User login
Competition Keeps Us on Our Toes
In July 2010, 443-bed Mary Washington Hospital in Fredericksburg, Va., decided to end its contract for hospitalist services with a local private practice, the Fredericksburg Hospitalist Group (FGH), and to contract instead with national management company HMG (now Cogent HMG).
“We thought the local group might fold and leave, even though they retained a contract with our smaller affiliated hospital,” the 100-bed Stafford Hospital in nearby Stafford, Va., says Rebecca Bigoney, MD, vice president of medical affairs at Mary Washington Hospital. But FHG chose to stay and started aggressively marketing its services to local physicians.
“Today, we have two hospitalist groups that are similar in size, with an almost identical number of patients. They are both competitive and collegial, and it works far better than we thought it would,” Dr. Bigoney says. “We have seen many benefits from having two hospitalist groups; it makes both of them try harder. They have good leaders and aligned incentives.”
The groups also work together on such projects as developing order sets, managing lengths of hospital stay, and implementing computerized physician order entry.
Both groups are represented on hospital committees and within the recently formed division of hospital medicine. Rules of engagement were negotiated with the leadership of the two groups, including a policy on hospitalist admissions and transfers, protocols for handling unassigned patients, a process for local medical groups and physicians to designate their preference for hospitalist coverage, and what to do if the patient is admitted to the wrong group because the primary-care physician is not known at time of admission. If no preference for hospitalist group is given by the primary-care physician, the referral goes to Cogent HMG.
Dr. Bigoney acknowledges FHG physicians had some hard feelings at first. That sentiment is confirmed by FHG founder and hospitalist Feroz Tamana, MD.
“Of course, there was some confusion and anxiety [over the transfer],” Dr. Tamana says. “But from Day One, it has worked pretty well.”
FHG initially downsized from 24 physicians to eight, but has since grown back to 14.
Kerry Lecky, MD, joined Mary Washington in November 2011 to lead the contracting Cogent HMG practice. Everyone was in agreement as to the rules of engagement at that time “and how to align with the hospital’s goals,” said Dr. Lecky, who has since moved on to another position. “The competition has been an opportunity to improve quality. It could be a problem if there were too many hospitalist groups. But two is a very manageable number.”
Is this approach sustainable for the long haul?
“With two groups, we keep each other on our toes,” she says. And the ability to offer a choice of hospitalists to primary-care physicians has been a plus. TH
Larry Beresford is a freelance writer in Oakland, Calif.
In July 2010, 443-bed Mary Washington Hospital in Fredericksburg, Va., decided to end its contract for hospitalist services with a local private practice, the Fredericksburg Hospitalist Group (FGH), and to contract instead with national management company HMG (now Cogent HMG).
“We thought the local group might fold and leave, even though they retained a contract with our smaller affiliated hospital,” the 100-bed Stafford Hospital in nearby Stafford, Va., says Rebecca Bigoney, MD, vice president of medical affairs at Mary Washington Hospital. But FHG chose to stay and started aggressively marketing its services to local physicians.
“Today, we have two hospitalist groups that are similar in size, with an almost identical number of patients. They are both competitive and collegial, and it works far better than we thought it would,” Dr. Bigoney says. “We have seen many benefits from having two hospitalist groups; it makes both of them try harder. They have good leaders and aligned incentives.”
The groups also work together on such projects as developing order sets, managing lengths of hospital stay, and implementing computerized physician order entry.
Both groups are represented on hospital committees and within the recently formed division of hospital medicine. Rules of engagement were negotiated with the leadership of the two groups, including a policy on hospitalist admissions and transfers, protocols for handling unassigned patients, a process for local medical groups and physicians to designate their preference for hospitalist coverage, and what to do if the patient is admitted to the wrong group because the primary-care physician is not known at time of admission. If no preference for hospitalist group is given by the primary-care physician, the referral goes to Cogent HMG.
Dr. Bigoney acknowledges FHG physicians had some hard feelings at first. That sentiment is confirmed by FHG founder and hospitalist Feroz Tamana, MD.
“Of course, there was some confusion and anxiety [over the transfer],” Dr. Tamana says. “But from Day One, it has worked pretty well.”
FHG initially downsized from 24 physicians to eight, but has since grown back to 14.
Kerry Lecky, MD, joined Mary Washington in November 2011 to lead the contracting Cogent HMG practice. Everyone was in agreement as to the rules of engagement at that time “and how to align with the hospital’s goals,” said Dr. Lecky, who has since moved on to another position. “The competition has been an opportunity to improve quality. It could be a problem if there were too many hospitalist groups. But two is a very manageable number.”
Is this approach sustainable for the long haul?
“With two groups, we keep each other on our toes,” she says. And the ability to offer a choice of hospitalists to primary-care physicians has been a plus. TH
Larry Beresford is a freelance writer in Oakland, Calif.
In July 2010, 443-bed Mary Washington Hospital in Fredericksburg, Va., decided to end its contract for hospitalist services with a local private practice, the Fredericksburg Hospitalist Group (FGH), and to contract instead with national management company HMG (now Cogent HMG).
“We thought the local group might fold and leave, even though they retained a contract with our smaller affiliated hospital,” the 100-bed Stafford Hospital in nearby Stafford, Va., says Rebecca Bigoney, MD, vice president of medical affairs at Mary Washington Hospital. But FHG chose to stay and started aggressively marketing its services to local physicians.
“Today, we have two hospitalist groups that are similar in size, with an almost identical number of patients. They are both competitive and collegial, and it works far better than we thought it would,” Dr. Bigoney says. “We have seen many benefits from having two hospitalist groups; it makes both of them try harder. They have good leaders and aligned incentives.”
The groups also work together on such projects as developing order sets, managing lengths of hospital stay, and implementing computerized physician order entry.
Both groups are represented on hospital committees and within the recently formed division of hospital medicine. Rules of engagement were negotiated with the leadership of the two groups, including a policy on hospitalist admissions and transfers, protocols for handling unassigned patients, a process for local medical groups and physicians to designate their preference for hospitalist coverage, and what to do if the patient is admitted to the wrong group because the primary-care physician is not known at time of admission. If no preference for hospitalist group is given by the primary-care physician, the referral goes to Cogent HMG.
Dr. Bigoney acknowledges FHG physicians had some hard feelings at first. That sentiment is confirmed by FHG founder and hospitalist Feroz Tamana, MD.
“Of course, there was some confusion and anxiety [over the transfer],” Dr. Tamana says. “But from Day One, it has worked pretty well.”
FHG initially downsized from 24 physicians to eight, but has since grown back to 14.
Kerry Lecky, MD, joined Mary Washington in November 2011 to lead the contracting Cogent HMG practice. Everyone was in agreement as to the rules of engagement at that time “and how to align with the hospital’s goals,” said Dr. Lecky, who has since moved on to another position. “The competition has been an opportunity to improve quality. It could be a problem if there were too many hospitalist groups. But two is a very manageable number.”
Is this approach sustainable for the long haul?
“With two groups, we keep each other on our toes,” she says. And the ability to offer a choice of hospitalists to primary-care physicians has been a plus. TH
Larry Beresford is a freelance writer in Oakland, Calif.
When Should Hospitalists Consult A Dermatologist About Pediatric Conditions?
Hospitalists sometimes come across skin problems in pediatric patients, and some of these issues fall outside the scope of their expertise.
“I find lesions incidentally that I recommend be referred to dermatologists for evaluation on an outpatient basis” more often than in inpatient dermatologic situations, says Logan Murray, MD, a pediatric hospitalist at the Barbara Bush Children’s Hospital at Maine Medical Center in Portland. “I recently managed a newborn with a 6 cm diameter brown patch in the lumbar area with fine, dark, vellus hair, which I suspect is a congenital giant melanocytic nevus,” he says. To properly evaluate the birthmark, he referred the patient’s parents to a dermatologist.
In these instances, it makes sense for a hospitalist to request that a dermatologist see the child and talk with the parents during hospitalization.
“We get many consults [that] are appropriate,” says Susan Bayliss, MD, a pediatric dermatologist at St. Louis Children’s Hospital. If a hospitalist can’t identify a particular skin issue and reassure parents, it’s time to call a dermatologist.
Distinguishing between acute and chronic dermatologic conditions is important. “The skin is often overlooked among hospitalists,” who are managing sicker patients nowadays, says Neera Agarwal-Antal, MD, head of the division of dermatology at Akron Children’s Hospital in Akron, Ohio.
One of the most dangerous and potentially fatal dermatologic emergencies is Stevens-Johnson syndrome, known in later stages as toxic epidermal necrolysis. Usually triggered by a drug-related reaction, the disease can cause large areas of skin to detach and lesions to develop in the mucous membranes. However, “the good news is most skin conditions are not acute or deadly,” Dr. Agarwal-Antal says.
Warts are very common and often can wait for examination in an outpatient setting. If an adolescent has significant acne, a hospitalist may ask gently, “Are you interested in doing something about your complexion?” To a patient who answers “yes,” a hospitalist could suggest over-the-counter benzoyl peroxide, says Dr. Bayliss, who is also professor of dermatology and pediatrics at Washington University School of Medicine in St. Louis.
“Pediatric dermatology is basically an outpatient specialty,” she adds. “Many kids have skin issues, but most of them do not need to be addressed by a hospitalist.” TH
Susan Kreimer is a freelance writer in New York.
Hospitalists sometimes come across skin problems in pediatric patients, and some of these issues fall outside the scope of their expertise.
“I find lesions incidentally that I recommend be referred to dermatologists for evaluation on an outpatient basis” more often than in inpatient dermatologic situations, says Logan Murray, MD, a pediatric hospitalist at the Barbara Bush Children’s Hospital at Maine Medical Center in Portland. “I recently managed a newborn with a 6 cm diameter brown patch in the lumbar area with fine, dark, vellus hair, which I suspect is a congenital giant melanocytic nevus,” he says. To properly evaluate the birthmark, he referred the patient’s parents to a dermatologist.
In these instances, it makes sense for a hospitalist to request that a dermatologist see the child and talk with the parents during hospitalization.
“We get many consults [that] are appropriate,” says Susan Bayliss, MD, a pediatric dermatologist at St. Louis Children’s Hospital. If a hospitalist can’t identify a particular skin issue and reassure parents, it’s time to call a dermatologist.
Distinguishing between acute and chronic dermatologic conditions is important. “The skin is often overlooked among hospitalists,” who are managing sicker patients nowadays, says Neera Agarwal-Antal, MD, head of the division of dermatology at Akron Children’s Hospital in Akron, Ohio.
One of the most dangerous and potentially fatal dermatologic emergencies is Stevens-Johnson syndrome, known in later stages as toxic epidermal necrolysis. Usually triggered by a drug-related reaction, the disease can cause large areas of skin to detach and lesions to develop in the mucous membranes. However, “the good news is most skin conditions are not acute or deadly,” Dr. Agarwal-Antal says.
Warts are very common and often can wait for examination in an outpatient setting. If an adolescent has significant acne, a hospitalist may ask gently, “Are you interested in doing something about your complexion?” To a patient who answers “yes,” a hospitalist could suggest over-the-counter benzoyl peroxide, says Dr. Bayliss, who is also professor of dermatology and pediatrics at Washington University School of Medicine in St. Louis.
“Pediatric dermatology is basically an outpatient specialty,” she adds. “Many kids have skin issues, but most of them do not need to be addressed by a hospitalist.” TH
Susan Kreimer is a freelance writer in New York.
Hospitalists sometimes come across skin problems in pediatric patients, and some of these issues fall outside the scope of their expertise.
“I find lesions incidentally that I recommend be referred to dermatologists for evaluation on an outpatient basis” more often than in inpatient dermatologic situations, says Logan Murray, MD, a pediatric hospitalist at the Barbara Bush Children’s Hospital at Maine Medical Center in Portland. “I recently managed a newborn with a 6 cm diameter brown patch in the lumbar area with fine, dark, vellus hair, which I suspect is a congenital giant melanocytic nevus,” he says. To properly evaluate the birthmark, he referred the patient’s parents to a dermatologist.
In these instances, it makes sense for a hospitalist to request that a dermatologist see the child and talk with the parents during hospitalization.
“We get many consults [that] are appropriate,” says Susan Bayliss, MD, a pediatric dermatologist at St. Louis Children’s Hospital. If a hospitalist can’t identify a particular skin issue and reassure parents, it’s time to call a dermatologist.
Distinguishing between acute and chronic dermatologic conditions is important. “The skin is often overlooked among hospitalists,” who are managing sicker patients nowadays, says Neera Agarwal-Antal, MD, head of the division of dermatology at Akron Children’s Hospital in Akron, Ohio.
One of the most dangerous and potentially fatal dermatologic emergencies is Stevens-Johnson syndrome, known in later stages as toxic epidermal necrolysis. Usually triggered by a drug-related reaction, the disease can cause large areas of skin to detach and lesions to develop in the mucous membranes. However, “the good news is most skin conditions are not acute or deadly,” Dr. Agarwal-Antal says.
Warts are very common and often can wait for examination in an outpatient setting. If an adolescent has significant acne, a hospitalist may ask gently, “Are you interested in doing something about your complexion?” To a patient who answers “yes,” a hospitalist could suggest over-the-counter benzoyl peroxide, says Dr. Bayliss, who is also professor of dermatology and pediatrics at Washington University School of Medicine in St. Louis.
“Pediatric dermatology is basically an outpatient specialty,” she adds. “Many kids have skin issues, but most of them do not need to be addressed by a hospitalist.” TH
Susan Kreimer is a freelance writer in New York.
Work-Hour Restrictions Impact Staffing, Education for Academic Hospital Medicine
Source: 2012 State of Hospital Medicine report


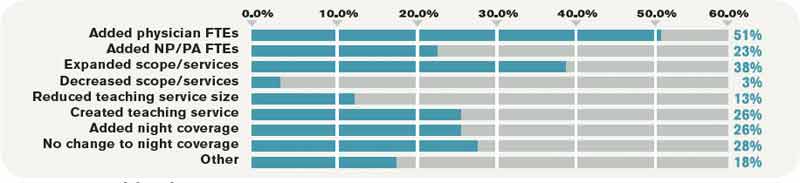
In July 2011, the Accreditation Council for Graduate Medical Education (ACGME) implemented new duty-hour restrictions on resident physicians. Among other changes, interns were restricted to a maximum of 16 hours of continuous duty. New rules also limited second-year residents and above to 24 hours of continuous duty, plus up to four additional hours for transition and educational activities. Recommendations were made for strategic napping, greater supervision requirements, and a minimum of eight to 10 hours off between shifts.
The 2012 State of Hospital Medicine report, which is based on 2011 data encompassing the period of these duty-hour changes, takes a systematic look at how academic HM practices have adjusted to the new resident rules. The most notable changes have been the addition of physician FTEs (51.3% of adult academic HM practices have done so) and nurse practitioners or physician assistants (23%). Additional common responses to resident work-hour limitations are listed in Table 1.
Source: 2012 State of Hospital Medicine report
These data underscore the immensity of changes academic HM groups have faced as a result of new work-hour limitations, as the majority of internal-medicine residents work with hospitalist attendings on inpatient medicine rotations. House staff no longer can be used as an inexpensive source of labor, given limitations on service and new expectations for resident education and supervision.
As others have commented on this topic in The Hospitalist, the role of the academic hospitalist is being redefined. No longer is academic HM synonymous with teaching alone; the clinical duties of many academic hospitalists now include a combination of teaching and non-teaching services, often with some night coverage. At our hospitals in San Diego and Boston, for instance, changes incurred due to work-hour restrictions include elimination of house staff coverage from one of the medical center’s hospitals and a significant increase in nonteaching service responsibilities across all hospitalists. An alternative approach that some programs have embraced is the recruitment of separate cadres of teaching and nonteaching hospitalists, which might result in markedly different professional expectations within the same group or institution.
Trends shifting clinical work from residents to hospitalists are likely to continue, no doubt increasing demand for hospitalists and physician extenders. In the past, the combination of less expensive resident labor and lower salaries in academia was financially favorable for hospitals. Due to resident duty-hour limitations, academic hospitalist groups have had to negotiate not only for additional hires, but, in many instances, also higher salaries commensurate with nonteaching work.
Given the impact on a hospital’s finances, academic HM practices have had to look more closely at clinical volumes and productivity, making protected time for nonclinical pursuits more difficult to come by. Alignment of hospitalists’ interests with those of hospital administrators through performance-improvement projects (e.g. reducing length of stay, readmissions, or nosocomial infections) will be crucial to the financial viability of the academic HM practice, and leadership in these areas will define and differentiate academic hospitalists in the future.
Dr. Bryan Huang, who works in Boston, and Dr. Grace Huang, who works in San Diego, both are members of SHM’s Practice Analysis Committee.
Source: 2012 State of Hospital Medicine report
In July 2011, the Accreditation Council for Graduate Medical Education (ACGME) implemented new duty-hour restrictions on resident physicians. Among other changes, interns were restricted to a maximum of 16 hours of continuous duty. New rules also limited second-year residents and above to 24 hours of continuous duty, plus up to four additional hours for transition and educational activities. Recommendations were made for strategic napping, greater supervision requirements, and a minimum of eight to 10 hours off between shifts.
The 2012 State of Hospital Medicine report, which is based on 2011 data encompassing the period of these duty-hour changes, takes a systematic look at how academic HM practices have adjusted to the new resident rules. The most notable changes have been the addition of physician FTEs (51.3% of adult academic HM practices have done so) and nurse practitioners or physician assistants (23%). Additional common responses to resident work-hour limitations are listed in Table 1.
Source: 2012 State of Hospital Medicine report
These data underscore the immensity of changes academic HM groups have faced as a result of new work-hour limitations, as the majority of internal-medicine residents work with hospitalist attendings on inpatient medicine rotations. House staff no longer can be used as an inexpensive source of labor, given limitations on service and new expectations for resident education and supervision.
As others have commented on this topic in The Hospitalist, the role of the academic hospitalist is being redefined. No longer is academic HM synonymous with teaching alone; the clinical duties of many academic hospitalists now include a combination of teaching and non-teaching services, often with some night coverage. At our hospitals in San Diego and Boston, for instance, changes incurred due to work-hour restrictions include elimination of house staff coverage from one of the medical center’s hospitals and a significant increase in nonteaching service responsibilities across all hospitalists. An alternative approach that some programs have embraced is the recruitment of separate cadres of teaching and nonteaching hospitalists, which might result in markedly different professional expectations within the same group or institution.
Trends shifting clinical work from residents to hospitalists are likely to continue, no doubt increasing demand for hospitalists and physician extenders. In the past, the combination of less expensive resident labor and lower salaries in academia was financially favorable for hospitals. Due to resident duty-hour limitations, academic hospitalist groups have had to negotiate not only for additional hires, but, in many instances, also higher salaries commensurate with nonteaching work.
Given the impact on a hospital’s finances, academic HM practices have had to look more closely at clinical volumes and productivity, making protected time for nonclinical pursuits more difficult to come by. Alignment of hospitalists’ interests with those of hospital administrators through performance-improvement projects (e.g. reducing length of stay, readmissions, or nosocomial infections) will be crucial to the financial viability of the academic HM practice, and leadership in these areas will define and differentiate academic hospitalists in the future.
Dr. Bryan Huang, who works in Boston, and Dr. Grace Huang, who works in San Diego, both are members of SHM’s Practice Analysis Committee.
Source: 2012 State of Hospital Medicine report
In July 2011, the Accreditation Council for Graduate Medical Education (ACGME) implemented new duty-hour restrictions on resident physicians. Among other changes, interns were restricted to a maximum of 16 hours of continuous duty. New rules also limited second-year residents and above to 24 hours of continuous duty, plus up to four additional hours for transition and educational activities. Recommendations were made for strategic napping, greater supervision requirements, and a minimum of eight to 10 hours off between shifts.
The 2012 State of Hospital Medicine report, which is based on 2011 data encompassing the period of these duty-hour changes, takes a systematic look at how academic HM practices have adjusted to the new resident rules. The most notable changes have been the addition of physician FTEs (51.3% of adult academic HM practices have done so) and nurse practitioners or physician assistants (23%). Additional common responses to resident work-hour limitations are listed in Table 1.
Source: 2012 State of Hospital Medicine report
These data underscore the immensity of changes academic HM groups have faced as a result of new work-hour limitations, as the majority of internal-medicine residents work with hospitalist attendings on inpatient medicine rotations. House staff no longer can be used as an inexpensive source of labor, given limitations on service and new expectations for resident education and supervision.
As others have commented on this topic in The Hospitalist, the role of the academic hospitalist is being redefined. No longer is academic HM synonymous with teaching alone; the clinical duties of many academic hospitalists now include a combination of teaching and non-teaching services, often with some night coverage. At our hospitals in San Diego and Boston, for instance, changes incurred due to work-hour restrictions include elimination of house staff coverage from one of the medical center’s hospitals and a significant increase in nonteaching service responsibilities across all hospitalists. An alternative approach that some programs have embraced is the recruitment of separate cadres of teaching and nonteaching hospitalists, which might result in markedly different professional expectations within the same group or institution.
Trends shifting clinical work from residents to hospitalists are likely to continue, no doubt increasing demand for hospitalists and physician extenders. In the past, the combination of less expensive resident labor and lower salaries in academia was financially favorable for hospitals. Due to resident duty-hour limitations, academic hospitalist groups have had to negotiate not only for additional hires, but, in many instances, also higher salaries commensurate with nonteaching work.
Given the impact on a hospital’s finances, academic HM practices have had to look more closely at clinical volumes and productivity, making protected time for nonclinical pursuits more difficult to come by. Alignment of hospitalists’ interests with those of hospital administrators through performance-improvement projects (e.g. reducing length of stay, readmissions, or nosocomial infections) will be crucial to the financial viability of the academic HM practice, and leadership in these areas will define and differentiate academic hospitalists in the future.
Dr. Bryan Huang, who works in Boston, and Dr. Grace Huang, who works in San Diego, both are members of SHM’s Practice Analysis Committee.
SHM Supports Clarification to Observational Status Loophole for Medicare Patients
Medicare requires beneficiaries to have at least three consecutive days as a hospital inpatient to qualify for Medicare-covered skilled nursing facility (SNF) care. As the use and duration of observation status continues to rise throughout the nation, patients have been getting caught more frequently within a policy trap: Even though they are physically within the hospital and generally receive care that is indistinguishable from the care received by other inpatients, Medicare is not covering their subsequent SNF stays.
Why? Observation status is considered “outpatient” by both the hospital and Medicare and, therefore, is not counted toward Medicare’s three-day rule.
This leaves seniors on the hook for their skilled nursing care costs, which often exceed their ability to pay. Further, this shortsighted policy might actually result in a net greater cost to Medicare and the health-care system. Faced with mounting costs, many seniors truncate or opt out of SNF care altogether, leaving them vulnerable to added health issues (e.g. dehydration, falls). With new conditions that were not present at the time of the original hospital stay, many of these seniors are at risk to return to the hospital and become another readmission statistic.
As key players in hospitals and, increasingly, in skilled nursing facilities, hospitalists are caught squarely in the middle of this policy. Transitions of care both in and out of these institutions should be guided by sound medical decision-making, not whether Medicare will cover the costs incurred. Although the three-day rule—and, indeed, observation status itself—was originally cast as a cost-containment policy, such policies should incorporate broader care process and delivery reforms that do not add burden to patients when they are at their most vulnerable.
SHM affirms that it is sensible for Medicare to provide coverage for skilled nursing care if a clinician recommends it as part of a treatment plan. Coverage determination should not be beholden to a patient status subject to other systemic pressures, but should reflect the best interest of the patient and the care ordered by providers.
The Improving Access to Medicare Coverage Act, sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio), would clarify the law to indicate that Medicare beneficiaries in observation status are deemed inpatients in the hospital for the purposes of the three-day requirement for SNF coverage. This simple adjustment would ensure that patients are able to access the skilled nursing care they need and that providers do not have to worry about this systemic barrier to patient care.
SHM is actively supporting this legislation. A letter of support was sent to Courtney and Brown earlier this year, and membership was mobilized to take action through our Legislative Action Center (www.hospitalmedicine.org/advocacy). Hospitalists also plan to voice their support for the legislation during Hospitalists on the Hill, to be held this month in conjunction with HM13.
As one of only a few specialty medical societies that are active on this issue, SHM stands out as a leader on health-care-system reforms that improve access to care for patients and reduce administrative barriers to medically appropriate care.
Joshua Lapps is SHM’s government relations specialist.
Medicare requires beneficiaries to have at least three consecutive days as a hospital inpatient to qualify for Medicare-covered skilled nursing facility (SNF) care. As the use and duration of observation status continues to rise throughout the nation, patients have been getting caught more frequently within a policy trap: Even though they are physically within the hospital and generally receive care that is indistinguishable from the care received by other inpatients, Medicare is not covering their subsequent SNF stays.
Why? Observation status is considered “outpatient” by both the hospital and Medicare and, therefore, is not counted toward Medicare’s three-day rule.
This leaves seniors on the hook for their skilled nursing care costs, which often exceed their ability to pay. Further, this shortsighted policy might actually result in a net greater cost to Medicare and the health-care system. Faced with mounting costs, many seniors truncate or opt out of SNF care altogether, leaving them vulnerable to added health issues (e.g. dehydration, falls). With new conditions that were not present at the time of the original hospital stay, many of these seniors are at risk to return to the hospital and become another readmission statistic.
As key players in hospitals and, increasingly, in skilled nursing facilities, hospitalists are caught squarely in the middle of this policy. Transitions of care both in and out of these institutions should be guided by sound medical decision-making, not whether Medicare will cover the costs incurred. Although the three-day rule—and, indeed, observation status itself—was originally cast as a cost-containment policy, such policies should incorporate broader care process and delivery reforms that do not add burden to patients when they are at their most vulnerable.
SHM affirms that it is sensible for Medicare to provide coverage for skilled nursing care if a clinician recommends it as part of a treatment plan. Coverage determination should not be beholden to a patient status subject to other systemic pressures, but should reflect the best interest of the patient and the care ordered by providers.
The Improving Access to Medicare Coverage Act, sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio), would clarify the law to indicate that Medicare beneficiaries in observation status are deemed inpatients in the hospital for the purposes of the three-day requirement for SNF coverage. This simple adjustment would ensure that patients are able to access the skilled nursing care they need and that providers do not have to worry about this systemic barrier to patient care.
SHM is actively supporting this legislation. A letter of support was sent to Courtney and Brown earlier this year, and membership was mobilized to take action through our Legislative Action Center (www.hospitalmedicine.org/advocacy). Hospitalists also plan to voice their support for the legislation during Hospitalists on the Hill, to be held this month in conjunction with HM13.
As one of only a few specialty medical societies that are active on this issue, SHM stands out as a leader on health-care-system reforms that improve access to care for patients and reduce administrative barriers to medically appropriate care.
Joshua Lapps is SHM’s government relations specialist.
Medicare requires beneficiaries to have at least three consecutive days as a hospital inpatient to qualify for Medicare-covered skilled nursing facility (SNF) care. As the use and duration of observation status continues to rise throughout the nation, patients have been getting caught more frequently within a policy trap: Even though they are physically within the hospital and generally receive care that is indistinguishable from the care received by other inpatients, Medicare is not covering their subsequent SNF stays.
Why? Observation status is considered “outpatient” by both the hospital and Medicare and, therefore, is not counted toward Medicare’s three-day rule.
This leaves seniors on the hook for their skilled nursing care costs, which often exceed their ability to pay. Further, this shortsighted policy might actually result in a net greater cost to Medicare and the health-care system. Faced with mounting costs, many seniors truncate or opt out of SNF care altogether, leaving them vulnerable to added health issues (e.g. dehydration, falls). With new conditions that were not present at the time of the original hospital stay, many of these seniors are at risk to return to the hospital and become another readmission statistic.
As key players in hospitals and, increasingly, in skilled nursing facilities, hospitalists are caught squarely in the middle of this policy. Transitions of care both in and out of these institutions should be guided by sound medical decision-making, not whether Medicare will cover the costs incurred. Although the three-day rule—and, indeed, observation status itself—was originally cast as a cost-containment policy, such policies should incorporate broader care process and delivery reforms that do not add burden to patients when they are at their most vulnerable.
SHM affirms that it is sensible for Medicare to provide coverage for skilled nursing care if a clinician recommends it as part of a treatment plan. Coverage determination should not be beholden to a patient status subject to other systemic pressures, but should reflect the best interest of the patient and the care ordered by providers.
The Improving Access to Medicare Coverage Act, sponsored by Rep. Joe Courtney (D-Conn.), Rep. Tom Latham (R-Iowa), and Sen. Sherrod Brown (D-Ohio), would clarify the law to indicate that Medicare beneficiaries in observation status are deemed inpatients in the hospital for the purposes of the three-day requirement for SNF coverage. This simple adjustment would ensure that patients are able to access the skilled nursing care they need and that providers do not have to worry about this systemic barrier to patient care.
SHM is actively supporting this legislation. A letter of support was sent to Courtney and Brown earlier this year, and membership was mobilized to take action through our Legislative Action Center (www.hospitalmedicine.org/advocacy). Hospitalists also plan to voice their support for the legislation during Hospitalists on the Hill, to be held this month in conjunction with HM13.
As one of only a few specialty medical societies that are active on this issue, SHM stands out as a leader on health-care-system reforms that improve access to care for patients and reduce administrative barriers to medically appropriate care.
Joshua Lapps is SHM’s government relations specialist.
SHM To Award First Certificates of Leadership at HM13
This month, Thomas McIlraith, MD, SFHM, will be on stage at HM13 accepting one of the first SHM Certificates in Leadership. As chair of hospital medicine at Sacramento, Calif.-based Mercy Medical Group, Dr. McIlraith already is familiar with the need for leadership in our specialty and shares why SHM’s Leadership Academy and new certification have helped his hospital and his career.
Question: What made you apply for the Certificate in Leadership in the first place?
Answer: I have always felt that a young field like hospital medicine needs to have resources to develop leadership; I don’t think there is another place in the field of medicine that has more shared responsibility requiring coordinated response than hospital medicine.
I have always been impressed and grateful that SHM recognized this and put forth the considerable effort required to create and develop the Leadership Academies into the premiere institution that they have evolved into. That is why I not only got involved in the leadership academies personally, but also had my entire leadership team complete the curriculum.
Certification is the culmination of that experience for me; I am hoping it is not the end, however. I have had other leadership training course work, and while the SHM Leadership Academies and the certification process were the best experience, I have learned that you can never have too much leadership training.
There are always new challenges a leader will be called on to face, and leadership skills need to continually grow.
Q: What’s been the biggest impact on your career so far? How do you plan on using it in the future?
A: It is not enough to be successful; you have to be able to tell the story of your success. Most of us want to be humble and focus on serving our patients, but the tree that falls in the woods is applicable to successful hospital medicine programs: If nobody hears about it, are you really successful? Can you really drive change?
Lenny Marcus put it best in his SHM Leadership Academy session on meta-leadership: Learning how to communicate to your boss is leading up; communicating across the silos of your organization is meta-leadership. The academies teach you about the skills you need for leadership; certification allows you to put those skills into action.
I vividly remember the day that academy instructor Eric Rice called me up to give me feedback on the first draft of my project. I was already stressed out because in four days I knew I had to give a critical presentation to top hospital leadership and health plan medical directors about our group. We had two new hospital presidents and a new service area senior vice president that had already terminated their contract with the ED group that covered three of the four hospitals. I knew they were scrutinizing my group; the pressure was on.
Eric gave the feedback that I had been focusing on the clinical aspects of my project and said I needed to tell the economic story—to measure the economic impact of my intervention. Further, he advised me on how to get the data to tell that story. I knew that he had just given me the material I needed to blow away the upcoming presentation to the hospital presidents, but would I get the data in time? I called up the CFO of the hospital as Eric advised, told him that I needed the data for a presentation I was giving to his boss in four days.
I got the data in time and blew away the presentation. I got to inform one of the new presidents that we had improved the contribution margin in his ICU by half a million dollars and cut length of stay by 0.9 days, while dramatically improving sepsis mortality. I was then able to go on and tell the HM leaders of our entire hospital system about our intervention and encouraged them to take similar steps.
Someday I hope I get the chance to tell Lenny Marcus this story; I hope he will consider me a meta-leader.
After the dust settled from those successes, I went back to my computer to write up the final draft of my project and I was able to tell a much better story than I ever could have without that advice Eric Rice and the committee [gave me].
My new boss was at the presentation that I gave. We went to the American Medical Group Association conference recently, and he did not hesitate to walk around bragging about what we had done, often quoting the numbers I delivered in my presentation. In another coda to the story, the new service area senior vice president asked my wife and I to join him and his wife for dinner; we have struck up a very valuable friendship.
—Thomas McIlraith, MD, SFHM
Q: What would you say to others who are thinking about applying for the certificate?
A: What are you waiting for?
On a more serious note, we are all engaged with important projects to make our hospitals run better, to keep our patients safer, and give our patients better experience. In the certification process, you continue with that work while top leaders from the field of hospital medicine coach and advise you.
Not only do you come out with a better product in the short term, but also you have better skills for taking on projects in the future; you know what questions to ask and what stories to tell and to whom. That stays with you long after the certification project is over.
Q: How are the results of your project benefiting your institution?
A: My hospitalists are seeing increased productivity and my hospitals are seeing stronger contribution margin in tough economic times. Further, the successful completion of the project has elevated the reputation of my department.
This month, Thomas McIlraith, MD, SFHM, will be on stage at HM13 accepting one of the first SHM Certificates in Leadership. As chair of hospital medicine at Sacramento, Calif.-based Mercy Medical Group, Dr. McIlraith already is familiar with the need for leadership in our specialty and shares why SHM’s Leadership Academy and new certification have helped his hospital and his career.
Question: What made you apply for the Certificate in Leadership in the first place?
Answer: I have always felt that a young field like hospital medicine needs to have resources to develop leadership; I don’t think there is another place in the field of medicine that has more shared responsibility requiring coordinated response than hospital medicine.
I have always been impressed and grateful that SHM recognized this and put forth the considerable effort required to create and develop the Leadership Academies into the premiere institution that they have evolved into. That is why I not only got involved in the leadership academies personally, but also had my entire leadership team complete the curriculum.
Certification is the culmination of that experience for me; I am hoping it is not the end, however. I have had other leadership training course work, and while the SHM Leadership Academies and the certification process were the best experience, I have learned that you can never have too much leadership training.
There are always new challenges a leader will be called on to face, and leadership skills need to continually grow.
Q: What’s been the biggest impact on your career so far? How do you plan on using it in the future?
A: It is not enough to be successful; you have to be able to tell the story of your success. Most of us want to be humble and focus on serving our patients, but the tree that falls in the woods is applicable to successful hospital medicine programs: If nobody hears about it, are you really successful? Can you really drive change?
Lenny Marcus put it best in his SHM Leadership Academy session on meta-leadership: Learning how to communicate to your boss is leading up; communicating across the silos of your organization is meta-leadership. The academies teach you about the skills you need for leadership; certification allows you to put those skills into action.
I vividly remember the day that academy instructor Eric Rice called me up to give me feedback on the first draft of my project. I was already stressed out because in four days I knew I had to give a critical presentation to top hospital leadership and health plan medical directors about our group. We had two new hospital presidents and a new service area senior vice president that had already terminated their contract with the ED group that covered three of the four hospitals. I knew they were scrutinizing my group; the pressure was on.
Eric gave the feedback that I had been focusing on the clinical aspects of my project and said I needed to tell the economic story—to measure the economic impact of my intervention. Further, he advised me on how to get the data to tell that story. I knew that he had just given me the material I needed to blow away the upcoming presentation to the hospital presidents, but would I get the data in time? I called up the CFO of the hospital as Eric advised, told him that I needed the data for a presentation I was giving to his boss in four days.
I got the data in time and blew away the presentation. I got to inform one of the new presidents that we had improved the contribution margin in his ICU by half a million dollars and cut length of stay by 0.9 days, while dramatically improving sepsis mortality. I was then able to go on and tell the HM leaders of our entire hospital system about our intervention and encouraged them to take similar steps.
Someday I hope I get the chance to tell Lenny Marcus this story; I hope he will consider me a meta-leader.
After the dust settled from those successes, I went back to my computer to write up the final draft of my project and I was able to tell a much better story than I ever could have without that advice Eric Rice and the committee [gave me].
My new boss was at the presentation that I gave. We went to the American Medical Group Association conference recently, and he did not hesitate to walk around bragging about what we had done, often quoting the numbers I delivered in my presentation. In another coda to the story, the new service area senior vice president asked my wife and I to join him and his wife for dinner; we have struck up a very valuable friendship.
—Thomas McIlraith, MD, SFHM
Q: What would you say to others who are thinking about applying for the certificate?
A: What are you waiting for?
On a more serious note, we are all engaged with important projects to make our hospitals run better, to keep our patients safer, and give our patients better experience. In the certification process, you continue with that work while top leaders from the field of hospital medicine coach and advise you.
Not only do you come out with a better product in the short term, but also you have better skills for taking on projects in the future; you know what questions to ask and what stories to tell and to whom. That stays with you long after the certification project is over.
Q: How are the results of your project benefiting your institution?
A: My hospitalists are seeing increased productivity and my hospitals are seeing stronger contribution margin in tough economic times. Further, the successful completion of the project has elevated the reputation of my department.
This month, Thomas McIlraith, MD, SFHM, will be on stage at HM13 accepting one of the first SHM Certificates in Leadership. As chair of hospital medicine at Sacramento, Calif.-based Mercy Medical Group, Dr. McIlraith already is familiar with the need for leadership in our specialty and shares why SHM’s Leadership Academy and new certification have helped his hospital and his career.
Question: What made you apply for the Certificate in Leadership in the first place?
Answer: I have always felt that a young field like hospital medicine needs to have resources to develop leadership; I don’t think there is another place in the field of medicine that has more shared responsibility requiring coordinated response than hospital medicine.
I have always been impressed and grateful that SHM recognized this and put forth the considerable effort required to create and develop the Leadership Academies into the premiere institution that they have evolved into. That is why I not only got involved in the leadership academies personally, but also had my entire leadership team complete the curriculum.
Certification is the culmination of that experience for me; I am hoping it is not the end, however. I have had other leadership training course work, and while the SHM Leadership Academies and the certification process were the best experience, I have learned that you can never have too much leadership training.
There are always new challenges a leader will be called on to face, and leadership skills need to continually grow.
Q: What’s been the biggest impact on your career so far? How do you plan on using it in the future?
A: It is not enough to be successful; you have to be able to tell the story of your success. Most of us want to be humble and focus on serving our patients, but the tree that falls in the woods is applicable to successful hospital medicine programs: If nobody hears about it, are you really successful? Can you really drive change?
Lenny Marcus put it best in his SHM Leadership Academy session on meta-leadership: Learning how to communicate to your boss is leading up; communicating across the silos of your organization is meta-leadership. The academies teach you about the skills you need for leadership; certification allows you to put those skills into action.
I vividly remember the day that academy instructor Eric Rice called me up to give me feedback on the first draft of my project. I was already stressed out because in four days I knew I had to give a critical presentation to top hospital leadership and health plan medical directors about our group. We had two new hospital presidents and a new service area senior vice president that had already terminated their contract with the ED group that covered three of the four hospitals. I knew they were scrutinizing my group; the pressure was on.
Eric gave the feedback that I had been focusing on the clinical aspects of my project and said I needed to tell the economic story—to measure the economic impact of my intervention. Further, he advised me on how to get the data to tell that story. I knew that he had just given me the material I needed to blow away the upcoming presentation to the hospital presidents, but would I get the data in time? I called up the CFO of the hospital as Eric advised, told him that I needed the data for a presentation I was giving to his boss in four days.
I got the data in time and blew away the presentation. I got to inform one of the new presidents that we had improved the contribution margin in his ICU by half a million dollars and cut length of stay by 0.9 days, while dramatically improving sepsis mortality. I was then able to go on and tell the HM leaders of our entire hospital system about our intervention and encouraged them to take similar steps.
Someday I hope I get the chance to tell Lenny Marcus this story; I hope he will consider me a meta-leader.
After the dust settled from those successes, I went back to my computer to write up the final draft of my project and I was able to tell a much better story than I ever could have without that advice Eric Rice and the committee [gave me].
My new boss was at the presentation that I gave. We went to the American Medical Group Association conference recently, and he did not hesitate to walk around bragging about what we had done, often quoting the numbers I delivered in my presentation. In another coda to the story, the new service area senior vice president asked my wife and I to join him and his wife for dinner; we have struck up a very valuable friendship.
—Thomas McIlraith, MD, SFHM
Q: What would you say to others who are thinking about applying for the certificate?
A: What are you waiting for?
On a more serious note, we are all engaged with important projects to make our hospitals run better, to keep our patients safer, and give our patients better experience. In the certification process, you continue with that work while top leaders from the field of hospital medicine coach and advise you.
Not only do you come out with a better product in the short term, but also you have better skills for taking on projects in the future; you know what questions to ask and what stories to tell and to whom. That stays with you long after the certification project is over.
Q: How are the results of your project benefiting your institution?
A: My hospitalists are seeing increased productivity and my hospitals are seeing stronger contribution margin in tough economic times. Further, the successful completion of the project has elevated the reputation of my department.
SHM Welcomes Nonphysician Fellows to Hospital Medicine
This year marks the first in which nonphysicians will be inducted as Fellows and senior Fellows in Hospital Medicine. SHM welcomes those nurse practitioners, physician assistants, and practice administrators who practice as hospitalists to the growing ranks of individuals committing their time and talent to the specialty.
NonPhysician SHM Fellows 2013
PRACTICE ADMINISTRATORS
- Kim Dickinson, SFHM
- Leslie L. Flores, MHA, SFHM
- Vicky-Lynne Gloger, MS, SFHM
- Roberta P. Himebaugh, MBA, SFHM
- Ajay Kharbanda, MBA, CMPE, SFHM
- Dave K. Dookeeram, MPH, FACHE, FHM
- Bradley J. Eshbaugh, MBA, FACMPE, FHM
- Lara Hauslaib, MPH, FHM
- Holly A. Hammond, MBA, FHM
NURSE PRACTITIONERS & PHYSICIAN ASSISTANTS
- Lorraine L. Britting, ANP, SFHM
- Jeanette Ann Kalupa, DNP, SFHM
- Mikkii Swanson, DNP, MSN, RN, SFHM
- Deborah Haywood, RN, MBA, FHM
- Julie Lepzinski, RN, BSN, MBA, FHM
- James W. Levy, PA-C, FHM
- Susan Willis, PhD, PA-C, FHM
This year marks the first in which nonphysicians will be inducted as Fellows and senior Fellows in Hospital Medicine. SHM welcomes those nurse practitioners, physician assistants, and practice administrators who practice as hospitalists to the growing ranks of individuals committing their time and talent to the specialty.
NonPhysician SHM Fellows 2013
PRACTICE ADMINISTRATORS
- Kim Dickinson, SFHM
- Leslie L. Flores, MHA, SFHM
- Vicky-Lynne Gloger, MS, SFHM
- Roberta P. Himebaugh, MBA, SFHM
- Ajay Kharbanda, MBA, CMPE, SFHM
- Dave K. Dookeeram, MPH, FACHE, FHM
- Bradley J. Eshbaugh, MBA, FACMPE, FHM
- Lara Hauslaib, MPH, FHM
- Holly A. Hammond, MBA, FHM
NURSE PRACTITIONERS & PHYSICIAN ASSISTANTS
- Lorraine L. Britting, ANP, SFHM
- Jeanette Ann Kalupa, DNP, SFHM
- Mikkii Swanson, DNP, MSN, RN, SFHM
- Deborah Haywood, RN, MBA, FHM
- Julie Lepzinski, RN, BSN, MBA, FHM
- James W. Levy, PA-C, FHM
- Susan Willis, PhD, PA-C, FHM
This year marks the first in which nonphysicians will be inducted as Fellows and senior Fellows in Hospital Medicine. SHM welcomes those nurse practitioners, physician assistants, and practice administrators who practice as hospitalists to the growing ranks of individuals committing their time and talent to the specialty.
NonPhysician SHM Fellows 2013
PRACTICE ADMINISTRATORS
- Kim Dickinson, SFHM
- Leslie L. Flores, MHA, SFHM
- Vicky-Lynne Gloger, MS, SFHM
- Roberta P. Himebaugh, MBA, SFHM
- Ajay Kharbanda, MBA, CMPE, SFHM
- Dave K. Dookeeram, MPH, FACHE, FHM
- Bradley J. Eshbaugh, MBA, FACMPE, FHM
- Lara Hauslaib, MPH, FHM
- Holly A. Hammond, MBA, FHM
NURSE PRACTITIONERS & PHYSICIAN ASSISTANTS
- Lorraine L. Britting, ANP, SFHM
- Jeanette Ann Kalupa, DNP, SFHM
- Mikkii Swanson, DNP, MSN, RN, SFHM
- Deborah Haywood, RN, MBA, FHM
- Julie Lepzinski, RN, BSN, MBA, FHM
- James W. Levy, PA-C, FHM
- Susan Willis, PhD, PA-C, FHM
Some Thoughts on the Patient-Doctor Relationship
There is an inherent power differential in the patient-doctor relationship: The patient comes to the doctor as an authority on his/her physical or emotional state and is thus either intellectually or emotionally dependent on the doctor’s treatment plan and advice. It is therefore absolutely essential that the doctor respect the patient as an equal participant in the treatment. Although the doctor certainly has knowledge about how similar conditions were successfully treated in the past, hopefully a medical professional will display an attitude of respect and mutual collaboration with the patient to resolve his/her problem.
Listening is a key component of conveying an attitude of respect toward the patient. Nowadays practitioners are most often taking notes at their computers while speaking with the patient. This is certainly time-efficient and may in fact be necessary in order for a medical practice to remain solvent with the demands of Medicare and insurance companies. However, multitasking does not convey to the patient that they are connecting with the doctor. Listening is a complex action, which not only involves the ears, but the eyes, the kinesthetic responses of the whole body, and attention to the patient’s nonverbal communication.
Some of the key faux pas to avoid when listening to the patient include:
- Not centering oneself before engaging in a “crucial conversation”;
- Not listening because one is thinking ahead to his/her own response;
- Not maintaining eye contact;
- Not being aware of when one feels challenged and/or defensive;
- Discouraging the patient from contributing his/her own ideas;
- Not allowing the patient to give feedback on what s/he heard as instructions; and
- Taking phone calls or allowing interruptions during a consultation.
It is always helpful to give a patient clear, written instructions about medications, diet, exercise, etc., that result from the consultation. Some doctors send this report via secure email to the patient for review, which is an excellent technique.
The art of apology is another topic that greatly impacts the doctor-patient relationship, as well as the doctor’s relationship with the patient’s family members. This art is a process that has recently emerged in the medical and medical insurance industries. Kaiser Permanente’s director of medical-legal affairs has adopted the practice of asking permission to videotape the actual conversation in which a physician apologizes to a patient for a mistake in a procedure. These conversations are meant to help medical professionals learn how to admit mistakes and ask for forgiveness. Oftentimes patients are looking for just such a communication, which may allow them to put to rest feelings of resentment, bitterness, and regret.
Our patients’ well-being is our ideal goal. Knowing that they have been heard and their feelings understood may in the long run allow patients and their families to heal mind/body/soul more powerfully than we had ever thought. Of course, in our litigious society this may well be an art that remains to be developed over the long term.
There is an inherent power differential in the patient-doctor relationship: The patient comes to the doctor as an authority on his/her physical or emotional state and is thus either intellectually or emotionally dependent on the doctor’s treatment plan and advice. It is therefore absolutely essential that the doctor respect the patient as an equal participant in the treatment. Although the doctor certainly has knowledge about how similar conditions were successfully treated in the past, hopefully a medical professional will display an attitude of respect and mutual collaboration with the patient to resolve his/her problem.
Listening is a key component of conveying an attitude of respect toward the patient. Nowadays practitioners are most often taking notes at their computers while speaking with the patient. This is certainly time-efficient and may in fact be necessary in order for a medical practice to remain solvent with the demands of Medicare and insurance companies. However, multitasking does not convey to the patient that they are connecting with the doctor. Listening is a complex action, which not only involves the ears, but the eyes, the kinesthetic responses of the whole body, and attention to the patient’s nonverbal communication.
Some of the key faux pas to avoid when listening to the patient include:
- Not centering oneself before engaging in a “crucial conversation”;
- Not listening because one is thinking ahead to his/her own response;
- Not maintaining eye contact;
- Not being aware of when one feels challenged and/or defensive;
- Discouraging the patient from contributing his/her own ideas;
- Not allowing the patient to give feedback on what s/he heard as instructions; and
- Taking phone calls or allowing interruptions during a consultation.
It is always helpful to give a patient clear, written instructions about medications, diet, exercise, etc., that result from the consultation. Some doctors send this report via secure email to the patient for review, which is an excellent technique.
The art of apology is another topic that greatly impacts the doctor-patient relationship, as well as the doctor’s relationship with the patient’s family members. This art is a process that has recently emerged in the medical and medical insurance industries. Kaiser Permanente’s director of medical-legal affairs has adopted the practice of asking permission to videotape the actual conversation in which a physician apologizes to a patient for a mistake in a procedure. These conversations are meant to help medical professionals learn how to admit mistakes and ask for forgiveness. Oftentimes patients are looking for just such a communication, which may allow them to put to rest feelings of resentment, bitterness, and regret.
Our patients’ well-being is our ideal goal. Knowing that they have been heard and their feelings understood may in the long run allow patients and their families to heal mind/body/soul more powerfully than we had ever thought. Of course, in our litigious society this may well be an art that remains to be developed over the long term.
There is an inherent power differential in the patient-doctor relationship: The patient comes to the doctor as an authority on his/her physical or emotional state and is thus either intellectually or emotionally dependent on the doctor’s treatment plan and advice. It is therefore absolutely essential that the doctor respect the patient as an equal participant in the treatment. Although the doctor certainly has knowledge about how similar conditions were successfully treated in the past, hopefully a medical professional will display an attitude of respect and mutual collaboration with the patient to resolve his/her problem.
Listening is a key component of conveying an attitude of respect toward the patient. Nowadays practitioners are most often taking notes at their computers while speaking with the patient. This is certainly time-efficient and may in fact be necessary in order for a medical practice to remain solvent with the demands of Medicare and insurance companies. However, multitasking does not convey to the patient that they are connecting with the doctor. Listening is a complex action, which not only involves the ears, but the eyes, the kinesthetic responses of the whole body, and attention to the patient’s nonverbal communication.
Some of the key faux pas to avoid when listening to the patient include:
- Not centering oneself before engaging in a “crucial conversation”;
- Not listening because one is thinking ahead to his/her own response;
- Not maintaining eye contact;
- Not being aware of when one feels challenged and/or defensive;
- Discouraging the patient from contributing his/her own ideas;
- Not allowing the patient to give feedback on what s/he heard as instructions; and
- Taking phone calls or allowing interruptions during a consultation.
It is always helpful to give a patient clear, written instructions about medications, diet, exercise, etc., that result from the consultation. Some doctors send this report via secure email to the patient for review, which is an excellent technique.
The art of apology is another topic that greatly impacts the doctor-patient relationship, as well as the doctor’s relationship with the patient’s family members. This art is a process that has recently emerged in the medical and medical insurance industries. Kaiser Permanente’s director of medical-legal affairs has adopted the practice of asking permission to videotape the actual conversation in which a physician apologizes to a patient for a mistake in a procedure. These conversations are meant to help medical professionals learn how to admit mistakes and ask for forgiveness. Oftentimes patients are looking for just such a communication, which may allow them to put to rest feelings of resentment, bitterness, and regret.
Our patients’ well-being is our ideal goal. Knowing that they have been heard and their feelings understood may in the long run allow patients and their families to heal mind/body/soul more powerfully than we had ever thought. Of course, in our litigious society this may well be an art that remains to be developed over the long term.
Coordinated Approach May Help in Caring for Hospitals’ Neediest Patients

To my way of thinking, a person’s diagnosis or pathophysiology is not as strong a predictor of needing inpatient hospital care as it might have been 10 or 20 years ago. Rather than the clinical diagnosis (e.g. pneumonia), it seems to me that frailty or social complexity often are the principal determinants of which patients are admitted to a hospital for medical conditions.
Some of these patients are admitted frequently but appear to realize little or no benefit from hospitalization. These patients typically have little or no social support, and they often have either significant mental health disorders or substance abuse, or both. Much has been written about these patients, and I recommend an article by Dr. Atul Gawande in the Jan. 24, 2011, issue of The New Yorker titled “The Hot Spotters: Can We Lower Medical Costs by Giving the Neediest Patients Better Care?”
The Agency for Healthcare Research and Quality’s “Statistical Brief 354” on how health-care expenditures are allocated across the population reported that 1% of the population accounted for more than 22% of health-care spending in 2008. One in 5 of those were in that category again in 2009. Some of these patients would benefit from care plans.
The Role of Care Plans
It seems that there may be few effective inpatient interventions that will benefit these patients. After all, they have chronic issues that require ongoing relationships with outpatient providers, something that many of these patients lack. But for some (most?) of these patients, it seems clear that frequent hospitalizations don’t help and sometimes just perpetuate or worsen the patient’s dependence on the hospital at a high financial cost to society—and significant frustration and burnout on the part of hospital caregivers, including hospitalists.
For most hospitals, this problem is significant enough to require some sort of coordinated approach to the care of the dozens of types of patients in this category. Implementing whatever plan of care seems appropriate to the caregivers during each admission is frustrating, ensures lots of variation in care, and makes it easier for manipulative patients to abuse the hospital resources and personnel.
A better approach is to follow the same plan of care from one hospital visit to the next. You already knew that. But developing a care plan to follow during each ED visit and admission is time-consuming and often fraught with uncertainty about where boundaries should be set. So if you’re like me, you might just try to guide the patient to discharge this time and hope that whoever sees the patient on the next admission will take the initiative to develop the care plan. The result is that few such plans are developed.
Your Hospital Needs a Care Plan
Relying on individual doctors or nurses to take the initiative to develop care plans will almost always mean few plans are developed, they will vary in their effectiveness, and other providers may not be aware a plan exists. This was the case at the hospital where I practice until I heard Dr. Rick Hilger, MD, SFHM, a hospitalist at Regions Hospital in Minneapolis, present on this topic at HM12 in San Diego.
Dr. Hilger led a multidisciplinary team to develop care plans (they call them “restriction care plans”) and found that they dramatically reduced the rate of hospital admissions and ED visits for these patients. Hearing about this experience served as a kick in the pants for me, so I did much the same thing at “my” hospital. We have now developed plans for more than 20 patients and found that they visit our ED and are admitted less often. And, anecdotally at least, hospitalists and other hospital staff find that the care plans reduce, at least a little, the stress of caring for these patients.
Unanswered Questions
Although it seems clear that care plans reduce visits to the hospital that develops them, I suspect that some of these patients aren’t consuming any fewer health-care resources. They may just seek care from a different hospital.
My home state of Washington is working to develop individual patient care plans available to all hospitals in the state. A system called the Emergency Department Information Exchange (EDIE) has been adopted by nearly all the hospitals in the state. It allows them to share information on ED visits and such things as care plans with one another. For example, through EDIE, each hospital could see the opiate dosing schedule and admission criteria agreed to by patient and primary-care physician.
So it seems that care plans and the technology to share them can make it more difficult for patients to harm themselves by visiting many hospitals to get excessive opiate prescriptions, for example. This should benefit the patient and lower ED and hospital expenditures for these patients. But we don’t know what portion of costs simply is shifted to other settings, so there is no easy way to know the net effect on health-care costs.
An important unanswered question is whether these care plans improve patient well-being. It seems clear they do in some cases, but it is hard to know whether some patients may be worse off because of the plan.
Conclusion
I think nearly every hospital would benefit from a care plan committee composed of at least one hospitalist, ED physician, a nursing representative, and potentially other disciplines (see “Care Plan Attributes,” above). Our committee includes our inpatient psychiatrist, a really valuable contributor.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
To my way of thinking, a person’s diagnosis or pathophysiology is not as strong a predictor of needing inpatient hospital care as it might have been 10 or 20 years ago. Rather than the clinical diagnosis (e.g. pneumonia), it seems to me that frailty or social complexity often are the principal determinants of which patients are admitted to a hospital for medical conditions.
Some of these patients are admitted frequently but appear to realize little or no benefit from hospitalization. These patients typically have little or no social support, and they often have either significant mental health disorders or substance abuse, or both. Much has been written about these patients, and I recommend an article by Dr. Atul Gawande in the Jan. 24, 2011, issue of The New Yorker titled “The Hot Spotters: Can We Lower Medical Costs by Giving the Neediest Patients Better Care?”
The Agency for Healthcare Research and Quality’s “Statistical Brief 354” on how health-care expenditures are allocated across the population reported that 1% of the population accounted for more than 22% of health-care spending in 2008. One in 5 of those were in that category again in 2009. Some of these patients would benefit from care plans.
The Role of Care Plans
It seems that there may be few effective inpatient interventions that will benefit these patients. After all, they have chronic issues that require ongoing relationships with outpatient providers, something that many of these patients lack. But for some (most?) of these patients, it seems clear that frequent hospitalizations don’t help and sometimes just perpetuate or worsen the patient’s dependence on the hospital at a high financial cost to society—and significant frustration and burnout on the part of hospital caregivers, including hospitalists.
For most hospitals, this problem is significant enough to require some sort of coordinated approach to the care of the dozens of types of patients in this category. Implementing whatever plan of care seems appropriate to the caregivers during each admission is frustrating, ensures lots of variation in care, and makes it easier for manipulative patients to abuse the hospital resources and personnel.
A better approach is to follow the same plan of care from one hospital visit to the next. You already knew that. But developing a care plan to follow during each ED visit and admission is time-consuming and often fraught with uncertainty about where boundaries should be set. So if you’re like me, you might just try to guide the patient to discharge this time and hope that whoever sees the patient on the next admission will take the initiative to develop the care plan. The result is that few such plans are developed.
Your Hospital Needs a Care Plan
Relying on individual doctors or nurses to take the initiative to develop care plans will almost always mean few plans are developed, they will vary in their effectiveness, and other providers may not be aware a plan exists. This was the case at the hospital where I practice until I heard Dr. Rick Hilger, MD, SFHM, a hospitalist at Regions Hospital in Minneapolis, present on this topic at HM12 in San Diego.
Dr. Hilger led a multidisciplinary team to develop care plans (they call them “restriction care plans”) and found that they dramatically reduced the rate of hospital admissions and ED visits for these patients. Hearing about this experience served as a kick in the pants for me, so I did much the same thing at “my” hospital. We have now developed plans for more than 20 patients and found that they visit our ED and are admitted less often. And, anecdotally at least, hospitalists and other hospital staff find that the care plans reduce, at least a little, the stress of caring for these patients.
Unanswered Questions
Although it seems clear that care plans reduce visits to the hospital that develops them, I suspect that some of these patients aren’t consuming any fewer health-care resources. They may just seek care from a different hospital.
My home state of Washington is working to develop individual patient care plans available to all hospitals in the state. A system called the Emergency Department Information Exchange (EDIE) has been adopted by nearly all the hospitals in the state. It allows them to share information on ED visits and such things as care plans with one another. For example, through EDIE, each hospital could see the opiate dosing schedule and admission criteria agreed to by patient and primary-care physician.
So it seems that care plans and the technology to share them can make it more difficult for patients to harm themselves by visiting many hospitals to get excessive opiate prescriptions, for example. This should benefit the patient and lower ED and hospital expenditures for these patients. But we don’t know what portion of costs simply is shifted to other settings, so there is no easy way to know the net effect on health-care costs.
An important unanswered question is whether these care plans improve patient well-being. It seems clear they do in some cases, but it is hard to know whether some patients may be worse off because of the plan.
Conclusion
I think nearly every hospital would benefit from a care plan committee composed of at least one hospitalist, ED physician, a nursing representative, and potentially other disciplines (see “Care Plan Attributes,” above). Our committee includes our inpatient psychiatrist, a really valuable contributor.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
To my way of thinking, a person’s diagnosis or pathophysiology is not as strong a predictor of needing inpatient hospital care as it might have been 10 or 20 years ago. Rather than the clinical diagnosis (e.g. pneumonia), it seems to me that frailty or social complexity often are the principal determinants of which patients are admitted to a hospital for medical conditions.
Some of these patients are admitted frequently but appear to realize little or no benefit from hospitalization. These patients typically have little or no social support, and they often have either significant mental health disorders or substance abuse, or both. Much has been written about these patients, and I recommend an article by Dr. Atul Gawande in the Jan. 24, 2011, issue of The New Yorker titled “The Hot Spotters: Can We Lower Medical Costs by Giving the Neediest Patients Better Care?”
The Agency for Healthcare Research and Quality’s “Statistical Brief 354” on how health-care expenditures are allocated across the population reported that 1% of the population accounted for more than 22% of health-care spending in 2008. One in 5 of those were in that category again in 2009. Some of these patients would benefit from care plans.
The Role of Care Plans
It seems that there may be few effective inpatient interventions that will benefit these patients. After all, they have chronic issues that require ongoing relationships with outpatient providers, something that many of these patients lack. But for some (most?) of these patients, it seems clear that frequent hospitalizations don’t help and sometimes just perpetuate or worsen the patient’s dependence on the hospital at a high financial cost to society—and significant frustration and burnout on the part of hospital caregivers, including hospitalists.
For most hospitals, this problem is significant enough to require some sort of coordinated approach to the care of the dozens of types of patients in this category. Implementing whatever plan of care seems appropriate to the caregivers during each admission is frustrating, ensures lots of variation in care, and makes it easier for manipulative patients to abuse the hospital resources and personnel.
A better approach is to follow the same plan of care from one hospital visit to the next. You already knew that. But developing a care plan to follow during each ED visit and admission is time-consuming and often fraught with uncertainty about where boundaries should be set. So if you’re like me, you might just try to guide the patient to discharge this time and hope that whoever sees the patient on the next admission will take the initiative to develop the care plan. The result is that few such plans are developed.
Your Hospital Needs a Care Plan
Relying on individual doctors or nurses to take the initiative to develop care plans will almost always mean few plans are developed, they will vary in their effectiveness, and other providers may not be aware a plan exists. This was the case at the hospital where I practice until I heard Dr. Rick Hilger, MD, SFHM, a hospitalist at Regions Hospital in Minneapolis, present on this topic at HM12 in San Diego.
Dr. Hilger led a multidisciplinary team to develop care plans (they call them “restriction care plans”) and found that they dramatically reduced the rate of hospital admissions and ED visits for these patients. Hearing about this experience served as a kick in the pants for me, so I did much the same thing at “my” hospital. We have now developed plans for more than 20 patients and found that they visit our ED and are admitted less often. And, anecdotally at least, hospitalists and other hospital staff find that the care plans reduce, at least a little, the stress of caring for these patients.
Unanswered Questions
Although it seems clear that care plans reduce visits to the hospital that develops them, I suspect that some of these patients aren’t consuming any fewer health-care resources. They may just seek care from a different hospital.
My home state of Washington is working to develop individual patient care plans available to all hospitals in the state. A system called the Emergency Department Information Exchange (EDIE) has been adopted by nearly all the hospitals in the state. It allows them to share information on ED visits and such things as care plans with one another. For example, through EDIE, each hospital could see the opiate dosing schedule and admission criteria agreed to by patient and primary-care physician.
So it seems that care plans and the technology to share them can make it more difficult for patients to harm themselves by visiting many hospitals to get excessive opiate prescriptions, for example. This should benefit the patient and lower ED and hospital expenditures for these patients. But we don’t know what portion of costs simply is shifted to other settings, so there is no easy way to know the net effect on health-care costs.
An important unanswered question is whether these care plans improve patient well-being. It seems clear they do in some cases, but it is hard to know whether some patients may be worse off because of the plan.
Conclusion
I think nearly every hospital would benefit from a care plan committee composed of at least one hospitalist, ED physician, a nursing representative, and potentially other disciplines (see “Care Plan Attributes,” above). Our committee includes our inpatient psychiatrist, a really valuable contributor.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Communication Key to Peaceful Coexistence for Competing Hospital Medicine Groups

Experienced hospitalists and medical directors agree that the key to multiple hospitalist groups coexisting effectively under one roof—whether directly competing or not—is good communication. Effective communication can take time to build.
“Start by working together on something—anything, [such as] a hospital committee of some sort where there’s not likely to be much tension,” says hospitalist pioneer and practice consultant John Nelson, MD, MHM.
Dr. Nelson practices at Overlake Hospital in Bellevue, Wash., which has a hospitalist group employed by the hospital and another employed by Group Health Cooperative, a nonprofit health system in Washington state. It is important to put some trust in the trust bank, he says, “and that’s hard if you have no social connections at all. At my hospital, we enjoy each other’s company, we visit each other at lunch, and we even tried to have a journal club.” The two hospitalist groups work together on developing care protocols. Dr. Nelson says it also makes sense for the groups’ leaders to sit down together on a regular basis and have a venue for discussing important issues and solving problems that may arise.
Other suggestions for hospitalist groups working together under one roof include:
- Clearly define each group’s territory. The groups’ representatives can go out and try to persuade health plans or physician groups to shift their hospitalist allegiances, but there should be no “trolling” or “poaching” of patients going on inside the hospital’s walls. That will only confuse patients and disrupt the hospital’s larger service goals.
- Inform the ED and other key staff of your schedules. It’s important that everyone know exactly who is supposed to get which patients, and how these referrals get made. But recognize that mistakes happen and, hopefully, these will even out between the groups over time.
- Transparency, honesty, and even-handed treatment of all hospitalists can prevent resentment. Clearly defined guidelines and expectations are helpful. If the policy spells out transfers for an incorrectly referred patient, both sides should be accessible and cooperative with that process.
- Identify areas of common interest and agree to work together on these areas (i.e. competition-free zones). It might be possible, for example, for competing groups to take each others’ after-hours call on a rotating basis, with a firm commitment not to steal patients along the way.
- Spell out responsibilities in a way that everyone can agree is fair, such as alternating referrals or taking call on alternating days. For example, if subsidies are paid to more than one hospitalist group, is this done equitably, such as based on the number of hospitalist FTEs or shifts?
- Restrictive covenants and contractual noncompete clauses could become an issue in areas where multiple groups practice. Rather than using overly broad, blanket language, it could be clarified that such pacts apply only to the hospital where the physician currently works, and within a reasonable time frame. But everyone involved should be aware of what these covenants contain and, if they appear unreasonable, don’t sign them.
—Larry Beresford
Experienced hospitalists and medical directors agree that the key to multiple hospitalist groups coexisting effectively under one roof—whether directly competing or not—is good communication. Effective communication can take time to build.
“Start by working together on something—anything, [such as] a hospital committee of some sort where there’s not likely to be much tension,” says hospitalist pioneer and practice consultant John Nelson, MD, MHM.
Dr. Nelson practices at Overlake Hospital in Bellevue, Wash., which has a hospitalist group employed by the hospital and another employed by Group Health Cooperative, a nonprofit health system in Washington state. It is important to put some trust in the trust bank, he says, “and that’s hard if you have no social connections at all. At my hospital, we enjoy each other’s company, we visit each other at lunch, and we even tried to have a journal club.” The two hospitalist groups work together on developing care protocols. Dr. Nelson says it also makes sense for the groups’ leaders to sit down together on a regular basis and have a venue for discussing important issues and solving problems that may arise.
Other suggestions for hospitalist groups working together under one roof include:
- Clearly define each group’s territory. The groups’ representatives can go out and try to persuade health plans or physician groups to shift their hospitalist allegiances, but there should be no “trolling” or “poaching” of patients going on inside the hospital’s walls. That will only confuse patients and disrupt the hospital’s larger service goals.
- Inform the ED and other key staff of your schedules. It’s important that everyone know exactly who is supposed to get which patients, and how these referrals get made. But recognize that mistakes happen and, hopefully, these will even out between the groups over time.
- Transparency, honesty, and even-handed treatment of all hospitalists can prevent resentment. Clearly defined guidelines and expectations are helpful. If the policy spells out transfers for an incorrectly referred patient, both sides should be accessible and cooperative with that process.
- Identify areas of common interest and agree to work together on these areas (i.e. competition-free zones). It might be possible, for example, for competing groups to take each others’ after-hours call on a rotating basis, with a firm commitment not to steal patients along the way.
- Spell out responsibilities in a way that everyone can agree is fair, such as alternating referrals or taking call on alternating days. For example, if subsidies are paid to more than one hospitalist group, is this done equitably, such as based on the number of hospitalist FTEs or shifts?
- Restrictive covenants and contractual noncompete clauses could become an issue in areas where multiple groups practice. Rather than using overly broad, blanket language, it could be clarified that such pacts apply only to the hospital where the physician currently works, and within a reasonable time frame. But everyone involved should be aware of what these covenants contain and, if they appear unreasonable, don’t sign them.
—Larry Beresford
Experienced hospitalists and medical directors agree that the key to multiple hospitalist groups coexisting effectively under one roof—whether directly competing or not—is good communication. Effective communication can take time to build.
“Start by working together on something—anything, [such as] a hospital committee of some sort where there’s not likely to be much tension,” says hospitalist pioneer and practice consultant John Nelson, MD, MHM.
Dr. Nelson practices at Overlake Hospital in Bellevue, Wash., which has a hospitalist group employed by the hospital and another employed by Group Health Cooperative, a nonprofit health system in Washington state. It is important to put some trust in the trust bank, he says, “and that’s hard if you have no social connections at all. At my hospital, we enjoy each other’s company, we visit each other at lunch, and we even tried to have a journal club.” The two hospitalist groups work together on developing care protocols. Dr. Nelson says it also makes sense for the groups’ leaders to sit down together on a regular basis and have a venue for discussing important issues and solving problems that may arise.
Other suggestions for hospitalist groups working together under one roof include:
- Clearly define each group’s territory. The groups’ representatives can go out and try to persuade health plans or physician groups to shift their hospitalist allegiances, but there should be no “trolling” or “poaching” of patients going on inside the hospital’s walls. That will only confuse patients and disrupt the hospital’s larger service goals.
- Inform the ED and other key staff of your schedules. It’s important that everyone know exactly who is supposed to get which patients, and how these referrals get made. But recognize that mistakes happen and, hopefully, these will even out between the groups over time.
- Transparency, honesty, and even-handed treatment of all hospitalists can prevent resentment. Clearly defined guidelines and expectations are helpful. If the policy spells out transfers for an incorrectly referred patient, both sides should be accessible and cooperative with that process.
- Identify areas of common interest and agree to work together on these areas (i.e. competition-free zones). It might be possible, for example, for competing groups to take each others’ after-hours call on a rotating basis, with a firm commitment not to steal patients along the way.
- Spell out responsibilities in a way that everyone can agree is fair, such as alternating referrals or taking call on alternating days. For example, if subsidies are paid to more than one hospitalist group, is this done equitably, such as based on the number of hospitalist FTEs or shifts?
- Restrictive covenants and contractual noncompete clauses could become an issue in areas where multiple groups practice. Rather than using overly broad, blanket language, it could be clarified that such pacts apply only to the hospital where the physician currently works, and within a reasonable time frame. But everyone involved should be aware of what these covenants contain and, if they appear unreasonable, don’t sign them.
—Larry Beresford
Documentation, CMS-Approved Language Key to Getting Paid for Hospitalist Teaching Services

When hospitalists work in academic centers, medical and surgical services are furnished, in part, by a resident within the scope of the hospitalists’ training program. A resident is “an individual who participates in an approved graduate medical education (GME) program or a physician who is not in an approved GME program but who is authorized to practice only in a hospital setting.”1 Resident services are covered by Centers for Medicare & Medicaid Services (CMS) and paid by the Fiscal Intermediary through direct GME and Indirect Medical Education (IME) payments. These services are not billed or paid using the Medicare Physician Fee Schedule. The teaching physician is responsible for supervising the resident’s health-care delivery but is not paid for the resident’s work. The teaching physician is paid for their personal and medically necessary service in providing patient care. The teaching physician has the option to perform the entire service, or perform the self-determined critical or key portion(s) of the service.
Comprehensive Service
Teaching physicians independently see the patient and perform all required elements to support the visit level (e.g. 99233: subsequent hospital care, per day, which requires at least two of the following three key components: a detailed interval history, a detailed examination, or high-complexity medical decision-making).2 The teaching physician writes a note independent of a resident encounter with the patient or documentation. The teaching physician note “stands alone” and does not rely on the resident’s documentation. If the resident saw the patient and documented the encounter, the teaching physician might choose to “link to” the resident note in lieu of personally documenting the entire service. The linking statement must demonstrate teaching physician involvement in the patient encounter and participation in patient management. Use of CMS-approved statements is best to meet these requirements. Statement examples include:3
- “I performed a history and physical examination of the patient and discussed his management with the resident. I reviewed the resident’s note and agree with the documented findings and plan of care.”
- “I saw and evaluated the patient. I agree with the findings and the plan of care as documented in the resident’s note.”
- “I saw and examined the patient. I agree with the resident’s note, except the heart murmur is louder, so I will obtain an echo to evaluate.”
Each of these statements meets the minimum requirements for billing. However, teaching physicians should offer more information in support of other clinical, quality, and regulatory initiatives and mandates, better exemplified in the last example. The reported visit level will be supported by the combined documentation (teaching physician and resident).
The teaching physician submits a claim in their name and, if it is a Medicare claim, appends modifier GC to the selected visit level (e.g. 99223-GC). This alerts the Medicare contractor that services were provided under teaching physician rules. Requests for documentation should include a response with medical record entries from the teaching physician and resident.
Critical/Key Portion
“Supervised” service: The resident and teaching physician can round together; they can see the patient at the same time. The teaching physician observes the resident’s performance during the patient encounter, or personally performs self-determined elements of patient care. The resident documents their patient care. The attending must still note their presence in the medical record, performance of the critical or key portions of the service, and involvement in patient management. CMS-accepted statements include:3
- “I was present with the resident during the history and exam. I discussed the case with the resident and agree with the findings and plan as documented in the resident’s note.”
- “I saw the patient with the resident and agree with the resident’s findings and plan.”
Although these statements demonstrate acceptable billing language, they lack patient-specific details that support the teaching physician’s personal contribution to patient care and the quality of their expertise. The teaching physician selects the visit level that represents the combined documentation and, if it is a Medicare claim, appends modifier GC to the selected visit level (e.g. 99232-GC).
“Shared” service: The resident sees the patient unaccompanied and documents the corresponding care provided. The teaching physician sees the patient at a different time but performs only the critical or key portions of the service. The case is subsequently discussed with the resident. The teaching physician must document their presence and performance of the critical or key portions of the service, along with any patient management. Using CMS-quoted statements ensures regulatory compliance:3
- “I saw and evaluated the patient. I reviewed the resident’s note and agree, except that the picture is more consistent with pericarditis than myocardial ischemia. Will begin NSAIDs.”
- “I saw and evaluated the patient. Discussed with resident and agree with resident’s findings and plan as documented in the resident’s note.”
- “See resident’s note for details. I saw and evaluated the patient and agree with the resident’s finding and plans as written.”
- “I saw and evaluated the patient. Agree with resident’s note, but lower extremities are weaker, now 3/5; MRI of L/S spine today.”
Once again, the teaching physician selects the visit level that represents the combined documentation and, if it is a Medicare claim, appends modifier GC to the selected visit level (e.g. 99233-GC).
EHR Considerations
When seeing patients independent of one another, the timing of the teaching physician and resident encounters does not impact billing. However, the time that the resident encounter is documented in the medical record can significantly impact the payment when reviewed by external auditors. When the resident note is dated and timed later than the teaching physician’s entry, the teaching physician cannot consider the resident’s note for visit-level selection. The teaching physician should not “link to” a resident note that is viewed as “not having been written” prior to the teaching physician note. This would not fulfill the requirements represented in the CMS-approved language “I reviewed the resident’s note and agree.”
Electronic health record (EHR) systems sometimes hinder compliance. If the resident completes the note but does not “finalize” or “close” the encounter until after the teaching physician documents their own note, it can falsely appear that the resident note did not exist at the time the teaching physician created their entry. Because an auditor can only view the finalized entries, the timing of each entry might be erroneously represented. Proper training and closing of encounters can diminish these issues.
Additionally, scribing the attestation is not permitted. Residents cannot document the teaching physician attestation on behalf of the physician under any circumstance. CMS rules require the teaching physician to document their presence, participation, and management of the patient. In an EHR, the teaching physician must document this entry under his/her own log-in and password, which is not to be shared with anyone.
Students
CMS defines student as “an individual who participates in an accredited educational program [e.g. a medical school] that is not an approved GME program.”1 A student is not regarded as a “physician in training,” and the service is not eligible for reimbursement consideration under the teaching physician rules.
Per CMS guidelines, students can document services in the medical record, but the teaching physician may only refer to the student’s systems review and past/family/social history entries. The teaching physician must verify and redocument the history of present illness. A student’s physical exam findings or medical decision-making are not suitable for tethering, and the teaching physician must personally perform and redocument the physical exam and medical decision-making. The visit level reflects only the teaching physician’s personally performed and documented service.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. Guidelines for Teaching Physicians, Interns, Residents. CMS website. Available at: http://www.cms.gov/MLNProducts/downloads/gdelinesteachgresfctsht.pdf. Accessed Jan. 8, 2013.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 100. CMS website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 8, 2013.
- Centers for Medicare and Medicaid Services. Medicare Benefit Policy Manual: Chapter 15, Section 30.2. CMS website. Available at: http://www.cms.hhs.gov/manuals/Downloads/bp102c15.pdf. Accessed Jan. 8, 2013.
When hospitalists work in academic centers, medical and surgical services are furnished, in part, by a resident within the scope of the hospitalists’ training program. A resident is “an individual who participates in an approved graduate medical education (GME) program or a physician who is not in an approved GME program but who is authorized to practice only in a hospital setting.”1 Resident services are covered by Centers for Medicare & Medicaid Services (CMS) and paid by the Fiscal Intermediary through direct GME and Indirect Medical Education (IME) payments. These services are not billed or paid using the Medicare Physician Fee Schedule. The teaching physician is responsible for supervising the resident’s health-care delivery but is not paid for the resident’s work. The teaching physician is paid for their personal and medically necessary service in providing patient care. The teaching physician has the option to perform the entire service, or perform the self-determined critical or key portion(s) of the service.
Comprehensive Service
Teaching physicians independently see the patient and perform all required elements to support the visit level (e.g. 99233: subsequent hospital care, per day, which requires at least two of the following three key components: a detailed interval history, a detailed examination, or high-complexity medical decision-making).2 The teaching physician writes a note independent of a resident encounter with the patient or documentation. The teaching physician note “stands alone” and does not rely on the resident’s documentation. If the resident saw the patient and documented the encounter, the teaching physician might choose to “link to” the resident note in lieu of personally documenting the entire service. The linking statement must demonstrate teaching physician involvement in the patient encounter and participation in patient management. Use of CMS-approved statements is best to meet these requirements. Statement examples include:3
- “I performed a history and physical examination of the patient and discussed his management with the resident. I reviewed the resident’s note and agree with the documented findings and plan of care.”
- “I saw and evaluated the patient. I agree with the findings and the plan of care as documented in the resident’s note.”
- “I saw and examined the patient. I agree with the resident’s note, except the heart murmur is louder, so I will obtain an echo to evaluate.”
Each of these statements meets the minimum requirements for billing. However, teaching physicians should offer more information in support of other clinical, quality, and regulatory initiatives and mandates, better exemplified in the last example. The reported visit level will be supported by the combined documentation (teaching physician and resident).
The teaching physician submits a claim in their name and, if it is a Medicare claim, appends modifier GC to the selected visit level (e.g. 99223-GC). This alerts the Medicare contractor that services were provided under teaching physician rules. Requests for documentation should include a response with medical record entries from the teaching physician and resident.
Critical/Key Portion
“Supervised” service: The resident and teaching physician can round together; they can see the patient at the same time. The teaching physician observes the resident’s performance during the patient encounter, or personally performs self-determined elements of patient care. The resident documents their patient care. The attending must still note their presence in the medical record, performance of the critical or key portions of the service, and involvement in patient management. CMS-accepted statements include:3
- “I was present with the resident during the history and exam. I discussed the case with the resident and agree with the findings and plan as documented in the resident’s note.”
- “I saw the patient with the resident and agree with the resident’s findings and plan.”
Although these statements demonstrate acceptable billing language, they lack patient-specific details that support the teaching physician’s personal contribution to patient care and the quality of their expertise. The teaching physician selects the visit level that represents the combined documentation and, if it is a Medicare claim, appends modifier GC to the selected visit level (e.g. 99232-GC).
“Shared” service: The resident sees the patient unaccompanied and documents the corresponding care provided. The teaching physician sees the patient at a different time but performs only the critical or key portions of the service. The case is subsequently discussed with the resident. The teaching physician must document their presence and performance of the critical or key portions of the service, along with any patient management. Using CMS-quoted statements ensures regulatory compliance:3
- “I saw and evaluated the patient. I reviewed the resident’s note and agree, except that the picture is more consistent with pericarditis than myocardial ischemia. Will begin NSAIDs.”
- “I saw and evaluated the patient. Discussed with resident and agree with resident’s findings and plan as documented in the resident’s note.”
- “See resident’s note for details. I saw and evaluated the patient and agree with the resident’s finding and plans as written.”
- “I saw and evaluated the patient. Agree with resident’s note, but lower extremities are weaker, now 3/5; MRI of L/S spine today.”
Once again, the teaching physician selects the visit level that represents the combined documentation and, if it is a Medicare claim, appends modifier GC to the selected visit level (e.g. 99233-GC).
EHR Considerations
When seeing patients independent of one another, the timing of the teaching physician and resident encounters does not impact billing. However, the time that the resident encounter is documented in the medical record can significantly impact the payment when reviewed by external auditors. When the resident note is dated and timed later than the teaching physician’s entry, the teaching physician cannot consider the resident’s note for visit-level selection. The teaching physician should not “link to” a resident note that is viewed as “not having been written” prior to the teaching physician note. This would not fulfill the requirements represented in the CMS-approved language “I reviewed the resident’s note and agree.”
Electronic health record (EHR) systems sometimes hinder compliance. If the resident completes the note but does not “finalize” or “close” the encounter until after the teaching physician documents their own note, it can falsely appear that the resident note did not exist at the time the teaching physician created their entry. Because an auditor can only view the finalized entries, the timing of each entry might be erroneously represented. Proper training and closing of encounters can diminish these issues.
Additionally, scribing the attestation is not permitted. Residents cannot document the teaching physician attestation on behalf of the physician under any circumstance. CMS rules require the teaching physician to document their presence, participation, and management of the patient. In an EHR, the teaching physician must document this entry under his/her own log-in and password, which is not to be shared with anyone.
Students
CMS defines student as “an individual who participates in an accredited educational program [e.g. a medical school] that is not an approved GME program.”1 A student is not regarded as a “physician in training,” and the service is not eligible for reimbursement consideration under the teaching physician rules.
Per CMS guidelines, students can document services in the medical record, but the teaching physician may only refer to the student’s systems review and past/family/social history entries. The teaching physician must verify and redocument the history of present illness. A student’s physical exam findings or medical decision-making are not suitable for tethering, and the teaching physician must personally perform and redocument the physical exam and medical decision-making. The visit level reflects only the teaching physician’s personally performed and documented service.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. Guidelines for Teaching Physicians, Interns, Residents. CMS website. Available at: http://www.cms.gov/MLNProducts/downloads/gdelinesteachgresfctsht.pdf. Accessed Jan. 8, 2013.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 100. CMS website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 8, 2013.
- Centers for Medicare and Medicaid Services. Medicare Benefit Policy Manual: Chapter 15, Section 30.2. CMS website. Available at: http://www.cms.hhs.gov/manuals/Downloads/bp102c15.pdf. Accessed Jan. 8, 2013.
When hospitalists work in academic centers, medical and surgical services are furnished, in part, by a resident within the scope of the hospitalists’ training program. A resident is “an individual who participates in an approved graduate medical education (GME) program or a physician who is not in an approved GME program but who is authorized to practice only in a hospital setting.”1 Resident services are covered by Centers for Medicare & Medicaid Services (CMS) and paid by the Fiscal Intermediary through direct GME and Indirect Medical Education (IME) payments. These services are not billed or paid using the Medicare Physician Fee Schedule. The teaching physician is responsible for supervising the resident’s health-care delivery but is not paid for the resident’s work. The teaching physician is paid for their personal and medically necessary service in providing patient care. The teaching physician has the option to perform the entire service, or perform the self-determined critical or key portion(s) of the service.
Comprehensive Service
Teaching physicians independently see the patient and perform all required elements to support the visit level (e.g. 99233: subsequent hospital care, per day, which requires at least two of the following three key components: a detailed interval history, a detailed examination, or high-complexity medical decision-making).2 The teaching physician writes a note independent of a resident encounter with the patient or documentation. The teaching physician note “stands alone” and does not rely on the resident’s documentation. If the resident saw the patient and documented the encounter, the teaching physician might choose to “link to” the resident note in lieu of personally documenting the entire service. The linking statement must demonstrate teaching physician involvement in the patient encounter and participation in patient management. Use of CMS-approved statements is best to meet these requirements. Statement examples include:3
- “I performed a history and physical examination of the patient and discussed his management with the resident. I reviewed the resident’s note and agree with the documented findings and plan of care.”
- “I saw and evaluated the patient. I agree with the findings and the plan of care as documented in the resident’s note.”
- “I saw and examined the patient. I agree with the resident’s note, except the heart murmur is louder, so I will obtain an echo to evaluate.”
Each of these statements meets the minimum requirements for billing. However, teaching physicians should offer more information in support of other clinical, quality, and regulatory initiatives and mandates, better exemplified in the last example. The reported visit level will be supported by the combined documentation (teaching physician and resident).
The teaching physician submits a claim in their name and, if it is a Medicare claim, appends modifier GC to the selected visit level (e.g. 99223-GC). This alerts the Medicare contractor that services were provided under teaching physician rules. Requests for documentation should include a response with medical record entries from the teaching physician and resident.
Critical/Key Portion
“Supervised” service: The resident and teaching physician can round together; they can see the patient at the same time. The teaching physician observes the resident’s performance during the patient encounter, or personally performs self-determined elements of patient care. The resident documents their patient care. The attending must still note their presence in the medical record, performance of the critical or key portions of the service, and involvement in patient management. CMS-accepted statements include:3
- “I was present with the resident during the history and exam. I discussed the case with the resident and agree with the findings and plan as documented in the resident’s note.”
- “I saw the patient with the resident and agree with the resident’s findings and plan.”
Although these statements demonstrate acceptable billing language, they lack patient-specific details that support the teaching physician’s personal contribution to patient care and the quality of their expertise. The teaching physician selects the visit level that represents the combined documentation and, if it is a Medicare claim, appends modifier GC to the selected visit level (e.g. 99232-GC).
“Shared” service: The resident sees the patient unaccompanied and documents the corresponding care provided. The teaching physician sees the patient at a different time but performs only the critical or key portions of the service. The case is subsequently discussed with the resident. The teaching physician must document their presence and performance of the critical or key portions of the service, along with any patient management. Using CMS-quoted statements ensures regulatory compliance:3
- “I saw and evaluated the patient. I reviewed the resident’s note and agree, except that the picture is more consistent with pericarditis than myocardial ischemia. Will begin NSAIDs.”
- “I saw and evaluated the patient. Discussed with resident and agree with resident’s findings and plan as documented in the resident’s note.”
- “See resident’s note for details. I saw and evaluated the patient and agree with the resident’s finding and plans as written.”
- “I saw and evaluated the patient. Agree with resident’s note, but lower extremities are weaker, now 3/5; MRI of L/S spine today.”
Once again, the teaching physician selects the visit level that represents the combined documentation and, if it is a Medicare claim, appends modifier GC to the selected visit level (e.g. 99233-GC).
EHR Considerations
When seeing patients independent of one another, the timing of the teaching physician and resident encounters does not impact billing. However, the time that the resident encounter is documented in the medical record can significantly impact the payment when reviewed by external auditors. When the resident note is dated and timed later than the teaching physician’s entry, the teaching physician cannot consider the resident’s note for visit-level selection. The teaching physician should not “link to” a resident note that is viewed as “not having been written” prior to the teaching physician note. This would not fulfill the requirements represented in the CMS-approved language “I reviewed the resident’s note and agree.”
Electronic health record (EHR) systems sometimes hinder compliance. If the resident completes the note but does not “finalize” or “close” the encounter until after the teaching physician documents their own note, it can falsely appear that the resident note did not exist at the time the teaching physician created their entry. Because an auditor can only view the finalized entries, the timing of each entry might be erroneously represented. Proper training and closing of encounters can diminish these issues.
Additionally, scribing the attestation is not permitted. Residents cannot document the teaching physician attestation on behalf of the physician under any circumstance. CMS rules require the teaching physician to document their presence, participation, and management of the patient. In an EHR, the teaching physician must document this entry under his/her own log-in and password, which is not to be shared with anyone.
Students
CMS defines student as “an individual who participates in an accredited educational program [e.g. a medical school] that is not an approved GME program.”1 A student is not regarded as a “physician in training,” and the service is not eligible for reimbursement consideration under the teaching physician rules.
Per CMS guidelines, students can document services in the medical record, but the teaching physician may only refer to the student’s systems review and past/family/social history entries. The teaching physician must verify and redocument the history of present illness. A student’s physical exam findings or medical decision-making are not suitable for tethering, and the teaching physician must personally perform and redocument the physical exam and medical decision-making. The visit level reflects only the teaching physician’s personally performed and documented service.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. Guidelines for Teaching Physicians, Interns, Residents. CMS website. Available at: http://www.cms.gov/MLNProducts/downloads/gdelinesteachgresfctsht.pdf. Accessed Jan. 8, 2013.
- Abraham M, Ahlman J, Anderson C, Boudreau A, Connelly J. Current Procedural Terminology 2012 Professional Edition. Chicago: American Medical Association Press; 2011.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 100. CMS website. Available at: http://www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 8, 2013.
- Centers for Medicare and Medicaid Services. Medicare Benefit Policy Manual: Chapter 15, Section 30.2. CMS website. Available at: http://www.cms.hhs.gov/manuals/Downloads/bp102c15.pdf. Accessed Jan. 8, 2013.