User login
Final Exam?
You enter a patient’s room with all your senses on alert. You absorb the environment quickly—even before addressing the patient. It is perhaps these “small moments in medicine,” the under-the-radar information, that a physician may best remember about individual people or cases, says Andrew Bomback, MD, a first-year fellow in nephrology at the University of North Carolina at Chapel Hill. “Not the details of a specific disease state,” he elaborates, “but the visceral memory, such as how someone smells.”
In his article, “The Physical Exam and the Sense of Smell,” published in the New England Journal of Medicine in January 2006, Dr. Bomback writes that his training by doctors who “preached the gospel of the physical exam” was intended so that he and his fellow students “would not forget that the best doctors help their patients with their eyes, ears, and hands, not just with numbers posted on a computer screen.”1
Those small moments are often usurped from doctors as they deal with the demands and obligations of their jobs in an often-hurried environment. Let’s face it, he says, “The physical exam has just been truncated to very brief encounters.”
In fact, facing this dilemma is one of the first remedies he would prescribe. In response to the article, “I got a lot of nice letters from [physicians] who related similar incidents that happened in their training, where they used smell to learn more about a patient,” he says.
In contrast, he also received “somewhat negative letters where the message from those mostly retired physicians was, ‘You’re just not spending enough time with patients.’ I think that is a very unrealistic piece of advice,” says Dr. Bomback. “It would be very interesting to see whether they could carry the pager of a hospitalist or resident for 12 hours and actually be able to do what that hospitalist or resident does.”
Physicians today must first acknowledge the reality “that we don’t have as much time as we need,” says Dr. Bomback. “And once you admit that you’re not going to be able to spend as much time as you ideally would like … that we only have a 12-hour work shift if you are a hospitalist or a 30-hour call shift if you are a resident,” you have to maximize the time with the patient by giving “a focused physical that it is well done, accurate, and respectful to the patient.”
—Tim Creamer, MD, director, hospital medicine program, Community General Hospital, Syracuse, NY
Crisis or Evolution?
Sandeep Jauhar, MD, director of the Heart Failure Program at Long Island Jewish Medical Center, New Hyde Park, N.Y., also had an article in last year’s NEJM “Perspective” series.1-4 In that piece, “The Demise of the Physical Exam,”2 Dr. Jauhar posed a question: Is the demise of physical diagnosis a crisis or a natural evolution? Now, a year later, The Hospitalist asked him that same question.
“I don’t view it as a crisis,” he says, “but maybe that’s because of my vantage point as a cardiologist. Cardiology is very technology-driven; very few diagnoses are made on the basis of the physical exam.”
Dr. Jauhar believes that the greatest benefit of performing a thorough physical exam is not necessarily to pin down a diagnosis, though it can expedite that process, but to limit the tests that are ordered.
William Dickey, MD, hospitalist and director of quality at Abbott Northwestern Medical Center, Minneapolis, Minn., agrees that the decision of what testing to do, if any, is still guided by the physical exam.
“The high-tech diagnostic testing doesn’t demean the importance of the exam of all,” he says, but its role may have changed.
Are the intricate skills of performing a physical exam imperative, or have they mostly been replaced by technology? “I would say they’re not fully imperative under the assumption that you have the technology and you want to get the job done,” says Dr. Bomback. “Are they desired? Absolutely. A good physical exam and a remarkable finding are about showing what goes on inside the body and manifests itself outside the body.”
The ability to adequately hear a heart murmur or detect tetany is based on the physiologic understanding of why that murmur occurs or how calcium metabolism works. With that in mind, Dr. Bomback believes all patients would want their doctors to have those skills. “But,” he quickly qualifies, “could you have a functioning doctor get through his or her workday without knowing that? Absolutely. Could a cardiologist treat CHF without being able to hear a murmur? Of course. … So it’s desirable, but it’s not totally necessary.”
One reason for the desirability of maintaining those skills, which require physicians to “get up close,” as Dr. Dickey puts it, pertains to the importance of touching, seeing, and listening and to the quality of the patient-physician interaction itself.4 All the physicians interviewed for this article concur that getting that physical sense of the patient will tell you things that other information will not, and involving this true sensitivity in the interaction will most likely put the patient at greater ease.
“Because, in addition to all the information that a physician can discover from doing a physical exam, there is also a sense of rapport that the physical exam builds,” says C. Martin Buchanan, MD, FACP, a hospitalist at Penrose Hospital in Colorado Springs, Colo. “The therapy of being there, being present at the patient’s side, touching the patient, doing something for them, having a kind of healing energy, if you will, that we … transmit to the patient and [which essentially communicates], ‘I’m here to help you, I accept you as a human being even though you’re ill; I’m willing to touch you, and I’m here to help you feel better.’”
Not a Demise, but Compromised
“The physical exam is compromised during patient assessment because of where it ranks in importance,” says Tim Creamer, MD, director of the hospital medicine program at Community General Hospital in Syracuse, N.Y. “There are people who say that history is 80% of the diagnosis, which makes the physical exam 20% of the diagnosis. Although you try to emphasize that diagnostics, such as X-rays and labs, should only confirm your history and physical, we still depend too much on the technology to diagnose for us.”
The physical exam is not emphasized after medical school, says Dr. Creamer, who teaches second-year family practice residents. The emphasis now has become the patient-doctor interface: educating and talking with the patient and family. “And even in the lay literature, they encourage consumers to ‘Get your doctor to spend time with you,’” he says. “They mean talking to you, not checking your neck veins for A, C, and V waves.” Hospitalists may also minimize the physical exam, he adds, “because we feel pressured to maximize the talking and listening.”
The Focused Physical
The newest title in the 2006 edition of the Medical Knowledge Self-Assessment Program (MKSAP), published by the American College of Physicians, “Foundations of Internal Medicine,” includes an extensive discussion about the evidence-based physical exam. A good deal of recent research has addressed the topic of which physical findings are truly important to assess various conditions.
“If internists will pay attention to what’s in the medical literature about reliable physical findings,” says Dr. Buchanan, “we can tailor our physical exam a bit better, make more efficient use of the [interview] time, and provide very useful information for our diagnostic assessment and treatment planning.”
The MKSAP-14 offers 11 print books, a CD-ROM, and a new online version. Information is available at www.acponline.org/catalog/mksap/14/.
Powers of Observation
Performing a good physical exam is “something that we all aspire to and something we always try to improve,” says Dr. Bomback. “Anytime I hear of someone with a good physical exam finding I will try to see that patient.” It’s one of the reasons he likes working in an academic center. “There are always interesting cases, and there is always someone who wants to teach someone else what they’re seeing. It’s a constant learning process.”
Dr. Creamer agrees. He used to veer from his day-to-day routine and “follow around Max Kutzer, an internist at Crouse Hospital here at Syracuse, who practiced for years and who taught the physical exam to medical students at Harvard in 1954,” a time—he points out—when little-to-no diagnostic technology existed. Accompanying this master of medical observation, he says, was a Zen-like experience. The elder doctor “would walk to a patient’s doorway and stand there and watch the person breathe and watch how disheveled the bed was, whether the chair had been sat in, and [after] a couple of minutes he would walk out and say, ‘Now tell me what you noticed.’ ”
Dr. Creamer remembers naming “two or three things. But [Dr. Kutzer] would say, ‘OK, but let me tell you 10 more.’ ” Dr. Kutzer, now 96 and still productive, Dr. Creamer says, has written a book, Observation and the Physical Exam, which is in the editing stage.
Because physicians are pressed for time, those powers of observation may be, if not lost, at least largely neglected or ignored. “But I still do those things,” says Dr. Creamer. “I’ll walk to the door and watch a person breathe while they’re sleeping … . You lose the anxiety overtones when you’re watching someone sleeping. ... In order to learn, you need to listen. Listening takes time. You’ve got to step back and take the time to learn, and that’s where it gets tricky.”
Dr. Bomback believes technology will never replace the power of observation. “Those are the unique skills that come with being a hospitalist or any physician … and a lot of the reason why most people become physicians,” he says. “It is a skill that [they have had] from early on. It’s empathy, that you can observe a patient and understand what’s going on—maybe not completely, and not totally consciously, but there is an empathic sensation.”
Conclusion
The traditional use of the physical exam may have changed, but its value is still important to patient care.
“The physical exam is part of the culture of medicine,” says Dr. Jauhar. “It may have started to lose some of its utility as we get more technology, but it can limit the use of technology and help us make diagnoses more quickly.”
Providers might also sometimes be in a place “where you don’t have a CT scan or an MRI machine,” he adds. The provider discovers things that machines can’t supply, and the contributions of even a brief physical exam can communicate humanity to the patient.
“I have always wondered how physicians can do telemedicine,” says Dr. Dickey, “because there is something about being there and being with the patient in terms of judging the severity of illness that is very important.”
“For all these reasons, it’s important for hospitalists to maintain their skills,” says Dr. Jauhar, “because otherwise we’re losing a big part of what it is to be a doctor. We’re just becoming technicians.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Bomback A. The physical exam and the sense of smell. N Engl J Med. 2006 Jan 26;354(4):327-329.
- Jauhar S. The demise of the physical exam. N Engl J Med. 2006;354(6):548-551.
- Markel H. The stethoscope and the art of listening. N Engl J Med. 2006;354(6):551-553.
- Treadway K. Becoming a physician: heart sounds. N Engl J Med. 2006 Mar 16;354(11):1112-1113.
You enter a patient’s room with all your senses on alert. You absorb the environment quickly—even before addressing the patient. It is perhaps these “small moments in medicine,” the under-the-radar information, that a physician may best remember about individual people or cases, says Andrew Bomback, MD, a first-year fellow in nephrology at the University of North Carolina at Chapel Hill. “Not the details of a specific disease state,” he elaborates, “but the visceral memory, such as how someone smells.”
In his article, “The Physical Exam and the Sense of Smell,” published in the New England Journal of Medicine in January 2006, Dr. Bomback writes that his training by doctors who “preached the gospel of the physical exam” was intended so that he and his fellow students “would not forget that the best doctors help their patients with their eyes, ears, and hands, not just with numbers posted on a computer screen.”1
Those small moments are often usurped from doctors as they deal with the demands and obligations of their jobs in an often-hurried environment. Let’s face it, he says, “The physical exam has just been truncated to very brief encounters.”
In fact, facing this dilemma is one of the first remedies he would prescribe. In response to the article, “I got a lot of nice letters from [physicians] who related similar incidents that happened in their training, where they used smell to learn more about a patient,” he says.
In contrast, he also received “somewhat negative letters where the message from those mostly retired physicians was, ‘You’re just not spending enough time with patients.’ I think that is a very unrealistic piece of advice,” says Dr. Bomback. “It would be very interesting to see whether they could carry the pager of a hospitalist or resident for 12 hours and actually be able to do what that hospitalist or resident does.”
Physicians today must first acknowledge the reality “that we don’t have as much time as we need,” says Dr. Bomback. “And once you admit that you’re not going to be able to spend as much time as you ideally would like … that we only have a 12-hour work shift if you are a hospitalist or a 30-hour call shift if you are a resident,” you have to maximize the time with the patient by giving “a focused physical that it is well done, accurate, and respectful to the patient.”
—Tim Creamer, MD, director, hospital medicine program, Community General Hospital, Syracuse, NY
Crisis or Evolution?
Sandeep Jauhar, MD, director of the Heart Failure Program at Long Island Jewish Medical Center, New Hyde Park, N.Y., also had an article in last year’s NEJM “Perspective” series.1-4 In that piece, “The Demise of the Physical Exam,”2 Dr. Jauhar posed a question: Is the demise of physical diagnosis a crisis or a natural evolution? Now, a year later, The Hospitalist asked him that same question.
“I don’t view it as a crisis,” he says, “but maybe that’s because of my vantage point as a cardiologist. Cardiology is very technology-driven; very few diagnoses are made on the basis of the physical exam.”
Dr. Jauhar believes that the greatest benefit of performing a thorough physical exam is not necessarily to pin down a diagnosis, though it can expedite that process, but to limit the tests that are ordered.
William Dickey, MD, hospitalist and director of quality at Abbott Northwestern Medical Center, Minneapolis, Minn., agrees that the decision of what testing to do, if any, is still guided by the physical exam.
“The high-tech diagnostic testing doesn’t demean the importance of the exam of all,” he says, but its role may have changed.
Are the intricate skills of performing a physical exam imperative, or have they mostly been replaced by technology? “I would say they’re not fully imperative under the assumption that you have the technology and you want to get the job done,” says Dr. Bomback. “Are they desired? Absolutely. A good physical exam and a remarkable finding are about showing what goes on inside the body and manifests itself outside the body.”
The ability to adequately hear a heart murmur or detect tetany is based on the physiologic understanding of why that murmur occurs or how calcium metabolism works. With that in mind, Dr. Bomback believes all patients would want their doctors to have those skills. “But,” he quickly qualifies, “could you have a functioning doctor get through his or her workday without knowing that? Absolutely. Could a cardiologist treat CHF without being able to hear a murmur? Of course. … So it’s desirable, but it’s not totally necessary.”
One reason for the desirability of maintaining those skills, which require physicians to “get up close,” as Dr. Dickey puts it, pertains to the importance of touching, seeing, and listening and to the quality of the patient-physician interaction itself.4 All the physicians interviewed for this article concur that getting that physical sense of the patient will tell you things that other information will not, and involving this true sensitivity in the interaction will most likely put the patient at greater ease.
“Because, in addition to all the information that a physician can discover from doing a physical exam, there is also a sense of rapport that the physical exam builds,” says C. Martin Buchanan, MD, FACP, a hospitalist at Penrose Hospital in Colorado Springs, Colo. “The therapy of being there, being present at the patient’s side, touching the patient, doing something for them, having a kind of healing energy, if you will, that we … transmit to the patient and [which essentially communicates], ‘I’m here to help you, I accept you as a human being even though you’re ill; I’m willing to touch you, and I’m here to help you feel better.’”
Not a Demise, but Compromised
“The physical exam is compromised during patient assessment because of where it ranks in importance,” says Tim Creamer, MD, director of the hospital medicine program at Community General Hospital in Syracuse, N.Y. “There are people who say that history is 80% of the diagnosis, which makes the physical exam 20% of the diagnosis. Although you try to emphasize that diagnostics, such as X-rays and labs, should only confirm your history and physical, we still depend too much on the technology to diagnose for us.”
The physical exam is not emphasized after medical school, says Dr. Creamer, who teaches second-year family practice residents. The emphasis now has become the patient-doctor interface: educating and talking with the patient and family. “And even in the lay literature, they encourage consumers to ‘Get your doctor to spend time with you,’” he says. “They mean talking to you, not checking your neck veins for A, C, and V waves.” Hospitalists may also minimize the physical exam, he adds, “because we feel pressured to maximize the talking and listening.”
The Focused Physical
The newest title in the 2006 edition of the Medical Knowledge Self-Assessment Program (MKSAP), published by the American College of Physicians, “Foundations of Internal Medicine,” includes an extensive discussion about the evidence-based physical exam. A good deal of recent research has addressed the topic of which physical findings are truly important to assess various conditions.
“If internists will pay attention to what’s in the medical literature about reliable physical findings,” says Dr. Buchanan, “we can tailor our physical exam a bit better, make more efficient use of the [interview] time, and provide very useful information for our diagnostic assessment and treatment planning.”
The MKSAP-14 offers 11 print books, a CD-ROM, and a new online version. Information is available at www.acponline.org/catalog/mksap/14/.
Powers of Observation
Performing a good physical exam is “something that we all aspire to and something we always try to improve,” says Dr. Bomback. “Anytime I hear of someone with a good physical exam finding I will try to see that patient.” It’s one of the reasons he likes working in an academic center. “There are always interesting cases, and there is always someone who wants to teach someone else what they’re seeing. It’s a constant learning process.”
Dr. Creamer agrees. He used to veer from his day-to-day routine and “follow around Max Kutzer, an internist at Crouse Hospital here at Syracuse, who practiced for years and who taught the physical exam to medical students at Harvard in 1954,” a time—he points out—when little-to-no diagnostic technology existed. Accompanying this master of medical observation, he says, was a Zen-like experience. The elder doctor “would walk to a patient’s doorway and stand there and watch the person breathe and watch how disheveled the bed was, whether the chair had been sat in, and [after] a couple of minutes he would walk out and say, ‘Now tell me what you noticed.’ ”
Dr. Creamer remembers naming “two or three things. But [Dr. Kutzer] would say, ‘OK, but let me tell you 10 more.’ ” Dr. Kutzer, now 96 and still productive, Dr. Creamer says, has written a book, Observation and the Physical Exam, which is in the editing stage.
Because physicians are pressed for time, those powers of observation may be, if not lost, at least largely neglected or ignored. “But I still do those things,” says Dr. Creamer. “I’ll walk to the door and watch a person breathe while they’re sleeping … . You lose the anxiety overtones when you’re watching someone sleeping. ... In order to learn, you need to listen. Listening takes time. You’ve got to step back and take the time to learn, and that’s where it gets tricky.”
Dr. Bomback believes technology will never replace the power of observation. “Those are the unique skills that come with being a hospitalist or any physician … and a lot of the reason why most people become physicians,” he says. “It is a skill that [they have had] from early on. It’s empathy, that you can observe a patient and understand what’s going on—maybe not completely, and not totally consciously, but there is an empathic sensation.”
Conclusion
The traditional use of the physical exam may have changed, but its value is still important to patient care.
“The physical exam is part of the culture of medicine,” says Dr. Jauhar. “It may have started to lose some of its utility as we get more technology, but it can limit the use of technology and help us make diagnoses more quickly.”
Providers might also sometimes be in a place “where you don’t have a CT scan or an MRI machine,” he adds. The provider discovers things that machines can’t supply, and the contributions of even a brief physical exam can communicate humanity to the patient.
“I have always wondered how physicians can do telemedicine,” says Dr. Dickey, “because there is something about being there and being with the patient in terms of judging the severity of illness that is very important.”
“For all these reasons, it’s important for hospitalists to maintain their skills,” says Dr. Jauhar, “because otherwise we’re losing a big part of what it is to be a doctor. We’re just becoming technicians.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Bomback A. The physical exam and the sense of smell. N Engl J Med. 2006 Jan 26;354(4):327-329.
- Jauhar S. The demise of the physical exam. N Engl J Med. 2006;354(6):548-551.
- Markel H. The stethoscope and the art of listening. N Engl J Med. 2006;354(6):551-553.
- Treadway K. Becoming a physician: heart sounds. N Engl J Med. 2006 Mar 16;354(11):1112-1113.
You enter a patient’s room with all your senses on alert. You absorb the environment quickly—even before addressing the patient. It is perhaps these “small moments in medicine,” the under-the-radar information, that a physician may best remember about individual people or cases, says Andrew Bomback, MD, a first-year fellow in nephrology at the University of North Carolina at Chapel Hill. “Not the details of a specific disease state,” he elaborates, “but the visceral memory, such as how someone smells.”
In his article, “The Physical Exam and the Sense of Smell,” published in the New England Journal of Medicine in January 2006, Dr. Bomback writes that his training by doctors who “preached the gospel of the physical exam” was intended so that he and his fellow students “would not forget that the best doctors help their patients with their eyes, ears, and hands, not just with numbers posted on a computer screen.”1
Those small moments are often usurped from doctors as they deal with the demands and obligations of their jobs in an often-hurried environment. Let’s face it, he says, “The physical exam has just been truncated to very brief encounters.”
In fact, facing this dilemma is one of the first remedies he would prescribe. In response to the article, “I got a lot of nice letters from [physicians] who related similar incidents that happened in their training, where they used smell to learn more about a patient,” he says.
In contrast, he also received “somewhat negative letters where the message from those mostly retired physicians was, ‘You’re just not spending enough time with patients.’ I think that is a very unrealistic piece of advice,” says Dr. Bomback. “It would be very interesting to see whether they could carry the pager of a hospitalist or resident for 12 hours and actually be able to do what that hospitalist or resident does.”
Physicians today must first acknowledge the reality “that we don’t have as much time as we need,” says Dr. Bomback. “And once you admit that you’re not going to be able to spend as much time as you ideally would like … that we only have a 12-hour work shift if you are a hospitalist or a 30-hour call shift if you are a resident,” you have to maximize the time with the patient by giving “a focused physical that it is well done, accurate, and respectful to the patient.”
—Tim Creamer, MD, director, hospital medicine program, Community General Hospital, Syracuse, NY
Crisis or Evolution?
Sandeep Jauhar, MD, director of the Heart Failure Program at Long Island Jewish Medical Center, New Hyde Park, N.Y., also had an article in last year’s NEJM “Perspective” series.1-4 In that piece, “The Demise of the Physical Exam,”2 Dr. Jauhar posed a question: Is the demise of physical diagnosis a crisis or a natural evolution? Now, a year later, The Hospitalist asked him that same question.
“I don’t view it as a crisis,” he says, “but maybe that’s because of my vantage point as a cardiologist. Cardiology is very technology-driven; very few diagnoses are made on the basis of the physical exam.”
Dr. Jauhar believes that the greatest benefit of performing a thorough physical exam is not necessarily to pin down a diagnosis, though it can expedite that process, but to limit the tests that are ordered.
William Dickey, MD, hospitalist and director of quality at Abbott Northwestern Medical Center, Minneapolis, Minn., agrees that the decision of what testing to do, if any, is still guided by the physical exam.
“The high-tech diagnostic testing doesn’t demean the importance of the exam of all,” he says, but its role may have changed.
Are the intricate skills of performing a physical exam imperative, or have they mostly been replaced by technology? “I would say they’re not fully imperative under the assumption that you have the technology and you want to get the job done,” says Dr. Bomback. “Are they desired? Absolutely. A good physical exam and a remarkable finding are about showing what goes on inside the body and manifests itself outside the body.”
The ability to adequately hear a heart murmur or detect tetany is based on the physiologic understanding of why that murmur occurs or how calcium metabolism works. With that in mind, Dr. Bomback believes all patients would want their doctors to have those skills. “But,” he quickly qualifies, “could you have a functioning doctor get through his or her workday without knowing that? Absolutely. Could a cardiologist treat CHF without being able to hear a murmur? Of course. … So it’s desirable, but it’s not totally necessary.”
One reason for the desirability of maintaining those skills, which require physicians to “get up close,” as Dr. Dickey puts it, pertains to the importance of touching, seeing, and listening and to the quality of the patient-physician interaction itself.4 All the physicians interviewed for this article concur that getting that physical sense of the patient will tell you things that other information will not, and involving this true sensitivity in the interaction will most likely put the patient at greater ease.
“Because, in addition to all the information that a physician can discover from doing a physical exam, there is also a sense of rapport that the physical exam builds,” says C. Martin Buchanan, MD, FACP, a hospitalist at Penrose Hospital in Colorado Springs, Colo. “The therapy of being there, being present at the patient’s side, touching the patient, doing something for them, having a kind of healing energy, if you will, that we … transmit to the patient and [which essentially communicates], ‘I’m here to help you, I accept you as a human being even though you’re ill; I’m willing to touch you, and I’m here to help you feel better.’”
Not a Demise, but Compromised
“The physical exam is compromised during patient assessment because of where it ranks in importance,” says Tim Creamer, MD, director of the hospital medicine program at Community General Hospital in Syracuse, N.Y. “There are people who say that history is 80% of the diagnosis, which makes the physical exam 20% of the diagnosis. Although you try to emphasize that diagnostics, such as X-rays and labs, should only confirm your history and physical, we still depend too much on the technology to diagnose for us.”
The physical exam is not emphasized after medical school, says Dr. Creamer, who teaches second-year family practice residents. The emphasis now has become the patient-doctor interface: educating and talking with the patient and family. “And even in the lay literature, they encourage consumers to ‘Get your doctor to spend time with you,’” he says. “They mean talking to you, not checking your neck veins for A, C, and V waves.” Hospitalists may also minimize the physical exam, he adds, “because we feel pressured to maximize the talking and listening.”
The Focused Physical
The newest title in the 2006 edition of the Medical Knowledge Self-Assessment Program (MKSAP), published by the American College of Physicians, “Foundations of Internal Medicine,” includes an extensive discussion about the evidence-based physical exam. A good deal of recent research has addressed the topic of which physical findings are truly important to assess various conditions.
“If internists will pay attention to what’s in the medical literature about reliable physical findings,” says Dr. Buchanan, “we can tailor our physical exam a bit better, make more efficient use of the [interview] time, and provide very useful information for our diagnostic assessment and treatment planning.”
The MKSAP-14 offers 11 print books, a CD-ROM, and a new online version. Information is available at www.acponline.org/catalog/mksap/14/.
Powers of Observation
Performing a good physical exam is “something that we all aspire to and something we always try to improve,” says Dr. Bomback. “Anytime I hear of someone with a good physical exam finding I will try to see that patient.” It’s one of the reasons he likes working in an academic center. “There are always interesting cases, and there is always someone who wants to teach someone else what they’re seeing. It’s a constant learning process.”
Dr. Creamer agrees. He used to veer from his day-to-day routine and “follow around Max Kutzer, an internist at Crouse Hospital here at Syracuse, who practiced for years and who taught the physical exam to medical students at Harvard in 1954,” a time—he points out—when little-to-no diagnostic technology existed. Accompanying this master of medical observation, he says, was a Zen-like experience. The elder doctor “would walk to a patient’s doorway and stand there and watch the person breathe and watch how disheveled the bed was, whether the chair had been sat in, and [after] a couple of minutes he would walk out and say, ‘Now tell me what you noticed.’ ”
Dr. Creamer remembers naming “two or three things. But [Dr. Kutzer] would say, ‘OK, but let me tell you 10 more.’ ” Dr. Kutzer, now 96 and still productive, Dr. Creamer says, has written a book, Observation and the Physical Exam, which is in the editing stage.
Because physicians are pressed for time, those powers of observation may be, if not lost, at least largely neglected or ignored. “But I still do those things,” says Dr. Creamer. “I’ll walk to the door and watch a person breathe while they’re sleeping … . You lose the anxiety overtones when you’re watching someone sleeping. ... In order to learn, you need to listen. Listening takes time. You’ve got to step back and take the time to learn, and that’s where it gets tricky.”
Dr. Bomback believes technology will never replace the power of observation. “Those are the unique skills that come with being a hospitalist or any physician … and a lot of the reason why most people become physicians,” he says. “It is a skill that [they have had] from early on. It’s empathy, that you can observe a patient and understand what’s going on—maybe not completely, and not totally consciously, but there is an empathic sensation.”
Conclusion
The traditional use of the physical exam may have changed, but its value is still important to patient care.
“The physical exam is part of the culture of medicine,” says Dr. Jauhar. “It may have started to lose some of its utility as we get more technology, but it can limit the use of technology and help us make diagnoses more quickly.”
Providers might also sometimes be in a place “where you don’t have a CT scan or an MRI machine,” he adds. The provider discovers things that machines can’t supply, and the contributions of even a brief physical exam can communicate humanity to the patient.
“I have always wondered how physicians can do telemedicine,” says Dr. Dickey, “because there is something about being there and being with the patient in terms of judging the severity of illness that is very important.”
“For all these reasons, it’s important for hospitalists to maintain their skills,” says Dr. Jauhar, “because otherwise we’re losing a big part of what it is to be a doctor. We’re just becoming technicians.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Bomback A. The physical exam and the sense of smell. N Engl J Med. 2006 Jan 26;354(4):327-329.
- Jauhar S. The demise of the physical exam. N Engl J Med. 2006;354(6):548-551.
- Markel H. The stethoscope and the art of listening. N Engl J Med. 2006;354(6):551-553.
- Treadway K. Becoming a physician: heart sounds. N Engl J Med. 2006 Mar 16;354(11):1112-1113.
The A to Z of Intellectual Disability
It is estimated that 17% of children in the United States have a developmental disability and that 1% to 2% of children are diagnosed with mental retardation.1 Of interest to hospitalists: Those with intellectual disability (ID) use healthcare services more than those in the general population.
During a 12-month period, 16% of adults with ID were hospitalized, and 30% were seen in an emergency department (ED).2 Because the average age at death in this population has increased—to 66.1 years in one study—hospitalists must become familiar with the medical management of these patients.3 Achieving comprehensive care presents a challenge because of the atypical presentation of symptoms and the behavioral and communication problems found in many hospitalized patients with ID.
In this article, I will address some of the major clinical issues hospitalists confront when caring for this population.
Where to Begin
One key to understanding how to care for this population is ascertaining whether there is underlying etiology of ID. A diagnosis can be established in approximately 50% of patients who have ID.4 For example, patients with Down syndrome are more likely to have celiac disease, hypothyroidism, leukemia, atlantoaxial subluxation, obstructive sleep apnea, Alzheimer’s dementia, seizure disorder, and behavioral and psychiatric disorders than are patients in the general population.5
Table 1 (see p. 21) lists common medical conditions found in patients with ID. Hospitalists should make it a priority to obtain a comprehensive medical record from the patient’s healthcare provider or to gather the necessary information from a caregiver who knows the patient well; this person may assist the hospitalist in interpreting mannerisms of the nonverbal patient that reflect symptoms such as pain.
Swallowing Difficulties: Problems and Solutions
The risk of aspiration and subsequent mortality because of oral dysfunction and dysphagia is increased in patients with profound ID. The presence of choking and coughing during feeds identifies patients at significant risk of asphyxiation.6
In one study involving patients with severe ID, the absence of respiratory distress during meals or the lack of chronic lung disease identified 85% of patients who did not aspirate.7 Clinical assessment by speech-language therapists and the use of video fluoroscopy may be helpful in patients who experience either frequent aspiration pneumonias or episodes of coughing or choking during feeds. Cramming food into the mouth, eating too fast, and losing the bolus into the pharynx prematurely were factors predictive of asphyxiation risk.6 Speech-language therapists and nutritionists may assist hospitalists by recommending diet and feeding modifications that ensure the safe speed and size of bolus delivery, along with adjustment in food textures to reduce the risk of asphyxiation.
Patients with swallowing difficulties are also vulnerable to dehydration and malnutrition. In fact, more than 60% of children and adults with ID are underweight, with a body mass index less than or equal to 20. Food-intake surveys have demonstrated adequate protein intake but reduced fat, carbohydrate, and energy-food intake. Increasing energy-dense fats and sugar-containing foods, while monitoring for adequate fluid intake, is recommended in these individuals.8
In patients who have worsening dysphagia associated with pneumonia, insertion of an enteral feeding tube, such as a percutaneous endoscopic gastrostomy (PEG) tube, can provide adequate nutrition and may reduce the risk of future episodes of pneumonia (although this practice is controversial).
In one study, there was a 45% reduction in the incidence of pneumonia in the year following feeding-tube insertion.9 Other investigators have not found that gastrostomy tubes prevent pneumonia, however.10 Instead, the presence or absence of gastroesophageal reflux and whether or not the patient has a prior history of aspiration pneumonia seem to be more important factors in determining if episodes of pneumonia will occur after feeding-tube placement.
The prevalence of gastroesophageal reflux (GER) in 435 institutionalized patients with IQ <50 ID was 48.2%.11 Almost 70% of patients with GER had reflux esophagitis, while 14% had Barrett’s esophagus, and 3.9% had peptic strictures. Bui and colleagues studied 105 ID patients with feeding gastrostomy, 45 of whom had dysphagia but no history of aspiration pneumonia and 60 who had recurrent aspiration, either alone or with dysphagia.12 Only two of 45 (4.4%) patients with dysphagia alone developed aspiration pneumonia, while 15 of 60 (25.0%) with a prior history of aspiration pneumonia had a future event.12
Continued aspiration pneumonia may be due to oral secretions and gastric contents entering the respiratory tract. Preoperative GER has been associated with postoperative aspiration pneumonia.10 Elevating the head of the bed, avoiding bolus feeding, treating constipation, discontinuing feeding promptly in cases of respiratory distress or increased gastric residual volume, and treating gastroesophageal reflux pharmacologically may decrease further pneumonia events in these patients.9
Treating Seizures
Another common issue hospitalists must be attuned to in adult patients with ID is epilepsy. Prevalent in as many as 40% of adult patients with mental retardation and cerebral palsy, uncontrolled epilepsy has been associated with increased mortality.13,14 Clinical guidelines for the management of epilepsy in this population have been published.15 Recommended first-line treatments of generalized seizures include sodium valproate and lamotrigine. If these medications are unsuccessful, or if side effects prohibit continued usage, then topiramate and carbamazepine are suggested. Do not use carbamazepine in myoclonic or absence seizures. Lennox-Gastaut syndrome can be treated with lamotrigine, while topiramate and felbamate can be used as add-on therapy to reduce atonic seizures.
For treatment of partial seizures, valproate, carbamazepine, and lamotrigine are recommended first-line treatments. Levetiracetam can be used as add-on therapy. The guidelines suggest that studies of add-on therapy failed to differentiate among lamotrigine, gabapentin, topiramate and tiagabine.
Adjust the initial anti-epileptic drug (AED) to the maximum tolerated dose before slowly introducing a second AED without tapering the first. If the patient responds to the second drug, consider a gradual tapering of the first drug. It is not uncommon for multiple AEDs to be used in patients with ID. In patients referred to a specialized epilepsy clinic, over 80% were on two or more AEDs; 43% became seizure-free for a year or more, while another 40% of patients had a 50% or greater reduction in seizure frequency.16
AEDs that induce the cytochrome P-450 system—particularly phenytoin—phenobarbital, and carbamazepine, have been associated with low bone mineral density (BMD) in patients with ID.17 Additional risk factors for low BMD, such as hypogonadism, low body mass, decreased mobility, and vitamin D deficiency may contribute to the increased incidence of non-traumatic fractures found in institutionalized adults with ID.18,19 In one study, the annual incidence of non-traumatic fracture was 7.3% among 391 institutionalized adults.18
In another study, however, researchers found that although 57% of patients who suffered a fracture were vitamin-D deficient there was no significant association between vitamin D deficiency and fractures.20 Although there are no specific guidelines designed to evaluate and treat bone-health-related issues in adults with ID, it seems prudent to ensure adequate calcium and vitamin D intake, to encourage exercise if possible, and, in patients who suffer non-traumatic fractures, to evaluate for osteoporosis and give appropriate therapy according to the recommendations of the National Institutes of Health Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy.21
Self-Injurious Behavior and the Risk of Polypharmacy
Adults with ID who are nonverbal may demonstrate self-injurious behavior (SIB) as a manifestation of pain from fracture, constipation, or other medical illnesses. The prevalence of SIB in this population ranges from 2% to 50%.22 Psychotropic medications are frequently used to protect patients from self-injury.23 The challenge for hospitalists is to keep patients from injuring themselves without masking underlying pathologic conditions.
Several hypotheses have tried to explain why patients engage in SIB: These include increased level of endogenous opioids leading to pain insensitivity, opioid release due to low endogenous opioid levels caused by the SIB itself, and reaction to pain. Breau and colleagues concluded that children with ID who suffered chronic pain self-injured less body surface area and fewer body sites than children without chronic pain. Patients without chronic pain who engaged in SIB were more likely to self-injure their heads and hands.22
If a medical etiology cannot be ascertained for aggressive, self-injurious, and destructive behavior, psychotropic agents are frequently employed, with rates that range from 18% to 49% in patients with ID.24 These medications should be prescribed in a start-low/go-slow manner and only after a thorough assessment has been performed and the physician has determined that the behavior cannot be redirected and poses an imminent risk to the patient.25
Because of ID patients’ decreased communication skills, polypharmacy is a significant risk; side effects of psychotropic agents may be mistakenly treated with additional agents. According to Janowsky and colleagues, the mean lowest effective dose of conventional antipsychotics such as haloperidol was 5.9 mg/day to maintain symptom suppression of maladaptive behavior, with relapse of symptoms occurring at a mean dose of 3.8 mg/day in an ID population.23 Atypical antipsychotics are now more widely used in adults with ID, and although they are less likely to cause extrapyramidal side effects, they can still lead to weight gain, sedation, increased lipid levels, and activation of diabetes mellitus. In one study, low dose risperidone (2 mg/day) reduced aberrant behavior by half in 57% of patients with ID. Increased appetite and weight gain were common side effects.26
Other agents such as benzodiazepines have been reported to have behavioral side effects as high as 13% when used in patients with ID; in one study, time to onset of side effects averaged 23 days.27 This may erroneously lead outpatient physicians to prescribe additional agents to counteract the behavioral side effects of the drugs that were initiated in the hospital. If you prescribe benzodiazepines then the patient’s side effects may be mitigated by using lower doses of lorazepam (3 mg/day or less). You may also consider naltrexone to treat patients with SIB. A review of 86 ID patients with SIB concluded that naltrexone was effective in reducing self-injury in 80% of subjects, with nearly half of the patients experiencing a 50% reduction in these types of behavior. The dose most studied was 50 mg.28
Palliative Care
Hospitalists should also be familiar with the palliative-care needs of patients with ID. A recent survey of directors providing services to older adults with ID identified the following as frequently cited obstacles to end-of-life care: availability of direct care staff, availability of nursing/medical staff, staff untrained in end-of-life care, anxiety about responding to families, and liability concerns.29
Because many patients with ID are unable to make medical decisions about their care, a surrogate (e.g., a family member, a judicially appointed guardian, or a court) must decide to initiate or maintain medical interventions. The prevailing standard that applies to surrogate decision-making in the ID population is identifying the patient’s best interests. The medical course chosen may not necessarily be the best option, but it should not be “antithetical to the patient’s interests as to constitute neglect or abuse.”30
A clinical scenario hospitalists may face in patients with profound ID that addresses this legal reasoning involves seeing a patient with respiratory distress in the ED who needs intubation and mechanical ventilation to have a chance at survival. Later, this patient is found to have metastatic cancer and is in significant pain and discomfort. Applying the best interests standard, the hospitalist may elect to intubate and treat the patient. Once the cancer is discovered, however, the physician does not insist that the patient undergo invasive treatment and, instead, focuses his/her efforts on providing palliative care.
Conclusion
As the number of patients with ID transitioning from pediatrics to medicine increases, hospitalists will be looked upon to develop a comprehensive approach to ensure their overall well-being. A systematic approach to caring for hospitalized adults is suggested in Table 2 (see p. 22). TH
Dr. Geskey is assistant professor, Pediatrics and Medicine, Penn State, Milton S. Hershey Medical Center, Penn State College of Medicine, Department of Pediatrics & Internal Medicine.
References
- Boyle CA, Decouflé P, Yeargin-Allsopp M. Prevalence and health impact of developmental disabilities in US children. Pediatrics. 1994;93(3):399-403.
- Janicki MP, Davidson PW, Henderson CM, et al. Health characteristics and health services utilization in older adults with intellectual disabilities living in community residences. J Intellect Disabil Res. 2002;46:287-298.
- Janicki MP, Dalton AJ, Henderson CM, et al. Mortality and morbidity among older adults with intellectual disability: health services considerations. Disabil Rehabil. 1999;21(5-6):284-294.
- van Karnebeek CD, Scheper FY, Abeling NG, et al. Etiology of mental retardation in children referred to a tertiary care center: a prospective study. Am J Ment Retard. 2005;110(4):253-267.
- Roizen NJ, Patterson D. Down’s syndrome. Lancet. 2003 Apr;361(9365):1281-1289. Comment in Lancet, 2003 Jul; 362(9365):1281-80-81.
- Samuels R, Chadwick DD. Predictors of asphyxiation risk in adults with intellectual disabilities and dysphagia. J Intellect Disabil Res. 2006 May;50(Pt 5):362-370.
- Rogers B, Stratton P, Msall M, et al. Long-term morbidity and management strategies of tracheal aspiration in adults with severe developmental disabilities. Am J Ment Retard. 1994 Jan:98(4):490-498.
- Kennedy M, McCombie L, Dawes P, et al. Nutritional support for patients with intellectual disability and nutrition/dysphagia disorders in community care. J Intellect Disabil Res. 1997 Oct;41(Pt 5):430-436.
- Gray DS, Kimmel D. Enteral tube feeding and pneumonia. Am J Ment Retard. 2006 Mar;111(2):113-120.
- Hassett JM, Sunby C, Flint LM. No elimination of aspiration pneumonia in neurologically disabled patients with feeding gastrostomy. Surg Gynecol Obstet. 1988 Nov;167(5):383-388.
- Böhmer CJM, Niezen-de Boer MC, Klinkenberg-Knol EC, et al. The prevalence of gastroesophageal reflux disease in institutionalized intellectually disabled individuals. Am J Gastroenterol. 1999;94(3):804-810.
- Bui HD, Dang CV, Chaney RH, et al. Does gastrostomy and fundoplication prevent aspiration pneumonia in mentally retarded persons? Am J Ment Retard. 1989 Jul;94(1):16-19.
- McDermott S, Moran R, Platt T, et al. Prevalence of epilepsy in adults with mental retardation and related disabilities in primary care. Am J Ment Retard. 2005 Jan;110(1):48-56.
- Forsgren L, Edvinsson SO, Nyström L, et al. Influence of epilepsy on mortality in mental retardation: an epidemiologic study. Epilepsia. 1996;37(19):956-963.
- Working group of the International Association of the Scientific Study of Intellectual Disability. Clinical guidelines for the management of epilepsy in adults with an intellectual disability. Seizure. 2001 Sep;10(6):401-409.
- Kelly K, Stephen LJ, Brodie MJ. Pharmacological outcomes in people with mental retardation and epilepsy. Epilepsy Behav. 2004 Feb;5(1):67-71.
- Sheth RD. Metabolic concerns associated with antiepileptic drugs. Neurology. 2004;63(Suppl 4):S24-29.
- Ryder KM, Williams J, Womack C, et al. Appendicular fractures: a significant problem among institutionalized adults with developmental disabilities. Am J Ment Retard. 2003 Sep;108(5):340-346.
- Jaffe JS, Timell AM, Elolia R, et al. Risk factors for low bone mineral density in individuals residing in a facility for the people with intellectual disability. J Intellect Disabil Res. 2005Jun;49(Pt 6):457-462.
- Vanlint S, Nugent N. Vitamin D and fractures in people with intellectual disability. J Intellect Disabil Res. 2006 Oct; 50(Pt 10):761-767.
- NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. Osteoporosis prevention, diagnosis, and therapy. JAMA. 2001;285:785-795.
- Breau LM, Camfield CS, Symons FJ, et al. Relation between pain and self-injurious behavior in nonverbal children with severe cognitive impairments. J Pediatr. 2003 May;142(5):498-503.
- Janowsky DS, Barnhill LJ, Shetty M, et al. Minimally effective doses of conventional antipsychotic medications used to treat aggression, self-injurious and destructive behaviors in mentally retarded adults. J Clin Psychopharmacol. 2005 Feb;25(1):19-25.
- Valdovinos MG, Schroeder SR, Kim G. Prevalence and correlates of psychotropic medication use among adults with developmental disabilities: 1970-2000. Int Rev Res Ment Retard. 2003;26:175-220.
- Szymanski L, King BH. Summary of the Practice Parameters for the Assessment and Treatment of Children, Adolescents, and Adults with Mental Retardation and Comorbid Mental Disorders. American Academy of Child and Adolescent Psychiatry. J Am Acad Child Adolesc Psychiatry. 1999;38:1606-1610.
- Hellings JA, Zarcone JR, Reese RM, et al. A crossover study of risperidone in children, adolescents and adults with mental retardation. J Autism Dev Disord. 2006;36(3):401-411.
- Kalachnik JE, Hanzel TE, Sevenich R, et al. Benzodiazepine behavioral side effects: review and implications for individuals with mental retardation. Am J Ment Retard. 2002 Sep;107(5):376-410.
- Symons FJ, Thompson A, Rodriguez MC. Self-injurious behavior and the efficacy of naltrexone treatment: a quantitative synthesis. Ment Retard Dev Disabil Res Rev. 2004;10(3):193-200.
- Botsford AL. Status of end of life care in organizations providing services for older people with a developmental disability. Am J Ment Retard. 2004;109(5):421-428.
- Cantor NL. The bane of surrogate decision-making defining the best interests of never-competent persons. J Leg Med. 2005 Jun;26(2):155-205.
It is estimated that 17% of children in the United States have a developmental disability and that 1% to 2% of children are diagnosed with mental retardation.1 Of interest to hospitalists: Those with intellectual disability (ID) use healthcare services more than those in the general population.
During a 12-month period, 16% of adults with ID were hospitalized, and 30% were seen in an emergency department (ED).2 Because the average age at death in this population has increased—to 66.1 years in one study—hospitalists must become familiar with the medical management of these patients.3 Achieving comprehensive care presents a challenge because of the atypical presentation of symptoms and the behavioral and communication problems found in many hospitalized patients with ID.
In this article, I will address some of the major clinical issues hospitalists confront when caring for this population.
Where to Begin
One key to understanding how to care for this population is ascertaining whether there is underlying etiology of ID. A diagnosis can be established in approximately 50% of patients who have ID.4 For example, patients with Down syndrome are more likely to have celiac disease, hypothyroidism, leukemia, atlantoaxial subluxation, obstructive sleep apnea, Alzheimer’s dementia, seizure disorder, and behavioral and psychiatric disorders than are patients in the general population.5
Table 1 (see p. 21) lists common medical conditions found in patients with ID. Hospitalists should make it a priority to obtain a comprehensive medical record from the patient’s healthcare provider or to gather the necessary information from a caregiver who knows the patient well; this person may assist the hospitalist in interpreting mannerisms of the nonverbal patient that reflect symptoms such as pain.
Swallowing Difficulties: Problems and Solutions
The risk of aspiration and subsequent mortality because of oral dysfunction and dysphagia is increased in patients with profound ID. The presence of choking and coughing during feeds identifies patients at significant risk of asphyxiation.6
In one study involving patients with severe ID, the absence of respiratory distress during meals or the lack of chronic lung disease identified 85% of patients who did not aspirate.7 Clinical assessment by speech-language therapists and the use of video fluoroscopy may be helpful in patients who experience either frequent aspiration pneumonias or episodes of coughing or choking during feeds. Cramming food into the mouth, eating too fast, and losing the bolus into the pharynx prematurely were factors predictive of asphyxiation risk.6 Speech-language therapists and nutritionists may assist hospitalists by recommending diet and feeding modifications that ensure the safe speed and size of bolus delivery, along with adjustment in food textures to reduce the risk of asphyxiation.
Patients with swallowing difficulties are also vulnerable to dehydration and malnutrition. In fact, more than 60% of children and adults with ID are underweight, with a body mass index less than or equal to 20. Food-intake surveys have demonstrated adequate protein intake but reduced fat, carbohydrate, and energy-food intake. Increasing energy-dense fats and sugar-containing foods, while monitoring for adequate fluid intake, is recommended in these individuals.8
In patients who have worsening dysphagia associated with pneumonia, insertion of an enteral feeding tube, such as a percutaneous endoscopic gastrostomy (PEG) tube, can provide adequate nutrition and may reduce the risk of future episodes of pneumonia (although this practice is controversial).
In one study, there was a 45% reduction in the incidence of pneumonia in the year following feeding-tube insertion.9 Other investigators have not found that gastrostomy tubes prevent pneumonia, however.10 Instead, the presence or absence of gastroesophageal reflux and whether or not the patient has a prior history of aspiration pneumonia seem to be more important factors in determining if episodes of pneumonia will occur after feeding-tube placement.
The prevalence of gastroesophageal reflux (GER) in 435 institutionalized patients with IQ <50 ID was 48.2%.11 Almost 70% of patients with GER had reflux esophagitis, while 14% had Barrett’s esophagus, and 3.9% had peptic strictures. Bui and colleagues studied 105 ID patients with feeding gastrostomy, 45 of whom had dysphagia but no history of aspiration pneumonia and 60 who had recurrent aspiration, either alone or with dysphagia.12 Only two of 45 (4.4%) patients with dysphagia alone developed aspiration pneumonia, while 15 of 60 (25.0%) with a prior history of aspiration pneumonia had a future event.12
Continued aspiration pneumonia may be due to oral secretions and gastric contents entering the respiratory tract. Preoperative GER has been associated with postoperative aspiration pneumonia.10 Elevating the head of the bed, avoiding bolus feeding, treating constipation, discontinuing feeding promptly in cases of respiratory distress or increased gastric residual volume, and treating gastroesophageal reflux pharmacologically may decrease further pneumonia events in these patients.9
Treating Seizures
Another common issue hospitalists must be attuned to in adult patients with ID is epilepsy. Prevalent in as many as 40% of adult patients with mental retardation and cerebral palsy, uncontrolled epilepsy has been associated with increased mortality.13,14 Clinical guidelines for the management of epilepsy in this population have been published.15 Recommended first-line treatments of generalized seizures include sodium valproate and lamotrigine. If these medications are unsuccessful, or if side effects prohibit continued usage, then topiramate and carbamazepine are suggested. Do not use carbamazepine in myoclonic or absence seizures. Lennox-Gastaut syndrome can be treated with lamotrigine, while topiramate and felbamate can be used as add-on therapy to reduce atonic seizures.
For treatment of partial seizures, valproate, carbamazepine, and lamotrigine are recommended first-line treatments. Levetiracetam can be used as add-on therapy. The guidelines suggest that studies of add-on therapy failed to differentiate among lamotrigine, gabapentin, topiramate and tiagabine.
Adjust the initial anti-epileptic drug (AED) to the maximum tolerated dose before slowly introducing a second AED without tapering the first. If the patient responds to the second drug, consider a gradual tapering of the first drug. It is not uncommon for multiple AEDs to be used in patients with ID. In patients referred to a specialized epilepsy clinic, over 80% were on two or more AEDs; 43% became seizure-free for a year or more, while another 40% of patients had a 50% or greater reduction in seizure frequency.16
AEDs that induce the cytochrome P-450 system—particularly phenytoin—phenobarbital, and carbamazepine, have been associated with low bone mineral density (BMD) in patients with ID.17 Additional risk factors for low BMD, such as hypogonadism, low body mass, decreased mobility, and vitamin D deficiency may contribute to the increased incidence of non-traumatic fractures found in institutionalized adults with ID.18,19 In one study, the annual incidence of non-traumatic fracture was 7.3% among 391 institutionalized adults.18
In another study, however, researchers found that although 57% of patients who suffered a fracture were vitamin-D deficient there was no significant association between vitamin D deficiency and fractures.20 Although there are no specific guidelines designed to evaluate and treat bone-health-related issues in adults with ID, it seems prudent to ensure adequate calcium and vitamin D intake, to encourage exercise if possible, and, in patients who suffer non-traumatic fractures, to evaluate for osteoporosis and give appropriate therapy according to the recommendations of the National Institutes of Health Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy.21
Self-Injurious Behavior and the Risk of Polypharmacy
Adults with ID who are nonverbal may demonstrate self-injurious behavior (SIB) as a manifestation of pain from fracture, constipation, or other medical illnesses. The prevalence of SIB in this population ranges from 2% to 50%.22 Psychotropic medications are frequently used to protect patients from self-injury.23 The challenge for hospitalists is to keep patients from injuring themselves without masking underlying pathologic conditions.
Several hypotheses have tried to explain why patients engage in SIB: These include increased level of endogenous opioids leading to pain insensitivity, opioid release due to low endogenous opioid levels caused by the SIB itself, and reaction to pain. Breau and colleagues concluded that children with ID who suffered chronic pain self-injured less body surface area and fewer body sites than children without chronic pain. Patients without chronic pain who engaged in SIB were more likely to self-injure their heads and hands.22
If a medical etiology cannot be ascertained for aggressive, self-injurious, and destructive behavior, psychotropic agents are frequently employed, with rates that range from 18% to 49% in patients with ID.24 These medications should be prescribed in a start-low/go-slow manner and only after a thorough assessment has been performed and the physician has determined that the behavior cannot be redirected and poses an imminent risk to the patient.25
Because of ID patients’ decreased communication skills, polypharmacy is a significant risk; side effects of psychotropic agents may be mistakenly treated with additional agents. According to Janowsky and colleagues, the mean lowest effective dose of conventional antipsychotics such as haloperidol was 5.9 mg/day to maintain symptom suppression of maladaptive behavior, with relapse of symptoms occurring at a mean dose of 3.8 mg/day in an ID population.23 Atypical antipsychotics are now more widely used in adults with ID, and although they are less likely to cause extrapyramidal side effects, they can still lead to weight gain, sedation, increased lipid levels, and activation of diabetes mellitus. In one study, low dose risperidone (2 mg/day) reduced aberrant behavior by half in 57% of patients with ID. Increased appetite and weight gain were common side effects.26
Other agents such as benzodiazepines have been reported to have behavioral side effects as high as 13% when used in patients with ID; in one study, time to onset of side effects averaged 23 days.27 This may erroneously lead outpatient physicians to prescribe additional agents to counteract the behavioral side effects of the drugs that were initiated in the hospital. If you prescribe benzodiazepines then the patient’s side effects may be mitigated by using lower doses of lorazepam (3 mg/day or less). You may also consider naltrexone to treat patients with SIB. A review of 86 ID patients with SIB concluded that naltrexone was effective in reducing self-injury in 80% of subjects, with nearly half of the patients experiencing a 50% reduction in these types of behavior. The dose most studied was 50 mg.28
Palliative Care
Hospitalists should also be familiar with the palliative-care needs of patients with ID. A recent survey of directors providing services to older adults with ID identified the following as frequently cited obstacles to end-of-life care: availability of direct care staff, availability of nursing/medical staff, staff untrained in end-of-life care, anxiety about responding to families, and liability concerns.29
Because many patients with ID are unable to make medical decisions about their care, a surrogate (e.g., a family member, a judicially appointed guardian, or a court) must decide to initiate or maintain medical interventions. The prevailing standard that applies to surrogate decision-making in the ID population is identifying the patient’s best interests. The medical course chosen may not necessarily be the best option, but it should not be “antithetical to the patient’s interests as to constitute neglect or abuse.”30
A clinical scenario hospitalists may face in patients with profound ID that addresses this legal reasoning involves seeing a patient with respiratory distress in the ED who needs intubation and mechanical ventilation to have a chance at survival. Later, this patient is found to have metastatic cancer and is in significant pain and discomfort. Applying the best interests standard, the hospitalist may elect to intubate and treat the patient. Once the cancer is discovered, however, the physician does not insist that the patient undergo invasive treatment and, instead, focuses his/her efforts on providing palliative care.
Conclusion
As the number of patients with ID transitioning from pediatrics to medicine increases, hospitalists will be looked upon to develop a comprehensive approach to ensure their overall well-being. A systematic approach to caring for hospitalized adults is suggested in Table 2 (see p. 22). TH
Dr. Geskey is assistant professor, Pediatrics and Medicine, Penn State, Milton S. Hershey Medical Center, Penn State College of Medicine, Department of Pediatrics & Internal Medicine.
References
- Boyle CA, Decouflé P, Yeargin-Allsopp M. Prevalence and health impact of developmental disabilities in US children. Pediatrics. 1994;93(3):399-403.
- Janicki MP, Davidson PW, Henderson CM, et al. Health characteristics and health services utilization in older adults with intellectual disabilities living in community residences. J Intellect Disabil Res. 2002;46:287-298.
- Janicki MP, Dalton AJ, Henderson CM, et al. Mortality and morbidity among older adults with intellectual disability: health services considerations. Disabil Rehabil. 1999;21(5-6):284-294.
- van Karnebeek CD, Scheper FY, Abeling NG, et al. Etiology of mental retardation in children referred to a tertiary care center: a prospective study. Am J Ment Retard. 2005;110(4):253-267.
- Roizen NJ, Patterson D. Down’s syndrome. Lancet. 2003 Apr;361(9365):1281-1289. Comment in Lancet, 2003 Jul; 362(9365):1281-80-81.
- Samuels R, Chadwick DD. Predictors of asphyxiation risk in adults with intellectual disabilities and dysphagia. J Intellect Disabil Res. 2006 May;50(Pt 5):362-370.
- Rogers B, Stratton P, Msall M, et al. Long-term morbidity and management strategies of tracheal aspiration in adults with severe developmental disabilities. Am J Ment Retard. 1994 Jan:98(4):490-498.
- Kennedy M, McCombie L, Dawes P, et al. Nutritional support for patients with intellectual disability and nutrition/dysphagia disorders in community care. J Intellect Disabil Res. 1997 Oct;41(Pt 5):430-436.
- Gray DS, Kimmel D. Enteral tube feeding and pneumonia. Am J Ment Retard. 2006 Mar;111(2):113-120.
- Hassett JM, Sunby C, Flint LM. No elimination of aspiration pneumonia in neurologically disabled patients with feeding gastrostomy. Surg Gynecol Obstet. 1988 Nov;167(5):383-388.
- Böhmer CJM, Niezen-de Boer MC, Klinkenberg-Knol EC, et al. The prevalence of gastroesophageal reflux disease in institutionalized intellectually disabled individuals. Am J Gastroenterol. 1999;94(3):804-810.
- Bui HD, Dang CV, Chaney RH, et al. Does gastrostomy and fundoplication prevent aspiration pneumonia in mentally retarded persons? Am J Ment Retard. 1989 Jul;94(1):16-19.
- McDermott S, Moran R, Platt T, et al. Prevalence of epilepsy in adults with mental retardation and related disabilities in primary care. Am J Ment Retard. 2005 Jan;110(1):48-56.
- Forsgren L, Edvinsson SO, Nyström L, et al. Influence of epilepsy on mortality in mental retardation: an epidemiologic study. Epilepsia. 1996;37(19):956-963.
- Working group of the International Association of the Scientific Study of Intellectual Disability. Clinical guidelines for the management of epilepsy in adults with an intellectual disability. Seizure. 2001 Sep;10(6):401-409.
- Kelly K, Stephen LJ, Brodie MJ. Pharmacological outcomes in people with mental retardation and epilepsy. Epilepsy Behav. 2004 Feb;5(1):67-71.
- Sheth RD. Metabolic concerns associated with antiepileptic drugs. Neurology. 2004;63(Suppl 4):S24-29.
- Ryder KM, Williams J, Womack C, et al. Appendicular fractures: a significant problem among institutionalized adults with developmental disabilities. Am J Ment Retard. 2003 Sep;108(5):340-346.
- Jaffe JS, Timell AM, Elolia R, et al. Risk factors for low bone mineral density in individuals residing in a facility for the people with intellectual disability. J Intellect Disabil Res. 2005Jun;49(Pt 6):457-462.
- Vanlint S, Nugent N. Vitamin D and fractures in people with intellectual disability. J Intellect Disabil Res. 2006 Oct; 50(Pt 10):761-767.
- NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. Osteoporosis prevention, diagnosis, and therapy. JAMA. 2001;285:785-795.
- Breau LM, Camfield CS, Symons FJ, et al. Relation between pain and self-injurious behavior in nonverbal children with severe cognitive impairments. J Pediatr. 2003 May;142(5):498-503.
- Janowsky DS, Barnhill LJ, Shetty M, et al. Minimally effective doses of conventional antipsychotic medications used to treat aggression, self-injurious and destructive behaviors in mentally retarded adults. J Clin Psychopharmacol. 2005 Feb;25(1):19-25.
- Valdovinos MG, Schroeder SR, Kim G. Prevalence and correlates of psychotropic medication use among adults with developmental disabilities: 1970-2000. Int Rev Res Ment Retard. 2003;26:175-220.
- Szymanski L, King BH. Summary of the Practice Parameters for the Assessment and Treatment of Children, Adolescents, and Adults with Mental Retardation and Comorbid Mental Disorders. American Academy of Child and Adolescent Psychiatry. J Am Acad Child Adolesc Psychiatry. 1999;38:1606-1610.
- Hellings JA, Zarcone JR, Reese RM, et al. A crossover study of risperidone in children, adolescents and adults with mental retardation. J Autism Dev Disord. 2006;36(3):401-411.
- Kalachnik JE, Hanzel TE, Sevenich R, et al. Benzodiazepine behavioral side effects: review and implications for individuals with mental retardation. Am J Ment Retard. 2002 Sep;107(5):376-410.
- Symons FJ, Thompson A, Rodriguez MC. Self-injurious behavior and the efficacy of naltrexone treatment: a quantitative synthesis. Ment Retard Dev Disabil Res Rev. 2004;10(3):193-200.
- Botsford AL. Status of end of life care in organizations providing services for older people with a developmental disability. Am J Ment Retard. 2004;109(5):421-428.
- Cantor NL. The bane of surrogate decision-making defining the best interests of never-competent persons. J Leg Med. 2005 Jun;26(2):155-205.
It is estimated that 17% of children in the United States have a developmental disability and that 1% to 2% of children are diagnosed with mental retardation.1 Of interest to hospitalists: Those with intellectual disability (ID) use healthcare services more than those in the general population.
During a 12-month period, 16% of adults with ID were hospitalized, and 30% were seen in an emergency department (ED).2 Because the average age at death in this population has increased—to 66.1 years in one study—hospitalists must become familiar with the medical management of these patients.3 Achieving comprehensive care presents a challenge because of the atypical presentation of symptoms and the behavioral and communication problems found in many hospitalized patients with ID.
In this article, I will address some of the major clinical issues hospitalists confront when caring for this population.
Where to Begin
One key to understanding how to care for this population is ascertaining whether there is underlying etiology of ID. A diagnosis can be established in approximately 50% of patients who have ID.4 For example, patients with Down syndrome are more likely to have celiac disease, hypothyroidism, leukemia, atlantoaxial subluxation, obstructive sleep apnea, Alzheimer’s dementia, seizure disorder, and behavioral and psychiatric disorders than are patients in the general population.5
Table 1 (see p. 21) lists common medical conditions found in patients with ID. Hospitalists should make it a priority to obtain a comprehensive medical record from the patient’s healthcare provider or to gather the necessary information from a caregiver who knows the patient well; this person may assist the hospitalist in interpreting mannerisms of the nonverbal patient that reflect symptoms such as pain.
Swallowing Difficulties: Problems and Solutions
The risk of aspiration and subsequent mortality because of oral dysfunction and dysphagia is increased in patients with profound ID. The presence of choking and coughing during feeds identifies patients at significant risk of asphyxiation.6
In one study involving patients with severe ID, the absence of respiratory distress during meals or the lack of chronic lung disease identified 85% of patients who did not aspirate.7 Clinical assessment by speech-language therapists and the use of video fluoroscopy may be helpful in patients who experience either frequent aspiration pneumonias or episodes of coughing or choking during feeds. Cramming food into the mouth, eating too fast, and losing the bolus into the pharynx prematurely were factors predictive of asphyxiation risk.6 Speech-language therapists and nutritionists may assist hospitalists by recommending diet and feeding modifications that ensure the safe speed and size of bolus delivery, along with adjustment in food textures to reduce the risk of asphyxiation.
Patients with swallowing difficulties are also vulnerable to dehydration and malnutrition. In fact, more than 60% of children and adults with ID are underweight, with a body mass index less than or equal to 20. Food-intake surveys have demonstrated adequate protein intake but reduced fat, carbohydrate, and energy-food intake. Increasing energy-dense fats and sugar-containing foods, while monitoring for adequate fluid intake, is recommended in these individuals.8
In patients who have worsening dysphagia associated with pneumonia, insertion of an enteral feeding tube, such as a percutaneous endoscopic gastrostomy (PEG) tube, can provide adequate nutrition and may reduce the risk of future episodes of pneumonia (although this practice is controversial).
In one study, there was a 45% reduction in the incidence of pneumonia in the year following feeding-tube insertion.9 Other investigators have not found that gastrostomy tubes prevent pneumonia, however.10 Instead, the presence or absence of gastroesophageal reflux and whether or not the patient has a prior history of aspiration pneumonia seem to be more important factors in determining if episodes of pneumonia will occur after feeding-tube placement.
The prevalence of gastroesophageal reflux (GER) in 435 institutionalized patients with IQ <50 ID was 48.2%.11 Almost 70% of patients with GER had reflux esophagitis, while 14% had Barrett’s esophagus, and 3.9% had peptic strictures. Bui and colleagues studied 105 ID patients with feeding gastrostomy, 45 of whom had dysphagia but no history of aspiration pneumonia and 60 who had recurrent aspiration, either alone or with dysphagia.12 Only two of 45 (4.4%) patients with dysphagia alone developed aspiration pneumonia, while 15 of 60 (25.0%) with a prior history of aspiration pneumonia had a future event.12
Continued aspiration pneumonia may be due to oral secretions and gastric contents entering the respiratory tract. Preoperative GER has been associated with postoperative aspiration pneumonia.10 Elevating the head of the bed, avoiding bolus feeding, treating constipation, discontinuing feeding promptly in cases of respiratory distress or increased gastric residual volume, and treating gastroesophageal reflux pharmacologically may decrease further pneumonia events in these patients.9
Treating Seizures
Another common issue hospitalists must be attuned to in adult patients with ID is epilepsy. Prevalent in as many as 40% of adult patients with mental retardation and cerebral palsy, uncontrolled epilepsy has been associated with increased mortality.13,14 Clinical guidelines for the management of epilepsy in this population have been published.15 Recommended first-line treatments of generalized seizures include sodium valproate and lamotrigine. If these medications are unsuccessful, or if side effects prohibit continued usage, then topiramate and carbamazepine are suggested. Do not use carbamazepine in myoclonic or absence seizures. Lennox-Gastaut syndrome can be treated with lamotrigine, while topiramate and felbamate can be used as add-on therapy to reduce atonic seizures.
For treatment of partial seizures, valproate, carbamazepine, and lamotrigine are recommended first-line treatments. Levetiracetam can be used as add-on therapy. The guidelines suggest that studies of add-on therapy failed to differentiate among lamotrigine, gabapentin, topiramate and tiagabine.
Adjust the initial anti-epileptic drug (AED) to the maximum tolerated dose before slowly introducing a second AED without tapering the first. If the patient responds to the second drug, consider a gradual tapering of the first drug. It is not uncommon for multiple AEDs to be used in patients with ID. In patients referred to a specialized epilepsy clinic, over 80% were on two or more AEDs; 43% became seizure-free for a year or more, while another 40% of patients had a 50% or greater reduction in seizure frequency.16
AEDs that induce the cytochrome P-450 system—particularly phenytoin—phenobarbital, and carbamazepine, have been associated with low bone mineral density (BMD) in patients with ID.17 Additional risk factors for low BMD, such as hypogonadism, low body mass, decreased mobility, and vitamin D deficiency may contribute to the increased incidence of non-traumatic fractures found in institutionalized adults with ID.18,19 In one study, the annual incidence of non-traumatic fracture was 7.3% among 391 institutionalized adults.18
In another study, however, researchers found that although 57% of patients who suffered a fracture were vitamin-D deficient there was no significant association between vitamin D deficiency and fractures.20 Although there are no specific guidelines designed to evaluate and treat bone-health-related issues in adults with ID, it seems prudent to ensure adequate calcium and vitamin D intake, to encourage exercise if possible, and, in patients who suffer non-traumatic fractures, to evaluate for osteoporosis and give appropriate therapy according to the recommendations of the National Institutes of Health Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy.21
Self-Injurious Behavior and the Risk of Polypharmacy
Adults with ID who are nonverbal may demonstrate self-injurious behavior (SIB) as a manifestation of pain from fracture, constipation, or other medical illnesses. The prevalence of SIB in this population ranges from 2% to 50%.22 Psychotropic medications are frequently used to protect patients from self-injury.23 The challenge for hospitalists is to keep patients from injuring themselves without masking underlying pathologic conditions.
Several hypotheses have tried to explain why patients engage in SIB: These include increased level of endogenous opioids leading to pain insensitivity, opioid release due to low endogenous opioid levels caused by the SIB itself, and reaction to pain. Breau and colleagues concluded that children with ID who suffered chronic pain self-injured less body surface area and fewer body sites than children without chronic pain. Patients without chronic pain who engaged in SIB were more likely to self-injure their heads and hands.22
If a medical etiology cannot be ascertained for aggressive, self-injurious, and destructive behavior, psychotropic agents are frequently employed, with rates that range from 18% to 49% in patients with ID.24 These medications should be prescribed in a start-low/go-slow manner and only after a thorough assessment has been performed and the physician has determined that the behavior cannot be redirected and poses an imminent risk to the patient.25
Because of ID patients’ decreased communication skills, polypharmacy is a significant risk; side effects of psychotropic agents may be mistakenly treated with additional agents. According to Janowsky and colleagues, the mean lowest effective dose of conventional antipsychotics such as haloperidol was 5.9 mg/day to maintain symptom suppression of maladaptive behavior, with relapse of symptoms occurring at a mean dose of 3.8 mg/day in an ID population.23 Atypical antipsychotics are now more widely used in adults with ID, and although they are less likely to cause extrapyramidal side effects, they can still lead to weight gain, sedation, increased lipid levels, and activation of diabetes mellitus. In one study, low dose risperidone (2 mg/day) reduced aberrant behavior by half in 57% of patients with ID. Increased appetite and weight gain were common side effects.26
Other agents such as benzodiazepines have been reported to have behavioral side effects as high as 13% when used in patients with ID; in one study, time to onset of side effects averaged 23 days.27 This may erroneously lead outpatient physicians to prescribe additional agents to counteract the behavioral side effects of the drugs that were initiated in the hospital. If you prescribe benzodiazepines then the patient’s side effects may be mitigated by using lower doses of lorazepam (3 mg/day or less). You may also consider naltrexone to treat patients with SIB. A review of 86 ID patients with SIB concluded that naltrexone was effective in reducing self-injury in 80% of subjects, with nearly half of the patients experiencing a 50% reduction in these types of behavior. The dose most studied was 50 mg.28
Palliative Care
Hospitalists should also be familiar with the palliative-care needs of patients with ID. A recent survey of directors providing services to older adults with ID identified the following as frequently cited obstacles to end-of-life care: availability of direct care staff, availability of nursing/medical staff, staff untrained in end-of-life care, anxiety about responding to families, and liability concerns.29
Because many patients with ID are unable to make medical decisions about their care, a surrogate (e.g., a family member, a judicially appointed guardian, or a court) must decide to initiate or maintain medical interventions. The prevailing standard that applies to surrogate decision-making in the ID population is identifying the patient’s best interests. The medical course chosen may not necessarily be the best option, but it should not be “antithetical to the patient’s interests as to constitute neglect or abuse.”30
A clinical scenario hospitalists may face in patients with profound ID that addresses this legal reasoning involves seeing a patient with respiratory distress in the ED who needs intubation and mechanical ventilation to have a chance at survival. Later, this patient is found to have metastatic cancer and is in significant pain and discomfort. Applying the best interests standard, the hospitalist may elect to intubate and treat the patient. Once the cancer is discovered, however, the physician does not insist that the patient undergo invasive treatment and, instead, focuses his/her efforts on providing palliative care.
Conclusion
As the number of patients with ID transitioning from pediatrics to medicine increases, hospitalists will be looked upon to develop a comprehensive approach to ensure their overall well-being. A systematic approach to caring for hospitalized adults is suggested in Table 2 (see p. 22). TH
Dr. Geskey is assistant professor, Pediatrics and Medicine, Penn State, Milton S. Hershey Medical Center, Penn State College of Medicine, Department of Pediatrics & Internal Medicine.
References
- Boyle CA, Decouflé P, Yeargin-Allsopp M. Prevalence and health impact of developmental disabilities in US children. Pediatrics. 1994;93(3):399-403.
- Janicki MP, Davidson PW, Henderson CM, et al. Health characteristics and health services utilization in older adults with intellectual disabilities living in community residences. J Intellect Disabil Res. 2002;46:287-298.
- Janicki MP, Dalton AJ, Henderson CM, et al. Mortality and morbidity among older adults with intellectual disability: health services considerations. Disabil Rehabil. 1999;21(5-6):284-294.
- van Karnebeek CD, Scheper FY, Abeling NG, et al. Etiology of mental retardation in children referred to a tertiary care center: a prospective study. Am J Ment Retard. 2005;110(4):253-267.
- Roizen NJ, Patterson D. Down’s syndrome. Lancet. 2003 Apr;361(9365):1281-1289. Comment in Lancet, 2003 Jul; 362(9365):1281-80-81.
- Samuels R, Chadwick DD. Predictors of asphyxiation risk in adults with intellectual disabilities and dysphagia. J Intellect Disabil Res. 2006 May;50(Pt 5):362-370.
- Rogers B, Stratton P, Msall M, et al. Long-term morbidity and management strategies of tracheal aspiration in adults with severe developmental disabilities. Am J Ment Retard. 1994 Jan:98(4):490-498.
- Kennedy M, McCombie L, Dawes P, et al. Nutritional support for patients with intellectual disability and nutrition/dysphagia disorders in community care. J Intellect Disabil Res. 1997 Oct;41(Pt 5):430-436.
- Gray DS, Kimmel D. Enteral tube feeding and pneumonia. Am J Ment Retard. 2006 Mar;111(2):113-120.
- Hassett JM, Sunby C, Flint LM. No elimination of aspiration pneumonia in neurologically disabled patients with feeding gastrostomy. Surg Gynecol Obstet. 1988 Nov;167(5):383-388.
- Böhmer CJM, Niezen-de Boer MC, Klinkenberg-Knol EC, et al. The prevalence of gastroesophageal reflux disease in institutionalized intellectually disabled individuals. Am J Gastroenterol. 1999;94(3):804-810.
- Bui HD, Dang CV, Chaney RH, et al. Does gastrostomy and fundoplication prevent aspiration pneumonia in mentally retarded persons? Am J Ment Retard. 1989 Jul;94(1):16-19.
- McDermott S, Moran R, Platt T, et al. Prevalence of epilepsy in adults with mental retardation and related disabilities in primary care. Am J Ment Retard. 2005 Jan;110(1):48-56.
- Forsgren L, Edvinsson SO, Nyström L, et al. Influence of epilepsy on mortality in mental retardation: an epidemiologic study. Epilepsia. 1996;37(19):956-963.
- Working group of the International Association of the Scientific Study of Intellectual Disability. Clinical guidelines for the management of epilepsy in adults with an intellectual disability. Seizure. 2001 Sep;10(6):401-409.
- Kelly K, Stephen LJ, Brodie MJ. Pharmacological outcomes in people with mental retardation and epilepsy. Epilepsy Behav. 2004 Feb;5(1):67-71.
- Sheth RD. Metabolic concerns associated with antiepileptic drugs. Neurology. 2004;63(Suppl 4):S24-29.
- Ryder KM, Williams J, Womack C, et al. Appendicular fractures: a significant problem among institutionalized adults with developmental disabilities. Am J Ment Retard. 2003 Sep;108(5):340-346.
- Jaffe JS, Timell AM, Elolia R, et al. Risk factors for low bone mineral density in individuals residing in a facility for the people with intellectual disability. J Intellect Disabil Res. 2005Jun;49(Pt 6):457-462.
- Vanlint S, Nugent N. Vitamin D and fractures in people with intellectual disability. J Intellect Disabil Res. 2006 Oct; 50(Pt 10):761-767.
- NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. Osteoporosis prevention, diagnosis, and therapy. JAMA. 2001;285:785-795.
- Breau LM, Camfield CS, Symons FJ, et al. Relation between pain and self-injurious behavior in nonverbal children with severe cognitive impairments. J Pediatr. 2003 May;142(5):498-503.
- Janowsky DS, Barnhill LJ, Shetty M, et al. Minimally effective doses of conventional antipsychotic medications used to treat aggression, self-injurious and destructive behaviors in mentally retarded adults. J Clin Psychopharmacol. 2005 Feb;25(1):19-25.
- Valdovinos MG, Schroeder SR, Kim G. Prevalence and correlates of psychotropic medication use among adults with developmental disabilities: 1970-2000. Int Rev Res Ment Retard. 2003;26:175-220.
- Szymanski L, King BH. Summary of the Practice Parameters for the Assessment and Treatment of Children, Adolescents, and Adults with Mental Retardation and Comorbid Mental Disorders. American Academy of Child and Adolescent Psychiatry. J Am Acad Child Adolesc Psychiatry. 1999;38:1606-1610.
- Hellings JA, Zarcone JR, Reese RM, et al. A crossover study of risperidone in children, adolescents and adults with mental retardation. J Autism Dev Disord. 2006;36(3):401-411.
- Kalachnik JE, Hanzel TE, Sevenich R, et al. Benzodiazepine behavioral side effects: review and implications for individuals with mental retardation. Am J Ment Retard. 2002 Sep;107(5):376-410.
- Symons FJ, Thompson A, Rodriguez MC. Self-injurious behavior and the efficacy of naltrexone treatment: a quantitative synthesis. Ment Retard Dev Disabil Res Rev. 2004;10(3):193-200.
- Botsford AL. Status of end of life care in organizations providing services for older people with a developmental disability. Am J Ment Retard. 2004;109(5):421-428.
- Cantor NL. The bane of surrogate decision-making defining the best interests of never-competent persons. J Leg Med. 2005 Jun;26(2):155-205.
Inflammatory Findings
Mrs. K, an 81-year-old golf-enthusiast admitted with congestive heart failure, now refuses to walk and complains of ankle pain. When you see her, she refuses to let even a bedsheet near her left ankle, and she claims that you did this to her.
Unfortunately, she’s probably right. Mrs. K also has a history of podagra, and she developed an acute gouty monoarthritis after receiving treatment with diuretics and aspirin. Gout—along with the other causes of inpatient acute monoarthritis (pseudogout, septic arthritis, and trauma)—are increasingly common diagnoses in the geriatric patient population. Because the elderly are uniquely predisposed to losing functional independence following an acute attack, making a timely diagnosis is particularly important in this age group. And though the patient’s clinical features may point toward an etiology, making the correct diagnosis ultimately depends on the results of the joint tap.
Gout
Gout occurs in patients with high serum levels of uric acid, though not all hyperuricemic patients develop gout. Among elderly hospitalized patients with hyperuricemia, approximately 65% have significant renal impairment, and others have advanced hypertension, coronary artery disease, and congestive heart failure. Over time, high serum uric acid levels may lead to the deposition of monosodium urate crystals in the joints; these lesions are the precursors of a gouty attack.
Gouty attacks occur when crystal deposits become inflamed. The inflammation may be triggered by a medication-induced change in uric acid concentration or by a medical condition, including acute illness, trauma, surgery, and dehydration. (See Table 1, p.18.) Though some elderly patients with acute gouty arthritis will manifest confusion or a sudden change in ambulatory status, most will present with a monoarthritis and a rise in temperature. Gout is suspected clinically when the first metatarsal phalangeal joint is involved (podagra), but other commonly involved joints include the ankle and the knee. Uric acid levels in the blood are usually elevated but can also temporarily normalize or even dip low during attacks. An X-ray of the involved joint may be normal or may already show the characteristic erosive lesion of gout, the “overhanging edge.”
Making the correct diagnosis is dependent upon visualizing intracellular, needle-shaped, negatively birefringent crystals in the synovial fluid. After the fluid is removed from the affected joint, it should be examined under polarized light within two hours; if more time is needed, the fluid can be refrigerated for up to 12 hours. Co-infection of a gouty joint has been described in the elderly population, and the synovial fluid should be sent to the laboratory for a cell count, Gram’s stain, and culture, as well as glucose and lactate levels. (See Table 2, below.)
Direct in-hospital treatment of gout toward alleviating the current attack, preventing future attacks, and providing appropriate antibiotic coverage in suspected co-infected cases until joint culture results are finalized. Treatment options for the acute attack include NSAIDs and corticosteroids—either oral or intra-articular. Hourly oral colchicine is not a good option for an elderly patient because the diarrhea that ensues is particularly disruptive. Nor is IV colchicine a good option thanks to its side-effect profile that renders it unusable in patients with reduced renal function. The treatment of hyperuricemia with allopurinol should not be undertaken during the acute attack because any change in the serum uric acid concentration will serve only to exacerbate the current inflammation.
Anti-inflammatory doses of NSAIDs are effective and will shorten the duration of symptoms substantially. Seven to 10 days of indomethacin at a dose of 50 mg taken orally three times daily is the traditional choice, and though it is generally conceded that ibuprofen and naproxen also work well, no comparative trials have been performed. Elderly patients are at increased risk for adverse effects from NSAIDs, particularly those patients with severely reduced renal function, gastropathy, asthma, congestive heart failure, or other intravascularly depleted states. Gastric mucosal protection, using proton-pump inhibitors, and careful monitoring of fluid status, renal function, and mental status are of particular concern in this population.
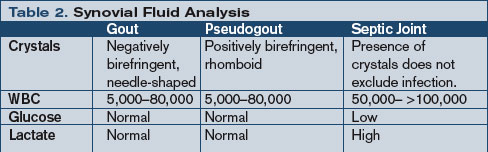
Because recent research indicates that COX-2 inhibitors have thrombotic potential and are contraindicated in patients at high risk for cardiovascular events or stroke, the extent to which they can be used in an elderly patient with an acute gouty attack is limited. A traditional NSAID in combination with a proton-pump inhibitor may be as effective as a COX-2 inhibitor in reducing the risk of gastroduodenal toxicity, however.
Corticosteroids—given either orally or intra-articularly—are an appropriate treatment for patients who can’t tolerate an NSAID. As long as a septic joint has been excluded, an intra-articular injection of 40–80 mg triamcinolone acetonide or 40 mg of methylprednisolone acetate will result in major improvement within 24 hours for most patients. Another option is a seven- to 10-day course of oral prednisone, starting with 40 mg on day one and reducing the dosage by 5 mg/day. Elderly patients taking oral prednisone should also receive adequate calcium, vitamin D, and a proton pump inhibitor for gastrointestinal protection, as well as close monitoring of blood pressure, glucose, and mental status.
If a patient has a history of frequent attacks or tophi, has a serum uric acid level higher than 12 mg/dl, or is consistently receiving high doses of diuretics, that person is at high risk for subsequent attacks and should receive prophylactic treatment with either a low-dose daily NSAID or a renally dosed oral colchicine.
Pseudogout
Pseudogout is the articular manifestation of calcium pyrophosphate dihydrate (CPPD) deposition, and this process is associated with aging as well as with various endocrinopathies, the most common of which is hyperparathyroidism. (See Table 3, below.) The shedding of CPPD crystals initiates an inflammatory process, and these crystals invoke an inflammatory response in much the same manner as uric acid crystals.
While the precipitants of a pseudogout attack are less well defined than those of gout, dehydration and joint surgery have both been identified as predisposing factors. The acute monoarticular pain and swelling (the knee is most common, followed by the ankle and then any other synovial joint) that ensues usually has a more insidious onset, and an X-ray may show chondrocalcinosis within the joint space. The diagnosis is confirmed by the demonstration of intracellular CPPD crystals in the aspirated joint fluid. Though less easily seen than monosodium urate crystals, rhomboidal crystals that display weakly positive birefringence under polarized light will be revealed with careful observation. Vitally important to the diagnosis of any crystal-associated arthritis is the exclusion of septic arthritis. To this end, conduct synovial fluid and blood cultures even if the suspicion of sepsis is low.
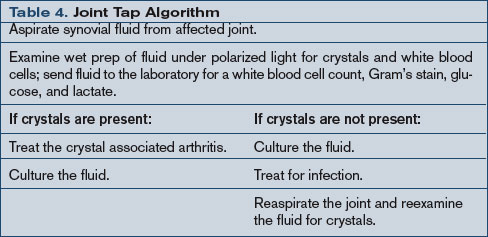
Treatment goals for pseudogout center on the abatement of the current arthritis and the exclusion of an infected joint or a concurrent metabolic syndrome. NSAIDs are the mainstay of therapy for the management of pseudogout; they are prescribed in anti-inflammatory doses similar to those used in the treatment of gout. Corticosteroids can also be used, particularly an intra-articular injection, as long as infection has been excluded. As with any crystal arthropathy, a septic joint should be considered and treated in high-risk patients even before the results of the joint fluid cultures are available. (See Table 4, above.)
Septic Arthritis
Even with timely antibacterial treatment, an elderly patient with a septic joint has a 7% to 32% mortality rate. Staphylococcus and Streptococcus are the most commonly cultured pathogens, but consider E. coli, Pseudomonas, and Klebsiella species in patients with diabetes mellitus, malignancy, or other debilitating chronic syndromes; less common agents include tuberculosis and gonococcus. Fever may be present, but a recent study revealed that fewer than 60% of geriatric patients with septic arthritis presented with a febrile illness. Thus, systemic features are not reliable enough to warrant making or excluding the diagnosis of septic arthritis without examination of the synovial fluid. (See Table 5, below.)
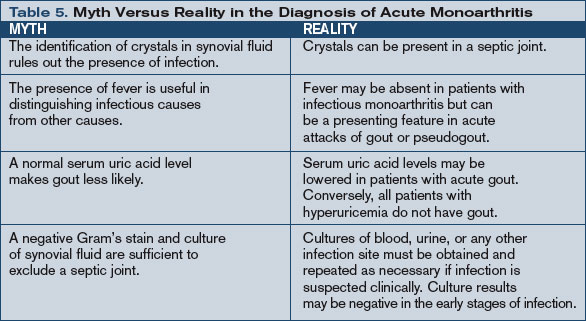
Send synovial fluid for leukocyte count, Gram’s stain, and culture in all suspected cases, and several studies suggest that the diagnostic yield may be improved with direct inoculation of fluid into blood culture vials or isolator tubes. Synovial fluid will also show very low glucose (less than 25% of simultaneous plasma glucose) and very high lactate (greater than 10 mm/l) in the untreated bacterial septic joint.
Treatment of a septic joint includes both appropriate antimicrobial therapy and joint drainage. Three weeks of parenteral antimicrobial therapy directed against the isolated pathogen is usually sufficient once the affected joint has been drained. Surgical drainage is indicated in joints—like the hip—that are difficult to aspirate or monitor. Other indications include pus in the synovial fluid, spread of infection to the soft tissues, or an inadequate clinical response to appropriate antibiotics after five to seven days. Otherwise, daily aspiration is the treatment of choice for an uncomplicated infected joint. Additionally, as is true in any acute monoarthritis, bed rest and optimal joint positioning are required to prevent the occurrence of joint deformation and harmful contractures. TH
Dr. Landis is a rheumatologist and a freelance writer.
Special thanks to Bradley Flansbaum, MD, for his assistance with this article.
References
- Tenenbaum J. Inflammatory musculoskeletal conditions in older adults. Geriatr Aging. 2005;8(3):14-17.
- Bieber JD, Terkeltaub RA. Gout: on the brink of novel therapeutic options for an ancient disease. Arthritis Rheum. 2004 Aug;50(8):2400-2414.
- Terkeltaub RA. Clinical practice. Gout. N Engl J Med. 2003 Oct 23;349(17):1647-1655.
- Leirisalo-Repo M. Early arthritis and infection. Curr Opin Rheumatol. 2005 Jul;17(4):433-439.
- Siva C, Velazquez C, Mody A, et al. Diagnosing acute monoarthritis in adults: a practical approach for the family physician. Am Fam Physician. 2003 Jul 1;68(1):83-90.
Mrs. K, an 81-year-old golf-enthusiast admitted with congestive heart failure, now refuses to walk and complains of ankle pain. When you see her, she refuses to let even a bedsheet near her left ankle, and she claims that you did this to her.
Unfortunately, she’s probably right. Mrs. K also has a history of podagra, and she developed an acute gouty monoarthritis after receiving treatment with diuretics and aspirin. Gout—along with the other causes of inpatient acute monoarthritis (pseudogout, septic arthritis, and trauma)—are increasingly common diagnoses in the geriatric patient population. Because the elderly are uniquely predisposed to losing functional independence following an acute attack, making a timely diagnosis is particularly important in this age group. And though the patient’s clinical features may point toward an etiology, making the correct diagnosis ultimately depends on the results of the joint tap.
Gout
Gout occurs in patients with high serum levels of uric acid, though not all hyperuricemic patients develop gout. Among elderly hospitalized patients with hyperuricemia, approximately 65% have significant renal impairment, and others have advanced hypertension, coronary artery disease, and congestive heart failure. Over time, high serum uric acid levels may lead to the deposition of monosodium urate crystals in the joints; these lesions are the precursors of a gouty attack.
Gouty attacks occur when crystal deposits become inflamed. The inflammation may be triggered by a medication-induced change in uric acid concentration or by a medical condition, including acute illness, trauma, surgery, and dehydration. (See Table 1, p.18.) Though some elderly patients with acute gouty arthritis will manifest confusion or a sudden change in ambulatory status, most will present with a monoarthritis and a rise in temperature. Gout is suspected clinically when the first metatarsal phalangeal joint is involved (podagra), but other commonly involved joints include the ankle and the knee. Uric acid levels in the blood are usually elevated but can also temporarily normalize or even dip low during attacks. An X-ray of the involved joint may be normal or may already show the characteristic erosive lesion of gout, the “overhanging edge.”
Making the correct diagnosis is dependent upon visualizing intracellular, needle-shaped, negatively birefringent crystals in the synovial fluid. After the fluid is removed from the affected joint, it should be examined under polarized light within two hours; if more time is needed, the fluid can be refrigerated for up to 12 hours. Co-infection of a gouty joint has been described in the elderly population, and the synovial fluid should be sent to the laboratory for a cell count, Gram’s stain, and culture, as well as glucose and lactate levels. (See Table 2, below.)
Direct in-hospital treatment of gout toward alleviating the current attack, preventing future attacks, and providing appropriate antibiotic coverage in suspected co-infected cases until joint culture results are finalized. Treatment options for the acute attack include NSAIDs and corticosteroids—either oral or intra-articular. Hourly oral colchicine is not a good option for an elderly patient because the diarrhea that ensues is particularly disruptive. Nor is IV colchicine a good option thanks to its side-effect profile that renders it unusable in patients with reduced renal function. The treatment of hyperuricemia with allopurinol should not be undertaken during the acute attack because any change in the serum uric acid concentration will serve only to exacerbate the current inflammation.
Anti-inflammatory doses of NSAIDs are effective and will shorten the duration of symptoms substantially. Seven to 10 days of indomethacin at a dose of 50 mg taken orally three times daily is the traditional choice, and though it is generally conceded that ibuprofen and naproxen also work well, no comparative trials have been performed. Elderly patients are at increased risk for adverse effects from NSAIDs, particularly those patients with severely reduced renal function, gastropathy, asthma, congestive heart failure, or other intravascularly depleted states. Gastric mucosal protection, using proton-pump inhibitors, and careful monitoring of fluid status, renal function, and mental status are of particular concern in this population.
Because recent research indicates that COX-2 inhibitors have thrombotic potential and are contraindicated in patients at high risk for cardiovascular events or stroke, the extent to which they can be used in an elderly patient with an acute gouty attack is limited. A traditional NSAID in combination with a proton-pump inhibitor may be as effective as a COX-2 inhibitor in reducing the risk of gastroduodenal toxicity, however.
Corticosteroids—given either orally or intra-articularly—are an appropriate treatment for patients who can’t tolerate an NSAID. As long as a septic joint has been excluded, an intra-articular injection of 40–80 mg triamcinolone acetonide or 40 mg of methylprednisolone acetate will result in major improvement within 24 hours for most patients. Another option is a seven- to 10-day course of oral prednisone, starting with 40 mg on day one and reducing the dosage by 5 mg/day. Elderly patients taking oral prednisone should also receive adequate calcium, vitamin D, and a proton pump inhibitor for gastrointestinal protection, as well as close monitoring of blood pressure, glucose, and mental status.
If a patient has a history of frequent attacks or tophi, has a serum uric acid level higher than 12 mg/dl, or is consistently receiving high doses of diuretics, that person is at high risk for subsequent attacks and should receive prophylactic treatment with either a low-dose daily NSAID or a renally dosed oral colchicine.
Pseudogout
Pseudogout is the articular manifestation of calcium pyrophosphate dihydrate (CPPD) deposition, and this process is associated with aging as well as with various endocrinopathies, the most common of which is hyperparathyroidism. (See Table 3, below.) The shedding of CPPD crystals initiates an inflammatory process, and these crystals invoke an inflammatory response in much the same manner as uric acid crystals.
While the precipitants of a pseudogout attack are less well defined than those of gout, dehydration and joint surgery have both been identified as predisposing factors. The acute monoarticular pain and swelling (the knee is most common, followed by the ankle and then any other synovial joint) that ensues usually has a more insidious onset, and an X-ray may show chondrocalcinosis within the joint space. The diagnosis is confirmed by the demonstration of intracellular CPPD crystals in the aspirated joint fluid. Though less easily seen than monosodium urate crystals, rhomboidal crystals that display weakly positive birefringence under polarized light will be revealed with careful observation. Vitally important to the diagnosis of any crystal-associated arthritis is the exclusion of septic arthritis. To this end, conduct synovial fluid and blood cultures even if the suspicion of sepsis is low.
Treatment goals for pseudogout center on the abatement of the current arthritis and the exclusion of an infected joint or a concurrent metabolic syndrome. NSAIDs are the mainstay of therapy for the management of pseudogout; they are prescribed in anti-inflammatory doses similar to those used in the treatment of gout. Corticosteroids can also be used, particularly an intra-articular injection, as long as infection has been excluded. As with any crystal arthropathy, a septic joint should be considered and treated in high-risk patients even before the results of the joint fluid cultures are available. (See Table 4, above.)
Septic Arthritis
Even with timely antibacterial treatment, an elderly patient with a septic joint has a 7% to 32% mortality rate. Staphylococcus and Streptococcus are the most commonly cultured pathogens, but consider E. coli, Pseudomonas, and Klebsiella species in patients with diabetes mellitus, malignancy, or other debilitating chronic syndromes; less common agents include tuberculosis and gonococcus. Fever may be present, but a recent study revealed that fewer than 60% of geriatric patients with septic arthritis presented with a febrile illness. Thus, systemic features are not reliable enough to warrant making or excluding the diagnosis of septic arthritis without examination of the synovial fluid. (See Table 5, below.)
Send synovial fluid for leukocyte count, Gram’s stain, and culture in all suspected cases, and several studies suggest that the diagnostic yield may be improved with direct inoculation of fluid into blood culture vials or isolator tubes. Synovial fluid will also show very low glucose (less than 25% of simultaneous plasma glucose) and very high lactate (greater than 10 mm/l) in the untreated bacterial septic joint.
Treatment of a septic joint includes both appropriate antimicrobial therapy and joint drainage. Three weeks of parenteral antimicrobial therapy directed against the isolated pathogen is usually sufficient once the affected joint has been drained. Surgical drainage is indicated in joints—like the hip—that are difficult to aspirate or monitor. Other indications include pus in the synovial fluid, spread of infection to the soft tissues, or an inadequate clinical response to appropriate antibiotics after five to seven days. Otherwise, daily aspiration is the treatment of choice for an uncomplicated infected joint. Additionally, as is true in any acute monoarthritis, bed rest and optimal joint positioning are required to prevent the occurrence of joint deformation and harmful contractures. TH
Dr. Landis is a rheumatologist and a freelance writer.
Special thanks to Bradley Flansbaum, MD, for his assistance with this article.
References
- Tenenbaum J. Inflammatory musculoskeletal conditions in older adults. Geriatr Aging. 2005;8(3):14-17.
- Bieber JD, Terkeltaub RA. Gout: on the brink of novel therapeutic options for an ancient disease. Arthritis Rheum. 2004 Aug;50(8):2400-2414.
- Terkeltaub RA. Clinical practice. Gout. N Engl J Med. 2003 Oct 23;349(17):1647-1655.
- Leirisalo-Repo M. Early arthritis and infection. Curr Opin Rheumatol. 2005 Jul;17(4):433-439.
- Siva C, Velazquez C, Mody A, et al. Diagnosing acute monoarthritis in adults: a practical approach for the family physician. Am Fam Physician. 2003 Jul 1;68(1):83-90.
Mrs. K, an 81-year-old golf-enthusiast admitted with congestive heart failure, now refuses to walk and complains of ankle pain. When you see her, she refuses to let even a bedsheet near her left ankle, and she claims that you did this to her.
Unfortunately, she’s probably right. Mrs. K also has a history of podagra, and she developed an acute gouty monoarthritis after receiving treatment with diuretics and aspirin. Gout—along with the other causes of inpatient acute monoarthritis (pseudogout, septic arthritis, and trauma)—are increasingly common diagnoses in the geriatric patient population. Because the elderly are uniquely predisposed to losing functional independence following an acute attack, making a timely diagnosis is particularly important in this age group. And though the patient’s clinical features may point toward an etiology, making the correct diagnosis ultimately depends on the results of the joint tap.
Gout
Gout occurs in patients with high serum levels of uric acid, though not all hyperuricemic patients develop gout. Among elderly hospitalized patients with hyperuricemia, approximately 65% have significant renal impairment, and others have advanced hypertension, coronary artery disease, and congestive heart failure. Over time, high serum uric acid levels may lead to the deposition of monosodium urate crystals in the joints; these lesions are the precursors of a gouty attack.
Gouty attacks occur when crystal deposits become inflamed. The inflammation may be triggered by a medication-induced change in uric acid concentration or by a medical condition, including acute illness, trauma, surgery, and dehydration. (See Table 1, p.18.) Though some elderly patients with acute gouty arthritis will manifest confusion or a sudden change in ambulatory status, most will present with a monoarthritis and a rise in temperature. Gout is suspected clinically when the first metatarsal phalangeal joint is involved (podagra), but other commonly involved joints include the ankle and the knee. Uric acid levels in the blood are usually elevated but can also temporarily normalize or even dip low during attacks. An X-ray of the involved joint may be normal or may already show the characteristic erosive lesion of gout, the “overhanging edge.”
Making the correct diagnosis is dependent upon visualizing intracellular, needle-shaped, negatively birefringent crystals in the synovial fluid. After the fluid is removed from the affected joint, it should be examined under polarized light within two hours; if more time is needed, the fluid can be refrigerated for up to 12 hours. Co-infection of a gouty joint has been described in the elderly population, and the synovial fluid should be sent to the laboratory for a cell count, Gram’s stain, and culture, as well as glucose and lactate levels. (See Table 2, below.)
Direct in-hospital treatment of gout toward alleviating the current attack, preventing future attacks, and providing appropriate antibiotic coverage in suspected co-infected cases until joint culture results are finalized. Treatment options for the acute attack include NSAIDs and corticosteroids—either oral or intra-articular. Hourly oral colchicine is not a good option for an elderly patient because the diarrhea that ensues is particularly disruptive. Nor is IV colchicine a good option thanks to its side-effect profile that renders it unusable in patients with reduced renal function. The treatment of hyperuricemia with allopurinol should not be undertaken during the acute attack because any change in the serum uric acid concentration will serve only to exacerbate the current inflammation.
Anti-inflammatory doses of NSAIDs are effective and will shorten the duration of symptoms substantially. Seven to 10 days of indomethacin at a dose of 50 mg taken orally three times daily is the traditional choice, and though it is generally conceded that ibuprofen and naproxen also work well, no comparative trials have been performed. Elderly patients are at increased risk for adverse effects from NSAIDs, particularly those patients with severely reduced renal function, gastropathy, asthma, congestive heart failure, or other intravascularly depleted states. Gastric mucosal protection, using proton-pump inhibitors, and careful monitoring of fluid status, renal function, and mental status are of particular concern in this population.
Because recent research indicates that COX-2 inhibitors have thrombotic potential and are contraindicated in patients at high risk for cardiovascular events or stroke, the extent to which they can be used in an elderly patient with an acute gouty attack is limited. A traditional NSAID in combination with a proton-pump inhibitor may be as effective as a COX-2 inhibitor in reducing the risk of gastroduodenal toxicity, however.
Corticosteroids—given either orally or intra-articularly—are an appropriate treatment for patients who can’t tolerate an NSAID. As long as a septic joint has been excluded, an intra-articular injection of 40–80 mg triamcinolone acetonide or 40 mg of methylprednisolone acetate will result in major improvement within 24 hours for most patients. Another option is a seven- to 10-day course of oral prednisone, starting with 40 mg on day one and reducing the dosage by 5 mg/day. Elderly patients taking oral prednisone should also receive adequate calcium, vitamin D, and a proton pump inhibitor for gastrointestinal protection, as well as close monitoring of blood pressure, glucose, and mental status.
If a patient has a history of frequent attacks or tophi, has a serum uric acid level higher than 12 mg/dl, or is consistently receiving high doses of diuretics, that person is at high risk for subsequent attacks and should receive prophylactic treatment with either a low-dose daily NSAID or a renally dosed oral colchicine.
Pseudogout
Pseudogout is the articular manifestation of calcium pyrophosphate dihydrate (CPPD) deposition, and this process is associated with aging as well as with various endocrinopathies, the most common of which is hyperparathyroidism. (See Table 3, below.) The shedding of CPPD crystals initiates an inflammatory process, and these crystals invoke an inflammatory response in much the same manner as uric acid crystals.
While the precipitants of a pseudogout attack are less well defined than those of gout, dehydration and joint surgery have both been identified as predisposing factors. The acute monoarticular pain and swelling (the knee is most common, followed by the ankle and then any other synovial joint) that ensues usually has a more insidious onset, and an X-ray may show chondrocalcinosis within the joint space. The diagnosis is confirmed by the demonstration of intracellular CPPD crystals in the aspirated joint fluid. Though less easily seen than monosodium urate crystals, rhomboidal crystals that display weakly positive birefringence under polarized light will be revealed with careful observation. Vitally important to the diagnosis of any crystal-associated arthritis is the exclusion of septic arthritis. To this end, conduct synovial fluid and blood cultures even if the suspicion of sepsis is low.
Treatment goals for pseudogout center on the abatement of the current arthritis and the exclusion of an infected joint or a concurrent metabolic syndrome. NSAIDs are the mainstay of therapy for the management of pseudogout; they are prescribed in anti-inflammatory doses similar to those used in the treatment of gout. Corticosteroids can also be used, particularly an intra-articular injection, as long as infection has been excluded. As with any crystal arthropathy, a septic joint should be considered and treated in high-risk patients even before the results of the joint fluid cultures are available. (See Table 4, above.)
Septic Arthritis
Even with timely antibacterial treatment, an elderly patient with a septic joint has a 7% to 32% mortality rate. Staphylococcus and Streptococcus are the most commonly cultured pathogens, but consider E. coli, Pseudomonas, and Klebsiella species in patients with diabetes mellitus, malignancy, or other debilitating chronic syndromes; less common agents include tuberculosis and gonococcus. Fever may be present, but a recent study revealed that fewer than 60% of geriatric patients with septic arthritis presented with a febrile illness. Thus, systemic features are not reliable enough to warrant making or excluding the diagnosis of septic arthritis without examination of the synovial fluid. (See Table 5, below.)
Send synovial fluid for leukocyte count, Gram’s stain, and culture in all suspected cases, and several studies suggest that the diagnostic yield may be improved with direct inoculation of fluid into blood culture vials or isolator tubes. Synovial fluid will also show very low glucose (less than 25% of simultaneous plasma glucose) and very high lactate (greater than 10 mm/l) in the untreated bacterial septic joint.
Treatment of a septic joint includes both appropriate antimicrobial therapy and joint drainage. Three weeks of parenteral antimicrobial therapy directed against the isolated pathogen is usually sufficient once the affected joint has been drained. Surgical drainage is indicated in joints—like the hip—that are difficult to aspirate or monitor. Other indications include pus in the synovial fluid, spread of infection to the soft tissues, or an inadequate clinical response to appropriate antibiotics after five to seven days. Otherwise, daily aspiration is the treatment of choice for an uncomplicated infected joint. Additionally, as is true in any acute monoarthritis, bed rest and optimal joint positioning are required to prevent the occurrence of joint deformation and harmful contractures. TH
Dr. Landis is a rheumatologist and a freelance writer.
Special thanks to Bradley Flansbaum, MD, for his assistance with this article.
References
- Tenenbaum J. Inflammatory musculoskeletal conditions in older adults. Geriatr Aging. 2005;8(3):14-17.
- Bieber JD, Terkeltaub RA. Gout: on the brink of novel therapeutic options for an ancient disease. Arthritis Rheum. 2004 Aug;50(8):2400-2414.
- Terkeltaub RA. Clinical practice. Gout. N Engl J Med. 2003 Oct 23;349(17):1647-1655.
- Leirisalo-Repo M. Early arthritis and infection. Curr Opin Rheumatol. 2005 Jul;17(4):433-439.
- Siva C, Velazquez C, Mody A, et al. Diagnosing acute monoarthritis in adults: a practical approach for the family physician. Am Fam Physician. 2003 Jul 1;68(1):83-90.
Status Report
The mission of the University HealthSystem Consortium, based in Chicago, is “to advance knowledge, foster collaboration, and promote change to help members succeed in their respective markets. UHC’s vision is to be a catalyst for change, accelerating the achievement of clinical and operational excellence.” (www.uhc.edu).
As part of UHC’s improvement and effectiveness initiatives, a benchmarking project (“Role of the Hospitalist 2006 Benchmarking Project Performance Scorecard”) was undertaken during the summer and fall of 2006 to examine what hospitalists nationwide do, as well as how they are incorporated into patient care and how they are funded by member hospitals. The benchmarking project articulated how hospitalist programs are measured and what they do to add value to their member organizations.
Methods
A seven-person steering committee was selected to provide guidance. Under the direction of Danielle Carrier, MBA, project manager, Operations Improvement; UHC, the committee developed a survey of hospitalist program characteristics, hospitalist value self-assessment, and hospitalist innovative strategies. Twenty-three member organizations participated.
Results
The most common reason for starting a hospitalist program was improving efficiency and reducing length of stay through enhanced on-site availability; however, the impetus for hospitalist services has changed in 81% of responding organizations. The most common changes were increasing the focus on teaching and academic pursuits, quality, and safety, and providing coverage for services to facilitate Accreditation Council for Graduate Medical Education (ACGME) compliance, including co-management of surgical patients. The direction of change differed by the age of the program and the hospitalist model (teaching, non-teaching, and mixed models).
The benchmarking project articulated the value that hospitalist programs bring to their organizations:
- Quality improvement initiatives (development of protocols or pathways, standardization of care, medication reconciliation, enhanced glycemic control, and physician availability at care transitions such as ICU and emergency department [ED], as well as for pre-operative consults);
- Development of new services (palliative care programs, surgical co-management); and
- Improvement of the educational process (through more contact with faculty, multidisciplinary team rounding, curriculum development around the core competencies, hospitalist training programs, and practice-based learning).
Of the respondents, 95% report that hospitalists assume leadership roles in quality and safety initiatives. For the key stakeholders (senior administrator or department chair) the aspects of the hospitalist program that bring the most value are quality of care and safety, throughput and LOS, and expanded admission capacity and coverage.
Measures of success include length of stay, relative value units and service workload, teaching evaluations, admission and consult volume, costs and cost savings, core measures and national quality indicators, patient satisfaction, referring physician satisfaction, and academic productivity.
Information on hospitalist program funding indicated the following:
- Sole funding of salaries by the hospital: 45% of respondents; and
- Joint funding (hospital and another organization such as a medical school, a practice plan, or a clinical department): 50% of respondents.
Although no organization offers incentives for the program itself, 35% of organizations offer incentives for individual hospitalists. Incentives for individual hospitalists include productivity and relative value units, LOS, budget, quality measures, and weekend work. Two-thirds of organizations with individual incentives reported that the incentives have altered behavior or helped achieve program objectives.
The survey of workload and schedule was notable for the following:
- An annual average of 10 weeks of protected non-direct patient-care time per hospitalist is offered at 52% percent of programs;
- A full-time hospitalist spends an average of 23 weeks attending on inpatient units; and
- Time spent on average for hospitalists: 2.5% administrative, 4.9% quality, 5.3% research, 14.9% teaching, 2.6% outpatient care.
Areas in which the hospitalist program needs to play a stronger or increased role include quality improvement and patient safety, non-internal medicine services, clinical education, research, and leadership within the health system. There was no major variation among hospital administrator and chair of medicine responses. Program directors of three years or less identified quality improvement and standardizing care as areas that need more emphasis. Program directors of more than three years identified quality, research, and health system leadership as areas they’d like to gain a more significant role.
The most common impediment to the continuation and growth of hospitalist programs: attracting and retaining physicians, given the ratio of salary to workload, the level of burnout, and the lack of a defined career path. Attracting quality candidates with academic skills and/or the ability to lead and manage change was identified as a major impediment.
Challenges included:
- Cultural and political issues;
- Inadequate commitment or support for the program;
- Lack of understanding with regard to the role of the hospitalist and the true value of the program;
- Lack of organizational clarity of program goals, expectations, and measures of success; and
- Improvement of academic and scholarly aspects of the program.
Conclusions
The “Role of the Hospitalist 2006 Benchmarking Project Performance Scorecard.” reported on the need to proactively manage the program direction and growth by developing and expanding lines of business, which may include:
- Non-internal medicine services such as co-management models, pre-operative clinics, and anticoagulation clinics;
- Palliative care services;
- Quality and safety improvement efforts;
- Facilitation of admissions from the emergency department and transfers both within and outside the network; and
- Care of extended care facility patients.
Hospitalist program satisfaction in academic models may be enhanced by increasing the academic and research presence and by supporting the role of the hospitalist in quality improvement. In addition, the project identifies the need to effectively manage increasing demand for hospitalists for other service lines.
Articulating the hospitalist program’s value is the first step in obtaining the resources to proactively manage the program’s direction and growth. UHC recommends clearly defining the hospitalist program goals, expectations, and measures of success. This requires obtaining input and buy-in from all key stakeholders and developing measures for all key aspects of the program, including intangible contributions. Key stakeholders should meet regularly with hospitalists to discuss program accomplishments. Hospitalist program representatives should assume leadership roles within the hospital and medical staff. For example, hospitalists should become members of the medical staff executive committee and the hospital’s operational committee, interwoven into the fabric of the hospital. It is also important to identify and monitor measures to support program funding and support, as well as to create a business case for new program roles.
Enhancing hospitalist career development and advancement is central to the recruitment and retention of experienced hospitalists. Development of effective recruitment and retention strategies includes creating a hospitalist career path, offering protected time for non-direct patient care activities, implementing innovative strategies to manage night and weekend coverage, defining and monitoring workload indicators, building reward and recognition programs, and implementing incentive programs. Training and education curriculum should focus on the needs of hospitalists and should include modules in areas of program growth such as palliative care and surgical co-management. TH
The mission of the University HealthSystem Consortium, based in Chicago, is “to advance knowledge, foster collaboration, and promote change to help members succeed in their respective markets. UHC’s vision is to be a catalyst for change, accelerating the achievement of clinical and operational excellence.” (www.uhc.edu).
As part of UHC’s improvement and effectiveness initiatives, a benchmarking project (“Role of the Hospitalist 2006 Benchmarking Project Performance Scorecard”) was undertaken during the summer and fall of 2006 to examine what hospitalists nationwide do, as well as how they are incorporated into patient care and how they are funded by member hospitals. The benchmarking project articulated how hospitalist programs are measured and what they do to add value to their member organizations.
Methods
A seven-person steering committee was selected to provide guidance. Under the direction of Danielle Carrier, MBA, project manager, Operations Improvement; UHC, the committee developed a survey of hospitalist program characteristics, hospitalist value self-assessment, and hospitalist innovative strategies. Twenty-three member organizations participated.
Results
The most common reason for starting a hospitalist program was improving efficiency and reducing length of stay through enhanced on-site availability; however, the impetus for hospitalist services has changed in 81% of responding organizations. The most common changes were increasing the focus on teaching and academic pursuits, quality, and safety, and providing coverage for services to facilitate Accreditation Council for Graduate Medical Education (ACGME) compliance, including co-management of surgical patients. The direction of change differed by the age of the program and the hospitalist model (teaching, non-teaching, and mixed models).
The benchmarking project articulated the value that hospitalist programs bring to their organizations:
- Quality improvement initiatives (development of protocols or pathways, standardization of care, medication reconciliation, enhanced glycemic control, and physician availability at care transitions such as ICU and emergency department [ED], as well as for pre-operative consults);
- Development of new services (palliative care programs, surgical co-management); and
- Improvement of the educational process (through more contact with faculty, multidisciplinary team rounding, curriculum development around the core competencies, hospitalist training programs, and practice-based learning).
Of the respondents, 95% report that hospitalists assume leadership roles in quality and safety initiatives. For the key stakeholders (senior administrator or department chair) the aspects of the hospitalist program that bring the most value are quality of care and safety, throughput and LOS, and expanded admission capacity and coverage.
Measures of success include length of stay, relative value units and service workload, teaching evaluations, admission and consult volume, costs and cost savings, core measures and national quality indicators, patient satisfaction, referring physician satisfaction, and academic productivity.
Information on hospitalist program funding indicated the following:
- Sole funding of salaries by the hospital: 45% of respondents; and
- Joint funding (hospital and another organization such as a medical school, a practice plan, or a clinical department): 50% of respondents.
Although no organization offers incentives for the program itself, 35% of organizations offer incentives for individual hospitalists. Incentives for individual hospitalists include productivity and relative value units, LOS, budget, quality measures, and weekend work. Two-thirds of organizations with individual incentives reported that the incentives have altered behavior or helped achieve program objectives.
The survey of workload and schedule was notable for the following:
- An annual average of 10 weeks of protected non-direct patient-care time per hospitalist is offered at 52% percent of programs;
- A full-time hospitalist spends an average of 23 weeks attending on inpatient units; and
- Time spent on average for hospitalists: 2.5% administrative, 4.9% quality, 5.3% research, 14.9% teaching, 2.6% outpatient care.
Areas in which the hospitalist program needs to play a stronger or increased role include quality improvement and patient safety, non-internal medicine services, clinical education, research, and leadership within the health system. There was no major variation among hospital administrator and chair of medicine responses. Program directors of three years or less identified quality improvement and standardizing care as areas that need more emphasis. Program directors of more than three years identified quality, research, and health system leadership as areas they’d like to gain a more significant role.
The most common impediment to the continuation and growth of hospitalist programs: attracting and retaining physicians, given the ratio of salary to workload, the level of burnout, and the lack of a defined career path. Attracting quality candidates with academic skills and/or the ability to lead and manage change was identified as a major impediment.
Challenges included:
- Cultural and political issues;
- Inadequate commitment or support for the program;
- Lack of understanding with regard to the role of the hospitalist and the true value of the program;
- Lack of organizational clarity of program goals, expectations, and measures of success; and
- Improvement of academic and scholarly aspects of the program.
Conclusions
The “Role of the Hospitalist 2006 Benchmarking Project Performance Scorecard.” reported on the need to proactively manage the program direction and growth by developing and expanding lines of business, which may include:
- Non-internal medicine services such as co-management models, pre-operative clinics, and anticoagulation clinics;
- Palliative care services;
- Quality and safety improvement efforts;
- Facilitation of admissions from the emergency department and transfers both within and outside the network; and
- Care of extended care facility patients.
Hospitalist program satisfaction in academic models may be enhanced by increasing the academic and research presence and by supporting the role of the hospitalist in quality improvement. In addition, the project identifies the need to effectively manage increasing demand for hospitalists for other service lines.
Articulating the hospitalist program’s value is the first step in obtaining the resources to proactively manage the program’s direction and growth. UHC recommends clearly defining the hospitalist program goals, expectations, and measures of success. This requires obtaining input and buy-in from all key stakeholders and developing measures for all key aspects of the program, including intangible contributions. Key stakeholders should meet regularly with hospitalists to discuss program accomplishments. Hospitalist program representatives should assume leadership roles within the hospital and medical staff. For example, hospitalists should become members of the medical staff executive committee and the hospital’s operational committee, interwoven into the fabric of the hospital. It is also important to identify and monitor measures to support program funding and support, as well as to create a business case for new program roles.
Enhancing hospitalist career development and advancement is central to the recruitment and retention of experienced hospitalists. Development of effective recruitment and retention strategies includes creating a hospitalist career path, offering protected time for non-direct patient care activities, implementing innovative strategies to manage night and weekend coverage, defining and monitoring workload indicators, building reward and recognition programs, and implementing incentive programs. Training and education curriculum should focus on the needs of hospitalists and should include modules in areas of program growth such as palliative care and surgical co-management. TH
The mission of the University HealthSystem Consortium, based in Chicago, is “to advance knowledge, foster collaboration, and promote change to help members succeed in their respective markets. UHC’s vision is to be a catalyst for change, accelerating the achievement of clinical and operational excellence.” (www.uhc.edu).
As part of UHC’s improvement and effectiveness initiatives, a benchmarking project (“Role of the Hospitalist 2006 Benchmarking Project Performance Scorecard”) was undertaken during the summer and fall of 2006 to examine what hospitalists nationwide do, as well as how they are incorporated into patient care and how they are funded by member hospitals. The benchmarking project articulated how hospitalist programs are measured and what they do to add value to their member organizations.
Methods
A seven-person steering committee was selected to provide guidance. Under the direction of Danielle Carrier, MBA, project manager, Operations Improvement; UHC, the committee developed a survey of hospitalist program characteristics, hospitalist value self-assessment, and hospitalist innovative strategies. Twenty-three member organizations participated.
Results
The most common reason for starting a hospitalist program was improving efficiency and reducing length of stay through enhanced on-site availability; however, the impetus for hospitalist services has changed in 81% of responding organizations. The most common changes were increasing the focus on teaching and academic pursuits, quality, and safety, and providing coverage for services to facilitate Accreditation Council for Graduate Medical Education (ACGME) compliance, including co-management of surgical patients. The direction of change differed by the age of the program and the hospitalist model (teaching, non-teaching, and mixed models).
The benchmarking project articulated the value that hospitalist programs bring to their organizations:
- Quality improvement initiatives (development of protocols or pathways, standardization of care, medication reconciliation, enhanced glycemic control, and physician availability at care transitions such as ICU and emergency department [ED], as well as for pre-operative consults);
- Development of new services (palliative care programs, surgical co-management); and
- Improvement of the educational process (through more contact with faculty, multidisciplinary team rounding, curriculum development around the core competencies, hospitalist training programs, and practice-based learning).
Of the respondents, 95% report that hospitalists assume leadership roles in quality and safety initiatives. For the key stakeholders (senior administrator or department chair) the aspects of the hospitalist program that bring the most value are quality of care and safety, throughput and LOS, and expanded admission capacity and coverage.
Measures of success include length of stay, relative value units and service workload, teaching evaluations, admission and consult volume, costs and cost savings, core measures and national quality indicators, patient satisfaction, referring physician satisfaction, and academic productivity.
Information on hospitalist program funding indicated the following:
- Sole funding of salaries by the hospital: 45% of respondents; and
- Joint funding (hospital and another organization such as a medical school, a practice plan, or a clinical department): 50% of respondents.
Although no organization offers incentives for the program itself, 35% of organizations offer incentives for individual hospitalists. Incentives for individual hospitalists include productivity and relative value units, LOS, budget, quality measures, and weekend work. Two-thirds of organizations with individual incentives reported that the incentives have altered behavior or helped achieve program objectives.
The survey of workload and schedule was notable for the following:
- An annual average of 10 weeks of protected non-direct patient-care time per hospitalist is offered at 52% percent of programs;
- A full-time hospitalist spends an average of 23 weeks attending on inpatient units; and
- Time spent on average for hospitalists: 2.5% administrative, 4.9% quality, 5.3% research, 14.9% teaching, 2.6% outpatient care.
Areas in which the hospitalist program needs to play a stronger or increased role include quality improvement and patient safety, non-internal medicine services, clinical education, research, and leadership within the health system. There was no major variation among hospital administrator and chair of medicine responses. Program directors of three years or less identified quality improvement and standardizing care as areas that need more emphasis. Program directors of more than three years identified quality, research, and health system leadership as areas they’d like to gain a more significant role.
The most common impediment to the continuation and growth of hospitalist programs: attracting and retaining physicians, given the ratio of salary to workload, the level of burnout, and the lack of a defined career path. Attracting quality candidates with academic skills and/or the ability to lead and manage change was identified as a major impediment.
Challenges included:
- Cultural and political issues;
- Inadequate commitment or support for the program;
- Lack of understanding with regard to the role of the hospitalist and the true value of the program;
- Lack of organizational clarity of program goals, expectations, and measures of success; and
- Improvement of academic and scholarly aspects of the program.
Conclusions
The “Role of the Hospitalist 2006 Benchmarking Project Performance Scorecard.” reported on the need to proactively manage the program direction and growth by developing and expanding lines of business, which may include:
- Non-internal medicine services such as co-management models, pre-operative clinics, and anticoagulation clinics;
- Palliative care services;
- Quality and safety improvement efforts;
- Facilitation of admissions from the emergency department and transfers both within and outside the network; and
- Care of extended care facility patients.
Hospitalist program satisfaction in academic models may be enhanced by increasing the academic and research presence and by supporting the role of the hospitalist in quality improvement. In addition, the project identifies the need to effectively manage increasing demand for hospitalists for other service lines.
Articulating the hospitalist program’s value is the first step in obtaining the resources to proactively manage the program’s direction and growth. UHC recommends clearly defining the hospitalist program goals, expectations, and measures of success. This requires obtaining input and buy-in from all key stakeholders and developing measures for all key aspects of the program, including intangible contributions. Key stakeholders should meet regularly with hospitalists to discuss program accomplishments. Hospitalist program representatives should assume leadership roles within the hospital and medical staff. For example, hospitalists should become members of the medical staff executive committee and the hospital’s operational committee, interwoven into the fabric of the hospital. It is also important to identify and monitor measures to support program funding and support, as well as to create a business case for new program roles.
Enhancing hospitalist career development and advancement is central to the recruitment and retention of experienced hospitalists. Development of effective recruitment and retention strategies includes creating a hospitalist career path, offering protected time for non-direct patient care activities, implementing innovative strategies to manage night and weekend coverage, defining and monitoring workload indicators, building reward and recognition programs, and implementing incentive programs. Training and education curriculum should focus on the needs of hospitalists and should include modules in areas of program growth such as palliative care and surgical co-management. TH
Reasons to Research

If you’re a community-based hospitalist who hasn’t conducted research since your residency or medical school, you may want to consider undertaking a research project to broaden your career and your skill set.
Why Add Research to Your Workload?
If you’re a non-researcher, why would you want to add this new component to an already busy workload?
“I think there are a number of reasons why a hospitalist might want to get involved in doing research,” says Peter Lindenauer, MD, MSc, FACP, medical director, Clinical and Quality Informatics, Baystate Health in Springfield, Mass., and assistant professor of medicine at Tufts University School of Medicine in Boston. You may decide to undertake research because you’re curious about a specific area and want to make some new discoveries—and expand the general body of knowledge in that area. Or you may undertake a research project, says Dr. Lindenauer, because of “a desire to help your patients more specifically—to provide better care based on your own research findings.”
But some non-academic hospitalists may decide to lead a research project for more personal reasons. “I’m someone whose career has benefited from doing research,” admits Dr. Lindenauer, pointing out that a published research study brings recognition to the study author. “It can help you establish a professional niche. By doing research, you can become a highly visible member of our professional society.”
And a more basic reason, says Dr. Lindenauer, is that “research is something that can provide diversification to your work life, and it can bring professional satisfaction. It spices up one’s career.”
QI: The Perfect Fit
A full-time hospitalist who is a novice or an inexperienced researcher obviously isn’t in a position to lead a multi-center, randomized trial or conduct extensive lab work. There is another type of research, however, that seems the perfect fit for a community-based hospitalist.
“Rather than setting the bar at an unattainable level, hospitalists should consider getting involved in quality improvement research, since hospitalists are often ideally suited to participate [in] and lead the interventions themselves,” says Dr. Lindenauer. “It’s not the only kind of research, but it’s a natural, given the roles that hospitalists play. However, hospitalists can be involved in clinical trials, in analyses of secondary data, and even in doing intervention studies at their own institutions.”
And a quality improvement project, if conducted correctly, is likely to be accepted for publication and/or presentation. “While QI research is somewhat different than traditional, clinical research, there’s an increasing interest in seeing [QI] research published in established medical journals,” explains Dr. Lindenauer. “Some hospitalists have been very successful at doing this and [in] publishing the results and … giving presentations.”
Steps to Get Started
So how should you go about setting up your first QI research project?
Your first step—and possibly the most important—is selecting a research topic. “It’s important to come up with good research questions,” says Dr. Lindenauer. “One framework for choosing a topic is the acronym FINER, which stands for: [is it] feasible, interesting, novel, ethical, and relevant?”
Once you have a likely focus for quality improvement, outline how you mean to go about the project. “You have to choose a study plan and make sure the plan matches the question,” says Dr. Lindenauer.
When you have a basic idea for your project, says Dr. Lindenauer, “You have to find time in an already busy life, and you have to find support.” For one thing, very few questions can be answered by a single physician. For another, you’ll need your hospital’s buy-in.
“For QI research, it’s natural to go to your hospital’s quality improvement department,” says Dr. Lindenauer. “Ask the director of the department to sit down, and then find out what’s on the hospital’s agenda. You’ll need to find some common ground, some overlap between your interests and the hospital’s. Support is so important, and given all the external pressures for improving quality, it’s unlikely that your quality improvement department will support a project that doesn’t align with their plans or focus. So align your interests with those of the hospital and go from there.”
Ideally, you’ll also find some mentorship before or during your first project. “At a community hospital, where no faculty is available, you must identify potential mentors from outside your hospital,” says Dr. Lindenauer. “Find faculty at a university that your hospital is affiliated with or someone who was a mentor to you during your residency or medical school. And sometimes a quality improvement department can supply a mentor.”
Lastly, “find some degree of training,” advises Dr. Lindenauer. “SHM has regularly offered workshops as a first step to starting research. Other societies offer short, intensive training—or a fellowship. If you get … charged up doing research, find a fellowship.”
Build in Review by an IRB
There’s one more crucial step involved in setting up and conducting a QI research project, assuming you want to get your results published: “You should notify [your institutional review board] and have them look at your project,” says Dr. Lindenauer. “The best time to do this is during the conceptualization, once you have your research protocol.”
You should take care of this on your own because your QI department isn’t likely to think it’s necessary. “There’s often a disconnect between the perceived need for the involvement of the IRB between researchers and QI folks,” explains Dr. Lindenauer. “Usually, QI departments don’t tend to seek IRB review for their projects. But if you’re contemplating publishing your research—which is typically the ultimate goal to a research project—this always requires IRB review. This is true even though the case is often that QI projects are exempt.”
One place to begin your education on QI research is on SHM’s Web site, under “Quality & Safety,” where you can browse quality improvement tools and several quality improvement resource rooms. TH
Jane Jerrard has written for The Hospitalist since 2005.
If you’re a community-based hospitalist who hasn’t conducted research since your residency or medical school, you may want to consider undertaking a research project to broaden your career and your skill set.
Why Add Research to Your Workload?
If you’re a non-researcher, why would you want to add this new component to an already busy workload?
“I think there are a number of reasons why a hospitalist might want to get involved in doing research,” says Peter Lindenauer, MD, MSc, FACP, medical director, Clinical and Quality Informatics, Baystate Health in Springfield, Mass., and assistant professor of medicine at Tufts University School of Medicine in Boston. You may decide to undertake research because you’re curious about a specific area and want to make some new discoveries—and expand the general body of knowledge in that area. Or you may undertake a research project, says Dr. Lindenauer, because of “a desire to help your patients more specifically—to provide better care based on your own research findings.”
But some non-academic hospitalists may decide to lead a research project for more personal reasons. “I’m someone whose career has benefited from doing research,” admits Dr. Lindenauer, pointing out that a published research study brings recognition to the study author. “It can help you establish a professional niche. By doing research, you can become a highly visible member of our professional society.”
And a more basic reason, says Dr. Lindenauer, is that “research is something that can provide diversification to your work life, and it can bring professional satisfaction. It spices up one’s career.”
QI: The Perfect Fit
A full-time hospitalist who is a novice or an inexperienced researcher obviously isn’t in a position to lead a multi-center, randomized trial or conduct extensive lab work. There is another type of research, however, that seems the perfect fit for a community-based hospitalist.
“Rather than setting the bar at an unattainable level, hospitalists should consider getting involved in quality improvement research, since hospitalists are often ideally suited to participate [in] and lead the interventions themselves,” says Dr. Lindenauer. “It’s not the only kind of research, but it’s a natural, given the roles that hospitalists play. However, hospitalists can be involved in clinical trials, in analyses of secondary data, and even in doing intervention studies at their own institutions.”
And a quality improvement project, if conducted correctly, is likely to be accepted for publication and/or presentation. “While QI research is somewhat different than traditional, clinical research, there’s an increasing interest in seeing [QI] research published in established medical journals,” explains Dr. Lindenauer. “Some hospitalists have been very successful at doing this and [in] publishing the results and … giving presentations.”
Steps to Get Started
So how should you go about setting up your first QI research project?
Your first step—and possibly the most important—is selecting a research topic. “It’s important to come up with good research questions,” says Dr. Lindenauer. “One framework for choosing a topic is the acronym FINER, which stands for: [is it] feasible, interesting, novel, ethical, and relevant?”
Once you have a likely focus for quality improvement, outline how you mean to go about the project. “You have to choose a study plan and make sure the plan matches the question,” says Dr. Lindenauer.
When you have a basic idea for your project, says Dr. Lindenauer, “You have to find time in an already busy life, and you have to find support.” For one thing, very few questions can be answered by a single physician. For another, you’ll need your hospital’s buy-in.
“For QI research, it’s natural to go to your hospital’s quality improvement department,” says Dr. Lindenauer. “Ask the director of the department to sit down, and then find out what’s on the hospital’s agenda. You’ll need to find some common ground, some overlap between your interests and the hospital’s. Support is so important, and given all the external pressures for improving quality, it’s unlikely that your quality improvement department will support a project that doesn’t align with their plans or focus. So align your interests with those of the hospital and go from there.”
Ideally, you’ll also find some mentorship before or during your first project. “At a community hospital, where no faculty is available, you must identify potential mentors from outside your hospital,” says Dr. Lindenauer. “Find faculty at a university that your hospital is affiliated with or someone who was a mentor to you during your residency or medical school. And sometimes a quality improvement department can supply a mentor.”
Lastly, “find some degree of training,” advises Dr. Lindenauer. “SHM has regularly offered workshops as a first step to starting research. Other societies offer short, intensive training—or a fellowship. If you get … charged up doing research, find a fellowship.”
Build in Review by an IRB
There’s one more crucial step involved in setting up and conducting a QI research project, assuming you want to get your results published: “You should notify [your institutional review board] and have them look at your project,” says Dr. Lindenauer. “The best time to do this is during the conceptualization, once you have your research protocol.”
You should take care of this on your own because your QI department isn’t likely to think it’s necessary. “There’s often a disconnect between the perceived need for the involvement of the IRB between researchers and QI folks,” explains Dr. Lindenauer. “Usually, QI departments don’t tend to seek IRB review for their projects. But if you’re contemplating publishing your research—which is typically the ultimate goal to a research project—this always requires IRB review. This is true even though the case is often that QI projects are exempt.”
One place to begin your education on QI research is on SHM’s Web site, under “Quality & Safety,” where you can browse quality improvement tools and several quality improvement resource rooms. TH
Jane Jerrard has written for The Hospitalist since 2005.
If you’re a community-based hospitalist who hasn’t conducted research since your residency or medical school, you may want to consider undertaking a research project to broaden your career and your skill set.
Why Add Research to Your Workload?
If you’re a non-researcher, why would you want to add this new component to an already busy workload?
“I think there are a number of reasons why a hospitalist might want to get involved in doing research,” says Peter Lindenauer, MD, MSc, FACP, medical director, Clinical and Quality Informatics, Baystate Health in Springfield, Mass., and assistant professor of medicine at Tufts University School of Medicine in Boston. You may decide to undertake research because you’re curious about a specific area and want to make some new discoveries—and expand the general body of knowledge in that area. Or you may undertake a research project, says Dr. Lindenauer, because of “a desire to help your patients more specifically—to provide better care based on your own research findings.”
But some non-academic hospitalists may decide to lead a research project for more personal reasons. “I’m someone whose career has benefited from doing research,” admits Dr. Lindenauer, pointing out that a published research study brings recognition to the study author. “It can help you establish a professional niche. By doing research, you can become a highly visible member of our professional society.”
And a more basic reason, says Dr. Lindenauer, is that “research is something that can provide diversification to your work life, and it can bring professional satisfaction. It spices up one’s career.”
QI: The Perfect Fit
A full-time hospitalist who is a novice or an inexperienced researcher obviously isn’t in a position to lead a multi-center, randomized trial or conduct extensive lab work. There is another type of research, however, that seems the perfect fit for a community-based hospitalist.
“Rather than setting the bar at an unattainable level, hospitalists should consider getting involved in quality improvement research, since hospitalists are often ideally suited to participate [in] and lead the interventions themselves,” says Dr. Lindenauer. “It’s not the only kind of research, but it’s a natural, given the roles that hospitalists play. However, hospitalists can be involved in clinical trials, in analyses of secondary data, and even in doing intervention studies at their own institutions.”
And a quality improvement project, if conducted correctly, is likely to be accepted for publication and/or presentation. “While QI research is somewhat different than traditional, clinical research, there’s an increasing interest in seeing [QI] research published in established medical journals,” explains Dr. Lindenauer. “Some hospitalists have been very successful at doing this and [in] publishing the results and … giving presentations.”
Steps to Get Started
So how should you go about setting up your first QI research project?
Your first step—and possibly the most important—is selecting a research topic. “It’s important to come up with good research questions,” says Dr. Lindenauer. “One framework for choosing a topic is the acronym FINER, which stands for: [is it] feasible, interesting, novel, ethical, and relevant?”
Once you have a likely focus for quality improvement, outline how you mean to go about the project. “You have to choose a study plan and make sure the plan matches the question,” says Dr. Lindenauer.
When you have a basic idea for your project, says Dr. Lindenauer, “You have to find time in an already busy life, and you have to find support.” For one thing, very few questions can be answered by a single physician. For another, you’ll need your hospital’s buy-in.
“For QI research, it’s natural to go to your hospital’s quality improvement department,” says Dr. Lindenauer. “Ask the director of the department to sit down, and then find out what’s on the hospital’s agenda. You’ll need to find some common ground, some overlap between your interests and the hospital’s. Support is so important, and given all the external pressures for improving quality, it’s unlikely that your quality improvement department will support a project that doesn’t align with their plans or focus. So align your interests with those of the hospital and go from there.”
Ideally, you’ll also find some mentorship before or during your first project. “At a community hospital, where no faculty is available, you must identify potential mentors from outside your hospital,” says Dr. Lindenauer. “Find faculty at a university that your hospital is affiliated with or someone who was a mentor to you during your residency or medical school. And sometimes a quality improvement department can supply a mentor.”
Lastly, “find some degree of training,” advises Dr. Lindenauer. “SHM has regularly offered workshops as a first step to starting research. Other societies offer short, intensive training—or a fellowship. If you get … charged up doing research, find a fellowship.”
Build in Review by an IRB
There’s one more crucial step involved in setting up and conducting a QI research project, assuming you want to get your results published: “You should notify [your institutional review board] and have them look at your project,” says Dr. Lindenauer. “The best time to do this is during the conceptualization, once you have your research protocol.”
You should take care of this on your own because your QI department isn’t likely to think it’s necessary. “There’s often a disconnect between the perceived need for the involvement of the IRB between researchers and QI folks,” explains Dr. Lindenauer. “Usually, QI departments don’t tend to seek IRB review for their projects. But if you’re contemplating publishing your research—which is typically the ultimate goal to a research project—this always requires IRB review. This is true even though the case is often that QI projects are exempt.”
One place to begin your education on QI research is on SHM’s Web site, under “Quality & Safety,” where you can browse quality improvement tools and several quality improvement resource rooms. TH
Jane Jerrard has written for The Hospitalist since 2005.
Don't Commit to Overcommit
There is never enough time, unless you’re serving it. —Malcolm Forbes (1919-1990)
Has this ever happened to you? You agree—months in advance—to write an article for The Hospitalist, thinking you will have plenty of time to research and write it. You hurriedly enter the item on your calendar and turn back to all your current commitments. Later, as the date approaches, you realize that you’re running out of time to do justice to the article to which you had committed.
Psychologists have explored the common human problem of overbooking and have found many contributing dynamics. A 2005 study in the Journal of Experimental Psychology suggested one explanation: Most of us, when accepting invitations weeks or months in advance, tend to view the future as more open and less busy than the present. “The nature of time fools us and we ‘forget’ about how things fill our days,” comment study authors Gal Zauberman and John Lynch.1
How do hospitalists weigh competing demands on their time? For answers to this question, naturally we asked several already-busy hospitalists to discuss the issue. They shared some lessons learned and a few strategies for managing their most precious commodity.
No Mystery
“Many things take longer than they’re supposed to,” points out S. Trent Rosenbloom, MD, MPH, a former hospitalist and currently assistant professor in the departments of Biomedical Informatics, Internal Medicine and Pediatrics, and the School of Nursing at Vanderbilt University Medical Center in Nashville, Tenn.
His situation on the morning of our interview necessitated a reschedule due to a longer-than-anticipated smog check the afternoon before. “I told myself, next year, I’ll take care of this before the deadline,” he says. “But I always end up doing this at the last minute because everything else gets in the way.”
“This interview is another example: overcommitting once more,” writes Michael J. Hovan, MD, when he agrees via e-mail to a telephone interview about the problem of overscheduling. Like most hospitalists, Dr. Hovan works with a perpetually full plate. He is inpatient director for the Hospital Family Medicine Service and assistant professor at Mayo Medical School in the Division of Family and Community Medicine at the Mayo Clinic in Scottsdale/Phoenix. Like his colleagues, Dr. Hovan has had to struggle with juggling multiple roles.
“The hospital is a far different practice environment than it was just a few years ago,” he remarks. The high intensity of patient management is now coupled with increasing administrative complexities due to a more heavily regulated environment.
As a relatively new specialty, hospital medicine requires more attention in order to establish its visibility and viability. Dr. Hovan feels this pressure keenly because, as a family medicine hospitalist, he’s in a minority position. (The majority of hospitalists trained in internal medicine, according to SHM’s 2006 Annual Survey.2)
“It’s even more important for my department, in a tertiary academic center, to maintain a visible presence on particular committees,” he says. The result of all these necessary roles? “There really are no weekends or defined time off,” says Dr. Hovan. “I’d estimate that 20% of what I do is done ‘off the clock.’ I have taken the Mayo computers to Hawaii, to family ski vacations, and [to] far less exotic locales away from the hospital setting.”
“Medicine Is Stressful”
Mary A. Dallas, MD, formerly medical director of the hospitalist service and currently medical information officer for Presbyterian Healthcare Services, an integrated healthcare delivery network in Albuquerque, N.M., noticed certain trends when she was creating schedules with the hospitalist group.
“Things sound really good on paper,” she says. “The reality is, the intensity of work is high, and sometimes you forget about that when you’re creating schedules. You might have set yourself up for three overnight shifts in order to compress work hours and expand off-time, and by the end of the second shift, you are really tired.”
Another factor is that employers expect hospitalists to see patients until the end of their shifts, and that’s when the off the clock paperwork occurs. A 40-hour workweek can easily balloon into 50 hours or more.
Physicians may also neglect to build in the emotional toll of their jobs when blocking in future schedules. “Medicine is stressful,” comments Sylvia C.W. McKean, MD, FACP, medical director, Brigham and Women’s Hospital/Faulkner Hospitalist Service in Boston. “It’s stressful to see people suffer and to deal with families who are stressed and sometimes not perfectly functional.”
In addition, she says, “Excellence in teaching and excellence in patient care require communication, and communication takes time. If physicians are up all night taking calls and then working all day so that there is continuity in patient care, you have to grapple with the issue of physician fatigue.”
And Then There Are Committees
Even though committee participation is technically considered “volunteer” time, physicians who are elected chiefs of their hospital sections are automatically expected to participate. It behooves hospitalists to participate in committee work at their institutions, believes Dr. Dallas, because this is often where governance decisions are made about how they will practice in the hospital.
Tom Baudendistel, MD, is associate residency program director at California Pacific Medical Center, a community-based hospital in San Francisco operated by Sutter Health. The hospitalists in his group are very involved in committee work. “The committees are important, and we want the administration to match our faces to our names, especially when it comes to budget negotiation time,” he explains. “That is a direct benefit of being visible participants in committees.”
Committee participation may be handled differently in purely academic settings. The time Dr. Rosenbloom spends in committees related to department support is credited to his work schedule. The problem comes when, once again, that participation takes more time than expected. One of his weekly committees routinely runs a half hour longer than its one-and-a-half hour time slot and requires five to eight hours of preparatory work. As is common with his peers, Dr. Rosenbloom has sometimes used his allotted consulting time to cover extra commitments related to his primary job.
Temptations to Say Yes
Invitations to participate in extra administrative or educational duties often naturally flow to productive people, observes Dr. Dallas. “You may be dragged into a lot of different work that you didn’t necessarily need to be into,” she says. “You just have to step back periodically and ask, ‘Is this right for me? Am I the right person to be involved? Are there other people who can do this? And then, say no. Really, that’s OK!” (See “Triage What’s Important,” p. 15, for tips.]
“It’s easy to get overloaded,” admits Dr. Baudendistel. “I certainly found myself overextended more often earlier in my career.” Saying yes to additional commitments can be related to workplace power dynamics, he believes. “When people who are in positions above you approach you about a project that is going to take time—whether or not it’s your passion or skill set—there is pressure to want to please that person. Saying no is a skill, and if you say ‘absolutely not’ early on in your career, you will not be asked to do other things. You may be shooting yourself in the foot.”
Defining Trails
It’s natural enough for hospitalists to feel optimistic about the openness of the future, says Dr. Hovan. Hospitalists may feel that the time investments they make now to nurture their profession within their institutions are temporary and may not always be as intense. The hope is that “the specialty is going to be more mature and [will] become more self-sustaining in the near future. Yet you glimpse over the horizon, and that’s not really true,” he says ruefully. “Everything in hospital medicine has nascency about it. There are no established trails. When we define one role, another one emerges.”
Many hospitalist services, for example, are now expanding beyond the medical floor to the surgical floor to perform consults to provide post-surgical management of medical issues.
Dr. McKean sees the “overwhelming demand for service” as one of hospital medicine’s trickiest challenges. “Basically, because hospitalists are young and energetic and wanting to please, it’s very easy for them to feel like they have to meet all the service obligations.” But this propensity can derail the overall mission of and vision for the hospitalist service if physicians do not set clear goals for themselves and their groups.
Physician, Know Thyself
Building in time to set and re-examine career goals is a skill that hospitalists should practice regularly, says Dr. McKean: “I learned the hard way that a hospitalist’s most important strategy is to be very self-reflective.”
She confesses that, in the past, she has often said yes to the point that her obligations became unmanageable. She advises young hospitalists to reflect on what is important to them and also “to recognize that during different times in their lives, they’re going to either have less free time or more free time, depending upon their families and other demands. So what might seem like a great opportunity might be an unrealistic one when you have three children under the age of five.” On the other hand, someone who is single might set a goal to make as much money as possible in the short term by taking on additional work shifts.
Dr. McKean also suggests that young hospitalists seek out not just one but multiple mentors. For example, “someone who wants to be a superstar in hospital medicine relating to quality improvement might naturally pick as a mentor somebody who is already doing quality improvement.”
A person who is having difficulty juggling family roles in addition to intensive work schedules might want to seek out someone who has … grappled successfully with those issues. Hospitalists should also consider seeking mentors outside the discipline of medicine—those in business, for instance, can contribute valuable insights to someone seeking a career in hospital administration.
Given the nature of hospital medicine, guarding one’s time will always be a concern, agree most of those interviewed for this article. “I think the juggling act is always there,” says Dr. Baudendistel. “There are usually up to six or more balls that you can simultaneously be juggling: administrative duties, family obligations, society commitments, teaching duties, your own academic agenda, and your professional agenda. You just have to know which ones are your priorities. And, sometimes, you have to acknowledge that maybe it’s time to say no or to stop doing one of those things.” TH
Contributing Writer Gretchen Henkel thanks the hospitalists who reshuffled their commitments in order to discuss overbooking with her and thanks her editor, Lisa Dionne, for the two extensions that allowed her to complete this assignment.
References
- Zauberman G, Lynch JG Jr. Resource slack and propensity to discount delayed investments of time versus money. J Exp Psychol Gen. 2005 Feb;134(1):23-37.
- Society of Hospital Medicine 2005-2006 Survey: State of the Hospital Medicine Movement. 2006. Available at: www.hospitalmedicine.org. Last accessed February 19, 2007.
There is never enough time, unless you’re serving it. —Malcolm Forbes (1919-1990)
Has this ever happened to you? You agree—months in advance—to write an article for The Hospitalist, thinking you will have plenty of time to research and write it. You hurriedly enter the item on your calendar and turn back to all your current commitments. Later, as the date approaches, you realize that you’re running out of time to do justice to the article to which you had committed.
Psychologists have explored the common human problem of overbooking and have found many contributing dynamics. A 2005 study in the Journal of Experimental Psychology suggested one explanation: Most of us, when accepting invitations weeks or months in advance, tend to view the future as more open and less busy than the present. “The nature of time fools us and we ‘forget’ about how things fill our days,” comment study authors Gal Zauberman and John Lynch.1
How do hospitalists weigh competing demands on their time? For answers to this question, naturally we asked several already-busy hospitalists to discuss the issue. They shared some lessons learned and a few strategies for managing their most precious commodity.
No Mystery
“Many things take longer than they’re supposed to,” points out S. Trent Rosenbloom, MD, MPH, a former hospitalist and currently assistant professor in the departments of Biomedical Informatics, Internal Medicine and Pediatrics, and the School of Nursing at Vanderbilt University Medical Center in Nashville, Tenn.
His situation on the morning of our interview necessitated a reschedule due to a longer-than-anticipated smog check the afternoon before. “I told myself, next year, I’ll take care of this before the deadline,” he says. “But I always end up doing this at the last minute because everything else gets in the way.”
“This interview is another example: overcommitting once more,” writes Michael J. Hovan, MD, when he agrees via e-mail to a telephone interview about the problem of overscheduling. Like most hospitalists, Dr. Hovan works with a perpetually full plate. He is inpatient director for the Hospital Family Medicine Service and assistant professor at Mayo Medical School in the Division of Family and Community Medicine at the Mayo Clinic in Scottsdale/Phoenix. Like his colleagues, Dr. Hovan has had to struggle with juggling multiple roles.
“The hospital is a far different practice environment than it was just a few years ago,” he remarks. The high intensity of patient management is now coupled with increasing administrative complexities due to a more heavily regulated environment.
As a relatively new specialty, hospital medicine requires more attention in order to establish its visibility and viability. Dr. Hovan feels this pressure keenly because, as a family medicine hospitalist, he’s in a minority position. (The majority of hospitalists trained in internal medicine, according to SHM’s 2006 Annual Survey.2)
“It’s even more important for my department, in a tertiary academic center, to maintain a visible presence on particular committees,” he says. The result of all these necessary roles? “There really are no weekends or defined time off,” says Dr. Hovan. “I’d estimate that 20% of what I do is done ‘off the clock.’ I have taken the Mayo computers to Hawaii, to family ski vacations, and [to] far less exotic locales away from the hospital setting.”
“Medicine Is Stressful”
Mary A. Dallas, MD, formerly medical director of the hospitalist service and currently medical information officer for Presbyterian Healthcare Services, an integrated healthcare delivery network in Albuquerque, N.M., noticed certain trends when she was creating schedules with the hospitalist group.
“Things sound really good on paper,” she says. “The reality is, the intensity of work is high, and sometimes you forget about that when you’re creating schedules. You might have set yourself up for three overnight shifts in order to compress work hours and expand off-time, and by the end of the second shift, you are really tired.”
Another factor is that employers expect hospitalists to see patients until the end of their shifts, and that’s when the off the clock paperwork occurs. A 40-hour workweek can easily balloon into 50 hours or more.
Physicians may also neglect to build in the emotional toll of their jobs when blocking in future schedules. “Medicine is stressful,” comments Sylvia C.W. McKean, MD, FACP, medical director, Brigham and Women’s Hospital/Faulkner Hospitalist Service in Boston. “It’s stressful to see people suffer and to deal with families who are stressed and sometimes not perfectly functional.”
In addition, she says, “Excellence in teaching and excellence in patient care require communication, and communication takes time. If physicians are up all night taking calls and then working all day so that there is continuity in patient care, you have to grapple with the issue of physician fatigue.”
And Then There Are Committees
Even though committee participation is technically considered “volunteer” time, physicians who are elected chiefs of their hospital sections are automatically expected to participate. It behooves hospitalists to participate in committee work at their institutions, believes Dr. Dallas, because this is often where governance decisions are made about how they will practice in the hospital.
Tom Baudendistel, MD, is associate residency program director at California Pacific Medical Center, a community-based hospital in San Francisco operated by Sutter Health. The hospitalists in his group are very involved in committee work. “The committees are important, and we want the administration to match our faces to our names, especially when it comes to budget negotiation time,” he explains. “That is a direct benefit of being visible participants in committees.”
Committee participation may be handled differently in purely academic settings. The time Dr. Rosenbloom spends in committees related to department support is credited to his work schedule. The problem comes when, once again, that participation takes more time than expected. One of his weekly committees routinely runs a half hour longer than its one-and-a-half hour time slot and requires five to eight hours of preparatory work. As is common with his peers, Dr. Rosenbloom has sometimes used his allotted consulting time to cover extra commitments related to his primary job.
Temptations to Say Yes
Invitations to participate in extra administrative or educational duties often naturally flow to productive people, observes Dr. Dallas. “You may be dragged into a lot of different work that you didn’t necessarily need to be into,” she says. “You just have to step back periodically and ask, ‘Is this right for me? Am I the right person to be involved? Are there other people who can do this? And then, say no. Really, that’s OK!” (See “Triage What’s Important,” p. 15, for tips.]
“It’s easy to get overloaded,” admits Dr. Baudendistel. “I certainly found myself overextended more often earlier in my career.” Saying yes to additional commitments can be related to workplace power dynamics, he believes. “When people who are in positions above you approach you about a project that is going to take time—whether or not it’s your passion or skill set—there is pressure to want to please that person. Saying no is a skill, and if you say ‘absolutely not’ early on in your career, you will not be asked to do other things. You may be shooting yourself in the foot.”
Defining Trails
It’s natural enough for hospitalists to feel optimistic about the openness of the future, says Dr. Hovan. Hospitalists may feel that the time investments they make now to nurture their profession within their institutions are temporary and may not always be as intense. The hope is that “the specialty is going to be more mature and [will] become more self-sustaining in the near future. Yet you glimpse over the horizon, and that’s not really true,” he says ruefully. “Everything in hospital medicine has nascency about it. There are no established trails. When we define one role, another one emerges.”
Many hospitalist services, for example, are now expanding beyond the medical floor to the surgical floor to perform consults to provide post-surgical management of medical issues.
Dr. McKean sees the “overwhelming demand for service” as one of hospital medicine’s trickiest challenges. “Basically, because hospitalists are young and energetic and wanting to please, it’s very easy for them to feel like they have to meet all the service obligations.” But this propensity can derail the overall mission of and vision for the hospitalist service if physicians do not set clear goals for themselves and their groups.
Physician, Know Thyself
Building in time to set and re-examine career goals is a skill that hospitalists should practice regularly, says Dr. McKean: “I learned the hard way that a hospitalist’s most important strategy is to be very self-reflective.”
She confesses that, in the past, she has often said yes to the point that her obligations became unmanageable. She advises young hospitalists to reflect on what is important to them and also “to recognize that during different times in their lives, they’re going to either have less free time or more free time, depending upon their families and other demands. So what might seem like a great opportunity might be an unrealistic one when you have three children under the age of five.” On the other hand, someone who is single might set a goal to make as much money as possible in the short term by taking on additional work shifts.
Dr. McKean also suggests that young hospitalists seek out not just one but multiple mentors. For example, “someone who wants to be a superstar in hospital medicine relating to quality improvement might naturally pick as a mentor somebody who is already doing quality improvement.”
A person who is having difficulty juggling family roles in addition to intensive work schedules might want to seek out someone who has … grappled successfully with those issues. Hospitalists should also consider seeking mentors outside the discipline of medicine—those in business, for instance, can contribute valuable insights to someone seeking a career in hospital administration.
Given the nature of hospital medicine, guarding one’s time will always be a concern, agree most of those interviewed for this article. “I think the juggling act is always there,” says Dr. Baudendistel. “There are usually up to six or more balls that you can simultaneously be juggling: administrative duties, family obligations, society commitments, teaching duties, your own academic agenda, and your professional agenda. You just have to know which ones are your priorities. And, sometimes, you have to acknowledge that maybe it’s time to say no or to stop doing one of those things.” TH
Contributing Writer Gretchen Henkel thanks the hospitalists who reshuffled their commitments in order to discuss overbooking with her and thanks her editor, Lisa Dionne, for the two extensions that allowed her to complete this assignment.
References
- Zauberman G, Lynch JG Jr. Resource slack and propensity to discount delayed investments of time versus money. J Exp Psychol Gen. 2005 Feb;134(1):23-37.
- Society of Hospital Medicine 2005-2006 Survey: State of the Hospital Medicine Movement. 2006. Available at: www.hospitalmedicine.org. Last accessed February 19, 2007.
There is never enough time, unless you’re serving it. —Malcolm Forbes (1919-1990)
Has this ever happened to you? You agree—months in advance—to write an article for The Hospitalist, thinking you will have plenty of time to research and write it. You hurriedly enter the item on your calendar and turn back to all your current commitments. Later, as the date approaches, you realize that you’re running out of time to do justice to the article to which you had committed.
Psychologists have explored the common human problem of overbooking and have found many contributing dynamics. A 2005 study in the Journal of Experimental Psychology suggested one explanation: Most of us, when accepting invitations weeks or months in advance, tend to view the future as more open and less busy than the present. “The nature of time fools us and we ‘forget’ about how things fill our days,” comment study authors Gal Zauberman and John Lynch.1
How do hospitalists weigh competing demands on their time? For answers to this question, naturally we asked several already-busy hospitalists to discuss the issue. They shared some lessons learned and a few strategies for managing their most precious commodity.
No Mystery
“Many things take longer than they’re supposed to,” points out S. Trent Rosenbloom, MD, MPH, a former hospitalist and currently assistant professor in the departments of Biomedical Informatics, Internal Medicine and Pediatrics, and the School of Nursing at Vanderbilt University Medical Center in Nashville, Tenn.
His situation on the morning of our interview necessitated a reschedule due to a longer-than-anticipated smog check the afternoon before. “I told myself, next year, I’ll take care of this before the deadline,” he says. “But I always end up doing this at the last minute because everything else gets in the way.”
“This interview is another example: overcommitting once more,” writes Michael J. Hovan, MD, when he agrees via e-mail to a telephone interview about the problem of overscheduling. Like most hospitalists, Dr. Hovan works with a perpetually full plate. He is inpatient director for the Hospital Family Medicine Service and assistant professor at Mayo Medical School in the Division of Family and Community Medicine at the Mayo Clinic in Scottsdale/Phoenix. Like his colleagues, Dr. Hovan has had to struggle with juggling multiple roles.
“The hospital is a far different practice environment than it was just a few years ago,” he remarks. The high intensity of patient management is now coupled with increasing administrative complexities due to a more heavily regulated environment.
As a relatively new specialty, hospital medicine requires more attention in order to establish its visibility and viability. Dr. Hovan feels this pressure keenly because, as a family medicine hospitalist, he’s in a minority position. (The majority of hospitalists trained in internal medicine, according to SHM’s 2006 Annual Survey.2)
“It’s even more important for my department, in a tertiary academic center, to maintain a visible presence on particular committees,” he says. The result of all these necessary roles? “There really are no weekends or defined time off,” says Dr. Hovan. “I’d estimate that 20% of what I do is done ‘off the clock.’ I have taken the Mayo computers to Hawaii, to family ski vacations, and [to] far less exotic locales away from the hospital setting.”
“Medicine Is Stressful”
Mary A. Dallas, MD, formerly medical director of the hospitalist service and currently medical information officer for Presbyterian Healthcare Services, an integrated healthcare delivery network in Albuquerque, N.M., noticed certain trends when she was creating schedules with the hospitalist group.
“Things sound really good on paper,” she says. “The reality is, the intensity of work is high, and sometimes you forget about that when you’re creating schedules. You might have set yourself up for three overnight shifts in order to compress work hours and expand off-time, and by the end of the second shift, you are really tired.”
Another factor is that employers expect hospitalists to see patients until the end of their shifts, and that’s when the off the clock paperwork occurs. A 40-hour workweek can easily balloon into 50 hours or more.
Physicians may also neglect to build in the emotional toll of their jobs when blocking in future schedules. “Medicine is stressful,” comments Sylvia C.W. McKean, MD, FACP, medical director, Brigham and Women’s Hospital/Faulkner Hospitalist Service in Boston. “It’s stressful to see people suffer and to deal with families who are stressed and sometimes not perfectly functional.”
In addition, she says, “Excellence in teaching and excellence in patient care require communication, and communication takes time. If physicians are up all night taking calls and then working all day so that there is continuity in patient care, you have to grapple with the issue of physician fatigue.”
And Then There Are Committees
Even though committee participation is technically considered “volunteer” time, physicians who are elected chiefs of their hospital sections are automatically expected to participate. It behooves hospitalists to participate in committee work at their institutions, believes Dr. Dallas, because this is often where governance decisions are made about how they will practice in the hospital.
Tom Baudendistel, MD, is associate residency program director at California Pacific Medical Center, a community-based hospital in San Francisco operated by Sutter Health. The hospitalists in his group are very involved in committee work. “The committees are important, and we want the administration to match our faces to our names, especially when it comes to budget negotiation time,” he explains. “That is a direct benefit of being visible participants in committees.”
Committee participation may be handled differently in purely academic settings. The time Dr. Rosenbloom spends in committees related to department support is credited to his work schedule. The problem comes when, once again, that participation takes more time than expected. One of his weekly committees routinely runs a half hour longer than its one-and-a-half hour time slot and requires five to eight hours of preparatory work. As is common with his peers, Dr. Rosenbloom has sometimes used his allotted consulting time to cover extra commitments related to his primary job.
Temptations to Say Yes
Invitations to participate in extra administrative or educational duties often naturally flow to productive people, observes Dr. Dallas. “You may be dragged into a lot of different work that you didn’t necessarily need to be into,” she says. “You just have to step back periodically and ask, ‘Is this right for me? Am I the right person to be involved? Are there other people who can do this? And then, say no. Really, that’s OK!” (See “Triage What’s Important,” p. 15, for tips.]
“It’s easy to get overloaded,” admits Dr. Baudendistel. “I certainly found myself overextended more often earlier in my career.” Saying yes to additional commitments can be related to workplace power dynamics, he believes. “When people who are in positions above you approach you about a project that is going to take time—whether or not it’s your passion or skill set—there is pressure to want to please that person. Saying no is a skill, and if you say ‘absolutely not’ early on in your career, you will not be asked to do other things. You may be shooting yourself in the foot.”
Defining Trails
It’s natural enough for hospitalists to feel optimistic about the openness of the future, says Dr. Hovan. Hospitalists may feel that the time investments they make now to nurture their profession within their institutions are temporary and may not always be as intense. The hope is that “the specialty is going to be more mature and [will] become more self-sustaining in the near future. Yet you glimpse over the horizon, and that’s not really true,” he says ruefully. “Everything in hospital medicine has nascency about it. There are no established trails. When we define one role, another one emerges.”
Many hospitalist services, for example, are now expanding beyond the medical floor to the surgical floor to perform consults to provide post-surgical management of medical issues.
Dr. McKean sees the “overwhelming demand for service” as one of hospital medicine’s trickiest challenges. “Basically, because hospitalists are young and energetic and wanting to please, it’s very easy for them to feel like they have to meet all the service obligations.” But this propensity can derail the overall mission of and vision for the hospitalist service if physicians do not set clear goals for themselves and their groups.
Physician, Know Thyself
Building in time to set and re-examine career goals is a skill that hospitalists should practice regularly, says Dr. McKean: “I learned the hard way that a hospitalist’s most important strategy is to be very self-reflective.”
She confesses that, in the past, she has often said yes to the point that her obligations became unmanageable. She advises young hospitalists to reflect on what is important to them and also “to recognize that during different times in their lives, they’re going to either have less free time or more free time, depending upon their families and other demands. So what might seem like a great opportunity might be an unrealistic one when you have three children under the age of five.” On the other hand, someone who is single might set a goal to make as much money as possible in the short term by taking on additional work shifts.
Dr. McKean also suggests that young hospitalists seek out not just one but multiple mentors. For example, “someone who wants to be a superstar in hospital medicine relating to quality improvement might naturally pick as a mentor somebody who is already doing quality improvement.”
A person who is having difficulty juggling family roles in addition to intensive work schedules might want to seek out someone who has … grappled successfully with those issues. Hospitalists should also consider seeking mentors outside the discipline of medicine—those in business, for instance, can contribute valuable insights to someone seeking a career in hospital administration.
Given the nature of hospital medicine, guarding one’s time will always be a concern, agree most of those interviewed for this article. “I think the juggling act is always there,” says Dr. Baudendistel. “There are usually up to six or more balls that you can simultaneously be juggling: administrative duties, family obligations, society commitments, teaching duties, your own academic agenda, and your professional agenda. You just have to know which ones are your priorities. And, sometimes, you have to acknowledge that maybe it’s time to say no or to stop doing one of those things.” TH
Contributing Writer Gretchen Henkel thanks the hospitalists who reshuffled their commitments in order to discuss overbooking with her and thanks her editor, Lisa Dionne, for the two extensions that allowed her to complete this assignment.
References
- Zauberman G, Lynch JG Jr. Resource slack and propensity to discount delayed investments of time versus money. J Exp Psychol Gen. 2005 Feb;134(1):23-37.
- Society of Hospital Medicine 2005-2006 Survey: State of the Hospital Medicine Movement. 2006. Available at: www.hospitalmedicine.org. Last accessed February 19, 2007.
Radiologic Images for Hospitalists

Patient History: A 68-year-old patient with systemic lupus erythematosus (SLE) has been referred for the evaluation of an asymptomatic right atrial mass found on an outside cardiac echocardiogram.
Salient findings: SSFGRE cardiac gated magnetic resonance and computed tomography of the heart with contrast demonstrate a large (3 cm x 4.5 cm) fusiform aneurysm of the right coronary artery (RCA). This should account for the atrial mass seen on the outside echocardiogram. Although there is marked circumferential mural thrombus (see horizontal arrows in Figs. 1 and 2, above), the vessel lumen is widely patent (see vertical arrows in Figs. 1 and 2, above), as evidenced by free flow of contrast within the center of the RCA.

Patient population and natural history of disease: Coronary artery aneurysms are defined as dilatation of the artery to greater than 1.5% to 2.0% of the normal artery diameter; however, they can be much larger. Coronary artery aneurysms are rare, occurring in 1.4 to 2.0% of the general population and in up to 5.3% of those undergoing cardiac catheterization. In North America, the most common etiology of coronary artery aneurysms is atherosclerosis. In Japan, the most common cause is likely Kawasaki disease. Other etiologies include congenital connective tissue diseases such as Marfan syndrome and Ehlers-Danlos syndrome, dissection, infections such as syphilis, vasculitis, and post-coronary intervention. The RCA is most commonly involved, followed by the left anterior descending artery (LAD). Consequences include thrombus formation and rupture with subsequent infarction, ischemia, and/or tamponade. SLE may be the culprit in this patient’s RCA aneurysm.
Management: Coronary artery aneurysms are often diagnosed incidentally, and rupture is rare. If symptoms of ischemia or impending rupture occur, bypass can be performed in selected patients. Some physicians advocate surgery in all patients with aneurysms that are greater than three to four times the normal native vessel diameter. Studies are limited, however, and treatment is often based on anecdotal evidence. Without symptoms and with a widely patent vessel lumen, as in this patient, many would advocate medical management with an antiplatelet +/- anticoagulant regimen. Some studies have shown an association of abdominal aortic aneurysm (AAA) in patients with coronary artery aneurysms and, therefore, advocate screening for AAA in these patients.
Take-home points:
- Coronary artery aneurysms are typically found incidentally, and rupture is rare;
- Surgery is indicated for symptoms of cardiac ischemia or in cases where there is concern for impending rupture; and
- Coronary artery aneurysms are associated with atherosclerosis, Kawasaki disease, connective tissue diseases, and post-coronary interventions. TH
Helena Summers is a radiology resident and Erik Summers is a hospitalist at the Mayo Clinic College of Medicine in Rochester, Minn.
References
- Collins MJ, Borges AJ, Singh G, et al. A giant coronary artery aneurysm in the right coronary artery. Cardiovasc Pathol. 2006 May-Jun;15(3):150-152.
- Mariscalco G, Mantovani V, Ferrarese S, et al. Coronary artery aneurysm: management and association with abdominal aortic aneurysm. Cardiovasc Pathol. 2006 Mar-Apr;15(2):100-104.
Patient History: A 68-year-old patient with systemic lupus erythematosus (SLE) has been referred for the evaluation of an asymptomatic right atrial mass found on an outside cardiac echocardiogram.
Salient findings: SSFGRE cardiac gated magnetic resonance and computed tomography of the heart with contrast demonstrate a large (3 cm x 4.5 cm) fusiform aneurysm of the right coronary artery (RCA). This should account for the atrial mass seen on the outside echocardiogram. Although there is marked circumferential mural thrombus (see horizontal arrows in Figs. 1 and 2, above), the vessel lumen is widely patent (see vertical arrows in Figs. 1 and 2, above), as evidenced by free flow of contrast within the center of the RCA.
Patient population and natural history of disease: Coronary artery aneurysms are defined as dilatation of the artery to greater than 1.5% to 2.0% of the normal artery diameter; however, they can be much larger. Coronary artery aneurysms are rare, occurring in 1.4 to 2.0% of the general population and in up to 5.3% of those undergoing cardiac catheterization. In North America, the most common etiology of coronary artery aneurysms is atherosclerosis. In Japan, the most common cause is likely Kawasaki disease. Other etiologies include congenital connective tissue diseases such as Marfan syndrome and Ehlers-Danlos syndrome, dissection, infections such as syphilis, vasculitis, and post-coronary intervention. The RCA is most commonly involved, followed by the left anterior descending artery (LAD). Consequences include thrombus formation and rupture with subsequent infarction, ischemia, and/or tamponade. SLE may be the culprit in this patient’s RCA aneurysm.
Management: Coronary artery aneurysms are often diagnosed incidentally, and rupture is rare. If symptoms of ischemia or impending rupture occur, bypass can be performed in selected patients. Some physicians advocate surgery in all patients with aneurysms that are greater than three to four times the normal native vessel diameter. Studies are limited, however, and treatment is often based on anecdotal evidence. Without symptoms and with a widely patent vessel lumen, as in this patient, many would advocate medical management with an antiplatelet +/- anticoagulant regimen. Some studies have shown an association of abdominal aortic aneurysm (AAA) in patients with coronary artery aneurysms and, therefore, advocate screening for AAA in these patients.
Take-home points:
- Coronary artery aneurysms are typically found incidentally, and rupture is rare;
- Surgery is indicated for symptoms of cardiac ischemia or in cases where there is concern for impending rupture; and
- Coronary artery aneurysms are associated with atherosclerosis, Kawasaki disease, connective tissue diseases, and post-coronary interventions. TH
Helena Summers is a radiology resident and Erik Summers is a hospitalist at the Mayo Clinic College of Medicine in Rochester, Minn.
References
- Collins MJ, Borges AJ, Singh G, et al. A giant coronary artery aneurysm in the right coronary artery. Cardiovasc Pathol. 2006 May-Jun;15(3):150-152.
- Mariscalco G, Mantovani V, Ferrarese S, et al. Coronary artery aneurysm: management and association with abdominal aortic aneurysm. Cardiovasc Pathol. 2006 Mar-Apr;15(2):100-104.
Patient History: A 68-year-old patient with systemic lupus erythematosus (SLE) has been referred for the evaluation of an asymptomatic right atrial mass found on an outside cardiac echocardiogram.
Salient findings: SSFGRE cardiac gated magnetic resonance and computed tomography of the heart with contrast demonstrate a large (3 cm x 4.5 cm) fusiform aneurysm of the right coronary artery (RCA). This should account for the atrial mass seen on the outside echocardiogram. Although there is marked circumferential mural thrombus (see horizontal arrows in Figs. 1 and 2, above), the vessel lumen is widely patent (see vertical arrows in Figs. 1 and 2, above), as evidenced by free flow of contrast within the center of the RCA.
Patient population and natural history of disease: Coronary artery aneurysms are defined as dilatation of the artery to greater than 1.5% to 2.0% of the normal artery diameter; however, they can be much larger. Coronary artery aneurysms are rare, occurring in 1.4 to 2.0% of the general population and in up to 5.3% of those undergoing cardiac catheterization. In North America, the most common etiology of coronary artery aneurysms is atherosclerosis. In Japan, the most common cause is likely Kawasaki disease. Other etiologies include congenital connective tissue diseases such as Marfan syndrome and Ehlers-Danlos syndrome, dissection, infections such as syphilis, vasculitis, and post-coronary intervention. The RCA is most commonly involved, followed by the left anterior descending artery (LAD). Consequences include thrombus formation and rupture with subsequent infarction, ischemia, and/or tamponade. SLE may be the culprit in this patient’s RCA aneurysm.
Management: Coronary artery aneurysms are often diagnosed incidentally, and rupture is rare. If symptoms of ischemia or impending rupture occur, bypass can be performed in selected patients. Some physicians advocate surgery in all patients with aneurysms that are greater than three to four times the normal native vessel diameter. Studies are limited, however, and treatment is often based on anecdotal evidence. Without symptoms and with a widely patent vessel lumen, as in this patient, many would advocate medical management with an antiplatelet +/- anticoagulant regimen. Some studies have shown an association of abdominal aortic aneurysm (AAA) in patients with coronary artery aneurysms and, therefore, advocate screening for AAA in these patients.
Take-home points:
- Coronary artery aneurysms are typically found incidentally, and rupture is rare;
- Surgery is indicated for symptoms of cardiac ischemia or in cases where there is concern for impending rupture; and
- Coronary artery aneurysms are associated with atherosclerosis, Kawasaki disease, connective tissue diseases, and post-coronary interventions. TH
Helena Summers is a radiology resident and Erik Summers is a hospitalist at the Mayo Clinic College of Medicine in Rochester, Minn.
References
- Collins MJ, Borges AJ, Singh G, et al. A giant coronary artery aneurysm in the right coronary artery. Cardiovasc Pathol. 2006 May-Jun;15(3):150-152.
- Mariscalco G, Mantovani V, Ferrarese S, et al. Coronary artery aneurysm: management and association with abdominal aortic aneurysm. Cardiovasc Pathol. 2006 Mar-Apr;15(2):100-104.
Federal Flu Fighters

Experts say that a pandemic flu outbreak will hit the United States—a pandemic large enough to stretch our healthcare resources to the breaking point and overwhelm hospitals.
“They say it’s not if, but when,” says James C. Pile, MD, FACP, Division of Hospital Medicine, Case Western Reserve University, MetroHealth Medical Center, Cleveland, Ohio, an infectious diseases specialist with a longstanding interest in bioterrorism/pandemic preparedness, and former editor of The Hospitalist.
Your Government at Work
The federal government is taking a lead role in preparing for this outbreak or outbreaks. President George W. Bush issued a National Strategy for Pandemic Influenza in November 2005, which focuses on measures to slow or stop the spread of a pandemic flu and on “sustaining infrastructure and mitigating impact to the economy and the functioning of society.”
That strategy charges the Department of Health and Human Services (HHS) with leading federal pandemic preparedness. The HHS is working with state and local agencies on planning and has made $600 million available for state and local preparedness efforts, including the exercising of pandemic plans across communities and at all levels of government.
Total congressional funding for pandemic flu preparedness, says Dr. Pile, is “somewhere in the neighborhood of $5 billion dollars.”
A Working Plan
In May 2006, President Bush released the Implementation Plan for the National Strategy, which stipulates more than 300 actions for federal departments and agencies and sets clear expectations for state and local governments. It also provides guidance for all federal departments and agencies on the development of their own plans.
The latest update on the Implementation Plan (released in December 2006) lists dozens of action items, including:
- The Department of Homeland Security will provide emergency response element training (e.g., incident management, triage, security, and communications) and provide assistance, when requested, to state, local, and public health entities within six months.
- HHS will work with state and local governments to develop protocols for the distribution of critical medical materials such as ventilators in times of medical emergency, also within six months.
- HHS will prepare guidance for local Medical Reserve Corps coordinators describing the role of the Corps during a pandemic. The Medical Reserve Corps comprises teams of local volunteer medical and public health professionals who can contribute their skills and expertise during times of need.
For the latest details on the Implementation Plan and the status of these and other action items, visit www.pandemicflu.gov.
Federal, State, and Local–A Crucial Mix
In addition to providing overall planning and support, says Dr. Pile, “the federal government will also be responsible for helping to supply assets to states and regions that may be overwhelmed” during a pandemic flu outbreak.
Specifically, the government oversees the Strategic National Stockpile (SNS) program, which manages large quantities of medicine and medical supplies. These materials are stockpiled, ready to use in the event of a public health emergency. When federal and local authorities agree that the SNS is needed, supplies will be delivered to any state within 12 hours. Each state has plans to distribute so-called push packs of medicine and medical supplies to affected communities as quickly as possible.
“I’m not sure the federal government will be able to reliably deliver these push packs in a timely manner in the event of a severe, multi-state pandemic,” says Dr. Pile. “During Hurricane Katrina, which certainly posed challenges different from a pandemic flu outbreak but also included a number of similarities, we saw the struggle of the national government to react quickly.” He believes that the stockpiles may not be adequate in a worst-case scenario, such as a pandemic flu on the scale of the 1918 flu epidemic.
“It’s clear there just aren’t enough mechanical ventilators in the country to provide adequate surge capacity in the event of a severe pandemic, with best estimates of 80,000 to 105,000 ventilators nationally, most of which are in use at any given time,” he says.
Another issue is how much help the federal government can actually provide in the event of a pandemic flu. “Some government agencies and individuals have stressed that if there is a really catastrophic national influenza pandemic, the cavalry is not necessarily going to be coming,” says Dr. Pile. “Individual hospitals and regions will very possibly need to rely on their intrinsic resources, at least initially.”
So when a pandemic flu outbreak begins, where can hospitals find support? “HHS will take the lead role at the federal level,” says Dr. Pile. “State departments of health will oversee the response for each state. And at the city and municipal level, it will vary.”
The Role of Hospitalists
At this point, while all levels of government are still shaping plans for handling pandemic flu, what should hospitalists do?
“Hopefully, they’re involved in planning within their own institutions and regionally,” says Dr. Pile. “If not, that’s a great role for them. However, a lot of the people involved in [pandemic flu response] planning are not familiar with hospitalists.”
Woodruff J. English II, MD, hospitalist and co-director of Hospitalist Program, Providence St. Vincent Medical Center, Portland, Ore., is in charge of emergency preparedness, including pandemic flu, for his institution. He worked with his state department of health and the CDC. After conducting a tabletop exercise, Providence St. Vincent Medical Center has a plan in place that includes a number of tents that can set up as triage space for admitting and screening patients, plans to secure the hospital against riots and looters, staffing issues, and much more. “We’re figuring out what questions to ask; I wouldn’t say we’re prepared,” says Dr. English. “We’re taking a careful look at how we do business.”
When a pandemic flu outbreak does occur, hospitalists throughout affected areas will definitely be involved.
“They’d play a front and center role,” speculates Dr. Pile. “Critical care would be rolled out of the critical care unit into other areas of the hospital. Clearly, there wouldn’t be enough critical care physicians, so hospitalists would have to step in.”
At this stage of the government’s Implementation Plan, your hospital medicine program may be called upon to help create your hospital’s preparedness plan for pandemic flu. If you haven’t been asked, check with your director or administrator to see if such a plan exists, perhaps as part of a general emergency preparedness plan.
With the support of the federal and state government, your hospital should be able to take some steps toward preparing for a major outbreak of pandemic flu. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
Experts say that a pandemic flu outbreak will hit the United States—a pandemic large enough to stretch our healthcare resources to the breaking point and overwhelm hospitals.
“They say it’s not if, but when,” says James C. Pile, MD, FACP, Division of Hospital Medicine, Case Western Reserve University, MetroHealth Medical Center, Cleveland, Ohio, an infectious diseases specialist with a longstanding interest in bioterrorism/pandemic preparedness, and former editor of The Hospitalist.
Your Government at Work
The federal government is taking a lead role in preparing for this outbreak or outbreaks. President George W. Bush issued a National Strategy for Pandemic Influenza in November 2005, which focuses on measures to slow or stop the spread of a pandemic flu and on “sustaining infrastructure and mitigating impact to the economy and the functioning of society.”
That strategy charges the Department of Health and Human Services (HHS) with leading federal pandemic preparedness. The HHS is working with state and local agencies on planning and has made $600 million available for state and local preparedness efforts, including the exercising of pandemic plans across communities and at all levels of government.
Total congressional funding for pandemic flu preparedness, says Dr. Pile, is “somewhere in the neighborhood of $5 billion dollars.”
A Working Plan
In May 2006, President Bush released the Implementation Plan for the National Strategy, which stipulates more than 300 actions for federal departments and agencies and sets clear expectations for state and local governments. It also provides guidance for all federal departments and agencies on the development of their own plans.
The latest update on the Implementation Plan (released in December 2006) lists dozens of action items, including:
- The Department of Homeland Security will provide emergency response element training (e.g., incident management, triage, security, and communications) and provide assistance, when requested, to state, local, and public health entities within six months.
- HHS will work with state and local governments to develop protocols for the distribution of critical medical materials such as ventilators in times of medical emergency, also within six months.
- HHS will prepare guidance for local Medical Reserve Corps coordinators describing the role of the Corps during a pandemic. The Medical Reserve Corps comprises teams of local volunteer medical and public health professionals who can contribute their skills and expertise during times of need.
For the latest details on the Implementation Plan and the status of these and other action items, visit www.pandemicflu.gov.
Federal, State, and Local–A Crucial Mix
In addition to providing overall planning and support, says Dr. Pile, “the federal government will also be responsible for helping to supply assets to states and regions that may be overwhelmed” during a pandemic flu outbreak.
Specifically, the government oversees the Strategic National Stockpile (SNS) program, which manages large quantities of medicine and medical supplies. These materials are stockpiled, ready to use in the event of a public health emergency. When federal and local authorities agree that the SNS is needed, supplies will be delivered to any state within 12 hours. Each state has plans to distribute so-called push packs of medicine and medical supplies to affected communities as quickly as possible.
“I’m not sure the federal government will be able to reliably deliver these push packs in a timely manner in the event of a severe, multi-state pandemic,” says Dr. Pile. “During Hurricane Katrina, which certainly posed challenges different from a pandemic flu outbreak but also included a number of similarities, we saw the struggle of the national government to react quickly.” He believes that the stockpiles may not be adequate in a worst-case scenario, such as a pandemic flu on the scale of the 1918 flu epidemic.
“It’s clear there just aren’t enough mechanical ventilators in the country to provide adequate surge capacity in the event of a severe pandemic, with best estimates of 80,000 to 105,000 ventilators nationally, most of which are in use at any given time,” he says.
Another issue is how much help the federal government can actually provide in the event of a pandemic flu. “Some government agencies and individuals have stressed that if there is a really catastrophic national influenza pandemic, the cavalry is not necessarily going to be coming,” says Dr. Pile. “Individual hospitals and regions will very possibly need to rely on their intrinsic resources, at least initially.”
So when a pandemic flu outbreak begins, where can hospitals find support? “HHS will take the lead role at the federal level,” says Dr. Pile. “State departments of health will oversee the response for each state. And at the city and municipal level, it will vary.”
The Role of Hospitalists
At this point, while all levels of government are still shaping plans for handling pandemic flu, what should hospitalists do?
“Hopefully, they’re involved in planning within their own institutions and regionally,” says Dr. Pile. “If not, that’s a great role for them. However, a lot of the people involved in [pandemic flu response] planning are not familiar with hospitalists.”
Woodruff J. English II, MD, hospitalist and co-director of Hospitalist Program, Providence St. Vincent Medical Center, Portland, Ore., is in charge of emergency preparedness, including pandemic flu, for his institution. He worked with his state department of health and the CDC. After conducting a tabletop exercise, Providence St. Vincent Medical Center has a plan in place that includes a number of tents that can set up as triage space for admitting and screening patients, plans to secure the hospital against riots and looters, staffing issues, and much more. “We’re figuring out what questions to ask; I wouldn’t say we’re prepared,” says Dr. English. “We’re taking a careful look at how we do business.”
When a pandemic flu outbreak does occur, hospitalists throughout affected areas will definitely be involved.
“They’d play a front and center role,” speculates Dr. Pile. “Critical care would be rolled out of the critical care unit into other areas of the hospital. Clearly, there wouldn’t be enough critical care physicians, so hospitalists would have to step in.”
At this stage of the government’s Implementation Plan, your hospital medicine program may be called upon to help create your hospital’s preparedness plan for pandemic flu. If you haven’t been asked, check with your director or administrator to see if such a plan exists, perhaps as part of a general emergency preparedness plan.
With the support of the federal and state government, your hospital should be able to take some steps toward preparing for a major outbreak of pandemic flu. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
Experts say that a pandemic flu outbreak will hit the United States—a pandemic large enough to stretch our healthcare resources to the breaking point and overwhelm hospitals.
“They say it’s not if, but when,” says James C. Pile, MD, FACP, Division of Hospital Medicine, Case Western Reserve University, MetroHealth Medical Center, Cleveland, Ohio, an infectious diseases specialist with a longstanding interest in bioterrorism/pandemic preparedness, and former editor of The Hospitalist.
Your Government at Work
The federal government is taking a lead role in preparing for this outbreak or outbreaks. President George W. Bush issued a National Strategy for Pandemic Influenza in November 2005, which focuses on measures to slow or stop the spread of a pandemic flu and on “sustaining infrastructure and mitigating impact to the economy and the functioning of society.”
That strategy charges the Department of Health and Human Services (HHS) with leading federal pandemic preparedness. The HHS is working with state and local agencies on planning and has made $600 million available for state and local preparedness efforts, including the exercising of pandemic plans across communities and at all levels of government.
Total congressional funding for pandemic flu preparedness, says Dr. Pile, is “somewhere in the neighborhood of $5 billion dollars.”
A Working Plan
In May 2006, President Bush released the Implementation Plan for the National Strategy, which stipulates more than 300 actions for federal departments and agencies and sets clear expectations for state and local governments. It also provides guidance for all federal departments and agencies on the development of their own plans.
The latest update on the Implementation Plan (released in December 2006) lists dozens of action items, including:
- The Department of Homeland Security will provide emergency response element training (e.g., incident management, triage, security, and communications) and provide assistance, when requested, to state, local, and public health entities within six months.
- HHS will work with state and local governments to develop protocols for the distribution of critical medical materials such as ventilators in times of medical emergency, also within six months.
- HHS will prepare guidance for local Medical Reserve Corps coordinators describing the role of the Corps during a pandemic. The Medical Reserve Corps comprises teams of local volunteer medical and public health professionals who can contribute their skills and expertise during times of need.
For the latest details on the Implementation Plan and the status of these and other action items, visit www.pandemicflu.gov.
Federal, State, and Local–A Crucial Mix
In addition to providing overall planning and support, says Dr. Pile, “the federal government will also be responsible for helping to supply assets to states and regions that may be overwhelmed” during a pandemic flu outbreak.
Specifically, the government oversees the Strategic National Stockpile (SNS) program, which manages large quantities of medicine and medical supplies. These materials are stockpiled, ready to use in the event of a public health emergency. When federal and local authorities agree that the SNS is needed, supplies will be delivered to any state within 12 hours. Each state has plans to distribute so-called push packs of medicine and medical supplies to affected communities as quickly as possible.
“I’m not sure the federal government will be able to reliably deliver these push packs in a timely manner in the event of a severe, multi-state pandemic,” says Dr. Pile. “During Hurricane Katrina, which certainly posed challenges different from a pandemic flu outbreak but also included a number of similarities, we saw the struggle of the national government to react quickly.” He believes that the stockpiles may not be adequate in a worst-case scenario, such as a pandemic flu on the scale of the 1918 flu epidemic.
“It’s clear there just aren’t enough mechanical ventilators in the country to provide adequate surge capacity in the event of a severe pandemic, with best estimates of 80,000 to 105,000 ventilators nationally, most of which are in use at any given time,” he says.
Another issue is how much help the federal government can actually provide in the event of a pandemic flu. “Some government agencies and individuals have stressed that if there is a really catastrophic national influenza pandemic, the cavalry is not necessarily going to be coming,” says Dr. Pile. “Individual hospitals and regions will very possibly need to rely on their intrinsic resources, at least initially.”
So when a pandemic flu outbreak begins, where can hospitals find support? “HHS will take the lead role at the federal level,” says Dr. Pile. “State departments of health will oversee the response for each state. And at the city and municipal level, it will vary.”
The Role of Hospitalists
At this point, while all levels of government are still shaping plans for handling pandemic flu, what should hospitalists do?
“Hopefully, they’re involved in planning within their own institutions and regionally,” says Dr. Pile. “If not, that’s a great role for them. However, a lot of the people involved in [pandemic flu response] planning are not familiar with hospitalists.”
Woodruff J. English II, MD, hospitalist and co-director of Hospitalist Program, Providence St. Vincent Medical Center, Portland, Ore., is in charge of emergency preparedness, including pandemic flu, for his institution. He worked with his state department of health and the CDC. After conducting a tabletop exercise, Providence St. Vincent Medical Center has a plan in place that includes a number of tents that can set up as triage space for admitting and screening patients, plans to secure the hospital against riots and looters, staffing issues, and much more. “We’re figuring out what questions to ask; I wouldn’t say we’re prepared,” says Dr. English. “We’re taking a careful look at how we do business.”
When a pandemic flu outbreak does occur, hospitalists throughout affected areas will definitely be involved.
“They’d play a front and center role,” speculates Dr. Pile. “Critical care would be rolled out of the critical care unit into other areas of the hospital. Clearly, there wouldn’t be enough critical care physicians, so hospitalists would have to step in.”
At this stage of the government’s Implementation Plan, your hospital medicine program may be called upon to help create your hospital’s preparedness plan for pandemic flu. If you haven’t been asked, check with your director or administrator to see if such a plan exists, perhaps as part of a general emergency preparedness plan.
With the support of the federal and state government, your hospital should be able to take some steps toward preparing for a major outbreak of pandemic flu. TH
Jane Jerrard writes “Public Policy” for The Hospitalist.
An Information Services Update

As I sit here brainstorming the latest and greatest news from SHM and the folks at Information Services, it surprised me to realize that I have been with SHM for exactly two years.
When I look back at some of our accomplishments—launching a brand new SHM Web site, creating six new Web-based resource rooms around specific disease states, launching an online career center for hospitalists, and opening a hospitalist legislative advocacy center—I can’t help but think about the talented people who have brought us this far and how they will make your experience with SHM even more valuable and exciting in the years to come.
Our interactive designer, Bruce Hansen, came to SHM with a variety of skills and life experiences, including time spent working with the Peace Corps in the Ukraine. Bruce is our ace Web guru at SHM, and not only is he responsible for SHM’s Web site, but he also leads the development of the resource rooms that many of our members have come to use as a resource in their daily professional lives. Through Bruce’s leadership and intense dedication to making our Web site as easy for each of you to use as possible, you will begin to see dramatic improvements in the format of SHM’s Web site homepage. Coming in the summer of 2007, we will also be launching improvements on how to navigate and move through the Web site, making it much easier to get to the information you need.
In the Web-sphere, cool graphics and easy-to-use links are important, but content is king, and that has been the primary focus of our project assistant, Lubna Manna. Lubna came to SHM with a background in creating programs for PDAs and phones, which she will be drawing from as SHM begins to introduce resources for iPods and other handheld devices. In addition to helping many of our members with questions about our Web site, Lubna has been working with the staff at SHM to find new and dynamic ways to present the information you need, when you need it, through our Web site. Understanding how many of you currently use our Web site has given us a glimpse into what matters most, and Lubna is finding ways to change how and where we deliver information via the Web to make sure it is easy for you to find the information you need.
Our most recent addition to the Information Services team, Travis Kamps, our Web production assistant, is a wizard of sorts when it comes to anything new or cool on the Web or in other technologies. Over the next couple of months, Travis will work hand in hand with Bruce to create resource rooms that are easier to use and provide you with ways to access these quality improvement resources, whether you are just starting out in QI or are an old pro. With Travis’ help and guidance, we will also begin to see how the Internet and SHM can foster an online community in which hospitalists can network, share ideas and questions, and create a collaborative environment from which all of our members can benefit.
Of course, in any organization, there are many things that go on behind the scenes that others don’t see or know about. Have you ever wondered where all the maintenance and support staff at Disneyworld work? Believe it or not, they are just below your feet as you stroll down Main Street. In Information Services, a lot of what we do is just below your feet or behind the scenes, but we are here, and we are dedicated to finding new, creative, and innovative ways to ensure that you get the biggest bang for your buck from your SHM membership.
In the coming months, you will see improvements to your membership experience through the Web site, at the 2007 Annual Meeting, and in the products and services that are all part of your SHM membership. We are always trying to find new ways to provide you with the resources you need to make a difference in your hospital and in the healthcare that you provide. With your help and support, I am confident that the next two years will be exciting and valuable to you. TH
As I sit here brainstorming the latest and greatest news from SHM and the folks at Information Services, it surprised me to realize that I have been with SHM for exactly two years.
When I look back at some of our accomplishments—launching a brand new SHM Web site, creating six new Web-based resource rooms around specific disease states, launching an online career center for hospitalists, and opening a hospitalist legislative advocacy center—I can’t help but think about the talented people who have brought us this far and how they will make your experience with SHM even more valuable and exciting in the years to come.
Our interactive designer, Bruce Hansen, came to SHM with a variety of skills and life experiences, including time spent working with the Peace Corps in the Ukraine. Bruce is our ace Web guru at SHM, and not only is he responsible for SHM’s Web site, but he also leads the development of the resource rooms that many of our members have come to use as a resource in their daily professional lives. Through Bruce’s leadership and intense dedication to making our Web site as easy for each of you to use as possible, you will begin to see dramatic improvements in the format of SHM’s Web site homepage. Coming in the summer of 2007, we will also be launching improvements on how to navigate and move through the Web site, making it much easier to get to the information you need.
In the Web-sphere, cool graphics and easy-to-use links are important, but content is king, and that has been the primary focus of our project assistant, Lubna Manna. Lubna came to SHM with a background in creating programs for PDAs and phones, which she will be drawing from as SHM begins to introduce resources for iPods and other handheld devices. In addition to helping many of our members with questions about our Web site, Lubna has been working with the staff at SHM to find new and dynamic ways to present the information you need, when you need it, through our Web site. Understanding how many of you currently use our Web site has given us a glimpse into what matters most, and Lubna is finding ways to change how and where we deliver information via the Web to make sure it is easy for you to find the information you need.
Our most recent addition to the Information Services team, Travis Kamps, our Web production assistant, is a wizard of sorts when it comes to anything new or cool on the Web or in other technologies. Over the next couple of months, Travis will work hand in hand with Bruce to create resource rooms that are easier to use and provide you with ways to access these quality improvement resources, whether you are just starting out in QI or are an old pro. With Travis’ help and guidance, we will also begin to see how the Internet and SHM can foster an online community in which hospitalists can network, share ideas and questions, and create a collaborative environment from which all of our members can benefit.
Of course, in any organization, there are many things that go on behind the scenes that others don’t see or know about. Have you ever wondered where all the maintenance and support staff at Disneyworld work? Believe it or not, they are just below your feet as you stroll down Main Street. In Information Services, a lot of what we do is just below your feet or behind the scenes, but we are here, and we are dedicated to finding new, creative, and innovative ways to ensure that you get the biggest bang for your buck from your SHM membership.
In the coming months, you will see improvements to your membership experience through the Web site, at the 2007 Annual Meeting, and in the products and services that are all part of your SHM membership. We are always trying to find new ways to provide you with the resources you need to make a difference in your hospital and in the healthcare that you provide. With your help and support, I am confident that the next two years will be exciting and valuable to you. TH
As I sit here brainstorming the latest and greatest news from SHM and the folks at Information Services, it surprised me to realize that I have been with SHM for exactly two years.
When I look back at some of our accomplishments—launching a brand new SHM Web site, creating six new Web-based resource rooms around specific disease states, launching an online career center for hospitalists, and opening a hospitalist legislative advocacy center—I can’t help but think about the talented people who have brought us this far and how they will make your experience with SHM even more valuable and exciting in the years to come.
Our interactive designer, Bruce Hansen, came to SHM with a variety of skills and life experiences, including time spent working with the Peace Corps in the Ukraine. Bruce is our ace Web guru at SHM, and not only is he responsible for SHM’s Web site, but he also leads the development of the resource rooms that many of our members have come to use as a resource in their daily professional lives. Through Bruce’s leadership and intense dedication to making our Web site as easy for each of you to use as possible, you will begin to see dramatic improvements in the format of SHM’s Web site homepage. Coming in the summer of 2007, we will also be launching improvements on how to navigate and move through the Web site, making it much easier to get to the information you need.
In the Web-sphere, cool graphics and easy-to-use links are important, but content is king, and that has been the primary focus of our project assistant, Lubna Manna. Lubna came to SHM with a background in creating programs for PDAs and phones, which she will be drawing from as SHM begins to introduce resources for iPods and other handheld devices. In addition to helping many of our members with questions about our Web site, Lubna has been working with the staff at SHM to find new and dynamic ways to present the information you need, when you need it, through our Web site. Understanding how many of you currently use our Web site has given us a glimpse into what matters most, and Lubna is finding ways to change how and where we deliver information via the Web to make sure it is easy for you to find the information you need.
Our most recent addition to the Information Services team, Travis Kamps, our Web production assistant, is a wizard of sorts when it comes to anything new or cool on the Web or in other technologies. Over the next couple of months, Travis will work hand in hand with Bruce to create resource rooms that are easier to use and provide you with ways to access these quality improvement resources, whether you are just starting out in QI or are an old pro. With Travis’ help and guidance, we will also begin to see how the Internet and SHM can foster an online community in which hospitalists can network, share ideas and questions, and create a collaborative environment from which all of our members can benefit.
Of course, in any organization, there are many things that go on behind the scenes that others don’t see or know about. Have you ever wondered where all the maintenance and support staff at Disneyworld work? Believe it or not, they are just below your feet as you stroll down Main Street. In Information Services, a lot of what we do is just below your feet or behind the scenes, but we are here, and we are dedicated to finding new, creative, and innovative ways to ensure that you get the biggest bang for your buck from your SHM membership.
In the coming months, you will see improvements to your membership experience through the Web site, at the 2007 Annual Meeting, and in the products and services that are all part of your SHM membership. We are always trying to find new ways to provide you with the resources you need to make a difference in your hospital and in the healthcare that you provide. With your help and support, I am confident that the next two years will be exciting and valuable to you. TH
Focus on Research

As hospital medicine progresses, it is important that our new specialty be seen as a true academic discipline—not just as a service specialty. Starting our own journal, the Journal of Hospital Medicine, in 2006 was an important step. While there are a growing number of hospitalist researchers around the country, it is important that SHM promote and support further development of researchers in hospital medicine.
This year, SHM’s research efforts will include the development of a wide research network, support for individual and organizational research initiatives, and a focus on strengthening the internal research organization. These efforts will necessarily be broad and will cut across and incorporate the efforts that are already underway in the areas of education and quality.
Goals for SHM Research Efforts
- Increase extramural research funding to SHM and its members;
- Contribute to the growing number of SHM members choosing the society for the career development and research opportunities it offers; and
- Improve visibility and credibility for SHM nationally (e.g., hospitalists in prominent academic leadership positions and on national panels).
The development of a wide research network will include the identification of researchers in the SHM membership with common research interests. A preliminary list has been generated from an e-mail sent to all SHM members in November 2006 promoting two NIH opportunities to study venous thromboembolism (VTE) and asking for a response from members interested in receiving similar information. A monthly grant opportunity bulletin is planned for release to this audience. As this Research Forum develops, a type of research dating service could match research interests and experience with those interested in funding such projects.
An important networking activity is finding ways to link academic and community sites. One possible mechanism to enable such collaboration is an Internet-based tool for abstracting information from a medical chart. The resulting data could be shared and used to validate quality measures, tailor therapies, or assess the prevalence of disease. Also, an inter-society Academic Summit is planned to investigate areas in which collaboration with other professional societies would be appropriate. Be sure to voice your opinions during the Special Interest Forum on Research at the 2007 Annual Meeting on May 24, 2007, in Dallas.
Support for individual and organizational research initiatives will take the form of identifying opportunities and showcasing more opportunities for research at national conferences and local meetings. By working closely to identify commonalities with the Hospital Quality and Patient Safety (HQPS) Committee around research, implementation, and education, this support is designed to be seamless and coordinated. Currently under consideration is the development of research pages on the SHM Web site to highlight ongoing research efforts, possibly including a searchable, online catalog or a database of research opportunities. As time allows, assistance with individual grant applications will be offered.
By focusing on strengthening the internal SHM research organization, an increasingly visible research committee will present a consistent message of support for research and will hopefully empower individual hospital researchers to access the resources of SHM in all possible ways, from using the resource rooms on the SHM Web site to reading the Journal of Hospital Medicine to attending chapter meetings. Strengthening the internal research infrastructure will extend the sphere of influence and raise the profile of SHM as hospitalists appear on national panels, co-authoring key papers, and participating in other research communities. Increased visibility will lead to more support for training, fellowships, and pilot grant programs for promising potential projects in high-priority areas such as health services, quality improvement, clinical epidemiologic studies (clinical trial, genomics, biomarkers), and educational and health technology research.
In 2007, expect to see a new emphasis on research at SHM. We’ll be busy developing funding streams to increase investment in promising researchers, particularly those whose projects may lead to grants and/or collaboration with other SHM researchers. Look for surveys designed to assess the unique academic and research needs of hospitalists and to find new opportunities to get involved in research at SHM conferences and the annual meeting. These efforts will be successful if they lead to an increase in the quality and the quantity of the dialogue around research in hospital medicine. Please contact Carolyn Brennan, director of Research Program Development, at [email protected] for more information or to get involved.
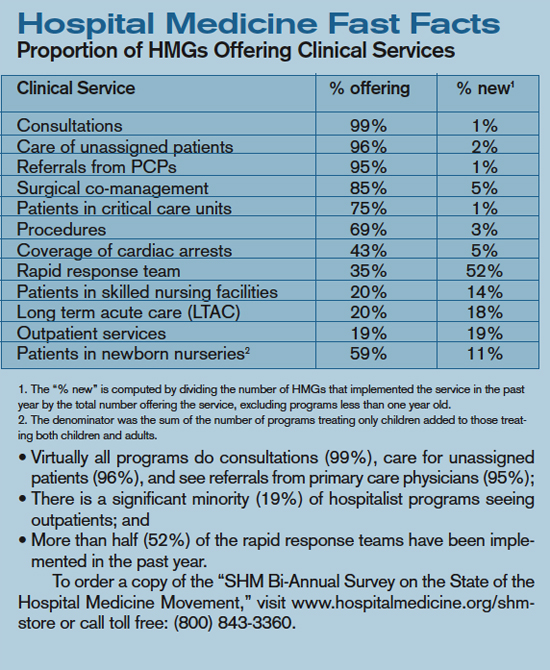
February Leadership Academy
SHM hosted another sold-out Level I Leadership Academy in sunny Orlando at the Gaylord Palms Resort and Convention Center. The meeting attracted more than 130 hospital medicine leaders who gathered to learn—among many things—how to evaluate personal leadership strengths and weaknesses and how to apply this knowledge to everyday leadership and management challenges.
Nationally respected speakers Mike Guthrie, MD; David Javitch, PhD; Jack Silversin, DMD; Tim Keogh, PhD; Eric Howell, MD; Larry Wellikson, MD; and Russell Holman, MD, led the group in discussions on a variety of different leadership topics. Dr. Keogh kept attendees intrigued by tackling the wide range of personality traits in the industry and instructing attendees in how to work effectively with others by using his DiSC survey. As always, the group was enthusiastic and worked collaboratively during Dr. Silversin’s infamous broken squares activity, in which attendees are involved in an eye-opening experience on effective communication.
“This is our fifth time hosting this course and, every time, I’m amazed to see how enthusiastic attendees are about what they have learned and how they plan to go back and improve their organizations,” says Dr. Holman, SHM Leadership Academy Course Director and president-elect of SHM.
Leadership Academy Level I is a great networking opportunity designed to provide leaders in hospital medicine with the tangible skills and resources required to successfully lead and manage hospitalist programs now and in the future. The intimate setting allows for small group sessions in which attendees have a chance to interact with faculty and share real-life situations from their own institutions. In addition to Level I, SHM will host the advanced course, Leadership Academy Level II, in the fall. This course will allow attendees to expand and enhance the skills learned in Level I and features keynote speaker Leonard Marcus, PhD, who defined the term “Meta-Leadership” in hospital medicine.
Don’t miss out on your chance to become a leader in hospital medicine. Mark your calendar for our next Leadership Academy, November 12-15, 2007, in San Antonio.
As hospital medicine progresses, it is important that our new specialty be seen as a true academic discipline—not just as a service specialty. Starting our own journal, the Journal of Hospital Medicine, in 2006 was an important step. While there are a growing number of hospitalist researchers around the country, it is important that SHM promote and support further development of researchers in hospital medicine.
This year, SHM’s research efforts will include the development of a wide research network, support for individual and organizational research initiatives, and a focus on strengthening the internal research organization. These efforts will necessarily be broad and will cut across and incorporate the efforts that are already underway in the areas of education and quality.
Goals for SHM Research Efforts
- Increase extramural research funding to SHM and its members;
- Contribute to the growing number of SHM members choosing the society for the career development and research opportunities it offers; and
- Improve visibility and credibility for SHM nationally (e.g., hospitalists in prominent academic leadership positions and on national panels).
The development of a wide research network will include the identification of researchers in the SHM membership with common research interests. A preliminary list has been generated from an e-mail sent to all SHM members in November 2006 promoting two NIH opportunities to study venous thromboembolism (VTE) and asking for a response from members interested in receiving similar information. A monthly grant opportunity bulletin is planned for release to this audience. As this Research Forum develops, a type of research dating service could match research interests and experience with those interested in funding such projects.
An important networking activity is finding ways to link academic and community sites. One possible mechanism to enable such collaboration is an Internet-based tool for abstracting information from a medical chart. The resulting data could be shared and used to validate quality measures, tailor therapies, or assess the prevalence of disease. Also, an inter-society Academic Summit is planned to investigate areas in which collaboration with other professional societies would be appropriate. Be sure to voice your opinions during the Special Interest Forum on Research at the 2007 Annual Meeting on May 24, 2007, in Dallas.
Support for individual and organizational research initiatives will take the form of identifying opportunities and showcasing more opportunities for research at national conferences and local meetings. By working closely to identify commonalities with the Hospital Quality and Patient Safety (HQPS) Committee around research, implementation, and education, this support is designed to be seamless and coordinated. Currently under consideration is the development of research pages on the SHM Web site to highlight ongoing research efforts, possibly including a searchable, online catalog or a database of research opportunities. As time allows, assistance with individual grant applications will be offered.
By focusing on strengthening the internal SHM research organization, an increasingly visible research committee will present a consistent message of support for research and will hopefully empower individual hospital researchers to access the resources of SHM in all possible ways, from using the resource rooms on the SHM Web site to reading the Journal of Hospital Medicine to attending chapter meetings. Strengthening the internal research infrastructure will extend the sphere of influence and raise the profile of SHM as hospitalists appear on national panels, co-authoring key papers, and participating in other research communities. Increased visibility will lead to more support for training, fellowships, and pilot grant programs for promising potential projects in high-priority areas such as health services, quality improvement, clinical epidemiologic studies (clinical trial, genomics, biomarkers), and educational and health technology research.
In 2007, expect to see a new emphasis on research at SHM. We’ll be busy developing funding streams to increase investment in promising researchers, particularly those whose projects may lead to grants and/or collaboration with other SHM researchers. Look for surveys designed to assess the unique academic and research needs of hospitalists and to find new opportunities to get involved in research at SHM conferences and the annual meeting. These efforts will be successful if they lead to an increase in the quality and the quantity of the dialogue around research in hospital medicine. Please contact Carolyn Brennan, director of Research Program Development, at [email protected] for more information or to get involved.
February Leadership Academy
SHM hosted another sold-out Level I Leadership Academy in sunny Orlando at the Gaylord Palms Resort and Convention Center. The meeting attracted more than 130 hospital medicine leaders who gathered to learn—among many things—how to evaluate personal leadership strengths and weaknesses and how to apply this knowledge to everyday leadership and management challenges.
Nationally respected speakers Mike Guthrie, MD; David Javitch, PhD; Jack Silversin, DMD; Tim Keogh, PhD; Eric Howell, MD; Larry Wellikson, MD; and Russell Holman, MD, led the group in discussions on a variety of different leadership topics. Dr. Keogh kept attendees intrigued by tackling the wide range of personality traits in the industry and instructing attendees in how to work effectively with others by using his DiSC survey. As always, the group was enthusiastic and worked collaboratively during Dr. Silversin’s infamous broken squares activity, in which attendees are involved in an eye-opening experience on effective communication.
“This is our fifth time hosting this course and, every time, I’m amazed to see how enthusiastic attendees are about what they have learned and how they plan to go back and improve their organizations,” says Dr. Holman, SHM Leadership Academy Course Director and president-elect of SHM.
Leadership Academy Level I is a great networking opportunity designed to provide leaders in hospital medicine with the tangible skills and resources required to successfully lead and manage hospitalist programs now and in the future. The intimate setting allows for small group sessions in which attendees have a chance to interact with faculty and share real-life situations from their own institutions. In addition to Level I, SHM will host the advanced course, Leadership Academy Level II, in the fall. This course will allow attendees to expand and enhance the skills learned in Level I and features keynote speaker Leonard Marcus, PhD, who defined the term “Meta-Leadership” in hospital medicine.
Don’t miss out on your chance to become a leader in hospital medicine. Mark your calendar for our next Leadership Academy, November 12-15, 2007, in San Antonio.
As hospital medicine progresses, it is important that our new specialty be seen as a true academic discipline—not just as a service specialty. Starting our own journal, the Journal of Hospital Medicine, in 2006 was an important step. While there are a growing number of hospitalist researchers around the country, it is important that SHM promote and support further development of researchers in hospital medicine.
This year, SHM’s research efforts will include the development of a wide research network, support for individual and organizational research initiatives, and a focus on strengthening the internal research organization. These efforts will necessarily be broad and will cut across and incorporate the efforts that are already underway in the areas of education and quality.
Goals for SHM Research Efforts
- Increase extramural research funding to SHM and its members;
- Contribute to the growing number of SHM members choosing the society for the career development and research opportunities it offers; and
- Improve visibility and credibility for SHM nationally (e.g., hospitalists in prominent academic leadership positions and on national panels).
The development of a wide research network will include the identification of researchers in the SHM membership with common research interests. A preliminary list has been generated from an e-mail sent to all SHM members in November 2006 promoting two NIH opportunities to study venous thromboembolism (VTE) and asking for a response from members interested in receiving similar information. A monthly grant opportunity bulletin is planned for release to this audience. As this Research Forum develops, a type of research dating service could match research interests and experience with those interested in funding such projects.
An important networking activity is finding ways to link academic and community sites. One possible mechanism to enable such collaboration is an Internet-based tool for abstracting information from a medical chart. The resulting data could be shared and used to validate quality measures, tailor therapies, or assess the prevalence of disease. Also, an inter-society Academic Summit is planned to investigate areas in which collaboration with other professional societies would be appropriate. Be sure to voice your opinions during the Special Interest Forum on Research at the 2007 Annual Meeting on May 24, 2007, in Dallas.
Support for individual and organizational research initiatives will take the form of identifying opportunities and showcasing more opportunities for research at national conferences and local meetings. By working closely to identify commonalities with the Hospital Quality and Patient Safety (HQPS) Committee around research, implementation, and education, this support is designed to be seamless and coordinated. Currently under consideration is the development of research pages on the SHM Web site to highlight ongoing research efforts, possibly including a searchable, online catalog or a database of research opportunities. As time allows, assistance with individual grant applications will be offered.
By focusing on strengthening the internal SHM research organization, an increasingly visible research committee will present a consistent message of support for research and will hopefully empower individual hospital researchers to access the resources of SHM in all possible ways, from using the resource rooms on the SHM Web site to reading the Journal of Hospital Medicine to attending chapter meetings. Strengthening the internal research infrastructure will extend the sphere of influence and raise the profile of SHM as hospitalists appear on national panels, co-authoring key papers, and participating in other research communities. Increased visibility will lead to more support for training, fellowships, and pilot grant programs for promising potential projects in high-priority areas such as health services, quality improvement, clinical epidemiologic studies (clinical trial, genomics, biomarkers), and educational and health technology research.
In 2007, expect to see a new emphasis on research at SHM. We’ll be busy developing funding streams to increase investment in promising researchers, particularly those whose projects may lead to grants and/or collaboration with other SHM researchers. Look for surveys designed to assess the unique academic and research needs of hospitalists and to find new opportunities to get involved in research at SHM conferences and the annual meeting. These efforts will be successful if they lead to an increase in the quality and the quantity of the dialogue around research in hospital medicine. Please contact Carolyn Brennan, director of Research Program Development, at [email protected] for more information or to get involved.
February Leadership Academy
SHM hosted another sold-out Level I Leadership Academy in sunny Orlando at the Gaylord Palms Resort and Convention Center. The meeting attracted more than 130 hospital medicine leaders who gathered to learn—among many things—how to evaluate personal leadership strengths and weaknesses and how to apply this knowledge to everyday leadership and management challenges.
Nationally respected speakers Mike Guthrie, MD; David Javitch, PhD; Jack Silversin, DMD; Tim Keogh, PhD; Eric Howell, MD; Larry Wellikson, MD; and Russell Holman, MD, led the group in discussions on a variety of different leadership topics. Dr. Keogh kept attendees intrigued by tackling the wide range of personality traits in the industry and instructing attendees in how to work effectively with others by using his DiSC survey. As always, the group was enthusiastic and worked collaboratively during Dr. Silversin’s infamous broken squares activity, in which attendees are involved in an eye-opening experience on effective communication.
“This is our fifth time hosting this course and, every time, I’m amazed to see how enthusiastic attendees are about what they have learned and how they plan to go back and improve their organizations,” says Dr. Holman, SHM Leadership Academy Course Director and president-elect of SHM.
Leadership Academy Level I is a great networking opportunity designed to provide leaders in hospital medicine with the tangible skills and resources required to successfully lead and manage hospitalist programs now and in the future. The intimate setting allows for small group sessions in which attendees have a chance to interact with faculty and share real-life situations from their own institutions. In addition to Level I, SHM will host the advanced course, Leadership Academy Level II, in the fall. This course will allow attendees to expand and enhance the skills learned in Level I and features keynote speaker Leonard Marcus, PhD, who defined the term “Meta-Leadership” in hospital medicine.
Don’t miss out on your chance to become a leader in hospital medicine. Mark your calendar for our next Leadership Academy, November 12-15, 2007, in San Antonio.