User login
Doctor, my breathing is better when I lie down
A 73‐year‐old female presented with progressive shortness of breath that was worse in the upright position and was relieved when she was lying flat (platypnea). Arterial blood gas analysis revealed a partial pressure of oxygen of 56 mm Hg in the supine position and 42 mm Hg when the patient was seated upright. Chest radiography revealed an ill‐defined density in the left lung base, and a high‐resolution computed tomography scan of the chest revealed dilated arteries and veins in the left lower lobe (Figure 1). Pulmonary angiography showed a huge pulmonary arteriovenous malformation (PAVM) with a nidus of 7 cm 8 cm involving the left lower lobe (Figure 2; the arrow points to the catheter tip). Embolization therapy was not an option because of the large size of the PAVM, which would have necessitated several coils with an increased risk of systemic embolization. Left lower lobectomy was performed with marked relief of the patient's dyspnea and hypoxemia.
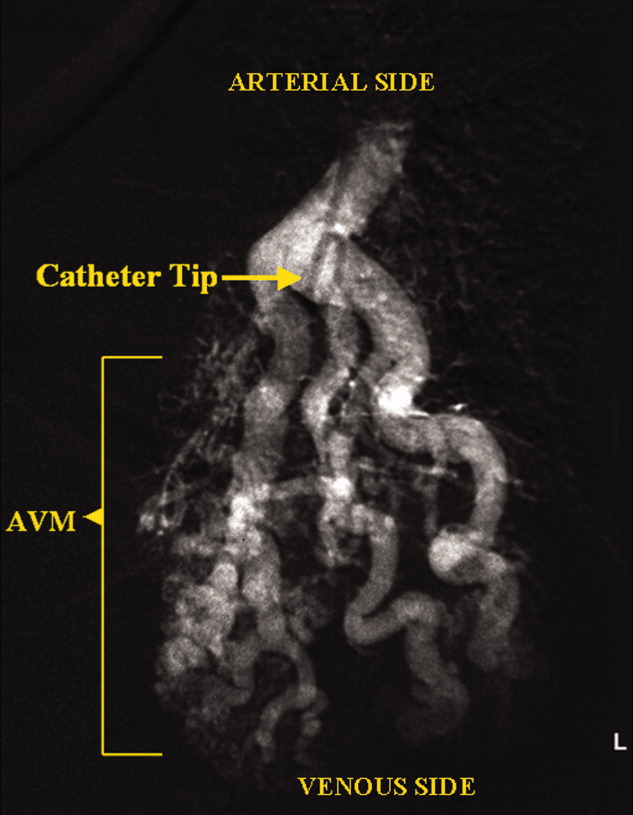
PAVMs are extracardiac shunts caused by abnormal communication between pulmonary arteries and pulmonary veins. Hereditary hemorrhagic telangiectasia accounts for nearly 84% of PAVMs. PAVMs as complications of the surgical treatment of complex cyanotic congenital heart disease, trauma, and liver disease and sporadic PAVMs, as in our case, are less common. There were no associated signs of hereditary hemorrhagic telangiectasia or liver disease in our patient, and gradual enlargement over time likely resulted in the late presentation. Common clinical manifestations of PAVMs include dyspnea, hemoptysis, and chest pain. A PAVM may also cause platypnea because of a decrease in blood flow through the PAVM in the dependent portions of the lungs when the patient changes from an upright position to a supine position. This decrease in blood flow though the PAVM causes an improvement in the shortness of breath and hypoxemia as there is decreased right‐to‐left shunting of blood. Treatment is initiated for all symptomatic patients and PAVMs more than 2 cm in diameter. Embolization therapy is preferable because it avoids the risks of major surgery. Surgery is performed for patients with an untreatable allergy to the contrast material and with large PAVMs not technically amenable to embolization therapy, as in our patient.
A 73‐year‐old female presented with progressive shortness of breath that was worse in the upright position and was relieved when she was lying flat (platypnea). Arterial blood gas analysis revealed a partial pressure of oxygen of 56 mm Hg in the supine position and 42 mm Hg when the patient was seated upright. Chest radiography revealed an ill‐defined density in the left lung base, and a high‐resolution computed tomography scan of the chest revealed dilated arteries and veins in the left lower lobe (Figure 1). Pulmonary angiography showed a huge pulmonary arteriovenous malformation (PAVM) with a nidus of 7 cm 8 cm involving the left lower lobe (Figure 2; the arrow points to the catheter tip). Embolization therapy was not an option because of the large size of the PAVM, which would have necessitated several coils with an increased risk of systemic embolization. Left lower lobectomy was performed with marked relief of the patient's dyspnea and hypoxemia.
PAVMs are extracardiac shunts caused by abnormal communication between pulmonary arteries and pulmonary veins. Hereditary hemorrhagic telangiectasia accounts for nearly 84% of PAVMs. PAVMs as complications of the surgical treatment of complex cyanotic congenital heart disease, trauma, and liver disease and sporadic PAVMs, as in our case, are less common. There were no associated signs of hereditary hemorrhagic telangiectasia or liver disease in our patient, and gradual enlargement over time likely resulted in the late presentation. Common clinical manifestations of PAVMs include dyspnea, hemoptysis, and chest pain. A PAVM may also cause platypnea because of a decrease in blood flow through the PAVM in the dependent portions of the lungs when the patient changes from an upright position to a supine position. This decrease in blood flow though the PAVM causes an improvement in the shortness of breath and hypoxemia as there is decreased right‐to‐left shunting of blood. Treatment is initiated for all symptomatic patients and PAVMs more than 2 cm in diameter. Embolization therapy is preferable because it avoids the risks of major surgery. Surgery is performed for patients with an untreatable allergy to the contrast material and with large PAVMs not technically amenable to embolization therapy, as in our patient.
A 73‐year‐old female presented with progressive shortness of breath that was worse in the upright position and was relieved when she was lying flat (platypnea). Arterial blood gas analysis revealed a partial pressure of oxygen of 56 mm Hg in the supine position and 42 mm Hg when the patient was seated upright. Chest radiography revealed an ill‐defined density in the left lung base, and a high‐resolution computed tomography scan of the chest revealed dilated arteries and veins in the left lower lobe (Figure 1). Pulmonary angiography showed a huge pulmonary arteriovenous malformation (PAVM) with a nidus of 7 cm 8 cm involving the left lower lobe (Figure 2; the arrow points to the catheter tip). Embolization therapy was not an option because of the large size of the PAVM, which would have necessitated several coils with an increased risk of systemic embolization. Left lower lobectomy was performed with marked relief of the patient's dyspnea and hypoxemia.
PAVMs are extracardiac shunts caused by abnormal communication between pulmonary arteries and pulmonary veins. Hereditary hemorrhagic telangiectasia accounts for nearly 84% of PAVMs. PAVMs as complications of the surgical treatment of complex cyanotic congenital heart disease, trauma, and liver disease and sporadic PAVMs, as in our case, are less common. There were no associated signs of hereditary hemorrhagic telangiectasia or liver disease in our patient, and gradual enlargement over time likely resulted in the late presentation. Common clinical manifestations of PAVMs include dyspnea, hemoptysis, and chest pain. A PAVM may also cause platypnea because of a decrease in blood flow through the PAVM in the dependent portions of the lungs when the patient changes from an upright position to a supine position. This decrease in blood flow though the PAVM causes an improvement in the shortness of breath and hypoxemia as there is decreased right‐to‐left shunting of blood. Treatment is initiated for all symptomatic patients and PAVMs more than 2 cm in diameter. Embolization therapy is preferable because it avoids the risks of major surgery. Surgery is performed for patients with an untreatable allergy to the contrast material and with large PAVMs not technically amenable to embolization therapy, as in our patient.
Plane Crash Highlights Hospitalists' Role in MCIs
Mass casualty incidents (MCIs), such as the landing of a US Airways jetliner in New York City's frigid Hudson River, showcase the role hospitalists can play in an ED scrambling to handle a triage scenario.
When the Airbus A320 and its 155 passengers crashed Jan. 15, New York and New Jersey hospitals braced for incoming patients. However, reports showed only a few dozen passengers were treated—the most serious for a fractured leg. Still, at Jersey City (N.J.) Medical Center (JCMC), eight victims brought to the ED meant half a dozen patients had to be discharged to make room.
"The hospitalists were involved only on the periphery this time, as we initially needed their approval to move patients out in anticipation of mass casualties," Douglas Ratner, MD, chairman and program director of JCMC's Department of Medicine, wrote in an e-mail. "They will be integral in future endeavors like this."
To that end, some hospitalists used the "Miracle on the Hudson" as a rallying cry for more training.
"How many of us have gone through rigorous teamwork training to learn to better communicate with our 'cabinmates' during times of stress? Remarkably few," Robert Wachter, MD, a hospitalist as well as a professor and associate chairman of the University of California at San Francisco’s department of medicine, wrote on his blog (the-hospitalist.org/blogs). "How often do we need to demonstrate our continued competency in our specialty? For most board-certified physicians, about every 10 years (up from 'never' 20 years ago). And how well do we learn from our errors? Well, never mind."
Mass casualty incidents (MCIs), such as the landing of a US Airways jetliner in New York City's frigid Hudson River, showcase the role hospitalists can play in an ED scrambling to handle a triage scenario.
When the Airbus A320 and its 155 passengers crashed Jan. 15, New York and New Jersey hospitals braced for incoming patients. However, reports showed only a few dozen passengers were treated—the most serious for a fractured leg. Still, at Jersey City (N.J.) Medical Center (JCMC), eight victims brought to the ED meant half a dozen patients had to be discharged to make room.
"The hospitalists were involved only on the periphery this time, as we initially needed their approval to move patients out in anticipation of mass casualties," Douglas Ratner, MD, chairman and program director of JCMC's Department of Medicine, wrote in an e-mail. "They will be integral in future endeavors like this."
To that end, some hospitalists used the "Miracle on the Hudson" as a rallying cry for more training.
"How many of us have gone through rigorous teamwork training to learn to better communicate with our 'cabinmates' during times of stress? Remarkably few," Robert Wachter, MD, a hospitalist as well as a professor and associate chairman of the University of California at San Francisco’s department of medicine, wrote on his blog (the-hospitalist.org/blogs). "How often do we need to demonstrate our continued competency in our specialty? For most board-certified physicians, about every 10 years (up from 'never' 20 years ago). And how well do we learn from our errors? Well, never mind."
Mass casualty incidents (MCIs), such as the landing of a US Airways jetliner in New York City's frigid Hudson River, showcase the role hospitalists can play in an ED scrambling to handle a triage scenario.
When the Airbus A320 and its 155 passengers crashed Jan. 15, New York and New Jersey hospitals braced for incoming patients. However, reports showed only a few dozen passengers were treated—the most serious for a fractured leg. Still, at Jersey City (N.J.) Medical Center (JCMC), eight victims brought to the ED meant half a dozen patients had to be discharged to make room.
"The hospitalists were involved only on the periphery this time, as we initially needed their approval to move patients out in anticipation of mass casualties," Douglas Ratner, MD, chairman and program director of JCMC's Department of Medicine, wrote in an e-mail. "They will be integral in future endeavors like this."
To that end, some hospitalists used the "Miracle on the Hudson" as a rallying cry for more training.
"How many of us have gone through rigorous teamwork training to learn to better communicate with our 'cabinmates' during times of stress? Remarkably few," Robert Wachter, MD, a hospitalist as well as a professor and associate chairman of the University of California at San Francisco’s department of medicine, wrote on his blog (the-hospitalist.org/blogs). "How often do we need to demonstrate our continued competency in our specialty? For most board-certified physicians, about every 10 years (up from 'never' 20 years ago). And how well do we learn from our errors? Well, never mind."
The Blog Rounds
Too busy rounding on patients to keep up with the blogosphere? We're doing the surfing for you in this first monthly roundup of what your colleagues are buzzing about in cyberspace.
First up: The Happy Hospitalist, who was not happy about Medco CEO Dave Snow's support of treatment protocols, had the following to say last week: "This guy doesn't get it. Cookbook medicine is but a tiny fraction of care. Perhaps 5% or less. I can admit a hemorrhagic stroke, follow standardized protocols, and the next 10 patients will have 10 different permutations of care. I can follow the guidelines to a T and every single patient's comorbid conditions will add layers upon layers of complication to the management."
On SHM's Hospitalist Leader blog, former SHM CEO Rusty Holman touched upon another frustration in the workplace: New hires who complain that "this isn't what I signed up for." Dr. Holman’s advice? When hiring explain that "the job you take today is likely— no, is certain— to be different a year from now." Dr. Holman assures practice managers that "as a leader, you will never be faulted for telling the truth."
Speaking of leaders, Health Beat's Maggie Mahar offered her thoughts on President Obama's inauguration speech: "When President Obama said, 'The time has come to put away childish things,' I couldn't help but recall healthcare reformer Don Berwick, sounding discouraged last winter, as he said, 'Maybe this country just isn't mature enough for healthcare reform.' Berwick, who is the president of the Institute for Healthcare Improvement, was referring to the fact that at times, it seems that everyone wants healthcare for all— but no one wants to pay for it."
Too busy rounding on patients to keep up with the blogosphere? We're doing the surfing for you in this first monthly roundup of what your colleagues are buzzing about in cyberspace.
First up: The Happy Hospitalist, who was not happy about Medco CEO Dave Snow's support of treatment protocols, had the following to say last week: "This guy doesn't get it. Cookbook medicine is but a tiny fraction of care. Perhaps 5% or less. I can admit a hemorrhagic stroke, follow standardized protocols, and the next 10 patients will have 10 different permutations of care. I can follow the guidelines to a T and every single patient's comorbid conditions will add layers upon layers of complication to the management."
On SHM's Hospitalist Leader blog, former SHM CEO Rusty Holman touched upon another frustration in the workplace: New hires who complain that "this isn't what I signed up for." Dr. Holman’s advice? When hiring explain that "the job you take today is likely— no, is certain— to be different a year from now." Dr. Holman assures practice managers that "as a leader, you will never be faulted for telling the truth."
Speaking of leaders, Health Beat's Maggie Mahar offered her thoughts on President Obama's inauguration speech: "When President Obama said, 'The time has come to put away childish things,' I couldn't help but recall healthcare reformer Don Berwick, sounding discouraged last winter, as he said, 'Maybe this country just isn't mature enough for healthcare reform.' Berwick, who is the president of the Institute for Healthcare Improvement, was referring to the fact that at times, it seems that everyone wants healthcare for all— but no one wants to pay for it."
Too busy rounding on patients to keep up with the blogosphere? We're doing the surfing for you in this first monthly roundup of what your colleagues are buzzing about in cyberspace.
First up: The Happy Hospitalist, who was not happy about Medco CEO Dave Snow's support of treatment protocols, had the following to say last week: "This guy doesn't get it. Cookbook medicine is but a tiny fraction of care. Perhaps 5% or less. I can admit a hemorrhagic stroke, follow standardized protocols, and the next 10 patients will have 10 different permutations of care. I can follow the guidelines to a T and every single patient's comorbid conditions will add layers upon layers of complication to the management."
On SHM's Hospitalist Leader blog, former SHM CEO Rusty Holman touched upon another frustration in the workplace: New hires who complain that "this isn't what I signed up for." Dr. Holman’s advice? When hiring explain that "the job you take today is likely— no, is certain— to be different a year from now." Dr. Holman assures practice managers that "as a leader, you will never be faulted for telling the truth."
Speaking of leaders, Health Beat's Maggie Mahar offered her thoughts on President Obama's inauguration speech: "When President Obama said, 'The time has come to put away childish things,' I couldn't help but recall healthcare reformer Don Berwick, sounding discouraged last winter, as he said, 'Maybe this country just isn't mature enough for healthcare reform.' Berwick, who is the president of the Institute for Healthcare Improvement, was referring to the fact that at times, it seems that everyone wants healthcare for all— but no one wants to pay for it."
Onward and Upward
New data from the American Hospital Association (AHA) showing hospitalists number 23,000 and now practice in 4 out of 5 large hospitals drew the same response from doctors and administrators alike: We know.
"I don’t think a hospitalist program is optional," says Mark Larey, MD, vice president of medical affairs at St. Joseph's Mercy Health Center in Hot Springs, Ark. "In today’s environment, due to the regulatory issues, trying to improve patient satisfaction, trying to manage the increased unassigned population, it would be increasingly difficult to keep everything balanced … without a hospitalist service."
Dr. Larey's 309-bed hospital has a team of five internists and one nurse practitioner, and is adding a sixth full-time position this fall to absorb increased stress on the emergency department. The situation is typical of the exponential growth of the industry since it started in 1996 with as few as 500 hospitalists, says Larry Wellikson, MD, CEO of SHM.
In many hospitals, hospital medicine has become a quality-care necessity—one that increases satisfaction scores, trims length of stay, and increases emergency-room throughputs, Dr. Wellikson says. AHA figures culled from the 2007 survey of nearly 5,000 community hospitals show that at hospitals with 200 or more beds, 83% have hospital medicine programs. SHM estimates the current hospitalist workforce at 29,000.
"It took emergency medicine 25, 30 years to get to the point hospital medicine got to in 10 years," Dr. Wellikson says. "It’s the growth of a specialty on steroids."
For more information, visit http://www.aha.org/aha/research-and-trends/health-and-hospital-trends/2008.html.
New data from the American Hospital Association (AHA) showing hospitalists number 23,000 and now practice in 4 out of 5 large hospitals drew the same response from doctors and administrators alike: We know.
"I don’t think a hospitalist program is optional," says Mark Larey, MD, vice president of medical affairs at St. Joseph's Mercy Health Center in Hot Springs, Ark. "In today’s environment, due to the regulatory issues, trying to improve patient satisfaction, trying to manage the increased unassigned population, it would be increasingly difficult to keep everything balanced … without a hospitalist service."
Dr. Larey's 309-bed hospital has a team of five internists and one nurse practitioner, and is adding a sixth full-time position this fall to absorb increased stress on the emergency department. The situation is typical of the exponential growth of the industry since it started in 1996 with as few as 500 hospitalists, says Larry Wellikson, MD, CEO of SHM.
In many hospitals, hospital medicine has become a quality-care necessity—one that increases satisfaction scores, trims length of stay, and increases emergency-room throughputs, Dr. Wellikson says. AHA figures culled from the 2007 survey of nearly 5,000 community hospitals show that at hospitals with 200 or more beds, 83% have hospital medicine programs. SHM estimates the current hospitalist workforce at 29,000.
"It took emergency medicine 25, 30 years to get to the point hospital medicine got to in 10 years," Dr. Wellikson says. "It’s the growth of a specialty on steroids."
For more information, visit http://www.aha.org/aha/research-and-trends/health-and-hospital-trends/2008.html.
New data from the American Hospital Association (AHA) showing hospitalists number 23,000 and now practice in 4 out of 5 large hospitals drew the same response from doctors and administrators alike: We know.
"I don’t think a hospitalist program is optional," says Mark Larey, MD, vice president of medical affairs at St. Joseph's Mercy Health Center in Hot Springs, Ark. "In today’s environment, due to the regulatory issues, trying to improve patient satisfaction, trying to manage the increased unassigned population, it would be increasingly difficult to keep everything balanced … without a hospitalist service."
Dr. Larey's 309-bed hospital has a team of five internists and one nurse practitioner, and is adding a sixth full-time position this fall to absorb increased stress on the emergency department. The situation is typical of the exponential growth of the industry since it started in 1996 with as few as 500 hospitalists, says Larry Wellikson, MD, CEO of SHM.
In many hospitals, hospital medicine has become a quality-care necessity—one that increases satisfaction scores, trims length of stay, and increases emergency-room throughputs, Dr. Wellikson says. AHA figures culled from the 2007 survey of nearly 5,000 community hospitals show that at hospitals with 200 or more beds, 83% have hospital medicine programs. SHM estimates the current hospitalist workforce at 29,000.
"It took emergency medicine 25, 30 years to get to the point hospital medicine got to in 10 years," Dr. Wellikson says. "It’s the growth of a specialty on steroids."
For more information, visit http://www.aha.org/aha/research-and-trends/health-and-hospital-trends/2008.html.
Research Roundup
Question: Can a D-dimer level assess the risk of recurrent venous thromboembolism (VTE) after a course of anticoagulation therapy has been completed?
Background: The duration of anticoagulation therapy for first unprovoked VTE is uncertain. Identifying risk of recurrent VTE will help clinicians make decisions on optimal duration of anticoagulation.
Study design: Systematic review and meta-analysis.
Setting: Patients who have completed therapy for an episode of VTE without known risks.
Synopsis: Seven high-quality studies totaling 1,888 patients with first unprovoked VTE were analyzed. All patients received standardized therapy for at least three months with warfarin (Coumadin). A D-dimer had been checked in all patients between three and six weeks after stopping anticoagulation. The annual rate of VTE recurrence among patients with a positive D-dimer result was 8.9% (confidence interval (CI), 5.8% to 11.9%) compared with 3.5% (CI, 2.7 to 4.3%) for those with a negative result.
False-positive or false-negative D-dimer results could have occurred due to the heterogeneity in duration of anticoagulation and timing of D-dimer testing among the various studies. Since none of the studies were blinded to a history of VTE, there is potential for outcome ascertainment bias due to studying a sample deemed susceptible to disease recurrence.
Bottom line: D-dimer testing holds promise in identifying risk of VTE recurrence and could aid therapeutic decision-making regarding duration of anticoagulation.
Citation: Ann Intern Med. 2008;149:481-490
–Reviewed for the eWire by Rebecca Allyn, MD, Smitha Chadaga, MD, Mary Dedecker, MD, Vignesh Narayanan, MD, Eugene S. Chu, MD, Division of Hospital Medicine, Denver Health and Hospital Authority
Question: Can a D-dimer level assess the risk of recurrent venous thromboembolism (VTE) after a course of anticoagulation therapy has been completed?
Background: The duration of anticoagulation therapy for first unprovoked VTE is uncertain. Identifying risk of recurrent VTE will help clinicians make decisions on optimal duration of anticoagulation.
Study design: Systematic review and meta-analysis.
Setting: Patients who have completed therapy for an episode of VTE without known risks.
Synopsis: Seven high-quality studies totaling 1,888 patients with first unprovoked VTE were analyzed. All patients received standardized therapy for at least three months with warfarin (Coumadin). A D-dimer had been checked in all patients between three and six weeks after stopping anticoagulation. The annual rate of VTE recurrence among patients with a positive D-dimer result was 8.9% (confidence interval (CI), 5.8% to 11.9%) compared with 3.5% (CI, 2.7 to 4.3%) for those with a negative result.
False-positive or false-negative D-dimer results could have occurred due to the heterogeneity in duration of anticoagulation and timing of D-dimer testing among the various studies. Since none of the studies were blinded to a history of VTE, there is potential for outcome ascertainment bias due to studying a sample deemed susceptible to disease recurrence.
Bottom line: D-dimer testing holds promise in identifying risk of VTE recurrence and could aid therapeutic decision-making regarding duration of anticoagulation.
Citation: Ann Intern Med. 2008;149:481-490
–Reviewed for the eWire by Rebecca Allyn, MD, Smitha Chadaga, MD, Mary Dedecker, MD, Vignesh Narayanan, MD, Eugene S. Chu, MD, Division of Hospital Medicine, Denver Health and Hospital Authority
Question: Can a D-dimer level assess the risk of recurrent venous thromboembolism (VTE) after a course of anticoagulation therapy has been completed?
Background: The duration of anticoagulation therapy for first unprovoked VTE is uncertain. Identifying risk of recurrent VTE will help clinicians make decisions on optimal duration of anticoagulation.
Study design: Systematic review and meta-analysis.
Setting: Patients who have completed therapy for an episode of VTE without known risks.
Synopsis: Seven high-quality studies totaling 1,888 patients with first unprovoked VTE were analyzed. All patients received standardized therapy for at least three months with warfarin (Coumadin). A D-dimer had been checked in all patients between three and six weeks after stopping anticoagulation. The annual rate of VTE recurrence among patients with a positive D-dimer result was 8.9% (confidence interval (CI), 5.8% to 11.9%) compared with 3.5% (CI, 2.7 to 4.3%) for those with a negative result.
False-positive or false-negative D-dimer results could have occurred due to the heterogeneity in duration of anticoagulation and timing of D-dimer testing among the various studies. Since none of the studies were blinded to a history of VTE, there is potential for outcome ascertainment bias due to studying a sample deemed susceptible to disease recurrence.
Bottom line: D-dimer testing holds promise in identifying risk of VTE recurrence and could aid therapeutic decision-making regarding duration of anticoagulation.
Citation: Ann Intern Med. 2008;149:481-490
–Reviewed for the eWire by Rebecca Allyn, MD, Smitha Chadaga, MD, Mary Dedecker, MD, Vignesh Narayanan, MD, Eugene S. Chu, MD, Division of Hospital Medicine, Denver Health and Hospital Authority
CPR for EHRs
The truth about EHR systems is that their implementation is never easy. It's a lot of work. It takes time and money, and despite the best laid plans there will be trauma and frustration. So expecting problems to arise is key to keeping perspective.
When our office implemented an electronic health records system in 2000, our system crashed 25–75 times a day for 5 months, and we lost patient data each time. I repeat: We lost patient data each time. Extensive troubleshooting ensued. Ceiling tiles were ripped out to see if the fluorescent lights were interfering with the network cables, a consultant was brought in, and our server and network were reinstalled. Finally, the cause of the crashes was determined to be a bug in our Microsoft program. As nightmarish as this situation was, I would say that such technology challenges were nothing compared to challenges in managing processes and people.
From a process perspective, a common mistake involves attempting to make the EHR system conform to what is done with paper. The whole point is to imagine a process that can help your office save time and money instead of mirroring what you did for years with a paper-based system.
Staff challenges are by far the toughest ones to manage because they require changing the minds and habits of individuals who don't feel comfortable giving up paper-based processes. Persistent naysayers can sabotage EHR implementation by convincing others that the changes cannot be made. Over the years, four of five staff members have left. When new staff members were hired, we emphasized the fact that our office was computerized and those individuals have successfully adapted to a paperless system. Among the lessons we've learned over the years are these:
▸ Don't skimp on training. When you're spending thousands of dollars on an EHR system it's tempting to shave costs and training may appear to be part of the discretionary spending budget. But giving training short shrift can cost you a lot more than you saved in the long run.
Even if you're the most technologically savvy physician, avoid the “I can do it all” mentality. Your time is best spent seeing patients and making money. Make sure that others are well trained so you feel comfortable delegating EHR responsibilities.
▸ Train the Luddites last. Once you've worked out all the kinks in the training process with those who are most comfortable using computers, it'll go a lot more smoothly for those who are less tech-savvy. Don't let anyone opt out of training. That can cost tens of thousands of dollars in the long run.
▸ Include everyone in brainstorming sessions. While no one likes meetings, get everyone involved in implementation meetings, not just the doctors and the office manager, because you will get good ideas from everyone. In addition, if they are involved in the brainstorming sessions, they are far more likely to adopt new behaviors.
▸ It doesn't have to be perfect. During the transition phase to an EHR system, there's a temptation to try to make everything perfect. Soon after we went live with our system, I spent a lot of time checking electronic charts to make sure the staff had included consultation notes. It was really a wasted step, because 99% of the time they had done it. In the rare event that the notes don't get into the chart, it doesn't affect patient care. The key is knowing when to accept a process as good enough and move on.
▸ Get a leader. You need a leader with a vision to organize the troubleshooting, both to build support and to keep everyone on track. The most common cause of EHR failure is lack of a leader.
The truth about EHR systems is that their implementation is never easy. It's a lot of work. It takes time and money, and despite the best laid plans there will be trauma and frustration. So expecting problems to arise is key to keeping perspective.
When our office implemented an electronic health records system in 2000, our system crashed 25–75 times a day for 5 months, and we lost patient data each time. I repeat: We lost patient data each time. Extensive troubleshooting ensued. Ceiling tiles were ripped out to see if the fluorescent lights were interfering with the network cables, a consultant was brought in, and our server and network were reinstalled. Finally, the cause of the crashes was determined to be a bug in our Microsoft program. As nightmarish as this situation was, I would say that such technology challenges were nothing compared to challenges in managing processes and people.
From a process perspective, a common mistake involves attempting to make the EHR system conform to what is done with paper. The whole point is to imagine a process that can help your office save time and money instead of mirroring what you did for years with a paper-based system.
Staff challenges are by far the toughest ones to manage because they require changing the minds and habits of individuals who don't feel comfortable giving up paper-based processes. Persistent naysayers can sabotage EHR implementation by convincing others that the changes cannot be made. Over the years, four of five staff members have left. When new staff members were hired, we emphasized the fact that our office was computerized and those individuals have successfully adapted to a paperless system. Among the lessons we've learned over the years are these:
▸ Don't skimp on training. When you're spending thousands of dollars on an EHR system it's tempting to shave costs and training may appear to be part of the discretionary spending budget. But giving training short shrift can cost you a lot more than you saved in the long run.
Even if you're the most technologically savvy physician, avoid the “I can do it all” mentality. Your time is best spent seeing patients and making money. Make sure that others are well trained so you feel comfortable delegating EHR responsibilities.
▸ Train the Luddites last. Once you've worked out all the kinks in the training process with those who are most comfortable using computers, it'll go a lot more smoothly for those who are less tech-savvy. Don't let anyone opt out of training. That can cost tens of thousands of dollars in the long run.
▸ Include everyone in brainstorming sessions. While no one likes meetings, get everyone involved in implementation meetings, not just the doctors and the office manager, because you will get good ideas from everyone. In addition, if they are involved in the brainstorming sessions, they are far more likely to adopt new behaviors.
▸ It doesn't have to be perfect. During the transition phase to an EHR system, there's a temptation to try to make everything perfect. Soon after we went live with our system, I spent a lot of time checking electronic charts to make sure the staff had included consultation notes. It was really a wasted step, because 99% of the time they had done it. In the rare event that the notes don't get into the chart, it doesn't affect patient care. The key is knowing when to accept a process as good enough and move on.
▸ Get a leader. You need a leader with a vision to organize the troubleshooting, both to build support and to keep everyone on track. The most common cause of EHR failure is lack of a leader.
The truth about EHR systems is that their implementation is never easy. It's a lot of work. It takes time and money, and despite the best laid plans there will be trauma and frustration. So expecting problems to arise is key to keeping perspective.
When our office implemented an electronic health records system in 2000, our system crashed 25–75 times a day for 5 months, and we lost patient data each time. I repeat: We lost patient data each time. Extensive troubleshooting ensued. Ceiling tiles were ripped out to see if the fluorescent lights were interfering with the network cables, a consultant was brought in, and our server and network were reinstalled. Finally, the cause of the crashes was determined to be a bug in our Microsoft program. As nightmarish as this situation was, I would say that such technology challenges were nothing compared to challenges in managing processes and people.
From a process perspective, a common mistake involves attempting to make the EHR system conform to what is done with paper. The whole point is to imagine a process that can help your office save time and money instead of mirroring what you did for years with a paper-based system.
Staff challenges are by far the toughest ones to manage because they require changing the minds and habits of individuals who don't feel comfortable giving up paper-based processes. Persistent naysayers can sabotage EHR implementation by convincing others that the changes cannot be made. Over the years, four of five staff members have left. When new staff members were hired, we emphasized the fact that our office was computerized and those individuals have successfully adapted to a paperless system. Among the lessons we've learned over the years are these:
▸ Don't skimp on training. When you're spending thousands of dollars on an EHR system it's tempting to shave costs and training may appear to be part of the discretionary spending budget. But giving training short shrift can cost you a lot more than you saved in the long run.
Even if you're the most technologically savvy physician, avoid the “I can do it all” mentality. Your time is best spent seeing patients and making money. Make sure that others are well trained so you feel comfortable delegating EHR responsibilities.
▸ Train the Luddites last. Once you've worked out all the kinks in the training process with those who are most comfortable using computers, it'll go a lot more smoothly for those who are less tech-savvy. Don't let anyone opt out of training. That can cost tens of thousands of dollars in the long run.
▸ Include everyone in brainstorming sessions. While no one likes meetings, get everyone involved in implementation meetings, not just the doctors and the office manager, because you will get good ideas from everyone. In addition, if they are involved in the brainstorming sessions, they are far more likely to adopt new behaviors.
▸ It doesn't have to be perfect. During the transition phase to an EHR system, there's a temptation to try to make everything perfect. Soon after we went live with our system, I spent a lot of time checking electronic charts to make sure the staff had included consultation notes. It was really a wasted step, because 99% of the time they had done it. In the rare event that the notes don't get into the chart, it doesn't affect patient care. The key is knowing when to accept a process as good enough and move on.
▸ Get a leader. You need a leader with a vision to organize the troubleshooting, both to build support and to keep everyone on track. The most common cause of EHR failure is lack of a leader.
A New Revenue Source?
A recently expanded palliative care program at University Hospital in Salt Lake City is the latest window into ancillary revenue streams hospitalists can tap during the continuing economic crisis.
Stephen Bekanich, MD, a hospitalist and medical director of the Utah center's palliative-care team, says his program saves money for the hospital and increases the value of its hospitalists. In October, Dr. Bekanich's team expanded into outpatient clinic treatment one half-day a week. While he plans to study the revenue generated through that month before expanding further, Dr. Bekanich thinks palliative-care teams are a strong revenue source for hospitalists.
"It’s a natural tie-in," he says. "The people that probably win the most with having palliative care established within the hospital is the hospital itself. We see that in our patient satisfaction."
Palliative care can lower hospital expenditures by cutting down on costly procedures that may not improve a patient's quality of life, as well as by trimming lengths of stay, Dr. Bekanich says. In the first half of 2008, Dr. Bekanich's team saved University Hospital about $600,000. The team’s 2008 budget was roughly $330,000 for about 500 encounters.
There are obstacles, though. Because palliative care is a recognized specialty, starting a program requires a hospitalist who is willing—and able—to become certified and hospital administration willing to front expenditures.
"The idea of starting this from scratch is going to become more difficult," Dr. Bekanich says, "but it’s worthwhile."
A recently expanded palliative care program at University Hospital in Salt Lake City is the latest window into ancillary revenue streams hospitalists can tap during the continuing economic crisis.
Stephen Bekanich, MD, a hospitalist and medical director of the Utah center's palliative-care team, says his program saves money for the hospital and increases the value of its hospitalists. In October, Dr. Bekanich's team expanded into outpatient clinic treatment one half-day a week. While he plans to study the revenue generated through that month before expanding further, Dr. Bekanich thinks palliative-care teams are a strong revenue source for hospitalists.
"It’s a natural tie-in," he says. "The people that probably win the most with having palliative care established within the hospital is the hospital itself. We see that in our patient satisfaction."
Palliative care can lower hospital expenditures by cutting down on costly procedures that may not improve a patient's quality of life, as well as by trimming lengths of stay, Dr. Bekanich says. In the first half of 2008, Dr. Bekanich's team saved University Hospital about $600,000. The team’s 2008 budget was roughly $330,000 for about 500 encounters.
There are obstacles, though. Because palliative care is a recognized specialty, starting a program requires a hospitalist who is willing—and able—to become certified and hospital administration willing to front expenditures.
"The idea of starting this from scratch is going to become more difficult," Dr. Bekanich says, "but it’s worthwhile."
A recently expanded palliative care program at University Hospital in Salt Lake City is the latest window into ancillary revenue streams hospitalists can tap during the continuing economic crisis.
Stephen Bekanich, MD, a hospitalist and medical director of the Utah center's palliative-care team, says his program saves money for the hospital and increases the value of its hospitalists. In October, Dr. Bekanich's team expanded into outpatient clinic treatment one half-day a week. While he plans to study the revenue generated through that month before expanding further, Dr. Bekanich thinks palliative-care teams are a strong revenue source for hospitalists.
"It’s a natural tie-in," he says. "The people that probably win the most with having palliative care established within the hospital is the hospital itself. We see that in our patient satisfaction."
Palliative care can lower hospital expenditures by cutting down on costly procedures that may not improve a patient's quality of life, as well as by trimming lengths of stay, Dr. Bekanich says. In the first half of 2008, Dr. Bekanich's team saved University Hospital about $600,000. The team’s 2008 budget was roughly $330,000 for about 500 encounters.
There are obstacles, though. Because palliative care is a recognized specialty, starting a program requires a hospitalist who is willing—and able—to become certified and hospital administration willing to front expenditures.
"The idea of starting this from scratch is going to become more difficult," Dr. Bekanich says, "but it’s worthwhile."
Ringing in the New Year
Garth King, MD, a hospitalist and medical director at Southwest General Medical Center in Lafayette, La., wasn’t surprised he was treating an inebriated 17-year-old who came to the hospital with his mother this past New Year's Eve. The intoxicated 14-year-old who came in shortly after, however, did throw him slightly off guard.
"We usually just send them to the emergency room, where they are monitored," Dr. King says. "It's a waste of resources to admit them."
Kenneth Patrick, MD, a hospitalist and ICU director at Chestnut Hill Hospital in Philadelphia, says alcohol-related conditions, including gastritis and pancreatitis, are the most common cases he sees on New Year's Eve and New Year's Day. The second-most common, he says, are fractures caused by slipping on ice or snow.
"New Year's Day is the busiest day of the year for inpatients," Dr. Patrick says.
National data on daily hospital visits don't exist, but Dr. King agrees with Dr. Patrick's assessment. He says the number of patients his group normally sees doubles between Christmas Eve and New Year’s Day. "In residency, I remember this would happen," he says. "It would seem like family members would bring in their family members, just because."
If you are one of the unfortunate members of your HM group scheduled to work next holiday season, Dr. Patrick offers a little advice: "Stay well-hydrated and get lots of rest, because you will be busy."
Garth King, MD, a hospitalist and medical director at Southwest General Medical Center in Lafayette, La., wasn’t surprised he was treating an inebriated 17-year-old who came to the hospital with his mother this past New Year's Eve. The intoxicated 14-year-old who came in shortly after, however, did throw him slightly off guard.
"We usually just send them to the emergency room, where they are monitored," Dr. King says. "It's a waste of resources to admit them."
Kenneth Patrick, MD, a hospitalist and ICU director at Chestnut Hill Hospital in Philadelphia, says alcohol-related conditions, including gastritis and pancreatitis, are the most common cases he sees on New Year's Eve and New Year's Day. The second-most common, he says, are fractures caused by slipping on ice or snow.
"New Year's Day is the busiest day of the year for inpatients," Dr. Patrick says.
National data on daily hospital visits don't exist, but Dr. King agrees with Dr. Patrick's assessment. He says the number of patients his group normally sees doubles between Christmas Eve and New Year’s Day. "In residency, I remember this would happen," he says. "It would seem like family members would bring in their family members, just because."
If you are one of the unfortunate members of your HM group scheduled to work next holiday season, Dr. Patrick offers a little advice: "Stay well-hydrated and get lots of rest, because you will be busy."
Garth King, MD, a hospitalist and medical director at Southwest General Medical Center in Lafayette, La., wasn’t surprised he was treating an inebriated 17-year-old who came to the hospital with his mother this past New Year's Eve. The intoxicated 14-year-old who came in shortly after, however, did throw him slightly off guard.
"We usually just send them to the emergency room, where they are monitored," Dr. King says. "It's a waste of resources to admit them."
Kenneth Patrick, MD, a hospitalist and ICU director at Chestnut Hill Hospital in Philadelphia, says alcohol-related conditions, including gastritis and pancreatitis, are the most common cases he sees on New Year's Eve and New Year's Day. The second-most common, he says, are fractures caused by slipping on ice or snow.
"New Year's Day is the busiest day of the year for inpatients," Dr. Patrick says.
National data on daily hospital visits don't exist, but Dr. King agrees with Dr. Patrick's assessment. He says the number of patients his group normally sees doubles between Christmas Eve and New Year’s Day. "In residency, I remember this would happen," he says. "It would seem like family members would bring in their family members, just because."
If you are one of the unfortunate members of your HM group scheduled to work next holiday season, Dr. Patrick offers a little advice: "Stay well-hydrated and get lots of rest, because you will be busy."
Methicillin‐resistant Staphylococcus aureus bacteremia due to prostatic abscess
Community‐associated methicillin‐resistant Staphylococcus aureus (MRSA) infection is an evolving disease that is changing medical practice. MRSA has become the most frequent cause of skin and soft‐tissue infections presenting to most emergency departments in the United States.1 In comparison with methicillin‐sensitive S. aureus, community‐associated MRSA is more likely to present as soft‐tissue abscesses or necrotizing pneumonia.2 In 2005 alone, 94,360 invasive MRSA infections were estimated to have occurred in the United States, most of which were associated with MRSA bacteremia.3 In the hospital, MRSA infections are associated with greater lengths of stay, higher mortality, and increased costs.3
We report a patient with persistent MRSA bacteremia due to a prostatic abscess. Prostatitis or prostatic abscess with MRSA has rarely been reported. Resolution of the bacteremia was achieved only after drainage of the abscess. This case highlights the importance of recognizing this clinical condition and draining any MRSA‐associated abscesses. In addition, the abscess‐forming characteristics of MRSA may suggest that the incidence of prostatic abscess due to this microbe is on the rise.
CASE REPORT
A 40‐year‐old human immunodeficiency viruspositive man presented with a 10‐day history of intermittent fever, urinary hesitancy, weak urinary stream, and intermittent abdominal pain relieved following urination. He denied dysuria, hematuria, chest pain, dyspnea, nausea, weight loss, diarrhea, or decreased functional status. His last CD4 count was 528/L on highly active antiretroviral therapy 1 year prior to presentation; however, he had run out of medications several months prior to presentation. His medical history was also significant for incision and drainage of skin abscesses with unknown microbiology several months prior to presentation. He currently used tobacco but denied illicit drug use. He was sexually abstinent for over a year prior to presentation but had a history of having unprotected sex with men.
On physical examination, his vital signs were as follows: temperature, 37.8C; blood pressure, 133/84 mm Hg; heart rate, 107 beats/minute; respiration rate, 16 breaths/minute; and oxygen saturation, 100% on room air. He was under no distress. His heart sound was tachycardic and regular with no murmur noted. Lung sounds were clear. Abdominal examination revealed no tenderness or organomegaly. His prostate was boggy, minimally tender, and slightly enlarged. The rest of his physical examination was normal. The white blood cell count was 7.5 109/L with 79% neutrophils. The serum chemistry was normal. The prostate‐specific antigen level was 2.9 ng/mL. A repeat CD4 count was 140/L. Urinalysis revealed large leukocyte esterase, no nitrites, and 60 white blood cells per high‐power field. He was diagnosed with prostatitis and discharged on levofloxacin.
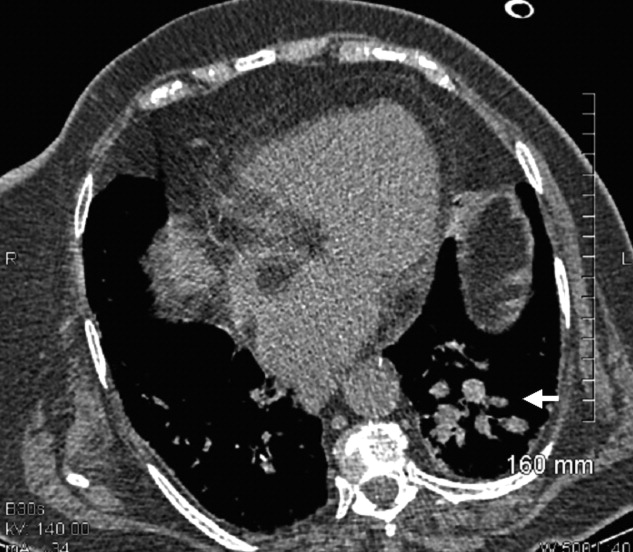
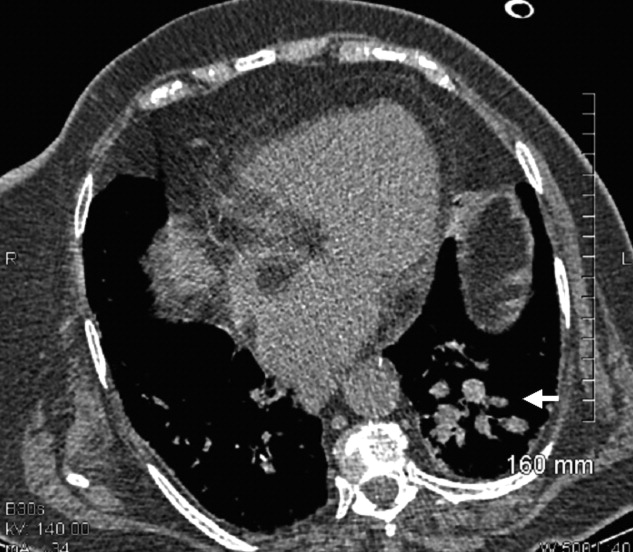
The subsequent day, he returned to the emergency department with an inability to void. A Foley catheter was placed with resolution of his symptoms. Later that day, blood cultures from his initial admission grew MRSA in 2 out of 4 bottles, and he was admitted to the hospital. A review of the prior urine culture showed no growth. Computed tomography (CT) of the abdomen and pelvis showed an enlarged prostate with multiple noncommunicating peripherally enhancing hypodensities consistent with prostatic abscesses (arrows in Figure 1). These abscesses were associated with periprostatic fat stranding, edematous seminal vesicles, diffuse urinary bladder wall thickening, and mild inguinal adenopathy. Therapy with intravenous vancomycin was initiated.

Over the next 6 days, the patient continued to have intermittent fevers. Blood cultures continued to grow MRSA. Gentamicin was added for possible synergy on hospital day 3 without improvement. A transesophageal echocardiogram was normal. On hospital day 6, repeat CT showed no change in the size of the prostatic abscesses but an increased capsular bulge along the right mid gland. The urology service was consulted. They performed bedside transperineal drainage of the largest abscess with transrectal ultrasound guidance. No indwelling drain was placed. A culture of the purulent drainage grew MRSA. Three days after the surgical drainage, the patient was afebrile, urinary symptoms had resolved, and serial blood cultures remained negative. He was discharged on hospital day 13 to complete a 4‐week course of intravenous vancomycin. The patient missed an appointment for follow‐up imaging.
DISCUSSION
We report a case of community‐associated MRSA bacteremia secondary to a prostatic abscess, as confirmed by cultures from serum and of the abscess. S. aureus bacteremia often stems from infections of the respiratory tract, skin, and soft tissues, endocarditis, or infections of indwelling devices.4S. aureus can then create embolic foci, including in the prostate, which can serve as sources of persistent bacteremia. However, new evidence suggests community‐associated MRSA might be sexually transmitted among men who have sex with men.5 An MRSA prostatic abscess could then potentially be related to an ascending urinary tract infection or translocation from the gastrointestinal tract.
The vast majority of prostatitis cases prostatic abscesses are caused by Escherichia coli and other gram‐negative bacilli.6 Staphylococcus species are less common, and MRSA isolates have been described as a rare etiologic agent. Only four other case reports describing MRSA bacteremia associated with prostatitis or prostatic abscesses have been published.710 Both our patient and the three other case reports in the literature with prostatic abscesses and MRSA bacteremia required drainage of the abscess as well as antibiotics for resolution. The other reported cases involved drainage by transurethral resection of the prostate,79 whereas our case used transperineal drainage of the prostatic abscess via transrectal ultrasound guidance. In addition to intravenous antibiotics, drainage appears to be a key therapeutic measure for resolution of MRSA prostatic abscesses.
With the increasing incidence of community‐associated and healthcare‐associated MRSA infections, the incidence of prostatitis or prostatic abscesses secondary to MRSA may be increasing. MRSA seems to have a specific predilection for abscess formation in skin and soft‐tissue infections and pneumonia.2 Clinicians must be alert to a potentially higher frequency of MRSA as a cause of prostatic abscesses and prostatitis.
In the evaluation of a patient with persistent MRSA bacteremia, the potential for the prostate as a source of infection should be considered. Urinary symptoms may be subtle. Clinicians should have a low threshold for imaging studies such as CT to evaluate for a possible source of MRSA bacteremia. If a prostatic abscess is found, prompt surgical drainage or debridement is necessary for cure.
- ,,, et al.Methicillin‐resistant S. aureus infections among patients in the emergency department.N Engl J Med.2006;355:666–674.
- ,,, et al.Comparison of both clinical features and mortality risk associated with bacteremia due to community‐acquired methicillin‐resistant Staphylococcus aureus and methicillin‐susceptible S. aureus.Clin Infect Dis.2008;46:799–806.
- ,,, et al.Invasive methicillin‐resistant Staphylococcus aureus infections in the United States.JAMA.2007;298:1763–1771.
- ,,,,,.The current spectrum of Staphylococcus aureus infection in a tertiary care hospital.Medicine (Baltimore).1994;73:186–208.
- ,,, et al.Emergence of multidrug‐resistant, community‐associated, methicillin‐resistant Staphylococcus aureus clone USA300 in men who have sex with men.Ann Intern Med.2008;148:249–257.
- ,,, et al.Prostatic abscess in the antibiotic era.Rev Infect Dis.1988;10:239–249.
- ,,.Community‐acquired methicillin‐resistant Staphylococcus aureus prostatic abscess.Urology.2004;64:808–810.
- ,,.Persistent methicillin‐resistant Staphylococcus aureus bacteremia due to a prostatic abscess.Scand J Infect Dis.2003;35:273–274.
- ,.Dual perinephric and prostatic abscesses from methicillin resistant Staphylococcus aureus.South Med J.2007;100:515–516.
- ,.Methicillin‐resistant Staphylococcus aureus prostatitis.Urology.2007;69:779.e1–779.e3.
Community‐associated methicillin‐resistant Staphylococcus aureus (MRSA) infection is an evolving disease that is changing medical practice. MRSA has become the most frequent cause of skin and soft‐tissue infections presenting to most emergency departments in the United States.1 In comparison with methicillin‐sensitive S. aureus, community‐associated MRSA is more likely to present as soft‐tissue abscesses or necrotizing pneumonia.2 In 2005 alone, 94,360 invasive MRSA infections were estimated to have occurred in the United States, most of which were associated with MRSA bacteremia.3 In the hospital, MRSA infections are associated with greater lengths of stay, higher mortality, and increased costs.3
We report a patient with persistent MRSA bacteremia due to a prostatic abscess. Prostatitis or prostatic abscess with MRSA has rarely been reported. Resolution of the bacteremia was achieved only after drainage of the abscess. This case highlights the importance of recognizing this clinical condition and draining any MRSA‐associated abscesses. In addition, the abscess‐forming characteristics of MRSA may suggest that the incidence of prostatic abscess due to this microbe is on the rise.
CASE REPORT
A 40‐year‐old human immunodeficiency viruspositive man presented with a 10‐day history of intermittent fever, urinary hesitancy, weak urinary stream, and intermittent abdominal pain relieved following urination. He denied dysuria, hematuria, chest pain, dyspnea, nausea, weight loss, diarrhea, or decreased functional status. His last CD4 count was 528/L on highly active antiretroviral therapy 1 year prior to presentation; however, he had run out of medications several months prior to presentation. His medical history was also significant for incision and drainage of skin abscesses with unknown microbiology several months prior to presentation. He currently used tobacco but denied illicit drug use. He was sexually abstinent for over a year prior to presentation but had a history of having unprotected sex with men.
On physical examination, his vital signs were as follows: temperature, 37.8C; blood pressure, 133/84 mm Hg; heart rate, 107 beats/minute; respiration rate, 16 breaths/minute; and oxygen saturation, 100% on room air. He was under no distress. His heart sound was tachycardic and regular with no murmur noted. Lung sounds were clear. Abdominal examination revealed no tenderness or organomegaly. His prostate was boggy, minimally tender, and slightly enlarged. The rest of his physical examination was normal. The white blood cell count was 7.5 109/L with 79% neutrophils. The serum chemistry was normal. The prostate‐specific antigen level was 2.9 ng/mL. A repeat CD4 count was 140/L. Urinalysis revealed large leukocyte esterase, no nitrites, and 60 white blood cells per high‐power field. He was diagnosed with prostatitis and discharged on levofloxacin.
The subsequent day, he returned to the emergency department with an inability to void. A Foley catheter was placed with resolution of his symptoms. Later that day, blood cultures from his initial admission grew MRSA in 2 out of 4 bottles, and he was admitted to the hospital. A review of the prior urine culture showed no growth. Computed tomography (CT) of the abdomen and pelvis showed an enlarged prostate with multiple noncommunicating peripherally enhancing hypodensities consistent with prostatic abscesses (arrows in Figure 1). These abscesses were associated with periprostatic fat stranding, edematous seminal vesicles, diffuse urinary bladder wall thickening, and mild inguinal adenopathy. Therapy with intravenous vancomycin was initiated.
Over the next 6 days, the patient continued to have intermittent fevers. Blood cultures continued to grow MRSA. Gentamicin was added for possible synergy on hospital day 3 without improvement. A transesophageal echocardiogram was normal. On hospital day 6, repeat CT showed no change in the size of the prostatic abscesses but an increased capsular bulge along the right mid gland. The urology service was consulted. They performed bedside transperineal drainage of the largest abscess with transrectal ultrasound guidance. No indwelling drain was placed. A culture of the purulent drainage grew MRSA. Three days after the surgical drainage, the patient was afebrile, urinary symptoms had resolved, and serial blood cultures remained negative. He was discharged on hospital day 13 to complete a 4‐week course of intravenous vancomycin. The patient missed an appointment for follow‐up imaging.
DISCUSSION
We report a case of community‐associated MRSA bacteremia secondary to a prostatic abscess, as confirmed by cultures from serum and of the abscess. S. aureus bacteremia often stems from infections of the respiratory tract, skin, and soft tissues, endocarditis, or infections of indwelling devices.4S. aureus can then create embolic foci, including in the prostate, which can serve as sources of persistent bacteremia. However, new evidence suggests community‐associated MRSA might be sexually transmitted among men who have sex with men.5 An MRSA prostatic abscess could then potentially be related to an ascending urinary tract infection or translocation from the gastrointestinal tract.
The vast majority of prostatitis cases prostatic abscesses are caused by Escherichia coli and other gram‐negative bacilli.6 Staphylococcus species are less common, and MRSA isolates have been described as a rare etiologic agent. Only four other case reports describing MRSA bacteremia associated with prostatitis or prostatic abscesses have been published.710 Both our patient and the three other case reports in the literature with prostatic abscesses and MRSA bacteremia required drainage of the abscess as well as antibiotics for resolution. The other reported cases involved drainage by transurethral resection of the prostate,79 whereas our case used transperineal drainage of the prostatic abscess via transrectal ultrasound guidance. In addition to intravenous antibiotics, drainage appears to be a key therapeutic measure for resolution of MRSA prostatic abscesses.
With the increasing incidence of community‐associated and healthcare‐associated MRSA infections, the incidence of prostatitis or prostatic abscesses secondary to MRSA may be increasing. MRSA seems to have a specific predilection for abscess formation in skin and soft‐tissue infections and pneumonia.2 Clinicians must be alert to a potentially higher frequency of MRSA as a cause of prostatic abscesses and prostatitis.
In the evaluation of a patient with persistent MRSA bacteremia, the potential for the prostate as a source of infection should be considered. Urinary symptoms may be subtle. Clinicians should have a low threshold for imaging studies such as CT to evaluate for a possible source of MRSA bacteremia. If a prostatic abscess is found, prompt surgical drainage or debridement is necessary for cure.
Community‐associated methicillin‐resistant Staphylococcus aureus (MRSA) infection is an evolving disease that is changing medical practice. MRSA has become the most frequent cause of skin and soft‐tissue infections presenting to most emergency departments in the United States.1 In comparison with methicillin‐sensitive S. aureus, community‐associated MRSA is more likely to present as soft‐tissue abscesses or necrotizing pneumonia.2 In 2005 alone, 94,360 invasive MRSA infections were estimated to have occurred in the United States, most of which were associated with MRSA bacteremia.3 In the hospital, MRSA infections are associated with greater lengths of stay, higher mortality, and increased costs.3
We report a patient with persistent MRSA bacteremia due to a prostatic abscess. Prostatitis or prostatic abscess with MRSA has rarely been reported. Resolution of the bacteremia was achieved only after drainage of the abscess. This case highlights the importance of recognizing this clinical condition and draining any MRSA‐associated abscesses. In addition, the abscess‐forming characteristics of MRSA may suggest that the incidence of prostatic abscess due to this microbe is on the rise.
CASE REPORT
A 40‐year‐old human immunodeficiency viruspositive man presented with a 10‐day history of intermittent fever, urinary hesitancy, weak urinary stream, and intermittent abdominal pain relieved following urination. He denied dysuria, hematuria, chest pain, dyspnea, nausea, weight loss, diarrhea, or decreased functional status. His last CD4 count was 528/L on highly active antiretroviral therapy 1 year prior to presentation; however, he had run out of medications several months prior to presentation. His medical history was also significant for incision and drainage of skin abscesses with unknown microbiology several months prior to presentation. He currently used tobacco but denied illicit drug use. He was sexually abstinent for over a year prior to presentation but had a history of having unprotected sex with men.
On physical examination, his vital signs were as follows: temperature, 37.8C; blood pressure, 133/84 mm Hg; heart rate, 107 beats/minute; respiration rate, 16 breaths/minute; and oxygen saturation, 100% on room air. He was under no distress. His heart sound was tachycardic and regular with no murmur noted. Lung sounds were clear. Abdominal examination revealed no tenderness or organomegaly. His prostate was boggy, minimally tender, and slightly enlarged. The rest of his physical examination was normal. The white blood cell count was 7.5 109/L with 79% neutrophils. The serum chemistry was normal. The prostate‐specific antigen level was 2.9 ng/mL. A repeat CD4 count was 140/L. Urinalysis revealed large leukocyte esterase, no nitrites, and 60 white blood cells per high‐power field. He was diagnosed with prostatitis and discharged on levofloxacin.
The subsequent day, he returned to the emergency department with an inability to void. A Foley catheter was placed with resolution of his symptoms. Later that day, blood cultures from his initial admission grew MRSA in 2 out of 4 bottles, and he was admitted to the hospital. A review of the prior urine culture showed no growth. Computed tomography (CT) of the abdomen and pelvis showed an enlarged prostate with multiple noncommunicating peripherally enhancing hypodensities consistent with prostatic abscesses (arrows in Figure 1). These abscesses were associated with periprostatic fat stranding, edematous seminal vesicles, diffuse urinary bladder wall thickening, and mild inguinal adenopathy. Therapy with intravenous vancomycin was initiated.
Over the next 6 days, the patient continued to have intermittent fevers. Blood cultures continued to grow MRSA. Gentamicin was added for possible synergy on hospital day 3 without improvement. A transesophageal echocardiogram was normal. On hospital day 6, repeat CT showed no change in the size of the prostatic abscesses but an increased capsular bulge along the right mid gland. The urology service was consulted. They performed bedside transperineal drainage of the largest abscess with transrectal ultrasound guidance. No indwelling drain was placed. A culture of the purulent drainage grew MRSA. Three days after the surgical drainage, the patient was afebrile, urinary symptoms had resolved, and serial blood cultures remained negative. He was discharged on hospital day 13 to complete a 4‐week course of intravenous vancomycin. The patient missed an appointment for follow‐up imaging.
DISCUSSION
We report a case of community‐associated MRSA bacteremia secondary to a prostatic abscess, as confirmed by cultures from serum and of the abscess. S. aureus bacteremia often stems from infections of the respiratory tract, skin, and soft tissues, endocarditis, or infections of indwelling devices.4S. aureus can then create embolic foci, including in the prostate, which can serve as sources of persistent bacteremia. However, new evidence suggests community‐associated MRSA might be sexually transmitted among men who have sex with men.5 An MRSA prostatic abscess could then potentially be related to an ascending urinary tract infection or translocation from the gastrointestinal tract.
The vast majority of prostatitis cases prostatic abscesses are caused by Escherichia coli and other gram‐negative bacilli.6 Staphylococcus species are less common, and MRSA isolates have been described as a rare etiologic agent. Only four other case reports describing MRSA bacteremia associated with prostatitis or prostatic abscesses have been published.710 Both our patient and the three other case reports in the literature with prostatic abscesses and MRSA bacteremia required drainage of the abscess as well as antibiotics for resolution. The other reported cases involved drainage by transurethral resection of the prostate,79 whereas our case used transperineal drainage of the prostatic abscess via transrectal ultrasound guidance. In addition to intravenous antibiotics, drainage appears to be a key therapeutic measure for resolution of MRSA prostatic abscesses.
With the increasing incidence of community‐associated and healthcare‐associated MRSA infections, the incidence of prostatitis or prostatic abscesses secondary to MRSA may be increasing. MRSA seems to have a specific predilection for abscess formation in skin and soft‐tissue infections and pneumonia.2 Clinicians must be alert to a potentially higher frequency of MRSA as a cause of prostatic abscesses and prostatitis.
In the evaluation of a patient with persistent MRSA bacteremia, the potential for the prostate as a source of infection should be considered. Urinary symptoms may be subtle. Clinicians should have a low threshold for imaging studies such as CT to evaluate for a possible source of MRSA bacteremia. If a prostatic abscess is found, prompt surgical drainage or debridement is necessary for cure.
- ,,, et al.Methicillin‐resistant S. aureus infections among patients in the emergency department.N Engl J Med.2006;355:666–674.
- ,,, et al.Comparison of both clinical features and mortality risk associated with bacteremia due to community‐acquired methicillin‐resistant Staphylococcus aureus and methicillin‐susceptible S. aureus.Clin Infect Dis.2008;46:799–806.
- ,,, et al.Invasive methicillin‐resistant Staphylococcus aureus infections in the United States.JAMA.2007;298:1763–1771.
- ,,,,,.The current spectrum of Staphylococcus aureus infection in a tertiary care hospital.Medicine (Baltimore).1994;73:186–208.
- ,,, et al.Emergence of multidrug‐resistant, community‐associated, methicillin‐resistant Staphylococcus aureus clone USA300 in men who have sex with men.Ann Intern Med.2008;148:249–257.
- ,,, et al.Prostatic abscess in the antibiotic era.Rev Infect Dis.1988;10:239–249.
- ,,.Community‐acquired methicillin‐resistant Staphylococcus aureus prostatic abscess.Urology.2004;64:808–810.
- ,,.Persistent methicillin‐resistant Staphylococcus aureus bacteremia due to a prostatic abscess.Scand J Infect Dis.2003;35:273–274.
- ,.Dual perinephric and prostatic abscesses from methicillin resistant Staphylococcus aureus.South Med J.2007;100:515–516.
- ,.Methicillin‐resistant Staphylococcus aureus prostatitis.Urology.2007;69:779.e1–779.e3.
- ,,, et al.Methicillin‐resistant S. aureus infections among patients in the emergency department.N Engl J Med.2006;355:666–674.
- ,,, et al.Comparison of both clinical features and mortality risk associated with bacteremia due to community‐acquired methicillin‐resistant Staphylococcus aureus and methicillin‐susceptible S. aureus.Clin Infect Dis.2008;46:799–806.
- ,,, et al.Invasive methicillin‐resistant Staphylococcus aureus infections in the United States.JAMA.2007;298:1763–1771.
- ,,,,,.The current spectrum of Staphylococcus aureus infection in a tertiary care hospital.Medicine (Baltimore).1994;73:186–208.
- ,,, et al.Emergence of multidrug‐resistant, community‐associated, methicillin‐resistant Staphylococcus aureus clone USA300 in men who have sex with men.Ann Intern Med.2008;148:249–257.
- ,,, et al.Prostatic abscess in the antibiotic era.Rev Infect Dis.1988;10:239–249.
- ,,.Community‐acquired methicillin‐resistant Staphylococcus aureus prostatic abscess.Urology.2004;64:808–810.
- ,,.Persistent methicillin‐resistant Staphylococcus aureus bacteremia due to a prostatic abscess.Scand J Infect Dis.2003;35:273–274.
- ,.Dual perinephric and prostatic abscesses from methicillin resistant Staphylococcus aureus.South Med J.2007;100:515–516.
- ,.Methicillin‐resistant Staphylococcus aureus prostatitis.Urology.2007;69:779.e1–779.e3.

Calcinosis universalis
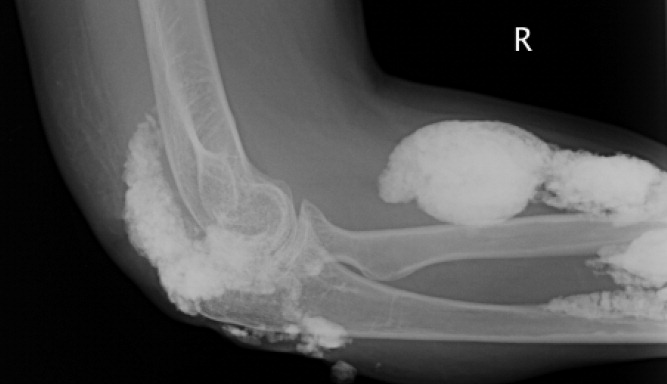
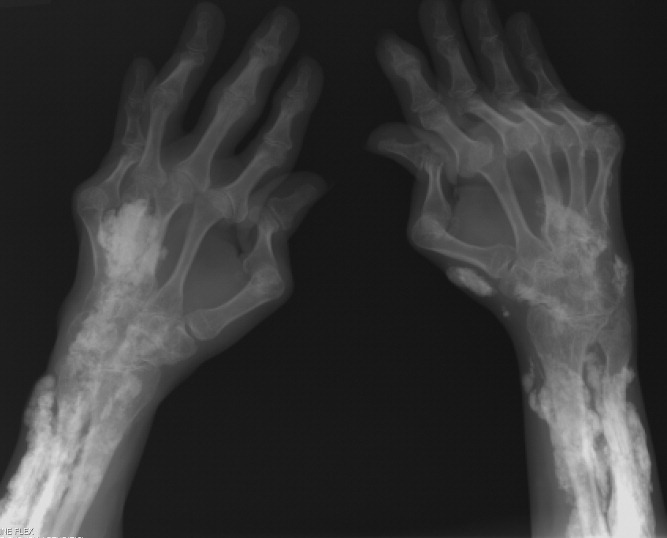
A 38‐year‐old woman with juvenile dermatomyositis (JDM) and calcinosis universalis presented with 3 days of drainage from a lesion on her right elbow. An examination of the elbow revealed diffuse and firm subcutaneous nodules with overlying erythema. X‐rays illustrated soft‐tissue calcifications in the forearm and elbow without evidence of osteomyelitis (Figure 1). Wound cultures grew Staphylococcus aureus, and the patient was started on intravenous antibiotics for abscess treatment.

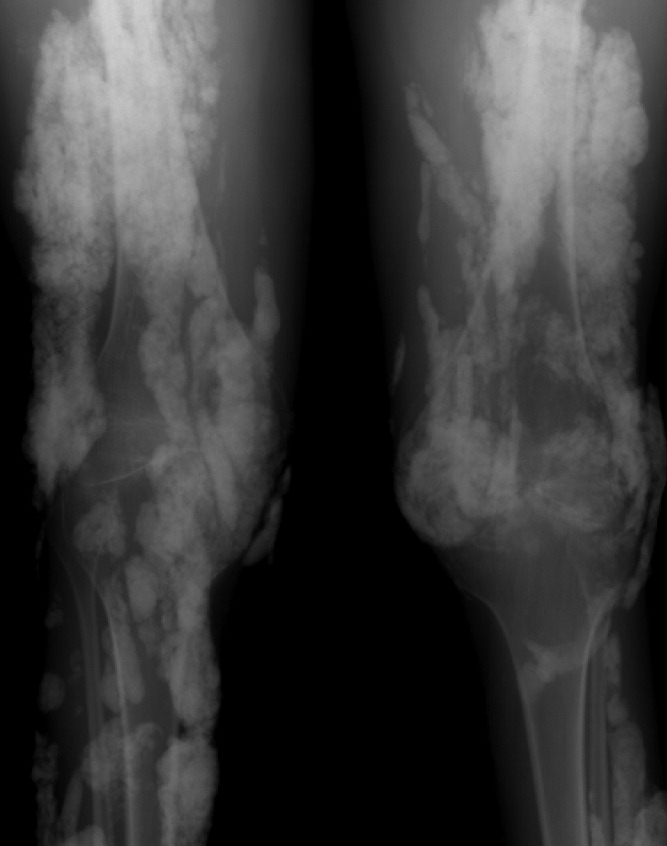
Calcinosis universalis is soft‐tissue calcification presenting as a complication of JDM. It is often detected in childhood in 30% to 70% of patients. It is hypothesized that calcinosis is due to chronic tissue inflammation, as seen in JDM, leading to muscle damage, releasing calcium, and inducing mineralization. Calcinosis universalis often presents as calcified nodules and plaques in areas of repeated trauma, such as joints, extremities, and buttocks (Figures 13). Calcification is localized in subcutaneous tissue, fascial planes, tendons, or intramuscular areas. It can cause debilitating secondary complications such as skin ulcerations expressing calcified material, superimposed infections of skin lesions, joint contractures with severe arthralgias, and muscle atrophy. Calcinosis has been correlated with severity of JDM with presence of cardiac involvement and use of more than one immunosuppression medication.1 It has also been associated with the degree of vasculopathy and delay in initiation of therapy for controlling inflammation in JDM.2
Soft‐tissue calcification can be classified into 5 categories:
-
Dystrophic calcification occurs in injured tissues with normal calcium, phosphorus, and parathyroid hormone levels, as seen in this patient. Calcified nodules or plaques occur in the extremities and buttocks. This is most often seen in JDM, scleroderma, and systemic lupus erythematosus.
-
Metastatic calcification affects normal tissues with abnormal levels of calcium and phosphorus. It is seen in large joints as well as arteries and visceral organs. It is associated with hyperparathyroidism, hypervitaminosis D, and malignancies.
-
Calciphylaxis with abnormal calcium and phosphorus metabolism causes small‐vessel calcification in patients with chronic renal failure.
-
Tumoral calcification is a familial condition with normal calcium levels but elevated phosphorus levels. Large subcutaneous calcifications are seen near high‐pressure areas and joints.
-
Idiopathic calcification is seen in healthy children and young adults with normal calcium metabolism and appears as multiple subcutaneous calcifications.2
Although multiple therapeutic options have been tried for the management or prevention of calcinosis, there is currently no accepted standard of treatment. In patients with calcinosis, warfarin, probenecid, colchicine, bisphosphonates, minocycline, diltiazem, aluminum hydroxide, corticosteroids, and salicylate have been attempted with variable results. Other therapeutic options include carbon dioxide laser treatments and surgical excision of large plaques. Decreasing muscle inflammation with aggressive treatment of JDM may improve outcomes and decrease the incidence of calcification.3 Unfortunately, once calcinosis has occurred, it is highly refractory to medical therapy.
Calcinosis universalis can lead to severe functional impairment. It can be distinguished from other types of calcinosis by diffuse involvement of muscle and fascia in connective tissue disease with normal calcium and phosphorus levels. New management modalities such as cyclosporine, intravenous immunoglobulin, and tumor necrosis factor alpha inhibitors are currently being evaluated.
- ,,, et al.Risk factors associated with calcinosis of juvenile dermatomyositis.JPediatr (Rio J).2008;84(1):68–74.
- ,,,.Calcinosis in rheumatic diseases.Semin Arthritis Rheum.2005;34(6):805–812.
- ,,, et al.Aggressive management of juvenile dermatomyositis results in improved outcome and decreased incidence of calcinosis.J Am Acad Dermatol.2002;47(4):505–511.
A 38‐year‐old woman with juvenile dermatomyositis (JDM) and calcinosis universalis presented with 3 days of drainage from a lesion on her right elbow. An examination of the elbow revealed diffuse and firm subcutaneous nodules with overlying erythema. X‐rays illustrated soft‐tissue calcifications in the forearm and elbow without evidence of osteomyelitis (Figure 1). Wound cultures grew Staphylococcus aureus, and the patient was started on intravenous antibiotics for abscess treatment.
Calcinosis universalis is soft‐tissue calcification presenting as a complication of JDM. It is often detected in childhood in 30% to 70% of patients. It is hypothesized that calcinosis is due to chronic tissue inflammation, as seen in JDM, leading to muscle damage, releasing calcium, and inducing mineralization. Calcinosis universalis often presents as calcified nodules and plaques in areas of repeated trauma, such as joints, extremities, and buttocks (Figures 13). Calcification is localized in subcutaneous tissue, fascial planes, tendons, or intramuscular areas. It can cause debilitating secondary complications such as skin ulcerations expressing calcified material, superimposed infections of skin lesions, joint contractures with severe arthralgias, and muscle atrophy. Calcinosis has been correlated with severity of JDM with presence of cardiac involvement and use of more than one immunosuppression medication.1 It has also been associated with the degree of vasculopathy and delay in initiation of therapy for controlling inflammation in JDM.2
Soft‐tissue calcification can be classified into 5 categories:
-
Dystrophic calcification occurs in injured tissues with normal calcium, phosphorus, and parathyroid hormone levels, as seen in this patient. Calcified nodules or plaques occur in the extremities and buttocks. This is most often seen in JDM, scleroderma, and systemic lupus erythematosus.
-
Metastatic calcification affects normal tissues with abnormal levels of calcium and phosphorus. It is seen in large joints as well as arteries and visceral organs. It is associated with hyperparathyroidism, hypervitaminosis D, and malignancies.
-
Calciphylaxis with abnormal calcium and phosphorus metabolism causes small‐vessel calcification in patients with chronic renal failure.
-
Tumoral calcification is a familial condition with normal calcium levels but elevated phosphorus levels. Large subcutaneous calcifications are seen near high‐pressure areas and joints.
-
Idiopathic calcification is seen in healthy children and young adults with normal calcium metabolism and appears as multiple subcutaneous calcifications.2
Although multiple therapeutic options have been tried for the management or prevention of calcinosis, there is currently no accepted standard of treatment. In patients with calcinosis, warfarin, probenecid, colchicine, bisphosphonates, minocycline, diltiazem, aluminum hydroxide, corticosteroids, and salicylate have been attempted with variable results. Other therapeutic options include carbon dioxide laser treatments and surgical excision of large plaques. Decreasing muscle inflammation with aggressive treatment of JDM may improve outcomes and decrease the incidence of calcification.3 Unfortunately, once calcinosis has occurred, it is highly refractory to medical therapy.
Calcinosis universalis can lead to severe functional impairment. It can be distinguished from other types of calcinosis by diffuse involvement of muscle and fascia in connective tissue disease with normal calcium and phosphorus levels. New management modalities such as cyclosporine, intravenous immunoglobulin, and tumor necrosis factor alpha inhibitors are currently being evaluated.
A 38‐year‐old woman with juvenile dermatomyositis (JDM) and calcinosis universalis presented with 3 days of drainage from a lesion on her right elbow. An examination of the elbow revealed diffuse and firm subcutaneous nodules with overlying erythema. X‐rays illustrated soft‐tissue calcifications in the forearm and elbow without evidence of osteomyelitis (Figure 1). Wound cultures grew Staphylococcus aureus, and the patient was started on intravenous antibiotics for abscess treatment.
Calcinosis universalis is soft‐tissue calcification presenting as a complication of JDM. It is often detected in childhood in 30% to 70% of patients. It is hypothesized that calcinosis is due to chronic tissue inflammation, as seen in JDM, leading to muscle damage, releasing calcium, and inducing mineralization. Calcinosis universalis often presents as calcified nodules and plaques in areas of repeated trauma, such as joints, extremities, and buttocks (Figures 13). Calcification is localized in subcutaneous tissue, fascial planes, tendons, or intramuscular areas. It can cause debilitating secondary complications such as skin ulcerations expressing calcified material, superimposed infections of skin lesions, joint contractures with severe arthralgias, and muscle atrophy. Calcinosis has been correlated with severity of JDM with presence of cardiac involvement and use of more than one immunosuppression medication.1 It has also been associated with the degree of vasculopathy and delay in initiation of therapy for controlling inflammation in JDM.2
Soft‐tissue calcification can be classified into 5 categories:
-
Dystrophic calcification occurs in injured tissues with normal calcium, phosphorus, and parathyroid hormone levels, as seen in this patient. Calcified nodules or plaques occur in the extremities and buttocks. This is most often seen in JDM, scleroderma, and systemic lupus erythematosus.
-
Metastatic calcification affects normal tissues with abnormal levels of calcium and phosphorus. It is seen in large joints as well as arteries and visceral organs. It is associated with hyperparathyroidism, hypervitaminosis D, and malignancies.
-
Calciphylaxis with abnormal calcium and phosphorus metabolism causes small‐vessel calcification in patients with chronic renal failure.
-
Tumoral calcification is a familial condition with normal calcium levels but elevated phosphorus levels. Large subcutaneous calcifications are seen near high‐pressure areas and joints.
-
Idiopathic calcification is seen in healthy children and young adults with normal calcium metabolism and appears as multiple subcutaneous calcifications.2
Although multiple therapeutic options have been tried for the management or prevention of calcinosis, there is currently no accepted standard of treatment. In patients with calcinosis, warfarin, probenecid, colchicine, bisphosphonates, minocycline, diltiazem, aluminum hydroxide, corticosteroids, and salicylate have been attempted with variable results. Other therapeutic options include carbon dioxide laser treatments and surgical excision of large plaques. Decreasing muscle inflammation with aggressive treatment of JDM may improve outcomes and decrease the incidence of calcification.3 Unfortunately, once calcinosis has occurred, it is highly refractory to medical therapy.
Calcinosis universalis can lead to severe functional impairment. It can be distinguished from other types of calcinosis by diffuse involvement of muscle and fascia in connective tissue disease with normal calcium and phosphorus levels. New management modalities such as cyclosporine, intravenous immunoglobulin, and tumor necrosis factor alpha inhibitors are currently being evaluated.
- ,,, et al.Risk factors associated with calcinosis of juvenile dermatomyositis.JPediatr (Rio J).2008;84(1):68–74.
- ,,,.Calcinosis in rheumatic diseases.Semin Arthritis Rheum.2005;34(6):805–812.
- ,,, et al.Aggressive management of juvenile dermatomyositis results in improved outcome and decreased incidence of calcinosis.J Am Acad Dermatol.2002;47(4):505–511.
- ,,, et al.Risk factors associated with calcinosis of juvenile dermatomyositis.JPediatr (Rio J).2008;84(1):68–74.
- ,,,.Calcinosis in rheumatic diseases.Semin Arthritis Rheum.2005;34(6):805–812.
- ,,, et al.Aggressive management of juvenile dermatomyositis results in improved outcome and decreased incidence of calcinosis.J Am Acad Dermatol.2002;47(4):505–511.