User login
Aesculapius, My Story

My father was a god; my grandfather was a god. My aunt killed my mother, and my grandfather plans on killing me. I guess you might call us a dysfunctional family. Some people also say I am a god, but I don’t see it that way. There’s no accounting for what people believe in. The ancient Greeks and Romans liked to make up stories about me; sometimes even I am not sure what is truth and what is fiction. I thought I’d take this chance to tell you about myself. If you are a modern-day proponent of the healing arts, perhaps you will find this of interest.
Dear Old Dad
My father was Apollo, son of Jupiter. He wasn’t a great dad; he was more interested in his godly duties and romantic liaisons than in my upbringing. My mother was a nymph named Coronis. I never met her. She was obviously beautiful and alluring; it’s a nymph thing. She met Apollo, and they spent many happy days in the olive groves. I was conceived on a beautiful hillside above the Aegean Sea.
Apollo soon lost interest in Coronis; he was busy with the family business: causing plagues, driving the chariot of fire across the sky, and so on. Coronis discovered she was pregnant and met a heroic mortal, Ischys; together, they tried to start a new life. There was no way Apollo was going to go along with this. No one leaves a god; it’s supposed to be the other way around. Apollo killed the mortal Ischys and had his sister Diana shoot an arrow into Coronis’ heart. As my mother’s body burned on a funeral pyre, Apollo had a fit of remorse and cut me from my mother’s womb—the first of what would eventually be called cesarean sections. Welcome to my life.

The Early Years
My home was on Mount Pelion. Chiron, a centaur, was my nanny and mentor. He was an expert hunter and was well versed in medicine and music. He was always horsing around. His daughter, Ocyrhoe, prophesied that I would become a great healer; with my heritage, it seemed a safe bet. When Chiron died, years later, Jupiter placed him in the sky; you might recognize him as Sagittarius. One day, millennia later, a company would take his name and would have trouble making influenza vaccine. I grew up under his tutelage and, in time, became an adequate healer myself.
The Wife and Kids
When I grew older, it was time to take a wife. I found a woman with an interest in botanicals. Her name was Epione. We had many children together, but things eroded in our relationship after that. It might have been a postpartum thing, or maybe I spent too much time at work. I’ll never know. She became more interested in soporifics—mandrake especially. She started spending a lot of time in her cave. She and Bacchus were always sitting around our home partying and listening to Pluto’s underworld band, The Dead, and enjoying their favorite song, “The Deadly Nightshade.”
I did pretty well with my children; they all went into the family healing business. My first daughter was named Hygeia. She was always by my side and a great help in my practice. She specialized in preventing disease. My second daughter was Panacea. She was pretty good with a cure and was always in high demand. She started hanging around with some chick named Placebo. Her name in Latin means “I will please,” and she always did. Two of my sons, Machaon and Podalirius, became naval surgeons; one was wounded at Troy but survived. My third son, Telosophorus, was born a dwarf and specialized in rehabilitation.
Things Take a Turn for the Worse
Life was going pretty well until I was lured into the shadowy realms of life and death. I had always believed that if the gods decided a patient was to get better, then I must use my skill to aid in this endeavor. If the Fates had decreed a patient was to die, there was little I could do against the will of the gods. Then events occurred that would enable me to take things to a whole new level, and—once again—it was because of sex.
Theseus was the king of Athens. He became king when his father committed suicide, thinking wrongly that Theseus was dead. This was not an auspicious start for a ruler. When Theseus’ first wife died, he married the princess Phaedra, daughter of the Cretan King Minos—a truly freaky chick. Theseus had a grown son, Hippolytus, who had rugged good looks and a bright future, a real stud. Phaedra decided Hippolytus would be a better husband for her than his father, but Hippolytus spurned her advances. Phaedra, in her wrath, turned Theseus against his son. Theseus used his own godly contacts and convinced Neptune to deal with Hippolytus. While Hippolytus was driving a chariot along a coastal road, Neptune set a sea monster to rise up from the ocean, scaring Theseus’ horse, which led to a fatal crash.
The goddess Diana, my aunt, came to me and taught me the secret to reviving the dead. Don’t expect me to share it with you. No “see one, do one, teach one” from me. I’ll just say it involves very small thunderbolts. I would have been better off without the knowledge. Using the new technique, I revived Hippolytus, who spent the rest of his days in Italy with a water nymph named Egeria. Not a bad afterlife. My trouble, on the other hand, had just begun. Pluto, god of the underworld, was furious. He thought no man should remove the dead from his realm. It was a classic turf battle, and I lost. Jupiter, my grandfather, was forced to put me to death with a thunderbolt.
Life after Death
My name lived on. The earliest places of healing were temples of Aesculapius; the Iatros, who worked there, were the earliest physicians. Yes, they did make me a god, but it’s not like I could stop them. On the island of Kós, my thousandth grandson was named Hippocrates—you may have heard of him. Another of my descendants, Galen, trained at my temple in Pergamon.
It’s been a few thousand years since all of this happened. Don’t ask how you can be reading my words—it’s a mythology thing. Things did not go well for Apollo after I died. When he heard I had been killed, my father lost his temper and took out his wrath on the cyclops who had made Jupiter’s thunderbolts on Mount Aetna. His punishment for that temper tantrum was to serve a mortal, Admetus, for a year. Admetus fell ill; near death, he convinced Apollo to appeal to the Fates. They agreed that someone would take his place. Nobody in the kingdom volunteered for this duty, not even his elderly parents. Finally his wife Alcestis volunteered, and her fate was set. When Death came for her, Hercules, who was passing through, seized Death and would not let him go until she was spared.
Lessons from the Past
You, the modern hospitalist, may read this tale and wonder what it has to do with modern-day medicine and why it is in this publication. Perhaps the Fates have had their way with the medical editor—hence this topic in this publication. Some parts of the tale are of etymological interest: Panacea, Hygeia, Iatros, Aesculapius, Chiron, and Aetna, to name a few. The bigger issue is the question of how your medical forefathers looked at life and death. Perhaps a patient might be healed, but if not, it was the gods’ will. Death was not easily cheated. Ademetus was saved by his wife’s sacrifice; she was willing to donate her life for his. There is something in this tale about futile resuscitation as well. And of course, the most important message: It never pays to get involved in sex or politics. TH
Dr. Newman is the physician editor of The Hospitalist. He’s also consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine, Rochester, Minn.
My father was a god; my grandfather was a god. My aunt killed my mother, and my grandfather plans on killing me. I guess you might call us a dysfunctional family. Some people also say I am a god, but I don’t see it that way. There’s no accounting for what people believe in. The ancient Greeks and Romans liked to make up stories about me; sometimes even I am not sure what is truth and what is fiction. I thought I’d take this chance to tell you about myself. If you are a modern-day proponent of the healing arts, perhaps you will find this of interest.
Dear Old Dad
My father was Apollo, son of Jupiter. He wasn’t a great dad; he was more interested in his godly duties and romantic liaisons than in my upbringing. My mother was a nymph named Coronis. I never met her. She was obviously beautiful and alluring; it’s a nymph thing. She met Apollo, and they spent many happy days in the olive groves. I was conceived on a beautiful hillside above the Aegean Sea.
Apollo soon lost interest in Coronis; he was busy with the family business: causing plagues, driving the chariot of fire across the sky, and so on. Coronis discovered she was pregnant and met a heroic mortal, Ischys; together, they tried to start a new life. There was no way Apollo was going to go along with this. No one leaves a god; it’s supposed to be the other way around. Apollo killed the mortal Ischys and had his sister Diana shoot an arrow into Coronis’ heart. As my mother’s body burned on a funeral pyre, Apollo had a fit of remorse and cut me from my mother’s womb—the first of what would eventually be called cesarean sections. Welcome to my life.
The Early Years
My home was on Mount Pelion. Chiron, a centaur, was my nanny and mentor. He was an expert hunter and was well versed in medicine and music. He was always horsing around. His daughter, Ocyrhoe, prophesied that I would become a great healer; with my heritage, it seemed a safe bet. When Chiron died, years later, Jupiter placed him in the sky; you might recognize him as Sagittarius. One day, millennia later, a company would take his name and would have trouble making influenza vaccine. I grew up under his tutelage and, in time, became an adequate healer myself.
The Wife and Kids
When I grew older, it was time to take a wife. I found a woman with an interest in botanicals. Her name was Epione. We had many children together, but things eroded in our relationship after that. It might have been a postpartum thing, or maybe I spent too much time at work. I’ll never know. She became more interested in soporifics—mandrake especially. She started spending a lot of time in her cave. She and Bacchus were always sitting around our home partying and listening to Pluto’s underworld band, The Dead, and enjoying their favorite song, “The Deadly Nightshade.”
I did pretty well with my children; they all went into the family healing business. My first daughter was named Hygeia. She was always by my side and a great help in my practice. She specialized in preventing disease. My second daughter was Panacea. She was pretty good with a cure and was always in high demand. She started hanging around with some chick named Placebo. Her name in Latin means “I will please,” and she always did. Two of my sons, Machaon and Podalirius, became naval surgeons; one was wounded at Troy but survived. My third son, Telosophorus, was born a dwarf and specialized in rehabilitation.
Things Take a Turn for the Worse
Life was going pretty well until I was lured into the shadowy realms of life and death. I had always believed that if the gods decided a patient was to get better, then I must use my skill to aid in this endeavor. If the Fates had decreed a patient was to die, there was little I could do against the will of the gods. Then events occurred that would enable me to take things to a whole new level, and—once again—it was because of sex.
Theseus was the king of Athens. He became king when his father committed suicide, thinking wrongly that Theseus was dead. This was not an auspicious start for a ruler. When Theseus’ first wife died, he married the princess Phaedra, daughter of the Cretan King Minos—a truly freaky chick. Theseus had a grown son, Hippolytus, who had rugged good looks and a bright future, a real stud. Phaedra decided Hippolytus would be a better husband for her than his father, but Hippolytus spurned her advances. Phaedra, in her wrath, turned Theseus against his son. Theseus used his own godly contacts and convinced Neptune to deal with Hippolytus. While Hippolytus was driving a chariot along a coastal road, Neptune set a sea monster to rise up from the ocean, scaring Theseus’ horse, which led to a fatal crash.
The goddess Diana, my aunt, came to me and taught me the secret to reviving the dead. Don’t expect me to share it with you. No “see one, do one, teach one” from me. I’ll just say it involves very small thunderbolts. I would have been better off without the knowledge. Using the new technique, I revived Hippolytus, who spent the rest of his days in Italy with a water nymph named Egeria. Not a bad afterlife. My trouble, on the other hand, had just begun. Pluto, god of the underworld, was furious. He thought no man should remove the dead from his realm. It was a classic turf battle, and I lost. Jupiter, my grandfather, was forced to put me to death with a thunderbolt.
Life after Death
My name lived on. The earliest places of healing were temples of Aesculapius; the Iatros, who worked there, were the earliest physicians. Yes, they did make me a god, but it’s not like I could stop them. On the island of Kós, my thousandth grandson was named Hippocrates—you may have heard of him. Another of my descendants, Galen, trained at my temple in Pergamon.
It’s been a few thousand years since all of this happened. Don’t ask how you can be reading my words—it’s a mythology thing. Things did not go well for Apollo after I died. When he heard I had been killed, my father lost his temper and took out his wrath on the cyclops who had made Jupiter’s thunderbolts on Mount Aetna. His punishment for that temper tantrum was to serve a mortal, Admetus, for a year. Admetus fell ill; near death, he convinced Apollo to appeal to the Fates. They agreed that someone would take his place. Nobody in the kingdom volunteered for this duty, not even his elderly parents. Finally his wife Alcestis volunteered, and her fate was set. When Death came for her, Hercules, who was passing through, seized Death and would not let him go until she was spared.
Lessons from the Past
You, the modern hospitalist, may read this tale and wonder what it has to do with modern-day medicine and why it is in this publication. Perhaps the Fates have had their way with the medical editor—hence this topic in this publication. Some parts of the tale are of etymological interest: Panacea, Hygeia, Iatros, Aesculapius, Chiron, and Aetna, to name a few. The bigger issue is the question of how your medical forefathers looked at life and death. Perhaps a patient might be healed, but if not, it was the gods’ will. Death was not easily cheated. Ademetus was saved by his wife’s sacrifice; she was willing to donate her life for his. There is something in this tale about futile resuscitation as well. And of course, the most important message: It never pays to get involved in sex or politics. TH
Dr. Newman is the physician editor of The Hospitalist. He’s also consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine, Rochester, Minn.
My father was a god; my grandfather was a god. My aunt killed my mother, and my grandfather plans on killing me. I guess you might call us a dysfunctional family. Some people also say I am a god, but I don’t see it that way. There’s no accounting for what people believe in. The ancient Greeks and Romans liked to make up stories about me; sometimes even I am not sure what is truth and what is fiction. I thought I’d take this chance to tell you about myself. If you are a modern-day proponent of the healing arts, perhaps you will find this of interest.
Dear Old Dad
My father was Apollo, son of Jupiter. He wasn’t a great dad; he was more interested in his godly duties and romantic liaisons than in my upbringing. My mother was a nymph named Coronis. I never met her. She was obviously beautiful and alluring; it’s a nymph thing. She met Apollo, and they spent many happy days in the olive groves. I was conceived on a beautiful hillside above the Aegean Sea.
Apollo soon lost interest in Coronis; he was busy with the family business: causing plagues, driving the chariot of fire across the sky, and so on. Coronis discovered she was pregnant and met a heroic mortal, Ischys; together, they tried to start a new life. There was no way Apollo was going to go along with this. No one leaves a god; it’s supposed to be the other way around. Apollo killed the mortal Ischys and had his sister Diana shoot an arrow into Coronis’ heart. As my mother’s body burned on a funeral pyre, Apollo had a fit of remorse and cut me from my mother’s womb—the first of what would eventually be called cesarean sections. Welcome to my life.
The Early Years
My home was on Mount Pelion. Chiron, a centaur, was my nanny and mentor. He was an expert hunter and was well versed in medicine and music. He was always horsing around. His daughter, Ocyrhoe, prophesied that I would become a great healer; with my heritage, it seemed a safe bet. When Chiron died, years later, Jupiter placed him in the sky; you might recognize him as Sagittarius. One day, millennia later, a company would take his name and would have trouble making influenza vaccine. I grew up under his tutelage and, in time, became an adequate healer myself.
The Wife and Kids
When I grew older, it was time to take a wife. I found a woman with an interest in botanicals. Her name was Epione. We had many children together, but things eroded in our relationship after that. It might have been a postpartum thing, or maybe I spent too much time at work. I’ll never know. She became more interested in soporifics—mandrake especially. She started spending a lot of time in her cave. She and Bacchus were always sitting around our home partying and listening to Pluto’s underworld band, The Dead, and enjoying their favorite song, “The Deadly Nightshade.”
I did pretty well with my children; they all went into the family healing business. My first daughter was named Hygeia. She was always by my side and a great help in my practice. She specialized in preventing disease. My second daughter was Panacea. She was pretty good with a cure and was always in high demand. She started hanging around with some chick named Placebo. Her name in Latin means “I will please,” and she always did. Two of my sons, Machaon and Podalirius, became naval surgeons; one was wounded at Troy but survived. My third son, Telosophorus, was born a dwarf and specialized in rehabilitation.
Things Take a Turn for the Worse
Life was going pretty well until I was lured into the shadowy realms of life and death. I had always believed that if the gods decided a patient was to get better, then I must use my skill to aid in this endeavor. If the Fates had decreed a patient was to die, there was little I could do against the will of the gods. Then events occurred that would enable me to take things to a whole new level, and—once again—it was because of sex.
Theseus was the king of Athens. He became king when his father committed suicide, thinking wrongly that Theseus was dead. This was not an auspicious start for a ruler. When Theseus’ first wife died, he married the princess Phaedra, daughter of the Cretan King Minos—a truly freaky chick. Theseus had a grown son, Hippolytus, who had rugged good looks and a bright future, a real stud. Phaedra decided Hippolytus would be a better husband for her than his father, but Hippolytus spurned her advances. Phaedra, in her wrath, turned Theseus against his son. Theseus used his own godly contacts and convinced Neptune to deal with Hippolytus. While Hippolytus was driving a chariot along a coastal road, Neptune set a sea monster to rise up from the ocean, scaring Theseus’ horse, which led to a fatal crash.
The goddess Diana, my aunt, came to me and taught me the secret to reviving the dead. Don’t expect me to share it with you. No “see one, do one, teach one” from me. I’ll just say it involves very small thunderbolts. I would have been better off without the knowledge. Using the new technique, I revived Hippolytus, who spent the rest of his days in Italy with a water nymph named Egeria. Not a bad afterlife. My trouble, on the other hand, had just begun. Pluto, god of the underworld, was furious. He thought no man should remove the dead from his realm. It was a classic turf battle, and I lost. Jupiter, my grandfather, was forced to put me to death with a thunderbolt.
Life after Death
My name lived on. The earliest places of healing were temples of Aesculapius; the Iatros, who worked there, were the earliest physicians. Yes, they did make me a god, but it’s not like I could stop them. On the island of Kós, my thousandth grandson was named Hippocrates—you may have heard of him. Another of my descendants, Galen, trained at my temple in Pergamon.
It’s been a few thousand years since all of this happened. Don’t ask how you can be reading my words—it’s a mythology thing. Things did not go well for Apollo after I died. When he heard I had been killed, my father lost his temper and took out his wrath on the cyclops who had made Jupiter’s thunderbolts on Mount Aetna. His punishment for that temper tantrum was to serve a mortal, Admetus, for a year. Admetus fell ill; near death, he convinced Apollo to appeal to the Fates. They agreed that someone would take his place. Nobody in the kingdom volunteered for this duty, not even his elderly parents. Finally his wife Alcestis volunteered, and her fate was set. When Death came for her, Hercules, who was passing through, seized Death and would not let him go until she was spared.
Lessons from the Past
You, the modern hospitalist, may read this tale and wonder what it has to do with modern-day medicine and why it is in this publication. Perhaps the Fates have had their way with the medical editor—hence this topic in this publication. Some parts of the tale are of etymological interest: Panacea, Hygeia, Iatros, Aesculapius, Chiron, and Aetna, to name a few. The bigger issue is the question of how your medical forefathers looked at life and death. Perhaps a patient might be healed, but if not, it was the gods’ will. Death was not easily cheated. Ademetus was saved by his wife’s sacrifice; she was willing to donate her life for his. There is something in this tale about futile resuscitation as well. And of course, the most important message: It never pays to get involved in sex or politics. TH
Dr. Newman is the physician editor of The Hospitalist. He’s also consultant, Hospital Internal Medicine, and assistant professor of internal medicine and medical history, Mayo Clinic College of Medicine, Rochester, Minn.
The Vacation Conundrum

The vacation conundrum most people face has to do with things like whether to drive or fly, or whether to sleep on the ground or in a hotel. But some hospitalists encounter tricky problems when figuring out how to operationalize their contractual provision for vacation time.
What is the Vacation Conundrum?
I’m a big believer in hospitalists having liberal amounts of time off, but I think most practices should avoid contractually specifying vacation time. This may sound contradictory and terribly unfair to the doctor. But avoiding a contractual guarantee of vacation time doesn’t mean the hospitalist gets any less time off. And the way hospitalist contracts address vacation time has gotten a lot of organizations in trouble. Let me explain.
Contracts often stipulate that a hospitalist will have a specified number of weeks of vacation time annually, and this language has usually been taken from the organization’s existing contracts with other physicians. But confusion often arises some time after the hospitalist practice is up and running. One big problem is deciding who will cover for the hospitalist on vacation. If all doctors work extra shifts to cover for a member of the practice who is on vacation, they will all take turns working extra—a practice that negates the effect of the promised holiday. Another problem is that most hospitalists follow non-traditional work schedules, making it difficult to determine which of the days not worked are vacation days and which are days the doctor just wasn’t scheduled to work.
To better understand this issue, it is worth thinking about how most hospitalist schedules differ from that of a typical office-based doctor or businessperson. Someone in business is usually expected to work every Monday through Friday of the year—except government holidays. Those weekdays that the business person doesn’t work are usually regarded as vacation days. (Note that I’m intentionally ignoring sick time in this discussion.) Weekend days are almost never regarded as vacation days in the business world.
But things are far more complicated for hospitalists because of the non-traditional—not always Monday through Friday—schedule they work. If a hospitalist has Tuesday and Wednesday off this week, should that be counted as vacation time or simply weekend days displaced into the middle of the week because the doctor worked the prior weekend? It is often impossible to answer this question unambiguously.
Another issue to be considered is that decisions about vacation time and the normal—non-vacation—schedule the hospitalists use are often made independently. For example, many groups use a seven days on-seven days off schedule, with 12-hour shifts on each worked day. This might lead to an agreement that every seven worked days will count as two weeks of work that has been compressed into one week on the calendar. If that’s the case, debate can arise when trying to figure out what one week of vacation really means.
One could reasonably argue that it means the doctor is relieved of five days of work, because in most jobs a week off means being off Monday through Friday. Or, because every seven worked days counts as two weeks of work, a week off could mean being relieved of half of those days—or 3.5 days off. Lastly, a hospitalist could reasonably argue that a week off means being relieved of all seven days of one of the worked weeks. This last approach is the most common way the issue is handled. Specifying vacation in numbers of days or hours, rather than in numbers of weeks, helps but does not eliminate this confusion.
Things can get really tricky when hospitalists start adjusting their standard work schedule. They might shorten or lengthen certain existing shifts or add new shifts (e.g., an evening admitting shift) all of which complicates figuring out what a day or week of vacation really means. Think about a group that has a standard schedule of 10-hour day shifts, 14-hour night shifts, and a six-hour evening admitting shift (e.g., 5 p.m. to 11 p.m.). What will a day or week of vacation mean for them? Maybe they could specify a certain number of hours of vacation rather than days or weeks. That would be useful only for practices that contract for doctors to work a specified number of hours annually, which is probably not the best way to organize a hospitalist’s work. And hours of vacation time can get pretty complicated because doctors usually don’t regard an hour of a day shift as equivalent to an hour of the night or evening shift.
I have a great relationship with a hospital executive who works a Monday-through-Friday schedule. For years, when she noticed that I had been off for a few days, she would always ask if I had just gotten back from “vacation.” I wouldn’t bother to explain to her that it usually wasn’t vacation; it was just days I wasn’t scheduled to work to make up for working 12 to 20 consecutive days. But after about a year of her asking me about my vacation every two or three weeks, she mentioned how much she envied that I had so much vacation time, when in fact I had worked more days that year—had less time off and less vacation time—than she had. I could have taken the time to respond to each of her inquiries about my vacations by explaining which were just days I wasn’t scheduled to work and which really were vacation days. But the distinction is really arbitrary. As long as I’m getting enough time off—a lot—how each of those days is labeled doesn’t really matter.
Solutions to the Vacation Conundrum
I think it’s best to use one of the following two approaches to avoid confusion about vacation time:
- Specify how many shifts—or other work periods—the hospitalist is expected to work monthly or annually; or
- Agree—perhaps in a contract—that each hospitalist will work the same number of days (shifts) annually unless doctors mutually decide to do otherwise.
All of the other days can be thought of as days not scheduled to work—weekends, if you will, even if the days off occur during the week instead of Saturday and Sunday—vacation days, or even CME days. That way there is no need to keep track of how the days not worked are labeled or classified.
Full-time hospitalists in the group I am part of work 210 days annually. After I explain our schedule to a prospective new member of the group, I’m often asked how much vacation a new hire will get. I explain that we just specify how much work is expected of a doctor, and the non-worked days can be classified any way they would like. Understandably, some people really want a provision for vacation in the contract, so I will sometimes ask them to tell me how many vacation days they would like annually. If they say they’d like 21 days of vacation, I tell them that will be fine. We will write the contract to reflect the 231 days they are expected to work annually, but they will have 21 days of vacation. So they’re back to working the same 210 days a year that the rest of us work.
Summary
If your current contract specifies numbers of days—or weeks or hours—of vacation time and that works well, without any confusion about what constitutes a vacation day, then there is no reason to change anything right now. But you should think about what a day of vacation might mean if you change your current schedule a great deal—if you changed the duration of shifts, for example. If that might cast uncertainty on what a day of vacation means, then consider developing a contract that is silent on vacation and just specifies how much work is expected of the doctor.
I want to emphasize again that a hospitalist will have exactly the same amount of time off for vacation or any other purpose in a contract that just specifies the number of shifts/days worked and is silent on vacation time. This does not take anything away from the doctor. It is simply a different way to address the issue in the contract, while eliminating a lot of potential confusion and frustration.
If you want to know if this is really a reasonable and workable approach to vacation time, you should talk with the emergency department (ED) doctors at your hospital. If you ask them how much vacation they get, they’re likely to look puzzled and say something like, “I don’t know how much vacation time I get. All I know is that I work 14 shifts a month.” Years ago, the non-traditional working schedule used by ED doctors led many or most groups to adopt the approach to vacation I’m suggesting for hospitalists. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
The vacation conundrum most people face has to do with things like whether to drive or fly, or whether to sleep on the ground or in a hotel. But some hospitalists encounter tricky problems when figuring out how to operationalize their contractual provision for vacation time.
What is the Vacation Conundrum?
I’m a big believer in hospitalists having liberal amounts of time off, but I think most practices should avoid contractually specifying vacation time. This may sound contradictory and terribly unfair to the doctor. But avoiding a contractual guarantee of vacation time doesn’t mean the hospitalist gets any less time off. And the way hospitalist contracts address vacation time has gotten a lot of organizations in trouble. Let me explain.
Contracts often stipulate that a hospitalist will have a specified number of weeks of vacation time annually, and this language has usually been taken from the organization’s existing contracts with other physicians. But confusion often arises some time after the hospitalist practice is up and running. One big problem is deciding who will cover for the hospitalist on vacation. If all doctors work extra shifts to cover for a member of the practice who is on vacation, they will all take turns working extra—a practice that negates the effect of the promised holiday. Another problem is that most hospitalists follow non-traditional work schedules, making it difficult to determine which of the days not worked are vacation days and which are days the doctor just wasn’t scheduled to work.
To better understand this issue, it is worth thinking about how most hospitalist schedules differ from that of a typical office-based doctor or businessperson. Someone in business is usually expected to work every Monday through Friday of the year—except government holidays. Those weekdays that the business person doesn’t work are usually regarded as vacation days. (Note that I’m intentionally ignoring sick time in this discussion.) Weekend days are almost never regarded as vacation days in the business world.
But things are far more complicated for hospitalists because of the non-traditional—not always Monday through Friday—schedule they work. If a hospitalist has Tuesday and Wednesday off this week, should that be counted as vacation time or simply weekend days displaced into the middle of the week because the doctor worked the prior weekend? It is often impossible to answer this question unambiguously.
Another issue to be considered is that decisions about vacation time and the normal—non-vacation—schedule the hospitalists use are often made independently. For example, many groups use a seven days on-seven days off schedule, with 12-hour shifts on each worked day. This might lead to an agreement that every seven worked days will count as two weeks of work that has been compressed into one week on the calendar. If that’s the case, debate can arise when trying to figure out what one week of vacation really means.
One could reasonably argue that it means the doctor is relieved of five days of work, because in most jobs a week off means being off Monday through Friday. Or, because every seven worked days counts as two weeks of work, a week off could mean being relieved of half of those days—or 3.5 days off. Lastly, a hospitalist could reasonably argue that a week off means being relieved of all seven days of one of the worked weeks. This last approach is the most common way the issue is handled. Specifying vacation in numbers of days or hours, rather than in numbers of weeks, helps but does not eliminate this confusion.
Things can get really tricky when hospitalists start adjusting their standard work schedule. They might shorten or lengthen certain existing shifts or add new shifts (e.g., an evening admitting shift) all of which complicates figuring out what a day or week of vacation really means. Think about a group that has a standard schedule of 10-hour day shifts, 14-hour night shifts, and a six-hour evening admitting shift (e.g., 5 p.m. to 11 p.m.). What will a day or week of vacation mean for them? Maybe they could specify a certain number of hours of vacation rather than days or weeks. That would be useful only for practices that contract for doctors to work a specified number of hours annually, which is probably not the best way to organize a hospitalist’s work. And hours of vacation time can get pretty complicated because doctors usually don’t regard an hour of a day shift as equivalent to an hour of the night or evening shift.
I have a great relationship with a hospital executive who works a Monday-through-Friday schedule. For years, when she noticed that I had been off for a few days, she would always ask if I had just gotten back from “vacation.” I wouldn’t bother to explain to her that it usually wasn’t vacation; it was just days I wasn’t scheduled to work to make up for working 12 to 20 consecutive days. But after about a year of her asking me about my vacation every two or three weeks, she mentioned how much she envied that I had so much vacation time, when in fact I had worked more days that year—had less time off and less vacation time—than she had. I could have taken the time to respond to each of her inquiries about my vacations by explaining which were just days I wasn’t scheduled to work and which really were vacation days. But the distinction is really arbitrary. As long as I’m getting enough time off—a lot—how each of those days is labeled doesn’t really matter.
Solutions to the Vacation Conundrum
I think it’s best to use one of the following two approaches to avoid confusion about vacation time:
- Specify how many shifts—or other work periods—the hospitalist is expected to work monthly or annually; or
- Agree—perhaps in a contract—that each hospitalist will work the same number of days (shifts) annually unless doctors mutually decide to do otherwise.
All of the other days can be thought of as days not scheduled to work—weekends, if you will, even if the days off occur during the week instead of Saturday and Sunday—vacation days, or even CME days. That way there is no need to keep track of how the days not worked are labeled or classified.
Full-time hospitalists in the group I am part of work 210 days annually. After I explain our schedule to a prospective new member of the group, I’m often asked how much vacation a new hire will get. I explain that we just specify how much work is expected of a doctor, and the non-worked days can be classified any way they would like. Understandably, some people really want a provision for vacation in the contract, so I will sometimes ask them to tell me how many vacation days they would like annually. If they say they’d like 21 days of vacation, I tell them that will be fine. We will write the contract to reflect the 231 days they are expected to work annually, but they will have 21 days of vacation. So they’re back to working the same 210 days a year that the rest of us work.
Summary
If your current contract specifies numbers of days—or weeks or hours—of vacation time and that works well, without any confusion about what constitutes a vacation day, then there is no reason to change anything right now. But you should think about what a day of vacation might mean if you change your current schedule a great deal—if you changed the duration of shifts, for example. If that might cast uncertainty on what a day of vacation means, then consider developing a contract that is silent on vacation and just specifies how much work is expected of the doctor.
I want to emphasize again that a hospitalist will have exactly the same amount of time off for vacation or any other purpose in a contract that just specifies the number of shifts/days worked and is silent on vacation time. This does not take anything away from the doctor. It is simply a different way to address the issue in the contract, while eliminating a lot of potential confusion and frustration.
If you want to know if this is really a reasonable and workable approach to vacation time, you should talk with the emergency department (ED) doctors at your hospital. If you ask them how much vacation they get, they’re likely to look puzzled and say something like, “I don’t know how much vacation time I get. All I know is that I work 14 shifts a month.” Years ago, the non-traditional working schedule used by ED doctors led many or most groups to adopt the approach to vacation I’m suggesting for hospitalists. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
The vacation conundrum most people face has to do with things like whether to drive or fly, or whether to sleep on the ground or in a hotel. But some hospitalists encounter tricky problems when figuring out how to operationalize their contractual provision for vacation time.
What is the Vacation Conundrum?
I’m a big believer in hospitalists having liberal amounts of time off, but I think most practices should avoid contractually specifying vacation time. This may sound contradictory and terribly unfair to the doctor. But avoiding a contractual guarantee of vacation time doesn’t mean the hospitalist gets any less time off. And the way hospitalist contracts address vacation time has gotten a lot of organizations in trouble. Let me explain.
Contracts often stipulate that a hospitalist will have a specified number of weeks of vacation time annually, and this language has usually been taken from the organization’s existing contracts with other physicians. But confusion often arises some time after the hospitalist practice is up and running. One big problem is deciding who will cover for the hospitalist on vacation. If all doctors work extra shifts to cover for a member of the practice who is on vacation, they will all take turns working extra—a practice that negates the effect of the promised holiday. Another problem is that most hospitalists follow non-traditional work schedules, making it difficult to determine which of the days not worked are vacation days and which are days the doctor just wasn’t scheduled to work.
To better understand this issue, it is worth thinking about how most hospitalist schedules differ from that of a typical office-based doctor or businessperson. Someone in business is usually expected to work every Monday through Friday of the year—except government holidays. Those weekdays that the business person doesn’t work are usually regarded as vacation days. (Note that I’m intentionally ignoring sick time in this discussion.) Weekend days are almost never regarded as vacation days in the business world.
But things are far more complicated for hospitalists because of the non-traditional—not always Monday through Friday—schedule they work. If a hospitalist has Tuesday and Wednesday off this week, should that be counted as vacation time or simply weekend days displaced into the middle of the week because the doctor worked the prior weekend? It is often impossible to answer this question unambiguously.
Another issue to be considered is that decisions about vacation time and the normal—non-vacation—schedule the hospitalists use are often made independently. For example, many groups use a seven days on-seven days off schedule, with 12-hour shifts on each worked day. This might lead to an agreement that every seven worked days will count as two weeks of work that has been compressed into one week on the calendar. If that’s the case, debate can arise when trying to figure out what one week of vacation really means.
One could reasonably argue that it means the doctor is relieved of five days of work, because in most jobs a week off means being off Monday through Friday. Or, because every seven worked days counts as two weeks of work, a week off could mean being relieved of half of those days—or 3.5 days off. Lastly, a hospitalist could reasonably argue that a week off means being relieved of all seven days of one of the worked weeks. This last approach is the most common way the issue is handled. Specifying vacation in numbers of days or hours, rather than in numbers of weeks, helps but does not eliminate this confusion.
Things can get really tricky when hospitalists start adjusting their standard work schedule. They might shorten or lengthen certain existing shifts or add new shifts (e.g., an evening admitting shift) all of which complicates figuring out what a day or week of vacation really means. Think about a group that has a standard schedule of 10-hour day shifts, 14-hour night shifts, and a six-hour evening admitting shift (e.g., 5 p.m. to 11 p.m.). What will a day or week of vacation mean for them? Maybe they could specify a certain number of hours of vacation rather than days or weeks. That would be useful only for practices that contract for doctors to work a specified number of hours annually, which is probably not the best way to organize a hospitalist’s work. And hours of vacation time can get pretty complicated because doctors usually don’t regard an hour of a day shift as equivalent to an hour of the night or evening shift.
I have a great relationship with a hospital executive who works a Monday-through-Friday schedule. For years, when she noticed that I had been off for a few days, she would always ask if I had just gotten back from “vacation.” I wouldn’t bother to explain to her that it usually wasn’t vacation; it was just days I wasn’t scheduled to work to make up for working 12 to 20 consecutive days. But after about a year of her asking me about my vacation every two or three weeks, she mentioned how much she envied that I had so much vacation time, when in fact I had worked more days that year—had less time off and less vacation time—than she had. I could have taken the time to respond to each of her inquiries about my vacations by explaining which were just days I wasn’t scheduled to work and which really were vacation days. But the distinction is really arbitrary. As long as I’m getting enough time off—a lot—how each of those days is labeled doesn’t really matter.
Solutions to the Vacation Conundrum
I think it’s best to use one of the following two approaches to avoid confusion about vacation time:
- Specify how many shifts—or other work periods—the hospitalist is expected to work monthly or annually; or
- Agree—perhaps in a contract—that each hospitalist will work the same number of days (shifts) annually unless doctors mutually decide to do otherwise.
All of the other days can be thought of as days not scheduled to work—weekends, if you will, even if the days off occur during the week instead of Saturday and Sunday—vacation days, or even CME days. That way there is no need to keep track of how the days not worked are labeled or classified.
Full-time hospitalists in the group I am part of work 210 days annually. After I explain our schedule to a prospective new member of the group, I’m often asked how much vacation a new hire will get. I explain that we just specify how much work is expected of a doctor, and the non-worked days can be classified any way they would like. Understandably, some people really want a provision for vacation in the contract, so I will sometimes ask them to tell me how many vacation days they would like annually. If they say they’d like 21 days of vacation, I tell them that will be fine. We will write the contract to reflect the 231 days they are expected to work annually, but they will have 21 days of vacation. So they’re back to working the same 210 days a year that the rest of us work.
Summary
If your current contract specifies numbers of days—or weeks or hours—of vacation time and that works well, without any confusion about what constitutes a vacation day, then there is no reason to change anything right now. But you should think about what a day of vacation might mean if you change your current schedule a great deal—if you changed the duration of shifts, for example. If that might cast uncertainty on what a day of vacation means, then consider developing a contract that is silent on vacation and just specifies how much work is expected of the doctor.
I want to emphasize again that a hospitalist will have exactly the same amount of time off for vacation or any other purpose in a contract that just specifies the number of shifts/days worked and is silent on vacation time. This does not take anything away from the doctor. It is simply a different way to address the issue in the contract, while eliminating a lot of potential confusion and frustration.
If you want to know if this is really a reasonable and workable approach to vacation time, you should talk with the emergency department (ED) doctors at your hospital. If you ask them how much vacation they get, they’re likely to look puzzled and say something like, “I don’t know how much vacation time I get. All I know is that I work 14 shifts a month.” Years ago, the non-traditional working schedule used by ED doctors led many or most groups to adopt the approach to vacation I’m suggesting for hospitalists. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is a co-founder and past-president of SHM. He is a principal in Nelson/Flores Associates, a national hospitalist practice management consulting firm. This column represents his views and is not intended to reflect an official position of SHM.
Reduce CR-BSI, Quality Performance Measures, Treat DVT. Plus Adult Bacterial Meningitis in “Classic Lit”

Reduce CR-BSI
Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006 Dec 28;355(26):2725-2732.
For practicing clinicians, quality improvement (QI) is a difficult and important task. There can be requirements for extra steps, additional forms, or new safety procedures when caring for patients; there is also the promise of improved clinical outcomes. This tradeoff can be justified when solid, evidence-based techniques are implemented, but—unfortunately—definitive evidence is not always available. Public reporting of a variety of quality indicators, now mandated by the Centers for Medicare and Medicaid Services (CMS), is likely to boost calls for changes in clinical medicine, and the pressure to adopt new safety practices is likely to increase.
Fortunately, this article by Pronovost and colleagues provides a test of state-of-the-art QI theory applied to an important QI target, catheter-related bloodstream infections (CR-BSI). Annually there are 80,000 CR-BSI in the United States, causing about 28,000 deaths in ICU patients; the medical costs to treat these infections is estimated at $2.3 billion. There have been numerous published and unpublished trials of QI methods that have reduced the incidence of such infections, but none have been as large as this one, a state-wide ICU trial conducted in Michigan and funded by the Agency for Healthcare Research and Quality (AHRQ).
One-hundred-three ICUs, representing 85% of ICU beds in the state, participated in the study. In addition to the intervention to reduce CR-BSI, a comprehensive program aimed at instilling a culture of safety was implemented, including the creation of a QI team with a physician and nurse as team leaders, use of a daily goals sheet to enhance clinician-clinician communication, an intervention to reduce ventilator-associated pneumonia, and a comprehensive safety program designed to improve the culture of safety.
The study intervention was designed to improve clinicians’ use of five evidence-based procedures recommended by the Centers for Disease Control and Prevention (CDC):
- Handwashing;
- Use of full barrier precautions;
- Use of chlorhexidine antiseptic;
- Avoidance of femoral line placement; and
- Removal of unnecessary catheters.
The strategies used to encourage these practices were technologically simple and easy to implement. They included the use of a central line kit with a procedure checklist, the termination of any procedure for failure to follow protocol, and daily discussions of line removal on rounds. Additionally, at regular meetings, all clinicians received feedback regarding numbers and rates of CR-BSI.
The results were impressive: The overall rate of CR-BSI decreased from a baseline median of 2.7 (mean, 7.7) infections per 1,000 catheter-days to 0 (mean, 2.3) during the first three-month period after implementation of the intervention (P<0.002). During the 18 months of follow-up, this reduction was sustained at 0 (mean, 1.4). The results applied in both academic and non-teaching hospitals, regardless of size.
Even with such simple methods, managing a statewide implementation of a comprehensive QI program is a feat of organization, as anyone who has implemented even small-scale projects knows. An accompanying editorial praised the effort, noting the magnitude of the accomplishment and recommending widespread adoption of these simple yet effective techniques. Given the push toward the adoption of similar methods, this demonstration is welcome and makes the wholesale acceptance of such measures not only easier but also imperative.
Quality Performance Measures across the Nation
Landon BE, Normand SL, Lessler A, et al. Quality of care for the treatment of acute medical conditions in US hospitals. Arch Intern Med. 2006 Dec 11;166(22):2511-2517.
Background
Current efforts have focused on examining and reporting indicators in order to increase the quality of care provided to patients in the United States. In January 2004 the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) began collecting monthly data from its accredited hospitals on performance measures across three of five select disease conditions. Similarly, since 2004, CMS has provided data from Hospital Quality Alliance members on 10 performance measures in the areas of congestive heart failure, acute myocardial infarction, and pneumonia. This study collected data from these reports to expand on previous work examining the quality of care in the United States on a national level. It also analyzed the characteristics of hospitals that have met these quality measures.
Methods
Overall, 4,856 different hospitals were included in the analysis. Data was obtained for all relevant discharges between January 1 and June 2004 from both CMS and JCAHO, with preference given to the JCAHO data. Discrepancies in reporting data between the two data sets were less than 1%. The 2003 Annual Survey of Hospitals from the American Hospital Association (AHA) was used to define the population of hospitals operating in the United States in terms of:
- Number of beds;
- Ownership (for-profit, not-for-profit, government, or military);
- Region;
- Metropolitan statistical area type (rural, small, medium, or large);
- Teaching status (major—member of the Council of Teaching Hospitals, minor—any other medical school affiliation or residency program, or non-teaching);
- Availability of advanced technology (MRI and PET scanning);
- Nurse staffing patterns; and
- Number of Medicaid and Medicare discharges.
These data sets were linked. Composite scales were created for each disease. Bivariate associations using two-tailed T-tests for continuous variables and chi-squared tests for categorical variables were made. For each individual and composite measure, the mean performance and the 25th and 75th percentiles were calculated. The top performing quintiles for each of the three diseases were taken and cross-tabulated across the three specific disease composites. A random-effects logistic regression model was estimated for each composite using a binary logistic model with SAS statistical software and the grouped hospital data that modeled the number of opportunities met in each hospital out of the total number of opportunities at the hospital.
Results
Hospitalized patients with congestive heart failure, acute myocardial infarction, and pneumonia received 75.9% of the recommended processes of care as a whole. Performance varied considerably, from a mean of 0.36 (0.00-0.67) for thrombolytic therapy administered within 30 minutes of arrival for an MI to a mean of 0.98 (0.98-1.00) for assessment of oxygen for patients with pneumonia. Mean composite scores were 0.85 (0.81-0.95) for acute myocardial infarction, 0.64 (0.52-0.78) for congestive heart failure, and 0.88 (0.80-0.97) for pneumonia.
When comparing hospitals in quintiles of performance, 10.5% were in the top quintile for two out of three diseases, but only 3.8% were in the top quintile for all three diseases. “Treatment and diagnosis” as well as “counseling and prevention” were correlated among all three conditions after factor analysis.
Multivariate analysis demonstrated for-profit hospitals as consistently performing worse than not-for-profit hospitals in meeting performance measures. Federal and military hospitals had the highest success in meeting the measures for the three diseases analyzed. Major teaching hospitals met more quality indicators for patients with acute MI and “treatment and diagnosis” but not for CHF, pneumonia, or “counseling and prevention” when compared with non-teaching hospitals. Performance decreased as the share of Medicaid patients increased. More technology and a registered nursing staff with more education were factors associated with higher success in meeting quality indicators.
Conclusions
This ambitious study evaluated the quality of hospital care across the nation using information collected from both JCAHO and CMS. It demonstrated room for improvement, with hospitals as a whole providing 76% of the recommended measures for acute MI, CHF, and pneumonia. The study suggests that ownership characteristics, teaching status, JCAHO accreditation, technology investments, and nursing staff with degrees strongly correlates to success in meeting performance measures.
The authors conclude that the findings have implications for public policy and patient choice. They hypothesize that regions of the country and rural locations more often associated with low performance could use additional resources aimed at bolstering performance. Patients living in rural areas have little choice without traveling great distances. The authors also state that the characteristics of hospitals that influence performance, such as ownership, teaching status, JCAHO accreditation, technology investments, and nursing status, are remediable.
It is important to bear in mind, however, given the cross-sectional nature of the data, that the associations reported are not proof of causality. Quality performance measures were not highly correlated among hospitals for the three conditions studied, with only 3.8% in the top quintile for all three diseases; this result demonstrates the difficulty inherent in generically rating hospitals. Additionally, this study makes no attempt to examine how meeting performance measures affects clinical outcomes, an important part of this ongoing national debate.
Treat DVT
Kearon C, Ginsberg JS, Julian JA, et al. Comparison of fixed-dose weight-adjusted unfractionated heparin and low-molecular-weight heparin for acute treatment of venous thromboembolism. JAMA. 2006 Aug 23;296(8):935-942.
Background
The current practice of treating DVT involves starting the patient on LMW (low molecular weight) heparin administered subcutaneously or initiating an IV drip of unfractionated heparin. The latter prevents the patient from being discharged as soon as treatment is initiated and requires repeat checking of aPTTs and drip adjustments, which may lead to over-shoot and/or sub-therapeutic dosage. On the other hand, treatment with LMW heparin is costly and can be tricky for patients with varying degrees of renal failure. Using fixed-dose subcutaneous injections of unfractionated heparin is a novel idea and could be the solution to the above-mentioned issues.
Methods
Eight hospitals in Canada and New Zealand with a total of 708 eligible and willing participants were involved in the study. The study design was a randomized, controlled, non-inferiority trial; the adjudication and monitoring committees were blinded. Patients older than 18 with a new diagnosis of DVT and/or pulmonary embolism were considered eligible. Patients with any of the usual contraindications for anticoagulation, including recent major bleeding events, were excluded, as were patients with renal failure and pregnancy.
Computerized randomization was done at a central location, and patients were started on either twice daily weight-based dosing of LMW heparin (100 IU/kg) or twice daily dosing of weight-based unfractionated heparin (first dose of 333 U/kg, subsequent doses of 250 U/kg). No coagulation testing was done to modify these doses. The patients were treated for at least five days, until the International Normalized Ratio (INR) was in the therapeutic range for two consecutive days. Patients were concomitantly started on warfarin. Recurrent venous thromboses, bleeding episodes—described as drop of hemoglobin >2.0—and death were primary endpoints.
Results
The assumption of non-inferiority was supported by the analysis of recurrent VTEs, which were 12 (3.4%) in the LMW heparin group and 13 (3.8%) in the unfractionated heparin group—clinically, a non-significant difference. Bleeding rates at 10 days or at three months were not significantly different for the two groups. Number of deaths was 18 in the unfractionated heparin group and 22 in the LMW heparin group. No patients were reported to have developed heparin-induced thrombocytopenia, a serious and often life-threatening complication of unfractionated heparin use.
Conclusions
This interesting study demonstrates that the use of fixed dose, unmonitored, subcutaneous unfractionated heparin in twice daily dosing is non-inferior to treatment with different kinds of LMW heparin. The authors have also analyzed the cost difference, which, at existing U.S. pricing, would be in the vicinity of $675 for the six-day treatment of an 80-kg patient. Though more data is needed on patients with special considerations such as renal failure, the results, which support non-inferiority and cite a major cost advantage, merit further studies to validate these conclusions and to further evaluate this approach in patient populations with special considerations.
Non-Invasive Testing Prior to Vascular Surgery
Poldermans D, Bax JJ, Schouten O, et al. Should major vascular surgery be delayed because of preoperative cardiac testing in intermediate-risk patients receiving beta-blocker therapy with tight heart rate control? J Am Coll Cardiol. 2006 Sep 5;48(5):964-969.
Background
Current guidelines from the AHA and the American College of Cardiology (ACC) recommend non-invasive testing for patients scheduled for major vascular surgery as part of the pre-operative work-up if they have clinical factors suggestive of increased cardiac risk. The study was performed to show that no testing combined with aggressive beta blockade is not inferior in comparison to non-invasive testing for patients in the intermediate risk group who are preparing to undergo major vascular surgery. Testing often results in delays that can result in poor outcomes; additionally, invasive intervention based upon non-invasive test results has not been clearly shown to add any benefit to the eventual outcome of the patient.
Methods
The study was conducted at five clinical centers in Europe and Brazil, where 1,476 patients undergoing elective open abdominal aortic or infrainguinal arterial reconstruction were enrolled. The design was a randomized, controlled, non-inferiority trial with the outcome assessors blinded. Inclusion criteria consisted of age older than 70, angina pectoris, prior myocardial infarction (MI), compensated or history of congestive heart failure, diabetes mellitus, renal dysfunction and prior stroke, or transient ischemic attack. Patients with one or two risk factors were labeled intermediate risk and were randomized to receive either just beta-blocker therapy or non-invasive testing with dobutamine echocardiography or dobutamine or dipyridamole perfusion scintigraphy.
Patients with limited or no ischemia were referred for surgery with beta-blocker therapy. In patients with extensive ischemia—five ischemic segments or more—coronary angiography and revascularization were performed if the main surgery could be delayed. Beta-blocker therapy was instituted in all patients, with a goal heart rate of 60-65. The beta-blocker therapy was continued postoperatively. IV metoprolol was used in the ICU if a patient could not take drugs orally. Primary endpoints were a combination of cardiac death and nonfatal MI at 30 days and two years.
Results
Of the 770 patients classified as intermediate risk, 386 received cardiac testing and 384 patients were not tested. There were no significant differences in the presence of ischemic heart disease in the two subsets. The time gap between screening to vascular surgery was 34 days (seven to 88 days) in the no testing group, compared with 53 days (1,321 days) in the testing group (P<0.001). There was no difference in the composite endpoints—either at 30 days or at two years—for the two groups.
Conclusions
This excellent study shows that the approach of no screening in patients with intermediate cardiac risk factors before vascular surgery is non-inferior. An interesting point elucidated by the authors in their discussion details why studies designed to achieve a goal heart rate, rather than those based on fixed dose beta-blockers, are ideal to show the benefits of beta blockade in this population subset. The benefit of coronary revascularization for intermediate risk patients with extensive ischemia could not be defined, however; the number was too small to show any significance.
Reduce CR-BSI
Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006 Dec 28;355(26):2725-2732.
For practicing clinicians, quality improvement (QI) is a difficult and important task. There can be requirements for extra steps, additional forms, or new safety procedures when caring for patients; there is also the promise of improved clinical outcomes. This tradeoff can be justified when solid, evidence-based techniques are implemented, but—unfortunately—definitive evidence is not always available. Public reporting of a variety of quality indicators, now mandated by the Centers for Medicare and Medicaid Services (CMS), is likely to boost calls for changes in clinical medicine, and the pressure to adopt new safety practices is likely to increase.
Fortunately, this article by Pronovost and colleagues provides a test of state-of-the-art QI theory applied to an important QI target, catheter-related bloodstream infections (CR-BSI). Annually there are 80,000 CR-BSI in the United States, causing about 28,000 deaths in ICU patients; the medical costs to treat these infections is estimated at $2.3 billion. There have been numerous published and unpublished trials of QI methods that have reduced the incidence of such infections, but none have been as large as this one, a state-wide ICU trial conducted in Michigan and funded by the Agency for Healthcare Research and Quality (AHRQ).
One-hundred-three ICUs, representing 85% of ICU beds in the state, participated in the study. In addition to the intervention to reduce CR-BSI, a comprehensive program aimed at instilling a culture of safety was implemented, including the creation of a QI team with a physician and nurse as team leaders, use of a daily goals sheet to enhance clinician-clinician communication, an intervention to reduce ventilator-associated pneumonia, and a comprehensive safety program designed to improve the culture of safety.
The study intervention was designed to improve clinicians’ use of five evidence-based procedures recommended by the Centers for Disease Control and Prevention (CDC):
- Handwashing;
- Use of full barrier precautions;
- Use of chlorhexidine antiseptic;
- Avoidance of femoral line placement; and
- Removal of unnecessary catheters.
The strategies used to encourage these practices were technologically simple and easy to implement. They included the use of a central line kit with a procedure checklist, the termination of any procedure for failure to follow protocol, and daily discussions of line removal on rounds. Additionally, at regular meetings, all clinicians received feedback regarding numbers and rates of CR-BSI.
The results were impressive: The overall rate of CR-BSI decreased from a baseline median of 2.7 (mean, 7.7) infections per 1,000 catheter-days to 0 (mean, 2.3) during the first three-month period after implementation of the intervention (P<0.002). During the 18 months of follow-up, this reduction was sustained at 0 (mean, 1.4). The results applied in both academic and non-teaching hospitals, regardless of size.
Even with such simple methods, managing a statewide implementation of a comprehensive QI program is a feat of organization, as anyone who has implemented even small-scale projects knows. An accompanying editorial praised the effort, noting the magnitude of the accomplishment and recommending widespread adoption of these simple yet effective techniques. Given the push toward the adoption of similar methods, this demonstration is welcome and makes the wholesale acceptance of such measures not only easier but also imperative.
Quality Performance Measures across the Nation
Landon BE, Normand SL, Lessler A, et al. Quality of care for the treatment of acute medical conditions in US hospitals. Arch Intern Med. 2006 Dec 11;166(22):2511-2517.
Background
Current efforts have focused on examining and reporting indicators in order to increase the quality of care provided to patients in the United States. In January 2004 the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) began collecting monthly data from its accredited hospitals on performance measures across three of five select disease conditions. Similarly, since 2004, CMS has provided data from Hospital Quality Alliance members on 10 performance measures in the areas of congestive heart failure, acute myocardial infarction, and pneumonia. This study collected data from these reports to expand on previous work examining the quality of care in the United States on a national level. It also analyzed the characteristics of hospitals that have met these quality measures.
Methods
Overall, 4,856 different hospitals were included in the analysis. Data was obtained for all relevant discharges between January 1 and June 2004 from both CMS and JCAHO, with preference given to the JCAHO data. Discrepancies in reporting data between the two data sets were less than 1%. The 2003 Annual Survey of Hospitals from the American Hospital Association (AHA) was used to define the population of hospitals operating in the United States in terms of:
- Number of beds;
- Ownership (for-profit, not-for-profit, government, or military);
- Region;
- Metropolitan statistical area type (rural, small, medium, or large);
- Teaching status (major—member of the Council of Teaching Hospitals, minor—any other medical school affiliation or residency program, or non-teaching);
- Availability of advanced technology (MRI and PET scanning);
- Nurse staffing patterns; and
- Number of Medicaid and Medicare discharges.
These data sets were linked. Composite scales were created for each disease. Bivariate associations using two-tailed T-tests for continuous variables and chi-squared tests for categorical variables were made. For each individual and composite measure, the mean performance and the 25th and 75th percentiles were calculated. The top performing quintiles for each of the three diseases were taken and cross-tabulated across the three specific disease composites. A random-effects logistic regression model was estimated for each composite using a binary logistic model with SAS statistical software and the grouped hospital data that modeled the number of opportunities met in each hospital out of the total number of opportunities at the hospital.
Results
Hospitalized patients with congestive heart failure, acute myocardial infarction, and pneumonia received 75.9% of the recommended processes of care as a whole. Performance varied considerably, from a mean of 0.36 (0.00-0.67) for thrombolytic therapy administered within 30 minutes of arrival for an MI to a mean of 0.98 (0.98-1.00) for assessment of oxygen for patients with pneumonia. Mean composite scores were 0.85 (0.81-0.95) for acute myocardial infarction, 0.64 (0.52-0.78) for congestive heart failure, and 0.88 (0.80-0.97) for pneumonia.
When comparing hospitals in quintiles of performance, 10.5% were in the top quintile for two out of three diseases, but only 3.8% were in the top quintile for all three diseases. “Treatment and diagnosis” as well as “counseling and prevention” were correlated among all three conditions after factor analysis.
Multivariate analysis demonstrated for-profit hospitals as consistently performing worse than not-for-profit hospitals in meeting performance measures. Federal and military hospitals had the highest success in meeting the measures for the three diseases analyzed. Major teaching hospitals met more quality indicators for patients with acute MI and “treatment and diagnosis” but not for CHF, pneumonia, or “counseling and prevention” when compared with non-teaching hospitals. Performance decreased as the share of Medicaid patients increased. More technology and a registered nursing staff with more education were factors associated with higher success in meeting quality indicators.
Conclusions
This ambitious study evaluated the quality of hospital care across the nation using information collected from both JCAHO and CMS. It demonstrated room for improvement, with hospitals as a whole providing 76% of the recommended measures for acute MI, CHF, and pneumonia. The study suggests that ownership characteristics, teaching status, JCAHO accreditation, technology investments, and nursing staff with degrees strongly correlates to success in meeting performance measures.
The authors conclude that the findings have implications for public policy and patient choice. They hypothesize that regions of the country and rural locations more often associated with low performance could use additional resources aimed at bolstering performance. Patients living in rural areas have little choice without traveling great distances. The authors also state that the characteristics of hospitals that influence performance, such as ownership, teaching status, JCAHO accreditation, technology investments, and nursing status, are remediable.
It is important to bear in mind, however, given the cross-sectional nature of the data, that the associations reported are not proof of causality. Quality performance measures were not highly correlated among hospitals for the three conditions studied, with only 3.8% in the top quintile for all three diseases; this result demonstrates the difficulty inherent in generically rating hospitals. Additionally, this study makes no attempt to examine how meeting performance measures affects clinical outcomes, an important part of this ongoing national debate.
Treat DVT
Kearon C, Ginsberg JS, Julian JA, et al. Comparison of fixed-dose weight-adjusted unfractionated heparin and low-molecular-weight heparin for acute treatment of venous thromboembolism. JAMA. 2006 Aug 23;296(8):935-942.
Background
The current practice of treating DVT involves starting the patient on LMW (low molecular weight) heparin administered subcutaneously or initiating an IV drip of unfractionated heparin. The latter prevents the patient from being discharged as soon as treatment is initiated and requires repeat checking of aPTTs and drip adjustments, which may lead to over-shoot and/or sub-therapeutic dosage. On the other hand, treatment with LMW heparin is costly and can be tricky for patients with varying degrees of renal failure. Using fixed-dose subcutaneous injections of unfractionated heparin is a novel idea and could be the solution to the above-mentioned issues.
Methods
Eight hospitals in Canada and New Zealand with a total of 708 eligible and willing participants were involved in the study. The study design was a randomized, controlled, non-inferiority trial; the adjudication and monitoring committees were blinded. Patients older than 18 with a new diagnosis of DVT and/or pulmonary embolism were considered eligible. Patients with any of the usual contraindications for anticoagulation, including recent major bleeding events, were excluded, as were patients with renal failure and pregnancy.
Computerized randomization was done at a central location, and patients were started on either twice daily weight-based dosing of LMW heparin (100 IU/kg) or twice daily dosing of weight-based unfractionated heparin (first dose of 333 U/kg, subsequent doses of 250 U/kg). No coagulation testing was done to modify these doses. The patients were treated for at least five days, until the International Normalized Ratio (INR) was in the therapeutic range for two consecutive days. Patients were concomitantly started on warfarin. Recurrent venous thromboses, bleeding episodes—described as drop of hemoglobin >2.0—and death were primary endpoints.
Results
The assumption of non-inferiority was supported by the analysis of recurrent VTEs, which were 12 (3.4%) in the LMW heparin group and 13 (3.8%) in the unfractionated heparin group—clinically, a non-significant difference. Bleeding rates at 10 days or at three months were not significantly different for the two groups. Number of deaths was 18 in the unfractionated heparin group and 22 in the LMW heparin group. No patients were reported to have developed heparin-induced thrombocytopenia, a serious and often life-threatening complication of unfractionated heparin use.
Conclusions
This interesting study demonstrates that the use of fixed dose, unmonitored, subcutaneous unfractionated heparin in twice daily dosing is non-inferior to treatment with different kinds of LMW heparin. The authors have also analyzed the cost difference, which, at existing U.S. pricing, would be in the vicinity of $675 for the six-day treatment of an 80-kg patient. Though more data is needed on patients with special considerations such as renal failure, the results, which support non-inferiority and cite a major cost advantage, merit further studies to validate these conclusions and to further evaluate this approach in patient populations with special considerations.
Non-Invasive Testing Prior to Vascular Surgery
Poldermans D, Bax JJ, Schouten O, et al. Should major vascular surgery be delayed because of preoperative cardiac testing in intermediate-risk patients receiving beta-blocker therapy with tight heart rate control? J Am Coll Cardiol. 2006 Sep 5;48(5):964-969.
Background
Current guidelines from the AHA and the American College of Cardiology (ACC) recommend non-invasive testing for patients scheduled for major vascular surgery as part of the pre-operative work-up if they have clinical factors suggestive of increased cardiac risk. The study was performed to show that no testing combined with aggressive beta blockade is not inferior in comparison to non-invasive testing for patients in the intermediate risk group who are preparing to undergo major vascular surgery. Testing often results in delays that can result in poor outcomes; additionally, invasive intervention based upon non-invasive test results has not been clearly shown to add any benefit to the eventual outcome of the patient.
Methods
The study was conducted at five clinical centers in Europe and Brazil, where 1,476 patients undergoing elective open abdominal aortic or infrainguinal arterial reconstruction were enrolled. The design was a randomized, controlled, non-inferiority trial with the outcome assessors blinded. Inclusion criteria consisted of age older than 70, angina pectoris, prior myocardial infarction (MI), compensated or history of congestive heart failure, diabetes mellitus, renal dysfunction and prior stroke, or transient ischemic attack. Patients with one or two risk factors were labeled intermediate risk and were randomized to receive either just beta-blocker therapy or non-invasive testing with dobutamine echocardiography or dobutamine or dipyridamole perfusion scintigraphy.
Patients with limited or no ischemia were referred for surgery with beta-blocker therapy. In patients with extensive ischemia—five ischemic segments or more—coronary angiography and revascularization were performed if the main surgery could be delayed. Beta-blocker therapy was instituted in all patients, with a goal heart rate of 60-65. The beta-blocker therapy was continued postoperatively. IV metoprolol was used in the ICU if a patient could not take drugs orally. Primary endpoints were a combination of cardiac death and nonfatal MI at 30 days and two years.
Results
Of the 770 patients classified as intermediate risk, 386 received cardiac testing and 384 patients were not tested. There were no significant differences in the presence of ischemic heart disease in the two subsets. The time gap between screening to vascular surgery was 34 days (seven to 88 days) in the no testing group, compared with 53 days (1,321 days) in the testing group (P<0.001). There was no difference in the composite endpoints—either at 30 days or at two years—for the two groups.
Conclusions
This excellent study shows that the approach of no screening in patients with intermediate cardiac risk factors before vascular surgery is non-inferior. An interesting point elucidated by the authors in their discussion details why studies designed to achieve a goal heart rate, rather than those based on fixed dose beta-blockers, are ideal to show the benefits of beta blockade in this population subset. The benefit of coronary revascularization for intermediate risk patients with extensive ischemia could not be defined, however; the number was too small to show any significance.
Reduce CR-BSI
Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006 Dec 28;355(26):2725-2732.
For practicing clinicians, quality improvement (QI) is a difficult and important task. There can be requirements for extra steps, additional forms, or new safety procedures when caring for patients; there is also the promise of improved clinical outcomes. This tradeoff can be justified when solid, evidence-based techniques are implemented, but—unfortunately—definitive evidence is not always available. Public reporting of a variety of quality indicators, now mandated by the Centers for Medicare and Medicaid Services (CMS), is likely to boost calls for changes in clinical medicine, and the pressure to adopt new safety practices is likely to increase.
Fortunately, this article by Pronovost and colleagues provides a test of state-of-the-art QI theory applied to an important QI target, catheter-related bloodstream infections (CR-BSI). Annually there are 80,000 CR-BSI in the United States, causing about 28,000 deaths in ICU patients; the medical costs to treat these infections is estimated at $2.3 billion. There have been numerous published and unpublished trials of QI methods that have reduced the incidence of such infections, but none have been as large as this one, a state-wide ICU trial conducted in Michigan and funded by the Agency for Healthcare Research and Quality (AHRQ).
One-hundred-three ICUs, representing 85% of ICU beds in the state, participated in the study. In addition to the intervention to reduce CR-BSI, a comprehensive program aimed at instilling a culture of safety was implemented, including the creation of a QI team with a physician and nurse as team leaders, use of a daily goals sheet to enhance clinician-clinician communication, an intervention to reduce ventilator-associated pneumonia, and a comprehensive safety program designed to improve the culture of safety.
The study intervention was designed to improve clinicians’ use of five evidence-based procedures recommended by the Centers for Disease Control and Prevention (CDC):
- Handwashing;
- Use of full barrier precautions;
- Use of chlorhexidine antiseptic;
- Avoidance of femoral line placement; and
- Removal of unnecessary catheters.
The strategies used to encourage these practices were technologically simple and easy to implement. They included the use of a central line kit with a procedure checklist, the termination of any procedure for failure to follow protocol, and daily discussions of line removal on rounds. Additionally, at regular meetings, all clinicians received feedback regarding numbers and rates of CR-BSI.
The results were impressive: The overall rate of CR-BSI decreased from a baseline median of 2.7 (mean, 7.7) infections per 1,000 catheter-days to 0 (mean, 2.3) during the first three-month period after implementation of the intervention (P<0.002). During the 18 months of follow-up, this reduction was sustained at 0 (mean, 1.4). The results applied in both academic and non-teaching hospitals, regardless of size.
Even with such simple methods, managing a statewide implementation of a comprehensive QI program is a feat of organization, as anyone who has implemented even small-scale projects knows. An accompanying editorial praised the effort, noting the magnitude of the accomplishment and recommending widespread adoption of these simple yet effective techniques. Given the push toward the adoption of similar methods, this demonstration is welcome and makes the wholesale acceptance of such measures not only easier but also imperative.
Quality Performance Measures across the Nation
Landon BE, Normand SL, Lessler A, et al. Quality of care for the treatment of acute medical conditions in US hospitals. Arch Intern Med. 2006 Dec 11;166(22):2511-2517.
Background
Current efforts have focused on examining and reporting indicators in order to increase the quality of care provided to patients in the United States. In January 2004 the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) began collecting monthly data from its accredited hospitals on performance measures across three of five select disease conditions. Similarly, since 2004, CMS has provided data from Hospital Quality Alliance members on 10 performance measures in the areas of congestive heart failure, acute myocardial infarction, and pneumonia. This study collected data from these reports to expand on previous work examining the quality of care in the United States on a national level. It also analyzed the characteristics of hospitals that have met these quality measures.
Methods
Overall, 4,856 different hospitals were included in the analysis. Data was obtained for all relevant discharges between January 1 and June 2004 from both CMS and JCAHO, with preference given to the JCAHO data. Discrepancies in reporting data between the two data sets were less than 1%. The 2003 Annual Survey of Hospitals from the American Hospital Association (AHA) was used to define the population of hospitals operating in the United States in terms of:
- Number of beds;
- Ownership (for-profit, not-for-profit, government, or military);
- Region;
- Metropolitan statistical area type (rural, small, medium, or large);
- Teaching status (major—member of the Council of Teaching Hospitals, minor—any other medical school affiliation or residency program, or non-teaching);
- Availability of advanced technology (MRI and PET scanning);
- Nurse staffing patterns; and
- Number of Medicaid and Medicare discharges.
These data sets were linked. Composite scales were created for each disease. Bivariate associations using two-tailed T-tests for continuous variables and chi-squared tests for categorical variables were made. For each individual and composite measure, the mean performance and the 25th and 75th percentiles were calculated. The top performing quintiles for each of the three diseases were taken and cross-tabulated across the three specific disease composites. A random-effects logistic regression model was estimated for each composite using a binary logistic model with SAS statistical software and the grouped hospital data that modeled the number of opportunities met in each hospital out of the total number of opportunities at the hospital.
Results
Hospitalized patients with congestive heart failure, acute myocardial infarction, and pneumonia received 75.9% of the recommended processes of care as a whole. Performance varied considerably, from a mean of 0.36 (0.00-0.67) for thrombolytic therapy administered within 30 minutes of arrival for an MI to a mean of 0.98 (0.98-1.00) for assessment of oxygen for patients with pneumonia. Mean composite scores were 0.85 (0.81-0.95) for acute myocardial infarction, 0.64 (0.52-0.78) for congestive heart failure, and 0.88 (0.80-0.97) for pneumonia.
When comparing hospitals in quintiles of performance, 10.5% were in the top quintile for two out of three diseases, but only 3.8% were in the top quintile for all three diseases. “Treatment and diagnosis” as well as “counseling and prevention” were correlated among all three conditions after factor analysis.
Multivariate analysis demonstrated for-profit hospitals as consistently performing worse than not-for-profit hospitals in meeting performance measures. Federal and military hospitals had the highest success in meeting the measures for the three diseases analyzed. Major teaching hospitals met more quality indicators for patients with acute MI and “treatment and diagnosis” but not for CHF, pneumonia, or “counseling and prevention” when compared with non-teaching hospitals. Performance decreased as the share of Medicaid patients increased. More technology and a registered nursing staff with more education were factors associated with higher success in meeting quality indicators.
Conclusions
This ambitious study evaluated the quality of hospital care across the nation using information collected from both JCAHO and CMS. It demonstrated room for improvement, with hospitals as a whole providing 76% of the recommended measures for acute MI, CHF, and pneumonia. The study suggests that ownership characteristics, teaching status, JCAHO accreditation, technology investments, and nursing staff with degrees strongly correlates to success in meeting performance measures.
The authors conclude that the findings have implications for public policy and patient choice. They hypothesize that regions of the country and rural locations more often associated with low performance could use additional resources aimed at bolstering performance. Patients living in rural areas have little choice without traveling great distances. The authors also state that the characteristics of hospitals that influence performance, such as ownership, teaching status, JCAHO accreditation, technology investments, and nursing status, are remediable.
It is important to bear in mind, however, given the cross-sectional nature of the data, that the associations reported are not proof of causality. Quality performance measures were not highly correlated among hospitals for the three conditions studied, with only 3.8% in the top quintile for all three diseases; this result demonstrates the difficulty inherent in generically rating hospitals. Additionally, this study makes no attempt to examine how meeting performance measures affects clinical outcomes, an important part of this ongoing national debate.
Treat DVT
Kearon C, Ginsberg JS, Julian JA, et al. Comparison of fixed-dose weight-adjusted unfractionated heparin and low-molecular-weight heparin for acute treatment of venous thromboembolism. JAMA. 2006 Aug 23;296(8):935-942.
Background
The current practice of treating DVT involves starting the patient on LMW (low molecular weight) heparin administered subcutaneously or initiating an IV drip of unfractionated heparin. The latter prevents the patient from being discharged as soon as treatment is initiated and requires repeat checking of aPTTs and drip adjustments, which may lead to over-shoot and/or sub-therapeutic dosage. On the other hand, treatment with LMW heparin is costly and can be tricky for patients with varying degrees of renal failure. Using fixed-dose subcutaneous injections of unfractionated heparin is a novel idea and could be the solution to the above-mentioned issues.
Methods
Eight hospitals in Canada and New Zealand with a total of 708 eligible and willing participants were involved in the study. The study design was a randomized, controlled, non-inferiority trial; the adjudication and monitoring committees were blinded. Patients older than 18 with a new diagnosis of DVT and/or pulmonary embolism were considered eligible. Patients with any of the usual contraindications for anticoagulation, including recent major bleeding events, were excluded, as were patients with renal failure and pregnancy.
Computerized randomization was done at a central location, and patients were started on either twice daily weight-based dosing of LMW heparin (100 IU/kg) or twice daily dosing of weight-based unfractionated heparin (first dose of 333 U/kg, subsequent doses of 250 U/kg). No coagulation testing was done to modify these doses. The patients were treated for at least five days, until the International Normalized Ratio (INR) was in the therapeutic range for two consecutive days. Patients were concomitantly started on warfarin. Recurrent venous thromboses, bleeding episodes—described as drop of hemoglobin >2.0—and death were primary endpoints.
Results
The assumption of non-inferiority was supported by the analysis of recurrent VTEs, which were 12 (3.4%) in the LMW heparin group and 13 (3.8%) in the unfractionated heparin group—clinically, a non-significant difference. Bleeding rates at 10 days or at three months were not significantly different for the two groups. Number of deaths was 18 in the unfractionated heparin group and 22 in the LMW heparin group. No patients were reported to have developed heparin-induced thrombocytopenia, a serious and often life-threatening complication of unfractionated heparin use.
Conclusions
This interesting study demonstrates that the use of fixed dose, unmonitored, subcutaneous unfractionated heparin in twice daily dosing is non-inferior to treatment with different kinds of LMW heparin. The authors have also analyzed the cost difference, which, at existing U.S. pricing, would be in the vicinity of $675 for the six-day treatment of an 80-kg patient. Though more data is needed on patients with special considerations such as renal failure, the results, which support non-inferiority and cite a major cost advantage, merit further studies to validate these conclusions and to further evaluate this approach in patient populations with special considerations.
Non-Invasive Testing Prior to Vascular Surgery
Poldermans D, Bax JJ, Schouten O, et al. Should major vascular surgery be delayed because of preoperative cardiac testing in intermediate-risk patients receiving beta-blocker therapy with tight heart rate control? J Am Coll Cardiol. 2006 Sep 5;48(5):964-969.
Background
Current guidelines from the AHA and the American College of Cardiology (ACC) recommend non-invasive testing for patients scheduled for major vascular surgery as part of the pre-operative work-up if they have clinical factors suggestive of increased cardiac risk. The study was performed to show that no testing combined with aggressive beta blockade is not inferior in comparison to non-invasive testing for patients in the intermediate risk group who are preparing to undergo major vascular surgery. Testing often results in delays that can result in poor outcomes; additionally, invasive intervention based upon non-invasive test results has not been clearly shown to add any benefit to the eventual outcome of the patient.
Methods
The study was conducted at five clinical centers in Europe and Brazil, where 1,476 patients undergoing elective open abdominal aortic or infrainguinal arterial reconstruction were enrolled. The design was a randomized, controlled, non-inferiority trial with the outcome assessors blinded. Inclusion criteria consisted of age older than 70, angina pectoris, prior myocardial infarction (MI), compensated or history of congestive heart failure, diabetes mellitus, renal dysfunction and prior stroke, or transient ischemic attack. Patients with one or two risk factors were labeled intermediate risk and were randomized to receive either just beta-blocker therapy or non-invasive testing with dobutamine echocardiography or dobutamine or dipyridamole perfusion scintigraphy.
Patients with limited or no ischemia were referred for surgery with beta-blocker therapy. In patients with extensive ischemia—five ischemic segments or more—coronary angiography and revascularization were performed if the main surgery could be delayed. Beta-blocker therapy was instituted in all patients, with a goal heart rate of 60-65. The beta-blocker therapy was continued postoperatively. IV metoprolol was used in the ICU if a patient could not take drugs orally. Primary endpoints were a combination of cardiac death and nonfatal MI at 30 days and two years.
Results
Of the 770 patients classified as intermediate risk, 386 received cardiac testing and 384 patients were not tested. There were no significant differences in the presence of ischemic heart disease in the two subsets. The time gap between screening to vascular surgery was 34 days (seven to 88 days) in the no testing group, compared with 53 days (1,321 days) in the testing group (P<0.001). There was no difference in the composite endpoints—either at 30 days or at two years—for the two groups.
Conclusions
This excellent study shows that the approach of no screening in patients with intermediate cardiac risk factors before vascular surgery is non-inferior. An interesting point elucidated by the authors in their discussion details why studies designed to achieve a goal heart rate, rather than those based on fixed dose beta-blockers, are ideal to show the benefits of beta blockade in this population subset. The benefit of coronary revascularization for intermediate risk patients with extensive ischemia could not be defined, however; the number was too small to show any significance.
Score!
Deciding to measure performance—whether by test scores or clinical indicators—is step one to improve what you’re measuring. So when the Centers for Medicare and Medicaid Services (CMS) awarded $8.85 million in incentives to hospitals that showed measurable care improvements in 2005, it was no surprise that industry stakeholders took notice. Top decile hospitals received a 3% bonus, while second decile winners received 1%; bonuses were based on the achievement of specific clinical quality indicators. CMS improved care quality in five targeted clinical areas by the percentages indicated: community-acquired pneumonia (CAP) by 10%, heart failure by 9%, hip/knee replacement and coronary artery bypass graft (CABG) by 5% each, and acute myocardial infarction (AMI) by 4%.
CMS’ core measures project encourages winners to tout their achievements to consumers, recruitable physicians, payers, and anyone else who will listen. Like any program based on achieving scores rather than identifying the processes necessary to achieve success, though, insiders can speculate about what variables are responsible for positive outcomes. In the case of CMS’ core measures, if hospitalist stakeholders can demonstrate that having hospitalists increases a hospital’s CMS core measure performance, they’ve earned important marketing and clinical leverage. Stacy Goldsholl, MD, of Wilmington, N.C.-based TeamHealth, estimates that more than 70% of TeamHealth’s potential clients now ask for her firm’s data on CMS core measures.
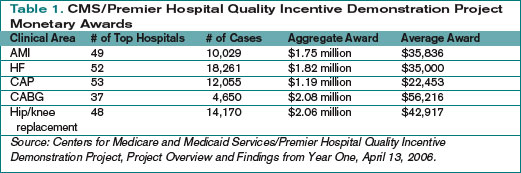
The Hospitalist’s Measures
To explore the relationship between a hospital’s position in the top two deciles on core measures with its hospitalist program, The Hospitalist extrapolated data from the CMS/Premier Hospital Quality Incentive Demonstration Project (www.premierinc.com/quality-safety) and SHM’s membership list, a proxy for a comprehensive list of hospitalist programs. All 44 hospitals in the top two deciles for heart failure core measures and the 49 hospitals listed for CAP were checked against the SHM list, as were their Web sites, for mention of a hospitalist program.
We compared data on two of the five core measures: heart failure and CAP. We expected a higher correlation for CAP because hospitalists are more likely to have primary inpatient responsibility for CAP patients than they are for heart failure patients, for whom cardiologists often have primary accountability. Here are the results of The Hospitalist’s analysis.
Hospitals in the top 10% for heart failure core measures are St. Helena Hospital (Calif.), Homestead Hospital (Fla.), Kootenai Medical Center (Idaho), Mission Hospital (N.C.), Staten Island University Hospital (N.Y.), Harris Methodist Fort Worth (Texas), and Harris Methodist Southwest (Texas).
Top decile performers in CAP are Methodist Medical Center of Illinois (Ill.), St. Vincent Memorial Hospital (Ill.), Heartland Regional Medical Center (Mo.), Stanly Memorial Hospital (N.C.), Alegent Health Immanuel Medical Center (Neb.), Staten Island University Hospital (N.Y.), Presbyterian Hospital of Kaufman (Texas), and Aurora Medical Center (Wis.).
Hospitals with some form of hospitalist program performed well, particularly on the second decile of the two core measures The Hospitalist examined: heart failure (44%) and community-acquired pneumonia (58%).
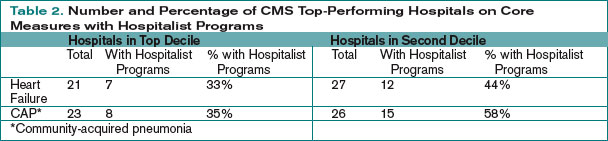
Complex Issues
Hospitalists expressed varied reactions to The Hospitalist’s correlation between a hospital’s core measures performance and its use of hospitalists. Adam Singer, MD, CEO of IPC-The Hospitalist Company of North Hollywood, Calif., scanned The Hospitalist’s lists and found a number of top-performing hospitals on its roster, including Methodist Forth Worth and Methodist Southwest in Texas.
According to Dr. Singer, none of IPC’s 105 hospitalist practices tie core measures to the group’s incentives, and prospective clients haven’t made core measures a top priority. Still, the firm has invested substantially in information technology (IT) infrastructure for hospitalists to track core measures compliance and other clinical indicators.
“In a pay-for-performance world, you need IT tools to help with core measures and DRG [diagnosis-related group] documentation, which will improve clinical and financial results dramatically.”
Ron Greeno, MD, CMO of Cogent Healthcare in Los Angeles, is dubious about tying core measures compliance to the presence of hospitalists. “The core measures are CMS’ attempt to devise a statistical representation of everything clinically relevant that a doctor does,” he says. “It’s like a quiz at school. You can memorize answers to the quiz without learning the subject … . It’s measuring quality by proxy.”
The fact that “hospitalist program” applies to a wide range of programs—from one emergency department doctor admitting patients to full-blown, highly organized, and well-resourced hospital medicine groups, also muddies the waters. “Comparing them on core measure compliance is not science,” concludes Dr. Greeno.
Team Health’s Dr. Goldsholl says that while hospitalists enhance core measures compliance many hospitals throw other resources at improving core measures compliance without much to show for it.
“Some hospitals have case managers telling doctors that they can’t discharge a patient without documenting core measure compliance, or [they] have hired one case manager per core measure,” she explains. “Others issue MD report cards. Some [hospitals] without strong quality improvement departments and strong governance aren’t sure what to do.”
Dr. Goldsholl points out that hospitalists, who routinely incorporate core measures compliance along with their other duties, give hospitals greater value for money spent than hiring case managers just for core measure compliance.
Then there are problems with the core measures themselves, as a recent JAMA study shows. Fonarow and colleagues examined the correlation between heart failure-related 60- to 90-day mortality and re-hospitalizations and CMS core measures.1 They concluded that “current heart failure performance measures, aside from prescription of an ACE inhibitor or angiotensin receptor blocker at discharge, have little relationship to mortality and combined mortality/rehospitalizations … post-hospitalization.” The authors urge the adoption of additional measures and better methods for identifying and validating heart failure performance measures.
More to Come
Core measure weakness notwithstanding, Dr. Greeno believes CMS core measures represent a major salvo in the pay-for-performance movement. “They’re the first step in changing the entire reimbursement system,” he says. “To succeed, a hospital will need the right doctors trained to work together as a team, with consensus on order sets, care protocols, excellent communication with primary care physicians, and statistical identification of obstacles to achieving quality within the hospitals.” TH
Marlene Piturro is a regular contributor to The Hospitalist.
Reference
- Fonarow GC, Abraham WT, Albert NM, et al. Association between performance measures and clinical outcomes for patients hospitalized with heart failure. JAMA. 2007 Jan 3;297(1):61-70.
Deciding to measure performance—whether by test scores or clinical indicators—is step one to improve what you’re measuring. So when the Centers for Medicare and Medicaid Services (CMS) awarded $8.85 million in incentives to hospitals that showed measurable care improvements in 2005, it was no surprise that industry stakeholders took notice. Top decile hospitals received a 3% bonus, while second decile winners received 1%; bonuses were based on the achievement of specific clinical quality indicators. CMS improved care quality in five targeted clinical areas by the percentages indicated: community-acquired pneumonia (CAP) by 10%, heart failure by 9%, hip/knee replacement and coronary artery bypass graft (CABG) by 5% each, and acute myocardial infarction (AMI) by 4%.
CMS’ core measures project encourages winners to tout their achievements to consumers, recruitable physicians, payers, and anyone else who will listen. Like any program based on achieving scores rather than identifying the processes necessary to achieve success, though, insiders can speculate about what variables are responsible for positive outcomes. In the case of CMS’ core measures, if hospitalist stakeholders can demonstrate that having hospitalists increases a hospital’s CMS core measure performance, they’ve earned important marketing and clinical leverage. Stacy Goldsholl, MD, of Wilmington, N.C.-based TeamHealth, estimates that more than 70% of TeamHealth’s potential clients now ask for her firm’s data on CMS core measures.
The Hospitalist’s Measures
To explore the relationship between a hospital’s position in the top two deciles on core measures with its hospitalist program, The Hospitalist extrapolated data from the CMS/Premier Hospital Quality Incentive Demonstration Project (www.premierinc.com/quality-safety) and SHM’s membership list, a proxy for a comprehensive list of hospitalist programs. All 44 hospitals in the top two deciles for heart failure core measures and the 49 hospitals listed for CAP were checked against the SHM list, as were their Web sites, for mention of a hospitalist program.
We compared data on two of the five core measures: heart failure and CAP. We expected a higher correlation for CAP because hospitalists are more likely to have primary inpatient responsibility for CAP patients than they are for heart failure patients, for whom cardiologists often have primary accountability. Here are the results of The Hospitalist’s analysis.
Hospitals in the top 10% for heart failure core measures are St. Helena Hospital (Calif.), Homestead Hospital (Fla.), Kootenai Medical Center (Idaho), Mission Hospital (N.C.), Staten Island University Hospital (N.Y.), Harris Methodist Fort Worth (Texas), and Harris Methodist Southwest (Texas).
Top decile performers in CAP are Methodist Medical Center of Illinois (Ill.), St. Vincent Memorial Hospital (Ill.), Heartland Regional Medical Center (Mo.), Stanly Memorial Hospital (N.C.), Alegent Health Immanuel Medical Center (Neb.), Staten Island University Hospital (N.Y.), Presbyterian Hospital of Kaufman (Texas), and Aurora Medical Center (Wis.).
Hospitals with some form of hospitalist program performed well, particularly on the second decile of the two core measures The Hospitalist examined: heart failure (44%) and community-acquired pneumonia (58%).
Complex Issues
Hospitalists expressed varied reactions to The Hospitalist’s correlation between a hospital’s core measures performance and its use of hospitalists. Adam Singer, MD, CEO of IPC-The Hospitalist Company of North Hollywood, Calif., scanned The Hospitalist’s lists and found a number of top-performing hospitals on its roster, including Methodist Forth Worth and Methodist Southwest in Texas.
According to Dr. Singer, none of IPC’s 105 hospitalist practices tie core measures to the group’s incentives, and prospective clients haven’t made core measures a top priority. Still, the firm has invested substantially in information technology (IT) infrastructure for hospitalists to track core measures compliance and other clinical indicators.
“In a pay-for-performance world, you need IT tools to help with core measures and DRG [diagnosis-related group] documentation, which will improve clinical and financial results dramatically.”
Ron Greeno, MD, CMO of Cogent Healthcare in Los Angeles, is dubious about tying core measures compliance to the presence of hospitalists. “The core measures are CMS’ attempt to devise a statistical representation of everything clinically relevant that a doctor does,” he says. “It’s like a quiz at school. You can memorize answers to the quiz without learning the subject … . It’s measuring quality by proxy.”
The fact that “hospitalist program” applies to a wide range of programs—from one emergency department doctor admitting patients to full-blown, highly organized, and well-resourced hospital medicine groups, also muddies the waters. “Comparing them on core measure compliance is not science,” concludes Dr. Greeno.
Team Health’s Dr. Goldsholl says that while hospitalists enhance core measures compliance many hospitals throw other resources at improving core measures compliance without much to show for it.
“Some hospitals have case managers telling doctors that they can’t discharge a patient without documenting core measure compliance, or [they] have hired one case manager per core measure,” she explains. “Others issue MD report cards. Some [hospitals] without strong quality improvement departments and strong governance aren’t sure what to do.”
Dr. Goldsholl points out that hospitalists, who routinely incorporate core measures compliance along with their other duties, give hospitals greater value for money spent than hiring case managers just for core measure compliance.
Then there are problems with the core measures themselves, as a recent JAMA study shows. Fonarow and colleagues examined the correlation between heart failure-related 60- to 90-day mortality and re-hospitalizations and CMS core measures.1 They concluded that “current heart failure performance measures, aside from prescription of an ACE inhibitor or angiotensin receptor blocker at discharge, have little relationship to mortality and combined mortality/rehospitalizations … post-hospitalization.” The authors urge the adoption of additional measures and better methods for identifying and validating heart failure performance measures.
More to Come
Core measure weakness notwithstanding, Dr. Greeno believes CMS core measures represent a major salvo in the pay-for-performance movement. “They’re the first step in changing the entire reimbursement system,” he says. “To succeed, a hospital will need the right doctors trained to work together as a team, with consensus on order sets, care protocols, excellent communication with primary care physicians, and statistical identification of obstacles to achieving quality within the hospitals.” TH
Marlene Piturro is a regular contributor to The Hospitalist.
Reference
- Fonarow GC, Abraham WT, Albert NM, et al. Association between performance measures and clinical outcomes for patients hospitalized with heart failure. JAMA. 2007 Jan 3;297(1):61-70.
Deciding to measure performance—whether by test scores or clinical indicators—is step one to improve what you’re measuring. So when the Centers for Medicare and Medicaid Services (CMS) awarded $8.85 million in incentives to hospitals that showed measurable care improvements in 2005, it was no surprise that industry stakeholders took notice. Top decile hospitals received a 3% bonus, while second decile winners received 1%; bonuses were based on the achievement of specific clinical quality indicators. CMS improved care quality in five targeted clinical areas by the percentages indicated: community-acquired pneumonia (CAP) by 10%, heart failure by 9%, hip/knee replacement and coronary artery bypass graft (CABG) by 5% each, and acute myocardial infarction (AMI) by 4%.
CMS’ core measures project encourages winners to tout their achievements to consumers, recruitable physicians, payers, and anyone else who will listen. Like any program based on achieving scores rather than identifying the processes necessary to achieve success, though, insiders can speculate about what variables are responsible for positive outcomes. In the case of CMS’ core measures, if hospitalist stakeholders can demonstrate that having hospitalists increases a hospital’s CMS core measure performance, they’ve earned important marketing and clinical leverage. Stacy Goldsholl, MD, of Wilmington, N.C.-based TeamHealth, estimates that more than 70% of TeamHealth’s potential clients now ask for her firm’s data on CMS core measures.
The Hospitalist’s Measures
To explore the relationship between a hospital’s position in the top two deciles on core measures with its hospitalist program, The Hospitalist extrapolated data from the CMS/Premier Hospital Quality Incentive Demonstration Project (www.premierinc.com/quality-safety) and SHM’s membership list, a proxy for a comprehensive list of hospitalist programs. All 44 hospitals in the top two deciles for heart failure core measures and the 49 hospitals listed for CAP were checked against the SHM list, as were their Web sites, for mention of a hospitalist program.
We compared data on two of the five core measures: heart failure and CAP. We expected a higher correlation for CAP because hospitalists are more likely to have primary inpatient responsibility for CAP patients than they are for heart failure patients, for whom cardiologists often have primary accountability. Here are the results of The Hospitalist’s analysis.
Hospitals in the top 10% for heart failure core measures are St. Helena Hospital (Calif.), Homestead Hospital (Fla.), Kootenai Medical Center (Idaho), Mission Hospital (N.C.), Staten Island University Hospital (N.Y.), Harris Methodist Fort Worth (Texas), and Harris Methodist Southwest (Texas).
Top decile performers in CAP are Methodist Medical Center of Illinois (Ill.), St. Vincent Memorial Hospital (Ill.), Heartland Regional Medical Center (Mo.), Stanly Memorial Hospital (N.C.), Alegent Health Immanuel Medical Center (Neb.), Staten Island University Hospital (N.Y.), Presbyterian Hospital of Kaufman (Texas), and Aurora Medical Center (Wis.).
Hospitals with some form of hospitalist program performed well, particularly on the second decile of the two core measures The Hospitalist examined: heart failure (44%) and community-acquired pneumonia (58%).
Complex Issues
Hospitalists expressed varied reactions to The Hospitalist’s correlation between a hospital’s core measures performance and its use of hospitalists. Adam Singer, MD, CEO of IPC-The Hospitalist Company of North Hollywood, Calif., scanned The Hospitalist’s lists and found a number of top-performing hospitals on its roster, including Methodist Forth Worth and Methodist Southwest in Texas.
According to Dr. Singer, none of IPC’s 105 hospitalist practices tie core measures to the group’s incentives, and prospective clients haven’t made core measures a top priority. Still, the firm has invested substantially in information technology (IT) infrastructure for hospitalists to track core measures compliance and other clinical indicators.
“In a pay-for-performance world, you need IT tools to help with core measures and DRG [diagnosis-related group] documentation, which will improve clinical and financial results dramatically.”
Ron Greeno, MD, CMO of Cogent Healthcare in Los Angeles, is dubious about tying core measures compliance to the presence of hospitalists. “The core measures are CMS’ attempt to devise a statistical representation of everything clinically relevant that a doctor does,” he says. “It’s like a quiz at school. You can memorize answers to the quiz without learning the subject … . It’s measuring quality by proxy.”
The fact that “hospitalist program” applies to a wide range of programs—from one emergency department doctor admitting patients to full-blown, highly organized, and well-resourced hospital medicine groups, also muddies the waters. “Comparing them on core measure compliance is not science,” concludes Dr. Greeno.
Team Health’s Dr. Goldsholl says that while hospitalists enhance core measures compliance many hospitals throw other resources at improving core measures compliance without much to show for it.
“Some hospitals have case managers telling doctors that they can’t discharge a patient without documenting core measure compliance, or [they] have hired one case manager per core measure,” she explains. “Others issue MD report cards. Some [hospitals] without strong quality improvement departments and strong governance aren’t sure what to do.”
Dr. Goldsholl points out that hospitalists, who routinely incorporate core measures compliance along with their other duties, give hospitals greater value for money spent than hiring case managers just for core measure compliance.
Then there are problems with the core measures themselves, as a recent JAMA study shows. Fonarow and colleagues examined the correlation between heart failure-related 60- to 90-day mortality and re-hospitalizations and CMS core measures.1 They concluded that “current heart failure performance measures, aside from prescription of an ACE inhibitor or angiotensin receptor blocker at discharge, have little relationship to mortality and combined mortality/rehospitalizations … post-hospitalization.” The authors urge the adoption of additional measures and better methods for identifying and validating heart failure performance measures.
More to Come
Core measure weakness notwithstanding, Dr. Greeno believes CMS core measures represent a major salvo in the pay-for-performance movement. “They’re the first step in changing the entire reimbursement system,” he says. “To succeed, a hospital will need the right doctors trained to work together as a team, with consensus on order sets, care protocols, excellent communication with primary care physicians, and statistical identification of obstacles to achieving quality within the hospitals.” TH
Marlene Piturro is a regular contributor to The Hospitalist.
Reference
- Fonarow GC, Abraham WT, Albert NM, et al. Association between performance measures and clinical outcomes for patients hospitalized with heart failure. JAMA. 2007 Jan 3;297(1):61-70.
A Sign-off Pace Car
Sign-offs, change of service, handoffs, inter-shift communications. Whatever the euphemism used, these occurrences symbolize the stigmata of disruption in the continuity of care for the hospitalized patient. The medical literature is saturated with studies pointing to the universal fact that disruption in the continuity of care leads to medical errors, and this ultimately contributes to compromise in patient care and safety. The New England Journal of Medicine article demonstrating that mortality rates are higher on the weekends than on weekdays is just a hint of the negative consequences that result from the disruption of the continuity of care in hospital medicine.1
Disruptions in continuity of care have been viewed as a necessary evil by the medical community. There is an ever-present diametric pull between physician hourly workload and continuity of care. Is the full potential of the hospitalist model undermined by the disruption in continuity of care? As hospitalists, we are fully aware of the inherent benefits of being in-house in terms of delivering efficiency and quality of care. Unfortunately, the weakness inherent in the hospitalist model has been the fragmented delivery of care it provides—a problem that is primarily due to the multiple changes in physician care that set it apart from the continuity of care that a primary care physician model can deliver. In the traditional primary care physician model, a patient is under the care of the primary care physician during hospitalization, with 24/7 pager coverage and occasional weekend sign-ons and sign-offs.
Decatur (Ill.) Memorial Hospital (DMH) is a 350-bed hospital; our facility serves a community of 100,000 and acts as a tertiary center for the smaller medical facilities in the collar counties. All specialty services are represented, including invasive cardiology, interventional radiology, neuro-interventional radiology, cardiothoracic surgery, and neurosurgery. Currently DMH Hospitalist Services has four physicians (with the addition of two more hospitalists planned for July 2007), two physician assistants, and an office manager. DMH Hospitalist Services utilizes a one-week-on/one-week-off system. Because Decatur has no traffic congestion, all hospitalists live 10 to 15 minutes from the hospital by car.

We in Hospitalist Services advocate a paradigm shift: Continuity-of-care disruptions should be minimized by eliminating the process entirely. We didn’t want to improve the sign-off process; instead, we eliminated it. We don’t use the traditional hospitalist model of shift work. Rather we have affected a marriage of the primary care physician model and the hospitalist model, utilizing the advantages of both models in a hybrid system.
In our model, we have eliminated the daily sign-off and sign-on process altogether. The only time there is a sign-off and sign-on is on a weekly basis, when the new service starts its weekly shift on Monday mornings. Instead of the 14 handoffs required in a week for a nocturnist shift model, there is only one physician sign-off and sign-on per patient per week. Because the number of handoffs has been reduced from 14 to one per week, the change of service sign-outs on Monday are performed face to face and at a deliberate pace, with sign-out averages of 15 patients sometimes taking a full hour or more. This luxurious pace is not possible with multiple handoffs per day.
For the patient admitted and discharged between Mondays, there is no disruption in continuity of care in terms of physicians. The hospitalist who accepts the patient on Monday morning will be on pager call for the patient until the next Monday morning when he or she signs off for the week—or until the patient is discharged, whichever comes first.
Responsibilities for new admissions and consults are divided into a 24-hour period, with the physician on call performing all the admissions and consults. During the next 24-hour period, the same hospitalist does not have any admission responsibilities. All new admissions are evaluated in real time by the admitting hospitalists; admissions between midnight and 7 a.m., however, can be evaluated in the morning at the discretion of the hospitalist in conjunction with the emergency department physician, who may write temporary holding orders. All critically ill patients are evaluated in real time.
We have found that there are some key advantages to our model. First, there is true continuity of care. As mentioned earlier, the admitting hospitalist will be the attending physician until the patient is discharged or until the following Monday morning when the relieving hospitalist accepts the patient.
Second, when the hospitalist is paged after hours, patient familiarity aids in the appropriate and efficient management of the patient, with reduction in unnecessary laboratory orders, redundant tests, and overcautious ICU transfers. “When our nurses call the hospitalist about their patients, especially in the evening and night shifts, the nurses are not wasting time and effort educating an on-call physician about the patient, but instead can focus on the acute medical issues at hand, knowing that the hospitalist intimately knows the patient’s background and current medical status,” says Chris Pope, RN, director of the Medical Nursing Unit at Decatur Memorial Hospital. “This gives confidence to our nursing staff that their interactions with the hospitalists will result in appropriate care delivered to the patient.”
Third, the hospitalist has a natural incentive to optimize patient care, knowing that a lackadaisical approach to patient care cannot be pawned to another physician at a later shift: The hospitalist has true ownership and attending status for the patient. I believe that the manner in which a hospitalist program’s infrastructure is set up plays a critical role in the hospitalists’ behavior. Just as collective farms in the communist system were far less efficient and more poorly run than privately owned farms in a capitalist system, hospitalist programs that have more of a collective approach to patient management may offer less motivation for the hospitalist.
Fourth, our relationships and ability to communicate with the patients and their families are strengthened because the confusion about exactly who is the hospitalist in charge of patient care has been eliminated with the removal of nocturnists and weekend coverage. We have found this to be one of the most rewarding aspects of this system because communication is the bedrock of any doctor-patient relationship and is especially important for the hospitalist, who must quickly develop a rapport with the patient. This success is reflected in the fact that our hospitalists have earned among them 20 Decatur Memorial Hospital Exceptional Service Recognition Awards from our patients in the last two years.
Fifth, the nurses and the primary care physician have a clear understanding of which hospitalist/attending is responsible for patient care. The nursing staff was initially shocked that there was no cross coverage, even on weekends and nights; the primary care physician, though, knows exactly which hospitalist is taking care of his or her patient, even after hours. In thinking about my time spent working at a major teaching hospital (a powerfully negative experience, by the way) I found there that, most of the time, I couldn’t get a clear answer from the internal medicine residents who were taking care of my patient. If I rounded early, the service had not picked up the patient from night float; and if I rounded in the afternoon, the service had signed out to the night float, and the night float had no medical knowledge of the patient. I made a personal commitment that this would not happen at DMH.
Sixth, we believe that the ultimate sign-out, the sign-out to the primary care physician on discharge of a patient, is just as critical as any in-house sign-out process. The Hospitalist Services at Decatur Memorial Hospital utilizes General Electric’s Centricity EMR, an electronic medical record system. With modification of the program, we perform our histories, physicals, and discharge summaries electronically.
We have modified the software so the discharge summary serves a triple purpose: The summary serves as a discharge instruction for the patient, including medication reconciliation with electronic prescription printout, as well as instructions for diet, follow-up care, and ancillary services. Secondly, the discharge summary is electronically sent to the medical records department to fulfill the discharge summary requirements of the hospitalization. Finally, the discharge summary is electronically mailed to primary care physicians who have Centricity EMR and is faxed to those who do not. All of these goals are achieved prior to patient discharge. And, as an additional courtesy, all primary care physicians receive a phone call in order to add a human element.
The success of DMH’s Hospitalist Services is directly attributable to the continuity of care that our schedule provides. The hospitalist model was a new concept among the medical staff at Decatur Memorial Hospital. It was met with skepticism among our primary care physicians, mostly because of the strong relationships the physicians had developed with their patients. With the continuity of care provided by our model, however, we were able to market the Hospitalist Services with great success.
“The continuity of care was something my group was very concerned about when we decided to utilize the services of our local hospitalists,” says Michael Wall, MD, FAAFP, who is part of a DMH call group consisting of six family practice physicians. “Prior to our move to the hospitalist model, we would normally cover our own patients throughout the week and sign out to the on-call physician in our group for weekend coverage. Those sign-outs were very detailed and specific, including the nuances involved in [the] care of our ‘special’ patients.
“When we began using the hospitalists, Dr. Yu assured us that the same high quality service that our patients have come to expect from us would continue, including [in] the area of continuity of care,” he explains. “Since our transition, both the physicians and patients have been pleased with the high level of service delivered by our hospitalists. The Hospitalist Services has truly kept their promise to us on all the issues we were most concerned about. Our patients are happy, and our group physicians are happy. It has been a win-win arrangement for everyone.”
According to James Neviackas, MD, who was head of nephrology at DMH before being recruited as a hospitalist in Hospitalist Services, “Actually, the patients in our service receive better continuity of care than the primary care model, since there are no changes of service, even on the weeknights or weekends.”
The obvious major disadvantage of the DMH model is the fact that the hospitalist is on continuous pager call for seven days. But it has been our experience that the incentive to “tuck in the patient” to minimize after-hours pages continuously challenges each hospitalist to optimize medical care for the patient. This is especially true for the critically ill patient, because DMH is a regional tertiary center, and our Hospitalist Services act as accepting physicians for regional transfers to our institution.
We have been successfully recruiting physicians as we expand our services, and our model has not been a source of candidate qualm, even among physicians coming out of residency. What has helped tremendously in the acceptance of our model has been the fact that three out of our four hospitalists have been in a solo practice environment and are used to the concept of continuity of care; they do not see it as a burden but as a duty.
Our service views itself as practice partners with the primary care physicians we provide service to and feel that we are part of their group, not just hospital consultants. “I don’t feel like a hospitalist at all but [instead like] an internist following his own patients through hospitalization,” says Larry Holder, MD, FACP, who was in a solo internal medicine practice before joining the Hospitalist Services. “The schedule gives me the chance to bond with my patients and give them the optimal care that they deserve. Patients and their families frequently ask anxiously if I’m going to be there tomorrow or if there are emergencies [will I] be around. And to be able to say, ‘I’ll be here if you need me,’ gives patients and their families a sense of reassurance and instant bonding with the physician. At the end of the day, our profession is about healing the patient in a compassionate manner and not just about length of stay and cost reductions.”
Using a hospitalist model with multiple disruptions in continuity of care is analogous to having a Formula One race car but only being able to drive in rush hour traffic. The true potential of a hospitalist is constantly hindered when there is disruption in continuity of care. We should not be asking ourselves how to reduce the negative consequences of the sign-off process but, rather, how we can eliminate the process altogether. TH
Dr. Yu is medical director, Hospitalist Services, Decatur (Ill.) Memorial Hospital.
References
- Bell CM, Redelmeier DA. Mortality among patients admitted to hospitals on weekends as compared with weekdays. N Engl J Med. 2001 Aug 30;345(9):663-668. Erratum in: N Engl J Med 2001 Nov 22;345(21):1580.
Sign-offs, change of service, handoffs, inter-shift communications. Whatever the euphemism used, these occurrences symbolize the stigmata of disruption in the continuity of care for the hospitalized patient. The medical literature is saturated with studies pointing to the universal fact that disruption in the continuity of care leads to medical errors, and this ultimately contributes to compromise in patient care and safety. The New England Journal of Medicine article demonstrating that mortality rates are higher on the weekends than on weekdays is just a hint of the negative consequences that result from the disruption of the continuity of care in hospital medicine.1
Disruptions in continuity of care have been viewed as a necessary evil by the medical community. There is an ever-present diametric pull between physician hourly workload and continuity of care. Is the full potential of the hospitalist model undermined by the disruption in continuity of care? As hospitalists, we are fully aware of the inherent benefits of being in-house in terms of delivering efficiency and quality of care. Unfortunately, the weakness inherent in the hospitalist model has been the fragmented delivery of care it provides—a problem that is primarily due to the multiple changes in physician care that set it apart from the continuity of care that a primary care physician model can deliver. In the traditional primary care physician model, a patient is under the care of the primary care physician during hospitalization, with 24/7 pager coverage and occasional weekend sign-ons and sign-offs.
Decatur (Ill.) Memorial Hospital (DMH) is a 350-bed hospital; our facility serves a community of 100,000 and acts as a tertiary center for the smaller medical facilities in the collar counties. All specialty services are represented, including invasive cardiology, interventional radiology, neuro-interventional radiology, cardiothoracic surgery, and neurosurgery. Currently DMH Hospitalist Services has four physicians (with the addition of two more hospitalists planned for July 2007), two physician assistants, and an office manager. DMH Hospitalist Services utilizes a one-week-on/one-week-off system. Because Decatur has no traffic congestion, all hospitalists live 10 to 15 minutes from the hospital by car.
We in Hospitalist Services advocate a paradigm shift: Continuity-of-care disruptions should be minimized by eliminating the process entirely. We didn’t want to improve the sign-off process; instead, we eliminated it. We don’t use the traditional hospitalist model of shift work. Rather we have affected a marriage of the primary care physician model and the hospitalist model, utilizing the advantages of both models in a hybrid system.
In our model, we have eliminated the daily sign-off and sign-on process altogether. The only time there is a sign-off and sign-on is on a weekly basis, when the new service starts its weekly shift on Monday mornings. Instead of the 14 handoffs required in a week for a nocturnist shift model, there is only one physician sign-off and sign-on per patient per week. Because the number of handoffs has been reduced from 14 to one per week, the change of service sign-outs on Monday are performed face to face and at a deliberate pace, with sign-out averages of 15 patients sometimes taking a full hour or more. This luxurious pace is not possible with multiple handoffs per day.
For the patient admitted and discharged between Mondays, there is no disruption in continuity of care in terms of physicians. The hospitalist who accepts the patient on Monday morning will be on pager call for the patient until the next Monday morning when he or she signs off for the week—or until the patient is discharged, whichever comes first.
Responsibilities for new admissions and consults are divided into a 24-hour period, with the physician on call performing all the admissions and consults. During the next 24-hour period, the same hospitalist does not have any admission responsibilities. All new admissions are evaluated in real time by the admitting hospitalists; admissions between midnight and 7 a.m., however, can be evaluated in the morning at the discretion of the hospitalist in conjunction with the emergency department physician, who may write temporary holding orders. All critically ill patients are evaluated in real time.
We have found that there are some key advantages to our model. First, there is true continuity of care. As mentioned earlier, the admitting hospitalist will be the attending physician until the patient is discharged or until the following Monday morning when the relieving hospitalist accepts the patient.
Second, when the hospitalist is paged after hours, patient familiarity aids in the appropriate and efficient management of the patient, with reduction in unnecessary laboratory orders, redundant tests, and overcautious ICU transfers. “When our nurses call the hospitalist about their patients, especially in the evening and night shifts, the nurses are not wasting time and effort educating an on-call physician about the patient, but instead can focus on the acute medical issues at hand, knowing that the hospitalist intimately knows the patient’s background and current medical status,” says Chris Pope, RN, director of the Medical Nursing Unit at Decatur Memorial Hospital. “This gives confidence to our nursing staff that their interactions with the hospitalists will result in appropriate care delivered to the patient.”
Third, the hospitalist has a natural incentive to optimize patient care, knowing that a lackadaisical approach to patient care cannot be pawned to another physician at a later shift: The hospitalist has true ownership and attending status for the patient. I believe that the manner in which a hospitalist program’s infrastructure is set up plays a critical role in the hospitalists’ behavior. Just as collective farms in the communist system were far less efficient and more poorly run than privately owned farms in a capitalist system, hospitalist programs that have more of a collective approach to patient management may offer less motivation for the hospitalist.
Fourth, our relationships and ability to communicate with the patients and their families are strengthened because the confusion about exactly who is the hospitalist in charge of patient care has been eliminated with the removal of nocturnists and weekend coverage. We have found this to be one of the most rewarding aspects of this system because communication is the bedrock of any doctor-patient relationship and is especially important for the hospitalist, who must quickly develop a rapport with the patient. This success is reflected in the fact that our hospitalists have earned among them 20 Decatur Memorial Hospital Exceptional Service Recognition Awards from our patients in the last two years.
Fifth, the nurses and the primary care physician have a clear understanding of which hospitalist/attending is responsible for patient care. The nursing staff was initially shocked that there was no cross coverage, even on weekends and nights; the primary care physician, though, knows exactly which hospitalist is taking care of his or her patient, even after hours. In thinking about my time spent working at a major teaching hospital (a powerfully negative experience, by the way) I found there that, most of the time, I couldn’t get a clear answer from the internal medicine residents who were taking care of my patient. If I rounded early, the service had not picked up the patient from night float; and if I rounded in the afternoon, the service had signed out to the night float, and the night float had no medical knowledge of the patient. I made a personal commitment that this would not happen at DMH.
Sixth, we believe that the ultimate sign-out, the sign-out to the primary care physician on discharge of a patient, is just as critical as any in-house sign-out process. The Hospitalist Services at Decatur Memorial Hospital utilizes General Electric’s Centricity EMR, an electronic medical record system. With modification of the program, we perform our histories, physicals, and discharge summaries electronically.
We have modified the software so the discharge summary serves a triple purpose: The summary serves as a discharge instruction for the patient, including medication reconciliation with electronic prescription printout, as well as instructions for diet, follow-up care, and ancillary services. Secondly, the discharge summary is electronically sent to the medical records department to fulfill the discharge summary requirements of the hospitalization. Finally, the discharge summary is electronically mailed to primary care physicians who have Centricity EMR and is faxed to those who do not. All of these goals are achieved prior to patient discharge. And, as an additional courtesy, all primary care physicians receive a phone call in order to add a human element.
The success of DMH’s Hospitalist Services is directly attributable to the continuity of care that our schedule provides. The hospitalist model was a new concept among the medical staff at Decatur Memorial Hospital. It was met with skepticism among our primary care physicians, mostly because of the strong relationships the physicians had developed with their patients. With the continuity of care provided by our model, however, we were able to market the Hospitalist Services with great success.
“The continuity of care was something my group was very concerned about when we decided to utilize the services of our local hospitalists,” says Michael Wall, MD, FAAFP, who is part of a DMH call group consisting of six family practice physicians. “Prior to our move to the hospitalist model, we would normally cover our own patients throughout the week and sign out to the on-call physician in our group for weekend coverage. Those sign-outs were very detailed and specific, including the nuances involved in [the] care of our ‘special’ patients.
“When we began using the hospitalists, Dr. Yu assured us that the same high quality service that our patients have come to expect from us would continue, including [in] the area of continuity of care,” he explains. “Since our transition, both the physicians and patients have been pleased with the high level of service delivered by our hospitalists. The Hospitalist Services has truly kept their promise to us on all the issues we were most concerned about. Our patients are happy, and our group physicians are happy. It has been a win-win arrangement for everyone.”
According to James Neviackas, MD, who was head of nephrology at DMH before being recruited as a hospitalist in Hospitalist Services, “Actually, the patients in our service receive better continuity of care than the primary care model, since there are no changes of service, even on the weeknights or weekends.”
The obvious major disadvantage of the DMH model is the fact that the hospitalist is on continuous pager call for seven days. But it has been our experience that the incentive to “tuck in the patient” to minimize after-hours pages continuously challenges each hospitalist to optimize medical care for the patient. This is especially true for the critically ill patient, because DMH is a regional tertiary center, and our Hospitalist Services act as accepting physicians for regional transfers to our institution.
We have been successfully recruiting physicians as we expand our services, and our model has not been a source of candidate qualm, even among physicians coming out of residency. What has helped tremendously in the acceptance of our model has been the fact that three out of our four hospitalists have been in a solo practice environment and are used to the concept of continuity of care; they do not see it as a burden but as a duty.
Our service views itself as practice partners with the primary care physicians we provide service to and feel that we are part of their group, not just hospital consultants. “I don’t feel like a hospitalist at all but [instead like] an internist following his own patients through hospitalization,” says Larry Holder, MD, FACP, who was in a solo internal medicine practice before joining the Hospitalist Services. “The schedule gives me the chance to bond with my patients and give them the optimal care that they deserve. Patients and their families frequently ask anxiously if I’m going to be there tomorrow or if there are emergencies [will I] be around. And to be able to say, ‘I’ll be here if you need me,’ gives patients and their families a sense of reassurance and instant bonding with the physician. At the end of the day, our profession is about healing the patient in a compassionate manner and not just about length of stay and cost reductions.”
Using a hospitalist model with multiple disruptions in continuity of care is analogous to having a Formula One race car but only being able to drive in rush hour traffic. The true potential of a hospitalist is constantly hindered when there is disruption in continuity of care. We should not be asking ourselves how to reduce the negative consequences of the sign-off process but, rather, how we can eliminate the process altogether. TH
Dr. Yu is medical director, Hospitalist Services, Decatur (Ill.) Memorial Hospital.
References
- Bell CM, Redelmeier DA. Mortality among patients admitted to hospitals on weekends as compared with weekdays. N Engl J Med. 2001 Aug 30;345(9):663-668. Erratum in: N Engl J Med 2001 Nov 22;345(21):1580.
Sign-offs, change of service, handoffs, inter-shift communications. Whatever the euphemism used, these occurrences symbolize the stigmata of disruption in the continuity of care for the hospitalized patient. The medical literature is saturated with studies pointing to the universal fact that disruption in the continuity of care leads to medical errors, and this ultimately contributes to compromise in patient care and safety. The New England Journal of Medicine article demonstrating that mortality rates are higher on the weekends than on weekdays is just a hint of the negative consequences that result from the disruption of the continuity of care in hospital medicine.1
Disruptions in continuity of care have been viewed as a necessary evil by the medical community. There is an ever-present diametric pull between physician hourly workload and continuity of care. Is the full potential of the hospitalist model undermined by the disruption in continuity of care? As hospitalists, we are fully aware of the inherent benefits of being in-house in terms of delivering efficiency and quality of care. Unfortunately, the weakness inherent in the hospitalist model has been the fragmented delivery of care it provides—a problem that is primarily due to the multiple changes in physician care that set it apart from the continuity of care that a primary care physician model can deliver. In the traditional primary care physician model, a patient is under the care of the primary care physician during hospitalization, with 24/7 pager coverage and occasional weekend sign-ons and sign-offs.
Decatur (Ill.) Memorial Hospital (DMH) is a 350-bed hospital; our facility serves a community of 100,000 and acts as a tertiary center for the smaller medical facilities in the collar counties. All specialty services are represented, including invasive cardiology, interventional radiology, neuro-interventional radiology, cardiothoracic surgery, and neurosurgery. Currently DMH Hospitalist Services has four physicians (with the addition of two more hospitalists planned for July 2007), two physician assistants, and an office manager. DMH Hospitalist Services utilizes a one-week-on/one-week-off system. Because Decatur has no traffic congestion, all hospitalists live 10 to 15 minutes from the hospital by car.
We in Hospitalist Services advocate a paradigm shift: Continuity-of-care disruptions should be minimized by eliminating the process entirely. We didn’t want to improve the sign-off process; instead, we eliminated it. We don’t use the traditional hospitalist model of shift work. Rather we have affected a marriage of the primary care physician model and the hospitalist model, utilizing the advantages of both models in a hybrid system.
In our model, we have eliminated the daily sign-off and sign-on process altogether. The only time there is a sign-off and sign-on is on a weekly basis, when the new service starts its weekly shift on Monday mornings. Instead of the 14 handoffs required in a week for a nocturnist shift model, there is only one physician sign-off and sign-on per patient per week. Because the number of handoffs has been reduced from 14 to one per week, the change of service sign-outs on Monday are performed face to face and at a deliberate pace, with sign-out averages of 15 patients sometimes taking a full hour or more. This luxurious pace is not possible with multiple handoffs per day.
For the patient admitted and discharged between Mondays, there is no disruption in continuity of care in terms of physicians. The hospitalist who accepts the patient on Monday morning will be on pager call for the patient until the next Monday morning when he or she signs off for the week—or until the patient is discharged, whichever comes first.
Responsibilities for new admissions and consults are divided into a 24-hour period, with the physician on call performing all the admissions and consults. During the next 24-hour period, the same hospitalist does not have any admission responsibilities. All new admissions are evaluated in real time by the admitting hospitalists; admissions between midnight and 7 a.m., however, can be evaluated in the morning at the discretion of the hospitalist in conjunction with the emergency department physician, who may write temporary holding orders. All critically ill patients are evaluated in real time.
We have found that there are some key advantages to our model. First, there is true continuity of care. As mentioned earlier, the admitting hospitalist will be the attending physician until the patient is discharged or until the following Monday morning when the relieving hospitalist accepts the patient.
Second, when the hospitalist is paged after hours, patient familiarity aids in the appropriate and efficient management of the patient, with reduction in unnecessary laboratory orders, redundant tests, and overcautious ICU transfers. “When our nurses call the hospitalist about their patients, especially in the evening and night shifts, the nurses are not wasting time and effort educating an on-call physician about the patient, but instead can focus on the acute medical issues at hand, knowing that the hospitalist intimately knows the patient’s background and current medical status,” says Chris Pope, RN, director of the Medical Nursing Unit at Decatur Memorial Hospital. “This gives confidence to our nursing staff that their interactions with the hospitalists will result in appropriate care delivered to the patient.”
Third, the hospitalist has a natural incentive to optimize patient care, knowing that a lackadaisical approach to patient care cannot be pawned to another physician at a later shift: The hospitalist has true ownership and attending status for the patient. I believe that the manner in which a hospitalist program’s infrastructure is set up plays a critical role in the hospitalists’ behavior. Just as collective farms in the communist system were far less efficient and more poorly run than privately owned farms in a capitalist system, hospitalist programs that have more of a collective approach to patient management may offer less motivation for the hospitalist.
Fourth, our relationships and ability to communicate with the patients and their families are strengthened because the confusion about exactly who is the hospitalist in charge of patient care has been eliminated with the removal of nocturnists and weekend coverage. We have found this to be one of the most rewarding aspects of this system because communication is the bedrock of any doctor-patient relationship and is especially important for the hospitalist, who must quickly develop a rapport with the patient. This success is reflected in the fact that our hospitalists have earned among them 20 Decatur Memorial Hospital Exceptional Service Recognition Awards from our patients in the last two years.
Fifth, the nurses and the primary care physician have a clear understanding of which hospitalist/attending is responsible for patient care. The nursing staff was initially shocked that there was no cross coverage, even on weekends and nights; the primary care physician, though, knows exactly which hospitalist is taking care of his or her patient, even after hours. In thinking about my time spent working at a major teaching hospital (a powerfully negative experience, by the way) I found there that, most of the time, I couldn’t get a clear answer from the internal medicine residents who were taking care of my patient. If I rounded early, the service had not picked up the patient from night float; and if I rounded in the afternoon, the service had signed out to the night float, and the night float had no medical knowledge of the patient. I made a personal commitment that this would not happen at DMH.
Sixth, we believe that the ultimate sign-out, the sign-out to the primary care physician on discharge of a patient, is just as critical as any in-house sign-out process. The Hospitalist Services at Decatur Memorial Hospital utilizes General Electric’s Centricity EMR, an electronic medical record system. With modification of the program, we perform our histories, physicals, and discharge summaries electronically.
We have modified the software so the discharge summary serves a triple purpose: The summary serves as a discharge instruction for the patient, including medication reconciliation with electronic prescription printout, as well as instructions for diet, follow-up care, and ancillary services. Secondly, the discharge summary is electronically sent to the medical records department to fulfill the discharge summary requirements of the hospitalization. Finally, the discharge summary is electronically mailed to primary care physicians who have Centricity EMR and is faxed to those who do not. All of these goals are achieved prior to patient discharge. And, as an additional courtesy, all primary care physicians receive a phone call in order to add a human element.
The success of DMH’s Hospitalist Services is directly attributable to the continuity of care that our schedule provides. The hospitalist model was a new concept among the medical staff at Decatur Memorial Hospital. It was met with skepticism among our primary care physicians, mostly because of the strong relationships the physicians had developed with their patients. With the continuity of care provided by our model, however, we were able to market the Hospitalist Services with great success.
“The continuity of care was something my group was very concerned about when we decided to utilize the services of our local hospitalists,” says Michael Wall, MD, FAAFP, who is part of a DMH call group consisting of six family practice physicians. “Prior to our move to the hospitalist model, we would normally cover our own patients throughout the week and sign out to the on-call physician in our group for weekend coverage. Those sign-outs were very detailed and specific, including the nuances involved in [the] care of our ‘special’ patients.
“When we began using the hospitalists, Dr. Yu assured us that the same high quality service that our patients have come to expect from us would continue, including [in] the area of continuity of care,” he explains. “Since our transition, both the physicians and patients have been pleased with the high level of service delivered by our hospitalists. The Hospitalist Services has truly kept their promise to us on all the issues we were most concerned about. Our patients are happy, and our group physicians are happy. It has been a win-win arrangement for everyone.”
According to James Neviackas, MD, who was head of nephrology at DMH before being recruited as a hospitalist in Hospitalist Services, “Actually, the patients in our service receive better continuity of care than the primary care model, since there are no changes of service, even on the weeknights or weekends.”
The obvious major disadvantage of the DMH model is the fact that the hospitalist is on continuous pager call for seven days. But it has been our experience that the incentive to “tuck in the patient” to minimize after-hours pages continuously challenges each hospitalist to optimize medical care for the patient. This is especially true for the critically ill patient, because DMH is a regional tertiary center, and our Hospitalist Services act as accepting physicians for regional transfers to our institution.
We have been successfully recruiting physicians as we expand our services, and our model has not been a source of candidate qualm, even among physicians coming out of residency. What has helped tremendously in the acceptance of our model has been the fact that three out of our four hospitalists have been in a solo practice environment and are used to the concept of continuity of care; they do not see it as a burden but as a duty.
Our service views itself as practice partners with the primary care physicians we provide service to and feel that we are part of their group, not just hospital consultants. “I don’t feel like a hospitalist at all but [instead like] an internist following his own patients through hospitalization,” says Larry Holder, MD, FACP, who was in a solo internal medicine practice before joining the Hospitalist Services. “The schedule gives me the chance to bond with my patients and give them the optimal care that they deserve. Patients and their families frequently ask anxiously if I’m going to be there tomorrow or if there are emergencies [will I] be around. And to be able to say, ‘I’ll be here if you need me,’ gives patients and their families a sense of reassurance and instant bonding with the physician. At the end of the day, our profession is about healing the patient in a compassionate manner and not just about length of stay and cost reductions.”
Using a hospitalist model with multiple disruptions in continuity of care is analogous to having a Formula One race car but only being able to drive in rush hour traffic. The true potential of a hospitalist is constantly hindered when there is disruption in continuity of care. We should not be asking ourselves how to reduce the negative consequences of the sign-off process but, rather, how we can eliminate the process altogether. TH
Dr. Yu is medical director, Hospitalist Services, Decatur (Ill.) Memorial Hospital.
References
- Bell CM, Redelmeier DA. Mortality among patients admitted to hospitals on weekends as compared with weekdays. N Engl J Med. 2001 Aug 30;345(9):663-668. Erratum in: N Engl J Med 2001 Nov 22;345(21):1580.
A Pennsylvania Practice

More than 20 years before the term hospitalist was coined, the Brockie Medical Group, a strong internal medicine practice led by Benjamin Hoover, MD, relished its hospital work at York Hospital in York, Pa. Back then, the doctors didn’t call themselves hospitalists, but the time they spent on hospital duties made them the forebears of today’s hospitalists.
According to John McConville, MD, chairman of York Hospital’s department of medicine and a hospital fixture since 1976, some of Brockie Internal Medicine group’s physicians devoted 60% to 70% of their practice time to inpatient tasks. “That was the culture when I arrived on the scene,” he recounts. Shortly thereafter, the group grew stronger when The Brockie Internal Medicine Group’s main competition—a sizable family practice group—fell apart. Brockie absorbed its like-minded physicians.
York, pa.
The Brockie Internal Medical Group is firmly anchored in York, Pa., home to factories that produce barbells and Harley-Davidson motorcycles. York has a soft side, though—it produced the first Peppermint Pattie, a mint-chocolate candy. It is an affordable, rapidly growing suburb, a place where commuters to Philadelphia, Baltimore, and Washington, D.C., can have a comfortable lifestyle without big city housing prices and the hassles of urban life.
The medical community is close-knit, described by Jonathan Whitney, MD, a Brockie hospitalist leader, as “a collegial environment with a growing population and plenty of patients, so there’s not a sense of competition among physicians.” Dr. Whitney, along with William “Tex” Landis, MD, and Michael Lamanteer, MD, form the Brockie Hospitalist Group’s executive committee, elected decision makers who deal with WellSpan Health and York Hospital on behalf of their colleagues.
WellSpan’s Role
As York grew, so did the Brockie Internal Medical Group. Then came managed care in the 1980s and 1990s, and Brockie’s internists were not happy. “We saw the medical landscape changing everywhere, and we didn’t want managed care pushing us around,” explains Dr. Landis, a Lancaster, Pa., native and now the Brockie Hospitalist Group’s lead physician. “Analyzing how medicine was changing, we felt vulnerable as a single specialty group. We considered various scenarios for becoming a multi-specialty practice, but decided that wasn’t right for us.”
So, in 1995, five group partners decided to sell the practice to WellSpan Health, an integrated nonprofit healthcare system located in South Central Pennsylvania. Their expectation? That WellSpan’s administrative support and financial muscle would protect them against managed care’s encroachment.
Affiliating with WellSpan Health aligned Brockie with the medical services line of York Hospital, providing the administrative support they needed to grow and thrive. Working together, Brockie’s medical leaders and WellSpan administrators oversee the following areas: strategic planning; budgeting, compensation, benefits, and incentives; collections and coding; care management and performance improvement; recruiting and other personnel issues; and scheduling and coverage.
The Hospitalist Program
York Hospital and its surrounding community continued to grow, as did the need for more office-based and inpatient physician services. By 2001, York Hospital’s top executives recognized that a dedicated hospitalist group was the best solution for its overflowing emergency department (ED), booming admissions, and climbing average daily census. As specialists in internal medicine already heavily involved in inpatient care, the Brockie Internal Medical Group was York Hospital’s obvious choice to pioneer a hospital medicine program. Five Brockie physicians chose to join the newly minted inpatient hospital group (the Brockie Hospitalist Group), with four others continuing outpatient care. Over time, seven more hospitalists came on board, with more anticipated in late 2006 through mid-2007.
Part of the York Hospital mindset is that the demand for inpatient services would keep climbing as the community continued to attract newcomers. An unanticipated consequence of having a hospital medicine program was that outpatient practices quickly grew by 20% because they had offloaded their hospital work, in turn generating more hospital admissions. Brockie and York leaders, recognizing the possibility of stress and burnout on hospitalists as their volume of work grew, took steps to avert problems. “We’re in a sustained growth mode and we need the hospitalists to be satisfied with their compensation and schedules to be able to recruit new physicians,” says Dr. McConville. “Hospital administration underwrites the hospitalist program’s shortfall so that we can pay [the hospitalists] a salary commensurate with MGMA [Medical Group Management Association] guidelines plus productivity. It’s a substantial amount annually and well worth it,” he adds.
Unlike many hospitalist programs, York Hospital’s did not arise because physicians wanted to avoid driving to the hospital to make rounds. “Some groups are five minutes away and they gave us their inpatient work, while a group that’s 45 minutes away still does hospital rounds. What drives physicians here is their view of continuity of care,” says Dr. McConville.
Brockie is York’s only hospitalist group, although three other medical groups have hired two doctors to handle their inpatient work. “It’s not a problem for us. We don’t have a sense of competition,” says Dr. Whitney.
The Nuts and Bolts
Perhaps it’s Brockie’s long tenure as a medical group, its acquisition by WellSpan and the performance expectations that such an acquisition denotes, the thoroughness of its hospitalist leaders, or some combination of the above, but the hospitalists have their schedules and compensation calculations down pat.
Dr. Lamanteer spends much time and thought on the hospitalists’ compensation package. He studies national salary data and factors them into a sophisticated system of relative value units (RVUs) and case-based data to maintain a “competitive compensation package that provides incentives for both our physicians and the hospital to balance productivity with keeping length of stay in check,” he says. That’s not as easy as he makes it sound, because bumping up RVUs and volume has to be balanced with a length of stay that is both efficient and safe for patients.
Compensation begins with base salary—either Level I for 132 hours or Level II for 147 hours over three weeks. Productivity bonuses start with one point awarded for each admission, discharge, consult, and ED evaluation. Point values are then adjusted for average professional revenue generated per patient. The threshold for bonus pay is 806 points. Additionally, three clinical performance criteria, chosen annually, impact the bonus. For example, recent targets include ordering a tentative discharge time one or more days in advance (>65%), abiding by the “do not use” abbreviation list created by the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) (>90%), and complying with diagnostic coding rules (>75% accuracy).
The hospitalists’ schedule is challenging, particularly for doctors way past residency, involving 8 a.m. to 10 p.m. shifts on a three-week cycle that starts on a Friday. Physicians work eight 14-hour days, followed by a weekend off, then five days on (Monday-Friday) and six days off (Saturday-Thursday). The hospitalists don’t routinely cover night call. A full-time nocturnist, who started in 1992, and moonlighters cover the 10 p.m. to 8 a.m. shift seven days a week, with hospitalists covering only for major emergencies.
Avoiding Burnout
York Hospital’s ED and a cap on residents’ hours keep the Brockie hospitalists busy. But, early in 2005, it looked as if the workload had reached a plateau. Although Dr. Whitney suspected that the breather wouldn’t last, the group had no evidence that the tempo would increase and voted to maintain the number of hospitalists. The tempo picked up.
“We had estimated an 11 percent growth in RVUs, which actually grew by 23 percent last year,” says Dr. Whitney. Then a large primary care group agreed to shift its inpatient work to Brockie in 2006. Dr. Whitney estimated that assuming that practice’s hospital patients would add 5,000 RVUs and 600 more admissions.
“We realized we could approach a point of stress and burnout with the increased workload, so we recruited two new hospitalists,” says Dr. Whitney.
Still, the hospitalists face a balancing act of census peaks and valleys. “The variations with census and admissions go well beyond the bell curve,” says Whitney, who prepares for crunches by finding volunteers among the hospitalists to cover unexpected peaks.
If Brockie sounds like a Harvard case study on hospitalist medicine, it should. Its long tenure, physician leadership, and administrative support have shaped the business practices that facilitated the program’s growth. For one, the sophisticated compensation/productivity scheme didn’t come about by accident. Dr. McConville, a representative of WellSpan’s medical service line, meets with three Brockie hospitalists to fine-tune the program’s metrics. QI measures that are newly written each year, regular individual feedback, and inclusion of evidence-based guidelines contribute to measures and practices that address many of hospital medicine’s problems.
A Big Step to Little Things
But Brockie isn’t perfect. The responsibility of 24/7 coverage and 14-hour days allows little things to fall through the cracks—things like finding the time to promote the hospitalist service on the Web site, getting new formulary updates out quickly, and immediately informing all of those concerned that a patient has died. Brockie has addressed those and other issues that are the mortar to the bricks of a hospitalist practice by hiring David Orskey, an ex-Navy corpsman, as its senior practice manager in July 2006.
Orskey, co-chair of the medical group’s process improvement committee, sees his work as finding efficiencies, working for better care, and increasing patient satisfaction, plus attending to the budget and human resources issues and networking with outpatient practices.
“Twenty-one years in Navy medicine prepared me for this job,” says Orskey. “I’m enjoying this community, which has everything from farmland to executive homes and an influx of Hispanic migrants.”
He’s able to focus on both the details and the big picture, such as making sure that everyone works toward implementing and using the electronic medical record and improving after-hours answering services, as well as refining credentialing and risk management.
LTAC Unit
Brockie’s hospitalists also serve Mechanicsburg, Pa.,-based Select Medical Corporation’s long-term acute care (LTAC) unit, a 30-bed unit within York Hospital that supports patients needing a bridge between an acute hospital and skilled nursing care. The patients run the gamut in their needs—some have pulmonary/ventilator issues; others present medically complex situations such as heart failure, multi-system organ impairment, and cancer; some are neurosurgical/post trauma; and others need specialized wound care.
Dr. Whitney explains that all Brockie hospitalists add the LTAC to their rounds, usually leaving them for the end of the day, when the physicians can better attend to their complex situations. “Many of these patients are older, have been in the ICU with complicated medical issues, and face weeks of care in the LTAC before they can go to a nursing home or another long-term care setting,” he says. “It’s a whole different LOS, and it’s good that we have the LTAC because it reduces the hospital’s burden of caring for them as acute patients, when they really need what the LTAC offers.”
Conclusion
Dr. Lamanteer keeps an eye on the Brockie hospitalists’ future. “It’s clear that we benefit patients, that we provide excellent care, and that we need a large subsidy to do it,” he says. And the big picture means keeping focused on the peaks and valleys of admissions and wondering how volume will grow in the next ten years. He’d like to limit the number of 14-hour shifts to help physicians avoid burnout and to limit weekend duty to one out of three (sustainable) or one out of four (heaven). TH
Marlene Piturro is based in New York.
More than 20 years before the term hospitalist was coined, the Brockie Medical Group, a strong internal medicine practice led by Benjamin Hoover, MD, relished its hospital work at York Hospital in York, Pa. Back then, the doctors didn’t call themselves hospitalists, but the time they spent on hospital duties made them the forebears of today’s hospitalists.
According to John McConville, MD, chairman of York Hospital’s department of medicine and a hospital fixture since 1976, some of Brockie Internal Medicine group’s physicians devoted 60% to 70% of their practice time to inpatient tasks. “That was the culture when I arrived on the scene,” he recounts. Shortly thereafter, the group grew stronger when The Brockie Internal Medicine Group’s main competition—a sizable family practice group—fell apart. Brockie absorbed its like-minded physicians.
York, pa.
The Brockie Internal Medical Group is firmly anchored in York, Pa., home to factories that produce barbells and Harley-Davidson motorcycles. York has a soft side, though—it produced the first Peppermint Pattie, a mint-chocolate candy. It is an affordable, rapidly growing suburb, a place where commuters to Philadelphia, Baltimore, and Washington, D.C., can have a comfortable lifestyle without big city housing prices and the hassles of urban life.
The medical community is close-knit, described by Jonathan Whitney, MD, a Brockie hospitalist leader, as “a collegial environment with a growing population and plenty of patients, so there’s not a sense of competition among physicians.” Dr. Whitney, along with William “Tex” Landis, MD, and Michael Lamanteer, MD, form the Brockie Hospitalist Group’s executive committee, elected decision makers who deal with WellSpan Health and York Hospital on behalf of their colleagues.
WellSpan’s Role
As York grew, so did the Brockie Internal Medical Group. Then came managed care in the 1980s and 1990s, and Brockie’s internists were not happy. “We saw the medical landscape changing everywhere, and we didn’t want managed care pushing us around,” explains Dr. Landis, a Lancaster, Pa., native and now the Brockie Hospitalist Group’s lead physician. “Analyzing how medicine was changing, we felt vulnerable as a single specialty group. We considered various scenarios for becoming a multi-specialty practice, but decided that wasn’t right for us.”
So, in 1995, five group partners decided to sell the practice to WellSpan Health, an integrated nonprofit healthcare system located in South Central Pennsylvania. Their expectation? That WellSpan’s administrative support and financial muscle would protect them against managed care’s encroachment.
Affiliating with WellSpan Health aligned Brockie with the medical services line of York Hospital, providing the administrative support they needed to grow and thrive. Working together, Brockie’s medical leaders and WellSpan administrators oversee the following areas: strategic planning; budgeting, compensation, benefits, and incentives; collections and coding; care management and performance improvement; recruiting and other personnel issues; and scheduling and coverage.
The Hospitalist Program
York Hospital and its surrounding community continued to grow, as did the need for more office-based and inpatient physician services. By 2001, York Hospital’s top executives recognized that a dedicated hospitalist group was the best solution for its overflowing emergency department (ED), booming admissions, and climbing average daily census. As specialists in internal medicine already heavily involved in inpatient care, the Brockie Internal Medical Group was York Hospital’s obvious choice to pioneer a hospital medicine program. Five Brockie physicians chose to join the newly minted inpatient hospital group (the Brockie Hospitalist Group), with four others continuing outpatient care. Over time, seven more hospitalists came on board, with more anticipated in late 2006 through mid-2007.
Part of the York Hospital mindset is that the demand for inpatient services would keep climbing as the community continued to attract newcomers. An unanticipated consequence of having a hospital medicine program was that outpatient practices quickly grew by 20% because they had offloaded their hospital work, in turn generating more hospital admissions. Brockie and York leaders, recognizing the possibility of stress and burnout on hospitalists as their volume of work grew, took steps to avert problems. “We’re in a sustained growth mode and we need the hospitalists to be satisfied with their compensation and schedules to be able to recruit new physicians,” says Dr. McConville. “Hospital administration underwrites the hospitalist program’s shortfall so that we can pay [the hospitalists] a salary commensurate with MGMA [Medical Group Management Association] guidelines plus productivity. It’s a substantial amount annually and well worth it,” he adds.
Unlike many hospitalist programs, York Hospital’s did not arise because physicians wanted to avoid driving to the hospital to make rounds. “Some groups are five minutes away and they gave us their inpatient work, while a group that’s 45 minutes away still does hospital rounds. What drives physicians here is their view of continuity of care,” says Dr. McConville.
Brockie is York’s only hospitalist group, although three other medical groups have hired two doctors to handle their inpatient work. “It’s not a problem for us. We don’t have a sense of competition,” says Dr. Whitney.
The Nuts and Bolts
Perhaps it’s Brockie’s long tenure as a medical group, its acquisition by WellSpan and the performance expectations that such an acquisition denotes, the thoroughness of its hospitalist leaders, or some combination of the above, but the hospitalists have their schedules and compensation calculations down pat.
Dr. Lamanteer spends much time and thought on the hospitalists’ compensation package. He studies national salary data and factors them into a sophisticated system of relative value units (RVUs) and case-based data to maintain a “competitive compensation package that provides incentives for both our physicians and the hospital to balance productivity with keeping length of stay in check,” he says. That’s not as easy as he makes it sound, because bumping up RVUs and volume has to be balanced with a length of stay that is both efficient and safe for patients.
Compensation begins with base salary—either Level I for 132 hours or Level II for 147 hours over three weeks. Productivity bonuses start with one point awarded for each admission, discharge, consult, and ED evaluation. Point values are then adjusted for average professional revenue generated per patient. The threshold for bonus pay is 806 points. Additionally, three clinical performance criteria, chosen annually, impact the bonus. For example, recent targets include ordering a tentative discharge time one or more days in advance (>65%), abiding by the “do not use” abbreviation list created by the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) (>90%), and complying with diagnostic coding rules (>75% accuracy).
The hospitalists’ schedule is challenging, particularly for doctors way past residency, involving 8 a.m. to 10 p.m. shifts on a three-week cycle that starts on a Friday. Physicians work eight 14-hour days, followed by a weekend off, then five days on (Monday-Friday) and six days off (Saturday-Thursday). The hospitalists don’t routinely cover night call. A full-time nocturnist, who started in 1992, and moonlighters cover the 10 p.m. to 8 a.m. shift seven days a week, with hospitalists covering only for major emergencies.
Avoiding Burnout
York Hospital’s ED and a cap on residents’ hours keep the Brockie hospitalists busy. But, early in 2005, it looked as if the workload had reached a plateau. Although Dr. Whitney suspected that the breather wouldn’t last, the group had no evidence that the tempo would increase and voted to maintain the number of hospitalists. The tempo picked up.
“We had estimated an 11 percent growth in RVUs, which actually grew by 23 percent last year,” says Dr. Whitney. Then a large primary care group agreed to shift its inpatient work to Brockie in 2006. Dr. Whitney estimated that assuming that practice’s hospital patients would add 5,000 RVUs and 600 more admissions.
“We realized we could approach a point of stress and burnout with the increased workload, so we recruited two new hospitalists,” says Dr. Whitney.
Still, the hospitalists face a balancing act of census peaks and valleys. “The variations with census and admissions go well beyond the bell curve,” says Whitney, who prepares for crunches by finding volunteers among the hospitalists to cover unexpected peaks.
If Brockie sounds like a Harvard case study on hospitalist medicine, it should. Its long tenure, physician leadership, and administrative support have shaped the business practices that facilitated the program’s growth. For one, the sophisticated compensation/productivity scheme didn’t come about by accident. Dr. McConville, a representative of WellSpan’s medical service line, meets with three Brockie hospitalists to fine-tune the program’s metrics. QI measures that are newly written each year, regular individual feedback, and inclusion of evidence-based guidelines contribute to measures and practices that address many of hospital medicine’s problems.
A Big Step to Little Things
But Brockie isn’t perfect. The responsibility of 24/7 coverage and 14-hour days allows little things to fall through the cracks—things like finding the time to promote the hospitalist service on the Web site, getting new formulary updates out quickly, and immediately informing all of those concerned that a patient has died. Brockie has addressed those and other issues that are the mortar to the bricks of a hospitalist practice by hiring David Orskey, an ex-Navy corpsman, as its senior practice manager in July 2006.
Orskey, co-chair of the medical group’s process improvement committee, sees his work as finding efficiencies, working for better care, and increasing patient satisfaction, plus attending to the budget and human resources issues and networking with outpatient practices.
“Twenty-one years in Navy medicine prepared me for this job,” says Orskey. “I’m enjoying this community, which has everything from farmland to executive homes and an influx of Hispanic migrants.”
He’s able to focus on both the details and the big picture, such as making sure that everyone works toward implementing and using the electronic medical record and improving after-hours answering services, as well as refining credentialing and risk management.
LTAC Unit
Brockie’s hospitalists also serve Mechanicsburg, Pa.,-based Select Medical Corporation’s long-term acute care (LTAC) unit, a 30-bed unit within York Hospital that supports patients needing a bridge between an acute hospital and skilled nursing care. The patients run the gamut in their needs—some have pulmonary/ventilator issues; others present medically complex situations such as heart failure, multi-system organ impairment, and cancer; some are neurosurgical/post trauma; and others need specialized wound care.
Dr. Whitney explains that all Brockie hospitalists add the LTAC to their rounds, usually leaving them for the end of the day, when the physicians can better attend to their complex situations. “Many of these patients are older, have been in the ICU with complicated medical issues, and face weeks of care in the LTAC before they can go to a nursing home or another long-term care setting,” he says. “It’s a whole different LOS, and it’s good that we have the LTAC because it reduces the hospital’s burden of caring for them as acute patients, when they really need what the LTAC offers.”
Conclusion
Dr. Lamanteer keeps an eye on the Brockie hospitalists’ future. “It’s clear that we benefit patients, that we provide excellent care, and that we need a large subsidy to do it,” he says. And the big picture means keeping focused on the peaks and valleys of admissions and wondering how volume will grow in the next ten years. He’d like to limit the number of 14-hour shifts to help physicians avoid burnout and to limit weekend duty to one out of three (sustainable) or one out of four (heaven). TH
Marlene Piturro is based in New York.
More than 20 years before the term hospitalist was coined, the Brockie Medical Group, a strong internal medicine practice led by Benjamin Hoover, MD, relished its hospital work at York Hospital in York, Pa. Back then, the doctors didn’t call themselves hospitalists, but the time they spent on hospital duties made them the forebears of today’s hospitalists.
According to John McConville, MD, chairman of York Hospital’s department of medicine and a hospital fixture since 1976, some of Brockie Internal Medicine group’s physicians devoted 60% to 70% of their practice time to inpatient tasks. “That was the culture when I arrived on the scene,” he recounts. Shortly thereafter, the group grew stronger when The Brockie Internal Medicine Group’s main competition—a sizable family practice group—fell apart. Brockie absorbed its like-minded physicians.
York, pa.
The Brockie Internal Medical Group is firmly anchored in York, Pa., home to factories that produce barbells and Harley-Davidson motorcycles. York has a soft side, though—it produced the first Peppermint Pattie, a mint-chocolate candy. It is an affordable, rapidly growing suburb, a place where commuters to Philadelphia, Baltimore, and Washington, D.C., can have a comfortable lifestyle without big city housing prices and the hassles of urban life.
The medical community is close-knit, described by Jonathan Whitney, MD, a Brockie hospitalist leader, as “a collegial environment with a growing population and plenty of patients, so there’s not a sense of competition among physicians.” Dr. Whitney, along with William “Tex” Landis, MD, and Michael Lamanteer, MD, form the Brockie Hospitalist Group’s executive committee, elected decision makers who deal with WellSpan Health and York Hospital on behalf of their colleagues.
WellSpan’s Role
As York grew, so did the Brockie Internal Medical Group. Then came managed care in the 1980s and 1990s, and Brockie’s internists were not happy. “We saw the medical landscape changing everywhere, and we didn’t want managed care pushing us around,” explains Dr. Landis, a Lancaster, Pa., native and now the Brockie Hospitalist Group’s lead physician. “Analyzing how medicine was changing, we felt vulnerable as a single specialty group. We considered various scenarios for becoming a multi-specialty practice, but decided that wasn’t right for us.”
So, in 1995, five group partners decided to sell the practice to WellSpan Health, an integrated nonprofit healthcare system located in South Central Pennsylvania. Their expectation? That WellSpan’s administrative support and financial muscle would protect them against managed care’s encroachment.
Affiliating with WellSpan Health aligned Brockie with the medical services line of York Hospital, providing the administrative support they needed to grow and thrive. Working together, Brockie’s medical leaders and WellSpan administrators oversee the following areas: strategic planning; budgeting, compensation, benefits, and incentives; collections and coding; care management and performance improvement; recruiting and other personnel issues; and scheduling and coverage.
The Hospitalist Program
York Hospital and its surrounding community continued to grow, as did the need for more office-based and inpatient physician services. By 2001, York Hospital’s top executives recognized that a dedicated hospitalist group was the best solution for its overflowing emergency department (ED), booming admissions, and climbing average daily census. As specialists in internal medicine already heavily involved in inpatient care, the Brockie Internal Medical Group was York Hospital’s obvious choice to pioneer a hospital medicine program. Five Brockie physicians chose to join the newly minted inpatient hospital group (the Brockie Hospitalist Group), with four others continuing outpatient care. Over time, seven more hospitalists came on board, with more anticipated in late 2006 through mid-2007.
Part of the York Hospital mindset is that the demand for inpatient services would keep climbing as the community continued to attract newcomers. An unanticipated consequence of having a hospital medicine program was that outpatient practices quickly grew by 20% because they had offloaded their hospital work, in turn generating more hospital admissions. Brockie and York leaders, recognizing the possibility of stress and burnout on hospitalists as their volume of work grew, took steps to avert problems. “We’re in a sustained growth mode and we need the hospitalists to be satisfied with their compensation and schedules to be able to recruit new physicians,” says Dr. McConville. “Hospital administration underwrites the hospitalist program’s shortfall so that we can pay [the hospitalists] a salary commensurate with MGMA [Medical Group Management Association] guidelines plus productivity. It’s a substantial amount annually and well worth it,” he adds.
Unlike many hospitalist programs, York Hospital’s did not arise because physicians wanted to avoid driving to the hospital to make rounds. “Some groups are five minutes away and they gave us their inpatient work, while a group that’s 45 minutes away still does hospital rounds. What drives physicians here is their view of continuity of care,” says Dr. McConville.
Brockie is York’s only hospitalist group, although three other medical groups have hired two doctors to handle their inpatient work. “It’s not a problem for us. We don’t have a sense of competition,” says Dr. Whitney.
The Nuts and Bolts
Perhaps it’s Brockie’s long tenure as a medical group, its acquisition by WellSpan and the performance expectations that such an acquisition denotes, the thoroughness of its hospitalist leaders, or some combination of the above, but the hospitalists have their schedules and compensation calculations down pat.
Dr. Lamanteer spends much time and thought on the hospitalists’ compensation package. He studies national salary data and factors them into a sophisticated system of relative value units (RVUs) and case-based data to maintain a “competitive compensation package that provides incentives for both our physicians and the hospital to balance productivity with keeping length of stay in check,” he says. That’s not as easy as he makes it sound, because bumping up RVUs and volume has to be balanced with a length of stay that is both efficient and safe for patients.
Compensation begins with base salary—either Level I for 132 hours or Level II for 147 hours over three weeks. Productivity bonuses start with one point awarded for each admission, discharge, consult, and ED evaluation. Point values are then adjusted for average professional revenue generated per patient. The threshold for bonus pay is 806 points. Additionally, three clinical performance criteria, chosen annually, impact the bonus. For example, recent targets include ordering a tentative discharge time one or more days in advance (>65%), abiding by the “do not use” abbreviation list created by the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) (>90%), and complying with diagnostic coding rules (>75% accuracy).
The hospitalists’ schedule is challenging, particularly for doctors way past residency, involving 8 a.m. to 10 p.m. shifts on a three-week cycle that starts on a Friday. Physicians work eight 14-hour days, followed by a weekend off, then five days on (Monday-Friday) and six days off (Saturday-Thursday). The hospitalists don’t routinely cover night call. A full-time nocturnist, who started in 1992, and moonlighters cover the 10 p.m. to 8 a.m. shift seven days a week, with hospitalists covering only for major emergencies.
Avoiding Burnout
York Hospital’s ED and a cap on residents’ hours keep the Brockie hospitalists busy. But, early in 2005, it looked as if the workload had reached a plateau. Although Dr. Whitney suspected that the breather wouldn’t last, the group had no evidence that the tempo would increase and voted to maintain the number of hospitalists. The tempo picked up.
“We had estimated an 11 percent growth in RVUs, which actually grew by 23 percent last year,” says Dr. Whitney. Then a large primary care group agreed to shift its inpatient work to Brockie in 2006. Dr. Whitney estimated that assuming that practice’s hospital patients would add 5,000 RVUs and 600 more admissions.
“We realized we could approach a point of stress and burnout with the increased workload, so we recruited two new hospitalists,” says Dr. Whitney.
Still, the hospitalists face a balancing act of census peaks and valleys. “The variations with census and admissions go well beyond the bell curve,” says Whitney, who prepares for crunches by finding volunteers among the hospitalists to cover unexpected peaks.
If Brockie sounds like a Harvard case study on hospitalist medicine, it should. Its long tenure, physician leadership, and administrative support have shaped the business practices that facilitated the program’s growth. For one, the sophisticated compensation/productivity scheme didn’t come about by accident. Dr. McConville, a representative of WellSpan’s medical service line, meets with three Brockie hospitalists to fine-tune the program’s metrics. QI measures that are newly written each year, regular individual feedback, and inclusion of evidence-based guidelines contribute to measures and practices that address many of hospital medicine’s problems.
A Big Step to Little Things
But Brockie isn’t perfect. The responsibility of 24/7 coverage and 14-hour days allows little things to fall through the cracks—things like finding the time to promote the hospitalist service on the Web site, getting new formulary updates out quickly, and immediately informing all of those concerned that a patient has died. Brockie has addressed those and other issues that are the mortar to the bricks of a hospitalist practice by hiring David Orskey, an ex-Navy corpsman, as its senior practice manager in July 2006.
Orskey, co-chair of the medical group’s process improvement committee, sees his work as finding efficiencies, working for better care, and increasing patient satisfaction, plus attending to the budget and human resources issues and networking with outpatient practices.
“Twenty-one years in Navy medicine prepared me for this job,” says Orskey. “I’m enjoying this community, which has everything from farmland to executive homes and an influx of Hispanic migrants.”
He’s able to focus on both the details and the big picture, such as making sure that everyone works toward implementing and using the electronic medical record and improving after-hours answering services, as well as refining credentialing and risk management.
LTAC Unit
Brockie’s hospitalists also serve Mechanicsburg, Pa.,-based Select Medical Corporation’s long-term acute care (LTAC) unit, a 30-bed unit within York Hospital that supports patients needing a bridge between an acute hospital and skilled nursing care. The patients run the gamut in their needs—some have pulmonary/ventilator issues; others present medically complex situations such as heart failure, multi-system organ impairment, and cancer; some are neurosurgical/post trauma; and others need specialized wound care.
Dr. Whitney explains that all Brockie hospitalists add the LTAC to their rounds, usually leaving them for the end of the day, when the physicians can better attend to their complex situations. “Many of these patients are older, have been in the ICU with complicated medical issues, and face weeks of care in the LTAC before they can go to a nursing home or another long-term care setting,” he says. “It’s a whole different LOS, and it’s good that we have the LTAC because it reduces the hospital’s burden of caring for them as acute patients, when they really need what the LTAC offers.”
Conclusion
Dr. Lamanteer keeps an eye on the Brockie hospitalists’ future. “It’s clear that we benefit patients, that we provide excellent care, and that we need a large subsidy to do it,” he says. And the big picture means keeping focused on the peaks and valleys of admissions and wondering how volume will grow in the next ten years. He’d like to limit the number of 14-hour shifts to help physicians avoid burnout and to limit weekend duty to one out of three (sustainable) or one out of four (heaven). TH
Marlene Piturro is based in New York.
Brazil Blossoms
The establishment of a hospital medicine program in Brazil and the attempt to develop the specialty nationwide is both fascinating and challenging. Brazil has about 7,155 hospitals, with 443,210 beds available (including 2,727 public hospitals with 148,966 beds and 4,428 private facilities with 294,244 beds). 1 (See Table 1, p. 44.)
Historical problems in the public health system—also found in private sectors—have motivated physicians to address and improve inefficient management, insufficient financial support, the high number of frequent unnecessary admissions and re-admissions, extended length of stays, limited access to beds and medical services of high complexity, and overcrowded emergency departments.
SUS—Principles and Problems
The Brazilian public health system, called Sistema Único de Saúde, or SUS, is based on universal care and health as a right of citizenship and a state responsibility. Its main principles are universality, integrality, equity, decentralization, and social control.2 Less than half of the Brazilian population uses the SUS system exclusively. They use private health systems as a complement. This situation reflects the difficulties in the Brazilian public health system. The reasons for this duplicity highlight the challenges of our situation.
At the same time, physicians face serious problems. Most are employed by both the public and private sectors. Average salaries in the public system (by far the largest employer) are extremely low. Medical doctors are forced to work many extra hours, including numerous night shifts, creating a major barrier to the growth of physicians dedicated to horizontal inpatient care.
The government, in an attempt to improve medical—and hospital—assistance in the country with “a new kind of health assistance focused on high quality and efficient services,” has created the following projects: Humaniza SUS and QualiSUS.3,4 Theoretical support, operational contours, extent, and applicability are still not clear, however. For many medical doctors, these are merely abstract ideas. QualiSUS has renovated emergency departments in Brazil, but service quality has not improved enough. In our opinion, there are no public policies capable of providing good hospital services and efficient management in Brazilian hospitals, and—even if they existed—we would need to stop corruption in order to meet public commitments.
In Rio Grande do Sul, the Brazilian state where we work as medical doctors, the inadequate SUS reimbursement points to a calamitous future. Here, most hospital care is provided by philanthropic hospitals, which are more vulnerable in financial terms.5 (See Table 2, p. 44.) Despite being in a pioneer state in terms of hospital administration schools, with more than 2,000 graduates in recent years, these philanthropic hospitals have an estimated reimbursement deficit of more than 80%, an unattainable amount even for the best administrator.

Could Hospitalists Be Part of a Solution?
On top of these growing deficits, we have witnessed the closing of more than 2,000 available beds in the last four years, as well as the loss of 10,000 hospital positions and the complete closing of eight hospitals. Aiming to ensure the survival of this hospital system, physicians, health professionals, and organizations involved with hospitals have joined forces to find a solution. Their logo is best translated as “More Health for the Hospitals,” and our group supports their goals.6
Looking at the situation from a different perspective, we see many opportunities for Brazilian hospitalists. Their potential contribution to the quality and safety of medical care is an obvious advantage for hospital management and patients. We predict that this scenario can be accomplished—even in our state. It is possible to make a profit in public as well as in lucrative private institutions. In public institutions, a profit can be made as long as hospital administrators use adequate policy. We believe that in private institutions, though not in philanthropic ones, the key point is hospital administration cooperation and goodwill. Elucidation of hospitalists’ capabilities will open the necessary doors. We are ready to reduce the hospitalization fee and length of stay—among other costs. In this way, we can work with the administrator to develop tools for systems and quality improvements.
Hospital Medicine’s Emergence in Brazil
The implementation of hospital medicine, especially those aspects that involve more than just having a general medicine physician dealing with inpatient care, is brand new in Brazil. So far, the U.S. hospitalist model of care is unfamiliar to most Brazilian medical doctors and healthcare managers. Some institutions have hired hospitalists to be part of rapid response teams, neglecting the more specialized dimension of this new model of care; they are not aware of this title’s real meaning. There is a long way to go until the hospitalist is seen as a specialist, and we hope all our efforts will earn this new specialty official recognition in Brazil.
Our group is based in the Brazilian state of Rio Grande do Sul, mainly in Porto Alegre, its capital. Most of our time is dedicated to inpatient care, and we started our movement after studying the model of care delineated by Wachter and Lee.7-9 In 2005, we formed a local association called GEAMH (Grupo de Estudos e Atualização em Medicina Hospitalar) to promote the understanding and diffusion of hospitalist principles, integrated by the professors and former and current residents of a large local internal medicine residence program from the Internal Medicine Department of Nossa Senhora da Conceição Hospital (HNSC).
We have created a Web site (www.medicinahospitalar.com.br) where you can find history, news, and information about hospital medicine fellowships in the United States, as well as online hospital medicine continuing education. As you can see, we are spreading SHM’s ideas.
The third year of the HNSC Internal Medicine Residence Program (R3) focused on hospital medicine was developed in 2005. We believe this to be the first initiative of its kind in Brazil. HNSC is part of Conceição Hospital Group, which is composed of four hospital units and is one of the biggest public hospital networks in Brazil.
The Internal Medicine Residence Program started at HNSC in 1968. The department itself has more than 100 hospital beds. Medical residents’ activities all take place in the hospital, and there are nine professors: Eduardo Fernandes, Guilherme Barcellos, Janete Brauner, José Luiz F. Soares, Nelson Roessler, Paulo Almeida, Paulo Ricardo Cardoso, Sergio Dedavid, and Sergio Prezzi. We would like to make special mention of our colleagues Eduardo Fernandes, current head of HNSC Internal Medicine Medical Residence Program, and Sergio Prezzi, the R3 coordinator.

Table 2. Philanthropic Hospitals5 Conditions: A hospital is considered philanthropic if at least 60% of its admissions are SUS patients or if it spends 5% to 20% of its income on health-related activities.
Advantages: Special reimbursement from state or city administrations and significant federal tax deductions.
The HNSC Internal Medicine Service is well known for graduating internists skilled in hospital practices, mainly because the program is run by professors who specialize in that area. The R3 is a one-year training program. Our goal is to train physicians to provide outstanding and comprehensive inpatient care. Through supervised training, our residents are able to treat common hospital illnesses; we are also training them in consultative medicine and in the clinical management of surgical patients. Other areas of medical residents’ education include medical ethics, end-of-life care, inpatient nutritional support, risk management, rational use of drugs, and technology and evidence-based medicine.
Our third-year residents have the opportunity to try bone marrow biopsy, pleural biopsy, and thorax draining—all of which are usually handled by other medical specialists. In general, residents also have many opportunities to learn about and practice endotracheal intubations, ventilator management, central vein access, and many other procedures.
Based on HNSC experience, a formal stage in hospital medicine under the supervision of Luciano Bauer Grohs, MD, one of the founders of GEAMH, has also been integrated into internal medicine training at Nossa Senhora de Pompéia Hospital in the city of Caxias do Sul, located 125 kilometers from Porto Alegre.
Our group has developed medical education in the inpatient setting. Because there is no hospital medicine society in Brazil, we have tried to coordinate with the Brazilian Society of Internal Medicine, encouraging discussions about hospital care and promoting workshops about mechanical ventilation, central vein access, and early goal-directed therapy for sepsis. More recently, we have chosen to work independently, believing that hospital medicine is distinct from internal medicine.
When we organized the Brazilian Annual Congress of Medical Residents in 2006, we had the opportunity to bring together medical residents and professors from different medical areas. The Congress’ main focuses were rational use of drugs and technology and the relationship between the young physician and the pharmaceutical industry. The participation of Robert Goodman (of No Free Lunch fame) was an important part of the convention.10
Slow and Steady Growth
We understand that there is a long journey ahead, beyond educational and medical assistance. Our group is still far from promoting research. But hospital medicine specialization has launched in Brazil. Dr. Watcher has said to us, “In the United States, the hospitalist field is the fastest growing specialty in the country—and probably in the history of the country. Hospitalists are transforming the delivery of American hospital care and improving quality, patient safety, education, end-of-life care, and more. We are thrilled to partner with our Brazilian colleagues as, together, we try to improve the quality of care for hospitalized patients everywhere.” We are confident that his vision will become a reality in Brazil in the near future. TH
Note: We are in debt to the professors at the Hospital Conceição Internal Medicine Residency Program, without whom our initiatives would never have blossomed. Special thanks to Eduardo Fernandes, Sergio Prezzi, and Paulo Ricardo Cardoso.
Dr. Barcellos is a specialist in internal medicine, emergency medicine, and critical care. He is professor in Nossa Senhora da Conceição Hospital’s Hospital Medicine Residence Program and president of GEAMH, a local association designed to promote the understanding and diffusion of hospitalist principles.
Dr. Wajner is a specialist in internal medicine and emergency medicine and a Master of Science student at Universidade Federal do Rio Grande do Sul.
Dr. de Waldemar is a specialist in internal medicine and emergency medicine.
References
- Departamento de População e Indicadores Sociais. Estatísticas da saúde: assistência médico-sanitária 2005/IBGE. Departamento de População e Indicadores Sociais. 2006. Available at: www.ibge.gov.br/home/estatistica/populacao/condicaodevida/ams/2005/ams2005.pdf. Last accessed January 28, 2007.
- Agência Nacional de Vigilância Sanitária. Lei nº 8080. D.O.U. - Diário Oficial da União; Poder Executivo. September 20, 1990. Available at: http://e-legis.bvs.br/leisref/public/showAct.php?id=16619&word=. Last accessed January 28, 2007.
- Brazilian Ministry of Health Web site. Available at: http://portal.saude.gov.br/saude. Last accessed January 28, 2007.
- Deslandes SF. Análise do discurso oficial sobre a humanização da assistência hospitalar. Ciência e saúde coletiva. 2004;9:7-14. Available at: www.scielo.br/pdf/csc/v9n1/19819.pdf. Last ccessed January 28, 2007.
- Portela MC, Lima SML, Barbosa PR, et al. Caracterização assistencial de hospitais filantrópicos no Brasil. Rev Saúde Pública. 2004;38:811-818. Available at: www.scielo.br/pdf/rsp/v38n6/09.pdf. Last accessed January 28, 2007.
- Sindicato Médico do Rio Grande do Sul Web site. Available at: www.simers.org.br/entquerem.php. Last accessed January 28, 2007.
- Wachter RM, Goldman L. The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996 Aug 15;335(7):514-517.
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002 Feb 16;287:487–494. Review.
- Wachter RM. An introduction to the hospitalist model. Ann Intern Med. 1999 Feb 16;130(4 Pt 2):338–342.
- No Free Lunch Web site. Available at: www.nofreelunch.org. Last accessed January 28, 2007.
The establishment of a hospital medicine program in Brazil and the attempt to develop the specialty nationwide is both fascinating and challenging. Brazil has about 7,155 hospitals, with 443,210 beds available (including 2,727 public hospitals with 148,966 beds and 4,428 private facilities with 294,244 beds). 1 (See Table 1, p. 44.)
Historical problems in the public health system—also found in private sectors—have motivated physicians to address and improve inefficient management, insufficient financial support, the high number of frequent unnecessary admissions and re-admissions, extended length of stays, limited access to beds and medical services of high complexity, and overcrowded emergency departments.
SUS—Principles and Problems
The Brazilian public health system, called Sistema Único de Saúde, or SUS, is based on universal care and health as a right of citizenship and a state responsibility. Its main principles are universality, integrality, equity, decentralization, and social control.2 Less than half of the Brazilian population uses the SUS system exclusively. They use private health systems as a complement. This situation reflects the difficulties in the Brazilian public health system. The reasons for this duplicity highlight the challenges of our situation.
At the same time, physicians face serious problems. Most are employed by both the public and private sectors. Average salaries in the public system (by far the largest employer) are extremely low. Medical doctors are forced to work many extra hours, including numerous night shifts, creating a major barrier to the growth of physicians dedicated to horizontal inpatient care.
The government, in an attempt to improve medical—and hospital—assistance in the country with “a new kind of health assistance focused on high quality and efficient services,” has created the following projects: Humaniza SUS and QualiSUS.3,4 Theoretical support, operational contours, extent, and applicability are still not clear, however. For many medical doctors, these are merely abstract ideas. QualiSUS has renovated emergency departments in Brazil, but service quality has not improved enough. In our opinion, there are no public policies capable of providing good hospital services and efficient management in Brazilian hospitals, and—even if they existed—we would need to stop corruption in order to meet public commitments.
In Rio Grande do Sul, the Brazilian state where we work as medical doctors, the inadequate SUS reimbursement points to a calamitous future. Here, most hospital care is provided by philanthropic hospitals, which are more vulnerable in financial terms.5 (See Table 2, p. 44.) Despite being in a pioneer state in terms of hospital administration schools, with more than 2,000 graduates in recent years, these philanthropic hospitals have an estimated reimbursement deficit of more than 80%, an unattainable amount even for the best administrator.
Could Hospitalists Be Part of a Solution?
On top of these growing deficits, we have witnessed the closing of more than 2,000 available beds in the last four years, as well as the loss of 10,000 hospital positions and the complete closing of eight hospitals. Aiming to ensure the survival of this hospital system, physicians, health professionals, and organizations involved with hospitals have joined forces to find a solution. Their logo is best translated as “More Health for the Hospitals,” and our group supports their goals.6
Looking at the situation from a different perspective, we see many opportunities for Brazilian hospitalists. Their potential contribution to the quality and safety of medical care is an obvious advantage for hospital management and patients. We predict that this scenario can be accomplished—even in our state. It is possible to make a profit in public as well as in lucrative private institutions. In public institutions, a profit can be made as long as hospital administrators use adequate policy. We believe that in private institutions, though not in philanthropic ones, the key point is hospital administration cooperation and goodwill. Elucidation of hospitalists’ capabilities will open the necessary doors. We are ready to reduce the hospitalization fee and length of stay—among other costs. In this way, we can work with the administrator to develop tools for systems and quality improvements.
Hospital Medicine’s Emergence in Brazil
The implementation of hospital medicine, especially those aspects that involve more than just having a general medicine physician dealing with inpatient care, is brand new in Brazil. So far, the U.S. hospitalist model of care is unfamiliar to most Brazilian medical doctors and healthcare managers. Some institutions have hired hospitalists to be part of rapid response teams, neglecting the more specialized dimension of this new model of care; they are not aware of this title’s real meaning. There is a long way to go until the hospitalist is seen as a specialist, and we hope all our efforts will earn this new specialty official recognition in Brazil.
Our group is based in the Brazilian state of Rio Grande do Sul, mainly in Porto Alegre, its capital. Most of our time is dedicated to inpatient care, and we started our movement after studying the model of care delineated by Wachter and Lee.7-9 In 2005, we formed a local association called GEAMH (Grupo de Estudos e Atualização em Medicina Hospitalar) to promote the understanding and diffusion of hospitalist principles, integrated by the professors and former and current residents of a large local internal medicine residence program from the Internal Medicine Department of Nossa Senhora da Conceição Hospital (HNSC).
We have created a Web site (www.medicinahospitalar.com.br) where you can find history, news, and information about hospital medicine fellowships in the United States, as well as online hospital medicine continuing education. As you can see, we are spreading SHM’s ideas.
The third year of the HNSC Internal Medicine Residence Program (R3) focused on hospital medicine was developed in 2005. We believe this to be the first initiative of its kind in Brazil. HNSC is part of Conceição Hospital Group, which is composed of four hospital units and is one of the biggest public hospital networks in Brazil.
The Internal Medicine Residence Program started at HNSC in 1968. The department itself has more than 100 hospital beds. Medical residents’ activities all take place in the hospital, and there are nine professors: Eduardo Fernandes, Guilherme Barcellos, Janete Brauner, José Luiz F. Soares, Nelson Roessler, Paulo Almeida, Paulo Ricardo Cardoso, Sergio Dedavid, and Sergio Prezzi. We would like to make special mention of our colleagues Eduardo Fernandes, current head of HNSC Internal Medicine Medical Residence Program, and Sergio Prezzi, the R3 coordinator.
Table 2. Philanthropic Hospitals5 Conditions: A hospital is considered philanthropic if at least 60% of its admissions are SUS patients or if it spends 5% to 20% of its income on health-related activities.
Advantages: Special reimbursement from state or city administrations and significant federal tax deductions.
The HNSC Internal Medicine Service is well known for graduating internists skilled in hospital practices, mainly because the program is run by professors who specialize in that area. The R3 is a one-year training program. Our goal is to train physicians to provide outstanding and comprehensive inpatient care. Through supervised training, our residents are able to treat common hospital illnesses; we are also training them in consultative medicine and in the clinical management of surgical patients. Other areas of medical residents’ education include medical ethics, end-of-life care, inpatient nutritional support, risk management, rational use of drugs, and technology and evidence-based medicine.
Our third-year residents have the opportunity to try bone marrow biopsy, pleural biopsy, and thorax draining—all of which are usually handled by other medical specialists. In general, residents also have many opportunities to learn about and practice endotracheal intubations, ventilator management, central vein access, and many other procedures.
Based on HNSC experience, a formal stage in hospital medicine under the supervision of Luciano Bauer Grohs, MD, one of the founders of GEAMH, has also been integrated into internal medicine training at Nossa Senhora de Pompéia Hospital in the city of Caxias do Sul, located 125 kilometers from Porto Alegre.
Our group has developed medical education in the inpatient setting. Because there is no hospital medicine society in Brazil, we have tried to coordinate with the Brazilian Society of Internal Medicine, encouraging discussions about hospital care and promoting workshops about mechanical ventilation, central vein access, and early goal-directed therapy for sepsis. More recently, we have chosen to work independently, believing that hospital medicine is distinct from internal medicine.
When we organized the Brazilian Annual Congress of Medical Residents in 2006, we had the opportunity to bring together medical residents and professors from different medical areas. The Congress’ main focuses were rational use of drugs and technology and the relationship between the young physician and the pharmaceutical industry. The participation of Robert Goodman (of No Free Lunch fame) was an important part of the convention.10
Slow and Steady Growth
We understand that there is a long journey ahead, beyond educational and medical assistance. Our group is still far from promoting research. But hospital medicine specialization has launched in Brazil. Dr. Watcher has said to us, “In the United States, the hospitalist field is the fastest growing specialty in the country—and probably in the history of the country. Hospitalists are transforming the delivery of American hospital care and improving quality, patient safety, education, end-of-life care, and more. We are thrilled to partner with our Brazilian colleagues as, together, we try to improve the quality of care for hospitalized patients everywhere.” We are confident that his vision will become a reality in Brazil in the near future. TH
Note: We are in debt to the professors at the Hospital Conceição Internal Medicine Residency Program, without whom our initiatives would never have blossomed. Special thanks to Eduardo Fernandes, Sergio Prezzi, and Paulo Ricardo Cardoso.
Dr. Barcellos is a specialist in internal medicine, emergency medicine, and critical care. He is professor in Nossa Senhora da Conceição Hospital’s Hospital Medicine Residence Program and president of GEAMH, a local association designed to promote the understanding and diffusion of hospitalist principles.
Dr. Wajner is a specialist in internal medicine and emergency medicine and a Master of Science student at Universidade Federal do Rio Grande do Sul.
Dr. de Waldemar is a specialist in internal medicine and emergency medicine.
References
- Departamento de População e Indicadores Sociais. Estatísticas da saúde: assistência médico-sanitária 2005/IBGE. Departamento de População e Indicadores Sociais. 2006. Available at: www.ibge.gov.br/home/estatistica/populacao/condicaodevida/ams/2005/ams2005.pdf. Last accessed January 28, 2007.
- Agência Nacional de Vigilância Sanitária. Lei nº 8080. D.O.U. - Diário Oficial da União; Poder Executivo. September 20, 1990. Available at: http://e-legis.bvs.br/leisref/public/showAct.php?id=16619&word=. Last accessed January 28, 2007.
- Brazilian Ministry of Health Web site. Available at: http://portal.saude.gov.br/saude. Last accessed January 28, 2007.
- Deslandes SF. Análise do discurso oficial sobre a humanização da assistência hospitalar. Ciência e saúde coletiva. 2004;9:7-14. Available at: www.scielo.br/pdf/csc/v9n1/19819.pdf. Last ccessed January 28, 2007.
- Portela MC, Lima SML, Barbosa PR, et al. Caracterização assistencial de hospitais filantrópicos no Brasil. Rev Saúde Pública. 2004;38:811-818. Available at: www.scielo.br/pdf/rsp/v38n6/09.pdf. Last accessed January 28, 2007.
- Sindicato Médico do Rio Grande do Sul Web site. Available at: www.simers.org.br/entquerem.php. Last accessed January 28, 2007.
- Wachter RM, Goldman L. The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996 Aug 15;335(7):514-517.
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002 Feb 16;287:487–494. Review.
- Wachter RM. An introduction to the hospitalist model. Ann Intern Med. 1999 Feb 16;130(4 Pt 2):338–342.
- No Free Lunch Web site. Available at: www.nofreelunch.org. Last accessed January 28, 2007.
The establishment of a hospital medicine program in Brazil and the attempt to develop the specialty nationwide is both fascinating and challenging. Brazil has about 7,155 hospitals, with 443,210 beds available (including 2,727 public hospitals with 148,966 beds and 4,428 private facilities with 294,244 beds). 1 (See Table 1, p. 44.)
Historical problems in the public health system—also found in private sectors—have motivated physicians to address and improve inefficient management, insufficient financial support, the high number of frequent unnecessary admissions and re-admissions, extended length of stays, limited access to beds and medical services of high complexity, and overcrowded emergency departments.
SUS—Principles and Problems
The Brazilian public health system, called Sistema Único de Saúde, or SUS, is based on universal care and health as a right of citizenship and a state responsibility. Its main principles are universality, integrality, equity, decentralization, and social control.2 Less than half of the Brazilian population uses the SUS system exclusively. They use private health systems as a complement. This situation reflects the difficulties in the Brazilian public health system. The reasons for this duplicity highlight the challenges of our situation.
At the same time, physicians face serious problems. Most are employed by both the public and private sectors. Average salaries in the public system (by far the largest employer) are extremely low. Medical doctors are forced to work many extra hours, including numerous night shifts, creating a major barrier to the growth of physicians dedicated to horizontal inpatient care.
The government, in an attempt to improve medical—and hospital—assistance in the country with “a new kind of health assistance focused on high quality and efficient services,” has created the following projects: Humaniza SUS and QualiSUS.3,4 Theoretical support, operational contours, extent, and applicability are still not clear, however. For many medical doctors, these are merely abstract ideas. QualiSUS has renovated emergency departments in Brazil, but service quality has not improved enough. In our opinion, there are no public policies capable of providing good hospital services and efficient management in Brazilian hospitals, and—even if they existed—we would need to stop corruption in order to meet public commitments.
In Rio Grande do Sul, the Brazilian state where we work as medical doctors, the inadequate SUS reimbursement points to a calamitous future. Here, most hospital care is provided by philanthropic hospitals, which are more vulnerable in financial terms.5 (See Table 2, p. 44.) Despite being in a pioneer state in terms of hospital administration schools, with more than 2,000 graduates in recent years, these philanthropic hospitals have an estimated reimbursement deficit of more than 80%, an unattainable amount even for the best administrator.
Could Hospitalists Be Part of a Solution?
On top of these growing deficits, we have witnessed the closing of more than 2,000 available beds in the last four years, as well as the loss of 10,000 hospital positions and the complete closing of eight hospitals. Aiming to ensure the survival of this hospital system, physicians, health professionals, and organizations involved with hospitals have joined forces to find a solution. Their logo is best translated as “More Health for the Hospitals,” and our group supports their goals.6
Looking at the situation from a different perspective, we see many opportunities for Brazilian hospitalists. Their potential contribution to the quality and safety of medical care is an obvious advantage for hospital management and patients. We predict that this scenario can be accomplished—even in our state. It is possible to make a profit in public as well as in lucrative private institutions. In public institutions, a profit can be made as long as hospital administrators use adequate policy. We believe that in private institutions, though not in philanthropic ones, the key point is hospital administration cooperation and goodwill. Elucidation of hospitalists’ capabilities will open the necessary doors. We are ready to reduce the hospitalization fee and length of stay—among other costs. In this way, we can work with the administrator to develop tools for systems and quality improvements.
Hospital Medicine’s Emergence in Brazil
The implementation of hospital medicine, especially those aspects that involve more than just having a general medicine physician dealing with inpatient care, is brand new in Brazil. So far, the U.S. hospitalist model of care is unfamiliar to most Brazilian medical doctors and healthcare managers. Some institutions have hired hospitalists to be part of rapid response teams, neglecting the more specialized dimension of this new model of care; they are not aware of this title’s real meaning. There is a long way to go until the hospitalist is seen as a specialist, and we hope all our efforts will earn this new specialty official recognition in Brazil.
Our group is based in the Brazilian state of Rio Grande do Sul, mainly in Porto Alegre, its capital. Most of our time is dedicated to inpatient care, and we started our movement after studying the model of care delineated by Wachter and Lee.7-9 In 2005, we formed a local association called GEAMH (Grupo de Estudos e Atualização em Medicina Hospitalar) to promote the understanding and diffusion of hospitalist principles, integrated by the professors and former and current residents of a large local internal medicine residence program from the Internal Medicine Department of Nossa Senhora da Conceição Hospital (HNSC).
We have created a Web site (www.medicinahospitalar.com.br) where you can find history, news, and information about hospital medicine fellowships in the United States, as well as online hospital medicine continuing education. As you can see, we are spreading SHM’s ideas.
The third year of the HNSC Internal Medicine Residence Program (R3) focused on hospital medicine was developed in 2005. We believe this to be the first initiative of its kind in Brazil. HNSC is part of Conceição Hospital Group, which is composed of four hospital units and is one of the biggest public hospital networks in Brazil.
The Internal Medicine Residence Program started at HNSC in 1968. The department itself has more than 100 hospital beds. Medical residents’ activities all take place in the hospital, and there are nine professors: Eduardo Fernandes, Guilherme Barcellos, Janete Brauner, José Luiz F. Soares, Nelson Roessler, Paulo Almeida, Paulo Ricardo Cardoso, Sergio Dedavid, and Sergio Prezzi. We would like to make special mention of our colleagues Eduardo Fernandes, current head of HNSC Internal Medicine Medical Residence Program, and Sergio Prezzi, the R3 coordinator.
Table 2. Philanthropic Hospitals5 Conditions: A hospital is considered philanthropic if at least 60% of its admissions are SUS patients or if it spends 5% to 20% of its income on health-related activities.
Advantages: Special reimbursement from state or city administrations and significant federal tax deductions.
The HNSC Internal Medicine Service is well known for graduating internists skilled in hospital practices, mainly because the program is run by professors who specialize in that area. The R3 is a one-year training program. Our goal is to train physicians to provide outstanding and comprehensive inpatient care. Through supervised training, our residents are able to treat common hospital illnesses; we are also training them in consultative medicine and in the clinical management of surgical patients. Other areas of medical residents’ education include medical ethics, end-of-life care, inpatient nutritional support, risk management, rational use of drugs, and technology and evidence-based medicine.
Our third-year residents have the opportunity to try bone marrow biopsy, pleural biopsy, and thorax draining—all of which are usually handled by other medical specialists. In general, residents also have many opportunities to learn about and practice endotracheal intubations, ventilator management, central vein access, and many other procedures.
Based on HNSC experience, a formal stage in hospital medicine under the supervision of Luciano Bauer Grohs, MD, one of the founders of GEAMH, has also been integrated into internal medicine training at Nossa Senhora de Pompéia Hospital in the city of Caxias do Sul, located 125 kilometers from Porto Alegre.
Our group has developed medical education in the inpatient setting. Because there is no hospital medicine society in Brazil, we have tried to coordinate with the Brazilian Society of Internal Medicine, encouraging discussions about hospital care and promoting workshops about mechanical ventilation, central vein access, and early goal-directed therapy for sepsis. More recently, we have chosen to work independently, believing that hospital medicine is distinct from internal medicine.
When we organized the Brazilian Annual Congress of Medical Residents in 2006, we had the opportunity to bring together medical residents and professors from different medical areas. The Congress’ main focuses were rational use of drugs and technology and the relationship between the young physician and the pharmaceutical industry. The participation of Robert Goodman (of No Free Lunch fame) was an important part of the convention.10
Slow and Steady Growth
We understand that there is a long journey ahead, beyond educational and medical assistance. Our group is still far from promoting research. But hospital medicine specialization has launched in Brazil. Dr. Watcher has said to us, “In the United States, the hospitalist field is the fastest growing specialty in the country—and probably in the history of the country. Hospitalists are transforming the delivery of American hospital care and improving quality, patient safety, education, end-of-life care, and more. We are thrilled to partner with our Brazilian colleagues as, together, we try to improve the quality of care for hospitalized patients everywhere.” We are confident that his vision will become a reality in Brazil in the near future. TH
Note: We are in debt to the professors at the Hospital Conceição Internal Medicine Residency Program, without whom our initiatives would never have blossomed. Special thanks to Eduardo Fernandes, Sergio Prezzi, and Paulo Ricardo Cardoso.
Dr. Barcellos is a specialist in internal medicine, emergency medicine, and critical care. He is professor in Nossa Senhora da Conceição Hospital’s Hospital Medicine Residence Program and president of GEAMH, a local association designed to promote the understanding and diffusion of hospitalist principles.
Dr. Wajner is a specialist in internal medicine and emergency medicine and a Master of Science student at Universidade Federal do Rio Grande do Sul.
Dr. de Waldemar is a specialist in internal medicine and emergency medicine.
References
- Departamento de População e Indicadores Sociais. Estatísticas da saúde: assistência médico-sanitária 2005/IBGE. Departamento de População e Indicadores Sociais. 2006. Available at: www.ibge.gov.br/home/estatistica/populacao/condicaodevida/ams/2005/ams2005.pdf. Last accessed January 28, 2007.
- Agência Nacional de Vigilância Sanitária. Lei nº 8080. D.O.U. - Diário Oficial da União; Poder Executivo. September 20, 1990. Available at: http://e-legis.bvs.br/leisref/public/showAct.php?id=16619&word=. Last accessed January 28, 2007.
- Brazilian Ministry of Health Web site. Available at: http://portal.saude.gov.br/saude. Last accessed January 28, 2007.
- Deslandes SF. Análise do discurso oficial sobre a humanização da assistência hospitalar. Ciência e saúde coletiva. 2004;9:7-14. Available at: www.scielo.br/pdf/csc/v9n1/19819.pdf. Last ccessed January 28, 2007.
- Portela MC, Lima SML, Barbosa PR, et al. Caracterização assistencial de hospitais filantrópicos no Brasil. Rev Saúde Pública. 2004;38:811-818. Available at: www.scielo.br/pdf/rsp/v38n6/09.pdf. Last accessed January 28, 2007.
- Sindicato Médico do Rio Grande do Sul Web site. Available at: www.simers.org.br/entquerem.php. Last accessed January 28, 2007.
- Wachter RM, Goldman L. The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996 Aug 15;335(7):514-517.
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002 Feb 16;287:487–494. Review.
- Wachter RM. An introduction to the hospitalist model. Ann Intern Med. 1999 Feb 16;130(4 Pt 2):338–342.
- No Free Lunch Web site. Available at: www.nofreelunch.org. Last accessed January 28, 2007.
Perfect Pain Control
Skillful use of intravenous pain medications can be a powerful tool in the clinician’s pain management armamentarium. Yet many physicians are uncomfortable prescribing IV pain medications, especially opioids, even when their patients are experiencing severe pain—7-10 on the verbal analogue scale (VAS). This reticence, say the palliative care specialists interviewed for this article, may be due to a lack of training and knowledge, as well as misperceptions about proper use of IV opioids. The end result for patients can be inadequate pain control, which, according to researchers, continues to be a problem in U.S. hospitals.1
Even hospitalists not affiliated with a surgical service who do not treat perioperative patients are likely to encounter many different scenarios in which IV pain medications could appropriately address patients’ discomfort. David Ling, MD, a member of SHM’s Palliative Care Task Force, a hospitalist at Baystate Medical Center in Springfield, Mass., and assistant professor of medicine at Tufts University School of Medicine (Boston), says patients who need IV pain medicines range from those with acute abdominal pain, pancreatitis, or small bowel obstructions to patients with end-stage cancer, renal disease, or congestive heart failure.
“It’s probably a bigger number on the medical service than most people realize,” he says.
The Short List
When it comes to effective IV pain medications very few choices exist, according to recommendations from the National Comprehensive Cancer Network and other pain advocacy organizations. An informal poll of interview sources corroborates this revelation.
“Morphine is the gold standard in pain control,” says Thomas Bookwalter, PharmD, clinical pharmacist on the General Medicine Service at the University of California at San Francisco (UCSF) Medical Center, a Health Sciences associate clinical professor at the UCSF School of Pharmacy, and a member of SHM’s Palliative Care Task Force.
Preferences for morphine or other opioids vary by practitioner and institution. For instance, says Dr. Bookwalter, the pain service at UCSF has been using hydromorphone more frequently of late.
Nicole L. Artz, MD, director of the Adult Sickle Cell Disease Care Team at the University of Chicago Hospitals and instructor of medicine at the University of Chicago Medical School, also occasionally uses IV infusions of ketorolac—a powerful NSAID designed for short-term management of moderately severe pain in adults. But, like morphine, it is contraindicated in patients with renal insufficiency and can have GI side effects.
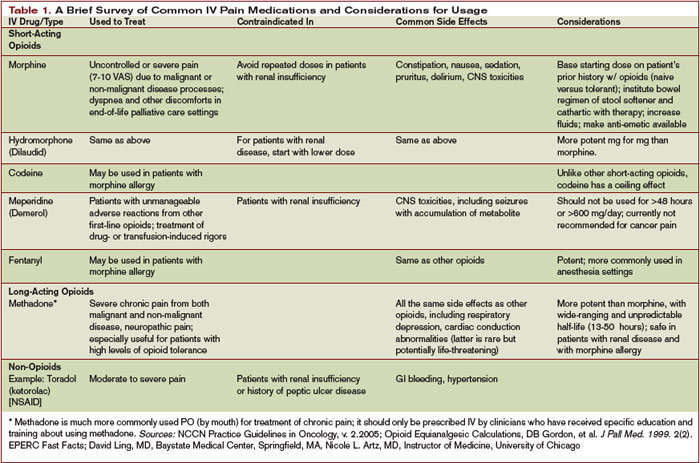
Common Missteps
That opioids remain the drugs of choice for controlling severe pain puts some physicians outside their comfort zone. Dr. Ling, who has extensive experience with IV opioids, has observed two common tendencies among physicians inexperienced with prescribing opioids. “There is a tendency, based on the traditional teaching, to prescribe a lower-than-necessary first dose and for those doses to not be frequent enough,” he says.
Dr. Artz, who has a special interest in pain management, lectures on effectively using opioids to house staff at the University of Chicago. She has observed a deficit in physician training in pain management and has seen physicians make many errors when writing orders for opioids, including mixing IV and short-acting oral opioids or two long-acting opioids, not distinguishing between patients who are opioid-naïve and opioid-tolerant in choosing a starting dose, failing to titrate short-acting opioids rapidly despite inadequate pain control, and giving orders for repeated doses of morphine in patients with renal insufficiency.
Dr. Bookwalter says the World Health Organization’s stepladder approach to treating pain (starting with oral NSAIDs and moving up to opioids) does not align with current scientific thinking on prescribing pain medication. For severe pain, a clinician should consider immediately starting an IV opioid, reassessing the patient every 15-30 minutes to see whether the dose is effectively decreasing the pain. National Comprehensive Cancer Network (NCCN) Guidelines for Adult Cancer Pain recommend rapid dose escalation to address the level of the patient’s pain.2
Skill Sets to Acquire
In addition to postgraduate and conference courses on pain control, another good first step in educating oneself about pain is to become familiar with equianalgesic doses of opioids. It is also mandatory to know not only how to convert between different opioids but between different routes of administration, Dr. Artz emphasizes. This step is crucial when patients have been stabilized and are ready for discharge. When conversions from IV opioids to equianalgesic doses of oral opioids are performed incorrectly, patients get the idea that the oral medication doesn’t work as well and that they need the IV pain medicine, “when, in reality, we didn’t give them an equivalent dose of oral pain medicine.”
Equianalgesic tables for use in converting 24-hour standing doses of an IV opioid to an oral formulation are readily available. Dr. Bookwalter offers a cautionary note about the use of conversion charts: “These charts are based on single-dose studies. The thing to remember is that these are ballpark numbers. Every place and every practitioner will use them in a slightly different way. The key thing is close monitoring to make sure the pain is relieved and that side effects are kept at a minimum.”
Familiarity with various pain intensity scales is also necessary. The Wong numerical rating scale—either written or verbal (0 = no pain and 10 = worst pain imaginable)—is the most commonly used. The Wong-Baker FACES Pain Rating Scale is helpful when assessing patients who are not English speakers or who have other impairments.3 Dr. Artz reminds hospitalists never to guess by just looking at their patients what their levels of pain are. Many patients have developed coping strategies to mask their pain.
Finally, Dr. Ling advises hospitalists to examine their own beliefs about using opioids for pain control. “Narcotics, in general, have a social stigma attached to them,” he points out. “I think most doctors, without additional experience and training [in prescribing IV opioids], will have a natural built-in response of, ‘Do I really want to give them that much?’ ”
Dr. Ling admits even he sometimes becomes a little uncomfortable with titrating to larger doses. “But some patients—especially those with a new diagnosis of metastatic cancer—or cancer that is invading an organ system, have appropriately high requirements for pain medication,” he stresses. Dr. Ling recalls one educational video made by the colleague of a patient who required a 400-mg dose of IV morphine daily. While the patient’s surgeon, anesthesiologist, and internist did not believe that the patient required that much morphine, her hospitalist finally convinced the treatment team by achieving adequate pain control using her own pain management skill.
“It’s not the dose so much as looking at the patient and talking with the patient” that should guide dosing decisions, says Eva Chittenden, MD, assistant director of the UCSF Palliative Care Service and chair of SHM’s Palliative Care Task Force. “You will know within 10 to 15 minutes if a dose is working.”
Adds Howard R. Epstein, MD, medical director of Care Management and Palliative Care at Regions Hospital in St. Paul, Minn., and also a member of SHM’s Palliative Care Task Force, “You have to assess your intervention: Was it effective? Did it relieve the patient’s pain? How long did it last?”
Dr. Bookwalter says hospitalists have an edge with pain patients. “The advantage that hospitalists have is that they can do more frequent monitoring,” he says. “The choice of drug is key, but frequent monitoring is even more key: You have to know if the patient is getting nauseated, or is still in pain, or how much the pain decreased with a certain dose.”
Special Considerations
Multiple variables influence a clinician’s decision to prescribe IV opioids for a patient—and at what dose and frequency. Basic principles of pain management dictate administering an initial IV bolus by a provider or by using patient-controlled analgesia (PCA) at lower doses if the patient is opioid-naïve, and at higher doses if a patient has already been taking oral narcotics. The NCCN recommends starting doses of 1-5 mg of IV morphine or equivalent for opioid-naïve patients, or a dose 10%-20% of a daily IV morphine equivalent for those already on opioids.2
The clinician should reassess the patient at 15 minutes to determine whether the pain score is unchanged, increased, or decreased. “If, after 15 minutes, that patient is still in severe pain, you want to be giving another dose,” emphasizes Dr. Chittenden. “You want to get the pain under control and then figure out what the standing dose should be.” The NCCN advises increasing the dose by 50%-100% if the pain score is unchanged or has increased after the initial dose.
IV opioids can also be indicated in elderly patients, unless they suffer from renal insufficiency. Palliative care specialists usually follow the maxim “start low and go slow” for elderly patients, and a 0.5 to 1-mg initial dose would be a reasonable place to begin treating an elderly patient in pain, says Dr. Chittenden. In addition to reassessing every 15 minutes for changes in the pain score, the hospitalist should also closely monitor the patient for sedation, respiratory rate, and other untoward side effects.
Hospitalists as Advocates
Hospitalists can play a vital role in advocating for better pain control for hospitalized patients. “Unfortunately,” notes Dr. Epstein, “pain management is not very well taught in most residency programs. But it’s an essential skill—not to mention a core competency—for hospitalists. If they don’t feel comfortable with their current fund of knowledge, there are plenty of resources out there to gain the skills or develop a higher comfort level and provide more competent pain management—to palliative as well as non-palliative patients.”
In actively dying patients, adequate pain control frees them from suffering. “If people have severe pain, they can’t talk with their families, and they can’t do the other things that might be important to them, whether they’re dying or not dying,” says Dr. Chittenden. “We should be trying to address pain in all patients in the hospital, not just those who are dying. Those in the ICU, those who have just had operations, those who have chronic pain—it’s not OK for them to come to the hospital and be having terrible pain.”
Dr. Artz agrees: “I cannot imagine that it is good for healing if a patient’s sympathetic nervous system is revved up because they’re in severe pain. I believe that adequate pain control is a really important piece of helping people get better.”
Dr. Ling urges colleagues to put themselves in the patient’s shoes, asking themselves, “If I were the patient, what would I need to control my pain?” Everyone’s pain threshold is different, he asserts, and physicians should listen to their patients’ reports. “Rather than asking why would we need to prescribe a large dose of narcotics, ask, ‘Why wouldn’t you want to control the pain?’ ” TH
Gretchen Henkel writes frequently for The Hospitalist.
References
- Gordon DB, Stevenson KK, Griffie J, et al. Opioid equianalgesic calculations. J Palliat Med. 1999 summer;2(2):209-218.
- National Comprehensive Cancer Network Practice Guidelines in Oncology. Adult cancer pain. Available at: www.nccn.org/professionals/physician_gls/PDF/pain.pdf. Last accessed January 28, 2007.
- Wong DL, Hockenberry-Eaton M, Wilson D, et al. Wong’s Essentials of Pediatric Nursing. 6th ed. St. Louis: Mosby;2001:1301.
Skillful use of intravenous pain medications can be a powerful tool in the clinician’s pain management armamentarium. Yet many physicians are uncomfortable prescribing IV pain medications, especially opioids, even when their patients are experiencing severe pain—7-10 on the verbal analogue scale (VAS). This reticence, say the palliative care specialists interviewed for this article, may be due to a lack of training and knowledge, as well as misperceptions about proper use of IV opioids. The end result for patients can be inadequate pain control, which, according to researchers, continues to be a problem in U.S. hospitals.1
Even hospitalists not affiliated with a surgical service who do not treat perioperative patients are likely to encounter many different scenarios in which IV pain medications could appropriately address patients’ discomfort. David Ling, MD, a member of SHM’s Palliative Care Task Force, a hospitalist at Baystate Medical Center in Springfield, Mass., and assistant professor of medicine at Tufts University School of Medicine (Boston), says patients who need IV pain medicines range from those with acute abdominal pain, pancreatitis, or small bowel obstructions to patients with end-stage cancer, renal disease, or congestive heart failure.
“It’s probably a bigger number on the medical service than most people realize,” he says.
The Short List
When it comes to effective IV pain medications very few choices exist, according to recommendations from the National Comprehensive Cancer Network and other pain advocacy organizations. An informal poll of interview sources corroborates this revelation.
“Morphine is the gold standard in pain control,” says Thomas Bookwalter, PharmD, clinical pharmacist on the General Medicine Service at the University of California at San Francisco (UCSF) Medical Center, a Health Sciences associate clinical professor at the UCSF School of Pharmacy, and a member of SHM’s Palliative Care Task Force.
Preferences for morphine or other opioids vary by practitioner and institution. For instance, says Dr. Bookwalter, the pain service at UCSF has been using hydromorphone more frequently of late.
Nicole L. Artz, MD, director of the Adult Sickle Cell Disease Care Team at the University of Chicago Hospitals and instructor of medicine at the University of Chicago Medical School, also occasionally uses IV infusions of ketorolac—a powerful NSAID designed for short-term management of moderately severe pain in adults. But, like morphine, it is contraindicated in patients with renal insufficiency and can have GI side effects.
Common Missteps
That opioids remain the drugs of choice for controlling severe pain puts some physicians outside their comfort zone. Dr. Ling, who has extensive experience with IV opioids, has observed two common tendencies among physicians inexperienced with prescribing opioids. “There is a tendency, based on the traditional teaching, to prescribe a lower-than-necessary first dose and for those doses to not be frequent enough,” he says.
Dr. Artz, who has a special interest in pain management, lectures on effectively using opioids to house staff at the University of Chicago. She has observed a deficit in physician training in pain management and has seen physicians make many errors when writing orders for opioids, including mixing IV and short-acting oral opioids or two long-acting opioids, not distinguishing between patients who are opioid-naïve and opioid-tolerant in choosing a starting dose, failing to titrate short-acting opioids rapidly despite inadequate pain control, and giving orders for repeated doses of morphine in patients with renal insufficiency.
Dr. Bookwalter says the World Health Organization’s stepladder approach to treating pain (starting with oral NSAIDs and moving up to opioids) does not align with current scientific thinking on prescribing pain medication. For severe pain, a clinician should consider immediately starting an IV opioid, reassessing the patient every 15-30 minutes to see whether the dose is effectively decreasing the pain. National Comprehensive Cancer Network (NCCN) Guidelines for Adult Cancer Pain recommend rapid dose escalation to address the level of the patient’s pain.2
Skill Sets to Acquire
In addition to postgraduate and conference courses on pain control, another good first step in educating oneself about pain is to become familiar with equianalgesic doses of opioids. It is also mandatory to know not only how to convert between different opioids but between different routes of administration, Dr. Artz emphasizes. This step is crucial when patients have been stabilized and are ready for discharge. When conversions from IV opioids to equianalgesic doses of oral opioids are performed incorrectly, patients get the idea that the oral medication doesn’t work as well and that they need the IV pain medicine, “when, in reality, we didn’t give them an equivalent dose of oral pain medicine.”
Equianalgesic tables for use in converting 24-hour standing doses of an IV opioid to an oral formulation are readily available. Dr. Bookwalter offers a cautionary note about the use of conversion charts: “These charts are based on single-dose studies. The thing to remember is that these are ballpark numbers. Every place and every practitioner will use them in a slightly different way. The key thing is close monitoring to make sure the pain is relieved and that side effects are kept at a minimum.”
Familiarity with various pain intensity scales is also necessary. The Wong numerical rating scale—either written or verbal (0 = no pain and 10 = worst pain imaginable)—is the most commonly used. The Wong-Baker FACES Pain Rating Scale is helpful when assessing patients who are not English speakers or who have other impairments.3 Dr. Artz reminds hospitalists never to guess by just looking at their patients what their levels of pain are. Many patients have developed coping strategies to mask their pain.
Finally, Dr. Ling advises hospitalists to examine their own beliefs about using opioids for pain control. “Narcotics, in general, have a social stigma attached to them,” he points out. “I think most doctors, without additional experience and training [in prescribing IV opioids], will have a natural built-in response of, ‘Do I really want to give them that much?’ ”
Dr. Ling admits even he sometimes becomes a little uncomfortable with titrating to larger doses. “But some patients—especially those with a new diagnosis of metastatic cancer—or cancer that is invading an organ system, have appropriately high requirements for pain medication,” he stresses. Dr. Ling recalls one educational video made by the colleague of a patient who required a 400-mg dose of IV morphine daily. While the patient’s surgeon, anesthesiologist, and internist did not believe that the patient required that much morphine, her hospitalist finally convinced the treatment team by achieving adequate pain control using her own pain management skill.
“It’s not the dose so much as looking at the patient and talking with the patient” that should guide dosing decisions, says Eva Chittenden, MD, assistant director of the UCSF Palliative Care Service and chair of SHM’s Palliative Care Task Force. “You will know within 10 to 15 minutes if a dose is working.”
Adds Howard R. Epstein, MD, medical director of Care Management and Palliative Care at Regions Hospital in St. Paul, Minn., and also a member of SHM’s Palliative Care Task Force, “You have to assess your intervention: Was it effective? Did it relieve the patient’s pain? How long did it last?”
Dr. Bookwalter says hospitalists have an edge with pain patients. “The advantage that hospitalists have is that they can do more frequent monitoring,” he says. “The choice of drug is key, but frequent monitoring is even more key: You have to know if the patient is getting nauseated, or is still in pain, or how much the pain decreased with a certain dose.”
Special Considerations
Multiple variables influence a clinician’s decision to prescribe IV opioids for a patient—and at what dose and frequency. Basic principles of pain management dictate administering an initial IV bolus by a provider or by using patient-controlled analgesia (PCA) at lower doses if the patient is opioid-naïve, and at higher doses if a patient has already been taking oral narcotics. The NCCN recommends starting doses of 1-5 mg of IV morphine or equivalent for opioid-naïve patients, or a dose 10%-20% of a daily IV morphine equivalent for those already on opioids.2
The clinician should reassess the patient at 15 minutes to determine whether the pain score is unchanged, increased, or decreased. “If, after 15 minutes, that patient is still in severe pain, you want to be giving another dose,” emphasizes Dr. Chittenden. “You want to get the pain under control and then figure out what the standing dose should be.” The NCCN advises increasing the dose by 50%-100% if the pain score is unchanged or has increased after the initial dose.
IV opioids can also be indicated in elderly patients, unless they suffer from renal insufficiency. Palliative care specialists usually follow the maxim “start low and go slow” for elderly patients, and a 0.5 to 1-mg initial dose would be a reasonable place to begin treating an elderly patient in pain, says Dr. Chittenden. In addition to reassessing every 15 minutes for changes in the pain score, the hospitalist should also closely monitor the patient for sedation, respiratory rate, and other untoward side effects.
Hospitalists as Advocates
Hospitalists can play a vital role in advocating for better pain control for hospitalized patients. “Unfortunately,” notes Dr. Epstein, “pain management is not very well taught in most residency programs. But it’s an essential skill—not to mention a core competency—for hospitalists. If they don’t feel comfortable with their current fund of knowledge, there are plenty of resources out there to gain the skills or develop a higher comfort level and provide more competent pain management—to palliative as well as non-palliative patients.”
In actively dying patients, adequate pain control frees them from suffering. “If people have severe pain, they can’t talk with their families, and they can’t do the other things that might be important to them, whether they’re dying or not dying,” says Dr. Chittenden. “We should be trying to address pain in all patients in the hospital, not just those who are dying. Those in the ICU, those who have just had operations, those who have chronic pain—it’s not OK for them to come to the hospital and be having terrible pain.”
Dr. Artz agrees: “I cannot imagine that it is good for healing if a patient’s sympathetic nervous system is revved up because they’re in severe pain. I believe that adequate pain control is a really important piece of helping people get better.”
Dr. Ling urges colleagues to put themselves in the patient’s shoes, asking themselves, “If I were the patient, what would I need to control my pain?” Everyone’s pain threshold is different, he asserts, and physicians should listen to their patients’ reports. “Rather than asking why would we need to prescribe a large dose of narcotics, ask, ‘Why wouldn’t you want to control the pain?’ ” TH
Gretchen Henkel writes frequently for The Hospitalist.
References
- Gordon DB, Stevenson KK, Griffie J, et al. Opioid equianalgesic calculations. J Palliat Med. 1999 summer;2(2):209-218.
- National Comprehensive Cancer Network Practice Guidelines in Oncology. Adult cancer pain. Available at: www.nccn.org/professionals/physician_gls/PDF/pain.pdf. Last accessed January 28, 2007.
- Wong DL, Hockenberry-Eaton M, Wilson D, et al. Wong’s Essentials of Pediatric Nursing. 6th ed. St. Louis: Mosby;2001:1301.
Skillful use of intravenous pain medications can be a powerful tool in the clinician’s pain management armamentarium. Yet many physicians are uncomfortable prescribing IV pain medications, especially opioids, even when their patients are experiencing severe pain—7-10 on the verbal analogue scale (VAS). This reticence, say the palliative care specialists interviewed for this article, may be due to a lack of training and knowledge, as well as misperceptions about proper use of IV opioids. The end result for patients can be inadequate pain control, which, according to researchers, continues to be a problem in U.S. hospitals.1
Even hospitalists not affiliated with a surgical service who do not treat perioperative patients are likely to encounter many different scenarios in which IV pain medications could appropriately address patients’ discomfort. David Ling, MD, a member of SHM’s Palliative Care Task Force, a hospitalist at Baystate Medical Center in Springfield, Mass., and assistant professor of medicine at Tufts University School of Medicine (Boston), says patients who need IV pain medicines range from those with acute abdominal pain, pancreatitis, or small bowel obstructions to patients with end-stage cancer, renal disease, or congestive heart failure.
“It’s probably a bigger number on the medical service than most people realize,” he says.
The Short List
When it comes to effective IV pain medications very few choices exist, according to recommendations from the National Comprehensive Cancer Network and other pain advocacy organizations. An informal poll of interview sources corroborates this revelation.
“Morphine is the gold standard in pain control,” says Thomas Bookwalter, PharmD, clinical pharmacist on the General Medicine Service at the University of California at San Francisco (UCSF) Medical Center, a Health Sciences associate clinical professor at the UCSF School of Pharmacy, and a member of SHM’s Palliative Care Task Force.
Preferences for morphine or other opioids vary by practitioner and institution. For instance, says Dr. Bookwalter, the pain service at UCSF has been using hydromorphone more frequently of late.
Nicole L. Artz, MD, director of the Adult Sickle Cell Disease Care Team at the University of Chicago Hospitals and instructor of medicine at the University of Chicago Medical School, also occasionally uses IV infusions of ketorolac—a powerful NSAID designed for short-term management of moderately severe pain in adults. But, like morphine, it is contraindicated in patients with renal insufficiency and can have GI side effects.
Common Missteps
That opioids remain the drugs of choice for controlling severe pain puts some physicians outside their comfort zone. Dr. Ling, who has extensive experience with IV opioids, has observed two common tendencies among physicians inexperienced with prescribing opioids. “There is a tendency, based on the traditional teaching, to prescribe a lower-than-necessary first dose and for those doses to not be frequent enough,” he says.
Dr. Artz, who has a special interest in pain management, lectures on effectively using opioids to house staff at the University of Chicago. She has observed a deficit in physician training in pain management and has seen physicians make many errors when writing orders for opioids, including mixing IV and short-acting oral opioids or two long-acting opioids, not distinguishing between patients who are opioid-naïve and opioid-tolerant in choosing a starting dose, failing to titrate short-acting opioids rapidly despite inadequate pain control, and giving orders for repeated doses of morphine in patients with renal insufficiency.
Dr. Bookwalter says the World Health Organization’s stepladder approach to treating pain (starting with oral NSAIDs and moving up to opioids) does not align with current scientific thinking on prescribing pain medication. For severe pain, a clinician should consider immediately starting an IV opioid, reassessing the patient every 15-30 minutes to see whether the dose is effectively decreasing the pain. National Comprehensive Cancer Network (NCCN) Guidelines for Adult Cancer Pain recommend rapid dose escalation to address the level of the patient’s pain.2
Skill Sets to Acquire
In addition to postgraduate and conference courses on pain control, another good first step in educating oneself about pain is to become familiar with equianalgesic doses of opioids. It is also mandatory to know not only how to convert between different opioids but between different routes of administration, Dr. Artz emphasizes. This step is crucial when patients have been stabilized and are ready for discharge. When conversions from IV opioids to equianalgesic doses of oral opioids are performed incorrectly, patients get the idea that the oral medication doesn’t work as well and that they need the IV pain medicine, “when, in reality, we didn’t give them an equivalent dose of oral pain medicine.”
Equianalgesic tables for use in converting 24-hour standing doses of an IV opioid to an oral formulation are readily available. Dr. Bookwalter offers a cautionary note about the use of conversion charts: “These charts are based on single-dose studies. The thing to remember is that these are ballpark numbers. Every place and every practitioner will use them in a slightly different way. The key thing is close monitoring to make sure the pain is relieved and that side effects are kept at a minimum.”
Familiarity with various pain intensity scales is also necessary. The Wong numerical rating scale—either written or verbal (0 = no pain and 10 = worst pain imaginable)—is the most commonly used. The Wong-Baker FACES Pain Rating Scale is helpful when assessing patients who are not English speakers or who have other impairments.3 Dr. Artz reminds hospitalists never to guess by just looking at their patients what their levels of pain are. Many patients have developed coping strategies to mask their pain.
Finally, Dr. Ling advises hospitalists to examine their own beliefs about using opioids for pain control. “Narcotics, in general, have a social stigma attached to them,” he points out. “I think most doctors, without additional experience and training [in prescribing IV opioids], will have a natural built-in response of, ‘Do I really want to give them that much?’ ”
Dr. Ling admits even he sometimes becomes a little uncomfortable with titrating to larger doses. “But some patients—especially those with a new diagnosis of metastatic cancer—or cancer that is invading an organ system, have appropriately high requirements for pain medication,” he stresses. Dr. Ling recalls one educational video made by the colleague of a patient who required a 400-mg dose of IV morphine daily. While the patient’s surgeon, anesthesiologist, and internist did not believe that the patient required that much morphine, her hospitalist finally convinced the treatment team by achieving adequate pain control using her own pain management skill.
“It’s not the dose so much as looking at the patient and talking with the patient” that should guide dosing decisions, says Eva Chittenden, MD, assistant director of the UCSF Palliative Care Service and chair of SHM’s Palliative Care Task Force. “You will know within 10 to 15 minutes if a dose is working.”
Adds Howard R. Epstein, MD, medical director of Care Management and Palliative Care at Regions Hospital in St. Paul, Minn., and also a member of SHM’s Palliative Care Task Force, “You have to assess your intervention: Was it effective? Did it relieve the patient’s pain? How long did it last?”
Dr. Bookwalter says hospitalists have an edge with pain patients. “The advantage that hospitalists have is that they can do more frequent monitoring,” he says. “The choice of drug is key, but frequent monitoring is even more key: You have to know if the patient is getting nauseated, or is still in pain, or how much the pain decreased with a certain dose.”
Special Considerations
Multiple variables influence a clinician’s decision to prescribe IV opioids for a patient—and at what dose and frequency. Basic principles of pain management dictate administering an initial IV bolus by a provider or by using patient-controlled analgesia (PCA) at lower doses if the patient is opioid-naïve, and at higher doses if a patient has already been taking oral narcotics. The NCCN recommends starting doses of 1-5 mg of IV morphine or equivalent for opioid-naïve patients, or a dose 10%-20% of a daily IV morphine equivalent for those already on opioids.2
The clinician should reassess the patient at 15 minutes to determine whether the pain score is unchanged, increased, or decreased. “If, after 15 minutes, that patient is still in severe pain, you want to be giving another dose,” emphasizes Dr. Chittenden. “You want to get the pain under control and then figure out what the standing dose should be.” The NCCN advises increasing the dose by 50%-100% if the pain score is unchanged or has increased after the initial dose.
IV opioids can also be indicated in elderly patients, unless they suffer from renal insufficiency. Palliative care specialists usually follow the maxim “start low and go slow” for elderly patients, and a 0.5 to 1-mg initial dose would be a reasonable place to begin treating an elderly patient in pain, says Dr. Chittenden. In addition to reassessing every 15 minutes for changes in the pain score, the hospitalist should also closely monitor the patient for sedation, respiratory rate, and other untoward side effects.
Hospitalists as Advocates
Hospitalists can play a vital role in advocating for better pain control for hospitalized patients. “Unfortunately,” notes Dr. Epstein, “pain management is not very well taught in most residency programs. But it’s an essential skill—not to mention a core competency—for hospitalists. If they don’t feel comfortable with their current fund of knowledge, there are plenty of resources out there to gain the skills or develop a higher comfort level and provide more competent pain management—to palliative as well as non-palliative patients.”
In actively dying patients, adequate pain control frees them from suffering. “If people have severe pain, they can’t talk with their families, and they can’t do the other things that might be important to them, whether they’re dying or not dying,” says Dr. Chittenden. “We should be trying to address pain in all patients in the hospital, not just those who are dying. Those in the ICU, those who have just had operations, those who have chronic pain—it’s not OK for them to come to the hospital and be having terrible pain.”
Dr. Artz agrees: “I cannot imagine that it is good for healing if a patient’s sympathetic nervous system is revved up because they’re in severe pain. I believe that adequate pain control is a really important piece of helping people get better.”
Dr. Ling urges colleagues to put themselves in the patient’s shoes, asking themselves, “If I were the patient, what would I need to control my pain?” Everyone’s pain threshold is different, he asserts, and physicians should listen to their patients’ reports. “Rather than asking why would we need to prescribe a large dose of narcotics, ask, ‘Why wouldn’t you want to control the pain?’ ” TH
Gretchen Henkel writes frequently for The Hospitalist.
References
- Gordon DB, Stevenson KK, Griffie J, et al. Opioid equianalgesic calculations. J Palliat Med. 1999 summer;2(2):209-218.
- National Comprehensive Cancer Network Practice Guidelines in Oncology. Adult cancer pain. Available at: www.nccn.org/professionals/physician_gls/PDF/pain.pdf. Last accessed January 28, 2007.
- Wong DL, Hockenberry-Eaton M, Wilson D, et al. Wong’s Essentials of Pediatric Nursing. 6th ed. St. Louis: Mosby;2001:1301.
Manage Sickle Cell Pain Crises
Standardized order sets reduce medication errors and create efficiency for physicians, nurses, and pharmacists.1 A less recognized benefit may be that standardized orders promote equity in care and may help to mitigate disparities that occur along racial and ethnic lines. Patients admitted with an acute pain crisis secondary to sickle cell disease (SCD) are often suspected of drug-seeking behavior and may be treated in a cursory manner because they are “frequent flyers” on the medical service. In view of these factors, this patient group may benefit more than others from a standardized treatment protocol. Over the past year, hospitalists and other clinicians at Novant Health in Charlotte, N.C., have composed an admission order set for SCD pain crisis in an effort to improve care for this underserved group.
Novant Health
Novant Health is a multi-hospital, non-profit system serving 3.5 million people from Virginia to South Carolina. Presbyterian Hospital, a 531-bed facility in Charlotte, N.C., is the flagship hospital for Novant’s Southern Piedmont Region (SPR). Presbyterian Inpatient Care Specialists (PICS) is a 44-provider group that offers hospitalist services for adult patients at Presbyterian Hospital, two community hospitals in Matthews and Huntersville, and Presbyterian Orthopedic Hospital.2 In 2005, 180 adult patients were discharged from the Novant-SPR hospitals with a principal diagnosis of SCD, and most of these patients were managed by PICS. This cohort of 180 patients accounted for more than 600 hospitalizations for SCD-related illness at the Novant-SPR facilities in 2005.
Process and Procedure
Standardized order sets have been in widespread use at the Novant-SPR facilities for a number of years. The process of order set development begins with patient needs as perceived by medical staff. Once a physician has drafted an order set, the draft is reviewed by the Order Set Subcommittee, a multidisciplinary team chaired by Susan Smith, RPh, PharmD, with nurses, physicians, and other support staff represented as needed. Once the subcommittee has approved the draft, it goes to the Pharmacy and Therapeutics Committee for final approval. In this fashion, more than 600 order sets have been developed and made available on the hospital’s intranet. The PICS team has helped to develop a number of disease management order sets and protocols, including the general medical admission orders. In addition, PICS has assisted in developing disease-specific orders for community-acquired pneumonia (CAP), CVA/TIA, and other common diseases admitted by the hospitalist service.
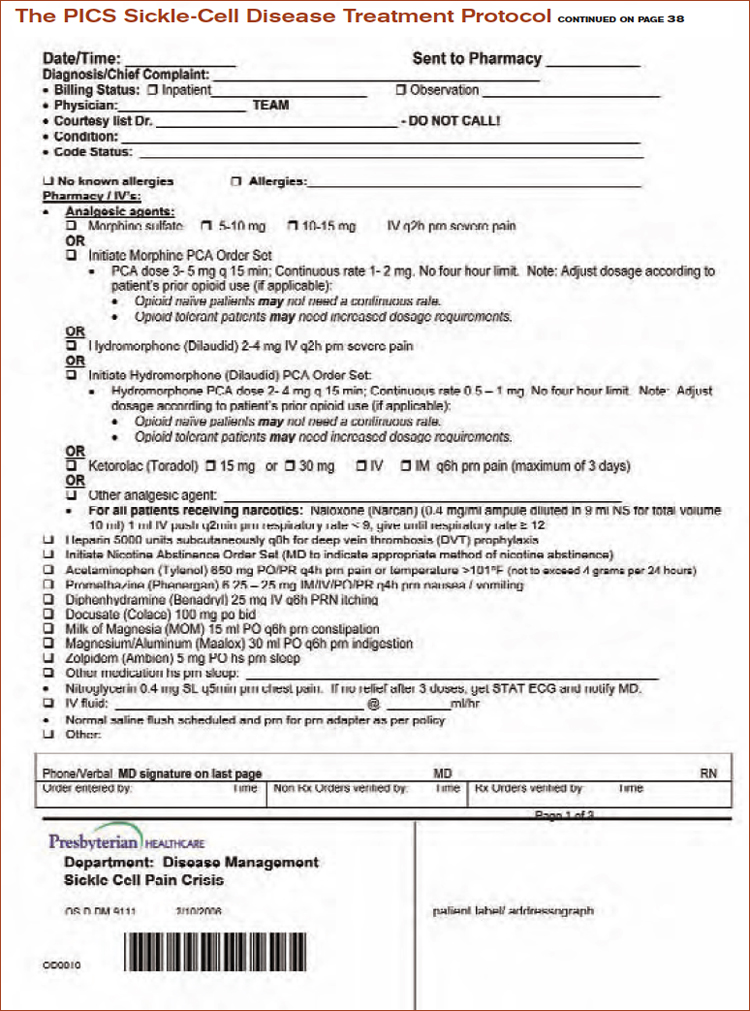
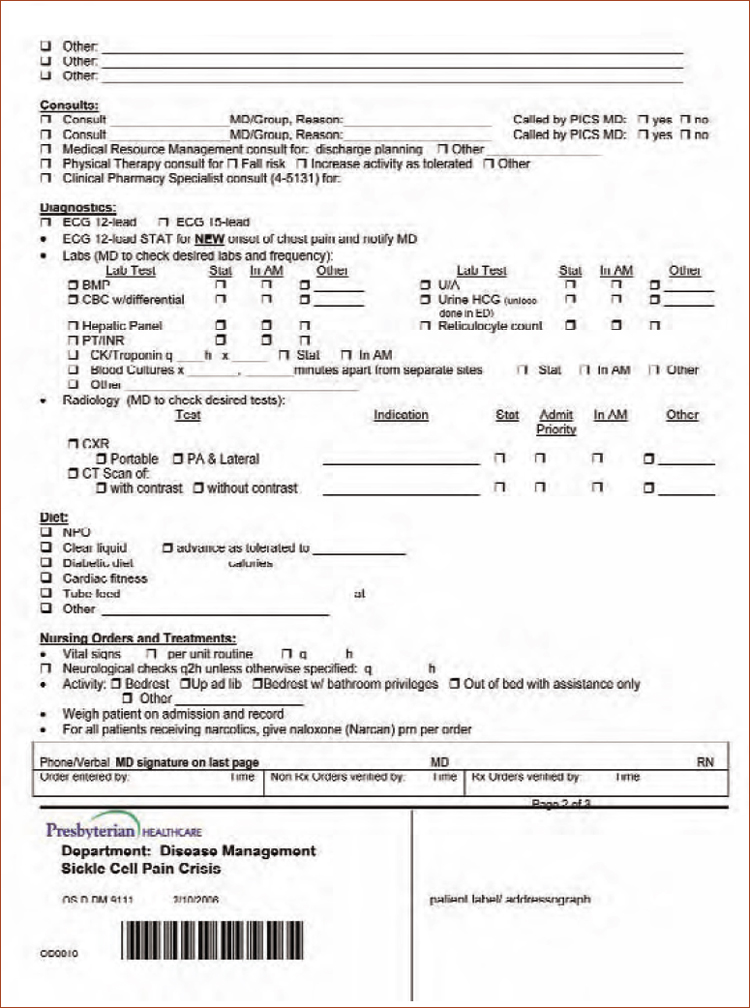
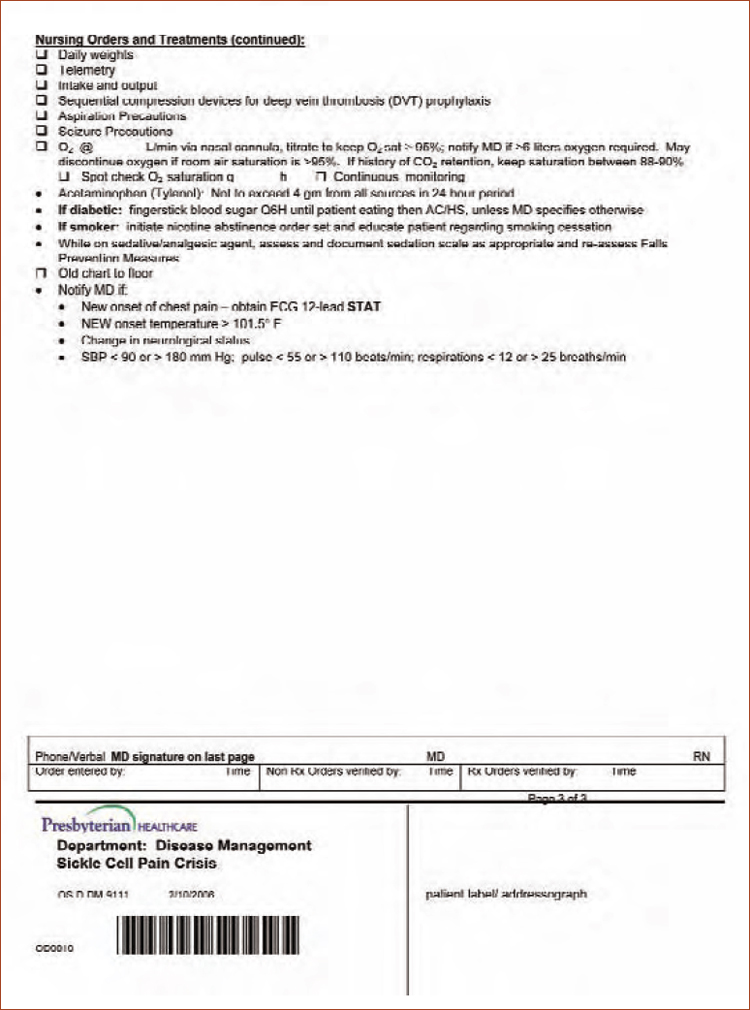
In the case of the adult SCD pain crisis order set, Stephen Wallenhaupt, MD, chief medical officer for Novant Health, recalls, “We recognize that SCD patients have unique needs in terms of pain management and that a standardized order set which incorporates aggressive pain management options is the best way to meet their needs.”
Fran Davis, RPh, PharmD, researched the pertinent literature and consulted the anesthesiologists on staff in an effort to tailor the pain management options for SCD patients. Using the recommendations of these specialists, the order set reflects the consensus that patients with a severe SCD pain crisis require parenteral opiate analgesia on admission.3
Because many patients admitted by PICS can be categorized as having severe pain, the order set contains choices for patient-controlled analgesia (PCA), in keeping with the recommendation for opiate administration at a fixed interval rather than on an as-needed basis.4 And because many hospitalists may not be familiar with ordering PCA, the SCD orders specify the dose ranges, as well as the lockout interval for morphine and hydromorphone PCA. With PCA options readily available, hospitalists need not delay therapy while awaiting a consultation from the pain management service. For all patients receiving opiates, the order set contains an automatic order for naloxone for respiratory depression manifested by a respiratory rate less than nine.
For patients with less severe pain, options for PRN (pro re nata, or as needed) bolus dose morphine and hydromorphone offer dose ranges that reflect the narcotic tolerance frequently observed in these patients. The order set includes options for non-opiate agents, including ketorolac and acetaminophen. Adjuvant therapies, including promethazine, zolpidem, and diphenhydramine, are also contained within the order set. Prompts for intravenous fluid replacement, oxygen therapy, and other supportive measures are incorporated into the orders as well.
The Novant-SPR hospitals have adopted a separate order set for the administration of pneumococcal vaccine. This order set allows for the automatic administration of pneumococcal vaccine, without a specific physician order, to every patient who meets criteria and who desires the vaccine. On admission, every patient is screened by a nurse regarding their need for pneumococcal vaccine; as a result, SCD patients who have not been immunized in the previous five years are offered the vaccine.
Day Hospital Model
In order to provide SCD patients with immediate and aggressive analgesic therapy and fluid replacement, some centers have adopted the Day Hospital (DH) model. The DH is a specific site at which patients with SCD pain crisis are treated by staff familiar with the patients and with their special analgesic needs.5 The DH model has been shown to provide rapid pain relief in an outpatient setting and to reduce the need for unnecessary hospitalizations. In addition, length of stay and cost per case are lower for DH patients admitted to the hospital than for patients not followed by DH staff. It has been suggested that the DH model is especially appropriate for centers with an emergency department too busy to begin treatment in a timely fashion.6
Novant Health has adopted the DH model in the urgent care setting. Patients with pain crises can be managed in one of Novant’s urgent care centers with a standard order set that includes options for IV hydration as well as parenteral morphine or hydromorphone. This outpatient order set parallels that designed for inpatients, because it prompts the physician to order aggressive analgesic therapy as well as adjuvant treatments for nausea and anxiety. Practitioners from Novant’s Sickle Cell Clinic often meet the patient at the urgent care center to assist with evaluation and management. In the past two years, approximately two-thirds of patients with SCD pain crisis have been discharged to home with good pain relief. The remaining one-third are referred to the hospital—usually to be admitted and managed by the PICS team.
Hope for the Future
It has been more than 50 years since the molecular defect in hemoglobin S was first described by Linus Pauling and 50 years since the genetic defect was first elucidated.7,8 Despite these and subsequent advances in understanding the pathogenesis of SCD at the cellular and molecular level, our treatment for SCD remains inadequate. It is akin to a “halfway technology” described by Lewis Thomas as, “the kinds of things that must be done … in order to compensate for the incapacitating effects of certain diseases whose course one is unable to do very much about. It is a technology designed to make up for disease, or to postpone death.”9
At present a number of agents designed to inhibit the sickling process are under investigation, including omega-3 fatty acids, Gardos channel blockers, and anti-adhesion therapies.10 In time, perhaps, one of these rational approaches to treatment will bridge the chasm in the halfway technology currently at our disposal. TH
Dr. Gardella is a board-certified internist and pulmonologist who currently serves as vice president for clinical improvement for Novant Health—Southern Piedmont Region.
Julie Swanger works with both pediatric and adult sickle cell populations through Presbyterian Community Care Services and Blume Pediatric Hematology and Oncology Clinic in Charlotte, N.C.
References
- Conlan M. Therapeutic interventions frequent among hospital pharmacists. Drug Top Hosp Pharmacist Rep. 2000;14(9):38-39.
- Piturro M. Top PICS: Presbyterian Inpatient Care Specialists bring high-quality hospitalist care to North Carolina. The Hospitalist. 2006;01(10):23-25.
- Elander J, Midence K. A review of evidence about factors affecting quality of pain management in sickle cell disease. Clin J Pain. 1996 Sep;12(3):180-193.
- Steinberg MH. Management of sickle cell disease. N Engl J Med. 1999;340:1021-1030.
- Sickle Cell Disease Association of America, Inc., Web site. Outpatient management issues in sickle cell disease. Available at: www.sicklecelldisease.org/research/scd_manage3.phtml. Last accessed January 26, 2007.
- Benjamin LJ, Swinson GI, Nagel RL. Sickle cell anemia day hospital: an approach for the management of uncomplicated painful crises. Blood. 2000 Feb;95(4):1130-1136.
- Pauling L, Itano HA, Singer SJ, et al. Sickle cell anemia a molecular disease. Science. 1949 Nov 25;110:543-548.
- Ingram VM. Gene mutations in human haemoglobin: the chemical difference between normal and sickle cell haemoglobin. Nature. 1957 Aug 17;180(4581):326-328.
- Thomas L. The technology of medicine. In: The Lives of a Cell. New York: Viking Press; 1974:31-36.
- Okpala IE. New therapies for sickle cell disease. Hematol Oncol Clin North Am. 2005 Oct;19(5):975-987.
Standardized order sets reduce medication errors and create efficiency for physicians, nurses, and pharmacists.1 A less recognized benefit may be that standardized orders promote equity in care and may help to mitigate disparities that occur along racial and ethnic lines. Patients admitted with an acute pain crisis secondary to sickle cell disease (SCD) are often suspected of drug-seeking behavior and may be treated in a cursory manner because they are “frequent flyers” on the medical service. In view of these factors, this patient group may benefit more than others from a standardized treatment protocol. Over the past year, hospitalists and other clinicians at Novant Health in Charlotte, N.C., have composed an admission order set for SCD pain crisis in an effort to improve care for this underserved group.
Novant Health
Novant Health is a multi-hospital, non-profit system serving 3.5 million people from Virginia to South Carolina. Presbyterian Hospital, a 531-bed facility in Charlotte, N.C., is the flagship hospital for Novant’s Southern Piedmont Region (SPR). Presbyterian Inpatient Care Specialists (PICS) is a 44-provider group that offers hospitalist services for adult patients at Presbyterian Hospital, two community hospitals in Matthews and Huntersville, and Presbyterian Orthopedic Hospital.2 In 2005, 180 adult patients were discharged from the Novant-SPR hospitals with a principal diagnosis of SCD, and most of these patients were managed by PICS. This cohort of 180 patients accounted for more than 600 hospitalizations for SCD-related illness at the Novant-SPR facilities in 2005.
Process and Procedure
Standardized order sets have been in widespread use at the Novant-SPR facilities for a number of years. The process of order set development begins with patient needs as perceived by medical staff. Once a physician has drafted an order set, the draft is reviewed by the Order Set Subcommittee, a multidisciplinary team chaired by Susan Smith, RPh, PharmD, with nurses, physicians, and other support staff represented as needed. Once the subcommittee has approved the draft, it goes to the Pharmacy and Therapeutics Committee for final approval. In this fashion, more than 600 order sets have been developed and made available on the hospital’s intranet. The PICS team has helped to develop a number of disease management order sets and protocols, including the general medical admission orders. In addition, PICS has assisted in developing disease-specific orders for community-acquired pneumonia (CAP), CVA/TIA, and other common diseases admitted by the hospitalist service.
In the case of the adult SCD pain crisis order set, Stephen Wallenhaupt, MD, chief medical officer for Novant Health, recalls, “We recognize that SCD patients have unique needs in terms of pain management and that a standardized order set which incorporates aggressive pain management options is the best way to meet their needs.”
Fran Davis, RPh, PharmD, researched the pertinent literature and consulted the anesthesiologists on staff in an effort to tailor the pain management options for SCD patients. Using the recommendations of these specialists, the order set reflects the consensus that patients with a severe SCD pain crisis require parenteral opiate analgesia on admission.3
Because many patients admitted by PICS can be categorized as having severe pain, the order set contains choices for patient-controlled analgesia (PCA), in keeping with the recommendation for opiate administration at a fixed interval rather than on an as-needed basis.4 And because many hospitalists may not be familiar with ordering PCA, the SCD orders specify the dose ranges, as well as the lockout interval for morphine and hydromorphone PCA. With PCA options readily available, hospitalists need not delay therapy while awaiting a consultation from the pain management service. For all patients receiving opiates, the order set contains an automatic order for naloxone for respiratory depression manifested by a respiratory rate less than nine.
For patients with less severe pain, options for PRN (pro re nata, or as needed) bolus dose morphine and hydromorphone offer dose ranges that reflect the narcotic tolerance frequently observed in these patients. The order set includes options for non-opiate agents, including ketorolac and acetaminophen. Adjuvant therapies, including promethazine, zolpidem, and diphenhydramine, are also contained within the order set. Prompts for intravenous fluid replacement, oxygen therapy, and other supportive measures are incorporated into the orders as well.
The Novant-SPR hospitals have adopted a separate order set for the administration of pneumococcal vaccine. This order set allows for the automatic administration of pneumococcal vaccine, without a specific physician order, to every patient who meets criteria and who desires the vaccine. On admission, every patient is screened by a nurse regarding their need for pneumococcal vaccine; as a result, SCD patients who have not been immunized in the previous five years are offered the vaccine.
Day Hospital Model
In order to provide SCD patients with immediate and aggressive analgesic therapy and fluid replacement, some centers have adopted the Day Hospital (DH) model. The DH is a specific site at which patients with SCD pain crisis are treated by staff familiar with the patients and with their special analgesic needs.5 The DH model has been shown to provide rapid pain relief in an outpatient setting and to reduce the need for unnecessary hospitalizations. In addition, length of stay and cost per case are lower for DH patients admitted to the hospital than for patients not followed by DH staff. It has been suggested that the DH model is especially appropriate for centers with an emergency department too busy to begin treatment in a timely fashion.6
Novant Health has adopted the DH model in the urgent care setting. Patients with pain crises can be managed in one of Novant’s urgent care centers with a standard order set that includes options for IV hydration as well as parenteral morphine or hydromorphone. This outpatient order set parallels that designed for inpatients, because it prompts the physician to order aggressive analgesic therapy as well as adjuvant treatments for nausea and anxiety. Practitioners from Novant’s Sickle Cell Clinic often meet the patient at the urgent care center to assist with evaluation and management. In the past two years, approximately two-thirds of patients with SCD pain crisis have been discharged to home with good pain relief. The remaining one-third are referred to the hospital—usually to be admitted and managed by the PICS team.
Hope for the Future
It has been more than 50 years since the molecular defect in hemoglobin S was first described by Linus Pauling and 50 years since the genetic defect was first elucidated.7,8 Despite these and subsequent advances in understanding the pathogenesis of SCD at the cellular and molecular level, our treatment for SCD remains inadequate. It is akin to a “halfway technology” described by Lewis Thomas as, “the kinds of things that must be done … in order to compensate for the incapacitating effects of certain diseases whose course one is unable to do very much about. It is a technology designed to make up for disease, or to postpone death.”9
At present a number of agents designed to inhibit the sickling process are under investigation, including omega-3 fatty acids, Gardos channel blockers, and anti-adhesion therapies.10 In time, perhaps, one of these rational approaches to treatment will bridge the chasm in the halfway technology currently at our disposal. TH
Dr. Gardella is a board-certified internist and pulmonologist who currently serves as vice president for clinical improvement for Novant Health—Southern Piedmont Region.
Julie Swanger works with both pediatric and adult sickle cell populations through Presbyterian Community Care Services and Blume Pediatric Hematology and Oncology Clinic in Charlotte, N.C.
References
- Conlan M. Therapeutic interventions frequent among hospital pharmacists. Drug Top Hosp Pharmacist Rep. 2000;14(9):38-39.
- Piturro M. Top PICS: Presbyterian Inpatient Care Specialists bring high-quality hospitalist care to North Carolina. The Hospitalist. 2006;01(10):23-25.
- Elander J, Midence K. A review of evidence about factors affecting quality of pain management in sickle cell disease. Clin J Pain. 1996 Sep;12(3):180-193.
- Steinberg MH. Management of sickle cell disease. N Engl J Med. 1999;340:1021-1030.
- Sickle Cell Disease Association of America, Inc., Web site. Outpatient management issues in sickle cell disease. Available at: www.sicklecelldisease.org/research/scd_manage3.phtml. Last accessed January 26, 2007.
- Benjamin LJ, Swinson GI, Nagel RL. Sickle cell anemia day hospital: an approach for the management of uncomplicated painful crises. Blood. 2000 Feb;95(4):1130-1136.
- Pauling L, Itano HA, Singer SJ, et al. Sickle cell anemia a molecular disease. Science. 1949 Nov 25;110:543-548.
- Ingram VM. Gene mutations in human haemoglobin: the chemical difference between normal and sickle cell haemoglobin. Nature. 1957 Aug 17;180(4581):326-328.
- Thomas L. The technology of medicine. In: The Lives of a Cell. New York: Viking Press; 1974:31-36.
- Okpala IE. New therapies for sickle cell disease. Hematol Oncol Clin North Am. 2005 Oct;19(5):975-987.
Standardized order sets reduce medication errors and create efficiency for physicians, nurses, and pharmacists.1 A less recognized benefit may be that standardized orders promote equity in care and may help to mitigate disparities that occur along racial and ethnic lines. Patients admitted with an acute pain crisis secondary to sickle cell disease (SCD) are often suspected of drug-seeking behavior and may be treated in a cursory manner because they are “frequent flyers” on the medical service. In view of these factors, this patient group may benefit more than others from a standardized treatment protocol. Over the past year, hospitalists and other clinicians at Novant Health in Charlotte, N.C., have composed an admission order set for SCD pain crisis in an effort to improve care for this underserved group.
Novant Health
Novant Health is a multi-hospital, non-profit system serving 3.5 million people from Virginia to South Carolina. Presbyterian Hospital, a 531-bed facility in Charlotte, N.C., is the flagship hospital for Novant’s Southern Piedmont Region (SPR). Presbyterian Inpatient Care Specialists (PICS) is a 44-provider group that offers hospitalist services for adult patients at Presbyterian Hospital, two community hospitals in Matthews and Huntersville, and Presbyterian Orthopedic Hospital.2 In 2005, 180 adult patients were discharged from the Novant-SPR hospitals with a principal diagnosis of SCD, and most of these patients were managed by PICS. This cohort of 180 patients accounted for more than 600 hospitalizations for SCD-related illness at the Novant-SPR facilities in 2005.
Process and Procedure
Standardized order sets have been in widespread use at the Novant-SPR facilities for a number of years. The process of order set development begins with patient needs as perceived by medical staff. Once a physician has drafted an order set, the draft is reviewed by the Order Set Subcommittee, a multidisciplinary team chaired by Susan Smith, RPh, PharmD, with nurses, physicians, and other support staff represented as needed. Once the subcommittee has approved the draft, it goes to the Pharmacy and Therapeutics Committee for final approval. In this fashion, more than 600 order sets have been developed and made available on the hospital’s intranet. The PICS team has helped to develop a number of disease management order sets and protocols, including the general medical admission orders. In addition, PICS has assisted in developing disease-specific orders for community-acquired pneumonia (CAP), CVA/TIA, and other common diseases admitted by the hospitalist service.
In the case of the adult SCD pain crisis order set, Stephen Wallenhaupt, MD, chief medical officer for Novant Health, recalls, “We recognize that SCD patients have unique needs in terms of pain management and that a standardized order set which incorporates aggressive pain management options is the best way to meet their needs.”
Fran Davis, RPh, PharmD, researched the pertinent literature and consulted the anesthesiologists on staff in an effort to tailor the pain management options for SCD patients. Using the recommendations of these specialists, the order set reflects the consensus that patients with a severe SCD pain crisis require parenteral opiate analgesia on admission.3
Because many patients admitted by PICS can be categorized as having severe pain, the order set contains choices for patient-controlled analgesia (PCA), in keeping with the recommendation for opiate administration at a fixed interval rather than on an as-needed basis.4 And because many hospitalists may not be familiar with ordering PCA, the SCD orders specify the dose ranges, as well as the lockout interval for morphine and hydromorphone PCA. With PCA options readily available, hospitalists need not delay therapy while awaiting a consultation from the pain management service. For all patients receiving opiates, the order set contains an automatic order for naloxone for respiratory depression manifested by a respiratory rate less than nine.
For patients with less severe pain, options for PRN (pro re nata, or as needed) bolus dose morphine and hydromorphone offer dose ranges that reflect the narcotic tolerance frequently observed in these patients. The order set includes options for non-opiate agents, including ketorolac and acetaminophen. Adjuvant therapies, including promethazine, zolpidem, and diphenhydramine, are also contained within the order set. Prompts for intravenous fluid replacement, oxygen therapy, and other supportive measures are incorporated into the orders as well.
The Novant-SPR hospitals have adopted a separate order set for the administration of pneumococcal vaccine. This order set allows for the automatic administration of pneumococcal vaccine, without a specific physician order, to every patient who meets criteria and who desires the vaccine. On admission, every patient is screened by a nurse regarding their need for pneumococcal vaccine; as a result, SCD patients who have not been immunized in the previous five years are offered the vaccine.
Day Hospital Model
In order to provide SCD patients with immediate and aggressive analgesic therapy and fluid replacement, some centers have adopted the Day Hospital (DH) model. The DH is a specific site at which patients with SCD pain crisis are treated by staff familiar with the patients and with their special analgesic needs.5 The DH model has been shown to provide rapid pain relief in an outpatient setting and to reduce the need for unnecessary hospitalizations. In addition, length of stay and cost per case are lower for DH patients admitted to the hospital than for patients not followed by DH staff. It has been suggested that the DH model is especially appropriate for centers with an emergency department too busy to begin treatment in a timely fashion.6
Novant Health has adopted the DH model in the urgent care setting. Patients with pain crises can be managed in one of Novant’s urgent care centers with a standard order set that includes options for IV hydration as well as parenteral morphine or hydromorphone. This outpatient order set parallels that designed for inpatients, because it prompts the physician to order aggressive analgesic therapy as well as adjuvant treatments for nausea and anxiety. Practitioners from Novant’s Sickle Cell Clinic often meet the patient at the urgent care center to assist with evaluation and management. In the past two years, approximately two-thirds of patients with SCD pain crisis have been discharged to home with good pain relief. The remaining one-third are referred to the hospital—usually to be admitted and managed by the PICS team.
Hope for the Future
It has been more than 50 years since the molecular defect in hemoglobin S was first described by Linus Pauling and 50 years since the genetic defect was first elucidated.7,8 Despite these and subsequent advances in understanding the pathogenesis of SCD at the cellular and molecular level, our treatment for SCD remains inadequate. It is akin to a “halfway technology” described by Lewis Thomas as, “the kinds of things that must be done … in order to compensate for the incapacitating effects of certain diseases whose course one is unable to do very much about. It is a technology designed to make up for disease, or to postpone death.”9
At present a number of agents designed to inhibit the sickling process are under investigation, including omega-3 fatty acids, Gardos channel blockers, and anti-adhesion therapies.10 In time, perhaps, one of these rational approaches to treatment will bridge the chasm in the halfway technology currently at our disposal. TH
Dr. Gardella is a board-certified internist and pulmonologist who currently serves as vice president for clinical improvement for Novant Health—Southern Piedmont Region.
Julie Swanger works with both pediatric and adult sickle cell populations through Presbyterian Community Care Services and Blume Pediatric Hematology and Oncology Clinic in Charlotte, N.C.
References
- Conlan M. Therapeutic interventions frequent among hospital pharmacists. Drug Top Hosp Pharmacist Rep. 2000;14(9):38-39.
- Piturro M. Top PICS: Presbyterian Inpatient Care Specialists bring high-quality hospitalist care to North Carolina. The Hospitalist. 2006;01(10):23-25.
- Elander J, Midence K. A review of evidence about factors affecting quality of pain management in sickle cell disease. Clin J Pain. 1996 Sep;12(3):180-193.
- Steinberg MH. Management of sickle cell disease. N Engl J Med. 1999;340:1021-1030.
- Sickle Cell Disease Association of America, Inc., Web site. Outpatient management issues in sickle cell disease. Available at: www.sicklecelldisease.org/research/scd_manage3.phtml. Last accessed January 26, 2007.
- Benjamin LJ, Swinson GI, Nagel RL. Sickle cell anemia day hospital: an approach for the management of uncomplicated painful crises. Blood. 2000 Feb;95(4):1130-1136.
- Pauling L, Itano HA, Singer SJ, et al. Sickle cell anemia a molecular disease. Science. 1949 Nov 25;110:543-548.
- Ingram VM. Gene mutations in human haemoglobin: the chemical difference between normal and sickle cell haemoglobin. Nature. 1957 Aug 17;180(4581):326-328.
- Thomas L. The technology of medicine. In: The Lives of a Cell. New York: Viking Press; 1974:31-36.
- Okpala IE. New therapies for sickle cell disease. Hematol Oncol Clin North Am. 2005 Oct;19(5):975-987.
Hospitalists & Handoffs
In the nearly 10 years since the word “hospitalist” entered our consciousness, it has been inspiring to witness the dramatic growth in the specialty and, accompanying it, the growth in the membership of SHM.1 Over this same period, the healthcare system has made progress toward ensuring that it provides the safest, highest quality healthcare possible.
In my mind, the two phenomena are related. SHM itself and—more generally—the hospitalist field have played a vital role in promoting the use of evidence-based care, improved teamwork, and health information technology. Each of these efforts has made a significant difference in the care patients receive in hospitals. Similarly, the mission of the Agency for Healthcare Research and Quality (AHRQ) is to improve the quality, safety, efficiency, and effectiveness of healthcare for all Americans. Both organizations are working to create positive change that will improve the health and healthcare of all patients.
As their numbers continue to grow, hospitalists are becoming integral members of the inpatient care team at many hospitals.
According to a recent survey conducted by SHM, a hospitalist averaged more than 2,300 inpatient encounters in 2005—a 7% increase over 2004.2 Today, hospital medicine groups practice not only in large metropolitan areas, but also in rural regions where one in three groups began operation during 2005.
In addition to their inpatient care responsibilities, the 15,000 hospitalists who practice today in the United States and Canada serve in key physician leadership roles that directly influence quality improvement and patient safety. Most hospitalists—86%—participate in quality improvement. More than half are involved in implementing information technology (54%) and teaching house staff (51%), and more than one-third—35%—are responsible for their organization’s rapid response team. The SHM survey found that nearly all hospital medicine groups provide round-the-clock patient care at their hospitals.
In this article I will emphasize two key areas relevant to improving patient safety for hospitalized patients: patient handoffs and communication.
Responsibility for Patient Handoffs
Hospitalists’ clinical and leadership roles are significant responsibilities for patient safety, including the critical period known as patient handoff or sign-out.
Patient handoffs refer to the interaction, communication, and planning required to achieve a seamless transition from one clinician to the next.3 When executed in a timely and thorough manner, patient handoffs can reduce the likelihood of medical errors and misinformation, prevent lost or missing clinical information, and maintain a high level of medical care.
Given today’s short hospital stays and the complex medical nature of the care necessary for many patients, timely and effective handoffs demand that hospitalists develop skills that extend beyond superior clinical care. They include:
- Communicating in an effective and efficient manner during patient sign-out;
- Demonstrating the use of “read-back” skills when communicating tasks;
- Developing oral and written patient summaries, including characteristics of the patient, provider, and time of the sign-out;
- Evaluating all medications for indication, dosing, and planned duration at the time of sign-out; and
- Anticipating what may go wrong with a patient after a transition in care occurs and clearly communicating this concern to the receiving clinician.
A Fumbled Handoff: A Case Study
A breakdown in communications—notably an error of omission in the patient handoff—contributed to a poor outcome for an elderly patient who was admitted to the hospital for an elective sigmoid resection.
The case, which was published in the AHRQ’s “Morbidity and Mortality Rounds on the Web” (developed by hospital medicine expert Robert Wachter, MD, and his team under contract to our agency), illustrates some of the challenges that face all clinicians in effectively transferring patient information and care responsibilities.4 It also underscores the need for close involvement by hospitalists in improving quality, teaching and supervising house staff, and implementing information systems.
According to the case study, a 73-year-old female patient with a history of hypertension, non-insulin dependent diabetes, and chronic renal insufficiency became tachycardic two days after surgery, despite receiving a low-dose beta-blocker. The same day, she informed her nurse that she had developed pain in her left leg.
Assuming the pain was related to the pre-operative epidural, the nurse contacted the anesthesia service, which responded by decreasing the epidural rate; the primary surgical team was not called. Late on the third day after surgery, the cross-covering intern was contacted about the patient’s left leg pain. No information about the intern’s findings was relayed to the primary team the following day.
On the fourth day, the patient complained to the nurse about mild chest discomfort, resulting in attention within 20 minutes by house staff and from the attending physician several hours later. The patient’s exam was unremarkable and a work-up was initiated.
Within an hour of the attending’s visit, the patient’s blood pressure dropped to 70/40, followed by a pulseless electrical activity arrest. The patient could not be resuscitated. A post-mortem examination revealed a pulmonary embolism.
Handoffs in an Era of Work-Hour Restrictions
Missing information about pain in the patient’s leg and a breakdown in communication between physicians contributed to the patient’s poor outcome. In this case, the breakdown may also have been influenced by the intern’s involvement on the third day. Like all medical residents this intern is subject to duty-hour restrictions.
Work-hour limits for all residents training in U.S. hospitals took effect in July 2003. Under these standards, created by the Accreditation Council for Graduate Medical Education (ACGME), residents are limited to a maximum of 30 consecutive work hours—known as the 30-hour rule, which includes time used for sign-out, teaching, and continuity of care. They are also prohibited from working more than 80 hours per week.
Despite the clear safety benefit of preventing fatigue-related mistakes, work-hour mandates have increased the number of patient handoffs and the potential for communication breakdowns.5 A survey of interns conducted at the hospital where this case study occurred identified a higher volume of sign-outs and the resulting potential for harm to patients as main concerns with the work-hour restrictions.6
Concerns about the quality and continuity of care that hospital patients receive are evident even among those medical residents whose work hours were restricted before the ACGME requirements took effect. (In New York state residents’ work hours have been restricted since 1998.)
A 2006 study of surgical residents at New York’s Beth Israel Hospital found that most believed that the quality of care patients received was either unchanged (63%) or worse (26%) since the work-hour restrictions took effect.7 Possible reasons for this perception include unresolved issues with continuity of care, miscommunication, and cross-coverage availability. The study concluded that interventions that target intern sign-out coverage constraints will be important for future efforts to improve the quality of care for hospital patients.
Written sign-outs appear to overcome some of the human errors that inevitably result from verbal patient summaries, such as disruptions and forgetfulness. Recent findings have, however, identified significant shortcomings in the quality and timeliness of written reports.
Critical information, such as code status and allergies, was missing in 80% of written sign-outs in one recent study.8 And in a 2006 study of the quality of discharge summaries, only 19% of hospital physicians with an outpatient practice reported being satisfied with the timeliness of discharge summaries. Only a third reported being satisfied with their quality of information. Most troubling, 41% believed that at least one of their patients hospitalized in the previous six months had experienced a preventable adverse event related to poor transfer of information at discharge.9
Use Redundancy and Simulation to Improve Safety
Given the clear challenges of providing quality and continuity of care in the inpatient setting, hospitalists are well positioned to identify strategies for safe and effective patient handoffs and advocate for a systems approach to their implementation.
Safety strategies that have been employed by industries outside of healthcare can provide a useful starting point. So-called “highly reliable” organizations use a variety of approaches to reduce the incidence of errors that occur during transitions in work staff. A recent review of transition methods used by NASA’s Johnson Space Center (Houston), Canadian nuclear power plants, and an ambulance dispatch center—organizations where lapses in transitions also have serious consequences—found that these entities used up to 21 handoff strategies.10 Techniques included verbal, face-to-face, and interactive questioning coordinated with written summaries just before a shift change.
Increasing redundancy is another technique used by highly reliable organizations to reduce the likelihood of missed, incomplete, or misinterpreted information. To create redundancy in clinical care, a physician would include more information at the outset of a procedure or medication order than is now typically provided. This additional information is then repeated and validated by other members of the care team throughout the process, reducing the likelihood of misinterpretation of an instruction or action based on incomplete information.
For example, if a physician always includes both the drug name and the condition for which it is prescribed, a medication order for “Celebrex, seizures,” instead of “Cerebyx, seizures,” would immediately indicate a mistake had occurred in ordering a pain medication instead of an anti-convulsant.11 Research has shown that increasing the amount of information about a medication order reduces the range of potentially valid clinical decisions.
Whether a hospital relies on verbal communication, written communication, computer-based communication, or a combination of all three, redundancy can be built into its sign-out processes. As PDAs become more widely used, structured sign-outs should incorporate redundancy into patient-specific checklists to include information on clinical status, recent and pending tests and study results, and similar, pertinent information.
Simulation-based training that incorporates redundancy and promotes read-back of patient information holds promise for error reduction, especially during patient handoffs.
AHRQ has recently funded research on simulation training projects that seek to:
- Reduce communication errors during patient handoffs in the emergency department by implementing a patient-specific checklist based on an electronic medical record and by testing the effect of companion simulation-based training; and
- Evaluate and improve safe communication and coordination between anesthesia providers and nurses during care transitions and during hand-offs between the operating room and the post-anesthesia care unit.12
The 24/7 role of hospital physicians brings unique experiences and insights to the challenges of patient safety that can test the feasibility of systems to reduce errors associated with care transitions. As their numbers and leadership roles expand, hospitalists are poised to make significant contributions to improving patient safety and outcomes.
We at AHRQ look forward to assisting hospitalists in making these contributions and to achieving these goals together. We also look forward to continuing our relationship with SHM and the hospitalist community as a whole. TH
Dr. Clancy is the director of the Agency for Healthcare Research and Quality.
References
- Wachter RM, Goldman L. The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996 Aug 15;335(7):514-517.
- Impact of the nation’s hospitalists continues to grow new society of hospital medicine survey says [press release]. Society of Hospital Medicine. May 4, 2006.
- Society of Hospital Medicine. The core competencies in hospital medicine: a framework for curriculum development by the society of hospital medicine. J Hosp Med. 2006;1;S1. Available at: http://onlinelibrary.wiley.com/doi/10.1002/jhm.72/pdf. Last accessed January 17, 2007.
- Vidyarthi A [commentary]. Agency for Healthcare Research and Quality Web M&M: Morbidity and Mortality Rounds on the Web. Fumbled handoff. March 2004. Available at: www.webmm.ahrq.gov/case.aspx?caseID=55. Last accessed January 17, 2007.
- Wachter RM, Shojania KG. Internal Bleeding: The Truth Behind America’s Terrifying Epidemic of Medical Mistakes. New York: Rugged Land LLG; 2004.
- Vidyarthi A. Morbidity and Mortality Rounds on the Web, “Fumbled Handoff,” unpublished data, 2004.
- Biller CK, Antonacci AC, Pelletier S, et al. The 80-hour work guidelines and resident survey perceptions of quality. J Surg Res. 2006 Oct;135(2):275-281. Epub 2006 Aug 24.
- Lee LH, Levine JA, Schultz HJ. Utility of a standardized sign-out card for new medical interns. J Gen Intern Med. 1996;11(12):753-755.
- O’Leary KJ, Leibovitz DM, Feinglass J, et al. Outpatient physicians’ satisfaction with discharge summaries and perceived need for an electronic discharge summary. J Hosp Med. 2006;1:317-320. Published online Oct. 11, 2006.
- Reason JT. Managing the Risks of Organizational Accidents. Aldershot, England: Ashgate Publishing Company; 1997:135.
- Bar-Yam Y. System care: multiscale analysis of medical errors–eliminating errors and improving organizational capabilities. New England Complex Systems Institute: Technical Report; Sept 2004. Available at: http://necsi.org/projects/yaneer/NECSITechnicalReport2004-09.pdf. Last accessed January 17, 2007.
- Agency for Healthcare Research and Quality. Improving patient safety through simulation research. 2006 Simulation Projects. Available at: www.ahrq.gov/qual/simulproj.htm. Last accessed January 17, 2007.
In the nearly 10 years since the word “hospitalist” entered our consciousness, it has been inspiring to witness the dramatic growth in the specialty and, accompanying it, the growth in the membership of SHM.1 Over this same period, the healthcare system has made progress toward ensuring that it provides the safest, highest quality healthcare possible.
In my mind, the two phenomena are related. SHM itself and—more generally—the hospitalist field have played a vital role in promoting the use of evidence-based care, improved teamwork, and health information technology. Each of these efforts has made a significant difference in the care patients receive in hospitals. Similarly, the mission of the Agency for Healthcare Research and Quality (AHRQ) is to improve the quality, safety, efficiency, and effectiveness of healthcare for all Americans. Both organizations are working to create positive change that will improve the health and healthcare of all patients.
As their numbers continue to grow, hospitalists are becoming integral members of the inpatient care team at many hospitals.
According to a recent survey conducted by SHM, a hospitalist averaged more than 2,300 inpatient encounters in 2005—a 7% increase over 2004.2 Today, hospital medicine groups practice not only in large metropolitan areas, but also in rural regions where one in three groups began operation during 2005.
In addition to their inpatient care responsibilities, the 15,000 hospitalists who practice today in the United States and Canada serve in key physician leadership roles that directly influence quality improvement and patient safety. Most hospitalists—86%—participate in quality improvement. More than half are involved in implementing information technology (54%) and teaching house staff (51%), and more than one-third—35%—are responsible for their organization’s rapid response team. The SHM survey found that nearly all hospital medicine groups provide round-the-clock patient care at their hospitals.
In this article I will emphasize two key areas relevant to improving patient safety for hospitalized patients: patient handoffs and communication.
Responsibility for Patient Handoffs
Hospitalists’ clinical and leadership roles are significant responsibilities for patient safety, including the critical period known as patient handoff or sign-out.
Patient handoffs refer to the interaction, communication, and planning required to achieve a seamless transition from one clinician to the next.3 When executed in a timely and thorough manner, patient handoffs can reduce the likelihood of medical errors and misinformation, prevent lost or missing clinical information, and maintain a high level of medical care.
Given today’s short hospital stays and the complex medical nature of the care necessary for many patients, timely and effective handoffs demand that hospitalists develop skills that extend beyond superior clinical care. They include:
- Communicating in an effective and efficient manner during patient sign-out;
- Demonstrating the use of “read-back” skills when communicating tasks;
- Developing oral and written patient summaries, including characteristics of the patient, provider, and time of the sign-out;
- Evaluating all medications for indication, dosing, and planned duration at the time of sign-out; and
- Anticipating what may go wrong with a patient after a transition in care occurs and clearly communicating this concern to the receiving clinician.
A Fumbled Handoff: A Case Study
A breakdown in communications—notably an error of omission in the patient handoff—contributed to a poor outcome for an elderly patient who was admitted to the hospital for an elective sigmoid resection.
The case, which was published in the AHRQ’s “Morbidity and Mortality Rounds on the Web” (developed by hospital medicine expert Robert Wachter, MD, and his team under contract to our agency), illustrates some of the challenges that face all clinicians in effectively transferring patient information and care responsibilities.4 It also underscores the need for close involvement by hospitalists in improving quality, teaching and supervising house staff, and implementing information systems.
According to the case study, a 73-year-old female patient with a history of hypertension, non-insulin dependent diabetes, and chronic renal insufficiency became tachycardic two days after surgery, despite receiving a low-dose beta-blocker. The same day, she informed her nurse that she had developed pain in her left leg.
Assuming the pain was related to the pre-operative epidural, the nurse contacted the anesthesia service, which responded by decreasing the epidural rate; the primary surgical team was not called. Late on the third day after surgery, the cross-covering intern was contacted about the patient’s left leg pain. No information about the intern’s findings was relayed to the primary team the following day.
On the fourth day, the patient complained to the nurse about mild chest discomfort, resulting in attention within 20 minutes by house staff and from the attending physician several hours later. The patient’s exam was unremarkable and a work-up was initiated.
Within an hour of the attending’s visit, the patient’s blood pressure dropped to 70/40, followed by a pulseless electrical activity arrest. The patient could not be resuscitated. A post-mortem examination revealed a pulmonary embolism.
Handoffs in an Era of Work-Hour Restrictions
Missing information about pain in the patient’s leg and a breakdown in communication between physicians contributed to the patient’s poor outcome. In this case, the breakdown may also have been influenced by the intern’s involvement on the third day. Like all medical residents this intern is subject to duty-hour restrictions.
Work-hour limits for all residents training in U.S. hospitals took effect in July 2003. Under these standards, created by the Accreditation Council for Graduate Medical Education (ACGME), residents are limited to a maximum of 30 consecutive work hours—known as the 30-hour rule, which includes time used for sign-out, teaching, and continuity of care. They are also prohibited from working more than 80 hours per week.
Despite the clear safety benefit of preventing fatigue-related mistakes, work-hour mandates have increased the number of patient handoffs and the potential for communication breakdowns.5 A survey of interns conducted at the hospital where this case study occurred identified a higher volume of sign-outs and the resulting potential for harm to patients as main concerns with the work-hour restrictions.6
Concerns about the quality and continuity of care that hospital patients receive are evident even among those medical residents whose work hours were restricted before the ACGME requirements took effect. (In New York state residents’ work hours have been restricted since 1998.)
A 2006 study of surgical residents at New York’s Beth Israel Hospital found that most believed that the quality of care patients received was either unchanged (63%) or worse (26%) since the work-hour restrictions took effect.7 Possible reasons for this perception include unresolved issues with continuity of care, miscommunication, and cross-coverage availability. The study concluded that interventions that target intern sign-out coverage constraints will be important for future efforts to improve the quality of care for hospital patients.
Written sign-outs appear to overcome some of the human errors that inevitably result from verbal patient summaries, such as disruptions and forgetfulness. Recent findings have, however, identified significant shortcomings in the quality and timeliness of written reports.
Critical information, such as code status and allergies, was missing in 80% of written sign-outs in one recent study.8 And in a 2006 study of the quality of discharge summaries, only 19% of hospital physicians with an outpatient practice reported being satisfied with the timeliness of discharge summaries. Only a third reported being satisfied with their quality of information. Most troubling, 41% believed that at least one of their patients hospitalized in the previous six months had experienced a preventable adverse event related to poor transfer of information at discharge.9
Use Redundancy and Simulation to Improve Safety
Given the clear challenges of providing quality and continuity of care in the inpatient setting, hospitalists are well positioned to identify strategies for safe and effective patient handoffs and advocate for a systems approach to their implementation.
Safety strategies that have been employed by industries outside of healthcare can provide a useful starting point. So-called “highly reliable” organizations use a variety of approaches to reduce the incidence of errors that occur during transitions in work staff. A recent review of transition methods used by NASA’s Johnson Space Center (Houston), Canadian nuclear power plants, and an ambulance dispatch center—organizations where lapses in transitions also have serious consequences—found that these entities used up to 21 handoff strategies.10 Techniques included verbal, face-to-face, and interactive questioning coordinated with written summaries just before a shift change.
Increasing redundancy is another technique used by highly reliable organizations to reduce the likelihood of missed, incomplete, or misinterpreted information. To create redundancy in clinical care, a physician would include more information at the outset of a procedure or medication order than is now typically provided. This additional information is then repeated and validated by other members of the care team throughout the process, reducing the likelihood of misinterpretation of an instruction or action based on incomplete information.
For example, if a physician always includes both the drug name and the condition for which it is prescribed, a medication order for “Celebrex, seizures,” instead of “Cerebyx, seizures,” would immediately indicate a mistake had occurred in ordering a pain medication instead of an anti-convulsant.11 Research has shown that increasing the amount of information about a medication order reduces the range of potentially valid clinical decisions.
Whether a hospital relies on verbal communication, written communication, computer-based communication, or a combination of all three, redundancy can be built into its sign-out processes. As PDAs become more widely used, structured sign-outs should incorporate redundancy into patient-specific checklists to include information on clinical status, recent and pending tests and study results, and similar, pertinent information.
Simulation-based training that incorporates redundancy and promotes read-back of patient information holds promise for error reduction, especially during patient handoffs.
AHRQ has recently funded research on simulation training projects that seek to:
- Reduce communication errors during patient handoffs in the emergency department by implementing a patient-specific checklist based on an electronic medical record and by testing the effect of companion simulation-based training; and
- Evaluate and improve safe communication and coordination between anesthesia providers and nurses during care transitions and during hand-offs between the operating room and the post-anesthesia care unit.12
The 24/7 role of hospital physicians brings unique experiences and insights to the challenges of patient safety that can test the feasibility of systems to reduce errors associated with care transitions. As their numbers and leadership roles expand, hospitalists are poised to make significant contributions to improving patient safety and outcomes.
We at AHRQ look forward to assisting hospitalists in making these contributions and to achieving these goals together. We also look forward to continuing our relationship with SHM and the hospitalist community as a whole. TH
Dr. Clancy is the director of the Agency for Healthcare Research and Quality.
References
- Wachter RM, Goldman L. The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996 Aug 15;335(7):514-517.
- Impact of the nation’s hospitalists continues to grow new society of hospital medicine survey says [press release]. Society of Hospital Medicine. May 4, 2006.
- Society of Hospital Medicine. The core competencies in hospital medicine: a framework for curriculum development by the society of hospital medicine. J Hosp Med. 2006;1;S1. Available at: http://onlinelibrary.wiley.com/doi/10.1002/jhm.72/pdf. Last accessed January 17, 2007.
- Vidyarthi A [commentary]. Agency for Healthcare Research and Quality Web M&M: Morbidity and Mortality Rounds on the Web. Fumbled handoff. March 2004. Available at: www.webmm.ahrq.gov/case.aspx?caseID=55. Last accessed January 17, 2007.
- Wachter RM, Shojania KG. Internal Bleeding: The Truth Behind America’s Terrifying Epidemic of Medical Mistakes. New York: Rugged Land LLG; 2004.
- Vidyarthi A. Morbidity and Mortality Rounds on the Web, “Fumbled Handoff,” unpublished data, 2004.
- Biller CK, Antonacci AC, Pelletier S, et al. The 80-hour work guidelines and resident survey perceptions of quality. J Surg Res. 2006 Oct;135(2):275-281. Epub 2006 Aug 24.
- Lee LH, Levine JA, Schultz HJ. Utility of a standardized sign-out card for new medical interns. J Gen Intern Med. 1996;11(12):753-755.
- O’Leary KJ, Leibovitz DM, Feinglass J, et al. Outpatient physicians’ satisfaction with discharge summaries and perceived need for an electronic discharge summary. J Hosp Med. 2006;1:317-320. Published online Oct. 11, 2006.
- Reason JT. Managing the Risks of Organizational Accidents. Aldershot, England: Ashgate Publishing Company; 1997:135.
- Bar-Yam Y. System care: multiscale analysis of medical errors–eliminating errors and improving organizational capabilities. New England Complex Systems Institute: Technical Report; Sept 2004. Available at: http://necsi.org/projects/yaneer/NECSITechnicalReport2004-09.pdf. Last accessed January 17, 2007.
- Agency for Healthcare Research and Quality. Improving patient safety through simulation research. 2006 Simulation Projects. Available at: www.ahrq.gov/qual/simulproj.htm. Last accessed January 17, 2007.
In the nearly 10 years since the word “hospitalist” entered our consciousness, it has been inspiring to witness the dramatic growth in the specialty and, accompanying it, the growth in the membership of SHM.1 Over this same period, the healthcare system has made progress toward ensuring that it provides the safest, highest quality healthcare possible.
In my mind, the two phenomena are related. SHM itself and—more generally—the hospitalist field have played a vital role in promoting the use of evidence-based care, improved teamwork, and health information technology. Each of these efforts has made a significant difference in the care patients receive in hospitals. Similarly, the mission of the Agency for Healthcare Research and Quality (AHRQ) is to improve the quality, safety, efficiency, and effectiveness of healthcare for all Americans. Both organizations are working to create positive change that will improve the health and healthcare of all patients.
As their numbers continue to grow, hospitalists are becoming integral members of the inpatient care team at many hospitals.
According to a recent survey conducted by SHM, a hospitalist averaged more than 2,300 inpatient encounters in 2005—a 7% increase over 2004.2 Today, hospital medicine groups practice not only in large metropolitan areas, but also in rural regions where one in three groups began operation during 2005.
In addition to their inpatient care responsibilities, the 15,000 hospitalists who practice today in the United States and Canada serve in key physician leadership roles that directly influence quality improvement and patient safety. Most hospitalists—86%—participate in quality improvement. More than half are involved in implementing information technology (54%) and teaching house staff (51%), and more than one-third—35%—are responsible for their organization’s rapid response team. The SHM survey found that nearly all hospital medicine groups provide round-the-clock patient care at their hospitals.
In this article I will emphasize two key areas relevant to improving patient safety for hospitalized patients: patient handoffs and communication.
Responsibility for Patient Handoffs
Hospitalists’ clinical and leadership roles are significant responsibilities for patient safety, including the critical period known as patient handoff or sign-out.
Patient handoffs refer to the interaction, communication, and planning required to achieve a seamless transition from one clinician to the next.3 When executed in a timely and thorough manner, patient handoffs can reduce the likelihood of medical errors and misinformation, prevent lost or missing clinical information, and maintain a high level of medical care.
Given today’s short hospital stays and the complex medical nature of the care necessary for many patients, timely and effective handoffs demand that hospitalists develop skills that extend beyond superior clinical care. They include:
- Communicating in an effective and efficient manner during patient sign-out;
- Demonstrating the use of “read-back” skills when communicating tasks;
- Developing oral and written patient summaries, including characteristics of the patient, provider, and time of the sign-out;
- Evaluating all medications for indication, dosing, and planned duration at the time of sign-out; and
- Anticipating what may go wrong with a patient after a transition in care occurs and clearly communicating this concern to the receiving clinician.
A Fumbled Handoff: A Case Study
A breakdown in communications—notably an error of omission in the patient handoff—contributed to a poor outcome for an elderly patient who was admitted to the hospital for an elective sigmoid resection.
The case, which was published in the AHRQ’s “Morbidity and Mortality Rounds on the Web” (developed by hospital medicine expert Robert Wachter, MD, and his team under contract to our agency), illustrates some of the challenges that face all clinicians in effectively transferring patient information and care responsibilities.4 It also underscores the need for close involvement by hospitalists in improving quality, teaching and supervising house staff, and implementing information systems.
According to the case study, a 73-year-old female patient with a history of hypertension, non-insulin dependent diabetes, and chronic renal insufficiency became tachycardic two days after surgery, despite receiving a low-dose beta-blocker. The same day, she informed her nurse that she had developed pain in her left leg.
Assuming the pain was related to the pre-operative epidural, the nurse contacted the anesthesia service, which responded by decreasing the epidural rate; the primary surgical team was not called. Late on the third day after surgery, the cross-covering intern was contacted about the patient’s left leg pain. No information about the intern’s findings was relayed to the primary team the following day.
On the fourth day, the patient complained to the nurse about mild chest discomfort, resulting in attention within 20 minutes by house staff and from the attending physician several hours later. The patient’s exam was unremarkable and a work-up was initiated.
Within an hour of the attending’s visit, the patient’s blood pressure dropped to 70/40, followed by a pulseless electrical activity arrest. The patient could not be resuscitated. A post-mortem examination revealed a pulmonary embolism.
Handoffs in an Era of Work-Hour Restrictions
Missing information about pain in the patient’s leg and a breakdown in communication between physicians contributed to the patient’s poor outcome. In this case, the breakdown may also have been influenced by the intern’s involvement on the third day. Like all medical residents this intern is subject to duty-hour restrictions.
Work-hour limits for all residents training in U.S. hospitals took effect in July 2003. Under these standards, created by the Accreditation Council for Graduate Medical Education (ACGME), residents are limited to a maximum of 30 consecutive work hours—known as the 30-hour rule, which includes time used for sign-out, teaching, and continuity of care. They are also prohibited from working more than 80 hours per week.
Despite the clear safety benefit of preventing fatigue-related mistakes, work-hour mandates have increased the number of patient handoffs and the potential for communication breakdowns.5 A survey of interns conducted at the hospital where this case study occurred identified a higher volume of sign-outs and the resulting potential for harm to patients as main concerns with the work-hour restrictions.6
Concerns about the quality and continuity of care that hospital patients receive are evident even among those medical residents whose work hours were restricted before the ACGME requirements took effect. (In New York state residents’ work hours have been restricted since 1998.)
A 2006 study of surgical residents at New York’s Beth Israel Hospital found that most believed that the quality of care patients received was either unchanged (63%) or worse (26%) since the work-hour restrictions took effect.7 Possible reasons for this perception include unresolved issues with continuity of care, miscommunication, and cross-coverage availability. The study concluded that interventions that target intern sign-out coverage constraints will be important for future efforts to improve the quality of care for hospital patients.
Written sign-outs appear to overcome some of the human errors that inevitably result from verbal patient summaries, such as disruptions and forgetfulness. Recent findings have, however, identified significant shortcomings in the quality and timeliness of written reports.
Critical information, such as code status and allergies, was missing in 80% of written sign-outs in one recent study.8 And in a 2006 study of the quality of discharge summaries, only 19% of hospital physicians with an outpatient practice reported being satisfied with the timeliness of discharge summaries. Only a third reported being satisfied with their quality of information. Most troubling, 41% believed that at least one of their patients hospitalized in the previous six months had experienced a preventable adverse event related to poor transfer of information at discharge.9
Use Redundancy and Simulation to Improve Safety
Given the clear challenges of providing quality and continuity of care in the inpatient setting, hospitalists are well positioned to identify strategies for safe and effective patient handoffs and advocate for a systems approach to their implementation.
Safety strategies that have been employed by industries outside of healthcare can provide a useful starting point. So-called “highly reliable” organizations use a variety of approaches to reduce the incidence of errors that occur during transitions in work staff. A recent review of transition methods used by NASA’s Johnson Space Center (Houston), Canadian nuclear power plants, and an ambulance dispatch center—organizations where lapses in transitions also have serious consequences—found that these entities used up to 21 handoff strategies.10 Techniques included verbal, face-to-face, and interactive questioning coordinated with written summaries just before a shift change.
Increasing redundancy is another technique used by highly reliable organizations to reduce the likelihood of missed, incomplete, or misinterpreted information. To create redundancy in clinical care, a physician would include more information at the outset of a procedure or medication order than is now typically provided. This additional information is then repeated and validated by other members of the care team throughout the process, reducing the likelihood of misinterpretation of an instruction or action based on incomplete information.
For example, if a physician always includes both the drug name and the condition for which it is prescribed, a medication order for “Celebrex, seizures,” instead of “Cerebyx, seizures,” would immediately indicate a mistake had occurred in ordering a pain medication instead of an anti-convulsant.11 Research has shown that increasing the amount of information about a medication order reduces the range of potentially valid clinical decisions.
Whether a hospital relies on verbal communication, written communication, computer-based communication, or a combination of all three, redundancy can be built into its sign-out processes. As PDAs become more widely used, structured sign-outs should incorporate redundancy into patient-specific checklists to include information on clinical status, recent and pending tests and study results, and similar, pertinent information.
Simulation-based training that incorporates redundancy and promotes read-back of patient information holds promise for error reduction, especially during patient handoffs.
AHRQ has recently funded research on simulation training projects that seek to:
- Reduce communication errors during patient handoffs in the emergency department by implementing a patient-specific checklist based on an electronic medical record and by testing the effect of companion simulation-based training; and
- Evaluate and improve safe communication and coordination between anesthesia providers and nurses during care transitions and during hand-offs between the operating room and the post-anesthesia care unit.12
The 24/7 role of hospital physicians brings unique experiences and insights to the challenges of patient safety that can test the feasibility of systems to reduce errors associated with care transitions. As their numbers and leadership roles expand, hospitalists are poised to make significant contributions to improving patient safety and outcomes.
We at AHRQ look forward to assisting hospitalists in making these contributions and to achieving these goals together. We also look forward to continuing our relationship with SHM and the hospitalist community as a whole. TH
Dr. Clancy is the director of the Agency for Healthcare Research and Quality.
References
- Wachter RM, Goldman L. The emerging role of “hospitalists” in the American health care system. N Engl J Med. 1996 Aug 15;335(7):514-517.
- Impact of the nation’s hospitalists continues to grow new society of hospital medicine survey says [press release]. Society of Hospital Medicine. May 4, 2006.
- Society of Hospital Medicine. The core competencies in hospital medicine: a framework for curriculum development by the society of hospital medicine. J Hosp Med. 2006;1;S1. Available at: http://onlinelibrary.wiley.com/doi/10.1002/jhm.72/pdf. Last accessed January 17, 2007.
- Vidyarthi A [commentary]. Agency for Healthcare Research and Quality Web M&M: Morbidity and Mortality Rounds on the Web. Fumbled handoff. March 2004. Available at: www.webmm.ahrq.gov/case.aspx?caseID=55. Last accessed January 17, 2007.
- Wachter RM, Shojania KG. Internal Bleeding: The Truth Behind America’s Terrifying Epidemic of Medical Mistakes. New York: Rugged Land LLG; 2004.
- Vidyarthi A. Morbidity and Mortality Rounds on the Web, “Fumbled Handoff,” unpublished data, 2004.
- Biller CK, Antonacci AC, Pelletier S, et al. The 80-hour work guidelines and resident survey perceptions of quality. J Surg Res. 2006 Oct;135(2):275-281. Epub 2006 Aug 24.
- Lee LH, Levine JA, Schultz HJ. Utility of a standardized sign-out card for new medical interns. J Gen Intern Med. 1996;11(12):753-755.
- O’Leary KJ, Leibovitz DM, Feinglass J, et al. Outpatient physicians’ satisfaction with discharge summaries and perceived need for an electronic discharge summary. J Hosp Med. 2006;1:317-320. Published online Oct. 11, 2006.
- Reason JT. Managing the Risks of Organizational Accidents. Aldershot, England: Ashgate Publishing Company; 1997:135.
- Bar-Yam Y. System care: multiscale analysis of medical errors–eliminating errors and improving organizational capabilities. New England Complex Systems Institute: Technical Report; Sept 2004. Available at: http://necsi.org/projects/yaneer/NECSITechnicalReport2004-09.pdf. Last accessed January 17, 2007.
- Agency for Healthcare Research and Quality. Improving patient safety through simulation research. 2006 Simulation Projects. Available at: www.ahrq.gov/qual/simulproj.htm. Last accessed January 17, 2007.