User login
In the Literature: The latest research you need to know
In This Edition
Literature At A Glance
A guide to this month’s studies
- High-dose vs. low-dose clopidogrel after cardiac stenting
- Rates of overdiagnosis of PE with CTPA
- Outcomes of hospitalists with PAs or residents
- White coats and MRSA
- Correlation of vital signs and pain
- Rate of asymptomatic perioperative MI
- Relationship of opioid prescription patterns and overdose
- Interdisciplinary rounds and rates of adverse events
High-Dose Clopidogrel Is Not Superior to Standard-Dose Clopidogrel in Patients with High On-Treatment Platelet Activity after Percutaneous Corona
Clinical question: In patients with high on-treatment platelet activity, does the use of high-dose clopidogrel after percutaneous coronary intervention (PCI) decrease the risk of cardiovascular events?
Background: In patients receiving clopidogrel, high platelet reactivity after PCI is associated with an increase in cardiovascular events. At present, treatments targeted at this population are not well-defined.
Study design: Randomized, double-blind, active-control trial.
Setting: Eighty-three centers in North America.
Synopsis: Researchers randomized 2,214 patients with drug-eluting stents to receive either high-dose clopidogrel (600 mg initial dose, 150 mg daily thereafter) or standard-dose clopidogrel (no additional loading dose, 75 mg daily). At six months, the primary endpoint of death from cardiovascular causes, nonfatal myocardial infarction, or stent thrombosis was no different in the two groups (2.3% in the high-dose group versus 2.3% in the standard-dose group; hazard ratio 1.01).
Bottom line: High-dose clopidogrel adds no benefit over standard-dose clopidogrel in patients with high platelet reactivity who have undergone PCI with drug-eluting stent placement.
Citation: Price MJ, Berger PB, Teirstein PS, et al. Standard- vs. high-dose clopidogrel based on platelet function testing after percutaneous coronary intervention: the GRAVITAS randomized trial. JAMA. 2011;305(11):1097-1105.
Computed Tomographic Pulmonary Angiography (CTPA) Is Associated with Overdiagnosis and Overtreatment of Pulmonary Embolism (PE)
Clinical question: Is the use of CTPA associated with increased incidence of PE and increased complications from anticoagulation treatment?
Background: CTPA is a sensitive, noninvasive test for diagnosing PE that could have a drawback: identifying potentially clinically unimportant (small) pulmonary emboli that subsequently are treated. Overtreatment might be associated with patient harm due to increased complications of anticoagulation therapy.
Study design: Time-trend analysis of PE between the pre-CTPA period (1993 to 1998) and the post-CTPA period (1998 to 2006).
Setting: Nongovernmental U.S. hospitals.
Synopsis: The Nationwide Inpatient Sample and Multiple Cause-of-Death databases were used to determine national estimates of hospitalization for PE, along with morbidity and mortality from PE.
The age-adjusted analysis revealed a statistically significant increase in the incidence of PE diagnosis after introduction of CTPA (to 112 per 100,000 from 62 per 100,000), with minimal change in overall PE mortality. This was accompanied by a substantial reduction in PE case-fatality rate, the rate of hospital deaths among patients with a diagnosis of pulmonary embolism.
Availability of CTPA was associated with a significant increase in anticoagulation complication rates (to 5.3 per 100,000 from 3.1 per 100,000), including statistically significant increases in gastrointestinal hemorrhage and secondary thrombocytopenia, and a trend toward higher rates of intracranial hemorrhage.
Bottom line: Introduction of CTPA was associated with changes suggestive of overdiagnosis (increased incidence, relatively unchanged mortality) and overtreatment (increased complication rates) of PE, but it remains unknown which small PEs are clinically significant.
Citation: Wiener RS, Schwartz LM, Woloshin S. Time trends in pulmonary embolism in the United States: evidence of overdiagnosis. Arch Intern Med. 2011;171(9):831-837.
Hospitalist-Physician Assistant Teams Associated with Longer Length of Stay, No Change in Mortality, Readmission Rates
Clinical question: Do length of stay (LOS), hospital mortality, or readmission rate change if hospitalists and physician assistants, or the traditional resident-hospitalist teams, provide the patient care?
Background: Resident work-hour limitations require new models of care for hospitalized patients. Many academic medical centers have hired physician assistants to work with hospitalists to provide care. Little is known about how these models affect such outcomes as LOS, inpatient mortality rates, and readmission rates.
Study design: Retrospective cohort.
Setting: A 430-bed urban academic medical center in Milwaukee.
Synopsis: Administrative data were gathered on 9,681 patients admitted to the general medical service. Of those enrolled, 2,171 were cared for by a hospitalist-physician assistant (H-PA) team, while resident-hospitalist teams cared for 7,510 patients. Patient assignment was dependent on time of admission but not on patient complexity. Patients admitted overnight after the resident team capped were assigned to the H-PA team the next morning, resulting in increased transitions of care for the H-PA team.
Adjusted analyses revealed a 6.45% increase in LOS for the H-PA team compared with the resident team. Charges, inpatient mortality, and readmission rates at seven, 14, and 30 days were unchanged. Subgroup analyses revealed smaller differences in LOS for H-PA teams and resident-hospitalist teams with the same hospitalist (LOS 5.44% higher, P=0.081).
Conclusions from this study are limited due to lack of randomization of assignment, the retrospective design, and the use of administrative data at one institution.
Bottom line: Hospitalist-PA teams might result in a slightly increased LOS compared with the traditional resident teams; however, inpatient mortality and readmission rates are similar.
Citation: Singh S, Fletcher KE, Schapira MM, et al. A comparison of outcomes of general medical inpatient care provided by a hospitalist-physician assistant model vs a traditional resident-based model. J Hosp Med. 2011;6:122-130.
Washing White Coats Does Not Lower MRSA Bacterial Contamination
Clinical question: Are clean, short-sleeved uniforms less likely to carry MRSA than regularly laundered long-sleeved white coats?
Background: Studies have shown that bacteria frequently colonize in physician garments. However, evidence that short-sleeved garments or newly laundered garments are less likely to be contaminated has been lacking. Despite the paucity of evidence, the British Department of Health barred the use of traditional white coats and long-sleeved garments in 2007.
Study design: Prospective, randomized, controlled trial.
Setting: Urban U.S. hospital.
Synopsis: Study authors randomized 100 internal-medicine residents and hospitalists to their own long-sleeved white coats or freshly laundered short-sleeved uniforms from August 2008 to November 2009. Swabs were taken from the sleeves of the white coats or uniform, the breast pocket, and the volar wrist surface of the dominant hand. Swabs were cultured for MRSA and for general colony count.
Results showed no significant difference in colony counts or MRSA colonization in any of the sites tested between the newly laundered uniforms and the white coats. Additionally, there was no effect in relation to the frequency of laundering the white coats. Notably, within three hours of donning freshly laundered uniforms, bacterial counts approached 50% of the total bacterial counts seen at eight hours.
Bottom line: Laundering of uniforms does not affect MRSA colonization rate or general bacterial burden on physician uniforms or skin surfaces, though the effect on nosocomial infection has not been established.
Citation: Burden M, Cervantes L, Weed D, Keniston A, Price CS, Albert RK. Newly cleaned physician uniforms and infrequently washed white coats have similar rates of bacterial contamination after an 8-hour workday: a randomized controlled trial. J Hosp Med. 2011;6:177-182.
Self-Reported Pain Severity Does Not Correlate with Heart Rate or Blood Pressure Measurements in Pre-Hospital Setting
Clinical question: Do measured vital signs, including heart rate, blood pressure, and respiratory rate, correlate with the degree of self-reported pain?
Background: Because pain often can be associated with alterations in autonomic tone, it has been hypothesized that alterations in vital signs will occur in patients who report pain.
Study design: Retrospective cohort study.
Setting: Pre-hospital in Melbourne, Australia.
Synopsis: The authors reviewed all ambulance patient care records for patients age >14 years with a Glasgow Coma Score (GCS) >12 transported to a hospital during a seven-day period in 2005. Patients were selected for analysis if their patient care record included an initial assessment of pain severity, as measured by a numeric rating scale (NRS), in which patients rate their pain from 0 to 10.
More than half of the 3,357 patients transported by paramedics during the period were included in this analysis (n=1286). There was no correlation between heart rate or systolic blood pressure with the degree of self-reported pain. Although an increased respiratory rate was statistically correlated with a higher rating of pain, this relationship was not clinically significant, as each one-point increase in the pain rating scale was associated with a 0.16-breaths-per-minute increase in the respiratory rate.
Limitations included the large number of records excluded from analysis because pain was not evaluated, as well as numerous unmeasured confounders, including active disease processes such as sepsis, that were not accounted for.
Bottom line: Severity of pain did not correlate with heart rate or systolic blood pressure in the pre-hospital setting.
Citation: Lord B, Woollard M. The reliability of vital signs in estimating pain severity among adult patients treated by paramedics. Emerg Med J. 2011;28:147-150.
Asymptomatic Perioperative Myocardial Infarction Is Common in Patients Undergoing Noncardiac Surgery
Clinical question: In patients undergoing noncardiac surgery, what is the incidence and clinical characteristics of perioperative myocardial infarction (MI)?
Background: Though millions of patients experience perioperative MI after noncardiac surgery, little is known about the characteristics and outcomes of these patients.
Study design: Cohort study.
Setting: One hundred ninety centers in 23 countries.
Synopsis: Using data from the 8,351 patients in the POISE (PeriOperative ISchemic Evaluation) trial, this study showed that perioperative MI occurred in 5% of patients; 65% were asymptomatic. Patients who experienced postoperative MI were older and had more cardiovascular risk factors when compared to those who did not. The 30-day mortality was higher in patients with a perioperative MI (11.6%) compared with those who did not (2.2%); the presence or absence of ischemic symptoms was not associated with mortality rate.
Of the 8.3% of patients who experienced an elevation in cardiac biomarkers but who did not meet the definition of MI, there was an increased risk of nonfatal cardiac arrest and nonacute coronary revascularization. Those in the highest quartile also had increased 30-day mortality.
Bottom line: Given the high proportion of asymptomatic MIs and isolated elevations in cardiac biomarkers and the association between these events and increased risk of death, hospitalists should consider routine monitoring of troponin in at-risk patients undergoing noncardiac surgery.
Citation: Devereaux PJ, Xavier D, Pogue J, et al. Characteristics and short-term prognosis of perioperative myocardial infarction in patients undergoing noncardiac surgery: a cohort study. Ann Intern Med. 2011;154(8):523-528.
Patients Prescribed Higher Opioid Doses Are at Increased Risk of Opioid Overdose Death
Clinical question: What is the association between opioid prescribing patterns and fatal opioid overdose?
Background: In the past 10 years, the rate of fatal overdose from opioid prescription for pain has more than doubled. Little is known about how the indications (substance abuse disorders, cancer-related pain, chronic pain, acute pain), maximal daily dose, and scheduling (standing, as-needed, or both) of opioid prescriptions relate to this increased risk.
Study design: Case-cohort study.
Setting: Veterans Health Administration (VHA) patients.
Synopsis: The VHA’s National Patient Care Database was used to randomly select a cohort of 154,684 nonhospice/nonpalliative-care patients who were prescribed opioids from 2004 to 2008. They were compared with 750 patients who were treated with prescription opioids who died from opioid overdose during this time.
Fatal opioid overdose was a rare event (0.04%), but risk increased with higher prescribed maximum daily morphine dose-equivalence, especially when greater than or equal to 50 mg/day in all subgroups (substance abuse, acute and chronic pain, and cancer). Fatal overdoses were higher in middle-aged white men with acute or chronic pain, substance abuse disorders, and other psychiatric illness. Patients with cancer were at increased risk of fatal overdose if they were prescribed as-needed opioids alone.
Treatment with both as-needed and standing opioids did not statistically affect risk of overdose death in any subgroup.
Bottom line: Although rare, risk of fatal opioid overdose in patients prescribed opiate medication increases with higher maximum prescribed daily dose.
Citation: Bohnert AS, Valenstein M, Bair M, et al. Association between opioid prescribing patterns and opioid overdose-related deaths. JAMA. 2011; 305:1315-1321.
Structured Interdisciplinary Rounds on Medical Teaching Unit Significantly Decrease Adverse Events
Clinical question: Do structured interdisciplinary rounds have an impact on the rate of adverse events?
Background: Many preventable adverse events occurring during hospitalization can be attributed to communication failures. Structured interdisciplinary rounds provide a format as well as a forum for team members to discuss patient care. Prior studies demonstrated improvements in collaboration; whether this translates to better patient care is not known.
Study design: Retrospective cohort using historic and concurrent control.
Setting: Tertiary-care teaching hospital in Chicago.
Synopsis: Structured interdisciplinary rounds, led by a nurse manager and medical director, and including nurses, residents, pharmacists, social workers, and case managers, were implemented on a medical teaching unit. New patients were discussed using a structured communication tool; existing patients were discussed in an unstructured format. Medical records were abstracted for 370 patients hospitalized after implementation of the intervention, equally divided between intervention and control units. One hundred eighty-five patients hospitalized on the intervention unit prior to the implementation of rounds served as a historic control.
Patients in the intervention unit had significantly lower rates of total adverse events (3.9 per 100 patient days in the intervention, compared with 7.2 and 7.7 per 100 patient days for the concurrent and historic control units, respectively), and preventable adverse events (0.9 per 100 patient days, compared with 2.8 and 2.1 per 100 patient days for the concurrent and historic controls, respectively).
Limitations of the study include lack of blinding of the medical record, slightly different patient populations in intervention and control groups, and the one-hospital setting, which could limit generalizability.
Bottom line: Structured interdisciplinary rounds might serve to improve communication between nurses, pharmacists, and physicians, resulting in decreases in adverse events.
Citation: O’Leary KJ, Buck R, Fligiel HM, et al. Structured interdisciplinary rounds in a medical teaching unit: improving patient safety. Arch Intern Med. 2011;171(7):678-684.
Pediatric HM Literature
Short-Course Antibiotic Therapy Effective for Bacterial Meningitis

Clinical question: Is five days of parenteral ceftriaxone as effective as 10 days for the treatment of bacterial meningitis in children?
Background: Morbidity and mortality in bacterial meningitis remain high, particularly in developing countries. Antibiotics are effective treatment, yet the optimal duration of treatment remains uncertain. Some data support a shorter duration of treatment (three to five days).
Study design: Multicountry, double-blind, placebo-controlled, randomized equivalence study.
Setting: Ten pediatric referral hospitals in Bangladesh, Egypt, Malawi, Pakistan, and Vietnam.
Synopsis: Children aged two months to 12 years with bacterial meningitis (due to Haemophilus influenza, Streptococcus pneumonia, Neisseria meningitidis, or culture-negative with indicative cerebrospinal fluid findings) and without complicating medical conditions were enrolled at participating centers. All children received 80 mg/kg to 100 mg/kg of parenteral ceftriaxone daily and a repeat lumbar puncture 48 to 72 hours after initiation of therapy.
Ultimately, 1,004 children without resistant organisms, persistently positive cultures, or suppurative complications were randomized on day five of therapy to placebo or continuance of ceftriaxone for five more days.
No bacteriologic failures (primary endpoint) were evident with either five or 10 days of treatment.
In addition, no statistically significant differences were found between the groups with respect to clinical treatment failure, hearing loss, neurological sequelae, or death. Secondary analysis by organism revealed similar results.
The primary limitation of this study is that it occurred in developing countries with a fair incidence of H. influenzae meningitis and a low rate of third-generation cephalosporin resistance.
However, pneumococcal and meningococcal disease remained prominent, and this study suggests that clinically stable patients might be treated with a shorter course of parenteral ceftriaxone therapy than currently is recommended.
Bottom line: Five days of ceftriaxone is as effective as 10 days for uncomplicated bacterial meningitis in children.
Citation: Molyneux E, Nizami SQ, Saha S, et al. 5 versus 10 days of treatment with ceftriaxone for bacterial meningitis in children: a double-blind randomised equivalence study. Lancet. 2011;377:1837-1845.
Reviewed by Pediatric Editor Mark Shen, MD, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
In This Edition
Literature At A Glance
A guide to this month’s studies
- High-dose vs. low-dose clopidogrel after cardiac stenting
- Rates of overdiagnosis of PE with CTPA
- Outcomes of hospitalists with PAs or residents
- White coats and MRSA
- Correlation of vital signs and pain
- Rate of asymptomatic perioperative MI
- Relationship of opioid prescription patterns and overdose
- Interdisciplinary rounds and rates of adverse events
High-Dose Clopidogrel Is Not Superior to Standard-Dose Clopidogrel in Patients with High On-Treatment Platelet Activity after Percutaneous Corona
Clinical question: In patients with high on-treatment platelet activity, does the use of high-dose clopidogrel after percutaneous coronary intervention (PCI) decrease the risk of cardiovascular events?
Background: In patients receiving clopidogrel, high platelet reactivity after PCI is associated with an increase in cardiovascular events. At present, treatments targeted at this population are not well-defined.
Study design: Randomized, double-blind, active-control trial.
Setting: Eighty-three centers in North America.
Synopsis: Researchers randomized 2,214 patients with drug-eluting stents to receive either high-dose clopidogrel (600 mg initial dose, 150 mg daily thereafter) or standard-dose clopidogrel (no additional loading dose, 75 mg daily). At six months, the primary endpoint of death from cardiovascular causes, nonfatal myocardial infarction, or stent thrombosis was no different in the two groups (2.3% in the high-dose group versus 2.3% in the standard-dose group; hazard ratio 1.01).
Bottom line: High-dose clopidogrel adds no benefit over standard-dose clopidogrel in patients with high platelet reactivity who have undergone PCI with drug-eluting stent placement.
Citation: Price MJ, Berger PB, Teirstein PS, et al. Standard- vs. high-dose clopidogrel based on platelet function testing after percutaneous coronary intervention: the GRAVITAS randomized trial. JAMA. 2011;305(11):1097-1105.
Computed Tomographic Pulmonary Angiography (CTPA) Is Associated with Overdiagnosis and Overtreatment of Pulmonary Embolism (PE)
Clinical question: Is the use of CTPA associated with increased incidence of PE and increased complications from anticoagulation treatment?
Background: CTPA is a sensitive, noninvasive test for diagnosing PE that could have a drawback: identifying potentially clinically unimportant (small) pulmonary emboli that subsequently are treated. Overtreatment might be associated with patient harm due to increased complications of anticoagulation therapy.
Study design: Time-trend analysis of PE between the pre-CTPA period (1993 to 1998) and the post-CTPA period (1998 to 2006).
Setting: Nongovernmental U.S. hospitals.
Synopsis: The Nationwide Inpatient Sample and Multiple Cause-of-Death databases were used to determine national estimates of hospitalization for PE, along with morbidity and mortality from PE.
The age-adjusted analysis revealed a statistically significant increase in the incidence of PE diagnosis after introduction of CTPA (to 112 per 100,000 from 62 per 100,000), with minimal change in overall PE mortality. This was accompanied by a substantial reduction in PE case-fatality rate, the rate of hospital deaths among patients with a diagnosis of pulmonary embolism.
Availability of CTPA was associated with a significant increase in anticoagulation complication rates (to 5.3 per 100,000 from 3.1 per 100,000), including statistically significant increases in gastrointestinal hemorrhage and secondary thrombocytopenia, and a trend toward higher rates of intracranial hemorrhage.
Bottom line: Introduction of CTPA was associated with changes suggestive of overdiagnosis (increased incidence, relatively unchanged mortality) and overtreatment (increased complication rates) of PE, but it remains unknown which small PEs are clinically significant.
Citation: Wiener RS, Schwartz LM, Woloshin S. Time trends in pulmonary embolism in the United States: evidence of overdiagnosis. Arch Intern Med. 2011;171(9):831-837.
Hospitalist-Physician Assistant Teams Associated with Longer Length of Stay, No Change in Mortality, Readmission Rates
Clinical question: Do length of stay (LOS), hospital mortality, or readmission rate change if hospitalists and physician assistants, or the traditional resident-hospitalist teams, provide the patient care?
Background: Resident work-hour limitations require new models of care for hospitalized patients. Many academic medical centers have hired physician assistants to work with hospitalists to provide care. Little is known about how these models affect such outcomes as LOS, inpatient mortality rates, and readmission rates.
Study design: Retrospective cohort.
Setting: A 430-bed urban academic medical center in Milwaukee.
Synopsis: Administrative data were gathered on 9,681 patients admitted to the general medical service. Of those enrolled, 2,171 were cared for by a hospitalist-physician assistant (H-PA) team, while resident-hospitalist teams cared for 7,510 patients. Patient assignment was dependent on time of admission but not on patient complexity. Patients admitted overnight after the resident team capped were assigned to the H-PA team the next morning, resulting in increased transitions of care for the H-PA team.
Adjusted analyses revealed a 6.45% increase in LOS for the H-PA team compared with the resident team. Charges, inpatient mortality, and readmission rates at seven, 14, and 30 days were unchanged. Subgroup analyses revealed smaller differences in LOS for H-PA teams and resident-hospitalist teams with the same hospitalist (LOS 5.44% higher, P=0.081).
Conclusions from this study are limited due to lack of randomization of assignment, the retrospective design, and the use of administrative data at one institution.
Bottom line: Hospitalist-PA teams might result in a slightly increased LOS compared with the traditional resident teams; however, inpatient mortality and readmission rates are similar.
Citation: Singh S, Fletcher KE, Schapira MM, et al. A comparison of outcomes of general medical inpatient care provided by a hospitalist-physician assistant model vs a traditional resident-based model. J Hosp Med. 2011;6:122-130.
Washing White Coats Does Not Lower MRSA Bacterial Contamination
Clinical question: Are clean, short-sleeved uniforms less likely to carry MRSA than regularly laundered long-sleeved white coats?
Background: Studies have shown that bacteria frequently colonize in physician garments. However, evidence that short-sleeved garments or newly laundered garments are less likely to be contaminated has been lacking. Despite the paucity of evidence, the British Department of Health barred the use of traditional white coats and long-sleeved garments in 2007.
Study design: Prospective, randomized, controlled trial.
Setting: Urban U.S. hospital.
Synopsis: Study authors randomized 100 internal-medicine residents and hospitalists to their own long-sleeved white coats or freshly laundered short-sleeved uniforms from August 2008 to November 2009. Swabs were taken from the sleeves of the white coats or uniform, the breast pocket, and the volar wrist surface of the dominant hand. Swabs were cultured for MRSA and for general colony count.
Results showed no significant difference in colony counts or MRSA colonization in any of the sites tested between the newly laundered uniforms and the white coats. Additionally, there was no effect in relation to the frequency of laundering the white coats. Notably, within three hours of donning freshly laundered uniforms, bacterial counts approached 50% of the total bacterial counts seen at eight hours.
Bottom line: Laundering of uniforms does not affect MRSA colonization rate or general bacterial burden on physician uniforms or skin surfaces, though the effect on nosocomial infection has not been established.
Citation: Burden M, Cervantes L, Weed D, Keniston A, Price CS, Albert RK. Newly cleaned physician uniforms and infrequently washed white coats have similar rates of bacterial contamination after an 8-hour workday: a randomized controlled trial. J Hosp Med. 2011;6:177-182.
Self-Reported Pain Severity Does Not Correlate with Heart Rate or Blood Pressure Measurements in Pre-Hospital Setting
Clinical question: Do measured vital signs, including heart rate, blood pressure, and respiratory rate, correlate with the degree of self-reported pain?
Background: Because pain often can be associated with alterations in autonomic tone, it has been hypothesized that alterations in vital signs will occur in patients who report pain.
Study design: Retrospective cohort study.
Setting: Pre-hospital in Melbourne, Australia.
Synopsis: The authors reviewed all ambulance patient care records for patients age >14 years with a Glasgow Coma Score (GCS) >12 transported to a hospital during a seven-day period in 2005. Patients were selected for analysis if their patient care record included an initial assessment of pain severity, as measured by a numeric rating scale (NRS), in which patients rate their pain from 0 to 10.
More than half of the 3,357 patients transported by paramedics during the period were included in this analysis (n=1286). There was no correlation between heart rate or systolic blood pressure with the degree of self-reported pain. Although an increased respiratory rate was statistically correlated with a higher rating of pain, this relationship was not clinically significant, as each one-point increase in the pain rating scale was associated with a 0.16-breaths-per-minute increase in the respiratory rate.
Limitations included the large number of records excluded from analysis because pain was not evaluated, as well as numerous unmeasured confounders, including active disease processes such as sepsis, that were not accounted for.
Bottom line: Severity of pain did not correlate with heart rate or systolic blood pressure in the pre-hospital setting.
Citation: Lord B, Woollard M. The reliability of vital signs in estimating pain severity among adult patients treated by paramedics. Emerg Med J. 2011;28:147-150.
Asymptomatic Perioperative Myocardial Infarction Is Common in Patients Undergoing Noncardiac Surgery
Clinical question: In patients undergoing noncardiac surgery, what is the incidence and clinical characteristics of perioperative myocardial infarction (MI)?
Background: Though millions of patients experience perioperative MI after noncardiac surgery, little is known about the characteristics and outcomes of these patients.
Study design: Cohort study.
Setting: One hundred ninety centers in 23 countries.
Synopsis: Using data from the 8,351 patients in the POISE (PeriOperative ISchemic Evaluation) trial, this study showed that perioperative MI occurred in 5% of patients; 65% were asymptomatic. Patients who experienced postoperative MI were older and had more cardiovascular risk factors when compared to those who did not. The 30-day mortality was higher in patients with a perioperative MI (11.6%) compared with those who did not (2.2%); the presence or absence of ischemic symptoms was not associated with mortality rate.
Of the 8.3% of patients who experienced an elevation in cardiac biomarkers but who did not meet the definition of MI, there was an increased risk of nonfatal cardiac arrest and nonacute coronary revascularization. Those in the highest quartile also had increased 30-day mortality.
Bottom line: Given the high proportion of asymptomatic MIs and isolated elevations in cardiac biomarkers and the association between these events and increased risk of death, hospitalists should consider routine monitoring of troponin in at-risk patients undergoing noncardiac surgery.
Citation: Devereaux PJ, Xavier D, Pogue J, et al. Characteristics and short-term prognosis of perioperative myocardial infarction in patients undergoing noncardiac surgery: a cohort study. Ann Intern Med. 2011;154(8):523-528.
Patients Prescribed Higher Opioid Doses Are at Increased Risk of Opioid Overdose Death
Clinical question: What is the association between opioid prescribing patterns and fatal opioid overdose?
Background: In the past 10 years, the rate of fatal overdose from opioid prescription for pain has more than doubled. Little is known about how the indications (substance abuse disorders, cancer-related pain, chronic pain, acute pain), maximal daily dose, and scheduling (standing, as-needed, or both) of opioid prescriptions relate to this increased risk.
Study design: Case-cohort study.
Setting: Veterans Health Administration (VHA) patients.
Synopsis: The VHA’s National Patient Care Database was used to randomly select a cohort of 154,684 nonhospice/nonpalliative-care patients who were prescribed opioids from 2004 to 2008. They were compared with 750 patients who were treated with prescription opioids who died from opioid overdose during this time.
Fatal opioid overdose was a rare event (0.04%), but risk increased with higher prescribed maximum daily morphine dose-equivalence, especially when greater than or equal to 50 mg/day in all subgroups (substance abuse, acute and chronic pain, and cancer). Fatal overdoses were higher in middle-aged white men with acute or chronic pain, substance abuse disorders, and other psychiatric illness. Patients with cancer were at increased risk of fatal overdose if they were prescribed as-needed opioids alone.
Treatment with both as-needed and standing opioids did not statistically affect risk of overdose death in any subgroup.
Bottom line: Although rare, risk of fatal opioid overdose in patients prescribed opiate medication increases with higher maximum prescribed daily dose.
Citation: Bohnert AS, Valenstein M, Bair M, et al. Association between opioid prescribing patterns and opioid overdose-related deaths. JAMA. 2011; 305:1315-1321.
Structured Interdisciplinary Rounds on Medical Teaching Unit Significantly Decrease Adverse Events
Clinical question: Do structured interdisciplinary rounds have an impact on the rate of adverse events?
Background: Many preventable adverse events occurring during hospitalization can be attributed to communication failures. Structured interdisciplinary rounds provide a format as well as a forum for team members to discuss patient care. Prior studies demonstrated improvements in collaboration; whether this translates to better patient care is not known.
Study design: Retrospective cohort using historic and concurrent control.
Setting: Tertiary-care teaching hospital in Chicago.
Synopsis: Structured interdisciplinary rounds, led by a nurse manager and medical director, and including nurses, residents, pharmacists, social workers, and case managers, were implemented on a medical teaching unit. New patients were discussed using a structured communication tool; existing patients were discussed in an unstructured format. Medical records were abstracted for 370 patients hospitalized after implementation of the intervention, equally divided between intervention and control units. One hundred eighty-five patients hospitalized on the intervention unit prior to the implementation of rounds served as a historic control.
Patients in the intervention unit had significantly lower rates of total adverse events (3.9 per 100 patient days in the intervention, compared with 7.2 and 7.7 per 100 patient days for the concurrent and historic control units, respectively), and preventable adverse events (0.9 per 100 patient days, compared with 2.8 and 2.1 per 100 patient days for the concurrent and historic controls, respectively).
Limitations of the study include lack of blinding of the medical record, slightly different patient populations in intervention and control groups, and the one-hospital setting, which could limit generalizability.
Bottom line: Structured interdisciplinary rounds might serve to improve communication between nurses, pharmacists, and physicians, resulting in decreases in adverse events.
Citation: O’Leary KJ, Buck R, Fligiel HM, et al. Structured interdisciplinary rounds in a medical teaching unit: improving patient safety. Arch Intern Med. 2011;171(7):678-684.
Pediatric HM Literature
Short-Course Antibiotic Therapy Effective for Bacterial Meningitis
Clinical question: Is five days of parenteral ceftriaxone as effective as 10 days for the treatment of bacterial meningitis in children?
Background: Morbidity and mortality in bacterial meningitis remain high, particularly in developing countries. Antibiotics are effective treatment, yet the optimal duration of treatment remains uncertain. Some data support a shorter duration of treatment (three to five days).
Study design: Multicountry, double-blind, placebo-controlled, randomized equivalence study.
Setting: Ten pediatric referral hospitals in Bangladesh, Egypt, Malawi, Pakistan, and Vietnam.
Synopsis: Children aged two months to 12 years with bacterial meningitis (due to Haemophilus influenza, Streptococcus pneumonia, Neisseria meningitidis, or culture-negative with indicative cerebrospinal fluid findings) and without complicating medical conditions were enrolled at participating centers. All children received 80 mg/kg to 100 mg/kg of parenteral ceftriaxone daily and a repeat lumbar puncture 48 to 72 hours after initiation of therapy.
Ultimately, 1,004 children without resistant organisms, persistently positive cultures, or suppurative complications were randomized on day five of therapy to placebo or continuance of ceftriaxone for five more days.
No bacteriologic failures (primary endpoint) were evident with either five or 10 days of treatment.
In addition, no statistically significant differences were found between the groups with respect to clinical treatment failure, hearing loss, neurological sequelae, or death. Secondary analysis by organism revealed similar results.
The primary limitation of this study is that it occurred in developing countries with a fair incidence of H. influenzae meningitis and a low rate of third-generation cephalosporin resistance.
However, pneumococcal and meningococcal disease remained prominent, and this study suggests that clinically stable patients might be treated with a shorter course of parenteral ceftriaxone therapy than currently is recommended.
Bottom line: Five days of ceftriaxone is as effective as 10 days for uncomplicated bacterial meningitis in children.
Citation: Molyneux E, Nizami SQ, Saha S, et al. 5 versus 10 days of treatment with ceftriaxone for bacterial meningitis in children: a double-blind randomised equivalence study. Lancet. 2011;377:1837-1845.
Reviewed by Pediatric Editor Mark Shen, MD, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
In This Edition
Literature At A Glance
A guide to this month’s studies
- High-dose vs. low-dose clopidogrel after cardiac stenting
- Rates of overdiagnosis of PE with CTPA
- Outcomes of hospitalists with PAs or residents
- White coats and MRSA
- Correlation of vital signs and pain
- Rate of asymptomatic perioperative MI
- Relationship of opioid prescription patterns and overdose
- Interdisciplinary rounds and rates of adverse events
High-Dose Clopidogrel Is Not Superior to Standard-Dose Clopidogrel in Patients with High On-Treatment Platelet Activity after Percutaneous Corona
Clinical question: In patients with high on-treatment platelet activity, does the use of high-dose clopidogrel after percutaneous coronary intervention (PCI) decrease the risk of cardiovascular events?
Background: In patients receiving clopidogrel, high platelet reactivity after PCI is associated with an increase in cardiovascular events. At present, treatments targeted at this population are not well-defined.
Study design: Randomized, double-blind, active-control trial.
Setting: Eighty-three centers in North America.
Synopsis: Researchers randomized 2,214 patients with drug-eluting stents to receive either high-dose clopidogrel (600 mg initial dose, 150 mg daily thereafter) or standard-dose clopidogrel (no additional loading dose, 75 mg daily). At six months, the primary endpoint of death from cardiovascular causes, nonfatal myocardial infarction, or stent thrombosis was no different in the two groups (2.3% in the high-dose group versus 2.3% in the standard-dose group; hazard ratio 1.01).
Bottom line: High-dose clopidogrel adds no benefit over standard-dose clopidogrel in patients with high platelet reactivity who have undergone PCI with drug-eluting stent placement.
Citation: Price MJ, Berger PB, Teirstein PS, et al. Standard- vs. high-dose clopidogrel based on platelet function testing after percutaneous coronary intervention: the GRAVITAS randomized trial. JAMA. 2011;305(11):1097-1105.
Computed Tomographic Pulmonary Angiography (CTPA) Is Associated with Overdiagnosis and Overtreatment of Pulmonary Embolism (PE)
Clinical question: Is the use of CTPA associated with increased incidence of PE and increased complications from anticoagulation treatment?
Background: CTPA is a sensitive, noninvasive test for diagnosing PE that could have a drawback: identifying potentially clinically unimportant (small) pulmonary emboli that subsequently are treated. Overtreatment might be associated with patient harm due to increased complications of anticoagulation therapy.
Study design: Time-trend analysis of PE between the pre-CTPA period (1993 to 1998) and the post-CTPA period (1998 to 2006).
Setting: Nongovernmental U.S. hospitals.
Synopsis: The Nationwide Inpatient Sample and Multiple Cause-of-Death databases were used to determine national estimates of hospitalization for PE, along with morbidity and mortality from PE.
The age-adjusted analysis revealed a statistically significant increase in the incidence of PE diagnosis after introduction of CTPA (to 112 per 100,000 from 62 per 100,000), with minimal change in overall PE mortality. This was accompanied by a substantial reduction in PE case-fatality rate, the rate of hospital deaths among patients with a diagnosis of pulmonary embolism.
Availability of CTPA was associated with a significant increase in anticoagulation complication rates (to 5.3 per 100,000 from 3.1 per 100,000), including statistically significant increases in gastrointestinal hemorrhage and secondary thrombocytopenia, and a trend toward higher rates of intracranial hemorrhage.
Bottom line: Introduction of CTPA was associated with changes suggestive of overdiagnosis (increased incidence, relatively unchanged mortality) and overtreatment (increased complication rates) of PE, but it remains unknown which small PEs are clinically significant.
Citation: Wiener RS, Schwartz LM, Woloshin S. Time trends in pulmonary embolism in the United States: evidence of overdiagnosis. Arch Intern Med. 2011;171(9):831-837.
Hospitalist-Physician Assistant Teams Associated with Longer Length of Stay, No Change in Mortality, Readmission Rates
Clinical question: Do length of stay (LOS), hospital mortality, or readmission rate change if hospitalists and physician assistants, or the traditional resident-hospitalist teams, provide the patient care?
Background: Resident work-hour limitations require new models of care for hospitalized patients. Many academic medical centers have hired physician assistants to work with hospitalists to provide care. Little is known about how these models affect such outcomes as LOS, inpatient mortality rates, and readmission rates.
Study design: Retrospective cohort.
Setting: A 430-bed urban academic medical center in Milwaukee.
Synopsis: Administrative data were gathered on 9,681 patients admitted to the general medical service. Of those enrolled, 2,171 were cared for by a hospitalist-physician assistant (H-PA) team, while resident-hospitalist teams cared for 7,510 patients. Patient assignment was dependent on time of admission but not on patient complexity. Patients admitted overnight after the resident team capped were assigned to the H-PA team the next morning, resulting in increased transitions of care for the H-PA team.
Adjusted analyses revealed a 6.45% increase in LOS for the H-PA team compared with the resident team. Charges, inpatient mortality, and readmission rates at seven, 14, and 30 days were unchanged. Subgroup analyses revealed smaller differences in LOS for H-PA teams and resident-hospitalist teams with the same hospitalist (LOS 5.44% higher, P=0.081).
Conclusions from this study are limited due to lack of randomization of assignment, the retrospective design, and the use of administrative data at one institution.
Bottom line: Hospitalist-PA teams might result in a slightly increased LOS compared with the traditional resident teams; however, inpatient mortality and readmission rates are similar.
Citation: Singh S, Fletcher KE, Schapira MM, et al. A comparison of outcomes of general medical inpatient care provided by a hospitalist-physician assistant model vs a traditional resident-based model. J Hosp Med. 2011;6:122-130.
Washing White Coats Does Not Lower MRSA Bacterial Contamination
Clinical question: Are clean, short-sleeved uniforms less likely to carry MRSA than regularly laundered long-sleeved white coats?
Background: Studies have shown that bacteria frequently colonize in physician garments. However, evidence that short-sleeved garments or newly laundered garments are less likely to be contaminated has been lacking. Despite the paucity of evidence, the British Department of Health barred the use of traditional white coats and long-sleeved garments in 2007.
Study design: Prospective, randomized, controlled trial.
Setting: Urban U.S. hospital.
Synopsis: Study authors randomized 100 internal-medicine residents and hospitalists to their own long-sleeved white coats or freshly laundered short-sleeved uniforms from August 2008 to November 2009. Swabs were taken from the sleeves of the white coats or uniform, the breast pocket, and the volar wrist surface of the dominant hand. Swabs were cultured for MRSA and for general colony count.
Results showed no significant difference in colony counts or MRSA colonization in any of the sites tested between the newly laundered uniforms and the white coats. Additionally, there was no effect in relation to the frequency of laundering the white coats. Notably, within three hours of donning freshly laundered uniforms, bacterial counts approached 50% of the total bacterial counts seen at eight hours.
Bottom line: Laundering of uniforms does not affect MRSA colonization rate or general bacterial burden on physician uniforms or skin surfaces, though the effect on nosocomial infection has not been established.
Citation: Burden M, Cervantes L, Weed D, Keniston A, Price CS, Albert RK. Newly cleaned physician uniforms and infrequently washed white coats have similar rates of bacterial contamination after an 8-hour workday: a randomized controlled trial. J Hosp Med. 2011;6:177-182.
Self-Reported Pain Severity Does Not Correlate with Heart Rate or Blood Pressure Measurements in Pre-Hospital Setting
Clinical question: Do measured vital signs, including heart rate, blood pressure, and respiratory rate, correlate with the degree of self-reported pain?
Background: Because pain often can be associated with alterations in autonomic tone, it has been hypothesized that alterations in vital signs will occur in patients who report pain.
Study design: Retrospective cohort study.
Setting: Pre-hospital in Melbourne, Australia.
Synopsis: The authors reviewed all ambulance patient care records for patients age >14 years with a Glasgow Coma Score (GCS) >12 transported to a hospital during a seven-day period in 2005. Patients were selected for analysis if their patient care record included an initial assessment of pain severity, as measured by a numeric rating scale (NRS), in which patients rate their pain from 0 to 10.
More than half of the 3,357 patients transported by paramedics during the period were included in this analysis (n=1286). There was no correlation between heart rate or systolic blood pressure with the degree of self-reported pain. Although an increased respiratory rate was statistically correlated with a higher rating of pain, this relationship was not clinically significant, as each one-point increase in the pain rating scale was associated with a 0.16-breaths-per-minute increase in the respiratory rate.
Limitations included the large number of records excluded from analysis because pain was not evaluated, as well as numerous unmeasured confounders, including active disease processes such as sepsis, that were not accounted for.
Bottom line: Severity of pain did not correlate with heart rate or systolic blood pressure in the pre-hospital setting.
Citation: Lord B, Woollard M. The reliability of vital signs in estimating pain severity among adult patients treated by paramedics. Emerg Med J. 2011;28:147-150.
Asymptomatic Perioperative Myocardial Infarction Is Common in Patients Undergoing Noncardiac Surgery
Clinical question: In patients undergoing noncardiac surgery, what is the incidence and clinical characteristics of perioperative myocardial infarction (MI)?
Background: Though millions of patients experience perioperative MI after noncardiac surgery, little is known about the characteristics and outcomes of these patients.
Study design: Cohort study.
Setting: One hundred ninety centers in 23 countries.
Synopsis: Using data from the 8,351 patients in the POISE (PeriOperative ISchemic Evaluation) trial, this study showed that perioperative MI occurred in 5% of patients; 65% were asymptomatic. Patients who experienced postoperative MI were older and had more cardiovascular risk factors when compared to those who did not. The 30-day mortality was higher in patients with a perioperative MI (11.6%) compared with those who did not (2.2%); the presence or absence of ischemic symptoms was not associated with mortality rate.
Of the 8.3% of patients who experienced an elevation in cardiac biomarkers but who did not meet the definition of MI, there was an increased risk of nonfatal cardiac arrest and nonacute coronary revascularization. Those in the highest quartile also had increased 30-day mortality.
Bottom line: Given the high proportion of asymptomatic MIs and isolated elevations in cardiac biomarkers and the association between these events and increased risk of death, hospitalists should consider routine monitoring of troponin in at-risk patients undergoing noncardiac surgery.
Citation: Devereaux PJ, Xavier D, Pogue J, et al. Characteristics and short-term prognosis of perioperative myocardial infarction in patients undergoing noncardiac surgery: a cohort study. Ann Intern Med. 2011;154(8):523-528.
Patients Prescribed Higher Opioid Doses Are at Increased Risk of Opioid Overdose Death
Clinical question: What is the association between opioid prescribing patterns and fatal opioid overdose?
Background: In the past 10 years, the rate of fatal overdose from opioid prescription for pain has more than doubled. Little is known about how the indications (substance abuse disorders, cancer-related pain, chronic pain, acute pain), maximal daily dose, and scheduling (standing, as-needed, or both) of opioid prescriptions relate to this increased risk.
Study design: Case-cohort study.
Setting: Veterans Health Administration (VHA) patients.
Synopsis: The VHA’s National Patient Care Database was used to randomly select a cohort of 154,684 nonhospice/nonpalliative-care patients who were prescribed opioids from 2004 to 2008. They were compared with 750 patients who were treated with prescription opioids who died from opioid overdose during this time.
Fatal opioid overdose was a rare event (0.04%), but risk increased with higher prescribed maximum daily morphine dose-equivalence, especially when greater than or equal to 50 mg/day in all subgroups (substance abuse, acute and chronic pain, and cancer). Fatal overdoses were higher in middle-aged white men with acute or chronic pain, substance abuse disorders, and other psychiatric illness. Patients with cancer were at increased risk of fatal overdose if they were prescribed as-needed opioids alone.
Treatment with both as-needed and standing opioids did not statistically affect risk of overdose death in any subgroup.
Bottom line: Although rare, risk of fatal opioid overdose in patients prescribed opiate medication increases with higher maximum prescribed daily dose.
Citation: Bohnert AS, Valenstein M, Bair M, et al. Association between opioid prescribing patterns and opioid overdose-related deaths. JAMA. 2011; 305:1315-1321.
Structured Interdisciplinary Rounds on Medical Teaching Unit Significantly Decrease Adverse Events
Clinical question: Do structured interdisciplinary rounds have an impact on the rate of adverse events?
Background: Many preventable adverse events occurring during hospitalization can be attributed to communication failures. Structured interdisciplinary rounds provide a format as well as a forum for team members to discuss patient care. Prior studies demonstrated improvements in collaboration; whether this translates to better patient care is not known.
Study design: Retrospective cohort using historic and concurrent control.
Setting: Tertiary-care teaching hospital in Chicago.
Synopsis: Structured interdisciplinary rounds, led by a nurse manager and medical director, and including nurses, residents, pharmacists, social workers, and case managers, were implemented on a medical teaching unit. New patients were discussed using a structured communication tool; existing patients were discussed in an unstructured format. Medical records were abstracted for 370 patients hospitalized after implementation of the intervention, equally divided between intervention and control units. One hundred eighty-five patients hospitalized on the intervention unit prior to the implementation of rounds served as a historic control.
Patients in the intervention unit had significantly lower rates of total adverse events (3.9 per 100 patient days in the intervention, compared with 7.2 and 7.7 per 100 patient days for the concurrent and historic control units, respectively), and preventable adverse events (0.9 per 100 patient days, compared with 2.8 and 2.1 per 100 patient days for the concurrent and historic controls, respectively).
Limitations of the study include lack of blinding of the medical record, slightly different patient populations in intervention and control groups, and the one-hospital setting, which could limit generalizability.
Bottom line: Structured interdisciplinary rounds might serve to improve communication between nurses, pharmacists, and physicians, resulting in decreases in adverse events.
Citation: O’Leary KJ, Buck R, Fligiel HM, et al. Structured interdisciplinary rounds in a medical teaching unit: improving patient safety. Arch Intern Med. 2011;171(7):678-684.
Pediatric HM Literature
Short-Course Antibiotic Therapy Effective for Bacterial Meningitis
Clinical question: Is five days of parenteral ceftriaxone as effective as 10 days for the treatment of bacterial meningitis in children?
Background: Morbidity and mortality in bacterial meningitis remain high, particularly in developing countries. Antibiotics are effective treatment, yet the optimal duration of treatment remains uncertain. Some data support a shorter duration of treatment (three to five days).
Study design: Multicountry, double-blind, placebo-controlled, randomized equivalence study.
Setting: Ten pediatric referral hospitals in Bangladesh, Egypt, Malawi, Pakistan, and Vietnam.
Synopsis: Children aged two months to 12 years with bacterial meningitis (due to Haemophilus influenza, Streptococcus pneumonia, Neisseria meningitidis, or culture-negative with indicative cerebrospinal fluid findings) and without complicating medical conditions were enrolled at participating centers. All children received 80 mg/kg to 100 mg/kg of parenteral ceftriaxone daily and a repeat lumbar puncture 48 to 72 hours after initiation of therapy.
Ultimately, 1,004 children without resistant organisms, persistently positive cultures, or suppurative complications were randomized on day five of therapy to placebo or continuance of ceftriaxone for five more days.
No bacteriologic failures (primary endpoint) were evident with either five or 10 days of treatment.
In addition, no statistically significant differences were found between the groups with respect to clinical treatment failure, hearing loss, neurological sequelae, or death. Secondary analysis by organism revealed similar results.
The primary limitation of this study is that it occurred in developing countries with a fair incidence of H. influenzae meningitis and a low rate of third-generation cephalosporin resistance.
However, pneumococcal and meningococcal disease remained prominent, and this study suggests that clinically stable patients might be treated with a shorter course of parenteral ceftriaxone therapy than currently is recommended.
Bottom line: Five days of ceftriaxone is as effective as 10 days for uncomplicated bacterial meningitis in children.
Citation: Molyneux E, Nizami SQ, Saha S, et al. 5 versus 10 days of treatment with ceftriaxone for bacterial meningitis in children: a double-blind randomised equivalence study. Lancet. 2011;377:1837-1845.
Reviewed by Pediatric Editor Mark Shen, MD, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
What Is the Best E&M of Heparin-Induced Thrombocytopenia?
Case
A 52-year-old white woman presents to the ED after a motor vehicle accident with a fractured left femur. After surgical repair of the fracture, she is treated with enoxaparin 40 mg daily for VTE prophylaxis. Upon admission to the hospital, her platelet count is 180x109/L. On postoperative day three, it is 140x109/L; on postoperative day six, it is 78x109/L. Because of persistent swelling of the left leg, a venous ultrasound is obtained; results are negative for DVT. Is the decrease in the platelet count concerning for heparin-induced thrombocytopenia?
Overview
Approximately one-third of hospitalized patients are exposed to heparin each year.1 A well-described, life-threatening adverse effect of heparin use is thrombocytopenia, also called heparin-induced thrombocytopenia (HIT). Studies suggest that the frequency of HIT in the U.S. is as high as 1% to 5% in patients exposed to unfractionated heparin.1,2
There are two types of HIT. Type 2 HIT is more serious, with risk for life- or limb-threatening complications. Type 1 HIT is a nonimmune disorder caused by the direct effect of heparin on platelet activation, which is characterized by a drop in thrombocyte count within the first 48 hours of heparin exposure. The platelet count is expected to normalize with continued heparin exposure in Type 1 HIT. Type 2 HIT is an immune-mediated disorder in which heparin-dependent IgG recognizes complexes of heparin and platelet factor 4 (PF4), which subsequently induce platelet activation via the platelet Fc gammaRIIa receptor. A positive feedback loop occurs, causing further release of PF4 and platelet activation, which can lead to devastating prothrombotic complications.
Individuals affected by Type 2 HIT have a 20% to 50% risk of developing new thrombotic events, and also have a 10% rate of major morbidity, including limb ischemia requiring amputation, cerebrovascular events, myocardial infarction, DVT, or pulmonary embolus.1,2
Until recently, the mortality rate in HIT has been reported as high as 20%; however, earlier diagnosis and treatment have resulted in a better prognosis, with mortality and major morbidity of 6% to 10%.2 Low-molecular-weight heparin (LMWH) carries a lower risk for development of HIT; as such, one measure to reduce the risk of HIT is to use LMWH in place of unfractionated heparin.3
Review of the Data
When to suspect HIT. HIT should be considered as a potential diagnosis anytime there is a drop in platelet count, either during or shortly following heparin exposure. The differential diagnosis for thrombocytopenia during heparin exposure is broad and includes:
- Disseminated intravascular coagulation;
- Drug-induced thrombocytopenia;
- Hemolytic-uremic syndrome;
- Immune thrombocytopenic purpura;
- Post-transfusion thrombocytopenia;
- Systemic lupus erythematosus; and
- Thrombotic thrombocytopenic purpura.
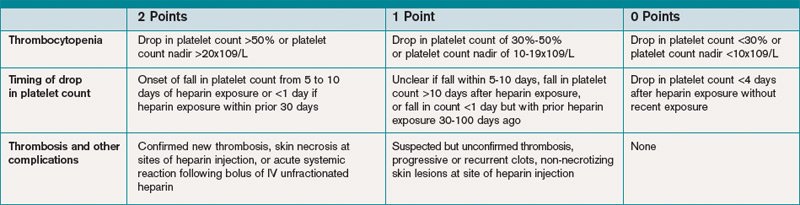
The 2009 Clinical Practice Guideline on Evaluation and Management of HIT provided by the American Society of Hematology recommends the use of Warkentin’s 4Ts clinical probability scoring system as a guide in determining the probability of HIT in patients with thrombocytopenia who are exposed to heparin.4 The 4Ts scoring system is detailed in Table 1.
In patients with intermediate to high clinical probability of HIT (4-5 points and 6-8 points, respectively, on the 4Ts scoring system), immunologic and functional assays could further guide management. In patients with a low probability of HIT (4Ts score <3), the diagnosis is unlikely and an alternative diagnoses should be considered. Immunologic and functional assays are not recommended for these patients, and heparin can be continued.
Laboratory and diagnostic workups. Immunologic assays (polyspecific ELISA, IgG-specific ELISA, and particle gel immunoassay) detect antibodies against the PF4 heparin complexes regardless of their capacity to activate platelets. These tests are highly sensitive but less specific for HIT because they also detect PF4-heparin antibodies in patients who do not have HIT; therefore, immunoassays have a lower positive predictive value but a high negative predictive value (>95%).5
Functional assays (serotonin release assay, heparin-induced platelet activation assay, and platelet aggregation test) detect antibodies that induce heparin-dependent platelet activation. These assays are highly sensitive and specific but are not available at many medical centers. The positive predictive value of these assays is higher (89% to 100%).5
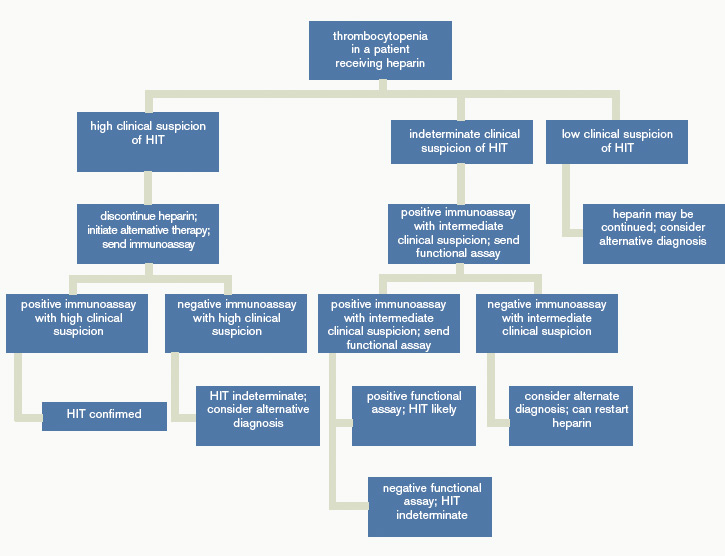
Figure 1 provides a diagnostic and initial treatment algorithm for suspected HIT. Immunoassays to detect PF4-heparin antibodies are recommended when clinical probability of HIT is intermediate to high. In these patients, a negative result on serologic testing has a high negative predictive value and suggests that an alternative diagnosis is more likely. In patients with a positive serologic test and intermediate probability of HIT, a functional assay might be beneficial, as a positive result increases the probability of HIT. For patients with high probability of HIT and a positive immunologic assay, functional assays might not be indicated as the diagnosis is likely.
Treatment. If the probability of HIT is intermediate to high based on the 4Ts scoring system, all heparin products, including heparin flushes, should be immediately discontinued and a laboratory investigation for HIT antibodies should be undertaken. An investigation for lower-limb DVT also should be pursued in patients with high probability of HIT, as the risk of thrombosis is more than 30-fold higher than controls, and studies show that approximately 25% of patients with HIT present with both thrombocytopenia and thrombosis.5 In addition, the presence of thrombosis might influence duration of anticoagulation.
Avoid platelet transfusions, as this might propagate thrombosis.
Anticoagulation. With a significant risk of thrombosis associated with this disorder, treatment with an alternative anticoagulant should be started. Vitamin K antagonists, such as warfarin, cannot be given in acute HIT because of the high risk of inducing skin necrosis and venous limb gangrene. Such anticoagulation should not be used until the platelet count increases to greater than 150x109/L. If warfarin already has been given, reversal with vitamin K is indicated.
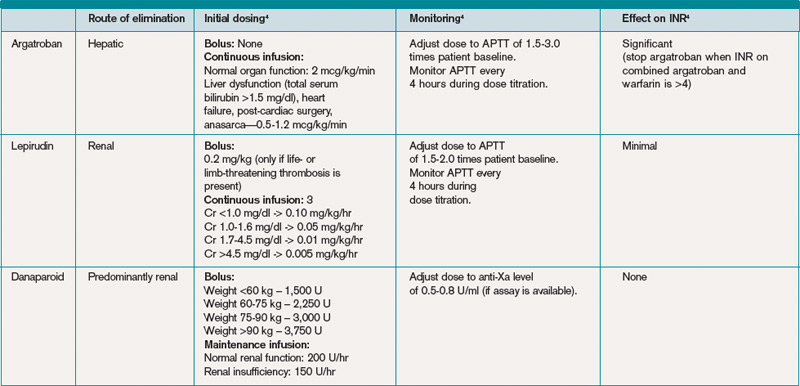
Consequently, an alternative anticoagulant bridge to warfarin therapy must be used. Usually, the bridging agent will be one of two intravenous direct thrombin inhibitors (argatroban and lepirudin) approved for this purpose.6 Both are associated with a higher risk of bleeding. Argatroban is hepatically cleared; lepirudin is renally cleared. Table 2 summarizes dosing information for these agents. A third direct thrombin inhibitor, bivalirudin, is approved for treatment of HIT, but only during percutaneous coronary intervention.6
Finally, the recently FDA-approved oral direct thrombin inhibitor dabigatrin has not been studied in or approved for HIT.
Other rational therapies include the factor Xa inhibitors danaparoid and fondaparinux. However, only danaparoid is FDA-approved for use in the treatment of HIT. It can, in cases of low or moderate suspicion of HIT, be given in prophylactic doses, lowering the risk of major bleeding.
Duration of treatment. Whichever bridging anticoagulant is chosen, it should be continued until the platelet count has fully recovered. Further, prior to discontinuation, warfarin therapy should be administered for at least five days and the international normalized ratio (INR) should be therapeutic for approximately 48 hours.
The subsequent length of warfarin therapy is dependent upon the presence or absence of an associated thrombosis. With the presence of a thrombus, the duration should be as defined for other provoked thromboses (three to six months). With no thrombus, the duration should be at least 30 days.
Future anticoagulation in patients with a prior diagnosis of HIT. A history of HIT does not appear to be a risk factor for a higher frequency of forming heparin antibodies upon re-exposure to heparin.7 Therefore, in patients with an important indication for heparin (i.e. cardiac or vascular surgery) and a remote history of HIT (>100 days), heparin can be used. In patients with a subacute history of HIT in whom surgery cannot be delayed, heparin products should be avoided and laboratory investigation should be pursued.
If the immunoassay is positive but the functional assay is negative, it is reasonable to use heparin. If both the immunologic and the functional assays are positive, the patient should be considered as having acute HIT, and bivalirudin is recommended.4
Back to the Case
Our patient has acute thrombocytopenia with a fall in platelets greater than 50% from baseline. The decrease is within the appropriate time frame for HIT. No thrombosis is found, but no alternate explanation for the thrombocytopenia is apparent. The 4Ts score of 6 indicates high risk for HIT. Heparin was discontinued, and argatroban at a rate of 2 mcg/kg/min was initiated. The immunoassay was positive.
Argatroban was continued until the platelet count reached 150x109/L, at which point warfarin therapy, 5 mg daily, was started. After four days, the INR was 2.2. After another 24 hours, argatroban was discontinued. She was instructed to continue warfarin for another 30 days.
Bottom Line
Evaluation for HIT combines clinical judgment, summarized in the 4Ts, with laboratory evaluation including an immunoassay and possibly a functional assay. Treatment requires immediate discontinuation of heparin, early initiation of a direct thrombin inhibitor, and bridging to warfarin to continue treatment for at least 30 days. TH
Drs. Smith and Rice are members of the Section of Hospital Medicine at Vanderbilt University in Nashville, Tenn.
References
- Heparin-Induced Thrombocytopenia. MedScape Reference website. Available at: http://emedicine.medscape.com/article/1357846. Accessed Aug. 31, 2010.
- Heparin-Induced Thrombocytopenia. Orpha.net website. Available at: http://www.orpha.net/data/patho/GB/uk-HIT.pdf. Accessed Aug. 31, 2010.
- Warkentin TE, Levine MN, Hirsh J, et al. Heparin-induced thrombocytopenia in patients treated with low-molecular-weight heparin or unfractionated heparin. N Engl J Med. 1995;332(20):1330-1335.
- American Society of Hematology Guidelines: Immune Thrombocytopenia (HIT). American Society of Hematology website. Available at: www.hematology.org/Practice/Guidelines/2934.aspx. Accessed Jan. 28, 2011.
- Arepally GM, Ortel TL. Heparin-induced thrombocytopenia. Annu Rev Med. 2010;61:77-90.
- Warkentin TE, Greinacher A, Koster A, Lincoff AM. Treatment and prevention of heparin-induced thrombocytopenia: American College of Chest Physicians Evidence-based Clinical Practice Guidelines (8th Edition). Chest. 2008;133:340S-380S.
- Warkentin TE. Agents for the treatment of heparin-induced thrombocytopenia. Hematol Oncol Clin N Am. 2010;24:755-775.
Case
A 52-year-old white woman presents to the ED after a motor vehicle accident with a fractured left femur. After surgical repair of the fracture, she is treated with enoxaparin 40 mg daily for VTE prophylaxis. Upon admission to the hospital, her platelet count is 180x109/L. On postoperative day three, it is 140x109/L; on postoperative day six, it is 78x109/L. Because of persistent swelling of the left leg, a venous ultrasound is obtained; results are negative for DVT. Is the decrease in the platelet count concerning for heparin-induced thrombocytopenia?
Overview
Approximately one-third of hospitalized patients are exposed to heparin each year.1 A well-described, life-threatening adverse effect of heparin use is thrombocytopenia, also called heparin-induced thrombocytopenia (HIT). Studies suggest that the frequency of HIT in the U.S. is as high as 1% to 5% in patients exposed to unfractionated heparin.1,2
There are two types of HIT. Type 2 HIT is more serious, with risk for life- or limb-threatening complications. Type 1 HIT is a nonimmune disorder caused by the direct effect of heparin on platelet activation, which is characterized by a drop in thrombocyte count within the first 48 hours of heparin exposure. The platelet count is expected to normalize with continued heparin exposure in Type 1 HIT. Type 2 HIT is an immune-mediated disorder in which heparin-dependent IgG recognizes complexes of heparin and platelet factor 4 (PF4), which subsequently induce platelet activation via the platelet Fc gammaRIIa receptor. A positive feedback loop occurs, causing further release of PF4 and platelet activation, which can lead to devastating prothrombotic complications.
Individuals affected by Type 2 HIT have a 20% to 50% risk of developing new thrombotic events, and also have a 10% rate of major morbidity, including limb ischemia requiring amputation, cerebrovascular events, myocardial infarction, DVT, or pulmonary embolus.1,2
Until recently, the mortality rate in HIT has been reported as high as 20%; however, earlier diagnosis and treatment have resulted in a better prognosis, with mortality and major morbidity of 6% to 10%.2 Low-molecular-weight heparin (LMWH) carries a lower risk for development of HIT; as such, one measure to reduce the risk of HIT is to use LMWH in place of unfractionated heparin.3
Review of the Data
When to suspect HIT. HIT should be considered as a potential diagnosis anytime there is a drop in platelet count, either during or shortly following heparin exposure. The differential diagnosis for thrombocytopenia during heparin exposure is broad and includes:
- Disseminated intravascular coagulation;
- Drug-induced thrombocytopenia;
- Hemolytic-uremic syndrome;
- Immune thrombocytopenic purpura;
- Post-transfusion thrombocytopenia;
- Systemic lupus erythematosus; and
- Thrombotic thrombocytopenic purpura.
The 2009 Clinical Practice Guideline on Evaluation and Management of HIT provided by the American Society of Hematology recommends the use of Warkentin’s 4Ts clinical probability scoring system as a guide in determining the probability of HIT in patients with thrombocytopenia who are exposed to heparin.4 The 4Ts scoring system is detailed in Table 1.
In patients with intermediate to high clinical probability of HIT (4-5 points and 6-8 points, respectively, on the 4Ts scoring system), immunologic and functional assays could further guide management. In patients with a low probability of HIT (4Ts score <3), the diagnosis is unlikely and an alternative diagnoses should be considered. Immunologic and functional assays are not recommended for these patients, and heparin can be continued.
Laboratory and diagnostic workups. Immunologic assays (polyspecific ELISA, IgG-specific ELISA, and particle gel immunoassay) detect antibodies against the PF4 heparin complexes regardless of their capacity to activate platelets. These tests are highly sensitive but less specific for HIT because they also detect PF4-heparin antibodies in patients who do not have HIT; therefore, immunoassays have a lower positive predictive value but a high negative predictive value (>95%).5
Functional assays (serotonin release assay, heparin-induced platelet activation assay, and platelet aggregation test) detect antibodies that induce heparin-dependent platelet activation. These assays are highly sensitive and specific but are not available at many medical centers. The positive predictive value of these assays is higher (89% to 100%).5
Figure 1 provides a diagnostic and initial treatment algorithm for suspected HIT. Immunoassays to detect PF4-heparin antibodies are recommended when clinical probability of HIT is intermediate to high. In these patients, a negative result on serologic testing has a high negative predictive value and suggests that an alternative diagnosis is more likely. In patients with a positive serologic test and intermediate probability of HIT, a functional assay might be beneficial, as a positive result increases the probability of HIT. For patients with high probability of HIT and a positive immunologic assay, functional assays might not be indicated as the diagnosis is likely.
Treatment. If the probability of HIT is intermediate to high based on the 4Ts scoring system, all heparin products, including heparin flushes, should be immediately discontinued and a laboratory investigation for HIT antibodies should be undertaken. An investigation for lower-limb DVT also should be pursued in patients with high probability of HIT, as the risk of thrombosis is more than 30-fold higher than controls, and studies show that approximately 25% of patients with HIT present with both thrombocytopenia and thrombosis.5 In addition, the presence of thrombosis might influence duration of anticoagulation.
Avoid platelet transfusions, as this might propagate thrombosis.
Anticoagulation. With a significant risk of thrombosis associated with this disorder, treatment with an alternative anticoagulant should be started. Vitamin K antagonists, such as warfarin, cannot be given in acute HIT because of the high risk of inducing skin necrosis and venous limb gangrene. Such anticoagulation should not be used until the platelet count increases to greater than 150x109/L. If warfarin already has been given, reversal with vitamin K is indicated.
Consequently, an alternative anticoagulant bridge to warfarin therapy must be used. Usually, the bridging agent will be one of two intravenous direct thrombin inhibitors (argatroban and lepirudin) approved for this purpose.6 Both are associated with a higher risk of bleeding. Argatroban is hepatically cleared; lepirudin is renally cleared. Table 2 summarizes dosing information for these agents. A third direct thrombin inhibitor, bivalirudin, is approved for treatment of HIT, but only during percutaneous coronary intervention.6
Finally, the recently FDA-approved oral direct thrombin inhibitor dabigatrin has not been studied in or approved for HIT.
Other rational therapies include the factor Xa inhibitors danaparoid and fondaparinux. However, only danaparoid is FDA-approved for use in the treatment of HIT. It can, in cases of low or moderate suspicion of HIT, be given in prophylactic doses, lowering the risk of major bleeding.
Duration of treatment. Whichever bridging anticoagulant is chosen, it should be continued until the platelet count has fully recovered. Further, prior to discontinuation, warfarin therapy should be administered for at least five days and the international normalized ratio (INR) should be therapeutic for approximately 48 hours.
The subsequent length of warfarin therapy is dependent upon the presence or absence of an associated thrombosis. With the presence of a thrombus, the duration should be as defined for other provoked thromboses (three to six months). With no thrombus, the duration should be at least 30 days.
Future anticoagulation in patients with a prior diagnosis of HIT. A history of HIT does not appear to be a risk factor for a higher frequency of forming heparin antibodies upon re-exposure to heparin.7 Therefore, in patients with an important indication for heparin (i.e. cardiac or vascular surgery) and a remote history of HIT (>100 days), heparin can be used. In patients with a subacute history of HIT in whom surgery cannot be delayed, heparin products should be avoided and laboratory investigation should be pursued.
If the immunoassay is positive but the functional assay is negative, it is reasonable to use heparin. If both the immunologic and the functional assays are positive, the patient should be considered as having acute HIT, and bivalirudin is recommended.4
Back to the Case
Our patient has acute thrombocytopenia with a fall in platelets greater than 50% from baseline. The decrease is within the appropriate time frame for HIT. No thrombosis is found, but no alternate explanation for the thrombocytopenia is apparent. The 4Ts score of 6 indicates high risk for HIT. Heparin was discontinued, and argatroban at a rate of 2 mcg/kg/min was initiated. The immunoassay was positive.
Argatroban was continued until the platelet count reached 150x109/L, at which point warfarin therapy, 5 mg daily, was started. After four days, the INR was 2.2. After another 24 hours, argatroban was discontinued. She was instructed to continue warfarin for another 30 days.
Bottom Line
Evaluation for HIT combines clinical judgment, summarized in the 4Ts, with laboratory evaluation including an immunoassay and possibly a functional assay. Treatment requires immediate discontinuation of heparin, early initiation of a direct thrombin inhibitor, and bridging to warfarin to continue treatment for at least 30 days. TH
Drs. Smith and Rice are members of the Section of Hospital Medicine at Vanderbilt University in Nashville, Tenn.
References
- Heparin-Induced Thrombocytopenia. MedScape Reference website. Available at: http://emedicine.medscape.com/article/1357846. Accessed Aug. 31, 2010.
- Heparin-Induced Thrombocytopenia. Orpha.net website. Available at: http://www.orpha.net/data/patho/GB/uk-HIT.pdf. Accessed Aug. 31, 2010.
- Warkentin TE, Levine MN, Hirsh J, et al. Heparin-induced thrombocytopenia in patients treated with low-molecular-weight heparin or unfractionated heparin. N Engl J Med. 1995;332(20):1330-1335.
- American Society of Hematology Guidelines: Immune Thrombocytopenia (HIT). American Society of Hematology website. Available at: www.hematology.org/Practice/Guidelines/2934.aspx. Accessed Jan. 28, 2011.
- Arepally GM, Ortel TL. Heparin-induced thrombocytopenia. Annu Rev Med. 2010;61:77-90.
- Warkentin TE, Greinacher A, Koster A, Lincoff AM. Treatment and prevention of heparin-induced thrombocytopenia: American College of Chest Physicians Evidence-based Clinical Practice Guidelines (8th Edition). Chest. 2008;133:340S-380S.
- Warkentin TE. Agents for the treatment of heparin-induced thrombocytopenia. Hematol Oncol Clin N Am. 2010;24:755-775.
Case
A 52-year-old white woman presents to the ED after a motor vehicle accident with a fractured left femur. After surgical repair of the fracture, she is treated with enoxaparin 40 mg daily for VTE prophylaxis. Upon admission to the hospital, her platelet count is 180x109/L. On postoperative day three, it is 140x109/L; on postoperative day six, it is 78x109/L. Because of persistent swelling of the left leg, a venous ultrasound is obtained; results are negative for DVT. Is the decrease in the platelet count concerning for heparin-induced thrombocytopenia?
Overview
Approximately one-third of hospitalized patients are exposed to heparin each year.1 A well-described, life-threatening adverse effect of heparin use is thrombocytopenia, also called heparin-induced thrombocytopenia (HIT). Studies suggest that the frequency of HIT in the U.S. is as high as 1% to 5% in patients exposed to unfractionated heparin.1,2
There are two types of HIT. Type 2 HIT is more serious, with risk for life- or limb-threatening complications. Type 1 HIT is a nonimmune disorder caused by the direct effect of heparin on platelet activation, which is characterized by a drop in thrombocyte count within the first 48 hours of heparin exposure. The platelet count is expected to normalize with continued heparin exposure in Type 1 HIT. Type 2 HIT is an immune-mediated disorder in which heparin-dependent IgG recognizes complexes of heparin and platelet factor 4 (PF4), which subsequently induce platelet activation via the platelet Fc gammaRIIa receptor. A positive feedback loop occurs, causing further release of PF4 and platelet activation, which can lead to devastating prothrombotic complications.
Individuals affected by Type 2 HIT have a 20% to 50% risk of developing new thrombotic events, and also have a 10% rate of major morbidity, including limb ischemia requiring amputation, cerebrovascular events, myocardial infarction, DVT, or pulmonary embolus.1,2
Until recently, the mortality rate in HIT has been reported as high as 20%; however, earlier diagnosis and treatment have resulted in a better prognosis, with mortality and major morbidity of 6% to 10%.2 Low-molecular-weight heparin (LMWH) carries a lower risk for development of HIT; as such, one measure to reduce the risk of HIT is to use LMWH in place of unfractionated heparin.3
Review of the Data
When to suspect HIT. HIT should be considered as a potential diagnosis anytime there is a drop in platelet count, either during or shortly following heparin exposure. The differential diagnosis for thrombocytopenia during heparin exposure is broad and includes:
- Disseminated intravascular coagulation;
- Drug-induced thrombocytopenia;
- Hemolytic-uremic syndrome;
- Immune thrombocytopenic purpura;
- Post-transfusion thrombocytopenia;
- Systemic lupus erythematosus; and
- Thrombotic thrombocytopenic purpura.
The 2009 Clinical Practice Guideline on Evaluation and Management of HIT provided by the American Society of Hematology recommends the use of Warkentin’s 4Ts clinical probability scoring system as a guide in determining the probability of HIT in patients with thrombocytopenia who are exposed to heparin.4 The 4Ts scoring system is detailed in Table 1.
In patients with intermediate to high clinical probability of HIT (4-5 points and 6-8 points, respectively, on the 4Ts scoring system), immunologic and functional assays could further guide management. In patients with a low probability of HIT (4Ts score <3), the diagnosis is unlikely and an alternative diagnoses should be considered. Immunologic and functional assays are not recommended for these patients, and heparin can be continued.
Laboratory and diagnostic workups. Immunologic assays (polyspecific ELISA, IgG-specific ELISA, and particle gel immunoassay) detect antibodies against the PF4 heparin complexes regardless of their capacity to activate platelets. These tests are highly sensitive but less specific for HIT because they also detect PF4-heparin antibodies in patients who do not have HIT; therefore, immunoassays have a lower positive predictive value but a high negative predictive value (>95%).5
Functional assays (serotonin release assay, heparin-induced platelet activation assay, and platelet aggregation test) detect antibodies that induce heparin-dependent platelet activation. These assays are highly sensitive and specific but are not available at many medical centers. The positive predictive value of these assays is higher (89% to 100%).5
Figure 1 provides a diagnostic and initial treatment algorithm for suspected HIT. Immunoassays to detect PF4-heparin antibodies are recommended when clinical probability of HIT is intermediate to high. In these patients, a negative result on serologic testing has a high negative predictive value and suggests that an alternative diagnosis is more likely. In patients with a positive serologic test and intermediate probability of HIT, a functional assay might be beneficial, as a positive result increases the probability of HIT. For patients with high probability of HIT and a positive immunologic assay, functional assays might not be indicated as the diagnosis is likely.
Treatment. If the probability of HIT is intermediate to high based on the 4Ts scoring system, all heparin products, including heparin flushes, should be immediately discontinued and a laboratory investigation for HIT antibodies should be undertaken. An investigation for lower-limb DVT also should be pursued in patients with high probability of HIT, as the risk of thrombosis is more than 30-fold higher than controls, and studies show that approximately 25% of patients with HIT present with both thrombocytopenia and thrombosis.5 In addition, the presence of thrombosis might influence duration of anticoagulation.
Avoid platelet transfusions, as this might propagate thrombosis.
Anticoagulation. With a significant risk of thrombosis associated with this disorder, treatment with an alternative anticoagulant should be started. Vitamin K antagonists, such as warfarin, cannot be given in acute HIT because of the high risk of inducing skin necrosis and venous limb gangrene. Such anticoagulation should not be used until the platelet count increases to greater than 150x109/L. If warfarin already has been given, reversal with vitamin K is indicated.
Consequently, an alternative anticoagulant bridge to warfarin therapy must be used. Usually, the bridging agent will be one of two intravenous direct thrombin inhibitors (argatroban and lepirudin) approved for this purpose.6 Both are associated with a higher risk of bleeding. Argatroban is hepatically cleared; lepirudin is renally cleared. Table 2 summarizes dosing information for these agents. A third direct thrombin inhibitor, bivalirudin, is approved for treatment of HIT, but only during percutaneous coronary intervention.6
Finally, the recently FDA-approved oral direct thrombin inhibitor dabigatrin has not been studied in or approved for HIT.
Other rational therapies include the factor Xa inhibitors danaparoid and fondaparinux. However, only danaparoid is FDA-approved for use in the treatment of HIT. It can, in cases of low or moderate suspicion of HIT, be given in prophylactic doses, lowering the risk of major bleeding.
Duration of treatment. Whichever bridging anticoagulant is chosen, it should be continued until the platelet count has fully recovered. Further, prior to discontinuation, warfarin therapy should be administered for at least five days and the international normalized ratio (INR) should be therapeutic for approximately 48 hours.
The subsequent length of warfarin therapy is dependent upon the presence or absence of an associated thrombosis. With the presence of a thrombus, the duration should be as defined for other provoked thromboses (three to six months). With no thrombus, the duration should be at least 30 days.
Future anticoagulation in patients with a prior diagnosis of HIT. A history of HIT does not appear to be a risk factor for a higher frequency of forming heparin antibodies upon re-exposure to heparin.7 Therefore, in patients with an important indication for heparin (i.e. cardiac or vascular surgery) and a remote history of HIT (>100 days), heparin can be used. In patients with a subacute history of HIT in whom surgery cannot be delayed, heparin products should be avoided and laboratory investigation should be pursued.
If the immunoassay is positive but the functional assay is negative, it is reasonable to use heparin. If both the immunologic and the functional assays are positive, the patient should be considered as having acute HIT, and bivalirudin is recommended.4
Back to the Case
Our patient has acute thrombocytopenia with a fall in platelets greater than 50% from baseline. The decrease is within the appropriate time frame for HIT. No thrombosis is found, but no alternate explanation for the thrombocytopenia is apparent. The 4Ts score of 6 indicates high risk for HIT. Heparin was discontinued, and argatroban at a rate of 2 mcg/kg/min was initiated. The immunoassay was positive.
Argatroban was continued until the platelet count reached 150x109/L, at which point warfarin therapy, 5 mg daily, was started. After four days, the INR was 2.2. After another 24 hours, argatroban was discontinued. She was instructed to continue warfarin for another 30 days.
Bottom Line
Evaluation for HIT combines clinical judgment, summarized in the 4Ts, with laboratory evaluation including an immunoassay and possibly a functional assay. Treatment requires immediate discontinuation of heparin, early initiation of a direct thrombin inhibitor, and bridging to warfarin to continue treatment for at least 30 days. TH
Drs. Smith and Rice are members of the Section of Hospital Medicine at Vanderbilt University in Nashville, Tenn.
References
- Heparin-Induced Thrombocytopenia. MedScape Reference website. Available at: http://emedicine.medscape.com/article/1357846. Accessed Aug. 31, 2010.
- Heparin-Induced Thrombocytopenia. Orpha.net website. Available at: http://www.orpha.net/data/patho/GB/uk-HIT.pdf. Accessed Aug. 31, 2010.
- Warkentin TE, Levine MN, Hirsh J, et al. Heparin-induced thrombocytopenia in patients treated with low-molecular-weight heparin or unfractionated heparin. N Engl J Med. 1995;332(20):1330-1335.
- American Society of Hematology Guidelines: Immune Thrombocytopenia (HIT). American Society of Hematology website. Available at: www.hematology.org/Practice/Guidelines/2934.aspx. Accessed Jan. 28, 2011.
- Arepally GM, Ortel TL. Heparin-induced thrombocytopenia. Annu Rev Med. 2010;61:77-90.
- Warkentin TE, Greinacher A, Koster A, Lincoff AM. Treatment and prevention of heparin-induced thrombocytopenia: American College of Chest Physicians Evidence-based Clinical Practice Guidelines (8th Edition). Chest. 2008;133:340S-380S.
- Warkentin TE. Agents for the treatment of heparin-induced thrombocytopenia. Hematol Oncol Clin N Am. 2010;24:755-775.
Exchange Anxiety
A 224-page document full of regulatory jargon might not be a fun summer read. Nevertheless, the U.S. Department of Health and Human Service’s (HHS) mid-July release of proposed rules for state-run health insurance exchanges (HIE) represents a major step toward expanding an insurance pool that could grow by an estimated 24 million Americans over the next eight years.
When the exchanges arrive in 2014, the single biggest impact is likely to be a major expansion of access, with 8.9 million individuals expected to sign up in the first year alone, according to projections by the Congressional Budget Office. A new report by PwC US Health Research Institute forecasts that a stunning 97% of those expected participants will be individuals who currently lack health insurance. A major driver of the new enrollments will be sliding-scale federal subsidies for individuals who earn from 138% to 400% of the federal poverty level, helping them buy insurance through the exchanges.
Experts say the exchanges also could directly impact hospitalists by bringing big changes to hospitals’ reimbursement revenue streams, spurring efforts to improve patient satisfaction metrics and increasing the momentum toward clinical comanagement agreements.
First, though, the public will get a chance to weigh in over rules that have been alternately lauded and derided, largely following the fault lines over the broader package of healthcare reforms. At a news conference set in front of a hardware store, HHS Secretary Kathleen Sebelius said competition on a level playing field would increase the purchasing power and drive down costs for individuals and small businesses. Websites for each of the exchanges would allow consumers to comparison-shop, with HHS ensuring that plans provide minimum standards for coverage. Patient groups, consumer organizations, and some small-business associations have welcomed the HHS rules, despite some concern that the exchanges could be tilted too far in favor of insurers. Overall, many analysts say, the rules have provided a fair amount of latitude over how the HIEs will be established and governed. Some business lobbyists, however, contend that the complex requirements will increase healthcare costs instead of lowering them. A July 16 editorial in the Wall Street Journal blasted the exchange rules as poorly designed and offering too little flexibility for states.
Two state-run ex-changes already exist, in Massachusetts and Utah. As of mid-July, however, states that had enacted laws to establish their own HIEs were outnumbered by those whose legislatures or governors had specifically blocked efforts to do likewise, according to the National Conference of State Legislatures. If states cannot or will not set up an exchange, HHS will step in and do it for them.
Reversal of Fortune?
Regardless of who ultimately oversees the exchanges, studies have begun suggesting who the most likely participants might be. An analysis by the Kaiser Family Foundation suggests that the newly insured are likely to be relatively older, less educated, more racially diverse, and in poorer health than those who currently carry private insurance but have fewer diagnosed conditions (www.kff.org/health reform/8147.cfm). Just as analysts, such as PwC, say that insurers will need to change their business strategy to lure and retain consumers, hospitals might need to redouble efforts to ensure high quality and patient satisfaction among a patient demographic that might be harder to please.
Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, says the shift could represent a boon for hospitals that have been forced to maximize efficiency. “In general, those hospitals that have a poorer payor mix have tended to become very efficient, and so they make money off of Medicare patients,” Dr. Williams, a former SHM president, says. “This is fascinating because, on the one hand, there may be a lot of patients for whom hospitalists can now get paid because they’re insured. But I personally think that, simultaneously, we’re going to be seeing cutbacks in payments for other patients who have private insurance.”
For some hospitals, the net effect on revenue might not be materially different, though Dr. Williams sees a potentially sizable benefit for “safety net” hospitals that care for a large proportion of uninsured patients and excel in making the most of limited resources. Some investors apparently agree. Last December, Nashville, Tenn.-based Vanguard Health Systems finalized a deal to buy Detroit Medical Center, with a total investment of nearly $1.5 billion. Dr. Williams says the expectation is that the medical center will suddenly see many more insured patients via an HIE. The result could be a dramatic boost to its finances.
Wealthier hospitals, by contrast, have had less incentive to maximize efficiency—and now are worried by the potential financial impacts of insurance exchanges. “Your classic, highly profitable community hospital that has a good payor mix loses money on Medicare patients and tends to subsidize that with their private patients,” Dr. Williams says. “The wealthier hospitals are nervous because they’re worried that this entire health insurance exchange is going to put downward pressure on reimbursements from the private insurers.”

—Mark Williams, MD, FACP, SFHM, chief, division of hospital medicine, Feinberg School of Medicine, Northwestern University, Chicago
Satisfaction Times Two
With Medicare’s value-based purchasing initiative on its way, hospitals are ramping up their attention to patient satisfaction scores. So how will an influx of potentially older and sicker patients insured through the exchanges affect hospitalists’ scores? No one knows, but because hospitalists already are known for their expertise in treating this very demographic, some experts expect hospitals to lean on them more for leading quality and satisfaction initiatives. This reliance could represent a major opportunity for HM, but faulty performance metrics could also bring danger (read more about this topic in next month’s The Hospitalist).
Cherilyn Murer, president and CEO of Joliet, Ill.-based Murer Consultants Inc., says the expected shift in the nature of inpatients could accelerate efforts to be more accurate about physicians’ performance measures. “Patients who may be in the ICU are at a higher level of crisis than a person who’s in and out for an appendectomy, and yet we’re using the same tool of satisfaction,” she says. Furthermore, she adds, many factors that contribute to patient satisfaction are highly subjective and have nothing to do with a specific physician. “We have to really question the tools now, moreso than only questioning the participation and the outcome,” she says. As with other aspects of healthcare reform, Murer says, the looming arrival of exchanges also should be prompting hospitalists to ask themselves: “What’s our game plan now?” One compelling answer, she contends, is a clinical comanagement agreement that takes a longer-term view of doctors’ relationships with hospitals and gives them more control over decision-making. After all, if HM is taking care of “the sickest of the sick patients,” she says, a comanagement agreement can mean more say in factors that will directly impact their jobs over the long haul. Strategic direction of product lines, space, and equipment-buying decisions are just a few examples.
Murer ultimately sees clinical comanagement as a precursor to more widespread bundling of payments to hospitals and physicians. The mix of private and public insurance reimbursements, already in flux, might be further clouded by the arrival of HIEs. But solidifying hospital-hospitalist alignment with a flexible comanagement agreement, she says, can offer some reassurance over job structure, rewards, and authority as healthcare continues hurtling toward profound change.
Bryn Nelson is a freelance medical writer based in Seattle.
A 224-page document full of regulatory jargon might not be a fun summer read. Nevertheless, the U.S. Department of Health and Human Service’s (HHS) mid-July release of proposed rules for state-run health insurance exchanges (HIE) represents a major step toward expanding an insurance pool that could grow by an estimated 24 million Americans over the next eight years.
When the exchanges arrive in 2014, the single biggest impact is likely to be a major expansion of access, with 8.9 million individuals expected to sign up in the first year alone, according to projections by the Congressional Budget Office. A new report by PwC US Health Research Institute forecasts that a stunning 97% of those expected participants will be individuals who currently lack health insurance. A major driver of the new enrollments will be sliding-scale federal subsidies for individuals who earn from 138% to 400% of the federal poverty level, helping them buy insurance through the exchanges.
Experts say the exchanges also could directly impact hospitalists by bringing big changes to hospitals’ reimbursement revenue streams, spurring efforts to improve patient satisfaction metrics and increasing the momentum toward clinical comanagement agreements.
First, though, the public will get a chance to weigh in over rules that have been alternately lauded and derided, largely following the fault lines over the broader package of healthcare reforms. At a news conference set in front of a hardware store, HHS Secretary Kathleen Sebelius said competition on a level playing field would increase the purchasing power and drive down costs for individuals and small businesses. Websites for each of the exchanges would allow consumers to comparison-shop, with HHS ensuring that plans provide minimum standards for coverage. Patient groups, consumer organizations, and some small-business associations have welcomed the HHS rules, despite some concern that the exchanges could be tilted too far in favor of insurers. Overall, many analysts say, the rules have provided a fair amount of latitude over how the HIEs will be established and governed. Some business lobbyists, however, contend that the complex requirements will increase healthcare costs instead of lowering them. A July 16 editorial in the Wall Street Journal blasted the exchange rules as poorly designed and offering too little flexibility for states.
Two state-run ex-changes already exist, in Massachusetts and Utah. As of mid-July, however, states that had enacted laws to establish their own HIEs were outnumbered by those whose legislatures or governors had specifically blocked efforts to do likewise, according to the National Conference of State Legislatures. If states cannot or will not set up an exchange, HHS will step in and do it for them.
Reversal of Fortune?
Regardless of who ultimately oversees the exchanges, studies have begun suggesting who the most likely participants might be. An analysis by the Kaiser Family Foundation suggests that the newly insured are likely to be relatively older, less educated, more racially diverse, and in poorer health than those who currently carry private insurance but have fewer diagnosed conditions (www.kff.org/health reform/8147.cfm). Just as analysts, such as PwC, say that insurers will need to change their business strategy to lure and retain consumers, hospitals might need to redouble efforts to ensure high quality and patient satisfaction among a patient demographic that might be harder to please.
Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, says the shift could represent a boon for hospitals that have been forced to maximize efficiency. “In general, those hospitals that have a poorer payor mix have tended to become very efficient, and so they make money off of Medicare patients,” Dr. Williams, a former SHM president, says. “This is fascinating because, on the one hand, there may be a lot of patients for whom hospitalists can now get paid because they’re insured. But I personally think that, simultaneously, we’re going to be seeing cutbacks in payments for other patients who have private insurance.”
For some hospitals, the net effect on revenue might not be materially different, though Dr. Williams sees a potentially sizable benefit for “safety net” hospitals that care for a large proportion of uninsured patients and excel in making the most of limited resources. Some investors apparently agree. Last December, Nashville, Tenn.-based Vanguard Health Systems finalized a deal to buy Detroit Medical Center, with a total investment of nearly $1.5 billion. Dr. Williams says the expectation is that the medical center will suddenly see many more insured patients via an HIE. The result could be a dramatic boost to its finances.
Wealthier hospitals, by contrast, have had less incentive to maximize efficiency—and now are worried by the potential financial impacts of insurance exchanges. “Your classic, highly profitable community hospital that has a good payor mix loses money on Medicare patients and tends to subsidize that with their private patients,” Dr. Williams says. “The wealthier hospitals are nervous because they’re worried that this entire health insurance exchange is going to put downward pressure on reimbursements from the private insurers.”
—Mark Williams, MD, FACP, SFHM, chief, division of hospital medicine, Feinberg School of Medicine, Northwestern University, Chicago
Satisfaction Times Two
With Medicare’s value-based purchasing initiative on its way, hospitals are ramping up their attention to patient satisfaction scores. So how will an influx of potentially older and sicker patients insured through the exchanges affect hospitalists’ scores? No one knows, but because hospitalists already are known for their expertise in treating this very demographic, some experts expect hospitals to lean on them more for leading quality and satisfaction initiatives. This reliance could represent a major opportunity for HM, but faulty performance metrics could also bring danger (read more about this topic in next month’s The Hospitalist).
Cherilyn Murer, president and CEO of Joliet, Ill.-based Murer Consultants Inc., says the expected shift in the nature of inpatients could accelerate efforts to be more accurate about physicians’ performance measures. “Patients who may be in the ICU are at a higher level of crisis than a person who’s in and out for an appendectomy, and yet we’re using the same tool of satisfaction,” she says. Furthermore, she adds, many factors that contribute to patient satisfaction are highly subjective and have nothing to do with a specific physician. “We have to really question the tools now, moreso than only questioning the participation and the outcome,” she says. As with other aspects of healthcare reform, Murer says, the looming arrival of exchanges also should be prompting hospitalists to ask themselves: “What’s our game plan now?” One compelling answer, she contends, is a clinical comanagement agreement that takes a longer-term view of doctors’ relationships with hospitals and gives them more control over decision-making. After all, if HM is taking care of “the sickest of the sick patients,” she says, a comanagement agreement can mean more say in factors that will directly impact their jobs over the long haul. Strategic direction of product lines, space, and equipment-buying decisions are just a few examples.
Murer ultimately sees clinical comanagement as a precursor to more widespread bundling of payments to hospitals and physicians. The mix of private and public insurance reimbursements, already in flux, might be further clouded by the arrival of HIEs. But solidifying hospital-hospitalist alignment with a flexible comanagement agreement, she says, can offer some reassurance over job structure, rewards, and authority as healthcare continues hurtling toward profound change.
Bryn Nelson is a freelance medical writer based in Seattle.
A 224-page document full of regulatory jargon might not be a fun summer read. Nevertheless, the U.S. Department of Health and Human Service’s (HHS) mid-July release of proposed rules for state-run health insurance exchanges (HIE) represents a major step toward expanding an insurance pool that could grow by an estimated 24 million Americans over the next eight years.
When the exchanges arrive in 2014, the single biggest impact is likely to be a major expansion of access, with 8.9 million individuals expected to sign up in the first year alone, according to projections by the Congressional Budget Office. A new report by PwC US Health Research Institute forecasts that a stunning 97% of those expected participants will be individuals who currently lack health insurance. A major driver of the new enrollments will be sliding-scale federal subsidies for individuals who earn from 138% to 400% of the federal poverty level, helping them buy insurance through the exchanges.
Experts say the exchanges also could directly impact hospitalists by bringing big changes to hospitals’ reimbursement revenue streams, spurring efforts to improve patient satisfaction metrics and increasing the momentum toward clinical comanagement agreements.
First, though, the public will get a chance to weigh in over rules that have been alternately lauded and derided, largely following the fault lines over the broader package of healthcare reforms. At a news conference set in front of a hardware store, HHS Secretary Kathleen Sebelius said competition on a level playing field would increase the purchasing power and drive down costs for individuals and small businesses. Websites for each of the exchanges would allow consumers to comparison-shop, with HHS ensuring that plans provide minimum standards for coverage. Patient groups, consumer organizations, and some small-business associations have welcomed the HHS rules, despite some concern that the exchanges could be tilted too far in favor of insurers. Overall, many analysts say, the rules have provided a fair amount of latitude over how the HIEs will be established and governed. Some business lobbyists, however, contend that the complex requirements will increase healthcare costs instead of lowering them. A July 16 editorial in the Wall Street Journal blasted the exchange rules as poorly designed and offering too little flexibility for states.
Two state-run ex-changes already exist, in Massachusetts and Utah. As of mid-July, however, states that had enacted laws to establish their own HIEs were outnumbered by those whose legislatures or governors had specifically blocked efforts to do likewise, according to the National Conference of State Legislatures. If states cannot or will not set up an exchange, HHS will step in and do it for them.
Reversal of Fortune?
Regardless of who ultimately oversees the exchanges, studies have begun suggesting who the most likely participants might be. An analysis by the Kaiser Family Foundation suggests that the newly insured are likely to be relatively older, less educated, more racially diverse, and in poorer health than those who currently carry private insurance but have fewer diagnosed conditions (www.kff.org/health reform/8147.cfm). Just as analysts, such as PwC, say that insurers will need to change their business strategy to lure and retain consumers, hospitals might need to redouble efforts to ensure high quality and patient satisfaction among a patient demographic that might be harder to please.
Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, says the shift could represent a boon for hospitals that have been forced to maximize efficiency. “In general, those hospitals that have a poorer payor mix have tended to become very efficient, and so they make money off of Medicare patients,” Dr. Williams, a former SHM president, says. “This is fascinating because, on the one hand, there may be a lot of patients for whom hospitalists can now get paid because they’re insured. But I personally think that, simultaneously, we’re going to be seeing cutbacks in payments for other patients who have private insurance.”
For some hospitals, the net effect on revenue might not be materially different, though Dr. Williams sees a potentially sizable benefit for “safety net” hospitals that care for a large proportion of uninsured patients and excel in making the most of limited resources. Some investors apparently agree. Last December, Nashville, Tenn.-based Vanguard Health Systems finalized a deal to buy Detroit Medical Center, with a total investment of nearly $1.5 billion. Dr. Williams says the expectation is that the medical center will suddenly see many more insured patients via an HIE. The result could be a dramatic boost to its finances.
Wealthier hospitals, by contrast, have had less incentive to maximize efficiency—and now are worried by the potential financial impacts of insurance exchanges. “Your classic, highly profitable community hospital that has a good payor mix loses money on Medicare patients and tends to subsidize that with their private patients,” Dr. Williams says. “The wealthier hospitals are nervous because they’re worried that this entire health insurance exchange is going to put downward pressure on reimbursements from the private insurers.”
—Mark Williams, MD, FACP, SFHM, chief, division of hospital medicine, Feinberg School of Medicine, Northwestern University, Chicago
Satisfaction Times Two
With Medicare’s value-based purchasing initiative on its way, hospitals are ramping up their attention to patient satisfaction scores. So how will an influx of potentially older and sicker patients insured through the exchanges affect hospitalists’ scores? No one knows, but because hospitalists already are known for their expertise in treating this very demographic, some experts expect hospitals to lean on them more for leading quality and satisfaction initiatives. This reliance could represent a major opportunity for HM, but faulty performance metrics could also bring danger (read more about this topic in next month’s The Hospitalist).
Cherilyn Murer, president and CEO of Joliet, Ill.-based Murer Consultants Inc., says the expected shift in the nature of inpatients could accelerate efforts to be more accurate about physicians’ performance measures. “Patients who may be in the ICU are at a higher level of crisis than a person who’s in and out for an appendectomy, and yet we’re using the same tool of satisfaction,” she says. Furthermore, she adds, many factors that contribute to patient satisfaction are highly subjective and have nothing to do with a specific physician. “We have to really question the tools now, moreso than only questioning the participation and the outcome,” she says. As with other aspects of healthcare reform, Murer says, the looming arrival of exchanges also should be prompting hospitalists to ask themselves: “What’s our game plan now?” One compelling answer, she contends, is a clinical comanagement agreement that takes a longer-term view of doctors’ relationships with hospitals and gives them more control over decision-making. After all, if HM is taking care of “the sickest of the sick patients,” she says, a comanagement agreement can mean more say in factors that will directly impact their jobs over the long haul. Strategic direction of product lines, space, and equipment-buying decisions are just a few examples.
Murer ultimately sees clinical comanagement as a precursor to more widespread bundling of payments to hospitals and physicians. The mix of private and public insurance reimbursements, already in flux, might be further clouded by the arrival of HIEs. But solidifying hospital-hospitalist alignment with a flexible comanagement agreement, she says, can offer some reassurance over job structure, rewards, and authority as healthcare continues hurtling toward profound change.
Bryn Nelson is a freelance medical writer based in Seattle.
Find Your Niche

“You must define yourself as a hospitalist.” I smiled uncomfortably at my colleagues across the table as I pondered how best to respond to this statement. This seemingly innocuous comment had me perplexed, despite the fact that I aced the “What I want to be when I grow up” question as a fifth-grader. What had changed in all these years?
It was my first job as a hospitalist. I was two months out of residency and had accepted a position at the large academic hospital where I’d spent the previous three years of my life. The comfort was alluring and the transition appeared mundane. However, I naively did not realize that the difference between residency and the launch of a professional career was far greater than a miraculous transformation of paychecks.
Don’t get me wrong—throughout residency, I knew that I had a wealth of untapped energy and ideas; I was just too exhausted from patient-care duties to put action and plans into place. But as I vaulted into my career, I realized I now had the opportunity to act on these ideas and transcend the physician-in-training stereotype.
And so here I was, sitting with colleagues, attempting to define what would occupy the nonclinical portion of my upcoming career.
You might be wondering, “Isn’t great patient care enough for me as a hospitalist?” Indeed, in residency, we are praised, ranked, and valued almost solely on clinical acuity. As a hospitalist, however, we have the unique opportunity of defining ourselves in ways beyond bedside skills. While we are all astute clinicians, an important secret was kept from you during residency: You can choose another hat to wear and—unlike during your training years—you will have the time to do so.
Not buying it? It’s true. Simply pause and reflect on the hospitalists or general internal-medicine physicians you once admired; odds are they weren’t just clinicians, but they were also clinician-educators, clinician-researchers, clinician-administrators, clinician-fill-in-the-blank. In essence, they found a niche, a path that defined their careers.
And now, it’s time you did the same. But how, you ask? Here are a few pointers to get you started:
No. 1: Take Your Time
Before you go off trying to find your claim to fame, keep in mind that the first few years out of residency are a time of transition. Simply put, taking on too much, too early, could capsize your vessel. Learning to become an attending comes with a myriad of diverse responsibilities and a slow march to confidence in your clinical skills. This is a full-time position and one that requires diligence, both to ensure that you gain a strong clinical footing and fully understand the dimensions and nuances of potential “niches.” Get secure in your new role before beginning the search for your new calling. Once you feel comfortable with the resident-to-attending transition, you might find yourself itching to take on that new role in the hospital.
No. 2: Identify Your Passion
My mentor in residency was Dr. M, an all-star attending who had the energy to inspire by building an effortless bridge over the intern-resident-attending communication gap. As I studied her actions during my intern year, I found myself asking, “Could I ever be that successful in my career?”
As we shared experiences, I realized Dr. M genuinely was happy and passionate about her job every day. Her ability to effectively communicate to residents, nurses, and patients was a simple segue to her niche. So what is her niche? Dr. M is a clinician-communicator. Whether it is blogging about a recent patient experience on the wards or appearing as a physician correspondent for an Atlanta news affiliate, Dr. M’s strength is effective communication. Despite being a great clinician, it was her drive outside the wards that helped me understand she had found, and was living, her passion.
During residency, every physician had that one thing that continued to drive us when the going got tough. For some, it was the eager medical student who deserved to learn about that critical aortic stenosis murmur, even if you were 28 hours into your shift. For others, it was quality-improvement (QI) projects that arose from experiencing firsthand the effects of haphazard care transitions. Still others became passionate about patient advocacy after watching patients struggle to understand complex diseases.
Why are these examples relevant? Because each example represents a pathway to your niche. The first person might find a niche as a clinician-educator, exploring opportunities with the medical school during their first year. The second might align themselves with like-minded colleagues in QI and begin projects that will solve frustrations or improve physician efficiency. The third might get involved with local health fairs or local news stations to promote health awareness. The common link between all of these examples is that a clinician’s niche is based on their passion.
No. 3: Stay in Your Own Orbit
We’ve all been go-getters. We’re used to stretching ourselves thin to show what efficient, all-around superdocs we are. And this drive to say yes to your boss, that clinical nurse specialist, and to your colleague who schedules medical student clinical exams will lead to fruitful clinical ventures. Ultimately, however, this approach will leave you exhausted and will leave your colleagues wondering what it is that you actually do with your nonclinical time.
The solution? Learn to invest yourself, and your time, wisely.
During the first week of my new career (when I was asked that fateful question to define myself), I received the best advice. Dr. S (yes, another mentor—it’s OK to have multiple mentors) drew a series of random dots on a sheet of paper. Each of these dots represented opportunities that would arise during my first year. Circling a dot in the middle of the page, Dr. S looked at me and said, “One of these dots represents your passion. The remaining dots are where others’ interests lie. Pick one of these and work in its orbit only. Sure, you may jump up to another dot for a project, but the more you stay within the orbit of your passion, the happier and more productive you’ll be.”
In your first few years on the job, do say yes to joining committees, taking on projects, and collaborating with colleagues. But as you do, ensure that each of these decisions is within your orbit. Saying yes is easy, but saying yes and making it count twice is a skill that you will develop as your career progresses.
Not sure what your orbit is? I encourage you to refer back to tip No. 2 and start seeking out opportunities that center around your passion, not someone else’s.
No. 4: Master the Network
Networking is an art in which our business-minded friends from college excel. Unfortunately, studying for exams and resting after a 30-hour MICU call is a solo venture that leaves little room to hone networking skills. But now, the onlooker must become the master … of networking.
Networking is an important skill to develop, and you start the very first day of your career. The relationships you forge with successful colleagues and superiors will provide you with opportunities beyond the clinical arena (see “Simple Strategies to Expand Your HM Network,” below).
Not sure where to start? A mentor can help. Look at the well-respected leaders in your department and institution, and take note of how each of these people always talk about their mentors and the role they played in crystallizing their career paths. Good mentors steer you toward other like-minded professionals. They help you navigate the complex relationships that are at the base of a successful networking strategy. A wise strategy is to find multiple mentors who serve different purposes in your career; this usually leads to untold opportunities.
Can’t find a suitable mentor at the workplace? Fear not. Consider networking at local, regional, and national society meetings (www.hospitalmedicine.org/events). When the opportunity arises, do more than just attend the clinical sessions during these meetings. Learn which committees are available through the various societies and contact their leaders to express interest in joining next year’s group. Your fellow committee members will be a natural place to practice your networking skills. High-quality relationships made during this time have the potential to grow, and they could lead to more opportunities as your career progresses.
No. 5: Take Calculated Risks
This might sound simple enough, but it is not easy. It is uncomfortable to make mistakes in front of a public audience (and believe me, we all make mistakes). But you will be successful, too, and you must learn how to promote yourself during these times.
Challenge yourself by attending SHM’s Academic Hospitalist Academy (www.academichospitalist.org), or by taking on that project discussed at the last committee meeting. Say yes to your mentor when they learn your passion is QI and appropriately volunteer you to lead a resident research project. Submit your most recent project to an abstract competition, such as SHM’s Research, Innovation, and Clinical Vignettes (RIV) competition. Before you go, research others in your field with similar interests and seek them out during the meeting to share your experiences. Be ready to explain your pitfalls as well, and use this as an opportunity to learn from experienced colleagues.
Whether it is speaking in front of a group of strangers at the academy, giving a presentation to your colleagues, or meeting HM leaders at the national meeting, opportunities abound and often pay off in the long run.
No. 6: Ready For Change
Wait, change? Back up to tip No. 2. I know you’re saying, “But I’m following my passion.” Remember that, fresh out of residency, your interests likely are somewhat different than those of your future self. Thus, as the saying goes, the only thing that is certain is change.
Through networking and putting yourself in new positions, you will discover a world that was never revealed to you in residency. Case in point: my friend and colleague Dr. H. As a chief resident, Dr. H was exposed to a year of educational opportunities before she embarked on a hospitalist career. Education seemed like a natural fit in her first year as a hospitalist. In fact, she never imagined that it would be her experience with the inner workings of her hospital’s electronic medical record (EMR) during her chief year that would catapult her career as the physician director for information services. Yes, she is now a hospitalist-administrator. The bottom line: Remain resilient and ready to take up that next interesting opportunity.
Residency provides you with the skills to be a confident and effective clinician. But as residency comes to a close, think about what really drives you. Where do you see yourself in five years? How about 10 years?
Plot your course to live your passion at work every day; as you start your new job, find, refine, and define your niche.
Dr. Payne is a hospitalist in the Department of Internal Medicine at Emory University Hospital in Atlanta, and a clinical instructor of medicine at Emory University School of Medicine.
“You must define yourself as a hospitalist.” I smiled uncomfortably at my colleagues across the table as I pondered how best to respond to this statement. This seemingly innocuous comment had me perplexed, despite the fact that I aced the “What I want to be when I grow up” question as a fifth-grader. What had changed in all these years?
It was my first job as a hospitalist. I was two months out of residency and had accepted a position at the large academic hospital where I’d spent the previous three years of my life. The comfort was alluring and the transition appeared mundane. However, I naively did not realize that the difference between residency and the launch of a professional career was far greater than a miraculous transformation of paychecks.
Don’t get me wrong—throughout residency, I knew that I had a wealth of untapped energy and ideas; I was just too exhausted from patient-care duties to put action and plans into place. But as I vaulted into my career, I realized I now had the opportunity to act on these ideas and transcend the physician-in-training stereotype.
And so here I was, sitting with colleagues, attempting to define what would occupy the nonclinical portion of my upcoming career.
You might be wondering, “Isn’t great patient care enough for me as a hospitalist?” Indeed, in residency, we are praised, ranked, and valued almost solely on clinical acuity. As a hospitalist, however, we have the unique opportunity of defining ourselves in ways beyond bedside skills. While we are all astute clinicians, an important secret was kept from you during residency: You can choose another hat to wear and—unlike during your training years—you will have the time to do so.
Not buying it? It’s true. Simply pause and reflect on the hospitalists or general internal-medicine physicians you once admired; odds are they weren’t just clinicians, but they were also clinician-educators, clinician-researchers, clinician-administrators, clinician-fill-in-the-blank. In essence, they found a niche, a path that defined their careers.
And now, it’s time you did the same. But how, you ask? Here are a few pointers to get you started:
No. 1: Take Your Time
Before you go off trying to find your claim to fame, keep in mind that the first few years out of residency are a time of transition. Simply put, taking on too much, too early, could capsize your vessel. Learning to become an attending comes with a myriad of diverse responsibilities and a slow march to confidence in your clinical skills. This is a full-time position and one that requires diligence, both to ensure that you gain a strong clinical footing and fully understand the dimensions and nuances of potential “niches.” Get secure in your new role before beginning the search for your new calling. Once you feel comfortable with the resident-to-attending transition, you might find yourself itching to take on that new role in the hospital.
No. 2: Identify Your Passion
My mentor in residency was Dr. M, an all-star attending who had the energy to inspire by building an effortless bridge over the intern-resident-attending communication gap. As I studied her actions during my intern year, I found myself asking, “Could I ever be that successful in my career?”
As we shared experiences, I realized Dr. M genuinely was happy and passionate about her job every day. Her ability to effectively communicate to residents, nurses, and patients was a simple segue to her niche. So what is her niche? Dr. M is a clinician-communicator. Whether it is blogging about a recent patient experience on the wards or appearing as a physician correspondent for an Atlanta news affiliate, Dr. M’s strength is effective communication. Despite being a great clinician, it was her drive outside the wards that helped me understand she had found, and was living, her passion.
During residency, every physician had that one thing that continued to drive us when the going got tough. For some, it was the eager medical student who deserved to learn about that critical aortic stenosis murmur, even if you were 28 hours into your shift. For others, it was quality-improvement (QI) projects that arose from experiencing firsthand the effects of haphazard care transitions. Still others became passionate about patient advocacy after watching patients struggle to understand complex diseases.
Why are these examples relevant? Because each example represents a pathway to your niche. The first person might find a niche as a clinician-educator, exploring opportunities with the medical school during their first year. The second might align themselves with like-minded colleagues in QI and begin projects that will solve frustrations or improve physician efficiency. The third might get involved with local health fairs or local news stations to promote health awareness. The common link between all of these examples is that a clinician’s niche is based on their passion.
No. 3: Stay in Your Own Orbit
We’ve all been go-getters. We’re used to stretching ourselves thin to show what efficient, all-around superdocs we are. And this drive to say yes to your boss, that clinical nurse specialist, and to your colleague who schedules medical student clinical exams will lead to fruitful clinical ventures. Ultimately, however, this approach will leave you exhausted and will leave your colleagues wondering what it is that you actually do with your nonclinical time.
The solution? Learn to invest yourself, and your time, wisely.
During the first week of my new career (when I was asked that fateful question to define myself), I received the best advice. Dr. S (yes, another mentor—it’s OK to have multiple mentors) drew a series of random dots on a sheet of paper. Each of these dots represented opportunities that would arise during my first year. Circling a dot in the middle of the page, Dr. S looked at me and said, “One of these dots represents your passion. The remaining dots are where others’ interests lie. Pick one of these and work in its orbit only. Sure, you may jump up to another dot for a project, but the more you stay within the orbit of your passion, the happier and more productive you’ll be.”
In your first few years on the job, do say yes to joining committees, taking on projects, and collaborating with colleagues. But as you do, ensure that each of these decisions is within your orbit. Saying yes is easy, but saying yes and making it count twice is a skill that you will develop as your career progresses.
Not sure what your orbit is? I encourage you to refer back to tip No. 2 and start seeking out opportunities that center around your passion, not someone else’s.
No. 4: Master the Network
Networking is an art in which our business-minded friends from college excel. Unfortunately, studying for exams and resting after a 30-hour MICU call is a solo venture that leaves little room to hone networking skills. But now, the onlooker must become the master … of networking.
Networking is an important skill to develop, and you start the very first day of your career. The relationships you forge with successful colleagues and superiors will provide you with opportunities beyond the clinical arena (see “Simple Strategies to Expand Your HM Network,” below).
Not sure where to start? A mentor can help. Look at the well-respected leaders in your department and institution, and take note of how each of these people always talk about their mentors and the role they played in crystallizing their career paths. Good mentors steer you toward other like-minded professionals. They help you navigate the complex relationships that are at the base of a successful networking strategy. A wise strategy is to find multiple mentors who serve different purposes in your career; this usually leads to untold opportunities.
Can’t find a suitable mentor at the workplace? Fear not. Consider networking at local, regional, and national society meetings (www.hospitalmedicine.org/events). When the opportunity arises, do more than just attend the clinical sessions during these meetings. Learn which committees are available through the various societies and contact their leaders to express interest in joining next year’s group. Your fellow committee members will be a natural place to practice your networking skills. High-quality relationships made during this time have the potential to grow, and they could lead to more opportunities as your career progresses.
No. 5: Take Calculated Risks
This might sound simple enough, but it is not easy. It is uncomfortable to make mistakes in front of a public audience (and believe me, we all make mistakes). But you will be successful, too, and you must learn how to promote yourself during these times.
Challenge yourself by attending SHM’s Academic Hospitalist Academy (www.academichospitalist.org), or by taking on that project discussed at the last committee meeting. Say yes to your mentor when they learn your passion is QI and appropriately volunteer you to lead a resident research project. Submit your most recent project to an abstract competition, such as SHM’s Research, Innovation, and Clinical Vignettes (RIV) competition. Before you go, research others in your field with similar interests and seek them out during the meeting to share your experiences. Be ready to explain your pitfalls as well, and use this as an opportunity to learn from experienced colleagues.
Whether it is speaking in front of a group of strangers at the academy, giving a presentation to your colleagues, or meeting HM leaders at the national meeting, opportunities abound and often pay off in the long run.
No. 6: Ready For Change
Wait, change? Back up to tip No. 2. I know you’re saying, “But I’m following my passion.” Remember that, fresh out of residency, your interests likely are somewhat different than those of your future self. Thus, as the saying goes, the only thing that is certain is change.
Through networking and putting yourself in new positions, you will discover a world that was never revealed to you in residency. Case in point: my friend and colleague Dr. H. As a chief resident, Dr. H was exposed to a year of educational opportunities before she embarked on a hospitalist career. Education seemed like a natural fit in her first year as a hospitalist. In fact, she never imagined that it would be her experience with the inner workings of her hospital’s electronic medical record (EMR) during her chief year that would catapult her career as the physician director for information services. Yes, she is now a hospitalist-administrator. The bottom line: Remain resilient and ready to take up that next interesting opportunity.
Residency provides you with the skills to be a confident and effective clinician. But as residency comes to a close, think about what really drives you. Where do you see yourself in five years? How about 10 years?
Plot your course to live your passion at work every day; as you start your new job, find, refine, and define your niche.
Dr. Payne is a hospitalist in the Department of Internal Medicine at Emory University Hospital in Atlanta, and a clinical instructor of medicine at Emory University School of Medicine.
“You must define yourself as a hospitalist.” I smiled uncomfortably at my colleagues across the table as I pondered how best to respond to this statement. This seemingly innocuous comment had me perplexed, despite the fact that I aced the “What I want to be when I grow up” question as a fifth-grader. What had changed in all these years?
It was my first job as a hospitalist. I was two months out of residency and had accepted a position at the large academic hospital where I’d spent the previous three years of my life. The comfort was alluring and the transition appeared mundane. However, I naively did not realize that the difference between residency and the launch of a professional career was far greater than a miraculous transformation of paychecks.
Don’t get me wrong—throughout residency, I knew that I had a wealth of untapped energy and ideas; I was just too exhausted from patient-care duties to put action and plans into place. But as I vaulted into my career, I realized I now had the opportunity to act on these ideas and transcend the physician-in-training stereotype.
And so here I was, sitting with colleagues, attempting to define what would occupy the nonclinical portion of my upcoming career.
You might be wondering, “Isn’t great patient care enough for me as a hospitalist?” Indeed, in residency, we are praised, ranked, and valued almost solely on clinical acuity. As a hospitalist, however, we have the unique opportunity of defining ourselves in ways beyond bedside skills. While we are all astute clinicians, an important secret was kept from you during residency: You can choose another hat to wear and—unlike during your training years—you will have the time to do so.
Not buying it? It’s true. Simply pause and reflect on the hospitalists or general internal-medicine physicians you once admired; odds are they weren’t just clinicians, but they were also clinician-educators, clinician-researchers, clinician-administrators, clinician-fill-in-the-blank. In essence, they found a niche, a path that defined their careers.
And now, it’s time you did the same. But how, you ask? Here are a few pointers to get you started:
No. 1: Take Your Time
Before you go off trying to find your claim to fame, keep in mind that the first few years out of residency are a time of transition. Simply put, taking on too much, too early, could capsize your vessel. Learning to become an attending comes with a myriad of diverse responsibilities and a slow march to confidence in your clinical skills. This is a full-time position and one that requires diligence, both to ensure that you gain a strong clinical footing and fully understand the dimensions and nuances of potential “niches.” Get secure in your new role before beginning the search for your new calling. Once you feel comfortable with the resident-to-attending transition, you might find yourself itching to take on that new role in the hospital.
No. 2: Identify Your Passion
My mentor in residency was Dr. M, an all-star attending who had the energy to inspire by building an effortless bridge over the intern-resident-attending communication gap. As I studied her actions during my intern year, I found myself asking, “Could I ever be that successful in my career?”
As we shared experiences, I realized Dr. M genuinely was happy and passionate about her job every day. Her ability to effectively communicate to residents, nurses, and patients was a simple segue to her niche. So what is her niche? Dr. M is a clinician-communicator. Whether it is blogging about a recent patient experience on the wards or appearing as a physician correspondent for an Atlanta news affiliate, Dr. M’s strength is effective communication. Despite being a great clinician, it was her drive outside the wards that helped me understand she had found, and was living, her passion.
During residency, every physician had that one thing that continued to drive us when the going got tough. For some, it was the eager medical student who deserved to learn about that critical aortic stenosis murmur, even if you were 28 hours into your shift. For others, it was quality-improvement (QI) projects that arose from experiencing firsthand the effects of haphazard care transitions. Still others became passionate about patient advocacy after watching patients struggle to understand complex diseases.
Why are these examples relevant? Because each example represents a pathway to your niche. The first person might find a niche as a clinician-educator, exploring opportunities with the medical school during their first year. The second might align themselves with like-minded colleagues in QI and begin projects that will solve frustrations or improve physician efficiency. The third might get involved with local health fairs or local news stations to promote health awareness. The common link between all of these examples is that a clinician’s niche is based on their passion.
No. 3: Stay in Your Own Orbit
We’ve all been go-getters. We’re used to stretching ourselves thin to show what efficient, all-around superdocs we are. And this drive to say yes to your boss, that clinical nurse specialist, and to your colleague who schedules medical student clinical exams will lead to fruitful clinical ventures. Ultimately, however, this approach will leave you exhausted and will leave your colleagues wondering what it is that you actually do with your nonclinical time.
The solution? Learn to invest yourself, and your time, wisely.
During the first week of my new career (when I was asked that fateful question to define myself), I received the best advice. Dr. S (yes, another mentor—it’s OK to have multiple mentors) drew a series of random dots on a sheet of paper. Each of these dots represented opportunities that would arise during my first year. Circling a dot in the middle of the page, Dr. S looked at me and said, “One of these dots represents your passion. The remaining dots are where others’ interests lie. Pick one of these and work in its orbit only. Sure, you may jump up to another dot for a project, but the more you stay within the orbit of your passion, the happier and more productive you’ll be.”
In your first few years on the job, do say yes to joining committees, taking on projects, and collaborating with colleagues. But as you do, ensure that each of these decisions is within your orbit. Saying yes is easy, but saying yes and making it count twice is a skill that you will develop as your career progresses.
Not sure what your orbit is? I encourage you to refer back to tip No. 2 and start seeking out opportunities that center around your passion, not someone else’s.
No. 4: Master the Network
Networking is an art in which our business-minded friends from college excel. Unfortunately, studying for exams and resting after a 30-hour MICU call is a solo venture that leaves little room to hone networking skills. But now, the onlooker must become the master … of networking.
Networking is an important skill to develop, and you start the very first day of your career. The relationships you forge with successful colleagues and superiors will provide you with opportunities beyond the clinical arena (see “Simple Strategies to Expand Your HM Network,” below).
Not sure where to start? A mentor can help. Look at the well-respected leaders in your department and institution, and take note of how each of these people always talk about their mentors and the role they played in crystallizing their career paths. Good mentors steer you toward other like-minded professionals. They help you navigate the complex relationships that are at the base of a successful networking strategy. A wise strategy is to find multiple mentors who serve different purposes in your career; this usually leads to untold opportunities.
Can’t find a suitable mentor at the workplace? Fear not. Consider networking at local, regional, and national society meetings (www.hospitalmedicine.org/events). When the opportunity arises, do more than just attend the clinical sessions during these meetings. Learn which committees are available through the various societies and contact their leaders to express interest in joining next year’s group. Your fellow committee members will be a natural place to practice your networking skills. High-quality relationships made during this time have the potential to grow, and they could lead to more opportunities as your career progresses.
No. 5: Take Calculated Risks
This might sound simple enough, but it is not easy. It is uncomfortable to make mistakes in front of a public audience (and believe me, we all make mistakes). But you will be successful, too, and you must learn how to promote yourself during these times.
Challenge yourself by attending SHM’s Academic Hospitalist Academy (www.academichospitalist.org), or by taking on that project discussed at the last committee meeting. Say yes to your mentor when they learn your passion is QI and appropriately volunteer you to lead a resident research project. Submit your most recent project to an abstract competition, such as SHM’s Research, Innovation, and Clinical Vignettes (RIV) competition. Before you go, research others in your field with similar interests and seek them out during the meeting to share your experiences. Be ready to explain your pitfalls as well, and use this as an opportunity to learn from experienced colleagues.
Whether it is speaking in front of a group of strangers at the academy, giving a presentation to your colleagues, or meeting HM leaders at the national meeting, opportunities abound and often pay off in the long run.
No. 6: Ready For Change
Wait, change? Back up to tip No. 2. I know you’re saying, “But I’m following my passion.” Remember that, fresh out of residency, your interests likely are somewhat different than those of your future self. Thus, as the saying goes, the only thing that is certain is change.
Through networking and putting yourself in new positions, you will discover a world that was never revealed to you in residency. Case in point: my friend and colleague Dr. H. As a chief resident, Dr. H was exposed to a year of educational opportunities before she embarked on a hospitalist career. Education seemed like a natural fit in her first year as a hospitalist. In fact, she never imagined that it would be her experience with the inner workings of her hospital’s electronic medical record (EMR) during her chief year that would catapult her career as the physician director for information services. Yes, she is now a hospitalist-administrator. The bottom line: Remain resilient and ready to take up that next interesting opportunity.
Residency provides you with the skills to be a confident and effective clinician. But as residency comes to a close, think about what really drives you. Where do you see yourself in five years? How about 10 years?
Plot your course to live your passion at work every day; as you start your new job, find, refine, and define your niche.
Dr. Payne is a hospitalist in the Department of Internal Medicine at Emory University Hospital in Atlanta, and a clinical instructor of medicine at Emory University School of Medicine.
Dr. Optimization
Like many physicians, Larry Holder, MD, FACP, FHM, entered the medical profession with the desire to make a difference. After completing a fellowship in hematology and oncology in 1988, he joined Cancer Care Specialists of Central Illinois, a community oncology practice based in Decatur, and anticipated a lengthy career in which he would contribute to significant breakthroughs in cancer treatment.
After 12 years, however, he changed direction.
“I had become a bit disillusioned and realized we weren’t making big impacts, especially on the more common cancers,” he says. “I also got very attached to my patients, and in oncology, that’s not always a good thing. It became very trying emotionally.”
Dr. Holder spent the next five years practicing internal medicine at Community Health Improvement Center in Decatur. In 2005, he joined the hospitalist program at Decatur Memorial Hospital. Last year, he became medical director of hospitalist services, chief medical informatics officer (CMIO), and medical director of information systems.
Although he has found a new niche, his philosophy remains the same.
“Everything I do comes down to the fact I still love taking care of patients,” says Dr. Holder, one of six new members of Team Hospitalist. “That’s why I became a doctor. It’s very rewarding, and I never want to give that up.”

Question: You left oncology partly because you became attached to your patients. Does that approach help you as a hospitalist?
Answer: Definitely. I try to teach younger hospitalists the value of developing a rapport with patients. I enjoy building that emotional or intellectual attachment. I’m a big believer in the human aspect of what we do, and it’s one of the aspects of my job I love the most.
Q: Did you join Decatur Memorial with aspirations of leading its hospitalist program?
A: No. My plan was to focus on giving good patient care, get involved on the quality side, and become the CMIO for the hospital. When the medical director role opened up, it seemed to be sitting there waiting to be filled. I structured it so I could continue to see patients and split my administrative time between being the medical director of the hospitalists and being the CMIO.
Q: Why is it so important for you to still see patients?
A: As a physician, I still find it extremely rewarding. As medical director, I need to be in the trenches to know what the hospitalists are going through and what problems they are having. As CMIO, it’s very important that I use the system I’m in charge of trying to optimize.
Q: What advice would you give to a physician who is about to become leader of a program?
A: You need to anticipate growth. I was caught off guard by how fast our program continued to grow, and how quickly we reached the point where we needed more hospitalists. In retrospect, I should have immediately started looking to recruit. I also was not prepared for the financial aspect. If you don’t have a financial background, I would very quickly get training in that area.
Q: What is your biggest challenge as medical director?
A: Getting others in the hospital to accept change, even when all indications are it’s for the better.
Q: Have you identified a strategy that helps make that process easier?
A: The first step is to establish a sense of urgency. Then I try to get people who will be involved in the process or people who don’t oppose change to help set up a vision for the project and communicate that vision. Once you get empowerment to do the project, go for a short, early win that shows the concept is viable and can make it.
Q: How did you develop your interest in information systems?
A: I’ve always been interested in computers and how we can use computerization and informatic systems to improve patient care. When I became a hospitalist, I got much more involved. Decatur Memorial implemented computer physician order entry (CPOE). I became the physician champion for that, and my interest grew from there. I’m fortunate our administration is very good at pushing to improve our information systems.
Q: Does that interest fit with your approach toward medicine?
A: Absolutely. I’m a big believer in evidenced-based medicine. I think computer systems complement that very well.
Q: You were a finalist for McKesson’s Distinguished Achieve-ment Award and received an award this year from the Association of Medical Directors of Information Systems. What were those honors for?
A: We did a complete cultural change with nurses and physicians in terms of how they deal with diabetes. As part of that project, I developed a CPOE order set that automatically calculated the basal, nutritional, and correctional insulin dosage for the physician based on the patient’s weight and height. It made the right thing to do the easy thing to do. The concept involved the use of evidence-based medicine, project improvement with the Six Sigma process, and the high-level use of informatics.
Q: Has that improved patient care?
A: I was able to demonstrate a statistically significant improvement in glucose control without a change in hypoglycemia, so I did demonstrate an improved clinical outcome.
Q: What’s next for you professionally?
A: I have no intention of changing jobs, but I will continue to be very involved in quality projects. The biggest long-term project is developing more patient- and family-centered care at our hospital. I went to a national conference in February, and a big component was patient-centered care. I was very intrigued by it and brought the vision back to our hospital.
Q: Where does the effort stand?
A: I thought our hospitalist group would be a good group to do an initial component of the project. It went over really well, and people started asking me to present it to others. It took on a life of its own, and I wound up on a bit of a lecture series. It has since become an official Six Sigma project. We got the charter for it and it’s going in the hospital’s strategic plan, which I’m very pleased about.
Q: You earned FHM designation earlier this year. What does that mean to you?
A: It means a great deal. It’s tremendous recognition for the work I’ve done, the quality improvement projects I’ve been involved with, and the leadership roles I’ve taken on. At the same time, when you are able to show a national society views your work as important, I think it gives me even more credibility with the administration and the support staff.
Mark Leiser is a freelance writer based in New Jersey.
Like many physicians, Larry Holder, MD, FACP, FHM, entered the medical profession with the desire to make a difference. After completing a fellowship in hematology and oncology in 1988, he joined Cancer Care Specialists of Central Illinois, a community oncology practice based in Decatur, and anticipated a lengthy career in which he would contribute to significant breakthroughs in cancer treatment.
After 12 years, however, he changed direction.
“I had become a bit disillusioned and realized we weren’t making big impacts, especially on the more common cancers,” he says. “I also got very attached to my patients, and in oncology, that’s not always a good thing. It became very trying emotionally.”
Dr. Holder spent the next five years practicing internal medicine at Community Health Improvement Center in Decatur. In 2005, he joined the hospitalist program at Decatur Memorial Hospital. Last year, he became medical director of hospitalist services, chief medical informatics officer (CMIO), and medical director of information systems.
Although he has found a new niche, his philosophy remains the same.
“Everything I do comes down to the fact I still love taking care of patients,” says Dr. Holder, one of six new members of Team Hospitalist. “That’s why I became a doctor. It’s very rewarding, and I never want to give that up.”
Question: You left oncology partly because you became attached to your patients. Does that approach help you as a hospitalist?
Answer: Definitely. I try to teach younger hospitalists the value of developing a rapport with patients. I enjoy building that emotional or intellectual attachment. I’m a big believer in the human aspect of what we do, and it’s one of the aspects of my job I love the most.
Q: Did you join Decatur Memorial with aspirations of leading its hospitalist program?
A: No. My plan was to focus on giving good patient care, get involved on the quality side, and become the CMIO for the hospital. When the medical director role opened up, it seemed to be sitting there waiting to be filled. I structured it so I could continue to see patients and split my administrative time between being the medical director of the hospitalists and being the CMIO.
Q: Why is it so important for you to still see patients?
A: As a physician, I still find it extremely rewarding. As medical director, I need to be in the trenches to know what the hospitalists are going through and what problems they are having. As CMIO, it’s very important that I use the system I’m in charge of trying to optimize.
Q: What advice would you give to a physician who is about to become leader of a program?
A: You need to anticipate growth. I was caught off guard by how fast our program continued to grow, and how quickly we reached the point where we needed more hospitalists. In retrospect, I should have immediately started looking to recruit. I also was not prepared for the financial aspect. If you don’t have a financial background, I would very quickly get training in that area.
Q: What is your biggest challenge as medical director?
A: Getting others in the hospital to accept change, even when all indications are it’s for the better.
Q: Have you identified a strategy that helps make that process easier?
A: The first step is to establish a sense of urgency. Then I try to get people who will be involved in the process or people who don’t oppose change to help set up a vision for the project and communicate that vision. Once you get empowerment to do the project, go for a short, early win that shows the concept is viable and can make it.
Q: How did you develop your interest in information systems?
A: I’ve always been interested in computers and how we can use computerization and informatic systems to improve patient care. When I became a hospitalist, I got much more involved. Decatur Memorial implemented computer physician order entry (CPOE). I became the physician champion for that, and my interest grew from there. I’m fortunate our administration is very good at pushing to improve our information systems.
Q: Does that interest fit with your approach toward medicine?
A: Absolutely. I’m a big believer in evidenced-based medicine. I think computer systems complement that very well.
Q: You were a finalist for McKesson’s Distinguished Achieve-ment Award and received an award this year from the Association of Medical Directors of Information Systems. What were those honors for?
A: We did a complete cultural change with nurses and physicians in terms of how they deal with diabetes. As part of that project, I developed a CPOE order set that automatically calculated the basal, nutritional, and correctional insulin dosage for the physician based on the patient’s weight and height. It made the right thing to do the easy thing to do. The concept involved the use of evidence-based medicine, project improvement with the Six Sigma process, and the high-level use of informatics.
Q: Has that improved patient care?
A: I was able to demonstrate a statistically significant improvement in glucose control without a change in hypoglycemia, so I did demonstrate an improved clinical outcome.
Q: What’s next for you professionally?
A: I have no intention of changing jobs, but I will continue to be very involved in quality projects. The biggest long-term project is developing more patient- and family-centered care at our hospital. I went to a national conference in February, and a big component was patient-centered care. I was very intrigued by it and brought the vision back to our hospital.
Q: Where does the effort stand?
A: I thought our hospitalist group would be a good group to do an initial component of the project. It went over really well, and people started asking me to present it to others. It took on a life of its own, and I wound up on a bit of a lecture series. It has since become an official Six Sigma project. We got the charter for it and it’s going in the hospital’s strategic plan, which I’m very pleased about.
Q: You earned FHM designation earlier this year. What does that mean to you?
A: It means a great deal. It’s tremendous recognition for the work I’ve done, the quality improvement projects I’ve been involved with, and the leadership roles I’ve taken on. At the same time, when you are able to show a national society views your work as important, I think it gives me even more credibility with the administration and the support staff.
Mark Leiser is a freelance writer based in New Jersey.
Like many physicians, Larry Holder, MD, FACP, FHM, entered the medical profession with the desire to make a difference. After completing a fellowship in hematology and oncology in 1988, he joined Cancer Care Specialists of Central Illinois, a community oncology practice based in Decatur, and anticipated a lengthy career in which he would contribute to significant breakthroughs in cancer treatment.
After 12 years, however, he changed direction.
“I had become a bit disillusioned and realized we weren’t making big impacts, especially on the more common cancers,” he says. “I also got very attached to my patients, and in oncology, that’s not always a good thing. It became very trying emotionally.”
Dr. Holder spent the next five years practicing internal medicine at Community Health Improvement Center in Decatur. In 2005, he joined the hospitalist program at Decatur Memorial Hospital. Last year, he became medical director of hospitalist services, chief medical informatics officer (CMIO), and medical director of information systems.
Although he has found a new niche, his philosophy remains the same.
“Everything I do comes down to the fact I still love taking care of patients,” says Dr. Holder, one of six new members of Team Hospitalist. “That’s why I became a doctor. It’s very rewarding, and I never want to give that up.”
Question: You left oncology partly because you became attached to your patients. Does that approach help you as a hospitalist?
Answer: Definitely. I try to teach younger hospitalists the value of developing a rapport with patients. I enjoy building that emotional or intellectual attachment. I’m a big believer in the human aspect of what we do, and it’s one of the aspects of my job I love the most.
Q: Did you join Decatur Memorial with aspirations of leading its hospitalist program?
A: No. My plan was to focus on giving good patient care, get involved on the quality side, and become the CMIO for the hospital. When the medical director role opened up, it seemed to be sitting there waiting to be filled. I structured it so I could continue to see patients and split my administrative time between being the medical director of the hospitalists and being the CMIO.
Q: Why is it so important for you to still see patients?
A: As a physician, I still find it extremely rewarding. As medical director, I need to be in the trenches to know what the hospitalists are going through and what problems they are having. As CMIO, it’s very important that I use the system I’m in charge of trying to optimize.
Q: What advice would you give to a physician who is about to become leader of a program?
A: You need to anticipate growth. I was caught off guard by how fast our program continued to grow, and how quickly we reached the point where we needed more hospitalists. In retrospect, I should have immediately started looking to recruit. I also was not prepared for the financial aspect. If you don’t have a financial background, I would very quickly get training in that area.
Q: What is your biggest challenge as medical director?
A: Getting others in the hospital to accept change, even when all indications are it’s for the better.
Q: Have you identified a strategy that helps make that process easier?
A: The first step is to establish a sense of urgency. Then I try to get people who will be involved in the process or people who don’t oppose change to help set up a vision for the project and communicate that vision. Once you get empowerment to do the project, go for a short, early win that shows the concept is viable and can make it.
Q: How did you develop your interest in information systems?
A: I’ve always been interested in computers and how we can use computerization and informatic systems to improve patient care. When I became a hospitalist, I got much more involved. Decatur Memorial implemented computer physician order entry (CPOE). I became the physician champion for that, and my interest grew from there. I’m fortunate our administration is very good at pushing to improve our information systems.
Q: Does that interest fit with your approach toward medicine?
A: Absolutely. I’m a big believer in evidenced-based medicine. I think computer systems complement that very well.
Q: You were a finalist for McKesson’s Distinguished Achieve-ment Award and received an award this year from the Association of Medical Directors of Information Systems. What were those honors for?
A: We did a complete cultural change with nurses and physicians in terms of how they deal with diabetes. As part of that project, I developed a CPOE order set that automatically calculated the basal, nutritional, and correctional insulin dosage for the physician based on the patient’s weight and height. It made the right thing to do the easy thing to do. The concept involved the use of evidence-based medicine, project improvement with the Six Sigma process, and the high-level use of informatics.
Q: Has that improved patient care?
A: I was able to demonstrate a statistically significant improvement in glucose control without a change in hypoglycemia, so I did demonstrate an improved clinical outcome.
Q: What’s next for you professionally?
A: I have no intention of changing jobs, but I will continue to be very involved in quality projects. The biggest long-term project is developing more patient- and family-centered care at our hospital. I went to a national conference in February, and a big component was patient-centered care. I was very intrigued by it and brought the vision back to our hospital.
Q: Where does the effort stand?
A: I thought our hospitalist group would be a good group to do an initial component of the project. It went over really well, and people started asking me to present it to others. It took on a life of its own, and I wound up on a bit of a lecture series. It has since become an official Six Sigma project. We got the charter for it and it’s going in the hospital’s strategic plan, which I’m very pleased about.
Q: You earned FHM designation earlier this year. What does that mean to you?
A: It means a great deal. It’s tremendous recognition for the work I’ve done, the quality improvement projects I’ve been involved with, and the leadership roles I’ve taken on. At the same time, when you are able to show a national society views your work as important, I think it gives me even more credibility with the administration and the support staff.
Mark Leiser is a freelance writer based in New Jersey.
Should You Report a Substance-Abusing Colleague to the State Licensing Board?

PRO
Hospitalists’ moral obligation is to protect the patient
In this era of historic budget deficits, wars, and political strife surrounding healthcare reform, one might ask if we can afford to spend valuable time and energy on the issue of reporting physicians who abuse substances.
At first glance, I certainly had skepticism about the subject, but then I dug deeper. To my surprise (and likely yours), studies indicate that physicians develop substance-abuse problems as often or more than the general population does.1 Recent reports detail horrific patient outcomes at the hands of health providers whose actions are compromised by drug use. With data showing the prevalence of substance abuse among physicians hovering around 10% to 12%, we must accept the reality that hospitalists are not exempt.2,3,4,5
As medical doctors, our promise to our patients is to provide care in an ethical manner. Even if we try to live in denial, most of us would agree that with great blessing (or power) comes great responsibility. So when the question of reporting a fellow hospitalist who is abusing substances was asked, my response was unequivocally yes.
In my opinion, this discussion can be limited to two overarching principles: First, we are compelled to put our patients first. As hospitalists, we are blessed to be caring for some of the most frail and vulnerable in our society. Fortunately, an overwhelming number of us do so with pride, skill, and integrity.
The task of providing high-quality care to an empowered patient population is difficult enough with us being physically, emotionally, and mentally exhausted. But to add substance abuse to this is just a complete and utter violation of our patients’ trust. We must agree that putting our patients’ well-being beyond reproach requires us to report any colleague who is compromised.
Second, delayed help for a colleague in trouble with substance-abuse issues could be fatal—and for more than just that single colleague. At some point, we are compelled to do more than just raise an eyebrow and shake our head. Usually at the time of discovery, months if not years of substance abuse already have gone by undetected. Deferring to the next person is just not an option. There is too much at stake. It is our moral duty to help our colleagues who are unable to realize the danger they are posing to themselves, the team, and, most importantly, the patients.
Certainly, physicians do not need another lecture about the perils of substance abuse. Whether discussing prescription drugs, alcohol, marijuana, cocaine, or the like, we all have witnessed the devastating effects of abuse. The fact is, any substance that alters our ability to perform our trusted duty must be avoided.
Colleagues, the algorithm is simple: Be vigilant, observe, confirm, and report. It is our moral and ethical imperative.
Dr. Pyke is chief medical officer of Medicus Consulting, LLC.

CON
Responsible, helpful action doesn’t always mean official involvement
Recognizing impairment in our colleagues is both difficult and ethically challenging. Despite national trends, medicine remains a largely self-regulated profession, and we have an ethical obligation to report impaired, incompetent, or unethical colleagues. Rarely are the indications for reporting or identifying a colleague clear.
As trained clinicians, we know the signs of substance abuse:6
- Frequent tardiness and absences;
- Unexplained disappearances during working hours;
- Inappropriate behavior;
- Affective lability or irritability;
- Interpersonal conflict;
- Avoidance of peers or supervisors;
- Keeping odd hours;
- Disorganized and forgetful;
- Incomplete charts and work performance;
- Heavy drinking at social functions;
- Unexplained changes in weight or energy level;
- Diminished personal hygiene;
- Slurred or rapid speech;
- Frequently dilated pupils or red, watery eyes and a runny nose;
- Defensiveness, anxiety, apathy, and manipulative behaviors; and
- Withdrawal from long-standing relationships.
Yet when it is a colleague, we are often in denial about their substance abuse. Certainly, simple seasonal allergies and allergy medications can cause a number of the above symptoms. We also are aware of and fear the potential impact of licensing board notification on a physician’s career. In fact, in a national survey of physicians, 45% of respondents who had encountered impaired or incompetent physicians had not reported them, even though 96% of those surveyed agreed that physicians should report impaired or incompetent colleagues.7
Similar to reporting child or elder abuse, you don’t want to be wrong.
At the same time, impaired physicians are disruptive. They negatively impact the lives of their patients, colleagues, and hospital staff.
It is possible to do both the responsible thing and not go directly to the licensing board. You are not responsible for diagnosing your colleagues, but rather recognizing possible impairment.
Check out the Federation of State Physician Health Programs’ website (www.fsphp.org) to identify a local physician health program. Call them and place a report of concern identifying your impaired colleague. While it’s possibly new to you, they have years of experience working with this situation. Trust these organizations, many of which are independent from licensing, to intervene responsibly and confidentially. They can evaluate your colleague and provide a treatment plan and monitoring, as needed. Their approach is rehabilitative rather than punitive, and they resist reporting to the medical board unless the physician-patient is noncompliant.
Physicians have better outcomes than the general population, with reported abstinence rates of 70% to 90% for those who complete treatment.8,9 Between 75% and 85% of physicians who complete rehabilitation and comply with close monitoring and follow-up care are able to return to work.9,10
There is hope for your impaired colleague. Contact your local physician health program.
Dr. Guerrasio is a hospitalist and director of resident and medical student remediation at the University of Colorado Denver.
References
- Hughes PH, Brandenburg N, Baldwin DC Jr., et al. Prevalence of substance use among US physicians. JAMA. 1992;267:2333-2339.
- Gold KB, Teitelbaum SA. Physicians impaired by substance abuse disorders. The Journal of Global Drug Policy and Practice website. Available at: http://www.globaldrugpolicy.org/2/2/3.php. Accessed June 27, 2011.
- Wolfgang AP. Substance abuse potential and job stress: a study of pharmacists, physicians, and nurses. J Pharm Mark Manage. 1989;3(4):97-110.
- Cicala RS. Substance abuse among physicians: What you need to know. Hosp Phys. 2003:39-46.
- Berge KH, Seppala MD, Schipper AM. Chemical dependency and the physician. Mayo Clin Proc. 2009;84(7):625-631.
- Bright RP, Krahn L. Impaired physicians: How to recognize, when to report, and where to refer. Curr Psy. 2010;9(6):11-20.
- Campbell EG, Regan S, Gruen RL, et al. Professionalism in medicine: results of a national survey of physicians. Ann Intern Med. 2007;147:795-802.
- Femino J, Nirenberg TD. Treatment outcome studies on physician impairment: a review of the literature. R I Med. 1994;77:345-350.
- Alpern F, Correnti CE, Dolan TE, Llufrio MC, Sill A. A survey of recovering Maryland physicians. Md Med J. 1992;41:301-303.
- Gallegos KV, Lubin BH, Bowers C, Blevins JW, Talbott GD, Wilson PO. Relapse and recovery: five to ten year follow-up study of chemically dependent physicians—the Georgia experience. Md Med J. 1992;41:315-319.
PRO
Hospitalists’ moral obligation is to protect the patient
In this era of historic budget deficits, wars, and political strife surrounding healthcare reform, one might ask if we can afford to spend valuable time and energy on the issue of reporting physicians who abuse substances.
At first glance, I certainly had skepticism about the subject, but then I dug deeper. To my surprise (and likely yours), studies indicate that physicians develop substance-abuse problems as often or more than the general population does.1 Recent reports detail horrific patient outcomes at the hands of health providers whose actions are compromised by drug use. With data showing the prevalence of substance abuse among physicians hovering around 10% to 12%, we must accept the reality that hospitalists are not exempt.2,3,4,5
As medical doctors, our promise to our patients is to provide care in an ethical manner. Even if we try to live in denial, most of us would agree that with great blessing (or power) comes great responsibility. So when the question of reporting a fellow hospitalist who is abusing substances was asked, my response was unequivocally yes.
In my opinion, this discussion can be limited to two overarching principles: First, we are compelled to put our patients first. As hospitalists, we are blessed to be caring for some of the most frail and vulnerable in our society. Fortunately, an overwhelming number of us do so with pride, skill, and integrity.
The task of providing high-quality care to an empowered patient population is difficult enough with us being physically, emotionally, and mentally exhausted. But to add substance abuse to this is just a complete and utter violation of our patients’ trust. We must agree that putting our patients’ well-being beyond reproach requires us to report any colleague who is compromised.
Second, delayed help for a colleague in trouble with substance-abuse issues could be fatal—and for more than just that single colleague. At some point, we are compelled to do more than just raise an eyebrow and shake our head. Usually at the time of discovery, months if not years of substance abuse already have gone by undetected. Deferring to the next person is just not an option. There is too much at stake. It is our moral duty to help our colleagues who are unable to realize the danger they are posing to themselves, the team, and, most importantly, the patients.
Certainly, physicians do not need another lecture about the perils of substance abuse. Whether discussing prescription drugs, alcohol, marijuana, cocaine, or the like, we all have witnessed the devastating effects of abuse. The fact is, any substance that alters our ability to perform our trusted duty must be avoided.
Colleagues, the algorithm is simple: Be vigilant, observe, confirm, and report. It is our moral and ethical imperative.
Dr. Pyke is chief medical officer of Medicus Consulting, LLC.
CON
Responsible, helpful action doesn’t always mean official involvement
Recognizing impairment in our colleagues is both difficult and ethically challenging. Despite national trends, medicine remains a largely self-regulated profession, and we have an ethical obligation to report impaired, incompetent, or unethical colleagues. Rarely are the indications for reporting or identifying a colleague clear.
As trained clinicians, we know the signs of substance abuse:6
- Frequent tardiness and absences;
- Unexplained disappearances during working hours;
- Inappropriate behavior;
- Affective lability or irritability;
- Interpersonal conflict;
- Avoidance of peers or supervisors;
- Keeping odd hours;
- Disorganized and forgetful;
- Incomplete charts and work performance;
- Heavy drinking at social functions;
- Unexplained changes in weight or energy level;
- Diminished personal hygiene;
- Slurred or rapid speech;
- Frequently dilated pupils or red, watery eyes and a runny nose;
- Defensiveness, anxiety, apathy, and manipulative behaviors; and
- Withdrawal from long-standing relationships.
Yet when it is a colleague, we are often in denial about their substance abuse. Certainly, simple seasonal allergies and allergy medications can cause a number of the above symptoms. We also are aware of and fear the potential impact of licensing board notification on a physician’s career. In fact, in a national survey of physicians, 45% of respondents who had encountered impaired or incompetent physicians had not reported them, even though 96% of those surveyed agreed that physicians should report impaired or incompetent colleagues.7
Similar to reporting child or elder abuse, you don’t want to be wrong.
At the same time, impaired physicians are disruptive. They negatively impact the lives of their patients, colleagues, and hospital staff.
It is possible to do both the responsible thing and not go directly to the licensing board. You are not responsible for diagnosing your colleagues, but rather recognizing possible impairment.
Check out the Federation of State Physician Health Programs’ website (www.fsphp.org) to identify a local physician health program. Call them and place a report of concern identifying your impaired colleague. While it’s possibly new to you, they have years of experience working with this situation. Trust these organizations, many of which are independent from licensing, to intervene responsibly and confidentially. They can evaluate your colleague and provide a treatment plan and monitoring, as needed. Their approach is rehabilitative rather than punitive, and they resist reporting to the medical board unless the physician-patient is noncompliant.
Physicians have better outcomes than the general population, with reported abstinence rates of 70% to 90% for those who complete treatment.8,9 Between 75% and 85% of physicians who complete rehabilitation and comply with close monitoring and follow-up care are able to return to work.9,10
There is hope for your impaired colleague. Contact your local physician health program.
Dr. Guerrasio is a hospitalist and director of resident and medical student remediation at the University of Colorado Denver.
References
- Hughes PH, Brandenburg N, Baldwin DC Jr., et al. Prevalence of substance use among US physicians. JAMA. 1992;267:2333-2339.
- Gold KB, Teitelbaum SA. Physicians impaired by substance abuse disorders. The Journal of Global Drug Policy and Practice website. Available at: http://www.globaldrugpolicy.org/2/2/3.php. Accessed June 27, 2011.
- Wolfgang AP. Substance abuse potential and job stress: a study of pharmacists, physicians, and nurses. J Pharm Mark Manage. 1989;3(4):97-110.
- Cicala RS. Substance abuse among physicians: What you need to know. Hosp Phys. 2003:39-46.
- Berge KH, Seppala MD, Schipper AM. Chemical dependency and the physician. Mayo Clin Proc. 2009;84(7):625-631.
- Bright RP, Krahn L. Impaired physicians: How to recognize, when to report, and where to refer. Curr Psy. 2010;9(6):11-20.
- Campbell EG, Regan S, Gruen RL, et al. Professionalism in medicine: results of a national survey of physicians. Ann Intern Med. 2007;147:795-802.
- Femino J, Nirenberg TD. Treatment outcome studies on physician impairment: a review of the literature. R I Med. 1994;77:345-350.
- Alpern F, Correnti CE, Dolan TE, Llufrio MC, Sill A. A survey of recovering Maryland physicians. Md Med J. 1992;41:301-303.
- Gallegos KV, Lubin BH, Bowers C, Blevins JW, Talbott GD, Wilson PO. Relapse and recovery: five to ten year follow-up study of chemically dependent physicians—the Georgia experience. Md Med J. 1992;41:315-319.
PRO
Hospitalists’ moral obligation is to protect the patient
In this era of historic budget deficits, wars, and political strife surrounding healthcare reform, one might ask if we can afford to spend valuable time and energy on the issue of reporting physicians who abuse substances.
At first glance, I certainly had skepticism about the subject, but then I dug deeper. To my surprise (and likely yours), studies indicate that physicians develop substance-abuse problems as often or more than the general population does.1 Recent reports detail horrific patient outcomes at the hands of health providers whose actions are compromised by drug use. With data showing the prevalence of substance abuse among physicians hovering around 10% to 12%, we must accept the reality that hospitalists are not exempt.2,3,4,5
As medical doctors, our promise to our patients is to provide care in an ethical manner. Even if we try to live in denial, most of us would agree that with great blessing (or power) comes great responsibility. So when the question of reporting a fellow hospitalist who is abusing substances was asked, my response was unequivocally yes.
In my opinion, this discussion can be limited to two overarching principles: First, we are compelled to put our patients first. As hospitalists, we are blessed to be caring for some of the most frail and vulnerable in our society. Fortunately, an overwhelming number of us do so with pride, skill, and integrity.
The task of providing high-quality care to an empowered patient population is difficult enough with us being physically, emotionally, and mentally exhausted. But to add substance abuse to this is just a complete and utter violation of our patients’ trust. We must agree that putting our patients’ well-being beyond reproach requires us to report any colleague who is compromised.
Second, delayed help for a colleague in trouble with substance-abuse issues could be fatal—and for more than just that single colleague. At some point, we are compelled to do more than just raise an eyebrow and shake our head. Usually at the time of discovery, months if not years of substance abuse already have gone by undetected. Deferring to the next person is just not an option. There is too much at stake. It is our moral duty to help our colleagues who are unable to realize the danger they are posing to themselves, the team, and, most importantly, the patients.
Certainly, physicians do not need another lecture about the perils of substance abuse. Whether discussing prescription drugs, alcohol, marijuana, cocaine, or the like, we all have witnessed the devastating effects of abuse. The fact is, any substance that alters our ability to perform our trusted duty must be avoided.
Colleagues, the algorithm is simple: Be vigilant, observe, confirm, and report. It is our moral and ethical imperative.
Dr. Pyke is chief medical officer of Medicus Consulting, LLC.
CON
Responsible, helpful action doesn’t always mean official involvement
Recognizing impairment in our colleagues is both difficult and ethically challenging. Despite national trends, medicine remains a largely self-regulated profession, and we have an ethical obligation to report impaired, incompetent, or unethical colleagues. Rarely are the indications for reporting or identifying a colleague clear.
As trained clinicians, we know the signs of substance abuse:6
- Frequent tardiness and absences;
- Unexplained disappearances during working hours;
- Inappropriate behavior;
- Affective lability or irritability;
- Interpersonal conflict;
- Avoidance of peers or supervisors;
- Keeping odd hours;
- Disorganized and forgetful;
- Incomplete charts and work performance;
- Heavy drinking at social functions;
- Unexplained changes in weight or energy level;
- Diminished personal hygiene;
- Slurred or rapid speech;
- Frequently dilated pupils or red, watery eyes and a runny nose;
- Defensiveness, anxiety, apathy, and manipulative behaviors; and
- Withdrawal from long-standing relationships.
Yet when it is a colleague, we are often in denial about their substance abuse. Certainly, simple seasonal allergies and allergy medications can cause a number of the above symptoms. We also are aware of and fear the potential impact of licensing board notification on a physician’s career. In fact, in a national survey of physicians, 45% of respondents who had encountered impaired or incompetent physicians had not reported them, even though 96% of those surveyed agreed that physicians should report impaired or incompetent colleagues.7
Similar to reporting child or elder abuse, you don’t want to be wrong.
At the same time, impaired physicians are disruptive. They negatively impact the lives of their patients, colleagues, and hospital staff.
It is possible to do both the responsible thing and not go directly to the licensing board. You are not responsible for diagnosing your colleagues, but rather recognizing possible impairment.
Check out the Federation of State Physician Health Programs’ website (www.fsphp.org) to identify a local physician health program. Call them and place a report of concern identifying your impaired colleague. While it’s possibly new to you, they have years of experience working with this situation. Trust these organizations, many of which are independent from licensing, to intervene responsibly and confidentially. They can evaluate your colleague and provide a treatment plan and monitoring, as needed. Their approach is rehabilitative rather than punitive, and they resist reporting to the medical board unless the physician-patient is noncompliant.
Physicians have better outcomes than the general population, with reported abstinence rates of 70% to 90% for those who complete treatment.8,9 Between 75% and 85% of physicians who complete rehabilitation and comply with close monitoring and follow-up care are able to return to work.9,10
There is hope for your impaired colleague. Contact your local physician health program.
Dr. Guerrasio is a hospitalist and director of resident and medical student remediation at the University of Colorado Denver.
References
- Hughes PH, Brandenburg N, Baldwin DC Jr., et al. Prevalence of substance use among US physicians. JAMA. 1992;267:2333-2339.
- Gold KB, Teitelbaum SA. Physicians impaired by substance abuse disorders. The Journal of Global Drug Policy and Practice website. Available at: http://www.globaldrugpolicy.org/2/2/3.php. Accessed June 27, 2011.
- Wolfgang AP. Substance abuse potential and job stress: a study of pharmacists, physicians, and nurses. J Pharm Mark Manage. 1989;3(4):97-110.
- Cicala RS. Substance abuse among physicians: What you need to know. Hosp Phys. 2003:39-46.
- Berge KH, Seppala MD, Schipper AM. Chemical dependency and the physician. Mayo Clin Proc. 2009;84(7):625-631.
- Bright RP, Krahn L. Impaired physicians: How to recognize, when to report, and where to refer. Curr Psy. 2010;9(6):11-20.
- Campbell EG, Regan S, Gruen RL, et al. Professionalism in medicine: results of a national survey of physicians. Ann Intern Med. 2007;147:795-802.
- Femino J, Nirenberg TD. Treatment outcome studies on physician impairment: a review of the literature. R I Med. 1994;77:345-350.
- Alpern F, Correnti CE, Dolan TE, Llufrio MC, Sill A. A survey of recovering Maryland physicians. Md Med J. 1992;41:301-303.
- Gallegos KV, Lubin BH, Bowers C, Blevins JW, Talbott GD, Wilson PO. Relapse and recovery: five to ten year follow-up study of chemically dependent physicians—the Georgia experience. Md Med J. 1992;41:315-319.
The Burden of Burnout
SHM’s Career Satisfaction Task Force is no longer active, but its mission—to help hospitalists and groups improve job and career satisfaction—continues with a small group of former members. Working behind the scenes, the group surveyed hospitalists across the nation and began analyzing the data, all with the goal of finding maximal approaches to preventing burnout among their peers and colleagues.
“It’s one thing to describe burnout as a problem, and it’s a second thing to say, ‘How do we minimize the risk of burnout for the individual and for the program?’ ” says Chad Whelan, MD, FHM, director of the division of hospital medicine at Loyola University Health System in Maywood, Ill.
Dr. Whelan is one of three people working on the Hospital Medicine Physician Worklife Survey project. The others are Keiki Hinami, MD, assistant professor in the division of hospital medicine at Northwestern Memorial Hospital in Chicago, and Tosha Wetterneck, MD, FACP, associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
They surveyed nearly 3,800 potential hospitalists, ultimately analyzing more than 800 responses, and Dr. Wetterneck presented results and analysis through two research abstracts at HM11. The first abstract was translated into a paper and published online in July by the Journal of General Internal Medicine.1
What they found was while 62.6% of respondents reported high satisfaction with their job and 69% with the HM specialty, there were certain satisfaction domains—such as organizational climate and personal time availability—that rated low. The authors suspect those low ratings could lead to burnout, but they also note the results provide a roadmap for HM groups looking to address the issue.
“Now we have a lot more needs and demands put upon us as a profession,” Dr. Wetterneck says. “We wanted to know what people were doing nowadays, what kind of work were they doing, and were they happy with it.”
One revealing result, she notes, is that some hospitalists are “not happy” with some of the reasons they initially chose a career in HM. For example, many physicians turn to HM because of the flexibility in scheduling and team approach to patient care and QI. Yet, survey results suggest hospitalists are unhappy with the amount of personal time they have and don’t feel like they are part of a team, she says.

—Tosha Wetterneck, MD, FACP, associate professor of medicine, University of Wisconsin School of Medicine and Public Health, Madison
Workload Worries
The JGIM article, which assessed hospitalists’ satisfaction with such aspects as workload, compensation, patient-care quality, organizational fairness, autonomy, availability of personal time, and work relationships, showed that while hospitalists rated care quality and relationships with staff and colleagues high, they ranked compensation, organizational climate, autonomy, and availability of personal time low.
“To have such low satisfaction scores with their climate and their organization is concerning,” Dr. Wetterneck says. “It’s very important for [hospitalists] to be able to feel like they’re part of a team, that they’re part of an organization, and that the work they do really matters within that organization.”
Dr. Wetterneck acknowledges schedule flexibility is a key factor in hospitalist career choice, and it worries her that a majority of hospitalists surveyed are unhappy with the amount of personal time they had.
“When I presented these findings at the meeting, I had a lot of people telling me that the field has grown so quickly and the demands on the hospitalist group have grown so much that they haven’t been able to keep pace with hiring hospitalists to meet the demands in the workplace,” she says. “So people have to work more than they thought they would in the beginning, and that’s impinging on their personal time. … The flexibility piece is lost.”
Most hospitalists asked to work more are resilient and adapt. But over time, Dr. Wetterneck says, they begin to lose the ability to balance the demands and rewards of the job, and burnout develops.
“The study that we’ve been conducting suggests that the rate of burnout among practicing hospitalists is about 30 percent, which is a significant proportion of us,” Dr. Hinami says. “[It appears] that the rate of burnout symptoms of practicing hospitalists has remained stable, or may have increased, since the last time the publication of a nationwide survey was done.”
The last time a large survey measuring satisfaction among hospitalists was published was in 2001.2 It found that about 13% of hospitalists were burned out and about 25% were at risk of burnout, says Winthrop Whitcomb, MD, MHM, medical director of healthcare quality at Baystate Medical Center in Springfield, Mass., and one of the authors of the 2001 study. Without question, burnout continues to be a major challenge for the entire field of HM, he says.
“Growth has always and will continue to fuel burnout,” says Dr. Whitcomb, cofounder and past president of SHM. “It’s a hard job, and as long as you’re growing, you’re not really getting your feet underneath you.”
The task force study found that hospitalists with burnout symptoms were much more likely to reduce work effort, leave their clinical situation, leave HM, and abandon direct patient care altogether than those without burnout symptoms.
Whereas the task force survey used a single-item question to ask hospitalists their level of burnout on a scale of 1 to 5, the 2001 study used a different scale and asked multiple questions to determine if respondents were burned out or at risk of burnout, Dr. Wetterneck explains.
“Even though it’s not a fair comparison, could it be that more hospitalists are burned out now than they were 10 years ago? I happen to think it probably is real … because of some of the satisfaction data we’re looking at,” she says.
Dr. Wetterneck’s group hasn’t analyzed if the reasons for burnout among hospitalists have changed over the years, but, anecdotally, Dr. Whelan has noticed a difference. Early hospitalists often burned out because they had to work day shifts and take night call. Today, far fewer hospitalists are always on. However, there are more hospitalists than ever before working in the hospital at off hours, which comes with different stressors, he says.
Greater Responsibility, Greater Dissatisfaction
As hospitalists’ roles expand, unpredictable interruptions are more frequent, says Sylvia McKean, MD, SFHM, FACP, a senior hospitalist at Brigham and Women’s Hospital in Boston, associate professor of medicine at Harvard Medical School, and former co-chair of the Career Satisfaction Task Force.
“For example, if you’re [scheduled] to admit patients to the hospital and you’re also on the rapid-response team and someone happens to need a rapid assessment, you can be interrupted,” she says. “If you’re a hospitalist taking care of someone who has had a subarachnoid hemorrhage and the neurosurgeon is going to come in the next morning but you’re uncertain about what to do or even to recognize a problem in that patient, those are the kinds of things that cause people to get anxious and feel more fatigued.”
As more subspecialists focus on consultations in the hospital, hospitalists are tending to see more specialty patients and, as a result, could feel overwhelmed, Dr. McKean says.
The new survey group is not yet in a position to be prescriptive about burnout, Dr. Hinami says. However, he and his colleagues hope to shed some light on possible solutions in the near future.
“What we understand about burnout is that it depends on both individual characteristics and characteristics of the work environment,” Dr. Hinami says. “We’re exploring the kind of ways in which job designs can be altered to help hospitalists—whatever their personal endowments are—to cope better with the stresses of the work.”
According to the research group, one thing is clear: Compensation is not a cure-all. One of the HM11 abstracts showed that satisfaction with compensation was correlated the least with both. “There’s only so much you can be paid more to do before it’s not enough anymore,” Dr. Wetterneck says. “There are some people who take money over a happy job, and that’s what they want to do for a couple of years. That’s not really going to grow our profession in the long run.”
Lisa Ryan is a freelance writer based in New Jersey.
Reference
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. July 2011 [epub ahead of print].
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
SHM’s Career Satisfaction Task Force is no longer active, but its mission—to help hospitalists and groups improve job and career satisfaction—continues with a small group of former members. Working behind the scenes, the group surveyed hospitalists across the nation and began analyzing the data, all with the goal of finding maximal approaches to preventing burnout among their peers and colleagues.
“It’s one thing to describe burnout as a problem, and it’s a second thing to say, ‘How do we minimize the risk of burnout for the individual and for the program?’ ” says Chad Whelan, MD, FHM, director of the division of hospital medicine at Loyola University Health System in Maywood, Ill.
Dr. Whelan is one of three people working on the Hospital Medicine Physician Worklife Survey project. The others are Keiki Hinami, MD, assistant professor in the division of hospital medicine at Northwestern Memorial Hospital in Chicago, and Tosha Wetterneck, MD, FACP, associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
They surveyed nearly 3,800 potential hospitalists, ultimately analyzing more than 800 responses, and Dr. Wetterneck presented results and analysis through two research abstracts at HM11. The first abstract was translated into a paper and published online in July by the Journal of General Internal Medicine.1
What they found was while 62.6% of respondents reported high satisfaction with their job and 69% with the HM specialty, there were certain satisfaction domains—such as organizational climate and personal time availability—that rated low. The authors suspect those low ratings could lead to burnout, but they also note the results provide a roadmap for HM groups looking to address the issue.
“Now we have a lot more needs and demands put upon us as a profession,” Dr. Wetterneck says. “We wanted to know what people were doing nowadays, what kind of work were they doing, and were they happy with it.”
One revealing result, she notes, is that some hospitalists are “not happy” with some of the reasons they initially chose a career in HM. For example, many physicians turn to HM because of the flexibility in scheduling and team approach to patient care and QI. Yet, survey results suggest hospitalists are unhappy with the amount of personal time they have and don’t feel like they are part of a team, she says.
—Tosha Wetterneck, MD, FACP, associate professor of medicine, University of Wisconsin School of Medicine and Public Health, Madison
Workload Worries
The JGIM article, which assessed hospitalists’ satisfaction with such aspects as workload, compensation, patient-care quality, organizational fairness, autonomy, availability of personal time, and work relationships, showed that while hospitalists rated care quality and relationships with staff and colleagues high, they ranked compensation, organizational climate, autonomy, and availability of personal time low.
“To have such low satisfaction scores with their climate and their organization is concerning,” Dr. Wetterneck says. “It’s very important for [hospitalists] to be able to feel like they’re part of a team, that they’re part of an organization, and that the work they do really matters within that organization.”
Dr. Wetterneck acknowledges schedule flexibility is a key factor in hospitalist career choice, and it worries her that a majority of hospitalists surveyed are unhappy with the amount of personal time they had.
“When I presented these findings at the meeting, I had a lot of people telling me that the field has grown so quickly and the demands on the hospitalist group have grown so much that they haven’t been able to keep pace with hiring hospitalists to meet the demands in the workplace,” she says. “So people have to work more than they thought they would in the beginning, and that’s impinging on their personal time. … The flexibility piece is lost.”
Most hospitalists asked to work more are resilient and adapt. But over time, Dr. Wetterneck says, they begin to lose the ability to balance the demands and rewards of the job, and burnout develops.
“The study that we’ve been conducting suggests that the rate of burnout among practicing hospitalists is about 30 percent, which is a significant proportion of us,” Dr. Hinami says. “[It appears] that the rate of burnout symptoms of practicing hospitalists has remained stable, or may have increased, since the last time the publication of a nationwide survey was done.”
The last time a large survey measuring satisfaction among hospitalists was published was in 2001.2 It found that about 13% of hospitalists were burned out and about 25% were at risk of burnout, says Winthrop Whitcomb, MD, MHM, medical director of healthcare quality at Baystate Medical Center in Springfield, Mass., and one of the authors of the 2001 study. Without question, burnout continues to be a major challenge for the entire field of HM, he says.
“Growth has always and will continue to fuel burnout,” says Dr. Whitcomb, cofounder and past president of SHM. “It’s a hard job, and as long as you’re growing, you’re not really getting your feet underneath you.”
The task force study found that hospitalists with burnout symptoms were much more likely to reduce work effort, leave their clinical situation, leave HM, and abandon direct patient care altogether than those without burnout symptoms.
Whereas the task force survey used a single-item question to ask hospitalists their level of burnout on a scale of 1 to 5, the 2001 study used a different scale and asked multiple questions to determine if respondents were burned out or at risk of burnout, Dr. Wetterneck explains.
“Even though it’s not a fair comparison, could it be that more hospitalists are burned out now than they were 10 years ago? I happen to think it probably is real … because of some of the satisfaction data we’re looking at,” she says.
Dr. Wetterneck’s group hasn’t analyzed if the reasons for burnout among hospitalists have changed over the years, but, anecdotally, Dr. Whelan has noticed a difference. Early hospitalists often burned out because they had to work day shifts and take night call. Today, far fewer hospitalists are always on. However, there are more hospitalists than ever before working in the hospital at off hours, which comes with different stressors, he says.
Greater Responsibility, Greater Dissatisfaction
As hospitalists’ roles expand, unpredictable interruptions are more frequent, says Sylvia McKean, MD, SFHM, FACP, a senior hospitalist at Brigham and Women’s Hospital in Boston, associate professor of medicine at Harvard Medical School, and former co-chair of the Career Satisfaction Task Force.
“For example, if you’re [scheduled] to admit patients to the hospital and you’re also on the rapid-response team and someone happens to need a rapid assessment, you can be interrupted,” she says. “If you’re a hospitalist taking care of someone who has had a subarachnoid hemorrhage and the neurosurgeon is going to come in the next morning but you’re uncertain about what to do or even to recognize a problem in that patient, those are the kinds of things that cause people to get anxious and feel more fatigued.”
As more subspecialists focus on consultations in the hospital, hospitalists are tending to see more specialty patients and, as a result, could feel overwhelmed, Dr. McKean says.
The new survey group is not yet in a position to be prescriptive about burnout, Dr. Hinami says. However, he and his colleagues hope to shed some light on possible solutions in the near future.
“What we understand about burnout is that it depends on both individual characteristics and characteristics of the work environment,” Dr. Hinami says. “We’re exploring the kind of ways in which job designs can be altered to help hospitalists—whatever their personal endowments are—to cope better with the stresses of the work.”
According to the research group, one thing is clear: Compensation is not a cure-all. One of the HM11 abstracts showed that satisfaction with compensation was correlated the least with both. “There’s only so much you can be paid more to do before it’s not enough anymore,” Dr. Wetterneck says. “There are some people who take money over a happy job, and that’s what they want to do for a couple of years. That’s not really going to grow our profession in the long run.”
Lisa Ryan is a freelance writer based in New Jersey.
Reference
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. July 2011 [epub ahead of print].
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
SHM’s Career Satisfaction Task Force is no longer active, but its mission—to help hospitalists and groups improve job and career satisfaction—continues with a small group of former members. Working behind the scenes, the group surveyed hospitalists across the nation and began analyzing the data, all with the goal of finding maximal approaches to preventing burnout among their peers and colleagues.
“It’s one thing to describe burnout as a problem, and it’s a second thing to say, ‘How do we minimize the risk of burnout for the individual and for the program?’ ” says Chad Whelan, MD, FHM, director of the division of hospital medicine at Loyola University Health System in Maywood, Ill.
Dr. Whelan is one of three people working on the Hospital Medicine Physician Worklife Survey project. The others are Keiki Hinami, MD, assistant professor in the division of hospital medicine at Northwestern Memorial Hospital in Chicago, and Tosha Wetterneck, MD, FACP, associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
They surveyed nearly 3,800 potential hospitalists, ultimately analyzing more than 800 responses, and Dr. Wetterneck presented results and analysis through two research abstracts at HM11. The first abstract was translated into a paper and published online in July by the Journal of General Internal Medicine.1
What they found was while 62.6% of respondents reported high satisfaction with their job and 69% with the HM specialty, there were certain satisfaction domains—such as organizational climate and personal time availability—that rated low. The authors suspect those low ratings could lead to burnout, but they also note the results provide a roadmap for HM groups looking to address the issue.
“Now we have a lot more needs and demands put upon us as a profession,” Dr. Wetterneck says. “We wanted to know what people were doing nowadays, what kind of work were they doing, and were they happy with it.”
One revealing result, she notes, is that some hospitalists are “not happy” with some of the reasons they initially chose a career in HM. For example, many physicians turn to HM because of the flexibility in scheduling and team approach to patient care and QI. Yet, survey results suggest hospitalists are unhappy with the amount of personal time they have and don’t feel like they are part of a team, she says.
—Tosha Wetterneck, MD, FACP, associate professor of medicine, University of Wisconsin School of Medicine and Public Health, Madison
Workload Worries
The JGIM article, which assessed hospitalists’ satisfaction with such aspects as workload, compensation, patient-care quality, organizational fairness, autonomy, availability of personal time, and work relationships, showed that while hospitalists rated care quality and relationships with staff and colleagues high, they ranked compensation, organizational climate, autonomy, and availability of personal time low.
“To have such low satisfaction scores with their climate and their organization is concerning,” Dr. Wetterneck says. “It’s very important for [hospitalists] to be able to feel like they’re part of a team, that they’re part of an organization, and that the work they do really matters within that organization.”
Dr. Wetterneck acknowledges schedule flexibility is a key factor in hospitalist career choice, and it worries her that a majority of hospitalists surveyed are unhappy with the amount of personal time they had.
“When I presented these findings at the meeting, I had a lot of people telling me that the field has grown so quickly and the demands on the hospitalist group have grown so much that they haven’t been able to keep pace with hiring hospitalists to meet the demands in the workplace,” she says. “So people have to work more than they thought they would in the beginning, and that’s impinging on their personal time. … The flexibility piece is lost.”
Most hospitalists asked to work more are resilient and adapt. But over time, Dr. Wetterneck says, they begin to lose the ability to balance the demands and rewards of the job, and burnout develops.
“The study that we’ve been conducting suggests that the rate of burnout among practicing hospitalists is about 30 percent, which is a significant proportion of us,” Dr. Hinami says. “[It appears] that the rate of burnout symptoms of practicing hospitalists has remained stable, or may have increased, since the last time the publication of a nationwide survey was done.”
The last time a large survey measuring satisfaction among hospitalists was published was in 2001.2 It found that about 13% of hospitalists were burned out and about 25% were at risk of burnout, says Winthrop Whitcomb, MD, MHM, medical director of healthcare quality at Baystate Medical Center in Springfield, Mass., and one of the authors of the 2001 study. Without question, burnout continues to be a major challenge for the entire field of HM, he says.
“Growth has always and will continue to fuel burnout,” says Dr. Whitcomb, cofounder and past president of SHM. “It’s a hard job, and as long as you’re growing, you’re not really getting your feet underneath you.”
The task force study found that hospitalists with burnout symptoms were much more likely to reduce work effort, leave their clinical situation, leave HM, and abandon direct patient care altogether than those without burnout symptoms.
Whereas the task force survey used a single-item question to ask hospitalists their level of burnout on a scale of 1 to 5, the 2001 study used a different scale and asked multiple questions to determine if respondents were burned out or at risk of burnout, Dr. Wetterneck explains.
“Even though it’s not a fair comparison, could it be that more hospitalists are burned out now than they were 10 years ago? I happen to think it probably is real … because of some of the satisfaction data we’re looking at,” she says.
Dr. Wetterneck’s group hasn’t analyzed if the reasons for burnout among hospitalists have changed over the years, but, anecdotally, Dr. Whelan has noticed a difference. Early hospitalists often burned out because they had to work day shifts and take night call. Today, far fewer hospitalists are always on. However, there are more hospitalists than ever before working in the hospital at off hours, which comes with different stressors, he says.
Greater Responsibility, Greater Dissatisfaction
As hospitalists’ roles expand, unpredictable interruptions are more frequent, says Sylvia McKean, MD, SFHM, FACP, a senior hospitalist at Brigham and Women’s Hospital in Boston, associate professor of medicine at Harvard Medical School, and former co-chair of the Career Satisfaction Task Force.
“For example, if you’re [scheduled] to admit patients to the hospital and you’re also on the rapid-response team and someone happens to need a rapid assessment, you can be interrupted,” she says. “If you’re a hospitalist taking care of someone who has had a subarachnoid hemorrhage and the neurosurgeon is going to come in the next morning but you’re uncertain about what to do or even to recognize a problem in that patient, those are the kinds of things that cause people to get anxious and feel more fatigued.”
As more subspecialists focus on consultations in the hospital, hospitalists are tending to see more specialty patients and, as a result, could feel overwhelmed, Dr. McKean says.
The new survey group is not yet in a position to be prescriptive about burnout, Dr. Hinami says. However, he and his colleagues hope to shed some light on possible solutions in the near future.
“What we understand about burnout is that it depends on both individual characteristics and characteristics of the work environment,” Dr. Hinami says. “We’re exploring the kind of ways in which job designs can be altered to help hospitalists—whatever their personal endowments are—to cope better with the stresses of the work.”
According to the research group, one thing is clear: Compensation is not a cure-all. One of the HM11 abstracts showed that satisfaction with compensation was correlated the least with both. “There’s only so much you can be paid more to do before it’s not enough anymore,” Dr. Wetterneck says. “There are some people who take money over a happy job, and that’s what they want to do for a couple of years. That’s not really going to grow our profession in the long run.”
Lisa Ryan is a freelance writer based in New Jersey.
Reference
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers. J Gen Intern Med. July 2011 [epub ahead of print].
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
Purposeful Visits Enhance Hospitalized Seniors’ Quality of Life
An abstract presented at HM11, “Purposeful Visits for Hospitalized Elderly Patients,” describes a service at the University of Colorado Hospital (UCH) in Denver that has shown improvements in participating patients’ mood, agitation, and orientation.
The purposeful-visit program was started, says senior author Ethan Cumbler, MD, a hospitalist at UCH and director of its Acute Care for the Elderly Service, because hospitals often are a profoundly unfriendly environment, especially for vulnerable, chronically ill patients. “It’s a social and intellectual desert where patients don’t get the stimulation they would receive at home,” he adds.
The program was established to leverage professional resources by training a core cadre of four to six volunteers in communication techniques (e.g. open-ended questioning), says the hospital’s recreational therapist, William Mramor, CTRS, MS. Charge nurses help identify patients and topics to explore, and the volunteers use a prepared script to help guide interactions, Mramor says.
“The purposeful visit directly addresses issues of patients’ feelings and promotes a patient-centered hospital experience,” he says.
Based on assessments using a five-point scale, with scores ranging from “worsening” (1 or 2) to “improving” (4 or 5), patient mood was rated 3.94 by the volunteers and 3.65 by the nurses. Slightly lower scores were recorded for patient agitation and patient orientation but in every case showed improvement.
“What distinguishes these purposeful visits is their goal of enhancing patients’ memory, decreasing their loneliness, and helping them understand the value of reconnecting to things they enjoy,” says Dr. Cumbler. —LB
Technology
New E-Pillbox Actively Monitors Med-Recon, Fights Readmissions
Electronic pillboxes are nothing new, but some hospitalists might not have seen the latest one.
Earlier this year, the FDA approved PillStation, a traditional pillbox married to a software system that uploads data to the system’s maker, SentiCare Inc., which then monitors how well a patient is following their medication regimen. The four-year-old medical firm is pitching the product to hospitals and accountable-care organizations (ACOs), among other potential clients.
And in a sales pitch practically tailored to HM, SentiCare bills itself as a medication adherence system that can help fight readmissions, particularly in cases of chronic disease or congestive heart failure. The device actually takes photographs of the pills to be taken and can record whether a patient has removed them from the device.
“Hospitals need to dramatically reduce their readmissions rates,” Yogendra Jain, chief technology officer and cofounder of SentiCare, wrote in an email to The Hospitalist. “One critical factor is medication and hospital discharge instruction adherence. Through its embedded camera, PillStation can confirm that from day one of departing the hospital... medications are loaded correctly and that the patient is taking it on time.”—RQ

Quality
Home Healthcare Has Fewer Rehospitalizations
A recent study by Avalere Health, a healthcare advisory firm based in Washington, D.C., found that providing home healthcare after hospital discharge for patients with three common conditions resulted in fewer hospital readmissions than for similar patients receiving other post-acute services. Those comparable services included long-term acute-care hospitals, inpatient rehabilitation facilities, skilled nursing facilities, and hospices.
“We tried to control for hospital DRG, severity of illness, and comorbidities,” says Emil Parker, Avalere’s director of post-acute and long-term-care practice, although he acknowledges the complexities of risk adjustment.
In comparing Medicare spending and rehospitalization rates after initial hospital visits for patients with diabetes, COPD, and congestive heart failure from 2006 to 2009, the study estimated that referrals to home healthcare resulted in $670 million in Medicare savings from 20,426 fewer readmissions.
“Hospitalists should think about the continuum of institutional support for patients discharged from the hospital with significant support needs,” Parker says. “Our study shows that in this population, provision of home healthcare is cost-effective and benefits patients by improving the continuity of their care.” —LB

Patient Safety
L.A. Hospitals Add HM for Medicaid Patients
In June, Anthem Blue Cross of Woodland Hills, Calif., began offering covered hospitalist services to its adult managed-care members covered by Medi-Cal, the Medicaid program for California residents, at 24 hospitals in Los Angeles County. The service is designed to take advantage of the existing hospitalist presence in those hospitals, which is provided by ApolloMed, a Glendale, Calif.-based medical management services company.
The hospitalist service is designed to enhance quality of care during hospitalization, reduce costs, and plan for more timely discharges and transitions to outpatient care. ApolloMed plans to add more hospitals in the region to the program, as well as additional post-discharge outpatient clinics. —LB

Technology
By the Numbers: 5.9
The percentage of total national health expenditures spent on medical devices in 2009, according to a report released in June by the Advanced Medical Technology Association.
The report highlights that while technology is washing over medicine, and HM in particular, with the adoption of electronic health records, portable ultrasounds, and tablet computing, the $147 billion spent on medical devices in 2009 represented just 5.9% of the $2.5 trillion in national health spending.
The trade group also reported that the average annual rate for medical device spending increased 7.5% in the 20-year period that ended in 2009. That outpaced the average annual rate for overall national heath expenditures, which ticked up 7% over the same time period. —RQ
An abstract presented at HM11, “Purposeful Visits for Hospitalized Elderly Patients,” describes a service at the University of Colorado Hospital (UCH) in Denver that has shown improvements in participating patients’ mood, agitation, and orientation.
The purposeful-visit program was started, says senior author Ethan Cumbler, MD, a hospitalist at UCH and director of its Acute Care for the Elderly Service, because hospitals often are a profoundly unfriendly environment, especially for vulnerable, chronically ill patients. “It’s a social and intellectual desert where patients don’t get the stimulation they would receive at home,” he adds.
The program was established to leverage professional resources by training a core cadre of four to six volunteers in communication techniques (e.g. open-ended questioning), says the hospital’s recreational therapist, William Mramor, CTRS, MS. Charge nurses help identify patients and topics to explore, and the volunteers use a prepared script to help guide interactions, Mramor says.
“The purposeful visit directly addresses issues of patients’ feelings and promotes a patient-centered hospital experience,” he says.
Based on assessments using a five-point scale, with scores ranging from “worsening” (1 or 2) to “improving” (4 or 5), patient mood was rated 3.94 by the volunteers and 3.65 by the nurses. Slightly lower scores were recorded for patient agitation and patient orientation but in every case showed improvement.
“What distinguishes these purposeful visits is their goal of enhancing patients’ memory, decreasing their loneliness, and helping them understand the value of reconnecting to things they enjoy,” says Dr. Cumbler. —LB
Technology
New E-Pillbox Actively Monitors Med-Recon, Fights Readmissions
Electronic pillboxes are nothing new, but some hospitalists might not have seen the latest one.
Earlier this year, the FDA approved PillStation, a traditional pillbox married to a software system that uploads data to the system’s maker, SentiCare Inc., which then monitors how well a patient is following their medication regimen. The four-year-old medical firm is pitching the product to hospitals and accountable-care organizations (ACOs), among other potential clients.
And in a sales pitch practically tailored to HM, SentiCare bills itself as a medication adherence system that can help fight readmissions, particularly in cases of chronic disease or congestive heart failure. The device actually takes photographs of the pills to be taken and can record whether a patient has removed them from the device.
“Hospitals need to dramatically reduce their readmissions rates,” Yogendra Jain, chief technology officer and cofounder of SentiCare, wrote in an email to The Hospitalist. “One critical factor is medication and hospital discharge instruction adherence. Through its embedded camera, PillStation can confirm that from day one of departing the hospital... medications are loaded correctly and that the patient is taking it on time.”—RQ
Quality
Home Healthcare Has Fewer Rehospitalizations
A recent study by Avalere Health, a healthcare advisory firm based in Washington, D.C., found that providing home healthcare after hospital discharge for patients with three common conditions resulted in fewer hospital readmissions than for similar patients receiving other post-acute services. Those comparable services included long-term acute-care hospitals, inpatient rehabilitation facilities, skilled nursing facilities, and hospices.
“We tried to control for hospital DRG, severity of illness, and comorbidities,” says Emil Parker, Avalere’s director of post-acute and long-term-care practice, although he acknowledges the complexities of risk adjustment.
In comparing Medicare spending and rehospitalization rates after initial hospital visits for patients with diabetes, COPD, and congestive heart failure from 2006 to 2009, the study estimated that referrals to home healthcare resulted in $670 million in Medicare savings from 20,426 fewer readmissions.
“Hospitalists should think about the continuum of institutional support for patients discharged from the hospital with significant support needs,” Parker says. “Our study shows that in this population, provision of home healthcare is cost-effective and benefits patients by improving the continuity of their care.” —LB
Patient Safety
L.A. Hospitals Add HM for Medicaid Patients
In June, Anthem Blue Cross of Woodland Hills, Calif., began offering covered hospitalist services to its adult managed-care members covered by Medi-Cal, the Medicaid program for California residents, at 24 hospitals in Los Angeles County. The service is designed to take advantage of the existing hospitalist presence in those hospitals, which is provided by ApolloMed, a Glendale, Calif.-based medical management services company.
The hospitalist service is designed to enhance quality of care during hospitalization, reduce costs, and plan for more timely discharges and transitions to outpatient care. ApolloMed plans to add more hospitals in the region to the program, as well as additional post-discharge outpatient clinics. —LB
Technology
By the Numbers: 5.9
The percentage of total national health expenditures spent on medical devices in 2009, according to a report released in June by the Advanced Medical Technology Association.
The report highlights that while technology is washing over medicine, and HM in particular, with the adoption of electronic health records, portable ultrasounds, and tablet computing, the $147 billion spent on medical devices in 2009 represented just 5.9% of the $2.5 trillion in national health spending.
The trade group also reported that the average annual rate for medical device spending increased 7.5% in the 20-year period that ended in 2009. That outpaced the average annual rate for overall national heath expenditures, which ticked up 7% over the same time period. —RQ
An abstract presented at HM11, “Purposeful Visits for Hospitalized Elderly Patients,” describes a service at the University of Colorado Hospital (UCH) in Denver that has shown improvements in participating patients’ mood, agitation, and orientation.
The purposeful-visit program was started, says senior author Ethan Cumbler, MD, a hospitalist at UCH and director of its Acute Care for the Elderly Service, because hospitals often are a profoundly unfriendly environment, especially for vulnerable, chronically ill patients. “It’s a social and intellectual desert where patients don’t get the stimulation they would receive at home,” he adds.
The program was established to leverage professional resources by training a core cadre of four to six volunteers in communication techniques (e.g. open-ended questioning), says the hospital’s recreational therapist, William Mramor, CTRS, MS. Charge nurses help identify patients and topics to explore, and the volunteers use a prepared script to help guide interactions, Mramor says.
“The purposeful visit directly addresses issues of patients’ feelings and promotes a patient-centered hospital experience,” he says.
Based on assessments using a five-point scale, with scores ranging from “worsening” (1 or 2) to “improving” (4 or 5), patient mood was rated 3.94 by the volunteers and 3.65 by the nurses. Slightly lower scores were recorded for patient agitation and patient orientation but in every case showed improvement.
“What distinguishes these purposeful visits is their goal of enhancing patients’ memory, decreasing their loneliness, and helping them understand the value of reconnecting to things they enjoy,” says Dr. Cumbler. —LB
Technology
New E-Pillbox Actively Monitors Med-Recon, Fights Readmissions
Electronic pillboxes are nothing new, but some hospitalists might not have seen the latest one.
Earlier this year, the FDA approved PillStation, a traditional pillbox married to a software system that uploads data to the system’s maker, SentiCare Inc., which then monitors how well a patient is following their medication regimen. The four-year-old medical firm is pitching the product to hospitals and accountable-care organizations (ACOs), among other potential clients.
And in a sales pitch practically tailored to HM, SentiCare bills itself as a medication adherence system that can help fight readmissions, particularly in cases of chronic disease or congestive heart failure. The device actually takes photographs of the pills to be taken and can record whether a patient has removed them from the device.
“Hospitals need to dramatically reduce their readmissions rates,” Yogendra Jain, chief technology officer and cofounder of SentiCare, wrote in an email to The Hospitalist. “One critical factor is medication and hospital discharge instruction adherence. Through its embedded camera, PillStation can confirm that from day one of departing the hospital... medications are loaded correctly and that the patient is taking it on time.”—RQ
Quality
Home Healthcare Has Fewer Rehospitalizations
A recent study by Avalere Health, a healthcare advisory firm based in Washington, D.C., found that providing home healthcare after hospital discharge for patients with three common conditions resulted in fewer hospital readmissions than for similar patients receiving other post-acute services. Those comparable services included long-term acute-care hospitals, inpatient rehabilitation facilities, skilled nursing facilities, and hospices.
“We tried to control for hospital DRG, severity of illness, and comorbidities,” says Emil Parker, Avalere’s director of post-acute and long-term-care practice, although he acknowledges the complexities of risk adjustment.
In comparing Medicare spending and rehospitalization rates after initial hospital visits for patients with diabetes, COPD, and congestive heart failure from 2006 to 2009, the study estimated that referrals to home healthcare resulted in $670 million in Medicare savings from 20,426 fewer readmissions.
“Hospitalists should think about the continuum of institutional support for patients discharged from the hospital with significant support needs,” Parker says. “Our study shows that in this population, provision of home healthcare is cost-effective and benefits patients by improving the continuity of their care.” —LB
Patient Safety
L.A. Hospitals Add HM for Medicaid Patients
In June, Anthem Blue Cross of Woodland Hills, Calif., began offering covered hospitalist services to its adult managed-care members covered by Medi-Cal, the Medicaid program for California residents, at 24 hospitals in Los Angeles County. The service is designed to take advantage of the existing hospitalist presence in those hospitals, which is provided by ApolloMed, a Glendale, Calif.-based medical management services company.
The hospitalist service is designed to enhance quality of care during hospitalization, reduce costs, and plan for more timely discharges and transitions to outpatient care. ApolloMed plans to add more hospitals in the region to the program, as well as additional post-discharge outpatient clinics. —LB
Technology
By the Numbers: 5.9
The percentage of total national health expenditures spent on medical devices in 2009, according to a report released in June by the Advanced Medical Technology Association.
The report highlights that while technology is washing over medicine, and HM in particular, with the adoption of electronic health records, portable ultrasounds, and tablet computing, the $147 billion spent on medical devices in 2009 represented just 5.9% of the $2.5 trillion in national health spending.
The trade group also reported that the average annual rate for medical device spending increased 7.5% in the 20-year period that ended in 2009. That outpaced the average annual rate for overall national heath expenditures, which ticked up 7% over the same time period. —RQ
Conglomerate HM?
William Geers, MD, finished up his residency in 2007, then went to work for a close-knit emergency-medicine group of about 25 doctors in Daytona Beach, Fla.
“Everybody was pretty tight,” he says of his first job.
He had met his wife in residency in Daytona, but after a while, they figured it was time for a change. “We’d been in Daytona for about six years and were ready to go try someplace different,” Dr. Geers says. “Tallahassee seemed like a good match because that’s kind of right in between our families.”
He soon landed a hospitalist job at Capital Regional Medical Center, and he suddenly was a part of EmCare, one of the biggest corporations in the emergency-medicine field and, more recently, in the field of hospital medicine. EmCare provides doctors to about 400 hospitals nationwide.
Dr. Geers said the corporate affiliation didn’t factor into his decision, adding that he took more of a traditional approach when choosing a new job.
“At the time, this program was a little bit smaller, which I liked,” says Dr. Geers, who also looked at the city’s other hospital, Tallahassee Memorial. “I met some of the physicians over here. I liked them.”
But he has noticed perks.
“I think we have some advantages working with EmCare in that we do have a pretty big group that’s backing us,” he explains. “I feel a little more secure with issues like malpractice. If things like that ever come up, I really feel like I have a lot of support with EmCare.”
With the corporate presence on the rise in HM, more and more hospitalists are entering the ranks of large companies. Some are doing so straight out of residency. Some are giving up their private practices and selling them to corporations looking to expand.
Corporations that provide hospitalists to hospitals are getting ever bigger, using sophisticated infrastructure and economies of scale, they say, to make life easier for the people who work for them, allowing the hospitalists to focus on patient care. Their efficiencies are attractive to hospitals looking to simplify.
Three years ago, North Hollywood, Calif.-based IPC: The Hospitalist Company became a publicly traded company. Its stock price has more than doubled since then.
In July, Eagle Hospital Physicians acquired North Carolina-based PrimeDoc and its 100 doctors covering seven hospitals. Similar acquisitions by larger corporations have become almost weekly news.
And, probably most significantly, Cogent Healthcare recently completed a merger with Hospitalists Management Group, a union of two of the biggest hospitalist companies in the U.S. The new company, Cogent HMG, now includes a corps of 1,000 doctors, nurses, and physician assistants (PAs), with client hospitals in 28 states.
Cogent had clients that were medium to large in size, generally in more urban areas but scattered geographically. HMG mostly served small- to medium-sized hospitals with densities in certain regions. With the merger came a recognition that the larger a company becomes, the greater the opportunity for efficiency and better services, says Rusty Holman, MD, MHM, chief clinical officer of the new company.
“The real value out of bringing these two companies together is bringing the best of different worlds together, creating new products and services for hospitals that don’t exist today, and to be able to serve a broader customer base,” says Dr. Holman, a former SHM president. “It’s also to leverage some of the infrastructure that has been built over a greater number of programs and hospitals to gain efficiency and scale that way. So that is the primary focus of the integration today.”
Cogent HMG CEO Steve Houff, MD, says the merger will mean investment in clinical support, physician recruiting, and technology, and will benefit patients and hospital partners alike.
“Both Cogent and HMG have a track record for delivering improvements in clinical quality and patient satisfaction at each of the hospitals we serve. The plan is for that to continue on a broader scale,” he wrote in an email to The Hospitalist.

—R. Jeffrey Taylor, president, chief operating officer, IPC: The Hospitalist Company, North Hollywood, Calif.
The Good, the Bad, the Oligopoly
The average size of a hospitalist group in the U.S. is about 10 full-time equivalents, according to recent survey data from SHM and MGMA. With the swelling of the size of HM’s biggest corporate players comes the question of how far the coalescing will go: Will most patient care eventually be provided by only a few groups?
R. Jeffrey Taylor, IPC’s president and chief operating officer, says the mergers and acquisitions will continue, but he doesn’t see a day when there will be just a few titans ruling all.
“I do think there will be more consolidation going forward than there is now, but I don’t see a future in which there are, you know, two or three groups that completely dominate the landscape,” he says. “There’s always that concern that that’s going to happen in the hospital industry, or that’s going to happen with payors. And there are always new entrants.”

For all the movement toward bigger companies, “this is still an unconsolidated industry,” and new physician practices will always continue to be formed, he says.
“We’re the largest group, and we’re maybe 3 1/2 percent of all the hospitals in the country. I wouldn’t consider this, today, a terribly consolidated industry,” he adds. “I do think it will move in that direction. I just don’t think it will get all the way there, because of the sort of private, entrepreneurial, independent spirit that’s common among physicians.”
Mike Tarwater, a board member of the American Hospital Association, says private hospitalist providers will only be an alternative to—and not a replacement provider for—large, self-contained systems like the Carolinas Medical Center (CMC), for which he serves as CEO. The health system has a wide spectrum of facilities—from large, urban academic centers like the 874-bed medical center in Charlotte, N.C., to 52-bed Anson Community Hospital in Wadesboro, N.C., population 5,780.
“As a system, we have the wherewithal and the recruiting expertise, and, with 1,700 physician associates across the system, we’ve kind of got critical mass,” Tarwater says. “So we will be an alternative to that in our region.”
Frank Michota, MD, FHM, director of academic affairs in the Department of Hospital Medicine at The Cleveland Clinic, says that the extensive training programs of many of the larger hospitalist groups (e.g. Cogent Academy, IPC’s extensive onboarding process and leadership conferences) could be a very good thing for the field.
“I have always thought that companies like Cogent did a very nice job in orienting their hospitalists to the patient-care goals and the process variables that were being measured,” Dr. Michota says. “I think that by making an even larger group, they have the opportunity to continue to standardize the approach to hospital care so that one hospitalist equals one hospitalist equals one hospitalist. I think that’s a positive.”
The flip side, though, is that anything that might be done wrong would be magnified in such a system.
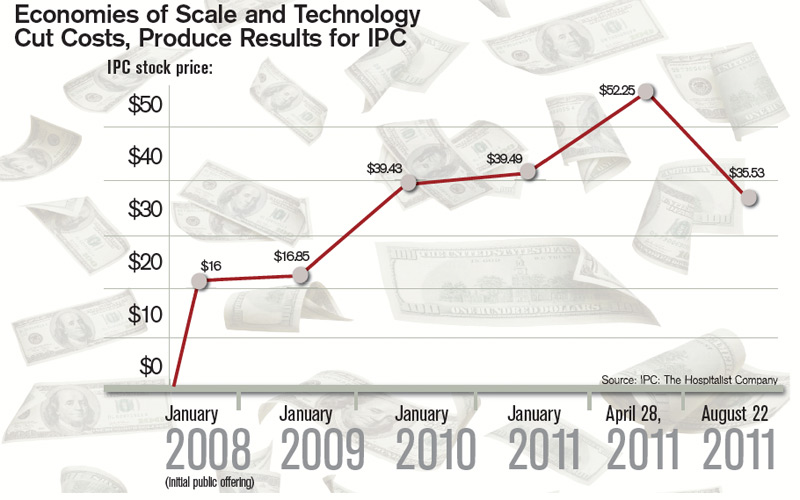
“I think that there are some dangers in how these large companies will incentivize their hospitalists,” he adds. “If they are consistent from hospitalist to hospitalist, but if there’s a perverse adverse effect from one of their financial incentives, it will be carried out across a lot of hospitals all at the same time. “But I think it’s a little early to tell what the impact of this might be. But, at least for right now, it’s actually a positive thing because it standardizes the hospitalist.”
Tarwater says that even when larger corporations buy smaller practices, familiarity tends to remain.
“Most of what I have seen are existing groups that join through merger or acquisition, and so we already have experience with the doctors, we already have long-standing relationships with the doctors,” he says. “I think any health system or hospital would be reticent to sign up with somebody that they’ve never heard of, that doesn’t have a track record, or that they don’t know already at least some of the players.” Hospitals looking to hire a private company have to exercise caution, particularly if the company is trying to break into a new region where it isn’t known.
“Those hospitals and healthcare systems just have to be really careful who they’re signing contracts with,” he said. “It’s no different than anything else we do. You just have to know who your partners are, and what drives them and where they stand on important issues.”
Executives say patient care is not at risk, even as consolidation continues. “With or without competition, we are relentlessly trying to improve our approach to patient care, our performance, and our hospital partnerships,” Cogent HMG’s Dr. Houff says.
Money Talks
It doesn’t appear that more hospitalist companies are planning to go public—at least for now.
The largest privately held company, Cogent HMG, is not planning an initial public offering anytime soon, Dr. Houff says. The company’s goal is to “continue investing in smart growth to capture more of the hospital medicine market, expand offerings to our existing hospital clients, and provide additional support to our clinical teams on the ground,” he says. “We have a strong capital partner to help us in that effort and are not looking at the public markets at this time.”
Taking on stockholders is a tricky business—one that requires careful planning and a willingness from practice leaders and administrators to relinquish some autonomy to outside interests. And then there are the financial requirements.
“They’ve really got to be able to produce some serious revenue in order for somebody to be willing to put some money into them,” says Mark Hamm, CEO of EmCare Inpatient Services.
The lure of working for a private hospitalist company promises to continue to be an attractive one. Some are drawn by the leadership possibilities—those who “aspire to be the true alpha doctor,” as IPC’s Taylor puts it. Others are drawn by the stability of a larger company.
There also is flexibility in location, Dr. Holman notes.
“Now, with Cogent HMG, [hospitalists] have even more choices in terms of relocating within the same company,” he says. “So they can keep all of the benefits, keep all of the knowledge and familiarity of the system and philosophy of care that we employ, and just be able to transfer.”
continued below...
Emergency-Medicine Companies Increasingly Venture into HM

Hollywood, Fla.-based Hospital Physician Partners (HPP) was an ED business when more opportunity came knocking: Hospitals started asking them to provide some hospitalists to go with their emergency-room doctors.
Today, HPP is firmly in the hospital medicine business. And all signs point toward more and more hospitals hiring companies to handle both emergency care and inpatient care.
“In many ways, we expanded our efforts into hospitalist medicine as a result of requests from our hospital partners where we are providing emergency, ER medicine,” said Ed Weinberg, HPP’s chief operating officer.
“Their needs were such that they asked us to provide hospital medicine services. So from that, it became clear that it was an area that was really growing.
And that is something we are pursuing as vigorously as we are emergency medicine.”
Handling both emergency care and hospital medicine can help with the transition of the patient from the emergency room to a bed upstairs, he says.
“The efficiency is being able to transition a patient from being in the emergency department as an inpatient very seamlessly,” he said. “That’s where our efficiencies are, because we have physicians working who are carrying out the same philosophy.”
Out of the company’s 120 contracts, 15 of them are in hospital medicine, but it’s growing quickly, he says.
At EmCare, traditionally an emergency-medicine company that is now getting into hospital medicine, there are about 400 emergency-medicine programs and more than 50 HM programs.
Mark Hamm, CEO of EmCare Inpatient Services, says that it can be much more cost-effective to contract with one company for both hospitalist and emergency-medicine services—which he said hospitals have found attractive.
Their arrangements range from completely separate emergency and hospital medicine staffs to small, rural hospitals where ER physicians also do rounds.
Some hospitals “just don’t have the money for a full-time hospitalist and don’t really need one,” Hamm says.
The patient transitions tend to go more smoothly when both types of care are provided by EmCare. When they’re not, there can be slowdowns.
“Our goal is to quickly and appropriately move patients through the system,” he says. “If we have a hospitalist provider that’s not really on the same page, that can create bottlenecks. . . . But it’s a blip.
“Our goal is to sit down, even if it’s not an EmCare hospitalist, to sit down with that director and say, ‘Hey, look, let’s be the leader here, let’s work together and appropriately expedite these patients.’ We do the same thing on the hospitalist side.”
Inpatient care promises to be a big part of their future business, most executives agree.
“Hospital medicine,” Weinberg says, “is growing by leaps and bounds.” —TC
Dr. Houff says the majority of newly recruited physicians are coming out of residency but that the company is attracting physicians in the middle of their careers, along with physicians having backgrounds beyond internal medicine.
In Tallahassee at Capital Regional, Dr. Geers says that he feels there is support from the company that can protect his job quality, with “a little bit more room to negotiate with the hospital if the hospital wants us to take on new responsibilities.
“Whereas if we worked directly for the hospital, I don’t think we’d have much say in the matter,” he says.
He also says he is happy with the predictable schedule; he’s responsible for 7 a.m. to 7 p.m. and nothing more.
“If you’re finished rounding and you’ve seen all your patients and tied up all your loose ends, you’re not always there till 7 p.m.,” he points out. “Sometimes you can leave a little early....Once 7 p.m. comes, you’re not going to get paged in the middle of the night.”
Thomas R. Collins is a freelance medical writer based in Florida.
Wall Street’s Rosy View of Hospital Medicine

When IPC: The Hospitalist Company went public in January 2008, its stock price was $16 a share. In late July of this year, it was hovering a tick below $50 a share.
It’s been an obvious financial success—a performance that speaks well of the hospitalist specialty as a whole, says analyst Kevin Campbell, who covers IPC for Avondale Partners.
“Investors like the industry,” Campbell explains. “They see the need for hospitalists....When investors look at that, they see the opportunity for continued growth.”
IPC’s management team, he adds, has done “an excellent job of growing both the revenues and the earnings.”
Revenues in 2008 were $251 million. This year, they’re projected to be $454 million, an increase of 80%.
Six of 10 analysts say the company is a “strong buy,” one says it’s a “buy,” and for three others, it’s a “hold,” according to research listed on the NASDAQ website.
One of the key reasons IPC has performed well, Campbell says, is that when it makes an acquisition, physicians whose practices are bought are not paid everything at once; a portion is paid out later. Because the payment is a factor of the company’s performance, that encourages the physicians to keep their newly acquired practices performing optimally.
That’s different from scenarios in which “doctors would take their big check and retire,” he says, “and the operations for the practice would decline significantly. This is one way that IPCM [the stock symbol] can ensure that that doesn’t happen.”
Campbell also says it probably is unlikely that there will be another public offering of a hospitalist company in the near future. “There’s not a lot of companies of scale,” he says. “You have to have some scale before you would consider going public.”
R. Jeffrey Taylor, IPC’s president and COO, says another public offering from a hospitalist company isn’t that far-fetched.
“I would not be at all surprised to see someone else follow that path,” he says. “Frankly, it will probably be a little easier for the second company to do it because we have helped educate people about the hospitalist model, and fortunately the company and the stock have performed well. So I think it would be an easier sell to the public market the second time around. And I expect that’s more likely than not in the next few years.” —TC
William Geers, MD, finished up his residency in 2007, then went to work for a close-knit emergency-medicine group of about 25 doctors in Daytona Beach, Fla.
“Everybody was pretty tight,” he says of his first job.
He had met his wife in residency in Daytona, but after a while, they figured it was time for a change. “We’d been in Daytona for about six years and were ready to go try someplace different,” Dr. Geers says. “Tallahassee seemed like a good match because that’s kind of right in between our families.”
He soon landed a hospitalist job at Capital Regional Medical Center, and he suddenly was a part of EmCare, one of the biggest corporations in the emergency-medicine field and, more recently, in the field of hospital medicine. EmCare provides doctors to about 400 hospitals nationwide.
Dr. Geers said the corporate affiliation didn’t factor into his decision, adding that he took more of a traditional approach when choosing a new job.
“At the time, this program was a little bit smaller, which I liked,” says Dr. Geers, who also looked at the city’s other hospital, Tallahassee Memorial. “I met some of the physicians over here. I liked them.”
But he has noticed perks.
“I think we have some advantages working with EmCare in that we do have a pretty big group that’s backing us,” he explains. “I feel a little more secure with issues like malpractice. If things like that ever come up, I really feel like I have a lot of support with EmCare.”
With the corporate presence on the rise in HM, more and more hospitalists are entering the ranks of large companies. Some are doing so straight out of residency. Some are giving up their private practices and selling them to corporations looking to expand.
Corporations that provide hospitalists to hospitals are getting ever bigger, using sophisticated infrastructure and economies of scale, they say, to make life easier for the people who work for them, allowing the hospitalists to focus on patient care. Their efficiencies are attractive to hospitals looking to simplify.
Three years ago, North Hollywood, Calif.-based IPC: The Hospitalist Company became a publicly traded company. Its stock price has more than doubled since then.
In July, Eagle Hospital Physicians acquired North Carolina-based PrimeDoc and its 100 doctors covering seven hospitals. Similar acquisitions by larger corporations have become almost weekly news.
And, probably most significantly, Cogent Healthcare recently completed a merger with Hospitalists Management Group, a union of two of the biggest hospitalist companies in the U.S. The new company, Cogent HMG, now includes a corps of 1,000 doctors, nurses, and physician assistants (PAs), with client hospitals in 28 states.
Cogent had clients that were medium to large in size, generally in more urban areas but scattered geographically. HMG mostly served small- to medium-sized hospitals with densities in certain regions. With the merger came a recognition that the larger a company becomes, the greater the opportunity for efficiency and better services, says Rusty Holman, MD, MHM, chief clinical officer of the new company.
“The real value out of bringing these two companies together is bringing the best of different worlds together, creating new products and services for hospitals that don’t exist today, and to be able to serve a broader customer base,” says Dr. Holman, a former SHM president. “It’s also to leverage some of the infrastructure that has been built over a greater number of programs and hospitals to gain efficiency and scale that way. So that is the primary focus of the integration today.”
Cogent HMG CEO Steve Houff, MD, says the merger will mean investment in clinical support, physician recruiting, and technology, and will benefit patients and hospital partners alike.
“Both Cogent and HMG have a track record for delivering improvements in clinical quality and patient satisfaction at each of the hospitals we serve. The plan is for that to continue on a broader scale,” he wrote in an email to The Hospitalist.
—R. Jeffrey Taylor, president, chief operating officer, IPC: The Hospitalist Company, North Hollywood, Calif.
The Good, the Bad, the Oligopoly
The average size of a hospitalist group in the U.S. is about 10 full-time equivalents, according to recent survey data from SHM and MGMA. With the swelling of the size of HM’s biggest corporate players comes the question of how far the coalescing will go: Will most patient care eventually be provided by only a few groups?
R. Jeffrey Taylor, IPC’s president and chief operating officer, says the mergers and acquisitions will continue, but he doesn’t see a day when there will be just a few titans ruling all.
“I do think there will be more consolidation going forward than there is now, but I don’t see a future in which there are, you know, two or three groups that completely dominate the landscape,” he says. “There’s always that concern that that’s going to happen in the hospital industry, or that’s going to happen with payors. And there are always new entrants.”
For all the movement toward bigger companies, “this is still an unconsolidated industry,” and new physician practices will always continue to be formed, he says.
“We’re the largest group, and we’re maybe 3 1/2 percent of all the hospitals in the country. I wouldn’t consider this, today, a terribly consolidated industry,” he adds. “I do think it will move in that direction. I just don’t think it will get all the way there, because of the sort of private, entrepreneurial, independent spirit that’s common among physicians.”
Mike Tarwater, a board member of the American Hospital Association, says private hospitalist providers will only be an alternative to—and not a replacement provider for—large, self-contained systems like the Carolinas Medical Center (CMC), for which he serves as CEO. The health system has a wide spectrum of facilities—from large, urban academic centers like the 874-bed medical center in Charlotte, N.C., to 52-bed Anson Community Hospital in Wadesboro, N.C., population 5,780.
“As a system, we have the wherewithal and the recruiting expertise, and, with 1,700 physician associates across the system, we’ve kind of got critical mass,” Tarwater says. “So we will be an alternative to that in our region.”
Frank Michota, MD, FHM, director of academic affairs in the Department of Hospital Medicine at The Cleveland Clinic, says that the extensive training programs of many of the larger hospitalist groups (e.g. Cogent Academy, IPC’s extensive onboarding process and leadership conferences) could be a very good thing for the field.
“I have always thought that companies like Cogent did a very nice job in orienting their hospitalists to the patient-care goals and the process variables that were being measured,” Dr. Michota says. “I think that by making an even larger group, they have the opportunity to continue to standardize the approach to hospital care so that one hospitalist equals one hospitalist equals one hospitalist. I think that’s a positive.”
The flip side, though, is that anything that might be done wrong would be magnified in such a system.
“I think that there are some dangers in how these large companies will incentivize their hospitalists,” he adds. “If they are consistent from hospitalist to hospitalist, but if there’s a perverse adverse effect from one of their financial incentives, it will be carried out across a lot of hospitals all at the same time. “But I think it’s a little early to tell what the impact of this might be. But, at least for right now, it’s actually a positive thing because it standardizes the hospitalist.”
Tarwater says that even when larger corporations buy smaller practices, familiarity tends to remain.
“Most of what I have seen are existing groups that join through merger or acquisition, and so we already have experience with the doctors, we already have long-standing relationships with the doctors,” he says. “I think any health system or hospital would be reticent to sign up with somebody that they’ve never heard of, that doesn’t have a track record, or that they don’t know already at least some of the players.” Hospitals looking to hire a private company have to exercise caution, particularly if the company is trying to break into a new region where it isn’t known.
“Those hospitals and healthcare systems just have to be really careful who they’re signing contracts with,” he said. “It’s no different than anything else we do. You just have to know who your partners are, and what drives them and where they stand on important issues.”
Executives say patient care is not at risk, even as consolidation continues. “With or without competition, we are relentlessly trying to improve our approach to patient care, our performance, and our hospital partnerships,” Cogent HMG’s Dr. Houff says.
Money Talks
It doesn’t appear that more hospitalist companies are planning to go public—at least for now.
The largest privately held company, Cogent HMG, is not planning an initial public offering anytime soon, Dr. Houff says. The company’s goal is to “continue investing in smart growth to capture more of the hospital medicine market, expand offerings to our existing hospital clients, and provide additional support to our clinical teams on the ground,” he says. “We have a strong capital partner to help us in that effort and are not looking at the public markets at this time.”
Taking on stockholders is a tricky business—one that requires careful planning and a willingness from practice leaders and administrators to relinquish some autonomy to outside interests. And then there are the financial requirements.
“They’ve really got to be able to produce some serious revenue in order for somebody to be willing to put some money into them,” says Mark Hamm, CEO of EmCare Inpatient Services.
The lure of working for a private hospitalist company promises to continue to be an attractive one. Some are drawn by the leadership possibilities—those who “aspire to be the true alpha doctor,” as IPC’s Taylor puts it. Others are drawn by the stability of a larger company.
There also is flexibility in location, Dr. Holman notes.
“Now, with Cogent HMG, [hospitalists] have even more choices in terms of relocating within the same company,” he says. “So they can keep all of the benefits, keep all of the knowledge and familiarity of the system and philosophy of care that we employ, and just be able to transfer.”
continued below...
Emergency-Medicine Companies Increasingly Venture into HM
Hollywood, Fla.-based Hospital Physician Partners (HPP) was an ED business when more opportunity came knocking: Hospitals started asking them to provide some hospitalists to go with their emergency-room doctors.
Today, HPP is firmly in the hospital medicine business. And all signs point toward more and more hospitals hiring companies to handle both emergency care and inpatient care.
“In many ways, we expanded our efforts into hospitalist medicine as a result of requests from our hospital partners where we are providing emergency, ER medicine,” said Ed Weinberg, HPP’s chief operating officer.
“Their needs were such that they asked us to provide hospital medicine services. So from that, it became clear that it was an area that was really growing.
And that is something we are pursuing as vigorously as we are emergency medicine.”
Handling both emergency care and hospital medicine can help with the transition of the patient from the emergency room to a bed upstairs, he says.
“The efficiency is being able to transition a patient from being in the emergency department as an inpatient very seamlessly,” he said. “That’s where our efficiencies are, because we have physicians working who are carrying out the same philosophy.”
Out of the company’s 120 contracts, 15 of them are in hospital medicine, but it’s growing quickly, he says.
At EmCare, traditionally an emergency-medicine company that is now getting into hospital medicine, there are about 400 emergency-medicine programs and more than 50 HM programs.
Mark Hamm, CEO of EmCare Inpatient Services, says that it can be much more cost-effective to contract with one company for both hospitalist and emergency-medicine services—which he said hospitals have found attractive.
Their arrangements range from completely separate emergency and hospital medicine staffs to small, rural hospitals where ER physicians also do rounds.
Some hospitals “just don’t have the money for a full-time hospitalist and don’t really need one,” Hamm says.
The patient transitions tend to go more smoothly when both types of care are provided by EmCare. When they’re not, there can be slowdowns.
“Our goal is to quickly and appropriately move patients through the system,” he says. “If we have a hospitalist provider that’s not really on the same page, that can create bottlenecks. . . . But it’s a blip.
“Our goal is to sit down, even if it’s not an EmCare hospitalist, to sit down with that director and say, ‘Hey, look, let’s be the leader here, let’s work together and appropriately expedite these patients.’ We do the same thing on the hospitalist side.”
Inpatient care promises to be a big part of their future business, most executives agree.
“Hospital medicine,” Weinberg says, “is growing by leaps and bounds.” —TC
Dr. Houff says the majority of newly recruited physicians are coming out of residency but that the company is attracting physicians in the middle of their careers, along with physicians having backgrounds beyond internal medicine.
In Tallahassee at Capital Regional, Dr. Geers says that he feels there is support from the company that can protect his job quality, with “a little bit more room to negotiate with the hospital if the hospital wants us to take on new responsibilities.
“Whereas if we worked directly for the hospital, I don’t think we’d have much say in the matter,” he says.
He also says he is happy with the predictable schedule; he’s responsible for 7 a.m. to 7 p.m. and nothing more.
“If you’re finished rounding and you’ve seen all your patients and tied up all your loose ends, you’re not always there till 7 p.m.,” he points out. “Sometimes you can leave a little early....Once 7 p.m. comes, you’re not going to get paged in the middle of the night.”
Thomas R. Collins is a freelance medical writer based in Florida.
Wall Street’s Rosy View of Hospital Medicine
When IPC: The Hospitalist Company went public in January 2008, its stock price was $16 a share. In late July of this year, it was hovering a tick below $50 a share.
It’s been an obvious financial success—a performance that speaks well of the hospitalist specialty as a whole, says analyst Kevin Campbell, who covers IPC for Avondale Partners.
“Investors like the industry,” Campbell explains. “They see the need for hospitalists....When investors look at that, they see the opportunity for continued growth.”
IPC’s management team, he adds, has done “an excellent job of growing both the revenues and the earnings.”
Revenues in 2008 were $251 million. This year, they’re projected to be $454 million, an increase of 80%.
Six of 10 analysts say the company is a “strong buy,” one says it’s a “buy,” and for three others, it’s a “hold,” according to research listed on the NASDAQ website.
One of the key reasons IPC has performed well, Campbell says, is that when it makes an acquisition, physicians whose practices are bought are not paid everything at once; a portion is paid out later. Because the payment is a factor of the company’s performance, that encourages the physicians to keep their newly acquired practices performing optimally.
That’s different from scenarios in which “doctors would take their big check and retire,” he says, “and the operations for the practice would decline significantly. This is one way that IPCM [the stock symbol] can ensure that that doesn’t happen.”
Campbell also says it probably is unlikely that there will be another public offering of a hospitalist company in the near future. “There’s not a lot of companies of scale,” he says. “You have to have some scale before you would consider going public.”
R. Jeffrey Taylor, IPC’s president and COO, says another public offering from a hospitalist company isn’t that far-fetched.
“I would not be at all surprised to see someone else follow that path,” he says. “Frankly, it will probably be a little easier for the second company to do it because we have helped educate people about the hospitalist model, and fortunately the company and the stock have performed well. So I think it would be an easier sell to the public market the second time around. And I expect that’s more likely than not in the next few years.” —TC
William Geers, MD, finished up his residency in 2007, then went to work for a close-knit emergency-medicine group of about 25 doctors in Daytona Beach, Fla.
“Everybody was pretty tight,” he says of his first job.
He had met his wife in residency in Daytona, but after a while, they figured it was time for a change. “We’d been in Daytona for about six years and were ready to go try someplace different,” Dr. Geers says. “Tallahassee seemed like a good match because that’s kind of right in between our families.”
He soon landed a hospitalist job at Capital Regional Medical Center, and he suddenly was a part of EmCare, one of the biggest corporations in the emergency-medicine field and, more recently, in the field of hospital medicine. EmCare provides doctors to about 400 hospitals nationwide.
Dr. Geers said the corporate affiliation didn’t factor into his decision, adding that he took more of a traditional approach when choosing a new job.
“At the time, this program was a little bit smaller, which I liked,” says Dr. Geers, who also looked at the city’s other hospital, Tallahassee Memorial. “I met some of the physicians over here. I liked them.”
But he has noticed perks.
“I think we have some advantages working with EmCare in that we do have a pretty big group that’s backing us,” he explains. “I feel a little more secure with issues like malpractice. If things like that ever come up, I really feel like I have a lot of support with EmCare.”
With the corporate presence on the rise in HM, more and more hospitalists are entering the ranks of large companies. Some are doing so straight out of residency. Some are giving up their private practices and selling them to corporations looking to expand.
Corporations that provide hospitalists to hospitals are getting ever bigger, using sophisticated infrastructure and economies of scale, they say, to make life easier for the people who work for them, allowing the hospitalists to focus on patient care. Their efficiencies are attractive to hospitals looking to simplify.
Three years ago, North Hollywood, Calif.-based IPC: The Hospitalist Company became a publicly traded company. Its stock price has more than doubled since then.
In July, Eagle Hospital Physicians acquired North Carolina-based PrimeDoc and its 100 doctors covering seven hospitals. Similar acquisitions by larger corporations have become almost weekly news.
And, probably most significantly, Cogent Healthcare recently completed a merger with Hospitalists Management Group, a union of two of the biggest hospitalist companies in the U.S. The new company, Cogent HMG, now includes a corps of 1,000 doctors, nurses, and physician assistants (PAs), with client hospitals in 28 states.
Cogent had clients that were medium to large in size, generally in more urban areas but scattered geographically. HMG mostly served small- to medium-sized hospitals with densities in certain regions. With the merger came a recognition that the larger a company becomes, the greater the opportunity for efficiency and better services, says Rusty Holman, MD, MHM, chief clinical officer of the new company.
“The real value out of bringing these two companies together is bringing the best of different worlds together, creating new products and services for hospitals that don’t exist today, and to be able to serve a broader customer base,” says Dr. Holman, a former SHM president. “It’s also to leverage some of the infrastructure that has been built over a greater number of programs and hospitals to gain efficiency and scale that way. So that is the primary focus of the integration today.”
Cogent HMG CEO Steve Houff, MD, says the merger will mean investment in clinical support, physician recruiting, and technology, and will benefit patients and hospital partners alike.
“Both Cogent and HMG have a track record for delivering improvements in clinical quality and patient satisfaction at each of the hospitals we serve. The plan is for that to continue on a broader scale,” he wrote in an email to The Hospitalist.
—R. Jeffrey Taylor, president, chief operating officer, IPC: The Hospitalist Company, North Hollywood, Calif.
The Good, the Bad, the Oligopoly
The average size of a hospitalist group in the U.S. is about 10 full-time equivalents, according to recent survey data from SHM and MGMA. With the swelling of the size of HM’s biggest corporate players comes the question of how far the coalescing will go: Will most patient care eventually be provided by only a few groups?
R. Jeffrey Taylor, IPC’s president and chief operating officer, says the mergers and acquisitions will continue, but he doesn’t see a day when there will be just a few titans ruling all.
“I do think there will be more consolidation going forward than there is now, but I don’t see a future in which there are, you know, two or three groups that completely dominate the landscape,” he says. “There’s always that concern that that’s going to happen in the hospital industry, or that’s going to happen with payors. And there are always new entrants.”
For all the movement toward bigger companies, “this is still an unconsolidated industry,” and new physician practices will always continue to be formed, he says.
“We’re the largest group, and we’re maybe 3 1/2 percent of all the hospitals in the country. I wouldn’t consider this, today, a terribly consolidated industry,” he adds. “I do think it will move in that direction. I just don’t think it will get all the way there, because of the sort of private, entrepreneurial, independent spirit that’s common among physicians.”
Mike Tarwater, a board member of the American Hospital Association, says private hospitalist providers will only be an alternative to—and not a replacement provider for—large, self-contained systems like the Carolinas Medical Center (CMC), for which he serves as CEO. The health system has a wide spectrum of facilities—from large, urban academic centers like the 874-bed medical center in Charlotte, N.C., to 52-bed Anson Community Hospital in Wadesboro, N.C., population 5,780.
“As a system, we have the wherewithal and the recruiting expertise, and, with 1,700 physician associates across the system, we’ve kind of got critical mass,” Tarwater says. “So we will be an alternative to that in our region.”
Frank Michota, MD, FHM, director of academic affairs in the Department of Hospital Medicine at The Cleveland Clinic, says that the extensive training programs of many of the larger hospitalist groups (e.g. Cogent Academy, IPC’s extensive onboarding process and leadership conferences) could be a very good thing for the field.
“I have always thought that companies like Cogent did a very nice job in orienting their hospitalists to the patient-care goals and the process variables that were being measured,” Dr. Michota says. “I think that by making an even larger group, they have the opportunity to continue to standardize the approach to hospital care so that one hospitalist equals one hospitalist equals one hospitalist. I think that’s a positive.”
The flip side, though, is that anything that might be done wrong would be magnified in such a system.
“I think that there are some dangers in how these large companies will incentivize their hospitalists,” he adds. “If they are consistent from hospitalist to hospitalist, but if there’s a perverse adverse effect from one of their financial incentives, it will be carried out across a lot of hospitals all at the same time. “But I think it’s a little early to tell what the impact of this might be. But, at least for right now, it’s actually a positive thing because it standardizes the hospitalist.”
Tarwater says that even when larger corporations buy smaller practices, familiarity tends to remain.
“Most of what I have seen are existing groups that join through merger or acquisition, and so we already have experience with the doctors, we already have long-standing relationships with the doctors,” he says. “I think any health system or hospital would be reticent to sign up with somebody that they’ve never heard of, that doesn’t have a track record, or that they don’t know already at least some of the players.” Hospitals looking to hire a private company have to exercise caution, particularly if the company is trying to break into a new region where it isn’t known.
“Those hospitals and healthcare systems just have to be really careful who they’re signing contracts with,” he said. “It’s no different than anything else we do. You just have to know who your partners are, and what drives them and where they stand on important issues.”
Executives say patient care is not at risk, even as consolidation continues. “With or without competition, we are relentlessly trying to improve our approach to patient care, our performance, and our hospital partnerships,” Cogent HMG’s Dr. Houff says.
Money Talks
It doesn’t appear that more hospitalist companies are planning to go public—at least for now.
The largest privately held company, Cogent HMG, is not planning an initial public offering anytime soon, Dr. Houff says. The company’s goal is to “continue investing in smart growth to capture more of the hospital medicine market, expand offerings to our existing hospital clients, and provide additional support to our clinical teams on the ground,” he says. “We have a strong capital partner to help us in that effort and are not looking at the public markets at this time.”
Taking on stockholders is a tricky business—one that requires careful planning and a willingness from practice leaders and administrators to relinquish some autonomy to outside interests. And then there are the financial requirements.
“They’ve really got to be able to produce some serious revenue in order for somebody to be willing to put some money into them,” says Mark Hamm, CEO of EmCare Inpatient Services.
The lure of working for a private hospitalist company promises to continue to be an attractive one. Some are drawn by the leadership possibilities—those who “aspire to be the true alpha doctor,” as IPC’s Taylor puts it. Others are drawn by the stability of a larger company.
There also is flexibility in location, Dr. Holman notes.
“Now, with Cogent HMG, [hospitalists] have even more choices in terms of relocating within the same company,” he says. “So they can keep all of the benefits, keep all of the knowledge and familiarity of the system and philosophy of care that we employ, and just be able to transfer.”
continued below...
Emergency-Medicine Companies Increasingly Venture into HM
Hollywood, Fla.-based Hospital Physician Partners (HPP) was an ED business when more opportunity came knocking: Hospitals started asking them to provide some hospitalists to go with their emergency-room doctors.
Today, HPP is firmly in the hospital medicine business. And all signs point toward more and more hospitals hiring companies to handle both emergency care and inpatient care.
“In many ways, we expanded our efforts into hospitalist medicine as a result of requests from our hospital partners where we are providing emergency, ER medicine,” said Ed Weinberg, HPP’s chief operating officer.
“Their needs were such that they asked us to provide hospital medicine services. So from that, it became clear that it was an area that was really growing.
And that is something we are pursuing as vigorously as we are emergency medicine.”
Handling both emergency care and hospital medicine can help with the transition of the patient from the emergency room to a bed upstairs, he says.
“The efficiency is being able to transition a patient from being in the emergency department as an inpatient very seamlessly,” he said. “That’s where our efficiencies are, because we have physicians working who are carrying out the same philosophy.”
Out of the company’s 120 contracts, 15 of them are in hospital medicine, but it’s growing quickly, he says.
At EmCare, traditionally an emergency-medicine company that is now getting into hospital medicine, there are about 400 emergency-medicine programs and more than 50 HM programs.
Mark Hamm, CEO of EmCare Inpatient Services, says that it can be much more cost-effective to contract with one company for both hospitalist and emergency-medicine services—which he said hospitals have found attractive.
Their arrangements range from completely separate emergency and hospital medicine staffs to small, rural hospitals where ER physicians also do rounds.
Some hospitals “just don’t have the money for a full-time hospitalist and don’t really need one,” Hamm says.
The patient transitions tend to go more smoothly when both types of care are provided by EmCare. When they’re not, there can be slowdowns.
“Our goal is to quickly and appropriately move patients through the system,” he says. “If we have a hospitalist provider that’s not really on the same page, that can create bottlenecks. . . . But it’s a blip.
“Our goal is to sit down, even if it’s not an EmCare hospitalist, to sit down with that director and say, ‘Hey, look, let’s be the leader here, let’s work together and appropriately expedite these patients.’ We do the same thing on the hospitalist side.”
Inpatient care promises to be a big part of their future business, most executives agree.
“Hospital medicine,” Weinberg says, “is growing by leaps and bounds.” —TC
Dr. Houff says the majority of newly recruited physicians are coming out of residency but that the company is attracting physicians in the middle of their careers, along with physicians having backgrounds beyond internal medicine.
In Tallahassee at Capital Regional, Dr. Geers says that he feels there is support from the company that can protect his job quality, with “a little bit more room to negotiate with the hospital if the hospital wants us to take on new responsibilities.
“Whereas if we worked directly for the hospital, I don’t think we’d have much say in the matter,” he says.
He also says he is happy with the predictable schedule; he’s responsible for 7 a.m. to 7 p.m. and nothing more.
“If you’re finished rounding and you’ve seen all your patients and tied up all your loose ends, you’re not always there till 7 p.m.,” he points out. “Sometimes you can leave a little early....Once 7 p.m. comes, you’re not going to get paged in the middle of the night.”
Thomas R. Collins is a freelance medical writer based in Florida.
Wall Street’s Rosy View of Hospital Medicine
When IPC: The Hospitalist Company went public in January 2008, its stock price was $16 a share. In late July of this year, it was hovering a tick below $50 a share.
It’s been an obvious financial success—a performance that speaks well of the hospitalist specialty as a whole, says analyst Kevin Campbell, who covers IPC for Avondale Partners.
“Investors like the industry,” Campbell explains. “They see the need for hospitalists....When investors look at that, they see the opportunity for continued growth.”
IPC’s management team, he adds, has done “an excellent job of growing both the revenues and the earnings.”
Revenues in 2008 were $251 million. This year, they’re projected to be $454 million, an increase of 80%.
Six of 10 analysts say the company is a “strong buy,” one says it’s a “buy,” and for three others, it’s a “hold,” according to research listed on the NASDAQ website.
One of the key reasons IPC has performed well, Campbell says, is that when it makes an acquisition, physicians whose practices are bought are not paid everything at once; a portion is paid out later. Because the payment is a factor of the company’s performance, that encourages the physicians to keep their newly acquired practices performing optimally.
That’s different from scenarios in which “doctors would take their big check and retire,” he says, “and the operations for the practice would decline significantly. This is one way that IPCM [the stock symbol] can ensure that that doesn’t happen.”
Campbell also says it probably is unlikely that there will be another public offering of a hospitalist company in the near future. “There’s not a lot of companies of scale,” he says. “You have to have some scale before you would consider going public.”
R. Jeffrey Taylor, IPC’s president and COO, says another public offering from a hospitalist company isn’t that far-fetched.
“I would not be at all surprised to see someone else follow that path,” he says. “Frankly, it will probably be a little easier for the second company to do it because we have helped educate people about the hospitalist model, and fortunately the company and the stock have performed well. So I think it would be an easier sell to the public market the second time around. And I expect that’s more likely than not in the next few years.” —TC
Modest Gains
Hospitalists are earning a little more, working a little harder, and are less likely to switch jobs or careers, according to the 2011 State of Hospital Medicine report. The annual report, based on data collected jointly by SHM and the Medical Group Management Association (MGMA), offers more than 10,000 compensation and productivity data points for all types of hospitalists, including, for the first time, an exclusive look at academic hospitalists.
As previously reported, median adult hospitalist compensation increased to $220,619, a 2.6% increase from the $215,000 figure reported last year. “I think that’s a reflection of the market and demand for hospitalists, and the value that hospitals and other healthcare payors see that hospitalists bring,” says William “Tex” Landis, MD, FHM, medical director of Wellspan Hospitalists in York, Pa., and chair of SHM’s Practice Analysis Committee.
The compensation increases for hospitalists reported in the SHM-MGMA survey mirror results in other recent surveys. The 2011 Medical Group Compensation and Financial Survey, produced by the American Medical Group Association, found the overall average increase in physician compensation was 2.4%. Primary-care physicians (PCPs) reported a 2.6% increase in 2010, while the “hospitalist-internal medicine” category saw one of the steepest increases at 6.29%, according to the report (www.amga.org).
According to the 2011 MedScape Physician Compensation Report, 27% of the more than 15,000 physicians surveyed said their income increased from 2009 to 2010, whereas 50% said they saw no change. About 23% reported a decline in income, the report showed (www.medscape.com/features/slideshow/compensation/2011/).
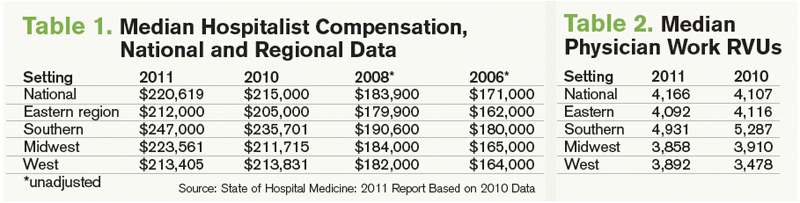
Continuing a decadelong trend, the SHM-MGMA report shows hospitalists in the South make the most (median compensation $247,000, up from $235,701 in 2010) and hospitalists in the East ($212,000, up from $205,000 in 2010) lag behind the other regions (see Table 1).

The Hospitalist spoke to five members of SHM’s Practice Analysis Committee (PAC) about the survey results, and each points to continued nationwide demand as the driver of increased compensation. However, the committee also cautions HM groups and directors to be leery of trending this data, as the report is based on a volunteer survey, the survey population changes year to year, and only two years of identical survey data are available.
“As hospital medicine continues to grow, the hospitals become so dependent on the services that the hospitalists provide,” says PAC member Scarlett Blue, RN-BC, MSN, NE-BC, CPHQ, vice president of quality and clinical development for Eagle Hospital Physicians. “[Hospitals] know HM is critical and…I think that hospitalists demonstrate tremendous value, which the hospitals and the management groups recognize.”
The 2011 report, available Sept. 14, compiled data about 4,633 hospitalists in 412 groups. Eighty-five percent of the respondents classified themselves as “adult” hospitalists, 5% as “pediatric” hospitalists, and 10% as both adult and pediatric. Of note, this is the first time SHM has produced compensation and productivity data in consecutive years. In addition to compensation, the survey provides drill-down capability on productivity and reimbursement metrics, along with specific data regarding night coverage arrangements (see “Survey Insights,”), financial support payments, physician turnover, and, for the first time, a look at nonphysician providers (NPPs) in HM practice (see “Nonphysician Provider Data Available for First Time,”).
continued below...
Nonphysician Provider Data Available for First Time

Hospitalist groups were asked about nurse practitioner (NP) and physician assistant (PA) employment, and 49% of HM groups reported having some type of nonphysician provider (NPP) on staff (see Figure 4). Those results, although not startling to some, should open the other half’s eyes, Dr. Landis says.
“Just looking to the future, I think most of us can see physician extenders¬⎯NPs and PAs⎯becoming more and more important in the delivery of hospital care,” he says. “We’re going to be looking to get more information about how that’s happening and what functions they’re performing and what resources, financially and otherwise, are required to help them be effective team members.”
Hawley says NPPs are a critical part of HM’s future but admits some hospitalists still are reluctant to work with NPPs because compensation and incentives are misaligned. “Oftentimes what a [physician] compensation plan will do is not provide for any work that is being done by the NPP,” she says. When physicians find out they also are being measured on patient satisfaction and other metrics, “then the NPP becomes very, very critical. So we’re seeing more and more acceptance. Our opinion, as a consulting group, is that there won’t be a [HM] program in this country that doesn’t somehow use nonphysician providers. There just aren’t enough hospitalists to go around.”
Dr. Landis says his committee is planning to collaborate with SHM’s Nonphysician Provider Committee to determine the best way to collect and disseminate NPP benchmarks. “That’s a future trend and everybody can see it,” he adds. “We have yet to solidify, though, how we’re going to measure and evaluate what’s going on there.” —JC
Hospitalist Productivity
Although hospitalists are earning more, the 2011 report also shows they are producing more work relative-value units (wRVUs) than ever before. The median physician wRVU rate annually for 2011 was 4,166, a 1.4% increase over the 2010 figure.
Hospitalists in the Eastern and Midwest regions reported relatively unchanged wRVUs when compared with 2010 figures. The Southern region, which outdistanced the other regions by more than 800 wRVUs per physician, reported a 6.7% decrease in wRVUs—4,931 in 2011 compared with 5,287 in 2010. On the flipside, the Western region showed a 11.9% increase per physician (see Table 2, left).
PAC committee members agree the wRVU variance between regions is difficult to explain, but most agree the slight year-over-year increase in productivity shows the specialty is stabilizing in terms of what productivity is expected from the average hospitalist.
“Maybe it is an indication that the field is maturing and we’re settling in at some data points that we can now potentially put some stock into,” says Beth E. Hawley, MBA, FACHE, senior vice president of The Cogent Group, a consulting division of Brentwood, Tenn.-based Cogent HMG. “Before, [the figures] changed dramatically from survey to survey; I think we’re seeing more stability now from last year to this year.

—Beth E. Hawley, MBA, FACHE, senior vice president, The Cogent Group, Brentwood, Tenn., SHM Practice Analysis Committee member
“It’s helpful to be able to sort [wRVUs] by employment model, by region, by large and small hospital. We can really get some better benchmarks, in terms of what should be the expectation.”
Chris Frost, MD, FHM, national medical director of hospital medicine services for HCA, says he remains somewhat hesitant to say HM is “settling into a number” for expected wRVUs, as he routinely hears from hospital administrators looking for “additional efficiencies that we can put in place to allow and position the hospitalists to be more productive” while maintaining a high quality care delivery model. He’s also puzzled by the geographic discrepancies. “I just have to scratch my head. I haven’t entirely figured that out yet,” he says.
That said, Dr. Frost agrees the wRVU benchmarks are the most useful in terms of “billable productivity. But I also would like to see—or believe—one of the reasons compensation is going up and the work RVU is flat is hospitalists are being recognized for their value in other arenas, as it relates to the transition from the fee-for-service to pay-for-value-type models, championing effective transitions of care, leading process improvement teams, etc. Those things can’t, or don’t, necessarily lend themselves well to a work RVU equivalent.”
The Buzz: Financial Support
First reported at HM11 in May, the survey shows hospitalist support payments increased more than 39%, to $136,403 per FTE hospitalist in 2011 from $98,253 in 2010. PAC members and other hospitalist experts in practice management attribute the startling increase in support payments to more accurate reporting. Others note that the rise in support payments could be attributed to the decline in collection of professional fees, a direct result of the economic downturn.
And, according to Dr. Landis, hospitals are more willing today to fund hospitalist services than ever before.
“I think [the rise in HM support] payments is because of the evolution of healthcare in the hospital as a whole,” he says. “Hospitals are looking to hospitalists to help them provide the care that that patients and families need, expect, and want. And we’re stepping up to the plate to do it, and they’re paying us to do it. I think that’s the story.
“If you want to tie that with why there’s $136,000 going per hospitalist, [it’s] because they want us there for that rapid-response team, and rapid-response teams don’t generate a lot of RVUs necessarily.”
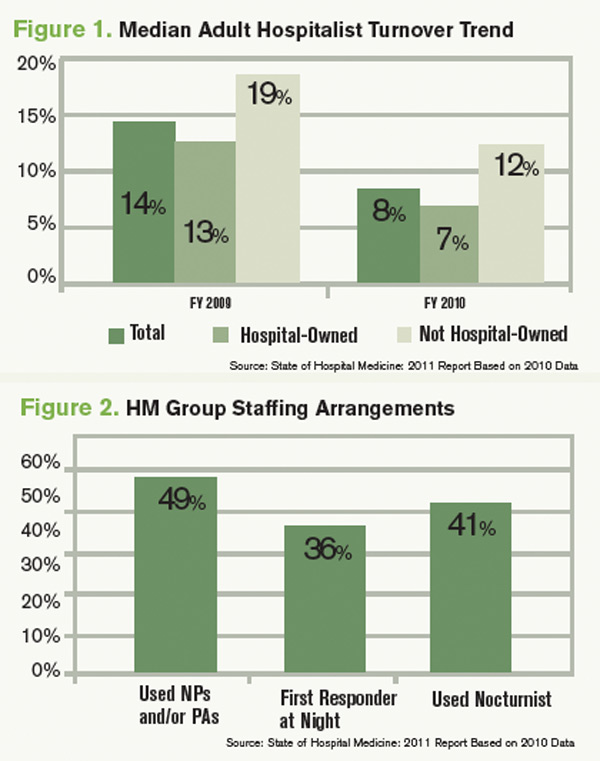
Hawley, the consultant, agrees the percentage increase in financial support is somewhat shocking, but she isn’t surprised by the median figure. She knows hospitals are asking more of HM groups, and all of those value-added, non-billable tasks and responsibilities come with a cost.
“It’s not totally surprising, but it’s a big leap,” she says. “I would say at least some of that has to be driven by the fact that we have hospitals and integrated delivery systems employing more and more of these physicians that responded to this survey, as well as physicians’ practices are perhaps becoming more educated as to what their finances are. There’s a better understanding of allocation of overhead, of billing fees, all of those things that go into a practice where … that may not have been as clear to folks when HM was a bit younger.”
Downward Trend: Hospitalist Turnover
In what some are calling a positive sign for the specialty, hospitalist turnover dropped to 8% in 2011, compared with a 14% turnover rate among hospitalist groups serving adults in 2010 (see Figure 1). Rates declined for both hospital-owned and non-hospital-owned groups, according to the report. Hawley, the consultant, says the decline in physician movement is “consistent” with what she sees in daily interactions with HM groups. Moreover, she considers that trend to be just as important as the overall decline in hospitalist turnover.
“[The survey indicates] more physicians are employed by a hospital or an integrated hospital system. With that, what we’re seeing on the consulting side is there are certain benefits with being employed by a hospital or healthcare system, in terms of retirement plans, things that [hospitalists] may not find as rich in a private practice or with a multispecialty group,” she says. When a hospitalist becomes employed with a hospital system, she hears them say, ‘This is where I want to live and raise my family.’ People choose this type of employment for a reason.”
That has been the experience of PAC member Tierza Stephan, MD, FACP, SFHM, who supervises more than 135 hospitalists as hospitalist district medical director for Minneapolis-based Allina Medical Clinic. Dr. Stephan currently has 15 openings at six of the eight HM groups she directs. Even so, she admits that her programs have been “blessed with low turnover.” The upshot: “We use that when we talk to the C-suite,” she says. “It’s way more costly to have one physician come in, train them, and then have them leave. The low turnover rate gets factored into the cost of what they’re paying.”
Dr. Frost says HM is becoming “less and less a stopover specialty,” as more physicians adopt HM as their career. Dr. Landis says that, although just two consecutive years of data are available, the decline in turnover rate is a good sign for the specialty.
“I think many of us suspect that as the hospitalist movement matures that there hopefully will be a stabilization of the turnover rate,” he says. “Hospitalists tend to be very portable, and when there’s a lot of open jobs and only a few hospitalists, there can be even more and more [turnover]. Typically, someone gets themselves into a situation, they feel that they’re overworked, underpaid, underappreciated, they’re going to look for another job, and those jobs are out there. As the market stabilizes, there will probably be less and less moving around.”
Interactive regional survey breakdowns
Jason Carris is editor of The Hospitalist.
Advice From a Numbers Guy

A self-described “numbers” guy, Troy Ahlstrom, MD, SFHM, agrees regional data is just as important as, if not more important than, the national numbers. He stresses knowing your market, your competitors, your hospital culture—and using that information along with the benchmarking data to formulate expectations for your group.
“Oftentimes you are measured against the guy next door,” says Dr. Ahlstrom, CFO of Traverse City-based Hospitalists of Northern Michigan. “You have to know the numbers, because [administrators] are going to know the numbers.”
Dr. Ahlstrom offers these tips for incorporating benchmarking data into your practice:
- Know your neighbors. “If you keep in mind your local needs, then you can look at the data and start to evaluate what parts are going to help you better formulate a practice that brings on the right people, does the right work, and continues to produce the amount of workload and compensation that makes sure they are happy in the future,” he says.
- Evaluate how applicable the data is. Pay attention to the total number of survey respondents in each category, and the standard deviation around the mean. “In other words, what is the central tendency of the data? You might find data in subsections that you find interesting, but it might not be data that has a central tendency,” he says. “Find data sets that are most applicable to your practice while assessing variations from the larger data sets. Consider how and why your practice might vary from the report as part of your evaluation.”
- Pick out trends and look at them in total. The key is to avoid looking at data points in isolation. “It’s important to look at trends in the data over time, and pick out where those trends are going to go,” he says.
- Involve your people. “I think that this data being available from the [provider] side and management side is a good thing,” Dr. Ahlstrom explains. “The more we are involved in understanding the trends in HM, the better we are going to plan where we are going in the future.”
—JC
Hospitalists are earning a little more, working a little harder, and are less likely to switch jobs or careers, according to the 2011 State of Hospital Medicine report. The annual report, based on data collected jointly by SHM and the Medical Group Management Association (MGMA), offers more than 10,000 compensation and productivity data points for all types of hospitalists, including, for the first time, an exclusive look at academic hospitalists.
As previously reported, median adult hospitalist compensation increased to $220,619, a 2.6% increase from the $215,000 figure reported last year. “I think that’s a reflection of the market and demand for hospitalists, and the value that hospitals and other healthcare payors see that hospitalists bring,” says William “Tex” Landis, MD, FHM, medical director of Wellspan Hospitalists in York, Pa., and chair of SHM’s Practice Analysis Committee.
The compensation increases for hospitalists reported in the SHM-MGMA survey mirror results in other recent surveys. The 2011 Medical Group Compensation and Financial Survey, produced by the American Medical Group Association, found the overall average increase in physician compensation was 2.4%. Primary-care physicians (PCPs) reported a 2.6% increase in 2010, while the “hospitalist-internal medicine” category saw one of the steepest increases at 6.29%, according to the report (www.amga.org).
According to the 2011 MedScape Physician Compensation Report, 27% of the more than 15,000 physicians surveyed said their income increased from 2009 to 2010, whereas 50% said they saw no change. About 23% reported a decline in income, the report showed (www.medscape.com/features/slideshow/compensation/2011/).
Continuing a decadelong trend, the SHM-MGMA report shows hospitalists in the South make the most (median compensation $247,000, up from $235,701 in 2010) and hospitalists in the East ($212,000, up from $205,000 in 2010) lag behind the other regions (see Table 1).
The Hospitalist spoke to five members of SHM’s Practice Analysis Committee (PAC) about the survey results, and each points to continued nationwide demand as the driver of increased compensation. However, the committee also cautions HM groups and directors to be leery of trending this data, as the report is based on a volunteer survey, the survey population changes year to year, and only two years of identical survey data are available.
“As hospital medicine continues to grow, the hospitals become so dependent on the services that the hospitalists provide,” says PAC member Scarlett Blue, RN-BC, MSN, NE-BC, CPHQ, vice president of quality and clinical development for Eagle Hospital Physicians. “[Hospitals] know HM is critical and…I think that hospitalists demonstrate tremendous value, which the hospitals and the management groups recognize.”
The 2011 report, available Sept. 14, compiled data about 4,633 hospitalists in 412 groups. Eighty-five percent of the respondents classified themselves as “adult” hospitalists, 5% as “pediatric” hospitalists, and 10% as both adult and pediatric. Of note, this is the first time SHM has produced compensation and productivity data in consecutive years. In addition to compensation, the survey provides drill-down capability on productivity and reimbursement metrics, along with specific data regarding night coverage arrangements (see “Survey Insights,”), financial support payments, physician turnover, and, for the first time, a look at nonphysician providers (NPPs) in HM practice (see “Nonphysician Provider Data Available for First Time,”).
continued below...
Nonphysician Provider Data Available for First Time
Hospitalist groups were asked about nurse practitioner (NP) and physician assistant (PA) employment, and 49% of HM groups reported having some type of nonphysician provider (NPP) on staff (see Figure 4). Those results, although not startling to some, should open the other half’s eyes, Dr. Landis says.
“Just looking to the future, I think most of us can see physician extenders¬⎯NPs and PAs⎯becoming more and more important in the delivery of hospital care,” he says. “We’re going to be looking to get more information about how that’s happening and what functions they’re performing and what resources, financially and otherwise, are required to help them be effective team members.”
Hawley says NPPs are a critical part of HM’s future but admits some hospitalists still are reluctant to work with NPPs because compensation and incentives are misaligned. “Oftentimes what a [physician] compensation plan will do is not provide for any work that is being done by the NPP,” she says. When physicians find out they also are being measured on patient satisfaction and other metrics, “then the NPP becomes very, very critical. So we’re seeing more and more acceptance. Our opinion, as a consulting group, is that there won’t be a [HM] program in this country that doesn’t somehow use nonphysician providers. There just aren’t enough hospitalists to go around.”
Dr. Landis says his committee is planning to collaborate with SHM’s Nonphysician Provider Committee to determine the best way to collect and disseminate NPP benchmarks. “That’s a future trend and everybody can see it,” he adds. “We have yet to solidify, though, how we’re going to measure and evaluate what’s going on there.” —JC
Hospitalist Productivity
Although hospitalists are earning more, the 2011 report also shows they are producing more work relative-value units (wRVUs) than ever before. The median physician wRVU rate annually for 2011 was 4,166, a 1.4% increase over the 2010 figure.
Hospitalists in the Eastern and Midwest regions reported relatively unchanged wRVUs when compared with 2010 figures. The Southern region, which outdistanced the other regions by more than 800 wRVUs per physician, reported a 6.7% decrease in wRVUs—4,931 in 2011 compared with 5,287 in 2010. On the flipside, the Western region showed a 11.9% increase per physician (see Table 2, left).
PAC committee members agree the wRVU variance between regions is difficult to explain, but most agree the slight year-over-year increase in productivity shows the specialty is stabilizing in terms of what productivity is expected from the average hospitalist.
“Maybe it is an indication that the field is maturing and we’re settling in at some data points that we can now potentially put some stock into,” says Beth E. Hawley, MBA, FACHE, senior vice president of The Cogent Group, a consulting division of Brentwood, Tenn.-based Cogent HMG. “Before, [the figures] changed dramatically from survey to survey; I think we’re seeing more stability now from last year to this year.
—Beth E. Hawley, MBA, FACHE, senior vice president, The Cogent Group, Brentwood, Tenn., SHM Practice Analysis Committee member
“It’s helpful to be able to sort [wRVUs] by employment model, by region, by large and small hospital. We can really get some better benchmarks, in terms of what should be the expectation.”
Chris Frost, MD, FHM, national medical director of hospital medicine services for HCA, says he remains somewhat hesitant to say HM is “settling into a number” for expected wRVUs, as he routinely hears from hospital administrators looking for “additional efficiencies that we can put in place to allow and position the hospitalists to be more productive” while maintaining a high quality care delivery model. He’s also puzzled by the geographic discrepancies. “I just have to scratch my head. I haven’t entirely figured that out yet,” he says.
That said, Dr. Frost agrees the wRVU benchmarks are the most useful in terms of “billable productivity. But I also would like to see—or believe—one of the reasons compensation is going up and the work RVU is flat is hospitalists are being recognized for their value in other arenas, as it relates to the transition from the fee-for-service to pay-for-value-type models, championing effective transitions of care, leading process improvement teams, etc. Those things can’t, or don’t, necessarily lend themselves well to a work RVU equivalent.”
The Buzz: Financial Support
First reported at HM11 in May, the survey shows hospitalist support payments increased more than 39%, to $136,403 per FTE hospitalist in 2011 from $98,253 in 2010. PAC members and other hospitalist experts in practice management attribute the startling increase in support payments to more accurate reporting. Others note that the rise in support payments could be attributed to the decline in collection of professional fees, a direct result of the economic downturn.
And, according to Dr. Landis, hospitals are more willing today to fund hospitalist services than ever before.
“I think [the rise in HM support] payments is because of the evolution of healthcare in the hospital as a whole,” he says. “Hospitals are looking to hospitalists to help them provide the care that that patients and families need, expect, and want. And we’re stepping up to the plate to do it, and they’re paying us to do it. I think that’s the story.
“If you want to tie that with why there’s $136,000 going per hospitalist, [it’s] because they want us there for that rapid-response team, and rapid-response teams don’t generate a lot of RVUs necessarily.”
Hawley, the consultant, agrees the percentage increase in financial support is somewhat shocking, but she isn’t surprised by the median figure. She knows hospitals are asking more of HM groups, and all of those value-added, non-billable tasks and responsibilities come with a cost.
“It’s not totally surprising, but it’s a big leap,” she says. “I would say at least some of that has to be driven by the fact that we have hospitals and integrated delivery systems employing more and more of these physicians that responded to this survey, as well as physicians’ practices are perhaps becoming more educated as to what their finances are. There’s a better understanding of allocation of overhead, of billing fees, all of those things that go into a practice where … that may not have been as clear to folks when HM was a bit younger.”
Downward Trend: Hospitalist Turnover
In what some are calling a positive sign for the specialty, hospitalist turnover dropped to 8% in 2011, compared with a 14% turnover rate among hospitalist groups serving adults in 2010 (see Figure 1). Rates declined for both hospital-owned and non-hospital-owned groups, according to the report. Hawley, the consultant, says the decline in physician movement is “consistent” with what she sees in daily interactions with HM groups. Moreover, she considers that trend to be just as important as the overall decline in hospitalist turnover.
“[The survey indicates] more physicians are employed by a hospital or an integrated hospital system. With that, what we’re seeing on the consulting side is there are certain benefits with being employed by a hospital or healthcare system, in terms of retirement plans, things that [hospitalists] may not find as rich in a private practice or with a multispecialty group,” she says. When a hospitalist becomes employed with a hospital system, she hears them say, ‘This is where I want to live and raise my family.’ People choose this type of employment for a reason.”
That has been the experience of PAC member Tierza Stephan, MD, FACP, SFHM, who supervises more than 135 hospitalists as hospitalist district medical director for Minneapolis-based Allina Medical Clinic. Dr. Stephan currently has 15 openings at six of the eight HM groups she directs. Even so, she admits that her programs have been “blessed with low turnover.” The upshot: “We use that when we talk to the C-suite,” she says. “It’s way more costly to have one physician come in, train them, and then have them leave. The low turnover rate gets factored into the cost of what they’re paying.”
Dr. Frost says HM is becoming “less and less a stopover specialty,” as more physicians adopt HM as their career. Dr. Landis says that, although just two consecutive years of data are available, the decline in turnover rate is a good sign for the specialty.
“I think many of us suspect that as the hospitalist movement matures that there hopefully will be a stabilization of the turnover rate,” he says. “Hospitalists tend to be very portable, and when there’s a lot of open jobs and only a few hospitalists, there can be even more and more [turnover]. Typically, someone gets themselves into a situation, they feel that they’re overworked, underpaid, underappreciated, they’re going to look for another job, and those jobs are out there. As the market stabilizes, there will probably be less and less moving around.”
Interactive regional survey breakdowns
Jason Carris is editor of The Hospitalist.
Advice From a Numbers Guy
A self-described “numbers” guy, Troy Ahlstrom, MD, SFHM, agrees regional data is just as important as, if not more important than, the national numbers. He stresses knowing your market, your competitors, your hospital culture—and using that information along with the benchmarking data to formulate expectations for your group.
“Oftentimes you are measured against the guy next door,” says Dr. Ahlstrom, CFO of Traverse City-based Hospitalists of Northern Michigan. “You have to know the numbers, because [administrators] are going to know the numbers.”
Dr. Ahlstrom offers these tips for incorporating benchmarking data into your practice:
- Know your neighbors. “If you keep in mind your local needs, then you can look at the data and start to evaluate what parts are going to help you better formulate a practice that brings on the right people, does the right work, and continues to produce the amount of workload and compensation that makes sure they are happy in the future,” he says.
- Evaluate how applicable the data is. Pay attention to the total number of survey respondents in each category, and the standard deviation around the mean. “In other words, what is the central tendency of the data? You might find data in subsections that you find interesting, but it might not be data that has a central tendency,” he says. “Find data sets that are most applicable to your practice while assessing variations from the larger data sets. Consider how and why your practice might vary from the report as part of your evaluation.”
- Pick out trends and look at them in total. The key is to avoid looking at data points in isolation. “It’s important to look at trends in the data over time, and pick out where those trends are going to go,” he says.
- Involve your people. “I think that this data being available from the [provider] side and management side is a good thing,” Dr. Ahlstrom explains. “The more we are involved in understanding the trends in HM, the better we are going to plan where we are going in the future.”
—JC
Hospitalists are earning a little more, working a little harder, and are less likely to switch jobs or careers, according to the 2011 State of Hospital Medicine report. The annual report, based on data collected jointly by SHM and the Medical Group Management Association (MGMA), offers more than 10,000 compensation and productivity data points for all types of hospitalists, including, for the first time, an exclusive look at academic hospitalists.
As previously reported, median adult hospitalist compensation increased to $220,619, a 2.6% increase from the $215,000 figure reported last year. “I think that’s a reflection of the market and demand for hospitalists, and the value that hospitals and other healthcare payors see that hospitalists bring,” says William “Tex” Landis, MD, FHM, medical director of Wellspan Hospitalists in York, Pa., and chair of SHM’s Practice Analysis Committee.
The compensation increases for hospitalists reported in the SHM-MGMA survey mirror results in other recent surveys. The 2011 Medical Group Compensation and Financial Survey, produced by the American Medical Group Association, found the overall average increase in physician compensation was 2.4%. Primary-care physicians (PCPs) reported a 2.6% increase in 2010, while the “hospitalist-internal medicine” category saw one of the steepest increases at 6.29%, according to the report (www.amga.org).
According to the 2011 MedScape Physician Compensation Report, 27% of the more than 15,000 physicians surveyed said their income increased from 2009 to 2010, whereas 50% said they saw no change. About 23% reported a decline in income, the report showed (www.medscape.com/features/slideshow/compensation/2011/).
Continuing a decadelong trend, the SHM-MGMA report shows hospitalists in the South make the most (median compensation $247,000, up from $235,701 in 2010) and hospitalists in the East ($212,000, up from $205,000 in 2010) lag behind the other regions (see Table 1).
The Hospitalist spoke to five members of SHM’s Practice Analysis Committee (PAC) about the survey results, and each points to continued nationwide demand as the driver of increased compensation. However, the committee also cautions HM groups and directors to be leery of trending this data, as the report is based on a volunteer survey, the survey population changes year to year, and only two years of identical survey data are available.
“As hospital medicine continues to grow, the hospitals become so dependent on the services that the hospitalists provide,” says PAC member Scarlett Blue, RN-BC, MSN, NE-BC, CPHQ, vice president of quality and clinical development for Eagle Hospital Physicians. “[Hospitals] know HM is critical and…I think that hospitalists demonstrate tremendous value, which the hospitals and the management groups recognize.”
The 2011 report, available Sept. 14, compiled data about 4,633 hospitalists in 412 groups. Eighty-five percent of the respondents classified themselves as “adult” hospitalists, 5% as “pediatric” hospitalists, and 10% as both adult and pediatric. Of note, this is the first time SHM has produced compensation and productivity data in consecutive years. In addition to compensation, the survey provides drill-down capability on productivity and reimbursement metrics, along with specific data regarding night coverage arrangements (see “Survey Insights,”), financial support payments, physician turnover, and, for the first time, a look at nonphysician providers (NPPs) in HM practice (see “Nonphysician Provider Data Available for First Time,”).
continued below...
Nonphysician Provider Data Available for First Time
Hospitalist groups were asked about nurse practitioner (NP) and physician assistant (PA) employment, and 49% of HM groups reported having some type of nonphysician provider (NPP) on staff (see Figure 4). Those results, although not startling to some, should open the other half’s eyes, Dr. Landis says.
“Just looking to the future, I think most of us can see physician extenders¬⎯NPs and PAs⎯becoming more and more important in the delivery of hospital care,” he says. “We’re going to be looking to get more information about how that’s happening and what functions they’re performing and what resources, financially and otherwise, are required to help them be effective team members.”
Hawley says NPPs are a critical part of HM’s future but admits some hospitalists still are reluctant to work with NPPs because compensation and incentives are misaligned. “Oftentimes what a [physician] compensation plan will do is not provide for any work that is being done by the NPP,” she says. When physicians find out they also are being measured on patient satisfaction and other metrics, “then the NPP becomes very, very critical. So we’re seeing more and more acceptance. Our opinion, as a consulting group, is that there won’t be a [HM] program in this country that doesn’t somehow use nonphysician providers. There just aren’t enough hospitalists to go around.”
Dr. Landis says his committee is planning to collaborate with SHM’s Nonphysician Provider Committee to determine the best way to collect and disseminate NPP benchmarks. “That’s a future trend and everybody can see it,” he adds. “We have yet to solidify, though, how we’re going to measure and evaluate what’s going on there.” —JC
Hospitalist Productivity
Although hospitalists are earning more, the 2011 report also shows they are producing more work relative-value units (wRVUs) than ever before. The median physician wRVU rate annually for 2011 was 4,166, a 1.4% increase over the 2010 figure.
Hospitalists in the Eastern and Midwest regions reported relatively unchanged wRVUs when compared with 2010 figures. The Southern region, which outdistanced the other regions by more than 800 wRVUs per physician, reported a 6.7% decrease in wRVUs—4,931 in 2011 compared with 5,287 in 2010. On the flipside, the Western region showed a 11.9% increase per physician (see Table 2, left).
PAC committee members agree the wRVU variance between regions is difficult to explain, but most agree the slight year-over-year increase in productivity shows the specialty is stabilizing in terms of what productivity is expected from the average hospitalist.
“Maybe it is an indication that the field is maturing and we’re settling in at some data points that we can now potentially put some stock into,” says Beth E. Hawley, MBA, FACHE, senior vice president of The Cogent Group, a consulting division of Brentwood, Tenn.-based Cogent HMG. “Before, [the figures] changed dramatically from survey to survey; I think we’re seeing more stability now from last year to this year.
—Beth E. Hawley, MBA, FACHE, senior vice president, The Cogent Group, Brentwood, Tenn., SHM Practice Analysis Committee member
“It’s helpful to be able to sort [wRVUs] by employment model, by region, by large and small hospital. We can really get some better benchmarks, in terms of what should be the expectation.”
Chris Frost, MD, FHM, national medical director of hospital medicine services for HCA, says he remains somewhat hesitant to say HM is “settling into a number” for expected wRVUs, as he routinely hears from hospital administrators looking for “additional efficiencies that we can put in place to allow and position the hospitalists to be more productive” while maintaining a high quality care delivery model. He’s also puzzled by the geographic discrepancies. “I just have to scratch my head. I haven’t entirely figured that out yet,” he says.
That said, Dr. Frost agrees the wRVU benchmarks are the most useful in terms of “billable productivity. But I also would like to see—or believe—one of the reasons compensation is going up and the work RVU is flat is hospitalists are being recognized for their value in other arenas, as it relates to the transition from the fee-for-service to pay-for-value-type models, championing effective transitions of care, leading process improvement teams, etc. Those things can’t, or don’t, necessarily lend themselves well to a work RVU equivalent.”
The Buzz: Financial Support
First reported at HM11 in May, the survey shows hospitalist support payments increased more than 39%, to $136,403 per FTE hospitalist in 2011 from $98,253 in 2010. PAC members and other hospitalist experts in practice management attribute the startling increase in support payments to more accurate reporting. Others note that the rise in support payments could be attributed to the decline in collection of professional fees, a direct result of the economic downturn.
And, according to Dr. Landis, hospitals are more willing today to fund hospitalist services than ever before.
“I think [the rise in HM support] payments is because of the evolution of healthcare in the hospital as a whole,” he says. “Hospitals are looking to hospitalists to help them provide the care that that patients and families need, expect, and want. And we’re stepping up to the plate to do it, and they’re paying us to do it. I think that’s the story.
“If you want to tie that with why there’s $136,000 going per hospitalist, [it’s] because they want us there for that rapid-response team, and rapid-response teams don’t generate a lot of RVUs necessarily.”
Hawley, the consultant, agrees the percentage increase in financial support is somewhat shocking, but she isn’t surprised by the median figure. She knows hospitals are asking more of HM groups, and all of those value-added, non-billable tasks and responsibilities come with a cost.
“It’s not totally surprising, but it’s a big leap,” she says. “I would say at least some of that has to be driven by the fact that we have hospitals and integrated delivery systems employing more and more of these physicians that responded to this survey, as well as physicians’ practices are perhaps becoming more educated as to what their finances are. There’s a better understanding of allocation of overhead, of billing fees, all of those things that go into a practice where … that may not have been as clear to folks when HM was a bit younger.”
Downward Trend: Hospitalist Turnover
In what some are calling a positive sign for the specialty, hospitalist turnover dropped to 8% in 2011, compared with a 14% turnover rate among hospitalist groups serving adults in 2010 (see Figure 1). Rates declined for both hospital-owned and non-hospital-owned groups, according to the report. Hawley, the consultant, says the decline in physician movement is “consistent” with what she sees in daily interactions with HM groups. Moreover, she considers that trend to be just as important as the overall decline in hospitalist turnover.
“[The survey indicates] more physicians are employed by a hospital or an integrated hospital system. With that, what we’re seeing on the consulting side is there are certain benefits with being employed by a hospital or healthcare system, in terms of retirement plans, things that [hospitalists] may not find as rich in a private practice or with a multispecialty group,” she says. When a hospitalist becomes employed with a hospital system, she hears them say, ‘This is where I want to live and raise my family.’ People choose this type of employment for a reason.”
That has been the experience of PAC member Tierza Stephan, MD, FACP, SFHM, who supervises more than 135 hospitalists as hospitalist district medical director for Minneapolis-based Allina Medical Clinic. Dr. Stephan currently has 15 openings at six of the eight HM groups she directs. Even so, she admits that her programs have been “blessed with low turnover.” The upshot: “We use that when we talk to the C-suite,” she says. “It’s way more costly to have one physician come in, train them, and then have them leave. The low turnover rate gets factored into the cost of what they’re paying.”
Dr. Frost says HM is becoming “less and less a stopover specialty,” as more physicians adopt HM as their career. Dr. Landis says that, although just two consecutive years of data are available, the decline in turnover rate is a good sign for the specialty.
“I think many of us suspect that as the hospitalist movement matures that there hopefully will be a stabilization of the turnover rate,” he says. “Hospitalists tend to be very portable, and when there’s a lot of open jobs and only a few hospitalists, there can be even more and more [turnover]. Typically, someone gets themselves into a situation, they feel that they’re overworked, underpaid, underappreciated, they’re going to look for another job, and those jobs are out there. As the market stabilizes, there will probably be less and less moving around.”
Interactive regional survey breakdowns
Jason Carris is editor of The Hospitalist.
Advice From a Numbers Guy
A self-described “numbers” guy, Troy Ahlstrom, MD, SFHM, agrees regional data is just as important as, if not more important than, the national numbers. He stresses knowing your market, your competitors, your hospital culture—and using that information along with the benchmarking data to formulate expectations for your group.
“Oftentimes you are measured against the guy next door,” says Dr. Ahlstrom, CFO of Traverse City-based Hospitalists of Northern Michigan. “You have to know the numbers, because [administrators] are going to know the numbers.”
Dr. Ahlstrom offers these tips for incorporating benchmarking data into your practice:
- Know your neighbors. “If you keep in mind your local needs, then you can look at the data and start to evaluate what parts are going to help you better formulate a practice that brings on the right people, does the right work, and continues to produce the amount of workload and compensation that makes sure they are happy in the future,” he says.
- Evaluate how applicable the data is. Pay attention to the total number of survey respondents in each category, and the standard deviation around the mean. “In other words, what is the central tendency of the data? You might find data in subsections that you find interesting, but it might not be data that has a central tendency,” he says. “Find data sets that are most applicable to your practice while assessing variations from the larger data sets. Consider how and why your practice might vary from the report as part of your evaluation.”
- Pick out trends and look at them in total. The key is to avoid looking at data points in isolation. “It’s important to look at trends in the data over time, and pick out where those trends are going to go,” he says.
- Involve your people. “I think that this data being available from the [provider] side and management side is a good thing,” Dr. Ahlstrom explains. “The more we are involved in understanding the trends in HM, the better we are going to plan where we are going in the future.”
—JC