User login
No-shows
Of all the headaches inherent in a private medical practice, few are more frustrating than patients who make appointments and then fail to keep them.
– almost double the average for all medical offices.

The problem has become so pervasive that many physicians are now charging a fee for missed appointments. I have never been a fan of such fees for a variety of reasons, starting with the anger and bad will that they engender; but also, in my experience, they seldom accomplish their intended goal of changing the behavior.
That’s because fees imply some sort of conscious decision made by a patient to miss an appointment, but studies show that this is rarely the case. Some patients cite transportation issues or childcare obligations. One Canadian study found that nearly a quarter of patients who missed an appointment felt too sick to keep it. Another reason is lack of insurance coverage. Studies have shown that the no-show rate is far higher when the patient is paying out-of-pocket for the visit.
Patients who don’t show up for appointments tend to be younger and poorer, and live farther away from the office than those who attend consistently. Some patients may be unaware that they need to cancel, while others report that they don’t feel obliged to keep appointments because they feel disrespected by the system. One person posted on a medical forum, “Everyone’s time is valuable. When the doctor makes me wait, there are consequences too. Why are there two standards in the situation?”
The most common reason for missed appointments, however, according to multiple studies, is that patients simply forget that they have one. One reason for that is a lag between appointment and visit. Many dermatologists are booked well in advance; by the time the appointment arrives, some patients’ complaints will have resolved spontaneously, while other patients will have found another office willing to see them sooner.
Another big reason is the absence of a strong physician-patient relationship. Perhaps the patient sees a different doctor or physician assistant at each visit and doesn’t feel a particular bond with any of them. Some patients may perceive a lack of concern on the part of the physician. And others may suffer from poor communication; for example, patients frequently become frustrated that a chronic condition has not resolved, when it has not been clearly explained to them that such problems cannot be expected to resolve rapidly or completely.
Whatever the reasons, no-shows are an economic and medicolegal liability. It is worth the considerable effort it often takes to minimize them.
Research suggests that no-show rates can be reduced by providing more same-day or next-day appointments. One large-scale analysis of national data found that same-day appointments accounted for just 2% of no-shows, while appointments booked 15 days or more in advance accounted for nearly a third of them. Canadian studies have likewise found the risk of no-shows increases the further in advance clinics book patients.
Deal with simple forgetfulness by calling your patients the day before to remind them of their appointments. Reasonably priced phone software is available from a variety of vendors to automate this process. Or hire a teenager to do it after school each day.
Whenever possible, use cellphone numbers for reminder calls. Patients often aren’t home during the day, and many don’t listen to their messages when they come in. And patients who have moved will often have a new home phone number, but their cellphone number will be the same.
Decrease the wait for new appointments. Keep some slots open each week for new patients, who will often “shop around” for a faster appointment while they’re waiting for an appointment they already have elsewhere.
But above all, seek to maximize the strength of your physician-patient relationships. Try not to shuttle patients between different physicians or PAs, and make it clear that you are genuinely concerned about their health. Impress upon them the crucial role they play in their own care, which includes keeping all their appointments.
In our office, significant no-shows (for example, a patient with a melanoma who misses a follow-up visit) receive a phone call and a certified letter, and their records go into a special file for close follow-up by the nursing staff.
If you choose to go the missed-appointment-fee route, be sure to post notices in your office and on your website clearly delineating your policy. Emphasize that it is not a service fee, and cannot be billed to insurance.
All missed appointments should be documented in the patient’s record; it’s important clinical and medicolegal information. And habitual no-shows should be dismissed from your practice. You cannot afford them.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Of all the headaches inherent in a private medical practice, few are more frustrating than patients who make appointments and then fail to keep them.
– almost double the average for all medical offices.
The problem has become so pervasive that many physicians are now charging a fee for missed appointments. I have never been a fan of such fees for a variety of reasons, starting with the anger and bad will that they engender; but also, in my experience, they seldom accomplish their intended goal of changing the behavior.
That’s because fees imply some sort of conscious decision made by a patient to miss an appointment, but studies show that this is rarely the case. Some patients cite transportation issues or childcare obligations. One Canadian study found that nearly a quarter of patients who missed an appointment felt too sick to keep it. Another reason is lack of insurance coverage. Studies have shown that the no-show rate is far higher when the patient is paying out-of-pocket for the visit.
Patients who don’t show up for appointments tend to be younger and poorer, and live farther away from the office than those who attend consistently. Some patients may be unaware that they need to cancel, while others report that they don’t feel obliged to keep appointments because they feel disrespected by the system. One person posted on a medical forum, “Everyone’s time is valuable. When the doctor makes me wait, there are consequences too. Why are there two standards in the situation?”
The most common reason for missed appointments, however, according to multiple studies, is that patients simply forget that they have one. One reason for that is a lag between appointment and visit. Many dermatologists are booked well in advance; by the time the appointment arrives, some patients’ complaints will have resolved spontaneously, while other patients will have found another office willing to see them sooner.
Another big reason is the absence of a strong physician-patient relationship. Perhaps the patient sees a different doctor or physician assistant at each visit and doesn’t feel a particular bond with any of them. Some patients may perceive a lack of concern on the part of the physician. And others may suffer from poor communication; for example, patients frequently become frustrated that a chronic condition has not resolved, when it has not been clearly explained to them that such problems cannot be expected to resolve rapidly or completely.
Whatever the reasons, no-shows are an economic and medicolegal liability. It is worth the considerable effort it often takes to minimize them.
Research suggests that no-show rates can be reduced by providing more same-day or next-day appointments. One large-scale analysis of national data found that same-day appointments accounted for just 2% of no-shows, while appointments booked 15 days or more in advance accounted for nearly a third of them. Canadian studies have likewise found the risk of no-shows increases the further in advance clinics book patients.
Deal with simple forgetfulness by calling your patients the day before to remind them of their appointments. Reasonably priced phone software is available from a variety of vendors to automate this process. Or hire a teenager to do it after school each day.
Whenever possible, use cellphone numbers for reminder calls. Patients often aren’t home during the day, and many don’t listen to their messages when they come in. And patients who have moved will often have a new home phone number, but their cellphone number will be the same.
Decrease the wait for new appointments. Keep some slots open each week for new patients, who will often “shop around” for a faster appointment while they’re waiting for an appointment they already have elsewhere.
But above all, seek to maximize the strength of your physician-patient relationships. Try not to shuttle patients between different physicians or PAs, and make it clear that you are genuinely concerned about their health. Impress upon them the crucial role they play in their own care, which includes keeping all their appointments.
In our office, significant no-shows (for example, a patient with a melanoma who misses a follow-up visit) receive a phone call and a certified letter, and their records go into a special file for close follow-up by the nursing staff.
If you choose to go the missed-appointment-fee route, be sure to post notices in your office and on your website clearly delineating your policy. Emphasize that it is not a service fee, and cannot be billed to insurance.
All missed appointments should be documented in the patient’s record; it’s important clinical and medicolegal information. And habitual no-shows should be dismissed from your practice. You cannot afford them.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Of all the headaches inherent in a private medical practice, few are more frustrating than patients who make appointments and then fail to keep them.
– almost double the average for all medical offices.
The problem has become so pervasive that many physicians are now charging a fee for missed appointments. I have never been a fan of such fees for a variety of reasons, starting with the anger and bad will that they engender; but also, in my experience, they seldom accomplish their intended goal of changing the behavior.
That’s because fees imply some sort of conscious decision made by a patient to miss an appointment, but studies show that this is rarely the case. Some patients cite transportation issues or childcare obligations. One Canadian study found that nearly a quarter of patients who missed an appointment felt too sick to keep it. Another reason is lack of insurance coverage. Studies have shown that the no-show rate is far higher when the patient is paying out-of-pocket for the visit.
Patients who don’t show up for appointments tend to be younger and poorer, and live farther away from the office than those who attend consistently. Some patients may be unaware that they need to cancel, while others report that they don’t feel obliged to keep appointments because they feel disrespected by the system. One person posted on a medical forum, “Everyone’s time is valuable. When the doctor makes me wait, there are consequences too. Why are there two standards in the situation?”
The most common reason for missed appointments, however, according to multiple studies, is that patients simply forget that they have one. One reason for that is a lag between appointment and visit. Many dermatologists are booked well in advance; by the time the appointment arrives, some patients’ complaints will have resolved spontaneously, while other patients will have found another office willing to see them sooner.
Another big reason is the absence of a strong physician-patient relationship. Perhaps the patient sees a different doctor or physician assistant at each visit and doesn’t feel a particular bond with any of them. Some patients may perceive a lack of concern on the part of the physician. And others may suffer from poor communication; for example, patients frequently become frustrated that a chronic condition has not resolved, when it has not been clearly explained to them that such problems cannot be expected to resolve rapidly or completely.
Whatever the reasons, no-shows are an economic and medicolegal liability. It is worth the considerable effort it often takes to minimize them.
Research suggests that no-show rates can be reduced by providing more same-day or next-day appointments. One large-scale analysis of national data found that same-day appointments accounted for just 2% of no-shows, while appointments booked 15 days or more in advance accounted for nearly a third of them. Canadian studies have likewise found the risk of no-shows increases the further in advance clinics book patients.
Deal with simple forgetfulness by calling your patients the day before to remind them of their appointments. Reasonably priced phone software is available from a variety of vendors to automate this process. Or hire a teenager to do it after school each day.
Whenever possible, use cellphone numbers for reminder calls. Patients often aren’t home during the day, and many don’t listen to their messages when they come in. And patients who have moved will often have a new home phone number, but their cellphone number will be the same.
Decrease the wait for new appointments. Keep some slots open each week for new patients, who will often “shop around” for a faster appointment while they’re waiting for an appointment they already have elsewhere.
But above all, seek to maximize the strength of your physician-patient relationships. Try not to shuttle patients between different physicians or PAs, and make it clear that you are genuinely concerned about their health. Impress upon them the crucial role they play in their own care, which includes keeping all their appointments.
In our office, significant no-shows (for example, a patient with a melanoma who misses a follow-up visit) receive a phone call and a certified letter, and their records go into a special file for close follow-up by the nursing staff.
If you choose to go the missed-appointment-fee route, be sure to post notices in your office and on your website clearly delineating your policy. Emphasize that it is not a service fee, and cannot be billed to insurance.
All missed appointments should be documented in the patient’s record; it’s important clinical and medicolegal information. And habitual no-shows should be dismissed from your practice. You cannot afford them.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].

Medical assistants identify strategies and barriers to clinic efficiency
ABSTRACT
Background: Medical assistant (MA) roles have expanded rapidly as primary care has evolved and MAs take on new patient care duties. Research that looks at the MA experience and factors that enhance or reduce efficiency among MAs is limited.
Methods: We surveyed all MAs working in 6 clinics run by a large academic family medicine department in Ann Arbor, Michigan. MAs deemed by peers as “most efficient” were selected for follow-up interviews. We evaluated personal strategies for efficiency, barriers to efficient care, impact of physician actions on efficiency, and satisfaction.
Results: A total of 75/86 MAs (87%) responded to at least some survey questions and 61/86 (71%) completed the full survey. We interviewed 18 MAs face to face. Most saw their role as essential to clinic functioning and viewed health care as a personal calling. MAs identified common strategies to improve efficiency and described the MA role to orchestrate the flow of the clinic day. Staff recognized differing priorities of patients, staff, and physicians and articulated frustrations with hierarchy and competing priorities as well as behaviors that impeded clinic efficiency. Respondents emphasized the importance of feeling valued by others on their team.
Conclusions: With the evolving demands made on MAs’ time, it is critical to understand how the most effective staff members manage their role and highlight the strategies they employ to provide efficient clinical care. Understanding factors that increase or decrease MA job satisfaction can help identify high-efficiency practices and promote a clinic culture that values and supports all staff.
As primary care continues to evolve into more team-based practice, the role of the medical assistant (MA) has rapidly transformed.1 Staff may assist with patient management, documentation in the electronic medical record, order entry, pre-visit planning, and fulfillment of quality metrics, particularly in a Primary Care Medical Home (PCMH).2 From 2012 through 2014, MA job postings per graduate increased from 1.3 to 2.3, suggesting twice as many job postings as graduates.3 As the demand for experienced MAs increases, the ability to recruit and retain high-performing staff members will be critical.
MAs are referenced in medical literature as early as the 1800s.4 The American Association of Medical Assistants was founded in 1956, which led to educational standardization and certifications.5 Despite the important role that MAs have long played in the proper functioning of a medical clinic—and the knowledge that team configurations impact a clinic’s efficiency and quality6,7—few investigations have sought out the MA’s perspective.8,9 Given the increasing clinical demands placed on all members of the primary care team (and the burnout that often results), it seems that MA insights into clinic efficiency could be valuable.
Continue to: Methods...
METHODS
This cross-sectional study was conducted from February to April 2019 at a large academic institution with 6 regional ambulatory care family medicine clinics, each one with 11,000 to 18,000 patient visits annually. Faculty work at all 6 clinics and residents at 2 of them. All MAs are hired, paid, and managed by a central administrative department rather than by the family medicine department. The family medicine clinics are currently PCMH certified, with a mix of fee-for-service and capitated reimbursement.
We developed and piloted a voluntary, anonymous 39-question (29 closed-ended and 10 brief open-ended) online Qualtrics survey, which we distributed via an email link to all the MAs in the department. The survey included clinic site, years as an MA, perceptions of the clinic environment, perception of teamwork at their site, identification of efficient practices, and feedback for physicians to improve efficiency and flow. Most questions were Likert-style with 5 choices ranging from “strongly agree” to “strongly disagree” or short answer. Age and gender were omitted to protect confidentiality, as most MAs in the department are female. Participants could opt to enter in a drawing for three $25 gift cards. The survey was reviewed by the University of Michigan Institutional Review Board and deemed exempt.
We asked MAs to nominate peers in their clinic who were “especially efficient and do their jobs well—people that others can learn from.” The staff members who were nominated most frequently by their peers were invited to share additional perspectives via a 10- to 30-minute semi-structured interview with the first author. Interviews covered highly efficient practices, barriers and facilitators to efficient care, and physician behaviors that impaired efficiency. We interviewed a minimum of 2 MAs per clinic and increased the number of interviews through snowball sampling, as needed, to reach data saturation (eg, the point at which we were no longer hearing new content). MAs were assured that all comments would be anonymized. There was no monetary incentive for the interviews. The interviewer had previously met only 3 of the 18 MAs interviewed.
Analysis. Summary statistics were calculated for quantitative data. To compare subgroups (such as individual clinics), a chi-square test was used. In cases when there were small cell sizes (< 5 subjects), we used the Fisher’s Exact test. Qualitative data was collected with real-time typewritten notes during the interviews to capture ideas and verbatim quotes when possible. We also included open-ended comments shared on the Qualtrics survey. Data were organized by theme using a deductive coding approach. Both authors reviewed and discussed observations, and coding was conducted by the first author. Reporting followed the STROBE Statement checklist for cross-sectional studies.10 Results were shared with MAs, supervisory staff, and physicians, which allowed for feedback and comments and served as “member-checking.” MAs reported that the data reflected their lived experiences.
Continue to: RESULTS...
RESULTS
Surveys were distributed to all 86 MAs working in family medicine clinics. A total of 75 (87%) responded to at least some questions (typically just demographics). We used those who completed the full survey (n = 61; 71%) for data analysis. Eighteen MAs participated in face-to-face interviews. Among respondents, 35 (47%) had worked at least 10 years as an MA and 21 (28%) had worked at least a decade in the family medicine department.
Perception of role
All respondents (n = 61; 100%) somewhat or strongly agreed that the MA role was “very important to keep the clinic functioning” and 58 (95%) reported that working in health care was “a calling” for them. Only 7 (11%) agreed that family medicine was an easier environment for MAs compared to a specialty clinic; 30 (49%) disagreed with this. Among respondents, 32 (53%) strongly or somewhat agreed that their work was very stressful and just half (n = 28; 46%) agreed there were adequate MA staff at their clinic.
Efficiency and competing priorities
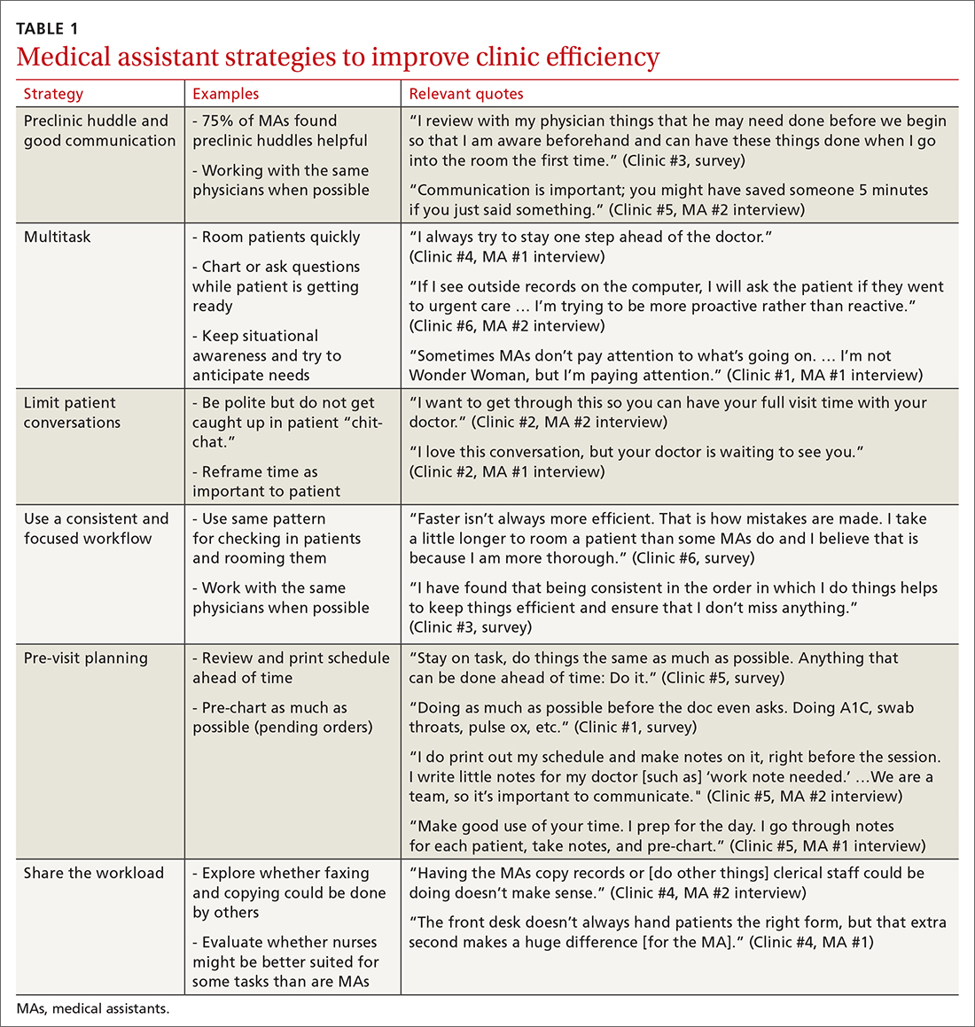
MAs described important work values that increased their efficiency. These included clinic culture (good communication and strong teamwork), as well as individual strategies such as multitasking, limiting patient conversations, and doing tasks in a consistent way to improve accuracy. (See TABLE 1.) They identified ways physicians bolster or hurt efficiency and ways in which the relationship between the physician and the MA shapes the MA’s perception of their value in clinic.
Communication was emphasized as critical for efficient care, and MAs encouraged the use of preclinic huddles and communication as priorities. Seventy-five percent of MAs reported preclinic huddles to plan for patient care were helpful, but only half said huddles took place “always” or “most of the time.” Many described reviewing the schedule and completing tasks ahead of patient arrival as critical to efficiency.
Participants described the tension between their identified role of orchestrating clinic flow and responding to directives by others that disrupted the flow. Several MAs found it challenging when physicians agreed to see very late patients and felt frustrated when decisions that changed the flow were made by the physician or front desk staff without including the MA. MAs were also able to articulate how they managed competing priorities within the clinic, such as when a patient- or physician-driven need to extend appointments was at odds with maintaining a timely schedule. They were eager to share personal tips for time management and prided themselves on careful and accurate performance and skills they had learned on the job. MAs also described how efficiency could be adversely affected by the behaviors or attitudes of physicians. (See TABLE 2.)
Continue to: Clinic environment...
Clinic environment
Thirty-six MAs (59%) reported that other MAs on their team were willing to help them out in clinic “a great deal” or “a lot” of the time, by helping to room a patient, acting as a chaperone for an exam, or doing a point-of-care lab. This sense of support varied across clinics (38% to 91% reported good support), suggesting that cultures vary by site. Some MAs expressed frustration at peers they saw as resistant to helping, exemplified by this verbatim quote from an interview:
“Some don’t want to help out. They may sigh. It’s how they react—you just know.” (Clinic #1, MA #2 interview)
Efficient MAs stressed the need for situational awareness to recognize when co-workers need help:
“[Peers often] are not aware that another MA is drowning. There’s 5 people who could have done that, and here I am running around and nobody budged.” (Clinic #5, MA #2 interview)
A minority of staff used the open-ended survey sections to describe clinic hierarchy. When asked about “pet peeves,” a few advised that physicians should not “talk down” to staff and should try to teach rather than criticize. Another asked that physicians not “bark orders” or have “low gratitude” for staff work. MAs found micromanaging stressful—particularly when the physician prompted the MA about patient arrivals:
“[I don’t like] when providers will make a comment about a patient arriving when you already know this information. You then rush to put [the] patient in [a] room, then [the] provider ends up making [the] patient wait an extensive amount of time. I’m perfectly capable of knowing when a patient arrives.” (Clinic #6, survey)
MAs did not like physicians “talking bad about us” or blaming the MA if the clinic is running behind.
Despite these concerns, most MAs reported feeling appreciated for the job they do. Only 10 (16%) reported that the people they work with rarely say “thank you,” and 2 (3%) stated they were not well supported by the physicians in clinic. Most (n = 38; 62%) strongly agreed or agreed that they felt part of the team and that their opinions matter. In the interviews, many expanded on this idea:
“I really feel like I’m valued, so I want to do everything I can to make [my doctor’s] day go better. If you want a good clinic, the best thing a doc can do is make the MA feel valued.” (Clinic #1, MA #1 interview)
Continue to: DISCUSSION...
DISCUSSION
Participants described their role much as an orchestra director, with MAs as the key to clinic flow and timeliness.9 Respondents articulated multiple common strategies used to increase their own efficiency and clinic flow; these may be considered best practices and incorporated as part of the basic training. Most MAs reported their day-to-day jobs were stressful and believed this was underrecognized, so efficiency strategies are critical. With staff completing multiple time-sensitive tasks during clinic, consistent co-worker support is crucial and may impact efficiency.8 Proper training of managers to provide that support and ensure equitable workloads may be one strategy to ensure that staff members feel the workplace is fair and collegial.
Several comments reflected the power differential within medical offices. One study reported that MAs and physicians “occupy roles at opposite ends of social and occupational hierarchies.”11 It’s important for physicians to be cognizant of these patterns and clinic culture, as reducing a hierarchy-based environment will be appreciated by MAs.9 Prior research has found that MAs have higher perceptions of their own competence than do the physicians working with them.12 If there is a fundamental lack of trust between the 2 groups, this will undoubtedly hinder team-building. Attention to this issue is key to a more favorable work environment.
Almost all respondents reported health care was a “calling,” which mirrors physician research that suggests seeing work as a “calling” is protective against burnout.13,14 Open-ended comments indicated great pride in contributions, and most staff members felt appreciated by their teams. Many described the working relationships with physicians as critical to their satisfaction at work and indicated that strong partnerships motivated them to do their best to make the physician’s day easier. Staff job satisfaction is linked to improved quality of care, so treating staff well contributes to high-value care for patients.15 We also uncovered some MA “pet peeves” that hinder efficiency and could be shared with physicians to emphasize the importance of patience and civility.
One barrier to expansion of MA roles within PCMH practices is the limited pay and career ladder for MAs who adopt new job responsibilities that require advanced skills or training.1,2 The mean MA salary at our institution ($37,372) is higher than in our state overall ($33,760), which may impact satisfaction.16 In addition, 93% of MAs are women; thus, they may continue to struggle more with lower pay than do workers in male- dominated professions.17,18 Expected job growth from 2018-2028 is predicted at 23%, which may help to boost salaries. 19 Prior studies describe the lack of a job ladder or promotion opportunities as a challenge1,20; this was not formally assessed in our study.
MAs see work in family medicine as much harder than it is in other specialty clinics. Being trusted with more responsibility, greater autonomy,21-23 and expanded patient care roles can boost MA self-efficacy, which can reduce burnout for both physicians and MAs. 8,24 However, new responsibilities should include appropriate training, support, and compensation, and match staff interests.7
Study limitations. The study was limited to 6 clinics in 1 department at a large academic medical center. Interviewed participants were selected by convenience and snowball sampling and thus, the results cannot be generalized to the population of MAs as a whole. As the initial interview goal was simply to gather efficiency tips, the project was not designed to be formal qualitative research. However, the discussions built on open-ended comments from the written survey helped contextualize our quantitative findings about efficiency. Notes were documented in real time by a single interviewer with rapid typing skills, which allowed capture of quotes verbatim. Subsequent studies would benefit from more formal qualitative research methods (recording and transcribing interviews, multiple coders to reduce risk of bias, and more complex thematic analysis).
Our research demonstrated how MAs perceive their roles in primary care and the facilitators and barriers to high efficiency in the workplace, which begins to fill an important knowledge gap in primary care. Disseminating practices that staff members themselves have identified as effective, and being attentive to how staff members are treated, may increase individual efficiency while improving staff retention and satisfaction.
CORRESPONDENCE Katherine J. Gold, MD, MSW, MS, Department of Family Medicine and Department of Obstetrics and Gynecology, University of Michigan, 1018 Fuller Street, Ann Arbor, MI 48104-1213; [email protected]
- Chapman SA, Blash LK. New roles for medical assistants in innovative primary care practices. Health Serv Res. 2017;52(suppl 1):383-406.
- Ferrante JM, Shaw EK, Bayly JE, et al. Barriers and facilitators to expanding roles of medical assistants in patient-centered medical homes (PCMHs). J Am Board Fam Med. 2018;31:226-235.
- Atkins B. The outlook for medical assisting in 2016 and beyond. Accessed January 27, 2022. www.medicalassistantdegrees.net/ articles/medical-assisting-trends/
- Unqualified medical “assistants.” Hospital (Lond 1886). 1897;23:163-164.
- Ameritech College of Healthcare. The origins of the AAMA. Accessed January 27, 2022. www.ameritech.edu/blog/medicalassisting-history/
- Dai M, Willard-Grace R, Knox M, et al. Team configurations, efficiency, and family physician burnout. J Am Board Fam Med. 2020;33:368-377.
- Harper PG, Van Riper K, Ramer T, et al. Team-based care: an expanded medical assistant role—enhanced rooming and visit assistance. J Interprof Care. 2018:1-7.
- Sheridan B, Chien AT, Peters AS, et al. Team-based primary care: the medical assistant perspective. Health Care Manage Rev. 2018;43:115-125.
- Tache S, Hill-Sakurai L. Medical assistants: the invisible “glue” of primary health care practices in the United States? J Health Organ Manag. 2010;24:288-305.
- STROBE checklist for cohort, case-control, and cross-sectional studies. Accessed January 27, 2022. www.strobe-statement.org/ fileadmin/Strobe/uploads/checklists/STROBE_checklist_v4_ combined.pdf
- Gray CP, Harrison MI, Hung D. Medical assistants as flow managers in primary care: challenges and recommendations. J Healthc Manag. 2016;61:181-191.
- Elder NC, Jacobson CJ, Bolon SK, et al. Patterns of relating between physicians and medical assistants in small family medicine offices. Ann Fam Med. 2014;12:150-157.
- Jager AJ, Tutty MA, Kao AC. Association between physician burnout and identification with medicine as a calling. Mayo Clinic Proc. 2017;92:415-422.
- Yoon JD, Daley BM, Curlin FA. The association between a sense of calling and physician well-being: a national study of primary care physicians and psychiatrists. Acad Psychiatry. 2017;41:167-173.
- Mohr DC, Young GJ, Meterko M, et al. Job satisfaction of primary care team members and quality of care. Am J Med Qual. 2011;26:18-25.
- US Bureau of Labor Statistics. Occupational employment and wage statistics. Accessed January 27, 2022. https://www.bls.gov/ oes/current/oes319092.htm
- Chapman SA, Marks A, Dower C. Positioning medical assistants for a greater role in the era of health reform. Acad Med. 2015;90:1347-1352.
- Mandel H. The role of occupational attributes in gender earnings inequality, 1970-2010. Soc Sci Res. 2016;55:122-138.
- US Bureau of Labor Statistics. Occupational outlook handbook: medical assistants. Accessed January 27, 2022. www.bls.gov/ooh/ healthcare/medical-assistants.htm
- Skillman SM, Dahal A, Frogner BK, et al. Frontline workers’ career pathways: a detailed look at Washington state’s medical assistant workforce. Med Care Res Rev. 2018:1077558718812950.
- Morse G, Salyers MP, Rollins AL, et al. Burnout in mental health services: a review of the problem and its remediation. Adm Policy Ment Health. 2012;39:341-352.
- Dubois CA, Bentein K, Ben Mansour JB, et al. Why some employees adopt or resist reorganization of work practices in health care: associations between perceived loss of resources, burnout, and attitudes to change. Int J Environ Res Pub Health. 2014;11: 187-201.
- Aronsson G, Theorell T, Grape T, et al. A systematic review including meta-analysis of work environment and burnout symptoms. BMC Public Health. 2017;17:264.
- O’Malley AS, Gourevitch R, Draper K, et al. Overcoming challenges to teamwork in patient-centered medical homes: a qualitative study. J Gen Intern Med. 2015;30:183-192.
ABSTRACT
Background: Medical assistant (MA) roles have expanded rapidly as primary care has evolved and MAs take on new patient care duties. Research that looks at the MA experience and factors that enhance or reduce efficiency among MAs is limited.
Methods: We surveyed all MAs working in 6 clinics run by a large academic family medicine department in Ann Arbor, Michigan. MAs deemed by peers as “most efficient” were selected for follow-up interviews. We evaluated personal strategies for efficiency, barriers to efficient care, impact of physician actions on efficiency, and satisfaction.
Results: A total of 75/86 MAs (87%) responded to at least some survey questions and 61/86 (71%) completed the full survey. We interviewed 18 MAs face to face. Most saw their role as essential to clinic functioning and viewed health care as a personal calling. MAs identified common strategies to improve efficiency and described the MA role to orchestrate the flow of the clinic day. Staff recognized differing priorities of patients, staff, and physicians and articulated frustrations with hierarchy and competing priorities as well as behaviors that impeded clinic efficiency. Respondents emphasized the importance of feeling valued by others on their team.
Conclusions: With the evolving demands made on MAs’ time, it is critical to understand how the most effective staff members manage their role and highlight the strategies they employ to provide efficient clinical care. Understanding factors that increase or decrease MA job satisfaction can help identify high-efficiency practices and promote a clinic culture that values and supports all staff.
As primary care continues to evolve into more team-based practice, the role of the medical assistant (MA) has rapidly transformed.1 Staff may assist with patient management, documentation in the electronic medical record, order entry, pre-visit planning, and fulfillment of quality metrics, particularly in a Primary Care Medical Home (PCMH).2 From 2012 through 2014, MA job postings per graduate increased from 1.3 to 2.3, suggesting twice as many job postings as graduates.3 As the demand for experienced MAs increases, the ability to recruit and retain high-performing staff members will be critical.
MAs are referenced in medical literature as early as the 1800s.4 The American Association of Medical Assistants was founded in 1956, which led to educational standardization and certifications.5 Despite the important role that MAs have long played in the proper functioning of a medical clinic—and the knowledge that team configurations impact a clinic’s efficiency and quality6,7—few investigations have sought out the MA’s perspective.8,9 Given the increasing clinical demands placed on all members of the primary care team (and the burnout that often results), it seems that MA insights into clinic efficiency could be valuable.
Continue to: Methods...
METHODS
This cross-sectional study was conducted from February to April 2019 at a large academic institution with 6 regional ambulatory care family medicine clinics, each one with 11,000 to 18,000 patient visits annually. Faculty work at all 6 clinics and residents at 2 of them. All MAs are hired, paid, and managed by a central administrative department rather than by the family medicine department. The family medicine clinics are currently PCMH certified, with a mix of fee-for-service and capitated reimbursement.
We developed and piloted a voluntary, anonymous 39-question (29 closed-ended and 10 brief open-ended) online Qualtrics survey, which we distributed via an email link to all the MAs in the department. The survey included clinic site, years as an MA, perceptions of the clinic environment, perception of teamwork at their site, identification of efficient practices, and feedback for physicians to improve efficiency and flow. Most questions were Likert-style with 5 choices ranging from “strongly agree” to “strongly disagree” or short answer. Age and gender were omitted to protect confidentiality, as most MAs in the department are female. Participants could opt to enter in a drawing for three $25 gift cards. The survey was reviewed by the University of Michigan Institutional Review Board and deemed exempt.
We asked MAs to nominate peers in their clinic who were “especially efficient and do their jobs well—people that others can learn from.” The staff members who were nominated most frequently by their peers were invited to share additional perspectives via a 10- to 30-minute semi-structured interview with the first author. Interviews covered highly efficient practices, barriers and facilitators to efficient care, and physician behaviors that impaired efficiency. We interviewed a minimum of 2 MAs per clinic and increased the number of interviews through snowball sampling, as needed, to reach data saturation (eg, the point at which we were no longer hearing new content). MAs were assured that all comments would be anonymized. There was no monetary incentive for the interviews. The interviewer had previously met only 3 of the 18 MAs interviewed.
Analysis. Summary statistics were calculated for quantitative data. To compare subgroups (such as individual clinics), a chi-square test was used. In cases when there were small cell sizes (< 5 subjects), we used the Fisher’s Exact test. Qualitative data was collected with real-time typewritten notes during the interviews to capture ideas and verbatim quotes when possible. We also included open-ended comments shared on the Qualtrics survey. Data were organized by theme using a deductive coding approach. Both authors reviewed and discussed observations, and coding was conducted by the first author. Reporting followed the STROBE Statement checklist for cross-sectional studies.10 Results were shared with MAs, supervisory staff, and physicians, which allowed for feedback and comments and served as “member-checking.” MAs reported that the data reflected their lived experiences.
Continue to: RESULTS...
RESULTS
Surveys were distributed to all 86 MAs working in family medicine clinics. A total of 75 (87%) responded to at least some questions (typically just demographics). We used those who completed the full survey (n = 61; 71%) for data analysis. Eighteen MAs participated in face-to-face interviews. Among respondents, 35 (47%) had worked at least 10 years as an MA and 21 (28%) had worked at least a decade in the family medicine department.
Perception of role
All respondents (n = 61; 100%) somewhat or strongly agreed that the MA role was “very important to keep the clinic functioning” and 58 (95%) reported that working in health care was “a calling” for them. Only 7 (11%) agreed that family medicine was an easier environment for MAs compared to a specialty clinic; 30 (49%) disagreed with this. Among respondents, 32 (53%) strongly or somewhat agreed that their work was very stressful and just half (n = 28; 46%) agreed there were adequate MA staff at their clinic.
Efficiency and competing priorities
MAs described important work values that increased their efficiency. These included clinic culture (good communication and strong teamwork), as well as individual strategies such as multitasking, limiting patient conversations, and doing tasks in a consistent way to improve accuracy. (See TABLE 1.) They identified ways physicians bolster or hurt efficiency and ways in which the relationship between the physician and the MA shapes the MA’s perception of their value in clinic.
Communication was emphasized as critical for efficient care, and MAs encouraged the use of preclinic huddles and communication as priorities. Seventy-five percent of MAs reported preclinic huddles to plan for patient care were helpful, but only half said huddles took place “always” or “most of the time.” Many described reviewing the schedule and completing tasks ahead of patient arrival as critical to efficiency.
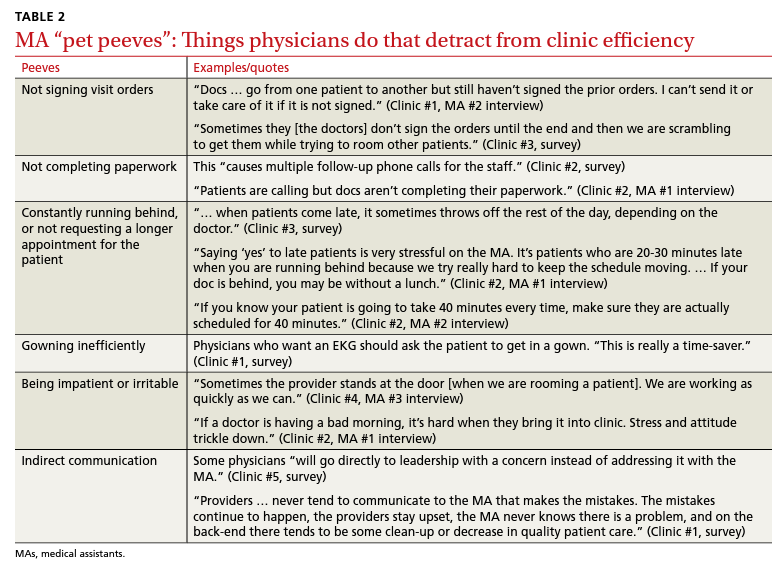
Participants described the tension between their identified role of orchestrating clinic flow and responding to directives by others that disrupted the flow. Several MAs found it challenging when physicians agreed to see very late patients and felt frustrated when decisions that changed the flow were made by the physician or front desk staff without including the MA. MAs were also able to articulate how they managed competing priorities within the clinic, such as when a patient- or physician-driven need to extend appointments was at odds with maintaining a timely schedule. They were eager to share personal tips for time management and prided themselves on careful and accurate performance and skills they had learned on the job. MAs also described how efficiency could be adversely affected by the behaviors or attitudes of physicians. (See TABLE 2.)
Continue to: Clinic environment...
Clinic environment
Thirty-six MAs (59%) reported that other MAs on their team were willing to help them out in clinic “a great deal” or “a lot” of the time, by helping to room a patient, acting as a chaperone for an exam, or doing a point-of-care lab. This sense of support varied across clinics (38% to 91% reported good support), suggesting that cultures vary by site. Some MAs expressed frustration at peers they saw as resistant to helping, exemplified by this verbatim quote from an interview:
“Some don’t want to help out. They may sigh. It’s how they react—you just know.” (Clinic #1, MA #2 interview)
Efficient MAs stressed the need for situational awareness to recognize when co-workers need help:
“[Peers often] are not aware that another MA is drowning. There’s 5 people who could have done that, and here I am running around and nobody budged.” (Clinic #5, MA #2 interview)
A minority of staff used the open-ended survey sections to describe clinic hierarchy. When asked about “pet peeves,” a few advised that physicians should not “talk down” to staff and should try to teach rather than criticize. Another asked that physicians not “bark orders” or have “low gratitude” for staff work. MAs found micromanaging stressful—particularly when the physician prompted the MA about patient arrivals:
“[I don’t like] when providers will make a comment about a patient arriving when you already know this information. You then rush to put [the] patient in [a] room, then [the] provider ends up making [the] patient wait an extensive amount of time. I’m perfectly capable of knowing when a patient arrives.” (Clinic #6, survey)
MAs did not like physicians “talking bad about us” or blaming the MA if the clinic is running behind.
Despite these concerns, most MAs reported feeling appreciated for the job they do. Only 10 (16%) reported that the people they work with rarely say “thank you,” and 2 (3%) stated they were not well supported by the physicians in clinic. Most (n = 38; 62%) strongly agreed or agreed that they felt part of the team and that their opinions matter. In the interviews, many expanded on this idea:
“I really feel like I’m valued, so I want to do everything I can to make [my doctor’s] day go better. If you want a good clinic, the best thing a doc can do is make the MA feel valued.” (Clinic #1, MA #1 interview)
Continue to: DISCUSSION...
DISCUSSION
Participants described their role much as an orchestra director, with MAs as the key to clinic flow and timeliness.9 Respondents articulated multiple common strategies used to increase their own efficiency and clinic flow; these may be considered best practices and incorporated as part of the basic training. Most MAs reported their day-to-day jobs were stressful and believed this was underrecognized, so efficiency strategies are critical. With staff completing multiple time-sensitive tasks during clinic, consistent co-worker support is crucial and may impact efficiency.8 Proper training of managers to provide that support and ensure equitable workloads may be one strategy to ensure that staff members feel the workplace is fair and collegial.
Several comments reflected the power differential within medical offices. One study reported that MAs and physicians “occupy roles at opposite ends of social and occupational hierarchies.”11 It’s important for physicians to be cognizant of these patterns and clinic culture, as reducing a hierarchy-based environment will be appreciated by MAs.9 Prior research has found that MAs have higher perceptions of their own competence than do the physicians working with them.12 If there is a fundamental lack of trust between the 2 groups, this will undoubtedly hinder team-building. Attention to this issue is key to a more favorable work environment.
Almost all respondents reported health care was a “calling,” which mirrors physician research that suggests seeing work as a “calling” is protective against burnout.13,14 Open-ended comments indicated great pride in contributions, and most staff members felt appreciated by their teams. Many described the working relationships with physicians as critical to their satisfaction at work and indicated that strong partnerships motivated them to do their best to make the physician’s day easier. Staff job satisfaction is linked to improved quality of care, so treating staff well contributes to high-value care for patients.15 We also uncovered some MA “pet peeves” that hinder efficiency and could be shared with physicians to emphasize the importance of patience and civility.
One barrier to expansion of MA roles within PCMH practices is the limited pay and career ladder for MAs who adopt new job responsibilities that require advanced skills or training.1,2 The mean MA salary at our institution ($37,372) is higher than in our state overall ($33,760), which may impact satisfaction.16 In addition, 93% of MAs are women; thus, they may continue to struggle more with lower pay than do workers in male- dominated professions.17,18 Expected job growth from 2018-2028 is predicted at 23%, which may help to boost salaries. 19 Prior studies describe the lack of a job ladder or promotion opportunities as a challenge1,20; this was not formally assessed in our study.
MAs see work in family medicine as much harder than it is in other specialty clinics. Being trusted with more responsibility, greater autonomy,21-23 and expanded patient care roles can boost MA self-efficacy, which can reduce burnout for both physicians and MAs. 8,24 However, new responsibilities should include appropriate training, support, and compensation, and match staff interests.7
Study limitations. The study was limited to 6 clinics in 1 department at a large academic medical center. Interviewed participants were selected by convenience and snowball sampling and thus, the results cannot be generalized to the population of MAs as a whole. As the initial interview goal was simply to gather efficiency tips, the project was not designed to be formal qualitative research. However, the discussions built on open-ended comments from the written survey helped contextualize our quantitative findings about efficiency. Notes were documented in real time by a single interviewer with rapid typing skills, which allowed capture of quotes verbatim. Subsequent studies would benefit from more formal qualitative research methods (recording and transcribing interviews, multiple coders to reduce risk of bias, and more complex thematic analysis).
Our research demonstrated how MAs perceive their roles in primary care and the facilitators and barriers to high efficiency in the workplace, which begins to fill an important knowledge gap in primary care. Disseminating practices that staff members themselves have identified as effective, and being attentive to how staff members are treated, may increase individual efficiency while improving staff retention and satisfaction.
CORRESPONDENCE Katherine J. Gold, MD, MSW, MS, Department of Family Medicine and Department of Obstetrics and Gynecology, University of Michigan, 1018 Fuller Street, Ann Arbor, MI 48104-1213; [email protected]
ABSTRACT
Background: Medical assistant (MA) roles have expanded rapidly as primary care has evolved and MAs take on new patient care duties. Research that looks at the MA experience and factors that enhance or reduce efficiency among MAs is limited.
Methods: We surveyed all MAs working in 6 clinics run by a large academic family medicine department in Ann Arbor, Michigan. MAs deemed by peers as “most efficient” were selected for follow-up interviews. We evaluated personal strategies for efficiency, barriers to efficient care, impact of physician actions on efficiency, and satisfaction.
Results: A total of 75/86 MAs (87%) responded to at least some survey questions and 61/86 (71%) completed the full survey. We interviewed 18 MAs face to face. Most saw their role as essential to clinic functioning and viewed health care as a personal calling. MAs identified common strategies to improve efficiency and described the MA role to orchestrate the flow of the clinic day. Staff recognized differing priorities of patients, staff, and physicians and articulated frustrations with hierarchy and competing priorities as well as behaviors that impeded clinic efficiency. Respondents emphasized the importance of feeling valued by others on their team.
Conclusions: With the evolving demands made on MAs’ time, it is critical to understand how the most effective staff members manage their role and highlight the strategies they employ to provide efficient clinical care. Understanding factors that increase or decrease MA job satisfaction can help identify high-efficiency practices and promote a clinic culture that values and supports all staff.
As primary care continues to evolve into more team-based practice, the role of the medical assistant (MA) has rapidly transformed.1 Staff may assist with patient management, documentation in the electronic medical record, order entry, pre-visit planning, and fulfillment of quality metrics, particularly in a Primary Care Medical Home (PCMH).2 From 2012 through 2014, MA job postings per graduate increased from 1.3 to 2.3, suggesting twice as many job postings as graduates.3 As the demand for experienced MAs increases, the ability to recruit and retain high-performing staff members will be critical.
MAs are referenced in medical literature as early as the 1800s.4 The American Association of Medical Assistants was founded in 1956, which led to educational standardization and certifications.5 Despite the important role that MAs have long played in the proper functioning of a medical clinic—and the knowledge that team configurations impact a clinic’s efficiency and quality6,7—few investigations have sought out the MA’s perspective.8,9 Given the increasing clinical demands placed on all members of the primary care team (and the burnout that often results), it seems that MA insights into clinic efficiency could be valuable.
Continue to: Methods...
METHODS
This cross-sectional study was conducted from February to April 2019 at a large academic institution with 6 regional ambulatory care family medicine clinics, each one with 11,000 to 18,000 patient visits annually. Faculty work at all 6 clinics and residents at 2 of them. All MAs are hired, paid, and managed by a central administrative department rather than by the family medicine department. The family medicine clinics are currently PCMH certified, with a mix of fee-for-service and capitated reimbursement.
We developed and piloted a voluntary, anonymous 39-question (29 closed-ended and 10 brief open-ended) online Qualtrics survey, which we distributed via an email link to all the MAs in the department. The survey included clinic site, years as an MA, perceptions of the clinic environment, perception of teamwork at their site, identification of efficient practices, and feedback for physicians to improve efficiency and flow. Most questions were Likert-style with 5 choices ranging from “strongly agree” to “strongly disagree” or short answer. Age and gender were omitted to protect confidentiality, as most MAs in the department are female. Participants could opt to enter in a drawing for three $25 gift cards. The survey was reviewed by the University of Michigan Institutional Review Board and deemed exempt.
We asked MAs to nominate peers in their clinic who were “especially efficient and do their jobs well—people that others can learn from.” The staff members who were nominated most frequently by their peers were invited to share additional perspectives via a 10- to 30-minute semi-structured interview with the first author. Interviews covered highly efficient practices, barriers and facilitators to efficient care, and physician behaviors that impaired efficiency. We interviewed a minimum of 2 MAs per clinic and increased the number of interviews through snowball sampling, as needed, to reach data saturation (eg, the point at which we were no longer hearing new content). MAs were assured that all comments would be anonymized. There was no monetary incentive for the interviews. The interviewer had previously met only 3 of the 18 MAs interviewed.
Analysis. Summary statistics were calculated for quantitative data. To compare subgroups (such as individual clinics), a chi-square test was used. In cases when there were small cell sizes (< 5 subjects), we used the Fisher’s Exact test. Qualitative data was collected with real-time typewritten notes during the interviews to capture ideas and verbatim quotes when possible. We also included open-ended comments shared on the Qualtrics survey. Data were organized by theme using a deductive coding approach. Both authors reviewed and discussed observations, and coding was conducted by the first author. Reporting followed the STROBE Statement checklist for cross-sectional studies.10 Results were shared with MAs, supervisory staff, and physicians, which allowed for feedback and comments and served as “member-checking.” MAs reported that the data reflected their lived experiences.
Continue to: RESULTS...
RESULTS
Surveys were distributed to all 86 MAs working in family medicine clinics. A total of 75 (87%) responded to at least some questions (typically just demographics). We used those who completed the full survey (n = 61; 71%) for data analysis. Eighteen MAs participated in face-to-face interviews. Among respondents, 35 (47%) had worked at least 10 years as an MA and 21 (28%) had worked at least a decade in the family medicine department.
Perception of role
All respondents (n = 61; 100%) somewhat or strongly agreed that the MA role was “very important to keep the clinic functioning” and 58 (95%) reported that working in health care was “a calling” for them. Only 7 (11%) agreed that family medicine was an easier environment for MAs compared to a specialty clinic; 30 (49%) disagreed with this. Among respondents, 32 (53%) strongly or somewhat agreed that their work was very stressful and just half (n = 28; 46%) agreed there were adequate MA staff at their clinic.
Efficiency and competing priorities
MAs described important work values that increased their efficiency. These included clinic culture (good communication and strong teamwork), as well as individual strategies such as multitasking, limiting patient conversations, and doing tasks in a consistent way to improve accuracy. (See TABLE 1.) They identified ways physicians bolster or hurt efficiency and ways in which the relationship between the physician and the MA shapes the MA’s perception of their value in clinic.
Communication was emphasized as critical for efficient care, and MAs encouraged the use of preclinic huddles and communication as priorities. Seventy-five percent of MAs reported preclinic huddles to plan for patient care were helpful, but only half said huddles took place “always” or “most of the time.” Many described reviewing the schedule and completing tasks ahead of patient arrival as critical to efficiency.
Participants described the tension between their identified role of orchestrating clinic flow and responding to directives by others that disrupted the flow. Several MAs found it challenging when physicians agreed to see very late patients and felt frustrated when decisions that changed the flow were made by the physician or front desk staff without including the MA. MAs were also able to articulate how they managed competing priorities within the clinic, such as when a patient- or physician-driven need to extend appointments was at odds with maintaining a timely schedule. They were eager to share personal tips for time management and prided themselves on careful and accurate performance and skills they had learned on the job. MAs also described how efficiency could be adversely affected by the behaviors or attitudes of physicians. (See TABLE 2.)
Continue to: Clinic environment...
Clinic environment
Thirty-six MAs (59%) reported that other MAs on their team were willing to help them out in clinic “a great deal” or “a lot” of the time, by helping to room a patient, acting as a chaperone for an exam, or doing a point-of-care lab. This sense of support varied across clinics (38% to 91% reported good support), suggesting that cultures vary by site. Some MAs expressed frustration at peers they saw as resistant to helping, exemplified by this verbatim quote from an interview:
“Some don’t want to help out. They may sigh. It’s how they react—you just know.” (Clinic #1, MA #2 interview)
Efficient MAs stressed the need for situational awareness to recognize when co-workers need help:
“[Peers often] are not aware that another MA is drowning. There’s 5 people who could have done that, and here I am running around and nobody budged.” (Clinic #5, MA #2 interview)
A minority of staff used the open-ended survey sections to describe clinic hierarchy. When asked about “pet peeves,” a few advised that physicians should not “talk down” to staff and should try to teach rather than criticize. Another asked that physicians not “bark orders” or have “low gratitude” for staff work. MAs found micromanaging stressful—particularly when the physician prompted the MA about patient arrivals:
“[I don’t like] when providers will make a comment about a patient arriving when you already know this information. You then rush to put [the] patient in [a] room, then [the] provider ends up making [the] patient wait an extensive amount of time. I’m perfectly capable of knowing when a patient arrives.” (Clinic #6, survey)
MAs did not like physicians “talking bad about us” or blaming the MA if the clinic is running behind.
Despite these concerns, most MAs reported feeling appreciated for the job they do. Only 10 (16%) reported that the people they work with rarely say “thank you,” and 2 (3%) stated they were not well supported by the physicians in clinic. Most (n = 38; 62%) strongly agreed or agreed that they felt part of the team and that their opinions matter. In the interviews, many expanded on this idea:
“I really feel like I’m valued, so I want to do everything I can to make [my doctor’s] day go better. If you want a good clinic, the best thing a doc can do is make the MA feel valued.” (Clinic #1, MA #1 interview)
Continue to: DISCUSSION...
DISCUSSION
Participants described their role much as an orchestra director, with MAs as the key to clinic flow and timeliness.9 Respondents articulated multiple common strategies used to increase their own efficiency and clinic flow; these may be considered best practices and incorporated as part of the basic training. Most MAs reported their day-to-day jobs were stressful and believed this was underrecognized, so efficiency strategies are critical. With staff completing multiple time-sensitive tasks during clinic, consistent co-worker support is crucial and may impact efficiency.8 Proper training of managers to provide that support and ensure equitable workloads may be one strategy to ensure that staff members feel the workplace is fair and collegial.
Several comments reflected the power differential within medical offices. One study reported that MAs and physicians “occupy roles at opposite ends of social and occupational hierarchies.”11 It’s important for physicians to be cognizant of these patterns and clinic culture, as reducing a hierarchy-based environment will be appreciated by MAs.9 Prior research has found that MAs have higher perceptions of their own competence than do the physicians working with them.12 If there is a fundamental lack of trust between the 2 groups, this will undoubtedly hinder team-building. Attention to this issue is key to a more favorable work environment.
Almost all respondents reported health care was a “calling,” which mirrors physician research that suggests seeing work as a “calling” is protective against burnout.13,14 Open-ended comments indicated great pride in contributions, and most staff members felt appreciated by their teams. Many described the working relationships with physicians as critical to their satisfaction at work and indicated that strong partnerships motivated them to do their best to make the physician’s day easier. Staff job satisfaction is linked to improved quality of care, so treating staff well contributes to high-value care for patients.15 We also uncovered some MA “pet peeves” that hinder efficiency and could be shared with physicians to emphasize the importance of patience and civility.
One barrier to expansion of MA roles within PCMH practices is the limited pay and career ladder for MAs who adopt new job responsibilities that require advanced skills or training.1,2 The mean MA salary at our institution ($37,372) is higher than in our state overall ($33,760), which may impact satisfaction.16 In addition, 93% of MAs are women; thus, they may continue to struggle more with lower pay than do workers in male- dominated professions.17,18 Expected job growth from 2018-2028 is predicted at 23%, which may help to boost salaries. 19 Prior studies describe the lack of a job ladder or promotion opportunities as a challenge1,20; this was not formally assessed in our study.
MAs see work in family medicine as much harder than it is in other specialty clinics. Being trusted with more responsibility, greater autonomy,21-23 and expanded patient care roles can boost MA self-efficacy, which can reduce burnout for both physicians and MAs. 8,24 However, new responsibilities should include appropriate training, support, and compensation, and match staff interests.7
Study limitations. The study was limited to 6 clinics in 1 department at a large academic medical center. Interviewed participants were selected by convenience and snowball sampling and thus, the results cannot be generalized to the population of MAs as a whole. As the initial interview goal was simply to gather efficiency tips, the project was not designed to be formal qualitative research. However, the discussions built on open-ended comments from the written survey helped contextualize our quantitative findings about efficiency. Notes were documented in real time by a single interviewer with rapid typing skills, which allowed capture of quotes verbatim. Subsequent studies would benefit from more formal qualitative research methods (recording and transcribing interviews, multiple coders to reduce risk of bias, and more complex thematic analysis).
Our research demonstrated how MAs perceive their roles in primary care and the facilitators and barriers to high efficiency in the workplace, which begins to fill an important knowledge gap in primary care. Disseminating practices that staff members themselves have identified as effective, and being attentive to how staff members are treated, may increase individual efficiency while improving staff retention and satisfaction.
CORRESPONDENCE Katherine J. Gold, MD, MSW, MS, Department of Family Medicine and Department of Obstetrics and Gynecology, University of Michigan, 1018 Fuller Street, Ann Arbor, MI 48104-1213; [email protected]
- Chapman SA, Blash LK. New roles for medical assistants in innovative primary care practices. Health Serv Res. 2017;52(suppl 1):383-406.
- Ferrante JM, Shaw EK, Bayly JE, et al. Barriers and facilitators to expanding roles of medical assistants in patient-centered medical homes (PCMHs). J Am Board Fam Med. 2018;31:226-235.
- Atkins B. The outlook for medical assisting in 2016 and beyond. Accessed January 27, 2022. www.medicalassistantdegrees.net/ articles/medical-assisting-trends/
- Unqualified medical “assistants.” Hospital (Lond 1886). 1897;23:163-164.
- Ameritech College of Healthcare. The origins of the AAMA. Accessed January 27, 2022. www.ameritech.edu/blog/medicalassisting-history/
- Dai M, Willard-Grace R, Knox M, et al. Team configurations, efficiency, and family physician burnout. J Am Board Fam Med. 2020;33:368-377.
- Harper PG, Van Riper K, Ramer T, et al. Team-based care: an expanded medical assistant role—enhanced rooming and visit assistance. J Interprof Care. 2018:1-7.
- Sheridan B, Chien AT, Peters AS, et al. Team-based primary care: the medical assistant perspective. Health Care Manage Rev. 2018;43:115-125.
- Tache S, Hill-Sakurai L. Medical assistants: the invisible “glue” of primary health care practices in the United States? J Health Organ Manag. 2010;24:288-305.
- STROBE checklist for cohort, case-control, and cross-sectional studies. Accessed January 27, 2022. www.strobe-statement.org/ fileadmin/Strobe/uploads/checklists/STROBE_checklist_v4_ combined.pdf
- Gray CP, Harrison MI, Hung D. Medical assistants as flow managers in primary care: challenges and recommendations. J Healthc Manag. 2016;61:181-191.
- Elder NC, Jacobson CJ, Bolon SK, et al. Patterns of relating between physicians and medical assistants in small family medicine offices. Ann Fam Med. 2014;12:150-157.
- Jager AJ, Tutty MA, Kao AC. Association between physician burnout and identification with medicine as a calling. Mayo Clinic Proc. 2017;92:415-422.
- Yoon JD, Daley BM, Curlin FA. The association between a sense of calling and physician well-being: a national study of primary care physicians and psychiatrists. Acad Psychiatry. 2017;41:167-173.
- Mohr DC, Young GJ, Meterko M, et al. Job satisfaction of primary care team members and quality of care. Am J Med Qual. 2011;26:18-25.
- US Bureau of Labor Statistics. Occupational employment and wage statistics. Accessed January 27, 2022. https://www.bls.gov/ oes/current/oes319092.htm
- Chapman SA, Marks A, Dower C. Positioning medical assistants for a greater role in the era of health reform. Acad Med. 2015;90:1347-1352.
- Mandel H. The role of occupational attributes in gender earnings inequality, 1970-2010. Soc Sci Res. 2016;55:122-138.
- US Bureau of Labor Statistics. Occupational outlook handbook: medical assistants. Accessed January 27, 2022. www.bls.gov/ooh/ healthcare/medical-assistants.htm
- Skillman SM, Dahal A, Frogner BK, et al. Frontline workers’ career pathways: a detailed look at Washington state’s medical assistant workforce. Med Care Res Rev. 2018:1077558718812950.
- Morse G, Salyers MP, Rollins AL, et al. Burnout in mental health services: a review of the problem and its remediation. Adm Policy Ment Health. 2012;39:341-352.
- Dubois CA, Bentein K, Ben Mansour JB, et al. Why some employees adopt or resist reorganization of work practices in health care: associations between perceived loss of resources, burnout, and attitudes to change. Int J Environ Res Pub Health. 2014;11: 187-201.
- Aronsson G, Theorell T, Grape T, et al. A systematic review including meta-analysis of work environment and burnout symptoms. BMC Public Health. 2017;17:264.
- O’Malley AS, Gourevitch R, Draper K, et al. Overcoming challenges to teamwork in patient-centered medical homes: a qualitative study. J Gen Intern Med. 2015;30:183-192.
- Chapman SA, Blash LK. New roles for medical assistants in innovative primary care practices. Health Serv Res. 2017;52(suppl 1):383-406.
- Ferrante JM, Shaw EK, Bayly JE, et al. Barriers and facilitators to expanding roles of medical assistants in patient-centered medical homes (PCMHs). J Am Board Fam Med. 2018;31:226-235.
- Atkins B. The outlook for medical assisting in 2016 and beyond. Accessed January 27, 2022. www.medicalassistantdegrees.net/ articles/medical-assisting-trends/
- Unqualified medical “assistants.” Hospital (Lond 1886). 1897;23:163-164.
- Ameritech College of Healthcare. The origins of the AAMA. Accessed January 27, 2022. www.ameritech.edu/blog/medicalassisting-history/
- Dai M, Willard-Grace R, Knox M, et al. Team configurations, efficiency, and family physician burnout. J Am Board Fam Med. 2020;33:368-377.
- Harper PG, Van Riper K, Ramer T, et al. Team-based care: an expanded medical assistant role—enhanced rooming and visit assistance. J Interprof Care. 2018:1-7.
- Sheridan B, Chien AT, Peters AS, et al. Team-based primary care: the medical assistant perspective. Health Care Manage Rev. 2018;43:115-125.
- Tache S, Hill-Sakurai L. Medical assistants: the invisible “glue” of primary health care practices in the United States? J Health Organ Manag. 2010;24:288-305.
- STROBE checklist for cohort, case-control, and cross-sectional studies. Accessed January 27, 2022. www.strobe-statement.org/ fileadmin/Strobe/uploads/checklists/STROBE_checklist_v4_ combined.pdf
- Gray CP, Harrison MI, Hung D. Medical assistants as flow managers in primary care: challenges and recommendations. J Healthc Manag. 2016;61:181-191.
- Elder NC, Jacobson CJ, Bolon SK, et al. Patterns of relating between physicians and medical assistants in small family medicine offices. Ann Fam Med. 2014;12:150-157.
- Jager AJ, Tutty MA, Kao AC. Association between physician burnout and identification with medicine as a calling. Mayo Clinic Proc. 2017;92:415-422.
- Yoon JD, Daley BM, Curlin FA. The association between a sense of calling and physician well-being: a national study of primary care physicians and psychiatrists. Acad Psychiatry. 2017;41:167-173.
- Mohr DC, Young GJ, Meterko M, et al. Job satisfaction of primary care team members and quality of care. Am J Med Qual. 2011;26:18-25.
- US Bureau of Labor Statistics. Occupational employment and wage statistics. Accessed January 27, 2022. https://www.bls.gov/ oes/current/oes319092.htm
- Chapman SA, Marks A, Dower C. Positioning medical assistants for a greater role in the era of health reform. Acad Med. 2015;90:1347-1352.
- Mandel H. The role of occupational attributes in gender earnings inequality, 1970-2010. Soc Sci Res. 2016;55:122-138.
- US Bureau of Labor Statistics. Occupational outlook handbook: medical assistants. Accessed January 27, 2022. www.bls.gov/ooh/ healthcare/medical-assistants.htm
- Skillman SM, Dahal A, Frogner BK, et al. Frontline workers’ career pathways: a detailed look at Washington state’s medical assistant workforce. Med Care Res Rev. 2018:1077558718812950.
- Morse G, Salyers MP, Rollins AL, et al. Burnout in mental health services: a review of the problem and its remediation. Adm Policy Ment Health. 2012;39:341-352.
- Dubois CA, Bentein K, Ben Mansour JB, et al. Why some employees adopt or resist reorganization of work practices in health care: associations between perceived loss of resources, burnout, and attitudes to change. Int J Environ Res Pub Health. 2014;11: 187-201.
- Aronsson G, Theorell T, Grape T, et al. A systematic review including meta-analysis of work environment and burnout symptoms. BMC Public Health. 2017;17:264.
- O’Malley AS, Gourevitch R, Draper K, et al. Overcoming challenges to teamwork in patient-centered medical homes: a qualitative study. J Gen Intern Med. 2015;30:183-192.
Medical assistants
When I began in private practice several eons ago, I employed only registered nurses (RNs) and licensed practical nurses (LPNs) in my office – as did, I think, most other physicians.
That is still the preferred way to go from an efficiency perspective, as well as the ability to delegate such tasks as blood collection and administering intramuscular injections. Unfortunately,
Given this reality, it makes sense to understand how the use of medical assistants has changed private medical practice, and how the most effective MAs manage their roles and maximize their efficiency in the office.
A recent article by two physicians at the University of Michigan, Ann Arbor, is one of the few published papers to address this issue. It presents the results of a cross-sectional study examining the MA’s experience and key factors that enhance or reduce efficiencies.
The authors sent an email survey to 86 MAs working in six clinics within the department of family medicine at the University of Michigan Medical Center, and received responses from 75 of them, including 61 who completed the entire survey. They then singled out 18 individuals deemed “most efficient” by their peers and conducted face-to-face interviews with them.
The surveys and interviews looked at how MAs identified personal strategies for efficiency, dealt with barriers to implementing those strategies, and navigated interoffice relationships, as well as how all of this affected overall job satisfaction.
All 61 respondents who completed the full survey agreed that the MA role was “very important to keep the clinic functioning” and nearly all said that working in health care was “a calling” for them. About half agreed that their work was very stressful, and about the same percentage reported that there was inadequate MA staffing at their clinic. Others complained of limited pay and promotion opportunities.
The surveyed MAs described important work values that increased their efficiency. These included good communication, strong teamwork, and workload sharing, as well as individual strategies such as multitasking, limiting patient conversations, and completing tasks in a consistent way to improve accuracy.
Other strategies identified as contributing to an efficient operation included preclinic huddles, reviews of patient records before the patient’s arrival, and completing routine office duties before the start of office hours.
Respondents were then asked to identify barriers to clinic efficiency, and most of them involved physicians who barked orders at them, did not complete paperwork or sign orders in a timely manner, and agreed to see late-arriving patients. Some MAs suggested that physicians refrain from “talking down” to them, and teach rather than criticize. They also faulted decisions affecting patient flow made by other staffers without soliciting the MAs’ input.
Despite these barriers, the authors found that most of the surveyed MAs agreed that their work was valued by doctors. “Proper training of managers to provide ... support and ensure equitable workloads may be one strategy to ensure that staff members feel the workplace is fair and collegial,” they said.
“Many described the working relationships with physicians as critical to their satisfaction at work and indicated that strong partnerships motivated them to do their best to make the physician’s day easier,” they added.
At the same time, the authors noted that most survey subjects reported that their jobs were “stressful,” and believed that their stress went underrecognized by physicians. They argued that “it’s important for physicians to be cognizant of these patterns and clinic culture, as reducing a hierarchy-based environment will be appreciated by MAs.”
Since this study involved only MAs in a family practice setting, further studies will be needed to determine whether these results translate to specialty offices – and whether the unique issues inherent in various specialty environments elicit different efficiency contributors and barriers.
Overall, though, “staff job satisfaction is linked to improved quality of care, so treating staff well contributes to high-value care for patients,” the authors wrote. “Disseminating practices that staff members themselves have identified as effective, and being attentive to how staff members are treated, may increase individual efficiency while improving staff retention and satisfaction.”
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
When I began in private practice several eons ago, I employed only registered nurses (RNs) and licensed practical nurses (LPNs) in my office – as did, I think, most other physicians.
That is still the preferred way to go from an efficiency perspective, as well as the ability to delegate such tasks as blood collection and administering intramuscular injections. Unfortunately,
Given this reality, it makes sense to understand how the use of medical assistants has changed private medical practice, and how the most effective MAs manage their roles and maximize their efficiency in the office.
A recent article by two physicians at the University of Michigan, Ann Arbor, is one of the few published papers to address this issue. It presents the results of a cross-sectional study examining the MA’s experience and key factors that enhance or reduce efficiencies.
The authors sent an email survey to 86 MAs working in six clinics within the department of family medicine at the University of Michigan Medical Center, and received responses from 75 of them, including 61 who completed the entire survey. They then singled out 18 individuals deemed “most efficient” by their peers and conducted face-to-face interviews with them.
The surveys and interviews looked at how MAs identified personal strategies for efficiency, dealt with barriers to implementing those strategies, and navigated interoffice relationships, as well as how all of this affected overall job satisfaction.
All 61 respondents who completed the full survey agreed that the MA role was “very important to keep the clinic functioning” and nearly all said that working in health care was “a calling” for them. About half agreed that their work was very stressful, and about the same percentage reported that there was inadequate MA staffing at their clinic. Others complained of limited pay and promotion opportunities.
The surveyed MAs described important work values that increased their efficiency. These included good communication, strong teamwork, and workload sharing, as well as individual strategies such as multitasking, limiting patient conversations, and completing tasks in a consistent way to improve accuracy.
Other strategies identified as contributing to an efficient operation included preclinic huddles, reviews of patient records before the patient’s arrival, and completing routine office duties before the start of office hours.
Respondents were then asked to identify barriers to clinic efficiency, and most of them involved physicians who barked orders at them, did not complete paperwork or sign orders in a timely manner, and agreed to see late-arriving patients. Some MAs suggested that physicians refrain from “talking down” to them, and teach rather than criticize. They also faulted decisions affecting patient flow made by other staffers without soliciting the MAs’ input.
Despite these barriers, the authors found that most of the surveyed MAs agreed that their work was valued by doctors. “Proper training of managers to provide ... support and ensure equitable workloads may be one strategy to ensure that staff members feel the workplace is fair and collegial,” they said.
“Many described the working relationships with physicians as critical to their satisfaction at work and indicated that strong partnerships motivated them to do their best to make the physician’s day easier,” they added.
At the same time, the authors noted that most survey subjects reported that their jobs were “stressful,” and believed that their stress went underrecognized by physicians. They argued that “it’s important for physicians to be cognizant of these patterns and clinic culture, as reducing a hierarchy-based environment will be appreciated by MAs.”
Since this study involved only MAs in a family practice setting, further studies will be needed to determine whether these results translate to specialty offices – and whether the unique issues inherent in various specialty environments elicit different efficiency contributors and barriers.
Overall, though, “staff job satisfaction is linked to improved quality of care, so treating staff well contributes to high-value care for patients,” the authors wrote. “Disseminating practices that staff members themselves have identified as effective, and being attentive to how staff members are treated, may increase individual efficiency while improving staff retention and satisfaction.”
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
When I began in private practice several eons ago, I employed only registered nurses (RNs) and licensed practical nurses (LPNs) in my office – as did, I think, most other physicians.
That is still the preferred way to go from an efficiency perspective, as well as the ability to delegate such tasks as blood collection and administering intramuscular injections. Unfortunately,
Given this reality, it makes sense to understand how the use of medical assistants has changed private medical practice, and how the most effective MAs manage their roles and maximize their efficiency in the office.
A recent article by two physicians at the University of Michigan, Ann Arbor, is one of the few published papers to address this issue. It presents the results of a cross-sectional study examining the MA’s experience and key factors that enhance or reduce efficiencies.
The authors sent an email survey to 86 MAs working in six clinics within the department of family medicine at the University of Michigan Medical Center, and received responses from 75 of them, including 61 who completed the entire survey. They then singled out 18 individuals deemed “most efficient” by their peers and conducted face-to-face interviews with them.
The surveys and interviews looked at how MAs identified personal strategies for efficiency, dealt with barriers to implementing those strategies, and navigated interoffice relationships, as well as how all of this affected overall job satisfaction.
All 61 respondents who completed the full survey agreed that the MA role was “very important to keep the clinic functioning” and nearly all said that working in health care was “a calling” for them. About half agreed that their work was very stressful, and about the same percentage reported that there was inadequate MA staffing at their clinic. Others complained of limited pay and promotion opportunities.
The surveyed MAs described important work values that increased their efficiency. These included good communication, strong teamwork, and workload sharing, as well as individual strategies such as multitasking, limiting patient conversations, and completing tasks in a consistent way to improve accuracy.
Other strategies identified as contributing to an efficient operation included preclinic huddles, reviews of patient records before the patient’s arrival, and completing routine office duties before the start of office hours.
Respondents were then asked to identify barriers to clinic efficiency, and most of them involved physicians who barked orders at them, did not complete paperwork or sign orders in a timely manner, and agreed to see late-arriving patients. Some MAs suggested that physicians refrain from “talking down” to them, and teach rather than criticize. They also faulted decisions affecting patient flow made by other staffers without soliciting the MAs’ input.
Despite these barriers, the authors found that most of the surveyed MAs agreed that their work was valued by doctors. “Proper training of managers to provide ... support and ensure equitable workloads may be one strategy to ensure that staff members feel the workplace is fair and collegial,” they said.
“Many described the working relationships with physicians as critical to their satisfaction at work and indicated that strong partnerships motivated them to do their best to make the physician’s day easier,” they added.
At the same time, the authors noted that most survey subjects reported that their jobs were “stressful,” and believed that their stress went underrecognized by physicians. They argued that “it’s important for physicians to be cognizant of these patterns and clinic culture, as reducing a hierarchy-based environment will be appreciated by MAs.”
Since this study involved only MAs in a family practice setting, further studies will be needed to determine whether these results translate to specialty offices – and whether the unique issues inherent in various specialty environments elicit different efficiency contributors and barriers.
Overall, though, “staff job satisfaction is linked to improved quality of care, so treating staff well contributes to high-value care for patients,” the authors wrote. “Disseminating practices that staff members themselves have identified as effective, and being attentive to how staff members are treated, may increase individual efficiency while improving staff retention and satisfaction.”
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Employment and buyout agreements
. The most common question was, “Do I really need to go to the trouble and expense of negotiating them?” If you have more than one physician in your group, you absolutely do need written contracts for a variety of reasons, but mostly to avoid conflicts later on. The proverbial “handshake agreement” is worthless in a major business dispute; everyone loses in such situations except the lawyers and accountants.
Mergers and buy-ins were covered at some length in my two previous columns. If the arrangement is to be one of employer and employees rather than a merger of equal partners, you will need an employment agreement to cover duties, requirements, expectations, and benefits. They define how each practitioner/employee will be paid, along with paid time off, health insurance, expense allowances, and malpractice coverage, among other basics. The more that is spelled out in the employment agreement, the fewer disagreements you are likely to have down the road.
Many employment contracts include a “termination without cause” clause, which benefits both the practice and the practitioners. It allows a practice to terminate a new associate if it feels a mistake has been made, even if he or she has done nothing wrong. On the other hand, the newcomer has the option to terminate if a better offer arises, their spouse hates the area, or for any other reason.
Buyouts should be addressed in advance as well. Several recent correspondents told me they didn’t see the necessity of writing a buyout agreement, because they plan to eventually sell their practice, rendering any buyout conditions moot. But what happens if an associate dies, becomes permanently disabled, or abruptly decides to leave the practice? If you haven’t prepared for such eventualities, you could find yourself receiving a demand from your ex-partner (or surviving spouse) for immediate payment of that partner’s portion of the practice’s value. And your valuation of the practice is likely to be severely at odds with the other party’s. Meanwhile, remaining partners must cover all the practice’s expenses and deal with an increased patient load.
A buyout agreement avoids these problems by planning for such eventualities in advance. You must agree on how a buyout amount will be valued. As I’ve said in previous columns, I strongly advise using a formula, not a fixed amount. If a buyout is based on 15- or 20-year-old reimbursements, the buyout will have no relationship to what the partners are currently being paid. Likewise, any buyout calculated at “appraised value” is a problem, because the buyout amount remains a mystery until an appraisal is performed. If the appraised value ends up being too high, the remaining owners may refuse to pay it. Have an actuary create a formula, so that a buyout figure can be calculated at any time. This area, especially, is where you need experienced, competent legal advice.
To avoid surprises, any buyout should require ample notice (6-12 months is common) to allow time to rearrange finances and recruit a new provider. Vesting schedules, similar to those used in retirement plans, are also popular. If a partner leaves before a prescribed time period has elapsed – say, 20 years – the buyout is proportionally reduced.
Buyouts can also be useful when dealing with noncompete agreements, which are notoriously difficult (and expensive) to enforce. One solution is a buyout penalty; a departing partner can compete with his or her former practice, but at the cost of a substantially reduced buyout. This permits competition, but discourages it, and compensates the targeted practice.
Buyouts are also a potential solution to some buy-in issues. A new associate entering an established practice may not be able to contribute assets equal to existing partners’ stakes and may lack the cash necessary to make up the difference. One alternative is to agree that any inequalities will be compensated at the other end in buyout value. Those partners contributing more assets will receive larger buyouts than those contributing less.
As I’ve said many times, these are not negotiations to undertake on your own. Enlist the aid of a consultant or attorney (or both) with ample medical practice experience.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
. The most common question was, “Do I really need to go to the trouble and expense of negotiating them?” If you have more than one physician in your group, you absolutely do need written contracts for a variety of reasons, but mostly to avoid conflicts later on. The proverbial “handshake agreement” is worthless in a major business dispute; everyone loses in such situations except the lawyers and accountants.
Mergers and buy-ins were covered at some length in my two previous columns. If the arrangement is to be one of employer and employees rather than a merger of equal partners, you will need an employment agreement to cover duties, requirements, expectations, and benefits. They define how each practitioner/employee will be paid, along with paid time off, health insurance, expense allowances, and malpractice coverage, among other basics. The more that is spelled out in the employment agreement, the fewer disagreements you are likely to have down the road.
Many employment contracts include a “termination without cause” clause, which benefits both the practice and the practitioners. It allows a practice to terminate a new associate if it feels a mistake has been made, even if he or she has done nothing wrong. On the other hand, the newcomer has the option to terminate if a better offer arises, their spouse hates the area, or for any other reason.
Buyouts should be addressed in advance as well. Several recent correspondents told me they didn’t see the necessity of writing a buyout agreement, because they plan to eventually sell their practice, rendering any buyout conditions moot. But what happens if an associate dies, becomes permanently disabled, or abruptly decides to leave the practice? If you haven’t prepared for such eventualities, you could find yourself receiving a demand from your ex-partner (or surviving spouse) for immediate payment of that partner’s portion of the practice’s value. And your valuation of the practice is likely to be severely at odds with the other party’s. Meanwhile, remaining partners must cover all the practice’s expenses and deal with an increased patient load.
A buyout agreement avoids these problems by planning for such eventualities in advance. You must agree on how a buyout amount will be valued. As I’ve said in previous columns, I strongly advise using a formula, not a fixed amount. If a buyout is based on 15- or 20-year-old reimbursements, the buyout will have no relationship to what the partners are currently being paid. Likewise, any buyout calculated at “appraised value” is a problem, because the buyout amount remains a mystery until an appraisal is performed. If the appraised value ends up being too high, the remaining owners may refuse to pay it. Have an actuary create a formula, so that a buyout figure can be calculated at any time. This area, especially, is where you need experienced, competent legal advice.
To avoid surprises, any buyout should require ample notice (6-12 months is common) to allow time to rearrange finances and recruit a new provider. Vesting schedules, similar to those used in retirement plans, are also popular. If a partner leaves before a prescribed time period has elapsed – say, 20 years – the buyout is proportionally reduced.
Buyouts can also be useful when dealing with noncompete agreements, which are notoriously difficult (and expensive) to enforce. One solution is a buyout penalty; a departing partner can compete with his or her former practice, but at the cost of a substantially reduced buyout. This permits competition, but discourages it, and compensates the targeted practice.
Buyouts are also a potential solution to some buy-in issues. A new associate entering an established practice may not be able to contribute assets equal to existing partners’ stakes and may lack the cash necessary to make up the difference. One alternative is to agree that any inequalities will be compensated at the other end in buyout value. Those partners contributing more assets will receive larger buyouts than those contributing less.
As I’ve said many times, these are not negotiations to undertake on your own. Enlist the aid of a consultant or attorney (or both) with ample medical practice experience.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
. The most common question was, “Do I really need to go to the trouble and expense of negotiating them?” If you have more than one physician in your group, you absolutely do need written contracts for a variety of reasons, but mostly to avoid conflicts later on. The proverbial “handshake agreement” is worthless in a major business dispute; everyone loses in such situations except the lawyers and accountants.
Mergers and buy-ins were covered at some length in my two previous columns. If the arrangement is to be one of employer and employees rather than a merger of equal partners, you will need an employment agreement to cover duties, requirements, expectations, and benefits. They define how each practitioner/employee will be paid, along with paid time off, health insurance, expense allowances, and malpractice coverage, among other basics. The more that is spelled out in the employment agreement, the fewer disagreements you are likely to have down the road.
Many employment contracts include a “termination without cause” clause, which benefits both the practice and the practitioners. It allows a practice to terminate a new associate if it feels a mistake has been made, even if he or she has done nothing wrong. On the other hand, the newcomer has the option to terminate if a better offer arises, their spouse hates the area, or for any other reason.
Buyouts should be addressed in advance as well. Several recent correspondents told me they didn’t see the necessity of writing a buyout agreement, because they plan to eventually sell their practice, rendering any buyout conditions moot. But what happens if an associate dies, becomes permanently disabled, or abruptly decides to leave the practice? If you haven’t prepared for such eventualities, you could find yourself receiving a demand from your ex-partner (or surviving spouse) for immediate payment of that partner’s portion of the practice’s value. And your valuation of the practice is likely to be severely at odds with the other party’s. Meanwhile, remaining partners must cover all the practice’s expenses and deal with an increased patient load.
A buyout agreement avoids these problems by planning for such eventualities in advance. You must agree on how a buyout amount will be valued. As I’ve said in previous columns, I strongly advise using a formula, not a fixed amount. If a buyout is based on 15- or 20-year-old reimbursements, the buyout will have no relationship to what the partners are currently being paid. Likewise, any buyout calculated at “appraised value” is a problem, because the buyout amount remains a mystery until an appraisal is performed. If the appraised value ends up being too high, the remaining owners may refuse to pay it. Have an actuary create a formula, so that a buyout figure can be calculated at any time. This area, especially, is where you need experienced, competent legal advice.
To avoid surprises, any buyout should require ample notice (6-12 months is common) to allow time to rearrange finances and recruit a new provider. Vesting schedules, similar to those used in retirement plans, are also popular. If a partner leaves before a prescribed time period has elapsed – say, 20 years – the buyout is proportionally reduced.
Buyouts can also be useful when dealing with noncompete agreements, which are notoriously difficult (and expensive) to enforce. One solution is a buyout penalty; a departing partner can compete with his or her former practice, but at the cost of a substantially reduced buyout. This permits competition, but discourages it, and compensates the targeted practice.
Buyouts are also a potential solution to some buy-in issues. A new associate entering an established practice may not be able to contribute assets equal to existing partners’ stakes and may lack the cash necessary to make up the difference. One alternative is to agree that any inequalities will be compensated at the other end in buyout value. Those partners contributing more assets will receive larger buyouts than those contributing less.
As I’ve said many times, these are not negotiations to undertake on your own. Enlist the aid of a consultant or attorney (or both) with ample medical practice experience.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Defending access to reproductive health care
The 1973 Supreme Court of the United States (SCOTUS) decision in Roe v Wade was a landmark ruling,1 establishing that the United States Constitution provides a fundamental “right to privacy,” protecting pregnant people’s freedom to access all available reproductive health care options. Recognizing that the right to abortion was not absolute, the majority of justices supported a trimester system. In the first trimester, decisions about abortion care are fully controlled by patients and clinicians, and no government could place restrictions on access to abortion. In the second trimester, SCOTUS ruled that states may choose to regulate abortion to protect maternal health. (As an example of such state restrictions, in Massachusetts, for many years, but no longer, the state required that abortions occur in a hospital when the patient was between 18 and 24 weeks’ gestation in order to facilitate comprehensive emergency care for complications.) Beginning in the third trimester, a point at which a fetus could be viable, the Court ruled that a government could prohibit abortion except when an abortion was necessary to protect the life or health of the pregnant person. In 1992, the SCOTUS decision in Planned Parenthood v Casey2 rejected the trimester system, reaffirming the right to an abortion before fetal viability, and adopting a new standard that states may not create an undue burden on a person seeking an abortion b
If, as anticipated, the 2022 SCOTUS decision in Dobbs v Jackson Women’s Health Organization3 overturns the precedents set in Roe v Wade and Planned Parenthood v Casey, decisions on abortion law will be relegated to elected legislators and state courts.4 It is expected that at least 26 state legislatures and governors will enact stringent new restrictions on access to abortion. This cataclysmic reversal of judicial opinion creates a historic challenge to obstetrician-gynecologists and their patients and could threaten access to other vital reproductive services beyond abortion, like contraception. We will be fighting, state by state, for people’s right to access all available reproductive health procedures. This will also significantly affect the ability for providers in women’s reproductive health to obtain appropriate and necessary education and training in a critical skills. If access to safe abortion is restricted, we fear patients may be forced to consider unsafe abortion, raising the specter of a return to the 1960s, when an epidemic of unsafe abortion caused countless injuries and deaths.5,6
How do we best prepare for these challenges?
- We will need to be flexible and continually evolve our clinical practices to be adherent with state and local legislation and regulation.
- To reduce unintended pregnancies, we need to strengthen our efforts to ensure that every patient has ready access to all available contraceptive options with no out-of-pocket cost.
- When a contraceptive is desired, we will focus on educating people about effectiveness, and offering them highly reliable contraception, such as the implant or intrauterine devices.
- We need to ensure timely access to abortion if state-based laws permit abortion before 6 or 7 weeks’ gestation. Providing medication abortion without an in-person visit using a telehealth option would be one option to expand rapid access to early first trimester abortion.
- Clinicians in states with access to abortion services will need to collaborate with colleagues in states with restrictions on abortion services to improve patient access across state borders.
On a national level, advancing our effective advocacy in Congress may lead to national legislation passed and signed by the President. This could supersede most state laws prohibiting access to comprehensive women’s reproductive health and create a unified, national approach to abortion care, allowing for the appropriate training of all obstetrician-gynecologists. We will also need to develop teams in every state capable of advocating for laws that ensure access to all reproductive health care options. The American College of Obstetricians and Gynecologists has leaders trained and tasked with legislative advocacy in every state.7 This network will be a foundation upon which to build additional advocacy efforts.
As women’s health care professionals, our responsibility to our patients, is to work to ensure universal access to safe and effective comprehensive reproductive options, and to ensure that our workforce is prepared to meet the needs of our patients by defending the patient-clinician relationship. Abortion care saves lives of pregnant patients and reduces maternal morbidity.8 Access to safe abortion care as part of comprehensive reproductive services is an important component of health care. ●
- Roe v Wade, 410 U.S. 113 (1973).
- Planned Parenthood v Casey, 505 U.S. 833 (1992).
- Dobbs v Jackson Women’s Health Organization, 19-1392. https://www.supremecourt.gov/search .aspx?filename=/docket/docketfiles/html /public/19-1392.html. Accessed May 18, 2022.
- Gerstein J, Ward A. Supreme Court has voted to overturn abortion rights, draft opinion shows. Politico. May 5, 2022. Updated May 3, 2022.
- Gold RB. Lessons from before Roe: will past be prologue? Guttmacher Institute. March 1, 2003. https://www.guttmacher.org/gpr/2003/03 /lessons-roe-will-past-be-prologue. Accessed May 18, 2022.
- Edelin KC. Broken Justice: A True Story of Race, Sex and Revenge in a Boston Courtroom. Pond View Press; 2007.
- The American College of Obstetricians and Gynecologists. Get involved in your state. ACOG web site. https://www.acog.org/advocacy /get-involved/get-involved-in-your-state. Accessed May 18, 2022.
- Institute of Medicine (US) Committee on Improving Birth Outcomes. Bale JR, Stoll BJ, Lucas AO, eds. Reducing maternal mortality and morbidity. In: Improving Birth Outcomes: Meeting the Challenge in the Developing World. Washington, DC: National Academies Press (US); 2003.
The 1973 Supreme Court of the United States (SCOTUS) decision in Roe v Wade was a landmark ruling,1 establishing that the United States Constitution provides a fundamental “right to privacy,” protecting pregnant people’s freedom to access all available reproductive health care options. Recognizing that the right to abortion was not absolute, the majority of justices supported a trimester system. In the first trimester, decisions about abortion care are fully controlled by patients and clinicians, and no government could place restrictions on access to abortion. In the second trimester, SCOTUS ruled that states may choose to regulate abortion to protect maternal health. (As an example of such state restrictions, in Massachusetts, for many years, but no longer, the state required that abortions occur in a hospital when the patient was between 18 and 24 weeks’ gestation in order to facilitate comprehensive emergency care for complications.) Beginning in the third trimester, a point at which a fetus could be viable, the Court ruled that a government could prohibit abortion except when an abortion was necessary to protect the life or health of the pregnant person. In 1992, the SCOTUS decision in Planned Parenthood v Casey2 rejected the trimester system, reaffirming the right to an abortion before fetal viability, and adopting a new standard that states may not create an undue burden on a person seeking an abortion b
If, as anticipated, the 2022 SCOTUS decision in Dobbs v Jackson Women’s Health Organization3 overturns the precedents set in Roe v Wade and Planned Parenthood v Casey, decisions on abortion law will be relegated to elected legislators and state courts.4 It is expected that at least 26 state legislatures and governors will enact stringent new restrictions on access to abortion. This cataclysmic reversal of judicial opinion creates a historic challenge to obstetrician-gynecologists and their patients and could threaten access to other vital reproductive services beyond abortion, like contraception. We will be fighting, state by state, for people’s right to access all available reproductive health procedures. This will also significantly affect the ability for providers in women’s reproductive health to obtain appropriate and necessary education and training in a critical skills. If access to safe abortion is restricted, we fear patients may be forced to consider unsafe abortion, raising the specter of a return to the 1960s, when an epidemic of unsafe abortion caused countless injuries and deaths.5,6
How do we best prepare for these challenges?
- We will need to be flexible and continually evolve our clinical practices to be adherent with state and local legislation and regulation.
- To reduce unintended pregnancies, we need to strengthen our efforts to ensure that every patient has ready access to all available contraceptive options with no out-of-pocket cost.
- When a contraceptive is desired, we will focus on educating people about effectiveness, and offering them highly reliable contraception, such as the implant or intrauterine devices.
- We need to ensure timely access to abortion if state-based laws permit abortion before 6 or 7 weeks’ gestation. Providing medication abortion without an in-person visit using a telehealth option would be one option to expand rapid access to early first trimester abortion.
- Clinicians in states with access to abortion services will need to collaborate with colleagues in states with restrictions on abortion services to improve patient access across state borders.
On a national level, advancing our effective advocacy in Congress may lead to national legislation passed and signed by the President. This could supersede most state laws prohibiting access to comprehensive women’s reproductive health and create a unified, national approach to abortion care, allowing for the appropriate training of all obstetrician-gynecologists. We will also need to develop teams in every state capable of advocating for laws that ensure access to all reproductive health care options. The American College of Obstetricians and Gynecologists has leaders trained and tasked with legislative advocacy in every state.7 This network will be a foundation upon which to build additional advocacy efforts.
As women’s health care professionals, our responsibility to our patients, is to work to ensure universal access to safe and effective comprehensive reproductive options, and to ensure that our workforce is prepared to meet the needs of our patients by defending the patient-clinician relationship. Abortion care saves lives of pregnant patients and reduces maternal morbidity.8 Access to safe abortion care as part of comprehensive reproductive services is an important component of health care. ●
The 1973 Supreme Court of the United States (SCOTUS) decision in Roe v Wade was a landmark ruling,1 establishing that the United States Constitution provides a fundamental “right to privacy,” protecting pregnant people’s freedom to access all available reproductive health care options. Recognizing that the right to abortion was not absolute, the majority of justices supported a trimester system. In the first trimester, decisions about abortion care are fully controlled by patients and clinicians, and no government could place restrictions on access to abortion. In the second trimester, SCOTUS ruled that states may choose to regulate abortion to protect maternal health. (As an example of such state restrictions, in Massachusetts, for many years, but no longer, the state required that abortions occur in a hospital when the patient was between 18 and 24 weeks’ gestation in order to facilitate comprehensive emergency care for complications.) Beginning in the third trimester, a point at which a fetus could be viable, the Court ruled that a government could prohibit abortion except when an abortion was necessary to protect the life or health of the pregnant person. In 1992, the SCOTUS decision in Planned Parenthood v Casey2 rejected the trimester system, reaffirming the right to an abortion before fetal viability, and adopting a new standard that states may not create an undue burden on a person seeking an abortion b
If, as anticipated, the 2022 SCOTUS decision in Dobbs v Jackson Women’s Health Organization3 overturns the precedents set in Roe v Wade and Planned Parenthood v Casey, decisions on abortion law will be relegated to elected legislators and state courts.4 It is expected that at least 26 state legislatures and governors will enact stringent new restrictions on access to abortion. This cataclysmic reversal of judicial opinion creates a historic challenge to obstetrician-gynecologists and their patients and could threaten access to other vital reproductive services beyond abortion, like contraception. We will be fighting, state by state, for people’s right to access all available reproductive health procedures. This will also significantly affect the ability for providers in women’s reproductive health to obtain appropriate and necessary education and training in a critical skills. If access to safe abortion is restricted, we fear patients may be forced to consider unsafe abortion, raising the specter of a return to the 1960s, when an epidemic of unsafe abortion caused countless injuries and deaths.5,6
How do we best prepare for these challenges?
- We will need to be flexible and continually evolve our clinical practices to be adherent with state and local legislation and regulation.
- To reduce unintended pregnancies, we need to strengthen our efforts to ensure that every patient has ready access to all available contraceptive options with no out-of-pocket cost.
- When a contraceptive is desired, we will focus on educating people about effectiveness, and offering them highly reliable contraception, such as the implant or intrauterine devices.
- We need to ensure timely access to abortion if state-based laws permit abortion before 6 or 7 weeks’ gestation. Providing medication abortion without an in-person visit using a telehealth option would be one option to expand rapid access to early first trimester abortion.
- Clinicians in states with access to abortion services will need to collaborate with colleagues in states with restrictions on abortion services to improve patient access across state borders.
On a national level, advancing our effective advocacy in Congress may lead to national legislation passed and signed by the President. This could supersede most state laws prohibiting access to comprehensive women’s reproductive health and create a unified, national approach to abortion care, allowing for the appropriate training of all obstetrician-gynecologists. We will also need to develop teams in every state capable of advocating for laws that ensure access to all reproductive health care options. The American College of Obstetricians and Gynecologists has leaders trained and tasked with legislative advocacy in every state.7 This network will be a foundation upon which to build additional advocacy efforts.
As women’s health care professionals, our responsibility to our patients, is to work to ensure universal access to safe and effective comprehensive reproductive options, and to ensure that our workforce is prepared to meet the needs of our patients by defending the patient-clinician relationship. Abortion care saves lives of pregnant patients and reduces maternal morbidity.8 Access to safe abortion care as part of comprehensive reproductive services is an important component of health care. ●
- Roe v Wade, 410 U.S. 113 (1973).
- Planned Parenthood v Casey, 505 U.S. 833 (1992).
- Dobbs v Jackson Women’s Health Organization, 19-1392. https://www.supremecourt.gov/search .aspx?filename=/docket/docketfiles/html /public/19-1392.html. Accessed May 18, 2022.
- Gerstein J, Ward A. Supreme Court has voted to overturn abortion rights, draft opinion shows. Politico. May 5, 2022. Updated May 3, 2022.
- Gold RB. Lessons from before Roe: will past be prologue? Guttmacher Institute. March 1, 2003. https://www.guttmacher.org/gpr/2003/03 /lessons-roe-will-past-be-prologue. Accessed May 18, 2022.
- Edelin KC. Broken Justice: A True Story of Race, Sex and Revenge in a Boston Courtroom. Pond View Press; 2007.
- The American College of Obstetricians and Gynecologists. Get involved in your state. ACOG web site. https://www.acog.org/advocacy /get-involved/get-involved-in-your-state. Accessed May 18, 2022.
- Institute of Medicine (US) Committee on Improving Birth Outcomes. Bale JR, Stoll BJ, Lucas AO, eds. Reducing maternal mortality and morbidity. In: Improving Birth Outcomes: Meeting the Challenge in the Developing World. Washington, DC: National Academies Press (US); 2003.
- Roe v Wade, 410 U.S. 113 (1973).
- Planned Parenthood v Casey, 505 U.S. 833 (1992).
- Dobbs v Jackson Women’s Health Organization, 19-1392. https://www.supremecourt.gov/search .aspx?filename=/docket/docketfiles/html /public/19-1392.html. Accessed May 18, 2022.
- Gerstein J, Ward A. Supreme Court has voted to overturn abortion rights, draft opinion shows. Politico. May 5, 2022. Updated May 3, 2022.
- Gold RB. Lessons from before Roe: will past be prologue? Guttmacher Institute. March 1, 2003. https://www.guttmacher.org/gpr/2003/03 /lessons-roe-will-past-be-prologue. Accessed May 18, 2022.
- Edelin KC. Broken Justice: A True Story of Race, Sex and Revenge in a Boston Courtroom. Pond View Press; 2007.
- The American College of Obstetricians and Gynecologists. Get involved in your state. ACOG web site. https://www.acog.org/advocacy /get-involved/get-involved-in-your-state. Accessed May 18, 2022.
- Institute of Medicine (US) Committee on Improving Birth Outcomes. Bale JR, Stoll BJ, Lucas AO, eds. Reducing maternal mortality and morbidity. In: Improving Birth Outcomes: Meeting the Challenge in the Developing World. Washington, DC: National Academies Press (US); 2003.

More practice merger options
The continuing than larger ones. While there are some smaller offices offering unique services that may be able to remain small, most small general practices will be forced to at least consider a larger alternative. Recently, I discussed one option – merging individual practices into a larger one – but others are available.
One alternate strategy is to form a cooperative group. If you look around your area of practice, you will likely find other small practices in similar situations that might be willing to collaborate with you for the purpose of pooling your billing and purchasing resources. This allows each participant to maintain independence, yet share office overhead expenses and employee salaries for mutual benefit. If that arrangement works, and remains satisfactory for all participants, you can consider expanding your sharing of expenditures, such as collective purchasing of supplies and equipment, and centralizing appointment scheduling. Such an arrangement might be particularly attractive to physicians in later stages of their careers who need to alleviate financial burdens but don’t wish to close up shop just yet.
After more time has passed, if everyone remains happy with the arrangement, an outright merger can be considered, allowing the group to negotiate higher insurance remunerations and even lower overhead costs. Obviously, projects of this size and scope require careful planning and implementation, and should not be undertaken without the help of competent legal counsel and an experienced business consultant.
Another option is to join an independent practice association (IPA), if one is operating in your area. IPAs are physician-directed legal entities, formed to provide the same advantages enjoyed by large group practices while allowing individual members to remain independent. IPAs have greater purchasing power, allowing members to cut costs on medical and office supplies. They can also negotiate more favorable contracts with insurance companies and other payers.
Before joining such an organization, examine its legal status carefully. Some IPAs have been charged with antitrust violations because their member practices are, in reality, competitors. Make certain that any IPA you consider joining abides by antitrust and price fixing laws. Look carefully at its financial solvency as well, as IPAs have also been known to fail, leaving former members to pick up the tab.
An alternative to the IPA is the accountable care organization (ACO), a relatively new entity created as part of the Affordable Care Act. Like an IPA, an ACO’s basic purpose is to limit unnecessary spending; but ACOs are typically limited to Medicare and Medicaid recipients, and involve a larger network of doctors and hospitals sharing financial and medical responsibility for patient care. Criteria for limits on spending are established by the Centers for Medicare & Medicaid Services (CMS).
ACOs offer financial incentives to cooperate, and to save money by avoiding unnecessary tests and procedures. A key component is the sharing of information. Providers who save money while also meeting quality targets are theoretically entitled to a portion of the savings. According to federal data, ACOs saved Medicare $4.1 billion in 2020). As of January 2022, 483 ACOs were participating in the Medicare Shared Savings Program. A similar entity designed for private-sector patients is the clinically integrated network (CIN), created by the Federal Trade Commission to serve the commercial or self-insured market, while ACOs treat Medicare and Medicaid patients. Like ACOs, the idea is to work together to improve care and reduce costs by sharing records and tracking data.
When joining any group, read the agreement carefully for any clauses that might infringe on your clinical judgment. In particular, be sure that there are no restrictions on patient treatment or physician referral options for your patients. You should also negotiate an escape clause, allowing you to opt out if you become unhappy with the arrangement.
Clearly, the price of remaining autonomous is significant, and many private practitioners are unwilling to pay it. In 2019, the American Medical Association reported that for the first time, there were fewer physician owners (45.9%) than employees (47.4%).
But as I have written many times, those of us who remain committed to independence will find ways to preserve it. In medicine, as in life, those most responsive to change will survive and flourish.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
The continuing than larger ones. While there are some smaller offices offering unique services that may be able to remain small, most small general practices will be forced to at least consider a larger alternative. Recently, I discussed one option – merging individual practices into a larger one – but others are available.
One alternate strategy is to form a cooperative group. If you look around your area of practice, you will likely find other small practices in similar situations that might be willing to collaborate with you for the purpose of pooling your billing and purchasing resources. This allows each participant to maintain independence, yet share office overhead expenses and employee salaries for mutual benefit. If that arrangement works, and remains satisfactory for all participants, you can consider expanding your sharing of expenditures, such as collective purchasing of supplies and equipment, and centralizing appointment scheduling. Such an arrangement might be particularly attractive to physicians in later stages of their careers who need to alleviate financial burdens but don’t wish to close up shop just yet.
After more time has passed, if everyone remains happy with the arrangement, an outright merger can be considered, allowing the group to negotiate higher insurance remunerations and even lower overhead costs. Obviously, projects of this size and scope require careful planning and implementation, and should not be undertaken without the help of competent legal counsel and an experienced business consultant.
Another option is to join an independent practice association (IPA), if one is operating in your area. IPAs are physician-directed legal entities, formed to provide the same advantages enjoyed by large group practices while allowing individual members to remain independent. IPAs have greater purchasing power, allowing members to cut costs on medical and office supplies. They can also negotiate more favorable contracts with insurance companies and other payers.
Before joining such an organization, examine its legal status carefully. Some IPAs have been charged with antitrust violations because their member practices are, in reality, competitors. Make certain that any IPA you consider joining abides by antitrust and price fixing laws. Look carefully at its financial solvency as well, as IPAs have also been known to fail, leaving former members to pick up the tab.
An alternative to the IPA is the accountable care organization (ACO), a relatively new entity created as part of the Affordable Care Act. Like an IPA, an ACO’s basic purpose is to limit unnecessary spending; but ACOs are typically limited to Medicare and Medicaid recipients, and involve a larger network of doctors and hospitals sharing financial and medical responsibility for patient care. Criteria for limits on spending are established by the Centers for Medicare & Medicaid Services (CMS).
ACOs offer financial incentives to cooperate, and to save money by avoiding unnecessary tests and procedures. A key component is the sharing of information. Providers who save money while also meeting quality targets are theoretically entitled to a portion of the savings. According to federal data, ACOs saved Medicare $4.1 billion in 2020). As of January 2022, 483 ACOs were participating in the Medicare Shared Savings Program. A similar entity designed for private-sector patients is the clinically integrated network (CIN), created by the Federal Trade Commission to serve the commercial or self-insured market, while ACOs treat Medicare and Medicaid patients. Like ACOs, the idea is to work together to improve care and reduce costs by sharing records and tracking data.
When joining any group, read the agreement carefully for any clauses that might infringe on your clinical judgment. In particular, be sure that there are no restrictions on patient treatment or physician referral options for your patients. You should also negotiate an escape clause, allowing you to opt out if you become unhappy with the arrangement.
Clearly, the price of remaining autonomous is significant, and many private practitioners are unwilling to pay it. In 2019, the American Medical Association reported that for the first time, there were fewer physician owners (45.9%) than employees (47.4%).
But as I have written many times, those of us who remain committed to independence will find ways to preserve it. In medicine, as in life, those most responsive to change will survive and flourish.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
The continuing than larger ones. While there are some smaller offices offering unique services that may be able to remain small, most small general practices will be forced to at least consider a larger alternative. Recently, I discussed one option – merging individual practices into a larger one – but others are available.
One alternate strategy is to form a cooperative group. If you look around your area of practice, you will likely find other small practices in similar situations that might be willing to collaborate with you for the purpose of pooling your billing and purchasing resources. This allows each participant to maintain independence, yet share office overhead expenses and employee salaries for mutual benefit. If that arrangement works, and remains satisfactory for all participants, you can consider expanding your sharing of expenditures, such as collective purchasing of supplies and equipment, and centralizing appointment scheduling. Such an arrangement might be particularly attractive to physicians in later stages of their careers who need to alleviate financial burdens but don’t wish to close up shop just yet.
After more time has passed, if everyone remains happy with the arrangement, an outright merger can be considered, allowing the group to negotiate higher insurance remunerations and even lower overhead costs. Obviously, projects of this size and scope require careful planning and implementation, and should not be undertaken without the help of competent legal counsel and an experienced business consultant.
Another option is to join an independent practice association (IPA), if one is operating in your area. IPAs are physician-directed legal entities, formed to provide the same advantages enjoyed by large group practices while allowing individual members to remain independent. IPAs have greater purchasing power, allowing members to cut costs on medical and office supplies. They can also negotiate more favorable contracts with insurance companies and other payers.
Before joining such an organization, examine its legal status carefully. Some IPAs have been charged with antitrust violations because their member practices are, in reality, competitors. Make certain that any IPA you consider joining abides by antitrust and price fixing laws. Look carefully at its financial solvency as well, as IPAs have also been known to fail, leaving former members to pick up the tab.
An alternative to the IPA is the accountable care organization (ACO), a relatively new entity created as part of the Affordable Care Act. Like an IPA, an ACO’s basic purpose is to limit unnecessary spending; but ACOs are typically limited to Medicare and Medicaid recipients, and involve a larger network of doctors and hospitals sharing financial and medical responsibility for patient care. Criteria for limits on spending are established by the Centers for Medicare & Medicaid Services (CMS).
ACOs offer financial incentives to cooperate, and to save money by avoiding unnecessary tests and procedures. A key component is the sharing of information. Providers who save money while also meeting quality targets are theoretically entitled to a portion of the savings. According to federal data, ACOs saved Medicare $4.1 billion in 2020). As of January 2022, 483 ACOs were participating in the Medicare Shared Savings Program. A similar entity designed for private-sector patients is the clinically integrated network (CIN), created by the Federal Trade Commission to serve the commercial or self-insured market, while ACOs treat Medicare and Medicaid patients. Like ACOs, the idea is to work together to improve care and reduce costs by sharing records and tracking data.
When joining any group, read the agreement carefully for any clauses that might infringe on your clinical judgment. In particular, be sure that there are no restrictions on patient treatment or physician referral options for your patients. You should also negotiate an escape clause, allowing you to opt out if you become unhappy with the arrangement.
Clearly, the price of remaining autonomous is significant, and many private practitioners are unwilling to pay it. In 2019, the American Medical Association reported that for the first time, there were fewer physician owners (45.9%) than employees (47.4%).
But as I have written many times, those of us who remain committed to independence will find ways to preserve it. In medicine, as in life, those most responsive to change will survive and flourish.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].