User login
Transitions Telethon

The headline was as biting as it was inciting. “Frustrations with hospitalist care: Need to improve transitions and communication,” it screamed from the cover of a recent issue of the Annals of Internal Medicine.1 Reading on the run, I thumbed to page 469 and glanced at the first few paragraphs, my mind spinning with the implications.
The article was an editorial following a recent thought piece by a primary-care physician (PCP) frustrated with his interactions with the HM model—mainly around the lack of communication from hospitalists about his patients, his marginalized role with his patients’ hospital care, and the lack of information transfer around transitions.2
Frustrations and Slapstick Comedy
Frustration with hospitalist care? Is this how PCPs see us? Are we really “frustrating” our outpatient colleagues? To an outsider, this presented a one-sided view of the issue—the side that sounds simplistically negative. What if someone important to our group should read this article, someone like my hospital CEO? I didn’t have to wonder for long as I looked up from my elevator reading to note my hospital CEO entering.
What followed eerily resembled one of those scenes from a slapstick comedy, as the boob, played perfectly by me, obviously fumbles something he intends to hide from his boss behind his back to escape the knowing eye of said boss. And, like a pornographic-magazine-sniffing parent, my CEO knowingly diagnosed the situation.
“Whatcha reading?” he sagely queried.
“Nothing,” I replied unconvincingly.
“Nothing? It sure looks like you hastily stuffed a magazine or something down the back of your pants as I walked in.”
“Oh, this?” I responded, unearthing a large medical journal from my pants, leaving an untucked shirt in its wake. “This is just a medical journal. You know, lots of medical stuff. It’s pretty complex. Probably hard for nonmedical types to understand,” I replied, employing a bit of professorial condescension to throw him off track.
“Annals of Internal Medicine,” he replied. “What a coincidence. I just received an e-mail from a friend with an Annals article about the issues of transitions of care with the hospitalist model. Sounds like a real problem. Maybe our new electronic health records will fix that. If not, you should fix it. Let’s chat about it soon.”
“Right,” I said as the elevator doors swished behind him, leaving me disheveled in both appearance and thoughts.
Testimonials?
The more recent Annals editorial summarized—and then printed—a few of the many online responses to the original thought piece.3 The responses ranged from outrage with the HM model of care to more measured discussions of the limitations of the “old” model it replaced. However, the tone and implications were clear: At least some, if not many, PCPs are displeased with the HM model.
One writer related a recent example in which his elderly patient was admitted unbeknownst to him. After receiving a query from a family member, he called the hospitalist on duty, who was uninformed about the patient details, had made questionable therapeutic changes, and was “unapologetic” about her team’s lack of communication, arguing that the ED physician “should have called.” That led this PCP to conclude that the system is “disjointed and isolating,” leaving “patients feeling abandoned.” Another writer commented that the current system of communication results in “potentially detrimental and demoralizing degrees of separation.” A response by a hospitalist detailed how they were able to put a system in place to contact PCPs with whom they are contracted 80% of the time.
The Annals editors concluded that the letters they received in response to the first article “reflect a schism that exists in internal medicine about the positive and negative effects of hospitalist care,” noting that “the evidence is still deficient about how to deliver care optimally when complex, seriously-ill patients must transition between multiple providers in diverse health care settings.” The authors go on to call for “intensive research and productive debates” about the HM model of care.
A Challenge to You
“Disjointed and isolating”? … “Detrimental and demoralizing”? … Lauding 80% PCP contact rates? … “Intensive research and debate”?
I get that this is a complex issue and that healthcare in the U.S. is fragmented to the point of fracture. To wit, it can be agonizingly time-consuming to track down PCPs and wade through their automated phone systems. And this assumes that your patient has a PCP, can identify that PCP, and has their phone number. If they don’t, you’re left to sift through online phone books, clinic websites, or Google searches with the hopes that you can summon the right Dr. Davis, Davies, or Daves—the patient’s not quite sure of the spelling but knows “she’s a nice lady doctor.” I know firsthand the tension between taking the time to make that PCP call and getting home in time for dinner with my family—I’m often guilty of choosing dinner.
However, I’m not sure “intensive research” is the answer. Nor is this a problem that can wait for technological solutions. I don’t want to diminish the great strides that have been made or understate the need to continue to innovate around transitions—this needs to be an area of ongoing study. But this is a problem that has at least one relatively simple, short-term solution: Just pick up the phone. As one Annals writer rightly questions: “How has inter-physician communication come to be regarded as an unexpected courtesy rather than an obligation?”
Good question.
So, I have a simple challenge for you: For one week, join me in committing to calling 100% of the available PCPs on patient discharge. I can guarantee you this will prove to be a hard, time-consuming, and, at times, migraine-inducing process. But it is an intervention that will make a difference, can be launched tomorrow, and does not require “intensive research and debate.”
We’ll no doubt gain some insight into our patients’ current therapeutic regimens, enlist PCPs’ help with the treatment decisions, and ensure that our patients’ transitions are as safe as possible. My guess is that we’ll also find it valuable to the point it becomes habit.
Start by committing with me to just one week.
Then go home and have dinner. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Frustrations with hospitalist care: need to improve transitions and communication. Ann Intern Med. 2010;152(7):469.
- Beckman H. Three degrees of separation. Ann Intern Med. 2009;151(12):890-891.
- The relationship between hospitalists and primary care physicians. Ann Intern Med. 2010;152(7):474-6.
The headline was as biting as it was inciting. “Frustrations with hospitalist care: Need to improve transitions and communication,” it screamed from the cover of a recent issue of the Annals of Internal Medicine.1 Reading on the run, I thumbed to page 469 and glanced at the first few paragraphs, my mind spinning with the implications.
The article was an editorial following a recent thought piece by a primary-care physician (PCP) frustrated with his interactions with the HM model—mainly around the lack of communication from hospitalists about his patients, his marginalized role with his patients’ hospital care, and the lack of information transfer around transitions.2
Frustrations and Slapstick Comedy
Frustration with hospitalist care? Is this how PCPs see us? Are we really “frustrating” our outpatient colleagues? To an outsider, this presented a one-sided view of the issue—the side that sounds simplistically negative. What if someone important to our group should read this article, someone like my hospital CEO? I didn’t have to wonder for long as I looked up from my elevator reading to note my hospital CEO entering.
What followed eerily resembled one of those scenes from a slapstick comedy, as the boob, played perfectly by me, obviously fumbles something he intends to hide from his boss behind his back to escape the knowing eye of said boss. And, like a pornographic-magazine-sniffing parent, my CEO knowingly diagnosed the situation.
“Whatcha reading?” he sagely queried.
“Nothing,” I replied unconvincingly.
“Nothing? It sure looks like you hastily stuffed a magazine or something down the back of your pants as I walked in.”
“Oh, this?” I responded, unearthing a large medical journal from my pants, leaving an untucked shirt in its wake. “This is just a medical journal. You know, lots of medical stuff. It’s pretty complex. Probably hard for nonmedical types to understand,” I replied, employing a bit of professorial condescension to throw him off track.
“Annals of Internal Medicine,” he replied. “What a coincidence. I just received an e-mail from a friend with an Annals article about the issues of transitions of care with the hospitalist model. Sounds like a real problem. Maybe our new electronic health records will fix that. If not, you should fix it. Let’s chat about it soon.”
“Right,” I said as the elevator doors swished behind him, leaving me disheveled in both appearance and thoughts.
Testimonials?
The more recent Annals editorial summarized—and then printed—a few of the many online responses to the original thought piece.3 The responses ranged from outrage with the HM model of care to more measured discussions of the limitations of the “old” model it replaced. However, the tone and implications were clear: At least some, if not many, PCPs are displeased with the HM model.
One writer related a recent example in which his elderly patient was admitted unbeknownst to him. After receiving a query from a family member, he called the hospitalist on duty, who was uninformed about the patient details, had made questionable therapeutic changes, and was “unapologetic” about her team’s lack of communication, arguing that the ED physician “should have called.” That led this PCP to conclude that the system is “disjointed and isolating,” leaving “patients feeling abandoned.” Another writer commented that the current system of communication results in “potentially detrimental and demoralizing degrees of separation.” A response by a hospitalist detailed how they were able to put a system in place to contact PCPs with whom they are contracted 80% of the time.
The Annals editors concluded that the letters they received in response to the first article “reflect a schism that exists in internal medicine about the positive and negative effects of hospitalist care,” noting that “the evidence is still deficient about how to deliver care optimally when complex, seriously-ill patients must transition between multiple providers in diverse health care settings.” The authors go on to call for “intensive research and productive debates” about the HM model of care.
A Challenge to You
“Disjointed and isolating”? … “Detrimental and demoralizing”? … Lauding 80% PCP contact rates? … “Intensive research and debate”?
I get that this is a complex issue and that healthcare in the U.S. is fragmented to the point of fracture. To wit, it can be agonizingly time-consuming to track down PCPs and wade through their automated phone systems. And this assumes that your patient has a PCP, can identify that PCP, and has their phone number. If they don’t, you’re left to sift through online phone books, clinic websites, or Google searches with the hopes that you can summon the right Dr. Davis, Davies, or Daves—the patient’s not quite sure of the spelling but knows “she’s a nice lady doctor.” I know firsthand the tension between taking the time to make that PCP call and getting home in time for dinner with my family—I’m often guilty of choosing dinner.
However, I’m not sure “intensive research” is the answer. Nor is this a problem that can wait for technological solutions. I don’t want to diminish the great strides that have been made or understate the need to continue to innovate around transitions—this needs to be an area of ongoing study. But this is a problem that has at least one relatively simple, short-term solution: Just pick up the phone. As one Annals writer rightly questions: “How has inter-physician communication come to be regarded as an unexpected courtesy rather than an obligation?”
Good question.
So, I have a simple challenge for you: For one week, join me in committing to calling 100% of the available PCPs on patient discharge. I can guarantee you this will prove to be a hard, time-consuming, and, at times, migraine-inducing process. But it is an intervention that will make a difference, can be launched tomorrow, and does not require “intensive research and debate.”
We’ll no doubt gain some insight into our patients’ current therapeutic regimens, enlist PCPs’ help with the treatment decisions, and ensure that our patients’ transitions are as safe as possible. My guess is that we’ll also find it valuable to the point it becomes habit.
Start by committing with me to just one week.
Then go home and have dinner. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Frustrations with hospitalist care: need to improve transitions and communication. Ann Intern Med. 2010;152(7):469.
- Beckman H. Three degrees of separation. Ann Intern Med. 2009;151(12):890-891.
- The relationship between hospitalists and primary care physicians. Ann Intern Med. 2010;152(7):474-6.
The headline was as biting as it was inciting. “Frustrations with hospitalist care: Need to improve transitions and communication,” it screamed from the cover of a recent issue of the Annals of Internal Medicine.1 Reading on the run, I thumbed to page 469 and glanced at the first few paragraphs, my mind spinning with the implications.
The article was an editorial following a recent thought piece by a primary-care physician (PCP) frustrated with his interactions with the HM model—mainly around the lack of communication from hospitalists about his patients, his marginalized role with his patients’ hospital care, and the lack of information transfer around transitions.2
Frustrations and Slapstick Comedy
Frustration with hospitalist care? Is this how PCPs see us? Are we really “frustrating” our outpatient colleagues? To an outsider, this presented a one-sided view of the issue—the side that sounds simplistically negative. What if someone important to our group should read this article, someone like my hospital CEO? I didn’t have to wonder for long as I looked up from my elevator reading to note my hospital CEO entering.
What followed eerily resembled one of those scenes from a slapstick comedy, as the boob, played perfectly by me, obviously fumbles something he intends to hide from his boss behind his back to escape the knowing eye of said boss. And, like a pornographic-magazine-sniffing parent, my CEO knowingly diagnosed the situation.
“Whatcha reading?” he sagely queried.
“Nothing,” I replied unconvincingly.
“Nothing? It sure looks like you hastily stuffed a magazine or something down the back of your pants as I walked in.”
“Oh, this?” I responded, unearthing a large medical journal from my pants, leaving an untucked shirt in its wake. “This is just a medical journal. You know, lots of medical stuff. It’s pretty complex. Probably hard for nonmedical types to understand,” I replied, employing a bit of professorial condescension to throw him off track.
“Annals of Internal Medicine,” he replied. “What a coincidence. I just received an e-mail from a friend with an Annals article about the issues of transitions of care with the hospitalist model. Sounds like a real problem. Maybe our new electronic health records will fix that. If not, you should fix it. Let’s chat about it soon.”
“Right,” I said as the elevator doors swished behind him, leaving me disheveled in both appearance and thoughts.
Testimonials?
The more recent Annals editorial summarized—and then printed—a few of the many online responses to the original thought piece.3 The responses ranged from outrage with the HM model of care to more measured discussions of the limitations of the “old” model it replaced. However, the tone and implications were clear: At least some, if not many, PCPs are displeased with the HM model.
One writer related a recent example in which his elderly patient was admitted unbeknownst to him. After receiving a query from a family member, he called the hospitalist on duty, who was uninformed about the patient details, had made questionable therapeutic changes, and was “unapologetic” about her team’s lack of communication, arguing that the ED physician “should have called.” That led this PCP to conclude that the system is “disjointed and isolating,” leaving “patients feeling abandoned.” Another writer commented that the current system of communication results in “potentially detrimental and demoralizing degrees of separation.” A response by a hospitalist detailed how they were able to put a system in place to contact PCPs with whom they are contracted 80% of the time.
The Annals editors concluded that the letters they received in response to the first article “reflect a schism that exists in internal medicine about the positive and negative effects of hospitalist care,” noting that “the evidence is still deficient about how to deliver care optimally when complex, seriously-ill patients must transition between multiple providers in diverse health care settings.” The authors go on to call for “intensive research and productive debates” about the HM model of care.
A Challenge to You
“Disjointed and isolating”? … “Detrimental and demoralizing”? … Lauding 80% PCP contact rates? … “Intensive research and debate”?
I get that this is a complex issue and that healthcare in the U.S. is fragmented to the point of fracture. To wit, it can be agonizingly time-consuming to track down PCPs and wade through their automated phone systems. And this assumes that your patient has a PCP, can identify that PCP, and has their phone number. If they don’t, you’re left to sift through online phone books, clinic websites, or Google searches with the hopes that you can summon the right Dr. Davis, Davies, or Daves—the patient’s not quite sure of the spelling but knows “she’s a nice lady doctor.” I know firsthand the tension between taking the time to make that PCP call and getting home in time for dinner with my family—I’m often guilty of choosing dinner.
However, I’m not sure “intensive research” is the answer. Nor is this a problem that can wait for technological solutions. I don’t want to diminish the great strides that have been made or understate the need to continue to innovate around transitions—this needs to be an area of ongoing study. But this is a problem that has at least one relatively simple, short-term solution: Just pick up the phone. As one Annals writer rightly questions: “How has inter-physician communication come to be regarded as an unexpected courtesy rather than an obligation?”
Good question.
So, I have a simple challenge for you: For one week, join me in committing to calling 100% of the available PCPs on patient discharge. I can guarantee you this will prove to be a hard, time-consuming, and, at times, migraine-inducing process. But it is an intervention that will make a difference, can be launched tomorrow, and does not require “intensive research and debate.”
We’ll no doubt gain some insight into our patients’ current therapeutic regimens, enlist PCPs’ help with the treatment decisions, and ensure that our patients’ transitions are as safe as possible. My guess is that we’ll also find it valuable to the point it becomes habit.
Start by committing with me to just one week.
Then go home and have dinner. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Frustrations with hospitalist care: need to improve transitions and communication. Ann Intern Med. 2010;152(7):469.
- Beckman H. Three degrees of separation. Ann Intern Med. 2009;151(12):890-891.
- The relationship between hospitalists and primary care physicians. Ann Intern Med. 2010;152(7):474-6.
Care Critical

There is a brewing crisis in critical-care medicine, a crisis that already is impacting HM. It would be easier for hospitalists to look the other way and say, “This is not our problem.” Make no mistake: It is our problem. There are not enough intensive-care physicians to go around.
In my generation, most physicians who trained in pulmonary and critical-care medicine thought they would do some office care, some bronchoscopies, and some critical care for the first several years of their professional lives. Few imagined that, in their 60s, their practice would still include rescuing patients from death at 2 a.m. Couple the intensity of care with such a demanding lifestyle, and it is hardly surprising that many critical-care doctors seek less-stressful practices (e.g., sleep medicine) or retirement.
New physicians who see the work-life imbalance are shying away from critical care in significant enough numbers, yet the demand for these doctors is growing. Whether that shift is due to the attraction of careers in HM, emergency medicine, or other IM specialties, or the perceived negatives to being a full-time intensivist, is beside the point. The medical workforce needs more critical-care physicians. And we are not going to be able to meet this need by assuming we will be able to recruit and train more surgeons, anesthesiologists, or pulmonary physicians in traditional critical-care pathways.
The situation is further complicated by workforce shortages on the rest of the ICU healthcare team. Many senior ICU nurses are reaching the end of their careers, and the pipeline to replace them is anything but robust. And all this comes at a time when the acuity of hospitalized patients is increasing and the demands for ICU expertise is at its height.
It is no surprise that hospitalists are called upon to fill the critical-care gap. SHM surveys show that 92% of hospitalists include ICU care in their practice. While hospitalists clearly do not have the training or skills to replace the intensivist, we clearly are witnessing a “scope creep.” Hospitalists are being asked to stretch their skills to fill the void in critical care.
Competence Question
The response to this is manifest in many ways. For example, steadily increasing numbers of hospitalists attend SHM’s annual critical-care precourses, and our procedures courses invariably sell out. These brief courses are important to hospitalists and their patients. Yet a day (or even two) of focused training for hospitalists will not raise their skill set to replace or even augment critical-care-trained physicians at their hospitals. The patients will keep coming and continue to need the expertise for their most-acute-care needs. Something must be done.
There are pockets of experiments on filling the increasing critical-care gap. Emory University’s Center for Critical Care in Atlanta will soon launch an experimental, HM-critical-care training program that will attempt to develop and verify critical-care competencies in just one postgraduate year after IM residency. A complementary approach could include a hospitalist-focused track within the three years of IM residency to include less outpatient medicine and more intensive-care training. This could be part of a broader restructuring of internal and family medicine residencies, which recognize the career paths (and needs) of their residents as some enter hospital-focused practice (e.g., as hospitalists, cardiologists, intensivists) and some concentrate more on the patient outside the hospital (e.g., primary care, endocrinology, rheumatology).
As training evolves, there will be practical issues of credentialing. Currently, a general-IM-trained hospitalist is required to complete a two-year fellowship in critical care to be a specialist. Interestingly, if one’s residency training is in surgery, anesthesia, or rheumatology, that physician requires only one additional year in critical care to become eligible for added/special qualifications in critical-care medicine. What, precisely, is the carryover of the longer residency experience that makes it possible to attain competency in critical care in half the training time?
There also is the risk that we will create a workforce that includes the intensivist-lite—someone who does not have complete, recognized training in critical care but has more than the typical hospitalist, and is perceived as “better than having no intensivist.” Is this in the best interest of our patients or our discipline?
Supply Solutions
There are other approaches to the workforce challenge beyond asking hospitalists to step away from practice for an additional year or two of training. As in other aspects of the hospital workforce, it is time to examine alternative deployment of the entire healthcare team. If intensivists and hospitalists are in limited supply, we need to revisit their roles and further look for opportunities to engage acute-care nurse practitioners, physician assistants, RNs, and others on the healthcare team to meet the expanding needs of our patients and our hospitals.
Another strategy would include regionalization of healthcare in population centers with multiple hospitals. In Orange County, Calif., where I live, there are 33 hospitals for 3 million people, each with some form of an ICU. Is it time to set standards of coverage and expertise so that 10 to 15 hospitals can provide a fully staffed ICU, and the other hospitals refer their most-acute patients rather than be stretched to staff their ICUs at a time of workforce shortages? Is it time to do what we did with trauma centers and set various levels of care so that not every hospital can or should be doing the most intense and costly level of care?
SHM, HM, and, most importantly, hospitalists find themselves in the midst of this growing problem. We must be part of the solution.
It is important to recognize the significant variability in the intensivist skill sets that individual hospitalists and HM groups currently possess; the variance creates hurdles in being able to step up and fill the critical-care gap. I’ve heard about hospitalists pausing their practices to obtain additional training in critical care. Hospitals across America are (or soon will be) scrambling to integrate their hospitalists and intensivists to maximize coverage and expertise. SHM has noticed an increased demand on hospitalists to increase knowledge and skills so they can extend the local coverage of critically ill patients.
It is time for SHM to clearly understand how this sea change is affecting you professionally and personally, because you practice on the frontlines of our nation’s hospitals.
It is time for SHM to engage our colleagues in the ICU—critical-care physicians and their professional societies—to understand their perspective and initiatives on this growing crisis.
It is time for SHM to engage medical educators in residency and fellowship training to explore potential changes in the curriculum—changes aimed at young physicians proceeding through their training that yield hospital-based physicians better prepared to enter the hospital environment of the 21st century.
And SHM may need to engage the boards and other credentialing bodies to look for flexibility that will reflect today’s realities, attract the best-trained physicians to care for the most-acutely-ill patients, and protect our patients by demanding expertise and training at the most appropriate levels. TH
Dr. Wellikson is CEO of SHM.
There is a brewing crisis in critical-care medicine, a crisis that already is impacting HM. It would be easier for hospitalists to look the other way and say, “This is not our problem.” Make no mistake: It is our problem. There are not enough intensive-care physicians to go around.
In my generation, most physicians who trained in pulmonary and critical-care medicine thought they would do some office care, some bronchoscopies, and some critical care for the first several years of their professional lives. Few imagined that, in their 60s, their practice would still include rescuing patients from death at 2 a.m. Couple the intensity of care with such a demanding lifestyle, and it is hardly surprising that many critical-care doctors seek less-stressful practices (e.g., sleep medicine) or retirement.
New physicians who see the work-life imbalance are shying away from critical care in significant enough numbers, yet the demand for these doctors is growing. Whether that shift is due to the attraction of careers in HM, emergency medicine, or other IM specialties, or the perceived negatives to being a full-time intensivist, is beside the point. The medical workforce needs more critical-care physicians. And we are not going to be able to meet this need by assuming we will be able to recruit and train more surgeons, anesthesiologists, or pulmonary physicians in traditional critical-care pathways.
The situation is further complicated by workforce shortages on the rest of the ICU healthcare team. Many senior ICU nurses are reaching the end of their careers, and the pipeline to replace them is anything but robust. And all this comes at a time when the acuity of hospitalized patients is increasing and the demands for ICU expertise is at its height.
It is no surprise that hospitalists are called upon to fill the critical-care gap. SHM surveys show that 92% of hospitalists include ICU care in their practice. While hospitalists clearly do not have the training or skills to replace the intensivist, we clearly are witnessing a “scope creep.” Hospitalists are being asked to stretch their skills to fill the void in critical care.
Competence Question
The response to this is manifest in many ways. For example, steadily increasing numbers of hospitalists attend SHM’s annual critical-care precourses, and our procedures courses invariably sell out. These brief courses are important to hospitalists and their patients. Yet a day (or even two) of focused training for hospitalists will not raise their skill set to replace or even augment critical-care-trained physicians at their hospitals. The patients will keep coming and continue to need the expertise for their most-acute-care needs. Something must be done.
There are pockets of experiments on filling the increasing critical-care gap. Emory University’s Center for Critical Care in Atlanta will soon launch an experimental, HM-critical-care training program that will attempt to develop and verify critical-care competencies in just one postgraduate year after IM residency. A complementary approach could include a hospitalist-focused track within the three years of IM residency to include less outpatient medicine and more intensive-care training. This could be part of a broader restructuring of internal and family medicine residencies, which recognize the career paths (and needs) of their residents as some enter hospital-focused practice (e.g., as hospitalists, cardiologists, intensivists) and some concentrate more on the patient outside the hospital (e.g., primary care, endocrinology, rheumatology).
As training evolves, there will be practical issues of credentialing. Currently, a general-IM-trained hospitalist is required to complete a two-year fellowship in critical care to be a specialist. Interestingly, if one’s residency training is in surgery, anesthesia, or rheumatology, that physician requires only one additional year in critical care to become eligible for added/special qualifications in critical-care medicine. What, precisely, is the carryover of the longer residency experience that makes it possible to attain competency in critical care in half the training time?
There also is the risk that we will create a workforce that includes the intensivist-lite—someone who does not have complete, recognized training in critical care but has more than the typical hospitalist, and is perceived as “better than having no intensivist.” Is this in the best interest of our patients or our discipline?
Supply Solutions
There are other approaches to the workforce challenge beyond asking hospitalists to step away from practice for an additional year or two of training. As in other aspects of the hospital workforce, it is time to examine alternative deployment of the entire healthcare team. If intensivists and hospitalists are in limited supply, we need to revisit their roles and further look for opportunities to engage acute-care nurse practitioners, physician assistants, RNs, and others on the healthcare team to meet the expanding needs of our patients and our hospitals.
Another strategy would include regionalization of healthcare in population centers with multiple hospitals. In Orange County, Calif., where I live, there are 33 hospitals for 3 million people, each with some form of an ICU. Is it time to set standards of coverage and expertise so that 10 to 15 hospitals can provide a fully staffed ICU, and the other hospitals refer their most-acute patients rather than be stretched to staff their ICUs at a time of workforce shortages? Is it time to do what we did with trauma centers and set various levels of care so that not every hospital can or should be doing the most intense and costly level of care?
SHM, HM, and, most importantly, hospitalists find themselves in the midst of this growing problem. We must be part of the solution.
It is important to recognize the significant variability in the intensivist skill sets that individual hospitalists and HM groups currently possess; the variance creates hurdles in being able to step up and fill the critical-care gap. I’ve heard about hospitalists pausing their practices to obtain additional training in critical care. Hospitals across America are (or soon will be) scrambling to integrate their hospitalists and intensivists to maximize coverage and expertise. SHM has noticed an increased demand on hospitalists to increase knowledge and skills so they can extend the local coverage of critically ill patients.
It is time for SHM to clearly understand how this sea change is affecting you professionally and personally, because you practice on the frontlines of our nation’s hospitals.
It is time for SHM to engage our colleagues in the ICU—critical-care physicians and their professional societies—to understand their perspective and initiatives on this growing crisis.
It is time for SHM to engage medical educators in residency and fellowship training to explore potential changes in the curriculum—changes aimed at young physicians proceeding through their training that yield hospital-based physicians better prepared to enter the hospital environment of the 21st century.
And SHM may need to engage the boards and other credentialing bodies to look for flexibility that will reflect today’s realities, attract the best-trained physicians to care for the most-acutely-ill patients, and protect our patients by demanding expertise and training at the most appropriate levels. TH
Dr. Wellikson is CEO of SHM.
There is a brewing crisis in critical-care medicine, a crisis that already is impacting HM. It would be easier for hospitalists to look the other way and say, “This is not our problem.” Make no mistake: It is our problem. There are not enough intensive-care physicians to go around.
In my generation, most physicians who trained in pulmonary and critical-care medicine thought they would do some office care, some bronchoscopies, and some critical care for the first several years of their professional lives. Few imagined that, in their 60s, their practice would still include rescuing patients from death at 2 a.m. Couple the intensity of care with such a demanding lifestyle, and it is hardly surprising that many critical-care doctors seek less-stressful practices (e.g., sleep medicine) or retirement.
New physicians who see the work-life imbalance are shying away from critical care in significant enough numbers, yet the demand for these doctors is growing. Whether that shift is due to the attraction of careers in HM, emergency medicine, or other IM specialties, or the perceived negatives to being a full-time intensivist, is beside the point. The medical workforce needs more critical-care physicians. And we are not going to be able to meet this need by assuming we will be able to recruit and train more surgeons, anesthesiologists, or pulmonary physicians in traditional critical-care pathways.
The situation is further complicated by workforce shortages on the rest of the ICU healthcare team. Many senior ICU nurses are reaching the end of their careers, and the pipeline to replace them is anything but robust. And all this comes at a time when the acuity of hospitalized patients is increasing and the demands for ICU expertise is at its height.
It is no surprise that hospitalists are called upon to fill the critical-care gap. SHM surveys show that 92% of hospitalists include ICU care in their practice. While hospitalists clearly do not have the training or skills to replace the intensivist, we clearly are witnessing a “scope creep.” Hospitalists are being asked to stretch their skills to fill the void in critical care.
Competence Question
The response to this is manifest in many ways. For example, steadily increasing numbers of hospitalists attend SHM’s annual critical-care precourses, and our procedures courses invariably sell out. These brief courses are important to hospitalists and their patients. Yet a day (or even two) of focused training for hospitalists will not raise their skill set to replace or even augment critical-care-trained physicians at their hospitals. The patients will keep coming and continue to need the expertise for their most-acute-care needs. Something must be done.
There are pockets of experiments on filling the increasing critical-care gap. Emory University’s Center for Critical Care in Atlanta will soon launch an experimental, HM-critical-care training program that will attempt to develop and verify critical-care competencies in just one postgraduate year after IM residency. A complementary approach could include a hospitalist-focused track within the three years of IM residency to include less outpatient medicine and more intensive-care training. This could be part of a broader restructuring of internal and family medicine residencies, which recognize the career paths (and needs) of their residents as some enter hospital-focused practice (e.g., as hospitalists, cardiologists, intensivists) and some concentrate more on the patient outside the hospital (e.g., primary care, endocrinology, rheumatology).
As training evolves, there will be practical issues of credentialing. Currently, a general-IM-trained hospitalist is required to complete a two-year fellowship in critical care to be a specialist. Interestingly, if one’s residency training is in surgery, anesthesia, or rheumatology, that physician requires only one additional year in critical care to become eligible for added/special qualifications in critical-care medicine. What, precisely, is the carryover of the longer residency experience that makes it possible to attain competency in critical care in half the training time?
There also is the risk that we will create a workforce that includes the intensivist-lite—someone who does not have complete, recognized training in critical care but has more than the typical hospitalist, and is perceived as “better than having no intensivist.” Is this in the best interest of our patients or our discipline?
Supply Solutions
There are other approaches to the workforce challenge beyond asking hospitalists to step away from practice for an additional year or two of training. As in other aspects of the hospital workforce, it is time to examine alternative deployment of the entire healthcare team. If intensivists and hospitalists are in limited supply, we need to revisit their roles and further look for opportunities to engage acute-care nurse practitioners, physician assistants, RNs, and others on the healthcare team to meet the expanding needs of our patients and our hospitals.
Another strategy would include regionalization of healthcare in population centers with multiple hospitals. In Orange County, Calif., where I live, there are 33 hospitals for 3 million people, each with some form of an ICU. Is it time to set standards of coverage and expertise so that 10 to 15 hospitals can provide a fully staffed ICU, and the other hospitals refer their most-acute patients rather than be stretched to staff their ICUs at a time of workforce shortages? Is it time to do what we did with trauma centers and set various levels of care so that not every hospital can or should be doing the most intense and costly level of care?
SHM, HM, and, most importantly, hospitalists find themselves in the midst of this growing problem. We must be part of the solution.
It is important to recognize the significant variability in the intensivist skill sets that individual hospitalists and HM groups currently possess; the variance creates hurdles in being able to step up and fill the critical-care gap. I’ve heard about hospitalists pausing their practices to obtain additional training in critical care. Hospitals across America are (or soon will be) scrambling to integrate their hospitalists and intensivists to maximize coverage and expertise. SHM has noticed an increased demand on hospitalists to increase knowledge and skills so they can extend the local coverage of critically ill patients.
It is time for SHM to clearly understand how this sea change is affecting you professionally and personally, because you practice on the frontlines of our nation’s hospitals.
It is time for SHM to engage our colleagues in the ICU—critical-care physicians and their professional societies—to understand their perspective and initiatives on this growing crisis.
It is time for SHM to engage medical educators in residency and fellowship training to explore potential changes in the curriculum—changes aimed at young physicians proceeding through their training that yield hospital-based physicians better prepared to enter the hospital environment of the 21st century.
And SHM may need to engage the boards and other credentialing bodies to look for flexibility that will reflect today’s realities, attract the best-trained physicians to care for the most-acutely-ill patients, and protect our patients by demanding expertise and training at the most appropriate levels. TH
Dr. Wellikson is CEO of SHM.
How should Parkinson’s disease be managed perioperatively?
Case
A 67-year-old female with moderately advanced Parkinson’s disease (PD) had a mechanical fall in her home, which resulted in a humeral fracture. The fall occurred in the morning before she was able to take her medications and was related to her difficulty in initiating movements.
On her current regimen, her PD symptoms are controlled. She is able to perform daily living activities independently and ambulates without assistance. She also performs more complex tasks (e.g., cooking and managing her finances). She has not exhibited any symptoms consistent with dementia. She occasionally experiences dyspnea on exertion and dysphagia, but she has not been evaluated for these complaints. She takes carbidopa/levodopa (CD/LD) 25 mg/100 mg four times a day, amantadine 100 mg twice daily, and ropinirole 3 mg three times a day.
She is scheduled for open reduction internal fixation of her fracture; the orthopedic surgeon has requested a perioperative risk assessment and recommendations concerning her medications. How should PD be managed perioperatively?
Overview
Advances in surgical and anesthetic techniques, in combination with an aging population, have contributed to an increasing number of geriatric patients undergoing surgery. As many as 50% of Americans older than 65 will undergo a surgical procedure; hospitalists will comanage many of these patients in the perioperative period.1
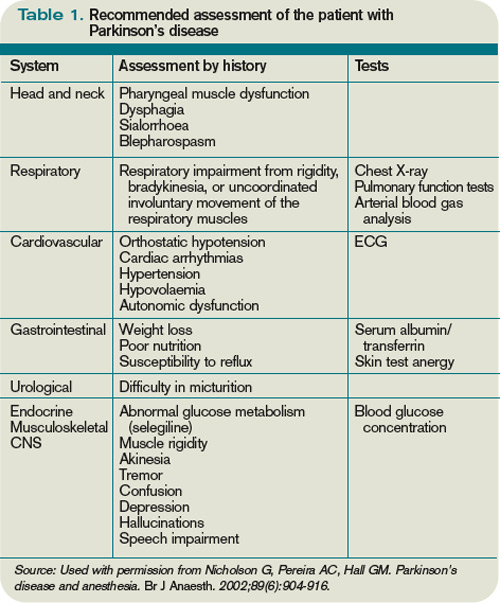
Although cardiopulmonary disorders receive a great deal of attention with regard to perioperative risk assessment, other comorbid conditions also contribute to perioperative risk—namely, disorders specific to the elderly population. Parkinson’s disease is one such condition that deserves attention.
PD is a progressive, neurodegenerative condition associated with loss of dopaminergic neurons and the presence of Lewy bodies within the substantia nigra and other areas of the brain and peripheral autonomic nervous system.2 Cardinal clinical features include rigidity, bradykinesia, and resting tremor. A supportive feature is a consistent response to levodopa. Postural instability, cognitive impairment, and autonomic dysfunction usually occur later in the disease.3,4
As the population ages, Parkinson’s disease is becoming more prevalent, affecting approximately 1% of individuals older than 60.5 These patients pose a specific challenge to the hospitalist, not only because the multiorgan system manifestations of PD can raise surgical risk, but also due to the direct effects of dopaminergic medications used to treat PD, lack of a parenteral route for these medications in NPO patients, and the risks associated with abrupt withdrawal of these medications.
Although surgical risk in PD patients has received intermittent attention in surgical, anesthesia, and neurology literature, there is no broad consensus statement or treatment guideline for the perioperative approach.
Literature Review
A retrospective cohort of 51 PD patients undergoing various types of surgery revealed that PD patients have a longer hospital stay than matched cohorts.6 Pepper et al studied a cohort of 234 PD patients in the Veterans Administration population who were undergoing a variety of surgeries.7 They found that patients with PD had a longer acute hospital stay and had higher in-hospital mortality.7 The multisystem manifestations of PD might account for this global increase in perioperative risk.
The following are reviews of organ-system manifestations of PD and their relevance to the perioperative period.
Motor: The motor symptoms of PD place patients at increased risk for falls and might impair their ability to participate in rehabilitation. Mueller et al demonstrated that there was a significantly increased risk of postoperative falls and a higher need for inpatient rehabilitation due to motor difficulties in the PD cohort.6
Pulmonary: PD patients have increased risk of abnormal pulmonary function secondary to rigidity and akinesia. Increased airway resistance and decreased lung elastic recoil lead to obstructive lung disease.8,9 Rigidity of voluntary chest wall and upper airway muscles leads to a restrictive lung disease pattern.8,10 Furthermore, respiratory dyskinesia is a common side effect of levodopa, which can result in restrictive and dyskinetic ventilation.11 As a consequence of disordered respiratory mechanics (especially in combination with disordered swallow mechanics), PD patients are at increased risk of lower respiratory infections. In fact, pneumonia remains the leading cause of mortality among PD patients.11
Not surprisingly, several cohorts have suggested that PD patients undergoing surgical procedures are at higher risk for atelectasis, pneumonia, and postoperative respiratory failure.7,12 Postoperative VTE rates are not statistically different between PD patients and matched cohorts.
Gastrointestinal: Abnor-malities in muscles of the mouth, pharynx, and esophagus account for the dysphagia commonly noted in PD.13 Barium swallow tests are abnormal in 80% or more of PD patients.14 Dysphagia can lead to aspiration, as well as inadequate oral intake, resulting in pneumonia and malnutrition, respectively.15 Dysfunction of the myenteric plexus (evidenced by Lewy Body deposition) accounts for gastrointestinal dysmotility manifested as gastroparesis, ileus, and slow colonic transit, which results in constipation.16
PD patients in the postoperative period are at risk for swallowing difficulties, which increases the risk of aspiration and might delay initiation of oral medications. Gastroparesis threatens appropriate delivery of oral medications for adequate absorption. In addition, postoperative ileus and constipation can pose challenges.
Cardiovascular: Such cardiac sympathetic abnormalities as orthostatic hypotension, postprandial or exercise-induced hypotension, impaired heart rate variability, and dysrhythmias are common in PD.17 Pepper et al found a trend toward increased risk of hypotension and acute myocardial infarction (MI) in PD patients undergoing surgery.7
Genitourinary: Urinary complaints (e.g., nocturia, frequency, urgency, and urge incontinence) are common in PD patients.18 These clinical complaints correspond to involuntary detrusor contractions (detrusor hyperreflexia).19 Pepper et al found an increased risk of postoperative urinary tract infection in PD patients.7

Cognitive: A recognized feature of advanced PD is cognitive impairment. Studies estimate the prevalence of dementia in cohorts of PD patients is from 28% to 44%. PD with dementia has been associated with shortened survival, impaired quality of life, and increased caregiver distress.20 Pepper et al noted a trend toward increased incidence of postoperative delirium in their cohort of 234 PD patients undergoing surgery.7
Medication: Management of anti-Parkinsonian medications in the perioperative period poses unique challenges. These medications’ prodopaminergic effects can lead to hemodynamic compromise and are potentially arrhythmogenic. At the same time, abrupt withdrawal of these medications can lead to a potentially lethal condition called Parkinsonism-hyperpyrexia syndrome (PHS), which is clinically similar to neuroleptic malignant syndrome.21 PHS is characterized by very high fever, extreme muscle rigidity, autonomic instability, altered consciousness, and multiple severe systemic complications (e.g., acute renal failure, disseminated intravascular coagulation, autonomic failure, aspiration pneumonia, and infections). PHS occurs in up to 4% of PD patients; mortality is reported to be from 4% for treated to 20% for untreated episodes.22-24
As many as 30% of patients who survive a PHS episode have worsening of their PD symptoms and never return to their pre-PHS baseline. PHS prevention in hospitalized patients by uninterrupted administration of PD medications should be the goal. Early recognition and aggressive treatment is key to successful recovery.
Furthermore, even brief interruption of medications can lead to decompensation of Parkinsonian symptoms, which not only delays recovery from surgery, but also increases the risk for multisystem complications as discussed above.25 Traditional anti-Parkinsonian medications can only be delivered orally, presenting significant challenges for NPO patients, especially those undergoing enteric surgery requiring bowel rest.
Case reports describe various approaches to medication management in the perioperative period, but no single consensus statement (or treatment guideline) exists. The most common clinical scenarios are:
- Patient undergoes short surgery and is able to take oral medication immediately after the procedure (e.g., orthopedic, eye);
- Patient undergoes more lengthy surgery and will be able to take enteric medications perioperatively (e.g., longer orthopedic surgeries, genitourinary); and
- Patient undergoes lengthy procedure in which they will be required to adhere to bowel rest (e.g., bowel resection).
Depending on the category, the approach to medication management might differ.
Furuya et al describe a 70-year-old male with PD who had previously experienced perioperative complications associated with his medication management, including postoperative rigidity, dysphagia, and difficulty maintaining respiratory secretions.26 These symptoms were reversed with intravenous levodopa. However, the patient experienced hypotension and premature ventricular contractions as side effects of this therapy. This patient was scheduled to undergo hepatic lobectomy. Given his previous complications, Furuya et al provided enteral administration of CD/LD via nasogastric tube every two hours during the surgery, with placement of a duodenostomy for postoperative administration of CD/LD. The patient maintained hemodynamic stability throughout the perioperative period and emerged from anesthesia smoothly with no muscle rigidity or postoperative complications.26
Fujii et al described three cases of PD patients undergoing gastrointestinal surgery. They suggested that the dose of medication required to control symptoms should be minimized before surgery to avoid withdrawal symptoms. They also described the use of intravenous levodopa immediately, postoperatively, while the patient was unable to tolerate enteric medications, and suggested the use of prokinetics to prevent ileus and maximize drug absorption.27
Gálvez-Jiménez et al discuss the limitations of intravenous levodopa, including hemodynamic compromise, need for escalating doses, frequent adjustments to maintain effect, and large amount of fluids required. They propose the use of subcutaneous apomorphine, which is a potent D1/D2 dopamine agonist in conjunction with rectal domeperidone, a D2 antagonist with poor blood-brain-barrier penetration, to counteract the peripheral dopaminergic side effects. The main limitation to this approach is that domeperidone is not available in the U.S.28
Intravenous antihistamines and anticholinergics are readily available. However, they show limited efficacy in halting Parkinsonian symptoms and carry multiple side effects (e.g., confusion, delay in gastrointestinal recovery, and urinary retention).28
Various anesthesiologists agree with administering anti-PD medications immediately, preoperatively, and restarting medications as soon as possible postoperatively. However, they do not provide uniform treatment guidelines regarding specific medication management.29,30
Deep-brain-stimulation (DBS) management: DBS is an effective treatment for advanced PD. There are more than 60,000 patients around the world who have DBS for various conditions, mostly for PD. Therefore, it is increasingly likely that hospitalists will encounter hospitalized patients with advanced PD who are treated both pharmacologically and with DBS. It is important to recognize that stimulation, just like PD medications, cannot be stopped suddenly. If there is any concern of the DBS system malfunctioning (i.e., fracture of the hardware during a fall), the neurologist or neurosurgeon managing the DBS should be contacted immediately. Certain diagnostic tests (MRI) and treatment procedures (diathermy) are contraindicated, and if done inappropriately, can result in permanent brain damage.31,32,33
During surgeries requiring blood-vessel cauterization, DBS should be temporarily turned off. This can be done with the patient’s handheld device or, preferably, by a trained technician usually available through 24/7 technical support services provided by the manufacturer.
Summary of recommendations: There are no clear treatment guidelines regarding the optimal perioperative management of PD patients. The following measures are based on available data and are extensions of routine perioperative management; however, there is no evidence to demonstrate their efficacy in decreasing complication rates among patients with PD:
- A thorough preoperative history and physical examination should include Parkinsonian signs and symptoms, precise medication regimen with doses and timing of intake, effects of medication withdrawal or missed doses, type of surgery planned, and comorbid conditions;
- Depending on symptoms mentioned in the history, consider further testing for dysphagia (preoperative swallow evaluation) and dyspnea (preoperative pulmonary function tests);
- The major goal of medication management in the perioperative period is to continue administration of dopamine replacement therapy as close to the outpatient regimen as possible.
- Titrate down dose of anti-Parkinsonian medications to lowest possible dose prior to surgery if prolonged NPO status is anticipated;
- Ensure medications are administered immediately prior to surgery;
- For short, nonenteric procedures, resume outpatient medication doses and timing of administration as soon as possible postoperatively. For longer, nonenteric surgeries, consider placement of nasogastric tube for medication delivery during procedure and immediately postoperatively;
- If the major limitation of oral medication intake is dysphagia, the use of orally disintegrated formulation CD/LD (parcopa) is helpful;
- For longer enteric surgeries in which patient must be on bowel rest, recommend consultation with neurologist specialized in movement disorders to guide use of intravenous or subcutaneous agents. Transdermal delivery systems of the dopamine agonist rotigotine are in the process of being approved in the U.S. market and might be helpful for this purpose;
- Initiation of tube feeding, when co-administered with levodopa, might result in sudden changes in medication absorption and potential worsening of PD symptoms; feeding should be started slowly and preferably at night when the body’s dopamine requirements are lower;
- Consider use of promotility agents;
- If apomorphine or intravenous LD are not available, consider trial of intravenous anticholinergics or antihistamines, carefully observing for potential cognitive and behavioral side effects;
- Avoid such dopamine antagonists as droperidol, haloperidol, risperidone, metaclopramide, prochlorperazine, or promethazine, as these medications can worsen Parkinsonian symptoms; and
- If patient was on MAO-B inhibitors (selegiline, rasagiline) before surgery, be aware of multiple potential interactions with various medications that are commonly used in perioperative period, including anesthesia agents and certain analgesics, specifically meperidine. These interactions include serotonin syndrome, and can be life-threatening.34
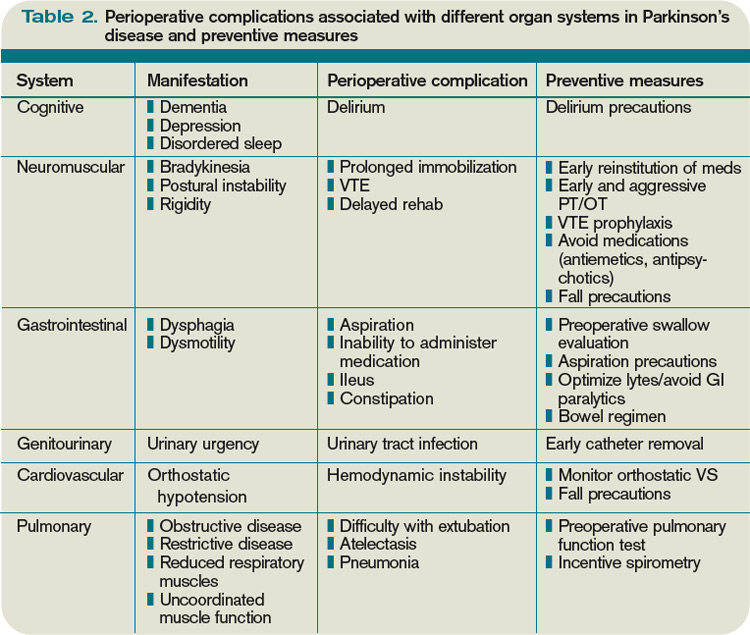
- Psychiatric considerations: delirium precautions;
- Motor considerations: early PT/OT, early referral to inpatient rehabilitation; fall precautions;
- Pulmonary considerations: institute aggressive incentive spirometry, postural drainage, management of respiratory secretions, and breathing exercises; VTE prophylaxis;
- Gastrointestinal considerations: aspiration precautions and prompt speech therapy to evaluate for aspiration and to teach appropriate swallow techniques (chin tuck); institute aggressive bowel regimen; maximize fluids, electrolytes, and avoid narcotics to prevent precipitating or exacerbating ileus;
- Cardiovascular considerations: monitor orthostatic vital signs; fall precautions to avoid syncopal falls; and
- Genitourinary considerations: early urinary catheter removal; vigilance in monitoring for urinary tract infection.
Back to the Case
The patient underwent repair of her fracture, was extubated, and recovered from general anesthesia without incident. She was evaluated in the postanesthesia care unit, at which time she had a slight tremor and mild rigidity. She was immediately given a dose of her CD/LD, and her evening doses of amantadine and ropinirole were resumed. The patient had no significant flare of her Parkinsonian symptoms and did not exhibit any evidence of PHS.
A postoperative consultation was placed for speech therapy, physical therapy, and occupational therapy. She was given low-molecular-weight heparin for VTE prophylaxis and asked to use incentive spirometry. On postoperative day one, she complained of urinary frequency. A urinalysis was consistent with possible infection. She was discharged home on her previous medication regimen, in addition to antibiotics for cystitis.
If the procedure had not been emergent, the patient might have benefited from a preoperative swallow evaluation, given her dysphagia. Consultation with a speech therapist would have ensured that the patient was educated regarding aspiration precautions. Although this patient did not have difficulty with extubation or experience postoperative respiratory failure, abnormal preoperative pulmonary function tests might have prompted the anesthesiologists to consider alternative low-risk techniques (e.g., a local nerve block).
Bottom Line
Perioperative management of patients with Parkinson’s disease requires knowledge of the multisystem disease characteristics that raise perioperative risk and the effects of the medications used to treat PD. To date, no clear treatment guidelines exist for the optimal perioperative management of PD patients.
However, vigilance in detecting possible complications and instituting attentive perioperative care can aid a hospitalist consultant in improving overall care for these patients. TH
Dr. Patel is a medical resident at the University of Colorado Denver. Dr. Stickrath is a hospitalist at the Denver VA Medical Center and instructor of medicine at the University of Colorado Denver. Dr. Anderson is a hospitalist at the Denver VA Medical Center and assistant professor of medicine at the University of Colorado Denver. Dr. Klepitskaya is a neurologist and assistant professor of neurology at the University of Colorado Denver.
References
- Ersan T. Perioperative management of the geriatric patient. Web MD website. Available at: http://emedicine.medscape.com/article/285433-overview. Accessed May 10, 2010.
- Braak H, Del Tredici K, Rüb U, de Vos RA, Jansen Steur EN, Braak E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging. 2003;24(2):197-211.
- Ward CD, Gibb WR. Research diagnostic criteria for Parkinson’s disease. Adv Neurol. 1990;53:245-249.
- Stern MB, Koller WC. Parkinsonian Syndromes. New York: Informa Healthcare Publishing; 1993.
- Nutt JG, Wooten GF. Clinical practice. Diagnosis and initial management of Parkinson’s disease. N Engl J Med. 2005;353(10):1021-1027.
- Mueller MC, Jüptner U, Wuellner U, et al. Parkinson’s disease influences the perioperative risk profile in surgery. Langenbecks Arch Surg. 2009;394(3):511-515.
- Pepper PV, Goldstein MK. Postoperative complications in Parkinson’s disease. J Am Geriatr Soc. 1999;47(8):967-972.
- Shill H, Stacy M. Respiratory function in Parkinson’s disease. Clin Neurosci. 1998;5(2):131-135.
- Neu HC, Connolly JJ Jr., Schwertley FW, Ladwig HA, Brody AW. Obstructive respiratory dysfunction in parkinsonian patients. Ann Rev Respir Dis. 1967;95(1):33-47.
- Chokroverty S. The spectrum of ventilatory disturbances in movement disorders. In: Chokroverty S, ed. Movement Disorders. Great Neck, New York: PMA Publishing Corp.; 1990:365-392.
- Shill H, Stacy M. Respiratory complications of Parkinson’s disease. Semin Respir Crit Care Med. 2002;23(3):261-265.
- Easdown LJ, Tessler KJ, Minuk J. Upper airway involvement in Parkinson’s disease resulting in postoperative respiratory failure. Can J Anaesth. 1995;42(4):344-347.
- Pfeiffer RF. Gastrointestinal dysfunction in Parkinson’s disease. Lancet Neurol. 2003;2(2):107-116.
- Castell JA, Johnston BT, Colcher A, Li Q, Gideon RM, Castell DO. Manometric abnormalities of the oesophagus in patients with Parkinson’s disease. Neurogastroenterol Motil. 2001;13(4):361-364.
- Marcason W. What are the primary nutritional issues for a patient with Parkinson’s disease? J Am Diet Assoc. 2009;109(7):1316.
- Djaldetti R, Lev N, Melamed E. Lesions outside the CNS in Parkinson’s disease. Mov Disord. 2009;24(6):793-800.
- Orimo S, Takahashi A, Uchihara T, Mori F, Kakita A, Wakabayashi K, Takahashi H. Degeneration of cardiac sympathetic nerve begins in the early disease process of Parkinson’s disease. Brain Pathol. 2007;17(1):24-30.
- Lemack GE, Dewey RB Jr., Roehrborn CG, O’Suilleabhain PE, Zimmern PE. Questionnaire-based assessment of bladder dysfunction in patients with mild to moderate Parkinson’s disease. Urology. 2000;56(2):250-254.
- Singer C. Urinary dysfunction in Parkinson’s disease. Clin Neurosci. 1998;5(2):78-86.
- Leverenz JB, Quinn JF, Zabetian C, Zhang J, Montine KS, Montine TJ. Cognitive impairment and dementia in patients with Parkinson disease. Curr Top Med Chem. 2009;9(10):903-912.
- Factor SA, Santiago A. Parkinson-hyperpyrexia syndrome in Parkinson’s disease. In: Frucht S, Fahn S, eds. Movement Disorder Emergencies: Diagnosis and Treatment. New York: Humana Press; 2005:29-40.
- Reed AP, Han DG: Intraoperative exacerbation of Parkinson’s disease. Anesth Analg. 1992;75(5):850-853.
- Harada T, Mitsuoka K, Kumagai R, et al. Clinical features of malignant syndrome in Parkinson’s disease and related neurological disorders. Parkinsonism Relat Disord. 2003;9(Suppl 1):S15-23.
- Onofrj M, Thomas A. Acute akinesia in Parkinson disease. Neurology. 2005;64(7):1162-1169.
- Serrano-Dueñas M. Neuroleptic malignant syndrome-like, or—dopaminergic malignant syndrome—due to levodopa therapy withdrawal. Clinical features in 11 patients. Parkinsonism Relat Disord. 2003;9(3):175-178.
- Furuya R, Hirai A, Andoh T, Kudoh I, Okumura F. Successful perioperative management of a patient with Parkinson’s disease by enteral levodopa administration under propofol anesthesia. Anesthesiology. 1998;89(1):261-263.
- Fujii T, Nakabayashi T, Hashimoto S, Kuwano H. Successful perioperative management of patients with Parkinson’s disease following gastrointestinal surgery: report of three cases. Surg Today. 2009;39(9):807-810.
- Gálvez-Jiménez N, Lang AE. The perioperative management of Parkinson’s disease revisited. Neurol Clin. 2004;22(2):367-377.
- Kalenka A, Schwarz A. Anasthesia and Parkinson’s disease: how to manage with new therapies? Curr Opin Anesthesiol. 2009;22(3):419-424.
- Nicholson G, Pereira AC, Hall GM. Parkinson’s disease and anesthesia. Br J Anaesthesia. 2002;89(6):904-916.
- Rezai AR, Baker KB, Tkach JA, et al. Is magnetic resonance imaging safe for patients with neurostimulation systems used for deep brain stimulation? Neurosurgery. 2005:57(5):1056-1062.
- Henderson JM, Tkach J, Phillips M, Baker K, Shellock FG, Rezai AR. Permanent neurological deficit related to magnetic resonance imaging in a patient with implanted deep brain stimulation electrodes for Parkinson’s disease: case report. Neurosurgery. 2005:57(5):E1063.
- Nutt JG, Anderson VC, Peacock JH, Hammerstad JP, Burchiel KJ. DBS and diathermy interaction induces severe CNS damage. Neurology. 2001;56 (10):1384-1386.
- Gordon PH, Frucht SJ. Neuroleptic malignant syndrome in advanced Parkinson’s disease. Mov Disord. 2001;16(5):960-962.
Case
A 67-year-old female with moderately advanced Parkinson’s disease (PD) had a mechanical fall in her home, which resulted in a humeral fracture. The fall occurred in the morning before she was able to take her medications and was related to her difficulty in initiating movements.
On her current regimen, her PD symptoms are controlled. She is able to perform daily living activities independently and ambulates without assistance. She also performs more complex tasks (e.g., cooking and managing her finances). She has not exhibited any symptoms consistent with dementia. She occasionally experiences dyspnea on exertion and dysphagia, but she has not been evaluated for these complaints. She takes carbidopa/levodopa (CD/LD) 25 mg/100 mg four times a day, amantadine 100 mg twice daily, and ropinirole 3 mg three times a day.
She is scheduled for open reduction internal fixation of her fracture; the orthopedic surgeon has requested a perioperative risk assessment and recommendations concerning her medications. How should PD be managed perioperatively?
Overview
Advances in surgical and anesthetic techniques, in combination with an aging population, have contributed to an increasing number of geriatric patients undergoing surgery. As many as 50% of Americans older than 65 will undergo a surgical procedure; hospitalists will comanage many of these patients in the perioperative period.1
Although cardiopulmonary disorders receive a great deal of attention with regard to perioperative risk assessment, other comorbid conditions also contribute to perioperative risk—namely, disorders specific to the elderly population. Parkinson’s disease is one such condition that deserves attention.
PD is a progressive, neurodegenerative condition associated with loss of dopaminergic neurons and the presence of Lewy bodies within the substantia nigra and other areas of the brain and peripheral autonomic nervous system.2 Cardinal clinical features include rigidity, bradykinesia, and resting tremor. A supportive feature is a consistent response to levodopa. Postural instability, cognitive impairment, and autonomic dysfunction usually occur later in the disease.3,4
As the population ages, Parkinson’s disease is becoming more prevalent, affecting approximately 1% of individuals older than 60.5 These patients pose a specific challenge to the hospitalist, not only because the multiorgan system manifestations of PD can raise surgical risk, but also due to the direct effects of dopaminergic medications used to treat PD, lack of a parenteral route for these medications in NPO patients, and the risks associated with abrupt withdrawal of these medications.
Although surgical risk in PD patients has received intermittent attention in surgical, anesthesia, and neurology literature, there is no broad consensus statement or treatment guideline for the perioperative approach.
Literature Review
A retrospective cohort of 51 PD patients undergoing various types of surgery revealed that PD patients have a longer hospital stay than matched cohorts.6 Pepper et al studied a cohort of 234 PD patients in the Veterans Administration population who were undergoing a variety of surgeries.7 They found that patients with PD had a longer acute hospital stay and had higher in-hospital mortality.7 The multisystem manifestations of PD might account for this global increase in perioperative risk.
The following are reviews of organ-system manifestations of PD and their relevance to the perioperative period.
Motor: The motor symptoms of PD place patients at increased risk for falls and might impair their ability to participate in rehabilitation. Mueller et al demonstrated that there was a significantly increased risk of postoperative falls and a higher need for inpatient rehabilitation due to motor difficulties in the PD cohort.6
Pulmonary: PD patients have increased risk of abnormal pulmonary function secondary to rigidity and akinesia. Increased airway resistance and decreased lung elastic recoil lead to obstructive lung disease.8,9 Rigidity of voluntary chest wall and upper airway muscles leads to a restrictive lung disease pattern.8,10 Furthermore, respiratory dyskinesia is a common side effect of levodopa, which can result in restrictive and dyskinetic ventilation.11 As a consequence of disordered respiratory mechanics (especially in combination with disordered swallow mechanics), PD patients are at increased risk of lower respiratory infections. In fact, pneumonia remains the leading cause of mortality among PD patients.11
Not surprisingly, several cohorts have suggested that PD patients undergoing surgical procedures are at higher risk for atelectasis, pneumonia, and postoperative respiratory failure.7,12 Postoperative VTE rates are not statistically different between PD patients and matched cohorts.
Gastrointestinal: Abnor-malities in muscles of the mouth, pharynx, and esophagus account for the dysphagia commonly noted in PD.13 Barium swallow tests are abnormal in 80% or more of PD patients.14 Dysphagia can lead to aspiration, as well as inadequate oral intake, resulting in pneumonia and malnutrition, respectively.15 Dysfunction of the myenteric plexus (evidenced by Lewy Body deposition) accounts for gastrointestinal dysmotility manifested as gastroparesis, ileus, and slow colonic transit, which results in constipation.16
PD patients in the postoperative period are at risk for swallowing difficulties, which increases the risk of aspiration and might delay initiation of oral medications. Gastroparesis threatens appropriate delivery of oral medications for adequate absorption. In addition, postoperative ileus and constipation can pose challenges.
Cardiovascular: Such cardiac sympathetic abnormalities as orthostatic hypotension, postprandial or exercise-induced hypotension, impaired heart rate variability, and dysrhythmias are common in PD.17 Pepper et al found a trend toward increased risk of hypotension and acute myocardial infarction (MI) in PD patients undergoing surgery.7
Genitourinary: Urinary complaints (e.g., nocturia, frequency, urgency, and urge incontinence) are common in PD patients.18 These clinical complaints correspond to involuntary detrusor contractions (detrusor hyperreflexia).19 Pepper et al found an increased risk of postoperative urinary tract infection in PD patients.7
Cognitive: A recognized feature of advanced PD is cognitive impairment. Studies estimate the prevalence of dementia in cohorts of PD patients is from 28% to 44%. PD with dementia has been associated with shortened survival, impaired quality of life, and increased caregiver distress.20 Pepper et al noted a trend toward increased incidence of postoperative delirium in their cohort of 234 PD patients undergoing surgery.7
Medication: Management of anti-Parkinsonian medications in the perioperative period poses unique challenges. These medications’ prodopaminergic effects can lead to hemodynamic compromise and are potentially arrhythmogenic. At the same time, abrupt withdrawal of these medications can lead to a potentially lethal condition called Parkinsonism-hyperpyrexia syndrome (PHS), which is clinically similar to neuroleptic malignant syndrome.21 PHS is characterized by very high fever, extreme muscle rigidity, autonomic instability, altered consciousness, and multiple severe systemic complications (e.g., acute renal failure, disseminated intravascular coagulation, autonomic failure, aspiration pneumonia, and infections). PHS occurs in up to 4% of PD patients; mortality is reported to be from 4% for treated to 20% for untreated episodes.22-24
As many as 30% of patients who survive a PHS episode have worsening of their PD symptoms and never return to their pre-PHS baseline. PHS prevention in hospitalized patients by uninterrupted administration of PD medications should be the goal. Early recognition and aggressive treatment is key to successful recovery.
Furthermore, even brief interruption of medications can lead to decompensation of Parkinsonian symptoms, which not only delays recovery from surgery, but also increases the risk for multisystem complications as discussed above.25 Traditional anti-Parkinsonian medications can only be delivered orally, presenting significant challenges for NPO patients, especially those undergoing enteric surgery requiring bowel rest.
Case reports describe various approaches to medication management in the perioperative period, but no single consensus statement (or treatment guideline) exists. The most common clinical scenarios are:
- Patient undergoes short surgery and is able to take oral medication immediately after the procedure (e.g., orthopedic, eye);
- Patient undergoes more lengthy surgery and will be able to take enteric medications perioperatively (e.g., longer orthopedic surgeries, genitourinary); and
- Patient undergoes lengthy procedure in which they will be required to adhere to bowel rest (e.g., bowel resection).
Depending on the category, the approach to medication management might differ.
Furuya et al describe a 70-year-old male with PD who had previously experienced perioperative complications associated with his medication management, including postoperative rigidity, dysphagia, and difficulty maintaining respiratory secretions.26 These symptoms were reversed with intravenous levodopa. However, the patient experienced hypotension and premature ventricular contractions as side effects of this therapy. This patient was scheduled to undergo hepatic lobectomy. Given his previous complications, Furuya et al provided enteral administration of CD/LD via nasogastric tube every two hours during the surgery, with placement of a duodenostomy for postoperative administration of CD/LD. The patient maintained hemodynamic stability throughout the perioperative period and emerged from anesthesia smoothly with no muscle rigidity or postoperative complications.26
Fujii et al described three cases of PD patients undergoing gastrointestinal surgery. They suggested that the dose of medication required to control symptoms should be minimized before surgery to avoid withdrawal symptoms. They also described the use of intravenous levodopa immediately, postoperatively, while the patient was unable to tolerate enteric medications, and suggested the use of prokinetics to prevent ileus and maximize drug absorption.27
Gálvez-Jiménez et al discuss the limitations of intravenous levodopa, including hemodynamic compromise, need for escalating doses, frequent adjustments to maintain effect, and large amount of fluids required. They propose the use of subcutaneous apomorphine, which is a potent D1/D2 dopamine agonist in conjunction with rectal domeperidone, a D2 antagonist with poor blood-brain-barrier penetration, to counteract the peripheral dopaminergic side effects. The main limitation to this approach is that domeperidone is not available in the U.S.28
Intravenous antihistamines and anticholinergics are readily available. However, they show limited efficacy in halting Parkinsonian symptoms and carry multiple side effects (e.g., confusion, delay in gastrointestinal recovery, and urinary retention).28
Various anesthesiologists agree with administering anti-PD medications immediately, preoperatively, and restarting medications as soon as possible postoperatively. However, they do not provide uniform treatment guidelines regarding specific medication management.29,30
Deep-brain-stimulation (DBS) management: DBS is an effective treatment for advanced PD. There are more than 60,000 patients around the world who have DBS for various conditions, mostly for PD. Therefore, it is increasingly likely that hospitalists will encounter hospitalized patients with advanced PD who are treated both pharmacologically and with DBS. It is important to recognize that stimulation, just like PD medications, cannot be stopped suddenly. If there is any concern of the DBS system malfunctioning (i.e., fracture of the hardware during a fall), the neurologist or neurosurgeon managing the DBS should be contacted immediately. Certain diagnostic tests (MRI) and treatment procedures (diathermy) are contraindicated, and if done inappropriately, can result in permanent brain damage.31,32,33
During surgeries requiring blood-vessel cauterization, DBS should be temporarily turned off. This can be done with the patient’s handheld device or, preferably, by a trained technician usually available through 24/7 technical support services provided by the manufacturer.
Summary of recommendations: There are no clear treatment guidelines regarding the optimal perioperative management of PD patients. The following measures are based on available data and are extensions of routine perioperative management; however, there is no evidence to demonstrate their efficacy in decreasing complication rates among patients with PD:
- A thorough preoperative history and physical examination should include Parkinsonian signs and symptoms, precise medication regimen with doses and timing of intake, effects of medication withdrawal or missed doses, type of surgery planned, and comorbid conditions;
- Depending on symptoms mentioned in the history, consider further testing for dysphagia (preoperative swallow evaluation) and dyspnea (preoperative pulmonary function tests);
- The major goal of medication management in the perioperative period is to continue administration of dopamine replacement therapy as close to the outpatient regimen as possible.
- Titrate down dose of anti-Parkinsonian medications to lowest possible dose prior to surgery if prolonged NPO status is anticipated;
- Ensure medications are administered immediately prior to surgery;
- For short, nonenteric procedures, resume outpatient medication doses and timing of administration as soon as possible postoperatively. For longer, nonenteric surgeries, consider placement of nasogastric tube for medication delivery during procedure and immediately postoperatively;
- If the major limitation of oral medication intake is dysphagia, the use of orally disintegrated formulation CD/LD (parcopa) is helpful;
- For longer enteric surgeries in which patient must be on bowel rest, recommend consultation with neurologist specialized in movement disorders to guide use of intravenous or subcutaneous agents. Transdermal delivery systems of the dopamine agonist rotigotine are in the process of being approved in the U.S. market and might be helpful for this purpose;
- Initiation of tube feeding, when co-administered with levodopa, might result in sudden changes in medication absorption and potential worsening of PD symptoms; feeding should be started slowly and preferably at night when the body’s dopamine requirements are lower;
- Consider use of promotility agents;
- If apomorphine or intravenous LD are not available, consider trial of intravenous anticholinergics or antihistamines, carefully observing for potential cognitive and behavioral side effects;
- Avoid such dopamine antagonists as droperidol, haloperidol, risperidone, metaclopramide, prochlorperazine, or promethazine, as these medications can worsen Parkinsonian symptoms; and
- If patient was on MAO-B inhibitors (selegiline, rasagiline) before surgery, be aware of multiple potential interactions with various medications that are commonly used in perioperative period, including anesthesia agents and certain analgesics, specifically meperidine. These interactions include serotonin syndrome, and can be life-threatening.34
- Psychiatric considerations: delirium precautions;
- Motor considerations: early PT/OT, early referral to inpatient rehabilitation; fall precautions;
- Pulmonary considerations: institute aggressive incentive spirometry, postural drainage, management of respiratory secretions, and breathing exercises; VTE prophylaxis;
- Gastrointestinal considerations: aspiration precautions and prompt speech therapy to evaluate for aspiration and to teach appropriate swallow techniques (chin tuck); institute aggressive bowel regimen; maximize fluids, electrolytes, and avoid narcotics to prevent precipitating or exacerbating ileus;
- Cardiovascular considerations: monitor orthostatic vital signs; fall precautions to avoid syncopal falls; and
- Genitourinary considerations: early urinary catheter removal; vigilance in monitoring for urinary tract infection.
Back to the Case
The patient underwent repair of her fracture, was extubated, and recovered from general anesthesia without incident. She was evaluated in the postanesthesia care unit, at which time she had a slight tremor and mild rigidity. She was immediately given a dose of her CD/LD, and her evening doses of amantadine and ropinirole were resumed. The patient had no significant flare of her Parkinsonian symptoms and did not exhibit any evidence of PHS.
A postoperative consultation was placed for speech therapy, physical therapy, and occupational therapy. She was given low-molecular-weight heparin for VTE prophylaxis and asked to use incentive spirometry. On postoperative day one, she complained of urinary frequency. A urinalysis was consistent with possible infection. She was discharged home on her previous medication regimen, in addition to antibiotics for cystitis.
If the procedure had not been emergent, the patient might have benefited from a preoperative swallow evaluation, given her dysphagia. Consultation with a speech therapist would have ensured that the patient was educated regarding aspiration precautions. Although this patient did not have difficulty with extubation or experience postoperative respiratory failure, abnormal preoperative pulmonary function tests might have prompted the anesthesiologists to consider alternative low-risk techniques (e.g., a local nerve block).
Bottom Line
Perioperative management of patients with Parkinson’s disease requires knowledge of the multisystem disease characteristics that raise perioperative risk and the effects of the medications used to treat PD. To date, no clear treatment guidelines exist for the optimal perioperative management of PD patients.
However, vigilance in detecting possible complications and instituting attentive perioperative care can aid a hospitalist consultant in improving overall care for these patients. TH
Dr. Patel is a medical resident at the University of Colorado Denver. Dr. Stickrath is a hospitalist at the Denver VA Medical Center and instructor of medicine at the University of Colorado Denver. Dr. Anderson is a hospitalist at the Denver VA Medical Center and assistant professor of medicine at the University of Colorado Denver. Dr. Klepitskaya is a neurologist and assistant professor of neurology at the University of Colorado Denver.
References
- Ersan T. Perioperative management of the geriatric patient. Web MD website. Available at: http://emedicine.medscape.com/article/285433-overview. Accessed May 10, 2010.
- Braak H, Del Tredici K, Rüb U, de Vos RA, Jansen Steur EN, Braak E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging. 2003;24(2):197-211.
- Ward CD, Gibb WR. Research diagnostic criteria for Parkinson’s disease. Adv Neurol. 1990;53:245-249.
- Stern MB, Koller WC. Parkinsonian Syndromes. New York: Informa Healthcare Publishing; 1993.
- Nutt JG, Wooten GF. Clinical practice. Diagnosis and initial management of Parkinson’s disease. N Engl J Med. 2005;353(10):1021-1027.
- Mueller MC, Jüptner U, Wuellner U, et al. Parkinson’s disease influences the perioperative risk profile in surgery. Langenbecks Arch Surg. 2009;394(3):511-515.
- Pepper PV, Goldstein MK. Postoperative complications in Parkinson’s disease. J Am Geriatr Soc. 1999;47(8):967-972.
- Shill H, Stacy M. Respiratory function in Parkinson’s disease. Clin Neurosci. 1998;5(2):131-135.
- Neu HC, Connolly JJ Jr., Schwertley FW, Ladwig HA, Brody AW. Obstructive respiratory dysfunction in parkinsonian patients. Ann Rev Respir Dis. 1967;95(1):33-47.
- Chokroverty S. The spectrum of ventilatory disturbances in movement disorders. In: Chokroverty S, ed. Movement Disorders. Great Neck, New York: PMA Publishing Corp.; 1990:365-392.
- Shill H, Stacy M. Respiratory complications of Parkinson’s disease. Semin Respir Crit Care Med. 2002;23(3):261-265.
- Easdown LJ, Tessler KJ, Minuk J. Upper airway involvement in Parkinson’s disease resulting in postoperative respiratory failure. Can J Anaesth. 1995;42(4):344-347.
- Pfeiffer RF. Gastrointestinal dysfunction in Parkinson’s disease. Lancet Neurol. 2003;2(2):107-116.
- Castell JA, Johnston BT, Colcher A, Li Q, Gideon RM, Castell DO. Manometric abnormalities of the oesophagus in patients with Parkinson’s disease. Neurogastroenterol Motil. 2001;13(4):361-364.
- Marcason W. What are the primary nutritional issues for a patient with Parkinson’s disease? J Am Diet Assoc. 2009;109(7):1316.
- Djaldetti R, Lev N, Melamed E. Lesions outside the CNS in Parkinson’s disease. Mov Disord. 2009;24(6):793-800.
- Orimo S, Takahashi A, Uchihara T, Mori F, Kakita A, Wakabayashi K, Takahashi H. Degeneration of cardiac sympathetic nerve begins in the early disease process of Parkinson’s disease. Brain Pathol. 2007;17(1):24-30.
- Lemack GE, Dewey RB Jr., Roehrborn CG, O’Suilleabhain PE, Zimmern PE. Questionnaire-based assessment of bladder dysfunction in patients with mild to moderate Parkinson’s disease. Urology. 2000;56(2):250-254.
- Singer C. Urinary dysfunction in Parkinson’s disease. Clin Neurosci. 1998;5(2):78-86.
- Leverenz JB, Quinn JF, Zabetian C, Zhang J, Montine KS, Montine TJ. Cognitive impairment and dementia in patients with Parkinson disease. Curr Top Med Chem. 2009;9(10):903-912.
- Factor SA, Santiago A. Parkinson-hyperpyrexia syndrome in Parkinson’s disease. In: Frucht S, Fahn S, eds. Movement Disorder Emergencies: Diagnosis and Treatment. New York: Humana Press; 2005:29-40.
- Reed AP, Han DG: Intraoperative exacerbation of Parkinson’s disease. Anesth Analg. 1992;75(5):850-853.
- Harada T, Mitsuoka K, Kumagai R, et al. Clinical features of malignant syndrome in Parkinson’s disease and related neurological disorders. Parkinsonism Relat Disord. 2003;9(Suppl 1):S15-23.
- Onofrj M, Thomas A. Acute akinesia in Parkinson disease. Neurology. 2005;64(7):1162-1169.
- Serrano-Dueñas M. Neuroleptic malignant syndrome-like, or—dopaminergic malignant syndrome—due to levodopa therapy withdrawal. Clinical features in 11 patients. Parkinsonism Relat Disord. 2003;9(3):175-178.
- Furuya R, Hirai A, Andoh T, Kudoh I, Okumura F. Successful perioperative management of a patient with Parkinson’s disease by enteral levodopa administration under propofol anesthesia. Anesthesiology. 1998;89(1):261-263.
- Fujii T, Nakabayashi T, Hashimoto S, Kuwano H. Successful perioperative management of patients with Parkinson’s disease following gastrointestinal surgery: report of three cases. Surg Today. 2009;39(9):807-810.
- Gálvez-Jiménez N, Lang AE. The perioperative management of Parkinson’s disease revisited. Neurol Clin. 2004;22(2):367-377.
- Kalenka A, Schwarz A. Anasthesia and Parkinson’s disease: how to manage with new therapies? Curr Opin Anesthesiol. 2009;22(3):419-424.
- Nicholson G, Pereira AC, Hall GM. Parkinson’s disease and anesthesia. Br J Anaesthesia. 2002;89(6):904-916.
- Rezai AR, Baker KB, Tkach JA, et al. Is magnetic resonance imaging safe for patients with neurostimulation systems used for deep brain stimulation? Neurosurgery. 2005:57(5):1056-1062.
- Henderson JM, Tkach J, Phillips M, Baker K, Shellock FG, Rezai AR. Permanent neurological deficit related to magnetic resonance imaging in a patient with implanted deep brain stimulation electrodes for Parkinson’s disease: case report. Neurosurgery. 2005:57(5):E1063.
- Nutt JG, Anderson VC, Peacock JH, Hammerstad JP, Burchiel KJ. DBS and diathermy interaction induces severe CNS damage. Neurology. 2001;56 (10):1384-1386.
- Gordon PH, Frucht SJ. Neuroleptic malignant syndrome in advanced Parkinson’s disease. Mov Disord. 2001;16(5):960-962.
Case
A 67-year-old female with moderately advanced Parkinson’s disease (PD) had a mechanical fall in her home, which resulted in a humeral fracture. The fall occurred in the morning before she was able to take her medications and was related to her difficulty in initiating movements.
On her current regimen, her PD symptoms are controlled. She is able to perform daily living activities independently and ambulates without assistance. She also performs more complex tasks (e.g., cooking and managing her finances). She has not exhibited any symptoms consistent with dementia. She occasionally experiences dyspnea on exertion and dysphagia, but she has not been evaluated for these complaints. She takes carbidopa/levodopa (CD/LD) 25 mg/100 mg four times a day, amantadine 100 mg twice daily, and ropinirole 3 mg three times a day.
She is scheduled for open reduction internal fixation of her fracture; the orthopedic surgeon has requested a perioperative risk assessment and recommendations concerning her medications. How should PD be managed perioperatively?
Overview
Advances in surgical and anesthetic techniques, in combination with an aging population, have contributed to an increasing number of geriatric patients undergoing surgery. As many as 50% of Americans older than 65 will undergo a surgical procedure; hospitalists will comanage many of these patients in the perioperative period.1
Although cardiopulmonary disorders receive a great deal of attention with regard to perioperative risk assessment, other comorbid conditions also contribute to perioperative risk—namely, disorders specific to the elderly population. Parkinson’s disease is one such condition that deserves attention.
PD is a progressive, neurodegenerative condition associated with loss of dopaminergic neurons and the presence of Lewy bodies within the substantia nigra and other areas of the brain and peripheral autonomic nervous system.2 Cardinal clinical features include rigidity, bradykinesia, and resting tremor. A supportive feature is a consistent response to levodopa. Postural instability, cognitive impairment, and autonomic dysfunction usually occur later in the disease.3,4
As the population ages, Parkinson’s disease is becoming more prevalent, affecting approximately 1% of individuals older than 60.5 These patients pose a specific challenge to the hospitalist, not only because the multiorgan system manifestations of PD can raise surgical risk, but also due to the direct effects of dopaminergic medications used to treat PD, lack of a parenteral route for these medications in NPO patients, and the risks associated with abrupt withdrawal of these medications.
Although surgical risk in PD patients has received intermittent attention in surgical, anesthesia, and neurology literature, there is no broad consensus statement or treatment guideline for the perioperative approach.
Literature Review
A retrospective cohort of 51 PD patients undergoing various types of surgery revealed that PD patients have a longer hospital stay than matched cohorts.6 Pepper et al studied a cohort of 234 PD patients in the Veterans Administration population who were undergoing a variety of surgeries.7 They found that patients with PD had a longer acute hospital stay and had higher in-hospital mortality.7 The multisystem manifestations of PD might account for this global increase in perioperative risk.
The following are reviews of organ-system manifestations of PD and their relevance to the perioperative period.
Motor: The motor symptoms of PD place patients at increased risk for falls and might impair their ability to participate in rehabilitation. Mueller et al demonstrated that there was a significantly increased risk of postoperative falls and a higher need for inpatient rehabilitation due to motor difficulties in the PD cohort.6
Pulmonary: PD patients have increased risk of abnormal pulmonary function secondary to rigidity and akinesia. Increased airway resistance and decreased lung elastic recoil lead to obstructive lung disease.8,9 Rigidity of voluntary chest wall and upper airway muscles leads to a restrictive lung disease pattern.8,10 Furthermore, respiratory dyskinesia is a common side effect of levodopa, which can result in restrictive and dyskinetic ventilation.11 As a consequence of disordered respiratory mechanics (especially in combination with disordered swallow mechanics), PD patients are at increased risk of lower respiratory infections. In fact, pneumonia remains the leading cause of mortality among PD patients.11
Not surprisingly, several cohorts have suggested that PD patients undergoing surgical procedures are at higher risk for atelectasis, pneumonia, and postoperative respiratory failure.7,12 Postoperative VTE rates are not statistically different between PD patients and matched cohorts.
Gastrointestinal: Abnor-malities in muscles of the mouth, pharynx, and esophagus account for the dysphagia commonly noted in PD.13 Barium swallow tests are abnormal in 80% or more of PD patients.14 Dysphagia can lead to aspiration, as well as inadequate oral intake, resulting in pneumonia and malnutrition, respectively.15 Dysfunction of the myenteric plexus (evidenced by Lewy Body deposition) accounts for gastrointestinal dysmotility manifested as gastroparesis, ileus, and slow colonic transit, which results in constipation.16
PD patients in the postoperative period are at risk for swallowing difficulties, which increases the risk of aspiration and might delay initiation of oral medications. Gastroparesis threatens appropriate delivery of oral medications for adequate absorption. In addition, postoperative ileus and constipation can pose challenges.
Cardiovascular: Such cardiac sympathetic abnormalities as orthostatic hypotension, postprandial or exercise-induced hypotension, impaired heart rate variability, and dysrhythmias are common in PD.17 Pepper et al found a trend toward increased risk of hypotension and acute myocardial infarction (MI) in PD patients undergoing surgery.7
Genitourinary: Urinary complaints (e.g., nocturia, frequency, urgency, and urge incontinence) are common in PD patients.18 These clinical complaints correspond to involuntary detrusor contractions (detrusor hyperreflexia).19 Pepper et al found an increased risk of postoperative urinary tract infection in PD patients.7
Cognitive: A recognized feature of advanced PD is cognitive impairment. Studies estimate the prevalence of dementia in cohorts of PD patients is from 28% to 44%. PD with dementia has been associated with shortened survival, impaired quality of life, and increased caregiver distress.20 Pepper et al noted a trend toward increased incidence of postoperative delirium in their cohort of 234 PD patients undergoing surgery.7
Medication: Management of anti-Parkinsonian medications in the perioperative period poses unique challenges. These medications’ prodopaminergic effects can lead to hemodynamic compromise and are potentially arrhythmogenic. At the same time, abrupt withdrawal of these medications can lead to a potentially lethal condition called Parkinsonism-hyperpyrexia syndrome (PHS), which is clinically similar to neuroleptic malignant syndrome.21 PHS is characterized by very high fever, extreme muscle rigidity, autonomic instability, altered consciousness, and multiple severe systemic complications (e.g., acute renal failure, disseminated intravascular coagulation, autonomic failure, aspiration pneumonia, and infections). PHS occurs in up to 4% of PD patients; mortality is reported to be from 4% for treated to 20% for untreated episodes.22-24
As many as 30% of patients who survive a PHS episode have worsening of their PD symptoms and never return to their pre-PHS baseline. PHS prevention in hospitalized patients by uninterrupted administration of PD medications should be the goal. Early recognition and aggressive treatment is key to successful recovery.
Furthermore, even brief interruption of medications can lead to decompensation of Parkinsonian symptoms, which not only delays recovery from surgery, but also increases the risk for multisystem complications as discussed above.25 Traditional anti-Parkinsonian medications can only be delivered orally, presenting significant challenges for NPO patients, especially those undergoing enteric surgery requiring bowel rest.
Case reports describe various approaches to medication management in the perioperative period, but no single consensus statement (or treatment guideline) exists. The most common clinical scenarios are:
- Patient undergoes short surgery and is able to take oral medication immediately after the procedure (e.g., orthopedic, eye);
- Patient undergoes more lengthy surgery and will be able to take enteric medications perioperatively (e.g., longer orthopedic surgeries, genitourinary); and
- Patient undergoes lengthy procedure in which they will be required to adhere to bowel rest (e.g., bowel resection).
Depending on the category, the approach to medication management might differ.
Furuya et al describe a 70-year-old male with PD who had previously experienced perioperative complications associated with his medication management, including postoperative rigidity, dysphagia, and difficulty maintaining respiratory secretions.26 These symptoms were reversed with intravenous levodopa. However, the patient experienced hypotension and premature ventricular contractions as side effects of this therapy. This patient was scheduled to undergo hepatic lobectomy. Given his previous complications, Furuya et al provided enteral administration of CD/LD via nasogastric tube every two hours during the surgery, with placement of a duodenostomy for postoperative administration of CD/LD. The patient maintained hemodynamic stability throughout the perioperative period and emerged from anesthesia smoothly with no muscle rigidity or postoperative complications.26
Fujii et al described three cases of PD patients undergoing gastrointestinal surgery. They suggested that the dose of medication required to control symptoms should be minimized before surgery to avoid withdrawal symptoms. They also described the use of intravenous levodopa immediately, postoperatively, while the patient was unable to tolerate enteric medications, and suggested the use of prokinetics to prevent ileus and maximize drug absorption.27
Gálvez-Jiménez et al discuss the limitations of intravenous levodopa, including hemodynamic compromise, need for escalating doses, frequent adjustments to maintain effect, and large amount of fluids required. They propose the use of subcutaneous apomorphine, which is a potent D1/D2 dopamine agonist in conjunction with rectal domeperidone, a D2 antagonist with poor blood-brain-barrier penetration, to counteract the peripheral dopaminergic side effects. The main limitation to this approach is that domeperidone is not available in the U.S.28
Intravenous antihistamines and anticholinergics are readily available. However, they show limited efficacy in halting Parkinsonian symptoms and carry multiple side effects (e.g., confusion, delay in gastrointestinal recovery, and urinary retention).28
Various anesthesiologists agree with administering anti-PD medications immediately, preoperatively, and restarting medications as soon as possible postoperatively. However, they do not provide uniform treatment guidelines regarding specific medication management.29,30
Deep-brain-stimulation (DBS) management: DBS is an effective treatment for advanced PD. There are more than 60,000 patients around the world who have DBS for various conditions, mostly for PD. Therefore, it is increasingly likely that hospitalists will encounter hospitalized patients with advanced PD who are treated both pharmacologically and with DBS. It is important to recognize that stimulation, just like PD medications, cannot be stopped suddenly. If there is any concern of the DBS system malfunctioning (i.e., fracture of the hardware during a fall), the neurologist or neurosurgeon managing the DBS should be contacted immediately. Certain diagnostic tests (MRI) and treatment procedures (diathermy) are contraindicated, and if done inappropriately, can result in permanent brain damage.31,32,33
During surgeries requiring blood-vessel cauterization, DBS should be temporarily turned off. This can be done with the patient’s handheld device or, preferably, by a trained technician usually available through 24/7 technical support services provided by the manufacturer.
Summary of recommendations: There are no clear treatment guidelines regarding the optimal perioperative management of PD patients. The following measures are based on available data and are extensions of routine perioperative management; however, there is no evidence to demonstrate their efficacy in decreasing complication rates among patients with PD:
- A thorough preoperative history and physical examination should include Parkinsonian signs and symptoms, precise medication regimen with doses and timing of intake, effects of medication withdrawal or missed doses, type of surgery planned, and comorbid conditions;
- Depending on symptoms mentioned in the history, consider further testing for dysphagia (preoperative swallow evaluation) and dyspnea (preoperative pulmonary function tests);
- The major goal of medication management in the perioperative period is to continue administration of dopamine replacement therapy as close to the outpatient regimen as possible.
- Titrate down dose of anti-Parkinsonian medications to lowest possible dose prior to surgery if prolonged NPO status is anticipated;
- Ensure medications are administered immediately prior to surgery;
- For short, nonenteric procedures, resume outpatient medication doses and timing of administration as soon as possible postoperatively. For longer, nonenteric surgeries, consider placement of nasogastric tube for medication delivery during procedure and immediately postoperatively;
- If the major limitation of oral medication intake is dysphagia, the use of orally disintegrated formulation CD/LD (parcopa) is helpful;
- For longer enteric surgeries in which patient must be on bowel rest, recommend consultation with neurologist specialized in movement disorders to guide use of intravenous or subcutaneous agents. Transdermal delivery systems of the dopamine agonist rotigotine are in the process of being approved in the U.S. market and might be helpful for this purpose;
- Initiation of tube feeding, when co-administered with levodopa, might result in sudden changes in medication absorption and potential worsening of PD symptoms; feeding should be started slowly and preferably at night when the body’s dopamine requirements are lower;
- Consider use of promotility agents;
- If apomorphine or intravenous LD are not available, consider trial of intravenous anticholinergics or antihistamines, carefully observing for potential cognitive and behavioral side effects;
- Avoid such dopamine antagonists as droperidol, haloperidol, risperidone, metaclopramide, prochlorperazine, or promethazine, as these medications can worsen Parkinsonian symptoms; and
- If patient was on MAO-B inhibitors (selegiline, rasagiline) before surgery, be aware of multiple potential interactions with various medications that are commonly used in perioperative period, including anesthesia agents and certain analgesics, specifically meperidine. These interactions include serotonin syndrome, and can be life-threatening.34
- Psychiatric considerations: delirium precautions;
- Motor considerations: early PT/OT, early referral to inpatient rehabilitation; fall precautions;
- Pulmonary considerations: institute aggressive incentive spirometry, postural drainage, management of respiratory secretions, and breathing exercises; VTE prophylaxis;
- Gastrointestinal considerations: aspiration precautions and prompt speech therapy to evaluate for aspiration and to teach appropriate swallow techniques (chin tuck); institute aggressive bowel regimen; maximize fluids, electrolytes, and avoid narcotics to prevent precipitating or exacerbating ileus;
- Cardiovascular considerations: monitor orthostatic vital signs; fall precautions to avoid syncopal falls; and
- Genitourinary considerations: early urinary catheter removal; vigilance in monitoring for urinary tract infection.
Back to the Case
The patient underwent repair of her fracture, was extubated, and recovered from general anesthesia without incident. She was evaluated in the postanesthesia care unit, at which time she had a slight tremor and mild rigidity. She was immediately given a dose of her CD/LD, and her evening doses of amantadine and ropinirole were resumed. The patient had no significant flare of her Parkinsonian symptoms and did not exhibit any evidence of PHS.
A postoperative consultation was placed for speech therapy, physical therapy, and occupational therapy. She was given low-molecular-weight heparin for VTE prophylaxis and asked to use incentive spirometry. On postoperative day one, she complained of urinary frequency. A urinalysis was consistent with possible infection. She was discharged home on her previous medication regimen, in addition to antibiotics for cystitis.
If the procedure had not been emergent, the patient might have benefited from a preoperative swallow evaluation, given her dysphagia. Consultation with a speech therapist would have ensured that the patient was educated regarding aspiration precautions. Although this patient did not have difficulty with extubation or experience postoperative respiratory failure, abnormal preoperative pulmonary function tests might have prompted the anesthesiologists to consider alternative low-risk techniques (e.g., a local nerve block).
Bottom Line
Perioperative management of patients with Parkinson’s disease requires knowledge of the multisystem disease characteristics that raise perioperative risk and the effects of the medications used to treat PD. To date, no clear treatment guidelines exist for the optimal perioperative management of PD patients.
However, vigilance in detecting possible complications and instituting attentive perioperative care can aid a hospitalist consultant in improving overall care for these patients. TH
Dr. Patel is a medical resident at the University of Colorado Denver. Dr. Stickrath is a hospitalist at the Denver VA Medical Center and instructor of medicine at the University of Colorado Denver. Dr. Anderson is a hospitalist at the Denver VA Medical Center and assistant professor of medicine at the University of Colorado Denver. Dr. Klepitskaya is a neurologist and assistant professor of neurology at the University of Colorado Denver.
References
- Ersan T. Perioperative management of the geriatric patient. Web MD website. Available at: http://emedicine.medscape.com/article/285433-overview. Accessed May 10, 2010.
- Braak H, Del Tredici K, Rüb U, de Vos RA, Jansen Steur EN, Braak E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging. 2003;24(2):197-211.
- Ward CD, Gibb WR. Research diagnostic criteria for Parkinson’s disease. Adv Neurol. 1990;53:245-249.
- Stern MB, Koller WC. Parkinsonian Syndromes. New York: Informa Healthcare Publishing; 1993.
- Nutt JG, Wooten GF. Clinical practice. Diagnosis and initial management of Parkinson’s disease. N Engl J Med. 2005;353(10):1021-1027.
- Mueller MC, Jüptner U, Wuellner U, et al. Parkinson’s disease influences the perioperative risk profile in surgery. Langenbecks Arch Surg. 2009;394(3):511-515.
- Pepper PV, Goldstein MK. Postoperative complications in Parkinson’s disease. J Am Geriatr Soc. 1999;47(8):967-972.
- Shill H, Stacy M. Respiratory function in Parkinson’s disease. Clin Neurosci. 1998;5(2):131-135.
- Neu HC, Connolly JJ Jr., Schwertley FW, Ladwig HA, Brody AW. Obstructive respiratory dysfunction in parkinsonian patients. Ann Rev Respir Dis. 1967;95(1):33-47.
- Chokroverty S. The spectrum of ventilatory disturbances in movement disorders. In: Chokroverty S, ed. Movement Disorders. Great Neck, New York: PMA Publishing Corp.; 1990:365-392.
- Shill H, Stacy M. Respiratory complications of Parkinson’s disease. Semin Respir Crit Care Med. 2002;23(3):261-265.
- Easdown LJ, Tessler KJ, Minuk J. Upper airway involvement in Parkinson’s disease resulting in postoperative respiratory failure. Can J Anaesth. 1995;42(4):344-347.
- Pfeiffer RF. Gastrointestinal dysfunction in Parkinson’s disease. Lancet Neurol. 2003;2(2):107-116.
- Castell JA, Johnston BT, Colcher A, Li Q, Gideon RM, Castell DO. Manometric abnormalities of the oesophagus in patients with Parkinson’s disease. Neurogastroenterol Motil. 2001;13(4):361-364.
- Marcason W. What are the primary nutritional issues for a patient with Parkinson’s disease? J Am Diet Assoc. 2009;109(7):1316.
- Djaldetti R, Lev N, Melamed E. Lesions outside the CNS in Parkinson’s disease. Mov Disord. 2009;24(6):793-800.
- Orimo S, Takahashi A, Uchihara T, Mori F, Kakita A, Wakabayashi K, Takahashi H. Degeneration of cardiac sympathetic nerve begins in the early disease process of Parkinson’s disease. Brain Pathol. 2007;17(1):24-30.
- Lemack GE, Dewey RB Jr., Roehrborn CG, O’Suilleabhain PE, Zimmern PE. Questionnaire-based assessment of bladder dysfunction in patients with mild to moderate Parkinson’s disease. Urology. 2000;56(2):250-254.
- Singer C. Urinary dysfunction in Parkinson’s disease. Clin Neurosci. 1998;5(2):78-86.
- Leverenz JB, Quinn JF, Zabetian C, Zhang J, Montine KS, Montine TJ. Cognitive impairment and dementia in patients with Parkinson disease. Curr Top Med Chem. 2009;9(10):903-912.
- Factor SA, Santiago A. Parkinson-hyperpyrexia syndrome in Parkinson’s disease. In: Frucht S, Fahn S, eds. Movement Disorder Emergencies: Diagnosis and Treatment. New York: Humana Press; 2005:29-40.
- Reed AP, Han DG: Intraoperative exacerbation of Parkinson’s disease. Anesth Analg. 1992;75(5):850-853.
- Harada T, Mitsuoka K, Kumagai R, et al. Clinical features of malignant syndrome in Parkinson’s disease and related neurological disorders. Parkinsonism Relat Disord. 2003;9(Suppl 1):S15-23.
- Onofrj M, Thomas A. Acute akinesia in Parkinson disease. Neurology. 2005;64(7):1162-1169.
- Serrano-Dueñas M. Neuroleptic malignant syndrome-like, or—dopaminergic malignant syndrome—due to levodopa therapy withdrawal. Clinical features in 11 patients. Parkinsonism Relat Disord. 2003;9(3):175-178.
- Furuya R, Hirai A, Andoh T, Kudoh I, Okumura F. Successful perioperative management of a patient with Parkinson’s disease by enteral levodopa administration under propofol anesthesia. Anesthesiology. 1998;89(1):261-263.
- Fujii T, Nakabayashi T, Hashimoto S, Kuwano H. Successful perioperative management of patients with Parkinson’s disease following gastrointestinal surgery: report of three cases. Surg Today. 2009;39(9):807-810.
- Gálvez-Jiménez N, Lang AE. The perioperative management of Parkinson’s disease revisited. Neurol Clin. 2004;22(2):367-377.
- Kalenka A, Schwarz A. Anasthesia and Parkinson’s disease: how to manage with new therapies? Curr Opin Anesthesiol. 2009;22(3):419-424.
- Nicholson G, Pereira AC, Hall GM. Parkinson’s disease and anesthesia. Br J Anaesthesia. 2002;89(6):904-916.
- Rezai AR, Baker KB, Tkach JA, et al. Is magnetic resonance imaging safe for patients with neurostimulation systems used for deep brain stimulation? Neurosurgery. 2005:57(5):1056-1062.
- Henderson JM, Tkach J, Phillips M, Baker K, Shellock FG, Rezai AR. Permanent neurological deficit related to magnetic resonance imaging in a patient with implanted deep brain stimulation electrodes for Parkinson’s disease: case report. Neurosurgery. 2005:57(5):E1063.
- Nutt JG, Anderson VC, Peacock JH, Hammerstad JP, Burchiel KJ. DBS and diathermy interaction induces severe CNS damage. Neurology. 2001;56 (10):1384-1386.
- Gordon PH, Frucht SJ. Neuroleptic malignant syndrome in advanced Parkinson’s disease. Mov Disord. 2001;16(5):960-962.
In the Literature: HM-Related Research You Need to Know
In This Edition:
- Catheter ablation for atrial fibrillation
- Noncontrast CT for appendicitis diagnosis
- Effectiveness of whole-leg ultrasound for DVT diagnosis
- Physician localization and nurse-physician communication
- PPI versus H2 blocker in patients with aspirin-related peptic ulcer disease
- Intensive insulin therapy in steroid-induced hyperglycemia associated with septic shock
- S. aureus decolonization and surgical-site infections
- ABCD2 score and risk of subsequent stroke
Catheter Ablation of Paroxysmal AF Might Be More Effective than Antiarrhythmic Therapy
Clinical question: In patients with paroxysmal atrial fibrillation (AF) unresponsive to initial antiarrhythmic therapy, what is the efficacy of catheter ablation compared with continued attempts at rhythm control?
Background: Although antiarrhythmic drug therapy (ADT) is generally first-line AF therapy, AF recurrence is high and treatment is associated with adverse effects. Catheter ablation is an alternative treatment. Recent studies comparing antiarrhythmic drugs and catheter ablation have involved small populations and have shown mixed results.
Study design: Prospective, multicenter, unblinded, randomized trial.
Setting: Nineteen hospitals—15 in the U.S.—with considerable experience in AF ablation.
Synopsis: This trial compared catheter ablation (n=106) vs. ADT (n=61) for symptomatic, paroxysmal AF refractory to at least one antiarrhythmic drug. Patients in the ablation arm were allowed up to three procedures within an 80-day period; patients in the ADT arm were treated with a previously unused class I or class III antiarrhythmic. After nine months, 34% of ablated patients had failed treatment compared with 84% of patients receiving ADT (HR 0.30 [95% CI, 0.19-0.47]).
While the results are encouraging, some limitations should be noted. Attempts to generalize the results of this study might be limited, as the hospitals had considerable experience in AF ablation, the patient population was relatively young (mean age=56 years), and patients with significant left ventrical dysfunction and persistent AF were excluded.
Furthermore, the long-term effectiveness of ablation was not evaluated, and the study did not assess such outcomes as mortality, stroke, or AF progression. The effectiveness of specific ablation techniques could not be determined because a variety of approaches was employed.
Bottom line: Patients with symptomatic paroxysmal AF without advanced heart failure might benefit from catheter ablation at experienced institutions.
Citation: Wilber DJ, Pappone C, Neuzil P, et al. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA. 2010;303(4):333-340.
Noncontrast CT Can Be Used to Evaluate Suspected Appendicitis
Clinical question: What is the diagnostic accuracy of noncontrast helical CT in the evaluation of suspected acute appendicitis in the ED?
Background: In the workup of acute appendicitis, various CT protocols are used, including combinations of oral, intravenous, and rectal contrast, as well as noncontrast protocols. Noncontrast CT is less time-consuming and avoids risk of allergic reaction or contrast-induced nephropathy. The diagnostic accuracy of noncontrast CT, however, is controversial.
Study design: Systematic review/meta-analysis.
Setting: Seven studies evaluating acute appendicitis with noncontrast CT in ED settings.
Synopsis: This is the first systematic review of noncontrast CT (helical/multislice) in adults with suspected appendicitis. The authors pooled seven studies (1,060 patients) comparing noncontrast CT with a reference standard of final diagnosis at surgery or followup at a minimum of two weeks. The review yielded the following pooled estimates: sensitivity 93%, specificity 96%, positive likelihood ratio 24, and negative likelihood ratio 0.08. Overall, the diagnostic accuracy of noncontrast CT was high.
A few limitations should be noted. In the original studies, results were reported inconsistently. In one study, 24% of scans were inconclusive, with an associated likelihood ratio of approximately 1. Future studies must address this important clinical question of how to treat patients with inconclusive scans. Another question is to what degree the accuracy reported in this study reflects the expertise of the institutions, the majority of which were university-affiliated. According to one study author, “a certain level of experience is required for skillful interpretation” of noncontrast CT.
Bottom line: Noncontrast CT has a high sensitivity and specificity for acute appendicitis, and should be considered an alternative to contrast CT, particularly in patients with contraindications to contrast or those at risk of contrast-induced nephropathy.
Citation: Hlibczuk V, Dattaro JA, Jin Z, Falzon L, Brown MD. Diagnostic accuracy of noncontrast computed tomography for appendicitis in adults: a systematic review. Ann Emerg Med. 2010;55(1):51-59.e1.
Whole-Leg Compression Ultrasound for DVT Has a Low Failure Rate in Outpatients
Clinical question: How useful is compression ultrasound (CUS) for diagnosing distal DVT?
Background: CUS can reliably evaluate proximal DVT, but its accuracy for distal DVT is controversial. Because of the risk of extension of distal DVT (up to 25%), guidelines recommend that some patients undergo serial proximal CUS after an initial negative result. As an alternative, recent studies have evaluated one-time, whole-leg CUS.
Study design: Systematic review and meta-analysis.
Setting: Review of randomized controlled trials and prospective cohort studies.
Synopsis: The study pooled data from seven studies and more than 4,700 patients with suspected DVT for whom anticoagulation was withheld after a single, negative, whole-leg CUS. At the three-month followup, the combined symptomatic VTE event rate was 0.57%, and the authors concluded that withholding anticoagulation was associated with a low VTE risk.
Although encouraging, this study had several limitations. First, whole-leg CUS is not widely performed or standardized, and the CUS technique varied slightly across the studies. Second, any attempt to generalize the results of this study might be limited, as the proportion of pregnant patients and those with malignancy was low. Furthermore, only one of the seven studies included inpatients that might be at higher VTE risk. Third, pre-test probability was assessed for only a subset of patients, limiting assessment of VTE by risk level. For example, the overall finding of the study—an event rate of 0.57%—appears low but is difficult to apply clinically when subset analyses for high-risk patients yielded a VTE rate of 2.5% with wide confidence intervals ranging from 0% to 7%.
Bottom line: Whole-leg CUS might be a practical alternative to serial proximal CUS, but more data incorporating pre-test probabilities and involving more inpatients are needed. Hospitalists should be cautious in applying pooled summary estimates.
Citation: Johnson SA, Stevens SM, Woller SC, et al. Risk of deep vein thrombosis following a single negative whole-leg compression ultrasound: a systematic review and meta-analysis. JAMA. 2010;303(5):438-445.
Localization of Inpatient Physicians on Hospital Units Increases Provider Communication Frequency
Clinical question: Does localization of inpatient physicians on hospital units improve communication with nursing staff?
Background: While nurses are typically localized on a hospital unit, inpatient physicians often care for patients on multiple units. This lack of regionalization makes it difficult for physicians and nurses to discuss care plans directly. No prior research has evaluated the effect of physician localization on nurse-physician communication.
Study design: Cross-sectional, pre- and postintervention study.
Setting: Tertiary-care teaching hospital, general medical service.
Synopsis: The study was a cross-sectional survey of nurses and physicians prelocalization (n=342 patients) and postlocalization (n=294 patients) of physicians on hospital units. Localization was associated with increased frequency of communication; however, it did not improve the consistency of nurse-physician agreement on the care plan. Nurse-physician agreement was improved on two aspects of the care plan—planned tests and anticipated length of stay—but not on primary diagnosis, planned procedures, medication changes, or consultations.
Limitations of the study were that it was conducted at a single teaching hospital, communication patterns might have changed during the year between pre- and postlocalization, and physicians were not completely localized to specific units (73% localization).
Despite the limitations, this study is the first to evaluate staff localization and communication on a general medical service. The findings suggest that localization is a first step toward interdisciplinary communication. It also shows that quality and content of communication require further assessment.
Future studies must assess the impact of communication on the quality of patient care.
Bottom line: Physician localization improved the frequency of nurse-physician dialogue but did not consistently facilitate a shared understanding of the care plan. Although not assessed in this study, the implication is that the quality of communication between providers needs improvement.
Citation: O’Leary KJ, Wayne DB, Landler MP, et al. J Gen Int Med. 2009;24(11):1223-1227.
Pantoprazole Better than Double-Dose Famotidine in Secondary Prevention of Aspirin-Related Injury
Clinical question: Is a twice-daily H2-receptor antagonist (H2RA) or a once-daily proton pump inhibitor (PPI) better in patients who must continue low-dose-aspirin therapy despite aspirin-related peptic ulcer disease?
Background: Some patients with aspirin-related peptic ulcer disease require continued aspirin therapy. It often is assumed that PPIs are superior to H2RAs in secondary prevention of low-dose aspirin-related injury, although no randomized trials have specifically addressed this question.
Study design: A prospective, double-blind, randomized controlled trial.
Setting: A university hospital in Hong Kong.
Synopsis: In this trial, 160 patients with aspirin-related peptic ulcers/erosions were randomized to 48 weeks of oral famotidine (40 mg twice daily) or pantoprazole (20 mg daily) after mucosal healing and eradication of H pylori. During this time, all patients continued to receive aspirin (80 mg daily).
The rates of recurrent dyspeptic or bleeding ulcers/erosions within 48 weeks were 20% with famotidine versus 0% with pantoprazole. The rates of gastrointestinal (GI) bleeding alone were 7.7% versus 0%, respectively.
Of note, none of the five patients with GI bleeding had significant dyspepsia, which is consistent with prior reports that NSAID-induced injury might be silent.
Overall, high-dose famotidine was inferior to pantoprazole in the prevention of recurrent aspirin-related injury. These findings support the ACCF/ACG/AHA 2008 recommendation of PPIs over double-dose H2RAs in this clinical setting. It is not known, however, whether the PPI strategy extends to average GI-risk patients taking aspirin.
Furthermore, although not demonstrated in this study, it is possible that the lower rates of dyspepsia with pantoprazole might facilitate adherence to prolonged aspirin therapy.
Bottom line: High-dose famotidine was inferior to pantoprazole in the prevention of recurrent low-dose-aspirin-related injury.
Citation: Ng FH, Wong SY, Lam KF, et al. Famotidine is inferior to pantoprazole in preventing recurrence of aspirin-related peptic ulcers or erosions. Gastroenterology. 2010;138
(1):82-88.
Intensive Insulin Therapy Is Not Beneficial in Corticosteroid-Induced Hyperglycemia Associated with Septic Shock
Clinical question: In septic shock treated with hydrocortisone, does intensive insulin therapy reduce in-hospital mortality compared with conventional glucose management?
Background: Corticosteroids might benefit patients with septic shock, but they also can exacerbate illness-induced hyperglycemia. It is hypothesized that normalization of blood glucose with intensive insulin might improve outcomes in these patients.
Study design: A multicenter, 2x2 factorial, randomized controlled trial.
Setting: Eleven ICUs in France.
Synopsis: In this 2x2 factorial comparison, 509 patients with septic shock treated with hydrocortisone were randomized to IV insulin, conventional insulin, fludrocortisone plus IV insulin, and fludrocortisone plus conventional insulin. The primary objective was to assess intensive IV versus conventional insulin, and a secondary objective was to assess the benefit of adding fludrocortisone to hydrocortisone therapy.
Overall, analysis showed no difference in in-hospital mortality in either of the two comparisons.
These null findings should be interpreted considering the following study limitations. In the intensive-insulin groups, there was a failure to reach target glucose levels of 80 mg/dL to 110 mg/dL (mean achieved levels 120 mg/dL to 130 mg/dL and higher). These levels overlapped to some degree with the control group, which targeted glucose levels <150 mg/dL and achieved mean levels of 140 mg/dL to 150 mg/dL.
The lack of substantial difference in glucose levels might have contributed to the null findings. Furthermore, the absolute risk reduction in the original sample-size calculations was overestimated. The result was an underpowered study, which also might have contributed to the null findings.
Bottom line: In septic shock treated with hydrocortisone, the optimal blood-glucose level and insulin strategy are unknown.
Citation: Annane D, Cariou A, Maxime V, et al. Corticosteroid treatment and intensive insulin therapy for septic shock in adults: a randomized controlled trial. JAMA. 2010;303(4):341-348.
Mupirocin-Chlorhexidine Decolonization of Nasal S. Aureus Carriers Reduces Surgical-Site Infections
Clinical question: Can rapid screening and decolonization of nasal carriers of Staphylococcus aureus on admission reduce surgical-site S. aureus infections?
Background: More than 80% of healthcare-associated (HCA) S. aureus infections are endogenous in origin. High-level nasal carriers have a three- to sixfold increased risk of infection with this organism compared with noncarriers and low-level carriers. Decolonization of nasal and extranasal S. aureus on admission might reduce this risk of infection.
Study design: Randomized, double-blinded, placebo-controlled, multicenter trial.
Setting: Three university hospitals and two general hospitals in the Netherlands.
Synopsis: In this study, 918 mostly surgical patients with nasal S. aureus identified preoperatively by PCR tests were randomized to decolonization versus placebo. The five-day decolonization protocol involved mupirocin nasal ointment and chlorhexidine soap baths. Decolonization reduced length of stay by nearly two days. Through six weeks postdischarge, the cumulative incidence of S. aureus infection was 3.4% after decolonization versus 7.7% with placebo (RR 0.42; 95% CI, 0.23-0.75). Among the sites of infection, deep surgical sites had the greatest risk reduction (RR 0.21; 95% CI, 0.07-0.62).
The results of this study are encouraging, but a few limitations should be noted. The decolonization protocol lasted five days, which might make implementation less practical. Also, the relative contributions of mupirocin and chlorhexidine are unclear.
S. aureus is important, but it represents a minority of surgical-site infections; the effect of the protocol on other organisms is unknown. Lastly, MRSA is not prevalent in the Netherlands and no carriers were identified in the study. Although the protocol was designed to eradicate MRSA, such carriers might have different carriage patterns requiring throat swabs in addition to nasal swabs.
Bottom line: Preoperative detection of S. aureus nasal carriage and nasal and extranasal decolonization significantly reduced endogenous S. aureus infection and length of stay. Decolonization might be most beneficial for carriers at increased risk of deep infection, such as those undergoing cardiac surgery.
Citation: Bode LG, Kluytmans JA, Wertheim HF, et al. Preventing surgical-site infections in nasal carriers of Staphylococcus aureus. N Engl J Med. 2010;362(1):9-17.
ABCD2 Is a Poor Predictor of Early Ischemic Stroke after Transient Ischemic Attack
Clinical question: How well does the ABCD2 score predict stroke risk within seven days of transient ischemic attack (TIA)?
Background: After TIA diagnosis, the seven-day risk of ischemic stroke is approximately 5%. Identifying these high-risk patients might facilitate ED decision-making. The ABCD2 score, a prediction tool for stroke after TIA, might be useful but has not been prospectively validated in a large, broad-patient population.
Study design: Prospective validation study, convenience sample.
Setting: Sixteen hospitals in North Carolina.
Synopsis: The ABCD2 score (range 0-7 points) predicts stroke risk after TIA. The investigators evaluated the accuracy of ABCD2 in predicting seven-day ischemic stroke risk in a convenience sample of 1,667 TIA patients. Strokes were categorized as disabling or nondisabling.
Overall, the score was poorly predictive of all ischemic stroke (c stat 0.59) and moderately predictive of the subset of disabling ischemic stroke (c stat 0.71). The ABCD2 had the most discriminatory power when used to identify patients at low risk of disabling stroke (0-3 points); for these patients, the negative likelihood ratio (LR) was 0.16 (0.04-0.64).
The study is the largest published external-validation study of the ABCD2 score, but it had significant limitations that should be considered. There was potential sampling bias because of nonconsecutive sampling, and unaccounted patients with TIA were discharged from the ED. Furthermore, ABCD2 scores were incalculable for 35% of patients, although the authors report that imputed data did not change the findings significantly.
Bottom line: The ABCD2 score does not sufficiently predict the seven-day risk of ischemic stroke after TIA. Further validation studies are needed.
Citation: Asimos AW, Johnson AM, Rosamond WD, et al. A multicenter evaluation of the ABCD2 score’s accuracy for predicting early ischemic stroke in admitted patients with transient ischemic attack. Ann Emerg Med. 2010;55(2):201-210.e5. TH
Dr. Kim is a hospitalist at Brigham and Women’s Hospital in Boston, and an instructor at Harvard Medical School.
In This Edition:
- Catheter ablation for atrial fibrillation
- Noncontrast CT for appendicitis diagnosis
- Effectiveness of whole-leg ultrasound for DVT diagnosis
- Physician localization and nurse-physician communication
- PPI versus H2 blocker in patients with aspirin-related peptic ulcer disease
- Intensive insulin therapy in steroid-induced hyperglycemia associated with septic shock
- S. aureus decolonization and surgical-site infections
- ABCD2 score and risk of subsequent stroke
Catheter Ablation of Paroxysmal AF Might Be More Effective than Antiarrhythmic Therapy
Clinical question: In patients with paroxysmal atrial fibrillation (AF) unresponsive to initial antiarrhythmic therapy, what is the efficacy of catheter ablation compared with continued attempts at rhythm control?
Background: Although antiarrhythmic drug therapy (ADT) is generally first-line AF therapy, AF recurrence is high and treatment is associated with adverse effects. Catheter ablation is an alternative treatment. Recent studies comparing antiarrhythmic drugs and catheter ablation have involved small populations and have shown mixed results.
Study design: Prospective, multicenter, unblinded, randomized trial.
Setting: Nineteen hospitals—15 in the U.S.—with considerable experience in AF ablation.
Synopsis: This trial compared catheter ablation (n=106) vs. ADT (n=61) for symptomatic, paroxysmal AF refractory to at least one antiarrhythmic drug. Patients in the ablation arm were allowed up to three procedures within an 80-day period; patients in the ADT arm were treated with a previously unused class I or class III antiarrhythmic. After nine months, 34% of ablated patients had failed treatment compared with 84% of patients receiving ADT (HR 0.30 [95% CI, 0.19-0.47]).
While the results are encouraging, some limitations should be noted. Attempts to generalize the results of this study might be limited, as the hospitals had considerable experience in AF ablation, the patient population was relatively young (mean age=56 years), and patients with significant left ventrical dysfunction and persistent AF were excluded.
Furthermore, the long-term effectiveness of ablation was not evaluated, and the study did not assess such outcomes as mortality, stroke, or AF progression. The effectiveness of specific ablation techniques could not be determined because a variety of approaches was employed.
Bottom line: Patients with symptomatic paroxysmal AF without advanced heart failure might benefit from catheter ablation at experienced institutions.
Citation: Wilber DJ, Pappone C, Neuzil P, et al. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA. 2010;303(4):333-340.
Noncontrast CT Can Be Used to Evaluate Suspected Appendicitis
Clinical question: What is the diagnostic accuracy of noncontrast helical CT in the evaluation of suspected acute appendicitis in the ED?
Background: In the workup of acute appendicitis, various CT protocols are used, including combinations of oral, intravenous, and rectal contrast, as well as noncontrast protocols. Noncontrast CT is less time-consuming and avoids risk of allergic reaction or contrast-induced nephropathy. The diagnostic accuracy of noncontrast CT, however, is controversial.
Study design: Systematic review/meta-analysis.
Setting: Seven studies evaluating acute appendicitis with noncontrast CT in ED settings.
Synopsis: This is the first systematic review of noncontrast CT (helical/multislice) in adults with suspected appendicitis. The authors pooled seven studies (1,060 patients) comparing noncontrast CT with a reference standard of final diagnosis at surgery or followup at a minimum of two weeks. The review yielded the following pooled estimates: sensitivity 93%, specificity 96%, positive likelihood ratio 24, and negative likelihood ratio 0.08. Overall, the diagnostic accuracy of noncontrast CT was high.
A few limitations should be noted. In the original studies, results were reported inconsistently. In one study, 24% of scans were inconclusive, with an associated likelihood ratio of approximately 1. Future studies must address this important clinical question of how to treat patients with inconclusive scans. Another question is to what degree the accuracy reported in this study reflects the expertise of the institutions, the majority of which were university-affiliated. According to one study author, “a certain level of experience is required for skillful interpretation” of noncontrast CT.
Bottom line: Noncontrast CT has a high sensitivity and specificity for acute appendicitis, and should be considered an alternative to contrast CT, particularly in patients with contraindications to contrast or those at risk of contrast-induced nephropathy.
Citation: Hlibczuk V, Dattaro JA, Jin Z, Falzon L, Brown MD. Diagnostic accuracy of noncontrast computed tomography for appendicitis in adults: a systematic review. Ann Emerg Med. 2010;55(1):51-59.e1.
Whole-Leg Compression Ultrasound for DVT Has a Low Failure Rate in Outpatients
Clinical question: How useful is compression ultrasound (CUS) for diagnosing distal DVT?
Background: CUS can reliably evaluate proximal DVT, but its accuracy for distal DVT is controversial. Because of the risk of extension of distal DVT (up to 25%), guidelines recommend that some patients undergo serial proximal CUS after an initial negative result. As an alternative, recent studies have evaluated one-time, whole-leg CUS.
Study design: Systematic review and meta-analysis.
Setting: Review of randomized controlled trials and prospective cohort studies.
Synopsis: The study pooled data from seven studies and more than 4,700 patients with suspected DVT for whom anticoagulation was withheld after a single, negative, whole-leg CUS. At the three-month followup, the combined symptomatic VTE event rate was 0.57%, and the authors concluded that withholding anticoagulation was associated with a low VTE risk.
Although encouraging, this study had several limitations. First, whole-leg CUS is not widely performed or standardized, and the CUS technique varied slightly across the studies. Second, any attempt to generalize the results of this study might be limited, as the proportion of pregnant patients and those with malignancy was low. Furthermore, only one of the seven studies included inpatients that might be at higher VTE risk. Third, pre-test probability was assessed for only a subset of patients, limiting assessment of VTE by risk level. For example, the overall finding of the study—an event rate of 0.57%—appears low but is difficult to apply clinically when subset analyses for high-risk patients yielded a VTE rate of 2.5% with wide confidence intervals ranging from 0% to 7%.
Bottom line: Whole-leg CUS might be a practical alternative to serial proximal CUS, but more data incorporating pre-test probabilities and involving more inpatients are needed. Hospitalists should be cautious in applying pooled summary estimates.
Citation: Johnson SA, Stevens SM, Woller SC, et al. Risk of deep vein thrombosis following a single negative whole-leg compression ultrasound: a systematic review and meta-analysis. JAMA. 2010;303(5):438-445.
Localization of Inpatient Physicians on Hospital Units Increases Provider Communication Frequency
Clinical question: Does localization of inpatient physicians on hospital units improve communication with nursing staff?
Background: While nurses are typically localized on a hospital unit, inpatient physicians often care for patients on multiple units. This lack of regionalization makes it difficult for physicians and nurses to discuss care plans directly. No prior research has evaluated the effect of physician localization on nurse-physician communication.
Study design: Cross-sectional, pre- and postintervention study.
Setting: Tertiary-care teaching hospital, general medical service.
Synopsis: The study was a cross-sectional survey of nurses and physicians prelocalization (n=342 patients) and postlocalization (n=294 patients) of physicians on hospital units. Localization was associated with increased frequency of communication; however, it did not improve the consistency of nurse-physician agreement on the care plan. Nurse-physician agreement was improved on two aspects of the care plan—planned tests and anticipated length of stay—but not on primary diagnosis, planned procedures, medication changes, or consultations.
Limitations of the study were that it was conducted at a single teaching hospital, communication patterns might have changed during the year between pre- and postlocalization, and physicians were not completely localized to specific units (73% localization).
Despite the limitations, this study is the first to evaluate staff localization and communication on a general medical service. The findings suggest that localization is a first step toward interdisciplinary communication. It also shows that quality and content of communication require further assessment.
Future studies must assess the impact of communication on the quality of patient care.
Bottom line: Physician localization improved the frequency of nurse-physician dialogue but did not consistently facilitate a shared understanding of the care plan. Although not assessed in this study, the implication is that the quality of communication between providers needs improvement.
Citation: O’Leary KJ, Wayne DB, Landler MP, et al. J Gen Int Med. 2009;24(11):1223-1227.
Pantoprazole Better than Double-Dose Famotidine in Secondary Prevention of Aspirin-Related Injury
Clinical question: Is a twice-daily H2-receptor antagonist (H2RA) or a once-daily proton pump inhibitor (PPI) better in patients who must continue low-dose-aspirin therapy despite aspirin-related peptic ulcer disease?
Background: Some patients with aspirin-related peptic ulcer disease require continued aspirin therapy. It often is assumed that PPIs are superior to H2RAs in secondary prevention of low-dose aspirin-related injury, although no randomized trials have specifically addressed this question.
Study design: A prospective, double-blind, randomized controlled trial.
Setting: A university hospital in Hong Kong.
Synopsis: In this trial, 160 patients with aspirin-related peptic ulcers/erosions were randomized to 48 weeks of oral famotidine (40 mg twice daily) or pantoprazole (20 mg daily) after mucosal healing and eradication of H pylori. During this time, all patients continued to receive aspirin (80 mg daily).
The rates of recurrent dyspeptic or bleeding ulcers/erosions within 48 weeks were 20% with famotidine versus 0% with pantoprazole. The rates of gastrointestinal (GI) bleeding alone were 7.7% versus 0%, respectively.
Of note, none of the five patients with GI bleeding had significant dyspepsia, which is consistent with prior reports that NSAID-induced injury might be silent.
Overall, high-dose famotidine was inferior to pantoprazole in the prevention of recurrent aspirin-related injury. These findings support the ACCF/ACG/AHA 2008 recommendation of PPIs over double-dose H2RAs in this clinical setting. It is not known, however, whether the PPI strategy extends to average GI-risk patients taking aspirin.
Furthermore, although not demonstrated in this study, it is possible that the lower rates of dyspepsia with pantoprazole might facilitate adherence to prolonged aspirin therapy.
Bottom line: High-dose famotidine was inferior to pantoprazole in the prevention of recurrent low-dose-aspirin-related injury.
Citation: Ng FH, Wong SY, Lam KF, et al. Famotidine is inferior to pantoprazole in preventing recurrence of aspirin-related peptic ulcers or erosions. Gastroenterology. 2010;138
(1):82-88.
Intensive Insulin Therapy Is Not Beneficial in Corticosteroid-Induced Hyperglycemia Associated with Septic Shock
Clinical question: In septic shock treated with hydrocortisone, does intensive insulin therapy reduce in-hospital mortality compared with conventional glucose management?
Background: Corticosteroids might benefit patients with septic shock, but they also can exacerbate illness-induced hyperglycemia. It is hypothesized that normalization of blood glucose with intensive insulin might improve outcomes in these patients.
Study design: A multicenter, 2x2 factorial, randomized controlled trial.
Setting: Eleven ICUs in France.
Synopsis: In this 2x2 factorial comparison, 509 patients with septic shock treated with hydrocortisone were randomized to IV insulin, conventional insulin, fludrocortisone plus IV insulin, and fludrocortisone plus conventional insulin. The primary objective was to assess intensive IV versus conventional insulin, and a secondary objective was to assess the benefit of adding fludrocortisone to hydrocortisone therapy.
Overall, analysis showed no difference in in-hospital mortality in either of the two comparisons.
These null findings should be interpreted considering the following study limitations. In the intensive-insulin groups, there was a failure to reach target glucose levels of 80 mg/dL to 110 mg/dL (mean achieved levels 120 mg/dL to 130 mg/dL and higher). These levels overlapped to some degree with the control group, which targeted glucose levels <150 mg/dL and achieved mean levels of 140 mg/dL to 150 mg/dL.
The lack of substantial difference in glucose levels might have contributed to the null findings. Furthermore, the absolute risk reduction in the original sample-size calculations was overestimated. The result was an underpowered study, which also might have contributed to the null findings.
Bottom line: In septic shock treated with hydrocortisone, the optimal blood-glucose level and insulin strategy are unknown.
Citation: Annane D, Cariou A, Maxime V, et al. Corticosteroid treatment and intensive insulin therapy for septic shock in adults: a randomized controlled trial. JAMA. 2010;303(4):341-348.
Mupirocin-Chlorhexidine Decolonization of Nasal S. Aureus Carriers Reduces Surgical-Site Infections
Clinical question: Can rapid screening and decolonization of nasal carriers of Staphylococcus aureus on admission reduce surgical-site S. aureus infections?
Background: More than 80% of healthcare-associated (HCA) S. aureus infections are endogenous in origin. High-level nasal carriers have a three- to sixfold increased risk of infection with this organism compared with noncarriers and low-level carriers. Decolonization of nasal and extranasal S. aureus on admission might reduce this risk of infection.
Study design: Randomized, double-blinded, placebo-controlled, multicenter trial.
Setting: Three university hospitals and two general hospitals in the Netherlands.
Synopsis: In this study, 918 mostly surgical patients with nasal S. aureus identified preoperatively by PCR tests were randomized to decolonization versus placebo. The five-day decolonization protocol involved mupirocin nasal ointment and chlorhexidine soap baths. Decolonization reduced length of stay by nearly two days. Through six weeks postdischarge, the cumulative incidence of S. aureus infection was 3.4% after decolonization versus 7.7% with placebo (RR 0.42; 95% CI, 0.23-0.75). Among the sites of infection, deep surgical sites had the greatest risk reduction (RR 0.21; 95% CI, 0.07-0.62).
The results of this study are encouraging, but a few limitations should be noted. The decolonization protocol lasted five days, which might make implementation less practical. Also, the relative contributions of mupirocin and chlorhexidine are unclear.
S. aureus is important, but it represents a minority of surgical-site infections; the effect of the protocol on other organisms is unknown. Lastly, MRSA is not prevalent in the Netherlands and no carriers were identified in the study. Although the protocol was designed to eradicate MRSA, such carriers might have different carriage patterns requiring throat swabs in addition to nasal swabs.
Bottom line: Preoperative detection of S. aureus nasal carriage and nasal and extranasal decolonization significantly reduced endogenous S. aureus infection and length of stay. Decolonization might be most beneficial for carriers at increased risk of deep infection, such as those undergoing cardiac surgery.
Citation: Bode LG, Kluytmans JA, Wertheim HF, et al. Preventing surgical-site infections in nasal carriers of Staphylococcus aureus. N Engl J Med. 2010;362(1):9-17.
ABCD2 Is a Poor Predictor of Early Ischemic Stroke after Transient Ischemic Attack
Clinical question: How well does the ABCD2 score predict stroke risk within seven days of transient ischemic attack (TIA)?
Background: After TIA diagnosis, the seven-day risk of ischemic stroke is approximately 5%. Identifying these high-risk patients might facilitate ED decision-making. The ABCD2 score, a prediction tool for stroke after TIA, might be useful but has not been prospectively validated in a large, broad-patient population.
Study design: Prospective validation study, convenience sample.
Setting: Sixteen hospitals in North Carolina.
Synopsis: The ABCD2 score (range 0-7 points) predicts stroke risk after TIA. The investigators evaluated the accuracy of ABCD2 in predicting seven-day ischemic stroke risk in a convenience sample of 1,667 TIA patients. Strokes were categorized as disabling or nondisabling.
Overall, the score was poorly predictive of all ischemic stroke (c stat 0.59) and moderately predictive of the subset of disabling ischemic stroke (c stat 0.71). The ABCD2 had the most discriminatory power when used to identify patients at low risk of disabling stroke (0-3 points); for these patients, the negative likelihood ratio (LR) was 0.16 (0.04-0.64).
The study is the largest published external-validation study of the ABCD2 score, but it had significant limitations that should be considered. There was potential sampling bias because of nonconsecutive sampling, and unaccounted patients with TIA were discharged from the ED. Furthermore, ABCD2 scores were incalculable for 35% of patients, although the authors report that imputed data did not change the findings significantly.
Bottom line: The ABCD2 score does not sufficiently predict the seven-day risk of ischemic stroke after TIA. Further validation studies are needed.
Citation: Asimos AW, Johnson AM, Rosamond WD, et al. A multicenter evaluation of the ABCD2 score’s accuracy for predicting early ischemic stroke in admitted patients with transient ischemic attack. Ann Emerg Med. 2010;55(2):201-210.e5. TH
Dr. Kim is a hospitalist at Brigham and Women’s Hospital in Boston, and an instructor at Harvard Medical School.
In This Edition:
- Catheter ablation for atrial fibrillation
- Noncontrast CT for appendicitis diagnosis
- Effectiveness of whole-leg ultrasound for DVT diagnosis
- Physician localization and nurse-physician communication
- PPI versus H2 blocker in patients with aspirin-related peptic ulcer disease
- Intensive insulin therapy in steroid-induced hyperglycemia associated with septic shock
- S. aureus decolonization and surgical-site infections
- ABCD2 score and risk of subsequent stroke
Catheter Ablation of Paroxysmal AF Might Be More Effective than Antiarrhythmic Therapy
Clinical question: In patients with paroxysmal atrial fibrillation (AF) unresponsive to initial antiarrhythmic therapy, what is the efficacy of catheter ablation compared with continued attempts at rhythm control?
Background: Although antiarrhythmic drug therapy (ADT) is generally first-line AF therapy, AF recurrence is high and treatment is associated with adverse effects. Catheter ablation is an alternative treatment. Recent studies comparing antiarrhythmic drugs and catheter ablation have involved small populations and have shown mixed results.
Study design: Prospective, multicenter, unblinded, randomized trial.
Setting: Nineteen hospitals—15 in the U.S.—with considerable experience in AF ablation.
Synopsis: This trial compared catheter ablation (n=106) vs. ADT (n=61) for symptomatic, paroxysmal AF refractory to at least one antiarrhythmic drug. Patients in the ablation arm were allowed up to three procedures within an 80-day period; patients in the ADT arm were treated with a previously unused class I or class III antiarrhythmic. After nine months, 34% of ablated patients had failed treatment compared with 84% of patients receiving ADT (HR 0.30 [95% CI, 0.19-0.47]).
While the results are encouraging, some limitations should be noted. Attempts to generalize the results of this study might be limited, as the hospitals had considerable experience in AF ablation, the patient population was relatively young (mean age=56 years), and patients with significant left ventrical dysfunction and persistent AF were excluded.
Furthermore, the long-term effectiveness of ablation was not evaluated, and the study did not assess such outcomes as mortality, stroke, or AF progression. The effectiveness of specific ablation techniques could not be determined because a variety of approaches was employed.
Bottom line: Patients with symptomatic paroxysmal AF without advanced heart failure might benefit from catheter ablation at experienced institutions.
Citation: Wilber DJ, Pappone C, Neuzil P, et al. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA. 2010;303(4):333-340.
Noncontrast CT Can Be Used to Evaluate Suspected Appendicitis
Clinical question: What is the diagnostic accuracy of noncontrast helical CT in the evaluation of suspected acute appendicitis in the ED?
Background: In the workup of acute appendicitis, various CT protocols are used, including combinations of oral, intravenous, and rectal contrast, as well as noncontrast protocols. Noncontrast CT is less time-consuming and avoids risk of allergic reaction or contrast-induced nephropathy. The diagnostic accuracy of noncontrast CT, however, is controversial.
Study design: Systematic review/meta-analysis.
Setting: Seven studies evaluating acute appendicitis with noncontrast CT in ED settings.
Synopsis: This is the first systematic review of noncontrast CT (helical/multislice) in adults with suspected appendicitis. The authors pooled seven studies (1,060 patients) comparing noncontrast CT with a reference standard of final diagnosis at surgery or followup at a minimum of two weeks. The review yielded the following pooled estimates: sensitivity 93%, specificity 96%, positive likelihood ratio 24, and negative likelihood ratio 0.08. Overall, the diagnostic accuracy of noncontrast CT was high.
A few limitations should be noted. In the original studies, results were reported inconsistently. In one study, 24% of scans were inconclusive, with an associated likelihood ratio of approximately 1. Future studies must address this important clinical question of how to treat patients with inconclusive scans. Another question is to what degree the accuracy reported in this study reflects the expertise of the institutions, the majority of which were university-affiliated. According to one study author, “a certain level of experience is required for skillful interpretation” of noncontrast CT.
Bottom line: Noncontrast CT has a high sensitivity and specificity for acute appendicitis, and should be considered an alternative to contrast CT, particularly in patients with contraindications to contrast or those at risk of contrast-induced nephropathy.
Citation: Hlibczuk V, Dattaro JA, Jin Z, Falzon L, Brown MD. Diagnostic accuracy of noncontrast computed tomography for appendicitis in adults: a systematic review. Ann Emerg Med. 2010;55(1):51-59.e1.
Whole-Leg Compression Ultrasound for DVT Has a Low Failure Rate in Outpatients
Clinical question: How useful is compression ultrasound (CUS) for diagnosing distal DVT?
Background: CUS can reliably evaluate proximal DVT, but its accuracy for distal DVT is controversial. Because of the risk of extension of distal DVT (up to 25%), guidelines recommend that some patients undergo serial proximal CUS after an initial negative result. As an alternative, recent studies have evaluated one-time, whole-leg CUS.
Study design: Systematic review and meta-analysis.
Setting: Review of randomized controlled trials and prospective cohort studies.
Synopsis: The study pooled data from seven studies and more than 4,700 patients with suspected DVT for whom anticoagulation was withheld after a single, negative, whole-leg CUS. At the three-month followup, the combined symptomatic VTE event rate was 0.57%, and the authors concluded that withholding anticoagulation was associated with a low VTE risk.
Although encouraging, this study had several limitations. First, whole-leg CUS is not widely performed or standardized, and the CUS technique varied slightly across the studies. Second, any attempt to generalize the results of this study might be limited, as the proportion of pregnant patients and those with malignancy was low. Furthermore, only one of the seven studies included inpatients that might be at higher VTE risk. Third, pre-test probability was assessed for only a subset of patients, limiting assessment of VTE by risk level. For example, the overall finding of the study—an event rate of 0.57%—appears low but is difficult to apply clinically when subset analyses for high-risk patients yielded a VTE rate of 2.5% with wide confidence intervals ranging from 0% to 7%.
Bottom line: Whole-leg CUS might be a practical alternative to serial proximal CUS, but more data incorporating pre-test probabilities and involving more inpatients are needed. Hospitalists should be cautious in applying pooled summary estimates.
Citation: Johnson SA, Stevens SM, Woller SC, et al. Risk of deep vein thrombosis following a single negative whole-leg compression ultrasound: a systematic review and meta-analysis. JAMA. 2010;303(5):438-445.
Localization of Inpatient Physicians on Hospital Units Increases Provider Communication Frequency
Clinical question: Does localization of inpatient physicians on hospital units improve communication with nursing staff?
Background: While nurses are typically localized on a hospital unit, inpatient physicians often care for patients on multiple units. This lack of regionalization makes it difficult for physicians and nurses to discuss care plans directly. No prior research has evaluated the effect of physician localization on nurse-physician communication.
Study design: Cross-sectional, pre- and postintervention study.
Setting: Tertiary-care teaching hospital, general medical service.
Synopsis: The study was a cross-sectional survey of nurses and physicians prelocalization (n=342 patients) and postlocalization (n=294 patients) of physicians on hospital units. Localization was associated with increased frequency of communication; however, it did not improve the consistency of nurse-physician agreement on the care plan. Nurse-physician agreement was improved on two aspects of the care plan—planned tests and anticipated length of stay—but not on primary diagnosis, planned procedures, medication changes, or consultations.
Limitations of the study were that it was conducted at a single teaching hospital, communication patterns might have changed during the year between pre- and postlocalization, and physicians were not completely localized to specific units (73% localization).
Despite the limitations, this study is the first to evaluate staff localization and communication on a general medical service. The findings suggest that localization is a first step toward interdisciplinary communication. It also shows that quality and content of communication require further assessment.
Future studies must assess the impact of communication on the quality of patient care.
Bottom line: Physician localization improved the frequency of nurse-physician dialogue but did not consistently facilitate a shared understanding of the care plan. Although not assessed in this study, the implication is that the quality of communication between providers needs improvement.
Citation: O’Leary KJ, Wayne DB, Landler MP, et al. J Gen Int Med. 2009;24(11):1223-1227.
Pantoprazole Better than Double-Dose Famotidine in Secondary Prevention of Aspirin-Related Injury
Clinical question: Is a twice-daily H2-receptor antagonist (H2RA) or a once-daily proton pump inhibitor (PPI) better in patients who must continue low-dose-aspirin therapy despite aspirin-related peptic ulcer disease?
Background: Some patients with aspirin-related peptic ulcer disease require continued aspirin therapy. It often is assumed that PPIs are superior to H2RAs in secondary prevention of low-dose aspirin-related injury, although no randomized trials have specifically addressed this question.
Study design: A prospective, double-blind, randomized controlled trial.
Setting: A university hospital in Hong Kong.
Synopsis: In this trial, 160 patients with aspirin-related peptic ulcers/erosions were randomized to 48 weeks of oral famotidine (40 mg twice daily) or pantoprazole (20 mg daily) after mucosal healing and eradication of H pylori. During this time, all patients continued to receive aspirin (80 mg daily).
The rates of recurrent dyspeptic or bleeding ulcers/erosions within 48 weeks were 20% with famotidine versus 0% with pantoprazole. The rates of gastrointestinal (GI) bleeding alone were 7.7% versus 0%, respectively.
Of note, none of the five patients with GI bleeding had significant dyspepsia, which is consistent with prior reports that NSAID-induced injury might be silent.
Overall, high-dose famotidine was inferior to pantoprazole in the prevention of recurrent aspirin-related injury. These findings support the ACCF/ACG/AHA 2008 recommendation of PPIs over double-dose H2RAs in this clinical setting. It is not known, however, whether the PPI strategy extends to average GI-risk patients taking aspirin.
Furthermore, although not demonstrated in this study, it is possible that the lower rates of dyspepsia with pantoprazole might facilitate adherence to prolonged aspirin therapy.
Bottom line: High-dose famotidine was inferior to pantoprazole in the prevention of recurrent low-dose-aspirin-related injury.
Citation: Ng FH, Wong SY, Lam KF, et al. Famotidine is inferior to pantoprazole in preventing recurrence of aspirin-related peptic ulcers or erosions. Gastroenterology. 2010;138
(1):82-88.
Intensive Insulin Therapy Is Not Beneficial in Corticosteroid-Induced Hyperglycemia Associated with Septic Shock
Clinical question: In septic shock treated with hydrocortisone, does intensive insulin therapy reduce in-hospital mortality compared with conventional glucose management?
Background: Corticosteroids might benefit patients with septic shock, but they also can exacerbate illness-induced hyperglycemia. It is hypothesized that normalization of blood glucose with intensive insulin might improve outcomes in these patients.
Study design: A multicenter, 2x2 factorial, randomized controlled trial.
Setting: Eleven ICUs in France.
Synopsis: In this 2x2 factorial comparison, 509 patients with septic shock treated with hydrocortisone were randomized to IV insulin, conventional insulin, fludrocortisone plus IV insulin, and fludrocortisone plus conventional insulin. The primary objective was to assess intensive IV versus conventional insulin, and a secondary objective was to assess the benefit of adding fludrocortisone to hydrocortisone therapy.
Overall, analysis showed no difference in in-hospital mortality in either of the two comparisons.
These null findings should be interpreted considering the following study limitations. In the intensive-insulin groups, there was a failure to reach target glucose levels of 80 mg/dL to 110 mg/dL (mean achieved levels 120 mg/dL to 130 mg/dL and higher). These levels overlapped to some degree with the control group, which targeted glucose levels <150 mg/dL and achieved mean levels of 140 mg/dL to 150 mg/dL.
The lack of substantial difference in glucose levels might have contributed to the null findings. Furthermore, the absolute risk reduction in the original sample-size calculations was overestimated. The result was an underpowered study, which also might have contributed to the null findings.
Bottom line: In septic shock treated with hydrocortisone, the optimal blood-glucose level and insulin strategy are unknown.
Citation: Annane D, Cariou A, Maxime V, et al. Corticosteroid treatment and intensive insulin therapy for septic shock in adults: a randomized controlled trial. JAMA. 2010;303(4):341-348.
Mupirocin-Chlorhexidine Decolonization of Nasal S. Aureus Carriers Reduces Surgical-Site Infections
Clinical question: Can rapid screening and decolonization of nasal carriers of Staphylococcus aureus on admission reduce surgical-site S. aureus infections?
Background: More than 80% of healthcare-associated (HCA) S. aureus infections are endogenous in origin. High-level nasal carriers have a three- to sixfold increased risk of infection with this organism compared with noncarriers and low-level carriers. Decolonization of nasal and extranasal S. aureus on admission might reduce this risk of infection.
Study design: Randomized, double-blinded, placebo-controlled, multicenter trial.
Setting: Three university hospitals and two general hospitals in the Netherlands.
Synopsis: In this study, 918 mostly surgical patients with nasal S. aureus identified preoperatively by PCR tests were randomized to decolonization versus placebo. The five-day decolonization protocol involved mupirocin nasal ointment and chlorhexidine soap baths. Decolonization reduced length of stay by nearly two days. Through six weeks postdischarge, the cumulative incidence of S. aureus infection was 3.4% after decolonization versus 7.7% with placebo (RR 0.42; 95% CI, 0.23-0.75). Among the sites of infection, deep surgical sites had the greatest risk reduction (RR 0.21; 95% CI, 0.07-0.62).
The results of this study are encouraging, but a few limitations should be noted. The decolonization protocol lasted five days, which might make implementation less practical. Also, the relative contributions of mupirocin and chlorhexidine are unclear.
S. aureus is important, but it represents a minority of surgical-site infections; the effect of the protocol on other organisms is unknown. Lastly, MRSA is not prevalent in the Netherlands and no carriers were identified in the study. Although the protocol was designed to eradicate MRSA, such carriers might have different carriage patterns requiring throat swabs in addition to nasal swabs.
Bottom line: Preoperative detection of S. aureus nasal carriage and nasal and extranasal decolonization significantly reduced endogenous S. aureus infection and length of stay. Decolonization might be most beneficial for carriers at increased risk of deep infection, such as those undergoing cardiac surgery.
Citation: Bode LG, Kluytmans JA, Wertheim HF, et al. Preventing surgical-site infections in nasal carriers of Staphylococcus aureus. N Engl J Med. 2010;362(1):9-17.
ABCD2 Is a Poor Predictor of Early Ischemic Stroke after Transient Ischemic Attack
Clinical question: How well does the ABCD2 score predict stroke risk within seven days of transient ischemic attack (TIA)?
Background: After TIA diagnosis, the seven-day risk of ischemic stroke is approximately 5%. Identifying these high-risk patients might facilitate ED decision-making. The ABCD2 score, a prediction tool for stroke after TIA, might be useful but has not been prospectively validated in a large, broad-patient population.
Study design: Prospective validation study, convenience sample.
Setting: Sixteen hospitals in North Carolina.
Synopsis: The ABCD2 score (range 0-7 points) predicts stroke risk after TIA. The investigators evaluated the accuracy of ABCD2 in predicting seven-day ischemic stroke risk in a convenience sample of 1,667 TIA patients. Strokes were categorized as disabling or nondisabling.
Overall, the score was poorly predictive of all ischemic stroke (c stat 0.59) and moderately predictive of the subset of disabling ischemic stroke (c stat 0.71). The ABCD2 had the most discriminatory power when used to identify patients at low risk of disabling stroke (0-3 points); for these patients, the negative likelihood ratio (LR) was 0.16 (0.04-0.64).
The study is the largest published external-validation study of the ABCD2 score, but it had significant limitations that should be considered. There was potential sampling bias because of nonconsecutive sampling, and unaccounted patients with TIA were discharged from the ED. Furthermore, ABCD2 scores were incalculable for 35% of patients, although the authors report that imputed data did not change the findings significantly.
Bottom line: The ABCD2 score does not sufficiently predict the seven-day risk of ischemic stroke after TIA. Further validation studies are needed.
Citation: Asimos AW, Johnson AM, Rosamond WD, et al. A multicenter evaluation of the ABCD2 score’s accuracy for predicting early ischemic stroke in admitted patients with transient ischemic attack. Ann Emerg Med. 2010;55(2):201-210.e5. TH
Dr. Kim is a hospitalist at Brigham and Women’s Hospital in Boston, and an instructor at Harvard Medical School.
Market Watch
New Generics
- Imiquimod cream 5% (generic Aldara)1
- Losartan tablets (generic Cozaar)2
- Losartan/hydrochlorothiazide tablets (generic Hyzaar)2
New Drugs, Indications, Approval Recommendations
- Olmesartan medoxomil (Benicar) has been approved by the FDA for treating hypertension in patients ages 6 to 16.3 It has been approved for treating hypertension in adults since 2002.
- Late last year, the prescribing information for rasagiline (Azilect) was updated to remove restrictions related to dietary tyramine ingestion (known as the “cheese reaction”), and removal of restrictions related to concomitant use of sympathomimetic amines (e.g., phenylephrine, pseudoephedrine, ephedrine, etc.) when used at the recommended doses of 0.5 mg and 1 mg.4,5
- Rifaximin (Xifaxin) has been approved by the FDA for treating hepatic encephalopathy.6 Twice-daily use of rifaximin 550 mg maintains remission from hepatic encephalopathy more effectively than placebo over a six-month period and significantly reduces the risk of hospitalization.7 In this study, more than 90% of patients also received lactulose. Rifaximin also has been approved by the FDA for treating travelers’ diarrhea.
- Earlier this year, rosuvastatin (Crestor) became the first statin to garner FDA approval for primary prevention of cardiovascular disease.8 Patients who might benefit from primary prevention include men 50 years or older and women 60 years or older with a fasting LDL <130 mg/dL, a highly-sensitive C-reactive protein level of greater than 2 mg/L, a triglyceride level lower than 500 mg/dL, and no prior history of stroke, myocardial infarction, or coronary heart-disease risk.
- Pipeline
- Fingolimod (FTY720, Gilenia), a once-daily oral disease modifying therapy for the treatment of multiple sclerosis, has been granted a priority review by the FDA. 9 The New Drug Application (NDA) was accepted in December 2009, but a priority review decreases the standard 10-month review to six months. The timeframe, however, could be extended to evaluate a risk evaluation and mitigation strategy (REMS) program. This sphingosine 1-phosphate receptor (S1P-R) has been shown to significantly reduce both relapses and disability progression (compared with placebo) in patients with relapsing remitting multiple sclerosis.
Safety Information
- Oral bisphosphonates: On March 11, the FDA posted information related to a possible connection between the use of bisphosphonates and the risk of developing atypical sub-trochanteric femur fractures.8 Two weeks later, a study and accompanying editorial described how there is no link between bisphosphonates and femur fractures.10,11 As of press time, the FDA had not commented on the study results.
- Clopidogrel has received a boxed warning related to decreased effectiveness when administered to patients who are poor metabolizers of the agent.12 Approximately 2% to 14% of the U.S. population are poor metabolizers due to a variation in CYP2C19 liver enzyme function. The warning includes information for prescribers about genetic testing for patients to identify those who might be poor metabolizers of clopidogrel; the information should assist providers with decision-making on the most appropriate therapy.
- Erythropoiesis-stimulating agents (ESAs): The FDA is requiring all ESAs to be prescribed and used under a REMS program to ensure their safe use.13 The measures were put in place after studies showed that ESA use can increase the risk of tumor growth and shorten survival in oncology patients. Only hospitals and healthcare professionals who enroll and complete specific training in the REMS program (known as ESA APPRISE Oncology) will be able to prescribe and dispense ESAs to healthcare professionals. All patients prescribed ESAs for any indication must receive a copy of the medication guide when the drug is dispensed. For prescribers using ESAs for noncancer indications (e.g., anemia related to HIV, chronic kidney disease patients, etc.), enrollment in the REMS program is not required; however, a medication guide must be given to patients when the drug is dispensed. For more information, visit www.esa-apprise.com/.
- Ritonavir (Norvir) and saquinavir (Invirase) combination and cardiac effects: The FDA is evaluating preliminary data that indicate the combined use of ritonavir and saquinavir might lead to prolongation of the QT and PR interval of the electrocardiogram, and might lead to Torsades de Pointes or heart block.14 Any patients receiving both of these agents should be evaluated for such symptoms as lightheadedness, fainting, or arrhythmias. The risk of arrhythmias may be increased in patients with a history of QT interval prolongation.
- Increased risk of muscle injury with high-dose simvastatin: The FDA has identified that the highest dose of simvastatin (80 mg) is associated with a greater risk of muscle injury, including rhabdomyolysis.15 The concern with simvastatin is as a single ingredient, and as part of combinations with ezetimibe or niacin. The FDA will publish a report when the review has been completed. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Fougera announces first generic approval of imiquimod cream 5% (Rx), equivalent to Aldara. Fougera website. Available at: http://www.fougera.com/news/release_detail.asp?id=1057. Accessed March 5, 2010.
- Dane L. US court ruling restores Teva’s marketing exclusivity for generics of Merck & Co. hypertension drugs. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=A9C69CCA747746D2832D25A523C54E63&logRowId=353155. Accessed March 23, 2010.
- FDA approves Benicar for the treatment of high blood pressure in children and adolescents aged 6-16. Available at: http://www.dsi.com/news/pdfs/FINAL_Benicar_Pediatric_Approval_Press_Release.pdf. Accessed March 23, 2010.
- FDA approves newly revised prescribing information for Azilect reducing medication and food restriction. Teva website. Available at: http://www.tevaneuroscience.com/NewsContent.aspx?Ispreview=No&Type=News&Id=251&Status=Current. Accessed March 23, 2010.
- Tilyou S. Tyramine-rich foods and rasagiline not always a bad mix. Pharmacy Practice News website. Available at: http://www.pharmacypracticenews.com/index.asp?section_id=50&show=dept&issue_id=618&article_id=14885. Accessed March 25, 2010.
- Drew J. FDA approves Salix drug Xifaxan as treatment for hepatic encephalopathy. Triangle Business Journal website. Available at: http://triangle.bizjournals.com/triangle/stories/2010/03/22/daily41.html?t=printable. Accessed March 25, 2010.
- Bass NM, Mullen KD, Sanyal A, et al. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010;362(12):1071-1081.
- Peck P, Agus ZS. FDA okays statin for primary prevention. MedPage Today website. Available at: http://www.medpagetoday.com/tbprint.cfm?tbid=18380. Accessed March 23, 2010.
- Novartis oral multiple sclerosis development compound Gilenia (FTY720) granted US priority review status. Novartis website. Available at: http://www.novartis.com/newsroom/media-releases/en/2010/1386852.shtml. Accessed March 23, 2010.
- Oral bisphosphonates: ongoing safety review of atypical subtrochanteric femur fractures. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm204127.htm. Accessed March 24, 2010.
- Black DM, Kelly MP, Genant HK, et al. Bisphosphonates and fractures of the subtrochanteric or diaphyseal femur. N Engl J Med. 2010 Mar 24.
- Shane E. Evolving data about subtrochanteric fractures and bisphosphonates. N Engl J Med. 2010 Mar 24.
- Dane L. FDA adds boxed warning to Plavix to advise of reduced effectiveness in some patients. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=7AD8DC1985644F1683D822FE7C1EC2B4&logRowId=355395. Accessed March 24, 2010.
- Drug safety communication: erythropoiesis-stimulating agents (ESAs): Procrit, Epogen and Aranesp. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm200297.htm. Accessed March 24, 2010.
- Jefferson E. FDA Announces Possible Safety Concern for HIV Drug Combination Published February 23, 2010 http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm201552.htm. Accessed March 24, 2010.
New Generics
- Imiquimod cream 5% (generic Aldara)1
- Losartan tablets (generic Cozaar)2
- Losartan/hydrochlorothiazide tablets (generic Hyzaar)2
New Drugs, Indications, Approval Recommendations
- Olmesartan medoxomil (Benicar) has been approved by the FDA for treating hypertension in patients ages 6 to 16.3 It has been approved for treating hypertension in adults since 2002.
- Late last year, the prescribing information for rasagiline (Azilect) was updated to remove restrictions related to dietary tyramine ingestion (known as the “cheese reaction”), and removal of restrictions related to concomitant use of sympathomimetic amines (e.g., phenylephrine, pseudoephedrine, ephedrine, etc.) when used at the recommended doses of 0.5 mg and 1 mg.4,5
- Rifaximin (Xifaxin) has been approved by the FDA for treating hepatic encephalopathy.6 Twice-daily use of rifaximin 550 mg maintains remission from hepatic encephalopathy more effectively than placebo over a six-month period and significantly reduces the risk of hospitalization.7 In this study, more than 90% of patients also received lactulose. Rifaximin also has been approved by the FDA for treating travelers’ diarrhea.
- Earlier this year, rosuvastatin (Crestor) became the first statin to garner FDA approval for primary prevention of cardiovascular disease.8 Patients who might benefit from primary prevention include men 50 years or older and women 60 years or older with a fasting LDL <130 mg/dL, a highly-sensitive C-reactive protein level of greater than 2 mg/L, a triglyceride level lower than 500 mg/dL, and no prior history of stroke, myocardial infarction, or coronary heart-disease risk.
- Pipeline
- Fingolimod (FTY720, Gilenia), a once-daily oral disease modifying therapy for the treatment of multiple sclerosis, has been granted a priority review by the FDA. 9 The New Drug Application (NDA) was accepted in December 2009, but a priority review decreases the standard 10-month review to six months. The timeframe, however, could be extended to evaluate a risk evaluation and mitigation strategy (REMS) program. This sphingosine 1-phosphate receptor (S1P-R) has been shown to significantly reduce both relapses and disability progression (compared with placebo) in patients with relapsing remitting multiple sclerosis.
Safety Information
- Oral bisphosphonates: On March 11, the FDA posted information related to a possible connection between the use of bisphosphonates and the risk of developing atypical sub-trochanteric femur fractures.8 Two weeks later, a study and accompanying editorial described how there is no link between bisphosphonates and femur fractures.10,11 As of press time, the FDA had not commented on the study results.
- Clopidogrel has received a boxed warning related to decreased effectiveness when administered to patients who are poor metabolizers of the agent.12 Approximately 2% to 14% of the U.S. population are poor metabolizers due to a variation in CYP2C19 liver enzyme function. The warning includes information for prescribers about genetic testing for patients to identify those who might be poor metabolizers of clopidogrel; the information should assist providers with decision-making on the most appropriate therapy.
- Erythropoiesis-stimulating agents (ESAs): The FDA is requiring all ESAs to be prescribed and used under a REMS program to ensure their safe use.13 The measures were put in place after studies showed that ESA use can increase the risk of tumor growth and shorten survival in oncology patients. Only hospitals and healthcare professionals who enroll and complete specific training in the REMS program (known as ESA APPRISE Oncology) will be able to prescribe and dispense ESAs to healthcare professionals. All patients prescribed ESAs for any indication must receive a copy of the medication guide when the drug is dispensed. For prescribers using ESAs for noncancer indications (e.g., anemia related to HIV, chronic kidney disease patients, etc.), enrollment in the REMS program is not required; however, a medication guide must be given to patients when the drug is dispensed. For more information, visit www.esa-apprise.com/.
- Ritonavir (Norvir) and saquinavir (Invirase) combination and cardiac effects: The FDA is evaluating preliminary data that indicate the combined use of ritonavir and saquinavir might lead to prolongation of the QT and PR interval of the electrocardiogram, and might lead to Torsades de Pointes or heart block.14 Any patients receiving both of these agents should be evaluated for such symptoms as lightheadedness, fainting, or arrhythmias. The risk of arrhythmias may be increased in patients with a history of QT interval prolongation.
- Increased risk of muscle injury with high-dose simvastatin: The FDA has identified that the highest dose of simvastatin (80 mg) is associated with a greater risk of muscle injury, including rhabdomyolysis.15 The concern with simvastatin is as a single ingredient, and as part of combinations with ezetimibe or niacin. The FDA will publish a report when the review has been completed. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Fougera announces first generic approval of imiquimod cream 5% (Rx), equivalent to Aldara. Fougera website. Available at: http://www.fougera.com/news/release_detail.asp?id=1057. Accessed March 5, 2010.
- Dane L. US court ruling restores Teva’s marketing exclusivity for generics of Merck & Co. hypertension drugs. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=A9C69CCA747746D2832D25A523C54E63&logRowId=353155. Accessed March 23, 2010.
- FDA approves Benicar for the treatment of high blood pressure in children and adolescents aged 6-16. Available at: http://www.dsi.com/news/pdfs/FINAL_Benicar_Pediatric_Approval_Press_Release.pdf. Accessed March 23, 2010.
- FDA approves newly revised prescribing information for Azilect reducing medication and food restriction. Teva website. Available at: http://www.tevaneuroscience.com/NewsContent.aspx?Ispreview=No&Type=News&Id=251&Status=Current. Accessed March 23, 2010.
- Tilyou S. Tyramine-rich foods and rasagiline not always a bad mix. Pharmacy Practice News website. Available at: http://www.pharmacypracticenews.com/index.asp?section_id=50&show=dept&issue_id=618&article_id=14885. Accessed March 25, 2010.
- Drew J. FDA approves Salix drug Xifaxan as treatment for hepatic encephalopathy. Triangle Business Journal website. Available at: http://triangle.bizjournals.com/triangle/stories/2010/03/22/daily41.html?t=printable. Accessed March 25, 2010.
- Bass NM, Mullen KD, Sanyal A, et al. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010;362(12):1071-1081.
- Peck P, Agus ZS. FDA okays statin for primary prevention. MedPage Today website. Available at: http://www.medpagetoday.com/tbprint.cfm?tbid=18380. Accessed March 23, 2010.
- Novartis oral multiple sclerosis development compound Gilenia (FTY720) granted US priority review status. Novartis website. Available at: http://www.novartis.com/newsroom/media-releases/en/2010/1386852.shtml. Accessed March 23, 2010.
- Oral bisphosphonates: ongoing safety review of atypical subtrochanteric femur fractures. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm204127.htm. Accessed March 24, 2010.
- Black DM, Kelly MP, Genant HK, et al. Bisphosphonates and fractures of the subtrochanteric or diaphyseal femur. N Engl J Med. 2010 Mar 24.
- Shane E. Evolving data about subtrochanteric fractures and bisphosphonates. N Engl J Med. 2010 Mar 24.
- Dane L. FDA adds boxed warning to Plavix to advise of reduced effectiveness in some patients. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=7AD8DC1985644F1683D822FE7C1EC2B4&logRowId=355395. Accessed March 24, 2010.
- Drug safety communication: erythropoiesis-stimulating agents (ESAs): Procrit, Epogen and Aranesp. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm200297.htm. Accessed March 24, 2010.
- Jefferson E. FDA Announces Possible Safety Concern for HIV Drug Combination Published February 23, 2010 http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm201552.htm. Accessed March 24, 2010.
New Generics
- Imiquimod cream 5% (generic Aldara)1
- Losartan tablets (generic Cozaar)2
- Losartan/hydrochlorothiazide tablets (generic Hyzaar)2
New Drugs, Indications, Approval Recommendations
- Olmesartan medoxomil (Benicar) has been approved by the FDA for treating hypertension in patients ages 6 to 16.3 It has been approved for treating hypertension in adults since 2002.
- Late last year, the prescribing information for rasagiline (Azilect) was updated to remove restrictions related to dietary tyramine ingestion (known as the “cheese reaction”), and removal of restrictions related to concomitant use of sympathomimetic amines (e.g., phenylephrine, pseudoephedrine, ephedrine, etc.) when used at the recommended doses of 0.5 mg and 1 mg.4,5
- Rifaximin (Xifaxin) has been approved by the FDA for treating hepatic encephalopathy.6 Twice-daily use of rifaximin 550 mg maintains remission from hepatic encephalopathy more effectively than placebo over a six-month period and significantly reduces the risk of hospitalization.7 In this study, more than 90% of patients also received lactulose. Rifaximin also has been approved by the FDA for treating travelers’ diarrhea.
- Earlier this year, rosuvastatin (Crestor) became the first statin to garner FDA approval for primary prevention of cardiovascular disease.8 Patients who might benefit from primary prevention include men 50 years or older and women 60 years or older with a fasting LDL <130 mg/dL, a highly-sensitive C-reactive protein level of greater than 2 mg/L, a triglyceride level lower than 500 mg/dL, and no prior history of stroke, myocardial infarction, or coronary heart-disease risk.
- Pipeline
- Fingolimod (FTY720, Gilenia), a once-daily oral disease modifying therapy for the treatment of multiple sclerosis, has been granted a priority review by the FDA. 9 The New Drug Application (NDA) was accepted in December 2009, but a priority review decreases the standard 10-month review to six months. The timeframe, however, could be extended to evaluate a risk evaluation and mitigation strategy (REMS) program. This sphingosine 1-phosphate receptor (S1P-R) has been shown to significantly reduce both relapses and disability progression (compared with placebo) in patients with relapsing remitting multiple sclerosis.
Safety Information
- Oral bisphosphonates: On March 11, the FDA posted information related to a possible connection between the use of bisphosphonates and the risk of developing atypical sub-trochanteric femur fractures.8 Two weeks later, a study and accompanying editorial described how there is no link between bisphosphonates and femur fractures.10,11 As of press time, the FDA had not commented on the study results.
- Clopidogrel has received a boxed warning related to decreased effectiveness when administered to patients who are poor metabolizers of the agent.12 Approximately 2% to 14% of the U.S. population are poor metabolizers due to a variation in CYP2C19 liver enzyme function. The warning includes information for prescribers about genetic testing for patients to identify those who might be poor metabolizers of clopidogrel; the information should assist providers with decision-making on the most appropriate therapy.
- Erythropoiesis-stimulating agents (ESAs): The FDA is requiring all ESAs to be prescribed and used under a REMS program to ensure their safe use.13 The measures were put in place after studies showed that ESA use can increase the risk of tumor growth and shorten survival in oncology patients. Only hospitals and healthcare professionals who enroll and complete specific training in the REMS program (known as ESA APPRISE Oncology) will be able to prescribe and dispense ESAs to healthcare professionals. All patients prescribed ESAs for any indication must receive a copy of the medication guide when the drug is dispensed. For prescribers using ESAs for noncancer indications (e.g., anemia related to HIV, chronic kidney disease patients, etc.), enrollment in the REMS program is not required; however, a medication guide must be given to patients when the drug is dispensed. For more information, visit www.esa-apprise.com/.
- Ritonavir (Norvir) and saquinavir (Invirase) combination and cardiac effects: The FDA is evaluating preliminary data that indicate the combined use of ritonavir and saquinavir might lead to prolongation of the QT and PR interval of the electrocardiogram, and might lead to Torsades de Pointes or heart block.14 Any patients receiving both of these agents should be evaluated for such symptoms as lightheadedness, fainting, or arrhythmias. The risk of arrhythmias may be increased in patients with a history of QT interval prolongation.
- Increased risk of muscle injury with high-dose simvastatin: The FDA has identified that the highest dose of simvastatin (80 mg) is associated with a greater risk of muscle injury, including rhabdomyolysis.15 The concern with simvastatin is as a single ingredient, and as part of combinations with ezetimibe or niacin. The FDA will publish a report when the review has been completed. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Fougera announces first generic approval of imiquimod cream 5% (Rx), equivalent to Aldara. Fougera website. Available at: http://www.fougera.com/news/release_detail.asp?id=1057. Accessed March 5, 2010.
- Dane L. US court ruling restores Teva’s marketing exclusivity for generics of Merck & Co. hypertension drugs. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=A9C69CCA747746D2832D25A523C54E63&logRowId=353155. Accessed March 23, 2010.
- FDA approves Benicar for the treatment of high blood pressure in children and adolescents aged 6-16. Available at: http://www.dsi.com/news/pdfs/FINAL_Benicar_Pediatric_Approval_Press_Release.pdf. Accessed March 23, 2010.
- FDA approves newly revised prescribing information for Azilect reducing medication and food restriction. Teva website. Available at: http://www.tevaneuroscience.com/NewsContent.aspx?Ispreview=No&Type=News&Id=251&Status=Current. Accessed March 23, 2010.
- Tilyou S. Tyramine-rich foods and rasagiline not always a bad mix. Pharmacy Practice News website. Available at: http://www.pharmacypracticenews.com/index.asp?section_id=50&show=dept&issue_id=618&article_id=14885. Accessed March 25, 2010.
- Drew J. FDA approves Salix drug Xifaxan as treatment for hepatic encephalopathy. Triangle Business Journal website. Available at: http://triangle.bizjournals.com/triangle/stories/2010/03/22/daily41.html?t=printable. Accessed March 25, 2010.
- Bass NM, Mullen KD, Sanyal A, et al. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010;362(12):1071-1081.
- Peck P, Agus ZS. FDA okays statin for primary prevention. MedPage Today website. Available at: http://www.medpagetoday.com/tbprint.cfm?tbid=18380. Accessed March 23, 2010.
- Novartis oral multiple sclerosis development compound Gilenia (FTY720) granted US priority review status. Novartis website. Available at: http://www.novartis.com/newsroom/media-releases/en/2010/1386852.shtml. Accessed March 23, 2010.
- Oral bisphosphonates: ongoing safety review of atypical subtrochanteric femur fractures. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm204127.htm. Accessed March 24, 2010.
- Black DM, Kelly MP, Genant HK, et al. Bisphosphonates and fractures of the subtrochanteric or diaphyseal femur. N Engl J Med. 2010 Mar 24.
- Shane E. Evolving data about subtrochanteric fractures and bisphosphonates. N Engl J Med. 2010 Mar 24.
- Dane L. FDA adds boxed warning to Plavix to advise of reduced effectiveness in some patients. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=7AD8DC1985644F1683D822FE7C1EC2B4&logRowId=355395. Accessed March 24, 2010.
- Drug safety communication: erythropoiesis-stimulating agents (ESAs): Procrit, Epogen and Aranesp. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm200297.htm. Accessed March 24, 2010.
- Jefferson E. FDA Announces Possible Safety Concern for HIV Drug Combination Published February 23, 2010 http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm201552.htm. Accessed March 24, 2010.
FPHM: Open for Business
2010 could be called the year of recognition for hospitalists. For the hundreds of hospitalists who were inducted as fellows, senior fellows, or master fellows in April, it has already been a momentous year. For some of them—and others, too—their journey toward full recognition of their efforts in the hospital will continue by taking the inaugural Focused Practice in Hospital Medicine (FPHM) Maintenance of Certification (MOC) secure examination administered by the American Board of Internal Medicine (ABIM).
Registration opened for eligible candidates May 1.
The registration period ends Aug. 1.
The first exam is Oct. 25.
In order to qualify for the FPHM MOC program, candidates must submit attestations to ABIM—both from themselves and a supervisor—that demonstrate that the applicant “meets thresholds for internal medicine practice in the hospital setting and professional commitment to hospital medicine,” according to ABIM’s Q&A document about the program.
In addition to attestations, program entrants must have served as a hospitalist for at least three years and fulfill ABIM’s basic requirements for the MOC (see “FPHM Eligibility Requirements,” p. 10).
Why Do It?
While HM has been gaining recognition in the healthcare arena for more than a decade, the FPHM MOC pathway is the first of its kind—and it represents the first time hospitalists will be recognized on an individual level by an independent evaluation organization like ABIM.
“This is a momentous opportunity at every level,” says SHM vice president of operations and general manager Todd Von Deak. “For the individual members, it provides a new kind of recognition of their expertise in a growing specialty. At a higher level, every applicant in the Hospital Medicine MOC program is helping to elevate the specialty among their peers and patients.”
For its part, SHM is helping to promote the program to its membership through informational e-mails to members and additional visibility on the website, www.hospitalmedicine. org.
“We are thrilled to introduce this program to our members,” Von Deak says. “We already have seen strong initial support for the program from SHM members, and we’re confident that even more will apply soon.”
Why Do It Now?
Participation in the first year of the FPHM program can influence the support the program receives in subsequent years, according to Von Deak. “A robust launch year is important to the success of a program like this,” he says. “SHM members can demonstrate to ABIM that this is a valuable program within the specialty by signing up soon. Strength in numbers is critical.”
Plus, hospitalists aren’t required to wait until their ABIM certification expires before registering for the FPHM program. While ABIM certification, which must be renewed every 10 years, is a prerequisite for the FPHM MOC, ABIM-certified hospitalists can register for the program at any time.
Hospitalists who don’t register soon will have to wait for more than 18 months before they can be recognized for their work by ABIM. Certificates for successful applicants in this year’s program will be distributed to hospitalists in early 2011.
For more details, visit www.abim.org, click the “Get Information by Specialty” box, then click the “Hospital Medicine, Focused Practice” section. TH
Brendon Shank is a freelance writer based in Philadelphia.
Fellow in Hospital medicine Spotlight

Margaret Fang, MD, FHM
Dr. Fang is assistant professor in residence, division of hospital medicine, and medical director of the anticoagulation clinic at the University of California at San Francisco.
Undergraduate: Northwestern Univer-sity, Evanston, Ill.
Medical school: Feinberg School of Medicine, Northwestern University, Chicago.
Notable: A practicing hospitalist and SHM member since 2003, Dr. Fang was the co-chair and founding member of SHM’s Young Physicians Task Force in 2003. She has been an active member of SHM’s Scientific Abstracts Committee since 2004 and the Research Committee since 2009. She also has been an assistant editor for the Journal of Hospital Medicine since 2006.
FYI: Outside of the hospital, Dr. Fang has developed a strong interest in food and wine, “which is only natural living in the beautiful bay area of San Francisco,” she says. She recently read “The Omnivore’s Dilemma” by Michael Pollan, and has subscribed to Community Supported Agriculture (CSA) ever since. She enjoys being adventurous and creative with her recipes, using locally grown ingredients supplied by the CSA. She indulges her interests in both cooking and eating, “with a bigger emphasis on eating.”
Quotable: “As a hospitalist that is actively involved in clinical research and administration, I get the opportunity to try out a lot of different things and pursue my many interests. SHM tries to embrace all aspects of the hospitalist field, and I am a big advocate of promoting clinical research and quality-improvement projects in our field.”
2010 could be called the year of recognition for hospitalists. For the hundreds of hospitalists who were inducted as fellows, senior fellows, or master fellows in April, it has already been a momentous year. For some of them—and others, too—their journey toward full recognition of their efforts in the hospital will continue by taking the inaugural Focused Practice in Hospital Medicine (FPHM) Maintenance of Certification (MOC) secure examination administered by the American Board of Internal Medicine (ABIM).
Registration opened for eligible candidates May 1.
The registration period ends Aug. 1.
The first exam is Oct. 25.
In order to qualify for the FPHM MOC program, candidates must submit attestations to ABIM—both from themselves and a supervisor—that demonstrate that the applicant “meets thresholds for internal medicine practice in the hospital setting and professional commitment to hospital medicine,” according to ABIM’s Q&A document about the program.
In addition to attestations, program entrants must have served as a hospitalist for at least three years and fulfill ABIM’s basic requirements for the MOC (see “FPHM Eligibility Requirements,” p. 10).
Why Do It?
While HM has been gaining recognition in the healthcare arena for more than a decade, the FPHM MOC pathway is the first of its kind—and it represents the first time hospitalists will be recognized on an individual level by an independent evaluation organization like ABIM.
“This is a momentous opportunity at every level,” says SHM vice president of operations and general manager Todd Von Deak. “For the individual members, it provides a new kind of recognition of their expertise in a growing specialty. At a higher level, every applicant in the Hospital Medicine MOC program is helping to elevate the specialty among their peers and patients.”
For its part, SHM is helping to promote the program to its membership through informational e-mails to members and additional visibility on the website, www.hospitalmedicine. org.
“We are thrilled to introduce this program to our members,” Von Deak says. “We already have seen strong initial support for the program from SHM members, and we’re confident that even more will apply soon.”
Why Do It Now?
Participation in the first year of the FPHM program can influence the support the program receives in subsequent years, according to Von Deak. “A robust launch year is important to the success of a program like this,” he says. “SHM members can demonstrate to ABIM that this is a valuable program within the specialty by signing up soon. Strength in numbers is critical.”
Plus, hospitalists aren’t required to wait until their ABIM certification expires before registering for the FPHM program. While ABIM certification, which must be renewed every 10 years, is a prerequisite for the FPHM MOC, ABIM-certified hospitalists can register for the program at any time.
Hospitalists who don’t register soon will have to wait for more than 18 months before they can be recognized for their work by ABIM. Certificates for successful applicants in this year’s program will be distributed to hospitalists in early 2011.
For more details, visit www.abim.org, click the “Get Information by Specialty” box, then click the “Hospital Medicine, Focused Practice” section. TH
Brendon Shank is a freelance writer based in Philadelphia.
Fellow in Hospital medicine Spotlight
Margaret Fang, MD, FHM
Dr. Fang is assistant professor in residence, division of hospital medicine, and medical director of the anticoagulation clinic at the University of California at San Francisco.
Undergraduate: Northwestern Univer-sity, Evanston, Ill.
Medical school: Feinberg School of Medicine, Northwestern University, Chicago.
Notable: A practicing hospitalist and SHM member since 2003, Dr. Fang was the co-chair and founding member of SHM’s Young Physicians Task Force in 2003. She has been an active member of SHM’s Scientific Abstracts Committee since 2004 and the Research Committee since 2009. She also has been an assistant editor for the Journal of Hospital Medicine since 2006.
FYI: Outside of the hospital, Dr. Fang has developed a strong interest in food and wine, “which is only natural living in the beautiful bay area of San Francisco,” she says. She recently read “The Omnivore’s Dilemma” by Michael Pollan, and has subscribed to Community Supported Agriculture (CSA) ever since. She enjoys being adventurous and creative with her recipes, using locally grown ingredients supplied by the CSA. She indulges her interests in both cooking and eating, “with a bigger emphasis on eating.”
Quotable: “As a hospitalist that is actively involved in clinical research and administration, I get the opportunity to try out a lot of different things and pursue my many interests. SHM tries to embrace all aspects of the hospitalist field, and I am a big advocate of promoting clinical research and quality-improvement projects in our field.”
2010 could be called the year of recognition for hospitalists. For the hundreds of hospitalists who were inducted as fellows, senior fellows, or master fellows in April, it has already been a momentous year. For some of them—and others, too—their journey toward full recognition of their efforts in the hospital will continue by taking the inaugural Focused Practice in Hospital Medicine (FPHM) Maintenance of Certification (MOC) secure examination administered by the American Board of Internal Medicine (ABIM).
Registration opened for eligible candidates May 1.
The registration period ends Aug. 1.
The first exam is Oct. 25.
In order to qualify for the FPHM MOC program, candidates must submit attestations to ABIM—both from themselves and a supervisor—that demonstrate that the applicant “meets thresholds for internal medicine practice in the hospital setting and professional commitment to hospital medicine,” according to ABIM’s Q&A document about the program.
In addition to attestations, program entrants must have served as a hospitalist for at least three years and fulfill ABIM’s basic requirements for the MOC (see “FPHM Eligibility Requirements,” p. 10).
Why Do It?
While HM has been gaining recognition in the healthcare arena for more than a decade, the FPHM MOC pathway is the first of its kind—and it represents the first time hospitalists will be recognized on an individual level by an independent evaluation organization like ABIM.
“This is a momentous opportunity at every level,” says SHM vice president of operations and general manager Todd Von Deak. “For the individual members, it provides a new kind of recognition of their expertise in a growing specialty. At a higher level, every applicant in the Hospital Medicine MOC program is helping to elevate the specialty among their peers and patients.”
For its part, SHM is helping to promote the program to its membership through informational e-mails to members and additional visibility on the website, www.hospitalmedicine. org.
“We are thrilled to introduce this program to our members,” Von Deak says. “We already have seen strong initial support for the program from SHM members, and we’re confident that even more will apply soon.”
Why Do It Now?
Participation in the first year of the FPHM program can influence the support the program receives in subsequent years, according to Von Deak. “A robust launch year is important to the success of a program like this,” he says. “SHM members can demonstrate to ABIM that this is a valuable program within the specialty by signing up soon. Strength in numbers is critical.”
Plus, hospitalists aren’t required to wait until their ABIM certification expires before registering for the FPHM program. While ABIM certification, which must be renewed every 10 years, is a prerequisite for the FPHM MOC, ABIM-certified hospitalists can register for the program at any time.
Hospitalists who don’t register soon will have to wait for more than 18 months before they can be recognized for their work by ABIM. Certificates for successful applicants in this year’s program will be distributed to hospitalists in early 2011.
For more details, visit www.abim.org, click the “Get Information by Specialty” box, then click the “Hospital Medicine, Focused Practice” section. TH
Brendon Shank is a freelance writer based in Philadelphia.
Fellow in Hospital medicine Spotlight
Margaret Fang, MD, FHM
Dr. Fang is assistant professor in residence, division of hospital medicine, and medical director of the anticoagulation clinic at the University of California at San Francisco.
Undergraduate: Northwestern Univer-sity, Evanston, Ill.
Medical school: Feinberg School of Medicine, Northwestern University, Chicago.
Notable: A practicing hospitalist and SHM member since 2003, Dr. Fang was the co-chair and founding member of SHM’s Young Physicians Task Force in 2003. She has been an active member of SHM’s Scientific Abstracts Committee since 2004 and the Research Committee since 2009. She also has been an assistant editor for the Journal of Hospital Medicine since 2006.
FYI: Outside of the hospital, Dr. Fang has developed a strong interest in food and wine, “which is only natural living in the beautiful bay area of San Francisco,” she says. She recently read “The Omnivore’s Dilemma” by Michael Pollan, and has subscribed to Community Supported Agriculture (CSA) ever since. She enjoys being adventurous and creative with her recipes, using locally grown ingredients supplied by the CSA. She indulges her interests in both cooking and eating, “with a bigger emphasis on eating.”
Quotable: “As a hospitalist that is actively involved in clinical research and administration, I get the opportunity to try out a lot of different things and pursue my many interests. SHM tries to embrace all aspects of the hospitalist field, and I am a big advocate of promoting clinical research and quality-improvement projects in our field.”
Team Hospitalist Seats 6 Members
Six hospitalists have joined Team Hospitalist, the only reader-involvement group of its kind in HM. Each of the new members has experience in the practice of HM; many offer specialized backgrounds in pediatrics, academics, and group administration. The new members will serve two-year terms on the 12-person board, and act as special editorial consultants to the magazine.

William D. Atchley Jr., MD, FACP, FHM
Division of Hospital Medicine
Sentara Medical Group Administration
Hampton, Va.

Weijen W. Chang, MD
Hospitalist/Pediatric
University of California at San Diego Medical Center and Rady Children’s Hospital

Kelly Cunningham, MD
Section of Hospital Medicine
Vanderbilt University
Nashville, Tenn.

Caitlin B. Foxley, MD
Medical Director
Inpatient Management, Inc.
The Nebraska Medical Center Hospitals
Omaha, Neb.

Rachel M. George, MD, MBA, FHM, CPE
Regional Medical Director/VP Operations
West Cogent Healthcare, Inc.
South Barrington, Ill.

Kenneth G. Simone, DO, FHM
Hospitalist Consultant
Hospitalist and Practice Solutions
Veazie, Me
Six hospitalists have joined Team Hospitalist, the only reader-involvement group of its kind in HM. Each of the new members has experience in the practice of HM; many offer specialized backgrounds in pediatrics, academics, and group administration. The new members will serve two-year terms on the 12-person board, and act as special editorial consultants to the magazine.
William D. Atchley Jr., MD, FACP, FHM
Division of Hospital Medicine
Sentara Medical Group Administration
Hampton, Va.
Weijen W. Chang, MD
Hospitalist/Pediatric
University of California at San Diego Medical Center and Rady Children’s Hospital
Kelly Cunningham, MD
Section of Hospital Medicine
Vanderbilt University
Nashville, Tenn.
Caitlin B. Foxley, MD
Medical Director
Inpatient Management, Inc.
The Nebraska Medical Center Hospitals
Omaha, Neb.
Rachel M. George, MD, MBA, FHM, CPE
Regional Medical Director/VP Operations
West Cogent Healthcare, Inc.
South Barrington, Ill.
Kenneth G. Simone, DO, FHM
Hospitalist Consultant
Hospitalist and Practice Solutions
Veazie, Me
Six hospitalists have joined Team Hospitalist, the only reader-involvement group of its kind in HM. Each of the new members has experience in the practice of HM; many offer specialized backgrounds in pediatrics, academics, and group administration. The new members will serve two-year terms on the 12-person board, and act as special editorial consultants to the magazine.
William D. Atchley Jr., MD, FACP, FHM
Division of Hospital Medicine
Sentara Medical Group Administration
Hampton, Va.
Weijen W. Chang, MD
Hospitalist/Pediatric
University of California at San Diego Medical Center and Rady Children’s Hospital
Kelly Cunningham, MD
Section of Hospital Medicine
Vanderbilt University
Nashville, Tenn.
Caitlin B. Foxley, MD
Medical Director
Inpatient Management, Inc.
The Nebraska Medical Center Hospitals
Omaha, Neb.
Rachel M. George, MD, MBA, FHM, CPE
Regional Medical Director/VP Operations
West Cogent Healthcare, Inc.
South Barrington, Ill.
Kenneth G. Simone, DO, FHM
Hospitalist Consultant
Hospitalist and Practice Solutions
Veazie, Me
Conference highlights growing HAI concerns
The Fifth Decennial International Conference on Healthcare-Associated Infections 2010, held in March in Atlanta, featured experts from several different fields discussing the significant prevalence of healthcare-associated infections (HAIs) and strategies that may be implemented to reduce their occurrence.
HAIs precipitated by the use of such devices as central venous catheters (CVCs), mechanical ventilators, and indwelling urinary catheters received special emphasis as important sources of patient morbidity and mortality.
Naomi O’Grady of the National Institutes of Health (NIH) summarized the current available knowledge regarding the prevention of central-line-associated bloodstream infections (CLABSIs). Strategies targeting appropriate line maintenance include:
- Chlorhexidine sponge dressings at the CVC insertion site in patients with short-term catheters;
- Cleanse catheter hubs and connectors with alcoholic-chlorhexidine (rather than alcohol alone) after each use; and
- Consider daily bathing of patients with chlorhexidine soap.
Speakers stressed that novel technologies, such as antimicrobial lock solutions and antiseptic- or antibiotic-impregnated catheters, should be considered when CLABSI rates remain high. Mark Shelly, MD, of Rochester, N.Y., emphasized awareness that CLABSIs occur frequently outside the ICU. “If you are only looking for CLABSI in the ICU, then you are missing more than half of the story,” Dr. Shelly said. Researchers from the National Health Safety Network (NHSN) provided more information about the substantial numbers of CLABSIs that occur on general medical wards.
Carolyn Gould, MD, MS, of the Centers for Disease Control and Prevention (CDC) confirmed that catheter-associated urinary tract infections (CAUTIs) are the most common type of HAI. CAUTIs occur at a frequency of >560,000 infections per year and cost as much as $500 million per year, she explained. Strategies to prevent CAUTIs include inserting urinary catheters only for appropriate indications and leaving them in place for the shortest possible duration.
In recent years, concern has grown about the prevalence of healthcare-associated Clostridium difficile infection (HA-CDI), which can lead to uncomplicated diarrhea, sepsis, or even death. Several speakers described strategies that reduce HA-CDI development, including the identification and removal of environmental sources of C. diff, accommodating CDI patients in a private room with contact precautions, and minimizing both the frequency and duration of antimicrobial therapy.
Uncertainty about the most reliable tests to confirm CDI was a topic of focus. Enzyme immunoassay (EIA) testing, cell cytotoxin assays, and polymerase chain reaction (PCR) testing are readily available in most U.S. hospitals; however, PCR testing might prove to be the most advantageous since it is rapid, sensitive, and specific.
Neil Fishman, MD, of the University of Pennsylvania School of Medicine in Philadelphia was one of several speakers to address the important role of antimicrobial stewardship program (ASP) development. According to Dr. Fishman, ASP goals should be to “ensure the proper use of antimicrobials” and to “promote cost-effectiveness.” By taking actions that promote the appropriate use of antimicrobials, the following positive consequences can be anticipated:
- Improved clinical outcomes;
- Reduced risk of adverse drug effects; and
- A reduction in, or stabilization of, the rate of antimicrobial resistance.
Multidrug-resistant (MDR) gram-negative Bacillus is a major challenge for hospitals worldwide. The CDC offers two guidelines for the optimal management and isolation of MDR organisms (MDRO): HICPAC 2006 (a management guideline) and HICPAC 2007 (MDRO isolation precaution guidelines). Consistent utilization of these guidelines is crucial to control the spread of MDRO.
The CDC’s Alexander Killen, MD, discussed the increasing proportion of MDR Acinetobacter and Enterobacteriaceae. Emerging issues among these organisms include the development of highly resistant strains, the incidence of which is increasing in nonacute-care settings.
The CDC’s Karen Anderson reported laboratory data on carbapenem-resistant Enterobacteriaceae (CRE) in a long-term-care facility. Her team demonstrated that CRE colonization can persist for up to six months. She speculated that the transfer of resistance between different species occurs, as does patient-to-patient transmission.
The CDC recommends the use of surveillance cultures as part of enhanced precautions. Surveillance is to continue until no new cases are detected.
Karen Clarke, MD, MS, MPH
Ketino Kobaidze, MD, PhD
Mohamad Moussa, MD
Sheri Tejedor, MD
Emory University
School of Medicine, Atlanta
The Fifth Decennial International Conference on Healthcare-Associated Infections 2010, held in March in Atlanta, featured experts from several different fields discussing the significant prevalence of healthcare-associated infections (HAIs) and strategies that may be implemented to reduce their occurrence.
HAIs precipitated by the use of such devices as central venous catheters (CVCs), mechanical ventilators, and indwelling urinary catheters received special emphasis as important sources of patient morbidity and mortality.
Naomi O’Grady of the National Institutes of Health (NIH) summarized the current available knowledge regarding the prevention of central-line-associated bloodstream infections (CLABSIs). Strategies targeting appropriate line maintenance include:
- Chlorhexidine sponge dressings at the CVC insertion site in patients with short-term catheters;
- Cleanse catheter hubs and connectors with alcoholic-chlorhexidine (rather than alcohol alone) after each use; and
- Consider daily bathing of patients with chlorhexidine soap.
Speakers stressed that novel technologies, such as antimicrobial lock solutions and antiseptic- or antibiotic-impregnated catheters, should be considered when CLABSI rates remain high. Mark Shelly, MD, of Rochester, N.Y., emphasized awareness that CLABSIs occur frequently outside the ICU. “If you are only looking for CLABSI in the ICU, then you are missing more than half of the story,” Dr. Shelly said. Researchers from the National Health Safety Network (NHSN) provided more information about the substantial numbers of CLABSIs that occur on general medical wards.
Carolyn Gould, MD, MS, of the Centers for Disease Control and Prevention (CDC) confirmed that catheter-associated urinary tract infections (CAUTIs) are the most common type of HAI. CAUTIs occur at a frequency of >560,000 infections per year and cost as much as $500 million per year, she explained. Strategies to prevent CAUTIs include inserting urinary catheters only for appropriate indications and leaving them in place for the shortest possible duration.
In recent years, concern has grown about the prevalence of healthcare-associated Clostridium difficile infection (HA-CDI), which can lead to uncomplicated diarrhea, sepsis, or even death. Several speakers described strategies that reduce HA-CDI development, including the identification and removal of environmental sources of C. diff, accommodating CDI patients in a private room with contact precautions, and minimizing both the frequency and duration of antimicrobial therapy.
Uncertainty about the most reliable tests to confirm CDI was a topic of focus. Enzyme immunoassay (EIA) testing, cell cytotoxin assays, and polymerase chain reaction (PCR) testing are readily available in most U.S. hospitals; however, PCR testing might prove to be the most advantageous since it is rapid, sensitive, and specific.
Neil Fishman, MD, of the University of Pennsylvania School of Medicine in Philadelphia was one of several speakers to address the important role of antimicrobial stewardship program (ASP) development. According to Dr. Fishman, ASP goals should be to “ensure the proper use of antimicrobials” and to “promote cost-effectiveness.” By taking actions that promote the appropriate use of antimicrobials, the following positive consequences can be anticipated:
- Improved clinical outcomes;
- Reduced risk of adverse drug effects; and
- A reduction in, or stabilization of, the rate of antimicrobial resistance.
Multidrug-resistant (MDR) gram-negative Bacillus is a major challenge for hospitals worldwide. The CDC offers two guidelines for the optimal management and isolation of MDR organisms (MDRO): HICPAC 2006 (a management guideline) and HICPAC 2007 (MDRO isolation precaution guidelines). Consistent utilization of these guidelines is crucial to control the spread of MDRO.
The CDC’s Alexander Killen, MD, discussed the increasing proportion of MDR Acinetobacter and Enterobacteriaceae. Emerging issues among these organisms include the development of highly resistant strains, the incidence of which is increasing in nonacute-care settings.
The CDC’s Karen Anderson reported laboratory data on carbapenem-resistant Enterobacteriaceae (CRE) in a long-term-care facility. Her team demonstrated that CRE colonization can persist for up to six months. She speculated that the transfer of resistance between different species occurs, as does patient-to-patient transmission.
The CDC recommends the use of surveillance cultures as part of enhanced precautions. Surveillance is to continue until no new cases are detected.
Karen Clarke, MD, MS, MPH
Ketino Kobaidze, MD, PhD
Mohamad Moussa, MD
Sheri Tejedor, MD
Emory University
School of Medicine, Atlanta
The Fifth Decennial International Conference on Healthcare-Associated Infections 2010, held in March in Atlanta, featured experts from several different fields discussing the significant prevalence of healthcare-associated infections (HAIs) and strategies that may be implemented to reduce their occurrence.
HAIs precipitated by the use of such devices as central venous catheters (CVCs), mechanical ventilators, and indwelling urinary catheters received special emphasis as important sources of patient morbidity and mortality.
Naomi O’Grady of the National Institutes of Health (NIH) summarized the current available knowledge regarding the prevention of central-line-associated bloodstream infections (CLABSIs). Strategies targeting appropriate line maintenance include:
- Chlorhexidine sponge dressings at the CVC insertion site in patients with short-term catheters;
- Cleanse catheter hubs and connectors with alcoholic-chlorhexidine (rather than alcohol alone) after each use; and
- Consider daily bathing of patients with chlorhexidine soap.
Speakers stressed that novel technologies, such as antimicrobial lock solutions and antiseptic- or antibiotic-impregnated catheters, should be considered when CLABSI rates remain high. Mark Shelly, MD, of Rochester, N.Y., emphasized awareness that CLABSIs occur frequently outside the ICU. “If you are only looking for CLABSI in the ICU, then you are missing more than half of the story,” Dr. Shelly said. Researchers from the National Health Safety Network (NHSN) provided more information about the substantial numbers of CLABSIs that occur on general medical wards.
Carolyn Gould, MD, MS, of the Centers for Disease Control and Prevention (CDC) confirmed that catheter-associated urinary tract infections (CAUTIs) are the most common type of HAI. CAUTIs occur at a frequency of >560,000 infections per year and cost as much as $500 million per year, she explained. Strategies to prevent CAUTIs include inserting urinary catheters only for appropriate indications and leaving them in place for the shortest possible duration.
In recent years, concern has grown about the prevalence of healthcare-associated Clostridium difficile infection (HA-CDI), which can lead to uncomplicated diarrhea, sepsis, or even death. Several speakers described strategies that reduce HA-CDI development, including the identification and removal of environmental sources of C. diff, accommodating CDI patients in a private room with contact precautions, and minimizing both the frequency and duration of antimicrobial therapy.
Uncertainty about the most reliable tests to confirm CDI was a topic of focus. Enzyme immunoassay (EIA) testing, cell cytotoxin assays, and polymerase chain reaction (PCR) testing are readily available in most U.S. hospitals; however, PCR testing might prove to be the most advantageous since it is rapid, sensitive, and specific.
Neil Fishman, MD, of the University of Pennsylvania School of Medicine in Philadelphia was one of several speakers to address the important role of antimicrobial stewardship program (ASP) development. According to Dr. Fishman, ASP goals should be to “ensure the proper use of antimicrobials” and to “promote cost-effectiveness.” By taking actions that promote the appropriate use of antimicrobials, the following positive consequences can be anticipated:
- Improved clinical outcomes;
- Reduced risk of adverse drug effects; and
- A reduction in, or stabilization of, the rate of antimicrobial resistance.
Multidrug-resistant (MDR) gram-negative Bacillus is a major challenge for hospitals worldwide. The CDC offers two guidelines for the optimal management and isolation of MDR organisms (MDRO): HICPAC 2006 (a management guideline) and HICPAC 2007 (MDRO isolation precaution guidelines). Consistent utilization of these guidelines is crucial to control the spread of MDRO.
The CDC’s Alexander Killen, MD, discussed the increasing proportion of MDR Acinetobacter and Enterobacteriaceae. Emerging issues among these organisms include the development of highly resistant strains, the incidence of which is increasing in nonacute-care settings.
The CDC’s Karen Anderson reported laboratory data on carbapenem-resistant Enterobacteriaceae (CRE) in a long-term-care facility. Her team demonstrated that CRE colonization can persist for up to six months. She speculated that the transfer of resistance between different species occurs, as does patient-to-patient transmission.
The CDC recommends the use of surveillance cultures as part of enhanced precautions. Surveillance is to continue until no new cases are detected.
Karen Clarke, MD, MS, MPH
Ketino Kobaidze, MD, PhD
Mohamad Moussa, MD
Sheri Tejedor, MD
Emory University
School of Medicine, Atlanta
Hospitalists’ Afghan Tour Atypical of Medical Missions in Active Combat Zones
As my wife is a hospitalist, I was taken aback to find pictures of Ghazni on the front cover of her trade publication for February 2010. Your article was interesting from the vantage point that I actually lived it. I would add the following clarifications:
Maj. (Ramey) Wilson was the battalion surgeon in Ghazni from 2007 to April of 2008. I succeeded him as the sole American physician in the province for 2008 until Ghazni was turned over to the Polish battle group in November of that year. During that time, combat with enemy forces and IED (improvised explosive device) attacks became significantly more common than in the preceding years.
As a neurologist and clinical neurophysiologist, my expertise prior to coming to Afghanistan in trauma care and first aid was quite limited. Our physician assistant was deployed to another base in the province. As indicated in your article, the practice environment was exceedingly crude, without radiologic, lab, or nursing support. While Dr. Wilson had made tremendous strides with the provincial hospital system, the local Afghan health officials encouraged their physicians to send patients to our base when they felt uncomfortable, rather than proceeding through the Afghan system. This overburdened the aid station when the Afghan facility had superior equipment and resources.
Certainly, both the local population and NATO forces in Ghazni were very fortunate to have a physician of Maj. Wilson’s caliber, as he was a one-man state department and Level I trauma center all wrapped into a single package. When the mission became more combat-focused, the humanitarian portion became both more difficult and more dangerous, and tensions increased between the provincial government and our battalion. Further, only briefly alluded to in your article was the additional effect of prolonged family separation, which adds significant and severe psychological stressors during deployment and on return to the U.S.
In short, I suspect that Maj. Wilson’s “challenges met, success exemplified” is atypical of battalion surgeons in the Middle East combat theatre, and definitely was at odds with my own experience in the same area just months later.
John Ney, MD
Former Maj., U.S. Army;
former Battalion Surgeon,
1-506th Infantry, 4th Brigade, 101st Airborne; senior fellow,
clinical research, University of Washington Department of Neurology, Seattle
Consider HM-Pharmacist Collaborations to Solve Manpower Issues, Improve LOS, and Reduce Medication Costs
The 2008 American Society of Hospital Pharmacists and the Society of Hospital Medicine (ASHP-SHM) Statement on Hospitalist-Pharmacist Collaboration encouraged the development of partnerships in order to optimize outcomes in hospitalized patients.1 This alliance comes naturally, as hospitalists and clinical pharmacists share a common goal: improve patient care through implementation of evidence-based medicine. Despite strong encouragement, little literature exists to describe successful collaborations.
In 2008, Mercy Hospital of Iowa City and the University of Iowa College of Pharmacy jointly hired a clinical pharmacist to be devoted to the hospitalist group at Mercy Hospital. This new hire also became a member of a multidisciplinary team. The pharmacists’ duties were established through implementation of facets of the 2008 ASHP-SHM statement.1 Each of the following duties is incorporated into daily practice:
- Attend daily hospitalist morning rounds and interdisciplinary rounds;
- Review patient records on daily basis; confer information or recommendations to physicians as needed throughout the day;
- Reconcile medication at admission and across the continuum of the hospital stay, including discharge;
- Provide patient education and counseling as needed;
- Serve as a drug information resource as needed to physicians, nurses, and other members of the interdisciplinary team;
- Review medication regimens and prescribing practices to ensure adherence to evidence-based medicine and core measures;
- Provide recommendations on pharmacokinetic drug monitoring, as well as renal dose adjustment or other dose adjustments; and
- Assist in the creation and implementation of medication-use policies and protocols, and participate in active, continued surveillance of medication protocols.
It might not be feasible to hire clinical pharmacists to be solely assigned to hospitalist teams, although success has been found at Mercy through the development of a shared clinical position with the College of Pharmacy. Although described as a 50-50 position, a majority of the teaching duties occur on-site at Mercy, working with fourth-year pharmacy students on clinical rotations. It has become a win-win situation: The hospitalist team benefits from a dedicated clinical pharmacist, and the students benefit from a clinical setting with vast opportunities to review general internal-medicine cases.
In contrast to developing a new position, reallocation of resources often is the route by which collaborations evolve. In a 2005 article by Cohen et al at Brookhaven Memorial Hospital in Patchogue, N.Y., patients treated by voluntary attending physicians were compared with patients treated by hospitalists who collaborated with residents from the institution’s accredited pharmacy residency program. Analyses revealed the hospitalist/pharmacist group achieved a 23% shorter length of stay, 21% lower cost of medication, and 1.5 fewer medications per patient.2 The hospitalist/pharmacist group also had a reduced length of IV antibiotic therapy and gastrointestinal medications by 1.7 and 0.9 days, respectively.2
Although anecdotal, an added benefit to having a clinical pharmacist assigned to the HM team at Mercy is continuity and familiarity with the physicians and patients. The clinical pharmacist inherently has a vested interest in the success of the hospitalists as well as the pharmacy department, which provides ongoing momentum for joint projects.
The recent development of the HM model of inpatient care has coincided with a rapid evolution in the role of hospital-based clinical pharmacists. Pharmacologic interventions are utilized for virtually all hospitalized patients, and they are inherently complex and potentially hazardous. Pharmacist involvement with the multidisciplinary hospitalist team provides a mechanism to address and minimize these complexities.
Innovative approaches to reallocate or create collaborative models are needed as the two disciplines, hospitalists and clinical pharmacists, continue to transform inpatient care.
Phyllis Hemerson, PharmD, BCPS
clinical pharmacy specialist
Mercy Hospital, Iowa City
assistant professor, University of Iowa College of Pharmacy
Martin Izakovic, MD, PhD, CPE, FHM, FACP, FACPE
vice president of medical staff affairs and chief medical officer
hospitalist program medical director, Mercy Hospital
References
- Cobaugh DJ, Amin A, Bookwalter T, et al. ASHP-SHM Joint Statement on Hospitalist-Pharmacist Collaboration. Am J Health Syst Pharm. 2008;65(3):260-263.
- Cohen K, Syed S. Hospitalists, pharmacists partner to cut errors. Healthcare Benchmarks Qual Improv. 2005;12(2):18-19.
As my wife is a hospitalist, I was taken aback to find pictures of Ghazni on the front cover of her trade publication for February 2010. Your article was interesting from the vantage point that I actually lived it. I would add the following clarifications:
Maj. (Ramey) Wilson was the battalion surgeon in Ghazni from 2007 to April of 2008. I succeeded him as the sole American physician in the province for 2008 until Ghazni was turned over to the Polish battle group in November of that year. During that time, combat with enemy forces and IED (improvised explosive device) attacks became significantly more common than in the preceding years.
As a neurologist and clinical neurophysiologist, my expertise prior to coming to Afghanistan in trauma care and first aid was quite limited. Our physician assistant was deployed to another base in the province. As indicated in your article, the practice environment was exceedingly crude, without radiologic, lab, or nursing support. While Dr. Wilson had made tremendous strides with the provincial hospital system, the local Afghan health officials encouraged their physicians to send patients to our base when they felt uncomfortable, rather than proceeding through the Afghan system. This overburdened the aid station when the Afghan facility had superior equipment and resources.
Certainly, both the local population and NATO forces in Ghazni were very fortunate to have a physician of Maj. Wilson’s caliber, as he was a one-man state department and Level I trauma center all wrapped into a single package. When the mission became more combat-focused, the humanitarian portion became both more difficult and more dangerous, and tensions increased between the provincial government and our battalion. Further, only briefly alluded to in your article was the additional effect of prolonged family separation, which adds significant and severe psychological stressors during deployment and on return to the U.S.
In short, I suspect that Maj. Wilson’s “challenges met, success exemplified” is atypical of battalion surgeons in the Middle East combat theatre, and definitely was at odds with my own experience in the same area just months later.
John Ney, MD
Former Maj., U.S. Army;
former Battalion Surgeon,
1-506th Infantry, 4th Brigade, 101st Airborne; senior fellow,
clinical research, University of Washington Department of Neurology, Seattle
Consider HM-Pharmacist Collaborations to Solve Manpower Issues, Improve LOS, and Reduce Medication Costs
The 2008 American Society of Hospital Pharmacists and the Society of Hospital Medicine (ASHP-SHM) Statement on Hospitalist-Pharmacist Collaboration encouraged the development of partnerships in order to optimize outcomes in hospitalized patients.1 This alliance comes naturally, as hospitalists and clinical pharmacists share a common goal: improve patient care through implementation of evidence-based medicine. Despite strong encouragement, little literature exists to describe successful collaborations.
In 2008, Mercy Hospital of Iowa City and the University of Iowa College of Pharmacy jointly hired a clinical pharmacist to be devoted to the hospitalist group at Mercy Hospital. This new hire also became a member of a multidisciplinary team. The pharmacists’ duties were established through implementation of facets of the 2008 ASHP-SHM statement.1 Each of the following duties is incorporated into daily practice:
- Attend daily hospitalist morning rounds and interdisciplinary rounds;
- Review patient records on daily basis; confer information or recommendations to physicians as needed throughout the day;
- Reconcile medication at admission and across the continuum of the hospital stay, including discharge;
- Provide patient education and counseling as needed;
- Serve as a drug information resource as needed to physicians, nurses, and other members of the interdisciplinary team;
- Review medication regimens and prescribing practices to ensure adherence to evidence-based medicine and core measures;
- Provide recommendations on pharmacokinetic drug monitoring, as well as renal dose adjustment or other dose adjustments; and
- Assist in the creation and implementation of medication-use policies and protocols, and participate in active, continued surveillance of medication protocols.
It might not be feasible to hire clinical pharmacists to be solely assigned to hospitalist teams, although success has been found at Mercy through the development of a shared clinical position with the College of Pharmacy. Although described as a 50-50 position, a majority of the teaching duties occur on-site at Mercy, working with fourth-year pharmacy students on clinical rotations. It has become a win-win situation: The hospitalist team benefits from a dedicated clinical pharmacist, and the students benefit from a clinical setting with vast opportunities to review general internal-medicine cases.
In contrast to developing a new position, reallocation of resources often is the route by which collaborations evolve. In a 2005 article by Cohen et al at Brookhaven Memorial Hospital in Patchogue, N.Y., patients treated by voluntary attending physicians were compared with patients treated by hospitalists who collaborated with residents from the institution’s accredited pharmacy residency program. Analyses revealed the hospitalist/pharmacist group achieved a 23% shorter length of stay, 21% lower cost of medication, and 1.5 fewer medications per patient.2 The hospitalist/pharmacist group also had a reduced length of IV antibiotic therapy and gastrointestinal medications by 1.7 and 0.9 days, respectively.2
Although anecdotal, an added benefit to having a clinical pharmacist assigned to the HM team at Mercy is continuity and familiarity with the physicians and patients. The clinical pharmacist inherently has a vested interest in the success of the hospitalists as well as the pharmacy department, which provides ongoing momentum for joint projects.
The recent development of the HM model of inpatient care has coincided with a rapid evolution in the role of hospital-based clinical pharmacists. Pharmacologic interventions are utilized for virtually all hospitalized patients, and they are inherently complex and potentially hazardous. Pharmacist involvement with the multidisciplinary hospitalist team provides a mechanism to address and minimize these complexities.
Innovative approaches to reallocate or create collaborative models are needed as the two disciplines, hospitalists and clinical pharmacists, continue to transform inpatient care.
Phyllis Hemerson, PharmD, BCPS
clinical pharmacy specialist
Mercy Hospital, Iowa City
assistant professor, University of Iowa College of Pharmacy
Martin Izakovic, MD, PhD, CPE, FHM, FACP, FACPE
vice president of medical staff affairs and chief medical officer
hospitalist program medical director, Mercy Hospital
References
- Cobaugh DJ, Amin A, Bookwalter T, et al. ASHP-SHM Joint Statement on Hospitalist-Pharmacist Collaboration. Am J Health Syst Pharm. 2008;65(3):260-263.
- Cohen K, Syed S. Hospitalists, pharmacists partner to cut errors. Healthcare Benchmarks Qual Improv. 2005;12(2):18-19.
As my wife is a hospitalist, I was taken aback to find pictures of Ghazni on the front cover of her trade publication for February 2010. Your article was interesting from the vantage point that I actually lived it. I would add the following clarifications:
Maj. (Ramey) Wilson was the battalion surgeon in Ghazni from 2007 to April of 2008. I succeeded him as the sole American physician in the province for 2008 until Ghazni was turned over to the Polish battle group in November of that year. During that time, combat with enemy forces and IED (improvised explosive device) attacks became significantly more common than in the preceding years.
As a neurologist and clinical neurophysiologist, my expertise prior to coming to Afghanistan in trauma care and first aid was quite limited. Our physician assistant was deployed to another base in the province. As indicated in your article, the practice environment was exceedingly crude, without radiologic, lab, or nursing support. While Dr. Wilson had made tremendous strides with the provincial hospital system, the local Afghan health officials encouraged their physicians to send patients to our base when they felt uncomfortable, rather than proceeding through the Afghan system. This overburdened the aid station when the Afghan facility had superior equipment and resources.
Certainly, both the local population and NATO forces in Ghazni were very fortunate to have a physician of Maj. Wilson’s caliber, as he was a one-man state department and Level I trauma center all wrapped into a single package. When the mission became more combat-focused, the humanitarian portion became both more difficult and more dangerous, and tensions increased between the provincial government and our battalion. Further, only briefly alluded to in your article was the additional effect of prolonged family separation, which adds significant and severe psychological stressors during deployment and on return to the U.S.
In short, I suspect that Maj. Wilson’s “challenges met, success exemplified” is atypical of battalion surgeons in the Middle East combat theatre, and definitely was at odds with my own experience in the same area just months later.
John Ney, MD
Former Maj., U.S. Army;
former Battalion Surgeon,
1-506th Infantry, 4th Brigade, 101st Airborne; senior fellow,
clinical research, University of Washington Department of Neurology, Seattle
Consider HM-Pharmacist Collaborations to Solve Manpower Issues, Improve LOS, and Reduce Medication Costs
The 2008 American Society of Hospital Pharmacists and the Society of Hospital Medicine (ASHP-SHM) Statement on Hospitalist-Pharmacist Collaboration encouraged the development of partnerships in order to optimize outcomes in hospitalized patients.1 This alliance comes naturally, as hospitalists and clinical pharmacists share a common goal: improve patient care through implementation of evidence-based medicine. Despite strong encouragement, little literature exists to describe successful collaborations.
In 2008, Mercy Hospital of Iowa City and the University of Iowa College of Pharmacy jointly hired a clinical pharmacist to be devoted to the hospitalist group at Mercy Hospital. This new hire also became a member of a multidisciplinary team. The pharmacists’ duties were established through implementation of facets of the 2008 ASHP-SHM statement.1 Each of the following duties is incorporated into daily practice:
- Attend daily hospitalist morning rounds and interdisciplinary rounds;
- Review patient records on daily basis; confer information or recommendations to physicians as needed throughout the day;
- Reconcile medication at admission and across the continuum of the hospital stay, including discharge;
- Provide patient education and counseling as needed;
- Serve as a drug information resource as needed to physicians, nurses, and other members of the interdisciplinary team;
- Review medication regimens and prescribing practices to ensure adherence to evidence-based medicine and core measures;
- Provide recommendations on pharmacokinetic drug monitoring, as well as renal dose adjustment or other dose adjustments; and
- Assist in the creation and implementation of medication-use policies and protocols, and participate in active, continued surveillance of medication protocols.
It might not be feasible to hire clinical pharmacists to be solely assigned to hospitalist teams, although success has been found at Mercy through the development of a shared clinical position with the College of Pharmacy. Although described as a 50-50 position, a majority of the teaching duties occur on-site at Mercy, working with fourth-year pharmacy students on clinical rotations. It has become a win-win situation: The hospitalist team benefits from a dedicated clinical pharmacist, and the students benefit from a clinical setting with vast opportunities to review general internal-medicine cases.
In contrast to developing a new position, reallocation of resources often is the route by which collaborations evolve. In a 2005 article by Cohen et al at Brookhaven Memorial Hospital in Patchogue, N.Y., patients treated by voluntary attending physicians were compared with patients treated by hospitalists who collaborated with residents from the institution’s accredited pharmacy residency program. Analyses revealed the hospitalist/pharmacist group achieved a 23% shorter length of stay, 21% lower cost of medication, and 1.5 fewer medications per patient.2 The hospitalist/pharmacist group also had a reduced length of IV antibiotic therapy and gastrointestinal medications by 1.7 and 0.9 days, respectively.2
Although anecdotal, an added benefit to having a clinical pharmacist assigned to the HM team at Mercy is continuity and familiarity with the physicians and patients. The clinical pharmacist inherently has a vested interest in the success of the hospitalists as well as the pharmacy department, which provides ongoing momentum for joint projects.
The recent development of the HM model of inpatient care has coincided with a rapid evolution in the role of hospital-based clinical pharmacists. Pharmacologic interventions are utilized for virtually all hospitalized patients, and they are inherently complex and potentially hazardous. Pharmacist involvement with the multidisciplinary hospitalist team provides a mechanism to address and minimize these complexities.
Innovative approaches to reallocate or create collaborative models are needed as the two disciplines, hospitalists and clinical pharmacists, continue to transform inpatient care.
Phyllis Hemerson, PharmD, BCPS
clinical pharmacy specialist
Mercy Hospital, Iowa City
assistant professor, University of Iowa College of Pharmacy
Martin Izakovic, MD, PhD, CPE, FHM, FACP, FACPE
vice president of medical staff affairs and chief medical officer
hospitalist program medical director, Mercy Hospital
References
- Cobaugh DJ, Amin A, Bookwalter T, et al. ASHP-SHM Joint Statement on Hospitalist-Pharmacist Collaboration. Am J Health Syst Pharm. 2008;65(3):260-263.
- Cohen K, Syed S. Hospitalists, pharmacists partner to cut errors. Healthcare Benchmarks Qual Improv. 2005;12(2):18-19.