User login
WATCH: Why Teaching Hospital Medicine Can Be a Rewarding Career
Two academic hospitalists talk about why they teach, what they're learning from their students, and what they see as the future of hospital medicine. Since academic HM is the new-hospitalist pipeline, hearing what they're seeing in their student and resident trainee corps is a snapshot of HM's sustainability.
Two academic hospitalists talk about why they teach, what they're learning from their students, and what they see as the future of hospital medicine. Since academic HM is the new-hospitalist pipeline, hearing what they're seeing in their student and resident trainee corps is a snapshot of HM's sustainability.
Two academic hospitalists talk about why they teach, what they're learning from their students, and what they see as the future of hospital medicine. Since academic HM is the new-hospitalist pipeline, hearing what they're seeing in their student and resident trainee corps is a snapshot of HM's sustainability.

Postoperative Clostridium Difficile Infection Associated with Number of Antibiotics, Surgical Procedure Complexity
Clinical question: What are the factors that increase risk of Clostridium difficile infection (CDI) in postoperative patients?

Background: CDI has become an important infectious etiology for morbidity, lengthy and costly hospital admissions, and mortality. This study focused on the risks for postoperative patients to be infected with C. diff. Awareness of the risk factors for CDI allows for processes to be implemented that can decrease the rate of infection.
Study design: Retrospective, observational study.
Setting: Multiple Veterans Health Administration surgery programs.
Synopsis: The study investigated 468,386 surgical procedures in 134 surgical programs in 12 subspecialties over a four-year period. Overall, the postoperative CDI rate was 0.4% per year. Rates were higher in emergency or complex procedures, older patients, patients with longer preoperative hospital stays, and those who received three or more classes of antibiotics. CDI in postoperative patients was associated with five times higher risk of mortality, a 12 times higher risk of morbidity, and longer hospital stays (17.9 versus 3.6 days) compared with those without CDI. Further studies with a larger population size will confirm the findings of this study.
The study was conducted on middle-aged to elderly male veterans, and it can only be assumed that these results will translate to other populations. Nevertheless, CDI can lead to significant morbidity and mortality, and the study reinforces the importance of infection control and prevention to reduce CDI incidence and disease severity.
Bottom line: Postoperative CDI is significantly associated with the number of postoperative antibiotics, surgical procedure complexity, preoperative length of stay, and patient comorbidities.
Citation: Li X, Wilson M, Nylander W, Smith T, Lynn M, Gunnar W. Analysis of morbidity and mortality outcomes in postoperative Clostridium difficile infection in the Veterans Health Administration. JAMA Surg. 2015;25:1-9.
Clinical question: What are the factors that increase risk of Clostridium difficile infection (CDI) in postoperative patients?
Background: CDI has become an important infectious etiology for morbidity, lengthy and costly hospital admissions, and mortality. This study focused on the risks for postoperative patients to be infected with C. diff. Awareness of the risk factors for CDI allows for processes to be implemented that can decrease the rate of infection.
Study design: Retrospective, observational study.
Setting: Multiple Veterans Health Administration surgery programs.
Synopsis: The study investigated 468,386 surgical procedures in 134 surgical programs in 12 subspecialties over a four-year period. Overall, the postoperative CDI rate was 0.4% per year. Rates were higher in emergency or complex procedures, older patients, patients with longer preoperative hospital stays, and those who received three or more classes of antibiotics. CDI in postoperative patients was associated with five times higher risk of mortality, a 12 times higher risk of morbidity, and longer hospital stays (17.9 versus 3.6 days) compared with those without CDI. Further studies with a larger population size will confirm the findings of this study.
The study was conducted on middle-aged to elderly male veterans, and it can only be assumed that these results will translate to other populations. Nevertheless, CDI can lead to significant morbidity and mortality, and the study reinforces the importance of infection control and prevention to reduce CDI incidence and disease severity.
Bottom line: Postoperative CDI is significantly associated with the number of postoperative antibiotics, surgical procedure complexity, preoperative length of stay, and patient comorbidities.
Citation: Li X, Wilson M, Nylander W, Smith T, Lynn M, Gunnar W. Analysis of morbidity and mortality outcomes in postoperative Clostridium difficile infection in the Veterans Health Administration. JAMA Surg. 2015;25:1-9.
Clinical question: What are the factors that increase risk of Clostridium difficile infection (CDI) in postoperative patients?
Background: CDI has become an important infectious etiology for morbidity, lengthy and costly hospital admissions, and mortality. This study focused on the risks for postoperative patients to be infected with C. diff. Awareness of the risk factors for CDI allows for processes to be implemented that can decrease the rate of infection.
Study design: Retrospective, observational study.
Setting: Multiple Veterans Health Administration surgery programs.
Synopsis: The study investigated 468,386 surgical procedures in 134 surgical programs in 12 subspecialties over a four-year period. Overall, the postoperative CDI rate was 0.4% per year. Rates were higher in emergency or complex procedures, older patients, patients with longer preoperative hospital stays, and those who received three or more classes of antibiotics. CDI in postoperative patients was associated with five times higher risk of mortality, a 12 times higher risk of morbidity, and longer hospital stays (17.9 versus 3.6 days) compared with those without CDI. Further studies with a larger population size will confirm the findings of this study.
The study was conducted on middle-aged to elderly male veterans, and it can only be assumed that these results will translate to other populations. Nevertheless, CDI can lead to significant morbidity and mortality, and the study reinforces the importance of infection control and prevention to reduce CDI incidence and disease severity.
Bottom line: Postoperative CDI is significantly associated with the number of postoperative antibiotics, surgical procedure complexity, preoperative length of stay, and patient comorbidities.
Citation: Li X, Wilson M, Nylander W, Smith T, Lynn M, Gunnar W. Analysis of morbidity and mortality outcomes in postoperative Clostridium difficile infection in the Veterans Health Administration. JAMA Surg. 2015;25:1-9.

Most Postoperative Readmissions Due to Patient Factors
Clinical question: What is the etiology of 30-day readmissions in postoperative patients?
Background: As the focus of healthcare changes to a quality-focused model, readmissions impact physicians, reimbursements, and patients. Understanding the cause of readmissions becomes essential to preventing them. The etiology of 30-day readmissions in postoperative patients has not specifically been studied.
Study design: Retrospective analysis.
Setting: Academic tertiary-care center.
Synopsis: Using administrative claims data, an analysis of 22,559 patients who underwent a major surgical procedure between 2009 and 2013 was performed. A total of 56 surgeons within eight surgical subspecialties were analyzed, showing that variation in 30-day readmissions was largely due to patient-specific factors (82.8%) while only a minority were attributable to surgical subspecialty (14.5%) and individual surgeon levels (2.8%). Factors associated with readmission included race/ethnicity, comorbidities, postoperative complications, and extended length of stay.
Further studies within this area will need to be conducted focusing on one specific subspecialty and one surgeon to exclude confounding factors. Additional meta-analysis can then compare these individual studies. A larger population and multiple care centers will also further validate the findings. Understanding the cause of the readmissions in postoperative patients can prevent further readmissions, improve quality of care, and decrease healthcare costs. If patient factors are identified as a major cause for readmissions in postoperative patients, changes in preoperative management may need to be made.
Bottom line: Postoperative readmissions are more dependent on patient factors than surgeon- or surgical subspecialty-specific factors.
Citation: Gani F, Lucas DJ, Kim Y, Schneider EB, Pawlik TM. Understanding variation in 30-day surgical readmission in the era of accountable care: effect of the patient, surgeon, and surgical subspecialties. JAMA Surg. 2015;150(11):1042-1049.
Clinical question: What is the etiology of 30-day readmissions in postoperative patients?
Background: As the focus of healthcare changes to a quality-focused model, readmissions impact physicians, reimbursements, and patients. Understanding the cause of readmissions becomes essential to preventing them. The etiology of 30-day readmissions in postoperative patients has not specifically been studied.
Study design: Retrospective analysis.
Setting: Academic tertiary-care center.
Synopsis: Using administrative claims data, an analysis of 22,559 patients who underwent a major surgical procedure between 2009 and 2013 was performed. A total of 56 surgeons within eight surgical subspecialties were analyzed, showing that variation in 30-day readmissions was largely due to patient-specific factors (82.8%) while only a minority were attributable to surgical subspecialty (14.5%) and individual surgeon levels (2.8%). Factors associated with readmission included race/ethnicity, comorbidities, postoperative complications, and extended length of stay.
Further studies within this area will need to be conducted focusing on one specific subspecialty and one surgeon to exclude confounding factors. Additional meta-analysis can then compare these individual studies. A larger population and multiple care centers will also further validate the findings. Understanding the cause of the readmissions in postoperative patients can prevent further readmissions, improve quality of care, and decrease healthcare costs. If patient factors are identified as a major cause for readmissions in postoperative patients, changes in preoperative management may need to be made.
Bottom line: Postoperative readmissions are more dependent on patient factors than surgeon- or surgical subspecialty-specific factors.
Citation: Gani F, Lucas DJ, Kim Y, Schneider EB, Pawlik TM. Understanding variation in 30-day surgical readmission in the era of accountable care: effect of the patient, surgeon, and surgical subspecialties. JAMA Surg. 2015;150(11):1042-1049.
Clinical question: What is the etiology of 30-day readmissions in postoperative patients?
Background: As the focus of healthcare changes to a quality-focused model, readmissions impact physicians, reimbursements, and patients. Understanding the cause of readmissions becomes essential to preventing them. The etiology of 30-day readmissions in postoperative patients has not specifically been studied.
Study design: Retrospective analysis.
Setting: Academic tertiary-care center.
Synopsis: Using administrative claims data, an analysis of 22,559 patients who underwent a major surgical procedure between 2009 and 2013 was performed. A total of 56 surgeons within eight surgical subspecialties were analyzed, showing that variation in 30-day readmissions was largely due to patient-specific factors (82.8%) while only a minority were attributable to surgical subspecialty (14.5%) and individual surgeon levels (2.8%). Factors associated with readmission included race/ethnicity, comorbidities, postoperative complications, and extended length of stay.
Further studies within this area will need to be conducted focusing on one specific subspecialty and one surgeon to exclude confounding factors. Additional meta-analysis can then compare these individual studies. A larger population and multiple care centers will also further validate the findings. Understanding the cause of the readmissions in postoperative patients can prevent further readmissions, improve quality of care, and decrease healthcare costs. If patient factors are identified as a major cause for readmissions in postoperative patients, changes in preoperative management may need to be made.
Bottom line: Postoperative readmissions are more dependent on patient factors than surgeon- or surgical subspecialty-specific factors.
Citation: Gani F, Lucas DJ, Kim Y, Schneider EB, Pawlik TM. Understanding variation in 30-day surgical readmission in the era of accountable care: effect of the patient, surgeon, and surgical subspecialties. JAMA Surg. 2015;150(11):1042-1049.
U.S. Hospitals Should Prepare for "ransomeware" Attacks by Cyber Criminals
(Reuters) - U.S. hospitals should brace for a surge in "ransomware" attacks by cyber criminals who infect and shut down computer networks, then demand payment in return for unlocking them, a non-profit healthcare group warned on Friday.
The Health Information Trust Alliance conducted a study of some 30 mid-sized U.S. hospitals late last year and found that 52 percent of them were infected with malicious software, HITRUST Chief Executive Daniel Nutkis told Reuters.
The most common type of malware was ransomware, Nutkis said, which was present in 35 percent of the hospitals included in the study of network traffic conducted by security software maker Trend Micro Inc.
Ransomware is malicious software that locks up data in computers and leaves messages demanding payment to recover the data. Last month, Hollywood Presbyterian Hospital in Los Angeles paid a ransom of $17,000 to regain access to its systems.
This week, an attack on MedStar Health forced the largest healthcare provider in Washington, D.C., to shut down much of its computer network. The Baltimore Sun reported a ransom of $18,500 was sought. MedStar declined to comment.
HITRUST said it expects such attacks to become more frequent because ransomware has turned into a profitable business for cyber criminals.
The results of the study, which HITRUST has yet to share with the public, demonstrate that hackers have moved away from focusing on stealing patient data, Nutkis said.
"If stuff isn't working, they move on. If stuff is working, they keep doing it," said Nutkis. "Organizations that are paying have considered their options, and unfortunately they don't have a lot of options."
Extortion has become more popular with cyber criminals because it is seen as a way to generate fast money, said Larry Whiteside, a healthcare expert with cyber security firm Optiv.
Stealing healthcare data is far more labour intensive, requiring attackers to keep their presence in a victim's network undetected for months as they steal data, then they need to find buyers, he added.
"With ransomware I'm going to get paid immediately," Whiteside said.
Frisco, Texas-based HITRUST's board includes executives from Anthem, Health Care Services, Humana, UnitedHealth and Walgreens.
(Reuters) - U.S. hospitals should brace for a surge in "ransomware" attacks by cyber criminals who infect and shut down computer networks, then demand payment in return for unlocking them, a non-profit healthcare group warned on Friday.
The Health Information Trust Alliance conducted a study of some 30 mid-sized U.S. hospitals late last year and found that 52 percent of them were infected with malicious software, HITRUST Chief Executive Daniel Nutkis told Reuters.
The most common type of malware was ransomware, Nutkis said, which was present in 35 percent of the hospitals included in the study of network traffic conducted by security software maker Trend Micro Inc.
Ransomware is malicious software that locks up data in computers and leaves messages demanding payment to recover the data. Last month, Hollywood Presbyterian Hospital in Los Angeles paid a ransom of $17,000 to regain access to its systems.
This week, an attack on MedStar Health forced the largest healthcare provider in Washington, D.C., to shut down much of its computer network. The Baltimore Sun reported a ransom of $18,500 was sought. MedStar declined to comment.
HITRUST said it expects such attacks to become more frequent because ransomware has turned into a profitable business for cyber criminals.
The results of the study, which HITRUST has yet to share with the public, demonstrate that hackers have moved away from focusing on stealing patient data, Nutkis said.
"If stuff isn't working, they move on. If stuff is working, they keep doing it," said Nutkis. "Organizations that are paying have considered their options, and unfortunately they don't have a lot of options."
Extortion has become more popular with cyber criminals because it is seen as a way to generate fast money, said Larry Whiteside, a healthcare expert with cyber security firm Optiv.
Stealing healthcare data is far more labour intensive, requiring attackers to keep their presence in a victim's network undetected for months as they steal data, then they need to find buyers, he added.
"With ransomware I'm going to get paid immediately," Whiteside said.
Frisco, Texas-based HITRUST's board includes executives from Anthem, Health Care Services, Humana, UnitedHealth and Walgreens.
(Reuters) - U.S. hospitals should brace for a surge in "ransomware" attacks by cyber criminals who infect and shut down computer networks, then demand payment in return for unlocking them, a non-profit healthcare group warned on Friday.
The Health Information Trust Alliance conducted a study of some 30 mid-sized U.S. hospitals late last year and found that 52 percent of them were infected with malicious software, HITRUST Chief Executive Daniel Nutkis told Reuters.
The most common type of malware was ransomware, Nutkis said, which was present in 35 percent of the hospitals included in the study of network traffic conducted by security software maker Trend Micro Inc.
Ransomware is malicious software that locks up data in computers and leaves messages demanding payment to recover the data. Last month, Hollywood Presbyterian Hospital in Los Angeles paid a ransom of $17,000 to regain access to its systems.
This week, an attack on MedStar Health forced the largest healthcare provider in Washington, D.C., to shut down much of its computer network. The Baltimore Sun reported a ransom of $18,500 was sought. MedStar declined to comment.
HITRUST said it expects such attacks to become more frequent because ransomware has turned into a profitable business for cyber criminals.
The results of the study, which HITRUST has yet to share with the public, demonstrate that hackers have moved away from focusing on stealing patient data, Nutkis said.
"If stuff isn't working, they move on. If stuff is working, they keep doing it," said Nutkis. "Organizations that are paying have considered their options, and unfortunately they don't have a lot of options."
Extortion has become more popular with cyber criminals because it is seen as a way to generate fast money, said Larry Whiteside, a healthcare expert with cyber security firm Optiv.
Stealing healthcare data is far more labour intensive, requiring attackers to keep their presence in a victim's network undetected for months as they steal data, then they need to find buyers, he added.
"With ransomware I'm going to get paid immediately," Whiteside said.
Frisco, Texas-based HITRUST's board includes executives from Anthem, Health Care Services, Humana, UnitedHealth and Walgreens.
Take Advantage of SHM's Volunteer Experiences
Are you interested in growing professionally and getting involved in work that you are excited about with colleagues across the country? You are in the driver’s seat as a hospitalist. You are in a position to lead, initiate quality improvement, impact patient outcomes, and advocate for your patients and your specialty in healthcare legislation.
SHM offers a wealth of volunteer experiences that will grow your strengths and interests, sharpen your professional acumen, and enhance your profile. New engagement opportunities are added regularly and represent unique ways to make a difference in hospital medicine. Check out some highlights:

These are just a few potential opportunities available from SHM. To learn more and find one that fits your interests, visit hospitalmedicine.org/professionalgrowth.
Are you interested in growing professionally and getting involved in work that you are excited about with colleagues across the country? You are in the driver’s seat as a hospitalist. You are in a position to lead, initiate quality improvement, impact patient outcomes, and advocate for your patients and your specialty in healthcare legislation.
SHM offers a wealth of volunteer experiences that will grow your strengths and interests, sharpen your professional acumen, and enhance your profile. New engagement opportunities are added regularly and represent unique ways to make a difference in hospital medicine. Check out some highlights:
These are just a few potential opportunities available from SHM. To learn more and find one that fits your interests, visit hospitalmedicine.org/professionalgrowth.
Are you interested in growing professionally and getting involved in work that you are excited about with colleagues across the country? You are in the driver’s seat as a hospitalist. You are in a position to lead, initiate quality improvement, impact patient outcomes, and advocate for your patients and your specialty in healthcare legislation.
SHM offers a wealth of volunteer experiences that will grow your strengths and interests, sharpen your professional acumen, and enhance your profile. New engagement opportunities are added regularly and represent unique ways to make a difference in hospital medicine. Check out some highlights:
These are just a few potential opportunities available from SHM. To learn more and find one that fits your interests, visit hospitalmedicine.org/professionalgrowth.
Administrators Share Strategies for High-Performing Hospitalist Groups at HM16
In November, Barbara Weisenbach took a new job as practice manager for the hospitalist group at Northwest Hospital in Seattle. She’s an experienced administrator but as for hospital medicine, not so much. And she is the group’s first full-fledged practice manager—as in, she’s not a physician taking on admin responsibilities and seeing a partial census.
She’s doing a lot of reshaping and a lot of learning, she said, standing outside Room 10 of the San Diego Convention Center, where a daylong pre-course on practice management was being held at SHM’s annual meeting.
“There have been a lot of business things that have been overlooked and not addressed ever before,” she said.
The pre-course, “The Highly Effective Hospital Medicine Group: Using SHM’s Key Characteristics to Drive Performance,” was led by John Nelson, MD, MHM, and Leslie Flores, MHA, SFHM, and offered one useful lesson after another, Weisenbach said.
“One of the most practical portions of the session this morning was about dashboards, which is something I’m currently working on and could definitely use some insight,” Weisenbach said, adding that a list of metrics a dashboard should include and general guidelines on effective dashboards were things she’ll find useful in her own implementation.
The pre-course expanded on the key principles and traits for effective groups, including effective leadership, engaged hospitalists, adequate resources, alignment with the hospital, and care coordination across settings.

HM16 also included two and a half days of practice management sessions. Plus, management themes were woven through workshops and sprinkled into other sessions.
In one session on handling change, presenters used a surfing analogy: Like a surfer’s intensity just before riding a wave, a laser focus is called for when the moment arrives to execute change.
“Get ready for the ride,” said Steve Behnke, MD, president of Columbus, Ohio–based MedOne Hospital Physicians.
He discussed details of introducing the electronic health record system Epic at their group. There was 18 months of planning involving the practice’s whole operational team, then a doubling of the staffing ratios when the system went live, followed by catered lunches to gather feedback and identify problems.
Presenters emphasized the idea of agility in responding to obstacles and realizing that change affects everyone. Successful change, they said, involves seeing the process from all perspectives and leaders should expect resistance.
“Court them. Listen to them. I can’t tell you how many times I’ve done that,” said Dea Robinson, MA, MedOne’s vice president of operations. “Just listening and giving a platform.”
Back at the pre-course, Dr. Nelson, a hospital medicine consultant, talked about the importance of effective leadership.

“An effective group leader is a really key element of a successful group,” said The Hospitalist’s resident practice management columnist. “I’ve worked on-site with many hundreds of hospitalist groups around the country. There’s pretty good correlation between the effectiveness of the leader and the success of the group overall. But a good leader alone is not enough.”
He added that there are too “few leaders to go around.”
A good leader is an active one, he said, adding with funny-because-it’s-true humor that a lot of leaders say their main job is to make the schedule. Good leaders, he said, need to be focused on making the group high-functioning, should be available for administrative work even when not on a clinical shift, and must be able to delegate.
Another critical ingredient for a successful group, he said, is having engaged frontline hospitalists. Reviews need to be meaningful, and meetings should be held regularly with attendance essentially mandatory. Meetings, he said, might need a “tune-up,” with actual voting, written agendas, minutes taken, and group problem-solving above one-way information.
Win Whitcomb, MD, MHM, on care coordination, said the relationship with primary care physicians is crucial though difficult.
“I think we have to go out of our way to build relationships,” he said. “And we don’t have occasion to see them, so we need to figure out a way to get to know our community.”
He suggested:
- Having dedicated transcriptionists for hospitalists,
- Tracking the rate at which discharge summaries are generated within 24 hours,
- Making sure PCPs know how to reach hospitalists, and
- Scheduling events—perhaps an annual event—for meeting PCPs and skill-nursing facility healthcare professionals.
It was clear that, in a field whose dimensions seem to be changing all the time, practice management remained a top interest at HM16. Robert Clothier, RN, a practice manager for the hospitalist group at ThedaCare in Wisconsin, recently switched from managing a cardiology clinic. He said there were huge differences in hospital medicine.
“The profession is growing so fast, and really nobody knows where the end is,” he said. “I can’t even think of anything where you could say, ‘Well, no, they’ll never do that.’ It’s endless. That’s going to be hardest thing. People are going to be pulling on us, and leadership from the hospital is going to be saying, ‘You guys need to do this.’
“So how can I control what we pick, and how can I make sure that we have the resources to do it?” TH
In November, Barbara Weisenbach took a new job as practice manager for the hospitalist group at Northwest Hospital in Seattle. She’s an experienced administrator but as for hospital medicine, not so much. And she is the group’s first full-fledged practice manager—as in, she’s not a physician taking on admin responsibilities and seeing a partial census.
She’s doing a lot of reshaping and a lot of learning, she said, standing outside Room 10 of the San Diego Convention Center, where a daylong pre-course on practice management was being held at SHM’s annual meeting.
“There have been a lot of business things that have been overlooked and not addressed ever before,” she said.
The pre-course, “The Highly Effective Hospital Medicine Group: Using SHM’s Key Characteristics to Drive Performance,” was led by John Nelson, MD, MHM, and Leslie Flores, MHA, SFHM, and offered one useful lesson after another, Weisenbach said.
“One of the most practical portions of the session this morning was about dashboards, which is something I’m currently working on and could definitely use some insight,” Weisenbach said, adding that a list of metrics a dashboard should include and general guidelines on effective dashboards were things she’ll find useful in her own implementation.
The pre-course expanded on the key principles and traits for effective groups, including effective leadership, engaged hospitalists, adequate resources, alignment with the hospital, and care coordination across settings.
HM16 also included two and a half days of practice management sessions. Plus, management themes were woven through workshops and sprinkled into other sessions.
In one session on handling change, presenters used a surfing analogy: Like a surfer’s intensity just before riding a wave, a laser focus is called for when the moment arrives to execute change.
“Get ready for the ride,” said Steve Behnke, MD, president of Columbus, Ohio–based MedOne Hospital Physicians.
He discussed details of introducing the electronic health record system Epic at their group. There was 18 months of planning involving the practice’s whole operational team, then a doubling of the staffing ratios when the system went live, followed by catered lunches to gather feedback and identify problems.
Presenters emphasized the idea of agility in responding to obstacles and realizing that change affects everyone. Successful change, they said, involves seeing the process from all perspectives and leaders should expect resistance.
“Court them. Listen to them. I can’t tell you how many times I’ve done that,” said Dea Robinson, MA, MedOne’s vice president of operations. “Just listening and giving a platform.”
Back at the pre-course, Dr. Nelson, a hospital medicine consultant, talked about the importance of effective leadership.
“An effective group leader is a really key element of a successful group,” said The Hospitalist’s resident practice management columnist. “I’ve worked on-site with many hundreds of hospitalist groups around the country. There’s pretty good correlation between the effectiveness of the leader and the success of the group overall. But a good leader alone is not enough.”
He added that there are too “few leaders to go around.”
A good leader is an active one, he said, adding with funny-because-it’s-true humor that a lot of leaders say their main job is to make the schedule. Good leaders, he said, need to be focused on making the group high-functioning, should be available for administrative work even when not on a clinical shift, and must be able to delegate.
Another critical ingredient for a successful group, he said, is having engaged frontline hospitalists. Reviews need to be meaningful, and meetings should be held regularly with attendance essentially mandatory. Meetings, he said, might need a “tune-up,” with actual voting, written agendas, minutes taken, and group problem-solving above one-way information.
Win Whitcomb, MD, MHM, on care coordination, said the relationship with primary care physicians is crucial though difficult.
“I think we have to go out of our way to build relationships,” he said. “And we don’t have occasion to see them, so we need to figure out a way to get to know our community.”
He suggested:
- Having dedicated transcriptionists for hospitalists,
- Tracking the rate at which discharge summaries are generated within 24 hours,
- Making sure PCPs know how to reach hospitalists, and
- Scheduling events—perhaps an annual event—for meeting PCPs and skill-nursing facility healthcare professionals.
It was clear that, in a field whose dimensions seem to be changing all the time, practice management remained a top interest at HM16. Robert Clothier, RN, a practice manager for the hospitalist group at ThedaCare in Wisconsin, recently switched from managing a cardiology clinic. He said there were huge differences in hospital medicine.
“The profession is growing so fast, and really nobody knows where the end is,” he said. “I can’t even think of anything where you could say, ‘Well, no, they’ll never do that.’ It’s endless. That’s going to be hardest thing. People are going to be pulling on us, and leadership from the hospital is going to be saying, ‘You guys need to do this.’
“So how can I control what we pick, and how can I make sure that we have the resources to do it?” TH
In November, Barbara Weisenbach took a new job as practice manager for the hospitalist group at Northwest Hospital in Seattle. She’s an experienced administrator but as for hospital medicine, not so much. And she is the group’s first full-fledged practice manager—as in, she’s not a physician taking on admin responsibilities and seeing a partial census.
She’s doing a lot of reshaping and a lot of learning, she said, standing outside Room 10 of the San Diego Convention Center, where a daylong pre-course on practice management was being held at SHM’s annual meeting.
“There have been a lot of business things that have been overlooked and not addressed ever before,” she said.
The pre-course, “The Highly Effective Hospital Medicine Group: Using SHM’s Key Characteristics to Drive Performance,” was led by John Nelson, MD, MHM, and Leslie Flores, MHA, SFHM, and offered one useful lesson after another, Weisenbach said.
“One of the most practical portions of the session this morning was about dashboards, which is something I’m currently working on and could definitely use some insight,” Weisenbach said, adding that a list of metrics a dashboard should include and general guidelines on effective dashboards were things she’ll find useful in her own implementation.
The pre-course expanded on the key principles and traits for effective groups, including effective leadership, engaged hospitalists, adequate resources, alignment with the hospital, and care coordination across settings.
HM16 also included two and a half days of practice management sessions. Plus, management themes were woven through workshops and sprinkled into other sessions.
In one session on handling change, presenters used a surfing analogy: Like a surfer’s intensity just before riding a wave, a laser focus is called for when the moment arrives to execute change.
“Get ready for the ride,” said Steve Behnke, MD, president of Columbus, Ohio–based MedOne Hospital Physicians.
He discussed details of introducing the electronic health record system Epic at their group. There was 18 months of planning involving the practice’s whole operational team, then a doubling of the staffing ratios when the system went live, followed by catered lunches to gather feedback and identify problems.
Presenters emphasized the idea of agility in responding to obstacles and realizing that change affects everyone. Successful change, they said, involves seeing the process from all perspectives and leaders should expect resistance.
“Court them. Listen to them. I can’t tell you how many times I’ve done that,” said Dea Robinson, MA, MedOne’s vice president of operations. “Just listening and giving a platform.”
Back at the pre-course, Dr. Nelson, a hospital medicine consultant, talked about the importance of effective leadership.
“An effective group leader is a really key element of a successful group,” said The Hospitalist’s resident practice management columnist. “I’ve worked on-site with many hundreds of hospitalist groups around the country. There’s pretty good correlation between the effectiveness of the leader and the success of the group overall. But a good leader alone is not enough.”
He added that there are too “few leaders to go around.”
A good leader is an active one, he said, adding with funny-because-it’s-true humor that a lot of leaders say their main job is to make the schedule. Good leaders, he said, need to be focused on making the group high-functioning, should be available for administrative work even when not on a clinical shift, and must be able to delegate.
Another critical ingredient for a successful group, he said, is having engaged frontline hospitalists. Reviews need to be meaningful, and meetings should be held regularly with attendance essentially mandatory. Meetings, he said, might need a “tune-up,” with actual voting, written agendas, minutes taken, and group problem-solving above one-way information.
Win Whitcomb, MD, MHM, on care coordination, said the relationship with primary care physicians is crucial though difficult.
“I think we have to go out of our way to build relationships,” he said. “And we don’t have occasion to see them, so we need to figure out a way to get to know our community.”
He suggested:
- Having dedicated transcriptionists for hospitalists,
- Tracking the rate at which discharge summaries are generated within 24 hours,
- Making sure PCPs know how to reach hospitalists, and
- Scheduling events—perhaps an annual event—for meeting PCPs and skill-nursing facility healthcare professionals.
It was clear that, in a field whose dimensions seem to be changing all the time, practice management remained a top interest at HM16. Robert Clothier, RN, a practice manager for the hospitalist group at ThedaCare in Wisconsin, recently switched from managing a cardiology clinic. He said there were huge differences in hospital medicine.
“The profession is growing so fast, and really nobody knows where the end is,” he said. “I can’t even think of anything where you could say, ‘Well, no, they’ll never do that.’ It’s endless. That’s going to be hardest thing. People are going to be pulling on us, and leadership from the hospital is going to be saying, ‘You guys need to do this.’
“So how can I control what we pick, and how can I make sure that we have the resources to do it?” TH
UK Report Shows Prevalence of Antibiotic Resistance in Pediatric Urinary Tract Infection
NEW YORK (Reuters Health) - The prevalence of antibiotic resistance in pediatric urinary tract infection (UTI) has reached such high levels in many countries that existing empiric therapies may no longer be effective, researchers from UK report."
Prevalence of resistance to commonly prescribed antibiotics in primary care in children with urinary tract infections caused by E. coli is high, and there was remarkable variability in E. coli resistance among countries in the study, particularly in countries outside the OECD (Organization for Economic Cooperation and Development), where one possible explanation is the availability of antibiotics over the counter," Ashley Bryce from the University of Bristol in the U.K. and Dr. Céire E. Costelloe from Imperial College London told Reuters Health in a joint email.
"This could render some antibiotics ineffective as first-line treatments for urinary tract infection," they said.
E. coli is responsible for more than 80% of all UTIs and is also the most common cause of bacteremia and foodborne infections and one cause of meningitis in neonates.
Bryce, Dr. Costelloe, and colleagues investigated the prevalence of resistance in community-acquired E. coli UTI to the most commonly prescribed antibiotics given to children in primary care in their systematic review of 58 published reports.
For all antibiotics tested, the prevalence of antibiotic resistance was higher in non-OECD countries than in OECD countries, the team reports in an article online March 15 in The BMJ.
The prevalence of resistance was highest for ampicillin, ranging from 41% in Switzerland to 100% in Ghana and Nigeria.
Resistance to co-trimoxazole and trimethoprim was 30% in OECD countries and 67% in Saudi Arabia, the only non-OECD country for which rates were available.
Pooled prevalences of resistance to ciprofloxacin and ceftazidime were around 2% in OECD countries but over 26% in non-OECD countries.
For all time periods analyzed, the odds of resistance were greater in children exposed to antibiotics than in those who were unexposed.
"The Infectious Diseases Society of America (IDSA) in collaboration with the European Society for Microbiology and Infectious Diseases (ESCMID) recommend that an antibiotic should be selected for first line empirical treatment of urinary tract infection only if the local prevalence of resistance is less than 20%," the researchers note.
"According to these guidelines, our review suggests ampicillin, co-trimoxazole, and trimethoprim are no longer suitable first line treatment options for urinary tract infection in many OECD countries and that as a result many guidelines, such as those published by the National Institute for Health and Care Excellence (NICE), might need updating," they write. "In non-OECD countries, resistance to all first line antibiotics specified for urinary tract infections was in excess of 20%, suggesting that choices of first line treatment might need to be re-evaluated in less well developed countries."
"We are not able to advise clinicians on which antibiotic is best to prescribe as this often depends on the individual case," Bryce and Dr. Costelloe said. "Clinicians should, however, adhere to local or national guidelines wherever possible, which is why it is of great importance that such guidelines are kept up to date and reflect current resistance rates."
"Clinicians may also wish to consider the antibiotic history of the child when they present to primary care with symptoms of an infection, especially in light of the suggestion of our results that previous treatment with an antibiotic is associated with resistance to that same antibiotic, and that this association may be present up to 6 months post treatment," they added.
Dr. Grant Russell from Monash University in Melbourne, Australia, wrote an editorial accompanying the report. He told Reuters Health by email, "I found the extent of the resistance (and the fact that it covered all of the regularly used empiric antibiotics) both concerning and surprising. The fact that choices are diminishing is disturbing, and the fact that the situation is dire in the developing world is deeply troubling."
"We need to do what we can do to prevent bacterial infections, and when treating them to consider that effective antibiotics are a finite resource," he said. "We all have a responsibility in attempting to conserve that resource."
"No new classes of antibiotics have been developed in the last 30 years - this and the dire situation in both the developed and the developing world suggests that the 'global problem' of antibiotic resistance is going to become more and more of an issue in years and decades to come," Dr. Russell concluded.
NEW YORK (Reuters Health) - The prevalence of antibiotic resistance in pediatric urinary tract infection (UTI) has reached such high levels in many countries that existing empiric therapies may no longer be effective, researchers from UK report."
Prevalence of resistance to commonly prescribed antibiotics in primary care in children with urinary tract infections caused by E. coli is high, and there was remarkable variability in E. coli resistance among countries in the study, particularly in countries outside the OECD (Organization for Economic Cooperation and Development), where one possible explanation is the availability of antibiotics over the counter," Ashley Bryce from the University of Bristol in the U.K. and Dr. Céire E. Costelloe from Imperial College London told Reuters Health in a joint email.
"This could render some antibiotics ineffective as first-line treatments for urinary tract infection," they said.
E. coli is responsible for more than 80% of all UTIs and is also the most common cause of bacteremia and foodborne infections and one cause of meningitis in neonates.
Bryce, Dr. Costelloe, and colleagues investigated the prevalence of resistance in community-acquired E. coli UTI to the most commonly prescribed antibiotics given to children in primary care in their systematic review of 58 published reports.
For all antibiotics tested, the prevalence of antibiotic resistance was higher in non-OECD countries than in OECD countries, the team reports in an article online March 15 in The BMJ.
The prevalence of resistance was highest for ampicillin, ranging from 41% in Switzerland to 100% in Ghana and Nigeria.
Resistance to co-trimoxazole and trimethoprim was 30% in OECD countries and 67% in Saudi Arabia, the only non-OECD country for which rates were available.
Pooled prevalences of resistance to ciprofloxacin and ceftazidime were around 2% in OECD countries but over 26% in non-OECD countries.
For all time periods analyzed, the odds of resistance were greater in children exposed to antibiotics than in those who were unexposed.
"The Infectious Diseases Society of America (IDSA) in collaboration with the European Society for Microbiology and Infectious Diseases (ESCMID) recommend that an antibiotic should be selected for first line empirical treatment of urinary tract infection only if the local prevalence of resistance is less than 20%," the researchers note.
"According to these guidelines, our review suggests ampicillin, co-trimoxazole, and trimethoprim are no longer suitable first line treatment options for urinary tract infection in many OECD countries and that as a result many guidelines, such as those published by the National Institute for Health and Care Excellence (NICE), might need updating," they write. "In non-OECD countries, resistance to all first line antibiotics specified for urinary tract infections was in excess of 20%, suggesting that choices of first line treatment might need to be re-evaluated in less well developed countries."
"We are not able to advise clinicians on which antibiotic is best to prescribe as this often depends on the individual case," Bryce and Dr. Costelloe said. "Clinicians should, however, adhere to local or national guidelines wherever possible, which is why it is of great importance that such guidelines are kept up to date and reflect current resistance rates."
"Clinicians may also wish to consider the antibiotic history of the child when they present to primary care with symptoms of an infection, especially in light of the suggestion of our results that previous treatment with an antibiotic is associated with resistance to that same antibiotic, and that this association may be present up to 6 months post treatment," they added.
Dr. Grant Russell from Monash University in Melbourne, Australia, wrote an editorial accompanying the report. He told Reuters Health by email, "I found the extent of the resistance (and the fact that it covered all of the regularly used empiric antibiotics) both concerning and surprising. The fact that choices are diminishing is disturbing, and the fact that the situation is dire in the developing world is deeply troubling."
"We need to do what we can do to prevent bacterial infections, and when treating them to consider that effective antibiotics are a finite resource," he said. "We all have a responsibility in attempting to conserve that resource."
"No new classes of antibiotics have been developed in the last 30 years - this and the dire situation in both the developed and the developing world suggests that the 'global problem' of antibiotic resistance is going to become more and more of an issue in years and decades to come," Dr. Russell concluded.
NEW YORK (Reuters Health) - The prevalence of antibiotic resistance in pediatric urinary tract infection (UTI) has reached such high levels in many countries that existing empiric therapies may no longer be effective, researchers from UK report."
Prevalence of resistance to commonly prescribed antibiotics in primary care in children with urinary tract infections caused by E. coli is high, and there was remarkable variability in E. coli resistance among countries in the study, particularly in countries outside the OECD (Organization for Economic Cooperation and Development), where one possible explanation is the availability of antibiotics over the counter," Ashley Bryce from the University of Bristol in the U.K. and Dr. Céire E. Costelloe from Imperial College London told Reuters Health in a joint email.
"This could render some antibiotics ineffective as first-line treatments for urinary tract infection," they said.
E. coli is responsible for more than 80% of all UTIs and is also the most common cause of bacteremia and foodborne infections and one cause of meningitis in neonates.
Bryce, Dr. Costelloe, and colleagues investigated the prevalence of resistance in community-acquired E. coli UTI to the most commonly prescribed antibiotics given to children in primary care in their systematic review of 58 published reports.
For all antibiotics tested, the prevalence of antibiotic resistance was higher in non-OECD countries than in OECD countries, the team reports in an article online March 15 in The BMJ.
The prevalence of resistance was highest for ampicillin, ranging from 41% in Switzerland to 100% in Ghana and Nigeria.
Resistance to co-trimoxazole and trimethoprim was 30% in OECD countries and 67% in Saudi Arabia, the only non-OECD country for which rates were available.
Pooled prevalences of resistance to ciprofloxacin and ceftazidime were around 2% in OECD countries but over 26% in non-OECD countries.
For all time periods analyzed, the odds of resistance were greater in children exposed to antibiotics than in those who were unexposed.
"The Infectious Diseases Society of America (IDSA) in collaboration with the European Society for Microbiology and Infectious Diseases (ESCMID) recommend that an antibiotic should be selected for first line empirical treatment of urinary tract infection only if the local prevalence of resistance is less than 20%," the researchers note.
"According to these guidelines, our review suggests ampicillin, co-trimoxazole, and trimethoprim are no longer suitable first line treatment options for urinary tract infection in many OECD countries and that as a result many guidelines, such as those published by the National Institute for Health and Care Excellence (NICE), might need updating," they write. "In non-OECD countries, resistance to all first line antibiotics specified for urinary tract infections was in excess of 20%, suggesting that choices of first line treatment might need to be re-evaluated in less well developed countries."
"We are not able to advise clinicians on which antibiotic is best to prescribe as this often depends on the individual case," Bryce and Dr. Costelloe said. "Clinicians should, however, adhere to local or national guidelines wherever possible, which is why it is of great importance that such guidelines are kept up to date and reflect current resistance rates."
"Clinicians may also wish to consider the antibiotic history of the child when they present to primary care with symptoms of an infection, especially in light of the suggestion of our results that previous treatment with an antibiotic is associated with resistance to that same antibiotic, and that this association may be present up to 6 months post treatment," they added.
Dr. Grant Russell from Monash University in Melbourne, Australia, wrote an editorial accompanying the report. He told Reuters Health by email, "I found the extent of the resistance (and the fact that it covered all of the regularly used empiric antibiotics) both concerning and surprising. The fact that choices are diminishing is disturbing, and the fact that the situation is dire in the developing world is deeply troubling."
"We need to do what we can do to prevent bacterial infections, and when treating them to consider that effective antibiotics are a finite resource," he said. "We all have a responsibility in attempting to conserve that resource."
"No new classes of antibiotics have been developed in the last 30 years - this and the dire situation in both the developed and the developing world suggests that the 'global problem' of antibiotic resistance is going to become more and more of an issue in years and decades to come," Dr. Russell concluded.
New Sepsis Definition, Bedside Screening to Identify Patients at High-Mortality Risk
Clinical question: What are the best criteria to identify sepsis and septic shock?
Bottom line: An international task force of experts has updated the definitions of sepsis and septic shock and created a new bedside scoring tool to identify patients with suspected infection who may be at high risk for poor outcomes. Based on the Sequential Organ Failure Assessment (SOFA) score, the new quickSOFA states that meeting 2 of 3 clinical criteria (respiratory rate of 22 per minute or greater, systolic blood pressure of 100 mg Hg or less, and altered mental status) identifies patients at high risk of poor outcomes from sepsis. This score will need to be validated further in multiple health care settings before it can be widely accepted in clinical practice. (LOE = 5)
References: Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016;315(8):801-810.
Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis (Sepsis-3). JAMA 2016;315(8):762-774.
Shankar-Hari M, Phillips GS, Levy ML, et al. Developing a new definition and assessing new clinical criteria for septic shock (Sepsis-3). JAMA 2016;315(8):775-787.
Study design: Other
Funding source: Foundation
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis: Systemic inflammatory response syndrome (SIRS) criteria are present in many hospitalized patients, even those without infections or life-threatening illnesses. The use of these criteria to identify sepsis may lead to misdiagnosis. Funded by the European Society of Intensive Care Medicine and the Society of Critical Care Medicine, an international task force consisting of 19 critical care, infectious disease, surgical, and pulmonary specialists convened to update the definitions of sepsis and septic shock and identify clinical criteria that can be used to recognize patients at high risk for mortality. Researchers conducted a systematic review and meta-analysis of observational studies followed by a Delphi consensus process to determine appropriate criteria for identifying septic shock. Furthermore, they validated and confirmed the ability of different clinical criteria, including the SIRS criteria and the SOFA score, to predict poor outcomes in patients with suspected infection.
Per the task force's recommendations, sepsis should be defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. Septic shock is a subset of sepsis in which there is an increased risk of mortality due to profound circulatory and cellular metabolism abnormalities. Sepsis can be identified by an increase in the SOFA score of 2 points or more. This is associated with an in-hospital mortality exceeding 10%. Septic shock can be identified by a vasopressor requirement to maintain a mean arterial pressure of 65 mm Hg or greater and a serum lactate level greater than 18 mg/dL (> 2 mmol/L) after adequate fluid resuscitation. This combination of clinical criteria is associated with a hospital mortality rate of 40%.
Using a derivation and validation cohort of approximately 75,000 patients, the group also developed a new bedside clinical measure termed quickSOFA, or qSOFA, which consists of a respiratory rate of 22 per minute or greater, altered mental status, and systolic blood pressure of 100 mm Hg or less. Patients with suspected infection who are not in the intensive care unit and have at least 2 of these 3 criteria are at higher risk of poor outcomes from sepsis (area under receiver operating characteristics curve = 0.81).
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: What are the best criteria to identify sepsis and septic shock?
Bottom line: An international task force of experts has updated the definitions of sepsis and septic shock and created a new bedside scoring tool to identify patients with suspected infection who may be at high risk for poor outcomes. Based on the Sequential Organ Failure Assessment (SOFA) score, the new quickSOFA states that meeting 2 of 3 clinical criteria (respiratory rate of 22 per minute or greater, systolic blood pressure of 100 mg Hg or less, and altered mental status) identifies patients at high risk of poor outcomes from sepsis. This score will need to be validated further in multiple health care settings before it can be widely accepted in clinical practice. (LOE = 5)
References: Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016;315(8):801-810.
Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis (Sepsis-3). JAMA 2016;315(8):762-774.
Shankar-Hari M, Phillips GS, Levy ML, et al. Developing a new definition and assessing new clinical criteria for septic shock (Sepsis-3). JAMA 2016;315(8):775-787.
Study design: Other
Funding source: Foundation
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis: Systemic inflammatory response syndrome (SIRS) criteria are present in many hospitalized patients, even those without infections or life-threatening illnesses. The use of these criteria to identify sepsis may lead to misdiagnosis. Funded by the European Society of Intensive Care Medicine and the Society of Critical Care Medicine, an international task force consisting of 19 critical care, infectious disease, surgical, and pulmonary specialists convened to update the definitions of sepsis and septic shock and identify clinical criteria that can be used to recognize patients at high risk for mortality. Researchers conducted a systematic review and meta-analysis of observational studies followed by a Delphi consensus process to determine appropriate criteria for identifying septic shock. Furthermore, they validated and confirmed the ability of different clinical criteria, including the SIRS criteria and the SOFA score, to predict poor outcomes in patients with suspected infection.
Per the task force's recommendations, sepsis should be defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. Septic shock is a subset of sepsis in which there is an increased risk of mortality due to profound circulatory and cellular metabolism abnormalities. Sepsis can be identified by an increase in the SOFA score of 2 points or more. This is associated with an in-hospital mortality exceeding 10%. Septic shock can be identified by a vasopressor requirement to maintain a mean arterial pressure of 65 mm Hg or greater and a serum lactate level greater than 18 mg/dL (> 2 mmol/L) after adequate fluid resuscitation. This combination of clinical criteria is associated with a hospital mortality rate of 40%.
Using a derivation and validation cohort of approximately 75,000 patients, the group also developed a new bedside clinical measure termed quickSOFA, or qSOFA, which consists of a respiratory rate of 22 per minute or greater, altered mental status, and systolic blood pressure of 100 mm Hg or less. Patients with suspected infection who are not in the intensive care unit and have at least 2 of these 3 criteria are at higher risk of poor outcomes from sepsis (area under receiver operating characteristics curve = 0.81).
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: What are the best criteria to identify sepsis and septic shock?
Bottom line: An international task force of experts has updated the definitions of sepsis and septic shock and created a new bedside scoring tool to identify patients with suspected infection who may be at high risk for poor outcomes. Based on the Sequential Organ Failure Assessment (SOFA) score, the new quickSOFA states that meeting 2 of 3 clinical criteria (respiratory rate of 22 per minute or greater, systolic blood pressure of 100 mg Hg or less, and altered mental status) identifies patients at high risk of poor outcomes from sepsis. This score will need to be validated further in multiple health care settings before it can be widely accepted in clinical practice. (LOE = 5)
References: Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016;315(8):801-810.
Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis (Sepsis-3). JAMA 2016;315(8):762-774.
Shankar-Hari M, Phillips GS, Levy ML, et al. Developing a new definition and assessing new clinical criteria for septic shock (Sepsis-3). JAMA 2016;315(8):775-787.
Study design: Other
Funding source: Foundation
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis: Systemic inflammatory response syndrome (SIRS) criteria are present in many hospitalized patients, even those without infections or life-threatening illnesses. The use of these criteria to identify sepsis may lead to misdiagnosis. Funded by the European Society of Intensive Care Medicine and the Society of Critical Care Medicine, an international task force consisting of 19 critical care, infectious disease, surgical, and pulmonary specialists convened to update the definitions of sepsis and septic shock and identify clinical criteria that can be used to recognize patients at high risk for mortality. Researchers conducted a systematic review and meta-analysis of observational studies followed by a Delphi consensus process to determine appropriate criteria for identifying septic shock. Furthermore, they validated and confirmed the ability of different clinical criteria, including the SIRS criteria and the SOFA score, to predict poor outcomes in patients with suspected infection.
Per the task force's recommendations, sepsis should be defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. Septic shock is a subset of sepsis in which there is an increased risk of mortality due to profound circulatory and cellular metabolism abnormalities. Sepsis can be identified by an increase in the SOFA score of 2 points or more. This is associated with an in-hospital mortality exceeding 10%. Septic shock can be identified by a vasopressor requirement to maintain a mean arterial pressure of 65 mm Hg or greater and a serum lactate level greater than 18 mg/dL (> 2 mmol/L) after adequate fluid resuscitation. This combination of clinical criteria is associated with a hospital mortality rate of 40%.
Using a derivation and validation cohort of approximately 75,000 patients, the group also developed a new bedside clinical measure termed quickSOFA, or qSOFA, which consists of a respiratory rate of 22 per minute or greater, altered mental status, and systolic blood pressure of 100 mm Hg or less. Patients with suspected infection who are not in the intensive care unit and have at least 2 of these 3 criteria are at higher risk of poor outcomes from sepsis (area under receiver operating characteristics curve = 0.81).
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Research Reaffirms Management of Hospitalized Patients with Community-Acquired Pneumonia
Clinical question: What is the best antibiotic strategy to improve outcomes in patients hospitalized with community-acquired pneumonia?
Bottom line: For patients hospitalized with community-acquired pneumonia (CAP), start antibiotics early, use either fluoroquinolone monotherapy or beta-lactam/macrolide combination therapy, and switch to oral antibiotics as soon as patients are hemodynamically stable and can take oral medications. Although the evidence is mostly of low quality, this review reaffirms what we already do. (LOE = 2a)
Reference: Lee JS, Giesler DL, Gellad WF, Fine MJ. Antibiotic therapy for adults hospitalized with community-acquired pneumonia. JAMA 2016;315(6):593-602.
Study design: Systematic review
Funding source: Unknown/not stated
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis: These investigators searched MEDLINE, EMBASE, and the Cochrane databases to identify studies that evaluated outcomes for patients hospitalized with CAP with regard to optimal timing of antibiotic initiation, initial antibiotic selection, and criteria for transition from intravenous to oral antibiotic therapy. Two authors independently reviewed studies for inclusion and assessed study quality.
Of 8 low-quality observational studies, 4 showed a significant association between initiating antibiotic therapy within 4 hours to 8 hours of hospital arrival and reduced mortality. When comparing 2 different antibiotic strategies, 6 of 8 observational studies showed mortality benefit with the use of beta-lactams plus macrolides as compared with beta-lactam monotherapy, though the 2 recent high-quality randomized trials had conflicting results. All three observational studies that compared fluoroquinolones with beta-lactam monotherapy for the treatment of CAP showed an association with fluoroquinolone use and decreased mortality.
Finally, one high-quality trial showed that transitioning patients to oral antibiotics once they meet clinical criteria for stability (stable vital signs, lack of confusion, ability to tolerate oral medications) leads to a shorter length of stay.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: What is the best antibiotic strategy to improve outcomes in patients hospitalized with community-acquired pneumonia?
Bottom line: For patients hospitalized with community-acquired pneumonia (CAP), start antibiotics early, use either fluoroquinolone monotherapy or beta-lactam/macrolide combination therapy, and switch to oral antibiotics as soon as patients are hemodynamically stable and can take oral medications. Although the evidence is mostly of low quality, this review reaffirms what we already do. (LOE = 2a)
Reference: Lee JS, Giesler DL, Gellad WF, Fine MJ. Antibiotic therapy for adults hospitalized with community-acquired pneumonia. JAMA 2016;315(6):593-602.
Study design: Systematic review
Funding source: Unknown/not stated
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis: These investigators searched MEDLINE, EMBASE, and the Cochrane databases to identify studies that evaluated outcomes for patients hospitalized with CAP with regard to optimal timing of antibiotic initiation, initial antibiotic selection, and criteria for transition from intravenous to oral antibiotic therapy. Two authors independently reviewed studies for inclusion and assessed study quality.
Of 8 low-quality observational studies, 4 showed a significant association between initiating antibiotic therapy within 4 hours to 8 hours of hospital arrival and reduced mortality. When comparing 2 different antibiotic strategies, 6 of 8 observational studies showed mortality benefit with the use of beta-lactams plus macrolides as compared with beta-lactam monotherapy, though the 2 recent high-quality randomized trials had conflicting results. All three observational studies that compared fluoroquinolones with beta-lactam monotherapy for the treatment of CAP showed an association with fluoroquinolone use and decreased mortality.
Finally, one high-quality trial showed that transitioning patients to oral antibiotics once they meet clinical criteria for stability (stable vital signs, lack of confusion, ability to tolerate oral medications) leads to a shorter length of stay.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: What is the best antibiotic strategy to improve outcomes in patients hospitalized with community-acquired pneumonia?
Bottom line: For patients hospitalized with community-acquired pneumonia (CAP), start antibiotics early, use either fluoroquinolone monotherapy or beta-lactam/macrolide combination therapy, and switch to oral antibiotics as soon as patients are hemodynamically stable and can take oral medications. Although the evidence is mostly of low quality, this review reaffirms what we already do. (LOE = 2a)
Reference: Lee JS, Giesler DL, Gellad WF, Fine MJ. Antibiotic therapy for adults hospitalized with community-acquired pneumonia. JAMA 2016;315(6):593-602.
Study design: Systematic review
Funding source: Unknown/not stated
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis: These investigators searched MEDLINE, EMBASE, and the Cochrane databases to identify studies that evaluated outcomes for patients hospitalized with CAP with regard to optimal timing of antibiotic initiation, initial antibiotic selection, and criteria for transition from intravenous to oral antibiotic therapy. Two authors independently reviewed studies for inclusion and assessed study quality.
Of 8 low-quality observational studies, 4 showed a significant association between initiating antibiotic therapy within 4 hours to 8 hours of hospital arrival and reduced mortality. When comparing 2 different antibiotic strategies, 6 of 8 observational studies showed mortality benefit with the use of beta-lactams plus macrolides as compared with beta-lactam monotherapy, though the 2 recent high-quality randomized trials had conflicting results. All three observational studies that compared fluoroquinolones with beta-lactam monotherapy for the treatment of CAP showed an association with fluoroquinolone use and decreased mortality.
Finally, one high-quality trial showed that transitioning patients to oral antibiotics once they meet clinical criteria for stability (stable vital signs, lack of confusion, ability to tolerate oral medications) leads to a shorter length of stay.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
When Should Harm-Reduction Strategies Be Used for Inpatients with Opioid Misuse?
Case
A 33-year-old male with a history of opioid overdose and opioid use disorder is admitted with IV heroin use complicated by injection site cellulitis. He is started on antibiotics with improvement in his cellulitis; however, his hospitalization is complicated by acute opioid withdrawal. Despite his history of opioid overdose and opioid use disorder, he has never seen a substance use disorder specialist nor received any education or treatment for his addiction. He reports that he will stop using illicit drugs but declines any further addiction treatment.
What strategies can be employed to reduce his risk of future harm from opioid misuse?
Background
Over the past decade, the U.S. has experienced a rapid increase in the rates of opioid prescriptions and opioid misuse.1 Consequently, the number of ED visits and hospitalizations for opioid-related complications has also increased.2 Many complications result from the practice of injection drug use (IDU), which predisposes individuals to serious blood-borne viral infections such as human immunodeficiency virus (HIV) and hepatitis C virus (HCV) as well as bacterial infections such as infective endocarditis. In addition, individuals who misuse opioids are at risk of death related to opioid overdose. In 2013, there were more than 24,000 deaths in the U.S. due to opioid overdose (see Figure 1).3
In response to the opioid epidemic, there have been a number of local, state, and federal public health initiatives to monitor and secure the opioid drug supply, improve treatment resources, and promulgate harm-reduction interventions. At a more individual level, hospitalists have an important role to play in combating the opioid epidemic. As frontline providers, hospitalists have access to hospitalized individuals with opioid misuse who may not otherwise be exposed to the healthcare system. Therefore, inpatient hospitalizations serve as a unique and important opportunity to engage individuals in the management of their addiction.
There are a number of interventions that hospitalists and substance use disorder specialists can pursue. Psychiatric evaluation and initiation of medication-assisted treatment often aim to aid patients in abstaining from further opioid misuse. However, many individuals with opioid use disorder are not ready for treatment or experience relapses of opioid misuse despite treatment. Given this, a secondary goal is to reduce any harm that may result from opioid misuse. This is done through the implementation of harm-reduction strategies. These strategies include teaching safe injection practices, facilitating the use of syringe exchange programs, and providing opioid overdose education and naloxone distribution.
Overview of Data
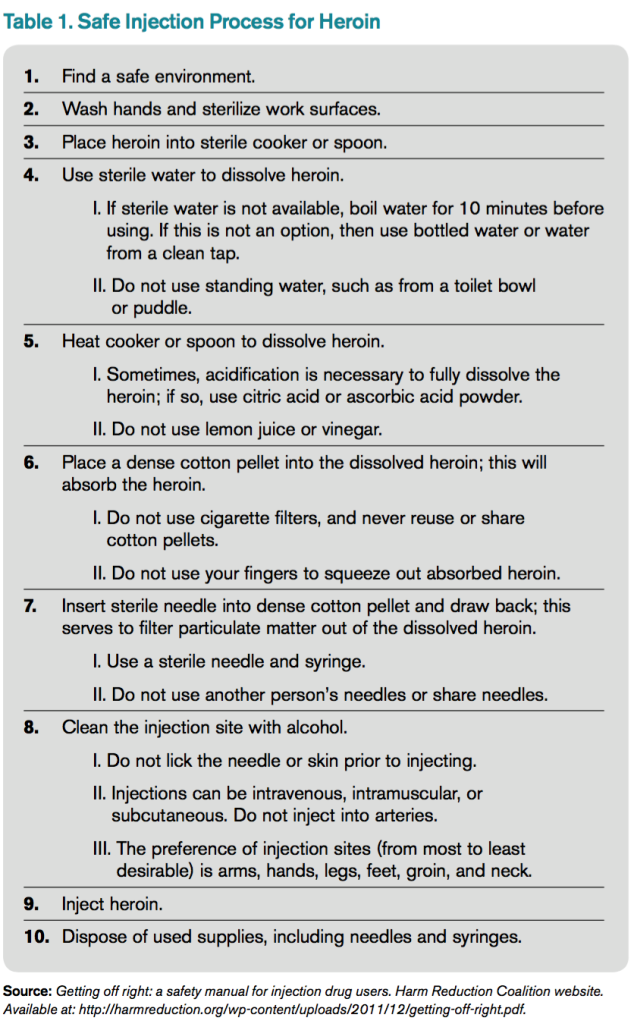
Safe Injection Education. People who inject drugs are at risk for viral, bacterial, and fungal infections. These infections are often the result of nonsterile injection and may be minimized by the utilization of safe injection practices. In order to educate people who inject drugs on safe injection practices, the hospitalist must first understand the process involved in injecting drugs. In Table 1, the process of injecting heroin is outlined (of note, other illicit drugs can be injected, and processes may vary).4

As evidenced by Table 1, the process of sterile injection can be complicated, especially for an individual who may be withdrawing from opioids. Table 1 is also optimistic in that it recommends new and sterile products be used with every injection. If new and sterile equipment is not available, another option is to clean the equipment after every use, which can be done by using bleach and water. This may mitigate the risk of viral, bacterial, and fungal infections. However, the risk is still present, so users should not share or use another individual’s equipment even if it has been cleaned. Due to the risk of viral, bacterial, and fungal infections, all hospitalized individuals who inject drugs should receive education on safe injection practices.
Syringe Exchange Programs. IDU accounts for up to 15% of all new HIV infections and is the primary risk factor for the transmission of HCV.5 These infections occur when people inject using equipment contaminated with blood that contains HIV and/or HCV. Given this, if people who inject drugs could access and consistently use sterile syringes and other injection paraphernalia, the risk of transmitting blood-borne infections would be dramatically reduced. This is the concept behind syringe exchange programs (also known as needle exchange programs), which serve to increase access to sterile syringes while removing contaminated or used syringes from the community.
There is compelling evidence that syringe exchange programs decrease the rate of HIV transmission and likely reduce the rate of HCV transmission as well.6 In addition, syringe exchange programs often provide other beneficial services, such as counseling, testing, and prevention efforts for HIV, HCV, and sexually transmitted infections; distribution of condoms; and referrals to treatment services for substance use disorder.5
Unfortunately, in the U.S., restrictive state laws and lack of funding limit the number of established syringe exchange programs. According to the North American Syringe Exchange Network, there are only 226 programs in 33 states and the District of Columbia. Hospitalists and social workers should be aware of available local resources, including syringe exchange programs, and distribute this information to hospitalized individuals who inject drugs.
Opioid Overdose Education and Naloxone Distribution. Syringe exchange programs and safe injection education aim to reduce harm by decreasing the transmission of infections; however, they do not address the problem of deaths related to opioid overdose. The primary harm-reduction strategy used to address deaths related to opioid overdose in the U.S is opioid overdose education and naloxone distribution (OEND). Naloxone is an opioid antagonist that reverses the respiratory depression and decreased consciousness caused by opioids. The OEND strategy involves educating first responders— including individuals and friends and family of individuals who use opioids—to recognize the signs of an opioid overdose, seek help, provide rescue breathing, administer naloxone, and stay with the individual until emergency medical services arrive.7 This strategy has been observed to decrease rates of death related to opioid overdose.7
Given the evolving opioid epidemic and effectiveness of the OEND strategy, it is not surprising that the number of local opioid overdose prevention programs adopting OEND has risen dramatically. As of 2014, there were 140 organizations, with 644 local sites providing naloxone in 29 states and the District of Columbia. These organizations have distributed 152,000 naloxone kits and have reported more than 26,000 reversals.8 Certainly, OEND has prevented morbidity and mortality in some of these patients.
The adoption of OEND can be performed by individual prescribers as well. Naloxone is U.S. FDA-approved for the treatment of opioid overdose, and thus the liability to prescribers is similar to that of other FDA-approved drugs. However, the distribution of naloxone to third parties, such as friends and family of individuals with opioid misuse, is more complex and regulated by state laws. Many states have created liability protection for naloxone prescription to third parties. Individual state laws and additional information can be found at prescribetoprevent.org.
Hospitalists should provide opioid overdose education to all individuals with opioid misuse and friends and family of individuals with opioid misuse. In addition, hospitalists should prescribe naloxone to individuals with opioid misuse and, in states where the law allows, distribute naloxone to friends and family of individuals with opioid misuse as well.
Controversies. In general, opioid use disorder treatment providers; public health officials; and local, state, and federal government agencies have increasingly embraced harm-reduction strategies. However, some feel that harm-reduction strategies are misguided or even detrimental due to concern that they implicitly condone or enable the use of illicit substances. There have been a number of studies to evaluate the potential unintended consequences of harm-reduction strategies, and overwhelmingly, these have been either neutral or have shown the benefit of harm-reduction interventions. At this point, there is no good evidence to prevent the widespread adoption of harm-reduction strategies for hospitalists.
Back to the Case
The case involves an individual who has already had at least two complications of his IV heroin use, including cellulitis and opioid overdose. Ideally, this individual would be willing to see an addiction specialist and start medication-assisted treatment. Unfortunately, he is unwilling to be further evaluated by a specialist at this time. Regardless, he remains at risk of future complications, and it is the hospitalist’s responsibility to intervene with a goal of reducing future harm that may result from his IV heroin use.
The hospitalist in this case advises the patient to abstain from heroin and IDU, encourages him to seek treatment for his opioid use disorder, and gives him resources for linkage to care if he becomes interested. In addition, the hospitalist educates the patient on safe injection practices and provides a list of local syringe exchange programs to decrease future risk of viral, bacterial, and fungal infections. Furthermore, the hospitalist provides opioid overdose education and distributes naloxone to the patient, along with friends and family of the patient, to reduce the risk of death related to opioid overdose.
Bottom Line
Hospitalists should utilize harm-reduction interventions in individuals hospitalized with opioid misuse. TH
Dr. Theisen-Toupal is a hospitalist at the Veterans Affairs Medical Center and assistant professor of medicine at the George Washington University School of Medicine & Health Sciences, both in Washington, D.C.
References
- Vital signs: overdoses of prescription opioid pain relievers—United States, 1999–2008. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6043a4.htm. Published November 4, 2011.
- Drug abuse warning network, 2011: national estimates of drug-related emergency department visits. Substance Abuse and Mental Health Services Administration website. Available at: http://www.samhsa.gov/data/2k13/DAWN2k11ED/DAWN2k11ED.htm#5. Accessed July 29, 2015.
- Hedergaard H, Chen LH, Warner M. Drug-poisoning deaths involving heroin: United States, 2000–2013. National Center for Health Statistics Data Brief. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/nchs/data/databriefs/db190.htm. Published March 2015.
- Getting off right: a safety manual for injection drug users. Harm Reduction Coalition website. Available at: http://harmreduction.org/wp-content/uploads/2011/12/getting-off-right.pdf.
- Syringe exchange programs—United States, 2008. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5945a4.htm/Syringe-Exchange-Programs-United-States-2008. Published November 19, 2010.
- Wodak A, Conney A. Effectiveness of sterile needle and syringe programming in reducing HIV/AIDS among injecting drug users. World Health Organization website. Available at: http://apps.who.int/iris/bitstream/10665/43107/1/9241591641.pdf. Published 2004.
- Walley AY, Xuan Z, Hackman HH, et al. Opioid overdose rates and implementation of overdose education and nasal naloxone distribution in Massachusetts: interrupted time series analysis. BMJ. 2013;346:f174.
- Wheeler E, Jones TS, Gilbert MK, Davidson PJ. Opioid overdose prevention programs providing naloxone to laypersons—United States, 2014. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6423a2.htm. Published June 19, 2015.
Case
A 33-year-old male with a history of opioid overdose and opioid use disorder is admitted with IV heroin use complicated by injection site cellulitis. He is started on antibiotics with improvement in his cellulitis; however, his hospitalization is complicated by acute opioid withdrawal. Despite his history of opioid overdose and opioid use disorder, he has never seen a substance use disorder specialist nor received any education or treatment for his addiction. He reports that he will stop using illicit drugs but declines any further addiction treatment.
What strategies can be employed to reduce his risk of future harm from opioid misuse?
Background
Over the past decade, the U.S. has experienced a rapid increase in the rates of opioid prescriptions and opioid misuse.1 Consequently, the number of ED visits and hospitalizations for opioid-related complications has also increased.2 Many complications result from the practice of injection drug use (IDU), which predisposes individuals to serious blood-borne viral infections such as human immunodeficiency virus (HIV) and hepatitis C virus (HCV) as well as bacterial infections such as infective endocarditis. In addition, individuals who misuse opioids are at risk of death related to opioid overdose. In 2013, there were more than 24,000 deaths in the U.S. due to opioid overdose (see Figure 1).3
In response to the opioid epidemic, there have been a number of local, state, and federal public health initiatives to monitor and secure the opioid drug supply, improve treatment resources, and promulgate harm-reduction interventions. At a more individual level, hospitalists have an important role to play in combating the opioid epidemic. As frontline providers, hospitalists have access to hospitalized individuals with opioid misuse who may not otherwise be exposed to the healthcare system. Therefore, inpatient hospitalizations serve as a unique and important opportunity to engage individuals in the management of their addiction.
There are a number of interventions that hospitalists and substance use disorder specialists can pursue. Psychiatric evaluation and initiation of medication-assisted treatment often aim to aid patients in abstaining from further opioid misuse. However, many individuals with opioid use disorder are not ready for treatment or experience relapses of opioid misuse despite treatment. Given this, a secondary goal is to reduce any harm that may result from opioid misuse. This is done through the implementation of harm-reduction strategies. These strategies include teaching safe injection practices, facilitating the use of syringe exchange programs, and providing opioid overdose education and naloxone distribution.
Overview of Data
Safe Injection Education. People who inject drugs are at risk for viral, bacterial, and fungal infections. These infections are often the result of nonsterile injection and may be minimized by the utilization of safe injection practices. In order to educate people who inject drugs on safe injection practices, the hospitalist must first understand the process involved in injecting drugs. In Table 1, the process of injecting heroin is outlined (of note, other illicit drugs can be injected, and processes may vary).4
As evidenced by Table 1, the process of sterile injection can be complicated, especially for an individual who may be withdrawing from opioids. Table 1 is also optimistic in that it recommends new and sterile products be used with every injection. If new and sterile equipment is not available, another option is to clean the equipment after every use, which can be done by using bleach and water. This may mitigate the risk of viral, bacterial, and fungal infections. However, the risk is still present, so users should not share or use another individual’s equipment even if it has been cleaned. Due to the risk of viral, bacterial, and fungal infections, all hospitalized individuals who inject drugs should receive education on safe injection practices.
Syringe Exchange Programs. IDU accounts for up to 15% of all new HIV infections and is the primary risk factor for the transmission of HCV.5 These infections occur when people inject using equipment contaminated with blood that contains HIV and/or HCV. Given this, if people who inject drugs could access and consistently use sterile syringes and other injection paraphernalia, the risk of transmitting blood-borne infections would be dramatically reduced. This is the concept behind syringe exchange programs (also known as needle exchange programs), which serve to increase access to sterile syringes while removing contaminated or used syringes from the community.
There is compelling evidence that syringe exchange programs decrease the rate of HIV transmission and likely reduce the rate of HCV transmission as well.6 In addition, syringe exchange programs often provide other beneficial services, such as counseling, testing, and prevention efforts for HIV, HCV, and sexually transmitted infections; distribution of condoms; and referrals to treatment services for substance use disorder.5
Unfortunately, in the U.S., restrictive state laws and lack of funding limit the number of established syringe exchange programs. According to the North American Syringe Exchange Network, there are only 226 programs in 33 states and the District of Columbia. Hospitalists and social workers should be aware of available local resources, including syringe exchange programs, and distribute this information to hospitalized individuals who inject drugs.
Opioid Overdose Education and Naloxone Distribution. Syringe exchange programs and safe injection education aim to reduce harm by decreasing the transmission of infections; however, they do not address the problem of deaths related to opioid overdose. The primary harm-reduction strategy used to address deaths related to opioid overdose in the U.S is opioid overdose education and naloxone distribution (OEND). Naloxone is an opioid antagonist that reverses the respiratory depression and decreased consciousness caused by opioids. The OEND strategy involves educating first responders— including individuals and friends and family of individuals who use opioids—to recognize the signs of an opioid overdose, seek help, provide rescue breathing, administer naloxone, and stay with the individual until emergency medical services arrive.7 This strategy has been observed to decrease rates of death related to opioid overdose.7
Given the evolving opioid epidemic and effectiveness of the OEND strategy, it is not surprising that the number of local opioid overdose prevention programs adopting OEND has risen dramatically. As of 2014, there were 140 organizations, with 644 local sites providing naloxone in 29 states and the District of Columbia. These organizations have distributed 152,000 naloxone kits and have reported more than 26,000 reversals.8 Certainly, OEND has prevented morbidity and mortality in some of these patients.
The adoption of OEND can be performed by individual prescribers as well. Naloxone is U.S. FDA-approved for the treatment of opioid overdose, and thus the liability to prescribers is similar to that of other FDA-approved drugs. However, the distribution of naloxone to third parties, such as friends and family of individuals with opioid misuse, is more complex and regulated by state laws. Many states have created liability protection for naloxone prescription to third parties. Individual state laws and additional information can be found at prescribetoprevent.org.
Hospitalists should provide opioid overdose education to all individuals with opioid misuse and friends and family of individuals with opioid misuse. In addition, hospitalists should prescribe naloxone to individuals with opioid misuse and, in states where the law allows, distribute naloxone to friends and family of individuals with opioid misuse as well.
Controversies. In general, opioid use disorder treatment providers; public health officials; and local, state, and federal government agencies have increasingly embraced harm-reduction strategies. However, some feel that harm-reduction strategies are misguided or even detrimental due to concern that they implicitly condone or enable the use of illicit substances. There have been a number of studies to evaluate the potential unintended consequences of harm-reduction strategies, and overwhelmingly, these have been either neutral or have shown the benefit of harm-reduction interventions. At this point, there is no good evidence to prevent the widespread adoption of harm-reduction strategies for hospitalists.
Back to the Case
The case involves an individual who has already had at least two complications of his IV heroin use, including cellulitis and opioid overdose. Ideally, this individual would be willing to see an addiction specialist and start medication-assisted treatment. Unfortunately, he is unwilling to be further evaluated by a specialist at this time. Regardless, he remains at risk of future complications, and it is the hospitalist’s responsibility to intervene with a goal of reducing future harm that may result from his IV heroin use.
The hospitalist in this case advises the patient to abstain from heroin and IDU, encourages him to seek treatment for his opioid use disorder, and gives him resources for linkage to care if he becomes interested. In addition, the hospitalist educates the patient on safe injection practices and provides a list of local syringe exchange programs to decrease future risk of viral, bacterial, and fungal infections. Furthermore, the hospitalist provides opioid overdose education and distributes naloxone to the patient, along with friends and family of the patient, to reduce the risk of death related to opioid overdose.
Bottom Line
Hospitalists should utilize harm-reduction interventions in individuals hospitalized with opioid misuse. TH
Dr. Theisen-Toupal is a hospitalist at the Veterans Affairs Medical Center and assistant professor of medicine at the George Washington University School of Medicine & Health Sciences, both in Washington, D.C.
References
- Vital signs: overdoses of prescription opioid pain relievers—United States, 1999–2008. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6043a4.htm. Published November 4, 2011.
- Drug abuse warning network, 2011: national estimates of drug-related emergency department visits. Substance Abuse and Mental Health Services Administration website. Available at: http://www.samhsa.gov/data/2k13/DAWN2k11ED/DAWN2k11ED.htm#5. Accessed July 29, 2015.
- Hedergaard H, Chen LH, Warner M. Drug-poisoning deaths involving heroin: United States, 2000–2013. National Center for Health Statistics Data Brief. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/nchs/data/databriefs/db190.htm. Published March 2015.
- Getting off right: a safety manual for injection drug users. Harm Reduction Coalition website. Available at: http://harmreduction.org/wp-content/uploads/2011/12/getting-off-right.pdf.
- Syringe exchange programs—United States, 2008. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5945a4.htm/Syringe-Exchange-Programs-United-States-2008. Published November 19, 2010.
- Wodak A, Conney A. Effectiveness of sterile needle and syringe programming in reducing HIV/AIDS among injecting drug users. World Health Organization website. Available at: http://apps.who.int/iris/bitstream/10665/43107/1/9241591641.pdf. Published 2004.
- Walley AY, Xuan Z, Hackman HH, et al. Opioid overdose rates and implementation of overdose education and nasal naloxone distribution in Massachusetts: interrupted time series analysis. BMJ. 2013;346:f174.
- Wheeler E, Jones TS, Gilbert MK, Davidson PJ. Opioid overdose prevention programs providing naloxone to laypersons—United States, 2014. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6423a2.htm. Published June 19, 2015.
Case
A 33-year-old male with a history of opioid overdose and opioid use disorder is admitted with IV heroin use complicated by injection site cellulitis. He is started on antibiotics with improvement in his cellulitis; however, his hospitalization is complicated by acute opioid withdrawal. Despite his history of opioid overdose and opioid use disorder, he has never seen a substance use disorder specialist nor received any education or treatment for his addiction. He reports that he will stop using illicit drugs but declines any further addiction treatment.
What strategies can be employed to reduce his risk of future harm from opioid misuse?
Background
Over the past decade, the U.S. has experienced a rapid increase in the rates of opioid prescriptions and opioid misuse.1 Consequently, the number of ED visits and hospitalizations for opioid-related complications has also increased.2 Many complications result from the practice of injection drug use (IDU), which predisposes individuals to serious blood-borne viral infections such as human immunodeficiency virus (HIV) and hepatitis C virus (HCV) as well as bacterial infections such as infective endocarditis. In addition, individuals who misuse opioids are at risk of death related to opioid overdose. In 2013, there were more than 24,000 deaths in the U.S. due to opioid overdose (see Figure 1).3
In response to the opioid epidemic, there have been a number of local, state, and federal public health initiatives to monitor and secure the opioid drug supply, improve treatment resources, and promulgate harm-reduction interventions. At a more individual level, hospitalists have an important role to play in combating the opioid epidemic. As frontline providers, hospitalists have access to hospitalized individuals with opioid misuse who may not otherwise be exposed to the healthcare system. Therefore, inpatient hospitalizations serve as a unique and important opportunity to engage individuals in the management of their addiction.
There are a number of interventions that hospitalists and substance use disorder specialists can pursue. Psychiatric evaluation and initiation of medication-assisted treatment often aim to aid patients in abstaining from further opioid misuse. However, many individuals with opioid use disorder are not ready for treatment or experience relapses of opioid misuse despite treatment. Given this, a secondary goal is to reduce any harm that may result from opioid misuse. This is done through the implementation of harm-reduction strategies. These strategies include teaching safe injection practices, facilitating the use of syringe exchange programs, and providing opioid overdose education and naloxone distribution.
Overview of Data
Safe Injection Education. People who inject drugs are at risk for viral, bacterial, and fungal infections. These infections are often the result of nonsterile injection and may be minimized by the utilization of safe injection practices. In order to educate people who inject drugs on safe injection practices, the hospitalist must first understand the process involved in injecting drugs. In Table 1, the process of injecting heroin is outlined (of note, other illicit drugs can be injected, and processes may vary).4
As evidenced by Table 1, the process of sterile injection can be complicated, especially for an individual who may be withdrawing from opioids. Table 1 is also optimistic in that it recommends new and sterile products be used with every injection. If new and sterile equipment is not available, another option is to clean the equipment after every use, which can be done by using bleach and water. This may mitigate the risk of viral, bacterial, and fungal infections. However, the risk is still present, so users should not share or use another individual’s equipment even if it has been cleaned. Due to the risk of viral, bacterial, and fungal infections, all hospitalized individuals who inject drugs should receive education on safe injection practices.
Syringe Exchange Programs. IDU accounts for up to 15% of all new HIV infections and is the primary risk factor for the transmission of HCV.5 These infections occur when people inject using equipment contaminated with blood that contains HIV and/or HCV. Given this, if people who inject drugs could access and consistently use sterile syringes and other injection paraphernalia, the risk of transmitting blood-borne infections would be dramatically reduced. This is the concept behind syringe exchange programs (also known as needle exchange programs), which serve to increase access to sterile syringes while removing contaminated or used syringes from the community.
There is compelling evidence that syringe exchange programs decrease the rate of HIV transmission and likely reduce the rate of HCV transmission as well.6 In addition, syringe exchange programs often provide other beneficial services, such as counseling, testing, and prevention efforts for HIV, HCV, and sexually transmitted infections; distribution of condoms; and referrals to treatment services for substance use disorder.5
Unfortunately, in the U.S., restrictive state laws and lack of funding limit the number of established syringe exchange programs. According to the North American Syringe Exchange Network, there are only 226 programs in 33 states and the District of Columbia. Hospitalists and social workers should be aware of available local resources, including syringe exchange programs, and distribute this information to hospitalized individuals who inject drugs.
Opioid Overdose Education and Naloxone Distribution. Syringe exchange programs and safe injection education aim to reduce harm by decreasing the transmission of infections; however, they do not address the problem of deaths related to opioid overdose. The primary harm-reduction strategy used to address deaths related to opioid overdose in the U.S is opioid overdose education and naloxone distribution (OEND). Naloxone is an opioid antagonist that reverses the respiratory depression and decreased consciousness caused by opioids. The OEND strategy involves educating first responders— including individuals and friends and family of individuals who use opioids—to recognize the signs of an opioid overdose, seek help, provide rescue breathing, administer naloxone, and stay with the individual until emergency medical services arrive.7 This strategy has been observed to decrease rates of death related to opioid overdose.7
Given the evolving opioid epidemic and effectiveness of the OEND strategy, it is not surprising that the number of local opioid overdose prevention programs adopting OEND has risen dramatically. As of 2014, there were 140 organizations, with 644 local sites providing naloxone in 29 states and the District of Columbia. These organizations have distributed 152,000 naloxone kits and have reported more than 26,000 reversals.8 Certainly, OEND has prevented morbidity and mortality in some of these patients.
The adoption of OEND can be performed by individual prescribers as well. Naloxone is U.S. FDA-approved for the treatment of opioid overdose, and thus the liability to prescribers is similar to that of other FDA-approved drugs. However, the distribution of naloxone to third parties, such as friends and family of individuals with opioid misuse, is more complex and regulated by state laws. Many states have created liability protection for naloxone prescription to third parties. Individual state laws and additional information can be found at prescribetoprevent.org.
Hospitalists should provide opioid overdose education to all individuals with opioid misuse and friends and family of individuals with opioid misuse. In addition, hospitalists should prescribe naloxone to individuals with opioid misuse and, in states where the law allows, distribute naloxone to friends and family of individuals with opioid misuse as well.
Controversies. In general, opioid use disorder treatment providers; public health officials; and local, state, and federal government agencies have increasingly embraced harm-reduction strategies. However, some feel that harm-reduction strategies are misguided or even detrimental due to concern that they implicitly condone or enable the use of illicit substances. There have been a number of studies to evaluate the potential unintended consequences of harm-reduction strategies, and overwhelmingly, these have been either neutral or have shown the benefit of harm-reduction interventions. At this point, there is no good evidence to prevent the widespread adoption of harm-reduction strategies for hospitalists.
Back to the Case
The case involves an individual who has already had at least two complications of his IV heroin use, including cellulitis and opioid overdose. Ideally, this individual would be willing to see an addiction specialist and start medication-assisted treatment. Unfortunately, he is unwilling to be further evaluated by a specialist at this time. Regardless, he remains at risk of future complications, and it is the hospitalist’s responsibility to intervene with a goal of reducing future harm that may result from his IV heroin use.
The hospitalist in this case advises the patient to abstain from heroin and IDU, encourages him to seek treatment for his opioid use disorder, and gives him resources for linkage to care if he becomes interested. In addition, the hospitalist educates the patient on safe injection practices and provides a list of local syringe exchange programs to decrease future risk of viral, bacterial, and fungal infections. Furthermore, the hospitalist provides opioid overdose education and distributes naloxone to the patient, along with friends and family of the patient, to reduce the risk of death related to opioid overdose.
Bottom Line
Hospitalists should utilize harm-reduction interventions in individuals hospitalized with opioid misuse. TH
Dr. Theisen-Toupal is a hospitalist at the Veterans Affairs Medical Center and assistant professor of medicine at the George Washington University School of Medicine & Health Sciences, both in Washington, D.C.
References
- Vital signs: overdoses of prescription opioid pain relievers—United States, 1999–2008. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6043a4.htm. Published November 4, 2011.
- Drug abuse warning network, 2011: national estimates of drug-related emergency department visits. Substance Abuse and Mental Health Services Administration website. Available at: http://www.samhsa.gov/data/2k13/DAWN2k11ED/DAWN2k11ED.htm#5. Accessed July 29, 2015.
- Hedergaard H, Chen LH, Warner M. Drug-poisoning deaths involving heroin: United States, 2000–2013. National Center for Health Statistics Data Brief. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/nchs/data/databriefs/db190.htm. Published March 2015.
- Getting off right: a safety manual for injection drug users. Harm Reduction Coalition website. Available at: http://harmreduction.org/wp-content/uploads/2011/12/getting-off-right.pdf.
- Syringe exchange programs—United States, 2008. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5945a4.htm/Syringe-Exchange-Programs-United-States-2008. Published November 19, 2010.
- Wodak A, Conney A. Effectiveness of sterile needle and syringe programming in reducing HIV/AIDS among injecting drug users. World Health Organization website. Available at: http://apps.who.int/iris/bitstream/10665/43107/1/9241591641.pdf. Published 2004.
- Walley AY, Xuan Z, Hackman HH, et al. Opioid overdose rates and implementation of overdose education and nasal naloxone distribution in Massachusetts: interrupted time series analysis. BMJ. 2013;346:f174.
- Wheeler E, Jones TS, Gilbert MK, Davidson PJ. Opioid overdose prevention programs providing naloxone to laypersons—United States, 2014. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6423a2.htm. Published June 19, 2015.