User login
Autar scale helps identify DVT risk, prevent DVT
The Autar scale is a successful tool for identifying orthopedic surgery patients at risk for deep vein thrombosis (DVT) – and can prevent DVT when patients follow prophylactic measures corresponding with their DVT risk level, according to researchers.
The study comprised 216 patients who were undergoing orthopedic surgery to the lower extremities in Henan, China. They were divided into a control group and an intervention group, consisting of 106 and 110 patients, respectively. Researchers used the Autar scale to assess the risk of a DVT occurring in all of the patients.
The scale is used mainly for evaluating the probability of DVT in a hospitalized patient undergoing surgery. It includes seven risk categories and 41 items, and is used to assign scores to patients indicating whether they are at no, low, moderate, or high risk of DVT.
Specific preventive measures were implemented among the intervention group’s members based on the Autar scale scores of each of these patients. The scores of patients in the control group were not used to implement DVT prophylaxis. Such patients, however, did receive routine nursing and mechanical and pharmacological prophylactic measures, if clinical experience and basic information caused their health care providers to identify them as being at high risk for DVT.
The Autar scale’s efficacy was confirmed by the fact that “the number of patients with DVT was in line with the number of high-risk patients in both groups,” according to Hui-Zhen Yin and Professor Ci-Ming Shan of Zhengzhou (China) University.
The numbers of DVTs that occurred in each group were significantly different from each other; 1.82% of patients in the intervention group got DVTs, compared to 9.43% of patients in the control group. Therefore, the study showed that the Autar scale is useful not only for predicting DVT, but also for preventing its incidence when patients receive the appropriate prophylactic and nursing interventions, the researchers noted.
They recommend wide use of the scale, because they believe it is “a comprehensive and valid instrument that improves the consistency of nursing assessment and creates a reference for preventing DVT in nursing practice.”
Read the full study in International Journal of Nursing Sciences (doi:10.1016/j.ijnss.2015.04.003).
The Autar scale is a successful tool for identifying orthopedic surgery patients at risk for deep vein thrombosis (DVT) – and can prevent DVT when patients follow prophylactic measures corresponding with their DVT risk level, according to researchers.
The study comprised 216 patients who were undergoing orthopedic surgery to the lower extremities in Henan, China. They were divided into a control group and an intervention group, consisting of 106 and 110 patients, respectively. Researchers used the Autar scale to assess the risk of a DVT occurring in all of the patients.
The scale is used mainly for evaluating the probability of DVT in a hospitalized patient undergoing surgery. It includes seven risk categories and 41 items, and is used to assign scores to patients indicating whether they are at no, low, moderate, or high risk of DVT.
Specific preventive measures were implemented among the intervention group’s members based on the Autar scale scores of each of these patients. The scores of patients in the control group were not used to implement DVT prophylaxis. Such patients, however, did receive routine nursing and mechanical and pharmacological prophylactic measures, if clinical experience and basic information caused their health care providers to identify them as being at high risk for DVT.
The Autar scale’s efficacy was confirmed by the fact that “the number of patients with DVT was in line with the number of high-risk patients in both groups,” according to Hui-Zhen Yin and Professor Ci-Ming Shan of Zhengzhou (China) University.
The numbers of DVTs that occurred in each group were significantly different from each other; 1.82% of patients in the intervention group got DVTs, compared to 9.43% of patients in the control group. Therefore, the study showed that the Autar scale is useful not only for predicting DVT, but also for preventing its incidence when patients receive the appropriate prophylactic and nursing interventions, the researchers noted.
They recommend wide use of the scale, because they believe it is “a comprehensive and valid instrument that improves the consistency of nursing assessment and creates a reference for preventing DVT in nursing practice.”
Read the full study in International Journal of Nursing Sciences (doi:10.1016/j.ijnss.2015.04.003).
The Autar scale is a successful tool for identifying orthopedic surgery patients at risk for deep vein thrombosis (DVT) – and can prevent DVT when patients follow prophylactic measures corresponding with their DVT risk level, according to researchers.
The study comprised 216 patients who were undergoing orthopedic surgery to the lower extremities in Henan, China. They were divided into a control group and an intervention group, consisting of 106 and 110 patients, respectively. Researchers used the Autar scale to assess the risk of a DVT occurring in all of the patients.
The scale is used mainly for evaluating the probability of DVT in a hospitalized patient undergoing surgery. It includes seven risk categories and 41 items, and is used to assign scores to patients indicating whether they are at no, low, moderate, or high risk of DVT.
Specific preventive measures were implemented among the intervention group’s members based on the Autar scale scores of each of these patients. The scores of patients in the control group were not used to implement DVT prophylaxis. Such patients, however, did receive routine nursing and mechanical and pharmacological prophylactic measures, if clinical experience and basic information caused their health care providers to identify them as being at high risk for DVT.
The Autar scale’s efficacy was confirmed by the fact that “the number of patients with DVT was in line with the number of high-risk patients in both groups,” according to Hui-Zhen Yin and Professor Ci-Ming Shan of Zhengzhou (China) University.
The numbers of DVTs that occurred in each group were significantly different from each other; 1.82% of patients in the intervention group got DVTs, compared to 9.43% of patients in the control group. Therefore, the study showed that the Autar scale is useful not only for predicting DVT, but also for preventing its incidence when patients receive the appropriate prophylactic and nursing interventions, the researchers noted.
They recommend wide use of the scale, because they believe it is “a comprehensive and valid instrument that improves the consistency of nursing assessment and creates a reference for preventing DVT in nursing practice.”
Read the full study in International Journal of Nursing Sciences (doi:10.1016/j.ijnss.2015.04.003).
Stricter DVT prophylaxis guidelines needed for cardiac and vascular surgery
Cardiac and vascular surgery patients should receive deep vein thrombosis (DVT) prophylaxis before and after surgery, say researchers who found a high incidence of postoperative DVT in these patients compared to general surgery patients.
The retrospective study of 2,669,772 surgery patients from the American College of Surgeons National Surgical Quality Improvement Program database found that 18,670 patients developed a DVT within 30 days of the operation.
The incidence of DVT according to the type of surgery was 2% for cardiac surgery, 0.99% for vascular surgery and 0.66% for general surgery, reported Dr. Faisal Aziz and his colleagues at Pennsylvania State University (Ann. Vasc. Surg. 2015; 29: 661-9).
Vascular surgery patients were at 1.5 times the risk of a postop DVT and cardiac surgery patients were at 3 times the risk compared with general surgery patients, a significant difference.
Preoperative factors associated with increased risk of developing DVT in the postoperative period included inpatient admission status (OR 7.8), general anesthesia (OR 2), and dyspnea at rest (OR 5).
“Despite the fact that most arterial surgery operations involve administration of therapeutic doses of anticoagulation therapy during the operations, incidence of postoperative DVT is high in these patients,” the study authors wrote.
“Intraoperative anticoagulation is not protective against development of DVT in the postoperative period” they said.
“Physicians should ensure adequate DVT prophylaxis in postoperative vascular surgery and cardiac surgery patients, according to established evidence based guidelines,” they concluded.
The authors did not report any financial disclosures.
Cardiac and vascular surgery patients should receive deep vein thrombosis (DVT) prophylaxis before and after surgery, say researchers who found a high incidence of postoperative DVT in these patients compared to general surgery patients.
The retrospective study of 2,669,772 surgery patients from the American College of Surgeons National Surgical Quality Improvement Program database found that 18,670 patients developed a DVT within 30 days of the operation.
The incidence of DVT according to the type of surgery was 2% for cardiac surgery, 0.99% for vascular surgery and 0.66% for general surgery, reported Dr. Faisal Aziz and his colleagues at Pennsylvania State University (Ann. Vasc. Surg. 2015; 29: 661-9).
Vascular surgery patients were at 1.5 times the risk of a postop DVT and cardiac surgery patients were at 3 times the risk compared with general surgery patients, a significant difference.
Preoperative factors associated with increased risk of developing DVT in the postoperative period included inpatient admission status (OR 7.8), general anesthesia (OR 2), and dyspnea at rest (OR 5).
“Despite the fact that most arterial surgery operations involve administration of therapeutic doses of anticoagulation therapy during the operations, incidence of postoperative DVT is high in these patients,” the study authors wrote.
“Intraoperative anticoagulation is not protective against development of DVT in the postoperative period” they said.
“Physicians should ensure adequate DVT prophylaxis in postoperative vascular surgery and cardiac surgery patients, according to established evidence based guidelines,” they concluded.
The authors did not report any financial disclosures.
Cardiac and vascular surgery patients should receive deep vein thrombosis (DVT) prophylaxis before and after surgery, say researchers who found a high incidence of postoperative DVT in these patients compared to general surgery patients.
The retrospective study of 2,669,772 surgery patients from the American College of Surgeons National Surgical Quality Improvement Program database found that 18,670 patients developed a DVT within 30 days of the operation.
The incidence of DVT according to the type of surgery was 2% for cardiac surgery, 0.99% for vascular surgery and 0.66% for general surgery, reported Dr. Faisal Aziz and his colleagues at Pennsylvania State University (Ann. Vasc. Surg. 2015; 29: 661-9).
Vascular surgery patients were at 1.5 times the risk of a postop DVT and cardiac surgery patients were at 3 times the risk compared with general surgery patients, a significant difference.
Preoperative factors associated with increased risk of developing DVT in the postoperative period included inpatient admission status (OR 7.8), general anesthesia (OR 2), and dyspnea at rest (OR 5).
“Despite the fact that most arterial surgery operations involve administration of therapeutic doses of anticoagulation therapy during the operations, incidence of postoperative DVT is high in these patients,” the study authors wrote.
“Intraoperative anticoagulation is not protective against development of DVT in the postoperative period” they said.
“Physicians should ensure adequate DVT prophylaxis in postoperative vascular surgery and cardiac surgery patients, according to established evidence based guidelines,” they concluded.
The authors did not report any financial disclosures.
FROM ANNALS OF VASCULAR SURGERY
Key clinical point: Intraoperative anticoagulation alone does not prevent DVT in patients undergoing vascular and cardiac surgery.
Major finding: The incidence of DVT according to the type of surgery was 2% for cardiac surgery, 0.99% for vascular surgery and 0.66% for general surgery.
Data source: Retrospective study of 2,669,772 surgery patients from the American College of Surgeons National Surgical Quality Improvement Program database.
Disclosures: The authors did not report any financial disclosures.
Larger-gauge PICCs, VTE history increase PICC-DVT risk
Risk factors of upper-extremity deep vein thrombosis associated with peripherally inserted central catheters include a history of venous thromboembolism and a larger-gauge catheter, according to Dr. Vineet Chopra and his associates at the University of Michigan Health System, Ann Arbor.
Compared to 4-Fr gauge PICCs, 5-Fr and 6-Fr PICCs significantly increased PICC-DVT risk, with odds ratios of 2.7 and 7.4, respectively. The OR for patients with a prior history of VTE was 1.7. While any surgery with a PICC in place increased risk, the OR was higher in surgery lasting less than 2 hours (2.75 vs. 2.17). PICCs inserted into the brachial or cephalic vein also increased PICC-DVT risk, compared with the basilic vein, with ORs of 6.8 and 5.8, respectively.
Patients who received both aspirin and statins were at a significantly lower risk of PICC-DVT than those who received only one drug or neither, with an OR of 0.31 for those who got both, compared with 0.77 for aspirin and 0.61 for statins. Pharmacologic VTE prophylaxis also benefited patients with an OR of DVT at 0.72.
“Given the existence of other supportive data regarding the influence of VTE prophylaxis on PICC-DVT and a potentially protective role of statins on thrombosis, further controlled studies of VTE prophylaxis, antiplatelet treatment, and statins to prevent PICC-DVT appear warranted,” the investigators recommended.
Find the full study in Thrombosis Research (doi:10.1016/j.thromres.2015.02.0120).
Risk factors of upper-extremity deep vein thrombosis associated with peripherally inserted central catheters include a history of venous thromboembolism and a larger-gauge catheter, according to Dr. Vineet Chopra and his associates at the University of Michigan Health System, Ann Arbor.
Compared to 4-Fr gauge PICCs, 5-Fr and 6-Fr PICCs significantly increased PICC-DVT risk, with odds ratios of 2.7 and 7.4, respectively. The OR for patients with a prior history of VTE was 1.7. While any surgery with a PICC in place increased risk, the OR was higher in surgery lasting less than 2 hours (2.75 vs. 2.17). PICCs inserted into the brachial or cephalic vein also increased PICC-DVT risk, compared with the basilic vein, with ORs of 6.8 and 5.8, respectively.
Patients who received both aspirin and statins were at a significantly lower risk of PICC-DVT than those who received only one drug or neither, with an OR of 0.31 for those who got both, compared with 0.77 for aspirin and 0.61 for statins. Pharmacologic VTE prophylaxis also benefited patients with an OR of DVT at 0.72.
“Given the existence of other supportive data regarding the influence of VTE prophylaxis on PICC-DVT and a potentially protective role of statins on thrombosis, further controlled studies of VTE prophylaxis, antiplatelet treatment, and statins to prevent PICC-DVT appear warranted,” the investigators recommended.
Find the full study in Thrombosis Research (doi:10.1016/j.thromres.2015.02.0120).
Risk factors of upper-extremity deep vein thrombosis associated with peripherally inserted central catheters include a history of venous thromboembolism and a larger-gauge catheter, according to Dr. Vineet Chopra and his associates at the University of Michigan Health System, Ann Arbor.
Compared to 4-Fr gauge PICCs, 5-Fr and 6-Fr PICCs significantly increased PICC-DVT risk, with odds ratios of 2.7 and 7.4, respectively. The OR for patients with a prior history of VTE was 1.7. While any surgery with a PICC in place increased risk, the OR was higher in surgery lasting less than 2 hours (2.75 vs. 2.17). PICCs inserted into the brachial or cephalic vein also increased PICC-DVT risk, compared with the basilic vein, with ORs of 6.8 and 5.8, respectively.
Patients who received both aspirin and statins were at a significantly lower risk of PICC-DVT than those who received only one drug or neither, with an OR of 0.31 for those who got both, compared with 0.77 for aspirin and 0.61 for statins. Pharmacologic VTE prophylaxis also benefited patients with an OR of DVT at 0.72.
“Given the existence of other supportive data regarding the influence of VTE prophylaxis on PICC-DVT and a potentially protective role of statins on thrombosis, further controlled studies of VTE prophylaxis, antiplatelet treatment, and statins to prevent PICC-DVT appear warranted,” the investigators recommended.
Find the full study in Thrombosis Research (doi:10.1016/j.thromres.2015.02.0120).
June 2015 Quiz 2
Q2: ANSWER: A
Critique
This pregnant patient has features compatible with Listeria monocytogenes infection. In any pregnant patient presenting with fever, Listeria needs to be considered after ruling out common conditions such as a urinary tract infection given the high morbidity associated with this condition. Blood cultures are used to make the diagnosis of Listeria, while stool and vaginal cultures are not helpful. While CSF cultures can be used in cases of Listeria meningitis, the yield of blood cultures is higher. Urine cultures are unlikely to add additional information in this patient’s case given the negative urine dipstick.
Reference
1. Jackson, K.A., Iwamoto, M., Swerdlow, D. Pregnancy-associated listeriosis. Epidemiol. Infect. 2010;138:1503-9.
Q2: ANSWER: A
Critique
This pregnant patient has features compatible with Listeria monocytogenes infection. In any pregnant patient presenting with fever, Listeria needs to be considered after ruling out common conditions such as a urinary tract infection given the high morbidity associated with this condition. Blood cultures are used to make the diagnosis of Listeria, while stool and vaginal cultures are not helpful. While CSF cultures can be used in cases of Listeria meningitis, the yield of blood cultures is higher. Urine cultures are unlikely to add additional information in this patient’s case given the negative urine dipstick.
Reference
1. Jackson, K.A., Iwamoto, M., Swerdlow, D. Pregnancy-associated listeriosis. Epidemiol. Infect. 2010;138:1503-9.
Q2: ANSWER: A
Critique
This pregnant patient has features compatible with Listeria monocytogenes infection. In any pregnant patient presenting with fever, Listeria needs to be considered after ruling out common conditions such as a urinary tract infection given the high morbidity associated with this condition. Blood cultures are used to make the diagnosis of Listeria, while stool and vaginal cultures are not helpful. While CSF cultures can be used in cases of Listeria meningitis, the yield of blood cultures is higher. Urine cultures are unlikely to add additional information in this patient’s case given the negative urine dipstick.
Reference
1. Jackson, K.A., Iwamoto, M., Swerdlow, D. Pregnancy-associated listeriosis. Epidemiol. Infect. 2010;138:1503-9.
June 2015 Quiz 1
Q1: ANSWER: D
Critique
The patient has had complicated recurrent Crohn’s disease and two resections. If this were his first resection of a short-segment ileal stricture, then choice (a) would be a reasonable alternative to starting medication at this time. This is based on the endoscopic scoring system of Rutgeerts in which endoscopic findings in the neoterminal ileum at 6-12 months postoperatively are somewhat predictive of clinical recurrence over the next 5 years. Short-term antibiotic therapy with ciprofloxacin has not been shown to be a good long-term solution to prevention of postoperative recurrence. Both azathioprine and 6-mercaptopurine have a modest effect on the prevention of postoperative recurrence of Crohn’s disease. Azathioprine at 1 mg/kg per day would be less than an optimal dose for this purpose. The D’Haens study used 1.5-2 mg/kg of azathioprine in combination with 3 months of metronidazole. At 1 year the endoscopic recurrence rate (i2-i4 lesions) was greater in the placebo group at 69% compared with 44% in the azathioprine-treated group. Infliximab has been shown in a small randomized trial to be very effective in preventing postoperative recurrence of Crohn’s disease. In a 24-subject randomized trial, 91% of the infliximab treated patients were free of endoscopic recurrence, compared to 9% of patients receiving placebo. In this patient, who is at a high risk for recurrence with recurrent inflammation, multiple surgeries, and continued smoking, anti-TNF therapy should be initiated within 4 weeks after surgery. Mesalamine has minimal postoperative preventative effects and would not be appropriate monotherapy to use in this high-risk patient.
References
1. D’Haens, G.R., Vermeire, S., Van Assche G., et al. Therapy of metronidazole with azathioprine to prevent postoperative recurrence of Crohn’s disease: a controlled randomized trial. Gastroenterology 2008;135:1123-9.
2. Regueiro, M., Schraut, W., Baidoo, L., et al. Infliximab prevents Crohn’s disease recurrence after ileal resection. Gastroenterology 2009;136:441-50.e1;quiz 716. Epub 2008 Oct 31.
3. Rutgeerts P, Geboes K, Vantrappen G, Beyls J, Kerremans R, Hiele M. Predictability of the postoperative course of Crohn’s disease. Gastroenterology 1990;99:956-63.
4. Schwartz M, Regueiro M. Prevention and treatment of postoperative Crohn’s disease recurrence: an update for a new decade. Curr. Gastroenterol. Rep. 2011;13:95-100.
Q1: ANSWER: D
Critique
The patient has had complicated recurrent Crohn’s disease and two resections. If this were his first resection of a short-segment ileal stricture, then choice (a) would be a reasonable alternative to starting medication at this time. This is based on the endoscopic scoring system of Rutgeerts in which endoscopic findings in the neoterminal ileum at 6-12 months postoperatively are somewhat predictive of clinical recurrence over the next 5 years. Short-term antibiotic therapy with ciprofloxacin has not been shown to be a good long-term solution to prevention of postoperative recurrence. Both azathioprine and 6-mercaptopurine have a modest effect on the prevention of postoperative recurrence of Crohn’s disease. Azathioprine at 1 mg/kg per day would be less than an optimal dose for this purpose. The D’Haens study used 1.5-2 mg/kg of azathioprine in combination with 3 months of metronidazole. At 1 year the endoscopic recurrence rate (i2-i4 lesions) was greater in the placebo group at 69% compared with 44% in the azathioprine-treated group. Infliximab has been shown in a small randomized trial to be very effective in preventing postoperative recurrence of Crohn’s disease. In a 24-subject randomized trial, 91% of the infliximab treated patients were free of endoscopic recurrence, compared to 9% of patients receiving placebo. In this patient, who is at a high risk for recurrence with recurrent inflammation, multiple surgeries, and continued smoking, anti-TNF therapy should be initiated within 4 weeks after surgery. Mesalamine has minimal postoperative preventative effects and would not be appropriate monotherapy to use in this high-risk patient.
References
1. D’Haens, G.R., Vermeire, S., Van Assche G., et al. Therapy of metronidazole with azathioprine to prevent postoperative recurrence of Crohn’s disease: a controlled randomized trial. Gastroenterology 2008;135:1123-9.
2. Regueiro, M., Schraut, W., Baidoo, L., et al. Infliximab prevents Crohn’s disease recurrence after ileal resection. Gastroenterology 2009;136:441-50.e1;quiz 716. Epub 2008 Oct 31.
3. Rutgeerts P, Geboes K, Vantrappen G, Beyls J, Kerremans R, Hiele M. Predictability of the postoperative course of Crohn’s disease. Gastroenterology 1990;99:956-63.
4. Schwartz M, Regueiro M. Prevention and treatment of postoperative Crohn’s disease recurrence: an update for a new decade. Curr. Gastroenterol. Rep. 2011;13:95-100.
Q1: ANSWER: D
Critique
The patient has had complicated recurrent Crohn’s disease and two resections. If this were his first resection of a short-segment ileal stricture, then choice (a) would be a reasonable alternative to starting medication at this time. This is based on the endoscopic scoring system of Rutgeerts in which endoscopic findings in the neoterminal ileum at 6-12 months postoperatively are somewhat predictive of clinical recurrence over the next 5 years. Short-term antibiotic therapy with ciprofloxacin has not been shown to be a good long-term solution to prevention of postoperative recurrence. Both azathioprine and 6-mercaptopurine have a modest effect on the prevention of postoperative recurrence of Crohn’s disease. Azathioprine at 1 mg/kg per day would be less than an optimal dose for this purpose. The D’Haens study used 1.5-2 mg/kg of azathioprine in combination with 3 months of metronidazole. At 1 year the endoscopic recurrence rate (i2-i4 lesions) was greater in the placebo group at 69% compared with 44% in the azathioprine-treated group. Infliximab has been shown in a small randomized trial to be very effective in preventing postoperative recurrence of Crohn’s disease. In a 24-subject randomized trial, 91% of the infliximab treated patients were free of endoscopic recurrence, compared to 9% of patients receiving placebo. In this patient, who is at a high risk for recurrence with recurrent inflammation, multiple surgeries, and continued smoking, anti-TNF therapy should be initiated within 4 weeks after surgery. Mesalamine has minimal postoperative preventative effects and would not be appropriate monotherapy to use in this high-risk patient.
References
1. D’Haens, G.R., Vermeire, S., Van Assche G., et al. Therapy of metronidazole with azathioprine to prevent postoperative recurrence of Crohn’s disease: a controlled randomized trial. Gastroenterology 2008;135:1123-9.
2. Regueiro, M., Schraut, W., Baidoo, L., et al. Infliximab prevents Crohn’s disease recurrence after ileal resection. Gastroenterology 2009;136:441-50.e1;quiz 716. Epub 2008 Oct 31.
3. Rutgeerts P, Geboes K, Vantrappen G, Beyls J, Kerremans R, Hiele M. Predictability of the postoperative course of Crohn’s disease. Gastroenterology 1990;99:956-63.
4. Schwartz M, Regueiro M. Prevention and treatment of postoperative Crohn’s disease recurrence: an update for a new decade. Curr. Gastroenterol. Rep. 2011;13:95-100.
Nanotherapy appears effective against MM

Photo by Aaron Logan
A nanoparticle-based therapy can effectively fight multiple myeloma (MM), according to preclinical research published in Molecular Cancer Therapy.
The nanoparticles protected their therapeutic cargo from degradation in the bloodstream and enhanced drug delivery into MM cells, thereby improving survival in mouse models of MM.
The nanoparticles carried an Sn 2 lipase-labile prodrug inhibitor of MYC-MAX dimerization (MI1-PD).
Researchers designed this prodrug for use in MM because MM pathogenesis is driven by the MYC oncoprotein, its dimerization with MAX, and the binding of this heterodimer to E-Boxes in the vicinity of target genes.
Previous research has shown that MYC inhibitors are extremely potent in vitro, but, when injected into the blood, they degrade immediately. The current study is the first to show that a MYC inhibitor can be effective in animals with cancer, as long as the drug has a vehicle to protect and deliver it into cancer cells.
“The nanoparticles serve as vehicles that protect the drug from the harsh environment of the blood,” said study author Gregory M. Lanza, MD, PhD, of the Washington University School of Medicine in St Louis, Missouri.
“In this case, the drug is modified into a prodrug and actually locked into the outer membrane of the particle.”
The nanoparticles are designed to carry targeting molecules that home in on and bind to MM cells that carry the complementary receptor. When a nanoparticle binds to an MM cell, their membranes fuse together, transferring MI1-PD to the malignant cell. When safely inside, MI1-PD is enzymatically freed to do its job, blocking MYC from activation.
In theory, noncancerous cells are unlikely to be adversely affected by MYC inhibition because healthy cells shouldn’t have highly activated MYC proteins to begin with, according to the researchers.
The team injected 2 sizes of MI1-PD-containing nanoparticles into mice with MM and found that the nanoparticles increased the animals’ median survival.
The median survival was 46 days for mice that received MI1-PD-containing, 200-nm nanoparticles and 28 days for mice that received control, 200-nm nanoparticles (P<0.05). For mice that received 20 nm nanoparticles, the median survival was 52 days and 29 days, respectively (P=0.001).
The researchers also pointed out that neither MI1 nor MI1-PD conferred a survival benefit for the mice when injected without nanoparticle protection.
“We’re excited about our results because there was no guarantee the nanotherapy would increase survival,” said study author Michael H. Tomasson, MD, of the Washington University School of Medicine.
“We injected the nanoparticles intravenously, and they found the tumors throughout the body, whether they were in the bone marrow, the spleen, or elsewhere.”
Drs Tomasson and Lanza said this technology is still years away from clinical trials, but they are optimistic about its future potential and are eager to begin that work. ![]()
Photo by Aaron Logan
A nanoparticle-based therapy can effectively fight multiple myeloma (MM), according to preclinical research published in Molecular Cancer Therapy.
The nanoparticles protected their therapeutic cargo from degradation in the bloodstream and enhanced drug delivery into MM cells, thereby improving survival in mouse models of MM.
The nanoparticles carried an Sn 2 lipase-labile prodrug inhibitor of MYC-MAX dimerization (MI1-PD).
Researchers designed this prodrug for use in MM because MM pathogenesis is driven by the MYC oncoprotein, its dimerization with MAX, and the binding of this heterodimer to E-Boxes in the vicinity of target genes.
Previous research has shown that MYC inhibitors are extremely potent in vitro, but, when injected into the blood, they degrade immediately. The current study is the first to show that a MYC inhibitor can be effective in animals with cancer, as long as the drug has a vehicle to protect and deliver it into cancer cells.
“The nanoparticles serve as vehicles that protect the drug from the harsh environment of the blood,” said study author Gregory M. Lanza, MD, PhD, of the Washington University School of Medicine in St Louis, Missouri.
“In this case, the drug is modified into a prodrug and actually locked into the outer membrane of the particle.”
The nanoparticles are designed to carry targeting molecules that home in on and bind to MM cells that carry the complementary receptor. When a nanoparticle binds to an MM cell, their membranes fuse together, transferring MI1-PD to the malignant cell. When safely inside, MI1-PD is enzymatically freed to do its job, blocking MYC from activation.
In theory, noncancerous cells are unlikely to be adversely affected by MYC inhibition because healthy cells shouldn’t have highly activated MYC proteins to begin with, according to the researchers.
The team injected 2 sizes of MI1-PD-containing nanoparticles into mice with MM and found that the nanoparticles increased the animals’ median survival.
The median survival was 46 days for mice that received MI1-PD-containing, 200-nm nanoparticles and 28 days for mice that received control, 200-nm nanoparticles (P<0.05). For mice that received 20 nm nanoparticles, the median survival was 52 days and 29 days, respectively (P=0.001).
The researchers also pointed out that neither MI1 nor MI1-PD conferred a survival benefit for the mice when injected without nanoparticle protection.
“We’re excited about our results because there was no guarantee the nanotherapy would increase survival,” said study author Michael H. Tomasson, MD, of the Washington University School of Medicine.
“We injected the nanoparticles intravenously, and they found the tumors throughout the body, whether they were in the bone marrow, the spleen, or elsewhere.”
Drs Tomasson and Lanza said this technology is still years away from clinical trials, but they are optimistic about its future potential and are eager to begin that work. ![]()
Photo by Aaron Logan
A nanoparticle-based therapy can effectively fight multiple myeloma (MM), according to preclinical research published in Molecular Cancer Therapy.
The nanoparticles protected their therapeutic cargo from degradation in the bloodstream and enhanced drug delivery into MM cells, thereby improving survival in mouse models of MM.
The nanoparticles carried an Sn 2 lipase-labile prodrug inhibitor of MYC-MAX dimerization (MI1-PD).
Researchers designed this prodrug for use in MM because MM pathogenesis is driven by the MYC oncoprotein, its dimerization with MAX, and the binding of this heterodimer to E-Boxes in the vicinity of target genes.
Previous research has shown that MYC inhibitors are extremely potent in vitro, but, when injected into the blood, they degrade immediately. The current study is the first to show that a MYC inhibitor can be effective in animals with cancer, as long as the drug has a vehicle to protect and deliver it into cancer cells.
“The nanoparticles serve as vehicles that protect the drug from the harsh environment of the blood,” said study author Gregory M. Lanza, MD, PhD, of the Washington University School of Medicine in St Louis, Missouri.
“In this case, the drug is modified into a prodrug and actually locked into the outer membrane of the particle.”
The nanoparticles are designed to carry targeting molecules that home in on and bind to MM cells that carry the complementary receptor. When a nanoparticle binds to an MM cell, their membranes fuse together, transferring MI1-PD to the malignant cell. When safely inside, MI1-PD is enzymatically freed to do its job, blocking MYC from activation.
In theory, noncancerous cells are unlikely to be adversely affected by MYC inhibition because healthy cells shouldn’t have highly activated MYC proteins to begin with, according to the researchers.
The team injected 2 sizes of MI1-PD-containing nanoparticles into mice with MM and found that the nanoparticles increased the animals’ median survival.
The median survival was 46 days for mice that received MI1-PD-containing, 200-nm nanoparticles and 28 days for mice that received control, 200-nm nanoparticles (P<0.05). For mice that received 20 nm nanoparticles, the median survival was 52 days and 29 days, respectively (P=0.001).
The researchers also pointed out that neither MI1 nor MI1-PD conferred a survival benefit for the mice when injected without nanoparticle protection.
“We’re excited about our results because there was no guarantee the nanotherapy would increase survival,” said study author Michael H. Tomasson, MD, of the Washington University School of Medicine.
“We injected the nanoparticles intravenously, and they found the tumors throughout the body, whether they were in the bone marrow, the spleen, or elsewhere.”
Drs Tomasson and Lanza said this technology is still years away from clinical trials, but they are optimistic about its future potential and are eager to begin that work. ![]()
CTLs captured on video destroying cancer cells
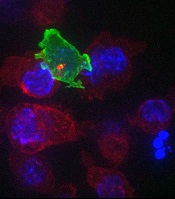
cancer cells (blue)
Image courtesy of Gillian
Griffiths and Jonny Settle
New research has illuminated the behavior of cytotoxic T cells (CTLs) as they hunt down and eliminate cancer cells.
Investigators used novel imaging techniques to capture the process on film and described their findings in an article published in Immunity.
The team captured the footage through high-resolution, 3D, time-lapse, multi-color imaging, making use of both spinning disk confocal microscopy and lattice light sheet microscopy.
These techniques involve capturing “slices” of an object and “stitching” them together to provide the final 3D images across the whole cell.
These approaches allowed the investigators to determine the order of events leading to the lethal “hit” CTLs deliver to cancer cells.
“Inside all of us lurks an army of ‘serial killers’ whose primary function is to kill again and again,” said study author Gillian Griffiths, PhD, of the Cambridge Institute for Medical Research in the UK.
“These [CTLs] patrol our bodies, identifying and destroying virally infected and cancer cells, and they do so with remarkable precision and efficiency.”
The CTLs, seen in the video as orange or green amorphous “blobs,” move around rapidly, investigating their environment as they travel.
When a CTL finds a cancer cell (blue), membrane protrusions rapidly explore the surface of the cell, checking for tell-tale signs that this is an uninvited guest.
The CTL binds to the cancer cell and injects cytotoxins (red) down microtubules to the interface between the T cell and the cancer cell, before puncturing the surface of the cancer cell and delivering its deadly cargo.
“In our bodies, where cells are packed together, it’s essential that the T cell focuses the lethal hit on its target,” Dr Griffiths explained. “Otherwise, it will cause collateral damage to neighboring, healthy cells.”
“Once the cytotoxins are injected into the cancer cell, its fate is sealed, and we can watch as it withers and dies. The T cell then moves on, hungry to find another victim.”
The investigators’ video is available on YouTube. ![]()
cancer cells (blue)
Image courtesy of Gillian
Griffiths and Jonny Settle
New research has illuminated the behavior of cytotoxic T cells (CTLs) as they hunt down and eliminate cancer cells.
Investigators used novel imaging techniques to capture the process on film and described their findings in an article published in Immunity.
The team captured the footage through high-resolution, 3D, time-lapse, multi-color imaging, making use of both spinning disk confocal microscopy and lattice light sheet microscopy.
These techniques involve capturing “slices” of an object and “stitching” them together to provide the final 3D images across the whole cell.
These approaches allowed the investigators to determine the order of events leading to the lethal “hit” CTLs deliver to cancer cells.
“Inside all of us lurks an army of ‘serial killers’ whose primary function is to kill again and again,” said study author Gillian Griffiths, PhD, of the Cambridge Institute for Medical Research in the UK.
“These [CTLs] patrol our bodies, identifying and destroying virally infected and cancer cells, and they do so with remarkable precision and efficiency.”
The CTLs, seen in the video as orange or green amorphous “blobs,” move around rapidly, investigating their environment as they travel.
When a CTL finds a cancer cell (blue), membrane protrusions rapidly explore the surface of the cell, checking for tell-tale signs that this is an uninvited guest.
The CTL binds to the cancer cell and injects cytotoxins (red) down microtubules to the interface between the T cell and the cancer cell, before puncturing the surface of the cancer cell and delivering its deadly cargo.
“In our bodies, where cells are packed together, it’s essential that the T cell focuses the lethal hit on its target,” Dr Griffiths explained. “Otherwise, it will cause collateral damage to neighboring, healthy cells.”
“Once the cytotoxins are injected into the cancer cell, its fate is sealed, and we can watch as it withers and dies. The T cell then moves on, hungry to find another victim.”
The investigators’ video is available on YouTube. ![]()
cancer cells (blue)
Image courtesy of Gillian
Griffiths and Jonny Settle
New research has illuminated the behavior of cytotoxic T cells (CTLs) as they hunt down and eliminate cancer cells.
Investigators used novel imaging techniques to capture the process on film and described their findings in an article published in Immunity.
The team captured the footage through high-resolution, 3D, time-lapse, multi-color imaging, making use of both spinning disk confocal microscopy and lattice light sheet microscopy.
These techniques involve capturing “slices” of an object and “stitching” them together to provide the final 3D images across the whole cell.
These approaches allowed the investigators to determine the order of events leading to the lethal “hit” CTLs deliver to cancer cells.
“Inside all of us lurks an army of ‘serial killers’ whose primary function is to kill again and again,” said study author Gillian Griffiths, PhD, of the Cambridge Institute for Medical Research in the UK.
“These [CTLs] patrol our bodies, identifying and destroying virally infected and cancer cells, and they do so with remarkable precision and efficiency.”
The CTLs, seen in the video as orange or green amorphous “blobs,” move around rapidly, investigating their environment as they travel.
When a CTL finds a cancer cell (blue), membrane protrusions rapidly explore the surface of the cell, checking for tell-tale signs that this is an uninvited guest.
The CTL binds to the cancer cell and injects cytotoxins (red) down microtubules to the interface between the T cell and the cancer cell, before puncturing the surface of the cancer cell and delivering its deadly cargo.
“In our bodies, where cells are packed together, it’s essential that the T cell focuses the lethal hit on its target,” Dr Griffiths explained. “Otherwise, it will cause collateral damage to neighboring, healthy cells.”
“Once the cytotoxins are injected into the cancer cell, its fate is sealed, and we can watch as it withers and dies. The T cell then moves on, hungry to find another victim.”
The investigators’ video is available on YouTube. ![]()
Approach could overcome drug resistance

Photo courtesy of the CDC
When treating patients with malaria and other infectious diseases, doctors should consider using drug combinations that reach similar parts of the body, according to researchers.
The group found that imperfect drug penetration—when drugs don’t reach all parts of the body—accelerates treatment resistance.
When there is a “pocket” of the body where only one drug is present, such as the brain or the digestive system, a pathogen can quickly develop resistance to one drug at a time.
“If there is a space where there is only one drug, that’s the place where the pathogen can start its escape,” said Pleuni Pennings, PhD, of San Francisco State University in California.
“Once it no longer has the first drug to deal with, it’s very easy for it to quickly become resistant to a second drug.”
Dr Pennings and her colleagues reported these findings in PNAS.
The team believes this research could have major implications for how treatment plans are designed and prescribed to patients with malaria, HIV, tuberculosis, and other ailments.
Because pathogens can quickly develop resistance to a single drug, providers often prescribe multiple drugs to increase their effectiveness.
The results of the study suggest that, when doing so, doctors should carefully consider which parts of the body each drug will reach and whether selecting medications with imperfect but similar penetrations might be the best treatment option.
“It may be better, in some cases, to leave a pocket of the body without any drugs instead of leaving a pocket with just one drug,” Dr Pennings said.
The study is the first to look at the connection between drug penetration and multidrug resistance. Dr Pennings and her colleagues ran computer simulations to observe the behavior of pathogens in response to changes in drugs and their levels of penetration.
The team found that, in instances where even small parts of the body could only be reached by one drug, the pathogen’s ability to build resistance to both drugs was accelerated compared to situations where no such pockets existed.
“This requires a new way of thinking about drug combinations that is a bit counterintuitive,” Dr Pennings said. “Suppose that drug A does not reach the brain, but drug B does. You’ll see the pathogen evolving resistance to drug B and assume that’s where the problem lies. But, in fact, it is drug A that is not doing its job because it’s not reaching the brain, and that’s the drug you may have to actually fix.”
With future research, Dr Pennings and her colleagues hope to outline the most effective drug combinations by exploring which parts of the body cannot be reached by specific drugs and where and how quickly specific pathogens are able to develop resistance. ![]()
Photo courtesy of the CDC
When treating patients with malaria and other infectious diseases, doctors should consider using drug combinations that reach similar parts of the body, according to researchers.
The group found that imperfect drug penetration—when drugs don’t reach all parts of the body—accelerates treatment resistance.
When there is a “pocket” of the body where only one drug is present, such as the brain or the digestive system, a pathogen can quickly develop resistance to one drug at a time.
“If there is a space where there is only one drug, that’s the place where the pathogen can start its escape,” said Pleuni Pennings, PhD, of San Francisco State University in California.
“Once it no longer has the first drug to deal with, it’s very easy for it to quickly become resistant to a second drug.”
Dr Pennings and her colleagues reported these findings in PNAS.
The team believes this research could have major implications for how treatment plans are designed and prescribed to patients with malaria, HIV, tuberculosis, and other ailments.
Because pathogens can quickly develop resistance to a single drug, providers often prescribe multiple drugs to increase their effectiveness.
The results of the study suggest that, when doing so, doctors should carefully consider which parts of the body each drug will reach and whether selecting medications with imperfect but similar penetrations might be the best treatment option.
“It may be better, in some cases, to leave a pocket of the body without any drugs instead of leaving a pocket with just one drug,” Dr Pennings said.
The study is the first to look at the connection between drug penetration and multidrug resistance. Dr Pennings and her colleagues ran computer simulations to observe the behavior of pathogens in response to changes in drugs and their levels of penetration.
The team found that, in instances where even small parts of the body could only be reached by one drug, the pathogen’s ability to build resistance to both drugs was accelerated compared to situations where no such pockets existed.
“This requires a new way of thinking about drug combinations that is a bit counterintuitive,” Dr Pennings said. “Suppose that drug A does not reach the brain, but drug B does. You’ll see the pathogen evolving resistance to drug B and assume that’s where the problem lies. But, in fact, it is drug A that is not doing its job because it’s not reaching the brain, and that’s the drug you may have to actually fix.”
With future research, Dr Pennings and her colleagues hope to outline the most effective drug combinations by exploring which parts of the body cannot be reached by specific drugs and where and how quickly specific pathogens are able to develop resistance. ![]()
Photo courtesy of the CDC
When treating patients with malaria and other infectious diseases, doctors should consider using drug combinations that reach similar parts of the body, according to researchers.
The group found that imperfect drug penetration—when drugs don’t reach all parts of the body—accelerates treatment resistance.
When there is a “pocket” of the body where only one drug is present, such as the brain or the digestive system, a pathogen can quickly develop resistance to one drug at a time.
“If there is a space where there is only one drug, that’s the place where the pathogen can start its escape,” said Pleuni Pennings, PhD, of San Francisco State University in California.
“Once it no longer has the first drug to deal with, it’s very easy for it to quickly become resistant to a second drug.”
Dr Pennings and her colleagues reported these findings in PNAS.
The team believes this research could have major implications for how treatment plans are designed and prescribed to patients with malaria, HIV, tuberculosis, and other ailments.
Because pathogens can quickly develop resistance to a single drug, providers often prescribe multiple drugs to increase their effectiveness.
The results of the study suggest that, when doing so, doctors should carefully consider which parts of the body each drug will reach and whether selecting medications with imperfect but similar penetrations might be the best treatment option.
“It may be better, in some cases, to leave a pocket of the body without any drugs instead of leaving a pocket with just one drug,” Dr Pennings said.
The study is the first to look at the connection between drug penetration and multidrug resistance. Dr Pennings and her colleagues ran computer simulations to observe the behavior of pathogens in response to changes in drugs and their levels of penetration.
The team found that, in instances where even small parts of the body could only be reached by one drug, the pathogen’s ability to build resistance to both drugs was accelerated compared to situations where no such pockets existed.
“This requires a new way of thinking about drug combinations that is a bit counterintuitive,” Dr Pennings said. “Suppose that drug A does not reach the brain, but drug B does. You’ll see the pathogen evolving resistance to drug B and assume that’s where the problem lies. But, in fact, it is drug A that is not doing its job because it’s not reaching the brain, and that’s the drug you may have to actually fix.”
With future research, Dr Pennings and her colleagues hope to outline the most effective drug combinations by exploring which parts of the body cannot be reached by specific drugs and where and how quickly specific pathogens are able to develop resistance. ![]()
Readmissions for severe sepsis fairly common

Photo courtesy of the CDC
DENVER—Severe sepsis is a significant cause of rehospitalization, along the lines of more commonly discussed conditions such as heart failure and pneumonia, according to research presented at the 2015 American Thoracic Society International Conference.
“Severe sepsis continues to be a common cause of hospitalization and has the associated high costs,” said Darya Rudym, MD, of New York University School of Medicine in New York.
She presented this finding at the meeting as publication number A3699.
Some quality measures associated with sepsis, such as length of hospital stay, have been studied previously. But Dr Rudym and her colleagues wanted to look at the rate of readmission within 30 days after discharge among patients with a diagnosis of severe sepsis.
The researchers also wanted to compare this rate to the readmission rates for outcomes reported by the Centers for Medicare and Medicaid Services, such as acute myocardial infarction, heart failure, and pneumonia.
The team examined inpatient discharges from Bellevue Hospital in New York City between July 2011 and July 2014 and identified subsequent readmissions to the hospital within 30 days.
During the 3-year study period, there were 22,712 discharges and an overall readmission rate of 15.31%, or 3477 patients.
The researchers used 3 different methods to identify patients with severe sepsis: Angus implementation, Martin implementation, and explicit ICD-9-CM sepsis codes.
There were 1801 cases of severe sepsis according to Angus implementation, 798 cases according to Martin implementation, and 579 cases according to ICD-9-CM sepsis codes.
In all, 266, 119, and 71 of these patients, respectively, were readmitted to the hospital within 30 days. This accounted for 14.77%, 14.91%, and 12.26% of cases, respectively.
The readmission rate for myocardial infarction was 8.67%. It was 14.46% for pneumonia, and 15% for heart failure.
“Readmission rates in severe sepsis are shown not to be significantly different from readmission rates in heart failure and pneumonia,” Dr Rudym noted. ![]()
Photo courtesy of the CDC
DENVER—Severe sepsis is a significant cause of rehospitalization, along the lines of more commonly discussed conditions such as heart failure and pneumonia, according to research presented at the 2015 American Thoracic Society International Conference.
“Severe sepsis continues to be a common cause of hospitalization and has the associated high costs,” said Darya Rudym, MD, of New York University School of Medicine in New York.
She presented this finding at the meeting as publication number A3699.
Some quality measures associated with sepsis, such as length of hospital stay, have been studied previously. But Dr Rudym and her colleagues wanted to look at the rate of readmission within 30 days after discharge among patients with a diagnosis of severe sepsis.
The researchers also wanted to compare this rate to the readmission rates for outcomes reported by the Centers for Medicare and Medicaid Services, such as acute myocardial infarction, heart failure, and pneumonia.
The team examined inpatient discharges from Bellevue Hospital in New York City between July 2011 and July 2014 and identified subsequent readmissions to the hospital within 30 days.
During the 3-year study period, there were 22,712 discharges and an overall readmission rate of 15.31%, or 3477 patients.
The researchers used 3 different methods to identify patients with severe sepsis: Angus implementation, Martin implementation, and explicit ICD-9-CM sepsis codes.
There were 1801 cases of severe sepsis according to Angus implementation, 798 cases according to Martin implementation, and 579 cases according to ICD-9-CM sepsis codes.
In all, 266, 119, and 71 of these patients, respectively, were readmitted to the hospital within 30 days. This accounted for 14.77%, 14.91%, and 12.26% of cases, respectively.
The readmission rate for myocardial infarction was 8.67%. It was 14.46% for pneumonia, and 15% for heart failure.
“Readmission rates in severe sepsis are shown not to be significantly different from readmission rates in heart failure and pneumonia,” Dr Rudym noted. ![]()
Photo courtesy of the CDC
DENVER—Severe sepsis is a significant cause of rehospitalization, along the lines of more commonly discussed conditions such as heart failure and pneumonia, according to research presented at the 2015 American Thoracic Society International Conference.
“Severe sepsis continues to be a common cause of hospitalization and has the associated high costs,” said Darya Rudym, MD, of New York University School of Medicine in New York.
She presented this finding at the meeting as publication number A3699.
Some quality measures associated with sepsis, such as length of hospital stay, have been studied previously. But Dr Rudym and her colleagues wanted to look at the rate of readmission within 30 days after discharge among patients with a diagnosis of severe sepsis.
The researchers also wanted to compare this rate to the readmission rates for outcomes reported by the Centers for Medicare and Medicaid Services, such as acute myocardial infarction, heart failure, and pneumonia.
The team examined inpatient discharges from Bellevue Hospital in New York City between July 2011 and July 2014 and identified subsequent readmissions to the hospital within 30 days.
During the 3-year study period, there were 22,712 discharges and an overall readmission rate of 15.31%, or 3477 patients.
The researchers used 3 different methods to identify patients with severe sepsis: Angus implementation, Martin implementation, and explicit ICD-9-CM sepsis codes.
There were 1801 cases of severe sepsis according to Angus implementation, 798 cases according to Martin implementation, and 579 cases according to ICD-9-CM sepsis codes.
In all, 266, 119, and 71 of these patients, respectively, were readmitted to the hospital within 30 days. This accounted for 14.77%, 14.91%, and 12.26% of cases, respectively.
The readmission rate for myocardial infarction was 8.67%. It was 14.46% for pneumonia, and 15% for heart failure.
“Readmission rates in severe sepsis are shown not to be significantly different from readmission rates in heart failure and pneumonia,” Dr Rudym noted. ![]()
Newest SHM Board Member Eager to Make Positive Impact
Christopher Frost, MD, FHM, has accomplished a lot in his career. He retired as a major from the U.S. Air Force Reserve. He's been an ED physician. And now he is the chief medical officer of hospital-based physicians for Hospital Corporation of America.
Yet, he considers being the newest member of SHM's Board of Directors a distinct honor.
"I am truly humbled to be participating with this group of energetic, intelligent, and wise individuals that comprise the SHM board," Dr. Frost says in an e-mail interview with The Hospitalist. "[I'm] very eager to participate with this group, and ultimately, I would like for us, not me, to be able to say we had some positive impact on the specialty, whether that be for our providers, patients, families, or some combination thereof."
Question: What drew you to hospital medicine?
Answer: During my chief [residency] year, I started moonlighting as a hospitalist for a large hematology/oncology group. I enjoyed the experience but did not really consider hospital medicine as a career option until I received a call asking if I knew of any residents who might be interested in joining a hospital medicine group undergoing rapid growth. Up until that moment, hospital medicine was just a moonlighting gig. It was still a relatively nascent specialty, and I did not realize it could be a career path. The call served as a catalyst to rethink my options.
Q: What keeps you engaged in the specialty?
A: The specialty attracts change agents. Individuals that are not necessarily satisfied with the status quo but instead are interested in collaborating with others to affect change. From a local level, in our community hospitals where hospitalists chair committees or serve as chiefs of staff, all the way to the national level where hospitalists are serving in such roles as the CMO of the Centers for Medicare & Medicaid Services or as the U.S. Surgeon General.
Q: As a new board member, what do you now realize that you didn’t before?
A: One is what it means to be a part of a “big tent” organization, and the other is an appreciation of the breadth and depth of the talent found among the SHM staff. I knew that SHM was involved in a lot of different activities and that several other specialty societies and organizations seek out SHM based on the collaborative nature of our specialty society; however, I didn't appreciate just how broad the scope of involvement extends. TH
Visit our website for more information on leadership.
Christopher Frost, MD, FHM, has accomplished a lot in his career. He retired as a major from the U.S. Air Force Reserve. He's been an ED physician. And now he is the chief medical officer of hospital-based physicians for Hospital Corporation of America.
Yet, he considers being the newest member of SHM's Board of Directors a distinct honor.
"I am truly humbled to be participating with this group of energetic, intelligent, and wise individuals that comprise the SHM board," Dr. Frost says in an e-mail interview with The Hospitalist. "[I'm] very eager to participate with this group, and ultimately, I would like for us, not me, to be able to say we had some positive impact on the specialty, whether that be for our providers, patients, families, or some combination thereof."
Question: What drew you to hospital medicine?
Answer: During my chief [residency] year, I started moonlighting as a hospitalist for a large hematology/oncology group. I enjoyed the experience but did not really consider hospital medicine as a career option until I received a call asking if I knew of any residents who might be interested in joining a hospital medicine group undergoing rapid growth. Up until that moment, hospital medicine was just a moonlighting gig. It was still a relatively nascent specialty, and I did not realize it could be a career path. The call served as a catalyst to rethink my options.
Q: What keeps you engaged in the specialty?
A: The specialty attracts change agents. Individuals that are not necessarily satisfied with the status quo but instead are interested in collaborating with others to affect change. From a local level, in our community hospitals where hospitalists chair committees or serve as chiefs of staff, all the way to the national level where hospitalists are serving in such roles as the CMO of the Centers for Medicare & Medicaid Services or as the U.S. Surgeon General.
Q: As a new board member, what do you now realize that you didn’t before?
A: One is what it means to be a part of a “big tent” organization, and the other is an appreciation of the breadth and depth of the talent found among the SHM staff. I knew that SHM was involved in a lot of different activities and that several other specialty societies and organizations seek out SHM based on the collaborative nature of our specialty society; however, I didn't appreciate just how broad the scope of involvement extends. TH
Visit our website for more information on leadership.
Christopher Frost, MD, FHM, has accomplished a lot in his career. He retired as a major from the U.S. Air Force Reserve. He's been an ED physician. And now he is the chief medical officer of hospital-based physicians for Hospital Corporation of America.
Yet, he considers being the newest member of SHM's Board of Directors a distinct honor.
"I am truly humbled to be participating with this group of energetic, intelligent, and wise individuals that comprise the SHM board," Dr. Frost says in an e-mail interview with The Hospitalist. "[I'm] very eager to participate with this group, and ultimately, I would like for us, not me, to be able to say we had some positive impact on the specialty, whether that be for our providers, patients, families, or some combination thereof."
Question: What drew you to hospital medicine?
Answer: During my chief [residency] year, I started moonlighting as a hospitalist for a large hematology/oncology group. I enjoyed the experience but did not really consider hospital medicine as a career option until I received a call asking if I knew of any residents who might be interested in joining a hospital medicine group undergoing rapid growth. Up until that moment, hospital medicine was just a moonlighting gig. It was still a relatively nascent specialty, and I did not realize it could be a career path. The call served as a catalyst to rethink my options.
Q: What keeps you engaged in the specialty?
A: The specialty attracts change agents. Individuals that are not necessarily satisfied with the status quo but instead are interested in collaborating with others to affect change. From a local level, in our community hospitals where hospitalists chair committees or serve as chiefs of staff, all the way to the national level where hospitalists are serving in such roles as the CMO of the Centers for Medicare & Medicaid Services or as the U.S. Surgeon General.
Q: As a new board member, what do you now realize that you didn’t before?
A: One is what it means to be a part of a “big tent” organization, and the other is an appreciation of the breadth and depth of the talent found among the SHM staff. I knew that SHM was involved in a lot of different activities and that several other specialty societies and organizations seek out SHM based on the collaborative nature of our specialty society; however, I didn't appreciate just how broad the scope of involvement extends. TH
Visit our website for more information on leadership.