User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Antibody cocktail reduces chance of developing COVID
A one-time dose of two long-acting monoclonal antibodies reduced the risk of developing symptomatic COVID by 77% in comparison with placebo (P < .001) in a randomized, double-blind, placebo-controlled, phase 3 trial in adults, according to researchers who presented results at IDWeek 2021, an annual scientific meeting on infectious diseases.
The mix of tixagevimab and cilgavimab (AZD7442, Astra Zeneca) in a 300-mg dose is delivered in two intramuscular injections.
“This is the first long-acting combination of monoclonal antibodies that represents a potential new option to augment COVID-19 prevention,” said lead author Myron J. Levin, MD, a professor and pediatric infectious disease specialist at the University of Colorado at Denver, Aurora, who presented the findings of the PROVENT trial.
Both antibodies were taken from B cells donated by patients who had been infected with SARS-CoV-2, and they work synergistically, Dr. Levin said.
“The combination of them is better than adding results of each individually,” he said. “In vitro experiments have already shown that variants of interest and concern, including the Delta variant, are successfully neutralized by this cocktail.”
The trial was conducted in 87 sites in the United States, the United Kingdom, Spain, France, and Belgium. Participants included 5,197 unvaccinated adults who had never been infected with SARS-CoV-2 and either were at higher risk for inadequate response to COVID-19 vaccines because they were immunocompromised or were at high risk for exposure.
“Efficacy was observed through at least 3 months,” Dr. Levin said. “Preliminary pharmacokinetic modeling predicts potential protection for up to 12 months.”
Raymund Razonable, MD, an infectious disease expert with the Mayo Clinic in Rochester, Minn., who was not involved with the trial, told this news organization he was particularly interested in this combination because the developers made use of novel technology that extends the half-life of the antibodies and because of the large number of participants in the study.
Modeling that shows protection could last up to a year is novel and important, he said.
“People won’t need frequent injections,” Dr. Razonable said. With postexposure prophylaxis monoclonal cocktails, people may be given a dose a month, he noted.
Dr. Razonable said, “This is something intended to prevent COVID in people who are unvaccinated. The downside to that is we want people to get vaccinated. The best strategy so far is really vaccination.”
He said AZD7442 could potentially help fill the void for patients who are not able to respond to the COVID vaccines, including some who are immunocompromised or are undergoing chemotherapy.
Dr. Razonable said that, although the 77% reduction for developing symptomatic COVID-19 (95% confidence interval vs. placebo, 46.0-90.0; P < .001) is impressive, it is a reduction in relative risk. Still unknown is how much an individual’s absolute risk is reduced.
He also said it would be helpful to know how many people in the study population were immunocompromised, “because I think that’s where this product will be useful for prevention.”
The primary study endpoints were the first case of SARS-CoV-2 RT-PCR-positive symptomatic illness post dose and prior to day 183 (efficacy) as well as the safety of the product.
The cocktail appeared to be well tolerated. Adverse events occurred in 35% of participants administered AZD7442 and in 34% of the placebo group. Injection-site reactions occurred in 2.4% of the AZD7442 group and in 2.1% of the placebo group. There was one case of severe or critical COVID-19; two COVID-19–related deaths occurred in the placebo group.
AZD7442 is being developed with the help of funding from the U.S. government. Dr. Levin has received support from GlaxoSmithKline companies. Many of the coauthors are employed by AstraZeneca and hold stock in the company. Dr. Razonable has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A one-time dose of two long-acting monoclonal antibodies reduced the risk of developing symptomatic COVID by 77% in comparison with placebo (P < .001) in a randomized, double-blind, placebo-controlled, phase 3 trial in adults, according to researchers who presented results at IDWeek 2021, an annual scientific meeting on infectious diseases.
The mix of tixagevimab and cilgavimab (AZD7442, Astra Zeneca) in a 300-mg dose is delivered in two intramuscular injections.
“This is the first long-acting combination of monoclonal antibodies that represents a potential new option to augment COVID-19 prevention,” said lead author Myron J. Levin, MD, a professor and pediatric infectious disease specialist at the University of Colorado at Denver, Aurora, who presented the findings of the PROVENT trial.
Both antibodies were taken from B cells donated by patients who had been infected with SARS-CoV-2, and they work synergistically, Dr. Levin said.
“The combination of them is better than adding results of each individually,” he said. “In vitro experiments have already shown that variants of interest and concern, including the Delta variant, are successfully neutralized by this cocktail.”
The trial was conducted in 87 sites in the United States, the United Kingdom, Spain, France, and Belgium. Participants included 5,197 unvaccinated adults who had never been infected with SARS-CoV-2 and either were at higher risk for inadequate response to COVID-19 vaccines because they were immunocompromised or were at high risk for exposure.
“Efficacy was observed through at least 3 months,” Dr. Levin said. “Preliminary pharmacokinetic modeling predicts potential protection for up to 12 months.”
Raymund Razonable, MD, an infectious disease expert with the Mayo Clinic in Rochester, Minn., who was not involved with the trial, told this news organization he was particularly interested in this combination because the developers made use of novel technology that extends the half-life of the antibodies and because of the large number of participants in the study.
Modeling that shows protection could last up to a year is novel and important, he said.
“People won’t need frequent injections,” Dr. Razonable said. With postexposure prophylaxis monoclonal cocktails, people may be given a dose a month, he noted.
Dr. Razonable said, “This is something intended to prevent COVID in people who are unvaccinated. The downside to that is we want people to get vaccinated. The best strategy so far is really vaccination.”
He said AZD7442 could potentially help fill the void for patients who are not able to respond to the COVID vaccines, including some who are immunocompromised or are undergoing chemotherapy.
Dr. Razonable said that, although the 77% reduction for developing symptomatic COVID-19 (95% confidence interval vs. placebo, 46.0-90.0; P < .001) is impressive, it is a reduction in relative risk. Still unknown is how much an individual’s absolute risk is reduced.
He also said it would be helpful to know how many people in the study population were immunocompromised, “because I think that’s where this product will be useful for prevention.”
The primary study endpoints were the first case of SARS-CoV-2 RT-PCR-positive symptomatic illness post dose and prior to day 183 (efficacy) as well as the safety of the product.
The cocktail appeared to be well tolerated. Adverse events occurred in 35% of participants administered AZD7442 and in 34% of the placebo group. Injection-site reactions occurred in 2.4% of the AZD7442 group and in 2.1% of the placebo group. There was one case of severe or critical COVID-19; two COVID-19–related deaths occurred in the placebo group.
AZD7442 is being developed with the help of funding from the U.S. government. Dr. Levin has received support from GlaxoSmithKline companies. Many of the coauthors are employed by AstraZeneca and hold stock in the company. Dr. Razonable has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A one-time dose of two long-acting monoclonal antibodies reduced the risk of developing symptomatic COVID by 77% in comparison with placebo (P < .001) in a randomized, double-blind, placebo-controlled, phase 3 trial in adults, according to researchers who presented results at IDWeek 2021, an annual scientific meeting on infectious diseases.
The mix of tixagevimab and cilgavimab (AZD7442, Astra Zeneca) in a 300-mg dose is delivered in two intramuscular injections.
“This is the first long-acting combination of monoclonal antibodies that represents a potential new option to augment COVID-19 prevention,” said lead author Myron J. Levin, MD, a professor and pediatric infectious disease specialist at the University of Colorado at Denver, Aurora, who presented the findings of the PROVENT trial.
Both antibodies were taken from B cells donated by patients who had been infected with SARS-CoV-2, and they work synergistically, Dr. Levin said.
“The combination of them is better than adding results of each individually,” he said. “In vitro experiments have already shown that variants of interest and concern, including the Delta variant, are successfully neutralized by this cocktail.”
The trial was conducted in 87 sites in the United States, the United Kingdom, Spain, France, and Belgium. Participants included 5,197 unvaccinated adults who had never been infected with SARS-CoV-2 and either were at higher risk for inadequate response to COVID-19 vaccines because they were immunocompromised or were at high risk for exposure.
“Efficacy was observed through at least 3 months,” Dr. Levin said. “Preliminary pharmacokinetic modeling predicts potential protection for up to 12 months.”
Raymund Razonable, MD, an infectious disease expert with the Mayo Clinic in Rochester, Minn., who was not involved with the trial, told this news organization he was particularly interested in this combination because the developers made use of novel technology that extends the half-life of the antibodies and because of the large number of participants in the study.
Modeling that shows protection could last up to a year is novel and important, he said.
“People won’t need frequent injections,” Dr. Razonable said. With postexposure prophylaxis monoclonal cocktails, people may be given a dose a month, he noted.
Dr. Razonable said, “This is something intended to prevent COVID in people who are unvaccinated. The downside to that is we want people to get vaccinated. The best strategy so far is really vaccination.”
He said AZD7442 could potentially help fill the void for patients who are not able to respond to the COVID vaccines, including some who are immunocompromised or are undergoing chemotherapy.
Dr. Razonable said that, although the 77% reduction for developing symptomatic COVID-19 (95% confidence interval vs. placebo, 46.0-90.0; P < .001) is impressive, it is a reduction in relative risk. Still unknown is how much an individual’s absolute risk is reduced.
He also said it would be helpful to know how many people in the study population were immunocompromised, “because I think that’s where this product will be useful for prevention.”
The primary study endpoints were the first case of SARS-CoV-2 RT-PCR-positive symptomatic illness post dose and prior to day 183 (efficacy) as well as the safety of the product.
The cocktail appeared to be well tolerated. Adverse events occurred in 35% of participants administered AZD7442 and in 34% of the placebo group. Injection-site reactions occurred in 2.4% of the AZD7442 group and in 2.1% of the placebo group. There was one case of severe or critical COVID-19; two COVID-19–related deaths occurred in the placebo group.
AZD7442 is being developed with the help of funding from the U.S. government. Dr. Levin has received support from GlaxoSmithKline companies. Many of the coauthors are employed by AstraZeneca and hold stock in the company. Dr. Razonable has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Drug cocktail significantly reduced severe COVID, death in outpatients
A monoclonal antibody combination of casirivimab and imdevimab (REGEN-COV) significantly reduced the risk of COVID-19–related hospitalizations and death from any cause in the phase 3 portion of an adaptive trial of outpatients.
Researchers, led by David Weinreich, MD, MBA, executive vice president of the drug cocktail’s manufacturer Regeneron, found in the randomized trial that the combination also resolved symptoms and reduced the SARS-CoV-2 viral load more quickly, compared with placebo.
Findings were published in the New England Journal of Medicine.
COVID-related hospitalization or death from any cause occurred in 18 of 1,355 patients (1.3%) in the group getting 2,400 mg infusions of the study drug, compared with 62 (4.6%) of 1,341 in the matching placebo group, indicating a relative risk reduction of 71.3%; P < .001.
Sunil Joshi, MD, president of the Duval County Medical Society Foundation and an immunologist in Jacksonville, Fla., said in an interview that these findings confirm benefits of REGEN-COV and are very good news for a patient group that includes those age 65 and older with high blood pressure, diabetes, or obesity; and for people not vaccinated, who are all at high risk of hospitalization or death if they get COVID-19.
“Vaccines are critically important,” he said, “but if you were to be infected and know that there’s a way to keep yourself out of the hospital, this is very good news.”
Researchers seek lowest doses
This trial found that the effect was similar when researchers cut the doses in half. These outcomes occurred in 7 of 736 (1%) of patients given 1,200 mg of REGEN-COV and in 24 (3.2%) of 748 in the matching placebo group (relative risk reduction, 70.4%; P = .002).
Symptoms were resolved on average 4 days earlier with each REGEN-COV dose than with placebo (10 days vs. 14 days; P < .001 for both comparisons).
Dr. Weinreich said in an interview that trials will continue to find the lowest effective doses that can stand up to all evolving variants.
“This is one of those settings where you don’t want to underdose. You’ve got one shot at this,” he said. “We’d love to do lower doses. It would be more convenient and we could treat more patients, but if it generates more clinical failures or doesn’t work with certain variants, then you’ve done a huge disservice to the world.”
Also new in this study is that researchers tested not only seronegative patients, but patients at high risk regardless of blood antibody status, he said.
“It’s the first suggestion of data that if you’re breaking through a vaccine and you’re at high risk, the use of the cocktail is something to strongly consider because treatment early is better than treatment later,” Dr. Weinreich said.
In addition to efficacy, the phase 3 trial demonstrated the cocktail had a good safety profile. Serious adverse events occurred more often in the placebo group (4%) than in the 1,200-mg group (1.1%) and the 2,400-mg group (1.3%). Infusion reactions (grade 2 or higher) occurred in less than 0.3% of patients in all groups.
William Fales, MD, state medical director for the Michigan Department of Health and Human Services, said the results confirm the promise of REGEN-COV for reducing hospitalizations and death in a peer-reviewed publication.
COVID-19 a moving target
However, Dr. Fales noted that COVID-19 is a moving target with emerging variants. The criteria for populations at high risk have also broadened since the start of the study, he said.
“A great example is pregnancy is now included as high risk, and that would have likely been a specific contraindication of patients in this clinical trial,” he said.
Dr. Fales said Michigan has been using both REGEN-COV and the Eli Lilly combination of bamlanivimab and etesevimab, which also has an emergency use authorization (EUA) from the Food and Drug Administration, with positive results.
REGEN-COV has an EUA to treat people who are at high risk of serious consequences from COVID-19, including those who are already infected (nonhospitalized) or those in certain postexposure prophylaxis settings.
“We’re seeing very low hospitalization rates and few deaths in a state that is predominately Delta,” Dr. Fales said. “So, this makes us feel that we’re doing the right thing and supports the current efforts around the country to make monoclonal antibody therapy available to high-risk patients.”
Dr. Joshi noted that trial results have been emerging from other monoclonal antibody cocktails with different COVID-19 patient groups.
However, he said in an interview, “how much more effective they would be than this is something we’d have to look at, as 71% effectiveness in keeping people out of the hospital is pretty good for any treatment.”
“These are great numbers, but vaccination itself keeps you from getting the disease in the first place and not just for a short time period. This treatment is just that – a treatment. It gets you through that episode but it doesn’t mean you won’t get sick again. You don’t develop an immune response as you do with the vaccine,” he said.
Dr. Weinreich agreed: “This is not a substitute for a vaccine except for the small group who get the vaccine and their bodies can’t respond to it because they’re significantly immunocompromised.”
The results from this paper “are one piece of a large, multistudy, phase 3 program that basically spans from prophylaxis all the way to hospitalization and pretty much the gamut – all of them – have worked. All of these studies have shown dramatic improvement in whatever the definitive regulatory endpoint is,” Dr. Weinreich said.
He said discussions are ongoing for full regulatory approval in the United States and for expanding the EUA for other populations, including pre-exposure prophylaxis, “which the [United Kingdom’s] authority has already granted us but the FDA has not.”
The study is funded by Regeneron and the Department of Health & Human Services. Dr. Weinreich is a vice president of Regeneron. Dr. Joshi reported no relevant financial relationships. Dr. Fales holds stock in Eli Lilly.
A version of this article first appeared on Medscape.com.
A monoclonal antibody combination of casirivimab and imdevimab (REGEN-COV) significantly reduced the risk of COVID-19–related hospitalizations and death from any cause in the phase 3 portion of an adaptive trial of outpatients.
Researchers, led by David Weinreich, MD, MBA, executive vice president of the drug cocktail’s manufacturer Regeneron, found in the randomized trial that the combination also resolved symptoms and reduced the SARS-CoV-2 viral load more quickly, compared with placebo.
Findings were published in the New England Journal of Medicine.
COVID-related hospitalization or death from any cause occurred in 18 of 1,355 patients (1.3%) in the group getting 2,400 mg infusions of the study drug, compared with 62 (4.6%) of 1,341 in the matching placebo group, indicating a relative risk reduction of 71.3%; P < .001.
Sunil Joshi, MD, president of the Duval County Medical Society Foundation and an immunologist in Jacksonville, Fla., said in an interview that these findings confirm benefits of REGEN-COV and are very good news for a patient group that includes those age 65 and older with high blood pressure, diabetes, or obesity; and for people not vaccinated, who are all at high risk of hospitalization or death if they get COVID-19.
“Vaccines are critically important,” he said, “but if you were to be infected and know that there’s a way to keep yourself out of the hospital, this is very good news.”
Researchers seek lowest doses
This trial found that the effect was similar when researchers cut the doses in half. These outcomes occurred in 7 of 736 (1%) of patients given 1,200 mg of REGEN-COV and in 24 (3.2%) of 748 in the matching placebo group (relative risk reduction, 70.4%; P = .002).
Symptoms were resolved on average 4 days earlier with each REGEN-COV dose than with placebo (10 days vs. 14 days; P < .001 for both comparisons).
Dr. Weinreich said in an interview that trials will continue to find the lowest effective doses that can stand up to all evolving variants.
“This is one of those settings where you don’t want to underdose. You’ve got one shot at this,” he said. “We’d love to do lower doses. It would be more convenient and we could treat more patients, but if it generates more clinical failures or doesn’t work with certain variants, then you’ve done a huge disservice to the world.”
Also new in this study is that researchers tested not only seronegative patients, but patients at high risk regardless of blood antibody status, he said.
“It’s the first suggestion of data that if you’re breaking through a vaccine and you’re at high risk, the use of the cocktail is something to strongly consider because treatment early is better than treatment later,” Dr. Weinreich said.
In addition to efficacy, the phase 3 trial demonstrated the cocktail had a good safety profile. Serious adverse events occurred more often in the placebo group (4%) than in the 1,200-mg group (1.1%) and the 2,400-mg group (1.3%). Infusion reactions (grade 2 or higher) occurred in less than 0.3% of patients in all groups.
William Fales, MD, state medical director for the Michigan Department of Health and Human Services, said the results confirm the promise of REGEN-COV for reducing hospitalizations and death in a peer-reviewed publication.
COVID-19 a moving target
However, Dr. Fales noted that COVID-19 is a moving target with emerging variants. The criteria for populations at high risk have also broadened since the start of the study, he said.
“A great example is pregnancy is now included as high risk, and that would have likely been a specific contraindication of patients in this clinical trial,” he said.
Dr. Fales said Michigan has been using both REGEN-COV and the Eli Lilly combination of bamlanivimab and etesevimab, which also has an emergency use authorization (EUA) from the Food and Drug Administration, with positive results.
REGEN-COV has an EUA to treat people who are at high risk of serious consequences from COVID-19, including those who are already infected (nonhospitalized) or those in certain postexposure prophylaxis settings.
“We’re seeing very low hospitalization rates and few deaths in a state that is predominately Delta,” Dr. Fales said. “So, this makes us feel that we’re doing the right thing and supports the current efforts around the country to make monoclonal antibody therapy available to high-risk patients.”
Dr. Joshi noted that trial results have been emerging from other monoclonal antibody cocktails with different COVID-19 patient groups.
However, he said in an interview, “how much more effective they would be than this is something we’d have to look at, as 71% effectiveness in keeping people out of the hospital is pretty good for any treatment.”
“These are great numbers, but vaccination itself keeps you from getting the disease in the first place and not just for a short time period. This treatment is just that – a treatment. It gets you through that episode but it doesn’t mean you won’t get sick again. You don’t develop an immune response as you do with the vaccine,” he said.
Dr. Weinreich agreed: “This is not a substitute for a vaccine except for the small group who get the vaccine and their bodies can’t respond to it because they’re significantly immunocompromised.”
The results from this paper “are one piece of a large, multistudy, phase 3 program that basically spans from prophylaxis all the way to hospitalization and pretty much the gamut – all of them – have worked. All of these studies have shown dramatic improvement in whatever the definitive regulatory endpoint is,” Dr. Weinreich said.
He said discussions are ongoing for full regulatory approval in the United States and for expanding the EUA for other populations, including pre-exposure prophylaxis, “which the [United Kingdom’s] authority has already granted us but the FDA has not.”
The study is funded by Regeneron and the Department of Health & Human Services. Dr. Weinreich is a vice president of Regeneron. Dr. Joshi reported no relevant financial relationships. Dr. Fales holds stock in Eli Lilly.
A version of this article first appeared on Medscape.com.
A monoclonal antibody combination of casirivimab and imdevimab (REGEN-COV) significantly reduced the risk of COVID-19–related hospitalizations and death from any cause in the phase 3 portion of an adaptive trial of outpatients.
Researchers, led by David Weinreich, MD, MBA, executive vice president of the drug cocktail’s manufacturer Regeneron, found in the randomized trial that the combination also resolved symptoms and reduced the SARS-CoV-2 viral load more quickly, compared with placebo.
Findings were published in the New England Journal of Medicine.
COVID-related hospitalization or death from any cause occurred in 18 of 1,355 patients (1.3%) in the group getting 2,400 mg infusions of the study drug, compared with 62 (4.6%) of 1,341 in the matching placebo group, indicating a relative risk reduction of 71.3%; P < .001.
Sunil Joshi, MD, president of the Duval County Medical Society Foundation and an immunologist in Jacksonville, Fla., said in an interview that these findings confirm benefits of REGEN-COV and are very good news for a patient group that includes those age 65 and older with high blood pressure, diabetes, or obesity; and for people not vaccinated, who are all at high risk of hospitalization or death if they get COVID-19.
“Vaccines are critically important,” he said, “but if you were to be infected and know that there’s a way to keep yourself out of the hospital, this is very good news.”
Researchers seek lowest doses
This trial found that the effect was similar when researchers cut the doses in half. These outcomes occurred in 7 of 736 (1%) of patients given 1,200 mg of REGEN-COV and in 24 (3.2%) of 748 in the matching placebo group (relative risk reduction, 70.4%; P = .002).
Symptoms were resolved on average 4 days earlier with each REGEN-COV dose than with placebo (10 days vs. 14 days; P < .001 for both comparisons).
Dr. Weinreich said in an interview that trials will continue to find the lowest effective doses that can stand up to all evolving variants.
“This is one of those settings where you don’t want to underdose. You’ve got one shot at this,” he said. “We’d love to do lower doses. It would be more convenient and we could treat more patients, but if it generates more clinical failures or doesn’t work with certain variants, then you’ve done a huge disservice to the world.”
Also new in this study is that researchers tested not only seronegative patients, but patients at high risk regardless of blood antibody status, he said.
“It’s the first suggestion of data that if you’re breaking through a vaccine and you’re at high risk, the use of the cocktail is something to strongly consider because treatment early is better than treatment later,” Dr. Weinreich said.
In addition to efficacy, the phase 3 trial demonstrated the cocktail had a good safety profile. Serious adverse events occurred more often in the placebo group (4%) than in the 1,200-mg group (1.1%) and the 2,400-mg group (1.3%). Infusion reactions (grade 2 or higher) occurred in less than 0.3% of patients in all groups.
William Fales, MD, state medical director for the Michigan Department of Health and Human Services, said the results confirm the promise of REGEN-COV for reducing hospitalizations and death in a peer-reviewed publication.
COVID-19 a moving target
However, Dr. Fales noted that COVID-19 is a moving target with emerging variants. The criteria for populations at high risk have also broadened since the start of the study, he said.
“A great example is pregnancy is now included as high risk, and that would have likely been a specific contraindication of patients in this clinical trial,” he said.
Dr. Fales said Michigan has been using both REGEN-COV and the Eli Lilly combination of bamlanivimab and etesevimab, which also has an emergency use authorization (EUA) from the Food and Drug Administration, with positive results.
REGEN-COV has an EUA to treat people who are at high risk of serious consequences from COVID-19, including those who are already infected (nonhospitalized) or those in certain postexposure prophylaxis settings.
“We’re seeing very low hospitalization rates and few deaths in a state that is predominately Delta,” Dr. Fales said. “So, this makes us feel that we’re doing the right thing and supports the current efforts around the country to make monoclonal antibody therapy available to high-risk patients.”
Dr. Joshi noted that trial results have been emerging from other monoclonal antibody cocktails with different COVID-19 patient groups.
However, he said in an interview, “how much more effective they would be than this is something we’d have to look at, as 71% effectiveness in keeping people out of the hospital is pretty good for any treatment.”
“These are great numbers, but vaccination itself keeps you from getting the disease in the first place and not just for a short time period. This treatment is just that – a treatment. It gets you through that episode but it doesn’t mean you won’t get sick again. You don’t develop an immune response as you do with the vaccine,” he said.
Dr. Weinreich agreed: “This is not a substitute for a vaccine except for the small group who get the vaccine and their bodies can’t respond to it because they’re significantly immunocompromised.”
The results from this paper “are one piece of a large, multistudy, phase 3 program that basically spans from prophylaxis all the way to hospitalization and pretty much the gamut – all of them – have worked. All of these studies have shown dramatic improvement in whatever the definitive regulatory endpoint is,” Dr. Weinreich said.
He said discussions are ongoing for full regulatory approval in the United States and for expanding the EUA for other populations, including pre-exposure prophylaxis, “which the [United Kingdom’s] authority has already granted us but the FDA has not.”
The study is funded by Regeneron and the Department of Health & Human Services. Dr. Weinreich is a vice president of Regeneron. Dr. Joshi reported no relevant financial relationships. Dr. Fales holds stock in Eli Lilly.
A version of this article first appeared on Medscape.com.
CVST after COVID-19 vaccine: New data confirm high mortality rate
, confirming the severity of the reaction and the associated high mortality rate.
The new series comes from an international registry of consecutive patients who experienced CVST within 28 days of COVID-19 vaccination between March 29 and June 18, 2021, from 81 hospitals in 19 countries.
The cases are described in an article published online on Sept. 28. in JAMA Neurology.
“This is a reliable description on the clinical condition of these patients with CVST associated with COVID-19 vaccination. It is striking that this a much worse condition than CVST not associated with COVID-19 vaccination, with a much higher rate of intracerebral hemorrhage and coma and a much higher mortality rate,” senior author Jonathan M. Coutinho, MD, Amsterdam University Medical Centers, told this news organization.
These data confirm the observations from an earlier U.K. cohort in which cases of cerebral venous thrombosis linked to COVID-19 vaccination occurred.
“This is the biggest series, and as an international series, it gives a broader perspective from a larger range of countries,” Dr. Coutinho said. “All the data together show that, although this side effect is rare, the consequences are very severe,” he added.
In the current study, the researchers regarded CVST as being linked to the vaccine if it was accompanied by thrombosis with thrombocytopenia syndrome (TTS), as evidenced by thrombosis and new-onset thrombocytopenia.
In the cohort of 116 patients with CVST after COVID-19 vaccination, 78 (67.2%) had thrombosis with TTS and were thus classified as having had a vaccine-related adverse event. These patients were frequently comatose at presentation (24%) and often had intracerebral hemorrhage (68%) and concomitant thromboembolism (36%); 47% died during hospitalization.
These patients were compared with the 38 patients in the same cohort who had CVST but in whom there was no indication of concomitant thrombosis and thrombocytopenia. The case patients were also compared with a control group of 207 patients with CVST who were included in a separate international registry before the COVID-19 pandemic.
Mortality rates were much higher among the patients deemed to have had a vaccine-related CVST. The in-hospital mortality rate was 47%, compared with 5% among the patients in the same cohort who did not have TTS and 3.9% among the prepandemic control group.
The mortality rate was even higher (61%) among patients in the TTS group for whom the diagnosis was made before the condition garnered attention in the scientific community. The mortality rate was 42% among patients diagnosed later.
Of the 78 patients in whom CVST and TTS occurred after COVID-19 vaccination in this cohort, 76 had received the AstraZeneca vaccine (in 75 patients, CVST and TTS occurred after the first vaccination; in one patient, they occurred after the second vaccination). One patient had received the Johnson & Johnson vaccine, and one had received the Pfizer vaccine.
“After more analysis, the case after the Pfizer vaccination is not believed to be caused by the vaccine,” Dr. Coutinho said. “In that case, the patient had a platelet count just below the lower limit and was taking an immunomodulator drug that is known to be associated with thrombocytopenia.”
For two patients who received the AstraZeneca vaccine, there was also an alternative explanation for the thrombocytopenia.
Dr. Coutinho also pointed out that the Johnson & Johnson vaccine has been used mainly in the United States, and these data were largely from other countries.
The median time from vaccination to CVST symptom onset was 9 days in the TTS group. The median platelet count at hospital admission among patients with postvaccination CVST-TTS was 45. Three patients presented with a normal platelet count and developed thrombocytopenia during admission; two patients presented with mild thrombocytopenia, 30 presented with moderate thrombocytopenia, and 43 presented with severe thrombocytopenia.
Antibodies against platelet factor 4 (PF4) were measured in 69 patients with TTS, of whom 63 (91%) tested positive (the one patient in whom TTS occurred after the patient received the Pfizer vaccine did not test positive). However, the researchers note that sensitivity varies among different PF4 ELISA tests. Findings of platelet activation assays were positive in all 36 tested patients.
In the TTS group, 52 patients (67%) received immunomodulation therapy, most often intravenous immunoglobulins (IVIG). Among patients treated with IVIG, the mortality rate was lower (28%).
Different from CVST linked to natural COVID-19 infection
Dr. Coutinho noted that CVST can occur in natural SARS-CoV-2 infection but that vaccine-associated CVST is very different.
“In natural COVID-19 infection, there is an increased risk of thrombosis, and some patients can get CVST as a part of this, but in these cases, this is not accompanied by thrombocytopenia. While the CVST in natural COVID-19 infection is also associated with a bad prognosis, this is more to do with the underlying disease. It is normally the very sick COVID patients who develop CVST, and these patients usually die from the underlying disease rather than the CVST itself,” he explained.
“Clinicians need to be aware of vaccine-related CVST, as it requires very specific and rapid treatment,” Dr. Coutinho stressed.
“Patients presenting with an extremely severe headache (unlike any headache they’ve had before) or with seizures or a focal deficit (weakness in arm or problems with speaking or vision) within 4 weeks of an adenovirus COVID-19 vaccination should ring alarm bells. It is important to do diagnostics quickly, with a platelet count the most important first step, and a rapid CT/MRI scan,” he said.
Other tests that should be conducted are D-dimer for thrombosis and the PF4 antibody test. But results for the PF4 antibody test can take days to come back, and clinicians shouldn’t wait for that, Dr. Coutinho notes.
“Specific treatment needs to be given immediately – with anticoagulation (preferably nonheparin) and immunomodulation with IVIG to stop the immune reaction. Platelets should not be given – that may seem counterintuitive in patients with a low platelet count, but giving platelets makes it worse,” he said.
Is there a geographic difference?
Dr. Coutinho pointed out that fewer cases of this vaccine-related CVST are being reported at the current time.
“We are not sure why this is the case. These adenovirus vaccines are not being used much now in Western countries, but our collaboration covers many less developed countries in South America and Asia, which are relying heavily on these vaccines. We are now shifting focus to these countries, but so far we have only seen a handful of cases from these areas,” he said.
He suggested that this may be because these countries started their vaccination programs later and are vaccinating their elderly (who are not so susceptible to this side effect) first, or it may be because of some environmental or genetic factor that has not yet been discovered.
“This is now an important research question – is the risk of vaccine-induced CVST the same in different countries or ethnicities? This could influence decisions on future vaccine strategies,” Dr. Coutinho said.
“So far, female sex is the strongest risk factor for vaccine-induced CVST. In our cohort, 81% of cases were in women. In addition, 95% were White, but that doesn’t allow us to conclude that this is a risk factor, as the majority of people who have been vaccinated are White. So, we have no clear insight into that yet,” he said.
In a comment for this news organization, the lead author of the previous U.K. report of a series of 70 cases of cerebral venous thrombosis linked to COVID-19 vaccination, Richard Perry, PhD, University College Hospital, London, described this new report as “an excellent study, with many of the same strengths and weaknesses as our study and has very similar results.”
Dr. Perry noted that the two studies used slightly different definitions of vaccine-induced thrombotic thrombocytopenia, but the cases reported appear to be very similar overall. “It is reassuring and gratifying to see that they have made such similar observations,” he said.
“And as they have drawn their cases from a broad range of countries whereas ours were all from the U.K., this provides evidence that the observations from both studies are reasonably generalizable,” he added.
Dr. Perry pointed out that this new report states that TTS occurred in one patient after the patient had received a second dose of the AstraZeneca vaccine. “I would like to know more about this case, because we didn’t see any cases after a second dose in our cohort,” he said.
Dr. Coutinho responded that he didn’t believe this was the first reported case after the second dose.
The study did not receive any specific funding. Dr. Coutinho has received grants paid to his institution from Boehringer Ingelheim and Bayer and payments paid to his institution for data safety monitoring board participation by Bayer.
A version of this article first appeared on Medscape.com.
, confirming the severity of the reaction and the associated high mortality rate.
The new series comes from an international registry of consecutive patients who experienced CVST within 28 days of COVID-19 vaccination between March 29 and June 18, 2021, from 81 hospitals in 19 countries.
The cases are described in an article published online on Sept. 28. in JAMA Neurology.
“This is a reliable description on the clinical condition of these patients with CVST associated with COVID-19 vaccination. It is striking that this a much worse condition than CVST not associated with COVID-19 vaccination, with a much higher rate of intracerebral hemorrhage and coma and a much higher mortality rate,” senior author Jonathan M. Coutinho, MD, Amsterdam University Medical Centers, told this news organization.
These data confirm the observations from an earlier U.K. cohort in which cases of cerebral venous thrombosis linked to COVID-19 vaccination occurred.
“This is the biggest series, and as an international series, it gives a broader perspective from a larger range of countries,” Dr. Coutinho said. “All the data together show that, although this side effect is rare, the consequences are very severe,” he added.
In the current study, the researchers regarded CVST as being linked to the vaccine if it was accompanied by thrombosis with thrombocytopenia syndrome (TTS), as evidenced by thrombosis and new-onset thrombocytopenia.
In the cohort of 116 patients with CVST after COVID-19 vaccination, 78 (67.2%) had thrombosis with TTS and were thus classified as having had a vaccine-related adverse event. These patients were frequently comatose at presentation (24%) and often had intracerebral hemorrhage (68%) and concomitant thromboembolism (36%); 47% died during hospitalization.
These patients were compared with the 38 patients in the same cohort who had CVST but in whom there was no indication of concomitant thrombosis and thrombocytopenia. The case patients were also compared with a control group of 207 patients with CVST who were included in a separate international registry before the COVID-19 pandemic.
Mortality rates were much higher among the patients deemed to have had a vaccine-related CVST. The in-hospital mortality rate was 47%, compared with 5% among the patients in the same cohort who did not have TTS and 3.9% among the prepandemic control group.
The mortality rate was even higher (61%) among patients in the TTS group for whom the diagnosis was made before the condition garnered attention in the scientific community. The mortality rate was 42% among patients diagnosed later.
Of the 78 patients in whom CVST and TTS occurred after COVID-19 vaccination in this cohort, 76 had received the AstraZeneca vaccine (in 75 patients, CVST and TTS occurred after the first vaccination; in one patient, they occurred after the second vaccination). One patient had received the Johnson & Johnson vaccine, and one had received the Pfizer vaccine.
“After more analysis, the case after the Pfizer vaccination is not believed to be caused by the vaccine,” Dr. Coutinho said. “In that case, the patient had a platelet count just below the lower limit and was taking an immunomodulator drug that is known to be associated with thrombocytopenia.”
For two patients who received the AstraZeneca vaccine, there was also an alternative explanation for the thrombocytopenia.
Dr. Coutinho also pointed out that the Johnson & Johnson vaccine has been used mainly in the United States, and these data were largely from other countries.
The median time from vaccination to CVST symptom onset was 9 days in the TTS group. The median platelet count at hospital admission among patients with postvaccination CVST-TTS was 45. Three patients presented with a normal platelet count and developed thrombocytopenia during admission; two patients presented with mild thrombocytopenia, 30 presented with moderate thrombocytopenia, and 43 presented with severe thrombocytopenia.
Antibodies against platelet factor 4 (PF4) were measured in 69 patients with TTS, of whom 63 (91%) tested positive (the one patient in whom TTS occurred after the patient received the Pfizer vaccine did not test positive). However, the researchers note that sensitivity varies among different PF4 ELISA tests. Findings of platelet activation assays were positive in all 36 tested patients.
In the TTS group, 52 patients (67%) received immunomodulation therapy, most often intravenous immunoglobulins (IVIG). Among patients treated with IVIG, the mortality rate was lower (28%).
Different from CVST linked to natural COVID-19 infection
Dr. Coutinho noted that CVST can occur in natural SARS-CoV-2 infection but that vaccine-associated CVST is very different.
“In natural COVID-19 infection, there is an increased risk of thrombosis, and some patients can get CVST as a part of this, but in these cases, this is not accompanied by thrombocytopenia. While the CVST in natural COVID-19 infection is also associated with a bad prognosis, this is more to do with the underlying disease. It is normally the very sick COVID patients who develop CVST, and these patients usually die from the underlying disease rather than the CVST itself,” he explained.
“Clinicians need to be aware of vaccine-related CVST, as it requires very specific and rapid treatment,” Dr. Coutinho stressed.
“Patients presenting with an extremely severe headache (unlike any headache they’ve had before) or with seizures or a focal deficit (weakness in arm or problems with speaking or vision) within 4 weeks of an adenovirus COVID-19 vaccination should ring alarm bells. It is important to do diagnostics quickly, with a platelet count the most important first step, and a rapid CT/MRI scan,” he said.
Other tests that should be conducted are D-dimer for thrombosis and the PF4 antibody test. But results for the PF4 antibody test can take days to come back, and clinicians shouldn’t wait for that, Dr. Coutinho notes.
“Specific treatment needs to be given immediately – with anticoagulation (preferably nonheparin) and immunomodulation with IVIG to stop the immune reaction. Platelets should not be given – that may seem counterintuitive in patients with a low platelet count, but giving platelets makes it worse,” he said.
Is there a geographic difference?
Dr. Coutinho pointed out that fewer cases of this vaccine-related CVST are being reported at the current time.
“We are not sure why this is the case. These adenovirus vaccines are not being used much now in Western countries, but our collaboration covers many less developed countries in South America and Asia, which are relying heavily on these vaccines. We are now shifting focus to these countries, but so far we have only seen a handful of cases from these areas,” he said.
He suggested that this may be because these countries started their vaccination programs later and are vaccinating their elderly (who are not so susceptible to this side effect) first, or it may be because of some environmental or genetic factor that has not yet been discovered.
“This is now an important research question – is the risk of vaccine-induced CVST the same in different countries or ethnicities? This could influence decisions on future vaccine strategies,” Dr. Coutinho said.
“So far, female sex is the strongest risk factor for vaccine-induced CVST. In our cohort, 81% of cases were in women. In addition, 95% were White, but that doesn’t allow us to conclude that this is a risk factor, as the majority of people who have been vaccinated are White. So, we have no clear insight into that yet,” he said.
In a comment for this news organization, the lead author of the previous U.K. report of a series of 70 cases of cerebral venous thrombosis linked to COVID-19 vaccination, Richard Perry, PhD, University College Hospital, London, described this new report as “an excellent study, with many of the same strengths and weaknesses as our study and has very similar results.”
Dr. Perry noted that the two studies used slightly different definitions of vaccine-induced thrombotic thrombocytopenia, but the cases reported appear to be very similar overall. “It is reassuring and gratifying to see that they have made such similar observations,” he said.
“And as they have drawn their cases from a broad range of countries whereas ours were all from the U.K., this provides evidence that the observations from both studies are reasonably generalizable,” he added.
Dr. Perry pointed out that this new report states that TTS occurred in one patient after the patient had received a second dose of the AstraZeneca vaccine. “I would like to know more about this case, because we didn’t see any cases after a second dose in our cohort,” he said.
Dr. Coutinho responded that he didn’t believe this was the first reported case after the second dose.
The study did not receive any specific funding. Dr. Coutinho has received grants paid to his institution from Boehringer Ingelheim and Bayer and payments paid to his institution for data safety monitoring board participation by Bayer.
A version of this article first appeared on Medscape.com.
, confirming the severity of the reaction and the associated high mortality rate.
The new series comes from an international registry of consecutive patients who experienced CVST within 28 days of COVID-19 vaccination between March 29 and June 18, 2021, from 81 hospitals in 19 countries.
The cases are described in an article published online on Sept. 28. in JAMA Neurology.
“This is a reliable description on the clinical condition of these patients with CVST associated with COVID-19 vaccination. It is striking that this a much worse condition than CVST not associated with COVID-19 vaccination, with a much higher rate of intracerebral hemorrhage and coma and a much higher mortality rate,” senior author Jonathan M. Coutinho, MD, Amsterdam University Medical Centers, told this news organization.
These data confirm the observations from an earlier U.K. cohort in which cases of cerebral venous thrombosis linked to COVID-19 vaccination occurred.
“This is the biggest series, and as an international series, it gives a broader perspective from a larger range of countries,” Dr. Coutinho said. “All the data together show that, although this side effect is rare, the consequences are very severe,” he added.
In the current study, the researchers regarded CVST as being linked to the vaccine if it was accompanied by thrombosis with thrombocytopenia syndrome (TTS), as evidenced by thrombosis and new-onset thrombocytopenia.
In the cohort of 116 patients with CVST after COVID-19 vaccination, 78 (67.2%) had thrombosis with TTS and were thus classified as having had a vaccine-related adverse event. These patients were frequently comatose at presentation (24%) and often had intracerebral hemorrhage (68%) and concomitant thromboembolism (36%); 47% died during hospitalization.
These patients were compared with the 38 patients in the same cohort who had CVST but in whom there was no indication of concomitant thrombosis and thrombocytopenia. The case patients were also compared with a control group of 207 patients with CVST who were included in a separate international registry before the COVID-19 pandemic.
Mortality rates were much higher among the patients deemed to have had a vaccine-related CVST. The in-hospital mortality rate was 47%, compared with 5% among the patients in the same cohort who did not have TTS and 3.9% among the prepandemic control group.
The mortality rate was even higher (61%) among patients in the TTS group for whom the diagnosis was made before the condition garnered attention in the scientific community. The mortality rate was 42% among patients diagnosed later.
Of the 78 patients in whom CVST and TTS occurred after COVID-19 vaccination in this cohort, 76 had received the AstraZeneca vaccine (in 75 patients, CVST and TTS occurred after the first vaccination; in one patient, they occurred after the second vaccination). One patient had received the Johnson & Johnson vaccine, and one had received the Pfizer vaccine.
“After more analysis, the case after the Pfizer vaccination is not believed to be caused by the vaccine,” Dr. Coutinho said. “In that case, the patient had a platelet count just below the lower limit and was taking an immunomodulator drug that is known to be associated with thrombocytopenia.”
For two patients who received the AstraZeneca vaccine, there was also an alternative explanation for the thrombocytopenia.
Dr. Coutinho also pointed out that the Johnson & Johnson vaccine has been used mainly in the United States, and these data were largely from other countries.
The median time from vaccination to CVST symptom onset was 9 days in the TTS group. The median platelet count at hospital admission among patients with postvaccination CVST-TTS was 45. Three patients presented with a normal platelet count and developed thrombocytopenia during admission; two patients presented with mild thrombocytopenia, 30 presented with moderate thrombocytopenia, and 43 presented with severe thrombocytopenia.
Antibodies against platelet factor 4 (PF4) were measured in 69 patients with TTS, of whom 63 (91%) tested positive (the one patient in whom TTS occurred after the patient received the Pfizer vaccine did not test positive). However, the researchers note that sensitivity varies among different PF4 ELISA tests. Findings of platelet activation assays were positive in all 36 tested patients.
In the TTS group, 52 patients (67%) received immunomodulation therapy, most often intravenous immunoglobulins (IVIG). Among patients treated with IVIG, the mortality rate was lower (28%).
Different from CVST linked to natural COVID-19 infection
Dr. Coutinho noted that CVST can occur in natural SARS-CoV-2 infection but that vaccine-associated CVST is very different.
“In natural COVID-19 infection, there is an increased risk of thrombosis, and some patients can get CVST as a part of this, but in these cases, this is not accompanied by thrombocytopenia. While the CVST in natural COVID-19 infection is also associated with a bad prognosis, this is more to do with the underlying disease. It is normally the very sick COVID patients who develop CVST, and these patients usually die from the underlying disease rather than the CVST itself,” he explained.
“Clinicians need to be aware of vaccine-related CVST, as it requires very specific and rapid treatment,” Dr. Coutinho stressed.
“Patients presenting with an extremely severe headache (unlike any headache they’ve had before) or with seizures or a focal deficit (weakness in arm or problems with speaking or vision) within 4 weeks of an adenovirus COVID-19 vaccination should ring alarm bells. It is important to do diagnostics quickly, with a platelet count the most important first step, and a rapid CT/MRI scan,” he said.
Other tests that should be conducted are D-dimer for thrombosis and the PF4 antibody test. But results for the PF4 antibody test can take days to come back, and clinicians shouldn’t wait for that, Dr. Coutinho notes.
“Specific treatment needs to be given immediately – with anticoagulation (preferably nonheparin) and immunomodulation with IVIG to stop the immune reaction. Platelets should not be given – that may seem counterintuitive in patients with a low platelet count, but giving platelets makes it worse,” he said.
Is there a geographic difference?
Dr. Coutinho pointed out that fewer cases of this vaccine-related CVST are being reported at the current time.
“We are not sure why this is the case. These adenovirus vaccines are not being used much now in Western countries, but our collaboration covers many less developed countries in South America and Asia, which are relying heavily on these vaccines. We are now shifting focus to these countries, but so far we have only seen a handful of cases from these areas,” he said.
He suggested that this may be because these countries started their vaccination programs later and are vaccinating their elderly (who are not so susceptible to this side effect) first, or it may be because of some environmental or genetic factor that has not yet been discovered.
“This is now an important research question – is the risk of vaccine-induced CVST the same in different countries or ethnicities? This could influence decisions on future vaccine strategies,” Dr. Coutinho said.
“So far, female sex is the strongest risk factor for vaccine-induced CVST. In our cohort, 81% of cases were in women. In addition, 95% were White, but that doesn’t allow us to conclude that this is a risk factor, as the majority of people who have been vaccinated are White. So, we have no clear insight into that yet,” he said.
In a comment for this news organization, the lead author of the previous U.K. report of a series of 70 cases of cerebral venous thrombosis linked to COVID-19 vaccination, Richard Perry, PhD, University College Hospital, London, described this new report as “an excellent study, with many of the same strengths and weaknesses as our study and has very similar results.”
Dr. Perry noted that the two studies used slightly different definitions of vaccine-induced thrombotic thrombocytopenia, but the cases reported appear to be very similar overall. “It is reassuring and gratifying to see that they have made such similar observations,” he said.
“And as they have drawn their cases from a broad range of countries whereas ours were all from the U.K., this provides evidence that the observations from both studies are reasonably generalizable,” he added.
Dr. Perry pointed out that this new report states that TTS occurred in one patient after the patient had received a second dose of the AstraZeneca vaccine. “I would like to know more about this case, because we didn’t see any cases after a second dose in our cohort,” he said.
Dr. Coutinho responded that he didn’t believe this was the first reported case after the second dose.
The study did not receive any specific funding. Dr. Coutinho has received grants paid to his institution from Boehringer Ingelheim and Bayer and payments paid to his institution for data safety monitoring board participation by Bayer.
A version of this article first appeared on Medscape.com.
Booster shot back-and-forth creates uncertainty, confusion
Many people are confused — patients and healthcare providers alike — in the wake of the U.S. Food and Drug Administration (FDA) and Centers for Disease Control and Prevention (CDC) announcements about who is authorized to get a third or ‘booster’ shot of the Pfizer/BioNTech COVID-19 vaccine.
, healthcare providers report. At the same time, the uncertainty from changing federal messages about boosters is causing some chaos, especially in the form of vaccine misinformation.
The confusion started, in part, with the August 13 announcement that immunocompromised Americans were eligible for a booster shot. Next came the initial Biden administration intention to provide most U.S. adults with a third shot starting September 20 — an announcement later rolled back — followed by the Food and Drug Administration (FDA) and Centers for Disease Control and Prevention (CDC) limiting boosters to select groups last week.
“It was only 3% of the population that was going to be getting a third dose, then it was back to everyone being able to get the booster, and then it’s back to a select crew,” Louito Edje, MD, a family physician in private practice in Cincinnati, said in an interview with this news organization.
This kind of mixed messaging is generating more questions than answers.
“Even though that is following the science, translating the science into policy, it’s really fraught with confusion for patients, especially,” added Dr. Edje, professor educator in the departments of medical education and family and community medicine at UC Health and a fellow of the American Academy of Family Physicians.
When asked if he’s seeing more uncertainty about boosters, community pharmacist Brian Caswell, RPh, said: “I’m going to have to say yes because I’ve been confused myself at times.”
“Yes, there is a lot of confusion,” added Mr. Caswell, owner or co-owner of four pharmacies in Kansas and Missouri and president of the National Community Pharmacists Association.
Boosting misinformation?
“Unfortunately, confusion leads to an acceleration of misinformation,” Mr. Caswell said.
Dr. Edje shared an example. “The folks who have been hesitant to even get the first vaccine appear now a little less likely to want to go ahead and get vaccinated.”
These patients point to breakthrough COVID-19 cases of the Delta variant, which “reinforces that they don’t need to get vaccinated in the first place,” Dr. Edje said.
“That’s unfortunate because it’s a complete fallacy.”
Clearer communication from the federal government could help alleviate confusion, Mr. Caswell said. “I would like to see an official CDC chart that states who is eligible as of a certain date. Something that is accessible through their webpage or a social media source that can be updated. That would help all of us.”
“For myself, I’ve got patients from Kansas, Oklahoma, and Missouri that might be operating under different guidelines. That makes it even more confusing,” he said.
More clarity is needed for individuals seeking boosters as well. “It would help to be very clear with the general public, who are becoming very knowledgeable within this vaccine realm,” Mr. Caswell said.
‘Gaming the system’
Although most people seeking a booster shot at one of Caswell’s pharmacies are following official recommendations, there are some who remain ineligible but nonetheless come in for an additional vaccine.
“Even before this announcement last Friday, in the latter part of August when the CDC talked about a booster for immunocompromised, we had interest from people who did not meet the criteria,” Mr. Caswell said.
To the ineligible, he and his staff explain the approval process, why certain decisions are made, and point out that the number of eligible Americans is likely to expand in the future.
“The vast majority of them are understanding,” Mr. Caswell said. “But we’ve had some people who really didn’t want to accept the information, and I don’t know what they’ve done.”
“Some people are gaming the system to get their booster or second shot of J&J,” he said.
For example, Mr. Caswell had a patient who crossed over state lines from Missouri seeking a vaccine booster at Wolkar Drug, a pharmacy in Baxter Springs, Kan. “We found out later he had a J&J shot at a facility or provider in Missouri. He came over to Kansas, signed up for it and got a booster with Moderna.”
“We called and asked him if he was aware of it. He said, ‘yes.’ When we questioned him more about it, he hung up.”
Dr. Edje is likewise seeing interest from some ineligible patients, she said.
Crossing a liability line?
Mr. Caswell has asked for advice from lawyers and the State Board of Pharmacy on potential liability if a pharmacist gives a booster to a patient not eligible under the official FDA and CDC guidance.
“We ask patients direct questions about whether they’ve had the COVID vaccine, COVID, and a whole litany of questions they must answer. And we’re assuming they are going to be honest and forthright,” he said. “The pharmacist needs to make sure they make every effort to get that information from the patient.”
Normally, healthcare providers like Mr. Caswell report each COVID-19 vaccination to the state registry after administration. “We have not gone through a police action and checked the registry first,” he said.
But, if people continue to try ‘gaming the system,’ he said, he might have to start checking the state registry before giving someone a booster.
The American Academy of Family Physicians offers advice from the CDC about legal protections for providers.
“As outlined by CDC, any off-label use of the Comirnaty/Pfizer-BioNTech COVID-19 vaccine is not authorized at this time and may not be covered under the PREP Act or the PREP Act declaration. This means that clinicians providing the vaccine outside of the authorized/approved use may not have immunity from claims,” the AAFP website states.
“Per CDC, individuals who receive a third dose may not be eligible for compensation after a possible adverse event. Such use would be in violation of the CDC COVID-19 vaccination program provider agreement and therefore may not be reimbursable and may impact the ability of a provider to remain in the CDC program, in addition to other potential sanctions. Administration fees for off-label doses may not be reimbursed by payers.”
Despite confusion, demand is up
Even amid all the uncertainty, there appears to be a jump in enthusiasm for the booster shots.
“The requests have gone up quite a bit. We’ve seen a number of requests from people in person and over the phone looking to get a booster,” Mr. Caswell said. “Since the discussion at the federal level...there has been a lot of interest in the third shot booster, itself, as well as about a booster for J&J.”
“There is quite a bit of excitement out there,” he said.
Dr. Edje agreed: “I take care of a fair number of folks...including the elderly and healthcare professionals. They are already asking for the booster.”
Interestingly, Dr. Edje would like to get a booster herself but is not eligible for the Pfizer third shot. She is a participant in a Moderna vaccine trial and can only receive additional immunization as part of the study.
‘Walk, don’t run’
To quell any potential early rush to get a third shot, U.S. health officials are reminding booster-ineligible people that they still have some protection against COVID-19.
“If you’re a person who ultimately might get a booster that will make you optimally protected, you don’t necessarily need to get it tomorrow,” Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases told CNN.
CDC Director Rochelle Walensky, MD, also weighed in. She told ABC that boosters for people who received a Moderna or Johnson & Johnson vaccine will be addressed with urgency.
“I want to reiterate that this is a very slow wane. There is no urgency here to go and get your booster immediately. You know, walk don’t run to your booster appointment,” she said.
“We will come and look at the data for Moderna and J&J in very short order.”
Dr. Edje and Mr. Caswell have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Many people are confused — patients and healthcare providers alike — in the wake of the U.S. Food and Drug Administration (FDA) and Centers for Disease Control and Prevention (CDC) announcements about who is authorized to get a third or ‘booster’ shot of the Pfizer/BioNTech COVID-19 vaccine.
, healthcare providers report. At the same time, the uncertainty from changing federal messages about boosters is causing some chaos, especially in the form of vaccine misinformation.
The confusion started, in part, with the August 13 announcement that immunocompromised Americans were eligible for a booster shot. Next came the initial Biden administration intention to provide most U.S. adults with a third shot starting September 20 — an announcement later rolled back — followed by the Food and Drug Administration (FDA) and Centers for Disease Control and Prevention (CDC) limiting boosters to select groups last week.
“It was only 3% of the population that was going to be getting a third dose, then it was back to everyone being able to get the booster, and then it’s back to a select crew,” Louito Edje, MD, a family physician in private practice in Cincinnati, said in an interview with this news organization.
This kind of mixed messaging is generating more questions than answers.
“Even though that is following the science, translating the science into policy, it’s really fraught with confusion for patients, especially,” added Dr. Edje, professor educator in the departments of medical education and family and community medicine at UC Health and a fellow of the American Academy of Family Physicians.
When asked if he’s seeing more uncertainty about boosters, community pharmacist Brian Caswell, RPh, said: “I’m going to have to say yes because I’ve been confused myself at times.”
“Yes, there is a lot of confusion,” added Mr. Caswell, owner or co-owner of four pharmacies in Kansas and Missouri and president of the National Community Pharmacists Association.
Boosting misinformation?
“Unfortunately, confusion leads to an acceleration of misinformation,” Mr. Caswell said.
Dr. Edje shared an example. “The folks who have been hesitant to even get the first vaccine appear now a little less likely to want to go ahead and get vaccinated.”
These patients point to breakthrough COVID-19 cases of the Delta variant, which “reinforces that they don’t need to get vaccinated in the first place,” Dr. Edje said.
“That’s unfortunate because it’s a complete fallacy.”
Clearer communication from the federal government could help alleviate confusion, Mr. Caswell said. “I would like to see an official CDC chart that states who is eligible as of a certain date. Something that is accessible through their webpage or a social media source that can be updated. That would help all of us.”
“For myself, I’ve got patients from Kansas, Oklahoma, and Missouri that might be operating under different guidelines. That makes it even more confusing,” he said.
More clarity is needed for individuals seeking boosters as well. “It would help to be very clear with the general public, who are becoming very knowledgeable within this vaccine realm,” Mr. Caswell said.
‘Gaming the system’
Although most people seeking a booster shot at one of Caswell’s pharmacies are following official recommendations, there are some who remain ineligible but nonetheless come in for an additional vaccine.
“Even before this announcement last Friday, in the latter part of August when the CDC talked about a booster for immunocompromised, we had interest from people who did not meet the criteria,” Mr. Caswell said.
To the ineligible, he and his staff explain the approval process, why certain decisions are made, and point out that the number of eligible Americans is likely to expand in the future.
“The vast majority of them are understanding,” Mr. Caswell said. “But we’ve had some people who really didn’t want to accept the information, and I don’t know what they’ve done.”
“Some people are gaming the system to get their booster or second shot of J&J,” he said.
For example, Mr. Caswell had a patient who crossed over state lines from Missouri seeking a vaccine booster at Wolkar Drug, a pharmacy in Baxter Springs, Kan. “We found out later he had a J&J shot at a facility or provider in Missouri. He came over to Kansas, signed up for it and got a booster with Moderna.”
“We called and asked him if he was aware of it. He said, ‘yes.’ When we questioned him more about it, he hung up.”
Dr. Edje is likewise seeing interest from some ineligible patients, she said.
Crossing a liability line?
Mr. Caswell has asked for advice from lawyers and the State Board of Pharmacy on potential liability if a pharmacist gives a booster to a patient not eligible under the official FDA and CDC guidance.
“We ask patients direct questions about whether they’ve had the COVID vaccine, COVID, and a whole litany of questions they must answer. And we’re assuming they are going to be honest and forthright,” he said. “The pharmacist needs to make sure they make every effort to get that information from the patient.”
Normally, healthcare providers like Mr. Caswell report each COVID-19 vaccination to the state registry after administration. “We have not gone through a police action and checked the registry first,” he said.
But, if people continue to try ‘gaming the system,’ he said, he might have to start checking the state registry before giving someone a booster.
The American Academy of Family Physicians offers advice from the CDC about legal protections for providers.
“As outlined by CDC, any off-label use of the Comirnaty/Pfizer-BioNTech COVID-19 vaccine is not authorized at this time and may not be covered under the PREP Act or the PREP Act declaration. This means that clinicians providing the vaccine outside of the authorized/approved use may not have immunity from claims,” the AAFP website states.
“Per CDC, individuals who receive a third dose may not be eligible for compensation after a possible adverse event. Such use would be in violation of the CDC COVID-19 vaccination program provider agreement and therefore may not be reimbursable and may impact the ability of a provider to remain in the CDC program, in addition to other potential sanctions. Administration fees for off-label doses may not be reimbursed by payers.”
Despite confusion, demand is up
Even amid all the uncertainty, there appears to be a jump in enthusiasm for the booster shots.
“The requests have gone up quite a bit. We’ve seen a number of requests from people in person and over the phone looking to get a booster,” Mr. Caswell said. “Since the discussion at the federal level...there has been a lot of interest in the third shot booster, itself, as well as about a booster for J&J.”
“There is quite a bit of excitement out there,” he said.
Dr. Edje agreed: “I take care of a fair number of folks...including the elderly and healthcare professionals. They are already asking for the booster.”
Interestingly, Dr. Edje would like to get a booster herself but is not eligible for the Pfizer third shot. She is a participant in a Moderna vaccine trial and can only receive additional immunization as part of the study.
‘Walk, don’t run’
To quell any potential early rush to get a third shot, U.S. health officials are reminding booster-ineligible people that they still have some protection against COVID-19.
“If you’re a person who ultimately might get a booster that will make you optimally protected, you don’t necessarily need to get it tomorrow,” Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases told CNN.
CDC Director Rochelle Walensky, MD, also weighed in. She told ABC that boosters for people who received a Moderna or Johnson & Johnson vaccine will be addressed with urgency.
“I want to reiterate that this is a very slow wane. There is no urgency here to go and get your booster immediately. You know, walk don’t run to your booster appointment,” she said.
“We will come and look at the data for Moderna and J&J in very short order.”
Dr. Edje and Mr. Caswell have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Many people are confused — patients and healthcare providers alike — in the wake of the U.S. Food and Drug Administration (FDA) and Centers for Disease Control and Prevention (CDC) announcements about who is authorized to get a third or ‘booster’ shot of the Pfizer/BioNTech COVID-19 vaccine.
, healthcare providers report. At the same time, the uncertainty from changing federal messages about boosters is causing some chaos, especially in the form of vaccine misinformation.
The confusion started, in part, with the August 13 announcement that immunocompromised Americans were eligible for a booster shot. Next came the initial Biden administration intention to provide most U.S. adults with a third shot starting September 20 — an announcement later rolled back — followed by the Food and Drug Administration (FDA) and Centers for Disease Control and Prevention (CDC) limiting boosters to select groups last week.
“It was only 3% of the population that was going to be getting a third dose, then it was back to everyone being able to get the booster, and then it’s back to a select crew,” Louito Edje, MD, a family physician in private practice in Cincinnati, said in an interview with this news organization.
This kind of mixed messaging is generating more questions than answers.
“Even though that is following the science, translating the science into policy, it’s really fraught with confusion for patients, especially,” added Dr. Edje, professor educator in the departments of medical education and family and community medicine at UC Health and a fellow of the American Academy of Family Physicians.
When asked if he’s seeing more uncertainty about boosters, community pharmacist Brian Caswell, RPh, said: “I’m going to have to say yes because I’ve been confused myself at times.”
“Yes, there is a lot of confusion,” added Mr. Caswell, owner or co-owner of four pharmacies in Kansas and Missouri and president of the National Community Pharmacists Association.
Boosting misinformation?
“Unfortunately, confusion leads to an acceleration of misinformation,” Mr. Caswell said.
Dr. Edje shared an example. “The folks who have been hesitant to even get the first vaccine appear now a little less likely to want to go ahead and get vaccinated.”
These patients point to breakthrough COVID-19 cases of the Delta variant, which “reinforces that they don’t need to get vaccinated in the first place,” Dr. Edje said.
“That’s unfortunate because it’s a complete fallacy.”
Clearer communication from the federal government could help alleviate confusion, Mr. Caswell said. “I would like to see an official CDC chart that states who is eligible as of a certain date. Something that is accessible through their webpage or a social media source that can be updated. That would help all of us.”
“For myself, I’ve got patients from Kansas, Oklahoma, and Missouri that might be operating under different guidelines. That makes it even more confusing,” he said.
More clarity is needed for individuals seeking boosters as well. “It would help to be very clear with the general public, who are becoming very knowledgeable within this vaccine realm,” Mr. Caswell said.
‘Gaming the system’
Although most people seeking a booster shot at one of Caswell’s pharmacies are following official recommendations, there are some who remain ineligible but nonetheless come in for an additional vaccine.
“Even before this announcement last Friday, in the latter part of August when the CDC talked about a booster for immunocompromised, we had interest from people who did not meet the criteria,” Mr. Caswell said.
To the ineligible, he and his staff explain the approval process, why certain decisions are made, and point out that the number of eligible Americans is likely to expand in the future.
“The vast majority of them are understanding,” Mr. Caswell said. “But we’ve had some people who really didn’t want to accept the information, and I don’t know what they’ve done.”
“Some people are gaming the system to get their booster or second shot of J&J,” he said.
For example, Mr. Caswell had a patient who crossed over state lines from Missouri seeking a vaccine booster at Wolkar Drug, a pharmacy in Baxter Springs, Kan. “We found out later he had a J&J shot at a facility or provider in Missouri. He came over to Kansas, signed up for it and got a booster with Moderna.”
“We called and asked him if he was aware of it. He said, ‘yes.’ When we questioned him more about it, he hung up.”
Dr. Edje is likewise seeing interest from some ineligible patients, she said.
Crossing a liability line?
Mr. Caswell has asked for advice from lawyers and the State Board of Pharmacy on potential liability if a pharmacist gives a booster to a patient not eligible under the official FDA and CDC guidance.
“We ask patients direct questions about whether they’ve had the COVID vaccine, COVID, and a whole litany of questions they must answer. And we’re assuming they are going to be honest and forthright,” he said. “The pharmacist needs to make sure they make every effort to get that information from the patient.”
Normally, healthcare providers like Mr. Caswell report each COVID-19 vaccination to the state registry after administration. “We have not gone through a police action and checked the registry first,” he said.
But, if people continue to try ‘gaming the system,’ he said, he might have to start checking the state registry before giving someone a booster.
The American Academy of Family Physicians offers advice from the CDC about legal protections for providers.
“As outlined by CDC, any off-label use of the Comirnaty/Pfizer-BioNTech COVID-19 vaccine is not authorized at this time and may not be covered under the PREP Act or the PREP Act declaration. This means that clinicians providing the vaccine outside of the authorized/approved use may not have immunity from claims,” the AAFP website states.
“Per CDC, individuals who receive a third dose may not be eligible for compensation after a possible adverse event. Such use would be in violation of the CDC COVID-19 vaccination program provider agreement and therefore may not be reimbursable and may impact the ability of a provider to remain in the CDC program, in addition to other potential sanctions. Administration fees for off-label doses may not be reimbursed by payers.”
Despite confusion, demand is up
Even amid all the uncertainty, there appears to be a jump in enthusiasm for the booster shots.
“The requests have gone up quite a bit. We’ve seen a number of requests from people in person and over the phone looking to get a booster,” Mr. Caswell said. “Since the discussion at the federal level...there has been a lot of interest in the third shot booster, itself, as well as about a booster for J&J.”
“There is quite a bit of excitement out there,” he said.
Dr. Edje agreed: “I take care of a fair number of folks...including the elderly and healthcare professionals. They are already asking for the booster.”
Interestingly, Dr. Edje would like to get a booster herself but is not eligible for the Pfizer third shot. She is a participant in a Moderna vaccine trial and can only receive additional immunization as part of the study.
‘Walk, don’t run’
To quell any potential early rush to get a third shot, U.S. health officials are reminding booster-ineligible people that they still have some protection against COVID-19.
“If you’re a person who ultimately might get a booster that will make you optimally protected, you don’t necessarily need to get it tomorrow,” Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases told CNN.
CDC Director Rochelle Walensky, MD, also weighed in. She told ABC that boosters for people who received a Moderna or Johnson & Johnson vaccine will be addressed with urgency.
“I want to reiterate that this is a very slow wane. There is no urgency here to go and get your booster immediately. You know, walk don’t run to your booster appointment,” she said.
“We will come and look at the data for Moderna and J&J in very short order.”
Dr. Edje and Mr. Caswell have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Age, C-reactive protein predict COVID-19 death in diabetes
The data, from the retrospective ACCREDIT cohort study, were presented at the virtual annual meeting of the European Association for the Study of Diabetes (EASD 2021) by Daniel Kevin Llanera, MD.
The combination of older age and high levels of the inflammatory marker CRP were linked to a tripled risk for death by day 7 after hospitalization for COVID-19 among people with diabetes. But, in contrast to other studies, recent A1c and body mass index did not predict COVID-19 outcomes.
“Both of these variables are easily available upon admission to hospital,” Dr. Llanera, who now works at Imperial College, London, said in an EASD press release.
“This means we can easily identify patients early on in their hospital stay who will likely require more aggressive interventions to try and improve survival.”
“It makes sense that CRP and age are important,” said Simon Heller, MB BChir, DM, of the University of Sheffield, England. “It may be that diabetes alone overwhelmed the additional effects of obesity and A1c.
“Certainly in other studies, age was the overwhelming bad prognostic sign among people with diabetes, and perhaps long-term diabetes has effects on the immune system which we haven’t yet identified.”
Kidney disease in younger patients also linked to poorer outcomes
The study, conducted when Dr. Llanera worked for the Countess of Chester NHS Foundation Trust, involved 1,004 patients with diabetes admitted with COVID-19 to seven hospitals in northwest England from Jan. 1 through June 30, 2020. The patients were a mean age of 74.1 years, 60.7% were male, and 45% were in the most deprived quintile based on the U.K. government deprivation index. Overall, 56.2% had macrovascular complications and 49.6% had microvascular complications.
They had a median BMI of 27.6 kg/m2, which is lower than that reported in previous studies and might explain the difference, Dr. Llanera noted.
The primary outcome, death within 7 days of admission, occurred in 24%. By day 30, 33% had died. These rates are higher than the rate found in previous studies, possibly because of greater socioeconomic deprivation and older age of the population, Dr. Llanera speculated.
A total of 7.5% of patients received intensive care by day 7 and 9.8% required intravenous insulin infusions.
On univariate analysis, insulin infusion was found to be protective, with those receiving it half as likely to die as those who didn’t need IV insulin (odds ratio [OR], 0.5).
In contrast, chronic kidney disease in people younger than 70 years increased the risk of death more than twofold (OR, 2.74), as did type 2 diabetes compared with other diabetes types (OR, 2.52).
As in previous studies, use of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers were not associated with COVID-19 outcomes, nor was the presence of diabetes-related complications.
In multivariate analysis, CRP and age emerged as the most significant predictors of the primary outcome, with those deemed high risk by a logistic regression model having an OR of 3.44 for death by day 7 compared with those at lower risk based on the two factors.
Data for glycemic control during the time of hospitalization weren’t available for this study, Dr. Llanera said in response to a question.
“We didn’t look into glycemic control during admission, just at entry, so I can’t answer whether strict glucose control is of benefit. I think it’s worth exploring further whether the use of IV insulin may be of benefit.”
Dr. Llanera also pointed out that people with diabetic kidney disease are in a chronic proinflammatory state and have immune dysregulation, thus potentially hindering their ability to “fight off” the virus.
“In addition, ACE2 receptors are upregulated in the kidneys of patients with diabetic kidney disease. These are molecules that facilitate entry of SARS-CoV-2 into the cells. This may lead to direct attack of the kidneys by the virus, possibly leading to worse overall outcomes,” he said.
Dr. Llanera has reported no relevant financial relationships. Dr. Heller has reported serving as consultant or speaker for Novo Nordisk, Eli Lilly, Sanofi Aventis, Mannkind, Zealand, MSD, and Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
The data, from the retrospective ACCREDIT cohort study, were presented at the virtual annual meeting of the European Association for the Study of Diabetes (EASD 2021) by Daniel Kevin Llanera, MD.
The combination of older age and high levels of the inflammatory marker CRP were linked to a tripled risk for death by day 7 after hospitalization for COVID-19 among people with diabetes. But, in contrast to other studies, recent A1c and body mass index did not predict COVID-19 outcomes.
“Both of these variables are easily available upon admission to hospital,” Dr. Llanera, who now works at Imperial College, London, said in an EASD press release.
“This means we can easily identify patients early on in their hospital stay who will likely require more aggressive interventions to try and improve survival.”
“It makes sense that CRP and age are important,” said Simon Heller, MB BChir, DM, of the University of Sheffield, England. “It may be that diabetes alone overwhelmed the additional effects of obesity and A1c.
“Certainly in other studies, age was the overwhelming bad prognostic sign among people with diabetes, and perhaps long-term diabetes has effects on the immune system which we haven’t yet identified.”
Kidney disease in younger patients also linked to poorer outcomes
The study, conducted when Dr. Llanera worked for the Countess of Chester NHS Foundation Trust, involved 1,004 patients with diabetes admitted with COVID-19 to seven hospitals in northwest England from Jan. 1 through June 30, 2020. The patients were a mean age of 74.1 years, 60.7% were male, and 45% were in the most deprived quintile based on the U.K. government deprivation index. Overall, 56.2% had macrovascular complications and 49.6% had microvascular complications.
They had a median BMI of 27.6 kg/m2, which is lower than that reported in previous studies and might explain the difference, Dr. Llanera noted.
The primary outcome, death within 7 days of admission, occurred in 24%. By day 30, 33% had died. These rates are higher than the rate found in previous studies, possibly because of greater socioeconomic deprivation and older age of the population, Dr. Llanera speculated.
A total of 7.5% of patients received intensive care by day 7 and 9.8% required intravenous insulin infusions.
On univariate analysis, insulin infusion was found to be protective, with those receiving it half as likely to die as those who didn’t need IV insulin (odds ratio [OR], 0.5).
In contrast, chronic kidney disease in people younger than 70 years increased the risk of death more than twofold (OR, 2.74), as did type 2 diabetes compared with other diabetes types (OR, 2.52).
As in previous studies, use of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers were not associated with COVID-19 outcomes, nor was the presence of diabetes-related complications.
In multivariate analysis, CRP and age emerged as the most significant predictors of the primary outcome, with those deemed high risk by a logistic regression model having an OR of 3.44 for death by day 7 compared with those at lower risk based on the two factors.
Data for glycemic control during the time of hospitalization weren’t available for this study, Dr. Llanera said in response to a question.
“We didn’t look into glycemic control during admission, just at entry, so I can’t answer whether strict glucose control is of benefit. I think it’s worth exploring further whether the use of IV insulin may be of benefit.”
Dr. Llanera also pointed out that people with diabetic kidney disease are in a chronic proinflammatory state and have immune dysregulation, thus potentially hindering their ability to “fight off” the virus.
“In addition, ACE2 receptors are upregulated in the kidneys of patients with diabetic kidney disease. These are molecules that facilitate entry of SARS-CoV-2 into the cells. This may lead to direct attack of the kidneys by the virus, possibly leading to worse overall outcomes,” he said.
Dr. Llanera has reported no relevant financial relationships. Dr. Heller has reported serving as consultant or speaker for Novo Nordisk, Eli Lilly, Sanofi Aventis, Mannkind, Zealand, MSD, and Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
The data, from the retrospective ACCREDIT cohort study, were presented at the virtual annual meeting of the European Association for the Study of Diabetes (EASD 2021) by Daniel Kevin Llanera, MD.
The combination of older age and high levels of the inflammatory marker CRP were linked to a tripled risk for death by day 7 after hospitalization for COVID-19 among people with diabetes. But, in contrast to other studies, recent A1c and body mass index did not predict COVID-19 outcomes.
“Both of these variables are easily available upon admission to hospital,” Dr. Llanera, who now works at Imperial College, London, said in an EASD press release.
“This means we can easily identify patients early on in their hospital stay who will likely require more aggressive interventions to try and improve survival.”
“It makes sense that CRP and age are important,” said Simon Heller, MB BChir, DM, of the University of Sheffield, England. “It may be that diabetes alone overwhelmed the additional effects of obesity and A1c.
“Certainly in other studies, age was the overwhelming bad prognostic sign among people with diabetes, and perhaps long-term diabetes has effects on the immune system which we haven’t yet identified.”
Kidney disease in younger patients also linked to poorer outcomes
The study, conducted when Dr. Llanera worked for the Countess of Chester NHS Foundation Trust, involved 1,004 patients with diabetes admitted with COVID-19 to seven hospitals in northwest England from Jan. 1 through June 30, 2020. The patients were a mean age of 74.1 years, 60.7% were male, and 45% were in the most deprived quintile based on the U.K. government deprivation index. Overall, 56.2% had macrovascular complications and 49.6% had microvascular complications.
They had a median BMI of 27.6 kg/m2, which is lower than that reported in previous studies and might explain the difference, Dr. Llanera noted.
The primary outcome, death within 7 days of admission, occurred in 24%. By day 30, 33% had died. These rates are higher than the rate found in previous studies, possibly because of greater socioeconomic deprivation and older age of the population, Dr. Llanera speculated.
A total of 7.5% of patients received intensive care by day 7 and 9.8% required intravenous insulin infusions.
On univariate analysis, insulin infusion was found to be protective, with those receiving it half as likely to die as those who didn’t need IV insulin (odds ratio [OR], 0.5).
In contrast, chronic kidney disease in people younger than 70 years increased the risk of death more than twofold (OR, 2.74), as did type 2 diabetes compared with other diabetes types (OR, 2.52).
As in previous studies, use of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers were not associated with COVID-19 outcomes, nor was the presence of diabetes-related complications.
In multivariate analysis, CRP and age emerged as the most significant predictors of the primary outcome, with those deemed high risk by a logistic regression model having an OR of 3.44 for death by day 7 compared with those at lower risk based on the two factors.
Data for glycemic control during the time of hospitalization weren’t available for this study, Dr. Llanera said in response to a question.
“We didn’t look into glycemic control during admission, just at entry, so I can’t answer whether strict glucose control is of benefit. I think it’s worth exploring further whether the use of IV insulin may be of benefit.”
Dr. Llanera also pointed out that people with diabetic kidney disease are in a chronic proinflammatory state and have immune dysregulation, thus potentially hindering their ability to “fight off” the virus.
“In addition, ACE2 receptors are upregulated in the kidneys of patients with diabetic kidney disease. These are molecules that facilitate entry of SARS-CoV-2 into the cells. This may lead to direct attack of the kidneys by the virus, possibly leading to worse overall outcomes,” he said.
Dr. Llanera has reported no relevant financial relationships. Dr. Heller has reported serving as consultant or speaker for Novo Nordisk, Eli Lilly, Sanofi Aventis, Mannkind, Zealand, MSD, and Boehringer Ingelheim.
A version of this article first appeared on Medscape.com.
COVID-19 hospitalization 80% more likely for smokers
Observational data was analyzed alongside hospital coronavirus test data and UK Biobank genetic information for the first time, and the findings are published in Thorax.
The data cover 421,469 people overall. Of these, 3.2% took a polymerase chain reaction swab test, 0.4% of these tested positive, 0.2% of them required hospitalization for COVID-19, and 0.1% of them died because of COVID-19.
When it came to smoking status, 59% had never smoked, 37% were ex-smokers, and 3% were current smokers.
Current smokers were 80% more likely to be admitted to hospital, and significantly more likely to die from COVID-19, than nonsmokers.
Time to quit
Heavy smokers who smoked more than 20 cigarettes a day were 6.11 times more likely to die from COVID-19 than people who had never smoked.
Analysis also showed those with a genetic predisposition to being smokers had a 45% higher infection risk, and 60% higher hospitalization risk.
The authors wrote: “Overall, the congruence of observational analyses indicating associations with recent smoking behaviors and [Mendelian randomization] analyses indicating associations with lifelong predisposition to smoking and smoking heaviness support a causal effect of smoking on COVID-19 severity.”
In a linked podcast, lead researcher Dr. Ashley Clift, said: “Our results strongly suggest that smoking is related to your risk of getting severe COVID, and just as smoking affects your risk of heart disease, different cancers, and all those other conditions we know smoking is linked to, it appears that it’s the same for COVID. So now might be as good a time as any to quit cigarettes and quit smoking.”
These results contrast with previous studies that have suggested a protective effect of smoking against COVID-19. In a linked editorial, Anthony Laverty, PhD, and Christopher Millet, PhD, Imperial College London, wrote: “The idea that tobacco smoking may protect against COVID-19 was always an improbable one.”
A version of this article first appeared on Medscape.com.
Observational data was analyzed alongside hospital coronavirus test data and UK Biobank genetic information for the first time, and the findings are published in Thorax.
The data cover 421,469 people overall. Of these, 3.2% took a polymerase chain reaction swab test, 0.4% of these tested positive, 0.2% of them required hospitalization for COVID-19, and 0.1% of them died because of COVID-19.
When it came to smoking status, 59% had never smoked, 37% were ex-smokers, and 3% were current smokers.
Current smokers were 80% more likely to be admitted to hospital, and significantly more likely to die from COVID-19, than nonsmokers.
Time to quit
Heavy smokers who smoked more than 20 cigarettes a day were 6.11 times more likely to die from COVID-19 than people who had never smoked.
Analysis also showed those with a genetic predisposition to being smokers had a 45% higher infection risk, and 60% higher hospitalization risk.
The authors wrote: “Overall, the congruence of observational analyses indicating associations with recent smoking behaviors and [Mendelian randomization] analyses indicating associations with lifelong predisposition to smoking and smoking heaviness support a causal effect of smoking on COVID-19 severity.”
In a linked podcast, lead researcher Dr. Ashley Clift, said: “Our results strongly suggest that smoking is related to your risk of getting severe COVID, and just as smoking affects your risk of heart disease, different cancers, and all those other conditions we know smoking is linked to, it appears that it’s the same for COVID. So now might be as good a time as any to quit cigarettes and quit smoking.”
These results contrast with previous studies that have suggested a protective effect of smoking against COVID-19. In a linked editorial, Anthony Laverty, PhD, and Christopher Millet, PhD, Imperial College London, wrote: “The idea that tobacco smoking may protect against COVID-19 was always an improbable one.”
A version of this article first appeared on Medscape.com.
Observational data was analyzed alongside hospital coronavirus test data and UK Biobank genetic information for the first time, and the findings are published in Thorax.
The data cover 421,469 people overall. Of these, 3.2% took a polymerase chain reaction swab test, 0.4% of these tested positive, 0.2% of them required hospitalization for COVID-19, and 0.1% of them died because of COVID-19.
When it came to smoking status, 59% had never smoked, 37% were ex-smokers, and 3% were current smokers.
Current smokers were 80% more likely to be admitted to hospital, and significantly more likely to die from COVID-19, than nonsmokers.
Time to quit
Heavy smokers who smoked more than 20 cigarettes a day were 6.11 times more likely to die from COVID-19 than people who had never smoked.
Analysis also showed those with a genetic predisposition to being smokers had a 45% higher infection risk, and 60% higher hospitalization risk.
The authors wrote: “Overall, the congruence of observational analyses indicating associations with recent smoking behaviors and [Mendelian randomization] analyses indicating associations with lifelong predisposition to smoking and smoking heaviness support a causal effect of smoking on COVID-19 severity.”
In a linked podcast, lead researcher Dr. Ashley Clift, said: “Our results strongly suggest that smoking is related to your risk of getting severe COVID, and just as smoking affects your risk of heart disease, different cancers, and all those other conditions we know smoking is linked to, it appears that it’s the same for COVID. So now might be as good a time as any to quit cigarettes and quit smoking.”
These results contrast with previous studies that have suggested a protective effect of smoking against COVID-19. In a linked editorial, Anthony Laverty, PhD, and Christopher Millet, PhD, Imperial College London, wrote: “The idea that tobacco smoking may protect against COVID-19 was always an improbable one.”
A version of this article first appeared on Medscape.com.
Children and COVID: New cases topped 200,000 after 3 weeks of declines
Weekly COVID-19 cases in children dropped again, but the count remained above 200,000 for the fifth consecutive week, according to the American Academy of Pediatrics and the Children’s Hospital Association.
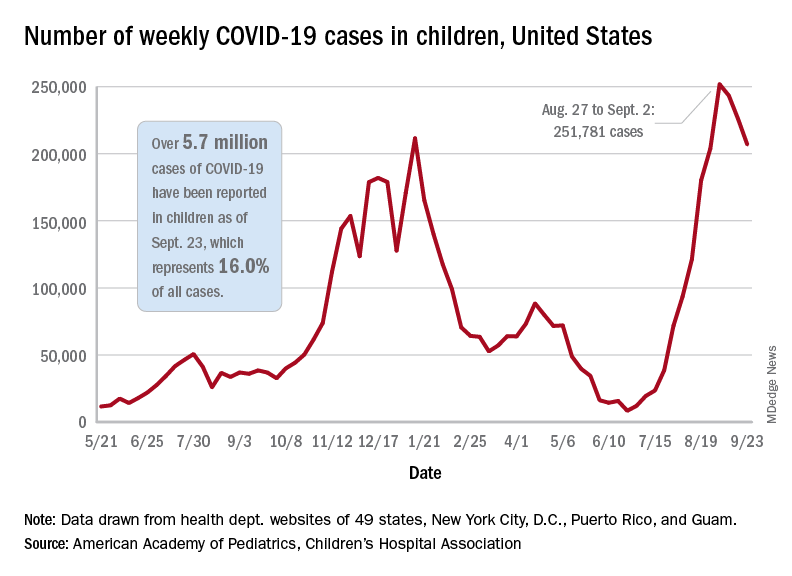
based on the data in the AAP/CHA joint weekly report on COVID in children.
In the most recent week, Sept. 17-23, there were almost 207,000 new cases of COVID-19 in children, which represented 26.7% of all cases reported in the 46 states that are currently posting data by age on their COVID dashboards, the AAP and CHA said. (New York has never reported such data by age, and Alabama, Nebraska, and Texas have not updated their websites since July 29, June 24, and Aug. 26, respectively.)
The decline in new vaccinations among children, however, began before the summer surge in new cases hit its peak – 251,781 during the week of Aug. 27 to Sept. 2 – and has continued for 7 straight weeks in children aged 12-17 years, based on data from the Centers for Disease Control and Prevention.
There were about 172,000 COVID vaccine initiations in children aged 12-17 for the week of Sept. 21-27, the lowest number since April, before it was approved for use in 12- to 15-year-olds. That figure is down by almost a third from the previous week and by more than two-thirds since early August, just before the decline in vaccinations began, according to the CDC’s COVID Data Tracker.
The cumulative vaccine situation looks like this: Just over 13 million children under age 18 years have received at least one dose as of Sept. 27, and almost 10.6 million are fully vaccinated. By age group, 53.9% of 12- to 15-year-olds and 61.6% of 16- to 17-year-olds have received at least one dose, with corresponding figures of 43.3% and 51.3% for full vaccination, the CDC said.
COVID-related hospital admissions also continue to fall after peaking at 0.51 children aged 0-17 per 100,000 population on Sept. 4. The admission rate was down to 0.45 per 100,000 as of Sept. 17, and the latest 7-day average (Sept. 19-25) was 258 admissions, compared with a peak of 371 for the week of Aug. 29 to Sept. 4, the CDC reported.
“Although we have seen slight improvements in COVID-19 volumes in the past week, we are at the beginning of an anticipated increase in” multi-inflammatory syndrome in children, Margaret Rush, MD, president of Monroe Carell Jr. Children’s Hospital at Vanderbilt University, Nashville, Tenn., said at a recent hearing of the House Committee on Energy and Commerce’s Oversight subcommittee. That increase would be expected to produce “a secondary wave of seriously ill children 3-6 weeks after acute infection peaks in the community,” the American Hospital Association said.
Meanwhile, Dr. Rush noted, there are signs that seasonal viruses are coming into play. “With the emergence of the Delta variant, we’ve experienced a steep increase in COVID-19 hospitalizations among children on top of an early surge of [respiratory syncytial virus], a serious respiratory illness we usually see in the winter months,” she said in a prepared statement before her testimony.
Weekly COVID-19 cases in children dropped again, but the count remained above 200,000 for the fifth consecutive week, according to the American Academy of Pediatrics and the Children’s Hospital Association.
based on the data in the AAP/CHA joint weekly report on COVID in children.
In the most recent week, Sept. 17-23, there were almost 207,000 new cases of COVID-19 in children, which represented 26.7% of all cases reported in the 46 states that are currently posting data by age on their COVID dashboards, the AAP and CHA said. (New York has never reported such data by age, and Alabama, Nebraska, and Texas have not updated their websites since July 29, June 24, and Aug. 26, respectively.)
The decline in new vaccinations among children, however, began before the summer surge in new cases hit its peak – 251,781 during the week of Aug. 27 to Sept. 2 – and has continued for 7 straight weeks in children aged 12-17 years, based on data from the Centers for Disease Control and Prevention.
There were about 172,000 COVID vaccine initiations in children aged 12-17 for the week of Sept. 21-27, the lowest number since April, before it was approved for use in 12- to 15-year-olds. That figure is down by almost a third from the previous week and by more than two-thirds since early August, just before the decline in vaccinations began, according to the CDC’s COVID Data Tracker.
The cumulative vaccine situation looks like this: Just over 13 million children under age 18 years have received at least one dose as of Sept. 27, and almost 10.6 million are fully vaccinated. By age group, 53.9% of 12- to 15-year-olds and 61.6% of 16- to 17-year-olds have received at least one dose, with corresponding figures of 43.3% and 51.3% for full vaccination, the CDC said.
COVID-related hospital admissions also continue to fall after peaking at 0.51 children aged 0-17 per 100,000 population on Sept. 4. The admission rate was down to 0.45 per 100,000 as of Sept. 17, and the latest 7-day average (Sept. 19-25) was 258 admissions, compared with a peak of 371 for the week of Aug. 29 to Sept. 4, the CDC reported.
“Although we have seen slight improvements in COVID-19 volumes in the past week, we are at the beginning of an anticipated increase in” multi-inflammatory syndrome in children, Margaret Rush, MD, president of Monroe Carell Jr. Children’s Hospital at Vanderbilt University, Nashville, Tenn., said at a recent hearing of the House Committee on Energy and Commerce’s Oversight subcommittee. That increase would be expected to produce “a secondary wave of seriously ill children 3-6 weeks after acute infection peaks in the community,” the American Hospital Association said.
Meanwhile, Dr. Rush noted, there are signs that seasonal viruses are coming into play. “With the emergence of the Delta variant, we’ve experienced a steep increase in COVID-19 hospitalizations among children on top of an early surge of [respiratory syncytial virus], a serious respiratory illness we usually see in the winter months,” she said in a prepared statement before her testimony.
Weekly COVID-19 cases in children dropped again, but the count remained above 200,000 for the fifth consecutive week, according to the American Academy of Pediatrics and the Children’s Hospital Association.
based on the data in the AAP/CHA joint weekly report on COVID in children.
In the most recent week, Sept. 17-23, there were almost 207,000 new cases of COVID-19 in children, which represented 26.7% of all cases reported in the 46 states that are currently posting data by age on their COVID dashboards, the AAP and CHA said. (New York has never reported such data by age, and Alabama, Nebraska, and Texas have not updated their websites since July 29, June 24, and Aug. 26, respectively.)
The decline in new vaccinations among children, however, began before the summer surge in new cases hit its peak – 251,781 during the week of Aug. 27 to Sept. 2 – and has continued for 7 straight weeks in children aged 12-17 years, based on data from the Centers for Disease Control and Prevention.
There were about 172,000 COVID vaccine initiations in children aged 12-17 for the week of Sept. 21-27, the lowest number since April, before it was approved for use in 12- to 15-year-olds. That figure is down by almost a third from the previous week and by more than two-thirds since early August, just before the decline in vaccinations began, according to the CDC’s COVID Data Tracker.
The cumulative vaccine situation looks like this: Just over 13 million children under age 18 years have received at least one dose as of Sept. 27, and almost 10.6 million are fully vaccinated. By age group, 53.9% of 12- to 15-year-olds and 61.6% of 16- to 17-year-olds have received at least one dose, with corresponding figures of 43.3% and 51.3% for full vaccination, the CDC said.
COVID-related hospital admissions also continue to fall after peaking at 0.51 children aged 0-17 per 100,000 population on Sept. 4. The admission rate was down to 0.45 per 100,000 as of Sept. 17, and the latest 7-day average (Sept. 19-25) was 258 admissions, compared with a peak of 371 for the week of Aug. 29 to Sept. 4, the CDC reported.
“Although we have seen slight improvements in COVID-19 volumes in the past week, we are at the beginning of an anticipated increase in” multi-inflammatory syndrome in children, Margaret Rush, MD, president of Monroe Carell Jr. Children’s Hospital at Vanderbilt University, Nashville, Tenn., said at a recent hearing of the House Committee on Energy and Commerce’s Oversight subcommittee. That increase would be expected to produce “a secondary wave of seriously ill children 3-6 weeks after acute infection peaks in the community,” the American Hospital Association said.
Meanwhile, Dr. Rush noted, there are signs that seasonal viruses are coming into play. “With the emergence of the Delta variant, we’ve experienced a steep increase in COVID-19 hospitalizations among children on top of an early surge of [respiratory syncytial virus], a serious respiratory illness we usually see in the winter months,” she said in a prepared statement before her testimony.
Polyethylene glycol linked to rare allergic reactions seen with mRNA COVID-19 vaccines
A common inert ingredient may be the culprit behind the rare allergic reactions reported among individuals who have received mRNA COVID-19 vaccines, according to investigators at a large regional health center that was among the first to administer the shots.
Blood samples from 10 of 11 individuals with suspected allergic reactions reacted to polyethylene glycol (PEG), a component of both the Pfizer and Moderna mRNA vaccines, according to a report in JAMA Network Open.
In total, only 22 individuals had suspected allergic reactions out of nearly 39,000 mRNA COVID-19 vaccine doses administered, the investigators reported, noting that the reactions were generally mild and all fully resolved.
Those findings should be reassuring to individuals who are reticent to sign up for a COVID-19 vaccine because of fear of an allergic reaction, said study senior author Kari Nadeau, MD, PhD, director of the Parker Center for Allergy and Asthma Research at Stanford (Calif.) University.
“We’re hoping that this word will get out and then that the companies could also think about making vaccines that have other products in them that don’t include polyethylene glycol,” Dr. Nadeau said in an interview.
PEG is a compound used in many products, including pharmaceuticals, cosmetics, and food. In the mRNA COVID-19 vaccines, PEG serves to stabilize the lipid nanoparticles that help protect and transport mRNA. However, its use in this setting has been linked to allergic reactions in this and previous studies.
No immunoglobulin E (IgE) antibodies to PEG were detected among the 22 individuals with suspected allergic reactions to mRNA COVID-19 vaccine, but PEG immunoglobulin G (IgG) was present. That suggests non-IgE mediated allergic reactions to PEG may be implicated for the majority of cases, Dr. Nadeau said.
This case series provides interesting new evidence to confirm previous reports that a mechanism other than the classic IgE-mediated allergic response is behind the suspected allergic reactions that are occurring after mRNA COVID-19 vaccine, said Aleena Banerji, MD, associate professor at Harvard Medical School, Boston, and clinical director of the Drug Allergy Program at Massachusetts General Hospital.
“We need to further understand the mechanism of these reactions, but what we know is that IGE mediated allergy to excipients like PEG is probably not the main cause,” Dr. Banerji, who was not involved in the study, said in an interview.
In a recent research letter published in JAMA Internal Medicine, Dr. Banerji and coauthors reported that all individuals with immediate suspected allergic reactions to mRNA COVID-19 vaccine went on to tolerate the second dose, with mild symptoms reported in the minority of patients (32 out of 159, or about 20%).
“Again, that is very consistent with not having an IgE-mediated allergy, so it seems to all be fitting with that picture,” Dr. Banerji said.
The case series by Dr. Nadeau and coauthors was based on review of nearly 39,000 mRNA COVID-19 vaccine doses administered between December 18, 2020 and January 26, 2021. Most mRNA vaccine recipients were Stanford-affiliated health care workers, according to the report.
Among recipients of those doses, they identified 148 individuals who had anaphylaxis-related ICD-10 codes recorded over the same time period. In a review of medical records, investigators pinpointed 22 individuals as having suspected allergy and invited them to participate in follow-up allergy testing.
A total of 11 individuals underwent skin prick testing, but none of them tested positive to PEG or to polysorbate 80, another excipient that has been linked to vaccine-related allergic reactions. One of the patients tested positive to the same mRNA vaccine they had previously received, according to the report.
Those same 11 individuals also underwent basophil activation testing (BAT). In contrast to the skin testing results, BAT results were positive for PEG in 10 of 11 cases (or 91%) and positive for their administered vaccine in all 11 cases, the report shows.
High levels of IgG to PEG were identified in blood samples of individuals with an allergy to the vaccine. Investigators said it’s possible that the BAT results were activated due to IgG via complement activation–related pseudoallergy, or CARPA, as has been hypothesized by some other investigators.
The negative skin prick testing results for PEG, which contrast with the positive BAT results to PEG, suggest that the former may not be appropriate for use as a predictive marker of potential vaccine allergy, according to Dr. Nadeau.
“The take-home message for doctors is to be careful,” she said. “Don’t assume that just because the person skin-tests negative to PEG or to the vaccine itself that you’re out of the woods, because the skin test would be often negative in those scenarios.”
The study was supported by a grants from the Asthma and Allergic Diseases Cooperative Research Centers, a grant from the National Institutes of Health, the National Institute of Allergy and Infectious Disease SARS Vaccine study, the Parker Foundation, the Crown Foundation, and the Sunshine Foundation. Dr. Nadeau reports numerous conflicts with various sources in the industry. Dr. Banerji has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A common inert ingredient may be the culprit behind the rare allergic reactions reported among individuals who have received mRNA COVID-19 vaccines, according to investigators at a large regional health center that was among the first to administer the shots.
Blood samples from 10 of 11 individuals with suspected allergic reactions reacted to polyethylene glycol (PEG), a component of both the Pfizer and Moderna mRNA vaccines, according to a report in JAMA Network Open.
In total, only 22 individuals had suspected allergic reactions out of nearly 39,000 mRNA COVID-19 vaccine doses administered, the investigators reported, noting that the reactions were generally mild and all fully resolved.
Those findings should be reassuring to individuals who are reticent to sign up for a COVID-19 vaccine because of fear of an allergic reaction, said study senior author Kari Nadeau, MD, PhD, director of the Parker Center for Allergy and Asthma Research at Stanford (Calif.) University.
“We’re hoping that this word will get out and then that the companies could also think about making vaccines that have other products in them that don’t include polyethylene glycol,” Dr. Nadeau said in an interview.
PEG is a compound used in many products, including pharmaceuticals, cosmetics, and food. In the mRNA COVID-19 vaccines, PEG serves to stabilize the lipid nanoparticles that help protect and transport mRNA. However, its use in this setting has been linked to allergic reactions in this and previous studies.
No immunoglobulin E (IgE) antibodies to PEG were detected among the 22 individuals with suspected allergic reactions to mRNA COVID-19 vaccine, but PEG immunoglobulin G (IgG) was present. That suggests non-IgE mediated allergic reactions to PEG may be implicated for the majority of cases, Dr. Nadeau said.
This case series provides interesting new evidence to confirm previous reports that a mechanism other than the classic IgE-mediated allergic response is behind the suspected allergic reactions that are occurring after mRNA COVID-19 vaccine, said Aleena Banerji, MD, associate professor at Harvard Medical School, Boston, and clinical director of the Drug Allergy Program at Massachusetts General Hospital.
“We need to further understand the mechanism of these reactions, but what we know is that IGE mediated allergy to excipients like PEG is probably not the main cause,” Dr. Banerji, who was not involved in the study, said in an interview.
In a recent research letter published in JAMA Internal Medicine, Dr. Banerji and coauthors reported that all individuals with immediate suspected allergic reactions to mRNA COVID-19 vaccine went on to tolerate the second dose, with mild symptoms reported in the minority of patients (32 out of 159, or about 20%).
“Again, that is very consistent with not having an IgE-mediated allergy, so it seems to all be fitting with that picture,” Dr. Banerji said.
The case series by Dr. Nadeau and coauthors was based on review of nearly 39,000 mRNA COVID-19 vaccine doses administered between December 18, 2020 and January 26, 2021. Most mRNA vaccine recipients were Stanford-affiliated health care workers, according to the report.
Among recipients of those doses, they identified 148 individuals who had anaphylaxis-related ICD-10 codes recorded over the same time period. In a review of medical records, investigators pinpointed 22 individuals as having suspected allergy and invited them to participate in follow-up allergy testing.
A total of 11 individuals underwent skin prick testing, but none of them tested positive to PEG or to polysorbate 80, another excipient that has been linked to vaccine-related allergic reactions. One of the patients tested positive to the same mRNA vaccine they had previously received, according to the report.
Those same 11 individuals also underwent basophil activation testing (BAT). In contrast to the skin testing results, BAT results were positive for PEG in 10 of 11 cases (or 91%) and positive for their administered vaccine in all 11 cases, the report shows.
High levels of IgG to PEG were identified in blood samples of individuals with an allergy to the vaccine. Investigators said it’s possible that the BAT results were activated due to IgG via complement activation–related pseudoallergy, or CARPA, as has been hypothesized by some other investigators.
The negative skin prick testing results for PEG, which contrast with the positive BAT results to PEG, suggest that the former may not be appropriate for use as a predictive marker of potential vaccine allergy, according to Dr. Nadeau.
“The take-home message for doctors is to be careful,” she said. “Don’t assume that just because the person skin-tests negative to PEG or to the vaccine itself that you’re out of the woods, because the skin test would be often negative in those scenarios.”
The study was supported by a grants from the Asthma and Allergic Diseases Cooperative Research Centers, a grant from the National Institutes of Health, the National Institute of Allergy and Infectious Disease SARS Vaccine study, the Parker Foundation, the Crown Foundation, and the Sunshine Foundation. Dr. Nadeau reports numerous conflicts with various sources in the industry. Dr. Banerji has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A common inert ingredient may be the culprit behind the rare allergic reactions reported among individuals who have received mRNA COVID-19 vaccines, according to investigators at a large regional health center that was among the first to administer the shots.
Blood samples from 10 of 11 individuals with suspected allergic reactions reacted to polyethylene glycol (PEG), a component of both the Pfizer and Moderna mRNA vaccines, according to a report in JAMA Network Open.
In total, only 22 individuals had suspected allergic reactions out of nearly 39,000 mRNA COVID-19 vaccine doses administered, the investigators reported, noting that the reactions were generally mild and all fully resolved.
Those findings should be reassuring to individuals who are reticent to sign up for a COVID-19 vaccine because of fear of an allergic reaction, said study senior author Kari Nadeau, MD, PhD, director of the Parker Center for Allergy and Asthma Research at Stanford (Calif.) University.
“We’re hoping that this word will get out and then that the companies could also think about making vaccines that have other products in them that don’t include polyethylene glycol,” Dr. Nadeau said in an interview.
PEG is a compound used in many products, including pharmaceuticals, cosmetics, and food. In the mRNA COVID-19 vaccines, PEG serves to stabilize the lipid nanoparticles that help protect and transport mRNA. However, its use in this setting has been linked to allergic reactions in this and previous studies.
No immunoglobulin E (IgE) antibodies to PEG were detected among the 22 individuals with suspected allergic reactions to mRNA COVID-19 vaccine, but PEG immunoglobulin G (IgG) was present. That suggests non-IgE mediated allergic reactions to PEG may be implicated for the majority of cases, Dr. Nadeau said.
This case series provides interesting new evidence to confirm previous reports that a mechanism other than the classic IgE-mediated allergic response is behind the suspected allergic reactions that are occurring after mRNA COVID-19 vaccine, said Aleena Banerji, MD, associate professor at Harvard Medical School, Boston, and clinical director of the Drug Allergy Program at Massachusetts General Hospital.
“We need to further understand the mechanism of these reactions, but what we know is that IGE mediated allergy to excipients like PEG is probably not the main cause,” Dr. Banerji, who was not involved in the study, said in an interview.
In a recent research letter published in JAMA Internal Medicine, Dr. Banerji and coauthors reported that all individuals with immediate suspected allergic reactions to mRNA COVID-19 vaccine went on to tolerate the second dose, with mild symptoms reported in the minority of patients (32 out of 159, or about 20%).
“Again, that is very consistent with not having an IgE-mediated allergy, so it seems to all be fitting with that picture,” Dr. Banerji said.
The case series by Dr. Nadeau and coauthors was based on review of nearly 39,000 mRNA COVID-19 vaccine doses administered between December 18, 2020 and January 26, 2021. Most mRNA vaccine recipients were Stanford-affiliated health care workers, according to the report.
Among recipients of those doses, they identified 148 individuals who had anaphylaxis-related ICD-10 codes recorded over the same time period. In a review of medical records, investigators pinpointed 22 individuals as having suspected allergy and invited them to participate in follow-up allergy testing.
A total of 11 individuals underwent skin prick testing, but none of them tested positive to PEG or to polysorbate 80, another excipient that has been linked to vaccine-related allergic reactions. One of the patients tested positive to the same mRNA vaccine they had previously received, according to the report.
Those same 11 individuals also underwent basophil activation testing (BAT). In contrast to the skin testing results, BAT results were positive for PEG in 10 of 11 cases (or 91%) and positive for their administered vaccine in all 11 cases, the report shows.
High levels of IgG to PEG were identified in blood samples of individuals with an allergy to the vaccine. Investigators said it’s possible that the BAT results were activated due to IgG via complement activation–related pseudoallergy, or CARPA, as has been hypothesized by some other investigators.
The negative skin prick testing results for PEG, which contrast with the positive BAT results to PEG, suggest that the former may not be appropriate for use as a predictive marker of potential vaccine allergy, according to Dr. Nadeau.
“The take-home message for doctors is to be careful,” she said. “Don’t assume that just because the person skin-tests negative to PEG or to the vaccine itself that you’re out of the woods, because the skin test would be often negative in those scenarios.”
The study was supported by a grants from the Asthma and Allergic Diseases Cooperative Research Centers, a grant from the National Institutes of Health, the National Institute of Allergy and Infectious Disease SARS Vaccine study, the Parker Foundation, the Crown Foundation, and the Sunshine Foundation. Dr. Nadeau reports numerous conflicts with various sources in the industry. Dr. Banerji has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Top questions answered about COVID-19 boosters for your patients
Confusion continues to circulate in the wake of decisions on booster doses of the Pfizer/BioNTech COVID-19 vaccine, all announced within 1 week. Many people – including those now eligible and those who officially have to wait for their shot at a third dose – have questions.

Multiple agencies are involved in the booster decisions, and they have put out multiple – and sometimes conflicting – messages about booster doses, leaving more questions than answers for many people.
On Sept. 22, the Food and Drug Administration granted an emergency use authorization (EUA) for a booster dose of the Pfizer mRNA COVID-19 vaccine for those 65 and older and those at high risk for severe illness from the coronavirus, including essential workers whose jobs increase their risk for infection – such as frontline health care workers.
The Centers for Disease Control and Prevention Director Rochelle Walensky, MD, then overruled advice from the agency’s Advisory Committee on Immunization Practices (ACIP) to recommend boosters for essential workers such as those working on the front lines during the pandemic.
As it stands now, the CDC recommends that the following groups should get a third dose of the Pfizer vaccine:
- People aged 65 years and older.
- People aged 18 years and older in long-term care settings.
- People aged 50-64 years with underlying medical conditions.
The CDC also recommends that the following groups may receive a booster shot of the Pfizer vaccine, based on their individual benefits and risks:
- People aged 18-49 years with underlying medical conditions.
- People aged 18-64 years at increased risk for COVID-19 exposure and transmission because of occupational or institutional setting.
The CDC currently considers the following groups at increased risk for COVID-19:
- First responders (health care workers, firefighters, police, congregate care staff).
- Education staff (teachers, support staff, day care workers).
- Food and agriculture workers.
- Manufacturing workers.
- Corrections workers.
- U.S. Postal Service workers.
- Public transit workers.
- Grocery store workers.
Health care professionals, among the most trusted sources of COVID-19 information, are likely to encounter a number of patients wondering how all this will work.
“It’s fantastic that boosters will be available for those who the data supports need [them],” Rachael Piltch-Loeb, PhD, said during a media briefing on Sept. 23, held between the FDA and CDC decisions.
“But we’re really in a place where we have a lot more questions and answers about what the next phase of the vaccine availability and updates are going to be in the United States,” added Dr. Piltch-Loeb, preparedness fellow in the division of policy translation and leadership development and a research associate in the department of biostatistics at the Harvard T. H. Chan School of Public Health in Boston.
1. What is the biggest concern you are hearing from patients about getting a booster?
“The biggest concerns are that everyone wants it and they don’t know where to get it. In health care’s defense, the CDC just figured out what to do,” said Janet Englund, MD, professor of pediatric infectious diseases and an infectious disease and virology expert at Seattle Children’s Hospital in Washington.
“Everyone thinks they should be eligible for a booster ... people in their 50s who are not yet 65+, people with young grandchildren, etc.,” she added. “I’m at Seattle Children’s Hospital, so people are asking about booster shots and about getting their children vaccinated.”
Boosters for all COVID-19 vaccines are completely free.
“All COVID-19 vaccines, including booster doses, will be provided free of charge to the U.S. population,” the CDC has said.
2. Will patients need to prove they meet eligibility criteria for a booster shot or will it be the honor system?
“No, patients will only need to attest that they fall into one of the high-risk groups for whom a booster vaccine is authorized,” said Robert Atmar, MD, professor of infectious diseases at Baylor College of Medicine in Houston.
Dr. Piltch-Loeb agreed. “It is likely to be an honor system. It is very unlikely that there will be punishments or other ramifications ... if doses are administered, beyond the approved usage.”
3. If a patient who had the Moderna or the Johnson and Johnson vaccination requests a booster, can health care workers give them Pfizer?
The short answer is no. “This only applies to individuals who have received the Pfizer vaccine,” Dr. Piltch-Loeb said.
More data will be needed before other vaccine boosters are authorized, she added.
“My understanding is the Moderna people have just recently submitted their information, all of their data to the FDA and J&J is in line to do that very shortly,” said William Schaffner, MD, professor of preventive medicine and infectious diseases at Vanderbilt University in Nashville, Tenn. “I would hope that within the next month to 6 weeks, we will get information about both of those vaccines,” Dr. Schaffner said.
4. When are the “mix-and-match” vaccine study results expected to come out?
“We expect that data from the study will be available in the coming weeks,” said Dr. Atmar, who is the national co-principal investigator of a mix-and-match booster trial launched in June 2021.
5. Are side effects of a booster vaccine expected to be about the same as what people experienced during their first or second immunization?
“I’m expecting the side effects will be similar to the second dose,” Dr. Englund said.
“The data presented ... at ACIP suggests that the side effects from the third shot are either the same or actually less than the first two shots,” said Carlos del Rio, MD, distinguished professor of medicine, epidemiology, and global health, and executive associate dean of Emory University School of Medicine at Grady Health System in Atlanta.
”Everyone reacts very differently to vaccines, regardless of vaccine type,” said Eric Ascher, MD, a family medicine physician at Lenox Hill Hospital in New York City. “I have had patients (as well as personal experience) where there were none to minimal symptoms, and others who felt they had a mild flu for 24 hours.”
“I expect no side effects greater than what was felt with you prior doses,” he said. “The vaccine is very safe and the benefit of vaccination outweighs the risks of any mild side effects.”
6. Is it unethical to give a booster to someone outside the approved groups if there are doses remaining at the end of the day in an open vial?
“Offering a booster shot to someone outside of approved groups if remaining doses will go to waste at the end of the day seems like a prudent decision, and relatively harmless action,” said Faith Fletcher, PhD, assistant professor at the Center for Medical Ethics and Health Policy at Baylor College of Medicine.
“However, if doses continue to fall in the laps of unapproved groups, we must evaluate the vaccine systems and structures that advantage some groups and disadvantage others,” she added. “We know that the distribution of COVID-19 vaccines has not been equitable – and some groups have been left behind.”
“I am not an ethicist and there are many competing concerns that this question addresses,” Dr. Atmar said. For example, “there is not a limitation of vaccine supply in the U.S., so that using leftover vaccine to prevent waste is no longer a major concern in the U.S.”
It could be more of a legal than ethical question, Dr. Atmar said. For an individual outside the authorized groups, legally, the FDA’s EUA for boosting does not allow the vaccine to be administered to this person, he said.
“The rationale for the restricted use in the EUA is that at this time the safety and risks associated with such administration are not known, and the benefits also have not been determined,” Dr. Atmar said. “Members of the ACIP raised concerns about other individuals who may potentially benefit from a booster but are not eligible and the importance of making boosters available to them, but from a legal standpoint – I am also not a lawyer, so this is my understanding – administration of the vaccine is limited to those identified in the EUA.”
7. What is the likelihood that one shot will combine COVID and flu protection in the near future?
It is not likely, Dr. Englund said. “The reason is that the flu vaccine changes so much, and it already has four different antigens. This is assuming we keep the same method of making the flu vaccine – the answer could be different if the flu vaccine becomes an mRNA vaccine in the future.”
Companies such as Moderna and Novavax are testing single-dose shots for COVID-19 and influenza, but they are still far from having anything ready for this flu season in the United States.
8. Is there any chance a booster shot distributed now will need to be redesigned for a future variant?
“Absolutely,” Dr. Englund said. “And a booster dose is the time we may want to consider re-engineering a vaccine.”
9. Do you think the FDA/CDC limitations on who is eligible for a booster was in any way influenced by the World Health Organization call for prioritizing shots for the unvaccinated in lower-resource countries?
“This is absolutely still a global problem,” Dr. Piltch-Loeb said. “We need to get more vaccine to more countries and more people as soon as possible, because if there’s anything we’ve seen about the variants it is that ... they can come from all different places.”
“That being said, I think that it is unlikely to change the course of action in the U.S.,” she added, when it comes to comparing the global need with the domestic policy priorities of the administration.
Dr. Atmar was more direct. “No,” he said. “The WHO recommends against boosting of anyone. The U.S. decisions about boosting those in this country who are eligible are aimed toward addressing perceived needs domestically at the same time that vaccines are being provided to other countries.
“The philosophy is to address both ‘needs’ at the same time,” Dr. Atmar said.
10. What does the future hold for booster shots?
“Predicting the future is really hard, especially when it involves COVID,” Dr. del Rio said.
“Having said that, COVID is not the flu, so I doubt there will be need for annual boosters. I think the population eligible for boosters will be expanded ... and the major population not addressed at this point is the people that received either Moderna or J&J [vaccines].”
Kelly Davis contributed to this feature. A version of this article first appeared on Medscape.com.
Confusion continues to circulate in the wake of decisions on booster doses of the Pfizer/BioNTech COVID-19 vaccine, all announced within 1 week. Many people – including those now eligible and those who officially have to wait for their shot at a third dose – have questions.
Multiple agencies are involved in the booster decisions, and they have put out multiple – and sometimes conflicting – messages about booster doses, leaving more questions than answers for many people.
On Sept. 22, the Food and Drug Administration granted an emergency use authorization (EUA) for a booster dose of the Pfizer mRNA COVID-19 vaccine for those 65 and older and those at high risk for severe illness from the coronavirus, including essential workers whose jobs increase their risk for infection – such as frontline health care workers.
The Centers for Disease Control and Prevention Director Rochelle Walensky, MD, then overruled advice from the agency’s Advisory Committee on Immunization Practices (ACIP) to recommend boosters for essential workers such as those working on the front lines during the pandemic.
As it stands now, the CDC recommends that the following groups should get a third dose of the Pfizer vaccine:
- People aged 65 years and older.
- People aged 18 years and older in long-term care settings.
- People aged 50-64 years with underlying medical conditions.
The CDC also recommends that the following groups may receive a booster shot of the Pfizer vaccine, based on their individual benefits and risks:
- People aged 18-49 years with underlying medical conditions.
- People aged 18-64 years at increased risk for COVID-19 exposure and transmission because of occupational or institutional setting.
The CDC currently considers the following groups at increased risk for COVID-19:
- First responders (health care workers, firefighters, police, congregate care staff).
- Education staff (teachers, support staff, day care workers).
- Food and agriculture workers.
- Manufacturing workers.
- Corrections workers.
- U.S. Postal Service workers.
- Public transit workers.
- Grocery store workers.
Health care professionals, among the most trusted sources of COVID-19 information, are likely to encounter a number of patients wondering how all this will work.
“It’s fantastic that boosters will be available for those who the data supports need [them],” Rachael Piltch-Loeb, PhD, said during a media briefing on Sept. 23, held between the FDA and CDC decisions.
“But we’re really in a place where we have a lot more questions and answers about what the next phase of the vaccine availability and updates are going to be in the United States,” added Dr. Piltch-Loeb, preparedness fellow in the division of policy translation and leadership development and a research associate in the department of biostatistics at the Harvard T. H. Chan School of Public Health in Boston.
1. What is the biggest concern you are hearing from patients about getting a booster?
“The biggest concerns are that everyone wants it and they don’t know where to get it. In health care’s defense, the CDC just figured out what to do,” said Janet Englund, MD, professor of pediatric infectious diseases and an infectious disease and virology expert at Seattle Children’s Hospital in Washington.
“Everyone thinks they should be eligible for a booster ... people in their 50s who are not yet 65+, people with young grandchildren, etc.,” she added. “I’m at Seattle Children’s Hospital, so people are asking about booster shots and about getting their children vaccinated.”
Boosters for all COVID-19 vaccines are completely free.
“All COVID-19 vaccines, including booster doses, will be provided free of charge to the U.S. population,” the CDC has said.
2. Will patients need to prove they meet eligibility criteria for a booster shot or will it be the honor system?
“No, patients will only need to attest that they fall into one of the high-risk groups for whom a booster vaccine is authorized,” said Robert Atmar, MD, professor of infectious diseases at Baylor College of Medicine in Houston.
Dr. Piltch-Loeb agreed. “It is likely to be an honor system. It is very unlikely that there will be punishments or other ramifications ... if doses are administered, beyond the approved usage.”
3. If a patient who had the Moderna or the Johnson and Johnson vaccination requests a booster, can health care workers give them Pfizer?
The short answer is no. “This only applies to individuals who have received the Pfizer vaccine,” Dr. Piltch-Loeb said.
More data will be needed before other vaccine boosters are authorized, she added.
“My understanding is the Moderna people have just recently submitted their information, all of their data to the FDA and J&J is in line to do that very shortly,” said William Schaffner, MD, professor of preventive medicine and infectious diseases at Vanderbilt University in Nashville, Tenn. “I would hope that within the next month to 6 weeks, we will get information about both of those vaccines,” Dr. Schaffner said.
4. When are the “mix-and-match” vaccine study results expected to come out?
“We expect that data from the study will be available in the coming weeks,” said Dr. Atmar, who is the national co-principal investigator of a mix-and-match booster trial launched in June 2021.
5. Are side effects of a booster vaccine expected to be about the same as what people experienced during their first or second immunization?
“I’m expecting the side effects will be similar to the second dose,” Dr. Englund said.
“The data presented ... at ACIP suggests that the side effects from the third shot are either the same or actually less than the first two shots,” said Carlos del Rio, MD, distinguished professor of medicine, epidemiology, and global health, and executive associate dean of Emory University School of Medicine at Grady Health System in Atlanta.
”Everyone reacts very differently to vaccines, regardless of vaccine type,” said Eric Ascher, MD, a family medicine physician at Lenox Hill Hospital in New York City. “I have had patients (as well as personal experience) where there were none to minimal symptoms, and others who felt they had a mild flu for 24 hours.”
“I expect no side effects greater than what was felt with you prior doses,” he said. “The vaccine is very safe and the benefit of vaccination outweighs the risks of any mild side effects.”
6. Is it unethical to give a booster to someone outside the approved groups if there are doses remaining at the end of the day in an open vial?
“Offering a booster shot to someone outside of approved groups if remaining doses will go to waste at the end of the day seems like a prudent decision, and relatively harmless action,” said Faith Fletcher, PhD, assistant professor at the Center for Medical Ethics and Health Policy at Baylor College of Medicine.
“However, if doses continue to fall in the laps of unapproved groups, we must evaluate the vaccine systems and structures that advantage some groups and disadvantage others,” she added. “We know that the distribution of COVID-19 vaccines has not been equitable – and some groups have been left behind.”
“I am not an ethicist and there are many competing concerns that this question addresses,” Dr. Atmar said. For example, “there is not a limitation of vaccine supply in the U.S., so that using leftover vaccine to prevent waste is no longer a major concern in the U.S.”
It could be more of a legal than ethical question, Dr. Atmar said. For an individual outside the authorized groups, legally, the FDA’s EUA for boosting does not allow the vaccine to be administered to this person, he said.
“The rationale for the restricted use in the EUA is that at this time the safety and risks associated with such administration are not known, and the benefits also have not been determined,” Dr. Atmar said. “Members of the ACIP raised concerns about other individuals who may potentially benefit from a booster but are not eligible and the importance of making boosters available to them, but from a legal standpoint – I am also not a lawyer, so this is my understanding – administration of the vaccine is limited to those identified in the EUA.”
7. What is the likelihood that one shot will combine COVID and flu protection in the near future?
It is not likely, Dr. Englund said. “The reason is that the flu vaccine changes so much, and it already has four different antigens. This is assuming we keep the same method of making the flu vaccine – the answer could be different if the flu vaccine becomes an mRNA vaccine in the future.”
Companies such as Moderna and Novavax are testing single-dose shots for COVID-19 and influenza, but they are still far from having anything ready for this flu season in the United States.
8. Is there any chance a booster shot distributed now will need to be redesigned for a future variant?
“Absolutely,” Dr. Englund said. “And a booster dose is the time we may want to consider re-engineering a vaccine.”
9. Do you think the FDA/CDC limitations on who is eligible for a booster was in any way influenced by the World Health Organization call for prioritizing shots for the unvaccinated in lower-resource countries?
“This is absolutely still a global problem,” Dr. Piltch-Loeb said. “We need to get more vaccine to more countries and more people as soon as possible, because if there’s anything we’ve seen about the variants it is that ... they can come from all different places.”
“That being said, I think that it is unlikely to change the course of action in the U.S.,” she added, when it comes to comparing the global need with the domestic policy priorities of the administration.
Dr. Atmar was more direct. “No,” he said. “The WHO recommends against boosting of anyone. The U.S. decisions about boosting those in this country who are eligible are aimed toward addressing perceived needs domestically at the same time that vaccines are being provided to other countries.
“The philosophy is to address both ‘needs’ at the same time,” Dr. Atmar said.
10. What does the future hold for booster shots?
“Predicting the future is really hard, especially when it involves COVID,” Dr. del Rio said.
“Having said that, COVID is not the flu, so I doubt there will be need for annual boosters. I think the population eligible for boosters will be expanded ... and the major population not addressed at this point is the people that received either Moderna or J&J [vaccines].”
Kelly Davis contributed to this feature. A version of this article first appeared on Medscape.com.
Confusion continues to circulate in the wake of decisions on booster doses of the Pfizer/BioNTech COVID-19 vaccine, all announced within 1 week. Many people – including those now eligible and those who officially have to wait for their shot at a third dose – have questions.
Multiple agencies are involved in the booster decisions, and they have put out multiple – and sometimes conflicting – messages about booster doses, leaving more questions than answers for many people.
On Sept. 22, the Food and Drug Administration granted an emergency use authorization (EUA) for a booster dose of the Pfizer mRNA COVID-19 vaccine for those 65 and older and those at high risk for severe illness from the coronavirus, including essential workers whose jobs increase their risk for infection – such as frontline health care workers.
The Centers for Disease Control and Prevention Director Rochelle Walensky, MD, then overruled advice from the agency’s Advisory Committee on Immunization Practices (ACIP) to recommend boosters for essential workers such as those working on the front lines during the pandemic.
As it stands now, the CDC recommends that the following groups should get a third dose of the Pfizer vaccine:
- People aged 65 years and older.
- People aged 18 years and older in long-term care settings.
- People aged 50-64 years with underlying medical conditions.
The CDC also recommends that the following groups may receive a booster shot of the Pfizer vaccine, based on their individual benefits and risks:
- People aged 18-49 years with underlying medical conditions.
- People aged 18-64 years at increased risk for COVID-19 exposure and transmission because of occupational or institutional setting.
The CDC currently considers the following groups at increased risk for COVID-19:
- First responders (health care workers, firefighters, police, congregate care staff).
- Education staff (teachers, support staff, day care workers).
- Food and agriculture workers.
- Manufacturing workers.
- Corrections workers.
- U.S. Postal Service workers.
- Public transit workers.
- Grocery store workers.
Health care professionals, among the most trusted sources of COVID-19 information, are likely to encounter a number of patients wondering how all this will work.
“It’s fantastic that boosters will be available for those who the data supports need [them],” Rachael Piltch-Loeb, PhD, said during a media briefing on Sept. 23, held between the FDA and CDC decisions.
“But we’re really in a place where we have a lot more questions and answers about what the next phase of the vaccine availability and updates are going to be in the United States,” added Dr. Piltch-Loeb, preparedness fellow in the division of policy translation and leadership development and a research associate in the department of biostatistics at the Harvard T. H. Chan School of Public Health in Boston.
1. What is the biggest concern you are hearing from patients about getting a booster?
“The biggest concerns are that everyone wants it and they don’t know where to get it. In health care’s defense, the CDC just figured out what to do,” said Janet Englund, MD, professor of pediatric infectious diseases and an infectious disease and virology expert at Seattle Children’s Hospital in Washington.
“Everyone thinks they should be eligible for a booster ... people in their 50s who are not yet 65+, people with young grandchildren, etc.,” she added. “I’m at Seattle Children’s Hospital, so people are asking about booster shots and about getting their children vaccinated.”
Boosters for all COVID-19 vaccines are completely free.
“All COVID-19 vaccines, including booster doses, will be provided free of charge to the U.S. population,” the CDC has said.
2. Will patients need to prove they meet eligibility criteria for a booster shot or will it be the honor system?
“No, patients will only need to attest that they fall into one of the high-risk groups for whom a booster vaccine is authorized,” said Robert Atmar, MD, professor of infectious diseases at Baylor College of Medicine in Houston.
Dr. Piltch-Loeb agreed. “It is likely to be an honor system. It is very unlikely that there will be punishments or other ramifications ... if doses are administered, beyond the approved usage.”
3. If a patient who had the Moderna or the Johnson and Johnson vaccination requests a booster, can health care workers give them Pfizer?
The short answer is no. “This only applies to individuals who have received the Pfizer vaccine,” Dr. Piltch-Loeb said.
More data will be needed before other vaccine boosters are authorized, she added.
“My understanding is the Moderna people have just recently submitted their information, all of their data to the FDA and J&J is in line to do that very shortly,” said William Schaffner, MD, professor of preventive medicine and infectious diseases at Vanderbilt University in Nashville, Tenn. “I would hope that within the next month to 6 weeks, we will get information about both of those vaccines,” Dr. Schaffner said.
4. When are the “mix-and-match” vaccine study results expected to come out?
“We expect that data from the study will be available in the coming weeks,” said Dr. Atmar, who is the national co-principal investigator of a mix-and-match booster trial launched in June 2021.
5. Are side effects of a booster vaccine expected to be about the same as what people experienced during their first or second immunization?
“I’m expecting the side effects will be similar to the second dose,” Dr. Englund said.
“The data presented ... at ACIP suggests that the side effects from the third shot are either the same or actually less than the first two shots,” said Carlos del Rio, MD, distinguished professor of medicine, epidemiology, and global health, and executive associate dean of Emory University School of Medicine at Grady Health System in Atlanta.
”Everyone reacts very differently to vaccines, regardless of vaccine type,” said Eric Ascher, MD, a family medicine physician at Lenox Hill Hospital in New York City. “I have had patients (as well as personal experience) where there were none to minimal symptoms, and others who felt they had a mild flu for 24 hours.”
“I expect no side effects greater than what was felt with you prior doses,” he said. “The vaccine is very safe and the benefit of vaccination outweighs the risks of any mild side effects.”
6. Is it unethical to give a booster to someone outside the approved groups if there are doses remaining at the end of the day in an open vial?
“Offering a booster shot to someone outside of approved groups if remaining doses will go to waste at the end of the day seems like a prudent decision, and relatively harmless action,” said Faith Fletcher, PhD, assistant professor at the Center for Medical Ethics and Health Policy at Baylor College of Medicine.
“However, if doses continue to fall in the laps of unapproved groups, we must evaluate the vaccine systems and structures that advantage some groups and disadvantage others,” she added. “We know that the distribution of COVID-19 vaccines has not been equitable – and some groups have been left behind.”
“I am not an ethicist and there are many competing concerns that this question addresses,” Dr. Atmar said. For example, “there is not a limitation of vaccine supply in the U.S., so that using leftover vaccine to prevent waste is no longer a major concern in the U.S.”
It could be more of a legal than ethical question, Dr. Atmar said. For an individual outside the authorized groups, legally, the FDA’s EUA for boosting does not allow the vaccine to be administered to this person, he said.
“The rationale for the restricted use in the EUA is that at this time the safety and risks associated with such administration are not known, and the benefits also have not been determined,” Dr. Atmar said. “Members of the ACIP raised concerns about other individuals who may potentially benefit from a booster but are not eligible and the importance of making boosters available to them, but from a legal standpoint – I am also not a lawyer, so this is my understanding – administration of the vaccine is limited to those identified in the EUA.”
7. What is the likelihood that one shot will combine COVID and flu protection in the near future?
It is not likely, Dr. Englund said. “The reason is that the flu vaccine changes so much, and it already has four different antigens. This is assuming we keep the same method of making the flu vaccine – the answer could be different if the flu vaccine becomes an mRNA vaccine in the future.”
Companies such as Moderna and Novavax are testing single-dose shots for COVID-19 and influenza, but they are still far from having anything ready for this flu season in the United States.
8. Is there any chance a booster shot distributed now will need to be redesigned for a future variant?
“Absolutely,” Dr. Englund said. “And a booster dose is the time we may want to consider re-engineering a vaccine.”
9. Do you think the FDA/CDC limitations on who is eligible for a booster was in any way influenced by the World Health Organization call for prioritizing shots for the unvaccinated in lower-resource countries?
“This is absolutely still a global problem,” Dr. Piltch-Loeb said. “We need to get more vaccine to more countries and more people as soon as possible, because if there’s anything we’ve seen about the variants it is that ... they can come from all different places.”
“That being said, I think that it is unlikely to change the course of action in the U.S.,” she added, when it comes to comparing the global need with the domestic policy priorities of the administration.
Dr. Atmar was more direct. “No,” he said. “The WHO recommends against boosting of anyone. The U.S. decisions about boosting those in this country who are eligible are aimed toward addressing perceived needs domestically at the same time that vaccines are being provided to other countries.
“The philosophy is to address both ‘needs’ at the same time,” Dr. Atmar said.
10. What does the future hold for booster shots?
“Predicting the future is really hard, especially when it involves COVID,” Dr. del Rio said.
“Having said that, COVID is not the flu, so I doubt there will be need for annual boosters. I think the population eligible for boosters will be expanded ... and the major population not addressed at this point is the people that received either Moderna or J&J [vaccines].”
Kelly Davis contributed to this feature. A version of this article first appeared on Medscape.com.
CDC chief overrules panel, OKs boosters for health care workers
The CDC’s Advisory Committee on Immunization Practices earlier Thursday voted to allow several groups of Americans to get a booster shot, but voted not to recommend it for adults age 18 to 64 who live or work in a place where the risk of COVID-19 is high. That would have included health care workers and other frontline employees.
But CDC Director Rochelle Walensky, MD, decided to reverse that recommendation and include the 18-to-64-year-olds in her final decision.
“As CDC Director, it is my job to recognize where our actions can have the greatest impact,” Dr. Walensky said in a statement late Thursday night, according to published reports. “At CDC, we are tasked with analyzing complex, often imperfect data to make concrete recommendations that optimize health. In a pandemic, even with uncertainty, we must take actions that we anticipate will do the greatest good.”
Dr. Walensky agreed with the rest of the advisory committee's decisions, which included recommendations that the following groups also be eligible for a booster shot:
- Adults ages 65 and up and residents of long-term care facilities
- Adults ages 50 to 64 who have an underlying medical condition that may increase their risk from a COVID infection
- Adults ages 18 to 49 who may be at increased risk from a COVID-19 infection because of an underlying medical condition, if a person feels like they need one based on a consideration of their individual benefit and risks.
About 26 million Americans are at least 6 months past the last dose of the Pfizer vaccines, making them eligible to receive a third dose. About 13.6 million of them are over the age of 65. Another 5.3 million are ages 50 to 64.
In making the recommendations, the committee left out healthcare workers. This was a departure from the Food and Drug Administration’s authorization which included boosters for those 65 and over, and for people 18 through 64 years of age who are at high risk for severe illness from the coronavirus, including essential workers – such as those in healthcare -- whose jobs increase their risk for infection.
This is the group Dr. Walensky added to the eligible list on her own.
Committee members “did not buy the need in occupational or institutional settings,” said William Schaffner, MD, an infectious disease specialist at Vanderbilt University in Nashville. Dr. Schaffner sits on the ACIP workgroup that considered the evidence behind boosters. He said that he would have voted yes to offer boosters to healthcare and other essential workers.
“There was a real split in the committee,” he said.
The vote on boosters for healthcare and other high-risk workers was rejected 9 to 6.
“I think that there is ample evidence that people such as healthcare workers do not have repeated exposure in the workplace,” said Beth Bell, MD, a clinical professor at the University of Washington. “They’re using PPE as they should and they’re following the other policies within the healthcare setting. There’s lots of evidence that suggest that health care workers who become infected become infected because of exposures in the community.”
She was not alone in feeling cautious.
“I think this is an extremely slippery slope,” said Sarah Long, MD, a pediatric infectious disease specialist at Drexel University in Philadelphia, before her vote to reject boosters for healthcare and other high-risk workers.
“We might as well just say, ‘Give it to everybody 18 and over.’ We have an extremely effective vaccine. It’s like saying it’s not working, and it is working.”
The committee saw data showing that all of the vaccines remain highly protective against hospitalization and death for all age groups, though protection against getting sick with COVID has waned slightly over time and with the dominance of the more contagious Delta variant. Those at highest risk for a severe breakthrough infection — those that cause hospitalization or death — are older adults.
How much will the U.S. benefit from boosters?
Some felt squeamish about broadly recommending boosters at all.
“We have too much hope on the line with these boosters,” said James Loehr, MD, who is a family physician in Ithaca, N.Y. Dr. Loehr said he felt the goal of giving boosters in the United States should be to decrease hospitalizations, and he felt they would, but that the impact would likely be smaller than appreciated.
Based on his calculations of the benefits of boosters for each age group, Dr. Loehr said if boosters were given to all 13 million seniors previously vaccinated with the Pfizer vaccine, we might prevent 200 hospitalizations a day, “which would be a lot,” he noted. But, he said, “considering that we have 10,000 hospitalizations a day now, it’s probably not that much.”
Others agreed.
“I really think this is a solution looking for a problem,” said Jason Goldman, MD, an associate professor at Florida Atlantic University who was representing the American College of Physicians. “You know, I don’t think it’s going to address the issue of the pandemic. I really think it’s just going to create more confusion on the provider from the position of implementation, and I really think it’s going really far afield of the data.”
ACIP Chair Grace Lee, MD, a pediatric infectious disease specialist at Stanford, said she had cared for children who had died of COVID.
“I can tell you that their family members really wished they had extra protection for their kids, because they weren’t symptomatic. Nobody else was sick at home,” she said.
Dr. Lee said for her, access was paramount, and she was in favor of expanding access to boosters for as many people as possible.
Next steps
People who were initially vaccinated with either Moderna or Johnson & Johnson vaccines are excluded from booster recommendations, something many on the committee were uncomfortable with.
The FDA is still considering Moderna’s application to market booster doses. Johnson & Johnson hasn’t yet applied to the FDA for permission to offer second doses in the United States.
While the ACIP’s recommendations are important, in this case, they may not have a huge practical effect, said Schaffner. The CDC has already approved third shots for people who are immunocompromised, and no proof of a medical condition is required to get one.
More than 2 million people have already gotten a third dose, he noted, and not all of them are immunocompromised.
“They have heard the president say that, you know, everybody should get a booster, and they’ve taken that at face value,” he said.
A version of this article first appeared on WebMD.com.
The CDC’s Advisory Committee on Immunization Practices earlier Thursday voted to allow several groups of Americans to get a booster shot, but voted not to recommend it for adults age 18 to 64 who live or work in a place where the risk of COVID-19 is high. That would have included health care workers and other frontline employees.
But CDC Director Rochelle Walensky, MD, decided to reverse that recommendation and include the 18-to-64-year-olds in her final decision.
“As CDC Director, it is my job to recognize where our actions can have the greatest impact,” Dr. Walensky said in a statement late Thursday night, according to published reports. “At CDC, we are tasked with analyzing complex, often imperfect data to make concrete recommendations that optimize health. In a pandemic, even with uncertainty, we must take actions that we anticipate will do the greatest good.”
Dr. Walensky agreed with the rest of the advisory committee's decisions, which included recommendations that the following groups also be eligible for a booster shot:
- Adults ages 65 and up and residents of long-term care facilities
- Adults ages 50 to 64 who have an underlying medical condition that may increase their risk from a COVID infection
- Adults ages 18 to 49 who may be at increased risk from a COVID-19 infection because of an underlying medical condition, if a person feels like they need one based on a consideration of their individual benefit and risks.
About 26 million Americans are at least 6 months past the last dose of the Pfizer vaccines, making them eligible to receive a third dose. About 13.6 million of them are over the age of 65. Another 5.3 million are ages 50 to 64.
In making the recommendations, the committee left out healthcare workers. This was a departure from the Food and Drug Administration’s authorization which included boosters for those 65 and over, and for people 18 through 64 years of age who are at high risk for severe illness from the coronavirus, including essential workers – such as those in healthcare -- whose jobs increase their risk for infection.
This is the group Dr. Walensky added to the eligible list on her own.
Committee members “did not buy the need in occupational or institutional settings,” said William Schaffner, MD, an infectious disease specialist at Vanderbilt University in Nashville. Dr. Schaffner sits on the ACIP workgroup that considered the evidence behind boosters. He said that he would have voted yes to offer boosters to healthcare and other essential workers.
“There was a real split in the committee,” he said.
The vote on boosters for healthcare and other high-risk workers was rejected 9 to 6.
“I think that there is ample evidence that people such as healthcare workers do not have repeated exposure in the workplace,” said Beth Bell, MD, a clinical professor at the University of Washington. “They’re using PPE as they should and they’re following the other policies within the healthcare setting. There’s lots of evidence that suggest that health care workers who become infected become infected because of exposures in the community.”
She was not alone in feeling cautious.
“I think this is an extremely slippery slope,” said Sarah Long, MD, a pediatric infectious disease specialist at Drexel University in Philadelphia, before her vote to reject boosters for healthcare and other high-risk workers.
“We might as well just say, ‘Give it to everybody 18 and over.’ We have an extremely effective vaccine. It’s like saying it’s not working, and it is working.”
The committee saw data showing that all of the vaccines remain highly protective against hospitalization and death for all age groups, though protection against getting sick with COVID has waned slightly over time and with the dominance of the more contagious Delta variant. Those at highest risk for a severe breakthrough infection — those that cause hospitalization or death — are older adults.
How much will the U.S. benefit from boosters?
Some felt squeamish about broadly recommending boosters at all.
“We have too much hope on the line with these boosters,” said James Loehr, MD, who is a family physician in Ithaca, N.Y. Dr. Loehr said he felt the goal of giving boosters in the United States should be to decrease hospitalizations, and he felt they would, but that the impact would likely be smaller than appreciated.
Based on his calculations of the benefits of boosters for each age group, Dr. Loehr said if boosters were given to all 13 million seniors previously vaccinated with the Pfizer vaccine, we might prevent 200 hospitalizations a day, “which would be a lot,” he noted. But, he said, “considering that we have 10,000 hospitalizations a day now, it’s probably not that much.”
Others agreed.
“I really think this is a solution looking for a problem,” said Jason Goldman, MD, an associate professor at Florida Atlantic University who was representing the American College of Physicians. “You know, I don’t think it’s going to address the issue of the pandemic. I really think it’s just going to create more confusion on the provider from the position of implementation, and I really think it’s going really far afield of the data.”
ACIP Chair Grace Lee, MD, a pediatric infectious disease specialist at Stanford, said she had cared for children who had died of COVID.
“I can tell you that their family members really wished they had extra protection for their kids, because they weren’t symptomatic. Nobody else was sick at home,” she said.
Dr. Lee said for her, access was paramount, and she was in favor of expanding access to boosters for as many people as possible.
Next steps
People who were initially vaccinated with either Moderna or Johnson & Johnson vaccines are excluded from booster recommendations, something many on the committee were uncomfortable with.
The FDA is still considering Moderna’s application to market booster doses. Johnson & Johnson hasn’t yet applied to the FDA for permission to offer second doses in the United States.
While the ACIP’s recommendations are important, in this case, they may not have a huge practical effect, said Schaffner. The CDC has already approved third shots for people who are immunocompromised, and no proof of a medical condition is required to get one.
More than 2 million people have already gotten a third dose, he noted, and not all of them are immunocompromised.
“They have heard the president say that, you know, everybody should get a booster, and they’ve taken that at face value,” he said.
A version of this article first appeared on WebMD.com.
The CDC’s Advisory Committee on Immunization Practices earlier Thursday voted to allow several groups of Americans to get a booster shot, but voted not to recommend it for adults age 18 to 64 who live or work in a place where the risk of COVID-19 is high. That would have included health care workers and other frontline employees.
But CDC Director Rochelle Walensky, MD, decided to reverse that recommendation and include the 18-to-64-year-olds in her final decision.
“As CDC Director, it is my job to recognize where our actions can have the greatest impact,” Dr. Walensky said in a statement late Thursday night, according to published reports. “At CDC, we are tasked with analyzing complex, often imperfect data to make concrete recommendations that optimize health. In a pandemic, even with uncertainty, we must take actions that we anticipate will do the greatest good.”
Dr. Walensky agreed with the rest of the advisory committee's decisions, which included recommendations that the following groups also be eligible for a booster shot:
- Adults ages 65 and up and residents of long-term care facilities
- Adults ages 50 to 64 who have an underlying medical condition that may increase their risk from a COVID infection
- Adults ages 18 to 49 who may be at increased risk from a COVID-19 infection because of an underlying medical condition, if a person feels like they need one based on a consideration of their individual benefit and risks.
About 26 million Americans are at least 6 months past the last dose of the Pfizer vaccines, making them eligible to receive a third dose. About 13.6 million of them are over the age of 65. Another 5.3 million are ages 50 to 64.
In making the recommendations, the committee left out healthcare workers. This was a departure from the Food and Drug Administration’s authorization which included boosters for those 65 and over, and for people 18 through 64 years of age who are at high risk for severe illness from the coronavirus, including essential workers – such as those in healthcare -- whose jobs increase their risk for infection.
This is the group Dr. Walensky added to the eligible list on her own.
Committee members “did not buy the need in occupational or institutional settings,” said William Schaffner, MD, an infectious disease specialist at Vanderbilt University in Nashville. Dr. Schaffner sits on the ACIP workgroup that considered the evidence behind boosters. He said that he would have voted yes to offer boosters to healthcare and other essential workers.
“There was a real split in the committee,” he said.
The vote on boosters for healthcare and other high-risk workers was rejected 9 to 6.
“I think that there is ample evidence that people such as healthcare workers do not have repeated exposure in the workplace,” said Beth Bell, MD, a clinical professor at the University of Washington. “They’re using PPE as they should and they’re following the other policies within the healthcare setting. There’s lots of evidence that suggest that health care workers who become infected become infected because of exposures in the community.”
She was not alone in feeling cautious.
“I think this is an extremely slippery slope,” said Sarah Long, MD, a pediatric infectious disease specialist at Drexel University in Philadelphia, before her vote to reject boosters for healthcare and other high-risk workers.
“We might as well just say, ‘Give it to everybody 18 and over.’ We have an extremely effective vaccine. It’s like saying it’s not working, and it is working.”
The committee saw data showing that all of the vaccines remain highly protective against hospitalization and death for all age groups, though protection against getting sick with COVID has waned slightly over time and with the dominance of the more contagious Delta variant. Those at highest risk for a severe breakthrough infection — those that cause hospitalization or death — are older adults.
How much will the U.S. benefit from boosters?
Some felt squeamish about broadly recommending boosters at all.
“We have too much hope on the line with these boosters,” said James Loehr, MD, who is a family physician in Ithaca, N.Y. Dr. Loehr said he felt the goal of giving boosters in the United States should be to decrease hospitalizations, and he felt they would, but that the impact would likely be smaller than appreciated.
Based on his calculations of the benefits of boosters for each age group, Dr. Loehr said if boosters were given to all 13 million seniors previously vaccinated with the Pfizer vaccine, we might prevent 200 hospitalizations a day, “which would be a lot,” he noted. But, he said, “considering that we have 10,000 hospitalizations a day now, it’s probably not that much.”
Others agreed.
“I really think this is a solution looking for a problem,” said Jason Goldman, MD, an associate professor at Florida Atlantic University who was representing the American College of Physicians. “You know, I don’t think it’s going to address the issue of the pandemic. I really think it’s just going to create more confusion on the provider from the position of implementation, and I really think it’s going really far afield of the data.”
ACIP Chair Grace Lee, MD, a pediatric infectious disease specialist at Stanford, said she had cared for children who had died of COVID.
“I can tell you that their family members really wished they had extra protection for their kids, because they weren’t symptomatic. Nobody else was sick at home,” she said.
Dr. Lee said for her, access was paramount, and she was in favor of expanding access to boosters for as many people as possible.
Next steps
People who were initially vaccinated with either Moderna or Johnson & Johnson vaccines are excluded from booster recommendations, something many on the committee were uncomfortable with.
The FDA is still considering Moderna’s application to market booster doses. Johnson & Johnson hasn’t yet applied to the FDA for permission to offer second doses in the United States.
While the ACIP’s recommendations are important, in this case, they may not have a huge practical effect, said Schaffner. The CDC has already approved third shots for people who are immunocompromised, and no proof of a medical condition is required to get one.
More than 2 million people have already gotten a third dose, he noted, and not all of them are immunocompromised.
“They have heard the president say that, you know, everybody should get a booster, and they’ve taken that at face value,” he said.
A version of this article first appeared on WebMD.com.