User login
Implementing an Alphanumeric Paging System
Effective communication between healthcare providers is essential to patient safety and quality of care.1, 2 Numeric pagers are commonly used communication devices in healthcare, but cannot convey important information such as the reason for the page, urgency of the page, or sender name. Physicians must respond to numeric pages, often disrupting patient encounters or educational activities.36 In a study of medical interns, disruptions to patient care occurred with up to 65% of pages received, two‐thirds of which were not felt to be urgent.5 In addition to causing frustration, frequent disruptions can contribute to medical errors.7, 8
Alphanumeric pagers can display both numbers and text, and may address some of the communication problems associated with numeric pagers. They also lay the groundwork for other patient safety initiatives such as automated paging of critical laboratory values9 and real‐time reporting of user‐requested laboratory data.10 Implementation of alphanumeric paging on a general surgery teaching service reduced disruptions to patient care and the number of pages requiring a return call.11
Our primary aim was to implement an alphanumeric paging system. We will describe our implementation strategies and barriers identified. We evaluated the implementation of alphanumeric paging by measuring (1) the proportion of pages sent as text pages, (2) the source of the pages (other physicians or from the general medicine [GM] ward), (3) the content of the text pages, (4) the number of pages that disrupted scheduled education activities, and (5) satisfaction with the alphanumeric paging system.
Materials and Methods
Setting
Sunnybrook Health Sciences Centre is a tertiary care academic teaching hospital affiliated with the University of Toronto (Toronto, Ontario, Canada). There are 4 physician teams that provide hospitalist care to admitted patients on the General Internal Medicine service. Each physician team consists of 1 attending physician, 1 second‐year or third‐year resident, 2 to 3 first‐year residents, and 3 to 4 third‐year and fourth‐year medical students. In total, 12 to 13 residents rotate through the General Internal Medicine service per month. Each physician team is assigned to 1 of 4 GM wards, which are staffed with nurses and allied health staff. Five to eight Internet‐enabled computer stations are located on each GM ward. All physicians, nurses, and allied health staff who worked on the 4 GM wards participated in the study.
Existing Paging System
Prior to July 2006, all physicians at our hospital carried numeric pagers. A physician could be paged by 3 methods: (1) through the hospital operator; (2) using the telephone; or (3) using an Internet‐based paging system (Smart Web 3.6.2, AmCom Software Inc.). Most pages were sent through the hospital operator or by telephone.
Intervention
The intervention included: (1) equipping resident physicians with alphanumeric pagers and (2) increasing the use of the existing Internet‐based paging system to send text pages. We equipped each resident with an alphanumeric pager (Motorola Flex Alphanumeric Pager). Users could send a text page using the existing Internet‐based application (Smart Web 3.6.2). This application allows users to search for a specific physician either by name or by on‐call assignment, and send a page up to 125 characters long from any Internet‐enabled computer in the hospital. Numeric pages could be sent by telephone, through the hospital operator, or by using the web‐based paging system throughout the study period.
Implementation Process
We provided alphanumeric pagers to the residents on the General Internal Medicine service in July 2006. Alphanumeric pagers were limited, so each resident traded their numeric pager for an alphanumeric pager at the start of each rotation. Once their rotation ended, they returned their alphanumeric pager for their original numeric pager. The communications department coordinated this process. The chief medical resident spent 10 minutes to teach the residents how to use the system at the beginning of the rotation. In August and September 2006, a member of the communications department trained the nurses on the 4 GM wards how to send a text page using the Internet‐based paging application. We scheduled these 15‐minute sessions throughout the day and evening in order to capture as many nurses as possible. We encouraged the nurses to include standardized information in the text message (eg, patient ID, issue, level of urgency, sender name, call‐back number).
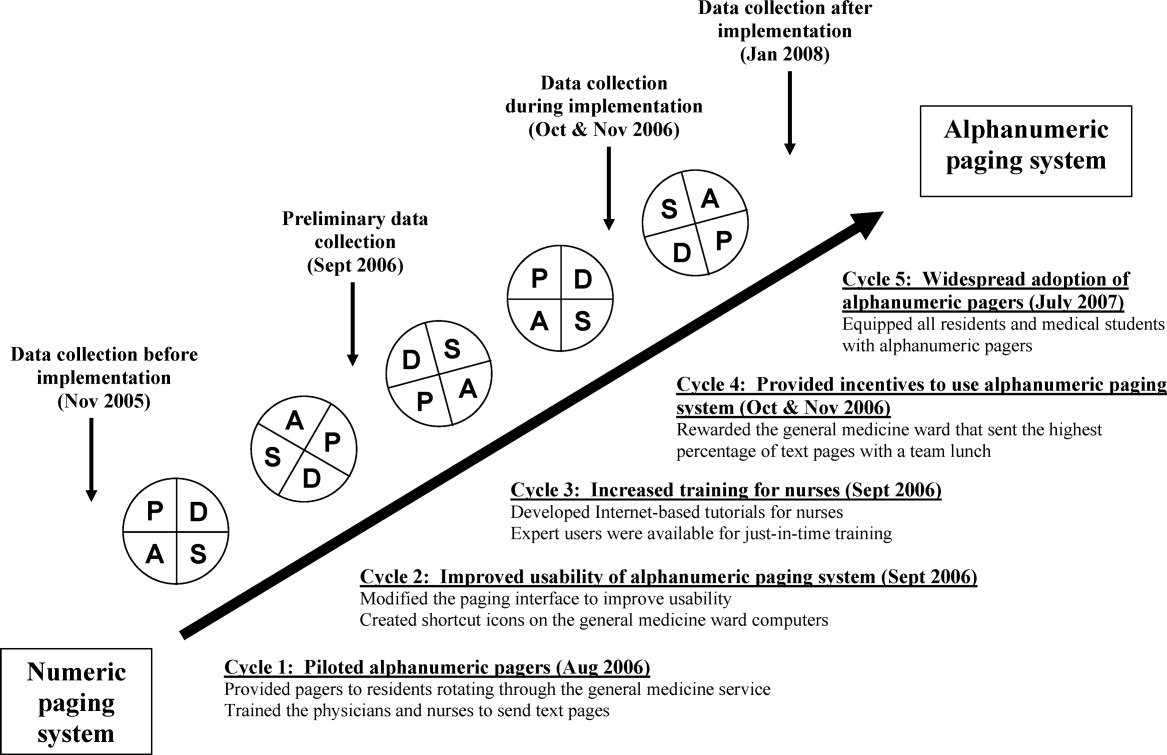
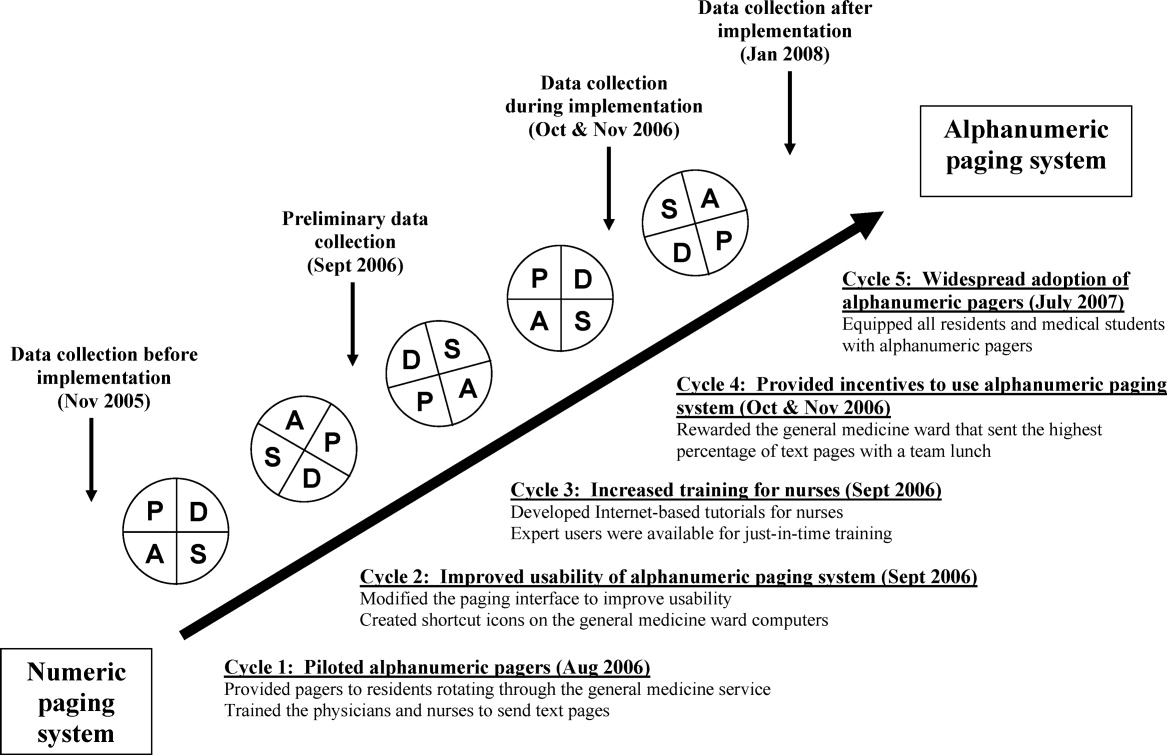
We used rapid‐cycle change methods12 to implement the alphanumeric system (Figure 1). The first change cycle in August 2006 consisted of providing pagers to residents and training the nurses and physicians to send text pages. Users reported that the paging interface was difficult to use. For the second change cycle in September 2006, the communications department modified the paging interface to improve usability and created shortcut icons on the GM ward computers. While the system was easier to access, the nurses reported that 1‐time training was insufficient. For the next change cycle in September 2006, we developed Internet‐based tutorials that could be accessed at any time, and made expert users (charge nurses) available for just‐in‐time training. We asked these charge nurses what they believed would encourage adoption of the system. They suggested that contests worked well with other initiatives. For the final change cycle in October and November 2006, we held a contest and rewarded the GM ward that sent the highest percentage of text pages with a team lunch.
Our results from November 2006 were presented to our hospital medical leaders, who approved widespread implementation of alphanumeric pagers for all residents and medical students in all programs. The cost of this upgrade was approximately $35,000 per year to lease 500 alphanumeric pagers. By July 2007, all residents and students in our hospital had alphanumeric pagers.
Measures
Our primary outcome measure was the percentage of pages sent as text pages. We chose November 2005 as our before implementation period to account for temporal variations in patient load, and secular trends in resident knowledge and experience during an academic year. We collected data during our rapid‐cycle improvement periods of implementation and testing in September to November 2006. We assessed sustainability after implementation by collecting data in January 2008, 6 months after hospital‐wide implementation of alphanumeric pagers, and 14 months after the initial implementation on the GIM service.
We reviewed weekday paging records from our communications department for each study period. For text pages, we reviewed the text message to determine whether the page was sent by a physician or by another health care professional. We established 5 mutually exclusive categories of messages prior to the study: (1) A GM ward‐to‐physician (GM ward‐to‐Doc) numeric page was any page that contained only a phone number for 1 of the 4 GM ward main telephone numbers; (2) A Doc‐to‐Doc numeric page was any page that was preceded by 000‐ (a convention used at our hospital to indicate a physician sender), or that contained a phone number used only by physicians, such as the doctor's lounge; (3) A GM ward‐to‐Doc text page was a text page sent by any GM ward health care professional; (4) A Doc‐to‐Doc text page was a text page sent by any physician or medical student; and (5) All other numeric pages, such as those with phone numbers from other hospital wards, were classified as numeric non‐GM ward and non‐Doc in‐hospital page.
We evaluated the impact of the alphanumeric system on disruptions by studying pages received during scheduled educational rounds that occur every weekday from 12:00 to 1:00 PM. We classified a page as disruptive if it required an immediate call‐back (ie, all numeric pages and urgent text pages).
We surveyed residents and daytime GM ward nursing staff during the implementation period (October and November 2006) to assess satisfaction with the alphanumeric paging system using a 5‐point Likert scale (1 = strongly disagree, 5 = strongly agree). We distributed paper surveys to nurses, and used an electronic web survey for residents.13
Statistical Analysis
We compared the paging data after implementation (January 2008) to the period before implementation (November 2005) using a Student t‐test for comparison of means, and chi‐square and Fisher's exact tests for categorical value comparisons. We assigned a significance level of P 0.05 for the t tests and chi‐square tests, and P 0.01 for the Fisher's exact tests. We used SPSS 11.0 to perform statistical analyses (Chicago, IL).
Results
Paging Patterns Before, During, and After Implementation
The number of pages per resident was similar before and during implementation, but higher afterwards. (46 16 pages/resident/week in November 2005, 47 20 pages/resident/week in November 2006, and 59 27 pages/resident/week in January 2008; P = 0.17; Table 1). The mean number of admissions per night was 8.0 2.7 before implementation, compared to 10.2 3.5 after implementation (P = 0.009).
| Before Implementation (all residents had numeric pagers) | During Implementation (all residents had alphanumeric pagers) | After Implementation (all residents had alphanumeric pagers) | |||
|---|---|---|---|---|---|
| Paging Characteristics | November 2005 | October 2006 | November 2006 | January 2008 | P Value |
| |||||
| Total number of pages | 1431 | 1879 | 1813 | 1269 | |
| Total number of resident weeks worked | 29 | 33 | 33 | 21 | |
| Pages per resident week, mean (SD) | 46.2 (16.3) | 57.9 (19.2) | 46.5 (20.2) | 59.0 (26.5) | 0.17* |
| Number of patients admitted per night, mean (SD) | 8.0 (2.7) | 10.2 (3.5) | 11.0 (2.9) | 10.2 (3.5) | 0.009* |
| Type of page, n (%) | |||||
| Numeric pages | 751 (53) | 462 (25) | 580 (32) | 374 (30) | 0.001 |
| GM wards‐to‐Doc | 584 (41) | 393 (21) | 538 (30) | 352 (28) | 0.001 |
| Doc‐to‐Doc | 167 (12) | 69 (4) | 42 (2) | 22 (2) | 0.001 |
| Non‐GM ward/Doc pages | 680 (47) | 1107 (59) | 809 (45) | 487 (38) | 0.001 |
| Text pages | 0 (0) | 310 (16) | 424 (23) | 408 (32) | 0.001 |
| GM wards‐to‐Doc | 0 (0) | 175 (9) | 221 (12) | 129 (10) | 0.001 |
| Doc‐to‐Doc | 0 (0) | 135 (7) | 203 (11) | 279 (22) | 0.001 |
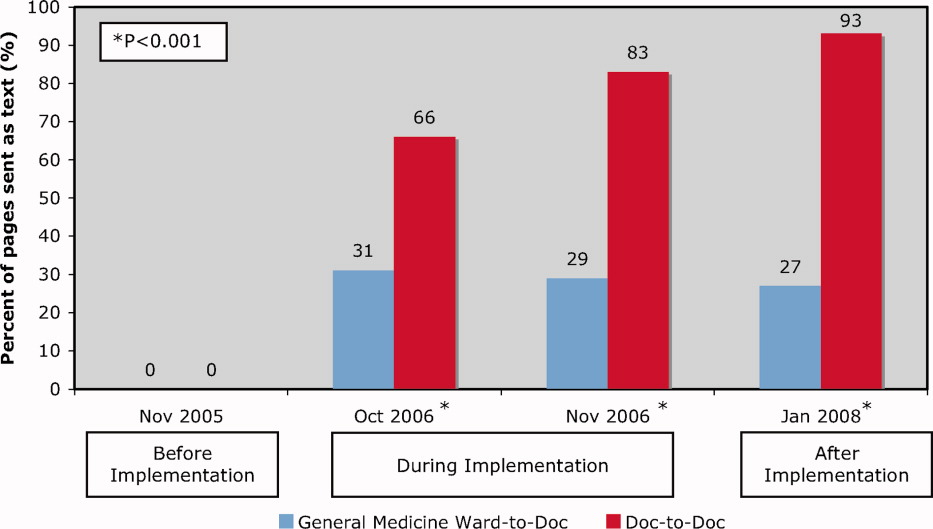
We observed a significant and sustained increase in the use of text paging during the study (Table 1). After implementation, 32% of all pages sent to our residents were text messages (P 0.001). Physicians almost exclusively sent text pages by the end of implementation (increase from 0% to 83% text paging rate during implementation, and 93% after implementation; P 0.001; Figure 2). GM ward text paging rates also increased from 0% to 29% during implementation, and 27% after implementation (P 0.001; Figure 2). The alphanumeric paging system was used to a greater degree by physicians compared to other workers on the GM ward after full implementation (93% vs. 27%; P 0.001). We explored the proportion of GM ward‐to‐Doc pages sent as text from different GM wards during implementation, and found significant variation, ranging from 14% to 57% (P 0.001).
The most common reasons for text paging from GM wards were to request a patient assessment or for notification of a patient's clinical status (25%), to clarify written orders (20%), and to request a medication prescription (13%) (Table 2). Among physicians, the most common reasons for text paging were to set up meetings for work or teaching rounds (33%), to relay patient‐care related messages (27%), and to sign‐over patients at the end of the day (23%) (Table 3). The remainder of the other Doc‐to‐Doc pages (18%) were mostly personal messages or team communication that was not related to clinical work.
| Reason for Paging | Number (%) | Examples |
|---|---|---|
| ||
| Requests for patient assessment or notification of a patient's clinical status | 55 (25) | Patient X. Temp 38.5. No other symptoms. [Nurse's name]. |
| The repeat CXR on Patient X has been completed. Please call [ward] if NG can be used. Thank you. | ||
| Clarification of a written order | 45 (20) | Would you like Patient X to get a second dose of Lasix? He has already had 100 mg and his output thus far is 500 cc. [Nurse's name] |
| Patient X. BP = 100/62, pulse 54. Patient is supposed to have metoprolol 50 mg tonight. Do you want me to hold it? [Nurse's name] | ||
| Request for a medication prescription | 28 (13) | Patient X needs an analgesic for pain in his arms and legs. Please call [ward]. |
| Patient X has a daily coumadin order. INR 2.14. Please call with dosage for 1800. Ask for [Nurse]. | ||
| Cosigning written order | 25 (11) | Please co‐sign neurology suggested orders for Patient X. [Nurse's name] |
| Not urgent at your leisure, please co‐sign Patient X orders on [ward] for medical student. Thanks. | ||
| Notification of a recent laboratory result | 23 (11) | Patient X's potassium is 3.0 today. Please call [ward]. |
| Patient X. Sodium 163. Troponin unchanged at 1.54. [ward]. | ||
| Arranging meetings with patients and/or family | 18 (8) | Meeting with Patient X's family and social worker at 2 pm tomorrow on [ward]. |
| [Social worker] is here. [Physiotherapist] expected any minute. We are going to meet in family room for Patient X. | ||
| Request to complete paperwork | 15 (7) | Patient X is ready to go home, and just needs discharge orders and prescriptions |
| Referral form for community palliative doctor on the front of the chart fill in where marked by arrows. Can you please put on form prognosis as well? [Social worker] | ||
| Other | 12 (6) | |
| Total | 221 (100) | |
| Reason for Paging | Number (%) | Examples |
|---|---|---|
| ||
| Setting up meetings for work or teaching rounds | 67 (33) | Confirmed diabetes teaching at 1400 hr in [room]. Please let medical students know. Thanks. |
| Please come to [lecture theatre] if you can in the next 10 minutes for the teleconferenced noon rounds. Thanks. | ||
| We are in the Emergency Department with [attending staff]. Come to meet us here if you can. | ||
| Relaying patient‐care related messages | 54 (27) | Patient X US query cholangitis, can we ask for a surgical consult. He may benefit from surgery or percutaneous drain. Please repeat his blood work. |
| Patient X in [room X]. Presented with DKA. pH 7.2. pCO2 23, bicarbonate 9. Lytes pending. Got IV insulin and NS. Need to check to clinical stability. [Resident] | ||
| Signing‐over patients at the end of the day | 46 (23) | I'm ready to sign out to you. Where are you? [Resident]. |
| Patient X is back from cardiac cath, and is stable. Please check Cr over WE, and watch for CHF. | ||
| Other | 36 (18) | |
| Total | 203 (100) | |
Impact of Alphanumeric Paging System on Disruptions
We evaluated the impact of the alphanumeric system on disruptions by studying pages received during scheduled educational rounds (Table 4). Prior to implementation, residents were paged 2.9 2.4 times per week during educational rounds, compared to 3.4 3.6 times per week after implementation (P = 0.66). Prior to implementation, all pages were numeric necessitating an immediate call‐back, causing an educational disruption. During the implementation period, 13% of pages received during educational rounds were nonurgent text pages that did not require an immediate call‐back, increasing to 29% after implementation (P 0.001).
| November 2005 (3 weeks)* | November 2006 (3 weeks) | January 2008 (2 weeks) | P Value* | |
|---|---|---|---|---|
| ||||
| Total number of pages received during scheduled educational rounds | 104 | 129 | 103 | |
| Total pages from GM ward or Doc | 61 (59%) | 76 (59%) | 62 (60%) | 0.888 |
| Numeric | 61 (59%) | 43 (33%) | 25 (24%) | 0.001 |
| Text | 0 (0%) | 33 (26%) | 37 (36%) | 0.001 |
| Urgent | 0 (0%) | 16 (13%) | 7 (7%) | 0.007 |
| Nonurgent | 0 (0%) | 17 (13%) | 30 (29%) | 0.001 |
| Numeric pages non‐GM ward and non‐Doc | 43 (41%) | 53 (41%) | 41 (40%) | 0.888 |
| Pages requiring an immediate call back | 104 (100%) | 112 (87%) | 73 (71%) | 0.001 |
User Satisfaction
Physicians (18/25; response rate = 72%) were very satisfied with the alphanumeric paging system (mean, 4.6/5), felt that the alphanumeric paging system minimized disruptions to patient care duties (4.1/5) as well as educational rounds (4.2/5), and allowed them to prioritize their tasks effectively (4.6/5). Nursing staff (32/80, response rate = 40%) were also satisfied with the alphanumeric paging system (4.1/5), and found the technology very easy to use (4.5/5).
Potential Barriers to and Unintended Downsides of Implementation
We identified a number of barriers that limited the broader adoption of alphanumeric paging at our hospital. Nursing staff expressed concerns about limited computer and typographical skills. We addressed this by involving nursing champions to promote the alphanumeric paging system and to assist with nurse training. There were insufficient computers available for the nurses to send text pages, so many opted to page the physician using the conventional telephone system. The limited number of alphanumeric pagers during the implementation period meant that cross‐covering and off‐service residents were not carrying alphanumeric pagers. This undermined our ability to encourage use of a single paging system. We addressed this by convincing the hospital to provide alphanumeric pagers to all residents and medical students at our institution, a practice that was adopted in July 2007.
We also identified several potential unintended downsides to the implementation of alphanumeric paging. Nurses received no confirmation that nonurgent pages had reached the residents. We asked the residents to close the communication loop by making a phone call or confirming in person at the next convenient opportunity. Pagers store confidential transmitted patient information unless the resident deletes it. Communication using the pagers may replace discussions that should occur in person. For example, residents might send a text page with brief updates about patients as the only form of sign‐over. Even though the majority of sign‐over pages in our study were simply a text message to arrange a place to meet for face‐to‐face sign‐over, we did encounter a small number of pages where it is unclear whether provision of actual sign‐over information via text message was in lieu of a formal handoff, or whether it was accompanied by an in‐person handoff as well. Finally, nurses had to leave the patient's bedside to send a text page from a computer workstation. We highlighted that sending a nonurgent text page allows nurses to return to the bedside rather than wait at the nursing station for a call‐back.
Our opinions regarding key elements of an alphanumeric paging system implementation are summarized in Table 5.
| Equip all members of the healthcare team with alphanumeric pagers | |
| Use a web‐based paging program that allows easy and accurate identification of the responsible physician 24 hours a day, 7 days a week | |
| Install sufficient computer terminals for accessing the paging program | |
| Provide 2‐way communication so the page recipient can acknowledge the receipt of the message | |
| Maintain patient confidentiality by encrypting or encoding messages and sending them via a secure server | |
| Choose pager technology that ensures reliable delivery of messages without dropped pages | |
| Ensure ongoing technical support and training services for health care team members |
Discussion
We successfully implemented an alphanumeric paging system on a resident inpatient internal medicine teaching service, with 42% of pages from our GM wards or physicians sent as text pages during implementation period. Six months after widespread use of alphanumeric pagers at our hospital (and 14 months after the initial implementation on the General Internal Medicine service) the text paging rate was 52%. Physicians have nearly universally adopted the use of alphanumeric paging as a means of communicating with one another, while the adoption by nursing staff was modest. The implementation of the alphanumeric paging system was associated with a significant reduction in disruptive pages.
We could identify only one prior study of alphanumeric paging implementation in a hospital setting. A general surgery teaching service in the United States demonstrated that 35% of all pages received by residents were text pages 3 months after implementation,11 similar to our result of 32% text paging rate after full implementation. We found a greater use of text paging among physicians in our study (93% of Doc‐to‐Doc pages were text), compared to 55% in this prior study. This difference may be partially explained by varied methods for identifying Doc‐to‐Doc pages between the studies.
A number of factors influence the adoption of new technology, such as the technology's features, end‐user characteristics, and dissemination strategies.14 During the implementation, even though the web‐based paging system was deemed easy to use, there was a lack of computers available to send text messages at each of our nursing stations. Residents were generally more familiar with technology and the use of computers for communication than nurses, and therefore more likely to use the technology. The presence of innovators influenced the success of adoption, evidenced by the fact that the GM ward that sent the highest percentage of pages as text was also the GM ward where the project leader (B.W.) worked as the attending staff during the implementation period.
Our study has several limitations. First, our method for classifying the source of numeric pages was imperfect. Our method systematically underestimates Doc‐to‐Doc numeric pages, because we assumed that all pages from GM ward phone numbers were not from physicians. We also may have misclassified the origin of some text messages. These limitations would not affect our conclusion that text messaging increased, but may overestimate the increase in Doc‐to‐Doc text messaging, and underestimate the increase in GM ward‐to‐Doc text messaging. The reasons for paging are not known for the numeric pages. The number of pages received per resident increased after implementation, so it is possible that alphanumeric pages increased calls for certain nonurgent issues, such as co‐signing orders. Finally, we assumed that residents were attending scheduled educational rounds, but were unable to confirm attendance, so we cannot be sure that disruptions actually were reduced.
In summary, we implemented an alphanumeric paging system, and observed a sustained use of text messaging after 1 year. The implementation of alphanumeric paging was associated with a reduction in disruptive pages sent during scheduled educational rounds.
Acknowledgements
Twenty alphanumeric pagers were provided in kind for the duration of the implementation period by PageNet Canada. The authors thank the Advance Practice Nurses from the 4 GM wards (Sonia Dyal, Jackie Griffin‐White, Tracey Kitchen‐Clark, and Trish Trieu) and members of the communications department (Jonathon Tunstead, Howard Golding, Joan Moodie, and Myles Leicester) for the instrumental role they played in the implementation of the alphanumeric paging system.
- , , , , .Teams: communication in multidisciplinary care.Oncologist.2006;11:520–526.
- .14,000 preventable deaths in Australian hospitals.BMJ.1995;310:1487.
- , .Interrupted care. The effects of paging on pediatric resident activities.Am J Dis Child.1992;146:806–808.
- , , .Patterns of paging medical interns during night calls at two teaching hospitals.CMAJ.1994;151:307–311.
- , .The sounds of the hospital. Paging patterns in three teaching hospitals.N Engl J Med.1988;319:1585–1589.
- , , .How hospitalists spend their time: insights on efficiency and safety.J Hosp Med.2006;1:88–93.
- , .Communication behaviours in a hospital setting: an observational study.BMJ.1998;316:673–676.
- , .Residents' suggestions for reducing errors in teaching hospitals.N Engl J Med.2003;348:851–855.
- , , et al.Improving response to critical laboratory results with automation: results of a randomized controlled trial.J Am Med Inform Assoc.1999;6:512–522.
- , , , .Real‐time notification of laboratory data requested by users through alphanumeric pagers.J Am Med Inform Assoc.2002;9:217–222.
- , , , , .Alphanumeric paging in an academic hospital setting.Am J Surg.2006;191:561–565.
- .A primer on leading the improvement of systems.BMJ.1996;312:619–622.
- SurveyMonkey.com. The simple way to create surveys. Available at: http://www.surveymonkey.com. Accessed September 2009.
- .Diffusion of innovations.New York:Free Press;1995.
Effective communication between healthcare providers is essential to patient safety and quality of care.1, 2 Numeric pagers are commonly used communication devices in healthcare, but cannot convey important information such as the reason for the page, urgency of the page, or sender name. Physicians must respond to numeric pages, often disrupting patient encounters or educational activities.36 In a study of medical interns, disruptions to patient care occurred with up to 65% of pages received, two‐thirds of which were not felt to be urgent.5 In addition to causing frustration, frequent disruptions can contribute to medical errors.7, 8
Alphanumeric pagers can display both numbers and text, and may address some of the communication problems associated with numeric pagers. They also lay the groundwork for other patient safety initiatives such as automated paging of critical laboratory values9 and real‐time reporting of user‐requested laboratory data.10 Implementation of alphanumeric paging on a general surgery teaching service reduced disruptions to patient care and the number of pages requiring a return call.11
Our primary aim was to implement an alphanumeric paging system. We will describe our implementation strategies and barriers identified. We evaluated the implementation of alphanumeric paging by measuring (1) the proportion of pages sent as text pages, (2) the source of the pages (other physicians or from the general medicine [GM] ward), (3) the content of the text pages, (4) the number of pages that disrupted scheduled education activities, and (5) satisfaction with the alphanumeric paging system.
Materials and Methods
Setting
Sunnybrook Health Sciences Centre is a tertiary care academic teaching hospital affiliated with the University of Toronto (Toronto, Ontario, Canada). There are 4 physician teams that provide hospitalist care to admitted patients on the General Internal Medicine service. Each physician team consists of 1 attending physician, 1 second‐year or third‐year resident, 2 to 3 first‐year residents, and 3 to 4 third‐year and fourth‐year medical students. In total, 12 to 13 residents rotate through the General Internal Medicine service per month. Each physician team is assigned to 1 of 4 GM wards, which are staffed with nurses and allied health staff. Five to eight Internet‐enabled computer stations are located on each GM ward. All physicians, nurses, and allied health staff who worked on the 4 GM wards participated in the study.
Existing Paging System
Prior to July 2006, all physicians at our hospital carried numeric pagers. A physician could be paged by 3 methods: (1) through the hospital operator; (2) using the telephone; or (3) using an Internet‐based paging system (Smart Web 3.6.2, AmCom Software Inc.). Most pages were sent through the hospital operator or by telephone.
Intervention
The intervention included: (1) equipping resident physicians with alphanumeric pagers and (2) increasing the use of the existing Internet‐based paging system to send text pages. We equipped each resident with an alphanumeric pager (Motorola Flex Alphanumeric Pager). Users could send a text page using the existing Internet‐based application (Smart Web 3.6.2). This application allows users to search for a specific physician either by name or by on‐call assignment, and send a page up to 125 characters long from any Internet‐enabled computer in the hospital. Numeric pages could be sent by telephone, through the hospital operator, or by using the web‐based paging system throughout the study period.
Implementation Process
We provided alphanumeric pagers to the residents on the General Internal Medicine service in July 2006. Alphanumeric pagers were limited, so each resident traded their numeric pager for an alphanumeric pager at the start of each rotation. Once their rotation ended, they returned their alphanumeric pager for their original numeric pager. The communications department coordinated this process. The chief medical resident spent 10 minutes to teach the residents how to use the system at the beginning of the rotation. In August and September 2006, a member of the communications department trained the nurses on the 4 GM wards how to send a text page using the Internet‐based paging application. We scheduled these 15‐minute sessions throughout the day and evening in order to capture as many nurses as possible. We encouraged the nurses to include standardized information in the text message (eg, patient ID, issue, level of urgency, sender name, call‐back number).
We used rapid‐cycle change methods12 to implement the alphanumeric system (Figure 1). The first change cycle in August 2006 consisted of providing pagers to residents and training the nurses and physicians to send text pages. Users reported that the paging interface was difficult to use. For the second change cycle in September 2006, the communications department modified the paging interface to improve usability and created shortcut icons on the GM ward computers. While the system was easier to access, the nurses reported that 1‐time training was insufficient. For the next change cycle in September 2006, we developed Internet‐based tutorials that could be accessed at any time, and made expert users (charge nurses) available for just‐in‐time training. We asked these charge nurses what they believed would encourage adoption of the system. They suggested that contests worked well with other initiatives. For the final change cycle in October and November 2006, we held a contest and rewarded the GM ward that sent the highest percentage of text pages with a team lunch.
Our results from November 2006 were presented to our hospital medical leaders, who approved widespread implementation of alphanumeric pagers for all residents and medical students in all programs. The cost of this upgrade was approximately $35,000 per year to lease 500 alphanumeric pagers. By July 2007, all residents and students in our hospital had alphanumeric pagers.
Measures
Our primary outcome measure was the percentage of pages sent as text pages. We chose November 2005 as our before implementation period to account for temporal variations in patient load, and secular trends in resident knowledge and experience during an academic year. We collected data during our rapid‐cycle improvement periods of implementation and testing in September to November 2006. We assessed sustainability after implementation by collecting data in January 2008, 6 months after hospital‐wide implementation of alphanumeric pagers, and 14 months after the initial implementation on the GIM service.
We reviewed weekday paging records from our communications department for each study period. For text pages, we reviewed the text message to determine whether the page was sent by a physician or by another health care professional. We established 5 mutually exclusive categories of messages prior to the study: (1) A GM ward‐to‐physician (GM ward‐to‐Doc) numeric page was any page that contained only a phone number for 1 of the 4 GM ward main telephone numbers; (2) A Doc‐to‐Doc numeric page was any page that was preceded by 000‐ (a convention used at our hospital to indicate a physician sender), or that contained a phone number used only by physicians, such as the doctor's lounge; (3) A GM ward‐to‐Doc text page was a text page sent by any GM ward health care professional; (4) A Doc‐to‐Doc text page was a text page sent by any physician or medical student; and (5) All other numeric pages, such as those with phone numbers from other hospital wards, were classified as numeric non‐GM ward and non‐Doc in‐hospital page.
We evaluated the impact of the alphanumeric system on disruptions by studying pages received during scheduled educational rounds that occur every weekday from 12:00 to 1:00 PM. We classified a page as disruptive if it required an immediate call‐back (ie, all numeric pages and urgent text pages).
We surveyed residents and daytime GM ward nursing staff during the implementation period (October and November 2006) to assess satisfaction with the alphanumeric paging system using a 5‐point Likert scale (1 = strongly disagree, 5 = strongly agree). We distributed paper surveys to nurses, and used an electronic web survey for residents.13
Statistical Analysis
We compared the paging data after implementation (January 2008) to the period before implementation (November 2005) using a Student t‐test for comparison of means, and chi‐square and Fisher's exact tests for categorical value comparisons. We assigned a significance level of P 0.05 for the t tests and chi‐square tests, and P 0.01 for the Fisher's exact tests. We used SPSS 11.0 to perform statistical analyses (Chicago, IL).
Results
Paging Patterns Before, During, and After Implementation
The number of pages per resident was similar before and during implementation, but higher afterwards. (46 16 pages/resident/week in November 2005, 47 20 pages/resident/week in November 2006, and 59 27 pages/resident/week in January 2008; P = 0.17; Table 1). The mean number of admissions per night was 8.0 2.7 before implementation, compared to 10.2 3.5 after implementation (P = 0.009).
| Before Implementation (all residents had numeric pagers) | During Implementation (all residents had alphanumeric pagers) | After Implementation (all residents had alphanumeric pagers) | |||
|---|---|---|---|---|---|
| Paging Characteristics | November 2005 | October 2006 | November 2006 | January 2008 | P Value |
| |||||
| Total number of pages | 1431 | 1879 | 1813 | 1269 | |
| Total number of resident weeks worked | 29 | 33 | 33 | 21 | |
| Pages per resident week, mean (SD) | 46.2 (16.3) | 57.9 (19.2) | 46.5 (20.2) | 59.0 (26.5) | 0.17* |
| Number of patients admitted per night, mean (SD) | 8.0 (2.7) | 10.2 (3.5) | 11.0 (2.9) | 10.2 (3.5) | 0.009* |
| Type of page, n (%) | |||||
| Numeric pages | 751 (53) | 462 (25) | 580 (32) | 374 (30) | 0.001 |
| GM wards‐to‐Doc | 584 (41) | 393 (21) | 538 (30) | 352 (28) | 0.001 |
| Doc‐to‐Doc | 167 (12) | 69 (4) | 42 (2) | 22 (2) | 0.001 |
| Non‐GM ward/Doc pages | 680 (47) | 1107 (59) | 809 (45) | 487 (38) | 0.001 |
| Text pages | 0 (0) | 310 (16) | 424 (23) | 408 (32) | 0.001 |
| GM wards‐to‐Doc | 0 (0) | 175 (9) | 221 (12) | 129 (10) | 0.001 |
| Doc‐to‐Doc | 0 (0) | 135 (7) | 203 (11) | 279 (22) | 0.001 |
We observed a significant and sustained increase in the use of text paging during the study (Table 1). After implementation, 32% of all pages sent to our residents were text messages (P 0.001). Physicians almost exclusively sent text pages by the end of implementation (increase from 0% to 83% text paging rate during implementation, and 93% after implementation; P 0.001; Figure 2). GM ward text paging rates also increased from 0% to 29% during implementation, and 27% after implementation (P 0.001; Figure 2). The alphanumeric paging system was used to a greater degree by physicians compared to other workers on the GM ward after full implementation (93% vs. 27%; P 0.001). We explored the proportion of GM ward‐to‐Doc pages sent as text from different GM wards during implementation, and found significant variation, ranging from 14% to 57% (P 0.001).
The most common reasons for text paging from GM wards were to request a patient assessment or for notification of a patient's clinical status (25%), to clarify written orders (20%), and to request a medication prescription (13%) (Table 2). Among physicians, the most common reasons for text paging were to set up meetings for work or teaching rounds (33%), to relay patient‐care related messages (27%), and to sign‐over patients at the end of the day (23%) (Table 3). The remainder of the other Doc‐to‐Doc pages (18%) were mostly personal messages or team communication that was not related to clinical work.
| Reason for Paging | Number (%) | Examples |
|---|---|---|
| ||
| Requests for patient assessment or notification of a patient's clinical status | 55 (25) | Patient X. Temp 38.5. No other symptoms. [Nurse's name]. |
| The repeat CXR on Patient X has been completed. Please call [ward] if NG can be used. Thank you. | ||
| Clarification of a written order | 45 (20) | Would you like Patient X to get a second dose of Lasix? He has already had 100 mg and his output thus far is 500 cc. [Nurse's name] |
| Patient X. BP = 100/62, pulse 54. Patient is supposed to have metoprolol 50 mg tonight. Do you want me to hold it? [Nurse's name] | ||
| Request for a medication prescription | 28 (13) | Patient X needs an analgesic for pain in his arms and legs. Please call [ward]. |
| Patient X has a daily coumadin order. INR 2.14. Please call with dosage for 1800. Ask for [Nurse]. | ||
| Cosigning written order | 25 (11) | Please co‐sign neurology suggested orders for Patient X. [Nurse's name] |
| Not urgent at your leisure, please co‐sign Patient X orders on [ward] for medical student. Thanks. | ||
| Notification of a recent laboratory result | 23 (11) | Patient X's potassium is 3.0 today. Please call [ward]. |
| Patient X. Sodium 163. Troponin unchanged at 1.54. [ward]. | ||
| Arranging meetings with patients and/or family | 18 (8) | Meeting with Patient X's family and social worker at 2 pm tomorrow on [ward]. |
| [Social worker] is here. [Physiotherapist] expected any minute. We are going to meet in family room for Patient X. | ||
| Request to complete paperwork | 15 (7) | Patient X is ready to go home, and just needs discharge orders and prescriptions |
| Referral form for community palliative doctor on the front of the chart fill in where marked by arrows. Can you please put on form prognosis as well? [Social worker] | ||
| Other | 12 (6) | |
| Total | 221 (100) | |
| Reason for Paging | Number (%) | Examples |
|---|---|---|
| ||
| Setting up meetings for work or teaching rounds | 67 (33) | Confirmed diabetes teaching at 1400 hr in [room]. Please let medical students know. Thanks. |
| Please come to [lecture theatre] if you can in the next 10 minutes for the teleconferenced noon rounds. Thanks. | ||
| We are in the Emergency Department with [attending staff]. Come to meet us here if you can. | ||
| Relaying patient‐care related messages | 54 (27) | Patient X US query cholangitis, can we ask for a surgical consult. He may benefit from surgery or percutaneous drain. Please repeat his blood work. |
| Patient X in [room X]. Presented with DKA. pH 7.2. pCO2 23, bicarbonate 9. Lytes pending. Got IV insulin and NS. Need to check to clinical stability. [Resident] | ||
| Signing‐over patients at the end of the day | 46 (23) | I'm ready to sign out to you. Where are you? [Resident]. |
| Patient X is back from cardiac cath, and is stable. Please check Cr over WE, and watch for CHF. | ||
| Other | 36 (18) | |
| Total | 203 (100) | |
Impact of Alphanumeric Paging System on Disruptions
We evaluated the impact of the alphanumeric system on disruptions by studying pages received during scheduled educational rounds (Table 4). Prior to implementation, residents were paged 2.9 2.4 times per week during educational rounds, compared to 3.4 3.6 times per week after implementation (P = 0.66). Prior to implementation, all pages were numeric necessitating an immediate call‐back, causing an educational disruption. During the implementation period, 13% of pages received during educational rounds were nonurgent text pages that did not require an immediate call‐back, increasing to 29% after implementation (P 0.001).
| November 2005 (3 weeks)* | November 2006 (3 weeks) | January 2008 (2 weeks) | P Value* | |
|---|---|---|---|---|
| ||||
| Total number of pages received during scheduled educational rounds | 104 | 129 | 103 | |
| Total pages from GM ward or Doc | 61 (59%) | 76 (59%) | 62 (60%) | 0.888 |
| Numeric | 61 (59%) | 43 (33%) | 25 (24%) | 0.001 |
| Text | 0 (0%) | 33 (26%) | 37 (36%) | 0.001 |
| Urgent | 0 (0%) | 16 (13%) | 7 (7%) | 0.007 |
| Nonurgent | 0 (0%) | 17 (13%) | 30 (29%) | 0.001 |
| Numeric pages non‐GM ward and non‐Doc | 43 (41%) | 53 (41%) | 41 (40%) | 0.888 |
| Pages requiring an immediate call back | 104 (100%) | 112 (87%) | 73 (71%) | 0.001 |
User Satisfaction
Physicians (18/25; response rate = 72%) were very satisfied with the alphanumeric paging system (mean, 4.6/5), felt that the alphanumeric paging system minimized disruptions to patient care duties (4.1/5) as well as educational rounds (4.2/5), and allowed them to prioritize their tasks effectively (4.6/5). Nursing staff (32/80, response rate = 40%) were also satisfied with the alphanumeric paging system (4.1/5), and found the technology very easy to use (4.5/5).
Potential Barriers to and Unintended Downsides of Implementation
We identified a number of barriers that limited the broader adoption of alphanumeric paging at our hospital. Nursing staff expressed concerns about limited computer and typographical skills. We addressed this by involving nursing champions to promote the alphanumeric paging system and to assist with nurse training. There were insufficient computers available for the nurses to send text pages, so many opted to page the physician using the conventional telephone system. The limited number of alphanumeric pagers during the implementation period meant that cross‐covering and off‐service residents were not carrying alphanumeric pagers. This undermined our ability to encourage use of a single paging system. We addressed this by convincing the hospital to provide alphanumeric pagers to all residents and medical students at our institution, a practice that was adopted in July 2007.
We also identified several potential unintended downsides to the implementation of alphanumeric paging. Nurses received no confirmation that nonurgent pages had reached the residents. We asked the residents to close the communication loop by making a phone call or confirming in person at the next convenient opportunity. Pagers store confidential transmitted patient information unless the resident deletes it. Communication using the pagers may replace discussions that should occur in person. For example, residents might send a text page with brief updates about patients as the only form of sign‐over. Even though the majority of sign‐over pages in our study were simply a text message to arrange a place to meet for face‐to‐face sign‐over, we did encounter a small number of pages where it is unclear whether provision of actual sign‐over information via text message was in lieu of a formal handoff, or whether it was accompanied by an in‐person handoff as well. Finally, nurses had to leave the patient's bedside to send a text page from a computer workstation. We highlighted that sending a nonurgent text page allows nurses to return to the bedside rather than wait at the nursing station for a call‐back.
Our opinions regarding key elements of an alphanumeric paging system implementation are summarized in Table 5.
| Equip all members of the healthcare team with alphanumeric pagers | |
| Use a web‐based paging program that allows easy and accurate identification of the responsible physician 24 hours a day, 7 days a week | |
| Install sufficient computer terminals for accessing the paging program | |
| Provide 2‐way communication so the page recipient can acknowledge the receipt of the message | |
| Maintain patient confidentiality by encrypting or encoding messages and sending them via a secure server | |
| Choose pager technology that ensures reliable delivery of messages without dropped pages | |
| Ensure ongoing technical support and training services for health care team members |
Discussion
We successfully implemented an alphanumeric paging system on a resident inpatient internal medicine teaching service, with 42% of pages from our GM wards or physicians sent as text pages during implementation period. Six months after widespread use of alphanumeric pagers at our hospital (and 14 months after the initial implementation on the General Internal Medicine service) the text paging rate was 52%. Physicians have nearly universally adopted the use of alphanumeric paging as a means of communicating with one another, while the adoption by nursing staff was modest. The implementation of the alphanumeric paging system was associated with a significant reduction in disruptive pages.
We could identify only one prior study of alphanumeric paging implementation in a hospital setting. A general surgery teaching service in the United States demonstrated that 35% of all pages received by residents were text pages 3 months after implementation,11 similar to our result of 32% text paging rate after full implementation. We found a greater use of text paging among physicians in our study (93% of Doc‐to‐Doc pages were text), compared to 55% in this prior study. This difference may be partially explained by varied methods for identifying Doc‐to‐Doc pages between the studies.
A number of factors influence the adoption of new technology, such as the technology's features, end‐user characteristics, and dissemination strategies.14 During the implementation, even though the web‐based paging system was deemed easy to use, there was a lack of computers available to send text messages at each of our nursing stations. Residents were generally more familiar with technology and the use of computers for communication than nurses, and therefore more likely to use the technology. The presence of innovators influenced the success of adoption, evidenced by the fact that the GM ward that sent the highest percentage of pages as text was also the GM ward where the project leader (B.W.) worked as the attending staff during the implementation period.
Our study has several limitations. First, our method for classifying the source of numeric pages was imperfect. Our method systematically underestimates Doc‐to‐Doc numeric pages, because we assumed that all pages from GM ward phone numbers were not from physicians. We also may have misclassified the origin of some text messages. These limitations would not affect our conclusion that text messaging increased, but may overestimate the increase in Doc‐to‐Doc text messaging, and underestimate the increase in GM ward‐to‐Doc text messaging. The reasons for paging are not known for the numeric pages. The number of pages received per resident increased after implementation, so it is possible that alphanumeric pages increased calls for certain nonurgent issues, such as co‐signing orders. Finally, we assumed that residents were attending scheduled educational rounds, but were unable to confirm attendance, so we cannot be sure that disruptions actually were reduced.
In summary, we implemented an alphanumeric paging system, and observed a sustained use of text messaging after 1 year. The implementation of alphanumeric paging was associated with a reduction in disruptive pages sent during scheduled educational rounds.
Acknowledgements
Twenty alphanumeric pagers were provided in kind for the duration of the implementation period by PageNet Canada. The authors thank the Advance Practice Nurses from the 4 GM wards (Sonia Dyal, Jackie Griffin‐White, Tracey Kitchen‐Clark, and Trish Trieu) and members of the communications department (Jonathon Tunstead, Howard Golding, Joan Moodie, and Myles Leicester) for the instrumental role they played in the implementation of the alphanumeric paging system.
Effective communication between healthcare providers is essential to patient safety and quality of care.1, 2 Numeric pagers are commonly used communication devices in healthcare, but cannot convey important information such as the reason for the page, urgency of the page, or sender name. Physicians must respond to numeric pages, often disrupting patient encounters or educational activities.36 In a study of medical interns, disruptions to patient care occurred with up to 65% of pages received, two‐thirds of which were not felt to be urgent.5 In addition to causing frustration, frequent disruptions can contribute to medical errors.7, 8
Alphanumeric pagers can display both numbers and text, and may address some of the communication problems associated with numeric pagers. They also lay the groundwork for other patient safety initiatives such as automated paging of critical laboratory values9 and real‐time reporting of user‐requested laboratory data.10 Implementation of alphanumeric paging on a general surgery teaching service reduced disruptions to patient care and the number of pages requiring a return call.11
Our primary aim was to implement an alphanumeric paging system. We will describe our implementation strategies and barriers identified. We evaluated the implementation of alphanumeric paging by measuring (1) the proportion of pages sent as text pages, (2) the source of the pages (other physicians or from the general medicine [GM] ward), (3) the content of the text pages, (4) the number of pages that disrupted scheduled education activities, and (5) satisfaction with the alphanumeric paging system.
Materials and Methods
Setting
Sunnybrook Health Sciences Centre is a tertiary care academic teaching hospital affiliated with the University of Toronto (Toronto, Ontario, Canada). There are 4 physician teams that provide hospitalist care to admitted patients on the General Internal Medicine service. Each physician team consists of 1 attending physician, 1 second‐year or third‐year resident, 2 to 3 first‐year residents, and 3 to 4 third‐year and fourth‐year medical students. In total, 12 to 13 residents rotate through the General Internal Medicine service per month. Each physician team is assigned to 1 of 4 GM wards, which are staffed with nurses and allied health staff. Five to eight Internet‐enabled computer stations are located on each GM ward. All physicians, nurses, and allied health staff who worked on the 4 GM wards participated in the study.
Existing Paging System
Prior to July 2006, all physicians at our hospital carried numeric pagers. A physician could be paged by 3 methods: (1) through the hospital operator; (2) using the telephone; or (3) using an Internet‐based paging system (Smart Web 3.6.2, AmCom Software Inc.). Most pages were sent through the hospital operator or by telephone.
Intervention
The intervention included: (1) equipping resident physicians with alphanumeric pagers and (2) increasing the use of the existing Internet‐based paging system to send text pages. We equipped each resident with an alphanumeric pager (Motorola Flex Alphanumeric Pager). Users could send a text page using the existing Internet‐based application (Smart Web 3.6.2). This application allows users to search for a specific physician either by name or by on‐call assignment, and send a page up to 125 characters long from any Internet‐enabled computer in the hospital. Numeric pages could be sent by telephone, through the hospital operator, or by using the web‐based paging system throughout the study period.
Implementation Process
We provided alphanumeric pagers to the residents on the General Internal Medicine service in July 2006. Alphanumeric pagers were limited, so each resident traded their numeric pager for an alphanumeric pager at the start of each rotation. Once their rotation ended, they returned their alphanumeric pager for their original numeric pager. The communications department coordinated this process. The chief medical resident spent 10 minutes to teach the residents how to use the system at the beginning of the rotation. In August and September 2006, a member of the communications department trained the nurses on the 4 GM wards how to send a text page using the Internet‐based paging application. We scheduled these 15‐minute sessions throughout the day and evening in order to capture as many nurses as possible. We encouraged the nurses to include standardized information in the text message (eg, patient ID, issue, level of urgency, sender name, call‐back number).
We used rapid‐cycle change methods12 to implement the alphanumeric system (Figure 1). The first change cycle in August 2006 consisted of providing pagers to residents and training the nurses and physicians to send text pages. Users reported that the paging interface was difficult to use. For the second change cycle in September 2006, the communications department modified the paging interface to improve usability and created shortcut icons on the GM ward computers. While the system was easier to access, the nurses reported that 1‐time training was insufficient. For the next change cycle in September 2006, we developed Internet‐based tutorials that could be accessed at any time, and made expert users (charge nurses) available for just‐in‐time training. We asked these charge nurses what they believed would encourage adoption of the system. They suggested that contests worked well with other initiatives. For the final change cycle in October and November 2006, we held a contest and rewarded the GM ward that sent the highest percentage of text pages with a team lunch.
Our results from November 2006 were presented to our hospital medical leaders, who approved widespread implementation of alphanumeric pagers for all residents and medical students in all programs. The cost of this upgrade was approximately $35,000 per year to lease 500 alphanumeric pagers. By July 2007, all residents and students in our hospital had alphanumeric pagers.
Measures
Our primary outcome measure was the percentage of pages sent as text pages. We chose November 2005 as our before implementation period to account for temporal variations in patient load, and secular trends in resident knowledge and experience during an academic year. We collected data during our rapid‐cycle improvement periods of implementation and testing in September to November 2006. We assessed sustainability after implementation by collecting data in January 2008, 6 months after hospital‐wide implementation of alphanumeric pagers, and 14 months after the initial implementation on the GIM service.
We reviewed weekday paging records from our communications department for each study period. For text pages, we reviewed the text message to determine whether the page was sent by a physician or by another health care professional. We established 5 mutually exclusive categories of messages prior to the study: (1) A GM ward‐to‐physician (GM ward‐to‐Doc) numeric page was any page that contained only a phone number for 1 of the 4 GM ward main telephone numbers; (2) A Doc‐to‐Doc numeric page was any page that was preceded by 000‐ (a convention used at our hospital to indicate a physician sender), or that contained a phone number used only by physicians, such as the doctor's lounge; (3) A GM ward‐to‐Doc text page was a text page sent by any GM ward health care professional; (4) A Doc‐to‐Doc text page was a text page sent by any physician or medical student; and (5) All other numeric pages, such as those with phone numbers from other hospital wards, were classified as numeric non‐GM ward and non‐Doc in‐hospital page.
We evaluated the impact of the alphanumeric system on disruptions by studying pages received during scheduled educational rounds that occur every weekday from 12:00 to 1:00 PM. We classified a page as disruptive if it required an immediate call‐back (ie, all numeric pages and urgent text pages).
We surveyed residents and daytime GM ward nursing staff during the implementation period (October and November 2006) to assess satisfaction with the alphanumeric paging system using a 5‐point Likert scale (1 = strongly disagree, 5 = strongly agree). We distributed paper surveys to nurses, and used an electronic web survey for residents.13
Statistical Analysis
We compared the paging data after implementation (January 2008) to the period before implementation (November 2005) using a Student t‐test for comparison of means, and chi‐square and Fisher's exact tests for categorical value comparisons. We assigned a significance level of P 0.05 for the t tests and chi‐square tests, and P 0.01 for the Fisher's exact tests. We used SPSS 11.0 to perform statistical analyses (Chicago, IL).
Results
Paging Patterns Before, During, and After Implementation
The number of pages per resident was similar before and during implementation, but higher afterwards. (46 16 pages/resident/week in November 2005, 47 20 pages/resident/week in November 2006, and 59 27 pages/resident/week in January 2008; P = 0.17; Table 1). The mean number of admissions per night was 8.0 2.7 before implementation, compared to 10.2 3.5 after implementation (P = 0.009).
| Before Implementation (all residents had numeric pagers) | During Implementation (all residents had alphanumeric pagers) | After Implementation (all residents had alphanumeric pagers) | |||
|---|---|---|---|---|---|
| Paging Characteristics | November 2005 | October 2006 | November 2006 | January 2008 | P Value |
| |||||
| Total number of pages | 1431 | 1879 | 1813 | 1269 | |
| Total number of resident weeks worked | 29 | 33 | 33 | 21 | |
| Pages per resident week, mean (SD) | 46.2 (16.3) | 57.9 (19.2) | 46.5 (20.2) | 59.0 (26.5) | 0.17* |
| Number of patients admitted per night, mean (SD) | 8.0 (2.7) | 10.2 (3.5) | 11.0 (2.9) | 10.2 (3.5) | 0.009* |
| Type of page, n (%) | |||||
| Numeric pages | 751 (53) | 462 (25) | 580 (32) | 374 (30) | 0.001 |
| GM wards‐to‐Doc | 584 (41) | 393 (21) | 538 (30) | 352 (28) | 0.001 |
| Doc‐to‐Doc | 167 (12) | 69 (4) | 42 (2) | 22 (2) | 0.001 |
| Non‐GM ward/Doc pages | 680 (47) | 1107 (59) | 809 (45) | 487 (38) | 0.001 |
| Text pages | 0 (0) | 310 (16) | 424 (23) | 408 (32) | 0.001 |
| GM wards‐to‐Doc | 0 (0) | 175 (9) | 221 (12) | 129 (10) | 0.001 |
| Doc‐to‐Doc | 0 (0) | 135 (7) | 203 (11) | 279 (22) | 0.001 |
We observed a significant and sustained increase in the use of text paging during the study (Table 1). After implementation, 32% of all pages sent to our residents were text messages (P 0.001). Physicians almost exclusively sent text pages by the end of implementation (increase from 0% to 83% text paging rate during implementation, and 93% after implementation; P 0.001; Figure 2). GM ward text paging rates also increased from 0% to 29% during implementation, and 27% after implementation (P 0.001; Figure 2). The alphanumeric paging system was used to a greater degree by physicians compared to other workers on the GM ward after full implementation (93% vs. 27%; P 0.001). We explored the proportion of GM ward‐to‐Doc pages sent as text from different GM wards during implementation, and found significant variation, ranging from 14% to 57% (P 0.001).
The most common reasons for text paging from GM wards were to request a patient assessment or for notification of a patient's clinical status (25%), to clarify written orders (20%), and to request a medication prescription (13%) (Table 2). Among physicians, the most common reasons for text paging were to set up meetings for work or teaching rounds (33%), to relay patient‐care related messages (27%), and to sign‐over patients at the end of the day (23%) (Table 3). The remainder of the other Doc‐to‐Doc pages (18%) were mostly personal messages or team communication that was not related to clinical work.
| Reason for Paging | Number (%) | Examples |
|---|---|---|
| ||
| Requests for patient assessment or notification of a patient's clinical status | 55 (25) | Patient X. Temp 38.5. No other symptoms. [Nurse's name]. |
| The repeat CXR on Patient X has been completed. Please call [ward] if NG can be used. Thank you. | ||
| Clarification of a written order | 45 (20) | Would you like Patient X to get a second dose of Lasix? He has already had 100 mg and his output thus far is 500 cc. [Nurse's name] |
| Patient X. BP = 100/62, pulse 54. Patient is supposed to have metoprolol 50 mg tonight. Do you want me to hold it? [Nurse's name] | ||
| Request for a medication prescription | 28 (13) | Patient X needs an analgesic for pain in his arms and legs. Please call [ward]. |
| Patient X has a daily coumadin order. INR 2.14. Please call with dosage for 1800. Ask for [Nurse]. | ||
| Cosigning written order | 25 (11) | Please co‐sign neurology suggested orders for Patient X. [Nurse's name] |
| Not urgent at your leisure, please co‐sign Patient X orders on [ward] for medical student. Thanks. | ||
| Notification of a recent laboratory result | 23 (11) | Patient X's potassium is 3.0 today. Please call [ward]. |
| Patient X. Sodium 163. Troponin unchanged at 1.54. [ward]. | ||
| Arranging meetings with patients and/or family | 18 (8) | Meeting with Patient X's family and social worker at 2 pm tomorrow on [ward]. |
| [Social worker] is here. [Physiotherapist] expected any minute. We are going to meet in family room for Patient X. | ||
| Request to complete paperwork | 15 (7) | Patient X is ready to go home, and just needs discharge orders and prescriptions |
| Referral form for community palliative doctor on the front of the chart fill in where marked by arrows. Can you please put on form prognosis as well? [Social worker] | ||
| Other | 12 (6) | |
| Total | 221 (100) | |
| Reason for Paging | Number (%) | Examples |
|---|---|---|
| ||
| Setting up meetings for work or teaching rounds | 67 (33) | Confirmed diabetes teaching at 1400 hr in [room]. Please let medical students know. Thanks. |
| Please come to [lecture theatre] if you can in the next 10 minutes for the teleconferenced noon rounds. Thanks. | ||
| We are in the Emergency Department with [attending staff]. Come to meet us here if you can. | ||
| Relaying patient‐care related messages | 54 (27) | Patient X US query cholangitis, can we ask for a surgical consult. He may benefit from surgery or percutaneous drain. Please repeat his blood work. |
| Patient X in [room X]. Presented with DKA. pH 7.2. pCO2 23, bicarbonate 9. Lytes pending. Got IV insulin and NS. Need to check to clinical stability. [Resident] | ||
| Signing‐over patients at the end of the day | 46 (23) | I'm ready to sign out to you. Where are you? [Resident]. |
| Patient X is back from cardiac cath, and is stable. Please check Cr over WE, and watch for CHF. | ||
| Other | 36 (18) | |
| Total | 203 (100) | |
Impact of Alphanumeric Paging System on Disruptions
We evaluated the impact of the alphanumeric system on disruptions by studying pages received during scheduled educational rounds (Table 4). Prior to implementation, residents were paged 2.9 2.4 times per week during educational rounds, compared to 3.4 3.6 times per week after implementation (P = 0.66). Prior to implementation, all pages were numeric necessitating an immediate call‐back, causing an educational disruption. During the implementation period, 13% of pages received during educational rounds were nonurgent text pages that did not require an immediate call‐back, increasing to 29% after implementation (P 0.001).
| November 2005 (3 weeks)* | November 2006 (3 weeks) | January 2008 (2 weeks) | P Value* | |
|---|---|---|---|---|
| ||||
| Total number of pages received during scheduled educational rounds | 104 | 129 | 103 | |
| Total pages from GM ward or Doc | 61 (59%) | 76 (59%) | 62 (60%) | 0.888 |
| Numeric | 61 (59%) | 43 (33%) | 25 (24%) | 0.001 |
| Text | 0 (0%) | 33 (26%) | 37 (36%) | 0.001 |
| Urgent | 0 (0%) | 16 (13%) | 7 (7%) | 0.007 |
| Nonurgent | 0 (0%) | 17 (13%) | 30 (29%) | 0.001 |
| Numeric pages non‐GM ward and non‐Doc | 43 (41%) | 53 (41%) | 41 (40%) | 0.888 |
| Pages requiring an immediate call back | 104 (100%) | 112 (87%) | 73 (71%) | 0.001 |
User Satisfaction
Physicians (18/25; response rate = 72%) were very satisfied with the alphanumeric paging system (mean, 4.6/5), felt that the alphanumeric paging system minimized disruptions to patient care duties (4.1/5) as well as educational rounds (4.2/5), and allowed them to prioritize their tasks effectively (4.6/5). Nursing staff (32/80, response rate = 40%) were also satisfied with the alphanumeric paging system (4.1/5), and found the technology very easy to use (4.5/5).
Potential Barriers to and Unintended Downsides of Implementation
We identified a number of barriers that limited the broader adoption of alphanumeric paging at our hospital. Nursing staff expressed concerns about limited computer and typographical skills. We addressed this by involving nursing champions to promote the alphanumeric paging system and to assist with nurse training. There were insufficient computers available for the nurses to send text pages, so many opted to page the physician using the conventional telephone system. The limited number of alphanumeric pagers during the implementation period meant that cross‐covering and off‐service residents were not carrying alphanumeric pagers. This undermined our ability to encourage use of a single paging system. We addressed this by convincing the hospital to provide alphanumeric pagers to all residents and medical students at our institution, a practice that was adopted in July 2007.
We also identified several potential unintended downsides to the implementation of alphanumeric paging. Nurses received no confirmation that nonurgent pages had reached the residents. We asked the residents to close the communication loop by making a phone call or confirming in person at the next convenient opportunity. Pagers store confidential transmitted patient information unless the resident deletes it. Communication using the pagers may replace discussions that should occur in person. For example, residents might send a text page with brief updates about patients as the only form of sign‐over. Even though the majority of sign‐over pages in our study were simply a text message to arrange a place to meet for face‐to‐face sign‐over, we did encounter a small number of pages where it is unclear whether provision of actual sign‐over information via text message was in lieu of a formal handoff, or whether it was accompanied by an in‐person handoff as well. Finally, nurses had to leave the patient's bedside to send a text page from a computer workstation. We highlighted that sending a nonurgent text page allows nurses to return to the bedside rather than wait at the nursing station for a call‐back.
Our opinions regarding key elements of an alphanumeric paging system implementation are summarized in Table 5.
| Equip all members of the healthcare team with alphanumeric pagers | |
| Use a web‐based paging program that allows easy and accurate identification of the responsible physician 24 hours a day, 7 days a week | |
| Install sufficient computer terminals for accessing the paging program | |
| Provide 2‐way communication so the page recipient can acknowledge the receipt of the message | |
| Maintain patient confidentiality by encrypting or encoding messages and sending them via a secure server | |
| Choose pager technology that ensures reliable delivery of messages without dropped pages | |
| Ensure ongoing technical support and training services for health care team members |
Discussion
We successfully implemented an alphanumeric paging system on a resident inpatient internal medicine teaching service, with 42% of pages from our GM wards or physicians sent as text pages during implementation period. Six months after widespread use of alphanumeric pagers at our hospital (and 14 months after the initial implementation on the General Internal Medicine service) the text paging rate was 52%. Physicians have nearly universally adopted the use of alphanumeric paging as a means of communicating with one another, while the adoption by nursing staff was modest. The implementation of the alphanumeric paging system was associated with a significant reduction in disruptive pages.
We could identify only one prior study of alphanumeric paging implementation in a hospital setting. A general surgery teaching service in the United States demonstrated that 35% of all pages received by residents were text pages 3 months after implementation,11 similar to our result of 32% text paging rate after full implementation. We found a greater use of text paging among physicians in our study (93% of Doc‐to‐Doc pages were text), compared to 55% in this prior study. This difference may be partially explained by varied methods for identifying Doc‐to‐Doc pages between the studies.
A number of factors influence the adoption of new technology, such as the technology's features, end‐user characteristics, and dissemination strategies.14 During the implementation, even though the web‐based paging system was deemed easy to use, there was a lack of computers available to send text messages at each of our nursing stations. Residents were generally more familiar with technology and the use of computers for communication than nurses, and therefore more likely to use the technology. The presence of innovators influenced the success of adoption, evidenced by the fact that the GM ward that sent the highest percentage of pages as text was also the GM ward where the project leader (B.W.) worked as the attending staff during the implementation period.
Our study has several limitations. First, our method for classifying the source of numeric pages was imperfect. Our method systematically underestimates Doc‐to‐Doc numeric pages, because we assumed that all pages from GM ward phone numbers were not from physicians. We also may have misclassified the origin of some text messages. These limitations would not affect our conclusion that text messaging increased, but may overestimate the increase in Doc‐to‐Doc text messaging, and underestimate the increase in GM ward‐to‐Doc text messaging. The reasons for paging are not known for the numeric pages. The number of pages received per resident increased after implementation, so it is possible that alphanumeric pages increased calls for certain nonurgent issues, such as co‐signing orders. Finally, we assumed that residents were attending scheduled educational rounds, but were unable to confirm attendance, so we cannot be sure that disruptions actually were reduced.
In summary, we implemented an alphanumeric paging system, and observed a sustained use of text messaging after 1 year. The implementation of alphanumeric paging was associated with a reduction in disruptive pages sent during scheduled educational rounds.
Acknowledgements
Twenty alphanumeric pagers were provided in kind for the duration of the implementation period by PageNet Canada. The authors thank the Advance Practice Nurses from the 4 GM wards (Sonia Dyal, Jackie Griffin‐White, Tracey Kitchen‐Clark, and Trish Trieu) and members of the communications department (Jonathon Tunstead, Howard Golding, Joan Moodie, and Myles Leicester) for the instrumental role they played in the implementation of the alphanumeric paging system.
- , , , , .Teams: communication in multidisciplinary care.Oncologist.2006;11:520–526.
- .14,000 preventable deaths in Australian hospitals.BMJ.1995;310:1487.
- , .Interrupted care. The effects of paging on pediatric resident activities.Am J Dis Child.1992;146:806–808.
- , , .Patterns of paging medical interns during night calls at two teaching hospitals.CMAJ.1994;151:307–311.
- , .The sounds of the hospital. Paging patterns in three teaching hospitals.N Engl J Med.1988;319:1585–1589.
- , , .How hospitalists spend their time: insights on efficiency and safety.J Hosp Med.2006;1:88–93.
- , .Communication behaviours in a hospital setting: an observational study.BMJ.1998;316:673–676.
- , .Residents' suggestions for reducing errors in teaching hospitals.N Engl J Med.2003;348:851–855.
- , , et al.Improving response to critical laboratory results with automation: results of a randomized controlled trial.J Am Med Inform Assoc.1999;6:512–522.
- , , , .Real‐time notification of laboratory data requested by users through alphanumeric pagers.J Am Med Inform Assoc.2002;9:217–222.
- , , , , .Alphanumeric paging in an academic hospital setting.Am J Surg.2006;191:561–565.
- .A primer on leading the improvement of systems.BMJ.1996;312:619–622.
- SurveyMonkey.com. The simple way to create surveys. Available at: http://www.surveymonkey.com. Accessed September 2009.
- .Diffusion of innovations.New York:Free Press;1995.
- , , , , .Teams: communication in multidisciplinary care.Oncologist.2006;11:520–526.
- .14,000 preventable deaths in Australian hospitals.BMJ.1995;310:1487.
- , .Interrupted care. The effects of paging on pediatric resident activities.Am J Dis Child.1992;146:806–808.
- , , .Patterns of paging medical interns during night calls at two teaching hospitals.CMAJ.1994;151:307–311.
- , .The sounds of the hospital. Paging patterns in three teaching hospitals.N Engl J Med.1988;319:1585–1589.
- , , .How hospitalists spend their time: insights on efficiency and safety.J Hosp Med.2006;1:88–93.
- , .Communication behaviours in a hospital setting: an observational study.BMJ.1998;316:673–676.
- , .Residents' suggestions for reducing errors in teaching hospitals.N Engl J Med.2003;348:851–855.
- , , et al.Improving response to critical laboratory results with automation: results of a randomized controlled trial.J Am Med Inform Assoc.1999;6:512–522.
- , , , .Real‐time notification of laboratory data requested by users through alphanumeric pagers.J Am Med Inform Assoc.2002;9:217–222.
- , , , , .Alphanumeric paging in an academic hospital setting.Am J Surg.2006;191:561–565.
- .A primer on leading the improvement of systems.BMJ.1996;312:619–622.
- SurveyMonkey.com. The simple way to create surveys. Available at: http://www.surveymonkey.com. Accessed September 2009.
- .Diffusion of innovations.New York:Free Press;1995.
Statin therapy: New data suggest effects on plaque volume and stability
| ||||||||||||||||
| ||||||||||||||||
Value‐Driven Health Care
It is estimated that the Medicare Part A trust fund will be exhausted by 2016 to 2019; also, the quality of care delivered in the United States is highly variable.13 Value is typically defined as the quality achieved for a given cost (ie, value = quality/cost). The focus on the 3 related concepts of value, quality, and cost of health care is likely to continue to increase. Previously, the U.S. Department of Health and Human Services (HHS) made value‐driven health care one of the Department's top priorities.4 Policymakers are in a period of transition but the publicly available plans of the President and Senate leadership indicate that the focus on value‐based initiatives will likely continue to increase as our nation strives to achieve better outcomes for our health care dollar.5, 6 Specifically, the federal government and other payers increasingly align payment incentives with value and quality, encourage public reporting on quality and Medicare payment costs, such as on the Hospital Compare website (
Since hospital care represented $648 billion in 2006, which is 37% of the total patient‐related U.S. health care expenditure, the trend to pay for value will likely have significant impact on hospitals and hospitalists.7 The Society of Hospital Medicine has a public policy committee that provides feedback to government on programs and policies related to value‐driven health care. The policies and programs need consideration and input from the broader community of hospitalists. This work outlines some of the major national initiatives and policies focused on value‐driven health care and their implications for hospitalists. Hospitalists will need to understand the policy landscape and trends, lead improvement in their individual hospitals to receive value‐based incentives, and assess the opportunities and challenges of current and potential payer programs and policies.
Policies and Initiatives: Implications for Hospitals and Hospitalists
Within the portfolio of value‐driven health care, there are at least 6 major government programs, initiatives, and policies with implications for hospitals and hospitalists: value‐based purchasing (VBP), quality and cost public reporting, Medicare demonstrations, hospital‐acquired conditions, incentives for use of effective HIT, and the physician quality reporting initiative (PQRI) (Table 1).
| Initiative or Policy | Description | Specific Examples | Potential Implications |
|---|---|---|---|
| Value‐based purchasing | At least a portion of hospital payment related to value instead of the traditional fee‐for‐service model | Performance score is based on domains such as process measures (eg, beta‐blocker at discharge for acute myocardial), outcome measures (eg, 30‐day AMI mortality), and satisfaction measures (eg, Consumer Assessment of Healthcare Providers and Hospital Survey, aka HCAHPS) | Hospitalists will influence hospital performance on Total Performance Score and could lead quality improvement efforts to improve score |
| Payment based on hospital Total Performance Score | |||
| Public reporting of quality and cost | Websites such as CMS HospitalCompare increasingly report on select quality and cost metrics | HospitalCompare reports process measures (eg, percent of heart failure patients given discharge instructions), outcome measures (eg, 30‐day risk‐adjusted mortality for AMI), survey of patients' hospital experience, and Medicare payment and volume for certain conditions | Many of these measures are directly related to care provided by hospitalists |
| Hospitalists could lead quality improvement initiatives focused on these measures | |||
| Medicare demonstrations | CMS has demonstration projects to test concepts, such as value‐based purchasing, incentive payments, and care management, aimed at improving the value of care delivered | Premier Hospital Quality Incentive Demonstration: Differentiates payment to hospitals based on performance on 30 metrics | Hospitals with their associated hospitalists can apply to participate in these and other demonstrations |
| Acute Care Episode (ACE) Demonstration: Provides bundled payments for select orthopedic and cardiovascular inpatient procedures | |||
| Medicare Hospital Gainsharing Demonstration: Hospitals can provide gainsharing payments to physicians based on savings from improving quality and efficiency | Successful demonstrations can be expanded or components incorporated into payment policy | ||
| Hospital‐acquired conditions | CMS rule that the presence of a select group of reasonably preventable conditions as the only complicating condition will not cause a higher‐paying diagnosis‐related group (DRG) to be assigned to the case | First 10 implemented: | Hospitalists can lead or participate in safety initiatives to decrease or eliminate these complications |
| Foreign object retained after surgery; | |||
| Air embolism; | |||
| Blood incompatibility; | |||
| Stage III and IV pressure ulcers; | |||
| Falls and trauma; | |||
| Manifestations of poor glycemic control; | |||
| Catheter‐associated urinary tract infections; | |||
| Vascular catheter‐associated infection; | |||
| Surgical site infection following specific surgeries; | |||
| Deep vein thrombosis and pulmonary embolus | |||
| Incentives for use of effective health information technology | Incentives for HIT use, often focused on certified interoperable systems and/or quality reporting, are provided by federal and private payers | The American Recovery and Reinvestment Act included over $17 billion of HIT incentives | Front line providers, including hospitalists, need to help guide implementation of HIT to be successful |
| Incentive money was directed at hospitals (hospital‐based physicians were excluded) and ambulatory physicians are eligible for direct incentives | Systems that include physician order entry, clinical decision support, and quality measurement capture and reporting can help hospitalists deliver higher quality care | ||
| Physician Quality Reporting Initiative (PQRI) | Quality measures linked to 2% incentive payment to physicians and other practitioners for reporting quality measures via claims or registry | Examples of measures hospitalists can report on include: | Hospitalists can drive performance on these measures, lead reporting efforts, and share in the financial rewards |
| Deep vein thrombosis prophylaxis for ischemic stroke or intracranial hemorrhage; | |||
| Medication reconciliation at discharge; | |||
| Advance care plan documented; | |||
| Oral antiplatelet therapy for patients discharged with stroke diagnosis |
Value‐Based Purchasing
The Deficit Reduction Act Section 5001(b) authorized the Centers for Medicare and Medicaid Services (CMS) to develop a Medicare hospital VBP plan. The VBP plan is currently in the Presidents FY10 budget and the senate Committee's specification for health reform. VBP involves at least a portion of the payment being related to value instead of the traditional fee‐for‐service (FFS) model. CMS has consulted with external stakeholders on the measures, data infrastructure and validation, and incentive structure for the proposed program. Hospitals would submit data for all VBP measures that apply and performance scores would be given based on both attainment and improvement. The higher of the 2 scores (ie, attainment or improvement) would represent the hospital's performance in a given domain and the weighted domain scores would determine the hospital's total performance score. This total performance score would then be translated into an incentive payment for the hospital. Measure domains would include process measures (eg, beta‐blocker at discharge for acute myocardial infarction [AMI]), outcome measures (eg, 30‐day AMI mortality), and satisfaction measures (eg, Consumer Assessment of Healthcare Providers and Systems Hospital survey [HCAHPS]). Hospitalists are in a unique position to impact and improve performance in all of the above domains for hospitals. This has the potential to increase the value of high‐performing hospitalist groups to their respective hospitals. Most importantly, this program aligns incentives with rewarding the provision of high‐quality care as defined by these measures. Over time, CMS may consider expanding the measures to other domains such as efficiency, more patient‐centered outcomes, and care coordination. In terms of efficiency measurement, the Medicare Improvements for Patients and Providers Act (MIPPA) passed in 2008 called for CMS to provide confidential reports to physicians or groups of physicians on their relative resource use. This legislation also called for HHS to develop a plan for transitioning to VBP for Medicare professional services and a report to Congress on this plan.9 This lays the foundation for transforming Medicare to focus more on quality, resource use, and value and less on FFS.
Public Reporting of Quality and Cost
CMS is beginning to empower consumers with information on quality and Medicare payment costs so they can make educated decisions on where and how they seek care. The CMS website focused on hospitals is HospitalCompare (
Medicare Demonstrations
Several Medicare demonstration projects already implemented or in the planning stages are particularly relevant to hospitals and hospitalist practice. These demonstrations test concepts, such as VBP, incentive payments, and care management, aimed at improving the value of care delivered. If demonstrations are successful, they have potential for incorporation into federal policy. The Premier Hospital Quality Incentive Demonstration is an incentive program that differentiates payment to hospitals based on performance on 30 quality measures. Participation is voluntary. The top 20% of hospitals receive incentive payments.11 The success of this demonstration led to its current second phase. The Acute Care Episode (ACE) Demonstration will provide bundled payments (including Part A and B services) for ACEs within Medicare FFS. The demonstration includes gainsharing by allowing sites to reward individual clinicians, teams of clinicians, or other hospital staff who show measurable clinical quality improvement. The focus is on select orthopedic and cardiovascular inpatient procedures (eg, hip/knee replacement surgery and coronary artery bypass graft surgery).12 The demonstration also has potential to increase volume to participant physician‐hospital organizations through financial incentives to beneficiaries via payments to offset their Medicare cost‐sharing obligations. If this demonstration is successful and the concept of bundled payment is expanded to other conditions and additional geographies, this could have significant impact on hospitalists. Specifically, programs for care coordination and reducing readmissions and complications after discharge would be directly incentivized. The demonstration focuses on Texas, Oklahoma, Colorado, and New Mexico. The Medicare Hospital Gainsharing Demonstration program to test and evaluate arrangements between hospitals and physicians is designed improve the quality and efficiency of care provided to beneficiaries. The demonstration allows hospitals to provide gainsharing payments to physicians that represent solely a share of the savings incurred as a result of collaborative efforts to improve overall quality and efficiency. The demonstration was launched in 2007.13 Finally, the upcoming Medicare Medical Home Demonstration has the potential for direct or indirect hospitalist participation as facilitators in Tier 2 medical homes that take into account care coordination across inpatient and outpatient settings.14 These demonstrations represent attempts by the federal government to align incentives with high‐quality, high‐value delivery of care.
Hospital‐Acquired Conditions
Hospital‐acquired conditions (HACs) have significant cost and quality implications for U.S. healthcare, such as the estimated 99,000 deaths associated with hospital‐acquired infections annually.15 Therefore, CMS received statutory authority to not pay additional charges for reasonably preventable HACs. Beginning October 1, 2008, CMS implemented a rule that the presence of selected reasonably preventable conditions as the only complicating condition would not cause a higher‐paying DRG to be assigned to the case; therefore, the case would be paid as though the secondary diagnosis were not present. CMS also required the reporting of a new data element to delineate HACs from conditions present on admission. Hospitals can indicate to CMS if a condition was present on admission as a secondary diagnosis, allowing reimbursement for care provided to treat any condition present on admission. The first 10 HACs to be implemented were: foreign object retained after surgery, air embolism, blood incompatibility, stage III and IV pressure ulcers, falls and trauma, manifestations of poor glycemic control, catheter‐associated urinary tract infections, vascular catheterassociated infection, surgical site infection following specific surgeries, and deep vein thrombosis and pulmonary embolus.16 Since some complications are not absolutely preventable and evidence‐based guidelines for the prevention of some complications are lacking, this has generated some resistance from the provider community.17 The HAC payment policy is a step toward aligning incentives with quality performance, but any further HACs will need to be evaluated for their level of preventability and potential for unintended consequences.
Incentives for Use of Effective HIT
The use of HIT can be incentivized in 3 main ways, all of which are likely to increase over time. First, incentives can be implemented to reward reporting quality metrics via electronic health records or registries. Second, incentives based on quality performance may indirectly encourage the adoption of HIT because an electronic medical record, especially with computerized provider order entry and decision support, may enable higher performance on quality metrics. Finally, CMS has provided direct incentives for information technology adoption, such as certified electronic health records.18 The American Recovery and Reinvestment Act of 2009 created over $17 billion of potential incentive payments for HIT use by physicians and hospitals.19 Hospitals are eligible for significant incentives reaching estimates over $6 million per year, phasing out by 2015, so Congress excluded hospital‐based physicians from direct payments. Ambulatory physicians are eligible for up to $18,000 per year, phasing out by 2015, with subsequent payment reductions for nonuse. Since hospitalists often function at the nexus of clinical care, quality improvement, and technology use, they have the opportunity to lead or facilitate effective implementation of information technology in their hospitals. These efforts may be rewarded by hospitals.
PQRI
PQRI was authorized in 2006 and included a 1.5% incentive payment for satisfactorily reporting quality data. The incentive payment will increase to 2% in 2009. There are 153 PQRI measures in 2009 and a significant number of the measures focus on hospital‐based care. Examples of measures hospitalists can help report include: deep vein thrombosis prophylaxis for ischemic stroke or intracranial hemorrhage, medication reconciliation at discharge, advance care plan documentation, oral antiplatelet therapy for patients discharged with stroke diagnosis, and anticoagulant therapy prescribed for atrial fibrillation in stroke patients at discharge. PQRI measures can be reported through claims‐based or registry‐based reporting. Reporting can be done on individual measures or for measure groups associated with specific conditions.20 Hospitalists have the potential to drive performance on these measures, lead reporting efforts, and share in the financial rewards.
Future Considerations
The political leadership at the federal and state level is beginning a new transition; however, the focus on quality and value for our health care dollar will likely continue to increase.5, 6 The U.S. health care system has untenable cost estimates, significant quality gaps, and a fractured payment system that fails to reward effective care coordination.2, 21, 22 This increased focus on quality and value should be viewed as an opportunity for hospitalists and hospitals. Hospitalist groups that can achieve high‐quality performance will be increasingly valued, and hospitals should further recognize the critical role hospitalists play in achieving high performance and the associated financial rewards. Hospitalists often lead quality improvement and safety programs in hospitals, and these programs are likely to be seen as progressively more important as payment is linked to performance. The Society of Hospital Medicine engages with policymakers and this role is increasingly significant as more policy and payment decisions impact hospitalists. The Society has focused on collaborative work with payers, policymakers, and other providers to find joint shared solutions. Hospitalists can serve as a link between providers and a focal point of care coordination, especially for the hospitalized patient. Finally, as our system and its incentives continue to progress toward alignment with value‐based high quality care, hospitalists should be leading the change and be an essential part of the solution to transform our health care system to provide high‐quality, efficient care to all Americans.
Acknowledgements
Dr. Tom Valuck is recognized for his thoughtful comments and edits in preparation, submission, and revision of this manuscript.
- Medicare Board of Trustees. A Summary of the 2008 Report. Available at: http://www.ssa.gov/OACT/TRSUM/trsummary.html. Accessed April 2009.
- , , , et al.The quality of health care delivered to adults in the United States.N Engl J Med.2003;348(26):2635–2645.
- Economy Likely to Move up Medicare's Insolvency. Available at: http://abcnews.go.com/Politics/Health/wireStory?id=6369658. Accessed April 2009.
- Value‐Driven Health Care. Available at: http://www.hhs.gov/valuedriven. Accessed April 2009.
- Obama‐Biden Full Health Care Plan. Available at: http://www.barackobama.com/issues/healthcare. Accessed April 2009.
- Senate Chairman Max Baucus Call to Action Health Reform 2009. Available at: http://finance.senate.gov/healthreform2009/finalwhitepaper.pdf. Accessed April 2009.
- , , , .National health spending in 2006: a year of change for prescription drugs.Health Aff (Millwood).2008;27(1):14–29.
- Medicare Hospital Value‐Based Purchasing Plan. October 31,2008. Available at: http://www.cms.hhs.gov/AcuteInpatientPPS/downloads/hospital_VBP_plan_issues_paper.pdf. Accessed April 2009.
- Medicare Improvements for Patients and Providers Act of 2008. Available at: http://www.asm.org/ASM/files/ccLibraryFiles/Filename/000000004120/HR6331.pdf. Accessed April 2009.
- HospitalCompare. Available at: www.hospitalcompare.hhs.gov. Accessed April 2009.
- Premier Hospital Quality Incentive Demonstration. Available at: http://www.cms.hhs.gov/HospitalQualityInits/35_hospitalpremier.asp. Accessed April 2009.
- Acute Care Episode Demonstration. Available at: http://www.cms.hhs.gov/DemoProjectsEvalRpts/MD/itemdetail.asp?filterType=none122(2):160–166.
- Hospital Acquired Conditions. Available at: http://www.cms.hhs.gov/HospitalAcqCond/06_Hospital‐Acquired_Conditions.asp. Accessed April 2009.
- , , .The wisdom and justice of not paying for “preventable complications”.JAMA.2008;299(18):2197–2199.
- E‐prescribing incentive program. Available at: http://www.cms.hhs.gov/ERXincentive. Accessed April 2009.
- American Recovery and Reinvestment Act. Available at: http://frwebgate.access.gpo.gov/cgi‐bin/getdoc.cgi?dbname=111_cong_bills299(19):2319–2321.
It is estimated that the Medicare Part A trust fund will be exhausted by 2016 to 2019; also, the quality of care delivered in the United States is highly variable.13 Value is typically defined as the quality achieved for a given cost (ie, value = quality/cost). The focus on the 3 related concepts of value, quality, and cost of health care is likely to continue to increase. Previously, the U.S. Department of Health and Human Services (HHS) made value‐driven health care one of the Department's top priorities.4 Policymakers are in a period of transition but the publicly available plans of the President and Senate leadership indicate that the focus on value‐based initiatives will likely continue to increase as our nation strives to achieve better outcomes for our health care dollar.5, 6 Specifically, the federal government and other payers increasingly align payment incentives with value and quality, encourage public reporting on quality and Medicare payment costs, such as on the Hospital Compare website (
Since hospital care represented $648 billion in 2006, which is 37% of the total patient‐related U.S. health care expenditure, the trend to pay for value will likely have significant impact on hospitals and hospitalists.7 The Society of Hospital Medicine has a public policy committee that provides feedback to government on programs and policies related to value‐driven health care. The policies and programs need consideration and input from the broader community of hospitalists. This work outlines some of the major national initiatives and policies focused on value‐driven health care and their implications for hospitalists. Hospitalists will need to understand the policy landscape and trends, lead improvement in their individual hospitals to receive value‐based incentives, and assess the opportunities and challenges of current and potential payer programs and policies.
Policies and Initiatives: Implications for Hospitals and Hospitalists
Within the portfolio of value‐driven health care, there are at least 6 major government programs, initiatives, and policies with implications for hospitals and hospitalists: value‐based purchasing (VBP), quality and cost public reporting, Medicare demonstrations, hospital‐acquired conditions, incentives for use of effective HIT, and the physician quality reporting initiative (PQRI) (Table 1).
| Initiative or Policy | Description | Specific Examples | Potential Implications |
|---|---|---|---|
| Value‐based purchasing | At least a portion of hospital payment related to value instead of the traditional fee‐for‐service model | Performance score is based on domains such as process measures (eg, beta‐blocker at discharge for acute myocardial), outcome measures (eg, 30‐day AMI mortality), and satisfaction measures (eg, Consumer Assessment of Healthcare Providers and Hospital Survey, aka HCAHPS) | Hospitalists will influence hospital performance on Total Performance Score and could lead quality improvement efforts to improve score |
| Payment based on hospital Total Performance Score | |||
| Public reporting of quality and cost | Websites such as CMS HospitalCompare increasingly report on select quality and cost metrics | HospitalCompare reports process measures (eg, percent of heart failure patients given discharge instructions), outcome measures (eg, 30‐day risk‐adjusted mortality for AMI), survey of patients' hospital experience, and Medicare payment and volume for certain conditions | Many of these measures are directly related to care provided by hospitalists |
| Hospitalists could lead quality improvement initiatives focused on these measures | |||
| Medicare demonstrations | CMS has demonstration projects to test concepts, such as value‐based purchasing, incentive payments, and care management, aimed at improving the value of care delivered | Premier Hospital Quality Incentive Demonstration: Differentiates payment to hospitals based on performance on 30 metrics | Hospitals with their associated hospitalists can apply to participate in these and other demonstrations |
| Acute Care Episode (ACE) Demonstration: Provides bundled payments for select orthopedic and cardiovascular inpatient procedures | |||
| Medicare Hospital Gainsharing Demonstration: Hospitals can provide gainsharing payments to physicians based on savings from improving quality and efficiency | Successful demonstrations can be expanded or components incorporated into payment policy | ||
| Hospital‐acquired conditions | CMS rule that the presence of a select group of reasonably preventable conditions as the only complicating condition will not cause a higher‐paying diagnosis‐related group (DRG) to be assigned to the case | First 10 implemented: | Hospitalists can lead or participate in safety initiatives to decrease or eliminate these complications |
| Foreign object retained after surgery; | |||
| Air embolism; | |||
| Blood incompatibility; | |||
| Stage III and IV pressure ulcers; | |||
| Falls and trauma; | |||
| Manifestations of poor glycemic control; | |||
| Catheter‐associated urinary tract infections; | |||
| Vascular catheter‐associated infection; | |||
| Surgical site infection following specific surgeries; | |||
| Deep vein thrombosis and pulmonary embolus | |||
| Incentives for use of effective health information technology | Incentives for HIT use, often focused on certified interoperable systems and/or quality reporting, are provided by federal and private payers | The American Recovery and Reinvestment Act included over $17 billion of HIT incentives | Front line providers, including hospitalists, need to help guide implementation of HIT to be successful |
| Incentive money was directed at hospitals (hospital‐based physicians were excluded) and ambulatory physicians are eligible for direct incentives | Systems that include physician order entry, clinical decision support, and quality measurement capture and reporting can help hospitalists deliver higher quality care | ||
| Physician Quality Reporting Initiative (PQRI) | Quality measures linked to 2% incentive payment to physicians and other practitioners for reporting quality measures via claims or registry | Examples of measures hospitalists can report on include: | Hospitalists can drive performance on these measures, lead reporting efforts, and share in the financial rewards |
| Deep vein thrombosis prophylaxis for ischemic stroke or intracranial hemorrhage; | |||
| Medication reconciliation at discharge; | |||
| Advance care plan documented; | |||
| Oral antiplatelet therapy for patients discharged with stroke diagnosis |
Value‐Based Purchasing
The Deficit Reduction Act Section 5001(b) authorized the Centers for Medicare and Medicaid Services (CMS) to develop a Medicare hospital VBP plan. The VBP plan is currently in the Presidents FY10 budget and the senate Committee's specification for health reform. VBP involves at least a portion of the payment being related to value instead of the traditional fee‐for‐service (FFS) model. CMS has consulted with external stakeholders on the measures, data infrastructure and validation, and incentive structure for the proposed program. Hospitals would submit data for all VBP measures that apply and performance scores would be given based on both attainment and improvement. The higher of the 2 scores (ie, attainment or improvement) would represent the hospital's performance in a given domain and the weighted domain scores would determine the hospital's total performance score. This total performance score would then be translated into an incentive payment for the hospital. Measure domains would include process measures (eg, beta‐blocker at discharge for acute myocardial infarction [AMI]), outcome measures (eg, 30‐day AMI mortality), and satisfaction measures (eg, Consumer Assessment of Healthcare Providers and Systems Hospital survey [HCAHPS]). Hospitalists are in a unique position to impact and improve performance in all of the above domains for hospitals. This has the potential to increase the value of high‐performing hospitalist groups to their respective hospitals. Most importantly, this program aligns incentives with rewarding the provision of high‐quality care as defined by these measures. Over time, CMS may consider expanding the measures to other domains such as efficiency, more patient‐centered outcomes, and care coordination. In terms of efficiency measurement, the Medicare Improvements for Patients and Providers Act (MIPPA) passed in 2008 called for CMS to provide confidential reports to physicians or groups of physicians on their relative resource use. This legislation also called for HHS to develop a plan for transitioning to VBP for Medicare professional services and a report to Congress on this plan.9 This lays the foundation for transforming Medicare to focus more on quality, resource use, and value and less on FFS.
Public Reporting of Quality and Cost
CMS is beginning to empower consumers with information on quality and Medicare payment costs so they can make educated decisions on where and how they seek care. The CMS website focused on hospitals is HospitalCompare (
Medicare Demonstrations
Several Medicare demonstration projects already implemented or in the planning stages are particularly relevant to hospitals and hospitalist practice. These demonstrations test concepts, such as VBP, incentive payments, and care management, aimed at improving the value of care delivered. If demonstrations are successful, they have potential for incorporation into federal policy. The Premier Hospital Quality Incentive Demonstration is an incentive program that differentiates payment to hospitals based on performance on 30 quality measures. Participation is voluntary. The top 20% of hospitals receive incentive payments.11 The success of this demonstration led to its current second phase. The Acute Care Episode (ACE) Demonstration will provide bundled payments (including Part A and B services) for ACEs within Medicare FFS. The demonstration includes gainsharing by allowing sites to reward individual clinicians, teams of clinicians, or other hospital staff who show measurable clinical quality improvement. The focus is on select orthopedic and cardiovascular inpatient procedures (eg, hip/knee replacement surgery and coronary artery bypass graft surgery).12 The demonstration also has potential to increase volume to participant physician‐hospital organizations through financial incentives to beneficiaries via payments to offset their Medicare cost‐sharing obligations. If this demonstration is successful and the concept of bundled payment is expanded to other conditions and additional geographies, this could have significant impact on hospitalists. Specifically, programs for care coordination and reducing readmissions and complications after discharge would be directly incentivized. The demonstration focuses on Texas, Oklahoma, Colorado, and New Mexico. The Medicare Hospital Gainsharing Demonstration program to test and evaluate arrangements between hospitals and physicians is designed improve the quality and efficiency of care provided to beneficiaries. The demonstration allows hospitals to provide gainsharing payments to physicians that represent solely a share of the savings incurred as a result of collaborative efforts to improve overall quality and efficiency. The demonstration was launched in 2007.13 Finally, the upcoming Medicare Medical Home Demonstration has the potential for direct or indirect hospitalist participation as facilitators in Tier 2 medical homes that take into account care coordination across inpatient and outpatient settings.14 These demonstrations represent attempts by the federal government to align incentives with high‐quality, high‐value delivery of care.
Hospital‐Acquired Conditions
Hospital‐acquired conditions (HACs) have significant cost and quality implications for U.S. healthcare, such as the estimated 99,000 deaths associated with hospital‐acquired infections annually.15 Therefore, CMS received statutory authority to not pay additional charges for reasonably preventable HACs. Beginning October 1, 2008, CMS implemented a rule that the presence of selected reasonably preventable conditions as the only complicating condition would not cause a higher‐paying DRG to be assigned to the case; therefore, the case would be paid as though the secondary diagnosis were not present. CMS also required the reporting of a new data element to delineate HACs from conditions present on admission. Hospitals can indicate to CMS if a condition was present on admission as a secondary diagnosis, allowing reimbursement for care provided to treat any condition present on admission. The first 10 HACs to be implemented were: foreign object retained after surgery, air embolism, blood incompatibility, stage III and IV pressure ulcers, falls and trauma, manifestations of poor glycemic control, catheter‐associated urinary tract infections, vascular catheterassociated infection, surgical site infection following specific surgeries, and deep vein thrombosis and pulmonary embolus.16 Since some complications are not absolutely preventable and evidence‐based guidelines for the prevention of some complications are lacking, this has generated some resistance from the provider community.17 The HAC payment policy is a step toward aligning incentives with quality performance, but any further HACs will need to be evaluated for their level of preventability and potential for unintended consequences.
Incentives for Use of Effective HIT
The use of HIT can be incentivized in 3 main ways, all of which are likely to increase over time. First, incentives can be implemented to reward reporting quality metrics via electronic health records or registries. Second, incentives based on quality performance may indirectly encourage the adoption of HIT because an electronic medical record, especially with computerized provider order entry and decision support, may enable higher performance on quality metrics. Finally, CMS has provided direct incentives for information technology adoption, such as certified electronic health records.18 The American Recovery and Reinvestment Act of 2009 created over $17 billion of potential incentive payments for HIT use by physicians and hospitals.19 Hospitals are eligible for significant incentives reaching estimates over $6 million per year, phasing out by 2015, so Congress excluded hospital‐based physicians from direct payments. Ambulatory physicians are eligible for up to $18,000 per year, phasing out by 2015, with subsequent payment reductions for nonuse. Since hospitalists often function at the nexus of clinical care, quality improvement, and technology use, they have the opportunity to lead or facilitate effective implementation of information technology in their hospitals. These efforts may be rewarded by hospitals.
PQRI
PQRI was authorized in 2006 and included a 1.5% incentive payment for satisfactorily reporting quality data. The incentive payment will increase to 2% in 2009. There are 153 PQRI measures in 2009 and a significant number of the measures focus on hospital‐based care. Examples of measures hospitalists can help report include: deep vein thrombosis prophylaxis for ischemic stroke or intracranial hemorrhage, medication reconciliation at discharge, advance care plan documentation, oral antiplatelet therapy for patients discharged with stroke diagnosis, and anticoagulant therapy prescribed for atrial fibrillation in stroke patients at discharge. PQRI measures can be reported through claims‐based or registry‐based reporting. Reporting can be done on individual measures or for measure groups associated with specific conditions.20 Hospitalists have the potential to drive performance on these measures, lead reporting efforts, and share in the financial rewards.
Future Considerations
The political leadership at the federal and state level is beginning a new transition; however, the focus on quality and value for our health care dollar will likely continue to increase.5, 6 The U.S. health care system has untenable cost estimates, significant quality gaps, and a fractured payment system that fails to reward effective care coordination.2, 21, 22 This increased focus on quality and value should be viewed as an opportunity for hospitalists and hospitals. Hospitalist groups that can achieve high‐quality performance will be increasingly valued, and hospitals should further recognize the critical role hospitalists play in achieving high performance and the associated financial rewards. Hospitalists often lead quality improvement and safety programs in hospitals, and these programs are likely to be seen as progressively more important as payment is linked to performance. The Society of Hospital Medicine engages with policymakers and this role is increasingly significant as more policy and payment decisions impact hospitalists. The Society has focused on collaborative work with payers, policymakers, and other providers to find joint shared solutions. Hospitalists can serve as a link between providers and a focal point of care coordination, especially for the hospitalized patient. Finally, as our system and its incentives continue to progress toward alignment with value‐based high quality care, hospitalists should be leading the change and be an essential part of the solution to transform our health care system to provide high‐quality, efficient care to all Americans.
Acknowledgements
Dr. Tom Valuck is recognized for his thoughtful comments and edits in preparation, submission, and revision of this manuscript.
It is estimated that the Medicare Part A trust fund will be exhausted by 2016 to 2019; also, the quality of care delivered in the United States is highly variable.13 Value is typically defined as the quality achieved for a given cost (ie, value = quality/cost). The focus on the 3 related concepts of value, quality, and cost of health care is likely to continue to increase. Previously, the U.S. Department of Health and Human Services (HHS) made value‐driven health care one of the Department's top priorities.4 Policymakers are in a period of transition but the publicly available plans of the President and Senate leadership indicate that the focus on value‐based initiatives will likely continue to increase as our nation strives to achieve better outcomes for our health care dollar.5, 6 Specifically, the federal government and other payers increasingly align payment incentives with value and quality, encourage public reporting on quality and Medicare payment costs, such as on the Hospital Compare website (
Since hospital care represented $648 billion in 2006, which is 37% of the total patient‐related U.S. health care expenditure, the trend to pay for value will likely have significant impact on hospitals and hospitalists.7 The Society of Hospital Medicine has a public policy committee that provides feedback to government on programs and policies related to value‐driven health care. The policies and programs need consideration and input from the broader community of hospitalists. This work outlines some of the major national initiatives and policies focused on value‐driven health care and their implications for hospitalists. Hospitalists will need to understand the policy landscape and trends, lead improvement in their individual hospitals to receive value‐based incentives, and assess the opportunities and challenges of current and potential payer programs and policies.
Policies and Initiatives: Implications for Hospitals and Hospitalists
Within the portfolio of value‐driven health care, there are at least 6 major government programs, initiatives, and policies with implications for hospitals and hospitalists: value‐based purchasing (VBP), quality and cost public reporting, Medicare demonstrations, hospital‐acquired conditions, incentives for use of effective HIT, and the physician quality reporting initiative (PQRI) (Table 1).
| Initiative or Policy | Description | Specific Examples | Potential Implications |
|---|---|---|---|
| Value‐based purchasing | At least a portion of hospital payment related to value instead of the traditional fee‐for‐service model | Performance score is based on domains such as process measures (eg, beta‐blocker at discharge for acute myocardial), outcome measures (eg, 30‐day AMI mortality), and satisfaction measures (eg, Consumer Assessment of Healthcare Providers and Hospital Survey, aka HCAHPS) | Hospitalists will influence hospital performance on Total Performance Score and could lead quality improvement efforts to improve score |
| Payment based on hospital Total Performance Score | |||
| Public reporting of quality and cost | Websites such as CMS HospitalCompare increasingly report on select quality and cost metrics | HospitalCompare reports process measures (eg, percent of heart failure patients given discharge instructions), outcome measures (eg, 30‐day risk‐adjusted mortality for AMI), survey of patients' hospital experience, and Medicare payment and volume for certain conditions | Many of these measures are directly related to care provided by hospitalists |
| Hospitalists could lead quality improvement initiatives focused on these measures | |||
| Medicare demonstrations | CMS has demonstration projects to test concepts, such as value‐based purchasing, incentive payments, and care management, aimed at improving the value of care delivered | Premier Hospital Quality Incentive Demonstration: Differentiates payment to hospitals based on performance on 30 metrics | Hospitals with their associated hospitalists can apply to participate in these and other demonstrations |
| Acute Care Episode (ACE) Demonstration: Provides bundled payments for select orthopedic and cardiovascular inpatient procedures | |||
| Medicare Hospital Gainsharing Demonstration: Hospitals can provide gainsharing payments to physicians based on savings from improving quality and efficiency | Successful demonstrations can be expanded or components incorporated into payment policy | ||
| Hospital‐acquired conditions | CMS rule that the presence of a select group of reasonably preventable conditions as the only complicating condition will not cause a higher‐paying diagnosis‐related group (DRG) to be assigned to the case | First 10 implemented: | Hospitalists can lead or participate in safety initiatives to decrease or eliminate these complications |
| Foreign object retained after surgery; | |||
| Air embolism; | |||
| Blood incompatibility; | |||
| Stage III and IV pressure ulcers; | |||
| Falls and trauma; | |||
| Manifestations of poor glycemic control; | |||
| Catheter‐associated urinary tract infections; | |||
| Vascular catheter‐associated infection; | |||
| Surgical site infection following specific surgeries; | |||
| Deep vein thrombosis and pulmonary embolus | |||
| Incentives for use of effective health information technology | Incentives for HIT use, often focused on certified interoperable systems and/or quality reporting, are provided by federal and private payers | The American Recovery and Reinvestment Act included over $17 billion of HIT incentives | Front line providers, including hospitalists, need to help guide implementation of HIT to be successful |
| Incentive money was directed at hospitals (hospital‐based physicians were excluded) and ambulatory physicians are eligible for direct incentives | Systems that include physician order entry, clinical decision support, and quality measurement capture and reporting can help hospitalists deliver higher quality care | ||
| Physician Quality Reporting Initiative (PQRI) | Quality measures linked to 2% incentive payment to physicians and other practitioners for reporting quality measures via claims or registry | Examples of measures hospitalists can report on include: | Hospitalists can drive performance on these measures, lead reporting efforts, and share in the financial rewards |
| Deep vein thrombosis prophylaxis for ischemic stroke or intracranial hemorrhage; | |||
| Medication reconciliation at discharge; | |||
| Advance care plan documented; | |||
| Oral antiplatelet therapy for patients discharged with stroke diagnosis |
Value‐Based Purchasing
The Deficit Reduction Act Section 5001(b) authorized the Centers for Medicare and Medicaid Services (CMS) to develop a Medicare hospital VBP plan. The VBP plan is currently in the Presidents FY10 budget and the senate Committee's specification for health reform. VBP involves at least a portion of the payment being related to value instead of the traditional fee‐for‐service (FFS) model. CMS has consulted with external stakeholders on the measures, data infrastructure and validation, and incentive structure for the proposed program. Hospitals would submit data for all VBP measures that apply and performance scores would be given based on both attainment and improvement. The higher of the 2 scores (ie, attainment or improvement) would represent the hospital's performance in a given domain and the weighted domain scores would determine the hospital's total performance score. This total performance score would then be translated into an incentive payment for the hospital. Measure domains would include process measures (eg, beta‐blocker at discharge for acute myocardial infarction [AMI]), outcome measures (eg, 30‐day AMI mortality), and satisfaction measures (eg, Consumer Assessment of Healthcare Providers and Systems Hospital survey [HCAHPS]). Hospitalists are in a unique position to impact and improve performance in all of the above domains for hospitals. This has the potential to increase the value of high‐performing hospitalist groups to their respective hospitals. Most importantly, this program aligns incentives with rewarding the provision of high‐quality care as defined by these measures. Over time, CMS may consider expanding the measures to other domains such as efficiency, more patient‐centered outcomes, and care coordination. In terms of efficiency measurement, the Medicare Improvements for Patients and Providers Act (MIPPA) passed in 2008 called for CMS to provide confidential reports to physicians or groups of physicians on their relative resource use. This legislation also called for HHS to develop a plan for transitioning to VBP for Medicare professional services and a report to Congress on this plan.9 This lays the foundation for transforming Medicare to focus more on quality, resource use, and value and less on FFS.
Public Reporting of Quality and Cost
CMS is beginning to empower consumers with information on quality and Medicare payment costs so they can make educated decisions on where and how they seek care. The CMS website focused on hospitals is HospitalCompare (
Medicare Demonstrations
Several Medicare demonstration projects already implemented or in the planning stages are particularly relevant to hospitals and hospitalist practice. These demonstrations test concepts, such as VBP, incentive payments, and care management, aimed at improving the value of care delivered. If demonstrations are successful, they have potential for incorporation into federal policy. The Premier Hospital Quality Incentive Demonstration is an incentive program that differentiates payment to hospitals based on performance on 30 quality measures. Participation is voluntary. The top 20% of hospitals receive incentive payments.11 The success of this demonstration led to its current second phase. The Acute Care Episode (ACE) Demonstration will provide bundled payments (including Part A and B services) for ACEs within Medicare FFS. The demonstration includes gainsharing by allowing sites to reward individual clinicians, teams of clinicians, or other hospital staff who show measurable clinical quality improvement. The focus is on select orthopedic and cardiovascular inpatient procedures (eg, hip/knee replacement surgery and coronary artery bypass graft surgery).12 The demonstration also has potential to increase volume to participant physician‐hospital organizations through financial incentives to beneficiaries via payments to offset their Medicare cost‐sharing obligations. If this demonstration is successful and the concept of bundled payment is expanded to other conditions and additional geographies, this could have significant impact on hospitalists. Specifically, programs for care coordination and reducing readmissions and complications after discharge would be directly incentivized. The demonstration focuses on Texas, Oklahoma, Colorado, and New Mexico. The Medicare Hospital Gainsharing Demonstration program to test and evaluate arrangements between hospitals and physicians is designed improve the quality and efficiency of care provided to beneficiaries. The demonstration allows hospitals to provide gainsharing payments to physicians that represent solely a share of the savings incurred as a result of collaborative efforts to improve overall quality and efficiency. The demonstration was launched in 2007.13 Finally, the upcoming Medicare Medical Home Demonstration has the potential for direct or indirect hospitalist participation as facilitators in Tier 2 medical homes that take into account care coordination across inpatient and outpatient settings.14 These demonstrations represent attempts by the federal government to align incentives with high‐quality, high‐value delivery of care.
Hospital‐Acquired Conditions
Hospital‐acquired conditions (HACs) have significant cost and quality implications for U.S. healthcare, such as the estimated 99,000 deaths associated with hospital‐acquired infections annually.15 Therefore, CMS received statutory authority to not pay additional charges for reasonably preventable HACs. Beginning October 1, 2008, CMS implemented a rule that the presence of selected reasonably preventable conditions as the only complicating condition would not cause a higher‐paying DRG to be assigned to the case; therefore, the case would be paid as though the secondary diagnosis were not present. CMS also required the reporting of a new data element to delineate HACs from conditions present on admission. Hospitals can indicate to CMS if a condition was present on admission as a secondary diagnosis, allowing reimbursement for care provided to treat any condition present on admission. The first 10 HACs to be implemented were: foreign object retained after surgery, air embolism, blood incompatibility, stage III and IV pressure ulcers, falls and trauma, manifestations of poor glycemic control, catheter‐associated urinary tract infections, vascular catheterassociated infection, surgical site infection following specific surgeries, and deep vein thrombosis and pulmonary embolus.16 Since some complications are not absolutely preventable and evidence‐based guidelines for the prevention of some complications are lacking, this has generated some resistance from the provider community.17 The HAC payment policy is a step toward aligning incentives with quality performance, but any further HACs will need to be evaluated for their level of preventability and potential for unintended consequences.
Incentives for Use of Effective HIT
The use of HIT can be incentivized in 3 main ways, all of which are likely to increase over time. First, incentives can be implemented to reward reporting quality metrics via electronic health records or registries. Second, incentives based on quality performance may indirectly encourage the adoption of HIT because an electronic medical record, especially with computerized provider order entry and decision support, may enable higher performance on quality metrics. Finally, CMS has provided direct incentives for information technology adoption, such as certified electronic health records.18 The American Recovery and Reinvestment Act of 2009 created over $17 billion of potential incentive payments for HIT use by physicians and hospitals.19 Hospitals are eligible for significant incentives reaching estimates over $6 million per year, phasing out by 2015, so Congress excluded hospital‐based physicians from direct payments. Ambulatory physicians are eligible for up to $18,000 per year, phasing out by 2015, with subsequent payment reductions for nonuse. Since hospitalists often function at the nexus of clinical care, quality improvement, and technology use, they have the opportunity to lead or facilitate effective implementation of information technology in their hospitals. These efforts may be rewarded by hospitals.
PQRI
PQRI was authorized in 2006 and included a 1.5% incentive payment for satisfactorily reporting quality data. The incentive payment will increase to 2% in 2009. There are 153 PQRI measures in 2009 and a significant number of the measures focus on hospital‐based care. Examples of measures hospitalists can help report include: deep vein thrombosis prophylaxis for ischemic stroke or intracranial hemorrhage, medication reconciliation at discharge, advance care plan documentation, oral antiplatelet therapy for patients discharged with stroke diagnosis, and anticoagulant therapy prescribed for atrial fibrillation in stroke patients at discharge. PQRI measures can be reported through claims‐based or registry‐based reporting. Reporting can be done on individual measures or for measure groups associated with specific conditions.20 Hospitalists have the potential to drive performance on these measures, lead reporting efforts, and share in the financial rewards.
Future Considerations
The political leadership at the federal and state level is beginning a new transition; however, the focus on quality and value for our health care dollar will likely continue to increase.5, 6 The U.S. health care system has untenable cost estimates, significant quality gaps, and a fractured payment system that fails to reward effective care coordination.2, 21, 22 This increased focus on quality and value should be viewed as an opportunity for hospitalists and hospitals. Hospitalist groups that can achieve high‐quality performance will be increasingly valued, and hospitals should further recognize the critical role hospitalists play in achieving high performance and the associated financial rewards. Hospitalists often lead quality improvement and safety programs in hospitals, and these programs are likely to be seen as progressively more important as payment is linked to performance. The Society of Hospital Medicine engages with policymakers and this role is increasingly significant as more policy and payment decisions impact hospitalists. The Society has focused on collaborative work with payers, policymakers, and other providers to find joint shared solutions. Hospitalists can serve as a link between providers and a focal point of care coordination, especially for the hospitalized patient. Finally, as our system and its incentives continue to progress toward alignment with value‐based high quality care, hospitalists should be leading the change and be an essential part of the solution to transform our health care system to provide high‐quality, efficient care to all Americans.
Acknowledgements
Dr. Tom Valuck is recognized for his thoughtful comments and edits in preparation, submission, and revision of this manuscript.
- Medicare Board of Trustees. A Summary of the 2008 Report. Available at: http://www.ssa.gov/OACT/TRSUM/trsummary.html. Accessed April 2009.
- , , , et al.The quality of health care delivered to adults in the United States.N Engl J Med.2003;348(26):2635–2645.
- Economy Likely to Move up Medicare's Insolvency. Available at: http://abcnews.go.com/Politics/Health/wireStory?id=6369658. Accessed April 2009.
- Value‐Driven Health Care. Available at: http://www.hhs.gov/valuedriven. Accessed April 2009.
- Obama‐Biden Full Health Care Plan. Available at: http://www.barackobama.com/issues/healthcare. Accessed April 2009.
- Senate Chairman Max Baucus Call to Action Health Reform 2009. Available at: http://finance.senate.gov/healthreform2009/finalwhitepaper.pdf. Accessed April 2009.
- , , , .National health spending in 2006: a year of change for prescription drugs.Health Aff (Millwood).2008;27(1):14–29.
- Medicare Hospital Value‐Based Purchasing Plan. October 31,2008. Available at: http://www.cms.hhs.gov/AcuteInpatientPPS/downloads/hospital_VBP_plan_issues_paper.pdf. Accessed April 2009.
- Medicare Improvements for Patients and Providers Act of 2008. Available at: http://www.asm.org/ASM/files/ccLibraryFiles/Filename/000000004120/HR6331.pdf. Accessed April 2009.
- HospitalCompare. Available at: www.hospitalcompare.hhs.gov. Accessed April 2009.
- Premier Hospital Quality Incentive Demonstration. Available at: http://www.cms.hhs.gov/HospitalQualityInits/35_hospitalpremier.asp. Accessed April 2009.
- Acute Care Episode Demonstration. Available at: http://www.cms.hhs.gov/DemoProjectsEvalRpts/MD/itemdetail.asp?filterType=none122(2):160–166.
- Hospital Acquired Conditions. Available at: http://www.cms.hhs.gov/HospitalAcqCond/06_Hospital‐Acquired_Conditions.asp. Accessed April 2009.
- , , .The wisdom and justice of not paying for “preventable complications”.JAMA.2008;299(18):2197–2199.
- E‐prescribing incentive program. Available at: http://www.cms.hhs.gov/ERXincentive. Accessed April 2009.
- American Recovery and Reinvestment Act. Available at: http://frwebgate.access.gpo.gov/cgi‐bin/getdoc.cgi?dbname=111_cong_bills299(19):2319–2321.
- Medicare Board of Trustees. A Summary of the 2008 Report. Available at: http://www.ssa.gov/OACT/TRSUM/trsummary.html. Accessed April 2009.
- , , , et al.The quality of health care delivered to adults in the United States.N Engl J Med.2003;348(26):2635–2645.
- Economy Likely to Move up Medicare's Insolvency. Available at: http://abcnews.go.com/Politics/Health/wireStory?id=6369658. Accessed April 2009.
- Value‐Driven Health Care. Available at: http://www.hhs.gov/valuedriven. Accessed April 2009.
- Obama‐Biden Full Health Care Plan. Available at: http://www.barackobama.com/issues/healthcare. Accessed April 2009.
- Senate Chairman Max Baucus Call to Action Health Reform 2009. Available at: http://finance.senate.gov/healthreform2009/finalwhitepaper.pdf. Accessed April 2009.
- , , , .National health spending in 2006: a year of change for prescription drugs.Health Aff (Millwood).2008;27(1):14–29.
- Medicare Hospital Value‐Based Purchasing Plan. October 31,2008. Available at: http://www.cms.hhs.gov/AcuteInpatientPPS/downloads/hospital_VBP_plan_issues_paper.pdf. Accessed April 2009.
- Medicare Improvements for Patients and Providers Act of 2008. Available at: http://www.asm.org/ASM/files/ccLibraryFiles/Filename/000000004120/HR6331.pdf. Accessed April 2009.
- HospitalCompare. Available at: www.hospitalcompare.hhs.gov. Accessed April 2009.
- Premier Hospital Quality Incentive Demonstration. Available at: http://www.cms.hhs.gov/HospitalQualityInits/35_hospitalpremier.asp. Accessed April 2009.
- Acute Care Episode Demonstration. Available at: http://www.cms.hhs.gov/DemoProjectsEvalRpts/MD/itemdetail.asp?filterType=none122(2):160–166.
- Hospital Acquired Conditions. Available at: http://www.cms.hhs.gov/HospitalAcqCond/06_Hospital‐Acquired_Conditions.asp. Accessed April 2009.
- , , .The wisdom and justice of not paying for “preventable complications”.JAMA.2008;299(18):2197–2199.
- E‐prescribing incentive program. Available at: http://www.cms.hhs.gov/ERXincentive. Accessed April 2009.
- American Recovery and Reinvestment Act. Available at: http://frwebgate.access.gpo.gov/cgi‐bin/getdoc.cgi?dbname=111_cong_bills299(19):2319–2321.
Hospitalists in Internal Medicine Residency
By the year 2010, more than 20,000 hospitalists will be in practice, compared to 5000 rheumatologists and 8000 pulmonologists.13 The growth of this career option has been driven by an industry need to reduce healthcare costs, increase the emphasis on quality improvement of healthcare services, and improve the efficiency and delivery of care between that provided in the hospital and that provided by the primary care physician.49
While hospitalists' roots can be traced back to community hospitals in the late 1980s and early 1990s, this career option is now flourishing in academic centers, with the rise of hospitalist faculty and hospitalist faculty tracks.10, 11 One potential advantage of having faculty who are hospitalists is the availability and expertise of physicians who specialize in the care of hospitalized patients.8, 12 Additionally, hospitalist faculty have been reported to achieve high resident satisfaction scores, increase understanding of cost‐effective measures, and improve the supervision of hospital procedures.12 To our knowledge, the medical literature does not provide an estimate of the percentage of internal medicine residency programs utilizing hospitalist faculty.
Critics of hospitalist faculty point to the potential loss of teaching opportunities from shorter hospital stays, bemoan the decreased physician‐patient continuity between inpatient and outpatient arenas, and fear that the hospitalists' presence may decrease resident autonomy and decrease subspecialty consultations by fellows.5, 13, 14 Hospitalist faculty need development, education, and training to match the teaching activities they are expected to fulfill. The challenge is for hospitalist societies and national residency organizations to define, plan for, and meet their faculty development needs.
Goals
The goals of this study were to describe the current involvement of hospitalists in internal medicine residencies. More specifically, we wanted to determine: (1) the percentage of programs with hospitalists as faculty, (2) the teaching activities of hospitalists, (3) regional differences in academic hospitalist activity, and (4) the number of programs with hospitalist training tracks.
Materials and Methods
Questionnaire Development
The Survey Committee of the Association of Program Directors in Internal Medicine (APDIM) is charged with developing questionnaires to track the baseline characteristics of the 391 internal medicine residencies in the United States as well as to address current issues facing residencies and residency directors. The Survey Committee's goal is to create a longitudinal data warehouse to: (1) track changes over time, (2) create valid outcome measures, and (3) facilitate educational studies and interventions. Two of the authors (B.B. and F.M.) were members of this committee. This work contains results from 2 successive questionnaires.
The first questionnaire, completed in 2005, and its administration have been described in our previous reports.1517 The second, completed in 2007, repeated many of the baseline characteristic questions, and introduced new questions regarding current residency issues, in particular hospitalism in residencies. Whereas the 2005 questionnaire was sent as an e‐mail attachment to the residency programs, the 2007 questionnaire used a web‐based format for completion and data collection. We e‐mailed a notification of the questionnaire with a link to the website in November 2006 to each member program of APDIM (total = 381 programs in 2006), representing 97% of the training programs in internal medicine. The directions and glossary for the questionnaire provided definitions and explained that the first section about the baseline characteristics could be completed by a program administrator or an associate program director. In both surveys, we defined the term faculty as any physician who serves as an attending or preceptor, provides lectures, noon conferences, physical diagnosis rounds, etc., or attends educational conferences (eg, morning report) on a regular basis. The survey assumed that program directors identified hospitalists as physicians whose primary professional focus is the general medical care of hospitalized patients. We asked that the program director review and approve the first section, and complete the remaining questions on his or her own. We sent subsequent request e‐mails in December 2006 and January 2007. The survey was confidential with respondents tracked by numerical codes.
Data Analysis
We used SPSS for Windows 15.0.0 (SPSS, Inc., Chicago, IL) statistics program for all analyses. Each program was categorized by setting (university‐based, community‐based, military, Veterans Administration, multispecialty group), number of residents, and the state in which the program was located. Respondents were assigned a region based upon the categorization used by the U.S. Census Bureau.18 We combined response categories for variables when we found sparsely selected responses. We examined continuous variables for evidence of skewness, outliers, and nonnormality.
In order to avoid misinterpretation of the results of multiple comparisons, we are reporting only bivariate associations that are significant at the P < 0.01 level. We used Spearman's rho to find correlations with the number of hospitalists and continuous variables. Chi‐square analyses were used to compare nominal variables. Fisher's exact test was used to compare the increase in the prevalence of hospitalists at primary teaching hospitals over time. For all the analyses we used 2‐sided tests.
Results
A total of 272 (response rate 70%) programs completed the 2005 survey, and 236 (response rate 62%) completed the 2007 survey. A total of 171 programs completed both surveys. In 2007, 15 (6%) program directors reported that they were hospitalists while 118 (50%) claimed to be traditional general internists.
For the program directors who answered both surveys, 57% indicated that their primary teaching hospital employed hospitalists before the residency work‐hour limits were implemented (before June 2002). At the time of the survey in 2005, 77% said that hospitalists were employed, a 20% increase in 3 years. When we surveyed these same programs again in 2007, the proportion had risen to 81% (Fisher's exact P = 0.02 compared to before work‐hour limits; Figure 1).

Hospitalist Data from 2007
Eighty‐three percent of program directors identified using hospitalists as a part of their residency faculty. There was no significant difference between community‐based and university‐based residency programs (Table 1). There was an expected positive correlation (Spearman rho = 0.39, P < 0.001) between the total number of hospital beds and the number of hospitalists. The number and proportion of hospitalists had no correlation with residency program size, Residency Review Committee (RRC) cycle length (P = 0.99), or the American Board of Internal Medicine (ABIM) board exam pass rate (P = 0.60).
| Community‐Based (n = 130) | University‐Based (n = 63) | Northeast Region (n = 76) | Midwest Region (n = 53) | Southern Region (n = 59) | Western Region (n = 30) | |
|---|---|---|---|---|---|---|
| ||||||
| Does your primary teaching hospital employ hospitalists now?* | 98 (75) | 54 (86) | 61 (80) | 41 (77) | 48 (81) | 22 (73) |
| Are the hospitalists involved in teaching residents?* | 90 (91) | 47 (87) | 60 (98) | 35 (85) | 38 (79) | 22 (100) |
| If Yes, what teaching activities?* | ||||||
| Hospitalists serve as attending on resident service | 81 (92) | 43 (91) | 57 (95) | 32 (91) | 33 (87) | 20 (91) |
| Hospitalists conduct teaching rounds | 71 (79) | 39 (83) | 55 (92) | 30 (86) | 24 (63) | 18 (82) |
| Hospitalists perform direct observation of inpatient clinical skills | 60 (67) | 32 (68) | 45 (75) | 26 (74) | 20 (53) | 17 (77) |
| Hospitalists provide lectures | 56 (67) | 35 (74) | 43 (72) | 26 (74) | 19 (50) | 18 (82) |
| Hospitalists attend morning report | 43 (49) | 27 (59) | 35 (58) | 19 (54) | 19 (50) | 13 (57) |
| Hospitalists teach physical diagnosis | 41 (46) | 23 (49) | 28 (47) | 21 (60) | 14 (37) | 13 (59) |
| Hospitalists conduct interdisciplinary education rounds | 25 (28) | 18 (38) | 24 (40) | 10 (29) | 11 (29) | 7 (32) |
| Do you have a hospitalist track/focus? | 13 (11) | 6 (10) | 6 (8) | 5 (9) | 7 (12) | 5 (17) |
Teaching hospitals of the university‐based residencies employed hospitalists more often than those of community‐based programs (87% vs. 76%, P = 0.07; Table 1). And, while programs across the United States employed hospitalists at near the same proportions, programs in the Northeast (92%) and the West coast (92%) trended toward involving them in teaching residents more often (vs. Midwest 78% and South 76%, P = 0.04). Compared to programs in the Northeast, those in the Southern region generally utilize hospitalists less for common teaching activities, and in particular, significantly less (63%, P = 0.001) for conducting teaching rounds. Eleven percent of residencies had a hospitalist track or a hospitalist training focus, and this did not vary between community‐based and university‐based programs, but the Western region trended toward a higher percentage (17%, P = 0.18, compared to the Northeast 8%).
Of those programs that utilize hospitalists, program directors indicated that hospitalists contributed the following teaching activities to their residency programs (Table 1): serve as attending on resident service (92%), conduct teaching rounds (81%), perform direct observation of inpatient clinical skills (67%), provide lectures (68%), attend morning report (52%), teach physical diagnosis (48%), and conduct interdisciplinary education rounds (31%). Notable comments provided by program directors about other teaching activities of hospitalists included: accept and review night float patients, residents do inpatient consultations with hospitalists, serve as one of the associate program directors, and write curriculum updates and develop evaluation methods (ie, oral exams, multiple choice questions, etc.).
Discussion
This is the first study to document the national rise of hospitalist faculty in internal medicine residency programs. Program directors noted a 20% increase in teaching hospitals that employed hospitalists after the work‐hour regulations went into effecta trend that continued to rise. The tendency was seen first on the coasts, where managed care has higher penetration, and particularly in the Northeast, where New York's resident work‐hour reforms occurred by state mandate prior to the residency accreditation action that affected the rest of the country. Not only have hospitalists picked up the burden of service at these hospitals,19, 20 but the vast majority of programs (>80%) have utilized hospitalists as teachers in important areas of their residency. The magnitude of hospitalist involvement in residency training may have important implications.
Beyond the financial significance of hospitalists at academic teaching hospitals,21 only a few studies have addressed their impact on resident education. On the monthly evaluations at the University of California, San Francisco (San Francisco, CA), residents' satisfaction with their attendings was significantly higher when the physician was a hospitalist rather than a traditional faculty member.22 Residents believed hospitalists were more effective teachers, and provided more effective feedback. At Emory University (Atlanta, GA), a methodologically more rigorous study of postrotation assessment of faculty demonstrated that ratings of hospitalists were not different from traditional general internists; both scored higher than subspecialists.23 The hospitalists as a group had completed training more recently, which also was associated with higher scores.
Even community hospitals that sponsor residency programs have benefited from hospitalist faculty. At Norwalk Hospital (Norwalk, CT), the program had used resident teams led by a group of community physicians and a small group of employed internists. But time pressures and reimbursement concerns created tension between the workload and education balance. After hiring 2 hospitalist clinician‐educators, the length of stay and cost per case were substantially reduced, while resident evaluations indicated improved teaching rounds, conferences, and bedside teaching.24
The results of our study fit with the role of hospitalists as well as what individual programs have reported about hospitalist faculty in the past. Hospitalist faculty serve by and large (92%) as attendings on the hospital ward services. Theoretically, who better to have round with residents in the hospital than the specialists of hospital medicine. For a pulmonary curricular experience, residents work with pulmonologists. But beyond serving as attendings in the hospital, they perform the traditional functions of hospital attendings: providing teaching rounds (>80%), evaluating clinical skills (67%), and even lecturing to residents (>65%). The Southern region trends toward slower adoption of hospitalists as faculty, particularly compared with the Northeast. Overall, what is striking is how much hospitalist faculty already are filling the roles expected of all academic faculty.
We found that only 11% of programs have a hospitalist track through which internal medicine residents may develop the specialized skills and knowledge needed to function optimally in a hospitalist career.25 But given the rapid growth of this specialty, we might expect to see a similar rise in programs providing such specialized training.
Are there risks to having hospitalists teaching residents? One concern is the potential to model fragmented medical care to trainees when hospitals and ambulatory health systems neglect to ensure quality handoffs.26 In an era that heralds the demise of the primary care general internist,27 the impact of hospitalist faculty on general internal medicine nationally, the gravitation of residents toward or away from hospitalist and ambulatory careers, and the role of the traditional general internist in residency training programs in the future remain to be seen. These were not addressed by our data, but are ripe areas for study.
This study has several limitations. It relies on self‐reported data from program directors that, while knowing the intimate details of their educational program, may not have exact knowledge of the number of hospitalists employed by their hospitals. There is also the potential for recall bias by asking the group to remember the number of hospitalists before duty‐hour implementation. Both points in time of our 2 surveys (2005 and 2007) were after the incident growth of hospital medicine as evidenced by the high prevalence of hospitalists in both surveys. Yet, most program directors know that the service needs of the hospitals were acutely increased when the duty‐hours policies went into affect, and probably were fairly involved in hospital decisions to utilize hospitalist physicians to meet these needs. Finally, our study does not address hospitalism within the family medicine and pediatric specialties, both of which have a significant stake in hospital medicine.
In conclusion, our study documents the recent growth and current prevalence of hospitalists' activities in the teaching hospitals of internal medicine residencies in the United States, the duties they perform in resident education, and the magnitude of their penetration in the geographic regions of the country, both in community‐based and university‐based programs. The high degree of involvement of hospitalists in resident education may have important implications for the future of internal medicine as a discipline both with regard to the need for academic faculty development of this important sector of the education community as well as for the education and career development of the residents whom they train.
Acknowledgements
The authors thank the Mayo Clinic Survey Research Center for their assistance with survey design and data collection.
- , , , et al.Implementation of a voluntary hospitalist service at a community teaching hospital; improved clinical efficiency and patient outcomes.Ann Intern Med.2002;137:859–865.
- , , , et al.The United States rheumatology workforce: supply and demand, 2005–2025.Arthritis Rheum.2007;56(3):722–729.
- , , , , ;Committee on Manpower for Pulmonary and Critical Care Societies.Caring for the critically ill patient. Current and projected workforce requirements for care of the critically ill and patients with pulmonary disease: can we meet the requirements of an aging population?JAMA.2000;284(21):2762–2770.
- , .The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- , , , , .Reorganizing an academic medical service: impact on cost, quality, patient satisfaction, and education.JAMA.1998;279:1560–1565.
- , , .The effect of full‐time faculty hospitalists on the efficiency of care at a community teaching hospital.Ann Intern Med.1998;129:197–203.
- .An introduction to the hospitalist model.Ann Intern Med.1999;130:338–342.
- , .The hospitalist movement 5 years later.JAMA.2002;287:487–494.
- , , , , .What effect does inpatient physician specialty and experience have on clinical outcomes and resource utilization on a general medical service?J Gen Intern Med.2004;19:395–401.
- , , , et al.The presence of hospitalists in medical education.Acad Med.2000;75(suppl):S34–S36.
- , , , et al.Assessing the value of hospitalists to academic health centers: Brigham and Women's Hospital and Harvard Medical School.Am J Med.1999;106:134–137.
- , .Role of hospitalists in medical education.Am J Med.1999;107(4):305–309.
- , .The hospitalists: new boon for internal medicine or retreat from primary care?Ann Intern Med.1999;130:382–387.
- .The hospitalist movement: caution lights flashing at the crossroads.Am J Med.1999;107:409–413.
- , , .The state of competency evaluation in internal medicine residency.J Gen Intern Med.2008;23(7):1010–1015.
- , , .Sources of satisfaction for residency program directors: a second administration of the PD‐Sat.Am J Med.2009;122(2):196–201.
- , , .What predicts residency accreditation cycle length?Acad Med.2009;84(3):356–361.
- U.S. Census Bureau. Census Regions and Divisions of the United States. Available at: http://www.census.gov/geo/www/us_regdiv.pdf. Accessed May 2009.
- , , , et al.Complying with ACGME resident duty hours restrictions: restructuring the 80‐hour workweek to enhance education and patient safety at Texas A81(12):1026–1031.
- Association of Program Directors in Internal Medicine;, , , , .Redesigning residency education in internal medicine: a position paper from the Association of Program Directors in Internal Medicine.Ann Intern Med.2006;144(12):920–926.
- , , , et al.Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists.Ann Intern Med.2002;137(11):866–874.
- , , , , .Effects of hospitalist attending physicians on trainee satisfaction with teaching and with internal medicine rotations.Arch Intern Med.2004;164:1866–1871.
- , , , et al.Hospitalists as teachers.J Gen Intern Med.2004;19(1):8–15.
- , , , et al.The positive impact of initiation of hospitalist clinician educators.J Gen Intern Med.2004;19(4):293–301.
- , , , , .How to use The core competencies in hospital medicine: a framework for curriculum development.J Hosp Med.2006;1:48–56.
- .The hospitalist model: perspectives of the patient, the internist, and internal medicine.Ann Intern Med.1999;130:368–372.
- American College of Physicians. The impending collapse of primary care medicine and its implications for the state of the nation's health care: a report from the American College of Physicians. January 30,2006. Available at: http://www.acponline.org/advocacy/events/state_of_healthcare/statehc06_1.pdf. Accessed May 2009.
By the year 2010, more than 20,000 hospitalists will be in practice, compared to 5000 rheumatologists and 8000 pulmonologists.13 The growth of this career option has been driven by an industry need to reduce healthcare costs, increase the emphasis on quality improvement of healthcare services, and improve the efficiency and delivery of care between that provided in the hospital and that provided by the primary care physician.49
While hospitalists' roots can be traced back to community hospitals in the late 1980s and early 1990s, this career option is now flourishing in academic centers, with the rise of hospitalist faculty and hospitalist faculty tracks.10, 11 One potential advantage of having faculty who are hospitalists is the availability and expertise of physicians who specialize in the care of hospitalized patients.8, 12 Additionally, hospitalist faculty have been reported to achieve high resident satisfaction scores, increase understanding of cost‐effective measures, and improve the supervision of hospital procedures.12 To our knowledge, the medical literature does not provide an estimate of the percentage of internal medicine residency programs utilizing hospitalist faculty.
Critics of hospitalist faculty point to the potential loss of teaching opportunities from shorter hospital stays, bemoan the decreased physician‐patient continuity between inpatient and outpatient arenas, and fear that the hospitalists' presence may decrease resident autonomy and decrease subspecialty consultations by fellows.5, 13, 14 Hospitalist faculty need development, education, and training to match the teaching activities they are expected to fulfill. The challenge is for hospitalist societies and national residency organizations to define, plan for, and meet their faculty development needs.
Goals
The goals of this study were to describe the current involvement of hospitalists in internal medicine residencies. More specifically, we wanted to determine: (1) the percentage of programs with hospitalists as faculty, (2) the teaching activities of hospitalists, (3) regional differences in academic hospitalist activity, and (4) the number of programs with hospitalist training tracks.
Materials and Methods
Questionnaire Development
The Survey Committee of the Association of Program Directors in Internal Medicine (APDIM) is charged with developing questionnaires to track the baseline characteristics of the 391 internal medicine residencies in the United States as well as to address current issues facing residencies and residency directors. The Survey Committee's goal is to create a longitudinal data warehouse to: (1) track changes over time, (2) create valid outcome measures, and (3) facilitate educational studies and interventions. Two of the authors (B.B. and F.M.) were members of this committee. This work contains results from 2 successive questionnaires.
The first questionnaire, completed in 2005, and its administration have been described in our previous reports.1517 The second, completed in 2007, repeated many of the baseline characteristic questions, and introduced new questions regarding current residency issues, in particular hospitalism in residencies. Whereas the 2005 questionnaire was sent as an e‐mail attachment to the residency programs, the 2007 questionnaire used a web‐based format for completion and data collection. We e‐mailed a notification of the questionnaire with a link to the website in November 2006 to each member program of APDIM (total = 381 programs in 2006), representing 97% of the training programs in internal medicine. The directions and glossary for the questionnaire provided definitions and explained that the first section about the baseline characteristics could be completed by a program administrator or an associate program director. In both surveys, we defined the term faculty as any physician who serves as an attending or preceptor, provides lectures, noon conferences, physical diagnosis rounds, etc., or attends educational conferences (eg, morning report) on a regular basis. The survey assumed that program directors identified hospitalists as physicians whose primary professional focus is the general medical care of hospitalized patients. We asked that the program director review and approve the first section, and complete the remaining questions on his or her own. We sent subsequent request e‐mails in December 2006 and January 2007. The survey was confidential with respondents tracked by numerical codes.
Data Analysis
We used SPSS for Windows 15.0.0 (SPSS, Inc., Chicago, IL) statistics program for all analyses. Each program was categorized by setting (university‐based, community‐based, military, Veterans Administration, multispecialty group), number of residents, and the state in which the program was located. Respondents were assigned a region based upon the categorization used by the U.S. Census Bureau.18 We combined response categories for variables when we found sparsely selected responses. We examined continuous variables for evidence of skewness, outliers, and nonnormality.
In order to avoid misinterpretation of the results of multiple comparisons, we are reporting only bivariate associations that are significant at the P < 0.01 level. We used Spearman's rho to find correlations with the number of hospitalists and continuous variables. Chi‐square analyses were used to compare nominal variables. Fisher's exact test was used to compare the increase in the prevalence of hospitalists at primary teaching hospitals over time. For all the analyses we used 2‐sided tests.
Results
A total of 272 (response rate 70%) programs completed the 2005 survey, and 236 (response rate 62%) completed the 2007 survey. A total of 171 programs completed both surveys. In 2007, 15 (6%) program directors reported that they were hospitalists while 118 (50%) claimed to be traditional general internists.
For the program directors who answered both surveys, 57% indicated that their primary teaching hospital employed hospitalists before the residency work‐hour limits were implemented (before June 2002). At the time of the survey in 2005, 77% said that hospitalists were employed, a 20% increase in 3 years. When we surveyed these same programs again in 2007, the proportion had risen to 81% (Fisher's exact P = 0.02 compared to before work‐hour limits; Figure 1).
Hospitalist Data from 2007
Eighty‐three percent of program directors identified using hospitalists as a part of their residency faculty. There was no significant difference between community‐based and university‐based residency programs (Table 1). There was an expected positive correlation (Spearman rho = 0.39, P < 0.001) between the total number of hospital beds and the number of hospitalists. The number and proportion of hospitalists had no correlation with residency program size, Residency Review Committee (RRC) cycle length (P = 0.99), or the American Board of Internal Medicine (ABIM) board exam pass rate (P = 0.60).
| Community‐Based (n = 130) | University‐Based (n = 63) | Northeast Region (n = 76) | Midwest Region (n = 53) | Southern Region (n = 59) | Western Region (n = 30) | |
|---|---|---|---|---|---|---|
| ||||||
| Does your primary teaching hospital employ hospitalists now?* | 98 (75) | 54 (86) | 61 (80) | 41 (77) | 48 (81) | 22 (73) |
| Are the hospitalists involved in teaching residents?* | 90 (91) | 47 (87) | 60 (98) | 35 (85) | 38 (79) | 22 (100) |
| If Yes, what teaching activities?* | ||||||
| Hospitalists serve as attending on resident service | 81 (92) | 43 (91) | 57 (95) | 32 (91) | 33 (87) | 20 (91) |
| Hospitalists conduct teaching rounds | 71 (79) | 39 (83) | 55 (92) | 30 (86) | 24 (63) | 18 (82) |
| Hospitalists perform direct observation of inpatient clinical skills | 60 (67) | 32 (68) | 45 (75) | 26 (74) | 20 (53) | 17 (77) |
| Hospitalists provide lectures | 56 (67) | 35 (74) | 43 (72) | 26 (74) | 19 (50) | 18 (82) |
| Hospitalists attend morning report | 43 (49) | 27 (59) | 35 (58) | 19 (54) | 19 (50) | 13 (57) |
| Hospitalists teach physical diagnosis | 41 (46) | 23 (49) | 28 (47) | 21 (60) | 14 (37) | 13 (59) |
| Hospitalists conduct interdisciplinary education rounds | 25 (28) | 18 (38) | 24 (40) | 10 (29) | 11 (29) | 7 (32) |
| Do you have a hospitalist track/focus? | 13 (11) | 6 (10) | 6 (8) | 5 (9) | 7 (12) | 5 (17) |
Teaching hospitals of the university‐based residencies employed hospitalists more often than those of community‐based programs (87% vs. 76%, P = 0.07; Table 1). And, while programs across the United States employed hospitalists at near the same proportions, programs in the Northeast (92%) and the West coast (92%) trended toward involving them in teaching residents more often (vs. Midwest 78% and South 76%, P = 0.04). Compared to programs in the Northeast, those in the Southern region generally utilize hospitalists less for common teaching activities, and in particular, significantly less (63%, P = 0.001) for conducting teaching rounds. Eleven percent of residencies had a hospitalist track or a hospitalist training focus, and this did not vary between community‐based and university‐based programs, but the Western region trended toward a higher percentage (17%, P = 0.18, compared to the Northeast 8%).
Of those programs that utilize hospitalists, program directors indicated that hospitalists contributed the following teaching activities to their residency programs (Table 1): serve as attending on resident service (92%), conduct teaching rounds (81%), perform direct observation of inpatient clinical skills (67%), provide lectures (68%), attend morning report (52%), teach physical diagnosis (48%), and conduct interdisciplinary education rounds (31%). Notable comments provided by program directors about other teaching activities of hospitalists included: accept and review night float patients, residents do inpatient consultations with hospitalists, serve as one of the associate program directors, and write curriculum updates and develop evaluation methods (ie, oral exams, multiple choice questions, etc.).
Discussion
This is the first study to document the national rise of hospitalist faculty in internal medicine residency programs. Program directors noted a 20% increase in teaching hospitals that employed hospitalists after the work‐hour regulations went into effecta trend that continued to rise. The tendency was seen first on the coasts, where managed care has higher penetration, and particularly in the Northeast, where New York's resident work‐hour reforms occurred by state mandate prior to the residency accreditation action that affected the rest of the country. Not only have hospitalists picked up the burden of service at these hospitals,19, 20 but the vast majority of programs (>80%) have utilized hospitalists as teachers in important areas of their residency. The magnitude of hospitalist involvement in residency training may have important implications.
Beyond the financial significance of hospitalists at academic teaching hospitals,21 only a few studies have addressed their impact on resident education. On the monthly evaluations at the University of California, San Francisco (San Francisco, CA), residents' satisfaction with their attendings was significantly higher when the physician was a hospitalist rather than a traditional faculty member.22 Residents believed hospitalists were more effective teachers, and provided more effective feedback. At Emory University (Atlanta, GA), a methodologically more rigorous study of postrotation assessment of faculty demonstrated that ratings of hospitalists were not different from traditional general internists; both scored higher than subspecialists.23 The hospitalists as a group had completed training more recently, which also was associated with higher scores.
Even community hospitals that sponsor residency programs have benefited from hospitalist faculty. At Norwalk Hospital (Norwalk, CT), the program had used resident teams led by a group of community physicians and a small group of employed internists. But time pressures and reimbursement concerns created tension between the workload and education balance. After hiring 2 hospitalist clinician‐educators, the length of stay and cost per case were substantially reduced, while resident evaluations indicated improved teaching rounds, conferences, and bedside teaching.24
The results of our study fit with the role of hospitalists as well as what individual programs have reported about hospitalist faculty in the past. Hospitalist faculty serve by and large (92%) as attendings on the hospital ward services. Theoretically, who better to have round with residents in the hospital than the specialists of hospital medicine. For a pulmonary curricular experience, residents work with pulmonologists. But beyond serving as attendings in the hospital, they perform the traditional functions of hospital attendings: providing teaching rounds (>80%), evaluating clinical skills (67%), and even lecturing to residents (>65%). The Southern region trends toward slower adoption of hospitalists as faculty, particularly compared with the Northeast. Overall, what is striking is how much hospitalist faculty already are filling the roles expected of all academic faculty.
We found that only 11% of programs have a hospitalist track through which internal medicine residents may develop the specialized skills and knowledge needed to function optimally in a hospitalist career.25 But given the rapid growth of this specialty, we might expect to see a similar rise in programs providing such specialized training.
Are there risks to having hospitalists teaching residents? One concern is the potential to model fragmented medical care to trainees when hospitals and ambulatory health systems neglect to ensure quality handoffs.26 In an era that heralds the demise of the primary care general internist,27 the impact of hospitalist faculty on general internal medicine nationally, the gravitation of residents toward or away from hospitalist and ambulatory careers, and the role of the traditional general internist in residency training programs in the future remain to be seen. These were not addressed by our data, but are ripe areas for study.
This study has several limitations. It relies on self‐reported data from program directors that, while knowing the intimate details of their educational program, may not have exact knowledge of the number of hospitalists employed by their hospitals. There is also the potential for recall bias by asking the group to remember the number of hospitalists before duty‐hour implementation. Both points in time of our 2 surveys (2005 and 2007) were after the incident growth of hospital medicine as evidenced by the high prevalence of hospitalists in both surveys. Yet, most program directors know that the service needs of the hospitals were acutely increased when the duty‐hours policies went into affect, and probably were fairly involved in hospital decisions to utilize hospitalist physicians to meet these needs. Finally, our study does not address hospitalism within the family medicine and pediatric specialties, both of which have a significant stake in hospital medicine.
In conclusion, our study documents the recent growth and current prevalence of hospitalists' activities in the teaching hospitals of internal medicine residencies in the United States, the duties they perform in resident education, and the magnitude of their penetration in the geographic regions of the country, both in community‐based and university‐based programs. The high degree of involvement of hospitalists in resident education may have important implications for the future of internal medicine as a discipline both with regard to the need for academic faculty development of this important sector of the education community as well as for the education and career development of the residents whom they train.
Acknowledgements
The authors thank the Mayo Clinic Survey Research Center for their assistance with survey design and data collection.
By the year 2010, more than 20,000 hospitalists will be in practice, compared to 5000 rheumatologists and 8000 pulmonologists.13 The growth of this career option has been driven by an industry need to reduce healthcare costs, increase the emphasis on quality improvement of healthcare services, and improve the efficiency and delivery of care between that provided in the hospital and that provided by the primary care physician.49
While hospitalists' roots can be traced back to community hospitals in the late 1980s and early 1990s, this career option is now flourishing in academic centers, with the rise of hospitalist faculty and hospitalist faculty tracks.10, 11 One potential advantage of having faculty who are hospitalists is the availability and expertise of physicians who specialize in the care of hospitalized patients.8, 12 Additionally, hospitalist faculty have been reported to achieve high resident satisfaction scores, increase understanding of cost‐effective measures, and improve the supervision of hospital procedures.12 To our knowledge, the medical literature does not provide an estimate of the percentage of internal medicine residency programs utilizing hospitalist faculty.
Critics of hospitalist faculty point to the potential loss of teaching opportunities from shorter hospital stays, bemoan the decreased physician‐patient continuity between inpatient and outpatient arenas, and fear that the hospitalists' presence may decrease resident autonomy and decrease subspecialty consultations by fellows.5, 13, 14 Hospitalist faculty need development, education, and training to match the teaching activities they are expected to fulfill. The challenge is for hospitalist societies and national residency organizations to define, plan for, and meet their faculty development needs.
Goals
The goals of this study were to describe the current involvement of hospitalists in internal medicine residencies. More specifically, we wanted to determine: (1) the percentage of programs with hospitalists as faculty, (2) the teaching activities of hospitalists, (3) regional differences in academic hospitalist activity, and (4) the number of programs with hospitalist training tracks.
Materials and Methods
Questionnaire Development
The Survey Committee of the Association of Program Directors in Internal Medicine (APDIM) is charged with developing questionnaires to track the baseline characteristics of the 391 internal medicine residencies in the United States as well as to address current issues facing residencies and residency directors. The Survey Committee's goal is to create a longitudinal data warehouse to: (1) track changes over time, (2) create valid outcome measures, and (3) facilitate educational studies and interventions. Two of the authors (B.B. and F.M.) were members of this committee. This work contains results from 2 successive questionnaires.
The first questionnaire, completed in 2005, and its administration have been described in our previous reports.1517 The second, completed in 2007, repeated many of the baseline characteristic questions, and introduced new questions regarding current residency issues, in particular hospitalism in residencies. Whereas the 2005 questionnaire was sent as an e‐mail attachment to the residency programs, the 2007 questionnaire used a web‐based format for completion and data collection. We e‐mailed a notification of the questionnaire with a link to the website in November 2006 to each member program of APDIM (total = 381 programs in 2006), representing 97% of the training programs in internal medicine. The directions and glossary for the questionnaire provided definitions and explained that the first section about the baseline characteristics could be completed by a program administrator or an associate program director. In both surveys, we defined the term faculty as any physician who serves as an attending or preceptor, provides lectures, noon conferences, physical diagnosis rounds, etc., or attends educational conferences (eg, morning report) on a regular basis. The survey assumed that program directors identified hospitalists as physicians whose primary professional focus is the general medical care of hospitalized patients. We asked that the program director review and approve the first section, and complete the remaining questions on his or her own. We sent subsequent request e‐mails in December 2006 and January 2007. The survey was confidential with respondents tracked by numerical codes.
Data Analysis
We used SPSS for Windows 15.0.0 (SPSS, Inc., Chicago, IL) statistics program for all analyses. Each program was categorized by setting (university‐based, community‐based, military, Veterans Administration, multispecialty group), number of residents, and the state in which the program was located. Respondents were assigned a region based upon the categorization used by the U.S. Census Bureau.18 We combined response categories for variables when we found sparsely selected responses. We examined continuous variables for evidence of skewness, outliers, and nonnormality.
In order to avoid misinterpretation of the results of multiple comparisons, we are reporting only bivariate associations that are significant at the P < 0.01 level. We used Spearman's rho to find correlations with the number of hospitalists and continuous variables. Chi‐square analyses were used to compare nominal variables. Fisher's exact test was used to compare the increase in the prevalence of hospitalists at primary teaching hospitals over time. For all the analyses we used 2‐sided tests.
Results
A total of 272 (response rate 70%) programs completed the 2005 survey, and 236 (response rate 62%) completed the 2007 survey. A total of 171 programs completed both surveys. In 2007, 15 (6%) program directors reported that they were hospitalists while 118 (50%) claimed to be traditional general internists.
For the program directors who answered both surveys, 57% indicated that their primary teaching hospital employed hospitalists before the residency work‐hour limits were implemented (before June 2002). At the time of the survey in 2005, 77% said that hospitalists were employed, a 20% increase in 3 years. When we surveyed these same programs again in 2007, the proportion had risen to 81% (Fisher's exact P = 0.02 compared to before work‐hour limits; Figure 1).
Hospitalist Data from 2007
Eighty‐three percent of program directors identified using hospitalists as a part of their residency faculty. There was no significant difference between community‐based and university‐based residency programs (Table 1). There was an expected positive correlation (Spearman rho = 0.39, P < 0.001) between the total number of hospital beds and the number of hospitalists. The number and proportion of hospitalists had no correlation with residency program size, Residency Review Committee (RRC) cycle length (P = 0.99), or the American Board of Internal Medicine (ABIM) board exam pass rate (P = 0.60).
| Community‐Based (n = 130) | University‐Based (n = 63) | Northeast Region (n = 76) | Midwest Region (n = 53) | Southern Region (n = 59) | Western Region (n = 30) | |
|---|---|---|---|---|---|---|
| ||||||
| Does your primary teaching hospital employ hospitalists now?* | 98 (75) | 54 (86) | 61 (80) | 41 (77) | 48 (81) | 22 (73) |
| Are the hospitalists involved in teaching residents?* | 90 (91) | 47 (87) | 60 (98) | 35 (85) | 38 (79) | 22 (100) |
| If Yes, what teaching activities?* | ||||||
| Hospitalists serve as attending on resident service | 81 (92) | 43 (91) | 57 (95) | 32 (91) | 33 (87) | 20 (91) |
| Hospitalists conduct teaching rounds | 71 (79) | 39 (83) | 55 (92) | 30 (86) | 24 (63) | 18 (82) |
| Hospitalists perform direct observation of inpatient clinical skills | 60 (67) | 32 (68) | 45 (75) | 26 (74) | 20 (53) | 17 (77) |
| Hospitalists provide lectures | 56 (67) | 35 (74) | 43 (72) | 26 (74) | 19 (50) | 18 (82) |
| Hospitalists attend morning report | 43 (49) | 27 (59) | 35 (58) | 19 (54) | 19 (50) | 13 (57) |
| Hospitalists teach physical diagnosis | 41 (46) | 23 (49) | 28 (47) | 21 (60) | 14 (37) | 13 (59) |
| Hospitalists conduct interdisciplinary education rounds | 25 (28) | 18 (38) | 24 (40) | 10 (29) | 11 (29) | 7 (32) |
| Do you have a hospitalist track/focus? | 13 (11) | 6 (10) | 6 (8) | 5 (9) | 7 (12) | 5 (17) |
Teaching hospitals of the university‐based residencies employed hospitalists more often than those of community‐based programs (87% vs. 76%, P = 0.07; Table 1). And, while programs across the United States employed hospitalists at near the same proportions, programs in the Northeast (92%) and the West coast (92%) trended toward involving them in teaching residents more often (vs. Midwest 78% and South 76%, P = 0.04). Compared to programs in the Northeast, those in the Southern region generally utilize hospitalists less for common teaching activities, and in particular, significantly less (63%, P = 0.001) for conducting teaching rounds. Eleven percent of residencies had a hospitalist track or a hospitalist training focus, and this did not vary between community‐based and university‐based programs, but the Western region trended toward a higher percentage (17%, P = 0.18, compared to the Northeast 8%).
Of those programs that utilize hospitalists, program directors indicated that hospitalists contributed the following teaching activities to their residency programs (Table 1): serve as attending on resident service (92%), conduct teaching rounds (81%), perform direct observation of inpatient clinical skills (67%), provide lectures (68%), attend morning report (52%), teach physical diagnosis (48%), and conduct interdisciplinary education rounds (31%). Notable comments provided by program directors about other teaching activities of hospitalists included: accept and review night float patients, residents do inpatient consultations with hospitalists, serve as one of the associate program directors, and write curriculum updates and develop evaluation methods (ie, oral exams, multiple choice questions, etc.).
Discussion
This is the first study to document the national rise of hospitalist faculty in internal medicine residency programs. Program directors noted a 20% increase in teaching hospitals that employed hospitalists after the work‐hour regulations went into effecta trend that continued to rise. The tendency was seen first on the coasts, where managed care has higher penetration, and particularly in the Northeast, where New York's resident work‐hour reforms occurred by state mandate prior to the residency accreditation action that affected the rest of the country. Not only have hospitalists picked up the burden of service at these hospitals,19, 20 but the vast majority of programs (>80%) have utilized hospitalists as teachers in important areas of their residency. The magnitude of hospitalist involvement in residency training may have important implications.
Beyond the financial significance of hospitalists at academic teaching hospitals,21 only a few studies have addressed their impact on resident education. On the monthly evaluations at the University of California, San Francisco (San Francisco, CA), residents' satisfaction with their attendings was significantly higher when the physician was a hospitalist rather than a traditional faculty member.22 Residents believed hospitalists were more effective teachers, and provided more effective feedback. At Emory University (Atlanta, GA), a methodologically more rigorous study of postrotation assessment of faculty demonstrated that ratings of hospitalists were not different from traditional general internists; both scored higher than subspecialists.23 The hospitalists as a group had completed training more recently, which also was associated with higher scores.
Even community hospitals that sponsor residency programs have benefited from hospitalist faculty. At Norwalk Hospital (Norwalk, CT), the program had used resident teams led by a group of community physicians and a small group of employed internists. But time pressures and reimbursement concerns created tension between the workload and education balance. After hiring 2 hospitalist clinician‐educators, the length of stay and cost per case were substantially reduced, while resident evaluations indicated improved teaching rounds, conferences, and bedside teaching.24
The results of our study fit with the role of hospitalists as well as what individual programs have reported about hospitalist faculty in the past. Hospitalist faculty serve by and large (92%) as attendings on the hospital ward services. Theoretically, who better to have round with residents in the hospital than the specialists of hospital medicine. For a pulmonary curricular experience, residents work with pulmonologists. But beyond serving as attendings in the hospital, they perform the traditional functions of hospital attendings: providing teaching rounds (>80%), evaluating clinical skills (67%), and even lecturing to residents (>65%). The Southern region trends toward slower adoption of hospitalists as faculty, particularly compared with the Northeast. Overall, what is striking is how much hospitalist faculty already are filling the roles expected of all academic faculty.
We found that only 11% of programs have a hospitalist track through which internal medicine residents may develop the specialized skills and knowledge needed to function optimally in a hospitalist career.25 But given the rapid growth of this specialty, we might expect to see a similar rise in programs providing such specialized training.
Are there risks to having hospitalists teaching residents? One concern is the potential to model fragmented medical care to trainees when hospitals and ambulatory health systems neglect to ensure quality handoffs.26 In an era that heralds the demise of the primary care general internist,27 the impact of hospitalist faculty on general internal medicine nationally, the gravitation of residents toward or away from hospitalist and ambulatory careers, and the role of the traditional general internist in residency training programs in the future remain to be seen. These were not addressed by our data, but are ripe areas for study.
This study has several limitations. It relies on self‐reported data from program directors that, while knowing the intimate details of their educational program, may not have exact knowledge of the number of hospitalists employed by their hospitals. There is also the potential for recall bias by asking the group to remember the number of hospitalists before duty‐hour implementation. Both points in time of our 2 surveys (2005 and 2007) were after the incident growth of hospital medicine as evidenced by the high prevalence of hospitalists in both surveys. Yet, most program directors know that the service needs of the hospitals were acutely increased when the duty‐hours policies went into affect, and probably were fairly involved in hospital decisions to utilize hospitalist physicians to meet these needs. Finally, our study does not address hospitalism within the family medicine and pediatric specialties, both of which have a significant stake in hospital medicine.
In conclusion, our study documents the recent growth and current prevalence of hospitalists' activities in the teaching hospitals of internal medicine residencies in the United States, the duties they perform in resident education, and the magnitude of their penetration in the geographic regions of the country, both in community‐based and university‐based programs. The high degree of involvement of hospitalists in resident education may have important implications for the future of internal medicine as a discipline both with regard to the need for academic faculty development of this important sector of the education community as well as for the education and career development of the residents whom they train.
Acknowledgements
The authors thank the Mayo Clinic Survey Research Center for their assistance with survey design and data collection.
- , , , et al.Implementation of a voluntary hospitalist service at a community teaching hospital; improved clinical efficiency and patient outcomes.Ann Intern Med.2002;137:859–865.
- , , , et al.The United States rheumatology workforce: supply and demand, 2005–2025.Arthritis Rheum.2007;56(3):722–729.
- , , , , ;Committee on Manpower for Pulmonary and Critical Care Societies.Caring for the critically ill patient. Current and projected workforce requirements for care of the critically ill and patients with pulmonary disease: can we meet the requirements of an aging population?JAMA.2000;284(21):2762–2770.
- , .The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- , , , , .Reorganizing an academic medical service: impact on cost, quality, patient satisfaction, and education.JAMA.1998;279:1560–1565.
- , , .The effect of full‐time faculty hospitalists on the efficiency of care at a community teaching hospital.Ann Intern Med.1998;129:197–203.
- .An introduction to the hospitalist model.Ann Intern Med.1999;130:338–342.
- , .The hospitalist movement 5 years later.JAMA.2002;287:487–494.
- , , , , .What effect does inpatient physician specialty and experience have on clinical outcomes and resource utilization on a general medical service?J Gen Intern Med.2004;19:395–401.
- , , , et al.The presence of hospitalists in medical education.Acad Med.2000;75(suppl):S34–S36.
- , , , et al.Assessing the value of hospitalists to academic health centers: Brigham and Women's Hospital and Harvard Medical School.Am J Med.1999;106:134–137.
- , .Role of hospitalists in medical education.Am J Med.1999;107(4):305–309.
- , .The hospitalists: new boon for internal medicine or retreat from primary care?Ann Intern Med.1999;130:382–387.
- .The hospitalist movement: caution lights flashing at the crossroads.Am J Med.1999;107:409–413.
- , , .The state of competency evaluation in internal medicine residency.J Gen Intern Med.2008;23(7):1010–1015.
- , , .Sources of satisfaction for residency program directors: a second administration of the PD‐Sat.Am J Med.2009;122(2):196–201.
- , , .What predicts residency accreditation cycle length?Acad Med.2009;84(3):356–361.
- U.S. Census Bureau. Census Regions and Divisions of the United States. Available at: http://www.census.gov/geo/www/us_regdiv.pdf. Accessed May 2009.
- , , , et al.Complying with ACGME resident duty hours restrictions: restructuring the 80‐hour workweek to enhance education and patient safety at Texas A81(12):1026–1031.
- Association of Program Directors in Internal Medicine;, , , , .Redesigning residency education in internal medicine: a position paper from the Association of Program Directors in Internal Medicine.Ann Intern Med.2006;144(12):920–926.
- , , , et al.Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists.Ann Intern Med.2002;137(11):866–874.
- , , , , .Effects of hospitalist attending physicians on trainee satisfaction with teaching and with internal medicine rotations.Arch Intern Med.2004;164:1866–1871.
- , , , et al.Hospitalists as teachers.J Gen Intern Med.2004;19(1):8–15.
- , , , et al.The positive impact of initiation of hospitalist clinician educators.J Gen Intern Med.2004;19(4):293–301.
- , , , , .How to use The core competencies in hospital medicine: a framework for curriculum development.J Hosp Med.2006;1:48–56.
- .The hospitalist model: perspectives of the patient, the internist, and internal medicine.Ann Intern Med.1999;130:368–372.
- American College of Physicians. The impending collapse of primary care medicine and its implications for the state of the nation's health care: a report from the American College of Physicians. January 30,2006. Available at: http://www.acponline.org/advocacy/events/state_of_healthcare/statehc06_1.pdf. Accessed May 2009.
- , , , et al.Implementation of a voluntary hospitalist service at a community teaching hospital; improved clinical efficiency and patient outcomes.Ann Intern Med.2002;137:859–865.
- , , , et al.The United States rheumatology workforce: supply and demand, 2005–2025.Arthritis Rheum.2007;56(3):722–729.
- , , , , ;Committee on Manpower for Pulmonary and Critical Care Societies.Caring for the critically ill patient. Current and projected workforce requirements for care of the critically ill and patients with pulmonary disease: can we meet the requirements of an aging population?JAMA.2000;284(21):2762–2770.
- , .The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- , , , , .Reorganizing an academic medical service: impact on cost, quality, patient satisfaction, and education.JAMA.1998;279:1560–1565.
- , , .The effect of full‐time faculty hospitalists on the efficiency of care at a community teaching hospital.Ann Intern Med.1998;129:197–203.
- .An introduction to the hospitalist model.Ann Intern Med.1999;130:338–342.
- , .The hospitalist movement 5 years later.JAMA.2002;287:487–494.
- , , , , .What effect does inpatient physician specialty and experience have on clinical outcomes and resource utilization on a general medical service?J Gen Intern Med.2004;19:395–401.
- , , , et al.The presence of hospitalists in medical education.Acad Med.2000;75(suppl):S34–S36.
- , , , et al.Assessing the value of hospitalists to academic health centers: Brigham and Women's Hospital and Harvard Medical School.Am J Med.1999;106:134–137.
- , .Role of hospitalists in medical education.Am J Med.1999;107(4):305–309.
- , .The hospitalists: new boon for internal medicine or retreat from primary care?Ann Intern Med.1999;130:382–387.
- .The hospitalist movement: caution lights flashing at the crossroads.Am J Med.1999;107:409–413.
- , , .The state of competency evaluation in internal medicine residency.J Gen Intern Med.2008;23(7):1010–1015.
- , , .Sources of satisfaction for residency program directors: a second administration of the PD‐Sat.Am J Med.2009;122(2):196–201.
- , , .What predicts residency accreditation cycle length?Acad Med.2009;84(3):356–361.
- U.S. Census Bureau. Census Regions and Divisions of the United States. Available at: http://www.census.gov/geo/www/us_regdiv.pdf. Accessed May 2009.
- , , , et al.Complying with ACGME resident duty hours restrictions: restructuring the 80‐hour workweek to enhance education and patient safety at Texas A81(12):1026–1031.
- Association of Program Directors in Internal Medicine;, , , , .Redesigning residency education in internal medicine: a position paper from the Association of Program Directors in Internal Medicine.Ann Intern Med.2006;144(12):920–926.
- , , , et al.Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists.Ann Intern Med.2002;137(11):866–874.
- , , , , .Effects of hospitalist attending physicians on trainee satisfaction with teaching and with internal medicine rotations.Arch Intern Med.2004;164:1866–1871.
- , , , et al.Hospitalists as teachers.J Gen Intern Med.2004;19(1):8–15.
- , , , et al.The positive impact of initiation of hospitalist clinician educators.J Gen Intern Med.2004;19(4):293–301.
- , , , , .How to use The core competencies in hospital medicine: a framework for curriculum development.J Hosp Med.2006;1:48–56.
- .The hospitalist model: perspectives of the patient, the internist, and internal medicine.Ann Intern Med.1999;130:368–372.
- American College of Physicians. The impending collapse of primary care medicine and its implications for the state of the nation's health care: a report from the American College of Physicians. January 30,2006. Available at: http://www.acponline.org/advocacy/events/state_of_healthcare/statehc06_1.pdf. Accessed May 2009.
Copyright © 2009 Society of Hospital Medicine
Hospitalists Best Educators in the Hospital
Hospitalists are increasingly assuming a primary role in medical education in the hospital setting, as they also steadily care for a larger portion of hospitalized patients.1 This issue of the Journal of Hospital Medicine highlights the role of hospitalists as teachers in academic medical centers, confirming their expanding and positive role in resident and medical student education. A survey of academic medical centers, a systematic review, an evaluation of the implementation of an educational curriculum, and a survey of residents hint at the challenges hospitalists face in teaching, but also expose us to a more advanced yet facile approach to evaluating the effectiveness of a teaching intervention.25 These publications provoke interesting questions about clinical teaching that hospital medicine educators and researchers should pursue answering. I believe they will also encourage us to innovate in medical education and assessment of that teaching.
Traditionally, teaching attendings for resident teams on medicine or pediatric services rotated through these duties for 1 to 3 months each year, while spending the majority of their time in clinic or research activities. The increasing complexity of hospitalized patients and the pressure to reduce length of stay prompted closer oversight of trainees. With the advent of resident work‐hour restrictions, the need for greater clinical involvement by attending physicians made it increasingly difficult to maintain the traditional model of limited engagement by faculty attendings. Simply put, the dwindling pool of willing and able teaching attendings encouraged teaching hospitals to employ hospitalists to fill the gap in teaching and supervision, as well as clinical coverage.6
Beasley et al.2 report that resident work‐hour restrictions were associated with an increase in the number of teaching hospitals employing hospitalists to 79% of 193 surveyed hospitals in 2007. Of those hospitals with hospitalists, 92% reported that hospitalists serve as attendings on the teaching service. Hospitalists also teach in a number of other venues within these programs, including formal teaching rounds without direct care responsibility, along with delivering didactic lectures and clinical skills education.
How well are teaching hospitalists performing compared to traditional teaching attendings? Natarajan et al.4 provide an important summary of the evidence in a systematic review of studies comparing teaching efforts of hospitalist attendings to those of nonhospitalist attendings. Eight studies from a variety of institutions measured trainee (resident or medical student) attitudes. It is gratifying to learn that hospitalists were generally rated higher at overall teaching effectiveness, provision of feedback, knowledge base, and involvement of the learner in patient care. It seems likely that publication bias would overestimate the positive effect of hospitalists on learner attitudes. However, there are plausible reasons that the positive effect is accurate. Because their professional responsibilities are focused in the hospital, hospitalists should naturally be more available to learners for teaching and feedback. Hospitalists tend to be younger in their academic careers, placing them closer to the cutting edge of knowledge gained during residency and possibly fellowship. They may be more in tune with the needs and pressures faced by their learners, having dealt with these same challenges either during recent training or during nonteaching rotations.
As a relatively young specialty with young and developing academic hospitalists, will the advantage suggested by the Natarajan et al.4 systematic review be sustained over the long term as careers in hospital medicine mature? A 2005 systematic review studying this question among practicing clinicians found, somewhat paradoxically, that older, more experienced clinicians appeared to be at risk for providing lower‐quality care.7 To avoid this decline in clinical effectiveness, hospitalists should proactively seek innovative ways to refresh and update their knowledge and skills throughout their careers. This is particularly critical for teaching physicians. We should seize the opportunity to study the relationship between advancing clinical/teaching experience and educational quality within our teaching programs.
The review by Natarajan et al.4 should also challenge the hospitalist community to achieve even higher levels of proficiency as teachers of medicine. The review alludes to bedside teaching and attention to psychosocial aspects of care as opportunities for improvement by hospitalist teachers. A recent study suggested that physical examination instruction receives declining attention from inpatient teachers and that there are opportunities to increase the amount of bedside teaching.8 A provocative study of inpatients admitted to a teaching service found that physical examination could substantially impact patient care, but that trainees often failed to appreciate significant findings on initial examination.9 How do teaching hospitalists become proficient at physical examination and bedside teaching? Are there models around the country that are successfully developing outstanding clinician educators, incorporating teach‐the‐teacher models to improve physical examination and bedside teaching?
A practical limitation of attitude surveys and learner evaluation is the well‐known phenomenon of grade inflation that resulted in high ratings for all attending groups in the studies summarized by Natarajan et al.4 This limits the ability of surveys or evaluations to distinguish truly outstanding teachers and consequently makes it difficult to analyze the attributes of these teachers. We need better tools to detect and learn teaching techniques from great teachers in the clinical environment. We need studies evaluating the effect of teaching hospitalists on learner knowledge or, even more importantly, learner outcomes. Ultimately, we need studies of educational interventions that evaluate the impact of these interventions on patient outcome.
Wright et al.5 provide guidance as they describe the evaluation of a teaching intervention that moves beyond measurement of knowledge or attitudes. The Johns Hopkins Bayview hospitalist group sought to improve the quality of medical consultations performed by hospitalists and by residents rotating on the consultation service using a case‐based teaching module with audits of recent notes. The participants then audited their most recent consultation notes with feedback from the module teacher. The study employed pretests and posttests of knowledgea standard evaluation for educational interventions. This tells us little about the true impact of the teaching module. However, the study then assessed the quality of written consultations done by hospitalists before and after the educational interventions. Scores of consult notes improved significantly after the intervention, although the number of assessments for each physician was limited. Importantly, we need to know if interventions such as this are sustained over time. Wright's well‐established medical education research group's study design assessed the impact of an intervention on physician performance and moves us closer to assessment of the impact on actual patient outcomes. As clinical teachers, we would like to believe that our teaching and our educational innovations are having a positive impact on patient care. Can we demonstrate this?
As academic medical centers contend with further resident work‐hour restrictions proposed by the Institute of Medicine (IOM),10 how will this affect hospitalist teachers? The study by Mazotti et al.3 from the University of California at San Francisco residency program found that about one‐quarter of residents reported spending less time teaching after implementation of the Accreditation Council for Graduate Medical Education (ACGME) duty‐hour restrictions in 2003. Interestingly, those residents reporting less time spent teaching also reported less emotional exhaustion and perceived that they were delivering higher‐quality patient care. This raises a fascinating question for academic hospitalists. Would these findings be similar among teaching hospitalists and nonteaching hospitalists? What about hospitalists who rotate through months of teaching and nonteaching services? Is teaching emotionally exhausting for experienced teachers? A Mayo Clinic study suggested that the extent that faculty physicians are able to engage in work that is most meaningful to them as individuals is a strong determinant of faculty burnout.11 Is the hospitalist who finds teaching most rewarding at risk of burnout if they are assigned only 2 weeks a year as a teaching attending? The answers to these questions will be critical to hospitalist program leaders trying to assure sustainable careers for hospitalists in their programs.
Although the study by Mazotti et al.3 did not assess the impact of the reduction in resident teaching time on the teaching responsibilities for academic hospitalists, previous studies suggest that faculty are also teaching less since the introduction of work‐hour restrictions.12, 13 If the new IOM recommendations are enacted, who will teach? Although the reported experience following the 2003 work‐hour restrictions begs pessimism, the anticipated changes represent an opportunity for creative hospitalist teachers to demonstrate effective adaptations to the changing and compressed inpatient teaching environment.
In summary, this issue of the Journal presents studies that praise the role hospitalists play in teaching the next generation of physicians, but also gives a glimpse of future challenges and opportunities. We should take advantage of hospitalists' central position in clinical education in the hospital to innovate, study the effect on both learner outcomes and patient outcomes, and share our experiences with the hospitalist and medical education communities.
- , , , .Growth in the care of older patients by hospitalists in the United States.N Engl J Med.2009;360(11):1102–1112.
- , , .Hospitalists involvement in internal medicine residencies.J Hosp Med.2009;4(8):471–475.
- , , , , .Impact of duty hour restriction on resident inpatient teaching.J Hosp Med.2009;4(8):476–480.
- , , , .Effect of hospitalist attending physicians on trainee educational experiences: a systematic review.J Hosp Med.2009;4(8):490–498.
- , , , , , .A case‐based teaching module combined with audit and feedback to improve the quality of consultations.J Hosp Med.2009;4(8):486–489.
- , , , , .Non‐housestaff medicine services in academic centers: models and challenges.J Hosp Med.2008;3(3):247–255.
- , , .Systematic review: the relationship between clinical experience and quality of health care.Ann Intern Med.2005;142(4):260–273.
- , , .Quantification of bedside teaching by an academic hospitalist group.J Hosp Med.2009;4(5):304–307.
- .Physical examination in the care of medical inpatients: an observational study.Lancet.2003;362(9390):1100–1105.
- Institute of Medicine. Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. 2008. Available at: http://www.iom.edu/CMS/3809/48553/60449.aspx. Accessed September2009.
- , , , et al.Career fit and burnout among academic faculty.Arch Intern Med.2009;169(10):990–995.
- , .Teaching internal medicine residents in the new era. Inpatient attending with duty‐hour regulations.J Gen Intern Med.2006;21(5):447–452.
- , , , .Effects of resident work hour limitations on faculty professional lives.J Gen Intern Med.2008;23(7):1077–1083.
Hospitalists are increasingly assuming a primary role in medical education in the hospital setting, as they also steadily care for a larger portion of hospitalized patients.1 This issue of the Journal of Hospital Medicine highlights the role of hospitalists as teachers in academic medical centers, confirming their expanding and positive role in resident and medical student education. A survey of academic medical centers, a systematic review, an evaluation of the implementation of an educational curriculum, and a survey of residents hint at the challenges hospitalists face in teaching, but also expose us to a more advanced yet facile approach to evaluating the effectiveness of a teaching intervention.25 These publications provoke interesting questions about clinical teaching that hospital medicine educators and researchers should pursue answering. I believe they will also encourage us to innovate in medical education and assessment of that teaching.
Traditionally, teaching attendings for resident teams on medicine or pediatric services rotated through these duties for 1 to 3 months each year, while spending the majority of their time in clinic or research activities. The increasing complexity of hospitalized patients and the pressure to reduce length of stay prompted closer oversight of trainees. With the advent of resident work‐hour restrictions, the need for greater clinical involvement by attending physicians made it increasingly difficult to maintain the traditional model of limited engagement by faculty attendings. Simply put, the dwindling pool of willing and able teaching attendings encouraged teaching hospitals to employ hospitalists to fill the gap in teaching and supervision, as well as clinical coverage.6
Beasley et al.2 report that resident work‐hour restrictions were associated with an increase in the number of teaching hospitals employing hospitalists to 79% of 193 surveyed hospitals in 2007. Of those hospitals with hospitalists, 92% reported that hospitalists serve as attendings on the teaching service. Hospitalists also teach in a number of other venues within these programs, including formal teaching rounds without direct care responsibility, along with delivering didactic lectures and clinical skills education.
How well are teaching hospitalists performing compared to traditional teaching attendings? Natarajan et al.4 provide an important summary of the evidence in a systematic review of studies comparing teaching efforts of hospitalist attendings to those of nonhospitalist attendings. Eight studies from a variety of institutions measured trainee (resident or medical student) attitudes. It is gratifying to learn that hospitalists were generally rated higher at overall teaching effectiveness, provision of feedback, knowledge base, and involvement of the learner in patient care. It seems likely that publication bias would overestimate the positive effect of hospitalists on learner attitudes. However, there are plausible reasons that the positive effect is accurate. Because their professional responsibilities are focused in the hospital, hospitalists should naturally be more available to learners for teaching and feedback. Hospitalists tend to be younger in their academic careers, placing them closer to the cutting edge of knowledge gained during residency and possibly fellowship. They may be more in tune with the needs and pressures faced by their learners, having dealt with these same challenges either during recent training or during nonteaching rotations.
As a relatively young specialty with young and developing academic hospitalists, will the advantage suggested by the Natarajan et al.4 systematic review be sustained over the long term as careers in hospital medicine mature? A 2005 systematic review studying this question among practicing clinicians found, somewhat paradoxically, that older, more experienced clinicians appeared to be at risk for providing lower‐quality care.7 To avoid this decline in clinical effectiveness, hospitalists should proactively seek innovative ways to refresh and update their knowledge and skills throughout their careers. This is particularly critical for teaching physicians. We should seize the opportunity to study the relationship between advancing clinical/teaching experience and educational quality within our teaching programs.
The review by Natarajan et al.4 should also challenge the hospitalist community to achieve even higher levels of proficiency as teachers of medicine. The review alludes to bedside teaching and attention to psychosocial aspects of care as opportunities for improvement by hospitalist teachers. A recent study suggested that physical examination instruction receives declining attention from inpatient teachers and that there are opportunities to increase the amount of bedside teaching.8 A provocative study of inpatients admitted to a teaching service found that physical examination could substantially impact patient care, but that trainees often failed to appreciate significant findings on initial examination.9 How do teaching hospitalists become proficient at physical examination and bedside teaching? Are there models around the country that are successfully developing outstanding clinician educators, incorporating teach‐the‐teacher models to improve physical examination and bedside teaching?
A practical limitation of attitude surveys and learner evaluation is the well‐known phenomenon of grade inflation that resulted in high ratings for all attending groups in the studies summarized by Natarajan et al.4 This limits the ability of surveys or evaluations to distinguish truly outstanding teachers and consequently makes it difficult to analyze the attributes of these teachers. We need better tools to detect and learn teaching techniques from great teachers in the clinical environment. We need studies evaluating the effect of teaching hospitalists on learner knowledge or, even more importantly, learner outcomes. Ultimately, we need studies of educational interventions that evaluate the impact of these interventions on patient outcome.
Wright et al.5 provide guidance as they describe the evaluation of a teaching intervention that moves beyond measurement of knowledge or attitudes. The Johns Hopkins Bayview hospitalist group sought to improve the quality of medical consultations performed by hospitalists and by residents rotating on the consultation service using a case‐based teaching module with audits of recent notes. The participants then audited their most recent consultation notes with feedback from the module teacher. The study employed pretests and posttests of knowledgea standard evaluation for educational interventions. This tells us little about the true impact of the teaching module. However, the study then assessed the quality of written consultations done by hospitalists before and after the educational interventions. Scores of consult notes improved significantly after the intervention, although the number of assessments for each physician was limited. Importantly, we need to know if interventions such as this are sustained over time. Wright's well‐established medical education research group's study design assessed the impact of an intervention on physician performance and moves us closer to assessment of the impact on actual patient outcomes. As clinical teachers, we would like to believe that our teaching and our educational innovations are having a positive impact on patient care. Can we demonstrate this?
As academic medical centers contend with further resident work‐hour restrictions proposed by the Institute of Medicine (IOM),10 how will this affect hospitalist teachers? The study by Mazotti et al.3 from the University of California at San Francisco residency program found that about one‐quarter of residents reported spending less time teaching after implementation of the Accreditation Council for Graduate Medical Education (ACGME) duty‐hour restrictions in 2003. Interestingly, those residents reporting less time spent teaching also reported less emotional exhaustion and perceived that they were delivering higher‐quality patient care. This raises a fascinating question for academic hospitalists. Would these findings be similar among teaching hospitalists and nonteaching hospitalists? What about hospitalists who rotate through months of teaching and nonteaching services? Is teaching emotionally exhausting for experienced teachers? A Mayo Clinic study suggested that the extent that faculty physicians are able to engage in work that is most meaningful to them as individuals is a strong determinant of faculty burnout.11 Is the hospitalist who finds teaching most rewarding at risk of burnout if they are assigned only 2 weeks a year as a teaching attending? The answers to these questions will be critical to hospitalist program leaders trying to assure sustainable careers for hospitalists in their programs.
Although the study by Mazotti et al.3 did not assess the impact of the reduction in resident teaching time on the teaching responsibilities for academic hospitalists, previous studies suggest that faculty are also teaching less since the introduction of work‐hour restrictions.12, 13 If the new IOM recommendations are enacted, who will teach? Although the reported experience following the 2003 work‐hour restrictions begs pessimism, the anticipated changes represent an opportunity for creative hospitalist teachers to demonstrate effective adaptations to the changing and compressed inpatient teaching environment.
In summary, this issue of the Journal presents studies that praise the role hospitalists play in teaching the next generation of physicians, but also gives a glimpse of future challenges and opportunities. We should take advantage of hospitalists' central position in clinical education in the hospital to innovate, study the effect on both learner outcomes and patient outcomes, and share our experiences with the hospitalist and medical education communities.
Hospitalists are increasingly assuming a primary role in medical education in the hospital setting, as they also steadily care for a larger portion of hospitalized patients.1 This issue of the Journal of Hospital Medicine highlights the role of hospitalists as teachers in academic medical centers, confirming their expanding and positive role in resident and medical student education. A survey of academic medical centers, a systematic review, an evaluation of the implementation of an educational curriculum, and a survey of residents hint at the challenges hospitalists face in teaching, but also expose us to a more advanced yet facile approach to evaluating the effectiveness of a teaching intervention.25 These publications provoke interesting questions about clinical teaching that hospital medicine educators and researchers should pursue answering. I believe they will also encourage us to innovate in medical education and assessment of that teaching.
Traditionally, teaching attendings for resident teams on medicine or pediatric services rotated through these duties for 1 to 3 months each year, while spending the majority of their time in clinic or research activities. The increasing complexity of hospitalized patients and the pressure to reduce length of stay prompted closer oversight of trainees. With the advent of resident work‐hour restrictions, the need for greater clinical involvement by attending physicians made it increasingly difficult to maintain the traditional model of limited engagement by faculty attendings. Simply put, the dwindling pool of willing and able teaching attendings encouraged teaching hospitals to employ hospitalists to fill the gap in teaching and supervision, as well as clinical coverage.6
Beasley et al.2 report that resident work‐hour restrictions were associated with an increase in the number of teaching hospitals employing hospitalists to 79% of 193 surveyed hospitals in 2007. Of those hospitals with hospitalists, 92% reported that hospitalists serve as attendings on the teaching service. Hospitalists also teach in a number of other venues within these programs, including formal teaching rounds without direct care responsibility, along with delivering didactic lectures and clinical skills education.
How well are teaching hospitalists performing compared to traditional teaching attendings? Natarajan et al.4 provide an important summary of the evidence in a systematic review of studies comparing teaching efforts of hospitalist attendings to those of nonhospitalist attendings. Eight studies from a variety of institutions measured trainee (resident or medical student) attitudes. It is gratifying to learn that hospitalists were generally rated higher at overall teaching effectiveness, provision of feedback, knowledge base, and involvement of the learner in patient care. It seems likely that publication bias would overestimate the positive effect of hospitalists on learner attitudes. However, there are plausible reasons that the positive effect is accurate. Because their professional responsibilities are focused in the hospital, hospitalists should naturally be more available to learners for teaching and feedback. Hospitalists tend to be younger in their academic careers, placing them closer to the cutting edge of knowledge gained during residency and possibly fellowship. They may be more in tune with the needs and pressures faced by their learners, having dealt with these same challenges either during recent training or during nonteaching rotations.
As a relatively young specialty with young and developing academic hospitalists, will the advantage suggested by the Natarajan et al.4 systematic review be sustained over the long term as careers in hospital medicine mature? A 2005 systematic review studying this question among practicing clinicians found, somewhat paradoxically, that older, more experienced clinicians appeared to be at risk for providing lower‐quality care.7 To avoid this decline in clinical effectiveness, hospitalists should proactively seek innovative ways to refresh and update their knowledge and skills throughout their careers. This is particularly critical for teaching physicians. We should seize the opportunity to study the relationship between advancing clinical/teaching experience and educational quality within our teaching programs.
The review by Natarajan et al.4 should also challenge the hospitalist community to achieve even higher levels of proficiency as teachers of medicine. The review alludes to bedside teaching and attention to psychosocial aspects of care as opportunities for improvement by hospitalist teachers. A recent study suggested that physical examination instruction receives declining attention from inpatient teachers and that there are opportunities to increase the amount of bedside teaching.8 A provocative study of inpatients admitted to a teaching service found that physical examination could substantially impact patient care, but that trainees often failed to appreciate significant findings on initial examination.9 How do teaching hospitalists become proficient at physical examination and bedside teaching? Are there models around the country that are successfully developing outstanding clinician educators, incorporating teach‐the‐teacher models to improve physical examination and bedside teaching?
A practical limitation of attitude surveys and learner evaluation is the well‐known phenomenon of grade inflation that resulted in high ratings for all attending groups in the studies summarized by Natarajan et al.4 This limits the ability of surveys or evaluations to distinguish truly outstanding teachers and consequently makes it difficult to analyze the attributes of these teachers. We need better tools to detect and learn teaching techniques from great teachers in the clinical environment. We need studies evaluating the effect of teaching hospitalists on learner knowledge or, even more importantly, learner outcomes. Ultimately, we need studies of educational interventions that evaluate the impact of these interventions on patient outcome.
Wright et al.5 provide guidance as they describe the evaluation of a teaching intervention that moves beyond measurement of knowledge or attitudes. The Johns Hopkins Bayview hospitalist group sought to improve the quality of medical consultations performed by hospitalists and by residents rotating on the consultation service using a case‐based teaching module with audits of recent notes. The participants then audited their most recent consultation notes with feedback from the module teacher. The study employed pretests and posttests of knowledgea standard evaluation for educational interventions. This tells us little about the true impact of the teaching module. However, the study then assessed the quality of written consultations done by hospitalists before and after the educational interventions. Scores of consult notes improved significantly after the intervention, although the number of assessments for each physician was limited. Importantly, we need to know if interventions such as this are sustained over time. Wright's well‐established medical education research group's study design assessed the impact of an intervention on physician performance and moves us closer to assessment of the impact on actual patient outcomes. As clinical teachers, we would like to believe that our teaching and our educational innovations are having a positive impact on patient care. Can we demonstrate this?
As academic medical centers contend with further resident work‐hour restrictions proposed by the Institute of Medicine (IOM),10 how will this affect hospitalist teachers? The study by Mazotti et al.3 from the University of California at San Francisco residency program found that about one‐quarter of residents reported spending less time teaching after implementation of the Accreditation Council for Graduate Medical Education (ACGME) duty‐hour restrictions in 2003. Interestingly, those residents reporting less time spent teaching also reported less emotional exhaustion and perceived that they were delivering higher‐quality patient care. This raises a fascinating question for academic hospitalists. Would these findings be similar among teaching hospitalists and nonteaching hospitalists? What about hospitalists who rotate through months of teaching and nonteaching services? Is teaching emotionally exhausting for experienced teachers? A Mayo Clinic study suggested that the extent that faculty physicians are able to engage in work that is most meaningful to them as individuals is a strong determinant of faculty burnout.11 Is the hospitalist who finds teaching most rewarding at risk of burnout if they are assigned only 2 weeks a year as a teaching attending? The answers to these questions will be critical to hospitalist program leaders trying to assure sustainable careers for hospitalists in their programs.
Although the study by Mazotti et al.3 did not assess the impact of the reduction in resident teaching time on the teaching responsibilities for academic hospitalists, previous studies suggest that faculty are also teaching less since the introduction of work‐hour restrictions.12, 13 If the new IOM recommendations are enacted, who will teach? Although the reported experience following the 2003 work‐hour restrictions begs pessimism, the anticipated changes represent an opportunity for creative hospitalist teachers to demonstrate effective adaptations to the changing and compressed inpatient teaching environment.
In summary, this issue of the Journal presents studies that praise the role hospitalists play in teaching the next generation of physicians, but also gives a glimpse of future challenges and opportunities. We should take advantage of hospitalists' central position in clinical education in the hospital to innovate, study the effect on both learner outcomes and patient outcomes, and share our experiences with the hospitalist and medical education communities.
- , , , .Growth in the care of older patients by hospitalists in the United States.N Engl J Med.2009;360(11):1102–1112.
- , , .Hospitalists involvement in internal medicine residencies.J Hosp Med.2009;4(8):471–475.
- , , , , .Impact of duty hour restriction on resident inpatient teaching.J Hosp Med.2009;4(8):476–480.
- , , , .Effect of hospitalist attending physicians on trainee educational experiences: a systematic review.J Hosp Med.2009;4(8):490–498.
- , , , , , .A case‐based teaching module combined with audit and feedback to improve the quality of consultations.J Hosp Med.2009;4(8):486–489.
- , , , , .Non‐housestaff medicine services in academic centers: models and challenges.J Hosp Med.2008;3(3):247–255.
- , , .Systematic review: the relationship between clinical experience and quality of health care.Ann Intern Med.2005;142(4):260–273.
- , , .Quantification of bedside teaching by an academic hospitalist group.J Hosp Med.2009;4(5):304–307.
- .Physical examination in the care of medical inpatients: an observational study.Lancet.2003;362(9390):1100–1105.
- Institute of Medicine. Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. 2008. Available at: http://www.iom.edu/CMS/3809/48553/60449.aspx. Accessed September2009.
- , , , et al.Career fit and burnout among academic faculty.Arch Intern Med.2009;169(10):990–995.
- , .Teaching internal medicine residents in the new era. Inpatient attending with duty‐hour regulations.J Gen Intern Med.2006;21(5):447–452.
- , , , .Effects of resident work hour limitations on faculty professional lives.J Gen Intern Med.2008;23(7):1077–1083.
- , , , .Growth in the care of older patients by hospitalists in the United States.N Engl J Med.2009;360(11):1102–1112.
- , , .Hospitalists involvement in internal medicine residencies.J Hosp Med.2009;4(8):471–475.
- , , , , .Impact of duty hour restriction on resident inpatient teaching.J Hosp Med.2009;4(8):476–480.
- , , , .Effect of hospitalist attending physicians on trainee educational experiences: a systematic review.J Hosp Med.2009;4(8):490–498.
- , , , , , .A case‐based teaching module combined with audit and feedback to improve the quality of consultations.J Hosp Med.2009;4(8):486–489.
- , , , , .Non‐housestaff medicine services in academic centers: models and challenges.J Hosp Med.2008;3(3):247–255.
- , , .Systematic review: the relationship between clinical experience and quality of health care.Ann Intern Med.2005;142(4):260–273.
- , , .Quantification of bedside teaching by an academic hospitalist group.J Hosp Med.2009;4(5):304–307.
- .Physical examination in the care of medical inpatients: an observational study.Lancet.2003;362(9390):1100–1105.
- Institute of Medicine. Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. 2008. Available at: http://www.iom.edu/CMS/3809/48553/60449.aspx. Accessed September2009.
- , , , et al.Career fit and burnout among academic faculty.Arch Intern Med.2009;169(10):990–995.
- , .Teaching internal medicine residents in the new era. Inpatient attending with duty‐hour regulations.J Gen Intern Med.2006;21(5):447–452.
- , , , .Effects of resident work hour limitations on faculty professional lives.J Gen Intern Med.2008;23(7):1077–1083.
The Third Time's the Charm
A 58‐year old woman was brought to the emergency department with confusion. Her husband stated that for several hours she had been drifting in and out at home, and that he had to shout to get her attention. He described no seizure activity, weakness, incontinence, or difficulty speaking, and had noted no complaints of headache, fevers, chest pain, shortness of breath, or gastrointestinal complaints.
Altered mental status in a middle‐aged woman can result from a diverse set of etiologies. A key distinction in the neurological examination will be to assure that the complaint of confusion is accurate as opposed to aphasia; the former is usually indicative of diffuse cerebral dysfunction while the latter suggests a focal lesion in the dominant hemisphere.
The acuity of the change in mental status is important, as are the fluctuations described by the husband. Unwitnessed or nonconvulsive seizure activity can present this way. Toxic/metabolic etiologies, infectious and inflammatory disorders of the central nervous system (CNS), and vascular diseases are also important considerations. Although stroke does not typically present with global encephalopathy, intermittent large vessel occlusion, especially in the posterior circulation, can disrupt cognition in this manner. Following a physical examination, initial workup should focus on toxic/metabolic etiologies, followed rapidly by head imaging if no cause is identified.
Her past medical history was notable for type 2 diabetes mellitus, coronary artery disease, hyperlipidemia, and an unspecified seizure disorder, which according to her husband was diagnosed during a recent hospitalization for a similar presentation. She also had a remote history of venous thromboembolism and antithrombin‐III deficiency. She was unemployed, lived with her husband, and spent most of her time at home. She never smoked, and rarely drank alcohol. Her family history was unobtainable, and her husband denied that she used any illicit drugs. Her medications included pioglitazone, aspirin, simvastatin, pregabalin, ferrous sulfate, levetiracetam, warfarin, and magnesium oxide, and she was allergic to sulfa.
While the differential diagnosis remains broad, 3 elements of the history are potentially relevant. The history of epilepsy based on a similar prior presentation increases the likelihood that the current spell is ictal in nature; examination of previous records would be important in order to document whether these spells have indeed been proven to be epileptic, as many conditions can mimic seizures. Given the history of venous thromboembolism and hypercoagulability, one must consider cerebral venous sinus thrombosis, which can present with global neurologic dysfunction and seizures. Prompt identification, usually via computed tomography (CT) or magnetic resonance angiography, is vital, because anticoagulation can mitigate this potentially life‐threatening illness. Finally, although many medications can cause encephalopathy in overdose, levetiracetam has well‐described cognitive side effects even at usual doses, including encephalopathy, irritability, and depression.
The records from that recent hospitalization remarked that she had presented confused and stuporous. Her potassium had been 2.7 mmol/L, international normalized ration (INR) 3.4, and hemoglobin 8 g/dL; other routine laboratory studies were normal. CT and magnetic resonance imaging (MRI) of the brain had been negative, and electroencephalogram (EEG) reportedly was performed but specific results were unknown. She was discharged alert and oriented 1 week prior to the current presentation on the above medications, including levetiracetam for this newly‐diagnosed seizure disorder.
Previous records confirm that the current presentation is that of a relapsing acute alteration in mental status. Regardless of the EEG findings or response to antiepileptic medications, a seizure disorder should remain a primary consideration, although relapsing inflammatory, toxic/metabolic conditions, and, rarely, vascular disorders can also present in this manner.
The neurologic manifestations of hypokalemia are usually peripheral in nature, including periodic paralysis; confusion accompanying hypokalemia is usually not a result of the low potassium itself but rather due to an underlying toxic or endocrinologic cause. Various causes of anemia can lead to mental status changes; the mean corpuscular volume (MCV) will be particularly helpful given known associations between megaloblastic anemia and confusional states.
On examination, she appeared to be in good health and in no distress. She was afebrile. Her blood pressure was 93/57, pulse 90 beats per minute, respiratory rate 16 per minute, and room air oxygen saturation 100%. She was oriented to her surroundings, but slow in her responses to questioning. There were no cranial nerve, motor, or sensory deficits, or abnormal reflexes or movements. Examination of the head, skin, chest, cardiovascular system, abdomen, and extremities was normal. Serum sodium was 136 mmol/L, creatinine 1.2 mg/dL, calcium 9.3 mg/dL, and glucose 81 mg/dL; other routine blood chemistries were normal. Her white blood cell (WBC) count was 7100/L, hemoglobin 9.2 g/dL with normal MCV, and platelet count 275,000/L. INR was 3.4, and liver function tests were normal. CT of the brain demonstrated no evidence of acute pathology.
Given that her laboratory results (aside from the hemoglobin) and CT were essentially normal, the most common etiology of a recurrent encephalopathy would be a toxic exposure including drugs, alcohol, and environmental toxins or poisons. A comprehensive serum drug screen, including heavy metals, could follow a basic urinary screen for drugs of abuse; specific etiologies may be suggested by patterns of injury seen on MRI such as those seen with carbon monoxide or methanol exposure. Other recurrent metabolic processes include the porphyrias and relapsing inflammatory disorders, which could be entertained if further diagnostics are unrevealing.
An EEG is warranted at this point and is a test that is underutilized in the workup of altered mental status. Patients who have a spell and do not quickly awaken should be considered to be in nonconvulsive status epilepticus until proven otherwise. This can be easily identified on the EEG and is an important entity to recognize quickly. Additional findings on EEG may suggest focal cerebral dysfunction (such as that following a seizure or acute unilateral injury), diffuse encephalopathy (eg, triphasic waves), or fairly specific diagnoses (eg, periodic lateralized epileptiform discharges from the temporal lobes in suspected herpes simplex meningoencephalitis). While the CT of the brain is a reasonable initial screen, MRI is more sensitive for structural disease and should be obtained if no etiology is rapidly identified.
Finally, acute infectious etiologies such as abscess, encephalitis, or meningoencephalitis need to be excluded via lumbar puncture. Spinal fluid examination also can be helpful in the consideration of inflammatory and autoimmune disorders.
Over the next several hours, while still in the emergency department, she became increasingly obtunded, to the point that she was unresponsive to all stimuli. No seizure activity was witnessed, her vital signs were unchanged, and no medications had been administered. She was urgently transferred to a tertiary care center, where, at the time of arrival, she was obtunded and nonverbal, and opened her eyes only to noxious stimuli. She would withdraw all 4 extremities in response to pain. Pupils were 2 mm and symmetrically reactive. Corneal reflexes were normal, and her gag reflex was diminished. Motor tone was decreased in all 4 extremities. No fasciculations were noted. Deep tendon reflexes were present but symmetrically diminished throughout, and Babinski testing demonstrated a withdrawal response bilaterally.
Coma is a state of profound unconsciousness where the patient is unarousable and unaware of her surroundings. Coma can result either from bihemispheric dysfunction or diffuse injury to the reticular activating system in the brainstem, and the physical examination should focus on distinguishing between these 2 sites. Because the nuclei of cranial nerves III through XII (excepting XI) reside in the brainstem, the coma examination emphasizes testing the cranial nerves; although all cranial nerves are not tested in this patient, the ones that are appear to be normal, making bihemispheric dysfunction most likely. Bihemispheric coma most commonly results from diffuse toxic or metabolic etiologies such as intoxication or hepatic encephalopathy, but it can also be caused by bilateral structural lesions (including the bilateral thalami) or ongoing seizure activity.
Although an EEG remains the key test in this patient given her past history and an MRI would prove extremely useful, her deterioration warrants a workup for CNS infection. Since the head CT was negative, it would be prudent to proceed with urgent lumbar puncture (although it should never be performed in a patient with significant coagulopathy due to risks of hemorrhage leading to spinal cord injury). She should be covered empirically with broad spectrum meningeal‐dose antibiotics, including acyclovir, until the results of the spinal fluid examination are known, given that bacterial meningitis and herpes meningoencephalitis carry a high morbidity and mortality if not treated promptly.
Routine blood tests were similar to her labs at the referring emergency room. Ammonia level was 10 mol/L. Urine toxicology screen was negative, and blood tests for ethanol, salicylates, lithium, and acetaminophen were negative. Chest X‐ray and urinalysis were normal, and electrocardiogram was notable only for a sinus tachycardia. Cultures of the blood were obtained and the patient was admitted to the intensive care unit.
Levetiracetam, vancomycin, piperacillin‐tazobactam, and acyclovir were initiated. A lumbar puncture was performed without reversing the anticoagulation, and the procedure was traumatic. The cerebrospinal fluid was bloody, with a clear supernatant. Cell count demonstrated a red blood cell (RBC) count of 1250/L and a WBC count of 9/L, with a WBC differential of 42% neutrophils, 48% lymphocytes, and 8% monocytes. The cerebrospinal fluid (CSF) glucose was 62 mg/dL (with a serum glucose of 74 mg/dL) and protein 41 mg/dL. The CSF Gram stain demonstrated no organisms, and fluid was sent for routine culture and polymerase chain reaction (PCR) to detect herpes simplex virus (HSV). A neurology consultation was urgently requested.
As mentioned, it would have been more appropriate to reverse the patient's anticoagulation prior to lumbar puncture. The absence of xanthochromia suggests that the RBCs seen in the sample were introduced at the time of the lumbar puncture, arguing against a hemorrhagic disorder of the CNS (occasionally seen with herpes simplex encephalitis) or spinal fluid (eg, subarachnoid hemorrhage).
A reasonable rule of thumb to correct for the number of RBCs in a traumatic lumbar puncture is to allow 1 WBC for every 700 RBCs/L. Given this conversion, there are still too many WBCs in this sample, indicating a mild pleocytosis that is approximately one‐half neutrophilic and one‐half lymphocytic. This profile is nonspecific and can occur with a variety of conditions including stroke, seizure, inflammatory disorders, and infections, including viruses such as West Nile virus.
While coverage with acyclovir and broad‐spectrum antibacterials is appropriate, it should be noted that piperacillin‐tazobactam has poor CSF penetration and therefore is not a good choice for empiric coverage of CNS infections.
The neurologist's examination additionally noted multifocal myoclonus with noxious stimuli, most prominent in the face and toes. An urgent EEG demonstrated continuous, slow, generalized triphasic wave activity (Figures 1 and 2); no epileptiform discharges were seen. The erythrocyte sedimentation rate (ESR) was 66 mm/hour (normal, 0‐30), and tests for antinuclear antibodies, serum levetiracetam level, and thyroid function studies were ordered.

Stimulus‐evoked multifocal myoclonus is a general marker of encephalopathy found in many conditions, including hepatic and renal failure, drug intoxication (eg, opiates), neurodegenerative disorders (eg, Creutzfeldt‐Jakob disease [CJD]), and postanoxic injury, the latter of which is termed the Lance‐Adams syndrome.
Triphasic waves on EEG, while commonly associated with hepatic encephalopathy, have a similarly broad differential diagnosis, although in a comatose patient, they must first and foremost be distinguished from the repetitive discharges characteristic of nonconvulsive status epilepticus. In addition to hepatic and renal failure, triphasic waves have also been described in medication toxicity (especially with anticonvulsants, lithium, and cephalosporins), CNS infections (including Lyme disease and West Nile virus), strokes involving the bilateral thalami (usually from deep venous thrombosis), inflammatory disorders (such as Hashimoto's encephalopathy [HE]), and neurodegenerative diseases. It is important to remember that a single EEG does not exclude the possibility of an episodic ictal disorder and longer‐term monitoring would be required to definitively exclude seizures.
At this point, although the myoclonus and triphasic waves most commonly would indicate a toxic/metabolic process, the elevated ESR and CSF pleocytosis argue for an inflammatory or infectious condition. An MRI remains the next most useful test to guide further workup because many such conditions have distinct signatures on MRI.
The following day, she was noted to have periods of alertnessopening her eyes and following some commandsbut at other times she was difficult to arouse or obtunded. Tremulous movements and sporadic myoclonic jerks continued but no focal neurologic signs were found. Although there was increased muscle tone throughout, she was intermittently seen moving her limbs spontaneously, but not to command. No new findings were appreciated on routine laboratory tests. Antinuclear antibody testing was negative. Serum levetiracetam level was 23.5 g/mL (reference range, 545). Serum thyroid‐stimulating hormone was less than 0.005 U/mL, but free T3 was 3.5 pg/mL (normal, 1.8‐4.6) and free T4 was 2.0 ng/dL (normal, 0.71.8). An MRI of the brain was compromised by motion artifact but no significant abnormalities were appreciated.
At this point, a family member in another state disclosed that the patient had also been hospitalized 2 months previously while visiting him. Her chief complaint had been shortness of breath. The records were obtained; a cardiac catheterization had revealed nonobstructive coronary disease, and medical management was recommended. The notes mentioned that during the hospitalization she developed altered mental status with disorientation and shaking. CT and MRI of the brain had been unremarkable. The confusion was not explained, but she was discharged in good condition, alert and fully‐oriented.
The additional history confirms a relapsing encephalopathy, now with at least 3 occurrences. The most common etiologies in the face of a normal MRI and basic labs would be recurrent intoxication or exposures, but the inflammatory CSF profile and elevated ESR are not consistent with this. A variety of inflammatory disorders can present with recurrent encephalopathy, including demyelinating diseases and neurosarcoidosis. Some systemic rheumatologic conditions, such as systemic lupus erythematosus, can present with relapsing neurologic symptoms due to seizures, vasculitis, or cerebritis. Vasculitis would fit this picture as well, except for the normal findings on 2 MRIs. In a patient with such dramatic symptoms of neurologic dysfunction, one would expect to see changes on the MRI of cerebral inflammation with probable ischemia.
Therefore, given the CSF, ESR, clinical course, and unrevealing MRI and EEG, the most likely group of disorders responsible would be the nonvasculitic autoimmune meningoencephalitides, which present with recurrent encephalopathy and feature spontaneous remissions and/or often‐dramatic responses to corticosteroids. Key disorders in this category include Sjogren's disease, lupus, and steroid responsive encephalopathy associated with autoimmune thyroiditis (Hashimoto's encephalopathy). The latter condition is the most common of the group and is suggested by the abnormal thyroid‐stimulating hormone testing, although it may occur in the setting of normal thyroid function. The diagnosis can be confirmed with thyroperoxidase and thyroglobulin antibody testing.
Three days into the hospitalization, her mental status had gradually improved such that she was more consistently awake and oriented to person and place, and she was transferred to a regular nursing unit. Final results from the CSF and blood cultures were negative, as was PCR for HSV. The antimicrobials were discontinued. Routine serum chemistries continued to be unremarkable. Additional studies recommended by the neurologist demonstrated an antithyroperoxidase antibody concentration of 587.1 IU/mL (normal, 5), and antithyroglobulin antibody level of 52.2 IU/mL (normal, 10).
These results confirm the diagnosis of HE which, in addition to its presentation as a recurrent illness, is an important treatable cause of dementia and should be considered in young patients, those with autoimmune and thyroid disorders, and those whose dementia is rapidly progressive. Most cases are thought to be steroid‐responsive, but some studies have defined the disorder based on this responsiveness, resulting in some nonresponders likely being overlooked.
A trial of corticosteroids should be considered if the patient does not quickly return to baseline given the potential morbidities associated with prolonged altered mental status to this degree. Whether initiation of chronic immunosuppression could prevent these attacks in the future is unclear from the literature but should be considered given the recurrent, dramatic presentation in this patient.
A diagnosis of HE was made, and she was prescribed corticosteroids. Twenty‐four hours later, she was alert and fully‐oriented. She was discharged to home on prednisone and seen in follow‐up in neurology clinic 1 month later. She had had no further episodes of confusion or stupor, but because of steroid‐induced hyperglycemia, her corticosteroids were decreased and mycophenolate mofetil added for chronic immunosuppression. Four months after discharge she was neurologically stable but continued to struggle with the adverse effects of chronic corticosteroid treatment.
COMMENTARY
HE is an uncommon condition that can present with a rapidly progressive decline and should be considered in patients who present with recurrent mental status change in the setting of normal imaging studies and routine laboratory results. The entity was initially described by Lord William Russell Brain in 1966, and in the most recent terminology is known as steroid‐responsive encephalopathy associated with autoimmune thyroiditis (SREAT).1 It is characterized by an acute or subacute encephalopathy associated with thyroid autoimmunity. Patients typically present with fluctuating symptoms, episodes of confusion, alterations of consciousness, and rapid cognitive decline.2 Common features include myoclonus, tremor, ataxia, speech disturbance, stroke‐like episodes, increased muscle tone, neuropsychiatric manifestations, and seizures, that in some cases may progress to status epilepticus.3, 4
Although serum antithyroglobulin and antithyroperoxidase antibodies are elevated in HE, their presence is thought to be an epiphenomenon of the condition rather than the direct cause. Supporting this are the facts that the incidence of encephalopathy is not increased in patients with established autoimmune thyroiditis, and the presence of antithyroid antibodies ranges from 5% to 20% in the general population.2, 5 There is also no evidence that thyroid antibodies directly react with brain tissue, and the levels of these antibodies do not correlate with either neurologic manifestations or clinical improvement.2, 4, 5 As HE has been reported in patients with euthyroidism, hypothyroidism, and hyperthyroidism (with hypothyroidismeither subclinical or activemost common), it is also unlikely that the level of thyroid hormones play a role in the etiology of this disease.2, 4, 6
The etiology and pathogenesis of HE are unclear, although an immune‐mediated process is generally implicated, either from an inflammatory vasculitis or as a form of acute disseminated encephalomyelitis.7‐9 Global hypoperfusion on single‐photon emission computed tomography (SPECT) studies has also been reported.10, 11 Patients with HE may have nonspecific evidence of inflammation, including an elevated ESR, CRP, and CSF protein.12 Other laboratory abnormalities may include a mild elevation of liver aminotransferase levels; renal impairment has also been reported in a few cases of HE in the form of glomerulonephritis, and may be related to deposition of immune complexes containing thyroglobulin antigen.6, 12‐14 MRI of the brain is normal or nonspecific in most cases, and the EEG most commonly shows diffuse slowing.
The differential for a rapidly progressive cognitive decline includes CJD, CNS vasculitis, paraneoplastic syndromes, and autoimmune and subacute infectious encephalopathies. In patients with CJD, T2‐weighted imaging may show hyperintense signals in the basal ganglia, while diffusion‐weighted sequences may reveal changes in the cortical ribbon and bilateral thalami.15 In CNS vasculitis, the imaging findings are variable and range from discrete areas of vascular infarcts to hemorrhagic lesions.16 In paraneoplastic and autoimmune encephalopathies (excluding HE), MRI often shows nonenhancing signal intensity changes in the mesial temporal lobes.12 This patient had repeatedly normal MRI studies of the brain, which in combination with the history of tremor, myoclonus, seizures, and interval return to baseline status, helped point to the diagnosis of HE.
Different approaches to treatment of HE have been recommended. As the acronym SREAT suggests, patients typically respond dramatically to high‐dose steroid therapy. Although a number of patients also improve spontaneously, up to 60% of patients experience a relapsing course and require chronic immunosuppressive agents for maintenance therapy, including long‐term steroids and azathioprine.2, 17 Treatment with plasma exchange and intravenous immune globulin have also been reported, but with mixed results.18, 19 Due to her history of multiple relapses, the patient was placed on mycophenolate mofetil for additional maintenance immunosuppression, as her corticosteroid dose was reduced due to adverse effects.
Acute mental status change is a potentially emergent situation that must be evaluated with careful history and studies to exclude life‐threatening metabolic, infectious, and vascular conditions. This patient presented similarly on 2 prior occasions, and each time her physician team evaluated what appeared to be a new onset of altered consciousness, reaching a plausible but ultimately incorrect diagnosis. The patient's third presentation was finally the charm, as her physicians learned of the repeated history of a confusional state, and in particular the return to baseline status, allowing them to create a differential that focused on etiologies of relapsing encephalopathy and make the correct diagnosis.
Key Points
-
Recurrent acute or subacute cognitive deterioration invokes a differential diagnosis of toxic/metabolic disorders and unusual inflammatory conditions.
-
The nonvasculitic autoimmune encephalopathies are a group of uncommon conditions characterized by nonspecific findings of inflammation and generally unremarkable CNS imaging studies.
-
HE, or SREAT, is the most common of these conditions, and is notable for mental status changes, various findings of increased muscular tone, thyroid autoimmunity, and generally a dramatic response to corticosteroids.
- , , .Hashimoto's disease and encephalopathy.Lancet.1966;2:512–514.
- , , .Hashimoto encephalopathy: syndrome or myth?Arch Neurol.2003;60:164–171.
- , , .Pisani F. Recurrent status epilepticus as the main feature of Hashimoto's encephalopathy.Epilepsy Behav.2006;8:328–330.
- , , , et al.Steroid‐responsive encephalopathy associated with autoimmune thyroiditis.Arch Neurol.2006;63:197–202.
- , , , , .Encephalopathy associated with Hashimoto thyroiditis: diagnosis and treatment.J Neurol.1996;243:585–593.
- , , , , .Hashimoto's encephalopathy: a steroid‐responsive disorder associated with high anti‐thyroid antibody titers‐report of 5 cases.Neurology.1991;41:228–233.
- , , , , .Hashimoto encephalopathy: a brainstem vasculitis?Neurology.2000;54:769–770.
- , , , , .Nonvasculitic autoimmune inflammatory meningoencephalitis (NAIM): A reversible form of encephalopathy.Neurology.1999;53:1579–1581.
- , , , .Hashimoto's encephalopathy: postmortem findings after fatal status epilepticus.Neurology.2003;61:1124–1126.
- , , .Autoimmune thyroiditis and a rapidly progressive dementia: global hypoperfusion on SPECT scanning suggests a possible mechanism.Neurology.1997;49:623–626.
- , , , , .Hashimoto's encephalopathy: clinical, SPECT and neurophysiologic data.QJM.2003;96:455–457.
- , , .Autoimmune Encephalopathies.The Neurologist.2007;13:140–147.
- , , , , , .Thyroid antigen‐antibody nephritis.Clin Immunol Immunopathol1976;6:341–346.
- , , .Immune complex glomerulonephritis mediated by thyroid antigens.Arch Pathol Lab Med1978;102:530–533.
- , , , et al.Diffusion‐weighted MR imaging of early‐stage Creutzfeldt‐Jakob disease: typical and atypical manifestations.Radiographics.2006;26:S191–S204.
- , , , , .CNS vasculitis in autoimmune disease: MR imaging findings and correlation with angiography.AJNR Am J Neuroradiol.1999;20:75–85.
- , .Long‐Term Treatment of Hashimoto's Encephalopathy.J Neuropsychiatry Clin Neurosci.2006;18:14–20.
- , .Hashimoto's encephalopathy: steroid resistance and response to intravenouc immunoglobulins.J Neurol Neurosurg Psychiatry.2005;76:455–456.
- , .Hashimoto's encephalopathy responding to plasmapheresis.J Neurol Neurosurg Psychiatry.2001;70:132.
A 58‐year old woman was brought to the emergency department with confusion. Her husband stated that for several hours she had been drifting in and out at home, and that he had to shout to get her attention. He described no seizure activity, weakness, incontinence, or difficulty speaking, and had noted no complaints of headache, fevers, chest pain, shortness of breath, or gastrointestinal complaints.
Altered mental status in a middle‐aged woman can result from a diverse set of etiologies. A key distinction in the neurological examination will be to assure that the complaint of confusion is accurate as opposed to aphasia; the former is usually indicative of diffuse cerebral dysfunction while the latter suggests a focal lesion in the dominant hemisphere.
The acuity of the change in mental status is important, as are the fluctuations described by the husband. Unwitnessed or nonconvulsive seizure activity can present this way. Toxic/metabolic etiologies, infectious and inflammatory disorders of the central nervous system (CNS), and vascular diseases are also important considerations. Although stroke does not typically present with global encephalopathy, intermittent large vessel occlusion, especially in the posterior circulation, can disrupt cognition in this manner. Following a physical examination, initial workup should focus on toxic/metabolic etiologies, followed rapidly by head imaging if no cause is identified.
Her past medical history was notable for type 2 diabetes mellitus, coronary artery disease, hyperlipidemia, and an unspecified seizure disorder, which according to her husband was diagnosed during a recent hospitalization for a similar presentation. She also had a remote history of venous thromboembolism and antithrombin‐III deficiency. She was unemployed, lived with her husband, and spent most of her time at home. She never smoked, and rarely drank alcohol. Her family history was unobtainable, and her husband denied that she used any illicit drugs. Her medications included pioglitazone, aspirin, simvastatin, pregabalin, ferrous sulfate, levetiracetam, warfarin, and magnesium oxide, and she was allergic to sulfa.
While the differential diagnosis remains broad, 3 elements of the history are potentially relevant. The history of epilepsy based on a similar prior presentation increases the likelihood that the current spell is ictal in nature; examination of previous records would be important in order to document whether these spells have indeed been proven to be epileptic, as many conditions can mimic seizures. Given the history of venous thromboembolism and hypercoagulability, one must consider cerebral venous sinus thrombosis, which can present with global neurologic dysfunction and seizures. Prompt identification, usually via computed tomography (CT) or magnetic resonance angiography, is vital, because anticoagulation can mitigate this potentially life‐threatening illness. Finally, although many medications can cause encephalopathy in overdose, levetiracetam has well‐described cognitive side effects even at usual doses, including encephalopathy, irritability, and depression.
The records from that recent hospitalization remarked that she had presented confused and stuporous. Her potassium had been 2.7 mmol/L, international normalized ration (INR) 3.4, and hemoglobin 8 g/dL; other routine laboratory studies were normal. CT and magnetic resonance imaging (MRI) of the brain had been negative, and electroencephalogram (EEG) reportedly was performed but specific results were unknown. She was discharged alert and oriented 1 week prior to the current presentation on the above medications, including levetiracetam for this newly‐diagnosed seizure disorder.
Previous records confirm that the current presentation is that of a relapsing acute alteration in mental status. Regardless of the EEG findings or response to antiepileptic medications, a seizure disorder should remain a primary consideration, although relapsing inflammatory, toxic/metabolic conditions, and, rarely, vascular disorders can also present in this manner.
The neurologic manifestations of hypokalemia are usually peripheral in nature, including periodic paralysis; confusion accompanying hypokalemia is usually not a result of the low potassium itself but rather due to an underlying toxic or endocrinologic cause. Various causes of anemia can lead to mental status changes; the mean corpuscular volume (MCV) will be particularly helpful given known associations between megaloblastic anemia and confusional states.
On examination, she appeared to be in good health and in no distress. She was afebrile. Her blood pressure was 93/57, pulse 90 beats per minute, respiratory rate 16 per minute, and room air oxygen saturation 100%. She was oriented to her surroundings, but slow in her responses to questioning. There were no cranial nerve, motor, or sensory deficits, or abnormal reflexes or movements. Examination of the head, skin, chest, cardiovascular system, abdomen, and extremities was normal. Serum sodium was 136 mmol/L, creatinine 1.2 mg/dL, calcium 9.3 mg/dL, and glucose 81 mg/dL; other routine blood chemistries were normal. Her white blood cell (WBC) count was 7100/L, hemoglobin 9.2 g/dL with normal MCV, and platelet count 275,000/L. INR was 3.4, and liver function tests were normal. CT of the brain demonstrated no evidence of acute pathology.
Given that her laboratory results (aside from the hemoglobin) and CT were essentially normal, the most common etiology of a recurrent encephalopathy would be a toxic exposure including drugs, alcohol, and environmental toxins or poisons. A comprehensive serum drug screen, including heavy metals, could follow a basic urinary screen for drugs of abuse; specific etiologies may be suggested by patterns of injury seen on MRI such as those seen with carbon monoxide or methanol exposure. Other recurrent metabolic processes include the porphyrias and relapsing inflammatory disorders, which could be entertained if further diagnostics are unrevealing.
An EEG is warranted at this point and is a test that is underutilized in the workup of altered mental status. Patients who have a spell and do not quickly awaken should be considered to be in nonconvulsive status epilepticus until proven otherwise. This can be easily identified on the EEG and is an important entity to recognize quickly. Additional findings on EEG may suggest focal cerebral dysfunction (such as that following a seizure or acute unilateral injury), diffuse encephalopathy (eg, triphasic waves), or fairly specific diagnoses (eg, periodic lateralized epileptiform discharges from the temporal lobes in suspected herpes simplex meningoencephalitis). While the CT of the brain is a reasonable initial screen, MRI is more sensitive for structural disease and should be obtained if no etiology is rapidly identified.
Finally, acute infectious etiologies such as abscess, encephalitis, or meningoencephalitis need to be excluded via lumbar puncture. Spinal fluid examination also can be helpful in the consideration of inflammatory and autoimmune disorders.
Over the next several hours, while still in the emergency department, she became increasingly obtunded, to the point that she was unresponsive to all stimuli. No seizure activity was witnessed, her vital signs were unchanged, and no medications had been administered. She was urgently transferred to a tertiary care center, where, at the time of arrival, she was obtunded and nonverbal, and opened her eyes only to noxious stimuli. She would withdraw all 4 extremities in response to pain. Pupils were 2 mm and symmetrically reactive. Corneal reflexes were normal, and her gag reflex was diminished. Motor tone was decreased in all 4 extremities. No fasciculations were noted. Deep tendon reflexes were present but symmetrically diminished throughout, and Babinski testing demonstrated a withdrawal response bilaterally.
Coma is a state of profound unconsciousness where the patient is unarousable and unaware of her surroundings. Coma can result either from bihemispheric dysfunction or diffuse injury to the reticular activating system in the brainstem, and the physical examination should focus on distinguishing between these 2 sites. Because the nuclei of cranial nerves III through XII (excepting XI) reside in the brainstem, the coma examination emphasizes testing the cranial nerves; although all cranial nerves are not tested in this patient, the ones that are appear to be normal, making bihemispheric dysfunction most likely. Bihemispheric coma most commonly results from diffuse toxic or metabolic etiologies such as intoxication or hepatic encephalopathy, but it can also be caused by bilateral structural lesions (including the bilateral thalami) or ongoing seizure activity.
Although an EEG remains the key test in this patient given her past history and an MRI would prove extremely useful, her deterioration warrants a workup for CNS infection. Since the head CT was negative, it would be prudent to proceed with urgent lumbar puncture (although it should never be performed in a patient with significant coagulopathy due to risks of hemorrhage leading to spinal cord injury). She should be covered empirically with broad spectrum meningeal‐dose antibiotics, including acyclovir, until the results of the spinal fluid examination are known, given that bacterial meningitis and herpes meningoencephalitis carry a high morbidity and mortality if not treated promptly.
Routine blood tests were similar to her labs at the referring emergency room. Ammonia level was 10 mol/L. Urine toxicology screen was negative, and blood tests for ethanol, salicylates, lithium, and acetaminophen were negative. Chest X‐ray and urinalysis were normal, and electrocardiogram was notable only for a sinus tachycardia. Cultures of the blood were obtained and the patient was admitted to the intensive care unit.
Levetiracetam, vancomycin, piperacillin‐tazobactam, and acyclovir were initiated. A lumbar puncture was performed without reversing the anticoagulation, and the procedure was traumatic. The cerebrospinal fluid was bloody, with a clear supernatant. Cell count demonstrated a red blood cell (RBC) count of 1250/L and a WBC count of 9/L, with a WBC differential of 42% neutrophils, 48% lymphocytes, and 8% monocytes. The cerebrospinal fluid (CSF) glucose was 62 mg/dL (with a serum glucose of 74 mg/dL) and protein 41 mg/dL. The CSF Gram stain demonstrated no organisms, and fluid was sent for routine culture and polymerase chain reaction (PCR) to detect herpes simplex virus (HSV). A neurology consultation was urgently requested.
As mentioned, it would have been more appropriate to reverse the patient's anticoagulation prior to lumbar puncture. The absence of xanthochromia suggests that the RBCs seen in the sample were introduced at the time of the lumbar puncture, arguing against a hemorrhagic disorder of the CNS (occasionally seen with herpes simplex encephalitis) or spinal fluid (eg, subarachnoid hemorrhage).
A reasonable rule of thumb to correct for the number of RBCs in a traumatic lumbar puncture is to allow 1 WBC for every 700 RBCs/L. Given this conversion, there are still too many WBCs in this sample, indicating a mild pleocytosis that is approximately one‐half neutrophilic and one‐half lymphocytic. This profile is nonspecific and can occur with a variety of conditions including stroke, seizure, inflammatory disorders, and infections, including viruses such as West Nile virus.
While coverage with acyclovir and broad‐spectrum antibacterials is appropriate, it should be noted that piperacillin‐tazobactam has poor CSF penetration and therefore is not a good choice for empiric coverage of CNS infections.
The neurologist's examination additionally noted multifocal myoclonus with noxious stimuli, most prominent in the face and toes. An urgent EEG demonstrated continuous, slow, generalized triphasic wave activity (Figures 1 and 2); no epileptiform discharges were seen. The erythrocyte sedimentation rate (ESR) was 66 mm/hour (normal, 0‐30), and tests for antinuclear antibodies, serum levetiracetam level, and thyroid function studies were ordered.
Stimulus‐evoked multifocal myoclonus is a general marker of encephalopathy found in many conditions, including hepatic and renal failure, drug intoxication (eg, opiates), neurodegenerative disorders (eg, Creutzfeldt‐Jakob disease [CJD]), and postanoxic injury, the latter of which is termed the Lance‐Adams syndrome.
Triphasic waves on EEG, while commonly associated with hepatic encephalopathy, have a similarly broad differential diagnosis, although in a comatose patient, they must first and foremost be distinguished from the repetitive discharges characteristic of nonconvulsive status epilepticus. In addition to hepatic and renal failure, triphasic waves have also been described in medication toxicity (especially with anticonvulsants, lithium, and cephalosporins), CNS infections (including Lyme disease and West Nile virus), strokes involving the bilateral thalami (usually from deep venous thrombosis), inflammatory disorders (such as Hashimoto's encephalopathy [HE]), and neurodegenerative diseases. It is important to remember that a single EEG does not exclude the possibility of an episodic ictal disorder and longer‐term monitoring would be required to definitively exclude seizures.
At this point, although the myoclonus and triphasic waves most commonly would indicate a toxic/metabolic process, the elevated ESR and CSF pleocytosis argue for an inflammatory or infectious condition. An MRI remains the next most useful test to guide further workup because many such conditions have distinct signatures on MRI.
The following day, she was noted to have periods of alertnessopening her eyes and following some commandsbut at other times she was difficult to arouse or obtunded. Tremulous movements and sporadic myoclonic jerks continued but no focal neurologic signs were found. Although there was increased muscle tone throughout, she was intermittently seen moving her limbs spontaneously, but not to command. No new findings were appreciated on routine laboratory tests. Antinuclear antibody testing was negative. Serum levetiracetam level was 23.5 g/mL (reference range, 545). Serum thyroid‐stimulating hormone was less than 0.005 U/mL, but free T3 was 3.5 pg/mL (normal, 1.8‐4.6) and free T4 was 2.0 ng/dL (normal, 0.71.8). An MRI of the brain was compromised by motion artifact but no significant abnormalities were appreciated.
At this point, a family member in another state disclosed that the patient had also been hospitalized 2 months previously while visiting him. Her chief complaint had been shortness of breath. The records were obtained; a cardiac catheterization had revealed nonobstructive coronary disease, and medical management was recommended. The notes mentioned that during the hospitalization she developed altered mental status with disorientation and shaking. CT and MRI of the brain had been unremarkable. The confusion was not explained, but she was discharged in good condition, alert and fully‐oriented.
The additional history confirms a relapsing encephalopathy, now with at least 3 occurrences. The most common etiologies in the face of a normal MRI and basic labs would be recurrent intoxication or exposures, but the inflammatory CSF profile and elevated ESR are not consistent with this. A variety of inflammatory disorders can present with recurrent encephalopathy, including demyelinating diseases and neurosarcoidosis. Some systemic rheumatologic conditions, such as systemic lupus erythematosus, can present with relapsing neurologic symptoms due to seizures, vasculitis, or cerebritis. Vasculitis would fit this picture as well, except for the normal findings on 2 MRIs. In a patient with such dramatic symptoms of neurologic dysfunction, one would expect to see changes on the MRI of cerebral inflammation with probable ischemia.
Therefore, given the CSF, ESR, clinical course, and unrevealing MRI and EEG, the most likely group of disorders responsible would be the nonvasculitic autoimmune meningoencephalitides, which present with recurrent encephalopathy and feature spontaneous remissions and/or often‐dramatic responses to corticosteroids. Key disorders in this category include Sjogren's disease, lupus, and steroid responsive encephalopathy associated with autoimmune thyroiditis (Hashimoto's encephalopathy). The latter condition is the most common of the group and is suggested by the abnormal thyroid‐stimulating hormone testing, although it may occur in the setting of normal thyroid function. The diagnosis can be confirmed with thyroperoxidase and thyroglobulin antibody testing.
Three days into the hospitalization, her mental status had gradually improved such that she was more consistently awake and oriented to person and place, and she was transferred to a regular nursing unit. Final results from the CSF and blood cultures were negative, as was PCR for HSV. The antimicrobials were discontinued. Routine serum chemistries continued to be unremarkable. Additional studies recommended by the neurologist demonstrated an antithyroperoxidase antibody concentration of 587.1 IU/mL (normal, 5), and antithyroglobulin antibody level of 52.2 IU/mL (normal, 10).
These results confirm the diagnosis of HE which, in addition to its presentation as a recurrent illness, is an important treatable cause of dementia and should be considered in young patients, those with autoimmune and thyroid disorders, and those whose dementia is rapidly progressive. Most cases are thought to be steroid‐responsive, but some studies have defined the disorder based on this responsiveness, resulting in some nonresponders likely being overlooked.
A trial of corticosteroids should be considered if the patient does not quickly return to baseline given the potential morbidities associated with prolonged altered mental status to this degree. Whether initiation of chronic immunosuppression could prevent these attacks in the future is unclear from the literature but should be considered given the recurrent, dramatic presentation in this patient.
A diagnosis of HE was made, and she was prescribed corticosteroids. Twenty‐four hours later, she was alert and fully‐oriented. She was discharged to home on prednisone and seen in follow‐up in neurology clinic 1 month later. She had had no further episodes of confusion or stupor, but because of steroid‐induced hyperglycemia, her corticosteroids were decreased and mycophenolate mofetil added for chronic immunosuppression. Four months after discharge she was neurologically stable but continued to struggle with the adverse effects of chronic corticosteroid treatment.
COMMENTARY
HE is an uncommon condition that can present with a rapidly progressive decline and should be considered in patients who present with recurrent mental status change in the setting of normal imaging studies and routine laboratory results. The entity was initially described by Lord William Russell Brain in 1966, and in the most recent terminology is known as steroid‐responsive encephalopathy associated with autoimmune thyroiditis (SREAT).1 It is characterized by an acute or subacute encephalopathy associated with thyroid autoimmunity. Patients typically present with fluctuating symptoms, episodes of confusion, alterations of consciousness, and rapid cognitive decline.2 Common features include myoclonus, tremor, ataxia, speech disturbance, stroke‐like episodes, increased muscle tone, neuropsychiatric manifestations, and seizures, that in some cases may progress to status epilepticus.3, 4
Although serum antithyroglobulin and antithyroperoxidase antibodies are elevated in HE, their presence is thought to be an epiphenomenon of the condition rather than the direct cause. Supporting this are the facts that the incidence of encephalopathy is not increased in patients with established autoimmune thyroiditis, and the presence of antithyroid antibodies ranges from 5% to 20% in the general population.2, 5 There is also no evidence that thyroid antibodies directly react with brain tissue, and the levels of these antibodies do not correlate with either neurologic manifestations or clinical improvement.2, 4, 5 As HE has been reported in patients with euthyroidism, hypothyroidism, and hyperthyroidism (with hypothyroidismeither subclinical or activemost common), it is also unlikely that the level of thyroid hormones play a role in the etiology of this disease.2, 4, 6
The etiology and pathogenesis of HE are unclear, although an immune‐mediated process is generally implicated, either from an inflammatory vasculitis or as a form of acute disseminated encephalomyelitis.7‐9 Global hypoperfusion on single‐photon emission computed tomography (SPECT) studies has also been reported.10, 11 Patients with HE may have nonspecific evidence of inflammation, including an elevated ESR, CRP, and CSF protein.12 Other laboratory abnormalities may include a mild elevation of liver aminotransferase levels; renal impairment has also been reported in a few cases of HE in the form of glomerulonephritis, and may be related to deposition of immune complexes containing thyroglobulin antigen.6, 12‐14 MRI of the brain is normal or nonspecific in most cases, and the EEG most commonly shows diffuse slowing.
The differential for a rapidly progressive cognitive decline includes CJD, CNS vasculitis, paraneoplastic syndromes, and autoimmune and subacute infectious encephalopathies. In patients with CJD, T2‐weighted imaging may show hyperintense signals in the basal ganglia, while diffusion‐weighted sequences may reveal changes in the cortical ribbon and bilateral thalami.15 In CNS vasculitis, the imaging findings are variable and range from discrete areas of vascular infarcts to hemorrhagic lesions.16 In paraneoplastic and autoimmune encephalopathies (excluding HE), MRI often shows nonenhancing signal intensity changes in the mesial temporal lobes.12 This patient had repeatedly normal MRI studies of the brain, which in combination with the history of tremor, myoclonus, seizures, and interval return to baseline status, helped point to the diagnosis of HE.
Different approaches to treatment of HE have been recommended. As the acronym SREAT suggests, patients typically respond dramatically to high‐dose steroid therapy. Although a number of patients also improve spontaneously, up to 60% of patients experience a relapsing course and require chronic immunosuppressive agents for maintenance therapy, including long‐term steroids and azathioprine.2, 17 Treatment with plasma exchange and intravenous immune globulin have also been reported, but with mixed results.18, 19 Due to her history of multiple relapses, the patient was placed on mycophenolate mofetil for additional maintenance immunosuppression, as her corticosteroid dose was reduced due to adverse effects.
Acute mental status change is a potentially emergent situation that must be evaluated with careful history and studies to exclude life‐threatening metabolic, infectious, and vascular conditions. This patient presented similarly on 2 prior occasions, and each time her physician team evaluated what appeared to be a new onset of altered consciousness, reaching a plausible but ultimately incorrect diagnosis. The patient's third presentation was finally the charm, as her physicians learned of the repeated history of a confusional state, and in particular the return to baseline status, allowing them to create a differential that focused on etiologies of relapsing encephalopathy and make the correct diagnosis.
Key Points
-
Recurrent acute or subacute cognitive deterioration invokes a differential diagnosis of toxic/metabolic disorders and unusual inflammatory conditions.
-
The nonvasculitic autoimmune encephalopathies are a group of uncommon conditions characterized by nonspecific findings of inflammation and generally unremarkable CNS imaging studies.
-
HE, or SREAT, is the most common of these conditions, and is notable for mental status changes, various findings of increased muscular tone, thyroid autoimmunity, and generally a dramatic response to corticosteroids.
A 58‐year old woman was brought to the emergency department with confusion. Her husband stated that for several hours she had been drifting in and out at home, and that he had to shout to get her attention. He described no seizure activity, weakness, incontinence, or difficulty speaking, and had noted no complaints of headache, fevers, chest pain, shortness of breath, or gastrointestinal complaints.
Altered mental status in a middle‐aged woman can result from a diverse set of etiologies. A key distinction in the neurological examination will be to assure that the complaint of confusion is accurate as opposed to aphasia; the former is usually indicative of diffuse cerebral dysfunction while the latter suggests a focal lesion in the dominant hemisphere.
The acuity of the change in mental status is important, as are the fluctuations described by the husband. Unwitnessed or nonconvulsive seizure activity can present this way. Toxic/metabolic etiologies, infectious and inflammatory disorders of the central nervous system (CNS), and vascular diseases are also important considerations. Although stroke does not typically present with global encephalopathy, intermittent large vessel occlusion, especially in the posterior circulation, can disrupt cognition in this manner. Following a physical examination, initial workup should focus on toxic/metabolic etiologies, followed rapidly by head imaging if no cause is identified.
Her past medical history was notable for type 2 diabetes mellitus, coronary artery disease, hyperlipidemia, and an unspecified seizure disorder, which according to her husband was diagnosed during a recent hospitalization for a similar presentation. She also had a remote history of venous thromboembolism and antithrombin‐III deficiency. She was unemployed, lived with her husband, and spent most of her time at home. She never smoked, and rarely drank alcohol. Her family history was unobtainable, and her husband denied that she used any illicit drugs. Her medications included pioglitazone, aspirin, simvastatin, pregabalin, ferrous sulfate, levetiracetam, warfarin, and magnesium oxide, and she was allergic to sulfa.
While the differential diagnosis remains broad, 3 elements of the history are potentially relevant. The history of epilepsy based on a similar prior presentation increases the likelihood that the current spell is ictal in nature; examination of previous records would be important in order to document whether these spells have indeed been proven to be epileptic, as many conditions can mimic seizures. Given the history of venous thromboembolism and hypercoagulability, one must consider cerebral venous sinus thrombosis, which can present with global neurologic dysfunction and seizures. Prompt identification, usually via computed tomography (CT) or magnetic resonance angiography, is vital, because anticoagulation can mitigate this potentially life‐threatening illness. Finally, although many medications can cause encephalopathy in overdose, levetiracetam has well‐described cognitive side effects even at usual doses, including encephalopathy, irritability, and depression.
The records from that recent hospitalization remarked that she had presented confused and stuporous. Her potassium had been 2.7 mmol/L, international normalized ration (INR) 3.4, and hemoglobin 8 g/dL; other routine laboratory studies were normal. CT and magnetic resonance imaging (MRI) of the brain had been negative, and electroencephalogram (EEG) reportedly was performed but specific results were unknown. She was discharged alert and oriented 1 week prior to the current presentation on the above medications, including levetiracetam for this newly‐diagnosed seizure disorder.
Previous records confirm that the current presentation is that of a relapsing acute alteration in mental status. Regardless of the EEG findings or response to antiepileptic medications, a seizure disorder should remain a primary consideration, although relapsing inflammatory, toxic/metabolic conditions, and, rarely, vascular disorders can also present in this manner.
The neurologic manifestations of hypokalemia are usually peripheral in nature, including periodic paralysis; confusion accompanying hypokalemia is usually not a result of the low potassium itself but rather due to an underlying toxic or endocrinologic cause. Various causes of anemia can lead to mental status changes; the mean corpuscular volume (MCV) will be particularly helpful given known associations between megaloblastic anemia and confusional states.
On examination, she appeared to be in good health and in no distress. She was afebrile. Her blood pressure was 93/57, pulse 90 beats per minute, respiratory rate 16 per minute, and room air oxygen saturation 100%. She was oriented to her surroundings, but slow in her responses to questioning. There were no cranial nerve, motor, or sensory deficits, or abnormal reflexes or movements. Examination of the head, skin, chest, cardiovascular system, abdomen, and extremities was normal. Serum sodium was 136 mmol/L, creatinine 1.2 mg/dL, calcium 9.3 mg/dL, and glucose 81 mg/dL; other routine blood chemistries were normal. Her white blood cell (WBC) count was 7100/L, hemoglobin 9.2 g/dL with normal MCV, and platelet count 275,000/L. INR was 3.4, and liver function tests were normal. CT of the brain demonstrated no evidence of acute pathology.
Given that her laboratory results (aside from the hemoglobin) and CT were essentially normal, the most common etiology of a recurrent encephalopathy would be a toxic exposure including drugs, alcohol, and environmental toxins or poisons. A comprehensive serum drug screen, including heavy metals, could follow a basic urinary screen for drugs of abuse; specific etiologies may be suggested by patterns of injury seen on MRI such as those seen with carbon monoxide or methanol exposure. Other recurrent metabolic processes include the porphyrias and relapsing inflammatory disorders, which could be entertained if further diagnostics are unrevealing.
An EEG is warranted at this point and is a test that is underutilized in the workup of altered mental status. Patients who have a spell and do not quickly awaken should be considered to be in nonconvulsive status epilepticus until proven otherwise. This can be easily identified on the EEG and is an important entity to recognize quickly. Additional findings on EEG may suggest focal cerebral dysfunction (such as that following a seizure or acute unilateral injury), diffuse encephalopathy (eg, triphasic waves), or fairly specific diagnoses (eg, periodic lateralized epileptiform discharges from the temporal lobes in suspected herpes simplex meningoencephalitis). While the CT of the brain is a reasonable initial screen, MRI is more sensitive for structural disease and should be obtained if no etiology is rapidly identified.
Finally, acute infectious etiologies such as abscess, encephalitis, or meningoencephalitis need to be excluded via lumbar puncture. Spinal fluid examination also can be helpful in the consideration of inflammatory and autoimmune disorders.
Over the next several hours, while still in the emergency department, she became increasingly obtunded, to the point that she was unresponsive to all stimuli. No seizure activity was witnessed, her vital signs were unchanged, and no medications had been administered. She was urgently transferred to a tertiary care center, where, at the time of arrival, she was obtunded and nonverbal, and opened her eyes only to noxious stimuli. She would withdraw all 4 extremities in response to pain. Pupils were 2 mm and symmetrically reactive. Corneal reflexes were normal, and her gag reflex was diminished. Motor tone was decreased in all 4 extremities. No fasciculations were noted. Deep tendon reflexes were present but symmetrically diminished throughout, and Babinski testing demonstrated a withdrawal response bilaterally.
Coma is a state of profound unconsciousness where the patient is unarousable and unaware of her surroundings. Coma can result either from bihemispheric dysfunction or diffuse injury to the reticular activating system in the brainstem, and the physical examination should focus on distinguishing between these 2 sites. Because the nuclei of cranial nerves III through XII (excepting XI) reside in the brainstem, the coma examination emphasizes testing the cranial nerves; although all cranial nerves are not tested in this patient, the ones that are appear to be normal, making bihemispheric dysfunction most likely. Bihemispheric coma most commonly results from diffuse toxic or metabolic etiologies such as intoxication or hepatic encephalopathy, but it can also be caused by bilateral structural lesions (including the bilateral thalami) or ongoing seizure activity.
Although an EEG remains the key test in this patient given her past history and an MRI would prove extremely useful, her deterioration warrants a workup for CNS infection. Since the head CT was negative, it would be prudent to proceed with urgent lumbar puncture (although it should never be performed in a patient with significant coagulopathy due to risks of hemorrhage leading to spinal cord injury). She should be covered empirically with broad spectrum meningeal‐dose antibiotics, including acyclovir, until the results of the spinal fluid examination are known, given that bacterial meningitis and herpes meningoencephalitis carry a high morbidity and mortality if not treated promptly.
Routine blood tests were similar to her labs at the referring emergency room. Ammonia level was 10 mol/L. Urine toxicology screen was negative, and blood tests for ethanol, salicylates, lithium, and acetaminophen were negative. Chest X‐ray and urinalysis were normal, and electrocardiogram was notable only for a sinus tachycardia. Cultures of the blood were obtained and the patient was admitted to the intensive care unit.
Levetiracetam, vancomycin, piperacillin‐tazobactam, and acyclovir were initiated. A lumbar puncture was performed without reversing the anticoagulation, and the procedure was traumatic. The cerebrospinal fluid was bloody, with a clear supernatant. Cell count demonstrated a red blood cell (RBC) count of 1250/L and a WBC count of 9/L, with a WBC differential of 42% neutrophils, 48% lymphocytes, and 8% monocytes. The cerebrospinal fluid (CSF) glucose was 62 mg/dL (with a serum glucose of 74 mg/dL) and protein 41 mg/dL. The CSF Gram stain demonstrated no organisms, and fluid was sent for routine culture and polymerase chain reaction (PCR) to detect herpes simplex virus (HSV). A neurology consultation was urgently requested.
As mentioned, it would have been more appropriate to reverse the patient's anticoagulation prior to lumbar puncture. The absence of xanthochromia suggests that the RBCs seen in the sample were introduced at the time of the lumbar puncture, arguing against a hemorrhagic disorder of the CNS (occasionally seen with herpes simplex encephalitis) or spinal fluid (eg, subarachnoid hemorrhage).
A reasonable rule of thumb to correct for the number of RBCs in a traumatic lumbar puncture is to allow 1 WBC for every 700 RBCs/L. Given this conversion, there are still too many WBCs in this sample, indicating a mild pleocytosis that is approximately one‐half neutrophilic and one‐half lymphocytic. This profile is nonspecific and can occur with a variety of conditions including stroke, seizure, inflammatory disorders, and infections, including viruses such as West Nile virus.
While coverage with acyclovir and broad‐spectrum antibacterials is appropriate, it should be noted that piperacillin‐tazobactam has poor CSF penetration and therefore is not a good choice for empiric coverage of CNS infections.
The neurologist's examination additionally noted multifocal myoclonus with noxious stimuli, most prominent in the face and toes. An urgent EEG demonstrated continuous, slow, generalized triphasic wave activity (Figures 1 and 2); no epileptiform discharges were seen. The erythrocyte sedimentation rate (ESR) was 66 mm/hour (normal, 0‐30), and tests for antinuclear antibodies, serum levetiracetam level, and thyroid function studies were ordered.
Stimulus‐evoked multifocal myoclonus is a general marker of encephalopathy found in many conditions, including hepatic and renal failure, drug intoxication (eg, opiates), neurodegenerative disorders (eg, Creutzfeldt‐Jakob disease [CJD]), and postanoxic injury, the latter of which is termed the Lance‐Adams syndrome.
Triphasic waves on EEG, while commonly associated with hepatic encephalopathy, have a similarly broad differential diagnosis, although in a comatose patient, they must first and foremost be distinguished from the repetitive discharges characteristic of nonconvulsive status epilepticus. In addition to hepatic and renal failure, triphasic waves have also been described in medication toxicity (especially with anticonvulsants, lithium, and cephalosporins), CNS infections (including Lyme disease and West Nile virus), strokes involving the bilateral thalami (usually from deep venous thrombosis), inflammatory disorders (such as Hashimoto's encephalopathy [HE]), and neurodegenerative diseases. It is important to remember that a single EEG does not exclude the possibility of an episodic ictal disorder and longer‐term monitoring would be required to definitively exclude seizures.
At this point, although the myoclonus and triphasic waves most commonly would indicate a toxic/metabolic process, the elevated ESR and CSF pleocytosis argue for an inflammatory or infectious condition. An MRI remains the next most useful test to guide further workup because many such conditions have distinct signatures on MRI.
The following day, she was noted to have periods of alertnessopening her eyes and following some commandsbut at other times she was difficult to arouse or obtunded. Tremulous movements and sporadic myoclonic jerks continued but no focal neurologic signs were found. Although there was increased muscle tone throughout, she was intermittently seen moving her limbs spontaneously, but not to command. No new findings were appreciated on routine laboratory tests. Antinuclear antibody testing was negative. Serum levetiracetam level was 23.5 g/mL (reference range, 545). Serum thyroid‐stimulating hormone was less than 0.005 U/mL, but free T3 was 3.5 pg/mL (normal, 1.8‐4.6) and free T4 was 2.0 ng/dL (normal, 0.71.8). An MRI of the brain was compromised by motion artifact but no significant abnormalities were appreciated.
At this point, a family member in another state disclosed that the patient had also been hospitalized 2 months previously while visiting him. Her chief complaint had been shortness of breath. The records were obtained; a cardiac catheterization had revealed nonobstructive coronary disease, and medical management was recommended. The notes mentioned that during the hospitalization she developed altered mental status with disorientation and shaking. CT and MRI of the brain had been unremarkable. The confusion was not explained, but she was discharged in good condition, alert and fully‐oriented.
The additional history confirms a relapsing encephalopathy, now with at least 3 occurrences. The most common etiologies in the face of a normal MRI and basic labs would be recurrent intoxication or exposures, but the inflammatory CSF profile and elevated ESR are not consistent with this. A variety of inflammatory disorders can present with recurrent encephalopathy, including demyelinating diseases and neurosarcoidosis. Some systemic rheumatologic conditions, such as systemic lupus erythematosus, can present with relapsing neurologic symptoms due to seizures, vasculitis, or cerebritis. Vasculitis would fit this picture as well, except for the normal findings on 2 MRIs. In a patient with such dramatic symptoms of neurologic dysfunction, one would expect to see changes on the MRI of cerebral inflammation with probable ischemia.
Therefore, given the CSF, ESR, clinical course, and unrevealing MRI and EEG, the most likely group of disorders responsible would be the nonvasculitic autoimmune meningoencephalitides, which present with recurrent encephalopathy and feature spontaneous remissions and/or often‐dramatic responses to corticosteroids. Key disorders in this category include Sjogren's disease, lupus, and steroid responsive encephalopathy associated with autoimmune thyroiditis (Hashimoto's encephalopathy). The latter condition is the most common of the group and is suggested by the abnormal thyroid‐stimulating hormone testing, although it may occur in the setting of normal thyroid function. The diagnosis can be confirmed with thyroperoxidase and thyroglobulin antibody testing.
Three days into the hospitalization, her mental status had gradually improved such that she was more consistently awake and oriented to person and place, and she was transferred to a regular nursing unit. Final results from the CSF and blood cultures were negative, as was PCR for HSV. The antimicrobials were discontinued. Routine serum chemistries continued to be unremarkable. Additional studies recommended by the neurologist demonstrated an antithyroperoxidase antibody concentration of 587.1 IU/mL (normal, 5), and antithyroglobulin antibody level of 52.2 IU/mL (normal, 10).
These results confirm the diagnosis of HE which, in addition to its presentation as a recurrent illness, is an important treatable cause of dementia and should be considered in young patients, those with autoimmune and thyroid disorders, and those whose dementia is rapidly progressive. Most cases are thought to be steroid‐responsive, but some studies have defined the disorder based on this responsiveness, resulting in some nonresponders likely being overlooked.
A trial of corticosteroids should be considered if the patient does not quickly return to baseline given the potential morbidities associated with prolonged altered mental status to this degree. Whether initiation of chronic immunosuppression could prevent these attacks in the future is unclear from the literature but should be considered given the recurrent, dramatic presentation in this patient.
A diagnosis of HE was made, and she was prescribed corticosteroids. Twenty‐four hours later, she was alert and fully‐oriented. She was discharged to home on prednisone and seen in follow‐up in neurology clinic 1 month later. She had had no further episodes of confusion or stupor, but because of steroid‐induced hyperglycemia, her corticosteroids were decreased and mycophenolate mofetil added for chronic immunosuppression. Four months after discharge she was neurologically stable but continued to struggle with the adverse effects of chronic corticosteroid treatment.
COMMENTARY
HE is an uncommon condition that can present with a rapidly progressive decline and should be considered in patients who present with recurrent mental status change in the setting of normal imaging studies and routine laboratory results. The entity was initially described by Lord William Russell Brain in 1966, and in the most recent terminology is known as steroid‐responsive encephalopathy associated with autoimmune thyroiditis (SREAT).1 It is characterized by an acute or subacute encephalopathy associated with thyroid autoimmunity. Patients typically present with fluctuating symptoms, episodes of confusion, alterations of consciousness, and rapid cognitive decline.2 Common features include myoclonus, tremor, ataxia, speech disturbance, stroke‐like episodes, increased muscle tone, neuropsychiatric manifestations, and seizures, that in some cases may progress to status epilepticus.3, 4
Although serum antithyroglobulin and antithyroperoxidase antibodies are elevated in HE, their presence is thought to be an epiphenomenon of the condition rather than the direct cause. Supporting this are the facts that the incidence of encephalopathy is not increased in patients with established autoimmune thyroiditis, and the presence of antithyroid antibodies ranges from 5% to 20% in the general population.2, 5 There is also no evidence that thyroid antibodies directly react with brain tissue, and the levels of these antibodies do not correlate with either neurologic manifestations or clinical improvement.2, 4, 5 As HE has been reported in patients with euthyroidism, hypothyroidism, and hyperthyroidism (with hypothyroidismeither subclinical or activemost common), it is also unlikely that the level of thyroid hormones play a role in the etiology of this disease.2, 4, 6
The etiology and pathogenesis of HE are unclear, although an immune‐mediated process is generally implicated, either from an inflammatory vasculitis or as a form of acute disseminated encephalomyelitis.7‐9 Global hypoperfusion on single‐photon emission computed tomography (SPECT) studies has also been reported.10, 11 Patients with HE may have nonspecific evidence of inflammation, including an elevated ESR, CRP, and CSF protein.12 Other laboratory abnormalities may include a mild elevation of liver aminotransferase levels; renal impairment has also been reported in a few cases of HE in the form of glomerulonephritis, and may be related to deposition of immune complexes containing thyroglobulin antigen.6, 12‐14 MRI of the brain is normal or nonspecific in most cases, and the EEG most commonly shows diffuse slowing.
The differential for a rapidly progressive cognitive decline includes CJD, CNS vasculitis, paraneoplastic syndromes, and autoimmune and subacute infectious encephalopathies. In patients with CJD, T2‐weighted imaging may show hyperintense signals in the basal ganglia, while diffusion‐weighted sequences may reveal changes in the cortical ribbon and bilateral thalami.15 In CNS vasculitis, the imaging findings are variable and range from discrete areas of vascular infarcts to hemorrhagic lesions.16 In paraneoplastic and autoimmune encephalopathies (excluding HE), MRI often shows nonenhancing signal intensity changes in the mesial temporal lobes.12 This patient had repeatedly normal MRI studies of the brain, which in combination with the history of tremor, myoclonus, seizures, and interval return to baseline status, helped point to the diagnosis of HE.
Different approaches to treatment of HE have been recommended. As the acronym SREAT suggests, patients typically respond dramatically to high‐dose steroid therapy. Although a number of patients also improve spontaneously, up to 60% of patients experience a relapsing course and require chronic immunosuppressive agents for maintenance therapy, including long‐term steroids and azathioprine.2, 17 Treatment with plasma exchange and intravenous immune globulin have also been reported, but with mixed results.18, 19 Due to her history of multiple relapses, the patient was placed on mycophenolate mofetil for additional maintenance immunosuppression, as her corticosteroid dose was reduced due to adverse effects.
Acute mental status change is a potentially emergent situation that must be evaluated with careful history and studies to exclude life‐threatening metabolic, infectious, and vascular conditions. This patient presented similarly on 2 prior occasions, and each time her physician team evaluated what appeared to be a new onset of altered consciousness, reaching a plausible but ultimately incorrect diagnosis. The patient's third presentation was finally the charm, as her physicians learned of the repeated history of a confusional state, and in particular the return to baseline status, allowing them to create a differential that focused on etiologies of relapsing encephalopathy and make the correct diagnosis.
Key Points
-
Recurrent acute or subacute cognitive deterioration invokes a differential diagnosis of toxic/metabolic disorders and unusual inflammatory conditions.
-
The nonvasculitic autoimmune encephalopathies are a group of uncommon conditions characterized by nonspecific findings of inflammation and generally unremarkable CNS imaging studies.
-
HE, or SREAT, is the most common of these conditions, and is notable for mental status changes, various findings of increased muscular tone, thyroid autoimmunity, and generally a dramatic response to corticosteroids.
- , , .Hashimoto's disease and encephalopathy.Lancet.1966;2:512–514.
- , , .Hashimoto encephalopathy: syndrome or myth?Arch Neurol.2003;60:164–171.
- , , .Pisani F. Recurrent status epilepticus as the main feature of Hashimoto's encephalopathy.Epilepsy Behav.2006;8:328–330.
- , , , et al.Steroid‐responsive encephalopathy associated with autoimmune thyroiditis.Arch Neurol.2006;63:197–202.
- , , , , .Encephalopathy associated with Hashimoto thyroiditis: diagnosis and treatment.J Neurol.1996;243:585–593.
- , , , , .Hashimoto's encephalopathy: a steroid‐responsive disorder associated with high anti‐thyroid antibody titers‐report of 5 cases.Neurology.1991;41:228–233.
- , , , , .Hashimoto encephalopathy: a brainstem vasculitis?Neurology.2000;54:769–770.
- , , , , .Nonvasculitic autoimmune inflammatory meningoencephalitis (NAIM): A reversible form of encephalopathy.Neurology.1999;53:1579–1581.
- , , , .Hashimoto's encephalopathy: postmortem findings after fatal status epilepticus.Neurology.2003;61:1124–1126.
- , , .Autoimmune thyroiditis and a rapidly progressive dementia: global hypoperfusion on SPECT scanning suggests a possible mechanism.Neurology.1997;49:623–626.
- , , , , .Hashimoto's encephalopathy: clinical, SPECT and neurophysiologic data.QJM.2003;96:455–457.
- , , .Autoimmune Encephalopathies.The Neurologist.2007;13:140–147.
- , , , , , .Thyroid antigen‐antibody nephritis.Clin Immunol Immunopathol1976;6:341–346.
- , , .Immune complex glomerulonephritis mediated by thyroid antigens.Arch Pathol Lab Med1978;102:530–533.
- , , , et al.Diffusion‐weighted MR imaging of early‐stage Creutzfeldt‐Jakob disease: typical and atypical manifestations.Radiographics.2006;26:S191–S204.
- , , , , .CNS vasculitis in autoimmune disease: MR imaging findings and correlation with angiography.AJNR Am J Neuroradiol.1999;20:75–85.
- , .Long‐Term Treatment of Hashimoto's Encephalopathy.J Neuropsychiatry Clin Neurosci.2006;18:14–20.
- , .Hashimoto's encephalopathy: steroid resistance and response to intravenouc immunoglobulins.J Neurol Neurosurg Psychiatry.2005;76:455–456.
- , .Hashimoto's encephalopathy responding to plasmapheresis.J Neurol Neurosurg Psychiatry.2001;70:132.
- , , .Hashimoto's disease and encephalopathy.Lancet.1966;2:512–514.
- , , .Hashimoto encephalopathy: syndrome or myth?Arch Neurol.2003;60:164–171.
- , , .Pisani F. Recurrent status epilepticus as the main feature of Hashimoto's encephalopathy.Epilepsy Behav.2006;8:328–330.
- , , , et al.Steroid‐responsive encephalopathy associated with autoimmune thyroiditis.Arch Neurol.2006;63:197–202.
- , , , , .Encephalopathy associated with Hashimoto thyroiditis: diagnosis and treatment.J Neurol.1996;243:585–593.
- , , , , .Hashimoto's encephalopathy: a steroid‐responsive disorder associated with high anti‐thyroid antibody titers‐report of 5 cases.Neurology.1991;41:228–233.
- , , , , .Hashimoto encephalopathy: a brainstem vasculitis?Neurology.2000;54:769–770.
- , , , , .Nonvasculitic autoimmune inflammatory meningoencephalitis (NAIM): A reversible form of encephalopathy.Neurology.1999;53:1579–1581.
- , , , .Hashimoto's encephalopathy: postmortem findings after fatal status epilepticus.Neurology.2003;61:1124–1126.
- , , .Autoimmune thyroiditis and a rapidly progressive dementia: global hypoperfusion on SPECT scanning suggests a possible mechanism.Neurology.1997;49:623–626.
- , , , , .Hashimoto's encephalopathy: clinical, SPECT and neurophysiologic data.QJM.2003;96:455–457.
- , , .Autoimmune Encephalopathies.The Neurologist.2007;13:140–147.
- , , , , , .Thyroid antigen‐antibody nephritis.Clin Immunol Immunopathol1976;6:341–346.
- , , .Immune complex glomerulonephritis mediated by thyroid antigens.Arch Pathol Lab Med1978;102:530–533.
- , , , et al.Diffusion‐weighted MR imaging of early‐stage Creutzfeldt‐Jakob disease: typical and atypical manifestations.Radiographics.2006;26:S191–S204.
- , , , , .CNS vasculitis in autoimmune disease: MR imaging findings and correlation with angiography.AJNR Am J Neuroradiol.1999;20:75–85.
- , .Long‐Term Treatment of Hashimoto's Encephalopathy.J Neuropsychiatry Clin Neurosci.2006;18:14–20.
- , .Hashimoto's encephalopathy: steroid resistance and response to intravenouc immunoglobulins.J Neurol Neurosurg Psychiatry.2005;76:455–456.
- , .Hashimoto's encephalopathy responding to plasmapheresis.J Neurol Neurosurg Psychiatry.2001;70:132.

Physician Engagement and Hospital PIM
Physicians play an important role in improving quality improvement (QI) through clinical expertise and leadership.1, 2 The role of the physician leader is dynamic and complex, yet key competencies have been described in terms of personal commitment, professional credibility, QI behaviors and skills, and institutional linkages.3 Several characteristics have also been identified in hospitals successful in implementing QI, including shared goals for improvement, substantial administrative support, use of credible data feedback, and strong physician leadership.4 Cultivating physician leadership in hospital QI via development of these competencies is crucial for ongoing efforts in hospital QI activities.
The American Board of Internal Medicine (ABIM) developed web‐based assessment tools called Practice Improvement Modules (PIMs), as part of the maintenance of certification (MOC) program. Designed to facilitate physician involvement in QI, most PIMs target a single medical condition in the ambulatory practice,5 and involve a medical record audit performed by the physician, a patient survey, and a systems readiness survey. Physicians use the results of this data collection to perform a single test of change, and receive MOC credit when they report on the results of their intervention. Recognizing that QI activities may be different in hospital settings, the ABIM subsequently developed a Hospital‐based PIM (Hospital PIM) that allows physicians to use nationally‐approved hospital‐level performance data to complete the module. The Hospital PIM requires physicians to carry out a single test of change, and report any change in the perception of the environment supporting QI activities.
The ABIM has also begun work on potentially creating a focused pathway for hospitalists in the MOC program.6 Practice‐based learning and improvement (PBLI), systems‐based practice (SBP),7 and QI8 are core competencies of hospital medicine, and assessment of these competencies would be an important component of the new, focused MOC pathway. The Hospital PIM potentially provides an assessment methodology, thus it is important to understand the impact and value of this web‐based assessment tool.
The objective of this study is to explore the impact of the Hospital PIM on physicians participating in hospital‐based QI, including facilitators and barriers to a successful experience. We highlight several case studies to describe this impact, which can be defined as learning about QI, value‐added to practice, or an enhanced QI experience. We also describe 3 pathways suggesting how physician engagement, which is an emerging theme of our research, mediates the impact of the Hospital PIM.
Methods
A nonprobability purposive sample of physicians who completed the Hospital PIM (n = 21) as part of MOC by January 2007 was interviewed using semistructured telephone interviews. At the time of data collection, 771 physicians completed the Hospital PIM, and our sample strategically reflects equal proportions of those currently active on a QI team, as well as those who formed a QI team. Physicians were contacted via e‐mail and telephone to arrange an interview. None of the physicians contacted declined. All physicians were informed about the purpose of the study and provided consent for the ABIM to analyze and report data for purposes of understanding the feasibility of the PIM at improving practice. No physician personal identifiers were used in data analysis.
The interviews focused on four domains: reasons for choosing the module, assembly and role on any quality improvement teams, the value and satisfaction with the experience of completing the Hospital PIM, and prior experience with QI. Interviews were conducted by 1 trained member of the research team, and lasted approximately 30 minutes. Data collection was terminated when theoretical saturation was reached, or when no new data was revealed during the interviews. Interviews were audio‐recorded, and data were transcribed verbatim to facilitate analysis. Through an inductive and iterative approach, 3 members of the research team (including the interviewer) coded the data to identify themes that were consistently grounded in the data.9 These themes were subsequently discussed with a fourth researcher to maximize interrater reliability. Codes were then checked against existing literature to confirm linkages and enhance interpretation.
Results
The mean age of the participants (n = 21) was 42 years and 81% were male. Primary certificates were issued a mean of 13 years prior and completers came from a wide variety of disciplines, hospitals, and areas of expertise. Overall, the majority of physicians found the Hospital PIM to be a valuable experience (n = 17; 81%), which is similar to ABIM Hospital PIM surveillance data in which 75% of all completers said they would recommend the PIM to a colleague.
The impact and value of completing the PIM is illustrated in a variety of ways. For some, particularly those with extensive QI backgrounds, the PIM organized and broadened documentation of ongoing work. Several physicians described their utilization of the Hospital PIM as a byproduct of their hospital's existing cultural norms and interest in QI, and many Hospital PIM projects dovetailed with ongoing hospital QI activities. In these cases, even though the PIM did not stimulate new ideas, there was still value among physicians in receiving recognition for their ongoing QI activities and, perhaps more importantly, in learning by reflecting on their work.10
For others, the Hospital PIM was a catalyst to change. Similar to the role of a catalyst in a chemical reaction, our data suggest that the Hospital PIM facilitated QI by lowering the energy necessary for the process to occur. Many physicians reported the process stimulated new interest in QI, (eg, [The process] gave me some ideas about future QI projects that I plan to do, or described how the experience was an extra boost or stimulus to help change their ways.) These findings are consistent with recent findings on the use of PIMs in residency,11 which describes the Preventive Cardiology PIM as a catalyst to change.
Several physicians were surprised at how easy it was to begin and initiate a QI project, acknowledging the importance of leadership and teamwork (n = 7; 33%). In addition, many physicians highlighted reflective processes (n = 8; 38%) whereby the PIM led to an increased awareness of their clinical environment, or QI in general, including how QI can affect patient care and/or patient outcomes.
The most frequently reported facilitators to a successful PIM experience were familiarity/access to QI resources and staff, institutional support and culture of QI, and documentation of ongoing QI activities. The most frequently reported barrier (n = 9; 43%) was the time that it took to complete the module. Other barriers included a lack of institutional support or negative culture supporting QI activities, a lack of familiarity/access to QI resources and staff, and perceived irrelevance of QI activities to clinical practice.
Physician Engagement
Our data revealed a critical theme, whereby a physician's engagement with the QI process (especially the utilization of existing QI resources) mediated the impact of the PIM. Physicians who we describe as active engagers (n = 8) exhibited personal involvement in the QI project, including a commitment to working within the QI team structure. Active engagers possessed familiarity or knowledge of basic QI behaviors and skills, and most reported enhanced awareness of ongoing QI activities and the clinical environment as a result of completing the PIM.
Passive engagers (n = 10) may not have possessed the skills or motivation to become involved in the QI process. In our study, passive engagers were more likely to report perceived lack of relevance of QI activities to patient care practices, and may have had difficulty demonstrating personal commitment to improvement. Interestingly, many passive engagers reported an overall negative Hospital PIM experience, yet documented impact from the PIM via learning about the QI processes (eg, teamwork, communication, documentation, use of data) or ongoing QI activities that occurred while completing the PIM.
Finally, physicians who failed to engage in the QI process, nonengagers (n = 3) documented no evidence of QI learning and reported little impact from completing the PIM. The following case studies illustrate how physician engagement relates to physicians' experiences with the Hospital PIM and describes the unique influence of facilitators and barriers on both engagement and impact.
Case Study A: Active Engagement
This hospitalist spends 100% of his time performing clinical work in a hospital. He denies formal training in QI principles and has no prior experience in QI, but has an interest in QI resulting from prior work on throughput activities as part of a patient safety initiative at his hospital. He possesses a positive perception of his hospital's leadership and culture supporting QI activities: the hospital administration is very supportive of any sort of QI initiatives. His chosen measure was administration of pneumococcal vaccine in patients admitted with community acquired pneumonia (CAP), for which his hospital performed at 36% compliance.
Despite a lack of formal training in QI, this physician actively engaged with the existing QI resources and was able to call together the people who are typically associated with [QI] initiatives in the hospital to work on [the PIM]. This supportive culture facilitated the navigation through the hospital system and the physician's active engagement in the QI process.
Another key aspect of this physician's experience was his interaction with the members of a multidisciplinary team. While he provided the creative initiative for the project itself, the assembled QI team quickly identified areas of need and moved on to a quality‐based initiative, while providing a framework to disseminate the ideas of the project. The PIM was a valuable experience and this physician noted that it was surprisingly easier to begin and initiate a quality improvement project than thought.
Despite a lack of formal QI training or experience, this physician utilized his personal commitment to the value of QI and the positive hospital culture to engage the existing QI resources and staff. Similar to other active engagers, he demonstrated relationship building, team formation, and effective communication in completing the PIM. His level of engagement facilitated learning about QI and enhanced his PIM experience.
Case Study B: Passive Engagement
This physician is a subspecialist in Infectious Diseases who spends 15% of his time in patient care in the hospital. Prior to completing the PIM, he identified his prior QI experience as receiving messages from the head of our department in the hospital hearing about these kinds of things from a bureaucratic stance. At the beginning, he strongly disagreed with the notion that the hospital had strong leadership and culture supporting QI activities. His measure was the appropriate choice of initial antibiotics in CAP, in which his hospital reported 24% compliance.
In order to complete the module, this physician successfully enlisted the help of an existing QI team stating, I joined the group for that period of time so I could complete my certification. Specifically, They helped me to understand the problems, the barriers to improvement, and helped me get a sense of the ways to better improve the management of pneumonia in the hospital setting but in the end it probably didn't really affect my practice very much. When questioned about this dichotomy, this physician stated that the information learned in completing the PIM was not particularly relevant to a subspecialist who practices inpatient medicine for only a short period of time and mainly does research. Interestingly, after completing the module, this physician had a significantly improved perception of his hospital's QI leadership and culture.
Like other passive engagers, this physician described some interaction with existing QI resources and staff, though to a lesser degree than the active engagers. Even though completing the PIM was perceived as an overall negative experience, his familiarity with QI resources, and his ability to successfully engage with those resources, allowed him to complete the module and document an impact (ie, new personal learning about hospital QI principles and team formation) in the process. Another important finding is that QI learning occurred despite the presence of multiple barriers.
Case Studies C and D: No Engagement
Case Study C
This physician has a small clinical practice and works mostly in the laboratory. He admits to very limited QI experience and, at the onset of the PIM, possessed a moderately negative opinion about his hospital administration and culture supporting QI. He also chose pneumococcal vaccine administration, for which his hospital was performing at 48% compliance.
He tried multiple times to enlist the help of a hospital QI officer but was told to assemble the team myself and was subsequently unable to do so. This physician ended up being disengaged with the PIM and the QI process because he had no buy‐in from the QI department. The experience was frustrating and at the completion of the module, his perception of the hospital's QI leadership and culture was rated as moderately worse. This physician documented no impact as a result of completing the PIM.
Case Study D
This physician chose to complete the Hospital PIM because he worked as a hospitalist 100% of the time. He claims experience in QI by participating in conferences, teaching students, reading literature, but had not led or organized any QI projects or activities. He generally rated his hospital leadership and QI culture in positive terms.
Overall, this physician failed to engage because he did not believe in the basic tenets of QI, and possessed a negative view of the Hospital PIM and its relevance to his practice. This perceived irrelevance was illustrated when, despite having a hospital baseline performance measure of 5% compliance for percutaneous coronary intervention in under 120 minutes, he stated, We don't need to improve we're at a terrific level right now. During the PIM, this physician chose not to work with a QI team because he [didn't] need a team everybody knows their own place and what to do in each situation. To achieve QI gains, physicians at this hospital discuss with administration what they need to do to improve quality. This physician did document a change in the hospital's QI environment, but did not attribute it to the Hospital PIM, rather, because we just became more experienced in our hospital. The overall impact on this physician was negative, a waste of time, highlighting the perceived irrelevance of the PIM and of QI activities.
For various reasons highlighted in these case studies (eg, institutional barriers, perceived irrelevance, redundancy with existing QI activities), the Hospital PIM may be unhelpful to nonengagers and as a result, physicians with no engagement in the QI process may not have a successful experience with the Hospital PIM.
In summary, physician engagement mediates the experience and impact of the Hospital PIM on the physician. Importantly, initial engagement by itself is not a powerful predictor; rather, the degree of engagement unfolds as the QI activity progresses. Physicians may elect to (at times not purposefully) actively, passively, or not engage in the QI process; however, simply enrolling in the PIM will not necessarily lead to engagement or to a successful experience. The physician must engage in the QI process in order to achieve learning. In all of these case studies, facilitators and barriers undoubtedly influence the Hospital PIM experience, as well as any subsequent impact on learning about QI. However, their presence or absence does not seem to be as powerful of a predictor of impact as is the degree of physician engagement.
Discussion
This study describes experiences for a small number of early‐completers of the Hospital PIM. For many, impact is described as an increased awareness of the hospital clinical environment, particularly an awareness of ongoing QI activities. For others, the primary impact was learning through an increased appreciation of the importance of QI activities and understanding of basic QI procedures (ie, interdisciplinary teamwork, enhanced communication, and documentation, buy‐in, using data). Still others described impact as an enhanced QI experience via reflection on current QI work or catalyzing change in their hospital environment. Further exploration of these findings will be important to determine the full impact of the PIM. An unanticipated finding, however, was the emerging theme of the role of physician engagement in mediating a successful experience with the Hospital PIM.
Prior research on physician engagement more generally demonstrates that increased physician engagement enhances interaction with nursing and other office staff,12 improves overall physician alignment,13 enhances QI,2 and may heighten physicians' willingness to participate in hospital administration and policy.14 Our data support these findings and further describe the importance of engagement in QI activities, whether it be through assembling and working in a team, helping analyze hospital systems, navigating existing institutional linkages, or simply becoming the creative initiative on a QI project. For completers of the Hospital PIM, engaging in any aspect of the QI process facilitates a successful PIM experience as documented by impact, and may stimulate physician leadership and hospital level change as well. Nonengaging physicians, in contrast, had a negative experience and documented little or no impact as a result of completing the PIM.
As our findings illustrate, engagement may not be a fixed construct, and may be acquired or generated through the QI process. In this context, physicians with varying levels of QI experience and expertise may learn and find value in completing the Hospital PIM, provided they become engaged with the process. Internal (ie, personal commitment, buy‐in, perceived relevance) and external (ie, hospital QI culture, access to QI team, access to data) factors may influence the degree of satisfaction and success with the Hospital PIM experience, thus maximizing facilitators and overcoming the barriers is also important for a positive outcome.
There are important limitations to this study. Most importantly, we acknowledge that the quality of the resources available between hospitals is highly variable. Therefore, our subjective assessment of whether or not someone was actively engaged is largely dependent on the quality of the available resources, and in a resource‐poor environment, this may not be a fair reflection of their engagement. We further recognize that coming to any broad or conclusive findings about the impact of the PIM is difficult given the qualitative nature of this study. However, our findings do suggest that the Hospital PIM may promote learning and value to completing physicians, especially those that engage in the QI process. Future studies should further explore the described impact and the relationship between engagement and QI.
To further enhance the Hospital PIM, consideration of prerequisite criteria for future completers, such as documentation of engagement, adequate access to hospital QI resources, and significant clinical work in the hospital setting, may be warranted. Additionally, consideration for alternative means of MOC credit may be warranted for physicians who demonstrate a proficiency in QI activities or who work in hospitals that efficiently participate in QI activities, such as a Health Maintenance Organization, for whom completion of the Hospital PIM may be redundant.
In conclusion, our findings suggest that the Hospital PIM is a useful component of MOC for appropriate groups of physicians despite the unique aspects of the Hospital PIM using hospital‐level outcomes data. Many physicians in our sample found it to be useful as a catalyst for learning about QI activities, which was facilitated through active engagement with the PIM QI process. While ongoing study is needed, it is anticipated that the findings from this study will help to inform the proposed pathway of focused practice in hospital medicine as part of MOC, particularly activities geared toward assessing competency in QI.
- , , , , , .The roles of senior management in quality improvement efforts: what are the key components?J Healthc Manag.2003;48:15–28.
- , , .Promoting clinical involvement in hospital quality improvement efforts: the effects of top management, board, and physician leadership.Health Serv Res.1997;32:491–510.
- , , , , , .Characteristics of physician leaders working to improve the quality of care in acute myocardial infarction.Jt Comm J Qual Saf.2003;29:289–296.
- , , , , , .A qualitative study of increasing beta‐blocker use after myocardial infarction: why do some hospitals succeed?JAMA.2001;285:2604–2611.
- , , .Improving the quality of care via maintenance of certification and the web: an early status report.Perspect Biol Med.2008;51:71–83.
- American Board of Internal Medicine. Questions and answers about ABIM recognition of focused practice in hospital medicine. Available at: http://www.abim.org/news/news/hospital‐medicine‐qa.aspx?wt.mc_id=hospital‐medicine‐qa. Accessed March 2009.
- Accreditation Council for Graduate Medical Education. The outcomes project. Available at: http://www.acgme.org/Outcome. Accessed March 2009.
- The core competencies in hospital medicine: a framework for curriculum development by the Society of Hospital Medicine.J Hosp Med.2006;1(suppl):2–95.
- , .Basics of Qualitative Research: Grounded Theory Procedures and Techniques.Newbury Park, CA:Sage Publications;1998.
- , , .Self‐monitoring in clinical practice: a challenge for medical educators.J Cont Educ Health Prof.2008;28:5–13.
- , , .The Impact of a preventive cardioloy quality improvement intervention on residents and clinics: a qualitative exploration.Am J of Med Qual.2009;24:99–107.
- , .Why do nurse managers stay? Building a model of engagement: Part 1. Dimensions of engagement.J Nurs Adm.2008;38:118–124.
- , .Involving physicians in total quality management: results of a study. In: Blumental D, Scheck AC, eds.Improving Clinical Practice: Total Quality Management and the Physician.San Francisco, CA:Jossey‐Bass;1995.
- , .Increasing physician engagement. using norms of physician culture to improve relationships with medical staff.Physician Exec.2007;33:38–45.
Physicians play an important role in improving quality improvement (QI) through clinical expertise and leadership.1, 2 The role of the physician leader is dynamic and complex, yet key competencies have been described in terms of personal commitment, professional credibility, QI behaviors and skills, and institutional linkages.3 Several characteristics have also been identified in hospitals successful in implementing QI, including shared goals for improvement, substantial administrative support, use of credible data feedback, and strong physician leadership.4 Cultivating physician leadership in hospital QI via development of these competencies is crucial for ongoing efforts in hospital QI activities.
The American Board of Internal Medicine (ABIM) developed web‐based assessment tools called Practice Improvement Modules (PIMs), as part of the maintenance of certification (MOC) program. Designed to facilitate physician involvement in QI, most PIMs target a single medical condition in the ambulatory practice,5 and involve a medical record audit performed by the physician, a patient survey, and a systems readiness survey. Physicians use the results of this data collection to perform a single test of change, and receive MOC credit when they report on the results of their intervention. Recognizing that QI activities may be different in hospital settings, the ABIM subsequently developed a Hospital‐based PIM (Hospital PIM) that allows physicians to use nationally‐approved hospital‐level performance data to complete the module. The Hospital PIM requires physicians to carry out a single test of change, and report any change in the perception of the environment supporting QI activities.
The ABIM has also begun work on potentially creating a focused pathway for hospitalists in the MOC program.6 Practice‐based learning and improvement (PBLI), systems‐based practice (SBP),7 and QI8 are core competencies of hospital medicine, and assessment of these competencies would be an important component of the new, focused MOC pathway. The Hospital PIM potentially provides an assessment methodology, thus it is important to understand the impact and value of this web‐based assessment tool.
The objective of this study is to explore the impact of the Hospital PIM on physicians participating in hospital‐based QI, including facilitators and barriers to a successful experience. We highlight several case studies to describe this impact, which can be defined as learning about QI, value‐added to practice, or an enhanced QI experience. We also describe 3 pathways suggesting how physician engagement, which is an emerging theme of our research, mediates the impact of the Hospital PIM.
Methods
A nonprobability purposive sample of physicians who completed the Hospital PIM (n = 21) as part of MOC by January 2007 was interviewed using semistructured telephone interviews. At the time of data collection, 771 physicians completed the Hospital PIM, and our sample strategically reflects equal proportions of those currently active on a QI team, as well as those who formed a QI team. Physicians were contacted via e‐mail and telephone to arrange an interview. None of the physicians contacted declined. All physicians were informed about the purpose of the study and provided consent for the ABIM to analyze and report data for purposes of understanding the feasibility of the PIM at improving practice. No physician personal identifiers were used in data analysis.
The interviews focused on four domains: reasons for choosing the module, assembly and role on any quality improvement teams, the value and satisfaction with the experience of completing the Hospital PIM, and prior experience with QI. Interviews were conducted by 1 trained member of the research team, and lasted approximately 30 minutes. Data collection was terminated when theoretical saturation was reached, or when no new data was revealed during the interviews. Interviews were audio‐recorded, and data were transcribed verbatim to facilitate analysis. Through an inductive and iterative approach, 3 members of the research team (including the interviewer) coded the data to identify themes that were consistently grounded in the data.9 These themes were subsequently discussed with a fourth researcher to maximize interrater reliability. Codes were then checked against existing literature to confirm linkages and enhance interpretation.
Results
The mean age of the participants (n = 21) was 42 years and 81% were male. Primary certificates were issued a mean of 13 years prior and completers came from a wide variety of disciplines, hospitals, and areas of expertise. Overall, the majority of physicians found the Hospital PIM to be a valuable experience (n = 17; 81%), which is similar to ABIM Hospital PIM surveillance data in which 75% of all completers said they would recommend the PIM to a colleague.
The impact and value of completing the PIM is illustrated in a variety of ways. For some, particularly those with extensive QI backgrounds, the PIM organized and broadened documentation of ongoing work. Several physicians described their utilization of the Hospital PIM as a byproduct of their hospital's existing cultural norms and interest in QI, and many Hospital PIM projects dovetailed with ongoing hospital QI activities. In these cases, even though the PIM did not stimulate new ideas, there was still value among physicians in receiving recognition for their ongoing QI activities and, perhaps more importantly, in learning by reflecting on their work.10
For others, the Hospital PIM was a catalyst to change. Similar to the role of a catalyst in a chemical reaction, our data suggest that the Hospital PIM facilitated QI by lowering the energy necessary for the process to occur. Many physicians reported the process stimulated new interest in QI, (eg, [The process] gave me some ideas about future QI projects that I plan to do, or described how the experience was an extra boost or stimulus to help change their ways.) These findings are consistent with recent findings on the use of PIMs in residency,11 which describes the Preventive Cardiology PIM as a catalyst to change.
Several physicians were surprised at how easy it was to begin and initiate a QI project, acknowledging the importance of leadership and teamwork (n = 7; 33%). In addition, many physicians highlighted reflective processes (n = 8; 38%) whereby the PIM led to an increased awareness of their clinical environment, or QI in general, including how QI can affect patient care and/or patient outcomes.
The most frequently reported facilitators to a successful PIM experience were familiarity/access to QI resources and staff, institutional support and culture of QI, and documentation of ongoing QI activities. The most frequently reported barrier (n = 9; 43%) was the time that it took to complete the module. Other barriers included a lack of institutional support or negative culture supporting QI activities, a lack of familiarity/access to QI resources and staff, and perceived irrelevance of QI activities to clinical practice.
Physician Engagement
Our data revealed a critical theme, whereby a physician's engagement with the QI process (especially the utilization of existing QI resources) mediated the impact of the PIM. Physicians who we describe as active engagers (n = 8) exhibited personal involvement in the QI project, including a commitment to working within the QI team structure. Active engagers possessed familiarity or knowledge of basic QI behaviors and skills, and most reported enhanced awareness of ongoing QI activities and the clinical environment as a result of completing the PIM.
Passive engagers (n = 10) may not have possessed the skills or motivation to become involved in the QI process. In our study, passive engagers were more likely to report perceived lack of relevance of QI activities to patient care practices, and may have had difficulty demonstrating personal commitment to improvement. Interestingly, many passive engagers reported an overall negative Hospital PIM experience, yet documented impact from the PIM via learning about the QI processes (eg, teamwork, communication, documentation, use of data) or ongoing QI activities that occurred while completing the PIM.
Finally, physicians who failed to engage in the QI process, nonengagers (n = 3) documented no evidence of QI learning and reported little impact from completing the PIM. The following case studies illustrate how physician engagement relates to physicians' experiences with the Hospital PIM and describes the unique influence of facilitators and barriers on both engagement and impact.
Case Study A: Active Engagement
This hospitalist spends 100% of his time performing clinical work in a hospital. He denies formal training in QI principles and has no prior experience in QI, but has an interest in QI resulting from prior work on throughput activities as part of a patient safety initiative at his hospital. He possesses a positive perception of his hospital's leadership and culture supporting QI activities: the hospital administration is very supportive of any sort of QI initiatives. His chosen measure was administration of pneumococcal vaccine in patients admitted with community acquired pneumonia (CAP), for which his hospital performed at 36% compliance.
Despite a lack of formal training in QI, this physician actively engaged with the existing QI resources and was able to call together the people who are typically associated with [QI] initiatives in the hospital to work on [the PIM]. This supportive culture facilitated the navigation through the hospital system and the physician's active engagement in the QI process.
Another key aspect of this physician's experience was his interaction with the members of a multidisciplinary team. While he provided the creative initiative for the project itself, the assembled QI team quickly identified areas of need and moved on to a quality‐based initiative, while providing a framework to disseminate the ideas of the project. The PIM was a valuable experience and this physician noted that it was surprisingly easier to begin and initiate a quality improvement project than thought.
Despite a lack of formal QI training or experience, this physician utilized his personal commitment to the value of QI and the positive hospital culture to engage the existing QI resources and staff. Similar to other active engagers, he demonstrated relationship building, team formation, and effective communication in completing the PIM. His level of engagement facilitated learning about QI and enhanced his PIM experience.
Case Study B: Passive Engagement
This physician is a subspecialist in Infectious Diseases who spends 15% of his time in patient care in the hospital. Prior to completing the PIM, he identified his prior QI experience as receiving messages from the head of our department in the hospital hearing about these kinds of things from a bureaucratic stance. At the beginning, he strongly disagreed with the notion that the hospital had strong leadership and culture supporting QI activities. His measure was the appropriate choice of initial antibiotics in CAP, in which his hospital reported 24% compliance.
In order to complete the module, this physician successfully enlisted the help of an existing QI team stating, I joined the group for that period of time so I could complete my certification. Specifically, They helped me to understand the problems, the barriers to improvement, and helped me get a sense of the ways to better improve the management of pneumonia in the hospital setting but in the end it probably didn't really affect my practice very much. When questioned about this dichotomy, this physician stated that the information learned in completing the PIM was not particularly relevant to a subspecialist who practices inpatient medicine for only a short period of time and mainly does research. Interestingly, after completing the module, this physician had a significantly improved perception of his hospital's QI leadership and culture.
Like other passive engagers, this physician described some interaction with existing QI resources and staff, though to a lesser degree than the active engagers. Even though completing the PIM was perceived as an overall negative experience, his familiarity with QI resources, and his ability to successfully engage with those resources, allowed him to complete the module and document an impact (ie, new personal learning about hospital QI principles and team formation) in the process. Another important finding is that QI learning occurred despite the presence of multiple barriers.
Case Studies C and D: No Engagement
Case Study C
This physician has a small clinical practice and works mostly in the laboratory. He admits to very limited QI experience and, at the onset of the PIM, possessed a moderately negative opinion about his hospital administration and culture supporting QI. He also chose pneumococcal vaccine administration, for which his hospital was performing at 48% compliance.
He tried multiple times to enlist the help of a hospital QI officer but was told to assemble the team myself and was subsequently unable to do so. This physician ended up being disengaged with the PIM and the QI process because he had no buy‐in from the QI department. The experience was frustrating and at the completion of the module, his perception of the hospital's QI leadership and culture was rated as moderately worse. This physician documented no impact as a result of completing the PIM.
Case Study D
This physician chose to complete the Hospital PIM because he worked as a hospitalist 100% of the time. He claims experience in QI by participating in conferences, teaching students, reading literature, but had not led or organized any QI projects or activities. He generally rated his hospital leadership and QI culture in positive terms.
Overall, this physician failed to engage because he did not believe in the basic tenets of QI, and possessed a negative view of the Hospital PIM and its relevance to his practice. This perceived irrelevance was illustrated when, despite having a hospital baseline performance measure of 5% compliance for percutaneous coronary intervention in under 120 minutes, he stated, We don't need to improve we're at a terrific level right now. During the PIM, this physician chose not to work with a QI team because he [didn't] need a team everybody knows their own place and what to do in each situation. To achieve QI gains, physicians at this hospital discuss with administration what they need to do to improve quality. This physician did document a change in the hospital's QI environment, but did not attribute it to the Hospital PIM, rather, because we just became more experienced in our hospital. The overall impact on this physician was negative, a waste of time, highlighting the perceived irrelevance of the PIM and of QI activities.
For various reasons highlighted in these case studies (eg, institutional barriers, perceived irrelevance, redundancy with existing QI activities), the Hospital PIM may be unhelpful to nonengagers and as a result, physicians with no engagement in the QI process may not have a successful experience with the Hospital PIM.
In summary, physician engagement mediates the experience and impact of the Hospital PIM on the physician. Importantly, initial engagement by itself is not a powerful predictor; rather, the degree of engagement unfolds as the QI activity progresses. Physicians may elect to (at times not purposefully) actively, passively, or not engage in the QI process; however, simply enrolling in the PIM will not necessarily lead to engagement or to a successful experience. The physician must engage in the QI process in order to achieve learning. In all of these case studies, facilitators and barriers undoubtedly influence the Hospital PIM experience, as well as any subsequent impact on learning about QI. However, their presence or absence does not seem to be as powerful of a predictor of impact as is the degree of physician engagement.
Discussion
This study describes experiences for a small number of early‐completers of the Hospital PIM. For many, impact is described as an increased awareness of the hospital clinical environment, particularly an awareness of ongoing QI activities. For others, the primary impact was learning through an increased appreciation of the importance of QI activities and understanding of basic QI procedures (ie, interdisciplinary teamwork, enhanced communication, and documentation, buy‐in, using data). Still others described impact as an enhanced QI experience via reflection on current QI work or catalyzing change in their hospital environment. Further exploration of these findings will be important to determine the full impact of the PIM. An unanticipated finding, however, was the emerging theme of the role of physician engagement in mediating a successful experience with the Hospital PIM.
Prior research on physician engagement more generally demonstrates that increased physician engagement enhances interaction with nursing and other office staff,12 improves overall physician alignment,13 enhances QI,2 and may heighten physicians' willingness to participate in hospital administration and policy.14 Our data support these findings and further describe the importance of engagement in QI activities, whether it be through assembling and working in a team, helping analyze hospital systems, navigating existing institutional linkages, or simply becoming the creative initiative on a QI project. For completers of the Hospital PIM, engaging in any aspect of the QI process facilitates a successful PIM experience as documented by impact, and may stimulate physician leadership and hospital level change as well. Nonengaging physicians, in contrast, had a negative experience and documented little or no impact as a result of completing the PIM.
As our findings illustrate, engagement may not be a fixed construct, and may be acquired or generated through the QI process. In this context, physicians with varying levels of QI experience and expertise may learn and find value in completing the Hospital PIM, provided they become engaged with the process. Internal (ie, personal commitment, buy‐in, perceived relevance) and external (ie, hospital QI culture, access to QI team, access to data) factors may influence the degree of satisfaction and success with the Hospital PIM experience, thus maximizing facilitators and overcoming the barriers is also important for a positive outcome.
There are important limitations to this study. Most importantly, we acknowledge that the quality of the resources available between hospitals is highly variable. Therefore, our subjective assessment of whether or not someone was actively engaged is largely dependent on the quality of the available resources, and in a resource‐poor environment, this may not be a fair reflection of their engagement. We further recognize that coming to any broad or conclusive findings about the impact of the PIM is difficult given the qualitative nature of this study. However, our findings do suggest that the Hospital PIM may promote learning and value to completing physicians, especially those that engage in the QI process. Future studies should further explore the described impact and the relationship between engagement and QI.
To further enhance the Hospital PIM, consideration of prerequisite criteria for future completers, such as documentation of engagement, adequate access to hospital QI resources, and significant clinical work in the hospital setting, may be warranted. Additionally, consideration for alternative means of MOC credit may be warranted for physicians who demonstrate a proficiency in QI activities or who work in hospitals that efficiently participate in QI activities, such as a Health Maintenance Organization, for whom completion of the Hospital PIM may be redundant.
In conclusion, our findings suggest that the Hospital PIM is a useful component of MOC for appropriate groups of physicians despite the unique aspects of the Hospital PIM using hospital‐level outcomes data. Many physicians in our sample found it to be useful as a catalyst for learning about QI activities, which was facilitated through active engagement with the PIM QI process. While ongoing study is needed, it is anticipated that the findings from this study will help to inform the proposed pathway of focused practice in hospital medicine as part of MOC, particularly activities geared toward assessing competency in QI.
Physicians play an important role in improving quality improvement (QI) through clinical expertise and leadership.1, 2 The role of the physician leader is dynamic and complex, yet key competencies have been described in terms of personal commitment, professional credibility, QI behaviors and skills, and institutional linkages.3 Several characteristics have also been identified in hospitals successful in implementing QI, including shared goals for improvement, substantial administrative support, use of credible data feedback, and strong physician leadership.4 Cultivating physician leadership in hospital QI via development of these competencies is crucial for ongoing efforts in hospital QI activities.
The American Board of Internal Medicine (ABIM) developed web‐based assessment tools called Practice Improvement Modules (PIMs), as part of the maintenance of certification (MOC) program. Designed to facilitate physician involvement in QI, most PIMs target a single medical condition in the ambulatory practice,5 and involve a medical record audit performed by the physician, a patient survey, and a systems readiness survey. Physicians use the results of this data collection to perform a single test of change, and receive MOC credit when they report on the results of their intervention. Recognizing that QI activities may be different in hospital settings, the ABIM subsequently developed a Hospital‐based PIM (Hospital PIM) that allows physicians to use nationally‐approved hospital‐level performance data to complete the module. The Hospital PIM requires physicians to carry out a single test of change, and report any change in the perception of the environment supporting QI activities.
The ABIM has also begun work on potentially creating a focused pathway for hospitalists in the MOC program.6 Practice‐based learning and improvement (PBLI), systems‐based practice (SBP),7 and QI8 are core competencies of hospital medicine, and assessment of these competencies would be an important component of the new, focused MOC pathway. The Hospital PIM potentially provides an assessment methodology, thus it is important to understand the impact and value of this web‐based assessment tool.
The objective of this study is to explore the impact of the Hospital PIM on physicians participating in hospital‐based QI, including facilitators and barriers to a successful experience. We highlight several case studies to describe this impact, which can be defined as learning about QI, value‐added to practice, or an enhanced QI experience. We also describe 3 pathways suggesting how physician engagement, which is an emerging theme of our research, mediates the impact of the Hospital PIM.
Methods
A nonprobability purposive sample of physicians who completed the Hospital PIM (n = 21) as part of MOC by January 2007 was interviewed using semistructured telephone interviews. At the time of data collection, 771 physicians completed the Hospital PIM, and our sample strategically reflects equal proportions of those currently active on a QI team, as well as those who formed a QI team. Physicians were contacted via e‐mail and telephone to arrange an interview. None of the physicians contacted declined. All physicians were informed about the purpose of the study and provided consent for the ABIM to analyze and report data for purposes of understanding the feasibility of the PIM at improving practice. No physician personal identifiers were used in data analysis.
The interviews focused on four domains: reasons for choosing the module, assembly and role on any quality improvement teams, the value and satisfaction with the experience of completing the Hospital PIM, and prior experience with QI. Interviews were conducted by 1 trained member of the research team, and lasted approximately 30 minutes. Data collection was terminated when theoretical saturation was reached, or when no new data was revealed during the interviews. Interviews were audio‐recorded, and data were transcribed verbatim to facilitate analysis. Through an inductive and iterative approach, 3 members of the research team (including the interviewer) coded the data to identify themes that were consistently grounded in the data.9 These themes were subsequently discussed with a fourth researcher to maximize interrater reliability. Codes were then checked against existing literature to confirm linkages and enhance interpretation.
Results
The mean age of the participants (n = 21) was 42 years and 81% were male. Primary certificates were issued a mean of 13 years prior and completers came from a wide variety of disciplines, hospitals, and areas of expertise. Overall, the majority of physicians found the Hospital PIM to be a valuable experience (n = 17; 81%), which is similar to ABIM Hospital PIM surveillance data in which 75% of all completers said they would recommend the PIM to a colleague.
The impact and value of completing the PIM is illustrated in a variety of ways. For some, particularly those with extensive QI backgrounds, the PIM organized and broadened documentation of ongoing work. Several physicians described their utilization of the Hospital PIM as a byproduct of their hospital's existing cultural norms and interest in QI, and many Hospital PIM projects dovetailed with ongoing hospital QI activities. In these cases, even though the PIM did not stimulate new ideas, there was still value among physicians in receiving recognition for their ongoing QI activities and, perhaps more importantly, in learning by reflecting on their work.10
For others, the Hospital PIM was a catalyst to change. Similar to the role of a catalyst in a chemical reaction, our data suggest that the Hospital PIM facilitated QI by lowering the energy necessary for the process to occur. Many physicians reported the process stimulated new interest in QI, (eg, [The process] gave me some ideas about future QI projects that I plan to do, or described how the experience was an extra boost or stimulus to help change their ways.) These findings are consistent with recent findings on the use of PIMs in residency,11 which describes the Preventive Cardiology PIM as a catalyst to change.
Several physicians were surprised at how easy it was to begin and initiate a QI project, acknowledging the importance of leadership and teamwork (n = 7; 33%). In addition, many physicians highlighted reflective processes (n = 8; 38%) whereby the PIM led to an increased awareness of their clinical environment, or QI in general, including how QI can affect patient care and/or patient outcomes.
The most frequently reported facilitators to a successful PIM experience were familiarity/access to QI resources and staff, institutional support and culture of QI, and documentation of ongoing QI activities. The most frequently reported barrier (n = 9; 43%) was the time that it took to complete the module. Other barriers included a lack of institutional support or negative culture supporting QI activities, a lack of familiarity/access to QI resources and staff, and perceived irrelevance of QI activities to clinical practice.
Physician Engagement
Our data revealed a critical theme, whereby a physician's engagement with the QI process (especially the utilization of existing QI resources) mediated the impact of the PIM. Physicians who we describe as active engagers (n = 8) exhibited personal involvement in the QI project, including a commitment to working within the QI team structure. Active engagers possessed familiarity or knowledge of basic QI behaviors and skills, and most reported enhanced awareness of ongoing QI activities and the clinical environment as a result of completing the PIM.
Passive engagers (n = 10) may not have possessed the skills or motivation to become involved in the QI process. In our study, passive engagers were more likely to report perceived lack of relevance of QI activities to patient care practices, and may have had difficulty demonstrating personal commitment to improvement. Interestingly, many passive engagers reported an overall negative Hospital PIM experience, yet documented impact from the PIM via learning about the QI processes (eg, teamwork, communication, documentation, use of data) or ongoing QI activities that occurred while completing the PIM.
Finally, physicians who failed to engage in the QI process, nonengagers (n = 3) documented no evidence of QI learning and reported little impact from completing the PIM. The following case studies illustrate how physician engagement relates to physicians' experiences with the Hospital PIM and describes the unique influence of facilitators and barriers on both engagement and impact.
Case Study A: Active Engagement
This hospitalist spends 100% of his time performing clinical work in a hospital. He denies formal training in QI principles and has no prior experience in QI, but has an interest in QI resulting from prior work on throughput activities as part of a patient safety initiative at his hospital. He possesses a positive perception of his hospital's leadership and culture supporting QI activities: the hospital administration is very supportive of any sort of QI initiatives. His chosen measure was administration of pneumococcal vaccine in patients admitted with community acquired pneumonia (CAP), for which his hospital performed at 36% compliance.
Despite a lack of formal training in QI, this physician actively engaged with the existing QI resources and was able to call together the people who are typically associated with [QI] initiatives in the hospital to work on [the PIM]. This supportive culture facilitated the navigation through the hospital system and the physician's active engagement in the QI process.
Another key aspect of this physician's experience was his interaction with the members of a multidisciplinary team. While he provided the creative initiative for the project itself, the assembled QI team quickly identified areas of need and moved on to a quality‐based initiative, while providing a framework to disseminate the ideas of the project. The PIM was a valuable experience and this physician noted that it was surprisingly easier to begin and initiate a quality improvement project than thought.
Despite a lack of formal QI training or experience, this physician utilized his personal commitment to the value of QI and the positive hospital culture to engage the existing QI resources and staff. Similar to other active engagers, he demonstrated relationship building, team formation, and effective communication in completing the PIM. His level of engagement facilitated learning about QI and enhanced his PIM experience.
Case Study B: Passive Engagement
This physician is a subspecialist in Infectious Diseases who spends 15% of his time in patient care in the hospital. Prior to completing the PIM, he identified his prior QI experience as receiving messages from the head of our department in the hospital hearing about these kinds of things from a bureaucratic stance. At the beginning, he strongly disagreed with the notion that the hospital had strong leadership and culture supporting QI activities. His measure was the appropriate choice of initial antibiotics in CAP, in which his hospital reported 24% compliance.
In order to complete the module, this physician successfully enlisted the help of an existing QI team stating, I joined the group for that period of time so I could complete my certification. Specifically, They helped me to understand the problems, the barriers to improvement, and helped me get a sense of the ways to better improve the management of pneumonia in the hospital setting but in the end it probably didn't really affect my practice very much. When questioned about this dichotomy, this physician stated that the information learned in completing the PIM was not particularly relevant to a subspecialist who practices inpatient medicine for only a short period of time and mainly does research. Interestingly, after completing the module, this physician had a significantly improved perception of his hospital's QI leadership and culture.
Like other passive engagers, this physician described some interaction with existing QI resources and staff, though to a lesser degree than the active engagers. Even though completing the PIM was perceived as an overall negative experience, his familiarity with QI resources, and his ability to successfully engage with those resources, allowed him to complete the module and document an impact (ie, new personal learning about hospital QI principles and team formation) in the process. Another important finding is that QI learning occurred despite the presence of multiple barriers.
Case Studies C and D: No Engagement
Case Study C
This physician has a small clinical practice and works mostly in the laboratory. He admits to very limited QI experience and, at the onset of the PIM, possessed a moderately negative opinion about his hospital administration and culture supporting QI. He also chose pneumococcal vaccine administration, for which his hospital was performing at 48% compliance.
He tried multiple times to enlist the help of a hospital QI officer but was told to assemble the team myself and was subsequently unable to do so. This physician ended up being disengaged with the PIM and the QI process because he had no buy‐in from the QI department. The experience was frustrating and at the completion of the module, his perception of the hospital's QI leadership and culture was rated as moderately worse. This physician documented no impact as a result of completing the PIM.
Case Study D
This physician chose to complete the Hospital PIM because he worked as a hospitalist 100% of the time. He claims experience in QI by participating in conferences, teaching students, reading literature, but had not led or organized any QI projects or activities. He generally rated his hospital leadership and QI culture in positive terms.
Overall, this physician failed to engage because he did not believe in the basic tenets of QI, and possessed a negative view of the Hospital PIM and its relevance to his practice. This perceived irrelevance was illustrated when, despite having a hospital baseline performance measure of 5% compliance for percutaneous coronary intervention in under 120 minutes, he stated, We don't need to improve we're at a terrific level right now. During the PIM, this physician chose not to work with a QI team because he [didn't] need a team everybody knows their own place and what to do in each situation. To achieve QI gains, physicians at this hospital discuss with administration what they need to do to improve quality. This physician did document a change in the hospital's QI environment, but did not attribute it to the Hospital PIM, rather, because we just became more experienced in our hospital. The overall impact on this physician was negative, a waste of time, highlighting the perceived irrelevance of the PIM and of QI activities.
For various reasons highlighted in these case studies (eg, institutional barriers, perceived irrelevance, redundancy with existing QI activities), the Hospital PIM may be unhelpful to nonengagers and as a result, physicians with no engagement in the QI process may not have a successful experience with the Hospital PIM.
In summary, physician engagement mediates the experience and impact of the Hospital PIM on the physician. Importantly, initial engagement by itself is not a powerful predictor; rather, the degree of engagement unfolds as the QI activity progresses. Physicians may elect to (at times not purposefully) actively, passively, or not engage in the QI process; however, simply enrolling in the PIM will not necessarily lead to engagement or to a successful experience. The physician must engage in the QI process in order to achieve learning. In all of these case studies, facilitators and barriers undoubtedly influence the Hospital PIM experience, as well as any subsequent impact on learning about QI. However, their presence or absence does not seem to be as powerful of a predictor of impact as is the degree of physician engagement.
Discussion
This study describes experiences for a small number of early‐completers of the Hospital PIM. For many, impact is described as an increased awareness of the hospital clinical environment, particularly an awareness of ongoing QI activities. For others, the primary impact was learning through an increased appreciation of the importance of QI activities and understanding of basic QI procedures (ie, interdisciplinary teamwork, enhanced communication, and documentation, buy‐in, using data). Still others described impact as an enhanced QI experience via reflection on current QI work or catalyzing change in their hospital environment. Further exploration of these findings will be important to determine the full impact of the PIM. An unanticipated finding, however, was the emerging theme of the role of physician engagement in mediating a successful experience with the Hospital PIM.
Prior research on physician engagement more generally demonstrates that increased physician engagement enhances interaction with nursing and other office staff,12 improves overall physician alignment,13 enhances QI,2 and may heighten physicians' willingness to participate in hospital administration and policy.14 Our data support these findings and further describe the importance of engagement in QI activities, whether it be through assembling and working in a team, helping analyze hospital systems, navigating existing institutional linkages, or simply becoming the creative initiative on a QI project. For completers of the Hospital PIM, engaging in any aspect of the QI process facilitates a successful PIM experience as documented by impact, and may stimulate physician leadership and hospital level change as well. Nonengaging physicians, in contrast, had a negative experience and documented little or no impact as a result of completing the PIM.
As our findings illustrate, engagement may not be a fixed construct, and may be acquired or generated through the QI process. In this context, physicians with varying levels of QI experience and expertise may learn and find value in completing the Hospital PIM, provided they become engaged with the process. Internal (ie, personal commitment, buy‐in, perceived relevance) and external (ie, hospital QI culture, access to QI team, access to data) factors may influence the degree of satisfaction and success with the Hospital PIM experience, thus maximizing facilitators and overcoming the barriers is also important for a positive outcome.
There are important limitations to this study. Most importantly, we acknowledge that the quality of the resources available between hospitals is highly variable. Therefore, our subjective assessment of whether or not someone was actively engaged is largely dependent on the quality of the available resources, and in a resource‐poor environment, this may not be a fair reflection of their engagement. We further recognize that coming to any broad or conclusive findings about the impact of the PIM is difficult given the qualitative nature of this study. However, our findings do suggest that the Hospital PIM may promote learning and value to completing physicians, especially those that engage in the QI process. Future studies should further explore the described impact and the relationship between engagement and QI.
To further enhance the Hospital PIM, consideration of prerequisite criteria for future completers, such as documentation of engagement, adequate access to hospital QI resources, and significant clinical work in the hospital setting, may be warranted. Additionally, consideration for alternative means of MOC credit may be warranted for physicians who demonstrate a proficiency in QI activities or who work in hospitals that efficiently participate in QI activities, such as a Health Maintenance Organization, for whom completion of the Hospital PIM may be redundant.
In conclusion, our findings suggest that the Hospital PIM is a useful component of MOC for appropriate groups of physicians despite the unique aspects of the Hospital PIM using hospital‐level outcomes data. Many physicians in our sample found it to be useful as a catalyst for learning about QI activities, which was facilitated through active engagement with the PIM QI process. While ongoing study is needed, it is anticipated that the findings from this study will help to inform the proposed pathway of focused practice in hospital medicine as part of MOC, particularly activities geared toward assessing competency in QI.
- , , , , , .The roles of senior management in quality improvement efforts: what are the key components?J Healthc Manag.2003;48:15–28.
- , , .Promoting clinical involvement in hospital quality improvement efforts: the effects of top management, board, and physician leadership.Health Serv Res.1997;32:491–510.
- , , , , , .Characteristics of physician leaders working to improve the quality of care in acute myocardial infarction.Jt Comm J Qual Saf.2003;29:289–296.
- , , , , , .A qualitative study of increasing beta‐blocker use after myocardial infarction: why do some hospitals succeed?JAMA.2001;285:2604–2611.
- , , .Improving the quality of care via maintenance of certification and the web: an early status report.Perspect Biol Med.2008;51:71–83.
- American Board of Internal Medicine. Questions and answers about ABIM recognition of focused practice in hospital medicine. Available at: http://www.abim.org/news/news/hospital‐medicine‐qa.aspx?wt.mc_id=hospital‐medicine‐qa. Accessed March 2009.
- Accreditation Council for Graduate Medical Education. The outcomes project. Available at: http://www.acgme.org/Outcome. Accessed March 2009.
- The core competencies in hospital medicine: a framework for curriculum development by the Society of Hospital Medicine.J Hosp Med.2006;1(suppl):2–95.
- , .Basics of Qualitative Research: Grounded Theory Procedures and Techniques.Newbury Park, CA:Sage Publications;1998.
- , , .Self‐monitoring in clinical practice: a challenge for medical educators.J Cont Educ Health Prof.2008;28:5–13.
- , , .The Impact of a preventive cardioloy quality improvement intervention on residents and clinics: a qualitative exploration.Am J of Med Qual.2009;24:99–107.
- , .Why do nurse managers stay? Building a model of engagement: Part 1. Dimensions of engagement.J Nurs Adm.2008;38:118–124.
- , .Involving physicians in total quality management: results of a study. In: Blumental D, Scheck AC, eds.Improving Clinical Practice: Total Quality Management and the Physician.San Francisco, CA:Jossey‐Bass;1995.
- , .Increasing physician engagement. using norms of physician culture to improve relationships with medical staff.Physician Exec.2007;33:38–45.
- , , , , , .The roles of senior management in quality improvement efforts: what are the key components?J Healthc Manag.2003;48:15–28.
- , , .Promoting clinical involvement in hospital quality improvement efforts: the effects of top management, board, and physician leadership.Health Serv Res.1997;32:491–510.
- , , , , , .Characteristics of physician leaders working to improve the quality of care in acute myocardial infarction.Jt Comm J Qual Saf.2003;29:289–296.
- , , , , , .A qualitative study of increasing beta‐blocker use after myocardial infarction: why do some hospitals succeed?JAMA.2001;285:2604–2611.
- , , .Improving the quality of care via maintenance of certification and the web: an early status report.Perspect Biol Med.2008;51:71–83.
- American Board of Internal Medicine. Questions and answers about ABIM recognition of focused practice in hospital medicine. Available at: http://www.abim.org/news/news/hospital‐medicine‐qa.aspx?wt.mc_id=hospital‐medicine‐qa. Accessed March 2009.
- Accreditation Council for Graduate Medical Education. The outcomes project. Available at: http://www.acgme.org/Outcome. Accessed March 2009.
- The core competencies in hospital medicine: a framework for curriculum development by the Society of Hospital Medicine.J Hosp Med.2006;1(suppl):2–95.
- , .Basics of Qualitative Research: Grounded Theory Procedures and Techniques.Newbury Park, CA:Sage Publications;1998.
- , , .Self‐monitoring in clinical practice: a challenge for medical educators.J Cont Educ Health Prof.2008;28:5–13.
- , , .The Impact of a preventive cardioloy quality improvement intervention on residents and clinics: a qualitative exploration.Am J of Med Qual.2009;24:99–107.
- , .Why do nurse managers stay? Building a model of engagement: Part 1. Dimensions of engagement.J Nurs Adm.2008;38:118–124.
- , .Involving physicians in total quality management: results of a study. In: Blumental D, Scheck AC, eds.Improving Clinical Practice: Total Quality Management and the Physician.San Francisco, CA:Jossey‐Bass;1995.
- , .Increasing physician engagement. using norms of physician culture to improve relationships with medical staff.Physician Exec.2007;33:38–45.
Copyright © 2009 Society of Hospital Medicine
Teaching Patient‐Centered Care
In recent years, medical educators have recognized the importance of the inclusion of patient‐centered care in the medical school curriculum.1 There is an increased awareness of the importance of patient involvement in medical decision‐making, as well as a realization that patient‐centered care positively affects patient satisfaction and outcomes measures.2 The Institute of Medicine, in its 2001 report Crossing the Quality Chasm: A New Health System for the 21st Century, included patient‐centered care as one of the areas for the development of quality measures, defining it as providing care that is respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions.3 Several organizations, such as the Institute for Healthcare Improvement,4 have initiatives related to achieving the goals of patient‐centered care. While not a new phenomenon, patient‐centered care is permeating many areas of the healthcare delivery system.5 The recognition of patient‐centered care as both a desirable and measurable outcome of the healthcare enterprise has also renewed interest in the field of medical humanities as a valid tool for the advancement of patient‐centered initiatives and goals.
The Basis for Patient‐centered Care
Stewart et al.,6 in their book Patient‐Centered Medicine: Transforming the Clinical Method, identify 6 essential components of the patient‐centered clinical method: exploration of the disease and illness experience; understanding of the whole person; finding common ground; incorporating prevention and health promotion; enhancing the patient‐doctor relationship; and being realistic. These recommendations seek to improve the patient‐physician relationship by empowering the patient to be an active participant in his/her own health care.
The American Academy of Pediatrics recently released a policy statement7 outlining the benefits of family‐centered care in patient‐family outcomes, as well as in staff satisfaction. The statement also highlights the importance of bedside rounding by the attending physician and the healthcare team. Bedside rounding involves the patient in management discussions and decision making, while allowing for the unfiltered exchange of information. Nurses, therapists, and ancillary staff involved in the care of the patient also participate in the presentation. After the presentation, goals for the hospitalization are established, and the patient and family are asked for permission to implement the plan of care. Educational discussions regarding the patient's diagnosis usually take place outside the room, unless the patient's physical exam warrants a bedside teaching moment. Regardless of the format, patient‐involvement in the decision process is the central objective.
The Basis for the Medical Humanities
At the same time, there is renewed interest in the inclusion of the humanities in medicine. There is a perceived gap between the technological emphasis of the current medical school curriculum and the human values integral to the patient‐physician relationship.8 Namely, there is a growing concern that medical technology has suffused medical education with a sort of trade mentality in which doctors are trained in the latest scientific medical breakthroughs without the proper contextualization of the patient as the center of the healthcare enterprise.9 The National Endowment for the Humanities, the Association of American Medical Colleges, the Accreditation Council on Graduate Medical Education, and the Society for Health and Human Values have all called for increased emphasis of the humanities in medical education.10
What are the medical humanities? There is no clear‐cut definition. Felice Aull11 correlates the term with various so‐called liberal arts disciplines and their application to medical education and practice. She develops the notion that the medical humanities contribute to medical education in areas pertinent to patient‐centered care: insight into the human condition, development of observational and analytical skills, development of empathy and self‐reflection, and intercultural understanding.
In general, the medical humanities provide broad educational perspectives, and allow learners to develop skills critical to the development of a humane approach to patients.12 The paradigm relies on the assumption that exposure to the humanities in medical schoolin the form of formal lectures dealing with topics such as philosophy and literature, or through the role‐modeling interactions of teaching physicians and their perceived empathy to their patientswill allow the students to become more humane, and therefore, better doctors.13 The medical humanities seek to equip doctors with the critical thinking incumbent to the conversation about human values in a scientific field, and to explore questions of value and purpose critical in the medical setting.14
Shared Values
What are the values associated with the medical humanities that make them ideal for the teaching of patient‐centered care? Lester Friedman15 delineates 2 domains pertaining to the intrinsic values of the medical humanities. He identifies an affective domain, corresponding to a loose interpretation of the traditional affective perspective identified in the patient‐physician relationship; and a cognitive domain, a refocusing of medicine to its so‐called traditional professional roots, contrasted with the trade mentality of some in the profession today. Donnie Self16 identifies 2 currents of thought regarding the medical humanities: the affective approach, related to the development of compassion, sensitivity, empathy between the patients and their care providers; and the cognitive approach, which pertains to the development of logical and critical thinking required by medical education. These correspond to the integral attributes of patient‐centered care: incorporating the patients' ideas and affective responses to their illness; and establishing common ground and goals agreed upon by both patient and physician.17
The medical humanities are used to address such patient‐centered issues as end‐of‐life care in children,18 the physician‐patient narrative interaction,19 and the patients' role in their own health care.20 Medical humanities courses are also used in the training of cultural competence.21 Of course, the best‐known contribution of the medical humanities to patient‐centered care is the continuing importance of bioethics programs and their interrelation with other humanities fields.22
One of the goals of patient‐centered care is the elimination of perceived barriers of communication between patient and healthcare providers, in order to create a partnership aimed at improving healthcare outcomes.2 Since one of the fundamental aspects of medical training is learning the language of medicine,23 enhancing the communication skills of future physicians is part of the educational goals pursued by medical humanities programs.24 Language and its applicationsfor example, courses on medical interviewing or narrative medicineserve as the link between patient care and the medical humanities. Effective communication with patients is a measurable predictor of patient satisfaction, patient outcomes, and occurrences of malpractice litigation.17 For example, a study examining communication behaviors between physicians and the occurrence of malpractice claims25 found that doctors who were not sued spent more time with patients, educating patients about what to expect, and asking patients their understanding and opinion of the situation. Another study26 demonstrated that a patient‐focused approach improved the management of asthma, decreasing emergency room visits and hospitalizations. Therefore, it is not surprising that the Institute of Medicine's Committee on Behavioral and Social Sciences in Medical School Curricula identified basic and complex communications skills as priorities for inclusion in the medical curriculum.27
Doubts About the Process
There are doubts as to whether the medical humanities can really instill humanistic qualities in doctors. There are also questions about the physician‐centric focus of the medical humanities.28 This physician‐centric attitude runs counter to the intent of the medical humanities. Edmund Pellegrino and David Thomasma29 define the patient‐physician interaction as a human relationship where 1 person in need of healing seeks out another who professes to heal, or to assist in healing. The act of medicine ties these 2 persons together. While acknowledging the basic imbalance of the physician‐patient relationship, Pellegrino and Thomasma29 strive to close the gap by establishing medicine as a relation of mutual consent to effect individualized well‐being by working in, with, and through the body. The individualized exercise of well‐being, framed in, with, and through the body of the patient is similar to the description used by Stewart et al.6 of the patient as the unit of analysis delineating patient‐centered care, as it incorporates the interactive components proposed for a successful patient‐centered interaction.
There is also confusion between the teaching of humanities in medical schoolfor example, courses in history of medicine, narrative medicine, and medicine and the artsand the attempt to train humanistic physicians.30 Although an examination of humanities texts is certainly useful, the focus of the teaching of the medical humanities should evolve beyond a simple lucubration based on liberal studies, to a focused interaction between patient and physician, and a recentralization of the patient as the focus of that relationship.31
Conclusions
There is general agreement that a humane doctor is a better doctor. There is less agreement on how to measure the impact of a humanities education, as a qualitative assessment of satisfactory health care.19, 22, 25 There has been great growth in the teaching of medical humanities in medical schools. Most of the focus has been on the inclusion of humanities textssuch as literary, philosophical, and historical documentsas tools to establish a correlation between the arts and medicine, in hopes that the clarification of such association will provide medical students a broad‐based assessment, a so‐called world‐view, from which they can become introspective and humanistic when faced with their patients.32 Although this is a desirable goal, the driving force behind the medical humanities should shift to a quantifiable, evidence‐based assessment of its goals. A tool to achieve this verification is through the process of patient‐centered care. There is evidence to suggest patient‐centered care improves satisfaction and outcomes measures. It also refocuses care on the patient, which is the same goal of the medical humanities. By focusing on the patient, instead of the physician, the medical humanities will gain verification and validation within the academic healthcare environment.
- .Integrating the teaching of basic sciences, clinical sciences, and biopsychosocial issues.Acad Med.1998;73:S24–S31.
- , , , et al.The impact of patient‐centered care on outcomes.J Fam Pract.2000;49:796–804.
- Institute of Medicine.Committee on Quality Health Care in America.Crossing the Quality Chasm: A New Health System for the 21st Century.Washington, DC:National Academy Press;2001.
- Institute for Healthcare Improvement. Available at: http://www.ihi.org/IHI/Topics/PatientCenteredCare/PatientCenteredCareGeneral. Accessed March2009.
- , .Patient‐centered medicine: a professional evolution.JAMA.1996;275:152–156.
- , , , et al.Patient‐Centered Medicine: Transforming the CLINICAL method.Abingdon, UK:Radcliffe Medical Press;2003.
- American Academy of Pediatrics.Committee on Hospital Care. Institute for Family‐Centered Care. Family‐centered care and the pediatrician's role.Pediatrics.2003;112:691–693.
- , .Teaching Ethics, the Humanities and Human Values in Medical Schools: A Ten‐Year Overview.Washington, DC:Institute on Human Values in Medicine, Society for Health and Human Values;1982.
- .Medical humanism and technological anxiety. In: Self DJ, ed.The Role of the Humanities in Medical Education.Norfolk VA:Teagle 1978:1–7.
- , .A community‐based approach to the medical humanities.Med Educ.2004;38:204–217.
- . NYU Medical Humanities website. Mission statement. Available at: http://medhum.med.nyu.edu. Accessed March2009.
- .The humanities in medical education: context, outcomes and structures.Med Humanit.2000;26:23–30.
- .The Place of the Humanities in Medicine.New York:The Hastings Center, Institute of Society Ethics and the Life Sciences;1984.
- .Humanism and the Physician.Knoxville, TN:University of Tennessee Press;1979.
- .The precarious position of the medical humanities in the medical school curriculum.Acad Med.2002;77:320–322.
- .The educational philosophies behind medical humanities programs in the United States.Theor Med.1993;14:221–229.
- .The science of patient‐centered care.J Fam Pract.2000;49:805–806.
- , , , , .Medical education about end‐of‐life care in the pediatric setting: principles, challenges, and opportunities.Pediatrics.2000;105:575–584.
- .The patient‐physician relationship. Narrative medicine: a model for empathy, reflection, profession, and trust.JAMA.2001;286(15):1897–1902.
- .Medical humanities: means, ends, and evaluation. In: Evans M, Finley IG, eds.Medical Humanities.London, UK:BMJ Books;2001:204–216.
- American Institutes for Research.Teaching Cultural Competence in Health Care: A Review of Current Concepts, Policies and Practices.Washington, DC:Office of Minority Health;2002.
- .Bioethics and humanities: what makes us one field?J Med Philos.1998;23(4):356–368.
- .A medical humanities course: a pertinent pause on the medical beat.J Assembly for Expended Perspectives on Learning.2000–2001;6:40–51.
- , , editors.The humanities and medicine: reports of forty‐one U.S., Canadian and international programs.Acad Med2003;78:951–952.
- , , , , .Physician‐patient communication: the relationship with malpractice claims among primary care physicians and surgeons.JAMA.1997;277(7):553–559.
- , .Patient‐focused care: using the right tools.Chest.2006;130(suppl):73S–82S.
- Cuff PA, Vanselow N, eds.Committee on Behavioral and Social Sciences in Medical School Curricula.Improving Medical Education, Enhancing the Behavioral and Social Science Content of Medical School Curricula.Washington, DC:Institute of Medicine of the National Academies, The National Academies Press;2004. Available at: http://www.nap.edu/catalog.php?record_id=10956. Accessed March 2009.
- .Teaching analysis: doubts about medical humanities.Health Care Anal.1994;2:347–350.
- , .A Philosophical Basis of Medical Practice.New York, NY:Oxford University Press;1981.
- , , .The humanities, humanistic behavior, and the humane physician: a cautionary note.Ann Intern Med.1987;106:313–318.
- .Humanity and the medical humanities.Lancet.1995;346:1143–1145.
In recent years, medical educators have recognized the importance of the inclusion of patient‐centered care in the medical school curriculum.1 There is an increased awareness of the importance of patient involvement in medical decision‐making, as well as a realization that patient‐centered care positively affects patient satisfaction and outcomes measures.2 The Institute of Medicine, in its 2001 report Crossing the Quality Chasm: A New Health System for the 21st Century, included patient‐centered care as one of the areas for the development of quality measures, defining it as providing care that is respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions.3 Several organizations, such as the Institute for Healthcare Improvement,4 have initiatives related to achieving the goals of patient‐centered care. While not a new phenomenon, patient‐centered care is permeating many areas of the healthcare delivery system.5 The recognition of patient‐centered care as both a desirable and measurable outcome of the healthcare enterprise has also renewed interest in the field of medical humanities as a valid tool for the advancement of patient‐centered initiatives and goals.
The Basis for Patient‐centered Care
Stewart et al.,6 in their book Patient‐Centered Medicine: Transforming the Clinical Method, identify 6 essential components of the patient‐centered clinical method: exploration of the disease and illness experience; understanding of the whole person; finding common ground; incorporating prevention and health promotion; enhancing the patient‐doctor relationship; and being realistic. These recommendations seek to improve the patient‐physician relationship by empowering the patient to be an active participant in his/her own health care.
The American Academy of Pediatrics recently released a policy statement7 outlining the benefits of family‐centered care in patient‐family outcomes, as well as in staff satisfaction. The statement also highlights the importance of bedside rounding by the attending physician and the healthcare team. Bedside rounding involves the patient in management discussions and decision making, while allowing for the unfiltered exchange of information. Nurses, therapists, and ancillary staff involved in the care of the patient also participate in the presentation. After the presentation, goals for the hospitalization are established, and the patient and family are asked for permission to implement the plan of care. Educational discussions regarding the patient's diagnosis usually take place outside the room, unless the patient's physical exam warrants a bedside teaching moment. Regardless of the format, patient‐involvement in the decision process is the central objective.
The Basis for the Medical Humanities
At the same time, there is renewed interest in the inclusion of the humanities in medicine. There is a perceived gap between the technological emphasis of the current medical school curriculum and the human values integral to the patient‐physician relationship.8 Namely, there is a growing concern that medical technology has suffused medical education with a sort of trade mentality in which doctors are trained in the latest scientific medical breakthroughs without the proper contextualization of the patient as the center of the healthcare enterprise.9 The National Endowment for the Humanities, the Association of American Medical Colleges, the Accreditation Council on Graduate Medical Education, and the Society for Health and Human Values have all called for increased emphasis of the humanities in medical education.10
What are the medical humanities? There is no clear‐cut definition. Felice Aull11 correlates the term with various so‐called liberal arts disciplines and their application to medical education and practice. She develops the notion that the medical humanities contribute to medical education in areas pertinent to patient‐centered care: insight into the human condition, development of observational and analytical skills, development of empathy and self‐reflection, and intercultural understanding.
In general, the medical humanities provide broad educational perspectives, and allow learners to develop skills critical to the development of a humane approach to patients.12 The paradigm relies on the assumption that exposure to the humanities in medical schoolin the form of formal lectures dealing with topics such as philosophy and literature, or through the role‐modeling interactions of teaching physicians and their perceived empathy to their patientswill allow the students to become more humane, and therefore, better doctors.13 The medical humanities seek to equip doctors with the critical thinking incumbent to the conversation about human values in a scientific field, and to explore questions of value and purpose critical in the medical setting.14
Shared Values
What are the values associated with the medical humanities that make them ideal for the teaching of patient‐centered care? Lester Friedman15 delineates 2 domains pertaining to the intrinsic values of the medical humanities. He identifies an affective domain, corresponding to a loose interpretation of the traditional affective perspective identified in the patient‐physician relationship; and a cognitive domain, a refocusing of medicine to its so‐called traditional professional roots, contrasted with the trade mentality of some in the profession today. Donnie Self16 identifies 2 currents of thought regarding the medical humanities: the affective approach, related to the development of compassion, sensitivity, empathy between the patients and their care providers; and the cognitive approach, which pertains to the development of logical and critical thinking required by medical education. These correspond to the integral attributes of patient‐centered care: incorporating the patients' ideas and affective responses to their illness; and establishing common ground and goals agreed upon by both patient and physician.17
The medical humanities are used to address such patient‐centered issues as end‐of‐life care in children,18 the physician‐patient narrative interaction,19 and the patients' role in their own health care.20 Medical humanities courses are also used in the training of cultural competence.21 Of course, the best‐known contribution of the medical humanities to patient‐centered care is the continuing importance of bioethics programs and their interrelation with other humanities fields.22
One of the goals of patient‐centered care is the elimination of perceived barriers of communication between patient and healthcare providers, in order to create a partnership aimed at improving healthcare outcomes.2 Since one of the fundamental aspects of medical training is learning the language of medicine,23 enhancing the communication skills of future physicians is part of the educational goals pursued by medical humanities programs.24 Language and its applicationsfor example, courses on medical interviewing or narrative medicineserve as the link between patient care and the medical humanities. Effective communication with patients is a measurable predictor of patient satisfaction, patient outcomes, and occurrences of malpractice litigation.17 For example, a study examining communication behaviors between physicians and the occurrence of malpractice claims25 found that doctors who were not sued spent more time with patients, educating patients about what to expect, and asking patients their understanding and opinion of the situation. Another study26 demonstrated that a patient‐focused approach improved the management of asthma, decreasing emergency room visits and hospitalizations. Therefore, it is not surprising that the Institute of Medicine's Committee on Behavioral and Social Sciences in Medical School Curricula identified basic and complex communications skills as priorities for inclusion in the medical curriculum.27
Doubts About the Process
There are doubts as to whether the medical humanities can really instill humanistic qualities in doctors. There are also questions about the physician‐centric focus of the medical humanities.28 This physician‐centric attitude runs counter to the intent of the medical humanities. Edmund Pellegrino and David Thomasma29 define the patient‐physician interaction as a human relationship where 1 person in need of healing seeks out another who professes to heal, or to assist in healing. The act of medicine ties these 2 persons together. While acknowledging the basic imbalance of the physician‐patient relationship, Pellegrino and Thomasma29 strive to close the gap by establishing medicine as a relation of mutual consent to effect individualized well‐being by working in, with, and through the body. The individualized exercise of well‐being, framed in, with, and through the body of the patient is similar to the description used by Stewart et al.6 of the patient as the unit of analysis delineating patient‐centered care, as it incorporates the interactive components proposed for a successful patient‐centered interaction.
There is also confusion between the teaching of humanities in medical schoolfor example, courses in history of medicine, narrative medicine, and medicine and the artsand the attempt to train humanistic physicians.30 Although an examination of humanities texts is certainly useful, the focus of the teaching of the medical humanities should evolve beyond a simple lucubration based on liberal studies, to a focused interaction between patient and physician, and a recentralization of the patient as the focus of that relationship.31
Conclusions
There is general agreement that a humane doctor is a better doctor. There is less agreement on how to measure the impact of a humanities education, as a qualitative assessment of satisfactory health care.19, 22, 25 There has been great growth in the teaching of medical humanities in medical schools. Most of the focus has been on the inclusion of humanities textssuch as literary, philosophical, and historical documentsas tools to establish a correlation between the arts and medicine, in hopes that the clarification of such association will provide medical students a broad‐based assessment, a so‐called world‐view, from which they can become introspective and humanistic when faced with their patients.32 Although this is a desirable goal, the driving force behind the medical humanities should shift to a quantifiable, evidence‐based assessment of its goals. A tool to achieve this verification is through the process of patient‐centered care. There is evidence to suggest patient‐centered care improves satisfaction and outcomes measures. It also refocuses care on the patient, which is the same goal of the medical humanities. By focusing on the patient, instead of the physician, the medical humanities will gain verification and validation within the academic healthcare environment.
In recent years, medical educators have recognized the importance of the inclusion of patient‐centered care in the medical school curriculum.1 There is an increased awareness of the importance of patient involvement in medical decision‐making, as well as a realization that patient‐centered care positively affects patient satisfaction and outcomes measures.2 The Institute of Medicine, in its 2001 report Crossing the Quality Chasm: A New Health System for the 21st Century, included patient‐centered care as one of the areas for the development of quality measures, defining it as providing care that is respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions.3 Several organizations, such as the Institute for Healthcare Improvement,4 have initiatives related to achieving the goals of patient‐centered care. While not a new phenomenon, patient‐centered care is permeating many areas of the healthcare delivery system.5 The recognition of patient‐centered care as both a desirable and measurable outcome of the healthcare enterprise has also renewed interest in the field of medical humanities as a valid tool for the advancement of patient‐centered initiatives and goals.
The Basis for Patient‐centered Care
Stewart et al.,6 in their book Patient‐Centered Medicine: Transforming the Clinical Method, identify 6 essential components of the patient‐centered clinical method: exploration of the disease and illness experience; understanding of the whole person; finding common ground; incorporating prevention and health promotion; enhancing the patient‐doctor relationship; and being realistic. These recommendations seek to improve the patient‐physician relationship by empowering the patient to be an active participant in his/her own health care.
The American Academy of Pediatrics recently released a policy statement7 outlining the benefits of family‐centered care in patient‐family outcomes, as well as in staff satisfaction. The statement also highlights the importance of bedside rounding by the attending physician and the healthcare team. Bedside rounding involves the patient in management discussions and decision making, while allowing for the unfiltered exchange of information. Nurses, therapists, and ancillary staff involved in the care of the patient also participate in the presentation. After the presentation, goals for the hospitalization are established, and the patient and family are asked for permission to implement the plan of care. Educational discussions regarding the patient's diagnosis usually take place outside the room, unless the patient's physical exam warrants a bedside teaching moment. Regardless of the format, patient‐involvement in the decision process is the central objective.
The Basis for the Medical Humanities
At the same time, there is renewed interest in the inclusion of the humanities in medicine. There is a perceived gap between the technological emphasis of the current medical school curriculum and the human values integral to the patient‐physician relationship.8 Namely, there is a growing concern that medical technology has suffused medical education with a sort of trade mentality in which doctors are trained in the latest scientific medical breakthroughs without the proper contextualization of the patient as the center of the healthcare enterprise.9 The National Endowment for the Humanities, the Association of American Medical Colleges, the Accreditation Council on Graduate Medical Education, and the Society for Health and Human Values have all called for increased emphasis of the humanities in medical education.10
What are the medical humanities? There is no clear‐cut definition. Felice Aull11 correlates the term with various so‐called liberal arts disciplines and their application to medical education and practice. She develops the notion that the medical humanities contribute to medical education in areas pertinent to patient‐centered care: insight into the human condition, development of observational and analytical skills, development of empathy and self‐reflection, and intercultural understanding.
In general, the medical humanities provide broad educational perspectives, and allow learners to develop skills critical to the development of a humane approach to patients.12 The paradigm relies on the assumption that exposure to the humanities in medical schoolin the form of formal lectures dealing with topics such as philosophy and literature, or through the role‐modeling interactions of teaching physicians and their perceived empathy to their patientswill allow the students to become more humane, and therefore, better doctors.13 The medical humanities seek to equip doctors with the critical thinking incumbent to the conversation about human values in a scientific field, and to explore questions of value and purpose critical in the medical setting.14
Shared Values
What are the values associated with the medical humanities that make them ideal for the teaching of patient‐centered care? Lester Friedman15 delineates 2 domains pertaining to the intrinsic values of the medical humanities. He identifies an affective domain, corresponding to a loose interpretation of the traditional affective perspective identified in the patient‐physician relationship; and a cognitive domain, a refocusing of medicine to its so‐called traditional professional roots, contrasted with the trade mentality of some in the profession today. Donnie Self16 identifies 2 currents of thought regarding the medical humanities: the affective approach, related to the development of compassion, sensitivity, empathy between the patients and their care providers; and the cognitive approach, which pertains to the development of logical and critical thinking required by medical education. These correspond to the integral attributes of patient‐centered care: incorporating the patients' ideas and affective responses to their illness; and establishing common ground and goals agreed upon by both patient and physician.17
The medical humanities are used to address such patient‐centered issues as end‐of‐life care in children,18 the physician‐patient narrative interaction,19 and the patients' role in their own health care.20 Medical humanities courses are also used in the training of cultural competence.21 Of course, the best‐known contribution of the medical humanities to patient‐centered care is the continuing importance of bioethics programs and their interrelation with other humanities fields.22
One of the goals of patient‐centered care is the elimination of perceived barriers of communication between patient and healthcare providers, in order to create a partnership aimed at improving healthcare outcomes.2 Since one of the fundamental aspects of medical training is learning the language of medicine,23 enhancing the communication skills of future physicians is part of the educational goals pursued by medical humanities programs.24 Language and its applicationsfor example, courses on medical interviewing or narrative medicineserve as the link between patient care and the medical humanities. Effective communication with patients is a measurable predictor of patient satisfaction, patient outcomes, and occurrences of malpractice litigation.17 For example, a study examining communication behaviors between physicians and the occurrence of malpractice claims25 found that doctors who were not sued spent more time with patients, educating patients about what to expect, and asking patients their understanding and opinion of the situation. Another study26 demonstrated that a patient‐focused approach improved the management of asthma, decreasing emergency room visits and hospitalizations. Therefore, it is not surprising that the Institute of Medicine's Committee on Behavioral and Social Sciences in Medical School Curricula identified basic and complex communications skills as priorities for inclusion in the medical curriculum.27
Doubts About the Process
There are doubts as to whether the medical humanities can really instill humanistic qualities in doctors. There are also questions about the physician‐centric focus of the medical humanities.28 This physician‐centric attitude runs counter to the intent of the medical humanities. Edmund Pellegrino and David Thomasma29 define the patient‐physician interaction as a human relationship where 1 person in need of healing seeks out another who professes to heal, or to assist in healing. The act of medicine ties these 2 persons together. While acknowledging the basic imbalance of the physician‐patient relationship, Pellegrino and Thomasma29 strive to close the gap by establishing medicine as a relation of mutual consent to effect individualized well‐being by working in, with, and through the body. The individualized exercise of well‐being, framed in, with, and through the body of the patient is similar to the description used by Stewart et al.6 of the patient as the unit of analysis delineating patient‐centered care, as it incorporates the interactive components proposed for a successful patient‐centered interaction.
There is also confusion between the teaching of humanities in medical schoolfor example, courses in history of medicine, narrative medicine, and medicine and the artsand the attempt to train humanistic physicians.30 Although an examination of humanities texts is certainly useful, the focus of the teaching of the medical humanities should evolve beyond a simple lucubration based on liberal studies, to a focused interaction between patient and physician, and a recentralization of the patient as the focus of that relationship.31
Conclusions
There is general agreement that a humane doctor is a better doctor. There is less agreement on how to measure the impact of a humanities education, as a qualitative assessment of satisfactory health care.19, 22, 25 There has been great growth in the teaching of medical humanities in medical schools. Most of the focus has been on the inclusion of humanities textssuch as literary, philosophical, and historical documentsas tools to establish a correlation between the arts and medicine, in hopes that the clarification of such association will provide medical students a broad‐based assessment, a so‐called world‐view, from which they can become introspective and humanistic when faced with their patients.32 Although this is a desirable goal, the driving force behind the medical humanities should shift to a quantifiable, evidence‐based assessment of its goals. A tool to achieve this verification is through the process of patient‐centered care. There is evidence to suggest patient‐centered care improves satisfaction and outcomes measures. It also refocuses care on the patient, which is the same goal of the medical humanities. By focusing on the patient, instead of the physician, the medical humanities will gain verification and validation within the academic healthcare environment.
- .Integrating the teaching of basic sciences, clinical sciences, and biopsychosocial issues.Acad Med.1998;73:S24–S31.
- , , , et al.The impact of patient‐centered care on outcomes.J Fam Pract.2000;49:796–804.
- Institute of Medicine.Committee on Quality Health Care in America.Crossing the Quality Chasm: A New Health System for the 21st Century.Washington, DC:National Academy Press;2001.
- Institute for Healthcare Improvement. Available at: http://www.ihi.org/IHI/Topics/PatientCenteredCare/PatientCenteredCareGeneral. Accessed March2009.
- , .Patient‐centered medicine: a professional evolution.JAMA.1996;275:152–156.
- , , , et al.Patient‐Centered Medicine: Transforming the CLINICAL method.Abingdon, UK:Radcliffe Medical Press;2003.
- American Academy of Pediatrics.Committee on Hospital Care. Institute for Family‐Centered Care. Family‐centered care and the pediatrician's role.Pediatrics.2003;112:691–693.
- , .Teaching Ethics, the Humanities and Human Values in Medical Schools: A Ten‐Year Overview.Washington, DC:Institute on Human Values in Medicine, Society for Health and Human Values;1982.
- .Medical humanism and technological anxiety. In: Self DJ, ed.The Role of the Humanities in Medical Education.Norfolk VA:Teagle 1978:1–7.
- , .A community‐based approach to the medical humanities.Med Educ.2004;38:204–217.
- . NYU Medical Humanities website. Mission statement. Available at: http://medhum.med.nyu.edu. Accessed March2009.
- .The humanities in medical education: context, outcomes and structures.Med Humanit.2000;26:23–30.
- .The Place of the Humanities in Medicine.New York:The Hastings Center, Institute of Society Ethics and the Life Sciences;1984.
- .Humanism and the Physician.Knoxville, TN:University of Tennessee Press;1979.
- .The precarious position of the medical humanities in the medical school curriculum.Acad Med.2002;77:320–322.
- .The educational philosophies behind medical humanities programs in the United States.Theor Med.1993;14:221–229.
- .The science of patient‐centered care.J Fam Pract.2000;49:805–806.
- , , , , .Medical education about end‐of‐life care in the pediatric setting: principles, challenges, and opportunities.Pediatrics.2000;105:575–584.
- .The patient‐physician relationship. Narrative medicine: a model for empathy, reflection, profession, and trust.JAMA.2001;286(15):1897–1902.
- .Medical humanities: means, ends, and evaluation. In: Evans M, Finley IG, eds.Medical Humanities.London, UK:BMJ Books;2001:204–216.
- American Institutes for Research.Teaching Cultural Competence in Health Care: A Review of Current Concepts, Policies and Practices.Washington, DC:Office of Minority Health;2002.
- .Bioethics and humanities: what makes us one field?J Med Philos.1998;23(4):356–368.
- .A medical humanities course: a pertinent pause on the medical beat.J Assembly for Expended Perspectives on Learning.2000–2001;6:40–51.
- , , editors.The humanities and medicine: reports of forty‐one U.S., Canadian and international programs.Acad Med2003;78:951–952.
- , , , , .Physician‐patient communication: the relationship with malpractice claims among primary care physicians and surgeons.JAMA.1997;277(7):553–559.
- , .Patient‐focused care: using the right tools.Chest.2006;130(suppl):73S–82S.
- Cuff PA, Vanselow N, eds.Committee on Behavioral and Social Sciences in Medical School Curricula.Improving Medical Education, Enhancing the Behavioral and Social Science Content of Medical School Curricula.Washington, DC:Institute of Medicine of the National Academies, The National Academies Press;2004. Available at: http://www.nap.edu/catalog.php?record_id=10956. Accessed March 2009.
- .Teaching analysis: doubts about medical humanities.Health Care Anal.1994;2:347–350.
- , .A Philosophical Basis of Medical Practice.New York, NY:Oxford University Press;1981.
- , , .The humanities, humanistic behavior, and the humane physician: a cautionary note.Ann Intern Med.1987;106:313–318.
- .Humanity and the medical humanities.Lancet.1995;346:1143–1145.
- .Integrating the teaching of basic sciences, clinical sciences, and biopsychosocial issues.Acad Med.1998;73:S24–S31.
- , , , et al.The impact of patient‐centered care on outcomes.J Fam Pract.2000;49:796–804.
- Institute of Medicine.Committee on Quality Health Care in America.Crossing the Quality Chasm: A New Health System for the 21st Century.Washington, DC:National Academy Press;2001.
- Institute for Healthcare Improvement. Available at: http://www.ihi.org/IHI/Topics/PatientCenteredCare/PatientCenteredCareGeneral. Accessed March2009.
- , .Patient‐centered medicine: a professional evolution.JAMA.1996;275:152–156.
- , , , et al.Patient‐Centered Medicine: Transforming the CLINICAL method.Abingdon, UK:Radcliffe Medical Press;2003.
- American Academy of Pediatrics.Committee on Hospital Care. Institute for Family‐Centered Care. Family‐centered care and the pediatrician's role.Pediatrics.2003;112:691–693.
- , .Teaching Ethics, the Humanities and Human Values in Medical Schools: A Ten‐Year Overview.Washington, DC:Institute on Human Values in Medicine, Society for Health and Human Values;1982.
- .Medical humanism and technological anxiety. In: Self DJ, ed.The Role of the Humanities in Medical Education.Norfolk VA:Teagle 1978:1–7.
- , .A community‐based approach to the medical humanities.Med Educ.2004;38:204–217.
- . NYU Medical Humanities website. Mission statement. Available at: http://medhum.med.nyu.edu. Accessed March2009.
- .The humanities in medical education: context, outcomes and structures.Med Humanit.2000;26:23–30.
- .The Place of the Humanities in Medicine.New York:The Hastings Center, Institute of Society Ethics and the Life Sciences;1984.
- .Humanism and the Physician.Knoxville, TN:University of Tennessee Press;1979.
- .The precarious position of the medical humanities in the medical school curriculum.Acad Med.2002;77:320–322.
- .The educational philosophies behind medical humanities programs in the United States.Theor Med.1993;14:221–229.
- .The science of patient‐centered care.J Fam Pract.2000;49:805–806.
- , , , , .Medical education about end‐of‐life care in the pediatric setting: principles, challenges, and opportunities.Pediatrics.2000;105:575–584.
- .The patient‐physician relationship. Narrative medicine: a model for empathy, reflection, profession, and trust.JAMA.2001;286(15):1897–1902.
- .Medical humanities: means, ends, and evaluation. In: Evans M, Finley IG, eds.Medical Humanities.London, UK:BMJ Books;2001:204–216.
- American Institutes for Research.Teaching Cultural Competence in Health Care: A Review of Current Concepts, Policies and Practices.Washington, DC:Office of Minority Health;2002.
- .Bioethics and humanities: what makes us one field?J Med Philos.1998;23(4):356–368.
- .A medical humanities course: a pertinent pause on the medical beat.J Assembly for Expended Perspectives on Learning.2000–2001;6:40–51.
- , , editors.The humanities and medicine: reports of forty‐one U.S., Canadian and international programs.Acad Med2003;78:951–952.
- , , , , .Physician‐patient communication: the relationship with malpractice claims among primary care physicians and surgeons.JAMA.1997;277(7):553–559.
- , .Patient‐focused care: using the right tools.Chest.2006;130(suppl):73S–82S.
- Cuff PA, Vanselow N, eds.Committee on Behavioral and Social Sciences in Medical School Curricula.Improving Medical Education, Enhancing the Behavioral and Social Science Content of Medical School Curricula.Washington, DC:Institute of Medicine of the National Academies, The National Academies Press;2004. Available at: http://www.nap.edu/catalog.php?record_id=10956. Accessed March 2009.
- .Teaching analysis: doubts about medical humanities.Health Care Anal.1994;2:347–350.
- , .A Philosophical Basis of Medical Practice.New York, NY:Oxford University Press;1981.
- , , .The humanities, humanistic behavior, and the humane physician: a cautionary note.Ann Intern Med.1987;106:313–318.
- .Humanity and the medical humanities.Lancet.1995;346:1143–1145.
Prevention of Radiocontrast Nephropathy
Since contrast nephropathy (CN) was recognized more than 50 years ago,1 there have been continuous efforts to chemically modify radiocontrast agents to be less nephrotoxic. Although radiocontrast media have indeed become safer, which reduces the likelihood of CN per procedure, the indications for radiocontrast administration have dramatically increased, since over 80 million doses are delivered in the world annually.2, 3 Furthermore, the number of patients with CN risks, which are mainly chronic renal insufficiency (CRI) and diabetes (Table 1), has also grown. Currently, more than 26 million people are estimated to have CRI in the United States4 and 200 million people have diabetes worldwide.5 The combination of increased radiocontrast administration frequency and greater prevalence of at‐risk patients is likely to result in continued increases in CN events.
| Clear Risks | Probable Risks | Questionable Risks |
|---|---|---|
| ||
| Estimated GFR 60 mL/minute/1.73 m2, especially if due to diabetic nephropathy* | Diabetes mellitus* | Repeat contrast procedures |
| Concomitant use of nephrotoxic drugs | Age >75 years | |
| Hemodynamic instability | Male gender | |
| Congestive heart failure | Intraaortic balloon pump | |
| Large contrast volume (>100 mL) | Liver disease | |
| Intraarterial contrast administration | Peripheral vascular disease | |
| Hypertension | ||
| Anemia | ||
| Bence‐Jones proteinuria | ||
| Hyperuricemia | ||
The incidence of CN varies between studies, depending on risk factors of the cohort and definition of CN, but figures have been reported to be as high as 50% in studies enriched with CRI and diabetic patients. However, a very recent study disputes such high incidence rates by demonstrating that patients receiving no radiocontrast media had a similar frequency of serum creatinine increases compared to a comparable group of historical CN patients.6 This study emphasizes that conventional definitions of CN, eg, 25% increase in serum creatinine above baseline, may be too conservative.
A retrospective study of 7586 patients showed 22% in‐hospital mortality in patients who developed CN vs. 1.4% in those who did not, after adjusting for comorbidities. One‐ and 5‐year mortality rates were also higher in the CN group (12.1% vs. 3.7% and 44.6% vs. 14.5%, respectively).7 Another study of 1826 patients, who underwent coronary artery intervention procedures, showed that 14.4% developed CN and 0.8% required hemodialysis. Mortality was 1.1% in patients who did not develop CN, 7.1% in those with CN, and 35.7% in the hemodialysis‐treated CN group.8 Moreover, studies by several other groups also support the position that CN is associated with increased in‐hospital and long‐term mortality.911 Although radiocontrast administration may not be a causal risk factor for mortality, since at‐risk patients have a number of comorbidities, radiocontrast media should nevertheless at least be viewed as an important marker of acute kidney injury and death risk.
Despite the enhanced morbidity and mortality associated with CN, there are no strict guidelines for prevention of CN. Part of the reason is that the literature is controversial regarding most prevention strategies. Several interventions are commonly proposed to help prevent CN, including discriminate selection of the type of radiocontrast, N‐acetylcysteine, volume expansion with saline and/or NaHCO3, and prophylactic hemofiltration. The major purpose of this review is to discuss these different approaches to CN prevention, with the ultimate goal of offering discrete recommendations.
The basis of this semisystematic review was a literature search using the PubMed database (
We report on prophylactic maneuvers that are either commonly considered by nephrology consultants or contain sufficient data to warrant a meta‐analysis study. Studies involving statins, ascorbic acid, dopamine analogs, endothelin antagonists, and theophylline were not addressed in this review due to insufficient, inconclusive, or predominantly negative data. Clinical characteristics and pathogenesis of CN, which include vasoconstriction, ischemia, production of oxygen free radicals, tubular cell apoptosis, and intratubular obstruction, are also not discussed in detail, but have recently been reviewed.12
Risk Associated with Different Types of Radiocontrast Media
There are 3 generations of radiocontrast media: hyperosmolar (14001800 mosm/kg), low osmolar (500850 mosm/kg) and isoosmolar (290 mosm/kg). Note that the low osmolar agents have lower osmolarity relative to the hyperosmolar agents, but are still hyperosmolar compared to serum. Multiple studies have compared effects of radiocontrast with different osmolarities.
The Iohexol Cooperative Study was a double‐blind, randomized, controlled trial (RCT) that randomized 1196 patients to Iohexol (low osmolarity) or diatrizoate (hyperosmolar). Definition of CN was a rise in serum creatinine by >1 mg/dL within 48 to 72 hours after the radiocontrast exposure. Results were in favor of the iohexol group (3% developed CN vs. 7% in the diatrizoate group; P = 0.002). Subgroup analysis of patients with CRI and CRI plus diabetes also revealed less CN in the iohexol vs. diatrizoate groups (7% vs. 16% and 12% vs. 27%, respectively).13
An earlier non‐RCT of 303 patients undergoing femoral angiography compared iohexol/emoxaglate (both are low osmolar) to diatrizoate (hyperosmolar). Six different CN definitions were used. Each comprised a combination of different magnitudes of rise of serum creatinine over various periods of time. Overall, the incidence of CN was 7% in the low osmolar group vs. 26% in the hyperosmolar group (P = 0.001). In subgroup analysis of patients with CRI, and of patients with diabetes, less CN was again observed with low osmolar agents (10% vs. 41%, P = 0.017, in the CRI group; and 10% vs. 31%, P = 0.012, in the diabetes group). Analysis of subjects with baseline serum creatinine 1.5 mg/dL showed no differences between the 2 groups, emphasizing that prior CRI is an important CN risk factor.14
The RECOVER study was a double‐blind RCT of 300 patients undergoing coronary angiography, who were randomized to iodixanol (isoosmolar) or ioxaglate (low osmolarity). CN was defined as a rise in serum creatinine by >25% or 0.5 mg/dL at 24 and 48 hours. CN incidence was 7.9% in the iodixanol group vs. 17% in the ioxaglate group (P = 0.021). Subgroup analyses of patients stratified by severe CRI, diabetes, and contrast volume also favored iodixanol.15 In a similarly designed, double‐blind RCT involving 129 patients with diabetes and CRI randomized to iodixanol or iohexol, CN developed in 3% of iodixanol group vs. 26% in the iohexol group (P = 0.002).16 These results were further supported by a very recent double‐blind RCT comparing iodixanol to iopromide (low osmolar) in 117 patients with baseline serum creatinine 1.5 mg/dL undergoing CT scans. The incidence of serum creatinine increases of 0.5 mg/dL or 25% above baseline or glomerular filtration rate (GFR) reduction of 5 mL/minute was significantly lower in the iodixanol group (P = 0.04, 0.01, and 0.04 respectively).17
In contrast to these reports, 2 double‐blind RCTs showed no differences in CN incidence between iodixanol and low osmolar agents. One study compared iodixanol to iopromide in 64 patients undergoing intravenous pyelography (IVP),18 and the other included 16 nondiabetic patients with CRI and compared iodixanol to iohexol.19 However, because of the small sample sizes, it is likely that neither study is adequately powered to detect differences in outcome between the 2 types of radiocontrast media.
Given the importance of the issue and conflicting results from individual studies, a meta‐analysis of 16 double‐blind RCTs was performed.20 This study included 2727 patients undergoing angiography, compared iodixanol (isoosmolar) to a variety of low osmolar agents, and demonstrated that iodixanol was less nephrotoxic compared to the low osmolarity agents in CRI patients (2.8% vs. 8.4%; P = 0.001) and in patients with CRI plus diabetes (3.5% vs. 15.5%; P = 0.003). Independent predictors of CN were CRI, CRI plus diabetes, and the use of low‐osmolarity media, whereas diabetes, age, and radiocontrast volume were not statistically significant independent predictors.20
Taken together, we conclude that isoosmolar media represents the lowest risk for CN. An additional benefit is that isoosmolar media, on the basis of diminished osmotic load, is less likely to precipitate extracellular fluid volume overload, which is particularly germane for patients with CRI, who have diminished capacity to excrete solute loads. Therefore, we recommend using isoosmolar media, particularly in patients at high risk for CN, such as those with CRI, especially due to diabetic nephropathy.
Oral N‐Acetylcysteine
Based primarily upon in vitro evidence, N‐acetylcysteine (NAC) may theoretically prevent CN by direct antioxidant and vasodilatory effects. However, in vivo, NAC is rapidly metabolized and inactivated by the liver. Therefore, it has been postulated that the mechanism of action may be indirect, and the cysteine metabolite of NAC may stimulate glutathione synthesis, which then inhibits cellular oxidation.21
The first clinical trial to address the prophylactic role of NAC in CN was an RCT of 83 patients with CRI (mean serum creatinine [Cr] = 2.4) undergoing CT scans, who were randomized to NAC plus 0.45% NaCl vs. placebo and 0.9% NaCl.22 The NAC dose was 600 mg orally twice daily for 2 doses before and 2 doses after the procedure. Intravenous fluids were started 12 hours before and stopped 12 hours after the procedure and infused at a rate of 1 ml/kg/hour. CN definition was rise in serum creatinine by >0.5 mg/dL at 48 hours. The results were statistically significant, with a relative risk of CN = 0.1 (95%CI, 0.020.9) in subjects treated with NAC.
There have been many subsequent reports that have evaluated NAC in small numbers of patients with mild to moderate CRI. In general, results from these trials have been inconsistent, which has led to several meta‐analyses to delineate NAC efficacy in CN prevention. The most recent and largest meta‐analysis included 26 NAC RCTs, and revealed a statistically significant benefit from NAC (relative risk [RR] = 0.62; 95%CI, 0.440.88).23 Twelve other meta‐analyses, which incorporated fewer studies, have been published,2435 and 7 of the 12 reported a benefit from NAC.25, 27, 29, 30, 32, 34, 35
Although meta‐analysis is considered the most accepted strategy to define conclusions from multiple trials, conflicting results between NAC meta‐analyses highlight the possibility that this approach may still not provide resolution to clinical questions, especially when inclusion criteria differ between meta‐analyses. Therefore, as discussed by Bagshaw et al.,36 meta‐analyses are not always a panacea, and should be avoided if the trials to be included exhibit significant statistical or clinical heterogeneity, as is the case with studies involving NAC prophylaxis of CN. Finally, because meta‐analyses require pooling of data from published studies, which tend to be positive, the possibility of publication bias exists.
In summary, conclusions from trials to assess efficacy of oral NAC in the prevention of CN have been inconsistent, though there has been a general trend toward benefit. Factors contributing to inconsistent results include variable definitions of CN, degree of CRI and diabetes in the cohort, amount and type of contrast used, NAC dosing and intravenous hydration protocols. As a result, a large multicenter RCT would certainly be helpful. However, the size of such trial might be cost‐prohibitive, and unlikely to be underwritten by the pharmaceutical industry because the patent for NAC has expired.36
Intravenous NAC
In addition to the vast literature on oral NAC for CN prophylaxis, there are now studies that have also evaluated efficacy of intravenous NAC. In one of the largest double‐blind RCTs,37 487 patients (mean baseline serum creatinine = 1.6 mg/dL) were randomized to NAC 500 mg intravenously vs. placebo before cardiac catheterization. Both groups received the same hydration protocols. The study was stopped when an interim analysis determined that there was no advantage to NAC (CN incidence, which was defined as a decrease in creatinine clearance by >5 mL/minute at days 1 to 8 postprocedure, was 23.3% vs. 20.7% in the placebo group).
The RAPPID study examined higher intravenous NAC doses in 80 patients undergoing cardiac catheterization.38 Subjects in this study were randomized to either NAC (150 mg/kg in 500 mL 0.9% NaCl before procedure and then 50 mg/kg in 500 mL 0.9% NaCl over 4 hours after procedure) or 0.9% NaCl 12 hours before and 12 hours after procedure. Despite the relatively small study size, intravenous NAC demonstrated a significant benefit in the prevention of CN (RR = 0.28; P = 0.045) defined as rise in serum creatinine by >25% at 2 or 4 days postexposure. Hypersensitivity‐like reactions were observed in 14.5% of patients receiving intravenous NAC, but symptoms were easily recognized and managed.38
A recent study of 354 patients undergoing primary angioplasty evaluated the combination of intravenous and oral NAC in different doses.39 Patients were randomized to 3 groups: (1) NAC 600 mg intravenously once before procedure and then 600 mg orally twice daily for 48 hours; (2) NAC 1200 mg intravenously once before procedure and then 1200 mg orally twice daily for 48 hours; or (3) placebo. The primary outcome was increase in Cr by >25% and secondary outcomes were in‐hospital death and a composite score that included death and need for renal replacement therapy. Results were significantly in favor of the 1200‐mg NAC regimen across all outcomes (P = 0.001, 0.02, and 0.002, respectively). It should be emphasized that this study was restricted to patients undergoing primary angioplasty, which is an emergent procedure. As a result, implementation of this protocol would necessarily require rapid administration of intravenous NAC prior to the procedure, which might even require maintenance of NAC stocks within the catheterization laboratory.
Because there is a trend toward benefit from oral NAC and the benefit from intravenous NAC in trials from limited settings, and both NAC formulations are inexpensive and safe, we recommend that NAC should be included in CN prophylaxis protocols.
Extracellular Fluid Volume Expansion
Since publication of work by Solomon et al.,40 which demonstrated a benefit of intravenous hydration with 0.45% NaCl in the prevention of CN in a group of CKD patients, it has been considered standard practice to prescribe intravenous fluid regimens for CN prophylaxis in high‐risk subjects. In the largest study to test the effect of different hydration protocols for CN prevention, Mueller et al.41 randomized 1620 patients with normal baseline serum creatinine to intravenous 0.9 % NaCl vs. 0.45% NaCl. The definition of CN was rise in serum creatinine by >0.5 mg/dL at 48 hours and the incidence was 0.7% for the 0.9% NaCl group and 2% for the 0.45% NaCl group (P = 0.04).
More recently, several trials have examined the relative efficacy of intravenous NaCl vs. NaHCO3 for CN prophylaxis. In the first NaHCO3 RCT, Merten et al.42 compared 0.9% NaHCO3 to 0.9% NaCl infusion in a population with a mean serum creatinine of 1.8 mg/dL. Both groups received 3 mL/kg intravenous bolus over 1 hour before the radiographic procedure followed by 1 mL/kg/hour for 6 hours. Urine pH was measured to confirm alkalinization of urine in the NaHCO3‐treated patients and the primary end point was increase in serum creatinine by >25% within 48 hours. The study was terminated early (after enrollment of 119 patients) when the interim analysis showed CN incidence was 1.7% in the NaHCO3 group vs. 13.6% in the NaCl group (P = 0.02).
These results were corroborated in the recent REMEDIAL trial,43 which enrolled 326 patients with serum creatinine >2 mg/dL, who were randomized to 1 of 3 arms. One group received intravenous saline (0.9% NaCl for 12 hours before and 12 hours after the procedure) and oral NAC; a second group received intravenous NaHCO3 (3 mL/kg intravenous bolus over 1 hour before the radiographic procedure followed by 1 mL/kg/hour for 6 hours) and oral NAC; and a third group received intravenous 0.9% NaCl plus oral NAC and ascorbic acid. Patients had similar baseline characteristics and the primary end point was an increase in serum creatinine by >25% within 48 hours. The best results were observed in the NaHCO3 plus NAC group; 1.9% developed CN in this group vs. 9.9% in the NaCl plus NAC group vs. 10.3% in the NaCl plus NAC plus ascorbic acid group (P = 0.019). Three additional prospective but smaller studies also showed the superiority of NaHCO3.4446
In contrast to studies supporting a role for prophylactic NaHCO3, a recent RCT showed no superiority of NaHCO3 infusion regimens.47 In this trial, 352 patients undergoing coronary angiography were randomized to receive either NaHCO3 or 0.9% NaCl. Both solutions were administered at rates of 3 mL/kg for 1 hour before the procedure and 1.5 mL/kg/hour for 4 hours postprocedure. The primary endpoint (>25% decrease in estimated GFR during the first 4 days after contrast exposure) was met in 13.3% of NaHCO3 group vs. 14.6% of the 0.9% NaCl group (P = 0.82). Moreover, there were no differences in the rates of secondary outcomes, which included death, dialysis, and cardiovascular and cerebrovascular events.
Results from a very recent retrospective cohort study of 7977 patients demonstrated that NaHCO3 infusion was associated with increased risk of CN compared to no treatment (odds ratio [OR] = 3.1; P 0.001), whereas NAC alone or in combination with NaHCO3 was associated with no significant difference in the incidence of CN.48 However, multiple weaknesses associated with the retrospective study design, such as inclusion of few patients at high CN risk, and acceptance of serum creatinine values within 7 days before and after the contrast procedure, which likely captures causes of acute kidney injury other than CN, preclude abandonment of NaHCO3 prophylaxis for CN solely on the basis of this study.
In an effort to resolve the conflicting NaHCO3 prophylaxis literature, a meta‐analysis was recently conducted.49 This study encompassed 1307 patients enrolled in 7 RCTs that examined outcomes for NaHCO3 vs. saline prevention of CN. The main finding was a significant benefit of NaHCO3 for protection against CN (RR = 0.37; P = 0.005). No benefit of NaHCO3 infusion could be shown for postprocedure renal replacement therapy or death.
Therefore, based upon the results of multiple prospective trials, the recent meta‐analysis, the relative safety of NaHCO3 infusion with appropriate monitoring, and a plausible biological mechanism whereby bicarbonate may have antioxidant properties and scavenge oxygen‐derived free radicals, which have been implicated in CN pathogenesis,50 we advocate a prophylactic regimen employing NaHCO3 for patients at high risk for CN.
Renal Replacement Therapies
Two studies have been conducted by the same group (Marenzi et al.51, 52) to examine efficacy of continuous hemofiltration (CVVH) in preventing CN (hemofiltration clears solute by convection, and involves administration of a HCO‐rich replacement solution, whereas hemodialysis clears solute by both diffusion and convection, and there is routinely no replacement fluid). In the first study,51 114 patients with baseline serum creatinine greater than 2 mg/dL undergoing coronary angiography were randomized to hemofiltration vs. 0.9% NaCl infusion. Isovolemic hemofiltration was implemented for 4 to 6 hours before and 18 to 24 hours after the radiographic procedure. The primary endpoint was increase in creatinine by >25% within 72 hours. CN incidence was 5% in the hemofiltration group vs. 50% in the 0.9% NaCl group (P 0.001). The secondary outcomes including in‐hospital mortality, 1‐year mortality and temporary renal replacement were also superior in the hemofiltration group. In the second study, the same investigators compared 2 different hemofiltration protocols, using the same definition of CN.52 Patients with baseline creatinine clearance 30 mL/minute (n = 92) were randomized to 0.9% NaCl infusion, postprocedure isovolemic hemofiltration only, or preprocedure plus postprocedure hemofiltration (same protocol as previous study). The incidence of CN was significantly lower in the preprocedure plus postprocedure hemofiltration group (3% vs. 26% in the postprocedure hemofiltration group vs. 40% in the 0.9% NaCl without hemofiltration group; P = 0.0001). The preprocedure plus postprocedure hemofiltration group also had reductions in in‐hospital mortality and temporary renal replacement therapy rates.
Although the mechanism of hemofiltration prevention of CN is unknown, it is certainly not enhanced clearance of contrast material, inasmuch as hemofiltration was discontinued during the angiography procedure in all protocols, and radiocontrast was therefore not cleared by hemofiltration until the process was reinstituted. Furthermore, the second study indicates that the major benefit was derived from the preprocedure hemofiltration component. Contributing factors might be control of extracellular pH and redox potential with bicarbonate replacement fluid during hemofiltration. Important confounding issues to consider are that patients receiving hemofiltration were in controlled, monitored settings and thus received more intensive care than the hydration group, and that serum creatinine, the major outcome parameter, is cleared by hemofiltration. Before hemofiltration can be recommended as routine prophylactic therapy for CN, the data will need to be corroborated by other groups, preferably involving larger numbers of study subjects and including cost‐benefit analyses.
Multiple small studies have examined the possibility that dialysis immediately following radiocontrast exposure could prevent CN, presumably by accelerating radiocontrast clearance. Most of these reports were negative, including a well‐designed meta‐analysis of RCTs, which showed no benefit of hemodialysis.53 Of note, one report suggested that hemodialysis might be potentially harmful.54 The single prospective trial that showed benefit from prophylactic hemodialysis analyzed 82 patients with advanced CRI (baseline creatinine clearance 13 mL/minute) referred for coronary angiography55 These subjects were randomly assigned to intravenous 0.9% NaCl and hemodialysis vs. intravenous 0.9% NaCl alone. Subsequent renal replacement therapy was required in 35% of control patients and in only 2% in the prophylactic dialysis group. One potential limitation of this study is that the investigators were more cognizant of volume status in the hemodialysis group to avoid fluid shifts and volume depletion during dialysis, while the control group appeared to experience no comparable intravascular volume management. Moreover, this study was conducted in patients with extremely advanced renal insufficiency, and therefore does not reflect the vast majority of patients at risk for CN.
Conclusions
CN is associated with increased morbidity and mortality, and efforts to minimize CN are therefore warranted. However, the overwhelming majority of CN trials were designed to investigate the effects of prophylaxis strategies on surrogate endpoints for estimates of GFR. Therefore, conclusions regarding the effect of these regimens on definitive outcomes, such as death and vascular events, cannot be drawn. On balance, there is evidence that oral and intravenous NAC, as well as extracellular volume expansion with intravenous NaHCO3 are effective measures to prevent CN, whereas the data for renal replacement therapies are more equivocal. We emphasize though, that the literature on this topic is vast, and includes a large number of conflicting studies, including multiple meta‐analyses. As a result, we refrain from being too dogmatic about the best approach, and therefore cautiously offer the following recommendations for prevention of CN.
The first step is to identify high‐risk patients, who are most likely to benefit from prophylaxis (Table 1). Although risk stratification was not the focus of this review, Mehran et al.56 have developed a scoring system to quantitatively predict CN risk, with weighted parameters including CRI, diabetes, radiocontrast volume, age, hypotension, congestive heart failure, treatment with an intraaortic balloon pump, and anemia. For low‐risk patients, hydration with saline is probably adequate. For high‐risk patients, it would be prudent to initially consider whether sufficient information could be obtained from an alternative, noncontrasted radiologic procedure. If not, it would behoove the prescribing physician to then treat modifiable risk factors, as well as to discontinue potentially nephrotoxic medications.
In high‐risk patients undergoing radiocontrast procedures, we recommend using NAC and volume expansion with NaHCO3 (Table 2). Although the evidence for this combined approach is limited,43 we believe it is biologically consistent, since the rationale for both strategies is primarily modification of redox state and inhibition of oxygen free radical generation. Because NAC formulations are generally effective, safe and inexpensive ($0.04 for 600 mg oral NAC and $24 for 1200 mg intravenous NAC at our hospital), we recommend the protocol used by Marenzi et al.,39 NAC 1200 mg intravenously once before procedure and then 1200 mg orally twice daily for 48 hours, as prophylaxis for all contrast procedures in high‐risk patients. However, we recognize that this regimen would require formal evaluation in procedures other than emergent coronary artery angioplasty before it could be enthusiastically endorsed. Therefore, if intravenous NAC is not available and/or the procedure is not emergent, NAC 6001200 mg orally twice a day, 2 doses before and 2 doses after the procedure would be a rational alternative. For the NaHCO3 infusion, we recommend 3 mL/kg for 1 hour before the procedure, followed by 1 mL/kg/hour for 6 hours after.
|
| Minimize radiocontrast dose. |
| Isoosmolar radiocontrast media preferred. |
| Intravenous NaHCO3 at 3 mL/kg/hour for 1 hour prior to radiocontrast exposure, then 1 mL/kg/hour for 6 hours after. |
| Intravenous N‐acetylcysteine 1200 mg before procedure, then 1200 mg orally twice daily for a total of 4 doses. |
| If intravenous N‐acetylcysteine is not available, then N‐acetylcysteine 6001200 mg orally for 2 doses before and 2 doses after procedure. |
| If already undergoing acute dialysis with catheter vascular access, consider CVVH 6 hours before and for 24 hours after procedure. |
Hemofiltration is labor‐intensive, expensive, and not readily available in all hospitals that renders it difficult to endorse as a definitive or routine CN prophylaxis modality. However, if a patient is already undergoing acute dialysis with catheter vascular access, it would be reasonable to consider CVVH 6 hours before and for 24 hours after the procedure (Table 2).
For high‐risk patients, we recommend minimizing the radiocontrast dose (reviewed in Ref.57). Although the dose has not consistently been identified as a risk factor (Table 1), we envision no harm in reducing the dose, particularly if adequate information can be obtained by other means, eg, coronary angiogram accompanied by an echocardiogram, rather than a ventriculogram. We would also consider the use of isoosmolar media in high‐risk patients, since the data are relatively compelling.20 Low doses of isoosmolar media should be particularly beneficial to patients with preexisting hypertension or congestive heart failure, for which the osmotic load and excess extracellular volume expansion might be deleterious. However, because isoosmolar media is expensive, a detailed cost‐benefit analysis would be required before definitive recommendations could be made, especially for patients at lower risk for CN. Finally, because of the complex literature, as well as budgetary issues, we encourage communication between the physician ordering the contrast study and the operator (radiologist or cardiologist) concerning the type of procedure and contrast media to be used.
- , , , .Acute anuria following intravenous pyelography in a patient with myelomatosis.Acta Med Scand.1954;150(4):297–302.
- .Editorial: Contrast medium‐induced nephropathy.Nephrol Dial Transplant.2005;20(suppl 1):i1.
- , .Contrast‐induced nephrotoxicity: clinical landscape.Kidney Int Suppl.2006;(100):S3–S7.
- , , , et al.Prevalence of chronic kidney disease in the United States.JAMA.2007;298(17):2038–2047.
- , , , et al.Estimation of glomerular filtration rate in diabetic subjects: Cockcroft formula or modification of Diet in Renal Disease study equation?Diabetes Care.2005;28(4):838–843.
- , , , .Frequency of serum creatinine changes in the absence of iodinated contrast material: implications for studies of contrast nephrotoxicity.AJR Am J Roentgenol.2008;191(2):376–382.
- , , , et al.Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention.Circulation.2002;105(19):2259–2264.
- , , , , .Acute renal failure after coronary intervention: incidence, risk factors, and relationship to mortality.Am J Med.1997;103(5):368–375.
- , , .The effect of acute renal failure on mortality. A cohort analysis.JAMA.1996;275(19):1489–1494.
- , , , et al.The prognostic implications of further renal function deterioration within 48 h of interventional coronary procedures in patients with pre‐existent chronic renal insufficiency.J Am Coll Cardiol.2000;36(5):1542–1548.
- , , , et al.Contrast‐induced nephropathy after percutaneous coronary interventions in relation to chronic kidney disease and hemodynamic variables.Am J Cardiol.2005;95(1):13–19.
- , , , et al.Renal parenchymal hypoxia, hypoxia adaptation, and the pathogenesis of radiocontrast nephropathy.Clin J Am Soc Nephrol.2008;3(1):288–296.
- , , , et al.Nephrotoxicity of ionic and nonionic contrast media in 1196 patients: a randomized trial. The Iohexol Cooperative Study.Kidney Int.1995;47(1):254–261.
- , , , et al.Radiocontrast‐associated renal dysfunction: a comparison of lower‐osmolality and conventional high‐osmolality contrast media.AJR Am J Roentgenol.1991;157(1):59–65.
- , , , et al.,Renal toxicity evaluation and comparison between visipaque (iodixanol) and hexabrix (ioxaglate) in patients with renal insufficiency undergoing coronary angiography: the RECOVER study: a randomized controlled trial.J Am Coll Cardiol.2006;48(5):924–930.
- , , , et al.Nephrotoxic effects in high‐risk patients undergoing angiography.N Engl J Med.2003;348(6):491–499.
- , , , et al.Iso‐osmolality vs. low‐osmolality iodinated contrast medium at intravenous contrast‐enhanced CT: effect on kidney function.Radiology.2008;248(1):97–105.
- , , , et al.Effects of a dimeric vs a monomeric nonionic contrast medium on renal function in patients with mild to moderate renal insufficiency: a double‐blind, randomized clinical trial.Eur Radiol.1998;8(1):144–147.
- , , .Angiography with nonionic X‐ray contrast media in severe chronic renal failure: renal function and contrast retention.Nephron.1996;73(4):549–556.
- , , , .A meta‐analysis of the renal safety of isoosmolar iodixanol compared with low‐osmolar contrast media.J Am Coll Cardiol.2006;48(4):692–699.
- .N‐acetylcysteine in the prevention of contrast‐induced nephropathy.Clin J Am Soc Nephrol.2008;3(1):281–287.
- , , , , , .Prevention of radiographic‐contrast‐agent‐induced reductions in renal function by acetylcysteine.N Engl J Med.2000;343(3):180–184.
- , , , , .Meta‐analysis: effectiveness of drugs for preventing contrast‐induced nephropathy.Ann Intern Med.2008;148(4):284–294.
- , , , et al.Is acetylcysteine effective in preventing contrast‐related nephropathy? A meta‐analysis.Am J Med.2004;117(12):938–947.
- , , , , , .Acetylcysteine for prevention of contrast nephropathy: meta‐analysis.Lancet.2003;362(9384):598–603.
- , , , .Systematic review of the impact of N‐acetylcysteine on contrast nephropathy.Kidney Int.2004;65(4):1366–1374.
- , , , , .N‐acetylcysteine for the prevention of contrast‐induced nephropathy. A systematic review and meta‐analysis.J Gen Intern Med.2005;20(2):193–200.
- , , , .N‐acetylcysteine and contrast‐induced nephropathy: a meta‐analysis of 13 randomized trials.Am Heart J.2006;151(1):140–145.
- , , .Meta‐analysis of randomized clinical trials on the usefulness of acetylcysteine for prevention of contrast nephropathy.Am J Cardiol.2003;92(12):1454–1458.
- , , , , .Prevention of radiocontrast nephropathy with N‐acetylcysteine in patients with chronic kidney disease: a meta‐analysis of randomized, controlled trials.Am J Kidney Dis.2004;43(1):1–9.
- , , , et al.N‐acetylcysteine for the prevention of radiocontrast induced nephropathy: a meta‐analysis of prospective controlled trials.J Am Soc Nephrol.2004;15(3):761–769.
- , .The role of N‐acetylcysteine in preventing radiographic contrast‐induced nephropathy.Clin Nephrol.2004;62(2):77–83.
- , .Acetylcysteine for prevention of contrast‐induced nephropathy after intravascular angiography: a systematic review and meta‐analysis.BMC Med.2004;2:38.
- , , , , .Role of N‐acetylcysteine in prevention of contrast‐induced nephropathy after cardiovascular procedures: a meta‐analysis.Clin Cardiol.2004;27(11):607–610.
- , , .N‐acetylcysteine prophylaxis significantly reduces the risk of radiocontrast‐induced nephropathy: comprehensive meta‐analysis.Catheter Cardiovasc Interv.2005;64(4):471–479.
- , , , .Acetylcysteine in the prevention of contrast‐induced nephropathy: a case study of the pitfalls in the evolution of evidence.Arch Intern Med.2006;166(2):161–166.
- , , , et al.A randomized controlled trial of intravenous N‐acetylcysteine for the prevention of contrast‐induced nephropathy after cardiac catheterization: lack of effect.Am Heart J.2004;148(3):422–429.
- , , , , , .A rapid protocol for the prevention of contrast‐induced renal dysfunction: the RAPPID study.J Am Coll Cardiol.2003;41(12):2114–2118.
- , , , et al.N‐acetylcysteine and contrast‐induced nephropathy in primary angioplasty.N Engl J Med.2006;354(26):2773–2782.
- , , , , .Effects of saline, mannitol, and furosemide to prevent acute decreases in renal function induced by radiocontrast agents.N Engl J Med.1994;331(21):1416–1420.
- , , .Prevention of contrast media‐associated nephropathy: randomized comparison of 2 hydration regimens in 1620 patients undergoing coronary angioplasty.Arch Intern Med.2002;162(3):329–336.
- , , , et al.Prevention of contrast‐induced nephropathy with sodium bicarbonate: a randomized controlled trial.JAMA.2004;291(19):2328–2334.
- , , , et al.Renal insufficiency following contrast media administration trial (REMEDIAL): a randomized comparison of 3 preventive strategies.Circulation.2007;115(10):1211–1217.
- , , , et al.Sodium bicarbonate, N‐acetylcysteine, and saline for prevention of radiocontrast‐induced nephropathy. A comparison of 3 regimens for protecting contrast‐induced nephropathy in patients undergoing coronary procedures. A single‐center prospective controlled trial.Am Heart J.2007;154(3):539–544.
- , , , et al.The reno‐protective effect of hydration with sodium bicarbonate plus N‐acetylcysteine in patients undergoing emergency percutaneous coronary intervention: the RENO Study.J Am Coll Cardiol.2007;49(12):1283–1288.
- , , , et al.Comparison of usefulness of sodium bicarbonate vs. sodium chloride to prevent contrast‐induced nephropathy in patients undergoing an emergent coronary procedure.Am J Cardiol.2007;100(5):781–786.
- , , , et al.Sodium bicarbonate vs sodium chloride for the prevention of contrast medium‐induced nephropathy in patients undergoing coronary angiography: a randomized trial.JAMA.2008;300(9):1038–1046.
- , , , , , .Sodium bicarbonate is associated with an increased incidence of contrast nephropathy: a retrospective cohort study of 7977 patients at Mayo clinic.Clin J Am Soc Nephrol.2008;3(1):10–18.
- , , , et al.Current role of sodium bicarbonate‐based preprocedural hydration for the prevention of contrast‐induced acute kidney injury: a meta‐analysis.Am Heart J.2008;156(3):414–421.
- .Effect of sodium bicarbonate preloading on ischemic renal failure.Nephron.1986;44(1):70–74.
- , , , et al.The prevention of radiocontrast‐agent‐induced nephropathy by hemofiltration.N Engl J Med.2003;349(14):1333–1340.
- , , , et al.Comparison of two hemofiltration protocols for prevention of contrast‐induced nephropathy in high‐risk patients.Am J Med.2006;119(2):155–162.
- , , , et al.Extracorporeal blood purification therapies for prevention of radiocontrast‐induced nephropathy: a systematic review.Am J Kidney Dis.2006;48(3):361–371.
- , , , et al.Prophylactic hemodialysis after radiocontrast media in patients with renal insufficiency is potentially harmful.Am J Med.2001;111(9):692–698.
- , , , et al.Renal protection for coronary angiography in advanced renal failure patients by prophylactic hemodialysis. A randomized controlled trial.J Am Coll Cardiol.2007;50(11):1015–1020.
- , , , et al.A simple risk score for prediction of contrast‐induced nephropathy after percutaneous coronary intervention: development and initial validation.J Am Coll Cardiol.2004;44(7):1393–1399.
- .Contrast‐induced acute kidney injury.J Am Coll Cardiol.2008;51(15):1419–1428.
Since contrast nephropathy (CN) was recognized more than 50 years ago,1 there have been continuous efforts to chemically modify radiocontrast agents to be less nephrotoxic. Although radiocontrast media have indeed become safer, which reduces the likelihood of CN per procedure, the indications for radiocontrast administration have dramatically increased, since over 80 million doses are delivered in the world annually.2, 3 Furthermore, the number of patients with CN risks, which are mainly chronic renal insufficiency (CRI) and diabetes (Table 1), has also grown. Currently, more than 26 million people are estimated to have CRI in the United States4 and 200 million people have diabetes worldwide.5 The combination of increased radiocontrast administration frequency and greater prevalence of at‐risk patients is likely to result in continued increases in CN events.
| Clear Risks | Probable Risks | Questionable Risks |
|---|---|---|
| ||
| Estimated GFR 60 mL/minute/1.73 m2, especially if due to diabetic nephropathy* | Diabetes mellitus* | Repeat contrast procedures |
| Concomitant use of nephrotoxic drugs | Age >75 years | |
| Hemodynamic instability | Male gender | |
| Congestive heart failure | Intraaortic balloon pump | |
| Large contrast volume (>100 mL) | Liver disease | |
| Intraarterial contrast administration | Peripheral vascular disease | |
| Hypertension | ||
| Anemia | ||
| Bence‐Jones proteinuria | ||
| Hyperuricemia | ||
The incidence of CN varies between studies, depending on risk factors of the cohort and definition of CN, but figures have been reported to be as high as 50% in studies enriched with CRI and diabetic patients. However, a very recent study disputes such high incidence rates by demonstrating that patients receiving no radiocontrast media had a similar frequency of serum creatinine increases compared to a comparable group of historical CN patients.6 This study emphasizes that conventional definitions of CN, eg, 25% increase in serum creatinine above baseline, may be too conservative.
A retrospective study of 7586 patients showed 22% in‐hospital mortality in patients who developed CN vs. 1.4% in those who did not, after adjusting for comorbidities. One‐ and 5‐year mortality rates were also higher in the CN group (12.1% vs. 3.7% and 44.6% vs. 14.5%, respectively).7 Another study of 1826 patients, who underwent coronary artery intervention procedures, showed that 14.4% developed CN and 0.8% required hemodialysis. Mortality was 1.1% in patients who did not develop CN, 7.1% in those with CN, and 35.7% in the hemodialysis‐treated CN group.8 Moreover, studies by several other groups also support the position that CN is associated with increased in‐hospital and long‐term mortality.911 Although radiocontrast administration may not be a causal risk factor for mortality, since at‐risk patients have a number of comorbidities, radiocontrast media should nevertheless at least be viewed as an important marker of acute kidney injury and death risk.
Despite the enhanced morbidity and mortality associated with CN, there are no strict guidelines for prevention of CN. Part of the reason is that the literature is controversial regarding most prevention strategies. Several interventions are commonly proposed to help prevent CN, including discriminate selection of the type of radiocontrast, N‐acetylcysteine, volume expansion with saline and/or NaHCO3, and prophylactic hemofiltration. The major purpose of this review is to discuss these different approaches to CN prevention, with the ultimate goal of offering discrete recommendations.
The basis of this semisystematic review was a literature search using the PubMed database (
We report on prophylactic maneuvers that are either commonly considered by nephrology consultants or contain sufficient data to warrant a meta‐analysis study. Studies involving statins, ascorbic acid, dopamine analogs, endothelin antagonists, and theophylline were not addressed in this review due to insufficient, inconclusive, or predominantly negative data. Clinical characteristics and pathogenesis of CN, which include vasoconstriction, ischemia, production of oxygen free radicals, tubular cell apoptosis, and intratubular obstruction, are also not discussed in detail, but have recently been reviewed.12
Risk Associated with Different Types of Radiocontrast Media
There are 3 generations of radiocontrast media: hyperosmolar (14001800 mosm/kg), low osmolar (500850 mosm/kg) and isoosmolar (290 mosm/kg). Note that the low osmolar agents have lower osmolarity relative to the hyperosmolar agents, but are still hyperosmolar compared to serum. Multiple studies have compared effects of radiocontrast with different osmolarities.
The Iohexol Cooperative Study was a double‐blind, randomized, controlled trial (RCT) that randomized 1196 patients to Iohexol (low osmolarity) or diatrizoate (hyperosmolar). Definition of CN was a rise in serum creatinine by >1 mg/dL within 48 to 72 hours after the radiocontrast exposure. Results were in favor of the iohexol group (3% developed CN vs. 7% in the diatrizoate group; P = 0.002). Subgroup analysis of patients with CRI and CRI plus diabetes also revealed less CN in the iohexol vs. diatrizoate groups (7% vs. 16% and 12% vs. 27%, respectively).13
An earlier non‐RCT of 303 patients undergoing femoral angiography compared iohexol/emoxaglate (both are low osmolar) to diatrizoate (hyperosmolar). Six different CN definitions were used. Each comprised a combination of different magnitudes of rise of serum creatinine over various periods of time. Overall, the incidence of CN was 7% in the low osmolar group vs. 26% in the hyperosmolar group (P = 0.001). In subgroup analysis of patients with CRI, and of patients with diabetes, less CN was again observed with low osmolar agents (10% vs. 41%, P = 0.017, in the CRI group; and 10% vs. 31%, P = 0.012, in the diabetes group). Analysis of subjects with baseline serum creatinine 1.5 mg/dL showed no differences between the 2 groups, emphasizing that prior CRI is an important CN risk factor.14
The RECOVER study was a double‐blind RCT of 300 patients undergoing coronary angiography, who were randomized to iodixanol (isoosmolar) or ioxaglate (low osmolarity). CN was defined as a rise in serum creatinine by >25% or 0.5 mg/dL at 24 and 48 hours. CN incidence was 7.9% in the iodixanol group vs. 17% in the ioxaglate group (P = 0.021). Subgroup analyses of patients stratified by severe CRI, diabetes, and contrast volume also favored iodixanol.15 In a similarly designed, double‐blind RCT involving 129 patients with diabetes and CRI randomized to iodixanol or iohexol, CN developed in 3% of iodixanol group vs. 26% in the iohexol group (P = 0.002).16 These results were further supported by a very recent double‐blind RCT comparing iodixanol to iopromide (low osmolar) in 117 patients with baseline serum creatinine 1.5 mg/dL undergoing CT scans. The incidence of serum creatinine increases of 0.5 mg/dL or 25% above baseline or glomerular filtration rate (GFR) reduction of 5 mL/minute was significantly lower in the iodixanol group (P = 0.04, 0.01, and 0.04 respectively).17
In contrast to these reports, 2 double‐blind RCTs showed no differences in CN incidence between iodixanol and low osmolar agents. One study compared iodixanol to iopromide in 64 patients undergoing intravenous pyelography (IVP),18 and the other included 16 nondiabetic patients with CRI and compared iodixanol to iohexol.19 However, because of the small sample sizes, it is likely that neither study is adequately powered to detect differences in outcome between the 2 types of radiocontrast media.
Given the importance of the issue and conflicting results from individual studies, a meta‐analysis of 16 double‐blind RCTs was performed.20 This study included 2727 patients undergoing angiography, compared iodixanol (isoosmolar) to a variety of low osmolar agents, and demonstrated that iodixanol was less nephrotoxic compared to the low osmolarity agents in CRI patients (2.8% vs. 8.4%; P = 0.001) and in patients with CRI plus diabetes (3.5% vs. 15.5%; P = 0.003). Independent predictors of CN were CRI, CRI plus diabetes, and the use of low‐osmolarity media, whereas diabetes, age, and radiocontrast volume were not statistically significant independent predictors.20
Taken together, we conclude that isoosmolar media represents the lowest risk for CN. An additional benefit is that isoosmolar media, on the basis of diminished osmotic load, is less likely to precipitate extracellular fluid volume overload, which is particularly germane for patients with CRI, who have diminished capacity to excrete solute loads. Therefore, we recommend using isoosmolar media, particularly in patients at high risk for CN, such as those with CRI, especially due to diabetic nephropathy.
Oral N‐Acetylcysteine
Based primarily upon in vitro evidence, N‐acetylcysteine (NAC) may theoretically prevent CN by direct antioxidant and vasodilatory effects. However, in vivo, NAC is rapidly metabolized and inactivated by the liver. Therefore, it has been postulated that the mechanism of action may be indirect, and the cysteine metabolite of NAC may stimulate glutathione synthesis, which then inhibits cellular oxidation.21
The first clinical trial to address the prophylactic role of NAC in CN was an RCT of 83 patients with CRI (mean serum creatinine [Cr] = 2.4) undergoing CT scans, who were randomized to NAC plus 0.45% NaCl vs. placebo and 0.9% NaCl.22 The NAC dose was 600 mg orally twice daily for 2 doses before and 2 doses after the procedure. Intravenous fluids were started 12 hours before and stopped 12 hours after the procedure and infused at a rate of 1 ml/kg/hour. CN definition was rise in serum creatinine by >0.5 mg/dL at 48 hours. The results were statistically significant, with a relative risk of CN = 0.1 (95%CI, 0.020.9) in subjects treated with NAC.
There have been many subsequent reports that have evaluated NAC in small numbers of patients with mild to moderate CRI. In general, results from these trials have been inconsistent, which has led to several meta‐analyses to delineate NAC efficacy in CN prevention. The most recent and largest meta‐analysis included 26 NAC RCTs, and revealed a statistically significant benefit from NAC (relative risk [RR] = 0.62; 95%CI, 0.440.88).23 Twelve other meta‐analyses, which incorporated fewer studies, have been published,2435 and 7 of the 12 reported a benefit from NAC.25, 27, 29, 30, 32, 34, 35
Although meta‐analysis is considered the most accepted strategy to define conclusions from multiple trials, conflicting results between NAC meta‐analyses highlight the possibility that this approach may still not provide resolution to clinical questions, especially when inclusion criteria differ between meta‐analyses. Therefore, as discussed by Bagshaw et al.,36 meta‐analyses are not always a panacea, and should be avoided if the trials to be included exhibit significant statistical or clinical heterogeneity, as is the case with studies involving NAC prophylaxis of CN. Finally, because meta‐analyses require pooling of data from published studies, which tend to be positive, the possibility of publication bias exists.
In summary, conclusions from trials to assess efficacy of oral NAC in the prevention of CN have been inconsistent, though there has been a general trend toward benefit. Factors contributing to inconsistent results include variable definitions of CN, degree of CRI and diabetes in the cohort, amount and type of contrast used, NAC dosing and intravenous hydration protocols. As a result, a large multicenter RCT would certainly be helpful. However, the size of such trial might be cost‐prohibitive, and unlikely to be underwritten by the pharmaceutical industry because the patent for NAC has expired.36
Intravenous NAC
In addition to the vast literature on oral NAC for CN prophylaxis, there are now studies that have also evaluated efficacy of intravenous NAC. In one of the largest double‐blind RCTs,37 487 patients (mean baseline serum creatinine = 1.6 mg/dL) were randomized to NAC 500 mg intravenously vs. placebo before cardiac catheterization. Both groups received the same hydration protocols. The study was stopped when an interim analysis determined that there was no advantage to NAC (CN incidence, which was defined as a decrease in creatinine clearance by >5 mL/minute at days 1 to 8 postprocedure, was 23.3% vs. 20.7% in the placebo group).
The RAPPID study examined higher intravenous NAC doses in 80 patients undergoing cardiac catheterization.38 Subjects in this study were randomized to either NAC (150 mg/kg in 500 mL 0.9% NaCl before procedure and then 50 mg/kg in 500 mL 0.9% NaCl over 4 hours after procedure) or 0.9% NaCl 12 hours before and 12 hours after procedure. Despite the relatively small study size, intravenous NAC demonstrated a significant benefit in the prevention of CN (RR = 0.28; P = 0.045) defined as rise in serum creatinine by >25% at 2 or 4 days postexposure. Hypersensitivity‐like reactions were observed in 14.5% of patients receiving intravenous NAC, but symptoms were easily recognized and managed.38
A recent study of 354 patients undergoing primary angioplasty evaluated the combination of intravenous and oral NAC in different doses.39 Patients were randomized to 3 groups: (1) NAC 600 mg intravenously once before procedure and then 600 mg orally twice daily for 48 hours; (2) NAC 1200 mg intravenously once before procedure and then 1200 mg orally twice daily for 48 hours; or (3) placebo. The primary outcome was increase in Cr by >25% and secondary outcomes were in‐hospital death and a composite score that included death and need for renal replacement therapy. Results were significantly in favor of the 1200‐mg NAC regimen across all outcomes (P = 0.001, 0.02, and 0.002, respectively). It should be emphasized that this study was restricted to patients undergoing primary angioplasty, which is an emergent procedure. As a result, implementation of this protocol would necessarily require rapid administration of intravenous NAC prior to the procedure, which might even require maintenance of NAC stocks within the catheterization laboratory.
Because there is a trend toward benefit from oral NAC and the benefit from intravenous NAC in trials from limited settings, and both NAC formulations are inexpensive and safe, we recommend that NAC should be included in CN prophylaxis protocols.
Extracellular Fluid Volume Expansion
Since publication of work by Solomon et al.,40 which demonstrated a benefit of intravenous hydration with 0.45% NaCl in the prevention of CN in a group of CKD patients, it has been considered standard practice to prescribe intravenous fluid regimens for CN prophylaxis in high‐risk subjects. In the largest study to test the effect of different hydration protocols for CN prevention, Mueller et al.41 randomized 1620 patients with normal baseline serum creatinine to intravenous 0.9 % NaCl vs. 0.45% NaCl. The definition of CN was rise in serum creatinine by >0.5 mg/dL at 48 hours and the incidence was 0.7% for the 0.9% NaCl group and 2% for the 0.45% NaCl group (P = 0.04).
More recently, several trials have examined the relative efficacy of intravenous NaCl vs. NaHCO3 for CN prophylaxis. In the first NaHCO3 RCT, Merten et al.42 compared 0.9% NaHCO3 to 0.9% NaCl infusion in a population with a mean serum creatinine of 1.8 mg/dL. Both groups received 3 mL/kg intravenous bolus over 1 hour before the radiographic procedure followed by 1 mL/kg/hour for 6 hours. Urine pH was measured to confirm alkalinization of urine in the NaHCO3‐treated patients and the primary end point was increase in serum creatinine by >25% within 48 hours. The study was terminated early (after enrollment of 119 patients) when the interim analysis showed CN incidence was 1.7% in the NaHCO3 group vs. 13.6% in the NaCl group (P = 0.02).
These results were corroborated in the recent REMEDIAL trial,43 which enrolled 326 patients with serum creatinine >2 mg/dL, who were randomized to 1 of 3 arms. One group received intravenous saline (0.9% NaCl for 12 hours before and 12 hours after the procedure) and oral NAC; a second group received intravenous NaHCO3 (3 mL/kg intravenous bolus over 1 hour before the radiographic procedure followed by 1 mL/kg/hour for 6 hours) and oral NAC; and a third group received intravenous 0.9% NaCl plus oral NAC and ascorbic acid. Patients had similar baseline characteristics and the primary end point was an increase in serum creatinine by >25% within 48 hours. The best results were observed in the NaHCO3 plus NAC group; 1.9% developed CN in this group vs. 9.9% in the NaCl plus NAC group vs. 10.3% in the NaCl plus NAC plus ascorbic acid group (P = 0.019). Three additional prospective but smaller studies also showed the superiority of NaHCO3.4446
In contrast to studies supporting a role for prophylactic NaHCO3, a recent RCT showed no superiority of NaHCO3 infusion regimens.47 In this trial, 352 patients undergoing coronary angiography were randomized to receive either NaHCO3 or 0.9% NaCl. Both solutions were administered at rates of 3 mL/kg for 1 hour before the procedure and 1.5 mL/kg/hour for 4 hours postprocedure. The primary endpoint (>25% decrease in estimated GFR during the first 4 days after contrast exposure) was met in 13.3% of NaHCO3 group vs. 14.6% of the 0.9% NaCl group (P = 0.82). Moreover, there were no differences in the rates of secondary outcomes, which included death, dialysis, and cardiovascular and cerebrovascular events.
Results from a very recent retrospective cohort study of 7977 patients demonstrated that NaHCO3 infusion was associated with increased risk of CN compared to no treatment (odds ratio [OR] = 3.1; P 0.001), whereas NAC alone or in combination with NaHCO3 was associated with no significant difference in the incidence of CN.48 However, multiple weaknesses associated with the retrospective study design, such as inclusion of few patients at high CN risk, and acceptance of serum creatinine values within 7 days before and after the contrast procedure, which likely captures causes of acute kidney injury other than CN, preclude abandonment of NaHCO3 prophylaxis for CN solely on the basis of this study.
In an effort to resolve the conflicting NaHCO3 prophylaxis literature, a meta‐analysis was recently conducted.49 This study encompassed 1307 patients enrolled in 7 RCTs that examined outcomes for NaHCO3 vs. saline prevention of CN. The main finding was a significant benefit of NaHCO3 for protection against CN (RR = 0.37; P = 0.005). No benefit of NaHCO3 infusion could be shown for postprocedure renal replacement therapy or death.
Therefore, based upon the results of multiple prospective trials, the recent meta‐analysis, the relative safety of NaHCO3 infusion with appropriate monitoring, and a plausible biological mechanism whereby bicarbonate may have antioxidant properties and scavenge oxygen‐derived free radicals, which have been implicated in CN pathogenesis,50 we advocate a prophylactic regimen employing NaHCO3 for patients at high risk for CN.
Renal Replacement Therapies
Two studies have been conducted by the same group (Marenzi et al.51, 52) to examine efficacy of continuous hemofiltration (CVVH) in preventing CN (hemofiltration clears solute by convection, and involves administration of a HCO‐rich replacement solution, whereas hemodialysis clears solute by both diffusion and convection, and there is routinely no replacement fluid). In the first study,51 114 patients with baseline serum creatinine greater than 2 mg/dL undergoing coronary angiography were randomized to hemofiltration vs. 0.9% NaCl infusion. Isovolemic hemofiltration was implemented for 4 to 6 hours before and 18 to 24 hours after the radiographic procedure. The primary endpoint was increase in creatinine by >25% within 72 hours. CN incidence was 5% in the hemofiltration group vs. 50% in the 0.9% NaCl group (P 0.001). The secondary outcomes including in‐hospital mortality, 1‐year mortality and temporary renal replacement were also superior in the hemofiltration group. In the second study, the same investigators compared 2 different hemofiltration protocols, using the same definition of CN.52 Patients with baseline creatinine clearance 30 mL/minute (n = 92) were randomized to 0.9% NaCl infusion, postprocedure isovolemic hemofiltration only, or preprocedure plus postprocedure hemofiltration (same protocol as previous study). The incidence of CN was significantly lower in the preprocedure plus postprocedure hemofiltration group (3% vs. 26% in the postprocedure hemofiltration group vs. 40% in the 0.9% NaCl without hemofiltration group; P = 0.0001). The preprocedure plus postprocedure hemofiltration group also had reductions in in‐hospital mortality and temporary renal replacement therapy rates.
Although the mechanism of hemofiltration prevention of CN is unknown, it is certainly not enhanced clearance of contrast material, inasmuch as hemofiltration was discontinued during the angiography procedure in all protocols, and radiocontrast was therefore not cleared by hemofiltration until the process was reinstituted. Furthermore, the second study indicates that the major benefit was derived from the preprocedure hemofiltration component. Contributing factors might be control of extracellular pH and redox potential with bicarbonate replacement fluid during hemofiltration. Important confounding issues to consider are that patients receiving hemofiltration were in controlled, monitored settings and thus received more intensive care than the hydration group, and that serum creatinine, the major outcome parameter, is cleared by hemofiltration. Before hemofiltration can be recommended as routine prophylactic therapy for CN, the data will need to be corroborated by other groups, preferably involving larger numbers of study subjects and including cost‐benefit analyses.
Multiple small studies have examined the possibility that dialysis immediately following radiocontrast exposure could prevent CN, presumably by accelerating radiocontrast clearance. Most of these reports were negative, including a well‐designed meta‐analysis of RCTs, which showed no benefit of hemodialysis.53 Of note, one report suggested that hemodialysis might be potentially harmful.54 The single prospective trial that showed benefit from prophylactic hemodialysis analyzed 82 patients with advanced CRI (baseline creatinine clearance 13 mL/minute) referred for coronary angiography55 These subjects were randomly assigned to intravenous 0.9% NaCl and hemodialysis vs. intravenous 0.9% NaCl alone. Subsequent renal replacement therapy was required in 35% of control patients and in only 2% in the prophylactic dialysis group. One potential limitation of this study is that the investigators were more cognizant of volume status in the hemodialysis group to avoid fluid shifts and volume depletion during dialysis, while the control group appeared to experience no comparable intravascular volume management. Moreover, this study was conducted in patients with extremely advanced renal insufficiency, and therefore does not reflect the vast majority of patients at risk for CN.
Conclusions
CN is associated with increased morbidity and mortality, and efforts to minimize CN are therefore warranted. However, the overwhelming majority of CN trials were designed to investigate the effects of prophylaxis strategies on surrogate endpoints for estimates of GFR. Therefore, conclusions regarding the effect of these regimens on definitive outcomes, such as death and vascular events, cannot be drawn. On balance, there is evidence that oral and intravenous NAC, as well as extracellular volume expansion with intravenous NaHCO3 are effective measures to prevent CN, whereas the data for renal replacement therapies are more equivocal. We emphasize though, that the literature on this topic is vast, and includes a large number of conflicting studies, including multiple meta‐analyses. As a result, we refrain from being too dogmatic about the best approach, and therefore cautiously offer the following recommendations for prevention of CN.
The first step is to identify high‐risk patients, who are most likely to benefit from prophylaxis (Table 1). Although risk stratification was not the focus of this review, Mehran et al.56 have developed a scoring system to quantitatively predict CN risk, with weighted parameters including CRI, diabetes, radiocontrast volume, age, hypotension, congestive heart failure, treatment with an intraaortic balloon pump, and anemia. For low‐risk patients, hydration with saline is probably adequate. For high‐risk patients, it would be prudent to initially consider whether sufficient information could be obtained from an alternative, noncontrasted radiologic procedure. If not, it would behoove the prescribing physician to then treat modifiable risk factors, as well as to discontinue potentially nephrotoxic medications.
In high‐risk patients undergoing radiocontrast procedures, we recommend using NAC and volume expansion with NaHCO3 (Table 2). Although the evidence for this combined approach is limited,43 we believe it is biologically consistent, since the rationale for both strategies is primarily modification of redox state and inhibition of oxygen free radical generation. Because NAC formulations are generally effective, safe and inexpensive ($0.04 for 600 mg oral NAC and $24 for 1200 mg intravenous NAC at our hospital), we recommend the protocol used by Marenzi et al.,39 NAC 1200 mg intravenously once before procedure and then 1200 mg orally twice daily for 48 hours, as prophylaxis for all contrast procedures in high‐risk patients. However, we recognize that this regimen would require formal evaluation in procedures other than emergent coronary artery angioplasty before it could be enthusiastically endorsed. Therefore, if intravenous NAC is not available and/or the procedure is not emergent, NAC 6001200 mg orally twice a day, 2 doses before and 2 doses after the procedure would be a rational alternative. For the NaHCO3 infusion, we recommend 3 mL/kg for 1 hour before the procedure, followed by 1 mL/kg/hour for 6 hours after.
|
| Minimize radiocontrast dose. |
| Isoosmolar radiocontrast media preferred. |
| Intravenous NaHCO3 at 3 mL/kg/hour for 1 hour prior to radiocontrast exposure, then 1 mL/kg/hour for 6 hours after. |
| Intravenous N‐acetylcysteine 1200 mg before procedure, then 1200 mg orally twice daily for a total of 4 doses. |
| If intravenous N‐acetylcysteine is not available, then N‐acetylcysteine 6001200 mg orally for 2 doses before and 2 doses after procedure. |
| If already undergoing acute dialysis with catheter vascular access, consider CVVH 6 hours before and for 24 hours after procedure. |
Hemofiltration is labor‐intensive, expensive, and not readily available in all hospitals that renders it difficult to endorse as a definitive or routine CN prophylaxis modality. However, if a patient is already undergoing acute dialysis with catheter vascular access, it would be reasonable to consider CVVH 6 hours before and for 24 hours after the procedure (Table 2).
For high‐risk patients, we recommend minimizing the radiocontrast dose (reviewed in Ref.57). Although the dose has not consistently been identified as a risk factor (Table 1), we envision no harm in reducing the dose, particularly if adequate information can be obtained by other means, eg, coronary angiogram accompanied by an echocardiogram, rather than a ventriculogram. We would also consider the use of isoosmolar media in high‐risk patients, since the data are relatively compelling.20 Low doses of isoosmolar media should be particularly beneficial to patients with preexisting hypertension or congestive heart failure, for which the osmotic load and excess extracellular volume expansion might be deleterious. However, because isoosmolar media is expensive, a detailed cost‐benefit analysis would be required before definitive recommendations could be made, especially for patients at lower risk for CN. Finally, because of the complex literature, as well as budgetary issues, we encourage communication between the physician ordering the contrast study and the operator (radiologist or cardiologist) concerning the type of procedure and contrast media to be used.
Since contrast nephropathy (CN) was recognized more than 50 years ago,1 there have been continuous efforts to chemically modify radiocontrast agents to be less nephrotoxic. Although radiocontrast media have indeed become safer, which reduces the likelihood of CN per procedure, the indications for radiocontrast administration have dramatically increased, since over 80 million doses are delivered in the world annually.2, 3 Furthermore, the number of patients with CN risks, which are mainly chronic renal insufficiency (CRI) and diabetes (Table 1), has also grown. Currently, more than 26 million people are estimated to have CRI in the United States4 and 200 million people have diabetes worldwide.5 The combination of increased radiocontrast administration frequency and greater prevalence of at‐risk patients is likely to result in continued increases in CN events.
| Clear Risks | Probable Risks | Questionable Risks |
|---|---|---|
| ||
| Estimated GFR 60 mL/minute/1.73 m2, especially if due to diabetic nephropathy* | Diabetes mellitus* | Repeat contrast procedures |
| Concomitant use of nephrotoxic drugs | Age >75 years | |
| Hemodynamic instability | Male gender | |
| Congestive heart failure | Intraaortic balloon pump | |
| Large contrast volume (>100 mL) | Liver disease | |
| Intraarterial contrast administration | Peripheral vascular disease | |
| Hypertension | ||
| Anemia | ||
| Bence‐Jones proteinuria | ||
| Hyperuricemia | ||
The incidence of CN varies between studies, depending on risk factors of the cohort and definition of CN, but figures have been reported to be as high as 50% in studies enriched with CRI and diabetic patients. However, a very recent study disputes such high incidence rates by demonstrating that patients receiving no radiocontrast media had a similar frequency of serum creatinine increases compared to a comparable group of historical CN patients.6 This study emphasizes that conventional definitions of CN, eg, 25% increase in serum creatinine above baseline, may be too conservative.
A retrospective study of 7586 patients showed 22% in‐hospital mortality in patients who developed CN vs. 1.4% in those who did not, after adjusting for comorbidities. One‐ and 5‐year mortality rates were also higher in the CN group (12.1% vs. 3.7% and 44.6% vs. 14.5%, respectively).7 Another study of 1826 patients, who underwent coronary artery intervention procedures, showed that 14.4% developed CN and 0.8% required hemodialysis. Mortality was 1.1% in patients who did not develop CN, 7.1% in those with CN, and 35.7% in the hemodialysis‐treated CN group.8 Moreover, studies by several other groups also support the position that CN is associated with increased in‐hospital and long‐term mortality.911 Although radiocontrast administration may not be a causal risk factor for mortality, since at‐risk patients have a number of comorbidities, radiocontrast media should nevertheless at least be viewed as an important marker of acute kidney injury and death risk.
Despite the enhanced morbidity and mortality associated with CN, there are no strict guidelines for prevention of CN. Part of the reason is that the literature is controversial regarding most prevention strategies. Several interventions are commonly proposed to help prevent CN, including discriminate selection of the type of radiocontrast, N‐acetylcysteine, volume expansion with saline and/or NaHCO3, and prophylactic hemofiltration. The major purpose of this review is to discuss these different approaches to CN prevention, with the ultimate goal of offering discrete recommendations.
The basis of this semisystematic review was a literature search using the PubMed database (
We report on prophylactic maneuvers that are either commonly considered by nephrology consultants or contain sufficient data to warrant a meta‐analysis study. Studies involving statins, ascorbic acid, dopamine analogs, endothelin antagonists, and theophylline were not addressed in this review due to insufficient, inconclusive, or predominantly negative data. Clinical characteristics and pathogenesis of CN, which include vasoconstriction, ischemia, production of oxygen free radicals, tubular cell apoptosis, and intratubular obstruction, are also not discussed in detail, but have recently been reviewed.12
Risk Associated with Different Types of Radiocontrast Media
There are 3 generations of radiocontrast media: hyperosmolar (14001800 mosm/kg), low osmolar (500850 mosm/kg) and isoosmolar (290 mosm/kg). Note that the low osmolar agents have lower osmolarity relative to the hyperosmolar agents, but are still hyperosmolar compared to serum. Multiple studies have compared effects of radiocontrast with different osmolarities.
The Iohexol Cooperative Study was a double‐blind, randomized, controlled trial (RCT) that randomized 1196 patients to Iohexol (low osmolarity) or diatrizoate (hyperosmolar). Definition of CN was a rise in serum creatinine by >1 mg/dL within 48 to 72 hours after the radiocontrast exposure. Results were in favor of the iohexol group (3% developed CN vs. 7% in the diatrizoate group; P = 0.002). Subgroup analysis of patients with CRI and CRI plus diabetes also revealed less CN in the iohexol vs. diatrizoate groups (7% vs. 16% and 12% vs. 27%, respectively).13
An earlier non‐RCT of 303 patients undergoing femoral angiography compared iohexol/emoxaglate (both are low osmolar) to diatrizoate (hyperosmolar). Six different CN definitions were used. Each comprised a combination of different magnitudes of rise of serum creatinine over various periods of time. Overall, the incidence of CN was 7% in the low osmolar group vs. 26% in the hyperosmolar group (P = 0.001). In subgroup analysis of patients with CRI, and of patients with diabetes, less CN was again observed with low osmolar agents (10% vs. 41%, P = 0.017, in the CRI group; and 10% vs. 31%, P = 0.012, in the diabetes group). Analysis of subjects with baseline serum creatinine 1.5 mg/dL showed no differences between the 2 groups, emphasizing that prior CRI is an important CN risk factor.14
The RECOVER study was a double‐blind RCT of 300 patients undergoing coronary angiography, who were randomized to iodixanol (isoosmolar) or ioxaglate (low osmolarity). CN was defined as a rise in serum creatinine by >25% or 0.5 mg/dL at 24 and 48 hours. CN incidence was 7.9% in the iodixanol group vs. 17% in the ioxaglate group (P = 0.021). Subgroup analyses of patients stratified by severe CRI, diabetes, and contrast volume also favored iodixanol.15 In a similarly designed, double‐blind RCT involving 129 patients with diabetes and CRI randomized to iodixanol or iohexol, CN developed in 3% of iodixanol group vs. 26% in the iohexol group (P = 0.002).16 These results were further supported by a very recent double‐blind RCT comparing iodixanol to iopromide (low osmolar) in 117 patients with baseline serum creatinine 1.5 mg/dL undergoing CT scans. The incidence of serum creatinine increases of 0.5 mg/dL or 25% above baseline or glomerular filtration rate (GFR) reduction of 5 mL/minute was significantly lower in the iodixanol group (P = 0.04, 0.01, and 0.04 respectively).17
In contrast to these reports, 2 double‐blind RCTs showed no differences in CN incidence between iodixanol and low osmolar agents. One study compared iodixanol to iopromide in 64 patients undergoing intravenous pyelography (IVP),18 and the other included 16 nondiabetic patients with CRI and compared iodixanol to iohexol.19 However, because of the small sample sizes, it is likely that neither study is adequately powered to detect differences in outcome between the 2 types of radiocontrast media.
Given the importance of the issue and conflicting results from individual studies, a meta‐analysis of 16 double‐blind RCTs was performed.20 This study included 2727 patients undergoing angiography, compared iodixanol (isoosmolar) to a variety of low osmolar agents, and demonstrated that iodixanol was less nephrotoxic compared to the low osmolarity agents in CRI patients (2.8% vs. 8.4%; P = 0.001) and in patients with CRI plus diabetes (3.5% vs. 15.5%; P = 0.003). Independent predictors of CN were CRI, CRI plus diabetes, and the use of low‐osmolarity media, whereas diabetes, age, and radiocontrast volume were not statistically significant independent predictors.20
Taken together, we conclude that isoosmolar media represents the lowest risk for CN. An additional benefit is that isoosmolar media, on the basis of diminished osmotic load, is less likely to precipitate extracellular fluid volume overload, which is particularly germane for patients with CRI, who have diminished capacity to excrete solute loads. Therefore, we recommend using isoosmolar media, particularly in patients at high risk for CN, such as those with CRI, especially due to diabetic nephropathy.
Oral N‐Acetylcysteine
Based primarily upon in vitro evidence, N‐acetylcysteine (NAC) may theoretically prevent CN by direct antioxidant and vasodilatory effects. However, in vivo, NAC is rapidly metabolized and inactivated by the liver. Therefore, it has been postulated that the mechanism of action may be indirect, and the cysteine metabolite of NAC may stimulate glutathione synthesis, which then inhibits cellular oxidation.21
The first clinical trial to address the prophylactic role of NAC in CN was an RCT of 83 patients with CRI (mean serum creatinine [Cr] = 2.4) undergoing CT scans, who were randomized to NAC plus 0.45% NaCl vs. placebo and 0.9% NaCl.22 The NAC dose was 600 mg orally twice daily for 2 doses before and 2 doses after the procedure. Intravenous fluids were started 12 hours before and stopped 12 hours after the procedure and infused at a rate of 1 ml/kg/hour. CN definition was rise in serum creatinine by >0.5 mg/dL at 48 hours. The results were statistically significant, with a relative risk of CN = 0.1 (95%CI, 0.020.9) in subjects treated with NAC.
There have been many subsequent reports that have evaluated NAC in small numbers of patients with mild to moderate CRI. In general, results from these trials have been inconsistent, which has led to several meta‐analyses to delineate NAC efficacy in CN prevention. The most recent and largest meta‐analysis included 26 NAC RCTs, and revealed a statistically significant benefit from NAC (relative risk [RR] = 0.62; 95%CI, 0.440.88).23 Twelve other meta‐analyses, which incorporated fewer studies, have been published,2435 and 7 of the 12 reported a benefit from NAC.25, 27, 29, 30, 32, 34, 35
Although meta‐analysis is considered the most accepted strategy to define conclusions from multiple trials, conflicting results between NAC meta‐analyses highlight the possibility that this approach may still not provide resolution to clinical questions, especially when inclusion criteria differ between meta‐analyses. Therefore, as discussed by Bagshaw et al.,36 meta‐analyses are not always a panacea, and should be avoided if the trials to be included exhibit significant statistical or clinical heterogeneity, as is the case with studies involving NAC prophylaxis of CN. Finally, because meta‐analyses require pooling of data from published studies, which tend to be positive, the possibility of publication bias exists.
In summary, conclusions from trials to assess efficacy of oral NAC in the prevention of CN have been inconsistent, though there has been a general trend toward benefit. Factors contributing to inconsistent results include variable definitions of CN, degree of CRI and diabetes in the cohort, amount and type of contrast used, NAC dosing and intravenous hydration protocols. As a result, a large multicenter RCT would certainly be helpful. However, the size of such trial might be cost‐prohibitive, and unlikely to be underwritten by the pharmaceutical industry because the patent for NAC has expired.36
Intravenous NAC
In addition to the vast literature on oral NAC for CN prophylaxis, there are now studies that have also evaluated efficacy of intravenous NAC. In one of the largest double‐blind RCTs,37 487 patients (mean baseline serum creatinine = 1.6 mg/dL) were randomized to NAC 500 mg intravenously vs. placebo before cardiac catheterization. Both groups received the same hydration protocols. The study was stopped when an interim analysis determined that there was no advantage to NAC (CN incidence, which was defined as a decrease in creatinine clearance by >5 mL/minute at days 1 to 8 postprocedure, was 23.3% vs. 20.7% in the placebo group).
The RAPPID study examined higher intravenous NAC doses in 80 patients undergoing cardiac catheterization.38 Subjects in this study were randomized to either NAC (150 mg/kg in 500 mL 0.9% NaCl before procedure and then 50 mg/kg in 500 mL 0.9% NaCl over 4 hours after procedure) or 0.9% NaCl 12 hours before and 12 hours after procedure. Despite the relatively small study size, intravenous NAC demonstrated a significant benefit in the prevention of CN (RR = 0.28; P = 0.045) defined as rise in serum creatinine by >25% at 2 or 4 days postexposure. Hypersensitivity‐like reactions were observed in 14.5% of patients receiving intravenous NAC, but symptoms were easily recognized and managed.38
A recent study of 354 patients undergoing primary angioplasty evaluated the combination of intravenous and oral NAC in different doses.39 Patients were randomized to 3 groups: (1) NAC 600 mg intravenously once before procedure and then 600 mg orally twice daily for 48 hours; (2) NAC 1200 mg intravenously once before procedure and then 1200 mg orally twice daily for 48 hours; or (3) placebo. The primary outcome was increase in Cr by >25% and secondary outcomes were in‐hospital death and a composite score that included death and need for renal replacement therapy. Results were significantly in favor of the 1200‐mg NAC regimen across all outcomes (P = 0.001, 0.02, and 0.002, respectively). It should be emphasized that this study was restricted to patients undergoing primary angioplasty, which is an emergent procedure. As a result, implementation of this protocol would necessarily require rapid administration of intravenous NAC prior to the procedure, which might even require maintenance of NAC stocks within the catheterization laboratory.
Because there is a trend toward benefit from oral NAC and the benefit from intravenous NAC in trials from limited settings, and both NAC formulations are inexpensive and safe, we recommend that NAC should be included in CN prophylaxis protocols.
Extracellular Fluid Volume Expansion
Since publication of work by Solomon et al.,40 which demonstrated a benefit of intravenous hydration with 0.45% NaCl in the prevention of CN in a group of CKD patients, it has been considered standard practice to prescribe intravenous fluid regimens for CN prophylaxis in high‐risk subjects. In the largest study to test the effect of different hydration protocols for CN prevention, Mueller et al.41 randomized 1620 patients with normal baseline serum creatinine to intravenous 0.9 % NaCl vs. 0.45% NaCl. The definition of CN was rise in serum creatinine by >0.5 mg/dL at 48 hours and the incidence was 0.7% for the 0.9% NaCl group and 2% for the 0.45% NaCl group (P = 0.04).
More recently, several trials have examined the relative efficacy of intravenous NaCl vs. NaHCO3 for CN prophylaxis. In the first NaHCO3 RCT, Merten et al.42 compared 0.9% NaHCO3 to 0.9% NaCl infusion in a population with a mean serum creatinine of 1.8 mg/dL. Both groups received 3 mL/kg intravenous bolus over 1 hour before the radiographic procedure followed by 1 mL/kg/hour for 6 hours. Urine pH was measured to confirm alkalinization of urine in the NaHCO3‐treated patients and the primary end point was increase in serum creatinine by >25% within 48 hours. The study was terminated early (after enrollment of 119 patients) when the interim analysis showed CN incidence was 1.7% in the NaHCO3 group vs. 13.6% in the NaCl group (P = 0.02).
These results were corroborated in the recent REMEDIAL trial,43 which enrolled 326 patients with serum creatinine >2 mg/dL, who were randomized to 1 of 3 arms. One group received intravenous saline (0.9% NaCl for 12 hours before and 12 hours after the procedure) and oral NAC; a second group received intravenous NaHCO3 (3 mL/kg intravenous bolus over 1 hour before the radiographic procedure followed by 1 mL/kg/hour for 6 hours) and oral NAC; and a third group received intravenous 0.9% NaCl plus oral NAC and ascorbic acid. Patients had similar baseline characteristics and the primary end point was an increase in serum creatinine by >25% within 48 hours. The best results were observed in the NaHCO3 plus NAC group; 1.9% developed CN in this group vs. 9.9% in the NaCl plus NAC group vs. 10.3% in the NaCl plus NAC plus ascorbic acid group (P = 0.019). Three additional prospective but smaller studies also showed the superiority of NaHCO3.4446
In contrast to studies supporting a role for prophylactic NaHCO3, a recent RCT showed no superiority of NaHCO3 infusion regimens.47 In this trial, 352 patients undergoing coronary angiography were randomized to receive either NaHCO3 or 0.9% NaCl. Both solutions were administered at rates of 3 mL/kg for 1 hour before the procedure and 1.5 mL/kg/hour for 4 hours postprocedure. The primary endpoint (>25% decrease in estimated GFR during the first 4 days after contrast exposure) was met in 13.3% of NaHCO3 group vs. 14.6% of the 0.9% NaCl group (P = 0.82). Moreover, there were no differences in the rates of secondary outcomes, which included death, dialysis, and cardiovascular and cerebrovascular events.
Results from a very recent retrospective cohort study of 7977 patients demonstrated that NaHCO3 infusion was associated with increased risk of CN compared to no treatment (odds ratio [OR] = 3.1; P 0.001), whereas NAC alone or in combination with NaHCO3 was associated with no significant difference in the incidence of CN.48 However, multiple weaknesses associated with the retrospective study design, such as inclusion of few patients at high CN risk, and acceptance of serum creatinine values within 7 days before and after the contrast procedure, which likely captures causes of acute kidney injury other than CN, preclude abandonment of NaHCO3 prophylaxis for CN solely on the basis of this study.
In an effort to resolve the conflicting NaHCO3 prophylaxis literature, a meta‐analysis was recently conducted.49 This study encompassed 1307 patients enrolled in 7 RCTs that examined outcomes for NaHCO3 vs. saline prevention of CN. The main finding was a significant benefit of NaHCO3 for protection against CN (RR = 0.37; P = 0.005). No benefit of NaHCO3 infusion could be shown for postprocedure renal replacement therapy or death.
Therefore, based upon the results of multiple prospective trials, the recent meta‐analysis, the relative safety of NaHCO3 infusion with appropriate monitoring, and a plausible biological mechanism whereby bicarbonate may have antioxidant properties and scavenge oxygen‐derived free radicals, which have been implicated in CN pathogenesis,50 we advocate a prophylactic regimen employing NaHCO3 for patients at high risk for CN.
Renal Replacement Therapies
Two studies have been conducted by the same group (Marenzi et al.51, 52) to examine efficacy of continuous hemofiltration (CVVH) in preventing CN (hemofiltration clears solute by convection, and involves administration of a HCO‐rich replacement solution, whereas hemodialysis clears solute by both diffusion and convection, and there is routinely no replacement fluid). In the first study,51 114 patients with baseline serum creatinine greater than 2 mg/dL undergoing coronary angiography were randomized to hemofiltration vs. 0.9% NaCl infusion. Isovolemic hemofiltration was implemented for 4 to 6 hours before and 18 to 24 hours after the radiographic procedure. The primary endpoint was increase in creatinine by >25% within 72 hours. CN incidence was 5% in the hemofiltration group vs. 50% in the 0.9% NaCl group (P 0.001). The secondary outcomes including in‐hospital mortality, 1‐year mortality and temporary renal replacement were also superior in the hemofiltration group. In the second study, the same investigators compared 2 different hemofiltration protocols, using the same definition of CN.52 Patients with baseline creatinine clearance 30 mL/minute (n = 92) were randomized to 0.9% NaCl infusion, postprocedure isovolemic hemofiltration only, or preprocedure plus postprocedure hemofiltration (same protocol as previous study). The incidence of CN was significantly lower in the preprocedure plus postprocedure hemofiltration group (3% vs. 26% in the postprocedure hemofiltration group vs. 40% in the 0.9% NaCl without hemofiltration group; P = 0.0001). The preprocedure plus postprocedure hemofiltration group also had reductions in in‐hospital mortality and temporary renal replacement therapy rates.
Although the mechanism of hemofiltration prevention of CN is unknown, it is certainly not enhanced clearance of contrast material, inasmuch as hemofiltration was discontinued during the angiography procedure in all protocols, and radiocontrast was therefore not cleared by hemofiltration until the process was reinstituted. Furthermore, the second study indicates that the major benefit was derived from the preprocedure hemofiltration component. Contributing factors might be control of extracellular pH and redox potential with bicarbonate replacement fluid during hemofiltration. Important confounding issues to consider are that patients receiving hemofiltration were in controlled, monitored settings and thus received more intensive care than the hydration group, and that serum creatinine, the major outcome parameter, is cleared by hemofiltration. Before hemofiltration can be recommended as routine prophylactic therapy for CN, the data will need to be corroborated by other groups, preferably involving larger numbers of study subjects and including cost‐benefit analyses.
Multiple small studies have examined the possibility that dialysis immediately following radiocontrast exposure could prevent CN, presumably by accelerating radiocontrast clearance. Most of these reports were negative, including a well‐designed meta‐analysis of RCTs, which showed no benefit of hemodialysis.53 Of note, one report suggested that hemodialysis might be potentially harmful.54 The single prospective trial that showed benefit from prophylactic hemodialysis analyzed 82 patients with advanced CRI (baseline creatinine clearance 13 mL/minute) referred for coronary angiography55 These subjects were randomly assigned to intravenous 0.9% NaCl and hemodialysis vs. intravenous 0.9% NaCl alone. Subsequent renal replacement therapy was required in 35% of control patients and in only 2% in the prophylactic dialysis group. One potential limitation of this study is that the investigators were more cognizant of volume status in the hemodialysis group to avoid fluid shifts and volume depletion during dialysis, while the control group appeared to experience no comparable intravascular volume management. Moreover, this study was conducted in patients with extremely advanced renal insufficiency, and therefore does not reflect the vast majority of patients at risk for CN.
Conclusions
CN is associated with increased morbidity and mortality, and efforts to minimize CN are therefore warranted. However, the overwhelming majority of CN trials were designed to investigate the effects of prophylaxis strategies on surrogate endpoints for estimates of GFR. Therefore, conclusions regarding the effect of these regimens on definitive outcomes, such as death and vascular events, cannot be drawn. On balance, there is evidence that oral and intravenous NAC, as well as extracellular volume expansion with intravenous NaHCO3 are effective measures to prevent CN, whereas the data for renal replacement therapies are more equivocal. We emphasize though, that the literature on this topic is vast, and includes a large number of conflicting studies, including multiple meta‐analyses. As a result, we refrain from being too dogmatic about the best approach, and therefore cautiously offer the following recommendations for prevention of CN.
The first step is to identify high‐risk patients, who are most likely to benefit from prophylaxis (Table 1). Although risk stratification was not the focus of this review, Mehran et al.56 have developed a scoring system to quantitatively predict CN risk, with weighted parameters including CRI, diabetes, radiocontrast volume, age, hypotension, congestive heart failure, treatment with an intraaortic balloon pump, and anemia. For low‐risk patients, hydration with saline is probably adequate. For high‐risk patients, it would be prudent to initially consider whether sufficient information could be obtained from an alternative, noncontrasted radiologic procedure. If not, it would behoove the prescribing physician to then treat modifiable risk factors, as well as to discontinue potentially nephrotoxic medications.
In high‐risk patients undergoing radiocontrast procedures, we recommend using NAC and volume expansion with NaHCO3 (Table 2). Although the evidence for this combined approach is limited,43 we believe it is biologically consistent, since the rationale for both strategies is primarily modification of redox state and inhibition of oxygen free radical generation. Because NAC formulations are generally effective, safe and inexpensive ($0.04 for 600 mg oral NAC and $24 for 1200 mg intravenous NAC at our hospital), we recommend the protocol used by Marenzi et al.,39 NAC 1200 mg intravenously once before procedure and then 1200 mg orally twice daily for 48 hours, as prophylaxis for all contrast procedures in high‐risk patients. However, we recognize that this regimen would require formal evaluation in procedures other than emergent coronary artery angioplasty before it could be enthusiastically endorsed. Therefore, if intravenous NAC is not available and/or the procedure is not emergent, NAC 6001200 mg orally twice a day, 2 doses before and 2 doses after the procedure would be a rational alternative. For the NaHCO3 infusion, we recommend 3 mL/kg for 1 hour before the procedure, followed by 1 mL/kg/hour for 6 hours after.
|
| Minimize radiocontrast dose. |
| Isoosmolar radiocontrast media preferred. |
| Intravenous NaHCO3 at 3 mL/kg/hour for 1 hour prior to radiocontrast exposure, then 1 mL/kg/hour for 6 hours after. |
| Intravenous N‐acetylcysteine 1200 mg before procedure, then 1200 mg orally twice daily for a total of 4 doses. |
| If intravenous N‐acetylcysteine is not available, then N‐acetylcysteine 6001200 mg orally for 2 doses before and 2 doses after procedure. |
| If already undergoing acute dialysis with catheter vascular access, consider CVVH 6 hours before and for 24 hours after procedure. |
Hemofiltration is labor‐intensive, expensive, and not readily available in all hospitals that renders it difficult to endorse as a definitive or routine CN prophylaxis modality. However, if a patient is already undergoing acute dialysis with catheter vascular access, it would be reasonable to consider CVVH 6 hours before and for 24 hours after the procedure (Table 2).
For high‐risk patients, we recommend minimizing the radiocontrast dose (reviewed in Ref.57). Although the dose has not consistently been identified as a risk factor (Table 1), we envision no harm in reducing the dose, particularly if adequate information can be obtained by other means, eg, coronary angiogram accompanied by an echocardiogram, rather than a ventriculogram. We would also consider the use of isoosmolar media in high‐risk patients, since the data are relatively compelling.20 Low doses of isoosmolar media should be particularly beneficial to patients with preexisting hypertension or congestive heart failure, for which the osmotic load and excess extracellular volume expansion might be deleterious. However, because isoosmolar media is expensive, a detailed cost‐benefit analysis would be required before definitive recommendations could be made, especially for patients at lower risk for CN. Finally, because of the complex literature, as well as budgetary issues, we encourage communication between the physician ordering the contrast study and the operator (radiologist or cardiologist) concerning the type of procedure and contrast media to be used.
- , , , .Acute anuria following intravenous pyelography in a patient with myelomatosis.Acta Med Scand.1954;150(4):297–302.
- .Editorial: Contrast medium‐induced nephropathy.Nephrol Dial Transplant.2005;20(suppl 1):i1.
- , .Contrast‐induced nephrotoxicity: clinical landscape.Kidney Int Suppl.2006;(100):S3–S7.
- , , , et al.Prevalence of chronic kidney disease in the United States.JAMA.2007;298(17):2038–2047.
- , , , et al.Estimation of glomerular filtration rate in diabetic subjects: Cockcroft formula or modification of Diet in Renal Disease study equation?Diabetes Care.2005;28(4):838–843.
- , , , .Frequency of serum creatinine changes in the absence of iodinated contrast material: implications for studies of contrast nephrotoxicity.AJR Am J Roentgenol.2008;191(2):376–382.
- , , , et al.Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention.Circulation.2002;105(19):2259–2264.
- , , , , .Acute renal failure after coronary intervention: incidence, risk factors, and relationship to mortality.Am J Med.1997;103(5):368–375.
- , , .The effect of acute renal failure on mortality. A cohort analysis.JAMA.1996;275(19):1489–1494.
- , , , et al.The prognostic implications of further renal function deterioration within 48 h of interventional coronary procedures in patients with pre‐existent chronic renal insufficiency.J Am Coll Cardiol.2000;36(5):1542–1548.
- , , , et al.Contrast‐induced nephropathy after percutaneous coronary interventions in relation to chronic kidney disease and hemodynamic variables.Am J Cardiol.2005;95(1):13–19.
- , , , et al.Renal parenchymal hypoxia, hypoxia adaptation, and the pathogenesis of radiocontrast nephropathy.Clin J Am Soc Nephrol.2008;3(1):288–296.
- , , , et al.Nephrotoxicity of ionic and nonionic contrast media in 1196 patients: a randomized trial. The Iohexol Cooperative Study.Kidney Int.1995;47(1):254–261.
- , , , et al.Radiocontrast‐associated renal dysfunction: a comparison of lower‐osmolality and conventional high‐osmolality contrast media.AJR Am J Roentgenol.1991;157(1):59–65.
- , , , et al.,Renal toxicity evaluation and comparison between visipaque (iodixanol) and hexabrix (ioxaglate) in patients with renal insufficiency undergoing coronary angiography: the RECOVER study: a randomized controlled trial.J Am Coll Cardiol.2006;48(5):924–930.
- , , , et al.Nephrotoxic effects in high‐risk patients undergoing angiography.N Engl J Med.2003;348(6):491–499.
- , , , et al.Iso‐osmolality vs. low‐osmolality iodinated contrast medium at intravenous contrast‐enhanced CT: effect on kidney function.Radiology.2008;248(1):97–105.
- , , , et al.Effects of a dimeric vs a monomeric nonionic contrast medium on renal function in patients with mild to moderate renal insufficiency: a double‐blind, randomized clinical trial.Eur Radiol.1998;8(1):144–147.
- , , .Angiography with nonionic X‐ray contrast media in severe chronic renal failure: renal function and contrast retention.Nephron.1996;73(4):549–556.
- , , , .A meta‐analysis of the renal safety of isoosmolar iodixanol compared with low‐osmolar contrast media.J Am Coll Cardiol.2006;48(4):692–699.
- .N‐acetylcysteine in the prevention of contrast‐induced nephropathy.Clin J Am Soc Nephrol.2008;3(1):281–287.
- , , , , , .Prevention of radiographic‐contrast‐agent‐induced reductions in renal function by acetylcysteine.N Engl J Med.2000;343(3):180–184.
- , , , , .Meta‐analysis: effectiveness of drugs for preventing contrast‐induced nephropathy.Ann Intern Med.2008;148(4):284–294.
- , , , et al.Is acetylcysteine effective in preventing contrast‐related nephropathy? A meta‐analysis.Am J Med.2004;117(12):938–947.
- , , , , , .Acetylcysteine for prevention of contrast nephropathy: meta‐analysis.Lancet.2003;362(9384):598–603.
- , , , .Systematic review of the impact of N‐acetylcysteine on contrast nephropathy.Kidney Int.2004;65(4):1366–1374.
- , , , , .N‐acetylcysteine for the prevention of contrast‐induced nephropathy. A systematic review and meta‐analysis.J Gen Intern Med.2005;20(2):193–200.
- , , , .N‐acetylcysteine and contrast‐induced nephropathy: a meta‐analysis of 13 randomized trials.Am Heart J.2006;151(1):140–145.
- , , .Meta‐analysis of randomized clinical trials on the usefulness of acetylcysteine for prevention of contrast nephropathy.Am J Cardiol.2003;92(12):1454–1458.
- , , , , .Prevention of radiocontrast nephropathy with N‐acetylcysteine in patients with chronic kidney disease: a meta‐analysis of randomized, controlled trials.Am J Kidney Dis.2004;43(1):1–9.
- , , , et al.N‐acetylcysteine for the prevention of radiocontrast induced nephropathy: a meta‐analysis of prospective controlled trials.J Am Soc Nephrol.2004;15(3):761–769.
- , .The role of N‐acetylcysteine in preventing radiographic contrast‐induced nephropathy.Clin Nephrol.2004;62(2):77–83.
- , .Acetylcysteine for prevention of contrast‐induced nephropathy after intravascular angiography: a systematic review and meta‐analysis.BMC Med.2004;2:38.
- , , , , .Role of N‐acetylcysteine in prevention of contrast‐induced nephropathy after cardiovascular procedures: a meta‐analysis.Clin Cardiol.2004;27(11):607–610.
- , , .N‐acetylcysteine prophylaxis significantly reduces the risk of radiocontrast‐induced nephropathy: comprehensive meta‐analysis.Catheter Cardiovasc Interv.2005;64(4):471–479.
- , , , .Acetylcysteine in the prevention of contrast‐induced nephropathy: a case study of the pitfalls in the evolution of evidence.Arch Intern Med.2006;166(2):161–166.
- , , , et al.A randomized controlled trial of intravenous N‐acetylcysteine for the prevention of contrast‐induced nephropathy after cardiac catheterization: lack of effect.Am Heart J.2004;148(3):422–429.
- , , , , , .A rapid protocol for the prevention of contrast‐induced renal dysfunction: the RAPPID study.J Am Coll Cardiol.2003;41(12):2114–2118.
- , , , et al.N‐acetylcysteine and contrast‐induced nephropathy in primary angioplasty.N Engl J Med.2006;354(26):2773–2782.
- , , , , .Effects of saline, mannitol, and furosemide to prevent acute decreases in renal function induced by radiocontrast agents.N Engl J Med.1994;331(21):1416–1420.
- , , .Prevention of contrast media‐associated nephropathy: randomized comparison of 2 hydration regimens in 1620 patients undergoing coronary angioplasty.Arch Intern Med.2002;162(3):329–336.
- , , , et al.Prevention of contrast‐induced nephropathy with sodium bicarbonate: a randomized controlled trial.JAMA.2004;291(19):2328–2334.
- , , , et al.Renal insufficiency following contrast media administration trial (REMEDIAL): a randomized comparison of 3 preventive strategies.Circulation.2007;115(10):1211–1217.
- , , , et al.Sodium bicarbonate, N‐acetylcysteine, and saline for prevention of radiocontrast‐induced nephropathy. A comparison of 3 regimens for protecting contrast‐induced nephropathy in patients undergoing coronary procedures. A single‐center prospective controlled trial.Am Heart J.2007;154(3):539–544.
- , , , et al.The reno‐protective effect of hydration with sodium bicarbonate plus N‐acetylcysteine in patients undergoing emergency percutaneous coronary intervention: the RENO Study.J Am Coll Cardiol.2007;49(12):1283–1288.
- , , , et al.Comparison of usefulness of sodium bicarbonate vs. sodium chloride to prevent contrast‐induced nephropathy in patients undergoing an emergent coronary procedure.Am J Cardiol.2007;100(5):781–786.
- , , , et al.Sodium bicarbonate vs sodium chloride for the prevention of contrast medium‐induced nephropathy in patients undergoing coronary angiography: a randomized trial.JAMA.2008;300(9):1038–1046.
- , , , , , .Sodium bicarbonate is associated with an increased incidence of contrast nephropathy: a retrospective cohort study of 7977 patients at Mayo clinic.Clin J Am Soc Nephrol.2008;3(1):10–18.
- , , , et al.Current role of sodium bicarbonate‐based preprocedural hydration for the prevention of contrast‐induced acute kidney injury: a meta‐analysis.Am Heart J.2008;156(3):414–421.
- .Effect of sodium bicarbonate preloading on ischemic renal failure.Nephron.1986;44(1):70–74.
- , , , et al.The prevention of radiocontrast‐agent‐induced nephropathy by hemofiltration.N Engl J Med.2003;349(14):1333–1340.
- , , , et al.Comparison of two hemofiltration protocols for prevention of contrast‐induced nephropathy in high‐risk patients.Am J Med.2006;119(2):155–162.
- , , , et al.Extracorporeal blood purification therapies for prevention of radiocontrast‐induced nephropathy: a systematic review.Am J Kidney Dis.2006;48(3):361–371.
- , , , et al.Prophylactic hemodialysis after radiocontrast media in patients with renal insufficiency is potentially harmful.Am J Med.2001;111(9):692–698.
- , , , et al.Renal protection for coronary angiography in advanced renal failure patients by prophylactic hemodialysis. A randomized controlled trial.J Am Coll Cardiol.2007;50(11):1015–1020.
- , , , et al.A simple risk score for prediction of contrast‐induced nephropathy after percutaneous coronary intervention: development and initial validation.J Am Coll Cardiol.2004;44(7):1393–1399.
- .Contrast‐induced acute kidney injury.J Am Coll Cardiol.2008;51(15):1419–1428.
- , , , .Acute anuria following intravenous pyelography in a patient with myelomatosis.Acta Med Scand.1954;150(4):297–302.
- .Editorial: Contrast medium‐induced nephropathy.Nephrol Dial Transplant.2005;20(suppl 1):i1.
- , .Contrast‐induced nephrotoxicity: clinical landscape.Kidney Int Suppl.2006;(100):S3–S7.
- , , , et al.Prevalence of chronic kidney disease in the United States.JAMA.2007;298(17):2038–2047.
- , , , et al.Estimation of glomerular filtration rate in diabetic subjects: Cockcroft formula or modification of Diet in Renal Disease study equation?Diabetes Care.2005;28(4):838–843.
- , , , .Frequency of serum creatinine changes in the absence of iodinated contrast material: implications for studies of contrast nephrotoxicity.AJR Am J Roentgenol.2008;191(2):376–382.
- , , , et al.Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention.Circulation.2002;105(19):2259–2264.
- , , , , .Acute renal failure after coronary intervention: incidence, risk factors, and relationship to mortality.Am J Med.1997;103(5):368–375.
- , , .The effect of acute renal failure on mortality. A cohort analysis.JAMA.1996;275(19):1489–1494.
- , , , et al.The prognostic implications of further renal function deterioration within 48 h of interventional coronary procedures in patients with pre‐existent chronic renal insufficiency.J Am Coll Cardiol.2000;36(5):1542–1548.
- , , , et al.Contrast‐induced nephropathy after percutaneous coronary interventions in relation to chronic kidney disease and hemodynamic variables.Am J Cardiol.2005;95(1):13–19.
- , , , et al.Renal parenchymal hypoxia, hypoxia adaptation, and the pathogenesis of radiocontrast nephropathy.Clin J Am Soc Nephrol.2008;3(1):288–296.
- , , , et al.Nephrotoxicity of ionic and nonionic contrast media in 1196 patients: a randomized trial. The Iohexol Cooperative Study.Kidney Int.1995;47(1):254–261.
- , , , et al.Radiocontrast‐associated renal dysfunction: a comparison of lower‐osmolality and conventional high‐osmolality contrast media.AJR Am J Roentgenol.1991;157(1):59–65.
- , , , et al.,Renal toxicity evaluation and comparison between visipaque (iodixanol) and hexabrix (ioxaglate) in patients with renal insufficiency undergoing coronary angiography: the RECOVER study: a randomized controlled trial.J Am Coll Cardiol.2006;48(5):924–930.
- , , , et al.Nephrotoxic effects in high‐risk patients undergoing angiography.N Engl J Med.2003;348(6):491–499.
- , , , et al.Iso‐osmolality vs. low‐osmolality iodinated contrast medium at intravenous contrast‐enhanced CT: effect on kidney function.Radiology.2008;248(1):97–105.
- , , , et al.Effects of a dimeric vs a monomeric nonionic contrast medium on renal function in patients with mild to moderate renal insufficiency: a double‐blind, randomized clinical trial.Eur Radiol.1998;8(1):144–147.
- , , .Angiography with nonionic X‐ray contrast media in severe chronic renal failure: renal function and contrast retention.Nephron.1996;73(4):549–556.
- , , , .A meta‐analysis of the renal safety of isoosmolar iodixanol compared with low‐osmolar contrast media.J Am Coll Cardiol.2006;48(4):692–699.
- .N‐acetylcysteine in the prevention of contrast‐induced nephropathy.Clin J Am Soc Nephrol.2008;3(1):281–287.
- , , , , , .Prevention of radiographic‐contrast‐agent‐induced reductions in renal function by acetylcysteine.N Engl J Med.2000;343(3):180–184.
- , , , , .Meta‐analysis: effectiveness of drugs for preventing contrast‐induced nephropathy.Ann Intern Med.2008;148(4):284–294.
- , , , et al.Is acetylcysteine effective in preventing contrast‐related nephropathy? A meta‐analysis.Am J Med.2004;117(12):938–947.
- , , , , , .Acetylcysteine for prevention of contrast nephropathy: meta‐analysis.Lancet.2003;362(9384):598–603.
- , , , .Systematic review of the impact of N‐acetylcysteine on contrast nephropathy.Kidney Int.2004;65(4):1366–1374.
- , , , , .N‐acetylcysteine for the prevention of contrast‐induced nephropathy. A systematic review and meta‐analysis.J Gen Intern Med.2005;20(2):193–200.
- , , , .N‐acetylcysteine and contrast‐induced nephropathy: a meta‐analysis of 13 randomized trials.Am Heart J.2006;151(1):140–145.
- , , .Meta‐analysis of randomized clinical trials on the usefulness of acetylcysteine for prevention of contrast nephropathy.Am J Cardiol.2003;92(12):1454–1458.
- , , , , .Prevention of radiocontrast nephropathy with N‐acetylcysteine in patients with chronic kidney disease: a meta‐analysis of randomized, controlled trials.Am J Kidney Dis.2004;43(1):1–9.
- , , , et al.N‐acetylcysteine for the prevention of radiocontrast induced nephropathy: a meta‐analysis of prospective controlled trials.J Am Soc Nephrol.2004;15(3):761–769.
- , .The role of N‐acetylcysteine in preventing radiographic contrast‐induced nephropathy.Clin Nephrol.2004;62(2):77–83.
- , .Acetylcysteine for prevention of contrast‐induced nephropathy after intravascular angiography: a systematic review and meta‐analysis.BMC Med.2004;2:38.
- , , , , .Role of N‐acetylcysteine in prevention of contrast‐induced nephropathy after cardiovascular procedures: a meta‐analysis.Clin Cardiol.2004;27(11):607–610.
- , , .N‐acetylcysteine prophylaxis significantly reduces the risk of radiocontrast‐induced nephropathy: comprehensive meta‐analysis.Catheter Cardiovasc Interv.2005;64(4):471–479.
- , , , .Acetylcysteine in the prevention of contrast‐induced nephropathy: a case study of the pitfalls in the evolution of evidence.Arch Intern Med.2006;166(2):161–166.
- , , , et al.A randomized controlled trial of intravenous N‐acetylcysteine for the prevention of contrast‐induced nephropathy after cardiac catheterization: lack of effect.Am Heart J.2004;148(3):422–429.
- , , , , , .A rapid protocol for the prevention of contrast‐induced renal dysfunction: the RAPPID study.J Am Coll Cardiol.2003;41(12):2114–2118.
- , , , et al.N‐acetylcysteine and contrast‐induced nephropathy in primary angioplasty.N Engl J Med.2006;354(26):2773–2782.
- , , , , .Effects of saline, mannitol, and furosemide to prevent acute decreases in renal function induced by radiocontrast agents.N Engl J Med.1994;331(21):1416–1420.
- , , .Prevention of contrast media‐associated nephropathy: randomized comparison of 2 hydration regimens in 1620 patients undergoing coronary angioplasty.Arch Intern Med.2002;162(3):329–336.
- , , , et al.Prevention of contrast‐induced nephropathy with sodium bicarbonate: a randomized controlled trial.JAMA.2004;291(19):2328–2334.
- , , , et al.Renal insufficiency following contrast media administration trial (REMEDIAL): a randomized comparison of 3 preventive strategies.Circulation.2007;115(10):1211–1217.
- , , , et al.Sodium bicarbonate, N‐acetylcysteine, and saline for prevention of radiocontrast‐induced nephropathy. A comparison of 3 regimens for protecting contrast‐induced nephropathy in patients undergoing coronary procedures. A single‐center prospective controlled trial.Am Heart J.2007;154(3):539–544.
- , , , et al.The reno‐protective effect of hydration with sodium bicarbonate plus N‐acetylcysteine in patients undergoing emergency percutaneous coronary intervention: the RENO Study.J Am Coll Cardiol.2007;49(12):1283–1288.
- , , , et al.Comparison of usefulness of sodium bicarbonate vs. sodium chloride to prevent contrast‐induced nephropathy in patients undergoing an emergent coronary procedure.Am J Cardiol.2007;100(5):781–786.
- , , , et al.Sodium bicarbonate vs sodium chloride for the prevention of contrast medium‐induced nephropathy in patients undergoing coronary angiography: a randomized trial.JAMA.2008;300(9):1038–1046.
- , , , , , .Sodium bicarbonate is associated with an increased incidence of contrast nephropathy: a retrospective cohort study of 7977 patients at Mayo clinic.Clin J Am Soc Nephrol.2008;3(1):10–18.
- , , , et al.Current role of sodium bicarbonate‐based preprocedural hydration for the prevention of contrast‐induced acute kidney injury: a meta‐analysis.Am Heart J.2008;156(3):414–421.
- .Effect of sodium bicarbonate preloading on ischemic renal failure.Nephron.1986;44(1):70–74.
- , , , et al.The prevention of radiocontrast‐agent‐induced nephropathy by hemofiltration.N Engl J Med.2003;349(14):1333–1340.
- , , , et al.Comparison of two hemofiltration protocols for prevention of contrast‐induced nephropathy in high‐risk patients.Am J Med.2006;119(2):155–162.
- , , , et al.Extracorporeal blood purification therapies for prevention of radiocontrast‐induced nephropathy: a systematic review.Am J Kidney Dis.2006;48(3):361–371.
- , , , et al.Prophylactic hemodialysis after radiocontrast media in patients with renal insufficiency is potentially harmful.Am J Med.2001;111(9):692–698.
- , , , et al.Renal protection for coronary angiography in advanced renal failure patients by prophylactic hemodialysis. A randomized controlled trial.J Am Coll Cardiol.2007;50(11):1015–1020.
- , , , et al.A simple risk score for prediction of contrast‐induced nephropathy after percutaneous coronary intervention: development and initial validation.J Am Coll Cardiol.2004;44(7):1393–1399.
- .Contrast‐induced acute kidney injury.J Am Coll Cardiol.2008;51(15):1419–1428.
BMI and Postoperative Complications
Public health concerns such as the aging population1 and the increasing prevalence of obesity2 are also important issues to hospitals. However, little attention has been given to the interface of obesity and the elderly, largely due to the dearth of studies that include elderly patients. An aging population leads to an increase in geriatric syndromes, such as osteoporosis3 and its most devastating complication, hip fracture.4 These frail, hip‐fracture patients pose management challenges to practicing geriatricians and hospitalists.5,6 Furthermore, although fracture risk is inversely correlated to body mass index (BMI),7 this relationship has yet to be fully examined in the postoperative hip‐fracture population. In other surgical settings, there is disagreement as to whether underweight or obese patients are at higher risk of developing medical complications,8‐11 but for orthopedic patients, data have been limited to elective orthopedic populations.12‐14 We previously demonstrated that underweight hip‐fracture patients are at higher risk of postoperative cardiac complications at 1 year,15 consistent with studies of cardiac risk indices determining long‐term events. Because of different pathophysiologic mechanisms, the purpose of this study was to ascertain the influence of BMI on inpatient postoperative noncardiac medical complications and to assess predictors of such complications following urgent hip fracture repair.
Patients and Methods
All Olmsted County, Minnesota, residents undergoing urgent hip repair due to fracture were identified using the Rochester Epidemiology Project, a medical‐record linkage system funded by the Federal government since 1966 to support disease‐related epidemiology studies.16 All patient medical care is indexed, and both inpatient and outpatient visits are captured and available for review, allowing for complete case ascertainment. Medical care in Olmsted County is primarily provided by Mayo Clinic with its affiliated hospitals (St. Mary's and Rochester Methodist) and the Olmsted Medical Center, in addition to a few individual providers. Over 95% of all Olmsted County hip fracture surgeries are ultimately managed at St. Mary's Hospital.
Following approval by the Institutional Review Board we used this unique data resource to identify all residents with an International Classification of Diseases, 9th edition (ICD‐9) diagnosis code of 820 to 829 for hip fracture (n = 1310). Both sexes were included, and all patients included in the study provided research authorization for use of their medical records for research purposes.17 We excluded patients who were managed conservatively (n = 56), had a pathological fracture (n = 20), had multiple injuries (n = 19), were operated on >72 hours after fracture (n = 5), were aged <65 years (n = 2), or were admitted for reasons other than a fracture and experienced an in‐hospital fracture (n = 3). We subsequently excluded patients with missing information (n = 10). World Health Organization (WHO) criteria were used for classifying BMI: underweight (BMI < 18.5); normal (BMI = 18.5‐24.9); overweight (BMI = 25.0‐29.9); and obese (BMI 30.0).18
All data were abstracted using standardized collection forms by trained nurse abstractors blinded to the study hypothesis. Patients' admission height and weight were documented; if unavailable, the nearest data within 2 months prior to surgery were recorded. Patients' preadmission residence, functional status, baseline comorbidities, admission medications, discharge destination, as well as whether patients had an intensive care unit stay or any major surgeries in the past 90 days were abstracted. In addition, American Society of Anesthesia (ASA) class, type of anesthesia, and length of stay were also obtained. Inpatient complications that had been identified by the treating physicians and documented in the medical record or identified on imaging studies were assessed from the time of hip fracture repair to the time of discharge using standardized clinical criteria (Table 1). For criteria that were based on either objective findings or clinical documentation/suspicion, the patient was considered to meet the criteria of having a complication if they fulfilled either one. We did not include any cardiac outcomes, including congestive heart failure, angina, myocardial infarction, or arrhythmias that had been previously reported.15 Noncardiac complications were classified broadly: respiratory (respiratory failure, respiratory depression, or pulmonary hypoxemia); neurologic (any cerebral event including hemorrhagic or ischemic stroke, transient ischemic attack, or delirium); gastrointestinal (ileus or gastrointestinal bleeding); vascular (pulmonary embolus, or deep vein thrombosis); infectious (pneumonia, sepsis, urinary tract, wound, or cellulitis); renal/metabolic (acute renal failure, dehydration, or electrolyte abnormalities); or other (fractures or falls).
| Definition | Symptom |
|---|---|
| |
| Gastrointestinal | |
| Ileus | Dilated loops of bowel on X‐ray; documented ileus with nausea, vomiting, no stool or inability to take oral intake |
| Gastrointestinal bleeding | Sudden appearance of frank blood on nasogastric lavage or by rectum AND a decrease in hemoglobin of 2 g/dL or greater with no other suspected source of ongoing blood loss |
| Infectious | |
| Pneumonia | New infiltrate on chest x‐ray plus 2 of the following 3 findings: temperature >38C, elevated white cell count, sputum pathogen that requires antibiotic treatment |
| Bacteremia/sepsis | Localized infection with positive blood culture for the same pathogen AND chills, rigors, fever, elevated white cell count AND intravenous antibiotic treatment |
| Urinary tract infection | Pyuria symptoms |
| Positive gram stain symptoms | |
| Wound | |
| Cellulitis | As documented in physician's note of a superficial skin infection |
| Neurologic | |
| Cerebral eventhypoxia, thrombosis or hemorrhage | New neurologic dysfunction (hemiplegia, hemianesthesia, hemianopia, aphasia, or unconsciousness) postoperatively |
| Transient ischemic attack | Any neurologic dysfunction resolving within a 24‐hour period |
| Delirium | Positive Confusion Assessment Method38 |
| Renal/metabolic | |
| Renal failure | A doubling of baseline value of creatinine; serum creatinine >3.0 mg/dL; acute need for dialysis |
| Dehydration | As documented in the physician's note |
| Electrolyte abnormalities | Any laboratory evidence of abnormal electrolytes compared to normal |
| Respiratory | |
| Respiratory failure | Need for intubation and ventilation >24 hours postoperatively; need for reintubation and ventilation after 1 hour postoperatively |
| Respiratory depression | Respiratory arrest; PaCO2 >60 mmHg that provider believed was associated with narcotics |
| Pulmonary hypoxemia | SaO2 <90% with or without supplemental oxygen; supplemental oxygen >24 hours |
| Vascular | |
| Deep vein thrombosis | Positive lower extremity venous Doppler |
| Pulmonary embolism | Acute onset dyspnea and tachycardia, increased central venous pressure AND (positive ventilation/perfusion scan OR positive computed tomography OR positive pulmonary angiogram) |
| Other | |
| Fractures | Any in‐hospital documented fracture of any bone |
| Falls | Patients descending to the ground from any position unintentionally |
Continuous data are presented as means standard deviation and categorical data as counts and percentages. In testing for differences in patient demographics, past medical history, and baseline clinical data among BMI groups, Kruskal‐Wallis tests were performed for continuous variables and Fisher's Exact or Cochran‐Mantel‐Haenszel tests were used for discrete variables. Bonferroni adjustments were performed where appropriate. The primary outcome was the risk of any noncardiac medical complication during the postoperative hospitalization, based on patients with complications. Incidence rates were calculated for the overall group as well as for each BMI category. BMI was evaluated categorically according to the WHO criteria, as a continuous variable dichotomized as a BMI 18.5 kg/m2 to 24.9 kg/m2 (normal) vs. all others, and above/below 25.0 kg/m2. The effect of BMI and other potential risk factors on the complication rate was evaluated using logistic regression. The effect of BMI category on the overall complication rate was adjusted for the a priori risk factors of age, sex, surgical year, and ASA class both univariately (Model 1) and multivariately (Model 2). In addition to these variables, we also evaluated other potential risk factors, including baseline demographic and baseline clinical variables that were significant (P < 0.05) univariately using a stepwise selection; first forcing in BMI as a categorical variable (Model 3), then repeating the stepwise selection process without forcing in BMI (Model 4). Using data from Lawrence et al.,19 we estimated that we would have 80% power to detect differences in rates of inpatient noncardiac complications equal to an odds ratio (OR) = 2.2 (normal vs. underweight), OR = 2.0 (normal vs. overweight), and OR = 2.4 (normal vs. obese). Finally, because of power considerations, as an exploratory analysis, we additionally identified predictors of inpatient complications within each BMI category using stepwise selection. All statistical tests were 2‐sided, and P values <0.05 were considered significant. All analyses were performed using SAS for UNIX (version 9.1.3; SAS Institute, Inc., Cary, NC).
Results
Between 1988 and 2002, 1195 urgent repairs for hip fracture met our inclusion/exclusion criteria. We subsequently excluded 15 repairs with missing BMI data, and, of the 7 patients with >1 repair, we included only their first fracture episode in our analysis. Two were subsequently excluded due to an administrative error. Ultimately, 1180 hip fracture repairs were included in the analysis cohort. There were 184 (15.6%) patients in the underweight group, 640 (54.2%) with normal BMI, 251 (21.3%) with a BMI 25.0 to 29.9 kg/m2, and 105 (8.9%) with a BMI 30 kg/m2. Baseline characteristics are otherwise shown in Table 2. Normal BMI patients were significantly older than the other groups, and underweight patients were less likely to be admitted from home. Past history of having a cardiovascular risk factor or a cardiovascular diagnosis appeared to increase with increasing BMI. Underweight patients were more likely to have chronic obstructive pulmonary disease (COPD) than patients with normal BMI (P = 0.03) or overweight patients (P = 0.009), but not more than obese patients (P = 0.21). There were no differences across BMI groups in ASA class, type of anesthesia, intensive care unit stay, or length of stay.
| Variable | Underweight (<18.5 kg/m2) n = 184 n (%) | Normal (18.5‐24.9 kg/m2) n = 640 n (%) | Overweight (25‐29.9 kg/m2) n = 251 n (%) | Obese (30 kg/m2) n = 105 n (%) | P Value* |
|---|---|---|---|---|---|
| |||||
| Age (years) | 84.8 8.0 | 85.0 7.2 | 83.1 7.3 | 80.7 7.4 | <0.001 |
| Female sex | 171 (92.9) | 525 (82) | 177 (70.5) | 76 (72.4) | <0.001 |
| Preadmission residence | |||||
| ALC/SNF | 79 (42.9) | 250 (39.1) | 83 (33.1) | 36 (34.3) | 0.024 |
| Home | 105 (57.1) | 390 (60.9) | 168 (66.9) | 69 (65.7) | |
| Functional status | |||||
| Dependent | 25 (13.6) | 80 (12.5) | 24 (9.6) | 7 (6.7) | 0.044 |
| Walking independently | 159 (86.4) | 560 (87.5) | 226 (90.4) | 97 (93.3) | |
| History of | |||||
| Hypertension | 84 (45.7) | 374 (58.4) | 159 (63.3) | 70 (66.7) | <0.001 |
| Diabetes | 9 (4.9) | 71 (11.1) | 30 (12) | 30 (28.6) | <0.001 |
| Cerebrovascular disease | 40 (21.7) | 175 (27.3) | 77 (30.7) | 33 (31.4) | 0.028 |
| Myocardial infarction | 44 (23.9) | 140 (21.9) | 61 (24.3) | 36 (34.3) | 0.106 |
| Congestive heart failure | 48 (26.1) | 150 (23.4) | 76 (30.3) | 44 (41.9) | 0.003 |
| Atrial fibrillation/flutter | 49 (26.6) | 118 (18.4) | 57 (22.7) | 26 (24.8) | 0.985 |
| Chronic renal insufficiency | 11 (6) | 64 (10) | 34 (13.5) | 20 (19) | <0.001 |
| Dementia | 63 (34.2) | 233 (36.4) | 74 (29.5) | 26 (24.8) | 0.031 |
| Obstructive sleep apnea | 2 (1.1) | 5 (0.8) | 5 (2.0) | 6 (5.7) | 0.005 |
| COPD | 41 (22.3) | 100 (15.6) | 32 (12.7) | 17 (16.2) | 0.032 |
| Asthma | 13 (7.1) | 47 (7.3) | 18 (7.2) | 12 (11.4) | 0.395 |
| COPD or asthma | 49 (26.6) | 133 (20.8) | 45 (17.9) | 23 (21.9) | 0.093 |
| Pulmonary embolism or deep vein thrombosis | 9 (4.9) | 21 (3.3) | 21 (8.4) | 17 (16.2) | <0.001 |
| Osteoporosis | 77 (41.8) | 253 (39.5) | 73 (29.1) | 31 (29.5) | <0.001 |
| Collagen vascular diseases | 10 (5.4) | 29 (4.5) | 9 (3.6) | 12 (11.4) | 0.34 |
| Cancer | 61 (33.2) | 169 (26.4) | 75 (29.9) | 32 (30.5) | 0.88 |
| Lymphoma | 2 (1.1) | 3 (0.5) | 2 (0.8) | 2 (1.9) | 0.25 |
| Leukemia | 2 (1.1) | 3 (0.5) | 1 (0.4) | 1 (1) | |
| Major surgery within 90 days | 3 (1.6) | 10 (1.6) | 8 (3.2) | 3 (2.9) | 0.366 |
| ASA class | |||||
| I or II | 19 (10.4) | 93 (14.5) | 46 (18.3) | 12 (11.4) | 0.144 |
| III, IV, or V | 164 (89.6) | 547 (85.5) | 205 (81.7) | 93 (88.6) | |
| Type of anesthesia | |||||
| General | 134 (72.8) | 477 (74.5) | 192 (76.5) | 84 (80) | |
| Other (spinal, epidural, local, combination) | 50 (27.2) | 163 (25.5) | 59 (23.5) | 21 (20) | 0.16 |
| Admission medications | |||||
| Insulin | 2 (1.1) | 18 (2.8) | 11 (4.4) | 17 (16.2) | <0.001 |
| Aspirin | 50 (27.2) | 197 (30.8) | 82 (32.7) | 37 (35.2) | 0.126 |
| Beta‐blockers | 18 (9.8) | 90 (14.1) | 50 (19.9) | 25 (23.8) | <0.001 |
| ACE/ARB | 32 (17.4) | 95 (14.8) | 55 (21.9) | 28 (26.7) | 0.009 |
| Calcium‐channel blocker | 26 (14.1) | 104 (16.3) | 39 (15.5) | 21 (20) | 0.38 |
| Intensive care unit stay | 63 (34.2) | 154 (24.1) | 61 (24.3) | 30 (28.6) | 0.16 |
| Length of stay, days | 10.3 (9.7) | 9.7 (6.8) | 10.2 (7.6) | 11.1 (8.6) | 0.10 |
| Discharge destination | |||||
| Home | 20 (10.9) | 65 (10.2) | 43 (17.1) | 19 (18.1) | |
| ALC/nursing home | 146 (79.8) | 547 (85.5) | 199 (79.3) | 83 (79) | <0.001 |
| In‐hospital death | 17 (9.3) | 28 (4.4) | 9 (3.6) | 3 (2.9) | |
There were 77 (41.8%) postoperative inpatient noncardiac complications in the underweight group, 234 (36.6%) in the normal BMI group, 90 (35.9%) in the overweight group, and 42 (40.0%) in the obese group (P = 0.49). Figure 1 demonstrates the main subcategory complication rates by BMI group, and Table 3 outlines the univariate unadjusted complication rates. Other than gastrointestinal complications being more prevalent as BMI increases (P = 0.005), there were no significant differences in crude complication rates across BMI categories (all P > 0.05) for the other complication subcategories. A multiple comparisons analysis did not demonstrate any differences between normal and any of the other BMI categories for ileus. Normal BMI patients were more likely to be discharged to a nursing facility than overweight or obese patients (85.5% vs. 79.3%, P = 0.03; and 85.5% vs. 79.0%, P = 0.03, respectively). The proportion of in‐hospital deaths among underweight patients was significantly higher than in any of the other groups (9.3% vs. 4.4%; P = 0.01), but mean length of stay was not significantly different.
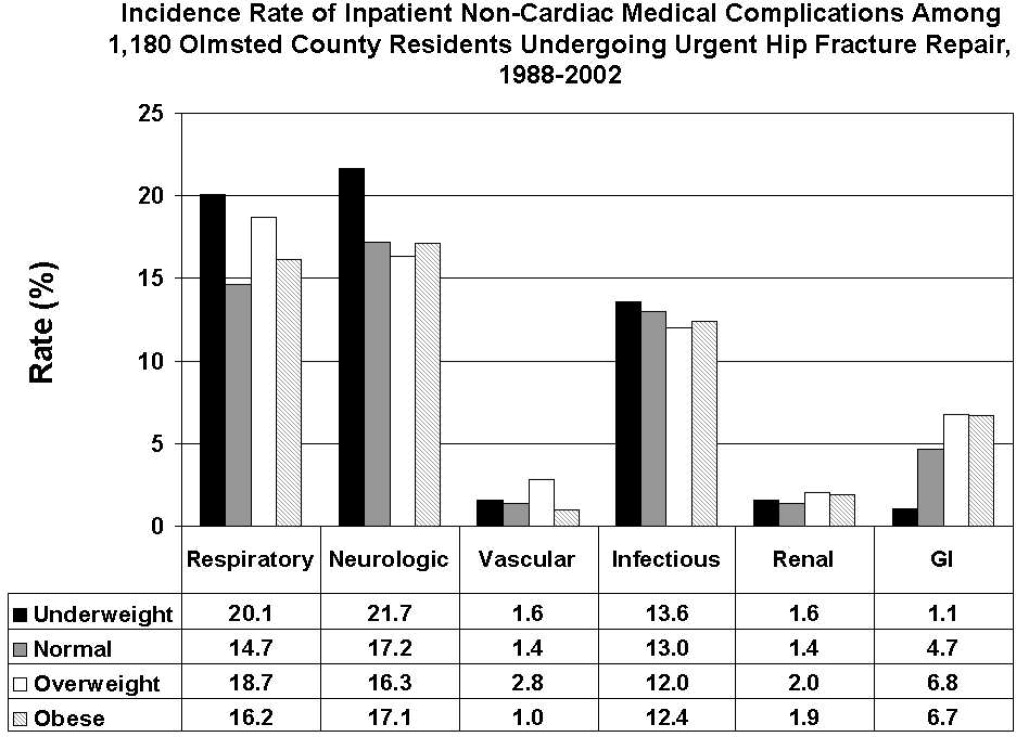
| Overall Cohort n (%) | Underweight (<18.5 kg/m2) n = 184 n (%) | Normal (18.5‐24.9 kg/m2) n = 640 n (%) | Overweight (25‐29.9 kg/m2) n = 251 n (%) | Obese (30 kg/m2) n = 105 n (%) | P Value | |
|---|---|---|---|---|---|---|
| ||||||
| Gastrointestinal | ||||||
| Ileus | 38 (3.2) | 1 (0.5) | 21 (3.3) | 12 (4.8) | 4 (3.8) | 0.03 |
| Gastrointestinal bleeding | 21 (1.8) | 1 (0.5) | 11 (1.7) | 6 (2.4) | 3 (2.9) | 0.35 |
| Infectious | ||||||
| Pneumonia | 69 (5.8) | 12 (6.5) | 39 (6.1) | 14 (5.6) | 4 (3.8) | 0.51 |
| Bacteremia/sepsis | 8 (0.7) | 1 (0.5) | 2 (0.3) | 5 (2.0) | 0 (0) | 0.06 |
| Urinary tract infection | 84 (7.1) | 12 (6.5) | 47 (7.3) | 15 (6) | 10 (9.5) | 0.78 |
| Wound | ||||||
| Cellulitis | ||||||
| Neurological | ||||||
| Cerebral event‐hypoxia, thrombosis or hemorrhage | 15 (1.3) | 1 (0.5) | 6 (0.9) | 6 (2.4) | 2 (1.9) | 0.21 |
| Transient ischemic attack | ||||||
| Delirium | 199 (16.9) | 40 (21.7) | 106 (16.6) | 36 (14.3) | 17 (16.2) | 0.08 |
| Renal/metabolic | ||||||
| Renal failure | 19 (1.6) | 3 (1.6) | 9 (1.4) | 5 (2.0) | 2 (1.9) | 0.82 |
| Dehydration | ||||||
| Electrolyte abnormalities | ||||||
| Respiratory | ||||||
| Respiratory failure | 53 (4.5) | 10 (5.4) | 23 (3.6) | 15 (6.0) | 5 (4.8) | 0.61 |
| Respiratory depression | 23 (1.9) | 3 (1.6) | 11 (1.7) | 8 (3.2) | 1 (1.0) | 0.50 |
| Pulmonary hypoxemia | 157 (13.3) | 33 (17.9) | 78 (12.2) | 34 (13.5) | 12 (11.4) | 0.22 |
| Vascular | ||||||
| Deep vein thrombosis | 5 (0.4) | 0 (0) | 2 (0.3) | 3 (1.2) | 0 (0) | 0.24 |
| Pulmonary embolism | 16 (1.4) | 3 (1.6) | 7 (1.1) | 5 (2.0) | 1 (1.0) | 0.65 |
| Other | ||||||
| Fractures | 6 (0.5) | 1 (0.5) | 5 (0.8) | 0 (0) | 0 (0) | 0.57 |
| Falls | ||||||
Significant univariate predictors of the composite outcome of any noncardiac complication included: age (OR, 1.04 95% confidence interval [CI>], 1.02‐1.06; P < 0.001), age 75 years (OR, 2.25; 95% CI, 1.52‐3.33; P < 0.001), age 85 years (OR, 1.49; 95% CI, 1.17‐1.89; P < 0.001), male sex (OR, 1.41; 95% CI, 1.05‐1.90; P = 0.02), admission from home (OR, 0.77; 95% CI, 0.61‐0.98; P = 0.03), a history of cerebrovascular disease (OR, 1.41; 95% CI, 1.08‐1.83; P = 0.01), myocardial infarction (OR, 1.41; 95% CI, 1.07‐1.86; P = 0.02), angina (OR, 1.32; 95% CI, 1.03‐1.69; P = 0.03), congestive heart failure (OR, 1.45; 95% CI, 1.11‐1.89; P = 0.006), dementia (OR, 1.39; 95% CI, 1.08‐1.78; P = 0.01), peripheral vascular disease (OR, 1.47; 95% CI, 1.06‐2.03; P = 0.02), COPD/asthma (OR, 1.56; 95% CI, 1.18‐2.08; P = 0.002), osteoarthritis (OR, 1.29; 95% CI, 1.01‐1.65; P = 0.04), code status as Do Not Resuscitate (OR, 0.74; 95% CI, 0.58‐0.94; P = 0.015), or ASA class III‐V (OR, 2.24; 95% CI, 1.53‐3.29; P < 0.001). Results were no different after using the Charlson comorbidity index in place of ASA class (data not shown). No significant differences in overall noncardiac complications were observed when examining BMI as a continuous variable, as a categorical variable, as 25 kg/m2 vs. <25 kg/m2, or as 18.5 kg/m2 to 24.9 kg/m2 vs. all others. Examining renal, respiratory, peripheral vascular, or neurologic complications univariately within these aforementioned strata also did not demonstrate any significant differences among BMI categories (data not shown).
Multivariable analyses (Models 1‐4) are shown for any overall noncardiac inpatient medical complication in Table 4. BMI was not a significant predictor in any of our models, specifically in our main model that examined the effect of BMI adjusting for a priori variables (Model 2). However, older age, male sex, and ASA class were highly significant predictors of complications in all four models; however, surgical year was nonsignificant. Notably, after stepwise selection for other demographic and premorbid variables, a history of COPD or asthma was found to be an additional significant factor both in Model 3 (forcing BMI in the model) and Model 4 (without BMI in the model). Exploratory analysis of individual predictors of inpatient noncardiac complications within each BMI category demonstrated that, in underweight patients, admission use of ‐blockers was a significant predictor of having any medical complication (OR, 3.1; 95% CI, 1.1‐8.60; P = 0.03). In normal BMI patients, age 75 years (OR, 2.6; 95% CI, 1.4‐4.9; P = 0.003), ASA class III‐V (OR, 2.3; 95% CI, 1.3‐3.9; P = 0.003), and a history of cerebrovascular disease (OR, 1.5; 95%CI, 1.04‐2.1; P = 0.03) were predictors; and, in obese patients, only age (OR, 1.1; 95% CI, 1.00‐1.12; P = 0.05) was significant. There were no significant predictors of having a medical complication in the overweight group.
| Underweight <18.5 kg/m2 n = 184* n (%) | Normal 18.5‐24.9 kg/m2 n = 640* n (%) | Overweight 25‐29.9 kg/m2 n = 251* n (%) | Obese 30 kg/m2 n = 105* n (%) | Age | Male Sex | Surgical Year | ASA Score, III‐V vs. I/II | COPD/ Asthma | |
|---|---|---|---|---|---|---|---|---|---|
| |||||||||
| Model 1a | 1.25 (0.89‐1.74) | Referent | 0.97 (0.72‐1.31) | 1.16 (0.76‐1.76) | |||||
| Model 1b | 1.26 (0.90‐1.77) | Referent | 1.05 (0.77‐1.43) | 1.38 (0.90‐2.13) | 1.04 (1.02‐1.06) | ||||
| Model 1c | 1.30 (0.93‐1.83) | Referent | 0.93 (0.68‐1.26) | 1.12 (0.73‐1.71) | 1.47 (1.09‐1.98) | ||||
| Model 1d | 1.28 (0.91‐1.79) | Referent | 0.97 (0.71‐1.31) | 1.13 (0.74‐1.73) | 1.03 (1.00‐1.06) | ||||
| Model 1e | 1.23 (0.88‐1.72) | Referent | 1.00 (0.73‐1.36) | 1.13 (0.74‐1.73) | 2.22 (1.52‐3.24) | ||||
| Model 2 | 1.33 (0.95‐1.88) | Referent | 1.01 (0.74‐1.38) | 1.28 (0.82‐1.98) | 1.04 (1.02‐1.06) | 1.59 (1.17‐2.17) | 1.02 (0.99‐1.05) | 1.89 (1.28‐2.79) | |
| Model 3∥ | 1.30 (0.92‐1.84) | Referent | 1.04 (0.76‐1.42) | 1.30 (0.84‐2.02) | 1.05 (1.03‐1.06) | 1.52 (1.11‐2.07) | 1.02 (0.99‐1.05) | 1.77 (1.20‐2.62) | 1.58 (1.17‐2.12) |
| Model 4 | 1.05 (1.03‐1.06) | 1.49 (1.10‐2.02) | 1.84 (1.25‐2.71) | 1.58 (1.18‐2.12) | |||||
Discussion
Most research describing the association of BMI with postoperative outcomes has concentrated on cardiac surgery, general surgical procedures, and intensive care unit utilization.8‐11,20 In the orthopedic literature, an elevated BMI has been associated with a higher number of short‐term complications, but this was limited to elective knee arthroplasty and spine surgery populations.12,13,21 Conversely, no differences were observed in obese patients undergoing hip arthroplasties.14,22 To the best of our knowledge, this study may be the first to examine the impact of BMI on inpatient hospital outcomes following urgent hip fracture repair. Our results suggest the risk of developing a noncardiac medical complication is the same regardless of BMI.
Our overall complication rate was higher (38%) than previous reports by others.19,23‐26 Thus, Lawrence et al.,19 in their retrospective study of 20 facilities, demonstrated an overall complication rate of 17%, even though they also included postoperative cardiac complications. Although their study period overlapped our own (1982‐1993), they additionally included patients aged 60 to 65 years, a population known to have fewer comorbidities and fewer postoperative complications than the elderly hip‐fracture patients studied here. In addition, their population may have been healthier at baseline, in that a higher proportion lived at home (73%) and a lower percentage were ASA class III‐V (71%) than our cohort. These differences in baseline characteristics may explain the higher complication rates observed in our study.
Our findings did not suggest any relationship of BMI with noncardiac postoperative medical complications in any of the 4 methods we used to stratify BMI (continuous, categorical, normal vs. abnormal, and 25 kg/m2). Evidence is contradictory as to what the effect of BMI has on postoperative complications. An elevated BMI (30 kg/m2) has been shown to lead to increased sternal wound infection and saphenous vein harvest infection in a cardiac surgery population,27 but other studies10,28,29 have demonstrated the opposite effect. Among 6336 patients undergoing elective general surgery procedures, the incidence of complications were similar by body mass.30 A matched study design that included urgent and emergent surgeries also did not find any appreciable increased perioperative risk in noncardiac surgery.28 Whether this may be due to the elective nature of the surgeries in these studies, hence leading to selection bias, is unknown.
In geriatric patients, multiple baseline comorbid conditions often are reflected in a higher ASA class, which increases the risk of significant perioperative complications. Our multivariate modeling showed that a high ASA class strongly predicts morbidity and mortality following hip fracture repair, in line with other studies.19,31,32 Although the Charlson comorbidity index could alternatively been used, we elected to adjust for ASA class as it is more commonly used and is simple to use. Interestingly, surgical year did not significantly predict any complication, which can suggest that practice changes play a minimal impact on patient outcomes. However, we caution that because the individual event rates, particularly vascular, were low, we were unable to fully determine whether changes in practice management, such as improved thromboprophylaxis, would impact event rates over time. Finally, other predictors such as older age33 and a concomitant history of either COPD or asthma,34 are well‐accepted predictors of inpatient complications. Our attempt to examine specific predictors of complications in each BMI category revealed differing results, making interpretations difficult. Because of power considerations, this was meant solely as an exploratory analysis, and larger cohorts are needed to further ascertain whether predictors are different in these groups. Such a study may in fact identify perioperative issues that allow practitioners caring for this population to modify these factors.
One of the major limitations in our study was our inability to adjust for individual complications using multivariable models, such as deep vein thrombosis or delirium, within each BMI stratum, because of statistical power issues. Such a study would require large numbers of individual complications or events to allow for appropriate adjustments. The authors acknowledge that such individual complication rates may vary dramatically. We were aware of this potential problem, and therefore a priori ascertained a composite outcome of any noncardiac medical complication. However, our results do provide preliminary information regarding the impact of BMI on noncardiac medical complications. Further studies would be needed, though, to fully determine the effect of BMI on the number of cases with each complication.
Obesity (or BMI) is a known cardiovascular risk factor, and our previous study's aim was to determine cardiovascular events in a comparable manner to the way risk indices, such as the Goldman, Lee, or the AHA preoperative algorithm function. The surgical literature often presents noncardiac complications separately, allowing us to directly compare our own data to other published studies. We used 2 separate approaches, focusing on the inpatient stay (ascertaining noncardiac complications) and 1‐year cardiac outcomes (cardiac complications), as these are mediated by different mechanisms and factors. Furthermore, the intent of both studies was to dispel any concerns that an elevated BMI would in fact lead to an increased number of complications. Whether cardiac complications, though, would impact noncardiac complications, or vice‐versa, is unknown, and would require further investigation.
Although we relied on well‐established definitions for body mass, they have often been challenged, as they may underestimate adiposity in the elderly population due to age‐related reductions in lean mass.35,36 Studies have demonstrated a poor correlation between percent body fat and BMI in the >65 year age group,37 which could impact our results and outcomes by misclassifying patients. Yet, as an anthropometric measurement, BMI is easily obtainable and its variables are routinely documented in patients' medical records, as compared to other anthropometric measurements. Other means of estimating adiposity, such as densitometry or computed tomography (CT) scanning, are impractical, expensive, and not used clinically but routinely in research settings. The lack of standardization in obtaining height and weight, despite nurse‐initiated protocols for bed calibration, may have introduced a degree of measurement bias. Furthermore, the extent of lean mass lost and volume status changes lead to further challenges of using BMI in hospital settings. Whether other anthropometric measurements, including hip circumference, waist circumference, or waist‐hip ratio, should be used in this group of patients requires further examination. However, despite its shortcomings in elderly patients, BMI is still deemed an appropriate surrogate for obesity.
Our main strength was the use of the Rochester Epidemiology Project medical record linkage system to ascertain all patient data. This focuses on patients from a single geographically‐defined community minimizing referral biases often observed in studies originating from a tertiary care referral center. Previous disease‐related epidemiology studies using the Olmsted County population have demonstrated excellent external validity to the U.S. white population.16 We relied on the medical documentation of the treating clinician for many diagnoses in our data abstraction. Although we attempted to use standardized definitions, clinicians may have inadvertently forgotten to document subjective signs or symptoms that would assist in the categorization of these complications. Hence, added inpatient complications may have been overlooked, suggesting that our results may slightly underestimate the true incidence in this population. Additionally, certain complications may overlap categories, such as pneumonia and infections. We agree with Lawrence et al.19 that long periods of time are necessary to accumulate data of this kind in an effort to describe complication rates epidemiologically.
Despite no difference in outcomes among BMI categories, our results have striking implications for the hospitalized patient. Thus, underweight elderly patients, often considered frail with minimal functional reserve, are at no higher risk for developing inpatient medical complications than patients with higher BMIs. This is contrary to our study focusing on cardiac complications, where underweight patients were at higher risk.15 Conversely, obese patients, who have been demonstrated to be at higher risk of medical complications (particularly pulmonary), had no greater risk than patients with normal BMI. To the practicing geriatrician and hospitalist, this information provides important prognostication regarding additional perioperative measures that need to be implemented in these different groups. Based on our results, BMI does not play a particular role in noncardiac medical complications, dispelling any myths of the added burden of excess weight on surgical outcomes in this population. From a hospital perspective, this may be important since additional testing or preventative management in these patients may lead to additional resource use. However, in‐hospital deaths were higher in underweight patients than in patients with a normal BMI. Although we were underpowered to detect any differences in mortality between groups and could therefore not adjust for additional variables, it is unknown whether cardiac or noncardiac complications may be a stronger predictor of death in the underweight patient population. Further studies would be needed to better ascertain this relationship.
Conclusions
In elderly patients undergoing urgent hip fracture repair, BMI does not appear to lead to an excess rate of inpatient noncardiac complications. Our results are the first to demonstrate that BMI has no impact on morbidity in this patient population. Further research on the influence of body composition on inpatient complications in this population is needed to accurately allow for appropriate perioperative prophylaxis. Whether BMI impacts specific complications or in‐patient mortality in this population still requires investigation.
Acknowledgements
The authors thank Donna K. Lawson, LPN, Kathy Wolfert, and Cherie Dolliver, for their assistance in data collection and management.
- , .The effect of longevity on spending for acute and long‐term care.N Engl J Med.2000;342(19):1409–1415.
- , , , .Excess deaths associated with underweight, overweight, and obesity.JAMA.2005;293(15):1861–1867.
- .Adverse outcomes of osteoporotic fractures in the general population.J Bone Miner Res.2003;18(6):1139–1141.
- , , , , , .Incidence and economic burden of osteoporosis‐related fractures in the United States, 2005–2025.J Bone Miner Res.2007;22(3):465–475.
- , .Medical care of elderly patients with hip fractures.Mayo Clin Proc.2001;76(3):295–298.
- , , , et al.Effects of a hospitalist model on elderly patients with hip fracture.Arch Intern Med.2005;165(7):796–801.
- , , , et al.Body mass index as a predictor of fracture risk: a meta‐analysis.Osteoporos Int.2005;16(11):1330–1338.
- , , , , .Increased body mass index predicts increased blood loss during radical cystectomy.J Urol.2004;171(3):1077–1079.
- , , , .Laparoscopic colorectal surgery in obese and nonobese patients: do differences in body mass indices lead to different outcomes?Surg Endosc.2004;18(10):1452–1456.
- , , , , , .The relationship of body mass index to outcomes after percutaneous coronary intervention.J Interv Cardiol.2006;19(5):388–395.
- , , , , , .Is extreme obesity a risk factor for cardiac surgery? An analysis of patients with a BMI ≥40.Eur J Cardiothorac Surg.2006;29(4):434–440.
- , , , , , .Perioperative morbidity following total knee arthroplasty among obese patients.J Knee Surg.2002;15(2):77–83.
- , , , et al.Obesity and spine surgery: relation to perioperative complications.J Neurosurg Spine.2007;6(4):291–297.
- , , , .The influence of obesity on perioperative morbidity and mortality in revision total hip arthroplasty.Arch Orthop Trauma Surg.2000;120(5–6):267–271.
- , , , et al.Body mass index and risk of adverse cardiac events in elderly hip fracture patients: a population‐based study.J Am Geriatr Soc.2009;57(3):419–426.
- .History of the Rochester Epidemiology Project.Mayo Clin Proc.1996;71(3):266–274.
- .The threat to medical‐records research.N Engl J Med.1997;337(20):1466–170.
- .A Treatise on Man and the Development of His Faculties.Brussels:Musquardt;1871.
- , , , , .Medical complications and outcomes after hip fracture repair.Arch Intern Med.2002;162(18):2053–2057.
- , , .Effect of obesity on intensive care morbidity and mortality: a meta‐analysis.Crit Care Med.2008;36(1):151–158.
- , .Relationship of body mass index to early complications in knee replacement surgery.Arch Orthop Trauma Surg.2008;128(1):5–9.
- , , , , , .Obesity in total hip replacement.J Bone Joint Surg Br.2008;90(4):424–429.
- , , , et al.Use of an intramedullary hip‐screw compared with a compression hip‐screw with a plate for intertrochanteric femoral fractures. A prospective, randomized study of one hundred patients.J Bone Joint Surg Am.1998;80(5):618–630.
- .Blood transfusion requirements in intracapsular femoral neck fractures.Injury.1996;27(10):709–711.
- , , , .Risk prediction in operatively treated fractures of the hip.Clin Orthop Relat Res.1993(293):148–152.
- .Internal fixation or arthroplasty for displaced subcapital fractures in the elderly?Injury.1992;23(8):521–524.
- , , , et al.Impact of body mass index and albumin on morbidity and mortality after cardiac surgery.J Thorac Cardiovasc Surg.1999;118(5):866–873.
- , , , et al.Increased body mass index and peri‐operative risk in patients undergoing non‐cardiac surgery.Obes Surg.2004;14(2):275–281.
- , , , et al.Effects of body size on operative, intermediate, and long‐term outcomes after coronary artery bypass operation.Ann Thorac Surg.2001;71(2):521–530; discussion 530–531.
- , , , .Obesity in general elective surgery.Lancet.2003;361(9374):2032–2035.
- , , , et al.Effects of a hospitalist care model on mortality of elderly patients with hip fractures.J Hosp Med.2007;2(4):219–225.
- , , , .Morbidity and mortality after hip fracture: the impact of operative delay.Arch Orthop Trauma Surg.2004;124(5):334–340.
- , , , , .Outcome after hip fracture in individuals ninety years of age and older.J Orthop Trauma.2001;15(1):34–39.
- , , , et al.Development and initial validation of a risk score for predicting in‐hospital and 1‐year mortality in patients with hip fractures.J Bone Miner Res.2005;20(3):494–500.
- , , , , , .How useful is body mass index for comparison of body fatness across age, sex, and ethnic groups?Am J Epidemiol.1996;143(3):228–239.
- , , , , .Reassessment of body mass indices.Am J Clin Nutr.1990;52(3):405–408.
- , , , et al.Accuracy of body mass index in diagnosing obesity in the adult general population.Int J Obes (Lond).2008;32(6):959–966.
- , , , , , .Clarifying confusion: the confusion assessment method. A new method for detection of delirium.Ann Intern Med.1990;113(12):941–948.
Public health concerns such as the aging population1 and the increasing prevalence of obesity2 are also important issues to hospitals. However, little attention has been given to the interface of obesity and the elderly, largely due to the dearth of studies that include elderly patients. An aging population leads to an increase in geriatric syndromes, such as osteoporosis3 and its most devastating complication, hip fracture.4 These frail, hip‐fracture patients pose management challenges to practicing geriatricians and hospitalists.5,6 Furthermore, although fracture risk is inversely correlated to body mass index (BMI),7 this relationship has yet to be fully examined in the postoperative hip‐fracture population. In other surgical settings, there is disagreement as to whether underweight or obese patients are at higher risk of developing medical complications,8‐11 but for orthopedic patients, data have been limited to elective orthopedic populations.12‐14 We previously demonstrated that underweight hip‐fracture patients are at higher risk of postoperative cardiac complications at 1 year,15 consistent with studies of cardiac risk indices determining long‐term events. Because of different pathophysiologic mechanisms, the purpose of this study was to ascertain the influence of BMI on inpatient postoperative noncardiac medical complications and to assess predictors of such complications following urgent hip fracture repair.
Patients and Methods
All Olmsted County, Minnesota, residents undergoing urgent hip repair due to fracture were identified using the Rochester Epidemiology Project, a medical‐record linkage system funded by the Federal government since 1966 to support disease‐related epidemiology studies.16 All patient medical care is indexed, and both inpatient and outpatient visits are captured and available for review, allowing for complete case ascertainment. Medical care in Olmsted County is primarily provided by Mayo Clinic with its affiliated hospitals (St. Mary's and Rochester Methodist) and the Olmsted Medical Center, in addition to a few individual providers. Over 95% of all Olmsted County hip fracture surgeries are ultimately managed at St. Mary's Hospital.
Following approval by the Institutional Review Board we used this unique data resource to identify all residents with an International Classification of Diseases, 9th edition (ICD‐9) diagnosis code of 820 to 829 for hip fracture (n = 1310). Both sexes were included, and all patients included in the study provided research authorization for use of their medical records for research purposes.17 We excluded patients who were managed conservatively (n = 56), had a pathological fracture (n = 20), had multiple injuries (n = 19), were operated on >72 hours after fracture (n = 5), were aged <65 years (n = 2), or were admitted for reasons other than a fracture and experienced an in‐hospital fracture (n = 3). We subsequently excluded patients with missing information (n = 10). World Health Organization (WHO) criteria were used for classifying BMI: underweight (BMI < 18.5); normal (BMI = 18.5‐24.9); overweight (BMI = 25.0‐29.9); and obese (BMI 30.0).18
All data were abstracted using standardized collection forms by trained nurse abstractors blinded to the study hypothesis. Patients' admission height and weight were documented; if unavailable, the nearest data within 2 months prior to surgery were recorded. Patients' preadmission residence, functional status, baseline comorbidities, admission medications, discharge destination, as well as whether patients had an intensive care unit stay or any major surgeries in the past 90 days were abstracted. In addition, American Society of Anesthesia (ASA) class, type of anesthesia, and length of stay were also obtained. Inpatient complications that had been identified by the treating physicians and documented in the medical record or identified on imaging studies were assessed from the time of hip fracture repair to the time of discharge using standardized clinical criteria (Table 1). For criteria that were based on either objective findings or clinical documentation/suspicion, the patient was considered to meet the criteria of having a complication if they fulfilled either one. We did not include any cardiac outcomes, including congestive heart failure, angina, myocardial infarction, or arrhythmias that had been previously reported.15 Noncardiac complications were classified broadly: respiratory (respiratory failure, respiratory depression, or pulmonary hypoxemia); neurologic (any cerebral event including hemorrhagic or ischemic stroke, transient ischemic attack, or delirium); gastrointestinal (ileus or gastrointestinal bleeding); vascular (pulmonary embolus, or deep vein thrombosis); infectious (pneumonia, sepsis, urinary tract, wound, or cellulitis); renal/metabolic (acute renal failure, dehydration, or electrolyte abnormalities); or other (fractures or falls).
| Definition | Symptom |
|---|---|
| |
| Gastrointestinal | |
| Ileus | Dilated loops of bowel on X‐ray; documented ileus with nausea, vomiting, no stool or inability to take oral intake |
| Gastrointestinal bleeding | Sudden appearance of frank blood on nasogastric lavage or by rectum AND a decrease in hemoglobin of 2 g/dL or greater with no other suspected source of ongoing blood loss |
| Infectious | |
| Pneumonia | New infiltrate on chest x‐ray plus 2 of the following 3 findings: temperature >38C, elevated white cell count, sputum pathogen that requires antibiotic treatment |
| Bacteremia/sepsis | Localized infection with positive blood culture for the same pathogen AND chills, rigors, fever, elevated white cell count AND intravenous antibiotic treatment |
| Urinary tract infection | Pyuria symptoms |
| Positive gram stain symptoms | |
| Wound | |
| Cellulitis | As documented in physician's note of a superficial skin infection |
| Neurologic | |
| Cerebral eventhypoxia, thrombosis or hemorrhage | New neurologic dysfunction (hemiplegia, hemianesthesia, hemianopia, aphasia, or unconsciousness) postoperatively |
| Transient ischemic attack | Any neurologic dysfunction resolving within a 24‐hour period |
| Delirium | Positive Confusion Assessment Method38 |
| Renal/metabolic | |
| Renal failure | A doubling of baseline value of creatinine; serum creatinine >3.0 mg/dL; acute need for dialysis |
| Dehydration | As documented in the physician's note |
| Electrolyte abnormalities | Any laboratory evidence of abnormal electrolytes compared to normal |
| Respiratory | |
| Respiratory failure | Need for intubation and ventilation >24 hours postoperatively; need for reintubation and ventilation after 1 hour postoperatively |
| Respiratory depression | Respiratory arrest; PaCO2 >60 mmHg that provider believed was associated with narcotics |
| Pulmonary hypoxemia | SaO2 <90% with or without supplemental oxygen; supplemental oxygen >24 hours |
| Vascular | |
| Deep vein thrombosis | Positive lower extremity venous Doppler |
| Pulmonary embolism | Acute onset dyspnea and tachycardia, increased central venous pressure AND (positive ventilation/perfusion scan OR positive computed tomography OR positive pulmonary angiogram) |
| Other | |
| Fractures | Any in‐hospital documented fracture of any bone |
| Falls | Patients descending to the ground from any position unintentionally |
Continuous data are presented as means standard deviation and categorical data as counts and percentages. In testing for differences in patient demographics, past medical history, and baseline clinical data among BMI groups, Kruskal‐Wallis tests were performed for continuous variables and Fisher's Exact or Cochran‐Mantel‐Haenszel tests were used for discrete variables. Bonferroni adjustments were performed where appropriate. The primary outcome was the risk of any noncardiac medical complication during the postoperative hospitalization, based on patients with complications. Incidence rates were calculated for the overall group as well as for each BMI category. BMI was evaluated categorically according to the WHO criteria, as a continuous variable dichotomized as a BMI 18.5 kg/m2 to 24.9 kg/m2 (normal) vs. all others, and above/below 25.0 kg/m2. The effect of BMI and other potential risk factors on the complication rate was evaluated using logistic regression. The effect of BMI category on the overall complication rate was adjusted for the a priori risk factors of age, sex, surgical year, and ASA class both univariately (Model 1) and multivariately (Model 2). In addition to these variables, we also evaluated other potential risk factors, including baseline demographic and baseline clinical variables that were significant (P < 0.05) univariately using a stepwise selection; first forcing in BMI as a categorical variable (Model 3), then repeating the stepwise selection process without forcing in BMI (Model 4). Using data from Lawrence et al.,19 we estimated that we would have 80% power to detect differences in rates of inpatient noncardiac complications equal to an odds ratio (OR) = 2.2 (normal vs. underweight), OR = 2.0 (normal vs. overweight), and OR = 2.4 (normal vs. obese). Finally, because of power considerations, as an exploratory analysis, we additionally identified predictors of inpatient complications within each BMI category using stepwise selection. All statistical tests were 2‐sided, and P values <0.05 were considered significant. All analyses were performed using SAS for UNIX (version 9.1.3; SAS Institute, Inc., Cary, NC).
Results
Between 1988 and 2002, 1195 urgent repairs for hip fracture met our inclusion/exclusion criteria. We subsequently excluded 15 repairs with missing BMI data, and, of the 7 patients with >1 repair, we included only their first fracture episode in our analysis. Two were subsequently excluded due to an administrative error. Ultimately, 1180 hip fracture repairs were included in the analysis cohort. There were 184 (15.6%) patients in the underweight group, 640 (54.2%) with normal BMI, 251 (21.3%) with a BMI 25.0 to 29.9 kg/m2, and 105 (8.9%) with a BMI 30 kg/m2. Baseline characteristics are otherwise shown in Table 2. Normal BMI patients were significantly older than the other groups, and underweight patients were less likely to be admitted from home. Past history of having a cardiovascular risk factor or a cardiovascular diagnosis appeared to increase with increasing BMI. Underweight patients were more likely to have chronic obstructive pulmonary disease (COPD) than patients with normal BMI (P = 0.03) or overweight patients (P = 0.009), but not more than obese patients (P = 0.21). There were no differences across BMI groups in ASA class, type of anesthesia, intensive care unit stay, or length of stay.
| Variable | Underweight (<18.5 kg/m2) n = 184 n (%) | Normal (18.5‐24.9 kg/m2) n = 640 n (%) | Overweight (25‐29.9 kg/m2) n = 251 n (%) | Obese (30 kg/m2) n = 105 n (%) | P Value* |
|---|---|---|---|---|---|
| |||||
| Age (years) | 84.8 8.0 | 85.0 7.2 | 83.1 7.3 | 80.7 7.4 | <0.001 |
| Female sex | 171 (92.9) | 525 (82) | 177 (70.5) | 76 (72.4) | <0.001 |
| Preadmission residence | |||||
| ALC/SNF | 79 (42.9) | 250 (39.1) | 83 (33.1) | 36 (34.3) | 0.024 |
| Home | 105 (57.1) | 390 (60.9) | 168 (66.9) | 69 (65.7) | |
| Functional status | |||||
| Dependent | 25 (13.6) | 80 (12.5) | 24 (9.6) | 7 (6.7) | 0.044 |
| Walking independently | 159 (86.4) | 560 (87.5) | 226 (90.4) | 97 (93.3) | |
| History of | |||||
| Hypertension | 84 (45.7) | 374 (58.4) | 159 (63.3) | 70 (66.7) | <0.001 |
| Diabetes | 9 (4.9) | 71 (11.1) | 30 (12) | 30 (28.6) | <0.001 |
| Cerebrovascular disease | 40 (21.7) | 175 (27.3) | 77 (30.7) | 33 (31.4) | 0.028 |
| Myocardial infarction | 44 (23.9) | 140 (21.9) | 61 (24.3) | 36 (34.3) | 0.106 |
| Congestive heart failure | 48 (26.1) | 150 (23.4) | 76 (30.3) | 44 (41.9) | 0.003 |
| Atrial fibrillation/flutter | 49 (26.6) | 118 (18.4) | 57 (22.7) | 26 (24.8) | 0.985 |
| Chronic renal insufficiency | 11 (6) | 64 (10) | 34 (13.5) | 20 (19) | <0.001 |
| Dementia | 63 (34.2) | 233 (36.4) | 74 (29.5) | 26 (24.8) | 0.031 |
| Obstructive sleep apnea | 2 (1.1) | 5 (0.8) | 5 (2.0) | 6 (5.7) | 0.005 |
| COPD | 41 (22.3) | 100 (15.6) | 32 (12.7) | 17 (16.2) | 0.032 |
| Asthma | 13 (7.1) | 47 (7.3) | 18 (7.2) | 12 (11.4) | 0.395 |
| COPD or asthma | 49 (26.6) | 133 (20.8) | 45 (17.9) | 23 (21.9) | 0.093 |
| Pulmonary embolism or deep vein thrombosis | 9 (4.9) | 21 (3.3) | 21 (8.4) | 17 (16.2) | <0.001 |
| Osteoporosis | 77 (41.8) | 253 (39.5) | 73 (29.1) | 31 (29.5) | <0.001 |
| Collagen vascular diseases | 10 (5.4) | 29 (4.5) | 9 (3.6) | 12 (11.4) | 0.34 |
| Cancer | 61 (33.2) | 169 (26.4) | 75 (29.9) | 32 (30.5) | 0.88 |
| Lymphoma | 2 (1.1) | 3 (0.5) | 2 (0.8) | 2 (1.9) | 0.25 |
| Leukemia | 2 (1.1) | 3 (0.5) | 1 (0.4) | 1 (1) | |
| Major surgery within 90 days | 3 (1.6) | 10 (1.6) | 8 (3.2) | 3 (2.9) | 0.366 |
| ASA class | |||||
| I or II | 19 (10.4) | 93 (14.5) | 46 (18.3) | 12 (11.4) | 0.144 |
| III, IV, or V | 164 (89.6) | 547 (85.5) | 205 (81.7) | 93 (88.6) | |
| Type of anesthesia | |||||
| General | 134 (72.8) | 477 (74.5) | 192 (76.5) | 84 (80) | |
| Other (spinal, epidural, local, combination) | 50 (27.2) | 163 (25.5) | 59 (23.5) | 21 (20) | 0.16 |
| Admission medications | |||||
| Insulin | 2 (1.1) | 18 (2.8) | 11 (4.4) | 17 (16.2) | <0.001 |
| Aspirin | 50 (27.2) | 197 (30.8) | 82 (32.7) | 37 (35.2) | 0.126 |
| Beta‐blockers | 18 (9.8) | 90 (14.1) | 50 (19.9) | 25 (23.8) | <0.001 |
| ACE/ARB | 32 (17.4) | 95 (14.8) | 55 (21.9) | 28 (26.7) | 0.009 |
| Calcium‐channel blocker | 26 (14.1) | 104 (16.3) | 39 (15.5) | 21 (20) | 0.38 |
| Intensive care unit stay | 63 (34.2) | 154 (24.1) | 61 (24.3) | 30 (28.6) | 0.16 |
| Length of stay, days | 10.3 (9.7) | 9.7 (6.8) | 10.2 (7.6) | 11.1 (8.6) | 0.10 |
| Discharge destination | |||||
| Home | 20 (10.9) | 65 (10.2) | 43 (17.1) | 19 (18.1) | |
| ALC/nursing home | 146 (79.8) | 547 (85.5) | 199 (79.3) | 83 (79) | <0.001 |
| In‐hospital death | 17 (9.3) | 28 (4.4) | 9 (3.6) | 3 (2.9) | |
There were 77 (41.8%) postoperative inpatient noncardiac complications in the underweight group, 234 (36.6%) in the normal BMI group, 90 (35.9%) in the overweight group, and 42 (40.0%) in the obese group (P = 0.49). Figure 1 demonstrates the main subcategory complication rates by BMI group, and Table 3 outlines the univariate unadjusted complication rates. Other than gastrointestinal complications being more prevalent as BMI increases (P = 0.005), there were no significant differences in crude complication rates across BMI categories (all P > 0.05) for the other complication subcategories. A multiple comparisons analysis did not demonstrate any differences between normal and any of the other BMI categories for ileus. Normal BMI patients were more likely to be discharged to a nursing facility than overweight or obese patients (85.5% vs. 79.3%, P = 0.03; and 85.5% vs. 79.0%, P = 0.03, respectively). The proportion of in‐hospital deaths among underweight patients was significantly higher than in any of the other groups (9.3% vs. 4.4%; P = 0.01), but mean length of stay was not significantly different.
| Overall Cohort n (%) | Underweight (<18.5 kg/m2) n = 184 n (%) | Normal (18.5‐24.9 kg/m2) n = 640 n (%) | Overweight (25‐29.9 kg/m2) n = 251 n (%) | Obese (30 kg/m2) n = 105 n (%) | P Value | |
|---|---|---|---|---|---|---|
| ||||||
| Gastrointestinal | ||||||
| Ileus | 38 (3.2) | 1 (0.5) | 21 (3.3) | 12 (4.8) | 4 (3.8) | 0.03 |
| Gastrointestinal bleeding | 21 (1.8) | 1 (0.5) | 11 (1.7) | 6 (2.4) | 3 (2.9) | 0.35 |
| Infectious | ||||||
| Pneumonia | 69 (5.8) | 12 (6.5) | 39 (6.1) | 14 (5.6) | 4 (3.8) | 0.51 |
| Bacteremia/sepsis | 8 (0.7) | 1 (0.5) | 2 (0.3) | 5 (2.0) | 0 (0) | 0.06 |
| Urinary tract infection | 84 (7.1) | 12 (6.5) | 47 (7.3) | 15 (6) | 10 (9.5) | 0.78 |
| Wound | ||||||
| Cellulitis | ||||||
| Neurological | ||||||
| Cerebral event‐hypoxia, thrombosis or hemorrhage | 15 (1.3) | 1 (0.5) | 6 (0.9) | 6 (2.4) | 2 (1.9) | 0.21 |
| Transient ischemic attack | ||||||
| Delirium | 199 (16.9) | 40 (21.7) | 106 (16.6) | 36 (14.3) | 17 (16.2) | 0.08 |
| Renal/metabolic | ||||||
| Renal failure | 19 (1.6) | 3 (1.6) | 9 (1.4) | 5 (2.0) | 2 (1.9) | 0.82 |
| Dehydration | ||||||
| Electrolyte abnormalities | ||||||
| Respiratory | ||||||
| Respiratory failure | 53 (4.5) | 10 (5.4) | 23 (3.6) | 15 (6.0) | 5 (4.8) | 0.61 |
| Respiratory depression | 23 (1.9) | 3 (1.6) | 11 (1.7) | 8 (3.2) | 1 (1.0) | 0.50 |
| Pulmonary hypoxemia | 157 (13.3) | 33 (17.9) | 78 (12.2) | 34 (13.5) | 12 (11.4) | 0.22 |
| Vascular | ||||||
| Deep vein thrombosis | 5 (0.4) | 0 (0) | 2 (0.3) | 3 (1.2) | 0 (0) | 0.24 |
| Pulmonary embolism | 16 (1.4) | 3 (1.6) | 7 (1.1) | 5 (2.0) | 1 (1.0) | 0.65 |
| Other | ||||||
| Fractures | 6 (0.5) | 1 (0.5) | 5 (0.8) | 0 (0) | 0 (0) | 0.57 |
| Falls | ||||||
Significant univariate predictors of the composite outcome of any noncardiac complication included: age (OR, 1.04 95% confidence interval [CI>], 1.02‐1.06; P < 0.001), age 75 years (OR, 2.25; 95% CI, 1.52‐3.33; P < 0.001), age 85 years (OR, 1.49; 95% CI, 1.17‐1.89; P < 0.001), male sex (OR, 1.41; 95% CI, 1.05‐1.90; P = 0.02), admission from home (OR, 0.77; 95% CI, 0.61‐0.98; P = 0.03), a history of cerebrovascular disease (OR, 1.41; 95% CI, 1.08‐1.83; P = 0.01), myocardial infarction (OR, 1.41; 95% CI, 1.07‐1.86; P = 0.02), angina (OR, 1.32; 95% CI, 1.03‐1.69; P = 0.03), congestive heart failure (OR, 1.45; 95% CI, 1.11‐1.89; P = 0.006), dementia (OR, 1.39; 95% CI, 1.08‐1.78; P = 0.01), peripheral vascular disease (OR, 1.47; 95% CI, 1.06‐2.03; P = 0.02), COPD/asthma (OR, 1.56; 95% CI, 1.18‐2.08; P = 0.002), osteoarthritis (OR, 1.29; 95% CI, 1.01‐1.65; P = 0.04), code status as Do Not Resuscitate (OR, 0.74; 95% CI, 0.58‐0.94; P = 0.015), or ASA class III‐V (OR, 2.24; 95% CI, 1.53‐3.29; P < 0.001). Results were no different after using the Charlson comorbidity index in place of ASA class (data not shown). No significant differences in overall noncardiac complications were observed when examining BMI as a continuous variable, as a categorical variable, as 25 kg/m2 vs. <25 kg/m2, or as 18.5 kg/m2 to 24.9 kg/m2 vs. all others. Examining renal, respiratory, peripheral vascular, or neurologic complications univariately within these aforementioned strata also did not demonstrate any significant differences among BMI categories (data not shown).
Multivariable analyses (Models 1‐4) are shown for any overall noncardiac inpatient medical complication in Table 4. BMI was not a significant predictor in any of our models, specifically in our main model that examined the effect of BMI adjusting for a priori variables (Model 2). However, older age, male sex, and ASA class were highly significant predictors of complications in all four models; however, surgical year was nonsignificant. Notably, after stepwise selection for other demographic and premorbid variables, a history of COPD or asthma was found to be an additional significant factor both in Model 3 (forcing BMI in the model) and Model 4 (without BMI in the model). Exploratory analysis of individual predictors of inpatient noncardiac complications within each BMI category demonstrated that, in underweight patients, admission use of ‐blockers was a significant predictor of having any medical complication (OR, 3.1; 95% CI, 1.1‐8.60; P = 0.03). In normal BMI patients, age 75 years (OR, 2.6; 95% CI, 1.4‐4.9; P = 0.003), ASA class III‐V (OR, 2.3; 95% CI, 1.3‐3.9; P = 0.003), and a history of cerebrovascular disease (OR, 1.5; 95%CI, 1.04‐2.1; P = 0.03) were predictors; and, in obese patients, only age (OR, 1.1; 95% CI, 1.00‐1.12; P = 0.05) was significant. There were no significant predictors of having a medical complication in the overweight group.
| Underweight <18.5 kg/m2 n = 184* n (%) | Normal 18.5‐24.9 kg/m2 n = 640* n (%) | Overweight 25‐29.9 kg/m2 n = 251* n (%) | Obese 30 kg/m2 n = 105* n (%) | Age | Male Sex | Surgical Year | ASA Score, III‐V vs. I/II | COPD/ Asthma | |
|---|---|---|---|---|---|---|---|---|---|
| |||||||||
| Model 1a | 1.25 (0.89‐1.74) | Referent | 0.97 (0.72‐1.31) | 1.16 (0.76‐1.76) | |||||
| Model 1b | 1.26 (0.90‐1.77) | Referent | 1.05 (0.77‐1.43) | 1.38 (0.90‐2.13) | 1.04 (1.02‐1.06) | ||||
| Model 1c | 1.30 (0.93‐1.83) | Referent | 0.93 (0.68‐1.26) | 1.12 (0.73‐1.71) | 1.47 (1.09‐1.98) | ||||
| Model 1d | 1.28 (0.91‐1.79) | Referent | 0.97 (0.71‐1.31) | 1.13 (0.74‐1.73) | 1.03 (1.00‐1.06) | ||||
| Model 1e | 1.23 (0.88‐1.72) | Referent | 1.00 (0.73‐1.36) | 1.13 (0.74‐1.73) | 2.22 (1.52‐3.24) | ||||
| Model 2 | 1.33 (0.95‐1.88) | Referent | 1.01 (0.74‐1.38) | 1.28 (0.82‐1.98) | 1.04 (1.02‐1.06) | 1.59 (1.17‐2.17) | 1.02 (0.99‐1.05) | 1.89 (1.28‐2.79) | |
| Model 3∥ | 1.30 (0.92‐1.84) | Referent | 1.04 (0.76‐1.42) | 1.30 (0.84‐2.02) | 1.05 (1.03‐1.06) | 1.52 (1.11‐2.07) | 1.02 (0.99‐1.05) | 1.77 (1.20‐2.62) | 1.58 (1.17‐2.12) |
| Model 4 | 1.05 (1.03‐1.06) | 1.49 (1.10‐2.02) | 1.84 (1.25‐2.71) | 1.58 (1.18‐2.12) | |||||
Discussion
Most research describing the association of BMI with postoperative outcomes has concentrated on cardiac surgery, general surgical procedures, and intensive care unit utilization.8‐11,20 In the orthopedic literature, an elevated BMI has been associated with a higher number of short‐term complications, but this was limited to elective knee arthroplasty and spine surgery populations.12,13,21 Conversely, no differences were observed in obese patients undergoing hip arthroplasties.14,22 To the best of our knowledge, this study may be the first to examine the impact of BMI on inpatient hospital outcomes following urgent hip fracture repair. Our results suggest the risk of developing a noncardiac medical complication is the same regardless of BMI.
Our overall complication rate was higher (38%) than previous reports by others.19,23‐26 Thus, Lawrence et al.,19 in their retrospective study of 20 facilities, demonstrated an overall complication rate of 17%, even though they also included postoperative cardiac complications. Although their study period overlapped our own (1982‐1993), they additionally included patients aged 60 to 65 years, a population known to have fewer comorbidities and fewer postoperative complications than the elderly hip‐fracture patients studied here. In addition, their population may have been healthier at baseline, in that a higher proportion lived at home (73%) and a lower percentage were ASA class III‐V (71%) than our cohort. These differences in baseline characteristics may explain the higher complication rates observed in our study.
Our findings did not suggest any relationship of BMI with noncardiac postoperative medical complications in any of the 4 methods we used to stratify BMI (continuous, categorical, normal vs. abnormal, and 25 kg/m2). Evidence is contradictory as to what the effect of BMI has on postoperative complications. An elevated BMI (30 kg/m2) has been shown to lead to increased sternal wound infection and saphenous vein harvest infection in a cardiac surgery population,27 but other studies10,28,29 have demonstrated the opposite effect. Among 6336 patients undergoing elective general surgery procedures, the incidence of complications were similar by body mass.30 A matched study design that included urgent and emergent surgeries also did not find any appreciable increased perioperative risk in noncardiac surgery.28 Whether this may be due to the elective nature of the surgeries in these studies, hence leading to selection bias, is unknown.
In geriatric patients, multiple baseline comorbid conditions often are reflected in a higher ASA class, which increases the risk of significant perioperative complications. Our multivariate modeling showed that a high ASA class strongly predicts morbidity and mortality following hip fracture repair, in line with other studies.19,31,32 Although the Charlson comorbidity index could alternatively been used, we elected to adjust for ASA class as it is more commonly used and is simple to use. Interestingly, surgical year did not significantly predict any complication, which can suggest that practice changes play a minimal impact on patient outcomes. However, we caution that because the individual event rates, particularly vascular, were low, we were unable to fully determine whether changes in practice management, such as improved thromboprophylaxis, would impact event rates over time. Finally, other predictors such as older age33 and a concomitant history of either COPD or asthma,34 are well‐accepted predictors of inpatient complications. Our attempt to examine specific predictors of complications in each BMI category revealed differing results, making interpretations difficult. Because of power considerations, this was meant solely as an exploratory analysis, and larger cohorts are needed to further ascertain whether predictors are different in these groups. Such a study may in fact identify perioperative issues that allow practitioners caring for this population to modify these factors.
One of the major limitations in our study was our inability to adjust for individual complications using multivariable models, such as deep vein thrombosis or delirium, within each BMI stratum, because of statistical power issues. Such a study would require large numbers of individual complications or events to allow for appropriate adjustments. The authors acknowledge that such individual complication rates may vary dramatically. We were aware of this potential problem, and therefore a priori ascertained a composite outcome of any noncardiac medical complication. However, our results do provide preliminary information regarding the impact of BMI on noncardiac medical complications. Further studies would be needed, though, to fully determine the effect of BMI on the number of cases with each complication.
Obesity (or BMI) is a known cardiovascular risk factor, and our previous study's aim was to determine cardiovascular events in a comparable manner to the way risk indices, such as the Goldman, Lee, or the AHA preoperative algorithm function. The surgical literature often presents noncardiac complications separately, allowing us to directly compare our own data to other published studies. We used 2 separate approaches, focusing on the inpatient stay (ascertaining noncardiac complications) and 1‐year cardiac outcomes (cardiac complications), as these are mediated by different mechanisms and factors. Furthermore, the intent of both studies was to dispel any concerns that an elevated BMI would in fact lead to an increased number of complications. Whether cardiac complications, though, would impact noncardiac complications, or vice‐versa, is unknown, and would require further investigation.
Although we relied on well‐established definitions for body mass, they have often been challenged, as they may underestimate adiposity in the elderly population due to age‐related reductions in lean mass.35,36 Studies have demonstrated a poor correlation between percent body fat and BMI in the >65 year age group,37 which could impact our results and outcomes by misclassifying patients. Yet, as an anthropometric measurement, BMI is easily obtainable and its variables are routinely documented in patients' medical records, as compared to other anthropometric measurements. Other means of estimating adiposity, such as densitometry or computed tomography (CT) scanning, are impractical, expensive, and not used clinically but routinely in research settings. The lack of standardization in obtaining height and weight, despite nurse‐initiated protocols for bed calibration, may have introduced a degree of measurement bias. Furthermore, the extent of lean mass lost and volume status changes lead to further challenges of using BMI in hospital settings. Whether other anthropometric measurements, including hip circumference, waist circumference, or waist‐hip ratio, should be used in this group of patients requires further examination. However, despite its shortcomings in elderly patients, BMI is still deemed an appropriate surrogate for obesity.
Our main strength was the use of the Rochester Epidemiology Project medical record linkage system to ascertain all patient data. This focuses on patients from a single geographically‐defined community minimizing referral biases often observed in studies originating from a tertiary care referral center. Previous disease‐related epidemiology studies using the Olmsted County population have demonstrated excellent external validity to the U.S. white population.16 We relied on the medical documentation of the treating clinician for many diagnoses in our data abstraction. Although we attempted to use standardized definitions, clinicians may have inadvertently forgotten to document subjective signs or symptoms that would assist in the categorization of these complications. Hence, added inpatient complications may have been overlooked, suggesting that our results may slightly underestimate the true incidence in this population. Additionally, certain complications may overlap categories, such as pneumonia and infections. We agree with Lawrence et al.19 that long periods of time are necessary to accumulate data of this kind in an effort to describe complication rates epidemiologically.
Despite no difference in outcomes among BMI categories, our results have striking implications for the hospitalized patient. Thus, underweight elderly patients, often considered frail with minimal functional reserve, are at no higher risk for developing inpatient medical complications than patients with higher BMIs. This is contrary to our study focusing on cardiac complications, where underweight patients were at higher risk.15 Conversely, obese patients, who have been demonstrated to be at higher risk of medical complications (particularly pulmonary), had no greater risk than patients with normal BMI. To the practicing geriatrician and hospitalist, this information provides important prognostication regarding additional perioperative measures that need to be implemented in these different groups. Based on our results, BMI does not play a particular role in noncardiac medical complications, dispelling any myths of the added burden of excess weight on surgical outcomes in this population. From a hospital perspective, this may be important since additional testing or preventative management in these patients may lead to additional resource use. However, in‐hospital deaths were higher in underweight patients than in patients with a normal BMI. Although we were underpowered to detect any differences in mortality between groups and could therefore not adjust for additional variables, it is unknown whether cardiac or noncardiac complications may be a stronger predictor of death in the underweight patient population. Further studies would be needed to better ascertain this relationship.
Conclusions
In elderly patients undergoing urgent hip fracture repair, BMI does not appear to lead to an excess rate of inpatient noncardiac complications. Our results are the first to demonstrate that BMI has no impact on morbidity in this patient population. Further research on the influence of body composition on inpatient complications in this population is needed to accurately allow for appropriate perioperative prophylaxis. Whether BMI impacts specific complications or in‐patient mortality in this population still requires investigation.
Acknowledgements
The authors thank Donna K. Lawson, LPN, Kathy Wolfert, and Cherie Dolliver, for their assistance in data collection and management.
Public health concerns such as the aging population1 and the increasing prevalence of obesity2 are also important issues to hospitals. However, little attention has been given to the interface of obesity and the elderly, largely due to the dearth of studies that include elderly patients. An aging population leads to an increase in geriatric syndromes, such as osteoporosis3 and its most devastating complication, hip fracture.4 These frail, hip‐fracture patients pose management challenges to practicing geriatricians and hospitalists.5,6 Furthermore, although fracture risk is inversely correlated to body mass index (BMI),7 this relationship has yet to be fully examined in the postoperative hip‐fracture population. In other surgical settings, there is disagreement as to whether underweight or obese patients are at higher risk of developing medical complications,8‐11 but for orthopedic patients, data have been limited to elective orthopedic populations.12‐14 We previously demonstrated that underweight hip‐fracture patients are at higher risk of postoperative cardiac complications at 1 year,15 consistent with studies of cardiac risk indices determining long‐term events. Because of different pathophysiologic mechanisms, the purpose of this study was to ascertain the influence of BMI on inpatient postoperative noncardiac medical complications and to assess predictors of such complications following urgent hip fracture repair.
Patients and Methods
All Olmsted County, Minnesota, residents undergoing urgent hip repair due to fracture were identified using the Rochester Epidemiology Project, a medical‐record linkage system funded by the Federal government since 1966 to support disease‐related epidemiology studies.16 All patient medical care is indexed, and both inpatient and outpatient visits are captured and available for review, allowing for complete case ascertainment. Medical care in Olmsted County is primarily provided by Mayo Clinic with its affiliated hospitals (St. Mary's and Rochester Methodist) and the Olmsted Medical Center, in addition to a few individual providers. Over 95% of all Olmsted County hip fracture surgeries are ultimately managed at St. Mary's Hospital.
Following approval by the Institutional Review Board we used this unique data resource to identify all residents with an International Classification of Diseases, 9th edition (ICD‐9) diagnosis code of 820 to 829 for hip fracture (n = 1310). Both sexes were included, and all patients included in the study provided research authorization for use of their medical records for research purposes.17 We excluded patients who were managed conservatively (n = 56), had a pathological fracture (n = 20), had multiple injuries (n = 19), were operated on >72 hours after fracture (n = 5), were aged <65 years (n = 2), or were admitted for reasons other than a fracture and experienced an in‐hospital fracture (n = 3). We subsequently excluded patients with missing information (n = 10). World Health Organization (WHO) criteria were used for classifying BMI: underweight (BMI < 18.5); normal (BMI = 18.5‐24.9); overweight (BMI = 25.0‐29.9); and obese (BMI 30.0).18
All data were abstracted using standardized collection forms by trained nurse abstractors blinded to the study hypothesis. Patients' admission height and weight were documented; if unavailable, the nearest data within 2 months prior to surgery were recorded. Patients' preadmission residence, functional status, baseline comorbidities, admission medications, discharge destination, as well as whether patients had an intensive care unit stay or any major surgeries in the past 90 days were abstracted. In addition, American Society of Anesthesia (ASA) class, type of anesthesia, and length of stay were also obtained. Inpatient complications that had been identified by the treating physicians and documented in the medical record or identified on imaging studies were assessed from the time of hip fracture repair to the time of discharge using standardized clinical criteria (Table 1). For criteria that were based on either objective findings or clinical documentation/suspicion, the patient was considered to meet the criteria of having a complication if they fulfilled either one. We did not include any cardiac outcomes, including congestive heart failure, angina, myocardial infarction, or arrhythmias that had been previously reported.15 Noncardiac complications were classified broadly: respiratory (respiratory failure, respiratory depression, or pulmonary hypoxemia); neurologic (any cerebral event including hemorrhagic or ischemic stroke, transient ischemic attack, or delirium); gastrointestinal (ileus or gastrointestinal bleeding); vascular (pulmonary embolus, or deep vein thrombosis); infectious (pneumonia, sepsis, urinary tract, wound, or cellulitis); renal/metabolic (acute renal failure, dehydration, or electrolyte abnormalities); or other (fractures or falls).
| Definition | Symptom |
|---|---|
| |
| Gastrointestinal | |
| Ileus | Dilated loops of bowel on X‐ray; documented ileus with nausea, vomiting, no stool or inability to take oral intake |
| Gastrointestinal bleeding | Sudden appearance of frank blood on nasogastric lavage or by rectum AND a decrease in hemoglobin of 2 g/dL or greater with no other suspected source of ongoing blood loss |
| Infectious | |
| Pneumonia | New infiltrate on chest x‐ray plus 2 of the following 3 findings: temperature >38C, elevated white cell count, sputum pathogen that requires antibiotic treatment |
| Bacteremia/sepsis | Localized infection with positive blood culture for the same pathogen AND chills, rigors, fever, elevated white cell count AND intravenous antibiotic treatment |
| Urinary tract infection | Pyuria symptoms |
| Positive gram stain symptoms | |
| Wound | |
| Cellulitis | As documented in physician's note of a superficial skin infection |
| Neurologic | |
| Cerebral eventhypoxia, thrombosis or hemorrhage | New neurologic dysfunction (hemiplegia, hemianesthesia, hemianopia, aphasia, or unconsciousness) postoperatively |
| Transient ischemic attack | Any neurologic dysfunction resolving within a 24‐hour period |
| Delirium | Positive Confusion Assessment Method38 |
| Renal/metabolic | |
| Renal failure | A doubling of baseline value of creatinine; serum creatinine >3.0 mg/dL; acute need for dialysis |
| Dehydration | As documented in the physician's note |
| Electrolyte abnormalities | Any laboratory evidence of abnormal electrolytes compared to normal |
| Respiratory | |
| Respiratory failure | Need for intubation and ventilation >24 hours postoperatively; need for reintubation and ventilation after 1 hour postoperatively |
| Respiratory depression | Respiratory arrest; PaCO2 >60 mmHg that provider believed was associated with narcotics |
| Pulmonary hypoxemia | SaO2 <90% with or without supplemental oxygen; supplemental oxygen >24 hours |
| Vascular | |
| Deep vein thrombosis | Positive lower extremity venous Doppler |
| Pulmonary embolism | Acute onset dyspnea and tachycardia, increased central venous pressure AND (positive ventilation/perfusion scan OR positive computed tomography OR positive pulmonary angiogram) |
| Other | |
| Fractures | Any in‐hospital documented fracture of any bone |
| Falls | Patients descending to the ground from any position unintentionally |
Continuous data are presented as means standard deviation and categorical data as counts and percentages. In testing for differences in patient demographics, past medical history, and baseline clinical data among BMI groups, Kruskal‐Wallis tests were performed for continuous variables and Fisher's Exact or Cochran‐Mantel‐Haenszel tests were used for discrete variables. Bonferroni adjustments were performed where appropriate. The primary outcome was the risk of any noncardiac medical complication during the postoperative hospitalization, based on patients with complications. Incidence rates were calculated for the overall group as well as for each BMI category. BMI was evaluated categorically according to the WHO criteria, as a continuous variable dichotomized as a BMI 18.5 kg/m2 to 24.9 kg/m2 (normal) vs. all others, and above/below 25.0 kg/m2. The effect of BMI and other potential risk factors on the complication rate was evaluated using logistic regression. The effect of BMI category on the overall complication rate was adjusted for the a priori risk factors of age, sex, surgical year, and ASA class both univariately (Model 1) and multivariately (Model 2). In addition to these variables, we also evaluated other potential risk factors, including baseline demographic and baseline clinical variables that were significant (P < 0.05) univariately using a stepwise selection; first forcing in BMI as a categorical variable (Model 3), then repeating the stepwise selection process without forcing in BMI (Model 4). Using data from Lawrence et al.,19 we estimated that we would have 80% power to detect differences in rates of inpatient noncardiac complications equal to an odds ratio (OR) = 2.2 (normal vs. underweight), OR = 2.0 (normal vs. overweight), and OR = 2.4 (normal vs. obese). Finally, because of power considerations, as an exploratory analysis, we additionally identified predictors of inpatient complications within each BMI category using stepwise selection. All statistical tests were 2‐sided, and P values <0.05 were considered significant. All analyses were performed using SAS for UNIX (version 9.1.3; SAS Institute, Inc., Cary, NC).
Results
Between 1988 and 2002, 1195 urgent repairs for hip fracture met our inclusion/exclusion criteria. We subsequently excluded 15 repairs with missing BMI data, and, of the 7 patients with >1 repair, we included only their first fracture episode in our analysis. Two were subsequently excluded due to an administrative error. Ultimately, 1180 hip fracture repairs were included in the analysis cohort. There were 184 (15.6%) patients in the underweight group, 640 (54.2%) with normal BMI, 251 (21.3%) with a BMI 25.0 to 29.9 kg/m2, and 105 (8.9%) with a BMI 30 kg/m2. Baseline characteristics are otherwise shown in Table 2. Normal BMI patients were significantly older than the other groups, and underweight patients were less likely to be admitted from home. Past history of having a cardiovascular risk factor or a cardiovascular diagnosis appeared to increase with increasing BMI. Underweight patients were more likely to have chronic obstructive pulmonary disease (COPD) than patients with normal BMI (P = 0.03) or overweight patients (P = 0.009), but not more than obese patients (P = 0.21). There were no differences across BMI groups in ASA class, type of anesthesia, intensive care unit stay, or length of stay.
| Variable | Underweight (<18.5 kg/m2) n = 184 n (%) | Normal (18.5‐24.9 kg/m2) n = 640 n (%) | Overweight (25‐29.9 kg/m2) n = 251 n (%) | Obese (30 kg/m2) n = 105 n (%) | P Value* |
|---|---|---|---|---|---|
| |||||
| Age (years) | 84.8 8.0 | 85.0 7.2 | 83.1 7.3 | 80.7 7.4 | <0.001 |
| Female sex | 171 (92.9) | 525 (82) | 177 (70.5) | 76 (72.4) | <0.001 |
| Preadmission residence | |||||
| ALC/SNF | 79 (42.9) | 250 (39.1) | 83 (33.1) | 36 (34.3) | 0.024 |
| Home | 105 (57.1) | 390 (60.9) | 168 (66.9) | 69 (65.7) | |
| Functional status | |||||
| Dependent | 25 (13.6) | 80 (12.5) | 24 (9.6) | 7 (6.7) | 0.044 |
| Walking independently | 159 (86.4) | 560 (87.5) | 226 (90.4) | 97 (93.3) | |
| History of | |||||
| Hypertension | 84 (45.7) | 374 (58.4) | 159 (63.3) | 70 (66.7) | <0.001 |
| Diabetes | 9 (4.9) | 71 (11.1) | 30 (12) | 30 (28.6) | <0.001 |
| Cerebrovascular disease | 40 (21.7) | 175 (27.3) | 77 (30.7) | 33 (31.4) | 0.028 |
| Myocardial infarction | 44 (23.9) | 140 (21.9) | 61 (24.3) | 36 (34.3) | 0.106 |
| Congestive heart failure | 48 (26.1) | 150 (23.4) | 76 (30.3) | 44 (41.9) | 0.003 |
| Atrial fibrillation/flutter | 49 (26.6) | 118 (18.4) | 57 (22.7) | 26 (24.8) | 0.985 |
| Chronic renal insufficiency | 11 (6) | 64 (10) | 34 (13.5) | 20 (19) | <0.001 |
| Dementia | 63 (34.2) | 233 (36.4) | 74 (29.5) | 26 (24.8) | 0.031 |
| Obstructive sleep apnea | 2 (1.1) | 5 (0.8) | 5 (2.0) | 6 (5.7) | 0.005 |
| COPD | 41 (22.3) | 100 (15.6) | 32 (12.7) | 17 (16.2) | 0.032 |
| Asthma | 13 (7.1) | 47 (7.3) | 18 (7.2) | 12 (11.4) | 0.395 |
| COPD or asthma | 49 (26.6) | 133 (20.8) | 45 (17.9) | 23 (21.9) | 0.093 |
| Pulmonary embolism or deep vein thrombosis | 9 (4.9) | 21 (3.3) | 21 (8.4) | 17 (16.2) | <0.001 |
| Osteoporosis | 77 (41.8) | 253 (39.5) | 73 (29.1) | 31 (29.5) | <0.001 |
| Collagen vascular diseases | 10 (5.4) | 29 (4.5) | 9 (3.6) | 12 (11.4) | 0.34 |
| Cancer | 61 (33.2) | 169 (26.4) | 75 (29.9) | 32 (30.5) | 0.88 |
| Lymphoma | 2 (1.1) | 3 (0.5) | 2 (0.8) | 2 (1.9) | 0.25 |
| Leukemia | 2 (1.1) | 3 (0.5) | 1 (0.4) | 1 (1) | |
| Major surgery within 90 days | 3 (1.6) | 10 (1.6) | 8 (3.2) | 3 (2.9) | 0.366 |
| ASA class | |||||
| I or II | 19 (10.4) | 93 (14.5) | 46 (18.3) | 12 (11.4) | 0.144 |
| III, IV, or V | 164 (89.6) | 547 (85.5) | 205 (81.7) | 93 (88.6) | |
| Type of anesthesia | |||||
| General | 134 (72.8) | 477 (74.5) | 192 (76.5) | 84 (80) | |
| Other (spinal, epidural, local, combination) | 50 (27.2) | 163 (25.5) | 59 (23.5) | 21 (20) | 0.16 |
| Admission medications | |||||
| Insulin | 2 (1.1) | 18 (2.8) | 11 (4.4) | 17 (16.2) | <0.001 |
| Aspirin | 50 (27.2) | 197 (30.8) | 82 (32.7) | 37 (35.2) | 0.126 |
| Beta‐blockers | 18 (9.8) | 90 (14.1) | 50 (19.9) | 25 (23.8) | <0.001 |
| ACE/ARB | 32 (17.4) | 95 (14.8) | 55 (21.9) | 28 (26.7) | 0.009 |
| Calcium‐channel blocker | 26 (14.1) | 104 (16.3) | 39 (15.5) | 21 (20) | 0.38 |
| Intensive care unit stay | 63 (34.2) | 154 (24.1) | 61 (24.3) | 30 (28.6) | 0.16 |
| Length of stay, days | 10.3 (9.7) | 9.7 (6.8) | 10.2 (7.6) | 11.1 (8.6) | 0.10 |
| Discharge destination | |||||
| Home | 20 (10.9) | 65 (10.2) | 43 (17.1) | 19 (18.1) | |
| ALC/nursing home | 146 (79.8) | 547 (85.5) | 199 (79.3) | 83 (79) | <0.001 |
| In‐hospital death | 17 (9.3) | 28 (4.4) | 9 (3.6) | 3 (2.9) | |
There were 77 (41.8%) postoperative inpatient noncardiac complications in the underweight group, 234 (36.6%) in the normal BMI group, 90 (35.9%) in the overweight group, and 42 (40.0%) in the obese group (P = 0.49). Figure 1 demonstrates the main subcategory complication rates by BMI group, and Table 3 outlines the univariate unadjusted complication rates. Other than gastrointestinal complications being more prevalent as BMI increases (P = 0.005), there were no significant differences in crude complication rates across BMI categories (all P > 0.05) for the other complication subcategories. A multiple comparisons analysis did not demonstrate any differences between normal and any of the other BMI categories for ileus. Normal BMI patients were more likely to be discharged to a nursing facility than overweight or obese patients (85.5% vs. 79.3%, P = 0.03; and 85.5% vs. 79.0%, P = 0.03, respectively). The proportion of in‐hospital deaths among underweight patients was significantly higher than in any of the other groups (9.3% vs. 4.4%; P = 0.01), but mean length of stay was not significantly different.
| Overall Cohort n (%) | Underweight (<18.5 kg/m2) n = 184 n (%) | Normal (18.5‐24.9 kg/m2) n = 640 n (%) | Overweight (25‐29.9 kg/m2) n = 251 n (%) | Obese (30 kg/m2) n = 105 n (%) | P Value | |
|---|---|---|---|---|---|---|
| ||||||
| Gastrointestinal | ||||||
| Ileus | 38 (3.2) | 1 (0.5) | 21 (3.3) | 12 (4.8) | 4 (3.8) | 0.03 |
| Gastrointestinal bleeding | 21 (1.8) | 1 (0.5) | 11 (1.7) | 6 (2.4) | 3 (2.9) | 0.35 |
| Infectious | ||||||
| Pneumonia | 69 (5.8) | 12 (6.5) | 39 (6.1) | 14 (5.6) | 4 (3.8) | 0.51 |
| Bacteremia/sepsis | 8 (0.7) | 1 (0.5) | 2 (0.3) | 5 (2.0) | 0 (0) | 0.06 |
| Urinary tract infection | 84 (7.1) | 12 (6.5) | 47 (7.3) | 15 (6) | 10 (9.5) | 0.78 |
| Wound | ||||||
| Cellulitis | ||||||
| Neurological | ||||||
| Cerebral event‐hypoxia, thrombosis or hemorrhage | 15 (1.3) | 1 (0.5) | 6 (0.9) | 6 (2.4) | 2 (1.9) | 0.21 |
| Transient ischemic attack | ||||||
| Delirium | 199 (16.9) | 40 (21.7) | 106 (16.6) | 36 (14.3) | 17 (16.2) | 0.08 |
| Renal/metabolic | ||||||
| Renal failure | 19 (1.6) | 3 (1.6) | 9 (1.4) | 5 (2.0) | 2 (1.9) | 0.82 |
| Dehydration | ||||||
| Electrolyte abnormalities | ||||||
| Respiratory | ||||||
| Respiratory failure | 53 (4.5) | 10 (5.4) | 23 (3.6) | 15 (6.0) | 5 (4.8) | 0.61 |
| Respiratory depression | 23 (1.9) | 3 (1.6) | 11 (1.7) | 8 (3.2) | 1 (1.0) | 0.50 |
| Pulmonary hypoxemia | 157 (13.3) | 33 (17.9) | 78 (12.2) | 34 (13.5) | 12 (11.4) | 0.22 |
| Vascular | ||||||
| Deep vein thrombosis | 5 (0.4) | 0 (0) | 2 (0.3) | 3 (1.2) | 0 (0) | 0.24 |
| Pulmonary embolism | 16 (1.4) | 3 (1.6) | 7 (1.1) | 5 (2.0) | 1 (1.0) | 0.65 |
| Other | ||||||
| Fractures | 6 (0.5) | 1 (0.5) | 5 (0.8) | 0 (0) | 0 (0) | 0.57 |
| Falls | ||||||
Significant univariate predictors of the composite outcome of any noncardiac complication included: age (OR, 1.04 95% confidence interval [CI>], 1.02‐1.06; P < 0.001), age 75 years (OR, 2.25; 95% CI, 1.52‐3.33; P < 0.001), age 85 years (OR, 1.49; 95% CI, 1.17‐1.89; P < 0.001), male sex (OR, 1.41; 95% CI, 1.05‐1.90; P = 0.02), admission from home (OR, 0.77; 95% CI, 0.61‐0.98; P = 0.03), a history of cerebrovascular disease (OR, 1.41; 95% CI, 1.08‐1.83; P = 0.01), myocardial infarction (OR, 1.41; 95% CI, 1.07‐1.86; P = 0.02), angina (OR, 1.32; 95% CI, 1.03‐1.69; P = 0.03), congestive heart failure (OR, 1.45; 95% CI, 1.11‐1.89; P = 0.006), dementia (OR, 1.39; 95% CI, 1.08‐1.78; P = 0.01), peripheral vascular disease (OR, 1.47; 95% CI, 1.06‐2.03; P = 0.02), COPD/asthma (OR, 1.56; 95% CI, 1.18‐2.08; P = 0.002), osteoarthritis (OR, 1.29; 95% CI, 1.01‐1.65; P = 0.04), code status as Do Not Resuscitate (OR, 0.74; 95% CI, 0.58‐0.94; P = 0.015), or ASA class III‐V (OR, 2.24; 95% CI, 1.53‐3.29; P < 0.001). Results were no different after using the Charlson comorbidity index in place of ASA class (data not shown). No significant differences in overall noncardiac complications were observed when examining BMI as a continuous variable, as a categorical variable, as 25 kg/m2 vs. <25 kg/m2, or as 18.5 kg/m2 to 24.9 kg/m2 vs. all others. Examining renal, respiratory, peripheral vascular, or neurologic complications univariately within these aforementioned strata also did not demonstrate any significant differences among BMI categories (data not shown).
Multivariable analyses (Models 1‐4) are shown for any overall noncardiac inpatient medical complication in Table 4. BMI was not a significant predictor in any of our models, specifically in our main model that examined the effect of BMI adjusting for a priori variables (Model 2). However, older age, male sex, and ASA class were highly significant predictors of complications in all four models; however, surgical year was nonsignificant. Notably, after stepwise selection for other demographic and premorbid variables, a history of COPD or asthma was found to be an additional significant factor both in Model 3 (forcing BMI in the model) and Model 4 (without BMI in the model). Exploratory analysis of individual predictors of inpatient noncardiac complications within each BMI category demonstrated that, in underweight patients, admission use of ‐blockers was a significant predictor of having any medical complication (OR, 3.1; 95% CI, 1.1‐8.60; P = 0.03). In normal BMI patients, age 75 years (OR, 2.6; 95% CI, 1.4‐4.9; P = 0.003), ASA class III‐V (OR, 2.3; 95% CI, 1.3‐3.9; P = 0.003), and a history of cerebrovascular disease (OR, 1.5; 95%CI, 1.04‐2.1; P = 0.03) were predictors; and, in obese patients, only age (OR, 1.1; 95% CI, 1.00‐1.12; P = 0.05) was significant. There were no significant predictors of having a medical complication in the overweight group.
| Underweight <18.5 kg/m2 n = 184* n (%) | Normal 18.5‐24.9 kg/m2 n = 640* n (%) | Overweight 25‐29.9 kg/m2 n = 251* n (%) | Obese 30 kg/m2 n = 105* n (%) | Age | Male Sex | Surgical Year | ASA Score, III‐V vs. I/II | COPD/ Asthma | |
|---|---|---|---|---|---|---|---|---|---|
| |||||||||
| Model 1a | 1.25 (0.89‐1.74) | Referent | 0.97 (0.72‐1.31) | 1.16 (0.76‐1.76) | |||||
| Model 1b | 1.26 (0.90‐1.77) | Referent | 1.05 (0.77‐1.43) | 1.38 (0.90‐2.13) | 1.04 (1.02‐1.06) | ||||
| Model 1c | 1.30 (0.93‐1.83) | Referent | 0.93 (0.68‐1.26) | 1.12 (0.73‐1.71) | 1.47 (1.09‐1.98) | ||||
| Model 1d | 1.28 (0.91‐1.79) | Referent | 0.97 (0.71‐1.31) | 1.13 (0.74‐1.73) | 1.03 (1.00‐1.06) | ||||
| Model 1e | 1.23 (0.88‐1.72) | Referent | 1.00 (0.73‐1.36) | 1.13 (0.74‐1.73) | 2.22 (1.52‐3.24) | ||||
| Model 2 | 1.33 (0.95‐1.88) | Referent | 1.01 (0.74‐1.38) | 1.28 (0.82‐1.98) | 1.04 (1.02‐1.06) | 1.59 (1.17‐2.17) | 1.02 (0.99‐1.05) | 1.89 (1.28‐2.79) | |
| Model 3∥ | 1.30 (0.92‐1.84) | Referent | 1.04 (0.76‐1.42) | 1.30 (0.84‐2.02) | 1.05 (1.03‐1.06) | 1.52 (1.11‐2.07) | 1.02 (0.99‐1.05) | 1.77 (1.20‐2.62) | 1.58 (1.17‐2.12) |
| Model 4 | 1.05 (1.03‐1.06) | 1.49 (1.10‐2.02) | 1.84 (1.25‐2.71) | 1.58 (1.18‐2.12) | |||||
Discussion
Most research describing the association of BMI with postoperative outcomes has concentrated on cardiac surgery, general surgical procedures, and intensive care unit utilization.8‐11,20 In the orthopedic literature, an elevated BMI has been associated with a higher number of short‐term complications, but this was limited to elective knee arthroplasty and spine surgery populations.12,13,21 Conversely, no differences were observed in obese patients undergoing hip arthroplasties.14,22 To the best of our knowledge, this study may be the first to examine the impact of BMI on inpatient hospital outcomes following urgent hip fracture repair. Our results suggest the risk of developing a noncardiac medical complication is the same regardless of BMI.
Our overall complication rate was higher (38%) than previous reports by others.19,23‐26 Thus, Lawrence et al.,19 in their retrospective study of 20 facilities, demonstrated an overall complication rate of 17%, even though they also included postoperative cardiac complications. Although their study period overlapped our own (1982‐1993), they additionally included patients aged 60 to 65 years, a population known to have fewer comorbidities and fewer postoperative complications than the elderly hip‐fracture patients studied here. In addition, their population may have been healthier at baseline, in that a higher proportion lived at home (73%) and a lower percentage were ASA class III‐V (71%) than our cohort. These differences in baseline characteristics may explain the higher complication rates observed in our study.
Our findings did not suggest any relationship of BMI with noncardiac postoperative medical complications in any of the 4 methods we used to stratify BMI (continuous, categorical, normal vs. abnormal, and 25 kg/m2). Evidence is contradictory as to what the effect of BMI has on postoperative complications. An elevated BMI (30 kg/m2) has been shown to lead to increased sternal wound infection and saphenous vein harvest infection in a cardiac surgery population,27 but other studies10,28,29 have demonstrated the opposite effect. Among 6336 patients undergoing elective general surgery procedures, the incidence of complications were similar by body mass.30 A matched study design that included urgent and emergent surgeries also did not find any appreciable increased perioperative risk in noncardiac surgery.28 Whether this may be due to the elective nature of the surgeries in these studies, hence leading to selection bias, is unknown.
In geriatric patients, multiple baseline comorbid conditions often are reflected in a higher ASA class, which increases the risk of significant perioperative complications. Our multivariate modeling showed that a high ASA class strongly predicts morbidity and mortality following hip fracture repair, in line with other studies.19,31,32 Although the Charlson comorbidity index could alternatively been used, we elected to adjust for ASA class as it is more commonly used and is simple to use. Interestingly, surgical year did not significantly predict any complication, which can suggest that practice changes play a minimal impact on patient outcomes. However, we caution that because the individual event rates, particularly vascular, were low, we were unable to fully determine whether changes in practice management, such as improved thromboprophylaxis, would impact event rates over time. Finally, other predictors such as older age33 and a concomitant history of either COPD or asthma,34 are well‐accepted predictors of inpatient complications. Our attempt to examine specific predictors of complications in each BMI category revealed differing results, making interpretations difficult. Because of power considerations, this was meant solely as an exploratory analysis, and larger cohorts are needed to further ascertain whether predictors are different in these groups. Such a study may in fact identify perioperative issues that allow practitioners caring for this population to modify these factors.
One of the major limitations in our study was our inability to adjust for individual complications using multivariable models, such as deep vein thrombosis or delirium, within each BMI stratum, because of statistical power issues. Such a study would require large numbers of individual complications or events to allow for appropriate adjustments. The authors acknowledge that such individual complication rates may vary dramatically. We were aware of this potential problem, and therefore a priori ascertained a composite outcome of any noncardiac medical complication. However, our results do provide preliminary information regarding the impact of BMI on noncardiac medical complications. Further studies would be needed, though, to fully determine the effect of BMI on the number of cases with each complication.
Obesity (or BMI) is a known cardiovascular risk factor, and our previous study's aim was to determine cardiovascular events in a comparable manner to the way risk indices, such as the Goldman, Lee, or the AHA preoperative algorithm function. The surgical literature often presents noncardiac complications separately, allowing us to directly compare our own data to other published studies. We used 2 separate approaches, focusing on the inpatient stay (ascertaining noncardiac complications) and 1‐year cardiac outcomes (cardiac complications), as these are mediated by different mechanisms and factors. Furthermore, the intent of both studies was to dispel any concerns that an elevated BMI would in fact lead to an increased number of complications. Whether cardiac complications, though, would impact noncardiac complications, or vice‐versa, is unknown, and would require further investigation.
Although we relied on well‐established definitions for body mass, they have often been challenged, as they may underestimate adiposity in the elderly population due to age‐related reductions in lean mass.35,36 Studies have demonstrated a poor correlation between percent body fat and BMI in the >65 year age group,37 which could impact our results and outcomes by misclassifying patients. Yet, as an anthropometric measurement, BMI is easily obtainable and its variables are routinely documented in patients' medical records, as compared to other anthropometric measurements. Other means of estimating adiposity, such as densitometry or computed tomography (CT) scanning, are impractical, expensive, and not used clinically but routinely in research settings. The lack of standardization in obtaining height and weight, despite nurse‐initiated protocols for bed calibration, may have introduced a degree of measurement bias. Furthermore, the extent of lean mass lost and volume status changes lead to further challenges of using BMI in hospital settings. Whether other anthropometric measurements, including hip circumference, waist circumference, or waist‐hip ratio, should be used in this group of patients requires further examination. However, despite its shortcomings in elderly patients, BMI is still deemed an appropriate surrogate for obesity.
Our main strength was the use of the Rochester Epidemiology Project medical record linkage system to ascertain all patient data. This focuses on patients from a single geographically‐defined community minimizing referral biases often observed in studies originating from a tertiary care referral center. Previous disease‐related epidemiology studies using the Olmsted County population have demonstrated excellent external validity to the U.S. white population.16 We relied on the medical documentation of the treating clinician for many diagnoses in our data abstraction. Although we attempted to use standardized definitions, clinicians may have inadvertently forgotten to document subjective signs or symptoms that would assist in the categorization of these complications. Hence, added inpatient complications may have been overlooked, suggesting that our results may slightly underestimate the true incidence in this population. Additionally, certain complications may overlap categories, such as pneumonia and infections. We agree with Lawrence et al.19 that long periods of time are necessary to accumulate data of this kind in an effort to describe complication rates epidemiologically.
Despite no difference in outcomes among BMI categories, our results have striking implications for the hospitalized patient. Thus, underweight elderly patients, often considered frail with minimal functional reserve, are at no higher risk for developing inpatient medical complications than patients with higher BMIs. This is contrary to our study focusing on cardiac complications, where underweight patients were at higher risk.15 Conversely, obese patients, who have been demonstrated to be at higher risk of medical complications (particularly pulmonary), had no greater risk than patients with normal BMI. To the practicing geriatrician and hospitalist, this information provides important prognostication regarding additional perioperative measures that need to be implemented in these different groups. Based on our results, BMI does not play a particular role in noncardiac medical complications, dispelling any myths of the added burden of excess weight on surgical outcomes in this population. From a hospital perspective, this may be important since additional testing or preventative management in these patients may lead to additional resource use. However, in‐hospital deaths were higher in underweight patients than in patients with a normal BMI. Although we were underpowered to detect any differences in mortality between groups and could therefore not adjust for additional variables, it is unknown whether cardiac or noncardiac complications may be a stronger predictor of death in the underweight patient population. Further studies would be needed to better ascertain this relationship.
Conclusions
In elderly patients undergoing urgent hip fracture repair, BMI does not appear to lead to an excess rate of inpatient noncardiac complications. Our results are the first to demonstrate that BMI has no impact on morbidity in this patient population. Further research on the influence of body composition on inpatient complications in this population is needed to accurately allow for appropriate perioperative prophylaxis. Whether BMI impacts specific complications or in‐patient mortality in this population still requires investigation.
Acknowledgements
The authors thank Donna K. Lawson, LPN, Kathy Wolfert, and Cherie Dolliver, for their assistance in data collection and management.
- , .The effect of longevity on spending for acute and long‐term care.N Engl J Med.2000;342(19):1409–1415.
- , , , .Excess deaths associated with underweight, overweight, and obesity.JAMA.2005;293(15):1861–1867.
- .Adverse outcomes of osteoporotic fractures in the general population.J Bone Miner Res.2003;18(6):1139–1141.
- , , , , , .Incidence and economic burden of osteoporosis‐related fractures in the United States, 2005–2025.J Bone Miner Res.2007;22(3):465–475.
- , .Medical care of elderly patients with hip fractures.Mayo Clin Proc.2001;76(3):295–298.
- , , , et al.Effects of a hospitalist model on elderly patients with hip fracture.Arch Intern Med.2005;165(7):796–801.
- , , , et al.Body mass index as a predictor of fracture risk: a meta‐analysis.Osteoporos Int.2005;16(11):1330–1338.
- , , , , .Increased body mass index predicts increased blood loss during radical cystectomy.J Urol.2004;171(3):1077–1079.
- , , , .Laparoscopic colorectal surgery in obese and nonobese patients: do differences in body mass indices lead to different outcomes?Surg Endosc.2004;18(10):1452–1456.
- , , , , , .The relationship of body mass index to outcomes after percutaneous coronary intervention.J Interv Cardiol.2006;19(5):388–395.
- , , , , , .Is extreme obesity a risk factor for cardiac surgery? An analysis of patients with a BMI ≥40.Eur J Cardiothorac Surg.2006;29(4):434–440.
- , , , , , .Perioperative morbidity following total knee arthroplasty among obese patients.J Knee Surg.2002;15(2):77–83.
- , , , et al.Obesity and spine surgery: relation to perioperative complications.J Neurosurg Spine.2007;6(4):291–297.
- , , , .The influence of obesity on perioperative morbidity and mortality in revision total hip arthroplasty.Arch Orthop Trauma Surg.2000;120(5–6):267–271.
- , , , et al.Body mass index and risk of adverse cardiac events in elderly hip fracture patients: a population‐based study.J Am Geriatr Soc.2009;57(3):419–426.
- .History of the Rochester Epidemiology Project.Mayo Clin Proc.1996;71(3):266–274.
- .The threat to medical‐records research.N Engl J Med.1997;337(20):1466–170.
- .A Treatise on Man and the Development of His Faculties.Brussels:Musquardt;1871.
- , , , , .Medical complications and outcomes after hip fracture repair.Arch Intern Med.2002;162(18):2053–2057.
- , , .Effect of obesity on intensive care morbidity and mortality: a meta‐analysis.Crit Care Med.2008;36(1):151–158.
- , .Relationship of body mass index to early complications in knee replacement surgery.Arch Orthop Trauma Surg.2008;128(1):5–9.
- , , , , , .Obesity in total hip replacement.J Bone Joint Surg Br.2008;90(4):424–429.
- , , , et al.Use of an intramedullary hip‐screw compared with a compression hip‐screw with a plate for intertrochanteric femoral fractures. A prospective, randomized study of one hundred patients.J Bone Joint Surg Am.1998;80(5):618–630.
- .Blood transfusion requirements in intracapsular femoral neck fractures.Injury.1996;27(10):709–711.
- , , , .Risk prediction in operatively treated fractures of the hip.Clin Orthop Relat Res.1993(293):148–152.
- .Internal fixation or arthroplasty for displaced subcapital fractures in the elderly?Injury.1992;23(8):521–524.
- , , , et al.Impact of body mass index and albumin on morbidity and mortality after cardiac surgery.J Thorac Cardiovasc Surg.1999;118(5):866–873.
- , , , et al.Increased body mass index and peri‐operative risk in patients undergoing non‐cardiac surgery.Obes Surg.2004;14(2):275–281.
- , , , et al.Effects of body size on operative, intermediate, and long‐term outcomes after coronary artery bypass operation.Ann Thorac Surg.2001;71(2):521–530; discussion 530–531.
- , , , .Obesity in general elective surgery.Lancet.2003;361(9374):2032–2035.
- , , , et al.Effects of a hospitalist care model on mortality of elderly patients with hip fractures.J Hosp Med.2007;2(4):219–225.
- , , , .Morbidity and mortality after hip fracture: the impact of operative delay.Arch Orthop Trauma Surg.2004;124(5):334–340.
- , , , , .Outcome after hip fracture in individuals ninety years of age and older.J Orthop Trauma.2001;15(1):34–39.
- , , , et al.Development and initial validation of a risk score for predicting in‐hospital and 1‐year mortality in patients with hip fractures.J Bone Miner Res.2005;20(3):494–500.
- , , , , , .How useful is body mass index for comparison of body fatness across age, sex, and ethnic groups?Am J Epidemiol.1996;143(3):228–239.
- , , , , .Reassessment of body mass indices.Am J Clin Nutr.1990;52(3):405–408.
- , , , et al.Accuracy of body mass index in diagnosing obesity in the adult general population.Int J Obes (Lond).2008;32(6):959–966.
- , , , , , .Clarifying confusion: the confusion assessment method. A new method for detection of delirium.Ann Intern Med.1990;113(12):941–948.
- , .The effect of longevity on spending for acute and long‐term care.N Engl J Med.2000;342(19):1409–1415.
- , , , .Excess deaths associated with underweight, overweight, and obesity.JAMA.2005;293(15):1861–1867.
- .Adverse outcomes of osteoporotic fractures in the general population.J Bone Miner Res.2003;18(6):1139–1141.
- , , , , , .Incidence and economic burden of osteoporosis‐related fractures in the United States, 2005–2025.J Bone Miner Res.2007;22(3):465–475.
- , .Medical care of elderly patients with hip fractures.Mayo Clin Proc.2001;76(3):295–298.
- , , , et al.Effects of a hospitalist model on elderly patients with hip fracture.Arch Intern Med.2005;165(7):796–801.
- , , , et al.Body mass index as a predictor of fracture risk: a meta‐analysis.Osteoporos Int.2005;16(11):1330–1338.
- , , , , .Increased body mass index predicts increased blood loss during radical cystectomy.J Urol.2004;171(3):1077–1079.
- , , , .Laparoscopic colorectal surgery in obese and nonobese patients: do differences in body mass indices lead to different outcomes?Surg Endosc.2004;18(10):1452–1456.
- , , , , , .The relationship of body mass index to outcomes after percutaneous coronary intervention.J Interv Cardiol.2006;19(5):388–395.
- , , , , , .Is extreme obesity a risk factor for cardiac surgery? An analysis of patients with a BMI ≥40.Eur J Cardiothorac Surg.2006;29(4):434–440.
- , , , , , .Perioperative morbidity following total knee arthroplasty among obese patients.J Knee Surg.2002;15(2):77–83.
- , , , et al.Obesity and spine surgery: relation to perioperative complications.J Neurosurg Spine.2007;6(4):291–297.
- , , , .The influence of obesity on perioperative morbidity and mortality in revision total hip arthroplasty.Arch Orthop Trauma Surg.2000;120(5–6):267–271.
- , , , et al.Body mass index and risk of adverse cardiac events in elderly hip fracture patients: a population‐based study.J Am Geriatr Soc.2009;57(3):419–426.
- .History of the Rochester Epidemiology Project.Mayo Clin Proc.1996;71(3):266–274.
- .The threat to medical‐records research.N Engl J Med.1997;337(20):1466–170.
- .A Treatise on Man and the Development of His Faculties.Brussels:Musquardt;1871.
- , , , , .Medical complications and outcomes after hip fracture repair.Arch Intern Med.2002;162(18):2053–2057.
- , , .Effect of obesity on intensive care morbidity and mortality: a meta‐analysis.Crit Care Med.2008;36(1):151–158.
- , .Relationship of body mass index to early complications in knee replacement surgery.Arch Orthop Trauma Surg.2008;128(1):5–9.
- , , , , , .Obesity in total hip replacement.J Bone Joint Surg Br.2008;90(4):424–429.
- , , , et al.Use of an intramedullary hip‐screw compared with a compression hip‐screw with a plate for intertrochanteric femoral fractures. A prospective, randomized study of one hundred patients.J Bone Joint Surg Am.1998;80(5):618–630.
- .Blood transfusion requirements in intracapsular femoral neck fractures.Injury.1996;27(10):709–711.
- , , , .Risk prediction in operatively treated fractures of the hip.Clin Orthop Relat Res.1993(293):148–152.
- .Internal fixation or arthroplasty for displaced subcapital fractures in the elderly?Injury.1992;23(8):521–524.
- , , , et al.Impact of body mass index and albumin on morbidity and mortality after cardiac surgery.J Thorac Cardiovasc Surg.1999;118(5):866–873.
- , , , et al.Increased body mass index and peri‐operative risk in patients undergoing non‐cardiac surgery.Obes Surg.2004;14(2):275–281.
- , , , et al.Effects of body size on operative, intermediate, and long‐term outcomes after coronary artery bypass operation.Ann Thorac Surg.2001;71(2):521–530; discussion 530–531.
- , , , .Obesity in general elective surgery.Lancet.2003;361(9374):2032–2035.
- , , , et al.Effects of a hospitalist care model on mortality of elderly patients with hip fractures.J Hosp Med.2007;2(4):219–225.
- , , , .Morbidity and mortality after hip fracture: the impact of operative delay.Arch Orthop Trauma Surg.2004;124(5):334–340.
- , , , , .Outcome after hip fracture in individuals ninety years of age and older.J Orthop Trauma.2001;15(1):34–39.
- , , , et al.Development and initial validation of a risk score for predicting in‐hospital and 1‐year mortality in patients with hip fractures.J Bone Miner Res.2005;20(3):494–500.
- , , , , , .How useful is body mass index for comparison of body fatness across age, sex, and ethnic groups?Am J Epidemiol.1996;143(3):228–239.
- , , , , .Reassessment of body mass indices.Am J Clin Nutr.1990;52(3):405–408.
- , , , et al.Accuracy of body mass index in diagnosing obesity in the adult general population.Int J Obes (Lond).2008;32(6):959–966.
- , , , , , .Clarifying confusion: the confusion assessment method. A new method for detection of delirium.Ann Intern Med.1990;113(12):941–948.
Copyright © 2009 Society of Hospital Medicine
Jeanne M. Huddleston, Division of Hospital Internal Medicine, Mayo Clinic, 200 First Street SW, Rochester, MN 55905