User login
Budget Checkup

Editor’s note: Part one of a two-part series.
Why does a particular hospitalist practice require more than the typical amount of financial support from a hospital? This is one of the most common questions I am asked. This month and next, I will provide a thorough list of potential answers.
SHM’s “2007-2008 Bi-annual Survey on the State of the Hospital Medicine Movement” showed that hospitals pay an average of $97,400 per year in support per full-time hospitalist. I suspect that amount is higher now. Nevertheless, hospital executives and hospitalists should understand the reasons why the hospital support that is required for their practice might be more or less.
A comprehensive list of potential reasons would include dozens of factors, and my intent is only to highlight some of the most common and significant ones.
Documentation, Coding, Billing, and Collecting
This is an area in which many, if not most, practices have room for improvement. One very simple way to estimate how your group is doing on these things is to think about how you’re performing on the following tasks:
- Do the hospitalists really understand the documentation requirements for each CPT code, and is their performance in selecting CPT codes audited regularly (e.g., annually)?1
- Does the group have a reliable method of charge capture that minimizes problems like lost charges? Is there an established “chain of custody” of this information, from the hospitalist to the biller?
- Is there a rigorous review or audit of the biller’s performance? Does the group monitor metrics, such as days in accounts receivable, collection rate, etc.? Is there a periodic audit of the biller? An audit could be as simple as tracking down five to 10 billed encounters from six months prior for each doctor in the practice, and reviewing the status of each bill (e.g., paid, written off, or perhaps the bill has vanished or never made it into the billing system).
- Is revenue appropriately applied to the hospitalist cost center? For many hospital-employed hospitalists, payors might be including their professional fee payments on the same remittance advice as hospital inpatient payments (due to same tax ID number). The hospital’s business office might be unable or unwilling to break these payments into hospital and professional fee portions and apply them correctly. Hospital-employed hospitalists should know whether their collections are being applied to their revenue center accurately.
Payor Mix
The two factors that govern the amount of professional fee revenues a hospitalist practice will collect are the integrity of the billing process (described above) and the payor mix. The payor mix for most hospitalist practices is roughly 55% to 60% Medicare, 5% to 10% self-pay, 5% to 10% Medicaid, and commercial insurance for the rest.
A hospitalist practice that is significantly different from this example should expect professional fee collections to vary accordingly.
Hospitalist Fee Schedule
My experience is that very few hospitalists know their own fee schedule. The term “fee schedule” is generally used to mean the billed charge for each type of service provided. A hospitalist fee schedule usually fits on a single page, with a list of CPT codes (admits, consults, followups, etc.) down one column and the charge for that service in a second column to the right. It would be reasonable to post the fee schedule in hospitalists’ offices.
Groups that use electronic charge capture, in which the doctor enters into a computer the CPT code to bill for each patient daily, can often see the related charge for each code as it is entered.
Someone connected to the practice, often in the billing office, should review the fee schedule—at least annually—to ensure that services aren’t being billed below the rate allowed by payors.
Negotiated Rates Paid by Commercial Insurance
Some hospitalist groups are able to negotiate higher payments than the typical rates paid by commercial payors. Because commercial insurance is a relatively small portion of most hospitalists’ payor mix, this might not have a large impact on the overall practice finances. So my sense is that most groups don’t pursue this opportunity.
Groups in markets with significant managed care are an exception. They usually are aggressive in negotiations for commercial payor rates.
Some hospital-employed HM groups might end up with lower commercial rates than they could have. Here is how it might happen: A hospital negotiates with Aetna to pay rates for hospital services (the bills submitted by the hospital, not the physician bills) that are attractive to the hospital. To make this proposal more palatable to Aetna, the hospital says it will accept lower rates for its employed physicians, including hospitalists. So the hospitalists’ collections end up lower, and the support paid by the hospital to the hospitalist group is correspondingly higher. The hospital ends up fine in this scenario, because it is being paid an attractive rate by Aetna for hospital services, but the hospitalist practice appears to be underperforming financially.
It is worth knowing if this is an issue at your practice, but in most cases it won’t explain larger problems in the hospitalist budget or amount of support required from the hospital.
Accounting Issues
Budgets and financial statements can be confusing, and revenues and expenses might not be what you expect. For example, in my practice, auditors told our accountants that we needed to accrue an extra month of salary into this year’s budget. So when looking at our fiscal year-end financial statement, the salary expense is for 13 months instead of 12 months. This quirk made it appear that we required more than the budgeted amount of support from our hospital, when in fact we performed better than budget this year.
I certainly can’t explain all the reasons for unusual accounting issues, and I still struggle to understand why accrual accounting is better than cash-basis accounting. My best advice is to have the lead hospitalist in your group get to know the accountant who handles your budget and financial statements. The accountant should explain all of these issues clearly.
In next month’s column, I’ll review how a hospitalist practice’s internal operations, such as staffing and scheduling, can have a major influence on the budget and the amount of support required from the hospital. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Centers for Medicare and Medicaid Services. Improper medicare fee-for-service payments report, November 2006: long report. CMS Web site. Available at: www.cms.hhs.gov/apps/er_report/preview_er_report_print.asp?from=public&which=long&reportID=5. Accessed Sept. 1, 2009.
Editor’s note: Part one of a two-part series.
Why does a particular hospitalist practice require more than the typical amount of financial support from a hospital? This is one of the most common questions I am asked. This month and next, I will provide a thorough list of potential answers.
SHM’s “2007-2008 Bi-annual Survey on the State of the Hospital Medicine Movement” showed that hospitals pay an average of $97,400 per year in support per full-time hospitalist. I suspect that amount is higher now. Nevertheless, hospital executives and hospitalists should understand the reasons why the hospital support that is required for their practice might be more or less.
A comprehensive list of potential reasons would include dozens of factors, and my intent is only to highlight some of the most common and significant ones.
Documentation, Coding, Billing, and Collecting
This is an area in which many, if not most, practices have room for improvement. One very simple way to estimate how your group is doing on these things is to think about how you’re performing on the following tasks:
- Do the hospitalists really understand the documentation requirements for each CPT code, and is their performance in selecting CPT codes audited regularly (e.g., annually)?1
- Does the group have a reliable method of charge capture that minimizes problems like lost charges? Is there an established “chain of custody” of this information, from the hospitalist to the biller?
- Is there a rigorous review or audit of the biller’s performance? Does the group monitor metrics, such as days in accounts receivable, collection rate, etc.? Is there a periodic audit of the biller? An audit could be as simple as tracking down five to 10 billed encounters from six months prior for each doctor in the practice, and reviewing the status of each bill (e.g., paid, written off, or perhaps the bill has vanished or never made it into the billing system).
- Is revenue appropriately applied to the hospitalist cost center? For many hospital-employed hospitalists, payors might be including their professional fee payments on the same remittance advice as hospital inpatient payments (due to same tax ID number). The hospital’s business office might be unable or unwilling to break these payments into hospital and professional fee portions and apply them correctly. Hospital-employed hospitalists should know whether their collections are being applied to their revenue center accurately.
Payor Mix
The two factors that govern the amount of professional fee revenues a hospitalist practice will collect are the integrity of the billing process (described above) and the payor mix. The payor mix for most hospitalist practices is roughly 55% to 60% Medicare, 5% to 10% self-pay, 5% to 10% Medicaid, and commercial insurance for the rest.
A hospitalist practice that is significantly different from this example should expect professional fee collections to vary accordingly.
Hospitalist Fee Schedule
My experience is that very few hospitalists know their own fee schedule. The term “fee schedule” is generally used to mean the billed charge for each type of service provided. A hospitalist fee schedule usually fits on a single page, with a list of CPT codes (admits, consults, followups, etc.) down one column and the charge for that service in a second column to the right. It would be reasonable to post the fee schedule in hospitalists’ offices.
Groups that use electronic charge capture, in which the doctor enters into a computer the CPT code to bill for each patient daily, can often see the related charge for each code as it is entered.
Someone connected to the practice, often in the billing office, should review the fee schedule—at least annually—to ensure that services aren’t being billed below the rate allowed by payors.
Negotiated Rates Paid by Commercial Insurance
Some hospitalist groups are able to negotiate higher payments than the typical rates paid by commercial payors. Because commercial insurance is a relatively small portion of most hospitalists’ payor mix, this might not have a large impact on the overall practice finances. So my sense is that most groups don’t pursue this opportunity.
Groups in markets with significant managed care are an exception. They usually are aggressive in negotiations for commercial payor rates.
Some hospital-employed HM groups might end up with lower commercial rates than they could have. Here is how it might happen: A hospital negotiates with Aetna to pay rates for hospital services (the bills submitted by the hospital, not the physician bills) that are attractive to the hospital. To make this proposal more palatable to Aetna, the hospital says it will accept lower rates for its employed physicians, including hospitalists. So the hospitalists’ collections end up lower, and the support paid by the hospital to the hospitalist group is correspondingly higher. The hospital ends up fine in this scenario, because it is being paid an attractive rate by Aetna for hospital services, but the hospitalist practice appears to be underperforming financially.
It is worth knowing if this is an issue at your practice, but in most cases it won’t explain larger problems in the hospitalist budget or amount of support required from the hospital.
Accounting Issues
Budgets and financial statements can be confusing, and revenues and expenses might not be what you expect. For example, in my practice, auditors told our accountants that we needed to accrue an extra month of salary into this year’s budget. So when looking at our fiscal year-end financial statement, the salary expense is for 13 months instead of 12 months. This quirk made it appear that we required more than the budgeted amount of support from our hospital, when in fact we performed better than budget this year.
I certainly can’t explain all the reasons for unusual accounting issues, and I still struggle to understand why accrual accounting is better than cash-basis accounting. My best advice is to have the lead hospitalist in your group get to know the accountant who handles your budget and financial statements. The accountant should explain all of these issues clearly.
In next month’s column, I’ll review how a hospitalist practice’s internal operations, such as staffing and scheduling, can have a major influence on the budget and the amount of support required from the hospital. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Centers for Medicare and Medicaid Services. Improper medicare fee-for-service payments report, November 2006: long report. CMS Web site. Available at: www.cms.hhs.gov/apps/er_report/preview_er_report_print.asp?from=public&which=long&reportID=5. Accessed Sept. 1, 2009.
Editor’s note: Part one of a two-part series.
Why does a particular hospitalist practice require more than the typical amount of financial support from a hospital? This is one of the most common questions I am asked. This month and next, I will provide a thorough list of potential answers.
SHM’s “2007-2008 Bi-annual Survey on the State of the Hospital Medicine Movement” showed that hospitals pay an average of $97,400 per year in support per full-time hospitalist. I suspect that amount is higher now. Nevertheless, hospital executives and hospitalists should understand the reasons why the hospital support that is required for their practice might be more or less.
A comprehensive list of potential reasons would include dozens of factors, and my intent is only to highlight some of the most common and significant ones.
Documentation, Coding, Billing, and Collecting
This is an area in which many, if not most, practices have room for improvement. One very simple way to estimate how your group is doing on these things is to think about how you’re performing on the following tasks:
- Do the hospitalists really understand the documentation requirements for each CPT code, and is their performance in selecting CPT codes audited regularly (e.g., annually)?1
- Does the group have a reliable method of charge capture that minimizes problems like lost charges? Is there an established “chain of custody” of this information, from the hospitalist to the biller?
- Is there a rigorous review or audit of the biller’s performance? Does the group monitor metrics, such as days in accounts receivable, collection rate, etc.? Is there a periodic audit of the biller? An audit could be as simple as tracking down five to 10 billed encounters from six months prior for each doctor in the practice, and reviewing the status of each bill (e.g., paid, written off, or perhaps the bill has vanished or never made it into the billing system).
- Is revenue appropriately applied to the hospitalist cost center? For many hospital-employed hospitalists, payors might be including their professional fee payments on the same remittance advice as hospital inpatient payments (due to same tax ID number). The hospital’s business office might be unable or unwilling to break these payments into hospital and professional fee portions and apply them correctly. Hospital-employed hospitalists should know whether their collections are being applied to their revenue center accurately.
Payor Mix
The two factors that govern the amount of professional fee revenues a hospitalist practice will collect are the integrity of the billing process (described above) and the payor mix. The payor mix for most hospitalist practices is roughly 55% to 60% Medicare, 5% to 10% self-pay, 5% to 10% Medicaid, and commercial insurance for the rest.
A hospitalist practice that is significantly different from this example should expect professional fee collections to vary accordingly.
Hospitalist Fee Schedule
My experience is that very few hospitalists know their own fee schedule. The term “fee schedule” is generally used to mean the billed charge for each type of service provided. A hospitalist fee schedule usually fits on a single page, with a list of CPT codes (admits, consults, followups, etc.) down one column and the charge for that service in a second column to the right. It would be reasonable to post the fee schedule in hospitalists’ offices.
Groups that use electronic charge capture, in which the doctor enters into a computer the CPT code to bill for each patient daily, can often see the related charge for each code as it is entered.
Someone connected to the practice, often in the billing office, should review the fee schedule—at least annually—to ensure that services aren’t being billed below the rate allowed by payors.
Negotiated Rates Paid by Commercial Insurance
Some hospitalist groups are able to negotiate higher payments than the typical rates paid by commercial payors. Because commercial insurance is a relatively small portion of most hospitalists’ payor mix, this might not have a large impact on the overall practice finances. So my sense is that most groups don’t pursue this opportunity.
Groups in markets with significant managed care are an exception. They usually are aggressive in negotiations for commercial payor rates.
Some hospital-employed HM groups might end up with lower commercial rates than they could have. Here is how it might happen: A hospital negotiates with Aetna to pay rates for hospital services (the bills submitted by the hospital, not the physician bills) that are attractive to the hospital. To make this proposal more palatable to Aetna, the hospital says it will accept lower rates for its employed physicians, including hospitalists. So the hospitalists’ collections end up lower, and the support paid by the hospital to the hospitalist group is correspondingly higher. The hospital ends up fine in this scenario, because it is being paid an attractive rate by Aetna for hospital services, but the hospitalist practice appears to be underperforming financially.
It is worth knowing if this is an issue at your practice, but in most cases it won’t explain larger problems in the hospitalist budget or amount of support required from the hospital.
Accounting Issues
Budgets and financial statements can be confusing, and revenues and expenses might not be what you expect. For example, in my practice, auditors told our accountants that we needed to accrue an extra month of salary into this year’s budget. So when looking at our fiscal year-end financial statement, the salary expense is for 13 months instead of 12 months. This quirk made it appear that we required more than the budgeted amount of support from our hospital, when in fact we performed better than budget this year.
I certainly can’t explain all the reasons for unusual accounting issues, and I still struggle to understand why accrual accounting is better than cash-basis accounting. My best advice is to have the lead hospitalist in your group get to know the accountant who handles your budget and financial statements. The accountant should explain all of these issues clearly.
In next month’s column, I’ll review how a hospitalist practice’s internal operations, such as staffing and scheduling, can have a major influence on the budget and the amount of support required from the hospital. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program.” This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Centers for Medicare and Medicaid Services. Improper medicare fee-for-service payments report, November 2006: long report. CMS Web site. Available at: www.cms.hhs.gov/apps/er_report/preview_er_report_print.asp?from=public&which=long&reportID=5. Accessed Sept. 1, 2009.
Spanish Flu Redux?

Apocalypse, pestilence, death. As I head back to work after a late-summer vacation, those words are on the tip of my tongue. Now before your mind drifts too far afield, this is not a synopsis of the time spent with family, or even my in-laws—although some have used similar words to describe my mother’s cooking. Rather, these are the descriptors of my vacation reading.
Summer Reading
I started the week relaxing contentedly with Cormac McCarthy’s “The Road.” I chose this book in part because I noticed that it soon will be released as a movie, but mostly because it had won the dustiest-book-in-my-office-reading-pile award. This tale of a young boy and his father traversing a post-apocalyptic America was shocking and surreal. I couldn’t help but interchange images of my 2-year-old son, Greyson, and me out on that road fighting for our existence. In my personal fictional account, I continuously, and heroically, MacGyver my way across a burned-out and treacherous landscape with death-defying adeptness—all the while Grey unknowingly totters, drooling and muttering in tow.

Reality, of course, would paint us in substantially different roles, with mine involving the lion’s share of muttering and drooling, leaving Grey wishing the apocalyptic dealer had dealt him his mother instead.
Next up, “The Last Town on Earth,” by Thomas Mullen. I don’t recall how this book got into my reading pile, but I’m glad it did. The story is set in the fictional city of Commonwealth in 1918. The small, isolated mill town makes the drastic decision to stanch the tide of Spanish flu by cutting itself off from civilization through a self-imposed quarantine.
It is here, on p. 98, that I was sidetracked by a family member’s question—“Do you think this swine flu will be as bad as the Spanish flu?” I was asked shortly after being inquired about my reading choice. “Of course not,” I replied knowingly, moments before realizing I didn’t know. In fact, I didn’t have the faintest idea—not because it’s tough to divine the future, but because I realized I had little more than a passing knowledge of the famous flu that raked the world early last century. And with that, I was off on my final vacation reading session—a quest to slake my thirst for influenza knowledge.
Flu Pandemic
The Spanish flu pandemic of 1918-1920 was the first of three to hit in the 20th century. It took its name not from its site of origin (debated but generally felt to be the U.S., Kansas specifically), but rather from the fact that Spain, a neutral country in World War I, had the most uncensored lines of communication, so the most credible news of the disease came from that country. This provided the false impression that Spain was the only—or at least most dramatically—affected country. Like today’s swine flu, the Spanish flu was an H1N1 influenza. To sate your inner microbiologist, this means the virus exhibits the first of 16 subtypes of hemagglutinin (H) and nine subtypes of neuraminidase (N). Generally, only H1, H2, H3, and N1 and N2 affect humans, and tend to cause mild disease in otherwise healthy populations, killing the immunocompromised, the very young, and the very old. This typically results in a case-fatality rate of about 0.1% and 250,000 to 500,000 deaths worldwide annually.
The Spanish flu, however, was different. For reasons that are not entirely clear, the Spanish flu struck in two waves. The first wave, in the spring of 1918, induced typical flu-like illness with generally mild outcomes, except for the immunocompromised. The second wave was unusual for two reasons. First, it began in the late summer of 1918, rather than the typical winter pattern seen in North America. Second, it was much more deadly, inducing what has been termed a cytokine storm. This immunological avalanche produced more severe disease in the immunopotent young, healthy populations—resulting in its unprecedented mortality in this cohort. In fact, upward of 99% of all Spanish flu deaths were in people younger than 65.
In the end, the pandemic left a broad swath of destruction in its wake. It is estimated that 500 million people—one-third of the world’s population at the time—were infected. The mortality rate was 10% to 20%, resulting in 50 million to 100 million deaths. Put another way, the Spanish flu killed 5% of humanity.
It did so rapidly. Nearly 1 million people died per week in the first 25 weeks of the second wave. To put it in perspective, it took HIV 25 years to reach that number. Thus, historians have termed the Spanish flu “the greatest medical holocaust in history.”
And then as quickly as it commenced, it abated. For example, in Philadelphia, there were about 5,000 flu deaths in one week in October 1918, yet a month later, the virus had nearly disappeared from the city. It’s not clear why this happened, but prevailing theories postulate that either the medical community got better at managing its mortal complications (e.g., bacterial pneumonia), or the bug itself mutated to a less virulent strain.
Is the Swine Flu our Spanish Flu?
On June 11, 2009, the World Health Organization (WHO) declared that the current H1N1 flu virus had reached pandemic status. This novel H1N1 serotype appears to be a direct descendent of the Spanish H1N1 subtype, but the new strain also combines genetic material culled from swine and birds reassorted in a manner that results in limited innate human defenses. And like the Spanish variant, it appears this new strain is hitting earlier in the year than usual and disproportionately affecting the young, with about two-thirds of U.S. deaths coming in the 25- to 64-year-old demographic.
So can we expect hundreds of millions of deaths from swine flu? Probably not. The WHO has been cautious to note that the upgrade to pandemic status was based on the rapidity and ease of spread, not the lethality of the virus. Furthermore, the Centers for Disease Control and Prevention (CDC)—which publishes a wonderful weekly update called FluView (www.cdc.gov/flu/weekly/)—notes that while the number of doctor’s visits for influenza-like illnesses through mid-August is unusually high, the rates of hospitalizations and proportion of deaths attributed to pneumonia and influenza are low and within normal limits for this time of year. Further, the virus continues in its original form, meaning it has not mutated, become more resistant to antiviral drugs, or been altered from the viruses selected for the 2009 vaccine.
So while we certainly must brace for the worst, I feel comfortable in the answer I provided my family member. I also am confident that Grey won’t be quarantined or left to roam the barren Earth anytime soon. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Apocalypse, pestilence, death. As I head back to work after a late-summer vacation, those words are on the tip of my tongue. Now before your mind drifts too far afield, this is not a synopsis of the time spent with family, or even my in-laws—although some have used similar words to describe my mother’s cooking. Rather, these are the descriptors of my vacation reading.
Summer Reading
I started the week relaxing contentedly with Cormac McCarthy’s “The Road.” I chose this book in part because I noticed that it soon will be released as a movie, but mostly because it had won the dustiest-book-in-my-office-reading-pile award. This tale of a young boy and his father traversing a post-apocalyptic America was shocking and surreal. I couldn’t help but interchange images of my 2-year-old son, Greyson, and me out on that road fighting for our existence. In my personal fictional account, I continuously, and heroically, MacGyver my way across a burned-out and treacherous landscape with death-defying adeptness—all the while Grey unknowingly totters, drooling and muttering in tow.
Reality, of course, would paint us in substantially different roles, with mine involving the lion’s share of muttering and drooling, leaving Grey wishing the apocalyptic dealer had dealt him his mother instead.
Next up, “The Last Town on Earth,” by Thomas Mullen. I don’t recall how this book got into my reading pile, but I’m glad it did. The story is set in the fictional city of Commonwealth in 1918. The small, isolated mill town makes the drastic decision to stanch the tide of Spanish flu by cutting itself off from civilization through a self-imposed quarantine.
It is here, on p. 98, that I was sidetracked by a family member’s question—“Do you think this swine flu will be as bad as the Spanish flu?” I was asked shortly after being inquired about my reading choice. “Of course not,” I replied knowingly, moments before realizing I didn’t know. In fact, I didn’t have the faintest idea—not because it’s tough to divine the future, but because I realized I had little more than a passing knowledge of the famous flu that raked the world early last century. And with that, I was off on my final vacation reading session—a quest to slake my thirst for influenza knowledge.
Flu Pandemic
The Spanish flu pandemic of 1918-1920 was the first of three to hit in the 20th century. It took its name not from its site of origin (debated but generally felt to be the U.S., Kansas specifically), but rather from the fact that Spain, a neutral country in World War I, had the most uncensored lines of communication, so the most credible news of the disease came from that country. This provided the false impression that Spain was the only—or at least most dramatically—affected country. Like today’s swine flu, the Spanish flu was an H1N1 influenza. To sate your inner microbiologist, this means the virus exhibits the first of 16 subtypes of hemagglutinin (H) and nine subtypes of neuraminidase (N). Generally, only H1, H2, H3, and N1 and N2 affect humans, and tend to cause mild disease in otherwise healthy populations, killing the immunocompromised, the very young, and the very old. This typically results in a case-fatality rate of about 0.1% and 250,000 to 500,000 deaths worldwide annually.
The Spanish flu, however, was different. For reasons that are not entirely clear, the Spanish flu struck in two waves. The first wave, in the spring of 1918, induced typical flu-like illness with generally mild outcomes, except for the immunocompromised. The second wave was unusual for two reasons. First, it began in the late summer of 1918, rather than the typical winter pattern seen in North America. Second, it was much more deadly, inducing what has been termed a cytokine storm. This immunological avalanche produced more severe disease in the immunopotent young, healthy populations—resulting in its unprecedented mortality in this cohort. In fact, upward of 99% of all Spanish flu deaths were in people younger than 65.
In the end, the pandemic left a broad swath of destruction in its wake. It is estimated that 500 million people—one-third of the world’s population at the time—were infected. The mortality rate was 10% to 20%, resulting in 50 million to 100 million deaths. Put another way, the Spanish flu killed 5% of humanity.
It did so rapidly. Nearly 1 million people died per week in the first 25 weeks of the second wave. To put it in perspective, it took HIV 25 years to reach that number. Thus, historians have termed the Spanish flu “the greatest medical holocaust in history.”
And then as quickly as it commenced, it abated. For example, in Philadelphia, there were about 5,000 flu deaths in one week in October 1918, yet a month later, the virus had nearly disappeared from the city. It’s not clear why this happened, but prevailing theories postulate that either the medical community got better at managing its mortal complications (e.g., bacterial pneumonia), or the bug itself mutated to a less virulent strain.
Is the Swine Flu our Spanish Flu?
On June 11, 2009, the World Health Organization (WHO) declared that the current H1N1 flu virus had reached pandemic status. This novel H1N1 serotype appears to be a direct descendent of the Spanish H1N1 subtype, but the new strain also combines genetic material culled from swine and birds reassorted in a manner that results in limited innate human defenses. And like the Spanish variant, it appears this new strain is hitting earlier in the year than usual and disproportionately affecting the young, with about two-thirds of U.S. deaths coming in the 25- to 64-year-old demographic.
So can we expect hundreds of millions of deaths from swine flu? Probably not. The WHO has been cautious to note that the upgrade to pandemic status was based on the rapidity and ease of spread, not the lethality of the virus. Furthermore, the Centers for Disease Control and Prevention (CDC)—which publishes a wonderful weekly update called FluView (www.cdc.gov/flu/weekly/)—notes that while the number of doctor’s visits for influenza-like illnesses through mid-August is unusually high, the rates of hospitalizations and proportion of deaths attributed to pneumonia and influenza are low and within normal limits for this time of year. Further, the virus continues in its original form, meaning it has not mutated, become more resistant to antiviral drugs, or been altered from the viruses selected for the 2009 vaccine.
So while we certainly must brace for the worst, I feel comfortable in the answer I provided my family member. I also am confident that Grey won’t be quarantined or left to roam the barren Earth anytime soon. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Apocalypse, pestilence, death. As I head back to work after a late-summer vacation, those words are on the tip of my tongue. Now before your mind drifts too far afield, this is not a synopsis of the time spent with family, or even my in-laws—although some have used similar words to describe my mother’s cooking. Rather, these are the descriptors of my vacation reading.
Summer Reading
I started the week relaxing contentedly with Cormac McCarthy’s “The Road.” I chose this book in part because I noticed that it soon will be released as a movie, but mostly because it had won the dustiest-book-in-my-office-reading-pile award. This tale of a young boy and his father traversing a post-apocalyptic America was shocking and surreal. I couldn’t help but interchange images of my 2-year-old son, Greyson, and me out on that road fighting for our existence. In my personal fictional account, I continuously, and heroically, MacGyver my way across a burned-out and treacherous landscape with death-defying adeptness—all the while Grey unknowingly totters, drooling and muttering in tow.
Reality, of course, would paint us in substantially different roles, with mine involving the lion’s share of muttering and drooling, leaving Grey wishing the apocalyptic dealer had dealt him his mother instead.
Next up, “The Last Town on Earth,” by Thomas Mullen. I don’t recall how this book got into my reading pile, but I’m glad it did. The story is set in the fictional city of Commonwealth in 1918. The small, isolated mill town makes the drastic decision to stanch the tide of Spanish flu by cutting itself off from civilization through a self-imposed quarantine.
It is here, on p. 98, that I was sidetracked by a family member’s question—“Do you think this swine flu will be as bad as the Spanish flu?” I was asked shortly after being inquired about my reading choice. “Of course not,” I replied knowingly, moments before realizing I didn’t know. In fact, I didn’t have the faintest idea—not because it’s tough to divine the future, but because I realized I had little more than a passing knowledge of the famous flu that raked the world early last century. And with that, I was off on my final vacation reading session—a quest to slake my thirst for influenza knowledge.
Flu Pandemic
The Spanish flu pandemic of 1918-1920 was the first of three to hit in the 20th century. It took its name not from its site of origin (debated but generally felt to be the U.S., Kansas specifically), but rather from the fact that Spain, a neutral country in World War I, had the most uncensored lines of communication, so the most credible news of the disease came from that country. This provided the false impression that Spain was the only—or at least most dramatically—affected country. Like today’s swine flu, the Spanish flu was an H1N1 influenza. To sate your inner microbiologist, this means the virus exhibits the first of 16 subtypes of hemagglutinin (H) and nine subtypes of neuraminidase (N). Generally, only H1, H2, H3, and N1 and N2 affect humans, and tend to cause mild disease in otherwise healthy populations, killing the immunocompromised, the very young, and the very old. This typically results in a case-fatality rate of about 0.1% and 250,000 to 500,000 deaths worldwide annually.
The Spanish flu, however, was different. For reasons that are not entirely clear, the Spanish flu struck in two waves. The first wave, in the spring of 1918, induced typical flu-like illness with generally mild outcomes, except for the immunocompromised. The second wave was unusual for two reasons. First, it began in the late summer of 1918, rather than the typical winter pattern seen in North America. Second, it was much more deadly, inducing what has been termed a cytokine storm. This immunological avalanche produced more severe disease in the immunopotent young, healthy populations—resulting in its unprecedented mortality in this cohort. In fact, upward of 99% of all Spanish flu deaths were in people younger than 65.
In the end, the pandemic left a broad swath of destruction in its wake. It is estimated that 500 million people—one-third of the world’s population at the time—were infected. The mortality rate was 10% to 20%, resulting in 50 million to 100 million deaths. Put another way, the Spanish flu killed 5% of humanity.
It did so rapidly. Nearly 1 million people died per week in the first 25 weeks of the second wave. To put it in perspective, it took HIV 25 years to reach that number. Thus, historians have termed the Spanish flu “the greatest medical holocaust in history.”
And then as quickly as it commenced, it abated. For example, in Philadelphia, there were about 5,000 flu deaths in one week in October 1918, yet a month later, the virus had nearly disappeared from the city. It’s not clear why this happened, but prevailing theories postulate that either the medical community got better at managing its mortal complications (e.g., bacterial pneumonia), or the bug itself mutated to a less virulent strain.
Is the Swine Flu our Spanish Flu?
On June 11, 2009, the World Health Organization (WHO) declared that the current H1N1 flu virus had reached pandemic status. This novel H1N1 serotype appears to be a direct descendent of the Spanish H1N1 subtype, but the new strain also combines genetic material culled from swine and birds reassorted in a manner that results in limited innate human defenses. And like the Spanish variant, it appears this new strain is hitting earlier in the year than usual and disproportionately affecting the young, with about two-thirds of U.S. deaths coming in the 25- to 64-year-old demographic.
So can we expect hundreds of millions of deaths from swine flu? Probably not. The WHO has been cautious to note that the upgrade to pandemic status was based on the rapidity and ease of spread, not the lethality of the virus. Furthermore, the Centers for Disease Control and Prevention (CDC)—which publishes a wonderful weekly update called FluView (www.cdc.gov/flu/weekly/)—notes that while the number of doctor’s visits for influenza-like illnesses through mid-August is unusually high, the rates of hospitalizations and proportion of deaths attributed to pneumonia and influenza are low and within normal limits for this time of year. Further, the virus continues in its original form, meaning it has not mutated, become more resistant to antiviral drugs, or been altered from the viruses selected for the 2009 vaccine.
So while we certainly must brace for the worst, I feel comfortable in the answer I provided my family member. I also am confident that Grey won’t be quarantined or left to roam the barren Earth anytime soon. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
The Time to Act Is Now

It should come as no surprise to most hospitalists that healthcare-associated infections (HAIs) are among the leading causes of death in the U.S. The Centers for Disease Control and Prevention (CDC) estimates that from 5% to 10% of hospitalized patients develops an HAI, which leads to nearly 100,000 deaths every year.
The big four infection categories are catheter-associated urinary tract infections (CAUTIs), ventilator-associated pneumonia (as well as non-ventilator-associated hospital-acquired pneumonia), central-line-associated bloodstream infections, and surgical-site infections. In addition, Clostridium difficile (C-diff) and methicillin-resistant Staphylococcus aureus (MRSA) infections add to the burden.
While the toll on patients is substantial, the financial burden is equally staggering. It is estimated that HAIs lead to $28 billion to $33 billion in excess healthcare costs each year. So what does this have to do with hospitalists? Everything.
National Efforts to Curb HAIs
The morbidity, mortality, and financial consequences of HAIs have not been lost on patients, payors, and policymakers; each group is demanding action. The Department of Health and Human Services (HHS) is coordinating a national effort addressing HAIs; it aims to bring together many of HHS’ agencies (CDC, Agency for Healthcare Research and Quality, National Institutes of Health, Centers for Medicare and Medicaid Services, etc.) and engage patients, payors, and care providers. As a show of support for these efforts, Congress provided HHS with more than $200 million to target HAIs. After much work, HHS released its action plan to prevent HAIs in January.
SHM was one of the organizations asked to comment on the prevention plan. We did.
- We supported HHS’ focus on process measures (rather than outcomes), which recognizes the inevitability of some HAIs;
- We asked to be more involved in the process of developing and implementing the action plan; and
- We specifically asked for hospitalist representation on the Healthcare Infection Control Practices Advisory Committee (HICPAC), which develops the guidelines and prioritizes national efforts targeting HAI prevention.
Wish granted. In June, I was invited to HHS’ offices in Washington, D.C., along with key stakeholders to hear details of the final plan of action and discuss implementation. The plan (www.hhs.gov/ophs/initiatives/hai/infection.html) addresses key HAIs, establishes baseline rates, and proposes five-year national targets for reductions in infections.
The National Quality Foundation (NQF) has endorsed most of the metrics. The targeted reductions seem reasonable, and they are mostly in line with current evidence on best practices.
Of note, HHS dropped ventilator-associated pneumonia as a target area because of feedback from stakeholders (e.g., SHM) who argued that current definitions of the condition were inadequate to allow accurate measurement of targeted performance improvement efforts. Also of note, SHM was offered a HICPAC seat, which will enhance our ability to further impact the development and evaluation of current and future metrics.
I was invited back to Washington in July to meet with Don Wright, MD, MPH, FAACP, HHS’ principal deputy assistant secretary for health. It’s obvious to me that HHS realizes that any effective campaign to reduce HAI incidence will require engaging hospitalists, and, interestingly, HHS has even heard from other professional societies that hospitalists are a key group to target if you plan to implement hospitalwide interventions that span the ED, hospital wards, ICUs, surgical patients, pediatrics, or any other nook or cranny in the hospital. Hospitalists and SHM appear to be at ground zero in the national effort to combat HAIs.
The Hospitalist’s Role
There are few medical conditions that impact more of SHM’s big tent of membership the way HAIs do. HAIs affect administrators, internists, family practitioners, pediatricians, physician assistants and nurse practitioners, nurses, residents, students, community practitioners, academics, and large management companies … the list goes on. Not surprisingly, efforts to combat HAIs will require teams composed of many of the groups highlighted above working together to create systems-based approaches in their own hospitals—in joint efforts to reduce the rate of preventable HAIs.
Take the most common HAI as an example: catheter-associated urinary tract infections. These infections affect patients in every hospital unit and are familiar to every care provider, regardless of background or practice setting. Administrators should care about CAUTIs in part because CMS no longer pays for a CAUTI when it complicates a hospitalization, but also because these infections adversely affect patient satisfaction. Efforts to reduce CAUTIs will need to address inappropriate catheter insertion, provide alternatives to catheter use (e.g., bladder scans), develop best practices for maintenance of necessary catheters, and facilitate timely removal of catheters no longer needed. Dealing with all of these issues will take a team-based systems approach.
I will not be surprised if hospitalists end up leading these initiatives across the country. Hospitalists will need to share best practices, collaborate in local or national initiatives, provide feedback to SHM and policymakers about what works and what doesn’t, and educate patients about HAIs and prevention. Every hospitalist in the country needs to understand the reasons HAIs develop, know strategies to prevent them, and work to implement these strategies in their hospitals.
Future Directions
Given the urgency, what can you expect next? The action plan is finalized, so HHS is turning its attention to implementation. HHS has reached out to SHM to see how we can get the word out to our members. Dissemination strategies include publication of key messages in The Hospitalist, the Journal of Hospital Medicine, Webinars, e-mail announcements, and presentations at our annual meeting.
And while HHS’ plan of action highlights the metrics, it does not provide detailed strategies to combat HAIs. Prevention tools will need to be developed, tested, and, if effective, disseminated. HHS has asked SHM to help in tool development and dissemination.
HHS will continue to work with CMS to align payment policies that incentivize prevention efforts, and SHM will need to follow these developments closely. In addition, AHRQ is dedicating substantial funds to support the development and dissemination of best practices to prevent HAIs.
HHS acknowledges we still have much to learn about HAIs and their prevention. I expect many hospitalists, as well as SHM, will be at the center of these initiatives. Healthcare-associated infections are a problem that can no longer be ignored. Prevention efforts need to be ramped up. Hospitalists around the country need to prepare to lead and champion these efforts. It is time to act. TH
Dr. Flanders is president of SHM.
It should come as no surprise to most hospitalists that healthcare-associated infections (HAIs) are among the leading causes of death in the U.S. The Centers for Disease Control and Prevention (CDC) estimates that from 5% to 10% of hospitalized patients develops an HAI, which leads to nearly 100,000 deaths every year.
The big four infection categories are catheter-associated urinary tract infections (CAUTIs), ventilator-associated pneumonia (as well as non-ventilator-associated hospital-acquired pneumonia), central-line-associated bloodstream infections, and surgical-site infections. In addition, Clostridium difficile (C-diff) and methicillin-resistant Staphylococcus aureus (MRSA) infections add to the burden.
While the toll on patients is substantial, the financial burden is equally staggering. It is estimated that HAIs lead to $28 billion to $33 billion in excess healthcare costs each year. So what does this have to do with hospitalists? Everything.
National Efforts to Curb HAIs
The morbidity, mortality, and financial consequences of HAIs have not been lost on patients, payors, and policymakers; each group is demanding action. The Department of Health and Human Services (HHS) is coordinating a national effort addressing HAIs; it aims to bring together many of HHS’ agencies (CDC, Agency for Healthcare Research and Quality, National Institutes of Health, Centers for Medicare and Medicaid Services, etc.) and engage patients, payors, and care providers. As a show of support for these efforts, Congress provided HHS with more than $200 million to target HAIs. After much work, HHS released its action plan to prevent HAIs in January.
SHM was one of the organizations asked to comment on the prevention plan. We did.
- We supported HHS’ focus on process measures (rather than outcomes), which recognizes the inevitability of some HAIs;
- We asked to be more involved in the process of developing and implementing the action plan; and
- We specifically asked for hospitalist representation on the Healthcare Infection Control Practices Advisory Committee (HICPAC), which develops the guidelines and prioritizes national efforts targeting HAI prevention.
Wish granted. In June, I was invited to HHS’ offices in Washington, D.C., along with key stakeholders to hear details of the final plan of action and discuss implementation. The plan (www.hhs.gov/ophs/initiatives/hai/infection.html) addresses key HAIs, establishes baseline rates, and proposes five-year national targets for reductions in infections.
The National Quality Foundation (NQF) has endorsed most of the metrics. The targeted reductions seem reasonable, and they are mostly in line with current evidence on best practices.
Of note, HHS dropped ventilator-associated pneumonia as a target area because of feedback from stakeholders (e.g., SHM) who argued that current definitions of the condition were inadequate to allow accurate measurement of targeted performance improvement efforts. Also of note, SHM was offered a HICPAC seat, which will enhance our ability to further impact the development and evaluation of current and future metrics.
I was invited back to Washington in July to meet with Don Wright, MD, MPH, FAACP, HHS’ principal deputy assistant secretary for health. It’s obvious to me that HHS realizes that any effective campaign to reduce HAI incidence will require engaging hospitalists, and, interestingly, HHS has even heard from other professional societies that hospitalists are a key group to target if you plan to implement hospitalwide interventions that span the ED, hospital wards, ICUs, surgical patients, pediatrics, or any other nook or cranny in the hospital. Hospitalists and SHM appear to be at ground zero in the national effort to combat HAIs.
The Hospitalist’s Role
There are few medical conditions that impact more of SHM’s big tent of membership the way HAIs do. HAIs affect administrators, internists, family practitioners, pediatricians, physician assistants and nurse practitioners, nurses, residents, students, community practitioners, academics, and large management companies … the list goes on. Not surprisingly, efforts to combat HAIs will require teams composed of many of the groups highlighted above working together to create systems-based approaches in their own hospitals—in joint efforts to reduce the rate of preventable HAIs.
Take the most common HAI as an example: catheter-associated urinary tract infections. These infections affect patients in every hospital unit and are familiar to every care provider, regardless of background or practice setting. Administrators should care about CAUTIs in part because CMS no longer pays for a CAUTI when it complicates a hospitalization, but also because these infections adversely affect patient satisfaction. Efforts to reduce CAUTIs will need to address inappropriate catheter insertion, provide alternatives to catheter use (e.g., bladder scans), develop best practices for maintenance of necessary catheters, and facilitate timely removal of catheters no longer needed. Dealing with all of these issues will take a team-based systems approach.
I will not be surprised if hospitalists end up leading these initiatives across the country. Hospitalists will need to share best practices, collaborate in local or national initiatives, provide feedback to SHM and policymakers about what works and what doesn’t, and educate patients about HAIs and prevention. Every hospitalist in the country needs to understand the reasons HAIs develop, know strategies to prevent them, and work to implement these strategies in their hospitals.
Future Directions
Given the urgency, what can you expect next? The action plan is finalized, so HHS is turning its attention to implementation. HHS has reached out to SHM to see how we can get the word out to our members. Dissemination strategies include publication of key messages in The Hospitalist, the Journal of Hospital Medicine, Webinars, e-mail announcements, and presentations at our annual meeting.
And while HHS’ plan of action highlights the metrics, it does not provide detailed strategies to combat HAIs. Prevention tools will need to be developed, tested, and, if effective, disseminated. HHS has asked SHM to help in tool development and dissemination.
HHS will continue to work with CMS to align payment policies that incentivize prevention efforts, and SHM will need to follow these developments closely. In addition, AHRQ is dedicating substantial funds to support the development and dissemination of best practices to prevent HAIs.
HHS acknowledges we still have much to learn about HAIs and their prevention. I expect many hospitalists, as well as SHM, will be at the center of these initiatives. Healthcare-associated infections are a problem that can no longer be ignored. Prevention efforts need to be ramped up. Hospitalists around the country need to prepare to lead and champion these efforts. It is time to act. TH
Dr. Flanders is president of SHM.
It should come as no surprise to most hospitalists that healthcare-associated infections (HAIs) are among the leading causes of death in the U.S. The Centers for Disease Control and Prevention (CDC) estimates that from 5% to 10% of hospitalized patients develops an HAI, which leads to nearly 100,000 deaths every year.
The big four infection categories are catheter-associated urinary tract infections (CAUTIs), ventilator-associated pneumonia (as well as non-ventilator-associated hospital-acquired pneumonia), central-line-associated bloodstream infections, and surgical-site infections. In addition, Clostridium difficile (C-diff) and methicillin-resistant Staphylococcus aureus (MRSA) infections add to the burden.
While the toll on patients is substantial, the financial burden is equally staggering. It is estimated that HAIs lead to $28 billion to $33 billion in excess healthcare costs each year. So what does this have to do with hospitalists? Everything.
National Efforts to Curb HAIs
The morbidity, mortality, and financial consequences of HAIs have not been lost on patients, payors, and policymakers; each group is demanding action. The Department of Health and Human Services (HHS) is coordinating a national effort addressing HAIs; it aims to bring together many of HHS’ agencies (CDC, Agency for Healthcare Research and Quality, National Institutes of Health, Centers for Medicare and Medicaid Services, etc.) and engage patients, payors, and care providers. As a show of support for these efforts, Congress provided HHS with more than $200 million to target HAIs. After much work, HHS released its action plan to prevent HAIs in January.
SHM was one of the organizations asked to comment on the prevention plan. We did.
- We supported HHS’ focus on process measures (rather than outcomes), which recognizes the inevitability of some HAIs;
- We asked to be more involved in the process of developing and implementing the action plan; and
- We specifically asked for hospitalist representation on the Healthcare Infection Control Practices Advisory Committee (HICPAC), which develops the guidelines and prioritizes national efforts targeting HAI prevention.
Wish granted. In June, I was invited to HHS’ offices in Washington, D.C., along with key stakeholders to hear details of the final plan of action and discuss implementation. The plan (www.hhs.gov/ophs/initiatives/hai/infection.html) addresses key HAIs, establishes baseline rates, and proposes five-year national targets for reductions in infections.
The National Quality Foundation (NQF) has endorsed most of the metrics. The targeted reductions seem reasonable, and they are mostly in line with current evidence on best practices.
Of note, HHS dropped ventilator-associated pneumonia as a target area because of feedback from stakeholders (e.g., SHM) who argued that current definitions of the condition were inadequate to allow accurate measurement of targeted performance improvement efforts. Also of note, SHM was offered a HICPAC seat, which will enhance our ability to further impact the development and evaluation of current and future metrics.
I was invited back to Washington in July to meet with Don Wright, MD, MPH, FAACP, HHS’ principal deputy assistant secretary for health. It’s obvious to me that HHS realizes that any effective campaign to reduce HAI incidence will require engaging hospitalists, and, interestingly, HHS has even heard from other professional societies that hospitalists are a key group to target if you plan to implement hospitalwide interventions that span the ED, hospital wards, ICUs, surgical patients, pediatrics, or any other nook or cranny in the hospital. Hospitalists and SHM appear to be at ground zero in the national effort to combat HAIs.
The Hospitalist’s Role
There are few medical conditions that impact more of SHM’s big tent of membership the way HAIs do. HAIs affect administrators, internists, family practitioners, pediatricians, physician assistants and nurse practitioners, nurses, residents, students, community practitioners, academics, and large management companies … the list goes on. Not surprisingly, efforts to combat HAIs will require teams composed of many of the groups highlighted above working together to create systems-based approaches in their own hospitals—in joint efforts to reduce the rate of preventable HAIs.
Take the most common HAI as an example: catheter-associated urinary tract infections. These infections affect patients in every hospital unit and are familiar to every care provider, regardless of background or practice setting. Administrators should care about CAUTIs in part because CMS no longer pays for a CAUTI when it complicates a hospitalization, but also because these infections adversely affect patient satisfaction. Efforts to reduce CAUTIs will need to address inappropriate catheter insertion, provide alternatives to catheter use (e.g., bladder scans), develop best practices for maintenance of necessary catheters, and facilitate timely removal of catheters no longer needed. Dealing with all of these issues will take a team-based systems approach.
I will not be surprised if hospitalists end up leading these initiatives across the country. Hospitalists will need to share best practices, collaborate in local or national initiatives, provide feedback to SHM and policymakers about what works and what doesn’t, and educate patients about HAIs and prevention. Every hospitalist in the country needs to understand the reasons HAIs develop, know strategies to prevent them, and work to implement these strategies in their hospitals.
Future Directions
Given the urgency, what can you expect next? The action plan is finalized, so HHS is turning its attention to implementation. HHS has reached out to SHM to see how we can get the word out to our members. Dissemination strategies include publication of key messages in The Hospitalist, the Journal of Hospital Medicine, Webinars, e-mail announcements, and presentations at our annual meeting.
And while HHS’ plan of action highlights the metrics, it does not provide detailed strategies to combat HAIs. Prevention tools will need to be developed, tested, and, if effective, disseminated. HHS has asked SHM to help in tool development and dissemination.
HHS will continue to work with CMS to align payment policies that incentivize prevention efforts, and SHM will need to follow these developments closely. In addition, AHRQ is dedicating substantial funds to support the development and dissemination of best practices to prevent HAIs.
HHS acknowledges we still have much to learn about HAIs and their prevention. I expect many hospitalists, as well as SHM, will be at the center of these initiatives. Healthcare-associated infections are a problem that can no longer be ignored. Prevention efforts need to be ramped up. Hospitalists around the country need to prepare to lead and champion these efforts. It is time to act. TH
Dr. Flanders is president of SHM.
Measures of Success
The headlines are harrowing: corporate layoffs; foreclosures on the rise; 401(k) retirement plans halved; government bailouts adding to the national debt. The worst economic downturn since the Great Depression has generated some unexpected outcomes, yet not all of them are bad for hospitalists. Below, four vignettes highlight HM groups that have achieved success despite—or in some cases because of—these troubled times.
A Better Business Agreement
It has taken nearly two years—and sometimes as many as four meetings a week—but Rajeev Alexander, MD, and his colleagues are nearing the finish line of an evolving business arrangement. The new arrangement has come about due to the economic downturn, which forced Oregon Medical Group (OMG), a multispecialty physician group serving hospitals in the Eugene/Springfield area and the HM group’s employer since 1988, to want to divest themselves of the hospitalist group. Now, after a lengthy negotiation, Dr. Alexander’s group of eight hospitalists is busier than ever.
Through what were essentially multiple quasi-buyouts, divestitures, and mergers, Dr. Alexander’s hospitalist group “spun off” from OMG and affiliated with PeaceHealth, a nonprofit health system serving seven hospitals in Oregon, Washington, and Alaska. The new contract means Dr. Alexander’s group is directly employed by Sacred Heart Hospital, a 541-bed PeaceHealth-owned facility in Eugene.
The new contract included a non-compete clause with OMG, which currently employs five hospitalists, yet Dr. Alexander’s group has maintained its patient volume. Compensation held steady and employee benefits improved. During an independent and slow-moving negotiation, Dr. Alexander’s group has merged with another HM service that originally was employed by PeaceHealth. The two HM groups (technically competitors) now practice in the same hospital and are ironing out the terms of the merger. At the moment, the groups have created a mutually respectful joint governance council.
“We’ve tackled the thorniest of problems,” Dr. Alexander says, “first, creating a combined work schedule to distribute patients and divide the work. Those of us on the governance council figured if we could get the docs to actually work together and share patients and communicate with each other as if they were one group, then the momentum for an actual administrative/contractual merger would feel inevitable.”

Although negotiations are expected to last through the end of the year to finalize such details as compensation, recruiting, and a group mission statement, the medical staff at Sacred Heart considers the merger a “done deal” and has thrown its support behind the effort. “Community outpatient docs have been clamoring for our services, and we have been having to hand out numbers and ask them to wait in line, so to speak,” Dr. Alexander says.
Dr. Alexander says he’s learned some lessons through the extensive negotiation process:
- Stay positive. In any business venture, absolutely nothing is impossible, even dodging a noncompete clause.
- Release your preconceptions. Conspiracy theories might abound, but most hospital administrators have the best of intentions. As highly regulated organizations, hospitals might simply be following their own bylaws and fulfilling responsibilities to stakeholders. Seek out at least one administrator whom you can trust, and with whom you can communicate effectively. A mutual understanding of intentions and objectives makes the process more successful for all concerned.
- Look beyond politics. Your trust and respect for administrators and fellow physicians will go a long way toward overcoming obstacles.
- Stick to your plan. Adhere to your goal of remaining independent, if that is important to you. “Our group resisted being funneled into becoming employed by a very large national hospitalist chain,” Dr. Alexander says, “and I would encourage physicians in other parts of the country to stick to their commitments as well.”
- Trust the negotiation process. Even if all goes well, what you’re shooting for at the beginning might not be exactly what you get after negotiations are over. This does not mean you’ve failed, or that hospital administration tricked you or failed to deliver on promises. It simply means you have created a negotiated settlement; both sides have come to a new appreciation for the other’s requirements and have made necessary and respectful accommodations.
Rural Rewards
Based in Traverse City, Hospitalists of Northwest Michigan (HNM) services four community hospitals and continues to witness solid growth. Since 2000, the group has grown from nine to nearly 40 providers, and from 2005 to 2008, patient encounters doubled. “In these hard economic times, hospitals are inviting us in because we provide value to the hospitals through leadership, increased hospital revenues, and improved recruiting and retention of specialists,” says Troy W. Ahlstrom, MD, president of HNM. “We continue to see healthy growth in patient volume as we align patient care goals with the needs of the hospitals and surrounding communities we serve.”
HNM, which established a service at the regional medical center and then assumed management of HM programs at three other rural hospitals, soon will add a fifth service to its ledger. HNM also began a pediatric program at the regional referral center, and the group is exploring the possibility of providing a network of pediatric care throughout the region.
Having grown up in the region, David Friar, MD, CEO of HNM, not only has a better understanding of the needs of rural hospitals, but also a personal investment in his group’s success. “These are our communities. We don’t view the hospitals as just a place to make a profit, but a place where our neighbors work and our families get their care,” he says.
Drs. Ahlstrom and Friar offer the following advice for achieving success in these economic times:
- Optimize receipts. Concern over compliance audits leads many hospitals to sacrifice group receipts by encouraging undercoding. “We’ve found hospitals do a poor job of negotiating the provider portion of third-party payer contracts and frequently lose provider charges because they focus on the much larger facility fees,” says Dr. Ahlstrom. The group’s receipts increased more than 30% when they began using an outside billing firm and adopted productivity incentives to encourage providers to practice better documentation and charge capture. Improving documentation also supports a hospital’s ability to accurately code its patients, which allows a hospital to bill for a more profitable diagnosis-related group (DRG), and improve its case-mix index. With these changes, Hospitalists of Northwest Michigan has increased provider pay and grown their practice while improving the hospitals’ profitability.
- Encourage frugality. The cost-plus model is popular, but it doesn’t incentivize programs to contain costs. In contrast, the fixed-price model encourages hospitalists to find cheaper ways to provide good care. “Because the money we save goes to us, we’ve all found creative ways to provide quality care for a third less money than similar cost-plus programs,” Dr. Ahlstrom says.
- Align incentives. Hospitals live or die on thin margins, Dr. Ahlstrom says. His group trains its employees to ask: What can I do to make the hospital stronger? “What’s good for the hospital is good for us, so we work with the hospitals, not for the hospitals,” Dr. Friar says.

At its smaller hospitals, HNM incentivized orthopedic admissions so that more surgical cases would stay local. Hospitalists were trained to perform stress tests so the hospital can provide testing on weekends. The group pays hospitalists a bonus for each admission, so when the ED calls, the hospitalists say, “Thanks! I’ll be right there.” The group also increased staffing on weekends.
The end result: It improves the hospital’s bottom line by shortening length of stay, and improving quality of care, patient satisfaction, and group morale.
“When we align the incentives, everybody wins,” says Dr. Friar. “The system has more capacity, the patients get better care, and the hospitalists no longer feel that weekend shifts are a huge burden.”
- Build “system-ness.” Sharing providers between hospitals has helped HNM build a cohesive system of quality care. What began as a way to cover shifts has created an interinstitutional camaraderie that allows for the easier flow of patients, improved communication, and widespread use of best-practice models. Sharing such resources as billing, credentialing, benefits, recruiting, and payroll has helped the group stay competitive, Dr. Ahlstrom says.
Growth in a Down Economy

Jude R. Alexander, MD, president of Inpatient Specialists in Rockville, Md., a bedroom community about 12 miles northwest of Washington, D.C., has continued to grow his group despite the down economy. Hospital admissions in the D.C. area decreased sharply in the second half of 2008, and patient volume rebounded slowly in the first half of 2009.
Inpatient Specialists initially downsized its staff, then it used flex physicians to meet demand as volume increased.
Despite national hospital trends of budget shortfalls, downgraded bond ratings, and increases in uninsured patients, two of Inpatient Specialists’ client hospitals chose to invest in the HM program. Dr. Alexander credits the vote of confidence to his group’s track record of optimal resource utilization, which has inherent cost savings in the millions.
Dr. Alexander also recommends HM groups in tough economic circumstances should:
- Maintain good relationships with partner hospitals;
- Run a lean business;
- Focus on excellent customer service to patients, their families, and their PCPs; and
- Build strong alliances with employed physicians by eliciting and giving constructive feedback.
“Following this basic strategy, Inpatient Specialists has experienced 7% growth in patient volume in the past 12 months,” Dr. Alexander says. “We’ve expanded to 40 full-time equivalent hospitalists, and 40 part-time employees.” Inpatient Specialists has its eye on geographic expansion, as well. The group is targeting services throughout the Capitol region—Maryland, Virginia, and the District of Columbia.
Bankruptcy to Profitability in One Year
In 2007, a few months after the 99-bed Auburn Memorial Hospital in Auburn, N.Y., was forced into bankruptcy, James Leyhane, MD, and his hospitalist group were displeased that they weren’t in control of their own program. Physicians had started leaving the hospital; Dr. Leyhane himself had interviewed at another hospital. “Our CEO approached me to ask what would make it right,” Dr. Leyhane recalls. “I said, ‘We’d need to be employed by the hospital.’ ”

The hospital and the private, six-physician internal-medicine group that employed the program entered bids on the HM group. In March 2008, the HM group became contractually employed by the hospital. Dr. Leyhane was given full control as hospitalist director of Auburn Memorial Hospitalists.

As a result of the new alignment, two major shifts took place. First, the hospital CEO more aggressively recruited subspecialists and surgeons. With the HM group now affiliated with the hospital, recruiting surgeons to Auburn Memorial became much easier. Second, more primary-care physicians (PCPs) began sending their patients to Auburn Memorial.
“We were all shocked at how quickly the administration was able to recruit new subspecialists to the area,” Dr. Leyhane says. “That helped get the profitable procedures back to the hospital.”
The biggest surprise came at the end of 2008. Patient volume had risen 11.5% higher than the hospital’s best-case predictions. “As a result of our emerging from under the umbrella of one physician group, the outlying physicians became less fearful that they might lose their patients to that group,” Dr. Leyhane says. “And in good faith, we still maintain a coverage arrangement with that IM group.”
Thus, what was first seen as a bad thing turned into a very good thing for both the hospitalist group and the hospital. Auburn Memorial posted a $3.1 million profit in 2008 (see Table 1).
Dr. Leyhane suggests HM group leaders facing similar financial crunches talk to area subspecialists and find out what it would take to get them affiliated with their institution.
“In our case, a stable hospitalist program was definitely one of their top requests,” Dr. Leyhane says, adding it also would be beneficial to include PCPs in the “what do you want from our hospital?” conversation. TH
Andrea M. Sattinger is a freelance writer based in North Carolina.
Image Source: COLIN ANDERSON/GETTYIMAGES
The headlines are harrowing: corporate layoffs; foreclosures on the rise; 401(k) retirement plans halved; government bailouts adding to the national debt. The worst economic downturn since the Great Depression has generated some unexpected outcomes, yet not all of them are bad for hospitalists. Below, four vignettes highlight HM groups that have achieved success despite—or in some cases because of—these troubled times.
A Better Business Agreement
It has taken nearly two years—and sometimes as many as four meetings a week—but Rajeev Alexander, MD, and his colleagues are nearing the finish line of an evolving business arrangement. The new arrangement has come about due to the economic downturn, which forced Oregon Medical Group (OMG), a multispecialty physician group serving hospitals in the Eugene/Springfield area and the HM group’s employer since 1988, to want to divest themselves of the hospitalist group. Now, after a lengthy negotiation, Dr. Alexander’s group of eight hospitalists is busier than ever.
Through what were essentially multiple quasi-buyouts, divestitures, and mergers, Dr. Alexander’s hospitalist group “spun off” from OMG and affiliated with PeaceHealth, a nonprofit health system serving seven hospitals in Oregon, Washington, and Alaska. The new contract means Dr. Alexander’s group is directly employed by Sacred Heart Hospital, a 541-bed PeaceHealth-owned facility in Eugene.
The new contract included a non-compete clause with OMG, which currently employs five hospitalists, yet Dr. Alexander’s group has maintained its patient volume. Compensation held steady and employee benefits improved. During an independent and slow-moving negotiation, Dr. Alexander’s group has merged with another HM service that originally was employed by PeaceHealth. The two HM groups (technically competitors) now practice in the same hospital and are ironing out the terms of the merger. At the moment, the groups have created a mutually respectful joint governance council.
“We’ve tackled the thorniest of problems,” Dr. Alexander says, “first, creating a combined work schedule to distribute patients and divide the work. Those of us on the governance council figured if we could get the docs to actually work together and share patients and communicate with each other as if they were one group, then the momentum for an actual administrative/contractual merger would feel inevitable.”
Although negotiations are expected to last through the end of the year to finalize such details as compensation, recruiting, and a group mission statement, the medical staff at Sacred Heart considers the merger a “done deal” and has thrown its support behind the effort. “Community outpatient docs have been clamoring for our services, and we have been having to hand out numbers and ask them to wait in line, so to speak,” Dr. Alexander says.
Dr. Alexander says he’s learned some lessons through the extensive negotiation process:
- Stay positive. In any business venture, absolutely nothing is impossible, even dodging a noncompete clause.
- Release your preconceptions. Conspiracy theories might abound, but most hospital administrators have the best of intentions. As highly regulated organizations, hospitals might simply be following their own bylaws and fulfilling responsibilities to stakeholders. Seek out at least one administrator whom you can trust, and with whom you can communicate effectively. A mutual understanding of intentions and objectives makes the process more successful for all concerned.
- Look beyond politics. Your trust and respect for administrators and fellow physicians will go a long way toward overcoming obstacles.
- Stick to your plan. Adhere to your goal of remaining independent, if that is important to you. “Our group resisted being funneled into becoming employed by a very large national hospitalist chain,” Dr. Alexander says, “and I would encourage physicians in other parts of the country to stick to their commitments as well.”
- Trust the negotiation process. Even if all goes well, what you’re shooting for at the beginning might not be exactly what you get after negotiations are over. This does not mean you’ve failed, or that hospital administration tricked you or failed to deliver on promises. It simply means you have created a negotiated settlement; both sides have come to a new appreciation for the other’s requirements and have made necessary and respectful accommodations.
Rural Rewards
Based in Traverse City, Hospitalists of Northwest Michigan (HNM) services four community hospitals and continues to witness solid growth. Since 2000, the group has grown from nine to nearly 40 providers, and from 2005 to 2008, patient encounters doubled. “In these hard economic times, hospitals are inviting us in because we provide value to the hospitals through leadership, increased hospital revenues, and improved recruiting and retention of specialists,” says Troy W. Ahlstrom, MD, president of HNM. “We continue to see healthy growth in patient volume as we align patient care goals with the needs of the hospitals and surrounding communities we serve.”
HNM, which established a service at the regional medical center and then assumed management of HM programs at three other rural hospitals, soon will add a fifth service to its ledger. HNM also began a pediatric program at the regional referral center, and the group is exploring the possibility of providing a network of pediatric care throughout the region.
Having grown up in the region, David Friar, MD, CEO of HNM, not only has a better understanding of the needs of rural hospitals, but also a personal investment in his group’s success. “These are our communities. We don’t view the hospitals as just a place to make a profit, but a place where our neighbors work and our families get their care,” he says.
Drs. Ahlstrom and Friar offer the following advice for achieving success in these economic times:
- Optimize receipts. Concern over compliance audits leads many hospitals to sacrifice group receipts by encouraging undercoding. “We’ve found hospitals do a poor job of negotiating the provider portion of third-party payer contracts and frequently lose provider charges because they focus on the much larger facility fees,” says Dr. Ahlstrom. The group’s receipts increased more than 30% when they began using an outside billing firm and adopted productivity incentives to encourage providers to practice better documentation and charge capture. Improving documentation also supports a hospital’s ability to accurately code its patients, which allows a hospital to bill for a more profitable diagnosis-related group (DRG), and improve its case-mix index. With these changes, Hospitalists of Northwest Michigan has increased provider pay and grown their practice while improving the hospitals’ profitability.
- Encourage frugality. The cost-plus model is popular, but it doesn’t incentivize programs to contain costs. In contrast, the fixed-price model encourages hospitalists to find cheaper ways to provide good care. “Because the money we save goes to us, we’ve all found creative ways to provide quality care for a third less money than similar cost-plus programs,” Dr. Ahlstrom says.
- Align incentives. Hospitals live or die on thin margins, Dr. Ahlstrom says. His group trains its employees to ask: What can I do to make the hospital stronger? “What’s good for the hospital is good for us, so we work with the hospitals, not for the hospitals,” Dr. Friar says.
At its smaller hospitals, HNM incentivized orthopedic admissions so that more surgical cases would stay local. Hospitalists were trained to perform stress tests so the hospital can provide testing on weekends. The group pays hospitalists a bonus for each admission, so when the ED calls, the hospitalists say, “Thanks! I’ll be right there.” The group also increased staffing on weekends.
The end result: It improves the hospital’s bottom line by shortening length of stay, and improving quality of care, patient satisfaction, and group morale.
“When we align the incentives, everybody wins,” says Dr. Friar. “The system has more capacity, the patients get better care, and the hospitalists no longer feel that weekend shifts are a huge burden.”
- Build “system-ness.” Sharing providers between hospitals has helped HNM build a cohesive system of quality care. What began as a way to cover shifts has created an interinstitutional camaraderie that allows for the easier flow of patients, improved communication, and widespread use of best-practice models. Sharing such resources as billing, credentialing, benefits, recruiting, and payroll has helped the group stay competitive, Dr. Ahlstrom says.
Growth in a Down Economy
Jude R. Alexander, MD, president of Inpatient Specialists in Rockville, Md., a bedroom community about 12 miles northwest of Washington, D.C., has continued to grow his group despite the down economy. Hospital admissions in the D.C. area decreased sharply in the second half of 2008, and patient volume rebounded slowly in the first half of 2009.
Inpatient Specialists initially downsized its staff, then it used flex physicians to meet demand as volume increased.
Despite national hospital trends of budget shortfalls, downgraded bond ratings, and increases in uninsured patients, two of Inpatient Specialists’ client hospitals chose to invest in the HM program. Dr. Alexander credits the vote of confidence to his group’s track record of optimal resource utilization, which has inherent cost savings in the millions.
Dr. Alexander also recommends HM groups in tough economic circumstances should:
- Maintain good relationships with partner hospitals;
- Run a lean business;
- Focus on excellent customer service to patients, their families, and their PCPs; and
- Build strong alliances with employed physicians by eliciting and giving constructive feedback.
“Following this basic strategy, Inpatient Specialists has experienced 7% growth in patient volume in the past 12 months,” Dr. Alexander says. “We’ve expanded to 40 full-time equivalent hospitalists, and 40 part-time employees.” Inpatient Specialists has its eye on geographic expansion, as well. The group is targeting services throughout the Capitol region—Maryland, Virginia, and the District of Columbia.
Bankruptcy to Profitability in One Year
In 2007, a few months after the 99-bed Auburn Memorial Hospital in Auburn, N.Y., was forced into bankruptcy, James Leyhane, MD, and his hospitalist group were displeased that they weren’t in control of their own program. Physicians had started leaving the hospital; Dr. Leyhane himself had interviewed at another hospital. “Our CEO approached me to ask what would make it right,” Dr. Leyhane recalls. “I said, ‘We’d need to be employed by the hospital.’ ”
The hospital and the private, six-physician internal-medicine group that employed the program entered bids on the HM group. In March 2008, the HM group became contractually employed by the hospital. Dr. Leyhane was given full control as hospitalist director of Auburn Memorial Hospitalists.
As a result of the new alignment, two major shifts took place. First, the hospital CEO more aggressively recruited subspecialists and surgeons. With the HM group now affiliated with the hospital, recruiting surgeons to Auburn Memorial became much easier. Second, more primary-care physicians (PCPs) began sending their patients to Auburn Memorial.
“We were all shocked at how quickly the administration was able to recruit new subspecialists to the area,” Dr. Leyhane says. “That helped get the profitable procedures back to the hospital.”
The biggest surprise came at the end of 2008. Patient volume had risen 11.5% higher than the hospital’s best-case predictions. “As a result of our emerging from under the umbrella of one physician group, the outlying physicians became less fearful that they might lose their patients to that group,” Dr. Leyhane says. “And in good faith, we still maintain a coverage arrangement with that IM group.”
Thus, what was first seen as a bad thing turned into a very good thing for both the hospitalist group and the hospital. Auburn Memorial posted a $3.1 million profit in 2008 (see Table 1).
Dr. Leyhane suggests HM group leaders facing similar financial crunches talk to area subspecialists and find out what it would take to get them affiliated with their institution.
“In our case, a stable hospitalist program was definitely one of their top requests,” Dr. Leyhane says, adding it also would be beneficial to include PCPs in the “what do you want from our hospital?” conversation. TH
Andrea M. Sattinger is a freelance writer based in North Carolina.
Image Source: COLIN ANDERSON/GETTYIMAGES
The headlines are harrowing: corporate layoffs; foreclosures on the rise; 401(k) retirement plans halved; government bailouts adding to the national debt. The worst economic downturn since the Great Depression has generated some unexpected outcomes, yet not all of them are bad for hospitalists. Below, four vignettes highlight HM groups that have achieved success despite—or in some cases because of—these troubled times.
A Better Business Agreement
It has taken nearly two years—and sometimes as many as four meetings a week—but Rajeev Alexander, MD, and his colleagues are nearing the finish line of an evolving business arrangement. The new arrangement has come about due to the economic downturn, which forced Oregon Medical Group (OMG), a multispecialty physician group serving hospitals in the Eugene/Springfield area and the HM group’s employer since 1988, to want to divest themselves of the hospitalist group. Now, after a lengthy negotiation, Dr. Alexander’s group of eight hospitalists is busier than ever.
Through what were essentially multiple quasi-buyouts, divestitures, and mergers, Dr. Alexander’s hospitalist group “spun off” from OMG and affiliated with PeaceHealth, a nonprofit health system serving seven hospitals in Oregon, Washington, and Alaska. The new contract means Dr. Alexander’s group is directly employed by Sacred Heart Hospital, a 541-bed PeaceHealth-owned facility in Eugene.
The new contract included a non-compete clause with OMG, which currently employs five hospitalists, yet Dr. Alexander’s group has maintained its patient volume. Compensation held steady and employee benefits improved. During an independent and slow-moving negotiation, Dr. Alexander’s group has merged with another HM service that originally was employed by PeaceHealth. The two HM groups (technically competitors) now practice in the same hospital and are ironing out the terms of the merger. At the moment, the groups have created a mutually respectful joint governance council.
“We’ve tackled the thorniest of problems,” Dr. Alexander says, “first, creating a combined work schedule to distribute patients and divide the work. Those of us on the governance council figured if we could get the docs to actually work together and share patients and communicate with each other as if they were one group, then the momentum for an actual administrative/contractual merger would feel inevitable.”
Although negotiations are expected to last through the end of the year to finalize such details as compensation, recruiting, and a group mission statement, the medical staff at Sacred Heart considers the merger a “done deal” and has thrown its support behind the effort. “Community outpatient docs have been clamoring for our services, and we have been having to hand out numbers and ask them to wait in line, so to speak,” Dr. Alexander says.
Dr. Alexander says he’s learned some lessons through the extensive negotiation process:
- Stay positive. In any business venture, absolutely nothing is impossible, even dodging a noncompete clause.
- Release your preconceptions. Conspiracy theories might abound, but most hospital administrators have the best of intentions. As highly regulated organizations, hospitals might simply be following their own bylaws and fulfilling responsibilities to stakeholders. Seek out at least one administrator whom you can trust, and with whom you can communicate effectively. A mutual understanding of intentions and objectives makes the process more successful for all concerned.
- Look beyond politics. Your trust and respect for administrators and fellow physicians will go a long way toward overcoming obstacles.
- Stick to your plan. Adhere to your goal of remaining independent, if that is important to you. “Our group resisted being funneled into becoming employed by a very large national hospitalist chain,” Dr. Alexander says, “and I would encourage physicians in other parts of the country to stick to their commitments as well.”
- Trust the negotiation process. Even if all goes well, what you’re shooting for at the beginning might not be exactly what you get after negotiations are over. This does not mean you’ve failed, or that hospital administration tricked you or failed to deliver on promises. It simply means you have created a negotiated settlement; both sides have come to a new appreciation for the other’s requirements and have made necessary and respectful accommodations.
Rural Rewards
Based in Traverse City, Hospitalists of Northwest Michigan (HNM) services four community hospitals and continues to witness solid growth. Since 2000, the group has grown from nine to nearly 40 providers, and from 2005 to 2008, patient encounters doubled. “In these hard economic times, hospitals are inviting us in because we provide value to the hospitals through leadership, increased hospital revenues, and improved recruiting and retention of specialists,” says Troy W. Ahlstrom, MD, president of HNM. “We continue to see healthy growth in patient volume as we align patient care goals with the needs of the hospitals and surrounding communities we serve.”
HNM, which established a service at the regional medical center and then assumed management of HM programs at three other rural hospitals, soon will add a fifth service to its ledger. HNM also began a pediatric program at the regional referral center, and the group is exploring the possibility of providing a network of pediatric care throughout the region.
Having grown up in the region, David Friar, MD, CEO of HNM, not only has a better understanding of the needs of rural hospitals, but also a personal investment in his group’s success. “These are our communities. We don’t view the hospitals as just a place to make a profit, but a place where our neighbors work and our families get their care,” he says.
Drs. Ahlstrom and Friar offer the following advice for achieving success in these economic times:
- Optimize receipts. Concern over compliance audits leads many hospitals to sacrifice group receipts by encouraging undercoding. “We’ve found hospitals do a poor job of negotiating the provider portion of third-party payer contracts and frequently lose provider charges because they focus on the much larger facility fees,” says Dr. Ahlstrom. The group’s receipts increased more than 30% when they began using an outside billing firm and adopted productivity incentives to encourage providers to practice better documentation and charge capture. Improving documentation also supports a hospital’s ability to accurately code its patients, which allows a hospital to bill for a more profitable diagnosis-related group (DRG), and improve its case-mix index. With these changes, Hospitalists of Northwest Michigan has increased provider pay and grown their practice while improving the hospitals’ profitability.
- Encourage frugality. The cost-plus model is popular, but it doesn’t incentivize programs to contain costs. In contrast, the fixed-price model encourages hospitalists to find cheaper ways to provide good care. “Because the money we save goes to us, we’ve all found creative ways to provide quality care for a third less money than similar cost-plus programs,” Dr. Ahlstrom says.
- Align incentives. Hospitals live or die on thin margins, Dr. Ahlstrom says. His group trains its employees to ask: What can I do to make the hospital stronger? “What’s good for the hospital is good for us, so we work with the hospitals, not for the hospitals,” Dr. Friar says.
At its smaller hospitals, HNM incentivized orthopedic admissions so that more surgical cases would stay local. Hospitalists were trained to perform stress tests so the hospital can provide testing on weekends. The group pays hospitalists a bonus for each admission, so when the ED calls, the hospitalists say, “Thanks! I’ll be right there.” The group also increased staffing on weekends.
The end result: It improves the hospital’s bottom line by shortening length of stay, and improving quality of care, patient satisfaction, and group morale.
“When we align the incentives, everybody wins,” says Dr. Friar. “The system has more capacity, the patients get better care, and the hospitalists no longer feel that weekend shifts are a huge burden.”
- Build “system-ness.” Sharing providers between hospitals has helped HNM build a cohesive system of quality care. What began as a way to cover shifts has created an interinstitutional camaraderie that allows for the easier flow of patients, improved communication, and widespread use of best-practice models. Sharing such resources as billing, credentialing, benefits, recruiting, and payroll has helped the group stay competitive, Dr. Ahlstrom says.
Growth in a Down Economy
Jude R. Alexander, MD, president of Inpatient Specialists in Rockville, Md., a bedroom community about 12 miles northwest of Washington, D.C., has continued to grow his group despite the down economy. Hospital admissions in the D.C. area decreased sharply in the second half of 2008, and patient volume rebounded slowly in the first half of 2009.
Inpatient Specialists initially downsized its staff, then it used flex physicians to meet demand as volume increased.
Despite national hospital trends of budget shortfalls, downgraded bond ratings, and increases in uninsured patients, two of Inpatient Specialists’ client hospitals chose to invest in the HM program. Dr. Alexander credits the vote of confidence to his group’s track record of optimal resource utilization, which has inherent cost savings in the millions.
Dr. Alexander also recommends HM groups in tough economic circumstances should:
- Maintain good relationships with partner hospitals;
- Run a lean business;
- Focus on excellent customer service to patients, their families, and their PCPs; and
- Build strong alliances with employed physicians by eliciting and giving constructive feedback.
“Following this basic strategy, Inpatient Specialists has experienced 7% growth in patient volume in the past 12 months,” Dr. Alexander says. “We’ve expanded to 40 full-time equivalent hospitalists, and 40 part-time employees.” Inpatient Specialists has its eye on geographic expansion, as well. The group is targeting services throughout the Capitol region—Maryland, Virginia, and the District of Columbia.
Bankruptcy to Profitability in One Year
In 2007, a few months after the 99-bed Auburn Memorial Hospital in Auburn, N.Y., was forced into bankruptcy, James Leyhane, MD, and his hospitalist group were displeased that they weren’t in control of their own program. Physicians had started leaving the hospital; Dr. Leyhane himself had interviewed at another hospital. “Our CEO approached me to ask what would make it right,” Dr. Leyhane recalls. “I said, ‘We’d need to be employed by the hospital.’ ”
The hospital and the private, six-physician internal-medicine group that employed the program entered bids on the HM group. In March 2008, the HM group became contractually employed by the hospital. Dr. Leyhane was given full control as hospitalist director of Auburn Memorial Hospitalists.
As a result of the new alignment, two major shifts took place. First, the hospital CEO more aggressively recruited subspecialists and surgeons. With the HM group now affiliated with the hospital, recruiting surgeons to Auburn Memorial became much easier. Second, more primary-care physicians (PCPs) began sending their patients to Auburn Memorial.
“We were all shocked at how quickly the administration was able to recruit new subspecialists to the area,” Dr. Leyhane says. “That helped get the profitable procedures back to the hospital.”
The biggest surprise came at the end of 2008. Patient volume had risen 11.5% higher than the hospital’s best-case predictions. “As a result of our emerging from under the umbrella of one physician group, the outlying physicians became less fearful that they might lose their patients to that group,” Dr. Leyhane says. “And in good faith, we still maintain a coverage arrangement with that IM group.”
Thus, what was first seen as a bad thing turned into a very good thing for both the hospitalist group and the hospital. Auburn Memorial posted a $3.1 million profit in 2008 (see Table 1).
Dr. Leyhane suggests HM group leaders facing similar financial crunches talk to area subspecialists and find out what it would take to get them affiliated with their institution.
“In our case, a stable hospitalist program was definitely one of their top requests,” Dr. Leyhane says, adding it also would be beneficial to include PCPs in the “what do you want from our hospital?” conversation. TH
Andrea M. Sattinger is a freelance writer based in North Carolina.
Image Source: COLIN ANDERSON/GETTYIMAGES
How should a patient with a new-onset seizure be managed?
Case
A 42-year-old man is brought to the hospital by his family after a reported seizure. The patient was found on the floor, unresponsive, and suffering convulsions lasting less than a minute. He suffered no apparent trauma before or during the event. He has no history of seizures. His mental status quickly improved; he experienced oriented lucidity with slight drowsiness. His neurological exam is nonfocal, and his vital signs and laboratory values are normal. A noncontrast head computed tomogram (CT) is normal.
What is the appropriate approach to diagnosis and management for this patient with a new-onset seizure?
Overview
A patient with a first seizure presents a dilemma. Underlying causes for seizure are potentially life-threatening, and must be identified if present. A patient whose first seizure is unprovoked is at risk for future seizures (i.e., epilepsy). However, long-term therapy with anticonvulsant medication has morbidity, side effects, and expense. Advising a patient on whether to drive has public safety and legal implications, as well as major lifestyle changes for the patient.
Seizures may be focal (limited to one area of the brain) or generalized (involving both hemispheres). For the most part, focal (also known as partial) seizures do not impair consciousness; generalized seizures do. Approximately 70% of first seizures are partial focal seizures.1 Such provoking causes as head trauma, stroke, alcohol withdrawal, brain tumors, and infections can be identified in about one-third of cases.1
Electroencephalogram (EEG) and computed tomogram (CT) of the brain should be obtained, but insufficient evidence exists to recommend other testing, which should be pursued according to the clinical context.2
Unprovoked seizures recur in about 25% to 50% of patients, resulting in a diagnosis of epilepsy.1,2,4-7
Therapy is unnecessary in patients whose seizures will not recur, but reliably identifying these patients is a challenge. Whether antiepileptic drug (AED) therapy should be initiated in patients with a first unprovoked seizure is controversial and will be reviewed below.
Review of the Data
History: No test or finding can reliably differentiate unwitnessed seizures from other events (e.g., syncope).2 History from a reliable observer often is necessary to determine whether the event actually was a seizure.2 In as many as 50% of patients with a “first” seizure, thorough history will likely reveal previously unrecognized seizures.1 Although most epilepsy syndromes begin in childhood or adolescence, a significant number of patients will experience their first seizure in adulthood.2
A thorough neurologic examination should be performed. In a minority of cases, an exam will suggest a focal lesion. An impaired level of consciousness might represent a post-ictal state or delirium.2
Diagnostic evaluation: If the history suggests a seizure, an EEG should be obtained. Although the EEG will be normal in 50% of patients following a first seizure, an abnormal EEG provides useful information about seizure type and the likelihood of recurrence.2 In nearly a quarter of patients, the EEG will show epileptiform abnormalities that predict future seizures.2
Generally, an EEG should be obtained as soon as feasible, once a seizure is suspected. Some evidence in children suggests that EEG yield is higher in the 24 hours after a first seizure.
A noncontrast head CT or magnetic resonance imaging (MRI) reveals a significant abnormality about 10% of the time.2 A CT or MRI should be obtained. Few studies have compared CT to MRI in terms of yield in determining first seizure etiology, and those that do compare the two suffer from selection bias.2 Although CT or MRI are appropriate in evaluating a patient with a first seizure, the MRI’s greater resolution might provide a higher diagnostic yield in terms of seizure etiology, and, therefore, some experts recommend MRI over CT in nonemergent cases.2
Insufficient data exist to support or refute diagnostic testing beyond brain imaging and EEG. Although electrolyte abnormalities, hypoglycemia, and infections might infrequently cause seizures, such routine blood tests as complete blood count (CBC) and chemistry panels are rarely helpful.
As many as 15% of patients with a seizure will have minor abnormalities on routine lab tests, but the abnormalities do not appear to be the cause of the seizure.2
Lumbar puncture (LP) is categorically recommended only in patients in whom there is a clinical suspicion for infection as a seizure etiology. Reviews suggest that signs and symptoms of infection are typically present in patients with meningitis or another infectious cause for seizure; LP generally has limited utility in other noninfectious causes of seizure.2
The utility of toxicology testing in a first seizure has not been studied widely. Testing urine or blood for the presence of alcohol, cocaine, methamphetamines, benzodiazepines, or drug metabolites could be useful in the appropriate clinical setting.2
It is unclear whether a patient with a first seizure requires hospitalization. If initial testing in the ED rules out serious causes of seizures, the yield for hospitalization is likely to be low. In clinical practice, however, hospitalization is common and often necessary to complete such diagnostic testing as EEG and MRI.
Medical therapy: Patients with suspected epilepsy (e.g., those whose presenting seizure is, in retrospect, not their first seizure) should begin antiepileptic drug therapy (AED).1
Typically, a broad-spectrum AED—one that is effective against both partial and generalized seizures—should be used as initial therapy for epilepsy. These include valproate, lamotrigine, topiramate, zonisamide, and levetiracetam (see Table 1, above). Valproate has the longest history of effectiveness; levetiracetam has fewer drug interactions, and randomized trials support its efficacy.1
Checking blood electrolytes and liver enzymes is recommended before beginning AED treatment. Significant hepatic or renal dysfunction might necessitate dosing adjustments in many AEDs.2
Inpatient consultation with a neurologist might be helpful, although insufficient evidence exists that such consultation improves patient outcomes or makes care more cost-efficient. A neurologist should follow up on patients with a first seizure after hospital discharge.2
Patients with a first seizure that likely was provoked by a reversible condition (e.g., hypotension, hypoglycemia, infection) should generally not begin AED therapy. This also includes patients with multiple seizures in a brief period of time (less than 24 hours), all attributed to the same reversible cause.1
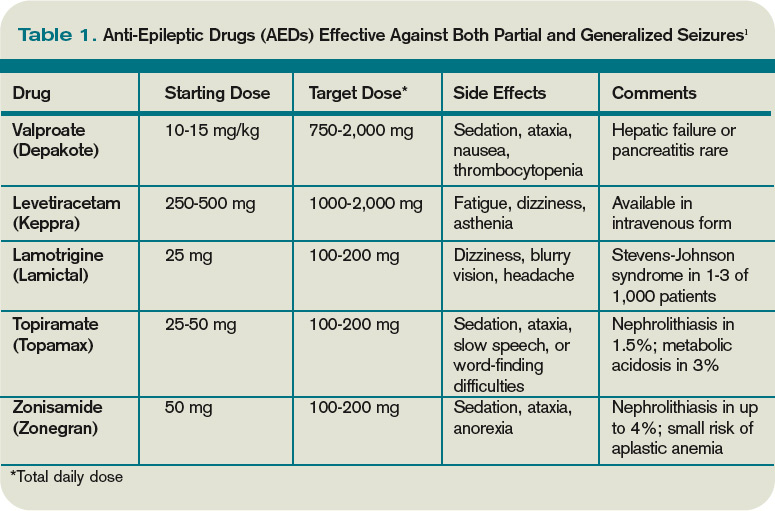
The decision to begin AED therapy after a first unprovoked seizure is controversial. Estimates of the likelihood of seizure recurrence range from 25% at two years to 50% at one year (in the absence of AED therapy).1-2,4-7 The decision to start AED therapy after a first seizure must therefore be individualized for each patient.
Patients at high risk for recurrent seizures should begin AED therapy.1 However, no test or prognostic tool reliably identifies these patients, and initiating therapy carries side effects and places psychological, financial, and social burdens on the patient. The prevailing clinical practice, therefore, has been watchful waiting, with a second seizure constituting proof of high risk for recurrence—and need for AED therapy. Three-quarters of patients with two or more unprovoked seizures likely will go on to have recurrent seizures.6
On the other hand, in patients believed to be at high risk for seizure recurrence, a more aggressive approach of initiating AED therapy after the first seizure is reasonable. A number of risk factors increasing risk for seizure recurrence have been identified (see Table 2, left).1,2 It is justified to initiate AED therapy if any of these factors are present, even after a single seizure. Still, it’s important to note that most people with risk factors will not benefit from AEDs, as only about 40% will have a seizure in the following two years.1
Early initiation of AED therapy might be appropriate for patients with occupations or hobbies in which seizures could be life-threatening (e.g., scuba divers, truck drivers).2
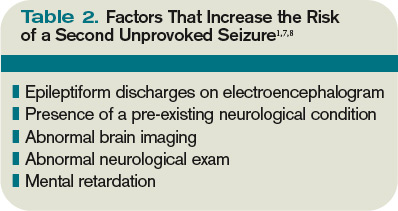
Low-risk patients still have a roughly 20% to 30% risk of seizure recurrence within three years.1 A second seizure that occurs while driving or while engaged in any hazardous activity could lead to serious injury.
Patients should be advised of this small but inescapable risk and instructed to contact their department of motor vehicles for specific legal restrictions, which vary by state. Once three seizure-free years have passed after a patient’s initial seizure, the chance of a recurrence falls to around 10% to 20%.6-7
Back to the Case
Our 42-year-old patient with a first seizure had normal findings on examination, laboratory studies, and brain imaging. An EEG showed epileptiform discharges in a spike and wave pattern. The attending hospitalist counseled him on his elevated risk of future seizures; the patient then elected to begin AED therapy, citing a fear of losing his driving privileges. Levetiracetam was started, which he tolerated despite mild sedation.
A year later, he suffered another seizure at his home. With regular followup and titration of his AED, he remained seizure-free for the next five years.
Bottom Line
Most patients with a single unprovoked seizure can be managed with watchful waiting, counseling, and neurological followup. Initiation of AED therapy is appropriate for patients with a high risk of seizure recurrence, or for whom another seizure could pose personal or social harm. TH
Dr. Hoffman is a hospitalist at Emory University School of Medicine in Atlanta.
References
- French JA, Pedley TA. Clinical practice: Initial management of epilepsy. N Engl J Med. 2008;359:166-176.
- Krumholz A, Wiebe S, Gronseth G, et al. Practice Parameter: evaluating an apparent unprovoked first seizure in adults (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Neurology. 2007;69:1996-2007.
- Schachter SC. Antiepileptic drug therapy: general treatment principles and application for special patient populations. Epilepsia. 1999;40(9):S20-25.
- Hauser WA, Rich SS, Annegers JF, et al. Seizure recurrence after a first unprovoked seizure: an extended follow-up. Neurology. 1990;40:1163-1170.
- Marson A, Jacoby A, Johnson A, et al. Immediate versus deferred antiepileptic drug treatment for epilepsy and single seizures: a randomized controlled trial. Lancet. 2005;365: 2007-2013.
- Hauser WA, Rich SS, Lee JR, Annegers JF, Anderson VE. Risk of recurrent seizures after two unprovoked seizures. N Engl J Med. 1998;338:429-434.
- Berg AT. Risk of recurrence after a first unprovoked seizure. Epilepsia. 2008;49:S13-18.
- Kim LG, Johnson TL, Marson AG, et al. Prediction of risk of seizure recurrence after a single seizure and early epilepsy: further results from the MESS trial. Lancet Neurology. 2006;5(4):317-322.
Case
A 42-year-old man is brought to the hospital by his family after a reported seizure. The patient was found on the floor, unresponsive, and suffering convulsions lasting less than a minute. He suffered no apparent trauma before or during the event. He has no history of seizures. His mental status quickly improved; he experienced oriented lucidity with slight drowsiness. His neurological exam is nonfocal, and his vital signs and laboratory values are normal. A noncontrast head computed tomogram (CT) is normal.
What is the appropriate approach to diagnosis and management for this patient with a new-onset seizure?
Overview
A patient with a first seizure presents a dilemma. Underlying causes for seizure are potentially life-threatening, and must be identified if present. A patient whose first seizure is unprovoked is at risk for future seizures (i.e., epilepsy). However, long-term therapy with anticonvulsant medication has morbidity, side effects, and expense. Advising a patient on whether to drive has public safety and legal implications, as well as major lifestyle changes for the patient.
Seizures may be focal (limited to one area of the brain) or generalized (involving both hemispheres). For the most part, focal (also known as partial) seizures do not impair consciousness; generalized seizures do. Approximately 70% of first seizures are partial focal seizures.1 Such provoking causes as head trauma, stroke, alcohol withdrawal, brain tumors, and infections can be identified in about one-third of cases.1
Electroencephalogram (EEG) and computed tomogram (CT) of the brain should be obtained, but insufficient evidence exists to recommend other testing, which should be pursued according to the clinical context.2
Unprovoked seizures recur in about 25% to 50% of patients, resulting in a diagnosis of epilepsy.1,2,4-7
Therapy is unnecessary in patients whose seizures will not recur, but reliably identifying these patients is a challenge. Whether antiepileptic drug (AED) therapy should be initiated in patients with a first unprovoked seizure is controversial and will be reviewed below.
Review of the Data
History: No test or finding can reliably differentiate unwitnessed seizures from other events (e.g., syncope).2 History from a reliable observer often is necessary to determine whether the event actually was a seizure.2 In as many as 50% of patients with a “first” seizure, thorough history will likely reveal previously unrecognized seizures.1 Although most epilepsy syndromes begin in childhood or adolescence, a significant number of patients will experience their first seizure in adulthood.2
A thorough neurologic examination should be performed. In a minority of cases, an exam will suggest a focal lesion. An impaired level of consciousness might represent a post-ictal state or delirium.2
Diagnostic evaluation: If the history suggests a seizure, an EEG should be obtained. Although the EEG will be normal in 50% of patients following a first seizure, an abnormal EEG provides useful information about seizure type and the likelihood of recurrence.2 In nearly a quarter of patients, the EEG will show epileptiform abnormalities that predict future seizures.2
Generally, an EEG should be obtained as soon as feasible, once a seizure is suspected. Some evidence in children suggests that EEG yield is higher in the 24 hours after a first seizure.
A noncontrast head CT or magnetic resonance imaging (MRI) reveals a significant abnormality about 10% of the time.2 A CT or MRI should be obtained. Few studies have compared CT to MRI in terms of yield in determining first seizure etiology, and those that do compare the two suffer from selection bias.2 Although CT or MRI are appropriate in evaluating a patient with a first seizure, the MRI’s greater resolution might provide a higher diagnostic yield in terms of seizure etiology, and, therefore, some experts recommend MRI over CT in nonemergent cases.2
Insufficient data exist to support or refute diagnostic testing beyond brain imaging and EEG. Although electrolyte abnormalities, hypoglycemia, and infections might infrequently cause seizures, such routine blood tests as complete blood count (CBC) and chemistry panels are rarely helpful.
As many as 15% of patients with a seizure will have minor abnormalities on routine lab tests, but the abnormalities do not appear to be the cause of the seizure.2
Lumbar puncture (LP) is categorically recommended only in patients in whom there is a clinical suspicion for infection as a seizure etiology. Reviews suggest that signs and symptoms of infection are typically present in patients with meningitis or another infectious cause for seizure; LP generally has limited utility in other noninfectious causes of seizure.2
The utility of toxicology testing in a first seizure has not been studied widely. Testing urine or blood for the presence of alcohol, cocaine, methamphetamines, benzodiazepines, or drug metabolites could be useful in the appropriate clinical setting.2
It is unclear whether a patient with a first seizure requires hospitalization. If initial testing in the ED rules out serious causes of seizures, the yield for hospitalization is likely to be low. In clinical practice, however, hospitalization is common and often necessary to complete such diagnostic testing as EEG and MRI.
Medical therapy: Patients with suspected epilepsy (e.g., those whose presenting seizure is, in retrospect, not their first seizure) should begin antiepileptic drug therapy (AED).1
Typically, a broad-spectrum AED—one that is effective against both partial and generalized seizures—should be used as initial therapy for epilepsy. These include valproate, lamotrigine, topiramate, zonisamide, and levetiracetam (see Table 1, above). Valproate has the longest history of effectiveness; levetiracetam has fewer drug interactions, and randomized trials support its efficacy.1
Checking blood electrolytes and liver enzymes is recommended before beginning AED treatment. Significant hepatic or renal dysfunction might necessitate dosing adjustments in many AEDs.2
Inpatient consultation with a neurologist might be helpful, although insufficient evidence exists that such consultation improves patient outcomes or makes care more cost-efficient. A neurologist should follow up on patients with a first seizure after hospital discharge.2
Patients with a first seizure that likely was provoked by a reversible condition (e.g., hypotension, hypoglycemia, infection) should generally not begin AED therapy. This also includes patients with multiple seizures in a brief period of time (less than 24 hours), all attributed to the same reversible cause.1
The decision to begin AED therapy after a first unprovoked seizure is controversial. Estimates of the likelihood of seizure recurrence range from 25% at two years to 50% at one year (in the absence of AED therapy).1-2,4-7 The decision to start AED therapy after a first seizure must therefore be individualized for each patient.
Patients at high risk for recurrent seizures should begin AED therapy.1 However, no test or prognostic tool reliably identifies these patients, and initiating therapy carries side effects and places psychological, financial, and social burdens on the patient. The prevailing clinical practice, therefore, has been watchful waiting, with a second seizure constituting proof of high risk for recurrence—and need for AED therapy. Three-quarters of patients with two or more unprovoked seizures likely will go on to have recurrent seizures.6
On the other hand, in patients believed to be at high risk for seizure recurrence, a more aggressive approach of initiating AED therapy after the first seizure is reasonable. A number of risk factors increasing risk for seizure recurrence have been identified (see Table 2, left).1,2 It is justified to initiate AED therapy if any of these factors are present, even after a single seizure. Still, it’s important to note that most people with risk factors will not benefit from AEDs, as only about 40% will have a seizure in the following two years.1
Early initiation of AED therapy might be appropriate for patients with occupations or hobbies in which seizures could be life-threatening (e.g., scuba divers, truck drivers).2
Low-risk patients still have a roughly 20% to 30% risk of seizure recurrence within three years.1 A second seizure that occurs while driving or while engaged in any hazardous activity could lead to serious injury.
Patients should be advised of this small but inescapable risk and instructed to contact their department of motor vehicles for specific legal restrictions, which vary by state. Once three seizure-free years have passed after a patient’s initial seizure, the chance of a recurrence falls to around 10% to 20%.6-7
Back to the Case
Our 42-year-old patient with a first seizure had normal findings on examination, laboratory studies, and brain imaging. An EEG showed epileptiform discharges in a spike and wave pattern. The attending hospitalist counseled him on his elevated risk of future seizures; the patient then elected to begin AED therapy, citing a fear of losing his driving privileges. Levetiracetam was started, which he tolerated despite mild sedation.
A year later, he suffered another seizure at his home. With regular followup and titration of his AED, he remained seizure-free for the next five years.
Bottom Line
Most patients with a single unprovoked seizure can be managed with watchful waiting, counseling, and neurological followup. Initiation of AED therapy is appropriate for patients with a high risk of seizure recurrence, or for whom another seizure could pose personal or social harm. TH
Dr. Hoffman is a hospitalist at Emory University School of Medicine in Atlanta.
References
- French JA, Pedley TA. Clinical practice: Initial management of epilepsy. N Engl J Med. 2008;359:166-176.
- Krumholz A, Wiebe S, Gronseth G, et al. Practice Parameter: evaluating an apparent unprovoked first seizure in adults (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Neurology. 2007;69:1996-2007.
- Schachter SC. Antiepileptic drug therapy: general treatment principles and application for special patient populations. Epilepsia. 1999;40(9):S20-25.
- Hauser WA, Rich SS, Annegers JF, et al. Seizure recurrence after a first unprovoked seizure: an extended follow-up. Neurology. 1990;40:1163-1170.
- Marson A, Jacoby A, Johnson A, et al. Immediate versus deferred antiepileptic drug treatment for epilepsy and single seizures: a randomized controlled trial. Lancet. 2005;365: 2007-2013.
- Hauser WA, Rich SS, Lee JR, Annegers JF, Anderson VE. Risk of recurrent seizures after two unprovoked seizures. N Engl J Med. 1998;338:429-434.
- Berg AT. Risk of recurrence after a first unprovoked seizure. Epilepsia. 2008;49:S13-18.
- Kim LG, Johnson TL, Marson AG, et al. Prediction of risk of seizure recurrence after a single seizure and early epilepsy: further results from the MESS trial. Lancet Neurology. 2006;5(4):317-322.
Case
A 42-year-old man is brought to the hospital by his family after a reported seizure. The patient was found on the floor, unresponsive, and suffering convulsions lasting less than a minute. He suffered no apparent trauma before or during the event. He has no history of seizures. His mental status quickly improved; he experienced oriented lucidity with slight drowsiness. His neurological exam is nonfocal, and his vital signs and laboratory values are normal. A noncontrast head computed tomogram (CT) is normal.
What is the appropriate approach to diagnosis and management for this patient with a new-onset seizure?
Overview
A patient with a first seizure presents a dilemma. Underlying causes for seizure are potentially life-threatening, and must be identified if present. A patient whose first seizure is unprovoked is at risk for future seizures (i.e., epilepsy). However, long-term therapy with anticonvulsant medication has morbidity, side effects, and expense. Advising a patient on whether to drive has public safety and legal implications, as well as major lifestyle changes for the patient.
Seizures may be focal (limited to one area of the brain) or generalized (involving both hemispheres). For the most part, focal (also known as partial) seizures do not impair consciousness; generalized seizures do. Approximately 70% of first seizures are partial focal seizures.1 Such provoking causes as head trauma, stroke, alcohol withdrawal, brain tumors, and infections can be identified in about one-third of cases.1
Electroencephalogram (EEG) and computed tomogram (CT) of the brain should be obtained, but insufficient evidence exists to recommend other testing, which should be pursued according to the clinical context.2
Unprovoked seizures recur in about 25% to 50% of patients, resulting in a diagnosis of epilepsy.1,2,4-7
Therapy is unnecessary in patients whose seizures will not recur, but reliably identifying these patients is a challenge. Whether antiepileptic drug (AED) therapy should be initiated in patients with a first unprovoked seizure is controversial and will be reviewed below.
Review of the Data
History: No test or finding can reliably differentiate unwitnessed seizures from other events (e.g., syncope).2 History from a reliable observer often is necessary to determine whether the event actually was a seizure.2 In as many as 50% of patients with a “first” seizure, thorough history will likely reveal previously unrecognized seizures.1 Although most epilepsy syndromes begin in childhood or adolescence, a significant number of patients will experience their first seizure in adulthood.2
A thorough neurologic examination should be performed. In a minority of cases, an exam will suggest a focal lesion. An impaired level of consciousness might represent a post-ictal state or delirium.2
Diagnostic evaluation: If the history suggests a seizure, an EEG should be obtained. Although the EEG will be normal in 50% of patients following a first seizure, an abnormal EEG provides useful information about seizure type and the likelihood of recurrence.2 In nearly a quarter of patients, the EEG will show epileptiform abnormalities that predict future seizures.2
Generally, an EEG should be obtained as soon as feasible, once a seizure is suspected. Some evidence in children suggests that EEG yield is higher in the 24 hours after a first seizure.
A noncontrast head CT or magnetic resonance imaging (MRI) reveals a significant abnormality about 10% of the time.2 A CT or MRI should be obtained. Few studies have compared CT to MRI in terms of yield in determining first seizure etiology, and those that do compare the two suffer from selection bias.2 Although CT or MRI are appropriate in evaluating a patient with a first seizure, the MRI’s greater resolution might provide a higher diagnostic yield in terms of seizure etiology, and, therefore, some experts recommend MRI over CT in nonemergent cases.2
Insufficient data exist to support or refute diagnostic testing beyond brain imaging and EEG. Although electrolyte abnormalities, hypoglycemia, and infections might infrequently cause seizures, such routine blood tests as complete blood count (CBC) and chemistry panels are rarely helpful.
As many as 15% of patients with a seizure will have minor abnormalities on routine lab tests, but the abnormalities do not appear to be the cause of the seizure.2
Lumbar puncture (LP) is categorically recommended only in patients in whom there is a clinical suspicion for infection as a seizure etiology. Reviews suggest that signs and symptoms of infection are typically present in patients with meningitis or another infectious cause for seizure; LP generally has limited utility in other noninfectious causes of seizure.2
The utility of toxicology testing in a first seizure has not been studied widely. Testing urine or blood for the presence of alcohol, cocaine, methamphetamines, benzodiazepines, or drug metabolites could be useful in the appropriate clinical setting.2
It is unclear whether a patient with a first seizure requires hospitalization. If initial testing in the ED rules out serious causes of seizures, the yield for hospitalization is likely to be low. In clinical practice, however, hospitalization is common and often necessary to complete such diagnostic testing as EEG and MRI.
Medical therapy: Patients with suspected epilepsy (e.g., those whose presenting seizure is, in retrospect, not their first seizure) should begin antiepileptic drug therapy (AED).1
Typically, a broad-spectrum AED—one that is effective against both partial and generalized seizures—should be used as initial therapy for epilepsy. These include valproate, lamotrigine, topiramate, zonisamide, and levetiracetam (see Table 1, above). Valproate has the longest history of effectiveness; levetiracetam has fewer drug interactions, and randomized trials support its efficacy.1
Checking blood electrolytes and liver enzymes is recommended before beginning AED treatment. Significant hepatic or renal dysfunction might necessitate dosing adjustments in many AEDs.2
Inpatient consultation with a neurologist might be helpful, although insufficient evidence exists that such consultation improves patient outcomes or makes care more cost-efficient. A neurologist should follow up on patients with a first seizure after hospital discharge.2
Patients with a first seizure that likely was provoked by a reversible condition (e.g., hypotension, hypoglycemia, infection) should generally not begin AED therapy. This also includes patients with multiple seizures in a brief period of time (less than 24 hours), all attributed to the same reversible cause.1
The decision to begin AED therapy after a first unprovoked seizure is controversial. Estimates of the likelihood of seizure recurrence range from 25% at two years to 50% at one year (in the absence of AED therapy).1-2,4-7 The decision to start AED therapy after a first seizure must therefore be individualized for each patient.
Patients at high risk for recurrent seizures should begin AED therapy.1 However, no test or prognostic tool reliably identifies these patients, and initiating therapy carries side effects and places psychological, financial, and social burdens on the patient. The prevailing clinical practice, therefore, has been watchful waiting, with a second seizure constituting proof of high risk for recurrence—and need for AED therapy. Three-quarters of patients with two or more unprovoked seizures likely will go on to have recurrent seizures.6
On the other hand, in patients believed to be at high risk for seizure recurrence, a more aggressive approach of initiating AED therapy after the first seizure is reasonable. A number of risk factors increasing risk for seizure recurrence have been identified (see Table 2, left).1,2 It is justified to initiate AED therapy if any of these factors are present, even after a single seizure. Still, it’s important to note that most people with risk factors will not benefit from AEDs, as only about 40% will have a seizure in the following two years.1
Early initiation of AED therapy might be appropriate for patients with occupations or hobbies in which seizures could be life-threatening (e.g., scuba divers, truck drivers).2
Low-risk patients still have a roughly 20% to 30% risk of seizure recurrence within three years.1 A second seizure that occurs while driving or while engaged in any hazardous activity could lead to serious injury.
Patients should be advised of this small but inescapable risk and instructed to contact their department of motor vehicles for specific legal restrictions, which vary by state. Once three seizure-free years have passed after a patient’s initial seizure, the chance of a recurrence falls to around 10% to 20%.6-7
Back to the Case
Our 42-year-old patient with a first seizure had normal findings on examination, laboratory studies, and brain imaging. An EEG showed epileptiform discharges in a spike and wave pattern. The attending hospitalist counseled him on his elevated risk of future seizures; the patient then elected to begin AED therapy, citing a fear of losing his driving privileges. Levetiracetam was started, which he tolerated despite mild sedation.
A year later, he suffered another seizure at his home. With regular followup and titration of his AED, he remained seizure-free for the next five years.
Bottom Line
Most patients with a single unprovoked seizure can be managed with watchful waiting, counseling, and neurological followup. Initiation of AED therapy is appropriate for patients with a high risk of seizure recurrence, or for whom another seizure could pose personal or social harm. TH
Dr. Hoffman is a hospitalist at Emory University School of Medicine in Atlanta.
References
- French JA, Pedley TA. Clinical practice: Initial management of epilepsy. N Engl J Med. 2008;359:166-176.
- Krumholz A, Wiebe S, Gronseth G, et al. Practice Parameter: evaluating an apparent unprovoked first seizure in adults (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Neurology. 2007;69:1996-2007.
- Schachter SC. Antiepileptic drug therapy: general treatment principles and application for special patient populations. Epilepsia. 1999;40(9):S20-25.
- Hauser WA, Rich SS, Annegers JF, et al. Seizure recurrence after a first unprovoked seizure: an extended follow-up. Neurology. 1990;40:1163-1170.
- Marson A, Jacoby A, Johnson A, et al. Immediate versus deferred antiepileptic drug treatment for epilepsy and single seizures: a randomized controlled trial. Lancet. 2005;365: 2007-2013.
- Hauser WA, Rich SS, Lee JR, Annegers JF, Anderson VE. Risk of recurrent seizures after two unprovoked seizures. N Engl J Med. 1998;338:429-434.
- Berg AT. Risk of recurrence after a first unprovoked seizure. Epilepsia. 2008;49:S13-18.
- Kim LG, Johnson TL, Marson AG, et al. Prediction of risk of seizure recurrence after a single seizure and early epilepsy: further results from the MESS trial. Lancet Neurology. 2006;5(4):317-322.
Should HM Be in the Comanagement Business?
PRO
Experience, availability make HM the perfect comanagement choice

Hospitalists should be in the business of comanagement, especially the comanagement of surgical patients. Thanks to modern medicine, people are living longer with a higher burden of comorbidity. Comanagement is intended to bring clinical acumen and experience to the bedside of a complex medical patient who is having surgery and needs acute medical care. Hospitalists must bring their extensive clinical experience and on-site availability to ensure the best outcomes.
The most important aspect of comanagement can be summed up in one phrase: right person, right place, and right time.
Right Person
The interaction between pre-existing comorbidities and the physiologic stress of anesthesia, volume shifts, narcotic therapy, sleep deprivation, postoperative anemia, and any number of other stressors can be complex.
Frankly, it is more appropriate for an experienced hospitalist to evaluate and manage these intricacies than a specialty surgeon, although general and critical-care surgeons are likely exceptions. Our internal medicine and geriatric training, not to mention experience, positions us to best meet the needs of these complex patients.
Right Place
Hospitalists are in the hospital and prepared to handle the unexpected. Surgeons cannot be in two places at once; they cannot leave the operating room with another patient on the table. Likewise, a general internist in a consultative role usually cannot leave the clinic on short notice. Hospitalists are physically present and available to go to a patient’s room when there is an immediate clinical need.
Right Time
Early evaluation and treatment are indicated when most postoperative complications occur. One of the defining characteristics of hospitalists is availability. Relying on a surgeon to be at the bedside immediately is inappropriate.
In traditional consultative roles, the medical consultant might also have clinical duties in an outpatient setting. Neither model allows an experienced physician to reliably get to the bedside, then evaluate, monitor, follow up on test results, and manage patient care. Hospitalists are available and can participate in all aspects of care until resolution of the complication.
Additional Opportunity
Another aspect of the comanagement model is the opportunity to extend beyond the postoperative setting to the preoperative evaluation. This brings with it the opportunity to identify possible problems before surgery. In addition, the business model for the preoperative consultation is quite strong.
Meeting patients’ clinical needs is the most important reason for engaging in a comanagement model of care in the perioperative setting. This model brings timely experience, evaluation, and management when and where it is needed. TH
CON
Establish rules of engagement before agreeing to share responsibilities

In the wee hours of a recent busy call night, the ED called me to admit a patient whose automatic implantable cardioverter cefibrillator (AICD) had fired repeatedly. The patient had no other active medical issues. When called, the electrophysiologist, who was on staff, demanded that I admit the patient for “medical comanagement.” The specialist agreed that I probably would have little to add to the care, but his firm expectation was that hospitalists admit his patients and he “consults” … especially at 2 a.m.
Job Description Defined
Comanagement, defined as shared responsibility, authority, and accountability for the management of a hospitalized patient, is an HM mainstay and a primary driver of the explosive growth of our field.1
While it stands to reason that surgical and specialty patients with active medical comorbidities likely fare better if hospitalists are integrated into their care, comanagement has broadened in its application to include scenarios in which the benefits are more dubious. Hospitalist comanagement now encompasses “management” of patients for whom hospitalists have little, if anything, to add.
At the other comanagement extreme, hospitalists, despite little or no formal training, primarily manage patients with acute neurologic, neurosurgical, psychiatric, and orthopedic diagnoses, often with inadequate surgical or specialty involvement.2,3 Although it makes sense for a hospital with only one neurosurgeon to have its hospitalists manage carefully selected neurosurgical patients, the justification for such scenarios becomes harder to reconcile at hospitals where there are no staffing shortages. I suspect the primary justification for hospitalist comanagement in such circumstances is to keep specialists doing lucrative procedures by day and in bed at night, and to ensure that someone manages the paperwork, discharge communication, and patient logistics that are often otherwise ignored.
Rules of Engagement
In well-designed comanagement arrangements, hospitalists and specialists work equitably under clearly defined and mutually agreed upon rules of engagement. They share responsibility for patients, collaborate to improve care, and teach and learn from each other. Unfortunately, in many instances, the power structure has tilted.
Practicing hospitalists frequently complain about their subordinate status and inability to control their working conditions; both are identified risk factors for career dissatisfaction and burnout.4,5
Before entering a comanagement relationship, hospitalists should gain a clear understanding of why they are being asked to comanage, what problems they are expected to fix by doing so, and what the consequences, intended or unintended, might be as a result. There should be mechanisms to ensure that the relationship is equitable and serves the best interests of the patient, rather than the care parties involved. TH
References
- 2007-2008 Bi-annual Survey on the State of the Hospital Medicine Movement. SHM Web site. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=Surveys2&Template=/CM/HTMLDisplay.cfm&ContentID=18419. Accessed July 26, 2009.
- Plauth WH, Pantilat SZ, Wachter RM, Fenton CL. Hospitalists’ perceptions of their residency training needs: results of a national survey. Am J Med. 2001;111:247-254.
- Glasheen JJ, Epstein KR, Siegal E, Kutner JS, Prochazka AV. The spectrum of community-based hospitalist practice: a call to tailor internal medicine residency training. Arch Intern Med. 2007;167(7):727-728.
- Linzer M , Gerrity M, Douglas JA, McMurray JE, Williams ES, Konrad TR. Physician stress: results from the physician work life study. Stress and Health. 2001;18(1)37-42.
- SHM Career Satisfaction White Paper. SHM Web site. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Practice_Resources& Template=/CM/ContentDisplay.cfm&ContentID=14631. Accessed July 26, 2009.
The opinions expressed herein are those of the authors and do not necessarily represent those of the Society of Hospital Medicine or The Hospitalist.
PRO
Experience, availability make HM the perfect comanagement choice
Hospitalists should be in the business of comanagement, especially the comanagement of surgical patients. Thanks to modern medicine, people are living longer with a higher burden of comorbidity. Comanagement is intended to bring clinical acumen and experience to the bedside of a complex medical patient who is having surgery and needs acute medical care. Hospitalists must bring their extensive clinical experience and on-site availability to ensure the best outcomes.
The most important aspect of comanagement can be summed up in one phrase: right person, right place, and right time.
Right Person
The interaction between pre-existing comorbidities and the physiologic stress of anesthesia, volume shifts, narcotic therapy, sleep deprivation, postoperative anemia, and any number of other stressors can be complex.
Frankly, it is more appropriate for an experienced hospitalist to evaluate and manage these intricacies than a specialty surgeon, although general and critical-care surgeons are likely exceptions. Our internal medicine and geriatric training, not to mention experience, positions us to best meet the needs of these complex patients.
Right Place
Hospitalists are in the hospital and prepared to handle the unexpected. Surgeons cannot be in two places at once; they cannot leave the operating room with another patient on the table. Likewise, a general internist in a consultative role usually cannot leave the clinic on short notice. Hospitalists are physically present and available to go to a patient’s room when there is an immediate clinical need.
Right Time
Early evaluation and treatment are indicated when most postoperative complications occur. One of the defining characteristics of hospitalists is availability. Relying on a surgeon to be at the bedside immediately is inappropriate.
In traditional consultative roles, the medical consultant might also have clinical duties in an outpatient setting. Neither model allows an experienced physician to reliably get to the bedside, then evaluate, monitor, follow up on test results, and manage patient care. Hospitalists are available and can participate in all aspects of care until resolution of the complication.
Additional Opportunity
Another aspect of the comanagement model is the opportunity to extend beyond the postoperative setting to the preoperative evaluation. This brings with it the opportunity to identify possible problems before surgery. In addition, the business model for the preoperative consultation is quite strong.
Meeting patients’ clinical needs is the most important reason for engaging in a comanagement model of care in the perioperative setting. This model brings timely experience, evaluation, and management when and where it is needed. TH
CON
Establish rules of engagement before agreeing to share responsibilities
In the wee hours of a recent busy call night, the ED called me to admit a patient whose automatic implantable cardioverter cefibrillator (AICD) had fired repeatedly. The patient had no other active medical issues. When called, the electrophysiologist, who was on staff, demanded that I admit the patient for “medical comanagement.” The specialist agreed that I probably would have little to add to the care, but his firm expectation was that hospitalists admit his patients and he “consults” … especially at 2 a.m.
Job Description Defined
Comanagement, defined as shared responsibility, authority, and accountability for the management of a hospitalized patient, is an HM mainstay and a primary driver of the explosive growth of our field.1
While it stands to reason that surgical and specialty patients with active medical comorbidities likely fare better if hospitalists are integrated into their care, comanagement has broadened in its application to include scenarios in which the benefits are more dubious. Hospitalist comanagement now encompasses “management” of patients for whom hospitalists have little, if anything, to add.
At the other comanagement extreme, hospitalists, despite little or no formal training, primarily manage patients with acute neurologic, neurosurgical, psychiatric, and orthopedic diagnoses, often with inadequate surgical or specialty involvement.2,3 Although it makes sense for a hospital with only one neurosurgeon to have its hospitalists manage carefully selected neurosurgical patients, the justification for such scenarios becomes harder to reconcile at hospitals where there are no staffing shortages. I suspect the primary justification for hospitalist comanagement in such circumstances is to keep specialists doing lucrative procedures by day and in bed at night, and to ensure that someone manages the paperwork, discharge communication, and patient logistics that are often otherwise ignored.
Rules of Engagement
In well-designed comanagement arrangements, hospitalists and specialists work equitably under clearly defined and mutually agreed upon rules of engagement. They share responsibility for patients, collaborate to improve care, and teach and learn from each other. Unfortunately, in many instances, the power structure has tilted.
Practicing hospitalists frequently complain about their subordinate status and inability to control their working conditions; both are identified risk factors for career dissatisfaction and burnout.4,5
Before entering a comanagement relationship, hospitalists should gain a clear understanding of why they are being asked to comanage, what problems they are expected to fix by doing so, and what the consequences, intended or unintended, might be as a result. There should be mechanisms to ensure that the relationship is equitable and serves the best interests of the patient, rather than the care parties involved. TH
References
- 2007-2008 Bi-annual Survey on the State of the Hospital Medicine Movement. SHM Web site. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=Surveys2&Template=/CM/HTMLDisplay.cfm&ContentID=18419. Accessed July 26, 2009.
- Plauth WH, Pantilat SZ, Wachter RM, Fenton CL. Hospitalists’ perceptions of their residency training needs: results of a national survey. Am J Med. 2001;111:247-254.
- Glasheen JJ, Epstein KR, Siegal E, Kutner JS, Prochazka AV. The spectrum of community-based hospitalist practice: a call to tailor internal medicine residency training. Arch Intern Med. 2007;167(7):727-728.
- Linzer M , Gerrity M, Douglas JA, McMurray JE, Williams ES, Konrad TR. Physician stress: results from the physician work life study. Stress and Health. 2001;18(1)37-42.
- SHM Career Satisfaction White Paper. SHM Web site. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Practice_Resources& Template=/CM/ContentDisplay.cfm&ContentID=14631. Accessed July 26, 2009.
The opinions expressed herein are those of the authors and do not necessarily represent those of the Society of Hospital Medicine or The Hospitalist.
PRO
Experience, availability make HM the perfect comanagement choice
Hospitalists should be in the business of comanagement, especially the comanagement of surgical patients. Thanks to modern medicine, people are living longer with a higher burden of comorbidity. Comanagement is intended to bring clinical acumen and experience to the bedside of a complex medical patient who is having surgery and needs acute medical care. Hospitalists must bring their extensive clinical experience and on-site availability to ensure the best outcomes.
The most important aspect of comanagement can be summed up in one phrase: right person, right place, and right time.
Right Person
The interaction between pre-existing comorbidities and the physiologic stress of anesthesia, volume shifts, narcotic therapy, sleep deprivation, postoperative anemia, and any number of other stressors can be complex.
Frankly, it is more appropriate for an experienced hospitalist to evaluate and manage these intricacies than a specialty surgeon, although general and critical-care surgeons are likely exceptions. Our internal medicine and geriatric training, not to mention experience, positions us to best meet the needs of these complex patients.
Right Place
Hospitalists are in the hospital and prepared to handle the unexpected. Surgeons cannot be in two places at once; they cannot leave the operating room with another patient on the table. Likewise, a general internist in a consultative role usually cannot leave the clinic on short notice. Hospitalists are physically present and available to go to a patient’s room when there is an immediate clinical need.
Right Time
Early evaluation and treatment are indicated when most postoperative complications occur. One of the defining characteristics of hospitalists is availability. Relying on a surgeon to be at the bedside immediately is inappropriate.
In traditional consultative roles, the medical consultant might also have clinical duties in an outpatient setting. Neither model allows an experienced physician to reliably get to the bedside, then evaluate, monitor, follow up on test results, and manage patient care. Hospitalists are available and can participate in all aspects of care until resolution of the complication.
Additional Opportunity
Another aspect of the comanagement model is the opportunity to extend beyond the postoperative setting to the preoperative evaluation. This brings with it the opportunity to identify possible problems before surgery. In addition, the business model for the preoperative consultation is quite strong.
Meeting patients’ clinical needs is the most important reason for engaging in a comanagement model of care in the perioperative setting. This model brings timely experience, evaluation, and management when and where it is needed. TH
CON
Establish rules of engagement before agreeing to share responsibilities
In the wee hours of a recent busy call night, the ED called me to admit a patient whose automatic implantable cardioverter cefibrillator (AICD) had fired repeatedly. The patient had no other active medical issues. When called, the electrophysiologist, who was on staff, demanded that I admit the patient for “medical comanagement.” The specialist agreed that I probably would have little to add to the care, but his firm expectation was that hospitalists admit his patients and he “consults” … especially at 2 a.m.
Job Description Defined
Comanagement, defined as shared responsibility, authority, and accountability for the management of a hospitalized patient, is an HM mainstay and a primary driver of the explosive growth of our field.1
While it stands to reason that surgical and specialty patients with active medical comorbidities likely fare better if hospitalists are integrated into their care, comanagement has broadened in its application to include scenarios in which the benefits are more dubious. Hospitalist comanagement now encompasses “management” of patients for whom hospitalists have little, if anything, to add.
At the other comanagement extreme, hospitalists, despite little or no formal training, primarily manage patients with acute neurologic, neurosurgical, psychiatric, and orthopedic diagnoses, often with inadequate surgical or specialty involvement.2,3 Although it makes sense for a hospital with only one neurosurgeon to have its hospitalists manage carefully selected neurosurgical patients, the justification for such scenarios becomes harder to reconcile at hospitals where there are no staffing shortages. I suspect the primary justification for hospitalist comanagement in such circumstances is to keep specialists doing lucrative procedures by day and in bed at night, and to ensure that someone manages the paperwork, discharge communication, and patient logistics that are often otherwise ignored.
Rules of Engagement
In well-designed comanagement arrangements, hospitalists and specialists work equitably under clearly defined and mutually agreed upon rules of engagement. They share responsibility for patients, collaborate to improve care, and teach and learn from each other. Unfortunately, in many instances, the power structure has tilted.
Practicing hospitalists frequently complain about their subordinate status and inability to control their working conditions; both are identified risk factors for career dissatisfaction and burnout.4,5
Before entering a comanagement relationship, hospitalists should gain a clear understanding of why they are being asked to comanage, what problems they are expected to fix by doing so, and what the consequences, intended or unintended, might be as a result. There should be mechanisms to ensure that the relationship is equitable and serves the best interests of the patient, rather than the care parties involved. TH
References
- 2007-2008 Bi-annual Survey on the State of the Hospital Medicine Movement. SHM Web site. Available at: www.hospitalmedicine.org/AM/Template.cfm?Section=Surveys2&Template=/CM/HTMLDisplay.cfm&ContentID=18419. Accessed July 26, 2009.
- Plauth WH, Pantilat SZ, Wachter RM, Fenton CL. Hospitalists’ perceptions of their residency training needs: results of a national survey. Am J Med. 2001;111:247-254.
- Glasheen JJ, Epstein KR, Siegal E, Kutner JS, Prochazka AV. The spectrum of community-based hospitalist practice: a call to tailor internal medicine residency training. Arch Intern Med. 2007;167(7):727-728.
- Linzer M , Gerrity M, Douglas JA, McMurray JE, Williams ES, Konrad TR. Physician stress: results from the physician work life study. Stress and Health. 2001;18(1)37-42.
- SHM Career Satisfaction White Paper. SHM Web site. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=Practice_Resources& Template=/CM/ContentDisplay.cfm&ContentID=14631. Accessed July 26, 2009.
The opinions expressed herein are those of the authors and do not necessarily represent those of the Society of Hospital Medicine or The Hospitalist.
Revenue Essentials
As physicians take on more extensive roles outside of patient care (e.g., administrative, academic, and billing compliance), involvement in the revenue cycle might diminish or even fail to commence. It is crucial for physicians to keep abreast of revenue cycle issues, but more often than not, they go unnoticed until a physician’s bottom line is affected.
The risk of inappropriately billed claims and corresponding reimbursement is increased until the problem is identified and resolved. In an effort to prevent this from occurring, physicians should get involved with or oversee their billing service or staff. Some of the revenue cycle essentials that require physician attention are:1
- Periodic reports of claims billed on the physician’s behalf and data regarding payments;
- Changes in procedure codes, diagnosis codes, or other information furnished by the physician without the physician’s knowledge and consent; and
- Information received from Medicare and other payors.
Feedback
One of the most common billing-related physician complaints involves the lack of feedback. Most physicians want to receive information regarding their quarterly billings: the volume and frequency of specific reported services, and corresponding payments or denials. Physicians prefer to know how they rank as individuals and as a group. Although they might not be experts in coding and documentation, this information offers physicians a feeling of security, as it permits them to identify typical billing patterns or highlight outlier patterns.
Establish communication with the manager/coder/biller to better assist with feedback. Appoint a physician leader to spearhead this effort; ensure feedback is provided quarterly, at a minimum. If the coders/billers feel that they have an approachable contact, they’re more likely to offer feedback before formal reports are generated. A quick resolution of potential problems lessens the financial burden on the HM group, as well as the resource-intensive education process that ensues.
Discrepancy Notation
Physicians should be notified whenever coding changes take place. Discrepancies occur when the physician employs coders to select the service or diagnosis codes, and the selected codes differ from the physician-intended codes. Discrepancies also occur when billers change the original physician-selected codes to codes that are considered covered or medically necessary by the pay0r. Physicians need to instruct coders to only report codes that are supported by the documentation.
Physicians must be aware that delegating any portion of the billing to an employee or a billing company does not alleviate physicians’ personal responsibility for erroneously submitted claims or receipt of overpayments. Physicians should regularly review information submitted by the designated employee or billing service to ensure consistency with their own records, and also keep complete administrative records for the claims a billing service files on their behalf.1 Physicians also should meet with staff to resolve discrepancies and reinforce the billing education process. If biller/coder performance becomes a recurring problem, the physician should question the competency of the employee or company with whom the billing is entrusted.
Accounts Receivable
Physicians do not necessarily recognize the need for involvement in the accounts receivable (A/R) component of the revenue cycle. Physicians should be aware of denials, and the reasons for the denials. Some services are denied because of issues that can be easily corrected (e.g., truncated diagnoses, two physicians of the same specialty billing on the same date, missing modifiers). These denial types might require physician assistance in changing the codes originally submitted. If the denied services can be corrected with the appropriate information and resubmitted electronically, payment might be recovered quickly. Other types of denials require submission of the documentation to support the service billed.
Billers should know the difference between the types of denials and the required action for each denial type. Physicians should feel confident that such denials will be handled in the correct manner. Be mindful of billing staff that accepts denials and surrenders the reimbursement efforts without hesitation. As a physician, do not default to the idea that “no news is good news.” Do not assume the billing manager (physician employee or outsourced firm) will let the group know if there is a problem. Develop a standard that requires monthly feedback of denials.
Only a short window of time exists for the appeals process to occur. Do not lose the potential to recover monies because the information was not provided to the physician in a timely manner. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. Protecting Your Practice. CMS Web site. Available at: www.cms.hhs.gov/MLNProducts/downloads/Protectingpracbroch508-09.pdf. Accessed Aug. 2, 2009.
- Office of Inspector General. Work Plan Health Care Financing Administration Projects Fiscal Year 1999. Physicians: Billing Service Companies. Available at: http://oig.hhs.gov/publications/docs/workplan/1999/99hcfawp.pdf. Accessed Aug. 2, 2009.
- Office of Inspector General. OIG Compliance Program Guidance for Third-Party Medical Billing Companies in Federal Register, December 1998, Vol. 63; pages 70138-70152. Available at: http://oig.hhs.gov/fraud/docs/complianceguidance/thirdparty.pdf. Accessed Aug. 2, 2009.
As physicians take on more extensive roles outside of patient care (e.g., administrative, academic, and billing compliance), involvement in the revenue cycle might diminish or even fail to commence. It is crucial for physicians to keep abreast of revenue cycle issues, but more often than not, they go unnoticed until a physician’s bottom line is affected.
The risk of inappropriately billed claims and corresponding reimbursement is increased until the problem is identified and resolved. In an effort to prevent this from occurring, physicians should get involved with or oversee their billing service or staff. Some of the revenue cycle essentials that require physician attention are:1
- Periodic reports of claims billed on the physician’s behalf and data regarding payments;
- Changes in procedure codes, diagnosis codes, or other information furnished by the physician without the physician’s knowledge and consent; and
- Information received from Medicare and other payors.
Feedback
One of the most common billing-related physician complaints involves the lack of feedback. Most physicians want to receive information regarding their quarterly billings: the volume and frequency of specific reported services, and corresponding payments or denials. Physicians prefer to know how they rank as individuals and as a group. Although they might not be experts in coding and documentation, this information offers physicians a feeling of security, as it permits them to identify typical billing patterns or highlight outlier patterns.
Establish communication with the manager/coder/biller to better assist with feedback. Appoint a physician leader to spearhead this effort; ensure feedback is provided quarterly, at a minimum. If the coders/billers feel that they have an approachable contact, they’re more likely to offer feedback before formal reports are generated. A quick resolution of potential problems lessens the financial burden on the HM group, as well as the resource-intensive education process that ensues.
Discrepancy Notation
Physicians should be notified whenever coding changes take place. Discrepancies occur when the physician employs coders to select the service or diagnosis codes, and the selected codes differ from the physician-intended codes. Discrepancies also occur when billers change the original physician-selected codes to codes that are considered covered or medically necessary by the pay0r. Physicians need to instruct coders to only report codes that are supported by the documentation.
Physicians must be aware that delegating any portion of the billing to an employee or a billing company does not alleviate physicians’ personal responsibility for erroneously submitted claims or receipt of overpayments. Physicians should regularly review information submitted by the designated employee or billing service to ensure consistency with their own records, and also keep complete administrative records for the claims a billing service files on their behalf.1 Physicians also should meet with staff to resolve discrepancies and reinforce the billing education process. If biller/coder performance becomes a recurring problem, the physician should question the competency of the employee or company with whom the billing is entrusted.
Accounts Receivable
Physicians do not necessarily recognize the need for involvement in the accounts receivable (A/R) component of the revenue cycle. Physicians should be aware of denials, and the reasons for the denials. Some services are denied because of issues that can be easily corrected (e.g., truncated diagnoses, two physicians of the same specialty billing on the same date, missing modifiers). These denial types might require physician assistance in changing the codes originally submitted. If the denied services can be corrected with the appropriate information and resubmitted electronically, payment might be recovered quickly. Other types of denials require submission of the documentation to support the service billed.
Billers should know the difference between the types of denials and the required action for each denial type. Physicians should feel confident that such denials will be handled in the correct manner. Be mindful of billing staff that accepts denials and surrenders the reimbursement efforts without hesitation. As a physician, do not default to the idea that “no news is good news.” Do not assume the billing manager (physician employee or outsourced firm) will let the group know if there is a problem. Develop a standard that requires monthly feedback of denials.
Only a short window of time exists for the appeals process to occur. Do not lose the potential to recover monies because the information was not provided to the physician in a timely manner. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. Protecting Your Practice. CMS Web site. Available at: www.cms.hhs.gov/MLNProducts/downloads/Protectingpracbroch508-09.pdf. Accessed Aug. 2, 2009.
- Office of Inspector General. Work Plan Health Care Financing Administration Projects Fiscal Year 1999. Physicians: Billing Service Companies. Available at: http://oig.hhs.gov/publications/docs/workplan/1999/99hcfawp.pdf. Accessed Aug. 2, 2009.
- Office of Inspector General. OIG Compliance Program Guidance for Third-Party Medical Billing Companies in Federal Register, December 1998, Vol. 63; pages 70138-70152. Available at: http://oig.hhs.gov/fraud/docs/complianceguidance/thirdparty.pdf. Accessed Aug. 2, 2009.
As physicians take on more extensive roles outside of patient care (e.g., administrative, academic, and billing compliance), involvement in the revenue cycle might diminish or even fail to commence. It is crucial for physicians to keep abreast of revenue cycle issues, but more often than not, they go unnoticed until a physician’s bottom line is affected.
The risk of inappropriately billed claims and corresponding reimbursement is increased until the problem is identified and resolved. In an effort to prevent this from occurring, physicians should get involved with or oversee their billing service or staff. Some of the revenue cycle essentials that require physician attention are:1
- Periodic reports of claims billed on the physician’s behalf and data regarding payments;
- Changes in procedure codes, diagnosis codes, or other information furnished by the physician without the physician’s knowledge and consent; and
- Information received from Medicare and other payors.
Feedback
One of the most common billing-related physician complaints involves the lack of feedback. Most physicians want to receive information regarding their quarterly billings: the volume and frequency of specific reported services, and corresponding payments or denials. Physicians prefer to know how they rank as individuals and as a group. Although they might not be experts in coding and documentation, this information offers physicians a feeling of security, as it permits them to identify typical billing patterns or highlight outlier patterns.
Establish communication with the manager/coder/biller to better assist with feedback. Appoint a physician leader to spearhead this effort; ensure feedback is provided quarterly, at a minimum. If the coders/billers feel that they have an approachable contact, they’re more likely to offer feedback before formal reports are generated. A quick resolution of potential problems lessens the financial burden on the HM group, as well as the resource-intensive education process that ensues.
Discrepancy Notation
Physicians should be notified whenever coding changes take place. Discrepancies occur when the physician employs coders to select the service or diagnosis codes, and the selected codes differ from the physician-intended codes. Discrepancies also occur when billers change the original physician-selected codes to codes that are considered covered or medically necessary by the pay0r. Physicians need to instruct coders to only report codes that are supported by the documentation.
Physicians must be aware that delegating any portion of the billing to an employee or a billing company does not alleviate physicians’ personal responsibility for erroneously submitted claims or receipt of overpayments. Physicians should regularly review information submitted by the designated employee or billing service to ensure consistency with their own records, and also keep complete administrative records for the claims a billing service files on their behalf.1 Physicians also should meet with staff to resolve discrepancies and reinforce the billing education process. If biller/coder performance becomes a recurring problem, the physician should question the competency of the employee or company with whom the billing is entrusted.
Accounts Receivable
Physicians do not necessarily recognize the need for involvement in the accounts receivable (A/R) component of the revenue cycle. Physicians should be aware of denials, and the reasons for the denials. Some services are denied because of issues that can be easily corrected (e.g., truncated diagnoses, two physicians of the same specialty billing on the same date, missing modifiers). These denial types might require physician assistance in changing the codes originally submitted. If the denied services can be corrected with the appropriate information and resubmitted electronically, payment might be recovered quickly. Other types of denials require submission of the documentation to support the service billed.
Billers should know the difference between the types of denials and the required action for each denial type. Physicians should feel confident that such denials will be handled in the correct manner. Be mindful of billing staff that accepts denials and surrenders the reimbursement efforts without hesitation. As a physician, do not default to the idea that “no news is good news.” Do not assume the billing manager (physician employee or outsourced firm) will let the group know if there is a problem. Develop a standard that requires monthly feedback of denials.
Only a short window of time exists for the appeals process to occur. Do not lose the potential to recover monies because the information was not provided to the physician in a timely manner. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. Protecting Your Practice. CMS Web site. Available at: www.cms.hhs.gov/MLNProducts/downloads/Protectingpracbroch508-09.pdf. Accessed Aug. 2, 2009.
- Office of Inspector General. Work Plan Health Care Financing Administration Projects Fiscal Year 1999. Physicians: Billing Service Companies. Available at: http://oig.hhs.gov/publications/docs/workplan/1999/99hcfawp.pdf. Accessed Aug. 2, 2009.
- Office of Inspector General. OIG Compliance Program Guidance for Third-Party Medical Billing Companies in Federal Register, December 1998, Vol. 63; pages 70138-70152. Available at: http://oig.hhs.gov/fraud/docs/complianceguidance/thirdparty.pdf. Accessed Aug. 2, 2009.
Payment Purgatory
It happens every year: A new Medicare physician fee schedule recommends a painful reduction in the rates the government doles out for more than 7,000 types of medical services performed by hospitalists, primary-care doctors, and other healthcare providers. And then Congress intervenes to keep the reduction from going into effect.
This year, however, the fee updates and policy proposals have become intertwined in the larger debate over comprehensive healthcare reform and a push toward what SHM calls a “value-based health delivery system.”
Few think the whopping 21.5% reduction proposed for 2010 rates, which are due to be published Nov. 1, actually will go into effect in January. A combination of other proposed changes to the fee schedule could soften any reduction. But the larger issue of how fees are currently calculated has become a rallying point for SHM and other healthcare-reform advocates who’d like to see the entire formula scrapped in favor of a more equitable distribution that focuses on outcomes. SHM has expressed concern that the current fee-for-service payment system “fails to provide providers with incentives to improve efficiency or quality of care, and encourages overutilization of services.”

—J. James Rohack, MD, AMA president
The current fee formula, known as the sustainable growth rate (SGR) and stipulated by the Balanced Budget Act of 1997, has resulted in a proposed rate cut every year since it went into effect in 2002. Congress consistently overrides the reimbursement cuts in one way or another, usually enacting modest increases or, such as in 2006 and 2007, an across-the-board freeze.
Hospitalists and other physicians have greeted another high-profile proposal with more enthusiasm: the removal of physician-administered drugs from the definition of “physician services,” thereby eliminating a high-cost item from the SGR formula. A Centers for Medicare and Medicaid Services (CMS) spokeswoman says the agency previously felt it lacked the authority to propose the removal. But a review earlier this year reversed that position, leading to the change. The removal, she says, “wouldn’t change the 21.5% percent decline in 2010, but it could have an impact in future years.”
American Medical Association President J. James Rohack, MD, joined the chorus of approval with a statement that asserted, “The removal of physician-administered drugs from the broken Medicare physician payment formula is a major victory for America’s seniors and their physicians.”
Consultation Change
A separate physician fee schedule proposal would eliminate payments for consultation codes in both outpatient and inpatient settings in favor of codes for evaluation and management services that carry lower reimbursement rates. Doctors would have a new way to bill for tele-health consultations, however. Leslie Flores, director of SHM’s Practice Management Institute, said the proposal has generated a high level of misinformation and misunderstanding among hospitalists who fear CMS will no longer reimburse for inpatient consultations. “It’s not that they won’t allow the work to be done anymore,” Flores says. “They’re just instructing people to bill in a different way for that work.”
CMS notes that the savings would be redistributed to increase payments for existing evaluation and management services codes, making the change cost-neutral. But Flores says a lack of details about the “crosswalk” from the old codes to the new codes, especially as they relate to transfers of care, is fueling hospitalists’ confusion over the true impact on their reimbursements.
“Our biggest concern with this consultation proposal that is now on the table is that CMS has not done anything to clarify how these transfers of care would be treated,” she says. For example, would hospitalists bill an admission code the first time they see a patient after being asked by a surgeon to take over that patient’s diabetes care? If so, “this proposal could actually result in some pretty good revenue increases for a lot of hospitalist practices that are doing a lot of surgical comanagement,” she says.
If hospitalists are instead required to bill a work-intensive transition of care under the code for a subsequent visit, which CMS has enforced since a 2006 rule clarification, Flores explains, HM could lose anywhere from 1% to 18% of reimbursements, depending on the exact code used.
Quality Reporting
The proposed fee schedule also is generating disappointment about what will not be included in Medicare’s Physician Quality Reporting Initiative (PQRI) for 2010. The pay-for-performance PQRI, which rewards physicians for reporting on quality measures by paying them an additional 2% of their estimated charges for covered services, will streamline some reporting requirements and increase the overall number of reportable measures. But several care-transition measures sought by SHM were not endorsed in time and will not be among them. Those measures include:
- Reconciled medication lists received by discharged patients;
- Transition records with specified elements received by discharged patients (including one measure for an inpatient discharge to home or self-care, and another for an ED discharge to home, ambulatory, or self-care); and
- Timely transmission of transition records.
“It was really a question of timing,” says Jill Epstein, senior advisor of SHM’s Performance and Standards Committee. The National Quality Forum, the nonprofit organization charged with signing off on all new measures, was not able to fully vet the recommended additions by the July 1 deadline, Epstein says, postponing their inclusion. “Our hope is that the measures will be included for 2011, of course.”
Separately, the PQRI proposal seeks to add an electronic-health-record-based mechanism to the list of eligible reporting methods. Although that addition is welcome news, Epstein says, SHM is expressing its concern about the shift toward patient-registry-based reporting, including a proposal to lessen or perhaps even discontinue claims-based reporting after 2010. “The issue for hospitalists, as well as for any specialty,” she says, “is that not every group will have access to a qualified PQRI registry as early as 2011,” particularly rural-based groups with fewer resources.
A similar change would streamline the E-Prescribing Incentive Program’s rules for how often e-prescribing codes must be reported. It also will offer more choices for how to report them, including through qualified registries. In the past, the program had little direct impact on hospitalists, but the new proposal recommends adding reporting codes specific to nursing homes, where some hospitalists provide care and could benefit from the incentives.
Paul Fishman, an economist at the Group Health Center for Health Studies in Seattle, says the increased focus on incentives in Medicare’s fee schedule suggests a growing realization of how such incentives can drive the delivery of healthcare services. “We know with absolute certainty that physicians make choices based on how things are reimbursed,” he says. Developing good outcome measures, then, will be critical for establishing pay-for-performance standards as part of a fee package that he says should include a blend of capitation and service-based and outcome-based reimbursements to strike a fairer balance.
“In healthcare, we’ve incented people to do more and more stuff, whether they improve outcomes or not, but we have to figure out a way to incent improvements in outcomes, while still retaining the long-term incentive to keep people healthy,” Fishman says. If better transitions of care result in a healthier population that is rehospitalized less often, for example, how can outcome-based incentives prevent hospitals from losing money in the long run? “We want to create the incentives to make the improvements in health outcomes, but we don’t want to punish the better actors because they are consistently lowering costs and also lowering reimbursement levels,” he says.
Achieving that balance in both Medicare and the broader healthcare system, he and other observers agree, is still very much a work in progress. TH
Bryn Nelson is a freelance writer based in Seattle.
It happens every year: A new Medicare physician fee schedule recommends a painful reduction in the rates the government doles out for more than 7,000 types of medical services performed by hospitalists, primary-care doctors, and other healthcare providers. And then Congress intervenes to keep the reduction from going into effect.
This year, however, the fee updates and policy proposals have become intertwined in the larger debate over comprehensive healthcare reform and a push toward what SHM calls a “value-based health delivery system.”
Few think the whopping 21.5% reduction proposed for 2010 rates, which are due to be published Nov. 1, actually will go into effect in January. A combination of other proposed changes to the fee schedule could soften any reduction. But the larger issue of how fees are currently calculated has become a rallying point for SHM and other healthcare-reform advocates who’d like to see the entire formula scrapped in favor of a more equitable distribution that focuses on outcomes. SHM has expressed concern that the current fee-for-service payment system “fails to provide providers with incentives to improve efficiency or quality of care, and encourages overutilization of services.”
—J. James Rohack, MD, AMA president
The current fee formula, known as the sustainable growth rate (SGR) and stipulated by the Balanced Budget Act of 1997, has resulted in a proposed rate cut every year since it went into effect in 2002. Congress consistently overrides the reimbursement cuts in one way or another, usually enacting modest increases or, such as in 2006 and 2007, an across-the-board freeze.
Hospitalists and other physicians have greeted another high-profile proposal with more enthusiasm: the removal of physician-administered drugs from the definition of “physician services,” thereby eliminating a high-cost item from the SGR formula. A Centers for Medicare and Medicaid Services (CMS) spokeswoman says the agency previously felt it lacked the authority to propose the removal. But a review earlier this year reversed that position, leading to the change. The removal, she says, “wouldn’t change the 21.5% percent decline in 2010, but it could have an impact in future years.”
American Medical Association President J. James Rohack, MD, joined the chorus of approval with a statement that asserted, “The removal of physician-administered drugs from the broken Medicare physician payment formula is a major victory for America’s seniors and their physicians.”
Consultation Change
A separate physician fee schedule proposal would eliminate payments for consultation codes in both outpatient and inpatient settings in favor of codes for evaluation and management services that carry lower reimbursement rates. Doctors would have a new way to bill for tele-health consultations, however. Leslie Flores, director of SHM’s Practice Management Institute, said the proposal has generated a high level of misinformation and misunderstanding among hospitalists who fear CMS will no longer reimburse for inpatient consultations. “It’s not that they won’t allow the work to be done anymore,” Flores says. “They’re just instructing people to bill in a different way for that work.”
CMS notes that the savings would be redistributed to increase payments for existing evaluation and management services codes, making the change cost-neutral. But Flores says a lack of details about the “crosswalk” from the old codes to the new codes, especially as they relate to transfers of care, is fueling hospitalists’ confusion over the true impact on their reimbursements.
“Our biggest concern with this consultation proposal that is now on the table is that CMS has not done anything to clarify how these transfers of care would be treated,” she says. For example, would hospitalists bill an admission code the first time they see a patient after being asked by a surgeon to take over that patient’s diabetes care? If so, “this proposal could actually result in some pretty good revenue increases for a lot of hospitalist practices that are doing a lot of surgical comanagement,” she says.
If hospitalists are instead required to bill a work-intensive transition of care under the code for a subsequent visit, which CMS has enforced since a 2006 rule clarification, Flores explains, HM could lose anywhere from 1% to 18% of reimbursements, depending on the exact code used.
Quality Reporting
The proposed fee schedule also is generating disappointment about what will not be included in Medicare’s Physician Quality Reporting Initiative (PQRI) for 2010. The pay-for-performance PQRI, which rewards physicians for reporting on quality measures by paying them an additional 2% of their estimated charges for covered services, will streamline some reporting requirements and increase the overall number of reportable measures. But several care-transition measures sought by SHM were not endorsed in time and will not be among them. Those measures include:
- Reconciled medication lists received by discharged patients;
- Transition records with specified elements received by discharged patients (including one measure for an inpatient discharge to home or self-care, and another for an ED discharge to home, ambulatory, or self-care); and
- Timely transmission of transition records.
“It was really a question of timing,” says Jill Epstein, senior advisor of SHM’s Performance and Standards Committee. The National Quality Forum, the nonprofit organization charged with signing off on all new measures, was not able to fully vet the recommended additions by the July 1 deadline, Epstein says, postponing their inclusion. “Our hope is that the measures will be included for 2011, of course.”
Separately, the PQRI proposal seeks to add an electronic-health-record-based mechanism to the list of eligible reporting methods. Although that addition is welcome news, Epstein says, SHM is expressing its concern about the shift toward patient-registry-based reporting, including a proposal to lessen or perhaps even discontinue claims-based reporting after 2010. “The issue for hospitalists, as well as for any specialty,” she says, “is that not every group will have access to a qualified PQRI registry as early as 2011,” particularly rural-based groups with fewer resources.
A similar change would streamline the E-Prescribing Incentive Program’s rules for how often e-prescribing codes must be reported. It also will offer more choices for how to report them, including through qualified registries. In the past, the program had little direct impact on hospitalists, but the new proposal recommends adding reporting codes specific to nursing homes, where some hospitalists provide care and could benefit from the incentives.
Paul Fishman, an economist at the Group Health Center for Health Studies in Seattle, says the increased focus on incentives in Medicare’s fee schedule suggests a growing realization of how such incentives can drive the delivery of healthcare services. “We know with absolute certainty that physicians make choices based on how things are reimbursed,” he says. Developing good outcome measures, then, will be critical for establishing pay-for-performance standards as part of a fee package that he says should include a blend of capitation and service-based and outcome-based reimbursements to strike a fairer balance.
“In healthcare, we’ve incented people to do more and more stuff, whether they improve outcomes or not, but we have to figure out a way to incent improvements in outcomes, while still retaining the long-term incentive to keep people healthy,” Fishman says. If better transitions of care result in a healthier population that is rehospitalized less often, for example, how can outcome-based incentives prevent hospitals from losing money in the long run? “We want to create the incentives to make the improvements in health outcomes, but we don’t want to punish the better actors because they are consistently lowering costs and also lowering reimbursement levels,” he says.
Achieving that balance in both Medicare and the broader healthcare system, he and other observers agree, is still very much a work in progress. TH
Bryn Nelson is a freelance writer based in Seattle.
It happens every year: A new Medicare physician fee schedule recommends a painful reduction in the rates the government doles out for more than 7,000 types of medical services performed by hospitalists, primary-care doctors, and other healthcare providers. And then Congress intervenes to keep the reduction from going into effect.
This year, however, the fee updates and policy proposals have become intertwined in the larger debate over comprehensive healthcare reform and a push toward what SHM calls a “value-based health delivery system.”
Few think the whopping 21.5% reduction proposed for 2010 rates, which are due to be published Nov. 1, actually will go into effect in January. A combination of other proposed changes to the fee schedule could soften any reduction. But the larger issue of how fees are currently calculated has become a rallying point for SHM and other healthcare-reform advocates who’d like to see the entire formula scrapped in favor of a more equitable distribution that focuses on outcomes. SHM has expressed concern that the current fee-for-service payment system “fails to provide providers with incentives to improve efficiency or quality of care, and encourages overutilization of services.”
—J. James Rohack, MD, AMA president
The current fee formula, known as the sustainable growth rate (SGR) and stipulated by the Balanced Budget Act of 1997, has resulted in a proposed rate cut every year since it went into effect in 2002. Congress consistently overrides the reimbursement cuts in one way or another, usually enacting modest increases or, such as in 2006 and 2007, an across-the-board freeze.
Hospitalists and other physicians have greeted another high-profile proposal with more enthusiasm: the removal of physician-administered drugs from the definition of “physician services,” thereby eliminating a high-cost item from the SGR formula. A Centers for Medicare and Medicaid Services (CMS) spokeswoman says the agency previously felt it lacked the authority to propose the removal. But a review earlier this year reversed that position, leading to the change. The removal, she says, “wouldn’t change the 21.5% percent decline in 2010, but it could have an impact in future years.”
American Medical Association President J. James Rohack, MD, joined the chorus of approval with a statement that asserted, “The removal of physician-administered drugs from the broken Medicare physician payment formula is a major victory for America’s seniors and their physicians.”
Consultation Change
A separate physician fee schedule proposal would eliminate payments for consultation codes in both outpatient and inpatient settings in favor of codes for evaluation and management services that carry lower reimbursement rates. Doctors would have a new way to bill for tele-health consultations, however. Leslie Flores, director of SHM’s Practice Management Institute, said the proposal has generated a high level of misinformation and misunderstanding among hospitalists who fear CMS will no longer reimburse for inpatient consultations. “It’s not that they won’t allow the work to be done anymore,” Flores says. “They’re just instructing people to bill in a different way for that work.”
CMS notes that the savings would be redistributed to increase payments for existing evaluation and management services codes, making the change cost-neutral. But Flores says a lack of details about the “crosswalk” from the old codes to the new codes, especially as they relate to transfers of care, is fueling hospitalists’ confusion over the true impact on their reimbursements.
“Our biggest concern with this consultation proposal that is now on the table is that CMS has not done anything to clarify how these transfers of care would be treated,” she says. For example, would hospitalists bill an admission code the first time they see a patient after being asked by a surgeon to take over that patient’s diabetes care? If so, “this proposal could actually result in some pretty good revenue increases for a lot of hospitalist practices that are doing a lot of surgical comanagement,” she says.
If hospitalists are instead required to bill a work-intensive transition of care under the code for a subsequent visit, which CMS has enforced since a 2006 rule clarification, Flores explains, HM could lose anywhere from 1% to 18% of reimbursements, depending on the exact code used.
Quality Reporting
The proposed fee schedule also is generating disappointment about what will not be included in Medicare’s Physician Quality Reporting Initiative (PQRI) for 2010. The pay-for-performance PQRI, which rewards physicians for reporting on quality measures by paying them an additional 2% of their estimated charges for covered services, will streamline some reporting requirements and increase the overall number of reportable measures. But several care-transition measures sought by SHM were not endorsed in time and will not be among them. Those measures include:
- Reconciled medication lists received by discharged patients;
- Transition records with specified elements received by discharged patients (including one measure for an inpatient discharge to home or self-care, and another for an ED discharge to home, ambulatory, or self-care); and
- Timely transmission of transition records.
“It was really a question of timing,” says Jill Epstein, senior advisor of SHM’s Performance and Standards Committee. The National Quality Forum, the nonprofit organization charged with signing off on all new measures, was not able to fully vet the recommended additions by the July 1 deadline, Epstein says, postponing their inclusion. “Our hope is that the measures will be included for 2011, of course.”
Separately, the PQRI proposal seeks to add an electronic-health-record-based mechanism to the list of eligible reporting methods. Although that addition is welcome news, Epstein says, SHM is expressing its concern about the shift toward patient-registry-based reporting, including a proposal to lessen or perhaps even discontinue claims-based reporting after 2010. “The issue for hospitalists, as well as for any specialty,” she says, “is that not every group will have access to a qualified PQRI registry as early as 2011,” particularly rural-based groups with fewer resources.
A similar change would streamline the E-Prescribing Incentive Program’s rules for how often e-prescribing codes must be reported. It also will offer more choices for how to report them, including through qualified registries. In the past, the program had little direct impact on hospitalists, but the new proposal recommends adding reporting codes specific to nursing homes, where some hospitalists provide care and could benefit from the incentives.
Paul Fishman, an economist at the Group Health Center for Health Studies in Seattle, says the increased focus on incentives in Medicare’s fee schedule suggests a growing realization of how such incentives can drive the delivery of healthcare services. “We know with absolute certainty that physicians make choices based on how things are reimbursed,” he says. Developing good outcome measures, then, will be critical for establishing pay-for-performance standards as part of a fee package that he says should include a blend of capitation and service-based and outcome-based reimbursements to strike a fairer balance.
“In healthcare, we’ve incented people to do more and more stuff, whether they improve outcomes or not, but we have to figure out a way to incent improvements in outcomes, while still retaining the long-term incentive to keep people healthy,” Fishman says. If better transitions of care result in a healthier population that is rehospitalized less often, for example, how can outcome-based incentives prevent hospitals from losing money in the long run? “We want to create the incentives to make the improvements in health outcomes, but we don’t want to punish the better actors because they are consistently lowering costs and also lowering reimbursement levels,” he says.
Achieving that balance in both Medicare and the broader healthcare system, he and other observers agree, is still very much a work in progress. TH
Bryn Nelson is a freelance writer based in Seattle.
Physician Engagement
There is a lot of talk in HM circles right now about quantifying such nebulous medical phrases as “meaningful use” and “healthcare reform.” A phrase heard less often, but potentially just as critical to HM’s future, is “physician engagement.”
A prod to help define the latter comes from Kelly Caverzagie, MD, an academic hospitalist in the division of hospital medicine at Henry Ford Hospital in Detroit. Dr. Caverzagie and staff from the American Board of Internal Medicine (ABIM) set out to attach some sort of metric quantification to that engagement, then determine what impact it had on QI programs. Hence the aptly named study to be published in the October edition of the Journal of Hospital Medicine: “The Role of Physician Engagement on the Impact of the Hospital Based Practice Improvement Module.”
Before joining Henry Ford in 2007 as a hospitalist and evaluation research specialist, Dr. Caverzagie had worked as a contractor with ABIM, completing a two-year fellowship at the University of Pennsylvania in Philadelphia. He remains under contract with ABIM, which still pays a “small portion” of his salary. That relationship and Dr. Caverzagie’s hospitalist-tinged view of evaluation techniques piqued his interest in the engagement issue.
“The physician needs to engage in the process,” Dr. Caverzagie says, defining that engagement as “active enrollment and doing it for the right reason. Just enrolling in it doesn’t make quality improvement happen. You actually need to be engaged. And then … there is added value.”
The study focused on 21 physicians who completed their Maintenance of Certification (MOC) to remain current with ABIM guidelines. The hospital-based practice improvement module (PIM) is a Web-based platform developed by ABIM that “allows physicians to use nationally-approved, hospital-level performance data to complete the module” as part of attaining their MOC.
Each of the doctors in Dr. Caverzagie’s study completed their PIM by January 2007 and were interviewed anonymously about their experience. Interviews were recorded and transcribed to better verify responses. Nearly all of the subjects found the PIM useful (n=17, 81%). But with more questioning, the authors determined that how valuable the module was viewed depended on how involved the physician was in its completion.

—Kelly Caverzagie, MD, academic hospitalist, Henry Ford Hospital, Detroit
“The impact of completing the hospital PIM is mediated by the degree of physician engagement with the QI process,” the authors conclude. “Physicians who become engaged with the hospital PIM and QI process may be more likely to report successful experiences … than those who do not become engaged.”
Dr. Caverzagie and three ABIM staffers understood the limits of their effort, which breaks little new ground but piles on further evidence to prove the efficacy of getting hospitalists and other physicians more engaged in QI. A sample size of fewer than two dozen anonymous physicians allows for too many variables to consider the data indefatigable, so Dr. Caverzagie leaves it up to such regulatory and advocacy bodies as ABIM and SHM to determine whether and how to make systemic and process changes that encourage more involvement. “I don’t know if you can force engagement,” he adds.
His team created a set of definitions to showcase how different physicians with different attitudes experience hospital PIMs differently.
The most successful category is defined as “active engagers,” physicians who exhibited personal involvement. Eight of the 21 physicians, or 38% of the sample population, fell into this grouping. Ten physicians (48%) fell under the heading of “passive engagers,” a somewhat ironic category in which physicians reported negative experiences even as they documented what they felt was the knowledge gained from their hospital PIM. Finally, the authors tagged three (14%) “non-engagers” who “documented no evidence of QI learning and reported little impact from completing the PIM.”
Correspondingly, case studies highlighted in the study showed that “active engagers” took advantage of existing QI resources and staff at their respective institutions. They sought out staff leadership and fed off positive hospital cultures where they existed. One physician said it was “surprisingly easier to begin and initiate a quality improvement project than thought.”
One “passive engager” described their previous QI experience in terms of mandates handed down from administration, although several in the subcategory acknowledged they learned new skills or new information about how QI programs operate in their hospital. There also was some dissatisfaction in this category about the leadership shown by institutional staff.
Still, Dr. Caverzagie expresses optimism with this middle grouping, the largest statistically. “QI learning occurred despite the presence of multiple barriers,” the authors wrote.
In the least successful category—the non-engagers—several physicians interviewed said they didn’t need QI projects or were unsatisfied with a past experience, so they didn’t bother to try again. One physician declared, “We’re at a terrific level right now,” despite a hospital baseline performance measure of 5% compliance for percutaneous coronary intervention in less than 120 minutes.
To be sure, all of the groupings were at the mercy of internal and external factors—hospital culture, perceived relevance, institutional bias, and access to QI leaders among them. What remains to be studied is how to overcome those hurdles. Dr. Caverzagie says more work is needed to determine just how effective PIMs can be. He thinks the next stage for the modules could include more quantifiable metrics, which would be reported and then analyzed to “take doctors to the next level.”
“The vast majority of physicians, hospitalists in particular, are very interested in improving the care that they provide for their patients,” Dr. Caverzagie says. “They’re just not necessarily sure how to get it done. A challenge for our profession is to try to find a way to facilitate becoming involved in activities.”TH
Richard Quinn is a freelance writer based in New Jersey.
There is a lot of talk in HM circles right now about quantifying such nebulous medical phrases as “meaningful use” and “healthcare reform.” A phrase heard less often, but potentially just as critical to HM’s future, is “physician engagement.”
A prod to help define the latter comes from Kelly Caverzagie, MD, an academic hospitalist in the division of hospital medicine at Henry Ford Hospital in Detroit. Dr. Caverzagie and staff from the American Board of Internal Medicine (ABIM) set out to attach some sort of metric quantification to that engagement, then determine what impact it had on QI programs. Hence the aptly named study to be published in the October edition of the Journal of Hospital Medicine: “The Role of Physician Engagement on the Impact of the Hospital Based Practice Improvement Module.”
Before joining Henry Ford in 2007 as a hospitalist and evaluation research specialist, Dr. Caverzagie had worked as a contractor with ABIM, completing a two-year fellowship at the University of Pennsylvania in Philadelphia. He remains under contract with ABIM, which still pays a “small portion” of his salary. That relationship and Dr. Caverzagie’s hospitalist-tinged view of evaluation techniques piqued his interest in the engagement issue.
“The physician needs to engage in the process,” Dr. Caverzagie says, defining that engagement as “active enrollment and doing it for the right reason. Just enrolling in it doesn’t make quality improvement happen. You actually need to be engaged. And then … there is added value.”
The study focused on 21 physicians who completed their Maintenance of Certification (MOC) to remain current with ABIM guidelines. The hospital-based practice improvement module (PIM) is a Web-based platform developed by ABIM that “allows physicians to use nationally-approved, hospital-level performance data to complete the module” as part of attaining their MOC.
Each of the doctors in Dr. Caverzagie’s study completed their PIM by January 2007 and were interviewed anonymously about their experience. Interviews were recorded and transcribed to better verify responses. Nearly all of the subjects found the PIM useful (n=17, 81%). But with more questioning, the authors determined that how valuable the module was viewed depended on how involved the physician was in its completion.
—Kelly Caverzagie, MD, academic hospitalist, Henry Ford Hospital, Detroit
“The impact of completing the hospital PIM is mediated by the degree of physician engagement with the QI process,” the authors conclude. “Physicians who become engaged with the hospital PIM and QI process may be more likely to report successful experiences … than those who do not become engaged.”
Dr. Caverzagie and three ABIM staffers understood the limits of their effort, which breaks little new ground but piles on further evidence to prove the efficacy of getting hospitalists and other physicians more engaged in QI. A sample size of fewer than two dozen anonymous physicians allows for too many variables to consider the data indefatigable, so Dr. Caverzagie leaves it up to such regulatory and advocacy bodies as ABIM and SHM to determine whether and how to make systemic and process changes that encourage more involvement. “I don’t know if you can force engagement,” he adds.
His team created a set of definitions to showcase how different physicians with different attitudes experience hospital PIMs differently.
The most successful category is defined as “active engagers,” physicians who exhibited personal involvement. Eight of the 21 physicians, or 38% of the sample population, fell into this grouping. Ten physicians (48%) fell under the heading of “passive engagers,” a somewhat ironic category in which physicians reported negative experiences even as they documented what they felt was the knowledge gained from their hospital PIM. Finally, the authors tagged three (14%) “non-engagers” who “documented no evidence of QI learning and reported little impact from completing the PIM.”
Correspondingly, case studies highlighted in the study showed that “active engagers” took advantage of existing QI resources and staff at their respective institutions. They sought out staff leadership and fed off positive hospital cultures where they existed. One physician said it was “surprisingly easier to begin and initiate a quality improvement project than thought.”
One “passive engager” described their previous QI experience in terms of mandates handed down from administration, although several in the subcategory acknowledged they learned new skills or new information about how QI programs operate in their hospital. There also was some dissatisfaction in this category about the leadership shown by institutional staff.
Still, Dr. Caverzagie expresses optimism with this middle grouping, the largest statistically. “QI learning occurred despite the presence of multiple barriers,” the authors wrote.
In the least successful category—the non-engagers—several physicians interviewed said they didn’t need QI projects or were unsatisfied with a past experience, so they didn’t bother to try again. One physician declared, “We’re at a terrific level right now,” despite a hospital baseline performance measure of 5% compliance for percutaneous coronary intervention in less than 120 minutes.
To be sure, all of the groupings were at the mercy of internal and external factors—hospital culture, perceived relevance, institutional bias, and access to QI leaders among them. What remains to be studied is how to overcome those hurdles. Dr. Caverzagie says more work is needed to determine just how effective PIMs can be. He thinks the next stage for the modules could include more quantifiable metrics, which would be reported and then analyzed to “take doctors to the next level.”
“The vast majority of physicians, hospitalists in particular, are very interested in improving the care that they provide for their patients,” Dr. Caverzagie says. “They’re just not necessarily sure how to get it done. A challenge for our profession is to try to find a way to facilitate becoming involved in activities.”TH
Richard Quinn is a freelance writer based in New Jersey.
There is a lot of talk in HM circles right now about quantifying such nebulous medical phrases as “meaningful use” and “healthcare reform.” A phrase heard less often, but potentially just as critical to HM’s future, is “physician engagement.”
A prod to help define the latter comes from Kelly Caverzagie, MD, an academic hospitalist in the division of hospital medicine at Henry Ford Hospital in Detroit. Dr. Caverzagie and staff from the American Board of Internal Medicine (ABIM) set out to attach some sort of metric quantification to that engagement, then determine what impact it had on QI programs. Hence the aptly named study to be published in the October edition of the Journal of Hospital Medicine: “The Role of Physician Engagement on the Impact of the Hospital Based Practice Improvement Module.”
Before joining Henry Ford in 2007 as a hospitalist and evaluation research specialist, Dr. Caverzagie had worked as a contractor with ABIM, completing a two-year fellowship at the University of Pennsylvania in Philadelphia. He remains under contract with ABIM, which still pays a “small portion” of his salary. That relationship and Dr. Caverzagie’s hospitalist-tinged view of evaluation techniques piqued his interest in the engagement issue.
“The physician needs to engage in the process,” Dr. Caverzagie says, defining that engagement as “active enrollment and doing it for the right reason. Just enrolling in it doesn’t make quality improvement happen. You actually need to be engaged. And then … there is added value.”
The study focused on 21 physicians who completed their Maintenance of Certification (MOC) to remain current with ABIM guidelines. The hospital-based practice improvement module (PIM) is a Web-based platform developed by ABIM that “allows physicians to use nationally-approved, hospital-level performance data to complete the module” as part of attaining their MOC.
Each of the doctors in Dr. Caverzagie’s study completed their PIM by January 2007 and were interviewed anonymously about their experience. Interviews were recorded and transcribed to better verify responses. Nearly all of the subjects found the PIM useful (n=17, 81%). But with more questioning, the authors determined that how valuable the module was viewed depended on how involved the physician was in its completion.
—Kelly Caverzagie, MD, academic hospitalist, Henry Ford Hospital, Detroit
“The impact of completing the hospital PIM is mediated by the degree of physician engagement with the QI process,” the authors conclude. “Physicians who become engaged with the hospital PIM and QI process may be more likely to report successful experiences … than those who do not become engaged.”
Dr. Caverzagie and three ABIM staffers understood the limits of their effort, which breaks little new ground but piles on further evidence to prove the efficacy of getting hospitalists and other physicians more engaged in QI. A sample size of fewer than two dozen anonymous physicians allows for too many variables to consider the data indefatigable, so Dr. Caverzagie leaves it up to such regulatory and advocacy bodies as ABIM and SHM to determine whether and how to make systemic and process changes that encourage more involvement. “I don’t know if you can force engagement,” he adds.
His team created a set of definitions to showcase how different physicians with different attitudes experience hospital PIMs differently.
The most successful category is defined as “active engagers,” physicians who exhibited personal involvement. Eight of the 21 physicians, or 38% of the sample population, fell into this grouping. Ten physicians (48%) fell under the heading of “passive engagers,” a somewhat ironic category in which physicians reported negative experiences even as they documented what they felt was the knowledge gained from their hospital PIM. Finally, the authors tagged three (14%) “non-engagers” who “documented no evidence of QI learning and reported little impact from completing the PIM.”
Correspondingly, case studies highlighted in the study showed that “active engagers” took advantage of existing QI resources and staff at their respective institutions. They sought out staff leadership and fed off positive hospital cultures where they existed. One physician said it was “surprisingly easier to begin and initiate a quality improvement project than thought.”
One “passive engager” described their previous QI experience in terms of mandates handed down from administration, although several in the subcategory acknowledged they learned new skills or new information about how QI programs operate in their hospital. There also was some dissatisfaction in this category about the leadership shown by institutional staff.
Still, Dr. Caverzagie expresses optimism with this middle grouping, the largest statistically. “QI learning occurred despite the presence of multiple barriers,” the authors wrote.
In the least successful category—the non-engagers—several physicians interviewed said they didn’t need QI projects or were unsatisfied with a past experience, so they didn’t bother to try again. One physician declared, “We’re at a terrific level right now,” despite a hospital baseline performance measure of 5% compliance for percutaneous coronary intervention in less than 120 minutes.
To be sure, all of the groupings were at the mercy of internal and external factors—hospital culture, perceived relevance, institutional bias, and access to QI leaders among them. What remains to be studied is how to overcome those hurdles. Dr. Caverzagie says more work is needed to determine just how effective PIMs can be. He thinks the next stage for the modules could include more quantifiable metrics, which would be reported and then analyzed to “take doctors to the next level.”
“The vast majority of physicians, hospitalists in particular, are very interested in improving the care that they provide for their patients,” Dr. Caverzagie says. “They’re just not necessarily sure how to get it done. A challenge for our profession is to try to find a way to facilitate becoming involved in activities.”TH
Richard Quinn is a freelance writer based in New Jersey.
Market Watch
In the Pipeline
- A new drug application (NDA) has been submitted to the Food and Drug Administration (FDA) for Acetavance, an intravenous (IV) form of acetaminophen used in the treatment of acute pain and fever in adults and children who cannot take oral medications.1
- An NDA for a low-dose aspirin and esomeprazole combination product has been submitted for risk reduction of low-dose-aspirin-associated gastric and/or duodenal ulcers. A supplemental NDA was submitted for esomeprazole for risk reduction of low-dose-aspirin-associated peptic ulcer disease.2
- An NDA for a new formulation of ondansetron, as an orally dissolving film strip, has been submitted to the FDA.3 The product has shown comparable bioequivalence to ondansetron (Zofran) as an anti-emetic for preventing chemotherapy-induced nausea and vomiting, nausea and vomiting associated with radiotherapy, and post-operative nausea and vomiting.
- An NDA for tesamorelin to treat HIV-lipodystrophy has been submitted to the FDA.4
New Generics
- Acarbose 25-, 50- and 100-mg tablets (generic precose)5
- Bicalutamide (Casodex)6
New Drugs, Indications and Dosage Forms
- Artemether and lumefantrine (Coartem) tablets have been approved by the FDA for the treatment of acute, uncomplicated malarial infections in adults and children who weigh at least 5 kg.7 Coartem should be taken with food, particularly food that contains fat, because it improves drug absorption. Common adverse effects include headache, anorexia, dizziness, asthenia, arthralgia, and myalgia.
- Besifloxacin 0.6% (Besivance) ophthalmic suspension has been approved by the FDA to treat bacterial conjunctivitis. Adverse effects include eye redness, blurred vision, eye pain, irritation, itching, and headache.8
- Dexamethasone intravitreal implant (Ozurdex) has been approved by the FDA for treating macular edema following branch retinal vein occlusion (BRVO) or central retinal vein occlusion (CRVO).9 The implant is biodegradable and delivers dexamethasone via an extended-release mechanism over one to three months. Ozurdex is administered as an in-office procedure and is expected to be available soon.
- Dronedarone (Multaq) tablets have been approved by the FDA as an antiarrhythmic agent.10 It is indicated to reduce the risk of cardiovascular hospitalization in patients with atrial flutter, or paroxysmal or persistent atrial fibrillation, with a recent episode of atrial fibrillation/atrial flutter and associated cardiovascular risk, who are in sinus rhythm or who will be cardioverted.11 Risk factors include age >70, hypertension, diabetes, prior cerebrovascular accident, a left atrial diameter ≥50 mm, and left ventricular ejection fraction [LVEF] <40%.
- Hyoscyamine sulfate (NuLev) chewable antispasmodic orally disintegrating tablets (0.125 mg) have been reintroduced and are available to treat patients age 2 and older with gastrointestinal spasticity disorders.12
- Lacosamide (Vimpat) has been approved by the FDA for add-on therapy in the treatment of partial-onset seizures in epilepsy patients age 17 and older.13
- Lamotrigine extended-release (Lamictal XR) has been approved by the FDA as a once-daily add-on therapy for partial-onset seizures in epilepsy patients age 13 and older.14
- Pioglitazone/metformin (ACTOplus met XR) combination tablets have been approved by the FDA for treating Type 2 diabetes.15 It should be available later this year.
- Risperidone (Risperdal Consta) has received additional FDA approval as a biweekly injection as monotherapy, and as adjunctive therapy to lithium or valproate, in the maintenance of bipolar I disorder.16
- Tadalafil (Adcirc) has been approved by the FDA for improving exercise ability in patients with pulmonary arterial hypertension (PAH).17 Tadalafil already is approved as brand-name Cialis for treating erectile dysfunction. Tadalafil is the first once-daily phosphodiesterase type-5 inhibitor for treating PAH, and it is hoped it will gain some of the sildenafil (Revatio) market.
Update
As a followup to the August “Market Watch,” pancrelipase (Creon) has been approved by the FDA and is available in three FDA-approved prescription strengths based on the lipase content (6,000, 12,000, and 24,000).18 TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
- NDA submitted for acetavance, a treatment for acute pain and fever. Monthly Prescribing Reference Web site. Available at: www.empr.com/NDA-submitted-for-Acetavance-a-treatment-for-acute-pain-and-fever/article/136799/. Accessed July 8, 2009.
- AstraZeneca submits NDA for low dose aspirin/esomeprazole combination product. AstraZeneca Web site. Available at: www.astrazeneca-us.com/about-astrazeneca-us/newsroom/all/5762542?itemId=5762542. Accessed July 8, 2009.
- MonoSol Rx and Strativa Pharmaceuticals submit new drug application for ondansetron orally dissolving film strip. Available at: www.monosolrx.com/news_09/news_040909.html. Accessed July 8, 2009.
- Theratech shares jump 8 pct on FDA filing. Reuters Web site. Available at: www.reuters.com/article/idUSN0126728920090601. Accessed July 8, 2009.
- Impax receives FDA approval for generic precos tablets, 25 mg, 50 mg and 100 mg. Available at: http://phx.corporate-ir.net/phoenix.zhtml?c=67240&p=irol-newsArticle&ID=1289907&highlight=. Accessed July 8, 2009.
- Caraco: FDA approves generic prostate cancer drug. Forbes Web site. Available at: www.forbes.com/feeds/ap/2009/07/07/ap6626628.html. Accessed July 8, 2009.
- Walsh S. FDA approved coartem tablets to treat malaria. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm149559.htm. Accessed July 8, 2009.
- Walsh S. FDA approves besivance to treat bacterial conjunctivitis. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm162486.htm. Accessed July 8, 2009.
- Ozurdex approved for treatment of macular edema. Monthly Prescribing Reference Web site. Available at: www.empr.com/Ozurdex-approved-for-treatment-of-macular-edema/article/138708/. Accessed July 8, 2009.
- Walsh S. FDA approves multaq to treat heart rhythm disorder. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm170276.htm. Accessed July 21, 2009.
- Multaq label. FDA Web site: Available at: www.accessdata.fda.gov/drugsatfda_docs/label/2009/022425lbl.pdf. Accessed July 21, 2009.
- NuLev chewable melt tablets available again. Monthly Prescribing Reference Web site. Available at: www.empr.com/NuLev-Chewable-Melt-Tablets-available-again/article/138396/?DCMP=EMC-MPR_WeeklyNewsbrief. Accessed July 8, 2009.
- UCB’s Vimpat (lacosamide) approved by FDA as add-on therapy for partial onset seizures in adults. Epilepsy Foundation Web site. Available at: www.epilepsyfoundation.org/epilepsyusa/news/UCB_Vimpat.cfm. Accessed July 8, 2009.
- Bratulic A. FDA approves GlaxoSmithKline’s lamictal XR. Available at: www.firstwordplus.com/Fws.do?articleid=62DD8DEA3F594BDC98DA97F80AB13ABB&logRowId=307825. Accessed July 8, 2009.
- FDA approves ACTOplus met XR (pioglitazone HCL and metformin HCl extended-release) tablets for the treatment of Type 2 diabetes. Available at: www.pipelinereview.com/index.php/2009051326959/Small-Molecules/FDA-Approves-ACTOplus-met-XR-pioglitazone-HCl-and-metformin-HCl-extended-release-Tablets-for-the-Treatment-of-Type-2-Diabetes.html. Accessed July 8, 2009.
- FDA approval letter for risperdal consta. FDA Web site. Available at: www.accessdata.fda.gov/drugsatfda_docs/appletter/2009/021346s025,021346s028ltr.pdf. Accessed July 8, 2009.
- Todoruk M. United Therapeutics’ Adcirca approved for pulmonary arterial hypertension in US. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=E71E91953E9844D2A776B021E19AEE22&logRowId=306627. Accessed July 8, 2009.
- Creon delayed-release capsules available for exocrine pancreatic insufficiency. Monthly Prescribing Reference Web site. Available at: www.empr.com/Creon-delayed-release-capsules-available-for-exocrine-pancreatic-insufficiency/article/139668/. Accessed August 10, 2009.
In the Pipeline
- A new drug application (NDA) has been submitted to the Food and Drug Administration (FDA) for Acetavance, an intravenous (IV) form of acetaminophen used in the treatment of acute pain and fever in adults and children who cannot take oral medications.1
- An NDA for a low-dose aspirin and esomeprazole combination product has been submitted for risk reduction of low-dose-aspirin-associated gastric and/or duodenal ulcers. A supplemental NDA was submitted for esomeprazole for risk reduction of low-dose-aspirin-associated peptic ulcer disease.2
- An NDA for a new formulation of ondansetron, as an orally dissolving film strip, has been submitted to the FDA.3 The product has shown comparable bioequivalence to ondansetron (Zofran) as an anti-emetic for preventing chemotherapy-induced nausea and vomiting, nausea and vomiting associated with radiotherapy, and post-operative nausea and vomiting.
- An NDA for tesamorelin to treat HIV-lipodystrophy has been submitted to the FDA.4
New Generics
- Acarbose 25-, 50- and 100-mg tablets (generic precose)5
- Bicalutamide (Casodex)6
New Drugs, Indications and Dosage Forms
- Artemether and lumefantrine (Coartem) tablets have been approved by the FDA for the treatment of acute, uncomplicated malarial infections in adults and children who weigh at least 5 kg.7 Coartem should be taken with food, particularly food that contains fat, because it improves drug absorption. Common adverse effects include headache, anorexia, dizziness, asthenia, arthralgia, and myalgia.
- Besifloxacin 0.6% (Besivance) ophthalmic suspension has been approved by the FDA to treat bacterial conjunctivitis. Adverse effects include eye redness, blurred vision, eye pain, irritation, itching, and headache.8
- Dexamethasone intravitreal implant (Ozurdex) has been approved by the FDA for treating macular edema following branch retinal vein occlusion (BRVO) or central retinal vein occlusion (CRVO).9 The implant is biodegradable and delivers dexamethasone via an extended-release mechanism over one to three months. Ozurdex is administered as an in-office procedure and is expected to be available soon.
- Dronedarone (Multaq) tablets have been approved by the FDA as an antiarrhythmic agent.10 It is indicated to reduce the risk of cardiovascular hospitalization in patients with atrial flutter, or paroxysmal or persistent atrial fibrillation, with a recent episode of atrial fibrillation/atrial flutter and associated cardiovascular risk, who are in sinus rhythm or who will be cardioverted.11 Risk factors include age >70, hypertension, diabetes, prior cerebrovascular accident, a left atrial diameter ≥50 mm, and left ventricular ejection fraction [LVEF] <40%.
- Hyoscyamine sulfate (NuLev) chewable antispasmodic orally disintegrating tablets (0.125 mg) have been reintroduced and are available to treat patients age 2 and older with gastrointestinal spasticity disorders.12
- Lacosamide (Vimpat) has been approved by the FDA for add-on therapy in the treatment of partial-onset seizures in epilepsy patients age 17 and older.13
- Lamotrigine extended-release (Lamictal XR) has been approved by the FDA as a once-daily add-on therapy for partial-onset seizures in epilepsy patients age 13 and older.14
- Pioglitazone/metformin (ACTOplus met XR) combination tablets have been approved by the FDA for treating Type 2 diabetes.15 It should be available later this year.
- Risperidone (Risperdal Consta) has received additional FDA approval as a biweekly injection as monotherapy, and as adjunctive therapy to lithium or valproate, in the maintenance of bipolar I disorder.16
- Tadalafil (Adcirc) has been approved by the FDA for improving exercise ability in patients with pulmonary arterial hypertension (PAH).17 Tadalafil already is approved as brand-name Cialis for treating erectile dysfunction. Tadalafil is the first once-daily phosphodiesterase type-5 inhibitor for treating PAH, and it is hoped it will gain some of the sildenafil (Revatio) market.
Update
As a followup to the August “Market Watch,” pancrelipase (Creon) has been approved by the FDA and is available in three FDA-approved prescription strengths based on the lipase content (6,000, 12,000, and 24,000).18 TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
- NDA submitted for acetavance, a treatment for acute pain and fever. Monthly Prescribing Reference Web site. Available at: www.empr.com/NDA-submitted-for-Acetavance-a-treatment-for-acute-pain-and-fever/article/136799/. Accessed July 8, 2009.
- AstraZeneca submits NDA for low dose aspirin/esomeprazole combination product. AstraZeneca Web site. Available at: www.astrazeneca-us.com/about-astrazeneca-us/newsroom/all/5762542?itemId=5762542. Accessed July 8, 2009.
- MonoSol Rx and Strativa Pharmaceuticals submit new drug application for ondansetron orally dissolving film strip. Available at: www.monosolrx.com/news_09/news_040909.html. Accessed July 8, 2009.
- Theratech shares jump 8 pct on FDA filing. Reuters Web site. Available at: www.reuters.com/article/idUSN0126728920090601. Accessed July 8, 2009.
- Impax receives FDA approval for generic precos tablets, 25 mg, 50 mg and 100 mg. Available at: http://phx.corporate-ir.net/phoenix.zhtml?c=67240&p=irol-newsArticle&ID=1289907&highlight=. Accessed July 8, 2009.
- Caraco: FDA approves generic prostate cancer drug. Forbes Web site. Available at: www.forbes.com/feeds/ap/2009/07/07/ap6626628.html. Accessed July 8, 2009.
- Walsh S. FDA approved coartem tablets to treat malaria. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm149559.htm. Accessed July 8, 2009.
- Walsh S. FDA approves besivance to treat bacterial conjunctivitis. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm162486.htm. Accessed July 8, 2009.
- Ozurdex approved for treatment of macular edema. Monthly Prescribing Reference Web site. Available at: www.empr.com/Ozurdex-approved-for-treatment-of-macular-edema/article/138708/. Accessed July 8, 2009.
- Walsh S. FDA approves multaq to treat heart rhythm disorder. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm170276.htm. Accessed July 21, 2009.
- Multaq label. FDA Web site: Available at: www.accessdata.fda.gov/drugsatfda_docs/label/2009/022425lbl.pdf. Accessed July 21, 2009.
- NuLev chewable melt tablets available again. Monthly Prescribing Reference Web site. Available at: www.empr.com/NuLev-Chewable-Melt-Tablets-available-again/article/138396/?DCMP=EMC-MPR_WeeklyNewsbrief. Accessed July 8, 2009.
- UCB’s Vimpat (lacosamide) approved by FDA as add-on therapy for partial onset seizures in adults. Epilepsy Foundation Web site. Available at: www.epilepsyfoundation.org/epilepsyusa/news/UCB_Vimpat.cfm. Accessed July 8, 2009.
- Bratulic A. FDA approves GlaxoSmithKline’s lamictal XR. Available at: www.firstwordplus.com/Fws.do?articleid=62DD8DEA3F594BDC98DA97F80AB13ABB&logRowId=307825. Accessed July 8, 2009.
- FDA approves ACTOplus met XR (pioglitazone HCL and metformin HCl extended-release) tablets for the treatment of Type 2 diabetes. Available at: www.pipelinereview.com/index.php/2009051326959/Small-Molecules/FDA-Approves-ACTOplus-met-XR-pioglitazone-HCl-and-metformin-HCl-extended-release-Tablets-for-the-Treatment-of-Type-2-Diabetes.html. Accessed July 8, 2009.
- FDA approval letter for risperdal consta. FDA Web site. Available at: www.accessdata.fda.gov/drugsatfda_docs/appletter/2009/021346s025,021346s028ltr.pdf. Accessed July 8, 2009.
- Todoruk M. United Therapeutics’ Adcirca approved for pulmonary arterial hypertension in US. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=E71E91953E9844D2A776B021E19AEE22&logRowId=306627. Accessed July 8, 2009.
- Creon delayed-release capsules available for exocrine pancreatic insufficiency. Monthly Prescribing Reference Web site. Available at: www.empr.com/Creon-delayed-release-capsules-available-for-exocrine-pancreatic-insufficiency/article/139668/. Accessed August 10, 2009.
In the Pipeline
- A new drug application (NDA) has been submitted to the Food and Drug Administration (FDA) for Acetavance, an intravenous (IV) form of acetaminophen used in the treatment of acute pain and fever in adults and children who cannot take oral medications.1
- An NDA for a low-dose aspirin and esomeprazole combination product has been submitted for risk reduction of low-dose-aspirin-associated gastric and/or duodenal ulcers. A supplemental NDA was submitted for esomeprazole for risk reduction of low-dose-aspirin-associated peptic ulcer disease.2
- An NDA for a new formulation of ondansetron, as an orally dissolving film strip, has been submitted to the FDA.3 The product has shown comparable bioequivalence to ondansetron (Zofran) as an anti-emetic for preventing chemotherapy-induced nausea and vomiting, nausea and vomiting associated with radiotherapy, and post-operative nausea and vomiting.
- An NDA for tesamorelin to treat HIV-lipodystrophy has been submitted to the FDA.4
New Generics
- Acarbose 25-, 50- and 100-mg tablets (generic precose)5
- Bicalutamide (Casodex)6
New Drugs, Indications and Dosage Forms
- Artemether and lumefantrine (Coartem) tablets have been approved by the FDA for the treatment of acute, uncomplicated malarial infections in adults and children who weigh at least 5 kg.7 Coartem should be taken with food, particularly food that contains fat, because it improves drug absorption. Common adverse effects include headache, anorexia, dizziness, asthenia, arthralgia, and myalgia.
- Besifloxacin 0.6% (Besivance) ophthalmic suspension has been approved by the FDA to treat bacterial conjunctivitis. Adverse effects include eye redness, blurred vision, eye pain, irritation, itching, and headache.8
- Dexamethasone intravitreal implant (Ozurdex) has been approved by the FDA for treating macular edema following branch retinal vein occlusion (BRVO) or central retinal vein occlusion (CRVO).9 The implant is biodegradable and delivers dexamethasone via an extended-release mechanism over one to three months. Ozurdex is administered as an in-office procedure and is expected to be available soon.
- Dronedarone (Multaq) tablets have been approved by the FDA as an antiarrhythmic agent.10 It is indicated to reduce the risk of cardiovascular hospitalization in patients with atrial flutter, or paroxysmal or persistent atrial fibrillation, with a recent episode of atrial fibrillation/atrial flutter and associated cardiovascular risk, who are in sinus rhythm or who will be cardioverted.11 Risk factors include age >70, hypertension, diabetes, prior cerebrovascular accident, a left atrial diameter ≥50 mm, and left ventricular ejection fraction [LVEF] <40%.
- Hyoscyamine sulfate (NuLev) chewable antispasmodic orally disintegrating tablets (0.125 mg) have been reintroduced and are available to treat patients age 2 and older with gastrointestinal spasticity disorders.12
- Lacosamide (Vimpat) has been approved by the FDA for add-on therapy in the treatment of partial-onset seizures in epilepsy patients age 17 and older.13
- Lamotrigine extended-release (Lamictal XR) has been approved by the FDA as a once-daily add-on therapy for partial-onset seizures in epilepsy patients age 13 and older.14
- Pioglitazone/metformin (ACTOplus met XR) combination tablets have been approved by the FDA for treating Type 2 diabetes.15 It should be available later this year.
- Risperidone (Risperdal Consta) has received additional FDA approval as a biweekly injection as monotherapy, and as adjunctive therapy to lithium or valproate, in the maintenance of bipolar I disorder.16
- Tadalafil (Adcirc) has been approved by the FDA for improving exercise ability in patients with pulmonary arterial hypertension (PAH).17 Tadalafil already is approved as brand-name Cialis for treating erectile dysfunction. Tadalafil is the first once-daily phosphodiesterase type-5 inhibitor for treating PAH, and it is hoped it will gain some of the sildenafil (Revatio) market.
Update
As a followup to the August “Market Watch,” pancrelipase (Creon) has been approved by the FDA and is available in three FDA-approved prescription strengths based on the lipase content (6,000, 12,000, and 24,000).18 TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City.
References
- NDA submitted for acetavance, a treatment for acute pain and fever. Monthly Prescribing Reference Web site. Available at: www.empr.com/NDA-submitted-for-Acetavance-a-treatment-for-acute-pain-and-fever/article/136799/. Accessed July 8, 2009.
- AstraZeneca submits NDA for low dose aspirin/esomeprazole combination product. AstraZeneca Web site. Available at: www.astrazeneca-us.com/about-astrazeneca-us/newsroom/all/5762542?itemId=5762542. Accessed July 8, 2009.
- MonoSol Rx and Strativa Pharmaceuticals submit new drug application for ondansetron orally dissolving film strip. Available at: www.monosolrx.com/news_09/news_040909.html. Accessed July 8, 2009.
- Theratech shares jump 8 pct on FDA filing. Reuters Web site. Available at: www.reuters.com/article/idUSN0126728920090601. Accessed July 8, 2009.
- Impax receives FDA approval for generic precos tablets, 25 mg, 50 mg and 100 mg. Available at: http://phx.corporate-ir.net/phoenix.zhtml?c=67240&p=irol-newsArticle&ID=1289907&highlight=. Accessed July 8, 2009.
- Caraco: FDA approves generic prostate cancer drug. Forbes Web site. Available at: www.forbes.com/feeds/ap/2009/07/07/ap6626628.html. Accessed July 8, 2009.
- Walsh S. FDA approved coartem tablets to treat malaria. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm149559.htm. Accessed July 8, 2009.
- Walsh S. FDA approves besivance to treat bacterial conjunctivitis. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm162486.htm. Accessed July 8, 2009.
- Ozurdex approved for treatment of macular edema. Monthly Prescribing Reference Web site. Available at: www.empr.com/Ozurdex-approved-for-treatment-of-macular-edema/article/138708/. Accessed July 8, 2009.
- Walsh S. FDA approves multaq to treat heart rhythm disorder. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm170276.htm. Accessed July 21, 2009.
- Multaq label. FDA Web site: Available at: www.accessdata.fda.gov/drugsatfda_docs/label/2009/022425lbl.pdf. Accessed July 21, 2009.
- NuLev chewable melt tablets available again. Monthly Prescribing Reference Web site. Available at: www.empr.com/NuLev-Chewable-Melt-Tablets-available-again/article/138396/?DCMP=EMC-MPR_WeeklyNewsbrief. Accessed July 8, 2009.
- UCB’s Vimpat (lacosamide) approved by FDA as add-on therapy for partial onset seizures in adults. Epilepsy Foundation Web site. Available at: www.epilepsyfoundation.org/epilepsyusa/news/UCB_Vimpat.cfm. Accessed July 8, 2009.
- Bratulic A. FDA approves GlaxoSmithKline’s lamictal XR. Available at: www.firstwordplus.com/Fws.do?articleid=62DD8DEA3F594BDC98DA97F80AB13ABB&logRowId=307825. Accessed July 8, 2009.
- FDA approves ACTOplus met XR (pioglitazone HCL and metformin HCl extended-release) tablets for the treatment of Type 2 diabetes. Available at: www.pipelinereview.com/index.php/2009051326959/Small-Molecules/FDA-Approves-ACTOplus-met-XR-pioglitazone-HCl-and-metformin-HCl-extended-release-Tablets-for-the-Treatment-of-Type-2-Diabetes.html. Accessed July 8, 2009.
- FDA approval letter for risperdal consta. FDA Web site. Available at: www.accessdata.fda.gov/drugsatfda_docs/appletter/2009/021346s025,021346s028ltr.pdf. Accessed July 8, 2009.
- Todoruk M. United Therapeutics’ Adcirca approved for pulmonary arterial hypertension in US. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=E71E91953E9844D2A776B021E19AEE22&logRowId=306627. Accessed July 8, 2009.
- Creon delayed-release capsules available for exocrine pancreatic insufficiency. Monthly Prescribing Reference Web site. Available at: www.empr.com/Creon-delayed-release-capsules-available-for-exocrine-pancreatic-insufficiency/article/139668/. Accessed August 10, 2009.