User login
Treatment-resistant OCD: Options beyond first-line medications
Obsessive-compulsive disorder (OCD) is marked by recurrent and persistent anxiety-provoking thoughts (obsessions) accompanied by repetitive behaviors (compulsions) that focus on alleviating distress caused by obsessive thoughts. Although patients recognize the obsessions and compulsions are unreasonable, these thoughts and behaviors remain time-consuming and impair function. Even when they appropriately identify and treat OCD, clinicians often face “treatment-resistant” (or “treatment-refractory”) patients who do not respond adequately to standard therapies (Box).1 Several factors contribute to treatment resistance, including those related to the patient, the environment, the clinician/health system, and pathology (Table 1).2 An estimated 10% to 40% of patients with OCD are treatment-resistant.2
This article discusses the range of options for addressing resistant OCD, including augmenting first-line treatments with pharmacotherapy, psychotherapy, or reversible or irreversible forms of neuromodulation.
Treatment resistance generally refers to lack of sufficient improvement despite multiple adequate and appropriate treatment trials. However, there are no universally accepted definitions or metrics of treatment resistance, and often it is operationally defined. For mood disorders, it may be defined by failure to remit or respond clinically (50% reduction in symptoms) despite ≥2 adequate antidepressant trials or failure to respond clinically despite adequate medication trials across several neurotransmitter classes. The terms treatment resistant and treatment refractory are synonymous; they refer to the same phenomenon and are used interchangeably in the literature. Including the terms “remission” and “recovery” when judging treatment efficacy for anxiety disorders can be limiting because of the chronic and often unrelenting nature of these conditions.
One review proposed categorizing obsessive-compulsive disorder treatment response into several stages along a spectrum, ranging from complete recovery (or remission) to full or partial response to non-response (or completely refractory).1 However it is defined, treatment resistance in anxiety disorders likely is characterized by minimal restoration of function despite several appropriate treatment exposures.
Table 1
Factors that contribute to treatment resistance in obsessive-compulsive disorder
| Patient |
| Disease severity Medical comorbidity Psychiatric comorbidity (mood, personality, and/or substance use disorders) Treatment nonadherence Cultural factors |
| Environment |
| Childhood stressors (trauma, abuse) Long-term persistent stressors (psychosocial, occupational, financial) Life stages |
| Clinician/health system |
| Lack of knowledge in primary care (brief treatment duration, subtherapeutic dosing) Lack of psychotherapeutic training Limited doctor-patient relationship (eg, availability/cost of treatment) |
| Pathology-related |
Underlying disease pathophysiology (largely unknown):
Syndromal variation (differing presentations over time) Treatment limitations (limited empirical studies, nonrepresentative study samples) |
| Source: Reference 2 |
First-line pharmacotherapy
Clomipramine or a selective serotonin reuptake inhibitor (SSRI) are considered first-line treatments for OCD. Although some evidence indicates that clomipramine may have greater efficacy than SSRIs, its poor tolerability and potential lethality in overdose make it a less practical first choice in treatment-naïve patients.3,4 SSRIs generally are well tolerated and have a favorable safety profile. Nearly all SSRIs have randomized clinical trials (RCTs) and FDA indications that support their use in OCD. SSRI choice may be guided by patient or prescriber preference because no evidence suggests that 1 SSRI is superior to another for treating OCD.5 In contrast to major depressive disorder, in OCD there is a dose-response relationship for SSRI treatment; higher doses typically are required to achieve response or remission.6,7
Augmentation and other options
Patients who have not responded to at least 2 adequate trials of first-line medications may benefit from an augmentation strategy or treatment with an unconventional agent. Such cases should be managed by a specialist who has experience in treating OCD and with careful consideration of potential risks of these interventions.
Evidence suggests the following pharmacotherapies may effectively treat OCD and may be warranted for treatment-resistant patients.
Serotonergic agents
Supratherapeutic SSRI doses. Evidence suggests that supratherapeutic doses of SSRIs may be effective, which may be a logical first step when treating patients already taking an SSRI who have not responded. In a multi-center, double-blind study comparing sertraline, 200 mg/d, to sertraline, 250 to 400 mg/d, the latter group showed significantly greater symptom improvement.8 Citalopram may not be suitable for this approach because of the recent FDA announcement regarding dose-dependent QTc prolongation associated with this medication.9
Serotonin-norepinephrine reuptake inhibitors (SNRIs). In the only double-blind, placebo-controlled study of venlafaxine for OCD, the drug was not significantly more effective than placebo.10 This study was small (N = 30). There are sufficient positive results from open-label and blinded comparator studies that venlafaxine generally is accepted as an effective and well-tolerated treatment for OCD at doses ≥225 mg/d.11
Duloxetine also may be effective in treating OCD. One case series reported improvement in 3 of 4 SSRI nonresponders who were switched to this medication and rapidly titrated to 120 mg/d.12
Clomipramine/SSRI augmentation. For patients who have not responded to an SSRI, several open-label trials support adding clomipramine.13 Conversely, SSRI augmentation for patients who have not adequately responded to clomipramine may be effective.14 With any dual therapy with serotonergic agents, monitor patients for signs and symptoms of serotonin syndrome.
IV clomipramine. By bypassing first-pass metabolism, IV clomipramine rapidly achieves high plasma levels. In a double-blind, placebo-controlled study of 54 OCD patients who were nonresponsive to oral clomipramine, IV clomipramine was more effective than placebo.15 An additional study found IV clomipramine is more effective when pulse loaded than when titrated gradually.16
Pindolol. The beta blocker pindolol acts as an antagonist of presynaptic 5-HT1A autoreceptors, increasing serotonergic signaling. A small double-blind, placebo-controlled trial (N = 14) found a significant decrease in Yale-Brown Obsessive Compulsive Scale (Y-BOCS) score with pindolol augmentation, 2.5 mg, 3 times daily, among patients who did not respond to ≥3 serotonin reuptake inhibitor (SRI) trials.17 Pindolol augmentation showed modest effects in 2 open-label studies.18,19 However, another small double-blind, placebo-controlled study (N = 15) found no difference between placebo and fluvoxamine augmented with pindolol.20
Ondansetron. A 5-HT3 receptor antagonist, ondansetron is used primarily as an antiemetic but has been shown to have anxiolytic properties in animal studies. In an open-label study of 8 patients with non–treatment refractory OCD, 3 achieved clinical response (at least 35% reduction in Y-BOCS score) with ondansetron monotherapy dosed at 1 mg, 3 times daily.21 In a subsequent single-blind trial with 14 treatment-resistant patients, 9 responded (at least 25% reduction in Y-BOCS score).22
Other medications
Antipsychotics. Most studies examining antipsychotic monotherapy for OCD have been negative. One exception was a small, open-label trial of aripiprazole monotherapy (N = 8) that found modest efficacy among non–treatment refractory patients.23 Augmentation with antipsychotics, however, has been well studied and there is good evidence of efficacy for this approach. Double-blind, placebo-controlled studies have supported the efficacy of augmenting SRIs with haloperidol, risperidone, olanzapine, quetiapine, and aripiprazole.24-26 Several case reports suggest ziprasidone may be an effective SRI adjunct, but 1 retrospective study found it was inferior to quetiapine.27
Benzodiazepines. Case reports present positive effects of clonazepam and alprazolam for OCD, but double-blind, placebo-controlled trials for monotherapy or adjunctive clonazepam have been negative.28,29 Furthermore, cognitive impairment and potential for dependence associated with benzodiazepines weigh against their use in OCD.
Opioids. A double-blind, placebo controlled crossover study of 23 patients with treatment-refractory OCD found once-weekly oral morphine added to patients’ current regimen significantly reduced Y-BOCS score vs placebo. Patients received 30 mg the first week and 15 to 45 mg the next week, depending on response or side effects.30 A case report and a small open-label trial support the efficacy of tramadol, a weak agonist of the μ opioid receptor and an inhibitor of serotonin and norepinephrine transporters, as monotherapy and as an adjunct to fluoxetine.31,32 Because patients with OCD may be particularly vulnerable to dependence and intentional or accidental overdose via opioid/benzodiazepine combinations, evaluate the risks and benefits before initiating an opioid.
Psychostimulants. Sparse but good evidence supports the efficacy of dextroamphetamine monotherapy for OCD.33,34 There are no positive studies of methylphenidate and several case reports of methylphenidate-induced OCD symptoms.35
N-methyl-D-aspartate (NMDA) antagonists. Increased glutamatergic neurotransmission has been implicated in the pathophysiology of OCD, which suggests a possible role for glutamate receptor antagonists. In an open-label trial, memantine, an NMDA antagonist used primarily to treat dementia, was associated with clinical response (>25% reduction in Y-BOCS scores) in 6 of 14 patients with treatment-refractory OCD.36 Several case reports and an open-label trial support the efficacy of riluzole—which is indicated for treating amyotrophic lateral sclerosis—as an adjunct for treatment-refractory OCD.37 Although its exact mechanism of action is unclear, riluzole’s effects are thought to be mediated via reduction in glutamatergic neurotransmission. IV ketamine has reported anti-OCD effects in a case report of a woman with treatment-resistant OCD. These effects occurred almost immediately and persisted for several days.38
Hallucinogens. Psilocybin, psilocin, and lysergic acid diethylamide have reported anti-OCD properties.39 As schedule I substances, however, they are not available outside of sanctioned research protocols and may carry substantial risk. Nonetheless, their efficacy suggests that other compounds that share their mechanism of action—namely agonism of 5-HT2A and 5-HT2C receptors—may merit investigation as potential treatments for OCD.
Psychotherapy
Cognitive-behavioral therapy (CBT) has been shown to be effective for OCD as monotherapy and augmentation to pharmacotherapy. CBT consists of cognitive and behavioral components, typically involving some form of cognitive restructuring and exposure response prevention. Although these 2 types of interventions arise from independent traditions, in CBT they are frequently intertwined, particularly when the focus of OCD patients’ anxiety is ego-dystonic thoughts.
One benefit of CBT over pharmacotherapy is that effects persist after treatment is terminated. A recent prospective study found CBT was effective for treatment-refractory OCD, with 74% of patients demonstrating clinical response after 20 to 25 sessions over 2 months and 61% maintaining clinical response 1 year after treatment.40 CBT administered remotely via teleconference, also known as “teletherapy,” has shown efficacy for OCD.41
Alternative medicine
Despite widespread use of herbal remedies for OCD, no trials have shown a strong positive effect. Both Hypericum perforatum (St. John’s wort) and Silybum marianum (milk thistle) have been used to treat obsessive and compulsive symptoms; however, placebo-controlled trials did not find any significant differences in symptoms or side effects between treatment groups.42,43 Lower-quality studies have reported modest effects for mindfulness meditation, yoga, and acupuncture.44
Because many patients continue to use complementary and alternative medicine therapies despite the lack of data on efficacy, it is important to monitor for potential interactions with prescription medications. St. John’s wort interacts with many medications because of induction of the cytochrome P450 (CYP) isoenzymes 3A4 and 2C9. This interaction may lower blood levels of alprazolam and clonazepam (3A4). Combining St. John’s wort with SSRIs increases the risk of serotonin syndrome. Milk thistle inhibits CYP450 isoenzyme 3A4, and may increase serum levels of other medications metabolized by this pathway.
Invasive therapies
Invasive options may be considered after several pharmacotherapeutic and psychotherapeutic approaches have not been effective or when significant functional impairment remains (Table 2). These therapies typically are reserved for patients whose treatment resistance is strongest.
Electroconvulsive therapy (ECT). Although ECT is an effective tool for treatment-resistant mood disorders or treatment-resistant anxiety complicated by severe depression, studies have not found ECT to be effective for OCD. One uncontrolled case series reported considerable improvements in OCD patients the year after ECT, although improvement was correlated with improved depression scores.45
Vagal nerve stimulation (VNS). In an open-label study of 7 OCD patients who received VNS, 3 were acute responders—characterized by a ≥25% improvement on the Y-BOCS—and 2 received continued benefits at 4-year follow up (2 patients dropped out).46
Repetitive transcranial magnetic stimulation (rTMS). A meta-analysis of 3 RCTs of rTMS for patients with OCD did not yield a large or statistically significant effect.47 Limitations of these trials included asymmetric stimulation sites (eg, left vs right only), limited stimulation sites (dorsolateral prefrontal cortex), different stimulation frequencies between studies, and a lack of sham stimulation conditions. A more recent RCT and subsequent review described moderate efficacy (defined by ≥25% decrease in Y-BOCS scores) compared with sham stimulations in OCD patients at 4 weeks, using the supplementary motor area as a stimulation site.48,49
The main limitation of rTMS is the inability to penetrate deeper brain structures implicated in OCD (eg, caudate nucleus, thalamus, anterior capsule fiber tracts), as well as a lack of specificity in stimulation site.
Surgical approaches. Cingulotomy is the most commonly employed surgical procedure for OCD in North America, likely because of a combination of clinical efficacy and low morbidity and mortality rates.50 Of the >1,000 cingulotomies that have been performed at Massachusetts General Hospital, no deaths or postoperative infections have been reported and 2 subdural hematomas have occurred.50 Common postsurgical side effects include transient headache, nausea, or difficulty urinating. The most serious common side effect—postoperative seizures—has been reported in 1% to 9% of cases.
Outcomes for these procedures cannot be fully assessed until at least 6 months to 2 years after the procedure, which suggests postoperative neural reorganization plays an important role in recovery. Direct comparisons of each lesion approach within studies are extremely rare. Overall, long-term outcomes of these approaches have demonstrated significant therapeutic effects of each of these procedures. Reported response rates vary between 30% to 70%, when applied to remission, response (≥35% Y-BOCS reduction), and functional improvements in quality of life.50
Deep brain stimulation (DBS). With this approach, small electrodes are inserted under precise stereotactic MRI guidance. The advantage of DBS over ablative surgery is the ability to adjust and customize neurostimulation. Following implantation, modifiable parameters of electrode stimulation include electrode polarity, intensity, frequency, and laterality. A specially trained psychiatrist can conduct parameter optimization during long-term follow-up.
The first trial of DBS for OCD was reported in 1999 (N = 4), with the initial target selected based on the site of anterior capsulotomy. Three patients derived clinically observed benefit, although no validated questionnaires were administered.51 Since then, at least 7 studies with blinded stimulation have been conducted, totaling 62 patients.52
In recent years, structures adjacent to the internal capsule also have been targeted based on the approach employed in ventral capsulotomy. Across all trials, response rates for this approach consistently have been in the 50% range, with average Y-BOCS score reductions ranging from 6.8 to 31 points.53 Some patients have reported rapid improvements in anhedonia, and this approach is being employed in treatment-resistant depression.
Postoperative complications occur more often with DBS than with lesion approaches because of the prosthetic nature of the procedure (eg, increased risk of infection, lead malfunction, etc.). Additionally, batteries must be periodically explanted and replaced. Reported stimulation-related side effects include mood changes (transient sadness, anxiety, euphoria, and hypomania), sensory disturbances (olfactory, gustatory, and motor sensations), and cognitive changes (confusion and forgetfulness). These side effects typically are stimulation-dependent and disappear after altering stimulation parameters.
Table 2
Invasive therapies for treatment-resistant OCD
| Therapy | Quality of evidence |
|---|---|
| Reversible | |
| Electroconvulsive therapy | Poor |
| Vagal nerve stimulation | Poor |
| Repetitive transcranial magnetic stimulation | Limited |
| Irreversible (surgical) | |
| Anterior capsulotomy. Target: anterior limb of the internal capsule | Fair |
| Anterior cingulotomy. Target: anterior cingulate and cingulum bundle | Fair |
| Subcaudate tractotomy. Target: substantia innominata, just inferior to the caudate nucleus | Fair |
| Limbic leucotomy. Target: anterior cingulotomy combined with subcaudate tractotomy | Fair |
| Deep brain stimulation. Multiple targets | Fair |
| OCD: obsessive-compulsive disorder | |
Related Resources
- American Psychiatric Association. Treatment of patients with obsessive-compulsive disorder. www.psychiatryonline.com/pracGuide/pracGuideTopic_10.aspx.
- Hyman BM, Pedrick C. The OCD workbook. Your guide to breaking free from obsessive compulsive disorder. 3rd ed. Oakland, CA: New Harbinger Publications Inc; 2010.
- Baer L. Getting control: overcoming your obsessions and compulsions. Revised ed. New York, NY: Plume; 2000.
Drug Brand Names
- Alprazolam • Xanax
- Aripiprazole • Abilify
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clonazepam • Klonopin
- Dextroamphetamine • Adderall
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Ketamine • Ketalar
- Memantine • Namenda
- Methylphenidate • Ritalin
- Morphine • MS Contin
- Olanzapine • Zyprexa
- Ondansetron • Zofran
- Pindolol • Visken
- Quetiapine • Seroquel
- Riluzole • Rilutek
- Risperidone • Risperdal
- Sertraline • Zoloft
- Tramadol • Ultram
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosures
Drs. Khalsa and Schiffman report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Bystritsky receives grant support from AstraZeneca, Brainways, Takeda, and Transcept and is a founder, stockholder, and consultant for BrainSonix.
1. Pallanti S, Quercioli L. Treatment-refractory obsessive-compulsive disorder: methodological issues operational definitions and therapeutic lines. Prog Neuropsychopharmacol Biol Psychiatry. 2006;30(3):400-412.
2. Bystritsky A. Treatment-resistant anxiety disorders. Mol Psychiatry. 2006;11(9):805-814.
3. Denys D. Pharmacotherapy of obsessive-compulsive disorder and obsessive-compulsive spectrum disorders. Psychiatr Clin North Am. 2006;29(2):553-584 xi.
4. Ackerman DL, Greenland S. Multivariate meta-analysis of controlled drug studies for obsessive-compulsive disorder. J Clin Psychopharmacol. 2002;22(3):309-317.
5. Soomro GM, Altman D, Rajagopal S, et al. Selective serotonin re-uptake inhibitors (SSRIs) versus placebo for obsessive compulsive disorder (OCD). Cochrane Database Syst Rev. 2008;(1):CD001765.-
6. Bloch MH, McGuire J, Landeros-Weisenberger A, et al. Meta-analysis of the dose-response relationship of SSRI in obsessive-compulsive disorder. Mol Psychiatry. 2010;15(8):850-855.
7. Koran LM, Hanna GL, Hollander E, et al. American Psychiatric Association. Practice guideline for the treatment of patients with obsessive-compulsive disorder. Am J Psychiatry. 2007;164(7 suppl):5-53.
8. Ninan PT, Koran LM, Kiev A, et al. High-dose sertraline strategy for nonresponders to acute treatment for obsessive-compulsive disorder: a multicenter double-blind trial. J Clin Psychiatry. 2006;67(1):15-22.
9. Food and Drug Administration. FDA drug safety communication: abnormal heart rhythms associated with high doses of Celexa (citalopram hydrobromide). http://www.fda.gov/Drugs/DrugSafety/ucm269086.htm#sa. Published August 24 2011. Accessed September 27, 2011.
10. Yaryura-Tobias JA, Neziroglu FA. Venlafaxine in obsessive-compulsive disorder. Arch Gen Psychiatry. 1996;53(7):653-654.
11. Phelps NJ, Cates ME. The role of venlafaxine in the treatment of obsessive-compulsive disorder. Ann Pharmacother. 2005;39(1):136-140.
12. Dell’osso B, Mundo E, Marazziti D, et al. Switching from serotonin reuptake inhibitors to duloxetine in patients with resistant obsessive compulsive disorder: a case series. J Psychopharmacol. 2008;22(2):210-213.
13. Pallanti S, Quercioli L, Paiva RS, et al. Citalopram for treatment-resistant obsessive-compulsive disorder. Eur Psychiatry. 1999;14:101-106.
14. Ravizza L, Barzega G, Bellino S, et al. Therapeutic effect and safety of adjunctive risperidone in refractory obsessive-compulsive disorder (OCD). Psychopharmacol Bull. 1996;32:677-682.
15. Fallon BA, Liebowitz MR, Campeas R, et al. Intravenous clomipramine for obsessive-compulsive disorder refractory to oral clomipramine: a placebo-controlled study. Arch Gen Psychiatry. 1998;55:918-924.
16. Koran LM, Pallanti S, Paiva RS, et al. Pulse loading versus gradual dosing of intravenous clomipramine in obsessive-compulsive disorder. Eur Neuropsychopharmacol. 1998;8:121-126.
17. Dannon PN, Sasson Y, Hirschmann S, et al. Pindolol augmentation in treatment-resistant obsessive compulsive disorder: a double-blind placebo controlled trial. Eur Neuropsychopharmacol. 2000;10:165-169.
18. Koran LM, Mueller K, Maloney A. Will pindolol augment the response to a serotonin reuptake inhibitor in obsessive-compulsive disorder? J Clin Psychopharmacol. 1996;16:253-254.
19. Hewlett WA, Vinogradov S, Agras WS. Clomipramine clonazepam, and clonidine treatment of obsessive-compulsive disorder. J Clin Psychopharmacol. 1992;12:420-430.
20. Mundo E, Guglielmo E, Bellodi L. Effect of adjuvant pindolol on the antiobsessional response to fluvoxamine: a double-blind placebo-controlled study. Int Clin Psychopharmacol. 1998;13:219-224.
21. Hewlett WA, Schmid SP, Salomon RM. Pilot trial of ondansetron in the treatment of 8 patients with obsessive-compulsive disorder. J Clin Psychiatry. 2003;64:1025-1030.
22. Pallanti S, Bernardi S, Antonini S, et al. Ondansetron augmentation in treatment-resistant obsessive-compulsive disorder: a preliminary, single-blind, prospective study. CNS Drugs. 2009;23(12):1047-1055.
23. Connor KM, Payne VM, Gadde KM, et al. The use of aripiprazole in obsessive-compulsive disorder: preliminary observations in 8 patients. J Clin Psychiatry. 2005;66:49-51.
24. Komossa K, Depping AM, Meyer M, et al. Second-generation antipsychotics for obsessive compulsive disorder. Cochrane Database Syst Rev. 2010;(12):CD008141.-
25. Bloch MH, Landeros-Weisenberger A, Kelmendi B, et al. A systematic review: antipsychotic augmentation with treatment refractory obsessive-compulsive disorder. Mol Psychiatry. 2006;11(7):622-632.
26. Muscatello MR, Bruno A, Pandolfo G, et al. Effect of aripiprazole augmentation of serotonin reuptake inhibitors or clomipramine in treatment-resistant obsessive-compulsive disorder: a double-blind, placebo-controlled study. J Clin Psychopharmacol. 2011;31(2):174-179.
27. Savas HA, Yumru M, Ozen ME. Quetiapine and ziprasidone as adjuncts in treatment-resistant obsessive-compulsive disorder: a retrospective comparative study. Clin Drug Investig. 2008;28(7):439-442.
28. Hollander E, Kaplan A, Stahl SM. A double-blind placebo-controlled trial of clonazepam in obsessive-compulsive disorder. World J Biol Psychiatry. 2003;4:30-34.
29. Crockett BA, Churchill E, Davidson JR. A double-blind combination study of clonazepam with sertraline in obsessive-compulsive disorder. Ann Clin Psychiatry. 2004;16(3):127-132.
30. Koran LM, Aboujaoude E, Bullock KD, et al. Double-blind treatment with oral morphine in treatment-resistant obsessive-compulsive disorder. J Clin Psychiatry. 2005;66(3):353-359.
31. Shapira NA, Keck PE Jr, Goldsmith TD, et al. Open-label pilot study of tramadol hydrochloride in treatment-refractory obsessive-compulsive disorder. Depress Anxiety. 1997;6:170-173.
32. Goldsmith TB, Shapira NA, Keck PE Jr. Rapid remission of OCD with tramadol hydrochloride. Am J Psychiatry. 1999;156(4):660-661.
33. Insel TR, Hamilton JA, Guttmacher LB, et al. D-amphetamine in obsessive-compulsive disorder. Psychopharmacology (Berl). 1983;80:231-235.
34. Joffe RT, Swinson RP, Levitt AJ. Acute psychostimulant challenge in primary obsessive-compulsive disorder. J Clin Psychopharmacol. 1991;11:237-241.
35. Woolley JB, Heyman I. Dexamphetamine for obsessive-compulsive disorder. Am J Psychiatry. 2003;160:183.-
36. Aboujaoude E, Barry JJ, Gamel N. Memantine augmentation in treatment-resistant obsessive-compulsive disorder: an open-label trial. J Clin Psychopharmacol. 2009;29(1):51-55.
37. Coric V, Taskiran S, Pittenger C, et al. Riluzole augmentation in treatment-resistant obsessive-compulsive disorder: an open-label trial. Biol Psychiatry. 2005;58(5):424-428.
38. Rodriguez CI, Kegeles LS, Flood P, et al. Rapid resolution of obsessions after an infusion of intravenous ketamine in a patient with treatment-resistant obsessive-compulsive disorder. J Clin Psychiatry. 2011;72(4):567-569.
39. Leonard HL, Rapoport JL. Relief of obsessive-compulsive symptoms by LSD and psilocin. Am J Psychiatry. 1987;144(9):1239-1240.
40. Anand N, Sudhir PM, Math SB, et al. Cognitive behavior therapy in medication non-responders with obsessive-compulsive disorder: a prospective 1-year follow-up study. J Anxiety Disord. 2011;25(7):939-945.
41. Himle JA, Fischer DJ, Muroff JR, et al. Videoconferencing-based cognitive-behavioral therapy for obsessive-compulsive disorder. Behav Res Ther. 2006;44(12):1821-1829.
42. Kobak KA, Taylor LV, Bystritsky A, et al. St John’s wort versus placebo in obsessive-compulsive disorder: results from a double-blind study. Int Clin Psychopharmacol. 2005;20(6):299-304.
43. Sayyah M, Boostani H, Pakseresht S, et al. Comparison of Silybum marianum (L.) Gaertn. with fluoxetine in the treatment of obsessive-compulsive Disorder. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(2):362-365.
44. Sarris J, Camfield D, Berk M. Complementary medicine self-help, and lifestyle interventions for obsessive compulsive disorder (OCD) and the OCD spectrum: a systematic review. J Affect Disord. 2011 (epub ahead of print).
45. Beale MD, Kellner CH, Pritchett JT, et al. ECT for OCD. J Clin Psychiatry. 1995;56(2):81-82.
46. George MS, Ward HE Jr, Ninan PT, et al. A pilot study of vagus nerve stimulation (VNS) for treatment-resistant anxiety disorders. Brain Stimul. 2008;1(2):112-121.
47. Slotema CW, Blom JD, Hoek HW, et al. Should we expand the toolbox of psychiatric treatment methods to include repetitive transcranial magnetic stimulation (rTMS)? A meta-analysis of the efficacy of rTMS in psychiatric disorders. J Clin Psychiatry. 2010;71(7):873-884.
48. Mantovani A, Simpson HB, Fallon BA, et al. Randomized sham-controlled trial of repetitive transcranial magnetic stimulation in treatment-resistant obsessive-compulsive disorder. Int J Neuropsychopharmacol. 2010;13(2):217-227.
49. Blom RM, Figee M, Vulink N, et al. Update on repetitive transcranial magnetic stimulation in obsessive-compulsive disorder: different targets. Curr Psychiatry Rep. 2011;13(4):289-294.
50. Greenberg BD, Rauch SL, Haber SN. Invasive circuitry-based neurotherapeutics: stereotactic ablation and deep brain stimulation for OCD. Neuropsychopharmacology. 2010;35(1):317-336.
51. Nuttin B, Cosyns P, Demeulemeester H, et al. Electrical stimulation in anterior limbs of internal capsules in patients with obsessive-compulsive disorder. Lancet. 1999;354(9189):1526.-
52. de Koning PP, Figee M, van den Munckhof P, et al. Current status of deep brain stimulation for obsessive-compulsive disorder: a clinical review of different targets. Curr Psychiatry Rep. 2011;13(4):274-282.
53. Greenberg BD, Gabriels LA, Malone DA, Jr, et al. Deep brain stimulation of the ventral internal capsule/ventral striatum for obsessive-compulsive disorder: worldwide experience. Mol Psychiatry. 2010;15(1):64-79.
Obsessive-compulsive disorder (OCD) is marked by recurrent and persistent anxiety-provoking thoughts (obsessions) accompanied by repetitive behaviors (compulsions) that focus on alleviating distress caused by obsessive thoughts. Although patients recognize the obsessions and compulsions are unreasonable, these thoughts and behaviors remain time-consuming and impair function. Even when they appropriately identify and treat OCD, clinicians often face “treatment-resistant” (or “treatment-refractory”) patients who do not respond adequately to standard therapies (Box).1 Several factors contribute to treatment resistance, including those related to the patient, the environment, the clinician/health system, and pathology (Table 1).2 An estimated 10% to 40% of patients with OCD are treatment-resistant.2
This article discusses the range of options for addressing resistant OCD, including augmenting first-line treatments with pharmacotherapy, psychotherapy, or reversible or irreversible forms of neuromodulation.
Treatment resistance generally refers to lack of sufficient improvement despite multiple adequate and appropriate treatment trials. However, there are no universally accepted definitions or metrics of treatment resistance, and often it is operationally defined. For mood disorders, it may be defined by failure to remit or respond clinically (50% reduction in symptoms) despite ≥2 adequate antidepressant trials or failure to respond clinically despite adequate medication trials across several neurotransmitter classes. The terms treatment resistant and treatment refractory are synonymous; they refer to the same phenomenon and are used interchangeably in the literature. Including the terms “remission” and “recovery” when judging treatment efficacy for anxiety disorders can be limiting because of the chronic and often unrelenting nature of these conditions.
One review proposed categorizing obsessive-compulsive disorder treatment response into several stages along a spectrum, ranging from complete recovery (or remission) to full or partial response to non-response (or completely refractory).1 However it is defined, treatment resistance in anxiety disorders likely is characterized by minimal restoration of function despite several appropriate treatment exposures.
Table 1
Factors that contribute to treatment resistance in obsessive-compulsive disorder
| Patient |
| Disease severity Medical comorbidity Psychiatric comorbidity (mood, personality, and/or substance use disorders) Treatment nonadherence Cultural factors |
| Environment |
| Childhood stressors (trauma, abuse) Long-term persistent stressors (psychosocial, occupational, financial) Life stages |
| Clinician/health system |
| Lack of knowledge in primary care (brief treatment duration, subtherapeutic dosing) Lack of psychotherapeutic training Limited doctor-patient relationship (eg, availability/cost of treatment) |
| Pathology-related |
Underlying disease pathophysiology (largely unknown):
Syndromal variation (differing presentations over time) Treatment limitations (limited empirical studies, nonrepresentative study samples) |
| Source: Reference 2 |
First-line pharmacotherapy
Clomipramine or a selective serotonin reuptake inhibitor (SSRI) are considered first-line treatments for OCD. Although some evidence indicates that clomipramine may have greater efficacy than SSRIs, its poor tolerability and potential lethality in overdose make it a less practical first choice in treatment-naïve patients.3,4 SSRIs generally are well tolerated and have a favorable safety profile. Nearly all SSRIs have randomized clinical trials (RCTs) and FDA indications that support their use in OCD. SSRI choice may be guided by patient or prescriber preference because no evidence suggests that 1 SSRI is superior to another for treating OCD.5 In contrast to major depressive disorder, in OCD there is a dose-response relationship for SSRI treatment; higher doses typically are required to achieve response or remission.6,7
Augmentation and other options
Patients who have not responded to at least 2 adequate trials of first-line medications may benefit from an augmentation strategy or treatment with an unconventional agent. Such cases should be managed by a specialist who has experience in treating OCD and with careful consideration of potential risks of these interventions.
Evidence suggests the following pharmacotherapies may effectively treat OCD and may be warranted for treatment-resistant patients.
Serotonergic agents
Supratherapeutic SSRI doses. Evidence suggests that supratherapeutic doses of SSRIs may be effective, which may be a logical first step when treating patients already taking an SSRI who have not responded. In a multi-center, double-blind study comparing sertraline, 200 mg/d, to sertraline, 250 to 400 mg/d, the latter group showed significantly greater symptom improvement.8 Citalopram may not be suitable for this approach because of the recent FDA announcement regarding dose-dependent QTc prolongation associated with this medication.9
Serotonin-norepinephrine reuptake inhibitors (SNRIs). In the only double-blind, placebo-controlled study of venlafaxine for OCD, the drug was not significantly more effective than placebo.10 This study was small (N = 30). There are sufficient positive results from open-label and blinded comparator studies that venlafaxine generally is accepted as an effective and well-tolerated treatment for OCD at doses ≥225 mg/d.11
Duloxetine also may be effective in treating OCD. One case series reported improvement in 3 of 4 SSRI nonresponders who were switched to this medication and rapidly titrated to 120 mg/d.12
Clomipramine/SSRI augmentation. For patients who have not responded to an SSRI, several open-label trials support adding clomipramine.13 Conversely, SSRI augmentation for patients who have not adequately responded to clomipramine may be effective.14 With any dual therapy with serotonergic agents, monitor patients for signs and symptoms of serotonin syndrome.
IV clomipramine. By bypassing first-pass metabolism, IV clomipramine rapidly achieves high plasma levels. In a double-blind, placebo-controlled study of 54 OCD patients who were nonresponsive to oral clomipramine, IV clomipramine was more effective than placebo.15 An additional study found IV clomipramine is more effective when pulse loaded than when titrated gradually.16
Pindolol. The beta blocker pindolol acts as an antagonist of presynaptic 5-HT1A autoreceptors, increasing serotonergic signaling. A small double-blind, placebo-controlled trial (N = 14) found a significant decrease in Yale-Brown Obsessive Compulsive Scale (Y-BOCS) score with pindolol augmentation, 2.5 mg, 3 times daily, among patients who did not respond to ≥3 serotonin reuptake inhibitor (SRI) trials.17 Pindolol augmentation showed modest effects in 2 open-label studies.18,19 However, another small double-blind, placebo-controlled study (N = 15) found no difference between placebo and fluvoxamine augmented with pindolol.20
Ondansetron. A 5-HT3 receptor antagonist, ondansetron is used primarily as an antiemetic but has been shown to have anxiolytic properties in animal studies. In an open-label study of 8 patients with non–treatment refractory OCD, 3 achieved clinical response (at least 35% reduction in Y-BOCS score) with ondansetron monotherapy dosed at 1 mg, 3 times daily.21 In a subsequent single-blind trial with 14 treatment-resistant patients, 9 responded (at least 25% reduction in Y-BOCS score).22
Other medications
Antipsychotics. Most studies examining antipsychotic monotherapy for OCD have been negative. One exception was a small, open-label trial of aripiprazole monotherapy (N = 8) that found modest efficacy among non–treatment refractory patients.23 Augmentation with antipsychotics, however, has been well studied and there is good evidence of efficacy for this approach. Double-blind, placebo-controlled studies have supported the efficacy of augmenting SRIs with haloperidol, risperidone, olanzapine, quetiapine, and aripiprazole.24-26 Several case reports suggest ziprasidone may be an effective SRI adjunct, but 1 retrospective study found it was inferior to quetiapine.27
Benzodiazepines. Case reports present positive effects of clonazepam and alprazolam for OCD, but double-blind, placebo-controlled trials for monotherapy or adjunctive clonazepam have been negative.28,29 Furthermore, cognitive impairment and potential for dependence associated with benzodiazepines weigh against their use in OCD.
Opioids. A double-blind, placebo controlled crossover study of 23 patients with treatment-refractory OCD found once-weekly oral morphine added to patients’ current regimen significantly reduced Y-BOCS score vs placebo. Patients received 30 mg the first week and 15 to 45 mg the next week, depending on response or side effects.30 A case report and a small open-label trial support the efficacy of tramadol, a weak agonist of the μ opioid receptor and an inhibitor of serotonin and norepinephrine transporters, as monotherapy and as an adjunct to fluoxetine.31,32 Because patients with OCD may be particularly vulnerable to dependence and intentional or accidental overdose via opioid/benzodiazepine combinations, evaluate the risks and benefits before initiating an opioid.
Psychostimulants. Sparse but good evidence supports the efficacy of dextroamphetamine monotherapy for OCD.33,34 There are no positive studies of methylphenidate and several case reports of methylphenidate-induced OCD symptoms.35
N-methyl-D-aspartate (NMDA) antagonists. Increased glutamatergic neurotransmission has been implicated in the pathophysiology of OCD, which suggests a possible role for glutamate receptor antagonists. In an open-label trial, memantine, an NMDA antagonist used primarily to treat dementia, was associated with clinical response (>25% reduction in Y-BOCS scores) in 6 of 14 patients with treatment-refractory OCD.36 Several case reports and an open-label trial support the efficacy of riluzole—which is indicated for treating amyotrophic lateral sclerosis—as an adjunct for treatment-refractory OCD.37 Although its exact mechanism of action is unclear, riluzole’s effects are thought to be mediated via reduction in glutamatergic neurotransmission. IV ketamine has reported anti-OCD effects in a case report of a woman with treatment-resistant OCD. These effects occurred almost immediately and persisted for several days.38
Hallucinogens. Psilocybin, psilocin, and lysergic acid diethylamide have reported anti-OCD properties.39 As schedule I substances, however, they are not available outside of sanctioned research protocols and may carry substantial risk. Nonetheless, their efficacy suggests that other compounds that share their mechanism of action—namely agonism of 5-HT2A and 5-HT2C receptors—may merit investigation as potential treatments for OCD.
Psychotherapy
Cognitive-behavioral therapy (CBT) has been shown to be effective for OCD as monotherapy and augmentation to pharmacotherapy. CBT consists of cognitive and behavioral components, typically involving some form of cognitive restructuring and exposure response prevention. Although these 2 types of interventions arise from independent traditions, in CBT they are frequently intertwined, particularly when the focus of OCD patients’ anxiety is ego-dystonic thoughts.
One benefit of CBT over pharmacotherapy is that effects persist after treatment is terminated. A recent prospective study found CBT was effective for treatment-refractory OCD, with 74% of patients demonstrating clinical response after 20 to 25 sessions over 2 months and 61% maintaining clinical response 1 year after treatment.40 CBT administered remotely via teleconference, also known as “teletherapy,” has shown efficacy for OCD.41
Alternative medicine
Despite widespread use of herbal remedies for OCD, no trials have shown a strong positive effect. Both Hypericum perforatum (St. John’s wort) and Silybum marianum (milk thistle) have been used to treat obsessive and compulsive symptoms; however, placebo-controlled trials did not find any significant differences in symptoms or side effects between treatment groups.42,43 Lower-quality studies have reported modest effects for mindfulness meditation, yoga, and acupuncture.44
Because many patients continue to use complementary and alternative medicine therapies despite the lack of data on efficacy, it is important to monitor for potential interactions with prescription medications. St. John’s wort interacts with many medications because of induction of the cytochrome P450 (CYP) isoenzymes 3A4 and 2C9. This interaction may lower blood levels of alprazolam and clonazepam (3A4). Combining St. John’s wort with SSRIs increases the risk of serotonin syndrome. Milk thistle inhibits CYP450 isoenzyme 3A4, and may increase serum levels of other medications metabolized by this pathway.
Invasive therapies
Invasive options may be considered after several pharmacotherapeutic and psychotherapeutic approaches have not been effective or when significant functional impairment remains (Table 2). These therapies typically are reserved for patients whose treatment resistance is strongest.
Electroconvulsive therapy (ECT). Although ECT is an effective tool for treatment-resistant mood disorders or treatment-resistant anxiety complicated by severe depression, studies have not found ECT to be effective for OCD. One uncontrolled case series reported considerable improvements in OCD patients the year after ECT, although improvement was correlated with improved depression scores.45
Vagal nerve stimulation (VNS). In an open-label study of 7 OCD patients who received VNS, 3 were acute responders—characterized by a ≥25% improvement on the Y-BOCS—and 2 received continued benefits at 4-year follow up (2 patients dropped out).46
Repetitive transcranial magnetic stimulation (rTMS). A meta-analysis of 3 RCTs of rTMS for patients with OCD did not yield a large or statistically significant effect.47 Limitations of these trials included asymmetric stimulation sites (eg, left vs right only), limited stimulation sites (dorsolateral prefrontal cortex), different stimulation frequencies between studies, and a lack of sham stimulation conditions. A more recent RCT and subsequent review described moderate efficacy (defined by ≥25% decrease in Y-BOCS scores) compared with sham stimulations in OCD patients at 4 weeks, using the supplementary motor area as a stimulation site.48,49
The main limitation of rTMS is the inability to penetrate deeper brain structures implicated in OCD (eg, caudate nucleus, thalamus, anterior capsule fiber tracts), as well as a lack of specificity in stimulation site.
Surgical approaches. Cingulotomy is the most commonly employed surgical procedure for OCD in North America, likely because of a combination of clinical efficacy and low morbidity and mortality rates.50 Of the >1,000 cingulotomies that have been performed at Massachusetts General Hospital, no deaths or postoperative infections have been reported and 2 subdural hematomas have occurred.50 Common postsurgical side effects include transient headache, nausea, or difficulty urinating. The most serious common side effect—postoperative seizures—has been reported in 1% to 9% of cases.
Outcomes for these procedures cannot be fully assessed until at least 6 months to 2 years after the procedure, which suggests postoperative neural reorganization plays an important role in recovery. Direct comparisons of each lesion approach within studies are extremely rare. Overall, long-term outcomes of these approaches have demonstrated significant therapeutic effects of each of these procedures. Reported response rates vary between 30% to 70%, when applied to remission, response (≥35% Y-BOCS reduction), and functional improvements in quality of life.50
Deep brain stimulation (DBS). With this approach, small electrodes are inserted under precise stereotactic MRI guidance. The advantage of DBS over ablative surgery is the ability to adjust and customize neurostimulation. Following implantation, modifiable parameters of electrode stimulation include electrode polarity, intensity, frequency, and laterality. A specially trained psychiatrist can conduct parameter optimization during long-term follow-up.
The first trial of DBS for OCD was reported in 1999 (N = 4), with the initial target selected based on the site of anterior capsulotomy. Three patients derived clinically observed benefit, although no validated questionnaires were administered.51 Since then, at least 7 studies with blinded stimulation have been conducted, totaling 62 patients.52
In recent years, structures adjacent to the internal capsule also have been targeted based on the approach employed in ventral capsulotomy. Across all trials, response rates for this approach consistently have been in the 50% range, with average Y-BOCS score reductions ranging from 6.8 to 31 points.53 Some patients have reported rapid improvements in anhedonia, and this approach is being employed in treatment-resistant depression.
Postoperative complications occur more often with DBS than with lesion approaches because of the prosthetic nature of the procedure (eg, increased risk of infection, lead malfunction, etc.). Additionally, batteries must be periodically explanted and replaced. Reported stimulation-related side effects include mood changes (transient sadness, anxiety, euphoria, and hypomania), sensory disturbances (olfactory, gustatory, and motor sensations), and cognitive changes (confusion and forgetfulness). These side effects typically are stimulation-dependent and disappear after altering stimulation parameters.
Table 2
Invasive therapies for treatment-resistant OCD
| Therapy | Quality of evidence |
|---|---|
| Reversible | |
| Electroconvulsive therapy | Poor |
| Vagal nerve stimulation | Poor |
| Repetitive transcranial magnetic stimulation | Limited |
| Irreversible (surgical) | |
| Anterior capsulotomy. Target: anterior limb of the internal capsule | Fair |
| Anterior cingulotomy. Target: anterior cingulate and cingulum bundle | Fair |
| Subcaudate tractotomy. Target: substantia innominata, just inferior to the caudate nucleus | Fair |
| Limbic leucotomy. Target: anterior cingulotomy combined with subcaudate tractotomy | Fair |
| Deep brain stimulation. Multiple targets | Fair |
| OCD: obsessive-compulsive disorder | |
Related Resources
- American Psychiatric Association. Treatment of patients with obsessive-compulsive disorder. www.psychiatryonline.com/pracGuide/pracGuideTopic_10.aspx.
- Hyman BM, Pedrick C. The OCD workbook. Your guide to breaking free from obsessive compulsive disorder. 3rd ed. Oakland, CA: New Harbinger Publications Inc; 2010.
- Baer L. Getting control: overcoming your obsessions and compulsions. Revised ed. New York, NY: Plume; 2000.
Drug Brand Names
- Alprazolam • Xanax
- Aripiprazole • Abilify
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clonazepam • Klonopin
- Dextroamphetamine • Adderall
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Ketamine • Ketalar
- Memantine • Namenda
- Methylphenidate • Ritalin
- Morphine • MS Contin
- Olanzapine • Zyprexa
- Ondansetron • Zofran
- Pindolol • Visken
- Quetiapine • Seroquel
- Riluzole • Rilutek
- Risperidone • Risperdal
- Sertraline • Zoloft
- Tramadol • Ultram
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosures
Drs. Khalsa and Schiffman report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Bystritsky receives grant support from AstraZeneca, Brainways, Takeda, and Transcept and is a founder, stockholder, and consultant for BrainSonix.
Obsessive-compulsive disorder (OCD) is marked by recurrent and persistent anxiety-provoking thoughts (obsessions) accompanied by repetitive behaviors (compulsions) that focus on alleviating distress caused by obsessive thoughts. Although patients recognize the obsessions and compulsions are unreasonable, these thoughts and behaviors remain time-consuming and impair function. Even when they appropriately identify and treat OCD, clinicians often face “treatment-resistant” (or “treatment-refractory”) patients who do not respond adequately to standard therapies (Box).1 Several factors contribute to treatment resistance, including those related to the patient, the environment, the clinician/health system, and pathology (Table 1).2 An estimated 10% to 40% of patients with OCD are treatment-resistant.2
This article discusses the range of options for addressing resistant OCD, including augmenting first-line treatments with pharmacotherapy, psychotherapy, or reversible or irreversible forms of neuromodulation.
Treatment resistance generally refers to lack of sufficient improvement despite multiple adequate and appropriate treatment trials. However, there are no universally accepted definitions or metrics of treatment resistance, and often it is operationally defined. For mood disorders, it may be defined by failure to remit or respond clinically (50% reduction in symptoms) despite ≥2 adequate antidepressant trials or failure to respond clinically despite adequate medication trials across several neurotransmitter classes. The terms treatment resistant and treatment refractory are synonymous; they refer to the same phenomenon and are used interchangeably in the literature. Including the terms “remission” and “recovery” when judging treatment efficacy for anxiety disorders can be limiting because of the chronic and often unrelenting nature of these conditions.
One review proposed categorizing obsessive-compulsive disorder treatment response into several stages along a spectrum, ranging from complete recovery (or remission) to full or partial response to non-response (or completely refractory).1 However it is defined, treatment resistance in anxiety disorders likely is characterized by minimal restoration of function despite several appropriate treatment exposures.
Table 1
Factors that contribute to treatment resistance in obsessive-compulsive disorder
| Patient |
| Disease severity Medical comorbidity Psychiatric comorbidity (mood, personality, and/or substance use disorders) Treatment nonadherence Cultural factors |
| Environment |
| Childhood stressors (trauma, abuse) Long-term persistent stressors (psychosocial, occupational, financial) Life stages |
| Clinician/health system |
| Lack of knowledge in primary care (brief treatment duration, subtherapeutic dosing) Lack of psychotherapeutic training Limited doctor-patient relationship (eg, availability/cost of treatment) |
| Pathology-related |
Underlying disease pathophysiology (largely unknown):
Syndromal variation (differing presentations over time) Treatment limitations (limited empirical studies, nonrepresentative study samples) |
| Source: Reference 2 |
First-line pharmacotherapy
Clomipramine or a selective serotonin reuptake inhibitor (SSRI) are considered first-line treatments for OCD. Although some evidence indicates that clomipramine may have greater efficacy than SSRIs, its poor tolerability and potential lethality in overdose make it a less practical first choice in treatment-naïve patients.3,4 SSRIs generally are well tolerated and have a favorable safety profile. Nearly all SSRIs have randomized clinical trials (RCTs) and FDA indications that support their use in OCD. SSRI choice may be guided by patient or prescriber preference because no evidence suggests that 1 SSRI is superior to another for treating OCD.5 In contrast to major depressive disorder, in OCD there is a dose-response relationship for SSRI treatment; higher doses typically are required to achieve response or remission.6,7
Augmentation and other options
Patients who have not responded to at least 2 adequate trials of first-line medications may benefit from an augmentation strategy or treatment with an unconventional agent. Such cases should be managed by a specialist who has experience in treating OCD and with careful consideration of potential risks of these interventions.
Evidence suggests the following pharmacotherapies may effectively treat OCD and may be warranted for treatment-resistant patients.
Serotonergic agents
Supratherapeutic SSRI doses. Evidence suggests that supratherapeutic doses of SSRIs may be effective, which may be a logical first step when treating patients already taking an SSRI who have not responded. In a multi-center, double-blind study comparing sertraline, 200 mg/d, to sertraline, 250 to 400 mg/d, the latter group showed significantly greater symptom improvement.8 Citalopram may not be suitable for this approach because of the recent FDA announcement regarding dose-dependent QTc prolongation associated with this medication.9
Serotonin-norepinephrine reuptake inhibitors (SNRIs). In the only double-blind, placebo-controlled study of venlafaxine for OCD, the drug was not significantly more effective than placebo.10 This study was small (N = 30). There are sufficient positive results from open-label and blinded comparator studies that venlafaxine generally is accepted as an effective and well-tolerated treatment for OCD at doses ≥225 mg/d.11
Duloxetine also may be effective in treating OCD. One case series reported improvement in 3 of 4 SSRI nonresponders who were switched to this medication and rapidly titrated to 120 mg/d.12
Clomipramine/SSRI augmentation. For patients who have not responded to an SSRI, several open-label trials support adding clomipramine.13 Conversely, SSRI augmentation for patients who have not adequately responded to clomipramine may be effective.14 With any dual therapy with serotonergic agents, monitor patients for signs and symptoms of serotonin syndrome.
IV clomipramine. By bypassing first-pass metabolism, IV clomipramine rapidly achieves high plasma levels. In a double-blind, placebo-controlled study of 54 OCD patients who were nonresponsive to oral clomipramine, IV clomipramine was more effective than placebo.15 An additional study found IV clomipramine is more effective when pulse loaded than when titrated gradually.16
Pindolol. The beta blocker pindolol acts as an antagonist of presynaptic 5-HT1A autoreceptors, increasing serotonergic signaling. A small double-blind, placebo-controlled trial (N = 14) found a significant decrease in Yale-Brown Obsessive Compulsive Scale (Y-BOCS) score with pindolol augmentation, 2.5 mg, 3 times daily, among patients who did not respond to ≥3 serotonin reuptake inhibitor (SRI) trials.17 Pindolol augmentation showed modest effects in 2 open-label studies.18,19 However, another small double-blind, placebo-controlled study (N = 15) found no difference between placebo and fluvoxamine augmented with pindolol.20
Ondansetron. A 5-HT3 receptor antagonist, ondansetron is used primarily as an antiemetic but has been shown to have anxiolytic properties in animal studies. In an open-label study of 8 patients with non–treatment refractory OCD, 3 achieved clinical response (at least 35% reduction in Y-BOCS score) with ondansetron monotherapy dosed at 1 mg, 3 times daily.21 In a subsequent single-blind trial with 14 treatment-resistant patients, 9 responded (at least 25% reduction in Y-BOCS score).22
Other medications
Antipsychotics. Most studies examining antipsychotic monotherapy for OCD have been negative. One exception was a small, open-label trial of aripiprazole monotherapy (N = 8) that found modest efficacy among non–treatment refractory patients.23 Augmentation with antipsychotics, however, has been well studied and there is good evidence of efficacy for this approach. Double-blind, placebo-controlled studies have supported the efficacy of augmenting SRIs with haloperidol, risperidone, olanzapine, quetiapine, and aripiprazole.24-26 Several case reports suggest ziprasidone may be an effective SRI adjunct, but 1 retrospective study found it was inferior to quetiapine.27
Benzodiazepines. Case reports present positive effects of clonazepam and alprazolam for OCD, but double-blind, placebo-controlled trials for monotherapy or adjunctive clonazepam have been negative.28,29 Furthermore, cognitive impairment and potential for dependence associated with benzodiazepines weigh against their use in OCD.
Opioids. A double-blind, placebo controlled crossover study of 23 patients with treatment-refractory OCD found once-weekly oral morphine added to patients’ current regimen significantly reduced Y-BOCS score vs placebo. Patients received 30 mg the first week and 15 to 45 mg the next week, depending on response or side effects.30 A case report and a small open-label trial support the efficacy of tramadol, a weak agonist of the μ opioid receptor and an inhibitor of serotonin and norepinephrine transporters, as monotherapy and as an adjunct to fluoxetine.31,32 Because patients with OCD may be particularly vulnerable to dependence and intentional or accidental overdose via opioid/benzodiazepine combinations, evaluate the risks and benefits before initiating an opioid.
Psychostimulants. Sparse but good evidence supports the efficacy of dextroamphetamine monotherapy for OCD.33,34 There are no positive studies of methylphenidate and several case reports of methylphenidate-induced OCD symptoms.35
N-methyl-D-aspartate (NMDA) antagonists. Increased glutamatergic neurotransmission has been implicated in the pathophysiology of OCD, which suggests a possible role for glutamate receptor antagonists. In an open-label trial, memantine, an NMDA antagonist used primarily to treat dementia, was associated with clinical response (>25% reduction in Y-BOCS scores) in 6 of 14 patients with treatment-refractory OCD.36 Several case reports and an open-label trial support the efficacy of riluzole—which is indicated for treating amyotrophic lateral sclerosis—as an adjunct for treatment-refractory OCD.37 Although its exact mechanism of action is unclear, riluzole’s effects are thought to be mediated via reduction in glutamatergic neurotransmission. IV ketamine has reported anti-OCD effects in a case report of a woman with treatment-resistant OCD. These effects occurred almost immediately and persisted for several days.38
Hallucinogens. Psilocybin, psilocin, and lysergic acid diethylamide have reported anti-OCD properties.39 As schedule I substances, however, they are not available outside of sanctioned research protocols and may carry substantial risk. Nonetheless, their efficacy suggests that other compounds that share their mechanism of action—namely agonism of 5-HT2A and 5-HT2C receptors—may merit investigation as potential treatments for OCD.
Psychotherapy
Cognitive-behavioral therapy (CBT) has been shown to be effective for OCD as monotherapy and augmentation to pharmacotherapy. CBT consists of cognitive and behavioral components, typically involving some form of cognitive restructuring and exposure response prevention. Although these 2 types of interventions arise from independent traditions, in CBT they are frequently intertwined, particularly when the focus of OCD patients’ anxiety is ego-dystonic thoughts.
One benefit of CBT over pharmacotherapy is that effects persist after treatment is terminated. A recent prospective study found CBT was effective for treatment-refractory OCD, with 74% of patients demonstrating clinical response after 20 to 25 sessions over 2 months and 61% maintaining clinical response 1 year after treatment.40 CBT administered remotely via teleconference, also known as “teletherapy,” has shown efficacy for OCD.41
Alternative medicine
Despite widespread use of herbal remedies for OCD, no trials have shown a strong positive effect. Both Hypericum perforatum (St. John’s wort) and Silybum marianum (milk thistle) have been used to treat obsessive and compulsive symptoms; however, placebo-controlled trials did not find any significant differences in symptoms or side effects between treatment groups.42,43 Lower-quality studies have reported modest effects for mindfulness meditation, yoga, and acupuncture.44
Because many patients continue to use complementary and alternative medicine therapies despite the lack of data on efficacy, it is important to monitor for potential interactions with prescription medications. St. John’s wort interacts with many medications because of induction of the cytochrome P450 (CYP) isoenzymes 3A4 and 2C9. This interaction may lower blood levels of alprazolam and clonazepam (3A4). Combining St. John’s wort with SSRIs increases the risk of serotonin syndrome. Milk thistle inhibits CYP450 isoenzyme 3A4, and may increase serum levels of other medications metabolized by this pathway.
Invasive therapies
Invasive options may be considered after several pharmacotherapeutic and psychotherapeutic approaches have not been effective or when significant functional impairment remains (Table 2). These therapies typically are reserved for patients whose treatment resistance is strongest.
Electroconvulsive therapy (ECT). Although ECT is an effective tool for treatment-resistant mood disorders or treatment-resistant anxiety complicated by severe depression, studies have not found ECT to be effective for OCD. One uncontrolled case series reported considerable improvements in OCD patients the year after ECT, although improvement was correlated with improved depression scores.45
Vagal nerve stimulation (VNS). In an open-label study of 7 OCD patients who received VNS, 3 were acute responders—characterized by a ≥25% improvement on the Y-BOCS—and 2 received continued benefits at 4-year follow up (2 patients dropped out).46
Repetitive transcranial magnetic stimulation (rTMS). A meta-analysis of 3 RCTs of rTMS for patients with OCD did not yield a large or statistically significant effect.47 Limitations of these trials included asymmetric stimulation sites (eg, left vs right only), limited stimulation sites (dorsolateral prefrontal cortex), different stimulation frequencies between studies, and a lack of sham stimulation conditions. A more recent RCT and subsequent review described moderate efficacy (defined by ≥25% decrease in Y-BOCS scores) compared with sham stimulations in OCD patients at 4 weeks, using the supplementary motor area as a stimulation site.48,49
The main limitation of rTMS is the inability to penetrate deeper brain structures implicated in OCD (eg, caudate nucleus, thalamus, anterior capsule fiber tracts), as well as a lack of specificity in stimulation site.
Surgical approaches. Cingulotomy is the most commonly employed surgical procedure for OCD in North America, likely because of a combination of clinical efficacy and low morbidity and mortality rates.50 Of the >1,000 cingulotomies that have been performed at Massachusetts General Hospital, no deaths or postoperative infections have been reported and 2 subdural hematomas have occurred.50 Common postsurgical side effects include transient headache, nausea, or difficulty urinating. The most serious common side effect—postoperative seizures—has been reported in 1% to 9% of cases.
Outcomes for these procedures cannot be fully assessed until at least 6 months to 2 years after the procedure, which suggests postoperative neural reorganization plays an important role in recovery. Direct comparisons of each lesion approach within studies are extremely rare. Overall, long-term outcomes of these approaches have demonstrated significant therapeutic effects of each of these procedures. Reported response rates vary between 30% to 70%, when applied to remission, response (≥35% Y-BOCS reduction), and functional improvements in quality of life.50
Deep brain stimulation (DBS). With this approach, small electrodes are inserted under precise stereotactic MRI guidance. The advantage of DBS over ablative surgery is the ability to adjust and customize neurostimulation. Following implantation, modifiable parameters of electrode stimulation include electrode polarity, intensity, frequency, and laterality. A specially trained psychiatrist can conduct parameter optimization during long-term follow-up.
The first trial of DBS for OCD was reported in 1999 (N = 4), with the initial target selected based on the site of anterior capsulotomy. Three patients derived clinically observed benefit, although no validated questionnaires were administered.51 Since then, at least 7 studies with blinded stimulation have been conducted, totaling 62 patients.52
In recent years, structures adjacent to the internal capsule also have been targeted based on the approach employed in ventral capsulotomy. Across all trials, response rates for this approach consistently have been in the 50% range, with average Y-BOCS score reductions ranging from 6.8 to 31 points.53 Some patients have reported rapid improvements in anhedonia, and this approach is being employed in treatment-resistant depression.
Postoperative complications occur more often with DBS than with lesion approaches because of the prosthetic nature of the procedure (eg, increased risk of infection, lead malfunction, etc.). Additionally, batteries must be periodically explanted and replaced. Reported stimulation-related side effects include mood changes (transient sadness, anxiety, euphoria, and hypomania), sensory disturbances (olfactory, gustatory, and motor sensations), and cognitive changes (confusion and forgetfulness). These side effects typically are stimulation-dependent and disappear after altering stimulation parameters.
Table 2
Invasive therapies for treatment-resistant OCD
| Therapy | Quality of evidence |
|---|---|
| Reversible | |
| Electroconvulsive therapy | Poor |
| Vagal nerve stimulation | Poor |
| Repetitive transcranial magnetic stimulation | Limited |
| Irreversible (surgical) | |
| Anterior capsulotomy. Target: anterior limb of the internal capsule | Fair |
| Anterior cingulotomy. Target: anterior cingulate and cingulum bundle | Fair |
| Subcaudate tractotomy. Target: substantia innominata, just inferior to the caudate nucleus | Fair |
| Limbic leucotomy. Target: anterior cingulotomy combined with subcaudate tractotomy | Fair |
| Deep brain stimulation. Multiple targets | Fair |
| OCD: obsessive-compulsive disorder | |
Related Resources
- American Psychiatric Association. Treatment of patients with obsessive-compulsive disorder. www.psychiatryonline.com/pracGuide/pracGuideTopic_10.aspx.
- Hyman BM, Pedrick C. The OCD workbook. Your guide to breaking free from obsessive compulsive disorder. 3rd ed. Oakland, CA: New Harbinger Publications Inc; 2010.
- Baer L. Getting control: overcoming your obsessions and compulsions. Revised ed. New York, NY: Plume; 2000.
Drug Brand Names
- Alprazolam • Xanax
- Aripiprazole • Abilify
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clonazepam • Klonopin
- Dextroamphetamine • Adderall
- Duloxetine • Cymbalta
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Ketamine • Ketalar
- Memantine • Namenda
- Methylphenidate • Ritalin
- Morphine • MS Contin
- Olanzapine • Zyprexa
- Ondansetron • Zofran
- Pindolol • Visken
- Quetiapine • Seroquel
- Riluzole • Rilutek
- Risperidone • Risperdal
- Sertraline • Zoloft
- Tramadol • Ultram
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Disclosures
Drs. Khalsa and Schiffman report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Bystritsky receives grant support from AstraZeneca, Brainways, Takeda, and Transcept and is a founder, stockholder, and consultant for BrainSonix.
1. Pallanti S, Quercioli L. Treatment-refractory obsessive-compulsive disorder: methodological issues operational definitions and therapeutic lines. Prog Neuropsychopharmacol Biol Psychiatry. 2006;30(3):400-412.
2. Bystritsky A. Treatment-resistant anxiety disorders. Mol Psychiatry. 2006;11(9):805-814.
3. Denys D. Pharmacotherapy of obsessive-compulsive disorder and obsessive-compulsive spectrum disorders. Psychiatr Clin North Am. 2006;29(2):553-584 xi.
4. Ackerman DL, Greenland S. Multivariate meta-analysis of controlled drug studies for obsessive-compulsive disorder. J Clin Psychopharmacol. 2002;22(3):309-317.
5. Soomro GM, Altman D, Rajagopal S, et al. Selective serotonin re-uptake inhibitors (SSRIs) versus placebo for obsessive compulsive disorder (OCD). Cochrane Database Syst Rev. 2008;(1):CD001765.-
6. Bloch MH, McGuire J, Landeros-Weisenberger A, et al. Meta-analysis of the dose-response relationship of SSRI in obsessive-compulsive disorder. Mol Psychiatry. 2010;15(8):850-855.
7. Koran LM, Hanna GL, Hollander E, et al. American Psychiatric Association. Practice guideline for the treatment of patients with obsessive-compulsive disorder. Am J Psychiatry. 2007;164(7 suppl):5-53.
8. Ninan PT, Koran LM, Kiev A, et al. High-dose sertraline strategy for nonresponders to acute treatment for obsessive-compulsive disorder: a multicenter double-blind trial. J Clin Psychiatry. 2006;67(1):15-22.
9. Food and Drug Administration. FDA drug safety communication: abnormal heart rhythms associated with high doses of Celexa (citalopram hydrobromide). http://www.fda.gov/Drugs/DrugSafety/ucm269086.htm#sa. Published August 24 2011. Accessed September 27, 2011.
10. Yaryura-Tobias JA, Neziroglu FA. Venlafaxine in obsessive-compulsive disorder. Arch Gen Psychiatry. 1996;53(7):653-654.
11. Phelps NJ, Cates ME. The role of venlafaxine in the treatment of obsessive-compulsive disorder. Ann Pharmacother. 2005;39(1):136-140.
12. Dell’osso B, Mundo E, Marazziti D, et al. Switching from serotonin reuptake inhibitors to duloxetine in patients with resistant obsessive compulsive disorder: a case series. J Psychopharmacol. 2008;22(2):210-213.
13. Pallanti S, Quercioli L, Paiva RS, et al. Citalopram for treatment-resistant obsessive-compulsive disorder. Eur Psychiatry. 1999;14:101-106.
14. Ravizza L, Barzega G, Bellino S, et al. Therapeutic effect and safety of adjunctive risperidone in refractory obsessive-compulsive disorder (OCD). Psychopharmacol Bull. 1996;32:677-682.
15. Fallon BA, Liebowitz MR, Campeas R, et al. Intravenous clomipramine for obsessive-compulsive disorder refractory to oral clomipramine: a placebo-controlled study. Arch Gen Psychiatry. 1998;55:918-924.
16. Koran LM, Pallanti S, Paiva RS, et al. Pulse loading versus gradual dosing of intravenous clomipramine in obsessive-compulsive disorder. Eur Neuropsychopharmacol. 1998;8:121-126.
17. Dannon PN, Sasson Y, Hirschmann S, et al. Pindolol augmentation in treatment-resistant obsessive compulsive disorder: a double-blind placebo controlled trial. Eur Neuropsychopharmacol. 2000;10:165-169.
18. Koran LM, Mueller K, Maloney A. Will pindolol augment the response to a serotonin reuptake inhibitor in obsessive-compulsive disorder? J Clin Psychopharmacol. 1996;16:253-254.
19. Hewlett WA, Vinogradov S, Agras WS. Clomipramine clonazepam, and clonidine treatment of obsessive-compulsive disorder. J Clin Psychopharmacol. 1992;12:420-430.
20. Mundo E, Guglielmo E, Bellodi L. Effect of adjuvant pindolol on the antiobsessional response to fluvoxamine: a double-blind placebo-controlled study. Int Clin Psychopharmacol. 1998;13:219-224.
21. Hewlett WA, Schmid SP, Salomon RM. Pilot trial of ondansetron in the treatment of 8 patients with obsessive-compulsive disorder. J Clin Psychiatry. 2003;64:1025-1030.
22. Pallanti S, Bernardi S, Antonini S, et al. Ondansetron augmentation in treatment-resistant obsessive-compulsive disorder: a preliminary, single-blind, prospective study. CNS Drugs. 2009;23(12):1047-1055.
23. Connor KM, Payne VM, Gadde KM, et al. The use of aripiprazole in obsessive-compulsive disorder: preliminary observations in 8 patients. J Clin Psychiatry. 2005;66:49-51.
24. Komossa K, Depping AM, Meyer M, et al. Second-generation antipsychotics for obsessive compulsive disorder. Cochrane Database Syst Rev. 2010;(12):CD008141.-
25. Bloch MH, Landeros-Weisenberger A, Kelmendi B, et al. A systematic review: antipsychotic augmentation with treatment refractory obsessive-compulsive disorder. Mol Psychiatry. 2006;11(7):622-632.
26. Muscatello MR, Bruno A, Pandolfo G, et al. Effect of aripiprazole augmentation of serotonin reuptake inhibitors or clomipramine in treatment-resistant obsessive-compulsive disorder: a double-blind, placebo-controlled study. J Clin Psychopharmacol. 2011;31(2):174-179.
27. Savas HA, Yumru M, Ozen ME. Quetiapine and ziprasidone as adjuncts in treatment-resistant obsessive-compulsive disorder: a retrospective comparative study. Clin Drug Investig. 2008;28(7):439-442.
28. Hollander E, Kaplan A, Stahl SM. A double-blind placebo-controlled trial of clonazepam in obsessive-compulsive disorder. World J Biol Psychiatry. 2003;4:30-34.
29. Crockett BA, Churchill E, Davidson JR. A double-blind combination study of clonazepam with sertraline in obsessive-compulsive disorder. Ann Clin Psychiatry. 2004;16(3):127-132.
30. Koran LM, Aboujaoude E, Bullock KD, et al. Double-blind treatment with oral morphine in treatment-resistant obsessive-compulsive disorder. J Clin Psychiatry. 2005;66(3):353-359.
31. Shapira NA, Keck PE Jr, Goldsmith TD, et al. Open-label pilot study of tramadol hydrochloride in treatment-refractory obsessive-compulsive disorder. Depress Anxiety. 1997;6:170-173.
32. Goldsmith TB, Shapira NA, Keck PE Jr. Rapid remission of OCD with tramadol hydrochloride. Am J Psychiatry. 1999;156(4):660-661.
33. Insel TR, Hamilton JA, Guttmacher LB, et al. D-amphetamine in obsessive-compulsive disorder. Psychopharmacology (Berl). 1983;80:231-235.
34. Joffe RT, Swinson RP, Levitt AJ. Acute psychostimulant challenge in primary obsessive-compulsive disorder. J Clin Psychopharmacol. 1991;11:237-241.
35. Woolley JB, Heyman I. Dexamphetamine for obsessive-compulsive disorder. Am J Psychiatry. 2003;160:183.-
36. Aboujaoude E, Barry JJ, Gamel N. Memantine augmentation in treatment-resistant obsessive-compulsive disorder: an open-label trial. J Clin Psychopharmacol. 2009;29(1):51-55.
37. Coric V, Taskiran S, Pittenger C, et al. Riluzole augmentation in treatment-resistant obsessive-compulsive disorder: an open-label trial. Biol Psychiatry. 2005;58(5):424-428.
38. Rodriguez CI, Kegeles LS, Flood P, et al. Rapid resolution of obsessions after an infusion of intravenous ketamine in a patient with treatment-resistant obsessive-compulsive disorder. J Clin Psychiatry. 2011;72(4):567-569.
39. Leonard HL, Rapoport JL. Relief of obsessive-compulsive symptoms by LSD and psilocin. Am J Psychiatry. 1987;144(9):1239-1240.
40. Anand N, Sudhir PM, Math SB, et al. Cognitive behavior therapy in medication non-responders with obsessive-compulsive disorder: a prospective 1-year follow-up study. J Anxiety Disord. 2011;25(7):939-945.
41. Himle JA, Fischer DJ, Muroff JR, et al. Videoconferencing-based cognitive-behavioral therapy for obsessive-compulsive disorder. Behav Res Ther. 2006;44(12):1821-1829.
42. Kobak KA, Taylor LV, Bystritsky A, et al. St John’s wort versus placebo in obsessive-compulsive disorder: results from a double-blind study. Int Clin Psychopharmacol. 2005;20(6):299-304.
43. Sayyah M, Boostani H, Pakseresht S, et al. Comparison of Silybum marianum (L.) Gaertn. with fluoxetine in the treatment of obsessive-compulsive Disorder. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(2):362-365.
44. Sarris J, Camfield D, Berk M. Complementary medicine self-help, and lifestyle interventions for obsessive compulsive disorder (OCD) and the OCD spectrum: a systematic review. J Affect Disord. 2011 (epub ahead of print).
45. Beale MD, Kellner CH, Pritchett JT, et al. ECT for OCD. J Clin Psychiatry. 1995;56(2):81-82.
46. George MS, Ward HE Jr, Ninan PT, et al. A pilot study of vagus nerve stimulation (VNS) for treatment-resistant anxiety disorders. Brain Stimul. 2008;1(2):112-121.
47. Slotema CW, Blom JD, Hoek HW, et al. Should we expand the toolbox of psychiatric treatment methods to include repetitive transcranial magnetic stimulation (rTMS)? A meta-analysis of the efficacy of rTMS in psychiatric disorders. J Clin Psychiatry. 2010;71(7):873-884.
48. Mantovani A, Simpson HB, Fallon BA, et al. Randomized sham-controlled trial of repetitive transcranial magnetic stimulation in treatment-resistant obsessive-compulsive disorder. Int J Neuropsychopharmacol. 2010;13(2):217-227.
49. Blom RM, Figee M, Vulink N, et al. Update on repetitive transcranial magnetic stimulation in obsessive-compulsive disorder: different targets. Curr Psychiatry Rep. 2011;13(4):289-294.
50. Greenberg BD, Rauch SL, Haber SN. Invasive circuitry-based neurotherapeutics: stereotactic ablation and deep brain stimulation for OCD. Neuropsychopharmacology. 2010;35(1):317-336.
51. Nuttin B, Cosyns P, Demeulemeester H, et al. Electrical stimulation in anterior limbs of internal capsules in patients with obsessive-compulsive disorder. Lancet. 1999;354(9189):1526.-
52. de Koning PP, Figee M, van den Munckhof P, et al. Current status of deep brain stimulation for obsessive-compulsive disorder: a clinical review of different targets. Curr Psychiatry Rep. 2011;13(4):274-282.
53. Greenberg BD, Gabriels LA, Malone DA, Jr, et al. Deep brain stimulation of the ventral internal capsule/ventral striatum for obsessive-compulsive disorder: worldwide experience. Mol Psychiatry. 2010;15(1):64-79.
1. Pallanti S, Quercioli L. Treatment-refractory obsessive-compulsive disorder: methodological issues operational definitions and therapeutic lines. Prog Neuropsychopharmacol Biol Psychiatry. 2006;30(3):400-412.
2. Bystritsky A. Treatment-resistant anxiety disorders. Mol Psychiatry. 2006;11(9):805-814.
3. Denys D. Pharmacotherapy of obsessive-compulsive disorder and obsessive-compulsive spectrum disorders. Psychiatr Clin North Am. 2006;29(2):553-584 xi.
4. Ackerman DL, Greenland S. Multivariate meta-analysis of controlled drug studies for obsessive-compulsive disorder. J Clin Psychopharmacol. 2002;22(3):309-317.
5. Soomro GM, Altman D, Rajagopal S, et al. Selective serotonin re-uptake inhibitors (SSRIs) versus placebo for obsessive compulsive disorder (OCD). Cochrane Database Syst Rev. 2008;(1):CD001765.-
6. Bloch MH, McGuire J, Landeros-Weisenberger A, et al. Meta-analysis of the dose-response relationship of SSRI in obsessive-compulsive disorder. Mol Psychiatry. 2010;15(8):850-855.
7. Koran LM, Hanna GL, Hollander E, et al. American Psychiatric Association. Practice guideline for the treatment of patients with obsessive-compulsive disorder. Am J Psychiatry. 2007;164(7 suppl):5-53.
8. Ninan PT, Koran LM, Kiev A, et al. High-dose sertraline strategy for nonresponders to acute treatment for obsessive-compulsive disorder: a multicenter double-blind trial. J Clin Psychiatry. 2006;67(1):15-22.
9. Food and Drug Administration. FDA drug safety communication: abnormal heart rhythms associated with high doses of Celexa (citalopram hydrobromide). http://www.fda.gov/Drugs/DrugSafety/ucm269086.htm#sa. Published August 24 2011. Accessed September 27, 2011.
10. Yaryura-Tobias JA, Neziroglu FA. Venlafaxine in obsessive-compulsive disorder. Arch Gen Psychiatry. 1996;53(7):653-654.
11. Phelps NJ, Cates ME. The role of venlafaxine in the treatment of obsessive-compulsive disorder. Ann Pharmacother. 2005;39(1):136-140.
12. Dell’osso B, Mundo E, Marazziti D, et al. Switching from serotonin reuptake inhibitors to duloxetine in patients with resistant obsessive compulsive disorder: a case series. J Psychopharmacol. 2008;22(2):210-213.
13. Pallanti S, Quercioli L, Paiva RS, et al. Citalopram for treatment-resistant obsessive-compulsive disorder. Eur Psychiatry. 1999;14:101-106.
14. Ravizza L, Barzega G, Bellino S, et al. Therapeutic effect and safety of adjunctive risperidone in refractory obsessive-compulsive disorder (OCD). Psychopharmacol Bull. 1996;32:677-682.
15. Fallon BA, Liebowitz MR, Campeas R, et al. Intravenous clomipramine for obsessive-compulsive disorder refractory to oral clomipramine: a placebo-controlled study. Arch Gen Psychiatry. 1998;55:918-924.
16. Koran LM, Pallanti S, Paiva RS, et al. Pulse loading versus gradual dosing of intravenous clomipramine in obsessive-compulsive disorder. Eur Neuropsychopharmacol. 1998;8:121-126.
17. Dannon PN, Sasson Y, Hirschmann S, et al. Pindolol augmentation in treatment-resistant obsessive compulsive disorder: a double-blind placebo controlled trial. Eur Neuropsychopharmacol. 2000;10:165-169.
18. Koran LM, Mueller K, Maloney A. Will pindolol augment the response to a serotonin reuptake inhibitor in obsessive-compulsive disorder? J Clin Psychopharmacol. 1996;16:253-254.
19. Hewlett WA, Vinogradov S, Agras WS. Clomipramine clonazepam, and clonidine treatment of obsessive-compulsive disorder. J Clin Psychopharmacol. 1992;12:420-430.
20. Mundo E, Guglielmo E, Bellodi L. Effect of adjuvant pindolol on the antiobsessional response to fluvoxamine: a double-blind placebo-controlled study. Int Clin Psychopharmacol. 1998;13:219-224.
21. Hewlett WA, Schmid SP, Salomon RM. Pilot trial of ondansetron in the treatment of 8 patients with obsessive-compulsive disorder. J Clin Psychiatry. 2003;64:1025-1030.
22. Pallanti S, Bernardi S, Antonini S, et al. Ondansetron augmentation in treatment-resistant obsessive-compulsive disorder: a preliminary, single-blind, prospective study. CNS Drugs. 2009;23(12):1047-1055.
23. Connor KM, Payne VM, Gadde KM, et al. The use of aripiprazole in obsessive-compulsive disorder: preliminary observations in 8 patients. J Clin Psychiatry. 2005;66:49-51.
24. Komossa K, Depping AM, Meyer M, et al. Second-generation antipsychotics for obsessive compulsive disorder. Cochrane Database Syst Rev. 2010;(12):CD008141.-
25. Bloch MH, Landeros-Weisenberger A, Kelmendi B, et al. A systematic review: antipsychotic augmentation with treatment refractory obsessive-compulsive disorder. Mol Psychiatry. 2006;11(7):622-632.
26. Muscatello MR, Bruno A, Pandolfo G, et al. Effect of aripiprazole augmentation of serotonin reuptake inhibitors or clomipramine in treatment-resistant obsessive-compulsive disorder: a double-blind, placebo-controlled study. J Clin Psychopharmacol. 2011;31(2):174-179.
27. Savas HA, Yumru M, Ozen ME. Quetiapine and ziprasidone as adjuncts in treatment-resistant obsessive-compulsive disorder: a retrospective comparative study. Clin Drug Investig. 2008;28(7):439-442.
28. Hollander E, Kaplan A, Stahl SM. A double-blind placebo-controlled trial of clonazepam in obsessive-compulsive disorder. World J Biol Psychiatry. 2003;4:30-34.
29. Crockett BA, Churchill E, Davidson JR. A double-blind combination study of clonazepam with sertraline in obsessive-compulsive disorder. Ann Clin Psychiatry. 2004;16(3):127-132.
30. Koran LM, Aboujaoude E, Bullock KD, et al. Double-blind treatment with oral morphine in treatment-resistant obsessive-compulsive disorder. J Clin Psychiatry. 2005;66(3):353-359.
31. Shapira NA, Keck PE Jr, Goldsmith TD, et al. Open-label pilot study of tramadol hydrochloride in treatment-refractory obsessive-compulsive disorder. Depress Anxiety. 1997;6:170-173.
32. Goldsmith TB, Shapira NA, Keck PE Jr. Rapid remission of OCD with tramadol hydrochloride. Am J Psychiatry. 1999;156(4):660-661.
33. Insel TR, Hamilton JA, Guttmacher LB, et al. D-amphetamine in obsessive-compulsive disorder. Psychopharmacology (Berl). 1983;80:231-235.
34. Joffe RT, Swinson RP, Levitt AJ. Acute psychostimulant challenge in primary obsessive-compulsive disorder. J Clin Psychopharmacol. 1991;11:237-241.
35. Woolley JB, Heyman I. Dexamphetamine for obsessive-compulsive disorder. Am J Psychiatry. 2003;160:183.-
36. Aboujaoude E, Barry JJ, Gamel N. Memantine augmentation in treatment-resistant obsessive-compulsive disorder: an open-label trial. J Clin Psychopharmacol. 2009;29(1):51-55.
37. Coric V, Taskiran S, Pittenger C, et al. Riluzole augmentation in treatment-resistant obsessive-compulsive disorder: an open-label trial. Biol Psychiatry. 2005;58(5):424-428.
38. Rodriguez CI, Kegeles LS, Flood P, et al. Rapid resolution of obsessions after an infusion of intravenous ketamine in a patient with treatment-resistant obsessive-compulsive disorder. J Clin Psychiatry. 2011;72(4):567-569.
39. Leonard HL, Rapoport JL. Relief of obsessive-compulsive symptoms by LSD and psilocin. Am J Psychiatry. 1987;144(9):1239-1240.
40. Anand N, Sudhir PM, Math SB, et al. Cognitive behavior therapy in medication non-responders with obsessive-compulsive disorder: a prospective 1-year follow-up study. J Anxiety Disord. 2011;25(7):939-945.
41. Himle JA, Fischer DJ, Muroff JR, et al. Videoconferencing-based cognitive-behavioral therapy for obsessive-compulsive disorder. Behav Res Ther. 2006;44(12):1821-1829.
42. Kobak KA, Taylor LV, Bystritsky A, et al. St John’s wort versus placebo in obsessive-compulsive disorder: results from a double-blind study. Int Clin Psychopharmacol. 2005;20(6):299-304.
43. Sayyah M, Boostani H, Pakseresht S, et al. Comparison of Silybum marianum (L.) Gaertn. with fluoxetine in the treatment of obsessive-compulsive Disorder. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(2):362-365.
44. Sarris J, Camfield D, Berk M. Complementary medicine self-help, and lifestyle interventions for obsessive compulsive disorder (OCD) and the OCD spectrum: a systematic review. J Affect Disord. 2011 (epub ahead of print).
45. Beale MD, Kellner CH, Pritchett JT, et al. ECT for OCD. J Clin Psychiatry. 1995;56(2):81-82.
46. George MS, Ward HE Jr, Ninan PT, et al. A pilot study of vagus nerve stimulation (VNS) for treatment-resistant anxiety disorders. Brain Stimul. 2008;1(2):112-121.
47. Slotema CW, Blom JD, Hoek HW, et al. Should we expand the toolbox of psychiatric treatment methods to include repetitive transcranial magnetic stimulation (rTMS)? A meta-analysis of the efficacy of rTMS in psychiatric disorders. J Clin Psychiatry. 2010;71(7):873-884.
48. Mantovani A, Simpson HB, Fallon BA, et al. Randomized sham-controlled trial of repetitive transcranial magnetic stimulation in treatment-resistant obsessive-compulsive disorder. Int J Neuropsychopharmacol. 2010;13(2):217-227.
49. Blom RM, Figee M, Vulink N, et al. Update on repetitive transcranial magnetic stimulation in obsessive-compulsive disorder: different targets. Curr Psychiatry Rep. 2011;13(4):289-294.
50. Greenberg BD, Rauch SL, Haber SN. Invasive circuitry-based neurotherapeutics: stereotactic ablation and deep brain stimulation for OCD. Neuropsychopharmacology. 2010;35(1):317-336.
51. Nuttin B, Cosyns P, Demeulemeester H, et al. Electrical stimulation in anterior limbs of internal capsules in patients with obsessive-compulsive disorder. Lancet. 1999;354(9189):1526.-
52. de Koning PP, Figee M, van den Munckhof P, et al. Current status of deep brain stimulation for obsessive-compulsive disorder: a clinical review of different targets. Curr Psychiatry Rep. 2011;13(4):274-282.
53. Greenberg BD, Gabriels LA, Malone DA, Jr, et al. Deep brain stimulation of the ventral internal capsule/ventral striatum for obsessive-compulsive disorder: worldwide experience. Mol Psychiatry. 2010;15(1):64-79.
Hallucinations: Common features and causes
Not all patients who experience hallucinations have a psychotic disorder. Many physical and psychiatric disorders can manifest with hallucinations, and some patients have >1 disorder that could cause different types of hallucinations. To avoid providing unnecessary or ineffective treatments—and to ensure that patients receive proper care for nonpsychiatric conditions—it is important to accurately diagnose the disorder causing a patient’s hallucinations.
In this article we describe common features and psychiatric and nonpsychiatric causes of auditory, visual, olfactory, gustatory, tactile, and somatic hallucinations. Awareness of typical presentations of hallucinations associated with specific disorders can help narrow the diagnosis and provide appropriate treatment.
Auditory hallucinations
Also known as paracusia, auditory hallucinations are perceptions of sounds without identifiable external stimuli. This type of hallucination has various causes (Table 1).1 A frequent symptom of schizophrenia, auditory hallucinations can cause substantial distress and functional disability.2 Approximately 60% to 90% of patients with schizophrenia and up to 80% of those with affective psychoses experience auditory hallucinations.1
Auditory hallucinations in psychosis usually are formed and complex.3 A common manifestation is hearing ≥1 voices. A patient might experience 2 voices talking about him in the third person. The voices may be perceived as coming from inside or outside the patient’s head. Some might hear their own thoughts spoken aloud. According to DSM-IV-TR, “hearing voices” is sufficient to diagnose schizophrenia if the hallucinations consist of a voice keeping up a running commentary on the person’s behavior or ≥2 voices conversing with each other.4 Auditory hallucinations also are seen in mood disorders but tend to be milder than their psychosis-induced counterparts.
Simple (unformed) auditory hallucinations—referred to as tinnitus—can be caused by disease of the middle ear (otosclerosis) or inner ear. These unformed hallucinations consist of buzzing or tones of varying pitch and timbre.1
Partial seizures may cause auditory hallucinations. Perceptions of music have been associated with partial seizures.5 Curie and colleagues found that 17% of 514 patients with temporal lobe epilepsy had auditory hallucinations as a component of their seizures.6 These hallucinations typically are brief, stereotyped sensory impressions and, if formed, may be trivial sentences, previously heard phrases, or commands.
Alcoholic hallucinosis is a hallucinatory syndrome caused by alcohol withdrawal. These hallucinations usually are vocal and typically consist of accusatory, threatening, and/or critical voices directed at the patient.1 Patients with alcohol hallucinosis also may experience musical auditory hallucinations.7,8
CNS neoplasms can produce auditory hallucinations in 3% to 10% of patients.9 Hemorrhages and arteriovenous malformations in the pontine tegmentum and lower midbrain have been associated with acute onset of auditory hallucinations. The sounds typically are unformed mechanical or seashell-like noises or music.10
Patients with migraines rarely report auditory hallucinations. When they occur, they typically consist of perceived unilateral tinnitus, phonophobia, or hearing loss.
Table 1
Common causes of auditory hallucinations
| Peripheral lesions |
| Middle ear disease |
| Inner ear disease |
| Auditory nerve disease |
| CNS disorders |
| Temporal lobe epilepsy |
| Pontine lesions |
| Stroke |
| Arteriovenous malformations |
| Syncope |
| Toxic metabolic disturbances |
| Alcoholic hallucinosis |
| Delirium |
| Hallucinogens |
| Schizophrenia |
| Mania |
| Psychotic depression |
| Dissociative identity disorder |
| Posttraumatic stress disorder |
| Source: Reference 1 |
Visual hallucinations
Visual hallucinations manifest as visual sensory perceptions in the absence of external stimuli.11 These false perceptions may consist of formed images (eg, people) or unformed images (eg, flashes of light).12 Visual hallucinations occur in numerous ophthalmologic, neurologic, medical, and psychiatric disorders (Table 2).13
DSM-IV-TR lists visual hallucinations as a primary diagnostic criterion for several psychotic disorders, including schizophrenia and schizoaffective disorder,4 and they occur in 16% to 72% of patients with these conditions.14,15 Patients with major depressive disorder or bipolar disorder also may experience visual hallucinations. Visual hallucinations in those with schizophrenia tend to involve vivid scenes with family members, religious figures, and/or animals.16
Delirium is a transient, reversible cause of cerebral dysfunction that often presents with hallucinations. Several studies have shown that visual hallucinations are the most common type among patients with delirium. Webster and Holroyd found visual hallucinations in 27% of 227 delirium patients.17
Delirium tremens typically is accompanied by visual hallucinations. Visions of small animals and crawling insects are common.18 Hallucinations due to drug intoxication or withdrawal generally vary in duration from brief to continuous; such experiences often contribute to agitation.19
Migraines are a well-recognized cause of visual hallucinations. Up to 31% of those with migraines experience an aura, and nearly 99% of those with aura have visual symptoms.20,21 The classic visual aura starts as an irregular colored crescent of light with multi-colored edges in the center of the visual field that gradually progresses toward the periphery, lasting <60 minutes. These simple visual hallucinations are most common; more complex hallucinations are seen more frequently in migraine coma and familial hemiplegic migraine.
Approximately 5% of patients with epilepsy have occipital seizures, which almost always have visual manifestations. Epileptic visual hallucinations often are simple, brief, stereotyped, and fragmentary. They usually consist of small, brightly colored spots or shapes that flash.22 Complex visual hallucinations in epilepsy are similar to hypnagogic hallucinations but are rare. Intracranial electroencephalography recordings have shown that pathological excitation of visual cortical areas may be responsible for complex visual hallucinations in epilepsy.19
Dementia with Lewy bodies (DLB) is associated with visual hallucinations.23 Visual hallucinations occur in >20% of patients with DLB.24 Patients with DLB may see complex scenarios of people and items that are not present. Visual hallucinations have an 83% positive predictive value for distinguishing DLB from dementia of the Alzheimer’s type.25 There is a strong correlation between Lewy bodies located in the amygdala and parahippocampus and well-formed visual hallucinations.26
Visual hallucinations are common in Parkinson’s disease and may occur in up to one-half of patients.27 Patients with Parkinson’s disease may experience hallucinations similar to those observed in DLB, which can range from seeing a person or animal to more complex, formed, and mobile people, animals, or objects.
Table 2
Common causes of visual hallucinations
| Neurologic disorders |
| Migraine |
| Epilepsy |
| Hemispheric lesions |
| Optic nerve disorders |
| Brain stem lesions (peduncular hallucinosis) |
| Narcolepsy |
| Ophthalmologic diseases |
| Glaucoma |
| Retinal disease |
| Enucleation |
| Cataract formation |
| Choroidal disorder |
| Macular abnormalities |
| Toxic and metabolic conditions |
| Toxic-metabolic encephalopathy |
| Drug and alcohol withdrawal syndromes |
| Hallucinogens |
| Schizophrenia |
| Affective disorders |
| Conversion disorders |
| Sensory deprivation |
| Sleep deprivation |
| Hypnosis |
| Intense emotional experiences |
| Source: Reference 13 |
Olfactory hallucinations
Also known as phantosmia, olfactory hallucinations involve smelling odors that are not derived from any physical stimulus. They can occur with several psychiatric conditions, including schizophrenia, depression, bipolar disorder, eating disorders, and substance abuse.28 Olfactory hallucinations caused by epileptic activity are rare. They constitute approximately 0.9% of all auras and typically are described as unpleasant. Tumors that affect the medial temporal lobe and mesial temporal sclerosis are associated with olfactory hallucinations.29 Olfactory hallucinations also have been reported in patients with multi-infarct dementia, Alzheimer’s disease, and alcoholic psychosyndromes. In patients with schizophrenia, the smell may be perceived as coming from an external source, whereas patients with depression may perceive the source as internal.30 Patients who perceive that they are the source of an offensive odor—a condition known as olfactory reference syndrome—may wash excessively, overuse deodorants and perfumes, or become socially withdrawn.30
Gustatory hallucinations
Patients with gustatory hallucinations may experience salivation, sensation of thirst, or taste alterations. These hallucinations can be observed when the sylvian fissure that extends to the insula is stimulated electrically.31 Similar to olfactory hallucinations, gustatory hallucinations are associated with temporal lobe disease and parietal operculum lesions.31,32 Sinus diseases have been associated with olfactory and gustatory hallucinations.33 Brief gustatory hallucinations can be elicited with stimulation of the right rolandic operculum, parietal operculum, amygdala, hippocampus, medial temporal gyrus, and anterior part of right temporal gyrus.34
Tactile hallucinations
These hallucinations may include perceptions of insects crawling over or under the skin (formication) or simulation of pressure on skin.35 They have been associated with substance abuse, toxicity, or withdrawal.28 Tactile hallucinations are characteristic of cocaine or amphetamine intoxication.35
Tactile hallucinations are a rare symptom of schizophrenia. Heveling and colleagues reported a case of a woman, age 68, with chronic schizophrenia who experienced touching and being touched by a “shadow man” several times a day in addition to auditory and visual hallucinations.36 Her symptoms disappeared after 4 weeks of antipsychotic and mood stabilizer therapy.
Tactile hallucinations have been associated with obsessive-compulsive disorder (OCD).37 Fontenelle and colleagues suggested that OCD and psychotic disorders may share dysfunctional dopaminergic circuits.37
Somatic hallucinations
Patients who have somatic hallucinations report perceptions of abnormal body sensations or physical experiences. For example, a patient may have sense of not having a stomach while eating.35
This type of hallucination has been associated with activation of postcentral gyrus, parietal operculum, insula, and inferior parietal lobule on stereoelectroencephalography.34 In a study of cerebral blood flow in 20 geriatric patients with delusional disorder, somatic type who were experiencing somatic hallucinations, positron emission testing scan demonstrated increased perfusion in somatic sensory processing regions, particularly the left postcentral gyrus and the right paracentral lobule.38 Other researchers have linked somatic hallucinations with activation in the primary somatosensory and posterior parietal cortex, areas that normally mediate tactile perception.39
Related Resource
- Teeple RC, Caplan JP, Stern TA. Visual hallucinations: differential diagnosis and treatment. Prim Care Companion J Clin Psychiatry. 2009;11(1):26-32.
Disclosures
Drs. Ali, Patel, Avenido, Bailey, and Jabeen report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Riley is on the board of directors for Vertex Pharmaceuticals.
Acknowledgment
The authors would like to thank Marwah Shahid, Research Associate, Vanderbilt University, Nashville, TN.
1. Cummings JL, Mega MS. Hallucinations. In: Cummings JL Mega MS, eds. Neuropsychiatry and behavioral neuroscience. New York, NY: Oxford University Press; 2003: 187–199.
2. Shergill SS, Murray RM, McGuire PK. Auditory hallucinations: a review of psychological treatments. Schizophr Res. 1998;32(3):137-150.
3. Goodwin DW, Alderson P, Rosenthal R. Clinical significance of hallucinations in psychiatric disorders. A study of 116 hallucinatory patients. Arch Gen Psychiatry. 1971;24(1):76-80.
4. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
5. Kasper BS, Kasper EM, Pauli E, et al. Phenomenology of hallucinations, illusions, and delusions as part of seizure semiology. Epilepsy Behav. 2010;18(1-2):13-23.
6. Currie S, Heathfield KW, Henson RA, et al. Clinical course and prognosis of temporal lobe epilepsy. A survey of 666 patients. Brain. 1971;94(1):173-190.
7. Keshavan MS, David AS, Steingard S, et al. Musical hallucinations: a review and synthesis. Cogn Behav Neurol. 1992;5(3):211-223.
8. Duncan R, Mitchell JD, Critchley EMR. Hallucinations and music. Behav Neurol. 1989;2(2):115-124.
9. Tarachow S. The clinical value of hallucinations in localizing brain tumors. Am J Psychiatry. 1941;97:1434-1442.
10. Lanska DJ, Lanska MJ, Mendez MF. Brainstem auditory hallucinosis. Neurology. 1987;37(10):1685.-
11. Norton JW, Corbett JJ. Visual perceptual abnormalities: hallucinations and illusions. Semin Neurol. 2000;20(1):111-121.
12. Kaplan HI, Sadock BJ, Grebb JA. Typical signs and symptoms of psychiatric illness defined. In: Kaplan HI Sadock BJ, Grebb JA, eds. Kaplan and Sadock’s synopsis of psychiatry: behavioral sciences, clinical psychiatry. Baltimore, MD: Williams and Wilkins; 1994:300.
13. Cummings JL, Miller BL. Visual hallucinations. Clinical occurrence and use in differential diagnosis. West J Med. 1987;146(1):46-51.
14. First MB, Tasman A. Schizophrenia and other psychoses. In: First MB Tasman A, eds. Clinical guide to the diagnosis and treatment of mental disorders. San Francisco, CA: John Wiley and Sons; 2009:245–278.
15. Mueser KT, Bellack AS, Brady EU. Hallucinations in schizophrenia. Acta Psychiatr Scand. 1990;82(1):26-29.
16. Small IF, Small JG, Andersen JM. Clinical characteristics of hallucinations of schizophrenia. Dis Nerv Syst. 1966;27(5):349-353.
17. Webster R, Holroyd S. Prevalence of psychotic symptoms in delirium. Psychosomatics. 2000;41(6):519-522.
18. Gastfriend DR, Renner JA, Hackett TP. Alcoholic patients: acute and chronic. In: Stern TA Fricchione G, Cassem NH, et al, eds. Massachusetts General Hospital handbook of general hospital psychiatry. 5th ed. Philadelphia, PA: Mosby; 2004:203–216.
19. Manford M, Andermann F. Complex visual hallucinations. Clinical and neurobiological insights. Brain. 1998;121(Pt 10):1819-1840.
20. Goadsby PJ, Lipton RB, Ferrari MD. Migraine—current understanding and treatment. N Engl J Med. 2002;346(4):257-270.
21. Russell MB, Olesen J. A nosographic analysis of the migraine aura in a general population. Brain. 1996;119(Pt 2):355-361.
22. Panayiotopoulos CP. Elementary visual hallucinations blindness, and headache in idiopathic occipital epilepsy: differentiation from migraine. J Neurol Neurosurg Psychiatry. 1999;66(4):536-540.
23. Ballard CG, O’Brien JT, Swann AG, et al. The natural history of psychosis and depression in dementia with Lewy bodies and Alzheimer’s disease: persistence and new cases over 1 year of follow-up. J Clin Psychiatry. 2001;62(1):46-49.
24. Ala TA, Yang KH, Sung JH, et al. Hallucinations and signs of parkinsonism help distinguish patients with dementia and cortical Lewy bodies from patients with Alzheimer’s disease at presentation: a clinicopathological study. J Neurol Neurosurg Psychiatry. 1997;62(1):16-21.
25. Tiraboschi P, Salmon DP, Hansen LA, et al. What best differentiates Lewy body from Alzheimer’s disease in early-stage dementia? Brain. 2006;129(Pt 3):729-735.
26. Harding AJ, Broe GA, Halliday GM. Visual hallucinations in Lewy body disease relate to Lewy bodies in the temporal lobe. Brain. 2002;125(Pt 2):391-403.
27. Williams DR, Lees AJ. Visual hallucinations in the diagnosis of idiopathic Parkinson’s disease: a retrospective autopsy study. Lancet Neurol. 2005;4(10):605-610.
28. Lewandowski KE, DePaola J, Camsari GB, et al. Tactile, olfactory, and gustatory hallucinations in psychotic disorders: a descriptive study. Ann Acad Med Singapore. 2009;38(5):383-385.
29. Acharya V, Acharya J, Lüders H. Olfactory epileptic auras. Neurology. 1998;51(1):56-61.
30. Ropper AH, Samuels MA. Disorders of smell and taste. In: Ropper AH Samuels MA, eds. Adams and Victor’s principles of neurology. 9th ed. New York, NY: McGraw-Hill Companies; 2009:216–224.
31. Ropper AH, Samuels MA. Epilepsy and other seizure disorders. In: Ropper AH Samuels MA, eds. Adams and Victor’s principles of neurology. 9th ed. New York, NY: McGraw-Hill Companies; 2009:304–338.
32. Capampangan DJ, Hoerth MT, Drazkowski JF, et al. Olfactory and gustatory hallucinations presenting as partial status epilepticus because of glioblastoma multiforme. Ann Emerg Med. 2010;56(4):374-377.
33. Frasnelli J, Reden J, Landis BN, et al. Comment on “Olfactory hallucinations as a manifestation of hidden rhinosinusitis”. J Clin Neurosci. 2010;17(4):543.-
34. Elliott B, Joyce E, Shorvon S. Delusions illusions and hallucinations in epilepsy: 1. Elementary phenomena. Epilepsy Res. 2009;85(2-3):162-171.
35. Nurcombe B, Ebert MH. The psychiatric interview. In: Ebert MH Nurcombe B, Loosen PT, et al, eds. Current diagnosis and treatment: psychiatry. 2nd ed. New York, NY: McGraw-Hill Companies; 2008:95–114.
36. Heveling T, Emrich HM, Dietrich DE. Treatment of a rare psychopathological phenomenon: tactile hallucinations and the delusional other. Eur Psychiatry. 2004;19(6):387-388.
37. Fontenelle LF, Lopes AP, Borges MC, et al. Auditory, visual, tactile, olfactory, and bodily hallucinations in patients with obsessive-compulsive disorder. CNS Spectr. 2008;13(2):125-130.
38. Nemoto K, Mizukami K, Hori T, et al. Hyperperfusion in primary somatosensory region related to somatic hallucination in the elderly. Psychiatry Clin Neurosci. 2010;64(4):421-425.
39. Shergill SS, Cameron LA, Brammer MJ, et al. Modality specific neural correlates of auditory and somatic hallucinations. J Neurol Neurosurg Psychiatry. 2001;71(5):688-690.
Not all patients who experience hallucinations have a psychotic disorder. Many physical and psychiatric disorders can manifest with hallucinations, and some patients have >1 disorder that could cause different types of hallucinations. To avoid providing unnecessary or ineffective treatments—and to ensure that patients receive proper care for nonpsychiatric conditions—it is important to accurately diagnose the disorder causing a patient’s hallucinations.
In this article we describe common features and psychiatric and nonpsychiatric causes of auditory, visual, olfactory, gustatory, tactile, and somatic hallucinations. Awareness of typical presentations of hallucinations associated with specific disorders can help narrow the diagnosis and provide appropriate treatment.
Auditory hallucinations
Also known as paracusia, auditory hallucinations are perceptions of sounds without identifiable external stimuli. This type of hallucination has various causes (Table 1).1 A frequent symptom of schizophrenia, auditory hallucinations can cause substantial distress and functional disability.2 Approximately 60% to 90% of patients with schizophrenia and up to 80% of those with affective psychoses experience auditory hallucinations.1
Auditory hallucinations in psychosis usually are formed and complex.3 A common manifestation is hearing ≥1 voices. A patient might experience 2 voices talking about him in the third person. The voices may be perceived as coming from inside or outside the patient’s head. Some might hear their own thoughts spoken aloud. According to DSM-IV-TR, “hearing voices” is sufficient to diagnose schizophrenia if the hallucinations consist of a voice keeping up a running commentary on the person’s behavior or ≥2 voices conversing with each other.4 Auditory hallucinations also are seen in mood disorders but tend to be milder than their psychosis-induced counterparts.
Simple (unformed) auditory hallucinations—referred to as tinnitus—can be caused by disease of the middle ear (otosclerosis) or inner ear. These unformed hallucinations consist of buzzing or tones of varying pitch and timbre.1
Partial seizures may cause auditory hallucinations. Perceptions of music have been associated with partial seizures.5 Curie and colleagues found that 17% of 514 patients with temporal lobe epilepsy had auditory hallucinations as a component of their seizures.6 These hallucinations typically are brief, stereotyped sensory impressions and, if formed, may be trivial sentences, previously heard phrases, or commands.
Alcoholic hallucinosis is a hallucinatory syndrome caused by alcohol withdrawal. These hallucinations usually are vocal and typically consist of accusatory, threatening, and/or critical voices directed at the patient.1 Patients with alcohol hallucinosis also may experience musical auditory hallucinations.7,8
CNS neoplasms can produce auditory hallucinations in 3% to 10% of patients.9 Hemorrhages and arteriovenous malformations in the pontine tegmentum and lower midbrain have been associated with acute onset of auditory hallucinations. The sounds typically are unformed mechanical or seashell-like noises or music.10
Patients with migraines rarely report auditory hallucinations. When they occur, they typically consist of perceived unilateral tinnitus, phonophobia, or hearing loss.
Table 1
Common causes of auditory hallucinations
| Peripheral lesions |
| Middle ear disease |
| Inner ear disease |
| Auditory nerve disease |
| CNS disorders |
| Temporal lobe epilepsy |
| Pontine lesions |
| Stroke |
| Arteriovenous malformations |
| Syncope |
| Toxic metabolic disturbances |
| Alcoholic hallucinosis |
| Delirium |
| Hallucinogens |
| Schizophrenia |
| Mania |
| Psychotic depression |
| Dissociative identity disorder |
| Posttraumatic stress disorder |
| Source: Reference 1 |
Visual hallucinations
Visual hallucinations manifest as visual sensory perceptions in the absence of external stimuli.11 These false perceptions may consist of formed images (eg, people) or unformed images (eg, flashes of light).12 Visual hallucinations occur in numerous ophthalmologic, neurologic, medical, and psychiatric disorders (Table 2).13
DSM-IV-TR lists visual hallucinations as a primary diagnostic criterion for several psychotic disorders, including schizophrenia and schizoaffective disorder,4 and they occur in 16% to 72% of patients with these conditions.14,15 Patients with major depressive disorder or bipolar disorder also may experience visual hallucinations. Visual hallucinations in those with schizophrenia tend to involve vivid scenes with family members, religious figures, and/or animals.16
Delirium is a transient, reversible cause of cerebral dysfunction that often presents with hallucinations. Several studies have shown that visual hallucinations are the most common type among patients with delirium. Webster and Holroyd found visual hallucinations in 27% of 227 delirium patients.17
Delirium tremens typically is accompanied by visual hallucinations. Visions of small animals and crawling insects are common.18 Hallucinations due to drug intoxication or withdrawal generally vary in duration from brief to continuous; such experiences often contribute to agitation.19
Migraines are a well-recognized cause of visual hallucinations. Up to 31% of those with migraines experience an aura, and nearly 99% of those with aura have visual symptoms.20,21 The classic visual aura starts as an irregular colored crescent of light with multi-colored edges in the center of the visual field that gradually progresses toward the periphery, lasting <60 minutes. These simple visual hallucinations are most common; more complex hallucinations are seen more frequently in migraine coma and familial hemiplegic migraine.
Approximately 5% of patients with epilepsy have occipital seizures, which almost always have visual manifestations. Epileptic visual hallucinations often are simple, brief, stereotyped, and fragmentary. They usually consist of small, brightly colored spots or shapes that flash.22 Complex visual hallucinations in epilepsy are similar to hypnagogic hallucinations but are rare. Intracranial electroencephalography recordings have shown that pathological excitation of visual cortical areas may be responsible for complex visual hallucinations in epilepsy.19
Dementia with Lewy bodies (DLB) is associated with visual hallucinations.23 Visual hallucinations occur in >20% of patients with DLB.24 Patients with DLB may see complex scenarios of people and items that are not present. Visual hallucinations have an 83% positive predictive value for distinguishing DLB from dementia of the Alzheimer’s type.25 There is a strong correlation between Lewy bodies located in the amygdala and parahippocampus and well-formed visual hallucinations.26
Visual hallucinations are common in Parkinson’s disease and may occur in up to one-half of patients.27 Patients with Parkinson’s disease may experience hallucinations similar to those observed in DLB, which can range from seeing a person or animal to more complex, formed, and mobile people, animals, or objects.
Table 2
Common causes of visual hallucinations
| Neurologic disorders |
| Migraine |
| Epilepsy |
| Hemispheric lesions |
| Optic nerve disorders |
| Brain stem lesions (peduncular hallucinosis) |
| Narcolepsy |
| Ophthalmologic diseases |
| Glaucoma |
| Retinal disease |
| Enucleation |
| Cataract formation |
| Choroidal disorder |
| Macular abnormalities |
| Toxic and metabolic conditions |
| Toxic-metabolic encephalopathy |
| Drug and alcohol withdrawal syndromes |
| Hallucinogens |
| Schizophrenia |
| Affective disorders |
| Conversion disorders |
| Sensory deprivation |
| Sleep deprivation |
| Hypnosis |
| Intense emotional experiences |
| Source: Reference 13 |
Olfactory hallucinations
Also known as phantosmia, olfactory hallucinations involve smelling odors that are not derived from any physical stimulus. They can occur with several psychiatric conditions, including schizophrenia, depression, bipolar disorder, eating disorders, and substance abuse.28 Olfactory hallucinations caused by epileptic activity are rare. They constitute approximately 0.9% of all auras and typically are described as unpleasant. Tumors that affect the medial temporal lobe and mesial temporal sclerosis are associated with olfactory hallucinations.29 Olfactory hallucinations also have been reported in patients with multi-infarct dementia, Alzheimer’s disease, and alcoholic psychosyndromes. In patients with schizophrenia, the smell may be perceived as coming from an external source, whereas patients with depression may perceive the source as internal.30 Patients who perceive that they are the source of an offensive odor—a condition known as olfactory reference syndrome—may wash excessively, overuse deodorants and perfumes, or become socially withdrawn.30
Gustatory hallucinations
Patients with gustatory hallucinations may experience salivation, sensation of thirst, or taste alterations. These hallucinations can be observed when the sylvian fissure that extends to the insula is stimulated electrically.31 Similar to olfactory hallucinations, gustatory hallucinations are associated with temporal lobe disease and parietal operculum lesions.31,32 Sinus diseases have been associated with olfactory and gustatory hallucinations.33 Brief gustatory hallucinations can be elicited with stimulation of the right rolandic operculum, parietal operculum, amygdala, hippocampus, medial temporal gyrus, and anterior part of right temporal gyrus.34
Tactile hallucinations
These hallucinations may include perceptions of insects crawling over or under the skin (formication) or simulation of pressure on skin.35 They have been associated with substance abuse, toxicity, or withdrawal.28 Tactile hallucinations are characteristic of cocaine or amphetamine intoxication.35
Tactile hallucinations are a rare symptom of schizophrenia. Heveling and colleagues reported a case of a woman, age 68, with chronic schizophrenia who experienced touching and being touched by a “shadow man” several times a day in addition to auditory and visual hallucinations.36 Her symptoms disappeared after 4 weeks of antipsychotic and mood stabilizer therapy.
Tactile hallucinations have been associated with obsessive-compulsive disorder (OCD).37 Fontenelle and colleagues suggested that OCD and psychotic disorders may share dysfunctional dopaminergic circuits.37
Somatic hallucinations
Patients who have somatic hallucinations report perceptions of abnormal body sensations or physical experiences. For example, a patient may have sense of not having a stomach while eating.35
This type of hallucination has been associated with activation of postcentral gyrus, parietal operculum, insula, and inferior parietal lobule on stereoelectroencephalography.34 In a study of cerebral blood flow in 20 geriatric patients with delusional disorder, somatic type who were experiencing somatic hallucinations, positron emission testing scan demonstrated increased perfusion in somatic sensory processing regions, particularly the left postcentral gyrus and the right paracentral lobule.38 Other researchers have linked somatic hallucinations with activation in the primary somatosensory and posterior parietal cortex, areas that normally mediate tactile perception.39
Related Resource
- Teeple RC, Caplan JP, Stern TA. Visual hallucinations: differential diagnosis and treatment. Prim Care Companion J Clin Psychiatry. 2009;11(1):26-32.
Disclosures
Drs. Ali, Patel, Avenido, Bailey, and Jabeen report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Riley is on the board of directors for Vertex Pharmaceuticals.
Acknowledgment
The authors would like to thank Marwah Shahid, Research Associate, Vanderbilt University, Nashville, TN.
Not all patients who experience hallucinations have a psychotic disorder. Many physical and psychiatric disorders can manifest with hallucinations, and some patients have >1 disorder that could cause different types of hallucinations. To avoid providing unnecessary or ineffective treatments—and to ensure that patients receive proper care for nonpsychiatric conditions—it is important to accurately diagnose the disorder causing a patient’s hallucinations.
In this article we describe common features and psychiatric and nonpsychiatric causes of auditory, visual, olfactory, gustatory, tactile, and somatic hallucinations. Awareness of typical presentations of hallucinations associated with specific disorders can help narrow the diagnosis and provide appropriate treatment.
Auditory hallucinations
Also known as paracusia, auditory hallucinations are perceptions of sounds without identifiable external stimuli. This type of hallucination has various causes (Table 1).1 A frequent symptom of schizophrenia, auditory hallucinations can cause substantial distress and functional disability.2 Approximately 60% to 90% of patients with schizophrenia and up to 80% of those with affective psychoses experience auditory hallucinations.1
Auditory hallucinations in psychosis usually are formed and complex.3 A common manifestation is hearing ≥1 voices. A patient might experience 2 voices talking about him in the third person. The voices may be perceived as coming from inside or outside the patient’s head. Some might hear their own thoughts spoken aloud. According to DSM-IV-TR, “hearing voices” is sufficient to diagnose schizophrenia if the hallucinations consist of a voice keeping up a running commentary on the person’s behavior or ≥2 voices conversing with each other.4 Auditory hallucinations also are seen in mood disorders but tend to be milder than their psychosis-induced counterparts.
Simple (unformed) auditory hallucinations—referred to as tinnitus—can be caused by disease of the middle ear (otosclerosis) or inner ear. These unformed hallucinations consist of buzzing or tones of varying pitch and timbre.1
Partial seizures may cause auditory hallucinations. Perceptions of music have been associated with partial seizures.5 Curie and colleagues found that 17% of 514 patients with temporal lobe epilepsy had auditory hallucinations as a component of their seizures.6 These hallucinations typically are brief, stereotyped sensory impressions and, if formed, may be trivial sentences, previously heard phrases, or commands.
Alcoholic hallucinosis is a hallucinatory syndrome caused by alcohol withdrawal. These hallucinations usually are vocal and typically consist of accusatory, threatening, and/or critical voices directed at the patient.1 Patients with alcohol hallucinosis also may experience musical auditory hallucinations.7,8
CNS neoplasms can produce auditory hallucinations in 3% to 10% of patients.9 Hemorrhages and arteriovenous malformations in the pontine tegmentum and lower midbrain have been associated with acute onset of auditory hallucinations. The sounds typically are unformed mechanical or seashell-like noises or music.10
Patients with migraines rarely report auditory hallucinations. When they occur, they typically consist of perceived unilateral tinnitus, phonophobia, or hearing loss.
Table 1
Common causes of auditory hallucinations
| Peripheral lesions |
| Middle ear disease |
| Inner ear disease |
| Auditory nerve disease |
| CNS disorders |
| Temporal lobe epilepsy |
| Pontine lesions |
| Stroke |
| Arteriovenous malformations |
| Syncope |
| Toxic metabolic disturbances |
| Alcoholic hallucinosis |
| Delirium |
| Hallucinogens |
| Schizophrenia |
| Mania |
| Psychotic depression |
| Dissociative identity disorder |
| Posttraumatic stress disorder |
| Source: Reference 1 |
Visual hallucinations
Visual hallucinations manifest as visual sensory perceptions in the absence of external stimuli.11 These false perceptions may consist of formed images (eg, people) or unformed images (eg, flashes of light).12 Visual hallucinations occur in numerous ophthalmologic, neurologic, medical, and psychiatric disorders (Table 2).13
DSM-IV-TR lists visual hallucinations as a primary diagnostic criterion for several psychotic disorders, including schizophrenia and schizoaffective disorder,4 and they occur in 16% to 72% of patients with these conditions.14,15 Patients with major depressive disorder or bipolar disorder also may experience visual hallucinations. Visual hallucinations in those with schizophrenia tend to involve vivid scenes with family members, religious figures, and/or animals.16
Delirium is a transient, reversible cause of cerebral dysfunction that often presents with hallucinations. Several studies have shown that visual hallucinations are the most common type among patients with delirium. Webster and Holroyd found visual hallucinations in 27% of 227 delirium patients.17
Delirium tremens typically is accompanied by visual hallucinations. Visions of small animals and crawling insects are common.18 Hallucinations due to drug intoxication or withdrawal generally vary in duration from brief to continuous; such experiences often contribute to agitation.19
Migraines are a well-recognized cause of visual hallucinations. Up to 31% of those with migraines experience an aura, and nearly 99% of those with aura have visual symptoms.20,21 The classic visual aura starts as an irregular colored crescent of light with multi-colored edges in the center of the visual field that gradually progresses toward the periphery, lasting <60 minutes. These simple visual hallucinations are most common; more complex hallucinations are seen more frequently in migraine coma and familial hemiplegic migraine.
Approximately 5% of patients with epilepsy have occipital seizures, which almost always have visual manifestations. Epileptic visual hallucinations often are simple, brief, stereotyped, and fragmentary. They usually consist of small, brightly colored spots or shapes that flash.22 Complex visual hallucinations in epilepsy are similar to hypnagogic hallucinations but are rare. Intracranial electroencephalography recordings have shown that pathological excitation of visual cortical areas may be responsible for complex visual hallucinations in epilepsy.19
Dementia with Lewy bodies (DLB) is associated with visual hallucinations.23 Visual hallucinations occur in >20% of patients with DLB.24 Patients with DLB may see complex scenarios of people and items that are not present. Visual hallucinations have an 83% positive predictive value for distinguishing DLB from dementia of the Alzheimer’s type.25 There is a strong correlation between Lewy bodies located in the amygdala and parahippocampus and well-formed visual hallucinations.26
Visual hallucinations are common in Parkinson’s disease and may occur in up to one-half of patients.27 Patients with Parkinson’s disease may experience hallucinations similar to those observed in DLB, which can range from seeing a person or animal to more complex, formed, and mobile people, animals, or objects.
Table 2
Common causes of visual hallucinations
| Neurologic disorders |
| Migraine |
| Epilepsy |
| Hemispheric lesions |
| Optic nerve disorders |
| Brain stem lesions (peduncular hallucinosis) |
| Narcolepsy |
| Ophthalmologic diseases |
| Glaucoma |
| Retinal disease |
| Enucleation |
| Cataract formation |
| Choroidal disorder |
| Macular abnormalities |
| Toxic and metabolic conditions |
| Toxic-metabolic encephalopathy |
| Drug and alcohol withdrawal syndromes |
| Hallucinogens |
| Schizophrenia |
| Affective disorders |
| Conversion disorders |
| Sensory deprivation |
| Sleep deprivation |
| Hypnosis |
| Intense emotional experiences |
| Source: Reference 13 |
Olfactory hallucinations
Also known as phantosmia, olfactory hallucinations involve smelling odors that are not derived from any physical stimulus. They can occur with several psychiatric conditions, including schizophrenia, depression, bipolar disorder, eating disorders, and substance abuse.28 Olfactory hallucinations caused by epileptic activity are rare. They constitute approximately 0.9% of all auras and typically are described as unpleasant. Tumors that affect the medial temporal lobe and mesial temporal sclerosis are associated with olfactory hallucinations.29 Olfactory hallucinations also have been reported in patients with multi-infarct dementia, Alzheimer’s disease, and alcoholic psychosyndromes. In patients with schizophrenia, the smell may be perceived as coming from an external source, whereas patients with depression may perceive the source as internal.30 Patients who perceive that they are the source of an offensive odor—a condition known as olfactory reference syndrome—may wash excessively, overuse deodorants and perfumes, or become socially withdrawn.30
Gustatory hallucinations
Patients with gustatory hallucinations may experience salivation, sensation of thirst, or taste alterations. These hallucinations can be observed when the sylvian fissure that extends to the insula is stimulated electrically.31 Similar to olfactory hallucinations, gustatory hallucinations are associated with temporal lobe disease and parietal operculum lesions.31,32 Sinus diseases have been associated with olfactory and gustatory hallucinations.33 Brief gustatory hallucinations can be elicited with stimulation of the right rolandic operculum, parietal operculum, amygdala, hippocampus, medial temporal gyrus, and anterior part of right temporal gyrus.34
Tactile hallucinations
These hallucinations may include perceptions of insects crawling over or under the skin (formication) or simulation of pressure on skin.35 They have been associated with substance abuse, toxicity, or withdrawal.28 Tactile hallucinations are characteristic of cocaine or amphetamine intoxication.35
Tactile hallucinations are a rare symptom of schizophrenia. Heveling and colleagues reported a case of a woman, age 68, with chronic schizophrenia who experienced touching and being touched by a “shadow man” several times a day in addition to auditory and visual hallucinations.36 Her symptoms disappeared after 4 weeks of antipsychotic and mood stabilizer therapy.
Tactile hallucinations have been associated with obsessive-compulsive disorder (OCD).37 Fontenelle and colleagues suggested that OCD and psychotic disorders may share dysfunctional dopaminergic circuits.37
Somatic hallucinations
Patients who have somatic hallucinations report perceptions of abnormal body sensations or physical experiences. For example, a patient may have sense of not having a stomach while eating.35
This type of hallucination has been associated with activation of postcentral gyrus, parietal operculum, insula, and inferior parietal lobule on stereoelectroencephalography.34 In a study of cerebral blood flow in 20 geriatric patients with delusional disorder, somatic type who were experiencing somatic hallucinations, positron emission testing scan demonstrated increased perfusion in somatic sensory processing regions, particularly the left postcentral gyrus and the right paracentral lobule.38 Other researchers have linked somatic hallucinations with activation in the primary somatosensory and posterior parietal cortex, areas that normally mediate tactile perception.39
Related Resource
- Teeple RC, Caplan JP, Stern TA. Visual hallucinations: differential diagnosis and treatment. Prim Care Companion J Clin Psychiatry. 2009;11(1):26-32.
Disclosures
Drs. Ali, Patel, Avenido, Bailey, and Jabeen report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Riley is on the board of directors for Vertex Pharmaceuticals.
Acknowledgment
The authors would like to thank Marwah Shahid, Research Associate, Vanderbilt University, Nashville, TN.
1. Cummings JL, Mega MS. Hallucinations. In: Cummings JL Mega MS, eds. Neuropsychiatry and behavioral neuroscience. New York, NY: Oxford University Press; 2003: 187–199.
2. Shergill SS, Murray RM, McGuire PK. Auditory hallucinations: a review of psychological treatments. Schizophr Res. 1998;32(3):137-150.
3. Goodwin DW, Alderson P, Rosenthal R. Clinical significance of hallucinations in psychiatric disorders. A study of 116 hallucinatory patients. Arch Gen Psychiatry. 1971;24(1):76-80.
4. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
5. Kasper BS, Kasper EM, Pauli E, et al. Phenomenology of hallucinations, illusions, and delusions as part of seizure semiology. Epilepsy Behav. 2010;18(1-2):13-23.
6. Currie S, Heathfield KW, Henson RA, et al. Clinical course and prognosis of temporal lobe epilepsy. A survey of 666 patients. Brain. 1971;94(1):173-190.
7. Keshavan MS, David AS, Steingard S, et al. Musical hallucinations: a review and synthesis. Cogn Behav Neurol. 1992;5(3):211-223.
8. Duncan R, Mitchell JD, Critchley EMR. Hallucinations and music. Behav Neurol. 1989;2(2):115-124.
9. Tarachow S. The clinical value of hallucinations in localizing brain tumors. Am J Psychiatry. 1941;97:1434-1442.
10. Lanska DJ, Lanska MJ, Mendez MF. Brainstem auditory hallucinosis. Neurology. 1987;37(10):1685.-
11. Norton JW, Corbett JJ. Visual perceptual abnormalities: hallucinations and illusions. Semin Neurol. 2000;20(1):111-121.
12. Kaplan HI, Sadock BJ, Grebb JA. Typical signs and symptoms of psychiatric illness defined. In: Kaplan HI Sadock BJ, Grebb JA, eds. Kaplan and Sadock’s synopsis of psychiatry: behavioral sciences, clinical psychiatry. Baltimore, MD: Williams and Wilkins; 1994:300.
13. Cummings JL, Miller BL. Visual hallucinations. Clinical occurrence and use in differential diagnosis. West J Med. 1987;146(1):46-51.
14. First MB, Tasman A. Schizophrenia and other psychoses. In: First MB Tasman A, eds. Clinical guide to the diagnosis and treatment of mental disorders. San Francisco, CA: John Wiley and Sons; 2009:245–278.
15. Mueser KT, Bellack AS, Brady EU. Hallucinations in schizophrenia. Acta Psychiatr Scand. 1990;82(1):26-29.
16. Small IF, Small JG, Andersen JM. Clinical characteristics of hallucinations of schizophrenia. Dis Nerv Syst. 1966;27(5):349-353.
17. Webster R, Holroyd S. Prevalence of psychotic symptoms in delirium. Psychosomatics. 2000;41(6):519-522.
18. Gastfriend DR, Renner JA, Hackett TP. Alcoholic patients: acute and chronic. In: Stern TA Fricchione G, Cassem NH, et al, eds. Massachusetts General Hospital handbook of general hospital psychiatry. 5th ed. Philadelphia, PA: Mosby; 2004:203–216.
19. Manford M, Andermann F. Complex visual hallucinations. Clinical and neurobiological insights. Brain. 1998;121(Pt 10):1819-1840.
20. Goadsby PJ, Lipton RB, Ferrari MD. Migraine—current understanding and treatment. N Engl J Med. 2002;346(4):257-270.
21. Russell MB, Olesen J. A nosographic analysis of the migraine aura in a general population. Brain. 1996;119(Pt 2):355-361.
22. Panayiotopoulos CP. Elementary visual hallucinations blindness, and headache in idiopathic occipital epilepsy: differentiation from migraine. J Neurol Neurosurg Psychiatry. 1999;66(4):536-540.
23. Ballard CG, O’Brien JT, Swann AG, et al. The natural history of psychosis and depression in dementia with Lewy bodies and Alzheimer’s disease: persistence and new cases over 1 year of follow-up. J Clin Psychiatry. 2001;62(1):46-49.
24. Ala TA, Yang KH, Sung JH, et al. Hallucinations and signs of parkinsonism help distinguish patients with dementia and cortical Lewy bodies from patients with Alzheimer’s disease at presentation: a clinicopathological study. J Neurol Neurosurg Psychiatry. 1997;62(1):16-21.
25. Tiraboschi P, Salmon DP, Hansen LA, et al. What best differentiates Lewy body from Alzheimer’s disease in early-stage dementia? Brain. 2006;129(Pt 3):729-735.
26. Harding AJ, Broe GA, Halliday GM. Visual hallucinations in Lewy body disease relate to Lewy bodies in the temporal lobe. Brain. 2002;125(Pt 2):391-403.
27. Williams DR, Lees AJ. Visual hallucinations in the diagnosis of idiopathic Parkinson’s disease: a retrospective autopsy study. Lancet Neurol. 2005;4(10):605-610.
28. Lewandowski KE, DePaola J, Camsari GB, et al. Tactile, olfactory, and gustatory hallucinations in psychotic disorders: a descriptive study. Ann Acad Med Singapore. 2009;38(5):383-385.
29. Acharya V, Acharya J, Lüders H. Olfactory epileptic auras. Neurology. 1998;51(1):56-61.
30. Ropper AH, Samuels MA. Disorders of smell and taste. In: Ropper AH Samuels MA, eds. Adams and Victor’s principles of neurology. 9th ed. New York, NY: McGraw-Hill Companies; 2009:216–224.
31. Ropper AH, Samuels MA. Epilepsy and other seizure disorders. In: Ropper AH Samuels MA, eds. Adams and Victor’s principles of neurology. 9th ed. New York, NY: McGraw-Hill Companies; 2009:304–338.
32. Capampangan DJ, Hoerth MT, Drazkowski JF, et al. Olfactory and gustatory hallucinations presenting as partial status epilepticus because of glioblastoma multiforme. Ann Emerg Med. 2010;56(4):374-377.
33. Frasnelli J, Reden J, Landis BN, et al. Comment on “Olfactory hallucinations as a manifestation of hidden rhinosinusitis”. J Clin Neurosci. 2010;17(4):543.-
34. Elliott B, Joyce E, Shorvon S. Delusions illusions and hallucinations in epilepsy: 1. Elementary phenomena. Epilepsy Res. 2009;85(2-3):162-171.
35. Nurcombe B, Ebert MH. The psychiatric interview. In: Ebert MH Nurcombe B, Loosen PT, et al, eds. Current diagnosis and treatment: psychiatry. 2nd ed. New York, NY: McGraw-Hill Companies; 2008:95–114.
36. Heveling T, Emrich HM, Dietrich DE. Treatment of a rare psychopathological phenomenon: tactile hallucinations and the delusional other. Eur Psychiatry. 2004;19(6):387-388.
37. Fontenelle LF, Lopes AP, Borges MC, et al. Auditory, visual, tactile, olfactory, and bodily hallucinations in patients with obsessive-compulsive disorder. CNS Spectr. 2008;13(2):125-130.
38. Nemoto K, Mizukami K, Hori T, et al. Hyperperfusion in primary somatosensory region related to somatic hallucination in the elderly. Psychiatry Clin Neurosci. 2010;64(4):421-425.
39. Shergill SS, Cameron LA, Brammer MJ, et al. Modality specific neural correlates of auditory and somatic hallucinations. J Neurol Neurosurg Psychiatry. 2001;71(5):688-690.
1. Cummings JL, Mega MS. Hallucinations. In: Cummings JL Mega MS, eds. Neuropsychiatry and behavioral neuroscience. New York, NY: Oxford University Press; 2003: 187–199.
2. Shergill SS, Murray RM, McGuire PK. Auditory hallucinations: a review of psychological treatments. Schizophr Res. 1998;32(3):137-150.
3. Goodwin DW, Alderson P, Rosenthal R. Clinical significance of hallucinations in psychiatric disorders. A study of 116 hallucinatory patients. Arch Gen Psychiatry. 1971;24(1):76-80.
4. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington DC: American Psychiatric Association; 2000.
5. Kasper BS, Kasper EM, Pauli E, et al. Phenomenology of hallucinations, illusions, and delusions as part of seizure semiology. Epilepsy Behav. 2010;18(1-2):13-23.
6. Currie S, Heathfield KW, Henson RA, et al. Clinical course and prognosis of temporal lobe epilepsy. A survey of 666 patients. Brain. 1971;94(1):173-190.
7. Keshavan MS, David AS, Steingard S, et al. Musical hallucinations: a review and synthesis. Cogn Behav Neurol. 1992;5(3):211-223.
8. Duncan R, Mitchell JD, Critchley EMR. Hallucinations and music. Behav Neurol. 1989;2(2):115-124.
9. Tarachow S. The clinical value of hallucinations in localizing brain tumors. Am J Psychiatry. 1941;97:1434-1442.
10. Lanska DJ, Lanska MJ, Mendez MF. Brainstem auditory hallucinosis. Neurology. 1987;37(10):1685.-
11. Norton JW, Corbett JJ. Visual perceptual abnormalities: hallucinations and illusions. Semin Neurol. 2000;20(1):111-121.
12. Kaplan HI, Sadock BJ, Grebb JA. Typical signs and symptoms of psychiatric illness defined. In: Kaplan HI Sadock BJ, Grebb JA, eds. Kaplan and Sadock’s synopsis of psychiatry: behavioral sciences, clinical psychiatry. Baltimore, MD: Williams and Wilkins; 1994:300.
13. Cummings JL, Miller BL. Visual hallucinations. Clinical occurrence and use in differential diagnosis. West J Med. 1987;146(1):46-51.
14. First MB, Tasman A. Schizophrenia and other psychoses. In: First MB Tasman A, eds. Clinical guide to the diagnosis and treatment of mental disorders. San Francisco, CA: John Wiley and Sons; 2009:245–278.
15. Mueser KT, Bellack AS, Brady EU. Hallucinations in schizophrenia. Acta Psychiatr Scand. 1990;82(1):26-29.
16. Small IF, Small JG, Andersen JM. Clinical characteristics of hallucinations of schizophrenia. Dis Nerv Syst. 1966;27(5):349-353.
17. Webster R, Holroyd S. Prevalence of psychotic symptoms in delirium. Psychosomatics. 2000;41(6):519-522.
18. Gastfriend DR, Renner JA, Hackett TP. Alcoholic patients: acute and chronic. In: Stern TA Fricchione G, Cassem NH, et al, eds. Massachusetts General Hospital handbook of general hospital psychiatry. 5th ed. Philadelphia, PA: Mosby; 2004:203–216.
19. Manford M, Andermann F. Complex visual hallucinations. Clinical and neurobiological insights. Brain. 1998;121(Pt 10):1819-1840.
20. Goadsby PJ, Lipton RB, Ferrari MD. Migraine—current understanding and treatment. N Engl J Med. 2002;346(4):257-270.
21. Russell MB, Olesen J. A nosographic analysis of the migraine aura in a general population. Brain. 1996;119(Pt 2):355-361.
22. Panayiotopoulos CP. Elementary visual hallucinations blindness, and headache in idiopathic occipital epilepsy: differentiation from migraine. J Neurol Neurosurg Psychiatry. 1999;66(4):536-540.
23. Ballard CG, O’Brien JT, Swann AG, et al. The natural history of psychosis and depression in dementia with Lewy bodies and Alzheimer’s disease: persistence and new cases over 1 year of follow-up. J Clin Psychiatry. 2001;62(1):46-49.
24. Ala TA, Yang KH, Sung JH, et al. Hallucinations and signs of parkinsonism help distinguish patients with dementia and cortical Lewy bodies from patients with Alzheimer’s disease at presentation: a clinicopathological study. J Neurol Neurosurg Psychiatry. 1997;62(1):16-21.
25. Tiraboschi P, Salmon DP, Hansen LA, et al. What best differentiates Lewy body from Alzheimer’s disease in early-stage dementia? Brain. 2006;129(Pt 3):729-735.
26. Harding AJ, Broe GA, Halliday GM. Visual hallucinations in Lewy body disease relate to Lewy bodies in the temporal lobe. Brain. 2002;125(Pt 2):391-403.
27. Williams DR, Lees AJ. Visual hallucinations in the diagnosis of idiopathic Parkinson’s disease: a retrospective autopsy study. Lancet Neurol. 2005;4(10):605-610.
28. Lewandowski KE, DePaola J, Camsari GB, et al. Tactile, olfactory, and gustatory hallucinations in psychotic disorders: a descriptive study. Ann Acad Med Singapore. 2009;38(5):383-385.
29. Acharya V, Acharya J, Lüders H. Olfactory epileptic auras. Neurology. 1998;51(1):56-61.
30. Ropper AH, Samuels MA. Disorders of smell and taste. In: Ropper AH Samuels MA, eds. Adams and Victor’s principles of neurology. 9th ed. New York, NY: McGraw-Hill Companies; 2009:216–224.
31. Ropper AH, Samuels MA. Epilepsy and other seizure disorders. In: Ropper AH Samuels MA, eds. Adams and Victor’s principles of neurology. 9th ed. New York, NY: McGraw-Hill Companies; 2009:304–338.
32. Capampangan DJ, Hoerth MT, Drazkowski JF, et al. Olfactory and gustatory hallucinations presenting as partial status epilepticus because of glioblastoma multiforme. Ann Emerg Med. 2010;56(4):374-377.
33. Frasnelli J, Reden J, Landis BN, et al. Comment on “Olfactory hallucinations as a manifestation of hidden rhinosinusitis”. J Clin Neurosci. 2010;17(4):543.-
34. Elliott B, Joyce E, Shorvon S. Delusions illusions and hallucinations in epilepsy: 1. Elementary phenomena. Epilepsy Res. 2009;85(2-3):162-171.
35. Nurcombe B, Ebert MH. The psychiatric interview. In: Ebert MH Nurcombe B, Loosen PT, et al, eds. Current diagnosis and treatment: psychiatry. 2nd ed. New York, NY: McGraw-Hill Companies; 2008:95–114.
36. Heveling T, Emrich HM, Dietrich DE. Treatment of a rare psychopathological phenomenon: tactile hallucinations and the delusional other. Eur Psychiatry. 2004;19(6):387-388.
37. Fontenelle LF, Lopes AP, Borges MC, et al. Auditory, visual, tactile, olfactory, and bodily hallucinations in patients with obsessive-compulsive disorder. CNS Spectr. 2008;13(2):125-130.
38. Nemoto K, Mizukami K, Hori T, et al. Hyperperfusion in primary somatosensory region related to somatic hallucination in the elderly. Psychiatry Clin Neurosci. 2010;64(4):421-425.
39. Shergill SS, Cameron LA, Brammer MJ, et al. Modality specific neural correlates of auditory and somatic hallucinations. J Neurol Neurosurg Psychiatry. 2001;71(5):688-690.
Beyond lithium: Using psychotherapy to reduce suicide risk in bipolar disorder
Discuss this article at www.facebook.com/CurrentPsychiatry
Patients with bipolar disorder (BD) have a high risk for suicidal ideation, suicide attempts, and suicide.1-3 Approximately 25% to 50% of BD patients attempt suicide at least once, and their attempts often are lethal—the ratio of attempts to completed suicides in BD patients is 3:1, compared with 30:1 in the general population.4 Lithium has been shown to effectively stabilize BD patients’ mood and significantly reduce the rates of suicide attempts and completed suicides,5-9 but does not reduce BD patients’ long-term suicide risk to that of the general population.
Literature on psychotherapeutic treatments for patients with BD primarily focuses on improving patients’ adherence to pharmacotherapy and achieving faster recovery and remission.10 Nonpharmacologic treatments for patients with BD include psychoeducation, family-focused psychoeducation, cognitive therapy, and interpersonal and social rhythm therapy (Table 1).11 Literature on nonpharmacologic treatments to address suicidality in BD patients is limited,12,13 and additional psychotherapeutic interventions to reduce suicide risk in BD patients are needed.14
In this article, I describe a novel psychotherapeutic intervention I use that integrates cognitive therapy principles with ideas derived from the psychosynthesis model.15,16 It consists of teaching patients to “disidentify” from suicidal thoughts, followed by a guided-imagery exercise in which patients experience a future positive life event with all 5 senses and internalize this experience. This creates a “hook into the future” that changes the present to match the future event and acts as an antidote to suicidal thoughts. I have used this strategy successfully in many patients as an adjunct to pharmacotherapy.
Table 1
Nonpharmacologic interventions for bipolar disorder
| Goals | Techniques |
|---|---|
| Psychoeducation | |
|
|
| Family-focused psychoeducation | |
|
|
| Cognitive therapy | |
|
|
| Interpersonal and social rhythm therapy | |
|
|
| BD: bipolar disorder Source: Reference 11 | |
A theoretical model
Roberto Assagioli, who established the approach to psychology called psychosynthesis, formulated a fundamental psychological principle in controlling one’s behavior: “We are dominated by everything with which our self becomes identified. We can dominate and control everything from which we disidentify ourselves.”15 According to the psychosynthesis model, it is easier to change thoughts we identify as foreign to “the self” (ego-dystonic) than thoughts we identify as being part of “the self” (ego-syntonic).
Patients whose suicidal thoughts are ego-syntonic identify with the thoughts as representing themselves and take ownership of these thoughts. Such patients are at a greater risk of acting on suicidal thoughts.
Patients whose suicidal thoughts are ego-dystonic consider the suicidal thoughts foreign to their core self and do not believe such thoughts represent them. In essence, they “disown” the thoughts and typically want to control and eliminate them. Examples of patients’ ego-syntonic vs ego-dystonic suicidal thoughts are listed in Table 2.
This construct calls for an intervention to help patients who have ego-syntonic suicidal thoughts restructure them as a manifestation of BD, rather then the patient’s core self belief. The intervention emphasizes the patient is not “a suicidal patient” but suffers from an illness that may manifest with suicidal ideation. Many BD patients overly identify with their disease, stating, “I am bipolar” or “I am suicidal.” The “I am” statement originates from the verb “to be,” which implies the disease is part of the patient’s identity. The goal of this intervention is to help the patient learn to disidentify from the disease and decide that suicidal thoughts do not represent their core self, but are a manifestation of the underlying disease.
The psychosynthesis model of helping patients disidentify and therefore disown suicidal thoughts is compatible with interventions that use mindfulness-based cognitive therapy training to teach patients to experience their thoughts as just passing through their consciousness without taking ownership of them.17
Table 2
Examples of ego-syntonic vs ego-dystonic suicidal thoughts
| Ego-syntonic | Ego-dystonic |
|---|---|
| ‘I want to be dead. I found a simple and sure way to do it’ | ‘I am having suicidal thoughts again and I don’t like it’ |
| ‘I know my family will be better off without me’ | ‘I’m afraid the illness is coming back. I can’t stop these images’ |
| ‘Life is too hard, too much pain. I just want to end it all’ | ‘I see my body in a coffin. It scares the hell out of me’ |
| ‘I’ve come to the end, life for me is over and done’ | ‘I don’t want to die. Please help me get well again’ |
| ‘I know my life is over. I just have to find the right way to do it’ | ‘It is as if a part of me wants to die but the rest of me wants to live’ |
| ‘Nobody cares about me. It is as if I am already dead’ | ‘I know my family needs me. I want to be there for them’ |
| ‘I have nothing to live for’ | ‘I have so much to live for, why am I having such crazy thoughts?’ |
The intervention
Assessment of suicidality is a fundamental skill for every mental health clinician.18 The psychotherapeutic intervention I use integrates the cognitive therapy principles of reframing, relabeling, and restructuring patients’ thoughts with disidentification from dysfunctional thoughts, feelings, and desires, based on psychosynthesis principles.
First, I conduct a comprehensive mental status examination that includes an in-depth exploration of the patient’s suicidal thoughts to determine if they are ego-syntonic or ego-dystonic. I begin by asking patients to clarify and elaborate on their statements referring to suicide, asking questions such as “Is there a part of you that objects to these thoughts?” and “Is there a part of you that wants to live?” If a patient indicates that he or she does experience inner conflict regarding such thoughts, these thoughts are classified as ego-dystonic. If a patient does not have any counter thoughts regarding the suicidal thoughts and fully identifies with them, the thoughts are classified as ego-syntonic.
I follow this with a treatment plan that helps patients change their view of their suicidal thoughts. I ask the patient to change these suicidal thoughts to ego-dystonic by focusing on the following statement: “I, (patient’s name), am a human being and like all human beings, I have thoughts; however, I am not my thoughts, I am much more than that.” I ask my patient to read this out loud and to mindfully meditate on this statement several times a day to reinforce the new understanding that these suicidal thoughts are a manifestation of the chemical imbalance of the mood disorder, and do not represent the patient as a person.
This intervention is paired with a future-focused internalized imagery experience I have described in previous articles.19,20 In this part of the treatment, the patient and I discuss a specific expected life milestone that is positive and for which he or she would want to be present (eg, children graduating from high school or college, a wedding, birth of a child/grandchild, etc.). Using guided imagery, the patient experiences this event with all 5 senses during the session. I instruct the patient to internalize the experience and bring it back from the future to the present. This creates a “hook into the future” that is coupled with this desired milestone event in the patient’s life.
The following 3 case studies provide examples of the application of this treatment intervention.
CASE 1: Disidentifying family history
Mrs. G, a 42-year-old mother of 2, suffers from bipolar II disorder with recurrent episodes of depression associated with ego-syntonic suicidal thoughts. She states that at times she feels she is a burden to her husband and children and believes they may be better off without her. She says she believes “ending it all” must be her destiny. After further investigation, I learn Mrs. G has a family history of BD and 3 relatives have committed suicide. This family history may partially explain her belief that suicide must be “in her genes.”
I discuss with Mrs. G the strategy of changing her thoughts. I tell her to write in her journal—which she brings to her sessions—the following statements: “I am a human being. I am an adult woman and mother of 2 children. I know I have thoughts but I am not my thoughts, I am much more than that. I know I have genes but I am not my genes, I am much more than that. I know I have feelings, but I am not my feelings, I am much more than that. I know I have cousins, uncles, aunts, and other relatives but I am not my relatives. I am uniquely myself, different from the others.”
I ask Mrs. G to read these statements out loud and repeat them several times a day to reinforce this new way of perceiving the suicidal thoughts and to disidentify from the thoughts and her family history as it relates to suicide.
Mrs. G and I talk about the future and expected family milestones. When I ask if her son would want her to be present at his college graduation, she says yes. We then discuss in detail the date, time of day, and location of this event, followed by a guided imagery exercise focused on the graduation. She is guided to experience this event with all 5 senses and describes the event in detail, including the expression on the faces of her husband and children, their voices, and the scent of their aftershave lotion. She hears her son saying, “Mom, I love you. Thank you for being there with me all these years. I could not have done it without you.” I ask Mrs. G to internalize these experiences and carve them into her memory. She is instructed to come back from this future-focused guided imagery experience. When her eyes open, she looks at me and describes her experience in great detail, at times using the past tense, which confirms that the future-focused event was internalized.
In her next session, Mrs. G reports an improvement in her sleep and a change in her suicidal thoughts, which now are only fleeting.
CASE 2: Experiencing graduation
Ms. J, age 17, was diagnosed with bipolar I disorder when she was 15. She has a family history of BD in her mother, 2 maternal aunts, her grandmother, and an older sister. All these women have a history of suicidal thoughts and suicide attempts requiring hospital treatment, but no completed suicides.
Ms. J has been taking an adequate combination of mood stabilizers. She has recovered from 2 previous depressive episodes and is experiencing a third relapse with suicidal thoughts. At times, she experiences these thoughts as ego-syntonic; at other times, they are ego-dystonic.
I first educate her about the nature of BD, explaining that her suicidal thoughts are a manifestation of a chemical imbalance in her brain as a result of the depressive relapse. I teach her to use guided imagery to focus on her favorite place of peace and serenity, the beach, which produces immediate relief of the intense anxiety she felt.
After we complete the disidentification exercise, I ask her to focus on her high school graduation ceremony, which is scheduled to take place in 1 year. In a state of guided imagery, she experiences her graduation from high school with all 5 senses. As she returns to a state of full alertness with her eyes open, she describes the graduation ceremony experience in detail using the past tense, as if it had already occurred, thereby creating her own hook into the future. I instruct her to write about this experience in her journal and bring it with her to the next session.
The following session, Ms. J reports that her suicide ideations have “disappeared.” She says this was accompanied by improvements in her overall mood and sleep.
CASE 3: Internalizing the future
Mr. C, a 38-year-old married father of 4 children, has bipolar II disorder and is in a depressed state. He has been treated with optimal doses of mood stabilizers and atypical antipsychotics but continues to have suicidal thoughts. These thoughts are at times ego-syntonic; he says, “My family would be better off without me.” When Mr. C’s mood improves, however, the suicidal thoughts become more ego-dystonic; he expresses fear that he might act out on the thoughts and states that he does not want to die, he really wants to live and get better. He has no history of suicide attempts.
During our session, I ask Mr. C to focus on a new perspective to understand his thoughts by repeating the following statements: “I, JC, am a human being. I know I have a bipolar mood disorder; however, I must remember I am not bipolar. I have suicidal thoughts; however, I am not my thoughts, I am much more than that. I know I want to live, to heal, and to get better. I want to be alive and well so I can see and participate in my children’s graduation from high school and be there when they get married and when my grandchildren are born.”
I teach Mr. C to use guided imagery, during which he experiences such future positive images and milestones in his life in all 5 senses and internalizes them by using the “back from the future” technique.17 By the end of the session, he reports feeling better, more hopeful, and confident in his abilities to control his suicidal thoughts. I instruct him to write in his diary about his experiences with the future-focused positive milestones and to bring this assignment to his next appointment.
At his next appointment, Mr. C reports that his suicidal thoughts have become more fleeting, lasting for 10 to 30 seconds, and then spontaneously change to focus on issues of the “here and now.” When I ask him to read what he’s written, what stands out is the use of past tense verbs to describe future-focused experiences. For me, this confirms that Mr. C has internalized the future, creating the desirable “future hook” that acts as an antidote to the suicidal thoughts.
Related Resources
- Rouget BW, Aubry JM. Efficacy of psychoeducational approaches on bipolar disorders: a review of the literature. J Affect Disord. 2007;98:11-27.
- Weinberg I, Ronningstam E, Goldblatt MJ, et al. Strategies in treatment of suicidality: identification of common and treatment-specific interventions in empirically supported treatment manuals. J Clin Psychiatry. 2010;71:699-706.
Drug Brand Name
- Lithium • Eskalith, Lithobid
Disclosure
Dr. Torem reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. McIntyre RS, Konarski JZ. Bipolar disorder: a national health concern. CNS Spectr. 2004;9(11 suppl 12):6-15.
2. Tsai SY, Lee CH, Kuo CJ, et al. A retrospective analysis of risk and protective factors for natural death in bipolar disorder. J Clin Psychiatry. 2005;66(12):1586-1591.
3. Osby U, Brandt L, Correia N, et al. Excess mortality in bipolar and unipolar disorder in Sweden. Arch Gen Psychiatry. 2001;58(9):844-850.
4. Baldessarini RJ, Pompili M, Tondo L. Suicide in bipolar disorder: risks and management. CNS Spectr. 2006;11(6):465-471.
5. Gelenberg AJ. Can lithium help to prevent suicide? Acta Psychiatr Scand. 2001;104(3):161-162.
6. Schou M. Suicidal behavior and prophylactic lithium treatment of major mood disorders: a review of reviews. Suicide Life Threat Behav. 2001;30(3):289-293.
7. Burgess S, Geddes J, Hawton K, et al. Lithium for maintenance treatment of mood disorders. Cochrane Database Syst Rev. 2001;(3):CD003013.-
8. Baldessarini RJ, Tondo L, Davis P, et al. Decreased risk of suicides and attempts during long-term lithium treatment: a meta-analytic review. Bipolar Disord. 2006;8(5 Pt 2):625-639.
9. Tondo L, Baldessarini RJ. Long-term lithium treatment in the prevention of suicidal behavior in bipolar disorder patients. Epidemiol Psichiatr Soc. 2009;18(3):179-183.
10. Miklowitz DJ. Adjunctive psychotherapy for bipolar disorder: state of the evidence. Am J Psychiatry. 2008;165(11):1408-1419.
11. Hirschfeld RMA, Harris TH, Davis HK. Making efficacious choices: the integration of pharmacotherapy and nonpharmacologic approaches to the treatment of patients with bipolar disorder. Current Psychiatry. 2009;8(10 suppl):S6-S11.
12. Rucci P, Frank E, Kostelnik B, et al. Suicide attempts in patients with bipolar I disorder during acute and maintenance phases of intensive treatment with pharmacotherapy and adjunctive psychotherapy. Am J Psychiatry. 2002;159(7):1160-1164.
13. Fountoulakis KN, Gonda X, Siamouli M, et al. Psychotherapeutic intervention and suicide risk reduction in bipolar disorder: a review of the evidence. J Affect Disord. 2009;113(1-2):21-29.
14. Pompili M, Rihmer Z, Innamorati M, et al. Assessment and treatment of suicide risk in bipolar disorders. Expert Rev Neurother. 2009;9(1):109-136.
15. Assagioli R. Psychosynthesis: a collection of basic writings. New York NY: The Viking Press Inc.; 1965.
16. Assagioli R. The act of will. New York NY: The Viking Press Inc.; 1973.
17. Williams JM, Alatiq Y, Crane C, et al. Mindfulness-based cognitive therapy (MBCT) in bipolar disorder: preliminary evaluation of immediate effects on between-episode functioning. J Affect Disord. 2008;107(1-3):275-279.
18. Shea SC. The delicate art of eliciting suicidal ideation. Psychiatric Annals. 2004;34:385-400.
19. Torem MS. “Back from the future”: a powerful age-progression technique. Am J Clin Hypn. 1992;35(2):81-88.
20. Torem MS. Treating depression: a remedy from the future. In: Yapko MD ed. Hypnosis and treating depression: applications in clinical practice. New York, NY: Routledge; 2006:97–119.
Discuss this article at www.facebook.com/CurrentPsychiatry
Patients with bipolar disorder (BD) have a high risk for suicidal ideation, suicide attempts, and suicide.1-3 Approximately 25% to 50% of BD patients attempt suicide at least once, and their attempts often are lethal—the ratio of attempts to completed suicides in BD patients is 3:1, compared with 30:1 in the general population.4 Lithium has been shown to effectively stabilize BD patients’ mood and significantly reduce the rates of suicide attempts and completed suicides,5-9 but does not reduce BD patients’ long-term suicide risk to that of the general population.
Literature on psychotherapeutic treatments for patients with BD primarily focuses on improving patients’ adherence to pharmacotherapy and achieving faster recovery and remission.10 Nonpharmacologic treatments for patients with BD include psychoeducation, family-focused psychoeducation, cognitive therapy, and interpersonal and social rhythm therapy (Table 1).11 Literature on nonpharmacologic treatments to address suicidality in BD patients is limited,12,13 and additional psychotherapeutic interventions to reduce suicide risk in BD patients are needed.14
In this article, I describe a novel psychotherapeutic intervention I use that integrates cognitive therapy principles with ideas derived from the psychosynthesis model.15,16 It consists of teaching patients to “disidentify” from suicidal thoughts, followed by a guided-imagery exercise in which patients experience a future positive life event with all 5 senses and internalize this experience. This creates a “hook into the future” that changes the present to match the future event and acts as an antidote to suicidal thoughts. I have used this strategy successfully in many patients as an adjunct to pharmacotherapy.
Table 1
Nonpharmacologic interventions for bipolar disorder
| Goals | Techniques |
|---|---|
| Psychoeducation | |
|
|
| Family-focused psychoeducation | |
|
|
| Cognitive therapy | |
|
|
| Interpersonal and social rhythm therapy | |
|
|
| BD: bipolar disorder Source: Reference 11 | |
A theoretical model
Roberto Assagioli, who established the approach to psychology called psychosynthesis, formulated a fundamental psychological principle in controlling one’s behavior: “We are dominated by everything with which our self becomes identified. We can dominate and control everything from which we disidentify ourselves.”15 According to the psychosynthesis model, it is easier to change thoughts we identify as foreign to “the self” (ego-dystonic) than thoughts we identify as being part of “the self” (ego-syntonic).
Patients whose suicidal thoughts are ego-syntonic identify with the thoughts as representing themselves and take ownership of these thoughts. Such patients are at a greater risk of acting on suicidal thoughts.
Patients whose suicidal thoughts are ego-dystonic consider the suicidal thoughts foreign to their core self and do not believe such thoughts represent them. In essence, they “disown” the thoughts and typically want to control and eliminate them. Examples of patients’ ego-syntonic vs ego-dystonic suicidal thoughts are listed in Table 2.
This construct calls for an intervention to help patients who have ego-syntonic suicidal thoughts restructure them as a manifestation of BD, rather then the patient’s core self belief. The intervention emphasizes the patient is not “a suicidal patient” but suffers from an illness that may manifest with suicidal ideation. Many BD patients overly identify with their disease, stating, “I am bipolar” or “I am suicidal.” The “I am” statement originates from the verb “to be,” which implies the disease is part of the patient’s identity. The goal of this intervention is to help the patient learn to disidentify from the disease and decide that suicidal thoughts do not represent their core self, but are a manifestation of the underlying disease.
The psychosynthesis model of helping patients disidentify and therefore disown suicidal thoughts is compatible with interventions that use mindfulness-based cognitive therapy training to teach patients to experience their thoughts as just passing through their consciousness without taking ownership of them.17
Table 2
Examples of ego-syntonic vs ego-dystonic suicidal thoughts
| Ego-syntonic | Ego-dystonic |
|---|---|
| ‘I want to be dead. I found a simple and sure way to do it’ | ‘I am having suicidal thoughts again and I don’t like it’ |
| ‘I know my family will be better off without me’ | ‘I’m afraid the illness is coming back. I can’t stop these images’ |
| ‘Life is too hard, too much pain. I just want to end it all’ | ‘I see my body in a coffin. It scares the hell out of me’ |
| ‘I’ve come to the end, life for me is over and done’ | ‘I don’t want to die. Please help me get well again’ |
| ‘I know my life is over. I just have to find the right way to do it’ | ‘It is as if a part of me wants to die but the rest of me wants to live’ |
| ‘Nobody cares about me. It is as if I am already dead’ | ‘I know my family needs me. I want to be there for them’ |
| ‘I have nothing to live for’ | ‘I have so much to live for, why am I having such crazy thoughts?’ |
The intervention
Assessment of suicidality is a fundamental skill for every mental health clinician.18 The psychotherapeutic intervention I use integrates the cognitive therapy principles of reframing, relabeling, and restructuring patients’ thoughts with disidentification from dysfunctional thoughts, feelings, and desires, based on psychosynthesis principles.
First, I conduct a comprehensive mental status examination that includes an in-depth exploration of the patient’s suicidal thoughts to determine if they are ego-syntonic or ego-dystonic. I begin by asking patients to clarify and elaborate on their statements referring to suicide, asking questions such as “Is there a part of you that objects to these thoughts?” and “Is there a part of you that wants to live?” If a patient indicates that he or she does experience inner conflict regarding such thoughts, these thoughts are classified as ego-dystonic. If a patient does not have any counter thoughts regarding the suicidal thoughts and fully identifies with them, the thoughts are classified as ego-syntonic.
I follow this with a treatment plan that helps patients change their view of their suicidal thoughts. I ask the patient to change these suicidal thoughts to ego-dystonic by focusing on the following statement: “I, (patient’s name), am a human being and like all human beings, I have thoughts; however, I am not my thoughts, I am much more than that.” I ask my patient to read this out loud and to mindfully meditate on this statement several times a day to reinforce the new understanding that these suicidal thoughts are a manifestation of the chemical imbalance of the mood disorder, and do not represent the patient as a person.
This intervention is paired with a future-focused internalized imagery experience I have described in previous articles.19,20 In this part of the treatment, the patient and I discuss a specific expected life milestone that is positive and for which he or she would want to be present (eg, children graduating from high school or college, a wedding, birth of a child/grandchild, etc.). Using guided imagery, the patient experiences this event with all 5 senses during the session. I instruct the patient to internalize the experience and bring it back from the future to the present. This creates a “hook into the future” that is coupled with this desired milestone event in the patient’s life.
The following 3 case studies provide examples of the application of this treatment intervention.
CASE 1: Disidentifying family history
Mrs. G, a 42-year-old mother of 2, suffers from bipolar II disorder with recurrent episodes of depression associated with ego-syntonic suicidal thoughts. She states that at times she feels she is a burden to her husband and children and believes they may be better off without her. She says she believes “ending it all” must be her destiny. After further investigation, I learn Mrs. G has a family history of BD and 3 relatives have committed suicide. This family history may partially explain her belief that suicide must be “in her genes.”
I discuss with Mrs. G the strategy of changing her thoughts. I tell her to write in her journal—which she brings to her sessions—the following statements: “I am a human being. I am an adult woman and mother of 2 children. I know I have thoughts but I am not my thoughts, I am much more than that. I know I have genes but I am not my genes, I am much more than that. I know I have feelings, but I am not my feelings, I am much more than that. I know I have cousins, uncles, aunts, and other relatives but I am not my relatives. I am uniquely myself, different from the others.”
I ask Mrs. G to read these statements out loud and repeat them several times a day to reinforce this new way of perceiving the suicidal thoughts and to disidentify from the thoughts and her family history as it relates to suicide.
Mrs. G and I talk about the future and expected family milestones. When I ask if her son would want her to be present at his college graduation, she says yes. We then discuss in detail the date, time of day, and location of this event, followed by a guided imagery exercise focused on the graduation. She is guided to experience this event with all 5 senses and describes the event in detail, including the expression on the faces of her husband and children, their voices, and the scent of their aftershave lotion. She hears her son saying, “Mom, I love you. Thank you for being there with me all these years. I could not have done it without you.” I ask Mrs. G to internalize these experiences and carve them into her memory. She is instructed to come back from this future-focused guided imagery experience. When her eyes open, she looks at me and describes her experience in great detail, at times using the past tense, which confirms that the future-focused event was internalized.
In her next session, Mrs. G reports an improvement in her sleep and a change in her suicidal thoughts, which now are only fleeting.
CASE 2: Experiencing graduation
Ms. J, age 17, was diagnosed with bipolar I disorder when she was 15. She has a family history of BD in her mother, 2 maternal aunts, her grandmother, and an older sister. All these women have a history of suicidal thoughts and suicide attempts requiring hospital treatment, but no completed suicides.
Ms. J has been taking an adequate combination of mood stabilizers. She has recovered from 2 previous depressive episodes and is experiencing a third relapse with suicidal thoughts. At times, she experiences these thoughts as ego-syntonic; at other times, they are ego-dystonic.
I first educate her about the nature of BD, explaining that her suicidal thoughts are a manifestation of a chemical imbalance in her brain as a result of the depressive relapse. I teach her to use guided imagery to focus on her favorite place of peace and serenity, the beach, which produces immediate relief of the intense anxiety she felt.
After we complete the disidentification exercise, I ask her to focus on her high school graduation ceremony, which is scheduled to take place in 1 year. In a state of guided imagery, she experiences her graduation from high school with all 5 senses. As she returns to a state of full alertness with her eyes open, she describes the graduation ceremony experience in detail using the past tense, as if it had already occurred, thereby creating her own hook into the future. I instruct her to write about this experience in her journal and bring it with her to the next session.
The following session, Ms. J reports that her suicide ideations have “disappeared.” She says this was accompanied by improvements in her overall mood and sleep.
CASE 3: Internalizing the future
Mr. C, a 38-year-old married father of 4 children, has bipolar II disorder and is in a depressed state. He has been treated with optimal doses of mood stabilizers and atypical antipsychotics but continues to have suicidal thoughts. These thoughts are at times ego-syntonic; he says, “My family would be better off without me.” When Mr. C’s mood improves, however, the suicidal thoughts become more ego-dystonic; he expresses fear that he might act out on the thoughts and states that he does not want to die, he really wants to live and get better. He has no history of suicide attempts.
During our session, I ask Mr. C to focus on a new perspective to understand his thoughts by repeating the following statements: “I, JC, am a human being. I know I have a bipolar mood disorder; however, I must remember I am not bipolar. I have suicidal thoughts; however, I am not my thoughts, I am much more than that. I know I want to live, to heal, and to get better. I want to be alive and well so I can see and participate in my children’s graduation from high school and be there when they get married and when my grandchildren are born.”
I teach Mr. C to use guided imagery, during which he experiences such future positive images and milestones in his life in all 5 senses and internalizes them by using the “back from the future” technique.17 By the end of the session, he reports feeling better, more hopeful, and confident in his abilities to control his suicidal thoughts. I instruct him to write in his diary about his experiences with the future-focused positive milestones and to bring this assignment to his next appointment.
At his next appointment, Mr. C reports that his suicidal thoughts have become more fleeting, lasting for 10 to 30 seconds, and then spontaneously change to focus on issues of the “here and now.” When I ask him to read what he’s written, what stands out is the use of past tense verbs to describe future-focused experiences. For me, this confirms that Mr. C has internalized the future, creating the desirable “future hook” that acts as an antidote to the suicidal thoughts.
Related Resources
- Rouget BW, Aubry JM. Efficacy of psychoeducational approaches on bipolar disorders: a review of the literature. J Affect Disord. 2007;98:11-27.
- Weinberg I, Ronningstam E, Goldblatt MJ, et al. Strategies in treatment of suicidality: identification of common and treatment-specific interventions in empirically supported treatment manuals. J Clin Psychiatry. 2010;71:699-706.
Drug Brand Name
- Lithium • Eskalith, Lithobid
Disclosure
Dr. Torem reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Discuss this article at www.facebook.com/CurrentPsychiatry
Patients with bipolar disorder (BD) have a high risk for suicidal ideation, suicide attempts, and suicide.1-3 Approximately 25% to 50% of BD patients attempt suicide at least once, and their attempts often are lethal—the ratio of attempts to completed suicides in BD patients is 3:1, compared with 30:1 in the general population.4 Lithium has been shown to effectively stabilize BD patients’ mood and significantly reduce the rates of suicide attempts and completed suicides,5-9 but does not reduce BD patients’ long-term suicide risk to that of the general population.
Literature on psychotherapeutic treatments for patients with BD primarily focuses on improving patients’ adherence to pharmacotherapy and achieving faster recovery and remission.10 Nonpharmacologic treatments for patients with BD include psychoeducation, family-focused psychoeducation, cognitive therapy, and interpersonal and social rhythm therapy (Table 1).11 Literature on nonpharmacologic treatments to address suicidality in BD patients is limited,12,13 and additional psychotherapeutic interventions to reduce suicide risk in BD patients are needed.14
In this article, I describe a novel psychotherapeutic intervention I use that integrates cognitive therapy principles with ideas derived from the psychosynthesis model.15,16 It consists of teaching patients to “disidentify” from suicidal thoughts, followed by a guided-imagery exercise in which patients experience a future positive life event with all 5 senses and internalize this experience. This creates a “hook into the future” that changes the present to match the future event and acts as an antidote to suicidal thoughts. I have used this strategy successfully in many patients as an adjunct to pharmacotherapy.
Table 1
Nonpharmacologic interventions for bipolar disorder
| Goals | Techniques |
|---|---|
| Psychoeducation | |
|
|
| Family-focused psychoeducation | |
|
|
| Cognitive therapy | |
|
|
| Interpersonal and social rhythm therapy | |
|
|
| BD: bipolar disorder Source: Reference 11 | |
A theoretical model
Roberto Assagioli, who established the approach to psychology called psychosynthesis, formulated a fundamental psychological principle in controlling one’s behavior: “We are dominated by everything with which our self becomes identified. We can dominate and control everything from which we disidentify ourselves.”15 According to the psychosynthesis model, it is easier to change thoughts we identify as foreign to “the self” (ego-dystonic) than thoughts we identify as being part of “the self” (ego-syntonic).
Patients whose suicidal thoughts are ego-syntonic identify with the thoughts as representing themselves and take ownership of these thoughts. Such patients are at a greater risk of acting on suicidal thoughts.
Patients whose suicidal thoughts are ego-dystonic consider the suicidal thoughts foreign to their core self and do not believe such thoughts represent them. In essence, they “disown” the thoughts and typically want to control and eliminate them. Examples of patients’ ego-syntonic vs ego-dystonic suicidal thoughts are listed in Table 2.
This construct calls for an intervention to help patients who have ego-syntonic suicidal thoughts restructure them as a manifestation of BD, rather then the patient’s core self belief. The intervention emphasizes the patient is not “a suicidal patient” but suffers from an illness that may manifest with suicidal ideation. Many BD patients overly identify with their disease, stating, “I am bipolar” or “I am suicidal.” The “I am” statement originates from the verb “to be,” which implies the disease is part of the patient’s identity. The goal of this intervention is to help the patient learn to disidentify from the disease and decide that suicidal thoughts do not represent their core self, but are a manifestation of the underlying disease.
The psychosynthesis model of helping patients disidentify and therefore disown suicidal thoughts is compatible with interventions that use mindfulness-based cognitive therapy training to teach patients to experience their thoughts as just passing through their consciousness without taking ownership of them.17
Table 2
Examples of ego-syntonic vs ego-dystonic suicidal thoughts
| Ego-syntonic | Ego-dystonic |
|---|---|
| ‘I want to be dead. I found a simple and sure way to do it’ | ‘I am having suicidal thoughts again and I don’t like it’ |
| ‘I know my family will be better off without me’ | ‘I’m afraid the illness is coming back. I can’t stop these images’ |
| ‘Life is too hard, too much pain. I just want to end it all’ | ‘I see my body in a coffin. It scares the hell out of me’ |
| ‘I’ve come to the end, life for me is over and done’ | ‘I don’t want to die. Please help me get well again’ |
| ‘I know my life is over. I just have to find the right way to do it’ | ‘It is as if a part of me wants to die but the rest of me wants to live’ |
| ‘Nobody cares about me. It is as if I am already dead’ | ‘I know my family needs me. I want to be there for them’ |
| ‘I have nothing to live for’ | ‘I have so much to live for, why am I having such crazy thoughts?’ |
The intervention
Assessment of suicidality is a fundamental skill for every mental health clinician.18 The psychotherapeutic intervention I use integrates the cognitive therapy principles of reframing, relabeling, and restructuring patients’ thoughts with disidentification from dysfunctional thoughts, feelings, and desires, based on psychosynthesis principles.
First, I conduct a comprehensive mental status examination that includes an in-depth exploration of the patient’s suicidal thoughts to determine if they are ego-syntonic or ego-dystonic. I begin by asking patients to clarify and elaborate on their statements referring to suicide, asking questions such as “Is there a part of you that objects to these thoughts?” and “Is there a part of you that wants to live?” If a patient indicates that he or she does experience inner conflict regarding such thoughts, these thoughts are classified as ego-dystonic. If a patient does not have any counter thoughts regarding the suicidal thoughts and fully identifies with them, the thoughts are classified as ego-syntonic.
I follow this with a treatment plan that helps patients change their view of their suicidal thoughts. I ask the patient to change these suicidal thoughts to ego-dystonic by focusing on the following statement: “I, (patient’s name), am a human being and like all human beings, I have thoughts; however, I am not my thoughts, I am much more than that.” I ask my patient to read this out loud and to mindfully meditate on this statement several times a day to reinforce the new understanding that these suicidal thoughts are a manifestation of the chemical imbalance of the mood disorder, and do not represent the patient as a person.
This intervention is paired with a future-focused internalized imagery experience I have described in previous articles.19,20 In this part of the treatment, the patient and I discuss a specific expected life milestone that is positive and for which he or she would want to be present (eg, children graduating from high school or college, a wedding, birth of a child/grandchild, etc.). Using guided imagery, the patient experiences this event with all 5 senses during the session. I instruct the patient to internalize the experience and bring it back from the future to the present. This creates a “hook into the future” that is coupled with this desired milestone event in the patient’s life.
The following 3 case studies provide examples of the application of this treatment intervention.
CASE 1: Disidentifying family history
Mrs. G, a 42-year-old mother of 2, suffers from bipolar II disorder with recurrent episodes of depression associated with ego-syntonic suicidal thoughts. She states that at times she feels she is a burden to her husband and children and believes they may be better off without her. She says she believes “ending it all” must be her destiny. After further investigation, I learn Mrs. G has a family history of BD and 3 relatives have committed suicide. This family history may partially explain her belief that suicide must be “in her genes.”
I discuss with Mrs. G the strategy of changing her thoughts. I tell her to write in her journal—which she brings to her sessions—the following statements: “I am a human being. I am an adult woman and mother of 2 children. I know I have thoughts but I am not my thoughts, I am much more than that. I know I have genes but I am not my genes, I am much more than that. I know I have feelings, but I am not my feelings, I am much more than that. I know I have cousins, uncles, aunts, and other relatives but I am not my relatives. I am uniquely myself, different from the others.”
I ask Mrs. G to read these statements out loud and repeat them several times a day to reinforce this new way of perceiving the suicidal thoughts and to disidentify from the thoughts and her family history as it relates to suicide.
Mrs. G and I talk about the future and expected family milestones. When I ask if her son would want her to be present at his college graduation, she says yes. We then discuss in detail the date, time of day, and location of this event, followed by a guided imagery exercise focused on the graduation. She is guided to experience this event with all 5 senses and describes the event in detail, including the expression on the faces of her husband and children, their voices, and the scent of their aftershave lotion. She hears her son saying, “Mom, I love you. Thank you for being there with me all these years. I could not have done it without you.” I ask Mrs. G to internalize these experiences and carve them into her memory. She is instructed to come back from this future-focused guided imagery experience. When her eyes open, she looks at me and describes her experience in great detail, at times using the past tense, which confirms that the future-focused event was internalized.
In her next session, Mrs. G reports an improvement in her sleep and a change in her suicidal thoughts, which now are only fleeting.
CASE 2: Experiencing graduation
Ms. J, age 17, was diagnosed with bipolar I disorder when she was 15. She has a family history of BD in her mother, 2 maternal aunts, her grandmother, and an older sister. All these women have a history of suicidal thoughts and suicide attempts requiring hospital treatment, but no completed suicides.
Ms. J has been taking an adequate combination of mood stabilizers. She has recovered from 2 previous depressive episodes and is experiencing a third relapse with suicidal thoughts. At times, she experiences these thoughts as ego-syntonic; at other times, they are ego-dystonic.
I first educate her about the nature of BD, explaining that her suicidal thoughts are a manifestation of a chemical imbalance in her brain as a result of the depressive relapse. I teach her to use guided imagery to focus on her favorite place of peace and serenity, the beach, which produces immediate relief of the intense anxiety she felt.
After we complete the disidentification exercise, I ask her to focus on her high school graduation ceremony, which is scheduled to take place in 1 year. In a state of guided imagery, she experiences her graduation from high school with all 5 senses. As she returns to a state of full alertness with her eyes open, she describes the graduation ceremony experience in detail using the past tense, as if it had already occurred, thereby creating her own hook into the future. I instruct her to write about this experience in her journal and bring it with her to the next session.
The following session, Ms. J reports that her suicide ideations have “disappeared.” She says this was accompanied by improvements in her overall mood and sleep.
CASE 3: Internalizing the future
Mr. C, a 38-year-old married father of 4 children, has bipolar II disorder and is in a depressed state. He has been treated with optimal doses of mood stabilizers and atypical antipsychotics but continues to have suicidal thoughts. These thoughts are at times ego-syntonic; he says, “My family would be better off without me.” When Mr. C’s mood improves, however, the suicidal thoughts become more ego-dystonic; he expresses fear that he might act out on the thoughts and states that he does not want to die, he really wants to live and get better. He has no history of suicide attempts.
During our session, I ask Mr. C to focus on a new perspective to understand his thoughts by repeating the following statements: “I, JC, am a human being. I know I have a bipolar mood disorder; however, I must remember I am not bipolar. I have suicidal thoughts; however, I am not my thoughts, I am much more than that. I know I want to live, to heal, and to get better. I want to be alive and well so I can see and participate in my children’s graduation from high school and be there when they get married and when my grandchildren are born.”
I teach Mr. C to use guided imagery, during which he experiences such future positive images and milestones in his life in all 5 senses and internalizes them by using the “back from the future” technique.17 By the end of the session, he reports feeling better, more hopeful, and confident in his abilities to control his suicidal thoughts. I instruct him to write in his diary about his experiences with the future-focused positive milestones and to bring this assignment to his next appointment.
At his next appointment, Mr. C reports that his suicidal thoughts have become more fleeting, lasting for 10 to 30 seconds, and then spontaneously change to focus on issues of the “here and now.” When I ask him to read what he’s written, what stands out is the use of past tense verbs to describe future-focused experiences. For me, this confirms that Mr. C has internalized the future, creating the desirable “future hook” that acts as an antidote to the suicidal thoughts.
Related Resources
- Rouget BW, Aubry JM. Efficacy of psychoeducational approaches on bipolar disorders: a review of the literature. J Affect Disord. 2007;98:11-27.
- Weinberg I, Ronningstam E, Goldblatt MJ, et al. Strategies in treatment of suicidality: identification of common and treatment-specific interventions in empirically supported treatment manuals. J Clin Psychiatry. 2010;71:699-706.
Drug Brand Name
- Lithium • Eskalith, Lithobid
Disclosure
Dr. Torem reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. McIntyre RS, Konarski JZ. Bipolar disorder: a national health concern. CNS Spectr. 2004;9(11 suppl 12):6-15.
2. Tsai SY, Lee CH, Kuo CJ, et al. A retrospective analysis of risk and protective factors for natural death in bipolar disorder. J Clin Psychiatry. 2005;66(12):1586-1591.
3. Osby U, Brandt L, Correia N, et al. Excess mortality in bipolar and unipolar disorder in Sweden. Arch Gen Psychiatry. 2001;58(9):844-850.
4. Baldessarini RJ, Pompili M, Tondo L. Suicide in bipolar disorder: risks and management. CNS Spectr. 2006;11(6):465-471.
5. Gelenberg AJ. Can lithium help to prevent suicide? Acta Psychiatr Scand. 2001;104(3):161-162.
6. Schou M. Suicidal behavior and prophylactic lithium treatment of major mood disorders: a review of reviews. Suicide Life Threat Behav. 2001;30(3):289-293.
7. Burgess S, Geddes J, Hawton K, et al. Lithium for maintenance treatment of mood disorders. Cochrane Database Syst Rev. 2001;(3):CD003013.-
8. Baldessarini RJ, Tondo L, Davis P, et al. Decreased risk of suicides and attempts during long-term lithium treatment: a meta-analytic review. Bipolar Disord. 2006;8(5 Pt 2):625-639.
9. Tondo L, Baldessarini RJ. Long-term lithium treatment in the prevention of suicidal behavior in bipolar disorder patients. Epidemiol Psichiatr Soc. 2009;18(3):179-183.
10. Miklowitz DJ. Adjunctive psychotherapy for bipolar disorder: state of the evidence. Am J Psychiatry. 2008;165(11):1408-1419.
11. Hirschfeld RMA, Harris TH, Davis HK. Making efficacious choices: the integration of pharmacotherapy and nonpharmacologic approaches to the treatment of patients with bipolar disorder. Current Psychiatry. 2009;8(10 suppl):S6-S11.
12. Rucci P, Frank E, Kostelnik B, et al. Suicide attempts in patients with bipolar I disorder during acute and maintenance phases of intensive treatment with pharmacotherapy and adjunctive psychotherapy. Am J Psychiatry. 2002;159(7):1160-1164.
13. Fountoulakis KN, Gonda X, Siamouli M, et al. Psychotherapeutic intervention and suicide risk reduction in bipolar disorder: a review of the evidence. J Affect Disord. 2009;113(1-2):21-29.
14. Pompili M, Rihmer Z, Innamorati M, et al. Assessment and treatment of suicide risk in bipolar disorders. Expert Rev Neurother. 2009;9(1):109-136.
15. Assagioli R. Psychosynthesis: a collection of basic writings. New York NY: The Viking Press Inc.; 1965.
16. Assagioli R. The act of will. New York NY: The Viking Press Inc.; 1973.
17. Williams JM, Alatiq Y, Crane C, et al. Mindfulness-based cognitive therapy (MBCT) in bipolar disorder: preliminary evaluation of immediate effects on between-episode functioning. J Affect Disord. 2008;107(1-3):275-279.
18. Shea SC. The delicate art of eliciting suicidal ideation. Psychiatric Annals. 2004;34:385-400.
19. Torem MS. “Back from the future”: a powerful age-progression technique. Am J Clin Hypn. 1992;35(2):81-88.
20. Torem MS. Treating depression: a remedy from the future. In: Yapko MD ed. Hypnosis and treating depression: applications in clinical practice. New York, NY: Routledge; 2006:97–119.
1. McIntyre RS, Konarski JZ. Bipolar disorder: a national health concern. CNS Spectr. 2004;9(11 suppl 12):6-15.
2. Tsai SY, Lee CH, Kuo CJ, et al. A retrospective analysis of risk and protective factors for natural death in bipolar disorder. J Clin Psychiatry. 2005;66(12):1586-1591.
3. Osby U, Brandt L, Correia N, et al. Excess mortality in bipolar and unipolar disorder in Sweden. Arch Gen Psychiatry. 2001;58(9):844-850.
4. Baldessarini RJ, Pompili M, Tondo L. Suicide in bipolar disorder: risks and management. CNS Spectr. 2006;11(6):465-471.
5. Gelenberg AJ. Can lithium help to prevent suicide? Acta Psychiatr Scand. 2001;104(3):161-162.
6. Schou M. Suicidal behavior and prophylactic lithium treatment of major mood disorders: a review of reviews. Suicide Life Threat Behav. 2001;30(3):289-293.
7. Burgess S, Geddes J, Hawton K, et al. Lithium for maintenance treatment of mood disorders. Cochrane Database Syst Rev. 2001;(3):CD003013.-
8. Baldessarini RJ, Tondo L, Davis P, et al. Decreased risk of suicides and attempts during long-term lithium treatment: a meta-analytic review. Bipolar Disord. 2006;8(5 Pt 2):625-639.
9. Tondo L, Baldessarini RJ. Long-term lithium treatment in the prevention of suicidal behavior in bipolar disorder patients. Epidemiol Psichiatr Soc. 2009;18(3):179-183.
10. Miklowitz DJ. Adjunctive psychotherapy for bipolar disorder: state of the evidence. Am J Psychiatry. 2008;165(11):1408-1419.
11. Hirschfeld RMA, Harris TH, Davis HK. Making efficacious choices: the integration of pharmacotherapy and nonpharmacologic approaches to the treatment of patients with bipolar disorder. Current Psychiatry. 2009;8(10 suppl):S6-S11.
12. Rucci P, Frank E, Kostelnik B, et al. Suicide attempts in patients with bipolar I disorder during acute and maintenance phases of intensive treatment with pharmacotherapy and adjunctive psychotherapy. Am J Psychiatry. 2002;159(7):1160-1164.
13. Fountoulakis KN, Gonda X, Siamouli M, et al. Psychotherapeutic intervention and suicide risk reduction in bipolar disorder: a review of the evidence. J Affect Disord. 2009;113(1-2):21-29.
14. Pompili M, Rihmer Z, Innamorati M, et al. Assessment and treatment of suicide risk in bipolar disorders. Expert Rev Neurother. 2009;9(1):109-136.
15. Assagioli R. Psychosynthesis: a collection of basic writings. New York NY: The Viking Press Inc.; 1965.
16. Assagioli R. The act of will. New York NY: The Viking Press Inc.; 1973.
17. Williams JM, Alatiq Y, Crane C, et al. Mindfulness-based cognitive therapy (MBCT) in bipolar disorder: preliminary evaluation of immediate effects on between-episode functioning. J Affect Disord. 2008;107(1-3):275-279.
18. Shea SC. The delicate art of eliciting suicidal ideation. Psychiatric Annals. 2004;34:385-400.
19. Torem MS. “Back from the future”: a powerful age-progression technique. Am J Clin Hypn. 1992;35(2):81-88.
20. Torem MS. Treating depression: a remedy from the future. In: Yapko MD ed. Hypnosis and treating depression: applications in clinical practice. New York, NY: Routledge; 2006:97–119.
Is there a rational management strategy for tardive dyskinesia?
Introduced into clinical practice more than a half century ago, antipsychotics are still the mainstay of schizophrenia treatment. However, from the earliest reports, antipsychotic efficacy was seemingly inseparable from extrapyramidal side effects (EPS) that manifested as acute and chronic involuntary movement disorders. Although acute extrapyramidal side effects could be prevented and treated, the late-arising symptoms of tardive dyskinesia (TD) seemed irreversible in most cases.
Concerns over TD stimulated extensive research and fueled efforts to develop new antipsychotics that spared the extrapyramidal motor system. Numerous industry-sponsored trials found a reduced risk of EPS—including TD—with newer, second-generation antipsychotics (SGAs), although this advantage diminished when modest doses of low- or mid-potency first-generation antipsychotics (FGAs) were used as the comparator.1-3 Nevertheless, in addition to the continued potential risk of introducing new cases of TD—even with SGAs—several other factors underscore the need to develop a rational strategy for clinical management of TD, including:
- thousands of patients are left with TD as a legacy of past treatment
- the neurophysiologic mechanisms underlying TD are not well understood
- there is no uniformly effective treatment to reverse TD
- TD may be irreversible in most cases.
Prevention
Because there is no “gold standard” treatment for TD, it is important to minimize the risk of TD by taking preventive measures and detecting incipient signs of the disorder. Preventive principles include:
- confirming and documenting the indication for antipsychotics
- using conservative maintenance doses and opting for lower potency or newer agents
- informing patients and caregivers of risk
- assessing for incipient signs of TD using the Abnormal Involuntary Movement Scale (AIMS),4 which should be administered at least every 3 to 6 months.
Confirming the diagnosis
TD presents as a polymorphous involuntary movement disorder,5-8 most often with nonrhythmic, repetitive, purposeless hyperkinetic symptoms. It usually affects orofacial and lingual musculature (“buccolinguomasticatory syndrome”) with chewing; bruxism; protrusion, curling, or twisting of the tongue; lip smacking, puckering, sucking, and pursing; retraction, grimacing or bridling of the mouth; bulging of the cheeks; or eye blinking and blepharospasm. Choreoathetoid movements of the fingers, hands, or upper or lower extremities also are common. Patients may experience axial symptoms affecting the neck, shoulders, spine, or pelvis. When severe, dyskinesias can affect breathing, swallowing, or speech, and interfere with walking and activities of daily living.
TD may present with nonchoreoathetoid symptoms that can be difficult to distinguish from acute EPS. These may co-exist with classic TD symptoms, but may represent separate subtypes with increased risk of progression, persistence, and severe disability. For example, tardive dystonia, which is estimated to occur in 1% to 4% of patients treated with antipsychotics,9 may be more generalized and disabling than TD, and may respond to anticholinergic agents. Akathisia and other movement disorders also occur as tardive variants.10
Multiple diagnostic schemes for TD have been proposed; criteria proposed by Schooler and Kane have been widely accepted (Table 1).11 TD onset occurs insidiously over ≥3 months of antipsychotic treatment and may begin with tic-like movements or increased eye blinking. TD often is suppressed or masked by ongoing antipsychotic treatment and becomes apparent only when the drug is reduced, switched, or discontinued. Dyskinesias increase with emotional arousal, activation, or distraction, and diminish with relaxation, sleep, or volitional effort. As a result, TD symptoms fluctuate over time; therefore, repeated measurements are necessary for reliable assessment of severity and persistence.
The differential diagnosis of TD necessitates conducting a careful medical and neurologic evaluation of all patients with new-onset movement disorders. Clues to neurologic causes include a family history of movement disorders, sudden onset or progressive course, associated medical or neurologic abnormalities, and asymmetry of symptoms. Some of the medical, neurologic, and psychiatric conditions to consider are listed in Table 2.12
Table 1
Schooler-Kane diagnostic criteria for TD
|
| Probable TD: meets criteria 1 through 3 Masked TD: meets criteria 1 through 3 but movements suppressed within 2 weeks by antipsychotic drugs Transient TD: movements not observed on subsequent examination within 3 months Withdrawal TD: movements observed within 2 weeks of antipsychotic drug discontinuation Persistent TD: movements persist for 3 months |
| TD: tardive dyskinesia Source: Reference 11 |
Table 2
Differential diagnosis of tardive dyskinesia
| Primary movement disorders |
|
| Secondary movement disorders |
|
| Source: Reference 12 |
Treatment decisions
If a patient develops TD, clinicians need to make several decisions (Algorithm). First, consider tapering any anticholinergic drugs unless acute EPS are prominent or tardive dystonia is present. Anticholinergic agents can worsen TD but not tardive dystonia; 60% of TD cases improve after discontinuing anticholinergics.13 Second, decide whether antipsychotics could be safely tapered or discontinued. If antipsychotics cannot be safely tapered, decide whether to maintain the patient’s present antipsychotic or switch to a more or less potent agent. Finally, decide whether a trial of an adjunctive antidyskinetic drug is warranted. All of these decisions require thorough discussion with patients and their families, accompanied by careful documentation.
Discontinuing, continuing, or switching antipsychotics. Discontinuing antipsychotics once TD becomes apparent is an option. However, the natural course of TD after drug withdrawal is unclear. Although drug withdrawal had been recommended to increase the odds of TD resolution, early studies showed withdrawing antipsychotics may lead to an initial worsening of TD in 33% to 53% of patients (unmasking or withdrawal dyskinesia).14 With long-term follow-up, 36% to 55% of patients eventually improved, which supports recommendations for drug reduction or withdrawal.14 However, complete and permanent reversibility beyond the withdrawal period is rare; Glazer et al found only 2% of patients showed complete reversal of TD after drug discontinuation.15,16 In a meta-analysis, Soares and McGrath17 reported 37% of patients assigned to placebo across studies showed at least some improvement in TD, but concluded insufficient evidence existed to support drug cessation or reduction as effective treatments for TD, especially when contrasted with robust evidence for the risk of psychotic relapse after drug withdrawal in patients with schizophrenia (53% within 9 months).18
A second option for a stable patient with good control of psychotic symptoms but established or long-term TD is to continue the antipsychotic, try to gradually reduce the dose, inform patients and caregivers of risks, document the decision, and monitor carefully. In most cases, TD may not progress even with continued antipsychotic treatment, although symptoms may worsen in some cases. However, in a patient with new-onset or early signs of TD, the clinician may be obligated to switch to a lower-potency antipsychotic or newer SGA to improve the chance of resolution; switching is discussed below.
Data on the change in prevalence of TD within a population during continued antipsychotic treatment have been inconsistent. Some studies show an increase, while others show a decrease or no change at all.19 However, prevalence rates obscure the dynamics of TD in individual patients. Roughly 50% of patients with TD have persistent symptoms, 10% to 30% have reduced symptoms, and 10% to 30% experience increased symptoms during treatment.13 Long-term studies estimated that up to 23% of patients may show loss of observable TD symptoms during treatment with FGAs in 1 year.19,20 Similarly, studies of SGAs have shown reduction of TD ratings; some found greater reductions, some found less reductions, and some no difference compared with FGAs.19,20 In some studies, improved TD outcomes were correlated with younger age, lower antipsychotic doses, reduced duration of drug treatment and dyskinesia, and increased length of follow-up.
In the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) study, there was a significant decline in TD severity ratings among 200 patients with TD at baseline who were randomized to receive 1 of 4 SGAs, but there were no significant differences among these SGAs in decline in AIMS scores (Figure).19 Fifty-five percent of these patients met criteria for TD at 2 consecutive post-baseline visits, 76% met criteria at some or all post-baseline visits, and 24% did not meet criteria at any subsequent visit. In addition, 32% showed ≥50% decrease and 7% showed ≥50% increase in AIMS score. Thus, similar to past evidence on the course of TD during treatment with FGAs or SGAs, most patients in this trial showed either persistence or fluctuation in observable TD symptoms.
Another alternative is to switch antipsychotics, keeping in mind the risk of destabilizing a patient and precipitating psychotic relapse. More potent antipsychotics—such as haloperidol—suppress TD in approximately 67% of patients and may be necessary to consider in patients with severe, disabling symptoms, although the safety of these drugs in relation to their impact on long-term TD outcome is unclear.13,21,22 On the other hand, lower-potency drugs and SGAs also have been associated with reduced TD symptoms23,24; this was confirmed by results of the CATIE trial cited above in which SGAs were associated with a significant reduction in TD severity ratings.19 Clozapine in particular has been recommended for suppressing TD, especially in cases of tardive dystonia.20 Surprisingly, data are limited and inconsistent in addressing whether high-potency FGAs suppress TD symptoms more than low-potency drugs or SGAs, and whether SGAs may suppress TD by mechanisms other than dopamine receptor blockade, which would enhance symptom remission.19,25,26
Apart from short-term suppression of TD symptoms, the advantage of switching to lower-potency antipsychotics or other SGAs would be to increase the odds of eventual TD resolution. Although there has been speculation that in contrast to high-potency FGAs, SGAs may increase the possibility of remission by actively reversing TD or by passively allowing time for TD to resolve, existing data are inconclusive as to whether treatment with SGAs or FGAs results in true recovery rather than symptom suppression. To distinguish remission from suppression, a few studies discontinued SGAs. Some reported continued absence of TD,27,28 but others found unmasking and reappearance of TD.29-31
Adjunctive antidyskinetic drugs. Agents that have been tested off-label for antidyskinetic effects could be considered if symptoms of TD remain problematic despite optimization of antipsychotic treatment, although none have been confirmed as uniformly effective in randomized controlled trials replicated by different investigators.13,17,22 These include dopamine-depleting agents, dopamine agonists, noradrenergic agonists and antagonists, GABAergic drugs (benzodiazepines, valproate, levetiracetam), lithium, calcium channel blockers, serotonergic drugs, antioxidants (vitamin E and B6), branched-chain amino acids, neuropeptides, cholinergic precursors, and cholinesterase inhibitors. Electroconvulsive therapy and botulinum toxin or surgical intervention (for tardive dystonia) also may be considered.
Hypotheses proposed to explain TD pathophysiology and thereby justify trials of specific antidyskinetic agents include dopamine receptor hypersensitivity, GABA insufficiency, and structural damage resulting from increased catecholamine metabolism and oxidative free radical production.32 Another hypothesis proposes that TD results from damage to striatal cholinergic interneurons due to loss of dopamine-mediated inhibition.33 If correct, this implies that cholinesterase inhibitors or cholinergic agonists may suppress TD by directly enhancing post-synaptic cholinergic activity, thereby compensating for the loss of pre-synaptic cholinergic neurons. Several preliminary trials that explored the use of cholinesterase inhibitors had mixed results.34-36 However, this hypothesis is supported by evidence from animal and human studies that correlated antipsychotic-induced changes in cholinergic activity with the delay in onset, irreversibility, and age-related risk of TD, the worsening of symptoms due to anticholinergic drugs, and the reduced liability of SGAs for causing TD. These findings suggest that further investigation of cholinergic mechanisms underlying TD may be worthwhile.35
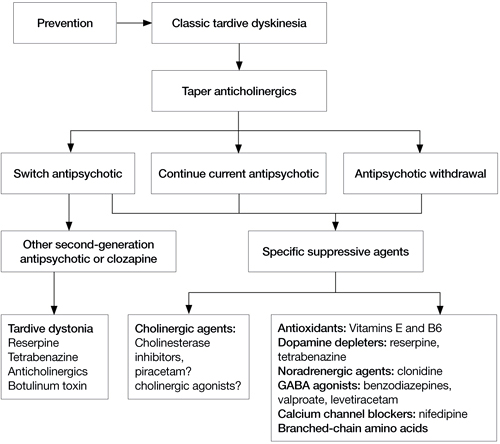
Algorithm: Proposed treatment algorithm for tardive dyskinesia
Source: Reprinted from Caroff SN, Hurford I, Lybrand J, et al. Movement disorders induced by antipsychotic drugs: implications of the CATIE Schizophrenia Trial. Neurol Clin. 2011;29:127-148 with permission from Elsevier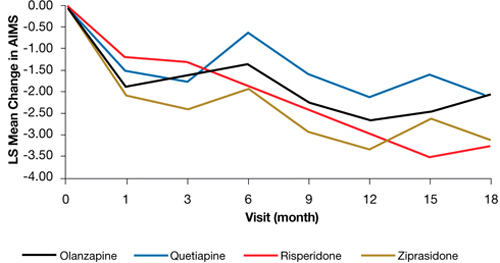
Figure: Adjusteda repeated measures model of change in total AIMS scores for patients with tardive dyskinesia at baseline in CATIE
a Model adjusted for baseline AIMS, baseline PANSS, and duration of illness. Adjusted P value for reduction in total AIMS score from baseline for all patients: P < .001. Treatment differences between the second-generation antipsychotics during the trial: P = .811
AIMS: Abnormal Involuntary Movement Scale; CATIE: Clinical Antipsychotic Trials of Intervention Effectiveness; PANSS: Positive and Negative Syndrome Scale
Source: Reprinted from Caroff SN, Davis VG, Miller DD, et al; for the CATIE Investigators. Treatment outcomes of patients with tardive dyskinesia and chronic schizophrenia. J Clin Psychiatry. 2011;72(3):295-303 with permission from Physician Postgraduate Press, Inc.Related Resources
- National Institute of Neurological Disorders and Stroke. NINDS Tardive Dyskinesia Information Page. www.ninds.nih.gov/disorders/tardive/tardive.htm.
- WE MOVE (Worldwide Education and Awareness for Movement Disorders). www.wemove.org.
Drug Brand Names
- Botulinum toxin • Botox, Dysport, others
- Clonidine • Catapres
- Clozapine • Clozaril
- Haloperidol • Haldol
- Levetiracetam • Keppra
- Levodopa • Dopar, Larodopa
- Lithium • Lithobid, Eskalith, others
- Nifedipine • Adalat, Afeditab CR, others
- Olanzapine • Zyprexa
- Phenytoin • Dilantin
- Quetiapine • Seroquel
- Reserpine • Serpasil
- Risperidone • Risperdal
- Tetrabenazine • Xenazine
- Valproate • Depakote
- Ziprasidone • Geodon
Disclosures
Drs. Caroff, Dhopesh, and Campbell report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Miller receives research/grant support from AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, Ortho-McNeil-Janssen, and Pfizer Inc. and is a consultant to GlaxoSmithKline and Otsuka.
1. Miller DD, Caroff SN, Davis SM, et al. Extrapyramidal side-effects of antipsychotics in a randomised trial. Br J Psychiatry. 2008;193(4):279-288.
2. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353(12):1209-1223.
3. Leucht S, Wahlbeck K, Hamann J, et al. New generation antipsychotics versus low-potency conventional antipsychotics: a systematic review and meta-analysis. Lancet. 2003;361(9369):1581-1589.
4. Guy W. Abnormal involuntary movement scale (AIMS). In: Guy W ed. ECDEU assessment manual for psychopharmacology. Rockville, MD: U.S. Department of Health, Education, and Welfare, Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration, National Institute of Mental Health, Psychopharmacology Research Branch, Division of Extramural Research Programs; 1976:534–537.
5. Tarsy D. Neuroleptic-induced extrapyramidal reactions: classification description, and diagnosis. Clin Neuropharmacol. 1983;6(1):9-26.
6. Kane JM. Tardive dyskinesia: epidemiological and clinical presentation. In: Bloom FE Kupfer DJ, eds. Psychopharmacology: the fourth generation of progress. New York, NY: Raven Press; 1995:1485–1495.
7. Casey DE. Neuroleptic drug-induced extrapyramidal syndromes and tardive dyskinesia. Schizophr Res. 1991;4(2):109-120.
8. Caroff SN, Hurford I, Lybrand J, et al. Movement disorders induced by antipsychotic drugs: implications of the CATIE schizophrenia trial. Neurol Clin. 2011;29(1):127-148.
9. Dayalu P, Chou KL. Antipsychotic-induced extrapyramidal symptoms and their management. Expert Opin Pharmacother. 2008;9(9):1451-1462.
10. Burke RE, Kang UJ, Jankovic J, et al. Tardive akathisia: an analysis of clinical features and response to open therapeutic trials. Mov Disord. 1989;4(2):157-175.
11. Schooler NR, Kane JM. Research diagnoses for tardive dyskinesia. Arch Gen Psychiatry. 1982;39(4):486-487.
12. American Psychiatric Association. Tardive dyskinesia: a task force report of the American Psychiatric Association. Washington DC: American Psychiatric Press, Inc; 1992.
13. Egan MF, Apud J, Wyatt RJ. Treatment of tardive dyskinesia. Schizophr Bull. 1997;23(4):583-609.
14. Casey DE, Gerlach J. Tardive dyskinesia: what is the long-term outcome? In: Casey DE Gardos G, eds. Tardive dyskinesia and neuroleptics: from dogma to reason. Washington, DC: American Psychiatric Press, Inc; 1986:76–97.
15. Glazer WM, Moore DC, Schooler NR, et al. Tardive dyskinesia. A discontinuation study. Arch Gen Psychiatry. 1984;41(6):623-627.
16. Glazer WM, Morgenstern H, Schooler N, et al. Predictors of improvement in tardive dyskinesia following discontinuation of neuroleptic medication. Br J Psychiatry. 1990;157:585-592.
17. Soares KV, McGrath JJ. The treatment of tardive dyskinesia—a systematic review and meta-analysis. Schizophr Res. 1999;39(1):1-16.
18. Gilbert PL, Harris MJ, McAdams LA, et al. Neuroleptic withdrawal in schizophrenic patients. A review of the literature. Arch Gen Psychiatry. 1995;52(3):173-188.
19. Caroff SN, Davis VG, Miller DD, et al. Treatment outcomes of patients with tardive dyskinesia and chronic schizophrenia. J Clin Psychiatry. 2011;72(3):295-303.
20. Lieberman JA, Saltz BL, Johns CA, et al. The effects of clozapine on tardive dyskinesia. Br J Psychiatry. 1991;158:503-510.
21. Jeste DV, Wyatt RJ. In search of treatment for tardive dyskinesia: review of the literature. Schizophr Bull. 1979;5(2):251-293.
22. Jeste DV, Lohr JB, Clark K, et al. Pharmacological treatments of tardive dyskinesia in the 1980s. J Clin Psychopharmacol. 1988;8(4 suppl):38S-48S.
23. Caroff SN, Mann SC, Campbell EC, et al. Movement disorders associated with atypical antipsychotic drugs. J Clin Psychiatry. 2002;63(suppl 4):12-19.
24. Tarsy D, Baldessarini RJ, Tarazi FI. Effects of newer antipsychotics on extrapyramidal function. CNS Drugs. 2002;16(1):23-45.
25. Emsley R, Turner HJ, Schronen J, et al. A single-blind, randomized trial comparing quetiapine and haloperidol in the treatment of tardive dyskinesia. J Clin Psychiatry. 2004;65(5):696-701.
26. Glazer WM, Hafez H. A comparison of masking effects of haloperidol versus molindone in tardive dyskinesia. Schizophr Res. 1990;3(5-6):315-320.
27. Kinon BJ, Jeste DV, Kollack-Walker S, et al. Olanzapine treatment for tardive dyskinesia in schizophrenia patients: a prospective clinical trial with patients randomized to blinded dose reduction periods. Prog Neuropsychopharmacol Biol Psychiatry. 2004;28(6):985-996.
28. Tamminga CA, Thaker GK, Moran M, et al. Clozapine in tardive dyskinesia: observations from human and animal model studies. J Clin Psychiatry. 1994;55(suppl B):102-106.
29. Simpson GM, Lee JH, Shrivastava RK. Clozapine in tardive dyskinesia. Psychopharmacology (Berl). 1978;56(1):75-80.
30. Ahmed S, Chengappa KN, Naidu VR, et al. Clozapine withdrawal-emergent dystonias and dyskinesias: a case series. J Clin Psychiatry. 1998;59(9):472-477.
31. Small JG, Milstein V, Marhenke JD, et al. Treatment outcome with clozapine in tardive dyskinesia, neuroleptic sensitivity, and treatment-resistant psychosis. J Clin Psychiatry. 1987;48(7):263-267.
32. Casey DE. Tardive dyskinesia: pathophysiology and animal models. J Clin Psychiatry. 2000;61(suppl 4):5-9.
33. Miller R, Chouinard G. Loss of striatal cholinergic neurons as a basis for tardive and L-dopa-induced dyskinesias neuroleptic-induced supersensitivity psychosis and refractory schizophrenia. Biol Psychiatry. 1993;34(10):713-738.
34. Caroff SN, Campbell EC, Havey J, et al. Treatment of tardive dyskinesia with donepezil: a pilot study. J Clin Psychiatry. 2001;62(10):772-775.
35. Caroff SN, Walker P, Campbell C, et al. Treatment of tardive dyskinesia with galantamine: a randomized controlled crossover trial. J Clin Psychiatry. 2007;68(3):410-415.
36. Caroff SN, Martine R, Kleiner-Fisman G, et al. Treatment of levodopa-induced dyskinesias with donepezil. Parkinsonism Relat Disord. 2006;12(4):261-263.
Introduced into clinical practice more than a half century ago, antipsychotics are still the mainstay of schizophrenia treatment. However, from the earliest reports, antipsychotic efficacy was seemingly inseparable from extrapyramidal side effects (EPS) that manifested as acute and chronic involuntary movement disorders. Although acute extrapyramidal side effects could be prevented and treated, the late-arising symptoms of tardive dyskinesia (TD) seemed irreversible in most cases.
Concerns over TD stimulated extensive research and fueled efforts to develop new antipsychotics that spared the extrapyramidal motor system. Numerous industry-sponsored trials found a reduced risk of EPS—including TD—with newer, second-generation antipsychotics (SGAs), although this advantage diminished when modest doses of low- or mid-potency first-generation antipsychotics (FGAs) were used as the comparator.1-3 Nevertheless, in addition to the continued potential risk of introducing new cases of TD—even with SGAs—several other factors underscore the need to develop a rational strategy for clinical management of TD, including:
- thousands of patients are left with TD as a legacy of past treatment
- the neurophysiologic mechanisms underlying TD are not well understood
- there is no uniformly effective treatment to reverse TD
- TD may be irreversible in most cases.
Prevention
Because there is no “gold standard” treatment for TD, it is important to minimize the risk of TD by taking preventive measures and detecting incipient signs of the disorder. Preventive principles include:
- confirming and documenting the indication for antipsychotics
- using conservative maintenance doses and opting for lower potency or newer agents
- informing patients and caregivers of risk
- assessing for incipient signs of TD using the Abnormal Involuntary Movement Scale (AIMS),4 which should be administered at least every 3 to 6 months.
Confirming the diagnosis
TD presents as a polymorphous involuntary movement disorder,5-8 most often with nonrhythmic, repetitive, purposeless hyperkinetic symptoms. It usually affects orofacial and lingual musculature (“buccolinguomasticatory syndrome”) with chewing; bruxism; protrusion, curling, or twisting of the tongue; lip smacking, puckering, sucking, and pursing; retraction, grimacing or bridling of the mouth; bulging of the cheeks; or eye blinking and blepharospasm. Choreoathetoid movements of the fingers, hands, or upper or lower extremities also are common. Patients may experience axial symptoms affecting the neck, shoulders, spine, or pelvis. When severe, dyskinesias can affect breathing, swallowing, or speech, and interfere with walking and activities of daily living.
TD may present with nonchoreoathetoid symptoms that can be difficult to distinguish from acute EPS. These may co-exist with classic TD symptoms, but may represent separate subtypes with increased risk of progression, persistence, and severe disability. For example, tardive dystonia, which is estimated to occur in 1% to 4% of patients treated with antipsychotics,9 may be more generalized and disabling than TD, and may respond to anticholinergic agents. Akathisia and other movement disorders also occur as tardive variants.10
Multiple diagnostic schemes for TD have been proposed; criteria proposed by Schooler and Kane have been widely accepted (Table 1).11 TD onset occurs insidiously over ≥3 months of antipsychotic treatment and may begin with tic-like movements or increased eye blinking. TD often is suppressed or masked by ongoing antipsychotic treatment and becomes apparent only when the drug is reduced, switched, or discontinued. Dyskinesias increase with emotional arousal, activation, or distraction, and diminish with relaxation, sleep, or volitional effort. As a result, TD symptoms fluctuate over time; therefore, repeated measurements are necessary for reliable assessment of severity and persistence.
The differential diagnosis of TD necessitates conducting a careful medical and neurologic evaluation of all patients with new-onset movement disorders. Clues to neurologic causes include a family history of movement disorders, sudden onset or progressive course, associated medical or neurologic abnormalities, and asymmetry of symptoms. Some of the medical, neurologic, and psychiatric conditions to consider are listed in Table 2.12
Table 1
Schooler-Kane diagnostic criteria for TD
|
| Probable TD: meets criteria 1 through 3 Masked TD: meets criteria 1 through 3 but movements suppressed within 2 weeks by antipsychotic drugs Transient TD: movements not observed on subsequent examination within 3 months Withdrawal TD: movements observed within 2 weeks of antipsychotic drug discontinuation Persistent TD: movements persist for 3 months |
| TD: tardive dyskinesia Source: Reference 11 |
Table 2
Differential diagnosis of tardive dyskinesia
| Primary movement disorders |
|
| Secondary movement disorders |
|
| Source: Reference 12 |
Treatment decisions
If a patient develops TD, clinicians need to make several decisions (Algorithm). First, consider tapering any anticholinergic drugs unless acute EPS are prominent or tardive dystonia is present. Anticholinergic agents can worsen TD but not tardive dystonia; 60% of TD cases improve after discontinuing anticholinergics.13 Second, decide whether antipsychotics could be safely tapered or discontinued. If antipsychotics cannot be safely tapered, decide whether to maintain the patient’s present antipsychotic or switch to a more or less potent agent. Finally, decide whether a trial of an adjunctive antidyskinetic drug is warranted. All of these decisions require thorough discussion with patients and their families, accompanied by careful documentation.
Discontinuing, continuing, or switching antipsychotics. Discontinuing antipsychotics once TD becomes apparent is an option. However, the natural course of TD after drug withdrawal is unclear. Although drug withdrawal had been recommended to increase the odds of TD resolution, early studies showed withdrawing antipsychotics may lead to an initial worsening of TD in 33% to 53% of patients (unmasking or withdrawal dyskinesia).14 With long-term follow-up, 36% to 55% of patients eventually improved, which supports recommendations for drug reduction or withdrawal.14 However, complete and permanent reversibility beyond the withdrawal period is rare; Glazer et al found only 2% of patients showed complete reversal of TD after drug discontinuation.15,16 In a meta-analysis, Soares and McGrath17 reported 37% of patients assigned to placebo across studies showed at least some improvement in TD, but concluded insufficient evidence existed to support drug cessation or reduction as effective treatments for TD, especially when contrasted with robust evidence for the risk of psychotic relapse after drug withdrawal in patients with schizophrenia (53% within 9 months).18
A second option for a stable patient with good control of psychotic symptoms but established or long-term TD is to continue the antipsychotic, try to gradually reduce the dose, inform patients and caregivers of risks, document the decision, and monitor carefully. In most cases, TD may not progress even with continued antipsychotic treatment, although symptoms may worsen in some cases. However, in a patient with new-onset or early signs of TD, the clinician may be obligated to switch to a lower-potency antipsychotic or newer SGA to improve the chance of resolution; switching is discussed below.
Data on the change in prevalence of TD within a population during continued antipsychotic treatment have been inconsistent. Some studies show an increase, while others show a decrease or no change at all.19 However, prevalence rates obscure the dynamics of TD in individual patients. Roughly 50% of patients with TD have persistent symptoms, 10% to 30% have reduced symptoms, and 10% to 30% experience increased symptoms during treatment.13 Long-term studies estimated that up to 23% of patients may show loss of observable TD symptoms during treatment with FGAs in 1 year.19,20 Similarly, studies of SGAs have shown reduction of TD ratings; some found greater reductions, some found less reductions, and some no difference compared with FGAs.19,20 In some studies, improved TD outcomes were correlated with younger age, lower antipsychotic doses, reduced duration of drug treatment and dyskinesia, and increased length of follow-up.
In the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) study, there was a significant decline in TD severity ratings among 200 patients with TD at baseline who were randomized to receive 1 of 4 SGAs, but there were no significant differences among these SGAs in decline in AIMS scores (Figure).19 Fifty-five percent of these patients met criteria for TD at 2 consecutive post-baseline visits, 76% met criteria at some or all post-baseline visits, and 24% did not meet criteria at any subsequent visit. In addition, 32% showed ≥50% decrease and 7% showed ≥50% increase in AIMS score. Thus, similar to past evidence on the course of TD during treatment with FGAs or SGAs, most patients in this trial showed either persistence or fluctuation in observable TD symptoms.
Another alternative is to switch antipsychotics, keeping in mind the risk of destabilizing a patient and precipitating psychotic relapse. More potent antipsychotics—such as haloperidol—suppress TD in approximately 67% of patients and may be necessary to consider in patients with severe, disabling symptoms, although the safety of these drugs in relation to their impact on long-term TD outcome is unclear.13,21,22 On the other hand, lower-potency drugs and SGAs also have been associated with reduced TD symptoms23,24; this was confirmed by results of the CATIE trial cited above in which SGAs were associated with a significant reduction in TD severity ratings.19 Clozapine in particular has been recommended for suppressing TD, especially in cases of tardive dystonia.20 Surprisingly, data are limited and inconsistent in addressing whether high-potency FGAs suppress TD symptoms more than low-potency drugs or SGAs, and whether SGAs may suppress TD by mechanisms other than dopamine receptor blockade, which would enhance symptom remission.19,25,26
Apart from short-term suppression of TD symptoms, the advantage of switching to lower-potency antipsychotics or other SGAs would be to increase the odds of eventual TD resolution. Although there has been speculation that in contrast to high-potency FGAs, SGAs may increase the possibility of remission by actively reversing TD or by passively allowing time for TD to resolve, existing data are inconclusive as to whether treatment with SGAs or FGAs results in true recovery rather than symptom suppression. To distinguish remission from suppression, a few studies discontinued SGAs. Some reported continued absence of TD,27,28 but others found unmasking and reappearance of TD.29-31
Adjunctive antidyskinetic drugs. Agents that have been tested off-label for antidyskinetic effects could be considered if symptoms of TD remain problematic despite optimization of antipsychotic treatment, although none have been confirmed as uniformly effective in randomized controlled trials replicated by different investigators.13,17,22 These include dopamine-depleting agents, dopamine agonists, noradrenergic agonists and antagonists, GABAergic drugs (benzodiazepines, valproate, levetiracetam), lithium, calcium channel blockers, serotonergic drugs, antioxidants (vitamin E and B6), branched-chain amino acids, neuropeptides, cholinergic precursors, and cholinesterase inhibitors. Electroconvulsive therapy and botulinum toxin or surgical intervention (for tardive dystonia) also may be considered.
Hypotheses proposed to explain TD pathophysiology and thereby justify trials of specific antidyskinetic agents include dopamine receptor hypersensitivity, GABA insufficiency, and structural damage resulting from increased catecholamine metabolism and oxidative free radical production.32 Another hypothesis proposes that TD results from damage to striatal cholinergic interneurons due to loss of dopamine-mediated inhibition.33 If correct, this implies that cholinesterase inhibitors or cholinergic agonists may suppress TD by directly enhancing post-synaptic cholinergic activity, thereby compensating for the loss of pre-synaptic cholinergic neurons. Several preliminary trials that explored the use of cholinesterase inhibitors had mixed results.34-36 However, this hypothesis is supported by evidence from animal and human studies that correlated antipsychotic-induced changes in cholinergic activity with the delay in onset, irreversibility, and age-related risk of TD, the worsening of symptoms due to anticholinergic drugs, and the reduced liability of SGAs for causing TD. These findings suggest that further investigation of cholinergic mechanisms underlying TD may be worthwhile.35
Algorithm: Proposed treatment algorithm for tardive dyskinesia
Source: Reprinted from Caroff SN, Hurford I, Lybrand J, et al. Movement disorders induced by antipsychotic drugs: implications of the CATIE Schizophrenia Trial. Neurol Clin. 2011;29:127-148 with permission from Elsevier
Figure: Adjusteda repeated measures model of change in total AIMS scores for patients with tardive dyskinesia at baseline in CATIE
a Model adjusted for baseline AIMS, baseline PANSS, and duration of illness. Adjusted P value for reduction in total AIMS score from baseline for all patients: P < .001. Treatment differences between the second-generation antipsychotics during the trial: P = .811
AIMS: Abnormal Involuntary Movement Scale; CATIE: Clinical Antipsychotic Trials of Intervention Effectiveness; PANSS: Positive and Negative Syndrome Scale
Source: Reprinted from Caroff SN, Davis VG, Miller DD, et al; for the CATIE Investigators. Treatment outcomes of patients with tardive dyskinesia and chronic schizophrenia. J Clin Psychiatry. 2011;72(3):295-303 with permission from Physician Postgraduate Press, Inc.Related Resources
- National Institute of Neurological Disorders and Stroke. NINDS Tardive Dyskinesia Information Page. www.ninds.nih.gov/disorders/tardive/tardive.htm.
- WE MOVE (Worldwide Education and Awareness for Movement Disorders). www.wemove.org.
Drug Brand Names
- Botulinum toxin • Botox, Dysport, others
- Clonidine • Catapres
- Clozapine • Clozaril
- Haloperidol • Haldol
- Levetiracetam • Keppra
- Levodopa • Dopar, Larodopa
- Lithium • Lithobid, Eskalith, others
- Nifedipine • Adalat, Afeditab CR, others
- Olanzapine • Zyprexa
- Phenytoin • Dilantin
- Quetiapine • Seroquel
- Reserpine • Serpasil
- Risperidone • Risperdal
- Tetrabenazine • Xenazine
- Valproate • Depakote
- Ziprasidone • Geodon
Disclosures
Drs. Caroff, Dhopesh, and Campbell report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Miller receives research/grant support from AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, Ortho-McNeil-Janssen, and Pfizer Inc. and is a consultant to GlaxoSmithKline and Otsuka.
Introduced into clinical practice more than a half century ago, antipsychotics are still the mainstay of schizophrenia treatment. However, from the earliest reports, antipsychotic efficacy was seemingly inseparable from extrapyramidal side effects (EPS) that manifested as acute and chronic involuntary movement disorders. Although acute extrapyramidal side effects could be prevented and treated, the late-arising symptoms of tardive dyskinesia (TD) seemed irreversible in most cases.
Concerns over TD stimulated extensive research and fueled efforts to develop new antipsychotics that spared the extrapyramidal motor system. Numerous industry-sponsored trials found a reduced risk of EPS—including TD—with newer, second-generation antipsychotics (SGAs), although this advantage diminished when modest doses of low- or mid-potency first-generation antipsychotics (FGAs) were used as the comparator.1-3 Nevertheless, in addition to the continued potential risk of introducing new cases of TD—even with SGAs—several other factors underscore the need to develop a rational strategy for clinical management of TD, including:
- thousands of patients are left with TD as a legacy of past treatment
- the neurophysiologic mechanisms underlying TD are not well understood
- there is no uniformly effective treatment to reverse TD
- TD may be irreversible in most cases.
Prevention
Because there is no “gold standard” treatment for TD, it is important to minimize the risk of TD by taking preventive measures and detecting incipient signs of the disorder. Preventive principles include:
- confirming and documenting the indication for antipsychotics
- using conservative maintenance doses and opting for lower potency or newer agents
- informing patients and caregivers of risk
- assessing for incipient signs of TD using the Abnormal Involuntary Movement Scale (AIMS),4 which should be administered at least every 3 to 6 months.
Confirming the diagnosis
TD presents as a polymorphous involuntary movement disorder,5-8 most often with nonrhythmic, repetitive, purposeless hyperkinetic symptoms. It usually affects orofacial and lingual musculature (“buccolinguomasticatory syndrome”) with chewing; bruxism; protrusion, curling, or twisting of the tongue; lip smacking, puckering, sucking, and pursing; retraction, grimacing or bridling of the mouth; bulging of the cheeks; or eye blinking and blepharospasm. Choreoathetoid movements of the fingers, hands, or upper or lower extremities also are common. Patients may experience axial symptoms affecting the neck, shoulders, spine, or pelvis. When severe, dyskinesias can affect breathing, swallowing, or speech, and interfere with walking and activities of daily living.
TD may present with nonchoreoathetoid symptoms that can be difficult to distinguish from acute EPS. These may co-exist with classic TD symptoms, but may represent separate subtypes with increased risk of progression, persistence, and severe disability. For example, tardive dystonia, which is estimated to occur in 1% to 4% of patients treated with antipsychotics,9 may be more generalized and disabling than TD, and may respond to anticholinergic agents. Akathisia and other movement disorders also occur as tardive variants.10
Multiple diagnostic schemes for TD have been proposed; criteria proposed by Schooler and Kane have been widely accepted (Table 1).11 TD onset occurs insidiously over ≥3 months of antipsychotic treatment and may begin with tic-like movements or increased eye blinking. TD often is suppressed or masked by ongoing antipsychotic treatment and becomes apparent only when the drug is reduced, switched, or discontinued. Dyskinesias increase with emotional arousal, activation, or distraction, and diminish with relaxation, sleep, or volitional effort. As a result, TD symptoms fluctuate over time; therefore, repeated measurements are necessary for reliable assessment of severity and persistence.
The differential diagnosis of TD necessitates conducting a careful medical and neurologic evaluation of all patients with new-onset movement disorders. Clues to neurologic causes include a family history of movement disorders, sudden onset or progressive course, associated medical or neurologic abnormalities, and asymmetry of symptoms. Some of the medical, neurologic, and psychiatric conditions to consider are listed in Table 2.12
Table 1
Schooler-Kane diagnostic criteria for TD
|
| Probable TD: meets criteria 1 through 3 Masked TD: meets criteria 1 through 3 but movements suppressed within 2 weeks by antipsychotic drugs Transient TD: movements not observed on subsequent examination within 3 months Withdrawal TD: movements observed within 2 weeks of antipsychotic drug discontinuation Persistent TD: movements persist for 3 months |
| TD: tardive dyskinesia Source: Reference 11 |
Table 2
Differential diagnosis of tardive dyskinesia
| Primary movement disorders |
|
| Secondary movement disorders |
|
| Source: Reference 12 |
Treatment decisions
If a patient develops TD, clinicians need to make several decisions (Algorithm). First, consider tapering any anticholinergic drugs unless acute EPS are prominent or tardive dystonia is present. Anticholinergic agents can worsen TD but not tardive dystonia; 60% of TD cases improve after discontinuing anticholinergics.13 Second, decide whether antipsychotics could be safely tapered or discontinued. If antipsychotics cannot be safely tapered, decide whether to maintain the patient’s present antipsychotic or switch to a more or less potent agent. Finally, decide whether a trial of an adjunctive antidyskinetic drug is warranted. All of these decisions require thorough discussion with patients and their families, accompanied by careful documentation.
Discontinuing, continuing, or switching antipsychotics. Discontinuing antipsychotics once TD becomes apparent is an option. However, the natural course of TD after drug withdrawal is unclear. Although drug withdrawal had been recommended to increase the odds of TD resolution, early studies showed withdrawing antipsychotics may lead to an initial worsening of TD in 33% to 53% of patients (unmasking or withdrawal dyskinesia).14 With long-term follow-up, 36% to 55% of patients eventually improved, which supports recommendations for drug reduction or withdrawal.14 However, complete and permanent reversibility beyond the withdrawal period is rare; Glazer et al found only 2% of patients showed complete reversal of TD after drug discontinuation.15,16 In a meta-analysis, Soares and McGrath17 reported 37% of patients assigned to placebo across studies showed at least some improvement in TD, but concluded insufficient evidence existed to support drug cessation or reduction as effective treatments for TD, especially when contrasted with robust evidence for the risk of psychotic relapse after drug withdrawal in patients with schizophrenia (53% within 9 months).18
A second option for a stable patient with good control of psychotic symptoms but established or long-term TD is to continue the antipsychotic, try to gradually reduce the dose, inform patients and caregivers of risks, document the decision, and monitor carefully. In most cases, TD may not progress even with continued antipsychotic treatment, although symptoms may worsen in some cases. However, in a patient with new-onset or early signs of TD, the clinician may be obligated to switch to a lower-potency antipsychotic or newer SGA to improve the chance of resolution; switching is discussed below.
Data on the change in prevalence of TD within a population during continued antipsychotic treatment have been inconsistent. Some studies show an increase, while others show a decrease or no change at all.19 However, prevalence rates obscure the dynamics of TD in individual patients. Roughly 50% of patients with TD have persistent symptoms, 10% to 30% have reduced symptoms, and 10% to 30% experience increased symptoms during treatment.13 Long-term studies estimated that up to 23% of patients may show loss of observable TD symptoms during treatment with FGAs in 1 year.19,20 Similarly, studies of SGAs have shown reduction of TD ratings; some found greater reductions, some found less reductions, and some no difference compared with FGAs.19,20 In some studies, improved TD outcomes were correlated with younger age, lower antipsychotic doses, reduced duration of drug treatment and dyskinesia, and increased length of follow-up.
In the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) study, there was a significant decline in TD severity ratings among 200 patients with TD at baseline who were randomized to receive 1 of 4 SGAs, but there were no significant differences among these SGAs in decline in AIMS scores (Figure).19 Fifty-five percent of these patients met criteria for TD at 2 consecutive post-baseline visits, 76% met criteria at some or all post-baseline visits, and 24% did not meet criteria at any subsequent visit. In addition, 32% showed ≥50% decrease and 7% showed ≥50% increase in AIMS score. Thus, similar to past evidence on the course of TD during treatment with FGAs or SGAs, most patients in this trial showed either persistence or fluctuation in observable TD symptoms.
Another alternative is to switch antipsychotics, keeping in mind the risk of destabilizing a patient and precipitating psychotic relapse. More potent antipsychotics—such as haloperidol—suppress TD in approximately 67% of patients and may be necessary to consider in patients with severe, disabling symptoms, although the safety of these drugs in relation to their impact on long-term TD outcome is unclear.13,21,22 On the other hand, lower-potency drugs and SGAs also have been associated with reduced TD symptoms23,24; this was confirmed by results of the CATIE trial cited above in which SGAs were associated with a significant reduction in TD severity ratings.19 Clozapine in particular has been recommended for suppressing TD, especially in cases of tardive dystonia.20 Surprisingly, data are limited and inconsistent in addressing whether high-potency FGAs suppress TD symptoms more than low-potency drugs or SGAs, and whether SGAs may suppress TD by mechanisms other than dopamine receptor blockade, which would enhance symptom remission.19,25,26
Apart from short-term suppression of TD symptoms, the advantage of switching to lower-potency antipsychotics or other SGAs would be to increase the odds of eventual TD resolution. Although there has been speculation that in contrast to high-potency FGAs, SGAs may increase the possibility of remission by actively reversing TD or by passively allowing time for TD to resolve, existing data are inconclusive as to whether treatment with SGAs or FGAs results in true recovery rather than symptom suppression. To distinguish remission from suppression, a few studies discontinued SGAs. Some reported continued absence of TD,27,28 but others found unmasking and reappearance of TD.29-31
Adjunctive antidyskinetic drugs. Agents that have been tested off-label for antidyskinetic effects could be considered if symptoms of TD remain problematic despite optimization of antipsychotic treatment, although none have been confirmed as uniformly effective in randomized controlled trials replicated by different investigators.13,17,22 These include dopamine-depleting agents, dopamine agonists, noradrenergic agonists and antagonists, GABAergic drugs (benzodiazepines, valproate, levetiracetam), lithium, calcium channel blockers, serotonergic drugs, antioxidants (vitamin E and B6), branched-chain amino acids, neuropeptides, cholinergic precursors, and cholinesterase inhibitors. Electroconvulsive therapy and botulinum toxin or surgical intervention (for tardive dystonia) also may be considered.
Hypotheses proposed to explain TD pathophysiology and thereby justify trials of specific antidyskinetic agents include dopamine receptor hypersensitivity, GABA insufficiency, and structural damage resulting from increased catecholamine metabolism and oxidative free radical production.32 Another hypothesis proposes that TD results from damage to striatal cholinergic interneurons due to loss of dopamine-mediated inhibition.33 If correct, this implies that cholinesterase inhibitors or cholinergic agonists may suppress TD by directly enhancing post-synaptic cholinergic activity, thereby compensating for the loss of pre-synaptic cholinergic neurons. Several preliminary trials that explored the use of cholinesterase inhibitors had mixed results.34-36 However, this hypothesis is supported by evidence from animal and human studies that correlated antipsychotic-induced changes in cholinergic activity with the delay in onset, irreversibility, and age-related risk of TD, the worsening of symptoms due to anticholinergic drugs, and the reduced liability of SGAs for causing TD. These findings suggest that further investigation of cholinergic mechanisms underlying TD may be worthwhile.35
Algorithm: Proposed treatment algorithm for tardive dyskinesia
Source: Reprinted from Caroff SN, Hurford I, Lybrand J, et al. Movement disorders induced by antipsychotic drugs: implications of the CATIE Schizophrenia Trial. Neurol Clin. 2011;29:127-148 with permission from Elsevier
Figure: Adjusteda repeated measures model of change in total AIMS scores for patients with tardive dyskinesia at baseline in CATIE
a Model adjusted for baseline AIMS, baseline PANSS, and duration of illness. Adjusted P value for reduction in total AIMS score from baseline for all patients: P < .001. Treatment differences between the second-generation antipsychotics during the trial: P = .811
AIMS: Abnormal Involuntary Movement Scale; CATIE: Clinical Antipsychotic Trials of Intervention Effectiveness; PANSS: Positive and Negative Syndrome Scale
Source: Reprinted from Caroff SN, Davis VG, Miller DD, et al; for the CATIE Investigators. Treatment outcomes of patients with tardive dyskinesia and chronic schizophrenia. J Clin Psychiatry. 2011;72(3):295-303 with permission from Physician Postgraduate Press, Inc.Related Resources
- National Institute of Neurological Disorders and Stroke. NINDS Tardive Dyskinesia Information Page. www.ninds.nih.gov/disorders/tardive/tardive.htm.
- WE MOVE (Worldwide Education and Awareness for Movement Disorders). www.wemove.org.
Drug Brand Names
- Botulinum toxin • Botox, Dysport, others
- Clonidine • Catapres
- Clozapine • Clozaril
- Haloperidol • Haldol
- Levetiracetam • Keppra
- Levodopa • Dopar, Larodopa
- Lithium • Lithobid, Eskalith, others
- Nifedipine • Adalat, Afeditab CR, others
- Olanzapine • Zyprexa
- Phenytoin • Dilantin
- Quetiapine • Seroquel
- Reserpine • Serpasil
- Risperidone • Risperdal
- Tetrabenazine • Xenazine
- Valproate • Depakote
- Ziprasidone • Geodon
Disclosures
Drs. Caroff, Dhopesh, and Campbell report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Miller receives research/grant support from AstraZeneca, Bristol-Myers Squibb, Eli Lilly and Company, Ortho-McNeil-Janssen, and Pfizer Inc. and is a consultant to GlaxoSmithKline and Otsuka.
1. Miller DD, Caroff SN, Davis SM, et al. Extrapyramidal side-effects of antipsychotics in a randomised trial. Br J Psychiatry. 2008;193(4):279-288.
2. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353(12):1209-1223.
3. Leucht S, Wahlbeck K, Hamann J, et al. New generation antipsychotics versus low-potency conventional antipsychotics: a systematic review and meta-analysis. Lancet. 2003;361(9369):1581-1589.
4. Guy W. Abnormal involuntary movement scale (AIMS). In: Guy W ed. ECDEU assessment manual for psychopharmacology. Rockville, MD: U.S. Department of Health, Education, and Welfare, Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration, National Institute of Mental Health, Psychopharmacology Research Branch, Division of Extramural Research Programs; 1976:534–537.
5. Tarsy D. Neuroleptic-induced extrapyramidal reactions: classification description, and diagnosis. Clin Neuropharmacol. 1983;6(1):9-26.
6. Kane JM. Tardive dyskinesia: epidemiological and clinical presentation. In: Bloom FE Kupfer DJ, eds. Psychopharmacology: the fourth generation of progress. New York, NY: Raven Press; 1995:1485–1495.
7. Casey DE. Neuroleptic drug-induced extrapyramidal syndromes and tardive dyskinesia. Schizophr Res. 1991;4(2):109-120.
8. Caroff SN, Hurford I, Lybrand J, et al. Movement disorders induced by antipsychotic drugs: implications of the CATIE schizophrenia trial. Neurol Clin. 2011;29(1):127-148.
9. Dayalu P, Chou KL. Antipsychotic-induced extrapyramidal symptoms and their management. Expert Opin Pharmacother. 2008;9(9):1451-1462.
10. Burke RE, Kang UJ, Jankovic J, et al. Tardive akathisia: an analysis of clinical features and response to open therapeutic trials. Mov Disord. 1989;4(2):157-175.
11. Schooler NR, Kane JM. Research diagnoses for tardive dyskinesia. Arch Gen Psychiatry. 1982;39(4):486-487.
12. American Psychiatric Association. Tardive dyskinesia: a task force report of the American Psychiatric Association. Washington DC: American Psychiatric Press, Inc; 1992.
13. Egan MF, Apud J, Wyatt RJ. Treatment of tardive dyskinesia. Schizophr Bull. 1997;23(4):583-609.
14. Casey DE, Gerlach J. Tardive dyskinesia: what is the long-term outcome? In: Casey DE Gardos G, eds. Tardive dyskinesia and neuroleptics: from dogma to reason. Washington, DC: American Psychiatric Press, Inc; 1986:76–97.
15. Glazer WM, Moore DC, Schooler NR, et al. Tardive dyskinesia. A discontinuation study. Arch Gen Psychiatry. 1984;41(6):623-627.
16. Glazer WM, Morgenstern H, Schooler N, et al. Predictors of improvement in tardive dyskinesia following discontinuation of neuroleptic medication. Br J Psychiatry. 1990;157:585-592.
17. Soares KV, McGrath JJ. The treatment of tardive dyskinesia—a systematic review and meta-analysis. Schizophr Res. 1999;39(1):1-16.
18. Gilbert PL, Harris MJ, McAdams LA, et al. Neuroleptic withdrawal in schizophrenic patients. A review of the literature. Arch Gen Psychiatry. 1995;52(3):173-188.
19. Caroff SN, Davis VG, Miller DD, et al. Treatment outcomes of patients with tardive dyskinesia and chronic schizophrenia. J Clin Psychiatry. 2011;72(3):295-303.
20. Lieberman JA, Saltz BL, Johns CA, et al. The effects of clozapine on tardive dyskinesia. Br J Psychiatry. 1991;158:503-510.
21. Jeste DV, Wyatt RJ. In search of treatment for tardive dyskinesia: review of the literature. Schizophr Bull. 1979;5(2):251-293.
22. Jeste DV, Lohr JB, Clark K, et al. Pharmacological treatments of tardive dyskinesia in the 1980s. J Clin Psychopharmacol. 1988;8(4 suppl):38S-48S.
23. Caroff SN, Mann SC, Campbell EC, et al. Movement disorders associated with atypical antipsychotic drugs. J Clin Psychiatry. 2002;63(suppl 4):12-19.
24. Tarsy D, Baldessarini RJ, Tarazi FI. Effects of newer antipsychotics on extrapyramidal function. CNS Drugs. 2002;16(1):23-45.
25. Emsley R, Turner HJ, Schronen J, et al. A single-blind, randomized trial comparing quetiapine and haloperidol in the treatment of tardive dyskinesia. J Clin Psychiatry. 2004;65(5):696-701.
26. Glazer WM, Hafez H. A comparison of masking effects of haloperidol versus molindone in tardive dyskinesia. Schizophr Res. 1990;3(5-6):315-320.
27. Kinon BJ, Jeste DV, Kollack-Walker S, et al. Olanzapine treatment for tardive dyskinesia in schizophrenia patients: a prospective clinical trial with patients randomized to blinded dose reduction periods. Prog Neuropsychopharmacol Biol Psychiatry. 2004;28(6):985-996.
28. Tamminga CA, Thaker GK, Moran M, et al. Clozapine in tardive dyskinesia: observations from human and animal model studies. J Clin Psychiatry. 1994;55(suppl B):102-106.
29. Simpson GM, Lee JH, Shrivastava RK. Clozapine in tardive dyskinesia. Psychopharmacology (Berl). 1978;56(1):75-80.
30. Ahmed S, Chengappa KN, Naidu VR, et al. Clozapine withdrawal-emergent dystonias and dyskinesias: a case series. J Clin Psychiatry. 1998;59(9):472-477.
31. Small JG, Milstein V, Marhenke JD, et al. Treatment outcome with clozapine in tardive dyskinesia, neuroleptic sensitivity, and treatment-resistant psychosis. J Clin Psychiatry. 1987;48(7):263-267.
32. Casey DE. Tardive dyskinesia: pathophysiology and animal models. J Clin Psychiatry. 2000;61(suppl 4):5-9.
33. Miller R, Chouinard G. Loss of striatal cholinergic neurons as a basis for tardive and L-dopa-induced dyskinesias neuroleptic-induced supersensitivity psychosis and refractory schizophrenia. Biol Psychiatry. 1993;34(10):713-738.
34. Caroff SN, Campbell EC, Havey J, et al. Treatment of tardive dyskinesia with donepezil: a pilot study. J Clin Psychiatry. 2001;62(10):772-775.
35. Caroff SN, Walker P, Campbell C, et al. Treatment of tardive dyskinesia with galantamine: a randomized controlled crossover trial. J Clin Psychiatry. 2007;68(3):410-415.
36. Caroff SN, Martine R, Kleiner-Fisman G, et al. Treatment of levodopa-induced dyskinesias with donepezil. Parkinsonism Relat Disord. 2006;12(4):261-263.
1. Miller DD, Caroff SN, Davis SM, et al. Extrapyramidal side-effects of antipsychotics in a randomised trial. Br J Psychiatry. 2008;193(4):279-288.
2. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353(12):1209-1223.
3. Leucht S, Wahlbeck K, Hamann J, et al. New generation antipsychotics versus low-potency conventional antipsychotics: a systematic review and meta-analysis. Lancet. 2003;361(9369):1581-1589.
4. Guy W. Abnormal involuntary movement scale (AIMS). In: Guy W ed. ECDEU assessment manual for psychopharmacology. Rockville, MD: U.S. Department of Health, Education, and Welfare, Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration, National Institute of Mental Health, Psychopharmacology Research Branch, Division of Extramural Research Programs; 1976:534–537.
5. Tarsy D. Neuroleptic-induced extrapyramidal reactions: classification description, and diagnosis. Clin Neuropharmacol. 1983;6(1):9-26.
6. Kane JM. Tardive dyskinesia: epidemiological and clinical presentation. In: Bloom FE Kupfer DJ, eds. Psychopharmacology: the fourth generation of progress. New York, NY: Raven Press; 1995:1485–1495.
7. Casey DE. Neuroleptic drug-induced extrapyramidal syndromes and tardive dyskinesia. Schizophr Res. 1991;4(2):109-120.
8. Caroff SN, Hurford I, Lybrand J, et al. Movement disorders induced by antipsychotic drugs: implications of the CATIE schizophrenia trial. Neurol Clin. 2011;29(1):127-148.
9. Dayalu P, Chou KL. Antipsychotic-induced extrapyramidal symptoms and their management. Expert Opin Pharmacother. 2008;9(9):1451-1462.
10. Burke RE, Kang UJ, Jankovic J, et al. Tardive akathisia: an analysis of clinical features and response to open therapeutic trials. Mov Disord. 1989;4(2):157-175.
11. Schooler NR, Kane JM. Research diagnoses for tardive dyskinesia. Arch Gen Psychiatry. 1982;39(4):486-487.
12. American Psychiatric Association. Tardive dyskinesia: a task force report of the American Psychiatric Association. Washington DC: American Psychiatric Press, Inc; 1992.
13. Egan MF, Apud J, Wyatt RJ. Treatment of tardive dyskinesia. Schizophr Bull. 1997;23(4):583-609.
14. Casey DE, Gerlach J. Tardive dyskinesia: what is the long-term outcome? In: Casey DE Gardos G, eds. Tardive dyskinesia and neuroleptics: from dogma to reason. Washington, DC: American Psychiatric Press, Inc; 1986:76–97.
15. Glazer WM, Moore DC, Schooler NR, et al. Tardive dyskinesia. A discontinuation study. Arch Gen Psychiatry. 1984;41(6):623-627.
16. Glazer WM, Morgenstern H, Schooler N, et al. Predictors of improvement in tardive dyskinesia following discontinuation of neuroleptic medication. Br J Psychiatry. 1990;157:585-592.
17. Soares KV, McGrath JJ. The treatment of tardive dyskinesia—a systematic review and meta-analysis. Schizophr Res. 1999;39(1):1-16.
18. Gilbert PL, Harris MJ, McAdams LA, et al. Neuroleptic withdrawal in schizophrenic patients. A review of the literature. Arch Gen Psychiatry. 1995;52(3):173-188.
19. Caroff SN, Davis VG, Miller DD, et al. Treatment outcomes of patients with tardive dyskinesia and chronic schizophrenia. J Clin Psychiatry. 2011;72(3):295-303.
20. Lieberman JA, Saltz BL, Johns CA, et al. The effects of clozapine on tardive dyskinesia. Br J Psychiatry. 1991;158:503-510.
21. Jeste DV, Wyatt RJ. In search of treatment for tardive dyskinesia: review of the literature. Schizophr Bull. 1979;5(2):251-293.
22. Jeste DV, Lohr JB, Clark K, et al. Pharmacological treatments of tardive dyskinesia in the 1980s. J Clin Psychopharmacol. 1988;8(4 suppl):38S-48S.
23. Caroff SN, Mann SC, Campbell EC, et al. Movement disorders associated with atypical antipsychotic drugs. J Clin Psychiatry. 2002;63(suppl 4):12-19.
24. Tarsy D, Baldessarini RJ, Tarazi FI. Effects of newer antipsychotics on extrapyramidal function. CNS Drugs. 2002;16(1):23-45.
25. Emsley R, Turner HJ, Schronen J, et al. A single-blind, randomized trial comparing quetiapine and haloperidol in the treatment of tardive dyskinesia. J Clin Psychiatry. 2004;65(5):696-701.
26. Glazer WM, Hafez H. A comparison of masking effects of haloperidol versus molindone in tardive dyskinesia. Schizophr Res. 1990;3(5-6):315-320.
27. Kinon BJ, Jeste DV, Kollack-Walker S, et al. Olanzapine treatment for tardive dyskinesia in schizophrenia patients: a prospective clinical trial with patients randomized to blinded dose reduction periods. Prog Neuropsychopharmacol Biol Psychiatry. 2004;28(6):985-996.
28. Tamminga CA, Thaker GK, Moran M, et al. Clozapine in tardive dyskinesia: observations from human and animal model studies. J Clin Psychiatry. 1994;55(suppl B):102-106.
29. Simpson GM, Lee JH, Shrivastava RK. Clozapine in tardive dyskinesia. Psychopharmacology (Berl). 1978;56(1):75-80.
30. Ahmed S, Chengappa KN, Naidu VR, et al. Clozapine withdrawal-emergent dystonias and dyskinesias: a case series. J Clin Psychiatry. 1998;59(9):472-477.
31. Small JG, Milstein V, Marhenke JD, et al. Treatment outcome with clozapine in tardive dyskinesia, neuroleptic sensitivity, and treatment-resistant psychosis. J Clin Psychiatry. 1987;48(7):263-267.
32. Casey DE. Tardive dyskinesia: pathophysiology and animal models. J Clin Psychiatry. 2000;61(suppl 4):5-9.
33. Miller R, Chouinard G. Loss of striatal cholinergic neurons as a basis for tardive and L-dopa-induced dyskinesias neuroleptic-induced supersensitivity psychosis and refractory schizophrenia. Biol Psychiatry. 1993;34(10):713-738.
34. Caroff SN, Campbell EC, Havey J, et al. Treatment of tardive dyskinesia with donepezil: a pilot study. J Clin Psychiatry. 2001;62(10):772-775.
35. Caroff SN, Walker P, Campbell C, et al. Treatment of tardive dyskinesia with galantamine: a randomized controlled crossover trial. J Clin Psychiatry. 2007;68(3):410-415.
36. Caroff SN, Martine R, Kleiner-Fisman G, et al. Treatment of levodopa-induced dyskinesias with donepezil. Parkinsonism Relat Disord. 2006;12(4):261-263.
Treating bipolar disorder during pregnancy
Discuss this article at www.facebook.com/CurrentPsychiatry
Ms. M, age 31, has bipolar I disorder and takes lamotrigine, 200 mg/d, and aripiprazole, 10 mg/d. She was first hospitalized at age 20 for a manic episode and was discharged on lithium, 1,200 mg/d. She was hospitalized again at age 25 for a depressive episode that occurred after she stopped taking lithium because of undesirable side effects. She was switched to lamotrigine, 200 mg/d, which she tolerated well. Aripiprazole, 10 mg/d, was added 1 year later to address emergence of mild mood elevation symptoms.
During a recent follow-up appointment, Ms. M expresses interest in getting pregnant in the next 6 months. Her mood has been stable for 5 years and she asks if she should stop taking her medications in preparation for pregnancy. What would you recommend?
Because the typical age of onset for bipolar disorder (BD) is late adolescence or early adulthood, women are at risk for new onset or recurrence of mood episodes throughout their peak reproductive years. This article updates practitioners on the treatment of BD during pregnancy, including preconception planning and the risks and benefits of medication use during pregnancy. We also cover treatment considerations during the postpartum period, such as prophylaxis of mood episodes and mood stabilizer treatment for women who breast-feed.
Prenatal planning
Ideally, “prenatal planning” should begin long before women with BD prepare to have children. Because one-half of pregnancies in the United States are unplanned1 and manic episodes may result in impulsivity and increased sexual activity, all women of reproductive age with BD should be counseled about birth control and risks of unplanned pregnancies. Discussions about risks of in utero exposure to psychotropics should occur when medications are first prescribed. Because certain mood stabilizers, (eg, carbamazepine) may decrease efficacy of oral contraceptives by inducing cytochrome P450 (CYP450) enzymes, women taking these medications also should be counseled about additional methods of birth control.2
Oral contraceptives also may affect mood stabilizer levels through similar mechanisms. Because of CYP450 induction, lamotrigine serum levels are lower during the 3 “active” weeks of exposure to exogenous estrogen. During the “pill-free” last week, lamotrigine levels may increase up to 54%.3
Because mood stabilizers such as valproate are associated with teratogenic risks, women with BD should be asked about contraception at every visit.4 Valproate also has been associated with an increased risk of menstrual cycle irregularity. Some studies have shown that even before initiating mood stabilizers, women with BD have a higher incidence of menstrual cycle irregularity than women without BD, which suggests the link between polycystic ovarian syndrome (PCOS) and BD may be independent of medications and part of the endophenotype.5
The importance of prenatal vitamins should be discussed. The recommended folate dosage for women planning to become pregnant is 0.4 to 1 mg/d and 0.8 to 5 mg/d for women with either a previous pregnancy with neural tube defects or those taking an antiepileptic medication.6
Table 17 summarizes recommendations to improve prenatal planning in women with BD. Goals include:
- meeting with the patient at least 3 months before conception to review current menstrual cycle functioning. If your patient exhibits any signs or symptoms of PCOS, consider referral to a gynecologist
- meeting with patient and partner/significant supports to discuss treatment decisions
- optimizing the patient’s mood before conception, preferably for at least 3 to 6 months
- prescribing monotherapy at the lowest therapeutic dose if clinically feasible
- assessing the patient’s personal preferences and beliefs regarding medication use during pregnancy and breast-feeding
- assessing the patient’s capacity to understand the risks and benefits of medication continuation/discontinuation during pregnancy, including risk for relapse, current literature on teratogenicity, perinatal complications, and neurodevelopmental studies. Document that the patient provides informed consent.
Table 1
Pregnancy and BD: Medication management guidelines
| Comprehensive prenatal counseling should begin at least 3 months before pregnancy. Folate supplementation is advised |
| Medication should be avoided if clinically feasible (particularly during the first trimester). Avoid abrupt discontinuation. Increase psychosocial and clinical supports |
If medication is pursued:
|
Comprehensive postpartum counseling should begin before and be reinforced throughout pregnancy, emphasizing:
|
| BD: bipolar disorder Source: Adapted from reference 7 |
CASE CONTINUED: Medication decisions
Ms. M’s first question is, “Should I stop taking my medications?” Ms. M and her psychiatrist review the risks and benefits of medication exposure during pregnancy (Table 2) and decide against discontinuing all medications because of her history of relapse when she stopped lithium. Because Ms. M’s mood has been stable for 5 years, she and her psychiatrist decide to limit her medications to lamotrigine monotherapy at her current dose, and agree to slowly taper aripiprazole. One week later, Ms. M calls and states she has a positive pregnancy test and is wondering if she should stop aripiprazole all at once. Ms. M is advised to continue with the original plan to slowly taper aripiprazole.
Table 2
Potential risks of continuing or discontinuing medications for BD during pregnancy
| Risks of discontinuing | Risks of continuing |
|---|---|
| Mood relapse during pregnancy or postpartum Risks of alternative treatment(s):
| Medication-specific risks:
|
| BD: bipolar disorder | |
Medication risks/benefits
Women with BD have a high rate of relapse associated with abrupt discontinuation of pharmacotherapy during pregnancy. As such, patients and their partners and families should be cautioned against rapid discontinuation of medications.8 The risk to mother and fetus is particularly high for women with a history of recurrent, severe mood episodes. These patients face not only a high risk of recurrence of mood episodes, but also the inherent danger of impulsivity, poor self-care, and suicidality associated with mania, depression, and mixed states. In these cases, continuing a medication (other than known teratogens such as valproate) that has effectively stabilized mood may be preferred to discontinuation; these decisions are made after careful risk/benefit assessment.
Carefully reviewing the patient’s history is essential to assessing the risks and benefits of tapering medications before pregnancy. Consider the frequency and severity of your patient’s mood episodes, and whether a switch in mood state was rapid or had a prodromal phase. If a patient currently has a stable mood, a history of mild to moderate mood episodes, a history of prodromal symptoms (eg, gradually increasing sleep disturbances and mood deterioration), and no history of rapid switches, gradually discontinuing medications before or during pregnancy may be considered. However, encourage women to enlist their partners and family members to monitor for warning symptoms and advocate for early medication intervention. Because insomnia is a sign of relapse for many patients, educate women and their families about the importance of maintaining a regular sleep/wake cycle and alerting care providers if this cycle changes.
Mood stabilizers with the greatest risk for teratogenicity are valproate, carbamazepine, and lithium.9 Valproate is associated with a 6% to 13% risk of congenital malformation, including neural tube defects (1% to 2%) and cardiac or craniofacial defects.3 Risks increase at doses >800 mg/d.10 Potential perinatal complications associated with valproate include heart rate deceleration, abnormal tone (hypotonia or hypertonia), and growth retardation.11 Neurobehavioral sequelae include lower IQ scores and increased risk of autism.12
Carbamazepine is associated with a 2% to 5% risk of congenital malformation, including neural tube defects and cardiac or craniofacial defects.4 Perinatal complications associated with carbamazepine include vitamin K deficiency.4 The neurobehavioral sequelae of carbamazepine are controversial; most prospective studies do not suggest long-term cognitive deficits.13 It is strongly recommended that valproate and carbamazepine be avoided, if possible, in women with BD who plan to become pregnant in the near future.
Prospective studies of lithium have shown a 2.8% rate of congenital malformations, which is much lower than the 11% rate found in retrospective studies.14 Ebstein’s anomaly—downward displacement of the tricuspid valve—is estimated to occur in .05% to 0.1% of infants exposed to lithium, which is 10 to 20 times the base rate, but a low absolute risk.11
It is recommended women taking lithium during pregnancy complete a fetal high resolution ultrasound and echocardiogram at 16 to 18 weeks.11 Perinatal complications associated with lithium include prematurity, hypotonia, hypothyroidism, hepatic abnormalities, respiratory distress, and nephrogenic diabetes insipidus.15 When prescribing lithium, divided doses are recommended to maintain a stable serum level. Serum lithium levels should be monitored frequently, and higher doses may be needed because of increased glomerular filtration rate and plasma volume throughout pregnancy.10 Because of fluid shifts at delivery—including blood loss during delivery and postpartum diuresis and diaphoresis—there is a risk of lithium toxicity at this time. Some researchers have suggested suspending lithium treatment during labor or 24 to 48 hours before planned induction or Caesarean section may lower this risk, with re-administration after delivery when medically stable.16 Women should be followed closely for signs of lithium toxicity and have lithium levels monitored as clinically indicated.16 There is insufficient data to support any neurobehavioral sequelae of in utero exposure to lithium; however, there are few long-term follow up studies using standardized measures.17
Lamotrigine is associated with a 1.9% to 4.6% rate of congenital malformations, including cleft lip/palate (8.9/1,000 vs 0.5 to 1.2/1,000 baseline).4 Studies suggest that rates of malformations (cardiac, genitourinary, gastrointestinal, neural tube defect) are dose-dependent: 1.3% at dosages <100 mg/d, 1.9% at 100 to 200 mg/d, and 5.4% at >200 mg/d.18 Because cleft lip and palate are formed by late second trimester, it is recommended to attempt to keep the lamotrigine dose <200 mg/d during the first and second trimesters. Higher doses of lamotrigine may be needed in the third trimester because of increased renal clearance.19 There is insufficient data to support any lamotrigine-associated neurobehavioral effects, and unlike studies of valproate, follow-up evaluations of lamotrigine-exposed children have not shown lower IQs.20
Evidence about the reproductive safety of other mood stabilizers used in BD is limited. A recent population-based cohort study did not show increased risk of major malformations in children exposed to topiramate, gabapentin, or oxcarbazepine during the first trimester of pregnancy.21 Topiramate often is used in combination with other mood stabilizers for weight control, and studies suggest that polypharmacy with topiramate, especially at higher doses and with valproate, increases the risk of major congenital malformations, especially cleft lip and cleft palate.22 Consequently, topiramate is not recommended for women planning to conceive.
Antipsychotics. Although there is increasing information about outcomes of neonates exposed to atypical antipsychotics during pregnancy, the literature still is limited. The greatest number of studies have evaluated olanzapine, risperidone, and quetiapine and show the rate of congenital malformations is 0.9% to 4.1%, which is consistent with general population rates.23-26 Perinatal complications associated with these atypical antipsychotics include neonatal extrapyramidal syndrome (EPS), possible neonatal adaptation/withdrawal syndrome, and an increased risk of the infant being either large or small for gestational age. Because atypical antipsychotics may increase the risk of metabolic syndrome, women should be counseled about the possible increased risk for gestational diabetes with these medications. None of these drugs have been associated with neurobehavioral sequelae, but long-term follow-up studies of exposed infants are lacking.
For aripiprazole, asenapine, ziprasidone, iloperidone, and lurasidone there is insufficient data about rate of congenital malformations, obstetric complications, and neurobehavioral sequelae. However, perinatal complications associated with these medications include risk of EPS and withdrawal symptoms.25,26
CASE CONTINUED: Worsening mood symptoms
During pregnancy, Ms. M’s mood is stable on lamotrigine, 200 mg/d, and she participates in individual interpersonally oriented psychotherapy to address anxieties related to becoming a mother. However, late in her third trimester, Ms. M reports worsening symptoms, including depressed mood, insomnia, fatigue, and poor motivation. She also learns her mother had an episode of postpartum depression. Ms. M and her doctor discuss the risks of postpartum relapse, but she declines additional medication for prophylaxis because she is concerned about its impact on breast-feeding.
Two days after delivery, Ms. M complains of increased insomnia and depressed mood, and her husband reports she is not getting out of bed. She describes thoughts and images of throwing her baby out the window, and feels her thoughts are controlled by something outside of herself. Ms. M suspects her husband is having an affair.
Postpartum risks
All women with BD should be counseled regarding prophylaxis with mood stabilizers during the postpartum period. Women with BD are at high risk of mania and psychosis postpartum, particularly those with a personal or family history of postpartum psychosis. Postpartum psychosis frequently presents with an abrupt onset, shortly after delivery (Table 3). Although it may present with the classic symptoms of mania or psychotic depression, it also may have features of delirium.27
Clinicians should immediately implement treatment with mood stabilizers and antipsychotics to manage acute psychotic symptoms, while also ruling out medical causes or comorbidities. Hospitalization should be considered. Aggressive treatment of insomnia will help stabilize mood. Electroconvulsive therapy can be used in treatment-refractory or urgent cases.10 Lastly, because approximately 4% of women with postpartum psychosis commit infanticide, all mother/child interactions should be closely supervised.27
In small prospective studies, use of lithium within 48 hours of delivery decreased the risk of relapse of postpartum psychosis within the first 3 months.28,29 In lower-risk patients who have discontinued pharmacotherapy during pregnancy, restarting medication before or immediately after delivery should be considered. At the same time, it is important to minimize sleep disruption, particularly postpartum. Psychoeducation—ideally begun in the preconception counseling visit—is extremely important for emphasizing the need for postpartum sleep.
Table 3
Consequences of postpartum mood relapse
| Suicide/infanticide |
| Reckless behavior/substance abuse |
| Poor self-care/care of infant |
| Difficulty with mother-infant bonding |
| Mood relapse more severe and difficult to treat than prior episodes |
| Possible hospitalization |
Breast-feeding concerns
Data on risks of infant exposure to medications through breast milk are largely limited to case reports and case series. All mood-stabilizing medications have been found to pass into breast milk at varying concentrations.28 If a patient chooses to breast-feed, she should inform her pediatrician of this decision, and she and her support system should be educated about signs of neonatal toxicity. Ideally, the psychiatrist should liaise with the patient’s pediatrician, especially when infants are premature, because the child’s liver metabolism may be immature, leading to higher serum drug levels and in some cases drug accumulation. Encourage patients to consider bottle feeding, either their own breast milk, pumped and stored, or formula. This will allow others to assist with feedings and the patient to have more consistent sleep, which could stabilize mood.
Lamotrigine concentrations in breast milk are highly variable.30 Lamotrigine is processed through glucuronidation, a process that is immature in neonates. One study found serum lamotrigine levels in infants were 23% to 33% of maternal serum levels and milk/plasma ratios were highly variable, ranging from 6% to 147%.30 Infants exposed to lamotrigine in breast milk should be monitored for rash and signs of thrombocytosis, and if clinically indicated, lamotrigine levels should be checked.30 Valproate has a low infant serum/maternal serum ratio; there are rare case reports of hepatotoxicity and thrombocytopenia. Although valproate can be reinitiated because of its lower breast milk concentration, it is not a drug of choice in reproductive-age women because of the many issues described above, including risks during pregnancy, PCOS, and effect on oral contraceptives.
Carbamazepine serum levels in breast-feeding infants range from 6% to 65%; hepatic dysfunction, sedation, and poor feeding have been reported in infants in rare instances.31
Historically, lithium has been considered incompatible with breast-feeding, but recent reports suggest with careful monitoring it may not be contraindicated. In 10 mother/infant pairs, lithium levels in breast milk and infant serum diminished over time, with no adverse neonatal effects.32 However, if an infant does breast-feed, it may be important to monitor thyroid-stimulating hormone, blood urea nitrogen-to-creatinine ratio, and ECG in both mother and infant, especially if the mother is taking high doses of lithium.
The safety of breast-feeding while treated with atypical antipsychotics is largely unknown. Case reports indicate low transmission of these medications into breast milk.28
CASE CONTINUED
Ms. M is admitted for psychiatric hospitalization because of worsening psychotic symptoms, poor self-care, and persistent thoughts of harming her baby. She agrees to restart aripiprazole, which is titrated to 20 mg/d. Breast-feeding is not pursued. She is discharged in 10 days after she no longer has thoughts of harming her baby, delusions, or psychotic or suicidal ideation. She and her family agree to close supervision by her family and outpatient follow-up.
Related Resources
- The Hospital for Sick Children. Pregnancy and breastfeeding resources. www.motherisk.org/women/pregnancyResources.jsp.
- U.S. National Library of Medicine. TOXNET toxicology data network. http://toxnet.nlm.nih.gov.
Drug Brand Names
- Aripiprazole • Abilify
- Asenapine • Saphris
- Carbamazepine • Equetro, Tegretol
- Gabapentin • Neurontin
- Iloperidone • Fanapt
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Lurasidone • Latuda
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Topiramate • Topamax
- Valproate • Depacon
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgement
The authors would like to thank Natasha Barthel, BS, for her assistance with this article.
1. Finer LB, Henshaw SK. Disparities in rates of unintended pregnancy in the United States, 1994 and 2001. Perspect Sex Reprod Health. 2006;38(2):90-96.
2. ACOG Committee on Practice Bulletins-Gynecology. ACOG practice bulletin. No. 73: use of hormonal contraception in women with coexisting medical conditions. Obstet Gynecol. 2006;107(6):1453-1472.
3. Wegner I, Edelbroek PM, Bulk S, et al. Lamotrigine kinetics within the menstrual cycle, after menopause, and with oral contraceptives. Neurology. 2009;73(17):1388-1393.
4. Tomson T, Battino D. Teratogenic effects of antiepileptic medications. Neurol Clin. 2009;27(4):993-1002.
5. Reynolds MF, Sisk EC, Rasgon NL. Valproate and neuroendocrine changes in relation to women treated for epilepsy and bipolar disorder: a review. Curr Med Chem. 2007;14(26):2799-2812.
6. Wilson RD, Johnson JA, Wyatt P, et al. Pre-conceptional vitamin/folic acid supplementation 2007: the use of folic acid in combination with a multivitamin supplement for the prevention of neural tube defects and other congenital anomalies. J Obstet Gynaecol Can. 2007;29(12):1003-1026.
7. Burt VK, Rasgon N. Special considerations in treating bipolar disorder in women. Bipolar Disord. 2004;6(1):2-13.
8. Viguera AC, Whitfield T, Baldessarini RJ, et al. Risk of recurrence in women with bipolar disorder during pregnancy: prospective study of mood stabilizer discontinuation. Am J Psychiatry. 2007;164(12):1817-1824.
9. Bowden CL, Singh V. Long-term management of bipolar disorder. In: Ketter T, ed. Advances in the treatment of bipolar disorder. Washington, DC: American Psychiatric Publishing, Inc.; 2005:111.
10. Wyszynski DF, Nambisan M, Surve T, et al. Increased rate of major malformations in offspring exposed to valproate during pregnancy. Neurology. 2005;64(6):961-965.
11. Yonkers KA, Wisner KL, Stowe Z, et al. Management of bipolar disorder during pregnancy and the postpartum period. Am J Psychiatry. 2004;161(4):608-620.
12. Meador KJ, Baker GA, Browning N, et al. Effects of breastfeeding in children of women taking antiepileptic drugs. Neurology. 2010;75(22):1954-1960.
13. Gentile S. Prophylactic treatment of bipolar disorder in pregnancy and breastfeeding: focus on emerging mood stabilizers. Bipolar Disord. 2006;8(3):207-220.
14. Iqbal MM, Gundlapalli SP, Ryan WG, et al. Effects of antimanic mood-stabilizing drugs on fetuses, neonates, and nursing infants. South Med J. 2001;94(3):304-322.
15. Kozma C. Neonatal toxicity and transient neurodevelopmental deficits following prenatal exposure to lithium: another clinical report and a review of the literature. Am J Med Genet A. 2005;132(4):441-444.
16. Newport DJ, Viguera AC, Beach AJ, et al. Lithium placental passage and obstetrical outcome: implications for clinical management during late pregnancy. Am J Psychiatry. 2005;162(11):2162-2170.
17. Schou M. What happened later to the lithium babies? A follow-up study of children born without malformations. Acta Psychiatr Scand. 1976;54(3):193-197.
18. Morrow J, Russell A, Guthrie E, et al. Malformation risks of antiepileptic drugs in pregnancy: a prospective study from the UK Epilepsy and Pregnancy Register. J Neurol Neurosurg Psychiatry. 2006;77(2):193-198.
19. Sabers A, Tomson T. Managing antiepileptic drugs during pregnancy and lactation. Curr Opin Neurol. 2009;22(2):157-161.
20. Cummings C, Stewart M, Stevenson M, et al. Neurodevelopment of children exposed in utero to lamotrigine, sodium valproate and carbamazepine. Arch Dis Child. 2011;96(7):643-647.
21. Mølgaard-Nielsen D, Hviid A. Newer-generation antiepileptic drugs and the risk of major birth defects. JAMA. 2011;305(19):1996-2002.
22. Martínez-Frías ML. Topiramate in pregnancy: preliminary experience from the UK Epilepsy and Pregnancy Register. Neurology. 2009;72(23):2054-2055.
23. McKenna K, Koren G, Tetelbaum M, et al. Pregnancy outcome of women using atypical antipsychotic drugs: a prospective comparative study. J Clin Psychiatry. 2005;66(4):444-449.
24. Reis M, Källén B. Maternal use of antipsychotics in early pregnancy and delivery outcome. J Clin Psychopharmacol. 2008;28(3):279-288.
25. Coppola D, Russo LJ, Kwarta RF, Jr, et al. Evaluating the postmarketing experience of risperidone use during pregnancy: pregnancy and neonatal outcomes. Drug Saf. 2007;30(3):247-264.
26. Einarson A, Boskovic R. Use and safety of antipsychotic drugs during pregnancy. J Psychiatr Pract. 2009;15(3):183-192.
27. Spinelli MG. Postpartum psychosis: detection of risk and management. Am J Psychiatry. 2009;166(4):405-408.
28. Yonkers KA, Vigod S, Ross LE. Diagnosis, pathophysiology, and management of mood disorders in pregnant and postpartum women. Obstet Gynecol. 2011;117(4):961-977.
29. Doucet S, Jones I, Letourneau N, et al. Interventions for the prevention and treatment of postpartum psychosis: a systematic review. Arch Womens Ment Health. 2011;14(2):89-98.
30. Newport DJ, Pennell PB, Calamaras MR, et al. Lamotrigine in breast milk and nursing infants: determination of exposure. Pediatrics. 2008;122(1):e223-231.
31. Gentile S. Prophylactic treatment of bipolar disorder in pregnancy and breastfeeding: focus on emerging mood stabilizers. Bipolar Disord. 2006;8(3):207-220.
32. Viguera AC, Newport DJ, Ritchie J, et al. Lithium in breast milk and nursing infants: clinical implications. Am J Psychiatry. 2007;164(2):342-345.
Discuss this article at www.facebook.com/CurrentPsychiatry
Ms. M, age 31, has bipolar I disorder and takes lamotrigine, 200 mg/d, and aripiprazole, 10 mg/d. She was first hospitalized at age 20 for a manic episode and was discharged on lithium, 1,200 mg/d. She was hospitalized again at age 25 for a depressive episode that occurred after she stopped taking lithium because of undesirable side effects. She was switched to lamotrigine, 200 mg/d, which she tolerated well. Aripiprazole, 10 mg/d, was added 1 year later to address emergence of mild mood elevation symptoms.
During a recent follow-up appointment, Ms. M expresses interest in getting pregnant in the next 6 months. Her mood has been stable for 5 years and she asks if she should stop taking her medications in preparation for pregnancy. What would you recommend?
Because the typical age of onset for bipolar disorder (BD) is late adolescence or early adulthood, women are at risk for new onset or recurrence of mood episodes throughout their peak reproductive years. This article updates practitioners on the treatment of BD during pregnancy, including preconception planning and the risks and benefits of medication use during pregnancy. We also cover treatment considerations during the postpartum period, such as prophylaxis of mood episodes and mood stabilizer treatment for women who breast-feed.
Prenatal planning
Ideally, “prenatal planning” should begin long before women with BD prepare to have children. Because one-half of pregnancies in the United States are unplanned1 and manic episodes may result in impulsivity and increased sexual activity, all women of reproductive age with BD should be counseled about birth control and risks of unplanned pregnancies. Discussions about risks of in utero exposure to psychotropics should occur when medications are first prescribed. Because certain mood stabilizers, (eg, carbamazepine) may decrease efficacy of oral contraceptives by inducing cytochrome P450 (CYP450) enzymes, women taking these medications also should be counseled about additional methods of birth control.2
Oral contraceptives also may affect mood stabilizer levels through similar mechanisms. Because of CYP450 induction, lamotrigine serum levels are lower during the 3 “active” weeks of exposure to exogenous estrogen. During the “pill-free” last week, lamotrigine levels may increase up to 54%.3
Because mood stabilizers such as valproate are associated with teratogenic risks, women with BD should be asked about contraception at every visit.4 Valproate also has been associated with an increased risk of menstrual cycle irregularity. Some studies have shown that even before initiating mood stabilizers, women with BD have a higher incidence of menstrual cycle irregularity than women without BD, which suggests the link between polycystic ovarian syndrome (PCOS) and BD may be independent of medications and part of the endophenotype.5
The importance of prenatal vitamins should be discussed. The recommended folate dosage for women planning to become pregnant is 0.4 to 1 mg/d and 0.8 to 5 mg/d for women with either a previous pregnancy with neural tube defects or those taking an antiepileptic medication.6
Table 17 summarizes recommendations to improve prenatal planning in women with BD. Goals include:
- meeting with the patient at least 3 months before conception to review current menstrual cycle functioning. If your patient exhibits any signs or symptoms of PCOS, consider referral to a gynecologist
- meeting with patient and partner/significant supports to discuss treatment decisions
- optimizing the patient’s mood before conception, preferably for at least 3 to 6 months
- prescribing monotherapy at the lowest therapeutic dose if clinically feasible
- assessing the patient’s personal preferences and beliefs regarding medication use during pregnancy and breast-feeding
- assessing the patient’s capacity to understand the risks and benefits of medication continuation/discontinuation during pregnancy, including risk for relapse, current literature on teratogenicity, perinatal complications, and neurodevelopmental studies. Document that the patient provides informed consent.
Table 1
Pregnancy and BD: Medication management guidelines
| Comprehensive prenatal counseling should begin at least 3 months before pregnancy. Folate supplementation is advised |
| Medication should be avoided if clinically feasible (particularly during the first trimester). Avoid abrupt discontinuation. Increase psychosocial and clinical supports |
If medication is pursued:
|
Comprehensive postpartum counseling should begin before and be reinforced throughout pregnancy, emphasizing:
|
| BD: bipolar disorder Source: Adapted from reference 7 |
CASE CONTINUED: Medication decisions
Ms. M’s first question is, “Should I stop taking my medications?” Ms. M and her psychiatrist review the risks and benefits of medication exposure during pregnancy (Table 2) and decide against discontinuing all medications because of her history of relapse when she stopped lithium. Because Ms. M’s mood has been stable for 5 years, she and her psychiatrist decide to limit her medications to lamotrigine monotherapy at her current dose, and agree to slowly taper aripiprazole. One week later, Ms. M calls and states she has a positive pregnancy test and is wondering if she should stop aripiprazole all at once. Ms. M is advised to continue with the original plan to slowly taper aripiprazole.
Table 2
Potential risks of continuing or discontinuing medications for BD during pregnancy
| Risks of discontinuing | Risks of continuing |
|---|---|
| Mood relapse during pregnancy or postpartum Risks of alternative treatment(s):
| Medication-specific risks:
|
| BD: bipolar disorder | |
Medication risks/benefits
Women with BD have a high rate of relapse associated with abrupt discontinuation of pharmacotherapy during pregnancy. As such, patients and their partners and families should be cautioned against rapid discontinuation of medications.8 The risk to mother and fetus is particularly high for women with a history of recurrent, severe mood episodes. These patients face not only a high risk of recurrence of mood episodes, but also the inherent danger of impulsivity, poor self-care, and suicidality associated with mania, depression, and mixed states. In these cases, continuing a medication (other than known teratogens such as valproate) that has effectively stabilized mood may be preferred to discontinuation; these decisions are made after careful risk/benefit assessment.
Carefully reviewing the patient’s history is essential to assessing the risks and benefits of tapering medications before pregnancy. Consider the frequency and severity of your patient’s mood episodes, and whether a switch in mood state was rapid or had a prodromal phase. If a patient currently has a stable mood, a history of mild to moderate mood episodes, a history of prodromal symptoms (eg, gradually increasing sleep disturbances and mood deterioration), and no history of rapid switches, gradually discontinuing medications before or during pregnancy may be considered. However, encourage women to enlist their partners and family members to monitor for warning symptoms and advocate for early medication intervention. Because insomnia is a sign of relapse for many patients, educate women and their families about the importance of maintaining a regular sleep/wake cycle and alerting care providers if this cycle changes.
Mood stabilizers with the greatest risk for teratogenicity are valproate, carbamazepine, and lithium.9 Valproate is associated with a 6% to 13% risk of congenital malformation, including neural tube defects (1% to 2%) and cardiac or craniofacial defects.3 Risks increase at doses >800 mg/d.10 Potential perinatal complications associated with valproate include heart rate deceleration, abnormal tone (hypotonia or hypertonia), and growth retardation.11 Neurobehavioral sequelae include lower IQ scores and increased risk of autism.12
Carbamazepine is associated with a 2% to 5% risk of congenital malformation, including neural tube defects and cardiac or craniofacial defects.4 Perinatal complications associated with carbamazepine include vitamin K deficiency.4 The neurobehavioral sequelae of carbamazepine are controversial; most prospective studies do not suggest long-term cognitive deficits.13 It is strongly recommended that valproate and carbamazepine be avoided, if possible, in women with BD who plan to become pregnant in the near future.
Prospective studies of lithium have shown a 2.8% rate of congenital malformations, which is much lower than the 11% rate found in retrospective studies.14 Ebstein’s anomaly—downward displacement of the tricuspid valve—is estimated to occur in .05% to 0.1% of infants exposed to lithium, which is 10 to 20 times the base rate, but a low absolute risk.11
It is recommended women taking lithium during pregnancy complete a fetal high resolution ultrasound and echocardiogram at 16 to 18 weeks.11 Perinatal complications associated with lithium include prematurity, hypotonia, hypothyroidism, hepatic abnormalities, respiratory distress, and nephrogenic diabetes insipidus.15 When prescribing lithium, divided doses are recommended to maintain a stable serum level. Serum lithium levels should be monitored frequently, and higher doses may be needed because of increased glomerular filtration rate and plasma volume throughout pregnancy.10 Because of fluid shifts at delivery—including blood loss during delivery and postpartum diuresis and diaphoresis—there is a risk of lithium toxicity at this time. Some researchers have suggested suspending lithium treatment during labor or 24 to 48 hours before planned induction or Caesarean section may lower this risk, with re-administration after delivery when medically stable.16 Women should be followed closely for signs of lithium toxicity and have lithium levels monitored as clinically indicated.16 There is insufficient data to support any neurobehavioral sequelae of in utero exposure to lithium; however, there are few long-term follow up studies using standardized measures.17
Lamotrigine is associated with a 1.9% to 4.6% rate of congenital malformations, including cleft lip/palate (8.9/1,000 vs 0.5 to 1.2/1,000 baseline).4 Studies suggest that rates of malformations (cardiac, genitourinary, gastrointestinal, neural tube defect) are dose-dependent: 1.3% at dosages <100 mg/d, 1.9% at 100 to 200 mg/d, and 5.4% at >200 mg/d.18 Because cleft lip and palate are formed by late second trimester, it is recommended to attempt to keep the lamotrigine dose <200 mg/d during the first and second trimesters. Higher doses of lamotrigine may be needed in the third trimester because of increased renal clearance.19 There is insufficient data to support any lamotrigine-associated neurobehavioral effects, and unlike studies of valproate, follow-up evaluations of lamotrigine-exposed children have not shown lower IQs.20
Evidence about the reproductive safety of other mood stabilizers used in BD is limited. A recent population-based cohort study did not show increased risk of major malformations in children exposed to topiramate, gabapentin, or oxcarbazepine during the first trimester of pregnancy.21 Topiramate often is used in combination with other mood stabilizers for weight control, and studies suggest that polypharmacy with topiramate, especially at higher doses and with valproate, increases the risk of major congenital malformations, especially cleft lip and cleft palate.22 Consequently, topiramate is not recommended for women planning to conceive.
Antipsychotics. Although there is increasing information about outcomes of neonates exposed to atypical antipsychotics during pregnancy, the literature still is limited. The greatest number of studies have evaluated olanzapine, risperidone, and quetiapine and show the rate of congenital malformations is 0.9% to 4.1%, which is consistent with general population rates.23-26 Perinatal complications associated with these atypical antipsychotics include neonatal extrapyramidal syndrome (EPS), possible neonatal adaptation/withdrawal syndrome, and an increased risk of the infant being either large or small for gestational age. Because atypical antipsychotics may increase the risk of metabolic syndrome, women should be counseled about the possible increased risk for gestational diabetes with these medications. None of these drugs have been associated with neurobehavioral sequelae, but long-term follow-up studies of exposed infants are lacking.
For aripiprazole, asenapine, ziprasidone, iloperidone, and lurasidone there is insufficient data about rate of congenital malformations, obstetric complications, and neurobehavioral sequelae. However, perinatal complications associated with these medications include risk of EPS and withdrawal symptoms.25,26
CASE CONTINUED: Worsening mood symptoms
During pregnancy, Ms. M’s mood is stable on lamotrigine, 200 mg/d, and she participates in individual interpersonally oriented psychotherapy to address anxieties related to becoming a mother. However, late in her third trimester, Ms. M reports worsening symptoms, including depressed mood, insomnia, fatigue, and poor motivation. She also learns her mother had an episode of postpartum depression. Ms. M and her doctor discuss the risks of postpartum relapse, but she declines additional medication for prophylaxis because she is concerned about its impact on breast-feeding.
Two days after delivery, Ms. M complains of increased insomnia and depressed mood, and her husband reports she is not getting out of bed. She describes thoughts and images of throwing her baby out the window, and feels her thoughts are controlled by something outside of herself. Ms. M suspects her husband is having an affair.
Postpartum risks
All women with BD should be counseled regarding prophylaxis with mood stabilizers during the postpartum period. Women with BD are at high risk of mania and psychosis postpartum, particularly those with a personal or family history of postpartum psychosis. Postpartum psychosis frequently presents with an abrupt onset, shortly after delivery (Table 3). Although it may present with the classic symptoms of mania or psychotic depression, it also may have features of delirium.27
Clinicians should immediately implement treatment with mood stabilizers and antipsychotics to manage acute psychotic symptoms, while also ruling out medical causes or comorbidities. Hospitalization should be considered. Aggressive treatment of insomnia will help stabilize mood. Electroconvulsive therapy can be used in treatment-refractory or urgent cases.10 Lastly, because approximately 4% of women with postpartum psychosis commit infanticide, all mother/child interactions should be closely supervised.27
In small prospective studies, use of lithium within 48 hours of delivery decreased the risk of relapse of postpartum psychosis within the first 3 months.28,29 In lower-risk patients who have discontinued pharmacotherapy during pregnancy, restarting medication before or immediately after delivery should be considered. At the same time, it is important to minimize sleep disruption, particularly postpartum. Psychoeducation—ideally begun in the preconception counseling visit—is extremely important for emphasizing the need for postpartum sleep.
Table 3
Consequences of postpartum mood relapse
| Suicide/infanticide |
| Reckless behavior/substance abuse |
| Poor self-care/care of infant |
| Difficulty with mother-infant bonding |
| Mood relapse more severe and difficult to treat than prior episodes |
| Possible hospitalization |
Breast-feeding concerns
Data on risks of infant exposure to medications through breast milk are largely limited to case reports and case series. All mood-stabilizing medications have been found to pass into breast milk at varying concentrations.28 If a patient chooses to breast-feed, she should inform her pediatrician of this decision, and she and her support system should be educated about signs of neonatal toxicity. Ideally, the psychiatrist should liaise with the patient’s pediatrician, especially when infants are premature, because the child’s liver metabolism may be immature, leading to higher serum drug levels and in some cases drug accumulation. Encourage patients to consider bottle feeding, either their own breast milk, pumped and stored, or formula. This will allow others to assist with feedings and the patient to have more consistent sleep, which could stabilize mood.
Lamotrigine concentrations in breast milk are highly variable.30 Lamotrigine is processed through glucuronidation, a process that is immature in neonates. One study found serum lamotrigine levels in infants were 23% to 33% of maternal serum levels and milk/plasma ratios were highly variable, ranging from 6% to 147%.30 Infants exposed to lamotrigine in breast milk should be monitored for rash and signs of thrombocytosis, and if clinically indicated, lamotrigine levels should be checked.30 Valproate has a low infant serum/maternal serum ratio; there are rare case reports of hepatotoxicity and thrombocytopenia. Although valproate can be reinitiated because of its lower breast milk concentration, it is not a drug of choice in reproductive-age women because of the many issues described above, including risks during pregnancy, PCOS, and effect on oral contraceptives.
Carbamazepine serum levels in breast-feeding infants range from 6% to 65%; hepatic dysfunction, sedation, and poor feeding have been reported in infants in rare instances.31
Historically, lithium has been considered incompatible with breast-feeding, but recent reports suggest with careful monitoring it may not be contraindicated. In 10 mother/infant pairs, lithium levels in breast milk and infant serum diminished over time, with no adverse neonatal effects.32 However, if an infant does breast-feed, it may be important to monitor thyroid-stimulating hormone, blood urea nitrogen-to-creatinine ratio, and ECG in both mother and infant, especially if the mother is taking high doses of lithium.
The safety of breast-feeding while treated with atypical antipsychotics is largely unknown. Case reports indicate low transmission of these medications into breast milk.28
CASE CONTINUED
Ms. M is admitted for psychiatric hospitalization because of worsening psychotic symptoms, poor self-care, and persistent thoughts of harming her baby. She agrees to restart aripiprazole, which is titrated to 20 mg/d. Breast-feeding is not pursued. She is discharged in 10 days after she no longer has thoughts of harming her baby, delusions, or psychotic or suicidal ideation. She and her family agree to close supervision by her family and outpatient follow-up.
Related Resources
- The Hospital for Sick Children. Pregnancy and breastfeeding resources. www.motherisk.org/women/pregnancyResources.jsp.
- U.S. National Library of Medicine. TOXNET toxicology data network. http://toxnet.nlm.nih.gov.
Drug Brand Names
- Aripiprazole • Abilify
- Asenapine • Saphris
- Carbamazepine • Equetro, Tegretol
- Gabapentin • Neurontin
- Iloperidone • Fanapt
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Lurasidone • Latuda
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Topiramate • Topamax
- Valproate • Depacon
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgement
The authors would like to thank Natasha Barthel, BS, for her assistance with this article.
Discuss this article at www.facebook.com/CurrentPsychiatry
Ms. M, age 31, has bipolar I disorder and takes lamotrigine, 200 mg/d, and aripiprazole, 10 mg/d. She was first hospitalized at age 20 for a manic episode and was discharged on lithium, 1,200 mg/d. She was hospitalized again at age 25 for a depressive episode that occurred after she stopped taking lithium because of undesirable side effects. She was switched to lamotrigine, 200 mg/d, which she tolerated well. Aripiprazole, 10 mg/d, was added 1 year later to address emergence of mild mood elevation symptoms.
During a recent follow-up appointment, Ms. M expresses interest in getting pregnant in the next 6 months. Her mood has been stable for 5 years and she asks if she should stop taking her medications in preparation for pregnancy. What would you recommend?
Because the typical age of onset for bipolar disorder (BD) is late adolescence or early adulthood, women are at risk for new onset or recurrence of mood episodes throughout their peak reproductive years. This article updates practitioners on the treatment of BD during pregnancy, including preconception planning and the risks and benefits of medication use during pregnancy. We also cover treatment considerations during the postpartum period, such as prophylaxis of mood episodes and mood stabilizer treatment for women who breast-feed.
Prenatal planning
Ideally, “prenatal planning” should begin long before women with BD prepare to have children. Because one-half of pregnancies in the United States are unplanned1 and manic episodes may result in impulsivity and increased sexual activity, all women of reproductive age with BD should be counseled about birth control and risks of unplanned pregnancies. Discussions about risks of in utero exposure to psychotropics should occur when medications are first prescribed. Because certain mood stabilizers, (eg, carbamazepine) may decrease efficacy of oral contraceptives by inducing cytochrome P450 (CYP450) enzymes, women taking these medications also should be counseled about additional methods of birth control.2
Oral contraceptives also may affect mood stabilizer levels through similar mechanisms. Because of CYP450 induction, lamotrigine serum levels are lower during the 3 “active” weeks of exposure to exogenous estrogen. During the “pill-free” last week, lamotrigine levels may increase up to 54%.3
Because mood stabilizers such as valproate are associated with teratogenic risks, women with BD should be asked about contraception at every visit.4 Valproate also has been associated with an increased risk of menstrual cycle irregularity. Some studies have shown that even before initiating mood stabilizers, women with BD have a higher incidence of menstrual cycle irregularity than women without BD, which suggests the link between polycystic ovarian syndrome (PCOS) and BD may be independent of medications and part of the endophenotype.5
The importance of prenatal vitamins should be discussed. The recommended folate dosage for women planning to become pregnant is 0.4 to 1 mg/d and 0.8 to 5 mg/d for women with either a previous pregnancy with neural tube defects or those taking an antiepileptic medication.6
Table 17 summarizes recommendations to improve prenatal planning in women with BD. Goals include:
- meeting with the patient at least 3 months before conception to review current menstrual cycle functioning. If your patient exhibits any signs or symptoms of PCOS, consider referral to a gynecologist
- meeting with patient and partner/significant supports to discuss treatment decisions
- optimizing the patient’s mood before conception, preferably for at least 3 to 6 months
- prescribing monotherapy at the lowest therapeutic dose if clinically feasible
- assessing the patient’s personal preferences and beliefs regarding medication use during pregnancy and breast-feeding
- assessing the patient’s capacity to understand the risks and benefits of medication continuation/discontinuation during pregnancy, including risk for relapse, current literature on teratogenicity, perinatal complications, and neurodevelopmental studies. Document that the patient provides informed consent.
Table 1
Pregnancy and BD: Medication management guidelines
| Comprehensive prenatal counseling should begin at least 3 months before pregnancy. Folate supplementation is advised |
| Medication should be avoided if clinically feasible (particularly during the first trimester). Avoid abrupt discontinuation. Increase psychosocial and clinical supports |
If medication is pursued:
|
Comprehensive postpartum counseling should begin before and be reinforced throughout pregnancy, emphasizing:
|
| BD: bipolar disorder Source: Adapted from reference 7 |
CASE CONTINUED: Medication decisions
Ms. M’s first question is, “Should I stop taking my medications?” Ms. M and her psychiatrist review the risks and benefits of medication exposure during pregnancy (Table 2) and decide against discontinuing all medications because of her history of relapse when she stopped lithium. Because Ms. M’s mood has been stable for 5 years, she and her psychiatrist decide to limit her medications to lamotrigine monotherapy at her current dose, and agree to slowly taper aripiprazole. One week later, Ms. M calls and states she has a positive pregnancy test and is wondering if she should stop aripiprazole all at once. Ms. M is advised to continue with the original plan to slowly taper aripiprazole.
Table 2
Potential risks of continuing or discontinuing medications for BD during pregnancy
| Risks of discontinuing | Risks of continuing |
|---|---|
| Mood relapse during pregnancy or postpartum Risks of alternative treatment(s):
| Medication-specific risks:
|
| BD: bipolar disorder | |
Medication risks/benefits
Women with BD have a high rate of relapse associated with abrupt discontinuation of pharmacotherapy during pregnancy. As such, patients and their partners and families should be cautioned against rapid discontinuation of medications.8 The risk to mother and fetus is particularly high for women with a history of recurrent, severe mood episodes. These patients face not only a high risk of recurrence of mood episodes, but also the inherent danger of impulsivity, poor self-care, and suicidality associated with mania, depression, and mixed states. In these cases, continuing a medication (other than known teratogens such as valproate) that has effectively stabilized mood may be preferred to discontinuation; these decisions are made after careful risk/benefit assessment.
Carefully reviewing the patient’s history is essential to assessing the risks and benefits of tapering medications before pregnancy. Consider the frequency and severity of your patient’s mood episodes, and whether a switch in mood state was rapid or had a prodromal phase. If a patient currently has a stable mood, a history of mild to moderate mood episodes, a history of prodromal symptoms (eg, gradually increasing sleep disturbances and mood deterioration), and no history of rapid switches, gradually discontinuing medications before or during pregnancy may be considered. However, encourage women to enlist their partners and family members to monitor for warning symptoms and advocate for early medication intervention. Because insomnia is a sign of relapse for many patients, educate women and their families about the importance of maintaining a regular sleep/wake cycle and alerting care providers if this cycle changes.
Mood stabilizers with the greatest risk for teratogenicity are valproate, carbamazepine, and lithium.9 Valproate is associated with a 6% to 13% risk of congenital malformation, including neural tube defects (1% to 2%) and cardiac or craniofacial defects.3 Risks increase at doses >800 mg/d.10 Potential perinatal complications associated with valproate include heart rate deceleration, abnormal tone (hypotonia or hypertonia), and growth retardation.11 Neurobehavioral sequelae include lower IQ scores and increased risk of autism.12
Carbamazepine is associated with a 2% to 5% risk of congenital malformation, including neural tube defects and cardiac or craniofacial defects.4 Perinatal complications associated with carbamazepine include vitamin K deficiency.4 The neurobehavioral sequelae of carbamazepine are controversial; most prospective studies do not suggest long-term cognitive deficits.13 It is strongly recommended that valproate and carbamazepine be avoided, if possible, in women with BD who plan to become pregnant in the near future.
Prospective studies of lithium have shown a 2.8% rate of congenital malformations, which is much lower than the 11% rate found in retrospective studies.14 Ebstein’s anomaly—downward displacement of the tricuspid valve—is estimated to occur in .05% to 0.1% of infants exposed to lithium, which is 10 to 20 times the base rate, but a low absolute risk.11
It is recommended women taking lithium during pregnancy complete a fetal high resolution ultrasound and echocardiogram at 16 to 18 weeks.11 Perinatal complications associated with lithium include prematurity, hypotonia, hypothyroidism, hepatic abnormalities, respiratory distress, and nephrogenic diabetes insipidus.15 When prescribing lithium, divided doses are recommended to maintain a stable serum level. Serum lithium levels should be monitored frequently, and higher doses may be needed because of increased glomerular filtration rate and plasma volume throughout pregnancy.10 Because of fluid shifts at delivery—including blood loss during delivery and postpartum diuresis and diaphoresis—there is a risk of lithium toxicity at this time. Some researchers have suggested suspending lithium treatment during labor or 24 to 48 hours before planned induction or Caesarean section may lower this risk, with re-administration after delivery when medically stable.16 Women should be followed closely for signs of lithium toxicity and have lithium levels monitored as clinically indicated.16 There is insufficient data to support any neurobehavioral sequelae of in utero exposure to lithium; however, there are few long-term follow up studies using standardized measures.17
Lamotrigine is associated with a 1.9% to 4.6% rate of congenital malformations, including cleft lip/palate (8.9/1,000 vs 0.5 to 1.2/1,000 baseline).4 Studies suggest that rates of malformations (cardiac, genitourinary, gastrointestinal, neural tube defect) are dose-dependent: 1.3% at dosages <100 mg/d, 1.9% at 100 to 200 mg/d, and 5.4% at >200 mg/d.18 Because cleft lip and palate are formed by late second trimester, it is recommended to attempt to keep the lamotrigine dose <200 mg/d during the first and second trimesters. Higher doses of lamotrigine may be needed in the third trimester because of increased renal clearance.19 There is insufficient data to support any lamotrigine-associated neurobehavioral effects, and unlike studies of valproate, follow-up evaluations of lamotrigine-exposed children have not shown lower IQs.20
Evidence about the reproductive safety of other mood stabilizers used in BD is limited. A recent population-based cohort study did not show increased risk of major malformations in children exposed to topiramate, gabapentin, or oxcarbazepine during the first trimester of pregnancy.21 Topiramate often is used in combination with other mood stabilizers for weight control, and studies suggest that polypharmacy with topiramate, especially at higher doses and with valproate, increases the risk of major congenital malformations, especially cleft lip and cleft palate.22 Consequently, topiramate is not recommended for women planning to conceive.
Antipsychotics. Although there is increasing information about outcomes of neonates exposed to atypical antipsychotics during pregnancy, the literature still is limited. The greatest number of studies have evaluated olanzapine, risperidone, and quetiapine and show the rate of congenital malformations is 0.9% to 4.1%, which is consistent with general population rates.23-26 Perinatal complications associated with these atypical antipsychotics include neonatal extrapyramidal syndrome (EPS), possible neonatal adaptation/withdrawal syndrome, and an increased risk of the infant being either large or small for gestational age. Because atypical antipsychotics may increase the risk of metabolic syndrome, women should be counseled about the possible increased risk for gestational diabetes with these medications. None of these drugs have been associated with neurobehavioral sequelae, but long-term follow-up studies of exposed infants are lacking.
For aripiprazole, asenapine, ziprasidone, iloperidone, and lurasidone there is insufficient data about rate of congenital malformations, obstetric complications, and neurobehavioral sequelae. However, perinatal complications associated with these medications include risk of EPS and withdrawal symptoms.25,26
CASE CONTINUED: Worsening mood symptoms
During pregnancy, Ms. M’s mood is stable on lamotrigine, 200 mg/d, and she participates in individual interpersonally oriented psychotherapy to address anxieties related to becoming a mother. However, late in her third trimester, Ms. M reports worsening symptoms, including depressed mood, insomnia, fatigue, and poor motivation. She also learns her mother had an episode of postpartum depression. Ms. M and her doctor discuss the risks of postpartum relapse, but she declines additional medication for prophylaxis because she is concerned about its impact on breast-feeding.
Two days after delivery, Ms. M complains of increased insomnia and depressed mood, and her husband reports she is not getting out of bed. She describes thoughts and images of throwing her baby out the window, and feels her thoughts are controlled by something outside of herself. Ms. M suspects her husband is having an affair.
Postpartum risks
All women with BD should be counseled regarding prophylaxis with mood stabilizers during the postpartum period. Women with BD are at high risk of mania and psychosis postpartum, particularly those with a personal or family history of postpartum psychosis. Postpartum psychosis frequently presents with an abrupt onset, shortly after delivery (Table 3). Although it may present with the classic symptoms of mania or psychotic depression, it also may have features of delirium.27
Clinicians should immediately implement treatment with mood stabilizers and antipsychotics to manage acute psychotic symptoms, while also ruling out medical causes or comorbidities. Hospitalization should be considered. Aggressive treatment of insomnia will help stabilize mood. Electroconvulsive therapy can be used in treatment-refractory or urgent cases.10 Lastly, because approximately 4% of women with postpartum psychosis commit infanticide, all mother/child interactions should be closely supervised.27
In small prospective studies, use of lithium within 48 hours of delivery decreased the risk of relapse of postpartum psychosis within the first 3 months.28,29 In lower-risk patients who have discontinued pharmacotherapy during pregnancy, restarting medication before or immediately after delivery should be considered. At the same time, it is important to minimize sleep disruption, particularly postpartum. Psychoeducation—ideally begun in the preconception counseling visit—is extremely important for emphasizing the need for postpartum sleep.
Table 3
Consequences of postpartum mood relapse
| Suicide/infanticide |
| Reckless behavior/substance abuse |
| Poor self-care/care of infant |
| Difficulty with mother-infant bonding |
| Mood relapse more severe and difficult to treat than prior episodes |
| Possible hospitalization |
Breast-feeding concerns
Data on risks of infant exposure to medications through breast milk are largely limited to case reports and case series. All mood-stabilizing medications have been found to pass into breast milk at varying concentrations.28 If a patient chooses to breast-feed, she should inform her pediatrician of this decision, and she and her support system should be educated about signs of neonatal toxicity. Ideally, the psychiatrist should liaise with the patient’s pediatrician, especially when infants are premature, because the child’s liver metabolism may be immature, leading to higher serum drug levels and in some cases drug accumulation. Encourage patients to consider bottle feeding, either their own breast milk, pumped and stored, or formula. This will allow others to assist with feedings and the patient to have more consistent sleep, which could stabilize mood.
Lamotrigine concentrations in breast milk are highly variable.30 Lamotrigine is processed through glucuronidation, a process that is immature in neonates. One study found serum lamotrigine levels in infants were 23% to 33% of maternal serum levels and milk/plasma ratios were highly variable, ranging from 6% to 147%.30 Infants exposed to lamotrigine in breast milk should be monitored for rash and signs of thrombocytosis, and if clinically indicated, lamotrigine levels should be checked.30 Valproate has a low infant serum/maternal serum ratio; there are rare case reports of hepatotoxicity and thrombocytopenia. Although valproate can be reinitiated because of its lower breast milk concentration, it is not a drug of choice in reproductive-age women because of the many issues described above, including risks during pregnancy, PCOS, and effect on oral contraceptives.
Carbamazepine serum levels in breast-feeding infants range from 6% to 65%; hepatic dysfunction, sedation, and poor feeding have been reported in infants in rare instances.31
Historically, lithium has been considered incompatible with breast-feeding, but recent reports suggest with careful monitoring it may not be contraindicated. In 10 mother/infant pairs, lithium levels in breast milk and infant serum diminished over time, with no adverse neonatal effects.32 However, if an infant does breast-feed, it may be important to monitor thyroid-stimulating hormone, blood urea nitrogen-to-creatinine ratio, and ECG in both mother and infant, especially if the mother is taking high doses of lithium.
The safety of breast-feeding while treated with atypical antipsychotics is largely unknown. Case reports indicate low transmission of these medications into breast milk.28
CASE CONTINUED
Ms. M is admitted for psychiatric hospitalization because of worsening psychotic symptoms, poor self-care, and persistent thoughts of harming her baby. She agrees to restart aripiprazole, which is titrated to 20 mg/d. Breast-feeding is not pursued. She is discharged in 10 days after she no longer has thoughts of harming her baby, delusions, or psychotic or suicidal ideation. She and her family agree to close supervision by her family and outpatient follow-up.
Related Resources
- The Hospital for Sick Children. Pregnancy and breastfeeding resources. www.motherisk.org/women/pregnancyResources.jsp.
- U.S. National Library of Medicine. TOXNET toxicology data network. http://toxnet.nlm.nih.gov.
Drug Brand Names
- Aripiprazole • Abilify
- Asenapine • Saphris
- Carbamazepine • Equetro, Tegretol
- Gabapentin • Neurontin
- Iloperidone • Fanapt
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Lurasidone • Latuda
- Olanzapine • Zyprexa
- Oxcarbazepine • Trileptal
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Topiramate • Topamax
- Valproate • Depacon
- Ziprasidone • Geodon
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgement
The authors would like to thank Natasha Barthel, BS, for her assistance with this article.
1. Finer LB, Henshaw SK. Disparities in rates of unintended pregnancy in the United States, 1994 and 2001. Perspect Sex Reprod Health. 2006;38(2):90-96.
2. ACOG Committee on Practice Bulletins-Gynecology. ACOG practice bulletin. No. 73: use of hormonal contraception in women with coexisting medical conditions. Obstet Gynecol. 2006;107(6):1453-1472.
3. Wegner I, Edelbroek PM, Bulk S, et al. Lamotrigine kinetics within the menstrual cycle, after menopause, and with oral contraceptives. Neurology. 2009;73(17):1388-1393.
4. Tomson T, Battino D. Teratogenic effects of antiepileptic medications. Neurol Clin. 2009;27(4):993-1002.
5. Reynolds MF, Sisk EC, Rasgon NL. Valproate and neuroendocrine changes in relation to women treated for epilepsy and bipolar disorder: a review. Curr Med Chem. 2007;14(26):2799-2812.
6. Wilson RD, Johnson JA, Wyatt P, et al. Pre-conceptional vitamin/folic acid supplementation 2007: the use of folic acid in combination with a multivitamin supplement for the prevention of neural tube defects and other congenital anomalies. J Obstet Gynaecol Can. 2007;29(12):1003-1026.
7. Burt VK, Rasgon N. Special considerations in treating bipolar disorder in women. Bipolar Disord. 2004;6(1):2-13.
8. Viguera AC, Whitfield T, Baldessarini RJ, et al. Risk of recurrence in women with bipolar disorder during pregnancy: prospective study of mood stabilizer discontinuation. Am J Psychiatry. 2007;164(12):1817-1824.
9. Bowden CL, Singh V. Long-term management of bipolar disorder. In: Ketter T, ed. Advances in the treatment of bipolar disorder. Washington, DC: American Psychiatric Publishing, Inc.; 2005:111.
10. Wyszynski DF, Nambisan M, Surve T, et al. Increased rate of major malformations in offspring exposed to valproate during pregnancy. Neurology. 2005;64(6):961-965.
11. Yonkers KA, Wisner KL, Stowe Z, et al. Management of bipolar disorder during pregnancy and the postpartum period. Am J Psychiatry. 2004;161(4):608-620.
12. Meador KJ, Baker GA, Browning N, et al. Effects of breastfeeding in children of women taking antiepileptic drugs. Neurology. 2010;75(22):1954-1960.
13. Gentile S. Prophylactic treatment of bipolar disorder in pregnancy and breastfeeding: focus on emerging mood stabilizers. Bipolar Disord. 2006;8(3):207-220.
14. Iqbal MM, Gundlapalli SP, Ryan WG, et al. Effects of antimanic mood-stabilizing drugs on fetuses, neonates, and nursing infants. South Med J. 2001;94(3):304-322.
15. Kozma C. Neonatal toxicity and transient neurodevelopmental deficits following prenatal exposure to lithium: another clinical report and a review of the literature. Am J Med Genet A. 2005;132(4):441-444.
16. Newport DJ, Viguera AC, Beach AJ, et al. Lithium placental passage and obstetrical outcome: implications for clinical management during late pregnancy. Am J Psychiatry. 2005;162(11):2162-2170.
17. Schou M. What happened later to the lithium babies? A follow-up study of children born without malformations. Acta Psychiatr Scand. 1976;54(3):193-197.
18. Morrow J, Russell A, Guthrie E, et al. Malformation risks of antiepileptic drugs in pregnancy: a prospective study from the UK Epilepsy and Pregnancy Register. J Neurol Neurosurg Psychiatry. 2006;77(2):193-198.
19. Sabers A, Tomson T. Managing antiepileptic drugs during pregnancy and lactation. Curr Opin Neurol. 2009;22(2):157-161.
20. Cummings C, Stewart M, Stevenson M, et al. Neurodevelopment of children exposed in utero to lamotrigine, sodium valproate and carbamazepine. Arch Dis Child. 2011;96(7):643-647.
21. Mølgaard-Nielsen D, Hviid A. Newer-generation antiepileptic drugs and the risk of major birth defects. JAMA. 2011;305(19):1996-2002.
22. Martínez-Frías ML. Topiramate in pregnancy: preliminary experience from the UK Epilepsy and Pregnancy Register. Neurology. 2009;72(23):2054-2055.
23. McKenna K, Koren G, Tetelbaum M, et al. Pregnancy outcome of women using atypical antipsychotic drugs: a prospective comparative study. J Clin Psychiatry. 2005;66(4):444-449.
24. Reis M, Källén B. Maternal use of antipsychotics in early pregnancy and delivery outcome. J Clin Psychopharmacol. 2008;28(3):279-288.
25. Coppola D, Russo LJ, Kwarta RF, Jr, et al. Evaluating the postmarketing experience of risperidone use during pregnancy: pregnancy and neonatal outcomes. Drug Saf. 2007;30(3):247-264.
26. Einarson A, Boskovic R. Use and safety of antipsychotic drugs during pregnancy. J Psychiatr Pract. 2009;15(3):183-192.
27. Spinelli MG. Postpartum psychosis: detection of risk and management. Am J Psychiatry. 2009;166(4):405-408.
28. Yonkers KA, Vigod S, Ross LE. Diagnosis, pathophysiology, and management of mood disorders in pregnant and postpartum women. Obstet Gynecol. 2011;117(4):961-977.
29. Doucet S, Jones I, Letourneau N, et al. Interventions for the prevention and treatment of postpartum psychosis: a systematic review. Arch Womens Ment Health. 2011;14(2):89-98.
30. Newport DJ, Pennell PB, Calamaras MR, et al. Lamotrigine in breast milk and nursing infants: determination of exposure. Pediatrics. 2008;122(1):e223-231.
31. Gentile S. Prophylactic treatment of bipolar disorder in pregnancy and breastfeeding: focus on emerging mood stabilizers. Bipolar Disord. 2006;8(3):207-220.
32. Viguera AC, Newport DJ, Ritchie J, et al. Lithium in breast milk and nursing infants: clinical implications. Am J Psychiatry. 2007;164(2):342-345.
1. Finer LB, Henshaw SK. Disparities in rates of unintended pregnancy in the United States, 1994 and 2001. Perspect Sex Reprod Health. 2006;38(2):90-96.
2. ACOG Committee on Practice Bulletins-Gynecology. ACOG practice bulletin. No. 73: use of hormonal contraception in women with coexisting medical conditions. Obstet Gynecol. 2006;107(6):1453-1472.
3. Wegner I, Edelbroek PM, Bulk S, et al. Lamotrigine kinetics within the menstrual cycle, after menopause, and with oral contraceptives. Neurology. 2009;73(17):1388-1393.
4. Tomson T, Battino D. Teratogenic effects of antiepileptic medications. Neurol Clin. 2009;27(4):993-1002.
5. Reynolds MF, Sisk EC, Rasgon NL. Valproate and neuroendocrine changes in relation to women treated for epilepsy and bipolar disorder: a review. Curr Med Chem. 2007;14(26):2799-2812.
6. Wilson RD, Johnson JA, Wyatt P, et al. Pre-conceptional vitamin/folic acid supplementation 2007: the use of folic acid in combination with a multivitamin supplement for the prevention of neural tube defects and other congenital anomalies. J Obstet Gynaecol Can. 2007;29(12):1003-1026.
7. Burt VK, Rasgon N. Special considerations in treating bipolar disorder in women. Bipolar Disord. 2004;6(1):2-13.
8. Viguera AC, Whitfield T, Baldessarini RJ, et al. Risk of recurrence in women with bipolar disorder during pregnancy: prospective study of mood stabilizer discontinuation. Am J Psychiatry. 2007;164(12):1817-1824.
9. Bowden CL, Singh V. Long-term management of bipolar disorder. In: Ketter T, ed. Advances in the treatment of bipolar disorder. Washington, DC: American Psychiatric Publishing, Inc.; 2005:111.
10. Wyszynski DF, Nambisan M, Surve T, et al. Increased rate of major malformations in offspring exposed to valproate during pregnancy. Neurology. 2005;64(6):961-965.
11. Yonkers KA, Wisner KL, Stowe Z, et al. Management of bipolar disorder during pregnancy and the postpartum period. Am J Psychiatry. 2004;161(4):608-620.
12. Meador KJ, Baker GA, Browning N, et al. Effects of breastfeeding in children of women taking antiepileptic drugs. Neurology. 2010;75(22):1954-1960.
13. Gentile S. Prophylactic treatment of bipolar disorder in pregnancy and breastfeeding: focus on emerging mood stabilizers. Bipolar Disord. 2006;8(3):207-220.
14. Iqbal MM, Gundlapalli SP, Ryan WG, et al. Effects of antimanic mood-stabilizing drugs on fetuses, neonates, and nursing infants. South Med J. 2001;94(3):304-322.
15. Kozma C. Neonatal toxicity and transient neurodevelopmental deficits following prenatal exposure to lithium: another clinical report and a review of the literature. Am J Med Genet A. 2005;132(4):441-444.
16. Newport DJ, Viguera AC, Beach AJ, et al. Lithium placental passage and obstetrical outcome: implications for clinical management during late pregnancy. Am J Psychiatry. 2005;162(11):2162-2170.
17. Schou M. What happened later to the lithium babies? A follow-up study of children born without malformations. Acta Psychiatr Scand. 1976;54(3):193-197.
18. Morrow J, Russell A, Guthrie E, et al. Malformation risks of antiepileptic drugs in pregnancy: a prospective study from the UK Epilepsy and Pregnancy Register. J Neurol Neurosurg Psychiatry. 2006;77(2):193-198.
19. Sabers A, Tomson T. Managing antiepileptic drugs during pregnancy and lactation. Curr Opin Neurol. 2009;22(2):157-161.
20. Cummings C, Stewart M, Stevenson M, et al. Neurodevelopment of children exposed in utero to lamotrigine, sodium valproate and carbamazepine. Arch Dis Child. 2011;96(7):643-647.
21. Mølgaard-Nielsen D, Hviid A. Newer-generation antiepileptic drugs and the risk of major birth defects. JAMA. 2011;305(19):1996-2002.
22. Martínez-Frías ML. Topiramate in pregnancy: preliminary experience from the UK Epilepsy and Pregnancy Register. Neurology. 2009;72(23):2054-2055.
23. McKenna K, Koren G, Tetelbaum M, et al. Pregnancy outcome of women using atypical antipsychotic drugs: a prospective comparative study. J Clin Psychiatry. 2005;66(4):444-449.
24. Reis M, Källén B. Maternal use of antipsychotics in early pregnancy and delivery outcome. J Clin Psychopharmacol. 2008;28(3):279-288.
25. Coppola D, Russo LJ, Kwarta RF, Jr, et al. Evaluating the postmarketing experience of risperidone use during pregnancy: pregnancy and neonatal outcomes. Drug Saf. 2007;30(3):247-264.
26. Einarson A, Boskovic R. Use and safety of antipsychotic drugs during pregnancy. J Psychiatr Pract. 2009;15(3):183-192.
27. Spinelli MG. Postpartum psychosis: detection of risk and management. Am J Psychiatry. 2009;166(4):405-408.
28. Yonkers KA, Vigod S, Ross LE. Diagnosis, pathophysiology, and management of mood disorders in pregnant and postpartum women. Obstet Gynecol. 2011;117(4):961-977.
29. Doucet S, Jones I, Letourneau N, et al. Interventions for the prevention and treatment of postpartum psychosis: a systematic review. Arch Womens Ment Health. 2011;14(2):89-98.
30. Newport DJ, Pennell PB, Calamaras MR, et al. Lamotrigine in breast milk and nursing infants: determination of exposure. Pediatrics. 2008;122(1):e223-231.
31. Gentile S. Prophylactic treatment of bipolar disorder in pregnancy and breastfeeding: focus on emerging mood stabilizers. Bipolar Disord. 2006;8(3):207-220.
32. Viguera AC, Newport DJ, Ritchie J, et al. Lithium in breast milk and nursing infants: clinical implications. Am J Psychiatry. 2007;164(2):342-345.
Cannabis, synthetic cannabinoids, and psychosis risk: What the evidence says
Discuss this article at www.facebook.com/CurrentPsychiatry
Over the past 50 years, anecdotal reports linking cannabis sativa (marijuana) and psychosis have been steadily accumulating, giving rise to the notion of “cannabis psychosis.” Despite this historic connection, marijuana often is regarded as a “soft drug” with few harmful effects. However, this benign view is now being revised, along with mounting research demonstrating a clear association between cannabis and psychosis.
In this article, I review evidence on marijuana’s impact on the risk of developing psychotic disorders, as well as the potential contributions of “medical” marijuana and other legally available products containing synthetic cannabinoids to psychosis risk.
Cannabis use and psychosis
Cannabis use has a largely deleterious effect on patients with psychotic disorders, and typically is associated with relapse, poor treatment adherence, and worsening psychotic symptoms.1,2 There is, however, evidence that some patients with schizophrenia might benefit from treatment with cannabidiol,3-5 another constituent of marijuana, as well as delta-9-tetrahydrocannabinol (Δ-9-THC), the principle psychoactive constituent of cannabis.6,7
The acute psychotic potential of cannabis has been demonstrated by studies that documented psychotic symptoms (eg, hallucinations, paranoid delusions, derealization) in a dose-dependent manner among healthy volunteers administered Δ-9-THC under experimental conditions.8-10 Various cross-sectional epidemiologic studies also have revealed an association between cannabis use and acute or chronic psychosis.11,12
In the absence of definitive evidence from randomized, long-term, placebo-controlled trials, the strongest evidence of a connection between cannabis use and development of a psychotic disorder comes from prospective, longitudinal cohort studies. In the past 15 years, new evidence has emerged from 7 such studies that cumulatively provide strong support for an association between cannabis use as an adolescent or young adult and a greater risk for developing a psychotic disorder such as schizophrenia.13-19 These longitudinal studies surveyed for self-reported cannabis use before psychosis onset and controlled for a variety of potential confounding factors (eg, other drug use and demographic, social, and psychological variables). Three meta-analyses of these and other studies concluded an increased risk of psychosis is associated with cannabis use, with an odds ratio of 1.4 to 2.9 (meaning the risk of developing psychosis with any history of cannabis use is up to 3-fold higher compared with those who did not use cannabis).11,20,21 In addition, this association appears to be dose-related, with increasing amounts of cannabis use linked to greater risk—1 study found an odds ratio of 7 for psychosis among daily cannabis users.16
There are several ways to explain the link between cannabis use and psychosis, and a causal relationship has not yet been firmly established (Table 1).1-7,11-19,21-25 Current evidence supports that cannabis is a “component cause” of chronic psychosis, meaning although neither necessary nor sufficient, cannabis use at a young age increases the likelihood of developing schizophrenia or other psychotic disorders.26 This risk may be greatest for young persons with some psychosis vulnerability (eg, those with attenuated psychotic symptoms).16,18
The overall magnitude of risk appears to be modest, and cannabis use is only 1 of myriad factors that increase the risk of psychosis.27 Furthermore, most cannabis users do not develop psychosis. However, the risk associated with cannabis occurs during a vulnerable time of development and is modifiable. Based on conservative estimates, 8% of emergent schizophrenia cases and 14% of more broadly defined emergent psychosis cases could be prevented if it were possible to eliminate cannabis use among young people.11,26 Therefore, reducing cannabis use among young people vulnerable to psychosis should be a clinical and public health priority.
Table 1
Hypotheses linking cannabis and psychosis
| Hypothesis | Strength of evidence | Evidence for | Evidence against |
|---|---|---|---|
| Cannabis does not cause chronic psychosis | Weak |
| |
| Cannabis can cause schizophrenia | Equivocal | Cannabis use precedes the onset of schizophrenia in longitudinal studies13-19 | The incidence of schizophrenia has not been clearly increasing as expected with increasing cannabis use11,21 |
| Cannabis worsens existing psychotic disorders | Strong | Cannabidiol and Δ-9-THC improve symptoms in some patients with schizophrenia3-7 | |
| Cannabis increases the risk of chronic psychosis among vulnerable individuals | Strong | Cannabis use is not always a risk factor for conversion to psychosis in studies of prodromal schizophrenia25 | |
| Δ-9-THC: delta-9-tetrahydrocannabinol | |||
Medical marijuana
Although cannabis extracts were marketed by major pharmaceutical companies and widely used by consumers for various ailments during the late 1800s, medicinal cannabis use in the United States declined significantly during the early 20th century. In 1937, the Marihuana Tax Act was passed, effectively putting a stop to physicians prescribing cannabis for medical purposes. The FDA currently classifies cannabis as a Schedule I drug (eg, high abuse potential, no currently accepted medical use, lack of safety data) and the use of cannabis and its prescription by physicians are prohibited under federal law.
However, in recognition of the potential medical benefits of cannabis, 16 states have legalized medicinal use (“medical marijuana”) over the past several years. Laws and regulations governing medical marijuana vary from state to state. For example, in California, adults who obtain a recommendation from a physician and register for a Medical Marijuana Identification Card can legally purchase cannabis from a state-recognized dispensary and use it in a non-public setting. The physician’s “recommendation” (not a prescription) is based upon the determination that “the person’s health would benefit from the use of marijuana in the treatment of cancer, anorexia, AIDS, chronic pain, spasticity, glaucoma, arthritis, migraine, or any other illness for which marijuana provides relief”28 (emphasis added). Although no state has yet legalized cannabis use for recreational purposes, with such regulations, an increasing number of jurisdictions have provided a way for consumers to easily obtain marijuana for loosely defined medical purposes.
Medical marijuana dispensaries offer a variety of cannabis strains, each with a different advertised “high” based upon variable proportions of Δ-9-THC and other constituents. The Δ-9-THC content of medical marijuana is about twice that of “street” marijuana, even with the latter’s Δ-9-THC content rising to >10% over the past 15 years.29,30 Therefore, medical marijuana is not only legal, but generally offers a more potent Δ-9-THC dose than typical street marijuana.
A single case of psychosis emerging in the context of medical marijuana has been reported in the literature.31 A 24-year-old man with mild, transient psychotic symptoms switched from street cannabis to medical marijuana for its superior potency and to conform with the law. He obtained a physician’s recommendation based on diagnoses of “posttraumatic stress disorder” and “pain.” After several months of increasingly frequent medical marijuana use, he developed florid and persistent psychotic symptoms necessitating antipsychotic medication, and was diagnosed with schizophrenia.
Although causality cannot be established based on this report, taken together with evidence that higher-potency cannabis is associated with a greater risk of psychotic emergence,32 this case raises concerns about the iatrogenic and psychotoxic liability of medical marijuana use among those vulnerable to psychosis. Policy decisions about medical marijuana and its use among patients with psychiatric illness must be informed by evidence of its psychotic potential.
Synthetic cannabinoids
Synthetic cannabinoids were developed in the 1960s for research purposes and potential clinical applications, but have not been FDA-approved for therapeutic use.33 Over the past 5 years, however, a variety of “herbal incense” products bearing names such as “Spice,” “K2,” and “Aroma” have emerged in Europe and the United States that contain botanicals laced with synthetic cannabinoids (Table 2).
Although herbal incense products are labeled “not for human consumption,” they are sold by “head shops” and on the Internet without age restrictions and typically are purchased for the sole purpose of ingesting them, usually by smoking. Their desired effects resemble cannabis intoxication, including sedation, relaxation, altered consciousness, and euphoria. The products initially had the added appeal of being legal and undetectable in routine drug screening. Although not listed among the product’s ingredients, chemical analyses confirmed these products typically contained 1 of 3 families of synthetic cannabinoid1 and cannabinoid2 (CB1/CB2) receptor agonists, designated by the prefixes JWH-, CP-, and HU-.34 The compounds most commonly found in these analyses (JWH-018; CP-47,497; HU-210) have significantly greater potency (ie, CB1 receptor affinity) compared with Δ-9-THC.33,34
The growing popularity of herbal incense products has prompted health concerns based on reports of emergency presentations for adverse effects, including tachycardia, agitation, excess sedation, and loss of consciousness.33,35,36 In addition, 8 anecdotal reports of psychosis associated with herbal incense (with a total of 33 patients) have emerged since 2010 (Table 3). Among them, a variety of psychotic symptoms are described in patients ranging in age from adolescence to adulthood, both with and without histories of psychosis. For those without a pre-existing psychotic disorder, symptoms were typically self-limited.
In the most recently presented case series of patients without pre-existing psychosis (N = 10), symptoms resolved in 70% of patients within 8 days, but 30% had psychosis that persisted beyond 5-month follow-up.37 Collectively, these reports suggest that synthetic cannabinoid intoxication is associated with acute psychosis as well as exacerbations of previously stable psychotic disorders, and also may have a propensity to trigger a chronic psychotic disorder among vulnerable individuals.
Because of health concerns and the abuse potential of herbal incense products, many have been banned in several European countries, 18 U.S. states, and the U.S. military.33,38 In March 2011, the FDA placed 5 synthetic cannabinoids (JWH-018, JWH-073, JWH-200, CP-47,497, and cannabicyclohexanol) on Schedule I, making them illegal to possess or sell in the United States.38 However, there are hundreds of synthetic cannabinoid homologues, and herbal incense manufacturers have rapidly adapted by substituting other synthetic cannabinoids not yet banned by existing legislation.34 The effects of these newly arising compounds in humans, including their psychotic potential, are largely unknown.
Table 2
Herbal incense products and synthetic cannabinoids
| Herbal incense brand names | Cannabinoids they may contain |
|---|---|
| Spice, K2, Mojo, Aroma, Dream, Chill, Chaos, Sence, Smoke, Skunk, Space Diamond, Silent Black, Genie, Algerian Blend, Yucatan Fire, Tai Fun, Sensation, SpicyXXX, Spike 99, Bonsai-18, Banana Cream Nuke, Wicked X, Natures Organic, Zen |
|
Table 3
Case reports of psychosis associated with synthetic cannabinoids
| Study | N (age) | Herbal product or suspected cannabinoid | Previous psychotic disorder | Symptoms |
|---|---|---|---|---|
| Müller et al, 2010a | 1 (25) | JWH-018 “Spice” | Yes | Anxiety, exacerbation of paranoid delusions, delusions of control, auditory hallucinations |
| Vearrier et al, 2010b | 1 (17) | JWH-018 | No | Tachycardia, hypokalemia, agitation, visual hallucinations |
| Every-Palmer, 2010c | 5 | JWH-018 CP-47,497 | Yes | Agitation, disorganization, paranoid and grandiose delusions |
| Rodgman et al, 2011d | 3 | JWH-018 (“Mojo”) | – | “Mojo psychosis” |
| Benford et al, 2011e | 1 (20) | JWH-018 (“Spice”) | – | Tachycardia, anxiety, paranoia, auditory and visual hallucinations |
| Van Der Veer et al, 2011f | 3 (20 to 30) | “Spice” “Spike 99” | No | Anxiety, disorganization, paranoia, Capgras delusion |
| Every-Palmer, 2011g | 9 (20s to 40s) | JWH-018 (“Aroma”) | Yes | Anxiety, agitation, paranoia |
| Hurst et al, 2011h | 10 (21 to 25) | “Spice” | No | Anxiety, agitation, confusion, disorganization, paranoia, ideas of reference, hallucinations |
| Source: References a. Müller H, Sperling W, Köhrmann M, et al. The synthetic cannabinoid Spice as a trigger for an acute exacerbation of cannabis induced recurrent psychotic episodes. Schizophr Res. 2010;118(1-3):309-310. b. Vearrier D, Osterhoudt KC. A teenager with agitation: higher than she should have climbed. Pediatr Emerg Care. 2010;26(6):462-465. c. Every-Palmer S. Warning: legal synthetic cannabinoid-receptor agonists such as JWH-018 may precipitate psychosis in vulnerable individuals. Addiction. 2010;105(10):1859-1860. d. Rodgman C, Kinzie E, Leimbach E. Bad Mojo: use of the new marijuana substitute leads to more and more ED visits for acute psychosis. Am J Emerg Med. 2011;29(2):232. e. Benford DM, Caplan JP. Psychiatric sequelae of spice, K2, and synthetic cannabinoid receptor agonists. Psychosomatics. 2011;52(3):295. f. Van Der Veer N, Friday J. Persistent psychosis following the use of Spice. Schizophr Res. 2011;130(1-3):285-286. g. Every-Palmer S. Synthetic cannabinoid JWH-018 and psychosis: an explorative study. Drug Alcohol Depend. 2011. [Epub ahead of print]. h. Hurst D, Loeffler G, McLay R. Synthetic cannabinoid agonist induced psychosis: a case series. Presented at: 164th Annual Meeting of the American Psychiatric Association; May 14-18, 2011; Honolulu, HI | ||||
Related Resources
- Murray RM, Morrison PD, Henquet C, et al. Cannabis, the mind and society: the hash realities. Nat Rev Neurosci. 2007;8(11):885-895.
- European Monitoring Centre for Drugs and Drug Addiction: Synthetic cannabinoids and “spice.” www.emcdda.europa.eu/publications/drug-profiles/synthetic-cannabinoids.
- U.S. Department of Justice, Drug Enforcement Agency, Office of Diversion Control: Schedules of controlled substances: temporary placement of five synthetic cannabinoids into Schedule I. www.deadiversion.usdoj.gov/fed_regs/rules/2011/fr0301.htm.
1. Degenhardt L, Tennant C, Gilmour S, et al. The temporal dynamics of relationships between cannabis, psychosis and depression among young adults with psychotic disorders: findings from a 10-month prospective study. Psychol Med. 2007;37(7):927-934.
2. Zammit S, Moore TH, Lingford-Hughes A, et al. Effects of cannabis use on outcomes of psychotic disorders: systematic review. Br J Psychiatry. 2008;193(5):357-363.
3. Zuardi AW, Crippa JA, Hallak JE, et al. Cannabidiol, a Cannabis sativa constituent, as an antipsychotic drug. Braz J Med Biol Res. 2006;39(4):421-429.
4. Zuardi AW, Hallak JE, Dursun SM, et al. Cannabidiol monotherapy for treatment-resistant schizophrenia. J Psychopharmacol. 2006;20(5):683-686.
5. Morgan CJ, Curran HV. Effects of cannabidiol on schizophrenia-like symptoms in people who use cannabis. Br J Psychiatry. 2008;192(4):306-307.
6. Schwarcz G, Karajgi B, McCarthy R. Synthetic delta-9-tetrahydrocannabinol (dronabinol) can improve the symptoms of schizophrenia. J Clin Psychopharmacol. 2009;29(3):255-258.
7. Schwarcz G, Karajgi B. Improvement in refractory psychosis with dronabinol: four case reports. J Clin Psychiatry. 2010;71(11):1552-1553.
8. D’Souza DC, Perry E, MacDougall L, et al. The psychotomimetic effects of intravenous delta-9-tetrahydrocannabinol in healthy individuals: implications for psychosis. Neuropsychopharmacology. 2004;29(8):1558-1572.
9. Morrison PD, Zois V, McKeown DA, et al. The acute effects of synthetic intravenous Delta9-tetrahydrocannabinol on psychosis, mood and cognitive functioning. Psychol Med. 2009;39(10):1607-1616.
10. Favrat B, Ménétrey A, Augsburger M, et al. Two cases of “cannabis acute psychosis” following the administration of oral cannabis. BMC Psychiatry. 2005;5:17.-
11. Moore TH, Zammit S, Lingford-Hughes A, et al. Cannabis use and risk of psychotic or affective mental health outcomes: a systematic review. Lancet. 2007;370(9584):319-328
12. Minozzi S, Davoli M, Bargagli AM, et al. An overview of systematic reviews on cannabis and psychosis: discussing apparently conflicting results. Drug Alcohol Rev. 2010;29(3):304-317.
13. Andréasson S, Allebeck P, Engström A, et al. Cannabis and schizophrenia. A longitudinal study of Swedish conscripts. Lancet. 1987;2(8574):1483-1486
14. Zammit S, Allebeck P, Andreasson S, et al. Self reported cannabis use as a risk factor for schizophrenia in Swedish conscripts of 1969: historical cohort study. BMJ. 2002;325(7374):1199.-
15. Arseneault L, Cannon M, Poulton R, et al. Cannabis use in adolescence and risk for adult psychosis: longitudinal prospective study. BMJ. 2002;325(7374):1212-1213
16. van Os J, Bak M, Hanssen M, et al. Cannabis use and psychosis: a longitudinal population-based study. Am J Epidemiol. 2002;156(4):319-327
17. Fergusson DM, Horwood LJ, Swain-Campbell NR. Cannabis dependence and psychotic symptoms in young people. Psychol Med. 2003;33(1):15-21
18. Henquet C, Krabbendam L, Spauwen J, et al. Prospective cohort study of cannabis use, predisposition for psychosis, and psychotic symptoms in young people. BMJ. 2005;330(7481):11.-
19. Kuepper R, van Os J, Lieb R, et al. Continued cannabis use and risk of incidence and persistence of psychotic symptoms: 10 year follow-up cohort study. BMJ. 2011;342:d738.-
20. Henquet C, Murray R, Linszen D, et al. The environment and schizophrenia: the role of cannabis use. Schizophr Bull. 2005;31(3):608-612
21. Semple DM, McIntosh AM, Lawrie SM. Cannabis as a risk factor for psychosis: systematic review. J Psychopharmacol. 2005;19(2):187-194
22. D’Souza DC, Abi-Saab WM, Madonick S, et al. Delta-9-tetrahydrocannabinol effects in schizophrenia: implications for cognition, psychosis, and addiction. Biol Psychiatry. 2005;57(6):594-608
23. Large M, Sharma S, Compton MT, et al. Cannabis use and earlier onset of psychosis: a systematic meta-analysis. Arch Gen Psychiatry. 2011;68(6):555-561
24. Kristensen K, Cadenhead KS. Cannabis abuse and risk for psychosis in a prodromal sample. Psychiatry Res. 2007;151(1-2):151-154.
25. Phillips LJ, Curry C, Yung AR, et al. Cannabis use is not associated with the development of psychosis in an “ultra” high-risk group. Aust N Z J Psychiatry. 2002;36(6):800-806
26. Arseneault L, Cannon M, Witton J, et al. Causal association between cannabis and psychosis: examination of the evidence. Br J Psychiatry. 2004;184:110-117.
27. Tandon R, Keshavan MS, Nasrallah HA. Schizophrenia, “just the facts” what we know in 2008. 2. Epidemiology and etiology. Schizophr Res. 2008;102(1-3):1-18.
28. California Secretary of State. California Proposition 215: Text of proposed law. Available at: http://vote96.sos.ca.gov/Vote96/html/BP/215text.htm. Accessed July 27, 2011.
29. Burgdorf JR, Kilmer B, Pacula RL. Heterogeneity in the composition of marijuana seized in California. Drug Alcohol Depend. 2011;117(1):59-61
30. Gieringer D. Medical cannabis potency testing project. Bulletin of the Multidisciplinary Association for Psychedelic Studies. 1999;9(3):20 22. Available at: http://www.maps.org/news-letters/v09n3/09320gie.html. Accessed July 27, 2011.
31. Pierre JM. Psychosis associated with medical marijuana: risk vs. benefits of medicinal cannabis use. Am J Psychiatry. 2010;167(5):598-599
32. Di Forti M, Morgan C, Dazzan P, et al. High-potency cannabis and the risk of psychosis. Br J Psychiatry. 2009;195(6):488-491.
33. Vardakou I, Pistos C, Spiliopoulou CH. Spice drugs as a new trend: mode of action, identification and legislation. Toxicol Lett. 2010;197(3):157-162
34. Dresen S, Ferreirós N, Pütz M, et al. Monitoring of herbal mixtures potentially containing synthetic cannabinoids as psychoactive compounds. J Mass Spectrom. 2010;45(10):1186-1194.
35. Simmons JR, Skinner CG, Williams J, et al. Intoxication from smoking “spice.” Ann Emerg Med. 2011;57(2):187-188
36. Schneir AB, Cullen J, Ly BT. “Spice” girls: synthetic cannabinoid intoxication. J Emerg Med. 2011;40(3):296-299
37. Hurst D, Loeffler G, McLay R. Synthetic cannabinoid agonist induced psychosis: a case series. Presented at: 164th Annual Meeting of the American Psychiatric Association; May 14-18, 2011; Honolulu, HI.
38. U.S. Department of Justice Drug Enforcement Agency. Temporary placement of five synthetic cannabinoids into schedule I. Available at: http://www.deadiversion.usdoj.gov/fed_regs/rules/2011/fr0301.htm. Accessed July 27, 2011.
Discuss this article at www.facebook.com/CurrentPsychiatry
Over the past 50 years, anecdotal reports linking cannabis sativa (marijuana) and psychosis have been steadily accumulating, giving rise to the notion of “cannabis psychosis.” Despite this historic connection, marijuana often is regarded as a “soft drug” with few harmful effects. However, this benign view is now being revised, along with mounting research demonstrating a clear association between cannabis and psychosis.
In this article, I review evidence on marijuana’s impact on the risk of developing psychotic disorders, as well as the potential contributions of “medical” marijuana and other legally available products containing synthetic cannabinoids to psychosis risk.
Cannabis use and psychosis
Cannabis use has a largely deleterious effect on patients with psychotic disorders, and typically is associated with relapse, poor treatment adherence, and worsening psychotic symptoms.1,2 There is, however, evidence that some patients with schizophrenia might benefit from treatment with cannabidiol,3-5 another constituent of marijuana, as well as delta-9-tetrahydrocannabinol (Δ-9-THC), the principle psychoactive constituent of cannabis.6,7
The acute psychotic potential of cannabis has been demonstrated by studies that documented psychotic symptoms (eg, hallucinations, paranoid delusions, derealization) in a dose-dependent manner among healthy volunteers administered Δ-9-THC under experimental conditions.8-10 Various cross-sectional epidemiologic studies also have revealed an association between cannabis use and acute or chronic psychosis.11,12
In the absence of definitive evidence from randomized, long-term, placebo-controlled trials, the strongest evidence of a connection between cannabis use and development of a psychotic disorder comes from prospective, longitudinal cohort studies. In the past 15 years, new evidence has emerged from 7 such studies that cumulatively provide strong support for an association between cannabis use as an adolescent or young adult and a greater risk for developing a psychotic disorder such as schizophrenia.13-19 These longitudinal studies surveyed for self-reported cannabis use before psychosis onset and controlled for a variety of potential confounding factors (eg, other drug use and demographic, social, and psychological variables). Three meta-analyses of these and other studies concluded an increased risk of psychosis is associated with cannabis use, with an odds ratio of 1.4 to 2.9 (meaning the risk of developing psychosis with any history of cannabis use is up to 3-fold higher compared with those who did not use cannabis).11,20,21 In addition, this association appears to be dose-related, with increasing amounts of cannabis use linked to greater risk—1 study found an odds ratio of 7 for psychosis among daily cannabis users.16
There are several ways to explain the link between cannabis use and psychosis, and a causal relationship has not yet been firmly established (Table 1).1-7,11-19,21-25 Current evidence supports that cannabis is a “component cause” of chronic psychosis, meaning although neither necessary nor sufficient, cannabis use at a young age increases the likelihood of developing schizophrenia or other psychotic disorders.26 This risk may be greatest for young persons with some psychosis vulnerability (eg, those with attenuated psychotic symptoms).16,18
The overall magnitude of risk appears to be modest, and cannabis use is only 1 of myriad factors that increase the risk of psychosis.27 Furthermore, most cannabis users do not develop psychosis. However, the risk associated with cannabis occurs during a vulnerable time of development and is modifiable. Based on conservative estimates, 8% of emergent schizophrenia cases and 14% of more broadly defined emergent psychosis cases could be prevented if it were possible to eliminate cannabis use among young people.11,26 Therefore, reducing cannabis use among young people vulnerable to psychosis should be a clinical and public health priority.
Table 1
Hypotheses linking cannabis and psychosis
| Hypothesis | Strength of evidence | Evidence for | Evidence against |
|---|---|---|---|
| Cannabis does not cause chronic psychosis | Weak |
| |
| Cannabis can cause schizophrenia | Equivocal | Cannabis use precedes the onset of schizophrenia in longitudinal studies13-19 | The incidence of schizophrenia has not been clearly increasing as expected with increasing cannabis use11,21 |
| Cannabis worsens existing psychotic disorders | Strong | Cannabidiol and Δ-9-THC improve symptoms in some patients with schizophrenia3-7 | |
| Cannabis increases the risk of chronic psychosis among vulnerable individuals | Strong | Cannabis use is not always a risk factor for conversion to psychosis in studies of prodromal schizophrenia25 | |
| Δ-9-THC: delta-9-tetrahydrocannabinol | |||
Medical marijuana
Although cannabis extracts were marketed by major pharmaceutical companies and widely used by consumers for various ailments during the late 1800s, medicinal cannabis use in the United States declined significantly during the early 20th century. In 1937, the Marihuana Tax Act was passed, effectively putting a stop to physicians prescribing cannabis for medical purposes. The FDA currently classifies cannabis as a Schedule I drug (eg, high abuse potential, no currently accepted medical use, lack of safety data) and the use of cannabis and its prescription by physicians are prohibited under federal law.
However, in recognition of the potential medical benefits of cannabis, 16 states have legalized medicinal use (“medical marijuana”) over the past several years. Laws and regulations governing medical marijuana vary from state to state. For example, in California, adults who obtain a recommendation from a physician and register for a Medical Marijuana Identification Card can legally purchase cannabis from a state-recognized dispensary and use it in a non-public setting. The physician’s “recommendation” (not a prescription) is based upon the determination that “the person’s health would benefit from the use of marijuana in the treatment of cancer, anorexia, AIDS, chronic pain, spasticity, glaucoma, arthritis, migraine, or any other illness for which marijuana provides relief”28 (emphasis added). Although no state has yet legalized cannabis use for recreational purposes, with such regulations, an increasing number of jurisdictions have provided a way for consumers to easily obtain marijuana for loosely defined medical purposes.
Medical marijuana dispensaries offer a variety of cannabis strains, each with a different advertised “high” based upon variable proportions of Δ-9-THC and other constituents. The Δ-9-THC content of medical marijuana is about twice that of “street” marijuana, even with the latter’s Δ-9-THC content rising to >10% over the past 15 years.29,30 Therefore, medical marijuana is not only legal, but generally offers a more potent Δ-9-THC dose than typical street marijuana.
A single case of psychosis emerging in the context of medical marijuana has been reported in the literature.31 A 24-year-old man with mild, transient psychotic symptoms switched from street cannabis to medical marijuana for its superior potency and to conform with the law. He obtained a physician’s recommendation based on diagnoses of “posttraumatic stress disorder” and “pain.” After several months of increasingly frequent medical marijuana use, he developed florid and persistent psychotic symptoms necessitating antipsychotic medication, and was diagnosed with schizophrenia.
Although causality cannot be established based on this report, taken together with evidence that higher-potency cannabis is associated with a greater risk of psychotic emergence,32 this case raises concerns about the iatrogenic and psychotoxic liability of medical marijuana use among those vulnerable to psychosis. Policy decisions about medical marijuana and its use among patients with psychiatric illness must be informed by evidence of its psychotic potential.
Synthetic cannabinoids
Synthetic cannabinoids were developed in the 1960s for research purposes and potential clinical applications, but have not been FDA-approved for therapeutic use.33 Over the past 5 years, however, a variety of “herbal incense” products bearing names such as “Spice,” “K2,” and “Aroma” have emerged in Europe and the United States that contain botanicals laced with synthetic cannabinoids (Table 2).
Although herbal incense products are labeled “not for human consumption,” they are sold by “head shops” and on the Internet without age restrictions and typically are purchased for the sole purpose of ingesting them, usually by smoking. Their desired effects resemble cannabis intoxication, including sedation, relaxation, altered consciousness, and euphoria. The products initially had the added appeal of being legal and undetectable in routine drug screening. Although not listed among the product’s ingredients, chemical analyses confirmed these products typically contained 1 of 3 families of synthetic cannabinoid1 and cannabinoid2 (CB1/CB2) receptor agonists, designated by the prefixes JWH-, CP-, and HU-.34 The compounds most commonly found in these analyses (JWH-018; CP-47,497; HU-210) have significantly greater potency (ie, CB1 receptor affinity) compared with Δ-9-THC.33,34
The growing popularity of herbal incense products has prompted health concerns based on reports of emergency presentations for adverse effects, including tachycardia, agitation, excess sedation, and loss of consciousness.33,35,36 In addition, 8 anecdotal reports of psychosis associated with herbal incense (with a total of 33 patients) have emerged since 2010 (Table 3). Among them, a variety of psychotic symptoms are described in patients ranging in age from adolescence to adulthood, both with and without histories of psychosis. For those without a pre-existing psychotic disorder, symptoms were typically self-limited.
In the most recently presented case series of patients without pre-existing psychosis (N = 10), symptoms resolved in 70% of patients within 8 days, but 30% had psychosis that persisted beyond 5-month follow-up.37 Collectively, these reports suggest that synthetic cannabinoid intoxication is associated with acute psychosis as well as exacerbations of previously stable psychotic disorders, and also may have a propensity to trigger a chronic psychotic disorder among vulnerable individuals.
Because of health concerns and the abuse potential of herbal incense products, many have been banned in several European countries, 18 U.S. states, and the U.S. military.33,38 In March 2011, the FDA placed 5 synthetic cannabinoids (JWH-018, JWH-073, JWH-200, CP-47,497, and cannabicyclohexanol) on Schedule I, making them illegal to possess or sell in the United States.38 However, there are hundreds of synthetic cannabinoid homologues, and herbal incense manufacturers have rapidly adapted by substituting other synthetic cannabinoids not yet banned by existing legislation.34 The effects of these newly arising compounds in humans, including their psychotic potential, are largely unknown.
Table 2
Herbal incense products and synthetic cannabinoids
| Herbal incense brand names | Cannabinoids they may contain |
|---|---|
| Spice, K2, Mojo, Aroma, Dream, Chill, Chaos, Sence, Smoke, Skunk, Space Diamond, Silent Black, Genie, Algerian Blend, Yucatan Fire, Tai Fun, Sensation, SpicyXXX, Spike 99, Bonsai-18, Banana Cream Nuke, Wicked X, Natures Organic, Zen |
|
Table 3
Case reports of psychosis associated with synthetic cannabinoids
| Study | N (age) | Herbal product or suspected cannabinoid | Previous psychotic disorder | Symptoms |
|---|---|---|---|---|
| Müller et al, 2010a | 1 (25) | JWH-018 “Spice” | Yes | Anxiety, exacerbation of paranoid delusions, delusions of control, auditory hallucinations |
| Vearrier et al, 2010b | 1 (17) | JWH-018 | No | Tachycardia, hypokalemia, agitation, visual hallucinations |
| Every-Palmer, 2010c | 5 | JWH-018 CP-47,497 | Yes | Agitation, disorganization, paranoid and grandiose delusions |
| Rodgman et al, 2011d | 3 | JWH-018 (“Mojo”) | – | “Mojo psychosis” |
| Benford et al, 2011e | 1 (20) | JWH-018 (“Spice”) | – | Tachycardia, anxiety, paranoia, auditory and visual hallucinations |
| Van Der Veer et al, 2011f | 3 (20 to 30) | “Spice” “Spike 99” | No | Anxiety, disorganization, paranoia, Capgras delusion |
| Every-Palmer, 2011g | 9 (20s to 40s) | JWH-018 (“Aroma”) | Yes | Anxiety, agitation, paranoia |
| Hurst et al, 2011h | 10 (21 to 25) | “Spice” | No | Anxiety, agitation, confusion, disorganization, paranoia, ideas of reference, hallucinations |
| Source: References a. Müller H, Sperling W, Köhrmann M, et al. The synthetic cannabinoid Spice as a trigger for an acute exacerbation of cannabis induced recurrent psychotic episodes. Schizophr Res. 2010;118(1-3):309-310. b. Vearrier D, Osterhoudt KC. A teenager with agitation: higher than she should have climbed. Pediatr Emerg Care. 2010;26(6):462-465. c. Every-Palmer S. Warning: legal synthetic cannabinoid-receptor agonists such as JWH-018 may precipitate psychosis in vulnerable individuals. Addiction. 2010;105(10):1859-1860. d. Rodgman C, Kinzie E, Leimbach E. Bad Mojo: use of the new marijuana substitute leads to more and more ED visits for acute psychosis. Am J Emerg Med. 2011;29(2):232. e. Benford DM, Caplan JP. Psychiatric sequelae of spice, K2, and synthetic cannabinoid receptor agonists. Psychosomatics. 2011;52(3):295. f. Van Der Veer N, Friday J. Persistent psychosis following the use of Spice. Schizophr Res. 2011;130(1-3):285-286. g. Every-Palmer S. Synthetic cannabinoid JWH-018 and psychosis: an explorative study. Drug Alcohol Depend. 2011. [Epub ahead of print]. h. Hurst D, Loeffler G, McLay R. Synthetic cannabinoid agonist induced psychosis: a case series. Presented at: 164th Annual Meeting of the American Psychiatric Association; May 14-18, 2011; Honolulu, HI | ||||
Related Resources
- Murray RM, Morrison PD, Henquet C, et al. Cannabis, the mind and society: the hash realities. Nat Rev Neurosci. 2007;8(11):885-895.
- European Monitoring Centre for Drugs and Drug Addiction: Synthetic cannabinoids and “spice.” www.emcdda.europa.eu/publications/drug-profiles/synthetic-cannabinoids.
- U.S. Department of Justice, Drug Enforcement Agency, Office of Diversion Control: Schedules of controlled substances: temporary placement of five synthetic cannabinoids into Schedule I. www.deadiversion.usdoj.gov/fed_regs/rules/2011/fr0301.htm.
Discuss this article at www.facebook.com/CurrentPsychiatry
Over the past 50 years, anecdotal reports linking cannabis sativa (marijuana) and psychosis have been steadily accumulating, giving rise to the notion of “cannabis psychosis.” Despite this historic connection, marijuana often is regarded as a “soft drug” with few harmful effects. However, this benign view is now being revised, along with mounting research demonstrating a clear association between cannabis and psychosis.
In this article, I review evidence on marijuana’s impact on the risk of developing psychotic disorders, as well as the potential contributions of “medical” marijuana and other legally available products containing synthetic cannabinoids to psychosis risk.
Cannabis use and psychosis
Cannabis use has a largely deleterious effect on patients with psychotic disorders, and typically is associated with relapse, poor treatment adherence, and worsening psychotic symptoms.1,2 There is, however, evidence that some patients with schizophrenia might benefit from treatment with cannabidiol,3-5 another constituent of marijuana, as well as delta-9-tetrahydrocannabinol (Δ-9-THC), the principle psychoactive constituent of cannabis.6,7
The acute psychotic potential of cannabis has been demonstrated by studies that documented psychotic symptoms (eg, hallucinations, paranoid delusions, derealization) in a dose-dependent manner among healthy volunteers administered Δ-9-THC under experimental conditions.8-10 Various cross-sectional epidemiologic studies also have revealed an association between cannabis use and acute or chronic psychosis.11,12
In the absence of definitive evidence from randomized, long-term, placebo-controlled trials, the strongest evidence of a connection between cannabis use and development of a psychotic disorder comes from prospective, longitudinal cohort studies. In the past 15 years, new evidence has emerged from 7 such studies that cumulatively provide strong support for an association between cannabis use as an adolescent or young adult and a greater risk for developing a psychotic disorder such as schizophrenia.13-19 These longitudinal studies surveyed for self-reported cannabis use before psychosis onset and controlled for a variety of potential confounding factors (eg, other drug use and demographic, social, and psychological variables). Three meta-analyses of these and other studies concluded an increased risk of psychosis is associated with cannabis use, with an odds ratio of 1.4 to 2.9 (meaning the risk of developing psychosis with any history of cannabis use is up to 3-fold higher compared with those who did not use cannabis).11,20,21 In addition, this association appears to be dose-related, with increasing amounts of cannabis use linked to greater risk—1 study found an odds ratio of 7 for psychosis among daily cannabis users.16
There are several ways to explain the link between cannabis use and psychosis, and a causal relationship has not yet been firmly established (Table 1).1-7,11-19,21-25 Current evidence supports that cannabis is a “component cause” of chronic psychosis, meaning although neither necessary nor sufficient, cannabis use at a young age increases the likelihood of developing schizophrenia or other psychotic disorders.26 This risk may be greatest for young persons with some psychosis vulnerability (eg, those with attenuated psychotic symptoms).16,18
The overall magnitude of risk appears to be modest, and cannabis use is only 1 of myriad factors that increase the risk of psychosis.27 Furthermore, most cannabis users do not develop psychosis. However, the risk associated with cannabis occurs during a vulnerable time of development and is modifiable. Based on conservative estimates, 8% of emergent schizophrenia cases and 14% of more broadly defined emergent psychosis cases could be prevented if it were possible to eliminate cannabis use among young people.11,26 Therefore, reducing cannabis use among young people vulnerable to psychosis should be a clinical and public health priority.
Table 1
Hypotheses linking cannabis and psychosis
| Hypothesis | Strength of evidence | Evidence for | Evidence against |
|---|---|---|---|
| Cannabis does not cause chronic psychosis | Weak |
| |
| Cannabis can cause schizophrenia | Equivocal | Cannabis use precedes the onset of schizophrenia in longitudinal studies13-19 | The incidence of schizophrenia has not been clearly increasing as expected with increasing cannabis use11,21 |
| Cannabis worsens existing psychotic disorders | Strong | Cannabidiol and Δ-9-THC improve symptoms in some patients with schizophrenia3-7 | |
| Cannabis increases the risk of chronic psychosis among vulnerable individuals | Strong | Cannabis use is not always a risk factor for conversion to psychosis in studies of prodromal schizophrenia25 | |
| Δ-9-THC: delta-9-tetrahydrocannabinol | |||
Medical marijuana
Although cannabis extracts were marketed by major pharmaceutical companies and widely used by consumers for various ailments during the late 1800s, medicinal cannabis use in the United States declined significantly during the early 20th century. In 1937, the Marihuana Tax Act was passed, effectively putting a stop to physicians prescribing cannabis for medical purposes. The FDA currently classifies cannabis as a Schedule I drug (eg, high abuse potential, no currently accepted medical use, lack of safety data) and the use of cannabis and its prescription by physicians are prohibited under federal law.
However, in recognition of the potential medical benefits of cannabis, 16 states have legalized medicinal use (“medical marijuana”) over the past several years. Laws and regulations governing medical marijuana vary from state to state. For example, in California, adults who obtain a recommendation from a physician and register for a Medical Marijuana Identification Card can legally purchase cannabis from a state-recognized dispensary and use it in a non-public setting. The physician’s “recommendation” (not a prescription) is based upon the determination that “the person’s health would benefit from the use of marijuana in the treatment of cancer, anorexia, AIDS, chronic pain, spasticity, glaucoma, arthritis, migraine, or any other illness for which marijuana provides relief”28 (emphasis added). Although no state has yet legalized cannabis use for recreational purposes, with such regulations, an increasing number of jurisdictions have provided a way for consumers to easily obtain marijuana for loosely defined medical purposes.
Medical marijuana dispensaries offer a variety of cannabis strains, each with a different advertised “high” based upon variable proportions of Δ-9-THC and other constituents. The Δ-9-THC content of medical marijuana is about twice that of “street” marijuana, even with the latter’s Δ-9-THC content rising to >10% over the past 15 years.29,30 Therefore, medical marijuana is not only legal, but generally offers a more potent Δ-9-THC dose than typical street marijuana.
A single case of psychosis emerging in the context of medical marijuana has been reported in the literature.31 A 24-year-old man with mild, transient psychotic symptoms switched from street cannabis to medical marijuana for its superior potency and to conform with the law. He obtained a physician’s recommendation based on diagnoses of “posttraumatic stress disorder” and “pain.” After several months of increasingly frequent medical marijuana use, he developed florid and persistent psychotic symptoms necessitating antipsychotic medication, and was diagnosed with schizophrenia.
Although causality cannot be established based on this report, taken together with evidence that higher-potency cannabis is associated with a greater risk of psychotic emergence,32 this case raises concerns about the iatrogenic and psychotoxic liability of medical marijuana use among those vulnerable to psychosis. Policy decisions about medical marijuana and its use among patients with psychiatric illness must be informed by evidence of its psychotic potential.
Synthetic cannabinoids
Synthetic cannabinoids were developed in the 1960s for research purposes and potential clinical applications, but have not been FDA-approved for therapeutic use.33 Over the past 5 years, however, a variety of “herbal incense” products bearing names such as “Spice,” “K2,” and “Aroma” have emerged in Europe and the United States that contain botanicals laced with synthetic cannabinoids (Table 2).
Although herbal incense products are labeled “not for human consumption,” they are sold by “head shops” and on the Internet without age restrictions and typically are purchased for the sole purpose of ingesting them, usually by smoking. Their desired effects resemble cannabis intoxication, including sedation, relaxation, altered consciousness, and euphoria. The products initially had the added appeal of being legal and undetectable in routine drug screening. Although not listed among the product’s ingredients, chemical analyses confirmed these products typically contained 1 of 3 families of synthetic cannabinoid1 and cannabinoid2 (CB1/CB2) receptor agonists, designated by the prefixes JWH-, CP-, and HU-.34 The compounds most commonly found in these analyses (JWH-018; CP-47,497; HU-210) have significantly greater potency (ie, CB1 receptor affinity) compared with Δ-9-THC.33,34
The growing popularity of herbal incense products has prompted health concerns based on reports of emergency presentations for adverse effects, including tachycardia, agitation, excess sedation, and loss of consciousness.33,35,36 In addition, 8 anecdotal reports of psychosis associated with herbal incense (with a total of 33 patients) have emerged since 2010 (Table 3). Among them, a variety of psychotic symptoms are described in patients ranging in age from adolescence to adulthood, both with and without histories of psychosis. For those without a pre-existing psychotic disorder, symptoms were typically self-limited.
In the most recently presented case series of patients without pre-existing psychosis (N = 10), symptoms resolved in 70% of patients within 8 days, but 30% had psychosis that persisted beyond 5-month follow-up.37 Collectively, these reports suggest that synthetic cannabinoid intoxication is associated with acute psychosis as well as exacerbations of previously stable psychotic disorders, and also may have a propensity to trigger a chronic psychotic disorder among vulnerable individuals.
Because of health concerns and the abuse potential of herbal incense products, many have been banned in several European countries, 18 U.S. states, and the U.S. military.33,38 In March 2011, the FDA placed 5 synthetic cannabinoids (JWH-018, JWH-073, JWH-200, CP-47,497, and cannabicyclohexanol) on Schedule I, making them illegal to possess or sell in the United States.38 However, there are hundreds of synthetic cannabinoid homologues, and herbal incense manufacturers have rapidly adapted by substituting other synthetic cannabinoids not yet banned by existing legislation.34 The effects of these newly arising compounds in humans, including their psychotic potential, are largely unknown.
Table 2
Herbal incense products and synthetic cannabinoids
| Herbal incense brand names | Cannabinoids they may contain |
|---|---|
| Spice, K2, Mojo, Aroma, Dream, Chill, Chaos, Sence, Smoke, Skunk, Space Diamond, Silent Black, Genie, Algerian Blend, Yucatan Fire, Tai Fun, Sensation, SpicyXXX, Spike 99, Bonsai-18, Banana Cream Nuke, Wicked X, Natures Organic, Zen |
|
Table 3
Case reports of psychosis associated with synthetic cannabinoids
| Study | N (age) | Herbal product or suspected cannabinoid | Previous psychotic disorder | Symptoms |
|---|---|---|---|---|
| Müller et al, 2010a | 1 (25) | JWH-018 “Spice” | Yes | Anxiety, exacerbation of paranoid delusions, delusions of control, auditory hallucinations |
| Vearrier et al, 2010b | 1 (17) | JWH-018 | No | Tachycardia, hypokalemia, agitation, visual hallucinations |
| Every-Palmer, 2010c | 5 | JWH-018 CP-47,497 | Yes | Agitation, disorganization, paranoid and grandiose delusions |
| Rodgman et al, 2011d | 3 | JWH-018 (“Mojo”) | – | “Mojo psychosis” |
| Benford et al, 2011e | 1 (20) | JWH-018 (“Spice”) | – | Tachycardia, anxiety, paranoia, auditory and visual hallucinations |
| Van Der Veer et al, 2011f | 3 (20 to 30) | “Spice” “Spike 99” | No | Anxiety, disorganization, paranoia, Capgras delusion |
| Every-Palmer, 2011g | 9 (20s to 40s) | JWH-018 (“Aroma”) | Yes | Anxiety, agitation, paranoia |
| Hurst et al, 2011h | 10 (21 to 25) | “Spice” | No | Anxiety, agitation, confusion, disorganization, paranoia, ideas of reference, hallucinations |
| Source: References a. Müller H, Sperling W, Köhrmann M, et al. The synthetic cannabinoid Spice as a trigger for an acute exacerbation of cannabis induced recurrent psychotic episodes. Schizophr Res. 2010;118(1-3):309-310. b. Vearrier D, Osterhoudt KC. A teenager with agitation: higher than she should have climbed. Pediatr Emerg Care. 2010;26(6):462-465. c. Every-Palmer S. Warning: legal synthetic cannabinoid-receptor agonists such as JWH-018 may precipitate psychosis in vulnerable individuals. Addiction. 2010;105(10):1859-1860. d. Rodgman C, Kinzie E, Leimbach E. Bad Mojo: use of the new marijuana substitute leads to more and more ED visits for acute psychosis. Am J Emerg Med. 2011;29(2):232. e. Benford DM, Caplan JP. Psychiatric sequelae of spice, K2, and synthetic cannabinoid receptor agonists. Psychosomatics. 2011;52(3):295. f. Van Der Veer N, Friday J. Persistent psychosis following the use of Spice. Schizophr Res. 2011;130(1-3):285-286. g. Every-Palmer S. Synthetic cannabinoid JWH-018 and psychosis: an explorative study. Drug Alcohol Depend. 2011. [Epub ahead of print]. h. Hurst D, Loeffler G, McLay R. Synthetic cannabinoid agonist induced psychosis: a case series. Presented at: 164th Annual Meeting of the American Psychiatric Association; May 14-18, 2011; Honolulu, HI | ||||
Related Resources
- Murray RM, Morrison PD, Henquet C, et al. Cannabis, the mind and society: the hash realities. Nat Rev Neurosci. 2007;8(11):885-895.
- European Monitoring Centre for Drugs and Drug Addiction: Synthetic cannabinoids and “spice.” www.emcdda.europa.eu/publications/drug-profiles/synthetic-cannabinoids.
- U.S. Department of Justice, Drug Enforcement Agency, Office of Diversion Control: Schedules of controlled substances: temporary placement of five synthetic cannabinoids into Schedule I. www.deadiversion.usdoj.gov/fed_regs/rules/2011/fr0301.htm.
1. Degenhardt L, Tennant C, Gilmour S, et al. The temporal dynamics of relationships between cannabis, psychosis and depression among young adults with psychotic disorders: findings from a 10-month prospective study. Psychol Med. 2007;37(7):927-934.
2. Zammit S, Moore TH, Lingford-Hughes A, et al. Effects of cannabis use on outcomes of psychotic disorders: systematic review. Br J Psychiatry. 2008;193(5):357-363.
3. Zuardi AW, Crippa JA, Hallak JE, et al. Cannabidiol, a Cannabis sativa constituent, as an antipsychotic drug. Braz J Med Biol Res. 2006;39(4):421-429.
4. Zuardi AW, Hallak JE, Dursun SM, et al. Cannabidiol monotherapy for treatment-resistant schizophrenia. J Psychopharmacol. 2006;20(5):683-686.
5. Morgan CJ, Curran HV. Effects of cannabidiol on schizophrenia-like symptoms in people who use cannabis. Br J Psychiatry. 2008;192(4):306-307.
6. Schwarcz G, Karajgi B, McCarthy R. Synthetic delta-9-tetrahydrocannabinol (dronabinol) can improve the symptoms of schizophrenia. J Clin Psychopharmacol. 2009;29(3):255-258.
7. Schwarcz G, Karajgi B. Improvement in refractory psychosis with dronabinol: four case reports. J Clin Psychiatry. 2010;71(11):1552-1553.
8. D’Souza DC, Perry E, MacDougall L, et al. The psychotomimetic effects of intravenous delta-9-tetrahydrocannabinol in healthy individuals: implications for psychosis. Neuropsychopharmacology. 2004;29(8):1558-1572.
9. Morrison PD, Zois V, McKeown DA, et al. The acute effects of synthetic intravenous Delta9-tetrahydrocannabinol on psychosis, mood and cognitive functioning. Psychol Med. 2009;39(10):1607-1616.
10. Favrat B, Ménétrey A, Augsburger M, et al. Two cases of “cannabis acute psychosis” following the administration of oral cannabis. BMC Psychiatry. 2005;5:17.-
11. Moore TH, Zammit S, Lingford-Hughes A, et al. Cannabis use and risk of psychotic or affective mental health outcomes: a systematic review. Lancet. 2007;370(9584):319-328
12. Minozzi S, Davoli M, Bargagli AM, et al. An overview of systematic reviews on cannabis and psychosis: discussing apparently conflicting results. Drug Alcohol Rev. 2010;29(3):304-317.
13. Andréasson S, Allebeck P, Engström A, et al. Cannabis and schizophrenia. A longitudinal study of Swedish conscripts. Lancet. 1987;2(8574):1483-1486
14. Zammit S, Allebeck P, Andreasson S, et al. Self reported cannabis use as a risk factor for schizophrenia in Swedish conscripts of 1969: historical cohort study. BMJ. 2002;325(7374):1199.-
15. Arseneault L, Cannon M, Poulton R, et al. Cannabis use in adolescence and risk for adult psychosis: longitudinal prospective study. BMJ. 2002;325(7374):1212-1213
16. van Os J, Bak M, Hanssen M, et al. Cannabis use and psychosis: a longitudinal population-based study. Am J Epidemiol. 2002;156(4):319-327
17. Fergusson DM, Horwood LJ, Swain-Campbell NR. Cannabis dependence and psychotic symptoms in young people. Psychol Med. 2003;33(1):15-21
18. Henquet C, Krabbendam L, Spauwen J, et al. Prospective cohort study of cannabis use, predisposition for psychosis, and psychotic symptoms in young people. BMJ. 2005;330(7481):11.-
19. Kuepper R, van Os J, Lieb R, et al. Continued cannabis use and risk of incidence and persistence of psychotic symptoms: 10 year follow-up cohort study. BMJ. 2011;342:d738.-
20. Henquet C, Murray R, Linszen D, et al. The environment and schizophrenia: the role of cannabis use. Schizophr Bull. 2005;31(3):608-612
21. Semple DM, McIntosh AM, Lawrie SM. Cannabis as a risk factor for psychosis: systematic review. J Psychopharmacol. 2005;19(2):187-194
22. D’Souza DC, Abi-Saab WM, Madonick S, et al. Delta-9-tetrahydrocannabinol effects in schizophrenia: implications for cognition, psychosis, and addiction. Biol Psychiatry. 2005;57(6):594-608
23. Large M, Sharma S, Compton MT, et al. Cannabis use and earlier onset of psychosis: a systematic meta-analysis. Arch Gen Psychiatry. 2011;68(6):555-561
24. Kristensen K, Cadenhead KS. Cannabis abuse and risk for psychosis in a prodromal sample. Psychiatry Res. 2007;151(1-2):151-154.
25. Phillips LJ, Curry C, Yung AR, et al. Cannabis use is not associated with the development of psychosis in an “ultra” high-risk group. Aust N Z J Psychiatry. 2002;36(6):800-806
26. Arseneault L, Cannon M, Witton J, et al. Causal association between cannabis and psychosis: examination of the evidence. Br J Psychiatry. 2004;184:110-117.
27. Tandon R, Keshavan MS, Nasrallah HA. Schizophrenia, “just the facts” what we know in 2008. 2. Epidemiology and etiology. Schizophr Res. 2008;102(1-3):1-18.
28. California Secretary of State. California Proposition 215: Text of proposed law. Available at: http://vote96.sos.ca.gov/Vote96/html/BP/215text.htm. Accessed July 27, 2011.
29. Burgdorf JR, Kilmer B, Pacula RL. Heterogeneity in the composition of marijuana seized in California. Drug Alcohol Depend. 2011;117(1):59-61
30. Gieringer D. Medical cannabis potency testing project. Bulletin of the Multidisciplinary Association for Psychedelic Studies. 1999;9(3):20 22. Available at: http://www.maps.org/news-letters/v09n3/09320gie.html. Accessed July 27, 2011.
31. Pierre JM. Psychosis associated with medical marijuana: risk vs. benefits of medicinal cannabis use. Am J Psychiatry. 2010;167(5):598-599
32. Di Forti M, Morgan C, Dazzan P, et al. High-potency cannabis and the risk of psychosis. Br J Psychiatry. 2009;195(6):488-491.
33. Vardakou I, Pistos C, Spiliopoulou CH. Spice drugs as a new trend: mode of action, identification and legislation. Toxicol Lett. 2010;197(3):157-162
34. Dresen S, Ferreirós N, Pütz M, et al. Monitoring of herbal mixtures potentially containing synthetic cannabinoids as psychoactive compounds. J Mass Spectrom. 2010;45(10):1186-1194.
35. Simmons JR, Skinner CG, Williams J, et al. Intoxication from smoking “spice.” Ann Emerg Med. 2011;57(2):187-188
36. Schneir AB, Cullen J, Ly BT. “Spice” girls: synthetic cannabinoid intoxication. J Emerg Med. 2011;40(3):296-299
37. Hurst D, Loeffler G, McLay R. Synthetic cannabinoid agonist induced psychosis: a case series. Presented at: 164th Annual Meeting of the American Psychiatric Association; May 14-18, 2011; Honolulu, HI.
38. U.S. Department of Justice Drug Enforcement Agency. Temporary placement of five synthetic cannabinoids into schedule I. Available at: http://www.deadiversion.usdoj.gov/fed_regs/rules/2011/fr0301.htm. Accessed July 27, 2011.
1. Degenhardt L, Tennant C, Gilmour S, et al. The temporal dynamics of relationships between cannabis, psychosis and depression among young adults with psychotic disorders: findings from a 10-month prospective study. Psychol Med. 2007;37(7):927-934.
2. Zammit S, Moore TH, Lingford-Hughes A, et al. Effects of cannabis use on outcomes of psychotic disorders: systematic review. Br J Psychiatry. 2008;193(5):357-363.
3. Zuardi AW, Crippa JA, Hallak JE, et al. Cannabidiol, a Cannabis sativa constituent, as an antipsychotic drug. Braz J Med Biol Res. 2006;39(4):421-429.
4. Zuardi AW, Hallak JE, Dursun SM, et al. Cannabidiol monotherapy for treatment-resistant schizophrenia. J Psychopharmacol. 2006;20(5):683-686.
5. Morgan CJ, Curran HV. Effects of cannabidiol on schizophrenia-like symptoms in people who use cannabis. Br J Psychiatry. 2008;192(4):306-307.
6. Schwarcz G, Karajgi B, McCarthy R. Synthetic delta-9-tetrahydrocannabinol (dronabinol) can improve the symptoms of schizophrenia. J Clin Psychopharmacol. 2009;29(3):255-258.
7. Schwarcz G, Karajgi B. Improvement in refractory psychosis with dronabinol: four case reports. J Clin Psychiatry. 2010;71(11):1552-1553.
8. D’Souza DC, Perry E, MacDougall L, et al. The psychotomimetic effects of intravenous delta-9-tetrahydrocannabinol in healthy individuals: implications for psychosis. Neuropsychopharmacology. 2004;29(8):1558-1572.
9. Morrison PD, Zois V, McKeown DA, et al. The acute effects of synthetic intravenous Delta9-tetrahydrocannabinol on psychosis, mood and cognitive functioning. Psychol Med. 2009;39(10):1607-1616.
10. Favrat B, Ménétrey A, Augsburger M, et al. Two cases of “cannabis acute psychosis” following the administration of oral cannabis. BMC Psychiatry. 2005;5:17.-
11. Moore TH, Zammit S, Lingford-Hughes A, et al. Cannabis use and risk of psychotic or affective mental health outcomes: a systematic review. Lancet. 2007;370(9584):319-328
12. Minozzi S, Davoli M, Bargagli AM, et al. An overview of systematic reviews on cannabis and psychosis: discussing apparently conflicting results. Drug Alcohol Rev. 2010;29(3):304-317.
13. Andréasson S, Allebeck P, Engström A, et al. Cannabis and schizophrenia. A longitudinal study of Swedish conscripts. Lancet. 1987;2(8574):1483-1486
14. Zammit S, Allebeck P, Andreasson S, et al. Self reported cannabis use as a risk factor for schizophrenia in Swedish conscripts of 1969: historical cohort study. BMJ. 2002;325(7374):1199.-
15. Arseneault L, Cannon M, Poulton R, et al. Cannabis use in adolescence and risk for adult psychosis: longitudinal prospective study. BMJ. 2002;325(7374):1212-1213
16. van Os J, Bak M, Hanssen M, et al. Cannabis use and psychosis: a longitudinal population-based study. Am J Epidemiol. 2002;156(4):319-327
17. Fergusson DM, Horwood LJ, Swain-Campbell NR. Cannabis dependence and psychotic symptoms in young people. Psychol Med. 2003;33(1):15-21
18. Henquet C, Krabbendam L, Spauwen J, et al. Prospective cohort study of cannabis use, predisposition for psychosis, and psychotic symptoms in young people. BMJ. 2005;330(7481):11.-
19. Kuepper R, van Os J, Lieb R, et al. Continued cannabis use and risk of incidence and persistence of psychotic symptoms: 10 year follow-up cohort study. BMJ. 2011;342:d738.-
20. Henquet C, Murray R, Linszen D, et al. The environment and schizophrenia: the role of cannabis use. Schizophr Bull. 2005;31(3):608-612
21. Semple DM, McIntosh AM, Lawrie SM. Cannabis as a risk factor for psychosis: systematic review. J Psychopharmacol. 2005;19(2):187-194
22. D’Souza DC, Abi-Saab WM, Madonick S, et al. Delta-9-tetrahydrocannabinol effects in schizophrenia: implications for cognition, psychosis, and addiction. Biol Psychiatry. 2005;57(6):594-608
23. Large M, Sharma S, Compton MT, et al. Cannabis use and earlier onset of psychosis: a systematic meta-analysis. Arch Gen Psychiatry. 2011;68(6):555-561
24. Kristensen K, Cadenhead KS. Cannabis abuse and risk for psychosis in a prodromal sample. Psychiatry Res. 2007;151(1-2):151-154.
25. Phillips LJ, Curry C, Yung AR, et al. Cannabis use is not associated with the development of psychosis in an “ultra” high-risk group. Aust N Z J Psychiatry. 2002;36(6):800-806
26. Arseneault L, Cannon M, Witton J, et al. Causal association between cannabis and psychosis: examination of the evidence. Br J Psychiatry. 2004;184:110-117.
27. Tandon R, Keshavan MS, Nasrallah HA. Schizophrenia, “just the facts” what we know in 2008. 2. Epidemiology and etiology. Schizophr Res. 2008;102(1-3):1-18.
28. California Secretary of State. California Proposition 215: Text of proposed law. Available at: http://vote96.sos.ca.gov/Vote96/html/BP/215text.htm. Accessed July 27, 2011.
29. Burgdorf JR, Kilmer B, Pacula RL. Heterogeneity in the composition of marijuana seized in California. Drug Alcohol Depend. 2011;117(1):59-61
30. Gieringer D. Medical cannabis potency testing project. Bulletin of the Multidisciplinary Association for Psychedelic Studies. 1999;9(3):20 22. Available at: http://www.maps.org/news-letters/v09n3/09320gie.html. Accessed July 27, 2011.
31. Pierre JM. Psychosis associated with medical marijuana: risk vs. benefits of medicinal cannabis use. Am J Psychiatry. 2010;167(5):598-599
32. Di Forti M, Morgan C, Dazzan P, et al. High-potency cannabis and the risk of psychosis. Br J Psychiatry. 2009;195(6):488-491.
33. Vardakou I, Pistos C, Spiliopoulou CH. Spice drugs as a new trend: mode of action, identification and legislation. Toxicol Lett. 2010;197(3):157-162
34. Dresen S, Ferreirós N, Pütz M, et al. Monitoring of herbal mixtures potentially containing synthetic cannabinoids as psychoactive compounds. J Mass Spectrom. 2010;45(10):1186-1194.
35. Simmons JR, Skinner CG, Williams J, et al. Intoxication from smoking “spice.” Ann Emerg Med. 2011;57(2):187-188
36. Schneir AB, Cullen J, Ly BT. “Spice” girls: synthetic cannabinoid intoxication. J Emerg Med. 2011;40(3):296-299
37. Hurst D, Loeffler G, McLay R. Synthetic cannabinoid agonist induced psychosis: a case series. Presented at: 164th Annual Meeting of the American Psychiatric Association; May 14-18, 2011; Honolulu, HI.
38. U.S. Department of Justice Drug Enforcement Agency. Temporary placement of five synthetic cannabinoids into schedule I. Available at: http://www.deadiversion.usdoj.gov/fed_regs/rules/2011/fr0301.htm. Accessed July 27, 2011.
Redefining personality disorders: Proposed revisions for DSM-5
A major update to the diagnostic manual used by mental health clinicians around the world is expected to inspire lively debate. Proposed revisions to the personality disorders (PD) section of the next edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), which is scheduled to be published in 2013, have generated great controversy because they would introduce a dimensional model to the categorical system and 4 PDs would be eliminated.
“The importance of personality functioning and personality traits is the major innovation here,” said Andrew Skodol, MD, the DSM-5 Personality and Personality Disorders Work Group’s chair and a Research Professor of Psychiatry at the University of Arizona College of Medicine. “In the past, we viewed personality disorders as binary. You either had one or you didn’t. But we now understand that personality pathology is a matter of degree.”1
Mark Zimmerman, MD, has written several papers—some of which are in press—about how these revisions might impact clinicians and whether the revisions are necessary. He is Director of the Rhode Island Methods to Improve Diagnostic Assessment and Services (MIDAS) project, an ongoing clinical research study involving the integration of research assessment methods into clinical practice.
Proposed revisions, rationale, and literature reviews for DSM-5 are available at www.DSM5.org and anyone, including the general public, was invited to provide feedback through the Web site. Current Psychiatry Associate Editor Donald W. Black, MD, interviewed Dr. Zimmerman on June 29, 2011, just a few days after the latest proposed revision was posted on June 21, 2011.
DR. BLACK: What is your understanding of the DSM-5 Personality Disorders Work Group proposal to revamp the PD category?
DR. ZIMMERMAN: The initial proposal, released in February 2010, was complex and generated a fair amount of critical commentary related to the marked changes in the approach toward diagnosis of PDs. That proposal replaced diagnostic criteria with a prototype description of personality types that patients would need to match. It also eliminated 5 PDs—paranoid, schizoid, histrionic, dependent, and narcissistic—retained antisocial, avoidant, borderline, obsessive-compulsive, and schizotypal, and introduced trait level ratings. The June 21 revision proposes eliminating only 4 disorders—narcissistic was retained—and the Work Group is no longer suggesting using prototypes but instead have diagnostic criteria (Table).2,3 We do not know if this is the final proposal because similar to the first proposal, it is not presented with much supporting empirical evidence that demonstrates its superiority toward diagnosing PDs compared with the DSM-IV approach.
Table
Personality disorder criteria: DSM-IV vs DSM-5
| DSM-IV | DSM-5 proposal (posted June 21, 2011) |
|---|---|
| General diagnostic criteria | |
|
|
| Personality disorders included | |
| Antisocial, avoidant, borderline, dependent, histrionic, narcissistic, obsessive-compulsive, paranoid, schizoid, schizotypal, personality disorder not otherwise specified | Antisocial, avoidant, borderline, narcissistic, obsessive-compulsive, schizotypal, personality disorder trait specified (requires a rating of significant impairment in personality functioning, combined with the presence of pathological trait domains or facets) |
| Source: References 2,3 | |
I’m not suggesting that the DSM-IV approach is without problems. My attitude is that before going forward with a change to the official diagnostic nomenclature, you need to clearly establish that the new way of doing things is better than the previous way by whatever metric you use.
DR. BLACK: Do you believe there is a need to revamp or revise the DSM-IV PD criteria?
DR. ZIMMERMAN: I think a number of the arguments put forth by the DSM-5 Work Group as justifications for revising the criteria do not hold up to empirical study.
One of the issues is the argument that there’s too much comorbidity among PDs. The theory is that disorders are not unique diagnostic entities if they are so frequently comorbid with other disorders. But how much comorbidity is too much? The DSM-5 Work Group doesn’t say. Oldham et al4 found comorbidity rates of 70% to 90%, depending on which semi-structured diagnostic interview was used; however, this was among individuals presenting for psychodynamic treatment of PDs.
I wanted to look at the comorbidity rates in nontreatment-seeking samples to find out if treatment seeking is associated with comorbidity. I reviewed the literature and identified 7 general population epidemiological studies that presented data on the number of individuals with ≥2 PD diagnoses. In these studies, the comorbidity rate is approximately 25%, which is one-half or less than the rates found in patient populations.5 This finding suggested to me that this may not be a nosology problem unless you think 25% comorbidity is too high. The DSM-5 people don’t speak to that, although quite frankly with 10 PDs I don’t think the 25% comorbidity rate is excessive. However, a comorbidity rate of 25% was much lower than that found in patient samples and suggests to me that one of the primary stated reasons of deleting 4 PDs may not be valid.
DR. BLACK: Assuming there is a need to revise the PD section, how would you have gone about that process?
DR. ZIMMERMAN: Whatever deficiencies you perceive in the criteria, the process should be that you come up with an alternative, examine the alternative empirically, and this is followed by independent replication that the new approach is superior to the prior one. My view is that it is not sufficient justification to make a change because there is a problem with the prior approach.
We can argue as to whether there really are problems with, for example, the categorical nature of classification. My research group and I wrote a paper arguing that DSM-IV can be interpreted as having a dimensional component (Box).6 DSM-IV suggests that clinicians record on axis II that a patient has some traits of a disorder even when the full criteria are not met. With that in mind, we conceptualized DSM-IV as having a 3-point dimension, where 0 means no traits of the disorder, 1 indicates subthreshold traits, and 2 indicates that the disorder is present. In a study of >2,000 patients, we found that DSM-IV’s 3-point dimensional approach was as highly associated with measures of psychosocial morbidity as more finely graded dimensional systems.6 We therefore concluded that DSM-IV already includes a dimensional system and questioned why we need to change that approach.
Zimmerman et al suggested that DSM-IV personality disorder (PD) criteria can be thought of as a dimensional system.6 They evaluated 2,150 psychiatric outpatients using semi-structured diagnostic interviews and computed dimensional PD scores in 3 ways:
- 3-point dimension, where 0 means no traits of the disorder, 1 indicates subthreshold traits, and 2 indicates that the disorder is present
- number of DSM-IV criteria met
- 5-point dimension analogous to what was being proposed for DSM-5.
Patients also were evaluated for the presence of a PD based on DSM-IV diagnostic threshold. They then correlated these assessment methods with 7 indices of psychosocial morbidity—the number of current axis I disorders, Global Assessment of Functioning scores, unemployment in the past 5 years, number of psychiatric hospitalizations, level of psychosocial functioning, suicidal ideation at the time of the evaluation, and number of lifetime suicide attempts. All methods of dimensional assessment were more highly correlated with psychosocial morbidity than categorical classification and there was no difference among the 3 dimensional methods.
One of my concerns with the dimensional system as currently proposed is the uncertain significance and possible implications of someone being given a low, non-zero rating. How might this play out in a custody evaluation of someone who is said to be “a little borderline”? What might the implications of non-zero ratings be in obtaining life insurance? The potential practical consequences of low ratings have not, to my knowledge, been discussed. Because of this concern we decided to do a study to determine if there was any clinical significance to low dimensional scores. I had hypothesized that if we compared individuals who had no criteria and only 1 BPD criterion, there would be no difference.
To be frank, I was seeking to show that there was no validity to low levels of pathology and therefore the DSM-5 group probably is getting into dangerous territory. In fact, we found that there were rather significant and robust differences between individuals with 0 criteria and 1 criterion.7 Even though this finding didn’t support my hypothesis, I thought it was significant because it supported the DSM-5 Work Group and I felt compelled to publish that data.
We now had 2 interesting pieces of information. A few years ago we published a study on borderline personality disorder (BPD) that found once you hit the diagnostic threshold it made no difference how many criteria you met.8 On the other hand, when you were below the diagnostic threshold, having 1 criterion vs 0 made a big difference. In addition, a fair number of studies show that dimensional models capture more of the variance in personality pathology than categorical variables.9-12
This lead to our next study in which we hypothesized that dimensionality was only important when the person didn’t meet criteria, not when they did meet criteria.13 So we divided patients in the MIDAS study into those with 0 to 4 BPD criteria and those with ≥5 and counted the number of criteria that were met. Then we correlated each of those 2 dimensional scores with various indicators of illness severity, such as number of suicide attempts, number of psychiatric hospitalizations, and amount of time missed from work in the past 5 years. We found that for individuals who already achieved the diagnostic threshold there were very low correlations with these psychosocial morbidity variables. But for patients with subthreshold symptomatology, there were significant correlations and those correlations were significantly higher than the correlations for the other group. We therefore suggested that dimensionality is important but only when you don’t meet the diagnostic threshold. Thus, we came to the conclusion that DSM-IV already provides for capturing the important dimensional nature of PDs.
DR. BLACK: I’ve discussed this issue with a number of people who basically say doctors tend to think categorically, they don’t think along dimensions. Would it be difficult for psychiatrists to accept this type of system because it’s so different from how physicians are trained to think?
DR. ZIMMERMAN: I think doctors do think categorically and about traits, not necessarily disorders. For example, we’ll see a patient and a clinician will say he’s overly perfectionistic, but there’s no perfectionistic disorder in DSM-IV. This patient may or may not have obsessive-compulsive personality disorder.
I think assessment and diagnosis in routine clinical practice are not nearly as comprehensive as in research. I think psychiatrists often are picking up on traits that they think are clinically significant, but even within that context, they’re thinking categorically, that the patient is perfectionistic rather than rating him a 7 on a scale from 0 to 10 in terms of perfectionism.
Eliminated disorders
DR. BLACK: The proposal will cut the number of PDs to 6 plus personality disorder trait specified and those remaining are to be called types. How did the DSM-5 Work Group select the 5 (now 4) disorders to get rid of? Did they just pick ones that were infrequently used?
DR. ZIMMERMAN: They retained the disorders that were studied in the Collaborative Longitudinal Personality Disorders Study study14 plus others with well established validity.
DR. BLACK: What do you think about that plan to reduce the number of PDs?
DR. ZIMMERMAN: The biggest problem I have is that the DSM-5 Work Group didn’t present any data on the implications of their plan. The conceptual justification was to reduce comorbidity rates. Well, you can hypothesize that comorbidity would actually increase if you retained only those disorders that are more frequently comorbid with other disorders. Would there be any individuals who only have 1 of the excluded diagnoses? Would there be false negatives? They didn’t indicate whether comorbidity would drop and by how much. And they didn’t indicate if there would be a potential impact on missing cases.
We did such an analysis because we had the data set available from the MIDAS project.15 We wanted to know if you excluded the 5 diagnoses that (at the time) were proposed for exclusion—narcissistic, paranoid, schizoid, dependent, and histrionic—what percentage of individuals would no longer be diagnosed with a PD? Second, how much would comorbidity rates change? And third, how did individuals who would no longer be diagnosed with a PD compare with individuals who never had a PD?
We found that the comorbidity rates did, in fact, drop from 30% to 21%. We found that the rate of PDs dropped only a little, but approximately 10% of individuals who previously would have been diagnosed with a PD would no longer be diagnosed. We compared individuals in the excluded group—those who had only 1 of the PDs that would no longer be considered a PD—with a group of patients who had a retained PD and also compared them to individuals with no PD. We found that the retained PD group and the excluded group did not differ on measures of psychosocial morbidity, such as Global Assessment of Functioning scores, hospitalizations, suicidality, number of current axis I disorders, etc. Also, the excluded group clearly was different than the no PD group. We questioned whether or not those in the excluded group might end up being false negative diagnoses in DSM-5. Certainly DSM-5 provides a provision to use trait ratings to still diagnose a PD, called personality disorder trait specified, which would be somewhat analogous to PD not otherwise specified (NOS).
It’s ironic insofar as another of the issues considered by the DSM-5 Work Group to be a problem with axis II is lack of coverage and that too many individuals are diagnosed with PD NOS. Their proposal to exclude PDs could result in more individuals being diagnosed with PD NOS. I know the group would disagree with that perspective, but they provided no evidence to support its view.
As I said at the beginning of this interview, I think we should be talking about this from a scientific perspective and nothing more than that.
Related Resource
- Widiger TA, Simonsen E, Sirovatka PJ, et al. Dimensional models of personality disorders: Refining the research agenda for DSM-V. Arlington, VA: American Psychiatric Publishing, Inc; 2007.
Disclosures
- Dr. Zimmerman reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
- Dr. Black receives research support from AstraZeneca and Psyadon.
1. DSM-5 revisions for personality disorders reflect major change. Public comment period for proposed diagnostic criteria extended through July 15 [news release]. Arlington, VA: American Psychiatric Association; July 7, 2011. http://www.psych.org/MainMenu/Newsroom/NewsReleases/2011-News-Releases_1/DSM-5-Revisions-for-Personality-Disorders-Reflect-Major-Change-.aspx?FT=.pdf. Accessed July 26, 2011.
2. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
3. Personality disorders. American Psychiatric Association DSM-5 development. http://www.dsm5.org/proposedrevision/Pages/PersonalityDisorders.aspx. Updated June 21, 2011. Accessed July 26, 2011.
4. Oldham JM, Skodol AE, Kellman HD, et al. Diagnosis of DSM-III-R personality disorders by two structured interviews: patterns of comorbidity. Am J Psychiatry. 1992;149(2):213-220.
5. Zimmerman M. Is there adequate empirical justification for radically revising the personality disorders section for DSM-5? Personality Disorders: Theory, Research and Treatment. In press.
6. Zimmerman M, Chelminski I, Young D, et al. Does DSM-IV already capture the dimensional nature of personality disorders? J Clin Psychiatry. In press.
7. Zimmerman M, Chelminski I, Young D, et al. Does the presence of one feature of borderline personality disorder have clinical significance?: Implications for dimensional ratings of personality disorders. J Clin Psychiatry. In press.
8. Asnaani A, Chelminski I, Young D, et al. Heterogeneity of borderline personality disorder: do the number of criteria met make a difference? J Pers Disord. 2007;21(6):615-625.
9. Skodol AE, Oldham JM, Bender DS, et al. Dimensional representations of DSM-IV personality disorders: relationships to functional impairment. Am J Psychiatry. 2005;162:1919-1925.
10. Durbin CE, Klein DN. Ten-year stability of personality disorders among outpatients with mood disorders. J Abnorm Psychol. 2006;115:75-84.
11. Grilo CM, Sanislow CA, Gunderson JG, et al. Two-year stability and change of schizotypal, borderline, avoidant, and obsessive-compulsive personality disorders. J Consult Clin Psychol. 2004;72:767-775.
12. Morey LC, Hopwood CJ, Gunderson JG, et al. Comparison of alternative models for personality disorders. Psychol Med. 2007;37:983-994.
13. Zimmerman M, Chelminski I, Young D, et al. Is dimensional scoring of borderline personality disorder only important for subthreshold levels of severity? J Pers Disord. In press.
14. Gunderson JG, Shea MT, Skodol AE, et al. The Collaborative Longitudinal Personality Disorders Study: development, aims, design, and sample characteristics. J Pers Disord. 2000;14(4):300-315.
15. Zimmerman M, Chelminski I, Young D, et al. Impact of deleting 5 DSM-IV personality disorders on prevalence, comorbidity, and the association between personality disorder pathology and psychosocial morbidity. J Clin Psychiatry. In press.

Donald W. Black, MD
Current Psychiatry Associate Editor, is Professor of Psychiatry and Director of the Residency Training Program at the University of Iowa, Iowa City, IA.
Mark Zimmerman, MD
Associate Professor of Psychiatry and Human Behavior at Brown University and Director of Outpatient Psychiatry at Rhode Island Hospital, Providence, RI.
Donald W. Black, MD
Current Psychiatry Associate Editor, is Professor of Psychiatry and Director of the Residency Training Program at the University of Iowa, Iowa City, IA.
Mark Zimmerman, MD
Associate Professor of Psychiatry and Human Behavior at Brown University and Director of Outpatient Psychiatry at Rhode Island Hospital, Providence, RI.
Donald W. Black, MD
Current Psychiatry Associate Editor, is Professor of Psychiatry and Director of the Residency Training Program at the University of Iowa, Iowa City, IA.
Mark Zimmerman, MD
Associate Professor of Psychiatry and Human Behavior at Brown University and Director of Outpatient Psychiatry at Rhode Island Hospital, Providence, RI.
A major update to the diagnostic manual used by mental health clinicians around the world is expected to inspire lively debate. Proposed revisions to the personality disorders (PD) section of the next edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), which is scheduled to be published in 2013, have generated great controversy because they would introduce a dimensional model to the categorical system and 4 PDs would be eliminated.
“The importance of personality functioning and personality traits is the major innovation here,” said Andrew Skodol, MD, the DSM-5 Personality and Personality Disorders Work Group’s chair and a Research Professor of Psychiatry at the University of Arizona College of Medicine. “In the past, we viewed personality disorders as binary. You either had one or you didn’t. But we now understand that personality pathology is a matter of degree.”1
Mark Zimmerman, MD, has written several papers—some of which are in press—about how these revisions might impact clinicians and whether the revisions are necessary. He is Director of the Rhode Island Methods to Improve Diagnostic Assessment and Services (MIDAS) project, an ongoing clinical research study involving the integration of research assessment methods into clinical practice.
Proposed revisions, rationale, and literature reviews for DSM-5 are available at www.DSM5.org and anyone, including the general public, was invited to provide feedback through the Web site. Current Psychiatry Associate Editor Donald W. Black, MD, interviewed Dr. Zimmerman on June 29, 2011, just a few days after the latest proposed revision was posted on June 21, 2011.
DR. BLACK: What is your understanding of the DSM-5 Personality Disorders Work Group proposal to revamp the PD category?
DR. ZIMMERMAN: The initial proposal, released in February 2010, was complex and generated a fair amount of critical commentary related to the marked changes in the approach toward diagnosis of PDs. That proposal replaced diagnostic criteria with a prototype description of personality types that patients would need to match. It also eliminated 5 PDs—paranoid, schizoid, histrionic, dependent, and narcissistic—retained antisocial, avoidant, borderline, obsessive-compulsive, and schizotypal, and introduced trait level ratings. The June 21 revision proposes eliminating only 4 disorders—narcissistic was retained—and the Work Group is no longer suggesting using prototypes but instead have diagnostic criteria (Table).2,3 We do not know if this is the final proposal because similar to the first proposal, it is not presented with much supporting empirical evidence that demonstrates its superiority toward diagnosing PDs compared with the DSM-IV approach.
Table
Personality disorder criteria: DSM-IV vs DSM-5
| DSM-IV | DSM-5 proposal (posted June 21, 2011) |
|---|---|
| General diagnostic criteria | |
|
|
| Personality disorders included | |
| Antisocial, avoidant, borderline, dependent, histrionic, narcissistic, obsessive-compulsive, paranoid, schizoid, schizotypal, personality disorder not otherwise specified | Antisocial, avoidant, borderline, narcissistic, obsessive-compulsive, schizotypal, personality disorder trait specified (requires a rating of significant impairment in personality functioning, combined with the presence of pathological trait domains or facets) |
| Source: References 2,3 | |
I’m not suggesting that the DSM-IV approach is without problems. My attitude is that before going forward with a change to the official diagnostic nomenclature, you need to clearly establish that the new way of doing things is better than the previous way by whatever metric you use.
DR. BLACK: Do you believe there is a need to revamp or revise the DSM-IV PD criteria?
DR. ZIMMERMAN: I think a number of the arguments put forth by the DSM-5 Work Group as justifications for revising the criteria do not hold up to empirical study.
One of the issues is the argument that there’s too much comorbidity among PDs. The theory is that disorders are not unique diagnostic entities if they are so frequently comorbid with other disorders. But how much comorbidity is too much? The DSM-5 Work Group doesn’t say. Oldham et al4 found comorbidity rates of 70% to 90%, depending on which semi-structured diagnostic interview was used; however, this was among individuals presenting for psychodynamic treatment of PDs.
I wanted to look at the comorbidity rates in nontreatment-seeking samples to find out if treatment seeking is associated with comorbidity. I reviewed the literature and identified 7 general population epidemiological studies that presented data on the number of individuals with ≥2 PD diagnoses. In these studies, the comorbidity rate is approximately 25%, which is one-half or less than the rates found in patient populations.5 This finding suggested to me that this may not be a nosology problem unless you think 25% comorbidity is too high. The DSM-5 people don’t speak to that, although quite frankly with 10 PDs I don’t think the 25% comorbidity rate is excessive. However, a comorbidity rate of 25% was much lower than that found in patient samples and suggests to me that one of the primary stated reasons of deleting 4 PDs may not be valid.
DR. BLACK: Assuming there is a need to revise the PD section, how would you have gone about that process?
DR. ZIMMERMAN: Whatever deficiencies you perceive in the criteria, the process should be that you come up with an alternative, examine the alternative empirically, and this is followed by independent replication that the new approach is superior to the prior one. My view is that it is not sufficient justification to make a change because there is a problem with the prior approach.
We can argue as to whether there really are problems with, for example, the categorical nature of classification. My research group and I wrote a paper arguing that DSM-IV can be interpreted as having a dimensional component (Box).6 DSM-IV suggests that clinicians record on axis II that a patient has some traits of a disorder even when the full criteria are not met. With that in mind, we conceptualized DSM-IV as having a 3-point dimension, where 0 means no traits of the disorder, 1 indicates subthreshold traits, and 2 indicates that the disorder is present. In a study of >2,000 patients, we found that DSM-IV’s 3-point dimensional approach was as highly associated with measures of psychosocial morbidity as more finely graded dimensional systems.6 We therefore concluded that DSM-IV already includes a dimensional system and questioned why we need to change that approach.
Zimmerman et al suggested that DSM-IV personality disorder (PD) criteria can be thought of as a dimensional system.6 They evaluated 2,150 psychiatric outpatients using semi-structured diagnostic interviews and computed dimensional PD scores in 3 ways:
- 3-point dimension, where 0 means no traits of the disorder, 1 indicates subthreshold traits, and 2 indicates that the disorder is present
- number of DSM-IV criteria met
- 5-point dimension analogous to what was being proposed for DSM-5.
Patients also were evaluated for the presence of a PD based on DSM-IV diagnostic threshold. They then correlated these assessment methods with 7 indices of psychosocial morbidity—the number of current axis I disorders, Global Assessment of Functioning scores, unemployment in the past 5 years, number of psychiatric hospitalizations, level of psychosocial functioning, suicidal ideation at the time of the evaluation, and number of lifetime suicide attempts. All methods of dimensional assessment were more highly correlated with psychosocial morbidity than categorical classification and there was no difference among the 3 dimensional methods.
One of my concerns with the dimensional system as currently proposed is the uncertain significance and possible implications of someone being given a low, non-zero rating. How might this play out in a custody evaluation of someone who is said to be “a little borderline”? What might the implications of non-zero ratings be in obtaining life insurance? The potential practical consequences of low ratings have not, to my knowledge, been discussed. Because of this concern we decided to do a study to determine if there was any clinical significance to low dimensional scores. I had hypothesized that if we compared individuals who had no criteria and only 1 BPD criterion, there would be no difference.
To be frank, I was seeking to show that there was no validity to low levels of pathology and therefore the DSM-5 group probably is getting into dangerous territory. In fact, we found that there were rather significant and robust differences between individuals with 0 criteria and 1 criterion.7 Even though this finding didn’t support my hypothesis, I thought it was significant because it supported the DSM-5 Work Group and I felt compelled to publish that data.
We now had 2 interesting pieces of information. A few years ago we published a study on borderline personality disorder (BPD) that found once you hit the diagnostic threshold it made no difference how many criteria you met.8 On the other hand, when you were below the diagnostic threshold, having 1 criterion vs 0 made a big difference. In addition, a fair number of studies show that dimensional models capture more of the variance in personality pathology than categorical variables.9-12
This lead to our next study in which we hypothesized that dimensionality was only important when the person didn’t meet criteria, not when they did meet criteria.13 So we divided patients in the MIDAS study into those with 0 to 4 BPD criteria and those with ≥5 and counted the number of criteria that were met. Then we correlated each of those 2 dimensional scores with various indicators of illness severity, such as number of suicide attempts, number of psychiatric hospitalizations, and amount of time missed from work in the past 5 years. We found that for individuals who already achieved the diagnostic threshold there were very low correlations with these psychosocial morbidity variables. But for patients with subthreshold symptomatology, there were significant correlations and those correlations were significantly higher than the correlations for the other group. We therefore suggested that dimensionality is important but only when you don’t meet the diagnostic threshold. Thus, we came to the conclusion that DSM-IV already provides for capturing the important dimensional nature of PDs.
DR. BLACK: I’ve discussed this issue with a number of people who basically say doctors tend to think categorically, they don’t think along dimensions. Would it be difficult for psychiatrists to accept this type of system because it’s so different from how physicians are trained to think?
DR. ZIMMERMAN: I think doctors do think categorically and about traits, not necessarily disorders. For example, we’ll see a patient and a clinician will say he’s overly perfectionistic, but there’s no perfectionistic disorder in DSM-IV. This patient may or may not have obsessive-compulsive personality disorder.
I think assessment and diagnosis in routine clinical practice are not nearly as comprehensive as in research. I think psychiatrists often are picking up on traits that they think are clinically significant, but even within that context, they’re thinking categorically, that the patient is perfectionistic rather than rating him a 7 on a scale from 0 to 10 in terms of perfectionism.
Eliminated disorders
DR. BLACK: The proposal will cut the number of PDs to 6 plus personality disorder trait specified and those remaining are to be called types. How did the DSM-5 Work Group select the 5 (now 4) disorders to get rid of? Did they just pick ones that were infrequently used?
DR. ZIMMERMAN: They retained the disorders that were studied in the Collaborative Longitudinal Personality Disorders Study study14 plus others with well established validity.
DR. BLACK: What do you think about that plan to reduce the number of PDs?
DR. ZIMMERMAN: The biggest problem I have is that the DSM-5 Work Group didn’t present any data on the implications of their plan. The conceptual justification was to reduce comorbidity rates. Well, you can hypothesize that comorbidity would actually increase if you retained only those disorders that are more frequently comorbid with other disorders. Would there be any individuals who only have 1 of the excluded diagnoses? Would there be false negatives? They didn’t indicate whether comorbidity would drop and by how much. And they didn’t indicate if there would be a potential impact on missing cases.
We did such an analysis because we had the data set available from the MIDAS project.15 We wanted to know if you excluded the 5 diagnoses that (at the time) were proposed for exclusion—narcissistic, paranoid, schizoid, dependent, and histrionic—what percentage of individuals would no longer be diagnosed with a PD? Second, how much would comorbidity rates change? And third, how did individuals who would no longer be diagnosed with a PD compare with individuals who never had a PD?
We found that the comorbidity rates did, in fact, drop from 30% to 21%. We found that the rate of PDs dropped only a little, but approximately 10% of individuals who previously would have been diagnosed with a PD would no longer be diagnosed. We compared individuals in the excluded group—those who had only 1 of the PDs that would no longer be considered a PD—with a group of patients who had a retained PD and also compared them to individuals with no PD. We found that the retained PD group and the excluded group did not differ on measures of psychosocial morbidity, such as Global Assessment of Functioning scores, hospitalizations, suicidality, number of current axis I disorders, etc. Also, the excluded group clearly was different than the no PD group. We questioned whether or not those in the excluded group might end up being false negative diagnoses in DSM-5. Certainly DSM-5 provides a provision to use trait ratings to still diagnose a PD, called personality disorder trait specified, which would be somewhat analogous to PD not otherwise specified (NOS).
It’s ironic insofar as another of the issues considered by the DSM-5 Work Group to be a problem with axis II is lack of coverage and that too many individuals are diagnosed with PD NOS. Their proposal to exclude PDs could result in more individuals being diagnosed with PD NOS. I know the group would disagree with that perspective, but they provided no evidence to support its view.
As I said at the beginning of this interview, I think we should be talking about this from a scientific perspective and nothing more than that.
Related Resource
- Widiger TA, Simonsen E, Sirovatka PJ, et al. Dimensional models of personality disorders: Refining the research agenda for DSM-V. Arlington, VA: American Psychiatric Publishing, Inc; 2007.
Disclosures
- Dr. Zimmerman reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
- Dr. Black receives research support from AstraZeneca and Psyadon.
A major update to the diagnostic manual used by mental health clinicians around the world is expected to inspire lively debate. Proposed revisions to the personality disorders (PD) section of the next edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), which is scheduled to be published in 2013, have generated great controversy because they would introduce a dimensional model to the categorical system and 4 PDs would be eliminated.
“The importance of personality functioning and personality traits is the major innovation here,” said Andrew Skodol, MD, the DSM-5 Personality and Personality Disorders Work Group’s chair and a Research Professor of Psychiatry at the University of Arizona College of Medicine. “In the past, we viewed personality disorders as binary. You either had one or you didn’t. But we now understand that personality pathology is a matter of degree.”1
Mark Zimmerman, MD, has written several papers—some of which are in press—about how these revisions might impact clinicians and whether the revisions are necessary. He is Director of the Rhode Island Methods to Improve Diagnostic Assessment and Services (MIDAS) project, an ongoing clinical research study involving the integration of research assessment methods into clinical practice.
Proposed revisions, rationale, and literature reviews for DSM-5 are available at www.DSM5.org and anyone, including the general public, was invited to provide feedback through the Web site. Current Psychiatry Associate Editor Donald W. Black, MD, interviewed Dr. Zimmerman on June 29, 2011, just a few days after the latest proposed revision was posted on June 21, 2011.
DR. BLACK: What is your understanding of the DSM-5 Personality Disorders Work Group proposal to revamp the PD category?
DR. ZIMMERMAN: The initial proposal, released in February 2010, was complex and generated a fair amount of critical commentary related to the marked changes in the approach toward diagnosis of PDs. That proposal replaced diagnostic criteria with a prototype description of personality types that patients would need to match. It also eliminated 5 PDs—paranoid, schizoid, histrionic, dependent, and narcissistic—retained antisocial, avoidant, borderline, obsessive-compulsive, and schizotypal, and introduced trait level ratings. The June 21 revision proposes eliminating only 4 disorders—narcissistic was retained—and the Work Group is no longer suggesting using prototypes but instead have diagnostic criteria (Table).2,3 We do not know if this is the final proposal because similar to the first proposal, it is not presented with much supporting empirical evidence that demonstrates its superiority toward diagnosing PDs compared with the DSM-IV approach.
Table
Personality disorder criteria: DSM-IV vs DSM-5
| DSM-IV | DSM-5 proposal (posted June 21, 2011) |
|---|---|
| General diagnostic criteria | |
|
|
| Personality disorders included | |
| Antisocial, avoidant, borderline, dependent, histrionic, narcissistic, obsessive-compulsive, paranoid, schizoid, schizotypal, personality disorder not otherwise specified | Antisocial, avoidant, borderline, narcissistic, obsessive-compulsive, schizotypal, personality disorder trait specified (requires a rating of significant impairment in personality functioning, combined with the presence of pathological trait domains or facets) |
| Source: References 2,3 | |
I’m not suggesting that the DSM-IV approach is without problems. My attitude is that before going forward with a change to the official diagnostic nomenclature, you need to clearly establish that the new way of doing things is better than the previous way by whatever metric you use.
DR. BLACK: Do you believe there is a need to revamp or revise the DSM-IV PD criteria?
DR. ZIMMERMAN: I think a number of the arguments put forth by the DSM-5 Work Group as justifications for revising the criteria do not hold up to empirical study.
One of the issues is the argument that there’s too much comorbidity among PDs. The theory is that disorders are not unique diagnostic entities if they are so frequently comorbid with other disorders. But how much comorbidity is too much? The DSM-5 Work Group doesn’t say. Oldham et al4 found comorbidity rates of 70% to 90%, depending on which semi-structured diagnostic interview was used; however, this was among individuals presenting for psychodynamic treatment of PDs.
I wanted to look at the comorbidity rates in nontreatment-seeking samples to find out if treatment seeking is associated with comorbidity. I reviewed the literature and identified 7 general population epidemiological studies that presented data on the number of individuals with ≥2 PD diagnoses. In these studies, the comorbidity rate is approximately 25%, which is one-half or less than the rates found in patient populations.5 This finding suggested to me that this may not be a nosology problem unless you think 25% comorbidity is too high. The DSM-5 people don’t speak to that, although quite frankly with 10 PDs I don’t think the 25% comorbidity rate is excessive. However, a comorbidity rate of 25% was much lower than that found in patient samples and suggests to me that one of the primary stated reasons of deleting 4 PDs may not be valid.
DR. BLACK: Assuming there is a need to revise the PD section, how would you have gone about that process?
DR. ZIMMERMAN: Whatever deficiencies you perceive in the criteria, the process should be that you come up with an alternative, examine the alternative empirically, and this is followed by independent replication that the new approach is superior to the prior one. My view is that it is not sufficient justification to make a change because there is a problem with the prior approach.
We can argue as to whether there really are problems with, for example, the categorical nature of classification. My research group and I wrote a paper arguing that DSM-IV can be interpreted as having a dimensional component (Box).6 DSM-IV suggests that clinicians record on axis II that a patient has some traits of a disorder even when the full criteria are not met. With that in mind, we conceptualized DSM-IV as having a 3-point dimension, where 0 means no traits of the disorder, 1 indicates subthreshold traits, and 2 indicates that the disorder is present. In a study of >2,000 patients, we found that DSM-IV’s 3-point dimensional approach was as highly associated with measures of psychosocial morbidity as more finely graded dimensional systems.6 We therefore concluded that DSM-IV already includes a dimensional system and questioned why we need to change that approach.
Zimmerman et al suggested that DSM-IV personality disorder (PD) criteria can be thought of as a dimensional system.6 They evaluated 2,150 psychiatric outpatients using semi-structured diagnostic interviews and computed dimensional PD scores in 3 ways:
- 3-point dimension, where 0 means no traits of the disorder, 1 indicates subthreshold traits, and 2 indicates that the disorder is present
- number of DSM-IV criteria met
- 5-point dimension analogous to what was being proposed for DSM-5.
Patients also were evaluated for the presence of a PD based on DSM-IV diagnostic threshold. They then correlated these assessment methods with 7 indices of psychosocial morbidity—the number of current axis I disorders, Global Assessment of Functioning scores, unemployment in the past 5 years, number of psychiatric hospitalizations, level of psychosocial functioning, suicidal ideation at the time of the evaluation, and number of lifetime suicide attempts. All methods of dimensional assessment were more highly correlated with psychosocial morbidity than categorical classification and there was no difference among the 3 dimensional methods.
One of my concerns with the dimensional system as currently proposed is the uncertain significance and possible implications of someone being given a low, non-zero rating. How might this play out in a custody evaluation of someone who is said to be “a little borderline”? What might the implications of non-zero ratings be in obtaining life insurance? The potential practical consequences of low ratings have not, to my knowledge, been discussed. Because of this concern we decided to do a study to determine if there was any clinical significance to low dimensional scores. I had hypothesized that if we compared individuals who had no criteria and only 1 BPD criterion, there would be no difference.
To be frank, I was seeking to show that there was no validity to low levels of pathology and therefore the DSM-5 group probably is getting into dangerous territory. In fact, we found that there were rather significant and robust differences between individuals with 0 criteria and 1 criterion.7 Even though this finding didn’t support my hypothesis, I thought it was significant because it supported the DSM-5 Work Group and I felt compelled to publish that data.
We now had 2 interesting pieces of information. A few years ago we published a study on borderline personality disorder (BPD) that found once you hit the diagnostic threshold it made no difference how many criteria you met.8 On the other hand, when you were below the diagnostic threshold, having 1 criterion vs 0 made a big difference. In addition, a fair number of studies show that dimensional models capture more of the variance in personality pathology than categorical variables.9-12
This lead to our next study in which we hypothesized that dimensionality was only important when the person didn’t meet criteria, not when they did meet criteria.13 So we divided patients in the MIDAS study into those with 0 to 4 BPD criteria and those with ≥5 and counted the number of criteria that were met. Then we correlated each of those 2 dimensional scores with various indicators of illness severity, such as number of suicide attempts, number of psychiatric hospitalizations, and amount of time missed from work in the past 5 years. We found that for individuals who already achieved the diagnostic threshold there were very low correlations with these psychosocial morbidity variables. But for patients with subthreshold symptomatology, there were significant correlations and those correlations were significantly higher than the correlations for the other group. We therefore suggested that dimensionality is important but only when you don’t meet the diagnostic threshold. Thus, we came to the conclusion that DSM-IV already provides for capturing the important dimensional nature of PDs.
DR. BLACK: I’ve discussed this issue with a number of people who basically say doctors tend to think categorically, they don’t think along dimensions. Would it be difficult for psychiatrists to accept this type of system because it’s so different from how physicians are trained to think?
DR. ZIMMERMAN: I think doctors do think categorically and about traits, not necessarily disorders. For example, we’ll see a patient and a clinician will say he’s overly perfectionistic, but there’s no perfectionistic disorder in DSM-IV. This patient may or may not have obsessive-compulsive personality disorder.
I think assessment and diagnosis in routine clinical practice are not nearly as comprehensive as in research. I think psychiatrists often are picking up on traits that they think are clinically significant, but even within that context, they’re thinking categorically, that the patient is perfectionistic rather than rating him a 7 on a scale from 0 to 10 in terms of perfectionism.
Eliminated disorders
DR. BLACK: The proposal will cut the number of PDs to 6 plus personality disorder trait specified and those remaining are to be called types. How did the DSM-5 Work Group select the 5 (now 4) disorders to get rid of? Did they just pick ones that were infrequently used?
DR. ZIMMERMAN: They retained the disorders that were studied in the Collaborative Longitudinal Personality Disorders Study study14 plus others with well established validity.
DR. BLACK: What do you think about that plan to reduce the number of PDs?
DR. ZIMMERMAN: The biggest problem I have is that the DSM-5 Work Group didn’t present any data on the implications of their plan. The conceptual justification was to reduce comorbidity rates. Well, you can hypothesize that comorbidity would actually increase if you retained only those disorders that are more frequently comorbid with other disorders. Would there be any individuals who only have 1 of the excluded diagnoses? Would there be false negatives? They didn’t indicate whether comorbidity would drop and by how much. And they didn’t indicate if there would be a potential impact on missing cases.
We did such an analysis because we had the data set available from the MIDAS project.15 We wanted to know if you excluded the 5 diagnoses that (at the time) were proposed for exclusion—narcissistic, paranoid, schizoid, dependent, and histrionic—what percentage of individuals would no longer be diagnosed with a PD? Second, how much would comorbidity rates change? And third, how did individuals who would no longer be diagnosed with a PD compare with individuals who never had a PD?
We found that the comorbidity rates did, in fact, drop from 30% to 21%. We found that the rate of PDs dropped only a little, but approximately 10% of individuals who previously would have been diagnosed with a PD would no longer be diagnosed. We compared individuals in the excluded group—those who had only 1 of the PDs that would no longer be considered a PD—with a group of patients who had a retained PD and also compared them to individuals with no PD. We found that the retained PD group and the excluded group did not differ on measures of psychosocial morbidity, such as Global Assessment of Functioning scores, hospitalizations, suicidality, number of current axis I disorders, etc. Also, the excluded group clearly was different than the no PD group. We questioned whether or not those in the excluded group might end up being false negative diagnoses in DSM-5. Certainly DSM-5 provides a provision to use trait ratings to still diagnose a PD, called personality disorder trait specified, which would be somewhat analogous to PD not otherwise specified (NOS).
It’s ironic insofar as another of the issues considered by the DSM-5 Work Group to be a problem with axis II is lack of coverage and that too many individuals are diagnosed with PD NOS. Their proposal to exclude PDs could result in more individuals being diagnosed with PD NOS. I know the group would disagree with that perspective, but they provided no evidence to support its view.
As I said at the beginning of this interview, I think we should be talking about this from a scientific perspective and nothing more than that.
Related Resource
- Widiger TA, Simonsen E, Sirovatka PJ, et al. Dimensional models of personality disorders: Refining the research agenda for DSM-V. Arlington, VA: American Psychiatric Publishing, Inc; 2007.
Disclosures
- Dr. Zimmerman reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
- Dr. Black receives research support from AstraZeneca and Psyadon.
1. DSM-5 revisions for personality disorders reflect major change. Public comment period for proposed diagnostic criteria extended through July 15 [news release]. Arlington, VA: American Psychiatric Association; July 7, 2011. http://www.psych.org/MainMenu/Newsroom/NewsReleases/2011-News-Releases_1/DSM-5-Revisions-for-Personality-Disorders-Reflect-Major-Change-.aspx?FT=.pdf. Accessed July 26, 2011.
2. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
3. Personality disorders. American Psychiatric Association DSM-5 development. http://www.dsm5.org/proposedrevision/Pages/PersonalityDisorders.aspx. Updated June 21, 2011. Accessed July 26, 2011.
4. Oldham JM, Skodol AE, Kellman HD, et al. Diagnosis of DSM-III-R personality disorders by two structured interviews: patterns of comorbidity. Am J Psychiatry. 1992;149(2):213-220.
5. Zimmerman M. Is there adequate empirical justification for radically revising the personality disorders section for DSM-5? Personality Disorders: Theory, Research and Treatment. In press.
6. Zimmerman M, Chelminski I, Young D, et al. Does DSM-IV already capture the dimensional nature of personality disorders? J Clin Psychiatry. In press.
7. Zimmerman M, Chelminski I, Young D, et al. Does the presence of one feature of borderline personality disorder have clinical significance?: Implications for dimensional ratings of personality disorders. J Clin Psychiatry. In press.
8. Asnaani A, Chelminski I, Young D, et al. Heterogeneity of borderline personality disorder: do the number of criteria met make a difference? J Pers Disord. 2007;21(6):615-625.
9. Skodol AE, Oldham JM, Bender DS, et al. Dimensional representations of DSM-IV personality disorders: relationships to functional impairment. Am J Psychiatry. 2005;162:1919-1925.
10. Durbin CE, Klein DN. Ten-year stability of personality disorders among outpatients with mood disorders. J Abnorm Psychol. 2006;115:75-84.
11. Grilo CM, Sanislow CA, Gunderson JG, et al. Two-year stability and change of schizotypal, borderline, avoidant, and obsessive-compulsive personality disorders. J Consult Clin Psychol. 2004;72:767-775.
12. Morey LC, Hopwood CJ, Gunderson JG, et al. Comparison of alternative models for personality disorders. Psychol Med. 2007;37:983-994.
13. Zimmerman M, Chelminski I, Young D, et al. Is dimensional scoring of borderline personality disorder only important for subthreshold levels of severity? J Pers Disord. In press.
14. Gunderson JG, Shea MT, Skodol AE, et al. The Collaborative Longitudinal Personality Disorders Study: development, aims, design, and sample characteristics. J Pers Disord. 2000;14(4):300-315.
15. Zimmerman M, Chelminski I, Young D, et al. Impact of deleting 5 DSM-IV personality disorders on prevalence, comorbidity, and the association between personality disorder pathology and psychosocial morbidity. J Clin Psychiatry. In press.
1. DSM-5 revisions for personality disorders reflect major change. Public comment period for proposed diagnostic criteria extended through July 15 [news release]. Arlington, VA: American Psychiatric Association; July 7, 2011. http://www.psych.org/MainMenu/Newsroom/NewsReleases/2011-News-Releases_1/DSM-5-Revisions-for-Personality-Disorders-Reflect-Major-Change-.aspx?FT=.pdf. Accessed July 26, 2011.
2. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
3. Personality disorders. American Psychiatric Association DSM-5 development. http://www.dsm5.org/proposedrevision/Pages/PersonalityDisorders.aspx. Updated June 21, 2011. Accessed July 26, 2011.
4. Oldham JM, Skodol AE, Kellman HD, et al. Diagnosis of DSM-III-R personality disorders by two structured interviews: patterns of comorbidity. Am J Psychiatry. 1992;149(2):213-220.
5. Zimmerman M. Is there adequate empirical justification for radically revising the personality disorders section for DSM-5? Personality Disorders: Theory, Research and Treatment. In press.
6. Zimmerman M, Chelminski I, Young D, et al. Does DSM-IV already capture the dimensional nature of personality disorders? J Clin Psychiatry. In press.
7. Zimmerman M, Chelminski I, Young D, et al. Does the presence of one feature of borderline personality disorder have clinical significance?: Implications for dimensional ratings of personality disorders. J Clin Psychiatry. In press.
8. Asnaani A, Chelminski I, Young D, et al. Heterogeneity of borderline personality disorder: do the number of criteria met make a difference? J Pers Disord. 2007;21(6):615-625.
9. Skodol AE, Oldham JM, Bender DS, et al. Dimensional representations of DSM-IV personality disorders: relationships to functional impairment. Am J Psychiatry. 2005;162:1919-1925.
10. Durbin CE, Klein DN. Ten-year stability of personality disorders among outpatients with mood disorders. J Abnorm Psychol. 2006;115:75-84.
11. Grilo CM, Sanislow CA, Gunderson JG, et al. Two-year stability and change of schizotypal, borderline, avoidant, and obsessive-compulsive personality disorders. J Consult Clin Psychol. 2004;72:767-775.
12. Morey LC, Hopwood CJ, Gunderson JG, et al. Comparison of alternative models for personality disorders. Psychol Med. 2007;37:983-994.
13. Zimmerman M, Chelminski I, Young D, et al. Is dimensional scoring of borderline personality disorder only important for subthreshold levels of severity? J Pers Disord. In press.
14. Gunderson JG, Shea MT, Skodol AE, et al. The Collaborative Longitudinal Personality Disorders Study: development, aims, design, and sample characteristics. J Pers Disord. 2000;14(4):300-315.
15. Zimmerman M, Chelminski I, Young D, et al. Impact of deleting 5 DSM-IV personality disorders on prevalence, comorbidity, and the association between personality disorder pathology and psychosocial morbidity. J Clin Psychiatry. In press.
Pharmacologic treatment of borderline personality disorder
As psychiatry’s understanding of borderline personality disorder (BPD) grows, the literature clearly describes the seriousness of BPD, as well as these patients’ high utilization of treatment. Pharmacotherapy for BPD remains controversial. The most recent American Psychiatric Association practice guidelines focus on using symptom domains of this heterogeneous illness to guide medication selection, yet when these guidelines were published, there was a lack of data to support this recommendation.1
This article evaluates medications for BPD and emerging data supporting matching medications to BPD symptom domains, with an emphasis on making choices that advance clinical practice. We conclude by reviewing studies of combined pharmacotherapy and dialectical behavior therapy (DBT) and describing how a multidisciplinary team approach can enhance BPD treatment.
Early research
Early studies of pharmacotherapy for BPD began after the development of the Diagnostic Interview for Borderlines2,3 and DSM-III criteria for BPD.4 Researchers recruited patients who fulfilled the diagnostic criteria; however, these participants’ symptom profiles were highly heterogeneous. Although such studies can be useful when starting to test new treatments—especially if they are able to show efficacy over placebo or explore safety—they are less helpful in guiding clinical practice.
During the 1980s, low doses of first-generation antipsychotics were evaluated based on hypotheses that BPD was related to schizophrenia. Case series5 and placebo-controlled trials6,7 pointed to symptom reduction over time and greater than placebo for BPD patients. Interestingly, in a small study of BPD inpatients, Soloff et al8 compared the first-generation antipsychotic haloperidol to amitriptyline and found amitriptyline led to symptom worsening in some patients. Cowdry and Gardner9 compared alprazolam, carbamazepine, trifluoperazine, and tranylcypromine in a double-blind, placebo-controlled crossover trial of 16 female BPD outpatients. They found antipsychotics were not useful. Further, the study found behavioral disinhibition when a benzodiazepine (alprazolam) was used alone in impulsive patients.
These studies provided a basis for the idea that medications could help reduce BPD symptoms. However, some early investigators noted that antipsychotics’ side effects led some patients to discontinue treatment.6
Next-generation studies
Antidepressants. Interest in exploring pharmacologic treatments for BPD diminished after the early efficacy trials. Several events led to a reemergence of this interest, including the FDA’s approval of the selective serotonin reuptake inhibitor fluoxetine for depression in 1987. Some investigators hypothesized fluoxetine’s antidepressant properties could help treat BPD symptoms and perhaps the serotonin reuptake action could diminish impulsivity.10 Case series and a double-blind, placebo-controlled trial11 demonstrated fluoxetine’s efficacy in BPD. In 1 study, Salzman et al12 found fluoxetine’s greatest impact was on “anger,” a major affective dimension of BPD.
Mood stabilizers. When valproic acid emerged as a successful treatment for bipolar disorder, researchers turned their attention to mood-stabilizing anticonvulsants for BPD. Numerous case series and controlled trials provided evidence of its efficacy.13,14 This was the first time subtypes of BPD patients were tested prospectively—with the hypothesis that the mood-stabilizing anticonvulsants would diminish impulsivity and aggression. The positive results of Hollander et al13 and Frankenburg and Zanarini14 in assessing divalproex in BPD patients with bipolar II disorder has implications for targeted treatment (discussed below).
Newer antipsychotics. The introduction of second-generation antipsychotics (SGA) led some researchers to explore whether these agents could decrease BPD symptoms. Case series15 and some (but not all) placebo-controlled trials have demonstrated benefit from SGAs such as olanzapine,16-18 aripiprazole,19 and quetiapine.20,21 Initial research on risperidone22 and ziprasidone also suggested efficacy for BPD. Two placebo-controlled studies of olanzapine examined which symptom groups were most helped; each reported a broad effect.16,17 However, not all studies of SGAs for BPD patients have been positive.18 Further, metabolic side effects have been noted for several SGAs, including olanzapine.18
Omega-3 fatty acids. Some studies examining omega-3 fatty acids have sparked an ongoing interest in this compound. In an 8-week, double-blind, pilot study of 30 women with BPD, Zanarini23 found omega-3 fatty acids demonstrated efficacy over placebo.
Most studies of BPD pharmacotherapy have used a classic clinical trial design, which does not easily translate into recommendations regarding medication selection for individual patients, especially those with BPD and comorbid illnesses. Also, existing trials have not fully explored starting doses, and no maintenance studies have been published. Therefore, many clinical application questions remain unresolved. However, some early treatment recommendations are supported by recent meta-analyses that demonstrate effects of medication classes for specific symptom domains.
Careful identification of comorbid psychiatric disorders is a rational first step. Diagnosing comorbid disorders, such as bipolar disorder, will determine medication choice and impact length of treatment. In a double-blind study of 30 women with BPD and comorbid bipolar II disorder, Frankenburg and Zanarini14 found divalproex had a statistically significant effect compared with placebo and could be considered for this specific population.
When treating a BPD patient who has a comorbid illness, it is important not to ignore BPD symptoms. The chronic emotional dysregulation and ongoing safety issues require psychiatrists to educate patients about these symptoms and to address them in a multidisciplinary manner.
Clarifying prominent symptom domains can help steer pharmacologic management. Many trials have attempted to focus on specific symptom domains, including cognitive-perceptual disturbances, impulsivity, and affective dysregulation. Table 124 lists BPD symptom domains and associated characteristics.
Table 1
Symptom domains of BPD
| Cognitive-perceptual symptoms |
| Suspiciousness |
| Referential thinking |
| Paranoid ideation |
| Illusions |
| Derealization |
| Depersonalization |
| Hallucination-like symptoms |
| Impulsive-behavioral dyscontrol |
| Impulsive aggression |
| Deliberate self-harm |
| Impulsive sexual behavior |
| Substance abuse |
| Impulsive spending |
| Affective dysregulation |
| Mood lability |
| Rejection sensitivity |
| Intense anger out of proportion to the stimuli |
| Sudden depressive mood episodes |
| BPD: borderline personality disorder Source: Reference 24 |
Dosing strategy
Developing a medication management strategy for BPD patients requires a thoughtful approach. When faced with a patient who has overwhelming distress, it is tempting to start with high medication doses; however, clinical experience suggests starting cautiously with lower doses will yield better tolerability and adherence. Based on our clinical experience, patients with BPD tend to be highly perceptive to physiologic stimuli and medication side effects.
Further research is needed to answer clinical questions regarding optimal dosing strategy and treatment, but some studies suggest when using SGAs, doses equivalent to one-third or one-half the dose used for treating schizophrenia may be appropriate.1,2,17,18 However, for fluoxetine, investigators have espoused using a dosage higher than generally used for depression.10 For mood-stabilizing anticonvulsants, almost all studies employed the same doses used for bipolar disorder.25 Some studies of valproic acid have verified appropriate blood levels—generally 50 to 100 μg/mL.
Controlled trials have not determined whether medications for patients with BPD should be used briefly during times of stress or for longer periods. Many studies of medication for BPD have been relatively brief trials that explored whether the drug has any potential efficacy. In our opinion, this issue currently is being addressed in clinical practice in a trial-and-error manner.
Clues to targeted treatment
Although pharmacotherapy for BPD subtypes remains controversial, recent meta-analyses by Ingenhoven24 and Nose26 and a Cochrane Review27 (with subsequent online update28) have identified evidence that supports the use of specific medications for treating BPD symptoms. These studies’ authors acknowledge replication studies are required because of the limited nature of the available data. In contrast, a meta-analysis conducted by the National Collaborating Centre for Mental Health29 did not identify sufficient evidence for medication use in BPD on which to base official guidelines to advise health care providers in the United Kingdom. The only medication recommendation in this meta-analysis is to consider prescribing short-term sedative antihistamines during crises; this recommendation is not supported by any clinical trial.
In a meta-analysis of 21 placebo-controlled trials of patients with BPD and/or schizotypal personality disorder, Inghoven et al24 used multiple domains and subdomains, including cognitive-perceptual symptoms, impulsive-behavioral dyscontrol, affective dysregulation, anger, and mood lability, to assess the efficacy of medication use (Table 2).24 They found:
- Antipsychotics seemed to have a moderate effect on cognitive-perceptual symptoms and a moderate-to-large effect on anger.
- Antidepressants had a small effect on anxiety, but no other domains.
- Mood stabilizers had a very large effect on impulsive-behavioral dyscontrol and anger, a large effect on anxiety, and a moderate effect on depressed mood.
- Regarding global functioning, mood stabilizers had a greater effect than antipsychotics. Both led to greater change than antidepressants.
A 2010 Cochrane Review meta-analysis initially conducted by Leib27 with subsequent online update by Stoffers28 included 28 studies with a total of 1,742 patients and also identified symptom-targeted BPD domains. This study analyzed pooled data and found support for the use of specific medications, including certain antipsychotics, mood stabilizers, and antidepressants, for specific BPD symptoms (Table 3).28 The authors recommended data be interpreted cautiously, however, because many of the clinical trials included in their meta-analysis have not been replicated and generalizability from research populations to clinical populations is not well understood.
Table 2
Which medications improve which BPD symptoms?
| Medication | Symptom domain | Effect |
|---|---|---|
| Antipsychotics | Cognitive-perceptual | Moderate |
| Anger | Moderate/large | |
| Antidepressants | Anxiety | Small |
| Anger | Small | |
| Mood stabilizers | Impulsive-behavioral dyscontrol | Very large |
| Anger | Very large | |
| Anxiety | Large | |
| Depressed mood | Moderate | |
| BPD: borderline personality disorder Source: Reference 24 | ||
Table 3
Pharmacotherapy for BPD: Results of a Cochrane review
| Class | Medication(s) |
|---|---|
| Cognitive-perceptual symptoms | |
| Antipsychotics | Olanzapine, aripiprazole |
| Impulsive-behavioral dyscontrol | |
| Mood stabilizers | Topiramate, lamotrigine |
| Antipsychotics | Aripiprazole |
| Affective dysregulation | |
| Antidepressants | Amitriptylinea (depressed mood) |
| Mood stabilizers | Topiramate, lamotrigine (anger), valproate (depressed mood) |
| Antipsychotics | Haloperidol (anger), olanzapine, aripiprazole |
| Omega-3 fatty acids | Fish oil (depression) |
| Suicidal behavior/suicidality | |
| Antipsychotics | Flupenthixol decanoate |
| Omega-3 fatty acids | Fish oil |
| Interpersonal problems | |
| Antipsychotics | Aripiprazole |
| Mood stabilizers | Valproate, topiramate |
| No improvement on any outcome: ziprasidone, thiothixene, phenelzine, fluoxetine, fluvoxamine, carbamazepine | |
| aDo not prescribe to suicidal patients BPD: borderline personality disorder Source: Reference 28 | |
DBT and pharmacotherapy
As is the case with many studies of psychiatric medications, early efficacy studies of pharmacotherapy for BPD did not include structured psychosocial treatment. In 2 double-blind, placebo-controlled trials with a total of 84 patients receiving DBT, those assigned to olanzapine had better outcomes on objective rating scales than those on placebo.30,31 Similar trials testing fluoxetine showed no advantage for the drug over placebo.32 In a pilot study by Moen et al,25 17 patients were assigned to “condensed DBT” before being randomized to divalproex extended release or placebo. Two patients remitted in the first 4 weeks and continued to improve without medication. If replicated, this finding may point to a targeted approach to the timing of medication initiation.
Clinical recommendations
Randomized, placebo-controlled BPD trials have demonstrated striking improvements in patients in placebo groups, which may be attributed to the powerful therapeutic impact of regular, structured, nonjudgmental interactions within a research protocol. Prescribers can enhance a medication’s therapeutic effect by keeping in mind the same principles that apply to treatment of other common psychiatric disorders.
Patients with BPD respond well to validation of their symptoms and their experience. Tell patients you take their BPD symptoms seriously and acknowledge their distress. The goal is to partner with patients to improve function, decrease reactivity, and reduce emotional pain. When working with BPD patients, it is appropriate to communicate a sense of optimism and hopefulness about their prognosis and treatment. Performing this approach in a caring way will better preserve the therapeutic alliance.
Additional suggestions based on our clinical experience include:
- Provide regular medication management visits.
- Consider using a structured symptom rating scale to evaluate symptoms over time, such as the Zanarini Rating Scale for Borderline Personality Disorder33 or Borderline Evaluation of Severity Over Time.34
- Educate patients with BPD about the disorder by making the appropriate diagnosis and providing reputable educational materials (see Related Resources).
- Do not diagnose a patient with BPD as having bipolar disorder unless they clearly meet criteria for bipolar disorder.
- Communicate your limitations in advance.
- Orient the patient to the possibility of needing to try different medications to determine the most helpful agent or combination.
- Do not de-emphasize risks of medications or side effects. Serious symptoms require medications that bear a risk of side effects; communicate these risks to patients and carefully weigh the risk-benefit profile.
- Inform patients you will be responsive to making appropriate changes if problems arise that are associated with pharmacotherapy and outweigh the benefit of medication.
Multidisciplinary teamwork
Best outcomes for patients with BPD are facilitated by a collaborative team effort. Such an approach addresses both the psychological and biologic underpinnings of the disorder and can significantly decrease the possibility of “splitting” among team members. To determine ways in which a therapist and physician may work together, clinicians should discuss the:
- meaning of medication to the therapist, psychiatrist, and patient
- potential benefits and limitations of medication
- the role of medication in the patient’s overall treatment.35
Patients with BPD experience emotional crisis. At times, prescribing patterns unfortunately reflect the practice of adding medications to address emotional crisis. This practice may partially account for the high rates of polypharmacy in BPD patients.36 Patients with BPD will benefit from interacting with a clinician whose approach is responsive, validating, and non-reactive to the patient’s symptoms and experiences. A comprehensive treatment approach includes screening and treating comorbid conditions, providing education about the diagnosis, and multidisciplinary involvement combined with rational, targeted pharmacotherapy.
- Friedel RO. Borderline personality disorder demystified: an essential guide for understanding and living with BPD. New York, NY: Marlowe & Company; 2004.
- Chapman A, Gratz K. Borderline personality disorder survival guide: everything you need to know about living with BPD. Oakland, CA: New Harbinger Publications, Inc; 2007.
- National Education Alliance for Borderline Personality Disorder. www.borderlinepersonalitydisorder.com.
Drug Brand Names
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Carbamazepine • Tegretol
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Lamotrigine • Lamictal
- Olanzapine • Zyprexa
- Phenelzine • Nardil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Thiothixene • Navane
- Topiramate • Topamax, Topiragen
- Tranylcypromine • Parnate
- Trifluoperazine • Stelazine
- Valproic acid • Depakote
- Ziprasidone • Geodon
Disclosure
Dr. Nelson receives research/grant support from the Minnesota Medical Foundation.
Dr. Schulz receives research/grant support from AstraZeneca, Otsuka, and Rules-Based Medicine and is a consultant to Bioavail, Bristol-Myers Squibb, and Eli Lilly and Company.
1. American Psychiatric Association Practice Guidelines. Practice guideline for the treatment of patients with borderline personality disorder. American Psychiatric Association. Am J Psychiatry. 2001;158(10 suppl):1-52.
2. Barrash J, Kroll J, Carey K, et al. Discriminating borderline disorder from other personality disorders. Cluster analysis of the diagnostic interview for borderlines. Arch Gen Psychiatry. 1983;40(12):1297-1302.
3. Kety SS, Rosenthal D, Wender PH, et al. Mental illness in the biological and adoptive families of adopted individuals who have become schizophrenic: a preliminary report based on psychiatric interviews. Proc Annu Meet Am Psychopathol Assoc. 1975;(63):147-165.
4. Diagnostic and statistical manual of mental disorders, 3rd ed. Washington DC: American Psychiatric Association; 1980.
5. Serban G, Siegel S. Response of borderline and schizotypal patients to small doses of thiothixene and haloperidol. Am J Psychiatry. 1984;141(11):1455-1458.
6. Goldberg SC, Schulz SC, Schulz PM, et al. Borderline and schizotypal personality disorders treated with low-dose thiothixene vs placebo. Arch Gen Psychiatry. 1986;43(7):680-686.
7. Soloff PH, George A, Nathan RS, et al. Progress in pharmacotherapy of borderline disorders. A double-blind study of amitriptyline, haloperidol, and placebo. Arch Gen Psychiatry. 1986;43(7):691-697.
8. Soloff PH, George A, Nathan RS, et al. Paradoxical effects of amitriptyline on borderline patients. Am J Psychiatry. 1986;143(12):1603-1635.
9. Cowdry RW, Gardner DL. Pharmacotherapy of borderline personality disorder. Alprazolam carbamazepine, trifluoperazine, and tranylcypromine. Arch Gen Psychiatry. 1988;45(2):111-119.
10. Markovitz PJ, Calabrese JR, Schulz SC, et al. Fluoxetine in the treatment of borderline and schizotypal personality disorders. Am J Psychiatry. 1991;148(8):1064-1067.
11. Coccaro EF, Kavoussi RJ. Fluoxetine and impulsive aggressive behavior in personality-disordered subjects. Arch Gen Psychiatry. 1997;54(12):1081-1088.
12. Salzman C, Wolfson AN, Schatzberg A, et al. Effect of fluoxetine on anger in symptomatic volunteers with borderline personality disorder. J Clin Psychopharmacol. 1995;15(1):23-29.
13. Hollander E, Tracy KA, Swann AC, et al. Divalproex in the treatment of impulsive aggression: efficacy in cluster B personality disorders. Neuropsychopharmacology. 2003;28(6):1186-1197.
14. Frankenburg FR, Zanarini MC. Divalproex sodium treatment of women with borderline personality disorder and bipolar II disorder: a double-blind placebo-controlled pilot study. J Clin Psychiatry. 2002;63(5):442-446.
15. Schulz SC, Camlin KL, Berry SA, et al. Olanzapine safety and efficacy in patients with borderline personality disorder and comorbid dysthymia. Biol Psychiatry. 1999;46(10):1429-1435.
16. Bogenschutz MP, George Nurnberg H. Olanzapine versus placebo in the treatment of borderline personality disorder. J Clin Psychiatry. 2004;65(1):104-109.
17. Zanarini MC, Frankenburg FR. Olanzapine treatment of female borderline personality disorder patients: a double-blind placebo-controlled pilot study. J Clin Psychiatry. 2001;62(11):849-854.
18. Schulz SC, Zanarini MC, Bateman A, et al. Olanzapine for the treatment of borderline personality disorder: variable dose 12-week randomised double-blind placebo-controlled study. Br J Psychiatry. 2008;193(6):485-492.
19. Nickel MK, Muehlbacher M, Nickel C, et al. Aripiprazole in the treatment of patients with borderline personality disorder: a double-blind, placebo-controlled study. Am J Psychiatry. 2006;163(5):833-838.
20. Adityanjee, Romine A, Brown E, et al. Quetiapine in patients with borderline personality disorder: an open-label trial. Ann Clin Psychiatry. 2008;20(4):219-226.
21. Villeneuve E, Lemelin S. Open-label study of atypical neuroleptic quetiapine for treatment of borderline personality disorder: impulsivity as main target. J Clin Psychiatry. 2005;66(10):1298-1303.
22. Rocca P, Marchiaro L, Cocuzza E, et al. Treatment of borderline personality disorder with risperidone. J Clin Psychiatry. 2002;63(3):241-244.
23. Zanarini MC, Frankenburg FR. Omega-3 fatty acid treatment of women with borderline personality disorder: a double-blind placebo-controlled pilot study. Am J Psychiatry. 2003;160(1):167-169.
24. Ingenhoven T, Lafay P, Rinne T, et al. Effectiveness of pharmacotherapy for severe personality disorders: meta-analyses of randomized controlled trials. J Clin Psychiatry. 2010;71(1):14-25.
25. Moen Moore R, Miller M, Lee S, et al. Extended release divalproex for borderline personality disorder. Poster presented at: U. S. Psychiatric and Mental Health Congress; October 13-16, 2007; Orlando, FL.
26. Nose M, Cipriani A, Biancosino B, et al. Efficacy of pharmacotherapy against core traits of borderline personality disorder: meta-analysis of randomized controlled trials. Int Clin Psychopharmacol. 2006;21(6):345-353.
27. Lieb K, Völlm B, Rücker G, et al. Pharmacotherapy for borderline personality disorder: Cochrane Systematic Review of Randomised Trials. Br J Psychiatry. 2010;196(1):4-12.
28. Stoffers J, Völlm BA, Rücker G, et al. Pharmacological interventions for borderline personality disorder. Cochrane Database Syst Rev. 2010;(6):CD005653.-
29. National Collaborating Centre for Mental Health. Borderline personality disorder: the NICE guideline on treatment and management. National clinical practice guideline no. 78. London United Kingdom: RCPsych Publications; 2009.
30. Linehan MM, McDavid JD, Brown MZ, et al. Olanzapine plus dialectical behavior therapy for women with high irritability who meet criteria for borderline personality disorder: a double-blind, placebo-controlled pilot study. J Clin Psychiatry. 2008;69(6):999-1005.
31. Soler J, Pascual JC, Campins J, et al. Double-blind, placebo-controlled study of dialectical behavior therapy plus olanzapine for borderline personality disorder. Am J Psychiatry. 2005;162(6):1221-1224.
32. Simpson EB, Yen S, Costello E, et al. Combined dialectical behavior therapy and fluoxetine in the treatment of borderline personality disorder. J Clin Psychiatry. 2004;65(3):379-385.
33. Zanarini MC, Vujanovic AA, Parachini EA, et al. Zanarini Rating Scale for Borderline Personality Disorder (ZAN-BPD): a continuous measure of DSM-IV borderline psychopathology. J Pers Disord. 2003;17(3):233-242.
34. Pfohl B, Blum N, St John D, et al. Reliability and validity of the Borderline Evaluation of Severity Over Time (BEST): a self-rated scale to measure severity and change in persons with borderline personality disorder. J Pers Disord. 2009;23(3):281-293.
35. Silk KR. Collaborative treatment for patients with personality disorders. In: Riba MB Balon R, eds. Psychopharmacology and psychotherapy: a collaborative approach. Washington, DC: American Psychiatric Press; 1999:221–277.
36. Zanarini MC. Update on pharmacotherapy of borderline personality disorder. Curr Psychiatry Rep. 2004;6(1):66-70.
As psychiatry’s understanding of borderline personality disorder (BPD) grows, the literature clearly describes the seriousness of BPD, as well as these patients’ high utilization of treatment. Pharmacotherapy for BPD remains controversial. The most recent American Psychiatric Association practice guidelines focus on using symptom domains of this heterogeneous illness to guide medication selection, yet when these guidelines were published, there was a lack of data to support this recommendation.1
This article evaluates medications for BPD and emerging data supporting matching medications to BPD symptom domains, with an emphasis on making choices that advance clinical practice. We conclude by reviewing studies of combined pharmacotherapy and dialectical behavior therapy (DBT) and describing how a multidisciplinary team approach can enhance BPD treatment.
Early research
Early studies of pharmacotherapy for BPD began after the development of the Diagnostic Interview for Borderlines2,3 and DSM-III criteria for BPD.4 Researchers recruited patients who fulfilled the diagnostic criteria; however, these participants’ symptom profiles were highly heterogeneous. Although such studies can be useful when starting to test new treatments—especially if they are able to show efficacy over placebo or explore safety—they are less helpful in guiding clinical practice.
During the 1980s, low doses of first-generation antipsychotics were evaluated based on hypotheses that BPD was related to schizophrenia. Case series5 and placebo-controlled trials6,7 pointed to symptom reduction over time and greater than placebo for BPD patients. Interestingly, in a small study of BPD inpatients, Soloff et al8 compared the first-generation antipsychotic haloperidol to amitriptyline and found amitriptyline led to symptom worsening in some patients. Cowdry and Gardner9 compared alprazolam, carbamazepine, trifluoperazine, and tranylcypromine in a double-blind, placebo-controlled crossover trial of 16 female BPD outpatients. They found antipsychotics were not useful. Further, the study found behavioral disinhibition when a benzodiazepine (alprazolam) was used alone in impulsive patients.
These studies provided a basis for the idea that medications could help reduce BPD symptoms. However, some early investigators noted that antipsychotics’ side effects led some patients to discontinue treatment.6
Next-generation studies
Antidepressants. Interest in exploring pharmacologic treatments for BPD diminished after the early efficacy trials. Several events led to a reemergence of this interest, including the FDA’s approval of the selective serotonin reuptake inhibitor fluoxetine for depression in 1987. Some investigators hypothesized fluoxetine’s antidepressant properties could help treat BPD symptoms and perhaps the serotonin reuptake action could diminish impulsivity.10 Case series and a double-blind, placebo-controlled trial11 demonstrated fluoxetine’s efficacy in BPD. In 1 study, Salzman et al12 found fluoxetine’s greatest impact was on “anger,” a major affective dimension of BPD.
Mood stabilizers. When valproic acid emerged as a successful treatment for bipolar disorder, researchers turned their attention to mood-stabilizing anticonvulsants for BPD. Numerous case series and controlled trials provided evidence of its efficacy.13,14 This was the first time subtypes of BPD patients were tested prospectively—with the hypothesis that the mood-stabilizing anticonvulsants would diminish impulsivity and aggression. The positive results of Hollander et al13 and Frankenburg and Zanarini14 in assessing divalproex in BPD patients with bipolar II disorder has implications for targeted treatment (discussed below).
Newer antipsychotics. The introduction of second-generation antipsychotics (SGA) led some researchers to explore whether these agents could decrease BPD symptoms. Case series15 and some (but not all) placebo-controlled trials have demonstrated benefit from SGAs such as olanzapine,16-18 aripiprazole,19 and quetiapine.20,21 Initial research on risperidone22 and ziprasidone also suggested efficacy for BPD. Two placebo-controlled studies of olanzapine examined which symptom groups were most helped; each reported a broad effect.16,17 However, not all studies of SGAs for BPD patients have been positive.18 Further, metabolic side effects have been noted for several SGAs, including olanzapine.18
Omega-3 fatty acids. Some studies examining omega-3 fatty acids have sparked an ongoing interest in this compound. In an 8-week, double-blind, pilot study of 30 women with BPD, Zanarini23 found omega-3 fatty acids demonstrated efficacy over placebo.
Most studies of BPD pharmacotherapy have used a classic clinical trial design, which does not easily translate into recommendations regarding medication selection for individual patients, especially those with BPD and comorbid illnesses. Also, existing trials have not fully explored starting doses, and no maintenance studies have been published. Therefore, many clinical application questions remain unresolved. However, some early treatment recommendations are supported by recent meta-analyses that demonstrate effects of medication classes for specific symptom domains.
Careful identification of comorbid psychiatric disorders is a rational first step. Diagnosing comorbid disorders, such as bipolar disorder, will determine medication choice and impact length of treatment. In a double-blind study of 30 women with BPD and comorbid bipolar II disorder, Frankenburg and Zanarini14 found divalproex had a statistically significant effect compared with placebo and could be considered for this specific population.
When treating a BPD patient who has a comorbid illness, it is important not to ignore BPD symptoms. The chronic emotional dysregulation and ongoing safety issues require psychiatrists to educate patients about these symptoms and to address them in a multidisciplinary manner.
Clarifying prominent symptom domains can help steer pharmacologic management. Many trials have attempted to focus on specific symptom domains, including cognitive-perceptual disturbances, impulsivity, and affective dysregulation. Table 124 lists BPD symptom domains and associated characteristics.
Table 1
Symptom domains of BPD
| Cognitive-perceptual symptoms |
| Suspiciousness |
| Referential thinking |
| Paranoid ideation |
| Illusions |
| Derealization |
| Depersonalization |
| Hallucination-like symptoms |
| Impulsive-behavioral dyscontrol |
| Impulsive aggression |
| Deliberate self-harm |
| Impulsive sexual behavior |
| Substance abuse |
| Impulsive spending |
| Affective dysregulation |
| Mood lability |
| Rejection sensitivity |
| Intense anger out of proportion to the stimuli |
| Sudden depressive mood episodes |
| BPD: borderline personality disorder Source: Reference 24 |
Dosing strategy
Developing a medication management strategy for BPD patients requires a thoughtful approach. When faced with a patient who has overwhelming distress, it is tempting to start with high medication doses; however, clinical experience suggests starting cautiously with lower doses will yield better tolerability and adherence. Based on our clinical experience, patients with BPD tend to be highly perceptive to physiologic stimuli and medication side effects.
Further research is needed to answer clinical questions regarding optimal dosing strategy and treatment, but some studies suggest when using SGAs, doses equivalent to one-third or one-half the dose used for treating schizophrenia may be appropriate.1,2,17,18 However, for fluoxetine, investigators have espoused using a dosage higher than generally used for depression.10 For mood-stabilizing anticonvulsants, almost all studies employed the same doses used for bipolar disorder.25 Some studies of valproic acid have verified appropriate blood levels—generally 50 to 100 μg/mL.
Controlled trials have not determined whether medications for patients with BPD should be used briefly during times of stress or for longer periods. Many studies of medication for BPD have been relatively brief trials that explored whether the drug has any potential efficacy. In our opinion, this issue currently is being addressed in clinical practice in a trial-and-error manner.
Clues to targeted treatment
Although pharmacotherapy for BPD subtypes remains controversial, recent meta-analyses by Ingenhoven24 and Nose26 and a Cochrane Review27 (with subsequent online update28) have identified evidence that supports the use of specific medications for treating BPD symptoms. These studies’ authors acknowledge replication studies are required because of the limited nature of the available data. In contrast, a meta-analysis conducted by the National Collaborating Centre for Mental Health29 did not identify sufficient evidence for medication use in BPD on which to base official guidelines to advise health care providers in the United Kingdom. The only medication recommendation in this meta-analysis is to consider prescribing short-term sedative antihistamines during crises; this recommendation is not supported by any clinical trial.
In a meta-analysis of 21 placebo-controlled trials of patients with BPD and/or schizotypal personality disorder, Inghoven et al24 used multiple domains and subdomains, including cognitive-perceptual symptoms, impulsive-behavioral dyscontrol, affective dysregulation, anger, and mood lability, to assess the efficacy of medication use (Table 2).24 They found:
- Antipsychotics seemed to have a moderate effect on cognitive-perceptual symptoms and a moderate-to-large effect on anger.
- Antidepressants had a small effect on anxiety, but no other domains.
- Mood stabilizers had a very large effect on impulsive-behavioral dyscontrol and anger, a large effect on anxiety, and a moderate effect on depressed mood.
- Regarding global functioning, mood stabilizers had a greater effect than antipsychotics. Both led to greater change than antidepressants.
A 2010 Cochrane Review meta-analysis initially conducted by Leib27 with subsequent online update by Stoffers28 included 28 studies with a total of 1,742 patients and also identified symptom-targeted BPD domains. This study analyzed pooled data and found support for the use of specific medications, including certain antipsychotics, mood stabilizers, and antidepressants, for specific BPD symptoms (Table 3).28 The authors recommended data be interpreted cautiously, however, because many of the clinical trials included in their meta-analysis have not been replicated and generalizability from research populations to clinical populations is not well understood.
Table 2
Which medications improve which BPD symptoms?
| Medication | Symptom domain | Effect |
|---|---|---|
| Antipsychotics | Cognitive-perceptual | Moderate |
| Anger | Moderate/large | |
| Antidepressants | Anxiety | Small |
| Anger | Small | |
| Mood stabilizers | Impulsive-behavioral dyscontrol | Very large |
| Anger | Very large | |
| Anxiety | Large | |
| Depressed mood | Moderate | |
| BPD: borderline personality disorder Source: Reference 24 | ||
Table 3
Pharmacotherapy for BPD: Results of a Cochrane review
| Class | Medication(s) |
|---|---|
| Cognitive-perceptual symptoms | |
| Antipsychotics | Olanzapine, aripiprazole |
| Impulsive-behavioral dyscontrol | |
| Mood stabilizers | Topiramate, lamotrigine |
| Antipsychotics | Aripiprazole |
| Affective dysregulation | |
| Antidepressants | Amitriptylinea (depressed mood) |
| Mood stabilizers | Topiramate, lamotrigine (anger), valproate (depressed mood) |
| Antipsychotics | Haloperidol (anger), olanzapine, aripiprazole |
| Omega-3 fatty acids | Fish oil (depression) |
| Suicidal behavior/suicidality | |
| Antipsychotics | Flupenthixol decanoate |
| Omega-3 fatty acids | Fish oil |
| Interpersonal problems | |
| Antipsychotics | Aripiprazole |
| Mood stabilizers | Valproate, topiramate |
| No improvement on any outcome: ziprasidone, thiothixene, phenelzine, fluoxetine, fluvoxamine, carbamazepine | |
| aDo not prescribe to suicidal patients BPD: borderline personality disorder Source: Reference 28 | |
DBT and pharmacotherapy
As is the case with many studies of psychiatric medications, early efficacy studies of pharmacotherapy for BPD did not include structured psychosocial treatment. In 2 double-blind, placebo-controlled trials with a total of 84 patients receiving DBT, those assigned to olanzapine had better outcomes on objective rating scales than those on placebo.30,31 Similar trials testing fluoxetine showed no advantage for the drug over placebo.32 In a pilot study by Moen et al,25 17 patients were assigned to “condensed DBT” before being randomized to divalproex extended release or placebo. Two patients remitted in the first 4 weeks and continued to improve without medication. If replicated, this finding may point to a targeted approach to the timing of medication initiation.
Clinical recommendations
Randomized, placebo-controlled BPD trials have demonstrated striking improvements in patients in placebo groups, which may be attributed to the powerful therapeutic impact of regular, structured, nonjudgmental interactions within a research protocol. Prescribers can enhance a medication’s therapeutic effect by keeping in mind the same principles that apply to treatment of other common psychiatric disorders.
Patients with BPD respond well to validation of their symptoms and their experience. Tell patients you take their BPD symptoms seriously and acknowledge their distress. The goal is to partner with patients to improve function, decrease reactivity, and reduce emotional pain. When working with BPD patients, it is appropriate to communicate a sense of optimism and hopefulness about their prognosis and treatment. Performing this approach in a caring way will better preserve the therapeutic alliance.
Additional suggestions based on our clinical experience include:
- Provide regular medication management visits.
- Consider using a structured symptom rating scale to evaluate symptoms over time, such as the Zanarini Rating Scale for Borderline Personality Disorder33 or Borderline Evaluation of Severity Over Time.34
- Educate patients with BPD about the disorder by making the appropriate diagnosis and providing reputable educational materials (see Related Resources).
- Do not diagnose a patient with BPD as having bipolar disorder unless they clearly meet criteria for bipolar disorder.
- Communicate your limitations in advance.
- Orient the patient to the possibility of needing to try different medications to determine the most helpful agent or combination.
- Do not de-emphasize risks of medications or side effects. Serious symptoms require medications that bear a risk of side effects; communicate these risks to patients and carefully weigh the risk-benefit profile.
- Inform patients you will be responsive to making appropriate changes if problems arise that are associated with pharmacotherapy and outweigh the benefit of medication.
Multidisciplinary teamwork
Best outcomes for patients with BPD are facilitated by a collaborative team effort. Such an approach addresses both the psychological and biologic underpinnings of the disorder and can significantly decrease the possibility of “splitting” among team members. To determine ways in which a therapist and physician may work together, clinicians should discuss the:
- meaning of medication to the therapist, psychiatrist, and patient
- potential benefits and limitations of medication
- the role of medication in the patient’s overall treatment.35
Patients with BPD experience emotional crisis. At times, prescribing patterns unfortunately reflect the practice of adding medications to address emotional crisis. This practice may partially account for the high rates of polypharmacy in BPD patients.36 Patients with BPD will benefit from interacting with a clinician whose approach is responsive, validating, and non-reactive to the patient’s symptoms and experiences. A comprehensive treatment approach includes screening and treating comorbid conditions, providing education about the diagnosis, and multidisciplinary involvement combined with rational, targeted pharmacotherapy.
- Friedel RO. Borderline personality disorder demystified: an essential guide for understanding and living with BPD. New York, NY: Marlowe & Company; 2004.
- Chapman A, Gratz K. Borderline personality disorder survival guide: everything you need to know about living with BPD. Oakland, CA: New Harbinger Publications, Inc; 2007.
- National Education Alliance for Borderline Personality Disorder. www.borderlinepersonalitydisorder.com.
Drug Brand Names
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Carbamazepine • Tegretol
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Lamotrigine • Lamictal
- Olanzapine • Zyprexa
- Phenelzine • Nardil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Thiothixene • Navane
- Topiramate • Topamax, Topiragen
- Tranylcypromine • Parnate
- Trifluoperazine • Stelazine
- Valproic acid • Depakote
- Ziprasidone • Geodon
Disclosure
Dr. Nelson receives research/grant support from the Minnesota Medical Foundation.
Dr. Schulz receives research/grant support from AstraZeneca, Otsuka, and Rules-Based Medicine and is a consultant to Bioavail, Bristol-Myers Squibb, and Eli Lilly and Company.
As psychiatry’s understanding of borderline personality disorder (BPD) grows, the literature clearly describes the seriousness of BPD, as well as these patients’ high utilization of treatment. Pharmacotherapy for BPD remains controversial. The most recent American Psychiatric Association practice guidelines focus on using symptom domains of this heterogeneous illness to guide medication selection, yet when these guidelines were published, there was a lack of data to support this recommendation.1
This article evaluates medications for BPD and emerging data supporting matching medications to BPD symptom domains, with an emphasis on making choices that advance clinical practice. We conclude by reviewing studies of combined pharmacotherapy and dialectical behavior therapy (DBT) and describing how a multidisciplinary team approach can enhance BPD treatment.
Early research
Early studies of pharmacotherapy for BPD began after the development of the Diagnostic Interview for Borderlines2,3 and DSM-III criteria for BPD.4 Researchers recruited patients who fulfilled the diagnostic criteria; however, these participants’ symptom profiles were highly heterogeneous. Although such studies can be useful when starting to test new treatments—especially if they are able to show efficacy over placebo or explore safety—they are less helpful in guiding clinical practice.
During the 1980s, low doses of first-generation antipsychotics were evaluated based on hypotheses that BPD was related to schizophrenia. Case series5 and placebo-controlled trials6,7 pointed to symptom reduction over time and greater than placebo for BPD patients. Interestingly, in a small study of BPD inpatients, Soloff et al8 compared the first-generation antipsychotic haloperidol to amitriptyline and found amitriptyline led to symptom worsening in some patients. Cowdry and Gardner9 compared alprazolam, carbamazepine, trifluoperazine, and tranylcypromine in a double-blind, placebo-controlled crossover trial of 16 female BPD outpatients. They found antipsychotics were not useful. Further, the study found behavioral disinhibition when a benzodiazepine (alprazolam) was used alone in impulsive patients.
These studies provided a basis for the idea that medications could help reduce BPD symptoms. However, some early investigators noted that antipsychotics’ side effects led some patients to discontinue treatment.6
Next-generation studies
Antidepressants. Interest in exploring pharmacologic treatments for BPD diminished after the early efficacy trials. Several events led to a reemergence of this interest, including the FDA’s approval of the selective serotonin reuptake inhibitor fluoxetine for depression in 1987. Some investigators hypothesized fluoxetine’s antidepressant properties could help treat BPD symptoms and perhaps the serotonin reuptake action could diminish impulsivity.10 Case series and a double-blind, placebo-controlled trial11 demonstrated fluoxetine’s efficacy in BPD. In 1 study, Salzman et al12 found fluoxetine’s greatest impact was on “anger,” a major affective dimension of BPD.
Mood stabilizers. When valproic acid emerged as a successful treatment for bipolar disorder, researchers turned their attention to mood-stabilizing anticonvulsants for BPD. Numerous case series and controlled trials provided evidence of its efficacy.13,14 This was the first time subtypes of BPD patients were tested prospectively—with the hypothesis that the mood-stabilizing anticonvulsants would diminish impulsivity and aggression. The positive results of Hollander et al13 and Frankenburg and Zanarini14 in assessing divalproex in BPD patients with bipolar II disorder has implications for targeted treatment (discussed below).
Newer antipsychotics. The introduction of second-generation antipsychotics (SGA) led some researchers to explore whether these agents could decrease BPD symptoms. Case series15 and some (but not all) placebo-controlled trials have demonstrated benefit from SGAs such as olanzapine,16-18 aripiprazole,19 and quetiapine.20,21 Initial research on risperidone22 and ziprasidone also suggested efficacy for BPD. Two placebo-controlled studies of olanzapine examined which symptom groups were most helped; each reported a broad effect.16,17 However, not all studies of SGAs for BPD patients have been positive.18 Further, metabolic side effects have been noted for several SGAs, including olanzapine.18
Omega-3 fatty acids. Some studies examining omega-3 fatty acids have sparked an ongoing interest in this compound. In an 8-week, double-blind, pilot study of 30 women with BPD, Zanarini23 found omega-3 fatty acids demonstrated efficacy over placebo.
Most studies of BPD pharmacotherapy have used a classic clinical trial design, which does not easily translate into recommendations regarding medication selection for individual patients, especially those with BPD and comorbid illnesses. Also, existing trials have not fully explored starting doses, and no maintenance studies have been published. Therefore, many clinical application questions remain unresolved. However, some early treatment recommendations are supported by recent meta-analyses that demonstrate effects of medication classes for specific symptom domains.
Careful identification of comorbid psychiatric disorders is a rational first step. Diagnosing comorbid disorders, such as bipolar disorder, will determine medication choice and impact length of treatment. In a double-blind study of 30 women with BPD and comorbid bipolar II disorder, Frankenburg and Zanarini14 found divalproex had a statistically significant effect compared with placebo and could be considered for this specific population.
When treating a BPD patient who has a comorbid illness, it is important not to ignore BPD symptoms. The chronic emotional dysregulation and ongoing safety issues require psychiatrists to educate patients about these symptoms and to address them in a multidisciplinary manner.
Clarifying prominent symptom domains can help steer pharmacologic management. Many trials have attempted to focus on specific symptom domains, including cognitive-perceptual disturbances, impulsivity, and affective dysregulation. Table 124 lists BPD symptom domains and associated characteristics.
Table 1
Symptom domains of BPD
| Cognitive-perceptual symptoms |
| Suspiciousness |
| Referential thinking |
| Paranoid ideation |
| Illusions |
| Derealization |
| Depersonalization |
| Hallucination-like symptoms |
| Impulsive-behavioral dyscontrol |
| Impulsive aggression |
| Deliberate self-harm |
| Impulsive sexual behavior |
| Substance abuse |
| Impulsive spending |
| Affective dysregulation |
| Mood lability |
| Rejection sensitivity |
| Intense anger out of proportion to the stimuli |
| Sudden depressive mood episodes |
| BPD: borderline personality disorder Source: Reference 24 |
Dosing strategy
Developing a medication management strategy for BPD patients requires a thoughtful approach. When faced with a patient who has overwhelming distress, it is tempting to start with high medication doses; however, clinical experience suggests starting cautiously with lower doses will yield better tolerability and adherence. Based on our clinical experience, patients with BPD tend to be highly perceptive to physiologic stimuli and medication side effects.
Further research is needed to answer clinical questions regarding optimal dosing strategy and treatment, but some studies suggest when using SGAs, doses equivalent to one-third or one-half the dose used for treating schizophrenia may be appropriate.1,2,17,18 However, for fluoxetine, investigators have espoused using a dosage higher than generally used for depression.10 For mood-stabilizing anticonvulsants, almost all studies employed the same doses used for bipolar disorder.25 Some studies of valproic acid have verified appropriate blood levels—generally 50 to 100 μg/mL.
Controlled trials have not determined whether medications for patients with BPD should be used briefly during times of stress or for longer periods. Many studies of medication for BPD have been relatively brief trials that explored whether the drug has any potential efficacy. In our opinion, this issue currently is being addressed in clinical practice in a trial-and-error manner.
Clues to targeted treatment
Although pharmacotherapy for BPD subtypes remains controversial, recent meta-analyses by Ingenhoven24 and Nose26 and a Cochrane Review27 (with subsequent online update28) have identified evidence that supports the use of specific medications for treating BPD symptoms. These studies’ authors acknowledge replication studies are required because of the limited nature of the available data. In contrast, a meta-analysis conducted by the National Collaborating Centre for Mental Health29 did not identify sufficient evidence for medication use in BPD on which to base official guidelines to advise health care providers in the United Kingdom. The only medication recommendation in this meta-analysis is to consider prescribing short-term sedative antihistamines during crises; this recommendation is not supported by any clinical trial.
In a meta-analysis of 21 placebo-controlled trials of patients with BPD and/or schizotypal personality disorder, Inghoven et al24 used multiple domains and subdomains, including cognitive-perceptual symptoms, impulsive-behavioral dyscontrol, affective dysregulation, anger, and mood lability, to assess the efficacy of medication use (Table 2).24 They found:
- Antipsychotics seemed to have a moderate effect on cognitive-perceptual symptoms and a moderate-to-large effect on anger.
- Antidepressants had a small effect on anxiety, but no other domains.
- Mood stabilizers had a very large effect on impulsive-behavioral dyscontrol and anger, a large effect on anxiety, and a moderate effect on depressed mood.
- Regarding global functioning, mood stabilizers had a greater effect than antipsychotics. Both led to greater change than antidepressants.
A 2010 Cochrane Review meta-analysis initially conducted by Leib27 with subsequent online update by Stoffers28 included 28 studies with a total of 1,742 patients and also identified symptom-targeted BPD domains. This study analyzed pooled data and found support for the use of specific medications, including certain antipsychotics, mood stabilizers, and antidepressants, for specific BPD symptoms (Table 3).28 The authors recommended data be interpreted cautiously, however, because many of the clinical trials included in their meta-analysis have not been replicated and generalizability from research populations to clinical populations is not well understood.
Table 2
Which medications improve which BPD symptoms?
| Medication | Symptom domain | Effect |
|---|---|---|
| Antipsychotics | Cognitive-perceptual | Moderate |
| Anger | Moderate/large | |
| Antidepressants | Anxiety | Small |
| Anger | Small | |
| Mood stabilizers | Impulsive-behavioral dyscontrol | Very large |
| Anger | Very large | |
| Anxiety | Large | |
| Depressed mood | Moderate | |
| BPD: borderline personality disorder Source: Reference 24 | ||
Table 3
Pharmacotherapy for BPD: Results of a Cochrane review
| Class | Medication(s) |
|---|---|
| Cognitive-perceptual symptoms | |
| Antipsychotics | Olanzapine, aripiprazole |
| Impulsive-behavioral dyscontrol | |
| Mood stabilizers | Topiramate, lamotrigine |
| Antipsychotics | Aripiprazole |
| Affective dysregulation | |
| Antidepressants | Amitriptylinea (depressed mood) |
| Mood stabilizers | Topiramate, lamotrigine (anger), valproate (depressed mood) |
| Antipsychotics | Haloperidol (anger), olanzapine, aripiprazole |
| Omega-3 fatty acids | Fish oil (depression) |
| Suicidal behavior/suicidality | |
| Antipsychotics | Flupenthixol decanoate |
| Omega-3 fatty acids | Fish oil |
| Interpersonal problems | |
| Antipsychotics | Aripiprazole |
| Mood stabilizers | Valproate, topiramate |
| No improvement on any outcome: ziprasidone, thiothixene, phenelzine, fluoxetine, fluvoxamine, carbamazepine | |
| aDo not prescribe to suicidal patients BPD: borderline personality disorder Source: Reference 28 | |
DBT and pharmacotherapy
As is the case with many studies of psychiatric medications, early efficacy studies of pharmacotherapy for BPD did not include structured psychosocial treatment. In 2 double-blind, placebo-controlled trials with a total of 84 patients receiving DBT, those assigned to olanzapine had better outcomes on objective rating scales than those on placebo.30,31 Similar trials testing fluoxetine showed no advantage for the drug over placebo.32 In a pilot study by Moen et al,25 17 patients were assigned to “condensed DBT” before being randomized to divalproex extended release or placebo. Two patients remitted in the first 4 weeks and continued to improve without medication. If replicated, this finding may point to a targeted approach to the timing of medication initiation.
Clinical recommendations
Randomized, placebo-controlled BPD trials have demonstrated striking improvements in patients in placebo groups, which may be attributed to the powerful therapeutic impact of regular, structured, nonjudgmental interactions within a research protocol. Prescribers can enhance a medication’s therapeutic effect by keeping in mind the same principles that apply to treatment of other common psychiatric disorders.
Patients with BPD respond well to validation of their symptoms and their experience. Tell patients you take their BPD symptoms seriously and acknowledge their distress. The goal is to partner with patients to improve function, decrease reactivity, and reduce emotional pain. When working with BPD patients, it is appropriate to communicate a sense of optimism and hopefulness about their prognosis and treatment. Performing this approach in a caring way will better preserve the therapeutic alliance.
Additional suggestions based on our clinical experience include:
- Provide regular medication management visits.
- Consider using a structured symptom rating scale to evaluate symptoms over time, such as the Zanarini Rating Scale for Borderline Personality Disorder33 or Borderline Evaluation of Severity Over Time.34
- Educate patients with BPD about the disorder by making the appropriate diagnosis and providing reputable educational materials (see Related Resources).
- Do not diagnose a patient with BPD as having bipolar disorder unless they clearly meet criteria for bipolar disorder.
- Communicate your limitations in advance.
- Orient the patient to the possibility of needing to try different medications to determine the most helpful agent or combination.
- Do not de-emphasize risks of medications or side effects. Serious symptoms require medications that bear a risk of side effects; communicate these risks to patients and carefully weigh the risk-benefit profile.
- Inform patients you will be responsive to making appropriate changes if problems arise that are associated with pharmacotherapy and outweigh the benefit of medication.
Multidisciplinary teamwork
Best outcomes for patients with BPD are facilitated by a collaborative team effort. Such an approach addresses both the psychological and biologic underpinnings of the disorder and can significantly decrease the possibility of “splitting” among team members. To determine ways in which a therapist and physician may work together, clinicians should discuss the:
- meaning of medication to the therapist, psychiatrist, and patient
- potential benefits and limitations of medication
- the role of medication in the patient’s overall treatment.35
Patients with BPD experience emotional crisis. At times, prescribing patterns unfortunately reflect the practice of adding medications to address emotional crisis. This practice may partially account for the high rates of polypharmacy in BPD patients.36 Patients with BPD will benefit from interacting with a clinician whose approach is responsive, validating, and non-reactive to the patient’s symptoms and experiences. A comprehensive treatment approach includes screening and treating comorbid conditions, providing education about the diagnosis, and multidisciplinary involvement combined with rational, targeted pharmacotherapy.
- Friedel RO. Borderline personality disorder demystified: an essential guide for understanding and living with BPD. New York, NY: Marlowe & Company; 2004.
- Chapman A, Gratz K. Borderline personality disorder survival guide: everything you need to know about living with BPD. Oakland, CA: New Harbinger Publications, Inc; 2007.
- National Education Alliance for Borderline Personality Disorder. www.borderlinepersonalitydisorder.com.
Drug Brand Names
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Aripiprazole • Abilify
- Carbamazepine • Tegretol
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Lamotrigine • Lamictal
- Olanzapine • Zyprexa
- Phenelzine • Nardil
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Thiothixene • Navane
- Topiramate • Topamax, Topiragen
- Tranylcypromine • Parnate
- Trifluoperazine • Stelazine
- Valproic acid • Depakote
- Ziprasidone • Geodon
Disclosure
Dr. Nelson receives research/grant support from the Minnesota Medical Foundation.
Dr. Schulz receives research/grant support from AstraZeneca, Otsuka, and Rules-Based Medicine and is a consultant to Bioavail, Bristol-Myers Squibb, and Eli Lilly and Company.
1. American Psychiatric Association Practice Guidelines. Practice guideline for the treatment of patients with borderline personality disorder. American Psychiatric Association. Am J Psychiatry. 2001;158(10 suppl):1-52.
2. Barrash J, Kroll J, Carey K, et al. Discriminating borderline disorder from other personality disorders. Cluster analysis of the diagnostic interview for borderlines. Arch Gen Psychiatry. 1983;40(12):1297-1302.
3. Kety SS, Rosenthal D, Wender PH, et al. Mental illness in the biological and adoptive families of adopted individuals who have become schizophrenic: a preliminary report based on psychiatric interviews. Proc Annu Meet Am Psychopathol Assoc. 1975;(63):147-165.
4. Diagnostic and statistical manual of mental disorders, 3rd ed. Washington DC: American Psychiatric Association; 1980.
5. Serban G, Siegel S. Response of borderline and schizotypal patients to small doses of thiothixene and haloperidol. Am J Psychiatry. 1984;141(11):1455-1458.
6. Goldberg SC, Schulz SC, Schulz PM, et al. Borderline and schizotypal personality disorders treated with low-dose thiothixene vs placebo. Arch Gen Psychiatry. 1986;43(7):680-686.
7. Soloff PH, George A, Nathan RS, et al. Progress in pharmacotherapy of borderline disorders. A double-blind study of amitriptyline, haloperidol, and placebo. Arch Gen Psychiatry. 1986;43(7):691-697.
8. Soloff PH, George A, Nathan RS, et al. Paradoxical effects of amitriptyline on borderline patients. Am J Psychiatry. 1986;143(12):1603-1635.
9. Cowdry RW, Gardner DL. Pharmacotherapy of borderline personality disorder. Alprazolam carbamazepine, trifluoperazine, and tranylcypromine. Arch Gen Psychiatry. 1988;45(2):111-119.
10. Markovitz PJ, Calabrese JR, Schulz SC, et al. Fluoxetine in the treatment of borderline and schizotypal personality disorders. Am J Psychiatry. 1991;148(8):1064-1067.
11. Coccaro EF, Kavoussi RJ. Fluoxetine and impulsive aggressive behavior in personality-disordered subjects. Arch Gen Psychiatry. 1997;54(12):1081-1088.
12. Salzman C, Wolfson AN, Schatzberg A, et al. Effect of fluoxetine on anger in symptomatic volunteers with borderline personality disorder. J Clin Psychopharmacol. 1995;15(1):23-29.
13. Hollander E, Tracy KA, Swann AC, et al. Divalproex in the treatment of impulsive aggression: efficacy in cluster B personality disorders. Neuropsychopharmacology. 2003;28(6):1186-1197.
14. Frankenburg FR, Zanarini MC. Divalproex sodium treatment of women with borderline personality disorder and bipolar II disorder: a double-blind placebo-controlled pilot study. J Clin Psychiatry. 2002;63(5):442-446.
15. Schulz SC, Camlin KL, Berry SA, et al. Olanzapine safety and efficacy in patients with borderline personality disorder and comorbid dysthymia. Biol Psychiatry. 1999;46(10):1429-1435.
16. Bogenschutz MP, George Nurnberg H. Olanzapine versus placebo in the treatment of borderline personality disorder. J Clin Psychiatry. 2004;65(1):104-109.
17. Zanarini MC, Frankenburg FR. Olanzapine treatment of female borderline personality disorder patients: a double-blind placebo-controlled pilot study. J Clin Psychiatry. 2001;62(11):849-854.
18. Schulz SC, Zanarini MC, Bateman A, et al. Olanzapine for the treatment of borderline personality disorder: variable dose 12-week randomised double-blind placebo-controlled study. Br J Psychiatry. 2008;193(6):485-492.
19. Nickel MK, Muehlbacher M, Nickel C, et al. Aripiprazole in the treatment of patients with borderline personality disorder: a double-blind, placebo-controlled study. Am J Psychiatry. 2006;163(5):833-838.
20. Adityanjee, Romine A, Brown E, et al. Quetiapine in patients with borderline personality disorder: an open-label trial. Ann Clin Psychiatry. 2008;20(4):219-226.
21. Villeneuve E, Lemelin S. Open-label study of atypical neuroleptic quetiapine for treatment of borderline personality disorder: impulsivity as main target. J Clin Psychiatry. 2005;66(10):1298-1303.
22. Rocca P, Marchiaro L, Cocuzza E, et al. Treatment of borderline personality disorder with risperidone. J Clin Psychiatry. 2002;63(3):241-244.
23. Zanarini MC, Frankenburg FR. Omega-3 fatty acid treatment of women with borderline personality disorder: a double-blind placebo-controlled pilot study. Am J Psychiatry. 2003;160(1):167-169.
24. Ingenhoven T, Lafay P, Rinne T, et al. Effectiveness of pharmacotherapy for severe personality disorders: meta-analyses of randomized controlled trials. J Clin Psychiatry. 2010;71(1):14-25.
25. Moen Moore R, Miller M, Lee S, et al. Extended release divalproex for borderline personality disorder. Poster presented at: U. S. Psychiatric and Mental Health Congress; October 13-16, 2007; Orlando, FL.
26. Nose M, Cipriani A, Biancosino B, et al. Efficacy of pharmacotherapy against core traits of borderline personality disorder: meta-analysis of randomized controlled trials. Int Clin Psychopharmacol. 2006;21(6):345-353.
27. Lieb K, Völlm B, Rücker G, et al. Pharmacotherapy for borderline personality disorder: Cochrane Systematic Review of Randomised Trials. Br J Psychiatry. 2010;196(1):4-12.
28. Stoffers J, Völlm BA, Rücker G, et al. Pharmacological interventions for borderline personality disorder. Cochrane Database Syst Rev. 2010;(6):CD005653.-
29. National Collaborating Centre for Mental Health. Borderline personality disorder: the NICE guideline on treatment and management. National clinical practice guideline no. 78. London United Kingdom: RCPsych Publications; 2009.
30. Linehan MM, McDavid JD, Brown MZ, et al. Olanzapine plus dialectical behavior therapy for women with high irritability who meet criteria for borderline personality disorder: a double-blind, placebo-controlled pilot study. J Clin Psychiatry. 2008;69(6):999-1005.
31. Soler J, Pascual JC, Campins J, et al. Double-blind, placebo-controlled study of dialectical behavior therapy plus olanzapine for borderline personality disorder. Am J Psychiatry. 2005;162(6):1221-1224.
32. Simpson EB, Yen S, Costello E, et al. Combined dialectical behavior therapy and fluoxetine in the treatment of borderline personality disorder. J Clin Psychiatry. 2004;65(3):379-385.
33. Zanarini MC, Vujanovic AA, Parachini EA, et al. Zanarini Rating Scale for Borderline Personality Disorder (ZAN-BPD): a continuous measure of DSM-IV borderline psychopathology. J Pers Disord. 2003;17(3):233-242.
34. Pfohl B, Blum N, St John D, et al. Reliability and validity of the Borderline Evaluation of Severity Over Time (BEST): a self-rated scale to measure severity and change in persons with borderline personality disorder. J Pers Disord. 2009;23(3):281-293.
35. Silk KR. Collaborative treatment for patients with personality disorders. In: Riba MB Balon R, eds. Psychopharmacology and psychotherapy: a collaborative approach. Washington, DC: American Psychiatric Press; 1999:221–277.
36. Zanarini MC. Update on pharmacotherapy of borderline personality disorder. Curr Psychiatry Rep. 2004;6(1):66-70.
1. American Psychiatric Association Practice Guidelines. Practice guideline for the treatment of patients with borderline personality disorder. American Psychiatric Association. Am J Psychiatry. 2001;158(10 suppl):1-52.
2. Barrash J, Kroll J, Carey K, et al. Discriminating borderline disorder from other personality disorders. Cluster analysis of the diagnostic interview for borderlines. Arch Gen Psychiatry. 1983;40(12):1297-1302.
3. Kety SS, Rosenthal D, Wender PH, et al. Mental illness in the biological and adoptive families of adopted individuals who have become schizophrenic: a preliminary report based on psychiatric interviews. Proc Annu Meet Am Psychopathol Assoc. 1975;(63):147-165.
4. Diagnostic and statistical manual of mental disorders, 3rd ed. Washington DC: American Psychiatric Association; 1980.
5. Serban G, Siegel S. Response of borderline and schizotypal patients to small doses of thiothixene and haloperidol. Am J Psychiatry. 1984;141(11):1455-1458.
6. Goldberg SC, Schulz SC, Schulz PM, et al. Borderline and schizotypal personality disorders treated with low-dose thiothixene vs placebo. Arch Gen Psychiatry. 1986;43(7):680-686.
7. Soloff PH, George A, Nathan RS, et al. Progress in pharmacotherapy of borderline disorders. A double-blind study of amitriptyline, haloperidol, and placebo. Arch Gen Psychiatry. 1986;43(7):691-697.
8. Soloff PH, George A, Nathan RS, et al. Paradoxical effects of amitriptyline on borderline patients. Am J Psychiatry. 1986;143(12):1603-1635.
9. Cowdry RW, Gardner DL. Pharmacotherapy of borderline personality disorder. Alprazolam carbamazepine, trifluoperazine, and tranylcypromine. Arch Gen Psychiatry. 1988;45(2):111-119.
10. Markovitz PJ, Calabrese JR, Schulz SC, et al. Fluoxetine in the treatment of borderline and schizotypal personality disorders. Am J Psychiatry. 1991;148(8):1064-1067.
11. Coccaro EF, Kavoussi RJ. Fluoxetine and impulsive aggressive behavior in personality-disordered subjects. Arch Gen Psychiatry. 1997;54(12):1081-1088.
12. Salzman C, Wolfson AN, Schatzberg A, et al. Effect of fluoxetine on anger in symptomatic volunteers with borderline personality disorder. J Clin Psychopharmacol. 1995;15(1):23-29.
13. Hollander E, Tracy KA, Swann AC, et al. Divalproex in the treatment of impulsive aggression: efficacy in cluster B personality disorders. Neuropsychopharmacology. 2003;28(6):1186-1197.
14. Frankenburg FR, Zanarini MC. Divalproex sodium treatment of women with borderline personality disorder and bipolar II disorder: a double-blind placebo-controlled pilot study. J Clin Psychiatry. 2002;63(5):442-446.
15. Schulz SC, Camlin KL, Berry SA, et al. Olanzapine safety and efficacy in patients with borderline personality disorder and comorbid dysthymia. Biol Psychiatry. 1999;46(10):1429-1435.
16. Bogenschutz MP, George Nurnberg H. Olanzapine versus placebo in the treatment of borderline personality disorder. J Clin Psychiatry. 2004;65(1):104-109.
17. Zanarini MC, Frankenburg FR. Olanzapine treatment of female borderline personality disorder patients: a double-blind placebo-controlled pilot study. J Clin Psychiatry. 2001;62(11):849-854.
18. Schulz SC, Zanarini MC, Bateman A, et al. Olanzapine for the treatment of borderline personality disorder: variable dose 12-week randomised double-blind placebo-controlled study. Br J Psychiatry. 2008;193(6):485-492.
19. Nickel MK, Muehlbacher M, Nickel C, et al. Aripiprazole in the treatment of patients with borderline personality disorder: a double-blind, placebo-controlled study. Am J Psychiatry. 2006;163(5):833-838.
20. Adityanjee, Romine A, Brown E, et al. Quetiapine in patients with borderline personality disorder: an open-label trial. Ann Clin Psychiatry. 2008;20(4):219-226.
21. Villeneuve E, Lemelin S. Open-label study of atypical neuroleptic quetiapine for treatment of borderline personality disorder: impulsivity as main target. J Clin Psychiatry. 2005;66(10):1298-1303.
22. Rocca P, Marchiaro L, Cocuzza E, et al. Treatment of borderline personality disorder with risperidone. J Clin Psychiatry. 2002;63(3):241-244.
23. Zanarini MC, Frankenburg FR. Omega-3 fatty acid treatment of women with borderline personality disorder: a double-blind placebo-controlled pilot study. Am J Psychiatry. 2003;160(1):167-169.
24. Ingenhoven T, Lafay P, Rinne T, et al. Effectiveness of pharmacotherapy for severe personality disorders: meta-analyses of randomized controlled trials. J Clin Psychiatry. 2010;71(1):14-25.
25. Moen Moore R, Miller M, Lee S, et al. Extended release divalproex for borderline personality disorder. Poster presented at: U. S. Psychiatric and Mental Health Congress; October 13-16, 2007; Orlando, FL.
26. Nose M, Cipriani A, Biancosino B, et al. Efficacy of pharmacotherapy against core traits of borderline personality disorder: meta-analysis of randomized controlled trials. Int Clin Psychopharmacol. 2006;21(6):345-353.
27. Lieb K, Völlm B, Rücker G, et al. Pharmacotherapy for borderline personality disorder: Cochrane Systematic Review of Randomised Trials. Br J Psychiatry. 2010;196(1):4-12.
28. Stoffers J, Völlm BA, Rücker G, et al. Pharmacological interventions for borderline personality disorder. Cochrane Database Syst Rev. 2010;(6):CD005653.-
29. National Collaborating Centre for Mental Health. Borderline personality disorder: the NICE guideline on treatment and management. National clinical practice guideline no. 78. London United Kingdom: RCPsych Publications; 2009.
30. Linehan MM, McDavid JD, Brown MZ, et al. Olanzapine plus dialectical behavior therapy for women with high irritability who meet criteria for borderline personality disorder: a double-blind, placebo-controlled pilot study. J Clin Psychiatry. 2008;69(6):999-1005.
31. Soler J, Pascual JC, Campins J, et al. Double-blind, placebo-controlled study of dialectical behavior therapy plus olanzapine for borderline personality disorder. Am J Psychiatry. 2005;162(6):1221-1224.
32. Simpson EB, Yen S, Costello E, et al. Combined dialectical behavior therapy and fluoxetine in the treatment of borderline personality disorder. J Clin Psychiatry. 2004;65(3):379-385.
33. Zanarini MC, Vujanovic AA, Parachini EA, et al. Zanarini Rating Scale for Borderline Personality Disorder (ZAN-BPD): a continuous measure of DSM-IV borderline psychopathology. J Pers Disord. 2003;17(3):233-242.
34. Pfohl B, Blum N, St John D, et al. Reliability and validity of the Borderline Evaluation of Severity Over Time (BEST): a self-rated scale to measure severity and change in persons with borderline personality disorder. J Pers Disord. 2009;23(3):281-293.
35. Silk KR. Collaborative treatment for patients with personality disorders. In: Riba MB Balon R, eds. Psychopharmacology and psychotherapy: a collaborative approach. Washington, DC: American Psychiatric Press; 1999:221–277.
36. Zanarini MC. Update on pharmacotherapy of borderline personality disorder. Curr Psychiatry Rep. 2004;6(1):66-70.
Do stimulants for ADHD increase the risk of substance use disorders?
Discuss this article at www.facebook.com/CurrentPsychiatry
Does prescribing stimulants to patients with attention-deficit/hyperactivity disorder (ADHD) increase their risk of future substance abuse? Because ADHD is a common pediatric condition with symptoms that often persist into adulthood, and stimulants are an efficacious first-line therapy, this possible association is a concern for psychiatrists whether they treat children or adults.
Some researchers have expressed concerns that stimulant exposure could predispose patients to future substance abuse.1 Proponents of the biologic model of “kindling” hypothesize early exposure to stimulants could increase the risk of later substance use disorders (SUDs) by modifying or “priming” the brain, which then becomes more receptive to illicit drug exposure. Although there is some evidence that stimulant use does increase SUD risk, other evidence suggests stimulant use does not increase susceptibility to SUDs2,3 and some studies have suggested stimulant use in ADHD patients may protect against SUDs.4,5
This article reviews shared characteristics of ADHD and SUDs and the latest research on the association between the clinical use of stimulants and later development of SUDs. We also offer clinical recommendations for assessing and treating ADHD and comorbid SUD.
ADHD/SUD overlap
Compared with those without the disorder, patients with ADHD have a 6.2 times higher risk of developing an SUD.6 Individuals with ADHD experience an earlier age of onset and a longer duration of SUDs.7 Several retrospective and prospective studies reveal ADHD is a risk factor for SUDs.8 A longitudinal study that tracked teenage males with or without ADHD into young adulthood found SUDs were 4 times more common among those with ADHD.9 Up to 45% of adults with ADHD have a history of alcohol abuse or dependence, and up to 30% have a history of illegal drug abuse or dependence.10
Conversely, an estimated 35% to 71% of alcohol abusers and 15% to 25% of substance-dependent patients have ADHD.11 Adults with ADHD and comorbid SUD report earlier onset12 and greater severity13 of substance abuse than adults without ADHD. Patients with ADHD experience earlier onset and higher rates of tobacco smoking by mid-adolescence.14
Developmental psychopathology. Longitudinal studies have suggested certain psychopathologic characteristics of ADHD can predispose an individual to SUDs independent of stimulant exposure. For example, inattention, impulsivity, and hyperactivity predispose an individual to develop an SUD and also are core symptoms of ADHD.15 Another study found impulsivity, impersistence, and difficulty sitting still at age 3 predicted alcohol abuse at age 21.16 A different longitudinal study found novelty-seeking behavior (restlessness, running/jumping and not keeping still, being squirmy and fidgety) between age 6 to 10 predicted adolescent drug abuse and cigarette smoking.17 Poor response inhibition is a key characteristic of ADHD and has been linked to adolescent drinking.18
ADHD may be an independent risk factor for SUD because a common neurobiologic psychopathology may predispose an individual to develop both conditions. The dopamine system has been implicated in SUD, and dysfunction in the dopaminergic circuits—mostly in basal and frontal cortex with consequent defects in executive function and reward system—also has been found in ADHD.19 Cognitive dysfunction associated with ADHD may decrease a patient’s ability to estimate the negative consequences of substance abuse and to delay immediate gratification from drug or alcohol use.
ADHD patients are more vulnerable to SUDs if they have a comorbid condition, such as oppositional defiant disorder,13,20 bipolar disorder,20,21 or conduct disorder (CD).20,22 Patients with ADHD and comorbid CD are estimated to be 8.8 times more likely to have an SUD before age 18 compared with those with ADHD alone.23 Comorbid ADHD and CD may increase patients’ predisposition to develop dependence on highly addictive drugs, such as cocaine or methamphetamine.24 Impaired executive function, behavioral dyscontrol, impulsivity, and peer rejection are common in both ADHD and CD and may increase the risk of developing SUDs in individuals who have both conditions.25 Other risk factors for SUDs in patients with ADHD are listed in Table 1.26
Table 1
Risk factors for SUDs in patients with ADHD
| Presence of comorbid conditions (ie, oppositional defiant disorder, conduct disorder, bipolar disorder, eating disorder) |
| White or Hispanic race |
| Partially treated or residual ADHD symptoms |
| Attending a competitive college program |
| College youth who had late onset of stimulant treatment |
| Member of a college sorority/fraternity |
| ADHD: attention-deficit/hyperactivity disorder; SUDs: substance use disorders Source: Reference 26 |
Stimulants’ affect on SUD risk
Increased risk. Limited studies suggest exposure to stimulants is a risk factor for developing SUDs. In a longitudinal study, Lambert et al27 followed 218 patients with ADHD and 182 without ADHD into adulthood and found a linear trend between duration of stimulant treatment and prevalence of cocaine dependence. ADHD patients exposed to stimulants for >1 year had the highest prevalence of cocaine abuse (27%), compared with untreated subjects (15%), or those treated with stimulants for <1 year (18%). However, the study did not control for comorbid contributing factors, such as CD.
No change. In a 10-year naturalistic study, Biederman et al28 followed 109 children with ADHD age 7 to 12 into adulthood. These children had a developmental reading disorder but no other psychiatric comorbidities. When comparing patients who were treated with methylphenidate (n = 43) with those who did not receive stimulants (n = 66), Bierderman et al found no significant difference between the 2 groups in the prevalence of SUD for any of the 7 drug categories studied.
Decreased risk. Two meta-analyses found children with ADHD who were treated with stimulants and followed until adolescence were 5.8 times less likely to develop SUDs compared with those who did not receive stimulants.28,29 This protective effect diminished when patients were followed into adulthood, but individuals treated with stimulants were 1.4 times less likely to develop SUDs than those not treated with stimulants.30 In a prospective case-control, 5-year follow-up study of 114 patients with ADHD treated with stimulants, Wilens et al31 found significant protective effects of stimulant treatment on the development of any SUD. They found no effects from time of onset or duration of stimulant therapy on subsequent risk of SUDs or cigarette smoking.
One possible explanation for stimulants’ apparently reduced protective effect among adults is for patients with ADHD, stimulant use might delay but not prevent SUDs. It also is likely that by adulthood, loss of parental supervision leads to poor medication adherence and increased susceptibility to SUDs.30
Other studies have found exposure to stimulants may protect against SUDs. Katusic et al23 reviewed medical records for documented SUDs in 295 adults with ADHD treated with stimulants and 84 who did not receive stimulants. They found 20% of patients who received stimulants had a documented SUD compared with 27% of those not treated with stimulants. Barkely et al32 followed 98 stimulant-treated and 21 untreated ADHD patients with a mean age of 15 and 21, respectively. They found stimulant treatment did not increase the risk for substance use or abuse in either group.
ADHD and stimulant abuse
The prevalence of stimulant misuse is as high as 9% in patients in grade school and high school and up to 35% in college-age individuals.33 ADHD patients who misuse stimulants (eg, escalating dose without authorization) or skip stimulant doses to use illicit drugs or alcohol are more likely to sell their medication.34 Immediate-release stimulant formulations are more liable to be abused than extended-release drugs because they achieve earlier peak drug concentrations and dopamine blockade, indicating rapid drug absorption and central drug activity. Close monitoring and use of extended-release formulations are useful deterrents against stimulant abuse.
Clinical recommendations
Detecting and treating SUDs in patients with ADHD can be challenging. Ideally, the best time to assess for ADHD symptoms is after a prolonged abstinence from any influencing substance. However, in most clinical situations this is not practical. A better approach is a longitudinal assessment for ADHD symptoms. Detecting evidence of early childhood onset of ADHD symptoms before the patient began using substances can be helpful in conducting a proper differential diagnosis. Assessing for symptoms of SUDs in early adolescence, along with serial assessment of ADHD symptoms, also can be helpful. Symptoms secondary to ADHD are likely to show a consistent pattern, whereas symptoms secondary to an SUD may be sporadic.
When assessing SUD risk, consider the patient’s clinical condition, history of comorbidities that suggest SUDs, and overall functional status. Collateral information about the patient’s behavior and substance abuse from family members is important. A history of CD, bipolar disorder, or antisocial personality disorder should raise concerns about potential future stimulant abuse or diversion. Close monitoring of patients suspected of having an SUD is essential to detect stimulant abuse or diversion, which often manifests as weight loss, requests for higher doses, requests to switch from long-acting or extended-release formulations to immediate-release formulations, and repeated and suspicious “lost prescriptions.” Close observation for other subtle signs—such as changes in personality or mood and unexplained accidents or injuries—also may be needed.35
Challenges of treating ADHD and co-occurring SUD include poor medication adherence, need for a higher therapeutic stimulant dose, and difficulty in assessing the therapeutic benefit of pharmacotherapy in the presence of an SUD.36 Treating ADHD comorbid with SUD requires a collaborative approach that involves a psychiatrist, family members, and a behavioral care provider in addition to frequent monitoring.34
In the absence of treatment guidelines for treating ADHD with comorbid SUDs, some clinicians prefer to stabilize the SUD before initiating stimulants. Others prefer to use nonstimulants (such as atomoxetine, guanfacine, bupropion, venlafaxine, tricyclic antidepressants, or modafinil) as a first-line treatment. However, nonstimulants have not demonstrated efficacy comparable to that of stimulants for ADHD.35
Table 2 offers clinical recommendations to minimize the risk of SUDs when treating ADHD patients with stimulants. Long-acting stimulant formulations are preferred over short-acting medications because they are less likely to be abused. Psychosocial interventions for treating ADHD and co-occurring SUD disorder include cognitive-behavioral therapy with emphasis on structured skills training and cognitive remediation.
Table 2
Minimizing SUD risk when treating ADHD patients with stimulants
| Assess symptom burden and psychosocial impairment |
| Establish a treatment contract and boundaries at the onset of treatment, including your right to terminate treatment if you suspect stimulant misuse |
| Assess for comorbidities that may increase your patient’s SUD risk (see Table 1) |
| Emphasize strict adherence to treatment recommendations |
| Involve the patient’s family as much as possible |
| Obtain collateral information on the patient’s history of ADHD-related symptoms from parents, siblings, significant others, etc. |
| Distinguish between patients with substance use vs an SUD or a history of an SUD |
| Obtain urine toxicology screening as appropriate |
| Carefully document dispensed stimulants– strength of medication, number of capsules, pills, patches, etc. Note date of dispensation and refill dates |
| Select delayed- or extended-release stimulant formulations |
| Consider prescribing nonstimulants if appropriate |
| Use rating scales such as Conners Adult ADHD Rating Scale to monitor ADHD symptom severity and response to treatment |
| Schedule frequent, face-to-face clinical monitoring visits |
| ADHD: attention-deficit/hyperactivity disorder; SUD: substance use disorder |
Related Resource
- Faraone SV, Wilens T. Does stimulant treatment lead to substance use disorders? J Clin Psychiatry. 2003;64(suppl 11):9-13.
- Upadhyaya HP, Rose K, Wang W, et al. Attention deficit hyperactivity disorder medication and substance use patterns among adolescents and young adults. J Child Adolesc Psychopharmacol. 2005;15:799-809.
- Mariani JJ, Levin FR. Treatment strategies for co-occurring ADHD and substance use disorders. Am J Addict. 2007;16(suppl 1):45-56.
Drug Brand Names
- Atomoxetine • Strattera
- Bupropion • Wellbutrin, Zyban
- Guanfacine • Tenex, Intuniv
- Methylphenidate • Ritalin
- Modafinil • Provigil
- Venlafaxine • Effexor
Disclosures
Dr. Shailesh Jain and Dr. Islam report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Rakesh Jain has received research support from, is a consultant to, and/or is a speaker for Addrenex Pharmaceuticals, AstraZeneca, Eli Lilly and Company, Forest Pharmaceuticals, Merck, Pamlab, Pfizer Inc., Shionogi Inc., Shire, and Sunovion Pharmaceuticals.
1. Lambert NM, McLeod M, Schenk S. Subjective responses to initial experience with cocaine: an exploration of the incentive-sensitization theory of drug abuse. Addiction. 2006;101(5):713-725.
2. Mannuzza S, Klein RG, Moulton JL. Does stimulant treatment place children at risk for adult substance abuse? A controlled prospective follow-up study. J Child Adolesc Psychopharmacol. 2003;13(3):273-282.
3. Katusic SK, Barbaresi WJ, Colligan RC, et al. Psychostimulant treatment and risk for substance abuse among young adults with a history of attention-deficit/hyperactivity disorder: a population-based, birth cohort study. J Child Adolesc Psychopharmacol. 2005;15(5):764-776.
4. Wilens TE, Faraone SV, Biederman J, et al. Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics. 2003;111(1):179-185.
5. Biederman J, Wilens T, Mick E, et al. Pharmacotherapy of attention-deficit/hyperactivity disorder reduces risk for substance use disorder. Pediatrics. 1999;104(2):e20.-
6. Katusic SK, Barbaresi WJ, Colligan RC, et al. Psychostimulant treatment and risk for substance abuse among young adults with a history of attention-deficit/hyperactivity disorder: a population-based, birth cohort study. J Child Adolesc Psychopharmacol. 2005;15(5):764-776.
7. Wilens TE. Impact of ADHD and its treatment on substance abuse in adults. J Clin Psychiatry. 2004;65(suppl 3):38-45.
8. Barkley RA, Fischer M, Smallish L, et al. Young adult follow-up of hyperactive children: antisocial activities and drug use. J Child Psychol Psychiatry. 2004;45(2):195-221.
9. Mannuzza S, Klein RG, Bessler A, et al. Adult outcome of hyperactive boys. Educational achievement, occupational rank, and psychiatric status. Arch Gen Psychiatry. 1993;50(7):565-576.
10. Wilens TE. Attention-deficit/hyperactivity disorder and the substance use disorders: the nature of the relationship subtypes at risk, and treatment issues. Psychiatr Clin North Am. 2004;27(2):283-301.
11. Wilens TE. AOD use and attention deficit/hyperactivity disorder. Alcohol Health Res World. 1998;22(2):127-130.
12. Wilens TE, Biederman J, Abrantes AM, et al. Clinical characteristics of psychiatrically referred adolescent outpatients with substance use disorder. J Am Acad Child Adolesc Psychiatry. 1997;36(7):941-947.
13. Schubiner H, Tzelepis A, Milberger S, et al. Prevalence of attention-deficit/hyperactivity disorder and conduct disorder among substance abusers. J Clin Psychiatry. 2000;61(4):244-251.
14. Lambert NM, Hartsough CS. Prospective study of tobacco smoking and substance dependencies among samples of ADHD and non-ADHD participants. J Learn Disabil. 1998;31(6):533-544.
15. Zucker RA. Alcohol use and the alcohol use disorders: a developmental biopsychosocial systems formulation covering the life course. In: Cicchetti D Cohen D, eds. Developmental psychopathology. 2nd ed. Hoboken, NJ: John Wiley & Sons Inc; 2006;620-656.
16. Caspi A, Moffitt TE, Newman DL, et al. Behavioral observations at age 3 years predict adult psychiatric disorders. Longitudinal evidence from a birth cohort. Arch Gen Psychiatry. 1996;53(11):1033-1039.
17. Màsse LC, Tremblay RE. Behavior of boys in kindergarten and the onset of substance use during adolescence. Arch Gen Psychiatry. 1997;54(1):62-68.
18. Nigg JT, Wong MM, Martel MM, et al. Poor response inhibition as a predictor of problem drinking and illicit drug use in adolescents at risk for alcoholism and other substance use disorders. J Am Acad Child Adolesc Psychiatry. 2006;45(4):468-475.
19. Seidman LJ, Valera EM, Makris N. Structural brain imaging of attention-deficit hyperactivity disorder. Biol Psychiatry. 2005;57(11):1263-1272.
20. Biederman J, Wilens T, Mick E, et al. Is ADHD a risk factor for psychoactive substance use disorders? Findings from a four-year prospective follow-up study. J Am Acad Child Adolesc Psychiatry. 1997;36(1):21-29.
21. Wilens TE, Biederman J, Millstein RB, et al. Risk for substance use disorders in youths with child- and adolescent-onset bipolar disorder. J Am Acad Child Adolesc Psychiatry. 1999;38(6):680-685.
22. Schubiner H, Saules KK, Arfken CL, et al. Double-blind placebo-controlled trial of methylphenidate in the treatment of adult ADHD patients with comorbid cocaine dependence. Exp Clin Psychopharmacol. 2002;10(3):286-294.
23. Katusic SK, Barbaresi WJ, Colligan RC, et al. Psychostimulant treatment and risk for substance abuse among young adults with a history of attention-deficit/hyperactivity disorder: a population-based, birth cohort study. J Child Adolesc Psychopharmacol. 2005;15(5):764-776.
24. Flory K, Milich R, Lynam DR, et al. Relation between childhood disruptive behavior disorders and substance use and dependence symptoms in young adulthood: individuals with symptoms of attention-deficit/hyperactivity disorder and conduct disorder are uniquely at risk. Psychol Addict Behav. 2003;17(2):151-158.
25. Wilens TE. Attention-deficit/hyperactivity disorder and the substance use disorders: the nature of the relationship subtypes at risk, and treatment issues. Psychiatr Clin North Am. 2004;27(2):283-301.
26. Wilson JJ. ADHD and substance use disorders: developmental aspects and the impact of stimulant treatment. Am J Addict. 2007;16(suppl 1):5-11.
27. Lambert NM, Hartsough CS. Prospective study of tobacco smoking and substance dependencies among samples of ADHD and non-ADHD participants. J Learn Disabil. 1998;31(6):533-544.
28. Biederman J, Monuteaux MC, Spencer T, et al. Stimulant therapy and risk for subsequent substance use disorders in male adults with ADHD: a naturalistic controlled 10-year follow-up study. Am J Psychiatry. 2008;165(5):597-603.
29. Wilens TE, Faraone SV, Biederman J, et al. Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics. 2003;111(1):179-185.
30. Faraone SV, Wilens TE. Effect of stimulant medications for attention-deficit/hyperactivity disorder on later substance use and the potential for stimulant misuse abuse, and diversion. J Clin Psychiatry. 2007;68(suppl 11):15-22.
31. Wilens TE, Adamson J, Monuteaux MC, et al. Effect of prior stimulant treatment for attention-deficit/hyperactivity disorder on subsequent risk for cigarette smoking and alcohol and drug use disorders in adolescents. Arch Pediatr Adolesc Med. 2008;162(10):916-921.
32. Barkley RA, Fischer M, Smallish L, et al. Does the treatment of attention-deficit/hyperactivity disorder with stimulants contribute to drug use/abuse? A 13-year prospective study. Pediatrics. 2003;111(1):97-109.
33. Wilens TE, Adler LA, Adams J, et al. Misuse and diversion of stimulants prescribed for ADHD: a systematic review of the literature. J Am Acad Child Adolesc Psychiatry. 2008;47(1):21-31.
34. Upadhyaya HP, Rose K, Wang W, et al. Attention-deficit/hyperactivity disorder, medication treatment, and substance use patterns among adolescents and young adults. J Child Adolesc Psychopharmacol. 2005;15(5):799-809.
35. Kollins SH. A qualitative review of issues arising in the use of psycho-stimulant medications in patients with ADHD and co-morbid substance use disorders. Curr Med Res Opin. 2008;24(5):1345-1357.
36. Faraone SV, Biederman J, Wilens TE, et al. A naturalistic study of the effects of pharmacotherapy on substance use disorders among ADHD adults. Psychol Med. 2007;37(12):1743-1752.
Discuss this article at www.facebook.com/CurrentPsychiatry
Does prescribing stimulants to patients with attention-deficit/hyperactivity disorder (ADHD) increase their risk of future substance abuse? Because ADHD is a common pediatric condition with symptoms that often persist into adulthood, and stimulants are an efficacious first-line therapy, this possible association is a concern for psychiatrists whether they treat children or adults.
Some researchers have expressed concerns that stimulant exposure could predispose patients to future substance abuse.1 Proponents of the biologic model of “kindling” hypothesize early exposure to stimulants could increase the risk of later substance use disorders (SUDs) by modifying or “priming” the brain, which then becomes more receptive to illicit drug exposure. Although there is some evidence that stimulant use does increase SUD risk, other evidence suggests stimulant use does not increase susceptibility to SUDs2,3 and some studies have suggested stimulant use in ADHD patients may protect against SUDs.4,5
This article reviews shared characteristics of ADHD and SUDs and the latest research on the association between the clinical use of stimulants and later development of SUDs. We also offer clinical recommendations for assessing and treating ADHD and comorbid SUD.
ADHD/SUD overlap
Compared with those without the disorder, patients with ADHD have a 6.2 times higher risk of developing an SUD.6 Individuals with ADHD experience an earlier age of onset and a longer duration of SUDs.7 Several retrospective and prospective studies reveal ADHD is a risk factor for SUDs.8 A longitudinal study that tracked teenage males with or without ADHD into young adulthood found SUDs were 4 times more common among those with ADHD.9 Up to 45% of adults with ADHD have a history of alcohol abuse or dependence, and up to 30% have a history of illegal drug abuse or dependence.10
Conversely, an estimated 35% to 71% of alcohol abusers and 15% to 25% of substance-dependent patients have ADHD.11 Adults with ADHD and comorbid SUD report earlier onset12 and greater severity13 of substance abuse than adults without ADHD. Patients with ADHD experience earlier onset and higher rates of tobacco smoking by mid-adolescence.14
Developmental psychopathology. Longitudinal studies have suggested certain psychopathologic characteristics of ADHD can predispose an individual to SUDs independent of stimulant exposure. For example, inattention, impulsivity, and hyperactivity predispose an individual to develop an SUD and also are core symptoms of ADHD.15 Another study found impulsivity, impersistence, and difficulty sitting still at age 3 predicted alcohol abuse at age 21.16 A different longitudinal study found novelty-seeking behavior (restlessness, running/jumping and not keeping still, being squirmy and fidgety) between age 6 to 10 predicted adolescent drug abuse and cigarette smoking.17 Poor response inhibition is a key characteristic of ADHD and has been linked to adolescent drinking.18
ADHD may be an independent risk factor for SUD because a common neurobiologic psychopathology may predispose an individual to develop both conditions. The dopamine system has been implicated in SUD, and dysfunction in the dopaminergic circuits—mostly in basal and frontal cortex with consequent defects in executive function and reward system—also has been found in ADHD.19 Cognitive dysfunction associated with ADHD may decrease a patient’s ability to estimate the negative consequences of substance abuse and to delay immediate gratification from drug or alcohol use.
ADHD patients are more vulnerable to SUDs if they have a comorbid condition, such as oppositional defiant disorder,13,20 bipolar disorder,20,21 or conduct disorder (CD).20,22 Patients with ADHD and comorbid CD are estimated to be 8.8 times more likely to have an SUD before age 18 compared with those with ADHD alone.23 Comorbid ADHD and CD may increase patients’ predisposition to develop dependence on highly addictive drugs, such as cocaine or methamphetamine.24 Impaired executive function, behavioral dyscontrol, impulsivity, and peer rejection are common in both ADHD and CD and may increase the risk of developing SUDs in individuals who have both conditions.25 Other risk factors for SUDs in patients with ADHD are listed in Table 1.26
Table 1
Risk factors for SUDs in patients with ADHD
| Presence of comorbid conditions (ie, oppositional defiant disorder, conduct disorder, bipolar disorder, eating disorder) |
| White or Hispanic race |
| Partially treated or residual ADHD symptoms |
| Attending a competitive college program |
| College youth who had late onset of stimulant treatment |
| Member of a college sorority/fraternity |
| ADHD: attention-deficit/hyperactivity disorder; SUDs: substance use disorders Source: Reference 26 |
Stimulants’ affect on SUD risk
Increased risk. Limited studies suggest exposure to stimulants is a risk factor for developing SUDs. In a longitudinal study, Lambert et al27 followed 218 patients with ADHD and 182 without ADHD into adulthood and found a linear trend between duration of stimulant treatment and prevalence of cocaine dependence. ADHD patients exposed to stimulants for >1 year had the highest prevalence of cocaine abuse (27%), compared with untreated subjects (15%), or those treated with stimulants for <1 year (18%). However, the study did not control for comorbid contributing factors, such as CD.
No change. In a 10-year naturalistic study, Biederman et al28 followed 109 children with ADHD age 7 to 12 into adulthood. These children had a developmental reading disorder but no other psychiatric comorbidities. When comparing patients who were treated with methylphenidate (n = 43) with those who did not receive stimulants (n = 66), Bierderman et al found no significant difference between the 2 groups in the prevalence of SUD for any of the 7 drug categories studied.
Decreased risk. Two meta-analyses found children with ADHD who were treated with stimulants and followed until adolescence were 5.8 times less likely to develop SUDs compared with those who did not receive stimulants.28,29 This protective effect diminished when patients were followed into adulthood, but individuals treated with stimulants were 1.4 times less likely to develop SUDs than those not treated with stimulants.30 In a prospective case-control, 5-year follow-up study of 114 patients with ADHD treated with stimulants, Wilens et al31 found significant protective effects of stimulant treatment on the development of any SUD. They found no effects from time of onset or duration of stimulant therapy on subsequent risk of SUDs or cigarette smoking.
One possible explanation for stimulants’ apparently reduced protective effect among adults is for patients with ADHD, stimulant use might delay but not prevent SUDs. It also is likely that by adulthood, loss of parental supervision leads to poor medication adherence and increased susceptibility to SUDs.30
Other studies have found exposure to stimulants may protect against SUDs. Katusic et al23 reviewed medical records for documented SUDs in 295 adults with ADHD treated with stimulants and 84 who did not receive stimulants. They found 20% of patients who received stimulants had a documented SUD compared with 27% of those not treated with stimulants. Barkely et al32 followed 98 stimulant-treated and 21 untreated ADHD patients with a mean age of 15 and 21, respectively. They found stimulant treatment did not increase the risk for substance use or abuse in either group.
ADHD and stimulant abuse
The prevalence of stimulant misuse is as high as 9% in patients in grade school and high school and up to 35% in college-age individuals.33 ADHD patients who misuse stimulants (eg, escalating dose without authorization) or skip stimulant doses to use illicit drugs or alcohol are more likely to sell their medication.34 Immediate-release stimulant formulations are more liable to be abused than extended-release drugs because they achieve earlier peak drug concentrations and dopamine blockade, indicating rapid drug absorption and central drug activity. Close monitoring and use of extended-release formulations are useful deterrents against stimulant abuse.
Clinical recommendations
Detecting and treating SUDs in patients with ADHD can be challenging. Ideally, the best time to assess for ADHD symptoms is after a prolonged abstinence from any influencing substance. However, in most clinical situations this is not practical. A better approach is a longitudinal assessment for ADHD symptoms. Detecting evidence of early childhood onset of ADHD symptoms before the patient began using substances can be helpful in conducting a proper differential diagnosis. Assessing for symptoms of SUDs in early adolescence, along with serial assessment of ADHD symptoms, also can be helpful. Symptoms secondary to ADHD are likely to show a consistent pattern, whereas symptoms secondary to an SUD may be sporadic.
When assessing SUD risk, consider the patient’s clinical condition, history of comorbidities that suggest SUDs, and overall functional status. Collateral information about the patient’s behavior and substance abuse from family members is important. A history of CD, bipolar disorder, or antisocial personality disorder should raise concerns about potential future stimulant abuse or diversion. Close monitoring of patients suspected of having an SUD is essential to detect stimulant abuse or diversion, which often manifests as weight loss, requests for higher doses, requests to switch from long-acting or extended-release formulations to immediate-release formulations, and repeated and suspicious “lost prescriptions.” Close observation for other subtle signs—such as changes in personality or mood and unexplained accidents or injuries—also may be needed.35
Challenges of treating ADHD and co-occurring SUD include poor medication adherence, need for a higher therapeutic stimulant dose, and difficulty in assessing the therapeutic benefit of pharmacotherapy in the presence of an SUD.36 Treating ADHD comorbid with SUD requires a collaborative approach that involves a psychiatrist, family members, and a behavioral care provider in addition to frequent monitoring.34
In the absence of treatment guidelines for treating ADHD with comorbid SUDs, some clinicians prefer to stabilize the SUD before initiating stimulants. Others prefer to use nonstimulants (such as atomoxetine, guanfacine, bupropion, venlafaxine, tricyclic antidepressants, or modafinil) as a first-line treatment. However, nonstimulants have not demonstrated efficacy comparable to that of stimulants for ADHD.35
Table 2 offers clinical recommendations to minimize the risk of SUDs when treating ADHD patients with stimulants. Long-acting stimulant formulations are preferred over short-acting medications because they are less likely to be abused. Psychosocial interventions for treating ADHD and co-occurring SUD disorder include cognitive-behavioral therapy with emphasis on structured skills training and cognitive remediation.
Table 2
Minimizing SUD risk when treating ADHD patients with stimulants
| Assess symptom burden and psychosocial impairment |
| Establish a treatment contract and boundaries at the onset of treatment, including your right to terminate treatment if you suspect stimulant misuse |
| Assess for comorbidities that may increase your patient’s SUD risk (see Table 1) |
| Emphasize strict adherence to treatment recommendations |
| Involve the patient’s family as much as possible |
| Obtain collateral information on the patient’s history of ADHD-related symptoms from parents, siblings, significant others, etc. |
| Distinguish between patients with substance use vs an SUD or a history of an SUD |
| Obtain urine toxicology screening as appropriate |
| Carefully document dispensed stimulants– strength of medication, number of capsules, pills, patches, etc. Note date of dispensation and refill dates |
| Select delayed- or extended-release stimulant formulations |
| Consider prescribing nonstimulants if appropriate |
| Use rating scales such as Conners Adult ADHD Rating Scale to monitor ADHD symptom severity and response to treatment |
| Schedule frequent, face-to-face clinical monitoring visits |
| ADHD: attention-deficit/hyperactivity disorder; SUD: substance use disorder |
Related Resource
- Faraone SV, Wilens T. Does stimulant treatment lead to substance use disorders? J Clin Psychiatry. 2003;64(suppl 11):9-13.
- Upadhyaya HP, Rose K, Wang W, et al. Attention deficit hyperactivity disorder medication and substance use patterns among adolescents and young adults. J Child Adolesc Psychopharmacol. 2005;15:799-809.
- Mariani JJ, Levin FR. Treatment strategies for co-occurring ADHD and substance use disorders. Am J Addict. 2007;16(suppl 1):45-56.
Drug Brand Names
- Atomoxetine • Strattera
- Bupropion • Wellbutrin, Zyban
- Guanfacine • Tenex, Intuniv
- Methylphenidate • Ritalin
- Modafinil • Provigil
- Venlafaxine • Effexor
Disclosures
Dr. Shailesh Jain and Dr. Islam report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Rakesh Jain has received research support from, is a consultant to, and/or is a speaker for Addrenex Pharmaceuticals, AstraZeneca, Eli Lilly and Company, Forest Pharmaceuticals, Merck, Pamlab, Pfizer Inc., Shionogi Inc., Shire, and Sunovion Pharmaceuticals.
Discuss this article at www.facebook.com/CurrentPsychiatry
Does prescribing stimulants to patients with attention-deficit/hyperactivity disorder (ADHD) increase their risk of future substance abuse? Because ADHD is a common pediatric condition with symptoms that often persist into adulthood, and stimulants are an efficacious first-line therapy, this possible association is a concern for psychiatrists whether they treat children or adults.
Some researchers have expressed concerns that stimulant exposure could predispose patients to future substance abuse.1 Proponents of the biologic model of “kindling” hypothesize early exposure to stimulants could increase the risk of later substance use disorders (SUDs) by modifying or “priming” the brain, which then becomes more receptive to illicit drug exposure. Although there is some evidence that stimulant use does increase SUD risk, other evidence suggests stimulant use does not increase susceptibility to SUDs2,3 and some studies have suggested stimulant use in ADHD patients may protect against SUDs.4,5
This article reviews shared characteristics of ADHD and SUDs and the latest research on the association between the clinical use of stimulants and later development of SUDs. We also offer clinical recommendations for assessing and treating ADHD and comorbid SUD.
ADHD/SUD overlap
Compared with those without the disorder, patients with ADHD have a 6.2 times higher risk of developing an SUD.6 Individuals with ADHD experience an earlier age of onset and a longer duration of SUDs.7 Several retrospective and prospective studies reveal ADHD is a risk factor for SUDs.8 A longitudinal study that tracked teenage males with or without ADHD into young adulthood found SUDs were 4 times more common among those with ADHD.9 Up to 45% of adults with ADHD have a history of alcohol abuse or dependence, and up to 30% have a history of illegal drug abuse or dependence.10
Conversely, an estimated 35% to 71% of alcohol abusers and 15% to 25% of substance-dependent patients have ADHD.11 Adults with ADHD and comorbid SUD report earlier onset12 and greater severity13 of substance abuse than adults without ADHD. Patients with ADHD experience earlier onset and higher rates of tobacco smoking by mid-adolescence.14
Developmental psychopathology. Longitudinal studies have suggested certain psychopathologic characteristics of ADHD can predispose an individual to SUDs independent of stimulant exposure. For example, inattention, impulsivity, and hyperactivity predispose an individual to develop an SUD and also are core symptoms of ADHD.15 Another study found impulsivity, impersistence, and difficulty sitting still at age 3 predicted alcohol abuse at age 21.16 A different longitudinal study found novelty-seeking behavior (restlessness, running/jumping and not keeping still, being squirmy and fidgety) between age 6 to 10 predicted adolescent drug abuse and cigarette smoking.17 Poor response inhibition is a key characteristic of ADHD and has been linked to adolescent drinking.18
ADHD may be an independent risk factor for SUD because a common neurobiologic psychopathology may predispose an individual to develop both conditions. The dopamine system has been implicated in SUD, and dysfunction in the dopaminergic circuits—mostly in basal and frontal cortex with consequent defects in executive function and reward system—also has been found in ADHD.19 Cognitive dysfunction associated with ADHD may decrease a patient’s ability to estimate the negative consequences of substance abuse and to delay immediate gratification from drug or alcohol use.
ADHD patients are more vulnerable to SUDs if they have a comorbid condition, such as oppositional defiant disorder,13,20 bipolar disorder,20,21 or conduct disorder (CD).20,22 Patients with ADHD and comorbid CD are estimated to be 8.8 times more likely to have an SUD before age 18 compared with those with ADHD alone.23 Comorbid ADHD and CD may increase patients’ predisposition to develop dependence on highly addictive drugs, such as cocaine or methamphetamine.24 Impaired executive function, behavioral dyscontrol, impulsivity, and peer rejection are common in both ADHD and CD and may increase the risk of developing SUDs in individuals who have both conditions.25 Other risk factors for SUDs in patients with ADHD are listed in Table 1.26
Table 1
Risk factors for SUDs in patients with ADHD
| Presence of comorbid conditions (ie, oppositional defiant disorder, conduct disorder, bipolar disorder, eating disorder) |
| White or Hispanic race |
| Partially treated or residual ADHD symptoms |
| Attending a competitive college program |
| College youth who had late onset of stimulant treatment |
| Member of a college sorority/fraternity |
| ADHD: attention-deficit/hyperactivity disorder; SUDs: substance use disorders Source: Reference 26 |
Stimulants’ affect on SUD risk
Increased risk. Limited studies suggest exposure to stimulants is a risk factor for developing SUDs. In a longitudinal study, Lambert et al27 followed 218 patients with ADHD and 182 without ADHD into adulthood and found a linear trend between duration of stimulant treatment and prevalence of cocaine dependence. ADHD patients exposed to stimulants for >1 year had the highest prevalence of cocaine abuse (27%), compared with untreated subjects (15%), or those treated with stimulants for <1 year (18%). However, the study did not control for comorbid contributing factors, such as CD.
No change. In a 10-year naturalistic study, Biederman et al28 followed 109 children with ADHD age 7 to 12 into adulthood. These children had a developmental reading disorder but no other psychiatric comorbidities. When comparing patients who were treated with methylphenidate (n = 43) with those who did not receive stimulants (n = 66), Bierderman et al found no significant difference between the 2 groups in the prevalence of SUD for any of the 7 drug categories studied.
Decreased risk. Two meta-analyses found children with ADHD who were treated with stimulants and followed until adolescence were 5.8 times less likely to develop SUDs compared with those who did not receive stimulants.28,29 This protective effect diminished when patients were followed into adulthood, but individuals treated with stimulants were 1.4 times less likely to develop SUDs than those not treated with stimulants.30 In a prospective case-control, 5-year follow-up study of 114 patients with ADHD treated with stimulants, Wilens et al31 found significant protective effects of stimulant treatment on the development of any SUD. They found no effects from time of onset or duration of stimulant therapy on subsequent risk of SUDs or cigarette smoking.
One possible explanation for stimulants’ apparently reduced protective effect among adults is for patients with ADHD, stimulant use might delay but not prevent SUDs. It also is likely that by adulthood, loss of parental supervision leads to poor medication adherence and increased susceptibility to SUDs.30
Other studies have found exposure to stimulants may protect against SUDs. Katusic et al23 reviewed medical records for documented SUDs in 295 adults with ADHD treated with stimulants and 84 who did not receive stimulants. They found 20% of patients who received stimulants had a documented SUD compared with 27% of those not treated with stimulants. Barkely et al32 followed 98 stimulant-treated and 21 untreated ADHD patients with a mean age of 15 and 21, respectively. They found stimulant treatment did not increase the risk for substance use or abuse in either group.
ADHD and stimulant abuse
The prevalence of stimulant misuse is as high as 9% in patients in grade school and high school and up to 35% in college-age individuals.33 ADHD patients who misuse stimulants (eg, escalating dose without authorization) or skip stimulant doses to use illicit drugs or alcohol are more likely to sell their medication.34 Immediate-release stimulant formulations are more liable to be abused than extended-release drugs because they achieve earlier peak drug concentrations and dopamine blockade, indicating rapid drug absorption and central drug activity. Close monitoring and use of extended-release formulations are useful deterrents against stimulant abuse.
Clinical recommendations
Detecting and treating SUDs in patients with ADHD can be challenging. Ideally, the best time to assess for ADHD symptoms is after a prolonged abstinence from any influencing substance. However, in most clinical situations this is not practical. A better approach is a longitudinal assessment for ADHD symptoms. Detecting evidence of early childhood onset of ADHD symptoms before the patient began using substances can be helpful in conducting a proper differential diagnosis. Assessing for symptoms of SUDs in early adolescence, along with serial assessment of ADHD symptoms, also can be helpful. Symptoms secondary to ADHD are likely to show a consistent pattern, whereas symptoms secondary to an SUD may be sporadic.
When assessing SUD risk, consider the patient’s clinical condition, history of comorbidities that suggest SUDs, and overall functional status. Collateral information about the patient’s behavior and substance abuse from family members is important. A history of CD, bipolar disorder, or antisocial personality disorder should raise concerns about potential future stimulant abuse or diversion. Close monitoring of patients suspected of having an SUD is essential to detect stimulant abuse or diversion, which often manifests as weight loss, requests for higher doses, requests to switch from long-acting or extended-release formulations to immediate-release formulations, and repeated and suspicious “lost prescriptions.” Close observation for other subtle signs—such as changes in personality or mood and unexplained accidents or injuries—also may be needed.35
Challenges of treating ADHD and co-occurring SUD include poor medication adherence, need for a higher therapeutic stimulant dose, and difficulty in assessing the therapeutic benefit of pharmacotherapy in the presence of an SUD.36 Treating ADHD comorbid with SUD requires a collaborative approach that involves a psychiatrist, family members, and a behavioral care provider in addition to frequent monitoring.34
In the absence of treatment guidelines for treating ADHD with comorbid SUDs, some clinicians prefer to stabilize the SUD before initiating stimulants. Others prefer to use nonstimulants (such as atomoxetine, guanfacine, bupropion, venlafaxine, tricyclic antidepressants, or modafinil) as a first-line treatment. However, nonstimulants have not demonstrated efficacy comparable to that of stimulants for ADHD.35
Table 2 offers clinical recommendations to minimize the risk of SUDs when treating ADHD patients with stimulants. Long-acting stimulant formulations are preferred over short-acting medications because they are less likely to be abused. Psychosocial interventions for treating ADHD and co-occurring SUD disorder include cognitive-behavioral therapy with emphasis on structured skills training and cognitive remediation.
Table 2
Minimizing SUD risk when treating ADHD patients with stimulants
| Assess symptom burden and psychosocial impairment |
| Establish a treatment contract and boundaries at the onset of treatment, including your right to terminate treatment if you suspect stimulant misuse |
| Assess for comorbidities that may increase your patient’s SUD risk (see Table 1) |
| Emphasize strict adherence to treatment recommendations |
| Involve the patient’s family as much as possible |
| Obtain collateral information on the patient’s history of ADHD-related symptoms from parents, siblings, significant others, etc. |
| Distinguish between patients with substance use vs an SUD or a history of an SUD |
| Obtain urine toxicology screening as appropriate |
| Carefully document dispensed stimulants– strength of medication, number of capsules, pills, patches, etc. Note date of dispensation and refill dates |
| Select delayed- or extended-release stimulant formulations |
| Consider prescribing nonstimulants if appropriate |
| Use rating scales such as Conners Adult ADHD Rating Scale to monitor ADHD symptom severity and response to treatment |
| Schedule frequent, face-to-face clinical monitoring visits |
| ADHD: attention-deficit/hyperactivity disorder; SUD: substance use disorder |
Related Resource
- Faraone SV, Wilens T. Does stimulant treatment lead to substance use disorders? J Clin Psychiatry. 2003;64(suppl 11):9-13.
- Upadhyaya HP, Rose K, Wang W, et al. Attention deficit hyperactivity disorder medication and substance use patterns among adolescents and young adults. J Child Adolesc Psychopharmacol. 2005;15:799-809.
- Mariani JJ, Levin FR. Treatment strategies for co-occurring ADHD and substance use disorders. Am J Addict. 2007;16(suppl 1):45-56.
Drug Brand Names
- Atomoxetine • Strattera
- Bupropion • Wellbutrin, Zyban
- Guanfacine • Tenex, Intuniv
- Methylphenidate • Ritalin
- Modafinil • Provigil
- Venlafaxine • Effexor
Disclosures
Dr. Shailesh Jain and Dr. Islam report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Rakesh Jain has received research support from, is a consultant to, and/or is a speaker for Addrenex Pharmaceuticals, AstraZeneca, Eli Lilly and Company, Forest Pharmaceuticals, Merck, Pamlab, Pfizer Inc., Shionogi Inc., Shire, and Sunovion Pharmaceuticals.
1. Lambert NM, McLeod M, Schenk S. Subjective responses to initial experience with cocaine: an exploration of the incentive-sensitization theory of drug abuse. Addiction. 2006;101(5):713-725.
2. Mannuzza S, Klein RG, Moulton JL. Does stimulant treatment place children at risk for adult substance abuse? A controlled prospective follow-up study. J Child Adolesc Psychopharmacol. 2003;13(3):273-282.
3. Katusic SK, Barbaresi WJ, Colligan RC, et al. Psychostimulant treatment and risk for substance abuse among young adults with a history of attention-deficit/hyperactivity disorder: a population-based, birth cohort study. J Child Adolesc Psychopharmacol. 2005;15(5):764-776.
4. Wilens TE, Faraone SV, Biederman J, et al. Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics. 2003;111(1):179-185.
5. Biederman J, Wilens T, Mick E, et al. Pharmacotherapy of attention-deficit/hyperactivity disorder reduces risk for substance use disorder. Pediatrics. 1999;104(2):e20.-
6. Katusic SK, Barbaresi WJ, Colligan RC, et al. Psychostimulant treatment and risk for substance abuse among young adults with a history of attention-deficit/hyperactivity disorder: a population-based, birth cohort study. J Child Adolesc Psychopharmacol. 2005;15(5):764-776.
7. Wilens TE. Impact of ADHD and its treatment on substance abuse in adults. J Clin Psychiatry. 2004;65(suppl 3):38-45.
8. Barkley RA, Fischer M, Smallish L, et al. Young adult follow-up of hyperactive children: antisocial activities and drug use. J Child Psychol Psychiatry. 2004;45(2):195-221.
9. Mannuzza S, Klein RG, Bessler A, et al. Adult outcome of hyperactive boys. Educational achievement, occupational rank, and psychiatric status. Arch Gen Psychiatry. 1993;50(7):565-576.
10. Wilens TE. Attention-deficit/hyperactivity disorder and the substance use disorders: the nature of the relationship subtypes at risk, and treatment issues. Psychiatr Clin North Am. 2004;27(2):283-301.
11. Wilens TE. AOD use and attention deficit/hyperactivity disorder. Alcohol Health Res World. 1998;22(2):127-130.
12. Wilens TE, Biederman J, Abrantes AM, et al. Clinical characteristics of psychiatrically referred adolescent outpatients with substance use disorder. J Am Acad Child Adolesc Psychiatry. 1997;36(7):941-947.
13. Schubiner H, Tzelepis A, Milberger S, et al. Prevalence of attention-deficit/hyperactivity disorder and conduct disorder among substance abusers. J Clin Psychiatry. 2000;61(4):244-251.
14. Lambert NM, Hartsough CS. Prospective study of tobacco smoking and substance dependencies among samples of ADHD and non-ADHD participants. J Learn Disabil. 1998;31(6):533-544.
15. Zucker RA. Alcohol use and the alcohol use disorders: a developmental biopsychosocial systems formulation covering the life course. In: Cicchetti D Cohen D, eds. Developmental psychopathology. 2nd ed. Hoboken, NJ: John Wiley & Sons Inc; 2006;620-656.
16. Caspi A, Moffitt TE, Newman DL, et al. Behavioral observations at age 3 years predict adult psychiatric disorders. Longitudinal evidence from a birth cohort. Arch Gen Psychiatry. 1996;53(11):1033-1039.
17. Màsse LC, Tremblay RE. Behavior of boys in kindergarten and the onset of substance use during adolescence. Arch Gen Psychiatry. 1997;54(1):62-68.
18. Nigg JT, Wong MM, Martel MM, et al. Poor response inhibition as a predictor of problem drinking and illicit drug use in adolescents at risk for alcoholism and other substance use disorders. J Am Acad Child Adolesc Psychiatry. 2006;45(4):468-475.
19. Seidman LJ, Valera EM, Makris N. Structural brain imaging of attention-deficit hyperactivity disorder. Biol Psychiatry. 2005;57(11):1263-1272.
20. Biederman J, Wilens T, Mick E, et al. Is ADHD a risk factor for psychoactive substance use disorders? Findings from a four-year prospective follow-up study. J Am Acad Child Adolesc Psychiatry. 1997;36(1):21-29.
21. Wilens TE, Biederman J, Millstein RB, et al. Risk for substance use disorders in youths with child- and adolescent-onset bipolar disorder. J Am Acad Child Adolesc Psychiatry. 1999;38(6):680-685.
22. Schubiner H, Saules KK, Arfken CL, et al. Double-blind placebo-controlled trial of methylphenidate in the treatment of adult ADHD patients with comorbid cocaine dependence. Exp Clin Psychopharmacol. 2002;10(3):286-294.
23. Katusic SK, Barbaresi WJ, Colligan RC, et al. Psychostimulant treatment and risk for substance abuse among young adults with a history of attention-deficit/hyperactivity disorder: a population-based, birth cohort study. J Child Adolesc Psychopharmacol. 2005;15(5):764-776.
24. Flory K, Milich R, Lynam DR, et al. Relation between childhood disruptive behavior disorders and substance use and dependence symptoms in young adulthood: individuals with symptoms of attention-deficit/hyperactivity disorder and conduct disorder are uniquely at risk. Psychol Addict Behav. 2003;17(2):151-158.
25. Wilens TE. Attention-deficit/hyperactivity disorder and the substance use disorders: the nature of the relationship subtypes at risk, and treatment issues. Psychiatr Clin North Am. 2004;27(2):283-301.
26. Wilson JJ. ADHD and substance use disorders: developmental aspects and the impact of stimulant treatment. Am J Addict. 2007;16(suppl 1):5-11.
27. Lambert NM, Hartsough CS. Prospective study of tobacco smoking and substance dependencies among samples of ADHD and non-ADHD participants. J Learn Disabil. 1998;31(6):533-544.
28. Biederman J, Monuteaux MC, Spencer T, et al. Stimulant therapy and risk for subsequent substance use disorders in male adults with ADHD: a naturalistic controlled 10-year follow-up study. Am J Psychiatry. 2008;165(5):597-603.
29. Wilens TE, Faraone SV, Biederman J, et al. Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics. 2003;111(1):179-185.
30. Faraone SV, Wilens TE. Effect of stimulant medications for attention-deficit/hyperactivity disorder on later substance use and the potential for stimulant misuse abuse, and diversion. J Clin Psychiatry. 2007;68(suppl 11):15-22.
31. Wilens TE, Adamson J, Monuteaux MC, et al. Effect of prior stimulant treatment for attention-deficit/hyperactivity disorder on subsequent risk for cigarette smoking and alcohol and drug use disorders in adolescents. Arch Pediatr Adolesc Med. 2008;162(10):916-921.
32. Barkley RA, Fischer M, Smallish L, et al. Does the treatment of attention-deficit/hyperactivity disorder with stimulants contribute to drug use/abuse? A 13-year prospective study. Pediatrics. 2003;111(1):97-109.
33. Wilens TE, Adler LA, Adams J, et al. Misuse and diversion of stimulants prescribed for ADHD: a systematic review of the literature. J Am Acad Child Adolesc Psychiatry. 2008;47(1):21-31.
34. Upadhyaya HP, Rose K, Wang W, et al. Attention-deficit/hyperactivity disorder, medication treatment, and substance use patterns among adolescents and young adults. J Child Adolesc Psychopharmacol. 2005;15(5):799-809.
35. Kollins SH. A qualitative review of issues arising in the use of psycho-stimulant medications in patients with ADHD and co-morbid substance use disorders. Curr Med Res Opin. 2008;24(5):1345-1357.
36. Faraone SV, Biederman J, Wilens TE, et al. A naturalistic study of the effects of pharmacotherapy on substance use disorders among ADHD adults. Psychol Med. 2007;37(12):1743-1752.
1. Lambert NM, McLeod M, Schenk S. Subjective responses to initial experience with cocaine: an exploration of the incentive-sensitization theory of drug abuse. Addiction. 2006;101(5):713-725.
2. Mannuzza S, Klein RG, Moulton JL. Does stimulant treatment place children at risk for adult substance abuse? A controlled prospective follow-up study. J Child Adolesc Psychopharmacol. 2003;13(3):273-282.
3. Katusic SK, Barbaresi WJ, Colligan RC, et al. Psychostimulant treatment and risk for substance abuse among young adults with a history of attention-deficit/hyperactivity disorder: a population-based, birth cohort study. J Child Adolesc Psychopharmacol. 2005;15(5):764-776.
4. Wilens TE, Faraone SV, Biederman J, et al. Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics. 2003;111(1):179-185.
5. Biederman J, Wilens T, Mick E, et al. Pharmacotherapy of attention-deficit/hyperactivity disorder reduces risk for substance use disorder. Pediatrics. 1999;104(2):e20.-
6. Katusic SK, Barbaresi WJ, Colligan RC, et al. Psychostimulant treatment and risk for substance abuse among young adults with a history of attention-deficit/hyperactivity disorder: a population-based, birth cohort study. J Child Adolesc Psychopharmacol. 2005;15(5):764-776.
7. Wilens TE. Impact of ADHD and its treatment on substance abuse in adults. J Clin Psychiatry. 2004;65(suppl 3):38-45.
8. Barkley RA, Fischer M, Smallish L, et al. Young adult follow-up of hyperactive children: antisocial activities and drug use. J Child Psychol Psychiatry. 2004;45(2):195-221.
9. Mannuzza S, Klein RG, Bessler A, et al. Adult outcome of hyperactive boys. Educational achievement, occupational rank, and psychiatric status. Arch Gen Psychiatry. 1993;50(7):565-576.
10. Wilens TE. Attention-deficit/hyperactivity disorder and the substance use disorders: the nature of the relationship subtypes at risk, and treatment issues. Psychiatr Clin North Am. 2004;27(2):283-301.
11. Wilens TE. AOD use and attention deficit/hyperactivity disorder. Alcohol Health Res World. 1998;22(2):127-130.
12. Wilens TE, Biederman J, Abrantes AM, et al. Clinical characteristics of psychiatrically referred adolescent outpatients with substance use disorder. J Am Acad Child Adolesc Psychiatry. 1997;36(7):941-947.
13. Schubiner H, Tzelepis A, Milberger S, et al. Prevalence of attention-deficit/hyperactivity disorder and conduct disorder among substance abusers. J Clin Psychiatry. 2000;61(4):244-251.
14. Lambert NM, Hartsough CS. Prospective study of tobacco smoking and substance dependencies among samples of ADHD and non-ADHD participants. J Learn Disabil. 1998;31(6):533-544.
15. Zucker RA. Alcohol use and the alcohol use disorders: a developmental biopsychosocial systems formulation covering the life course. In: Cicchetti D Cohen D, eds. Developmental psychopathology. 2nd ed. Hoboken, NJ: John Wiley & Sons Inc; 2006;620-656.
16. Caspi A, Moffitt TE, Newman DL, et al. Behavioral observations at age 3 years predict adult psychiatric disorders. Longitudinal evidence from a birth cohort. Arch Gen Psychiatry. 1996;53(11):1033-1039.
17. Màsse LC, Tremblay RE. Behavior of boys in kindergarten and the onset of substance use during adolescence. Arch Gen Psychiatry. 1997;54(1):62-68.
18. Nigg JT, Wong MM, Martel MM, et al. Poor response inhibition as a predictor of problem drinking and illicit drug use in adolescents at risk for alcoholism and other substance use disorders. J Am Acad Child Adolesc Psychiatry. 2006;45(4):468-475.
19. Seidman LJ, Valera EM, Makris N. Structural brain imaging of attention-deficit hyperactivity disorder. Biol Psychiatry. 2005;57(11):1263-1272.
20. Biederman J, Wilens T, Mick E, et al. Is ADHD a risk factor for psychoactive substance use disorders? Findings from a four-year prospective follow-up study. J Am Acad Child Adolesc Psychiatry. 1997;36(1):21-29.
21. Wilens TE, Biederman J, Millstein RB, et al. Risk for substance use disorders in youths with child- and adolescent-onset bipolar disorder. J Am Acad Child Adolesc Psychiatry. 1999;38(6):680-685.
22. Schubiner H, Saules KK, Arfken CL, et al. Double-blind placebo-controlled trial of methylphenidate in the treatment of adult ADHD patients with comorbid cocaine dependence. Exp Clin Psychopharmacol. 2002;10(3):286-294.
23. Katusic SK, Barbaresi WJ, Colligan RC, et al. Psychostimulant treatment and risk for substance abuse among young adults with a history of attention-deficit/hyperactivity disorder: a population-based, birth cohort study. J Child Adolesc Psychopharmacol. 2005;15(5):764-776.
24. Flory K, Milich R, Lynam DR, et al. Relation between childhood disruptive behavior disorders and substance use and dependence symptoms in young adulthood: individuals with symptoms of attention-deficit/hyperactivity disorder and conduct disorder are uniquely at risk. Psychol Addict Behav. 2003;17(2):151-158.
25. Wilens TE. Attention-deficit/hyperactivity disorder and the substance use disorders: the nature of the relationship subtypes at risk, and treatment issues. Psychiatr Clin North Am. 2004;27(2):283-301.
26. Wilson JJ. ADHD and substance use disorders: developmental aspects and the impact of stimulant treatment. Am J Addict. 2007;16(suppl 1):5-11.
27. Lambert NM, Hartsough CS. Prospective study of tobacco smoking and substance dependencies among samples of ADHD and non-ADHD participants. J Learn Disabil. 1998;31(6):533-544.
28. Biederman J, Monuteaux MC, Spencer T, et al. Stimulant therapy and risk for subsequent substance use disorders in male adults with ADHD: a naturalistic controlled 10-year follow-up study. Am J Psychiatry. 2008;165(5):597-603.
29. Wilens TE, Faraone SV, Biederman J, et al. Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics. 2003;111(1):179-185.
30. Faraone SV, Wilens TE. Effect of stimulant medications for attention-deficit/hyperactivity disorder on later substance use and the potential for stimulant misuse abuse, and diversion. J Clin Psychiatry. 2007;68(suppl 11):15-22.
31. Wilens TE, Adamson J, Monuteaux MC, et al. Effect of prior stimulant treatment for attention-deficit/hyperactivity disorder on subsequent risk for cigarette smoking and alcohol and drug use disorders in adolescents. Arch Pediatr Adolesc Med. 2008;162(10):916-921.
32. Barkley RA, Fischer M, Smallish L, et al. Does the treatment of attention-deficit/hyperactivity disorder with stimulants contribute to drug use/abuse? A 13-year prospective study. Pediatrics. 2003;111(1):97-109.
33. Wilens TE, Adler LA, Adams J, et al. Misuse and diversion of stimulants prescribed for ADHD: a systematic review of the literature. J Am Acad Child Adolesc Psychiatry. 2008;47(1):21-31.
34. Upadhyaya HP, Rose K, Wang W, et al. Attention-deficit/hyperactivity disorder, medication treatment, and substance use patterns among adolescents and young adults. J Child Adolesc Psychopharmacol. 2005;15(5):799-809.
35. Kollins SH. A qualitative review of issues arising in the use of psycho-stimulant medications in patients with ADHD and co-morbid substance use disorders. Curr Med Res Opin. 2008;24(5):1345-1357.
36. Faraone SV, Biederman J, Wilens TE, et al. A naturalistic study of the effects of pharmacotherapy on substance use disorders among ADHD adults. Psychol Med. 2007;37(12):1743-1752.
Strategies to help patients break the chains of tobacco addiction
Discuss this article at www.facebook.com/CurrentPsychiatry
You are treating Mr. P, age 34, for schizoaffective disorder. He smokes 1 pack of cigarettes per day and has smoked for approximately 17 years. He has tried to stop but never has been able to quit for more than a few weeks. He reveals whenever he tries to quit, he starts feeling extremely lethargic and “depressed” and resumes smoking to prevent these symptoms from worsening. However, Mr. P expresses some interest in trying to quit again and asks whether any medications could prevent him from becoming depressed while he tries to quit.
Cigarette smoking is overrepresented and undertreated among individuals with psychiatric illness, in part because of the largely unfounded belief held by some patients and clinicians that smoking cessation might worsen psychiatric symptoms. In this article, we argue this challenge can be overcome and psychiatrists and other mental health professionals can and should help their patients reap the innumerable benefits of quitting smoking. We discuss:
- the short- and long-term effects of smoking cessation
- evidence-based treatment guidelines for working with motivated and unmotivated smokers
- unique issues that may arise when treating smokers who have psychiatric disorders.
Quitting: Profound benefits
Quitting smoking has substantial benefits beginning within minutes after taking the last puff. Some of the benefits that occur within the first few days of quitting include:
- decreased blood pressure and pulse rate
- improved circulation
- improved ability to smell and taste
- easier breathing.
Longer-term smoking abstinence drastically reduces risk of heart attack, stroke, cancer, respiratory disease, and a host of other illnesses that affect—and kill—individuals with psychiatric disorders several decades earlier than their counterparts in the general population.1 There also are financial benefits to quitting; using the 2009 national average of $5.33 per pack, a 1-pack-per-day smoker who quits would save >$150 per month, which accounts for only the direct cost of cigarettes.2
Although the beneficial effects of quitting smoking are profound and far-reaching, in the short-term they are counterbalanced by nicotine withdrawal symptoms—including restlessness, irritability, depressed mood, concentration problems, and increased appetite/weight gain—that are formidable distractions from the positive aspects of quitting. Additionally, nicotine withdrawal symptoms tend to be more severe in smokers who have a psychiatric disorder.3 Fortunately, there are effective, evidence-based methods of reducing withdrawal symptoms and helping smokers cope with these and other challenges of quitting.
Combined treatment is best
Current treatment guidelines4 suggest all smokers should be offered pharmacotherapy and counseling to aid quitting because this combined approach has the highest success rate (Algorithm). Table 1 4 provides information about dosing, efficacy, and side effect profile of each of the 7 FDA-approved medications for smoking cessation. Using any of the approved medications at least doubles the odds of successful quitting compared with placebo.4 These pharmacotherapies can reduce or prevent nicotine withdrawal symptoms and—at least in the case of bupropion and varenicline—decrease reinforcement from smoking, thereby lowering the likelihood a lapse (ie, smoking ≥1 cigarettes without returning to regular smoking) will develop into a full-blown relapse (ie, return to regular smoking).
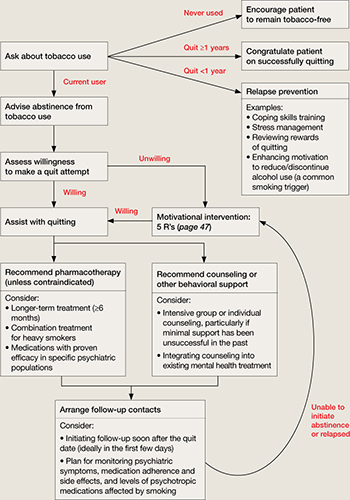
Algorithm: Tobacco cessation treatment for psychiatric patients
Source: Adapted from reference 4 Medication selection depends on many factors, including:
- the patient’s psychiatric illness
- her/his prior response to smoking cessation pharmacotherapies
- concomitant psychiatric medications
- patient preference.5
Placebo-controlled trials of smoking cessation aids in psychiatrically ill patients are limited, but several studies of smokers with a history of major depression indicate treatment with bupropion SR or nortriptyline is effective.6 Similarly, although relapse rates generally are higher in patients with schizophrenia compared with non-mentally ill smokers, nicotine replacement therapy and bupropion SR are more effective than placebo in patients with this disorder.7,8 When we prescribe these treatments, we tend to extend the duration of treatment beyond those described in Table 1 ,4 and to use combined treatments (eg, a transdermal patch with a shorter-acting gum or lozenge preparation) to better target the marked withdrawal symptoms more severely nicotine-dependent patients frequently experience.
Table 1
First-line pharmacotherapies for smoking cessation
| Medication | Standard dosage | Efficacy (OR, % abstinent at 6 mos. [with 95% CI]) | Contraindications (C) and precautions (P) | Common side effects |
|---|---|---|---|---|
| Non-nicotine medications | ||||
| Bupropion | Days 1-3: 150 mg/d Days 4-8: 150 mg bid Continue for 7-12 weeks at 150 mg bid | 2.0 (1.8-2.2), 24% (22%-26%) | C: Eating disorders, seizure history, taking bupropion, MAOI in past 2 weeks P: Pregnancy, cardiovascular disease, warning for emergent psychiatric symptoms | Insomnia, dry mouth |
| Varenicline | Days 1-3: 0.5 mg/d Days 4-7: 0.5 mg bid Day 8+: 1 mg bid Continue 11 weeks at 1 mg bid; up to 6 months for maintenance | 3.1 (2.5-3.8), 33% (29%-38%) | P: Warning for emergent psychiatric symptoms | Nausea, sleep problems, abnormal dreams |
| Nicotine replacement therapies | ||||
| Nicotine gum | 1 piece every 1-2 hours for 6-12 weeks <20 cigarettes/d: 2 mg gum ≥20 cigarettes/d: 4 mg gum | 1.5 (1.2-1.7), 19% (17%-22%) | P: Pregnancy, recent myocardial infarction, serious arrhythmia, unstable angina | Mouth soreness, hiccups, dyspepsia |
| Nicotine inhaler | 6-16 cartridges/d, up to 6 months | 2.1 (1.5-2.9), 25% (19%-32%) | Same as above | Mouth/throat irritation, coughing, rhinitis |
| Nicotine lozenge | 9-20 lozenges/d, up to 12 weeks Smoke ≤30 minutes after waking: 4 mg lozenge Smoke >30 minutes after waking: 2 mg lozenge | 2.0 (1.6-2.5)a | Same as above | Nausea, hiccups, heartburn |
| Nicotine nasal spray | 1-2 doses/hour, 8-40 doses/d for 3-6 months | 2.3 (1.7-3.0), 27% (22%-33%) | C: Severe reactive airway disease P: Same as above | Nasal irritation, higher risk of dependency |
| Nicotine patch | 1 patch/d, step-down dosing over 8 weeks Weeks 1-4: 21 mg patch Weeks 5-6: 14 mg patch Weeks 7-8: 7 mg patch | 1.9 (1.7-2.2) 23% (21%-26%) | P: Same as above | Skin reactions, sleep problems, abnormal dreams |
| aStead LF, Perera R, Bullen C, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2008;1:CD000146. bid: twice a day; CI: confidence interval; MAOI: monoamine oxidase inhibitor; OR: odds ratio Source: Adapted from reference 4 | ||||
Counseling. All smokers should be provided with brief interventions consistent with the 5 A’s—Ask, Advise, Assess, Assist, and Arrange (Table 2).4 For smokers who are not motivated to quit, the recommended approach follows the principles of the 5 R’s—Relevance, Risks, Rewards, Roadblocks, and Repetition (Table 3).4 Smokers who are motivated to quit and willing to participate in more intensive treatment may be offered face-to-face individual or group counseling (depending upon availability) or referred to a telephone quit line (see Related Resources). Intensive treatments such as these typically provide social support and assistance overcoming barriers to cessation and developing skills to initiate and maintain abstinence (eg, coping with a lapse or handling cravings, identifying and avoiding high-risk situations for smoking). As a general rule, greater intensity of counseling is associated with a greater likelihood of quitting.4
Table 2
The 5 A’s of tobacco treatment
| Intervention | Example | |
|---|---|---|
| Ask | Systematically inquire about tobacco use | “Do you currently use, or have you ever used, tobacco products?” |
| Advise | Counsel all tobacco users to quit in a clear, strong, and personalized manner | “I think it is very important for you quit smoking to keep your breathing problems from getting any worse” |
| Assess | Determine the tobacco user’s willingness to make a quit attempt | “What do you think? Are you ready to quit?” |
| Assist | Offer or refer to treatment/support (if ready to quit; if not ready, see Table 3 for recommended interventions) | “I’m here to help you with this. Let me start by letting you know about the many options available to help you quit” |
| Arrange | Plan for follow-up contacts (at least 1, preferably within 1 week of the quit date) | “I would like to give you a call within the next week to see how you did with your quit date. Would that be OK with you?” |
| Source: Adapted from reference 4 | ||
Table 3
The 5 R’s: Principles of interventions for smokers not ready to quit
| Principle | Example | |
|---|---|---|
| Relevance | Why is quitting smoking personally relevant? | “You’ve told me your kids sometimes make comments to you about quitting smoking. How does that affect you?” |
| Risks | What are the negative consequences of smoking? | “What don’t you like about smoking? What problems have you had from smoking?” |
| Rewards | What are the benefits of quitting smoking? | “Can you think of anything that would be good about quitting? Tell me about that” |
| Roadblocks | What are the barriers to quitting? | “What worries do you have about trying to quit? What happened the last time you tried to quit smoking?” |
| Repetition | Message repeated at every visit | “I know we have talked about quitting smoking before, but things may have changed since then. I also think that this is such an important issue we should keep it on the table for discussion. What do you think?” |
| Source: Adapted from reference 4 | ||
Q&A about treatment
How effective are smoking cessation interventions for individuals with psychiatric disorders? Several studies have demonstrated, on any given quit attempt, smokers with psychiatric or substance use disorders can be as successful as smokers without these disorders.9-11 In fact, quit rates as high as approximately 70% for end-of-treatment11 and 30% for 6-month follow-up10 have been reported. Of course, effectiveness varies by type and intensity of treatment as well as by individual characteristics of the smoker. Smokers with psychiatric disorders may fare better with more intensive interventions than briefer ones,12,13 and factors such as high levels of nicotine dependence and exposure to smoking environments—both of which are characteristic of smokers with serious mental illness—can negatively impact treatment outcomes.4
Should the nature of the psychiatric disorder(s) guide decisions about the optimal pharmacotherapy or counseling approach? There have been numerous attempts to investigate the effectiveness of targeted interventions for particular subgroups of smokers with psychiatric disorders, including:
- studies of the efficacy of the antidepressants bupropion14 and nortriptyline15 as well as cognitive-behavioral therapy-based mood management counseling16 for depressed smokers
- integrative treatment approaches for smokers with posttraumatic stress disorder (PTSD)17
- group counseling designed specifically for smokers with schizophrenia.18,19
Although more research is needed and there have been some promising early results (eg, McFall et al17), current literature does not provide consistent evidence supporting treatment matching solely on the basis of the psychiatric disorder. Rather, patient preference, safety considerations (eg, use of medications in children/adolescents, pregnant women), medication side effect profiles, prior experience with the treatment approach, and cost/availability of treatment should guide development of the treatment plan. When results from placebo-controlled trials are available for subgroups of patients (eg, those with a history of major depression), consider this information when selecting a pharmacologic smoking cessation aid.
What is the risk of psychiatric symptoms worsening as a result of quitting smoking? Little research on this topic is available because more often than not, smokers with psychiatric disorders are excluded from tobacco treatment studies. However, research examining psychiatric status changes among recent quitters with schizophrenia,20,21 depression,22,23 PTSD,17 and substance use disorders24 suggests smoking cessation does not worsen symptoms of these disorders, and may be associated with symptom improvement.17 Nonetheless, driven largely by anecdotal evidence, the misconception that smoking cessation worsens psychiatric symptoms remains a substantial barrier to treatment.
Mr. P’s case is an example of how not probing about the nature of psychiatric complaints can be problematic. Mr. P reported what on first glance appeared to be a worsening of psychiatric symptoms starting when he stopped smoking and resolved when he resumed smoking. However, without gathering additional information about these events, we cannot conclude stopping smoking caused his psychiatric symptoms to worsen. Other potential explanations include nicotine withdrawal symptoms, side effects of smoking cessation medications, an increase in levels of psychotropic medications for which metabolism is affected by tobacco smoke, or the natural course of his mood disorder. The timing of the onset and offset of symptoms seems to argue against Mr. P’s symptoms reflecting the natural course of his mood disorder, but the other 3 explanations remain plausible.
It is important to distinguish whether Mr. P’s worsening symptoms are consistent with a depressive episode or whether they are a manifestation of the transient dysphoria that accompanies nicotine withdrawal. Assessing the severity and persistence of the mood disturbance as well as the timing of onset could help make this determination. Nicotine withdrawal symptoms typically emerge within 24 hours of quitting or significantly reducing smoking and tend to peak within approximately 1 week. Thus, depressive symptoms that develop after weeks or months of abstinence would be less consistent with nicotine withdrawal. Additionally, the lethargy Mr. P reported may be a symptom of depression, or it may stem from a cessation-induced increase in antipsychotic serum levels. Because tobacco smoke increases the metabolism of several antipsychotics and antidepressants—including olanzapine, clozapine, haloperidol, and fluoxetine25—stopping smoking may increase medication levels and side effects. To rule out medication side effects as a cause of post-cessation mood changes, the psychiatrist should ask Mr. P about which smoking cessation pharmacotherapies (if any) he was using and which psychotropic medications he was taking. Unfortunately, such a detailed history is not always taken, and patient-generated theories of smoking cessation causing worsening psychiatric symptoms often are taken at face value.
When should smokers with psychiatric disorders be encouraged to quit? Are there times when smoking cessation should be discouraged? Tobacco treatment guidelines4 recommend advising users to quit at every clinical encounter, but there has been some debate about the timing of tobacco treatment for smokers with psychiatric disorders. There is minimal research to guide such treatment decisions. However, even if quit attempts are more successful during times of symptomatic stability—and there is no conclusive evidence to indicate they are—waiting for perfect mental health before initiating smoking cessation treatment is unnecessary and ill-advised. In some situations, such as when a patient has experienced an acute increase in psychiatric symptoms or when psychotropics are being titrated, a short-term postponement of quitting may be reasonable. However, discouraging smokers from trying to quit when they express readiness to try should be done sparingly, because it is uncertain how long that window of opportunity will be open, and the consequences of missed opportunities can be fatal.
- National Tobacco Quitline. 1-800-QUIT-NOW. www.smokefree.gov.
- University of California, San Francisco, Schools of Pharmacy and Medicine. Rx for Change (free online training program for clinicians). http://rxforchange.ucsf.edu.
- National Association of State Mental Health Program Directors. Tobacco-free living in psychiatric settings: a best-practices toolkit promoting wellness and recovery. www.nasmhpd.org/general_files/publications/NASMHPD.toolkitfinalupdated90707.pdf.
Drug Brand Names
- Bupropion • Wellbutrin, Zyban
- Clozapine • Clozaril
- Fluoxetine • Prozac
- Haloperidol • Haldol
- Nortriptyline • Aventyl, Pamelor
- Olanzapine • Zyprexa
- Varenicline • Chantix
Disclosures
Dr. Heffner was supported by National Institute on Drug Abuse grant#026517. She is a consultant to Pfizer Inc.
Dr. Anthenelli is supported by National Institute on Alcohol Abuse and Alcoholism grant#AA19720 and by the Department of Veterans Affairs. He is a consultant to GlaxoSmithKline and Pfizer Inc.
The Tri-State Tobacco and Alcohol Research Center receives research support from Eli Lilly and Company, Nabi Biopharmaceuticals, Pfizer Inc., and sanofi-aventis.
1. Colton CW, Manderscheid RW. Congruencies in increased mortality rates years of potential life lost, and causes of death among public mental health clients in eight states. Prev Chronic Dis. 2006;3(2):A42.-
2. Centers for Disease Control and Prevention. Trends in state and federal cigarette tax and retail price—1970-2009. 2010. Available at: http://www.cdc.gov/tobacco/data_statistics/tables/economics/trends. Accessed June 28 2011.
3. Xian H, Scherrer JF, Eisen SA, et al. Nicotine dependence subtypes: association with smoking history, diagnostic criteria and psychiatric disorders in 5440 regular smokers from the Vietnam Era Twin Registry. Addict Behav. 2007;32(1):137-147.
4. Fiore MC, Jaén CR, Baker TB, et al. A clinical practice guideline for treating tobacco use and dependence: 2008 update. A U. S. Public Health Service report. Am J Prev Med. 2008;35(2):158-176.
5. Anthenelli RM. How–and why–to help psychiatric patients stop smoking. Current Psychiatry. 2005;4(1):77-87.
6. Hughes JR, Stead LF, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2007;1:CD000031.-
7. Williams JM, Foulds J. Successful tobacco dependence treatment in schizophrenia. Am J Psychiatry. 2007;164(2):222-227.
8. George TP, Vessicchio JC, Termine A, et al. A placebo controlled trial of bupropion for smoking cessation in schizophrenia. Biol Psychiatry. 2002;52(1):53-61.
9. Hughes JR, Kalman D. Do smokers with alcohol problems have more difficulty quitting? Drug Alcohol Depend. 2006;82(2):91-102.
10. McClure JB, Swan GE, Catz SL, et al. Smoking outcome by psychiatric history after behavioral and varenicline treatment. J Subst Abuse Treat. 2010;38(4):394-402.
11. Stapleton JA, Watson L, Spirling LI, et al. Varenicline in the routine treatment of tobacco dependence: a pre-post comparison with nicotine replacement therapy and an evaluation in those with mental illness. Addiction. 2008;103(1):146-154.
12. Hall SM, Muñoz RF, Reus VI. Cognitive-behavioral intervention increases abstinence rates for depressive-history smokers. J Consult Clin Psychol. 1994;62(1):141-146.
13. Hall SM, Muñoz RF, Reus VI, et al. Mood management and nicotine gum in smoking treatment: a therapeutic contact and placebo-controlled study. J Consult Clin Psychol. 1996;64(5):1003-1009.
14. Evins AE, Culhane MA, Alpert JE, et al. A controlled trial of bupropion added to nicotine patch and behavioral therapy for smoking cessation in adults with unipolar depressive disorders. J Clin Psychopharmacol. 2008;28(6):660-666.
15. Hall SM, Reus VI, Muñoz RF, et al. Nortriptyline and cognitive-behavioral therapy in the treatment of cigarette smoking. Arch Gen Psychiatry. 1998;55(8):683-690.
16. Brown RA, Kahler CW, Niaura R, et al. Cognitive-behavioral treatment for depression in smoking cessation. J Consult Clin Psychol. 2001;69(3):471-480.
17. McFall M, Saxon AJ, Malte CA, et al. Integrating tobacco cessation into mental health care for posttraumatic stress disorder: a randomized controlled trial. JAMA. 2010;304(22):2485-2493.
18. George TP, Ziedonis DM, Feingold A, et al. Nicotine transdermal patch and atypical antipsychotic medications for smoking cessation in schizophrenia. Am J Psychiatry. 2000;157(11):1835-1842.
19. Williams JM, Steinberg ML, Zimmermann MH, et al. Comparison of two intensities of tobacco dependence counseling in schizophrenia and schizoaffective disorder. J Subst Abuse Treat. 2010;38(4):384-393.
20. Evins AE, Cather C, Culhane MA, et al. A 12-week double-blind, placebo-controlled study of bupropion sr added to high-dose dual nicotine replacement therapy for smoking cessation or reduction in schizophrenia. J Clin Psychopharmacol. 2007;27(4):380-386.
21. Weinberger AH, Hitsman B, Papandonatos GD, et al. Predictors of abstinence and changes in psychiatric symptoms in a pooled sample of smokers with schizophrenia receiving combination pharmacotherapy and behavioral therapy for smoking cessation. J Clin Psychopharmacol. 2009;29(6):601-603.
22. Prochaska JJ, Hall SM, Tsoh JY, et al. Treating tobacco dependence in clinically depressed smokers: effect of smoking cessation on mental health functioning. Am J Public Health. 2008;98(3):446-448.
23. Tsoh JY, Humfleet GL, Muñoz RF, et al. Development of major depression after treatment for smoking cessation. Am J Psychiatry. 2000;157(3):368-374.
24. Prochaska JJ, Delucchi K, Hall SM. A meta-analysis of smoking cessation interventions with individuals in substance abuse treatment or recovery. J Consult Clin Psychol. 2004;72(6):1144-1156.
25. Zevin S, Benowitz NL. Drug interactions with tobacco smoking. An update. Clin Pharmacokinet. 1999;36(6):425-438.
Discuss this article at www.facebook.com/CurrentPsychiatry
You are treating Mr. P, age 34, for schizoaffective disorder. He smokes 1 pack of cigarettes per day and has smoked for approximately 17 years. He has tried to stop but never has been able to quit for more than a few weeks. He reveals whenever he tries to quit, he starts feeling extremely lethargic and “depressed” and resumes smoking to prevent these symptoms from worsening. However, Mr. P expresses some interest in trying to quit again and asks whether any medications could prevent him from becoming depressed while he tries to quit.
Cigarette smoking is overrepresented and undertreated among individuals with psychiatric illness, in part because of the largely unfounded belief held by some patients and clinicians that smoking cessation might worsen psychiatric symptoms. In this article, we argue this challenge can be overcome and psychiatrists and other mental health professionals can and should help their patients reap the innumerable benefits of quitting smoking. We discuss:
- the short- and long-term effects of smoking cessation
- evidence-based treatment guidelines for working with motivated and unmotivated smokers
- unique issues that may arise when treating smokers who have psychiatric disorders.
Quitting: Profound benefits
Quitting smoking has substantial benefits beginning within minutes after taking the last puff. Some of the benefits that occur within the first few days of quitting include:
- decreased blood pressure and pulse rate
- improved circulation
- improved ability to smell and taste
- easier breathing.
Longer-term smoking abstinence drastically reduces risk of heart attack, stroke, cancer, respiratory disease, and a host of other illnesses that affect—and kill—individuals with psychiatric disorders several decades earlier than their counterparts in the general population.1 There also are financial benefits to quitting; using the 2009 national average of $5.33 per pack, a 1-pack-per-day smoker who quits would save >$150 per month, which accounts for only the direct cost of cigarettes.2
Although the beneficial effects of quitting smoking are profound and far-reaching, in the short-term they are counterbalanced by nicotine withdrawal symptoms—including restlessness, irritability, depressed mood, concentration problems, and increased appetite/weight gain—that are formidable distractions from the positive aspects of quitting. Additionally, nicotine withdrawal symptoms tend to be more severe in smokers who have a psychiatric disorder.3 Fortunately, there are effective, evidence-based methods of reducing withdrawal symptoms and helping smokers cope with these and other challenges of quitting.
Combined treatment is best
Current treatment guidelines4 suggest all smokers should be offered pharmacotherapy and counseling to aid quitting because this combined approach has the highest success rate (Algorithm). Table 1 4 provides information about dosing, efficacy, and side effect profile of each of the 7 FDA-approved medications for smoking cessation. Using any of the approved medications at least doubles the odds of successful quitting compared with placebo.4 These pharmacotherapies can reduce or prevent nicotine withdrawal symptoms and—at least in the case of bupropion and varenicline—decrease reinforcement from smoking, thereby lowering the likelihood a lapse (ie, smoking ≥1 cigarettes without returning to regular smoking) will develop into a full-blown relapse (ie, return to regular smoking).
Algorithm: Tobacco cessation treatment for psychiatric patients
Source: Adapted from reference 4 Medication selection depends on many factors, including:
- the patient’s psychiatric illness
- her/his prior response to smoking cessation pharmacotherapies
- concomitant psychiatric medications
- patient preference.5
Placebo-controlled trials of smoking cessation aids in psychiatrically ill patients are limited, but several studies of smokers with a history of major depression indicate treatment with bupropion SR or nortriptyline is effective.6 Similarly, although relapse rates generally are higher in patients with schizophrenia compared with non-mentally ill smokers, nicotine replacement therapy and bupropion SR are more effective than placebo in patients with this disorder.7,8 When we prescribe these treatments, we tend to extend the duration of treatment beyond those described in Table 1 ,4 and to use combined treatments (eg, a transdermal patch with a shorter-acting gum or lozenge preparation) to better target the marked withdrawal symptoms more severely nicotine-dependent patients frequently experience.
Table 1
First-line pharmacotherapies for smoking cessation
| Medication | Standard dosage | Efficacy (OR, % abstinent at 6 mos. [with 95% CI]) | Contraindications (C) and precautions (P) | Common side effects |
|---|---|---|---|---|
| Non-nicotine medications | ||||
| Bupropion | Days 1-3: 150 mg/d Days 4-8: 150 mg bid Continue for 7-12 weeks at 150 mg bid | 2.0 (1.8-2.2), 24% (22%-26%) | C: Eating disorders, seizure history, taking bupropion, MAOI in past 2 weeks P: Pregnancy, cardiovascular disease, warning for emergent psychiatric symptoms | Insomnia, dry mouth |
| Varenicline | Days 1-3: 0.5 mg/d Days 4-7: 0.5 mg bid Day 8+: 1 mg bid Continue 11 weeks at 1 mg bid; up to 6 months for maintenance | 3.1 (2.5-3.8), 33% (29%-38%) | P: Warning for emergent psychiatric symptoms | Nausea, sleep problems, abnormal dreams |
| Nicotine replacement therapies | ||||
| Nicotine gum | 1 piece every 1-2 hours for 6-12 weeks <20 cigarettes/d: 2 mg gum ≥20 cigarettes/d: 4 mg gum | 1.5 (1.2-1.7), 19% (17%-22%) | P: Pregnancy, recent myocardial infarction, serious arrhythmia, unstable angina | Mouth soreness, hiccups, dyspepsia |
| Nicotine inhaler | 6-16 cartridges/d, up to 6 months | 2.1 (1.5-2.9), 25% (19%-32%) | Same as above | Mouth/throat irritation, coughing, rhinitis |
| Nicotine lozenge | 9-20 lozenges/d, up to 12 weeks Smoke ≤30 minutes after waking: 4 mg lozenge Smoke >30 minutes after waking: 2 mg lozenge | 2.0 (1.6-2.5)a | Same as above | Nausea, hiccups, heartburn |
| Nicotine nasal spray | 1-2 doses/hour, 8-40 doses/d for 3-6 months | 2.3 (1.7-3.0), 27% (22%-33%) | C: Severe reactive airway disease P: Same as above | Nasal irritation, higher risk of dependency |
| Nicotine patch | 1 patch/d, step-down dosing over 8 weeks Weeks 1-4: 21 mg patch Weeks 5-6: 14 mg patch Weeks 7-8: 7 mg patch | 1.9 (1.7-2.2) 23% (21%-26%) | P: Same as above | Skin reactions, sleep problems, abnormal dreams |
| aStead LF, Perera R, Bullen C, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2008;1:CD000146. bid: twice a day; CI: confidence interval; MAOI: monoamine oxidase inhibitor; OR: odds ratio Source: Adapted from reference 4 | ||||
Counseling. All smokers should be provided with brief interventions consistent with the 5 A’s—Ask, Advise, Assess, Assist, and Arrange (Table 2).4 For smokers who are not motivated to quit, the recommended approach follows the principles of the 5 R’s—Relevance, Risks, Rewards, Roadblocks, and Repetition (Table 3).4 Smokers who are motivated to quit and willing to participate in more intensive treatment may be offered face-to-face individual or group counseling (depending upon availability) or referred to a telephone quit line (see Related Resources). Intensive treatments such as these typically provide social support and assistance overcoming barriers to cessation and developing skills to initiate and maintain abstinence (eg, coping with a lapse or handling cravings, identifying and avoiding high-risk situations for smoking). As a general rule, greater intensity of counseling is associated with a greater likelihood of quitting.4
Table 2
The 5 A’s of tobacco treatment
| Intervention | Example | |
|---|---|---|
| Ask | Systematically inquire about tobacco use | “Do you currently use, or have you ever used, tobacco products?” |
| Advise | Counsel all tobacco users to quit in a clear, strong, and personalized manner | “I think it is very important for you quit smoking to keep your breathing problems from getting any worse” |
| Assess | Determine the tobacco user’s willingness to make a quit attempt | “What do you think? Are you ready to quit?” |
| Assist | Offer or refer to treatment/support (if ready to quit; if not ready, see Table 3 for recommended interventions) | “I’m here to help you with this. Let me start by letting you know about the many options available to help you quit” |
| Arrange | Plan for follow-up contacts (at least 1, preferably within 1 week of the quit date) | “I would like to give you a call within the next week to see how you did with your quit date. Would that be OK with you?” |
| Source: Adapted from reference 4 | ||
Table 3
The 5 R’s: Principles of interventions for smokers not ready to quit
| Principle | Example | |
|---|---|---|
| Relevance | Why is quitting smoking personally relevant? | “You’ve told me your kids sometimes make comments to you about quitting smoking. How does that affect you?” |
| Risks | What are the negative consequences of smoking? | “What don’t you like about smoking? What problems have you had from smoking?” |
| Rewards | What are the benefits of quitting smoking? | “Can you think of anything that would be good about quitting? Tell me about that” |
| Roadblocks | What are the barriers to quitting? | “What worries do you have about trying to quit? What happened the last time you tried to quit smoking?” |
| Repetition | Message repeated at every visit | “I know we have talked about quitting smoking before, but things may have changed since then. I also think that this is such an important issue we should keep it on the table for discussion. What do you think?” |
| Source: Adapted from reference 4 | ||
Q&A about treatment
How effective are smoking cessation interventions for individuals with psychiatric disorders? Several studies have demonstrated, on any given quit attempt, smokers with psychiatric or substance use disorders can be as successful as smokers without these disorders.9-11 In fact, quit rates as high as approximately 70% for end-of-treatment11 and 30% for 6-month follow-up10 have been reported. Of course, effectiveness varies by type and intensity of treatment as well as by individual characteristics of the smoker. Smokers with psychiatric disorders may fare better with more intensive interventions than briefer ones,12,13 and factors such as high levels of nicotine dependence and exposure to smoking environments—both of which are characteristic of smokers with serious mental illness—can negatively impact treatment outcomes.4
Should the nature of the psychiatric disorder(s) guide decisions about the optimal pharmacotherapy or counseling approach? There have been numerous attempts to investigate the effectiveness of targeted interventions for particular subgroups of smokers with psychiatric disorders, including:
- studies of the efficacy of the antidepressants bupropion14 and nortriptyline15 as well as cognitive-behavioral therapy-based mood management counseling16 for depressed smokers
- integrative treatment approaches for smokers with posttraumatic stress disorder (PTSD)17
- group counseling designed specifically for smokers with schizophrenia.18,19
Although more research is needed and there have been some promising early results (eg, McFall et al17), current literature does not provide consistent evidence supporting treatment matching solely on the basis of the psychiatric disorder. Rather, patient preference, safety considerations (eg, use of medications in children/adolescents, pregnant women), medication side effect profiles, prior experience with the treatment approach, and cost/availability of treatment should guide development of the treatment plan. When results from placebo-controlled trials are available for subgroups of patients (eg, those with a history of major depression), consider this information when selecting a pharmacologic smoking cessation aid.
What is the risk of psychiatric symptoms worsening as a result of quitting smoking? Little research on this topic is available because more often than not, smokers with psychiatric disorders are excluded from tobacco treatment studies. However, research examining psychiatric status changes among recent quitters with schizophrenia,20,21 depression,22,23 PTSD,17 and substance use disorders24 suggests smoking cessation does not worsen symptoms of these disorders, and may be associated with symptom improvement.17 Nonetheless, driven largely by anecdotal evidence, the misconception that smoking cessation worsens psychiatric symptoms remains a substantial barrier to treatment.
Mr. P’s case is an example of how not probing about the nature of psychiatric complaints can be problematic. Mr. P reported what on first glance appeared to be a worsening of psychiatric symptoms starting when he stopped smoking and resolved when he resumed smoking. However, without gathering additional information about these events, we cannot conclude stopping smoking caused his psychiatric symptoms to worsen. Other potential explanations include nicotine withdrawal symptoms, side effects of smoking cessation medications, an increase in levels of psychotropic medications for which metabolism is affected by tobacco smoke, or the natural course of his mood disorder. The timing of the onset and offset of symptoms seems to argue against Mr. P’s symptoms reflecting the natural course of his mood disorder, but the other 3 explanations remain plausible.
It is important to distinguish whether Mr. P’s worsening symptoms are consistent with a depressive episode or whether they are a manifestation of the transient dysphoria that accompanies nicotine withdrawal. Assessing the severity and persistence of the mood disturbance as well as the timing of onset could help make this determination. Nicotine withdrawal symptoms typically emerge within 24 hours of quitting or significantly reducing smoking and tend to peak within approximately 1 week. Thus, depressive symptoms that develop after weeks or months of abstinence would be less consistent with nicotine withdrawal. Additionally, the lethargy Mr. P reported may be a symptom of depression, or it may stem from a cessation-induced increase in antipsychotic serum levels. Because tobacco smoke increases the metabolism of several antipsychotics and antidepressants—including olanzapine, clozapine, haloperidol, and fluoxetine25—stopping smoking may increase medication levels and side effects. To rule out medication side effects as a cause of post-cessation mood changes, the psychiatrist should ask Mr. P about which smoking cessation pharmacotherapies (if any) he was using and which psychotropic medications he was taking. Unfortunately, such a detailed history is not always taken, and patient-generated theories of smoking cessation causing worsening psychiatric symptoms often are taken at face value.
When should smokers with psychiatric disorders be encouraged to quit? Are there times when smoking cessation should be discouraged? Tobacco treatment guidelines4 recommend advising users to quit at every clinical encounter, but there has been some debate about the timing of tobacco treatment for smokers with psychiatric disorders. There is minimal research to guide such treatment decisions. However, even if quit attempts are more successful during times of symptomatic stability—and there is no conclusive evidence to indicate they are—waiting for perfect mental health before initiating smoking cessation treatment is unnecessary and ill-advised. In some situations, such as when a patient has experienced an acute increase in psychiatric symptoms or when psychotropics are being titrated, a short-term postponement of quitting may be reasonable. However, discouraging smokers from trying to quit when they express readiness to try should be done sparingly, because it is uncertain how long that window of opportunity will be open, and the consequences of missed opportunities can be fatal.
- National Tobacco Quitline. 1-800-QUIT-NOW. www.smokefree.gov.
- University of California, San Francisco, Schools of Pharmacy and Medicine. Rx for Change (free online training program for clinicians). http://rxforchange.ucsf.edu.
- National Association of State Mental Health Program Directors. Tobacco-free living in psychiatric settings: a best-practices toolkit promoting wellness and recovery. www.nasmhpd.org/general_files/publications/NASMHPD.toolkitfinalupdated90707.pdf.
Drug Brand Names
- Bupropion • Wellbutrin, Zyban
- Clozapine • Clozaril
- Fluoxetine • Prozac
- Haloperidol • Haldol
- Nortriptyline • Aventyl, Pamelor
- Olanzapine • Zyprexa
- Varenicline • Chantix
Disclosures
Dr. Heffner was supported by National Institute on Drug Abuse grant#026517. She is a consultant to Pfizer Inc.
Dr. Anthenelli is supported by National Institute on Alcohol Abuse and Alcoholism grant#AA19720 and by the Department of Veterans Affairs. He is a consultant to GlaxoSmithKline and Pfizer Inc.
The Tri-State Tobacco and Alcohol Research Center receives research support from Eli Lilly and Company, Nabi Biopharmaceuticals, Pfizer Inc., and sanofi-aventis.
Discuss this article at www.facebook.com/CurrentPsychiatry
You are treating Mr. P, age 34, for schizoaffective disorder. He smokes 1 pack of cigarettes per day and has smoked for approximately 17 years. He has tried to stop but never has been able to quit for more than a few weeks. He reveals whenever he tries to quit, he starts feeling extremely lethargic and “depressed” and resumes smoking to prevent these symptoms from worsening. However, Mr. P expresses some interest in trying to quit again and asks whether any medications could prevent him from becoming depressed while he tries to quit.
Cigarette smoking is overrepresented and undertreated among individuals with psychiatric illness, in part because of the largely unfounded belief held by some patients and clinicians that smoking cessation might worsen psychiatric symptoms. In this article, we argue this challenge can be overcome and psychiatrists and other mental health professionals can and should help their patients reap the innumerable benefits of quitting smoking. We discuss:
- the short- and long-term effects of smoking cessation
- evidence-based treatment guidelines for working with motivated and unmotivated smokers
- unique issues that may arise when treating smokers who have psychiatric disorders.
Quitting: Profound benefits
Quitting smoking has substantial benefits beginning within minutes after taking the last puff. Some of the benefits that occur within the first few days of quitting include:
- decreased blood pressure and pulse rate
- improved circulation
- improved ability to smell and taste
- easier breathing.
Longer-term smoking abstinence drastically reduces risk of heart attack, stroke, cancer, respiratory disease, and a host of other illnesses that affect—and kill—individuals with psychiatric disorders several decades earlier than their counterparts in the general population.1 There also are financial benefits to quitting; using the 2009 national average of $5.33 per pack, a 1-pack-per-day smoker who quits would save >$150 per month, which accounts for only the direct cost of cigarettes.2
Although the beneficial effects of quitting smoking are profound and far-reaching, in the short-term they are counterbalanced by nicotine withdrawal symptoms—including restlessness, irritability, depressed mood, concentration problems, and increased appetite/weight gain—that are formidable distractions from the positive aspects of quitting. Additionally, nicotine withdrawal symptoms tend to be more severe in smokers who have a psychiatric disorder.3 Fortunately, there are effective, evidence-based methods of reducing withdrawal symptoms and helping smokers cope with these and other challenges of quitting.
Combined treatment is best
Current treatment guidelines4 suggest all smokers should be offered pharmacotherapy and counseling to aid quitting because this combined approach has the highest success rate (Algorithm). Table 1 4 provides information about dosing, efficacy, and side effect profile of each of the 7 FDA-approved medications for smoking cessation. Using any of the approved medications at least doubles the odds of successful quitting compared with placebo.4 These pharmacotherapies can reduce or prevent nicotine withdrawal symptoms and—at least in the case of bupropion and varenicline—decrease reinforcement from smoking, thereby lowering the likelihood a lapse (ie, smoking ≥1 cigarettes without returning to regular smoking) will develop into a full-blown relapse (ie, return to regular smoking).
Algorithm: Tobacco cessation treatment for psychiatric patients
Source: Adapted from reference 4 Medication selection depends on many factors, including:
- the patient’s psychiatric illness
- her/his prior response to smoking cessation pharmacotherapies
- concomitant psychiatric medications
- patient preference.5
Placebo-controlled trials of smoking cessation aids in psychiatrically ill patients are limited, but several studies of smokers with a history of major depression indicate treatment with bupropion SR or nortriptyline is effective.6 Similarly, although relapse rates generally are higher in patients with schizophrenia compared with non-mentally ill smokers, nicotine replacement therapy and bupropion SR are more effective than placebo in patients with this disorder.7,8 When we prescribe these treatments, we tend to extend the duration of treatment beyond those described in Table 1 ,4 and to use combined treatments (eg, a transdermal patch with a shorter-acting gum or lozenge preparation) to better target the marked withdrawal symptoms more severely nicotine-dependent patients frequently experience.
Table 1
First-line pharmacotherapies for smoking cessation
| Medication | Standard dosage | Efficacy (OR, % abstinent at 6 mos. [with 95% CI]) | Contraindications (C) and precautions (P) | Common side effects |
|---|---|---|---|---|
| Non-nicotine medications | ||||
| Bupropion | Days 1-3: 150 mg/d Days 4-8: 150 mg bid Continue for 7-12 weeks at 150 mg bid | 2.0 (1.8-2.2), 24% (22%-26%) | C: Eating disorders, seizure history, taking bupropion, MAOI in past 2 weeks P: Pregnancy, cardiovascular disease, warning for emergent psychiatric symptoms | Insomnia, dry mouth |
| Varenicline | Days 1-3: 0.5 mg/d Days 4-7: 0.5 mg bid Day 8+: 1 mg bid Continue 11 weeks at 1 mg bid; up to 6 months for maintenance | 3.1 (2.5-3.8), 33% (29%-38%) | P: Warning for emergent psychiatric symptoms | Nausea, sleep problems, abnormal dreams |
| Nicotine replacement therapies | ||||
| Nicotine gum | 1 piece every 1-2 hours for 6-12 weeks <20 cigarettes/d: 2 mg gum ≥20 cigarettes/d: 4 mg gum | 1.5 (1.2-1.7), 19% (17%-22%) | P: Pregnancy, recent myocardial infarction, serious arrhythmia, unstable angina | Mouth soreness, hiccups, dyspepsia |
| Nicotine inhaler | 6-16 cartridges/d, up to 6 months | 2.1 (1.5-2.9), 25% (19%-32%) | Same as above | Mouth/throat irritation, coughing, rhinitis |
| Nicotine lozenge | 9-20 lozenges/d, up to 12 weeks Smoke ≤30 minutes after waking: 4 mg lozenge Smoke >30 minutes after waking: 2 mg lozenge | 2.0 (1.6-2.5)a | Same as above | Nausea, hiccups, heartburn |
| Nicotine nasal spray | 1-2 doses/hour, 8-40 doses/d for 3-6 months | 2.3 (1.7-3.0), 27% (22%-33%) | C: Severe reactive airway disease P: Same as above | Nasal irritation, higher risk of dependency |
| Nicotine patch | 1 patch/d, step-down dosing over 8 weeks Weeks 1-4: 21 mg patch Weeks 5-6: 14 mg patch Weeks 7-8: 7 mg patch | 1.9 (1.7-2.2) 23% (21%-26%) | P: Same as above | Skin reactions, sleep problems, abnormal dreams |
| aStead LF, Perera R, Bullen C, et al. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2008;1:CD000146. bid: twice a day; CI: confidence interval; MAOI: monoamine oxidase inhibitor; OR: odds ratio Source: Adapted from reference 4 | ||||
Counseling. All smokers should be provided with brief interventions consistent with the 5 A’s—Ask, Advise, Assess, Assist, and Arrange (Table 2).4 For smokers who are not motivated to quit, the recommended approach follows the principles of the 5 R’s—Relevance, Risks, Rewards, Roadblocks, and Repetition (Table 3).4 Smokers who are motivated to quit and willing to participate in more intensive treatment may be offered face-to-face individual or group counseling (depending upon availability) or referred to a telephone quit line (see Related Resources). Intensive treatments such as these typically provide social support and assistance overcoming barriers to cessation and developing skills to initiate and maintain abstinence (eg, coping with a lapse or handling cravings, identifying and avoiding high-risk situations for smoking). As a general rule, greater intensity of counseling is associated with a greater likelihood of quitting.4
Table 2
The 5 A’s of tobacco treatment
| Intervention | Example | |
|---|---|---|
| Ask | Systematically inquire about tobacco use | “Do you currently use, or have you ever used, tobacco products?” |
| Advise | Counsel all tobacco users to quit in a clear, strong, and personalized manner | “I think it is very important for you quit smoking to keep your breathing problems from getting any worse” |
| Assess | Determine the tobacco user’s willingness to make a quit attempt | “What do you think? Are you ready to quit?” |
| Assist | Offer or refer to treatment/support (if ready to quit; if not ready, see Table 3 for recommended interventions) | “I’m here to help you with this. Let me start by letting you know about the many options available to help you quit” |
| Arrange | Plan for follow-up contacts (at least 1, preferably within 1 week of the quit date) | “I would like to give you a call within the next week to see how you did with your quit date. Would that be OK with you?” |
| Source: Adapted from reference 4 | ||
Table 3
The 5 R’s: Principles of interventions for smokers not ready to quit
| Principle | Example | |
|---|---|---|
| Relevance | Why is quitting smoking personally relevant? | “You’ve told me your kids sometimes make comments to you about quitting smoking. How does that affect you?” |
| Risks | What are the negative consequences of smoking? | “What don’t you like about smoking? What problems have you had from smoking?” |
| Rewards | What are the benefits of quitting smoking? | “Can you think of anything that would be good about quitting? Tell me about that” |
| Roadblocks | What are the barriers to quitting? | “What worries do you have about trying to quit? What happened the last time you tried to quit smoking?” |
| Repetition | Message repeated at every visit | “I know we have talked about quitting smoking before, but things may have changed since then. I also think that this is such an important issue we should keep it on the table for discussion. What do you think?” |
| Source: Adapted from reference 4 | ||
Q&A about treatment
How effective are smoking cessation interventions for individuals with psychiatric disorders? Several studies have demonstrated, on any given quit attempt, smokers with psychiatric or substance use disorders can be as successful as smokers without these disorders.9-11 In fact, quit rates as high as approximately 70% for end-of-treatment11 and 30% for 6-month follow-up10 have been reported. Of course, effectiveness varies by type and intensity of treatment as well as by individual characteristics of the smoker. Smokers with psychiatric disorders may fare better with more intensive interventions than briefer ones,12,13 and factors such as high levels of nicotine dependence and exposure to smoking environments—both of which are characteristic of smokers with serious mental illness—can negatively impact treatment outcomes.4
Should the nature of the psychiatric disorder(s) guide decisions about the optimal pharmacotherapy or counseling approach? There have been numerous attempts to investigate the effectiveness of targeted interventions for particular subgroups of smokers with psychiatric disorders, including:
- studies of the efficacy of the antidepressants bupropion14 and nortriptyline15 as well as cognitive-behavioral therapy-based mood management counseling16 for depressed smokers
- integrative treatment approaches for smokers with posttraumatic stress disorder (PTSD)17
- group counseling designed specifically for smokers with schizophrenia.18,19
Although more research is needed and there have been some promising early results (eg, McFall et al17), current literature does not provide consistent evidence supporting treatment matching solely on the basis of the psychiatric disorder. Rather, patient preference, safety considerations (eg, use of medications in children/adolescents, pregnant women), medication side effect profiles, prior experience with the treatment approach, and cost/availability of treatment should guide development of the treatment plan. When results from placebo-controlled trials are available for subgroups of patients (eg, those with a history of major depression), consider this information when selecting a pharmacologic smoking cessation aid.
What is the risk of psychiatric symptoms worsening as a result of quitting smoking? Little research on this topic is available because more often than not, smokers with psychiatric disorders are excluded from tobacco treatment studies. However, research examining psychiatric status changes among recent quitters with schizophrenia,20,21 depression,22,23 PTSD,17 and substance use disorders24 suggests smoking cessation does not worsen symptoms of these disorders, and may be associated with symptom improvement.17 Nonetheless, driven largely by anecdotal evidence, the misconception that smoking cessation worsens psychiatric symptoms remains a substantial barrier to treatment.
Mr. P’s case is an example of how not probing about the nature of psychiatric complaints can be problematic. Mr. P reported what on first glance appeared to be a worsening of psychiatric symptoms starting when he stopped smoking and resolved when he resumed smoking. However, without gathering additional information about these events, we cannot conclude stopping smoking caused his psychiatric symptoms to worsen. Other potential explanations include nicotine withdrawal symptoms, side effects of smoking cessation medications, an increase in levels of psychotropic medications for which metabolism is affected by tobacco smoke, or the natural course of his mood disorder. The timing of the onset and offset of symptoms seems to argue against Mr. P’s symptoms reflecting the natural course of his mood disorder, but the other 3 explanations remain plausible.
It is important to distinguish whether Mr. P’s worsening symptoms are consistent with a depressive episode or whether they are a manifestation of the transient dysphoria that accompanies nicotine withdrawal. Assessing the severity and persistence of the mood disturbance as well as the timing of onset could help make this determination. Nicotine withdrawal symptoms typically emerge within 24 hours of quitting or significantly reducing smoking and tend to peak within approximately 1 week. Thus, depressive symptoms that develop after weeks or months of abstinence would be less consistent with nicotine withdrawal. Additionally, the lethargy Mr. P reported may be a symptom of depression, or it may stem from a cessation-induced increase in antipsychotic serum levels. Because tobacco smoke increases the metabolism of several antipsychotics and antidepressants—including olanzapine, clozapine, haloperidol, and fluoxetine25—stopping smoking may increase medication levels and side effects. To rule out medication side effects as a cause of post-cessation mood changes, the psychiatrist should ask Mr. P about which smoking cessation pharmacotherapies (if any) he was using and which psychotropic medications he was taking. Unfortunately, such a detailed history is not always taken, and patient-generated theories of smoking cessation causing worsening psychiatric symptoms often are taken at face value.
When should smokers with psychiatric disorders be encouraged to quit? Are there times when smoking cessation should be discouraged? Tobacco treatment guidelines4 recommend advising users to quit at every clinical encounter, but there has been some debate about the timing of tobacco treatment for smokers with psychiatric disorders. There is minimal research to guide such treatment decisions. However, even if quit attempts are more successful during times of symptomatic stability—and there is no conclusive evidence to indicate they are—waiting for perfect mental health before initiating smoking cessation treatment is unnecessary and ill-advised. In some situations, such as when a patient has experienced an acute increase in psychiatric symptoms or when psychotropics are being titrated, a short-term postponement of quitting may be reasonable. However, discouraging smokers from trying to quit when they express readiness to try should be done sparingly, because it is uncertain how long that window of opportunity will be open, and the consequences of missed opportunities can be fatal.
- National Tobacco Quitline. 1-800-QUIT-NOW. www.smokefree.gov.
- University of California, San Francisco, Schools of Pharmacy and Medicine. Rx for Change (free online training program for clinicians). http://rxforchange.ucsf.edu.
- National Association of State Mental Health Program Directors. Tobacco-free living in psychiatric settings: a best-practices toolkit promoting wellness and recovery. www.nasmhpd.org/general_files/publications/NASMHPD.toolkitfinalupdated90707.pdf.
Drug Brand Names
- Bupropion • Wellbutrin, Zyban
- Clozapine • Clozaril
- Fluoxetine • Prozac
- Haloperidol • Haldol
- Nortriptyline • Aventyl, Pamelor
- Olanzapine • Zyprexa
- Varenicline • Chantix
Disclosures
Dr. Heffner was supported by National Institute on Drug Abuse grant#026517. She is a consultant to Pfizer Inc.
Dr. Anthenelli is supported by National Institute on Alcohol Abuse and Alcoholism grant#AA19720 and by the Department of Veterans Affairs. He is a consultant to GlaxoSmithKline and Pfizer Inc.
The Tri-State Tobacco and Alcohol Research Center receives research support from Eli Lilly and Company, Nabi Biopharmaceuticals, Pfizer Inc., and sanofi-aventis.
1. Colton CW, Manderscheid RW. Congruencies in increased mortality rates years of potential life lost, and causes of death among public mental health clients in eight states. Prev Chronic Dis. 2006;3(2):A42.-
2. Centers for Disease Control and Prevention. Trends in state and federal cigarette tax and retail price—1970-2009. 2010. Available at: http://www.cdc.gov/tobacco/data_statistics/tables/economics/trends. Accessed June 28 2011.
3. Xian H, Scherrer JF, Eisen SA, et al. Nicotine dependence subtypes: association with smoking history, diagnostic criteria and psychiatric disorders in 5440 regular smokers from the Vietnam Era Twin Registry. Addict Behav. 2007;32(1):137-147.
4. Fiore MC, Jaén CR, Baker TB, et al. A clinical practice guideline for treating tobacco use and dependence: 2008 update. A U. S. Public Health Service report. Am J Prev Med. 2008;35(2):158-176.
5. Anthenelli RM. How–and why–to help psychiatric patients stop smoking. Current Psychiatry. 2005;4(1):77-87.
6. Hughes JR, Stead LF, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2007;1:CD000031.-
7. Williams JM, Foulds J. Successful tobacco dependence treatment in schizophrenia. Am J Psychiatry. 2007;164(2):222-227.
8. George TP, Vessicchio JC, Termine A, et al. A placebo controlled trial of bupropion for smoking cessation in schizophrenia. Biol Psychiatry. 2002;52(1):53-61.
9. Hughes JR, Kalman D. Do smokers with alcohol problems have more difficulty quitting? Drug Alcohol Depend. 2006;82(2):91-102.
10. McClure JB, Swan GE, Catz SL, et al. Smoking outcome by psychiatric history after behavioral and varenicline treatment. J Subst Abuse Treat. 2010;38(4):394-402.
11. Stapleton JA, Watson L, Spirling LI, et al. Varenicline in the routine treatment of tobacco dependence: a pre-post comparison with nicotine replacement therapy and an evaluation in those with mental illness. Addiction. 2008;103(1):146-154.
12. Hall SM, Muñoz RF, Reus VI. Cognitive-behavioral intervention increases abstinence rates for depressive-history smokers. J Consult Clin Psychol. 1994;62(1):141-146.
13. Hall SM, Muñoz RF, Reus VI, et al. Mood management and nicotine gum in smoking treatment: a therapeutic contact and placebo-controlled study. J Consult Clin Psychol. 1996;64(5):1003-1009.
14. Evins AE, Culhane MA, Alpert JE, et al. A controlled trial of bupropion added to nicotine patch and behavioral therapy for smoking cessation in adults with unipolar depressive disorders. J Clin Psychopharmacol. 2008;28(6):660-666.
15. Hall SM, Reus VI, Muñoz RF, et al. Nortriptyline and cognitive-behavioral therapy in the treatment of cigarette smoking. Arch Gen Psychiatry. 1998;55(8):683-690.
16. Brown RA, Kahler CW, Niaura R, et al. Cognitive-behavioral treatment for depression in smoking cessation. J Consult Clin Psychol. 2001;69(3):471-480.
17. McFall M, Saxon AJ, Malte CA, et al. Integrating tobacco cessation into mental health care for posttraumatic stress disorder: a randomized controlled trial. JAMA. 2010;304(22):2485-2493.
18. George TP, Ziedonis DM, Feingold A, et al. Nicotine transdermal patch and atypical antipsychotic medications for smoking cessation in schizophrenia. Am J Psychiatry. 2000;157(11):1835-1842.
19. Williams JM, Steinberg ML, Zimmermann MH, et al. Comparison of two intensities of tobacco dependence counseling in schizophrenia and schizoaffective disorder. J Subst Abuse Treat. 2010;38(4):384-393.
20. Evins AE, Cather C, Culhane MA, et al. A 12-week double-blind, placebo-controlled study of bupropion sr added to high-dose dual nicotine replacement therapy for smoking cessation or reduction in schizophrenia. J Clin Psychopharmacol. 2007;27(4):380-386.
21. Weinberger AH, Hitsman B, Papandonatos GD, et al. Predictors of abstinence and changes in psychiatric symptoms in a pooled sample of smokers with schizophrenia receiving combination pharmacotherapy and behavioral therapy for smoking cessation. J Clin Psychopharmacol. 2009;29(6):601-603.
22. Prochaska JJ, Hall SM, Tsoh JY, et al. Treating tobacco dependence in clinically depressed smokers: effect of smoking cessation on mental health functioning. Am J Public Health. 2008;98(3):446-448.
23. Tsoh JY, Humfleet GL, Muñoz RF, et al. Development of major depression after treatment for smoking cessation. Am J Psychiatry. 2000;157(3):368-374.
24. Prochaska JJ, Delucchi K, Hall SM. A meta-analysis of smoking cessation interventions with individuals in substance abuse treatment or recovery. J Consult Clin Psychol. 2004;72(6):1144-1156.
25. Zevin S, Benowitz NL. Drug interactions with tobacco smoking. An update. Clin Pharmacokinet. 1999;36(6):425-438.
1. Colton CW, Manderscheid RW. Congruencies in increased mortality rates years of potential life lost, and causes of death among public mental health clients in eight states. Prev Chronic Dis. 2006;3(2):A42.-
2. Centers for Disease Control and Prevention. Trends in state and federal cigarette tax and retail price—1970-2009. 2010. Available at: http://www.cdc.gov/tobacco/data_statistics/tables/economics/trends. Accessed June 28 2011.
3. Xian H, Scherrer JF, Eisen SA, et al. Nicotine dependence subtypes: association with smoking history, diagnostic criteria and psychiatric disorders in 5440 regular smokers from the Vietnam Era Twin Registry. Addict Behav. 2007;32(1):137-147.
4. Fiore MC, Jaén CR, Baker TB, et al. A clinical practice guideline for treating tobacco use and dependence: 2008 update. A U. S. Public Health Service report. Am J Prev Med. 2008;35(2):158-176.
5. Anthenelli RM. How–and why–to help psychiatric patients stop smoking. Current Psychiatry. 2005;4(1):77-87.
6. Hughes JR, Stead LF, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2007;1:CD000031.-
7. Williams JM, Foulds J. Successful tobacco dependence treatment in schizophrenia. Am J Psychiatry. 2007;164(2):222-227.
8. George TP, Vessicchio JC, Termine A, et al. A placebo controlled trial of bupropion for smoking cessation in schizophrenia. Biol Psychiatry. 2002;52(1):53-61.
9. Hughes JR, Kalman D. Do smokers with alcohol problems have more difficulty quitting? Drug Alcohol Depend. 2006;82(2):91-102.
10. McClure JB, Swan GE, Catz SL, et al. Smoking outcome by psychiatric history after behavioral and varenicline treatment. J Subst Abuse Treat. 2010;38(4):394-402.
11. Stapleton JA, Watson L, Spirling LI, et al. Varenicline in the routine treatment of tobacco dependence: a pre-post comparison with nicotine replacement therapy and an evaluation in those with mental illness. Addiction. 2008;103(1):146-154.
12. Hall SM, Muñoz RF, Reus VI. Cognitive-behavioral intervention increases abstinence rates for depressive-history smokers. J Consult Clin Psychol. 1994;62(1):141-146.
13. Hall SM, Muñoz RF, Reus VI, et al. Mood management and nicotine gum in smoking treatment: a therapeutic contact and placebo-controlled study. J Consult Clin Psychol. 1996;64(5):1003-1009.
14. Evins AE, Culhane MA, Alpert JE, et al. A controlled trial of bupropion added to nicotine patch and behavioral therapy for smoking cessation in adults with unipolar depressive disorders. J Clin Psychopharmacol. 2008;28(6):660-666.
15. Hall SM, Reus VI, Muñoz RF, et al. Nortriptyline and cognitive-behavioral therapy in the treatment of cigarette smoking. Arch Gen Psychiatry. 1998;55(8):683-690.
16. Brown RA, Kahler CW, Niaura R, et al. Cognitive-behavioral treatment for depression in smoking cessation. J Consult Clin Psychol. 2001;69(3):471-480.
17. McFall M, Saxon AJ, Malte CA, et al. Integrating tobacco cessation into mental health care for posttraumatic stress disorder: a randomized controlled trial. JAMA. 2010;304(22):2485-2493.
18. George TP, Ziedonis DM, Feingold A, et al. Nicotine transdermal patch and atypical antipsychotic medications for smoking cessation in schizophrenia. Am J Psychiatry. 2000;157(11):1835-1842.
19. Williams JM, Steinberg ML, Zimmermann MH, et al. Comparison of two intensities of tobacco dependence counseling in schizophrenia and schizoaffective disorder. J Subst Abuse Treat. 2010;38(4):384-393.
20. Evins AE, Cather C, Culhane MA, et al. A 12-week double-blind, placebo-controlled study of bupropion sr added to high-dose dual nicotine replacement therapy for smoking cessation or reduction in schizophrenia. J Clin Psychopharmacol. 2007;27(4):380-386.
21. Weinberger AH, Hitsman B, Papandonatos GD, et al. Predictors of abstinence and changes in psychiatric symptoms in a pooled sample of smokers with schizophrenia receiving combination pharmacotherapy and behavioral therapy for smoking cessation. J Clin Psychopharmacol. 2009;29(6):601-603.
22. Prochaska JJ, Hall SM, Tsoh JY, et al. Treating tobacco dependence in clinically depressed smokers: effect of smoking cessation on mental health functioning. Am J Public Health. 2008;98(3):446-448.
23. Tsoh JY, Humfleet GL, Muñoz RF, et al. Development of major depression after treatment for smoking cessation. Am J Psychiatry. 2000;157(3):368-374.
24. Prochaska JJ, Delucchi K, Hall SM. A meta-analysis of smoking cessation interventions with individuals in substance abuse treatment or recovery. J Consult Clin Psychol. 2004;72(6):1144-1156.
25. Zevin S, Benowitz NL. Drug interactions with tobacco smoking. An update. Clin Pharmacokinet. 1999;36(6):425-438.