User login
Sooner may not be better: Study shows no benefit of urgent colonoscopy for lower GI bleeding
Clinical Question: In patients hospitalized for a lower gastrointestinal bleeding (LGIB), does an urgent colonoscopy (less than 24 hours after admission) result in any clinical benefits, compared with waiting for an elective colonoscopy?
Background: LGIB is a common cause of morbidity and mortality, often requiring hospitalization. While colonoscopy is necessary for appropriate work-up and treatment, it remains unclear if time to colonoscopy (urgent vs. elective) confers any clinical benefit in hospitalized patients.
Study Design: Systematic review and meta-analysis.
Setting: Twelve studies meeting inclusion criteria.
Synopsis: Computerized bibliography databases were searched for appropriate studies, and 12 met inclusion criteria, resulting in a total sample size of 10,172 patients in the urgent colonoscopy arm and 14,224 patients in the elective colonoscopy.
Outcome measures included bleeding source identified on colonoscopy, therapeutic endoscopic interventions performed, patients requiring blood transfusions, rebleeding, adverse events, and mortality.
Urgent colonoscopy was associated with increased use of endoscopic therapeutic intervention (relative risk, 1.70; 95% CI, 1.08-2.67). There were no significant differences in bleeding source localization (RR, 1.08; 95% CI, 0.92-1.25), adverse event rates (RR, 1.05; 95% CI, 0.65-1.71), rebleeding rates (RR, 1.14; 95% CI, 0.74-1.78), transfusion requirement (RR, 1.02; 95% CI, 0.73-1.41), or mortality (RR, 1.17; 95% CI, 0.45-3.02) between urgent and elective colonoscopy.
Limitations of the study comprise of inclusion of small number of studies, underpowered statistical analysis, and possible variation in quality assessment of articles evaluated.
Bottom Line: Urgent colonoscopy is safe and usually well tolerated in hospitalized patients with LGIB, but, compared with elective colonoscopy, there is no clear evidence it alters important clinical outcomes.
Reference: Kouanda AM, Somsouk M, Sewell JL, Day LW. Urgent colonoscopy in patients with lower GI bleeding: A systematic review and meta-analysis. Gastrointest Endosc. Published online Feb 4, 2017. doi: 10.1016/j.gie.2017.01.035.
Dr. Martin is clinical professor in the division of hospital medicine, department of medicine, University of California, San Diego.
Clinical Question: In patients hospitalized for a lower gastrointestinal bleeding (LGIB), does an urgent colonoscopy (less than 24 hours after admission) result in any clinical benefits, compared with waiting for an elective colonoscopy?
Background: LGIB is a common cause of morbidity and mortality, often requiring hospitalization. While colonoscopy is necessary for appropriate work-up and treatment, it remains unclear if time to colonoscopy (urgent vs. elective) confers any clinical benefit in hospitalized patients.
Study Design: Systematic review and meta-analysis.
Setting: Twelve studies meeting inclusion criteria.
Synopsis: Computerized bibliography databases were searched for appropriate studies, and 12 met inclusion criteria, resulting in a total sample size of 10,172 patients in the urgent colonoscopy arm and 14,224 patients in the elective colonoscopy.
Outcome measures included bleeding source identified on colonoscopy, therapeutic endoscopic interventions performed, patients requiring blood transfusions, rebleeding, adverse events, and mortality.
Urgent colonoscopy was associated with increased use of endoscopic therapeutic intervention (relative risk, 1.70; 95% CI, 1.08-2.67). There were no significant differences in bleeding source localization (RR, 1.08; 95% CI, 0.92-1.25), adverse event rates (RR, 1.05; 95% CI, 0.65-1.71), rebleeding rates (RR, 1.14; 95% CI, 0.74-1.78), transfusion requirement (RR, 1.02; 95% CI, 0.73-1.41), or mortality (RR, 1.17; 95% CI, 0.45-3.02) between urgent and elective colonoscopy.
Limitations of the study comprise of inclusion of small number of studies, underpowered statistical analysis, and possible variation in quality assessment of articles evaluated.
Bottom Line: Urgent colonoscopy is safe and usually well tolerated in hospitalized patients with LGIB, but, compared with elective colonoscopy, there is no clear evidence it alters important clinical outcomes.
Reference: Kouanda AM, Somsouk M, Sewell JL, Day LW. Urgent colonoscopy in patients with lower GI bleeding: A systematic review and meta-analysis. Gastrointest Endosc. Published online Feb 4, 2017. doi: 10.1016/j.gie.2017.01.035.
Dr. Martin is clinical professor in the division of hospital medicine, department of medicine, University of California, San Diego.
Clinical Question: In patients hospitalized for a lower gastrointestinal bleeding (LGIB), does an urgent colonoscopy (less than 24 hours after admission) result in any clinical benefits, compared with waiting for an elective colonoscopy?
Background: LGIB is a common cause of morbidity and mortality, often requiring hospitalization. While colonoscopy is necessary for appropriate work-up and treatment, it remains unclear if time to colonoscopy (urgent vs. elective) confers any clinical benefit in hospitalized patients.
Study Design: Systematic review and meta-analysis.
Setting: Twelve studies meeting inclusion criteria.
Synopsis: Computerized bibliography databases were searched for appropriate studies, and 12 met inclusion criteria, resulting in a total sample size of 10,172 patients in the urgent colonoscopy arm and 14,224 patients in the elective colonoscopy.
Outcome measures included bleeding source identified on colonoscopy, therapeutic endoscopic interventions performed, patients requiring blood transfusions, rebleeding, adverse events, and mortality.
Urgent colonoscopy was associated with increased use of endoscopic therapeutic intervention (relative risk, 1.70; 95% CI, 1.08-2.67). There were no significant differences in bleeding source localization (RR, 1.08; 95% CI, 0.92-1.25), adverse event rates (RR, 1.05; 95% CI, 0.65-1.71), rebleeding rates (RR, 1.14; 95% CI, 0.74-1.78), transfusion requirement (RR, 1.02; 95% CI, 0.73-1.41), or mortality (RR, 1.17; 95% CI, 0.45-3.02) between urgent and elective colonoscopy.
Limitations of the study comprise of inclusion of small number of studies, underpowered statistical analysis, and possible variation in quality assessment of articles evaluated.
Bottom Line: Urgent colonoscopy is safe and usually well tolerated in hospitalized patients with LGIB, but, compared with elective colonoscopy, there is no clear evidence it alters important clinical outcomes.
Reference: Kouanda AM, Somsouk M, Sewell JL, Day LW. Urgent colonoscopy in patients with lower GI bleeding: A systematic review and meta-analysis. Gastrointest Endosc. Published online Feb 4, 2017. doi: 10.1016/j.gie.2017.01.035.
Dr. Martin is clinical professor in the division of hospital medicine, department of medicine, University of California, San Diego.
Angiotensin II may improve vasopressors’ efficacy
WASHINGTON – Adding angiotensin II to available vasopressor therapies correlated with significantly improved arterial pressure in patients with catecholamine-resistant vasodilatory shock and less adverse effects, according to a study presented at the recent international conference of the American Thoracic Society.
In a double blind, controlled, phase III study, 70% of 163 patients given angiotensin II reached arterial pressure of at least 75 mm HG or improved by at least 10 mm Hg three hours later, compared with 23.4% of the 158 patients given a placebo (P less than .001).
Those in the angiotensin II group also saw a mean pressure increase of 12.5 mm Hg in the first 3 hours after initiating treatment, compared with 2.9 mm Hg in the placebo group (P less than .001), according to Ashish Khanna, MD, FCCP, of the Cleveland Clinic, and his fellow researchers (N Engl J Med. 2017 May 21. doi: 10.1056/NEJMoa1704154).
Current vasopressor therapies for vasodilatory patients are associated with dangerous side effects and a 30-day mortality rate of more than 50%, which is a major concern for patients who do not have many options to begin with, the researchers noted.
“Treatment options for patients with catecholamine-resistant vasodilatory shock are limited, and the treatments that are available are often associated with side effects,” said Dr. Khanna and his colleagues.
The researchers added the naturally occurring peptide hormone angiotensin II to vasodilatory patients’ treatment regimen in order to “more closely [mimic] natural physiologic responses to shock, which include increased secretion of catecholamines, vasopressin, and RAAS hormones.”
To test the efficacy of angiotensin II, researchers gathered patients with a median age of 64 years and a mean arterial pressure of 66.3 mm Hg.
Sepsis was the predominant cause of shock for 80.7% of the study’s participants.
Patients were injected with either 20 ng/kg of body weight per minute of angiotensin II or an equivalent dose of a placebo until mean arterial pressure reached 75 mm Hg. After 3 hours and 15 minutes of treatment, the dosages were adjusted to keep pressure between 65 and 75 mm Hg for the next 48 hours.
Among patients in the angiotensin II group, 67% of patients were able to decrease angiotensin II and vasopressor doses within 30 minutes of injection, according to researchers.
When researchers measured improvement using the cardiovascular Sequential Organ Failure Assessment, patients in the angiotensin II group saw an average decrease of 1.75 points, compared with 1.28 points in patients in the placebo group (P = .01) 48 hours after treatment.
The Sequential Organ Failure Assessment is scaled from 0-4, with higher scores indicating more severe organ failure.
When measuring for adverse affects, serious effects occurred in 60.7% of the angiotensin II patients, compared with in 67.1% of those in the placebo group.
At the 28-day mark, 75 angiotensin II patients (46.0%) died, compared with 85 patients (53.8%) of the placebo group.
This study was limited by the small sample size, “so the possibility of clinically important side effects attributable to angiotensin II therapy cannot be exuded,” the researches warned.
Also, the follow-up timeline of 28 days, may not have given researchers enough time to uncover the full extent of positive and negative long-term effects associated with angiotensin II.
This study was supported by La Jolla Pharmaceutical, from which multiple researchers reported receiving financial support in the form of personal fees and grants. Two of the researchers reported having patents related to administering angiotensin II and additional patents pending.
[email protected]
On Twitter @eaztweets
WASHINGTON – Adding angiotensin II to available vasopressor therapies correlated with significantly improved arterial pressure in patients with catecholamine-resistant vasodilatory shock and less adverse effects, according to a study presented at the recent international conference of the American Thoracic Society.
In a double blind, controlled, phase III study, 70% of 163 patients given angiotensin II reached arterial pressure of at least 75 mm HG or improved by at least 10 mm Hg three hours later, compared with 23.4% of the 158 patients given a placebo (P less than .001).
Those in the angiotensin II group also saw a mean pressure increase of 12.5 mm Hg in the first 3 hours after initiating treatment, compared with 2.9 mm Hg in the placebo group (P less than .001), according to Ashish Khanna, MD, FCCP, of the Cleveland Clinic, and his fellow researchers (N Engl J Med. 2017 May 21. doi: 10.1056/NEJMoa1704154).
Current vasopressor therapies for vasodilatory patients are associated with dangerous side effects and a 30-day mortality rate of more than 50%, which is a major concern for patients who do not have many options to begin with, the researchers noted.
“Treatment options for patients with catecholamine-resistant vasodilatory shock are limited, and the treatments that are available are often associated with side effects,” said Dr. Khanna and his colleagues.
The researchers added the naturally occurring peptide hormone angiotensin II to vasodilatory patients’ treatment regimen in order to “more closely [mimic] natural physiologic responses to shock, which include increased secretion of catecholamines, vasopressin, and RAAS hormones.”
To test the efficacy of angiotensin II, researchers gathered patients with a median age of 64 years and a mean arterial pressure of 66.3 mm Hg.
Sepsis was the predominant cause of shock for 80.7% of the study’s participants.
Patients were injected with either 20 ng/kg of body weight per minute of angiotensin II or an equivalent dose of a placebo until mean arterial pressure reached 75 mm Hg. After 3 hours and 15 minutes of treatment, the dosages were adjusted to keep pressure between 65 and 75 mm Hg for the next 48 hours.
Among patients in the angiotensin II group, 67% of patients were able to decrease angiotensin II and vasopressor doses within 30 minutes of injection, according to researchers.
When researchers measured improvement using the cardiovascular Sequential Organ Failure Assessment, patients in the angiotensin II group saw an average decrease of 1.75 points, compared with 1.28 points in patients in the placebo group (P = .01) 48 hours after treatment.
The Sequential Organ Failure Assessment is scaled from 0-4, with higher scores indicating more severe organ failure.
When measuring for adverse affects, serious effects occurred in 60.7% of the angiotensin II patients, compared with in 67.1% of those in the placebo group.
At the 28-day mark, 75 angiotensin II patients (46.0%) died, compared with 85 patients (53.8%) of the placebo group.
This study was limited by the small sample size, “so the possibility of clinically important side effects attributable to angiotensin II therapy cannot be exuded,” the researches warned.
Also, the follow-up timeline of 28 days, may not have given researchers enough time to uncover the full extent of positive and negative long-term effects associated with angiotensin II.
This study was supported by La Jolla Pharmaceutical, from which multiple researchers reported receiving financial support in the form of personal fees and grants. Two of the researchers reported having patents related to administering angiotensin II and additional patents pending.
[email protected]
On Twitter @eaztweets
WASHINGTON – Adding angiotensin II to available vasopressor therapies correlated with significantly improved arterial pressure in patients with catecholamine-resistant vasodilatory shock and less adverse effects, according to a study presented at the recent international conference of the American Thoracic Society.
In a double blind, controlled, phase III study, 70% of 163 patients given angiotensin II reached arterial pressure of at least 75 mm HG or improved by at least 10 mm Hg three hours later, compared with 23.4% of the 158 patients given a placebo (P less than .001).
Those in the angiotensin II group also saw a mean pressure increase of 12.5 mm Hg in the first 3 hours after initiating treatment, compared with 2.9 mm Hg in the placebo group (P less than .001), according to Ashish Khanna, MD, FCCP, of the Cleveland Clinic, and his fellow researchers (N Engl J Med. 2017 May 21. doi: 10.1056/NEJMoa1704154).
Current vasopressor therapies for vasodilatory patients are associated with dangerous side effects and a 30-day mortality rate of more than 50%, which is a major concern for patients who do not have many options to begin with, the researchers noted.
“Treatment options for patients with catecholamine-resistant vasodilatory shock are limited, and the treatments that are available are often associated with side effects,” said Dr. Khanna and his colleagues.
The researchers added the naturally occurring peptide hormone angiotensin II to vasodilatory patients’ treatment regimen in order to “more closely [mimic] natural physiologic responses to shock, which include increased secretion of catecholamines, vasopressin, and RAAS hormones.”
To test the efficacy of angiotensin II, researchers gathered patients with a median age of 64 years and a mean arterial pressure of 66.3 mm Hg.
Sepsis was the predominant cause of shock for 80.7% of the study’s participants.
Patients were injected with either 20 ng/kg of body weight per minute of angiotensin II or an equivalent dose of a placebo until mean arterial pressure reached 75 mm Hg. After 3 hours and 15 minutes of treatment, the dosages were adjusted to keep pressure between 65 and 75 mm Hg for the next 48 hours.
Among patients in the angiotensin II group, 67% of patients were able to decrease angiotensin II and vasopressor doses within 30 minutes of injection, according to researchers.
When researchers measured improvement using the cardiovascular Sequential Organ Failure Assessment, patients in the angiotensin II group saw an average decrease of 1.75 points, compared with 1.28 points in patients in the placebo group (P = .01) 48 hours after treatment.
The Sequential Organ Failure Assessment is scaled from 0-4, with higher scores indicating more severe organ failure.
When measuring for adverse affects, serious effects occurred in 60.7% of the angiotensin II patients, compared with in 67.1% of those in the placebo group.
At the 28-day mark, 75 angiotensin II patients (46.0%) died, compared with 85 patients (53.8%) of the placebo group.
This study was limited by the small sample size, “so the possibility of clinically important side effects attributable to angiotensin II therapy cannot be exuded,” the researches warned.
Also, the follow-up timeline of 28 days, may not have given researchers enough time to uncover the full extent of positive and negative long-term effects associated with angiotensin II.
This study was supported by La Jolla Pharmaceutical, from which multiple researchers reported receiving financial support in the form of personal fees and grants. Two of the researchers reported having patents related to administering angiotensin II and additional patents pending.
[email protected]
On Twitter @eaztweets
At ATS 2017
Key clinical point:
Major finding: In the first 3 hours, patients taking angiotensin II improved arterial pressure by an average of 12.5 mm Hg, compared with 2.9 mm Hg in patients taking the placebo (P less than .001)
Data source: Double blind, randomized, control trial of 321 patients with catecholamine-resistant vasodilatory shock collected from 75 intensive care units globally during May 2015-January 2017.
Disclosures: Multiple investigators reported receiving support from La Jolla Pharmaceutical and similar companies in the form of grants and/or personal fees. Two of the researchers reported having patents related to administering angiotensin II and additional patents pending.
Assessing the risks associated with MRI patients with a pacemaker or defibrillator
Clinical Question: What are the risks of nonthoracic MRI in patients with pacemakers or implantable cardioverter-defibrillators (ICD) who are not preapproved by the Food and Drug Administration for MRI scanning?
Background: Implantable cardiovascular devices could suffer heating in MRI magnetic fields leading to cardiac thermal injury and changes in pacing properties. The FDA approves “MRI-conditional devices” deemed safe for MRI, but up to six million patients worldwide (and two million in the United States) have non–MRI conditional devices.
Setting: U.S. Centers participating in the MagnaSafe registry.
Synopsis: Adults with non–MRI conditional pacemakers (1000 cases) or ICDs (500 cases) implanted in the thorax after 2001 were scanned with nonthoracic MRI at 1.5 Tesla. Patients with abandoned or inactive leads, other implantable devices, and low batteries and pacing-dependent patients with ICDs were excluded.
Devices were interrogated before each MRI and set to either no pacing or asynchronous pacing with all tachycardia and bradycardia therapies deactivated. Primary endpoints included immediate death, generator or lead failure, loss of capture in paced patients, new arrhythmia, and generator reset.
No patients suffered death or device or lead failure. Six patients developed self-terminating atrial arrhythmias, while an additional six had partial pacemaker electrical reset. Several devices had detectable changes in battery voltage, lead impedance, pacing threshold, and P- or R-wave amplitude without evident clinical significance. Multiple MRIs caused no increase in adverse outcomes. This study suggests that patients with non–MRI conditional devices may be at low risk from nonthoracic imaging if appropriately screened with temporary pacemaker function modification before MRI.
Bottom Line: Appropriately screened and prepared patients with non–MRI conditional thoracic pacemakers or ICDs may be at low risk for complications from nonthoracic MRI at 1.5 Tesla.
Reference: Russo RJ, Costa HS, Silva PD, et al. Assessing the risks associated with MRI in patients with a pacemaker or defibrillator. N Engl J Med. 2017;376:755-64.
Dr. Frederick is assistant clinical professor in the division of hospital Medicine, department of medicine, University of California, San Diego.
Clinical Question: What are the risks of nonthoracic MRI in patients with pacemakers or implantable cardioverter-defibrillators (ICD) who are not preapproved by the Food and Drug Administration for MRI scanning?
Background: Implantable cardiovascular devices could suffer heating in MRI magnetic fields leading to cardiac thermal injury and changes in pacing properties. The FDA approves “MRI-conditional devices” deemed safe for MRI, but up to six million patients worldwide (and two million in the United States) have non–MRI conditional devices.
Setting: U.S. Centers participating in the MagnaSafe registry.
Synopsis: Adults with non–MRI conditional pacemakers (1000 cases) or ICDs (500 cases) implanted in the thorax after 2001 were scanned with nonthoracic MRI at 1.5 Tesla. Patients with abandoned or inactive leads, other implantable devices, and low batteries and pacing-dependent patients with ICDs were excluded.
Devices were interrogated before each MRI and set to either no pacing or asynchronous pacing with all tachycardia and bradycardia therapies deactivated. Primary endpoints included immediate death, generator or lead failure, loss of capture in paced patients, new arrhythmia, and generator reset.
No patients suffered death or device or lead failure. Six patients developed self-terminating atrial arrhythmias, while an additional six had partial pacemaker electrical reset. Several devices had detectable changes in battery voltage, lead impedance, pacing threshold, and P- or R-wave amplitude without evident clinical significance. Multiple MRIs caused no increase in adverse outcomes. This study suggests that patients with non–MRI conditional devices may be at low risk from nonthoracic imaging if appropriately screened with temporary pacemaker function modification before MRI.
Bottom Line: Appropriately screened and prepared patients with non–MRI conditional thoracic pacemakers or ICDs may be at low risk for complications from nonthoracic MRI at 1.5 Tesla.
Reference: Russo RJ, Costa HS, Silva PD, et al. Assessing the risks associated with MRI in patients with a pacemaker or defibrillator. N Engl J Med. 2017;376:755-64.
Dr. Frederick is assistant clinical professor in the division of hospital Medicine, department of medicine, University of California, San Diego.
Clinical Question: What are the risks of nonthoracic MRI in patients with pacemakers or implantable cardioverter-defibrillators (ICD) who are not preapproved by the Food and Drug Administration for MRI scanning?
Background: Implantable cardiovascular devices could suffer heating in MRI magnetic fields leading to cardiac thermal injury and changes in pacing properties. The FDA approves “MRI-conditional devices” deemed safe for MRI, but up to six million patients worldwide (and two million in the United States) have non–MRI conditional devices.
Setting: U.S. Centers participating in the MagnaSafe registry.
Synopsis: Adults with non–MRI conditional pacemakers (1000 cases) or ICDs (500 cases) implanted in the thorax after 2001 were scanned with nonthoracic MRI at 1.5 Tesla. Patients with abandoned or inactive leads, other implantable devices, and low batteries and pacing-dependent patients with ICDs were excluded.
Devices were interrogated before each MRI and set to either no pacing or asynchronous pacing with all tachycardia and bradycardia therapies deactivated. Primary endpoints included immediate death, generator or lead failure, loss of capture in paced patients, new arrhythmia, and generator reset.
No patients suffered death or device or lead failure. Six patients developed self-terminating atrial arrhythmias, while an additional six had partial pacemaker electrical reset. Several devices had detectable changes in battery voltage, lead impedance, pacing threshold, and P- or R-wave amplitude without evident clinical significance. Multiple MRIs caused no increase in adverse outcomes. This study suggests that patients with non–MRI conditional devices may be at low risk from nonthoracic imaging if appropriately screened with temporary pacemaker function modification before MRI.
Bottom Line: Appropriately screened and prepared patients with non–MRI conditional thoracic pacemakers or ICDs may be at low risk for complications from nonthoracic MRI at 1.5 Tesla.
Reference: Russo RJ, Costa HS, Silva PD, et al. Assessing the risks associated with MRI in patients with a pacemaker or defibrillator. N Engl J Med. 2017;376:755-64.
Dr. Frederick is assistant clinical professor in the division of hospital Medicine, department of medicine, University of California, San Diego.
Hospitalists and cost control in the U.S. health care system
The rising cost of care has been a major concern in the U.S. health care system. In 1990, about $714 million was spent on health care. In 2010, the cost had risen exponentially to about $2.6 trillion.1 An estimated $750 billion dollars is attributed to health care waste.2
Health care waste includes spending on laboratory testing, diagnostic imaging, procedures or other treatments. Below is a list of the various sources that contribute to health care spending waste:2
1. Unnecessary Services ($210 billion)
2. Excessive Administrative Costs (190 billion)
3. Inefficient Service Delivery ($130 billion)
4. Overpricing ($105 billion)
5. Fraud ($75 billion)
6. Treatment for services that could have been prevented ($55 billion)

Reducing the cost of care
The predominant fee-for-service method of reimbursement does not encourage hospitals or providers to try to control areas of waste. One strategy that puts pressure on the providers of health care to control these areas of waste is the bundled payment system. Bundled payment systems deter unnecessary testing and procedures and encourage care coordination between care providers to promote efficiency.
As hospitalists, we play a key role in the bundled payment arena. Hospitalists are strategically placed to ensure that each episode of care is provided in the most cost-efficient way possible without sacrificing quality.
Training about the evidence supporting bundled payments can be incorporated into medical school and the residency curriculum. Hospitalists can serve as educators for trainees regarding the benefits of bundled payments. This will help drive sustainability by making sure new doctors entering the health field are already equipped with knowledge about bundled payments and their advantages.
Hospitalists can also help spur innovation by engaging with hospital leadership to develop new bundled systems. Payment incentives to organizations that participate will help to drive hospitalist engagement. Hospitalists can also advocate for the development of a risk adjustment system to ensure that each patient’s severity is reflected in the payment. This will allow for more buy-in by hospitals and providers.
Improving the quality of care
The Institute of Medicine published a report that made recommendations for improving the quality of the U.S. health care system by identifying six dimensions that need to be addressed:
1. Safety
2. Effectiveness
3. Patient-centeredness
4. Timeliness
5. Efficiency
6. Equity
The Value Based Purchasing program aims to address these dimensions. The fee-for-service system does not provide an incentive to provide quality care, similar to the way it does not drive cost-conscious care. By linking reimbursement to quality care, hospitals and providers have a significant incentive to ensure that their patients receive high quality care. The passage of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) is another step in the direction of rewarding providers for quality of care rendered, not just quantity.
Role of hospitalists
Again, hospitalists should serve as educators about the importance of value based purchasing on quality outcomes,\ and its potential for cost savings through rendering appropriate and effective care.
Hospitalists should advocate for expanding value based purchasing across all payers. This will encourage providers to treat all their patients the same, with the expectation of improving quality of care for all patients and not just a limited insurance pool.
Hospitalists can also advocate for the utilization of the same measure for determining quality across all payers. This will allow for more efficient administrative efforts by eliminating the time used to report different measures to different insurance companies.
Unfortunately, the digital era has not made the same advances in the field of medicine as it has in other areas of life. As hospitalists, our clinical perspective puts us in a position of leadership in the area of informatics. We are uniquely qualified to exploit the power of the hospital’s information technology service and push it to its full potential.
Dr. Arole is chief hospitalist, Griffin Faculty Physicians, at Griffin Hospital in Derby, Conn.
References
1. The Healthcare Imperative: Lowering Costs and Improving Outcomes – Workshop Series Summary. 2011 Feb 24. The Institute of Medicine.
2. Health Affairs Policy Brief; Reducing Waste in Health Care. http://www.healthaffairs.org/healthpolicybriefs/brief.
The rising cost of care has been a major concern in the U.S. health care system. In 1990, about $714 million was spent on health care. In 2010, the cost had risen exponentially to about $2.6 trillion.1 An estimated $750 billion dollars is attributed to health care waste.2
Health care waste includes spending on laboratory testing, diagnostic imaging, procedures or other treatments. Below is a list of the various sources that contribute to health care spending waste:2
1. Unnecessary Services ($210 billion)
2. Excessive Administrative Costs (190 billion)
3. Inefficient Service Delivery ($130 billion)
4. Overpricing ($105 billion)
5. Fraud ($75 billion)
6. Treatment for services that could have been prevented ($55 billion)
Reducing the cost of care
The predominant fee-for-service method of reimbursement does not encourage hospitals or providers to try to control areas of waste. One strategy that puts pressure on the providers of health care to control these areas of waste is the bundled payment system. Bundled payment systems deter unnecessary testing and procedures and encourage care coordination between care providers to promote efficiency.
As hospitalists, we play a key role in the bundled payment arena. Hospitalists are strategically placed to ensure that each episode of care is provided in the most cost-efficient way possible without sacrificing quality.
Training about the evidence supporting bundled payments can be incorporated into medical school and the residency curriculum. Hospitalists can serve as educators for trainees regarding the benefits of bundled payments. This will help drive sustainability by making sure new doctors entering the health field are already equipped with knowledge about bundled payments and their advantages.
Hospitalists can also help spur innovation by engaging with hospital leadership to develop new bundled systems. Payment incentives to organizations that participate will help to drive hospitalist engagement. Hospitalists can also advocate for the development of a risk adjustment system to ensure that each patient’s severity is reflected in the payment. This will allow for more buy-in by hospitals and providers.
Improving the quality of care
The Institute of Medicine published a report that made recommendations for improving the quality of the U.S. health care system by identifying six dimensions that need to be addressed:
1. Safety
2. Effectiveness
3. Patient-centeredness
4. Timeliness
5. Efficiency
6. Equity
The Value Based Purchasing program aims to address these dimensions. The fee-for-service system does not provide an incentive to provide quality care, similar to the way it does not drive cost-conscious care. By linking reimbursement to quality care, hospitals and providers have a significant incentive to ensure that their patients receive high quality care. The passage of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) is another step in the direction of rewarding providers for quality of care rendered, not just quantity.
Role of hospitalists
Again, hospitalists should serve as educators about the importance of value based purchasing on quality outcomes,\ and its potential for cost savings through rendering appropriate and effective care.
Hospitalists should advocate for expanding value based purchasing across all payers. This will encourage providers to treat all their patients the same, with the expectation of improving quality of care for all patients and not just a limited insurance pool.
Hospitalists can also advocate for the utilization of the same measure for determining quality across all payers. This will allow for more efficient administrative efforts by eliminating the time used to report different measures to different insurance companies.
Unfortunately, the digital era has not made the same advances in the field of medicine as it has in other areas of life. As hospitalists, our clinical perspective puts us in a position of leadership in the area of informatics. We are uniquely qualified to exploit the power of the hospital’s information technology service and push it to its full potential.
Dr. Arole is chief hospitalist, Griffin Faculty Physicians, at Griffin Hospital in Derby, Conn.
References
1. The Healthcare Imperative: Lowering Costs and Improving Outcomes – Workshop Series Summary. 2011 Feb 24. The Institute of Medicine.
2. Health Affairs Policy Brief; Reducing Waste in Health Care. http://www.healthaffairs.org/healthpolicybriefs/brief.
The rising cost of care has been a major concern in the U.S. health care system. In 1990, about $714 million was spent on health care. In 2010, the cost had risen exponentially to about $2.6 trillion.1 An estimated $750 billion dollars is attributed to health care waste.2
Health care waste includes spending on laboratory testing, diagnostic imaging, procedures or other treatments. Below is a list of the various sources that contribute to health care spending waste:2
1. Unnecessary Services ($210 billion)
2. Excessive Administrative Costs (190 billion)
3. Inefficient Service Delivery ($130 billion)
4. Overpricing ($105 billion)
5. Fraud ($75 billion)
6. Treatment for services that could have been prevented ($55 billion)
Reducing the cost of care
The predominant fee-for-service method of reimbursement does not encourage hospitals or providers to try to control areas of waste. One strategy that puts pressure on the providers of health care to control these areas of waste is the bundled payment system. Bundled payment systems deter unnecessary testing and procedures and encourage care coordination between care providers to promote efficiency.
As hospitalists, we play a key role in the bundled payment arena. Hospitalists are strategically placed to ensure that each episode of care is provided in the most cost-efficient way possible without sacrificing quality.
Training about the evidence supporting bundled payments can be incorporated into medical school and the residency curriculum. Hospitalists can serve as educators for trainees regarding the benefits of bundled payments. This will help drive sustainability by making sure new doctors entering the health field are already equipped with knowledge about bundled payments and their advantages.
Hospitalists can also help spur innovation by engaging with hospital leadership to develop new bundled systems. Payment incentives to organizations that participate will help to drive hospitalist engagement. Hospitalists can also advocate for the development of a risk adjustment system to ensure that each patient’s severity is reflected in the payment. This will allow for more buy-in by hospitals and providers.
Improving the quality of care
The Institute of Medicine published a report that made recommendations for improving the quality of the U.S. health care system by identifying six dimensions that need to be addressed:
1. Safety
2. Effectiveness
3. Patient-centeredness
4. Timeliness
5. Efficiency
6. Equity
The Value Based Purchasing program aims to address these dimensions. The fee-for-service system does not provide an incentive to provide quality care, similar to the way it does not drive cost-conscious care. By linking reimbursement to quality care, hospitals and providers have a significant incentive to ensure that their patients receive high quality care. The passage of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) is another step in the direction of rewarding providers for quality of care rendered, not just quantity.
Role of hospitalists
Again, hospitalists should serve as educators about the importance of value based purchasing on quality outcomes,\ and its potential for cost savings through rendering appropriate and effective care.
Hospitalists should advocate for expanding value based purchasing across all payers. This will encourage providers to treat all their patients the same, with the expectation of improving quality of care for all patients and not just a limited insurance pool.
Hospitalists can also advocate for the utilization of the same measure for determining quality across all payers. This will allow for more efficient administrative efforts by eliminating the time used to report different measures to different insurance companies.
Unfortunately, the digital era has not made the same advances in the field of medicine as it has in other areas of life. As hospitalists, our clinical perspective puts us in a position of leadership in the area of informatics. We are uniquely qualified to exploit the power of the hospital’s information technology service and push it to its full potential.
Dr. Arole is chief hospitalist, Griffin Faculty Physicians, at Griffin Hospital in Derby, Conn.
References
1. The Healthcare Imperative: Lowering Costs and Improving Outcomes – Workshop Series Summary. 2011 Feb 24. The Institute of Medicine.
2. Health Affairs Policy Brief; Reducing Waste in Health Care. http://www.healthaffairs.org/healthpolicybriefs/brief.
Application of the MASCC and CISNE risk-stratification scores to identify low-risk febrile neutropenic patients in the emergency department
Clinical Question: Does the Multinational Association for Supportive Care in Cancer (MASCC) or Clinical Index of Stable Febrile Neutropenia (CISNE) risk-stratification score better predict patient outcomes in patients presenting to emergency departments with febrile neutropenia?
Background: Risk-stratification metrics like the MASCC and CISNE identify subsets of relatively low-risk patients with febrile neutropenia after chemotherapy for treatment at home with empiric oral antibiotic therapy and close follow-up while awaiting results of infectious work-up. Prior studies have validated these tools for admitted, but not for ED, patients.

Setting: Two academic ED at National Institutes of Health–designated cancer centers.
Synopsis: Included patients (n = 230) were at least 16 years old with a documented fever of 38° C or greater related to chemotherapy and an absolute neutrophil count less than 1,000 cells/μL. MASCC and CISNE risk stratification scores were calculated based on the documentation from the ED and recent oncology clinic visits. Outcome measures included length of stay, upgrade in level of care, positive blood cultures, clinical deterioration, and death and were assessed for up to 30 days following discharge. Low-risk patients were defined as those who experienced no negative endpoints. The CISNE score was more specific than the MASCC in identifying low-risk patients (98.1% vs. 54.2%), suggesting that the CISNE may be useful for hospitalists in identifying patients who may be safely discharged with oral antibiotics and close follow-up.
Limitations include possible misclassification bias from indirect assessment of symptom severity, lack of recent ECOG scores for six patients in the CISNE arm, and possible undocumented symptoms during ED evaluation required for subsequent score calculation. Additionally, most patients in this study reported mild symptoms which weighted their MASCC classification toward low-risk.
Bottom Line: The CISNE score may aid in risk-stratification of patients with chemotherapy-related febrile neutropenia presenting to the ED.
Reference: Coyne CJ, Le V, Brennan JJ, et al. Application of the MASCC and CISNE risk-stratification scores to identify low-risk febrile neutropenic patients in the emergency department. Ann Emerg Med. Published online 29 Dec 2016. doi: 10.1016/j.annemergmed.2016.11.007.
Dr. Frederick is assistant clinical professor in the division of hospital Medicine, department of medicine, University of California, San Diego.
Clinical Question: Does the Multinational Association for Supportive Care in Cancer (MASCC) or Clinical Index of Stable Febrile Neutropenia (CISNE) risk-stratification score better predict patient outcomes in patients presenting to emergency departments with febrile neutropenia?
Background: Risk-stratification metrics like the MASCC and CISNE identify subsets of relatively low-risk patients with febrile neutropenia after chemotherapy for treatment at home with empiric oral antibiotic therapy and close follow-up while awaiting results of infectious work-up. Prior studies have validated these tools for admitted, but not for ED, patients.
Setting: Two academic ED at National Institutes of Health–designated cancer centers.
Synopsis: Included patients (n = 230) were at least 16 years old with a documented fever of 38° C or greater related to chemotherapy and an absolute neutrophil count less than 1,000 cells/μL. MASCC and CISNE risk stratification scores were calculated based on the documentation from the ED and recent oncology clinic visits. Outcome measures included length of stay, upgrade in level of care, positive blood cultures, clinical deterioration, and death and were assessed for up to 30 days following discharge. Low-risk patients were defined as those who experienced no negative endpoints. The CISNE score was more specific than the MASCC in identifying low-risk patients (98.1% vs. 54.2%), suggesting that the CISNE may be useful for hospitalists in identifying patients who may be safely discharged with oral antibiotics and close follow-up.
Limitations include possible misclassification bias from indirect assessment of symptom severity, lack of recent ECOG scores for six patients in the CISNE arm, and possible undocumented symptoms during ED evaluation required for subsequent score calculation. Additionally, most patients in this study reported mild symptoms which weighted their MASCC classification toward low-risk.
Bottom Line: The CISNE score may aid in risk-stratification of patients with chemotherapy-related febrile neutropenia presenting to the ED.
Reference: Coyne CJ, Le V, Brennan JJ, et al. Application of the MASCC and CISNE risk-stratification scores to identify low-risk febrile neutropenic patients in the emergency department. Ann Emerg Med. Published online 29 Dec 2016. doi: 10.1016/j.annemergmed.2016.11.007.
Dr. Frederick is assistant clinical professor in the division of hospital Medicine, department of medicine, University of California, San Diego.
Clinical Question: Does the Multinational Association for Supportive Care in Cancer (MASCC) or Clinical Index of Stable Febrile Neutropenia (CISNE) risk-stratification score better predict patient outcomes in patients presenting to emergency departments with febrile neutropenia?
Background: Risk-stratification metrics like the MASCC and CISNE identify subsets of relatively low-risk patients with febrile neutropenia after chemotherapy for treatment at home with empiric oral antibiotic therapy and close follow-up while awaiting results of infectious work-up. Prior studies have validated these tools for admitted, but not for ED, patients.
Setting: Two academic ED at National Institutes of Health–designated cancer centers.
Synopsis: Included patients (n = 230) were at least 16 years old with a documented fever of 38° C or greater related to chemotherapy and an absolute neutrophil count less than 1,000 cells/μL. MASCC and CISNE risk stratification scores were calculated based on the documentation from the ED and recent oncology clinic visits. Outcome measures included length of stay, upgrade in level of care, positive blood cultures, clinical deterioration, and death and were assessed for up to 30 days following discharge. Low-risk patients were defined as those who experienced no negative endpoints. The CISNE score was more specific than the MASCC in identifying low-risk patients (98.1% vs. 54.2%), suggesting that the CISNE may be useful for hospitalists in identifying patients who may be safely discharged with oral antibiotics and close follow-up.
Limitations include possible misclassification bias from indirect assessment of symptom severity, lack of recent ECOG scores for six patients in the CISNE arm, and possible undocumented symptoms during ED evaluation required for subsequent score calculation. Additionally, most patients in this study reported mild symptoms which weighted their MASCC classification toward low-risk.
Bottom Line: The CISNE score may aid in risk-stratification of patients with chemotherapy-related febrile neutropenia presenting to the ED.
Reference: Coyne CJ, Le V, Brennan JJ, et al. Application of the MASCC and CISNE risk-stratification scores to identify low-risk febrile neutropenic patients in the emergency department. Ann Emerg Med. Published online 29 Dec 2016. doi: 10.1016/j.annemergmed.2016.11.007.
Dr. Frederick is assistant clinical professor in the division of hospital Medicine, department of medicine, University of California, San Diego.
Atrial fibrillation blunts beta-blockers for HFrEF
PARIS – Maximal beta-blocker treatment and lower heart rates are effective at cutting all-cause mortality in patients with heart failure with reduced ejection fraction (HFrEF) who are also in sinus rhythm, but it’s a totally different story for patients with similar heart failure plus atrial fibrillation. In the atrial fibrillation subgroup, treatment with a beta-blocker linked with no mortality benefit, and lower heart rates – below 70 beats per minute – appeared to actually link with worse patient survival, based on a meta-analysis of data from 11 beta-blocker trials with a total of more than 17,000 patients.
“Beta blockers may be doing good in heart failure patients with atrial fibrillation, but they also are doing harm that neutralizes any good they do.” In patients with HFrEF and atrial fibrillation, “I don’t like to see the heart rate below 80 beats per minute,” John G.F. Cleland, MD, said at a meeting held by the Heart Failure Association of the ESC.

“We’ve perhaps been too aggressive with heart-rate control in HFrEF patients with atrial fibrillation,” he added in an interview. In these patients “in the range of 60-100 bpm it doesn’t seem to make a lot of difference what the heart rate is, and, if it is less than 70 bpm, patients seem to do a little worse. When we treat these patients with a beta-blocker we don’t see benefit in any way that we’ve looked at the data.”
In contrast, among HFrEF patients in sinus rhythm “beta-blocker treatment is similarly effective regardless of what the baseline heart rate was. The benefit was as great when the baseline rate was 70 bpm or 90 bpm, so heart rate is not a great predictor of beta-blocker benefit in these patients. Patients who tolerated the full beta-blocker dosage had the greatest benefit, and patients who achieved the slowest heart rates also had the greatest benefit.”
In the multivariate models that Dr. Cleland and his associates tested in their meta-analysis, in HFrEF patients in sinus rhythm, the relationship between reduced heart rate and mortality benefit was stronger statistically than between beta-blocker dosage and reduced mortality, he said. “This suggests to me that, while we should use the targeted beta-blocker dosages when we can, it’s more important to achieve a target heart rate in these patients of 55-65 bpm.”
Dr. Cleland hypothesized, based on a report presented at the same meeting by a different research group, that reduced heart rate is not beneficial in HFrEF patients with atrial fibrillation because in this subgroup slower heart rates linked with an increased number of brief pauses in left ventricular pumping. These pauses may result in ventricular arrhythmias, he speculated. “It may be that beta-blockers are equally effective at slowing heart rate in patients with or without atrial fibrillation, but there is also harm from beta-blockers because they’re causing pauses in patients with atrial fibrillation,” he said.
These days, if he has a HFrEF patient with atrial fibrillation whose heart rate slows to 60 bpm, he will stop digoxin treatment if the patient is on that drug, and he will also reduce the beta-blocker dosage but not discontinue it.
The findings came from the Collaborative Systematic Overview of Randomized Controlled Trials of Beta-Blockers in the Treatment of Heart Failure (BB-META-HF), which included data from 11 large beta-blocker randomized trials in heart failure that had been published during 1993-2005. The analysis included data from 17,378 HFrEF patients, with 14,313 (82%) in sinus rhythm and 3,065 (18%) with atrial fibrillation. Follow-up data of patients on treatment was available for 15,007 of these patients.
Dr. Cleland and his associates showed in multivariate analyses that, when they controlled for several baseline demographic and clinical variables among patients in sinus rhythm who received a beta-blocker, the follow-up all-cause mortality fell by 36%, compared with placebo, in patients with a resting baseline heart rate of less than 70 bpm; by 21%, compared with placebo, in patients with a baseline heart rate of 70-90 bpm; and by 38%, compared with placebo, in patients with a baseline heart rate of more than 90 bpm. All three reductions were statistically significant. In contrast, among patients who also had atrial fibrillation beta-blocker treatment linked with no significant mortality reduction, compared with placebo, for patients with any baseline heart rate. Concurrently with Dr. Cleland’s report at the meeting the results appeared online (J Amer Coll Cardiol. 2017 Apr 30. doi: 10.1016/j.jacc.2017.04.001).
[email protected]
On Twitter @mitchelzoler
The findings from this analysis have several implications. First, the association of reduced mortality with reduced heart rate occurred only in patients in sinus rhythm. The irregular heart rhythms in patients with atrial fibrillation may counterbalance any reverse remodeling effects that come from reducing heart rate.
Also, the beneficial effect of beta-blocker treatment was roughly similar regardless of whether baseline heart rate was high or low. This distinguishes beta-blockers from ivabradine, a drug that only reduces heart rate. The magnitude of benefit from ivabradine treatment depends on a patient’s baseline heart rate. The observation that beta-blockers do not have the same limitation suggests that the mechanism of action of beta-blockers may go beyond their heart rate effect. It may also result from the effect of beta-blockers on antagonizing toxic effects from beta-adrenergic stimulation.
The pooled analysis also showed that many patients with HFrEF in sinus rhythm continued to have a high heart rate despite beta-blocker treatment. These patients may get additional benefit from further treatment to reduce their heart rate, with an agent like ivabradine.
But we must be cautious in interpreting the findings because they represent a secondary analysis, and the endpoint studied does not take into account quality of life, exercise tolerance, heart rate control, and tachyarrhythmias. We need prospective, randomized trials of HFrEF patients in sinus rhythm and with atrial fibrillation to better understand how to optimally treat these different types of patients.
The findings highlight that beta-blockers remain a mainstay of treatment for patients with HFrEF in sinus rhythm, and that we have more limited treatment options for HFrEF patients with atrial fibrillation.
Michael Böhm, MD, is professor and director of the cardiology clinic at Saarland University Hospital in Homburg, Germany. He has received honoraria from Bayer, Medtronic, Servier, and Pfizer, and he was a coauthor on the report presented by Dr. Cleland. He made these comments as designated discussant for the study.
The findings from this analysis have several implications. First, the association of reduced mortality with reduced heart rate occurred only in patients in sinus rhythm. The irregular heart rhythms in patients with atrial fibrillation may counterbalance any reverse remodeling effects that come from reducing heart rate.
Also, the beneficial effect of beta-blocker treatment was roughly similar regardless of whether baseline heart rate was high or low. This distinguishes beta-blockers from ivabradine, a drug that only reduces heart rate. The magnitude of benefit from ivabradine treatment depends on a patient’s baseline heart rate. The observation that beta-blockers do not have the same limitation suggests that the mechanism of action of beta-blockers may go beyond their heart rate effect. It may also result from the effect of beta-blockers on antagonizing toxic effects from beta-adrenergic stimulation.
The pooled analysis also showed that many patients with HFrEF in sinus rhythm continued to have a high heart rate despite beta-blocker treatment. These patients may get additional benefit from further treatment to reduce their heart rate, with an agent like ivabradine.
But we must be cautious in interpreting the findings because they represent a secondary analysis, and the endpoint studied does not take into account quality of life, exercise tolerance, heart rate control, and tachyarrhythmias. We need prospective, randomized trials of HFrEF patients in sinus rhythm and with atrial fibrillation to better understand how to optimally treat these different types of patients.
The findings highlight that beta-blockers remain a mainstay of treatment for patients with HFrEF in sinus rhythm, and that we have more limited treatment options for HFrEF patients with atrial fibrillation.
Michael Böhm, MD, is professor and director of the cardiology clinic at Saarland University Hospital in Homburg, Germany. He has received honoraria from Bayer, Medtronic, Servier, and Pfizer, and he was a coauthor on the report presented by Dr. Cleland. He made these comments as designated discussant for the study.
The findings from this analysis have several implications. First, the association of reduced mortality with reduced heart rate occurred only in patients in sinus rhythm. The irregular heart rhythms in patients with atrial fibrillation may counterbalance any reverse remodeling effects that come from reducing heart rate.
Also, the beneficial effect of beta-blocker treatment was roughly similar regardless of whether baseline heart rate was high or low. This distinguishes beta-blockers from ivabradine, a drug that only reduces heart rate. The magnitude of benefit from ivabradine treatment depends on a patient’s baseline heart rate. The observation that beta-blockers do not have the same limitation suggests that the mechanism of action of beta-blockers may go beyond their heart rate effect. It may also result from the effect of beta-blockers on antagonizing toxic effects from beta-adrenergic stimulation.
The pooled analysis also showed that many patients with HFrEF in sinus rhythm continued to have a high heart rate despite beta-blocker treatment. These patients may get additional benefit from further treatment to reduce their heart rate, with an agent like ivabradine.
But we must be cautious in interpreting the findings because they represent a secondary analysis, and the endpoint studied does not take into account quality of life, exercise tolerance, heart rate control, and tachyarrhythmias. We need prospective, randomized trials of HFrEF patients in sinus rhythm and with atrial fibrillation to better understand how to optimally treat these different types of patients.
The findings highlight that beta-blockers remain a mainstay of treatment for patients with HFrEF in sinus rhythm, and that we have more limited treatment options for HFrEF patients with atrial fibrillation.
Michael Böhm, MD, is professor and director of the cardiology clinic at Saarland University Hospital in Homburg, Germany. He has received honoraria from Bayer, Medtronic, Servier, and Pfizer, and he was a coauthor on the report presented by Dr. Cleland. He made these comments as designated discussant for the study.
PARIS – Maximal beta-blocker treatment and lower heart rates are effective at cutting all-cause mortality in patients with heart failure with reduced ejection fraction (HFrEF) who are also in sinus rhythm, but it’s a totally different story for patients with similar heart failure plus atrial fibrillation. In the atrial fibrillation subgroup, treatment with a beta-blocker linked with no mortality benefit, and lower heart rates – below 70 beats per minute – appeared to actually link with worse patient survival, based on a meta-analysis of data from 11 beta-blocker trials with a total of more than 17,000 patients.
“Beta blockers may be doing good in heart failure patients with atrial fibrillation, but they also are doing harm that neutralizes any good they do.” In patients with HFrEF and atrial fibrillation, “I don’t like to see the heart rate below 80 beats per minute,” John G.F. Cleland, MD, said at a meeting held by the Heart Failure Association of the ESC.
“We’ve perhaps been too aggressive with heart-rate control in HFrEF patients with atrial fibrillation,” he added in an interview. In these patients “in the range of 60-100 bpm it doesn’t seem to make a lot of difference what the heart rate is, and, if it is less than 70 bpm, patients seem to do a little worse. When we treat these patients with a beta-blocker we don’t see benefit in any way that we’ve looked at the data.”
In contrast, among HFrEF patients in sinus rhythm “beta-blocker treatment is similarly effective regardless of what the baseline heart rate was. The benefit was as great when the baseline rate was 70 bpm or 90 bpm, so heart rate is not a great predictor of beta-blocker benefit in these patients. Patients who tolerated the full beta-blocker dosage had the greatest benefit, and patients who achieved the slowest heart rates also had the greatest benefit.”
In the multivariate models that Dr. Cleland and his associates tested in their meta-analysis, in HFrEF patients in sinus rhythm, the relationship between reduced heart rate and mortality benefit was stronger statistically than between beta-blocker dosage and reduced mortality, he said. “This suggests to me that, while we should use the targeted beta-blocker dosages when we can, it’s more important to achieve a target heart rate in these patients of 55-65 bpm.”
Dr. Cleland hypothesized, based on a report presented at the same meeting by a different research group, that reduced heart rate is not beneficial in HFrEF patients with atrial fibrillation because in this subgroup slower heart rates linked with an increased number of brief pauses in left ventricular pumping. These pauses may result in ventricular arrhythmias, he speculated. “It may be that beta-blockers are equally effective at slowing heart rate in patients with or without atrial fibrillation, but there is also harm from beta-blockers because they’re causing pauses in patients with atrial fibrillation,” he said.
These days, if he has a HFrEF patient with atrial fibrillation whose heart rate slows to 60 bpm, he will stop digoxin treatment if the patient is on that drug, and he will also reduce the beta-blocker dosage but not discontinue it.
The findings came from the Collaborative Systematic Overview of Randomized Controlled Trials of Beta-Blockers in the Treatment of Heart Failure (BB-META-HF), which included data from 11 large beta-blocker randomized trials in heart failure that had been published during 1993-2005. The analysis included data from 17,378 HFrEF patients, with 14,313 (82%) in sinus rhythm and 3,065 (18%) with atrial fibrillation. Follow-up data of patients on treatment was available for 15,007 of these patients.
Dr. Cleland and his associates showed in multivariate analyses that, when they controlled for several baseline demographic and clinical variables among patients in sinus rhythm who received a beta-blocker, the follow-up all-cause mortality fell by 36%, compared with placebo, in patients with a resting baseline heart rate of less than 70 bpm; by 21%, compared with placebo, in patients with a baseline heart rate of 70-90 bpm; and by 38%, compared with placebo, in patients with a baseline heart rate of more than 90 bpm. All three reductions were statistically significant. In contrast, among patients who also had atrial fibrillation beta-blocker treatment linked with no significant mortality reduction, compared with placebo, for patients with any baseline heart rate. Concurrently with Dr. Cleland’s report at the meeting the results appeared online (J Amer Coll Cardiol. 2017 Apr 30. doi: 10.1016/j.jacc.2017.04.001).
[email protected]
On Twitter @mitchelzoler
PARIS – Maximal beta-blocker treatment and lower heart rates are effective at cutting all-cause mortality in patients with heart failure with reduced ejection fraction (HFrEF) who are also in sinus rhythm, but it’s a totally different story for patients with similar heart failure plus atrial fibrillation. In the atrial fibrillation subgroup, treatment with a beta-blocker linked with no mortality benefit, and lower heart rates – below 70 beats per minute – appeared to actually link with worse patient survival, based on a meta-analysis of data from 11 beta-blocker trials with a total of more than 17,000 patients.
“Beta blockers may be doing good in heart failure patients with atrial fibrillation, but they also are doing harm that neutralizes any good they do.” In patients with HFrEF and atrial fibrillation, “I don’t like to see the heart rate below 80 beats per minute,” John G.F. Cleland, MD, said at a meeting held by the Heart Failure Association of the ESC.
“We’ve perhaps been too aggressive with heart-rate control in HFrEF patients with atrial fibrillation,” he added in an interview. In these patients “in the range of 60-100 bpm it doesn’t seem to make a lot of difference what the heart rate is, and, if it is less than 70 bpm, patients seem to do a little worse. When we treat these patients with a beta-blocker we don’t see benefit in any way that we’ve looked at the data.”
In contrast, among HFrEF patients in sinus rhythm “beta-blocker treatment is similarly effective regardless of what the baseline heart rate was. The benefit was as great when the baseline rate was 70 bpm or 90 bpm, so heart rate is not a great predictor of beta-blocker benefit in these patients. Patients who tolerated the full beta-blocker dosage had the greatest benefit, and patients who achieved the slowest heart rates also had the greatest benefit.”
In the multivariate models that Dr. Cleland and his associates tested in their meta-analysis, in HFrEF patients in sinus rhythm, the relationship between reduced heart rate and mortality benefit was stronger statistically than between beta-blocker dosage and reduced mortality, he said. “This suggests to me that, while we should use the targeted beta-blocker dosages when we can, it’s more important to achieve a target heart rate in these patients of 55-65 bpm.”
Dr. Cleland hypothesized, based on a report presented at the same meeting by a different research group, that reduced heart rate is not beneficial in HFrEF patients with atrial fibrillation because in this subgroup slower heart rates linked with an increased number of brief pauses in left ventricular pumping. These pauses may result in ventricular arrhythmias, he speculated. “It may be that beta-blockers are equally effective at slowing heart rate in patients with or without atrial fibrillation, but there is also harm from beta-blockers because they’re causing pauses in patients with atrial fibrillation,” he said.
These days, if he has a HFrEF patient with atrial fibrillation whose heart rate slows to 60 bpm, he will stop digoxin treatment if the patient is on that drug, and he will also reduce the beta-blocker dosage but not discontinue it.
The findings came from the Collaborative Systematic Overview of Randomized Controlled Trials of Beta-Blockers in the Treatment of Heart Failure (BB-META-HF), which included data from 11 large beta-blocker randomized trials in heart failure that had been published during 1993-2005. The analysis included data from 17,378 HFrEF patients, with 14,313 (82%) in sinus rhythm and 3,065 (18%) with atrial fibrillation. Follow-up data of patients on treatment was available for 15,007 of these patients.
Dr. Cleland and his associates showed in multivariate analyses that, when they controlled for several baseline demographic and clinical variables among patients in sinus rhythm who received a beta-blocker, the follow-up all-cause mortality fell by 36%, compared with placebo, in patients with a resting baseline heart rate of less than 70 bpm; by 21%, compared with placebo, in patients with a baseline heart rate of 70-90 bpm; and by 38%, compared with placebo, in patients with a baseline heart rate of more than 90 bpm. All three reductions were statistically significant. In contrast, among patients who also had atrial fibrillation beta-blocker treatment linked with no significant mortality reduction, compared with placebo, for patients with any baseline heart rate. Concurrently with Dr. Cleland’s report at the meeting the results appeared online (J Amer Coll Cardiol. 2017 Apr 30. doi: 10.1016/j.jacc.2017.04.001).
[email protected]
On Twitter @mitchelzoler
AT HEART FAILURE 2017
Key clinical point:
Major finding: All-cause mortality was similar in patients with HFrEF and atrial fibrillation regardless of whether they received a beta-blocker or placebo.
Data source: BB-META-HF, a meta-analysis of 11 beta-blocker treatment trials with 17,378 HFrEF patients.
Disclosures: BB-META-HF received funding from Menarini and GlaxoSmithKline. Dr. Cleland has received research funding and honoraria from GlaxoSmithKline.
Bedside CGM boosts glucose control in hospital
BY RANDY DOTINGA
SAN DIEGO – Bedside continuous glucose monitoring (CGM) with a wireless hookup to a response team allowed doctors and nurses to gain better blood sugar control in hospitalized high-risk patients with diabetes, according to research reported at the annual scientific sessions of the American Diabetes Association.
“Continuous glucose monitoring and wireless connections can be useful in the hospital setting, not just in the outpatient setting,” said Maria Isabel Garcia, RN, of Scripps Whittier Diabetes Institute. “They help us to prevent problems rather than fixing them after they happen.”

Research suggests that complications due to dangerous blood sugar levels can lead to longer hospital stays, she noted.
For the study, researchers assigned 45 high-risk hospitalized patients with type 2 diabetes to be monitored by DexCom G4 CGM devices. The patients were being treated for a variety of conditions, and all were expected to be hospitalized for more than 2 days.
Researchers housed the normal-sized CGM devices in toolbox-sized containers at bedside. “We don’t want the equipment to get misplaced if the patient has to go from room to room or if the patient is discharged and takes the equipment by mistake,” Ms. Garcia said.
The patients were 43-82 years old (median, 61.4 years; standard deviation, 9.8), 56% male, 73% Hispanic (with 60% preferring to speak Spanish). The mean hemoglobin A1c was 10.2% (SD, 2.3), and the mean body mass index was 32.9 (SD, 8).
The patients were randomized to two groups. In both, the CGM devices were operative and tracked blood sugar levels. In one group, the information was transmitted via wireless hookup to a team of researchers (during the day) or a telemetry team (at night), who were alerted via alarms if blood sugar levels seemed too high or low. The teams would then alert nurses who’d confirm the levels via bedside testing and take appropriate action.
CGM data were gathered from the patients for an average of 4.2 days each (SD, 2.49; range 2-10), and the number of readings per patient ranged from 102 to 2,334 each (median 859.4; SD, 627.8).
The findings suggest that wireless transmission of CGM allowed hospital staff to improve blood sugar control. Readings under 70 mg/dL occurred 0.7% of the time in patients monitored via wireless hookup and 1.4% in the others. Readings over 250 mg/dL appeared 9.8% and 13.2% of the time, respectively and readings over 300 mg/dL appeared 2.6% and 5.1% of the time, respectively.
The investigators plan to recruit 460 patients for the study, Ms. Garcia said. Results may be available within a couple of years, she said.
DexCom provided the CGM devices for the study, which was funded by Diabetes Research Connection and the Confidence Foundation. Ms. Garcia reports no disclosures.
BY RANDY DOTINGA
SAN DIEGO – Bedside continuous glucose monitoring (CGM) with a wireless hookup to a response team allowed doctors and nurses to gain better blood sugar control in hospitalized high-risk patients with diabetes, according to research reported at the annual scientific sessions of the American Diabetes Association.
“Continuous glucose monitoring and wireless connections can be useful in the hospital setting, not just in the outpatient setting,” said Maria Isabel Garcia, RN, of Scripps Whittier Diabetes Institute. “They help us to prevent problems rather than fixing them after they happen.”
Research suggests that complications due to dangerous blood sugar levels can lead to longer hospital stays, she noted.
For the study, researchers assigned 45 high-risk hospitalized patients with type 2 diabetes to be monitored by DexCom G4 CGM devices. The patients were being treated for a variety of conditions, and all were expected to be hospitalized for more than 2 days.
Researchers housed the normal-sized CGM devices in toolbox-sized containers at bedside. “We don’t want the equipment to get misplaced if the patient has to go from room to room or if the patient is discharged and takes the equipment by mistake,” Ms. Garcia said.
The patients were 43-82 years old (median, 61.4 years; standard deviation, 9.8), 56% male, 73% Hispanic (with 60% preferring to speak Spanish). The mean hemoglobin A1c was 10.2% (SD, 2.3), and the mean body mass index was 32.9 (SD, 8).
The patients were randomized to two groups. In both, the CGM devices were operative and tracked blood sugar levels. In one group, the information was transmitted via wireless hookup to a team of researchers (during the day) or a telemetry team (at night), who were alerted via alarms if blood sugar levels seemed too high or low. The teams would then alert nurses who’d confirm the levels via bedside testing and take appropriate action.
CGM data were gathered from the patients for an average of 4.2 days each (SD, 2.49; range 2-10), and the number of readings per patient ranged from 102 to 2,334 each (median 859.4; SD, 627.8).
The findings suggest that wireless transmission of CGM allowed hospital staff to improve blood sugar control. Readings under 70 mg/dL occurred 0.7% of the time in patients monitored via wireless hookup and 1.4% in the others. Readings over 250 mg/dL appeared 9.8% and 13.2% of the time, respectively and readings over 300 mg/dL appeared 2.6% and 5.1% of the time, respectively.
The investigators plan to recruit 460 patients for the study, Ms. Garcia said. Results may be available within a couple of years, she said.
DexCom provided the CGM devices for the study, which was funded by Diabetes Research Connection and the Confidence Foundation. Ms. Garcia reports no disclosures.
BY RANDY DOTINGA
SAN DIEGO – Bedside continuous glucose monitoring (CGM) with a wireless hookup to a response team allowed doctors and nurses to gain better blood sugar control in hospitalized high-risk patients with diabetes, according to research reported at the annual scientific sessions of the American Diabetes Association.
“Continuous glucose monitoring and wireless connections can be useful in the hospital setting, not just in the outpatient setting,” said Maria Isabel Garcia, RN, of Scripps Whittier Diabetes Institute. “They help us to prevent problems rather than fixing them after they happen.”
Research suggests that complications due to dangerous blood sugar levels can lead to longer hospital stays, she noted.
For the study, researchers assigned 45 high-risk hospitalized patients with type 2 diabetes to be monitored by DexCom G4 CGM devices. The patients were being treated for a variety of conditions, and all were expected to be hospitalized for more than 2 days.
Researchers housed the normal-sized CGM devices in toolbox-sized containers at bedside. “We don’t want the equipment to get misplaced if the patient has to go from room to room or if the patient is discharged and takes the equipment by mistake,” Ms. Garcia said.
The patients were 43-82 years old (median, 61.4 years; standard deviation, 9.8), 56% male, 73% Hispanic (with 60% preferring to speak Spanish). The mean hemoglobin A1c was 10.2% (SD, 2.3), and the mean body mass index was 32.9 (SD, 8).
The patients were randomized to two groups. In both, the CGM devices were operative and tracked blood sugar levels. In one group, the information was transmitted via wireless hookup to a team of researchers (during the day) or a telemetry team (at night), who were alerted via alarms if blood sugar levels seemed too high or low. The teams would then alert nurses who’d confirm the levels via bedside testing and take appropriate action.
CGM data were gathered from the patients for an average of 4.2 days each (SD, 2.49; range 2-10), and the number of readings per patient ranged from 102 to 2,334 each (median 859.4; SD, 627.8).
The findings suggest that wireless transmission of CGM allowed hospital staff to improve blood sugar control. Readings under 70 mg/dL occurred 0.7% of the time in patients monitored via wireless hookup and 1.4% in the others. Readings over 250 mg/dL appeared 9.8% and 13.2% of the time, respectively and readings over 300 mg/dL appeared 2.6% and 5.1% of the time, respectively.
The investigators plan to recruit 460 patients for the study, Ms. Garcia said. Results may be available within a couple of years, she said.
DexCom provided the CGM devices for the study, which was funded by Diabetes Research Connection and the Confidence Foundation. Ms. Garcia reports no disclosures.
AT THE ADA ANNUAL SCIENTIFIC SESSIONS
Key clinical point: about high or low readings.
Major finding: Readings under 70 mg/dL occurred 0.7% of the time in patients monitored via wireless hookup and 1.4% in other patients. Readings over 250 mg/dL appeared 9.8% and 13.2% of the time, respectively, and readings over 300 mg/dL appeared 2.6% and 5.1% of the time, respectively.
Data source: Early results from a pilot randomized, controlled study of 45 hospitalized, high-risk patients with type 2 diabetes. CGM devices measured glucose levels in all patients, but they were only transmitted via wireless hookup to teams in one group.
Disclosures: DexCom provided the CGM machines for the study, which was funded by Diabetes Research Connection and the Confidence Foundation. Garcia reports no disclosures.
Crossing the personal quality chasm: QI enthusiast to QI leader
Editor’s Note: This new series highlights the professional pathways of quality improvement leaders. This month features the story of Eric Howell, MD, MHM, professor of medicine at Johns Hopkins University, Baltimore.
For Eric Howell, MD, MHM, the journey to becoming a professor of medicine at Johns Hopkins University, past president of SHM, and director of SHM’s Leadership Academies commenced with a major quality improvement (QI) challenge.
Johns Hopkins Bayview Medical Center was struggling with throughput from the emergency department when Dr. Howell began practicing there in the early days of hospital medicine. “The ED said the medicine service was too slow, and the hospitalists said, ‘We’re working as fast as we can,’ ” Dr. Howell recalled of his real-world introduction to implementation science. “So, I took on triage oversight in 2000 and began streamlining flow.”

With a growing reputation for finding solutions to reduce readmissions and improve care transitions, Dr. Howell joined the Better Outcomes by Optimizing Safe Transitions (Project BOOST) project team in 2007 to codevelop one of SHM’s most successful programs. He humbly attributes some of this success to luck. “I happened to be at the right place at the right time. There was a problem, opportunity knocked, and I opened the door,” he said.
After some reflection, he pinpoints more tangible factors – a gift for innovative thinking and finding options that unify, rather than polarize, people and departments.
“I always ensure a solution makes the pie bigger, so that everyone benefits from it,” he said. “I don’t approach a problem like a sporting event, where one group wins and another loses.”
Dr. Howell says that an inclusive mindset is an important characteristic for anyone on a QI track because “it encourages buy-in from everyone who is impacted by a problem, and their investment in making the outcome successful.”
Skill development in areas such as leadership principles and processes such as lean will benefit those on a QI pathway, but finding the right mentors is just as critical. Dr. Howell looked to multiple people from diverse backgrounds, none of which included QI, to “help me move my skill set forward,” he said. “A clinical educator helped me to interact with other people, learn to facilitate an educational initiative, and lead people to change.”
Another mentor, he recalled, was an engineer who helped him figure out how to measure the success of his projects. And a third mentor cleared the pathway of obstructions, providing access to the people who would make his projects successful.
Being able to pivot is also important, Dr. Howell said. “Whether it is looking at data or the people you need to approach to solve a problem, be able to change your approach. Flip-flopping is a good thing in QI, because you’re always adjusting your tactics based on new information.”
Today, as SHM’s senior physician advisor to its Center for Quality Improvement, Dr. Howell holds multiple roles within the Johns Hopkins system and has received numerous awards for excellence in teaching and practice. The core principles that he started with on the path remain the same: “Be humble,” he said, “and give away credit. We are often collaborating with other professionals, so shining a light on the great work that they do will make projects more successful and improve the likelihood that they will want to collaborate with you in the future.”
Claudia Stahl is a content manager for the Society of Hospital Medicine.
Editor’s Note: This new series highlights the professional pathways of quality improvement leaders. This month features the story of Eric Howell, MD, MHM, professor of medicine at Johns Hopkins University, Baltimore.
For Eric Howell, MD, MHM, the journey to becoming a professor of medicine at Johns Hopkins University, past president of SHM, and director of SHM’s Leadership Academies commenced with a major quality improvement (QI) challenge.
Johns Hopkins Bayview Medical Center was struggling with throughput from the emergency department when Dr. Howell began practicing there in the early days of hospital medicine. “The ED said the medicine service was too slow, and the hospitalists said, ‘We’re working as fast as we can,’ ” Dr. Howell recalled of his real-world introduction to implementation science. “So, I took on triage oversight in 2000 and began streamlining flow.”
With a growing reputation for finding solutions to reduce readmissions and improve care transitions, Dr. Howell joined the Better Outcomes by Optimizing Safe Transitions (Project BOOST) project team in 2007 to codevelop one of SHM’s most successful programs. He humbly attributes some of this success to luck. “I happened to be at the right place at the right time. There was a problem, opportunity knocked, and I opened the door,” he said.
After some reflection, he pinpoints more tangible factors – a gift for innovative thinking and finding options that unify, rather than polarize, people and departments.
“I always ensure a solution makes the pie bigger, so that everyone benefits from it,” he said. “I don’t approach a problem like a sporting event, where one group wins and another loses.”
Dr. Howell says that an inclusive mindset is an important characteristic for anyone on a QI track because “it encourages buy-in from everyone who is impacted by a problem, and their investment in making the outcome successful.”
Skill development in areas such as leadership principles and processes such as lean will benefit those on a QI pathway, but finding the right mentors is just as critical. Dr. Howell looked to multiple people from diverse backgrounds, none of which included QI, to “help me move my skill set forward,” he said. “A clinical educator helped me to interact with other people, learn to facilitate an educational initiative, and lead people to change.”
Another mentor, he recalled, was an engineer who helped him figure out how to measure the success of his projects. And a third mentor cleared the pathway of obstructions, providing access to the people who would make his projects successful.
Being able to pivot is also important, Dr. Howell said. “Whether it is looking at data or the people you need to approach to solve a problem, be able to change your approach. Flip-flopping is a good thing in QI, because you’re always adjusting your tactics based on new information.”
Today, as SHM’s senior physician advisor to its Center for Quality Improvement, Dr. Howell holds multiple roles within the Johns Hopkins system and has received numerous awards for excellence in teaching and practice. The core principles that he started with on the path remain the same: “Be humble,” he said, “and give away credit. We are often collaborating with other professionals, so shining a light on the great work that they do will make projects more successful and improve the likelihood that they will want to collaborate with you in the future.”
Claudia Stahl is a content manager for the Society of Hospital Medicine.
Editor’s Note: This new series highlights the professional pathways of quality improvement leaders. This month features the story of Eric Howell, MD, MHM, professor of medicine at Johns Hopkins University, Baltimore.
For Eric Howell, MD, MHM, the journey to becoming a professor of medicine at Johns Hopkins University, past president of SHM, and director of SHM’s Leadership Academies commenced with a major quality improvement (QI) challenge.
Johns Hopkins Bayview Medical Center was struggling with throughput from the emergency department when Dr. Howell began practicing there in the early days of hospital medicine. “The ED said the medicine service was too slow, and the hospitalists said, ‘We’re working as fast as we can,’ ” Dr. Howell recalled of his real-world introduction to implementation science. “So, I took on triage oversight in 2000 and began streamlining flow.”
With a growing reputation for finding solutions to reduce readmissions and improve care transitions, Dr. Howell joined the Better Outcomes by Optimizing Safe Transitions (Project BOOST) project team in 2007 to codevelop one of SHM’s most successful programs. He humbly attributes some of this success to luck. “I happened to be at the right place at the right time. There was a problem, opportunity knocked, and I opened the door,” he said.
After some reflection, he pinpoints more tangible factors – a gift for innovative thinking and finding options that unify, rather than polarize, people and departments.
“I always ensure a solution makes the pie bigger, so that everyone benefits from it,” he said. “I don’t approach a problem like a sporting event, where one group wins and another loses.”
Dr. Howell says that an inclusive mindset is an important characteristic for anyone on a QI track because “it encourages buy-in from everyone who is impacted by a problem, and their investment in making the outcome successful.”
Skill development in areas such as leadership principles and processes such as lean will benefit those on a QI pathway, but finding the right mentors is just as critical. Dr. Howell looked to multiple people from diverse backgrounds, none of which included QI, to “help me move my skill set forward,” he said. “A clinical educator helped me to interact with other people, learn to facilitate an educational initiative, and lead people to change.”
Another mentor, he recalled, was an engineer who helped him figure out how to measure the success of his projects. And a third mentor cleared the pathway of obstructions, providing access to the people who would make his projects successful.
Being able to pivot is also important, Dr. Howell said. “Whether it is looking at data or the people you need to approach to solve a problem, be able to change your approach. Flip-flopping is a good thing in QI, because you’re always adjusting your tactics based on new information.”
Today, as SHM’s senior physician advisor to its Center for Quality Improvement, Dr. Howell holds multiple roles within the Johns Hopkins system and has received numerous awards for excellence in teaching and practice. The core principles that he started with on the path remain the same: “Be humble,” he said, “and give away credit. We are often collaborating with other professionals, so shining a light on the great work that they do will make projects more successful and improve the likelihood that they will want to collaborate with you in the future.”
Claudia Stahl is a content manager for the Society of Hospital Medicine.
Low-dose aspirin bests dual-antiplatelet therapy in TAVR
PARIS – Single-antiplatelet therapy with low-dose aspirin following transcatheter aortic valve replacement (TAVR) reduced the occurrence of major adverse events, compared with guideline-recommended dual-antiplatelet therapy (DAPT), in the randomized ARTE trial.
The TAVR guideline recommendation for DAPT with low-dose aspirin plus clopidogrel is not based on evidence. It relies on expert opinion. ARTE (Aspirin Versus Aspirin + Clopidogrel Following TAVR) is the first sizable randomized trial to address the safety and efficacy of aspirin alone versus DAPT in the setting of TAVR, Josep Rodés-Cabau, MD, noted in presenting the ARTE results at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.

ARTE was a multicenter, prospective, international open-label study of 222 TAVR patients who were randomized to 3 months of single-antiplatelet therapy (SAPT) with aspirin at 80-100 mg/day or to DAPT with aspirin at 80-100 mg/day plus clopidogrel at 75 mg/day after a single 300-mg loading dose. Participants had a mean Society of Thoracic Surgery Predicted Risk of Mortality score of 6.3%. The vast majority of participants received the balloon-expandable Edwards Lifesciences Sapien XT valve. The remainder got the Sapien 3 valve.
The primary outcome was the 3-month composite of death, MI, major or life-threatening bleeding, or stroke or transient ischemic attack. It occurred in 15.3% of the DAPT group and 7.2% on SAPT, a difference that didn’t reach statistical significance (P = .065) because of small patient numbers.
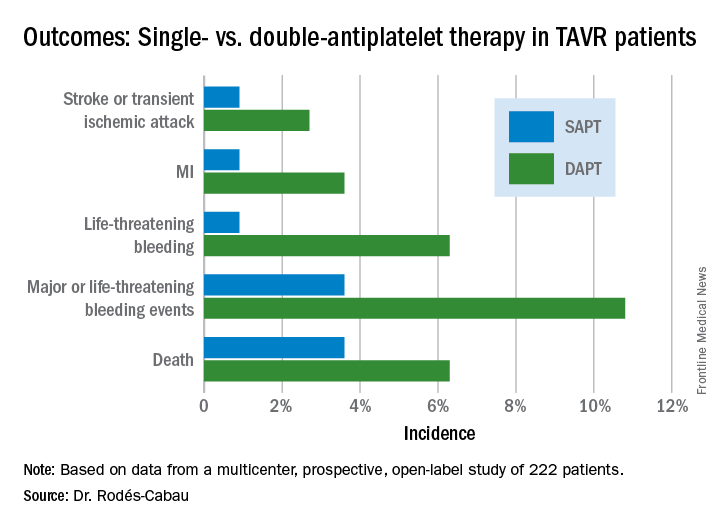
All subjects were on a proton pump inhibitor. The type, timing, and severity of bleeding events differed between the two study arms. All 4 bleeding events in the SAPT group were vascular in nature, while 5 of the 12 in the DAPT group were gastrointestinal. All the bleeding events in the SAPT group occurred within 72 hours after TAVR, whereas 5 of 12 in the DAPT recipients occurred later. Only one patient on SAPT experienced life-threatening bleeding, compared with seven DAPT patients who did.
“There were two prior smaller studies before ours,” according to Dr. Rodés-Cabau of Laval University in Quebec City. “One showed no differences, and an Italian one showed a tendency toward more bleeding with DAPT. So, I think there has been no sign to date that adding clopidogrel protects this group of patients from anything.”
Discussant Luis Nombela-Franco, MD, an interventional cardiologist at San Carlos Hospital in Madrid, pronounced the ARTE trial guideline-changing despite its limitations.
ARTE was supported by grants from Edwards Lifesciences and the Quebec Heart and Lung Institute.
Simultaneous with Dr. Rodés-Cabau’s presentation in Paris, the ARTE trial was published online (JACC Cardiovasc Interv. 2017 May 11. pii: S1936-8798[17]30812-9).

PARIS – Single-antiplatelet therapy with low-dose aspirin following transcatheter aortic valve replacement (TAVR) reduced the occurrence of major adverse events, compared with guideline-recommended dual-antiplatelet therapy (DAPT), in the randomized ARTE trial.
The TAVR guideline recommendation for DAPT with low-dose aspirin plus clopidogrel is not based on evidence. It relies on expert opinion. ARTE (Aspirin Versus Aspirin + Clopidogrel Following TAVR) is the first sizable randomized trial to address the safety and efficacy of aspirin alone versus DAPT in the setting of TAVR, Josep Rodés-Cabau, MD, noted in presenting the ARTE results at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
ARTE was a multicenter, prospective, international open-label study of 222 TAVR patients who were randomized to 3 months of single-antiplatelet therapy (SAPT) with aspirin at 80-100 mg/day or to DAPT with aspirin at 80-100 mg/day plus clopidogrel at 75 mg/day after a single 300-mg loading dose. Participants had a mean Society of Thoracic Surgery Predicted Risk of Mortality score of 6.3%. The vast majority of participants received the balloon-expandable Edwards Lifesciences Sapien XT valve. The remainder got the Sapien 3 valve.
The primary outcome was the 3-month composite of death, MI, major or life-threatening bleeding, or stroke or transient ischemic attack. It occurred in 15.3% of the DAPT group and 7.2% on SAPT, a difference that didn’t reach statistical significance (P = .065) because of small patient numbers.
All subjects were on a proton pump inhibitor. The type, timing, and severity of bleeding events differed between the two study arms. All 4 bleeding events in the SAPT group were vascular in nature, while 5 of the 12 in the DAPT group were gastrointestinal. All the bleeding events in the SAPT group occurred within 72 hours after TAVR, whereas 5 of 12 in the DAPT recipients occurred later. Only one patient on SAPT experienced life-threatening bleeding, compared with seven DAPT patients who did.
“There were two prior smaller studies before ours,” according to Dr. Rodés-Cabau of Laval University in Quebec City. “One showed no differences, and an Italian one showed a tendency toward more bleeding with DAPT. So, I think there has been no sign to date that adding clopidogrel protects this group of patients from anything.”
Discussant Luis Nombela-Franco, MD, an interventional cardiologist at San Carlos Hospital in Madrid, pronounced the ARTE trial guideline-changing despite its limitations.
ARTE was supported by grants from Edwards Lifesciences and the Quebec Heart and Lung Institute.
Simultaneous with Dr. Rodés-Cabau’s presentation in Paris, the ARTE trial was published online (JACC Cardiovasc Interv. 2017 May 11. pii: S1936-8798[17]30812-9).
PARIS – Single-antiplatelet therapy with low-dose aspirin following transcatheter aortic valve replacement (TAVR) reduced the occurrence of major adverse events, compared with guideline-recommended dual-antiplatelet therapy (DAPT), in the randomized ARTE trial.
The TAVR guideline recommendation for DAPT with low-dose aspirin plus clopidogrel is not based on evidence. It relies on expert opinion. ARTE (Aspirin Versus Aspirin + Clopidogrel Following TAVR) is the first sizable randomized trial to address the safety and efficacy of aspirin alone versus DAPT in the setting of TAVR, Josep Rodés-Cabau, MD, noted in presenting the ARTE results at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
ARTE was a multicenter, prospective, international open-label study of 222 TAVR patients who were randomized to 3 months of single-antiplatelet therapy (SAPT) with aspirin at 80-100 mg/day or to DAPT with aspirin at 80-100 mg/day plus clopidogrel at 75 mg/day after a single 300-mg loading dose. Participants had a mean Society of Thoracic Surgery Predicted Risk of Mortality score of 6.3%. The vast majority of participants received the balloon-expandable Edwards Lifesciences Sapien XT valve. The remainder got the Sapien 3 valve.
The primary outcome was the 3-month composite of death, MI, major or life-threatening bleeding, or stroke or transient ischemic attack. It occurred in 15.3% of the DAPT group and 7.2% on SAPT, a difference that didn’t reach statistical significance (P = .065) because of small patient numbers.
All subjects were on a proton pump inhibitor. The type, timing, and severity of bleeding events differed between the two study arms. All 4 bleeding events in the SAPT group were vascular in nature, while 5 of the 12 in the DAPT group were gastrointestinal. All the bleeding events in the SAPT group occurred within 72 hours after TAVR, whereas 5 of 12 in the DAPT recipients occurred later. Only one patient on SAPT experienced life-threatening bleeding, compared with seven DAPT patients who did.
“There were two prior smaller studies before ours,” according to Dr. Rodés-Cabau of Laval University in Quebec City. “One showed no differences, and an Italian one showed a tendency toward more bleeding with DAPT. So, I think there has been no sign to date that adding clopidogrel protects this group of patients from anything.”
Discussant Luis Nombela-Franco, MD, an interventional cardiologist at San Carlos Hospital in Madrid, pronounced the ARTE trial guideline-changing despite its limitations.
ARTE was supported by grants from Edwards Lifesciences and the Quebec Heart and Lung Institute.
Simultaneous with Dr. Rodés-Cabau’s presentation in Paris, the ARTE trial was published online (JACC Cardiovasc Interv. 2017 May 11. pii: S1936-8798[17]30812-9).
AT EUROPCR
Key clinical point:
Major finding: The 3-month composite of death, MI, major or life-threatening bleeding, or stroke or transient ischemic attack occurred in 15.3% of TAVR patients randomized to DAPT with low-dose aspirin plus clopidogrel, compared with 7.2% on aspirin only.
Data source: A randomized, multicenter, international, prospective open-label trial in 222 TAVR patients.
Disclosures: The presenter reported receiving research grants from Edwards Lifesciences and the Quebec Heart and Lung Institute, which supported the ARTE trial.
Everything We Say and Do: Setting discharge goals and visit expectations
Editor’s note: “Everything We Say and Do” is an informational series developed by SHM’s Patient Experience Committee to provide readers with thoughtful and actionable communication tactics that have great potential to positively impact patients’ experience of care. Each article will focus on how the contributor applies one or more of the “key communication” tactics in practice to maintain provider accountability for “everything we say and do that affects our patients’ thoughts, feelings, and well-being.”
What I say and do
I always ensure at the end of my visit with a patient and their family that they know when to expect me to return to see their child again.
Why I do it
One of the biggest frustrations I hear from families pertains to the discharge process. In talking with families, they want to know the approximate time for discharge. Often, during morning rounds, we mention that the patient may be able to go home later in the day and we say that we will come in again later to check on them. However, unless we give families a time frame for when we will come back and do that check, they are left waiting without any clear expectations.

How I do it
One of our goals during morning family-centered rounds is to discuss discharge for every patient, every day. Along with discussing the possibility of going home, we try to give the family goals that they can work on throughout the day that are tied to discharge – for example, the approximate by-mouth intake for a toddler admitted for gastroenteritis and dehydration.
I also give the family an approximate time when either I or the resident team will come back to see if they have achieved this goal. This may be either late afternoon or first thing in the morning if we are planning an early-morning discharge before rounds. The families seem to find this helpful because they are not tied to the room all day waiting for the doctor to come back.
I also make sure that the families know they can contact their nurse any time if they need to see any of the doctors sooner than we planned. I let them know that a physician is here on the floor 24 hours a day and that the nurses can easily reach us at any time if they have further concerns. In my experience, this is reassuring to our families.
Christine Hrach is a pediatric hospitalist at Washington University School of Medicine in St. Louis.
Editor’s note: “Everything We Say and Do” is an informational series developed by SHM’s Patient Experience Committee to provide readers with thoughtful and actionable communication tactics that have great potential to positively impact patients’ experience of care. Each article will focus on how the contributor applies one or more of the “key communication” tactics in practice to maintain provider accountability for “everything we say and do that affects our patients’ thoughts, feelings, and well-being.”
What I say and do
I always ensure at the end of my visit with a patient and their family that they know when to expect me to return to see their child again.
Why I do it
One of the biggest frustrations I hear from families pertains to the discharge process. In talking with families, they want to know the approximate time for discharge. Often, during morning rounds, we mention that the patient may be able to go home later in the day and we say that we will come in again later to check on them. However, unless we give families a time frame for when we will come back and do that check, they are left waiting without any clear expectations.
How I do it
One of our goals during morning family-centered rounds is to discuss discharge for every patient, every day. Along with discussing the possibility of going home, we try to give the family goals that they can work on throughout the day that are tied to discharge – for example, the approximate by-mouth intake for a toddler admitted for gastroenteritis and dehydration.
I also give the family an approximate time when either I or the resident team will come back to see if they have achieved this goal. This may be either late afternoon or first thing in the morning if we are planning an early-morning discharge before rounds. The families seem to find this helpful because they are not tied to the room all day waiting for the doctor to come back.
I also make sure that the families know they can contact their nurse any time if they need to see any of the doctors sooner than we planned. I let them know that a physician is here on the floor 24 hours a day and that the nurses can easily reach us at any time if they have further concerns. In my experience, this is reassuring to our families.
Christine Hrach is a pediatric hospitalist at Washington University School of Medicine in St. Louis.
Editor’s note: “Everything We Say and Do” is an informational series developed by SHM’s Patient Experience Committee to provide readers with thoughtful and actionable communication tactics that have great potential to positively impact patients’ experience of care. Each article will focus on how the contributor applies one or more of the “key communication” tactics in practice to maintain provider accountability for “everything we say and do that affects our patients’ thoughts, feelings, and well-being.”
What I say and do
I always ensure at the end of my visit with a patient and their family that they know when to expect me to return to see their child again.
Why I do it
One of the biggest frustrations I hear from families pertains to the discharge process. In talking with families, they want to know the approximate time for discharge. Often, during morning rounds, we mention that the patient may be able to go home later in the day and we say that we will come in again later to check on them. However, unless we give families a time frame for when we will come back and do that check, they are left waiting without any clear expectations.
How I do it
One of our goals during morning family-centered rounds is to discuss discharge for every patient, every day. Along with discussing the possibility of going home, we try to give the family goals that they can work on throughout the day that are tied to discharge – for example, the approximate by-mouth intake for a toddler admitted for gastroenteritis and dehydration.
I also give the family an approximate time when either I or the resident team will come back to see if they have achieved this goal. This may be either late afternoon or first thing in the morning if we are planning an early-morning discharge before rounds. The families seem to find this helpful because they are not tied to the room all day waiting for the doctor to come back.
I also make sure that the families know they can contact their nurse any time if they need to see any of the doctors sooner than we planned. I let them know that a physician is here on the floor 24 hours a day and that the nurses can easily reach us at any time if they have further concerns. In my experience, this is reassuring to our families.
Christine Hrach is a pediatric hospitalist at Washington University School of Medicine in St. Louis.