User login
Pros and Cons of Clinical Observation Units

Hospitals nationwide face significant capacity constraints in emergency departments. High hospitalization rates can have a ripple effect, leading to long wait times, frequent diversion of patients to other hospitals, and higher patient-care expenses. However, a sizable number of inpatient admissions can be prevented through dedicated clinical observation units, or COUs. Such a strategy is likely to be more efficient, can result in shorter lengths of stay, and can decrease health-care costs.1
Also known as clinical decision units, “obs” units, or short-stay observation units, these hospital-based units lend themselves as a feasible solution. Many of the COU success stories come from “chest pain” units, along with ED-based observation units. Over time, the COUs have been expanded to include many more conditions and have enjoyed success when dealing with asthma exacerbations, transient ischemic attacks, bronchiolitis in pediatric populations, and congestive-heart-failure exacerbation, to name a few.
Most COUs use a window of six to 24 hours to carry out triaging, diagnosing, treating, and monitoring the patient response. Anytime before the 24-hour mark, a decision is made whether to discharge or admit the patient. The success of dedicated COUs relies heavily on strong leadership, strict treatment protocols, and well-defined inclusion/exclusion criteria.
COU utilization has been well received by several professional bodies. Both emergency medicine physicians and hospitalists are natural key players in the widespread utilization of COUs. SHM, in a white paper, concluded: “Collaboration between hospitalists, emergency physicians, hospital administrators, and academicians will serve not only to promote outstanding observation care, but also to focus quality improvement and research efforts for the observation unit of the 21st century.”2 The American College of Emergency Physicians (ACEP), in its position statement, said the “observation of appropriate ED patients in a dedicated ED observation area, instead of a general inpatient bed or an acute care ED bed, is a ‘best practice’ that requires a commitment of staff and hospital resources.”3
As promising as the COUs appear, it is estimated that only one-third of hospitals have them in place.4 And while much of the COU story is good, there are concerns with the patient-care model.
The Good
Instinctively, a COU is a win-win proposition for all stakeholders. Essentially, many see these units as a fine blend of clinical care, fiscal responsibility, and patient accountability. Among the benefits:
Reduced admissions. On average, the admission rates from ED to inpatient services are 13.3%.5 In contrast, in hospitals that have a robust COU in place, the admission rates are much lower. As an example, Cook County Hospital in Chicago in the mid-1990s saw a decline in the admission rates from the emergency room following implementation of a COU, along with an increase in bed capacity due to the efficient, protocol-driven approach that goes along with successful ED observation units.6 With well-structured and managed observation units, such a reduction in hospitalization rates has been shown, is reproducible, and is achievable.
Improved case-mix multiplier. Inpatient reimbursements from the Centers for Medicare and Medicaid Services (CMS) and private insurers frequently are tied to the acuity of care a hospital provides. Critical to making that determination is the case mix that a given hospital sees. Usually, the more complex patients a hospital admits, the higher the reimbursements are. With a successful COU, a hospital can expect a case-mix multiplier representing patients with greater complexity and higher acuity.
What a successful COU essentially does is lead to the admission of patients with greater comorbidities—those who are sicker than the average patient. In doing so, COUs also facilitate safe discharges of the patients who do not necessarily need to be admitted. As an average, the cohort of patients who are admitted as inpatients then consists of patients who are sick enough and absolutely need to be admitted.
Resource utilization. When a patient is admitted from the ED to an inpatient floor, a lot of resources are utilized. These include expenses related to transportation, housekeeping, nursing, and ancillary services. Each of these additional resources comes with an expense. The more resources that are put in motion, the greater the expense a hospital incurs. With effective COUs, it is generally expected that suitable patients will get the care in a specific geographic area by the same set of providers. COUs tend to reduce unnecessary hospitalizations, redundancy of manpower utilization, and duplication of documentation—therefore reducing the expenses incurred by the hospital.
Infection control. The COUs operate based on minimizing the stay of the patients who can be safely discharged after a brief observation period. Decreased duration of stay also means decreased movement and unique provider contact/exposure—thus decreasing the chances for acquiring health-care-related infections. Besides, most COUs are restricted to a certain geographic area within the hospital, which helps to restrict patients to a limited area. This again may be helpful in better overall infection-control practices. More research is necessary to establish this association of the infection-control advantages of COUs. The hypothesis, however, does appear very promising.
Prompt and standardized care. Most COUs use an evidence-based, standardized approach toward the patients seen in the ED. Several professional bodies have endorsed the use of protocol-driven care for the conditions seen in the COU. Most professional organizations that have a key role in COUs advocate this approach, and include the ACEP, AHA, and SHM. When a COU has established itself, it likely is to use specific, expedited, protocol-driven approaches. This allows for care to be focused and standardized. This also is an opportunity to avoid redundant imaging and lab testing.
Patient safety. In its landmark publication “To Err is Human: Building a Safer Health System,” the Institute of Medicine identified communication error as one of the factors that lead to mistakes in patient care.7 COUs often tend to provide bulk of care at a given geographical area; this minimizes the transfer of patients from one place to another, thereby decreasing communication errors.
By providing more time to make decisions, COUs afford a greater diagnostic certainty. In the long run, this also helps a hospital minimize costly lawsuits.
The Bad
Not everything about COUs is great. There are certain areas that dull the luster of an observation unit.
Overzealous approaches. COUs are designed to allow more time to make clinical decisions when the triaging is in a gray area: whether to admit or not. Also, COUs provide clinicians with more time to follow the response to the care the patients receive in an emergent fashion. It needs to be emphasized that COUs are designed neither to replace hospitalization, nor to act as urgent care. As a corollary, there is a chance clinicians may be overzealous in discharging patients from COUs close to the 24-hour mark—even though it might not be clear whether the patient needs to be admitted or discharged. Overzealous discharging of COU patients can damage the premise of these units: to determine the need for admission and ensure patient safety. Having strict inclusion and exclusion criteria and good management can prevent these problems.
Staffing. Introduction of a COU can strain an already short-staffed ED. No different from any other novel approach, COU staffers need to be afforded a learning curve. This requires training personnel and establishing a robust team to staff COUs. It can be a strenuous process, at least in the beginning. Strong leadership and support of hospital, physician, and nursing leadership all play a role in the successful implementation and ongoing utilization of COUs.
Logistics. Coordination of people, facilities, and supplies that go into instituting a COU might be a challenge. Also, there may be times where patient ownership may not be very clear. Logistical concerns can include:
- Who owns the patient?
- How much of a role does a consulting service have?
- Who oversees the follow-up plans?
Although a popular COU setup is to have a dedicated observation unit adjacent to the ED, it is not a standard.
Reimbursement. Unfortunately, there is some degree of negative incentive built into reimbursements for COU operations. To understand why this is a bad thing for a hospital, let’s examine how hospitals are paid for services provided in a COU.
Frequently, COU patients are treated as “outpatients.” The operating formula is based on the Hospital Outpatient Prospective Payment System (OPPS), which is based on Ambulatory Payment Classification, or APC.8 Reimbursement differences in these two approaches can be quite sizable. Depending on what condition is being treated, the hospital reimbursement can be as little as half to a quarter of the payment for inpatient treatment.9 Essentially, the patient would have received very similar care, diagnostic work-up, antibiotics, imaging, lab work, and equally qualified clinicians as caretakers in both the settings. The payments need to account for the care in the COUs, which is usually more acute than in the ambulatory setting and potentially more efficient than an inpatient setting. The payments, therefore, should be sensitive to these factors.
The Ugly
COUs are intended to address many of the challenges facing the healthcare system, and in large part, that is what they do. However, some hospitals could be penalized for providing care through COUs. An efficient COU means that the patients who are admitted are, in fact, sicker. Logically, these patients will have a higher chance of being readmitted. Because the “not so sick” patients were successfully intervened and discharged from COUs, the patients that did get admitted must be pretty sick and must have higher comorbidities.
According to CMS, a readmission occurs if a patient has “an admission to a subsection hospital within 30 days of a discharge from the same or another subsection hospital.”10 The denominator here consists of all the patients who were discharged from the hospital inpatient stay. If a hospital does not have a robust COU, a large number of “not so sick” patients will be admitted as inpatients and will provide a larger denominator for calculating the readmission rates.
In contrast, a successful COU will allow for a large number of “not so sick” and “borderline” patients to be discharged, shrinking the denominator base, and “very sick” patients who are likely to be readmitted. This may erroneously cause the hospital to appear to have higher 30-day readmission rates. These hospitals may risk substantial readmission-related penalties.
This issue, along with a lopsided payment model, makes the COU landscape murky. With a greater share of pie being the “Il buono” in Il buono, il brutto, il cattivo, clinical observation units are certain to take a prominent position in addressing many of the issues that plague current healthcare facilities—capacity constraints, long ED wait times, limited inpatient beds, and soaring health-care expenditures.
Most important, COUs can lead to better and more efficient patient care.11 It is, therefore, not surprising that the IOM, in its report “Hospital Based Emergency Care—At the Breaking Point,” has identified clinical decision units as a “particularly promising” technique to improve patient flow.12
Dr. Asudani is a hospitalist in the division of hospital medicine in the department of internal medicine at the University of California San Diego Health System. Dr. Tolia is director of observation medicine in the department of emergency medicine and internal medicine at UCSD Health System.
References
- Baugh CW, Venkatesh AK, Hilton JA, Samuel PA, Schuur JD, Bohan JS. Making greater use of dedicated hospital observation units for many short-stay patients could save $3.1 billion a year. Health Aff (Millwood). 2012;31(10):2314-2323.
- Society of Hospital Medicine. The observation unit white paper. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=White_Papers&Template=/CM/ContentDisplay.cfm&ContentID=21890. Accessed April 3, 2013.
- American College of Emergency Physicians. Emergency department observation services. American College of Emergency Physicians website. Available at: http://www.acep.org/Clinical—Practice-Management/Emergency-Department-Observation-Services. Accessed April 10, 2013.
- Niska R, Bhuiya F, Xu J. National Hospital Ambulatory Medical Care Survey: 2007 emergency department summary. Hyattsville, Md.: National Center for Health Statistics; 2010.
- Centers for Disease Control and Prevention. Fast stats. Centers for Disease Control and Prevention. Available at: http://www.cdc.gov/nchs/fastats/ervisits.htm. Accessed April 9, 2013.
- Martinez E, Reilly BM, Evans AT, Roberts RR. The observation unit: a new interface between inpatient and outpatient care. Am J Med. 2001;110(4):274-277.
- To err is human: building a safer health system. Institute of Medicine. Washington (DC): National Academies Press; 2000.
- Centers for Medicare & Medicaid Services. Hospital outpatient prospective payment system. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/hospitaloutpaysysfctsht.pdf. Accessed April 2, 2013.
- Runy L. Clinical observation units: Building a bridge between outpatient and inpatient services. Hospitals and Health Networks website. Available at: http://www.hhnmag.com/hhnmag/jsp/articledisplay.jsp?dcrpath=HHNMAG/PubsNewsArticle/data/2006March/0603HHN_FEA_gatefold&domain=HHNMAG. Accessed April 9, 2013.
- Centers for Medicare & Medicaid Services. Readmissions reduction program. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html. Accessed May 6, 2013.
- Baugh CW, Venkatesh AK, Bohan JS. Emergency department observation nits: a clinical and financial benefit for hospitals. Health Care Manage Rev. 2011;36(1):28-37.
- Institute of Medicine. Hospital-based emergency care: at the breaking point. Washington: National Academies Press; 2007.
Hospitals nationwide face significant capacity constraints in emergency departments. High hospitalization rates can have a ripple effect, leading to long wait times, frequent diversion of patients to other hospitals, and higher patient-care expenses. However, a sizable number of inpatient admissions can be prevented through dedicated clinical observation units, or COUs. Such a strategy is likely to be more efficient, can result in shorter lengths of stay, and can decrease health-care costs.1
Also known as clinical decision units, “obs” units, or short-stay observation units, these hospital-based units lend themselves as a feasible solution. Many of the COU success stories come from “chest pain” units, along with ED-based observation units. Over time, the COUs have been expanded to include many more conditions and have enjoyed success when dealing with asthma exacerbations, transient ischemic attacks, bronchiolitis in pediatric populations, and congestive-heart-failure exacerbation, to name a few.
Most COUs use a window of six to 24 hours to carry out triaging, diagnosing, treating, and monitoring the patient response. Anytime before the 24-hour mark, a decision is made whether to discharge or admit the patient. The success of dedicated COUs relies heavily on strong leadership, strict treatment protocols, and well-defined inclusion/exclusion criteria.
COU utilization has been well received by several professional bodies. Both emergency medicine physicians and hospitalists are natural key players in the widespread utilization of COUs. SHM, in a white paper, concluded: “Collaboration between hospitalists, emergency physicians, hospital administrators, and academicians will serve not only to promote outstanding observation care, but also to focus quality improvement and research efforts for the observation unit of the 21st century.”2 The American College of Emergency Physicians (ACEP), in its position statement, said the “observation of appropriate ED patients in a dedicated ED observation area, instead of a general inpatient bed or an acute care ED bed, is a ‘best practice’ that requires a commitment of staff and hospital resources.”3
As promising as the COUs appear, it is estimated that only one-third of hospitals have them in place.4 And while much of the COU story is good, there are concerns with the patient-care model.
The Good
Instinctively, a COU is a win-win proposition for all stakeholders. Essentially, many see these units as a fine blend of clinical care, fiscal responsibility, and patient accountability. Among the benefits:
Reduced admissions. On average, the admission rates from ED to inpatient services are 13.3%.5 In contrast, in hospitals that have a robust COU in place, the admission rates are much lower. As an example, Cook County Hospital in Chicago in the mid-1990s saw a decline in the admission rates from the emergency room following implementation of a COU, along with an increase in bed capacity due to the efficient, protocol-driven approach that goes along with successful ED observation units.6 With well-structured and managed observation units, such a reduction in hospitalization rates has been shown, is reproducible, and is achievable.
Improved case-mix multiplier. Inpatient reimbursements from the Centers for Medicare and Medicaid Services (CMS) and private insurers frequently are tied to the acuity of care a hospital provides. Critical to making that determination is the case mix that a given hospital sees. Usually, the more complex patients a hospital admits, the higher the reimbursements are. With a successful COU, a hospital can expect a case-mix multiplier representing patients with greater complexity and higher acuity.
What a successful COU essentially does is lead to the admission of patients with greater comorbidities—those who are sicker than the average patient. In doing so, COUs also facilitate safe discharges of the patients who do not necessarily need to be admitted. As an average, the cohort of patients who are admitted as inpatients then consists of patients who are sick enough and absolutely need to be admitted.
Resource utilization. When a patient is admitted from the ED to an inpatient floor, a lot of resources are utilized. These include expenses related to transportation, housekeeping, nursing, and ancillary services. Each of these additional resources comes with an expense. The more resources that are put in motion, the greater the expense a hospital incurs. With effective COUs, it is generally expected that suitable patients will get the care in a specific geographic area by the same set of providers. COUs tend to reduce unnecessary hospitalizations, redundancy of manpower utilization, and duplication of documentation—therefore reducing the expenses incurred by the hospital.
Infection control. The COUs operate based on minimizing the stay of the patients who can be safely discharged after a brief observation period. Decreased duration of stay also means decreased movement and unique provider contact/exposure—thus decreasing the chances for acquiring health-care-related infections. Besides, most COUs are restricted to a certain geographic area within the hospital, which helps to restrict patients to a limited area. This again may be helpful in better overall infection-control practices. More research is necessary to establish this association of the infection-control advantages of COUs. The hypothesis, however, does appear very promising.
Prompt and standardized care. Most COUs use an evidence-based, standardized approach toward the patients seen in the ED. Several professional bodies have endorsed the use of protocol-driven care for the conditions seen in the COU. Most professional organizations that have a key role in COUs advocate this approach, and include the ACEP, AHA, and SHM. When a COU has established itself, it likely is to use specific, expedited, protocol-driven approaches. This allows for care to be focused and standardized. This also is an opportunity to avoid redundant imaging and lab testing.
Patient safety. In its landmark publication “To Err is Human: Building a Safer Health System,” the Institute of Medicine identified communication error as one of the factors that lead to mistakes in patient care.7 COUs often tend to provide bulk of care at a given geographical area; this minimizes the transfer of patients from one place to another, thereby decreasing communication errors.
By providing more time to make decisions, COUs afford a greater diagnostic certainty. In the long run, this also helps a hospital minimize costly lawsuits.
The Bad
Not everything about COUs is great. There are certain areas that dull the luster of an observation unit.
Overzealous approaches. COUs are designed to allow more time to make clinical decisions when the triaging is in a gray area: whether to admit or not. Also, COUs provide clinicians with more time to follow the response to the care the patients receive in an emergent fashion. It needs to be emphasized that COUs are designed neither to replace hospitalization, nor to act as urgent care. As a corollary, there is a chance clinicians may be overzealous in discharging patients from COUs close to the 24-hour mark—even though it might not be clear whether the patient needs to be admitted or discharged. Overzealous discharging of COU patients can damage the premise of these units: to determine the need for admission and ensure patient safety. Having strict inclusion and exclusion criteria and good management can prevent these problems.
Staffing. Introduction of a COU can strain an already short-staffed ED. No different from any other novel approach, COU staffers need to be afforded a learning curve. This requires training personnel and establishing a robust team to staff COUs. It can be a strenuous process, at least in the beginning. Strong leadership and support of hospital, physician, and nursing leadership all play a role in the successful implementation and ongoing utilization of COUs.
Logistics. Coordination of people, facilities, and supplies that go into instituting a COU might be a challenge. Also, there may be times where patient ownership may not be very clear. Logistical concerns can include:
- Who owns the patient?
- How much of a role does a consulting service have?
- Who oversees the follow-up plans?
Although a popular COU setup is to have a dedicated observation unit adjacent to the ED, it is not a standard.
Reimbursement. Unfortunately, there is some degree of negative incentive built into reimbursements for COU operations. To understand why this is a bad thing for a hospital, let’s examine how hospitals are paid for services provided in a COU.
Frequently, COU patients are treated as “outpatients.” The operating formula is based on the Hospital Outpatient Prospective Payment System (OPPS), which is based on Ambulatory Payment Classification, or APC.8 Reimbursement differences in these two approaches can be quite sizable. Depending on what condition is being treated, the hospital reimbursement can be as little as half to a quarter of the payment for inpatient treatment.9 Essentially, the patient would have received very similar care, diagnostic work-up, antibiotics, imaging, lab work, and equally qualified clinicians as caretakers in both the settings. The payments need to account for the care in the COUs, which is usually more acute than in the ambulatory setting and potentially more efficient than an inpatient setting. The payments, therefore, should be sensitive to these factors.
The Ugly
COUs are intended to address many of the challenges facing the healthcare system, and in large part, that is what they do. However, some hospitals could be penalized for providing care through COUs. An efficient COU means that the patients who are admitted are, in fact, sicker. Logically, these patients will have a higher chance of being readmitted. Because the “not so sick” patients were successfully intervened and discharged from COUs, the patients that did get admitted must be pretty sick and must have higher comorbidities.
According to CMS, a readmission occurs if a patient has “an admission to a subsection hospital within 30 days of a discharge from the same or another subsection hospital.”10 The denominator here consists of all the patients who were discharged from the hospital inpatient stay. If a hospital does not have a robust COU, a large number of “not so sick” patients will be admitted as inpatients and will provide a larger denominator for calculating the readmission rates.
In contrast, a successful COU will allow for a large number of “not so sick” and “borderline” patients to be discharged, shrinking the denominator base, and “very sick” patients who are likely to be readmitted. This may erroneously cause the hospital to appear to have higher 30-day readmission rates. These hospitals may risk substantial readmission-related penalties.
This issue, along with a lopsided payment model, makes the COU landscape murky. With a greater share of pie being the “Il buono” in Il buono, il brutto, il cattivo, clinical observation units are certain to take a prominent position in addressing many of the issues that plague current healthcare facilities—capacity constraints, long ED wait times, limited inpatient beds, and soaring health-care expenditures.
Most important, COUs can lead to better and more efficient patient care.11 It is, therefore, not surprising that the IOM, in its report “Hospital Based Emergency Care—At the Breaking Point,” has identified clinical decision units as a “particularly promising” technique to improve patient flow.12
Dr. Asudani is a hospitalist in the division of hospital medicine in the department of internal medicine at the University of California San Diego Health System. Dr. Tolia is director of observation medicine in the department of emergency medicine and internal medicine at UCSD Health System.
References
- Baugh CW, Venkatesh AK, Hilton JA, Samuel PA, Schuur JD, Bohan JS. Making greater use of dedicated hospital observation units for many short-stay patients could save $3.1 billion a year. Health Aff (Millwood). 2012;31(10):2314-2323.
- Society of Hospital Medicine. The observation unit white paper. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=White_Papers&Template=/CM/ContentDisplay.cfm&ContentID=21890. Accessed April 3, 2013.
- American College of Emergency Physicians. Emergency department observation services. American College of Emergency Physicians website. Available at: http://www.acep.org/Clinical—Practice-Management/Emergency-Department-Observation-Services. Accessed April 10, 2013.
- Niska R, Bhuiya F, Xu J. National Hospital Ambulatory Medical Care Survey: 2007 emergency department summary. Hyattsville, Md.: National Center for Health Statistics; 2010.
- Centers for Disease Control and Prevention. Fast stats. Centers for Disease Control and Prevention. Available at: http://www.cdc.gov/nchs/fastats/ervisits.htm. Accessed April 9, 2013.
- Martinez E, Reilly BM, Evans AT, Roberts RR. The observation unit: a new interface between inpatient and outpatient care. Am J Med. 2001;110(4):274-277.
- To err is human: building a safer health system. Institute of Medicine. Washington (DC): National Academies Press; 2000.
- Centers for Medicare & Medicaid Services. Hospital outpatient prospective payment system. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/hospitaloutpaysysfctsht.pdf. Accessed April 2, 2013.
- Runy L. Clinical observation units: Building a bridge between outpatient and inpatient services. Hospitals and Health Networks website. Available at: http://www.hhnmag.com/hhnmag/jsp/articledisplay.jsp?dcrpath=HHNMAG/PubsNewsArticle/data/2006March/0603HHN_FEA_gatefold&domain=HHNMAG. Accessed April 9, 2013.
- Centers for Medicare & Medicaid Services. Readmissions reduction program. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html. Accessed May 6, 2013.
- Baugh CW, Venkatesh AK, Bohan JS. Emergency department observation nits: a clinical and financial benefit for hospitals. Health Care Manage Rev. 2011;36(1):28-37.
- Institute of Medicine. Hospital-based emergency care: at the breaking point. Washington: National Academies Press; 2007.
Hospitals nationwide face significant capacity constraints in emergency departments. High hospitalization rates can have a ripple effect, leading to long wait times, frequent diversion of patients to other hospitals, and higher patient-care expenses. However, a sizable number of inpatient admissions can be prevented through dedicated clinical observation units, or COUs. Such a strategy is likely to be more efficient, can result in shorter lengths of stay, and can decrease health-care costs.1
Also known as clinical decision units, “obs” units, or short-stay observation units, these hospital-based units lend themselves as a feasible solution. Many of the COU success stories come from “chest pain” units, along with ED-based observation units. Over time, the COUs have been expanded to include many more conditions and have enjoyed success when dealing with asthma exacerbations, transient ischemic attacks, bronchiolitis in pediatric populations, and congestive-heart-failure exacerbation, to name a few.
Most COUs use a window of six to 24 hours to carry out triaging, diagnosing, treating, and monitoring the patient response. Anytime before the 24-hour mark, a decision is made whether to discharge or admit the patient. The success of dedicated COUs relies heavily on strong leadership, strict treatment protocols, and well-defined inclusion/exclusion criteria.
COU utilization has been well received by several professional bodies. Both emergency medicine physicians and hospitalists are natural key players in the widespread utilization of COUs. SHM, in a white paper, concluded: “Collaboration between hospitalists, emergency physicians, hospital administrators, and academicians will serve not only to promote outstanding observation care, but also to focus quality improvement and research efforts for the observation unit of the 21st century.”2 The American College of Emergency Physicians (ACEP), in its position statement, said the “observation of appropriate ED patients in a dedicated ED observation area, instead of a general inpatient bed or an acute care ED bed, is a ‘best practice’ that requires a commitment of staff and hospital resources.”3
As promising as the COUs appear, it is estimated that only one-third of hospitals have them in place.4 And while much of the COU story is good, there are concerns with the patient-care model.
The Good
Instinctively, a COU is a win-win proposition for all stakeholders. Essentially, many see these units as a fine blend of clinical care, fiscal responsibility, and patient accountability. Among the benefits:
Reduced admissions. On average, the admission rates from ED to inpatient services are 13.3%.5 In contrast, in hospitals that have a robust COU in place, the admission rates are much lower. As an example, Cook County Hospital in Chicago in the mid-1990s saw a decline in the admission rates from the emergency room following implementation of a COU, along with an increase in bed capacity due to the efficient, protocol-driven approach that goes along with successful ED observation units.6 With well-structured and managed observation units, such a reduction in hospitalization rates has been shown, is reproducible, and is achievable.
Improved case-mix multiplier. Inpatient reimbursements from the Centers for Medicare and Medicaid Services (CMS) and private insurers frequently are tied to the acuity of care a hospital provides. Critical to making that determination is the case mix that a given hospital sees. Usually, the more complex patients a hospital admits, the higher the reimbursements are. With a successful COU, a hospital can expect a case-mix multiplier representing patients with greater complexity and higher acuity.
What a successful COU essentially does is lead to the admission of patients with greater comorbidities—those who are sicker than the average patient. In doing so, COUs also facilitate safe discharges of the patients who do not necessarily need to be admitted. As an average, the cohort of patients who are admitted as inpatients then consists of patients who are sick enough and absolutely need to be admitted.
Resource utilization. When a patient is admitted from the ED to an inpatient floor, a lot of resources are utilized. These include expenses related to transportation, housekeeping, nursing, and ancillary services. Each of these additional resources comes with an expense. The more resources that are put in motion, the greater the expense a hospital incurs. With effective COUs, it is generally expected that suitable patients will get the care in a specific geographic area by the same set of providers. COUs tend to reduce unnecessary hospitalizations, redundancy of manpower utilization, and duplication of documentation—therefore reducing the expenses incurred by the hospital.
Infection control. The COUs operate based on minimizing the stay of the patients who can be safely discharged after a brief observation period. Decreased duration of stay also means decreased movement and unique provider contact/exposure—thus decreasing the chances for acquiring health-care-related infections. Besides, most COUs are restricted to a certain geographic area within the hospital, which helps to restrict patients to a limited area. This again may be helpful in better overall infection-control practices. More research is necessary to establish this association of the infection-control advantages of COUs. The hypothesis, however, does appear very promising.
Prompt and standardized care. Most COUs use an evidence-based, standardized approach toward the patients seen in the ED. Several professional bodies have endorsed the use of protocol-driven care for the conditions seen in the COU. Most professional organizations that have a key role in COUs advocate this approach, and include the ACEP, AHA, and SHM. When a COU has established itself, it likely is to use specific, expedited, protocol-driven approaches. This allows for care to be focused and standardized. This also is an opportunity to avoid redundant imaging and lab testing.
Patient safety. In its landmark publication “To Err is Human: Building a Safer Health System,” the Institute of Medicine identified communication error as one of the factors that lead to mistakes in patient care.7 COUs often tend to provide bulk of care at a given geographical area; this minimizes the transfer of patients from one place to another, thereby decreasing communication errors.
By providing more time to make decisions, COUs afford a greater diagnostic certainty. In the long run, this also helps a hospital minimize costly lawsuits.
The Bad
Not everything about COUs is great. There are certain areas that dull the luster of an observation unit.
Overzealous approaches. COUs are designed to allow more time to make clinical decisions when the triaging is in a gray area: whether to admit or not. Also, COUs provide clinicians with more time to follow the response to the care the patients receive in an emergent fashion. It needs to be emphasized that COUs are designed neither to replace hospitalization, nor to act as urgent care. As a corollary, there is a chance clinicians may be overzealous in discharging patients from COUs close to the 24-hour mark—even though it might not be clear whether the patient needs to be admitted or discharged. Overzealous discharging of COU patients can damage the premise of these units: to determine the need for admission and ensure patient safety. Having strict inclusion and exclusion criteria and good management can prevent these problems.
Staffing. Introduction of a COU can strain an already short-staffed ED. No different from any other novel approach, COU staffers need to be afforded a learning curve. This requires training personnel and establishing a robust team to staff COUs. It can be a strenuous process, at least in the beginning. Strong leadership and support of hospital, physician, and nursing leadership all play a role in the successful implementation and ongoing utilization of COUs.
Logistics. Coordination of people, facilities, and supplies that go into instituting a COU might be a challenge. Also, there may be times where patient ownership may not be very clear. Logistical concerns can include:
- Who owns the patient?
- How much of a role does a consulting service have?
- Who oversees the follow-up plans?
Although a popular COU setup is to have a dedicated observation unit adjacent to the ED, it is not a standard.
Reimbursement. Unfortunately, there is some degree of negative incentive built into reimbursements for COU operations. To understand why this is a bad thing for a hospital, let’s examine how hospitals are paid for services provided in a COU.
Frequently, COU patients are treated as “outpatients.” The operating formula is based on the Hospital Outpatient Prospective Payment System (OPPS), which is based on Ambulatory Payment Classification, or APC.8 Reimbursement differences in these two approaches can be quite sizable. Depending on what condition is being treated, the hospital reimbursement can be as little as half to a quarter of the payment for inpatient treatment.9 Essentially, the patient would have received very similar care, diagnostic work-up, antibiotics, imaging, lab work, and equally qualified clinicians as caretakers in both the settings. The payments need to account for the care in the COUs, which is usually more acute than in the ambulatory setting and potentially more efficient than an inpatient setting. The payments, therefore, should be sensitive to these factors.
The Ugly
COUs are intended to address many of the challenges facing the healthcare system, and in large part, that is what they do. However, some hospitals could be penalized for providing care through COUs. An efficient COU means that the patients who are admitted are, in fact, sicker. Logically, these patients will have a higher chance of being readmitted. Because the “not so sick” patients were successfully intervened and discharged from COUs, the patients that did get admitted must be pretty sick and must have higher comorbidities.
According to CMS, a readmission occurs if a patient has “an admission to a subsection hospital within 30 days of a discharge from the same or another subsection hospital.”10 The denominator here consists of all the patients who were discharged from the hospital inpatient stay. If a hospital does not have a robust COU, a large number of “not so sick” patients will be admitted as inpatients and will provide a larger denominator for calculating the readmission rates.
In contrast, a successful COU will allow for a large number of “not so sick” and “borderline” patients to be discharged, shrinking the denominator base, and “very sick” patients who are likely to be readmitted. This may erroneously cause the hospital to appear to have higher 30-day readmission rates. These hospitals may risk substantial readmission-related penalties.
This issue, along with a lopsided payment model, makes the COU landscape murky. With a greater share of pie being the “Il buono” in Il buono, il brutto, il cattivo, clinical observation units are certain to take a prominent position in addressing many of the issues that plague current healthcare facilities—capacity constraints, long ED wait times, limited inpatient beds, and soaring health-care expenditures.
Most important, COUs can lead to better and more efficient patient care.11 It is, therefore, not surprising that the IOM, in its report “Hospital Based Emergency Care—At the Breaking Point,” has identified clinical decision units as a “particularly promising” technique to improve patient flow.12
Dr. Asudani is a hospitalist in the division of hospital medicine in the department of internal medicine at the University of California San Diego Health System. Dr. Tolia is director of observation medicine in the department of emergency medicine and internal medicine at UCSD Health System.
References
- Baugh CW, Venkatesh AK, Hilton JA, Samuel PA, Schuur JD, Bohan JS. Making greater use of dedicated hospital observation units for many short-stay patients could save $3.1 billion a year. Health Aff (Millwood). 2012;31(10):2314-2323.
- Society of Hospital Medicine. The observation unit white paper. Society of Hospital Medicine website. Available at: http://www.hospitalmedicine.org/AM/Template.cfm?Section=White_Papers&Template=/CM/ContentDisplay.cfm&ContentID=21890. Accessed April 3, 2013.
- American College of Emergency Physicians. Emergency department observation services. American College of Emergency Physicians website. Available at: http://www.acep.org/Clinical—Practice-Management/Emergency-Department-Observation-Services. Accessed April 10, 2013.
- Niska R, Bhuiya F, Xu J. National Hospital Ambulatory Medical Care Survey: 2007 emergency department summary. Hyattsville, Md.: National Center for Health Statistics; 2010.
- Centers for Disease Control and Prevention. Fast stats. Centers for Disease Control and Prevention. Available at: http://www.cdc.gov/nchs/fastats/ervisits.htm. Accessed April 9, 2013.
- Martinez E, Reilly BM, Evans AT, Roberts RR. The observation unit: a new interface between inpatient and outpatient care. Am J Med. 2001;110(4):274-277.
- To err is human: building a safer health system. Institute of Medicine. Washington (DC): National Academies Press; 2000.
- Centers for Medicare & Medicaid Services. Hospital outpatient prospective payment system. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/hospitaloutpaysysfctsht.pdf. Accessed April 2, 2013.
- Runy L. Clinical observation units: Building a bridge between outpatient and inpatient services. Hospitals and Health Networks website. Available at: http://www.hhnmag.com/hhnmag/jsp/articledisplay.jsp?dcrpath=HHNMAG/PubsNewsArticle/data/2006March/0603HHN_FEA_gatefold&domain=HHNMAG. Accessed April 9, 2013.
- Centers for Medicare & Medicaid Services. Readmissions reduction program. Centers for Medicare & Medicaid Services website. Available at: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html. Accessed May 6, 2013.
- Baugh CW, Venkatesh AK, Bohan JS. Emergency department observation nits: a clinical and financial benefit for hospitals. Health Care Manage Rev. 2011;36(1):28-37.
- Institute of Medicine. Hospital-based emergency care: at the breaking point. Washington: National Academies Press; 2007.
Hospitalist Greg Harlan Embraces Everything Hospital Medicine Career Offers

If he wasn’t a physician administrator working for one of the largest physician management companies in the country, or a clinical instructor at a medical school, or a pediatric hospitalist picking up shifts at a children’s hospital, Greg Harlan, MD, MPH, would have a very different life.
He says he’d “promote vegetable gardens to kindergartners, hike the West Coast Trail, fight the obesity epidemic, and play lots of golf.”
Oh, yeah, one more: “Give every kid a bicycle.”
It’s quite the altruistic—some might say enviable—list. Instead, Dr. Harlan is hard at work as director of medical affairs at North Hollywood, Calif.-based IPC The Hospitalist Company. He is also a clinical instructor at the University of Southern California Medical School and moonlights as a pediatric hospitalist in Los Angeles.
He says he chose to focus on hospital medicine as a career while working as a young faculty member at the University of Utah.
“I noticed that lots of innovation, experimentation, and energy was coming from the newly formed hospitalist division,” says Dr. Harlan, one of nine new members of Team Hospitalist, The Hospitalist’s volunteer editorial advisory group. “I tried it out and loved it, especially getting to teach the students and residents for intense periods of time.”
At IPC, Dr. Harlan leads company-wide quality improvement (QI) initiatives, coordinates risk reduction activities, and directs the IPC-University of California San Francisco Fellowship for Hospitalist Leaders. He says he has a growing interest in “physician leadership, high-functioning teams, and physician groups’ well-being.”

“I am using my QI background to apply these principles to better understanding how teams and leaders can thrive,” he says.
Question: Why did you choose a career in medicine?
A: Medicine is a cool combination of hard science, psychology, counseling, and teaching. It’s an amazing way to combine multiple passions and get to be involved on a very intimate level with many people.
Q: What do you like most about working as a hospitalist?
A: The focus on improving the system as a whole. Ultimately, the patients benefit, but so do many of the other stakeholders in the processes we touch.
Q: What do you dislike most?
A: It’s tough to take in-house call at night. It’s also hard to step in to many sick patients’ care for a short period of time, especially midway through their hospitalization.
Q: What’s the best advice you ever received?
A: Find the people who actually do the work. This is the concept of going to the front line, to see where the real work is being done. It never ceases to amaze me to find out the difference between what we think is going on and what is actually going on.
Q: What’s the biggest change you’ve seen in HM in your career?
A: Providers are getting squeezed a little more each year. There are growing pressures from many sides, and the providers are feeling “crunched.”
Q: Why is it important for you to continue seeing patients?
A: Feeling the joy and pain of actually providing care for patients is integral to leading the hospitalist movement. By acutely experiencing an electronic health record, or dealing with medication authorizations or handoffs, one stays in the real world of hospital medicine.
Q: What is your biggest professional challenge?
A: Balancing my multiple passions. I love being a teacher and still teach young med students at USC med school (my alma mater). I still enjoy seeing patients, too. I am most excited by a growing interest in leadership and teamwork, but it’s still in its development stage as a career path.
Q: What is your biggest professional reward?
A: Being able to see others flourish. Whether it’s beginning med students, professional colleagues, or administrative staff, I truly beam when someone I’ve helped succeeds.
Q: When you aren’t working, what is important to you?
A: My family, my health, and staying balanced. I am learning the importance of listening to my body, trusting my intuition, and finding true “balance.” It’s not easy, but it’s imperative.
Q: What’s next professionally?
A: I am really excited to put some science behind “leadership in medicine” and “optimal teamwork in medicine.” I think there is so much more we can learn and implement.
Q: What’s the best book you’ve read recently? Why?
A: A few come to mind: “18 Minutes” by Peter Bregman offers some really easy steps to getting organized and focused; “Six Thinking Hats” by Edward de Bono is a great framework for approaching problems and innovations; “The Inner Game of Golf” by W. Timothy Gallwey makes me realize how amazing our bodies and minds truly are.
Q: How many Apple products do you interface with in a given week?
A: I only have an iPhone. Amazing little gadget, but I don’t want to become wedded to it. Maybe I’ll get a MacBook soon.
Q: What’s next in your Netflix queue?
A: We use Netflix mainly for their drama series. I prefer foreign films and documentaries. My wife and I love “Breaking Bad.” My kids and I are working our way through the “Star Wars” episodes.
Richard Quinn is a freelance writer in New Jersey.
If he wasn’t a physician administrator working for one of the largest physician management companies in the country, or a clinical instructor at a medical school, or a pediatric hospitalist picking up shifts at a children’s hospital, Greg Harlan, MD, MPH, would have a very different life.
He says he’d “promote vegetable gardens to kindergartners, hike the West Coast Trail, fight the obesity epidemic, and play lots of golf.”
Oh, yeah, one more: “Give every kid a bicycle.”
It’s quite the altruistic—some might say enviable—list. Instead, Dr. Harlan is hard at work as director of medical affairs at North Hollywood, Calif.-based IPC The Hospitalist Company. He is also a clinical instructor at the University of Southern California Medical School and moonlights as a pediatric hospitalist in Los Angeles.
He says he chose to focus on hospital medicine as a career while working as a young faculty member at the University of Utah.
“I noticed that lots of innovation, experimentation, and energy was coming from the newly formed hospitalist division,” says Dr. Harlan, one of nine new members of Team Hospitalist, The Hospitalist’s volunteer editorial advisory group. “I tried it out and loved it, especially getting to teach the students and residents for intense periods of time.”
At IPC, Dr. Harlan leads company-wide quality improvement (QI) initiatives, coordinates risk reduction activities, and directs the IPC-University of California San Francisco Fellowship for Hospitalist Leaders. He says he has a growing interest in “physician leadership, high-functioning teams, and physician groups’ well-being.”
“I am using my QI background to apply these principles to better understanding how teams and leaders can thrive,” he says.
Question: Why did you choose a career in medicine?
A: Medicine is a cool combination of hard science, psychology, counseling, and teaching. It’s an amazing way to combine multiple passions and get to be involved on a very intimate level with many people.
Q: What do you like most about working as a hospitalist?
A: The focus on improving the system as a whole. Ultimately, the patients benefit, but so do many of the other stakeholders in the processes we touch.
Q: What do you dislike most?
A: It’s tough to take in-house call at night. It’s also hard to step in to many sick patients’ care for a short period of time, especially midway through their hospitalization.
Q: What’s the best advice you ever received?
A: Find the people who actually do the work. This is the concept of going to the front line, to see where the real work is being done. It never ceases to amaze me to find out the difference between what we think is going on and what is actually going on.
Q: What’s the biggest change you’ve seen in HM in your career?
A: Providers are getting squeezed a little more each year. There are growing pressures from many sides, and the providers are feeling “crunched.”
Q: Why is it important for you to continue seeing patients?
A: Feeling the joy and pain of actually providing care for patients is integral to leading the hospitalist movement. By acutely experiencing an electronic health record, or dealing with medication authorizations or handoffs, one stays in the real world of hospital medicine.
Q: What is your biggest professional challenge?
A: Balancing my multiple passions. I love being a teacher and still teach young med students at USC med school (my alma mater). I still enjoy seeing patients, too. I am most excited by a growing interest in leadership and teamwork, but it’s still in its development stage as a career path.
Q: What is your biggest professional reward?
A: Being able to see others flourish. Whether it’s beginning med students, professional colleagues, or administrative staff, I truly beam when someone I’ve helped succeeds.
Q: When you aren’t working, what is important to you?
A: My family, my health, and staying balanced. I am learning the importance of listening to my body, trusting my intuition, and finding true “balance.” It’s not easy, but it’s imperative.
Q: What’s next professionally?
A: I am really excited to put some science behind “leadership in medicine” and “optimal teamwork in medicine.” I think there is so much more we can learn and implement.
Q: What’s the best book you’ve read recently? Why?
A: A few come to mind: “18 Minutes” by Peter Bregman offers some really easy steps to getting organized and focused; “Six Thinking Hats” by Edward de Bono is a great framework for approaching problems and innovations; “The Inner Game of Golf” by W. Timothy Gallwey makes me realize how amazing our bodies and minds truly are.
Q: How many Apple products do you interface with in a given week?
A: I only have an iPhone. Amazing little gadget, but I don’t want to become wedded to it. Maybe I’ll get a MacBook soon.
Q: What’s next in your Netflix queue?
A: We use Netflix mainly for their drama series. I prefer foreign films and documentaries. My wife and I love “Breaking Bad.” My kids and I are working our way through the “Star Wars” episodes.
Richard Quinn is a freelance writer in New Jersey.
If he wasn’t a physician administrator working for one of the largest physician management companies in the country, or a clinical instructor at a medical school, or a pediatric hospitalist picking up shifts at a children’s hospital, Greg Harlan, MD, MPH, would have a very different life.
He says he’d “promote vegetable gardens to kindergartners, hike the West Coast Trail, fight the obesity epidemic, and play lots of golf.”
Oh, yeah, one more: “Give every kid a bicycle.”
It’s quite the altruistic—some might say enviable—list. Instead, Dr. Harlan is hard at work as director of medical affairs at North Hollywood, Calif.-based IPC The Hospitalist Company. He is also a clinical instructor at the University of Southern California Medical School and moonlights as a pediatric hospitalist in Los Angeles.
He says he chose to focus on hospital medicine as a career while working as a young faculty member at the University of Utah.
“I noticed that lots of innovation, experimentation, and energy was coming from the newly formed hospitalist division,” says Dr. Harlan, one of nine new members of Team Hospitalist, The Hospitalist’s volunteer editorial advisory group. “I tried it out and loved it, especially getting to teach the students and residents for intense periods of time.”
At IPC, Dr. Harlan leads company-wide quality improvement (QI) initiatives, coordinates risk reduction activities, and directs the IPC-University of California San Francisco Fellowship for Hospitalist Leaders. He says he has a growing interest in “physician leadership, high-functioning teams, and physician groups’ well-being.”
“I am using my QI background to apply these principles to better understanding how teams and leaders can thrive,” he says.
Question: Why did you choose a career in medicine?
A: Medicine is a cool combination of hard science, psychology, counseling, and teaching. It’s an amazing way to combine multiple passions and get to be involved on a very intimate level with many people.
Q: What do you like most about working as a hospitalist?
A: The focus on improving the system as a whole. Ultimately, the patients benefit, but so do many of the other stakeholders in the processes we touch.
Q: What do you dislike most?
A: It’s tough to take in-house call at night. It’s also hard to step in to many sick patients’ care for a short period of time, especially midway through their hospitalization.
Q: What’s the best advice you ever received?
A: Find the people who actually do the work. This is the concept of going to the front line, to see where the real work is being done. It never ceases to amaze me to find out the difference between what we think is going on and what is actually going on.
Q: What’s the biggest change you’ve seen in HM in your career?
A: Providers are getting squeezed a little more each year. There are growing pressures from many sides, and the providers are feeling “crunched.”
Q: Why is it important for you to continue seeing patients?
A: Feeling the joy and pain of actually providing care for patients is integral to leading the hospitalist movement. By acutely experiencing an electronic health record, or dealing with medication authorizations or handoffs, one stays in the real world of hospital medicine.
Q: What is your biggest professional challenge?
A: Balancing my multiple passions. I love being a teacher and still teach young med students at USC med school (my alma mater). I still enjoy seeing patients, too. I am most excited by a growing interest in leadership and teamwork, but it’s still in its development stage as a career path.
Q: What is your biggest professional reward?
A: Being able to see others flourish. Whether it’s beginning med students, professional colleagues, or administrative staff, I truly beam when someone I’ve helped succeeds.
Q: When you aren’t working, what is important to you?
A: My family, my health, and staying balanced. I am learning the importance of listening to my body, trusting my intuition, and finding true “balance.” It’s not easy, but it’s imperative.
Q: What’s next professionally?
A: I am really excited to put some science behind “leadership in medicine” and “optimal teamwork in medicine.” I think there is so much more we can learn and implement.
Q: What’s the best book you’ve read recently? Why?
A: A few come to mind: “18 Minutes” by Peter Bregman offers some really easy steps to getting organized and focused; “Six Thinking Hats” by Edward de Bono is a great framework for approaching problems and innovations; “The Inner Game of Golf” by W. Timothy Gallwey makes me realize how amazing our bodies and minds truly are.
Q: How many Apple products do you interface with in a given week?
A: I only have an iPhone. Amazing little gadget, but I don’t want to become wedded to it. Maybe I’ll get a MacBook soon.
Q: What’s next in your Netflix queue?
A: We use Netflix mainly for their drama series. I prefer foreign films and documentaries. My wife and I love “Breaking Bad.” My kids and I are working our way through the “Star Wars” episodes.
Richard Quinn is a freelance writer in New Jersey.
How to Handle Medicare Documentation Audits

The recent announcement of a settlement by a physician firm should cause the HM community to pause and take inventory. The settlement “addressed allegations that, between 2004 and 2012, [the firm] knowingly submitted to federal health benefits programs inflated claims on behalf of its hospitalist employees for higher and more expensive levels of service than were documented by hospitalists in patient medical records.”1
This civil settlement highlights the vigilance being exercised against healthcare fraud and demonstrates the coordinated efforts in place to tackle the issue. To put the weight of this case in perspective, consider the breadth of legal entities involved: the U.S. Department of Justice; the U.S. Attorney’s Office; the U.S. Department of Health and Human Services; the U.S. Department of Defense; the U.S. Office of Personnel Management; the U.S. Department of Veterans’ Affairs; and the TRICARE Management Activity Office of General Counsel.1
The underlying factor in the settlement is a common issue routinely identified by Medicare-initiated review programs such as CERT (Comprehensive Error Rate Testing). CERT selects a stratified, random sample of approximately 40,000 claims submitted to Part A/B Medicare Administrative Contractors (MACs) and Durable Medical Equipment MACs (DME MACs) during each reporting period and allows the Centers for Medicare and Medicaid Services (CMS) to calculate a national improper payment rate and contractor- and service-specific improper payment rates.2 The CERT-determined improper payment rate identifies services that have not satisfied Medicare requirements, but it cannot label a claim fraudulent.2
Incorrect coding errors involving hospitalists are related to inpatient evaluation and management (E/M) services that do not adequately reflect the documentation in the medical record. For example, WPS Medicare identified the following error rates for claims submitted 7/1/11 to 6/30/12: 45% of 99223 (initial hospital care, per day, for the evaluation and management of a patient, which requires these three key components: a comprehensive history, a comprehensive exam, and medical decision-making of high complexity); and 34% of 99233 (subsequent hospital care, per day, for the evaluation and management of a patient, which requires at least two of these three key components: a detailed interval history, a detailed examination, and medical decision-making of high complexity).3,4 More recent WPS Medicare data in first quarter of FY2013 reveals a continuing problem but an improved error rate.5 Novitas Solutions offers additional support of these findings.6
Based on efforts that identify improper payments, MACs are encouraged to initiate targeted service-specific prepayment review to prevent improper payments for services identified by CERT or recovery audit contractors (RACs) as problem areas, as well as problem areas identified by their own data analysis.7 For this reason, hospitalists may see prepayment requests for documentation by Medicare for services that are most “problematic” (e.g., 99223 and 99233). This occurs when a claim involving these services is submitted to Medicare. The MAC suspends all or part of a claim so that a trained clinician or claims analyst can review the claim and associated documentation in order to make determinations about coverage and payment.7 Responding to these requests in a timely manner is crucial in preventing claim denials.
Responding to Requests
When documentation is requested by the payor, take note of the date and the provider for whom the service is requested. Be certain to include all pertinent information in support of the claim. The payor request letter will typically include a generic list of items that should be submitted with the documentation request. Consider these particular items when submitting documentation for targeted services typically provided by hospitalists:
- Initial Hospital Care (99223)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify any referenced sources of information (e.g., physician referencing a family history documented in the ED record);
- Dictations, when performed;
- Admitting orders; and
- Labs or diagnostic test reports performed on admission.
- Subsequent Hospital Care (99233)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify multiple encounters/entries recorded on a given date;
- Physician orders; and
- Labs or diagnostic test reports performed on the requested date.
Documentation Tips
Because it is the primary communication tool for providers involved in the patient’s care, documentation must be entered in a timely manner and must be decipherable to members of the healthcare team as well as other individuals who may need to review the information (e.g., auditors). Proper credit cannot be given for documentation that is difficult to read.
Information should include historical review of past/interim events, a physical exam, medical decision-making as related to the patient’s progress/response to intervention, and modification of the care plan (as necessary). The reason for the encounter should be evident to support the medical necessity of the service. Because various specialists may participate in patient care, documentation for each provider’s encounter should demonstrate personalized and non-duplicative care.
Each individual provider must exhibit a personal contribution to the case to prevent payors from viewing the documentation as overlapping and indistinguishable from care already provided by another physician. Each entry should be dated and signed with a legible identifier (i.e., signature with a printed name).
The next several articles will address each of the key components (history, exam, and decision-making) and serve as a “documentation refresher” for providers who wish to compare their documentation to current standards.
References
- Department of Justice, Office of Public Affairs. Tacoma, Wash., Medical Firm to Pay $14.5 Million to Settle Overbilling Allegations. Available at: www.justice.gov/opa/pr/2013/July/13-civ-758.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Comprehensive Error Rate Testing (CERT). Available at: www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/CERT/index.html?redirect=/cert. Accessed September 20, 2013.
- WPS Medicare, Legacy Part B. Are you billing these evaluation and management (e/m) services correctly? Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2011-0912-billemservices.shtml. Accessed September 20, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis, L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012:15-17.
- WPS Medicare, Legacy Part B. 1st Qtr. 2013 (Jan. - Mar.) - CERT Error Summary. Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2013-1st-quarter-summary.shtml. Accessed September 20, 2013.
- Novitas Solutions. Analysis of JL Part B Comprehensive Error Rate Testing (CERT) Data - January thru March 2013. Available at: https://www.novitas-solutions.com/cert/errors/2013/b-jan-mar-j12.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Program Integrity Manual, Chapter 3, Section 3.2. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/pim83c03.pdf. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual, Chapter 11, Section 40.1.2 Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed September 20, 2013.
The recent announcement of a settlement by a physician firm should cause the HM community to pause and take inventory. The settlement “addressed allegations that, between 2004 and 2012, [the firm] knowingly submitted to federal health benefits programs inflated claims on behalf of its hospitalist employees for higher and more expensive levels of service than were documented by hospitalists in patient medical records.”1
This civil settlement highlights the vigilance being exercised against healthcare fraud and demonstrates the coordinated efforts in place to tackle the issue. To put the weight of this case in perspective, consider the breadth of legal entities involved: the U.S. Department of Justice; the U.S. Attorney’s Office; the U.S. Department of Health and Human Services; the U.S. Department of Defense; the U.S. Office of Personnel Management; the U.S. Department of Veterans’ Affairs; and the TRICARE Management Activity Office of General Counsel.1
The underlying factor in the settlement is a common issue routinely identified by Medicare-initiated review programs such as CERT (Comprehensive Error Rate Testing). CERT selects a stratified, random sample of approximately 40,000 claims submitted to Part A/B Medicare Administrative Contractors (MACs) and Durable Medical Equipment MACs (DME MACs) during each reporting period and allows the Centers for Medicare and Medicaid Services (CMS) to calculate a national improper payment rate and contractor- and service-specific improper payment rates.2 The CERT-determined improper payment rate identifies services that have not satisfied Medicare requirements, but it cannot label a claim fraudulent.2
Incorrect coding errors involving hospitalists are related to inpatient evaluation and management (E/M) services that do not adequately reflect the documentation in the medical record. For example, WPS Medicare identified the following error rates for claims submitted 7/1/11 to 6/30/12: 45% of 99223 (initial hospital care, per day, for the evaluation and management of a patient, which requires these three key components: a comprehensive history, a comprehensive exam, and medical decision-making of high complexity); and 34% of 99233 (subsequent hospital care, per day, for the evaluation and management of a patient, which requires at least two of these three key components: a detailed interval history, a detailed examination, and medical decision-making of high complexity).3,4 More recent WPS Medicare data in first quarter of FY2013 reveals a continuing problem but an improved error rate.5 Novitas Solutions offers additional support of these findings.6
Based on efforts that identify improper payments, MACs are encouraged to initiate targeted service-specific prepayment review to prevent improper payments for services identified by CERT or recovery audit contractors (RACs) as problem areas, as well as problem areas identified by their own data analysis.7 For this reason, hospitalists may see prepayment requests for documentation by Medicare for services that are most “problematic” (e.g., 99223 and 99233). This occurs when a claim involving these services is submitted to Medicare. The MAC suspends all or part of a claim so that a trained clinician or claims analyst can review the claim and associated documentation in order to make determinations about coverage and payment.7 Responding to these requests in a timely manner is crucial in preventing claim denials.
Responding to Requests
When documentation is requested by the payor, take note of the date and the provider for whom the service is requested. Be certain to include all pertinent information in support of the claim. The payor request letter will typically include a generic list of items that should be submitted with the documentation request. Consider these particular items when submitting documentation for targeted services typically provided by hospitalists:
- Initial Hospital Care (99223)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify any referenced sources of information (e.g., physician referencing a family history documented in the ED record);
- Dictations, when performed;
- Admitting orders; and
- Labs or diagnostic test reports performed on admission.
- Subsequent Hospital Care (99233)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify multiple encounters/entries recorded on a given date;
- Physician orders; and
- Labs or diagnostic test reports performed on the requested date.
Documentation Tips
Because it is the primary communication tool for providers involved in the patient’s care, documentation must be entered in a timely manner and must be decipherable to members of the healthcare team as well as other individuals who may need to review the information (e.g., auditors). Proper credit cannot be given for documentation that is difficult to read.
Information should include historical review of past/interim events, a physical exam, medical decision-making as related to the patient’s progress/response to intervention, and modification of the care plan (as necessary). The reason for the encounter should be evident to support the medical necessity of the service. Because various specialists may participate in patient care, documentation for each provider’s encounter should demonstrate personalized and non-duplicative care.
Each individual provider must exhibit a personal contribution to the case to prevent payors from viewing the documentation as overlapping and indistinguishable from care already provided by another physician. Each entry should be dated and signed with a legible identifier (i.e., signature with a printed name).
The next several articles will address each of the key components (history, exam, and decision-making) and serve as a “documentation refresher” for providers who wish to compare their documentation to current standards.
References
- Department of Justice, Office of Public Affairs. Tacoma, Wash., Medical Firm to Pay $14.5 Million to Settle Overbilling Allegations. Available at: www.justice.gov/opa/pr/2013/July/13-civ-758.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Comprehensive Error Rate Testing (CERT). Available at: www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/CERT/index.html?redirect=/cert. Accessed September 20, 2013.
- WPS Medicare, Legacy Part B. Are you billing these evaluation and management (e/m) services correctly? Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2011-0912-billemservices.shtml. Accessed September 20, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis, L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012:15-17.
- WPS Medicare, Legacy Part B. 1st Qtr. 2013 (Jan. - Mar.) - CERT Error Summary. Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2013-1st-quarter-summary.shtml. Accessed September 20, 2013.
- Novitas Solutions. Analysis of JL Part B Comprehensive Error Rate Testing (CERT) Data - January thru March 2013. Available at: https://www.novitas-solutions.com/cert/errors/2013/b-jan-mar-j12.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Program Integrity Manual, Chapter 3, Section 3.2. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/pim83c03.pdf. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual, Chapter 11, Section 40.1.2 Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed September 20, 2013.
The recent announcement of a settlement by a physician firm should cause the HM community to pause and take inventory. The settlement “addressed allegations that, between 2004 and 2012, [the firm] knowingly submitted to federal health benefits programs inflated claims on behalf of its hospitalist employees for higher and more expensive levels of service than were documented by hospitalists in patient medical records.”1
This civil settlement highlights the vigilance being exercised against healthcare fraud and demonstrates the coordinated efforts in place to tackle the issue. To put the weight of this case in perspective, consider the breadth of legal entities involved: the U.S. Department of Justice; the U.S. Attorney’s Office; the U.S. Department of Health and Human Services; the U.S. Department of Defense; the U.S. Office of Personnel Management; the U.S. Department of Veterans’ Affairs; and the TRICARE Management Activity Office of General Counsel.1
The underlying factor in the settlement is a common issue routinely identified by Medicare-initiated review programs such as CERT (Comprehensive Error Rate Testing). CERT selects a stratified, random sample of approximately 40,000 claims submitted to Part A/B Medicare Administrative Contractors (MACs) and Durable Medical Equipment MACs (DME MACs) during each reporting period and allows the Centers for Medicare and Medicaid Services (CMS) to calculate a national improper payment rate and contractor- and service-specific improper payment rates.2 The CERT-determined improper payment rate identifies services that have not satisfied Medicare requirements, but it cannot label a claim fraudulent.2
Incorrect coding errors involving hospitalists are related to inpatient evaluation and management (E/M) services that do not adequately reflect the documentation in the medical record. For example, WPS Medicare identified the following error rates for claims submitted 7/1/11 to 6/30/12: 45% of 99223 (initial hospital care, per day, for the evaluation and management of a patient, which requires these three key components: a comprehensive history, a comprehensive exam, and medical decision-making of high complexity); and 34% of 99233 (subsequent hospital care, per day, for the evaluation and management of a patient, which requires at least two of these three key components: a detailed interval history, a detailed examination, and medical decision-making of high complexity).3,4 More recent WPS Medicare data in first quarter of FY2013 reveals a continuing problem but an improved error rate.5 Novitas Solutions offers additional support of these findings.6
Based on efforts that identify improper payments, MACs are encouraged to initiate targeted service-specific prepayment review to prevent improper payments for services identified by CERT or recovery audit contractors (RACs) as problem areas, as well as problem areas identified by their own data analysis.7 For this reason, hospitalists may see prepayment requests for documentation by Medicare for services that are most “problematic” (e.g., 99223 and 99233). This occurs when a claim involving these services is submitted to Medicare. The MAC suspends all or part of a claim so that a trained clinician or claims analyst can review the claim and associated documentation in order to make determinations about coverage and payment.7 Responding to these requests in a timely manner is crucial in preventing claim denials.
Responding to Requests
When documentation is requested by the payor, take note of the date and the provider for whom the service is requested. Be certain to include all pertinent information in support of the claim. The payor request letter will typically include a generic list of items that should be submitted with the documentation request. Consider these particular items when submitting documentation for targeted services typically provided by hospitalists:
- Initial Hospital Care (99223)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify any referenced sources of information (e.g., physician referencing a family history documented in the ED record);
- Dictations, when performed;
- Admitting orders; and
- Labs or diagnostic test reports performed on admission.
- Subsequent Hospital Care (99233)
- Physician notes (including resident, nurse practitioner, or physician assistant notes);
- Identify multiple encounters/entries recorded on a given date;
- Physician orders; and
- Labs or diagnostic test reports performed on the requested date.
Documentation Tips
Because it is the primary communication tool for providers involved in the patient’s care, documentation must be entered in a timely manner and must be decipherable to members of the healthcare team as well as other individuals who may need to review the information (e.g., auditors). Proper credit cannot be given for documentation that is difficult to read.
Information should include historical review of past/interim events, a physical exam, medical decision-making as related to the patient’s progress/response to intervention, and modification of the care plan (as necessary). The reason for the encounter should be evident to support the medical necessity of the service. Because various specialists may participate in patient care, documentation for each provider’s encounter should demonstrate personalized and non-duplicative care.
Each individual provider must exhibit a personal contribution to the case to prevent payors from viewing the documentation as overlapping and indistinguishable from care already provided by another physician. Each entry should be dated and signed with a legible identifier (i.e., signature with a printed name).
The next several articles will address each of the key components (history, exam, and decision-making) and serve as a “documentation refresher” for providers who wish to compare their documentation to current standards.
References
- Department of Justice, Office of Public Affairs. Tacoma, Wash., Medical Firm to Pay $14.5 Million to Settle Overbilling Allegations. Available at: www.justice.gov/opa/pr/2013/July/13-civ-758.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Comprehensive Error Rate Testing (CERT). Available at: www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/CERT/index.html?redirect=/cert. Accessed September 20, 2013.
- WPS Medicare, Legacy Part B. Are you billing these evaluation and management (e/m) services correctly? Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2011-0912-billemservices.shtml. Accessed September 20, 2013.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Levreau-Davis, L. Current Procedural Terminology 2013 Professional Edition. Chicago: American Medical Association Press; 2012:15-17.
- WPS Medicare, Legacy Part B. 1st Qtr. 2013 (Jan. - Mar.) - CERT Error Summary. Available at: http://www.wpsmedicare.com/j5macpartb/departments/cert/2013-1st-quarter-summary.shtml. Accessed September 20, 2013.
- Novitas Solutions. Analysis of JL Part B Comprehensive Error Rate Testing (CERT) Data - January thru March 2013. Available at: https://www.novitas-solutions.com/cert/errors/2013/b-jan-mar-j12.html. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Program Integrity Manual, Chapter 3, Section 3.2. Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/pim83c03.pdf. Accessed September 20, 2013.
- Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual, Chapter 11, Section 40.1.2 Available at: www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c11.pdf. Accessed September 20, 2013.
San Francisco Medical Center Adapts Choosing Wisely List for Waste Reduction Campaign


A University of California at San Francisco (UCSF) quality initiative targeting waste and overuse of healthcare resources plans to focus on four of five questionable treatments identified by the Society of Hospital Medicine for the ABIM Foundation’s Choosing Wisely campaign. The UCSF Division of Hospital Medicine’s High Value Care Committee grew out of efforts to operationalize a curriculum for teaching medical trainees about the actual costs of treatments they commonly order. UCSF hospitalist Christopher Moriates, MD, developed the curriculum when he was a resident.
The committee brings together physicians, who have historically focused on quality improvement, and finance administrators, who focus on cost reduction. Together they are pursuing performance improvement projects serving both goals, Dr. Moriates says. The committee identified six waste targets initially and has already reduced the use of ionized calcium blood tests, formerly administered to numerous patients at UCSF Medical Center whether they needed it or not, and the unnecessary use of nebulizers, by more than half.
“When the Choosing Wisely list came out, it fit with what we were doing, although I wasn’t sure that these things were problems for us,” Dr. Moriates explains.
The data, however, show that UCSF was significantly better than its peers for only one of the five treatments on the list: utilization of Foley catheters and corresponding rates of catheter-related urinary tract infections. The committee is focused on more judicious, evidence-based ordering of the other Choosing Wisely treatments: medications for stress ulcer prophylaxis, blood transfusions, continuous telemetry monitoring outside of the ICU, and certain lab tests.
Dr. Moriates recommends the Choosing Wisely list for other hospitals and hospitalists starting to tackle unnecessary medical treatments and tests. Data is essential to these efforts, he says, stressing the need to consider not just utilization rates but actual dollars spent.
“That shouldn’t be a major hurdle, given hospital information technology, but often it is,” he says, adding that waste initiatives are more successful when they are led by frontline champions, rather than just assigned by the department’s chair.
Read more about Dr. Moriates’ waste control efforts in HealthLeaders Media, and learn about another waste reduction strategy called the Teaching Value Project at www.teachingvalue.org.1
Reference
A University of California at San Francisco (UCSF) quality initiative targeting waste and overuse of healthcare resources plans to focus on four of five questionable treatments identified by the Society of Hospital Medicine for the ABIM Foundation’s Choosing Wisely campaign. The UCSF Division of Hospital Medicine’s High Value Care Committee grew out of efforts to operationalize a curriculum for teaching medical trainees about the actual costs of treatments they commonly order. UCSF hospitalist Christopher Moriates, MD, developed the curriculum when he was a resident.
The committee brings together physicians, who have historically focused on quality improvement, and finance administrators, who focus on cost reduction. Together they are pursuing performance improvement projects serving both goals, Dr. Moriates says. The committee identified six waste targets initially and has already reduced the use of ionized calcium blood tests, formerly administered to numerous patients at UCSF Medical Center whether they needed it or not, and the unnecessary use of nebulizers, by more than half.
“When the Choosing Wisely list came out, it fit with what we were doing, although I wasn’t sure that these things were problems for us,” Dr. Moriates explains.
The data, however, show that UCSF was significantly better than its peers for only one of the five treatments on the list: utilization of Foley catheters and corresponding rates of catheter-related urinary tract infections. The committee is focused on more judicious, evidence-based ordering of the other Choosing Wisely treatments: medications for stress ulcer prophylaxis, blood transfusions, continuous telemetry monitoring outside of the ICU, and certain lab tests.
Dr. Moriates recommends the Choosing Wisely list for other hospitals and hospitalists starting to tackle unnecessary medical treatments and tests. Data is essential to these efforts, he says, stressing the need to consider not just utilization rates but actual dollars spent.
“That shouldn’t be a major hurdle, given hospital information technology, but often it is,” he says, adding that waste initiatives are more successful when they are led by frontline champions, rather than just assigned by the department’s chair.
Read more about Dr. Moriates’ waste control efforts in HealthLeaders Media, and learn about another waste reduction strategy called the Teaching Value Project at www.teachingvalue.org.1
Reference
A University of California at San Francisco (UCSF) quality initiative targeting waste and overuse of healthcare resources plans to focus on four of five questionable treatments identified by the Society of Hospital Medicine for the ABIM Foundation’s Choosing Wisely campaign. The UCSF Division of Hospital Medicine’s High Value Care Committee grew out of efforts to operationalize a curriculum for teaching medical trainees about the actual costs of treatments they commonly order. UCSF hospitalist Christopher Moriates, MD, developed the curriculum when he was a resident.
The committee brings together physicians, who have historically focused on quality improvement, and finance administrators, who focus on cost reduction. Together they are pursuing performance improvement projects serving both goals, Dr. Moriates says. The committee identified six waste targets initially and has already reduced the use of ionized calcium blood tests, formerly administered to numerous patients at UCSF Medical Center whether they needed it or not, and the unnecessary use of nebulizers, by more than half.
“When the Choosing Wisely list came out, it fit with what we were doing, although I wasn’t sure that these things were problems for us,” Dr. Moriates explains.
The data, however, show that UCSF was significantly better than its peers for only one of the five treatments on the list: utilization of Foley catheters and corresponding rates of catheter-related urinary tract infections. The committee is focused on more judicious, evidence-based ordering of the other Choosing Wisely treatments: medications for stress ulcer prophylaxis, blood transfusions, continuous telemetry monitoring outside of the ICU, and certain lab tests.
Dr. Moriates recommends the Choosing Wisely list for other hospitals and hospitalists starting to tackle unnecessary medical treatments and tests. Data is essential to these efforts, he says, stressing the need to consider not just utilization rates but actual dollars spent.
“That shouldn’t be a major hurdle, given hospital information technology, but often it is,” he says, adding that waste initiatives are more successful when they are led by frontline champions, rather than just assigned by the department’s chair.
Read more about Dr. Moriates’ waste control efforts in HealthLeaders Media, and learn about another waste reduction strategy called the Teaching Value Project at www.teachingvalue.org.1
Reference
PIAA Director of Research and Loss Prevention Discusses Hospitalist Insurance Premiums
Click here to listen to more of our interview with Divya Parikh
Click here to listen to more of our interview with Divya Parikh
Click here to listen to more of our interview with Divya Parikh
SHM Report Provides New Insights About Physician Practice Leaders
The Society of Hospital Medicine’s 2012 State of Hospital Medicine report (SOHM) offers new insights about physician practice leaders.
Physician Leader Presence
“Choose a hospitalist leader with the right skills and experience. Selecting the right leader is fundamental to a successful hospitalist practice. These individuals are hard to find. They must be excellent clinically and have superb communication skills.”1
The SOHM survey shows that the vast majority (97%) of hospital medicine groups (HMGs) in the U.S. now have a designated physician leader (see Figure 1). Given this high percentage, examining the outliers is intriguing. Of the 13 adult medicine HMGs that reported not having a physician leader, the large majority were hospital-owned, located in the South region, and situated in non-teaching hospitals. The size of the HMG impacted the presence of a physician leader: 100% of groups with 20 or more full-time equivalents had physician leaders.
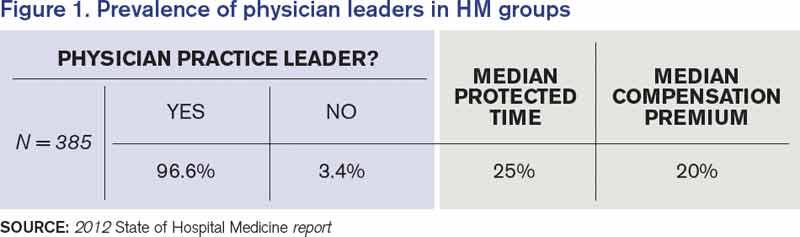
Source: 2012 State of Hospital Medicine report
Dedicated Leadership Time
“The medical director of the hospitalist program needs sufficient, non-clinical time to address administrative and leadership issues.”1
The 2007/2008 SOHM survey reported a median of 20% administrative time for physician leaders. In the 2012 survey, the median amount of time was 25% for adult medicine HMGs. The percentages were higher in the East and West regions, in hospital-owned programs, and in non- academic programs. The percentage of protected time also went up with group size.

Compensation
The 2012 SOHM shows median compensation premiums for physician leaders of 20%; that is, leader compensation is 120% of the average salary in their group. The numbers across regions and sizes were remarkably consistent. Overall, it seems that a 15% to 20% compensation premium for hospitalist leaders is standard.
Key Takeaways
No. 1, hospitalist groups need physician hospitalist leaders with protected leadership, but who also work clinically as a hospitalist. Why? Because hospitalists need a leader they respect, someone that they believe understands their specific issues. Unless the physician in charge has worked those 12-hour overnight shifts, argued with the consultants, tried to discharge an ornery patient, received 20 pages in an hour about medication reconciliation, or disagreed with an ED doc about the appropriateness of an admission, it would be hard for that leader to fully understand the stresses hospitalists encounter on a daily basis.
Hospitalist leaders are taking on increasingly important roles to help their organizations realize key performance improvement goals.
Additionally, the roles of outpatient doctors are changing: “Many physicians are no longer able or willing to serve on hospital committees or play a leadership role for the medical staff. Hospitalists have the potential to step in and help address these key issues”1
No. 2, size matters. Given increased responsibilities that include handling focused and ongoing professional practice evaluations, designing pathways to reduce adverse events, counseling, mentoring, disciplining, conducting yearly reviews, and investigating patient and staff complaints, it makes sense that larger programs also have leaders with more protected time and commensurate compensation.
As our healthcare systems ask hospitalists to offer higher reliability and to champion more administrative, safety, and quality projects, HM leaders—who are perfectly placed to organize and manage those projects—need the time and the compensation to do so. To borrow from hospitalist pioneer Bob Wachter, MD, MHM, our future C-suite leaders are percolating in hospitalist programs, learning the skills we will need to participate in the high reliability hospitals of our present and future.
Dr. Lovins is chief of hospital medicine at Middlesex Hospital in Middletown, Conn., and assistant clinical professor of medicine at Yale University School of Medicine. She is a member of SHM’s Practice Analysis Committee.
Reference
The Society of Hospital Medicine’s 2012 State of Hospital Medicine report (SOHM) offers new insights about physician practice leaders.
Physician Leader Presence
“Choose a hospitalist leader with the right skills and experience. Selecting the right leader is fundamental to a successful hospitalist practice. These individuals are hard to find. They must be excellent clinically and have superb communication skills.”1
The SOHM survey shows that the vast majority (97%) of hospital medicine groups (HMGs) in the U.S. now have a designated physician leader (see Figure 1). Given this high percentage, examining the outliers is intriguing. Of the 13 adult medicine HMGs that reported not having a physician leader, the large majority were hospital-owned, located in the South region, and situated in non-teaching hospitals. The size of the HMG impacted the presence of a physician leader: 100% of groups with 20 or more full-time equivalents had physician leaders.
Source: 2012 State of Hospital Medicine report
Dedicated Leadership Time
“The medical director of the hospitalist program needs sufficient, non-clinical time to address administrative and leadership issues.”1
The 2007/2008 SOHM survey reported a median of 20% administrative time for physician leaders. In the 2012 survey, the median amount of time was 25% for adult medicine HMGs. The percentages were higher in the East and West regions, in hospital-owned programs, and in non- academic programs. The percentage of protected time also went up with group size.
Compensation
The 2012 SOHM shows median compensation premiums for physician leaders of 20%; that is, leader compensation is 120% of the average salary in their group. The numbers across regions and sizes were remarkably consistent. Overall, it seems that a 15% to 20% compensation premium for hospitalist leaders is standard.
Key Takeaways
No. 1, hospitalist groups need physician hospitalist leaders with protected leadership, but who also work clinically as a hospitalist. Why? Because hospitalists need a leader they respect, someone that they believe understands their specific issues. Unless the physician in charge has worked those 12-hour overnight shifts, argued with the consultants, tried to discharge an ornery patient, received 20 pages in an hour about medication reconciliation, or disagreed with an ED doc about the appropriateness of an admission, it would be hard for that leader to fully understand the stresses hospitalists encounter on a daily basis.
Hospitalist leaders are taking on increasingly important roles to help their organizations realize key performance improvement goals.
Additionally, the roles of outpatient doctors are changing: “Many physicians are no longer able or willing to serve on hospital committees or play a leadership role for the medical staff. Hospitalists have the potential to step in and help address these key issues”1
No. 2, size matters. Given increased responsibilities that include handling focused and ongoing professional practice evaluations, designing pathways to reduce adverse events, counseling, mentoring, disciplining, conducting yearly reviews, and investigating patient and staff complaints, it makes sense that larger programs also have leaders with more protected time and commensurate compensation.
As our healthcare systems ask hospitalists to offer higher reliability and to champion more administrative, safety, and quality projects, HM leaders—who are perfectly placed to organize and manage those projects—need the time and the compensation to do so. To borrow from hospitalist pioneer Bob Wachter, MD, MHM, our future C-suite leaders are percolating in hospitalist programs, learning the skills we will need to participate in the high reliability hospitals of our present and future.
Dr. Lovins is chief of hospital medicine at Middlesex Hospital in Middletown, Conn., and assistant clinical professor of medicine at Yale University School of Medicine. She is a member of SHM’s Practice Analysis Committee.
Reference
The Society of Hospital Medicine’s 2012 State of Hospital Medicine report (SOHM) offers new insights about physician practice leaders.
Physician Leader Presence
“Choose a hospitalist leader with the right skills and experience. Selecting the right leader is fundamental to a successful hospitalist practice. These individuals are hard to find. They must be excellent clinically and have superb communication skills.”1
The SOHM survey shows that the vast majority (97%) of hospital medicine groups (HMGs) in the U.S. now have a designated physician leader (see Figure 1). Given this high percentage, examining the outliers is intriguing. Of the 13 adult medicine HMGs that reported not having a physician leader, the large majority were hospital-owned, located in the South region, and situated in non-teaching hospitals. The size of the HMG impacted the presence of a physician leader: 100% of groups with 20 or more full-time equivalents had physician leaders.
Source: 2012 State of Hospital Medicine report
Dedicated Leadership Time
“The medical director of the hospitalist program needs sufficient, non-clinical time to address administrative and leadership issues.”1
The 2007/2008 SOHM survey reported a median of 20% administrative time for physician leaders. In the 2012 survey, the median amount of time was 25% for adult medicine HMGs. The percentages were higher in the East and West regions, in hospital-owned programs, and in non- academic programs. The percentage of protected time also went up with group size.
Compensation
The 2012 SOHM shows median compensation premiums for physician leaders of 20%; that is, leader compensation is 120% of the average salary in their group. The numbers across regions and sizes were remarkably consistent. Overall, it seems that a 15% to 20% compensation premium for hospitalist leaders is standard.
Key Takeaways
No. 1, hospitalist groups need physician hospitalist leaders with protected leadership, but who also work clinically as a hospitalist. Why? Because hospitalists need a leader they respect, someone that they believe understands their specific issues. Unless the physician in charge has worked those 12-hour overnight shifts, argued with the consultants, tried to discharge an ornery patient, received 20 pages in an hour about medication reconciliation, or disagreed with an ED doc about the appropriateness of an admission, it would be hard for that leader to fully understand the stresses hospitalists encounter on a daily basis.
Hospitalist leaders are taking on increasingly important roles to help their organizations realize key performance improvement goals.
Additionally, the roles of outpatient doctors are changing: “Many physicians are no longer able or willing to serve on hospital committees or play a leadership role for the medical staff. Hospitalists have the potential to step in and help address these key issues”1
No. 2, size matters. Given increased responsibilities that include handling focused and ongoing professional practice evaluations, designing pathways to reduce adverse events, counseling, mentoring, disciplining, conducting yearly reviews, and investigating patient and staff complaints, it makes sense that larger programs also have leaders with more protected time and commensurate compensation.
As our healthcare systems ask hospitalists to offer higher reliability and to champion more administrative, safety, and quality projects, HM leaders—who are perfectly placed to organize and manage those projects—need the time and the compensation to do so. To borrow from hospitalist pioneer Bob Wachter, MD, MHM, our future C-suite leaders are percolating in hospitalist programs, learning the skills we will need to participate in the high reliability hospitals of our present and future.
Dr. Lovins is chief of hospital medicine at Middlesex Hospital in Middletown, Conn., and assistant clinical professor of medicine at Yale University School of Medicine. She is a member of SHM’s Practice Analysis Committee.
Reference
Culture Shift Required to Defeat Defensive Medicine
Hospitalist Allen Kachalia, MD, JD, of Brigham and Women’s Hospital in Boston, sees defensive medicine as a source of unnecessary costs—and a threat to patient safety.
In fact, he and his colleagues offered an oral presentation at HM13 earlier this year titled, “Overutilization and Defensive Medicine in U.S. Hospitals: A Randomized National Survey of Hospitalists.” In a survey of 1,020 hospitalists, it was reported that defensive medicine was practiced in 37% of pre-operative evaluations and 58% of syncope cases.
Dr. Kachalia says he understands the pressures that can lead physicians to order unnecessary tests, particularly when patients request them. So what does he say about those requests?

“The answer is a simple one but takes time and effort: If you don’t think that something is clinically indicated, you should talk with the patient, explaining to them why you don’t think it’s necessary,” he says. “And, hopefully, you can come to mutual agreement. Ordering things just for the sake of preventing legal liability is just not the right thing to do.”
Dr. Kachalia says he believes that a paradigm shift in how medical liability is handled in this country is needed to change those habits.
But culture change also takes time.
Bryan Weiss, MBA, managing director of the consulting services practice at Irving, Texas-based MedSynergies, says the first step of that change may be having physicians admit that few doctors know a lot about malpractice issues, because they are typically negotiated, arranged, and paid for by their employers, whether that’s a hospital or large management companies.
“It’s not me versus them,” says Weiss, a Team Hospitalist member. “As a specialty, we need to be in this together, to push the education and awareness that it’s OK not to know, so let’s work together to make it better. But it’s not going to happen overnight.”
Hospitalist Allen Kachalia, MD, JD, of Brigham and Women’s Hospital in Boston, sees defensive medicine as a source of unnecessary costs—and a threat to patient safety.
In fact, he and his colleagues offered an oral presentation at HM13 earlier this year titled, “Overutilization and Defensive Medicine in U.S. Hospitals: A Randomized National Survey of Hospitalists.” In a survey of 1,020 hospitalists, it was reported that defensive medicine was practiced in 37% of pre-operative evaluations and 58% of syncope cases.
Dr. Kachalia says he understands the pressures that can lead physicians to order unnecessary tests, particularly when patients request them. So what does he say about those requests?
“The answer is a simple one but takes time and effort: If you don’t think that something is clinically indicated, you should talk with the patient, explaining to them why you don’t think it’s necessary,” he says. “And, hopefully, you can come to mutual agreement. Ordering things just for the sake of preventing legal liability is just not the right thing to do.”
Dr. Kachalia says he believes that a paradigm shift in how medical liability is handled in this country is needed to change those habits.
But culture change also takes time.
Bryan Weiss, MBA, managing director of the consulting services practice at Irving, Texas-based MedSynergies, says the first step of that change may be having physicians admit that few doctors know a lot about malpractice issues, because they are typically negotiated, arranged, and paid for by their employers, whether that’s a hospital or large management companies.
“It’s not me versus them,” says Weiss, a Team Hospitalist member. “As a specialty, we need to be in this together, to push the education and awareness that it’s OK not to know, so let’s work together to make it better. But it’s not going to happen overnight.”
Hospitalist Allen Kachalia, MD, JD, of Brigham and Women’s Hospital in Boston, sees defensive medicine as a source of unnecessary costs—and a threat to patient safety.
In fact, he and his colleagues offered an oral presentation at HM13 earlier this year titled, “Overutilization and Defensive Medicine in U.S. Hospitals: A Randomized National Survey of Hospitalists.” In a survey of 1,020 hospitalists, it was reported that defensive medicine was practiced in 37% of pre-operative evaluations and 58% of syncope cases.
Dr. Kachalia says he understands the pressures that can lead physicians to order unnecessary tests, particularly when patients request them. So what does he say about those requests?
“The answer is a simple one but takes time and effort: If you don’t think that something is clinically indicated, you should talk with the patient, explaining to them why you don’t think it’s necessary,” he says. “And, hopefully, you can come to mutual agreement. Ordering things just for the sake of preventing legal liability is just not the right thing to do.”
Dr. Kachalia says he believes that a paradigm shift in how medical liability is handled in this country is needed to change those habits.
But culture change also takes time.
Bryan Weiss, MBA, managing director of the consulting services practice at Irving, Texas-based MedSynergies, says the first step of that change may be having physicians admit that few doctors know a lot about malpractice issues, because they are typically negotiated, arranged, and paid for by their employers, whether that’s a hospital or large management companies.
“It’s not me versus them,” says Weiss, a Team Hospitalist member. “As a specialty, we need to be in this together, to push the education and awareness that it’s OK not to know, so let’s work together to make it better. But it’s not going to happen overnight.”
Why Hospitalists Remain Outside Malpractice Insurers' High-Risk Categories, For Now

Source: The Doctors Company
Ten years ago, the national headlines on malpractice insurance were staggering. Media reports catalogued OB-GYNs who proclaimed they were shutting down their private practices in the face of runaway premiums. Surgeons and other proceduralists decried payments tied to lawsuits they’d argue were arbitrary and capricious. And the American Medical Association (AMA) made announcement after announcement about states being in a “malpractice crisis.”
In recent years, premiums have actually dropped and stabilized at levels that most physicians agree are manageable for bottom lines. But, in that time, there has been scant discussion about hospital medicine’s relationship with malpractice. It’s not because the issue isn’t omnipresent for all healthcare practitioners, including the relatively nascent specialty that is HM.
Practice management experts say anecdotally that delayed diagnosis of, or treatment for, a spinal epidural abscess (SEA) is likely to get more than a few hospitalists sued. And, the proliferation of co-management of other specialties—particularly those with higher risk of incidence and higher premiums than internal medicine—open up hospitalists to further liability.
The issue is that at less than 20 years as a specialty, HM is in its infancy when it comes to its interaction with malpractice premiums. Health insurance companies and trade groups that track the insurance industry are just beginning to have enough data on claims, premiums, and payouts to make recommendations on risk factors, risk mitigation, and potential trends.
Still, even in a landscape of limited information, there are a few rules of thumb hospitalist group leaders should live by when it comes to managing exposure to malpractice cases, according to interviews with a half dozen healthcare professionals:
- Know how your coverage works. Is there “tail coverage” that ensures you have protection for incidents that happened at an institution where you no longer practice? Even though hospital-employed physicians rarely have rate discussions directly (the hospital typically covers premiums as part of the compensation package), take the time to learn the basic details.
- Be diligent in documentation. Note concerns in charts when appropriate, and stand up for your point of view. There’s a fine line between picking fights with other physicians involved in a patient’s care and making your concerns known, but don’t be afraid to put your clinical view on the record.
- Avoid the practice of “defensive medicine.” Ordering tests and procedures that aren’t clinically necessary might seem like it can serve as a protection from later lawsuits, but it adds to healthcare costs and is just not the right thing to do, says hospitalist Allen Kachalia, MD, JD, of Brigham and Women’s Hospital in Boston, who has studied the phenomenon (see “Culture Shift Necessary to Defeat “Defensive” Medicine,” on p. 38).
- Recognize the risks associated with co-management. Caring for neurology, cardiology, and other subspecialty patients is a revenue boost for HM groups, but when some of those complex cases have adverse events, the hospitalist who interacted with the patient daily could be included in a lawsuit.
- Focus on communication skills. An analysis of claims data by The Doctors Company (TDC) (www.thedoctors.com), a medical malpractice insurance company exclusively endorsed by SHM, reports that the second most common factor contributing to patient injury by hospitalists is “communication breakdown among healthcare professionals.”
- Manage workloads to avoid burnout. Don’t take on too many patients at the expense of being involved in hospital committees or quality initiatives.
To be sure, many of the same tenets of being a productive hospitalist with high patient satisfaction scores—maintain manageable censuses; focus on patient centeredness; and use checklists, technology, and regimented protocols to reduce adverse events—translate very well to being a lower-risk hospitalist in relation to malpractice cases.
When you’re “thinking of patient satisfaction strategies, also think of them as risk mitigation strategies,” says John Nelson, MD, MHM, FACP, medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash., an SHM co-founder and practice management columnist for The Hospitalist. “They overlap tremendously.”
A History Lesson
Medical malpractice has been around for centuries and has two prevailing goals: 1) to provide monetary remuneration to patients who have been injured via substandard care and 2) to deter that poor treatment through fiscal punishment.
Malpractice lawsuits were not prevalent enough to be a major medical concern until the early 1800s. By the middle of the 19th century, the country hit its first periods of crisis.1 Cycles ebbed and flowed from there, with malpractice premiums causing crises in the 1980s and again in the early 2000s.
continued below...
Now, rates for medical professional liability insurance have been dropping for seven years, and an eighth straight annual decline is expected this year, according to Mike Matray, the editor of trade publication Medical Liability Monitor and the chief content officer of its associated website, www.mymedicalmalpracticeinsurance.com.
“We are in the longest, deepest soft market that the malpractice insurance industry has ever been in,” he says. “Right now, things are really good for the doctors, as far as rates coming down.”
Matray says he understands that declining rates may seem immaterial to a physician who receives an insurance bill that eats into the bottom line. For some specialties, that premium can be as high as $200,000 per physician, per year—or more.
“I’m not saying it isn’t expensive,” he adds. “It’s expensive to run a medical practice. At the same time, medical malpractice insurance is less expensive in today’s dollars than it was in 2005.”
The reduction in rates is multi-faceted. Prominently, state-level tort reforms like non-economic damage caps, health courts, and arbitration hearings are making it harder to bring cases to trial, particularly for lawyers who take cases on contingency. Second, frivolous lawsuits “are making an impression on jury pools,” Matray says, which means fewer filed claims and fewer cases that make it to trial. Third, this soft cycle has outlasted the typical pattern of rates falling for three to four years before rebounding.
“A lot of smart actuaries keep saying this has to change soon, because in a soft market there is a lot of competition,” he says, noting that in order to compete for low rates, insurance companies offer credits to clients and use their own reserve cash piles. “So things are really going to change in the next couple of years.”

—Robin Diamond, senior vice president and chief patient safety officer, The Doctors Company
In Need of Data, Patience
So what does it all mean for hospitalists and HM group leaders looking to be proactive about medical malpractice liability insurance? Patience is required.
For starters, there is no designated premium category for hospitalists. Much like the situation that exists for coding issues, the closest proxy for HM is internal medicine. According to Medical Liability Monitor, the premium paid by internal medicine physicians as of July 1, 2012, varied widely across the country. In South Florida, internal medicine insurance premiums in Miami, Dade, and Broward counties were between $42,000 and $46,000 per year. In South Dakota, one insurer reported rates of just under $4,000 per year. There is no average or median figure available, and Matray notes that actual rates paid can vary from county to county.
Moreover, it is difficult for group leaders or hospital executives to use past history to negotiate rates with insurers because of a shortage of reliable data. In its spring 2013 newsletter, the PIAA (formerly known as the Physician Insurers Association of America) published its first report on hospitalist claims reported to its Data Sharing Project. Of the 92,868 closed claims reported from 2002-2011, just 312, or 0.3%, named hospitalists as the defendant.
The data also showed that, of those claims, 20% were settled through insurance company payments. Those payments totaled $17.1 million, with an average payout to a claimant (known as the indemnity) of $272,553 per claim. Overall, hospitalists had a 20% paid-to-closed ratio, totaling more than $17.1 million. By comparison, the percent of paid-to-closed claims for all physicians was 29.3%, according to PIAA.
In a separate data set compiled this year by TDC, 34% of allegations against hospitalists were related to missed or failed diagnoses, with 28% tied to “improper management of treatment.” Twelve percent of allegations were the result of either improper medication management or ordering errors.
Robin Diamond, TDC’s senior vice president and chief patient safety officer, says that teasing out trends from the initial data can be challenging. Hospitalists, she says, can deal with so many different patients, diseases, and severity levels that it is difficult to draw conclusions.
“Hospital medicine is different than other specialties, because the hospitalist treats a broad range of patients in an acute care setting—from a pediatric patient to an adult patient with many chronic illnesses,” she says.
Divya Parikh, PIAA’s director of research and loss prevention, says HM group leaders should avoid reading too much into the first batch of data, because it’s a small sample size.
“A big part of that is we feel that a lot of hospitalists are intermingled into the other medical specialties,” she says. “So this becomes a very small subset where they are distinctly identified as hospitalists. And that’s the challenge.”
In particular, Parikh is curious to see whether HM’s rate of claims paid through insurance payments drops from 20% (already below the overall healthcare industry average). “It will be interesting as we proceed...to see if they begin to mitigate areas of risk where we used to see a lot of claims,” she adds. “If you look at a hospital setting, there has been some shift change in what the errors are. And, what you’d hope with hospitalists within these environments who are really owning this specialty, is that you’d see a decrease in that. There would be that connective care. There would be the patient that felt that they had an individual who was their go-to individual throughout their care at a hospital.”
A Peek at the Future
Insurers have begun compiling claims data on hospitalists and are taking a longer-term view of the specialty. TDC, for example, has analyzed its data and identified characteristics it says make a low-risk hospitalist, an analysis the company says is the first of its kind (see Figure 1). The insurer adds that it sees its responsibility as making sure everyone understands the hospitalist’s role within the acute care setting so that its pricing is commensurate with the liability risk.
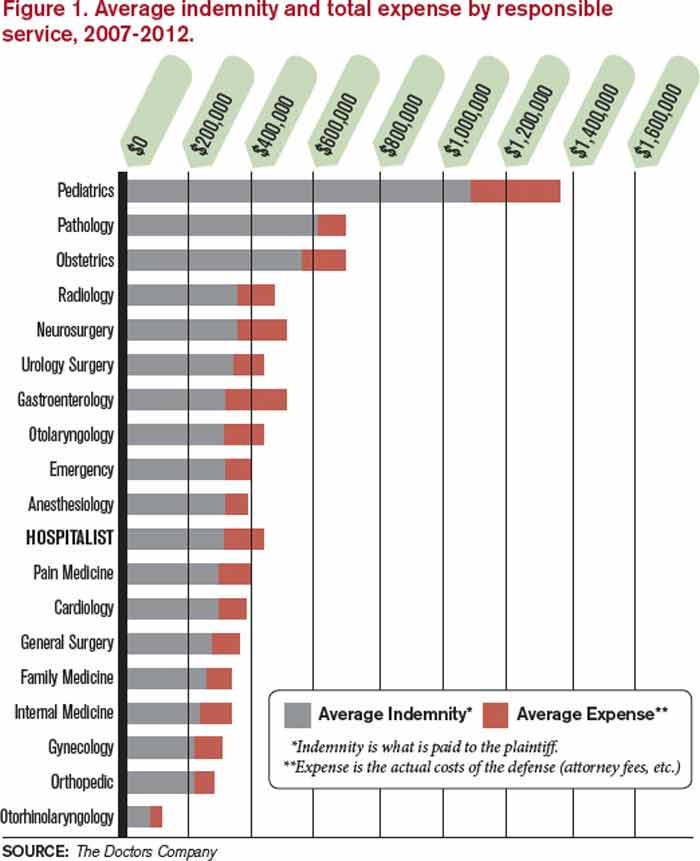
Source: The Doctors Company
“We’re looking at the systems within the hospitalist group, as well as how well that group is integrating with the hospital where they’re practicing,” Diamond says. “What kind of patient mix is this particular hospitalist group seeing in that particular hospital, because it can be different in a large healthcare corporation in Manhattan, New York, from a community hospital in rural Texas.”
The growing popularity of hospitalists taking on co-management responsibilities for other specialties is another trend to keep an eye on, as it creates what insurers call “vicarious liability.” Working together in teams with other specialties can improve communication, reduce errors during transitions of care, and create better outcomes. However, in instances where there are problems, being on a care team means hospitalists can open themselves to liability. To mitigate that risk, hospitalists can look to other groups that have dealt with shared liability issues in the past, Parikh says.
“Historically, you would have seen it with anesthesiology,” she explains. “And one huge improvement anesthesiologists have made when a patient comes in for a surgery now is they come out, introduce themselves, say hello, and tell you what’s going on. They put a face to the name, so that it’s not just a no-name anesthesiologist who gets included in the lawsuit as well because they’re naming everybody in the group.”
But, holistically, the best long-term mitigation strategy appears to be tort reform and new ways of looking at the way in which healthcare liability issues are handled in the U.S., says Anupam Jena, MD, PhD, assistant professor of healthcare policy and medicine at Harvard Medical School, and an internist at Massachusetts General Hospital, both in Boston. Dr. Jena says that there is limited evidence that enacted malpractice reforms have produced more than a 2% to 5% reduction in healthcare spending compared to states that have not.2 Instead, healthcare leaders should push for the elimination of defensive medicine, which he says contributes the lion’s share of the estimated $50 billion annual cost of malpractice liability across the country.
“Do I think the country is in a malpractice crisis? No,” he says. “Do I think that defensive medicine is larger than we think it is? Yes.
“If physicians practice as they felt they should practice without ordering extra tests and procedures, my guess would be you could reduce healthcare spending by substantially more than $50 billion.”
Richard Quinn is a freelance writer in New Jersey.
References
- Spiegel AD, Kavaler F. America’s first medical malpractice crisis, 1835-1865. J Community Health. 1997;22:283-308.
- Chandra A, Jena A, Seabury, S. Defensive medicine may be costlier than it seems. The Wall Street Journal website. http://online.wsj.com/article/SB10001424127887323701904578280112638373302.html. Accessed September 21, 2013.
Source: The Doctors Company
Ten years ago, the national headlines on malpractice insurance were staggering. Media reports catalogued OB-GYNs who proclaimed they were shutting down their private practices in the face of runaway premiums. Surgeons and other proceduralists decried payments tied to lawsuits they’d argue were arbitrary and capricious. And the American Medical Association (AMA) made announcement after announcement about states being in a “malpractice crisis.”
In recent years, premiums have actually dropped and stabilized at levels that most physicians agree are manageable for bottom lines. But, in that time, there has been scant discussion about hospital medicine’s relationship with malpractice. It’s not because the issue isn’t omnipresent for all healthcare practitioners, including the relatively nascent specialty that is HM.
Practice management experts say anecdotally that delayed diagnosis of, or treatment for, a spinal epidural abscess (SEA) is likely to get more than a few hospitalists sued. And, the proliferation of co-management of other specialties—particularly those with higher risk of incidence and higher premiums than internal medicine—open up hospitalists to further liability.
The issue is that at less than 20 years as a specialty, HM is in its infancy when it comes to its interaction with malpractice premiums. Health insurance companies and trade groups that track the insurance industry are just beginning to have enough data on claims, premiums, and payouts to make recommendations on risk factors, risk mitigation, and potential trends.
Still, even in a landscape of limited information, there are a few rules of thumb hospitalist group leaders should live by when it comes to managing exposure to malpractice cases, according to interviews with a half dozen healthcare professionals:
- Know how your coverage works. Is there “tail coverage” that ensures you have protection for incidents that happened at an institution where you no longer practice? Even though hospital-employed physicians rarely have rate discussions directly (the hospital typically covers premiums as part of the compensation package), take the time to learn the basic details.
- Be diligent in documentation. Note concerns in charts when appropriate, and stand up for your point of view. There’s a fine line between picking fights with other physicians involved in a patient’s care and making your concerns known, but don’t be afraid to put your clinical view on the record.
- Avoid the practice of “defensive medicine.” Ordering tests and procedures that aren’t clinically necessary might seem like it can serve as a protection from later lawsuits, but it adds to healthcare costs and is just not the right thing to do, says hospitalist Allen Kachalia, MD, JD, of Brigham and Women’s Hospital in Boston, who has studied the phenomenon (see “Culture Shift Necessary to Defeat “Defensive” Medicine,” on p. 38).
- Recognize the risks associated with co-management. Caring for neurology, cardiology, and other subspecialty patients is a revenue boost for HM groups, but when some of those complex cases have adverse events, the hospitalist who interacted with the patient daily could be included in a lawsuit.
- Focus on communication skills. An analysis of claims data by The Doctors Company (TDC) (www.thedoctors.com), a medical malpractice insurance company exclusively endorsed by SHM, reports that the second most common factor contributing to patient injury by hospitalists is “communication breakdown among healthcare professionals.”
- Manage workloads to avoid burnout. Don’t take on too many patients at the expense of being involved in hospital committees or quality initiatives.
To be sure, many of the same tenets of being a productive hospitalist with high patient satisfaction scores—maintain manageable censuses; focus on patient centeredness; and use checklists, technology, and regimented protocols to reduce adverse events—translate very well to being a lower-risk hospitalist in relation to malpractice cases.
When you’re “thinking of patient satisfaction strategies, also think of them as risk mitigation strategies,” says John Nelson, MD, MHM, FACP, medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash., an SHM co-founder and practice management columnist for The Hospitalist. “They overlap tremendously.”
A History Lesson
Medical malpractice has been around for centuries and has two prevailing goals: 1) to provide monetary remuneration to patients who have been injured via substandard care and 2) to deter that poor treatment through fiscal punishment.
Malpractice lawsuits were not prevalent enough to be a major medical concern until the early 1800s. By the middle of the 19th century, the country hit its first periods of crisis.1 Cycles ebbed and flowed from there, with malpractice premiums causing crises in the 1980s and again in the early 2000s.
continued below...
Now, rates for medical professional liability insurance have been dropping for seven years, and an eighth straight annual decline is expected this year, according to Mike Matray, the editor of trade publication Medical Liability Monitor and the chief content officer of its associated website, www.mymedicalmalpracticeinsurance.com.
“We are in the longest, deepest soft market that the malpractice insurance industry has ever been in,” he says. “Right now, things are really good for the doctors, as far as rates coming down.”
Matray says he understands that declining rates may seem immaterial to a physician who receives an insurance bill that eats into the bottom line. For some specialties, that premium can be as high as $200,000 per physician, per year—or more.
“I’m not saying it isn’t expensive,” he adds. “It’s expensive to run a medical practice. At the same time, medical malpractice insurance is less expensive in today’s dollars than it was in 2005.”
The reduction in rates is multi-faceted. Prominently, state-level tort reforms like non-economic damage caps, health courts, and arbitration hearings are making it harder to bring cases to trial, particularly for lawyers who take cases on contingency. Second, frivolous lawsuits “are making an impression on jury pools,” Matray says, which means fewer filed claims and fewer cases that make it to trial. Third, this soft cycle has outlasted the typical pattern of rates falling for three to four years before rebounding.
“A lot of smart actuaries keep saying this has to change soon, because in a soft market there is a lot of competition,” he says, noting that in order to compete for low rates, insurance companies offer credits to clients and use their own reserve cash piles. “So things are really going to change in the next couple of years.”
—Robin Diamond, senior vice president and chief patient safety officer, The Doctors Company
In Need of Data, Patience
So what does it all mean for hospitalists and HM group leaders looking to be proactive about medical malpractice liability insurance? Patience is required.
For starters, there is no designated premium category for hospitalists. Much like the situation that exists for coding issues, the closest proxy for HM is internal medicine. According to Medical Liability Monitor, the premium paid by internal medicine physicians as of July 1, 2012, varied widely across the country. In South Florida, internal medicine insurance premiums in Miami, Dade, and Broward counties were between $42,000 and $46,000 per year. In South Dakota, one insurer reported rates of just under $4,000 per year. There is no average or median figure available, and Matray notes that actual rates paid can vary from county to county.
Moreover, it is difficult for group leaders or hospital executives to use past history to negotiate rates with insurers because of a shortage of reliable data. In its spring 2013 newsletter, the PIAA (formerly known as the Physician Insurers Association of America) published its first report on hospitalist claims reported to its Data Sharing Project. Of the 92,868 closed claims reported from 2002-2011, just 312, or 0.3%, named hospitalists as the defendant.
The data also showed that, of those claims, 20% were settled through insurance company payments. Those payments totaled $17.1 million, with an average payout to a claimant (known as the indemnity) of $272,553 per claim. Overall, hospitalists had a 20% paid-to-closed ratio, totaling more than $17.1 million. By comparison, the percent of paid-to-closed claims for all physicians was 29.3%, according to PIAA.
In a separate data set compiled this year by TDC, 34% of allegations against hospitalists were related to missed or failed diagnoses, with 28% tied to “improper management of treatment.” Twelve percent of allegations were the result of either improper medication management or ordering errors.
Robin Diamond, TDC’s senior vice president and chief patient safety officer, says that teasing out trends from the initial data can be challenging. Hospitalists, she says, can deal with so many different patients, diseases, and severity levels that it is difficult to draw conclusions.
“Hospital medicine is different than other specialties, because the hospitalist treats a broad range of patients in an acute care setting—from a pediatric patient to an adult patient with many chronic illnesses,” she says.
Divya Parikh, PIAA’s director of research and loss prevention, says HM group leaders should avoid reading too much into the first batch of data, because it’s a small sample size.
“A big part of that is we feel that a lot of hospitalists are intermingled into the other medical specialties,” she says. “So this becomes a very small subset where they are distinctly identified as hospitalists. And that’s the challenge.”
In particular, Parikh is curious to see whether HM’s rate of claims paid through insurance payments drops from 20% (already below the overall healthcare industry average). “It will be interesting as we proceed...to see if they begin to mitigate areas of risk where we used to see a lot of claims,” she adds. “If you look at a hospital setting, there has been some shift change in what the errors are. And, what you’d hope with hospitalists within these environments who are really owning this specialty, is that you’d see a decrease in that. There would be that connective care. There would be the patient that felt that they had an individual who was their go-to individual throughout their care at a hospital.”
A Peek at the Future
Insurers have begun compiling claims data on hospitalists and are taking a longer-term view of the specialty. TDC, for example, has analyzed its data and identified characteristics it says make a low-risk hospitalist, an analysis the company says is the first of its kind (see Figure 1). The insurer adds that it sees its responsibility as making sure everyone understands the hospitalist’s role within the acute care setting so that its pricing is commensurate with the liability risk.
Source: The Doctors Company
“We’re looking at the systems within the hospitalist group, as well as how well that group is integrating with the hospital where they’re practicing,” Diamond says. “What kind of patient mix is this particular hospitalist group seeing in that particular hospital, because it can be different in a large healthcare corporation in Manhattan, New York, from a community hospital in rural Texas.”
The growing popularity of hospitalists taking on co-management responsibilities for other specialties is another trend to keep an eye on, as it creates what insurers call “vicarious liability.” Working together in teams with other specialties can improve communication, reduce errors during transitions of care, and create better outcomes. However, in instances where there are problems, being on a care team means hospitalists can open themselves to liability. To mitigate that risk, hospitalists can look to other groups that have dealt with shared liability issues in the past, Parikh says.
“Historically, you would have seen it with anesthesiology,” she explains. “And one huge improvement anesthesiologists have made when a patient comes in for a surgery now is they come out, introduce themselves, say hello, and tell you what’s going on. They put a face to the name, so that it’s not just a no-name anesthesiologist who gets included in the lawsuit as well because they’re naming everybody in the group.”
But, holistically, the best long-term mitigation strategy appears to be tort reform and new ways of looking at the way in which healthcare liability issues are handled in the U.S., says Anupam Jena, MD, PhD, assistant professor of healthcare policy and medicine at Harvard Medical School, and an internist at Massachusetts General Hospital, both in Boston. Dr. Jena says that there is limited evidence that enacted malpractice reforms have produced more than a 2% to 5% reduction in healthcare spending compared to states that have not.2 Instead, healthcare leaders should push for the elimination of defensive medicine, which he says contributes the lion’s share of the estimated $50 billion annual cost of malpractice liability across the country.
“Do I think the country is in a malpractice crisis? No,” he says. “Do I think that defensive medicine is larger than we think it is? Yes.
“If physicians practice as they felt they should practice without ordering extra tests and procedures, my guess would be you could reduce healthcare spending by substantially more than $50 billion.”
Richard Quinn is a freelance writer in New Jersey.
References
- Spiegel AD, Kavaler F. America’s first medical malpractice crisis, 1835-1865. J Community Health. 1997;22:283-308.
- Chandra A, Jena A, Seabury, S. Defensive medicine may be costlier than it seems. The Wall Street Journal website. http://online.wsj.com/article/SB10001424127887323701904578280112638373302.html. Accessed September 21, 2013.
Source: The Doctors Company
Ten years ago, the national headlines on malpractice insurance were staggering. Media reports catalogued OB-GYNs who proclaimed they were shutting down their private practices in the face of runaway premiums. Surgeons and other proceduralists decried payments tied to lawsuits they’d argue were arbitrary and capricious. And the American Medical Association (AMA) made announcement after announcement about states being in a “malpractice crisis.”
In recent years, premiums have actually dropped and stabilized at levels that most physicians agree are manageable for bottom lines. But, in that time, there has been scant discussion about hospital medicine’s relationship with malpractice. It’s not because the issue isn’t omnipresent for all healthcare practitioners, including the relatively nascent specialty that is HM.
Practice management experts say anecdotally that delayed diagnosis of, or treatment for, a spinal epidural abscess (SEA) is likely to get more than a few hospitalists sued. And, the proliferation of co-management of other specialties—particularly those with higher risk of incidence and higher premiums than internal medicine—open up hospitalists to further liability.
The issue is that at less than 20 years as a specialty, HM is in its infancy when it comes to its interaction with malpractice premiums. Health insurance companies and trade groups that track the insurance industry are just beginning to have enough data on claims, premiums, and payouts to make recommendations on risk factors, risk mitigation, and potential trends.
Still, even in a landscape of limited information, there are a few rules of thumb hospitalist group leaders should live by when it comes to managing exposure to malpractice cases, according to interviews with a half dozen healthcare professionals:
- Know how your coverage works. Is there “tail coverage” that ensures you have protection for incidents that happened at an institution where you no longer practice? Even though hospital-employed physicians rarely have rate discussions directly (the hospital typically covers premiums as part of the compensation package), take the time to learn the basic details.
- Be diligent in documentation. Note concerns in charts when appropriate, and stand up for your point of view. There’s a fine line between picking fights with other physicians involved in a patient’s care and making your concerns known, but don’t be afraid to put your clinical view on the record.
- Avoid the practice of “defensive medicine.” Ordering tests and procedures that aren’t clinically necessary might seem like it can serve as a protection from later lawsuits, but it adds to healthcare costs and is just not the right thing to do, says hospitalist Allen Kachalia, MD, JD, of Brigham and Women’s Hospital in Boston, who has studied the phenomenon (see “Culture Shift Necessary to Defeat “Defensive” Medicine,” on p. 38).
- Recognize the risks associated with co-management. Caring for neurology, cardiology, and other subspecialty patients is a revenue boost for HM groups, but when some of those complex cases have adverse events, the hospitalist who interacted with the patient daily could be included in a lawsuit.
- Focus on communication skills. An analysis of claims data by The Doctors Company (TDC) (www.thedoctors.com), a medical malpractice insurance company exclusively endorsed by SHM, reports that the second most common factor contributing to patient injury by hospitalists is “communication breakdown among healthcare professionals.”
- Manage workloads to avoid burnout. Don’t take on too many patients at the expense of being involved in hospital committees or quality initiatives.
To be sure, many of the same tenets of being a productive hospitalist with high patient satisfaction scores—maintain manageable censuses; focus on patient centeredness; and use checklists, technology, and regimented protocols to reduce adverse events—translate very well to being a lower-risk hospitalist in relation to malpractice cases.
When you’re “thinking of patient satisfaction strategies, also think of them as risk mitigation strategies,” says John Nelson, MD, MHM, FACP, medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash., an SHM co-founder and practice management columnist for The Hospitalist. “They overlap tremendously.”
A History Lesson
Medical malpractice has been around for centuries and has two prevailing goals: 1) to provide monetary remuneration to patients who have been injured via substandard care and 2) to deter that poor treatment through fiscal punishment.
Malpractice lawsuits were not prevalent enough to be a major medical concern until the early 1800s. By the middle of the 19th century, the country hit its first periods of crisis.1 Cycles ebbed and flowed from there, with malpractice premiums causing crises in the 1980s and again in the early 2000s.
continued below...
Now, rates for medical professional liability insurance have been dropping for seven years, and an eighth straight annual decline is expected this year, according to Mike Matray, the editor of trade publication Medical Liability Monitor and the chief content officer of its associated website, www.mymedicalmalpracticeinsurance.com.
“We are in the longest, deepest soft market that the malpractice insurance industry has ever been in,” he says. “Right now, things are really good for the doctors, as far as rates coming down.”
Matray says he understands that declining rates may seem immaterial to a physician who receives an insurance bill that eats into the bottom line. For some specialties, that premium can be as high as $200,000 per physician, per year—or more.
“I’m not saying it isn’t expensive,” he adds. “It’s expensive to run a medical practice. At the same time, medical malpractice insurance is less expensive in today’s dollars than it was in 2005.”
The reduction in rates is multi-faceted. Prominently, state-level tort reforms like non-economic damage caps, health courts, and arbitration hearings are making it harder to bring cases to trial, particularly for lawyers who take cases on contingency. Second, frivolous lawsuits “are making an impression on jury pools,” Matray says, which means fewer filed claims and fewer cases that make it to trial. Third, this soft cycle has outlasted the typical pattern of rates falling for three to four years before rebounding.
“A lot of smart actuaries keep saying this has to change soon, because in a soft market there is a lot of competition,” he says, noting that in order to compete for low rates, insurance companies offer credits to clients and use their own reserve cash piles. “So things are really going to change in the next couple of years.”
—Robin Diamond, senior vice president and chief patient safety officer, The Doctors Company
In Need of Data, Patience
So what does it all mean for hospitalists and HM group leaders looking to be proactive about medical malpractice liability insurance? Patience is required.
For starters, there is no designated premium category for hospitalists. Much like the situation that exists for coding issues, the closest proxy for HM is internal medicine. According to Medical Liability Monitor, the premium paid by internal medicine physicians as of July 1, 2012, varied widely across the country. In South Florida, internal medicine insurance premiums in Miami, Dade, and Broward counties were between $42,000 and $46,000 per year. In South Dakota, one insurer reported rates of just under $4,000 per year. There is no average or median figure available, and Matray notes that actual rates paid can vary from county to county.
Moreover, it is difficult for group leaders or hospital executives to use past history to negotiate rates with insurers because of a shortage of reliable data. In its spring 2013 newsletter, the PIAA (formerly known as the Physician Insurers Association of America) published its first report on hospitalist claims reported to its Data Sharing Project. Of the 92,868 closed claims reported from 2002-2011, just 312, or 0.3%, named hospitalists as the defendant.
The data also showed that, of those claims, 20% were settled through insurance company payments. Those payments totaled $17.1 million, with an average payout to a claimant (known as the indemnity) of $272,553 per claim. Overall, hospitalists had a 20% paid-to-closed ratio, totaling more than $17.1 million. By comparison, the percent of paid-to-closed claims for all physicians was 29.3%, according to PIAA.
In a separate data set compiled this year by TDC, 34% of allegations against hospitalists were related to missed or failed diagnoses, with 28% tied to “improper management of treatment.” Twelve percent of allegations were the result of either improper medication management or ordering errors.
Robin Diamond, TDC’s senior vice president and chief patient safety officer, says that teasing out trends from the initial data can be challenging. Hospitalists, she says, can deal with so many different patients, diseases, and severity levels that it is difficult to draw conclusions.
“Hospital medicine is different than other specialties, because the hospitalist treats a broad range of patients in an acute care setting—from a pediatric patient to an adult patient with many chronic illnesses,” she says.
Divya Parikh, PIAA’s director of research and loss prevention, says HM group leaders should avoid reading too much into the first batch of data, because it’s a small sample size.
“A big part of that is we feel that a lot of hospitalists are intermingled into the other medical specialties,” she says. “So this becomes a very small subset where they are distinctly identified as hospitalists. And that’s the challenge.”
In particular, Parikh is curious to see whether HM’s rate of claims paid through insurance payments drops from 20% (already below the overall healthcare industry average). “It will be interesting as we proceed...to see if they begin to mitigate areas of risk where we used to see a lot of claims,” she adds. “If you look at a hospital setting, there has been some shift change in what the errors are. And, what you’d hope with hospitalists within these environments who are really owning this specialty, is that you’d see a decrease in that. There would be that connective care. There would be the patient that felt that they had an individual who was their go-to individual throughout their care at a hospital.”
A Peek at the Future
Insurers have begun compiling claims data on hospitalists and are taking a longer-term view of the specialty. TDC, for example, has analyzed its data and identified characteristics it says make a low-risk hospitalist, an analysis the company says is the first of its kind (see Figure 1). The insurer adds that it sees its responsibility as making sure everyone understands the hospitalist’s role within the acute care setting so that its pricing is commensurate with the liability risk.
Source: The Doctors Company
“We’re looking at the systems within the hospitalist group, as well as how well that group is integrating with the hospital where they’re practicing,” Diamond says. “What kind of patient mix is this particular hospitalist group seeing in that particular hospital, because it can be different in a large healthcare corporation in Manhattan, New York, from a community hospital in rural Texas.”
The growing popularity of hospitalists taking on co-management responsibilities for other specialties is another trend to keep an eye on, as it creates what insurers call “vicarious liability.” Working together in teams with other specialties can improve communication, reduce errors during transitions of care, and create better outcomes. However, in instances where there are problems, being on a care team means hospitalists can open themselves to liability. To mitigate that risk, hospitalists can look to other groups that have dealt with shared liability issues in the past, Parikh says.
“Historically, you would have seen it with anesthesiology,” she explains. “And one huge improvement anesthesiologists have made when a patient comes in for a surgery now is they come out, introduce themselves, say hello, and tell you what’s going on. They put a face to the name, so that it’s not just a no-name anesthesiologist who gets included in the lawsuit as well because they’re naming everybody in the group.”
But, holistically, the best long-term mitigation strategy appears to be tort reform and new ways of looking at the way in which healthcare liability issues are handled in the U.S., says Anupam Jena, MD, PhD, assistant professor of healthcare policy and medicine at Harvard Medical School, and an internist at Massachusetts General Hospital, both in Boston. Dr. Jena says that there is limited evidence that enacted malpractice reforms have produced more than a 2% to 5% reduction in healthcare spending compared to states that have not.2 Instead, healthcare leaders should push for the elimination of defensive medicine, which he says contributes the lion’s share of the estimated $50 billion annual cost of malpractice liability across the country.
“Do I think the country is in a malpractice crisis? No,” he says. “Do I think that defensive medicine is larger than we think it is? Yes.
“If physicians practice as they felt they should practice without ordering extra tests and procedures, my guess would be you could reduce healthcare spending by substantially more than $50 billion.”
Richard Quinn is a freelance writer in New Jersey.
References
- Spiegel AD, Kavaler F. America’s first medical malpractice crisis, 1835-1865. J Community Health. 1997;22:283-308.
- Chandra A, Jena A, Seabury, S. Defensive medicine may be costlier than it seems. The Wall Street Journal website. http://online.wsj.com/article/SB10001424127887323701904578280112638373302.html. Accessed September 21, 2013.
Did poor communication lead to her death?

A woman in her 50s underwent hysterectomy performed by a surgeon, who then assigned an ObGyn to her follow-up care. The day after surgery, the patient had severe abdominal pain with decreased blood pressure and increased heart and respiration rates. The ObGyn admitted the patient to the intensive care unit (ICU), and then designated Dr. A, the patient’s family practitioner to continue her care. Dr. A was not available, so his associate, Dr. B, took over. Over the phone, Dr. B requested pulmonary, cardiology, and infectious disease consults. In the ICU the next day, the patient suffered respiratory arrest and was intubated. When her abdomen became rigid and swollen, emergency surgery revealed that a colon perforation had allowed fecal matter to reach the abdominal cavity. The woman died the next day from complications of sepsis, peritonitis, and multiple organ failure.
ESTATE’S CLAIM None of the physicians assigned to her care ever saw the patient in the ICU. Earlier surgery could have prevented her death. The physicians involved in her care failed to communicate with each other properly.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $3.2 million Illinois settlement was reached with the hospital.
BOTH PARENTS HAD PLATELET ANTIBODIES
When a 32-year-old woman became pregnant with her third child, she sought treatment at a clinic. The mother informed the nurse practi-tioner that her two other children had been diagnosed with low platelets at birth, but they were now healthy and had no further problems.
The woman gave birth vaginally to her third child at term. The newborn had Apgar scores of 8 and 8, at 1 and 5 minutes, respectively. However, the child’s platelet level was 26 x 103/µL. The baby was transferred to another hospital the next day, where he was diagnosed with hydrocephalus and neonatal alloimmune thrombocytopenia. He suffered a massive intracranial hemorrhage, which caused severe neurologic injuries and brain damage. A shunt was placed. The child has significant cognitive deficits as well as cerebral palsy with mild developmental delays. Testing showed that each parent had a different genotype for platelet antibodies.
PARENTS’ CLAIM The parents should have been tested for platelet antibodies prior to this birth due to the family’s history. A prenatal diagnosis of neonatal alloimmune thrombocytopenia would have allowed for treatment with gamma globulin, which could have avoided the intracranial hemorrhage.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $4.8 million California settlement was reached.
CORD PROLAPSE NOT CARED FOR IN AMBULANCE
At 36 weeks’ gestation, a mother called an ambulance when her membranes ruptured and she noticed an umbilical cord prolapse.
The child was in a breech presentation, experienced oxygen deprivation, and sustained severe neurologic damage.
PARENTS’ CLAIM The ambulance service was negligent in its care. The ambulance service dispatcher advised the mother to stand, squat, and push before the ambulance arrived. The ambulance attendants failed to take basic actions to relieve pressure on the prolapsed umbilical cord. The ambulance did not stop at two closer hospitals, which delayed arrival for an additional 20 minutes.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $2.7 million settlement was reached, but before it was submitted to the court for approval, the child died. The defendants then sought to revoke the settlement, but the parents claimed breach of contract. The defendants claimed that the agreement was orally negotiated independent of defense counsel and was unenforceable due to the child’s death and lack of court approval. A Texas judge issued summary judgment on breach of contract and awarded $2.7 million plus $40,000 in attorney fees to the parents.

SECOND- AND THIRD-DEGREE BURNS TO PERINEUM
A mother received an epidural injection during vaginal delivery. Six hours later, the patient asked a nurse for a warm compress to place on her perineum. The nurse heated the compress in a microwave and then applied it to the perineal area. The compress caused second- and third-degree burns to the patient’s labia and inner left thigh. She underwent surgical repair of the burned area, and, a year later, had plastic surgery.
PATIENT’S CLAIM The nurse was negligent in overheating the compress.
DEFENDANTS’ DEFENSE The hospital agreed that the nurse who heated and applied the compress had been negligent. The hospital paid all medical expenses relating to the burns, including follow-up surgeries.
VERDICT A $190,000 Utah verdict was returned for noneconomic damages.
DOCUMENTATION MAKES A DIFFERENCE FOR OBGYN AFTER CHILD DIES
A 30-year-old physician was pregnant with her first child. Due to a low amniotic fluid index and lagging fetal growth, she saw a maternal-fetal medicine specialist, who suggested labor induction at 39 weeks.
Labor progressed slowly. After three attempts at vacuum-assisted delivery, the ObGyn recommended cesarean delivery. The parents eventually consented to cesarean delivery after another failed vacuum-assisted attempt. Although the ObGyn had recommended cesarean 2 hours earlier, surgery was not ordered on an emergent basis.
At birth, the baby’s resuscitation took more than 20 minutes. The child lost nearly one-third of her blood volume; she had a subgaleal hemorrhage. Both parties agreed that the vacuum device probably caused the bleeding.
The child had hypoxic ischemic encephalopathy and disseminated intravascular coagulation. She suffered a myocardial infarction at 3 days of age. Without electrical brain activity, life support was removed, and the child died at 5 days of age. An autopsy found possible hypereosinophilic syndrome as the concurrent cause of death.
PARENTS’ CLAIM The mother claimed she was not informed of the risks, benefits, and alternatives to vacuum extraction; she would not have consented had she known the risks. The mother, her husband, and two family members maintained that the ObGyn offered the possibility of cesarean delivery as a question, but did not insist on it. The mother claimed she wanted what was best for the baby, and never refused a cesarean. The resuscitation efforts caused eosinophilic infiltration into several organs.
PHYSICIAN’S DEFENSE The ObGyn charted that the parents were “adamant about having a vaginal delivery,” and said she told the parents what she charted. The obstetric nurse testified that the mother delayed consent because she felt vaginal delivery was imminent. The ObGyn acted properly; eosinophilia caused the baby’s death.
VERDICT An Illinois defense verdict was returned.
HIGH BP TO BLAME FOR DEATHS OF BOTH MOTHER AND CHILD
A 23-year-old woman’s pregnancy was at high risk because of very high blood pressure (BP). At 34 weeks’ gestation, she went to a county hospital with symptoms of high BP; she was treated and discharged 3 days later. She returned to the hospital to be checked twice more within a month. The day after the third visit, she suffered a seizure and was taken to a university hospital, where emergency cesarean delivery was performed. The mother died from an aortic rupture during delivery.
The child was born with brain injuries and died at age 4 years due to neurologic complications.
ESTATE’S CLAIM The mother was not properly treated at the county hospital, resulting in both deaths; she should not have been discharged. Under monitoring, she would have undergone delivery before the aortic rupture occurred, avoiding the baby’s brain injury.
DEFENDANTS’ DEFENSE The mother was stable when released; aortic rupture is unpredictable and unpreventable, and would have occurred under any circumstances. It is highly unusual that a woman of her age would have an aortic rupture.
VERDICT A $3,062,803 California verdict was returned. The parties then settled for $1,782,000 (with the county assuming the medical lien).
NECROTIZING FASCIITIS FROM PERFORATED COLON
A woman underwent laparoscopic-assisted vaginal hysterectomy performed by her ObGyn, and was discharged after 3 days. The next day, she went to another hospital’s emergency department (ED) with abdominal distention and rigidity, severe abdominal pain, and vomiting. She had a toxic appearance, rapid pulse rate, and hypotension. In emergency surgery, several liters of dark brown, foul-smelling fluid were found in her abdomen, and feculent peritonitis and necrotizing fasciitis were diagnosed due to a perforated sigmoid colon. She required multiple hospitalizations and operations.
PATIENT’S CLAIM Perforation occurred during hysterectomy. The ObGyn failed to recognize the injury prior to discharge. The hospital staff did not properly assess her or communicate her symptoms to the ObGyn.
DEFENDANTS’ DEFENSE There was no negligence; proper care was given.
VERDICT A $2,922,503 Florida verdict was returned, with the jury finding the ObGyn 30% at fault and the hospital 70% at fault.
FAILURE TO REACT TO FETAL DISTRESS: $15.6M
After delivery at full term, a child suffered convulsions and seizures on her second day of life. A CT scan showed brain injuries. At age 11 years, she has severe learning and developmental delays, and requires 24-hour care.
PARENTS’ CLAIM Severe decelerations with slow return to baseline occurred several times during labor and delivery. The nurse midwife failed to recognize and react to fetal distress. A cesarean delivery should have been performed instead of a vaginal delivery. The delay in delivery caused the child’s injuries.
DEFENDANTS’ DEFENSE A prenatal neurogenetic disorder caused the child’s injuries.
VERDICT A $15.6 million Maryland verdict was returned. It will not be automatically reduced; the awarded noneconomic damages do not exceed the state cap.
LATE DELIVERY; SEVERE INJURY TO CHILD
At 40 weeks’ gestation, a woman was admitted to the hospital in labor. When the mother’s membranes were ruptured, a small amount of meconium was noted, but the fetal monitor strips were reassuring. Two hours later, the nurse and midwife noted a pattern of decelerations, but they felt the pattern was nonrepetitive and reactive. Thirty minutes later, the nurse and midwife noted decelerations to 90 bpm with pushing, but did not call a physician.
Another midwife arrived to assist the first midwife who was new to practice. The mother was given oxygen, her position was changed, and an IV fluid bolus was administered. Thirty minutes later, the nurses recognized late decelerations and called a Code White twice while the fetal heart rate continued to decelerate. After the attending physician unsuccessfully attempted vacuum extraction, an emergency cesarean delivery was performed.
The child’s Apgar scores were 2, 3, and 3, at 1, 5, and 10 minutes, respectively. The cord blood pH was 6.66, indicating severe metabolic acidosis. She developed seizures within the first few minutes of life. Imaging studies showed global hypoxic ischemic encephalopathy. The child cannot walk, talk, or sit up unsupported at age 8, and requires a G-tube. She is cortically blind and requires antiseizure medication.
PARENTS’ CLAIM The nurse, two midwives, and physician were negligent in their care of the mother and child.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $5 million Massachusetts settlement was reached.
WHAT CAUSED INFECTION AFTER ABORTION?
A 20-year-old woman underwent a surgical termination of pregnancy performed by an ObGyn. After discharge, the patient developed pain and other complications requiring rehospitalization and additional surgery for a pelvic infection.
PATIENT’S CLAIM Complications were due to a uterine perforation that spontaneously sealed before it could be detected. The ObGyn was negligent in the performance of the elective abortion. The patient has a large scar on her abdomen because of the additional operation.
PHYSICIAN’S DEFENSE Perforation of the uterus is a known complication of the procedure. However, no perforation occurred; it was not found on imaging, and spontaneous sealing of a perforation cannot occur. The patient’s complications were due to a subclinical infection that was activated by the surgery.
VERDICT A New York defense verdict was returned.
We want to hear from you. Tell us what you think!
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
A woman in her 50s underwent hysterectomy performed by a surgeon, who then assigned an ObGyn to her follow-up care. The day after surgery, the patient had severe abdominal pain with decreased blood pressure and increased heart and respiration rates. The ObGyn admitted the patient to the intensive care unit (ICU), and then designated Dr. A, the patient’s family practitioner to continue her care. Dr. A was not available, so his associate, Dr. B, took over. Over the phone, Dr. B requested pulmonary, cardiology, and infectious disease consults. In the ICU the next day, the patient suffered respiratory arrest and was intubated. When her abdomen became rigid and swollen, emergency surgery revealed that a colon perforation had allowed fecal matter to reach the abdominal cavity. The woman died the next day from complications of sepsis, peritonitis, and multiple organ failure.
ESTATE’S CLAIM None of the physicians assigned to her care ever saw the patient in the ICU. Earlier surgery could have prevented her death. The physicians involved in her care failed to communicate with each other properly.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $3.2 million Illinois settlement was reached with the hospital.
BOTH PARENTS HAD PLATELET ANTIBODIES
When a 32-year-old woman became pregnant with her third child, she sought treatment at a clinic. The mother informed the nurse practi-tioner that her two other children had been diagnosed with low platelets at birth, but they were now healthy and had no further problems.
The woman gave birth vaginally to her third child at term. The newborn had Apgar scores of 8 and 8, at 1 and 5 minutes, respectively. However, the child’s platelet level was 26 x 103/µL. The baby was transferred to another hospital the next day, where he was diagnosed with hydrocephalus and neonatal alloimmune thrombocytopenia. He suffered a massive intracranial hemorrhage, which caused severe neurologic injuries and brain damage. A shunt was placed. The child has significant cognitive deficits as well as cerebral palsy with mild developmental delays. Testing showed that each parent had a different genotype for platelet antibodies.
PARENTS’ CLAIM The parents should have been tested for platelet antibodies prior to this birth due to the family’s history. A prenatal diagnosis of neonatal alloimmune thrombocytopenia would have allowed for treatment with gamma globulin, which could have avoided the intracranial hemorrhage.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $4.8 million California settlement was reached.
CORD PROLAPSE NOT CARED FOR IN AMBULANCE
At 36 weeks’ gestation, a mother called an ambulance when her membranes ruptured and she noticed an umbilical cord prolapse.
The child was in a breech presentation, experienced oxygen deprivation, and sustained severe neurologic damage.
PARENTS’ CLAIM The ambulance service was negligent in its care. The ambulance service dispatcher advised the mother to stand, squat, and push before the ambulance arrived. The ambulance attendants failed to take basic actions to relieve pressure on the prolapsed umbilical cord. The ambulance did not stop at two closer hospitals, which delayed arrival for an additional 20 minutes.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $2.7 million settlement was reached, but before it was submitted to the court for approval, the child died. The defendants then sought to revoke the settlement, but the parents claimed breach of contract. The defendants claimed that the agreement was orally negotiated independent of defense counsel and was unenforceable due to the child’s death and lack of court approval. A Texas judge issued summary judgment on breach of contract and awarded $2.7 million plus $40,000 in attorney fees to the parents.
SECOND- AND THIRD-DEGREE BURNS TO PERINEUM
A mother received an epidural injection during vaginal delivery. Six hours later, the patient asked a nurse for a warm compress to place on her perineum. The nurse heated the compress in a microwave and then applied it to the perineal area. The compress caused second- and third-degree burns to the patient’s labia and inner left thigh. She underwent surgical repair of the burned area, and, a year later, had plastic surgery.
PATIENT’S CLAIM The nurse was negligent in overheating the compress.
DEFENDANTS’ DEFENSE The hospital agreed that the nurse who heated and applied the compress had been negligent. The hospital paid all medical expenses relating to the burns, including follow-up surgeries.
VERDICT A $190,000 Utah verdict was returned for noneconomic damages.
DOCUMENTATION MAKES A DIFFERENCE FOR OBGYN AFTER CHILD DIES
A 30-year-old physician was pregnant with her first child. Due to a low amniotic fluid index and lagging fetal growth, she saw a maternal-fetal medicine specialist, who suggested labor induction at 39 weeks.
Labor progressed slowly. After three attempts at vacuum-assisted delivery, the ObGyn recommended cesarean delivery. The parents eventually consented to cesarean delivery after another failed vacuum-assisted attempt. Although the ObGyn had recommended cesarean 2 hours earlier, surgery was not ordered on an emergent basis.
At birth, the baby’s resuscitation took more than 20 minutes. The child lost nearly one-third of her blood volume; she had a subgaleal hemorrhage. Both parties agreed that the vacuum device probably caused the bleeding.
The child had hypoxic ischemic encephalopathy and disseminated intravascular coagulation. She suffered a myocardial infarction at 3 days of age. Without electrical brain activity, life support was removed, and the child died at 5 days of age. An autopsy found possible hypereosinophilic syndrome as the concurrent cause of death.
PARENTS’ CLAIM The mother claimed she was not informed of the risks, benefits, and alternatives to vacuum extraction; she would not have consented had she known the risks. The mother, her husband, and two family members maintained that the ObGyn offered the possibility of cesarean delivery as a question, but did not insist on it. The mother claimed she wanted what was best for the baby, and never refused a cesarean. The resuscitation efforts caused eosinophilic infiltration into several organs.
PHYSICIAN’S DEFENSE The ObGyn charted that the parents were “adamant about having a vaginal delivery,” and said she told the parents what she charted. The obstetric nurse testified that the mother delayed consent because she felt vaginal delivery was imminent. The ObGyn acted properly; eosinophilia caused the baby’s death.
VERDICT An Illinois defense verdict was returned.
HIGH BP TO BLAME FOR DEATHS OF BOTH MOTHER AND CHILD
A 23-year-old woman’s pregnancy was at high risk because of very high blood pressure (BP). At 34 weeks’ gestation, she went to a county hospital with symptoms of high BP; she was treated and discharged 3 days later. She returned to the hospital to be checked twice more within a month. The day after the third visit, she suffered a seizure and was taken to a university hospital, where emergency cesarean delivery was performed. The mother died from an aortic rupture during delivery.
The child was born with brain injuries and died at age 4 years due to neurologic complications.
ESTATE’S CLAIM The mother was not properly treated at the county hospital, resulting in both deaths; she should not have been discharged. Under monitoring, she would have undergone delivery before the aortic rupture occurred, avoiding the baby’s brain injury.
DEFENDANTS’ DEFENSE The mother was stable when released; aortic rupture is unpredictable and unpreventable, and would have occurred under any circumstances. It is highly unusual that a woman of her age would have an aortic rupture.
VERDICT A $3,062,803 California verdict was returned. The parties then settled for $1,782,000 (with the county assuming the medical lien).
NECROTIZING FASCIITIS FROM PERFORATED COLON
A woman underwent laparoscopic-assisted vaginal hysterectomy performed by her ObGyn, and was discharged after 3 days. The next day, she went to another hospital’s emergency department (ED) with abdominal distention and rigidity, severe abdominal pain, and vomiting. She had a toxic appearance, rapid pulse rate, and hypotension. In emergency surgery, several liters of dark brown, foul-smelling fluid were found in her abdomen, and feculent peritonitis and necrotizing fasciitis were diagnosed due to a perforated sigmoid colon. She required multiple hospitalizations and operations.
PATIENT’S CLAIM Perforation occurred during hysterectomy. The ObGyn failed to recognize the injury prior to discharge. The hospital staff did not properly assess her or communicate her symptoms to the ObGyn.
DEFENDANTS’ DEFENSE There was no negligence; proper care was given.
VERDICT A $2,922,503 Florida verdict was returned, with the jury finding the ObGyn 30% at fault and the hospital 70% at fault.
FAILURE TO REACT TO FETAL DISTRESS: $15.6M
After delivery at full term, a child suffered convulsions and seizures on her second day of life. A CT scan showed brain injuries. At age 11 years, she has severe learning and developmental delays, and requires 24-hour care.
PARENTS’ CLAIM Severe decelerations with slow return to baseline occurred several times during labor and delivery. The nurse midwife failed to recognize and react to fetal distress. A cesarean delivery should have been performed instead of a vaginal delivery. The delay in delivery caused the child’s injuries.
DEFENDANTS’ DEFENSE A prenatal neurogenetic disorder caused the child’s injuries.
VERDICT A $15.6 million Maryland verdict was returned. It will not be automatically reduced; the awarded noneconomic damages do not exceed the state cap.
LATE DELIVERY; SEVERE INJURY TO CHILD
At 40 weeks’ gestation, a woman was admitted to the hospital in labor. When the mother’s membranes were ruptured, a small amount of meconium was noted, but the fetal monitor strips were reassuring. Two hours later, the nurse and midwife noted a pattern of decelerations, but they felt the pattern was nonrepetitive and reactive. Thirty minutes later, the nurse and midwife noted decelerations to 90 bpm with pushing, but did not call a physician.
Another midwife arrived to assist the first midwife who was new to practice. The mother was given oxygen, her position was changed, and an IV fluid bolus was administered. Thirty minutes later, the nurses recognized late decelerations and called a Code White twice while the fetal heart rate continued to decelerate. After the attending physician unsuccessfully attempted vacuum extraction, an emergency cesarean delivery was performed.
The child’s Apgar scores were 2, 3, and 3, at 1, 5, and 10 minutes, respectively. The cord blood pH was 6.66, indicating severe metabolic acidosis. She developed seizures within the first few minutes of life. Imaging studies showed global hypoxic ischemic encephalopathy. The child cannot walk, talk, or sit up unsupported at age 8, and requires a G-tube. She is cortically blind and requires antiseizure medication.
PARENTS’ CLAIM The nurse, two midwives, and physician were negligent in their care of the mother and child.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $5 million Massachusetts settlement was reached.
WHAT CAUSED INFECTION AFTER ABORTION?
A 20-year-old woman underwent a surgical termination of pregnancy performed by an ObGyn. After discharge, the patient developed pain and other complications requiring rehospitalization and additional surgery for a pelvic infection.
PATIENT’S CLAIM Complications were due to a uterine perforation that spontaneously sealed before it could be detected. The ObGyn was negligent in the performance of the elective abortion. The patient has a large scar on her abdomen because of the additional operation.
PHYSICIAN’S DEFENSE Perforation of the uterus is a known complication of the procedure. However, no perforation occurred; it was not found on imaging, and spontaneous sealing of a perforation cannot occur. The patient’s complications were due to a subclinical infection that was activated by the surgery.
VERDICT A New York defense verdict was returned.
We want to hear from you. Tell us what you think!
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
A woman in her 50s underwent hysterectomy performed by a surgeon, who then assigned an ObGyn to her follow-up care. The day after surgery, the patient had severe abdominal pain with decreased blood pressure and increased heart and respiration rates. The ObGyn admitted the patient to the intensive care unit (ICU), and then designated Dr. A, the patient’s family practitioner to continue her care. Dr. A was not available, so his associate, Dr. B, took over. Over the phone, Dr. B requested pulmonary, cardiology, and infectious disease consults. In the ICU the next day, the patient suffered respiratory arrest and was intubated. When her abdomen became rigid and swollen, emergency surgery revealed that a colon perforation had allowed fecal matter to reach the abdominal cavity. The woman died the next day from complications of sepsis, peritonitis, and multiple organ failure.
ESTATE’S CLAIM None of the physicians assigned to her care ever saw the patient in the ICU. Earlier surgery could have prevented her death. The physicians involved in her care failed to communicate with each other properly.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $3.2 million Illinois settlement was reached with the hospital.
BOTH PARENTS HAD PLATELET ANTIBODIES
When a 32-year-old woman became pregnant with her third child, she sought treatment at a clinic. The mother informed the nurse practi-tioner that her two other children had been diagnosed with low platelets at birth, but they were now healthy and had no further problems.
The woman gave birth vaginally to her third child at term. The newborn had Apgar scores of 8 and 8, at 1 and 5 minutes, respectively. However, the child’s platelet level was 26 x 103/µL. The baby was transferred to another hospital the next day, where he was diagnosed with hydrocephalus and neonatal alloimmune thrombocytopenia. He suffered a massive intracranial hemorrhage, which caused severe neurologic injuries and brain damage. A shunt was placed. The child has significant cognitive deficits as well as cerebral palsy with mild developmental delays. Testing showed that each parent had a different genotype for platelet antibodies.
PARENTS’ CLAIM The parents should have been tested for platelet antibodies prior to this birth due to the family’s history. A prenatal diagnosis of neonatal alloimmune thrombocytopenia would have allowed for treatment with gamma globulin, which could have avoided the intracranial hemorrhage.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $4.8 million California settlement was reached.
CORD PROLAPSE NOT CARED FOR IN AMBULANCE
At 36 weeks’ gestation, a mother called an ambulance when her membranes ruptured and she noticed an umbilical cord prolapse.
The child was in a breech presentation, experienced oxygen deprivation, and sustained severe neurologic damage.
PARENTS’ CLAIM The ambulance service was negligent in its care. The ambulance service dispatcher advised the mother to stand, squat, and push before the ambulance arrived. The ambulance attendants failed to take basic actions to relieve pressure on the prolapsed umbilical cord. The ambulance did not stop at two closer hospitals, which delayed arrival for an additional 20 minutes.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $2.7 million settlement was reached, but before it was submitted to the court for approval, the child died. The defendants then sought to revoke the settlement, but the parents claimed breach of contract. The defendants claimed that the agreement was orally negotiated independent of defense counsel and was unenforceable due to the child’s death and lack of court approval. A Texas judge issued summary judgment on breach of contract and awarded $2.7 million plus $40,000 in attorney fees to the parents.
SECOND- AND THIRD-DEGREE BURNS TO PERINEUM
A mother received an epidural injection during vaginal delivery. Six hours later, the patient asked a nurse for a warm compress to place on her perineum. The nurse heated the compress in a microwave and then applied it to the perineal area. The compress caused second- and third-degree burns to the patient’s labia and inner left thigh. She underwent surgical repair of the burned area, and, a year later, had plastic surgery.
PATIENT’S CLAIM The nurse was negligent in overheating the compress.
DEFENDANTS’ DEFENSE The hospital agreed that the nurse who heated and applied the compress had been negligent. The hospital paid all medical expenses relating to the burns, including follow-up surgeries.
VERDICT A $190,000 Utah verdict was returned for noneconomic damages.
DOCUMENTATION MAKES A DIFFERENCE FOR OBGYN AFTER CHILD DIES
A 30-year-old physician was pregnant with her first child. Due to a low amniotic fluid index and lagging fetal growth, she saw a maternal-fetal medicine specialist, who suggested labor induction at 39 weeks.
Labor progressed slowly. After three attempts at vacuum-assisted delivery, the ObGyn recommended cesarean delivery. The parents eventually consented to cesarean delivery after another failed vacuum-assisted attempt. Although the ObGyn had recommended cesarean 2 hours earlier, surgery was not ordered on an emergent basis.
At birth, the baby’s resuscitation took more than 20 minutes. The child lost nearly one-third of her blood volume; she had a subgaleal hemorrhage. Both parties agreed that the vacuum device probably caused the bleeding.
The child had hypoxic ischemic encephalopathy and disseminated intravascular coagulation. She suffered a myocardial infarction at 3 days of age. Without electrical brain activity, life support was removed, and the child died at 5 days of age. An autopsy found possible hypereosinophilic syndrome as the concurrent cause of death.
PARENTS’ CLAIM The mother claimed she was not informed of the risks, benefits, and alternatives to vacuum extraction; she would not have consented had she known the risks. The mother, her husband, and two family members maintained that the ObGyn offered the possibility of cesarean delivery as a question, but did not insist on it. The mother claimed she wanted what was best for the baby, and never refused a cesarean. The resuscitation efforts caused eosinophilic infiltration into several organs.
PHYSICIAN’S DEFENSE The ObGyn charted that the parents were “adamant about having a vaginal delivery,” and said she told the parents what she charted. The obstetric nurse testified that the mother delayed consent because she felt vaginal delivery was imminent. The ObGyn acted properly; eosinophilia caused the baby’s death.
VERDICT An Illinois defense verdict was returned.
HIGH BP TO BLAME FOR DEATHS OF BOTH MOTHER AND CHILD
A 23-year-old woman’s pregnancy was at high risk because of very high blood pressure (BP). At 34 weeks’ gestation, she went to a county hospital with symptoms of high BP; she was treated and discharged 3 days later. She returned to the hospital to be checked twice more within a month. The day after the third visit, she suffered a seizure and was taken to a university hospital, where emergency cesarean delivery was performed. The mother died from an aortic rupture during delivery.
The child was born with brain injuries and died at age 4 years due to neurologic complications.
ESTATE’S CLAIM The mother was not properly treated at the county hospital, resulting in both deaths; she should not have been discharged. Under monitoring, she would have undergone delivery before the aortic rupture occurred, avoiding the baby’s brain injury.
DEFENDANTS’ DEFENSE The mother was stable when released; aortic rupture is unpredictable and unpreventable, and would have occurred under any circumstances. It is highly unusual that a woman of her age would have an aortic rupture.
VERDICT A $3,062,803 California verdict was returned. The parties then settled for $1,782,000 (with the county assuming the medical lien).
NECROTIZING FASCIITIS FROM PERFORATED COLON
A woman underwent laparoscopic-assisted vaginal hysterectomy performed by her ObGyn, and was discharged after 3 days. The next day, she went to another hospital’s emergency department (ED) with abdominal distention and rigidity, severe abdominal pain, and vomiting. She had a toxic appearance, rapid pulse rate, and hypotension. In emergency surgery, several liters of dark brown, foul-smelling fluid were found in her abdomen, and feculent peritonitis and necrotizing fasciitis were diagnosed due to a perforated sigmoid colon. She required multiple hospitalizations and operations.
PATIENT’S CLAIM Perforation occurred during hysterectomy. The ObGyn failed to recognize the injury prior to discharge. The hospital staff did not properly assess her or communicate her symptoms to the ObGyn.
DEFENDANTS’ DEFENSE There was no negligence; proper care was given.
VERDICT A $2,922,503 Florida verdict was returned, with the jury finding the ObGyn 30% at fault and the hospital 70% at fault.
FAILURE TO REACT TO FETAL DISTRESS: $15.6M
After delivery at full term, a child suffered convulsions and seizures on her second day of life. A CT scan showed brain injuries. At age 11 years, she has severe learning and developmental delays, and requires 24-hour care.
PARENTS’ CLAIM Severe decelerations with slow return to baseline occurred several times during labor and delivery. The nurse midwife failed to recognize and react to fetal distress. A cesarean delivery should have been performed instead of a vaginal delivery. The delay in delivery caused the child’s injuries.
DEFENDANTS’ DEFENSE A prenatal neurogenetic disorder caused the child’s injuries.
VERDICT A $15.6 million Maryland verdict was returned. It will not be automatically reduced; the awarded noneconomic damages do not exceed the state cap.
LATE DELIVERY; SEVERE INJURY TO CHILD
At 40 weeks’ gestation, a woman was admitted to the hospital in labor. When the mother’s membranes were ruptured, a small amount of meconium was noted, but the fetal monitor strips were reassuring. Two hours later, the nurse and midwife noted a pattern of decelerations, but they felt the pattern was nonrepetitive and reactive. Thirty minutes later, the nurse and midwife noted decelerations to 90 bpm with pushing, but did not call a physician.
Another midwife arrived to assist the first midwife who was new to practice. The mother was given oxygen, her position was changed, and an IV fluid bolus was administered. Thirty minutes later, the nurses recognized late decelerations and called a Code White twice while the fetal heart rate continued to decelerate. After the attending physician unsuccessfully attempted vacuum extraction, an emergency cesarean delivery was performed.
The child’s Apgar scores were 2, 3, and 3, at 1, 5, and 10 minutes, respectively. The cord blood pH was 6.66, indicating severe metabolic acidosis. She developed seizures within the first few minutes of life. Imaging studies showed global hypoxic ischemic encephalopathy. The child cannot walk, talk, or sit up unsupported at age 8, and requires a G-tube. She is cortically blind and requires antiseizure medication.
PARENTS’ CLAIM The nurse, two midwives, and physician were negligent in their care of the mother and child.
DEFENDANTS’ DEFENSE The case was settled during the trial.
VERDICT A $5 million Massachusetts settlement was reached.
WHAT CAUSED INFECTION AFTER ABORTION?
A 20-year-old woman underwent a surgical termination of pregnancy performed by an ObGyn. After discharge, the patient developed pain and other complications requiring rehospitalization and additional surgery for a pelvic infection.
PATIENT’S CLAIM Complications were due to a uterine perforation that spontaneously sealed before it could be detected. The ObGyn was negligent in the performance of the elective abortion. The patient has a large scar on her abdomen because of the additional operation.
PHYSICIAN’S DEFENSE Perforation of the uterus is a known complication of the procedure. However, no perforation occurred; it was not found on imaging, and spontaneous sealing of a perforation cannot occur. The patient’s complications were due to a subclinical infection that was activated by the surgery.
VERDICT A New York defense verdict was returned.
We want to hear from you. Tell us what you think!
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Dos, don’ts, and dollars: Making the switch to an EHR
More and more ObGyns are adopting electronic health records (EHRs), not only to meet a government mandate but also with the hope of making their practice more efficient and productive. While it is likely that EHRs enhance qualitative benefits, such as safety, patient satisfaction, 24/7 availability of medical records, and patient access to medical data, it isn’t always clear how they boost the financial bottom line. For this reason, we recommend that every practice “run the numbers” before making the transition from paper to paperless records. That means estimating the cost, expenses, and potential for added income associated with the EHR before embarking on the change.
In this article, we explain five ways a switch to EHRs can reduce costs. We also offer strategies for choosing and implementing an EHR, from information gathering to motivating your staff.

Transcription costs are lower
The estimated cost of dictating a letter to a referring physician using conventional means is $12 to $15. That estimate includes the doctor’s time, the cost of the transcriptionist, the stationery, and the postage or cost of faxing the letter. An ObGyn may generate five to 10 letters per day. That’s $60 to $150 in expenses.
Most EHRs can generate a referral letter at no additional cost, provided the diagnosis, prescribed medications, and treatment plan have been entered in the system. Not only that, but each referral letter can be transmitted immediately to the recipient by email (or fax; the referring doctor’s preference). In the past, it may have taken as long as several weeks for the letter to be generated and make its way to the recipient by conventional means.
This use of the EHR can save a practice as much as $1,000 per physician every month.
Chart maintenance is no longer an issue
It sometimes can be a challenge for an ObGyn office to locate a paper chart. Any record lost in the “black hole” can wreak havoc with the schedule. It becomes even more problematic if the practice has multiple locations where charts are kept, delaying its recovery.
When a temporary chart must be created, it costs the practice time and dollars. It also becomes necessary to transfer the data into the permanent record, once it is located—another expense—not to mention the need to create a chart for every new patient.
It is not unusual for a busy practice to misplace as many as five charts a day, representing expenses of $25 to $50 per chart. With an EHR, this expense is reduced to $0, and the chart can be accessed 24/7 from multiple locations, including the physician’s home or mobile phone, provided the EHR is networked between practices and the data are secured on the cloud (with encryption to ensure patient confidentiality and compliance with the Health Insurance Portability and Accountability Act, or HIPAA).
Another expense with paper records: pulling charts for the day’s patients and returning them to the file rack at the conclusion of the day. These steps require additional employees and do nothing to improve patient care.
Coding is more accurate with an EHR
Prior to the development of EHRs, physicians had to guess the level of care that was provided and tended to “under-code” the visit, leading to a loss of income that the physician rightfully earned but didn’t document fully. As one coding expert has noted, if you didn’t document it, you didn’t do it, and if the record reflects that you didn’t do it, you can’t be paid for it.
In general, the higher the level of care and the higher the code used, the more extensive documentation should be. Today’s EHRs can automatically calculate the code best supported by the documentation entered at the time of the visit. After implementing an EHR, an ObGyn can ensure that accurate codes are submitted to payers, with higher levels of reimbursement honestly and ethically achieved.
A shift to EHRs frees up valuable square footage
It is not unusual for a practice to consume several hundred square feet of space for the storage of conventional medical records. Once a practice transitions to electronic records, however, these files are stored at a remote site or shredded once the entire paper record has been scanned into the EHR. The office space once required for paper record storage can then be converted into examination rooms or devoted to a laboratory, imaging center, or procedure room to generate ancillary income.
There’s an incentive involved
On February 17, 2009, the US government passed the Health Information Technology for Economic and Clinical Health (HITECH) Act in an effort to reduce the barriers to EHR implementation by outlining programs for standardization and funding of EHR programs.1,2 The HITECH Act contained meaningful-use incentives to reward participants for the adoption of EHRs, with payments disbursed through Medicare and Medicaid.2 By meeting several core objectives, individuals in private practice can earn as much as $44,000 over 5 years through the Medicare EHR incentive program and $63,750 over 6 years by participating in the Medicaid incentive program.3 Hospitals can earn more than $2 million over the same period. The objectives differ slightly for hospitals and individuals but are intended to improve quality, coordination, and safety of care while promoting patient involvement and public health.3
Related article: The Affordable Care Act and the drive for EHRs: Are small practices being squeezed? Lucia DiVenere, MD (July 2013)
The HITECH Act also sought to increase the security of EHRs to ensure patient privacy through standardization of EHR products. To become eligible for meaningful-use incentives, EHR software must meet government standards and specifications.3 Common requirements include the ability to document:
- vital signs
- test results
- all medications and allergies.
Another requirement is the ability to generate lists of patients with common conditions.3
By standardizing the EHR format, the HITECH Act improved networking by physicians by ensuring common capabilities among various EHR products.
The funding and standardization established by the HITECH Act increased the usage of EHRs among physicians to 57% by 2011.2
How did we get here? A history of the EHR
Computers and electronics originally were used for administrative purposes and did not offer meaningful clinical applications when they first were introduced to health care during the 1960s and 70s.8 These early machines were large, expensive, and slow and did not meet the practical needs of clinicians. During the 1980s and 90s, however, with networking capability and development of the World Wide Web, the potential for an electronic health record (EHR) became clearer. In 1991, an Institute of Medicine (IOM) report listed the “computer-based patient record” as “an essential technology for health care.”8 The authors of the IOM report envisioned a true network of practices and hospitals that seamlessly and efficiently share information and insight to increase quality of care, reduce medical errors, and improve patient safety.1
Despite advances in EHR technology, one major hurdle remained: cost. For many clinicians, the time and resources required for installation of the program, transfer of records to the electronic format, and training of staff was too high. By 2001, only 18% of physicians had incorporated the EHR.2 Today, nearly 60% of practices use an EHR.
Related article: EHRS and medicolegal risk: How they help, when they could hurt Martin Gimovsky, MD, and Baohuong N. Tran, DO (March 2013)
How to implement an EHR
The first step is to narrow your options to a few vendors that best suit the needs of your office. This process is beyond the scope of this article, but your ultimate objective should be to choose a user-friendly interface from a vendor that offers excellent document security, customer assistance, and support.4
Form an implementation team for your practice, and have it begin by consulting ObGyn practices of similar size that have recently installed one of the EHRs you are considering. By asking about other practices’ experiences and any pitfalls they encountered, you can greatly ease your transition to EHRs.
If possible, the physicians in your practice should visit the office of any colleagues who have implemented one of the EHRs you are considering to see how they like the product. Your office manager, nurses, and receptionist also should visit their counterparts in the other practice to ask about their experiences and opinions. The more information you glean from other ObGyn practices, the easier it will be to make your decision.
Be sure to check with your hospital to ensure compatibility with its system.
Ensure adequate technical support
One of the most important considerations in selecting a product is the availability and quality of tech support from the home office of the vendor. When you talk to other users of a product, ask how quickly tech support calls are returned and how efficiently problems are solved.
There will always be technical problems during the transition away from paper records. Ensuring their prompt resolution will be critical to your success.
Assign project management
After deciding on a particular product, create a project team to manage the complex, lengthy implementation process.4–6 This team should include a project manager who has the experience and skills to coordinate a complex plan, a well-respected product champion who can help maintain staff support for the change, and several information technology (IT) specialists who can manage the software and hardware challenges.4–6
Related article: What can "meaningful use" of an EHR mean for your bottom line? Robert L. Barbieri, MD (Editorial, February 2011)
Rally the troops
The most vital part of any implementation plan is staff “buy-in.”4–6 It is incumbent upon the project-management team to determine what effects EHR implementation will have on workflow and to explain to employees how the process ultimately will increase efficiency and reduce work time and cost. And the project champion must remind employees of these goals during the transition.4–6
Develop a backup system
Work with your IT staff to create a backup system for the EHR to protect against system malfunction.4 In the past, offices backed up their data to tapes or disks. Today, it probably is safer to back up to the cloud. Cloud computing, which allows for automatic back-up, is tightly regulated by HIPAA, so be sure to choose an approved vendor.7
Preload your data
Before going live with the EHR, data must be integrated and preloaded into the electronic format. This means integrating billing, lab results, orders, scheduling, and encounter templates into the EHR interface.4,6 When data are preloaded, employees can practice on the software before the launch date, ensuring a seamless transition.6
No “teeth-gnashing” necessary
The transition to an EHR system can be intimidating and may affect your staff’s productivity, efficiency, and morale. By following a few careful steps, the process can proceed without teeth-gnashing and loss of productivity. In fact, the suggestions offered here should improve productivity, office efficiency, and patient safety over the long term.
Who could ask for anything more?
We want to hear from you! Tell us what you think.
- Thakkar M, Davis DC. Risks, barriers, and benefits of EHR systems: a comparative study based on size of hospital. Perspect Health Inf Manag. 2006;3(5):1–19.
- Hsiao CJ, Hing E, Socey TC, et al. Electronic health record systems and intent to apply meaningful use incentives among office-based physician practices: United States, 2001–2011. NCHS Data Brief. 2011;(79):1–8.
- Terry NP. Anticipating stage two: assessing the development of meaningful use and EMR deployment. St. Louis University School of Law Legal Studies Research Paper Series. 2011;21.
- Keshavjee K, Bosomworth J, Copen J, et al. Best practices in EMR implementation: a systematic review. AMIA Annu Symp Proc. 2006;982.
- Lorenzi NM, Kouroubali A, Detmer DE, et al. How to successfully select and implement electronic health records (EHR) in small ambulatory practice settings. BMC Medical Informatics Decision Making. 2009;9(15):1–13.
- Smith PD. Implementing an EMR system: one clinic’s experience. Fam Pract Manag. 2003;10(5):37–42.
- Raheja D, Escano MC. Hazards in electronic medical records. J System Safety. 2010;46(4):1–4. http://system-safety.org/ejss/past/novdec2010ejss/pdf/health.pdf. Accessed October 8, 2013.
- Berner ES, Detmer DE, Simborg D. Will the wave finally break? A brief view of the adoption of electronic medical records in the United States. J Am Med Inform Assoc. 2005;12(1):3–7.

Neil H. Baum, MD, practices urology in New Orleans, Louisiana. He is Associate Clinical Professor of Urology at Tulane Medical School and Louisiana State University School of Medicine, both in New Orleans. He is also on the medical staff at Touro Infirmary in New Orleans, and East Jefferson General Hospital in Metairie, Louisiana. And he is the author of Marketing Your Clinical Practice: Ethically, Effectively, Economically (4th edition, 2009; Jones & Bartlett).

Paul Kepper has a Master’s of Science degree from Tulane University in New Orleans, Louisiana.
The authors report no financial relationships relevant to this article.
Neil H. Baum, MD, practices urology in New Orleans, Louisiana. He is Associate Clinical Professor of Urology at Tulane Medical School and Louisiana State University School of Medicine, both in New Orleans. He is also on the medical staff at Touro Infirmary in New Orleans, and East Jefferson General Hospital in Metairie, Louisiana. And he is the author of Marketing Your Clinical Practice: Ethically, Effectively, Economically (4th edition, 2009; Jones & Bartlett).
Paul Kepper has a Master’s of Science degree from Tulane University in New Orleans, Louisiana.
The authors report no financial relationships relevant to this article.
Neil H. Baum, MD, practices urology in New Orleans, Louisiana. He is Associate Clinical Professor of Urology at Tulane Medical School and Louisiana State University School of Medicine, both in New Orleans. He is also on the medical staff at Touro Infirmary in New Orleans, and East Jefferson General Hospital in Metairie, Louisiana. And he is the author of Marketing Your Clinical Practice: Ethically, Effectively, Economically (4th edition, 2009; Jones & Bartlett).
Paul Kepper has a Master’s of Science degree from Tulane University in New Orleans, Louisiana.
The authors report no financial relationships relevant to this article.
More and more ObGyns are adopting electronic health records (EHRs), not only to meet a government mandate but also with the hope of making their practice more efficient and productive. While it is likely that EHRs enhance qualitative benefits, such as safety, patient satisfaction, 24/7 availability of medical records, and patient access to medical data, it isn’t always clear how they boost the financial bottom line. For this reason, we recommend that every practice “run the numbers” before making the transition from paper to paperless records. That means estimating the cost, expenses, and potential for added income associated with the EHR before embarking on the change.
In this article, we explain five ways a switch to EHRs can reduce costs. We also offer strategies for choosing and implementing an EHR, from information gathering to motivating your staff.
Transcription costs are lower
The estimated cost of dictating a letter to a referring physician using conventional means is $12 to $15. That estimate includes the doctor’s time, the cost of the transcriptionist, the stationery, and the postage or cost of faxing the letter. An ObGyn may generate five to 10 letters per day. That’s $60 to $150 in expenses.
Most EHRs can generate a referral letter at no additional cost, provided the diagnosis, prescribed medications, and treatment plan have been entered in the system. Not only that, but each referral letter can be transmitted immediately to the recipient by email (or fax; the referring doctor’s preference). In the past, it may have taken as long as several weeks for the letter to be generated and make its way to the recipient by conventional means.
This use of the EHR can save a practice as much as $1,000 per physician every month.
Chart maintenance is no longer an issue
It sometimes can be a challenge for an ObGyn office to locate a paper chart. Any record lost in the “black hole” can wreak havoc with the schedule. It becomes even more problematic if the practice has multiple locations where charts are kept, delaying its recovery.
When a temporary chart must be created, it costs the practice time and dollars. It also becomes necessary to transfer the data into the permanent record, once it is located—another expense—not to mention the need to create a chart for every new patient.
It is not unusual for a busy practice to misplace as many as five charts a day, representing expenses of $25 to $50 per chart. With an EHR, this expense is reduced to $0, and the chart can be accessed 24/7 from multiple locations, including the physician’s home or mobile phone, provided the EHR is networked between practices and the data are secured on the cloud (with encryption to ensure patient confidentiality and compliance with the Health Insurance Portability and Accountability Act, or HIPAA).
Another expense with paper records: pulling charts for the day’s patients and returning them to the file rack at the conclusion of the day. These steps require additional employees and do nothing to improve patient care.
Coding is more accurate with an EHR
Prior to the development of EHRs, physicians had to guess the level of care that was provided and tended to “under-code” the visit, leading to a loss of income that the physician rightfully earned but didn’t document fully. As one coding expert has noted, if you didn’t document it, you didn’t do it, and if the record reflects that you didn’t do it, you can’t be paid for it.
In general, the higher the level of care and the higher the code used, the more extensive documentation should be. Today’s EHRs can automatically calculate the code best supported by the documentation entered at the time of the visit. After implementing an EHR, an ObGyn can ensure that accurate codes are submitted to payers, with higher levels of reimbursement honestly and ethically achieved.
A shift to EHRs frees up valuable square footage
It is not unusual for a practice to consume several hundred square feet of space for the storage of conventional medical records. Once a practice transitions to electronic records, however, these files are stored at a remote site or shredded once the entire paper record has been scanned into the EHR. The office space once required for paper record storage can then be converted into examination rooms or devoted to a laboratory, imaging center, or procedure room to generate ancillary income.
There’s an incentive involved
On February 17, 2009, the US government passed the Health Information Technology for Economic and Clinical Health (HITECH) Act in an effort to reduce the barriers to EHR implementation by outlining programs for standardization and funding of EHR programs.1,2 The HITECH Act contained meaningful-use incentives to reward participants for the adoption of EHRs, with payments disbursed through Medicare and Medicaid.2 By meeting several core objectives, individuals in private practice can earn as much as $44,000 over 5 years through the Medicare EHR incentive program and $63,750 over 6 years by participating in the Medicaid incentive program.3 Hospitals can earn more than $2 million over the same period. The objectives differ slightly for hospitals and individuals but are intended to improve quality, coordination, and safety of care while promoting patient involvement and public health.3
Related article: The Affordable Care Act and the drive for EHRs: Are small practices being squeezed? Lucia DiVenere, MD (July 2013)
The HITECH Act also sought to increase the security of EHRs to ensure patient privacy through standardization of EHR products. To become eligible for meaningful-use incentives, EHR software must meet government standards and specifications.3 Common requirements include the ability to document:
- vital signs
- test results
- all medications and allergies.
Another requirement is the ability to generate lists of patients with common conditions.3
By standardizing the EHR format, the HITECH Act improved networking by physicians by ensuring common capabilities among various EHR products.
The funding and standardization established by the HITECH Act increased the usage of EHRs among physicians to 57% by 2011.2
How did we get here? A history of the EHR
Computers and electronics originally were used for administrative purposes and did not offer meaningful clinical applications when they first were introduced to health care during the 1960s and 70s.8 These early machines were large, expensive, and slow and did not meet the practical needs of clinicians. During the 1980s and 90s, however, with networking capability and development of the World Wide Web, the potential for an electronic health record (EHR) became clearer. In 1991, an Institute of Medicine (IOM) report listed the “computer-based patient record” as “an essential technology for health care.”8 The authors of the IOM report envisioned a true network of practices and hospitals that seamlessly and efficiently share information and insight to increase quality of care, reduce medical errors, and improve patient safety.1
Despite advances in EHR technology, one major hurdle remained: cost. For many clinicians, the time and resources required for installation of the program, transfer of records to the electronic format, and training of staff was too high. By 2001, only 18% of physicians had incorporated the EHR.2 Today, nearly 60% of practices use an EHR.
Related article: EHRS and medicolegal risk: How they help, when they could hurt Martin Gimovsky, MD, and Baohuong N. Tran, DO (March 2013)
How to implement an EHR
The first step is to narrow your options to a few vendors that best suit the needs of your office. This process is beyond the scope of this article, but your ultimate objective should be to choose a user-friendly interface from a vendor that offers excellent document security, customer assistance, and support.4
Form an implementation team for your practice, and have it begin by consulting ObGyn practices of similar size that have recently installed one of the EHRs you are considering. By asking about other practices’ experiences and any pitfalls they encountered, you can greatly ease your transition to EHRs.
If possible, the physicians in your practice should visit the office of any colleagues who have implemented one of the EHRs you are considering to see how they like the product. Your office manager, nurses, and receptionist also should visit their counterparts in the other practice to ask about their experiences and opinions. The more information you glean from other ObGyn practices, the easier it will be to make your decision.
Be sure to check with your hospital to ensure compatibility with its system.
Ensure adequate technical support
One of the most important considerations in selecting a product is the availability and quality of tech support from the home office of the vendor. When you talk to other users of a product, ask how quickly tech support calls are returned and how efficiently problems are solved.
There will always be technical problems during the transition away from paper records. Ensuring their prompt resolution will be critical to your success.
Assign project management
After deciding on a particular product, create a project team to manage the complex, lengthy implementation process.4–6 This team should include a project manager who has the experience and skills to coordinate a complex plan, a well-respected product champion who can help maintain staff support for the change, and several information technology (IT) specialists who can manage the software and hardware challenges.4–6
Related article: What can "meaningful use" of an EHR mean for your bottom line? Robert L. Barbieri, MD (Editorial, February 2011)
Rally the troops
The most vital part of any implementation plan is staff “buy-in.”4–6 It is incumbent upon the project-management team to determine what effects EHR implementation will have on workflow and to explain to employees how the process ultimately will increase efficiency and reduce work time and cost. And the project champion must remind employees of these goals during the transition.4–6
Develop a backup system
Work with your IT staff to create a backup system for the EHR to protect against system malfunction.4 In the past, offices backed up their data to tapes or disks. Today, it probably is safer to back up to the cloud. Cloud computing, which allows for automatic back-up, is tightly regulated by HIPAA, so be sure to choose an approved vendor.7
Preload your data
Before going live with the EHR, data must be integrated and preloaded into the electronic format. This means integrating billing, lab results, orders, scheduling, and encounter templates into the EHR interface.4,6 When data are preloaded, employees can practice on the software before the launch date, ensuring a seamless transition.6
No “teeth-gnashing” necessary
The transition to an EHR system can be intimidating and may affect your staff’s productivity, efficiency, and morale. By following a few careful steps, the process can proceed without teeth-gnashing and loss of productivity. In fact, the suggestions offered here should improve productivity, office efficiency, and patient safety over the long term.
Who could ask for anything more?
We want to hear from you! Tell us what you think.
More and more ObGyns are adopting electronic health records (EHRs), not only to meet a government mandate but also with the hope of making their practice more efficient and productive. While it is likely that EHRs enhance qualitative benefits, such as safety, patient satisfaction, 24/7 availability of medical records, and patient access to medical data, it isn’t always clear how they boost the financial bottom line. For this reason, we recommend that every practice “run the numbers” before making the transition from paper to paperless records. That means estimating the cost, expenses, and potential for added income associated with the EHR before embarking on the change.
In this article, we explain five ways a switch to EHRs can reduce costs. We also offer strategies for choosing and implementing an EHR, from information gathering to motivating your staff.
Transcription costs are lower
The estimated cost of dictating a letter to a referring physician using conventional means is $12 to $15. That estimate includes the doctor’s time, the cost of the transcriptionist, the stationery, and the postage or cost of faxing the letter. An ObGyn may generate five to 10 letters per day. That’s $60 to $150 in expenses.
Most EHRs can generate a referral letter at no additional cost, provided the diagnosis, prescribed medications, and treatment plan have been entered in the system. Not only that, but each referral letter can be transmitted immediately to the recipient by email (or fax; the referring doctor’s preference). In the past, it may have taken as long as several weeks for the letter to be generated and make its way to the recipient by conventional means.
This use of the EHR can save a practice as much as $1,000 per physician every month.
Chart maintenance is no longer an issue
It sometimes can be a challenge for an ObGyn office to locate a paper chart. Any record lost in the “black hole” can wreak havoc with the schedule. It becomes even more problematic if the practice has multiple locations where charts are kept, delaying its recovery.
When a temporary chart must be created, it costs the practice time and dollars. It also becomes necessary to transfer the data into the permanent record, once it is located—another expense—not to mention the need to create a chart for every new patient.
It is not unusual for a busy practice to misplace as many as five charts a day, representing expenses of $25 to $50 per chart. With an EHR, this expense is reduced to $0, and the chart can be accessed 24/7 from multiple locations, including the physician’s home or mobile phone, provided the EHR is networked between practices and the data are secured on the cloud (with encryption to ensure patient confidentiality and compliance with the Health Insurance Portability and Accountability Act, or HIPAA).
Another expense with paper records: pulling charts for the day’s patients and returning them to the file rack at the conclusion of the day. These steps require additional employees and do nothing to improve patient care.
Coding is more accurate with an EHR
Prior to the development of EHRs, physicians had to guess the level of care that was provided and tended to “under-code” the visit, leading to a loss of income that the physician rightfully earned but didn’t document fully. As one coding expert has noted, if you didn’t document it, you didn’t do it, and if the record reflects that you didn’t do it, you can’t be paid for it.
In general, the higher the level of care and the higher the code used, the more extensive documentation should be. Today’s EHRs can automatically calculate the code best supported by the documentation entered at the time of the visit. After implementing an EHR, an ObGyn can ensure that accurate codes are submitted to payers, with higher levels of reimbursement honestly and ethically achieved.
A shift to EHRs frees up valuable square footage
It is not unusual for a practice to consume several hundred square feet of space for the storage of conventional medical records. Once a practice transitions to electronic records, however, these files are stored at a remote site or shredded once the entire paper record has been scanned into the EHR. The office space once required for paper record storage can then be converted into examination rooms or devoted to a laboratory, imaging center, or procedure room to generate ancillary income.
There’s an incentive involved
On February 17, 2009, the US government passed the Health Information Technology for Economic and Clinical Health (HITECH) Act in an effort to reduce the barriers to EHR implementation by outlining programs for standardization and funding of EHR programs.1,2 The HITECH Act contained meaningful-use incentives to reward participants for the adoption of EHRs, with payments disbursed through Medicare and Medicaid.2 By meeting several core objectives, individuals in private practice can earn as much as $44,000 over 5 years through the Medicare EHR incentive program and $63,750 over 6 years by participating in the Medicaid incentive program.3 Hospitals can earn more than $2 million over the same period. The objectives differ slightly for hospitals and individuals but are intended to improve quality, coordination, and safety of care while promoting patient involvement and public health.3
Related article: The Affordable Care Act and the drive for EHRs: Are small practices being squeezed? Lucia DiVenere, MD (July 2013)
The HITECH Act also sought to increase the security of EHRs to ensure patient privacy through standardization of EHR products. To become eligible for meaningful-use incentives, EHR software must meet government standards and specifications.3 Common requirements include the ability to document:
- vital signs
- test results
- all medications and allergies.
Another requirement is the ability to generate lists of patients with common conditions.3
By standardizing the EHR format, the HITECH Act improved networking by physicians by ensuring common capabilities among various EHR products.
The funding and standardization established by the HITECH Act increased the usage of EHRs among physicians to 57% by 2011.2
How did we get here? A history of the EHR
Computers and electronics originally were used for administrative purposes and did not offer meaningful clinical applications when they first were introduced to health care during the 1960s and 70s.8 These early machines were large, expensive, and slow and did not meet the practical needs of clinicians. During the 1980s and 90s, however, with networking capability and development of the World Wide Web, the potential for an electronic health record (EHR) became clearer. In 1991, an Institute of Medicine (IOM) report listed the “computer-based patient record” as “an essential technology for health care.”8 The authors of the IOM report envisioned a true network of practices and hospitals that seamlessly and efficiently share information and insight to increase quality of care, reduce medical errors, and improve patient safety.1
Despite advances in EHR technology, one major hurdle remained: cost. For many clinicians, the time and resources required for installation of the program, transfer of records to the electronic format, and training of staff was too high. By 2001, only 18% of physicians had incorporated the EHR.2 Today, nearly 60% of practices use an EHR.
Related article: EHRS and medicolegal risk: How they help, when they could hurt Martin Gimovsky, MD, and Baohuong N. Tran, DO (March 2013)
How to implement an EHR
The first step is to narrow your options to a few vendors that best suit the needs of your office. This process is beyond the scope of this article, but your ultimate objective should be to choose a user-friendly interface from a vendor that offers excellent document security, customer assistance, and support.4
Form an implementation team for your practice, and have it begin by consulting ObGyn practices of similar size that have recently installed one of the EHRs you are considering. By asking about other practices’ experiences and any pitfalls they encountered, you can greatly ease your transition to EHRs.
If possible, the physicians in your practice should visit the office of any colleagues who have implemented one of the EHRs you are considering to see how they like the product. Your office manager, nurses, and receptionist also should visit their counterparts in the other practice to ask about their experiences and opinions. The more information you glean from other ObGyn practices, the easier it will be to make your decision.
Be sure to check with your hospital to ensure compatibility with its system.
Ensure adequate technical support
One of the most important considerations in selecting a product is the availability and quality of tech support from the home office of the vendor. When you talk to other users of a product, ask how quickly tech support calls are returned and how efficiently problems are solved.
There will always be technical problems during the transition away from paper records. Ensuring their prompt resolution will be critical to your success.
Assign project management
After deciding on a particular product, create a project team to manage the complex, lengthy implementation process.4–6 This team should include a project manager who has the experience and skills to coordinate a complex plan, a well-respected product champion who can help maintain staff support for the change, and several information technology (IT) specialists who can manage the software and hardware challenges.4–6
Related article: What can "meaningful use" of an EHR mean for your bottom line? Robert L. Barbieri, MD (Editorial, February 2011)
Rally the troops
The most vital part of any implementation plan is staff “buy-in.”4–6 It is incumbent upon the project-management team to determine what effects EHR implementation will have on workflow and to explain to employees how the process ultimately will increase efficiency and reduce work time and cost. And the project champion must remind employees of these goals during the transition.4–6
Develop a backup system
Work with your IT staff to create a backup system for the EHR to protect against system malfunction.4 In the past, offices backed up their data to tapes or disks. Today, it probably is safer to back up to the cloud. Cloud computing, which allows for automatic back-up, is tightly regulated by HIPAA, so be sure to choose an approved vendor.7
Preload your data
Before going live with the EHR, data must be integrated and preloaded into the electronic format. This means integrating billing, lab results, orders, scheduling, and encounter templates into the EHR interface.4,6 When data are preloaded, employees can practice on the software before the launch date, ensuring a seamless transition.6
No “teeth-gnashing” necessary
The transition to an EHR system can be intimidating and may affect your staff’s productivity, efficiency, and morale. By following a few careful steps, the process can proceed without teeth-gnashing and loss of productivity. In fact, the suggestions offered here should improve productivity, office efficiency, and patient safety over the long term.
Who could ask for anything more?
We want to hear from you! Tell us what you think.
- Thakkar M, Davis DC. Risks, barriers, and benefits of EHR systems: a comparative study based on size of hospital. Perspect Health Inf Manag. 2006;3(5):1–19.
- Hsiao CJ, Hing E, Socey TC, et al. Electronic health record systems and intent to apply meaningful use incentives among office-based physician practices: United States, 2001–2011. NCHS Data Brief. 2011;(79):1–8.
- Terry NP. Anticipating stage two: assessing the development of meaningful use and EMR deployment. St. Louis University School of Law Legal Studies Research Paper Series. 2011;21.
- Keshavjee K, Bosomworth J, Copen J, et al. Best practices in EMR implementation: a systematic review. AMIA Annu Symp Proc. 2006;982.
- Lorenzi NM, Kouroubali A, Detmer DE, et al. How to successfully select and implement electronic health records (EHR) in small ambulatory practice settings. BMC Medical Informatics Decision Making. 2009;9(15):1–13.
- Smith PD. Implementing an EMR system: one clinic’s experience. Fam Pract Manag. 2003;10(5):37–42.
- Raheja D, Escano MC. Hazards in electronic medical records. J System Safety. 2010;46(4):1–4. http://system-safety.org/ejss/past/novdec2010ejss/pdf/health.pdf. Accessed October 8, 2013.
- Berner ES, Detmer DE, Simborg D. Will the wave finally break? A brief view of the adoption of electronic medical records in the United States. J Am Med Inform Assoc. 2005;12(1):3–7.
- Thakkar M, Davis DC. Risks, barriers, and benefits of EHR systems: a comparative study based on size of hospital. Perspect Health Inf Manag. 2006;3(5):1–19.
- Hsiao CJ, Hing E, Socey TC, et al. Electronic health record systems and intent to apply meaningful use incentives among office-based physician practices: United States, 2001–2011. NCHS Data Brief. 2011;(79):1–8.
- Terry NP. Anticipating stage two: assessing the development of meaningful use and EMR deployment. St. Louis University School of Law Legal Studies Research Paper Series. 2011;21.
- Keshavjee K, Bosomworth J, Copen J, et al. Best practices in EMR implementation: a systematic review. AMIA Annu Symp Proc. 2006;982.
- Lorenzi NM, Kouroubali A, Detmer DE, et al. How to successfully select and implement electronic health records (EHR) in small ambulatory practice settings. BMC Medical Informatics Decision Making. 2009;9(15):1–13.
- Smith PD. Implementing an EMR system: one clinic’s experience. Fam Pract Manag. 2003;10(5):37–42.
- Raheja D, Escano MC. Hazards in electronic medical records. J System Safety. 2010;46(4):1–4. http://system-safety.org/ejss/past/novdec2010ejss/pdf/health.pdf. Accessed October 8, 2013.
- Berner ES, Detmer DE, Simborg D. Will the wave finally break? A brief view of the adoption of electronic medical records in the United States. J Am Med Inform Assoc. 2005;12(1):3–7.
