User login
Back to School
Patience Agborbesong, MD, didn't go to SHM's "Essential Procedures for the Hospitalist" seminar on a whim. In fact, the medical director of Wake Forest Inpatient Physicians of Winston-Salem, N.C., skipped her own hospital's career day to attend the society's One-Day Hospitalist University (ODHU) session where she received four hours of hands-on training in the use of ultrasound equipment for vascular access, paracentesis, and thoracentesis.
"When I was training, we didn't use ultrasounds to routinely do central lines," says Dr. Agborbesong, an ODHU rookie. "Now that is something that is recommended as a patient safety measure. When we do the procedure without ultrasounds, you're blind-sticking and going by the anatomic landmarks."
The course was one of four one-day seminars that drew nearly 200 hospitalists to Atlanta. CME credit is awarded for all of the ODHU courses. The program also included "Best Practices in Managing a Hospital Medicine Program," "Critical Care Medicine for the Hospitalist," and "Fundamentals of Inpatient Coding and Documentation."
Like many hospitalists, Dr. Agborbesong used ODHU as a chance to expand the skill set of her 15-hospitalist group. In addition to relaying what she learned during the ultrasound course to her colleagues, she's also planning to hone her skills with help from radiologists at Wake Forest University Baptist Medical Center.
"I didn't come here thinking I would be an expert," she says. "It was a very good place to start."
To stay updated on SHM-sponsored training programs, visit the SHM Web site.
Patience Agborbesong, MD, didn't go to SHM's "Essential Procedures for the Hospitalist" seminar on a whim. In fact, the medical director of Wake Forest Inpatient Physicians of Winston-Salem, N.C., skipped her own hospital's career day to attend the society's One-Day Hospitalist University (ODHU) session where she received four hours of hands-on training in the use of ultrasound equipment for vascular access, paracentesis, and thoracentesis.
"When I was training, we didn't use ultrasounds to routinely do central lines," says Dr. Agborbesong, an ODHU rookie. "Now that is something that is recommended as a patient safety measure. When we do the procedure without ultrasounds, you're blind-sticking and going by the anatomic landmarks."
The course was one of four one-day seminars that drew nearly 200 hospitalists to Atlanta. CME credit is awarded for all of the ODHU courses. The program also included "Best Practices in Managing a Hospital Medicine Program," "Critical Care Medicine for the Hospitalist," and "Fundamentals of Inpatient Coding and Documentation."
Like many hospitalists, Dr. Agborbesong used ODHU as a chance to expand the skill set of her 15-hospitalist group. In addition to relaying what she learned during the ultrasound course to her colleagues, she's also planning to hone her skills with help from radiologists at Wake Forest University Baptist Medical Center.
"I didn't come here thinking I would be an expert," she says. "It was a very good place to start."
To stay updated on SHM-sponsored training programs, visit the SHM Web site.
Patience Agborbesong, MD, didn't go to SHM's "Essential Procedures for the Hospitalist" seminar on a whim. In fact, the medical director of Wake Forest Inpatient Physicians of Winston-Salem, N.C., skipped her own hospital's career day to attend the society's One-Day Hospitalist University (ODHU) session where she received four hours of hands-on training in the use of ultrasound equipment for vascular access, paracentesis, and thoracentesis.
"When I was training, we didn't use ultrasounds to routinely do central lines," says Dr. Agborbesong, an ODHU rookie. "Now that is something that is recommended as a patient safety measure. When we do the procedure without ultrasounds, you're blind-sticking and going by the anatomic landmarks."
The course was one of four one-day seminars that drew nearly 200 hospitalists to Atlanta. CME credit is awarded for all of the ODHU courses. The program also included "Best Practices in Managing a Hospital Medicine Program," "Critical Care Medicine for the Hospitalist," and "Fundamentals of Inpatient Coding and Documentation."
Like many hospitalists, Dr. Agborbesong used ODHU as a chance to expand the skill set of her 15-hospitalist group. In addition to relaying what she learned during the ultrasound course to her colleagues, she's also planning to hone her skills with help from radiologists at Wake Forest University Baptist Medical Center.
"I didn't come here thinking I would be an expert," she says. "It was a very good place to start."
To stay updated on SHM-sponsored training programs, visit the SHM Web site.
Transparent Hospitalists
Six weeks ago hospitalist Frank Michota Jr., MD, posted on the Cleveland Clinic's Web site that he receives at least $5,000 per year in fees from pharmaceutical firms Sanofi-Aventis U.S. Inc. and Scios Inc. Since then, not one of the 100 or so patients he's encountered has asked about it.
Still, hospitalists and specialists at the teaching hospital now are required to publicly disclose their financial ties to the pharmaceutical and medical device industries. The effort is aimed at increasing physician transparency and avoiding conflicts of interest—real or perceived.
As director of academic affairs for the hospital's Department of Hospital Medicine, Dr. Michota appreciates the credibility that the disclosure provides for research. But he thinks it does little to forward patient care. Because most hospitalists are required to use drugs or devices based on formularies, whether they have financial ties to the companies making the drugs or devices is irrelevant, he says.
"It’s not the patient that's looking at this stuff," Dr. Michota says, adding, "the disclosures are more for the ethereal discussions."
He emphasizes most physicians don’t seek out relationships with drug- and device-makers.
"I use Drug A because it's on my formulary," he says. "I have a lot of experience with [Drug A] because it's on my formulary. I'm then asked by the company to research it, because I have experience with Drug A. That's how it works, not the other way around."
Check out the Cleveland Clinic’s physician directory at http://my.clevelandclinic.org/staff_directory/default.aspx.
Six weeks ago hospitalist Frank Michota Jr., MD, posted on the Cleveland Clinic's Web site that he receives at least $5,000 per year in fees from pharmaceutical firms Sanofi-Aventis U.S. Inc. and Scios Inc. Since then, not one of the 100 or so patients he's encountered has asked about it.
Still, hospitalists and specialists at the teaching hospital now are required to publicly disclose their financial ties to the pharmaceutical and medical device industries. The effort is aimed at increasing physician transparency and avoiding conflicts of interest—real or perceived.
As director of academic affairs for the hospital's Department of Hospital Medicine, Dr. Michota appreciates the credibility that the disclosure provides for research. But he thinks it does little to forward patient care. Because most hospitalists are required to use drugs or devices based on formularies, whether they have financial ties to the companies making the drugs or devices is irrelevant, he says.
"It’s not the patient that's looking at this stuff," Dr. Michota says, adding, "the disclosures are more for the ethereal discussions."
He emphasizes most physicians don’t seek out relationships with drug- and device-makers.
"I use Drug A because it's on my formulary," he says. "I have a lot of experience with [Drug A] because it's on my formulary. I'm then asked by the company to research it, because I have experience with Drug A. That's how it works, not the other way around."
Check out the Cleveland Clinic’s physician directory at http://my.clevelandclinic.org/staff_directory/default.aspx.
Six weeks ago hospitalist Frank Michota Jr., MD, posted on the Cleveland Clinic's Web site that he receives at least $5,000 per year in fees from pharmaceutical firms Sanofi-Aventis U.S. Inc. and Scios Inc. Since then, not one of the 100 or so patients he's encountered has asked about it.
Still, hospitalists and specialists at the teaching hospital now are required to publicly disclose their financial ties to the pharmaceutical and medical device industries. The effort is aimed at increasing physician transparency and avoiding conflicts of interest—real or perceived.
As director of academic affairs for the hospital's Department of Hospital Medicine, Dr. Michota appreciates the credibility that the disclosure provides for research. But he thinks it does little to forward patient care. Because most hospitalists are required to use drugs or devices based on formularies, whether they have financial ties to the companies making the drugs or devices is irrelevant, he says.
"It’s not the patient that's looking at this stuff," Dr. Michota says, adding, "the disclosures are more for the ethereal discussions."
He emphasizes most physicians don’t seek out relationships with drug- and device-makers.
"I use Drug A because it's on my formulary," he says. "I have a lot of experience with [Drug A] because it's on my formulary. I'm then asked by the company to research it, because I have experience with Drug A. That's how it works, not the other way around."
Check out the Cleveland Clinic’s physician directory at http://my.clevelandclinic.org/staff_directory/default.aspx.
Research Roundup
Clinical question: Is low molecular weight heparin (LMWH) safe for deep vein thrombosis (DVT) prophylaxis in patients with severe renal insufficiency?
Background: LMWH is avoided in patients with severe renal insufficiency due to concerns about increased bleeding risk caused by delayed renal excretion.
Study design: Multi center, prospective, single-arm trial.
Setting: Several Canadian intensive-care units (ICUs).
Synopsis: 138 critically ill patients with a creatinine clearance lower than 30 mL/min received open-labeled dalteparin, 5,000 IU once daily for DVT prophylaxis for a median duration of seven days. Peak and trough anti-Xa levels were measured to assess for efficacy and evidence of bioaccumulation, respectively. Patients were monitored for DVT development, heparin-induced thrombocytopenia (HIT), and bleeding. None of the patients (0%, CI, 0%-3%) had evidence of bioaccumulation. Seven patients (5.1%) developed DVT and only two patients (1.4%) developed HIT. Of the 10 patients who bled (7.2%), two died.
Of note, 62% of patients in this study had acute renal failure and their improvement in renal function during their ICU stay might have contributed to lack of bioaccumulation. Another limitation is the lack of comparison with other DVT prophylaxis strategies, especially unfractionated heparin.
Bottom line: Using dalteparin for DVT prophylaxis is unlikely to increase bleeding risk in patients with severe renal insufficiency. However, this finding cannot be generalized to dialysis-dependent patients or those with chronic kidney disease.
Citation: Arch Intern Med. 2008;168(16):1805-1812
—Reviewed by Rebecca Allyn, MD, Smitha Chadaga, MD, Mary Dedecker, MD, Vignesh Narayanan, MD, Eugene S. Chu, MD, Division of Hospital Medicine, Denver Health and Hospital Authority
Clinical question: Is low molecular weight heparin (LMWH) safe for deep vein thrombosis (DVT) prophylaxis in patients with severe renal insufficiency?
Background: LMWH is avoided in patients with severe renal insufficiency due to concerns about increased bleeding risk caused by delayed renal excretion.
Study design: Multi center, prospective, single-arm trial.
Setting: Several Canadian intensive-care units (ICUs).
Synopsis: 138 critically ill patients with a creatinine clearance lower than 30 mL/min received open-labeled dalteparin, 5,000 IU once daily for DVT prophylaxis for a median duration of seven days. Peak and trough anti-Xa levels were measured to assess for efficacy and evidence of bioaccumulation, respectively. Patients were monitored for DVT development, heparin-induced thrombocytopenia (HIT), and bleeding. None of the patients (0%, CI, 0%-3%) had evidence of bioaccumulation. Seven patients (5.1%) developed DVT and only two patients (1.4%) developed HIT. Of the 10 patients who bled (7.2%), two died.
Of note, 62% of patients in this study had acute renal failure and their improvement in renal function during their ICU stay might have contributed to lack of bioaccumulation. Another limitation is the lack of comparison with other DVT prophylaxis strategies, especially unfractionated heparin.
Bottom line: Using dalteparin for DVT prophylaxis is unlikely to increase bleeding risk in patients with severe renal insufficiency. However, this finding cannot be generalized to dialysis-dependent patients or those with chronic kidney disease.
Citation: Arch Intern Med. 2008;168(16):1805-1812
—Reviewed by Rebecca Allyn, MD, Smitha Chadaga, MD, Mary Dedecker, MD, Vignesh Narayanan, MD, Eugene S. Chu, MD, Division of Hospital Medicine, Denver Health and Hospital Authority
Clinical question: Is low molecular weight heparin (LMWH) safe for deep vein thrombosis (DVT) prophylaxis in patients with severe renal insufficiency?
Background: LMWH is avoided in patients with severe renal insufficiency due to concerns about increased bleeding risk caused by delayed renal excretion.
Study design: Multi center, prospective, single-arm trial.
Setting: Several Canadian intensive-care units (ICUs).
Synopsis: 138 critically ill patients with a creatinine clearance lower than 30 mL/min received open-labeled dalteparin, 5,000 IU once daily for DVT prophylaxis for a median duration of seven days. Peak and trough anti-Xa levels were measured to assess for efficacy and evidence of bioaccumulation, respectively. Patients were monitored for DVT development, heparin-induced thrombocytopenia (HIT), and bleeding. None of the patients (0%, CI, 0%-3%) had evidence of bioaccumulation. Seven patients (5.1%) developed DVT and only two patients (1.4%) developed HIT. Of the 10 patients who bled (7.2%), two died.
Of note, 62% of patients in this study had acute renal failure and their improvement in renal function during their ICU stay might have contributed to lack of bioaccumulation. Another limitation is the lack of comparison with other DVT prophylaxis strategies, especially unfractionated heparin.
Bottom line: Using dalteparin for DVT prophylaxis is unlikely to increase bleeding risk in patients with severe renal insufficiency. However, this finding cannot be generalized to dialysis-dependent patients or those with chronic kidney disease.
Citation: Arch Intern Med. 2008;168(16):1805-1812
—Reviewed by Rebecca Allyn, MD, Smitha Chadaga, MD, Mary Dedecker, MD, Vignesh Narayanan, MD, Eugene S. Chu, MD, Division of Hospital Medicine, Denver Health and Hospital Authority
Mismatched Cord Blood
Dr. Mary Eapen reports findings that mismatched umbilical cord blood is as effective as mismatched bone marrow or peripheral blood in allogeneic stem cell transplantation in adults with acute leukemia.
Dr. Mary Eapen reports findings that mismatched umbilical cord blood is as effective as mismatched bone marrow or peripheral blood in allogeneic stem cell transplantation in adults with acute leukemia.
Dr. Mary Eapen reports findings that mismatched umbilical cord blood is as effective as mismatched bone marrow or peripheral blood in allogeneic stem cell transplantation in adults with acute leukemia.
Prepare to react to a medical malpractice lawsuit

Prepare to react to a medical malpractice lawsuit
One of my colleagues is being sued for medical malpractice. After he was notified of the lawsuit, his lawyer immediately advised him of some things he should and should not do. Can you help me understand what those might be?
J. Boggs, Fort Smith, Ark.
Dr. Hospitalist responds: Lawsuits alleging medical malpractice are common—probably more common than most of us realize. Most physicians either know someone who has been sued or is currently being sued for medical malpractice. Unfortunately, malpractice is not something most medical schools or postgraduate training programs address sufficiently as part of a curriculum.
To be clear, I am not an attorney. I advise you to speak with an attorney familiar with medical malpractice statutes in your state regarding any legal action. But in my discussions with medical malpractice lawyers and with physicians who have been sued, I have come to understand the process can be an emotional and lengthy experience for everyone involved.
Attorneys often advise medical malpractice defendants of several things:
- Immediately contact your risk manager. If you do not know who your risk manager is or do not have one, contact your medical malpractice carrier. Your risk manager will open a file and notify your medical malpractice carrier. They will ask an attorney to contact you. This attorney will advise you of the most appropriate steps to take.
- It is normal to feel a wide range of emotions when you learn you are being sued. You might be very angry with the plaintiff (the party filing the suit), especially if you believe you provided appropriate care. At times like this, many physicians want to vent and speak with friends, family, colleagues, or even the plaintiff. That leads to a second piece of advice: Don’t speak with ANYONE except your attorney about the case. This might be difficult and seem counterintuitive, but you can harm your case if you talk to others about it. As the lawsuit evolves, both parties will undergo a discovery process to learn everyone’s perspectives. Defendants likely will be asked to provide answers at a deposition. Plaintiff’s counsel will ask defendants whether they spoke with anyone about the case. If they learn defendants spoke with others about the case, they may depose those individuals to learn what was discussed in those private conversations with the defendants. As you can imagine, it can get messy when private conversations are revealed in depositions.
- The last piece of advice attorneys often given new clients: Never alter the record. This seems crazy, right? What intelligent doctor would actually go back and alter the record? Well, silly as it might sound, many providers do go back and change something in the record. Most of the time, the change was something the physician thought was innocuous, such as adding a date to a note. By the time a physician has been sued, the medical record in question probably has been copied, likely more than once. It’s fairly simple to recognize when the original record has been altered. But regardless of how innocent any change may seem, the perception is the alteration was meant to deceive. Jurors normally do not view such instances favorably. Defendants can only hurt themselves when they alter the record.
So, if you are ever a defendant in a case, contact your risk manager immediately, don’t talk to anyone about the case, and stay away from the medical records office.
Take extra precautions to prevent C. difficile infections
I work at a hospital where the infection control officer advocates universal use of alcohol-based hand gels to prevent transmission of infectious pathogens. I previously had been told alcohol-based gels might be insufficient to kill C. difficile. Is this true?
C. Nelson, Atlanta
Dr. Hospitalist responds: You bring up an important question. The role of hand hygiene as a measure to control hospital-acquired infections has become increasingly visible. This is long overdue. The thought of healthcare providers transmitting diseases because they didn’t clean their hands is abhorrent.
Many institutions around the country have adopted policies similar to your hospital’s, encouraging the use of alcohol-based hand gels over the use of soap and water. Hospitals have done this for several reasons:
- Healthcare providers are more likely to use alcohol-based gels than cleanse with soap and water;
- Rubbing your hands with gel takes less time than washing with soap and water;
- Hospitals can place gel dispensers in convenient locations outside each doorway, whereas there are only so many faucets and sinks on any given floor; and
- Even those who do wash their hands with soap and water often do not spend enough time adequately cleaning them.
Alcohol-based gels are effective against a wide range of bacteria that cause hospital-acquired infections, particularly against Staph, including MRSA. But C. difficile may be different. The control of C. difficile in hospitals is difficult because the organism can produce highly resistant spores, which can survive for long periods of time in a hospital environment, such as in mattresses, equipment, furniture, etc. Alcohol-based gels might be less effective against C. difficile spores than other organisms that cause healthcare-associated infections. Providers caring for patients with C. difficile should wear protective clothing, such as gloves and gowns, as well as clean their hands with soap and water.
For additional information on this subject, I suggest you check out Morbidity and Mortality Weekly Report’s “Guideline for Hand Hygiene in Health-Care Settings” (Oct. 25, 2002). You can access it online at the Infectious Disease Society of America’s Web site at www.idsociety.org/ content.aspx?id=4434#hh. TH
Prepare to react to a medical malpractice lawsuit
One of my colleagues is being sued for medical malpractice. After he was notified of the lawsuit, his lawyer immediately advised him of some things he should and should not do. Can you help me understand what those might be?
J. Boggs, Fort Smith, Ark.
Dr. Hospitalist responds: Lawsuits alleging medical malpractice are common—probably more common than most of us realize. Most physicians either know someone who has been sued or is currently being sued for medical malpractice. Unfortunately, malpractice is not something most medical schools or postgraduate training programs address sufficiently as part of a curriculum.
To be clear, I am not an attorney. I advise you to speak with an attorney familiar with medical malpractice statutes in your state regarding any legal action. But in my discussions with medical malpractice lawyers and with physicians who have been sued, I have come to understand the process can be an emotional and lengthy experience for everyone involved.
Attorneys often advise medical malpractice defendants of several things:
- Immediately contact your risk manager. If you do not know who your risk manager is or do not have one, contact your medical malpractice carrier. Your risk manager will open a file and notify your medical malpractice carrier. They will ask an attorney to contact you. This attorney will advise you of the most appropriate steps to take.
- It is normal to feel a wide range of emotions when you learn you are being sued. You might be very angry with the plaintiff (the party filing the suit), especially if you believe you provided appropriate care. At times like this, many physicians want to vent and speak with friends, family, colleagues, or even the plaintiff. That leads to a second piece of advice: Don’t speak with ANYONE except your attorney about the case. This might be difficult and seem counterintuitive, but you can harm your case if you talk to others about it. As the lawsuit evolves, both parties will undergo a discovery process to learn everyone’s perspectives. Defendants likely will be asked to provide answers at a deposition. Plaintiff’s counsel will ask defendants whether they spoke with anyone about the case. If they learn defendants spoke with others about the case, they may depose those individuals to learn what was discussed in those private conversations with the defendants. As you can imagine, it can get messy when private conversations are revealed in depositions.
- The last piece of advice attorneys often given new clients: Never alter the record. This seems crazy, right? What intelligent doctor would actually go back and alter the record? Well, silly as it might sound, many providers do go back and change something in the record. Most of the time, the change was something the physician thought was innocuous, such as adding a date to a note. By the time a physician has been sued, the medical record in question probably has been copied, likely more than once. It’s fairly simple to recognize when the original record has been altered. But regardless of how innocent any change may seem, the perception is the alteration was meant to deceive. Jurors normally do not view such instances favorably. Defendants can only hurt themselves when they alter the record.
So, if you are ever a defendant in a case, contact your risk manager immediately, don’t talk to anyone about the case, and stay away from the medical records office.
Take extra precautions to prevent C. difficile infections
I work at a hospital where the infection control officer advocates universal use of alcohol-based hand gels to prevent transmission of infectious pathogens. I previously had been told alcohol-based gels might be insufficient to kill C. difficile. Is this true?
C. Nelson, Atlanta
Dr. Hospitalist responds: You bring up an important question. The role of hand hygiene as a measure to control hospital-acquired infections has become increasingly visible. This is long overdue. The thought of healthcare providers transmitting diseases because they didn’t clean their hands is abhorrent.
Many institutions around the country have adopted policies similar to your hospital’s, encouraging the use of alcohol-based hand gels over the use of soap and water. Hospitals have done this for several reasons:
- Healthcare providers are more likely to use alcohol-based gels than cleanse with soap and water;
- Rubbing your hands with gel takes less time than washing with soap and water;
- Hospitals can place gel dispensers in convenient locations outside each doorway, whereas there are only so many faucets and sinks on any given floor; and
- Even those who do wash their hands with soap and water often do not spend enough time adequately cleaning them.
Alcohol-based gels are effective against a wide range of bacteria that cause hospital-acquired infections, particularly against Staph, including MRSA. But C. difficile may be different. The control of C. difficile in hospitals is difficult because the organism can produce highly resistant spores, which can survive for long periods of time in a hospital environment, such as in mattresses, equipment, furniture, etc. Alcohol-based gels might be less effective against C. difficile spores than other organisms that cause healthcare-associated infections. Providers caring for patients with C. difficile should wear protective clothing, such as gloves and gowns, as well as clean their hands with soap and water.
For additional information on this subject, I suggest you check out Morbidity and Mortality Weekly Report’s “Guideline for Hand Hygiene in Health-Care Settings” (Oct. 25, 2002). You can access it online at the Infectious Disease Society of America’s Web site at www.idsociety.org/ content.aspx?id=4434#hh. TH
Prepare to react to a medical malpractice lawsuit
One of my colleagues is being sued for medical malpractice. After he was notified of the lawsuit, his lawyer immediately advised him of some things he should and should not do. Can you help me understand what those might be?
J. Boggs, Fort Smith, Ark.
Dr. Hospitalist responds: Lawsuits alleging medical malpractice are common—probably more common than most of us realize. Most physicians either know someone who has been sued or is currently being sued for medical malpractice. Unfortunately, malpractice is not something most medical schools or postgraduate training programs address sufficiently as part of a curriculum.
To be clear, I am not an attorney. I advise you to speak with an attorney familiar with medical malpractice statutes in your state regarding any legal action. But in my discussions with medical malpractice lawyers and with physicians who have been sued, I have come to understand the process can be an emotional and lengthy experience for everyone involved.
Attorneys often advise medical malpractice defendants of several things:
- Immediately contact your risk manager. If you do not know who your risk manager is or do not have one, contact your medical malpractice carrier. Your risk manager will open a file and notify your medical malpractice carrier. They will ask an attorney to contact you. This attorney will advise you of the most appropriate steps to take.
- It is normal to feel a wide range of emotions when you learn you are being sued. You might be very angry with the plaintiff (the party filing the suit), especially if you believe you provided appropriate care. At times like this, many physicians want to vent and speak with friends, family, colleagues, or even the plaintiff. That leads to a second piece of advice: Don’t speak with ANYONE except your attorney about the case. This might be difficult and seem counterintuitive, but you can harm your case if you talk to others about it. As the lawsuit evolves, both parties will undergo a discovery process to learn everyone’s perspectives. Defendants likely will be asked to provide answers at a deposition. Plaintiff’s counsel will ask defendants whether they spoke with anyone about the case. If they learn defendants spoke with others about the case, they may depose those individuals to learn what was discussed in those private conversations with the defendants. As you can imagine, it can get messy when private conversations are revealed in depositions.
- The last piece of advice attorneys often given new clients: Never alter the record. This seems crazy, right? What intelligent doctor would actually go back and alter the record? Well, silly as it might sound, many providers do go back and change something in the record. Most of the time, the change was something the physician thought was innocuous, such as adding a date to a note. By the time a physician has been sued, the medical record in question probably has been copied, likely more than once. It’s fairly simple to recognize when the original record has been altered. But regardless of how innocent any change may seem, the perception is the alteration was meant to deceive. Jurors normally do not view such instances favorably. Defendants can only hurt themselves when they alter the record.
So, if you are ever a defendant in a case, contact your risk manager immediately, don’t talk to anyone about the case, and stay away from the medical records office.
Take extra precautions to prevent C. difficile infections
I work at a hospital where the infection control officer advocates universal use of alcohol-based hand gels to prevent transmission of infectious pathogens. I previously had been told alcohol-based gels might be insufficient to kill C. difficile. Is this true?
C. Nelson, Atlanta
Dr. Hospitalist responds: You bring up an important question. The role of hand hygiene as a measure to control hospital-acquired infections has become increasingly visible. This is long overdue. The thought of healthcare providers transmitting diseases because they didn’t clean their hands is abhorrent.
Many institutions around the country have adopted policies similar to your hospital’s, encouraging the use of alcohol-based hand gels over the use of soap and water. Hospitals have done this for several reasons:
- Healthcare providers are more likely to use alcohol-based gels than cleanse with soap and water;
- Rubbing your hands with gel takes less time than washing with soap and water;
- Hospitals can place gel dispensers in convenient locations outside each doorway, whereas there are only so many faucets and sinks on any given floor; and
- Even those who do wash their hands with soap and water often do not spend enough time adequately cleaning them.
Alcohol-based gels are effective against a wide range of bacteria that cause hospital-acquired infections, particularly against Staph, including MRSA. But C. difficile may be different. The control of C. difficile in hospitals is difficult because the organism can produce highly resistant spores, which can survive for long periods of time in a hospital environment, such as in mattresses, equipment, furniture, etc. Alcohol-based gels might be less effective against C. difficile spores than other organisms that cause healthcare-associated infections. Providers caring for patients with C. difficile should wear protective clothing, such as gloves and gowns, as well as clean their hands with soap and water.
For additional information on this subject, I suggest you check out Morbidity and Mortality Weekly Report’s “Guideline for Hand Hygiene in Health-Care Settings” (Oct. 25, 2002). You can access it online at the Infectious Disease Society of America’s Web site at www.idsociety.org/ content.aspx?id=4434#hh. TH
Bonus-Pay Bonanza

Although there is a lot of debate about the effectiveness of pay-for-performance (P4P) plans, I think the plans are only going to increase in the foreseeable future.
We need more research to tell us the relative impact of public reporting of performance data and P4P programs. Most importantly, the details of how these plans are set up, how and what they measure, and the dollar amount involved will have everything to do with whether they are successful in improving the value of care we provide.
SHM’S Practice Management Committee conducted a mini-survey of hospitalist group leaders in 2006. Here are some of the key findings.
P4P Prevalence
Forty-one percent (60 out of 146) of hospital medicine group (HMG) leaders reported their groups have a quality-incentive program. Of those HMG leaders more likely to report participation in a quality-incentive program:
- 60% were at hospitals participating in a P4P program;
- 50% were at multispecialty/PCP medical groups; and
- 50% were in the Southern region.
Of those HMG leaders less likely to report participation in P4P programs, 28% were at academic programs and 31% were at local hospitalist-only groups.
Group vs. Individual Incentives
Of the HMG leaders participating in a quality-incentive program:
- 43% reported it was an individual incentive;
- 35% reported it was a group incentive;
- 10% reported the plan had elements of both individual and group incentives; and
- 12% were not sure if their plans had individual or group incentives.
Basis of Quality Targets
Of the HMG leaders reporting that they participate in a quality-incentive program (respondents could indicate one or more answers):
- 60% of the programs have targets based on national benchmarks;
- 23% have targets based on local or regional benchmarks;
- 37% have targets based on their hospital’s previous experience; and
- 47% have targets based on improvement over a baseline.
Maximum Impact of Incentives
Of the HMG leaders reporting that they participate in a quality-incentive program:
- 16% report the maximum impact is less than 3%;
- 24% report the maximum impact is from 3% to 7%;
- 35% report the maximum impact is from 8% to 10%;
- 17% report the maximum impact is from 11% to 20%;
- 3% report the maximum impact is more than 20%; and
- 5% report they do not know the maximum impact.
Group vs. Individual Incentives
Of the HMG leaders reporting that they participate in a quality-incentive program:
- 61% said they have received an incentive payment;
- 37% have not received an incentive payment; and
- 2% were unsure if they have received an incentive payment.
Quality Metrics
The most common metrics used in P4P programs, based on 29 responses to the SHM survey:
- 93% of HM programs have metrics based on The Joint Commission’s (JCAHO) heart failure measures;
- 86% have metrics based on JCAHO pneumonia measures;
- 79% have metrics based on JCAHO myocardial infarction measures;
- 28% have metrics based on a measure of medication reconciliation;
- 24% have metrics based on avoidance of unapproved abbreviations;
- 24% have metrics based on 100,000 Lives Campaign measures;
- 21% have metrics based on patient satisfaction measures;
- 17% have metrics based on transitions-of-care measures;
- 10% have metrics based on throughput measures;
- 7% have metrics based on end-of-life measures;
- 7% have metrics based on “good citizenship” measures;
- 7% have metrics based on mortality rate measures; and
- 7% have metrics based on readmission rate measures.
The most common metrics used in quality-incentive programs, based on 45 responses to SHM’s survey:
- 73% of programs use JCAHO heart failure measures;
- 73% use “good citizenship” measures;
- 73% use patient satisfaction measures;
- 67% use JCAHO pneumonia measures;
- 51% use transitions-of-care measures;
- 44% use JCAHO M.I. measures;
- 31% use throughput measures;
- 27% use avoidance of unapproved abbreviations;
- 24% use a measure based on medication reconciliation;
- 11% use 100,000 Lives Campaign measures;
- 9% use readmission rate measures;
- 7% use mortality rate measures; and
- 2% use end-of-life measures.
Recommendations
The prevalence of hospitalist quality-based compensation plans is continuing to grow rapidly, but the details of the plans’ structure will govern whether they benefit our patients, improve the overall value of the care we provide, and serve as a meaningful component of our compensation. I suggest each practice consider implementing plans with the following attributes:
A total dollar amount available for performance that is enough to influence hospitalist behavior. I think quality incentives should compose as much as 15% to 20% of a hospitalist’s annual income. Plans connecting quality performance to equal to or less than 7% of annual compensation (the case for 40% of groups in the above survey) rarely are effective.
Money vs. metrics. It usually is better to establish a plan based on a sliding scale of improved performance rather than a single threshold. For example, if all of the bonus money is available for a 10% improvement in performance, consider providing 10% of the total available money for each 1% improvement in performance.
Degree of difficulty. Performance thresholds should be set so that hospitalists need to change their practices to achieve them, but not so far out of reach that hospitalists give up on them. This can get tricky. Many practices set thresholds that are very easy to reach (e.g., they may be near the current level of performance).
Metrics for which trusted data is readily available. In most cases, this means using data already being collected. Avoid hard-to-track metrics, as they are likely to lead to disagreements about their accuracy.
Group vs. individual measures. Most performance metrics can’t be clearly attributed to one hospitalist as compared to another. For example, who gets the credit or blame for Ms. Smith getting or not getting a pneumovax? The majority of performance metrics are best measured and paid on a group basis. Some metrics, such as documenting medicine reconciliation on admission and discharge, can be effectively attributed to a single hospitalist and could be paid on an individual basis.
Small number of metrics, A meaningfully large amount of money should be connected to each one. Don’t make the mistake of having a $10,000 per doctor annual quality bonus pool divided among 20 metrics (each metric would pay a maximum of $500 per year).
Rotating metrics. Consider an annual meeting with members of your hospital’s administration to jointly establish the metrics used in the hospitalist quality incentive for that year. It is reasonable to change the metrics periodically.
It seems to me P4P programs are in their infancy, and will continue to evolve rapidly. Plans that fail to improve outcomes enough to justify the complexity of implementing, tracking, and paying for them will disappear slowly. (I wonder if payment for pneumovax administration during the hospital stay will be in this category.) And new, more effective, and more valuable programs will be developed.
Hospitalist practices will need to be nimble to keep pace with all of this change. Although SHM can alert you to how new P4P initiatives might affect your practice, and even recommend methods to improve your performance, you and your hospitalist colleagues still will have a lot of work to operationalize these programs in your practice. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He is part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Although there is a lot of debate about the effectiveness of pay-for-performance (P4P) plans, I think the plans are only going to increase in the foreseeable future.
We need more research to tell us the relative impact of public reporting of performance data and P4P programs. Most importantly, the details of how these plans are set up, how and what they measure, and the dollar amount involved will have everything to do with whether they are successful in improving the value of care we provide.
SHM’S Practice Management Committee conducted a mini-survey of hospitalist group leaders in 2006. Here are some of the key findings.
P4P Prevalence
Forty-one percent (60 out of 146) of hospital medicine group (HMG) leaders reported their groups have a quality-incentive program. Of those HMG leaders more likely to report participation in a quality-incentive program:
- 60% were at hospitals participating in a P4P program;
- 50% were at multispecialty/PCP medical groups; and
- 50% were in the Southern region.
Of those HMG leaders less likely to report participation in P4P programs, 28% were at academic programs and 31% were at local hospitalist-only groups.
Group vs. Individual Incentives
Of the HMG leaders participating in a quality-incentive program:
- 43% reported it was an individual incentive;
- 35% reported it was a group incentive;
- 10% reported the plan had elements of both individual and group incentives; and
- 12% were not sure if their plans had individual or group incentives.
Basis of Quality Targets
Of the HMG leaders reporting that they participate in a quality-incentive program (respondents could indicate one or more answers):
- 60% of the programs have targets based on national benchmarks;
- 23% have targets based on local or regional benchmarks;
- 37% have targets based on their hospital’s previous experience; and
- 47% have targets based on improvement over a baseline.
Maximum Impact of Incentives
Of the HMG leaders reporting that they participate in a quality-incentive program:
- 16% report the maximum impact is less than 3%;
- 24% report the maximum impact is from 3% to 7%;
- 35% report the maximum impact is from 8% to 10%;
- 17% report the maximum impact is from 11% to 20%;
- 3% report the maximum impact is more than 20%; and
- 5% report they do not know the maximum impact.
Group vs. Individual Incentives
Of the HMG leaders reporting that they participate in a quality-incentive program:
- 61% said they have received an incentive payment;
- 37% have not received an incentive payment; and
- 2% were unsure if they have received an incentive payment.
Quality Metrics
The most common metrics used in P4P programs, based on 29 responses to the SHM survey:
- 93% of HM programs have metrics based on The Joint Commission’s (JCAHO) heart failure measures;
- 86% have metrics based on JCAHO pneumonia measures;
- 79% have metrics based on JCAHO myocardial infarction measures;
- 28% have metrics based on a measure of medication reconciliation;
- 24% have metrics based on avoidance of unapproved abbreviations;
- 24% have metrics based on 100,000 Lives Campaign measures;
- 21% have metrics based on patient satisfaction measures;
- 17% have metrics based on transitions-of-care measures;
- 10% have metrics based on throughput measures;
- 7% have metrics based on end-of-life measures;
- 7% have metrics based on “good citizenship” measures;
- 7% have metrics based on mortality rate measures; and
- 7% have metrics based on readmission rate measures.
The most common metrics used in quality-incentive programs, based on 45 responses to SHM’s survey:
- 73% of programs use JCAHO heart failure measures;
- 73% use “good citizenship” measures;
- 73% use patient satisfaction measures;
- 67% use JCAHO pneumonia measures;
- 51% use transitions-of-care measures;
- 44% use JCAHO M.I. measures;
- 31% use throughput measures;
- 27% use avoidance of unapproved abbreviations;
- 24% use a measure based on medication reconciliation;
- 11% use 100,000 Lives Campaign measures;
- 9% use readmission rate measures;
- 7% use mortality rate measures; and
- 2% use end-of-life measures.
Recommendations
The prevalence of hospitalist quality-based compensation plans is continuing to grow rapidly, but the details of the plans’ structure will govern whether they benefit our patients, improve the overall value of the care we provide, and serve as a meaningful component of our compensation. I suggest each practice consider implementing plans with the following attributes:
A total dollar amount available for performance that is enough to influence hospitalist behavior. I think quality incentives should compose as much as 15% to 20% of a hospitalist’s annual income. Plans connecting quality performance to equal to or less than 7% of annual compensation (the case for 40% of groups in the above survey) rarely are effective.
Money vs. metrics. It usually is better to establish a plan based on a sliding scale of improved performance rather than a single threshold. For example, if all of the bonus money is available for a 10% improvement in performance, consider providing 10% of the total available money for each 1% improvement in performance.
Degree of difficulty. Performance thresholds should be set so that hospitalists need to change their practices to achieve them, but not so far out of reach that hospitalists give up on them. This can get tricky. Many practices set thresholds that are very easy to reach (e.g., they may be near the current level of performance).
Metrics for which trusted data is readily available. In most cases, this means using data already being collected. Avoid hard-to-track metrics, as they are likely to lead to disagreements about their accuracy.
Group vs. individual measures. Most performance metrics can’t be clearly attributed to one hospitalist as compared to another. For example, who gets the credit or blame for Ms. Smith getting or not getting a pneumovax? The majority of performance metrics are best measured and paid on a group basis. Some metrics, such as documenting medicine reconciliation on admission and discharge, can be effectively attributed to a single hospitalist and could be paid on an individual basis.
Small number of metrics, A meaningfully large amount of money should be connected to each one. Don’t make the mistake of having a $10,000 per doctor annual quality bonus pool divided among 20 metrics (each metric would pay a maximum of $500 per year).
Rotating metrics. Consider an annual meeting with members of your hospital’s administration to jointly establish the metrics used in the hospitalist quality incentive for that year. It is reasonable to change the metrics periodically.
It seems to me P4P programs are in their infancy, and will continue to evolve rapidly. Plans that fail to improve outcomes enough to justify the complexity of implementing, tracking, and paying for them will disappear slowly. (I wonder if payment for pneumovax administration during the hospital stay will be in this category.) And new, more effective, and more valuable programs will be developed.
Hospitalist practices will need to be nimble to keep pace with all of this change. Although SHM can alert you to how new P4P initiatives might affect your practice, and even recommend methods to improve your performance, you and your hospitalist colleagues still will have a lot of work to operationalize these programs in your practice. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He is part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Although there is a lot of debate about the effectiveness of pay-for-performance (P4P) plans, I think the plans are only going to increase in the foreseeable future.
We need more research to tell us the relative impact of public reporting of performance data and P4P programs. Most importantly, the details of how these plans are set up, how and what they measure, and the dollar amount involved will have everything to do with whether they are successful in improving the value of care we provide.
SHM’S Practice Management Committee conducted a mini-survey of hospitalist group leaders in 2006. Here are some of the key findings.
P4P Prevalence
Forty-one percent (60 out of 146) of hospital medicine group (HMG) leaders reported their groups have a quality-incentive program. Of those HMG leaders more likely to report participation in a quality-incentive program:
- 60% were at hospitals participating in a P4P program;
- 50% were at multispecialty/PCP medical groups; and
- 50% were in the Southern region.
Of those HMG leaders less likely to report participation in P4P programs, 28% were at academic programs and 31% were at local hospitalist-only groups.
Group vs. Individual Incentives
Of the HMG leaders participating in a quality-incentive program:
- 43% reported it was an individual incentive;
- 35% reported it was a group incentive;
- 10% reported the plan had elements of both individual and group incentives; and
- 12% were not sure if their plans had individual or group incentives.
Basis of Quality Targets
Of the HMG leaders reporting that they participate in a quality-incentive program (respondents could indicate one or more answers):
- 60% of the programs have targets based on national benchmarks;
- 23% have targets based on local or regional benchmarks;
- 37% have targets based on their hospital’s previous experience; and
- 47% have targets based on improvement over a baseline.
Maximum Impact of Incentives
Of the HMG leaders reporting that they participate in a quality-incentive program:
- 16% report the maximum impact is less than 3%;
- 24% report the maximum impact is from 3% to 7%;
- 35% report the maximum impact is from 8% to 10%;
- 17% report the maximum impact is from 11% to 20%;
- 3% report the maximum impact is more than 20%; and
- 5% report they do not know the maximum impact.
Group vs. Individual Incentives
Of the HMG leaders reporting that they participate in a quality-incentive program:
- 61% said they have received an incentive payment;
- 37% have not received an incentive payment; and
- 2% were unsure if they have received an incentive payment.
Quality Metrics
The most common metrics used in P4P programs, based on 29 responses to the SHM survey:
- 93% of HM programs have metrics based on The Joint Commission’s (JCAHO) heart failure measures;
- 86% have metrics based on JCAHO pneumonia measures;
- 79% have metrics based on JCAHO myocardial infarction measures;
- 28% have metrics based on a measure of medication reconciliation;
- 24% have metrics based on avoidance of unapproved abbreviations;
- 24% have metrics based on 100,000 Lives Campaign measures;
- 21% have metrics based on patient satisfaction measures;
- 17% have metrics based on transitions-of-care measures;
- 10% have metrics based on throughput measures;
- 7% have metrics based on end-of-life measures;
- 7% have metrics based on “good citizenship” measures;
- 7% have metrics based on mortality rate measures; and
- 7% have metrics based on readmission rate measures.
The most common metrics used in quality-incentive programs, based on 45 responses to SHM’s survey:
- 73% of programs use JCAHO heart failure measures;
- 73% use “good citizenship” measures;
- 73% use patient satisfaction measures;
- 67% use JCAHO pneumonia measures;
- 51% use transitions-of-care measures;
- 44% use JCAHO M.I. measures;
- 31% use throughput measures;
- 27% use avoidance of unapproved abbreviations;
- 24% use a measure based on medication reconciliation;
- 11% use 100,000 Lives Campaign measures;
- 9% use readmission rate measures;
- 7% use mortality rate measures; and
- 2% use end-of-life measures.
Recommendations
The prevalence of hospitalist quality-based compensation plans is continuing to grow rapidly, but the details of the plans’ structure will govern whether they benefit our patients, improve the overall value of the care we provide, and serve as a meaningful component of our compensation. I suggest each practice consider implementing plans with the following attributes:
A total dollar amount available for performance that is enough to influence hospitalist behavior. I think quality incentives should compose as much as 15% to 20% of a hospitalist’s annual income. Plans connecting quality performance to equal to or less than 7% of annual compensation (the case for 40% of groups in the above survey) rarely are effective.
Money vs. metrics. It usually is better to establish a plan based on a sliding scale of improved performance rather than a single threshold. For example, if all of the bonus money is available for a 10% improvement in performance, consider providing 10% of the total available money for each 1% improvement in performance.
Degree of difficulty. Performance thresholds should be set so that hospitalists need to change their practices to achieve them, but not so far out of reach that hospitalists give up on them. This can get tricky. Many practices set thresholds that are very easy to reach (e.g., they may be near the current level of performance).
Metrics for which trusted data is readily available. In most cases, this means using data already being collected. Avoid hard-to-track metrics, as they are likely to lead to disagreements about their accuracy.
Group vs. individual measures. Most performance metrics can’t be clearly attributed to one hospitalist as compared to another. For example, who gets the credit or blame for Ms. Smith getting or not getting a pneumovax? The majority of performance metrics are best measured and paid on a group basis. Some metrics, such as documenting medicine reconciliation on admission and discharge, can be effectively attributed to a single hospitalist and could be paid on an individual basis.
Small number of metrics, A meaningfully large amount of money should be connected to each one. Don’t make the mistake of having a $10,000 per doctor annual quality bonus pool divided among 20 metrics (each metric would pay a maximum of $500 per year).
Rotating metrics. Consider an annual meeting with members of your hospital’s administration to jointly establish the metrics used in the hospitalist quality incentive for that year. It is reasonable to change the metrics periodically.
It seems to me P4P programs are in their infancy, and will continue to evolve rapidly. Plans that fail to improve outcomes enough to justify the complexity of implementing, tracking, and paying for them will disappear slowly. (I wonder if payment for pneumovax administration during the hospital stay will be in this category.) And new, more effective, and more valuable programs will be developed.
Hospitalist practices will need to be nimble to keep pace with all of this change. Although SHM can alert you to how new P4P initiatives might affect your practice, and even recommend methods to improve your performance, you and your hospitalist colleagues still will have a lot of work to operationalize these programs in your practice. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. He is part of the faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Don’t Be Afraid to Fear Fear

As the New Year dawns I, like many Americans, am afraid.
Over the past year we’ve experienced a global financial meltdown, a deepening recession, rampant home foreclosures, Humpty Dumpty-like nest eggs, and the once-proud American auto industry gasping for breath. All of this is balanced against the hope that springs from the election of the first black President, who promises “change we can believe in.”
Hospitals are in growing financial straits and those in charge are deeply concerned, if not downright scared. In some ways, this is hard to imagine. Most hospitals reported outstanding, if not record, profits for the 2007 and 2008 fiscal years. However, change is afoot. Hospital admissions are down at nearly a third of hospitals, with a similar number of hospitals reporting declines in lucrative elective procedures. Additionally, recession-induced layoffs have resulted in a sharp rise in the proportion of uncompensated care that, when coupled with mushrooming debt and tighter credit, is propelling many hospitals into the red.
As a result, Moody’s, the credit-rating giant, has reported a rash of hospital credit downgrades. In October and November alone, Moody’s downgraded 18 hospitals and upgraded only one. At the same time, Fitch, another credit agency, downgraded the entire hospital sector from “stable” to “negative.” Although the subject of credit downgrades is somewhat abstract for many practicing physicians, the upshot is that it will be more expensive to finance hospital debt.
Coming on the heels of the largest hospital-building boom in American history, billions of dollars of debt present a very thorny fiscal rose. When this coalesces with less hospital utilization, more nonpaying patients, and potential decreases in federal reimbursement, it represents a financial crunch of catastrophic proportions.
Thus, it is no surprise our hospital administrators are on edge.
Hospitalist Impact
Enter me, the director of a money-losing service line, into an executive-filled room to propose expansion of hospital support for my hospitalist program. With average hospital support running a tad under $100,000 per hospitalist nationally, and overall support of about a million dollars per hospitalist group a year, any request for expansion will be scrutinized with a jaundiced eye.
In my experience, growing our hospitalist group was welcomed when the hospital’s coffers were bulging, the ED was overcrowded, and hospital beds were expanding. Granted, we had robust data showing our presence cut the average length of stay, increased throughput, and improved patient satisfaction—in other words, we paid for ourselves through enhanced efficiencies and cost savings. Still, the current economic realities dictate an unprecedented level of cost-consciousness and fiscal diligence. The result is my negotiations with my hospital administration have intensified, with an increased examination of expansion proposals, infrastructure development, and salary support.
Opportunity Abounds
So what are we—or I, in this case—to do? As I look at the potential of a prolonged recession, I am convinced this situation offers us a profound opportunity. Let’s face it: The hospital medicine boom was born out of opportunity. Early hospitalists took advantage of the opportunity to staff unassigned patients in the ED, backfill the migration of primary care doctors out of the hospital, enhance DRG reimbursements, reduce length of stay, and improve patient, staff, and subspecialist satisfaction because of our ability and willingness to staff inpatients around the clock.
In the coming years, we will again be offered opportunities, although they likely will come disguised as challenges. Some will choose to ignore these challenges in the hope they just go away, preferring instead to fear the unknown. Others will turn this fear into action and prosper. Opportunities will center on our ability to enhance patient outcomes and experiences. As federal dollars dry up and more and more Americans become uninsured or underinsured, hospitals will be pushed to augment the level of service and care they provide.
On one hand, payors have determined (appropriately so) that they want quality over quantity, and those who can provide superior outcomes will be better reimbursed. With thinning margins, hospitals will look for effector arms to engage the type of process improvement necessary to improve outcomes and, subsequently, revenue. We should not cower from this challenge, rather, embrace it; this is our chance to shine. Hospitalists are better positioned, better than any other medical group, to re-engineer the processes of care required to improve the quality of hospital care.
At the same time, our customers—the patients—likely will be footing more of the bill. As such, this new breed of healthcare consumer will expect a higher level of service than previously delivered. Again, hospitals that can provide five-star service will be better positioned to capture this coveted but ever-shrinking cohort of paying patients. This again positions hospitalists well. In my hospital, our group cares for just over 25% of all hospitalized patients, about 5,500 admissions per year.
Many hospitalist groups have a reach well beyond that, perhaps approaching 75%. Consider the type of bargaining power a hospitalist group could have by systematically showing that your work improves patient satisfaction, retention, and referral.
Measurement Is Crucial
Which brings me to my final point: As the economy tightens further, we will feel a heretofore-unrealized pressure to document our benefit. If we cannot document the fact our work improves processes, reduces length of stay, enhances the quality of patient care, and increases patient satisfaction, then we run the risk of being a glaringly large, negative budgetary line item waiting to be slashed.
With resolutions in the air, I resolve to work closely with my group and our hospital to document our value, prove our worth, do it better. Indubitably, this will meet with resistance, as some will advocate turning a blind eye, afraid of the challenges we might encounter. I, however, am going to choose to embrace these opportunities by fearing the known, rather than the unknown.
I have no doubt an honest assessment of the work we do and the value we provide might be anxiety provoking. It will force us to evaluate our care in ways we fear, measure our outcomes in ways we fear, push ourselves to improve in ways we fear.
In a word, change. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
As the New Year dawns I, like many Americans, am afraid.
Over the past year we’ve experienced a global financial meltdown, a deepening recession, rampant home foreclosures, Humpty Dumpty-like nest eggs, and the once-proud American auto industry gasping for breath. All of this is balanced against the hope that springs from the election of the first black President, who promises “change we can believe in.”
Hospitals are in growing financial straits and those in charge are deeply concerned, if not downright scared. In some ways, this is hard to imagine. Most hospitals reported outstanding, if not record, profits for the 2007 and 2008 fiscal years. However, change is afoot. Hospital admissions are down at nearly a third of hospitals, with a similar number of hospitals reporting declines in lucrative elective procedures. Additionally, recession-induced layoffs have resulted in a sharp rise in the proportion of uncompensated care that, when coupled with mushrooming debt and tighter credit, is propelling many hospitals into the red.
As a result, Moody’s, the credit-rating giant, has reported a rash of hospital credit downgrades. In October and November alone, Moody’s downgraded 18 hospitals and upgraded only one. At the same time, Fitch, another credit agency, downgraded the entire hospital sector from “stable” to “negative.” Although the subject of credit downgrades is somewhat abstract for many practicing physicians, the upshot is that it will be more expensive to finance hospital debt.
Coming on the heels of the largest hospital-building boom in American history, billions of dollars of debt present a very thorny fiscal rose. When this coalesces with less hospital utilization, more nonpaying patients, and potential decreases in federal reimbursement, it represents a financial crunch of catastrophic proportions.
Thus, it is no surprise our hospital administrators are on edge.
Hospitalist Impact
Enter me, the director of a money-losing service line, into an executive-filled room to propose expansion of hospital support for my hospitalist program. With average hospital support running a tad under $100,000 per hospitalist nationally, and overall support of about a million dollars per hospitalist group a year, any request for expansion will be scrutinized with a jaundiced eye.
In my experience, growing our hospitalist group was welcomed when the hospital’s coffers were bulging, the ED was overcrowded, and hospital beds were expanding. Granted, we had robust data showing our presence cut the average length of stay, increased throughput, and improved patient satisfaction—in other words, we paid for ourselves through enhanced efficiencies and cost savings. Still, the current economic realities dictate an unprecedented level of cost-consciousness and fiscal diligence. The result is my negotiations with my hospital administration have intensified, with an increased examination of expansion proposals, infrastructure development, and salary support.
Opportunity Abounds
So what are we—or I, in this case—to do? As I look at the potential of a prolonged recession, I am convinced this situation offers us a profound opportunity. Let’s face it: The hospital medicine boom was born out of opportunity. Early hospitalists took advantage of the opportunity to staff unassigned patients in the ED, backfill the migration of primary care doctors out of the hospital, enhance DRG reimbursements, reduce length of stay, and improve patient, staff, and subspecialist satisfaction because of our ability and willingness to staff inpatients around the clock.
In the coming years, we will again be offered opportunities, although they likely will come disguised as challenges. Some will choose to ignore these challenges in the hope they just go away, preferring instead to fear the unknown. Others will turn this fear into action and prosper. Opportunities will center on our ability to enhance patient outcomes and experiences. As federal dollars dry up and more and more Americans become uninsured or underinsured, hospitals will be pushed to augment the level of service and care they provide.
On one hand, payors have determined (appropriately so) that they want quality over quantity, and those who can provide superior outcomes will be better reimbursed. With thinning margins, hospitals will look for effector arms to engage the type of process improvement necessary to improve outcomes and, subsequently, revenue. We should not cower from this challenge, rather, embrace it; this is our chance to shine. Hospitalists are better positioned, better than any other medical group, to re-engineer the processes of care required to improve the quality of hospital care.
At the same time, our customers—the patients—likely will be footing more of the bill. As such, this new breed of healthcare consumer will expect a higher level of service than previously delivered. Again, hospitals that can provide five-star service will be better positioned to capture this coveted but ever-shrinking cohort of paying patients. This again positions hospitalists well. In my hospital, our group cares for just over 25% of all hospitalized patients, about 5,500 admissions per year.
Many hospitalist groups have a reach well beyond that, perhaps approaching 75%. Consider the type of bargaining power a hospitalist group could have by systematically showing that your work improves patient satisfaction, retention, and referral.
Measurement Is Crucial
Which brings me to my final point: As the economy tightens further, we will feel a heretofore-unrealized pressure to document our benefit. If we cannot document the fact our work improves processes, reduces length of stay, enhances the quality of patient care, and increases patient satisfaction, then we run the risk of being a glaringly large, negative budgetary line item waiting to be slashed.
With resolutions in the air, I resolve to work closely with my group and our hospital to document our value, prove our worth, do it better. Indubitably, this will meet with resistance, as some will advocate turning a blind eye, afraid of the challenges we might encounter. I, however, am going to choose to embrace these opportunities by fearing the known, rather than the unknown.
I have no doubt an honest assessment of the work we do and the value we provide might be anxiety provoking. It will force us to evaluate our care in ways we fear, measure our outcomes in ways we fear, push ourselves to improve in ways we fear.
In a word, change. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
As the New Year dawns I, like many Americans, am afraid.
Over the past year we’ve experienced a global financial meltdown, a deepening recession, rampant home foreclosures, Humpty Dumpty-like nest eggs, and the once-proud American auto industry gasping for breath. All of this is balanced against the hope that springs from the election of the first black President, who promises “change we can believe in.”
Hospitals are in growing financial straits and those in charge are deeply concerned, if not downright scared. In some ways, this is hard to imagine. Most hospitals reported outstanding, if not record, profits for the 2007 and 2008 fiscal years. However, change is afoot. Hospital admissions are down at nearly a third of hospitals, with a similar number of hospitals reporting declines in lucrative elective procedures. Additionally, recession-induced layoffs have resulted in a sharp rise in the proportion of uncompensated care that, when coupled with mushrooming debt and tighter credit, is propelling many hospitals into the red.
As a result, Moody’s, the credit-rating giant, has reported a rash of hospital credit downgrades. In October and November alone, Moody’s downgraded 18 hospitals and upgraded only one. At the same time, Fitch, another credit agency, downgraded the entire hospital sector from “stable” to “negative.” Although the subject of credit downgrades is somewhat abstract for many practicing physicians, the upshot is that it will be more expensive to finance hospital debt.
Coming on the heels of the largest hospital-building boom in American history, billions of dollars of debt present a very thorny fiscal rose. When this coalesces with less hospital utilization, more nonpaying patients, and potential decreases in federal reimbursement, it represents a financial crunch of catastrophic proportions.
Thus, it is no surprise our hospital administrators are on edge.
Hospitalist Impact
Enter me, the director of a money-losing service line, into an executive-filled room to propose expansion of hospital support for my hospitalist program. With average hospital support running a tad under $100,000 per hospitalist nationally, and overall support of about a million dollars per hospitalist group a year, any request for expansion will be scrutinized with a jaundiced eye.
In my experience, growing our hospitalist group was welcomed when the hospital’s coffers were bulging, the ED was overcrowded, and hospital beds were expanding. Granted, we had robust data showing our presence cut the average length of stay, increased throughput, and improved patient satisfaction—in other words, we paid for ourselves through enhanced efficiencies and cost savings. Still, the current economic realities dictate an unprecedented level of cost-consciousness and fiscal diligence. The result is my negotiations with my hospital administration have intensified, with an increased examination of expansion proposals, infrastructure development, and salary support.
Opportunity Abounds
So what are we—or I, in this case—to do? As I look at the potential of a prolonged recession, I am convinced this situation offers us a profound opportunity. Let’s face it: The hospital medicine boom was born out of opportunity. Early hospitalists took advantage of the opportunity to staff unassigned patients in the ED, backfill the migration of primary care doctors out of the hospital, enhance DRG reimbursements, reduce length of stay, and improve patient, staff, and subspecialist satisfaction because of our ability and willingness to staff inpatients around the clock.
In the coming years, we will again be offered opportunities, although they likely will come disguised as challenges. Some will choose to ignore these challenges in the hope they just go away, preferring instead to fear the unknown. Others will turn this fear into action and prosper. Opportunities will center on our ability to enhance patient outcomes and experiences. As federal dollars dry up and more and more Americans become uninsured or underinsured, hospitals will be pushed to augment the level of service and care they provide.
On one hand, payors have determined (appropriately so) that they want quality over quantity, and those who can provide superior outcomes will be better reimbursed. With thinning margins, hospitals will look for effector arms to engage the type of process improvement necessary to improve outcomes and, subsequently, revenue. We should not cower from this challenge, rather, embrace it; this is our chance to shine. Hospitalists are better positioned, better than any other medical group, to re-engineer the processes of care required to improve the quality of hospital care.
At the same time, our customers—the patients—likely will be footing more of the bill. As such, this new breed of healthcare consumer will expect a higher level of service than previously delivered. Again, hospitals that can provide five-star service will be better positioned to capture this coveted but ever-shrinking cohort of paying patients. This again positions hospitalists well. In my hospital, our group cares for just over 25% of all hospitalized patients, about 5,500 admissions per year.
Many hospitalist groups have a reach well beyond that, perhaps approaching 75%. Consider the type of bargaining power a hospitalist group could have by systematically showing that your work improves patient satisfaction, retention, and referral.
Measurement Is Crucial
Which brings me to my final point: As the economy tightens further, we will feel a heretofore-unrealized pressure to document our benefit. If we cannot document the fact our work improves processes, reduces length of stay, enhances the quality of patient care, and increases patient satisfaction, then we run the risk of being a glaringly large, negative budgetary line item waiting to be slashed.
With resolutions in the air, I resolve to work closely with my group and our hospital to document our value, prove our worth, do it better. Indubitably, this will meet with resistance, as some will advocate turning a blind eye, afraid of the challenges we might encounter. I, however, am going to choose to embrace these opportunities by fearing the known, rather than the unknown.
I have no doubt an honest assessment of the work we do and the value we provide might be anxiety provoking. It will force us to evaluate our care in ways we fear, measure our outcomes in ways we fear, push ourselves to improve in ways we fear.
In a word, change. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Accountability in Action
“What we’ve got here is failure to communicate …”
(Cool Hand Luke)

Every three months, the personnel in my office get a little nervous as we send out the quarterly personal e-mails to physicians. These e-mails, titled “Quality Indicator Deficiency,” are generated from the quality department’s abstraction of quality measures. The e-mails are personally sent from me, the chief medical officer, to the attending physician. For each measure abstracted, an attending is assigned responsibility (some like to call it “blame”). Despite the fact that we are a teaching hospital, we focus on the attendings who oversee the residents, but residents are copied on the e-mail. The deficiency assignment is based on the physician deemed most critical to the delivery of the measure.
For example, for a patient with pneumonia admitted through the ED, the ED physician is assigned the correct antibiotics measure. If the patient was directly admitted to a nursing unit, the admitting attending is assigned the correct antibiotic measure. Similarly, the anesthesia attending, not the surgeon, is given the pre-operative antibiotic measure.
Why the anxiety from my office? Because when the letters go out, there usually is a very rapid response by many physicians, which results in significant scrutiny of the letters. I refer to this as “good conflict.” Not everyone in my office always agrees with the good part, but there is agreement that this leads to significant discussion and awareness. Prior to the letters, we were like many organizations: We reported aggregate data regularly in a variety of forums and formats in order to promote awareness. We had regular conversations with physicians, physician leaders, and hospital staff. There were numerous quality-improvement efforts in measure areas. We continue to do all of these things, but it is the letters that have turned it up a notch.
Assign Responsibility
Responses fall into three categories. First, “The data is wrong.” Second, “This is not my fault. It was so-and-so’s fault.” Third, “A hospital process prevented me from doing the right thing.” The responses have proven so predictable that I have developed standard scripting for my responses.
Occasionally, the data are wrong. All letters are sent after the charts are initially abstracted. The accuracy of a chart abstractor is close to 100%. Addition of a nurse reviewer and a physician reviewer will help us achieve perfection, but the cost of doing this is significant. I find that many physicians, including myself, want perfection when it gets personal, but I just can’t justify the expense. Moreover, when a physician states that the data are wrong, it is more likely that the data are correct, but the physician does not fully understand the specifications of the measure.
Fault is a more interesting response. Deliberately, our quality committee, which determines the assignment rules, has chosen to attach an attending to every single measure, even those driven by hospital staff. This is done because we feel the healthcare team needs to solve these deficiencies, and often this forces a discussion. For deficiencies that are more staff-related, we do send the letter to the physician and unit manager simultaneously. The usual response by the manager is to contact the physician, apologize, then work on a plan that will remedy the situation.
As a recent example, a nurse chose to give a medication prior to an antibiotic for pneumonia and thus missed the six-hour deadline. This resulted in a change in protocol in the ED.
The hospital process response is the most useful to me because for every quarter that we send letters, there are multiple hospital processes that are modified as a result of this response. It is always fascinating to me because almost all of these measures have had good quality-improvement teams, but there are always missed subtle issues or unintended consequences. Because physicians respond quickly and often passionately, the urgency to fix these processes is present, hence facilitating rapid change.
Kill Them with Kindness
When I suggested sending these letters a few years ago, many on the quality staff cringed. Their reluctance was not unfounded: My original letter was a tad abrasive. I have toned down the letter, even to the point that I am now asking for help rather than directly pointing the finger: “I need your help in reviewing the following patient’s chart. In an initial review of quality indicators, a deficiency is noted. This may be because of simple oversight, or the patient might have had a contraindication for therapy for which we cannot find documentation. A physician must document all contraindications. Please review this chart as soon as possible, and if you feel this deficiency is in error, please let me or one of the outcomes managers know immediately. This deficiency has not yet been reported to the federal quality-improvement organization. We may be able to correct the error prior to final submission.”
The last line of the response attaches responsibility: “If we do not hear from you, we will assume the deficiency stands.”
This whole plan is part of a campaign in our hospital to personalize quality data. Recently, several studies have shown that consumers do not review quality data. Other evidence is increasingly backing up the “embarrassment” approach, as some would like to label my methodology. I prefer to call it the “personalizing method.” Physician education these days is largely based on case studies and the evidence-based approach. Personalizing quality data combines both, and might be the ideal approach to taking great leaps in quality.
Some experts have lamented this approach, but I can tell you that when I received two letters regarding the omission of offering a patient with heart failure weight-monitoring instructions, I quickly changed my approach and now make sure that the residents and nurses are giving those instructions. Initially, I was a little defensive about it, but I did the right thing and made modifications. Personalizing does work, and we should embrace it more fully.
It is not easy to personalize. Our present systems—or lack thereof—require abstracting and the review of written notes to achieve high levels of accuracy in personalizing. Without these high levels of accuracy, it is difficult to engage physicians with this data. The future is in electronic capture, but none of this is perfect, either. Hospitals must develop and hone systems to catch physician assignment during multiple interventions of a typical patient stay.
The cost of all this is unknown and most likely significant. But one could easily imagine a tremendous improvement in quality.
My message to hospitalists and hospitalist leaders is “Make the data personal!” Start working on this today, so that within a few years, you, too, will have regular reports. Continue to aggregate quality data based on group performance and review it frequently. If you want more significant impact and greater physician engagement, make it personal. TH
Dr. Cawley is president of SHM.
“What we’ve got here is failure to communicate …”
(Cool Hand Luke)
Every three months, the personnel in my office get a little nervous as we send out the quarterly personal e-mails to physicians. These e-mails, titled “Quality Indicator Deficiency,” are generated from the quality department’s abstraction of quality measures. The e-mails are personally sent from me, the chief medical officer, to the attending physician. For each measure abstracted, an attending is assigned responsibility (some like to call it “blame”). Despite the fact that we are a teaching hospital, we focus on the attendings who oversee the residents, but residents are copied on the e-mail. The deficiency assignment is based on the physician deemed most critical to the delivery of the measure.
For example, for a patient with pneumonia admitted through the ED, the ED physician is assigned the correct antibiotics measure. If the patient was directly admitted to a nursing unit, the admitting attending is assigned the correct antibiotic measure. Similarly, the anesthesia attending, not the surgeon, is given the pre-operative antibiotic measure.
Why the anxiety from my office? Because when the letters go out, there usually is a very rapid response by many physicians, which results in significant scrutiny of the letters. I refer to this as “good conflict.” Not everyone in my office always agrees with the good part, but there is agreement that this leads to significant discussion and awareness. Prior to the letters, we were like many organizations: We reported aggregate data regularly in a variety of forums and formats in order to promote awareness. We had regular conversations with physicians, physician leaders, and hospital staff. There were numerous quality-improvement efforts in measure areas. We continue to do all of these things, but it is the letters that have turned it up a notch.
Assign Responsibility
Responses fall into three categories. First, “The data is wrong.” Second, “This is not my fault. It was so-and-so’s fault.” Third, “A hospital process prevented me from doing the right thing.” The responses have proven so predictable that I have developed standard scripting for my responses.
Occasionally, the data are wrong. All letters are sent after the charts are initially abstracted. The accuracy of a chart abstractor is close to 100%. Addition of a nurse reviewer and a physician reviewer will help us achieve perfection, but the cost of doing this is significant. I find that many physicians, including myself, want perfection when it gets personal, but I just can’t justify the expense. Moreover, when a physician states that the data are wrong, it is more likely that the data are correct, but the physician does not fully understand the specifications of the measure.
Fault is a more interesting response. Deliberately, our quality committee, which determines the assignment rules, has chosen to attach an attending to every single measure, even those driven by hospital staff. This is done because we feel the healthcare team needs to solve these deficiencies, and often this forces a discussion. For deficiencies that are more staff-related, we do send the letter to the physician and unit manager simultaneously. The usual response by the manager is to contact the physician, apologize, then work on a plan that will remedy the situation.
As a recent example, a nurse chose to give a medication prior to an antibiotic for pneumonia and thus missed the six-hour deadline. This resulted in a change in protocol in the ED.
The hospital process response is the most useful to me because for every quarter that we send letters, there are multiple hospital processes that are modified as a result of this response. It is always fascinating to me because almost all of these measures have had good quality-improvement teams, but there are always missed subtle issues or unintended consequences. Because physicians respond quickly and often passionately, the urgency to fix these processes is present, hence facilitating rapid change.
Kill Them with Kindness
When I suggested sending these letters a few years ago, many on the quality staff cringed. Their reluctance was not unfounded: My original letter was a tad abrasive. I have toned down the letter, even to the point that I am now asking for help rather than directly pointing the finger: “I need your help in reviewing the following patient’s chart. In an initial review of quality indicators, a deficiency is noted. This may be because of simple oversight, or the patient might have had a contraindication for therapy for which we cannot find documentation. A physician must document all contraindications. Please review this chart as soon as possible, and if you feel this deficiency is in error, please let me or one of the outcomes managers know immediately. This deficiency has not yet been reported to the federal quality-improvement organization. We may be able to correct the error prior to final submission.”
The last line of the response attaches responsibility: “If we do not hear from you, we will assume the deficiency stands.”
This whole plan is part of a campaign in our hospital to personalize quality data. Recently, several studies have shown that consumers do not review quality data. Other evidence is increasingly backing up the “embarrassment” approach, as some would like to label my methodology. I prefer to call it the “personalizing method.” Physician education these days is largely based on case studies and the evidence-based approach. Personalizing quality data combines both, and might be the ideal approach to taking great leaps in quality.
Some experts have lamented this approach, but I can tell you that when I received two letters regarding the omission of offering a patient with heart failure weight-monitoring instructions, I quickly changed my approach and now make sure that the residents and nurses are giving those instructions. Initially, I was a little defensive about it, but I did the right thing and made modifications. Personalizing does work, and we should embrace it more fully.
It is not easy to personalize. Our present systems—or lack thereof—require abstracting and the review of written notes to achieve high levels of accuracy in personalizing. Without these high levels of accuracy, it is difficult to engage physicians with this data. The future is in electronic capture, but none of this is perfect, either. Hospitals must develop and hone systems to catch physician assignment during multiple interventions of a typical patient stay.
The cost of all this is unknown and most likely significant. But one could easily imagine a tremendous improvement in quality.
My message to hospitalists and hospitalist leaders is “Make the data personal!” Start working on this today, so that within a few years, you, too, will have regular reports. Continue to aggregate quality data based on group performance and review it frequently. If you want more significant impact and greater physician engagement, make it personal. TH
Dr. Cawley is president of SHM.
“What we’ve got here is failure to communicate …”
(Cool Hand Luke)
Every three months, the personnel in my office get a little nervous as we send out the quarterly personal e-mails to physicians. These e-mails, titled “Quality Indicator Deficiency,” are generated from the quality department’s abstraction of quality measures. The e-mails are personally sent from me, the chief medical officer, to the attending physician. For each measure abstracted, an attending is assigned responsibility (some like to call it “blame”). Despite the fact that we are a teaching hospital, we focus on the attendings who oversee the residents, but residents are copied on the e-mail. The deficiency assignment is based on the physician deemed most critical to the delivery of the measure.
For example, for a patient with pneumonia admitted through the ED, the ED physician is assigned the correct antibiotics measure. If the patient was directly admitted to a nursing unit, the admitting attending is assigned the correct antibiotic measure. Similarly, the anesthesia attending, not the surgeon, is given the pre-operative antibiotic measure.
Why the anxiety from my office? Because when the letters go out, there usually is a very rapid response by many physicians, which results in significant scrutiny of the letters. I refer to this as “good conflict.” Not everyone in my office always agrees with the good part, but there is agreement that this leads to significant discussion and awareness. Prior to the letters, we were like many organizations: We reported aggregate data regularly in a variety of forums and formats in order to promote awareness. We had regular conversations with physicians, physician leaders, and hospital staff. There were numerous quality-improvement efforts in measure areas. We continue to do all of these things, but it is the letters that have turned it up a notch.
Assign Responsibility
Responses fall into three categories. First, “The data is wrong.” Second, “This is not my fault. It was so-and-so’s fault.” Third, “A hospital process prevented me from doing the right thing.” The responses have proven so predictable that I have developed standard scripting for my responses.
Occasionally, the data are wrong. All letters are sent after the charts are initially abstracted. The accuracy of a chart abstractor is close to 100%. Addition of a nurse reviewer and a physician reviewer will help us achieve perfection, but the cost of doing this is significant. I find that many physicians, including myself, want perfection when it gets personal, but I just can’t justify the expense. Moreover, when a physician states that the data are wrong, it is more likely that the data are correct, but the physician does not fully understand the specifications of the measure.
Fault is a more interesting response. Deliberately, our quality committee, which determines the assignment rules, has chosen to attach an attending to every single measure, even those driven by hospital staff. This is done because we feel the healthcare team needs to solve these deficiencies, and often this forces a discussion. For deficiencies that are more staff-related, we do send the letter to the physician and unit manager simultaneously. The usual response by the manager is to contact the physician, apologize, then work on a plan that will remedy the situation.
As a recent example, a nurse chose to give a medication prior to an antibiotic for pneumonia and thus missed the six-hour deadline. This resulted in a change in protocol in the ED.
The hospital process response is the most useful to me because for every quarter that we send letters, there are multiple hospital processes that are modified as a result of this response. It is always fascinating to me because almost all of these measures have had good quality-improvement teams, but there are always missed subtle issues or unintended consequences. Because physicians respond quickly and often passionately, the urgency to fix these processes is present, hence facilitating rapid change.
Kill Them with Kindness
When I suggested sending these letters a few years ago, many on the quality staff cringed. Their reluctance was not unfounded: My original letter was a tad abrasive. I have toned down the letter, even to the point that I am now asking for help rather than directly pointing the finger: “I need your help in reviewing the following patient’s chart. In an initial review of quality indicators, a deficiency is noted. This may be because of simple oversight, or the patient might have had a contraindication for therapy for which we cannot find documentation. A physician must document all contraindications. Please review this chart as soon as possible, and if you feel this deficiency is in error, please let me or one of the outcomes managers know immediately. This deficiency has not yet been reported to the federal quality-improvement organization. We may be able to correct the error prior to final submission.”
The last line of the response attaches responsibility: “If we do not hear from you, we will assume the deficiency stands.”
This whole plan is part of a campaign in our hospital to personalize quality data. Recently, several studies have shown that consumers do not review quality data. Other evidence is increasingly backing up the “embarrassment” approach, as some would like to label my methodology. I prefer to call it the “personalizing method.” Physician education these days is largely based on case studies and the evidence-based approach. Personalizing quality data combines both, and might be the ideal approach to taking great leaps in quality.
Some experts have lamented this approach, but I can tell you that when I received two letters regarding the omission of offering a patient with heart failure weight-monitoring instructions, I quickly changed my approach and now make sure that the residents and nurses are giving those instructions. Initially, I was a little defensive about it, but I did the right thing and made modifications. Personalizing does work, and we should embrace it more fully.
It is not easy to personalize. Our present systems—or lack thereof—require abstracting and the review of written notes to achieve high levels of accuracy in personalizing. Without these high levels of accuracy, it is difficult to engage physicians with this data. The future is in electronic capture, but none of this is perfect, either. Hospitals must develop and hone systems to catch physician assignment during multiple interventions of a typical patient stay.
The cost of all this is unknown and most likely significant. But one could easily imagine a tremendous improvement in quality.
My message to hospitalists and hospitalist leaders is “Make the data personal!” Start working on this today, so that within a few years, you, too, will have regular reports. Continue to aggregate quality data based on group performance and review it frequently. If you want more significant impact and greater physician engagement, make it personal. TH
Dr. Cawley is president of SHM.
One Hospital's Trash, Another Hospital's Treasure
The day after the Tepa District Hospital in Ghana, on the west coast of Africa, received its first sonogram machine, a life was saved. The scan picked up placenta previa in a young woman who was seven months pregnant, a complication that causes hundreds of maternal and fetal deaths each year in rural Africa.
Not this time. The ultrasound’s advance warning gave Isaac Boetang, MD, chief medical officer at Tepa District Hospital, the ability to plan ahead. Instead of facing a life-threatening hemorrhage at birth, which likely would tax his hospital’s limited resources, Dr. Boetang had time to prepare for a C-section and deliver a healthy baby to a healthy mother. In the seven months since the donated instrument arrived, Dr. Boetang estimates at least 30 more babies and mothers have been saved. Tepa’s sonogram machine was supplied by Doc to Dock, a non-profit organization working on a simple premise: Collect unused, surplus supplies from U.S. hospitals for distribution to needy hospitals in emerging countries.
Doc to Dock was born as the result of a call to charitable arms sounded by former President Bill Clinton in 2005 at his first summit meeting for the Clinton Global Initiative. He told the gathering his new foundation’s goal was “to help turn good intentions into good action and results.” Among the elite crowd of CEOs and celebrities in attendance that day was an unassuming New York cardiologist, Bruce Charash, MD, a clinical associate professor at New York University and former chief of cardiac care at Lenox Hospital in New York City. “It’s possible that year I was the only person who wasn’t a celebrity,” Dr. Charash says with a humble laugh. “They were asking us to do something to make an impact on the world, but until then my only developing world experience was spring break in 1975.”
As the former president challenged his guests to change the world, an idea Dr. Charash had long been mulling over crystallized. “I took it seriously and created a new charity,” he explains. “Send medical supplies to Africa.” When he was asked about a name, he thought slowly—and out loud. Doc, of course, his profession, to Dock, he says, as the image of a ship at a foreign port popped into his head. And that is how Dr. Charash made his own personal commitment to the Clinton Global Initiative. Doc to Dock was incorporated as a 501(c)(3) non-profit organization in February 2006. “We were the first charity formed under their umbrella,” he says. “and though we have no affiliation with them, they are an amazing support group.”

Good Deeds
The Greek poet Homer noted some 3,000 years ago, “the charity that is a trifle to us can be precious to others.” Dr. Charash knew American hospitals, doctors’ offices, pharmacies, and clinics, housed tons of unused medical supplies. In fact, the United Way estimates more than 7,000 tons of unused medical supplies and outdated equipment are discarded every day, either incinerated or carted off to landfills. At the same time in developing countries, thousands of patients are turned away from hospitals and medical centers due to a lack of medical supplies and equipment. Doc to Dock’s mission is to correct this imbalance.
Dr. Charash began conceiving a plan to somehow turn America’s trash—precious medical resources—into treasure, channeling the leftover sutures, scalpel blades, IV tubing, bandages, outdated equipment and machinery, old hospital beds and wheelchairs to hospitals in Africa.
Then Dr. Charash stumbled across a program, aptly named Merci, at The University of Virginia Medical Center, which collects its surplus supplies and used equipment for distribution to non-profit organizations, such as the Red Cross and Project Smile. The hospital invited Dr. Charash to take a look, and he was impressed by what he saw. Since its inception in 1992, Merci has collected more than 400 tons of medical materials worth more than $80 million.

Dr. Charash then set about soliciting donations from hospitals in his own backyard, New York City. It was a tall order. He and his small staff (one doctor, five staffers) needed to gather the surplus supplies and equipment, find a place to store it, recruit volunteers to inventory the items, and then enlist trucking and shipping companies to move the donations overseas. To find his supplies, he turned to hospitals, corporations, pharmaceutical companies, and even medical meetings. He found government and non-governmental organization partners willing to help him identify hospitals in need of and willing to receive the supplies. And, once identified, his team of volunteers began the process of matching the need with the goods collected, utilizing an online ordering system to supply the hospitals in Africa.
The Clinton name helped the cause enormously. In March, 2006, Dr. Charash reported to the Clinton Global Initiative (CGI) “the prestige of being a CGI commitment has opened many corporate doors that I do not necessarily believe would have opened without being identified with this effort.” Those open doors, coupled with Dr. Charash’s persistence, set Doc to Dock in motion.
It is proving a worthwhile voyage. One of the first partners to jump on board was Franklin Hospital in Valley Stream, N.Y., which is a part of the 305-bed North Shore Hospital System. Mary Hynes, a perioperative nurse educator, long had been discouraged by the waste of perfectly good supplies, some never even opened or routinely discarded from operating room packs. “I embraced it the nanosecond I heard it. We’d been wanting something for so long,” Hynes says. “For years, we had been throwing out stuff. It was almost criminal.”
Super Simple System
The Doc to Dock system is simple. Bright, electric-blue recycling barrels, emblazoned with the Doc to Dock logo, are stationed in the operating room and other easily accessible areas where hospital personnel can toss surplus supplies. Wrapped, sterile items, such as latex gloves, suture packs, scalpels, and bandages, routinely are overstocked in customized sterile packs as a bit of surgical “insurance.” Anything not used is discarded, still in a sterile wrap. “If a case is cancelled or something else happens,” Hynes says, “there is a sterile field with hundreds of dollars worth of supplies, which could not be reused. Everything has to be discarded and thrown away. You can’t reprocess it because there is too much liability involved.”
When Hynes switched jobs a few months ago, she transported her enthusiasm for Doc to Dock with her to the 371-bed Southside Hospital in Bay Shore, N.Y. Aided by a documentary DVD, which she showed her new colleagues, she instituted the Doc to Dock program at her new hospital. To date, the operating room and radiology department are donating excess supplies, and Hynes is planning to talk to the delivery room nurses soon.
“The barrels get filled right up,” Hynes explains. “This one hospital fills about six bins a week. Every two weeks, I call a trucker to pick them up.” Doc to Dock has arrangements with a dozen New York-area hospitals, thus far, including partnerships with the North Shore System and the Greater New York Hospital Association.
Make a Donation
The supplies may be donated, but it takes money to truck them, warehouse them and ship them to Africa. Doc to Dock relies on funding raised from corporations and philanthropic sources, plus in-kind donations from trucking and shipping companies who often move supplies for minimal or no cost.
In addition to supplies, Dr. Charash is looking for equipment. Many hospitals and clinics replace equipment, still in perfect working order, with newer models. Anesthesia machines, cryosurgery machines, mammogram machines, and cancer screening equipment, have found their way to African hospitals.
The sonogram traveled to Tepa District Hospital by way of a 40-foot shipping container, along with other supplies and equipment once destined for a U.S. scrap heap. The district serves about 100,000 villagers, and the hospital had been saving its nickels—one at a time—to purchase its own sonogram. The fundraising drive would have taken 10 years. One can only guess how many babies would have died in the meantime.
Through 2008, Doc to Dock had shipped nine containers to Ghana, Benin, Liberia, East Africa, Ethiopia, Kenya, and Uganda. Another container went to Haiti following a devastating hurricane. Four or five additional containers are just about ready to ship, Dr. Charash says. Each container costs about $25,000 per shipment. Dr. Charash estimates each shipment delivers approximately $500,000 worth of supplies and equipment.
Dr. Charash, who maintains privileges at Lenox and Mt. Sinai Medical Center in Manhattan, dreams big. He defines success by growing Doc to Dock to 100 containers per year within five years. He also wants to increase the number of hospitals donating goods, and the number of third-world hospitals receiving the supplies. Additionally, he wants to make the charity self-sustaining, as the need is always greater than the resources available.
“It’s a moral issue,” he says. “I have an obligation not to let it go to waste.” TH
Carol Berczuk is a freelance writer in New York CIty.
The day after the Tepa District Hospital in Ghana, on the west coast of Africa, received its first sonogram machine, a life was saved. The scan picked up placenta previa in a young woman who was seven months pregnant, a complication that causes hundreds of maternal and fetal deaths each year in rural Africa.
Not this time. The ultrasound’s advance warning gave Isaac Boetang, MD, chief medical officer at Tepa District Hospital, the ability to plan ahead. Instead of facing a life-threatening hemorrhage at birth, which likely would tax his hospital’s limited resources, Dr. Boetang had time to prepare for a C-section and deliver a healthy baby to a healthy mother. In the seven months since the donated instrument arrived, Dr. Boetang estimates at least 30 more babies and mothers have been saved. Tepa’s sonogram machine was supplied by Doc to Dock, a non-profit organization working on a simple premise: Collect unused, surplus supplies from U.S. hospitals for distribution to needy hospitals in emerging countries.
Doc to Dock was born as the result of a call to charitable arms sounded by former President Bill Clinton in 2005 at his first summit meeting for the Clinton Global Initiative. He told the gathering his new foundation’s goal was “to help turn good intentions into good action and results.” Among the elite crowd of CEOs and celebrities in attendance that day was an unassuming New York cardiologist, Bruce Charash, MD, a clinical associate professor at New York University and former chief of cardiac care at Lenox Hospital in New York City. “It’s possible that year I was the only person who wasn’t a celebrity,” Dr. Charash says with a humble laugh. “They were asking us to do something to make an impact on the world, but until then my only developing world experience was spring break in 1975.”
As the former president challenged his guests to change the world, an idea Dr. Charash had long been mulling over crystallized. “I took it seriously and created a new charity,” he explains. “Send medical supplies to Africa.” When he was asked about a name, he thought slowly—and out loud. Doc, of course, his profession, to Dock, he says, as the image of a ship at a foreign port popped into his head. And that is how Dr. Charash made his own personal commitment to the Clinton Global Initiative. Doc to Dock was incorporated as a 501(c)(3) non-profit organization in February 2006. “We were the first charity formed under their umbrella,” he says. “and though we have no affiliation with them, they are an amazing support group.”
Good Deeds
The Greek poet Homer noted some 3,000 years ago, “the charity that is a trifle to us can be precious to others.” Dr. Charash knew American hospitals, doctors’ offices, pharmacies, and clinics, housed tons of unused medical supplies. In fact, the United Way estimates more than 7,000 tons of unused medical supplies and outdated equipment are discarded every day, either incinerated or carted off to landfills. At the same time in developing countries, thousands of patients are turned away from hospitals and medical centers due to a lack of medical supplies and equipment. Doc to Dock’s mission is to correct this imbalance.
Dr. Charash began conceiving a plan to somehow turn America’s trash—precious medical resources—into treasure, channeling the leftover sutures, scalpel blades, IV tubing, bandages, outdated equipment and machinery, old hospital beds and wheelchairs to hospitals in Africa.
Then Dr. Charash stumbled across a program, aptly named Merci, at The University of Virginia Medical Center, which collects its surplus supplies and used equipment for distribution to non-profit organizations, such as the Red Cross and Project Smile. The hospital invited Dr. Charash to take a look, and he was impressed by what he saw. Since its inception in 1992, Merci has collected more than 400 tons of medical materials worth more than $80 million.
Dr. Charash then set about soliciting donations from hospitals in his own backyard, New York City. It was a tall order. He and his small staff (one doctor, five staffers) needed to gather the surplus supplies and equipment, find a place to store it, recruit volunteers to inventory the items, and then enlist trucking and shipping companies to move the donations overseas. To find his supplies, he turned to hospitals, corporations, pharmaceutical companies, and even medical meetings. He found government and non-governmental organization partners willing to help him identify hospitals in need of and willing to receive the supplies. And, once identified, his team of volunteers began the process of matching the need with the goods collected, utilizing an online ordering system to supply the hospitals in Africa.
The Clinton name helped the cause enormously. In March, 2006, Dr. Charash reported to the Clinton Global Initiative (CGI) “the prestige of being a CGI commitment has opened many corporate doors that I do not necessarily believe would have opened without being identified with this effort.” Those open doors, coupled with Dr. Charash’s persistence, set Doc to Dock in motion.
It is proving a worthwhile voyage. One of the first partners to jump on board was Franklin Hospital in Valley Stream, N.Y., which is a part of the 305-bed North Shore Hospital System. Mary Hynes, a perioperative nurse educator, long had been discouraged by the waste of perfectly good supplies, some never even opened or routinely discarded from operating room packs. “I embraced it the nanosecond I heard it. We’d been wanting something for so long,” Hynes says. “For years, we had been throwing out stuff. It was almost criminal.”
Super Simple System
The Doc to Dock system is simple. Bright, electric-blue recycling barrels, emblazoned with the Doc to Dock logo, are stationed in the operating room and other easily accessible areas where hospital personnel can toss surplus supplies. Wrapped, sterile items, such as latex gloves, suture packs, scalpels, and bandages, routinely are overstocked in customized sterile packs as a bit of surgical “insurance.” Anything not used is discarded, still in a sterile wrap. “If a case is cancelled or something else happens,” Hynes says, “there is a sterile field with hundreds of dollars worth of supplies, which could not be reused. Everything has to be discarded and thrown away. You can’t reprocess it because there is too much liability involved.”
When Hynes switched jobs a few months ago, she transported her enthusiasm for Doc to Dock with her to the 371-bed Southside Hospital in Bay Shore, N.Y. Aided by a documentary DVD, which she showed her new colleagues, she instituted the Doc to Dock program at her new hospital. To date, the operating room and radiology department are donating excess supplies, and Hynes is planning to talk to the delivery room nurses soon.
“The barrels get filled right up,” Hynes explains. “This one hospital fills about six bins a week. Every two weeks, I call a trucker to pick them up.” Doc to Dock has arrangements with a dozen New York-area hospitals, thus far, including partnerships with the North Shore System and the Greater New York Hospital Association.
Make a Donation
The supplies may be donated, but it takes money to truck them, warehouse them and ship them to Africa. Doc to Dock relies on funding raised from corporations and philanthropic sources, plus in-kind donations from trucking and shipping companies who often move supplies for minimal or no cost.
In addition to supplies, Dr. Charash is looking for equipment. Many hospitals and clinics replace equipment, still in perfect working order, with newer models. Anesthesia machines, cryosurgery machines, mammogram machines, and cancer screening equipment, have found their way to African hospitals.
The sonogram traveled to Tepa District Hospital by way of a 40-foot shipping container, along with other supplies and equipment once destined for a U.S. scrap heap. The district serves about 100,000 villagers, and the hospital had been saving its nickels—one at a time—to purchase its own sonogram. The fundraising drive would have taken 10 years. One can only guess how many babies would have died in the meantime.
Through 2008, Doc to Dock had shipped nine containers to Ghana, Benin, Liberia, East Africa, Ethiopia, Kenya, and Uganda. Another container went to Haiti following a devastating hurricane. Four or five additional containers are just about ready to ship, Dr. Charash says. Each container costs about $25,000 per shipment. Dr. Charash estimates each shipment delivers approximately $500,000 worth of supplies and equipment.
Dr. Charash, who maintains privileges at Lenox and Mt. Sinai Medical Center in Manhattan, dreams big. He defines success by growing Doc to Dock to 100 containers per year within five years. He also wants to increase the number of hospitals donating goods, and the number of third-world hospitals receiving the supplies. Additionally, he wants to make the charity self-sustaining, as the need is always greater than the resources available.
“It’s a moral issue,” he says. “I have an obligation not to let it go to waste.” TH
Carol Berczuk is a freelance writer in New York CIty.
The day after the Tepa District Hospital in Ghana, on the west coast of Africa, received its first sonogram machine, a life was saved. The scan picked up placenta previa in a young woman who was seven months pregnant, a complication that causes hundreds of maternal and fetal deaths each year in rural Africa.
Not this time. The ultrasound’s advance warning gave Isaac Boetang, MD, chief medical officer at Tepa District Hospital, the ability to plan ahead. Instead of facing a life-threatening hemorrhage at birth, which likely would tax his hospital’s limited resources, Dr. Boetang had time to prepare for a C-section and deliver a healthy baby to a healthy mother. In the seven months since the donated instrument arrived, Dr. Boetang estimates at least 30 more babies and mothers have been saved. Tepa’s sonogram machine was supplied by Doc to Dock, a non-profit organization working on a simple premise: Collect unused, surplus supplies from U.S. hospitals for distribution to needy hospitals in emerging countries.
Doc to Dock was born as the result of a call to charitable arms sounded by former President Bill Clinton in 2005 at his first summit meeting for the Clinton Global Initiative. He told the gathering his new foundation’s goal was “to help turn good intentions into good action and results.” Among the elite crowd of CEOs and celebrities in attendance that day was an unassuming New York cardiologist, Bruce Charash, MD, a clinical associate professor at New York University and former chief of cardiac care at Lenox Hospital in New York City. “It’s possible that year I was the only person who wasn’t a celebrity,” Dr. Charash says with a humble laugh. “They were asking us to do something to make an impact on the world, but until then my only developing world experience was spring break in 1975.”
As the former president challenged his guests to change the world, an idea Dr. Charash had long been mulling over crystallized. “I took it seriously and created a new charity,” he explains. “Send medical supplies to Africa.” When he was asked about a name, he thought slowly—and out loud. Doc, of course, his profession, to Dock, he says, as the image of a ship at a foreign port popped into his head. And that is how Dr. Charash made his own personal commitment to the Clinton Global Initiative. Doc to Dock was incorporated as a 501(c)(3) non-profit organization in February 2006. “We were the first charity formed under their umbrella,” he says. “and though we have no affiliation with them, they are an amazing support group.”
Good Deeds
The Greek poet Homer noted some 3,000 years ago, “the charity that is a trifle to us can be precious to others.” Dr. Charash knew American hospitals, doctors’ offices, pharmacies, and clinics, housed tons of unused medical supplies. In fact, the United Way estimates more than 7,000 tons of unused medical supplies and outdated equipment are discarded every day, either incinerated or carted off to landfills. At the same time in developing countries, thousands of patients are turned away from hospitals and medical centers due to a lack of medical supplies and equipment. Doc to Dock’s mission is to correct this imbalance.
Dr. Charash began conceiving a plan to somehow turn America’s trash—precious medical resources—into treasure, channeling the leftover sutures, scalpel blades, IV tubing, bandages, outdated equipment and machinery, old hospital beds and wheelchairs to hospitals in Africa.
Then Dr. Charash stumbled across a program, aptly named Merci, at The University of Virginia Medical Center, which collects its surplus supplies and used equipment for distribution to non-profit organizations, such as the Red Cross and Project Smile. The hospital invited Dr. Charash to take a look, and he was impressed by what he saw. Since its inception in 1992, Merci has collected more than 400 tons of medical materials worth more than $80 million.
Dr. Charash then set about soliciting donations from hospitals in his own backyard, New York City. It was a tall order. He and his small staff (one doctor, five staffers) needed to gather the surplus supplies and equipment, find a place to store it, recruit volunteers to inventory the items, and then enlist trucking and shipping companies to move the donations overseas. To find his supplies, he turned to hospitals, corporations, pharmaceutical companies, and even medical meetings. He found government and non-governmental organization partners willing to help him identify hospitals in need of and willing to receive the supplies. And, once identified, his team of volunteers began the process of matching the need with the goods collected, utilizing an online ordering system to supply the hospitals in Africa.
The Clinton name helped the cause enormously. In March, 2006, Dr. Charash reported to the Clinton Global Initiative (CGI) “the prestige of being a CGI commitment has opened many corporate doors that I do not necessarily believe would have opened without being identified with this effort.” Those open doors, coupled with Dr. Charash’s persistence, set Doc to Dock in motion.
It is proving a worthwhile voyage. One of the first partners to jump on board was Franklin Hospital in Valley Stream, N.Y., which is a part of the 305-bed North Shore Hospital System. Mary Hynes, a perioperative nurse educator, long had been discouraged by the waste of perfectly good supplies, some never even opened or routinely discarded from operating room packs. “I embraced it the nanosecond I heard it. We’d been wanting something for so long,” Hynes says. “For years, we had been throwing out stuff. It was almost criminal.”
Super Simple System
The Doc to Dock system is simple. Bright, electric-blue recycling barrels, emblazoned with the Doc to Dock logo, are stationed in the operating room and other easily accessible areas where hospital personnel can toss surplus supplies. Wrapped, sterile items, such as latex gloves, suture packs, scalpels, and bandages, routinely are overstocked in customized sterile packs as a bit of surgical “insurance.” Anything not used is discarded, still in a sterile wrap. “If a case is cancelled or something else happens,” Hynes says, “there is a sterile field with hundreds of dollars worth of supplies, which could not be reused. Everything has to be discarded and thrown away. You can’t reprocess it because there is too much liability involved.”
When Hynes switched jobs a few months ago, she transported her enthusiasm for Doc to Dock with her to the 371-bed Southside Hospital in Bay Shore, N.Y. Aided by a documentary DVD, which she showed her new colleagues, she instituted the Doc to Dock program at her new hospital. To date, the operating room and radiology department are donating excess supplies, and Hynes is planning to talk to the delivery room nurses soon.
“The barrels get filled right up,” Hynes explains. “This one hospital fills about six bins a week. Every two weeks, I call a trucker to pick them up.” Doc to Dock has arrangements with a dozen New York-area hospitals, thus far, including partnerships with the North Shore System and the Greater New York Hospital Association.
Make a Donation
The supplies may be donated, but it takes money to truck them, warehouse them and ship them to Africa. Doc to Dock relies on funding raised from corporations and philanthropic sources, plus in-kind donations from trucking and shipping companies who often move supplies for minimal or no cost.
In addition to supplies, Dr. Charash is looking for equipment. Many hospitals and clinics replace equipment, still in perfect working order, with newer models. Anesthesia machines, cryosurgery machines, mammogram machines, and cancer screening equipment, have found their way to African hospitals.
The sonogram traveled to Tepa District Hospital by way of a 40-foot shipping container, along with other supplies and equipment once destined for a U.S. scrap heap. The district serves about 100,000 villagers, and the hospital had been saving its nickels—one at a time—to purchase its own sonogram. The fundraising drive would have taken 10 years. One can only guess how many babies would have died in the meantime.
Through 2008, Doc to Dock had shipped nine containers to Ghana, Benin, Liberia, East Africa, Ethiopia, Kenya, and Uganda. Another container went to Haiti following a devastating hurricane. Four or five additional containers are just about ready to ship, Dr. Charash says. Each container costs about $25,000 per shipment. Dr. Charash estimates each shipment delivers approximately $500,000 worth of supplies and equipment.
Dr. Charash, who maintains privileges at Lenox and Mt. Sinai Medical Center in Manhattan, dreams big. He defines success by growing Doc to Dock to 100 containers per year within five years. He also wants to increase the number of hospitals donating goods, and the number of third-world hospitals receiving the supplies. Additionally, he wants to make the charity self-sustaining, as the need is always greater than the resources available.
“It’s a moral issue,” he says. “I have an obligation not to let it go to waste.” TH
Carol Berczuk is a freelance writer in New York CIty.
What is the proper duration of antibiotic treatment in adults hospitalized with community-acquired pneumonia?
Case
An 83-year-old male with hypertension, coronary artery disease, and obstructive sleep apnea presents with progressive shortness of breath, a productive cough, wheezing, and tachypnea. His blood pressure is 158/70 mm/Hg; temperature is 101.8; respirations are 26 breaths per minute; and oxygen saturation is 87% on room air. He has coarse breath sounds bilaterally, and decreased breath sounds over the right lower lung fields. His chest X-ray reveals a right lower lobe infiltrate. He is admitted to the hospital with a diagnosis of community-acquired pneumonia (CAP), and medical therapy is started. How should his antibiotic treatment be managed?
Overview
Community-acquired pneumonia is the most common infection-related cause of death in the U.S., and the eighth-leading cause of mortality overall.1 According to a 2006 survey, CAP results in more than 1.2 million hospital admissions annually, with an average length of stay of 5.1 days.2 Though less than 20% of CAP patients require hospitalization, cases necessitating admission contribute to more than 90% of the overall cost of pneumonia care.3
During the past several years, the availability of new antibiotics and the evolution of microbial resistance patterns have changed CAP treatment strategies. Furthermore, the development of prognostic scoring systems and increasing pressure to streamline resource utilization while improving quality of care have led to new treatment considerations, such as managing low-risk cases as outpatients.
More recently, attention has been directed to the optimal duration of antibiotic treatment, with a focus on shortening the duration of therapy. Historically, CAP treatment duration has been variable and not evidence-based. Shortening the course of antibiotics might limit antibiotic resistance, decrease costs, and improve patient adherence and tolerability.4 However, before defining the appropriate antibiotic duration for a patient hospitalized with CAP, other factors must be considered, such as the choice of empiric antibiotics, the patient’s initial response to treatment, severity of the disease, and presence of co-morbidities.
Review of the Data
Antibiotic choice. The most widely referenced practice guidelines for the management of CAP patients were published in 2007 by representatives of the Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS).5 Table 1 (above, right) summarizes the recommendations for empiric antibiotics for patients requiring inpatient treatment.
Time to clinical stability. A patient’s clinical response to empiric antibiotic therapy contributes heavily to the decision regarding treatment course and duration. The IDSA/ATS guidelines recommend patients be afebrile for 48 to 72 hours and have no more than one CAP-associated sign of clinical instability before discontinuation of therapy. Although studies have used different definitions of clinical stability, the consensus guidelines refer to six parameters, which are summarized in Table 2 (right).
With appropriate antibiotic therapy, most patients hospitalized with CAP achieve clinical stability in approximately three days.6,7 Providers should expect to see some improvement in vital signs within 48 to 72 hours of admission. Should a patient fail to demonstrate objective improvement during that time, providers should look for unusual pathogens, resistant organisms, nosocomial superinfections, or noninfectious conditions.5 Certain patients, such as those with multilobar pneumonia, associated pleural effusion, or higher pneumonia-severity index scores, also take longer to reach clinical stability.8
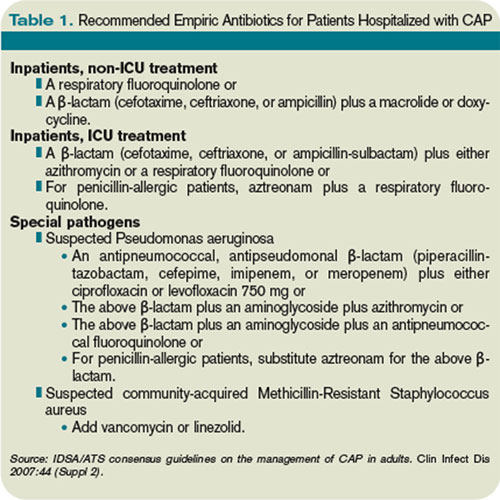
Switch to oral therapy. The ability to achieve clinical stability has important implications for hospital length of stay. Most patients hospitalized with CAP initially are treated with intravenous (IV) antibiotics and require transition to oral therapy in anticipation of discharge. Several studies have found there is no advantage to continuing IV medication once a patient is deemed clinically stable and is able to tolerate oral medication.9,10 There are no specific guidelines regarding choice of oral antibiotics, but it is common practice, supported by the IDSA/ATS recommendations, to use the same agent as the IV antibiotic or a medication in the same drug class. For patients started on β-lactam and macrolide combination therapy, it usually is appropriate to switch to a macrolide alone.5 In cases in which a pathogen has been identified, antibiotic selection should be based on the susceptibility profile.
Once patients are switched to oral antibiotics, it is not necessary for them to remain in the hospital for further observation, provided they have no other active medical problems or social needs. A retrospective analysis of 39,232 patients hospitalized with CAP compared those who were observed overnight after switching to oral antibiotics with those who were not and found no difference in 14-day readmission rate or 30-day mortality rate.11 These findings, in conjunction with the strategy of an early switch to oral therapy, suggest hospital length of stay may be safely reduced for many patients with uncomplicated CAP.
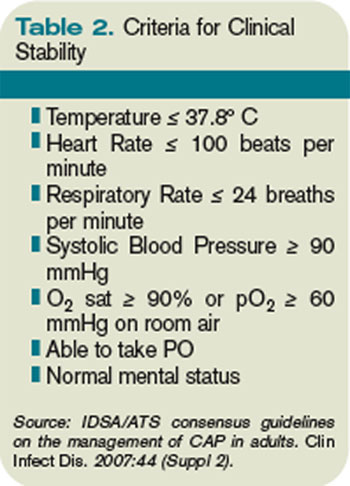
Duration of therapy. After a patient becomes clinically stable and a decision is made to switch to oral medication and a plan for hospital discharge, the question becomes how long to continue the course of antibiotics. Historically, clinical practice has extended treatment for up to two weeks, despite lack of evidence for this duration of therapy. The IDSA/ATS guidelines offer some general recommendations, noting patients should be treated for a minimum of five days, in addition to being afebrile for 48 to 72 hours and meet other criteria for clinical stability.5
Li and colleagues conducted a systematic review evaluating 15 randomized controlled trials comparing short-course (less than seven days) with extended (more than seven days) monotherapy for CAP in adults.4 Overall, the authors found no difference in the risk of treatment failure between short-course and extended-course antibiotic therapy, and they found no difference in bacteriologic eradication or mortality. It is important to note the studies included in this analysis enrolled patients with mild to moderate CAP, including those treated as outpatients, which limits the ability to extrapolate to exclusively inpatient populations and more severely ill patients.
Another meta-analysis, published shortly thereafter, examined randomized controlled trials in outpatients and inpatients not requiring intensive care. It compared different durations of treatment with the same agent in the same dosage. The authors similarly found no difference in effectiveness or safety of short (less than seven days) versus longer (at least two additional days of therapy) courses.12 Table 3 (above) reviews selected trials of short courses of antibiotics, which have been studied in inpatient populations.
The trials summarized in these meta-analyses examined monotherapy with levofloxacin for five days; gemifloxacin for seven days, azithromycin for three to five days; ceftriaxone for five days; cefuroxime for seven days; amoxicillin for three days; or telithromycin for five to seven days. The variety of antibiotics in these studies contrasts the IDSA/ATS guidelines, which recommend only fluoroquinolones as monotherapy for inpatient CAP.
One important randomized, double-blind study of fluoroquinolones compared a five-day course of levofloxacin 750 mg daily, with a 10-day course of levofloxacin, 500 mg daily, in 528 patients with mild to severe CAP.13 The authors found no difference in clinical success or microbiologic eradication between the two groups, concluding high-dose levofloxacin for five days is an effective and well-tolerated alternative to a longer course of a lower dose, likely related to the drug’s concentration-dependent properties.

Azithromycin also offers potential for short courses of therapy, as pulmonary concentrations of azithromycin remain elevated for as many as five days following a single oral dose.14 Several small studies have demonstrated the safety, efficacy, and cost-effectiveness of three to five days of azithromycin, as summarized in a meta-analysis by Contopoulos-Ioannidis and colleagues.15 Most of these trials, however, were limited to outpatients or inpatients with mild disease or confirmed atypical pneumonia. One randomized trial of 40 inpatients with mild to moderately severe CAP found comparable clinical outcomes with a three-day course of oral azithromycin 500 mg daily versus clarithromycin for at least eight days.16 Larger studies in more severely ill patients must be completed before routinely recommending this approach in hospitalized patients. Furthermore, due to the rising prevalence of macrolide resistance, empiric therapy with a macrolide alone can only be used for the treatment of carefully selected hospitalized patients with nonsevere diseases and without risk factors for drug-resistant Streptococcus pneumoniae.5
Telithromycin is a ketolide antibiotic, which has been studied in mild to moderate CAP, including multidrug-resistant strains of S. pneumoniae, in courses of five to seven days.17 However, severe adverse reactions, including hepatotoxicity, have been reported. At the time of the 2007 guidelines, the IDSA/ATS committee waited for additional safety data before making any recommendations on its use.
One additional study of note was a trial of amoxicillin in adult inpatients with mild to moderately severe CAP.18 One hundred twenty-one patients who clinically improved (based on a composite score of pulmonary symptoms and general improvement) following three days of IV amoxicillin were randomized to oral amoxicillin for an additional five days or given a placebo. At days 10 and 28, there was no difference in clinical success between the two groups. The authors concluded that a total of three days of treatment was not inferior to eight days in patients who substantially improved after the first 72 hours of empiric treatment. This trial was conducted in the Netherlands, where amoxicillin is the preferred empiric antibiotic for CAP and patterns of antimicrobial resistance differ greatly from those found in the U.S.
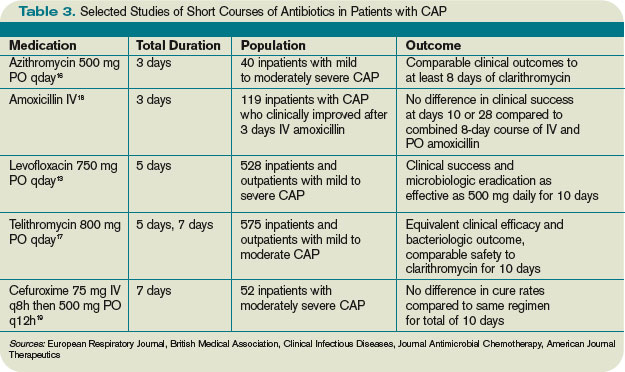
Other considerations. While some evidence supports shorter courses of antibiotics, many of the existing studies are limited by their inclusion of outpatients, adults with mild to moderate CAP, or small sample size. Hence, clinical judgment continues to play an important role in determining the appropriate duration of therapy. Factors such as pre-existing co-morbidities, severity of illness, and occurrence of complications should be considered. Data is limited on the appropriate duration of antibiotics in CAP patients requiring intensive care. It also is important to note the IDSA/ATS recommendations and most of the studies reviewed exclude patients with human immunodeficiency virus (HIV), and it is unknown whether these shorter courses of antibiotics are appropriate in the HIV population.
Lastly, the IDSA/ATS guidelines note longer durations of treatment may be required if the initial therapy was not active against the identified pathogen, or in cases complicated by extrapulmonary infections, such as endocarditis or meningitis.
Back to the Case
Our patient with moderately severe CAP was hospitalized based on his age and hypoxia. He was immediately treated with supplemental oxygen by nasal cannula, IV fluids, and a dose of IV levofloxacin 750 mg. Within 48 hours he met criteria for clinical stability, including defervescence, a decline in his respiratory rate to 19 breaths per minute, and improvement in oxygen saturation to 95% on room air. At this point, he was changed from IV to oral antibiotics. He continued on levofloxacin 750 mg daily and later that day was discharged home in good condition to complete a five-day course.
Bottom Line
For hospitalized adults with mild to moderately severe CAP, five to seven days of treatment, depending on the antibiotic selected, appears to be effective in most cases. Patients should be afebrile for 48 to 72 hours and demonstrate signs of clinical stability before therapy is discontinued. TH
Kelly Cunningham, MD, and Shelley Ellis, MD, MPH, are members of the Section of Hospital Medicine at Vanderbilt University in Nashville, Tenn. Sunil Kripalani, MD, MSc, serves as the section chief.
References
1. Kung HC, Hoyert DL, Xu J, Murphy SL. Deaths: final data for 2005. Natl Vital Stat Rep. 2008;56.
2. DeFrances CJ, Lucas CA, Buie VC, Golosinskiy A. 2006 National Hospital Discharge Survey. Natl Health Stat Report. 2008;5.
3. Niederman MS. Recent advances in community-acquired pneumonia: inpatient and outpatient. Chest. 2007;131:1205-1215.
4. Li JZ, Winston LG, Moore DH, Bent S. Efficacy of short-course antibiotic regimens for community-acquired pneumonia: a meta-analysis. Am J Med. 2007;120:783-790.
5. Mandell LA, Wunderink RG, Anzueto A et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl 2):S27-72.
6. Ramirez JA, Bordon J. Early switch from intravenous to oral antibiotics in hospitalized patients with bacteremic community-acquired Streptococcus pneumoniae pneumonia. Arch Intern Med. 2001;161:848-850.
7. Halm EA, Fine MJ, Marrie TJ et al. Time to clinical stability in patients hospitalized with community-acquired pneumonia: implications for practice guidelines. JAMA. 1998;279:1452-1457.
8. Menendez R, Torres A, Rodriguez de Castro F et al. Reaching stability in community-acquired pneumonia: the effects of the severity of disease, treatment, and the characteristics of patients. Clin Infect Dis. 2004;39:1783-1790.
9. Siegal RE, Halpern NA, Almenoff PL et al. A prospective randomised study of inpatient IV antibiotics for community-acquired pneumonia: the optimal duration of therapy. Chest. 1996;110:965-971.
10. Oosterheert JJ, Bonten MJ, Schneider MM et al. Effectiveness of early switch from intravenous to oral antibiotics in severe community acquired pneumonia: multicentre randomized trial. BMJ. 2006;333:1193-1197.
11. Nathan RV, Rhew DC, Murray C et al. In-hospital observation after antibiotic switch in pneumonia: a national evaluation. Am J Med. 2006;119:512-518.
12. Dimopoulos G, Matthaiou DK, Karageorgopoulos DE, et al. Short- versus long-course antibacterial therapy for community-acquired pneumonia: a meta-analysis. Drugs. 2008;68:1841-1854.
13. Dunbar LM, Wunderink RG, Habib MP et al. High-dose, short-course levofloxacin for community-acquired pneumonia: a new treatment paradigm. Clin Infect Dis. 2003;37:752-760.
14. Morris DL, De Souza A, Jones JA, Morgan WE. High and prolonged pulmonary tissue concentrations of azithromycin following a single oral dose. Eur J Clin Microbiol Infect Dis. 1991;10:859-861.
15. Contopoulos-Ioannidis DG, Ioannidis JPA, Chew P, Lau J. Meta-analysis of randomized controlled trials on the comparative efficacy and safety of azithromycin against other antibiotics for lower respiratory tract infections. J Antimicrob Chemother. 2001;48:691-703.
16. Rizzato G, Montemurro L, Fraioli P et al. Efficacy of a three-day course of azithromycin in moderately severe community-acquired pneumonia. Eur Respir J. 1995;8:398-402.
17. Tellier G, Niederman MS, Nusrat R et al. Clinical and bacteriological efficacy and safety of 5- and 7-day regimens of telithromycin once daily compared with a 10-day regimen of clarithromycin twice daily in patients with mild to moderate community-acquired pneumonia. J Antimicrob Chemother. 2004;54:515.
18. El Moussaoui R, de Borgie CA, van den Broek P et al. Effectiveness of discontinuing antibiotic treatment after three days versus eight days in mild to moderate-severe community acquired pneumonia: randomised, double blind study. BMJ. 2006;332:1355-1361.
19. Siegel RE, Alicea M, Lee A, Blaiklock R. Comparison of 7 versus 10 days of antibiotic therapy for hospitalized patients with uncomplicated community-acquired pneumonia: a prospective, randomized double-blind study. Am J Ther. 1999;6:217-222.
Case
An 83-year-old male with hypertension, coronary artery disease, and obstructive sleep apnea presents with progressive shortness of breath, a productive cough, wheezing, and tachypnea. His blood pressure is 158/70 mm/Hg; temperature is 101.8; respirations are 26 breaths per minute; and oxygen saturation is 87% on room air. He has coarse breath sounds bilaterally, and decreased breath sounds over the right lower lung fields. His chest X-ray reveals a right lower lobe infiltrate. He is admitted to the hospital with a diagnosis of community-acquired pneumonia (CAP), and medical therapy is started. How should his antibiotic treatment be managed?
Overview
Community-acquired pneumonia is the most common infection-related cause of death in the U.S., and the eighth-leading cause of mortality overall.1 According to a 2006 survey, CAP results in more than 1.2 million hospital admissions annually, with an average length of stay of 5.1 days.2 Though less than 20% of CAP patients require hospitalization, cases necessitating admission contribute to more than 90% of the overall cost of pneumonia care.3
During the past several years, the availability of new antibiotics and the evolution of microbial resistance patterns have changed CAP treatment strategies. Furthermore, the development of prognostic scoring systems and increasing pressure to streamline resource utilization while improving quality of care have led to new treatment considerations, such as managing low-risk cases as outpatients.
More recently, attention has been directed to the optimal duration of antibiotic treatment, with a focus on shortening the duration of therapy. Historically, CAP treatment duration has been variable and not evidence-based. Shortening the course of antibiotics might limit antibiotic resistance, decrease costs, and improve patient adherence and tolerability.4 However, before defining the appropriate antibiotic duration for a patient hospitalized with CAP, other factors must be considered, such as the choice of empiric antibiotics, the patient’s initial response to treatment, severity of the disease, and presence of co-morbidities.
Review of the Data
Antibiotic choice. The most widely referenced practice guidelines for the management of CAP patients were published in 2007 by representatives of the Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS).5 Table 1 (above, right) summarizes the recommendations for empiric antibiotics for patients requiring inpatient treatment.
Time to clinical stability. A patient’s clinical response to empiric antibiotic therapy contributes heavily to the decision regarding treatment course and duration. The IDSA/ATS guidelines recommend patients be afebrile for 48 to 72 hours and have no more than one CAP-associated sign of clinical instability before discontinuation of therapy. Although studies have used different definitions of clinical stability, the consensus guidelines refer to six parameters, which are summarized in Table 2 (right).
With appropriate antibiotic therapy, most patients hospitalized with CAP achieve clinical stability in approximately three days.6,7 Providers should expect to see some improvement in vital signs within 48 to 72 hours of admission. Should a patient fail to demonstrate objective improvement during that time, providers should look for unusual pathogens, resistant organisms, nosocomial superinfections, or noninfectious conditions.5 Certain patients, such as those with multilobar pneumonia, associated pleural effusion, or higher pneumonia-severity index scores, also take longer to reach clinical stability.8
Switch to oral therapy. The ability to achieve clinical stability has important implications for hospital length of stay. Most patients hospitalized with CAP initially are treated with intravenous (IV) antibiotics and require transition to oral therapy in anticipation of discharge. Several studies have found there is no advantage to continuing IV medication once a patient is deemed clinically stable and is able to tolerate oral medication.9,10 There are no specific guidelines regarding choice of oral antibiotics, but it is common practice, supported by the IDSA/ATS recommendations, to use the same agent as the IV antibiotic or a medication in the same drug class. For patients started on β-lactam and macrolide combination therapy, it usually is appropriate to switch to a macrolide alone.5 In cases in which a pathogen has been identified, antibiotic selection should be based on the susceptibility profile.
Once patients are switched to oral antibiotics, it is not necessary for them to remain in the hospital for further observation, provided they have no other active medical problems or social needs. A retrospective analysis of 39,232 patients hospitalized with CAP compared those who were observed overnight after switching to oral antibiotics with those who were not and found no difference in 14-day readmission rate or 30-day mortality rate.11 These findings, in conjunction with the strategy of an early switch to oral therapy, suggest hospital length of stay may be safely reduced for many patients with uncomplicated CAP.
Duration of therapy. After a patient becomes clinically stable and a decision is made to switch to oral medication and a plan for hospital discharge, the question becomes how long to continue the course of antibiotics. Historically, clinical practice has extended treatment for up to two weeks, despite lack of evidence for this duration of therapy. The IDSA/ATS guidelines offer some general recommendations, noting patients should be treated for a minimum of five days, in addition to being afebrile for 48 to 72 hours and meet other criteria for clinical stability.5
Li and colleagues conducted a systematic review evaluating 15 randomized controlled trials comparing short-course (less than seven days) with extended (more than seven days) monotherapy for CAP in adults.4 Overall, the authors found no difference in the risk of treatment failure between short-course and extended-course antibiotic therapy, and they found no difference in bacteriologic eradication or mortality. It is important to note the studies included in this analysis enrolled patients with mild to moderate CAP, including those treated as outpatients, which limits the ability to extrapolate to exclusively inpatient populations and more severely ill patients.
Another meta-analysis, published shortly thereafter, examined randomized controlled trials in outpatients and inpatients not requiring intensive care. It compared different durations of treatment with the same agent in the same dosage. The authors similarly found no difference in effectiveness or safety of short (less than seven days) versus longer (at least two additional days of therapy) courses.12 Table 3 (above) reviews selected trials of short courses of antibiotics, which have been studied in inpatient populations.
The trials summarized in these meta-analyses examined monotherapy with levofloxacin for five days; gemifloxacin for seven days, azithromycin for three to five days; ceftriaxone for five days; cefuroxime for seven days; amoxicillin for three days; or telithromycin for five to seven days. The variety of antibiotics in these studies contrasts the IDSA/ATS guidelines, which recommend only fluoroquinolones as monotherapy for inpatient CAP.
One important randomized, double-blind study of fluoroquinolones compared a five-day course of levofloxacin 750 mg daily, with a 10-day course of levofloxacin, 500 mg daily, in 528 patients with mild to severe CAP.13 The authors found no difference in clinical success or microbiologic eradication between the two groups, concluding high-dose levofloxacin for five days is an effective and well-tolerated alternative to a longer course of a lower dose, likely related to the drug’s concentration-dependent properties.
Azithromycin also offers potential for short courses of therapy, as pulmonary concentrations of azithromycin remain elevated for as many as five days following a single oral dose.14 Several small studies have demonstrated the safety, efficacy, and cost-effectiveness of three to five days of azithromycin, as summarized in a meta-analysis by Contopoulos-Ioannidis and colleagues.15 Most of these trials, however, were limited to outpatients or inpatients with mild disease or confirmed atypical pneumonia. One randomized trial of 40 inpatients with mild to moderately severe CAP found comparable clinical outcomes with a three-day course of oral azithromycin 500 mg daily versus clarithromycin for at least eight days.16 Larger studies in more severely ill patients must be completed before routinely recommending this approach in hospitalized patients. Furthermore, due to the rising prevalence of macrolide resistance, empiric therapy with a macrolide alone can only be used for the treatment of carefully selected hospitalized patients with nonsevere diseases and without risk factors for drug-resistant Streptococcus pneumoniae.5
Telithromycin is a ketolide antibiotic, which has been studied in mild to moderate CAP, including multidrug-resistant strains of S. pneumoniae, in courses of five to seven days.17 However, severe adverse reactions, including hepatotoxicity, have been reported. At the time of the 2007 guidelines, the IDSA/ATS committee waited for additional safety data before making any recommendations on its use.
One additional study of note was a trial of amoxicillin in adult inpatients with mild to moderately severe CAP.18 One hundred twenty-one patients who clinically improved (based on a composite score of pulmonary symptoms and general improvement) following three days of IV amoxicillin were randomized to oral amoxicillin for an additional five days or given a placebo. At days 10 and 28, there was no difference in clinical success between the two groups. The authors concluded that a total of three days of treatment was not inferior to eight days in patients who substantially improved after the first 72 hours of empiric treatment. This trial was conducted in the Netherlands, where amoxicillin is the preferred empiric antibiotic for CAP and patterns of antimicrobial resistance differ greatly from those found in the U.S.
Other considerations. While some evidence supports shorter courses of antibiotics, many of the existing studies are limited by their inclusion of outpatients, adults with mild to moderate CAP, or small sample size. Hence, clinical judgment continues to play an important role in determining the appropriate duration of therapy. Factors such as pre-existing co-morbidities, severity of illness, and occurrence of complications should be considered. Data is limited on the appropriate duration of antibiotics in CAP patients requiring intensive care. It also is important to note the IDSA/ATS recommendations and most of the studies reviewed exclude patients with human immunodeficiency virus (HIV), and it is unknown whether these shorter courses of antibiotics are appropriate in the HIV population.
Lastly, the IDSA/ATS guidelines note longer durations of treatment may be required if the initial therapy was not active against the identified pathogen, or in cases complicated by extrapulmonary infections, such as endocarditis or meningitis.
Back to the Case
Our patient with moderately severe CAP was hospitalized based on his age and hypoxia. He was immediately treated with supplemental oxygen by nasal cannula, IV fluids, and a dose of IV levofloxacin 750 mg. Within 48 hours he met criteria for clinical stability, including defervescence, a decline in his respiratory rate to 19 breaths per minute, and improvement in oxygen saturation to 95% on room air. At this point, he was changed from IV to oral antibiotics. He continued on levofloxacin 750 mg daily and later that day was discharged home in good condition to complete a five-day course.
Bottom Line
For hospitalized adults with mild to moderately severe CAP, five to seven days of treatment, depending on the antibiotic selected, appears to be effective in most cases. Patients should be afebrile for 48 to 72 hours and demonstrate signs of clinical stability before therapy is discontinued. TH
Kelly Cunningham, MD, and Shelley Ellis, MD, MPH, are members of the Section of Hospital Medicine at Vanderbilt University in Nashville, Tenn. Sunil Kripalani, MD, MSc, serves as the section chief.
References
1. Kung HC, Hoyert DL, Xu J, Murphy SL. Deaths: final data for 2005. Natl Vital Stat Rep. 2008;56.
2. DeFrances CJ, Lucas CA, Buie VC, Golosinskiy A. 2006 National Hospital Discharge Survey. Natl Health Stat Report. 2008;5.
3. Niederman MS. Recent advances in community-acquired pneumonia: inpatient and outpatient. Chest. 2007;131:1205-1215.
4. Li JZ, Winston LG, Moore DH, Bent S. Efficacy of short-course antibiotic regimens for community-acquired pneumonia: a meta-analysis. Am J Med. 2007;120:783-790.
5. Mandell LA, Wunderink RG, Anzueto A et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl 2):S27-72.
6. Ramirez JA, Bordon J. Early switch from intravenous to oral antibiotics in hospitalized patients with bacteremic community-acquired Streptococcus pneumoniae pneumonia. Arch Intern Med. 2001;161:848-850.
7. Halm EA, Fine MJ, Marrie TJ et al. Time to clinical stability in patients hospitalized with community-acquired pneumonia: implications for practice guidelines. JAMA. 1998;279:1452-1457.
8. Menendez R, Torres A, Rodriguez de Castro F et al. Reaching stability in community-acquired pneumonia: the effects of the severity of disease, treatment, and the characteristics of patients. Clin Infect Dis. 2004;39:1783-1790.
9. Siegal RE, Halpern NA, Almenoff PL et al. A prospective randomised study of inpatient IV antibiotics for community-acquired pneumonia: the optimal duration of therapy. Chest. 1996;110:965-971.
10. Oosterheert JJ, Bonten MJ, Schneider MM et al. Effectiveness of early switch from intravenous to oral antibiotics in severe community acquired pneumonia: multicentre randomized trial. BMJ. 2006;333:1193-1197.
11. Nathan RV, Rhew DC, Murray C et al. In-hospital observation after antibiotic switch in pneumonia: a national evaluation. Am J Med. 2006;119:512-518.
12. Dimopoulos G, Matthaiou DK, Karageorgopoulos DE, et al. Short- versus long-course antibacterial therapy for community-acquired pneumonia: a meta-analysis. Drugs. 2008;68:1841-1854.
13. Dunbar LM, Wunderink RG, Habib MP et al. High-dose, short-course levofloxacin for community-acquired pneumonia: a new treatment paradigm. Clin Infect Dis. 2003;37:752-760.
14. Morris DL, De Souza A, Jones JA, Morgan WE. High and prolonged pulmonary tissue concentrations of azithromycin following a single oral dose. Eur J Clin Microbiol Infect Dis. 1991;10:859-861.
15. Contopoulos-Ioannidis DG, Ioannidis JPA, Chew P, Lau J. Meta-analysis of randomized controlled trials on the comparative efficacy and safety of azithromycin against other antibiotics for lower respiratory tract infections. J Antimicrob Chemother. 2001;48:691-703.
16. Rizzato G, Montemurro L, Fraioli P et al. Efficacy of a three-day course of azithromycin in moderately severe community-acquired pneumonia. Eur Respir J. 1995;8:398-402.
17. Tellier G, Niederman MS, Nusrat R et al. Clinical and bacteriological efficacy and safety of 5- and 7-day regimens of telithromycin once daily compared with a 10-day regimen of clarithromycin twice daily in patients with mild to moderate community-acquired pneumonia. J Antimicrob Chemother. 2004;54:515.
18. El Moussaoui R, de Borgie CA, van den Broek P et al. Effectiveness of discontinuing antibiotic treatment after three days versus eight days in mild to moderate-severe community acquired pneumonia: randomised, double blind study. BMJ. 2006;332:1355-1361.
19. Siegel RE, Alicea M, Lee A, Blaiklock R. Comparison of 7 versus 10 days of antibiotic therapy for hospitalized patients with uncomplicated community-acquired pneumonia: a prospective, randomized double-blind study. Am J Ther. 1999;6:217-222.
Case
An 83-year-old male with hypertension, coronary artery disease, and obstructive sleep apnea presents with progressive shortness of breath, a productive cough, wheezing, and tachypnea. His blood pressure is 158/70 mm/Hg; temperature is 101.8; respirations are 26 breaths per minute; and oxygen saturation is 87% on room air. He has coarse breath sounds bilaterally, and decreased breath sounds over the right lower lung fields. His chest X-ray reveals a right lower lobe infiltrate. He is admitted to the hospital with a diagnosis of community-acquired pneumonia (CAP), and medical therapy is started. How should his antibiotic treatment be managed?
Overview
Community-acquired pneumonia is the most common infection-related cause of death in the U.S., and the eighth-leading cause of mortality overall.1 According to a 2006 survey, CAP results in more than 1.2 million hospital admissions annually, with an average length of stay of 5.1 days.2 Though less than 20% of CAP patients require hospitalization, cases necessitating admission contribute to more than 90% of the overall cost of pneumonia care.3
During the past several years, the availability of new antibiotics and the evolution of microbial resistance patterns have changed CAP treatment strategies. Furthermore, the development of prognostic scoring systems and increasing pressure to streamline resource utilization while improving quality of care have led to new treatment considerations, such as managing low-risk cases as outpatients.
More recently, attention has been directed to the optimal duration of antibiotic treatment, with a focus on shortening the duration of therapy. Historically, CAP treatment duration has been variable and not evidence-based. Shortening the course of antibiotics might limit antibiotic resistance, decrease costs, and improve patient adherence and tolerability.4 However, before defining the appropriate antibiotic duration for a patient hospitalized with CAP, other factors must be considered, such as the choice of empiric antibiotics, the patient’s initial response to treatment, severity of the disease, and presence of co-morbidities.
Review of the Data
Antibiotic choice. The most widely referenced practice guidelines for the management of CAP patients were published in 2007 by representatives of the Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS).5 Table 1 (above, right) summarizes the recommendations for empiric antibiotics for patients requiring inpatient treatment.
Time to clinical stability. A patient’s clinical response to empiric antibiotic therapy contributes heavily to the decision regarding treatment course and duration. The IDSA/ATS guidelines recommend patients be afebrile for 48 to 72 hours and have no more than one CAP-associated sign of clinical instability before discontinuation of therapy. Although studies have used different definitions of clinical stability, the consensus guidelines refer to six parameters, which are summarized in Table 2 (right).
With appropriate antibiotic therapy, most patients hospitalized with CAP achieve clinical stability in approximately three days.6,7 Providers should expect to see some improvement in vital signs within 48 to 72 hours of admission. Should a patient fail to demonstrate objective improvement during that time, providers should look for unusual pathogens, resistant organisms, nosocomial superinfections, or noninfectious conditions.5 Certain patients, such as those with multilobar pneumonia, associated pleural effusion, or higher pneumonia-severity index scores, also take longer to reach clinical stability.8
Switch to oral therapy. The ability to achieve clinical stability has important implications for hospital length of stay. Most patients hospitalized with CAP initially are treated with intravenous (IV) antibiotics and require transition to oral therapy in anticipation of discharge. Several studies have found there is no advantage to continuing IV medication once a patient is deemed clinically stable and is able to tolerate oral medication.9,10 There are no specific guidelines regarding choice of oral antibiotics, but it is common practice, supported by the IDSA/ATS recommendations, to use the same agent as the IV antibiotic or a medication in the same drug class. For patients started on β-lactam and macrolide combination therapy, it usually is appropriate to switch to a macrolide alone.5 In cases in which a pathogen has been identified, antibiotic selection should be based on the susceptibility profile.
Once patients are switched to oral antibiotics, it is not necessary for them to remain in the hospital for further observation, provided they have no other active medical problems or social needs. A retrospective analysis of 39,232 patients hospitalized with CAP compared those who were observed overnight after switching to oral antibiotics with those who were not and found no difference in 14-day readmission rate or 30-day mortality rate.11 These findings, in conjunction with the strategy of an early switch to oral therapy, suggest hospital length of stay may be safely reduced for many patients with uncomplicated CAP.
Duration of therapy. After a patient becomes clinically stable and a decision is made to switch to oral medication and a plan for hospital discharge, the question becomes how long to continue the course of antibiotics. Historically, clinical practice has extended treatment for up to two weeks, despite lack of evidence for this duration of therapy. The IDSA/ATS guidelines offer some general recommendations, noting patients should be treated for a minimum of five days, in addition to being afebrile for 48 to 72 hours and meet other criteria for clinical stability.5
Li and colleagues conducted a systematic review evaluating 15 randomized controlled trials comparing short-course (less than seven days) with extended (more than seven days) monotherapy for CAP in adults.4 Overall, the authors found no difference in the risk of treatment failure between short-course and extended-course antibiotic therapy, and they found no difference in bacteriologic eradication or mortality. It is important to note the studies included in this analysis enrolled patients with mild to moderate CAP, including those treated as outpatients, which limits the ability to extrapolate to exclusively inpatient populations and more severely ill patients.
Another meta-analysis, published shortly thereafter, examined randomized controlled trials in outpatients and inpatients not requiring intensive care. It compared different durations of treatment with the same agent in the same dosage. The authors similarly found no difference in effectiveness or safety of short (less than seven days) versus longer (at least two additional days of therapy) courses.12 Table 3 (above) reviews selected trials of short courses of antibiotics, which have been studied in inpatient populations.
The trials summarized in these meta-analyses examined monotherapy with levofloxacin for five days; gemifloxacin for seven days, azithromycin for three to five days; ceftriaxone for five days; cefuroxime for seven days; amoxicillin for three days; or telithromycin for five to seven days. The variety of antibiotics in these studies contrasts the IDSA/ATS guidelines, which recommend only fluoroquinolones as monotherapy for inpatient CAP.
One important randomized, double-blind study of fluoroquinolones compared a five-day course of levofloxacin 750 mg daily, with a 10-day course of levofloxacin, 500 mg daily, in 528 patients with mild to severe CAP.13 The authors found no difference in clinical success or microbiologic eradication between the two groups, concluding high-dose levofloxacin for five days is an effective and well-tolerated alternative to a longer course of a lower dose, likely related to the drug’s concentration-dependent properties.
Azithromycin also offers potential for short courses of therapy, as pulmonary concentrations of azithromycin remain elevated for as many as five days following a single oral dose.14 Several small studies have demonstrated the safety, efficacy, and cost-effectiveness of three to five days of azithromycin, as summarized in a meta-analysis by Contopoulos-Ioannidis and colleagues.15 Most of these trials, however, were limited to outpatients or inpatients with mild disease or confirmed atypical pneumonia. One randomized trial of 40 inpatients with mild to moderately severe CAP found comparable clinical outcomes with a three-day course of oral azithromycin 500 mg daily versus clarithromycin for at least eight days.16 Larger studies in more severely ill patients must be completed before routinely recommending this approach in hospitalized patients. Furthermore, due to the rising prevalence of macrolide resistance, empiric therapy with a macrolide alone can only be used for the treatment of carefully selected hospitalized patients with nonsevere diseases and without risk factors for drug-resistant Streptococcus pneumoniae.5
Telithromycin is a ketolide antibiotic, which has been studied in mild to moderate CAP, including multidrug-resistant strains of S. pneumoniae, in courses of five to seven days.17 However, severe adverse reactions, including hepatotoxicity, have been reported. At the time of the 2007 guidelines, the IDSA/ATS committee waited for additional safety data before making any recommendations on its use.
One additional study of note was a trial of amoxicillin in adult inpatients with mild to moderately severe CAP.18 One hundred twenty-one patients who clinically improved (based on a composite score of pulmonary symptoms and general improvement) following three days of IV amoxicillin were randomized to oral amoxicillin for an additional five days or given a placebo. At days 10 and 28, there was no difference in clinical success between the two groups. The authors concluded that a total of three days of treatment was not inferior to eight days in patients who substantially improved after the first 72 hours of empiric treatment. This trial was conducted in the Netherlands, where amoxicillin is the preferred empiric antibiotic for CAP and patterns of antimicrobial resistance differ greatly from those found in the U.S.
Other considerations. While some evidence supports shorter courses of antibiotics, many of the existing studies are limited by their inclusion of outpatients, adults with mild to moderate CAP, or small sample size. Hence, clinical judgment continues to play an important role in determining the appropriate duration of therapy. Factors such as pre-existing co-morbidities, severity of illness, and occurrence of complications should be considered. Data is limited on the appropriate duration of antibiotics in CAP patients requiring intensive care. It also is important to note the IDSA/ATS recommendations and most of the studies reviewed exclude patients with human immunodeficiency virus (HIV), and it is unknown whether these shorter courses of antibiotics are appropriate in the HIV population.
Lastly, the IDSA/ATS guidelines note longer durations of treatment may be required if the initial therapy was not active against the identified pathogen, or in cases complicated by extrapulmonary infections, such as endocarditis or meningitis.
Back to the Case
Our patient with moderately severe CAP was hospitalized based on his age and hypoxia. He was immediately treated with supplemental oxygen by nasal cannula, IV fluids, and a dose of IV levofloxacin 750 mg. Within 48 hours he met criteria for clinical stability, including defervescence, a decline in his respiratory rate to 19 breaths per minute, and improvement in oxygen saturation to 95% on room air. At this point, he was changed from IV to oral antibiotics. He continued on levofloxacin 750 mg daily and later that day was discharged home in good condition to complete a five-day course.
Bottom Line
For hospitalized adults with mild to moderately severe CAP, five to seven days of treatment, depending on the antibiotic selected, appears to be effective in most cases. Patients should be afebrile for 48 to 72 hours and demonstrate signs of clinical stability before therapy is discontinued. TH
Kelly Cunningham, MD, and Shelley Ellis, MD, MPH, are members of the Section of Hospital Medicine at Vanderbilt University in Nashville, Tenn. Sunil Kripalani, MD, MSc, serves as the section chief.
References
1. Kung HC, Hoyert DL, Xu J, Murphy SL. Deaths: final data for 2005. Natl Vital Stat Rep. 2008;56.
2. DeFrances CJ, Lucas CA, Buie VC, Golosinskiy A. 2006 National Hospital Discharge Survey. Natl Health Stat Report. 2008;5.
3. Niederman MS. Recent advances in community-acquired pneumonia: inpatient and outpatient. Chest. 2007;131:1205-1215.
4. Li JZ, Winston LG, Moore DH, Bent S. Efficacy of short-course antibiotic regimens for community-acquired pneumonia: a meta-analysis. Am J Med. 2007;120:783-790.
5. Mandell LA, Wunderink RG, Anzueto A et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl 2):S27-72.
6. Ramirez JA, Bordon J. Early switch from intravenous to oral antibiotics in hospitalized patients with bacteremic community-acquired Streptococcus pneumoniae pneumonia. Arch Intern Med. 2001;161:848-850.
7. Halm EA, Fine MJ, Marrie TJ et al. Time to clinical stability in patients hospitalized with community-acquired pneumonia: implications for practice guidelines. JAMA. 1998;279:1452-1457.
8. Menendez R, Torres A, Rodriguez de Castro F et al. Reaching stability in community-acquired pneumonia: the effects of the severity of disease, treatment, and the characteristics of patients. Clin Infect Dis. 2004;39:1783-1790.
9. Siegal RE, Halpern NA, Almenoff PL et al. A prospective randomised study of inpatient IV antibiotics for community-acquired pneumonia: the optimal duration of therapy. Chest. 1996;110:965-971.
10. Oosterheert JJ, Bonten MJ, Schneider MM et al. Effectiveness of early switch from intravenous to oral antibiotics in severe community acquired pneumonia: multicentre randomized trial. BMJ. 2006;333:1193-1197.
11. Nathan RV, Rhew DC, Murray C et al. In-hospital observation after antibiotic switch in pneumonia: a national evaluation. Am J Med. 2006;119:512-518.
12. Dimopoulos G, Matthaiou DK, Karageorgopoulos DE, et al. Short- versus long-course antibacterial therapy for community-acquired pneumonia: a meta-analysis. Drugs. 2008;68:1841-1854.
13. Dunbar LM, Wunderink RG, Habib MP et al. High-dose, short-course levofloxacin for community-acquired pneumonia: a new treatment paradigm. Clin Infect Dis. 2003;37:752-760.
14. Morris DL, De Souza A, Jones JA, Morgan WE. High and prolonged pulmonary tissue concentrations of azithromycin following a single oral dose. Eur J Clin Microbiol Infect Dis. 1991;10:859-861.
15. Contopoulos-Ioannidis DG, Ioannidis JPA, Chew P, Lau J. Meta-analysis of randomized controlled trials on the comparative efficacy and safety of azithromycin against other antibiotics for lower respiratory tract infections. J Antimicrob Chemother. 2001;48:691-703.
16. Rizzato G, Montemurro L, Fraioli P et al. Efficacy of a three-day course of azithromycin in moderately severe community-acquired pneumonia. Eur Respir J. 1995;8:398-402.
17. Tellier G, Niederman MS, Nusrat R et al. Clinical and bacteriological efficacy and safety of 5- and 7-day regimens of telithromycin once daily compared with a 10-day regimen of clarithromycin twice daily in patients with mild to moderate community-acquired pneumonia. J Antimicrob Chemother. 2004;54:515.
18. El Moussaoui R, de Borgie CA, van den Broek P et al. Effectiveness of discontinuing antibiotic treatment after three days versus eight days in mild to moderate-severe community acquired pneumonia: randomised, double blind study. BMJ. 2006;332:1355-1361.
19. Siegel RE, Alicea M, Lee A, Blaiklock R. Comparison of 7 versus 10 days of antibiotic therapy for hospitalized patients with uncomplicated community-acquired pneumonia: a prospective, randomized double-blind study. Am J Ther. 1999;6:217-222.