User login
Supreme Court Ruling Just the Beginning for Health Reform
Days after the landmark Supreme Court ruling declaring the Affordable Care Act to be constitutional, some uncertainties remain. While most of the law was upheld, the Court did strike down the provision withholding Medicaid funding from states who opt out of the expansion. It's unclear, yet, how many states will choose to opt out.
Meanwhile, many physician groups have voiced support for the Court's ruling. However, they continue to call for eliminating the law's Independent Payment Advisory board, implementing malpractice reform, and finding a permanent replacement to Medicare's Sustainable Growth Rate formula.
Check out our video for more details.
Days after the landmark Supreme Court ruling declaring the Affordable Care Act to be constitutional, some uncertainties remain. While most of the law was upheld, the Court did strike down the provision withholding Medicaid funding from states who opt out of the expansion. It's unclear, yet, how many states will choose to opt out.
Meanwhile, many physician groups have voiced support for the Court's ruling. However, they continue to call for eliminating the law's Independent Payment Advisory board, implementing malpractice reform, and finding a permanent replacement to Medicare's Sustainable Growth Rate formula.
Check out our video for more details.
Days after the landmark Supreme Court ruling declaring the Affordable Care Act to be constitutional, some uncertainties remain. While most of the law was upheld, the Court did strike down the provision withholding Medicaid funding from states who opt out of the expansion. It's unclear, yet, how many states will choose to opt out.
Meanwhile, many physician groups have voiced support for the Court's ruling. However, they continue to call for eliminating the law's Independent Payment Advisory board, implementing malpractice reform, and finding a permanent replacement to Medicare's Sustainable Growth Rate formula.
Check out our video for more details.
Anticoagulation in Portal Vein Thrombosis Safe, Effective
More than half of a group of cirrhosis patients with portal vein thrombosis achieved recanalization with anticoagulation treatment maintained for at least 12 months.
"Moreover, when complete recanalization is achieved, therapy with anticoagulants should be maintained throughout life in order to prevent recurrent thrombosis," wrote Dr. María Gabriela Delgado and Dr. Susana Seijo along with their colleagues in the July issue of Clinical Gastroenterology and Hepatology (doi: 10.1016/j.cgh.2012.01.012).
In the largest study to date to evaluate the safety and efficacy of anticoagulation for portal vein thrombosis in cirrhosis (for which there are no guidelines, according to the authors), the investigators looked at 55 patients with portal vein thrombosis and cirrhosis from four centers in Spain between June 2003 and September 2010.
All patients received anticoagulation according to the protocol of each hospital after the initiation of prophylaxis of variceal bleeding. For 31 patients, anticoagulation was indicated because of acute or subacute thrombosis, and in the remaining 24 patients, anticoagulation was started because of thrombosis progression.
Anticoagulant agents included low-molecular-weight heparin and vitamin K antagonists, wrote Dr. Delgado and Dr. Seijo, both of the University of Barcelona.
Over a mean 19 months of follow-up, half (n = 28) of the patients remained on anticoagulation until either the end of the study or liver transplant. The remaining 27 patients stopped treatment after a median of 6.3 months (range, 1-24 months).
A total of 33 patients achieved either complete or partial recanalization of the portal vein during the study period; 22 patients did not have a response.
There were three complete recanalizations that occurred within 1 month of anticoagulation initiation, and two patients achieved complete recanalization at month 12.
"Early initiation of anticoagulation therapy after the identification of thrombosis in an imaging study, especially in the first 2 weeks, was the only factor significantly associated with recanalization," wrote the authors.
A total of 17 patients had 30 clinical events during anticoagulation treatment. In 13 patients, these events were "liver related," according to the authors: six variceal bleeding episodes, eight new or worsening ascites cases, five hepatic encephalopathy cases, two spontaneous bacterial peritonitis cases, and two hepatocellular carcinoma cases (several patients had multiple events).
"Liver events were more frequent in patients not achieving recanalization (8/22) than in those achieving partial/complete recanalization (5/33)," added the investigators, though the difference between these groups did not reach significance (P = 0.1).
Non-liver-related events included five bleeding episodes, which the authors attributed to anticoagulation; one acute cholecystitis case; and one duodenal ulcer.
Overall, among the 11 total bleeding events (6 of which were liver related), the authors reported that all took place during the first year after starting anticoagulation, and five events occurred in the first 3 months of treatment.
Furthermore, the only significant predictor of bleeding was a platelet count below 50 × 109/L (P = .018).
Six patients died, none of whom were receiving anticoagulation at the time of death.
Despite its retrospective design and the fact that no comparison group was available, this study shows that "recanalization can be achieved very early after starting anticoagulation treatment; however, those patients who do not present early recanalization may finally achieve it when long-term anticoagulation therapy is maintained," wrote the authors.
More importantly, anticoagulation is "relatively safe" in this population, they added, except in cases of severely depressed platelet counts.
The authors disclosed no conflicts of interest related to this study, and indicated that the research was supported by public grants.
More than half of a group of cirrhosis patients with portal vein thrombosis achieved recanalization with anticoagulation treatment maintained for at least 12 months.
"Moreover, when complete recanalization is achieved, therapy with anticoagulants should be maintained throughout life in order to prevent recurrent thrombosis," wrote Dr. María Gabriela Delgado and Dr. Susana Seijo along with their colleagues in the July issue of Clinical Gastroenterology and Hepatology (doi: 10.1016/j.cgh.2012.01.012).
In the largest study to date to evaluate the safety and efficacy of anticoagulation for portal vein thrombosis in cirrhosis (for which there are no guidelines, according to the authors), the investigators looked at 55 patients with portal vein thrombosis and cirrhosis from four centers in Spain between June 2003 and September 2010.
All patients received anticoagulation according to the protocol of each hospital after the initiation of prophylaxis of variceal bleeding. For 31 patients, anticoagulation was indicated because of acute or subacute thrombosis, and in the remaining 24 patients, anticoagulation was started because of thrombosis progression.
Anticoagulant agents included low-molecular-weight heparin and vitamin K antagonists, wrote Dr. Delgado and Dr. Seijo, both of the University of Barcelona.
Over a mean 19 months of follow-up, half (n = 28) of the patients remained on anticoagulation until either the end of the study or liver transplant. The remaining 27 patients stopped treatment after a median of 6.3 months (range, 1-24 months).
A total of 33 patients achieved either complete or partial recanalization of the portal vein during the study period; 22 patients did not have a response.
There were three complete recanalizations that occurred within 1 month of anticoagulation initiation, and two patients achieved complete recanalization at month 12.
"Early initiation of anticoagulation therapy after the identification of thrombosis in an imaging study, especially in the first 2 weeks, was the only factor significantly associated with recanalization," wrote the authors.
A total of 17 patients had 30 clinical events during anticoagulation treatment. In 13 patients, these events were "liver related," according to the authors: six variceal bleeding episodes, eight new or worsening ascites cases, five hepatic encephalopathy cases, two spontaneous bacterial peritonitis cases, and two hepatocellular carcinoma cases (several patients had multiple events).
"Liver events were more frequent in patients not achieving recanalization (8/22) than in those achieving partial/complete recanalization (5/33)," added the investigators, though the difference between these groups did not reach significance (P = 0.1).
Non-liver-related events included five bleeding episodes, which the authors attributed to anticoagulation; one acute cholecystitis case; and one duodenal ulcer.
Overall, among the 11 total bleeding events (6 of which were liver related), the authors reported that all took place during the first year after starting anticoagulation, and five events occurred in the first 3 months of treatment.
Furthermore, the only significant predictor of bleeding was a platelet count below 50 × 109/L (P = .018).
Six patients died, none of whom were receiving anticoagulation at the time of death.
Despite its retrospective design and the fact that no comparison group was available, this study shows that "recanalization can be achieved very early after starting anticoagulation treatment; however, those patients who do not present early recanalization may finally achieve it when long-term anticoagulation therapy is maintained," wrote the authors.
More importantly, anticoagulation is "relatively safe" in this population, they added, except in cases of severely depressed platelet counts.
The authors disclosed no conflicts of interest related to this study, and indicated that the research was supported by public grants.
More than half of a group of cirrhosis patients with portal vein thrombosis achieved recanalization with anticoagulation treatment maintained for at least 12 months.
"Moreover, when complete recanalization is achieved, therapy with anticoagulants should be maintained throughout life in order to prevent recurrent thrombosis," wrote Dr. María Gabriela Delgado and Dr. Susana Seijo along with their colleagues in the July issue of Clinical Gastroenterology and Hepatology (doi: 10.1016/j.cgh.2012.01.012).
In the largest study to date to evaluate the safety and efficacy of anticoagulation for portal vein thrombosis in cirrhosis (for which there are no guidelines, according to the authors), the investigators looked at 55 patients with portal vein thrombosis and cirrhosis from four centers in Spain between June 2003 and September 2010.
All patients received anticoagulation according to the protocol of each hospital after the initiation of prophylaxis of variceal bleeding. For 31 patients, anticoagulation was indicated because of acute or subacute thrombosis, and in the remaining 24 patients, anticoagulation was started because of thrombosis progression.
Anticoagulant agents included low-molecular-weight heparin and vitamin K antagonists, wrote Dr. Delgado and Dr. Seijo, both of the University of Barcelona.
Over a mean 19 months of follow-up, half (n = 28) of the patients remained on anticoagulation until either the end of the study or liver transplant. The remaining 27 patients stopped treatment after a median of 6.3 months (range, 1-24 months).
A total of 33 patients achieved either complete or partial recanalization of the portal vein during the study period; 22 patients did not have a response.
There were three complete recanalizations that occurred within 1 month of anticoagulation initiation, and two patients achieved complete recanalization at month 12.
"Early initiation of anticoagulation therapy after the identification of thrombosis in an imaging study, especially in the first 2 weeks, was the only factor significantly associated with recanalization," wrote the authors.
A total of 17 patients had 30 clinical events during anticoagulation treatment. In 13 patients, these events were "liver related," according to the authors: six variceal bleeding episodes, eight new or worsening ascites cases, five hepatic encephalopathy cases, two spontaneous bacterial peritonitis cases, and two hepatocellular carcinoma cases (several patients had multiple events).
"Liver events were more frequent in patients not achieving recanalization (8/22) than in those achieving partial/complete recanalization (5/33)," added the investigators, though the difference between these groups did not reach significance (P = 0.1).
Non-liver-related events included five bleeding episodes, which the authors attributed to anticoagulation; one acute cholecystitis case; and one duodenal ulcer.
Overall, among the 11 total bleeding events (6 of which were liver related), the authors reported that all took place during the first year after starting anticoagulation, and five events occurred in the first 3 months of treatment.
Furthermore, the only significant predictor of bleeding was a platelet count below 50 × 109/L (P = .018).
Six patients died, none of whom were receiving anticoagulation at the time of death.
Despite its retrospective design and the fact that no comparison group was available, this study shows that "recanalization can be achieved very early after starting anticoagulation treatment; however, those patients who do not present early recanalization may finally achieve it when long-term anticoagulation therapy is maintained," wrote the authors.
More importantly, anticoagulation is "relatively safe" in this population, they added, except in cases of severely depressed platelet counts.
The authors disclosed no conflicts of interest related to this study, and indicated that the research was supported by public grants.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Hospitalists Should Prepare for the Patient-Centered Medical Home
In 2009, five of the primary-care health centers in Wisconsin-based Dean Health System began to transform into an increasingly popular—but, to many, still somewhat fuzzy—feature of the new healthcare landscape: the “patient-centered medical home.”
The goals are noble: Orient and guide the patient through the healthcare system. Don’t repeat tests already performed. Keep costs down. Prevent illnesses that are, in fact, preventable. And reward doctors for doing so rather than encouraging visit after visit and test after test.
The hospitalists in the Dean system were brought late into the patient-centered medical home, or PCMH, project, but are now more involved:
- They participate in discussions about impending hospitalizations for patients to determine whether hospitalization is really needed;
- They make every effort to assign the same doctor to a patient each time the patient is hospitalized; and
- They also are part of admissions and discharges that are smoother due to efforts to keep information flowing and keep patients in formed.
There have been hiccups, though. Dean hasn’t tracked readmission rates, so it isn’t known whether they’ve improved. And satisfaction ratings from patients haven’t improved—in part, says Kevin Eichhorn, MD, chief of the hospitalist division at Dean, because patients don’t fully appreciate the changes that have been made, although there is an effort to tell them.

—Ken Simone, DO, SFHM, principal, Hospitalist and Practice Solutions
“But we’ve also only been doing this routinely for about a year,” Dr. Eichhorn says. “My hope is that, as we get better at it, we will see some improvement in terms of patient satisfaction with their hospitalization and improvement in other quality metrics as well.”
If hospitalists already working in a PCMH model are struggling with the changes, imagine the question marks for hospitalists who aren’t familiar with the concept yet (see “The Patient-Centered Medical Home: A Primer,” below). Joseph Ming Wah Li, MD, SFHM, immediate past president of SHM, says most hospitalists are not.
“I think it’s fair to say that most hospitalists lack awareness and insight into what the patient-centered medical home will mean for patients and for hospitalists,” he says.
But it’s a concept HM as a whole should bone up on quickly. As attention to reducing healthcare costs intensifies and the PCMH model becomes more commonplace, hospitalists’ roles within such practices will increase.
Some say hospitalists will be hired by primary-care practices that previously did not employ hospitalists. They might provide extra help during transitions by following patients as they are discharged to skilled rehab units or nursing homes. They also might provide preoperative histories for elective surgeries.
“I believe the hospitalist will be right at the center of the model, along with the PCPs [primary-care physicians],” says Ken Simone, DO, SFHM, a national hospitalist practice management consultant and principal at Maine-based Hospitalist and Practice Solutions. “In my opinion, the PCMH model will expand the hospitalist’s role outside the four walls of the hospital.”
Time to Prepare
Dr. Simone and others say that now is the time for hospitalists to begin exploring the PCMH model and its implications in their locales. HM groups should:
Familiarize themselves with the PCMH concept.
Although the model continues to evolve, the main components can be found in a 2007 joint statement by the American Academy of Family Physicians, American Academy of Pediatrics, American College of Physicians, and American Osteopathic Association.1 They include the principles of a personal physician with whom the patient has an ongoing relationship; coordinated care across all elements of the healthcare system; better quality and safety; enhanced access to doctors and their teams; and a payment system that factors in the role of physicians and nonphysicians alike, as well as the role of technology and rewards for good outcomes.
“In a patient-centered medical home, there is a strong emphasis on coordination of care and communication between all members of a patient’s healthcare team,” says Jeffrey Cain, MD, president-elect of the American Academy of Family Physicians (AAFP). “Patients receive the highest-quality, patient-centered care when the primary-care physician takes the lead in coordinating care. This means keeping patients, specialists, hospitalists, and other health providers informed of all test results, treatment plans, expectations, progress, and outcomes.”
Find out about the PCMH activity in their own communities.
Dr. Cain said that the degree of PCMH adoption depends on where you work.
“It is spotty throughout the United States,” he notes. “There are areas of tremendous growth and areas that are waiting to have that happen.”
Dr. Simone, a Team Hospitalist member, says the degree to which hospitalists are familiar with PCMH depends on the level of adoption in the area.
“I have found greater hospitalist awareness in communities that have integrated healthcare delivery systems,” he says. “This makes sense, because these are the communities that are aggressively pursing the patient-centered home.”
Forge relationships with primary-care providers.
Dr. Simone encourages hospitalist groups to make marketing visits to local PCP offices. During these visits, hospitalists should discuss the services they provide, their staffing model, admission and communication protocols—and, “most importantly, ask what the hospitalist practice can do to meet the needs of both the patient and the referring providers.”
Dr. Li says it’s always been important to have open lines of communication with your PCPs—but now more than ever.
“If you don’t have this already, you’re already behind in the ballgame,” he says. “But it’s never too late. It’s critically important to have those communication systems in place so that patients get the best care possible.”
Talk to hospital administrators about clinical and financial links with PCMH practices.
The time to do this, Dr. Simone says, is when a local PCMH is being created, or at contract renewal time, if a PCMH is already exists.
“Hospitalists will obviously need to have a voice within the organization and some autonomy for them to commit to such an integrated relationship,” Dr. Simone says.
Prepare for the demands of sicker patients.
If better primary care means fewer hospitalizations, the patients who are admitted will be sicker, posing more challenges to hospitalists.
“Make sure each individual provider has the skill set and schedule that allows them to take care of these patients,” Dr. Li says.
Embrace the possibilities this model offers.
In the PCMH model, the coordination between the hospitalist and the PCP can only help a hospitalist at the time of discharge.
“It will be easier to get their patients into a primary-care office,” says Dr. Cain of AAFP.
David Meyers, MD, director of the Center for Primary Care, Prevention and Clinical Partnerships at the federal Agency for Healthcare Research and Quality (AHRQ), which provides tools and information that support primary care’s redesign and the PCMH, says the model essentially adds a member to the hospitalist’s team.
“If done well, it gives the hospitalist a partner in the community with whom to establish joint accountability,” Dr. Meyers explains. “In addition to establishing accountability, the PCMH helps ensure information flows both into and out of the hospital.”
A Growth Spurt
As of March 1, the nonprofit National Committee on Quality Assurance had recognized 3,979 practices across the country as “patient-centered medical homes.” And that doesn’t include practices that function according to PCMH principles but are not officially recognized.
The Mayo Clinic recently began a three-year pilot PCMH project in Wisconsin, in conjunction with Group Health Cooperative of Eau Claire.
Crucially, insurance companies are coming on board. In January, Indianapolis-based benefits company WellPoint announced a new payment system designed to promote better primary care, with increases to regular fees, payments for “non-visit” services, and shared savings payments based on quality outcomes and reduced medical costs.
Blue Cross and Blue Shield has reported success with PCMH models.
Meanwhile, the Centers for Medicare & Medicaid Services (CMS) is testing a PCMH model to see whether it generates higher quality of care and cost savings. So is the Department of Veterans Affairs.
—David Meyers, MD, director, Center for Primary Care, Prevention and Clinical Partnerships, Agency for Healthcare Research and Quality, Washington, D.C.
Primary-care doctors, hospitalists and government officials say the concept is likely here to stay. “We’re in a period of change,” Dr. Meyers says. “I don’t know where we’re going to be in five years from now, but forces are aligning such that this may really work.”
And hospitalists are vital to the success of any PCMH.
“The patient-centered medical home,” he says, “to be effective on what it can do, has to be integrated into a patient-centered medical neighborhood—the partnership between primary care or ambulatory care and inpatient care, and specifically the hospitalists and those folks working in nursing homes and skilled nursing facilities.”
Gordon Chen, MD, a cardiologist and senior vice president of medical affairs at Chen Medical in Miami, where a number of PCMH concepts have been in place for 10 years, says that he works both with hospitalists employed by Chen Medical and some not employed by Chen Medical. And he notices the difference.
“It can be a little bit more difficult to reach and to coordinate and collaborate with other physicians, but we can do it,” he says.
A tighter connection allows information to flow better between the PCPs and the hospitalists, he points out.
“One of the most frustrating things as a physician is to find out that your patient had a prolonged hospitalization and they come to see you in the clinic and you don’t have any information,” Dr. Chen says. “You look at this new medication list and you’re trying to put the pieces together. When a doctor doesn’t have all the information, and is guessing … it leads to poor decisions being made.”
Back at Dean Health System in Wisconsin, Dr. Eichhorn is confident that the concepts behind the patient-centered medical home can only be good for patients. Still, the project there—as at many other places—is a work in progress.
“Emphasizing wellness and preventative health certainly conveys significant benefits,” he says. “The challenge is defining what is a patient-centered medical home. It sounds like every group is struggling what that means and how to define it and then how to track your outcomes. And then does the patient have a sense of that? Are they appreciating something different in what’s happening to their healthcare?”
Thomas R. Collins is a freelance writer in South Florida.
Reference
In 2009, five of the primary-care health centers in Wisconsin-based Dean Health System began to transform into an increasingly popular—but, to many, still somewhat fuzzy—feature of the new healthcare landscape: the “patient-centered medical home.”
The goals are noble: Orient and guide the patient through the healthcare system. Don’t repeat tests already performed. Keep costs down. Prevent illnesses that are, in fact, preventable. And reward doctors for doing so rather than encouraging visit after visit and test after test.
The hospitalists in the Dean system were brought late into the patient-centered medical home, or PCMH, project, but are now more involved:
- They participate in discussions about impending hospitalizations for patients to determine whether hospitalization is really needed;
- They make every effort to assign the same doctor to a patient each time the patient is hospitalized; and
- They also are part of admissions and discharges that are smoother due to efforts to keep information flowing and keep patients in formed.
There have been hiccups, though. Dean hasn’t tracked readmission rates, so it isn’t known whether they’ve improved. And satisfaction ratings from patients haven’t improved—in part, says Kevin Eichhorn, MD, chief of the hospitalist division at Dean, because patients don’t fully appreciate the changes that have been made, although there is an effort to tell them.
—Ken Simone, DO, SFHM, principal, Hospitalist and Practice Solutions
“But we’ve also only been doing this routinely for about a year,” Dr. Eichhorn says. “My hope is that, as we get better at it, we will see some improvement in terms of patient satisfaction with their hospitalization and improvement in other quality metrics as well.”
If hospitalists already working in a PCMH model are struggling with the changes, imagine the question marks for hospitalists who aren’t familiar with the concept yet (see “The Patient-Centered Medical Home: A Primer,” below). Joseph Ming Wah Li, MD, SFHM, immediate past president of SHM, says most hospitalists are not.
“I think it’s fair to say that most hospitalists lack awareness and insight into what the patient-centered medical home will mean for patients and for hospitalists,” he says.
But it’s a concept HM as a whole should bone up on quickly. As attention to reducing healthcare costs intensifies and the PCMH model becomes more commonplace, hospitalists’ roles within such practices will increase.
Some say hospitalists will be hired by primary-care practices that previously did not employ hospitalists. They might provide extra help during transitions by following patients as they are discharged to skilled rehab units or nursing homes. They also might provide preoperative histories for elective surgeries.
“I believe the hospitalist will be right at the center of the model, along with the PCPs [primary-care physicians],” says Ken Simone, DO, SFHM, a national hospitalist practice management consultant and principal at Maine-based Hospitalist and Practice Solutions. “In my opinion, the PCMH model will expand the hospitalist’s role outside the four walls of the hospital.”
Time to Prepare
Dr. Simone and others say that now is the time for hospitalists to begin exploring the PCMH model and its implications in their locales. HM groups should:
Familiarize themselves with the PCMH concept.
Although the model continues to evolve, the main components can be found in a 2007 joint statement by the American Academy of Family Physicians, American Academy of Pediatrics, American College of Physicians, and American Osteopathic Association.1 They include the principles of a personal physician with whom the patient has an ongoing relationship; coordinated care across all elements of the healthcare system; better quality and safety; enhanced access to doctors and their teams; and a payment system that factors in the role of physicians and nonphysicians alike, as well as the role of technology and rewards for good outcomes.
“In a patient-centered medical home, there is a strong emphasis on coordination of care and communication between all members of a patient’s healthcare team,” says Jeffrey Cain, MD, president-elect of the American Academy of Family Physicians (AAFP). “Patients receive the highest-quality, patient-centered care when the primary-care physician takes the lead in coordinating care. This means keeping patients, specialists, hospitalists, and other health providers informed of all test results, treatment plans, expectations, progress, and outcomes.”
Find out about the PCMH activity in their own communities.
Dr. Cain said that the degree of PCMH adoption depends on where you work.
“It is spotty throughout the United States,” he notes. “There are areas of tremendous growth and areas that are waiting to have that happen.”
Dr. Simone, a Team Hospitalist member, says the degree to which hospitalists are familiar with PCMH depends on the level of adoption in the area.
“I have found greater hospitalist awareness in communities that have integrated healthcare delivery systems,” he says. “This makes sense, because these are the communities that are aggressively pursing the patient-centered home.”
Forge relationships with primary-care providers.
Dr. Simone encourages hospitalist groups to make marketing visits to local PCP offices. During these visits, hospitalists should discuss the services they provide, their staffing model, admission and communication protocols—and, “most importantly, ask what the hospitalist practice can do to meet the needs of both the patient and the referring providers.”
Dr. Li says it’s always been important to have open lines of communication with your PCPs—but now more than ever.
“If you don’t have this already, you’re already behind in the ballgame,” he says. “But it’s never too late. It’s critically important to have those communication systems in place so that patients get the best care possible.”
Talk to hospital administrators about clinical and financial links with PCMH practices.
The time to do this, Dr. Simone says, is when a local PCMH is being created, or at contract renewal time, if a PCMH is already exists.
“Hospitalists will obviously need to have a voice within the organization and some autonomy for them to commit to such an integrated relationship,” Dr. Simone says.
Prepare for the demands of sicker patients.
If better primary care means fewer hospitalizations, the patients who are admitted will be sicker, posing more challenges to hospitalists.
“Make sure each individual provider has the skill set and schedule that allows them to take care of these patients,” Dr. Li says.
Embrace the possibilities this model offers.
In the PCMH model, the coordination between the hospitalist and the PCP can only help a hospitalist at the time of discharge.
“It will be easier to get their patients into a primary-care office,” says Dr. Cain of AAFP.
David Meyers, MD, director of the Center for Primary Care, Prevention and Clinical Partnerships at the federal Agency for Healthcare Research and Quality (AHRQ), which provides tools and information that support primary care’s redesign and the PCMH, says the model essentially adds a member to the hospitalist’s team.
“If done well, it gives the hospitalist a partner in the community with whom to establish joint accountability,” Dr. Meyers explains. “In addition to establishing accountability, the PCMH helps ensure information flows both into and out of the hospital.”
A Growth Spurt
As of March 1, the nonprofit National Committee on Quality Assurance had recognized 3,979 practices across the country as “patient-centered medical homes.” And that doesn’t include practices that function according to PCMH principles but are not officially recognized.
The Mayo Clinic recently began a three-year pilot PCMH project in Wisconsin, in conjunction with Group Health Cooperative of Eau Claire.
Crucially, insurance companies are coming on board. In January, Indianapolis-based benefits company WellPoint announced a new payment system designed to promote better primary care, with increases to regular fees, payments for “non-visit” services, and shared savings payments based on quality outcomes and reduced medical costs.
Blue Cross and Blue Shield has reported success with PCMH models.
Meanwhile, the Centers for Medicare & Medicaid Services (CMS) is testing a PCMH model to see whether it generates higher quality of care and cost savings. So is the Department of Veterans Affairs.
—David Meyers, MD, director, Center for Primary Care, Prevention and Clinical Partnerships, Agency for Healthcare Research and Quality, Washington, D.C.
Primary-care doctors, hospitalists and government officials say the concept is likely here to stay. “We’re in a period of change,” Dr. Meyers says. “I don’t know where we’re going to be in five years from now, but forces are aligning such that this may really work.”
And hospitalists are vital to the success of any PCMH.
“The patient-centered medical home,” he says, “to be effective on what it can do, has to be integrated into a patient-centered medical neighborhood—the partnership between primary care or ambulatory care and inpatient care, and specifically the hospitalists and those folks working in nursing homes and skilled nursing facilities.”
Gordon Chen, MD, a cardiologist and senior vice president of medical affairs at Chen Medical in Miami, where a number of PCMH concepts have been in place for 10 years, says that he works both with hospitalists employed by Chen Medical and some not employed by Chen Medical. And he notices the difference.
“It can be a little bit more difficult to reach and to coordinate and collaborate with other physicians, but we can do it,” he says.
A tighter connection allows information to flow better between the PCPs and the hospitalists, he points out.
“One of the most frustrating things as a physician is to find out that your patient had a prolonged hospitalization and they come to see you in the clinic and you don’t have any information,” Dr. Chen says. “You look at this new medication list and you’re trying to put the pieces together. When a doctor doesn’t have all the information, and is guessing … it leads to poor decisions being made.”
Back at Dean Health System in Wisconsin, Dr. Eichhorn is confident that the concepts behind the patient-centered medical home can only be good for patients. Still, the project there—as at many other places—is a work in progress.
“Emphasizing wellness and preventative health certainly conveys significant benefits,” he says. “The challenge is defining what is a patient-centered medical home. It sounds like every group is struggling what that means and how to define it and then how to track your outcomes. And then does the patient have a sense of that? Are they appreciating something different in what’s happening to their healthcare?”
Thomas R. Collins is a freelance writer in South Florida.
Reference
In 2009, five of the primary-care health centers in Wisconsin-based Dean Health System began to transform into an increasingly popular—but, to many, still somewhat fuzzy—feature of the new healthcare landscape: the “patient-centered medical home.”
The goals are noble: Orient and guide the patient through the healthcare system. Don’t repeat tests already performed. Keep costs down. Prevent illnesses that are, in fact, preventable. And reward doctors for doing so rather than encouraging visit after visit and test after test.
The hospitalists in the Dean system were brought late into the patient-centered medical home, or PCMH, project, but are now more involved:
- They participate in discussions about impending hospitalizations for patients to determine whether hospitalization is really needed;
- They make every effort to assign the same doctor to a patient each time the patient is hospitalized; and
- They also are part of admissions and discharges that are smoother due to efforts to keep information flowing and keep patients in formed.
There have been hiccups, though. Dean hasn’t tracked readmission rates, so it isn’t known whether they’ve improved. And satisfaction ratings from patients haven’t improved—in part, says Kevin Eichhorn, MD, chief of the hospitalist division at Dean, because patients don’t fully appreciate the changes that have been made, although there is an effort to tell them.
—Ken Simone, DO, SFHM, principal, Hospitalist and Practice Solutions
“But we’ve also only been doing this routinely for about a year,” Dr. Eichhorn says. “My hope is that, as we get better at it, we will see some improvement in terms of patient satisfaction with their hospitalization and improvement in other quality metrics as well.”
If hospitalists already working in a PCMH model are struggling with the changes, imagine the question marks for hospitalists who aren’t familiar with the concept yet (see “The Patient-Centered Medical Home: A Primer,” below). Joseph Ming Wah Li, MD, SFHM, immediate past president of SHM, says most hospitalists are not.
“I think it’s fair to say that most hospitalists lack awareness and insight into what the patient-centered medical home will mean for patients and for hospitalists,” he says.
But it’s a concept HM as a whole should bone up on quickly. As attention to reducing healthcare costs intensifies and the PCMH model becomes more commonplace, hospitalists’ roles within such practices will increase.
Some say hospitalists will be hired by primary-care practices that previously did not employ hospitalists. They might provide extra help during transitions by following patients as they are discharged to skilled rehab units or nursing homes. They also might provide preoperative histories for elective surgeries.
“I believe the hospitalist will be right at the center of the model, along with the PCPs [primary-care physicians],” says Ken Simone, DO, SFHM, a national hospitalist practice management consultant and principal at Maine-based Hospitalist and Practice Solutions. “In my opinion, the PCMH model will expand the hospitalist’s role outside the four walls of the hospital.”
Time to Prepare
Dr. Simone and others say that now is the time for hospitalists to begin exploring the PCMH model and its implications in their locales. HM groups should:
Familiarize themselves with the PCMH concept.
Although the model continues to evolve, the main components can be found in a 2007 joint statement by the American Academy of Family Physicians, American Academy of Pediatrics, American College of Physicians, and American Osteopathic Association.1 They include the principles of a personal physician with whom the patient has an ongoing relationship; coordinated care across all elements of the healthcare system; better quality and safety; enhanced access to doctors and their teams; and a payment system that factors in the role of physicians and nonphysicians alike, as well as the role of technology and rewards for good outcomes.
“In a patient-centered medical home, there is a strong emphasis on coordination of care and communication between all members of a patient’s healthcare team,” says Jeffrey Cain, MD, president-elect of the American Academy of Family Physicians (AAFP). “Patients receive the highest-quality, patient-centered care when the primary-care physician takes the lead in coordinating care. This means keeping patients, specialists, hospitalists, and other health providers informed of all test results, treatment plans, expectations, progress, and outcomes.”
Find out about the PCMH activity in their own communities.
Dr. Cain said that the degree of PCMH adoption depends on where you work.
“It is spotty throughout the United States,” he notes. “There are areas of tremendous growth and areas that are waiting to have that happen.”
Dr. Simone, a Team Hospitalist member, says the degree to which hospitalists are familiar with PCMH depends on the level of adoption in the area.
“I have found greater hospitalist awareness in communities that have integrated healthcare delivery systems,” he says. “This makes sense, because these are the communities that are aggressively pursing the patient-centered home.”
Forge relationships with primary-care providers.
Dr. Simone encourages hospitalist groups to make marketing visits to local PCP offices. During these visits, hospitalists should discuss the services they provide, their staffing model, admission and communication protocols—and, “most importantly, ask what the hospitalist practice can do to meet the needs of both the patient and the referring providers.”
Dr. Li says it’s always been important to have open lines of communication with your PCPs—but now more than ever.
“If you don’t have this already, you’re already behind in the ballgame,” he says. “But it’s never too late. It’s critically important to have those communication systems in place so that patients get the best care possible.”
Talk to hospital administrators about clinical and financial links with PCMH practices.
The time to do this, Dr. Simone says, is when a local PCMH is being created, or at contract renewal time, if a PCMH is already exists.
“Hospitalists will obviously need to have a voice within the organization and some autonomy for them to commit to such an integrated relationship,” Dr. Simone says.
Prepare for the demands of sicker patients.
If better primary care means fewer hospitalizations, the patients who are admitted will be sicker, posing more challenges to hospitalists.
“Make sure each individual provider has the skill set and schedule that allows them to take care of these patients,” Dr. Li says.
Embrace the possibilities this model offers.
In the PCMH model, the coordination between the hospitalist and the PCP can only help a hospitalist at the time of discharge.
“It will be easier to get their patients into a primary-care office,” says Dr. Cain of AAFP.
David Meyers, MD, director of the Center for Primary Care, Prevention and Clinical Partnerships at the federal Agency for Healthcare Research and Quality (AHRQ), which provides tools and information that support primary care’s redesign and the PCMH, says the model essentially adds a member to the hospitalist’s team.
“If done well, it gives the hospitalist a partner in the community with whom to establish joint accountability,” Dr. Meyers explains. “In addition to establishing accountability, the PCMH helps ensure information flows both into and out of the hospital.”
A Growth Spurt
As of March 1, the nonprofit National Committee on Quality Assurance had recognized 3,979 practices across the country as “patient-centered medical homes.” And that doesn’t include practices that function according to PCMH principles but are not officially recognized.
The Mayo Clinic recently began a three-year pilot PCMH project in Wisconsin, in conjunction with Group Health Cooperative of Eau Claire.
Crucially, insurance companies are coming on board. In January, Indianapolis-based benefits company WellPoint announced a new payment system designed to promote better primary care, with increases to regular fees, payments for “non-visit” services, and shared savings payments based on quality outcomes and reduced medical costs.
Blue Cross and Blue Shield has reported success with PCMH models.
Meanwhile, the Centers for Medicare & Medicaid Services (CMS) is testing a PCMH model to see whether it generates higher quality of care and cost savings. So is the Department of Veterans Affairs.
—David Meyers, MD, director, Center for Primary Care, Prevention and Clinical Partnerships, Agency for Healthcare Research and Quality, Washington, D.C.
Primary-care doctors, hospitalists and government officials say the concept is likely here to stay. “We’re in a period of change,” Dr. Meyers says. “I don’t know where we’re going to be in five years from now, but forces are aligning such that this may really work.”
And hospitalists are vital to the success of any PCMH.
“The patient-centered medical home,” he says, “to be effective on what it can do, has to be integrated into a patient-centered medical neighborhood—the partnership between primary care or ambulatory care and inpatient care, and specifically the hospitalists and those folks working in nursing homes and skilled nursing facilities.”
Gordon Chen, MD, a cardiologist and senior vice president of medical affairs at Chen Medical in Miami, where a number of PCMH concepts have been in place for 10 years, says that he works both with hospitalists employed by Chen Medical and some not employed by Chen Medical. And he notices the difference.
“It can be a little bit more difficult to reach and to coordinate and collaborate with other physicians, but we can do it,” he says.
A tighter connection allows information to flow better between the PCPs and the hospitalists, he points out.
“One of the most frustrating things as a physician is to find out that your patient had a prolonged hospitalization and they come to see you in the clinic and you don’t have any information,” Dr. Chen says. “You look at this new medication list and you’re trying to put the pieces together. When a doctor doesn’t have all the information, and is guessing … it leads to poor decisions being made.”
Back at Dean Health System in Wisconsin, Dr. Eichhorn is confident that the concepts behind the patient-centered medical home can only be good for patients. Still, the project there—as at many other places—is a work in progress.
“Emphasizing wellness and preventative health certainly conveys significant benefits,” he says. “The challenge is defining what is a patient-centered medical home. It sounds like every group is struggling what that means and how to define it and then how to track your outcomes. And then does the patient have a sense of that? Are they appreciating something different in what’s happening to their healthcare?”
Thomas R. Collins is a freelance writer in South Florida.
Reference
Rural Hospitalists Face Myriad Challenges, Rewards
Michael McMahon, MD, one of two hospitalists at Carilion Giles Community Hospital (CGCH), a 25-bed critical-access hospital in Pearisburg, Va., started practicing HM two years ago after spending three decades as a family physician in the town of 2,761. Although he feels a strong connection with his close-knit community, Dr. McMahon faces the overriding challenge many rural hospitalists encounter daily: lack of immediate, on-site access to essential medical specialty resources.
“In a setting like this, it’s just me and the emergency department doctor. There are no specialists,” Dr. McMahon says. “Our nearest general surgeon is responsive but lives 30 miles away. So I have to wear a lot of hats.”
The biggest question Dr. McMahon deals with regularly is whether patients can be taken care of in-house or need to be transferred to a larger hospital, such as Carilion Roanoke Memorial Hospital, a 700-bed CGCH affiliate that is 60 miles away.
“Some decisions are obvious, and others are gray areas,” he explains. “We don’t do dialysis here. If it’s serious trauma, they go. If it’s a [myocardial infarction] needing acute cardiac intervention, they go.”
But some patients don’t want to go and would rather rely on what Dr. McMahon can achieve with his practice-honed diagnostic skills. He also uses relationships developed over the years with cardiologists, nephrologists, neurologists, and others in Roanoke—about 60 miles away—for telephone consultations on tough cases.
“This job requires much more clinical judgment than you would need in other settings where you can lean on other people or on the medical technology,” Dr. McMahon explains. “I have a good feel for where my own line is and for what this facility can handle.”
Dr. McMahon is part of a growing rural HM movement. According to a recent survey by the American Hospital Association, the number of rural hospitals with HM coverage is growing. One in 6 hospitals with fewer than 25 beds had HM programs in 2009, double the penetration of six years before. For hospitals with 25 to 49 beds, nearly 1 in 3 had a hospitalist presence in 2009—twice the number as in 2003.
—Brian Bossard, MD, FACP, FHM, director, Inpatient Physician Associates, Lincoln, Neb.
In addition to the lack of specialist backup, recruiting doctors to fill hospitalist positions in rural settings can be a major challenge. Other issues include staffing and scheduling, providing on-call and off-hours backup, and the economic stressors on small hospitals that constrain their ability to offer competitive compensation.
But rural hospitalists also emphasize the lifestyle benefits of calling a rural community home, such as the absence of crime, a slower pace, easy access to outdoor recreation, and the satisfying personal relationships that can develop in smaller communities.
“I like rural hospital medicine,” says Larry Labul, DO, FACOI, SFHM, a hospitalist at Franklin Memorial Hospital in Farmington, Maine, population 7,760. “I like being a big fish in a small pond, doing my own procedures, managing patients in the ICU. If I sometimes don’t know how to manage a procedure, I have a choice: Learn how to do it or send the patients somewhere else.”
Hospitalists in rural areas often become integral parts of their communities, says John Nelson, MD, MHM, medical director of the hospitalist program at Overlake Hospital in Bellevue, Wash., a Seattle suburb.
“There’s a reasonable chance you know your patients socially,” says Dr. Nelson, co-founder and past president of SHM and practice-management columnist for The Hospitalist. “I’ve been in the same place for 11 years, and if I have any connection with my patient, it’s a strange coincidence.”

Too often for urban hospitalists, he says, the next patient is just the next patient, whereas in a rural community, the odds are better than even that the doctor at least knows someone in the patient’s family. “That gives you a whole different perspective on the work.”
The Challenge: Recruitment
Despite the virtues of small towns for those who can appreciate them, rural hospitals face an uphill battle in attracting the desired complement of hospitalists to staff their programs. HM’s explosive growth means the field generally has benefited from a seller’s market, and rural communities have struggled to fill both inpatient and outpatient positions.
“Recruiting is tough in rural areas, even as some metro areas are starting to fill up with hospitalists,” Dr. Nelson says. Michael Manning, MD, a hospitalist at Murphy Medical Center in Murphy, the westernmost town in North Carolina (population 1,568), says it’s especially hard if the nearest airport is hours away. “A small hospital’s efforts to advertise just gets lost unless the candidate is actively looking for a rural setting to practice. Here we’ve got hunting and fishing. I came for the whitewater kayaking,” Dr. Manning says.
The challenge is to convince people who have never visited the area that a rural hospital is a great place to practice, says Brian Bossard, MD, FACP, FHM, director of Inpatient Physician Associates in Lincoln, Neb. “There are lots of barriers to address in order to negotiate a positive outcome. The more rural it is, the harder the job of recruiting. What more can we offer a recruit? Sometimes it’s money, a signing bonus, a benefit package. With many recruiting efforts, the spouse is part of the equation.”
Recruiting doctors to rural areas starts by leading with the hospital’s strengths, such as high-quality care, manageable workloads, or sustainable schedules, Dr. Bossard says. Recruiters also focus on the advantages of living and raising children away from the big city. International medical school graduates have long been a recruitment target of rural hospitals, but they present bureaucratic hoops that some hospitals are unwilling to jump through. (Visit the-hospitalist.org to learn why Foreign Medical Grads can bolster your HM group staffing.) Other hospitals employ recruiting staff, recruitment firms, paid advertising, and old-fashioned word of mouth—talking with anyone and everyone who might know a physician who could be interested.
Fannie Vavoulis, medical recruiter for Chatham-Kent Health Alliance in Chatham, Ontario, agrees that it can be difficult to recruit physicians to a setting like her predominantly agricultural community. But she has enjoyed recent success, in part due to the efforts of a 25-member community volunteer group of local business and health leaders who woo physician candidates. “We use the volunteers to show them around, help find opportunities for their spouses, and offering ongoing mentorship once they come here,” Vavoulis relates.
continued below...
A Little Like Home

Rapid City, S.D., with a population of 68,000, isn’t the most rural of settings, although Rapid City Regional Hospital (RCRH) also serves a large rural catchment area, with affiliated rural satellites. But the Black Hills are worlds away from places like Chicago or Dallas or New York City, where many future hospitalists do their residencies.
Pushpa Poudel, MD, came to 400-bed RCRH in 2010 following a residency at Wyckoff Heights Medical Center in Brooklyn, N.Y. “The people I met on my interview days were nice, but I was more attracted to the work environment and the dedication I found in the hospital here,” he says.

Dr. Poudel, who is from Nepal and attended medical school in Kathmandu, says the scenic Black Hills reminded him a little of home. After interviewing at RCRH, he went back to New York and talked two Nepalese physician friends into joining him there. Today, the multinational HM group at RCRH includes six hospitalists from Nepal, as well as others from India, Egypt, Costa Rica, and the Republic of Georgia. “We now have 28 hospitalists, and in the seven years since the program started, we’ve only lost one of them,” says Kristi Gylten, MBA, the service’s director.
All of the hospitalist group’s members meet candidates when they come for interviews. “They are the biggest sellers of the program,” Gylten says, although work-life balance, recreation in the Black Hills, and the reputation of the local school system are also draws. “Often the hardest part is just getting them to come out here. Once they come to Rapid City and see the community, it surprises them.”
—Larry Beresford
The Challenge: Expanded Scope
“This is a different brand of hospital medicine, with the potential for an expanded scope of practice,” says Dr. Bossard, whose group staffs hospitalist programs in Lincoln, Neb., and two rural communities in that state. “Physicians looking at your program need to understand that. Every hospital medicine program has its own identity and culture, but rural programs definitely have a culture of greater independence and autonomy.
“It’s a different breed of physician—a different culture and different standards of what hospitalists do and don’t do,” he explains.
Rural hospitalists often need to master procedures and medical specializations (including critical care) that many of their urban counterparts hand off to specialists. For conditions they can’t manage, the alternative is transferring the patient to a larger hospital, sometimes by ambulance or helicopter.
“Some physicians are uncomfortable with the level of expertise and procedural skills required to manage in this setting,” says Dr. Nelson, whose consulting firm regularly works with HM programs in rural areas. “But the hospital and the physician community are looking to the hospitalists as a resource to keep patients in the community as much as possible. If the hospitalists are too risk-averse, that may be a problem.”
—John Nelson, MD, MHM, hospitalist program medical director, Overlake Hospital, Bellevue, Wash., co-founder and past president of SHM
Dale Vizcarra, MD, a hospitalist at 60-bed St. Mary’s Healthcare Center in Pierre, S.D., has gotten used to not having on-site access to cardiology, anesthesiology, ENT, psychiatry, or pulmonology. “So you’re kind of piloting on your own,” she explains. “That could be hard for a new graduate who’s not used to flying solo.”
Dr. Vizcarra and a hospitalist partner navigate the lack of in-house specialist support by utilizing technology—for example, eICU-monitored beds or phoning physician colleagues in Sioux Falls. “The big question is, Do people know what they don’t know? It’s possible to be too quick—or not quick enough—to pick up the phone and ask for help,” she says.
Rural hospitals also face many of the same quality expectations and looming financial disincentives as their urban counterparts, but with fewer resources to devote to them. They conduct quality and safety projects and participate in SHM’s Project BOOST and similar quality initiatives. Three rural hospitals—Mariners Hospital in Tavernier, Fla., Miles Memorial Hospital in Damariscotta, Maine, and Sebasticook Valley Hospital in Palmyra, Maine—recently were named among the Leapfrog Group’s 65 top hospitals for 2011.1
A recent study by Karen Joynt, MD, MPH, of the Harvard School of Public Health and colleagues found that rural critical-access hospitals overall had fewer clinical capabilities, worse outcomes, and higher death rates for patients with heart attack, congestive heart failure, or pneumonia than their more urban counterparts.2 But Dr. Vizcarra says hospitalists can bring higher quality of care to rural hospitals.

“I also think staff satisfaction is better,” she says, adding that rural hospitals can try quality approaches tailored to the unique setting. “For example, because we have a lot of diabetic patients who are often noncompliant, we established a goal to have multiple members of our hospital team—from nurses to housekeeping—receive extra training in diabetes management and share it with patients. Sometimes it’s the person who hands out the food trays who has the best chance to reach the patient with this information.”
Dr. Vizcarra has lived in Pierre for 20 years and just became a hospitalist in April 2011. She loved primary care, but she says that “being a hospitalist in a clinical setting is a blast. There’s so much you can do—so many areas where you can improve care.”
The Challenge: Schedules
For a hospital to offer 24/7 hospitalist coverage on site, it generally requires at least three, if not four, full-time physicians dividing up days, nights, and weekends, allowing for vacations, sick days, and training time. Even so, a group of three or four hospitalists providing round-the-clock coverage is more likely to encounter some burnout than those programs that work seven-on/seven-off schedules. If the hospital is not able to afford four FTEs of salary—or to find physicians to fill those FTEs—it might decide that it doesn’t need hospitalists on site at night, Dr. Nelson says.
Alternatives include having the hospitalists take call from home, letting ED physicians do after-hours admits, or mobilizing community PCPs to divide up some of the coverage and call responsibility. Locums physicians are popular at rural hospitals, but they come at the expense of the personal relations and community integration that are counted among rural hospital medicine’s assets. Another approach, tried in some small hospitals where the caseload is insufficient to keep both a hospitalist and emergency doctor busy, is to combine the positions of ED doctor and hospitalist, then find physicians with the skills to fill both roles.
Increasingly, an alternative to supplementing hospitalists on the ground is telemedicine, which brings specialist expertise to rural hospitals long distance via telephone lines and video equipment. This concept may be more familiar in eICUs, but Atlanta-based Eagle Hospital Physicians also offers the services of hospitalists and neurologists via telemedicine links, says Richard Sanders, MPH, FACHE, the company’s director of telemedicine services. Specialists from Eagle’s pool of physicians serving hospitals across the Southeast work from wherever they have access to a telephone and Internet service.
“In order to address the issues rural hospitals and hospitalists face, we have to be innovative in our approach. Our hospital partners struggle with having patient volumes that require more hospitalists than they can recruit for, a problem exacerbated by the need for taking call at night, which can scare off some candidates,” Sanders says.
The peak time for telemedicine for the hospital that can manage partial on-site hospitalist coverage is the night shift—“typically the least productive time for hospitalists, with unpredictable volumes,” he says, “although you still need access to someone who can respond quickly.” Eagle also uses physician extenders as key members of its team and a video-equipped RP-7 robot that can move around the hospital as directed by the remote physician.
The Challenge: Extinction
Dr. McMahon, a Virginia native who practiced in the military after attending Medical College of Virginia, was recruited in 1980 by two residency colleagues who had secured jobs in Pearisburg, a small town in the western part of the state. “I’ve been here ever since,” he says. “I live and work with these people. I’m intimately involved in this community. I attend a lot of funerals. I’m the football team’s doctor, and I teach at the college of nursing.”
Dr. McMahon says that close-knit communities, such as Pearisburg, offer a different kind of medical care; he also says that kind of care is in danger of extinction. And he says something important will be lost if that happens.
Primary-care physicians (PCPs) help supplement the after-hours coverage provided by CGCH’s two staff hospitalists. “This is a community hospital, and we all work together,” Dr. McMahon says. “I know the family practice and internal medicine physicians and they know me.” But he also fears that this level of commitment may not continue much longer.
“We’re all aging in this community, and in another three to five years, the physicians are going to start to retire,” he says. “ … We’re a dying breed from the school of hard knocks and experience, and we’re being phased out in favor of technology-savvy younger doctors, for whom basic diagnostic skills are downplayed.
“There used to be more of a sense of camaraderie in medicine,” he notes. “Back in the day, when I first started here, we considered medicine a calling and not a job.”
For Dr. Vizcarra, the HM model of inpatient care represents a sea change in the connections between physicians and their patients.
“Now, in many small towns, you don’t see your doctor anymore when you’re in the hospital,” she says, adding disconnects can be magnified in small towns. “I try to compensate by providing patients with caring, compassionate, common-sense medicine when they are in the hospital. Usually, after the first day, it’s not an issue.”
Larry Beresford is a freelance writer in Oakland, Calif.
References
- The Leapfrog Group announces annual top hospitals list. The Leapfrog Group website. Available at: http://www.leapfroggroup.org/news/leapfrog_news/4810593. Accessed March 31, 2012.
- Joynt KE, Harris Y, Orav EJ, Jha AK. Quality of care and patient outcomes in critical access rural hospitals. JAMA. 2011;306(1):45-52.
Michael McMahon, MD, one of two hospitalists at Carilion Giles Community Hospital (CGCH), a 25-bed critical-access hospital in Pearisburg, Va., started practicing HM two years ago after spending three decades as a family physician in the town of 2,761. Although he feels a strong connection with his close-knit community, Dr. McMahon faces the overriding challenge many rural hospitalists encounter daily: lack of immediate, on-site access to essential medical specialty resources.
“In a setting like this, it’s just me and the emergency department doctor. There are no specialists,” Dr. McMahon says. “Our nearest general surgeon is responsive but lives 30 miles away. So I have to wear a lot of hats.”
The biggest question Dr. McMahon deals with regularly is whether patients can be taken care of in-house or need to be transferred to a larger hospital, such as Carilion Roanoke Memorial Hospital, a 700-bed CGCH affiliate that is 60 miles away.
“Some decisions are obvious, and others are gray areas,” he explains. “We don’t do dialysis here. If it’s serious trauma, they go. If it’s a [myocardial infarction] needing acute cardiac intervention, they go.”
But some patients don’t want to go and would rather rely on what Dr. McMahon can achieve with his practice-honed diagnostic skills. He also uses relationships developed over the years with cardiologists, nephrologists, neurologists, and others in Roanoke—about 60 miles away—for telephone consultations on tough cases.
“This job requires much more clinical judgment than you would need in other settings where you can lean on other people or on the medical technology,” Dr. McMahon explains. “I have a good feel for where my own line is and for what this facility can handle.”
Dr. McMahon is part of a growing rural HM movement. According to a recent survey by the American Hospital Association, the number of rural hospitals with HM coverage is growing. One in 6 hospitals with fewer than 25 beds had HM programs in 2009, double the penetration of six years before. For hospitals with 25 to 49 beds, nearly 1 in 3 had a hospitalist presence in 2009—twice the number as in 2003.
—Brian Bossard, MD, FACP, FHM, director, Inpatient Physician Associates, Lincoln, Neb.
In addition to the lack of specialist backup, recruiting doctors to fill hospitalist positions in rural settings can be a major challenge. Other issues include staffing and scheduling, providing on-call and off-hours backup, and the economic stressors on small hospitals that constrain their ability to offer competitive compensation.
But rural hospitalists also emphasize the lifestyle benefits of calling a rural community home, such as the absence of crime, a slower pace, easy access to outdoor recreation, and the satisfying personal relationships that can develop in smaller communities.
“I like rural hospital medicine,” says Larry Labul, DO, FACOI, SFHM, a hospitalist at Franklin Memorial Hospital in Farmington, Maine, population 7,760. “I like being a big fish in a small pond, doing my own procedures, managing patients in the ICU. If I sometimes don’t know how to manage a procedure, I have a choice: Learn how to do it or send the patients somewhere else.”
Hospitalists in rural areas often become integral parts of their communities, says John Nelson, MD, MHM, medical director of the hospitalist program at Overlake Hospital in Bellevue, Wash., a Seattle suburb.
“There’s a reasonable chance you know your patients socially,” says Dr. Nelson, co-founder and past president of SHM and practice-management columnist for The Hospitalist. “I’ve been in the same place for 11 years, and if I have any connection with my patient, it’s a strange coincidence.”
Too often for urban hospitalists, he says, the next patient is just the next patient, whereas in a rural community, the odds are better than even that the doctor at least knows someone in the patient’s family. “That gives you a whole different perspective on the work.”
The Challenge: Recruitment
Despite the virtues of small towns for those who can appreciate them, rural hospitals face an uphill battle in attracting the desired complement of hospitalists to staff their programs. HM’s explosive growth means the field generally has benefited from a seller’s market, and rural communities have struggled to fill both inpatient and outpatient positions.
“Recruiting is tough in rural areas, even as some metro areas are starting to fill up with hospitalists,” Dr. Nelson says. Michael Manning, MD, a hospitalist at Murphy Medical Center in Murphy, the westernmost town in North Carolina (population 1,568), says it’s especially hard if the nearest airport is hours away. “A small hospital’s efforts to advertise just gets lost unless the candidate is actively looking for a rural setting to practice. Here we’ve got hunting and fishing. I came for the whitewater kayaking,” Dr. Manning says.
The challenge is to convince people who have never visited the area that a rural hospital is a great place to practice, says Brian Bossard, MD, FACP, FHM, director of Inpatient Physician Associates in Lincoln, Neb. “There are lots of barriers to address in order to negotiate a positive outcome. The more rural it is, the harder the job of recruiting. What more can we offer a recruit? Sometimes it’s money, a signing bonus, a benefit package. With many recruiting efforts, the spouse is part of the equation.”
Recruiting doctors to rural areas starts by leading with the hospital’s strengths, such as high-quality care, manageable workloads, or sustainable schedules, Dr. Bossard says. Recruiters also focus on the advantages of living and raising children away from the big city. International medical school graduates have long been a recruitment target of rural hospitals, but they present bureaucratic hoops that some hospitals are unwilling to jump through. (Visit the-hospitalist.org to learn why Foreign Medical Grads can bolster your HM group staffing.) Other hospitals employ recruiting staff, recruitment firms, paid advertising, and old-fashioned word of mouth—talking with anyone and everyone who might know a physician who could be interested.
Fannie Vavoulis, medical recruiter for Chatham-Kent Health Alliance in Chatham, Ontario, agrees that it can be difficult to recruit physicians to a setting like her predominantly agricultural community. But she has enjoyed recent success, in part due to the efforts of a 25-member community volunteer group of local business and health leaders who woo physician candidates. “We use the volunteers to show them around, help find opportunities for their spouses, and offering ongoing mentorship once they come here,” Vavoulis relates.
continued below...
A Little Like Home
Rapid City, S.D., with a population of 68,000, isn’t the most rural of settings, although Rapid City Regional Hospital (RCRH) also serves a large rural catchment area, with affiliated rural satellites. But the Black Hills are worlds away from places like Chicago or Dallas or New York City, where many future hospitalists do their residencies.
Pushpa Poudel, MD, came to 400-bed RCRH in 2010 following a residency at Wyckoff Heights Medical Center in Brooklyn, N.Y. “The people I met on my interview days were nice, but I was more attracted to the work environment and the dedication I found in the hospital here,” he says.
Dr. Poudel, who is from Nepal and attended medical school in Kathmandu, says the scenic Black Hills reminded him a little of home. After interviewing at RCRH, he went back to New York and talked two Nepalese physician friends into joining him there. Today, the multinational HM group at RCRH includes six hospitalists from Nepal, as well as others from India, Egypt, Costa Rica, and the Republic of Georgia. “We now have 28 hospitalists, and in the seven years since the program started, we’ve only lost one of them,” says Kristi Gylten, MBA, the service’s director.
All of the hospitalist group’s members meet candidates when they come for interviews. “They are the biggest sellers of the program,” Gylten says, although work-life balance, recreation in the Black Hills, and the reputation of the local school system are also draws. “Often the hardest part is just getting them to come out here. Once they come to Rapid City and see the community, it surprises them.”
—Larry Beresford
The Challenge: Expanded Scope
“This is a different brand of hospital medicine, with the potential for an expanded scope of practice,” says Dr. Bossard, whose group staffs hospitalist programs in Lincoln, Neb., and two rural communities in that state. “Physicians looking at your program need to understand that. Every hospital medicine program has its own identity and culture, but rural programs definitely have a culture of greater independence and autonomy.
“It’s a different breed of physician—a different culture and different standards of what hospitalists do and don’t do,” he explains.
Rural hospitalists often need to master procedures and medical specializations (including critical care) that many of their urban counterparts hand off to specialists. For conditions they can’t manage, the alternative is transferring the patient to a larger hospital, sometimes by ambulance or helicopter.
“Some physicians are uncomfortable with the level of expertise and procedural skills required to manage in this setting,” says Dr. Nelson, whose consulting firm regularly works with HM programs in rural areas. “But the hospital and the physician community are looking to the hospitalists as a resource to keep patients in the community as much as possible. If the hospitalists are too risk-averse, that may be a problem.”
—John Nelson, MD, MHM, hospitalist program medical director, Overlake Hospital, Bellevue, Wash., co-founder and past president of SHM
Dale Vizcarra, MD, a hospitalist at 60-bed St. Mary’s Healthcare Center in Pierre, S.D., has gotten used to not having on-site access to cardiology, anesthesiology, ENT, psychiatry, or pulmonology. “So you’re kind of piloting on your own,” she explains. “That could be hard for a new graduate who’s not used to flying solo.”
Dr. Vizcarra and a hospitalist partner navigate the lack of in-house specialist support by utilizing technology—for example, eICU-monitored beds or phoning physician colleagues in Sioux Falls. “The big question is, Do people know what they don’t know? It’s possible to be too quick—or not quick enough—to pick up the phone and ask for help,” she says.
Rural hospitals also face many of the same quality expectations and looming financial disincentives as their urban counterparts, but with fewer resources to devote to them. They conduct quality and safety projects and participate in SHM’s Project BOOST and similar quality initiatives. Three rural hospitals—Mariners Hospital in Tavernier, Fla., Miles Memorial Hospital in Damariscotta, Maine, and Sebasticook Valley Hospital in Palmyra, Maine—recently were named among the Leapfrog Group’s 65 top hospitals for 2011.1
A recent study by Karen Joynt, MD, MPH, of the Harvard School of Public Health and colleagues found that rural critical-access hospitals overall had fewer clinical capabilities, worse outcomes, and higher death rates for patients with heart attack, congestive heart failure, or pneumonia than their more urban counterparts.2 But Dr. Vizcarra says hospitalists can bring higher quality of care to rural hospitals.
“I also think staff satisfaction is better,” she says, adding that rural hospitals can try quality approaches tailored to the unique setting. “For example, because we have a lot of diabetic patients who are often noncompliant, we established a goal to have multiple members of our hospital team—from nurses to housekeeping—receive extra training in diabetes management and share it with patients. Sometimes it’s the person who hands out the food trays who has the best chance to reach the patient with this information.”
Dr. Vizcarra has lived in Pierre for 20 years and just became a hospitalist in April 2011. She loved primary care, but she says that “being a hospitalist in a clinical setting is a blast. There’s so much you can do—so many areas where you can improve care.”
The Challenge: Schedules
For a hospital to offer 24/7 hospitalist coverage on site, it generally requires at least three, if not four, full-time physicians dividing up days, nights, and weekends, allowing for vacations, sick days, and training time. Even so, a group of three or four hospitalists providing round-the-clock coverage is more likely to encounter some burnout than those programs that work seven-on/seven-off schedules. If the hospital is not able to afford four FTEs of salary—or to find physicians to fill those FTEs—it might decide that it doesn’t need hospitalists on site at night, Dr. Nelson says.
Alternatives include having the hospitalists take call from home, letting ED physicians do after-hours admits, or mobilizing community PCPs to divide up some of the coverage and call responsibility. Locums physicians are popular at rural hospitals, but they come at the expense of the personal relations and community integration that are counted among rural hospital medicine’s assets. Another approach, tried in some small hospitals where the caseload is insufficient to keep both a hospitalist and emergency doctor busy, is to combine the positions of ED doctor and hospitalist, then find physicians with the skills to fill both roles.
Increasingly, an alternative to supplementing hospitalists on the ground is telemedicine, which brings specialist expertise to rural hospitals long distance via telephone lines and video equipment. This concept may be more familiar in eICUs, but Atlanta-based Eagle Hospital Physicians also offers the services of hospitalists and neurologists via telemedicine links, says Richard Sanders, MPH, FACHE, the company’s director of telemedicine services. Specialists from Eagle’s pool of physicians serving hospitals across the Southeast work from wherever they have access to a telephone and Internet service.
“In order to address the issues rural hospitals and hospitalists face, we have to be innovative in our approach. Our hospital partners struggle with having patient volumes that require more hospitalists than they can recruit for, a problem exacerbated by the need for taking call at night, which can scare off some candidates,” Sanders says.
The peak time for telemedicine for the hospital that can manage partial on-site hospitalist coverage is the night shift—“typically the least productive time for hospitalists, with unpredictable volumes,” he says, “although you still need access to someone who can respond quickly.” Eagle also uses physician extenders as key members of its team and a video-equipped RP-7 robot that can move around the hospital as directed by the remote physician.
The Challenge: Extinction
Dr. McMahon, a Virginia native who practiced in the military after attending Medical College of Virginia, was recruited in 1980 by two residency colleagues who had secured jobs in Pearisburg, a small town in the western part of the state. “I’ve been here ever since,” he says. “I live and work with these people. I’m intimately involved in this community. I attend a lot of funerals. I’m the football team’s doctor, and I teach at the college of nursing.”
Dr. McMahon says that close-knit communities, such as Pearisburg, offer a different kind of medical care; he also says that kind of care is in danger of extinction. And he says something important will be lost if that happens.
Primary-care physicians (PCPs) help supplement the after-hours coverage provided by CGCH’s two staff hospitalists. “This is a community hospital, and we all work together,” Dr. McMahon says. “I know the family practice and internal medicine physicians and they know me.” But he also fears that this level of commitment may not continue much longer.
“We’re all aging in this community, and in another three to five years, the physicians are going to start to retire,” he says. “ … We’re a dying breed from the school of hard knocks and experience, and we’re being phased out in favor of technology-savvy younger doctors, for whom basic diagnostic skills are downplayed.
“There used to be more of a sense of camaraderie in medicine,” he notes. “Back in the day, when I first started here, we considered medicine a calling and not a job.”
For Dr. Vizcarra, the HM model of inpatient care represents a sea change in the connections between physicians and their patients.
“Now, in many small towns, you don’t see your doctor anymore when you’re in the hospital,” she says, adding disconnects can be magnified in small towns. “I try to compensate by providing patients with caring, compassionate, common-sense medicine when they are in the hospital. Usually, after the first day, it’s not an issue.”
Larry Beresford is a freelance writer in Oakland, Calif.
References
- The Leapfrog Group announces annual top hospitals list. The Leapfrog Group website. Available at: http://www.leapfroggroup.org/news/leapfrog_news/4810593. Accessed March 31, 2012.
- Joynt KE, Harris Y, Orav EJ, Jha AK. Quality of care and patient outcomes in critical access rural hospitals. JAMA. 2011;306(1):45-52.
Michael McMahon, MD, one of two hospitalists at Carilion Giles Community Hospital (CGCH), a 25-bed critical-access hospital in Pearisburg, Va., started practicing HM two years ago after spending three decades as a family physician in the town of 2,761. Although he feels a strong connection with his close-knit community, Dr. McMahon faces the overriding challenge many rural hospitalists encounter daily: lack of immediate, on-site access to essential medical specialty resources.
“In a setting like this, it’s just me and the emergency department doctor. There are no specialists,” Dr. McMahon says. “Our nearest general surgeon is responsive but lives 30 miles away. So I have to wear a lot of hats.”
The biggest question Dr. McMahon deals with regularly is whether patients can be taken care of in-house or need to be transferred to a larger hospital, such as Carilion Roanoke Memorial Hospital, a 700-bed CGCH affiliate that is 60 miles away.
“Some decisions are obvious, and others are gray areas,” he explains. “We don’t do dialysis here. If it’s serious trauma, they go. If it’s a [myocardial infarction] needing acute cardiac intervention, they go.”
But some patients don’t want to go and would rather rely on what Dr. McMahon can achieve with his practice-honed diagnostic skills. He also uses relationships developed over the years with cardiologists, nephrologists, neurologists, and others in Roanoke—about 60 miles away—for telephone consultations on tough cases.
“This job requires much more clinical judgment than you would need in other settings where you can lean on other people or on the medical technology,” Dr. McMahon explains. “I have a good feel for where my own line is and for what this facility can handle.”
Dr. McMahon is part of a growing rural HM movement. According to a recent survey by the American Hospital Association, the number of rural hospitals with HM coverage is growing. One in 6 hospitals with fewer than 25 beds had HM programs in 2009, double the penetration of six years before. For hospitals with 25 to 49 beds, nearly 1 in 3 had a hospitalist presence in 2009—twice the number as in 2003.
—Brian Bossard, MD, FACP, FHM, director, Inpatient Physician Associates, Lincoln, Neb.
In addition to the lack of specialist backup, recruiting doctors to fill hospitalist positions in rural settings can be a major challenge. Other issues include staffing and scheduling, providing on-call and off-hours backup, and the economic stressors on small hospitals that constrain their ability to offer competitive compensation.
But rural hospitalists also emphasize the lifestyle benefits of calling a rural community home, such as the absence of crime, a slower pace, easy access to outdoor recreation, and the satisfying personal relationships that can develop in smaller communities.
“I like rural hospital medicine,” says Larry Labul, DO, FACOI, SFHM, a hospitalist at Franklin Memorial Hospital in Farmington, Maine, population 7,760. “I like being a big fish in a small pond, doing my own procedures, managing patients in the ICU. If I sometimes don’t know how to manage a procedure, I have a choice: Learn how to do it or send the patients somewhere else.”
Hospitalists in rural areas often become integral parts of their communities, says John Nelson, MD, MHM, medical director of the hospitalist program at Overlake Hospital in Bellevue, Wash., a Seattle suburb.
“There’s a reasonable chance you know your patients socially,” says Dr. Nelson, co-founder and past president of SHM and practice-management columnist for The Hospitalist. “I’ve been in the same place for 11 years, and if I have any connection with my patient, it’s a strange coincidence.”
Too often for urban hospitalists, he says, the next patient is just the next patient, whereas in a rural community, the odds are better than even that the doctor at least knows someone in the patient’s family. “That gives you a whole different perspective on the work.”
The Challenge: Recruitment
Despite the virtues of small towns for those who can appreciate them, rural hospitals face an uphill battle in attracting the desired complement of hospitalists to staff their programs. HM’s explosive growth means the field generally has benefited from a seller’s market, and rural communities have struggled to fill both inpatient and outpatient positions.
“Recruiting is tough in rural areas, even as some metro areas are starting to fill up with hospitalists,” Dr. Nelson says. Michael Manning, MD, a hospitalist at Murphy Medical Center in Murphy, the westernmost town in North Carolina (population 1,568), says it’s especially hard if the nearest airport is hours away. “A small hospital’s efforts to advertise just gets lost unless the candidate is actively looking for a rural setting to practice. Here we’ve got hunting and fishing. I came for the whitewater kayaking,” Dr. Manning says.
The challenge is to convince people who have never visited the area that a rural hospital is a great place to practice, says Brian Bossard, MD, FACP, FHM, director of Inpatient Physician Associates in Lincoln, Neb. “There are lots of barriers to address in order to negotiate a positive outcome. The more rural it is, the harder the job of recruiting. What more can we offer a recruit? Sometimes it’s money, a signing bonus, a benefit package. With many recruiting efforts, the spouse is part of the equation.”
Recruiting doctors to rural areas starts by leading with the hospital’s strengths, such as high-quality care, manageable workloads, or sustainable schedules, Dr. Bossard says. Recruiters also focus on the advantages of living and raising children away from the big city. International medical school graduates have long been a recruitment target of rural hospitals, but they present bureaucratic hoops that some hospitals are unwilling to jump through. (Visit the-hospitalist.org to learn why Foreign Medical Grads can bolster your HM group staffing.) Other hospitals employ recruiting staff, recruitment firms, paid advertising, and old-fashioned word of mouth—talking with anyone and everyone who might know a physician who could be interested.
Fannie Vavoulis, medical recruiter for Chatham-Kent Health Alliance in Chatham, Ontario, agrees that it can be difficult to recruit physicians to a setting like her predominantly agricultural community. But she has enjoyed recent success, in part due to the efforts of a 25-member community volunteer group of local business and health leaders who woo physician candidates. “We use the volunteers to show them around, help find opportunities for their spouses, and offering ongoing mentorship once they come here,” Vavoulis relates.
continued below...
A Little Like Home
Rapid City, S.D., with a population of 68,000, isn’t the most rural of settings, although Rapid City Regional Hospital (RCRH) also serves a large rural catchment area, with affiliated rural satellites. But the Black Hills are worlds away from places like Chicago or Dallas or New York City, where many future hospitalists do their residencies.
Pushpa Poudel, MD, came to 400-bed RCRH in 2010 following a residency at Wyckoff Heights Medical Center in Brooklyn, N.Y. “The people I met on my interview days were nice, but I was more attracted to the work environment and the dedication I found in the hospital here,” he says.
Dr. Poudel, who is from Nepal and attended medical school in Kathmandu, says the scenic Black Hills reminded him a little of home. After interviewing at RCRH, he went back to New York and talked two Nepalese physician friends into joining him there. Today, the multinational HM group at RCRH includes six hospitalists from Nepal, as well as others from India, Egypt, Costa Rica, and the Republic of Georgia. “We now have 28 hospitalists, and in the seven years since the program started, we’ve only lost one of them,” says Kristi Gylten, MBA, the service’s director.
All of the hospitalist group’s members meet candidates when they come for interviews. “They are the biggest sellers of the program,” Gylten says, although work-life balance, recreation in the Black Hills, and the reputation of the local school system are also draws. “Often the hardest part is just getting them to come out here. Once they come to Rapid City and see the community, it surprises them.”
—Larry Beresford
The Challenge: Expanded Scope
“This is a different brand of hospital medicine, with the potential for an expanded scope of practice,” says Dr. Bossard, whose group staffs hospitalist programs in Lincoln, Neb., and two rural communities in that state. “Physicians looking at your program need to understand that. Every hospital medicine program has its own identity and culture, but rural programs definitely have a culture of greater independence and autonomy.
“It’s a different breed of physician—a different culture and different standards of what hospitalists do and don’t do,” he explains.
Rural hospitalists often need to master procedures and medical specializations (including critical care) that many of their urban counterparts hand off to specialists. For conditions they can’t manage, the alternative is transferring the patient to a larger hospital, sometimes by ambulance or helicopter.
“Some physicians are uncomfortable with the level of expertise and procedural skills required to manage in this setting,” says Dr. Nelson, whose consulting firm regularly works with HM programs in rural areas. “But the hospital and the physician community are looking to the hospitalists as a resource to keep patients in the community as much as possible. If the hospitalists are too risk-averse, that may be a problem.”
—John Nelson, MD, MHM, hospitalist program medical director, Overlake Hospital, Bellevue, Wash., co-founder and past president of SHM
Dale Vizcarra, MD, a hospitalist at 60-bed St. Mary’s Healthcare Center in Pierre, S.D., has gotten used to not having on-site access to cardiology, anesthesiology, ENT, psychiatry, or pulmonology. “So you’re kind of piloting on your own,” she explains. “That could be hard for a new graduate who’s not used to flying solo.”
Dr. Vizcarra and a hospitalist partner navigate the lack of in-house specialist support by utilizing technology—for example, eICU-monitored beds or phoning physician colleagues in Sioux Falls. “The big question is, Do people know what they don’t know? It’s possible to be too quick—or not quick enough—to pick up the phone and ask for help,” she says.
Rural hospitals also face many of the same quality expectations and looming financial disincentives as their urban counterparts, but with fewer resources to devote to them. They conduct quality and safety projects and participate in SHM’s Project BOOST and similar quality initiatives. Three rural hospitals—Mariners Hospital in Tavernier, Fla., Miles Memorial Hospital in Damariscotta, Maine, and Sebasticook Valley Hospital in Palmyra, Maine—recently were named among the Leapfrog Group’s 65 top hospitals for 2011.1
A recent study by Karen Joynt, MD, MPH, of the Harvard School of Public Health and colleagues found that rural critical-access hospitals overall had fewer clinical capabilities, worse outcomes, and higher death rates for patients with heart attack, congestive heart failure, or pneumonia than their more urban counterparts.2 But Dr. Vizcarra says hospitalists can bring higher quality of care to rural hospitals.
“I also think staff satisfaction is better,” she says, adding that rural hospitals can try quality approaches tailored to the unique setting. “For example, because we have a lot of diabetic patients who are often noncompliant, we established a goal to have multiple members of our hospital team—from nurses to housekeeping—receive extra training in diabetes management and share it with patients. Sometimes it’s the person who hands out the food trays who has the best chance to reach the patient with this information.”
Dr. Vizcarra has lived in Pierre for 20 years and just became a hospitalist in April 2011. She loved primary care, but she says that “being a hospitalist in a clinical setting is a blast. There’s so much you can do—so many areas where you can improve care.”
The Challenge: Schedules
For a hospital to offer 24/7 hospitalist coverage on site, it generally requires at least three, if not four, full-time physicians dividing up days, nights, and weekends, allowing for vacations, sick days, and training time. Even so, a group of three or four hospitalists providing round-the-clock coverage is more likely to encounter some burnout than those programs that work seven-on/seven-off schedules. If the hospital is not able to afford four FTEs of salary—or to find physicians to fill those FTEs—it might decide that it doesn’t need hospitalists on site at night, Dr. Nelson says.
Alternatives include having the hospitalists take call from home, letting ED physicians do after-hours admits, or mobilizing community PCPs to divide up some of the coverage and call responsibility. Locums physicians are popular at rural hospitals, but they come at the expense of the personal relations and community integration that are counted among rural hospital medicine’s assets. Another approach, tried in some small hospitals where the caseload is insufficient to keep both a hospitalist and emergency doctor busy, is to combine the positions of ED doctor and hospitalist, then find physicians with the skills to fill both roles.
Increasingly, an alternative to supplementing hospitalists on the ground is telemedicine, which brings specialist expertise to rural hospitals long distance via telephone lines and video equipment. This concept may be more familiar in eICUs, but Atlanta-based Eagle Hospital Physicians also offers the services of hospitalists and neurologists via telemedicine links, says Richard Sanders, MPH, FACHE, the company’s director of telemedicine services. Specialists from Eagle’s pool of physicians serving hospitals across the Southeast work from wherever they have access to a telephone and Internet service.
“In order to address the issues rural hospitals and hospitalists face, we have to be innovative in our approach. Our hospital partners struggle with having patient volumes that require more hospitalists than they can recruit for, a problem exacerbated by the need for taking call at night, which can scare off some candidates,” Sanders says.
The peak time for telemedicine for the hospital that can manage partial on-site hospitalist coverage is the night shift—“typically the least productive time for hospitalists, with unpredictable volumes,” he says, “although you still need access to someone who can respond quickly.” Eagle also uses physician extenders as key members of its team and a video-equipped RP-7 robot that can move around the hospital as directed by the remote physician.
The Challenge: Extinction
Dr. McMahon, a Virginia native who practiced in the military after attending Medical College of Virginia, was recruited in 1980 by two residency colleagues who had secured jobs in Pearisburg, a small town in the western part of the state. “I’ve been here ever since,” he says. “I live and work with these people. I’m intimately involved in this community. I attend a lot of funerals. I’m the football team’s doctor, and I teach at the college of nursing.”
Dr. McMahon says that close-knit communities, such as Pearisburg, offer a different kind of medical care; he also says that kind of care is in danger of extinction. And he says something important will be lost if that happens.
Primary-care physicians (PCPs) help supplement the after-hours coverage provided by CGCH’s two staff hospitalists. “This is a community hospital, and we all work together,” Dr. McMahon says. “I know the family practice and internal medicine physicians and they know me.” But he also fears that this level of commitment may not continue much longer.
“We’re all aging in this community, and in another three to five years, the physicians are going to start to retire,” he says. “ … We’re a dying breed from the school of hard knocks and experience, and we’re being phased out in favor of technology-savvy younger doctors, for whom basic diagnostic skills are downplayed.
“There used to be more of a sense of camaraderie in medicine,” he notes. “Back in the day, when I first started here, we considered medicine a calling and not a job.”
For Dr. Vizcarra, the HM model of inpatient care represents a sea change in the connections between physicians and their patients.
“Now, in many small towns, you don’t see your doctor anymore when you’re in the hospital,” she says, adding disconnects can be magnified in small towns. “I try to compensate by providing patients with caring, compassionate, common-sense medicine when they are in the hospital. Usually, after the first day, it’s not an issue.”
Larry Beresford is a freelance writer in Oakland, Calif.
References
- The Leapfrog Group announces annual top hospitals list. The Leapfrog Group website. Available at: http://www.leapfroggroup.org/news/leapfrog_news/4810593. Accessed March 31, 2012.
- Joynt KE, Harris Y, Orav EJ, Jha AK. Quality of care and patient outcomes in critical access rural hospitals. JAMA. 2011;306(1):45-52.
ITL: Physician Reviews of HM-Relevant Research
In This Edition
Literature At A Glance
A guide to this month’s studies
- Nearly all CDIs Related to Exposure in Healthcare Setting
- In Suspected Acute Coronary Syndrome, CT Angiography Identifies Patients Safe for Discharge
- Impending Physiological Deterioration Can Be Predicted Using Data from a Comprehensive EHR
- Rapid Influenza Diagnostic Tests Have Low Sensitivity and High Specificity
- Multifaceted QI Intervention Increases Adherence to Evidence-Based Therapy in Acute Coronary Syndrome
- Rivaroxaban for the Treatment of Acute Pulmonary Embolism
- Coronary Stent Implantation Provides No Additional Benefit when Compared with Medical Therapy Alone in Patients with Stable Coronary Artery Disease
- Prolonged Versus Standard Duration Venous Thromboprophylaxis after Major Orthopedic Surgery
Nearly all CDIs Related to Exposure in Healthcare Setting
Clinical question: What is the contribution of non-hospital healthcare exposures to the burden of Clostridium difficile infection (CDI)?
Background: CDI is common among hospitalized patients and is associated with high rates of morbidity. Most CDI prevention programs are aimed at hospital-based risk factors. However, non-hospital healthcare exposures might contribute significantly to the burden of CDI, and hospital-based prevention programs might not address these risks.
Study design: Retrospective analysis of three population-based data sets.
Setting: Three population data sets tracking infections on a national and state level in the U.S.
Synopsis: This study analyzed two data sets to determine the contribution of non-hospital healthcare exposure to CDIs, and examined a third to determine whether a program addressing hospital-based exposures reduced the rate of CDI.Using data from the CDC’s Emerging Infections Program, 10,342 CDI cases from 111 hospitals were examined. Each case was classified as hospital onset (i.e. occurring three days after admission), nursing home onset, or community onset. A total of 94% of cases were associated with recent exposure to healthcare, 75% were classified as non-hospital onset, and 20% of hospital-onset cases were in patients who had recently been in a nursing home, suggesting that non-hospital-based healthcare exposures play a significant role. The second analysis used data from the National Healthcare Safety Network to examine 42,157 CDIs in 711 hospitals.
The authors found that 52% of CDIs were present on admission. The pooled rate of hospital-onset CDI was low (7.4 per 10,000 patient-days). The final analysis examined hospital-onset CDI rates across three hospital-based prevention programs over a period of nearly two years. The interventions were associated with a 20% decrease in CDI rates (to 7.5 from 9.3 per 10,000 patient days).
Bottom line: Nearly all CDIs are related to exposure in healthcare settings. Exposure to nursing home and ambulatory care seem to play a major role, and infection-control measures in addition to hospital-based strategies need to target these areas. Hospital-based interventions moderately decreased overall rates of CDI.
Citation: Centers for Disease Control and Prevention. Vital signs: preventing Clostridium difficile infections. MMWR Morb Mortal Wkly Rep. 2012;61:157-162.
In Suspected Acute Coronary Syndrome, CT Angiography Identifies Patients Safe for Discharge
Clinical question: Is a strategy utilizing CT angiography safe to allow discharge from the emergency department low- to intermediate-risk patients with possible acute coronary syndrome (ACS)?
Background: Admission rates for patients with possible acute coronary syndrome are high, but the majority of patients will not have cardiac causes of the symptoms. Coronary computed tomographic angiography (CCTA) has a high negative predictive value for the detection of coronary artery disease, but its utility in determining if a patient can be safely discharged from the emergency department has not been established.
Study design: Prospective, randomized, controlled, multicenter trial.
Setting: Five EDs in the U.S.; three included observation units.
Synopsis: The study enrolled 1,392 patients in a 2:1 ratio, with two-thirds undergoing CCTA and the other third treated with usual care (those admitted for possible ACS with a TIMI score of 0 to 2). Of 908 patients assigned to CCTA, 640 had a negative test, and none of them died or had a myocardial infarction within 30 days. Patients in the CCTA group were more likely than the group undergoing usual care to be discharged from the ED (49.6% vs. 22.7%), have a shorter length of stay (18 hours vs. 24.8 hours, P<.0001), and receive a coronary disease diagnosis.
Bottom line: In a randomized controlled trial, the use of CCTA to evaluate low- to intermediate-risk emergency department patients with possible ACS appears to be safe and effective, and leads to more discharges from the ED.
Citation: Litt HI, Gatsonis C, Snyder B, et al. CT angiography for safe discharge of patients with possible acute coronary syndromes. N Engl J Med. 2012;366:1393-1403.
Impending Physiological Deterioration Can Be Predicted Using Data from a Comprehensive EHR
Clinical question: Can impending physiological deterioration be predicted in medical-surgical ward patients using data from a comprehensive electronic health record (EHR)?
Background: Unplanned ICU transfer is associated with increased mortality and morbidity. Previous studies have examined physiological variables and track-and-trigger systems that might help in the identification of ward patients who are at risk for deterioration and transfer to a higher level of care. More hospitals across the U.S. are using EHRs, and eventually all hospitals are expected to be using one. However, it is unclear if an EHR-based model can accurately predict patients’ clinical deterioration.
Study design: Retrospective case-control study; the unit of analysis was the “patient shift,” each defined by a particular 12-hour period and patient. A complex model to predict patient deterioration and transfer to the ICU was developed and validated using EHR data that was available prior to the deterioration shift.
Setting: Fourteen hospitals of the Northern California Kaiser Permanente Medical Care Program (an integrated healthcare delivery system) that have used an operational EHR for at least three months.
Synopsis: The study identified 4,036 patient-shifts during which a transfer to the ICU occurred, and compared these with 39,782 patient-shifts during which no transfer occurred. Variables in the model included patient demographic data, diagnoses, comorbidities, lab results, and vital signs. The EHR-based predictive model performed well at predicting clinical deterioration and transfer to the ICU (derivation c-statistic 0.84, validation c-statistic 0.77). The model performed best among patients with gastrointestinal diseases (c-statistic 0.84) and worst in patients with acute myocardial infarction (c-statistic 0.57).
Bottom line: Impending physiologic deterioration can be predicted using EHR-based models.
Citation: Escobar GJ, Laguardia JC, Turk BJ, et al. Early detection of impending physiologic deterioration among patients who are not in intensive care: Development of predictive models using data from an automated electronic medical record. J Hosp Med. 2012:doi:10.1002/jhm.1929 [Epub ahead of print].
Rapid Influenza Diagnostic Tests Have Low Sensitivity and High Specificity
Clinical question: How accurate are rapid influenza diagnostic tests, and can they be used to guide further management?
Background: Three million to 5 million people a year develop influenza, which has a high mortality rate and potential global implications. The gold-standard diagnostic tests, PCR and viral culture, have a long turnaround time and are expensive. There have been limited systematic reviews addressing the accuracy of various rapid influenza diagnostic tests (RIDTs), especially in adults.
Study design: Systematic review and meta-analysis.
Setting: Varied.
Synopsis: Studies that compared commercial rapid influenza tests versus reference standards of PCR or viral culture were included. The 159 rapid tests were evaluated in 119 studies representing 26 different brands of commercial tests. Sixty-two of 119 studies included both adults and children, and 41 studies included children only. Overall, rapid influenza tests had a sensitivity of 62.3% and a specificity of 98.2%. There was a higher sensitivity for children than adults (67% vs. 54%) and a higher sensitivity for influenza A than influenza B (65% vs. 52%). The brand of rapid test made little difference. Most articles reviewed did not include a direct comparison between individual brands of RIDTs.
Bottom line: Rapid influenza diagnostic tests have low sensitivity and high specificity. A positive rapid test indicates likely influenza, but a negative test does not rule it out.
Citation: Chartrand C, Leeflang MM, Minion J, Brewer T, Pai M. Accuracy of rapid influenza diagnostic tests: a meta-analysis. Ann Intern Med. 2012;156:500-511.
Multifaceted QI Intervention Increases Adherence to Evidence-Based Therapy in Acute Coronary Syndrome
Clinical question: Does a multipronged approach to QI interventions improve the adherence to evidence-based therapies in acute coronary syndromes?
Background: Despite evidence-based recommendations for the use of antiplatelet medication, anticoagulants, beta-blockers, and statins in the setting of an acute coronary syndrome, adherence to these recommendations is poor, especially in low- to middle-income patients.
Study design: Cluster-randomized, prospective, blinded trial.
Setting: Thirty-six urban, public hospitals in Brazil.
Synopsis: Hospitals were randomly allocated to a multifaceted QI strategy versus routine practice. At each hospital, patients were enrolled in a consecutive manner when they presented to the emergency department with an acute coronary syndrome. The QI intervention included multiple modalities, including checklists in the ED, reminders, case management (by a trained RN) to ensure compliance, and educational materials to the staff (pocket algorithms and interactive web programs).
The primary endpoint was adherence to all available evidence-based therapies in the first 24 hours of management. Patients were more likely to receive all evidence-based therapies in hospitals that received the intervention (67.9% vs. 49.5%, P=0.01). The secondary endpoint (adherence at 24 hours and at discharge) was also significantly in favor of the intervention group (50.9% vs. 31.9%, P=0.03).
The findings might not be applicable to institutions with high adherence rates to evidence-based therapy.
Bottom line: A multifaceted QI intervention improves adherence to evidence-based therapies in urban hospitals in medium-income countries.
Citation: Berwanger O, Guimaraes HP, Lanranjeira LN, et al. Effect of a multifaceted intervention on use of evidence-based therapies in patients with acute coronary syndromes in Brazil: the BRIDGE-ACS randomized trial. JAMA. 2012 [Epub ahead of print].
Rivaroxaban for the Treatment of Acute Pulmonary Embolism
Clinical question: How does the efficacy and safety of rivaroxaban compare with low-molecular-weight heparin (LMWH) plus vitamin K antagonist (VKA) for treatment of acute pulmonary embolism (PE)?
Background: Data support the use of rivaroxaban for stroke prevention in atrial fibrillation, for VTE prophylaxis after orthopedic surgery, and for the treatment of acute coronary syndromes and acute deep vein thromboses. The EINSTEIN-PE investigators now study rivaroxaban for the treatment of acute symptomatic PE.
Study design: Randomized, open-label, noninferiority trial.
Setting: Two hundred sixty-three sites in 38 countries.
Synopsis: The investigators enrolled 4,832 patients with acute symptomatic PE (with or without DVT). Rivaroxaban alone was compared with standard therapy (enoxaparin followed by VKA to an international normalized ratio [INR] of 2 to 3) for three, six, or 12 months. The mean study duration was nine months. INR was in the therapeutic range 62.7% of the time.
The combined primary endpoint of fatal or nonfatal PE, or DVT, occurred in 2.1% in the rivaroxaban group and 1.8% in the standard-therapy group, meeting the pre-specified criteria for non-inferiority (HR 1.12; 95% CI: 0.75-1.68). There were no significant differences in the primary safety outcome of bleeding (HR, 0.90; 95% CI: 0.76-1.07). However, major bleeding events favored rivaroxaban, with events in 1.1% vs. 2.2% of those on VKA (HR 0.49, CI 0.31-0.79, P=0.003). Efficacy and safety of fixed-dose rivaroxaban did not vary by age, sex, weight, glomerular filtration rate, or extent of initial PE.
Bottom line: In patients with symptomatic acute PE, rivaroxaban is noninferior to standard treatment with LMWH plus VKA and might have a safety benefit of less major bleeding. Rivaroxaban and other new oral anticoagulants are likely to be used more frequently as more data is accumulated, but at this time, the guidelines continue to recommend VKA and LMWH as first-line agents.
Citation: The EINSTEIN-PE Investigators, Büller HR, Prins MH, et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med. 2012;366:1287-1297.
Coronary Stent Implantation Provides No Additional Benefit when Compared with Medical Therapy Alone in Patients with Stable Coronary Artery Disease
Clinical question: Does stent implantation lead to better outcomes when compared to medical therapy in patients with stable coronary artery disease (CAD)?
Background: It is unclear whether stent implantation improves outcomes any more than medical therapy in patients with stable CAD. This is a meta-analysis of trials comparing outcomes of coronary stent implantation with optimal medical therapy.
Study design: Meta-analysis of eight prospective randomized nonblinded trials comparing stent implantation plus medical therapy to medical therapy alone in patients with stable CAD. Outcomes of death, nonfatal myocardial infarction, unplanned revascularization, and persistent angina were compared between the two groups.
Setting: Varied.
Synopsis: Eight trials with 7,229 patients were included with an average follow-up of 4.3 years. In a pooled analysis, coronary stenting versus medical therapy was associated with similar risk of death (8.9% vs. 9.1% P=0.83); nonfatal myocardial infarction (8.9% vs. 8.1%, P=0.22); and persistent angina (29% vs. 33%, P=0.10). Coronary stenting was associated with decreased risk of unplanned revascularization, but the difference was not significant (21.4% vs. 30.7%, P=0.11).
Bottom line: In stable CAD, coronary stent implantation provides no additional benefit when compared to medical therapy.
Citation: Stergiopoulos K, Brown DL. Initial coronary stent implantation with medical therapy vs. medical therapy alone for stable coronary artery disease: meta-analysis of randomized controlled trials. Arch Intern Med. 2012;172:312-319.
Prolonged Versus Standard Duration Venous Thromboprophylaxis after Major Orthopedic Surgery
Clinical question: Should patients with hip or knee surgery receive venous thromboprophylaxis (VTE) prophylaxis for seven to 10 days post-operatively or for 21 days or more?
Background: Venous thromboembolism is the most frequent medical complication of knee and hip surgeries. Routine prophylaxis is recommended for minimum of seven to 10 days, but a longer duration might be more beneficial.
Study design: Systemic review and meta-analysis of eight randomized, controlled trials comparing different duration of VTE prophylaxis after hip fracture surgery and total hip or knee replacement.
Setting: Varied.
Synopsis: Eight trials with 2,917 patients met inclusion criteria. Pharmacological agents used for VTE prophylaxis in these trials were coumadin, enoxaparin, dalteparin, and fondaparinux. In patients with hip replacement, undergoing VTE prophylaxis for ≥21 days (compared with seven to 10 days) was associated with a decreased risk of pulmonary embolism (odds ratio [OR] 0.14, 95% CI 0.04-0.47), symptomatic DVTs (OR 0.36, 95% CI 0.16-0.81), asymptomatic DVTs (OR 0.48, 95% CI 0.31-0.75), and proximal DVTs (RR 0.29, CI 0.16-0.52). Prophylaxis for ≥21 days was also associated with an increased risk of minor bleeding (OR 7.55, 95% CI 1.51-37.64).
Data were not sufficient for evaluation of prolonged prophylaxis for total knee replacement and hip fracture surgery.
Bottom line: Prolonged prophylaxis is associated with fewer VTE events in patients with hip replacement but also carries increased risk of minor bleeding.
Citation: Sobieraj DM, Lee S, Coleman CI, et al. Prolonged versus standard-duration venous thromboprophylaxis in major orthopedic surgery: a systematic review. Ann Intern Med. 2012 May 15 [Epub ahead of print].
In This Edition
Literature At A Glance
A guide to this month’s studies
- Nearly all CDIs Related to Exposure in Healthcare Setting
- In Suspected Acute Coronary Syndrome, CT Angiography Identifies Patients Safe for Discharge
- Impending Physiological Deterioration Can Be Predicted Using Data from a Comprehensive EHR
- Rapid Influenza Diagnostic Tests Have Low Sensitivity and High Specificity
- Multifaceted QI Intervention Increases Adherence to Evidence-Based Therapy in Acute Coronary Syndrome
- Rivaroxaban for the Treatment of Acute Pulmonary Embolism
- Coronary Stent Implantation Provides No Additional Benefit when Compared with Medical Therapy Alone in Patients with Stable Coronary Artery Disease
- Prolonged Versus Standard Duration Venous Thromboprophylaxis after Major Orthopedic Surgery
Nearly all CDIs Related to Exposure in Healthcare Setting
Clinical question: What is the contribution of non-hospital healthcare exposures to the burden of Clostridium difficile infection (CDI)?
Background: CDI is common among hospitalized patients and is associated with high rates of morbidity. Most CDI prevention programs are aimed at hospital-based risk factors. However, non-hospital healthcare exposures might contribute significantly to the burden of CDI, and hospital-based prevention programs might not address these risks.
Study design: Retrospective analysis of three population-based data sets.
Setting: Three population data sets tracking infections on a national and state level in the U.S.
Synopsis: This study analyzed two data sets to determine the contribution of non-hospital healthcare exposure to CDIs, and examined a third to determine whether a program addressing hospital-based exposures reduced the rate of CDI.Using data from the CDC’s Emerging Infections Program, 10,342 CDI cases from 111 hospitals were examined. Each case was classified as hospital onset (i.e. occurring three days after admission), nursing home onset, or community onset. A total of 94% of cases were associated with recent exposure to healthcare, 75% were classified as non-hospital onset, and 20% of hospital-onset cases were in patients who had recently been in a nursing home, suggesting that non-hospital-based healthcare exposures play a significant role. The second analysis used data from the National Healthcare Safety Network to examine 42,157 CDIs in 711 hospitals.
The authors found that 52% of CDIs were present on admission. The pooled rate of hospital-onset CDI was low (7.4 per 10,000 patient-days). The final analysis examined hospital-onset CDI rates across three hospital-based prevention programs over a period of nearly two years. The interventions were associated with a 20% decrease in CDI rates (to 7.5 from 9.3 per 10,000 patient days).
Bottom line: Nearly all CDIs are related to exposure in healthcare settings. Exposure to nursing home and ambulatory care seem to play a major role, and infection-control measures in addition to hospital-based strategies need to target these areas. Hospital-based interventions moderately decreased overall rates of CDI.
Citation: Centers for Disease Control and Prevention. Vital signs: preventing Clostridium difficile infections. MMWR Morb Mortal Wkly Rep. 2012;61:157-162.
In Suspected Acute Coronary Syndrome, CT Angiography Identifies Patients Safe for Discharge
Clinical question: Is a strategy utilizing CT angiography safe to allow discharge from the emergency department low- to intermediate-risk patients with possible acute coronary syndrome (ACS)?
Background: Admission rates for patients with possible acute coronary syndrome are high, but the majority of patients will not have cardiac causes of the symptoms. Coronary computed tomographic angiography (CCTA) has a high negative predictive value for the detection of coronary artery disease, but its utility in determining if a patient can be safely discharged from the emergency department has not been established.
Study design: Prospective, randomized, controlled, multicenter trial.
Setting: Five EDs in the U.S.; three included observation units.
Synopsis: The study enrolled 1,392 patients in a 2:1 ratio, with two-thirds undergoing CCTA and the other third treated with usual care (those admitted for possible ACS with a TIMI score of 0 to 2). Of 908 patients assigned to CCTA, 640 had a negative test, and none of them died or had a myocardial infarction within 30 days. Patients in the CCTA group were more likely than the group undergoing usual care to be discharged from the ED (49.6% vs. 22.7%), have a shorter length of stay (18 hours vs. 24.8 hours, P<.0001), and receive a coronary disease diagnosis.
Bottom line: In a randomized controlled trial, the use of CCTA to evaluate low- to intermediate-risk emergency department patients with possible ACS appears to be safe and effective, and leads to more discharges from the ED.
Citation: Litt HI, Gatsonis C, Snyder B, et al. CT angiography for safe discharge of patients with possible acute coronary syndromes. N Engl J Med. 2012;366:1393-1403.
Impending Physiological Deterioration Can Be Predicted Using Data from a Comprehensive EHR
Clinical question: Can impending physiological deterioration be predicted in medical-surgical ward patients using data from a comprehensive electronic health record (EHR)?
Background: Unplanned ICU transfer is associated with increased mortality and morbidity. Previous studies have examined physiological variables and track-and-trigger systems that might help in the identification of ward patients who are at risk for deterioration and transfer to a higher level of care. More hospitals across the U.S. are using EHRs, and eventually all hospitals are expected to be using one. However, it is unclear if an EHR-based model can accurately predict patients’ clinical deterioration.
Study design: Retrospective case-control study; the unit of analysis was the “patient shift,” each defined by a particular 12-hour period and patient. A complex model to predict patient deterioration and transfer to the ICU was developed and validated using EHR data that was available prior to the deterioration shift.
Setting: Fourteen hospitals of the Northern California Kaiser Permanente Medical Care Program (an integrated healthcare delivery system) that have used an operational EHR for at least three months.
Synopsis: The study identified 4,036 patient-shifts during which a transfer to the ICU occurred, and compared these with 39,782 patient-shifts during which no transfer occurred. Variables in the model included patient demographic data, diagnoses, comorbidities, lab results, and vital signs. The EHR-based predictive model performed well at predicting clinical deterioration and transfer to the ICU (derivation c-statistic 0.84, validation c-statistic 0.77). The model performed best among patients with gastrointestinal diseases (c-statistic 0.84) and worst in patients with acute myocardial infarction (c-statistic 0.57).
Bottom line: Impending physiologic deterioration can be predicted using EHR-based models.
Citation: Escobar GJ, Laguardia JC, Turk BJ, et al. Early detection of impending physiologic deterioration among patients who are not in intensive care: Development of predictive models using data from an automated electronic medical record. J Hosp Med. 2012:doi:10.1002/jhm.1929 [Epub ahead of print].
Rapid Influenza Diagnostic Tests Have Low Sensitivity and High Specificity
Clinical question: How accurate are rapid influenza diagnostic tests, and can they be used to guide further management?
Background: Three million to 5 million people a year develop influenza, which has a high mortality rate and potential global implications. The gold-standard diagnostic tests, PCR and viral culture, have a long turnaround time and are expensive. There have been limited systematic reviews addressing the accuracy of various rapid influenza diagnostic tests (RIDTs), especially in adults.
Study design: Systematic review and meta-analysis.
Setting: Varied.
Synopsis: Studies that compared commercial rapid influenza tests versus reference standards of PCR or viral culture were included. The 159 rapid tests were evaluated in 119 studies representing 26 different brands of commercial tests. Sixty-two of 119 studies included both adults and children, and 41 studies included children only. Overall, rapid influenza tests had a sensitivity of 62.3% and a specificity of 98.2%. There was a higher sensitivity for children than adults (67% vs. 54%) and a higher sensitivity for influenza A than influenza B (65% vs. 52%). The brand of rapid test made little difference. Most articles reviewed did not include a direct comparison between individual brands of RIDTs.
Bottom line: Rapid influenza diagnostic tests have low sensitivity and high specificity. A positive rapid test indicates likely influenza, but a negative test does not rule it out.
Citation: Chartrand C, Leeflang MM, Minion J, Brewer T, Pai M. Accuracy of rapid influenza diagnostic tests: a meta-analysis. Ann Intern Med. 2012;156:500-511.
Multifaceted QI Intervention Increases Adherence to Evidence-Based Therapy in Acute Coronary Syndrome
Clinical question: Does a multipronged approach to QI interventions improve the adherence to evidence-based therapies in acute coronary syndromes?
Background: Despite evidence-based recommendations for the use of antiplatelet medication, anticoagulants, beta-blockers, and statins in the setting of an acute coronary syndrome, adherence to these recommendations is poor, especially in low- to middle-income patients.
Study design: Cluster-randomized, prospective, blinded trial.
Setting: Thirty-six urban, public hospitals in Brazil.
Synopsis: Hospitals were randomly allocated to a multifaceted QI strategy versus routine practice. At each hospital, patients were enrolled in a consecutive manner when they presented to the emergency department with an acute coronary syndrome. The QI intervention included multiple modalities, including checklists in the ED, reminders, case management (by a trained RN) to ensure compliance, and educational materials to the staff (pocket algorithms and interactive web programs).
The primary endpoint was adherence to all available evidence-based therapies in the first 24 hours of management. Patients were more likely to receive all evidence-based therapies in hospitals that received the intervention (67.9% vs. 49.5%, P=0.01). The secondary endpoint (adherence at 24 hours and at discharge) was also significantly in favor of the intervention group (50.9% vs. 31.9%, P=0.03).
The findings might not be applicable to institutions with high adherence rates to evidence-based therapy.
Bottom line: A multifaceted QI intervention improves adherence to evidence-based therapies in urban hospitals in medium-income countries.
Citation: Berwanger O, Guimaraes HP, Lanranjeira LN, et al. Effect of a multifaceted intervention on use of evidence-based therapies in patients with acute coronary syndromes in Brazil: the BRIDGE-ACS randomized trial. JAMA. 2012 [Epub ahead of print].
Rivaroxaban for the Treatment of Acute Pulmonary Embolism
Clinical question: How does the efficacy and safety of rivaroxaban compare with low-molecular-weight heparin (LMWH) plus vitamin K antagonist (VKA) for treatment of acute pulmonary embolism (PE)?
Background: Data support the use of rivaroxaban for stroke prevention in atrial fibrillation, for VTE prophylaxis after orthopedic surgery, and for the treatment of acute coronary syndromes and acute deep vein thromboses. The EINSTEIN-PE investigators now study rivaroxaban for the treatment of acute symptomatic PE.
Study design: Randomized, open-label, noninferiority trial.
Setting: Two hundred sixty-three sites in 38 countries.
Synopsis: The investigators enrolled 4,832 patients with acute symptomatic PE (with or without DVT). Rivaroxaban alone was compared with standard therapy (enoxaparin followed by VKA to an international normalized ratio [INR] of 2 to 3) for three, six, or 12 months. The mean study duration was nine months. INR was in the therapeutic range 62.7% of the time.
The combined primary endpoint of fatal or nonfatal PE, or DVT, occurred in 2.1% in the rivaroxaban group and 1.8% in the standard-therapy group, meeting the pre-specified criteria for non-inferiority (HR 1.12; 95% CI: 0.75-1.68). There were no significant differences in the primary safety outcome of bleeding (HR, 0.90; 95% CI: 0.76-1.07). However, major bleeding events favored rivaroxaban, with events in 1.1% vs. 2.2% of those on VKA (HR 0.49, CI 0.31-0.79, P=0.003). Efficacy and safety of fixed-dose rivaroxaban did not vary by age, sex, weight, glomerular filtration rate, or extent of initial PE.
Bottom line: In patients with symptomatic acute PE, rivaroxaban is noninferior to standard treatment with LMWH plus VKA and might have a safety benefit of less major bleeding. Rivaroxaban and other new oral anticoagulants are likely to be used more frequently as more data is accumulated, but at this time, the guidelines continue to recommend VKA and LMWH as first-line agents.
Citation: The EINSTEIN-PE Investigators, Büller HR, Prins MH, et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med. 2012;366:1287-1297.
Coronary Stent Implantation Provides No Additional Benefit when Compared with Medical Therapy Alone in Patients with Stable Coronary Artery Disease
Clinical question: Does stent implantation lead to better outcomes when compared to medical therapy in patients with stable coronary artery disease (CAD)?
Background: It is unclear whether stent implantation improves outcomes any more than medical therapy in patients with stable CAD. This is a meta-analysis of trials comparing outcomes of coronary stent implantation with optimal medical therapy.
Study design: Meta-analysis of eight prospective randomized nonblinded trials comparing stent implantation plus medical therapy to medical therapy alone in patients with stable CAD. Outcomes of death, nonfatal myocardial infarction, unplanned revascularization, and persistent angina were compared between the two groups.
Setting: Varied.
Synopsis: Eight trials with 7,229 patients were included with an average follow-up of 4.3 years. In a pooled analysis, coronary stenting versus medical therapy was associated with similar risk of death (8.9% vs. 9.1% P=0.83); nonfatal myocardial infarction (8.9% vs. 8.1%, P=0.22); and persistent angina (29% vs. 33%, P=0.10). Coronary stenting was associated with decreased risk of unplanned revascularization, but the difference was not significant (21.4% vs. 30.7%, P=0.11).
Bottom line: In stable CAD, coronary stent implantation provides no additional benefit when compared to medical therapy.
Citation: Stergiopoulos K, Brown DL. Initial coronary stent implantation with medical therapy vs. medical therapy alone for stable coronary artery disease: meta-analysis of randomized controlled trials. Arch Intern Med. 2012;172:312-319.
Prolonged Versus Standard Duration Venous Thromboprophylaxis after Major Orthopedic Surgery
Clinical question: Should patients with hip or knee surgery receive venous thromboprophylaxis (VTE) prophylaxis for seven to 10 days post-operatively or for 21 days or more?
Background: Venous thromboembolism is the most frequent medical complication of knee and hip surgeries. Routine prophylaxis is recommended for minimum of seven to 10 days, but a longer duration might be more beneficial.
Study design: Systemic review and meta-analysis of eight randomized, controlled trials comparing different duration of VTE prophylaxis after hip fracture surgery and total hip or knee replacement.
Setting: Varied.
Synopsis: Eight trials with 2,917 patients met inclusion criteria. Pharmacological agents used for VTE prophylaxis in these trials were coumadin, enoxaparin, dalteparin, and fondaparinux. In patients with hip replacement, undergoing VTE prophylaxis for ≥21 days (compared with seven to 10 days) was associated with a decreased risk of pulmonary embolism (odds ratio [OR] 0.14, 95% CI 0.04-0.47), symptomatic DVTs (OR 0.36, 95% CI 0.16-0.81), asymptomatic DVTs (OR 0.48, 95% CI 0.31-0.75), and proximal DVTs (RR 0.29, CI 0.16-0.52). Prophylaxis for ≥21 days was also associated with an increased risk of minor bleeding (OR 7.55, 95% CI 1.51-37.64).
Data were not sufficient for evaluation of prolonged prophylaxis for total knee replacement and hip fracture surgery.
Bottom line: Prolonged prophylaxis is associated with fewer VTE events in patients with hip replacement but also carries increased risk of minor bleeding.
Citation: Sobieraj DM, Lee S, Coleman CI, et al. Prolonged versus standard-duration venous thromboprophylaxis in major orthopedic surgery: a systematic review. Ann Intern Med. 2012 May 15 [Epub ahead of print].
In This Edition
Literature At A Glance
A guide to this month’s studies
- Nearly all CDIs Related to Exposure in Healthcare Setting
- In Suspected Acute Coronary Syndrome, CT Angiography Identifies Patients Safe for Discharge
- Impending Physiological Deterioration Can Be Predicted Using Data from a Comprehensive EHR
- Rapid Influenza Diagnostic Tests Have Low Sensitivity and High Specificity
- Multifaceted QI Intervention Increases Adherence to Evidence-Based Therapy in Acute Coronary Syndrome
- Rivaroxaban for the Treatment of Acute Pulmonary Embolism
- Coronary Stent Implantation Provides No Additional Benefit when Compared with Medical Therapy Alone in Patients with Stable Coronary Artery Disease
- Prolonged Versus Standard Duration Venous Thromboprophylaxis after Major Orthopedic Surgery
Nearly all CDIs Related to Exposure in Healthcare Setting
Clinical question: What is the contribution of non-hospital healthcare exposures to the burden of Clostridium difficile infection (CDI)?
Background: CDI is common among hospitalized patients and is associated with high rates of morbidity. Most CDI prevention programs are aimed at hospital-based risk factors. However, non-hospital healthcare exposures might contribute significantly to the burden of CDI, and hospital-based prevention programs might not address these risks.
Study design: Retrospective analysis of three population-based data sets.
Setting: Three population data sets tracking infections on a national and state level in the U.S.
Synopsis: This study analyzed two data sets to determine the contribution of non-hospital healthcare exposure to CDIs, and examined a third to determine whether a program addressing hospital-based exposures reduced the rate of CDI.Using data from the CDC’s Emerging Infections Program, 10,342 CDI cases from 111 hospitals were examined. Each case was classified as hospital onset (i.e. occurring three days after admission), nursing home onset, or community onset. A total of 94% of cases were associated with recent exposure to healthcare, 75% were classified as non-hospital onset, and 20% of hospital-onset cases were in patients who had recently been in a nursing home, suggesting that non-hospital-based healthcare exposures play a significant role. The second analysis used data from the National Healthcare Safety Network to examine 42,157 CDIs in 711 hospitals.
The authors found that 52% of CDIs were present on admission. The pooled rate of hospital-onset CDI was low (7.4 per 10,000 patient-days). The final analysis examined hospital-onset CDI rates across three hospital-based prevention programs over a period of nearly two years. The interventions were associated with a 20% decrease in CDI rates (to 7.5 from 9.3 per 10,000 patient days).
Bottom line: Nearly all CDIs are related to exposure in healthcare settings. Exposure to nursing home and ambulatory care seem to play a major role, and infection-control measures in addition to hospital-based strategies need to target these areas. Hospital-based interventions moderately decreased overall rates of CDI.
Citation: Centers for Disease Control and Prevention. Vital signs: preventing Clostridium difficile infections. MMWR Morb Mortal Wkly Rep. 2012;61:157-162.
In Suspected Acute Coronary Syndrome, CT Angiography Identifies Patients Safe for Discharge
Clinical question: Is a strategy utilizing CT angiography safe to allow discharge from the emergency department low- to intermediate-risk patients with possible acute coronary syndrome (ACS)?
Background: Admission rates for patients with possible acute coronary syndrome are high, but the majority of patients will not have cardiac causes of the symptoms. Coronary computed tomographic angiography (CCTA) has a high negative predictive value for the detection of coronary artery disease, but its utility in determining if a patient can be safely discharged from the emergency department has not been established.
Study design: Prospective, randomized, controlled, multicenter trial.
Setting: Five EDs in the U.S.; three included observation units.
Synopsis: The study enrolled 1,392 patients in a 2:1 ratio, with two-thirds undergoing CCTA and the other third treated with usual care (those admitted for possible ACS with a TIMI score of 0 to 2). Of 908 patients assigned to CCTA, 640 had a negative test, and none of them died or had a myocardial infarction within 30 days. Patients in the CCTA group were more likely than the group undergoing usual care to be discharged from the ED (49.6% vs. 22.7%), have a shorter length of stay (18 hours vs. 24.8 hours, P<.0001), and receive a coronary disease diagnosis.
Bottom line: In a randomized controlled trial, the use of CCTA to evaluate low- to intermediate-risk emergency department patients with possible ACS appears to be safe and effective, and leads to more discharges from the ED.
Citation: Litt HI, Gatsonis C, Snyder B, et al. CT angiography for safe discharge of patients with possible acute coronary syndromes. N Engl J Med. 2012;366:1393-1403.
Impending Physiological Deterioration Can Be Predicted Using Data from a Comprehensive EHR
Clinical question: Can impending physiological deterioration be predicted in medical-surgical ward patients using data from a comprehensive electronic health record (EHR)?
Background: Unplanned ICU transfer is associated with increased mortality and morbidity. Previous studies have examined physiological variables and track-and-trigger systems that might help in the identification of ward patients who are at risk for deterioration and transfer to a higher level of care. More hospitals across the U.S. are using EHRs, and eventually all hospitals are expected to be using one. However, it is unclear if an EHR-based model can accurately predict patients’ clinical deterioration.
Study design: Retrospective case-control study; the unit of analysis was the “patient shift,” each defined by a particular 12-hour period and patient. A complex model to predict patient deterioration and transfer to the ICU was developed and validated using EHR data that was available prior to the deterioration shift.
Setting: Fourteen hospitals of the Northern California Kaiser Permanente Medical Care Program (an integrated healthcare delivery system) that have used an operational EHR for at least three months.
Synopsis: The study identified 4,036 patient-shifts during which a transfer to the ICU occurred, and compared these with 39,782 patient-shifts during which no transfer occurred. Variables in the model included patient demographic data, diagnoses, comorbidities, lab results, and vital signs. The EHR-based predictive model performed well at predicting clinical deterioration and transfer to the ICU (derivation c-statistic 0.84, validation c-statistic 0.77). The model performed best among patients with gastrointestinal diseases (c-statistic 0.84) and worst in patients with acute myocardial infarction (c-statistic 0.57).
Bottom line: Impending physiologic deterioration can be predicted using EHR-based models.
Citation: Escobar GJ, Laguardia JC, Turk BJ, et al. Early detection of impending physiologic deterioration among patients who are not in intensive care: Development of predictive models using data from an automated electronic medical record. J Hosp Med. 2012:doi:10.1002/jhm.1929 [Epub ahead of print].
Rapid Influenza Diagnostic Tests Have Low Sensitivity and High Specificity
Clinical question: How accurate are rapid influenza diagnostic tests, and can they be used to guide further management?
Background: Three million to 5 million people a year develop influenza, which has a high mortality rate and potential global implications. The gold-standard diagnostic tests, PCR and viral culture, have a long turnaround time and are expensive. There have been limited systematic reviews addressing the accuracy of various rapid influenza diagnostic tests (RIDTs), especially in adults.
Study design: Systematic review and meta-analysis.
Setting: Varied.
Synopsis: Studies that compared commercial rapid influenza tests versus reference standards of PCR or viral culture were included. The 159 rapid tests were evaluated in 119 studies representing 26 different brands of commercial tests. Sixty-two of 119 studies included both adults and children, and 41 studies included children only. Overall, rapid influenza tests had a sensitivity of 62.3% and a specificity of 98.2%. There was a higher sensitivity for children than adults (67% vs. 54%) and a higher sensitivity for influenza A than influenza B (65% vs. 52%). The brand of rapid test made little difference. Most articles reviewed did not include a direct comparison between individual brands of RIDTs.
Bottom line: Rapid influenza diagnostic tests have low sensitivity and high specificity. A positive rapid test indicates likely influenza, but a negative test does not rule it out.
Citation: Chartrand C, Leeflang MM, Minion J, Brewer T, Pai M. Accuracy of rapid influenza diagnostic tests: a meta-analysis. Ann Intern Med. 2012;156:500-511.
Multifaceted QI Intervention Increases Adherence to Evidence-Based Therapy in Acute Coronary Syndrome
Clinical question: Does a multipronged approach to QI interventions improve the adherence to evidence-based therapies in acute coronary syndromes?
Background: Despite evidence-based recommendations for the use of antiplatelet medication, anticoagulants, beta-blockers, and statins in the setting of an acute coronary syndrome, adherence to these recommendations is poor, especially in low- to middle-income patients.
Study design: Cluster-randomized, prospective, blinded trial.
Setting: Thirty-six urban, public hospitals in Brazil.
Synopsis: Hospitals were randomly allocated to a multifaceted QI strategy versus routine practice. At each hospital, patients were enrolled in a consecutive manner when they presented to the emergency department with an acute coronary syndrome. The QI intervention included multiple modalities, including checklists in the ED, reminders, case management (by a trained RN) to ensure compliance, and educational materials to the staff (pocket algorithms and interactive web programs).
The primary endpoint was adherence to all available evidence-based therapies in the first 24 hours of management. Patients were more likely to receive all evidence-based therapies in hospitals that received the intervention (67.9% vs. 49.5%, P=0.01). The secondary endpoint (adherence at 24 hours and at discharge) was also significantly in favor of the intervention group (50.9% vs. 31.9%, P=0.03).
The findings might not be applicable to institutions with high adherence rates to evidence-based therapy.
Bottom line: A multifaceted QI intervention improves adherence to evidence-based therapies in urban hospitals in medium-income countries.
Citation: Berwanger O, Guimaraes HP, Lanranjeira LN, et al. Effect of a multifaceted intervention on use of evidence-based therapies in patients with acute coronary syndromes in Brazil: the BRIDGE-ACS randomized trial. JAMA. 2012 [Epub ahead of print].
Rivaroxaban for the Treatment of Acute Pulmonary Embolism
Clinical question: How does the efficacy and safety of rivaroxaban compare with low-molecular-weight heparin (LMWH) plus vitamin K antagonist (VKA) for treatment of acute pulmonary embolism (PE)?
Background: Data support the use of rivaroxaban for stroke prevention in atrial fibrillation, for VTE prophylaxis after orthopedic surgery, and for the treatment of acute coronary syndromes and acute deep vein thromboses. The EINSTEIN-PE investigators now study rivaroxaban for the treatment of acute symptomatic PE.
Study design: Randomized, open-label, noninferiority trial.
Setting: Two hundred sixty-three sites in 38 countries.
Synopsis: The investigators enrolled 4,832 patients with acute symptomatic PE (with or without DVT). Rivaroxaban alone was compared with standard therapy (enoxaparin followed by VKA to an international normalized ratio [INR] of 2 to 3) for three, six, or 12 months. The mean study duration was nine months. INR was in the therapeutic range 62.7% of the time.
The combined primary endpoint of fatal or nonfatal PE, or DVT, occurred in 2.1% in the rivaroxaban group and 1.8% in the standard-therapy group, meeting the pre-specified criteria for non-inferiority (HR 1.12; 95% CI: 0.75-1.68). There were no significant differences in the primary safety outcome of bleeding (HR, 0.90; 95% CI: 0.76-1.07). However, major bleeding events favored rivaroxaban, with events in 1.1% vs. 2.2% of those on VKA (HR 0.49, CI 0.31-0.79, P=0.003). Efficacy and safety of fixed-dose rivaroxaban did not vary by age, sex, weight, glomerular filtration rate, or extent of initial PE.
Bottom line: In patients with symptomatic acute PE, rivaroxaban is noninferior to standard treatment with LMWH plus VKA and might have a safety benefit of less major bleeding. Rivaroxaban and other new oral anticoagulants are likely to be used more frequently as more data is accumulated, but at this time, the guidelines continue to recommend VKA and LMWH as first-line agents.
Citation: The EINSTEIN-PE Investigators, Büller HR, Prins MH, et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med. 2012;366:1287-1297.
Coronary Stent Implantation Provides No Additional Benefit when Compared with Medical Therapy Alone in Patients with Stable Coronary Artery Disease
Clinical question: Does stent implantation lead to better outcomes when compared to medical therapy in patients with stable coronary artery disease (CAD)?
Background: It is unclear whether stent implantation improves outcomes any more than medical therapy in patients with stable CAD. This is a meta-analysis of trials comparing outcomes of coronary stent implantation with optimal medical therapy.
Study design: Meta-analysis of eight prospective randomized nonblinded trials comparing stent implantation plus medical therapy to medical therapy alone in patients with stable CAD. Outcomes of death, nonfatal myocardial infarction, unplanned revascularization, and persistent angina were compared between the two groups.
Setting: Varied.
Synopsis: Eight trials with 7,229 patients were included with an average follow-up of 4.3 years. In a pooled analysis, coronary stenting versus medical therapy was associated with similar risk of death (8.9% vs. 9.1% P=0.83); nonfatal myocardial infarction (8.9% vs. 8.1%, P=0.22); and persistent angina (29% vs. 33%, P=0.10). Coronary stenting was associated with decreased risk of unplanned revascularization, but the difference was not significant (21.4% vs. 30.7%, P=0.11).
Bottom line: In stable CAD, coronary stent implantation provides no additional benefit when compared to medical therapy.
Citation: Stergiopoulos K, Brown DL. Initial coronary stent implantation with medical therapy vs. medical therapy alone for stable coronary artery disease: meta-analysis of randomized controlled trials. Arch Intern Med. 2012;172:312-319.
Prolonged Versus Standard Duration Venous Thromboprophylaxis after Major Orthopedic Surgery
Clinical question: Should patients with hip or knee surgery receive venous thromboprophylaxis (VTE) prophylaxis for seven to 10 days post-operatively or for 21 days or more?
Background: Venous thromboembolism is the most frequent medical complication of knee and hip surgeries. Routine prophylaxis is recommended for minimum of seven to 10 days, but a longer duration might be more beneficial.
Study design: Systemic review and meta-analysis of eight randomized, controlled trials comparing different duration of VTE prophylaxis after hip fracture surgery and total hip or knee replacement.
Setting: Varied.
Synopsis: Eight trials with 2,917 patients met inclusion criteria. Pharmacological agents used for VTE prophylaxis in these trials were coumadin, enoxaparin, dalteparin, and fondaparinux. In patients with hip replacement, undergoing VTE prophylaxis for ≥21 days (compared with seven to 10 days) was associated with a decreased risk of pulmonary embolism (odds ratio [OR] 0.14, 95% CI 0.04-0.47), symptomatic DVTs (OR 0.36, 95% CI 0.16-0.81), asymptomatic DVTs (OR 0.48, 95% CI 0.31-0.75), and proximal DVTs (RR 0.29, CI 0.16-0.52). Prophylaxis for ≥21 days was also associated with an increased risk of minor bleeding (OR 7.55, 95% CI 1.51-37.64).
Data were not sufficient for evaluation of prolonged prophylaxis for total knee replacement and hip fracture surgery.
Bottom line: Prolonged prophylaxis is associated with fewer VTE events in patients with hip replacement but also carries increased risk of minor bleeding.
Citation: Sobieraj DM, Lee S, Coleman CI, et al. Prolonged versus standard-duration venous thromboprophylaxis in major orthopedic surgery: a systematic review. Ann Intern Med. 2012 May 15 [Epub ahead of print].
How is Graves' Disease Diagnosed and Evaluated?
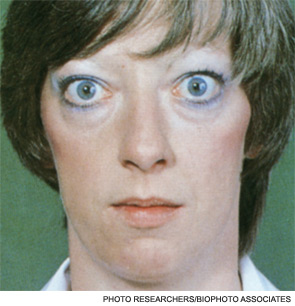
Case
A 25-year-old, previously healthy woman presents with one month of anxiety, palpitations, intermittent loose non-dysenteriform stools, fine tremors, and hair loss. She has had a 20-pound weight loss in the previous four months, even though she reports an increased appetite. Her heart rate ranges from 115 to 130 beats per minute, and her temperature is 37.5oC. An exam is notable for mild bilateral proptosis, thin hair, and moist skin. A goiter is visible; it has increased consistency on palpation with an audible bruit over it. She has hyperreflexia and fine tremors. An EKG reveals sinus tachycardia. How should this patient be evaluated? What treatment should be initiated?
Overview
Graves’ disease, the most common cause of hyperthyroidism, is caused by autoimmune stimulation of the thyrotropin (TSH) receptor. It generally presents with a variety of signs and symptoms found with hyperthyroidism, but it can also carry unique clinical features unrelated to thyrotoxicosis, such as ophthalmopathy and dermopathy.
Graves’ disease diagnosis mainly is clinical, but also is supported by elevated free levels of thyroid hormones (mainly triiodothyronine [T3]) and suppressed TSH levels. Anti-thyrotropin receptor antibodies generally are present. Imaging in Graves’ disease is characterized by increased radioiodine uptake, as well as increased perfusion by Doppler ultrasonography.
Treatment can be pharmacologic, using anti-thyroid drugs, or ablative, with either radioiodine or thyroidectomy. Adjunctive therapy includes symptom control with beta-blocker agents, as well as steroid supplementation, especially in patients with orbitopathy undergoing radioablative treatment.
The Data
Epidemiology. Graves’ disease is the most common cause of hyperthyroidism, with a prevalence of ~0.5% of the population. Women are most commonly affected, with a prevalence five to 10 times higher than in male peers. The most common age of presentation is between the fifth and sixth decades of life.1-3
The fact that Graves’ disease occurs with higher incidence in patients with a family history of thyroid disease—and that concordance rates of up to 35% are seen with monozygotic twins—suggests that both genetic and environmental factors influence disease susceptibility.2,4
Pathophysiology. Graves’ disease occurs as a result of direct activation of the G-protein-coupled adenylate cyclase in the thyrotropin receptor by circulating IgG antibodies.2,3 Follicular hypertrophy and hyperplasia, and increased vascularity, cause goiter formation and an increased production of T3 and thyroxine (T4). The increase in T3 and T4 subsequently suppress TSH production.
Graves’ disease also is associated with unique clinical manifestations unrelated to the circulating levels of thyroid hormones, such as Graves’ ophthalmopathy and infiltrative dermopathy (localized or pretibial myxedema). Both of these occur as a result of local tissue infiltration by inflammatory cells and deposition of glycosaminglycanes.5
Clinical manifestations. Graves’ disease is characterized by a constellation of clinical findings and patient symptoms (see Table 1).1-3 The clinical presentation could differ in elderly patients, who present more commonly with weight loss or depression (also known as apathetic hyperthyroidism) and less commonly with tachycardia and tremor.2,3

Although clinically apparent, exophtalmos is detected in 30% to 50% of patients; when using orbital imaging, it is identified in ≥80% of patients.5 Ophthalmopathy has a clinical course typically independent of the thyroid activity; its manifestations include proptosis, periorbital edema and inflammation, exposure keratitis, photophobia, extraocular muscle infiltration, and eyelid lag.5-8
Thyroid dermopathy (localized dermal myxedema) can occur in 0.5% to 4.3% of patients with Graves’ disease; it occurs most commonly among patients with Graves’ ophthalmopathy, in whom it occurs in up to 13% of cases. About 20% of patients with dermal myxedema have associated thyroid acropachy.3,9

Hospitalists should be aware of thyroid storm. Although rare, occurring in only 1% to 2% of patients with hyperthyroidism, it can be a medical emergency. It is generally manifested by fever (due to severe thermogenesis), atrial tachyarrhythmias (due to hyperadrenergic response), mental status changes, and liver dysfunction.
In addition, patients with thyroid storm might present with hyperglycemia, hypercalcemia, hypocortisolism, and hypokalemia.10 Thyroid storm requires prompt treatment of both the clinical manifestations and the underlying condition.
Differential Diagnosis from Other Causes of Thyroiditis
Laboratory. The classic presentation of Graves’ disease is a suppressed TSH and elevated serum T3 and T4 levels.1-3 Generally, T3 is higher than T4, which also occurs in toxic multinodular goiter, solitary hyperfunctioning nodule, and iodine-induced hyperthyroidism.2,6 The free T3 and T4 levels should be obtained, as these are useful for monitoring response to therapy.1-3
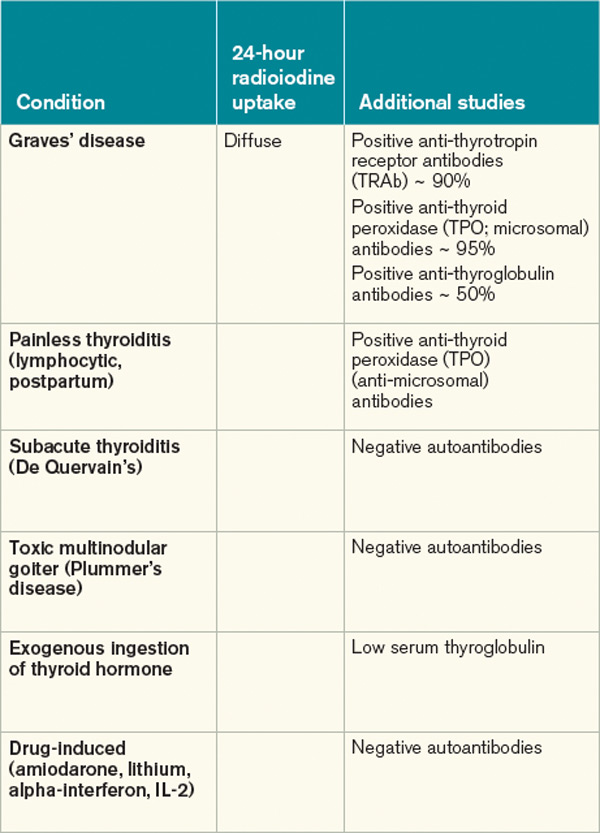
Most patients with Graves’ disease also have anti-thyroid antibodies (see Table 2), although these are not required for the diagnosis.1-3,11
Following initiation of treatment, TSH levels remain suppressed for approximately two to three months, even after free T3 and T4 levels return to normal or below normal. After this period of suppression is over, TSH levels can be used to adjust therapy.1-3
Imaging. A thyroid radioiodine-uptake study provides a measure of iodine uptake, as well as an image of functioning thyroid tissue; the imaging is done 24 hours after the intake of iodine-123 or iodine-131. Generalized increased uptake is characteristic of Graves’ disease.1-3,12 In comparison, patients with thyroiditis have decreased radioiodine uptake as well as low blood flow in Doppler ultrasonography.13
In patients with large goiters, when there are signs or symptoms of upper airway or thoracic outlet obstruction, imaging with a neck and upper-chest CT scan is recommended.2 In patients with unilateral proptosis, asymmetric ophthalmopathy, or visual loss, orbital imaging is advised (CT scan or MRI).2,5 In patients with tachyarrhythmias, an electrocardiogram should evaluate for the presence of atrial fibrillation.2 Table 2 illustrates how Graves’ disease can be distinguished from other causes of thyroiditis.1-3
Initial Treatment
Treatment of Graves’ disease has two main tenets: treating the underlying thyroid disorder and quickly controlling symptoms. The underlying thyroid disorder can be treated with such anti-thyroid drugs as thionamides (methimazole or propylthiouracil), ablative radioiodine, or surgical excision of the thyroid. Adjunct symptom therapy can include beta-blockers, organic iodide, and glucocorticoids.11,14 Thionamides are preferred in young patients, pregnant women, and cases with orbital involvement.14
In pregnancy, treatment with propylthiouracil is preferred, especially during the first two trimesters due to the risk of teratogenicity with methimazole (there have been associated case reports of choanal atresia, aplasia cutis, and facial malformations).15
Steroid prophylaxis is used in patients with prominent ocular symptoms who undergo radioiodine ablation to minimize risk of worsening of ophthalmopathy.16
Back to the Case
The patient was admitted; free T3 and T4 levels were elevated, TSH was suppressed, and anti-thyroid antibodies (anti-TPO, anti-TG, and anti-TRAb) were positive. An I-123 radioiodine uptake scan showed diffuse thyroid gland uptake. Beta-blockers were initiated for heart-rate control (atenolol 25 mg) with adequate response.
Given the patient’s young age, it was decided to initiate thionamides. A pregnancy test was negative, so methimazole was initiated at a dose of 10 mg orally once daily.
Dr. Auron is a hospitalist in the Department of Hospital Medicine and the Center for Pediatric Hospital Medicine at Cleveland Clinic. Dr. Hamilton is a hospitalist in the Department of Hospital Medicine at Cleveland Clinic.
References
- Baskin HJ, Cobin RH, Duick DS, et al. American Association of Clinical Endocrinologists medical guidelines for clinical practice for the evaluation and treatment of hyperthyroidism and hypothyroidism. (2006 Amended version). Endocr Pract. 2002;8:457-469.
- Brent GA. Clinical practice. Graves’ disease. N Engl J Med. 2008;358:2594-2605.
- Nayak B, Hodak SP. Hyperthyroidism. Endocrinol Metab Clin North Am. 2007;36:617-656.
- Manji N, Carr-Smith JD, Boelaert K, et al. Influences of age, gender, smoking, and family history on autoimmune thyroid disease phenotype. J Clin Endocrinol Metab. 2006;91:4873-4880.
- Bahn RS. Graves’ ophthalmopathy. N Engl J Med. 2010;362:726-738.
- Woeber KA. Triiodothyronine production in Graves’ hyperthyroidism. Thyroid. 2006;16:687-690.
- Osman F, Franklyn JA, Holder RL, Sheppard MC, Gammage MD. Cardiovascular manifestations of hyperthyroidism before and after antithyroid therapy: a matched case-control study. J Am Coll Cardiol. 2007;49:71-81.
- Wiersinga WM, Bartalena L. Epidemiology and prevention of Graves’ ophthalmopathy. Thyroid. 2002;12:855-860.
- Fatourechi V. Pretibial myxedema: pathophysiology and treatment options. Am J Clin Dermatol. 2005;6:295-309.
- Chong HW, See KC, Phua J. Thyroid storm with multiorgan failure. Thyroid. 2010;20:333-336.
- De Groot L. Diagnosis and treatment of Graves’ disease. Thyroid Disease Manager website. Available at: http://www.thyroidmanager.org/chapter/diagnosis-and-treatment-of-graves-disease/. Accessed Jan. 20, 2012.
- Cappelli C, Pirola I, De Martino E, et al. The role of imaging in Graves’ disease: a cost-effectiveness analysis. Eur J Radiol. 2008;65:99-103.
- Ota H, Amino N, Morita S, et al. Quantitative measurement of thyroid blood flow for differentiation of painless thyroiditis from Graves’ disease. Clin Endocrinol (Oxf). 2007;67:41-45.
- Fumarola A, Di Fiore A, Dainelli M, Grani G, Calvanese A. Medical treatment of hyperthyroidism: state of the art. Exp Clin Endocrinol Diabetes. 2010;118:678-684.
- Fitzpatrick DL, Russell MA. Diagnosis and management of thyroid disease in pregnancy. Obstet Gynecol Clin North Am. 2010;37:173-193.
- Bartalena L. The dilemma of how to manage Graves’ hyperthyroidism in patients with associated orbitopathy. J Clin Endocrinol Metab. 2011;96:592-599.
Case
A 25-year-old, previously healthy woman presents with one month of anxiety, palpitations, intermittent loose non-dysenteriform stools, fine tremors, and hair loss. She has had a 20-pound weight loss in the previous four months, even though she reports an increased appetite. Her heart rate ranges from 115 to 130 beats per minute, and her temperature is 37.5oC. An exam is notable for mild bilateral proptosis, thin hair, and moist skin. A goiter is visible; it has increased consistency on palpation with an audible bruit over it. She has hyperreflexia and fine tremors. An EKG reveals sinus tachycardia. How should this patient be evaluated? What treatment should be initiated?
Overview
Graves’ disease, the most common cause of hyperthyroidism, is caused by autoimmune stimulation of the thyrotropin (TSH) receptor. It generally presents with a variety of signs and symptoms found with hyperthyroidism, but it can also carry unique clinical features unrelated to thyrotoxicosis, such as ophthalmopathy and dermopathy.
Graves’ disease diagnosis mainly is clinical, but also is supported by elevated free levels of thyroid hormones (mainly triiodothyronine [T3]) and suppressed TSH levels. Anti-thyrotropin receptor antibodies generally are present. Imaging in Graves’ disease is characterized by increased radioiodine uptake, as well as increased perfusion by Doppler ultrasonography.
Treatment can be pharmacologic, using anti-thyroid drugs, or ablative, with either radioiodine or thyroidectomy. Adjunctive therapy includes symptom control with beta-blocker agents, as well as steroid supplementation, especially in patients with orbitopathy undergoing radioablative treatment.
The Data
Epidemiology. Graves’ disease is the most common cause of hyperthyroidism, with a prevalence of ~0.5% of the population. Women are most commonly affected, with a prevalence five to 10 times higher than in male peers. The most common age of presentation is between the fifth and sixth decades of life.1-3
The fact that Graves’ disease occurs with higher incidence in patients with a family history of thyroid disease—and that concordance rates of up to 35% are seen with monozygotic twins—suggests that both genetic and environmental factors influence disease susceptibility.2,4
Pathophysiology. Graves’ disease occurs as a result of direct activation of the G-protein-coupled adenylate cyclase in the thyrotropin receptor by circulating IgG antibodies.2,3 Follicular hypertrophy and hyperplasia, and increased vascularity, cause goiter formation and an increased production of T3 and thyroxine (T4). The increase in T3 and T4 subsequently suppress TSH production.
Graves’ disease also is associated with unique clinical manifestations unrelated to the circulating levels of thyroid hormones, such as Graves’ ophthalmopathy and infiltrative dermopathy (localized or pretibial myxedema). Both of these occur as a result of local tissue infiltration by inflammatory cells and deposition of glycosaminglycanes.5
Clinical manifestations. Graves’ disease is characterized by a constellation of clinical findings and patient symptoms (see Table 1).1-3 The clinical presentation could differ in elderly patients, who present more commonly with weight loss or depression (also known as apathetic hyperthyroidism) and less commonly with tachycardia and tremor.2,3
Although clinically apparent, exophtalmos is detected in 30% to 50% of patients; when using orbital imaging, it is identified in ≥80% of patients.5 Ophthalmopathy has a clinical course typically independent of the thyroid activity; its manifestations include proptosis, periorbital edema and inflammation, exposure keratitis, photophobia, extraocular muscle infiltration, and eyelid lag.5-8
Thyroid dermopathy (localized dermal myxedema) can occur in 0.5% to 4.3% of patients with Graves’ disease; it occurs most commonly among patients with Graves’ ophthalmopathy, in whom it occurs in up to 13% of cases. About 20% of patients with dermal myxedema have associated thyroid acropachy.3,9
Hospitalists should be aware of thyroid storm. Although rare, occurring in only 1% to 2% of patients with hyperthyroidism, it can be a medical emergency. It is generally manifested by fever (due to severe thermogenesis), atrial tachyarrhythmias (due to hyperadrenergic response), mental status changes, and liver dysfunction.
In addition, patients with thyroid storm might present with hyperglycemia, hypercalcemia, hypocortisolism, and hypokalemia.10 Thyroid storm requires prompt treatment of both the clinical manifestations and the underlying condition.
Differential Diagnosis from Other Causes of Thyroiditis
Laboratory. The classic presentation of Graves’ disease is a suppressed TSH and elevated serum T3 and T4 levels.1-3 Generally, T3 is higher than T4, which also occurs in toxic multinodular goiter, solitary hyperfunctioning nodule, and iodine-induced hyperthyroidism.2,6 The free T3 and T4 levels should be obtained, as these are useful for monitoring response to therapy.1-3
Most patients with Graves’ disease also have anti-thyroid antibodies (see Table 2), although these are not required for the diagnosis.1-3,11
Following initiation of treatment, TSH levels remain suppressed for approximately two to three months, even after free T3 and T4 levels return to normal or below normal. After this period of suppression is over, TSH levels can be used to adjust therapy.1-3
Imaging. A thyroid radioiodine-uptake study provides a measure of iodine uptake, as well as an image of functioning thyroid tissue; the imaging is done 24 hours after the intake of iodine-123 or iodine-131. Generalized increased uptake is characteristic of Graves’ disease.1-3,12 In comparison, patients with thyroiditis have decreased radioiodine uptake as well as low blood flow in Doppler ultrasonography.13
In patients with large goiters, when there are signs or symptoms of upper airway or thoracic outlet obstruction, imaging with a neck and upper-chest CT scan is recommended.2 In patients with unilateral proptosis, asymmetric ophthalmopathy, or visual loss, orbital imaging is advised (CT scan or MRI).2,5 In patients with tachyarrhythmias, an electrocardiogram should evaluate for the presence of atrial fibrillation.2 Table 2 illustrates how Graves’ disease can be distinguished from other causes of thyroiditis.1-3
Initial Treatment
Treatment of Graves’ disease has two main tenets: treating the underlying thyroid disorder and quickly controlling symptoms. The underlying thyroid disorder can be treated with such anti-thyroid drugs as thionamides (methimazole or propylthiouracil), ablative radioiodine, or surgical excision of the thyroid. Adjunct symptom therapy can include beta-blockers, organic iodide, and glucocorticoids.11,14 Thionamides are preferred in young patients, pregnant women, and cases with orbital involvement.14
In pregnancy, treatment with propylthiouracil is preferred, especially during the first two trimesters due to the risk of teratogenicity with methimazole (there have been associated case reports of choanal atresia, aplasia cutis, and facial malformations).15
Steroid prophylaxis is used in patients with prominent ocular symptoms who undergo radioiodine ablation to minimize risk of worsening of ophthalmopathy.16
Back to the Case
The patient was admitted; free T3 and T4 levels were elevated, TSH was suppressed, and anti-thyroid antibodies (anti-TPO, anti-TG, and anti-TRAb) were positive. An I-123 radioiodine uptake scan showed diffuse thyroid gland uptake. Beta-blockers were initiated for heart-rate control (atenolol 25 mg) with adequate response.
Given the patient’s young age, it was decided to initiate thionamides. A pregnancy test was negative, so methimazole was initiated at a dose of 10 mg orally once daily.
Dr. Auron is a hospitalist in the Department of Hospital Medicine and the Center for Pediatric Hospital Medicine at Cleveland Clinic. Dr. Hamilton is a hospitalist in the Department of Hospital Medicine at Cleveland Clinic.
References
- Baskin HJ, Cobin RH, Duick DS, et al. American Association of Clinical Endocrinologists medical guidelines for clinical practice for the evaluation and treatment of hyperthyroidism and hypothyroidism. (2006 Amended version). Endocr Pract. 2002;8:457-469.
- Brent GA. Clinical practice. Graves’ disease. N Engl J Med. 2008;358:2594-2605.
- Nayak B, Hodak SP. Hyperthyroidism. Endocrinol Metab Clin North Am. 2007;36:617-656.
- Manji N, Carr-Smith JD, Boelaert K, et al. Influences of age, gender, smoking, and family history on autoimmune thyroid disease phenotype. J Clin Endocrinol Metab. 2006;91:4873-4880.
- Bahn RS. Graves’ ophthalmopathy. N Engl J Med. 2010;362:726-738.
- Woeber KA. Triiodothyronine production in Graves’ hyperthyroidism. Thyroid. 2006;16:687-690.
- Osman F, Franklyn JA, Holder RL, Sheppard MC, Gammage MD. Cardiovascular manifestations of hyperthyroidism before and after antithyroid therapy: a matched case-control study. J Am Coll Cardiol. 2007;49:71-81.
- Wiersinga WM, Bartalena L. Epidemiology and prevention of Graves’ ophthalmopathy. Thyroid. 2002;12:855-860.
- Fatourechi V. Pretibial myxedema: pathophysiology and treatment options. Am J Clin Dermatol. 2005;6:295-309.
- Chong HW, See KC, Phua J. Thyroid storm with multiorgan failure. Thyroid. 2010;20:333-336.
- De Groot L. Diagnosis and treatment of Graves’ disease. Thyroid Disease Manager website. Available at: http://www.thyroidmanager.org/chapter/diagnosis-and-treatment-of-graves-disease/. Accessed Jan. 20, 2012.
- Cappelli C, Pirola I, De Martino E, et al. The role of imaging in Graves’ disease: a cost-effectiveness analysis. Eur J Radiol. 2008;65:99-103.
- Ota H, Amino N, Morita S, et al. Quantitative measurement of thyroid blood flow for differentiation of painless thyroiditis from Graves’ disease. Clin Endocrinol (Oxf). 2007;67:41-45.
- Fumarola A, Di Fiore A, Dainelli M, Grani G, Calvanese A. Medical treatment of hyperthyroidism: state of the art. Exp Clin Endocrinol Diabetes. 2010;118:678-684.
- Fitzpatrick DL, Russell MA. Diagnosis and management of thyroid disease in pregnancy. Obstet Gynecol Clin North Am. 2010;37:173-193.
- Bartalena L. The dilemma of how to manage Graves’ hyperthyroidism in patients with associated orbitopathy. J Clin Endocrinol Metab. 2011;96:592-599.
Case
A 25-year-old, previously healthy woman presents with one month of anxiety, palpitations, intermittent loose non-dysenteriform stools, fine tremors, and hair loss. She has had a 20-pound weight loss in the previous four months, even though she reports an increased appetite. Her heart rate ranges from 115 to 130 beats per minute, and her temperature is 37.5oC. An exam is notable for mild bilateral proptosis, thin hair, and moist skin. A goiter is visible; it has increased consistency on palpation with an audible bruit over it. She has hyperreflexia and fine tremors. An EKG reveals sinus tachycardia. How should this patient be evaluated? What treatment should be initiated?
Overview
Graves’ disease, the most common cause of hyperthyroidism, is caused by autoimmune stimulation of the thyrotropin (TSH) receptor. It generally presents with a variety of signs and symptoms found with hyperthyroidism, but it can also carry unique clinical features unrelated to thyrotoxicosis, such as ophthalmopathy and dermopathy.
Graves’ disease diagnosis mainly is clinical, but also is supported by elevated free levels of thyroid hormones (mainly triiodothyronine [T3]) and suppressed TSH levels. Anti-thyrotropin receptor antibodies generally are present. Imaging in Graves’ disease is characterized by increased radioiodine uptake, as well as increased perfusion by Doppler ultrasonography.
Treatment can be pharmacologic, using anti-thyroid drugs, or ablative, with either radioiodine or thyroidectomy. Adjunctive therapy includes symptom control with beta-blocker agents, as well as steroid supplementation, especially in patients with orbitopathy undergoing radioablative treatment.
The Data
Epidemiology. Graves’ disease is the most common cause of hyperthyroidism, with a prevalence of ~0.5% of the population. Women are most commonly affected, with a prevalence five to 10 times higher than in male peers. The most common age of presentation is between the fifth and sixth decades of life.1-3
The fact that Graves’ disease occurs with higher incidence in patients with a family history of thyroid disease—and that concordance rates of up to 35% are seen with monozygotic twins—suggests that both genetic and environmental factors influence disease susceptibility.2,4
Pathophysiology. Graves’ disease occurs as a result of direct activation of the G-protein-coupled adenylate cyclase in the thyrotropin receptor by circulating IgG antibodies.2,3 Follicular hypertrophy and hyperplasia, and increased vascularity, cause goiter formation and an increased production of T3 and thyroxine (T4). The increase in T3 and T4 subsequently suppress TSH production.
Graves’ disease also is associated with unique clinical manifestations unrelated to the circulating levels of thyroid hormones, such as Graves’ ophthalmopathy and infiltrative dermopathy (localized or pretibial myxedema). Both of these occur as a result of local tissue infiltration by inflammatory cells and deposition of glycosaminglycanes.5
Clinical manifestations. Graves’ disease is characterized by a constellation of clinical findings and patient symptoms (see Table 1).1-3 The clinical presentation could differ in elderly patients, who present more commonly with weight loss or depression (also known as apathetic hyperthyroidism) and less commonly with tachycardia and tremor.2,3
Although clinically apparent, exophtalmos is detected in 30% to 50% of patients; when using orbital imaging, it is identified in ≥80% of patients.5 Ophthalmopathy has a clinical course typically independent of the thyroid activity; its manifestations include proptosis, periorbital edema and inflammation, exposure keratitis, photophobia, extraocular muscle infiltration, and eyelid lag.5-8
Thyroid dermopathy (localized dermal myxedema) can occur in 0.5% to 4.3% of patients with Graves’ disease; it occurs most commonly among patients with Graves’ ophthalmopathy, in whom it occurs in up to 13% of cases. About 20% of patients with dermal myxedema have associated thyroid acropachy.3,9
Hospitalists should be aware of thyroid storm. Although rare, occurring in only 1% to 2% of patients with hyperthyroidism, it can be a medical emergency. It is generally manifested by fever (due to severe thermogenesis), atrial tachyarrhythmias (due to hyperadrenergic response), mental status changes, and liver dysfunction.
In addition, patients with thyroid storm might present with hyperglycemia, hypercalcemia, hypocortisolism, and hypokalemia.10 Thyroid storm requires prompt treatment of both the clinical manifestations and the underlying condition.
Differential Diagnosis from Other Causes of Thyroiditis
Laboratory. The classic presentation of Graves’ disease is a suppressed TSH and elevated serum T3 and T4 levels.1-3 Generally, T3 is higher than T4, which also occurs in toxic multinodular goiter, solitary hyperfunctioning nodule, and iodine-induced hyperthyroidism.2,6 The free T3 and T4 levels should be obtained, as these are useful for monitoring response to therapy.1-3
Most patients with Graves’ disease also have anti-thyroid antibodies (see Table 2), although these are not required for the diagnosis.1-3,11
Following initiation of treatment, TSH levels remain suppressed for approximately two to three months, even after free T3 and T4 levels return to normal or below normal. After this period of suppression is over, TSH levels can be used to adjust therapy.1-3
Imaging. A thyroid radioiodine-uptake study provides a measure of iodine uptake, as well as an image of functioning thyroid tissue; the imaging is done 24 hours after the intake of iodine-123 or iodine-131. Generalized increased uptake is characteristic of Graves’ disease.1-3,12 In comparison, patients with thyroiditis have decreased radioiodine uptake as well as low blood flow in Doppler ultrasonography.13
In patients with large goiters, when there are signs or symptoms of upper airway or thoracic outlet obstruction, imaging with a neck and upper-chest CT scan is recommended.2 In patients with unilateral proptosis, asymmetric ophthalmopathy, or visual loss, orbital imaging is advised (CT scan or MRI).2,5 In patients with tachyarrhythmias, an electrocardiogram should evaluate for the presence of atrial fibrillation.2 Table 2 illustrates how Graves’ disease can be distinguished from other causes of thyroiditis.1-3
Initial Treatment
Treatment of Graves’ disease has two main tenets: treating the underlying thyroid disorder and quickly controlling symptoms. The underlying thyroid disorder can be treated with such anti-thyroid drugs as thionamides (methimazole or propylthiouracil), ablative radioiodine, or surgical excision of the thyroid. Adjunct symptom therapy can include beta-blockers, organic iodide, and glucocorticoids.11,14 Thionamides are preferred in young patients, pregnant women, and cases with orbital involvement.14
In pregnancy, treatment with propylthiouracil is preferred, especially during the first two trimesters due to the risk of teratogenicity with methimazole (there have been associated case reports of choanal atresia, aplasia cutis, and facial malformations).15
Steroid prophylaxis is used in patients with prominent ocular symptoms who undergo radioiodine ablation to minimize risk of worsening of ophthalmopathy.16
Back to the Case
The patient was admitted; free T3 and T4 levels were elevated, TSH was suppressed, and anti-thyroid antibodies (anti-TPO, anti-TG, and anti-TRAb) were positive. An I-123 radioiodine uptake scan showed diffuse thyroid gland uptake. Beta-blockers were initiated for heart-rate control (atenolol 25 mg) with adequate response.
Given the patient’s young age, it was decided to initiate thionamides. A pregnancy test was negative, so methimazole was initiated at a dose of 10 mg orally once daily.
Dr. Auron is a hospitalist in the Department of Hospital Medicine and the Center for Pediatric Hospital Medicine at Cleveland Clinic. Dr. Hamilton is a hospitalist in the Department of Hospital Medicine at Cleveland Clinic.
References
- Baskin HJ, Cobin RH, Duick DS, et al. American Association of Clinical Endocrinologists medical guidelines for clinical practice for the evaluation and treatment of hyperthyroidism and hypothyroidism. (2006 Amended version). Endocr Pract. 2002;8:457-469.
- Brent GA. Clinical practice. Graves’ disease. N Engl J Med. 2008;358:2594-2605.
- Nayak B, Hodak SP. Hyperthyroidism. Endocrinol Metab Clin North Am. 2007;36:617-656.
- Manji N, Carr-Smith JD, Boelaert K, et al. Influences of age, gender, smoking, and family history on autoimmune thyroid disease phenotype. J Clin Endocrinol Metab. 2006;91:4873-4880.
- Bahn RS. Graves’ ophthalmopathy. N Engl J Med. 2010;362:726-738.
- Woeber KA. Triiodothyronine production in Graves’ hyperthyroidism. Thyroid. 2006;16:687-690.
- Osman F, Franklyn JA, Holder RL, Sheppard MC, Gammage MD. Cardiovascular manifestations of hyperthyroidism before and after antithyroid therapy: a matched case-control study. J Am Coll Cardiol. 2007;49:71-81.
- Wiersinga WM, Bartalena L. Epidemiology and prevention of Graves’ ophthalmopathy. Thyroid. 2002;12:855-860.
- Fatourechi V. Pretibial myxedema: pathophysiology and treatment options. Am J Clin Dermatol. 2005;6:295-309.
- Chong HW, See KC, Phua J. Thyroid storm with multiorgan failure. Thyroid. 2010;20:333-336.
- De Groot L. Diagnosis and treatment of Graves’ disease. Thyroid Disease Manager website. Available at: http://www.thyroidmanager.org/chapter/diagnosis-and-treatment-of-graves-disease/. Accessed Jan. 20, 2012.
- Cappelli C, Pirola I, De Martino E, et al. The role of imaging in Graves’ disease: a cost-effectiveness analysis. Eur J Radiol. 2008;65:99-103.
- Ota H, Amino N, Morita S, et al. Quantitative measurement of thyroid blood flow for differentiation of painless thyroiditis from Graves’ disease. Clin Endocrinol (Oxf). 2007;67:41-45.
- Fumarola A, Di Fiore A, Dainelli M, Grani G, Calvanese A. Medical treatment of hyperthyroidism: state of the art. Exp Clin Endocrinol Diabetes. 2010;118:678-684.
- Fitzpatrick DL, Russell MA. Diagnosis and management of thyroid disease in pregnancy. Obstet Gynecol Clin North Am. 2010;37:173-193.
- Bartalena L. The dilemma of how to manage Graves’ hyperthyroidism in patients with associated orbitopathy. J Clin Endocrinol Metab. 2011;96:592-599.
Hospitalists On the Move

Hospitalist Martha Buckley, MD, was named the 2011 Gordon B. Snider, MD, Physician Teammate of the Year among her peers at Fairfield Medical Center (FMC) in Lancaster, Ohio. Dr. Buckley has been a hospitalist at FMC for two years as part of Colonnade Medical Group, also based in Lancaster.

Hospitalist Scott Stuart, MD, has assumed the role of medical director for the PCU and care management at Evergreen Hospital in Kirkland, Wash. Dr. Stuart has worked for Evergreen as an internal-medicine hospitalist since 2005, and previously served as the managing physician and medical director of the hospitalist group from 2007 to 2010. He began his new roles earlier this month and continues as a hospitalist at Evergreen on a part-time basis.
Hospitalist Brian Clonts, MD, was honored with the Medical Innovator Award at the inaugural Champions of Health Care awards ceremony by the Branson/Lakes Area Chamber of Commerce. Dr. Clonts has worked at Skaggs Regional Medical Center in Branson, Mo., since 2008. He is the medical director for the Skaggs Hospitalist Department and the Skaggs Stroke Program, serves on several committees, and serves as a physician in the U.S. Air Force Reserves.
Marc B. Westle, DO, FACP, FHM, has been appointed senior vice president of innovation at Mission Health in Asheville, N.C. A board-certified internist, Dr. Westle is charged with exploring “new options to improve delivery of healthcare” and moving Mission Health to an “outcome- accountable, risk-bearing capable organization” to serve western North Carolina, according to a release.

Hospitalist Rashid Ehsan, MD, has been named the 2011 Physician of the Year at Culpeper Regional Hospital in Culpeper, Va. Dr. Ehsan is chair of the Department of Medicine and a member of the hospital’s Medical Executive and CME committees. According to a release, he was honored for his professionalism, compassion, and popularity with patients, nurses, and support staff.
Marvin Trotter, MD, an ED doctor and hospitalist at Ukiah Valley (Calif.) Medical Center, has been named chief medical officer. Dr. Trotter will be a member of the executive team and will represent the medical staff in areas of vision, quality, and growth. He will continue to serve as a hospitalist for inpatient care. A graduate of the University of Texas Southwestern Medical School, Dr. Trotter is board-certified in internal medicine and has been a member of the Ukiah Valley team since 1986.
Hospitalist Martha Buckley, MD, was named the 2011 Gordon B. Snider, MD, Physician Teammate of the Year among her peers at Fairfield Medical Center (FMC) in Lancaster, Ohio. Dr. Buckley has been a hospitalist at FMC for two years as part of Colonnade Medical Group, also based in Lancaster.
Hospitalist Scott Stuart, MD, has assumed the role of medical director for the PCU and care management at Evergreen Hospital in Kirkland, Wash. Dr. Stuart has worked for Evergreen as an internal-medicine hospitalist since 2005, and previously served as the managing physician and medical director of the hospitalist group from 2007 to 2010. He began his new roles earlier this month and continues as a hospitalist at Evergreen on a part-time basis.
Hospitalist Brian Clonts, MD, was honored with the Medical Innovator Award at the inaugural Champions of Health Care awards ceremony by the Branson/Lakes Area Chamber of Commerce. Dr. Clonts has worked at Skaggs Regional Medical Center in Branson, Mo., since 2008. He is the medical director for the Skaggs Hospitalist Department and the Skaggs Stroke Program, serves on several committees, and serves as a physician in the U.S. Air Force Reserves.
Marc B. Westle, DO, FACP, FHM, has been appointed senior vice president of innovation at Mission Health in Asheville, N.C. A board-certified internist, Dr. Westle is charged with exploring “new options to improve delivery of healthcare” and moving Mission Health to an “outcome- accountable, risk-bearing capable organization” to serve western North Carolina, according to a release.
Hospitalist Rashid Ehsan, MD, has been named the 2011 Physician of the Year at Culpeper Regional Hospital in Culpeper, Va. Dr. Ehsan is chair of the Department of Medicine and a member of the hospital’s Medical Executive and CME committees. According to a release, he was honored for his professionalism, compassion, and popularity with patients, nurses, and support staff.
Marvin Trotter, MD, an ED doctor and hospitalist at Ukiah Valley (Calif.) Medical Center, has been named chief medical officer. Dr. Trotter will be a member of the executive team and will represent the medical staff in areas of vision, quality, and growth. He will continue to serve as a hospitalist for inpatient care. A graduate of the University of Texas Southwestern Medical School, Dr. Trotter is board-certified in internal medicine and has been a member of the Ukiah Valley team since 1986.
Hospitalist Martha Buckley, MD, was named the 2011 Gordon B. Snider, MD, Physician Teammate of the Year among her peers at Fairfield Medical Center (FMC) in Lancaster, Ohio. Dr. Buckley has been a hospitalist at FMC for two years as part of Colonnade Medical Group, also based in Lancaster.
Hospitalist Scott Stuart, MD, has assumed the role of medical director for the PCU and care management at Evergreen Hospital in Kirkland, Wash. Dr. Stuart has worked for Evergreen as an internal-medicine hospitalist since 2005, and previously served as the managing physician and medical director of the hospitalist group from 2007 to 2010. He began his new roles earlier this month and continues as a hospitalist at Evergreen on a part-time basis.
Hospitalist Brian Clonts, MD, was honored with the Medical Innovator Award at the inaugural Champions of Health Care awards ceremony by the Branson/Lakes Area Chamber of Commerce. Dr. Clonts has worked at Skaggs Regional Medical Center in Branson, Mo., since 2008. He is the medical director for the Skaggs Hospitalist Department and the Skaggs Stroke Program, serves on several committees, and serves as a physician in the U.S. Air Force Reserves.
Marc B. Westle, DO, FACP, FHM, has been appointed senior vice president of innovation at Mission Health in Asheville, N.C. A board-certified internist, Dr. Westle is charged with exploring “new options to improve delivery of healthcare” and moving Mission Health to an “outcome- accountable, risk-bearing capable organization” to serve western North Carolina, according to a release.
Hospitalist Rashid Ehsan, MD, has been named the 2011 Physician of the Year at Culpeper Regional Hospital in Culpeper, Va. Dr. Ehsan is chair of the Department of Medicine and a member of the hospital’s Medical Executive and CME committees. According to a release, he was honored for his professionalism, compassion, and popularity with patients, nurses, and support staff.
Marvin Trotter, MD, an ED doctor and hospitalist at Ukiah Valley (Calif.) Medical Center, has been named chief medical officer. Dr. Trotter will be a member of the executive team and will represent the medical staff in areas of vision, quality, and growth. He will continue to serve as a hospitalist for inpatient care. A graduate of the University of Texas Southwestern Medical School, Dr. Trotter is board-certified in internal medicine and has been a member of the Ukiah Valley team since 1986.
SHM's Leadership Academy: Everything They Don't Teach in Medical School
Hospital medicine groups continue to grow and thrive across the country. And as they do, HM groups need experienced leaders to drive them toward continued success.
After all, the skills needed to lead hospitalist groups rarely are taught in medical school. And before employers—or potential employers—elevate hospitalists to senior positions, they need to be assured that their up-and-coming leaders can meet the challenge.
SHM’s specialty-leading Leadership Academy gives employers the confidence they want and new leaders the skill sets they need. The academy’s three courses comprise the only leadership-training program specifically designed for the challenges hospitalists face.
In the past, SHM has presented the Leadership Academy twice a year—once in the spring and once in fall. Now, SHM offers Leadership Academy once a year in the fall.
This year, hospitalists attending the Leadership Academy can take advantage of the majestic setting of the Hyatt Regency Scottsdale Resort and Spa at Gainey Ranch in Arizona, a 27-acre hotel-resort near the scenic McDowell Mountains.
The 2012 Leadership Academy will feature the entry-level course “Foundations of Leadership,” which helps hospitalists begin their leadership journey, and “Advanced Leadership: Strategies and Tools for Personal Leadership Excellence,” which enables hospitalists who have taken “Foundations of Leadership” to use their own personal leadership styles to drive culture change in their organizations.
Brendon Shank is SHM’s associate vice president of communications.
Hospital medicine groups continue to grow and thrive across the country. And as they do, HM groups need experienced leaders to drive them toward continued success.
After all, the skills needed to lead hospitalist groups rarely are taught in medical school. And before employers—or potential employers—elevate hospitalists to senior positions, they need to be assured that their up-and-coming leaders can meet the challenge.
SHM’s specialty-leading Leadership Academy gives employers the confidence they want and new leaders the skill sets they need. The academy’s three courses comprise the only leadership-training program specifically designed for the challenges hospitalists face.
In the past, SHM has presented the Leadership Academy twice a year—once in the spring and once in fall. Now, SHM offers Leadership Academy once a year in the fall.
This year, hospitalists attending the Leadership Academy can take advantage of the majestic setting of the Hyatt Regency Scottsdale Resort and Spa at Gainey Ranch in Arizona, a 27-acre hotel-resort near the scenic McDowell Mountains.
The 2012 Leadership Academy will feature the entry-level course “Foundations of Leadership,” which helps hospitalists begin their leadership journey, and “Advanced Leadership: Strategies and Tools for Personal Leadership Excellence,” which enables hospitalists who have taken “Foundations of Leadership” to use their own personal leadership styles to drive culture change in their organizations.
Brendon Shank is SHM’s associate vice president of communications.
Hospital medicine groups continue to grow and thrive across the country. And as they do, HM groups need experienced leaders to drive them toward continued success.
After all, the skills needed to lead hospitalist groups rarely are taught in medical school. And before employers—or potential employers—elevate hospitalists to senior positions, they need to be assured that their up-and-coming leaders can meet the challenge.
SHM’s specialty-leading Leadership Academy gives employers the confidence they want and new leaders the skill sets they need. The academy’s three courses comprise the only leadership-training program specifically designed for the challenges hospitalists face.
In the past, SHM has presented the Leadership Academy twice a year—once in the spring and once in fall. Now, SHM offers Leadership Academy once a year in the fall.
This year, hospitalists attending the Leadership Academy can take advantage of the majestic setting of the Hyatt Regency Scottsdale Resort and Spa at Gainey Ranch in Arizona, a 27-acre hotel-resort near the scenic McDowell Mountains.
The 2012 Leadership Academy will feature the entry-level course “Foundations of Leadership,” which helps hospitalists begin their leadership journey, and “Advanced Leadership: Strategies and Tools for Personal Leadership Excellence,” which enables hospitalists who have taken “Foundations of Leadership” to use their own personal leadership styles to drive culture change in their organizations.
Brendon Shank is SHM’s associate vice president of communications.
Welcome, New Residents
Every summer, a crop of fresh-faced residents greets the medical world. Freed from the travails of medical school, these new physicians embark on a journey of learning by doing, experiencing firsthand the successes and pitfalls of our medical system. Undoubtedly, the vast majority of residents enter the profession with a desire to do good, to heal.
What might not be of immediate concern to the newly minted, patient-focused doctor, however, is the need to heal the medical system.
For residents, policy might seem slightly tangential to the practice of medicine. Indeed, it is possible to practice medicine without becoming involved in policymaking; however, changes in policies and regulations affect the practice of medicine every day.
Whether at the organizational, local, or national level, policy is a vital consideration for practicing physicians. As a new resident, policy helps shape your day-to-day life, from how you interact with patients to the number of hours you are working.
In New York, for example, the 1989 Libby Zion law restricts the number of hours a resident may work to 80 hours per week, a limit formally endorsed in 2003 by the Accreditation Council for Graduate Medical Education (ACGME) for all accredited residency programs nationwide. These standards, which safeguard against the negative effects of sleep deprivation and chronic sleep loss, encourage better physical and mental care for residents and, ideally, promote better patient care. On the other hand, this rule changes the structure of residency programs and increases the number of patient handoffs to conform to hour restrictions. The challenge inherent in policy work is weighing competing interests and positions to find balance, or to justify imbalance.
When you sit down at a computer to input information about a patient, you will be using an electronic health record (EHR). This program is governed by regulations for health information technology (HIT). In fact, SHM commented on a recent proposed rule for the Stage 2 EHR Meaningful Use incentive program and whether hospitalists qualify for a hospital-based provider exemption from the program. By providing feedback to federal agencies, SHM actively influences the development of regulations, changing the impact of policies for hospitalists nationwide.
Your paycheck, too, is directly influenced by health policy, with much of the funds for residency programs coming from the federal Department of Health and Human Services and the rest coming from hospital sources. Recently, SHM supported U.S. Reps. Allyson Schwartz (D-Pa.) and Joe Heck (R-Nev.) in their introduction of H.R. 5707, the Medicare Physician Payment Innovation Act, which would repeal the sustainable growth rate (SGR) that threatens deep cuts to Medicare reimbursements originally intended to control spending. SHM actively advocates for rewarding high-value not simply high quantities of care, reflecting the orientation of hospitalists’ desire to improve the healthcare system.
Try as you might to avoid it, policy is all around you.
Even if such macro-level policy issues as value-based purchasing, payment bundling, or quality reporting initiatives seem beyond your scope of influence, it is important to stay involved and informed. SHM provides a conduit for hospitalists to become involved on large-scale policy issues. Ultimately, the strength of our organizational policy positions and influence grows with increased physician engagement.
More robust participation and more voices represented at the discussion increase the likelihood that meaningful and productive changes will occur.
As the next generation of hospitalists, today’s residents will be agents of change in their hospitals, improving patient care and advancing quality initiatives. By sharing these experiences, hospitalists can expand the policy conversation to reflect their work on the front lines—and help shape the reality for residents to come.
Every summer, a crop of fresh-faced residents greets the medical world. Freed from the travails of medical school, these new physicians embark on a journey of learning by doing, experiencing firsthand the successes and pitfalls of our medical system. Undoubtedly, the vast majority of residents enter the profession with a desire to do good, to heal.
What might not be of immediate concern to the newly minted, patient-focused doctor, however, is the need to heal the medical system.
For residents, policy might seem slightly tangential to the practice of medicine. Indeed, it is possible to practice medicine without becoming involved in policymaking; however, changes in policies and regulations affect the practice of medicine every day.
Whether at the organizational, local, or national level, policy is a vital consideration for practicing physicians. As a new resident, policy helps shape your day-to-day life, from how you interact with patients to the number of hours you are working.
In New York, for example, the 1989 Libby Zion law restricts the number of hours a resident may work to 80 hours per week, a limit formally endorsed in 2003 by the Accreditation Council for Graduate Medical Education (ACGME) for all accredited residency programs nationwide. These standards, which safeguard against the negative effects of sleep deprivation and chronic sleep loss, encourage better physical and mental care for residents and, ideally, promote better patient care. On the other hand, this rule changes the structure of residency programs and increases the number of patient handoffs to conform to hour restrictions. The challenge inherent in policy work is weighing competing interests and positions to find balance, or to justify imbalance.
When you sit down at a computer to input information about a patient, you will be using an electronic health record (EHR). This program is governed by regulations for health information technology (HIT). In fact, SHM commented on a recent proposed rule for the Stage 2 EHR Meaningful Use incentive program and whether hospitalists qualify for a hospital-based provider exemption from the program. By providing feedback to federal agencies, SHM actively influences the development of regulations, changing the impact of policies for hospitalists nationwide.
Your paycheck, too, is directly influenced by health policy, with much of the funds for residency programs coming from the federal Department of Health and Human Services and the rest coming from hospital sources. Recently, SHM supported U.S. Reps. Allyson Schwartz (D-Pa.) and Joe Heck (R-Nev.) in their introduction of H.R. 5707, the Medicare Physician Payment Innovation Act, which would repeal the sustainable growth rate (SGR) that threatens deep cuts to Medicare reimbursements originally intended to control spending. SHM actively advocates for rewarding high-value not simply high quantities of care, reflecting the orientation of hospitalists’ desire to improve the healthcare system.
Try as you might to avoid it, policy is all around you.
Even if such macro-level policy issues as value-based purchasing, payment bundling, or quality reporting initiatives seem beyond your scope of influence, it is important to stay involved and informed. SHM provides a conduit for hospitalists to become involved on large-scale policy issues. Ultimately, the strength of our organizational policy positions and influence grows with increased physician engagement.
More robust participation and more voices represented at the discussion increase the likelihood that meaningful and productive changes will occur.
As the next generation of hospitalists, today’s residents will be agents of change in their hospitals, improving patient care and advancing quality initiatives. By sharing these experiences, hospitalists can expand the policy conversation to reflect their work on the front lines—and help shape the reality for residents to come.
Every summer, a crop of fresh-faced residents greets the medical world. Freed from the travails of medical school, these new physicians embark on a journey of learning by doing, experiencing firsthand the successes and pitfalls of our medical system. Undoubtedly, the vast majority of residents enter the profession with a desire to do good, to heal.
What might not be of immediate concern to the newly minted, patient-focused doctor, however, is the need to heal the medical system.
For residents, policy might seem slightly tangential to the practice of medicine. Indeed, it is possible to practice medicine without becoming involved in policymaking; however, changes in policies and regulations affect the practice of medicine every day.
Whether at the organizational, local, or national level, policy is a vital consideration for practicing physicians. As a new resident, policy helps shape your day-to-day life, from how you interact with patients to the number of hours you are working.
In New York, for example, the 1989 Libby Zion law restricts the number of hours a resident may work to 80 hours per week, a limit formally endorsed in 2003 by the Accreditation Council for Graduate Medical Education (ACGME) for all accredited residency programs nationwide. These standards, which safeguard against the negative effects of sleep deprivation and chronic sleep loss, encourage better physical and mental care for residents and, ideally, promote better patient care. On the other hand, this rule changes the structure of residency programs and increases the number of patient handoffs to conform to hour restrictions. The challenge inherent in policy work is weighing competing interests and positions to find balance, or to justify imbalance.
When you sit down at a computer to input information about a patient, you will be using an electronic health record (EHR). This program is governed by regulations for health information technology (HIT). In fact, SHM commented on a recent proposed rule for the Stage 2 EHR Meaningful Use incentive program and whether hospitalists qualify for a hospital-based provider exemption from the program. By providing feedback to federal agencies, SHM actively influences the development of regulations, changing the impact of policies for hospitalists nationwide.
Your paycheck, too, is directly influenced by health policy, with much of the funds for residency programs coming from the federal Department of Health and Human Services and the rest coming from hospital sources. Recently, SHM supported U.S. Reps. Allyson Schwartz (D-Pa.) and Joe Heck (R-Nev.) in their introduction of H.R. 5707, the Medicare Physician Payment Innovation Act, which would repeal the sustainable growth rate (SGR) that threatens deep cuts to Medicare reimbursements originally intended to control spending. SHM actively advocates for rewarding high-value not simply high quantities of care, reflecting the orientation of hospitalists’ desire to improve the healthcare system.
Try as you might to avoid it, policy is all around you.
Even if such macro-level policy issues as value-based purchasing, payment bundling, or quality reporting initiatives seem beyond your scope of influence, it is important to stay involved and informed. SHM provides a conduit for hospitalists to become involved on large-scale policy issues. Ultimately, the strength of our organizational policy positions and influence grows with increased physician engagement.
More robust participation and more voices represented at the discussion increase the likelihood that meaningful and productive changes will occur.
As the next generation of hospitalists, today’s residents will be agents of change in their hospitals, improving patient care and advancing quality initiatives. By sharing these experiences, hospitalists can expand the policy conversation to reflect their work on the front lines—and help shape the reality for residents to come.
Project BOOST: Application deadline is Sep. 1
Almost every hospitalist knows what it’s like to see a familiar face that of a patient back in the hospital. Hundreds of hospitals across the country are learning that readmissions not only are a drain on hospitals and hospitalists, but they’re also preventable.
Now, thanks to the next cohort of SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions), which starts in October, even more hospitals can participate in this nationally recognized program to help reduce readmissions.
Sept. 1 is the deadline for Project BOOST applications, but now is the time to begin assembling applications. The Project BOOST application requires letters of support from hospital leadership and other elements that make last-minute applications difficult, if not impossible.
Project BOOST is a mentored-implementation, quality-improvement (QI) project. Here is what the program offers:
- A comprehensive intervention developed by a panel of nationally recognized experts based on the best-available evidence;
- Step-by-step instructions and project management tools, such as the Teachback Training Curriculum, to help interdisciplinary teams redesign workflow and plan, implement, and evaluate the intervention;
- Longitudinal technical assistance that provides face-to-face training and a year of expert mentoring and coaching to implement BOOST interventions that build a culture that supports safe and complete transitions. The mentoring program provides a “train the trainer” DVD and a curriculum for nurses and case managers on using the Teachback process, and webinars targeting the educational needs of other team members, including administrators, data analysts, physicians, nurses, and others;
- The ability for sites to communicate with and learn from each other via the BOOST listserv, BOOST community site, and quarterly all-site teleconferences and webinars; and
- The BOOST Data Center, an online resource center that allows sites to store and benchmark data against control units and other sites and generate reports.
Almost every hospitalist knows what it’s like to see a familiar face that of a patient back in the hospital. Hundreds of hospitals across the country are learning that readmissions not only are a drain on hospitals and hospitalists, but they’re also preventable.
Now, thanks to the next cohort of SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions), which starts in October, even more hospitals can participate in this nationally recognized program to help reduce readmissions.
Sept. 1 is the deadline for Project BOOST applications, but now is the time to begin assembling applications. The Project BOOST application requires letters of support from hospital leadership and other elements that make last-minute applications difficult, if not impossible.
Project BOOST is a mentored-implementation, quality-improvement (QI) project. Here is what the program offers:
- A comprehensive intervention developed by a panel of nationally recognized experts based on the best-available evidence;
- Step-by-step instructions and project management tools, such as the Teachback Training Curriculum, to help interdisciplinary teams redesign workflow and plan, implement, and evaluate the intervention;
- Longitudinal technical assistance that provides face-to-face training and a year of expert mentoring and coaching to implement BOOST interventions that build a culture that supports safe and complete transitions. The mentoring program provides a “train the trainer” DVD and a curriculum for nurses and case managers on using the Teachback process, and webinars targeting the educational needs of other team members, including administrators, data analysts, physicians, nurses, and others;
- The ability for sites to communicate with and learn from each other via the BOOST listserv, BOOST community site, and quarterly all-site teleconferences and webinars; and
- The BOOST Data Center, an online resource center that allows sites to store and benchmark data against control units and other sites and generate reports.
Almost every hospitalist knows what it’s like to see a familiar face that of a patient back in the hospital. Hundreds of hospitals across the country are learning that readmissions not only are a drain on hospitals and hospitalists, but they’re also preventable.
Now, thanks to the next cohort of SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions), which starts in October, even more hospitals can participate in this nationally recognized program to help reduce readmissions.
Sept. 1 is the deadline for Project BOOST applications, but now is the time to begin assembling applications. The Project BOOST application requires letters of support from hospital leadership and other elements that make last-minute applications difficult, if not impossible.
Project BOOST is a mentored-implementation, quality-improvement (QI) project. Here is what the program offers:
- A comprehensive intervention developed by a panel of nationally recognized experts based on the best-available evidence;
- Step-by-step instructions and project management tools, such as the Teachback Training Curriculum, to help interdisciplinary teams redesign workflow and plan, implement, and evaluate the intervention;
- Longitudinal technical assistance that provides face-to-face training and a year of expert mentoring and coaching to implement BOOST interventions that build a culture that supports safe and complete transitions. The mentoring program provides a “train the trainer” DVD and a curriculum for nurses and case managers on using the Teachback process, and webinars targeting the educational needs of other team members, including administrators, data analysts, physicians, nurses, and others;
- The ability for sites to communicate with and learn from each other via the BOOST listserv, BOOST community site, and quarterly all-site teleconferences and webinars; and
- The BOOST Data Center, an online resource center that allows sites to store and benchmark data against control units and other sites and generate reports.