therapeutic Unit.
“The randomized, phase 2 study of alisertib in small-cell lung cancer will continue as planned and is currently underway. Takeda also continues to support investigator-initiated research with alisertib and will evaluate its potential use in other oncology indications going forward.” ![]()