User login
Portulaca oleracea (purslane)
Portulaca oleracea, also known as purslane, has long been used in various traditional medicine systems to relieve pain and edema.1Portulaca oleracea is a warm-climate annual plant originally found in the Middle East, North Africa, and the Indian subcontinent and now cultivated in the Arabian peninsula; Japan, where it is an abundant garden plant from spring to fall;2,3 and throughout the world.
The use of P. oleracea, a member of the Portulacaceae family, as a vegetable as well as herbal medicine dates back several centuries.4 In modern times, purslane has been found to be rich in antioxidants, particularly omega-3 fatty acids, vitamins C and E, beta-carotene, melatonin, and glutathione, as well as several minerals.5,6,7 Currently, it is considered one of the top ten most common plants in the world, and one of the most-used medical plants according to the World Health Organization.6 It is considered a weed in the United States, but is eaten in many parts of the world.

Antioxidant activity
Using two different assays, Uddin et al. determined in 2012 that P. oleracea cultivars exhibited significant antioxidant activity through various growth stages. In addition, the researchers suggested that purslane could provide multiple minerals as well as antioxidants in the context of nutraceutical products and functional food.7 Early this year, Silva et al. studied the antioxidant activity of P. oleracea leaves, flowers, and stems from two different locations in Portugal, with assays revealing significantly greater antioxidant activity in the stems of both samples compared to the leaves and flowers. However, the phenolic extracts of all three plant sections from both samples were found to protect DNA against hydroxyl radicals. The investigators concluded that their findings, particularly related to high antioxidant activity, support the potential benefits of purslane consumption to human health.8
A 2014 analysis of 13 collected purslane accessions revealed significant mineral content (particularly potassium, followed by nitrogen, sodium, calcium, magnesium, phosphorus, iron, zinc, and manganese) and showed that antioxidant activity was more strongly associated with ornamental as opposed to common purslane, the latter of which was richer in mineral content.6
Anti-inflammatory activity
In 2000, Chan et al. found that a 10% ethanolic extract of the dried leaves and stem of a P. oleracea cultivar displayed significant anti-inflammatory and analgesic properties after topical and intraperitoneal, but not oral, administration in comparison to diclofenac sodium, a synthetic drug used as active control. They added that these activities corresponded to the reputed effects of the traditional uses of the wild species.9
Wound healing activity
Rashed et al. reported in 2003 that a crude extract of P. oleracea accelerates wound healing. They used Mus musculus JVI-1 to show that fresh homogenized crude aerial parts of the plant topically applied on excision wound surfaces reduced wound surface areas and increased tensile strength. The best documented contraction was associated with a single dose of 50 mg, followed by two doses of 25 mg each.10
Oral lichen planus treatment
In 2010, Agha-Hosseini et al. conducted a randomized double-blind placebo-controlled 3-month study to assess the effectiveness of purslane in the treatment of oral lichen planus. Thirty-seven symptomatic patients (confirmed by biopsy) were divided into a purslane treatment group (n = 20) and a placebo group (n = 17). The investigators reported that partial to complete clinical improvement was observed in 83% of the treatment group, with no response in the remaining 17%, whereas partial improvement was seen in 17% of the placebo group, 73% had no response, and the condition was aggravated in 10% of the placebo group. No adverse side effects were reported in either group, and the researchers concluded that purslane was clinically effective in treating oral lichen planus and warrants consideration as a treatment option for the disorder.5
Other activities
In 2001, Radhakrishnan et al. identified several neuropharmacological actions, particularly anti-nociceptive and muscle-relaxing activity, with a range of effects on the central and peripheral nervous system observed in animal studies.1 The betacyanins found in P. oleracea have subsequently been found to confer a protective effect against neurotoxicity, specifically, ameliorating the D-galactose-induced cognitive deficits in senescent mice.11P. oleracea also has been shown to efficiently eliminate the endocrine-disrupting chemical bisphenol A from a hydroponic solution.12
In 2012, Yan et al. showed that three newly isolated homoisoflavonoids, known as portulacanones, and the compound 2,2’-dihydroxy-4’,6’-dimethoxychalcone selectively exhibited in vitro cytotoxic activities against four human cancer cell lines.2
Conclusions
This antioxidant-rich plant is found throughout the world and has long been associated with traditional health care. Modern research into its potential dermatologic uses is ongoing, but the evidence is relatively scarce. There are indications that the antioxidant, anti-inflammatory, and wound healing activity reportedly exhibited by purslane may be harnessed for various cutaneous applications. However, much more research is necessary to determine how extensive a role purslane may play in skin care.
References
1.J. Ethnopharmacol. 2001;76:171-6
2.Phytochemistry 2012;80:37-41
3.J. Biosci. Bioeng. 2007;103:420-6
4.J. Ethnopharmacol. 2000;73:445-51
5.Phytother. Res. 2010;24:240-4
6.Biomed. Res. Int. 2014;2014:296063
7.Int. J. Mol. Sci. 2012;13:10257-67
8.Nat Prod. Commun. 2014;9:45-50
9. J. Ethnopharmacol. 2000;73:445-51
10. J. Ethnopharmacol. 2003;88:131-6
11. Phytomedicine. 2010 Jun;17:527-32
12. Biosci. Biotechnol. Biochem. 2012;76:1015-7
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). She has contributed to the Cosmeceutical Critique column in Dermatology News since January 2001. Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever.
Portulaca oleracea, also known as purslane, has long been used in various traditional medicine systems to relieve pain and edema.1Portulaca oleracea is a warm-climate annual plant originally found in the Middle East, North Africa, and the Indian subcontinent and now cultivated in the Arabian peninsula; Japan, where it is an abundant garden plant from spring to fall;2,3 and throughout the world.
The use of P. oleracea, a member of the Portulacaceae family, as a vegetable as well as herbal medicine dates back several centuries.4 In modern times, purslane has been found to be rich in antioxidants, particularly omega-3 fatty acids, vitamins C and E, beta-carotene, melatonin, and glutathione, as well as several minerals.5,6,7 Currently, it is considered one of the top ten most common plants in the world, and one of the most-used medical plants according to the World Health Organization.6 It is considered a weed in the United States, but is eaten in many parts of the world.
Antioxidant activity
Using two different assays, Uddin et al. determined in 2012 that P. oleracea cultivars exhibited significant antioxidant activity through various growth stages. In addition, the researchers suggested that purslane could provide multiple minerals as well as antioxidants in the context of nutraceutical products and functional food.7 Early this year, Silva et al. studied the antioxidant activity of P. oleracea leaves, flowers, and stems from two different locations in Portugal, with assays revealing significantly greater antioxidant activity in the stems of both samples compared to the leaves and flowers. However, the phenolic extracts of all three plant sections from both samples were found to protect DNA against hydroxyl radicals. The investigators concluded that their findings, particularly related to high antioxidant activity, support the potential benefits of purslane consumption to human health.8
A 2014 analysis of 13 collected purslane accessions revealed significant mineral content (particularly potassium, followed by nitrogen, sodium, calcium, magnesium, phosphorus, iron, zinc, and manganese) and showed that antioxidant activity was more strongly associated with ornamental as opposed to common purslane, the latter of which was richer in mineral content.6
Anti-inflammatory activity
In 2000, Chan et al. found that a 10% ethanolic extract of the dried leaves and stem of a P. oleracea cultivar displayed significant anti-inflammatory and analgesic properties after topical and intraperitoneal, but not oral, administration in comparison to diclofenac sodium, a synthetic drug used as active control. They added that these activities corresponded to the reputed effects of the traditional uses of the wild species.9
Wound healing activity
Rashed et al. reported in 2003 that a crude extract of P. oleracea accelerates wound healing. They used Mus musculus JVI-1 to show that fresh homogenized crude aerial parts of the plant topically applied on excision wound surfaces reduced wound surface areas and increased tensile strength. The best documented contraction was associated with a single dose of 50 mg, followed by two doses of 25 mg each.10
Oral lichen planus treatment
In 2010, Agha-Hosseini et al. conducted a randomized double-blind placebo-controlled 3-month study to assess the effectiveness of purslane in the treatment of oral lichen planus. Thirty-seven symptomatic patients (confirmed by biopsy) were divided into a purslane treatment group (n = 20) and a placebo group (n = 17). The investigators reported that partial to complete clinical improvement was observed in 83% of the treatment group, with no response in the remaining 17%, whereas partial improvement was seen in 17% of the placebo group, 73% had no response, and the condition was aggravated in 10% of the placebo group. No adverse side effects were reported in either group, and the researchers concluded that purslane was clinically effective in treating oral lichen planus and warrants consideration as a treatment option for the disorder.5
Other activities
In 2001, Radhakrishnan et al. identified several neuropharmacological actions, particularly anti-nociceptive and muscle-relaxing activity, with a range of effects on the central and peripheral nervous system observed in animal studies.1 The betacyanins found in P. oleracea have subsequently been found to confer a protective effect against neurotoxicity, specifically, ameliorating the D-galactose-induced cognitive deficits in senescent mice.11P. oleracea also has been shown to efficiently eliminate the endocrine-disrupting chemical bisphenol A from a hydroponic solution.12
In 2012, Yan et al. showed that three newly isolated homoisoflavonoids, known as portulacanones, and the compound 2,2’-dihydroxy-4’,6’-dimethoxychalcone selectively exhibited in vitro cytotoxic activities against four human cancer cell lines.2
Conclusions
This antioxidant-rich plant is found throughout the world and has long been associated with traditional health care. Modern research into its potential dermatologic uses is ongoing, but the evidence is relatively scarce. There are indications that the antioxidant, anti-inflammatory, and wound healing activity reportedly exhibited by purslane may be harnessed for various cutaneous applications. However, much more research is necessary to determine how extensive a role purslane may play in skin care.
References
1.J. Ethnopharmacol. 2001;76:171-6
2.Phytochemistry 2012;80:37-41
3.J. Biosci. Bioeng. 2007;103:420-6
4.J. Ethnopharmacol. 2000;73:445-51
5.Phytother. Res. 2010;24:240-4
6.Biomed. Res. Int. 2014;2014:296063
7.Int. J. Mol. Sci. 2012;13:10257-67
8.Nat Prod. Commun. 2014;9:45-50
9. J. Ethnopharmacol. 2000;73:445-51
10. J. Ethnopharmacol. 2003;88:131-6
11. Phytomedicine. 2010 Jun;17:527-32
12. Biosci. Biotechnol. Biochem. 2012;76:1015-7
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). She has contributed to the Cosmeceutical Critique column in Dermatology News since January 2001. Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever.
Portulaca oleracea, also known as purslane, has long been used in various traditional medicine systems to relieve pain and edema.1Portulaca oleracea is a warm-climate annual plant originally found in the Middle East, North Africa, and the Indian subcontinent and now cultivated in the Arabian peninsula; Japan, where it is an abundant garden plant from spring to fall;2,3 and throughout the world.
The use of P. oleracea, a member of the Portulacaceae family, as a vegetable as well as herbal medicine dates back several centuries.4 In modern times, purslane has been found to be rich in antioxidants, particularly omega-3 fatty acids, vitamins C and E, beta-carotene, melatonin, and glutathione, as well as several minerals.5,6,7 Currently, it is considered one of the top ten most common plants in the world, and one of the most-used medical plants according to the World Health Organization.6 It is considered a weed in the United States, but is eaten in many parts of the world.
Antioxidant activity
Using two different assays, Uddin et al. determined in 2012 that P. oleracea cultivars exhibited significant antioxidant activity through various growth stages. In addition, the researchers suggested that purslane could provide multiple minerals as well as antioxidants in the context of nutraceutical products and functional food.7 Early this year, Silva et al. studied the antioxidant activity of P. oleracea leaves, flowers, and stems from two different locations in Portugal, with assays revealing significantly greater antioxidant activity in the stems of both samples compared to the leaves and flowers. However, the phenolic extracts of all three plant sections from both samples were found to protect DNA against hydroxyl radicals. The investigators concluded that their findings, particularly related to high antioxidant activity, support the potential benefits of purslane consumption to human health.8
A 2014 analysis of 13 collected purslane accessions revealed significant mineral content (particularly potassium, followed by nitrogen, sodium, calcium, magnesium, phosphorus, iron, zinc, and manganese) and showed that antioxidant activity was more strongly associated with ornamental as opposed to common purslane, the latter of which was richer in mineral content.6
Anti-inflammatory activity
In 2000, Chan et al. found that a 10% ethanolic extract of the dried leaves and stem of a P. oleracea cultivar displayed significant anti-inflammatory and analgesic properties after topical and intraperitoneal, but not oral, administration in comparison to diclofenac sodium, a synthetic drug used as active control. They added that these activities corresponded to the reputed effects of the traditional uses of the wild species.9
Wound healing activity
Rashed et al. reported in 2003 that a crude extract of P. oleracea accelerates wound healing. They used Mus musculus JVI-1 to show that fresh homogenized crude aerial parts of the plant topically applied on excision wound surfaces reduced wound surface areas and increased tensile strength. The best documented contraction was associated with a single dose of 50 mg, followed by two doses of 25 mg each.10
Oral lichen planus treatment
In 2010, Agha-Hosseini et al. conducted a randomized double-blind placebo-controlled 3-month study to assess the effectiveness of purslane in the treatment of oral lichen planus. Thirty-seven symptomatic patients (confirmed by biopsy) were divided into a purslane treatment group (n = 20) and a placebo group (n = 17). The investigators reported that partial to complete clinical improvement was observed in 83% of the treatment group, with no response in the remaining 17%, whereas partial improvement was seen in 17% of the placebo group, 73% had no response, and the condition was aggravated in 10% of the placebo group. No adverse side effects were reported in either group, and the researchers concluded that purslane was clinically effective in treating oral lichen planus and warrants consideration as a treatment option for the disorder.5
Other activities
In 2001, Radhakrishnan et al. identified several neuropharmacological actions, particularly anti-nociceptive and muscle-relaxing activity, with a range of effects on the central and peripheral nervous system observed in animal studies.1 The betacyanins found in P. oleracea have subsequently been found to confer a protective effect against neurotoxicity, specifically, ameliorating the D-galactose-induced cognitive deficits in senescent mice.11P. oleracea also has been shown to efficiently eliminate the endocrine-disrupting chemical bisphenol A from a hydroponic solution.12
In 2012, Yan et al. showed that three newly isolated homoisoflavonoids, known as portulacanones, and the compound 2,2’-dihydroxy-4’,6’-dimethoxychalcone selectively exhibited in vitro cytotoxic activities against four human cancer cell lines.2
Conclusions
This antioxidant-rich plant is found throughout the world and has long been associated with traditional health care. Modern research into its potential dermatologic uses is ongoing, but the evidence is relatively scarce. There are indications that the antioxidant, anti-inflammatory, and wound healing activity reportedly exhibited by purslane may be harnessed for various cutaneous applications. However, much more research is necessary to determine how extensive a role purslane may play in skin care.
References
1.J. Ethnopharmacol. 2001;76:171-6
2.Phytochemistry 2012;80:37-41
3.J. Biosci. Bioeng. 2007;103:420-6
4.J. Ethnopharmacol. 2000;73:445-51
5.Phytother. Res. 2010;24:240-4
6.Biomed. Res. Int. 2014;2014:296063
7.Int. J. Mol. Sci. 2012;13:10257-67
8.Nat Prod. Commun. 2014;9:45-50
9. J. Ethnopharmacol. 2000;73:445-51
10. J. Ethnopharmacol. 2003;88:131-6
11. Phytomedicine. 2010 Jun;17:527-32
12. Biosci. Biotechnol. Biochem. 2012;76:1015-7
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in the Design District in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote the textbook “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002), and a book for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). She has contributed to the Cosmeceutical Critique column in Dermatology News since January 2001. Her latest book, “Cosmeceuticals and Cosmetic Ingredients,” was published in November 2014. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Evolus, Galderma, GlaxoSmithKline, Kythera Biopharmaceuticals, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Topix Pharmaceuticals, and Unilever.

NASPAG: Obesity raises unique contraceptive concerns in teens
ORLANDO – The data with respect to the effects of obesity on the efficacy of contraceptives in adolescents are limited, but the general consensus is that if efficacy is reduced, it isn’t by enough to make a real difference, according to Dr. Alene Toulany.
The effect of obesity is likely to be very small, and studies that have looked at pharmacokinetics in obesity have estimated that body weight accounts for only about 10%-20% of the variability of hormone levels, Dr. Toulany said at the North American Society for Pediatric and Adolescent Gynecology annual meeting.
“We know that this is within the normal range for individuals who are not obese, she said.

The concerns regarding efficacy in obese patients are understandable, as obesity increases the metabolic rate, increases clearance of hepatically metabolized drugs, increases circulating blood volume, and affects the absorption of contraceptive steroids through the adipose tissue, she said, adding that “it makes sense that the serum drug levels may be insufficient to maintain contraceptive effects, but the data are very limited and inconsistent.”
That’s not to say obesity isn’t a concern, added Dr. Toulany, an adolescent medicine specialist at the Hospital for Sick Children, Toronto, and the University of Toronto.
“Without fail, all of us will be seeing patients with obesity,” she said. The rate of adolescent obesity has quadrupled in the last 3 decades, increasing from 5% among those aged 12-19 years in 1980 to more than 20% now. A third are currently overweight or obese.
Further, sexually active obese women, regardless of age, are significantly less likely to use contraception, and obese teens are more likely to engage in risky sexual behaviors than are nonobese teens.
For these reasons, it is important to find the most effective contraceptive method, taking into account other risk factors and the likelihood of compliance, she said, noting that obesity is an independent risk factor for venous thromboembolism (VTE) and that studies suggest the risk is additive in users of estrogen-containing contraceptives.
However, she said, the benefits outweigh the risks of pregnancy in obesity – especially of unintended pregnancy.
The absolute risk of VTE in healthy women of reproductive age is small, and in adolescents it’s even smaller, she explained.
“The presence of risk factors for VTE should be taken into account when we see these youth in our clinics, but we can and should offer estrogen-containing contraceptives as long as there are no other risk factors,” she said.
Contraceptive options in young obese patients include:
• Intrauterine devices. There is no evidence that either copper IUDs or progestin-releasing IUDs have reduced efficacy in obese adolescents.
• Implants. These are highly effective in obese women, and even though the concentrations may be 30%-60% lower in obese women, they do remain above the contraceptive threshold for at least the first 3 years, Dr. Toulany said.
• Depot medroxyprogesterone acetate. There is some concern about weight gain with this injectable progestin-only contraceptive, particularly in those who are already obese, but it remains an option, as the levels do remain above what is needed to prevent ovulation. Interestingly, the persistence of ovulation suppression following discontinuation is different in obese women, and may be prolonged, compared with nonobese women; it is important to counsel patients about this, she said.
“So although randomized, controlled trials report no significant weight gain, we do agree with these observational studies that show that overweight and obese teens gain more weight with Depo-Provera than with oral contraceptives or with no contraceptives,” she said.
• Oral contraceptive pills. Although these may be less effective in obese adolescents, they remain an option and may be the best option in a given patient. Combined oral contraceptives are believed to be generally effective for pregnancy prevention, but “may be less forgiving of imperfect use,” and thus may not be the best choice in those who may have problems with adherence, for example.
The contraceptive patch is probably not a good option, because efficacy may be diminished as a result of absorption through the adipose tissues in those weighing more than 90 kg, Dr .Toulany said. Evidence is insufficient regarding the use of contraceptive rings in obese patients.
Bariatric surgery is increasingly being performed in adolescents, and this raises unique concerns with respect to contraception, Dr. Toulany said.
“We recommend discontinuing estrogen-containing contraceptives 1 month before surgery to reduce the risk of VTE postoperatively,” she said.
After bariatric surgery, those who undergo a restrictive procedure such as gastric banding or a gastric sleeve procedure that reduces the volume of the stomach can use oral contraceptives, but postsurgery vomiting and diarrhea could increase the risk of complications. In those who undergo surgery using a technique that involves a significant malabsorption component, such as Roux-en-Y gastric bypass, nonoral contraceptives are the best option.
“Most patients going for bariatric surgery have an IUD inserted at the time of surgery, and that’s what we would recommend,” Dr. Toulany said.
She reported having no relevant financial disclosures.
ORLANDO – The data with respect to the effects of obesity on the efficacy of contraceptives in adolescents are limited, but the general consensus is that if efficacy is reduced, it isn’t by enough to make a real difference, according to Dr. Alene Toulany.
The effect of obesity is likely to be very small, and studies that have looked at pharmacokinetics in obesity have estimated that body weight accounts for only about 10%-20% of the variability of hormone levels, Dr. Toulany said at the North American Society for Pediatric and Adolescent Gynecology annual meeting.
“We know that this is within the normal range for individuals who are not obese, she said.
The concerns regarding efficacy in obese patients are understandable, as obesity increases the metabolic rate, increases clearance of hepatically metabolized drugs, increases circulating blood volume, and affects the absorption of contraceptive steroids through the adipose tissue, she said, adding that “it makes sense that the serum drug levels may be insufficient to maintain contraceptive effects, but the data are very limited and inconsistent.”
That’s not to say obesity isn’t a concern, added Dr. Toulany, an adolescent medicine specialist at the Hospital for Sick Children, Toronto, and the University of Toronto.
“Without fail, all of us will be seeing patients with obesity,” she said. The rate of adolescent obesity has quadrupled in the last 3 decades, increasing from 5% among those aged 12-19 years in 1980 to more than 20% now. A third are currently overweight or obese.
Further, sexually active obese women, regardless of age, are significantly less likely to use contraception, and obese teens are more likely to engage in risky sexual behaviors than are nonobese teens.
For these reasons, it is important to find the most effective contraceptive method, taking into account other risk factors and the likelihood of compliance, she said, noting that obesity is an independent risk factor for venous thromboembolism (VTE) and that studies suggest the risk is additive in users of estrogen-containing contraceptives.
However, she said, the benefits outweigh the risks of pregnancy in obesity – especially of unintended pregnancy.
The absolute risk of VTE in healthy women of reproductive age is small, and in adolescents it’s even smaller, she explained.
“The presence of risk factors for VTE should be taken into account when we see these youth in our clinics, but we can and should offer estrogen-containing contraceptives as long as there are no other risk factors,” she said.
Contraceptive options in young obese patients include:
• Intrauterine devices. There is no evidence that either copper IUDs or progestin-releasing IUDs have reduced efficacy in obese adolescents.
• Implants. These are highly effective in obese women, and even though the concentrations may be 30%-60% lower in obese women, they do remain above the contraceptive threshold for at least the first 3 years, Dr. Toulany said.
• Depot medroxyprogesterone acetate. There is some concern about weight gain with this injectable progestin-only contraceptive, particularly in those who are already obese, but it remains an option, as the levels do remain above what is needed to prevent ovulation. Interestingly, the persistence of ovulation suppression following discontinuation is different in obese women, and may be prolonged, compared with nonobese women; it is important to counsel patients about this, she said.
“So although randomized, controlled trials report no significant weight gain, we do agree with these observational studies that show that overweight and obese teens gain more weight with Depo-Provera than with oral contraceptives or with no contraceptives,” she said.
• Oral contraceptive pills. Although these may be less effective in obese adolescents, they remain an option and may be the best option in a given patient. Combined oral contraceptives are believed to be generally effective for pregnancy prevention, but “may be less forgiving of imperfect use,” and thus may not be the best choice in those who may have problems with adherence, for example.
The contraceptive patch is probably not a good option, because efficacy may be diminished as a result of absorption through the adipose tissues in those weighing more than 90 kg, Dr .Toulany said. Evidence is insufficient regarding the use of contraceptive rings in obese patients.
Bariatric surgery is increasingly being performed in adolescents, and this raises unique concerns with respect to contraception, Dr. Toulany said.
“We recommend discontinuing estrogen-containing contraceptives 1 month before surgery to reduce the risk of VTE postoperatively,” she said.
After bariatric surgery, those who undergo a restrictive procedure such as gastric banding or a gastric sleeve procedure that reduces the volume of the stomach can use oral contraceptives, but postsurgery vomiting and diarrhea could increase the risk of complications. In those who undergo surgery using a technique that involves a significant malabsorption component, such as Roux-en-Y gastric bypass, nonoral contraceptives are the best option.
“Most patients going for bariatric surgery have an IUD inserted at the time of surgery, and that’s what we would recommend,” Dr. Toulany said.
She reported having no relevant financial disclosures.
ORLANDO – The data with respect to the effects of obesity on the efficacy of contraceptives in adolescents are limited, but the general consensus is that if efficacy is reduced, it isn’t by enough to make a real difference, according to Dr. Alene Toulany.
The effect of obesity is likely to be very small, and studies that have looked at pharmacokinetics in obesity have estimated that body weight accounts for only about 10%-20% of the variability of hormone levels, Dr. Toulany said at the North American Society for Pediatric and Adolescent Gynecology annual meeting.
“We know that this is within the normal range for individuals who are not obese, she said.
The concerns regarding efficacy in obese patients are understandable, as obesity increases the metabolic rate, increases clearance of hepatically metabolized drugs, increases circulating blood volume, and affects the absorption of contraceptive steroids through the adipose tissue, she said, adding that “it makes sense that the serum drug levels may be insufficient to maintain contraceptive effects, but the data are very limited and inconsistent.”
That’s not to say obesity isn’t a concern, added Dr. Toulany, an adolescent medicine specialist at the Hospital for Sick Children, Toronto, and the University of Toronto.
“Without fail, all of us will be seeing patients with obesity,” she said. The rate of adolescent obesity has quadrupled in the last 3 decades, increasing from 5% among those aged 12-19 years in 1980 to more than 20% now. A third are currently overweight or obese.
Further, sexually active obese women, regardless of age, are significantly less likely to use contraception, and obese teens are more likely to engage in risky sexual behaviors than are nonobese teens.
For these reasons, it is important to find the most effective contraceptive method, taking into account other risk factors and the likelihood of compliance, she said, noting that obesity is an independent risk factor for venous thromboembolism (VTE) and that studies suggest the risk is additive in users of estrogen-containing contraceptives.
However, she said, the benefits outweigh the risks of pregnancy in obesity – especially of unintended pregnancy.
The absolute risk of VTE in healthy women of reproductive age is small, and in adolescents it’s even smaller, she explained.
“The presence of risk factors for VTE should be taken into account when we see these youth in our clinics, but we can and should offer estrogen-containing contraceptives as long as there are no other risk factors,” she said.
Contraceptive options in young obese patients include:
• Intrauterine devices. There is no evidence that either copper IUDs or progestin-releasing IUDs have reduced efficacy in obese adolescents.
• Implants. These are highly effective in obese women, and even though the concentrations may be 30%-60% lower in obese women, they do remain above the contraceptive threshold for at least the first 3 years, Dr. Toulany said.
• Depot medroxyprogesterone acetate. There is some concern about weight gain with this injectable progestin-only contraceptive, particularly in those who are already obese, but it remains an option, as the levels do remain above what is needed to prevent ovulation. Interestingly, the persistence of ovulation suppression following discontinuation is different in obese women, and may be prolonged, compared with nonobese women; it is important to counsel patients about this, she said.
“So although randomized, controlled trials report no significant weight gain, we do agree with these observational studies that show that overweight and obese teens gain more weight with Depo-Provera than with oral contraceptives or with no contraceptives,” she said.
• Oral contraceptive pills. Although these may be less effective in obese adolescents, they remain an option and may be the best option in a given patient. Combined oral contraceptives are believed to be generally effective for pregnancy prevention, but “may be less forgiving of imperfect use,” and thus may not be the best choice in those who may have problems with adherence, for example.
The contraceptive patch is probably not a good option, because efficacy may be diminished as a result of absorption through the adipose tissues in those weighing more than 90 kg, Dr .Toulany said. Evidence is insufficient regarding the use of contraceptive rings in obese patients.
Bariatric surgery is increasingly being performed in adolescents, and this raises unique concerns with respect to contraception, Dr. Toulany said.
“We recommend discontinuing estrogen-containing contraceptives 1 month before surgery to reduce the risk of VTE postoperatively,” she said.
After bariatric surgery, those who undergo a restrictive procedure such as gastric banding or a gastric sleeve procedure that reduces the volume of the stomach can use oral contraceptives, but postsurgery vomiting and diarrhea could increase the risk of complications. In those who undergo surgery using a technique that involves a significant malabsorption component, such as Roux-en-Y gastric bypass, nonoral contraceptives are the best option.
“Most patients going for bariatric surgery have an IUD inserted at the time of surgery, and that’s what we would recommend,” Dr. Toulany said.
She reported having no relevant financial disclosures.
EXPERT ANALYSIS FROM THE NASPAG ANNUAL MEETING

Vitiligo Disease Triggers: Psychological Stressors Preceding the Onset of Disease
Vitiligo is the loss of skin pigmentation caused by autoimmune destruction of melanocytes. Multiple pathogenic factors for vitiligo have been described, including CD8+ T lymphocyte/T helper 1 infiltrates in lesional skin1,2 with increased expression of IFN-γ3 and tumor necrosis factor α,3-6 decreased transforming growth factor β,7 and circulating autoantibodies against tyrosine hydroxylase.8 Additionally, several studies have found a high prevalence of antecedent psychological stressors in vitiligo patients, suggesting that specific stressors may trigger and/or exacerbate vitiligo.9-12
The relationship between antecedent psychological stressors and vitiligo extent has not been well studied. Potential mechanisms for stress-triggered vitiligo include increased catecholamines13 and neuropeptides,14 which have been found in vitiligo patients. However, the complex relationship between stressors and subsequent vitiligo is not well defined. We hypothesized that persistent stressors are associated with increased vitiligo extent.
Vitiligo is classically considered to be a silent pigmentary disorder with few or no symptoms. Prior studies have demonstrated that one-third of vitiligo patients report skin symptoms (eg, pruritus, burning), which may be specifically associated with early-onset disease.15-17 Further, we observed that some vitiligo patients report abdominal cramping associated with their disease. Few studies have described the burden of skin symptoms and other associated symptoms in vitiligo or their determinants.
We conducted a prospective questionnaire-based study of 1541 adult vitiligo patients to identify psychological factors that may precede vitiligo onset. We hypothesized that some types of stressors that occur within 2 years prior to disease onset would have specific associations with vitiligo and/or somatic symptoms.
Methods
Study Population and Questionnaire Distribution
This prospective questionnaire-based study was approved by the institutional review board at St. Luke’s-Roosevelt Hospital Center (now Mount Sinai St. Luke’s-Roosevelt) (New York, New York) for adults (>18 years; male or female) with vitiligo. The survey was validated in paper format at St. Luke’s-Roosevelt Hospital Center and distributed online to members of nonprofit support groups for vitiligo vulgaris, as previously described.15
Questionnaire
The a priori aim of this questionnaire was to identify psychological factors that may precede vitiligo onset. The questionnaire consisted of 77 items (55 closed questions and 22 open questions) pertaining to participant demographics/vitiligo phenotype and psychological stressors preceding vitiligo onset. The questions related to this study and response rates are listed in eTable 1. Responses were verified by screening for noninteger or implausible values (eg, <0 or >100 years of age).
Sample Size
The primary outcome used for sample size calculation was the potential association between vitiligo and the presence of antecedent psychological stressors. Using a 2-tailed test, we determined that a sample size of 1264 participants would have 90% power at α=.05 and a baseline proportion of 0.01 (1% presumed prevalence of vitiligo) to detect an odds ratio (OR) of 2.5 or higher.18
Data and Statistical Analysis
Closed question responses were analyzed using descriptive statistics. Open-ended question responses were analyzed using content analysis. Related comments were coded and grouped, with similarities and differences noted. All data processing and statistics were done with SAS version 9.2. Age at diagnosis (years) and number of anatomic sites affected were divided into tertiles for statistical analysis due to wide skewing.
Logistic regression models were constructed with numbers of reported deaths or stressors per participant within the 2 years prior to vitiligo onset as independent variables (0, 1, or ≥2), and symptoms associated with vitiligo as dependent variables. Adjusted ORs were calculated from multivariate models that included sex, current age (continuous), and comorbid autoimmune disease (binary) as covariates. Linear interaction terms were tested and were included in final models if statistically significant (P<.05).
Ordinal logistic regression was used to analyze the relationship between stressors (and other independent variables) and number of anatomic sites affected with vitiligo (tertiles). Ordinal logistic regression models were constructed to examine the impact of psychological stressors on pruritus secondary to vitiligo (not relevant combined with not at all, a little, a lot, very much) as the dependent variable. The proportional odds assumption was met in both models, as judged by score testing (P>.05). Binary logistic regression was used to analyze laterality, body surface area (BSA) greater than 25%, and involvement of the face and/or body with vitiligo lesions (binary).
Binary logistic regression models were constructed with impact of psychological stressors preceding vitiligo onset on comorbid abdominal cramping and specific etiologies as the dependent variables. There were 20 candidate stressors occurring within the 2 years prior to vitiligo onset. Selection methods for predictors were used to identify significant covariates within the context of the other covariates included in the final models. The results of forward, backward, and stepwise approaches were similar, and the stepwise selection output was presented.
Missing values were encountered because some participants did not respond to all the questionnaire items. A complete case analysis was performed (ie, missing values were ignored throughout the study). Data imputation was considered by multiple imputations; however, there were few or no differences between the estimates from the 2 approaches. Therefore, final models did not involve data imputation.
The statistical significance for all estimates was considered to be P<.05. However, a P value near .05 should be interpreted with caution given the multiple dependent tests performed in this study with increased risk for falsely rejecting the null hypothesis.
Results
Survey Population Characteristics
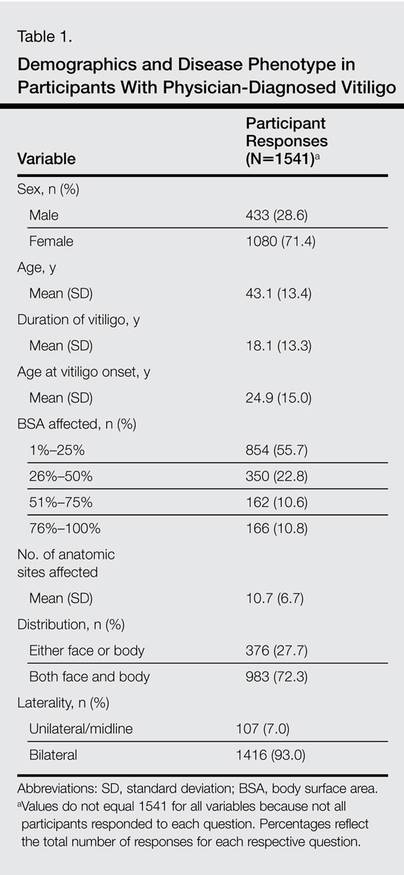
One thousand seven hundred participants started the survey; 1632 completed the survey (96.0% completion rate) and 1553 had been diagnosed with vitiligo by a physician. Twelve participants were excluded because they were younger than 18 years, leaving 1541 evaluable participants. Five hundred thirty-eight participants (34.9%) had comorbid autoimmune disorders. Demographics and disease phenotypes of the study participants are listed in Table 1.
Stressors Preceding Vitiligo Onset
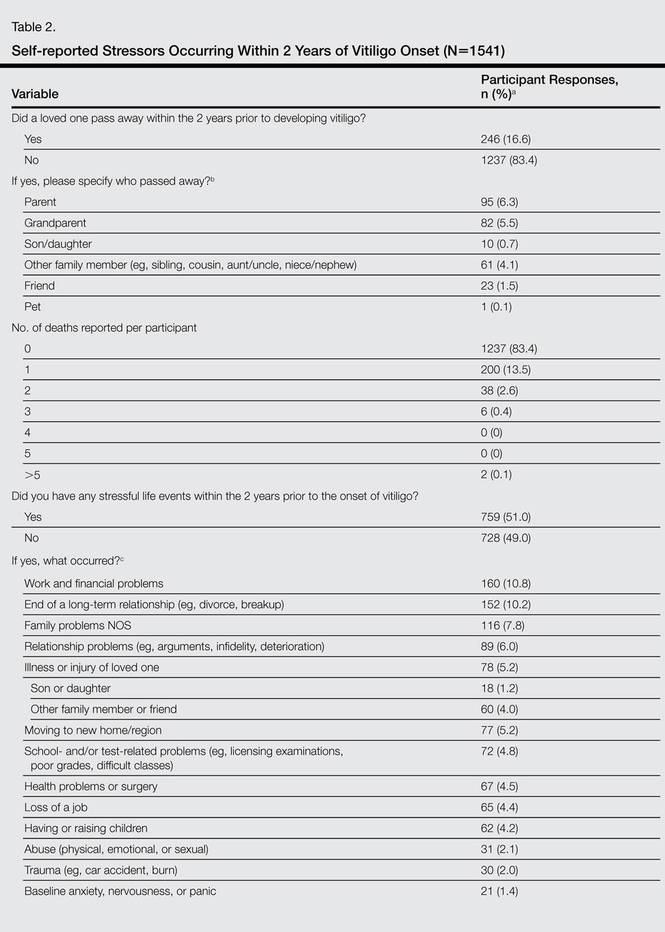
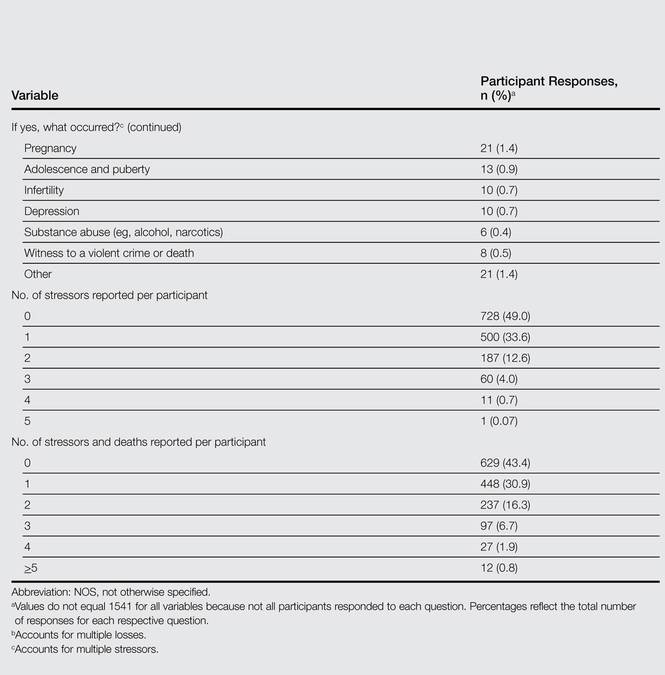
Eight hundred twenty-one participants (56.6%) experienced at least one death or stressor within 2 years prior to vitiligo onset (Table 2), including death of a loved one (16.6%) and stressful life events (51.0%) within the 2 years prior to the onset of vitiligo, especially work/financial problems (10.8%), end of a long-term relationship (10.2%), and family problems (not otherwise specified)(7.8%). Two hundred (13.5%) participants reported experiencing 1 death and 46 (3.1%) reported multiple deaths. Five hundred participants (33.6%) reported experiencing 1 stressor and 259 (17.4%) reported multiple stressors.
Stressors Not Associated With Vitiligo Extent
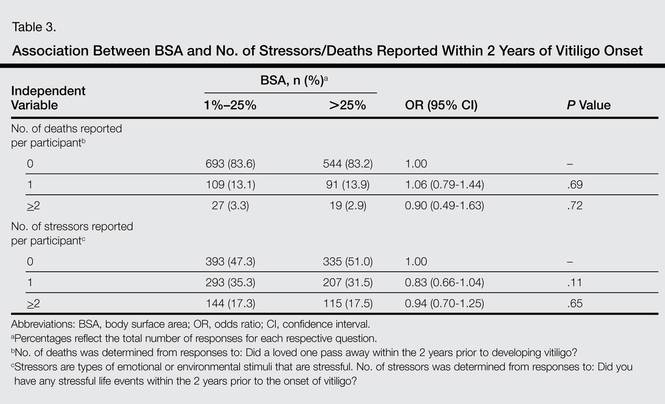
The number of deaths or stressors reported per participant within the 2 years prior to vitiligo onset were not associated with BSA, laterality, or distribution of lesions (Table 3 and eTable 2–eTable 4).
Symptoms Associated With Vitiligo
Five hundred twenty-two participants (34.5%) reported intermittent abdominal cramping, including premenstrual and/or menstrual cramping in women (9.7%), food-related abdominal cramping (4.4%), inflammatory bowel syndrome (IBS)(2.6%), anxiety-related abdominal cramping (1.5%), autoimmune gastrointestinal disorders (1.2%), and “other” etiologies (20.4%). Five hundred ten participants reported itching and/or burning associated with vitiligo lesions (35.1%).
Intermittent abdominal cramping overall was associated with a BSA greater than 75% (OR, 1.65; 95% confidence interval (CI), 1.17-2.32; P=.004). However, specific etiologies of abdominal cramping were not significantly associated with BSA (P≥.11). In contrast, itching and/or burning from vitiligo lesions was associated with a BSA greater than 25% (OR, 1.53; 95% CI, 1.23-1.90; P<.0001).
Association Between Number of Stressors and Symptoms in Vitiligo
A history of multiple stressors (≥2) within the 2 years prior to vitiligo onset was associated with intermittent abdominal cramping overall (OR, 1.84; 95% CI, 1.38-2.47; P<.0001), including premenstrual and/or menstrual cramping in women (OR, 1.84; 95% CI, 1.15-2.95; P=.01), IBS (OR, 3.29; 95% CI, 1.34-8.05; P=.01), and autoimmune gastrointestinal disorders (OR, 4.02; 95% CI, 1.27-12.80; P=.02)(eTable 5). These associations remained significant in multivariate models that included age, sex, and BSA as covariates. However, a history of 1 stressor or death or multiple deaths in the 2 years prior to vitiligo onset was not associated with any etiology of abdominal cramping.
Experiencing 1 (OR, 1.43; 95% CI, 1.12-1.82; P=.005) or multiple stressors (OR, 1.51; 95% CI, 1.12-2.04; P=.007) also was associated with itching and/or burning secondary to vitiligo. This association remained significant in a multivariate model that included age, sex, and BSA as covariates. However, a history of 1 or multiple deaths in the 2 years prior to vitiligo onset was not associated with itching and/or burning.
Association Between Specific Stressors and Vitiligo Symptoms
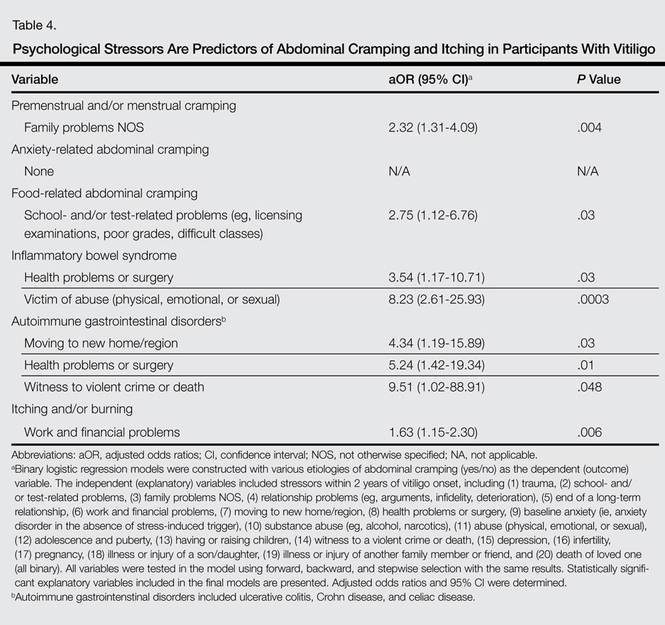
Perimenstrual (premenstrual and/or menstrual) cramping in women was associated with family problems (not otherwise specified) within the 2 years prior to vitiligo onset (Table 4). Food-related abdominal cramping was associated with school- and/or test-related stressors. Diagnosis of IBS was associated with health problems or surgery and being a victim of abuse within the 2 years prior to onset of vitiligo. Autoimmune gastrointestinal disorders were associated with moving to a new home/region, health problems or surgery, and witness to a violent crime or death. Finally, itching and/or burning of vitiligo lesions was associated with work and financial problems.
Comment
The present study found a high frequency of stressful life events and deaths of loved ones occurring within the 2 years preceding vitiligo onset. A history of multiple stressors but not deaths of loved ones was associated with more frequent symptoms in vitiligo patients, including itching and/or burning and intermittent abdominal pain. Specific stressors were associated with intermittent abdominal cramping, which occurred in approximately one-third of vitiligo patients. Abdominal cramping was related to menses in women, anxiety, foods, IBS, autoimmune gastrointestinal disorders, and other etiologies of abdominal cramping, which underscores the complex relationship between stressors, vitiligo, and inflammation. It is possible that stress-related immune abnormalities occur in vitiligo, which may influence the development of other autoimmune disorders. Alternatively, abdominal symptoms may precede and perhaps contribute to psychological stressors and impaired quality of life in vitiligo patients; however, the cross-sectional nature of the study did not allow us to elucidate this temporal relationship.
The present study found that 56.6% of participants experienced 1 or more deaths (17%) and/or stressful life events (51%) within the 2 years prior to vitiligo onset. These results are consistent with prior smaller studies that demonstrated a high frequency of stressful events preceding vitiligo onset. A case-controlled study found stressful events in 12 of 21 (57%) Romanian children with vitiligo, which was higher than controls.19 Another questionnaire-based, case-controlled study compared a heterogeneous group of 32 adolescent and adult Romanian patients with vitiligo and found higher odds of a stressful event in women preceding vitiligo diagnosis compared to controls.10 A retrospective analysis of 65 Croatian patients with vitiligo also reported that 56.9% (37/65) had some associated psychological factors.9 Another retrospective study of 31 adults with vitiligo found increased occurrence of 3 or more uncontrollable events, decreased perceived social support, and increased anxiety in vitiligo patients versus 116 other dermatologic disease controls.12 A questionnaire-based study found increased bereavements, changes in sleeping and eating habits, and personal injuries/illnesses in 73 British adults with vitiligo compared to 73 other age- and sex-matched dermatologic disease controls.11 All of these studies were limited by a small sample size, and the patient populations were localized to a regional dermatology referral center. The present study provided a larger analysis of stressful life events preceding vitiligo onset and included a diverse patient population.
The present study found that stressful life events and deaths of a loved one are not associated with vitiligo extent and distribution. This finding suggests that stressful life events may act as vitiligo triggers in genetically predisposed individuals, but ultimately the disease course and prognosis are driven by other factors, such as increased systemic inflammation or other immunologic abnormalities. Indeed, Silverberg and Silverberg20 and other investigators21,22 reported relative deficiencies of 25-hydroxyvitamin D,23 vitamins B6 and B12, and folic acid,20 as well as elevated serum homocysteine levels in vitiligo patients. Increased serum homocysteine levels were associated with increased BSA of vitiligo lesions.20 Elevated serum homocysteine levels also have been associated with increased inflammation in coronary artery disease,24 psoriasis,25,26 and in vitro.27 These laboratory anomalies likely reflect an underlying predisposition toward vitiligo, which might be triggered by stress responses or secondarily altered immune responses.
The present study had several strengths, including being prospective with a large sample size. The patient population included a large sample of men and women with representation of various adult ages and vitiligo extent. However, this study also had potential limitations. Measures of vitiligo extent were self-reported and were not clinically assessed. To address this limitation, we validated the questionnaire before posting it online.15 Invitation to participate in the survey was distributed by vitiligo support groups, which may have resulted in a selection bias toward participants with greater disease severity or with a poorer quality of life associated with vitiligo. Invitation to participate in this study was sent to members of vitiligo support groups, which allowed for recruitment of a large number of vitiligo patients despite a relatively low prevalence of disease in the general population. However, there are several challenges using this approach for nonvitiligo controls. Using participants with another dermatological disease as a control group may yield spurious results. Ideally, a large randomized sample of healthy participants with minimization of bias should be used for controls, which is an ambitious undertaking that was beyond the scope of this pilot study and will be the subject of future studies. Finally, this analysis found associations between stressors that occurred in the 2 years prior to vitiligo onset with symptomatic disease. We chose a broad interval for stressors because early vitiligo lesions may go unnoticed, making recognition of stressors occurring within days or weeks of onset infeasible. Further, we considered that chronic and prolonged stressors are more likely to have harmful consequences than acute stressors. Thus, stressors occurring within a more narrow interval (eg, 2 months) may not have the same association with vitiligo. Future studies are warranted to precisely identify the type and timing of psychological stressors preceding vitiligo onset.
Conclusion
In conclusion, there is a high prevalence of stressful life events preceding vitiligo, which may play an important role as disease triggers as well as predict the presence of intermittent abdominal cramping and itching or burning of skin. These associations indicate that screening of vitiligo patients for psychological stressors, abdominal cramping, and itching and/or burning of skin should be included in the routine assessment of vitiligo patients.
Appendix
1. Goronzy J, Weyand CM, Waase I. T cell subpopulations in inflammatory bowel disease: evidence for a defective induction of T8+ suppressor/cytotoxic T lymphocytes. Clin Exp Immunol. 1985;61:593-600.
2. Ongenae K, Van Geel N, Naeyaert JM. Evidence for an autoimmune pathogenesis of vitiligo. Pigment Cell Res. 2003;16:90-100.
3. Grimes PE, Morris R, Avaniss-Aghajani E, et al. Topical tacrolimus therapy for vitiligo: therapeutic responses and skin messenger RNA expression of proinflammatory cytokines. J Am Acad Dermatol. 2004;51:52-61.
4. Birol A, Kisa U, Kurtipek GS, et al. Increased tumor necrosis factor alpha (TNF-alpha) and interleukin 1 alpha (IL1-alpha) levels in the lesional skin of patients with nonsegmental vitiligo. Int J Dermatol. 2006;45:992-993.
5. Moretti S, Spallanzani A, Amato L, et al. New insights into the pathogenesis of vitiligo: imbalance of epidermal cytokines at sites of lesions. Pigment Cell Res. 2002;15:87-92.
6. Zailaie MZ. Decreased proinflammatory cytokine production by peripheral blood mononuclear cells from vitiligo patients following aspirin treatment. Saudi Med J. 2005;26:799-805.
7. Basak PY, Adiloglu AK, Ceyhan AM, et al. The role of helper and regulatory T cells in the pathogenesis of vitiligo. J Am Acad Dermatol. 2009;60:256-260.
8. Kemp EH, Emhemad S, Akhtar S, et al. Autoantibodies against tyrosine hydroxylase in patients with non-segmental (generalised) vitiligo. Exp Dermatol. 2011;20:35-40.
9. Barisic´-Drusko V, Rucevic I. Trigger factors in childhood psoriasis and vitiligo. Coll Antropol. 2004;28:277-285.
10. Manolache L, Benea V. Stress in patients with alopecia areata and vitiligo. J Eur Acad Dermatol Venereol. 2007;21:921-928.
11. Papadopoulos L, Bor R, Legg C, et al. Impact of life events on the onset of vitiligo in adults: preliminary evidence for a psychological dimension in aetiology. Clin Exp Dermatol. 1998;23:243-248.
12. Picardi A, Pasquini P, Cattaruzza MS, et al. Stressful life events, social support, attachment security and alexithymia in vitiligo. a case-control study. Psychother Psychosom. 2003;72:150-158.
13. Salzer BA, Schallreuter KU. Investigation of the personality structure in patients with vitiligo and a possible association with impaired catecholamine metabolism. Dermatology. 1995;190:109-115.
14. Al’Abadie MS, Senior HJ, Bleehen SS, et al. Neuropeptide and neuronal marker studies in vitiligo. Br J Dermatol. 1994;131:160-165.
15. Silverberg JI, Silverberg NB. Association between vitiligo extent and distribution and quality-of-life impairment. JAMA Dermatol. 2013;149:159-164.
16. Silverberg JI, Silverberg NB. Quality of life impairments in children and adolescents with vitiligo. Pediatr Dermatol. 2014;31:309-318.
17. Kanwar AJ, Mahajan R, Parsad D. Effect of age at onset on disease characteristics in vitiligo. J Cutan Med Surg. 2013;17:253-258.
18. Hsieh FY, Bloch DA, Larsen MD. A simple method of sample size calculation for linear and logistic regression. Stat Med. 1998;17:1623-1634.
19. Manolache L, Petrescu-Seceleanu D, Benea V. Correlation of stressful events with onset of vitiligo in children. J Eur Acad Dermatol Venereol. 2009;23:187-188.
20. Silverberg JI, Silverberg NB. Serum homocysteine as a biomarker of vitiligo vulgaris severity: a pilot study. J Am Acad Dermatol. 2011;64:445-447.
21. Shaker OG, El-Tahlawi SM. Is there a relationship between homocysteine and vitiligo? a pilot study. Br J Dermatol. 2008;159:720-724.
22. Balci DD, Yonden Z, Yenin JZ, et al. Serum homocysteine, folic acid and vitamin B12 levels in vitiligo. Eur J Dermatol. 2009;19:382-383.
23. Silverberg JI, Silverberg AI, Malka E, et al. A pilot study assessing the role of 25 hydroxy vitamin D levels in patients with vitiligo vulgaris. J Am Acad Dermatol. 2010;62:937-941.
24. Jonasson T, Ohlin AK, Gottsater A, et al. Plasma homocysteine and markers for oxidative stress and inflammation in patients with coronary artery disease—a prospective randomized study of vitamin supplementation. Clin Chem Lab Med. 2005;43:628-634.
25. Cakmak SK, Gul U, Kilic C, et al. Homocysteine, vitamin B12 and folic acid levels in psoriasis patients. J Eur Acad Dermatol Venereol. 2009;23:300-303.
26. Malerba M, Gisondi P, Radaeli A, et al. Plasma homocysteine and folate levels in patients with chronic plaque psoriasis. Br J Dermatol. 2006;155:1165-1169.
27. Shastry S, James LR. Homocysteine-induced macrophage inflammatory protein-2 production by glomerular mesangial cells is mediated by PI3 Kinase and p38 MAPK. J Inflamm (Lond). 2009;6:27.
Vitiligo is the loss of skin pigmentation caused by autoimmune destruction of melanocytes. Multiple pathogenic factors for vitiligo have been described, including CD8+ T lymphocyte/T helper 1 infiltrates in lesional skin1,2 with increased expression of IFN-γ3 and tumor necrosis factor α,3-6 decreased transforming growth factor β,7 and circulating autoantibodies against tyrosine hydroxylase.8 Additionally, several studies have found a high prevalence of antecedent psychological stressors in vitiligo patients, suggesting that specific stressors may trigger and/or exacerbate vitiligo.9-12
The relationship between antecedent psychological stressors and vitiligo extent has not been well studied. Potential mechanisms for stress-triggered vitiligo include increased catecholamines13 and neuropeptides,14 which have been found in vitiligo patients. However, the complex relationship between stressors and subsequent vitiligo is not well defined. We hypothesized that persistent stressors are associated with increased vitiligo extent.
Vitiligo is classically considered to be a silent pigmentary disorder with few or no symptoms. Prior studies have demonstrated that one-third of vitiligo patients report skin symptoms (eg, pruritus, burning), which may be specifically associated with early-onset disease.15-17 Further, we observed that some vitiligo patients report abdominal cramping associated with their disease. Few studies have described the burden of skin symptoms and other associated symptoms in vitiligo or their determinants.
We conducted a prospective questionnaire-based study of 1541 adult vitiligo patients to identify psychological factors that may precede vitiligo onset. We hypothesized that some types of stressors that occur within 2 years prior to disease onset would have specific associations with vitiligo and/or somatic symptoms.
Methods
Study Population and Questionnaire Distribution
This prospective questionnaire-based study was approved by the institutional review board at St. Luke’s-Roosevelt Hospital Center (now Mount Sinai St. Luke’s-Roosevelt) (New York, New York) for adults (>18 years; male or female) with vitiligo. The survey was validated in paper format at St. Luke’s-Roosevelt Hospital Center and distributed online to members of nonprofit support groups for vitiligo vulgaris, as previously described.15
Questionnaire
The a priori aim of this questionnaire was to identify psychological factors that may precede vitiligo onset. The questionnaire consisted of 77 items (55 closed questions and 22 open questions) pertaining to participant demographics/vitiligo phenotype and psychological stressors preceding vitiligo onset. The questions related to this study and response rates are listed in eTable 1. Responses were verified by screening for noninteger or implausible values (eg, <0 or >100 years of age).
Sample Size
The primary outcome used for sample size calculation was the potential association between vitiligo and the presence of antecedent psychological stressors. Using a 2-tailed test, we determined that a sample size of 1264 participants would have 90% power at α=.05 and a baseline proportion of 0.01 (1% presumed prevalence of vitiligo) to detect an odds ratio (OR) of 2.5 or higher.18
Data and Statistical Analysis
Closed question responses were analyzed using descriptive statistics. Open-ended question responses were analyzed using content analysis. Related comments were coded and grouped, with similarities and differences noted. All data processing and statistics were done with SAS version 9.2. Age at diagnosis (years) and number of anatomic sites affected were divided into tertiles for statistical analysis due to wide skewing.
Logistic regression models were constructed with numbers of reported deaths or stressors per participant within the 2 years prior to vitiligo onset as independent variables (0, 1, or ≥2), and symptoms associated with vitiligo as dependent variables. Adjusted ORs were calculated from multivariate models that included sex, current age (continuous), and comorbid autoimmune disease (binary) as covariates. Linear interaction terms were tested and were included in final models if statistically significant (P<.05).
Ordinal logistic regression was used to analyze the relationship between stressors (and other independent variables) and number of anatomic sites affected with vitiligo (tertiles). Ordinal logistic regression models were constructed to examine the impact of psychological stressors on pruritus secondary to vitiligo (not relevant combined with not at all, a little, a lot, very much) as the dependent variable. The proportional odds assumption was met in both models, as judged by score testing (P>.05). Binary logistic regression was used to analyze laterality, body surface area (BSA) greater than 25%, and involvement of the face and/or body with vitiligo lesions (binary).
Binary logistic regression models were constructed with impact of psychological stressors preceding vitiligo onset on comorbid abdominal cramping and specific etiologies as the dependent variables. There were 20 candidate stressors occurring within the 2 years prior to vitiligo onset. Selection methods for predictors were used to identify significant covariates within the context of the other covariates included in the final models. The results of forward, backward, and stepwise approaches were similar, and the stepwise selection output was presented.
Missing values were encountered because some participants did not respond to all the questionnaire items. A complete case analysis was performed (ie, missing values were ignored throughout the study). Data imputation was considered by multiple imputations; however, there were few or no differences between the estimates from the 2 approaches. Therefore, final models did not involve data imputation.
The statistical significance for all estimates was considered to be P<.05. However, a P value near .05 should be interpreted with caution given the multiple dependent tests performed in this study with increased risk for falsely rejecting the null hypothesis.
Results
Survey Population Characteristics
One thousand seven hundred participants started the survey; 1632 completed the survey (96.0% completion rate) and 1553 had been diagnosed with vitiligo by a physician. Twelve participants were excluded because they were younger than 18 years, leaving 1541 evaluable participants. Five hundred thirty-eight participants (34.9%) had comorbid autoimmune disorders. Demographics and disease phenotypes of the study participants are listed in Table 1.
Stressors Preceding Vitiligo Onset
Eight hundred twenty-one participants (56.6%) experienced at least one death or stressor within 2 years prior to vitiligo onset (Table 2), including death of a loved one (16.6%) and stressful life events (51.0%) within the 2 years prior to the onset of vitiligo, especially work/financial problems (10.8%), end of a long-term relationship (10.2%), and family problems (not otherwise specified)(7.8%). Two hundred (13.5%) participants reported experiencing 1 death and 46 (3.1%) reported multiple deaths. Five hundred participants (33.6%) reported experiencing 1 stressor and 259 (17.4%) reported multiple stressors.
Stressors Not Associated With Vitiligo Extent
The number of deaths or stressors reported per participant within the 2 years prior to vitiligo onset were not associated with BSA, laterality, or distribution of lesions (Table 3 and eTable 2–eTable 4).
Symptoms Associated With Vitiligo
Five hundred twenty-two participants (34.5%) reported intermittent abdominal cramping, including premenstrual and/or menstrual cramping in women (9.7%), food-related abdominal cramping (4.4%), inflammatory bowel syndrome (IBS)(2.6%), anxiety-related abdominal cramping (1.5%), autoimmune gastrointestinal disorders (1.2%), and “other” etiologies (20.4%). Five hundred ten participants reported itching and/or burning associated with vitiligo lesions (35.1%).
Intermittent abdominal cramping overall was associated with a BSA greater than 75% (OR, 1.65; 95% confidence interval (CI), 1.17-2.32; P=.004). However, specific etiologies of abdominal cramping were not significantly associated with BSA (P≥.11). In contrast, itching and/or burning from vitiligo lesions was associated with a BSA greater than 25% (OR, 1.53; 95% CI, 1.23-1.90; P<.0001).
Association Between Number of Stressors and Symptoms in Vitiligo
A history of multiple stressors (≥2) within the 2 years prior to vitiligo onset was associated with intermittent abdominal cramping overall (OR, 1.84; 95% CI, 1.38-2.47; P<.0001), including premenstrual and/or menstrual cramping in women (OR, 1.84; 95% CI, 1.15-2.95; P=.01), IBS (OR, 3.29; 95% CI, 1.34-8.05; P=.01), and autoimmune gastrointestinal disorders (OR, 4.02; 95% CI, 1.27-12.80; P=.02)(eTable 5). These associations remained significant in multivariate models that included age, sex, and BSA as covariates. However, a history of 1 stressor or death or multiple deaths in the 2 years prior to vitiligo onset was not associated with any etiology of abdominal cramping.
Experiencing 1 (OR, 1.43; 95% CI, 1.12-1.82; P=.005) or multiple stressors (OR, 1.51; 95% CI, 1.12-2.04; P=.007) also was associated with itching and/or burning secondary to vitiligo. This association remained significant in a multivariate model that included age, sex, and BSA as covariates. However, a history of 1 or multiple deaths in the 2 years prior to vitiligo onset was not associated with itching and/or burning.
Association Between Specific Stressors and Vitiligo Symptoms
Perimenstrual (premenstrual and/or menstrual) cramping in women was associated with family problems (not otherwise specified) within the 2 years prior to vitiligo onset (Table 4). Food-related abdominal cramping was associated with school- and/or test-related stressors. Diagnosis of IBS was associated with health problems or surgery and being a victim of abuse within the 2 years prior to onset of vitiligo. Autoimmune gastrointestinal disorders were associated with moving to a new home/region, health problems or surgery, and witness to a violent crime or death. Finally, itching and/or burning of vitiligo lesions was associated with work and financial problems.
Comment
The present study found a high frequency of stressful life events and deaths of loved ones occurring within the 2 years preceding vitiligo onset. A history of multiple stressors but not deaths of loved ones was associated with more frequent symptoms in vitiligo patients, including itching and/or burning and intermittent abdominal pain. Specific stressors were associated with intermittent abdominal cramping, which occurred in approximately one-third of vitiligo patients. Abdominal cramping was related to menses in women, anxiety, foods, IBS, autoimmune gastrointestinal disorders, and other etiologies of abdominal cramping, which underscores the complex relationship between stressors, vitiligo, and inflammation. It is possible that stress-related immune abnormalities occur in vitiligo, which may influence the development of other autoimmune disorders. Alternatively, abdominal symptoms may precede and perhaps contribute to psychological stressors and impaired quality of life in vitiligo patients; however, the cross-sectional nature of the study did not allow us to elucidate this temporal relationship.
The present study found that 56.6% of participants experienced 1 or more deaths (17%) and/or stressful life events (51%) within the 2 years prior to vitiligo onset. These results are consistent with prior smaller studies that demonstrated a high frequency of stressful events preceding vitiligo onset. A case-controlled study found stressful events in 12 of 21 (57%) Romanian children with vitiligo, which was higher than controls.19 Another questionnaire-based, case-controlled study compared a heterogeneous group of 32 adolescent and adult Romanian patients with vitiligo and found higher odds of a stressful event in women preceding vitiligo diagnosis compared to controls.10 A retrospective analysis of 65 Croatian patients with vitiligo also reported that 56.9% (37/65) had some associated psychological factors.9 Another retrospective study of 31 adults with vitiligo found increased occurrence of 3 or more uncontrollable events, decreased perceived social support, and increased anxiety in vitiligo patients versus 116 other dermatologic disease controls.12 A questionnaire-based study found increased bereavements, changes in sleeping and eating habits, and personal injuries/illnesses in 73 British adults with vitiligo compared to 73 other age- and sex-matched dermatologic disease controls.11 All of these studies were limited by a small sample size, and the patient populations were localized to a regional dermatology referral center. The present study provided a larger analysis of stressful life events preceding vitiligo onset and included a diverse patient population.
The present study found that stressful life events and deaths of a loved one are not associated with vitiligo extent and distribution. This finding suggests that stressful life events may act as vitiligo triggers in genetically predisposed individuals, but ultimately the disease course and prognosis are driven by other factors, such as increased systemic inflammation or other immunologic abnormalities. Indeed, Silverberg and Silverberg20 and other investigators21,22 reported relative deficiencies of 25-hydroxyvitamin D,23 vitamins B6 and B12, and folic acid,20 as well as elevated serum homocysteine levels in vitiligo patients. Increased serum homocysteine levels were associated with increased BSA of vitiligo lesions.20 Elevated serum homocysteine levels also have been associated with increased inflammation in coronary artery disease,24 psoriasis,25,26 and in vitro.27 These laboratory anomalies likely reflect an underlying predisposition toward vitiligo, which might be triggered by stress responses or secondarily altered immune responses.
The present study had several strengths, including being prospective with a large sample size. The patient population included a large sample of men and women with representation of various adult ages and vitiligo extent. However, this study also had potential limitations. Measures of vitiligo extent were self-reported and were not clinically assessed. To address this limitation, we validated the questionnaire before posting it online.15 Invitation to participate in the survey was distributed by vitiligo support groups, which may have resulted in a selection bias toward participants with greater disease severity or with a poorer quality of life associated with vitiligo. Invitation to participate in this study was sent to members of vitiligo support groups, which allowed for recruitment of a large number of vitiligo patients despite a relatively low prevalence of disease in the general population. However, there are several challenges using this approach for nonvitiligo controls. Using participants with another dermatological disease as a control group may yield spurious results. Ideally, a large randomized sample of healthy participants with minimization of bias should be used for controls, which is an ambitious undertaking that was beyond the scope of this pilot study and will be the subject of future studies. Finally, this analysis found associations between stressors that occurred in the 2 years prior to vitiligo onset with symptomatic disease. We chose a broad interval for stressors because early vitiligo lesions may go unnoticed, making recognition of stressors occurring within days or weeks of onset infeasible. Further, we considered that chronic and prolonged stressors are more likely to have harmful consequences than acute stressors. Thus, stressors occurring within a more narrow interval (eg, 2 months) may not have the same association with vitiligo. Future studies are warranted to precisely identify the type and timing of psychological stressors preceding vitiligo onset.
Conclusion
In conclusion, there is a high prevalence of stressful life events preceding vitiligo, which may play an important role as disease triggers as well as predict the presence of intermittent abdominal cramping and itching or burning of skin. These associations indicate that screening of vitiligo patients for psychological stressors, abdominal cramping, and itching and/or burning of skin should be included in the routine assessment of vitiligo patients.
Appendix
Vitiligo is the loss of skin pigmentation caused by autoimmune destruction of melanocytes. Multiple pathogenic factors for vitiligo have been described, including CD8+ T lymphocyte/T helper 1 infiltrates in lesional skin1,2 with increased expression of IFN-γ3 and tumor necrosis factor α,3-6 decreased transforming growth factor β,7 and circulating autoantibodies against tyrosine hydroxylase.8 Additionally, several studies have found a high prevalence of antecedent psychological stressors in vitiligo patients, suggesting that specific stressors may trigger and/or exacerbate vitiligo.9-12
The relationship between antecedent psychological stressors and vitiligo extent has not been well studied. Potential mechanisms for stress-triggered vitiligo include increased catecholamines13 and neuropeptides,14 which have been found in vitiligo patients. However, the complex relationship between stressors and subsequent vitiligo is not well defined. We hypothesized that persistent stressors are associated with increased vitiligo extent.
Vitiligo is classically considered to be a silent pigmentary disorder with few or no symptoms. Prior studies have demonstrated that one-third of vitiligo patients report skin symptoms (eg, pruritus, burning), which may be specifically associated with early-onset disease.15-17 Further, we observed that some vitiligo patients report abdominal cramping associated with their disease. Few studies have described the burden of skin symptoms and other associated symptoms in vitiligo or their determinants.
We conducted a prospective questionnaire-based study of 1541 adult vitiligo patients to identify psychological factors that may precede vitiligo onset. We hypothesized that some types of stressors that occur within 2 years prior to disease onset would have specific associations with vitiligo and/or somatic symptoms.
Methods
Study Population and Questionnaire Distribution
This prospective questionnaire-based study was approved by the institutional review board at St. Luke’s-Roosevelt Hospital Center (now Mount Sinai St. Luke’s-Roosevelt) (New York, New York) for adults (>18 years; male or female) with vitiligo. The survey was validated in paper format at St. Luke’s-Roosevelt Hospital Center and distributed online to members of nonprofit support groups for vitiligo vulgaris, as previously described.15
Questionnaire
The a priori aim of this questionnaire was to identify psychological factors that may precede vitiligo onset. The questionnaire consisted of 77 items (55 closed questions and 22 open questions) pertaining to participant demographics/vitiligo phenotype and psychological stressors preceding vitiligo onset. The questions related to this study and response rates are listed in eTable 1. Responses were verified by screening for noninteger or implausible values (eg, <0 or >100 years of age).
Sample Size
The primary outcome used for sample size calculation was the potential association between vitiligo and the presence of antecedent psychological stressors. Using a 2-tailed test, we determined that a sample size of 1264 participants would have 90% power at α=.05 and a baseline proportion of 0.01 (1% presumed prevalence of vitiligo) to detect an odds ratio (OR) of 2.5 or higher.18
Data and Statistical Analysis
Closed question responses were analyzed using descriptive statistics. Open-ended question responses were analyzed using content analysis. Related comments were coded and grouped, with similarities and differences noted. All data processing and statistics were done with SAS version 9.2. Age at diagnosis (years) and number of anatomic sites affected were divided into tertiles for statistical analysis due to wide skewing.
Logistic regression models were constructed with numbers of reported deaths or stressors per participant within the 2 years prior to vitiligo onset as independent variables (0, 1, or ≥2), and symptoms associated with vitiligo as dependent variables. Adjusted ORs were calculated from multivariate models that included sex, current age (continuous), and comorbid autoimmune disease (binary) as covariates. Linear interaction terms were tested and were included in final models if statistically significant (P<.05).
Ordinal logistic regression was used to analyze the relationship between stressors (and other independent variables) and number of anatomic sites affected with vitiligo (tertiles). Ordinal logistic regression models were constructed to examine the impact of psychological stressors on pruritus secondary to vitiligo (not relevant combined with not at all, a little, a lot, very much) as the dependent variable. The proportional odds assumption was met in both models, as judged by score testing (P>.05). Binary logistic regression was used to analyze laterality, body surface area (BSA) greater than 25%, and involvement of the face and/or body with vitiligo lesions (binary).
Binary logistic regression models were constructed with impact of psychological stressors preceding vitiligo onset on comorbid abdominal cramping and specific etiologies as the dependent variables. There were 20 candidate stressors occurring within the 2 years prior to vitiligo onset. Selection methods for predictors were used to identify significant covariates within the context of the other covariates included in the final models. The results of forward, backward, and stepwise approaches were similar, and the stepwise selection output was presented.
Missing values were encountered because some participants did not respond to all the questionnaire items. A complete case analysis was performed (ie, missing values were ignored throughout the study). Data imputation was considered by multiple imputations; however, there were few or no differences between the estimates from the 2 approaches. Therefore, final models did not involve data imputation.
The statistical significance for all estimates was considered to be P<.05. However, a P value near .05 should be interpreted with caution given the multiple dependent tests performed in this study with increased risk for falsely rejecting the null hypothesis.
Results
Survey Population Characteristics
One thousand seven hundred participants started the survey; 1632 completed the survey (96.0% completion rate) and 1553 had been diagnosed with vitiligo by a physician. Twelve participants were excluded because they were younger than 18 years, leaving 1541 evaluable participants. Five hundred thirty-eight participants (34.9%) had comorbid autoimmune disorders. Demographics and disease phenotypes of the study participants are listed in Table 1.
Stressors Preceding Vitiligo Onset
Eight hundred twenty-one participants (56.6%) experienced at least one death or stressor within 2 years prior to vitiligo onset (Table 2), including death of a loved one (16.6%) and stressful life events (51.0%) within the 2 years prior to the onset of vitiligo, especially work/financial problems (10.8%), end of a long-term relationship (10.2%), and family problems (not otherwise specified)(7.8%). Two hundred (13.5%) participants reported experiencing 1 death and 46 (3.1%) reported multiple deaths. Five hundred participants (33.6%) reported experiencing 1 stressor and 259 (17.4%) reported multiple stressors.
Stressors Not Associated With Vitiligo Extent
The number of deaths or stressors reported per participant within the 2 years prior to vitiligo onset were not associated with BSA, laterality, or distribution of lesions (Table 3 and eTable 2–eTable 4).
Symptoms Associated With Vitiligo
Five hundred twenty-two participants (34.5%) reported intermittent abdominal cramping, including premenstrual and/or menstrual cramping in women (9.7%), food-related abdominal cramping (4.4%), inflammatory bowel syndrome (IBS)(2.6%), anxiety-related abdominal cramping (1.5%), autoimmune gastrointestinal disorders (1.2%), and “other” etiologies (20.4%). Five hundred ten participants reported itching and/or burning associated with vitiligo lesions (35.1%).
Intermittent abdominal cramping overall was associated with a BSA greater than 75% (OR, 1.65; 95% confidence interval (CI), 1.17-2.32; P=.004). However, specific etiologies of abdominal cramping were not significantly associated with BSA (P≥.11). In contrast, itching and/or burning from vitiligo lesions was associated with a BSA greater than 25% (OR, 1.53; 95% CI, 1.23-1.90; P<.0001).
Association Between Number of Stressors and Symptoms in Vitiligo
A history of multiple stressors (≥2) within the 2 years prior to vitiligo onset was associated with intermittent abdominal cramping overall (OR, 1.84; 95% CI, 1.38-2.47; P<.0001), including premenstrual and/or menstrual cramping in women (OR, 1.84; 95% CI, 1.15-2.95; P=.01), IBS (OR, 3.29; 95% CI, 1.34-8.05; P=.01), and autoimmune gastrointestinal disorders (OR, 4.02; 95% CI, 1.27-12.80; P=.02)(eTable 5). These associations remained significant in multivariate models that included age, sex, and BSA as covariates. However, a history of 1 stressor or death or multiple deaths in the 2 years prior to vitiligo onset was not associated with any etiology of abdominal cramping.
Experiencing 1 (OR, 1.43; 95% CI, 1.12-1.82; P=.005) or multiple stressors (OR, 1.51; 95% CI, 1.12-2.04; P=.007) also was associated with itching and/or burning secondary to vitiligo. This association remained significant in a multivariate model that included age, sex, and BSA as covariates. However, a history of 1 or multiple deaths in the 2 years prior to vitiligo onset was not associated with itching and/or burning.
Association Between Specific Stressors and Vitiligo Symptoms
Perimenstrual (premenstrual and/or menstrual) cramping in women was associated with family problems (not otherwise specified) within the 2 years prior to vitiligo onset (Table 4). Food-related abdominal cramping was associated with school- and/or test-related stressors. Diagnosis of IBS was associated with health problems or surgery and being a victim of abuse within the 2 years prior to onset of vitiligo. Autoimmune gastrointestinal disorders were associated with moving to a new home/region, health problems or surgery, and witness to a violent crime or death. Finally, itching and/or burning of vitiligo lesions was associated with work and financial problems.
Comment
The present study found a high frequency of stressful life events and deaths of loved ones occurring within the 2 years preceding vitiligo onset. A history of multiple stressors but not deaths of loved ones was associated with more frequent symptoms in vitiligo patients, including itching and/or burning and intermittent abdominal pain. Specific stressors were associated with intermittent abdominal cramping, which occurred in approximately one-third of vitiligo patients. Abdominal cramping was related to menses in women, anxiety, foods, IBS, autoimmune gastrointestinal disorders, and other etiologies of abdominal cramping, which underscores the complex relationship between stressors, vitiligo, and inflammation. It is possible that stress-related immune abnormalities occur in vitiligo, which may influence the development of other autoimmune disorders. Alternatively, abdominal symptoms may precede and perhaps contribute to psychological stressors and impaired quality of life in vitiligo patients; however, the cross-sectional nature of the study did not allow us to elucidate this temporal relationship.
The present study found that 56.6% of participants experienced 1 or more deaths (17%) and/or stressful life events (51%) within the 2 years prior to vitiligo onset. These results are consistent with prior smaller studies that demonstrated a high frequency of stressful events preceding vitiligo onset. A case-controlled study found stressful events in 12 of 21 (57%) Romanian children with vitiligo, which was higher than controls.19 Another questionnaire-based, case-controlled study compared a heterogeneous group of 32 adolescent and adult Romanian patients with vitiligo and found higher odds of a stressful event in women preceding vitiligo diagnosis compared to controls.10 A retrospective analysis of 65 Croatian patients with vitiligo also reported that 56.9% (37/65) had some associated psychological factors.9 Another retrospective study of 31 adults with vitiligo found increased occurrence of 3 or more uncontrollable events, decreased perceived social support, and increased anxiety in vitiligo patients versus 116 other dermatologic disease controls.12 A questionnaire-based study found increased bereavements, changes in sleeping and eating habits, and personal injuries/illnesses in 73 British adults with vitiligo compared to 73 other age- and sex-matched dermatologic disease controls.11 All of these studies were limited by a small sample size, and the patient populations were localized to a regional dermatology referral center. The present study provided a larger analysis of stressful life events preceding vitiligo onset and included a diverse patient population.
The present study found that stressful life events and deaths of a loved one are not associated with vitiligo extent and distribution. This finding suggests that stressful life events may act as vitiligo triggers in genetically predisposed individuals, but ultimately the disease course and prognosis are driven by other factors, such as increased systemic inflammation or other immunologic abnormalities. Indeed, Silverberg and Silverberg20 and other investigators21,22 reported relative deficiencies of 25-hydroxyvitamin D,23 vitamins B6 and B12, and folic acid,20 as well as elevated serum homocysteine levels in vitiligo patients. Increased serum homocysteine levels were associated with increased BSA of vitiligo lesions.20 Elevated serum homocysteine levels also have been associated with increased inflammation in coronary artery disease,24 psoriasis,25,26 and in vitro.27 These laboratory anomalies likely reflect an underlying predisposition toward vitiligo, which might be triggered by stress responses or secondarily altered immune responses.
The present study had several strengths, including being prospective with a large sample size. The patient population included a large sample of men and women with representation of various adult ages and vitiligo extent. However, this study also had potential limitations. Measures of vitiligo extent were self-reported and were not clinically assessed. To address this limitation, we validated the questionnaire before posting it online.15 Invitation to participate in the survey was distributed by vitiligo support groups, which may have resulted in a selection bias toward participants with greater disease severity or with a poorer quality of life associated with vitiligo. Invitation to participate in this study was sent to members of vitiligo support groups, which allowed for recruitment of a large number of vitiligo patients despite a relatively low prevalence of disease in the general population. However, there are several challenges using this approach for nonvitiligo controls. Using participants with another dermatological disease as a control group may yield spurious results. Ideally, a large randomized sample of healthy participants with minimization of bias should be used for controls, which is an ambitious undertaking that was beyond the scope of this pilot study and will be the subject of future studies. Finally, this analysis found associations between stressors that occurred in the 2 years prior to vitiligo onset with symptomatic disease. We chose a broad interval for stressors because early vitiligo lesions may go unnoticed, making recognition of stressors occurring within days or weeks of onset infeasible. Further, we considered that chronic and prolonged stressors are more likely to have harmful consequences than acute stressors. Thus, stressors occurring within a more narrow interval (eg, 2 months) may not have the same association with vitiligo. Future studies are warranted to precisely identify the type and timing of psychological stressors preceding vitiligo onset.
Conclusion
In conclusion, there is a high prevalence of stressful life events preceding vitiligo, which may play an important role as disease triggers as well as predict the presence of intermittent abdominal cramping and itching or burning of skin. These associations indicate that screening of vitiligo patients for psychological stressors, abdominal cramping, and itching and/or burning of skin should be included in the routine assessment of vitiligo patients.
Appendix
1. Goronzy J, Weyand CM, Waase I. T cell subpopulations in inflammatory bowel disease: evidence for a defective induction of T8+ suppressor/cytotoxic T lymphocytes. Clin Exp Immunol. 1985;61:593-600.
2. Ongenae K, Van Geel N, Naeyaert JM. Evidence for an autoimmune pathogenesis of vitiligo. Pigment Cell Res. 2003;16:90-100.
3. Grimes PE, Morris R, Avaniss-Aghajani E, et al. Topical tacrolimus therapy for vitiligo: therapeutic responses and skin messenger RNA expression of proinflammatory cytokines. J Am Acad Dermatol. 2004;51:52-61.
4. Birol A, Kisa U, Kurtipek GS, et al. Increased tumor necrosis factor alpha (TNF-alpha) and interleukin 1 alpha (IL1-alpha) levels in the lesional skin of patients with nonsegmental vitiligo. Int J Dermatol. 2006;45:992-993.
5. Moretti S, Spallanzani A, Amato L, et al. New insights into the pathogenesis of vitiligo: imbalance of epidermal cytokines at sites of lesions. Pigment Cell Res. 2002;15:87-92.
6. Zailaie MZ. Decreased proinflammatory cytokine production by peripheral blood mononuclear cells from vitiligo patients following aspirin treatment. Saudi Med J. 2005;26:799-805.
7. Basak PY, Adiloglu AK, Ceyhan AM, et al. The role of helper and regulatory T cells in the pathogenesis of vitiligo. J Am Acad Dermatol. 2009;60:256-260.
8. Kemp EH, Emhemad S, Akhtar S, et al. Autoantibodies against tyrosine hydroxylase in patients with non-segmental (generalised) vitiligo. Exp Dermatol. 2011;20:35-40.
9. Barisic´-Drusko V, Rucevic I. Trigger factors in childhood psoriasis and vitiligo. Coll Antropol. 2004;28:277-285.
10. Manolache L, Benea V. Stress in patients with alopecia areata and vitiligo. J Eur Acad Dermatol Venereol. 2007;21:921-928.
11. Papadopoulos L, Bor R, Legg C, et al. Impact of life events on the onset of vitiligo in adults: preliminary evidence for a psychological dimension in aetiology. Clin Exp Dermatol. 1998;23:243-248.
12. Picardi A, Pasquini P, Cattaruzza MS, et al. Stressful life events, social support, attachment security and alexithymia in vitiligo. a case-control study. Psychother Psychosom. 2003;72:150-158.
13. Salzer BA, Schallreuter KU. Investigation of the personality structure in patients with vitiligo and a possible association with impaired catecholamine metabolism. Dermatology. 1995;190:109-115.
14. Al’Abadie MS, Senior HJ, Bleehen SS, et al. Neuropeptide and neuronal marker studies in vitiligo. Br J Dermatol. 1994;131:160-165.
15. Silverberg JI, Silverberg NB. Association between vitiligo extent and distribution and quality-of-life impairment. JAMA Dermatol. 2013;149:159-164.
16. Silverberg JI, Silverberg NB. Quality of life impairments in children and adolescents with vitiligo. Pediatr Dermatol. 2014;31:309-318.
17. Kanwar AJ, Mahajan R, Parsad D. Effect of age at onset on disease characteristics in vitiligo. J Cutan Med Surg. 2013;17:253-258.
18. Hsieh FY, Bloch DA, Larsen MD. A simple method of sample size calculation for linear and logistic regression. Stat Med. 1998;17:1623-1634.
19. Manolache L, Petrescu-Seceleanu D, Benea V. Correlation of stressful events with onset of vitiligo in children. J Eur Acad Dermatol Venereol. 2009;23:187-188.
20. Silverberg JI, Silverberg NB. Serum homocysteine as a biomarker of vitiligo vulgaris severity: a pilot study. J Am Acad Dermatol. 2011;64:445-447.
21. Shaker OG, El-Tahlawi SM. Is there a relationship between homocysteine and vitiligo? a pilot study. Br J Dermatol. 2008;159:720-724.
22. Balci DD, Yonden Z, Yenin JZ, et al. Serum homocysteine, folic acid and vitamin B12 levels in vitiligo. Eur J Dermatol. 2009;19:382-383.
23. Silverberg JI, Silverberg AI, Malka E, et al. A pilot study assessing the role of 25 hydroxy vitamin D levels in patients with vitiligo vulgaris. J Am Acad Dermatol. 2010;62:937-941.
24. Jonasson T, Ohlin AK, Gottsater A, et al. Plasma homocysteine and markers for oxidative stress and inflammation in patients with coronary artery disease—a prospective randomized study of vitamin supplementation. Clin Chem Lab Med. 2005;43:628-634.
25. Cakmak SK, Gul U, Kilic C, et al. Homocysteine, vitamin B12 and folic acid levels in psoriasis patients. J Eur Acad Dermatol Venereol. 2009;23:300-303.
26. Malerba M, Gisondi P, Radaeli A, et al. Plasma homocysteine and folate levels in patients with chronic plaque psoriasis. Br J Dermatol. 2006;155:1165-1169.
27. Shastry S, James LR. Homocysteine-induced macrophage inflammatory protein-2 production by glomerular mesangial cells is mediated by PI3 Kinase and p38 MAPK. J Inflamm (Lond). 2009;6:27.
1. Goronzy J, Weyand CM, Waase I. T cell subpopulations in inflammatory bowel disease: evidence for a defective induction of T8+ suppressor/cytotoxic T lymphocytes. Clin Exp Immunol. 1985;61:593-600.
2. Ongenae K, Van Geel N, Naeyaert JM. Evidence for an autoimmune pathogenesis of vitiligo. Pigment Cell Res. 2003;16:90-100.
3. Grimes PE, Morris R, Avaniss-Aghajani E, et al. Topical tacrolimus therapy for vitiligo: therapeutic responses and skin messenger RNA expression of proinflammatory cytokines. J Am Acad Dermatol. 2004;51:52-61.
4. Birol A, Kisa U, Kurtipek GS, et al. Increased tumor necrosis factor alpha (TNF-alpha) and interleukin 1 alpha (IL1-alpha) levels in the lesional skin of patients with nonsegmental vitiligo. Int J Dermatol. 2006;45:992-993.
5. Moretti S, Spallanzani A, Amato L, et al. New insights into the pathogenesis of vitiligo: imbalance of epidermal cytokines at sites of lesions. Pigment Cell Res. 2002;15:87-92.
6. Zailaie MZ. Decreased proinflammatory cytokine production by peripheral blood mononuclear cells from vitiligo patients following aspirin treatment. Saudi Med J. 2005;26:799-805.
7. Basak PY, Adiloglu AK, Ceyhan AM, et al. The role of helper and regulatory T cells in the pathogenesis of vitiligo. J Am Acad Dermatol. 2009;60:256-260.
8. Kemp EH, Emhemad S, Akhtar S, et al. Autoantibodies against tyrosine hydroxylase in patients with non-segmental (generalised) vitiligo. Exp Dermatol. 2011;20:35-40.
9. Barisic´-Drusko V, Rucevic I. Trigger factors in childhood psoriasis and vitiligo. Coll Antropol. 2004;28:277-285.
10. Manolache L, Benea V. Stress in patients with alopecia areata and vitiligo. J Eur Acad Dermatol Venereol. 2007;21:921-928.
11. Papadopoulos L, Bor R, Legg C, et al. Impact of life events on the onset of vitiligo in adults: preliminary evidence for a psychological dimension in aetiology. Clin Exp Dermatol. 1998;23:243-248.
12. Picardi A, Pasquini P, Cattaruzza MS, et al. Stressful life events, social support, attachment security and alexithymia in vitiligo. a case-control study. Psychother Psychosom. 2003;72:150-158.
13. Salzer BA, Schallreuter KU. Investigation of the personality structure in patients with vitiligo and a possible association with impaired catecholamine metabolism. Dermatology. 1995;190:109-115.
14. Al’Abadie MS, Senior HJ, Bleehen SS, et al. Neuropeptide and neuronal marker studies in vitiligo. Br J Dermatol. 1994;131:160-165.
15. Silverberg JI, Silverberg NB. Association between vitiligo extent and distribution and quality-of-life impairment. JAMA Dermatol. 2013;149:159-164.
16. Silverberg JI, Silverberg NB. Quality of life impairments in children and adolescents with vitiligo. Pediatr Dermatol. 2014;31:309-318.
17. Kanwar AJ, Mahajan R, Parsad D. Effect of age at onset on disease characteristics in vitiligo. J Cutan Med Surg. 2013;17:253-258.
18. Hsieh FY, Bloch DA, Larsen MD. A simple method of sample size calculation for linear and logistic regression. Stat Med. 1998;17:1623-1634.
19. Manolache L, Petrescu-Seceleanu D, Benea V. Correlation of stressful events with onset of vitiligo in children. J Eur Acad Dermatol Venereol. 2009;23:187-188.
20. Silverberg JI, Silverberg NB. Serum homocysteine as a biomarker of vitiligo vulgaris severity: a pilot study. J Am Acad Dermatol. 2011;64:445-447.
21. Shaker OG, El-Tahlawi SM. Is there a relationship between homocysteine and vitiligo? a pilot study. Br J Dermatol. 2008;159:720-724.
22. Balci DD, Yonden Z, Yenin JZ, et al. Serum homocysteine, folic acid and vitamin B12 levels in vitiligo. Eur J Dermatol. 2009;19:382-383.
23. Silverberg JI, Silverberg AI, Malka E, et al. A pilot study assessing the role of 25 hydroxy vitamin D levels in patients with vitiligo vulgaris. J Am Acad Dermatol. 2010;62:937-941.
24. Jonasson T, Ohlin AK, Gottsater A, et al. Plasma homocysteine and markers for oxidative stress and inflammation in patients with coronary artery disease—a prospective randomized study of vitamin supplementation. Clin Chem Lab Med. 2005;43:628-634.
25. Cakmak SK, Gul U, Kilic C, et al. Homocysteine, vitamin B12 and folic acid levels in psoriasis patients. J Eur Acad Dermatol Venereol. 2009;23:300-303.
26. Malerba M, Gisondi P, Radaeli A, et al. Plasma homocysteine and folate levels in patients with chronic plaque psoriasis. Br J Dermatol. 2006;155:1165-1169.
27. Shastry S, James LR. Homocysteine-induced macrophage inflammatory protein-2 production by glomerular mesangial cells is mediated by PI3 Kinase and p38 MAPK. J Inflamm (Lond). 2009;6:27.
Practice Points
- Psychological stressors (eg, loss of a loved one) that occurred within 2 years prior to vitiligo onset should be considered as potential disease triggers.
- Psychological stressors have been associated with symptoms of abdominal cramping and itching/burning in vitiligo patients but not disease extent or distribution.

Aesthetic Dermatology: Sun protection after aesthetic procedures
As summertime approaches, opportunities for outdoor activities increase. For many of our patients, summer inspires a desire to have aesthetic procedures in preparation for outdoor events, such as weddings and vacations. We must, however, be mindful that increased sun exposure after some aesthetic procedures can mean an increased risk of complications.
The main complication we worry about with sun exposure is, of course, hyperpigmentation. The risk is low with injectable procedures such as botulinum toxin and fillers, but sun protection is still encouraged, especially in skin types III-VI. The risk increases greatly with chemical peels and laser and light-based procedures, such as intense pulsed light, vascular lasers, pigment lasers, laser hair removal, and especially nonablative and ablative resurfacing (including nonlaser resurfacing such as dermabrasion).
Sun protection should be encouraged, even with seemingly less invasive procedures, such as electrodessication. I once had a patient with type-IV skin tell me at her first visit that, years before, she had electrodessication on her face for DPN (dermatosis papulosa nigra), a procedure she had done on several occasions without complications and great results. However, she went to a party on a boat the weekend after the procedure and developed hyperpigmentation at the procedure areas, and she still had a few dark macules several years later.
At a follow-up visit, she said the doctor told her she should not have gone out on the boat and should have worn sunscreen. Of course, she was highly upset that she wasn’t advised about sun protection at the time of the procedure. This is one of several stories I’ve heard or seen of complications and postinflammatory hyperpigmentation after an aesthetic procedure, when the patients felt that the treating physician or practitioner did not counsel them about sun exposure during the consultation or treatment visit. It seems intuitive, but I’ve made it a habit to make sun protection part of my counseling routine.
In my practice, we often give patients sunscreen to apply immediately after a procedure. Specifically encouraging the use of zinc- and/or titanium-based, broad-spectrum, noncomedogenic physical blockers that are SPF 30 or higher may help reduce the risk of potential irritation or allergy and subsequent postinflammatory pigmentary alteration from chemical blocking ingredients. We provide a postprocedure handout, and the medical assistant also will counsel about sun protection when applying it to the patient or reviewing postprocedure instructions. So the patient is counseled at least three times: By me during consultation or pre-procedure, by the medical assistant post procedure, and by written instructions.
Vigorous sun protection is encouraged for at least 1 week after any aesthetic procedure (and longer if the downtime is longer or if multiple treatments are required). Some practices also use antioxidant serums to reduce free radicals, encourage healing, and reduce the risk of hyperpigmentation after procedures. Wide-brimmed hats also are encouraged, particularly after resurfacing or photodynamic therapy (PDT). We give patients sun-protective hats when they leave our office after PDT. We counsel them to practice vigorous sun protection for at least 1 week and to avoid sitting by a window for 48 hours after the procedure so as to not reactivate the levulan.
Delaying more high-risk procedures, such as laser treatments, until after the summer months may be appropriate if sun cannot be avoided to mitigate the risk of complications. If a patient comes to the office for a laser procedure and is visibly more tan than at the time of the last treatment, I will counsel about risks, adjust the settings appropriately, or even delay the treatment altogether to a time when the tan has faded. This is particularly important for lasers and light treatments for which melanin is the target chromosphere, such as intense pulsed light and laser hair removal. Although UV exposure is more intense in the summer, in our practice in Southern California we follow these principles year-round for the safety of our patients.
Dr. Wesley and Dr. Talakoub are co-contributors to a monthly Aesthetic Dermatology column in Dermatology News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Wesley.
As summertime approaches, opportunities for outdoor activities increase. For many of our patients, summer inspires a desire to have aesthetic procedures in preparation for outdoor events, such as weddings and vacations. We must, however, be mindful that increased sun exposure after some aesthetic procedures can mean an increased risk of complications.
The main complication we worry about with sun exposure is, of course, hyperpigmentation. The risk is low with injectable procedures such as botulinum toxin and fillers, but sun protection is still encouraged, especially in skin types III-VI. The risk increases greatly with chemical peels and laser and light-based procedures, such as intense pulsed light, vascular lasers, pigment lasers, laser hair removal, and especially nonablative and ablative resurfacing (including nonlaser resurfacing such as dermabrasion).
Sun protection should be encouraged, even with seemingly less invasive procedures, such as electrodessication. I once had a patient with type-IV skin tell me at her first visit that, years before, she had electrodessication on her face for DPN (dermatosis papulosa nigra), a procedure she had done on several occasions without complications and great results. However, she went to a party on a boat the weekend after the procedure and developed hyperpigmentation at the procedure areas, and she still had a few dark macules several years later.
At a follow-up visit, she said the doctor told her she should not have gone out on the boat and should have worn sunscreen. Of course, she was highly upset that she wasn’t advised about sun protection at the time of the procedure. This is one of several stories I’ve heard or seen of complications and postinflammatory hyperpigmentation after an aesthetic procedure, when the patients felt that the treating physician or practitioner did not counsel them about sun exposure during the consultation or treatment visit. It seems intuitive, but I’ve made it a habit to make sun protection part of my counseling routine.
In my practice, we often give patients sunscreen to apply immediately after a procedure. Specifically encouraging the use of zinc- and/or titanium-based, broad-spectrum, noncomedogenic physical blockers that are SPF 30 or higher may help reduce the risk of potential irritation or allergy and subsequent postinflammatory pigmentary alteration from chemical blocking ingredients. We provide a postprocedure handout, and the medical assistant also will counsel about sun protection when applying it to the patient or reviewing postprocedure instructions. So the patient is counseled at least three times: By me during consultation or pre-procedure, by the medical assistant post procedure, and by written instructions.
Vigorous sun protection is encouraged for at least 1 week after any aesthetic procedure (and longer if the downtime is longer or if multiple treatments are required). Some practices also use antioxidant serums to reduce free radicals, encourage healing, and reduce the risk of hyperpigmentation after procedures. Wide-brimmed hats also are encouraged, particularly after resurfacing or photodynamic therapy (PDT). We give patients sun-protective hats when they leave our office after PDT. We counsel them to practice vigorous sun protection for at least 1 week and to avoid sitting by a window for 48 hours after the procedure so as to not reactivate the levulan.
Delaying more high-risk procedures, such as laser treatments, until after the summer months may be appropriate if sun cannot be avoided to mitigate the risk of complications. If a patient comes to the office for a laser procedure and is visibly more tan than at the time of the last treatment, I will counsel about risks, adjust the settings appropriately, or even delay the treatment altogether to a time when the tan has faded. This is particularly important for lasers and light treatments for which melanin is the target chromosphere, such as intense pulsed light and laser hair removal. Although UV exposure is more intense in the summer, in our practice in Southern California we follow these principles year-round for the safety of our patients.
Dr. Wesley and Dr. Talakoub are co-contributors to a monthly Aesthetic Dermatology column in Dermatology News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Wesley.
As summertime approaches, opportunities for outdoor activities increase. For many of our patients, summer inspires a desire to have aesthetic procedures in preparation for outdoor events, such as weddings and vacations. We must, however, be mindful that increased sun exposure after some aesthetic procedures can mean an increased risk of complications.
The main complication we worry about with sun exposure is, of course, hyperpigmentation. The risk is low with injectable procedures such as botulinum toxin and fillers, but sun protection is still encouraged, especially in skin types III-VI. The risk increases greatly with chemical peels and laser and light-based procedures, such as intense pulsed light, vascular lasers, pigment lasers, laser hair removal, and especially nonablative and ablative resurfacing (including nonlaser resurfacing such as dermabrasion).
Sun protection should be encouraged, even with seemingly less invasive procedures, such as electrodessication. I once had a patient with type-IV skin tell me at her first visit that, years before, she had electrodessication on her face for DPN (dermatosis papulosa nigra), a procedure she had done on several occasions without complications and great results. However, she went to a party on a boat the weekend after the procedure and developed hyperpigmentation at the procedure areas, and she still had a few dark macules several years later.
At a follow-up visit, she said the doctor told her she should not have gone out on the boat and should have worn sunscreen. Of course, she was highly upset that she wasn’t advised about sun protection at the time of the procedure. This is one of several stories I’ve heard or seen of complications and postinflammatory hyperpigmentation after an aesthetic procedure, when the patients felt that the treating physician or practitioner did not counsel them about sun exposure during the consultation or treatment visit. It seems intuitive, but I’ve made it a habit to make sun protection part of my counseling routine.
In my practice, we often give patients sunscreen to apply immediately after a procedure. Specifically encouraging the use of zinc- and/or titanium-based, broad-spectrum, noncomedogenic physical blockers that are SPF 30 or higher may help reduce the risk of potential irritation or allergy and subsequent postinflammatory pigmentary alteration from chemical blocking ingredients. We provide a postprocedure handout, and the medical assistant also will counsel about sun protection when applying it to the patient or reviewing postprocedure instructions. So the patient is counseled at least three times: By me during consultation or pre-procedure, by the medical assistant post procedure, and by written instructions.
Vigorous sun protection is encouraged for at least 1 week after any aesthetic procedure (and longer if the downtime is longer or if multiple treatments are required). Some practices also use antioxidant serums to reduce free radicals, encourage healing, and reduce the risk of hyperpigmentation after procedures. Wide-brimmed hats also are encouraged, particularly after resurfacing or photodynamic therapy (PDT). We give patients sun-protective hats when they leave our office after PDT. We counsel them to practice vigorous sun protection for at least 1 week and to avoid sitting by a window for 48 hours after the procedure so as to not reactivate the levulan.
Delaying more high-risk procedures, such as laser treatments, until after the summer months may be appropriate if sun cannot be avoided to mitigate the risk of complications. If a patient comes to the office for a laser procedure and is visibly more tan than at the time of the last treatment, I will counsel about risks, adjust the settings appropriately, or even delay the treatment altogether to a time when the tan has faded. This is particularly important for lasers and light treatments for which melanin is the target chromosphere, such as intense pulsed light and laser hair removal. Although UV exposure is more intense in the summer, in our practice in Southern California we follow these principles year-round for the safety of our patients.
Dr. Wesley and Dr. Talakoub are co-contributors to a monthly Aesthetic Dermatology column in Dermatology News. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Wesley.

The dangers of desonide
In a previous column, I warned about the high cost of generic desonide. This month, I alert you to the many potential dangers of this drug. By the time I’m done, you may not want to go near the stuff.
To approve e-scribe refills, we all need to acknowledge warnings and dangers and click “Benefit outweighs risk” or “Previously tolerated” or some other option. But some of these warnings make me wonder who on earth writes them.
Desonide comes with more warnings than almost any other medicine I prescribe electronically. I counted 21 such warnings. Here are some examples:
1. Desonide External Cream 0.05% should be used cautiously in Bacterial Infection, especially in Systemic Bacterial Infection. Since Folliculitis is a specific form of Bacterial Infection, the same precaution may apply.
I confess that I never thought of prescribing desonide for Bacterial Infection, Systemic or otherwise. Have you? (By the way, what’s with the excess use of capital letters?)
The second warning is even more dramatic.
2. Desonide External Cream 0.05% should be used cautiously in Viral Infection, especially in Systemic Viral Infection.
What makes this even more curious is the Viral Infections the warnings go on to enumerate.
2a. Since Actinic Keratosis is a specific form of Viral Infection, the same precaution may apply.
Actinic Keratosis is a Viral Infection? I didn’t know that.
3. Since Actinic Keratosis of the Hands and Arms is a specific form of Viral Infection, the same precaution may apply.
Now we learn of different subgroups of Actinic Keratoses that are Viral Infections. Did they teach you these in Dermatology School? (Please see Warnings 6-10, below.)
4. This warning refers to a specific Bacterial Infection called Folliculitis Nares Perforans. I don’t know what that is, but it sounds bad. Glad they warned me.
5. Since Pseudofolliculitis Barbae is a specific form of Bacterial Infection, the same precaution may apply.
I never used much desonide for pseudofolliculitis, cautiously or otherwise.
Warnings 6-10 describe more specific forms of Viral Infection: (6) Non-Hyperkeratotic Actinic Keratosis, (7) Actinic Keratosis of Face and Anterior Scalp, (8) Non-Hyperkeratotic Non-Pigmented Actinic Keratosis, (9) Non-Hyperkeratotic Face and Scalp Actinic Keratosis, (10) Pigmented Actinic Keratosis.
This is most disturbing. What Systemic Viral Infections did they leave me to use desonide on? Hyperkeratotic Non-Pigmented Actinic Keratoses of the Posterior Scalp?
Warning 11 is another specific Bacterial Infection: Local Folliculitis. What is the opposite of Local Folliculitis? Express Folliculitis?
Warning 12 is Perioral Dermatitis. Steroids on rosacea? Really? Maybe a cheaper one.
I will now skip to warning 16: Hirsutism has been associated with Desonide External Cream 0.05%. Since Hair Disease is a more general form of Hirsutism, it may also be considered a drug-related medical condition.
Did you know that desonide causes unwanted hair growth? Or realize that Hair Disease is a more general form of Hirsutism? I myself have male-pattern baldness. (Sorry, Male-Pattern BALDNESS.) Since Baldness is a Hair Disease, is it also a more general form of Hirsutism? Instead of having too little hair, do I now have too much?
The same is true for warning 17, which is identical to 16, except that it substitutes “Hypertrichosis” for “Hirsutism.”
Okay, colleagues, it’s time for a personal reckoning. You trained, practiced, took CME, but you didn’t know about any of these risks, did you? You’ve just been just heedlessly, incautiously, throwing around desonide, producing hairy patients with Systemic Bacterial and Viral Infections. And on “Non-Hyperkeratotic Non-Pigmented Actinic Keratosis,” no less. Aren’t you disappointed in yourselves?
When I first read warnings like these, I wrote my EMR provider to ask who puts together this stuff, and which consultants vet it. They never answered. It is very hard to believe that a dermatologist was involved at any stage of developing these warnings, with their irrelevant caveats and absurd classification schemes.
Who would develop electronic prescribing guidelines without at least consulting the physicians who do the prescribing? Why would they want to?
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years.
In a previous column, I warned about the high cost of generic desonide. This month, I alert you to the many potential dangers of this drug. By the time I’m done, you may not want to go near the stuff.
To approve e-scribe refills, we all need to acknowledge warnings and dangers and click “Benefit outweighs risk” or “Previously tolerated” or some other option. But some of these warnings make me wonder who on earth writes them.
Desonide comes with more warnings than almost any other medicine I prescribe electronically. I counted 21 such warnings. Here are some examples:
1. Desonide External Cream 0.05% should be used cautiously in Bacterial Infection, especially in Systemic Bacterial Infection. Since Folliculitis is a specific form of Bacterial Infection, the same precaution may apply.
I confess that I never thought of prescribing desonide for Bacterial Infection, Systemic or otherwise. Have you? (By the way, what’s with the excess use of capital letters?)
The second warning is even more dramatic.
2. Desonide External Cream 0.05% should be used cautiously in Viral Infection, especially in Systemic Viral Infection.
What makes this even more curious is the Viral Infections the warnings go on to enumerate.
2a. Since Actinic Keratosis is a specific form of Viral Infection, the same precaution may apply.
Actinic Keratosis is a Viral Infection? I didn’t know that.
3. Since Actinic Keratosis of the Hands and Arms is a specific form of Viral Infection, the same precaution may apply.
Now we learn of different subgroups of Actinic Keratoses that are Viral Infections. Did they teach you these in Dermatology School? (Please see Warnings 6-10, below.)
4. This warning refers to a specific Bacterial Infection called Folliculitis Nares Perforans. I don’t know what that is, but it sounds bad. Glad they warned me.
5. Since Pseudofolliculitis Barbae is a specific form of Bacterial Infection, the same precaution may apply.
I never used much desonide for pseudofolliculitis, cautiously or otherwise.
Warnings 6-10 describe more specific forms of Viral Infection: (6) Non-Hyperkeratotic Actinic Keratosis, (7) Actinic Keratosis of Face and Anterior Scalp, (8) Non-Hyperkeratotic Non-Pigmented Actinic Keratosis, (9) Non-Hyperkeratotic Face and Scalp Actinic Keratosis, (10) Pigmented Actinic Keratosis.
This is most disturbing. What Systemic Viral Infections did they leave me to use desonide on? Hyperkeratotic Non-Pigmented Actinic Keratoses of the Posterior Scalp?
Warning 11 is another specific Bacterial Infection: Local Folliculitis. What is the opposite of Local Folliculitis? Express Folliculitis?
Warning 12 is Perioral Dermatitis. Steroids on rosacea? Really? Maybe a cheaper one.
I will now skip to warning 16: Hirsutism has been associated with Desonide External Cream 0.05%. Since Hair Disease is a more general form of Hirsutism, it may also be considered a drug-related medical condition.
Did you know that desonide causes unwanted hair growth? Or realize that Hair Disease is a more general form of Hirsutism? I myself have male-pattern baldness. (Sorry, Male-Pattern BALDNESS.) Since Baldness is a Hair Disease, is it also a more general form of Hirsutism? Instead of having too little hair, do I now have too much?
The same is true for warning 17, which is identical to 16, except that it substitutes “Hypertrichosis” for “Hirsutism.”
Okay, colleagues, it’s time for a personal reckoning. You trained, practiced, took CME, but you didn’t know about any of these risks, did you? You’ve just been just heedlessly, incautiously, throwing around desonide, producing hairy patients with Systemic Bacterial and Viral Infections. And on “Non-Hyperkeratotic Non-Pigmented Actinic Keratosis,” no less. Aren’t you disappointed in yourselves?
When I first read warnings like these, I wrote my EMR provider to ask who puts together this stuff, and which consultants vet it. They never answered. It is very hard to believe that a dermatologist was involved at any stage of developing these warnings, with their irrelevant caveats and absurd classification schemes.
Who would develop electronic prescribing guidelines without at least consulting the physicians who do the prescribing? Why would they want to?
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years.
In a previous column, I warned about the high cost of generic desonide. This month, I alert you to the many potential dangers of this drug. By the time I’m done, you may not want to go near the stuff.
To approve e-scribe refills, we all need to acknowledge warnings and dangers and click “Benefit outweighs risk” or “Previously tolerated” or some other option. But some of these warnings make me wonder who on earth writes them.
Desonide comes with more warnings than almost any other medicine I prescribe electronically. I counted 21 such warnings. Here are some examples:
1. Desonide External Cream 0.05% should be used cautiously in Bacterial Infection, especially in Systemic Bacterial Infection. Since Folliculitis is a specific form of Bacterial Infection, the same precaution may apply.
I confess that I never thought of prescribing desonide for Bacterial Infection, Systemic or otherwise. Have you? (By the way, what’s with the excess use of capital letters?)
The second warning is even more dramatic.
2. Desonide External Cream 0.05% should be used cautiously in Viral Infection, especially in Systemic Viral Infection.
What makes this even more curious is the Viral Infections the warnings go on to enumerate.
2a. Since Actinic Keratosis is a specific form of Viral Infection, the same precaution may apply.
Actinic Keratosis is a Viral Infection? I didn’t know that.
3. Since Actinic Keratosis of the Hands and Arms is a specific form of Viral Infection, the same precaution may apply.
Now we learn of different subgroups of Actinic Keratoses that are Viral Infections. Did they teach you these in Dermatology School? (Please see Warnings 6-10, below.)
4. This warning refers to a specific Bacterial Infection called Folliculitis Nares Perforans. I don’t know what that is, but it sounds bad. Glad they warned me.
5. Since Pseudofolliculitis Barbae is a specific form of Bacterial Infection, the same precaution may apply.
I never used much desonide for pseudofolliculitis, cautiously or otherwise.
Warnings 6-10 describe more specific forms of Viral Infection: (6) Non-Hyperkeratotic Actinic Keratosis, (7) Actinic Keratosis of Face and Anterior Scalp, (8) Non-Hyperkeratotic Non-Pigmented Actinic Keratosis, (9) Non-Hyperkeratotic Face and Scalp Actinic Keratosis, (10) Pigmented Actinic Keratosis.
This is most disturbing. What Systemic Viral Infections did they leave me to use desonide on? Hyperkeratotic Non-Pigmented Actinic Keratoses of the Posterior Scalp?
Warning 11 is another specific Bacterial Infection: Local Folliculitis. What is the opposite of Local Folliculitis? Express Folliculitis?
Warning 12 is Perioral Dermatitis. Steroids on rosacea? Really? Maybe a cheaper one.
I will now skip to warning 16: Hirsutism has been associated with Desonide External Cream 0.05%. Since Hair Disease is a more general form of Hirsutism, it may also be considered a drug-related medical condition.
Did you know that desonide causes unwanted hair growth? Or realize that Hair Disease is a more general form of Hirsutism? I myself have male-pattern baldness. (Sorry, Male-Pattern BALDNESS.) Since Baldness is a Hair Disease, is it also a more general form of Hirsutism? Instead of having too little hair, do I now have too much?
The same is true for warning 17, which is identical to 16, except that it substitutes “Hypertrichosis” for “Hirsutism.”
Okay, colleagues, it’s time for a personal reckoning. You trained, practiced, took CME, but you didn’t know about any of these risks, did you? You’ve just been just heedlessly, incautiously, throwing around desonide, producing hairy patients with Systemic Bacterial and Viral Infections. And on “Non-Hyperkeratotic Non-Pigmented Actinic Keratosis,” no less. Aren’t you disappointed in yourselves?
When I first read warnings like these, I wrote my EMR provider to ask who puts together this stuff, and which consultants vet it. They never answered. It is very hard to believe that a dermatologist was involved at any stage of developing these warnings, with their irrelevant caveats and absurd classification schemes.
Who would develop electronic prescribing guidelines without at least consulting the physicians who do the prescribing? Why would they want to?
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years.

Resident debt is ruining medicine
Most physicians accumulate near $300,000 in debt by the time they finish residency and go to work. This debt is crushing, and it is having negative effects.
College and medical school tuition has soared in the last 20 years, keeping pace with federal loan availability. There is no clear relationship with increased quality of the educational experience or with increased knowledge of the students. Colleges are part of the problem, but, in my opinion, the medical schools are even more egregious. After all, how much does it cost to rent a lecture hall for 2 years and provide some lecturers?

I will never forget when I complained about the increasing expense of medical school to a dean once. He explained that all of the faculty’s salary is considered an expense to the medical school, and that students are only paying a fraction of the true cost.
I must object! If a professor makes a guest appearance for an afternoon or two, the medical students are expected to pay him for a year of work?
I will never forget the goofy physiology professor who gave us two afternoons of demonstrations and lectures. He hooked live frogs to electrodes and made waves on a monitor. It was interesting, but his salary is $200,000 a year. Was it worth $2,000 a student (a class of 100 medical students) to watch him make frogs twitch two afternoons? I think not.
Caribbean medical schools charge about the same as those in North America and make a large profit. Medical students have become a “profit center.” This is occurring in an age when medical students write and share much of their own educational content in an interactive environment. This cannot be sustained.
For the last 2 years of medical school, the students are turned loose on the hospital wards and become slaves. This is called running scut, and it includes running specimens to the lab, wheeling patients to x-ray, drawing blood, fetching lab results, doing much chart work (completing the chart is the most important thing), and learning a lot in spite of the grunt work. The older physicians do teach on rounds, and there is always a resident physician around.
Again, these practicing physicians (they bill for their services) would be there anyway for the residents, and if there were not residents, would have to be there for their patients. The medical students cannot possibly add much additional cost, but these attending physicians and residents salaries are included in the educational cost justification.
The debt introduces a toxic calculus to specialty selection. Residencies are chosen for their fiscal attractiveness, which is not a correct or sustaining reason in a long hard career. Also, it may become economically impossible to practice in a lower-paying specialty.
Let me tell you about Razor Rick, a college student I mentored for several years. I hire these kids in their college summers and breaks to do not much but make a little money, and in exchange they let me pontificate and smile at me. Well, Rick got through med school and then dropped out of his primary care residency, owing several hundred thousand dollars. I was stunned when his parents called me, and I insisted he come in to talk to me.
He patiently explained that his board scores were passing but not good enough to get into to a well-paying specialty. He logically explained that he would have a better life, and have a better return on his investment, if he simply went into pharma with his expensive degree.
I helped him find some interviews.
Some criticize this generation of doctors for not being engaged, for not joining organized medicine, and for avoiding the glorious heart of difficult medicine. I don’t blame them for being distracted. They have, on average, 300,000 good reasons to be more self-concerned.
Dermatology News is proud to introduce the inaugural column of Cold Iron Truth by Dr. Brett Coldiron. Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of over 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
Most physicians accumulate near $300,000 in debt by the time they finish residency and go to work. This debt is crushing, and it is having negative effects.
College and medical school tuition has soared in the last 20 years, keeping pace with federal loan availability. There is no clear relationship with increased quality of the educational experience or with increased knowledge of the students. Colleges are part of the problem, but, in my opinion, the medical schools are even more egregious. After all, how much does it cost to rent a lecture hall for 2 years and provide some lecturers?
I will never forget when I complained about the increasing expense of medical school to a dean once. He explained that all of the faculty’s salary is considered an expense to the medical school, and that students are only paying a fraction of the true cost.
I must object! If a professor makes a guest appearance for an afternoon or two, the medical students are expected to pay him for a year of work?
I will never forget the goofy physiology professor who gave us two afternoons of demonstrations and lectures. He hooked live frogs to electrodes and made waves on a monitor. It was interesting, but his salary is $200,000 a year. Was it worth $2,000 a student (a class of 100 medical students) to watch him make frogs twitch two afternoons? I think not.
Caribbean medical schools charge about the same as those in North America and make a large profit. Medical students have become a “profit center.” This is occurring in an age when medical students write and share much of their own educational content in an interactive environment. This cannot be sustained.
For the last 2 years of medical school, the students are turned loose on the hospital wards and become slaves. This is called running scut, and it includes running specimens to the lab, wheeling patients to x-ray, drawing blood, fetching lab results, doing much chart work (completing the chart is the most important thing), and learning a lot in spite of the grunt work. The older physicians do teach on rounds, and there is always a resident physician around.
Again, these practicing physicians (they bill for their services) would be there anyway for the residents, and if there were not residents, would have to be there for their patients. The medical students cannot possibly add much additional cost, but these attending physicians and residents salaries are included in the educational cost justification.
The debt introduces a toxic calculus to specialty selection. Residencies are chosen for their fiscal attractiveness, which is not a correct or sustaining reason in a long hard career. Also, it may become economically impossible to practice in a lower-paying specialty.
Let me tell you about Razor Rick, a college student I mentored for several years. I hire these kids in their college summers and breaks to do not much but make a little money, and in exchange they let me pontificate and smile at me. Well, Rick got through med school and then dropped out of his primary care residency, owing several hundred thousand dollars. I was stunned when his parents called me, and I insisted he come in to talk to me.
He patiently explained that his board scores were passing but not good enough to get into to a well-paying specialty. He logically explained that he would have a better life, and have a better return on his investment, if he simply went into pharma with his expensive degree.
I helped him find some interviews.
Some criticize this generation of doctors for not being engaged, for not joining organized medicine, and for avoiding the glorious heart of difficult medicine. I don’t blame them for being distracted. They have, on average, 300,000 good reasons to be more self-concerned.
Dermatology News is proud to introduce the inaugural column of Cold Iron Truth by Dr. Brett Coldiron. Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of over 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.
Most physicians accumulate near $300,000 in debt by the time they finish residency and go to work. This debt is crushing, and it is having negative effects.
College and medical school tuition has soared in the last 20 years, keeping pace with federal loan availability. There is no clear relationship with increased quality of the educational experience or with increased knowledge of the students. Colleges are part of the problem, but, in my opinion, the medical schools are even more egregious. After all, how much does it cost to rent a lecture hall for 2 years and provide some lecturers?
I will never forget when I complained about the increasing expense of medical school to a dean once. He explained that all of the faculty’s salary is considered an expense to the medical school, and that students are only paying a fraction of the true cost.
I must object! If a professor makes a guest appearance for an afternoon or two, the medical students are expected to pay him for a year of work?
I will never forget the goofy physiology professor who gave us two afternoons of demonstrations and lectures. He hooked live frogs to electrodes and made waves on a monitor. It was interesting, but his salary is $200,000 a year. Was it worth $2,000 a student (a class of 100 medical students) to watch him make frogs twitch two afternoons? I think not.
Caribbean medical schools charge about the same as those in North America and make a large profit. Medical students have become a “profit center.” This is occurring in an age when medical students write and share much of their own educational content in an interactive environment. This cannot be sustained.
For the last 2 years of medical school, the students are turned loose on the hospital wards and become slaves. This is called running scut, and it includes running specimens to the lab, wheeling patients to x-ray, drawing blood, fetching lab results, doing much chart work (completing the chart is the most important thing), and learning a lot in spite of the grunt work. The older physicians do teach on rounds, and there is always a resident physician around.
Again, these practicing physicians (they bill for their services) would be there anyway for the residents, and if there were not residents, would have to be there for their patients. The medical students cannot possibly add much additional cost, but these attending physicians and residents salaries are included in the educational cost justification.
The debt introduces a toxic calculus to specialty selection. Residencies are chosen for their fiscal attractiveness, which is not a correct or sustaining reason in a long hard career. Also, it may become economically impossible to practice in a lower-paying specialty.
Let me tell you about Razor Rick, a college student I mentored for several years. I hire these kids in their college summers and breaks to do not much but make a little money, and in exchange they let me pontificate and smile at me. Well, Rick got through med school and then dropped out of his primary care residency, owing several hundred thousand dollars. I was stunned when his parents called me, and I insisted he come in to talk to me.
He patiently explained that his board scores were passing but not good enough to get into to a well-paying specialty. He logically explained that he would have a better life, and have a better return on his investment, if he simply went into pharma with his expensive degree.
I helped him find some interviews.
Some criticize this generation of doctors for not being engaged, for not joining organized medicine, and for avoiding the glorious heart of difficult medicine. I don’t blame them for being distracted. They have, on average, 300,000 good reasons to be more self-concerned.
Dermatology News is proud to introduce the inaugural column of Cold Iron Truth by Dr. Brett Coldiron. Dr. Coldiron is a past president of the American Academy of Dermatology. He is currently in private practice, but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of over 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics.

Familial factors linked to child’s risk of blood cancer

A new study has linked a father’s age at his child’s birth to the risk that the child will develop a hematologic malignancy as an adult, but this risk only proved significant among children without siblings.
Only-children whose fathers were 35 or older at the child’s birth were significantly more likely to develop hematologic malignancies than only-children with fathers who were younger than 25 at the child’s birth.
There was no association between these cancers and a mother’s age, either among only-children or those with siblings.
A previous study of more than 100,000 women also showed an association between paternal—but not maternal—age at a child’s birth and the risk of hematologic malignancy.
To further investigate the association, Lauren Teras, PhD, of the American Cancer Society in Atlanta, Georgia, and her colleagues analyzed data from women and men enrolled in the American Cancer Society Cancer Prevention Study-II Nutrition Cohort.
The team reported their findings in the American Journal of Epidemiology.
Among the 138,003 participants, there were 2532 cases of hematologic malignancies diagnosed between 1992 and 2009.
Subjects’ mothers tended to be younger at their birth than fathers, with median ages of 27 and 31, respectively. Almost a third of the fathers were 35 or older when a subject was born, compared with 17% of the mothers.
In the categorical analysis, the researchers found a positive association between older paternal age at a subject’s birth and the risk of hematologic malignancies in male, but not female, subjects. The hazard ratio (HR) was 1.35 for male subjects with fathers aged 35 and older compared to those whose fathers were younger than 25.
On the other hand, when paternal age was modeled as a continuous variable, there was no association with the risk of hematologic malignancy for males or females. Likewise, there was no association between maternal age at a subject’s birth and the risk of hematologic malignancy in male or female subjects.
However, among subjects without siblings, there was a significant, positive association with paternal age and the risk of hematologic malignancy (P=0.002).
When the researchers separated only-children by sex, they found a suggestive positive association between paternal age and hematologic malignancy for females (HR=1.40) and a significant association for males (HR=1.84). However, the linear spline was significant for males (P=0.01) and females (P=0.04).
There was no association between paternal age at a subject’s birth and the risk of hematologic malignancy among subjects with at least 1 sibling (HR=1.06).
The researchers said the fact that the association between paternal age and malignancy was significant in subjects with no siblings suggests it may be related to the “hygiene hypothesis”—the idea that exposure to mild infections in childhood, which might be more numerous with more siblings, are important to immune system development and may reduce the risk of immune-related diseases.
It is possible that the combination of having an older father and no siblings may promote cell proliferation in those individuals with an underdeveloped immune system and, as such, favors the development of cancers related to the immune system, the team said.
They added that this study suggests a need for further research to better understand the association between paternal age at a child’s birth and hematologic malignancies.
“The lifetime risk of these cancers is fairly low—about 1 in 20 men and women will be diagnosed with lymphoma, leukemia, or myeloma at some point during their lifetime—so people born to older fathers should not be alarmed,” Dr Teras said.
“Still, the study does highlight the need for more research to confirm these findings and to clarify the biologic underpinning for this association, given the growing number of children born to older fathers in the United States and worldwide.” ![]()
A new study has linked a father’s age at his child’s birth to the risk that the child will develop a hematologic malignancy as an adult, but this risk only proved significant among children without siblings.
Only-children whose fathers were 35 or older at the child’s birth were significantly more likely to develop hematologic malignancies than only-children with fathers who were younger than 25 at the child’s birth.
There was no association between these cancers and a mother’s age, either among only-children or those with siblings.
A previous study of more than 100,000 women also showed an association between paternal—but not maternal—age at a child’s birth and the risk of hematologic malignancy.
To further investigate the association, Lauren Teras, PhD, of the American Cancer Society in Atlanta, Georgia, and her colleagues analyzed data from women and men enrolled in the American Cancer Society Cancer Prevention Study-II Nutrition Cohort.
The team reported their findings in the American Journal of Epidemiology.
Among the 138,003 participants, there were 2532 cases of hematologic malignancies diagnosed between 1992 and 2009.
Subjects’ mothers tended to be younger at their birth than fathers, with median ages of 27 and 31, respectively. Almost a third of the fathers were 35 or older when a subject was born, compared with 17% of the mothers.
In the categorical analysis, the researchers found a positive association between older paternal age at a subject’s birth and the risk of hematologic malignancies in male, but not female, subjects. The hazard ratio (HR) was 1.35 for male subjects with fathers aged 35 and older compared to those whose fathers were younger than 25.
On the other hand, when paternal age was modeled as a continuous variable, there was no association with the risk of hematologic malignancy for males or females. Likewise, there was no association between maternal age at a subject’s birth and the risk of hematologic malignancy in male or female subjects.
However, among subjects without siblings, there was a significant, positive association with paternal age and the risk of hematologic malignancy (P=0.002).
When the researchers separated only-children by sex, they found a suggestive positive association between paternal age and hematologic malignancy for females (HR=1.40) and a significant association for males (HR=1.84). However, the linear spline was significant for males (P=0.01) and females (P=0.04).
There was no association between paternal age at a subject’s birth and the risk of hematologic malignancy among subjects with at least 1 sibling (HR=1.06).
The researchers said the fact that the association between paternal age and malignancy was significant in subjects with no siblings suggests it may be related to the “hygiene hypothesis”—the idea that exposure to mild infections in childhood, which might be more numerous with more siblings, are important to immune system development and may reduce the risk of immune-related diseases.
It is possible that the combination of having an older father and no siblings may promote cell proliferation in those individuals with an underdeveloped immune system and, as such, favors the development of cancers related to the immune system, the team said.
They added that this study suggests a need for further research to better understand the association between paternal age at a child’s birth and hematologic malignancies.
“The lifetime risk of these cancers is fairly low—about 1 in 20 men and women will be diagnosed with lymphoma, leukemia, or myeloma at some point during their lifetime—so people born to older fathers should not be alarmed,” Dr Teras said.
“Still, the study does highlight the need for more research to confirm these findings and to clarify the biologic underpinning for this association, given the growing number of children born to older fathers in the United States and worldwide.” ![]()
A new study has linked a father’s age at his child’s birth to the risk that the child will develop a hematologic malignancy as an adult, but this risk only proved significant among children without siblings.
Only-children whose fathers were 35 or older at the child’s birth were significantly more likely to develop hematologic malignancies than only-children with fathers who were younger than 25 at the child’s birth.
There was no association between these cancers and a mother’s age, either among only-children or those with siblings.
A previous study of more than 100,000 women also showed an association between paternal—but not maternal—age at a child’s birth and the risk of hematologic malignancy.
To further investigate the association, Lauren Teras, PhD, of the American Cancer Society in Atlanta, Georgia, and her colleagues analyzed data from women and men enrolled in the American Cancer Society Cancer Prevention Study-II Nutrition Cohort.
The team reported their findings in the American Journal of Epidemiology.
Among the 138,003 participants, there were 2532 cases of hematologic malignancies diagnosed between 1992 and 2009.
Subjects’ mothers tended to be younger at their birth than fathers, with median ages of 27 and 31, respectively. Almost a third of the fathers were 35 or older when a subject was born, compared with 17% of the mothers.
In the categorical analysis, the researchers found a positive association between older paternal age at a subject’s birth and the risk of hematologic malignancies in male, but not female, subjects. The hazard ratio (HR) was 1.35 for male subjects with fathers aged 35 and older compared to those whose fathers were younger than 25.
On the other hand, when paternal age was modeled as a continuous variable, there was no association with the risk of hematologic malignancy for males or females. Likewise, there was no association between maternal age at a subject’s birth and the risk of hematologic malignancy in male or female subjects.
However, among subjects without siblings, there was a significant, positive association with paternal age and the risk of hematologic malignancy (P=0.002).
When the researchers separated only-children by sex, they found a suggestive positive association between paternal age and hematologic malignancy for females (HR=1.40) and a significant association for males (HR=1.84). However, the linear spline was significant for males (P=0.01) and females (P=0.04).
There was no association between paternal age at a subject’s birth and the risk of hematologic malignancy among subjects with at least 1 sibling (HR=1.06).
The researchers said the fact that the association between paternal age and malignancy was significant in subjects with no siblings suggests it may be related to the “hygiene hypothesis”—the idea that exposure to mild infections in childhood, which might be more numerous with more siblings, are important to immune system development and may reduce the risk of immune-related diseases.
It is possible that the combination of having an older father and no siblings may promote cell proliferation in those individuals with an underdeveloped immune system and, as such, favors the development of cancers related to the immune system, the team said.
They added that this study suggests a need for further research to better understand the association between paternal age at a child’s birth and hematologic malignancies.
“The lifetime risk of these cancers is fairly low—about 1 in 20 men and women will be diagnosed with lymphoma, leukemia, or myeloma at some point during their lifetime—so people born to older fathers should not be alarmed,” Dr Teras said.
“Still, the study does highlight the need for more research to confirm these findings and to clarify the biologic underpinning for this association, given the growing number of children born to older fathers in the United States and worldwide.” ![]()
New method to assess cancer risk from pollutants

Photo by Tiffany Dawn Nicholson
Scientists say they have developed a faster, more accurate method to assess cancer risk from certain common environmental pollutants.
The group found they could analyze the immediate genetic responses of the skin cells of exposed mice and apply statistical approaches to determine whether or not those cells would eventually become cancerous.
The study focused on a class of pollutants known as polycyclic aromatic hydrocarbons (PAHs) that commonly occur in the environment as mixtures such as diesel exhaust and cigarette smoke.
“After only 12 hours, we could predict the ability of certain PAH mixtures to cause cancer, rather than waiting 25 weeks for tumors to develop,” said study author Susan Tilton, PhD, of Oregon State University in Corvallis.
For at least some PAH mixtures, the new method is not only quicker but produces more accurate cancer-risk assessments than are currently possible, she added.
Dr Tilton and her colleagues described the method in Toxicological Sciences.
“Our work was intended as a proof of concept,” Dr Tilton noted. “The method needs to be tested with a larger group of chemicals and mixtures. But we now have a model that we can use to develop larger-scale screening tests with human cells in a laboratory dish.”
The researchers believe the model will be particularly useful for screening PAHs, a large class of pollutants that result from combustion of organic matter and fossil fuels. PAHs are widespread contaminants of air, water, and soil. There are hundreds of different kinds, and some are known carcinogens, but many have not been tested.
Humans are primarily exposed to PAHs in the environment as mixtures, which makes it harder to assess their cancer risk. The standard calculation, Dr Tilton said, is to identify the risk of each element in the mix—if it’s known—and add them together.
But this method doesn’t work with most PAH mixes. It assumes the risk for each component is known, as well as which components are in a given mix. Often, that information is not available.
For this study, Dr Tilton and her colleagues examined 3 PAH mixtures that are common in the environment—coal tar, diesel exhaust, and cigarette smoke—and various mixtures of them.
The group found that each substance touched off a rapid and distinctive cascade of biological and metabolic changes in the skin cells of a mouse. The response amounted to a unique “fingerprint” of the genetic changes that occur as cells reacted to exposure to each chemical.
By matching patterns of genetic changes known to occur as cells become cancerous, the researchers found that some of the cellular responses were early indicators of developing cancers.
They also found that the standard method to calculate carcinogenic material underestimated the cancer risk of some mixtures and overestimated the combined risk of others.
“Our study is a first step in moving away from risk assessments based on individual components of these PAH mixtures and developing more accurate methods that look at the mixture as a whole,” Dr Tilton said. “We’re hoping to bring the methodology to the point where we no longer need to use tumors as our endpoint.” ![]()
Photo by Tiffany Dawn Nicholson
Scientists say they have developed a faster, more accurate method to assess cancer risk from certain common environmental pollutants.
The group found they could analyze the immediate genetic responses of the skin cells of exposed mice and apply statistical approaches to determine whether or not those cells would eventually become cancerous.
The study focused on a class of pollutants known as polycyclic aromatic hydrocarbons (PAHs) that commonly occur in the environment as mixtures such as diesel exhaust and cigarette smoke.
“After only 12 hours, we could predict the ability of certain PAH mixtures to cause cancer, rather than waiting 25 weeks for tumors to develop,” said study author Susan Tilton, PhD, of Oregon State University in Corvallis.
For at least some PAH mixtures, the new method is not only quicker but produces more accurate cancer-risk assessments than are currently possible, she added.
Dr Tilton and her colleagues described the method in Toxicological Sciences.
“Our work was intended as a proof of concept,” Dr Tilton noted. “The method needs to be tested with a larger group of chemicals and mixtures. But we now have a model that we can use to develop larger-scale screening tests with human cells in a laboratory dish.”
The researchers believe the model will be particularly useful for screening PAHs, a large class of pollutants that result from combustion of organic matter and fossil fuels. PAHs are widespread contaminants of air, water, and soil. There are hundreds of different kinds, and some are known carcinogens, but many have not been tested.
Humans are primarily exposed to PAHs in the environment as mixtures, which makes it harder to assess their cancer risk. The standard calculation, Dr Tilton said, is to identify the risk of each element in the mix—if it’s known—and add them together.
But this method doesn’t work with most PAH mixes. It assumes the risk for each component is known, as well as which components are in a given mix. Often, that information is not available.
For this study, Dr Tilton and her colleagues examined 3 PAH mixtures that are common in the environment—coal tar, diesel exhaust, and cigarette smoke—and various mixtures of them.
The group found that each substance touched off a rapid and distinctive cascade of biological and metabolic changes in the skin cells of a mouse. The response amounted to a unique “fingerprint” of the genetic changes that occur as cells reacted to exposure to each chemical.
By matching patterns of genetic changes known to occur as cells become cancerous, the researchers found that some of the cellular responses were early indicators of developing cancers.
They also found that the standard method to calculate carcinogenic material underestimated the cancer risk of some mixtures and overestimated the combined risk of others.
“Our study is a first step in moving away from risk assessments based on individual components of these PAH mixtures and developing more accurate methods that look at the mixture as a whole,” Dr Tilton said. “We’re hoping to bring the methodology to the point where we no longer need to use tumors as our endpoint.” ![]()
Photo by Tiffany Dawn Nicholson
Scientists say they have developed a faster, more accurate method to assess cancer risk from certain common environmental pollutants.
The group found they could analyze the immediate genetic responses of the skin cells of exposed mice and apply statistical approaches to determine whether or not those cells would eventually become cancerous.
The study focused on a class of pollutants known as polycyclic aromatic hydrocarbons (PAHs) that commonly occur in the environment as mixtures such as diesel exhaust and cigarette smoke.
“After only 12 hours, we could predict the ability of certain PAH mixtures to cause cancer, rather than waiting 25 weeks for tumors to develop,” said study author Susan Tilton, PhD, of Oregon State University in Corvallis.
For at least some PAH mixtures, the new method is not only quicker but produces more accurate cancer-risk assessments than are currently possible, she added.
Dr Tilton and her colleagues described the method in Toxicological Sciences.
“Our work was intended as a proof of concept,” Dr Tilton noted. “The method needs to be tested with a larger group of chemicals and mixtures. But we now have a model that we can use to develop larger-scale screening tests with human cells in a laboratory dish.”
The researchers believe the model will be particularly useful for screening PAHs, a large class of pollutants that result from combustion of organic matter and fossil fuels. PAHs are widespread contaminants of air, water, and soil. There are hundreds of different kinds, and some are known carcinogens, but many have not been tested.
Humans are primarily exposed to PAHs in the environment as mixtures, which makes it harder to assess their cancer risk. The standard calculation, Dr Tilton said, is to identify the risk of each element in the mix—if it’s known—and add them together.
But this method doesn’t work with most PAH mixes. It assumes the risk for each component is known, as well as which components are in a given mix. Often, that information is not available.
For this study, Dr Tilton and her colleagues examined 3 PAH mixtures that are common in the environment—coal tar, diesel exhaust, and cigarette smoke—and various mixtures of them.
The group found that each substance touched off a rapid and distinctive cascade of biological and metabolic changes in the skin cells of a mouse. The response amounted to a unique “fingerprint” of the genetic changes that occur as cells reacted to exposure to each chemical.
By matching patterns of genetic changes known to occur as cells become cancerous, the researchers found that some of the cellular responses were early indicators of developing cancers.
They also found that the standard method to calculate carcinogenic material underestimated the cancer risk of some mixtures and overestimated the combined risk of others.
“Our study is a first step in moving away from risk assessments based on individual components of these PAH mixtures and developing more accurate methods that look at the mixture as a whole,” Dr Tilton said. “We’re hoping to bring the methodology to the point where we no longer need to use tumors as our endpoint.” ![]()
Microbubbles can treat, track thrombosis

Image by Andre E.X. Brown
SAN FRANCISCO—Microbubbles can be used to simultaneously treat and monitor thrombosis, according to preclinical research presented at the ATVB/PVD 2015 Scientific Sessions.
The microbubbles double as agents for contrast-enhanced ultrasound imaging and targeted drug-delivery vehicles.
Experiments in mice showed that the microbubbles could deliver treatment directly to a blood clot, noticeably reducing its size without causing abnormal bleeding.
Karlheinz Peter, MD, PhD, of Baker IDI Heart and Diabetes Institute in Melbourne, Victoria, Australia, presented these results at the meeting as abstract 36.
He and his colleagues combined the thrombolytic agent urokinase with an activated-platelet-specific, single-chain antibody and placed the duo on the surface of microbubbles.
The researchers then tracked the microbubbles’ progress in a mouse model of carotid artery thrombosis induced by ferric-chloride.
The team monitored clot size in these mice with ultrasound imaging and measured bleeding time after experimental injury, while comparing 4 treatment groups:
- Microbubbles coated with both the targeting antibody and urokinase
- Targeted microbubbles and a high dose of urokinase administered separately
- Targeted microbubbles and a low dose of urokinase administered separately
- A control group with targeted microbubbles and no urokinase.
Microbubbles with urokinase on their surface significantly reduced clot size after 45 minutes, but microbubbles without urokinase did not. The mean percentage change in thrombus size from baseline was 97.16 ± 4.3 and 37.09 ± 5.6, respectively (P<0.001).
Urokinase administered alone could only match the efficacy of the treatment-loaded microbubbles if the drug was administered at a high dose. However, that significantly prolonged bleeding time from baseline—1079.25 ± 260.7 seconds vs 79.25 ± 6.5 seconds (P<0.001)—whereas, treatment with microbubbles did not.
While this research is in the early stages, the researchers believe the technology could help patients who develop venous thromboembolism and related conditions, such as heart attack and stroke. The team also believes the technology could have a major impact on treatment of patients in the emergency department. ![]()
Image by Andre E.X. Brown
SAN FRANCISCO—Microbubbles can be used to simultaneously treat and monitor thrombosis, according to preclinical research presented at the ATVB/PVD 2015 Scientific Sessions.
The microbubbles double as agents for contrast-enhanced ultrasound imaging and targeted drug-delivery vehicles.
Experiments in mice showed that the microbubbles could deliver treatment directly to a blood clot, noticeably reducing its size without causing abnormal bleeding.
Karlheinz Peter, MD, PhD, of Baker IDI Heart and Diabetes Institute in Melbourne, Victoria, Australia, presented these results at the meeting as abstract 36.
He and his colleagues combined the thrombolytic agent urokinase with an activated-platelet-specific, single-chain antibody and placed the duo on the surface of microbubbles.
The researchers then tracked the microbubbles’ progress in a mouse model of carotid artery thrombosis induced by ferric-chloride.
The team monitored clot size in these mice with ultrasound imaging and measured bleeding time after experimental injury, while comparing 4 treatment groups:
- Microbubbles coated with both the targeting antibody and urokinase
- Targeted microbubbles and a high dose of urokinase administered separately
- Targeted microbubbles and a low dose of urokinase administered separately
- A control group with targeted microbubbles and no urokinase.
Microbubbles with urokinase on their surface significantly reduced clot size after 45 minutes, but microbubbles without urokinase did not. The mean percentage change in thrombus size from baseline was 97.16 ± 4.3 and 37.09 ± 5.6, respectively (P<0.001).
Urokinase administered alone could only match the efficacy of the treatment-loaded microbubbles if the drug was administered at a high dose. However, that significantly prolonged bleeding time from baseline—1079.25 ± 260.7 seconds vs 79.25 ± 6.5 seconds (P<0.001)—whereas, treatment with microbubbles did not.
While this research is in the early stages, the researchers believe the technology could help patients who develop venous thromboembolism and related conditions, such as heart attack and stroke. The team also believes the technology could have a major impact on treatment of patients in the emergency department. ![]()
Image by Andre E.X. Brown
SAN FRANCISCO—Microbubbles can be used to simultaneously treat and monitor thrombosis, according to preclinical research presented at the ATVB/PVD 2015 Scientific Sessions.
The microbubbles double as agents for contrast-enhanced ultrasound imaging and targeted drug-delivery vehicles.
Experiments in mice showed that the microbubbles could deliver treatment directly to a blood clot, noticeably reducing its size without causing abnormal bleeding.
Karlheinz Peter, MD, PhD, of Baker IDI Heart and Diabetes Institute in Melbourne, Victoria, Australia, presented these results at the meeting as abstract 36.
He and his colleagues combined the thrombolytic agent urokinase with an activated-platelet-specific, single-chain antibody and placed the duo on the surface of microbubbles.
The researchers then tracked the microbubbles’ progress in a mouse model of carotid artery thrombosis induced by ferric-chloride.
The team monitored clot size in these mice with ultrasound imaging and measured bleeding time after experimental injury, while comparing 4 treatment groups:
- Microbubbles coated with both the targeting antibody and urokinase
- Targeted microbubbles and a high dose of urokinase administered separately
- Targeted microbubbles and a low dose of urokinase administered separately
- A control group with targeted microbubbles and no urokinase.
Microbubbles with urokinase on their surface significantly reduced clot size after 45 minutes, but microbubbles without urokinase did not. The mean percentage change in thrombus size from baseline was 97.16 ± 4.3 and 37.09 ± 5.6, respectively (P<0.001).
Urokinase administered alone could only match the efficacy of the treatment-loaded microbubbles if the drug was administered at a high dose. However, that significantly prolonged bleeding time from baseline—1079.25 ± 260.7 seconds vs 79.25 ± 6.5 seconds (P<0.001)—whereas, treatment with microbubbles did not.
While this research is in the early stages, the researchers believe the technology could help patients who develop venous thromboembolism and related conditions, such as heart attack and stroke. The team also believes the technology could have a major impact on treatment of patients in the emergency department. ![]()
FDA issues draft guidance on blood donation

The US Food and Drug Administration (FDA) has released a draft guidance recommending changes to current policies aimed at reducing the risk of HIV transmission via blood products.
Among the recommended changes is a proposal to alter the policy that prevents men who have sex with men (MSM) from donating blood.
The FDA’s draft guidance is recommending that MSM be allowed to donate blood if they have abstained from sexual contact for 1 year.
If this draft guidance is implemented, the US would follow other countries that have lifted the lifetime ban on MSM blood donors in recent years, such as the UK, Canada, and South Africa.
Human rights groups—such as the Human Rights Campaign, the US’s largest lesbian, gay, bisexual, and transgender civil rights organization—have said the FDA’s proposed policy change is still discriminatory.
“While the new policy is a step in the right direction toward an ideal policy that reflects the best scientific research, it still falls far short of a fully acceptable solution because it continues to stigmatize gay and bisexual men,” said Human Rights Campaign Government Affairs Director David Stacy.
“This policy prevents men from donating life-saving blood based solely on their sexual orientation rather than actual risk to the blood supply. It simply cannot be justified in light of current scientific research and updated blood screening technology.”
On the other side of the debate, blood banking groups—including the American Red Cross, America’s Blood Centers, and the American Association of Blood Banks—have voiced their support of a 1-year deferral period for MSM, as data have suggested this group has an increased risk of contracting HIV.
According to the Centers for Disease Control and Prevention, MSM are more severely affected by HIV than any other group in the US.
“This change in policy would align the donor deferral period for MSM with criteria for other activities that may pose a similar risk of transfusion-transmissible infections,” the blood banking groups said in a joint statement.
“We believe the current FDA indefinite blood donation deferral for a man who has [had] sex with another man since 1977 is medically and scientifically unwarranted. The blood banking community strongly supports the use of rational, scientifically based deferral periods that are applied fairly and consistently among blood donors who engage in similar-risk activities.”
The FDA’s draft guidance seems to reflect that idea, as the 1-year deferral period does not only pertain to MSM. It also pertains to individuals who have a history of receiving a transfusion of whole blood or blood components, individuals with a history of syphilis or gonorrhea, and individuals who have had a tattoo or piercing in the last year, among others.
The draft guidance also includes recommendations pertaining to donor education material and donor history questionnaires, donor requalification, product retrieval and quarantine, testing requirements, and other issues.
The full guidance, available here, is open for comment. ![]()
The US Food and Drug Administration (FDA) has released a draft guidance recommending changes to current policies aimed at reducing the risk of HIV transmission via blood products.
Among the recommended changes is a proposal to alter the policy that prevents men who have sex with men (MSM) from donating blood.
The FDA’s draft guidance is recommending that MSM be allowed to donate blood if they have abstained from sexual contact for 1 year.
If this draft guidance is implemented, the US would follow other countries that have lifted the lifetime ban on MSM blood donors in recent years, such as the UK, Canada, and South Africa.
Human rights groups—such as the Human Rights Campaign, the US’s largest lesbian, gay, bisexual, and transgender civil rights organization—have said the FDA’s proposed policy change is still discriminatory.
“While the new policy is a step in the right direction toward an ideal policy that reflects the best scientific research, it still falls far short of a fully acceptable solution because it continues to stigmatize gay and bisexual men,” said Human Rights Campaign Government Affairs Director David Stacy.
“This policy prevents men from donating life-saving blood based solely on their sexual orientation rather than actual risk to the blood supply. It simply cannot be justified in light of current scientific research and updated blood screening technology.”
On the other side of the debate, blood banking groups—including the American Red Cross, America’s Blood Centers, and the American Association of Blood Banks—have voiced their support of a 1-year deferral period for MSM, as data have suggested this group has an increased risk of contracting HIV.
According to the Centers for Disease Control and Prevention, MSM are more severely affected by HIV than any other group in the US.
“This change in policy would align the donor deferral period for MSM with criteria for other activities that may pose a similar risk of transfusion-transmissible infections,” the blood banking groups said in a joint statement.
“We believe the current FDA indefinite blood donation deferral for a man who has [had] sex with another man since 1977 is medically and scientifically unwarranted. The blood banking community strongly supports the use of rational, scientifically based deferral periods that are applied fairly and consistently among blood donors who engage in similar-risk activities.”
The FDA’s draft guidance seems to reflect that idea, as the 1-year deferral period does not only pertain to MSM. It also pertains to individuals who have a history of receiving a transfusion of whole blood or blood components, individuals with a history of syphilis or gonorrhea, and individuals who have had a tattoo or piercing in the last year, among others.
The draft guidance also includes recommendations pertaining to donor education material and donor history questionnaires, donor requalification, product retrieval and quarantine, testing requirements, and other issues.
The full guidance, available here, is open for comment. ![]()
The US Food and Drug Administration (FDA) has released a draft guidance recommending changes to current policies aimed at reducing the risk of HIV transmission via blood products.
Among the recommended changes is a proposal to alter the policy that prevents men who have sex with men (MSM) from donating blood.
The FDA’s draft guidance is recommending that MSM be allowed to donate blood if they have abstained from sexual contact for 1 year.
If this draft guidance is implemented, the US would follow other countries that have lifted the lifetime ban on MSM blood donors in recent years, such as the UK, Canada, and South Africa.
Human rights groups—such as the Human Rights Campaign, the US’s largest lesbian, gay, bisexual, and transgender civil rights organization—have said the FDA’s proposed policy change is still discriminatory.
“While the new policy is a step in the right direction toward an ideal policy that reflects the best scientific research, it still falls far short of a fully acceptable solution because it continues to stigmatize gay and bisexual men,” said Human Rights Campaign Government Affairs Director David Stacy.
“This policy prevents men from donating life-saving blood based solely on their sexual orientation rather than actual risk to the blood supply. It simply cannot be justified in light of current scientific research and updated blood screening technology.”
On the other side of the debate, blood banking groups—including the American Red Cross, America’s Blood Centers, and the American Association of Blood Banks—have voiced their support of a 1-year deferral period for MSM, as data have suggested this group has an increased risk of contracting HIV.
According to the Centers for Disease Control and Prevention, MSM are more severely affected by HIV than any other group in the US.
“This change in policy would align the donor deferral period for MSM with criteria for other activities that may pose a similar risk of transfusion-transmissible infections,” the blood banking groups said in a joint statement.
“We believe the current FDA indefinite blood donation deferral for a man who has [had] sex with another man since 1977 is medically and scientifically unwarranted. The blood banking community strongly supports the use of rational, scientifically based deferral periods that are applied fairly and consistently among blood donors who engage in similar-risk activities.”
The FDA’s draft guidance seems to reflect that idea, as the 1-year deferral period does not only pertain to MSM. It also pertains to individuals who have a history of receiving a transfusion of whole blood or blood components, individuals with a history of syphilis or gonorrhea, and individuals who have had a tattoo or piercing in the last year, among others.
The draft guidance also includes recommendations pertaining to donor education material and donor history questionnaires, donor requalification, product retrieval and quarantine, testing requirements, and other issues.
The full guidance, available here, is open for comment. ![]()