User login
Brain Tumors Glow 'Like Lava' With New Surgical Probe
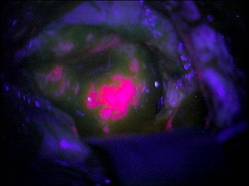
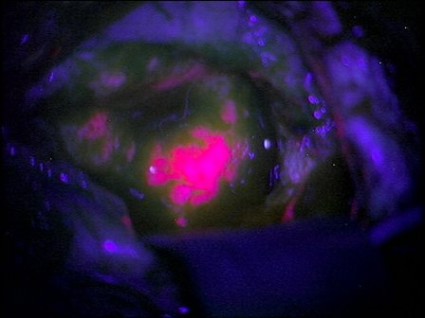
Neurosurgeons can now follow a glowing road map that points the way to cancerous brain tissue, leading thereby to a more effective surgical excision.
Researchers at the Norris Cotton Cancer Center and the Thayer School of Engineering at Dartmouth College, Hanover, N.H., have developed a probe that uses protoporphyrin IX fluorescence, oxygen saturation, hemoglobin concentration, and cell morphology to differentiate cancerous tissue from normal.
The probe identified 94% of glioma tissue in a small pilot study (J. Biomed. Opt. 2012 May 4 [doi:10.1117/1.JBO.17.5.056008]).
Research in Germany 15 years ago suggested that such a tool would identify only highly metabolic primary tumors. But augmenting the fluorescence technique with a computer algorithm that added the other cellular features gave surgeons a "jaw-dropping" view of low-grade tumors.
"The tumor glowed like lava," said Keith Paulsen, Ph.D., a professor of biomedical engineering at the school of engineering and a member of the cancer imaging and radiobiology research program at Norris Cotton Cancer Center.
The team will next evaluate their technique on lung cancers, with investigations of other tumor types to follow.
Neurosurgeons can now follow a glowing road map that points the way to cancerous brain tissue, leading thereby to a more effective surgical excision.
Researchers at the Norris Cotton Cancer Center and the Thayer School of Engineering at Dartmouth College, Hanover, N.H., have developed a probe that uses protoporphyrin IX fluorescence, oxygen saturation, hemoglobin concentration, and cell morphology to differentiate cancerous tissue from normal.
The probe identified 94% of glioma tissue in a small pilot study (J. Biomed. Opt. 2012 May 4 [doi:10.1117/1.JBO.17.5.056008]).
Research in Germany 15 years ago suggested that such a tool would identify only highly metabolic primary tumors. But augmenting the fluorescence technique with a computer algorithm that added the other cellular features gave surgeons a "jaw-dropping" view of low-grade tumors.
"The tumor glowed like lava," said Keith Paulsen, Ph.D., a professor of biomedical engineering at the school of engineering and a member of the cancer imaging and radiobiology research program at Norris Cotton Cancer Center.
The team will next evaluate their technique on lung cancers, with investigations of other tumor types to follow.
Neurosurgeons can now follow a glowing road map that points the way to cancerous brain tissue, leading thereby to a more effective surgical excision.
Researchers at the Norris Cotton Cancer Center and the Thayer School of Engineering at Dartmouth College, Hanover, N.H., have developed a probe that uses protoporphyrin IX fluorescence, oxygen saturation, hemoglobin concentration, and cell morphology to differentiate cancerous tissue from normal.
The probe identified 94% of glioma tissue in a small pilot study (J. Biomed. Opt. 2012 May 4 [doi:10.1117/1.JBO.17.5.056008]).
Research in Germany 15 years ago suggested that such a tool would identify only highly metabolic primary tumors. But augmenting the fluorescence technique with a computer algorithm that added the other cellular features gave surgeons a "jaw-dropping" view of low-grade tumors.
"The tumor glowed like lava," said Keith Paulsen, Ph.D., a professor of biomedical engineering at the school of engineering and a member of the cancer imaging and radiobiology research program at Norris Cotton Cancer Center.
The team will next evaluate their technique on lung cancers, with investigations of other tumor types to follow.
FROM THE JOURNAL OF BIOMEDICAL OPTICS
Discordant Antibiotics in Pediatric UTI
Urinary tract infections (UTIs) are one of the most common reasons for pediatric hospitalizations.1 Bacterial infections require prompt treatment with appropriate antimicrobial agents. Results from culture and susceptibility testing, however, are often unavailable until 48 hours after initial presentation. Therefore, the clinician must select antimicrobials empirically, basing decisions on likely pathogens and local resistance patterns.2 This decision is challenging because the effect of treatment delay on clinical outcomes is difficult to determine and resistance among uropathogens is increasing. Resistance rates have doubled over the past several years.3, 4 For common first‐line antibiotics, such as ampicillin and trimethoprim‐sulfamethoxazole, resistance rates for Escherichia coli, the most common uropathogen, exceed 25%.4, 5 While resistance to third‐generation cephalosporins remains low, rates in the United States have increased from <1% in 1999 to 4% in 2010. International data shows much higher resistance rates for cephalosporins in general.6, 7 This high prevalence of resistance may prompt the use of broad‐spectrum antibiotics for patients with UTI. For example, the use of third‐generation cephalosporins for UTI has doubled in recent years.3 Untreated, UTIs can lead to serious illness, but the consequences of inadequate initial antibiotic coverage are unknown.8, 9
Discordant antibiotic therapy, initial antibiotic therapy to which the causative bacterium is not susceptible, occurs in up to 9% of children hospitalized for UTI.10 However, there is reason to believe that discordant therapy may matter less for UTIs than for infections at other sites. First, in adults hospitalized with UTIs, discordant initial therapy did not affect the time to resolution of symptoms.11, 12 Second, most antibiotics used to treat UTIs are renally excreted and, thus, antibiotic concentrations at the site of infection are higher than can be achieved in the serum or cerebrospinal fluid.13 The Clinical and Laboratory Standard Institute has acknowledged that traditional susceptibility breakpoints may be too conservative for some non‐central nervous system infections; such as non‐central nervous system infections caused by Streptococcus pneumoniae.14
As resistance rates increase, more patients are likely to be treated with discordant therapy. Therefore, we sought to identify the clinical consequences of discordant antimicrobial therapy for patients hospitalized with a UTI.
METHODS
Design and Setting
We conducted a multicenter, retrospective cohort study. Data for this study were originally collected for a study that determined the accuracy of individual and combined International Classification of Diseases, Ninth Revision (ICD‐9) discharge diagnosis codes for children with laboratory tests for a UTI, in order to develop national quality measures for children hospitalized with UTIs.15 The institutional review board for each hospital (Seattle Children's Hospital, Seattle, WA; Monroe Carell Jr Children's Hospital at Vanderbilt, Nashville, TN; Cincinnati Children's Hospital Medical Center, Cincinnati, OH; Children's Mercy Hospital, Kansas City, MO; Children's Hospital of Philadelphia, Philadelphia, PA) approved the study.
Data Sources
Data were obtained from the Pediatric Health Information System (PHIS) and medical records for patients at the 5 participating hospitals. PHIS contains clinical and billing data from hospitalized children at 43 freestanding children's hospitals. Data quality and coding reliability are assured through a joint effort between the Children's Hospital Association (Shawnee Mission, KS) and participating hospitals.16 PHIS was used to identify participants based on presence of discharge diagnosis code and laboratory tests indicating possible UTI, patient demographics, antibiotic administration date, and utilization of hospital resources (length of stay [LOS], laboratory testing).
Medical records for each participant were reviewed to obtain laboratory and clinical information such as past medical history (including vesicoureteral reflux [VUR], abnormal genitourinary [GU] anatomy, use of prophylactic antibiotic), culture data, and fever data. Data were entered into a secured centrally housed web‐based data collection system. To assure consistency of chart review, all investigators responsible for data collection underwent training. In addition, 2 pilot medical record reviews were performed, followed by group discussion, to reach consensus on questions, preselected answers, interpretation of medical record data, and parameters for free text data entry.
Subjects
The initial cohort included 460 hospitalized patients, aged 3 days to 18 years of age, discharged from participating hospitals between July 1, 2008 and June 30, 2009 with a positive urine culture at any time during hospitalization.15 We excluded patients under 3 days of age because patients this young are more likely to have been transferred from the birthing hospital for a complication related to birth or a congenital anomaly. For this secondary analysis of patients from a prior study, our target population included patients admitted for management of UTI.15 We excluded patients with a negative initial urine culture (n = 59) or if their initial urine culture did not meet definition of laboratory‐confirmed UTI, defined as urine culture with >50,000 colony‐forming units (CFU) with an abnormal urinalysis (UA) (n = 77).1, 1719 An abnormal UA was defined by presence of white blood cells, leukocyte esterase, bacteria, and/or nitrites. For our cohort, all cultures with >50,000 CFU also had an abnormal urinalysis. We excluded 19 patients with cultures classified as 10,000100,000 CFU because we could not confirm that the CFU was >50,000. We excluded 30 patients with urine cultures classified as normal or mixed flora, positive for a mixture of organisms not further identified, or if results were unavailable. Additionally, coagulase‐negative Staphylococcus species (n = 8) were excluded, as these are typically considered contaminants in the setting of urine cultures.2 Patients likely to have received antibiotics prior to admission, or develop a UTI after admission, were identified and removed from the cohort if they had a urine culture performed more than 1 day before, or 2 days after, admission (n = 35). Cultures without resistance testing to the initial antibiotic selection were also excluded (n = 16).
Main Outcome Measures
The primary outcome measure was hospital LOS. Time to fever resolution was a secondary outcome measure. Fever was defined as temperature 38C. Fever duration was defined as number of hours until resolution of fever; only patients with fever at admission were included in this subanalysis.
Main Exposure
The main exposure was initial antibiotic therapy. Patients were classified into 3 groups according to initial antibiotic selection: those receiving 1) concordant; 2) discordant; or 3) delayed initial therapy. Concordance was defined as in vitro susceptibility to the initial antibiotic or class of antibiotic. If the uropathogen was sensitive to a narrow‐spectrum antibiotic (eg, first‐generation cephalosporin), but was not tested against a more broad‐spectrum antibiotic of the same class (eg, third‐generation cephalosporin), concordance was based on the sensitivity to the narrow‐spectrum antibiotic. If the uropathogen was sensitive to a broad‐spectrum antibiotic (eg, third‐generation cephalosporin), concordance to a more narrow‐spectrum antibiotic was not assumed. Discordance was defined as laboratory confirmation of in vitro resistance, or intermediate sensitivity of the pathogen to the initial antibiotic or class of antibiotics. Patients were considered to have a delay in antibiotic therapy if they did not receive antibiotics on the day of, or day after, collection of UA and culture. Patients with more than 1 uropathogen identified in a single culture were classified as discordant if any of the organisms was discordant to the initial antibiotic; they were classified as concordant if all organisms were concordant to the initial antibiotic. Antibiotic susceptibility was not tested in some cases (n = 16).
Initial antibiotic was defined as the antibiotic(s) billed on the same day or day after the UA was billed. If the patient had the UA completed on the day prior to admission, we used the antibiotic administered on the day of admission as the initial antibiotic.
Covariates
Covariates were selected a priori to include patient characteristics likely to affect patient outcomes; all were included in the final analysis. These were age, race, sex, insurance, disposition, prophylactic antibiotic use for any reason (VUR, oncologic process, etc), presence of a chronic care condition, and presence of VUR or GU anatomic abnormality. Age, race, sex, and insurance were obtained from PHIS. Medical record review was used to determine prophylactic antibiotic use, and presence of VUR or GU abnormalities (eg, posterior urethral valves). Chronic care conditions were defined using a previously reported method.20
Data Analysis
Continuous variables were described using median and interquartile range (IQR). Categorical variables were described using frequencies. Multivariable analyses were used to determine the independent association of discordant antibiotic therapy and the outcomes of interest. Poisson regression was used to fit the skewed LOS distribution. The effect of antibiotic concordance or discordance on LOS was determined for all patients in our sample, as well as for those with a urine culture positive for a single identified organism. We used the KruskalWallis test statistic to determine the association between duration of fever and discordant antibiotic therapy, given that duration of fever is a continuous variable. Generalized estimating equations accounted for clustering by hospital and the variability that exists between hospitals.
RESULTS
Of the initial 460 cases with positive urine culture growth at any time during admission, 216 met inclusion criteria for a laboratory‐confirmed UTI from urine culture completed at admission. The median age was 2.46 years (IQR: 0.27,8.89). In the study population, 25.0% were male, 31.0% were receiving prophylactic antibiotics, 13.0% had any grade of VUR, and 16.7% had abnormal GU anatomy (Table 1). A total of 82.4% of patients were treated with concordant initial therapy, 10.2% with discordant initial therapy, and 7.4% received delayed initial antibiotic therapy. There were no significant differences between the groups for any of the covariates. Discordant antibiotic cases ranged from 4.9% to 21.7% across hospitals.
| Overall | Concordant* | Discordant | Delayed Antibiotics | P Value | |
|---|---|---|---|---|---|
| |||||
| N | 216 | 178 (82.4) | 22 (10.2) | 16 (7.4) | |
| Gender | |||||
| Male | 54 (25.0) | 40 (22.5) | 8 (36.4) | 6 (37.5) | 0.18 |
| Female | 162 (75.0) | 138 (77.5) | 14 (63.64) | 10 (62.5) | |
| Race | |||||
| Non‐Hispanic white | 136 (63.9) | 110 (62.5) | 15 (71.4) | 11 (68.8) | 0.83 |
| Non‐Hispanic black | 28 (13.2) | 24 (13.6) | 2 (9.5) | 2 (12.5) | |
| Hispanic | 20 (9.4) | 16 (9.1) | 3 (14.3) | 1 (6.3) | |
| Asian | 10 (4.7) | 9 (5.1) | 1 (4.7) | ||
| Other | 19 (8.9) | 17 (9.7) | 2 (12.5) | ||
| Payor | |||||
| Government | 97 (44.9) | 80 (44.9) | 11 (50.0) | 6 (37.5) | 0.58 |
| Private | 70 (32.4) | 56 (31.5) | 6 (27.3) | 8 (50.0) | |
| Other | 49 (22.7) | 42 (23.6) | 5 (22.7) | 2 (12.5) | |
| Disposition | |||||
| Home | 204 (94.4) | 168 (94.4) | 21 (95.5) | 15 (93.8) | 0.99 |
| Died | 1 (0.5) | 1 (0.6) | |||
| Other | 11 (5.1) | 9 (5.1) | 1 (4.6) | 1 (6.3) | |
| Age | |||||
| 3 d60 d | 40 (18.5) | 35 (19.7) | 3 (13.6) | 2 (12.5) | 0.53 |
| 61 d2 y | 62 (28.7) | 54 (30.3) | 4 (18.2) | 4 (25.0) | |
| 3 y12 y | 75 (34.7) | 61 (34.3) | 8 (36.4) | 6 (37.5) | |
| 13 y18 y | 39 (18.1) | 28 (15.7) | 7 (31.8) | 4 (25.0) | |
| Length of stay | |||||
| 1 d5 d | 171 (79.2) | 147 (82.6) | 12 (54.6) | 12 (75.0) | 0.03 |
| 6 d10 d | 24 (11.1) | 17 (9.6) | 5 (22.7) | 2 (12.5) | |
| 11 d15 d | 10 (4.6) | 5 (2.8) | 3 (13.6) | 2 (12.5) | |
| 16 d+ | 11 (5.1) | 9 (5.1) | 2 (9.1) | 0 | |
| Complex chronic conditions | |||||
| Any CCC | 94 (43.5) | 77 (43.3) | 12 (54.6) | 5 (31.3) | 0.35 |
| Cardiovascular | 20 (9.3) | 19 (10.7) | 1 (6.3) | 0.24 | |
| Neuromuscular | 34 (15.7) | 26 (14.6) | 7 (31.8) | 1 (6.3) | 0.06 |
| Respiratory | 6 (2.8) | 6 (3.4) | 0.52 | ||
| Renal | 26 (12.0) | 21 (11.8) | 4 (18.2) | 1 (6.3) | 0.52 |
| Gastrointestinal | 3 (1.4) | 3 (1.7) | 0.72 | ||
| Hematologic/ immunologic | 1 (0.5) | 1 (4.6) | 0.01 | ||
| Metabolic | 8 (3.7) | 6 (3.4) | 1 (4.6) | 1 (6.3) | 0.82 |
| Congenital or genetic | 15 (6.9) | 11 (6.2) | 3 (13.6) | 1 (6.3) | 0.43 |
| Malignancy | 5 (2.3) | 3 (1.7) | 2 (9.1) | 0.08 | |
| VUR | 28 (13.0) | 23 (12.9) | 3 (13.6) | 2 (12.5) | 0.99 |
| Abnormal GU | 36 (16.7) | 31 (17.4) | 4 (18.2) | 1 (6.3) | 0.51 |
| Prophylactic antibiotics | 67 (31.0) | 53 (29.8) | 10 (45.5) | 4 (25.0) | 0.28 |
The most common causative organisms were E. coli (65.7%) and Klebsiella spp (9.7%) (Table 2). The most common initial antibiotics were a third‐generation cephalosporin (39.1%), combination of ampicillin and a third‐ or fourth‐generation cephalosporin (16.7%), and combination of ampicillin with gentamicin (11.1%). A third‐generation cephalosporin was the initial antibiotic for 46.1% of the E. coli and 56.9% of Klebsiella spp UTIs. Resistance to third‐generation cephalosporins but carbapenem susceptibility was noted for 4.5% of E. coli and 7.7% of Klebsiella spp isolates. Patients with UTIs caused by Klebsiella spp, mixed organisms, and Enterobacter spp were more likely to receive discordant antibiotic therapy. Patients with Enterobacter spp and mixed‐organism UTIs were more likely to have delayed antibiotic therapy. Nineteen patients (8.8%) had positive blood cultures. Fifteen (6.9%) required intensive care unit (ICU) admission during hospitalization.
| Organism | Cases | Concordant* No. (%) | Discordant No. (%) | Delayed Antibiotics No. (%) |
|---|---|---|---|---|
| ||||
| E. coli | 142 | 129 (90.8) | 3 (2.1) | 10 (7.0) |
| Klebsiella spp | 21 | 14 (66.7) | 7 (33.3) | 0 (0) |
| Enterococcus spp | 12 | 9 (75.0) | 3 (25.0) | 0 (0) |
| Enterobacter spp | 10 | 5 (50.0) | 3 (30.0) | 2 (20.0) |
| Pseudomonas spp | 10 | 9 (90.0) | 1 (10.0) | 0 (0) |
| Other single organisms | 6 | 5 (83.3) | 0 (0) | 1 (16.7) |
| Other identified multiple organisms | 15 | 7 (46.7) | 5 (33.3) | 3 (20.0) |
Unadjusted results are shown in Supporting Appendix 1, in the online version of this article. In the adjusted analysis, discordant antibiotic therapy was associated with a significantly longer LOS, compared with concordant therapy for all UTIs and for all UTIs caused by a single organism (Table 3). In adjusted analysis, discordant therapy was also associated with a 3.1 day (IQR: 2.0, 4.7) longer length of stay compared with concordant therapy for all E. coli UTIs.
| Bacteria | Difference in LOS (95% CI)* | P Value |
|---|---|---|
| ||
| All organisms | ||
| Concordant vs discordant | 1.8 (2.1, 1.5) | <0.0001 |
| Concordant vs delayed antibiotics | 1.4 (1.7, 1.1) | 0.01 |
| Single organisms | ||
| Concordant vs discordant | 1.9 (2.4, 1.5) | <0.0001 |
| Concordant vs delayed antibiotics | 1.2 (1.6, 1.2) | 0.37 |
Time to fever resolution was analyzed for patients with a documented fever at presentation for each treatment subgroup. One hundred thirty‐six patients were febrile at admission and 122 were febrile beyond the first recorded vital signs. Fever was present at admission in 60% of the concordant group and 55% of the discordant group (P = 0.6). The median duration of fever was 48 hours for the concordant group (n = 107; IQR: 24, 240) and 78 hours for the discordant group (n = 12; IQR: 48, 132). All patients were afebrile at discharge. Differences in fever duration between treatment groups were not statistically significant (P = 0.7).
DISCUSSION
Across 5 children's hospitals, 1 out of every 10 children hospitalized for UTI received discordant initial antibiotic therapy. Children receiving discordant antibiotic therapy had a 1.8 day longer LOS when compared with those on concordant therapy. However, there was no significant difference in time to fever resolution between the groups, suggesting that the increase in LOS was not explained by increased fever duration.
The overall rate of discordant therapy in this study is consistent with prior studies, as was the more common association of discordant therapy with non‐E. coli UTIs.10 According to the Kids' Inpatient Database 2009, there are 48,100 annual admissions for patients less than 20 years of age with a discharge diagnosis code of UTI in the United States.1 This suggests that nearly 4800 children with UTI could be affected by discordant therapy annually.
Children treated with discordant antibiotic therapy had a significantly longer LOS compared to those treated with concordant therapy. However, differences in time to fever resolution between the groups were not statistically significant. While resolution of fever may suggest clinical improvement and adequate empiric therapy, the lack of association with antibiotic concordance was not unexpected, since the relationship between fever resolution, clinical improvement, and LOS is complex and thus challenging to measure.21 These results support the notion that fever resolution alone may not be an adequate measure of clinical response.
It is possible that variability in discharge decision‐making may contribute to increased length of stay. Some clinicians may delay a patient's discharge until complete resolution of symptoms or knowledge of susceptibilities, while others may discharge patients that are still febrile and/or still receiving empiric antibiotics. Evidence‐based guidelines that address the appropriate time to discharge a patient with UTI are lacking. The American Academy of Pediatrics provides recommendations for use of parenteral antibiotics and hospital admission for patients with UTI, but does not address discharge decision‐making or patient management in the setting of discordant antibiotic therapy.2, 21
This study must be interpreted in the context of several limitations. First, our primary and secondary outcomes, LOS and fever duration, were surrogate measures for clinical response. We were not able to measure all clinical factors that may contribute to LOS, such as the patient's ability to tolerate oral fluids and antibiotics. Also, there may have been too few patients to detect a clinically important difference in fever duration between the concordant and discordant groups, especially for individual organisms. Although we did find a significant difference in LOS between patients treated with concordant compared with discordant therapy, there may be residual confounding from unobserved differences. This confounding, in conjunction with the small sample size, may cause us to underestimate the magnitude of the difference in LOS resulting from discordant therapy. Second, short‐term outcomes such as ICU admission were not investigated in this study; however, the proportion of patients admitted to the ICU in our population was quite small, precluding its use as a meaningful outcome measure. Third, the potential benefits to patients who were not exposed to unnecessary antibiotics, or harm to those that were exposed, could not be measured. Finally, our study was obtained using data from 5 free‐standing tertiary care pediatric facilities, thereby limiting its generalizability to other settings. Still, our rates of prophylactic antibiotic use, VUR, and GU abnormalities are similar to others reported in tertiary care children's hospitals, and we accounted for these covariates in our model.2225
As the frequency of infections caused by resistant bacteria increase, so will the number of patients receiving discordant antibiotics for UTI, compounding the challenge of empiric antimicrobial selection. Further research is needed to better understand how discordant initial antibiotic therapy contributes to LOS and whether it is associated with adverse short‐ and long‐term clinical outcomes. Such research could also aid in weighing the risk of broader‐spectrum prescribing on antimicrobial resistance patterns. While we identified an association between discordant initial antibiotic therapy and LOS, we were unable to determine the ideal empiric antibiotic therapy for patients hospitalized with UTI. Further investigation is needed to inform local and national practice guidelines for empiric antibiotic selection in patients with UTIs. This may also be an opportunity to decrease discordant empiric antibiotic selection, perhaps through use of antibiograms that stratify patients based on known factors, to lead to more specific initial therapy.
CONCLUSIONS
This study demonstrates that discordant antibiotic selection for UTI at admission is associated with longer hospital stay, but not fever duration. The full clinical consequences of discordant therapy, and the effects on length of stay, need to be better understood. Our findings, taken in combination with careful consideration of patient characteristics and prior history, may provide an opportunity to improve the hospital care for patients with UTIs.
Acknowledgements
Disclosure: Nothing to report.
- HCUP Kids' Inpatient Database (KID). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality; 2006 and 2009. Available at: http://www.hcup‐us.ahrq.gov/kidoverview.jsp.
- Subcommitee on Urinary Tract Infection, Steering Committee on Quality Improvement and Management. Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics. 2011;128(3)595–610. doi: 10.1542/peds.2011–1330. Available at: http://pediatrics.aappublications.org/content/128/3/595.full.html.
- , , . National ambulatory antibiotic prescribing patterns for pediatric urinary tract infection, 1998–2007. Pediatrics. 2011;127(6):1027–1033.
- , , , , . Previous antimicrobial exposure is associated with drug‐resistant urinary tract infections in children. Pediatrics. 2010;125(4):664–672.
- CDC. National Antimicrobial Resistance Monitoring System for Enteric Bacteria (NARMS): Human Isolates Final Report. Atlanta, GA: US Department of Health and Human Services, CDC; 2009.
- , , , , . Increasing antibiotic resistance among uropathogens isolated during years 2006–2009: impact on the empirical management. Int Braz J Urol. 2012;38(1):25–32.
- . 3rd Generation Cephalosporin‐Resistant Escherichia coli. 2010. Available at: http://www.cddep.org/ResistanceMap/bug‐drug/EC‐CS. Accessed May 14, 2012.
- , , , . Risk of renal scarring in children with a first urinary tract infection: a systematic review. Pediatrics. 2010;126(6):1084–1091.
- , . Treatment of urinary tract infections. Pediatr Infect Dis J. 1999;18(11):1020–1021.
- , , , , . Non‐Escherichia coli versus Escherichia coli community‐acquired urinary tract infections in children hospitalized in a tertiary center: relative frequency, risk factors, antimicrobial resistance and outcome. Pediatr Infect Dis J. 2005;24(7):581–585.
- , , , , , . Prognosis of urinary tract infections with discordant antibiotic treatment [in Spanish]. Rev Clin Esp. 2010;210(11):545–549.
- , , , et al. Appropriateness of empiric antibiotic therapy in urinary tract infection in emergency room [in Spanish]. Rev Clin Esp. 2010;210(1):11–16.
- , , . Principles and Practice of Pediatric Infectious Diseases. 3rd ed. New York, NY: Churchill Livingstone/Elsevier; 2009.
- National Committee for Clinical Laboratory Standards. Performance Standards for Antimicrobial Susceptibility Testing; Twelfth Informational Supplement.Vol M100‐S12. Wayne, PA: NCCLS; 2002.
- , , , et al. Accuracy of administrative billing codes to detect urinary tract infection hospitalizations. Pediatrics. 2011;128(2):323–330.
- , , , . Corticosteroids and mortality in children with bacterial meningitis. JAMA. 2008;299(17):2048–2055.
- , , , , . Enhanced urinalysis as a screening test for urinary tract infection. Pediatrics. 1993;91(6):1196–1199.
- , , , , . Pyuria and bacteriuria in urine specimens obtained by catheter from young children with fever. J Pediatr. 1994;124(4):513–519.
- , , , et al. Clinical and demographic factors associated with urinary tract infection in young febrile infants. Pediatrics. 2005;116(3):644–648.
- , , , , , . Deaths attributed to pediatric complex chronic conditions: national trends and implications for supportive care services. Pediatrics. 2001;107(6):E99.
- Committee on Quality Improvement. Subcommittee on Urinary Tract Infection. Practice parameter: the diagnosis, treatment, and evaluation of the initial urinary tract infection in febrile infants and young children. Pediatrics. 1999;103:843–852.
- , . Antibiotics or surgery for vesicoureteric reflux in children. Lancet. 2004;364(9446):1720–1722.
- , , , et al. Randomized intervention for children with vesicoureteral reflux (RIVUR): background commentary of RIVUR investigators. Pediatrics. 2008;122(suppl 5):S233–S239.
- , , . Length of intravenous antibiotic therapy and treatment failure in infants with urinary tract infections. Pediatrics. 2010;126(2):196–203.
- , , , , , . Vesicoureteral reflux in children with suspected and proven urinary tract infection. Pediatr Nephrol. 2010;25(8):1463–1469.
Urinary tract infections (UTIs) are one of the most common reasons for pediatric hospitalizations.1 Bacterial infections require prompt treatment with appropriate antimicrobial agents. Results from culture and susceptibility testing, however, are often unavailable until 48 hours after initial presentation. Therefore, the clinician must select antimicrobials empirically, basing decisions on likely pathogens and local resistance patterns.2 This decision is challenging because the effect of treatment delay on clinical outcomes is difficult to determine and resistance among uropathogens is increasing. Resistance rates have doubled over the past several years.3, 4 For common first‐line antibiotics, such as ampicillin and trimethoprim‐sulfamethoxazole, resistance rates for Escherichia coli, the most common uropathogen, exceed 25%.4, 5 While resistance to third‐generation cephalosporins remains low, rates in the United States have increased from <1% in 1999 to 4% in 2010. International data shows much higher resistance rates for cephalosporins in general.6, 7 This high prevalence of resistance may prompt the use of broad‐spectrum antibiotics for patients with UTI. For example, the use of third‐generation cephalosporins for UTI has doubled in recent years.3 Untreated, UTIs can lead to serious illness, but the consequences of inadequate initial antibiotic coverage are unknown.8, 9
Discordant antibiotic therapy, initial antibiotic therapy to which the causative bacterium is not susceptible, occurs in up to 9% of children hospitalized for UTI.10 However, there is reason to believe that discordant therapy may matter less for UTIs than for infections at other sites. First, in adults hospitalized with UTIs, discordant initial therapy did not affect the time to resolution of symptoms.11, 12 Second, most antibiotics used to treat UTIs are renally excreted and, thus, antibiotic concentrations at the site of infection are higher than can be achieved in the serum or cerebrospinal fluid.13 The Clinical and Laboratory Standard Institute has acknowledged that traditional susceptibility breakpoints may be too conservative for some non‐central nervous system infections; such as non‐central nervous system infections caused by Streptococcus pneumoniae.14
As resistance rates increase, more patients are likely to be treated with discordant therapy. Therefore, we sought to identify the clinical consequences of discordant antimicrobial therapy for patients hospitalized with a UTI.
METHODS
Design and Setting
We conducted a multicenter, retrospective cohort study. Data for this study were originally collected for a study that determined the accuracy of individual and combined International Classification of Diseases, Ninth Revision (ICD‐9) discharge diagnosis codes for children with laboratory tests for a UTI, in order to develop national quality measures for children hospitalized with UTIs.15 The institutional review board for each hospital (Seattle Children's Hospital, Seattle, WA; Monroe Carell Jr Children's Hospital at Vanderbilt, Nashville, TN; Cincinnati Children's Hospital Medical Center, Cincinnati, OH; Children's Mercy Hospital, Kansas City, MO; Children's Hospital of Philadelphia, Philadelphia, PA) approved the study.
Data Sources
Data were obtained from the Pediatric Health Information System (PHIS) and medical records for patients at the 5 participating hospitals. PHIS contains clinical and billing data from hospitalized children at 43 freestanding children's hospitals. Data quality and coding reliability are assured through a joint effort between the Children's Hospital Association (Shawnee Mission, KS) and participating hospitals.16 PHIS was used to identify participants based on presence of discharge diagnosis code and laboratory tests indicating possible UTI, patient demographics, antibiotic administration date, and utilization of hospital resources (length of stay [LOS], laboratory testing).
Medical records for each participant were reviewed to obtain laboratory and clinical information such as past medical history (including vesicoureteral reflux [VUR], abnormal genitourinary [GU] anatomy, use of prophylactic antibiotic), culture data, and fever data. Data were entered into a secured centrally housed web‐based data collection system. To assure consistency of chart review, all investigators responsible for data collection underwent training. In addition, 2 pilot medical record reviews were performed, followed by group discussion, to reach consensus on questions, preselected answers, interpretation of medical record data, and parameters for free text data entry.
Subjects
The initial cohort included 460 hospitalized patients, aged 3 days to 18 years of age, discharged from participating hospitals between July 1, 2008 and June 30, 2009 with a positive urine culture at any time during hospitalization.15 We excluded patients under 3 days of age because patients this young are more likely to have been transferred from the birthing hospital for a complication related to birth or a congenital anomaly. For this secondary analysis of patients from a prior study, our target population included patients admitted for management of UTI.15 We excluded patients with a negative initial urine culture (n = 59) or if their initial urine culture did not meet definition of laboratory‐confirmed UTI, defined as urine culture with >50,000 colony‐forming units (CFU) with an abnormal urinalysis (UA) (n = 77).1, 1719 An abnormal UA was defined by presence of white blood cells, leukocyte esterase, bacteria, and/or nitrites. For our cohort, all cultures with >50,000 CFU also had an abnormal urinalysis. We excluded 19 patients with cultures classified as 10,000100,000 CFU because we could not confirm that the CFU was >50,000. We excluded 30 patients with urine cultures classified as normal or mixed flora, positive for a mixture of organisms not further identified, or if results were unavailable. Additionally, coagulase‐negative Staphylococcus species (n = 8) were excluded, as these are typically considered contaminants in the setting of urine cultures.2 Patients likely to have received antibiotics prior to admission, or develop a UTI after admission, were identified and removed from the cohort if they had a urine culture performed more than 1 day before, or 2 days after, admission (n = 35). Cultures without resistance testing to the initial antibiotic selection were also excluded (n = 16).
Main Outcome Measures
The primary outcome measure was hospital LOS. Time to fever resolution was a secondary outcome measure. Fever was defined as temperature 38C. Fever duration was defined as number of hours until resolution of fever; only patients with fever at admission were included in this subanalysis.
Main Exposure
The main exposure was initial antibiotic therapy. Patients were classified into 3 groups according to initial antibiotic selection: those receiving 1) concordant; 2) discordant; or 3) delayed initial therapy. Concordance was defined as in vitro susceptibility to the initial antibiotic or class of antibiotic. If the uropathogen was sensitive to a narrow‐spectrum antibiotic (eg, first‐generation cephalosporin), but was not tested against a more broad‐spectrum antibiotic of the same class (eg, third‐generation cephalosporin), concordance was based on the sensitivity to the narrow‐spectrum antibiotic. If the uropathogen was sensitive to a broad‐spectrum antibiotic (eg, third‐generation cephalosporin), concordance to a more narrow‐spectrum antibiotic was not assumed. Discordance was defined as laboratory confirmation of in vitro resistance, or intermediate sensitivity of the pathogen to the initial antibiotic or class of antibiotics. Patients were considered to have a delay in antibiotic therapy if they did not receive antibiotics on the day of, or day after, collection of UA and culture. Patients with more than 1 uropathogen identified in a single culture were classified as discordant if any of the organisms was discordant to the initial antibiotic; they were classified as concordant if all organisms were concordant to the initial antibiotic. Antibiotic susceptibility was not tested in some cases (n = 16).
Initial antibiotic was defined as the antibiotic(s) billed on the same day or day after the UA was billed. If the patient had the UA completed on the day prior to admission, we used the antibiotic administered on the day of admission as the initial antibiotic.
Covariates
Covariates were selected a priori to include patient characteristics likely to affect patient outcomes; all were included in the final analysis. These were age, race, sex, insurance, disposition, prophylactic antibiotic use for any reason (VUR, oncologic process, etc), presence of a chronic care condition, and presence of VUR or GU anatomic abnormality. Age, race, sex, and insurance were obtained from PHIS. Medical record review was used to determine prophylactic antibiotic use, and presence of VUR or GU abnormalities (eg, posterior urethral valves). Chronic care conditions were defined using a previously reported method.20
Data Analysis
Continuous variables were described using median and interquartile range (IQR). Categorical variables were described using frequencies. Multivariable analyses were used to determine the independent association of discordant antibiotic therapy and the outcomes of interest. Poisson regression was used to fit the skewed LOS distribution. The effect of antibiotic concordance or discordance on LOS was determined for all patients in our sample, as well as for those with a urine culture positive for a single identified organism. We used the KruskalWallis test statistic to determine the association between duration of fever and discordant antibiotic therapy, given that duration of fever is a continuous variable. Generalized estimating equations accounted for clustering by hospital and the variability that exists between hospitals.
RESULTS
Of the initial 460 cases with positive urine culture growth at any time during admission, 216 met inclusion criteria for a laboratory‐confirmed UTI from urine culture completed at admission. The median age was 2.46 years (IQR: 0.27,8.89). In the study population, 25.0% were male, 31.0% were receiving prophylactic antibiotics, 13.0% had any grade of VUR, and 16.7% had abnormal GU anatomy (Table 1). A total of 82.4% of patients were treated with concordant initial therapy, 10.2% with discordant initial therapy, and 7.4% received delayed initial antibiotic therapy. There were no significant differences between the groups for any of the covariates. Discordant antibiotic cases ranged from 4.9% to 21.7% across hospitals.
| Overall | Concordant* | Discordant | Delayed Antibiotics | P Value | |
|---|---|---|---|---|---|
| |||||
| N | 216 | 178 (82.4) | 22 (10.2) | 16 (7.4) | |
| Gender | |||||
| Male | 54 (25.0) | 40 (22.5) | 8 (36.4) | 6 (37.5) | 0.18 |
| Female | 162 (75.0) | 138 (77.5) | 14 (63.64) | 10 (62.5) | |
| Race | |||||
| Non‐Hispanic white | 136 (63.9) | 110 (62.5) | 15 (71.4) | 11 (68.8) | 0.83 |
| Non‐Hispanic black | 28 (13.2) | 24 (13.6) | 2 (9.5) | 2 (12.5) | |
| Hispanic | 20 (9.4) | 16 (9.1) | 3 (14.3) | 1 (6.3) | |
| Asian | 10 (4.7) | 9 (5.1) | 1 (4.7) | ||
| Other | 19 (8.9) | 17 (9.7) | 2 (12.5) | ||
| Payor | |||||
| Government | 97 (44.9) | 80 (44.9) | 11 (50.0) | 6 (37.5) | 0.58 |
| Private | 70 (32.4) | 56 (31.5) | 6 (27.3) | 8 (50.0) | |
| Other | 49 (22.7) | 42 (23.6) | 5 (22.7) | 2 (12.5) | |
| Disposition | |||||
| Home | 204 (94.4) | 168 (94.4) | 21 (95.5) | 15 (93.8) | 0.99 |
| Died | 1 (0.5) | 1 (0.6) | |||
| Other | 11 (5.1) | 9 (5.1) | 1 (4.6) | 1 (6.3) | |
| Age | |||||
| 3 d60 d | 40 (18.5) | 35 (19.7) | 3 (13.6) | 2 (12.5) | 0.53 |
| 61 d2 y | 62 (28.7) | 54 (30.3) | 4 (18.2) | 4 (25.0) | |
| 3 y12 y | 75 (34.7) | 61 (34.3) | 8 (36.4) | 6 (37.5) | |
| 13 y18 y | 39 (18.1) | 28 (15.7) | 7 (31.8) | 4 (25.0) | |
| Length of stay | |||||
| 1 d5 d | 171 (79.2) | 147 (82.6) | 12 (54.6) | 12 (75.0) | 0.03 |
| 6 d10 d | 24 (11.1) | 17 (9.6) | 5 (22.7) | 2 (12.5) | |
| 11 d15 d | 10 (4.6) | 5 (2.8) | 3 (13.6) | 2 (12.5) | |
| 16 d+ | 11 (5.1) | 9 (5.1) | 2 (9.1) | 0 | |
| Complex chronic conditions | |||||
| Any CCC | 94 (43.5) | 77 (43.3) | 12 (54.6) | 5 (31.3) | 0.35 |
| Cardiovascular | 20 (9.3) | 19 (10.7) | 1 (6.3) | 0.24 | |
| Neuromuscular | 34 (15.7) | 26 (14.6) | 7 (31.8) | 1 (6.3) | 0.06 |
| Respiratory | 6 (2.8) | 6 (3.4) | 0.52 | ||
| Renal | 26 (12.0) | 21 (11.8) | 4 (18.2) | 1 (6.3) | 0.52 |
| Gastrointestinal | 3 (1.4) | 3 (1.7) | 0.72 | ||
| Hematologic/ immunologic | 1 (0.5) | 1 (4.6) | 0.01 | ||
| Metabolic | 8 (3.7) | 6 (3.4) | 1 (4.6) | 1 (6.3) | 0.82 |
| Congenital or genetic | 15 (6.9) | 11 (6.2) | 3 (13.6) | 1 (6.3) | 0.43 |
| Malignancy | 5 (2.3) | 3 (1.7) | 2 (9.1) | 0.08 | |
| VUR | 28 (13.0) | 23 (12.9) | 3 (13.6) | 2 (12.5) | 0.99 |
| Abnormal GU | 36 (16.7) | 31 (17.4) | 4 (18.2) | 1 (6.3) | 0.51 |
| Prophylactic antibiotics | 67 (31.0) | 53 (29.8) | 10 (45.5) | 4 (25.0) | 0.28 |
The most common causative organisms were E. coli (65.7%) and Klebsiella spp (9.7%) (Table 2). The most common initial antibiotics were a third‐generation cephalosporin (39.1%), combination of ampicillin and a third‐ or fourth‐generation cephalosporin (16.7%), and combination of ampicillin with gentamicin (11.1%). A third‐generation cephalosporin was the initial antibiotic for 46.1% of the E. coli and 56.9% of Klebsiella spp UTIs. Resistance to third‐generation cephalosporins but carbapenem susceptibility was noted for 4.5% of E. coli and 7.7% of Klebsiella spp isolates. Patients with UTIs caused by Klebsiella spp, mixed organisms, and Enterobacter spp were more likely to receive discordant antibiotic therapy. Patients with Enterobacter spp and mixed‐organism UTIs were more likely to have delayed antibiotic therapy. Nineteen patients (8.8%) had positive blood cultures. Fifteen (6.9%) required intensive care unit (ICU) admission during hospitalization.
| Organism | Cases | Concordant* No. (%) | Discordant No. (%) | Delayed Antibiotics No. (%) |
|---|---|---|---|---|
| ||||
| E. coli | 142 | 129 (90.8) | 3 (2.1) | 10 (7.0) |
| Klebsiella spp | 21 | 14 (66.7) | 7 (33.3) | 0 (0) |
| Enterococcus spp | 12 | 9 (75.0) | 3 (25.0) | 0 (0) |
| Enterobacter spp | 10 | 5 (50.0) | 3 (30.0) | 2 (20.0) |
| Pseudomonas spp | 10 | 9 (90.0) | 1 (10.0) | 0 (0) |
| Other single organisms | 6 | 5 (83.3) | 0 (0) | 1 (16.7) |
| Other identified multiple organisms | 15 | 7 (46.7) | 5 (33.3) | 3 (20.0) |
Unadjusted results are shown in Supporting Appendix 1, in the online version of this article. In the adjusted analysis, discordant antibiotic therapy was associated with a significantly longer LOS, compared with concordant therapy for all UTIs and for all UTIs caused by a single organism (Table 3). In adjusted analysis, discordant therapy was also associated with a 3.1 day (IQR: 2.0, 4.7) longer length of stay compared with concordant therapy for all E. coli UTIs.
| Bacteria | Difference in LOS (95% CI)* | P Value |
|---|---|---|
| ||
| All organisms | ||
| Concordant vs discordant | 1.8 (2.1, 1.5) | <0.0001 |
| Concordant vs delayed antibiotics | 1.4 (1.7, 1.1) | 0.01 |
| Single organisms | ||
| Concordant vs discordant | 1.9 (2.4, 1.5) | <0.0001 |
| Concordant vs delayed antibiotics | 1.2 (1.6, 1.2) | 0.37 |
Time to fever resolution was analyzed for patients with a documented fever at presentation for each treatment subgroup. One hundred thirty‐six patients were febrile at admission and 122 were febrile beyond the first recorded vital signs. Fever was present at admission in 60% of the concordant group and 55% of the discordant group (P = 0.6). The median duration of fever was 48 hours for the concordant group (n = 107; IQR: 24, 240) and 78 hours for the discordant group (n = 12; IQR: 48, 132). All patients were afebrile at discharge. Differences in fever duration between treatment groups were not statistically significant (P = 0.7).
DISCUSSION
Across 5 children's hospitals, 1 out of every 10 children hospitalized for UTI received discordant initial antibiotic therapy. Children receiving discordant antibiotic therapy had a 1.8 day longer LOS when compared with those on concordant therapy. However, there was no significant difference in time to fever resolution between the groups, suggesting that the increase in LOS was not explained by increased fever duration.
The overall rate of discordant therapy in this study is consistent with prior studies, as was the more common association of discordant therapy with non‐E. coli UTIs.10 According to the Kids' Inpatient Database 2009, there are 48,100 annual admissions for patients less than 20 years of age with a discharge diagnosis code of UTI in the United States.1 This suggests that nearly 4800 children with UTI could be affected by discordant therapy annually.
Children treated with discordant antibiotic therapy had a significantly longer LOS compared to those treated with concordant therapy. However, differences in time to fever resolution between the groups were not statistically significant. While resolution of fever may suggest clinical improvement and adequate empiric therapy, the lack of association with antibiotic concordance was not unexpected, since the relationship between fever resolution, clinical improvement, and LOS is complex and thus challenging to measure.21 These results support the notion that fever resolution alone may not be an adequate measure of clinical response.
It is possible that variability in discharge decision‐making may contribute to increased length of stay. Some clinicians may delay a patient's discharge until complete resolution of symptoms or knowledge of susceptibilities, while others may discharge patients that are still febrile and/or still receiving empiric antibiotics. Evidence‐based guidelines that address the appropriate time to discharge a patient with UTI are lacking. The American Academy of Pediatrics provides recommendations for use of parenteral antibiotics and hospital admission for patients with UTI, but does not address discharge decision‐making or patient management in the setting of discordant antibiotic therapy.2, 21
This study must be interpreted in the context of several limitations. First, our primary and secondary outcomes, LOS and fever duration, were surrogate measures for clinical response. We were not able to measure all clinical factors that may contribute to LOS, such as the patient's ability to tolerate oral fluids and antibiotics. Also, there may have been too few patients to detect a clinically important difference in fever duration between the concordant and discordant groups, especially for individual organisms. Although we did find a significant difference in LOS between patients treated with concordant compared with discordant therapy, there may be residual confounding from unobserved differences. This confounding, in conjunction with the small sample size, may cause us to underestimate the magnitude of the difference in LOS resulting from discordant therapy. Second, short‐term outcomes such as ICU admission were not investigated in this study; however, the proportion of patients admitted to the ICU in our population was quite small, precluding its use as a meaningful outcome measure. Third, the potential benefits to patients who were not exposed to unnecessary antibiotics, or harm to those that were exposed, could not be measured. Finally, our study was obtained using data from 5 free‐standing tertiary care pediatric facilities, thereby limiting its generalizability to other settings. Still, our rates of prophylactic antibiotic use, VUR, and GU abnormalities are similar to others reported in tertiary care children's hospitals, and we accounted for these covariates in our model.2225
As the frequency of infections caused by resistant bacteria increase, so will the number of patients receiving discordant antibiotics for UTI, compounding the challenge of empiric antimicrobial selection. Further research is needed to better understand how discordant initial antibiotic therapy contributes to LOS and whether it is associated with adverse short‐ and long‐term clinical outcomes. Such research could also aid in weighing the risk of broader‐spectrum prescribing on antimicrobial resistance patterns. While we identified an association between discordant initial antibiotic therapy and LOS, we were unable to determine the ideal empiric antibiotic therapy for patients hospitalized with UTI. Further investigation is needed to inform local and national practice guidelines for empiric antibiotic selection in patients with UTIs. This may also be an opportunity to decrease discordant empiric antibiotic selection, perhaps through use of antibiograms that stratify patients based on known factors, to lead to more specific initial therapy.
CONCLUSIONS
This study demonstrates that discordant antibiotic selection for UTI at admission is associated with longer hospital stay, but not fever duration. The full clinical consequences of discordant therapy, and the effects on length of stay, need to be better understood. Our findings, taken in combination with careful consideration of patient characteristics and prior history, may provide an opportunity to improve the hospital care for patients with UTIs.
Acknowledgements
Disclosure: Nothing to report.
Urinary tract infections (UTIs) are one of the most common reasons for pediatric hospitalizations.1 Bacterial infections require prompt treatment with appropriate antimicrobial agents. Results from culture and susceptibility testing, however, are often unavailable until 48 hours after initial presentation. Therefore, the clinician must select antimicrobials empirically, basing decisions on likely pathogens and local resistance patterns.2 This decision is challenging because the effect of treatment delay on clinical outcomes is difficult to determine and resistance among uropathogens is increasing. Resistance rates have doubled over the past several years.3, 4 For common first‐line antibiotics, such as ampicillin and trimethoprim‐sulfamethoxazole, resistance rates for Escherichia coli, the most common uropathogen, exceed 25%.4, 5 While resistance to third‐generation cephalosporins remains low, rates in the United States have increased from <1% in 1999 to 4% in 2010. International data shows much higher resistance rates for cephalosporins in general.6, 7 This high prevalence of resistance may prompt the use of broad‐spectrum antibiotics for patients with UTI. For example, the use of third‐generation cephalosporins for UTI has doubled in recent years.3 Untreated, UTIs can lead to serious illness, but the consequences of inadequate initial antibiotic coverage are unknown.8, 9
Discordant antibiotic therapy, initial antibiotic therapy to which the causative bacterium is not susceptible, occurs in up to 9% of children hospitalized for UTI.10 However, there is reason to believe that discordant therapy may matter less for UTIs than for infections at other sites. First, in adults hospitalized with UTIs, discordant initial therapy did not affect the time to resolution of symptoms.11, 12 Second, most antibiotics used to treat UTIs are renally excreted and, thus, antibiotic concentrations at the site of infection are higher than can be achieved in the serum or cerebrospinal fluid.13 The Clinical and Laboratory Standard Institute has acknowledged that traditional susceptibility breakpoints may be too conservative for some non‐central nervous system infections; such as non‐central nervous system infections caused by Streptococcus pneumoniae.14
As resistance rates increase, more patients are likely to be treated with discordant therapy. Therefore, we sought to identify the clinical consequences of discordant antimicrobial therapy for patients hospitalized with a UTI.
METHODS
Design and Setting
We conducted a multicenter, retrospective cohort study. Data for this study were originally collected for a study that determined the accuracy of individual and combined International Classification of Diseases, Ninth Revision (ICD‐9) discharge diagnosis codes for children with laboratory tests for a UTI, in order to develop national quality measures for children hospitalized with UTIs.15 The institutional review board for each hospital (Seattle Children's Hospital, Seattle, WA; Monroe Carell Jr Children's Hospital at Vanderbilt, Nashville, TN; Cincinnati Children's Hospital Medical Center, Cincinnati, OH; Children's Mercy Hospital, Kansas City, MO; Children's Hospital of Philadelphia, Philadelphia, PA) approved the study.
Data Sources
Data were obtained from the Pediatric Health Information System (PHIS) and medical records for patients at the 5 participating hospitals. PHIS contains clinical and billing data from hospitalized children at 43 freestanding children's hospitals. Data quality and coding reliability are assured through a joint effort between the Children's Hospital Association (Shawnee Mission, KS) and participating hospitals.16 PHIS was used to identify participants based on presence of discharge diagnosis code and laboratory tests indicating possible UTI, patient demographics, antibiotic administration date, and utilization of hospital resources (length of stay [LOS], laboratory testing).
Medical records for each participant were reviewed to obtain laboratory and clinical information such as past medical history (including vesicoureteral reflux [VUR], abnormal genitourinary [GU] anatomy, use of prophylactic antibiotic), culture data, and fever data. Data were entered into a secured centrally housed web‐based data collection system. To assure consistency of chart review, all investigators responsible for data collection underwent training. In addition, 2 pilot medical record reviews were performed, followed by group discussion, to reach consensus on questions, preselected answers, interpretation of medical record data, and parameters for free text data entry.
Subjects
The initial cohort included 460 hospitalized patients, aged 3 days to 18 years of age, discharged from participating hospitals between July 1, 2008 and June 30, 2009 with a positive urine culture at any time during hospitalization.15 We excluded patients under 3 days of age because patients this young are more likely to have been transferred from the birthing hospital for a complication related to birth or a congenital anomaly. For this secondary analysis of patients from a prior study, our target population included patients admitted for management of UTI.15 We excluded patients with a negative initial urine culture (n = 59) or if their initial urine culture did not meet definition of laboratory‐confirmed UTI, defined as urine culture with >50,000 colony‐forming units (CFU) with an abnormal urinalysis (UA) (n = 77).1, 1719 An abnormal UA was defined by presence of white blood cells, leukocyte esterase, bacteria, and/or nitrites. For our cohort, all cultures with >50,000 CFU also had an abnormal urinalysis. We excluded 19 patients with cultures classified as 10,000100,000 CFU because we could not confirm that the CFU was >50,000. We excluded 30 patients with urine cultures classified as normal or mixed flora, positive for a mixture of organisms not further identified, or if results were unavailable. Additionally, coagulase‐negative Staphylococcus species (n = 8) were excluded, as these are typically considered contaminants in the setting of urine cultures.2 Patients likely to have received antibiotics prior to admission, or develop a UTI after admission, were identified and removed from the cohort if they had a urine culture performed more than 1 day before, or 2 days after, admission (n = 35). Cultures without resistance testing to the initial antibiotic selection were also excluded (n = 16).
Main Outcome Measures
The primary outcome measure was hospital LOS. Time to fever resolution was a secondary outcome measure. Fever was defined as temperature 38C. Fever duration was defined as number of hours until resolution of fever; only patients with fever at admission were included in this subanalysis.
Main Exposure
The main exposure was initial antibiotic therapy. Patients were classified into 3 groups according to initial antibiotic selection: those receiving 1) concordant; 2) discordant; or 3) delayed initial therapy. Concordance was defined as in vitro susceptibility to the initial antibiotic or class of antibiotic. If the uropathogen was sensitive to a narrow‐spectrum antibiotic (eg, first‐generation cephalosporin), but was not tested against a more broad‐spectrum antibiotic of the same class (eg, third‐generation cephalosporin), concordance was based on the sensitivity to the narrow‐spectrum antibiotic. If the uropathogen was sensitive to a broad‐spectrum antibiotic (eg, third‐generation cephalosporin), concordance to a more narrow‐spectrum antibiotic was not assumed. Discordance was defined as laboratory confirmation of in vitro resistance, or intermediate sensitivity of the pathogen to the initial antibiotic or class of antibiotics. Patients were considered to have a delay in antibiotic therapy if they did not receive antibiotics on the day of, or day after, collection of UA and culture. Patients with more than 1 uropathogen identified in a single culture were classified as discordant if any of the organisms was discordant to the initial antibiotic; they were classified as concordant if all organisms were concordant to the initial antibiotic. Antibiotic susceptibility was not tested in some cases (n = 16).
Initial antibiotic was defined as the antibiotic(s) billed on the same day or day after the UA was billed. If the patient had the UA completed on the day prior to admission, we used the antibiotic administered on the day of admission as the initial antibiotic.
Covariates
Covariates were selected a priori to include patient characteristics likely to affect patient outcomes; all were included in the final analysis. These were age, race, sex, insurance, disposition, prophylactic antibiotic use for any reason (VUR, oncologic process, etc), presence of a chronic care condition, and presence of VUR or GU anatomic abnormality. Age, race, sex, and insurance were obtained from PHIS. Medical record review was used to determine prophylactic antibiotic use, and presence of VUR or GU abnormalities (eg, posterior urethral valves). Chronic care conditions were defined using a previously reported method.20
Data Analysis
Continuous variables were described using median and interquartile range (IQR). Categorical variables were described using frequencies. Multivariable analyses were used to determine the independent association of discordant antibiotic therapy and the outcomes of interest. Poisson regression was used to fit the skewed LOS distribution. The effect of antibiotic concordance or discordance on LOS was determined for all patients in our sample, as well as for those with a urine culture positive for a single identified organism. We used the KruskalWallis test statistic to determine the association between duration of fever and discordant antibiotic therapy, given that duration of fever is a continuous variable. Generalized estimating equations accounted for clustering by hospital and the variability that exists between hospitals.
RESULTS
Of the initial 460 cases with positive urine culture growth at any time during admission, 216 met inclusion criteria for a laboratory‐confirmed UTI from urine culture completed at admission. The median age was 2.46 years (IQR: 0.27,8.89). In the study population, 25.0% were male, 31.0% were receiving prophylactic antibiotics, 13.0% had any grade of VUR, and 16.7% had abnormal GU anatomy (Table 1). A total of 82.4% of patients were treated with concordant initial therapy, 10.2% with discordant initial therapy, and 7.4% received delayed initial antibiotic therapy. There were no significant differences between the groups for any of the covariates. Discordant antibiotic cases ranged from 4.9% to 21.7% across hospitals.
| Overall | Concordant* | Discordant | Delayed Antibiotics | P Value | |
|---|---|---|---|---|---|
| |||||
| N | 216 | 178 (82.4) | 22 (10.2) | 16 (7.4) | |
| Gender | |||||
| Male | 54 (25.0) | 40 (22.5) | 8 (36.4) | 6 (37.5) | 0.18 |
| Female | 162 (75.0) | 138 (77.5) | 14 (63.64) | 10 (62.5) | |
| Race | |||||
| Non‐Hispanic white | 136 (63.9) | 110 (62.5) | 15 (71.4) | 11 (68.8) | 0.83 |
| Non‐Hispanic black | 28 (13.2) | 24 (13.6) | 2 (9.5) | 2 (12.5) | |
| Hispanic | 20 (9.4) | 16 (9.1) | 3 (14.3) | 1 (6.3) | |
| Asian | 10 (4.7) | 9 (5.1) | 1 (4.7) | ||
| Other | 19 (8.9) | 17 (9.7) | 2 (12.5) | ||
| Payor | |||||
| Government | 97 (44.9) | 80 (44.9) | 11 (50.0) | 6 (37.5) | 0.58 |
| Private | 70 (32.4) | 56 (31.5) | 6 (27.3) | 8 (50.0) | |
| Other | 49 (22.7) | 42 (23.6) | 5 (22.7) | 2 (12.5) | |
| Disposition | |||||
| Home | 204 (94.4) | 168 (94.4) | 21 (95.5) | 15 (93.8) | 0.99 |
| Died | 1 (0.5) | 1 (0.6) | |||
| Other | 11 (5.1) | 9 (5.1) | 1 (4.6) | 1 (6.3) | |
| Age | |||||
| 3 d60 d | 40 (18.5) | 35 (19.7) | 3 (13.6) | 2 (12.5) | 0.53 |
| 61 d2 y | 62 (28.7) | 54 (30.3) | 4 (18.2) | 4 (25.0) | |
| 3 y12 y | 75 (34.7) | 61 (34.3) | 8 (36.4) | 6 (37.5) | |
| 13 y18 y | 39 (18.1) | 28 (15.7) | 7 (31.8) | 4 (25.0) | |
| Length of stay | |||||
| 1 d5 d | 171 (79.2) | 147 (82.6) | 12 (54.6) | 12 (75.0) | 0.03 |
| 6 d10 d | 24 (11.1) | 17 (9.6) | 5 (22.7) | 2 (12.5) | |
| 11 d15 d | 10 (4.6) | 5 (2.8) | 3 (13.6) | 2 (12.5) | |
| 16 d+ | 11 (5.1) | 9 (5.1) | 2 (9.1) | 0 | |
| Complex chronic conditions | |||||
| Any CCC | 94 (43.5) | 77 (43.3) | 12 (54.6) | 5 (31.3) | 0.35 |
| Cardiovascular | 20 (9.3) | 19 (10.7) | 1 (6.3) | 0.24 | |
| Neuromuscular | 34 (15.7) | 26 (14.6) | 7 (31.8) | 1 (6.3) | 0.06 |
| Respiratory | 6 (2.8) | 6 (3.4) | 0.52 | ||
| Renal | 26 (12.0) | 21 (11.8) | 4 (18.2) | 1 (6.3) | 0.52 |
| Gastrointestinal | 3 (1.4) | 3 (1.7) | 0.72 | ||
| Hematologic/ immunologic | 1 (0.5) | 1 (4.6) | 0.01 | ||
| Metabolic | 8 (3.7) | 6 (3.4) | 1 (4.6) | 1 (6.3) | 0.82 |
| Congenital or genetic | 15 (6.9) | 11 (6.2) | 3 (13.6) | 1 (6.3) | 0.43 |
| Malignancy | 5 (2.3) | 3 (1.7) | 2 (9.1) | 0.08 | |
| VUR | 28 (13.0) | 23 (12.9) | 3 (13.6) | 2 (12.5) | 0.99 |
| Abnormal GU | 36 (16.7) | 31 (17.4) | 4 (18.2) | 1 (6.3) | 0.51 |
| Prophylactic antibiotics | 67 (31.0) | 53 (29.8) | 10 (45.5) | 4 (25.0) | 0.28 |
The most common causative organisms were E. coli (65.7%) and Klebsiella spp (9.7%) (Table 2). The most common initial antibiotics were a third‐generation cephalosporin (39.1%), combination of ampicillin and a third‐ or fourth‐generation cephalosporin (16.7%), and combination of ampicillin with gentamicin (11.1%). A third‐generation cephalosporin was the initial antibiotic for 46.1% of the E. coli and 56.9% of Klebsiella spp UTIs. Resistance to third‐generation cephalosporins but carbapenem susceptibility was noted for 4.5% of E. coli and 7.7% of Klebsiella spp isolates. Patients with UTIs caused by Klebsiella spp, mixed organisms, and Enterobacter spp were more likely to receive discordant antibiotic therapy. Patients with Enterobacter spp and mixed‐organism UTIs were more likely to have delayed antibiotic therapy. Nineteen patients (8.8%) had positive blood cultures. Fifteen (6.9%) required intensive care unit (ICU) admission during hospitalization.
| Organism | Cases | Concordant* No. (%) | Discordant No. (%) | Delayed Antibiotics No. (%) |
|---|---|---|---|---|
| ||||
| E. coli | 142 | 129 (90.8) | 3 (2.1) | 10 (7.0) |
| Klebsiella spp | 21 | 14 (66.7) | 7 (33.3) | 0 (0) |
| Enterococcus spp | 12 | 9 (75.0) | 3 (25.0) | 0 (0) |
| Enterobacter spp | 10 | 5 (50.0) | 3 (30.0) | 2 (20.0) |
| Pseudomonas spp | 10 | 9 (90.0) | 1 (10.0) | 0 (0) |
| Other single organisms | 6 | 5 (83.3) | 0 (0) | 1 (16.7) |
| Other identified multiple organisms | 15 | 7 (46.7) | 5 (33.3) | 3 (20.0) |
Unadjusted results are shown in Supporting Appendix 1, in the online version of this article. In the adjusted analysis, discordant antibiotic therapy was associated with a significantly longer LOS, compared with concordant therapy for all UTIs and for all UTIs caused by a single organism (Table 3). In adjusted analysis, discordant therapy was also associated with a 3.1 day (IQR: 2.0, 4.7) longer length of stay compared with concordant therapy for all E. coli UTIs.
| Bacteria | Difference in LOS (95% CI)* | P Value |
|---|---|---|
| ||
| All organisms | ||
| Concordant vs discordant | 1.8 (2.1, 1.5) | <0.0001 |
| Concordant vs delayed antibiotics | 1.4 (1.7, 1.1) | 0.01 |
| Single organisms | ||
| Concordant vs discordant | 1.9 (2.4, 1.5) | <0.0001 |
| Concordant vs delayed antibiotics | 1.2 (1.6, 1.2) | 0.37 |
Time to fever resolution was analyzed for patients with a documented fever at presentation for each treatment subgroup. One hundred thirty‐six patients were febrile at admission and 122 were febrile beyond the first recorded vital signs. Fever was present at admission in 60% of the concordant group and 55% of the discordant group (P = 0.6). The median duration of fever was 48 hours for the concordant group (n = 107; IQR: 24, 240) and 78 hours for the discordant group (n = 12; IQR: 48, 132). All patients were afebrile at discharge. Differences in fever duration between treatment groups were not statistically significant (P = 0.7).
DISCUSSION
Across 5 children's hospitals, 1 out of every 10 children hospitalized for UTI received discordant initial antibiotic therapy. Children receiving discordant antibiotic therapy had a 1.8 day longer LOS when compared with those on concordant therapy. However, there was no significant difference in time to fever resolution between the groups, suggesting that the increase in LOS was not explained by increased fever duration.
The overall rate of discordant therapy in this study is consistent with prior studies, as was the more common association of discordant therapy with non‐E. coli UTIs.10 According to the Kids' Inpatient Database 2009, there are 48,100 annual admissions for patients less than 20 years of age with a discharge diagnosis code of UTI in the United States.1 This suggests that nearly 4800 children with UTI could be affected by discordant therapy annually.
Children treated with discordant antibiotic therapy had a significantly longer LOS compared to those treated with concordant therapy. However, differences in time to fever resolution between the groups were not statistically significant. While resolution of fever may suggest clinical improvement and adequate empiric therapy, the lack of association with antibiotic concordance was not unexpected, since the relationship between fever resolution, clinical improvement, and LOS is complex and thus challenging to measure.21 These results support the notion that fever resolution alone may not be an adequate measure of clinical response.
It is possible that variability in discharge decision‐making may contribute to increased length of stay. Some clinicians may delay a patient's discharge until complete resolution of symptoms or knowledge of susceptibilities, while others may discharge patients that are still febrile and/or still receiving empiric antibiotics. Evidence‐based guidelines that address the appropriate time to discharge a patient with UTI are lacking. The American Academy of Pediatrics provides recommendations for use of parenteral antibiotics and hospital admission for patients with UTI, but does not address discharge decision‐making or patient management in the setting of discordant antibiotic therapy.2, 21
This study must be interpreted in the context of several limitations. First, our primary and secondary outcomes, LOS and fever duration, were surrogate measures for clinical response. We were not able to measure all clinical factors that may contribute to LOS, such as the patient's ability to tolerate oral fluids and antibiotics. Also, there may have been too few patients to detect a clinically important difference in fever duration between the concordant and discordant groups, especially for individual organisms. Although we did find a significant difference in LOS between patients treated with concordant compared with discordant therapy, there may be residual confounding from unobserved differences. This confounding, in conjunction with the small sample size, may cause us to underestimate the magnitude of the difference in LOS resulting from discordant therapy. Second, short‐term outcomes such as ICU admission were not investigated in this study; however, the proportion of patients admitted to the ICU in our population was quite small, precluding its use as a meaningful outcome measure. Third, the potential benefits to patients who were not exposed to unnecessary antibiotics, or harm to those that were exposed, could not be measured. Finally, our study was obtained using data from 5 free‐standing tertiary care pediatric facilities, thereby limiting its generalizability to other settings. Still, our rates of prophylactic antibiotic use, VUR, and GU abnormalities are similar to others reported in tertiary care children's hospitals, and we accounted for these covariates in our model.2225
As the frequency of infections caused by resistant bacteria increase, so will the number of patients receiving discordant antibiotics for UTI, compounding the challenge of empiric antimicrobial selection. Further research is needed to better understand how discordant initial antibiotic therapy contributes to LOS and whether it is associated with adverse short‐ and long‐term clinical outcomes. Such research could also aid in weighing the risk of broader‐spectrum prescribing on antimicrobial resistance patterns. While we identified an association between discordant initial antibiotic therapy and LOS, we were unable to determine the ideal empiric antibiotic therapy for patients hospitalized with UTI. Further investigation is needed to inform local and national practice guidelines for empiric antibiotic selection in patients with UTIs. This may also be an opportunity to decrease discordant empiric antibiotic selection, perhaps through use of antibiograms that stratify patients based on known factors, to lead to more specific initial therapy.
CONCLUSIONS
This study demonstrates that discordant antibiotic selection for UTI at admission is associated with longer hospital stay, but not fever duration. The full clinical consequences of discordant therapy, and the effects on length of stay, need to be better understood. Our findings, taken in combination with careful consideration of patient characteristics and prior history, may provide an opportunity to improve the hospital care for patients with UTIs.
Acknowledgements
Disclosure: Nothing to report.
- HCUP Kids' Inpatient Database (KID). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality; 2006 and 2009. Available at: http://www.hcup‐us.ahrq.gov/kidoverview.jsp.
- Subcommitee on Urinary Tract Infection, Steering Committee on Quality Improvement and Management. Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics. 2011;128(3)595–610. doi: 10.1542/peds.2011–1330. Available at: http://pediatrics.aappublications.org/content/128/3/595.full.html.
- , , . National ambulatory antibiotic prescribing patterns for pediatric urinary tract infection, 1998–2007. Pediatrics. 2011;127(6):1027–1033.
- , , , , . Previous antimicrobial exposure is associated with drug‐resistant urinary tract infections in children. Pediatrics. 2010;125(4):664–672.
- CDC. National Antimicrobial Resistance Monitoring System for Enteric Bacteria (NARMS): Human Isolates Final Report. Atlanta, GA: US Department of Health and Human Services, CDC; 2009.
- , , , , . Increasing antibiotic resistance among uropathogens isolated during years 2006–2009: impact on the empirical management. Int Braz J Urol. 2012;38(1):25–32.
- . 3rd Generation Cephalosporin‐Resistant Escherichia coli. 2010. Available at: http://www.cddep.org/ResistanceMap/bug‐drug/EC‐CS. Accessed May 14, 2012.
- , , , . Risk of renal scarring in children with a first urinary tract infection: a systematic review. Pediatrics. 2010;126(6):1084–1091.
- , . Treatment of urinary tract infections. Pediatr Infect Dis J. 1999;18(11):1020–1021.
- , , , , . Non‐Escherichia coli versus Escherichia coli community‐acquired urinary tract infections in children hospitalized in a tertiary center: relative frequency, risk factors, antimicrobial resistance and outcome. Pediatr Infect Dis J. 2005;24(7):581–585.
- , , , , , . Prognosis of urinary tract infections with discordant antibiotic treatment [in Spanish]. Rev Clin Esp. 2010;210(11):545–549.
- , , , et al. Appropriateness of empiric antibiotic therapy in urinary tract infection in emergency room [in Spanish]. Rev Clin Esp. 2010;210(1):11–16.
- , , . Principles and Practice of Pediatric Infectious Diseases. 3rd ed. New York, NY: Churchill Livingstone/Elsevier; 2009.
- National Committee for Clinical Laboratory Standards. Performance Standards for Antimicrobial Susceptibility Testing; Twelfth Informational Supplement.Vol M100‐S12. Wayne, PA: NCCLS; 2002.
- , , , et al. Accuracy of administrative billing codes to detect urinary tract infection hospitalizations. Pediatrics. 2011;128(2):323–330.
- , , , . Corticosteroids and mortality in children with bacterial meningitis. JAMA. 2008;299(17):2048–2055.
- , , , , . Enhanced urinalysis as a screening test for urinary tract infection. Pediatrics. 1993;91(6):1196–1199.
- , , , , . Pyuria and bacteriuria in urine specimens obtained by catheter from young children with fever. J Pediatr. 1994;124(4):513–519.
- , , , et al. Clinical and demographic factors associated with urinary tract infection in young febrile infants. Pediatrics. 2005;116(3):644–648.
- , , , , , . Deaths attributed to pediatric complex chronic conditions: national trends and implications for supportive care services. Pediatrics. 2001;107(6):E99.
- Committee on Quality Improvement. Subcommittee on Urinary Tract Infection. Practice parameter: the diagnosis, treatment, and evaluation of the initial urinary tract infection in febrile infants and young children. Pediatrics. 1999;103:843–852.
- , . Antibiotics or surgery for vesicoureteric reflux in children. Lancet. 2004;364(9446):1720–1722.
- , , , et al. Randomized intervention for children with vesicoureteral reflux (RIVUR): background commentary of RIVUR investigators. Pediatrics. 2008;122(suppl 5):S233–S239.
- , , . Length of intravenous antibiotic therapy and treatment failure in infants with urinary tract infections. Pediatrics. 2010;126(2):196–203.
- , , , , , . Vesicoureteral reflux in children with suspected and proven urinary tract infection. Pediatr Nephrol. 2010;25(8):1463–1469.
- HCUP Kids' Inpatient Database (KID). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Healthcare Research and Quality; 2006 and 2009. Available at: http://www.hcup‐us.ahrq.gov/kidoverview.jsp.
- Subcommitee on Urinary Tract Infection, Steering Committee on Quality Improvement and Management. Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics. 2011;128(3)595–610. doi: 10.1542/peds.2011–1330. Available at: http://pediatrics.aappublications.org/content/128/3/595.full.html.
- , , . National ambulatory antibiotic prescribing patterns for pediatric urinary tract infection, 1998–2007. Pediatrics. 2011;127(6):1027–1033.
- , , , , . Previous antimicrobial exposure is associated with drug‐resistant urinary tract infections in children. Pediatrics. 2010;125(4):664–672.
- CDC. National Antimicrobial Resistance Monitoring System for Enteric Bacteria (NARMS): Human Isolates Final Report. Atlanta, GA: US Department of Health and Human Services, CDC; 2009.
- , , , , . Increasing antibiotic resistance among uropathogens isolated during years 2006–2009: impact on the empirical management. Int Braz J Urol. 2012;38(1):25–32.
- . 3rd Generation Cephalosporin‐Resistant Escherichia coli. 2010. Available at: http://www.cddep.org/ResistanceMap/bug‐drug/EC‐CS. Accessed May 14, 2012.
- , , , . Risk of renal scarring in children with a first urinary tract infection: a systematic review. Pediatrics. 2010;126(6):1084–1091.
- , . Treatment of urinary tract infections. Pediatr Infect Dis J. 1999;18(11):1020–1021.
- , , , , . Non‐Escherichia coli versus Escherichia coli community‐acquired urinary tract infections in children hospitalized in a tertiary center: relative frequency, risk factors, antimicrobial resistance and outcome. Pediatr Infect Dis J. 2005;24(7):581–585.
- , , , , , . Prognosis of urinary tract infections with discordant antibiotic treatment [in Spanish]. Rev Clin Esp. 2010;210(11):545–549.
- , , , et al. Appropriateness of empiric antibiotic therapy in urinary tract infection in emergency room [in Spanish]. Rev Clin Esp. 2010;210(1):11–16.
- , , . Principles and Practice of Pediatric Infectious Diseases. 3rd ed. New York, NY: Churchill Livingstone/Elsevier; 2009.
- National Committee for Clinical Laboratory Standards. Performance Standards for Antimicrobial Susceptibility Testing; Twelfth Informational Supplement.Vol M100‐S12. Wayne, PA: NCCLS; 2002.
- , , , et al. Accuracy of administrative billing codes to detect urinary tract infection hospitalizations. Pediatrics. 2011;128(2):323–330.
- , , , . Corticosteroids and mortality in children with bacterial meningitis. JAMA. 2008;299(17):2048–2055.
- , , , , . Enhanced urinalysis as a screening test for urinary tract infection. Pediatrics. 1993;91(6):1196–1199.
- , , , , . Pyuria and bacteriuria in urine specimens obtained by catheter from young children with fever. J Pediatr. 1994;124(4):513–519.
- , , , et al. Clinical and demographic factors associated with urinary tract infection in young febrile infants. Pediatrics. 2005;116(3):644–648.
- , , , , , . Deaths attributed to pediatric complex chronic conditions: national trends and implications for supportive care services. Pediatrics. 2001;107(6):E99.
- Committee on Quality Improvement. Subcommittee on Urinary Tract Infection. Practice parameter: the diagnosis, treatment, and evaluation of the initial urinary tract infection in febrile infants and young children. Pediatrics. 1999;103:843–852.
- , . Antibiotics or surgery for vesicoureteric reflux in children. Lancet. 2004;364(9446):1720–1722.
- , , , et al. Randomized intervention for children with vesicoureteral reflux (RIVUR): background commentary of RIVUR investigators. Pediatrics. 2008;122(suppl 5):S233–S239.
- , , . Length of intravenous antibiotic therapy and treatment failure in infants with urinary tract infections. Pediatrics. 2010;126(2):196–203.
- , , , , , . Vesicoureteral reflux in children with suspected and proven urinary tract infection. Pediatr Nephrol. 2010;25(8):1463–1469.
Copyright © 2012 Society of Hospital Medicine
Report: Wrong-Patient Orders Occur Frequently with CPOE Systems
Hospitalist Jason Adelman, MD, MS, believes computerized physician order-entry (CPOE) systems improve workflow and help prevent many mistakes, but the automation also causes mistakes as physicians toggle back and forth between screens in the system interface.
Dr. Adelman, patient safety officer at Montefiore Medical Center in the Bronx, N.Y., and colleagues developed an automated method for measuring wrong-patient electronic orders. They found that systems that compel physicians to re-enter certain information reduced errors.
CPOE systems have "certainly prevented errors," he says, "but they've unintentionally caused errors, and the name of the game is to keep working on ways to prevent more and more errors and minimize those errors unintentionally caused by these systems."
The researchers hypothesized that some wrong-patient orders are recognized by the orderer shortly after entry, promptly retracted, then re-entered on the correct patient. Their study results, published in the Journal of the American Medical Informatics Association, used a "retract and reorder" measurement tool that flagged any orders placed on a patient that were quickly retracted and replaced with a new order set.
Using the tool, Dr. Adleman and his research team estimated that 5,246 orders were placed on the wrong patients in 2009 at Montefiore.
The study also showed that interventions helped lower the odds of wrong-patient errors. One method made physicians click on a link to verify a patient’s identity, while another required the physician to manually input information to confirm the patient’s identity. Potential other interventions included using photo identification to ensure that physicians entered orders correctly.
"I think the goal is to try to get perfection," Dr. Adelman says. "I don't know if you could ever get totally there ... but you try."
Hospitalist Jason Adelman, MD, MS, believes computerized physician order-entry (CPOE) systems improve workflow and help prevent many mistakes, but the automation also causes mistakes as physicians toggle back and forth between screens in the system interface.
Dr. Adelman, patient safety officer at Montefiore Medical Center in the Bronx, N.Y., and colleagues developed an automated method for measuring wrong-patient electronic orders. They found that systems that compel physicians to re-enter certain information reduced errors.
CPOE systems have "certainly prevented errors," he says, "but they've unintentionally caused errors, and the name of the game is to keep working on ways to prevent more and more errors and minimize those errors unintentionally caused by these systems."
The researchers hypothesized that some wrong-patient orders are recognized by the orderer shortly after entry, promptly retracted, then re-entered on the correct patient. Their study results, published in the Journal of the American Medical Informatics Association, used a "retract and reorder" measurement tool that flagged any orders placed on a patient that were quickly retracted and replaced with a new order set.
Using the tool, Dr. Adleman and his research team estimated that 5,246 orders were placed on the wrong patients in 2009 at Montefiore.
The study also showed that interventions helped lower the odds of wrong-patient errors. One method made physicians click on a link to verify a patient’s identity, while another required the physician to manually input information to confirm the patient’s identity. Potential other interventions included using photo identification to ensure that physicians entered orders correctly.
"I think the goal is to try to get perfection," Dr. Adelman says. "I don't know if you could ever get totally there ... but you try."
Hospitalist Jason Adelman, MD, MS, believes computerized physician order-entry (CPOE) systems improve workflow and help prevent many mistakes, but the automation also causes mistakes as physicians toggle back and forth between screens in the system interface.
Dr. Adelman, patient safety officer at Montefiore Medical Center in the Bronx, N.Y., and colleagues developed an automated method for measuring wrong-patient electronic orders. They found that systems that compel physicians to re-enter certain information reduced errors.
CPOE systems have "certainly prevented errors," he says, "but they've unintentionally caused errors, and the name of the game is to keep working on ways to prevent more and more errors and minimize those errors unintentionally caused by these systems."
The researchers hypothesized that some wrong-patient orders are recognized by the orderer shortly after entry, promptly retracted, then re-entered on the correct patient. Their study results, published in the Journal of the American Medical Informatics Association, used a "retract and reorder" measurement tool that flagged any orders placed on a patient that were quickly retracted and replaced with a new order set.
Using the tool, Dr. Adleman and his research team estimated that 5,246 orders were placed on the wrong patients in 2009 at Montefiore.
The study also showed that interventions helped lower the odds of wrong-patient errors. One method made physicians click on a link to verify a patient’s identity, while another required the physician to manually input information to confirm the patient’s identity. Potential other interventions included using photo identification to ensure that physicians entered orders correctly.
"I think the goal is to try to get perfection," Dr. Adelman says. "I don't know if you could ever get totally there ... but you try."
International Concern: Hospitalists around the globe face similar issues, seek answers in U.S.
They hailed from such places as Germany, Bermuda, and Brazil, yet they were searching for the same answers as their American counterparts. How do I improve our better discharge process? How can we work better with administrators or primary-care physicians (PCPs)? How can we recruit better clinicians or see more patients in a day?
Nearly 20 international hospitalists gathered to discuss ideas, exchange business cards, and report on the growth of the hospitalist model in their countries at a Special Interest Forum at HM12 in April in San Diego.
“I’m here to get together with hospitalists, colleagues in the same field. We have a new program, and I thought I could learn from meeting people already in the field,” said David McGowan, MD, a hospitalist at the only HM group in Bermuda.
Dr. McGowan, attending his first SHM annual meeting, focused his attention on practice management, leadership and quality-initiative (QI) topics. His four-doctor HM group is relatively new, and he planned to “take some stuff back to my group.”
—Rafaela Komorowski Dal Molin, hospitalist, Hospital Mae de Deus, Porto Alegre, Brazil, scientific director, Brazilian Society of Hospital Medicine
Bermuda has one hospital, in the capital city of Hamilton, for the entire island of nearly 65,000 residents. Administration has been very supportive of the HM model, according to Dr. McGowan, although the group has faced challenges in the community.
“The system is new and people are used to their primary-care physicians being in the hospital,” he said. “We have been working on that through public relations, providing good care, and ramping up our communication with the primary-care physicians in the community.
“We set the standard for the island, and I think we are making progress. The quality of care is better. … I think the potential is there for things to be better, and outcomes are going to [get] better.”
Euro Development
Not so new to the HM model of care was Stefan Reinecke, MBA, chief of the division of general internal medicine at St. Mary’s Hospital in Stuttgart, Germany. HM12 marked the third time he’d traveled to the U.S. for an HM-focused meeting, and, as before, his areas of focus were on practice management and quality.
“I think there is a need for well-trained physicians in internal medicine, with a high knowledge of quality, methods of quality measurement, and outcome measurement,” said Dr. Reinecke, whose division has 35 inpatient physicians and 20 residents.
As in the U.S., a hospitalist model requires upfront costs to the German healthcare system, and Dr. Reinecke said he and other group leaders are feeling “strong financial pressures” from administration. He said he hoped to build new quality- and systems-improvement structures into his division, and “to do it daily,” he said.
South America
One way to validate a hospitalist service is to demonstrate improvements in quality and cost of care. That’s exactly what Rafaela Komorowski Dal Molin’s group at Hospital Mae de Deus in Porto Alegre, Brazil, has done─and her chief medical officer noticed.
“Our HM service reduced length of stay,” she said, noting hospitals and payors in her country are “thinking more and more about costs of care.”
She also said administrators are learning why the HM model of care is important. “HM in USA proved we can reduce the costs, and proved we influence the length of stay,” she said. “That’s interesting to medical directors.”
Dr. Dal Molin’s six-hospitalist group began in 2009 and includes an intensivist and pulmonologist. Starting this summer, the group will begin training four residents in an HM-focused program.
Dr. Dal Molin admitted Brazil’s healthcare system is just learning about the HM model, and groups face myriad clinical, financial, and professional issues. “HM in Brazil is not recognized as a specialty yet,” she said. “We’re working on it. I’m thinking maybe in the next two years it will be recognized.”
As scientific director of the Brazilian Society of Hospital Medicine, Dr. Dal Molin was one of a small contingency of hospitalists from the Southern Hemisphere at HM12. The group is planning its second Brazilian Congress of HM Nov. 15-16 in Sao Paulo.
Richard Quinn is a freelance writer based in New Jersey.
They hailed from such places as Germany, Bermuda, and Brazil, yet they were searching for the same answers as their American counterparts. How do I improve our better discharge process? How can we work better with administrators or primary-care physicians (PCPs)? How can we recruit better clinicians or see more patients in a day?
Nearly 20 international hospitalists gathered to discuss ideas, exchange business cards, and report on the growth of the hospitalist model in their countries at a Special Interest Forum at HM12 in April in San Diego.
“I’m here to get together with hospitalists, colleagues in the same field. We have a new program, and I thought I could learn from meeting people already in the field,” said David McGowan, MD, a hospitalist at the only HM group in Bermuda.
Dr. McGowan, attending his first SHM annual meeting, focused his attention on practice management, leadership and quality-initiative (QI) topics. His four-doctor HM group is relatively new, and he planned to “take some stuff back to my group.”
—Rafaela Komorowski Dal Molin, hospitalist, Hospital Mae de Deus, Porto Alegre, Brazil, scientific director, Brazilian Society of Hospital Medicine
Bermuda has one hospital, in the capital city of Hamilton, for the entire island of nearly 65,000 residents. Administration has been very supportive of the HM model, according to Dr. McGowan, although the group has faced challenges in the community.
“The system is new and people are used to their primary-care physicians being in the hospital,” he said. “We have been working on that through public relations, providing good care, and ramping up our communication with the primary-care physicians in the community.
“We set the standard for the island, and I think we are making progress. The quality of care is better. … I think the potential is there for things to be better, and outcomes are going to [get] better.”
Euro Development
Not so new to the HM model of care was Stefan Reinecke, MBA, chief of the division of general internal medicine at St. Mary’s Hospital in Stuttgart, Germany. HM12 marked the third time he’d traveled to the U.S. for an HM-focused meeting, and, as before, his areas of focus were on practice management and quality.
“I think there is a need for well-trained physicians in internal medicine, with a high knowledge of quality, methods of quality measurement, and outcome measurement,” said Dr. Reinecke, whose division has 35 inpatient physicians and 20 residents.
As in the U.S., a hospitalist model requires upfront costs to the German healthcare system, and Dr. Reinecke said he and other group leaders are feeling “strong financial pressures” from administration. He said he hoped to build new quality- and systems-improvement structures into his division, and “to do it daily,” he said.
South America
One way to validate a hospitalist service is to demonstrate improvements in quality and cost of care. That’s exactly what Rafaela Komorowski Dal Molin’s group at Hospital Mae de Deus in Porto Alegre, Brazil, has done─and her chief medical officer noticed.
“Our HM service reduced length of stay,” she said, noting hospitals and payors in her country are “thinking more and more about costs of care.”
She also said administrators are learning why the HM model of care is important. “HM in USA proved we can reduce the costs, and proved we influence the length of stay,” she said. “That’s interesting to medical directors.”
Dr. Dal Molin’s six-hospitalist group began in 2009 and includes an intensivist and pulmonologist. Starting this summer, the group will begin training four residents in an HM-focused program.
Dr. Dal Molin admitted Brazil’s healthcare system is just learning about the HM model, and groups face myriad clinical, financial, and professional issues. “HM in Brazil is not recognized as a specialty yet,” she said. “We’re working on it. I’m thinking maybe in the next two years it will be recognized.”
As scientific director of the Brazilian Society of Hospital Medicine, Dr. Dal Molin was one of a small contingency of hospitalists from the Southern Hemisphere at HM12. The group is planning its second Brazilian Congress of HM Nov. 15-16 in Sao Paulo.
Richard Quinn is a freelance writer based in New Jersey.
They hailed from such places as Germany, Bermuda, and Brazil, yet they were searching for the same answers as their American counterparts. How do I improve our better discharge process? How can we work better with administrators or primary-care physicians (PCPs)? How can we recruit better clinicians or see more patients in a day?
Nearly 20 international hospitalists gathered to discuss ideas, exchange business cards, and report on the growth of the hospitalist model in their countries at a Special Interest Forum at HM12 in April in San Diego.
“I’m here to get together with hospitalists, colleagues in the same field. We have a new program, and I thought I could learn from meeting people already in the field,” said David McGowan, MD, a hospitalist at the only HM group in Bermuda.
Dr. McGowan, attending his first SHM annual meeting, focused his attention on practice management, leadership and quality-initiative (QI) topics. His four-doctor HM group is relatively new, and he planned to “take some stuff back to my group.”
—Rafaela Komorowski Dal Molin, hospitalist, Hospital Mae de Deus, Porto Alegre, Brazil, scientific director, Brazilian Society of Hospital Medicine
Bermuda has one hospital, in the capital city of Hamilton, for the entire island of nearly 65,000 residents. Administration has been very supportive of the HM model, according to Dr. McGowan, although the group has faced challenges in the community.
“The system is new and people are used to their primary-care physicians being in the hospital,” he said. “We have been working on that through public relations, providing good care, and ramping up our communication with the primary-care physicians in the community.
“We set the standard for the island, and I think we are making progress. The quality of care is better. … I think the potential is there for things to be better, and outcomes are going to [get] better.”
Euro Development
Not so new to the HM model of care was Stefan Reinecke, MBA, chief of the division of general internal medicine at St. Mary’s Hospital in Stuttgart, Germany. HM12 marked the third time he’d traveled to the U.S. for an HM-focused meeting, and, as before, his areas of focus were on practice management and quality.
“I think there is a need for well-trained physicians in internal medicine, with a high knowledge of quality, methods of quality measurement, and outcome measurement,” said Dr. Reinecke, whose division has 35 inpatient physicians and 20 residents.
As in the U.S., a hospitalist model requires upfront costs to the German healthcare system, and Dr. Reinecke said he and other group leaders are feeling “strong financial pressures” from administration. He said he hoped to build new quality- and systems-improvement structures into his division, and “to do it daily,” he said.
South America
One way to validate a hospitalist service is to demonstrate improvements in quality and cost of care. That’s exactly what Rafaela Komorowski Dal Molin’s group at Hospital Mae de Deus in Porto Alegre, Brazil, has done─and her chief medical officer noticed.
“Our HM service reduced length of stay,” she said, noting hospitals and payors in her country are “thinking more and more about costs of care.”
She also said administrators are learning why the HM model of care is important. “HM in USA proved we can reduce the costs, and proved we influence the length of stay,” she said. “That’s interesting to medical directors.”
Dr. Dal Molin’s six-hospitalist group began in 2009 and includes an intensivist and pulmonologist. Starting this summer, the group will begin training four residents in an HM-focused program.
Dr. Dal Molin admitted Brazil’s healthcare system is just learning about the HM model, and groups face myriad clinical, financial, and professional issues. “HM in Brazil is not recognized as a specialty yet,” she said. “We’re working on it. I’m thinking maybe in the next two years it will be recognized.”
As scientific director of the Brazilian Society of Hospital Medicine, Dr. Dal Molin was one of a small contingency of hospitalists from the Southern Hemisphere at HM12. The group is planning its second Brazilian Congress of HM Nov. 15-16 in Sao Paulo.
Richard Quinn is a freelance writer based in New Jersey.
ITL: Physician Reviews of HM-Relevant Research
Clinical question: Does supported self-management of patients with chronic obstructive pulmonary disease (COPD) decrease COPD-related hospital readmission or death?
Clinical background: Supported self-management has benefited patients with such chronic diseases as heart failure and asthma. Evidence to support such a strategy for patients with COPD is relatively lacking.
Study design: Randomized, controlled trial.
Setting: Community-based care following urban hospitalization in western Scotland.
Synopsis: From June 2007 to May 2009, and following hospitalization for COPD exacerbation, 464 patients were randomized to receive routine community-based care with or without 12 months of support and training to detect, and promptly treat, recurrent exacerbations. Independent of disease severity or demographics, investigators found no difference in combined readmission rates (48% vs. 47%, 95% confidence interval [CI] 0.80-1.38) or death (10% vs. 7%, 95% CI 0.71-2.61).
Based on review of appropriateness of self-management strategies used by the intervention group, unplanned exploratory subgroup analysis classified a minority of the intervention group as “successful” (42%) supported self-managers, and demonstrated decreased COPD readmissions and deaths (27% vs. 49%, 95% CI 0.25-0.76, P=0.003) vs. “unsuccessful” self-managers. This successful group was younger and tended to live with others. Further research to define characteristics of patients who benefit from self-management is needed.
Bottom line: Supported self-management of COPD does not reduce COPD-related readmissions or deaths in a large population.
Citation: Bucknall CE, Miller G, Lloyd SM, et al. Glasgow supported self-management trial (GSuST) for patients with moderate to severe COPD: randomised controlled trial. BMJ. 2012;344:e1060.
Check out more physician reviews of HM-relevant research.
Clinical question: Does supported self-management of patients with chronic obstructive pulmonary disease (COPD) decrease COPD-related hospital readmission or death?
Clinical background: Supported self-management has benefited patients with such chronic diseases as heart failure and asthma. Evidence to support such a strategy for patients with COPD is relatively lacking.
Study design: Randomized, controlled trial.
Setting: Community-based care following urban hospitalization in western Scotland.
Synopsis: From June 2007 to May 2009, and following hospitalization for COPD exacerbation, 464 patients were randomized to receive routine community-based care with or without 12 months of support and training to detect, and promptly treat, recurrent exacerbations. Independent of disease severity or demographics, investigators found no difference in combined readmission rates (48% vs. 47%, 95% confidence interval [CI] 0.80-1.38) or death (10% vs. 7%, 95% CI 0.71-2.61).
Based on review of appropriateness of self-management strategies used by the intervention group, unplanned exploratory subgroup analysis classified a minority of the intervention group as “successful” (42%) supported self-managers, and demonstrated decreased COPD readmissions and deaths (27% vs. 49%, 95% CI 0.25-0.76, P=0.003) vs. “unsuccessful” self-managers. This successful group was younger and tended to live with others. Further research to define characteristics of patients who benefit from self-management is needed.
Bottom line: Supported self-management of COPD does not reduce COPD-related readmissions or deaths in a large population.
Citation: Bucknall CE, Miller G, Lloyd SM, et al. Glasgow supported self-management trial (GSuST) for patients with moderate to severe COPD: randomised controlled trial. BMJ. 2012;344:e1060.
Check out more physician reviews of HM-relevant research.
Clinical question: Does supported self-management of patients with chronic obstructive pulmonary disease (COPD) decrease COPD-related hospital readmission or death?
Clinical background: Supported self-management has benefited patients with such chronic diseases as heart failure and asthma. Evidence to support such a strategy for patients with COPD is relatively lacking.
Study design: Randomized, controlled trial.
Setting: Community-based care following urban hospitalization in western Scotland.
Synopsis: From June 2007 to May 2009, and following hospitalization for COPD exacerbation, 464 patients were randomized to receive routine community-based care with or without 12 months of support and training to detect, and promptly treat, recurrent exacerbations. Independent of disease severity or demographics, investigators found no difference in combined readmission rates (48% vs. 47%, 95% confidence interval [CI] 0.80-1.38) or death (10% vs. 7%, 95% CI 0.71-2.61).
Based on review of appropriateness of self-management strategies used by the intervention group, unplanned exploratory subgroup analysis classified a minority of the intervention group as “successful” (42%) supported self-managers, and demonstrated decreased COPD readmissions and deaths (27% vs. 49%, 95% CI 0.25-0.76, P=0.003) vs. “unsuccessful” self-managers. This successful group was younger and tended to live with others. Further research to define characteristics of patients who benefit from self-management is needed.
Bottom line: Supported self-management of COPD does not reduce COPD-related readmissions or deaths in a large population.
Citation: Bucknall CE, Miller G, Lloyd SM, et al. Glasgow supported self-management trial (GSuST) for patients with moderate to severe COPD: randomised controlled trial. BMJ. 2012;344:e1060.
Check out more physician reviews of HM-relevant research.
FDA grants drug accelerated approval for relapsed/refractory MM

The FDA has announced accelerated approval of carfilzomib (Kyprolis) as treatment for relapsed or refractory multiple myeloma (MM).
The drug is indicated for MM patients who have received at least 2 prior therapies, including bortezomib and an immunomodulatory agent, and have demonstrated disease progression on or within 60 days of completing their last treatment.
Carfilzomib was approved under the FDA’s accelerated approval program, which allows the agency to approve a drug based on data suggesting a clinical benefit. The drug’s maker is required to submit additional information after the approval to confirm that benefit.
Carfilzomib’s approval was based on efficacy data from a trial of 266 patients and safety data from 526 patients who received the drug.
The 266 patients had relapsed MM and had received at least 2 prior therapies, including bortezomib and an immunomodulatory agent (either thalidomide or lenalidomide). Patients received carfilzomib intravenously over a period of 2 to 10 minutes on 2 consecutive days a week for 3 weeks, followed by a 12-day rest period.
Patients received 20 mg/m2 at each dose in cycle 1 and 27 mg/m2 in subsequent cycles. They continued to receive treatment until their disease progressed, they developed unacceptable toxicity, or they completed 12 cycles.
Following treatment, the overall response rate was 22.9%. One patient achieved a complete response, 13 had very good partial responses, and 47 achieved partial responses. The median response duration was 7.8 months.
Researchers also evaluated carfilzomib’s safety in 526 patients with relapsed MM. Patients received a median of 4 treatment cycles and a median cumulative carfilzomib dose of 993.4 mg.
The most common adverse reactions—with an incidence of 30% or greater—were fatigue, anemia, nausea, thrombocytopenia, dyspnea, diarrhea, and pyrexia.
In addition, 45% of patients experienced serious adverse reactions. The most common were pneumonia, acute renal failure, pyrexia, and congestive heart failure.
Seven percent of patients (n=37) died on study. The most common causes of death, other than underlying disease, were cardiac (n=5), end-organ failure (n=4), and infection (n=4).
Carfilzomib will be marketed as Kyprolis by Onyx Pharmaceuticals. As a condition of the drug’s accelerated approval, Onyx is required to submit the complete analysis of an ongoing phase 3 trial comparing lenalidomide plus low-dose dexamethasone to lenalidomide, low-dose dexamethasone, and carfilzomib.
For more information on carfilzomib, consult the FDA website. ![]()
The FDA has announced accelerated approval of carfilzomib (Kyprolis) as treatment for relapsed or refractory multiple myeloma (MM).
The drug is indicated for MM patients who have received at least 2 prior therapies, including bortezomib and an immunomodulatory agent, and have demonstrated disease progression on or within 60 days of completing their last treatment.
Carfilzomib was approved under the FDA’s accelerated approval program, which allows the agency to approve a drug based on data suggesting a clinical benefit. The drug’s maker is required to submit additional information after the approval to confirm that benefit.
Carfilzomib’s approval was based on efficacy data from a trial of 266 patients and safety data from 526 patients who received the drug.
The 266 patients had relapsed MM and had received at least 2 prior therapies, including bortezomib and an immunomodulatory agent (either thalidomide or lenalidomide). Patients received carfilzomib intravenously over a period of 2 to 10 minutes on 2 consecutive days a week for 3 weeks, followed by a 12-day rest period.
Patients received 20 mg/m2 at each dose in cycle 1 and 27 mg/m2 in subsequent cycles. They continued to receive treatment until their disease progressed, they developed unacceptable toxicity, or they completed 12 cycles.
Following treatment, the overall response rate was 22.9%. One patient achieved a complete response, 13 had very good partial responses, and 47 achieved partial responses. The median response duration was 7.8 months.
Researchers also evaluated carfilzomib’s safety in 526 patients with relapsed MM. Patients received a median of 4 treatment cycles and a median cumulative carfilzomib dose of 993.4 mg.
The most common adverse reactions—with an incidence of 30% or greater—were fatigue, anemia, nausea, thrombocytopenia, dyspnea, diarrhea, and pyrexia.
In addition, 45% of patients experienced serious adverse reactions. The most common were pneumonia, acute renal failure, pyrexia, and congestive heart failure.
Seven percent of patients (n=37) died on study. The most common causes of death, other than underlying disease, were cardiac (n=5), end-organ failure (n=4), and infection (n=4).
Carfilzomib will be marketed as Kyprolis by Onyx Pharmaceuticals. As a condition of the drug’s accelerated approval, Onyx is required to submit the complete analysis of an ongoing phase 3 trial comparing lenalidomide plus low-dose dexamethasone to lenalidomide, low-dose dexamethasone, and carfilzomib.
For more information on carfilzomib, consult the FDA website. ![]()
The FDA has announced accelerated approval of carfilzomib (Kyprolis) as treatment for relapsed or refractory multiple myeloma (MM).
The drug is indicated for MM patients who have received at least 2 prior therapies, including bortezomib and an immunomodulatory agent, and have demonstrated disease progression on or within 60 days of completing their last treatment.
Carfilzomib was approved under the FDA’s accelerated approval program, which allows the agency to approve a drug based on data suggesting a clinical benefit. The drug’s maker is required to submit additional information after the approval to confirm that benefit.
Carfilzomib’s approval was based on efficacy data from a trial of 266 patients and safety data from 526 patients who received the drug.
The 266 patients had relapsed MM and had received at least 2 prior therapies, including bortezomib and an immunomodulatory agent (either thalidomide or lenalidomide). Patients received carfilzomib intravenously over a period of 2 to 10 minutes on 2 consecutive days a week for 3 weeks, followed by a 12-day rest period.
Patients received 20 mg/m2 at each dose in cycle 1 and 27 mg/m2 in subsequent cycles. They continued to receive treatment until their disease progressed, they developed unacceptable toxicity, or they completed 12 cycles.
Following treatment, the overall response rate was 22.9%. One patient achieved a complete response, 13 had very good partial responses, and 47 achieved partial responses. The median response duration was 7.8 months.
Researchers also evaluated carfilzomib’s safety in 526 patients with relapsed MM. Patients received a median of 4 treatment cycles and a median cumulative carfilzomib dose of 993.4 mg.
The most common adverse reactions—with an incidence of 30% or greater—were fatigue, anemia, nausea, thrombocytopenia, dyspnea, diarrhea, and pyrexia.
In addition, 45% of patients experienced serious adverse reactions. The most common were pneumonia, acute renal failure, pyrexia, and congestive heart failure.
Seven percent of patients (n=37) died on study. The most common causes of death, other than underlying disease, were cardiac (n=5), end-organ failure (n=4), and infection (n=4).
Carfilzomib will be marketed as Kyprolis by Onyx Pharmaceuticals. As a condition of the drug’s accelerated approval, Onyx is required to submit the complete analysis of an ongoing phase 3 trial comparing lenalidomide plus low-dose dexamethasone to lenalidomide, low-dose dexamethasone, and carfilzomib.
For more information on carfilzomib, consult the FDA website. ![]()
Best Treatment Approach Controversial in HCC
ORLANDO – Treatment centers and surgeons tend to play to their strengths when choosing therapy for patients with well-compensated cirrhosis of the liver and early hepatocellular carcinoma, investigators reported at a symposium sponsored by the Society of Surgical Oncology.
Therapy for early HCC with well-compensated cirrhosis is controversial; there is little agreement on when resection, transplantation, or radiofrequency ablation becomes the best approach. Choice of therapy for early HCC often depends on the surgeon’s repertoire of techniques and the therapeutic services the hospital offers, based on the findings of a web-based survey of centers that had at least five HCC cases per year.
"This study demonstrates that nonclinical factors have an important effect of therapy for early HCC, and in particular the choice of therapy depends in part on the surgeon’s portfolio of techniques, as well as the availability of transplantation services," said Dr. Hari Nathan of the department of surgery at Johns Hopkins Hospital in Baltimore.
In a previous analysis of the data from their web-based survey, Dr. Nathan and colleagues found that surgeon specialty was more important than certain patient-specific factors when determining treatment choice (J. Clin. Oncol. 2011;29:619-25).
"Differences in choice of therapy for nontransplant and transplant surgeons were not the result of an across-the-board preference for one therapy vs. another. Rather, some clinical factors impacted surgeons differently, depending on their specialty," he said.
In the new analysis, the authors used the survey data to assess the effect of surgeon and hospital factors on the choice of therapy for early, well-compensated HCC, and the effect of regional liver transplantation services on the surgeon’s choice of therapy.
They defined early HCC according to the Milan criteria as a single tumor less than 5 cm in its largest dimension, or two to three tumors less than 3 cm. Cirrhosis was considered to be well compensated if it was Child-Pugh class A, with no varices, ascites, or encephalopathy.
They presented respondents with case scenarios factoring in age, tumor number and size, type of resection required, etiology of cirrhosis (hepatitis B or C, or alcoholic), biological MELD (Model for End-Stage Liver Disease) score, platelet count, and anticipated transplantation waiting time.
Of the 1,032 invitations they extended, 336 surgeons (33%) responded. Of the respondents, 284 (85%) were in academic practices and 52 (15%) were in community practices for a median of 10 years (range, 4-17 years). About two-thirds (65%) were trained in liver transplantation. Procedures performed for HCC included transplantation and radiofrequency ablation (41% of responders), transplantation alone (14%), or liver resection but not transplantation (45%). Asked which procedures were available at their primary hospital (regardless of whether the respondent performed them personally), 100% said that resections were available, and 99% said that ablations were available. In contrast, transplantations were available at 71% of respondents’ hospitals.
The authors found that neither years in practice, surgical oncology training, nor liver transplantation training had a significant effect on treatment choice. Similarly, regional transplantation variables – such as number of procedures, percentage of transplant recipients with HCC, 30th percentile of liver transplantation wait time, and severity of illness by median MELD score – did not significantly predict treatment choice.
There was, however, significant variation in therapeutic choice based on practice type, adjusted for case presentation, with surgeons in academic practices favoring transplantation 57% of the time, compared with 47% for those in community practice. Community-based surgeons were more likely to favor liver resection (45% vs. 38% for academic surgeons), and radiofrequency ablation (9% vs. 4%).
In regression analysis that controlled for clinical factors, they found that surgeons in academic setting were significantly less likely than community-based surgeons to recommend ablation over liver transplantation (relative risk ratio [RRR], 0.41; P = .01). When they looked at the effect of practice types’ controlling for surgeons’ specialties, however, the significance of the practice type on treatment choice disappeared.
Regression analysis also showed that "higher volume surgeons prefer transplantation over resection more strongly than lower-volume surgeons," Dr. Nathan said.
High-volume surgeons (defined as those performing 30 or more cases annually) were overwhelmingly transplantation surgeons; when the authors adjusted for whether the surgeon performed transplantations, the preference for transplantation disappeared.
Additionally, nontransplantation surgeons who worked at hospitals where transplantations were available were more likely to recommend transplantation over ablation, compared with surgeons working at nontransplantation hospitals.
"Interestingly, they also favored resection over radiofrequency ablation more strongly. This appeared to be a separate phenomenon than the one that we observed for the portfolio – that’s personally performed by each surgeon – and in regression analyses these effects were independent," he said.
Coauthor John F.P. Bridges, Ph.D., provided financial and administrative support for the study. Dr. Nathan reported no relevant financial disclosures.
ORLANDO – Treatment centers and surgeons tend to play to their strengths when choosing therapy for patients with well-compensated cirrhosis of the liver and early hepatocellular carcinoma, investigators reported at a symposium sponsored by the Society of Surgical Oncology.
Therapy for early HCC with well-compensated cirrhosis is controversial; there is little agreement on when resection, transplantation, or radiofrequency ablation becomes the best approach. Choice of therapy for early HCC often depends on the surgeon’s repertoire of techniques and the therapeutic services the hospital offers, based on the findings of a web-based survey of centers that had at least five HCC cases per year.
"This study demonstrates that nonclinical factors have an important effect of therapy for early HCC, and in particular the choice of therapy depends in part on the surgeon’s portfolio of techniques, as well as the availability of transplantation services," said Dr. Hari Nathan of the department of surgery at Johns Hopkins Hospital in Baltimore.
In a previous analysis of the data from their web-based survey, Dr. Nathan and colleagues found that surgeon specialty was more important than certain patient-specific factors when determining treatment choice (J. Clin. Oncol. 2011;29:619-25).
"Differences in choice of therapy for nontransplant and transplant surgeons were not the result of an across-the-board preference for one therapy vs. another. Rather, some clinical factors impacted surgeons differently, depending on their specialty," he said.
In the new analysis, the authors used the survey data to assess the effect of surgeon and hospital factors on the choice of therapy for early, well-compensated HCC, and the effect of regional liver transplantation services on the surgeon’s choice of therapy.
They defined early HCC according to the Milan criteria as a single tumor less than 5 cm in its largest dimension, or two to three tumors less than 3 cm. Cirrhosis was considered to be well compensated if it was Child-Pugh class A, with no varices, ascites, or encephalopathy.
They presented respondents with case scenarios factoring in age, tumor number and size, type of resection required, etiology of cirrhosis (hepatitis B or C, or alcoholic), biological MELD (Model for End-Stage Liver Disease) score, platelet count, and anticipated transplantation waiting time.
Of the 1,032 invitations they extended, 336 surgeons (33%) responded. Of the respondents, 284 (85%) were in academic practices and 52 (15%) were in community practices for a median of 10 years (range, 4-17 years). About two-thirds (65%) were trained in liver transplantation. Procedures performed for HCC included transplantation and radiofrequency ablation (41% of responders), transplantation alone (14%), or liver resection but not transplantation (45%). Asked which procedures were available at their primary hospital (regardless of whether the respondent performed them personally), 100% said that resections were available, and 99% said that ablations were available. In contrast, transplantations were available at 71% of respondents’ hospitals.
The authors found that neither years in practice, surgical oncology training, nor liver transplantation training had a significant effect on treatment choice. Similarly, regional transplantation variables – such as number of procedures, percentage of transplant recipients with HCC, 30th percentile of liver transplantation wait time, and severity of illness by median MELD score – did not significantly predict treatment choice.
There was, however, significant variation in therapeutic choice based on practice type, adjusted for case presentation, with surgeons in academic practices favoring transplantation 57% of the time, compared with 47% for those in community practice. Community-based surgeons were more likely to favor liver resection (45% vs. 38% for academic surgeons), and radiofrequency ablation (9% vs. 4%).
In regression analysis that controlled for clinical factors, they found that surgeons in academic setting were significantly less likely than community-based surgeons to recommend ablation over liver transplantation (relative risk ratio [RRR], 0.41; P = .01). When they looked at the effect of practice types’ controlling for surgeons’ specialties, however, the significance of the practice type on treatment choice disappeared.
Regression analysis also showed that "higher volume surgeons prefer transplantation over resection more strongly than lower-volume surgeons," Dr. Nathan said.
High-volume surgeons (defined as those performing 30 or more cases annually) were overwhelmingly transplantation surgeons; when the authors adjusted for whether the surgeon performed transplantations, the preference for transplantation disappeared.
Additionally, nontransplantation surgeons who worked at hospitals where transplantations were available were more likely to recommend transplantation over ablation, compared with surgeons working at nontransplantation hospitals.
"Interestingly, they also favored resection over radiofrequency ablation more strongly. This appeared to be a separate phenomenon than the one that we observed for the portfolio – that’s personally performed by each surgeon – and in regression analyses these effects were independent," he said.
Coauthor John F.P. Bridges, Ph.D., provided financial and administrative support for the study. Dr. Nathan reported no relevant financial disclosures.
ORLANDO – Treatment centers and surgeons tend to play to their strengths when choosing therapy for patients with well-compensated cirrhosis of the liver and early hepatocellular carcinoma, investigators reported at a symposium sponsored by the Society of Surgical Oncology.
Therapy for early HCC with well-compensated cirrhosis is controversial; there is little agreement on when resection, transplantation, or radiofrequency ablation becomes the best approach. Choice of therapy for early HCC often depends on the surgeon’s repertoire of techniques and the therapeutic services the hospital offers, based on the findings of a web-based survey of centers that had at least five HCC cases per year.
"This study demonstrates that nonclinical factors have an important effect of therapy for early HCC, and in particular the choice of therapy depends in part on the surgeon’s portfolio of techniques, as well as the availability of transplantation services," said Dr. Hari Nathan of the department of surgery at Johns Hopkins Hospital in Baltimore.
In a previous analysis of the data from their web-based survey, Dr. Nathan and colleagues found that surgeon specialty was more important than certain patient-specific factors when determining treatment choice (J. Clin. Oncol. 2011;29:619-25).
"Differences in choice of therapy for nontransplant and transplant surgeons were not the result of an across-the-board preference for one therapy vs. another. Rather, some clinical factors impacted surgeons differently, depending on their specialty," he said.
In the new analysis, the authors used the survey data to assess the effect of surgeon and hospital factors on the choice of therapy for early, well-compensated HCC, and the effect of regional liver transplantation services on the surgeon’s choice of therapy.
They defined early HCC according to the Milan criteria as a single tumor less than 5 cm in its largest dimension, or two to three tumors less than 3 cm. Cirrhosis was considered to be well compensated if it was Child-Pugh class A, with no varices, ascites, or encephalopathy.
They presented respondents with case scenarios factoring in age, tumor number and size, type of resection required, etiology of cirrhosis (hepatitis B or C, or alcoholic), biological MELD (Model for End-Stage Liver Disease) score, platelet count, and anticipated transplantation waiting time.
Of the 1,032 invitations they extended, 336 surgeons (33%) responded. Of the respondents, 284 (85%) were in academic practices and 52 (15%) were in community practices for a median of 10 years (range, 4-17 years). About two-thirds (65%) were trained in liver transplantation. Procedures performed for HCC included transplantation and radiofrequency ablation (41% of responders), transplantation alone (14%), or liver resection but not transplantation (45%). Asked which procedures were available at their primary hospital (regardless of whether the respondent performed them personally), 100% said that resections were available, and 99% said that ablations were available. In contrast, transplantations were available at 71% of respondents’ hospitals.
The authors found that neither years in practice, surgical oncology training, nor liver transplantation training had a significant effect on treatment choice. Similarly, regional transplantation variables – such as number of procedures, percentage of transplant recipients with HCC, 30th percentile of liver transplantation wait time, and severity of illness by median MELD score – did not significantly predict treatment choice.
There was, however, significant variation in therapeutic choice based on practice type, adjusted for case presentation, with surgeons in academic practices favoring transplantation 57% of the time, compared with 47% for those in community practice. Community-based surgeons were more likely to favor liver resection (45% vs. 38% for academic surgeons), and radiofrequency ablation (9% vs. 4%).
In regression analysis that controlled for clinical factors, they found that surgeons in academic setting were significantly less likely than community-based surgeons to recommend ablation over liver transplantation (relative risk ratio [RRR], 0.41; P = .01). When they looked at the effect of practice types’ controlling for surgeons’ specialties, however, the significance of the practice type on treatment choice disappeared.
Regression analysis also showed that "higher volume surgeons prefer transplantation over resection more strongly than lower-volume surgeons," Dr. Nathan said.
High-volume surgeons (defined as those performing 30 or more cases annually) were overwhelmingly transplantation surgeons; when the authors adjusted for whether the surgeon performed transplantations, the preference for transplantation disappeared.
Additionally, nontransplantation surgeons who worked at hospitals where transplantations were available were more likely to recommend transplantation over ablation, compared with surgeons working at nontransplantation hospitals.
"Interestingly, they also favored resection over radiofrequency ablation more strongly. This appeared to be a separate phenomenon than the one that we observed for the portfolio – that’s personally performed by each surgeon – and in regression analyses these effects were independent," he said.
Coauthor John F.P. Bridges, Ph.D., provided financial and administrative support for the study. Dr. Nathan reported no relevant financial disclosures.
FROM A SYMPOSIUM SPONSORED BY THE SOCIETY OF SURGICAL ONCOLOGY
Major Finding: Surgeons in academic practices favor liver transplantation for early, well-compensated hepatocellular carcinoma 57% of the time; surgeons in community practice favor transplantation 47% of the time.
Data Source: Data were taken from a web-based survey of 284 surgeons in academic practices and 52 in community practices.
Disclosures: Coauthor John F. P. Bridges, Ph.D., provided financial and administrative support for the study. Dr. Nathan reported no relevant financial disclosures.
Do You Dare Visit a Hospital in July?
There was a piece in last Sunday’s New York Times written by an oncology nurse with an injunction to avoid getting sick in July. She wrote about her experience with a fresh resident who would not give her dying patient enough pain medications. She proceeded to remind readers that in July, when the academic year starts, the people taking care of sick patients in the hospital are fresh graduates who know nothing about the art of doctoring.
We’ve all heard this before. And, frankly, it is annoying.
In the article she wrote: "Any nurse who has worked in a teaching hospital is likely to have found July an especially difficult month because ... the first-year residents are calling the plays, but they have little real knowledge of the game."
I would like to counter that any new medical trainees who have worked in a teaching hospital are likely to have found July an especially difficult month, because on top of being concerned with patient well-being, they are also being constantly reminded by nurses that they don’t know what they are doing.
The truth is medical school in the United States is structured such that a medical student spends most of his 3rd year and all of his 4th year of medical school in clinical work. So when July comes around, the "brand-new intern" in fact is not "brand new." He has spent the last 2 years of his life in hospitals. He may not have as much experience as nurses that have worked the floors for years, but he is no greenhorn either.
In addition, there are the years of medical education. There has been so much focus on clinical skills – talking with patients, listening, sleuthing around for clues, even prettifying the narrative – that we forget that in order for any of these skills even to be useful, there is a basic knowledge set upon which these clinical skills are built. That knowledge base is what we earn from 2-3 years of didactic work, which is qualitatively different from clinical work, to be sure, but indispensable. The ability to combine clinical skills with sound medical knowledge is part of what makes a good physician good.
New graduates offer a fresh look at habits that have grown petrified. I remember an ICU intern being asked by a family if she could turn the ventilator off but keep tube feeds going. Being young and deferential, the intern asked the nurse about this. The nurse looked at the intern as if she had two heads. "Do they think palliative care can be à la carte?" When I heard the story I was shocked by the strong negative reaction to a request that I thought was reasonable. The patient is dying. Why can’t it be à la carte?
Finally, interns are not unsupervised. Beside the fact that they are not "brand new" and indeed have already had some experience working the floors, they also do not go around without oversight. Interns are accountable to their medical residents, and medical residents are accountable to their attending physicians. Nothing happens without the knowledge of the senior house staff.
Telling the general public that hospitals are not a safe place in July sends a dangerous and irresponsible message. The article is, as with most anecdotes (mine included!), hyperbolic. There is little evidence that medical errors are committed in excess in July, compared with the rest of the year.
We are in training because we want to become doctors, good doctors. Starting a new job is intimidating enough as it is without nurses telling us that we don’t know what we’re doing. What we need, more than being undermined, is guidance. It’s infinitely more productive and makes July a much less harrowing place in time.
Dr. Chan is in practice in Pawtucket, R.I.
There was a piece in last Sunday’s New York Times written by an oncology nurse with an injunction to avoid getting sick in July. She wrote about her experience with a fresh resident who would not give her dying patient enough pain medications. She proceeded to remind readers that in July, when the academic year starts, the people taking care of sick patients in the hospital are fresh graduates who know nothing about the art of doctoring.
We’ve all heard this before. And, frankly, it is annoying.
In the article she wrote: "Any nurse who has worked in a teaching hospital is likely to have found July an especially difficult month because ... the first-year residents are calling the plays, but they have little real knowledge of the game."
I would like to counter that any new medical trainees who have worked in a teaching hospital are likely to have found July an especially difficult month, because on top of being concerned with patient well-being, they are also being constantly reminded by nurses that they don’t know what they are doing.
The truth is medical school in the United States is structured such that a medical student spends most of his 3rd year and all of his 4th year of medical school in clinical work. So when July comes around, the "brand-new intern" in fact is not "brand new." He has spent the last 2 years of his life in hospitals. He may not have as much experience as nurses that have worked the floors for years, but he is no greenhorn either.
In addition, there are the years of medical education. There has been so much focus on clinical skills – talking with patients, listening, sleuthing around for clues, even prettifying the narrative – that we forget that in order for any of these skills even to be useful, there is a basic knowledge set upon which these clinical skills are built. That knowledge base is what we earn from 2-3 years of didactic work, which is qualitatively different from clinical work, to be sure, but indispensable. The ability to combine clinical skills with sound medical knowledge is part of what makes a good physician good.
New graduates offer a fresh look at habits that have grown petrified. I remember an ICU intern being asked by a family if she could turn the ventilator off but keep tube feeds going. Being young and deferential, the intern asked the nurse about this. The nurse looked at the intern as if she had two heads. "Do they think palliative care can be à la carte?" When I heard the story I was shocked by the strong negative reaction to a request that I thought was reasonable. The patient is dying. Why can’t it be à la carte?
Finally, interns are not unsupervised. Beside the fact that they are not "brand new" and indeed have already had some experience working the floors, they also do not go around without oversight. Interns are accountable to their medical residents, and medical residents are accountable to their attending physicians. Nothing happens without the knowledge of the senior house staff.
Telling the general public that hospitals are not a safe place in July sends a dangerous and irresponsible message. The article is, as with most anecdotes (mine included!), hyperbolic. There is little evidence that medical errors are committed in excess in July, compared with the rest of the year.
We are in training because we want to become doctors, good doctors. Starting a new job is intimidating enough as it is without nurses telling us that we don’t know what we’re doing. What we need, more than being undermined, is guidance. It’s infinitely more productive and makes July a much less harrowing place in time.
Dr. Chan is in practice in Pawtucket, R.I.
There was a piece in last Sunday’s New York Times written by an oncology nurse with an injunction to avoid getting sick in July. She wrote about her experience with a fresh resident who would not give her dying patient enough pain medications. She proceeded to remind readers that in July, when the academic year starts, the people taking care of sick patients in the hospital are fresh graduates who know nothing about the art of doctoring.
We’ve all heard this before. And, frankly, it is annoying.
In the article she wrote: "Any nurse who has worked in a teaching hospital is likely to have found July an especially difficult month because ... the first-year residents are calling the plays, but they have little real knowledge of the game."
I would like to counter that any new medical trainees who have worked in a teaching hospital are likely to have found July an especially difficult month, because on top of being concerned with patient well-being, they are also being constantly reminded by nurses that they don’t know what they are doing.
The truth is medical school in the United States is structured such that a medical student spends most of his 3rd year and all of his 4th year of medical school in clinical work. So when July comes around, the "brand-new intern" in fact is not "brand new." He has spent the last 2 years of his life in hospitals. He may not have as much experience as nurses that have worked the floors for years, but he is no greenhorn either.
In addition, there are the years of medical education. There has been so much focus on clinical skills – talking with patients, listening, sleuthing around for clues, even prettifying the narrative – that we forget that in order for any of these skills even to be useful, there is a basic knowledge set upon which these clinical skills are built. That knowledge base is what we earn from 2-3 years of didactic work, which is qualitatively different from clinical work, to be sure, but indispensable. The ability to combine clinical skills with sound medical knowledge is part of what makes a good physician good.
New graduates offer a fresh look at habits that have grown petrified. I remember an ICU intern being asked by a family if she could turn the ventilator off but keep tube feeds going. Being young and deferential, the intern asked the nurse about this. The nurse looked at the intern as if she had two heads. "Do they think palliative care can be à la carte?" When I heard the story I was shocked by the strong negative reaction to a request that I thought was reasonable. The patient is dying. Why can’t it be à la carte?
Finally, interns are not unsupervised. Beside the fact that they are not "brand new" and indeed have already had some experience working the floors, they also do not go around without oversight. Interns are accountable to their medical residents, and medical residents are accountable to their attending physicians. Nothing happens without the knowledge of the senior house staff.
Telling the general public that hospitals are not a safe place in July sends a dangerous and irresponsible message. The article is, as with most anecdotes (mine included!), hyperbolic. There is little evidence that medical errors are committed in excess in July, compared with the rest of the year.
We are in training because we want to become doctors, good doctors. Starting a new job is intimidating enough as it is without nurses telling us that we don’t know what we’re doing. What we need, more than being undermined, is guidance. It’s infinitely more productive and makes July a much less harrowing place in time.
Dr. Chan is in practice in Pawtucket, R.I.

Veith's Viewpoint: Vascular Surgery and Creativity
Vascular surgery is an exciting field. It also faces enormous challenges. These include a difficult economic climate and intense competition from other specialties, both interventional and surgical. Vascular surgery has certain assets, such as its commitment only to the management of vascular disease and its ability to provide medical, open surgical and interventional treatments, depending on which is best for the patient. However, these assets are balanced by liabilities, such as impaired access to interventional suites, the public perception that other specialties can provide better less invasive treatments, and weak influence or power within institutions or departments.
These liabilities are real and impact on both individual vascular surgeons and the specialty as a whole. It is because of these liabilities that vascular surgery has only maintained a degree of stability despite the enormous growth in the number of vascular patients and the introduction of exciting new means of treating these patients less invasively, more safely and more effectively.

How can we overcome these liabilities and make our specialty survive and prosper? The answer is creativity. If we develop new and better ways to manage and treat vascular patients and let the world know we are the innovators, our specialty will grow and prosper. Patients will seek out those that developed the new and better treatments and come to them. Having more patients needing treatment will increase the influence and power of vascular surgeons within institutions and departments.
Let’s look at some examples. I have had experience with three. The first was so-called limb salvage surgery. In the 1960s and 1970s, no one was interested in patients with toe and foot gangrene. However, as techniques were developed to improve the limb circulation in such patients, they flocked to those who could provide these treatments, even though many physicians and surgeons expressed doubts and skepticism about their value.
Later, when less invasive interventional treatments were also developed for improving the circulation, again patients sought out the centers that could provide them. Sure, the open and endovascular treatments for these ischemic problems were difficult to perform. They required skill and commitment. But when they worked, patients found out about them and requested them. The skeptics were eventually proven wrong, and creativity was rewarded.
However, even today skeptics exist with regard to some newer endovascular treatments below the inguinal ligament. I suspect they will again be proven wrong as the treatments improve and indications for use are crystalized.
A second example was endovascular grafts and EVAR. In the beginning, after Juan Parodi’s first demonstration of feasibility, these procedures were regarded with enormous skepticism and even derision. Complications and failures were highlighted by many. But as the techniques and devices were made better, results improved. Innovating vascular surgeons and centers gained in stature, and their patient loads increased. Creativity in developing new and better treatments reaped its rewards for individual surgeons, institutions, and our specialty.
A third example is the newer endovenous treatments to ablate the greater saphenous and other veins less invasively. These treatments work, and because of their less invasive nature, patients seek out those who perform them. This has opened up a new treatment area of opportunity for vascular surgeons. It now comprises a large portion of many vascular surgeons’ practices.
The three examples I have mentioned are now accepted areas of treatment in vascular surgery – all introduced largely by vascular surgeons. All three have also been adopted by other specialists, and there is nothing wrong with that. However, what are we to do about the uncertain future?
We vascular surgeons must continue to be creative. We must devise newer and better techniques for treating vascular disease. We must publicize and document the fact that these innovations have been made by vascular surgeons. This requires not only scientific publication but also an effective public relations campaign on all levels.
For vascular surgeons these new or better techniques can be medical, interventional or open surgical. Examples of medical treatment are those that slow the growth of aneurysms or the development and progression of atherosclerotic lesions.
Patients will seek out these creative improvements and come to the practitioners or centers that provide them. When they do, they will also return when they need a subsequent intervention or open surgical treatment. Our success as vascular surgeons will be enhanced.
The same is true for innovative, safer or better endovascular or open surgical procedures. When properly documented in the scientific peer-reviewed literature and appropriately publicized in the lay media, this creativity will enhance the stature and importance of Vascular Surgery.
Even though we exist in a highly competitive and difficult environment, this creativity more than anything else will help individual vascular surgeons and vascular surgery in general to survive and prosper.n
Dr. Frank J. Veith is Professor of Surgery at New York University Medical Center and the Cleveland Clinic. He is an associate medical editor for Vascular Specialist.
The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or publisher.
Vascular surgery is an exciting field. It also faces enormous challenges. These include a difficult economic climate and intense competition from other specialties, both interventional and surgical. Vascular surgery has certain assets, such as its commitment only to the management of vascular disease and its ability to provide medical, open surgical and interventional treatments, depending on which is best for the patient. However, these assets are balanced by liabilities, such as impaired access to interventional suites, the public perception that other specialties can provide better less invasive treatments, and weak influence or power within institutions or departments.
These liabilities are real and impact on both individual vascular surgeons and the specialty as a whole. It is because of these liabilities that vascular surgery has only maintained a degree of stability despite the enormous growth in the number of vascular patients and the introduction of exciting new means of treating these patients less invasively, more safely and more effectively.
How can we overcome these liabilities and make our specialty survive and prosper? The answer is creativity. If we develop new and better ways to manage and treat vascular patients and let the world know we are the innovators, our specialty will grow and prosper. Patients will seek out those that developed the new and better treatments and come to them. Having more patients needing treatment will increase the influence and power of vascular surgeons within institutions and departments.
Let’s look at some examples. I have had experience with three. The first was so-called limb salvage surgery. In the 1960s and 1970s, no one was interested in patients with toe and foot gangrene. However, as techniques were developed to improve the limb circulation in such patients, they flocked to those who could provide these treatments, even though many physicians and surgeons expressed doubts and skepticism about their value.
Later, when less invasive interventional treatments were also developed for improving the circulation, again patients sought out the centers that could provide them. Sure, the open and endovascular treatments for these ischemic problems were difficult to perform. They required skill and commitment. But when they worked, patients found out about them and requested them. The skeptics were eventually proven wrong, and creativity was rewarded.
However, even today skeptics exist with regard to some newer endovascular treatments below the inguinal ligament. I suspect they will again be proven wrong as the treatments improve and indications for use are crystalized.
A second example was endovascular grafts and EVAR. In the beginning, after Juan Parodi’s first demonstration of feasibility, these procedures were regarded with enormous skepticism and even derision. Complications and failures were highlighted by many. But as the techniques and devices were made better, results improved. Innovating vascular surgeons and centers gained in stature, and their patient loads increased. Creativity in developing new and better treatments reaped its rewards for individual surgeons, institutions, and our specialty.
A third example is the newer endovenous treatments to ablate the greater saphenous and other veins less invasively. These treatments work, and because of their less invasive nature, patients seek out those who perform them. This has opened up a new treatment area of opportunity for vascular surgeons. It now comprises a large portion of many vascular surgeons’ practices.
The three examples I have mentioned are now accepted areas of treatment in vascular surgery – all introduced largely by vascular surgeons. All three have also been adopted by other specialists, and there is nothing wrong with that. However, what are we to do about the uncertain future?
We vascular surgeons must continue to be creative. We must devise newer and better techniques for treating vascular disease. We must publicize and document the fact that these innovations have been made by vascular surgeons. This requires not only scientific publication but also an effective public relations campaign on all levels.
For vascular surgeons these new or better techniques can be medical, interventional or open surgical. Examples of medical treatment are those that slow the growth of aneurysms or the development and progression of atherosclerotic lesions.
Patients will seek out these creative improvements and come to the practitioners or centers that provide them. When they do, they will also return when they need a subsequent intervention or open surgical treatment. Our success as vascular surgeons will be enhanced.
The same is true for innovative, safer or better endovascular or open surgical procedures. When properly documented in the scientific peer-reviewed literature and appropriately publicized in the lay media, this creativity will enhance the stature and importance of Vascular Surgery.
Even though we exist in a highly competitive and difficult environment, this creativity more than anything else will help individual vascular surgeons and vascular surgery in general to survive and prosper.n
Dr. Frank J. Veith is Professor of Surgery at New York University Medical Center and the Cleveland Clinic. He is an associate medical editor for Vascular Specialist.
The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or publisher.
Vascular surgery is an exciting field. It also faces enormous challenges. These include a difficult economic climate and intense competition from other specialties, both interventional and surgical. Vascular surgery has certain assets, such as its commitment only to the management of vascular disease and its ability to provide medical, open surgical and interventional treatments, depending on which is best for the patient. However, these assets are balanced by liabilities, such as impaired access to interventional suites, the public perception that other specialties can provide better less invasive treatments, and weak influence or power within institutions or departments.
These liabilities are real and impact on both individual vascular surgeons and the specialty as a whole. It is because of these liabilities that vascular surgery has only maintained a degree of stability despite the enormous growth in the number of vascular patients and the introduction of exciting new means of treating these patients less invasively, more safely and more effectively.
How can we overcome these liabilities and make our specialty survive and prosper? The answer is creativity. If we develop new and better ways to manage and treat vascular patients and let the world know we are the innovators, our specialty will grow and prosper. Patients will seek out those that developed the new and better treatments and come to them. Having more patients needing treatment will increase the influence and power of vascular surgeons within institutions and departments.
Let’s look at some examples. I have had experience with three. The first was so-called limb salvage surgery. In the 1960s and 1970s, no one was interested in patients with toe and foot gangrene. However, as techniques were developed to improve the limb circulation in such patients, they flocked to those who could provide these treatments, even though many physicians and surgeons expressed doubts and skepticism about their value.
Later, when less invasive interventional treatments were also developed for improving the circulation, again patients sought out the centers that could provide them. Sure, the open and endovascular treatments for these ischemic problems were difficult to perform. They required skill and commitment. But when they worked, patients found out about them and requested them. The skeptics were eventually proven wrong, and creativity was rewarded.
However, even today skeptics exist with regard to some newer endovascular treatments below the inguinal ligament. I suspect they will again be proven wrong as the treatments improve and indications for use are crystalized.
A second example was endovascular grafts and EVAR. In the beginning, after Juan Parodi’s first demonstration of feasibility, these procedures were regarded with enormous skepticism and even derision. Complications and failures were highlighted by many. But as the techniques and devices were made better, results improved. Innovating vascular surgeons and centers gained in stature, and their patient loads increased. Creativity in developing new and better treatments reaped its rewards for individual surgeons, institutions, and our specialty.
A third example is the newer endovenous treatments to ablate the greater saphenous and other veins less invasively. These treatments work, and because of their less invasive nature, patients seek out those who perform them. This has opened up a new treatment area of opportunity for vascular surgeons. It now comprises a large portion of many vascular surgeons’ practices.
The three examples I have mentioned are now accepted areas of treatment in vascular surgery – all introduced largely by vascular surgeons. All three have also been adopted by other specialists, and there is nothing wrong with that. However, what are we to do about the uncertain future?
We vascular surgeons must continue to be creative. We must devise newer and better techniques for treating vascular disease. We must publicize and document the fact that these innovations have been made by vascular surgeons. This requires not only scientific publication but also an effective public relations campaign on all levels.
For vascular surgeons these new or better techniques can be medical, interventional or open surgical. Examples of medical treatment are those that slow the growth of aneurysms or the development and progression of atherosclerotic lesions.
Patients will seek out these creative improvements and come to the practitioners or centers that provide them. When they do, they will also return when they need a subsequent intervention or open surgical treatment. Our success as vascular surgeons will be enhanced.
The same is true for innovative, safer or better endovascular or open surgical procedures. When properly documented in the scientific peer-reviewed literature and appropriately publicized in the lay media, this creativity will enhance the stature and importance of Vascular Surgery.
Even though we exist in a highly competitive and difficult environment, this creativity more than anything else will help individual vascular surgeons and vascular surgery in general to survive and prosper.n
Dr. Frank J. Veith is Professor of Surgery at New York University Medical Center and the Cleveland Clinic. He is an associate medical editor for Vascular Specialist.
The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or publisher.

From The Vascular Community
Making history and recording history are rarely thought of in the same context; however occasionally the two are one and the same. Such is the case as the the Michigan Vascular Center, a private vascular practice located in Flint, Michigan, enters its 50th year of service to its community and state. Barring documentation to the contrary, we believe the Michigan Vascular Center is the oldest and longest running private practice vascular surgery group in the country. What follows is a brief summary of its remarkable history.
Its founder was Dr. Albert Macksood, the son of a Lebanese immigrant-physician Joseph Macksood, who returned home to Flint on July 1, 1963, after completing his surgical training with Dr. Emerick Szilagyi’s group at the Henry Ford Hospital in Detroit, Michigan. Those were the formative years of our specialty and Dr. Macksood brought to Flint skills few in the country possessed. Confident in his ability, imbued with boundless energy and an uncanny ability to engage any and all in meaningful dialogue.
Dr. Al was advised by his father to only practice vascular surgery, unusual for those years, so as not to compete with the general surgeons who lacked his vascular skills. Most remarkable about Dr. Macksood, however, was his simple, yet revolutionary, philosophy: “cover the waterfront” ( three Flint area hospitals which have had continuous emergency coverage since) , add only fellowship trained physicians as the need dictated and create a true group practice such that the patients belonged to, and were treated by, all partners. This created an equal work load and compensation and allowed all to have a life by making time for family and interests predictable. It also created power in numbers with the opportunity and support to broaden our horizons.
As the practice grew, Dr. Macksood tapped Dr. Szilagyi’s program for recruits. By 1975 three additional vascular surgeons – Dr. Al Morgan (’65), Dr. Rick Sherrin (’70) and I (’75) joined. This fact- that the first four members came from Dr. Szilagyi’s program- was important to our early success because all shared a common culture and work ethic- we were in synch- we shared the same philosophical approach to the patient and the practice of our specialty. This made incorporating a new partner a seamless experience. Since then vascular surgeons from other institutions have joined- Drs. Ippolito and McIlduff and Fortin from the Cleveland Clinic, Dr. Kinning from Ohio, Dr. Molnar from Vanderbuilt, Dr. Becker from Wayne State and Dr. Malhotra from the Albany Vascular Group. Currently we are recruiting fellows from the Medical College of Wisconsin and the Mayo Clinic.
As with all vascular practices, the transition into the endovascular arena during the ‘90s and early 2000 presented challenges’ Thanks to our networking with reps from the various medical device companies (Kathy Patterson then with Bard, Cheryl Lubin from Boston Scientific and Amy Ketola/John Toddhunter/ Matt Borenzweig then with Medtronic), vascular surgeons such as Dr. Vic Burnhardt, Dr. Ted Diethrich in Arizona and international physicians such as Dr. Antonio in Modena, Italy and Drs. Cremonesi and Castriota in Ravenna, Italy, our members were able to travel nationally and internationally to work with these men and gain the necessary skills for aortic endografting and carotid stenting.
By 2002 we established our Michigan Vascular Research Center for the numerous clinical trials we were involved in and offered hands on experience to teach other vascular surgeons the art of carotid stenting.
Our center has grown in response to the needs of our vascular practice and the vascular patient. Over the past several years we have added two free standing outpatient diagnostic/angioaccess centers and a free standing VeinSolutions Center. Our latest addition is a Mobility Center to enable the amputee to regain mobility. It has proven to be a great psychological boost to the amputee. On November 5, 2012, we will know if we are approved for a 5-2 vascular fellowship program.
As with any endeavor, the owners have to “tend to the store.” As a private practice group we realize we are responsible to each other and for the success of our practice. We risk our capital in our expansion decisions and this provides us with the opportunity to move swiftly, without layers of bureaucratic approval. We meet every two weeks to review and plan medical and business issues, always with an eye toward future developments and opportunities to improve the care of our patients.
We are very proud of our independent, private practice vascular center, planning for another 50 years, and believe that by adhering to our cultural values, we will make The Michigan Vascular Center a member of the 100 year club. The current health reform agenda presents challenges yet given the size of our group, we feel confident in the value and cost-effective systems we provide and believe we will find opportunity. We look forward to the future.
Carlo A. Dall’Olmo, MD,
For the Michigan Vascular Center Group
[For the complete story of the Center by Dr. Dall’Olmo, please visit our website at www.vascularspecialistonline.com.]
Making history and recording history are rarely thought of in the same context; however occasionally the two are one and the same. Such is the case as the the Michigan Vascular Center, a private vascular practice located in Flint, Michigan, enters its 50th year of service to its community and state. Barring documentation to the contrary, we believe the Michigan Vascular Center is the oldest and longest running private practice vascular surgery group in the country. What follows is a brief summary of its remarkable history.
Its founder was Dr. Albert Macksood, the son of a Lebanese immigrant-physician Joseph Macksood, who returned home to Flint on July 1, 1963, after completing his surgical training with Dr. Emerick Szilagyi’s group at the Henry Ford Hospital in Detroit, Michigan. Those were the formative years of our specialty and Dr. Macksood brought to Flint skills few in the country possessed. Confident in his ability, imbued with boundless energy and an uncanny ability to engage any and all in meaningful dialogue.
Dr. Al was advised by his father to only practice vascular surgery, unusual for those years, so as not to compete with the general surgeons who lacked his vascular skills. Most remarkable about Dr. Macksood, however, was his simple, yet revolutionary, philosophy: “cover the waterfront” ( three Flint area hospitals which have had continuous emergency coverage since) , add only fellowship trained physicians as the need dictated and create a true group practice such that the patients belonged to, and were treated by, all partners. This created an equal work load and compensation and allowed all to have a life by making time for family and interests predictable. It also created power in numbers with the opportunity and support to broaden our horizons.
As the practice grew, Dr. Macksood tapped Dr. Szilagyi’s program for recruits. By 1975 three additional vascular surgeons – Dr. Al Morgan (’65), Dr. Rick Sherrin (’70) and I (’75) joined. This fact- that the first four members came from Dr. Szilagyi’s program- was important to our early success because all shared a common culture and work ethic- we were in synch- we shared the same philosophical approach to the patient and the practice of our specialty. This made incorporating a new partner a seamless experience. Since then vascular surgeons from other institutions have joined- Drs. Ippolito and McIlduff and Fortin from the Cleveland Clinic, Dr. Kinning from Ohio, Dr. Molnar from Vanderbuilt, Dr. Becker from Wayne State and Dr. Malhotra from the Albany Vascular Group. Currently we are recruiting fellows from the Medical College of Wisconsin and the Mayo Clinic.
As with all vascular practices, the transition into the endovascular arena during the ‘90s and early 2000 presented challenges’ Thanks to our networking with reps from the various medical device companies (Kathy Patterson then with Bard, Cheryl Lubin from Boston Scientific and Amy Ketola/John Toddhunter/ Matt Borenzweig then with Medtronic), vascular surgeons such as Dr. Vic Burnhardt, Dr. Ted Diethrich in Arizona and international physicians such as Dr. Antonio in Modena, Italy and Drs. Cremonesi and Castriota in Ravenna, Italy, our members were able to travel nationally and internationally to work with these men and gain the necessary skills for aortic endografting and carotid stenting.
By 2002 we established our Michigan Vascular Research Center for the numerous clinical trials we were involved in and offered hands on experience to teach other vascular surgeons the art of carotid stenting.
Our center has grown in response to the needs of our vascular practice and the vascular patient. Over the past several years we have added two free standing outpatient diagnostic/angioaccess centers and a free standing VeinSolutions Center. Our latest addition is a Mobility Center to enable the amputee to regain mobility. It has proven to be a great psychological boost to the amputee. On November 5, 2012, we will know if we are approved for a 5-2 vascular fellowship program.
As with any endeavor, the owners have to “tend to the store.” As a private practice group we realize we are responsible to each other and for the success of our practice. We risk our capital in our expansion decisions and this provides us with the opportunity to move swiftly, without layers of bureaucratic approval. We meet every two weeks to review and plan medical and business issues, always with an eye toward future developments and opportunities to improve the care of our patients.
We are very proud of our independent, private practice vascular center, planning for another 50 years, and believe that by adhering to our cultural values, we will make The Michigan Vascular Center a member of the 100 year club. The current health reform agenda presents challenges yet given the size of our group, we feel confident in the value and cost-effective systems we provide and believe we will find opportunity. We look forward to the future.
Carlo A. Dall’Olmo, MD,
For the Michigan Vascular Center Group
[For the complete story of the Center by Dr. Dall’Olmo, please visit our website at www.vascularspecialistonline.com.]
Making history and recording history are rarely thought of in the same context; however occasionally the two are one and the same. Such is the case as the the Michigan Vascular Center, a private vascular practice located in Flint, Michigan, enters its 50th year of service to its community and state. Barring documentation to the contrary, we believe the Michigan Vascular Center is the oldest and longest running private practice vascular surgery group in the country. What follows is a brief summary of its remarkable history.
Its founder was Dr. Albert Macksood, the son of a Lebanese immigrant-physician Joseph Macksood, who returned home to Flint on July 1, 1963, after completing his surgical training with Dr. Emerick Szilagyi’s group at the Henry Ford Hospital in Detroit, Michigan. Those were the formative years of our specialty and Dr. Macksood brought to Flint skills few in the country possessed. Confident in his ability, imbued with boundless energy and an uncanny ability to engage any and all in meaningful dialogue.
Dr. Al was advised by his father to only practice vascular surgery, unusual for those years, so as not to compete with the general surgeons who lacked his vascular skills. Most remarkable about Dr. Macksood, however, was his simple, yet revolutionary, philosophy: “cover the waterfront” ( three Flint area hospitals which have had continuous emergency coverage since) , add only fellowship trained physicians as the need dictated and create a true group practice such that the patients belonged to, and were treated by, all partners. This created an equal work load and compensation and allowed all to have a life by making time for family and interests predictable. It also created power in numbers with the opportunity and support to broaden our horizons.
As the practice grew, Dr. Macksood tapped Dr. Szilagyi’s program for recruits. By 1975 three additional vascular surgeons – Dr. Al Morgan (’65), Dr. Rick Sherrin (’70) and I (’75) joined. This fact- that the first four members came from Dr. Szilagyi’s program- was important to our early success because all shared a common culture and work ethic- we were in synch- we shared the same philosophical approach to the patient and the practice of our specialty. This made incorporating a new partner a seamless experience. Since then vascular surgeons from other institutions have joined- Drs. Ippolito and McIlduff and Fortin from the Cleveland Clinic, Dr. Kinning from Ohio, Dr. Molnar from Vanderbuilt, Dr. Becker from Wayne State and Dr. Malhotra from the Albany Vascular Group. Currently we are recruiting fellows from the Medical College of Wisconsin and the Mayo Clinic.
As with all vascular practices, the transition into the endovascular arena during the ‘90s and early 2000 presented challenges’ Thanks to our networking with reps from the various medical device companies (Kathy Patterson then with Bard, Cheryl Lubin from Boston Scientific and Amy Ketola/John Toddhunter/ Matt Borenzweig then with Medtronic), vascular surgeons such as Dr. Vic Burnhardt, Dr. Ted Diethrich in Arizona and international physicians such as Dr. Antonio in Modena, Italy and Drs. Cremonesi and Castriota in Ravenna, Italy, our members were able to travel nationally and internationally to work with these men and gain the necessary skills for aortic endografting and carotid stenting.
By 2002 we established our Michigan Vascular Research Center for the numerous clinical trials we were involved in and offered hands on experience to teach other vascular surgeons the art of carotid stenting.
Our center has grown in response to the needs of our vascular practice and the vascular patient. Over the past several years we have added two free standing outpatient diagnostic/angioaccess centers and a free standing VeinSolutions Center. Our latest addition is a Mobility Center to enable the amputee to regain mobility. It has proven to be a great psychological boost to the amputee. On November 5, 2012, we will know if we are approved for a 5-2 vascular fellowship program.
As with any endeavor, the owners have to “tend to the store.” As a private practice group we realize we are responsible to each other and for the success of our practice. We risk our capital in our expansion decisions and this provides us with the opportunity to move swiftly, without layers of bureaucratic approval. We meet every two weeks to review and plan medical and business issues, always with an eye toward future developments and opportunities to improve the care of our patients.
We are very proud of our independent, private practice vascular center, planning for another 50 years, and believe that by adhering to our cultural values, we will make The Michigan Vascular Center a member of the 100 year club. The current health reform agenda presents challenges yet given the size of our group, we feel confident in the value and cost-effective systems we provide and believe we will find opportunity. We look forward to the future.
Carlo A. Dall’Olmo, MD,
For the Michigan Vascular Center Group
[For the complete story of the Center by Dr. Dall’Olmo, please visit our website at www.vascularspecialistonline.com.]