User login
Reimbursement Readiness

Doctors shouldn’t have to worry about financial issues. The welfare of our patients should be our only concern.
We should be able to devote our full attention to studying how best to serve the needs of the people we care for. We shouldn’t need to spend time learning about healthcare reform or things like ICD-9 (or ICD-10!)—things that don’t help us provide better care to patients.
But these are pie-in-the-sky dreams. As far as I can tell, all healthcare systems require caregivers to attend to economics and data management that aren’t directly tied to clinical care. Our system depends on all caregivers devoting some time to learn how the system is organized, and keeping up with how it evolves. And the crisis in runaway costs in U.S. healthcare only increases the need for all who work in healthcare to devote significant time (too much) to the operational (nonclinical side) of healthcare.
Hospitalist practice is a much simpler business to manage and operate than most forms of clinical practice. There usually is no building to rent, few nonclinical employees to manage, and a comparatively simple financial model. And if employed by a hospital or other large entity, nonclinicians handle most of the “business management.” So when it comes to the number of brain cells diverted to business rather than clinical concerns, hospitalists start with an advantage over most other specialties.
Still, we have a lot of nonclinical stuff to keep up with. Consider the concept of “managing to Medicare reimbursement.” This means managing a practice or hospital in a way that minimizes the failure to capture all appropriate Medicare reimbursement dollars. Even if you’ve never heard of this concept before, there are probably a lot of people at your hospital who have this as their main responsibility, and clinicians should know something about it.
So in an effort to distract the fewest brain cells away from clinical matters, here is a very simple overview of some components of managing to Medicare reimbursement relevant to hospitalists. This isn’t a comprehensive list, only some hospitalist-relevant highlights.
Medicare Reimbursement Today
Accurate determination of inpatient vs. observation status. Wow, this can get complicated. Most hospitals have people who devote significant time to doing this for patients every day, and even those experts sometimes disagree on the appropriate status. But all hospitalists should have a basic understanding of how this works and a willingness to answer questions from the hospital’s experts, and, when appropriate, write additional information in the chart to clarify the appropriate status.
Optimal resource utilization, including length of stay. Because Medicare pays an essentially fixed amount based on the diagnoses for each inpatient admission, managing costs is critical to a hospital’s financial well-being. Hospitalists have a huge role in this. And regardless of how Medicare reimburses for services, there is clinical rationale for being careful about resources used and how long someone stays in a hospital. In many cases, more is not better—and it even could be worse—for the patient.
Optimal clinical documentation and accurate DRG assignment. Good documentation is important for clinical care, but beyond that, the precise way things are documented can have significant influence on Medicare reimbursement. Low potassium might in some cases lead to higher reimbursement, but a doctor must write “hypokalemia”; simply writing K+ means the hospital can’t include hypokalemia as a diagnosis. (A doctor, nurse practitioner, or physician assistant must write out “hypokalemia” only once for Medicare purposes; it would then be fine to use K+ in the chart every other time.)
Say you have a patient with a UTI and sepsis. Write only “urosepsis,” and the hospital must bill for cystitis—low reimbursement. Write “urinary tract infection with sepsis,” and the hospital can bill for higher reimbursement.
There should be people at your hospital who are experts at this, and all hospitalists should work with them to learn appropriate documentation language to describe illnesses correctly for billing purposes. Many hospitals use a system of “DRG queries,” which hospitalists should always respond to (though they should agree with the issue raised, such as “was the pneumonia likely due to aspiration?” only when clinically appropriate).
Change Is Coming
Don’t make the mistake of thinking Medicare reimbursement is a static phenomenon. It is undergoing rapid and significant evolution. For example, the Affordable Care Act, aka healthcare reform legislation, provides for a number of changes hospitalists need to understand.
I suggest that you make sure to understand your hospital’s or medical group’s position on accountable-care organizations (ACOs). It is a pretty complicated program that, in the first few years, has modest impact on reimbursement. If the ACO performs well, the additional reimbursement to an organization might pay for little more than the staff salaries of the staff that managed the considerable complexity of enrolling in and reporting for the program. And there is a risk the organization could lose money if it doesn’t perform well. So many organizations have decided not to pursue participation as an ACO, but they may decide to put in place most of the elements of an ACO without enrolling in the program. Some refer to this as an “aco” rather than an “ACO.”
Value-based purchasing (VBP) is set to influence hospital reimbursement rates starting in 2013 based on a hospital’s performance in 2012. SHM has a terrific VBP toolkit available online.
Bundled payments and financial penalties for readmissions also take effect in 2013. Now is the time ensure that you understand the implications of these programs; they are designed so that the financial impact to most organizations will be modest.
Reimbursement penalties for a specified list of hospital-acquired conditions (HACs) will begin in 2015. Conditions most relevant for hospitalists include vascular catheter-related bloodstream infections, catheter-related urinary infection, or manifestations of poor glycemic control (HONK, DKA, hypo-/hyperglycemia).
I plan to address some of these programs in greater detail in future practice management columns.
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Doctors shouldn’t have to worry about financial issues. The welfare of our patients should be our only concern.
We should be able to devote our full attention to studying how best to serve the needs of the people we care for. We shouldn’t need to spend time learning about healthcare reform or things like ICD-9 (or ICD-10!)—things that don’t help us provide better care to patients.
But these are pie-in-the-sky dreams. As far as I can tell, all healthcare systems require caregivers to attend to economics and data management that aren’t directly tied to clinical care. Our system depends on all caregivers devoting some time to learn how the system is organized, and keeping up with how it evolves. And the crisis in runaway costs in U.S. healthcare only increases the need for all who work in healthcare to devote significant time (too much) to the operational (nonclinical side) of healthcare.
Hospitalist practice is a much simpler business to manage and operate than most forms of clinical practice. There usually is no building to rent, few nonclinical employees to manage, and a comparatively simple financial model. And if employed by a hospital or other large entity, nonclinicians handle most of the “business management.” So when it comes to the number of brain cells diverted to business rather than clinical concerns, hospitalists start with an advantage over most other specialties.
Still, we have a lot of nonclinical stuff to keep up with. Consider the concept of “managing to Medicare reimbursement.” This means managing a practice or hospital in a way that minimizes the failure to capture all appropriate Medicare reimbursement dollars. Even if you’ve never heard of this concept before, there are probably a lot of people at your hospital who have this as their main responsibility, and clinicians should know something about it.
So in an effort to distract the fewest brain cells away from clinical matters, here is a very simple overview of some components of managing to Medicare reimbursement relevant to hospitalists. This isn’t a comprehensive list, only some hospitalist-relevant highlights.
Medicare Reimbursement Today
Accurate determination of inpatient vs. observation status. Wow, this can get complicated. Most hospitals have people who devote significant time to doing this for patients every day, and even those experts sometimes disagree on the appropriate status. But all hospitalists should have a basic understanding of how this works and a willingness to answer questions from the hospital’s experts, and, when appropriate, write additional information in the chart to clarify the appropriate status.
Optimal resource utilization, including length of stay. Because Medicare pays an essentially fixed amount based on the diagnoses for each inpatient admission, managing costs is critical to a hospital’s financial well-being. Hospitalists have a huge role in this. And regardless of how Medicare reimburses for services, there is clinical rationale for being careful about resources used and how long someone stays in a hospital. In many cases, more is not better—and it even could be worse—for the patient.
Optimal clinical documentation and accurate DRG assignment. Good documentation is important for clinical care, but beyond that, the precise way things are documented can have significant influence on Medicare reimbursement. Low potassium might in some cases lead to higher reimbursement, but a doctor must write “hypokalemia”; simply writing K+ means the hospital can’t include hypokalemia as a diagnosis. (A doctor, nurse practitioner, or physician assistant must write out “hypokalemia” only once for Medicare purposes; it would then be fine to use K+ in the chart every other time.)
Say you have a patient with a UTI and sepsis. Write only “urosepsis,” and the hospital must bill for cystitis—low reimbursement. Write “urinary tract infection with sepsis,” and the hospital can bill for higher reimbursement.
There should be people at your hospital who are experts at this, and all hospitalists should work with them to learn appropriate documentation language to describe illnesses correctly for billing purposes. Many hospitals use a system of “DRG queries,” which hospitalists should always respond to (though they should agree with the issue raised, such as “was the pneumonia likely due to aspiration?” only when clinically appropriate).
Change Is Coming
Don’t make the mistake of thinking Medicare reimbursement is a static phenomenon. It is undergoing rapid and significant evolution. For example, the Affordable Care Act, aka healthcare reform legislation, provides for a number of changes hospitalists need to understand.
I suggest that you make sure to understand your hospital’s or medical group’s position on accountable-care organizations (ACOs). It is a pretty complicated program that, in the first few years, has modest impact on reimbursement. If the ACO performs well, the additional reimbursement to an organization might pay for little more than the staff salaries of the staff that managed the considerable complexity of enrolling in and reporting for the program. And there is a risk the organization could lose money if it doesn’t perform well. So many organizations have decided not to pursue participation as an ACO, but they may decide to put in place most of the elements of an ACO without enrolling in the program. Some refer to this as an “aco” rather than an “ACO.”
Value-based purchasing (VBP) is set to influence hospital reimbursement rates starting in 2013 based on a hospital’s performance in 2012. SHM has a terrific VBP toolkit available online.
Bundled payments and financial penalties for readmissions also take effect in 2013. Now is the time ensure that you understand the implications of these programs; they are designed so that the financial impact to most organizations will be modest.
Reimbursement penalties for a specified list of hospital-acquired conditions (HACs) will begin in 2015. Conditions most relevant for hospitalists include vascular catheter-related bloodstream infections, catheter-related urinary infection, or manifestations of poor glycemic control (HONK, DKA, hypo-/hyperglycemia).
I plan to address some of these programs in greater detail in future practice management columns.
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Doctors shouldn’t have to worry about financial issues. The welfare of our patients should be our only concern.
We should be able to devote our full attention to studying how best to serve the needs of the people we care for. We shouldn’t need to spend time learning about healthcare reform or things like ICD-9 (or ICD-10!)—things that don’t help us provide better care to patients.
But these are pie-in-the-sky dreams. As far as I can tell, all healthcare systems require caregivers to attend to economics and data management that aren’t directly tied to clinical care. Our system depends on all caregivers devoting some time to learn how the system is organized, and keeping up with how it evolves. And the crisis in runaway costs in U.S. healthcare only increases the need for all who work in healthcare to devote significant time (too much) to the operational (nonclinical side) of healthcare.
Hospitalist practice is a much simpler business to manage and operate than most forms of clinical practice. There usually is no building to rent, few nonclinical employees to manage, and a comparatively simple financial model. And if employed by a hospital or other large entity, nonclinicians handle most of the “business management.” So when it comes to the number of brain cells diverted to business rather than clinical concerns, hospitalists start with an advantage over most other specialties.
Still, we have a lot of nonclinical stuff to keep up with. Consider the concept of “managing to Medicare reimbursement.” This means managing a practice or hospital in a way that minimizes the failure to capture all appropriate Medicare reimbursement dollars. Even if you’ve never heard of this concept before, there are probably a lot of people at your hospital who have this as their main responsibility, and clinicians should know something about it.
So in an effort to distract the fewest brain cells away from clinical matters, here is a very simple overview of some components of managing to Medicare reimbursement relevant to hospitalists. This isn’t a comprehensive list, only some hospitalist-relevant highlights.
Medicare Reimbursement Today
Accurate determination of inpatient vs. observation status. Wow, this can get complicated. Most hospitals have people who devote significant time to doing this for patients every day, and even those experts sometimes disagree on the appropriate status. But all hospitalists should have a basic understanding of how this works and a willingness to answer questions from the hospital’s experts, and, when appropriate, write additional information in the chart to clarify the appropriate status.
Optimal resource utilization, including length of stay. Because Medicare pays an essentially fixed amount based on the diagnoses for each inpatient admission, managing costs is critical to a hospital’s financial well-being. Hospitalists have a huge role in this. And regardless of how Medicare reimburses for services, there is clinical rationale for being careful about resources used and how long someone stays in a hospital. In many cases, more is not better—and it even could be worse—for the patient.
Optimal clinical documentation and accurate DRG assignment. Good documentation is important for clinical care, but beyond that, the precise way things are documented can have significant influence on Medicare reimbursement. Low potassium might in some cases lead to higher reimbursement, but a doctor must write “hypokalemia”; simply writing K+ means the hospital can’t include hypokalemia as a diagnosis. (A doctor, nurse practitioner, or physician assistant must write out “hypokalemia” only once for Medicare purposes; it would then be fine to use K+ in the chart every other time.)
Say you have a patient with a UTI and sepsis. Write only “urosepsis,” and the hospital must bill for cystitis—low reimbursement. Write “urinary tract infection with sepsis,” and the hospital can bill for higher reimbursement.
There should be people at your hospital who are experts at this, and all hospitalists should work with them to learn appropriate documentation language to describe illnesses correctly for billing purposes. Many hospitals use a system of “DRG queries,” which hospitalists should always respond to (though they should agree with the issue raised, such as “was the pneumonia likely due to aspiration?” only when clinically appropriate).
Change Is Coming
Don’t make the mistake of thinking Medicare reimbursement is a static phenomenon. It is undergoing rapid and significant evolution. For example, the Affordable Care Act, aka healthcare reform legislation, provides for a number of changes hospitalists need to understand.
I suggest that you make sure to understand your hospital’s or medical group’s position on accountable-care organizations (ACOs). It is a pretty complicated program that, in the first few years, has modest impact on reimbursement. If the ACO performs well, the additional reimbursement to an organization might pay for little more than the staff salaries of the staff that managed the considerable complexity of enrolling in and reporting for the program. And there is a risk the organization could lose money if it doesn’t perform well. So many organizations have decided not to pursue participation as an ACO, but they may decide to put in place most of the elements of an ACO without enrolling in the program. Some refer to this as an “aco” rather than an “ACO.”
Value-based purchasing (VBP) is set to influence hospital reimbursement rates starting in 2013 based on a hospital’s performance in 2012. SHM has a terrific VBP toolkit available online.
Bundled payments and financial penalties for readmissions also take effect in 2013. Now is the time ensure that you understand the implications of these programs; they are designed so that the financial impact to most organizations will be modest.
Reimbursement penalties for a specified list of hospital-acquired conditions (HACs) will begin in 2015. Conditions most relevant for hospitalists include vascular catheter-related bloodstream infections, catheter-related urinary infection, or manifestations of poor glycemic control (HONK, DKA, hypo-/hyperglycemia).
I plan to address some of these programs in greater detail in future practice management columns.
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Leadership, Experience, Quality Factor into HM Compensation Formula

Last month, we looked at the three main factors affecting workload variability across different HM practices and its relationship to compensation. This month we will examine how physician pay varies within a single site.
For the purposes of this discussion, we will ignore volume of encounters by physician. It goes without saying that if two physicians are working and producing an equal amount at the same site, their compensation will be similar. Outside of volume variability, then, what causes differences in compensation?
Leadership: This is a hugely important piece of the puzzle, and one that merits some attention. There always should be differential pay attached to those physicians willing to shoulder the leadership burden. In my honest opinion, local HM group leaders are horrifically, grotesquely, and shockingly underpaid. They tend to be very hard-working, almost servants to the other members of the group, and usually are vastly underappreciated.
Money isn’t necessarily the answer here; maybe the reward is a lighter schedule or lighter rounding load, but the bottom line is that there should be a substantial differential for leaders. Unfortunately, I think that still tends to be the exception rather than the rule. Hospitalist group leaders have a heck of a hard job trying to lead other physicians, and they should be paid accordingly.
At the same time, the best leaders are the ones that are still working a clinical schedule and, because of that, still understand the day-to-day demands of the job. I am always a bit skeptical of the folks who are in positions of power but aren’t experiencing the daily workload.
Experience: This is a little bit tricky. In their simplest form, physician practices tend to have partners and non-partners. The timeline from employment to partnership is about two to three years. Upon becoming partner, additional benefits accrue, generally in the form of higher compensation or the ability to work a reduced schedule.
However, “experience” prima facie will not vault one into the partnership level upon joining a new group. That experience only counts for the group you are in. (And the partner collections from the insurance payor system? No change in reimbursement. We have a payor system that, at this point, does not adequately recognize experience or quality. I always have fun trying to explain this to my friends outside of healthcare. They tend to just shake their head and sigh. Hopefully we can get somewhere new with value-based purchasing and ACOs.) Anyway, enough digressing...
Nights: A fair number of groups use a night shift model. These shifts, due to their timing, will generate a lower volume of encounters and require a commensurately higher pay. As a result, the inclusion of nocturnist compensation in a pay model will skew the numbers. In a practice with a large number of hospitals and night shifts, nocturnists are a sought-after commodity.
Quality: Here is where things are going to get interesting in the very near future. A lot of hospitalist groups have quality measures that play a part in compensation, but it’s mostly small numbers, maybe 10% of total compensation. These measures tend to be internal quality metrics for things like chart completion, citizenship, or meeting attendance. Now, with the Centers for Medicare & Medicaid Services (CMS) getting into the game, hospitals are starting to sit up and pay attention. That means administrators want hospitalists to pay attention, too. Exactly how data for each physician will be extracted from the group, which typically is extracted from the hospital as a whole, is a valid question. However, expect quality measures to persistently factor into the compensation equation.
The response I’ve laid out is meant to foster discussion, not serve as a final determination, and represents only one hospitalist’s view on the subject.
Last month, we looked at the three main factors affecting workload variability across different HM practices and its relationship to compensation. This month we will examine how physician pay varies within a single site.
For the purposes of this discussion, we will ignore volume of encounters by physician. It goes without saying that if two physicians are working and producing an equal amount at the same site, their compensation will be similar. Outside of volume variability, then, what causes differences in compensation?
Leadership: This is a hugely important piece of the puzzle, and one that merits some attention. There always should be differential pay attached to those physicians willing to shoulder the leadership burden. In my honest opinion, local HM group leaders are horrifically, grotesquely, and shockingly underpaid. They tend to be very hard-working, almost servants to the other members of the group, and usually are vastly underappreciated.
Money isn’t necessarily the answer here; maybe the reward is a lighter schedule or lighter rounding load, but the bottom line is that there should be a substantial differential for leaders. Unfortunately, I think that still tends to be the exception rather than the rule. Hospitalist group leaders have a heck of a hard job trying to lead other physicians, and they should be paid accordingly.
At the same time, the best leaders are the ones that are still working a clinical schedule and, because of that, still understand the day-to-day demands of the job. I am always a bit skeptical of the folks who are in positions of power but aren’t experiencing the daily workload.
Experience: This is a little bit tricky. In their simplest form, physician practices tend to have partners and non-partners. The timeline from employment to partnership is about two to three years. Upon becoming partner, additional benefits accrue, generally in the form of higher compensation or the ability to work a reduced schedule.
However, “experience” prima facie will not vault one into the partnership level upon joining a new group. That experience only counts for the group you are in. (And the partner collections from the insurance payor system? No change in reimbursement. We have a payor system that, at this point, does not adequately recognize experience or quality. I always have fun trying to explain this to my friends outside of healthcare. They tend to just shake their head and sigh. Hopefully we can get somewhere new with value-based purchasing and ACOs.) Anyway, enough digressing...
Nights: A fair number of groups use a night shift model. These shifts, due to their timing, will generate a lower volume of encounters and require a commensurately higher pay. As a result, the inclusion of nocturnist compensation in a pay model will skew the numbers. In a practice with a large number of hospitals and night shifts, nocturnists are a sought-after commodity.
Quality: Here is where things are going to get interesting in the very near future. A lot of hospitalist groups have quality measures that play a part in compensation, but it’s mostly small numbers, maybe 10% of total compensation. These measures tend to be internal quality metrics for things like chart completion, citizenship, or meeting attendance. Now, with the Centers for Medicare & Medicaid Services (CMS) getting into the game, hospitals are starting to sit up and pay attention. That means administrators want hospitalists to pay attention, too. Exactly how data for each physician will be extracted from the group, which typically is extracted from the hospital as a whole, is a valid question. However, expect quality measures to persistently factor into the compensation equation.
The response I’ve laid out is meant to foster discussion, not serve as a final determination, and represents only one hospitalist’s view on the subject.
Last month, we looked at the three main factors affecting workload variability across different HM practices and its relationship to compensation. This month we will examine how physician pay varies within a single site.
For the purposes of this discussion, we will ignore volume of encounters by physician. It goes without saying that if two physicians are working and producing an equal amount at the same site, their compensation will be similar. Outside of volume variability, then, what causes differences in compensation?
Leadership: This is a hugely important piece of the puzzle, and one that merits some attention. There always should be differential pay attached to those physicians willing to shoulder the leadership burden. In my honest opinion, local HM group leaders are horrifically, grotesquely, and shockingly underpaid. They tend to be very hard-working, almost servants to the other members of the group, and usually are vastly underappreciated.
Money isn’t necessarily the answer here; maybe the reward is a lighter schedule or lighter rounding load, but the bottom line is that there should be a substantial differential for leaders. Unfortunately, I think that still tends to be the exception rather than the rule. Hospitalist group leaders have a heck of a hard job trying to lead other physicians, and they should be paid accordingly.
At the same time, the best leaders are the ones that are still working a clinical schedule and, because of that, still understand the day-to-day demands of the job. I am always a bit skeptical of the folks who are in positions of power but aren’t experiencing the daily workload.
Experience: This is a little bit tricky. In their simplest form, physician practices tend to have partners and non-partners. The timeline from employment to partnership is about two to three years. Upon becoming partner, additional benefits accrue, generally in the form of higher compensation or the ability to work a reduced schedule.
However, “experience” prima facie will not vault one into the partnership level upon joining a new group. That experience only counts for the group you are in. (And the partner collections from the insurance payor system? No change in reimbursement. We have a payor system that, at this point, does not adequately recognize experience or quality. I always have fun trying to explain this to my friends outside of healthcare. They tend to just shake their head and sigh. Hopefully we can get somewhere new with value-based purchasing and ACOs.) Anyway, enough digressing...
Nights: A fair number of groups use a night shift model. These shifts, due to their timing, will generate a lower volume of encounters and require a commensurately higher pay. As a result, the inclusion of nocturnist compensation in a pay model will skew the numbers. In a practice with a large number of hospitals and night shifts, nocturnists are a sought-after commodity.
Quality: Here is where things are going to get interesting in the very near future. A lot of hospitalist groups have quality measures that play a part in compensation, but it’s mostly small numbers, maybe 10% of total compensation. These measures tend to be internal quality metrics for things like chart completion, citizenship, or meeting attendance. Now, with the Centers for Medicare & Medicaid Services (CMS) getting into the game, hospitals are starting to sit up and pay attention. That means administrators want hospitalists to pay attention, too. Exactly how data for each physician will be extracted from the group, which typically is extracted from the hospital as a whole, is a valid question. However, expect quality measures to persistently factor into the compensation equation.
The response I’ve laid out is meant to foster discussion, not serve as a final determination, and represents only one hospitalist’s view on the subject.
Managing Your Dermatology Practice: Employee Rewards
Another holiday season is here, and I’ll bet many of you – more than would probably admit – will be handing out the usual holiday bonuses to your employees.
I revive my complaint about this tired old tradition every few years because it remains so inexplicably entrenched and because it is such a good illustration of the definition of insanity: doing the same thing over and over, but expecting a different result.
Why are holiday bonuses so ineffective? Because doling out a predictable reward at the same time every year – consultants call it "jelly bean motivation" – is not only a poor motivator, but can actually have the opposite effect on excellent employees who see no appreciation or acknowledgement of their beyond-the-call performance. Why work your tail off when the slackers are getting the same "reward?" Even mediocre employees don’t see it as a reward; it becomes an entitlement – an expected, meaningless component of their normal compensation.
In "1001 Ways to Reward Employees" (Workman Publishing, 1994), Bob Nelson wrote: "While money is important to employees, what tends to motivate them to perform – and to perform at higher levels – is the thoughtful, personal kind of recognition that signifies true appreciation for a job well done."
He lists three simple guidelines for effectively rewarding employees:
• Match the reward to the individual. Reward each person in ways that each individual employee finds rewarding.
• Match the reward to the achievement. An employee who successfully completes a yearlong medical records reorganization deserves a more substantial reward than one who simply runs an errand for you.
• Be timely and specific. To be effective, rewards must be given as soon as possible after a specific laudable behavior or achievement, and the employee should always be told why he or she is receiving it. A reward coming weeks or months later, for no particular reason, is no reward at all.
So how do you know what rewards your employees will find rewarding? Ask them! I periodically solicit suggestions for non-monetary rewards from my staff. "I can’t give you money," I tell them, "but I’ll consider just about anything else."
Some of their ideas have been surprisingly creative – and cheap. For example, my employees are required to park their cars each day on the other side of the hospital campus from my office building. One of them suggested that a closer parking space would be a good reward. So I obtained an extra access card for the doctors’ lot right next to my building, and each month one "Employee of the Month" gets to park there. This reward – which costs me nothing – has become the most hotly contested in the office.
A lot of good rewards cost little or nothing. As Bob Nelson put it, "A sincere word of thanks from the right person at the right time can mean more to an employee than a raise, a formal award, or a whole wall of certificates or plaques." One of the strongest motivators is the confidence that you, the boss, will take the time to notice a job well done and praise it publicly, in a timely manner.
Time off is another powerful motivator; who (including you) doesn’t appreciate a bit more free time?
Michael LeBoeuf, author of "The Greatest Management Principle in the World" (Putnam, 1985), recommended assigning deadlines to specific tasks; if the task is finished ahead of deadline, the extra time is the employee’s reward. Or each time a deadline is met, give a predetermined amount of time off as the reward. Or set up a scoring system in which employees earn an hour off for a specified period of productive work. When they have earned 4 hours they can have a half day off; 8 hours earns a day off, and so on.
LeBoeuf's greatest management principle is: "The things that get rewarded get done." Psychology 101, remember?
Creative reward options are abundant and easily found; a fast Internet search will give you plenty of ideas. Virtually anything you choose, if given with sincerity, will yield far better results than holiday bonuses and other empty gestures tossed out in a thoughtless manner for no particular reason.
Another holiday season is here, and I’ll bet many of you – more than would probably admit – will be handing out the usual holiday bonuses to your employees.
I revive my complaint about this tired old tradition every few years because it remains so inexplicably entrenched and because it is such a good illustration of the definition of insanity: doing the same thing over and over, but expecting a different result.
Why are holiday bonuses so ineffective? Because doling out a predictable reward at the same time every year – consultants call it "jelly bean motivation" – is not only a poor motivator, but can actually have the opposite effect on excellent employees who see no appreciation or acknowledgement of their beyond-the-call performance. Why work your tail off when the slackers are getting the same "reward?" Even mediocre employees don’t see it as a reward; it becomes an entitlement – an expected, meaningless component of their normal compensation.
In "1001 Ways to Reward Employees" (Workman Publishing, 1994), Bob Nelson wrote: "While money is important to employees, what tends to motivate them to perform – and to perform at higher levels – is the thoughtful, personal kind of recognition that signifies true appreciation for a job well done."
He lists three simple guidelines for effectively rewarding employees:
• Match the reward to the individual. Reward each person in ways that each individual employee finds rewarding.
• Match the reward to the achievement. An employee who successfully completes a yearlong medical records reorganization deserves a more substantial reward than one who simply runs an errand for you.
• Be timely and specific. To be effective, rewards must be given as soon as possible after a specific laudable behavior or achievement, and the employee should always be told why he or she is receiving it. A reward coming weeks or months later, for no particular reason, is no reward at all.
So how do you know what rewards your employees will find rewarding? Ask them! I periodically solicit suggestions for non-monetary rewards from my staff. "I can’t give you money," I tell them, "but I’ll consider just about anything else."
Some of their ideas have been surprisingly creative – and cheap. For example, my employees are required to park their cars each day on the other side of the hospital campus from my office building. One of them suggested that a closer parking space would be a good reward. So I obtained an extra access card for the doctors’ lot right next to my building, and each month one "Employee of the Month" gets to park there. This reward – which costs me nothing – has become the most hotly contested in the office.
A lot of good rewards cost little or nothing. As Bob Nelson put it, "A sincere word of thanks from the right person at the right time can mean more to an employee than a raise, a formal award, or a whole wall of certificates or plaques." One of the strongest motivators is the confidence that you, the boss, will take the time to notice a job well done and praise it publicly, in a timely manner.
Time off is another powerful motivator; who (including you) doesn’t appreciate a bit more free time?
Michael LeBoeuf, author of "The Greatest Management Principle in the World" (Putnam, 1985), recommended assigning deadlines to specific tasks; if the task is finished ahead of deadline, the extra time is the employee’s reward. Or each time a deadline is met, give a predetermined amount of time off as the reward. Or set up a scoring system in which employees earn an hour off for a specified period of productive work. When they have earned 4 hours they can have a half day off; 8 hours earns a day off, and so on.
LeBoeuf's greatest management principle is: "The things that get rewarded get done." Psychology 101, remember?
Creative reward options are abundant and easily found; a fast Internet search will give you plenty of ideas. Virtually anything you choose, if given with sincerity, will yield far better results than holiday bonuses and other empty gestures tossed out in a thoughtless manner for no particular reason.
Another holiday season is here, and I’ll bet many of you – more than would probably admit – will be handing out the usual holiday bonuses to your employees.
I revive my complaint about this tired old tradition every few years because it remains so inexplicably entrenched and because it is such a good illustration of the definition of insanity: doing the same thing over and over, but expecting a different result.
Why are holiday bonuses so ineffective? Because doling out a predictable reward at the same time every year – consultants call it "jelly bean motivation" – is not only a poor motivator, but can actually have the opposite effect on excellent employees who see no appreciation or acknowledgement of their beyond-the-call performance. Why work your tail off when the slackers are getting the same "reward?" Even mediocre employees don’t see it as a reward; it becomes an entitlement – an expected, meaningless component of their normal compensation.
In "1001 Ways to Reward Employees" (Workman Publishing, 1994), Bob Nelson wrote: "While money is important to employees, what tends to motivate them to perform – and to perform at higher levels – is the thoughtful, personal kind of recognition that signifies true appreciation for a job well done."
He lists three simple guidelines for effectively rewarding employees:
• Match the reward to the individual. Reward each person in ways that each individual employee finds rewarding.
• Match the reward to the achievement. An employee who successfully completes a yearlong medical records reorganization deserves a more substantial reward than one who simply runs an errand for you.
• Be timely and specific. To be effective, rewards must be given as soon as possible after a specific laudable behavior or achievement, and the employee should always be told why he or she is receiving it. A reward coming weeks or months later, for no particular reason, is no reward at all.
So how do you know what rewards your employees will find rewarding? Ask them! I periodically solicit suggestions for non-monetary rewards from my staff. "I can’t give you money," I tell them, "but I’ll consider just about anything else."
Some of their ideas have been surprisingly creative – and cheap. For example, my employees are required to park their cars each day on the other side of the hospital campus from my office building. One of them suggested that a closer parking space would be a good reward. So I obtained an extra access card for the doctors’ lot right next to my building, and each month one "Employee of the Month" gets to park there. This reward – which costs me nothing – has become the most hotly contested in the office.
A lot of good rewards cost little or nothing. As Bob Nelson put it, "A sincere word of thanks from the right person at the right time can mean more to an employee than a raise, a formal award, or a whole wall of certificates or plaques." One of the strongest motivators is the confidence that you, the boss, will take the time to notice a job well done and praise it publicly, in a timely manner.
Time off is another powerful motivator; who (including you) doesn’t appreciate a bit more free time?
Michael LeBoeuf, author of "The Greatest Management Principle in the World" (Putnam, 1985), recommended assigning deadlines to specific tasks; if the task is finished ahead of deadline, the extra time is the employee’s reward. Or each time a deadline is met, give a predetermined amount of time off as the reward. Or set up a scoring system in which employees earn an hour off for a specified period of productive work. When they have earned 4 hours they can have a half day off; 8 hours earns a day off, and so on.
LeBoeuf's greatest management principle is: "The things that get rewarded get done." Psychology 101, remember?
Creative reward options are abundant and easily found; a fast Internet search will give you plenty of ideas. Virtually anything you choose, if given with sincerity, will yield far better results than holiday bonuses and other empty gestures tossed out in a thoughtless manner for no particular reason.
Had C difficile cleared before chemotherapy? ... and more

THE DIAGNOSIS WAS BREAST CANCER for a 54-year-old woman. In May 2006, a surgeon performed a mastectomy and prescribed postoperative antibiotics.
In July, the patient became ill and was treated for Clostridium difficile infection. She began a course of chemotherapy in August, after telling her oncologist about the earlier infection. The patient later developed acute colitis and underwent emergency colectomy. She has a permanent ileostomy, has had 14 additional operations, and continues to suffer complications of severe colitis.
PATIENT’S CLAIM The surgeon was at fault for prescribing antibiotics after mastectomy. The oncologist was negligent in failing to test for C difficile before starting chemotherapy. The antibiotics caused C difficile infection. Because her immune system was compromised by chemotherapy, C difficile caused colitis.
PHYSICIANS’ DEFENSE The surgeon’s defense was not reported. The oncologist claimed he was not negligent; he questioned whether the patient had C difficile infection at all.
VERDICT The surgeon settled for an undisclosed amount before trial. A $4.5 million Oklahoma verdict was returned against the oncologist.
Uterine rupture and placental abruption found at C-section
A WOMAN WAS IN ACTIVE LABOR at 41 weeks’ gestation when admitted to the hospital. After 9 hours of labor, cesarean delivery was performed because the fetal heart-rate tracing showed tachycardia, with potential fetal distress.
At delivery, it was discovered that the uterus had ruptured and the placenta had abrupted. The child was asphyxic and bradycardic at birth. She suffered brain damage that resulted in severe cognitive deficits and cerebral palsy. At 5 years, she is unable to speak, walk, sit up, or feed herself.
PATIENT’S CLAIM Although the fetal heart-rate tracing showed fetal distress, several hours passed before cesarean delivery was performed. Oxytocin should not have been administered during labor because the drug is contraindicated in the presence of an abnormal fetal heart rate.
DEFENDANTS’ DEFENSE Hospital physicians and staff reacted properly and in a timely manner when the heart-rate tracing showed fetal distress. Uterine rupture and placental abruption could not have been foreseen.
VERDICT A $5.8 million Texas settlement was reached.
Fibrocystic mass becomes cancerous
A WOMAN UNDERWENT regular annual breast exams because of fibrocystic breast disease. Her primary care physician noted a breast mass in 1997, and continued to follow the mass. A biopsy in 1999 revealed fibrosis. In January 2002, breast cancer was diagnosed in the same mass, and the woman underwent mastectomy.
PATIENT’S CLAIM The physician was negligent in failing to diagnose breast cancer earlier. She had classic signs of cancer, including a persistent mass with changing symptoms.
PHYSICIAN’S DEFENSE The mass had been closely monitored, so that when changes were noted in December 2001, a referral was made and cancer diagnosed.
VERDICT A Louisiana defense verdict was returned.
Was mother’s labor monitored properly?
DURING DELIVERY, a woman experienced vaginal bleeding without pain or contractions. The nurses did not consider the bleeding excessive and did not detect any urgency to her labor until several hours later. The baby did not survive, and it was determined the mother suffered from vasa previa. She had been given a diagnosis of placenta previa at 15 weeks, but a sonogram at 20 weeks showed resolution.
PATIENT’S CLAIM The mother’s condition should have been monitored more closely. Vaginal bleeding during labor and delivery should have been responded to more urgently, given the history of placenta previa.
DEFENDANTS’ DEFENSE The hospital and the nurses claimed that the woman was properly treated.
VERDICT An Alabama defense verdict was returned.
Heart attack and death after epidural
AT AGE 34, A WOMAN WENT to the hospital for cesarean delivery of her third child. Within minutes of receiving epidural anesthesia, she became agitated and complained of difficulty breathing. She went into cardiopulmonary arrest, and resuscitation efforts were unsuccessful. The child survived.
ESTATE’S CLAIM A total spinal block occurred; the anesthesiologist failed to recognize and treat it in a timely manner.
PHYSICIAN’S DEFENSE Medications were properly administered; a total spinal block had not occurred. The patient had a history of Hodgkin’s lymphoma with chemotherapy, and radiation treatment of the chest. Autopsy indicated the cause of death was Castleman’s disease, a rare lymphoproliferative disease, which had not been diagnosed during her life.
VERDICT A $800,000 Virginia verdict was returned.
Retained sponge causes obstruction
AFTER CESAREAN DELIVERY, the nurses reported a complete sponge count. Immediately after surgery, the mother reported lower-left quadrant pain that resolved, then recurred. Several complaints to her ObGyn were dismissed. After 2.5 months, the ObGyn referred the patient to her primary care physician. An abdominal CT scan revealed a retained surgical sponge, with bowel perforation. The ObGyn attempted surgery, but the sponge was partially adhered to bowel. Colorectal surgeons had to resect two sections of small intestine to remove the infected sponge and abscess. She continues to have medical problems and has been hospitalized for an obstruction.
PATIENT’S CLAIM The nurses were negligent in failing to correctly count the sponges. The ObGyn was negligent for leaving the sponge in the patient’s abdomen, and for not responding to her complaints by determining the cause of her pain.
DEFENDANTS’ DEFENSE The nurses admitted liability but contended that the ObGyn was also at fault under the captain-of-the-ship doctrine. The ObGyn denied negligence, arguing that it was the nurses’ responsibility to count the sponges and that he acted properly by referring the patient to her primary care physician.
VERDICT The Pennsylvania jury found the hospital and nurses negligent and awarded a $525,000 verdict. A defense verdict was returned for the ObGyn.
Hypoxic ischemic encephalopathy
A WOMAN WENT TO THE HOSPITAL in labor. Her ObGyn was consulted by telephone at 10:20 pm. At 5:40 am, a positive scalp stimulation test indicated the fetus was healthy. The nurse called the ObGyn, who was en route to the hospital. At 6:04 am, the fetal heart rate dropped to 60 bpm. The nurse again contacted the ObGyn, and then called in a midwife, who took no effective action to complete delivery.
At 6:16 am, the covering physician was summoned, but the ObGyn arrived and took charge. When he saw that the fetal heart rate was still 60 bpm, he performed a central episiotomy and delivered the infant at 6:23 am using vacuum extraction. The infant suffered perinatal depression with hypoxic ischemic encephalopathy and brain damage.
PATIENT’S CLAIM The injuries were caused by continued low fetal heart rate. The hospital nurse, midwife, and covering physician were negligent in not reacting to the low fetal heart rate by performing emergency cesarean delivery. The ObGyn was negligent for not coming to the hospital earlier.
DEFENDANTS’ DEFENSE The hospital staff acted properly. The ObGyn was in touch with the hospital staff and came when labor became active. When he saw that the fetal heart rate was low, he saved the child’s life.
VERDICT A $7 million settlement was reached with the hospital; a defense verdict was returned for the ObGyn.
Incontinence or ovarian cancer?
A WOMAN IN HER 50s saw a urologist in November 2004 because of urinary incontinence. The urologist prescribed medication. During the next 2 years, there were additional examinations and treatment, but incontinence continued. In January 2007, a diagnosis of ovarian cancer was made. She died after the suit was filed.
ESTATE’S CLAIM Ovarian cancer should have been diagnosed in November 2004. The cancer could have been treated, and the patient would have survived. Incontinence is a symptom of that type of ovarian cancer.
PHYSICIAN’S DEFENSE The tests in November 2004 indicated that the decedent’s incontinence was from muscle weakness. Cancer did not develop until late 2006.
VERDICT A New York defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
THE DIAGNOSIS WAS BREAST CANCER for a 54-year-old woman. In May 2006, a surgeon performed a mastectomy and prescribed postoperative antibiotics.
In July, the patient became ill and was treated for Clostridium difficile infection. She began a course of chemotherapy in August, after telling her oncologist about the earlier infection. The patient later developed acute colitis and underwent emergency colectomy. She has a permanent ileostomy, has had 14 additional operations, and continues to suffer complications of severe colitis.
PATIENT’S CLAIM The surgeon was at fault for prescribing antibiotics after mastectomy. The oncologist was negligent in failing to test for C difficile before starting chemotherapy. The antibiotics caused C difficile infection. Because her immune system was compromised by chemotherapy, C difficile caused colitis.
PHYSICIANS’ DEFENSE The surgeon’s defense was not reported. The oncologist claimed he was not negligent; he questioned whether the patient had C difficile infection at all.
VERDICT The surgeon settled for an undisclosed amount before trial. A $4.5 million Oklahoma verdict was returned against the oncologist.
Uterine rupture and placental abruption found at C-section
A WOMAN WAS IN ACTIVE LABOR at 41 weeks’ gestation when admitted to the hospital. After 9 hours of labor, cesarean delivery was performed because the fetal heart-rate tracing showed tachycardia, with potential fetal distress.
At delivery, it was discovered that the uterus had ruptured and the placenta had abrupted. The child was asphyxic and bradycardic at birth. She suffered brain damage that resulted in severe cognitive deficits and cerebral palsy. At 5 years, she is unable to speak, walk, sit up, or feed herself.
PATIENT’S CLAIM Although the fetal heart-rate tracing showed fetal distress, several hours passed before cesarean delivery was performed. Oxytocin should not have been administered during labor because the drug is contraindicated in the presence of an abnormal fetal heart rate.
DEFENDANTS’ DEFENSE Hospital physicians and staff reacted properly and in a timely manner when the heart-rate tracing showed fetal distress. Uterine rupture and placental abruption could not have been foreseen.
VERDICT A $5.8 million Texas settlement was reached.
Fibrocystic mass becomes cancerous
A WOMAN UNDERWENT regular annual breast exams because of fibrocystic breast disease. Her primary care physician noted a breast mass in 1997, and continued to follow the mass. A biopsy in 1999 revealed fibrosis. In January 2002, breast cancer was diagnosed in the same mass, and the woman underwent mastectomy.
PATIENT’S CLAIM The physician was negligent in failing to diagnose breast cancer earlier. She had classic signs of cancer, including a persistent mass with changing symptoms.
PHYSICIAN’S DEFENSE The mass had been closely monitored, so that when changes were noted in December 2001, a referral was made and cancer diagnosed.
VERDICT A Louisiana defense verdict was returned.
Was mother’s labor monitored properly?
DURING DELIVERY, a woman experienced vaginal bleeding without pain or contractions. The nurses did not consider the bleeding excessive and did not detect any urgency to her labor until several hours later. The baby did not survive, and it was determined the mother suffered from vasa previa. She had been given a diagnosis of placenta previa at 15 weeks, but a sonogram at 20 weeks showed resolution.
PATIENT’S CLAIM The mother’s condition should have been monitored more closely. Vaginal bleeding during labor and delivery should have been responded to more urgently, given the history of placenta previa.
DEFENDANTS’ DEFENSE The hospital and the nurses claimed that the woman was properly treated.
VERDICT An Alabama defense verdict was returned.
Heart attack and death after epidural
AT AGE 34, A WOMAN WENT to the hospital for cesarean delivery of her third child. Within minutes of receiving epidural anesthesia, she became agitated and complained of difficulty breathing. She went into cardiopulmonary arrest, and resuscitation efforts were unsuccessful. The child survived.
ESTATE’S CLAIM A total spinal block occurred; the anesthesiologist failed to recognize and treat it in a timely manner.
PHYSICIAN’S DEFENSE Medications were properly administered; a total spinal block had not occurred. The patient had a history of Hodgkin’s lymphoma with chemotherapy, and radiation treatment of the chest. Autopsy indicated the cause of death was Castleman’s disease, a rare lymphoproliferative disease, which had not been diagnosed during her life.
VERDICT A $800,000 Virginia verdict was returned.
Retained sponge causes obstruction
AFTER CESAREAN DELIVERY, the nurses reported a complete sponge count. Immediately after surgery, the mother reported lower-left quadrant pain that resolved, then recurred. Several complaints to her ObGyn were dismissed. After 2.5 months, the ObGyn referred the patient to her primary care physician. An abdominal CT scan revealed a retained surgical sponge, with bowel perforation. The ObGyn attempted surgery, but the sponge was partially adhered to bowel. Colorectal surgeons had to resect two sections of small intestine to remove the infected sponge and abscess. She continues to have medical problems and has been hospitalized for an obstruction.
PATIENT’S CLAIM The nurses were negligent in failing to correctly count the sponges. The ObGyn was negligent for leaving the sponge in the patient’s abdomen, and for not responding to her complaints by determining the cause of her pain.
DEFENDANTS’ DEFENSE The nurses admitted liability but contended that the ObGyn was also at fault under the captain-of-the-ship doctrine. The ObGyn denied negligence, arguing that it was the nurses’ responsibility to count the sponges and that he acted properly by referring the patient to her primary care physician.
VERDICT The Pennsylvania jury found the hospital and nurses negligent and awarded a $525,000 verdict. A defense verdict was returned for the ObGyn.
Hypoxic ischemic encephalopathy
A WOMAN WENT TO THE HOSPITAL in labor. Her ObGyn was consulted by telephone at 10:20 pm. At 5:40 am, a positive scalp stimulation test indicated the fetus was healthy. The nurse called the ObGyn, who was en route to the hospital. At 6:04 am, the fetal heart rate dropped to 60 bpm. The nurse again contacted the ObGyn, and then called in a midwife, who took no effective action to complete delivery.
At 6:16 am, the covering physician was summoned, but the ObGyn arrived and took charge. When he saw that the fetal heart rate was still 60 bpm, he performed a central episiotomy and delivered the infant at 6:23 am using vacuum extraction. The infant suffered perinatal depression with hypoxic ischemic encephalopathy and brain damage.
PATIENT’S CLAIM The injuries were caused by continued low fetal heart rate. The hospital nurse, midwife, and covering physician were negligent in not reacting to the low fetal heart rate by performing emergency cesarean delivery. The ObGyn was negligent for not coming to the hospital earlier.
DEFENDANTS’ DEFENSE The hospital staff acted properly. The ObGyn was in touch with the hospital staff and came when labor became active. When he saw that the fetal heart rate was low, he saved the child’s life.
VERDICT A $7 million settlement was reached with the hospital; a defense verdict was returned for the ObGyn.
Incontinence or ovarian cancer?
A WOMAN IN HER 50s saw a urologist in November 2004 because of urinary incontinence. The urologist prescribed medication. During the next 2 years, there were additional examinations and treatment, but incontinence continued. In January 2007, a diagnosis of ovarian cancer was made. She died after the suit was filed.
ESTATE’S CLAIM Ovarian cancer should have been diagnosed in November 2004. The cancer could have been treated, and the patient would have survived. Incontinence is a symptom of that type of ovarian cancer.
PHYSICIAN’S DEFENSE The tests in November 2004 indicated that the decedent’s incontinence was from muscle weakness. Cancer did not develop until late 2006.
VERDICT A New York defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
THE DIAGNOSIS WAS BREAST CANCER for a 54-year-old woman. In May 2006, a surgeon performed a mastectomy and prescribed postoperative antibiotics.
In July, the patient became ill and was treated for Clostridium difficile infection. She began a course of chemotherapy in August, after telling her oncologist about the earlier infection. The patient later developed acute colitis and underwent emergency colectomy. She has a permanent ileostomy, has had 14 additional operations, and continues to suffer complications of severe colitis.
PATIENT’S CLAIM The surgeon was at fault for prescribing antibiotics after mastectomy. The oncologist was negligent in failing to test for C difficile before starting chemotherapy. The antibiotics caused C difficile infection. Because her immune system was compromised by chemotherapy, C difficile caused colitis.
PHYSICIANS’ DEFENSE The surgeon’s defense was not reported. The oncologist claimed he was not negligent; he questioned whether the patient had C difficile infection at all.
VERDICT The surgeon settled for an undisclosed amount before trial. A $4.5 million Oklahoma verdict was returned against the oncologist.
Uterine rupture and placental abruption found at C-section
A WOMAN WAS IN ACTIVE LABOR at 41 weeks’ gestation when admitted to the hospital. After 9 hours of labor, cesarean delivery was performed because the fetal heart-rate tracing showed tachycardia, with potential fetal distress.
At delivery, it was discovered that the uterus had ruptured and the placenta had abrupted. The child was asphyxic and bradycardic at birth. She suffered brain damage that resulted in severe cognitive deficits and cerebral palsy. At 5 years, she is unable to speak, walk, sit up, or feed herself.
PATIENT’S CLAIM Although the fetal heart-rate tracing showed fetal distress, several hours passed before cesarean delivery was performed. Oxytocin should not have been administered during labor because the drug is contraindicated in the presence of an abnormal fetal heart rate.
DEFENDANTS’ DEFENSE Hospital physicians and staff reacted properly and in a timely manner when the heart-rate tracing showed fetal distress. Uterine rupture and placental abruption could not have been foreseen.
VERDICT A $5.8 million Texas settlement was reached.
Fibrocystic mass becomes cancerous
A WOMAN UNDERWENT regular annual breast exams because of fibrocystic breast disease. Her primary care physician noted a breast mass in 1997, and continued to follow the mass. A biopsy in 1999 revealed fibrosis. In January 2002, breast cancer was diagnosed in the same mass, and the woman underwent mastectomy.
PATIENT’S CLAIM The physician was negligent in failing to diagnose breast cancer earlier. She had classic signs of cancer, including a persistent mass with changing symptoms.
PHYSICIAN’S DEFENSE The mass had been closely monitored, so that when changes were noted in December 2001, a referral was made and cancer diagnosed.
VERDICT A Louisiana defense verdict was returned.
Was mother’s labor monitored properly?
DURING DELIVERY, a woman experienced vaginal bleeding without pain or contractions. The nurses did not consider the bleeding excessive and did not detect any urgency to her labor until several hours later. The baby did not survive, and it was determined the mother suffered from vasa previa. She had been given a diagnosis of placenta previa at 15 weeks, but a sonogram at 20 weeks showed resolution.
PATIENT’S CLAIM The mother’s condition should have been monitored more closely. Vaginal bleeding during labor and delivery should have been responded to more urgently, given the history of placenta previa.
DEFENDANTS’ DEFENSE The hospital and the nurses claimed that the woman was properly treated.
VERDICT An Alabama defense verdict was returned.
Heart attack and death after epidural
AT AGE 34, A WOMAN WENT to the hospital for cesarean delivery of her third child. Within minutes of receiving epidural anesthesia, she became agitated and complained of difficulty breathing. She went into cardiopulmonary arrest, and resuscitation efforts were unsuccessful. The child survived.
ESTATE’S CLAIM A total spinal block occurred; the anesthesiologist failed to recognize and treat it in a timely manner.
PHYSICIAN’S DEFENSE Medications were properly administered; a total spinal block had not occurred. The patient had a history of Hodgkin’s lymphoma with chemotherapy, and radiation treatment of the chest. Autopsy indicated the cause of death was Castleman’s disease, a rare lymphoproliferative disease, which had not been diagnosed during her life.
VERDICT A $800,000 Virginia verdict was returned.
Retained sponge causes obstruction
AFTER CESAREAN DELIVERY, the nurses reported a complete sponge count. Immediately after surgery, the mother reported lower-left quadrant pain that resolved, then recurred. Several complaints to her ObGyn were dismissed. After 2.5 months, the ObGyn referred the patient to her primary care physician. An abdominal CT scan revealed a retained surgical sponge, with bowel perforation. The ObGyn attempted surgery, but the sponge was partially adhered to bowel. Colorectal surgeons had to resect two sections of small intestine to remove the infected sponge and abscess. She continues to have medical problems and has been hospitalized for an obstruction.
PATIENT’S CLAIM The nurses were negligent in failing to correctly count the sponges. The ObGyn was negligent for leaving the sponge in the patient’s abdomen, and for not responding to her complaints by determining the cause of her pain.
DEFENDANTS’ DEFENSE The nurses admitted liability but contended that the ObGyn was also at fault under the captain-of-the-ship doctrine. The ObGyn denied negligence, arguing that it was the nurses’ responsibility to count the sponges and that he acted properly by referring the patient to her primary care physician.
VERDICT The Pennsylvania jury found the hospital and nurses negligent and awarded a $525,000 verdict. A defense verdict was returned for the ObGyn.
Hypoxic ischemic encephalopathy
A WOMAN WENT TO THE HOSPITAL in labor. Her ObGyn was consulted by telephone at 10:20 pm. At 5:40 am, a positive scalp stimulation test indicated the fetus was healthy. The nurse called the ObGyn, who was en route to the hospital. At 6:04 am, the fetal heart rate dropped to 60 bpm. The nurse again contacted the ObGyn, and then called in a midwife, who took no effective action to complete delivery.
At 6:16 am, the covering physician was summoned, but the ObGyn arrived and took charge. When he saw that the fetal heart rate was still 60 bpm, he performed a central episiotomy and delivered the infant at 6:23 am using vacuum extraction. The infant suffered perinatal depression with hypoxic ischemic encephalopathy and brain damage.
PATIENT’S CLAIM The injuries were caused by continued low fetal heart rate. The hospital nurse, midwife, and covering physician were negligent in not reacting to the low fetal heart rate by performing emergency cesarean delivery. The ObGyn was negligent for not coming to the hospital earlier.
DEFENDANTS’ DEFENSE The hospital staff acted properly. The ObGyn was in touch with the hospital staff and came when labor became active. When he saw that the fetal heart rate was low, he saved the child’s life.
VERDICT A $7 million settlement was reached with the hospital; a defense verdict was returned for the ObGyn.
Incontinence or ovarian cancer?
A WOMAN IN HER 50s saw a urologist in November 2004 because of urinary incontinence. The urologist prescribed medication. During the next 2 years, there were additional examinations and treatment, but incontinence continued. In January 2007, a diagnosis of ovarian cancer was made. She died after the suit was filed.
ESTATE’S CLAIM Ovarian cancer should have been diagnosed in November 2004. The cancer could have been treated, and the patient would have survived. Incontinence is a symptom of that type of ovarian cancer.
PHYSICIAN’S DEFENSE The tests in November 2004 indicated that the decedent’s incontinence was from muscle weakness. Cancer did not develop until late 2006.
VERDICT A New York defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
We want to hear from you! Tell us what you think.
Why (and how) you should encourage your patients’ search for health information on the Web
CASE: The Internet has (at least) two faces
Both Patient A and Patient B are 8 weeks pregnant with their first baby. At an office visit, you discuss influenza vaccination.
Patient A tells you: “I was undecided about the vaccine until I read all these horror stories about the H1N1 vaccine. A Web site, organichealthadviser.com, says vaccines and pregnancies don’t mix safely.1 It says that if the flu vaccine isn’t safe for a baby less than 6 months old, how can it be safe during pregnancy?1 I read story after story of women who got the vaccine and miscarried. Why would I want to be injected with a toxin?”
Patient B explains: “I was undecided about the vaccine until I read the information on the Centers for Disease Control and Prevention (CDC) Web site.2 I didn’t know that pregnant women are more likely to get really sick from the flu. The CDC says the vaccine is safe during pregnancy, will not harm my baby, and not only reduces my chance of getting sick from the flu, but will give my baby protection for 6 months after she is born.2 When and where can I get my shot?”
Sixty-nine percent of Americans (80% of those who have Internet access) turn to the Web for information about their health care, and 23% of people who have a major medical illness or other health condition report that the Internet plays a major role in helping them deal with their health issue.3,4 They might research symptoms, diagnosis, tests, and therapies before a visit to your office; many come armed with questions, sometimes bringing reams of pages downloaded from various sites. Among women receiving ObGyn care, almost 60% have accessed Web-based information before their visit.5 Others take to the Internet after their appointment to confirm or refute what they have heard in the office.
Regardless of what a patient researches or when she does it, the why is because she wants to be an active participant in her medical care. That is a good thing because participatory medicine (shared decision-making) leads to improved outcomes. However, the key to truly informed decision-making is content: A patient can be fully empowered to participate in her health care only if she has information that is accurate, understandable, and current.
Web-based health information: Entirely factual?
Not only do patients research health online, 60% of people believe what they read to be factual and at least as good as the information they receive from you in your office. In fact, there is evidence that only 6% believe the health information they gather online is lacking in quality.5,6
However, studies reveal that the accuracy of medical content on the Web varies greatly from site to site. For example, among women seeking information on the Internet about potential teratogenic agents, 40% found incorrect information, some of which was potentially harmful.7
In addition to the problem of potentially suspect content, more than 50% of patients don’t disclose with you the information that they find online.7 Ever encounter a patient you just couldn’t sway from a diagnosis she believed she had but you knew she didn’t? If your patient tells you where she got the information, you can walk her through the diagnosis and treatment step by step, pointing out where her information might not be accurate (or, sometimes, even medically plausible)—but it’s hard to undo what you don’t know about.
The ideal scenario. Discuss Web-based information as part of your visit, thereby acknowledging that the Internet is a valid place to investigate personal health care. You can also preemptively provide tools for tracking down the most accurate and understandable content. See, for example, the patient handout.
Let’s face it: Physicians have an advantage when it comes to weeding out the wisdom from the woo. To supplement our baseline knowledge, we can easily research facts on PubMed, check our medical societies for guidelines, or, simply, ask a colleague. Our patients don’t have these same resources, but with some guidance from you, their Internet health experience can be greatly enhanced.
Are your searches on the Internet turning up reliable health advice? Watch for these 10 red flags of bad information
- Sensationalized content Is the information on the site presented in an alarmist tone? Is it loaded with scary stories and extreme outcomes? Are the issues presented in terms of black and white, with no shades of gray? If the answer to any of these questions is “Yes,” the author may have an axe to grind or a hidden leaning. Suspect the accuracy of the information you obtain!
- No date This may seem like a minor problem, but the world of health care moves swiftly. Treatments and approaches that are reliable one day can be discredited in the blink of an eye. If the site does not date its content, or indicate when it was last updated, you have no way of knowing how current it is. Move on!
- No author credentials The author or authors of material on the Web site should clearly, and visibly, present their credentials—that is, their education and training, their title, and where they work. If they do not, it is impossible to judge their expertise—in fact, expertise may be lacking.
- Buzz words The use of quasi-scientific buzz words such as “toxins,” “heavy metals,” and “detoxification” should draw your attention. These words have no meaning, so they should lead to you question what else on the site might be fiction.
- Patient testimonials Three people may have improved with a particular drug, but what about those who haven’t? Using unverified personal experiences is a sign of advertising, not good medicine.
- For sale sign If you can’t easily tell the difference between the medical content and products for sale, move along. Even when products don’t appear prominently, chances are that the bottom line of the Web site is profit, not education.
- All benefits and no risks Sites that have a stake in a particular treatment—be it monetary, emotional, or some other involvement—usually provide a lot of information on benefits but not so much about risks. Every treatment has risks.
- No sources When physicians scrutinize an article or study, they make it a point to check the list of sources at the end, to ensure that it contains legitimate information, such as reports from a medical journal or government publication. A Web site that presents detailed medical information without providing links to the references or comparable detail about the sources of that information is highly suspect.
- Conflict of interest Most reputable health sites not only provide information from experts, they list any so-called potential conflicts of interest that those experts may have. For example, if a medication made by XYZ Pharmaceuticals is recommended by Dr. Smith, who is also a consultant to XYZ, you should know. Articles and presentations at scientific meetings require these disclosures for a reason: Financial ties can produce bias.
- The Web site or product is listed on QuackWatch This Web site is dedicated to exposing unproven and scientifically questionable medical claims (http://www.quackwatch.com).
Where can you turn for help?
- An excellent starting place is the National Medical Library Web site at http://www.mlanet.org/resources/userguide.html, which provides resources for obtaining reliable health information.
- The National Library of Medicine and National Institutes of Health also provide an outstanding 16-minute lesson on how you can evaluate online health information. Find it at http://www.nlm.nih.gov/medlineplus/webeval/webeval.html.
- healthfinder.gov is a Web “encyclopedia” offering entries on more than 1,600 health topics.
© Copyright 2011 Quadrant HealthCom, Inc. This “Guide” may be reproduced by clinicians without permission or fee for single-copy distribution to patients. All other uses require the written permission of the publisher.
To obtain a PDF of this Patient Guide, click here .
Four tips for evaluating online content
Consider the source
The very first thing to consider is the domain name—e.g., “.gov,” “.org,” “.edu,” “.com,” or .anythingelse.
.gov sites are owned and maintained by the US government. From a medical standpoint, the .gov designation means that a site contains evidence-based information maintained by medical librarians that is written at a level that most people can read.
It’s a common misperception that the .org designation indicates a not-for-profit site that is therefore “looking out for the public’s best interest.” But anyone can purchase an .org domain. Even if a particular site really is administered by a not-for-profit organization, that status does not ensure that the content is of high quality.
.edu sites are affiliated with academic institutions.
.com and .anythingelse are, like .org, free for anyone to purchase.
Evidence-based medicine tells us that .gov sites are the most accurate for content—anything else is buyer beware (interestingly, .edu sites fared the worst in one study for accuracy).7,8 This doesn’t mean that sites that are not .gov have no value! On the contrary, non-governmental Web sites, blogs, and news articles are often the first place a search starts. That’s because current content, such as a new site, is more likely to feature prominently in a search engine response. But non-governmental sites do require an additional level of scrutiny. For example, in one study, only 55% of health information on news Web sites was medically accurate.8
Who is the author? Does she have financial ties or bias?
Think about who is running the Web site, why they are doing it, and what they are trying to achieve. Is the author a doctor, a health reporter, an advocate, or a drug company? The credentials of any physicians associated with the site should be listed as well as credentials and affiliations of authors, if they are non-physicians. Sites that list physician credentials tend to rate higher in accuracy of content.7
Talk with your patients about the importance of financial ties. The sponsor of the Web site should be listed (drug company, university, or a physician blogging without reimbursement). Bias and money go hand in hand, so be careful in evaluating whether the information provided favors the sponsor. If there are products for sale that are recommended by the medical content, bias is implied and, in my opinion, that site is not informational but commercial.
Bias can also be non-commercial, which is why authors of academic papers are not only supposed to report financial ties but also any real or perceived conflict of interest. This can be hard to discern at times, but the Web site should disclose why it exists. If the message is muddied by advertising and other commercial content, it’s best to just move along.
How current is the content?
We all know that new studies constantly reshape the way we practice (and sometimes guidelines from professional societies seem to change with the wind), and what is new quickly becomes out of date. The good and bad with online information is that it is always there. A permanent record is in many ways a good thing, but content from 2004 may not be applicable in 2011. This is a particular issue with news sites. They may report on a fascinating study in 2007, but if a retraction later appears or a new study refutes the findings, that information may not warrant an article on the Web. A good rule of thumb: Anything older than 2 years requires an additional level of scrutiny.
Be wary when the subject is complementary and alternative medicine
Online content related to complementary and alternative medicine (CAM) should be approached with a higher degree of caution. One study found that 25% of CAM sites presented information that could cause physical harm if acted upon, and almost all CAM sites omitted vital warnings, such as drug interactions, contraindications, and adverse reactions. The quality of CAM sites doesn’t improve even when they meet three or four of the JAMA benchmarks for information quality (see page 40).9 In one study of breast cancer sites, Web pages with CAM content were 15 times more likely to contain inaccurate content, compared with sites without CAM content.7

Instruments and tools for evaluating online content
Three tools are available to help patients and providers judge the quality of written online information:
Discern is a 16-question tool designed to assess the quality of online health information. You will find it at http://www.discern.org.uk/discern_instrument.php. I recommend that you mention this tool to patients, even if you are uncertain whether they will use it. Certainly, any patient wedded to what seems like questionable content from a specific Web site should be encouraged to evaluate the site using the Discern tool. In addition, if you have Web sites other than .gov sites that you like to share with patients, it might be wise to personally review them with Discern so that you can reaffirm that you are directing patients to reliable content rather than a quagmire of misinformation.10
The Health on the Net Foundation (HON) is an independent, seven-person, Geneva-based panel that evaluates accuracy of medical Web sites based on specific guiding principles. It can be accessed at http://www.hon.ch/. Web sites that meet these criteria are awarded seals of approval. Only one problem: Not all sites that carry the seal are compliant with HON, and sites that don’t carry the seal can nevertheless be complete and accurate.11,12
JAMA benchmarks are four disclosures intended to help ensure the quality of a Web site: authorship, references, conflict of interest, and currency of content. Some research suggests that sites that have three or four of the benchmarks are more likely to have accurate content, but there is also evidence to suggest that JAMA benchmarks may not always reliably identify inaccurate information.7,13
Recommend a mini-course
Because these tools may be difficult to use or unreliable at identifying quality content, I recommend that every patient spend time on the National Medical Library Web site learning how to look up information. The other benefit of this site is that it lists top 10 Web sites for content, so it is a great launching point for a multitude of searches. It can be found at http://www.mlanet.org/resources/userguide.html.
If the patient finds the information at this portal too dry, there is a fantastic 16-minute tutorial about evaluating online health information; it’s a service of the National Library of Medicine and the National Institutes of Health. I recommend that every provider do this tutorial. Why? So you can better educate yourself on how to use the Internet and so you can tell your patients how great it is. It’s available at http://www.nlm.nih.gov/medlineplus/webeval/webeval.html.
Take the bull by the horns
Discuss the Internet with every one of your patients. Specifically, ask if she has read any information online and, if she has, how it stacks up with what you have just discussed during her office visit. That’s what I do. Explain that accurate content is critical in health-care decisions, guide your patient to sites that are more likely to be accurate, and teach her how to maximize the Internet to enhance her health care.
In my experience, patients are thrilled to be pointed in the right direction.
We want to hear from you! Tell us what you think.
1. H1N1 vaccine and pregnancy. Organic Health Adviser. http://organichealthadviser.com/archives/h1n1-vaccine-and-pregnancy. Accessed November 12 2011.
2. Pregnant women and influenza. Centers for Disease Control and Prevention. http://www.cdc.gov/flu/protect/vaccine/pregnant.htm. Accessed November 12 2011.
3. Fox S. The social life of health information 2011. Pew Internet and American Life Project. http://pewresearch.org/pubs/1989/health-care-online-social-network-users. Accessed November 12, 2011.
4. Horrigan J, Rainie L. The Internet’s growing role in life’s major moments. Decision-making Communities, Health. Pew Internet and American Life Project. http://www.pewinternet.org/Reports/2006/The-Internets-Growing-Role-in-Lifes-Major-Moments.aspx. Accessed November 12, 2011.
5. Neelapala P, Duvvi SK, Kumar G, Kumar BN. Do gynaecology outpatients use the Internet to seek health information? A questionnaire survey. J Eval Clin Pract. 2008;14(2):300-304.
6. Diaz JA, Griffith RA, Ng JJ, Reinert SE, Friedmann PD, Moulton AW. Patients’ use of the Internet for medical information. J Gen Intern Med. 2001;17(3):180-185.
7. Bernstam EV, Walji MF, Sagaram S, Sagaram D, Johnson CW, Meric-Bernstam F. Commonly cited website quality criteria are not effective at identifying inaccurate online information about breast cancer. Cancer. 2008;112(6):1206-1213.
8. Scullard P, Peacock C, Davies P. Googling children’s health: reliability of medical information on the Internet. Arch Dis Child. 2010;95(8):580-582.
9. Walji M, Sagaram S, Sagaram D, et al. Efficacy of quality criteria to identify potentially harmful information: a cross-sectional survey of complementary and alternative medicine web sites. J Med Internet Res. 2004;6(2):e21.-
10. Charnock D, Shepperd S, Needham G, Gann R. Discern: an instrument for judging the quality of written consumer health information on treatment choices. J Epidemiol Community Health. 1999;53(2):105-111.
11. Hardwick JC, MacKenzie FM. Information contained in miscarriage-related websites and the predictive value of website scoring systems. Eur J Gynecol Reprod Biol. 2003;106(1):60-63.
12. Khazaal Y, Chatton A, Zullino D. HON label and Discern as content quality indicators of health-related websites [published online ahead of print May 2011]. Psychiatr Q. doi: 10.1007/s11126-011-9179-x.
13. Meric F, Bernstam EV, Mirza NQ, et al. Breast cancer on the world wide web: cross sectional survey of quality of information and popularity of websites. BMJ. 2002;324(7337):577-581.

Jennifer Gunter, MD
Dr. Gunter is an ObGyn in San Francisco. She is the author of The Preemie Primer: A Complete Guide for Parents of Premature Babies—from Birth through the Toddler Years and Beyond (Da Capo Press, 2010). Dr. Gunter blogs at http://www.drjengunter.com/ and you can find her on Twitter at @DrJenGunter.
Dr. Gunter reports no financial relationships relevant to this article.
Jennifer Gunter, MD
Dr. Gunter is an ObGyn in San Francisco. She is the author of The Preemie Primer: A Complete Guide for Parents of Premature Babies—from Birth through the Toddler Years and Beyond (Da Capo Press, 2010). Dr. Gunter blogs at http://www.drjengunter.com/ and you can find her on Twitter at @DrJenGunter.
Dr. Gunter reports no financial relationships relevant to this article.
Jennifer Gunter, MD
Dr. Gunter is an ObGyn in San Francisco. She is the author of The Preemie Primer: A Complete Guide for Parents of Premature Babies—from Birth through the Toddler Years and Beyond (Da Capo Press, 2010). Dr. Gunter blogs at http://www.drjengunter.com/ and you can find her on Twitter at @DrJenGunter.
Dr. Gunter reports no financial relationships relevant to this article.
CASE: The Internet has (at least) two faces
Both Patient A and Patient B are 8 weeks pregnant with their first baby. At an office visit, you discuss influenza vaccination.
Patient A tells you: “I was undecided about the vaccine until I read all these horror stories about the H1N1 vaccine. A Web site, organichealthadviser.com, says vaccines and pregnancies don’t mix safely.1 It says that if the flu vaccine isn’t safe for a baby less than 6 months old, how can it be safe during pregnancy?1 I read story after story of women who got the vaccine and miscarried. Why would I want to be injected with a toxin?”
Patient B explains: “I was undecided about the vaccine until I read the information on the Centers for Disease Control and Prevention (CDC) Web site.2 I didn’t know that pregnant women are more likely to get really sick from the flu. The CDC says the vaccine is safe during pregnancy, will not harm my baby, and not only reduces my chance of getting sick from the flu, but will give my baby protection for 6 months after she is born.2 When and where can I get my shot?”
Sixty-nine percent of Americans (80% of those who have Internet access) turn to the Web for information about their health care, and 23% of people who have a major medical illness or other health condition report that the Internet plays a major role in helping them deal with their health issue.3,4 They might research symptoms, diagnosis, tests, and therapies before a visit to your office; many come armed with questions, sometimes bringing reams of pages downloaded from various sites. Among women receiving ObGyn care, almost 60% have accessed Web-based information before their visit.5 Others take to the Internet after their appointment to confirm or refute what they have heard in the office.
Regardless of what a patient researches or when she does it, the why is because she wants to be an active participant in her medical care. That is a good thing because participatory medicine (shared decision-making) leads to improved outcomes. However, the key to truly informed decision-making is content: A patient can be fully empowered to participate in her health care only if she has information that is accurate, understandable, and current.
Web-based health information: Entirely factual?
Not only do patients research health online, 60% of people believe what they read to be factual and at least as good as the information they receive from you in your office. In fact, there is evidence that only 6% believe the health information they gather online is lacking in quality.5,6
However, studies reveal that the accuracy of medical content on the Web varies greatly from site to site. For example, among women seeking information on the Internet about potential teratogenic agents, 40% found incorrect information, some of which was potentially harmful.7
In addition to the problem of potentially suspect content, more than 50% of patients don’t disclose with you the information that they find online.7 Ever encounter a patient you just couldn’t sway from a diagnosis she believed she had but you knew she didn’t? If your patient tells you where she got the information, you can walk her through the diagnosis and treatment step by step, pointing out where her information might not be accurate (or, sometimes, even medically plausible)—but it’s hard to undo what you don’t know about.
The ideal scenario. Discuss Web-based information as part of your visit, thereby acknowledging that the Internet is a valid place to investigate personal health care. You can also preemptively provide tools for tracking down the most accurate and understandable content. See, for example, the patient handout.
Let’s face it: Physicians have an advantage when it comes to weeding out the wisdom from the woo. To supplement our baseline knowledge, we can easily research facts on PubMed, check our medical societies for guidelines, or, simply, ask a colleague. Our patients don’t have these same resources, but with some guidance from you, their Internet health experience can be greatly enhanced.
Are your searches on the Internet turning up reliable health advice? Watch for these 10 red flags of bad information
- Sensationalized content Is the information on the site presented in an alarmist tone? Is it loaded with scary stories and extreme outcomes? Are the issues presented in terms of black and white, with no shades of gray? If the answer to any of these questions is “Yes,” the author may have an axe to grind or a hidden leaning. Suspect the accuracy of the information you obtain!
- No date This may seem like a minor problem, but the world of health care moves swiftly. Treatments and approaches that are reliable one day can be discredited in the blink of an eye. If the site does not date its content, or indicate when it was last updated, you have no way of knowing how current it is. Move on!
- No author credentials The author or authors of material on the Web site should clearly, and visibly, present their credentials—that is, their education and training, their title, and where they work. If they do not, it is impossible to judge their expertise—in fact, expertise may be lacking.
- Buzz words The use of quasi-scientific buzz words such as “toxins,” “heavy metals,” and “detoxification” should draw your attention. These words have no meaning, so they should lead to you question what else on the site might be fiction.
- Patient testimonials Three people may have improved with a particular drug, but what about those who haven’t? Using unverified personal experiences is a sign of advertising, not good medicine.
- For sale sign If you can’t easily tell the difference between the medical content and products for sale, move along. Even when products don’t appear prominently, chances are that the bottom line of the Web site is profit, not education.
- All benefits and no risks Sites that have a stake in a particular treatment—be it monetary, emotional, or some other involvement—usually provide a lot of information on benefits but not so much about risks. Every treatment has risks.
- No sources When physicians scrutinize an article or study, they make it a point to check the list of sources at the end, to ensure that it contains legitimate information, such as reports from a medical journal or government publication. A Web site that presents detailed medical information without providing links to the references or comparable detail about the sources of that information is highly suspect.
- Conflict of interest Most reputable health sites not only provide information from experts, they list any so-called potential conflicts of interest that those experts may have. For example, if a medication made by XYZ Pharmaceuticals is recommended by Dr. Smith, who is also a consultant to XYZ, you should know. Articles and presentations at scientific meetings require these disclosures for a reason: Financial ties can produce bias.
- The Web site or product is listed on QuackWatch This Web site is dedicated to exposing unproven and scientifically questionable medical claims (http://www.quackwatch.com).
Where can you turn for help?
- An excellent starting place is the National Medical Library Web site at http://www.mlanet.org/resources/userguide.html, which provides resources for obtaining reliable health information.
- The National Library of Medicine and National Institutes of Health also provide an outstanding 16-minute lesson on how you can evaluate online health information. Find it at http://www.nlm.nih.gov/medlineplus/webeval/webeval.html.
- healthfinder.gov is a Web “encyclopedia” offering entries on more than 1,600 health topics.
© Copyright 2011 Quadrant HealthCom, Inc. This “Guide” may be reproduced by clinicians without permission or fee for single-copy distribution to patients. All other uses require the written permission of the publisher.
To obtain a PDF of this Patient Guide, click here .
Four tips for evaluating online content
Consider the source
The very first thing to consider is the domain name—e.g., “.gov,” “.org,” “.edu,” “.com,” or .anythingelse.
.gov sites are owned and maintained by the US government. From a medical standpoint, the .gov designation means that a site contains evidence-based information maintained by medical librarians that is written at a level that most people can read.
It’s a common misperception that the .org designation indicates a not-for-profit site that is therefore “looking out for the public’s best interest.” But anyone can purchase an .org domain. Even if a particular site really is administered by a not-for-profit organization, that status does not ensure that the content is of high quality.
.edu sites are affiliated with academic institutions.
.com and .anythingelse are, like .org, free for anyone to purchase.
Evidence-based medicine tells us that .gov sites are the most accurate for content—anything else is buyer beware (interestingly, .edu sites fared the worst in one study for accuracy).7,8 This doesn’t mean that sites that are not .gov have no value! On the contrary, non-governmental Web sites, blogs, and news articles are often the first place a search starts. That’s because current content, such as a new site, is more likely to feature prominently in a search engine response. But non-governmental sites do require an additional level of scrutiny. For example, in one study, only 55% of health information on news Web sites was medically accurate.8
Who is the author? Does she have financial ties or bias?
Think about who is running the Web site, why they are doing it, and what they are trying to achieve. Is the author a doctor, a health reporter, an advocate, or a drug company? The credentials of any physicians associated with the site should be listed as well as credentials and affiliations of authors, if they are non-physicians. Sites that list physician credentials tend to rate higher in accuracy of content.7
Talk with your patients about the importance of financial ties. The sponsor of the Web site should be listed (drug company, university, or a physician blogging without reimbursement). Bias and money go hand in hand, so be careful in evaluating whether the information provided favors the sponsor. If there are products for sale that are recommended by the medical content, bias is implied and, in my opinion, that site is not informational but commercial.
Bias can also be non-commercial, which is why authors of academic papers are not only supposed to report financial ties but also any real or perceived conflict of interest. This can be hard to discern at times, but the Web site should disclose why it exists. If the message is muddied by advertising and other commercial content, it’s best to just move along.
How current is the content?
We all know that new studies constantly reshape the way we practice (and sometimes guidelines from professional societies seem to change with the wind), and what is new quickly becomes out of date. The good and bad with online information is that it is always there. A permanent record is in many ways a good thing, but content from 2004 may not be applicable in 2011. This is a particular issue with news sites. They may report on a fascinating study in 2007, but if a retraction later appears or a new study refutes the findings, that information may not warrant an article on the Web. A good rule of thumb: Anything older than 2 years requires an additional level of scrutiny.
Be wary when the subject is complementary and alternative medicine
Online content related to complementary and alternative medicine (CAM) should be approached with a higher degree of caution. One study found that 25% of CAM sites presented information that could cause physical harm if acted upon, and almost all CAM sites omitted vital warnings, such as drug interactions, contraindications, and adverse reactions. The quality of CAM sites doesn’t improve even when they meet three or four of the JAMA benchmarks for information quality (see page 40).9 In one study of breast cancer sites, Web pages with CAM content were 15 times more likely to contain inaccurate content, compared with sites without CAM content.7
Instruments and tools for evaluating online content
Three tools are available to help patients and providers judge the quality of written online information:
Discern is a 16-question tool designed to assess the quality of online health information. You will find it at http://www.discern.org.uk/discern_instrument.php. I recommend that you mention this tool to patients, even if you are uncertain whether they will use it. Certainly, any patient wedded to what seems like questionable content from a specific Web site should be encouraged to evaluate the site using the Discern tool. In addition, if you have Web sites other than .gov sites that you like to share with patients, it might be wise to personally review them with Discern so that you can reaffirm that you are directing patients to reliable content rather than a quagmire of misinformation.10
The Health on the Net Foundation (HON) is an independent, seven-person, Geneva-based panel that evaluates accuracy of medical Web sites based on specific guiding principles. It can be accessed at http://www.hon.ch/. Web sites that meet these criteria are awarded seals of approval. Only one problem: Not all sites that carry the seal are compliant with HON, and sites that don’t carry the seal can nevertheless be complete and accurate.11,12
JAMA benchmarks are four disclosures intended to help ensure the quality of a Web site: authorship, references, conflict of interest, and currency of content. Some research suggests that sites that have three or four of the benchmarks are more likely to have accurate content, but there is also evidence to suggest that JAMA benchmarks may not always reliably identify inaccurate information.7,13
Recommend a mini-course
Because these tools may be difficult to use or unreliable at identifying quality content, I recommend that every patient spend time on the National Medical Library Web site learning how to look up information. The other benefit of this site is that it lists top 10 Web sites for content, so it is a great launching point for a multitude of searches. It can be found at http://www.mlanet.org/resources/userguide.html.
If the patient finds the information at this portal too dry, there is a fantastic 16-minute tutorial about evaluating online health information; it’s a service of the National Library of Medicine and the National Institutes of Health. I recommend that every provider do this tutorial. Why? So you can better educate yourself on how to use the Internet and so you can tell your patients how great it is. It’s available at http://www.nlm.nih.gov/medlineplus/webeval/webeval.html.
Take the bull by the horns
Discuss the Internet with every one of your patients. Specifically, ask if she has read any information online and, if she has, how it stacks up with what you have just discussed during her office visit. That’s what I do. Explain that accurate content is critical in health-care decisions, guide your patient to sites that are more likely to be accurate, and teach her how to maximize the Internet to enhance her health care.
In my experience, patients are thrilled to be pointed in the right direction.
We want to hear from you! Tell us what you think.
CASE: The Internet has (at least) two faces
Both Patient A and Patient B are 8 weeks pregnant with their first baby. At an office visit, you discuss influenza vaccination.
Patient A tells you: “I was undecided about the vaccine until I read all these horror stories about the H1N1 vaccine. A Web site, organichealthadviser.com, says vaccines and pregnancies don’t mix safely.1 It says that if the flu vaccine isn’t safe for a baby less than 6 months old, how can it be safe during pregnancy?1 I read story after story of women who got the vaccine and miscarried. Why would I want to be injected with a toxin?”
Patient B explains: “I was undecided about the vaccine until I read the information on the Centers for Disease Control and Prevention (CDC) Web site.2 I didn’t know that pregnant women are more likely to get really sick from the flu. The CDC says the vaccine is safe during pregnancy, will not harm my baby, and not only reduces my chance of getting sick from the flu, but will give my baby protection for 6 months after she is born.2 When and where can I get my shot?”
Sixty-nine percent of Americans (80% of those who have Internet access) turn to the Web for information about their health care, and 23% of people who have a major medical illness or other health condition report that the Internet plays a major role in helping them deal with their health issue.3,4 They might research symptoms, diagnosis, tests, and therapies before a visit to your office; many come armed with questions, sometimes bringing reams of pages downloaded from various sites. Among women receiving ObGyn care, almost 60% have accessed Web-based information before their visit.5 Others take to the Internet after their appointment to confirm or refute what they have heard in the office.
Regardless of what a patient researches or when she does it, the why is because she wants to be an active participant in her medical care. That is a good thing because participatory medicine (shared decision-making) leads to improved outcomes. However, the key to truly informed decision-making is content: A patient can be fully empowered to participate in her health care only if she has information that is accurate, understandable, and current.
Web-based health information: Entirely factual?
Not only do patients research health online, 60% of people believe what they read to be factual and at least as good as the information they receive from you in your office. In fact, there is evidence that only 6% believe the health information they gather online is lacking in quality.5,6
However, studies reveal that the accuracy of medical content on the Web varies greatly from site to site. For example, among women seeking information on the Internet about potential teratogenic agents, 40% found incorrect information, some of which was potentially harmful.7
In addition to the problem of potentially suspect content, more than 50% of patients don’t disclose with you the information that they find online.7 Ever encounter a patient you just couldn’t sway from a diagnosis she believed she had but you knew she didn’t? If your patient tells you where she got the information, you can walk her through the diagnosis and treatment step by step, pointing out where her information might not be accurate (or, sometimes, even medically plausible)—but it’s hard to undo what you don’t know about.
The ideal scenario. Discuss Web-based information as part of your visit, thereby acknowledging that the Internet is a valid place to investigate personal health care. You can also preemptively provide tools for tracking down the most accurate and understandable content. See, for example, the patient handout.
Let’s face it: Physicians have an advantage when it comes to weeding out the wisdom from the woo. To supplement our baseline knowledge, we can easily research facts on PubMed, check our medical societies for guidelines, or, simply, ask a colleague. Our patients don’t have these same resources, but with some guidance from you, their Internet health experience can be greatly enhanced.
Are your searches on the Internet turning up reliable health advice? Watch for these 10 red flags of bad information
- Sensationalized content Is the information on the site presented in an alarmist tone? Is it loaded with scary stories and extreme outcomes? Are the issues presented in terms of black and white, with no shades of gray? If the answer to any of these questions is “Yes,” the author may have an axe to grind or a hidden leaning. Suspect the accuracy of the information you obtain!
- No date This may seem like a minor problem, but the world of health care moves swiftly. Treatments and approaches that are reliable one day can be discredited in the blink of an eye. If the site does not date its content, or indicate when it was last updated, you have no way of knowing how current it is. Move on!
- No author credentials The author or authors of material on the Web site should clearly, and visibly, present their credentials—that is, their education and training, their title, and where they work. If they do not, it is impossible to judge their expertise—in fact, expertise may be lacking.
- Buzz words The use of quasi-scientific buzz words such as “toxins,” “heavy metals,” and “detoxification” should draw your attention. These words have no meaning, so they should lead to you question what else on the site might be fiction.
- Patient testimonials Three people may have improved with a particular drug, but what about those who haven’t? Using unverified personal experiences is a sign of advertising, not good medicine.
- For sale sign If you can’t easily tell the difference between the medical content and products for sale, move along. Even when products don’t appear prominently, chances are that the bottom line of the Web site is profit, not education.
- All benefits and no risks Sites that have a stake in a particular treatment—be it monetary, emotional, or some other involvement—usually provide a lot of information on benefits but not so much about risks. Every treatment has risks.
- No sources When physicians scrutinize an article or study, they make it a point to check the list of sources at the end, to ensure that it contains legitimate information, such as reports from a medical journal or government publication. A Web site that presents detailed medical information without providing links to the references or comparable detail about the sources of that information is highly suspect.
- Conflict of interest Most reputable health sites not only provide information from experts, they list any so-called potential conflicts of interest that those experts may have. For example, if a medication made by XYZ Pharmaceuticals is recommended by Dr. Smith, who is also a consultant to XYZ, you should know. Articles and presentations at scientific meetings require these disclosures for a reason: Financial ties can produce bias.
- The Web site or product is listed on QuackWatch This Web site is dedicated to exposing unproven and scientifically questionable medical claims (http://www.quackwatch.com).
Where can you turn for help?
- An excellent starting place is the National Medical Library Web site at http://www.mlanet.org/resources/userguide.html, which provides resources for obtaining reliable health information.
- The National Library of Medicine and National Institutes of Health also provide an outstanding 16-minute lesson on how you can evaluate online health information. Find it at http://www.nlm.nih.gov/medlineplus/webeval/webeval.html.
- healthfinder.gov is a Web “encyclopedia” offering entries on more than 1,600 health topics.
© Copyright 2011 Quadrant HealthCom, Inc. This “Guide” may be reproduced by clinicians without permission or fee for single-copy distribution to patients. All other uses require the written permission of the publisher.
To obtain a PDF of this Patient Guide, click here .
Four tips for evaluating online content
Consider the source
The very first thing to consider is the domain name—e.g., “.gov,” “.org,” “.edu,” “.com,” or .anythingelse.
.gov sites are owned and maintained by the US government. From a medical standpoint, the .gov designation means that a site contains evidence-based information maintained by medical librarians that is written at a level that most people can read.
It’s a common misperception that the .org designation indicates a not-for-profit site that is therefore “looking out for the public’s best interest.” But anyone can purchase an .org domain. Even if a particular site really is administered by a not-for-profit organization, that status does not ensure that the content is of high quality.
.edu sites are affiliated with academic institutions.
.com and .anythingelse are, like .org, free for anyone to purchase.
Evidence-based medicine tells us that .gov sites are the most accurate for content—anything else is buyer beware (interestingly, .edu sites fared the worst in one study for accuracy).7,8 This doesn’t mean that sites that are not .gov have no value! On the contrary, non-governmental Web sites, blogs, and news articles are often the first place a search starts. That’s because current content, such as a new site, is more likely to feature prominently in a search engine response. But non-governmental sites do require an additional level of scrutiny. For example, in one study, only 55% of health information on news Web sites was medically accurate.8
Who is the author? Does she have financial ties or bias?
Think about who is running the Web site, why they are doing it, and what they are trying to achieve. Is the author a doctor, a health reporter, an advocate, or a drug company? The credentials of any physicians associated with the site should be listed as well as credentials and affiliations of authors, if they are non-physicians. Sites that list physician credentials tend to rate higher in accuracy of content.7
Talk with your patients about the importance of financial ties. The sponsor of the Web site should be listed (drug company, university, or a physician blogging without reimbursement). Bias and money go hand in hand, so be careful in evaluating whether the information provided favors the sponsor. If there are products for sale that are recommended by the medical content, bias is implied and, in my opinion, that site is not informational but commercial.
Bias can also be non-commercial, which is why authors of academic papers are not only supposed to report financial ties but also any real or perceived conflict of interest. This can be hard to discern at times, but the Web site should disclose why it exists. If the message is muddied by advertising and other commercial content, it’s best to just move along.
How current is the content?
We all know that new studies constantly reshape the way we practice (and sometimes guidelines from professional societies seem to change with the wind), and what is new quickly becomes out of date. The good and bad with online information is that it is always there. A permanent record is in many ways a good thing, but content from 2004 may not be applicable in 2011. This is a particular issue with news sites. They may report on a fascinating study in 2007, but if a retraction later appears or a new study refutes the findings, that information may not warrant an article on the Web. A good rule of thumb: Anything older than 2 years requires an additional level of scrutiny.
Be wary when the subject is complementary and alternative medicine
Online content related to complementary and alternative medicine (CAM) should be approached with a higher degree of caution. One study found that 25% of CAM sites presented information that could cause physical harm if acted upon, and almost all CAM sites omitted vital warnings, such as drug interactions, contraindications, and adverse reactions. The quality of CAM sites doesn’t improve even when they meet three or four of the JAMA benchmarks for information quality (see page 40).9 In one study of breast cancer sites, Web pages with CAM content were 15 times more likely to contain inaccurate content, compared with sites without CAM content.7
Instruments and tools for evaluating online content
Three tools are available to help patients and providers judge the quality of written online information:
Discern is a 16-question tool designed to assess the quality of online health information. You will find it at http://www.discern.org.uk/discern_instrument.php. I recommend that you mention this tool to patients, even if you are uncertain whether they will use it. Certainly, any patient wedded to what seems like questionable content from a specific Web site should be encouraged to evaluate the site using the Discern tool. In addition, if you have Web sites other than .gov sites that you like to share with patients, it might be wise to personally review them with Discern so that you can reaffirm that you are directing patients to reliable content rather than a quagmire of misinformation.10
The Health on the Net Foundation (HON) is an independent, seven-person, Geneva-based panel that evaluates accuracy of medical Web sites based on specific guiding principles. It can be accessed at http://www.hon.ch/. Web sites that meet these criteria are awarded seals of approval. Only one problem: Not all sites that carry the seal are compliant with HON, and sites that don’t carry the seal can nevertheless be complete and accurate.11,12
JAMA benchmarks are four disclosures intended to help ensure the quality of a Web site: authorship, references, conflict of interest, and currency of content. Some research suggests that sites that have three or four of the benchmarks are more likely to have accurate content, but there is also evidence to suggest that JAMA benchmarks may not always reliably identify inaccurate information.7,13
Recommend a mini-course
Because these tools may be difficult to use or unreliable at identifying quality content, I recommend that every patient spend time on the National Medical Library Web site learning how to look up information. The other benefit of this site is that it lists top 10 Web sites for content, so it is a great launching point for a multitude of searches. It can be found at http://www.mlanet.org/resources/userguide.html.
If the patient finds the information at this portal too dry, there is a fantastic 16-minute tutorial about evaluating online health information; it’s a service of the National Library of Medicine and the National Institutes of Health. I recommend that every provider do this tutorial. Why? So you can better educate yourself on how to use the Internet and so you can tell your patients how great it is. It’s available at http://www.nlm.nih.gov/medlineplus/webeval/webeval.html.
Take the bull by the horns
Discuss the Internet with every one of your patients. Specifically, ask if she has read any information online and, if she has, how it stacks up with what you have just discussed during her office visit. That’s what I do. Explain that accurate content is critical in health-care decisions, guide your patient to sites that are more likely to be accurate, and teach her how to maximize the Internet to enhance her health care.
In my experience, patients are thrilled to be pointed in the right direction.
We want to hear from you! Tell us what you think.
1. H1N1 vaccine and pregnancy. Organic Health Adviser. http://organichealthadviser.com/archives/h1n1-vaccine-and-pregnancy. Accessed November 12 2011.
2. Pregnant women and influenza. Centers for Disease Control and Prevention. http://www.cdc.gov/flu/protect/vaccine/pregnant.htm. Accessed November 12 2011.
3. Fox S. The social life of health information 2011. Pew Internet and American Life Project. http://pewresearch.org/pubs/1989/health-care-online-social-network-users. Accessed November 12, 2011.
4. Horrigan J, Rainie L. The Internet’s growing role in life’s major moments. Decision-making Communities, Health. Pew Internet and American Life Project. http://www.pewinternet.org/Reports/2006/The-Internets-Growing-Role-in-Lifes-Major-Moments.aspx. Accessed November 12, 2011.
5. Neelapala P, Duvvi SK, Kumar G, Kumar BN. Do gynaecology outpatients use the Internet to seek health information? A questionnaire survey. J Eval Clin Pract. 2008;14(2):300-304.
6. Diaz JA, Griffith RA, Ng JJ, Reinert SE, Friedmann PD, Moulton AW. Patients’ use of the Internet for medical information. J Gen Intern Med. 2001;17(3):180-185.
7. Bernstam EV, Walji MF, Sagaram S, Sagaram D, Johnson CW, Meric-Bernstam F. Commonly cited website quality criteria are not effective at identifying inaccurate online information about breast cancer. Cancer. 2008;112(6):1206-1213.
8. Scullard P, Peacock C, Davies P. Googling children’s health: reliability of medical information on the Internet. Arch Dis Child. 2010;95(8):580-582.
9. Walji M, Sagaram S, Sagaram D, et al. Efficacy of quality criteria to identify potentially harmful information: a cross-sectional survey of complementary and alternative medicine web sites. J Med Internet Res. 2004;6(2):e21.-
10. Charnock D, Shepperd S, Needham G, Gann R. Discern: an instrument for judging the quality of written consumer health information on treatment choices. J Epidemiol Community Health. 1999;53(2):105-111.
11. Hardwick JC, MacKenzie FM. Information contained in miscarriage-related websites and the predictive value of website scoring systems. Eur J Gynecol Reprod Biol. 2003;106(1):60-63.
12. Khazaal Y, Chatton A, Zullino D. HON label and Discern as content quality indicators of health-related websites [published online ahead of print May 2011]. Psychiatr Q. doi: 10.1007/s11126-011-9179-x.
13. Meric F, Bernstam EV, Mirza NQ, et al. Breast cancer on the world wide web: cross sectional survey of quality of information and popularity of websites. BMJ. 2002;324(7337):577-581.
1. H1N1 vaccine and pregnancy. Organic Health Adviser. http://organichealthadviser.com/archives/h1n1-vaccine-and-pregnancy. Accessed November 12 2011.
2. Pregnant women and influenza. Centers for Disease Control and Prevention. http://www.cdc.gov/flu/protect/vaccine/pregnant.htm. Accessed November 12 2011.
3. Fox S. The social life of health information 2011. Pew Internet and American Life Project. http://pewresearch.org/pubs/1989/health-care-online-social-network-users. Accessed November 12, 2011.
4. Horrigan J, Rainie L. The Internet’s growing role in life’s major moments. Decision-making Communities, Health. Pew Internet and American Life Project. http://www.pewinternet.org/Reports/2006/The-Internets-Growing-Role-in-Lifes-Major-Moments.aspx. Accessed November 12, 2011.
5. Neelapala P, Duvvi SK, Kumar G, Kumar BN. Do gynaecology outpatients use the Internet to seek health information? A questionnaire survey. J Eval Clin Pract. 2008;14(2):300-304.
6. Diaz JA, Griffith RA, Ng JJ, Reinert SE, Friedmann PD, Moulton AW. Patients’ use of the Internet for medical information. J Gen Intern Med. 2001;17(3):180-185.
7. Bernstam EV, Walji MF, Sagaram S, Sagaram D, Johnson CW, Meric-Bernstam F. Commonly cited website quality criteria are not effective at identifying inaccurate online information about breast cancer. Cancer. 2008;112(6):1206-1213.
8. Scullard P, Peacock C, Davies P. Googling children’s health: reliability of medical information on the Internet. Arch Dis Child. 2010;95(8):580-582.
9. Walji M, Sagaram S, Sagaram D, et al. Efficacy of quality criteria to identify potentially harmful information: a cross-sectional survey of complementary and alternative medicine web sites. J Med Internet Res. 2004;6(2):e21.-
10. Charnock D, Shepperd S, Needham G, Gann R. Discern: an instrument for judging the quality of written consumer health information on treatment choices. J Epidemiol Community Health. 1999;53(2):105-111.
11. Hardwick JC, MacKenzie FM. Information contained in miscarriage-related websites and the predictive value of website scoring systems. Eur J Gynecol Reprod Biol. 2003;106(1):60-63.
12. Khazaal Y, Chatton A, Zullino D. HON label and Discern as content quality indicators of health-related websites [published online ahead of print May 2011]. Psychiatr Q. doi: 10.1007/s11126-011-9179-x.
13. Meric F, Bernstam EV, Mirza NQ, et al. Breast cancer on the world wide web: cross sectional survey of quality of information and popularity of websites. BMJ. 2002;324(7337):577-581.
The Buck Starts Here
Some of the best companies in America started in a garage or a basement with an individual who had a great idea and the ability to grow it into a progressively larger business.
“It takes a leader with different capabilities to take a company to the next level,” says Martin Buser, MPH, FACHE, a partner with Hospitalist Management Resources LLC in San Diego, which has helped more than 350 HM programs nationwide in the past 15 years. “It’s an attitude of never stop learning, an ability to look at issues from 30,000 feet instead of ground zero so you can see the whole picture.”
Similarly, the most important predictor of an HM program’s success is its director, Buser says. If directors know how to communicate, innovate, facilitate, problem-solve, and inspire, they are much more likely to run a high-performing hospitalist program, says David Lee, MD, MBA, FACP, FHM, vice chairman of the Hospital Medicine Department at Ochsner Health System in New Orleans.
If group directors lack the skills and fail to adapt to change, the program’s outlook is far from certain. “We unfortunately get involved with these programs,” Buser says. “It’s painful to see.” Bad behavior is nothing new to the hospital setting, and HM is not immune to poor management. The following are common examples of bad behaviors and how groups can avoid the mishaps.
Scenario No. 1 : Great Clinician, Nice Person, Weak Advocate

—Martin Buser, MPH, FACHE, partner, Hospitalist Management Resources LLC, San Diego
The case: Earlier this year, medical center administrators asked the hospitalist program to do more with less, explaining the hospital was having a bad financial year. Administration approached the HM director, an exceptional, gregarious clinician who was named to the position years ago to help the program gain acceptance. The director agreed to indefinitely postpone two much-needed hirings, deciding it was better to share in the sacrifice than protest the cuts to the program’s budget. Hospitalists have since been working more shifts without a pay increase, and burnout symptoms have emerged with no signs of a thaw in the hiring freeze.
Expert advice: Buser says the “weak advocate” is a common issue among hospitalist groups, many of which he says are “going to hell” when he gets a rescue call. When a hospital is facing financial hardship, it is imperative that the HM director stand up for the program by explaining in detail the ramifications of each level of budget cuts. That’s because administrators might not realize the long-term damage that would result from such actions, he says. Being a strong, savvy advocate is even more important now since the financial future of many hospitals is ominous.
“With all of our hospitalist clients, we ask the CFO what is happening in the future…and the numbers are phenomenal,” says Buser. “They are seeing reductions of $10 million to $30 million off their bottom line.”
Administrators’ knee-jerk reaction is to cut costs. But there is another option: Grow the hospital out of its financial difficulties. It is up to the HM director to show administrators how the HM group has strategically gained them market share and how it will continue to do so. Good directors are in near constant contact with administrators, demonstrating the value their hospitalist program brings to the hospital, Buser says.
“You’re having regular meetings with the administrator, you’re producing the dashboard on a regular basis, you’re giving him trends that are going on,” he explains. “Show that you understand the hospital’s issues. Certain things you want to compromise on, but other things you have to say, ‘If we do that, the ramifications are such that it’s just not going to work.’”
Scenario No. 2 : Recruiting Roulette

—David Friar, MD, SFHM, CEO, Hospitalists of Northern Michigan, Traverse City
The case: The HM director felt pressure to hire. The program’s hospitalists were seeing two to three patients a day more than they should have been, and hospital administrators were worried the program was losing ground to the other hospitalist group in the community. Using an outside recruiter, the director hired two adept physicians with stellar CVs after an expedited review process that included a background check, a few phone interviews, and day of in-person interviews with some administrators and a hospitalist on the team. Now, nearly a year later, one of the physicians is about to leave because her family doesn’t like the community, and the other new hire’s abrasive personality has caused considerable damage to the team’s cohesion.
Expert advice: A big part of an HM program’s value is how it practices as a unified team, and directors need to recognize how vital the “team fit” is to hospitalists, says David Friar, MD, SFHM, CEO of Hospitalists of Northern Michigan in Traverse City.
“A bad team fit is often worse than being short-staffed because it can literally destroy the team spirit,” he says.
Directors should have a standardized recruitment process that includes a comprehensive background screening where references are closely checked, a round of interviews by people outside the HM program (nurses and referring physicians), and substantial time spent with hospitalists in the program, says Bryce Gartland, MD, FHM, associate director of the hospital medicine division and medical director of care coordination at Emory Healthcare in Atlanta.
“We put [candidates] with one of our physicians to actually go around the hospital,” he says. “It’s amazing to me the number of things you can pick up by that broader exposure that you may not pick up sitting in a room with a candidate across the table for an hour.”
If a recruitment service is used, the director must describe the HM program in detail to the recruiter and even have them meet hospitalists on the staff, Dr. Friar says.
“Sending them a memo saying ‘We need three new hospitalists ASAP’ isn’t helping them find you the perfect candidate,” he says. “Even the best recruiter can only do a great job for you if they really know your team and what it is you need in a candidate.”
A director also is well served to make recruiting a family event where spouses and even children are part of the interview process.
“By including the entire family and then supporting them after the move, we are much more likely to recruit providers that will stay good members of our team for years to come,” Dr. Friar says.
Scenario No. 3 : Amitte Diem

—John Bulger, DO, FACP, FHM, chief quality officer, director, hospital medicine service line, Geisinger Health System, Danville, Pa.
The case: For months, the medical center has been receiving an increased number of referrals from outlying hospitals, and no end is in sight. The extra patient load, much of it involving complex cases, has agitated the medical center’s staff, particularly the specialists, and they’ve begun to complain to hospital administrators. Seeking an ally, the specialists reach out to the HM director to present their case. Without doing independent analysis, the HM director sides with the specialists. Hospital administrators, facing growing resistance, work to decrease the referrals and are successful.
Expert advice: Consider working in the opposite direction, one that might turn a referral challenge into a profitable opportunity, Buser says. One of his firm’s clients, after thorough research, established a transfer center and set up an activation fee for the specialists who took the referrals. Hospitalists admitted about 90% of the cases, called consults, and named specialists so they received full fee-for-service at Medicare rates if they saw uninsured patients.
“That hospital is now making about $78 million a year, and the medical staff is saying, ‘How can we grow this?’” Buser says. “Here’s an example of how the hospital medicine director was key to turning the bad into something good.”
Because physicians tend to be reticent to change, it’s critical for hospitalist directors who want to seize an opportunity to thoroughly plan out how the change will occur and to prepare for potential obstacles along the way, says John Bulger, DO, FACP, FHM, chief quality officer and director of the hospital medicine service line for Geisinger Health System in Danville, Pa.
“You really need to be prepared with your rationale of why you’re doing it, if there’s data behind why you’re doing it, what the data is that’s driving it, and really what you hope to do with that change,” he says. “If you don’t get buy in from your staff, the change is doomed to fail from the beginning.”
Directors must embrace being a change agent if they want their HM programs to continue to be successful. In the minds of many hospital administrators, a program is only as good as its last achievement.
“It’s kind of like, ‘What have you done for me lately?’” Buser says. “You want to stay ahead of the curve and be alert to what’s going on and not be caught keeping your eyes off the ball and, as a result, not moving your program forward.”
Scenario No. 4 : Fumbling the Handoff

—Daniel Cusator, MD, MBA, vice president, Camden Group, El Segundo, Calif.
The case: The medical center’s monthly data for the past year has shown that hospitalists are taking care of their patients efficiently and getting them out of the hospital more quickly. However, mixed in with the positive numbers is a stubbornly high 30-day readmission rate. Indeed, some primary care groups and referring geriatricians have begun to grouse to the HM director about the discharge notes, complaining they aren’t as comprehensive as they would like.
Plus, the notes always arrive via office fax, which makes them more likely to get misplaced and harder to receive when doctors are out of the office.
Expert advice: Handoffs from discharge to pickup are where a lot of complications, errors, and safety issues arise, and poor handoffs are one of the largest drivers of readmission rates, especially in the elderly patient population, says Daniel Cusator, MD, MBA, vice president of the Camden Group, a healthcare consulting firm in El Segundo, Calif.
If the hospitalist director doesn’t provide the leadership and resources to help the HM team better coordinate with patients’ regular doctors, handoffs won’t be a priority throughout the group.
The HM director must recognize that the term “discharge note” is a misnomer.
What referring physicians really want is a care plan, which includes information about testing done in the hospital, testing that might be needed in the outpatient setting, medications the patient is on, complications the patient had in the hospital, potential problems to monitor, and any necessary follow-up, says Dr. Cusator, formerly the chief medical officer of clinical integration at Providence Health & Services in Southern California.
PCPs also want the care plan transmitted in their preferred method, whether that is text messaging, HIPAA-compliant email messaging, secure messaging, or fax.
“What I’ve seen some hospitalist groups do is create a menu capability for each of the physicians to choose their preferred method of notification of discharge of their patient,” Dr. Cusator says. Results suggest such a menu leads to improved physician satisfaction and reduced patient complications after discharge, he adds.
With today’s technological innovations, HM directors are unlimited in their ability to improve handoffs between their team and patients’ PCPs and specialists, Dr. Cusator says. Some HM directors, for example, are leading efforts to link electronic medical records systems to hospital-based health information exchange hubs that are accessible to physicians in the community.
“Notes and clinical information are submitted to this health information exchange and made available to any of the physicians who are caring for the patient almost immediately upon dictation and notation,” he says.
Scenario No. 5 : Protect Your Assets

—David Lee, MD, MBA, FACP, FHM, vice chairman, Hospital Medicine Department, Ochsner Health System, New Orleans.
The case: A physician isn’t sure she wants a career in hospital medicine. She finds the specialty rewarding but is looking for a different challenge, something beyond exclusively seeing patients. The HM director notices the physician has an aptitude for finding ways to do tasks more efficiently.
The director privately thinks the physician would be a good fit for a quality improvement project that’s about to start but doesn’t pursue it. The HM team just added a primary care group, and its patient census is quickly rising, requiring the hospitalists to devote their entire shifts to patient care. Within the year, the physician leaves the team for a fellowship program outside hospital medicine.
Expert advice: There are three communities in hospital medicine, Dr. Bulger says: people who want to be hospitalists, people who are passing through on their way to something else, and people who sit somewhere in the middle.
HM directors, he says, should do everything they can to develop not only the career hospitalists but also those on the fence.
“A lot of them you can turn into people who are going to be hospitalists if they are doing something that is rewarding for them,” Dr. Bulger says. “Many times rewarding for them is being involved more in the leadership of the group, being involved in quality improvement projects, really seeing how they can impact the care for populations of patients—and not just the patient who happens to be sitting in front of them.”
It’s incumbent on HM group leaders to link hospitalists with mentors and help them find a niche, Dr. Lee says. It keeps people interested and makes them feel part of a group.
“They need to feel they belong,” he says. “There has to be a cohesiveness in order for your department to excel. You have to protect your assets in the group, which is your physicians.”
Sending hospitalists to professional development training, such as SHM’s Leadership Academy (see “Leadership Academy Adds ‘Women in HM Issues’ to Schedule,” p. 9) or QI-focused webinars offered by SHM or the Institute of Healthcare Improvement, and following up with day-to-day coaching is a solid physician-development strategy, Dr. Gartland says. By virtue of their job, hospitalists are expected to lead and manage people in interactions with the ED, primary care, non-physician providers, nursing staff, and beyond, he says.
Directors also have to stop assuming that competent physicians are competent managers. “A lot of physicians don’t have those core skill sets, and we’ve got to pay conscious attention toward spending time dedicated to developing those,” Dr. Gartland says.
If directors don’t make professional development a priority or provide hospitalists with the flexibility to do non-clinical activities, retention may become an issue, Dr. Bulger says. “They could leave and go somewhere else,” he says, yet perhaps the more significant danger is losing hospitalists to programs and specialties outside hospital medicine.
Lisa Ryan is a freelance writer based in New Jersey.
THE FUNDAMENTALS
As hospitals position themselves for healthcare reform, they increasingly will turn to HM for strategies on how to provide high-quality patient care at a lower cost, Buser says. To meet hospitals’ needs and enhance the value of their programs, hospitalist directors should consider adopting these strategies recommended by HM leaders:
- Align compensation with the HM program’s goals. For example, if quality improvement is the priority, directors should financially reward hospitalists on quality performance, Dr. Lee says.
- Boost support staff and functions. For example, directors should ensure their team has access to the hospital’s case managers, who can handle discharge logistics so the hospitalist can focus on clinical issues, Dr. Cusator says.
- Control program growth. To borrow a popular line from the movie Field of Dreams: “If you build it, they will come.” Directors should be deliberate with group expansion and ensure enough staff is in place before adding to their referral base or adding a new service line, Dr. Bulger says. This reduces hospitalist burnout and preserves the group’s quality of patient care.
- Define two to three targets for success in the upcoming year and concentrate on accomplishing them. Start by consolidating what your team is working on, says Steven Deitelzweig, MD, SFHM, chairman of the Department of Hospital Medicine at Ochsner Health System in New Orleans. Pick too many things to master, and you end up excelling in none, he adds.
- Evaluate performance beyond a scorecard. Using constructive criticism grounded with examples, HM directors should provide feedback about what a physician is doing well and what can be done better so they can improve, Dr. Gartland says.
- Foster creative problem solving by including hospitalists in decisions. Directors should encourage the expression of different opinions and ideas, which helps the program avoid “group think” and allows innovation to occur, Dr. Lee says.
- Galvanize the new generation. To retain young physicians and make them feel part of the program, directors should learn how they communicate, how they work, and how they view work, Dr. Lee says.
- Help your hospital accurately measure reimbursement and mortality rates. Directors should make coding a priority and provide hospitalists with the tools they need to capture correct ICD-9 and CPT codes for their patients, Dr. Cusator says.
- Identify missing core capabilities and dedicate resources for it. For example, if HM programs have a high census of chronically ill and end-of-life patients, directors should assist the hospital in establishing a palliative care or hospice program, Dr. Cusator says.
Some of the best companies in America started in a garage or a basement with an individual who had a great idea and the ability to grow it into a progressively larger business.
“It takes a leader with different capabilities to take a company to the next level,” says Martin Buser, MPH, FACHE, a partner with Hospitalist Management Resources LLC in San Diego, which has helped more than 350 HM programs nationwide in the past 15 years. “It’s an attitude of never stop learning, an ability to look at issues from 30,000 feet instead of ground zero so you can see the whole picture.”
Similarly, the most important predictor of an HM program’s success is its director, Buser says. If directors know how to communicate, innovate, facilitate, problem-solve, and inspire, they are much more likely to run a high-performing hospitalist program, says David Lee, MD, MBA, FACP, FHM, vice chairman of the Hospital Medicine Department at Ochsner Health System in New Orleans.
If group directors lack the skills and fail to adapt to change, the program’s outlook is far from certain. “We unfortunately get involved with these programs,” Buser says. “It’s painful to see.” Bad behavior is nothing new to the hospital setting, and HM is not immune to poor management. The following are common examples of bad behaviors and how groups can avoid the mishaps.
Scenario No. 1 : Great Clinician, Nice Person, Weak Advocate
—Martin Buser, MPH, FACHE, partner, Hospitalist Management Resources LLC, San Diego
The case: Earlier this year, medical center administrators asked the hospitalist program to do more with less, explaining the hospital was having a bad financial year. Administration approached the HM director, an exceptional, gregarious clinician who was named to the position years ago to help the program gain acceptance. The director agreed to indefinitely postpone two much-needed hirings, deciding it was better to share in the sacrifice than protest the cuts to the program’s budget. Hospitalists have since been working more shifts without a pay increase, and burnout symptoms have emerged with no signs of a thaw in the hiring freeze.
Expert advice: Buser says the “weak advocate” is a common issue among hospitalist groups, many of which he says are “going to hell” when he gets a rescue call. When a hospital is facing financial hardship, it is imperative that the HM director stand up for the program by explaining in detail the ramifications of each level of budget cuts. That’s because administrators might not realize the long-term damage that would result from such actions, he says. Being a strong, savvy advocate is even more important now since the financial future of many hospitals is ominous.
“With all of our hospitalist clients, we ask the CFO what is happening in the future…and the numbers are phenomenal,” says Buser. “They are seeing reductions of $10 million to $30 million off their bottom line.”
Administrators’ knee-jerk reaction is to cut costs. But there is another option: Grow the hospital out of its financial difficulties. It is up to the HM director to show administrators how the HM group has strategically gained them market share and how it will continue to do so. Good directors are in near constant contact with administrators, demonstrating the value their hospitalist program brings to the hospital, Buser says.
“You’re having regular meetings with the administrator, you’re producing the dashboard on a regular basis, you’re giving him trends that are going on,” he explains. “Show that you understand the hospital’s issues. Certain things you want to compromise on, but other things you have to say, ‘If we do that, the ramifications are such that it’s just not going to work.’”
Scenario No. 2 : Recruiting Roulette
—David Friar, MD, SFHM, CEO, Hospitalists of Northern Michigan, Traverse City
The case: The HM director felt pressure to hire. The program’s hospitalists were seeing two to three patients a day more than they should have been, and hospital administrators were worried the program was losing ground to the other hospitalist group in the community. Using an outside recruiter, the director hired two adept physicians with stellar CVs after an expedited review process that included a background check, a few phone interviews, and day of in-person interviews with some administrators and a hospitalist on the team. Now, nearly a year later, one of the physicians is about to leave because her family doesn’t like the community, and the other new hire’s abrasive personality has caused considerable damage to the team’s cohesion.
Expert advice: A big part of an HM program’s value is how it practices as a unified team, and directors need to recognize how vital the “team fit” is to hospitalists, says David Friar, MD, SFHM, CEO of Hospitalists of Northern Michigan in Traverse City.
“A bad team fit is often worse than being short-staffed because it can literally destroy the team spirit,” he says.
Directors should have a standardized recruitment process that includes a comprehensive background screening where references are closely checked, a round of interviews by people outside the HM program (nurses and referring physicians), and substantial time spent with hospitalists in the program, says Bryce Gartland, MD, FHM, associate director of the hospital medicine division and medical director of care coordination at Emory Healthcare in Atlanta.
“We put [candidates] with one of our physicians to actually go around the hospital,” he says. “It’s amazing to me the number of things you can pick up by that broader exposure that you may not pick up sitting in a room with a candidate across the table for an hour.”
If a recruitment service is used, the director must describe the HM program in detail to the recruiter and even have them meet hospitalists on the staff, Dr. Friar says.
“Sending them a memo saying ‘We need three new hospitalists ASAP’ isn’t helping them find you the perfect candidate,” he says. “Even the best recruiter can only do a great job for you if they really know your team and what it is you need in a candidate.”
A director also is well served to make recruiting a family event where spouses and even children are part of the interview process.
“By including the entire family and then supporting them after the move, we are much more likely to recruit providers that will stay good members of our team for years to come,” Dr. Friar says.
Scenario No. 3 : Amitte Diem
—John Bulger, DO, FACP, FHM, chief quality officer, director, hospital medicine service line, Geisinger Health System, Danville, Pa.
The case: For months, the medical center has been receiving an increased number of referrals from outlying hospitals, and no end is in sight. The extra patient load, much of it involving complex cases, has agitated the medical center’s staff, particularly the specialists, and they’ve begun to complain to hospital administrators. Seeking an ally, the specialists reach out to the HM director to present their case. Without doing independent analysis, the HM director sides with the specialists. Hospital administrators, facing growing resistance, work to decrease the referrals and are successful.
Expert advice: Consider working in the opposite direction, one that might turn a referral challenge into a profitable opportunity, Buser says. One of his firm’s clients, after thorough research, established a transfer center and set up an activation fee for the specialists who took the referrals. Hospitalists admitted about 90% of the cases, called consults, and named specialists so they received full fee-for-service at Medicare rates if they saw uninsured patients.
“That hospital is now making about $78 million a year, and the medical staff is saying, ‘How can we grow this?’” Buser says. “Here’s an example of how the hospital medicine director was key to turning the bad into something good.”
Because physicians tend to be reticent to change, it’s critical for hospitalist directors who want to seize an opportunity to thoroughly plan out how the change will occur and to prepare for potential obstacles along the way, says John Bulger, DO, FACP, FHM, chief quality officer and director of the hospital medicine service line for Geisinger Health System in Danville, Pa.
“You really need to be prepared with your rationale of why you’re doing it, if there’s data behind why you’re doing it, what the data is that’s driving it, and really what you hope to do with that change,” he says. “If you don’t get buy in from your staff, the change is doomed to fail from the beginning.”
Directors must embrace being a change agent if they want their HM programs to continue to be successful. In the minds of many hospital administrators, a program is only as good as its last achievement.
“It’s kind of like, ‘What have you done for me lately?’” Buser says. “You want to stay ahead of the curve and be alert to what’s going on and not be caught keeping your eyes off the ball and, as a result, not moving your program forward.”
Scenario No. 4 : Fumbling the Handoff
—Daniel Cusator, MD, MBA, vice president, Camden Group, El Segundo, Calif.
The case: The medical center’s monthly data for the past year has shown that hospitalists are taking care of their patients efficiently and getting them out of the hospital more quickly. However, mixed in with the positive numbers is a stubbornly high 30-day readmission rate. Indeed, some primary care groups and referring geriatricians have begun to grouse to the HM director about the discharge notes, complaining they aren’t as comprehensive as they would like.
Plus, the notes always arrive via office fax, which makes them more likely to get misplaced and harder to receive when doctors are out of the office.
Expert advice: Handoffs from discharge to pickup are where a lot of complications, errors, and safety issues arise, and poor handoffs are one of the largest drivers of readmission rates, especially in the elderly patient population, says Daniel Cusator, MD, MBA, vice president of the Camden Group, a healthcare consulting firm in El Segundo, Calif.
If the hospitalist director doesn’t provide the leadership and resources to help the HM team better coordinate with patients’ regular doctors, handoffs won’t be a priority throughout the group.
The HM director must recognize that the term “discharge note” is a misnomer.
What referring physicians really want is a care plan, which includes information about testing done in the hospital, testing that might be needed in the outpatient setting, medications the patient is on, complications the patient had in the hospital, potential problems to monitor, and any necessary follow-up, says Dr. Cusator, formerly the chief medical officer of clinical integration at Providence Health & Services in Southern California.
PCPs also want the care plan transmitted in their preferred method, whether that is text messaging, HIPAA-compliant email messaging, secure messaging, or fax.
“What I’ve seen some hospitalist groups do is create a menu capability for each of the physicians to choose their preferred method of notification of discharge of their patient,” Dr. Cusator says. Results suggest such a menu leads to improved physician satisfaction and reduced patient complications after discharge, he adds.
With today’s technological innovations, HM directors are unlimited in their ability to improve handoffs between their team and patients’ PCPs and specialists, Dr. Cusator says. Some HM directors, for example, are leading efforts to link electronic medical records systems to hospital-based health information exchange hubs that are accessible to physicians in the community.
“Notes and clinical information are submitted to this health information exchange and made available to any of the physicians who are caring for the patient almost immediately upon dictation and notation,” he says.
Scenario No. 5 : Protect Your Assets
—David Lee, MD, MBA, FACP, FHM, vice chairman, Hospital Medicine Department, Ochsner Health System, New Orleans.
The case: A physician isn’t sure she wants a career in hospital medicine. She finds the specialty rewarding but is looking for a different challenge, something beyond exclusively seeing patients. The HM director notices the physician has an aptitude for finding ways to do tasks more efficiently.
The director privately thinks the physician would be a good fit for a quality improvement project that’s about to start but doesn’t pursue it. The HM team just added a primary care group, and its patient census is quickly rising, requiring the hospitalists to devote their entire shifts to patient care. Within the year, the physician leaves the team for a fellowship program outside hospital medicine.
Expert advice: There are three communities in hospital medicine, Dr. Bulger says: people who want to be hospitalists, people who are passing through on their way to something else, and people who sit somewhere in the middle.
HM directors, he says, should do everything they can to develop not only the career hospitalists but also those on the fence.
“A lot of them you can turn into people who are going to be hospitalists if they are doing something that is rewarding for them,” Dr. Bulger says. “Many times rewarding for them is being involved more in the leadership of the group, being involved in quality improvement projects, really seeing how they can impact the care for populations of patients—and not just the patient who happens to be sitting in front of them.”
It’s incumbent on HM group leaders to link hospitalists with mentors and help them find a niche, Dr. Lee says. It keeps people interested and makes them feel part of a group.
“They need to feel they belong,” he says. “There has to be a cohesiveness in order for your department to excel. You have to protect your assets in the group, which is your physicians.”
Sending hospitalists to professional development training, such as SHM’s Leadership Academy (see “Leadership Academy Adds ‘Women in HM Issues’ to Schedule,” p. 9) or QI-focused webinars offered by SHM or the Institute of Healthcare Improvement, and following up with day-to-day coaching is a solid physician-development strategy, Dr. Gartland says. By virtue of their job, hospitalists are expected to lead and manage people in interactions with the ED, primary care, non-physician providers, nursing staff, and beyond, he says.
Directors also have to stop assuming that competent physicians are competent managers. “A lot of physicians don’t have those core skill sets, and we’ve got to pay conscious attention toward spending time dedicated to developing those,” Dr. Gartland says.
If directors don’t make professional development a priority or provide hospitalists with the flexibility to do non-clinical activities, retention may become an issue, Dr. Bulger says. “They could leave and go somewhere else,” he says, yet perhaps the more significant danger is losing hospitalists to programs and specialties outside hospital medicine.
Lisa Ryan is a freelance writer based in New Jersey.
THE FUNDAMENTALS
As hospitals position themselves for healthcare reform, they increasingly will turn to HM for strategies on how to provide high-quality patient care at a lower cost, Buser says. To meet hospitals’ needs and enhance the value of their programs, hospitalist directors should consider adopting these strategies recommended by HM leaders:
- Align compensation with the HM program’s goals. For example, if quality improvement is the priority, directors should financially reward hospitalists on quality performance, Dr. Lee says.
- Boost support staff and functions. For example, directors should ensure their team has access to the hospital’s case managers, who can handle discharge logistics so the hospitalist can focus on clinical issues, Dr. Cusator says.
- Control program growth. To borrow a popular line from the movie Field of Dreams: “If you build it, they will come.” Directors should be deliberate with group expansion and ensure enough staff is in place before adding to their referral base or adding a new service line, Dr. Bulger says. This reduces hospitalist burnout and preserves the group’s quality of patient care.
- Define two to three targets for success in the upcoming year and concentrate on accomplishing them. Start by consolidating what your team is working on, says Steven Deitelzweig, MD, SFHM, chairman of the Department of Hospital Medicine at Ochsner Health System in New Orleans. Pick too many things to master, and you end up excelling in none, he adds.
- Evaluate performance beyond a scorecard. Using constructive criticism grounded with examples, HM directors should provide feedback about what a physician is doing well and what can be done better so they can improve, Dr. Gartland says.
- Foster creative problem solving by including hospitalists in decisions. Directors should encourage the expression of different opinions and ideas, which helps the program avoid “group think” and allows innovation to occur, Dr. Lee says.
- Galvanize the new generation. To retain young physicians and make them feel part of the program, directors should learn how they communicate, how they work, and how they view work, Dr. Lee says.
- Help your hospital accurately measure reimbursement and mortality rates. Directors should make coding a priority and provide hospitalists with the tools they need to capture correct ICD-9 and CPT codes for their patients, Dr. Cusator says.
- Identify missing core capabilities and dedicate resources for it. For example, if HM programs have a high census of chronically ill and end-of-life patients, directors should assist the hospital in establishing a palliative care or hospice program, Dr. Cusator says.
Some of the best companies in America started in a garage or a basement with an individual who had a great idea and the ability to grow it into a progressively larger business.
“It takes a leader with different capabilities to take a company to the next level,” says Martin Buser, MPH, FACHE, a partner with Hospitalist Management Resources LLC in San Diego, which has helped more than 350 HM programs nationwide in the past 15 years. “It’s an attitude of never stop learning, an ability to look at issues from 30,000 feet instead of ground zero so you can see the whole picture.”
Similarly, the most important predictor of an HM program’s success is its director, Buser says. If directors know how to communicate, innovate, facilitate, problem-solve, and inspire, they are much more likely to run a high-performing hospitalist program, says David Lee, MD, MBA, FACP, FHM, vice chairman of the Hospital Medicine Department at Ochsner Health System in New Orleans.
If group directors lack the skills and fail to adapt to change, the program’s outlook is far from certain. “We unfortunately get involved with these programs,” Buser says. “It’s painful to see.” Bad behavior is nothing new to the hospital setting, and HM is not immune to poor management. The following are common examples of bad behaviors and how groups can avoid the mishaps.
Scenario No. 1 : Great Clinician, Nice Person, Weak Advocate
—Martin Buser, MPH, FACHE, partner, Hospitalist Management Resources LLC, San Diego
The case: Earlier this year, medical center administrators asked the hospitalist program to do more with less, explaining the hospital was having a bad financial year. Administration approached the HM director, an exceptional, gregarious clinician who was named to the position years ago to help the program gain acceptance. The director agreed to indefinitely postpone two much-needed hirings, deciding it was better to share in the sacrifice than protest the cuts to the program’s budget. Hospitalists have since been working more shifts without a pay increase, and burnout symptoms have emerged with no signs of a thaw in the hiring freeze.
Expert advice: Buser says the “weak advocate” is a common issue among hospitalist groups, many of which he says are “going to hell” when he gets a rescue call. When a hospital is facing financial hardship, it is imperative that the HM director stand up for the program by explaining in detail the ramifications of each level of budget cuts. That’s because administrators might not realize the long-term damage that would result from such actions, he says. Being a strong, savvy advocate is even more important now since the financial future of many hospitals is ominous.
“With all of our hospitalist clients, we ask the CFO what is happening in the future…and the numbers are phenomenal,” says Buser. “They are seeing reductions of $10 million to $30 million off their bottom line.”
Administrators’ knee-jerk reaction is to cut costs. But there is another option: Grow the hospital out of its financial difficulties. It is up to the HM director to show administrators how the HM group has strategically gained them market share and how it will continue to do so. Good directors are in near constant contact with administrators, demonstrating the value their hospitalist program brings to the hospital, Buser says.
“You’re having regular meetings with the administrator, you’re producing the dashboard on a regular basis, you’re giving him trends that are going on,” he explains. “Show that you understand the hospital’s issues. Certain things you want to compromise on, but other things you have to say, ‘If we do that, the ramifications are such that it’s just not going to work.’”
Scenario No. 2 : Recruiting Roulette
—David Friar, MD, SFHM, CEO, Hospitalists of Northern Michigan, Traverse City
The case: The HM director felt pressure to hire. The program’s hospitalists were seeing two to three patients a day more than they should have been, and hospital administrators were worried the program was losing ground to the other hospitalist group in the community. Using an outside recruiter, the director hired two adept physicians with stellar CVs after an expedited review process that included a background check, a few phone interviews, and day of in-person interviews with some administrators and a hospitalist on the team. Now, nearly a year later, one of the physicians is about to leave because her family doesn’t like the community, and the other new hire’s abrasive personality has caused considerable damage to the team’s cohesion.
Expert advice: A big part of an HM program’s value is how it practices as a unified team, and directors need to recognize how vital the “team fit” is to hospitalists, says David Friar, MD, SFHM, CEO of Hospitalists of Northern Michigan in Traverse City.
“A bad team fit is often worse than being short-staffed because it can literally destroy the team spirit,” he says.
Directors should have a standardized recruitment process that includes a comprehensive background screening where references are closely checked, a round of interviews by people outside the HM program (nurses and referring physicians), and substantial time spent with hospitalists in the program, says Bryce Gartland, MD, FHM, associate director of the hospital medicine division and medical director of care coordination at Emory Healthcare in Atlanta.
“We put [candidates] with one of our physicians to actually go around the hospital,” he says. “It’s amazing to me the number of things you can pick up by that broader exposure that you may not pick up sitting in a room with a candidate across the table for an hour.”
If a recruitment service is used, the director must describe the HM program in detail to the recruiter and even have them meet hospitalists on the staff, Dr. Friar says.
“Sending them a memo saying ‘We need three new hospitalists ASAP’ isn’t helping them find you the perfect candidate,” he says. “Even the best recruiter can only do a great job for you if they really know your team and what it is you need in a candidate.”
A director also is well served to make recruiting a family event where spouses and even children are part of the interview process.
“By including the entire family and then supporting them after the move, we are much more likely to recruit providers that will stay good members of our team for years to come,” Dr. Friar says.
Scenario No. 3 : Amitte Diem
—John Bulger, DO, FACP, FHM, chief quality officer, director, hospital medicine service line, Geisinger Health System, Danville, Pa.
The case: For months, the medical center has been receiving an increased number of referrals from outlying hospitals, and no end is in sight. The extra patient load, much of it involving complex cases, has agitated the medical center’s staff, particularly the specialists, and they’ve begun to complain to hospital administrators. Seeking an ally, the specialists reach out to the HM director to present their case. Without doing independent analysis, the HM director sides with the specialists. Hospital administrators, facing growing resistance, work to decrease the referrals and are successful.
Expert advice: Consider working in the opposite direction, one that might turn a referral challenge into a profitable opportunity, Buser says. One of his firm’s clients, after thorough research, established a transfer center and set up an activation fee for the specialists who took the referrals. Hospitalists admitted about 90% of the cases, called consults, and named specialists so they received full fee-for-service at Medicare rates if they saw uninsured patients.
“That hospital is now making about $78 million a year, and the medical staff is saying, ‘How can we grow this?’” Buser says. “Here’s an example of how the hospital medicine director was key to turning the bad into something good.”
Because physicians tend to be reticent to change, it’s critical for hospitalist directors who want to seize an opportunity to thoroughly plan out how the change will occur and to prepare for potential obstacles along the way, says John Bulger, DO, FACP, FHM, chief quality officer and director of the hospital medicine service line for Geisinger Health System in Danville, Pa.
“You really need to be prepared with your rationale of why you’re doing it, if there’s data behind why you’re doing it, what the data is that’s driving it, and really what you hope to do with that change,” he says. “If you don’t get buy in from your staff, the change is doomed to fail from the beginning.”
Directors must embrace being a change agent if they want their HM programs to continue to be successful. In the minds of many hospital administrators, a program is only as good as its last achievement.
“It’s kind of like, ‘What have you done for me lately?’” Buser says. “You want to stay ahead of the curve and be alert to what’s going on and not be caught keeping your eyes off the ball and, as a result, not moving your program forward.”
Scenario No. 4 : Fumbling the Handoff
—Daniel Cusator, MD, MBA, vice president, Camden Group, El Segundo, Calif.
The case: The medical center’s monthly data for the past year has shown that hospitalists are taking care of their patients efficiently and getting them out of the hospital more quickly. However, mixed in with the positive numbers is a stubbornly high 30-day readmission rate. Indeed, some primary care groups and referring geriatricians have begun to grouse to the HM director about the discharge notes, complaining they aren’t as comprehensive as they would like.
Plus, the notes always arrive via office fax, which makes them more likely to get misplaced and harder to receive when doctors are out of the office.
Expert advice: Handoffs from discharge to pickup are where a lot of complications, errors, and safety issues arise, and poor handoffs are one of the largest drivers of readmission rates, especially in the elderly patient population, says Daniel Cusator, MD, MBA, vice president of the Camden Group, a healthcare consulting firm in El Segundo, Calif.
If the hospitalist director doesn’t provide the leadership and resources to help the HM team better coordinate with patients’ regular doctors, handoffs won’t be a priority throughout the group.
The HM director must recognize that the term “discharge note” is a misnomer.
What referring physicians really want is a care plan, which includes information about testing done in the hospital, testing that might be needed in the outpatient setting, medications the patient is on, complications the patient had in the hospital, potential problems to monitor, and any necessary follow-up, says Dr. Cusator, formerly the chief medical officer of clinical integration at Providence Health & Services in Southern California.
PCPs also want the care plan transmitted in their preferred method, whether that is text messaging, HIPAA-compliant email messaging, secure messaging, or fax.
“What I’ve seen some hospitalist groups do is create a menu capability for each of the physicians to choose their preferred method of notification of discharge of their patient,” Dr. Cusator says. Results suggest such a menu leads to improved physician satisfaction and reduced patient complications after discharge, he adds.
With today’s technological innovations, HM directors are unlimited in their ability to improve handoffs between their team and patients’ PCPs and specialists, Dr. Cusator says. Some HM directors, for example, are leading efforts to link electronic medical records systems to hospital-based health information exchange hubs that are accessible to physicians in the community.
“Notes and clinical information are submitted to this health information exchange and made available to any of the physicians who are caring for the patient almost immediately upon dictation and notation,” he says.
Scenario No. 5 : Protect Your Assets
—David Lee, MD, MBA, FACP, FHM, vice chairman, Hospital Medicine Department, Ochsner Health System, New Orleans.
The case: A physician isn’t sure she wants a career in hospital medicine. She finds the specialty rewarding but is looking for a different challenge, something beyond exclusively seeing patients. The HM director notices the physician has an aptitude for finding ways to do tasks more efficiently.
The director privately thinks the physician would be a good fit for a quality improvement project that’s about to start but doesn’t pursue it. The HM team just added a primary care group, and its patient census is quickly rising, requiring the hospitalists to devote their entire shifts to patient care. Within the year, the physician leaves the team for a fellowship program outside hospital medicine.
Expert advice: There are three communities in hospital medicine, Dr. Bulger says: people who want to be hospitalists, people who are passing through on their way to something else, and people who sit somewhere in the middle.
HM directors, he says, should do everything they can to develop not only the career hospitalists but also those on the fence.
“A lot of them you can turn into people who are going to be hospitalists if they are doing something that is rewarding for them,” Dr. Bulger says. “Many times rewarding for them is being involved more in the leadership of the group, being involved in quality improvement projects, really seeing how they can impact the care for populations of patients—and not just the patient who happens to be sitting in front of them.”
It’s incumbent on HM group leaders to link hospitalists with mentors and help them find a niche, Dr. Lee says. It keeps people interested and makes them feel part of a group.
“They need to feel they belong,” he says. “There has to be a cohesiveness in order for your department to excel. You have to protect your assets in the group, which is your physicians.”
Sending hospitalists to professional development training, such as SHM’s Leadership Academy (see “Leadership Academy Adds ‘Women in HM Issues’ to Schedule,” p. 9) or QI-focused webinars offered by SHM or the Institute of Healthcare Improvement, and following up with day-to-day coaching is a solid physician-development strategy, Dr. Gartland says. By virtue of their job, hospitalists are expected to lead and manage people in interactions with the ED, primary care, non-physician providers, nursing staff, and beyond, he says.
Directors also have to stop assuming that competent physicians are competent managers. “A lot of physicians don’t have those core skill sets, and we’ve got to pay conscious attention toward spending time dedicated to developing those,” Dr. Gartland says.
If directors don’t make professional development a priority or provide hospitalists with the flexibility to do non-clinical activities, retention may become an issue, Dr. Bulger says. “They could leave and go somewhere else,” he says, yet perhaps the more significant danger is losing hospitalists to programs and specialties outside hospital medicine.
Lisa Ryan is a freelance writer based in New Jersey.
THE FUNDAMENTALS
As hospitals position themselves for healthcare reform, they increasingly will turn to HM for strategies on how to provide high-quality patient care at a lower cost, Buser says. To meet hospitals’ needs and enhance the value of their programs, hospitalist directors should consider adopting these strategies recommended by HM leaders:
- Align compensation with the HM program’s goals. For example, if quality improvement is the priority, directors should financially reward hospitalists on quality performance, Dr. Lee says.
- Boost support staff and functions. For example, directors should ensure their team has access to the hospital’s case managers, who can handle discharge logistics so the hospitalist can focus on clinical issues, Dr. Cusator says.
- Control program growth. To borrow a popular line from the movie Field of Dreams: “If you build it, they will come.” Directors should be deliberate with group expansion and ensure enough staff is in place before adding to their referral base or adding a new service line, Dr. Bulger says. This reduces hospitalist burnout and preserves the group’s quality of patient care.
- Define two to three targets for success in the upcoming year and concentrate on accomplishing them. Start by consolidating what your team is working on, says Steven Deitelzweig, MD, SFHM, chairman of the Department of Hospital Medicine at Ochsner Health System in New Orleans. Pick too many things to master, and you end up excelling in none, he adds.
- Evaluate performance beyond a scorecard. Using constructive criticism grounded with examples, HM directors should provide feedback about what a physician is doing well and what can be done better so they can improve, Dr. Gartland says.
- Foster creative problem solving by including hospitalists in decisions. Directors should encourage the expression of different opinions and ideas, which helps the program avoid “group think” and allows innovation to occur, Dr. Lee says.
- Galvanize the new generation. To retain young physicians and make them feel part of the program, directors should learn how they communicate, how they work, and how they view work, Dr. Lee says.
- Help your hospital accurately measure reimbursement and mortality rates. Directors should make coding a priority and provide hospitalists with the tools they need to capture correct ICD-9 and CPT codes for their patients, Dr. Cusator says.
- Identify missing core capabilities and dedicate resources for it. For example, if HM programs have a high census of chronically ill and end-of-life patients, directors should assist the hospital in establishing a palliative care or hospice program, Dr. Cusator says.
Dr. Hospitalist: Multiple Variables Factor into HM Compensation

I work with a number of health systems on determining full-market-value (FMV) compensation related to stipends paid to hospital-based specialists. What is your opinion on how compensation should be determined for the physicians to staff hospitals? Would you say that the busier the location, the higher the compensation? Would you say that the more hours the physician works (regardless of productivity), the more pay they receive? Would you say that the more years of experience that a physician has should result in higher compensation?
Curtis H. Bernstein, CPA/ABV, ASA, CVA, MBA,
director, valuation services,
Sinaiko Healthcare Consulting Inc.,
Los Angeles
Dr. Hospitalist responds:
The topic of physician compensation and workload comes up frequently, but this question frames it a bit differently. Namely, what are the external and internal factors at work in determining compensation? Let’s tackle the response in two parts: 1) How do you account for the variability across sites? and 2) How does physician pay vary within a single site? The crux of the first question comes down to trying to interpret physician workload across disparate locations. It’s not laden with quite the same complexity as Gordian’s knot, but it’s close. One could easily answer this question with a lot of “Yes, but ... ” in reference to the all the factors that go into determining compensation. Yes, a busier site would generate more encounters, thus more revenue, and thus more pay. However, that same site might also be so busy as to require more than one physician on at night. A higher-paid, but lower-volume, nocturnist would then skew the workload/pay scale. Same thing with the ICU; if it is fully staffed with intensivists (more likely in a higher-volume setting), then that would remove the single highest paying code for a hospitalist (the 99291: critical care time 35-74 minutes, 4.50 wRVU), and that has the potential to drop reimbursement. Practice management columnist John Nelson, MD, MHM, has written more than a few fantastic columns addressing just these sorts of issues, but let’s concentrate on just the key factors:
- Volume;
- Payor mix/collections;
- Ratio of day shifts to night shifts (optimal is 4:1), assuming that there are dedicated night shifts; and
- Value-added services.
Volume is fairly straightforward, with most hospitalists seeing around 15 patients per day. Now, an average is just that, and practices exist where the daily number is 10 and where the census is 25. Still, it’s an easy number to understand.
Payor mix is a little more complex but should not vary substantially quarter by quarter, though it could vary greatly year to year. (Note: This is independent of collection rate percentage, which is a completely artificial variable.) If Medicare pays $1 for a certain code and the charges are set at $1, then the collection rate is 100%. If the charges are set at $2, then the collection rate will be 50% but bring in the same amount of money. Arcane billing convention aside, from hospital to hospital and region to region, the payor mix and attendant collections will vary. Ratio of day shifts to night shifts posits that there is an optimal ratio of roughly four day shifts for every one night shift. Night shifts are more expensive, in general, so the more day shifts you have to cover your fixed cost of covering the nights, the better. The reason the ratio can’t be 10:1 is that 10 day-rounding hospitalists would generate a daily service of 150+ patients, and there is no way for one nocturnist to safely cross-cover all those folks, much less see new admissions.
Lastly, there are the value-added services that provide the raison d’être for hospitalists. We are fundamentally different from the procedure-based specialties in that our value comes not from increasing revenue (more procedures) but from decreasing costs. Initially, a lot of this focused on length of stay, and now it’s shifting to discussions of core measures, readmission rates, and other quality metrics. What a hospital is willing to pay for this service, which goes above and beyond taking call for unassigned patients, will go a long way toward determining the overall stipend and resultant physician compensation. (For more information on hospitalist compensation and productivity, check out the 2011 State of Hospital Medicine report, www.hospitalmedicine.org/survey)
Those are the basic underpinnings that will determine most of the variable compensation across disparate sites. Still, there can be other local factors (ancillary services, specialty support, EMRs, etc.) that come into play. Any practicing hospitalist can quickly discourse on what makes their job unique. And they are probably right—healthcare, like politics, is local.
I’ve run out of room to answer the second part of the question, which addresses the variable pay for physicians at the same site. Check back for that response next month.
I work with a number of health systems on determining full-market-value (FMV) compensation related to stipends paid to hospital-based specialists. What is your opinion on how compensation should be determined for the physicians to staff hospitals? Would you say that the busier the location, the higher the compensation? Would you say that the more hours the physician works (regardless of productivity), the more pay they receive? Would you say that the more years of experience that a physician has should result in higher compensation?
Curtis H. Bernstein, CPA/ABV, ASA, CVA, MBA,
director, valuation services,
Sinaiko Healthcare Consulting Inc.,
Los Angeles
Dr. Hospitalist responds:
The topic of physician compensation and workload comes up frequently, but this question frames it a bit differently. Namely, what are the external and internal factors at work in determining compensation? Let’s tackle the response in two parts: 1) How do you account for the variability across sites? and 2) How does physician pay vary within a single site? The crux of the first question comes down to trying to interpret physician workload across disparate locations. It’s not laden with quite the same complexity as Gordian’s knot, but it’s close. One could easily answer this question with a lot of “Yes, but ... ” in reference to the all the factors that go into determining compensation. Yes, a busier site would generate more encounters, thus more revenue, and thus more pay. However, that same site might also be so busy as to require more than one physician on at night. A higher-paid, but lower-volume, nocturnist would then skew the workload/pay scale. Same thing with the ICU; if it is fully staffed with intensivists (more likely in a higher-volume setting), then that would remove the single highest paying code for a hospitalist (the 99291: critical care time 35-74 minutes, 4.50 wRVU), and that has the potential to drop reimbursement. Practice management columnist John Nelson, MD, MHM, has written more than a few fantastic columns addressing just these sorts of issues, but let’s concentrate on just the key factors:
- Volume;
- Payor mix/collections;
- Ratio of day shifts to night shifts (optimal is 4:1), assuming that there are dedicated night shifts; and
- Value-added services.
Volume is fairly straightforward, with most hospitalists seeing around 15 patients per day. Now, an average is just that, and practices exist where the daily number is 10 and where the census is 25. Still, it’s an easy number to understand.
Payor mix is a little more complex but should not vary substantially quarter by quarter, though it could vary greatly year to year. (Note: This is independent of collection rate percentage, which is a completely artificial variable.) If Medicare pays $1 for a certain code and the charges are set at $1, then the collection rate is 100%. If the charges are set at $2, then the collection rate will be 50% but bring in the same amount of money. Arcane billing convention aside, from hospital to hospital and region to region, the payor mix and attendant collections will vary. Ratio of day shifts to night shifts posits that there is an optimal ratio of roughly four day shifts for every one night shift. Night shifts are more expensive, in general, so the more day shifts you have to cover your fixed cost of covering the nights, the better. The reason the ratio can’t be 10:1 is that 10 day-rounding hospitalists would generate a daily service of 150+ patients, and there is no way for one nocturnist to safely cross-cover all those folks, much less see new admissions.
Lastly, there are the value-added services that provide the raison d’être for hospitalists. We are fundamentally different from the procedure-based specialties in that our value comes not from increasing revenue (more procedures) but from decreasing costs. Initially, a lot of this focused on length of stay, and now it’s shifting to discussions of core measures, readmission rates, and other quality metrics. What a hospital is willing to pay for this service, which goes above and beyond taking call for unassigned patients, will go a long way toward determining the overall stipend and resultant physician compensation. (For more information on hospitalist compensation and productivity, check out the 2011 State of Hospital Medicine report, www.hospitalmedicine.org/survey)
Those are the basic underpinnings that will determine most of the variable compensation across disparate sites. Still, there can be other local factors (ancillary services, specialty support, EMRs, etc.) that come into play. Any practicing hospitalist can quickly discourse on what makes their job unique. And they are probably right—healthcare, like politics, is local.
I’ve run out of room to answer the second part of the question, which addresses the variable pay for physicians at the same site. Check back for that response next month.
I work with a number of health systems on determining full-market-value (FMV) compensation related to stipends paid to hospital-based specialists. What is your opinion on how compensation should be determined for the physicians to staff hospitals? Would you say that the busier the location, the higher the compensation? Would you say that the more hours the physician works (regardless of productivity), the more pay they receive? Would you say that the more years of experience that a physician has should result in higher compensation?
Curtis H. Bernstein, CPA/ABV, ASA, CVA, MBA,
director, valuation services,
Sinaiko Healthcare Consulting Inc.,
Los Angeles
Dr. Hospitalist responds:
The topic of physician compensation and workload comes up frequently, but this question frames it a bit differently. Namely, what are the external and internal factors at work in determining compensation? Let’s tackle the response in two parts: 1) How do you account for the variability across sites? and 2) How does physician pay vary within a single site? The crux of the first question comes down to trying to interpret physician workload across disparate locations. It’s not laden with quite the same complexity as Gordian’s knot, but it’s close. One could easily answer this question with a lot of “Yes, but ... ” in reference to the all the factors that go into determining compensation. Yes, a busier site would generate more encounters, thus more revenue, and thus more pay. However, that same site might also be so busy as to require more than one physician on at night. A higher-paid, but lower-volume, nocturnist would then skew the workload/pay scale. Same thing with the ICU; if it is fully staffed with intensivists (more likely in a higher-volume setting), then that would remove the single highest paying code for a hospitalist (the 99291: critical care time 35-74 minutes, 4.50 wRVU), and that has the potential to drop reimbursement. Practice management columnist John Nelson, MD, MHM, has written more than a few fantastic columns addressing just these sorts of issues, but let’s concentrate on just the key factors:
- Volume;
- Payor mix/collections;
- Ratio of day shifts to night shifts (optimal is 4:1), assuming that there are dedicated night shifts; and
- Value-added services.
Volume is fairly straightforward, with most hospitalists seeing around 15 patients per day. Now, an average is just that, and practices exist where the daily number is 10 and where the census is 25. Still, it’s an easy number to understand.
Payor mix is a little more complex but should not vary substantially quarter by quarter, though it could vary greatly year to year. (Note: This is independent of collection rate percentage, which is a completely artificial variable.) If Medicare pays $1 for a certain code and the charges are set at $1, then the collection rate is 100%. If the charges are set at $2, then the collection rate will be 50% but bring in the same amount of money. Arcane billing convention aside, from hospital to hospital and region to region, the payor mix and attendant collections will vary. Ratio of day shifts to night shifts posits that there is an optimal ratio of roughly four day shifts for every one night shift. Night shifts are more expensive, in general, so the more day shifts you have to cover your fixed cost of covering the nights, the better. The reason the ratio can’t be 10:1 is that 10 day-rounding hospitalists would generate a daily service of 150+ patients, and there is no way for one nocturnist to safely cross-cover all those folks, much less see new admissions.
Lastly, there are the value-added services that provide the raison d’être for hospitalists. We are fundamentally different from the procedure-based specialties in that our value comes not from increasing revenue (more procedures) but from decreasing costs. Initially, a lot of this focused on length of stay, and now it’s shifting to discussions of core measures, readmission rates, and other quality metrics. What a hospital is willing to pay for this service, which goes above and beyond taking call for unassigned patients, will go a long way toward determining the overall stipend and resultant physician compensation. (For more information on hospitalist compensation and productivity, check out the 2011 State of Hospital Medicine report, www.hospitalmedicine.org/survey)
Those are the basic underpinnings that will determine most of the variable compensation across disparate sites. Still, there can be other local factors (ancillary services, specialty support, EMRs, etc.) that come into play. Any practicing hospitalist can quickly discourse on what makes their job unique. And they are probably right—healthcare, like politics, is local.
I’ve run out of room to answer the second part of the question, which addresses the variable pay for physicians at the same site. Check back for that response next month.
Survey Insights: It's All Written in Code
One of the questions I am often asked is “What is the typical distribution of CPT codes for hospitalists?” Prior to publication of the 2011 State of Hospital Medicine report, no one could answer that question with any authority. The Centers for Medicare & Medicaid Services (CMS) publishes some Healthcare Procedure Code (HCPC) distribution information by specialty, but because CMS does not recognize HM as a specialty, the closest proxies are the reported distributions for internal medicine (or pediatrics). And hospitalists argue that because their patient population and the work they do are different, typical distributions for those specialties might not be applicable to hospitalists.
“Coding for hospitalists has to be different from other internists,” says SHM Practice Analysis Committee (PAC) member Rachel Lovins, MD, SFHM. “Because we take responsibility for unfamiliar patients that we hand back to other providers, our level of admission and discharge documentation in particular needs to be higher, in order to ensure excellent communication between hospitalists and PCPs.”
We finally have information about hospitalist coding practices, because both the academic and non-academic Hospital Medicine Supplements captured information about the distribution of inpatient admissions (CPT codes 99221, 99222, and 99223), subsequent visits (99231, 99232, and 99233), and discharges (99238 and 99239). Figure 1 shows the average CPT code distribution for non-academic HM groups serving adults only.
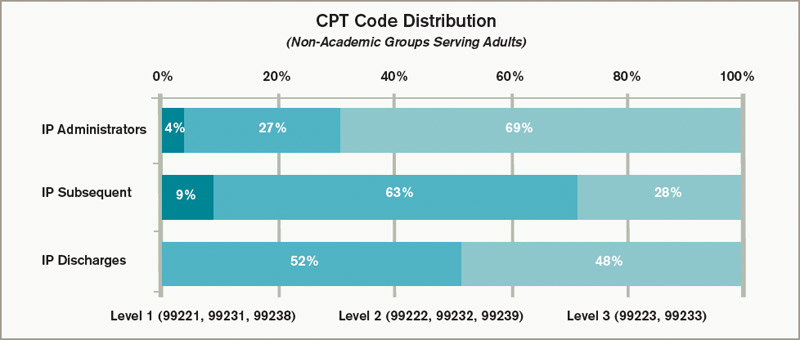
Figure 1. CPT code distribution for non-academic HM groups serving adults
The 2011 State of Hospital Medicine report also shows how CPT distribution varied based on some key practice characteristics. For example, HM practices that are not owned by hospitals/integrated delivery systems tend to code more of their services at higher service levels than do hospital-owned practices. And practices in the Western section of the country tend to code more services at higher levels than other parts of the country.
Other factors are certainly at play as well. “Whether a physician receives training in documentation and coding can have a tremendous impact on CPT distributions,” PAC member Beth Papetti says. “Historically, there has been a tendency for hospitalists to under-code, but through education and enhancements like electronic charge capture, hospitalists can more accurately substantiate the services they provided to the patient.”
Other committee members have speculated that a hospitalist’s compensation model might influence coding patterns, with those who receive less of their total compensation in the form of base salary (and more in the form of productivity and/or performance-based pay) tending to code more of their services at higher levels. But, in fact, the survey data don’t reveal any clear relationship between compensation structure and the average number of work RVUs (relative value units) per encounter.
Interestingly, coding patterns of academic HM practices were similar to those of non-academic practices for admissions and subsequent visits, but academic hospitalists tend to code a higher proportion of discharges at the <30-minute level (99238). PAC members speculate that residents and hospital support staff might perform a larger portion of the discharge coordination and paperwork in academic centers, and attendings can only bill based on their personal time, not time spent by others.
To contribute to a robust CPT distribution database, be sure to participate in the next State of Hospital Medicine survey, scheduled to launch in January 2012.
Leslie Flores, SHM senior advisor, practice management
One of the questions I am often asked is “What is the typical distribution of CPT codes for hospitalists?” Prior to publication of the 2011 State of Hospital Medicine report, no one could answer that question with any authority. The Centers for Medicare & Medicaid Services (CMS) publishes some Healthcare Procedure Code (HCPC) distribution information by specialty, but because CMS does not recognize HM as a specialty, the closest proxies are the reported distributions for internal medicine (or pediatrics). And hospitalists argue that because their patient population and the work they do are different, typical distributions for those specialties might not be applicable to hospitalists.
“Coding for hospitalists has to be different from other internists,” says SHM Practice Analysis Committee (PAC) member Rachel Lovins, MD, SFHM. “Because we take responsibility for unfamiliar patients that we hand back to other providers, our level of admission and discharge documentation in particular needs to be higher, in order to ensure excellent communication between hospitalists and PCPs.”
We finally have information about hospitalist coding practices, because both the academic and non-academic Hospital Medicine Supplements captured information about the distribution of inpatient admissions (CPT codes 99221, 99222, and 99223), subsequent visits (99231, 99232, and 99233), and discharges (99238 and 99239). Figure 1 shows the average CPT code distribution for non-academic HM groups serving adults only.
Figure 1. CPT code distribution for non-academic HM groups serving adults
The 2011 State of Hospital Medicine report also shows how CPT distribution varied based on some key practice characteristics. For example, HM practices that are not owned by hospitals/integrated delivery systems tend to code more of their services at higher service levels than do hospital-owned practices. And practices in the Western section of the country tend to code more services at higher levels than other parts of the country.
Other factors are certainly at play as well. “Whether a physician receives training in documentation and coding can have a tremendous impact on CPT distributions,” PAC member Beth Papetti says. “Historically, there has been a tendency for hospitalists to under-code, but through education and enhancements like electronic charge capture, hospitalists can more accurately substantiate the services they provided to the patient.”
Other committee members have speculated that a hospitalist’s compensation model might influence coding patterns, with those who receive less of their total compensation in the form of base salary (and more in the form of productivity and/or performance-based pay) tending to code more of their services at higher levels. But, in fact, the survey data don’t reveal any clear relationship between compensation structure and the average number of work RVUs (relative value units) per encounter.
Interestingly, coding patterns of academic HM practices were similar to those of non-academic practices for admissions and subsequent visits, but academic hospitalists tend to code a higher proportion of discharges at the <30-minute level (99238). PAC members speculate that residents and hospital support staff might perform a larger portion of the discharge coordination and paperwork in academic centers, and attendings can only bill based on their personal time, not time spent by others.
To contribute to a robust CPT distribution database, be sure to participate in the next State of Hospital Medicine survey, scheduled to launch in January 2012.
Leslie Flores, SHM senior advisor, practice management
One of the questions I am often asked is “What is the typical distribution of CPT codes for hospitalists?” Prior to publication of the 2011 State of Hospital Medicine report, no one could answer that question with any authority. The Centers for Medicare & Medicaid Services (CMS) publishes some Healthcare Procedure Code (HCPC) distribution information by specialty, but because CMS does not recognize HM as a specialty, the closest proxies are the reported distributions for internal medicine (or pediatrics). And hospitalists argue that because their patient population and the work they do are different, typical distributions for those specialties might not be applicable to hospitalists.
“Coding for hospitalists has to be different from other internists,” says SHM Practice Analysis Committee (PAC) member Rachel Lovins, MD, SFHM. “Because we take responsibility for unfamiliar patients that we hand back to other providers, our level of admission and discharge documentation in particular needs to be higher, in order to ensure excellent communication between hospitalists and PCPs.”
We finally have information about hospitalist coding practices, because both the academic and non-academic Hospital Medicine Supplements captured information about the distribution of inpatient admissions (CPT codes 99221, 99222, and 99223), subsequent visits (99231, 99232, and 99233), and discharges (99238 and 99239). Figure 1 shows the average CPT code distribution for non-academic HM groups serving adults only.
Figure 1. CPT code distribution for non-academic HM groups serving adults
The 2011 State of Hospital Medicine report also shows how CPT distribution varied based on some key practice characteristics. For example, HM practices that are not owned by hospitals/integrated delivery systems tend to code more of their services at higher service levels than do hospital-owned practices. And practices in the Western section of the country tend to code more services at higher levels than other parts of the country.
Other factors are certainly at play as well. “Whether a physician receives training in documentation and coding can have a tremendous impact on CPT distributions,” PAC member Beth Papetti says. “Historically, there has been a tendency for hospitalists to under-code, but through education and enhancements like electronic charge capture, hospitalists can more accurately substantiate the services they provided to the patient.”
Other committee members have speculated that a hospitalist’s compensation model might influence coding patterns, with those who receive less of their total compensation in the form of base salary (and more in the form of productivity and/or performance-based pay) tending to code more of their services at higher levels. But, in fact, the survey data don’t reveal any clear relationship between compensation structure and the average number of work RVUs (relative value units) per encounter.
Interestingly, coding patterns of academic HM practices were similar to those of non-academic practices for admissions and subsequent visits, but academic hospitalists tend to code a higher proportion of discharges at the <30-minute level (99238). PAC members speculate that residents and hospital support staff might perform a larger portion of the discharge coordination and paperwork in academic centers, and attendings can only bill based on their personal time, not time spent by others.
To contribute to a robust CPT distribution database, be sure to participate in the next State of Hospital Medicine survey, scheduled to launch in January 2012.
Leslie Flores, SHM senior advisor, practice management
Holdout Hospitals

I think 70% to 80% of U.S. hospitals now have a hospitalist practice. (Some have more than one hospitalist group operating within their walls.) I arrived at this estimate by relying on both my anecdotal experience and on the annual American Hospital Association survey, which in 2009 showed 58% of hospitals have hospitalists, with an ongoing rapid rate of adoption.
No regular reader of The Hospitalist should be surprised that most U.S. hospitals now have hospitalists, but some might be surprised that 20% to 30% don’t. There are about 5,800 hospitals in the U.S. (a ballpark figure), so that means about 1,100 to 1,800 don’t have hospitalists. What is unique about them?
For some hospitals, the answer is easy. For example, the U.S. has something like 450 psychiatric hospitals. They vary a lot, but many simply don’t accept patients with active medical problems, so these facilities would have little need for medical hospitalists.
Variations in how the term “hospitalist” is used probably account for some facilities reporting no hospitalists. For example, long-term acute-care hospitals (LTACs) might have dedicated inpatient providers but simply don’t call them hospitalists.
Even accounting for these things, there are still a lot of “med-surg” hospitals that say they don’t have hospitalists.
The Holdouts
My experience suggests the two most important reasons some hospitals have not yet developed a hospitalist practice are an oversupply of primary-care physicians (PCPs) and an attractive payor mix in the unassigned patient population. In fact, it is hard for me to imagine a hospital that enjoys both of these attributes ever being able to support hospitalists.
Although it isn’t a common problem, an excess of PCPs (or dearth of patients) removes the most universal and powerful stimulus to develop a hospitalist practice: the desire of PCPs to be relieved of hospital work. And in most cases, those PCPs can offset the loss of hospital work and its associated revenue, with more work in the office. This can mean a better lifestyle (e.g. no trips to the hospital on nights and weekends) and the same or higher income. But if there are too many PCPs in the community, they may be unwilling to give up the hospital work, as there might be no way to replace it in the office. End result: no hospitalists.
For the rare hospital that has an attractive ED-unassigned payor mix, PCPs are more likely to want to continue taking ED call and not support a proposal to develop a hospitalist practice. And access to the ED call roster can be important to new PCPs building a community practice. I have seen situations in which a hospital has addressed the poor reimbursement of unattached ED admissions by paying PCPs to provide that care. Even though that same hospital might want a hospitalist practice, the ED call payment it is providing to PCPs may create a barrier that can’t be overcome. Such a hospital will face the very difficult decision of terminating the payments for ED call and redirecting that money to a hospitalist practice—something that is likely to lead to a lot of frustration on the part of PCPs who depend on the pay-for-call arrangement. A common outcome: no hospitalists.
An occasional reason hospitals are late to the hospitalist party is one or two (rarely more than that) of its private PCPs have simply chosen to work heroic amounts, and in addition to office and hospital care of their private patients, they accept referrals from other PCPs. I have met a number of doctors like this. Some are terrific doctors who actively participate in hospital initiatives; many appear chronically tired and harried, and hospital staff express frustration that they do things like make rounds at 3 a.m., take hours to respond to urgent calls, refuse to use protocols, etc. But because they’ve responded to the PCPs’ desire to be relieved of hospital work, other doctors may rally to their support and prevent the hospital from moving forward with a hospitalist program.
Will Every Hospital Have Hospitalists Eventually?
It is really interesting to think about whether every hospital, outside narrow specialty hospitals, will have hospitalists in the future. I wonder what informed people in the 1970s and early 1980s were predicting for emergency medicine’s future. At that point it probably wasn’t clear that, in the future, dedicated ED doctors essentially would staff every ED in the country, but I think that is exactly what has happened. (I once worked with an approximately 100-bed rural hospital that didn’t have ED physicians until 1999. I wonder if they were the last adopter.)
I think hospitalists are critically important for nearly all med-surg hospitals; however, maybe there will always be a small number that either have PCPs continue to practice in the traditional model, working both outpatient and inpatient, or some other effective configuration that makes hospitalists less necessary. We’ll have to wait and see. But I’m pretty confident
that almost no institutions that have hospitalists will ever return to the pre-hospitalist model of care. It seems there is no going back.
For those hospitals without hospitalists currently who will at some future time have hospitalists, the right time for this to happen is dependent on a combination of local factors. It could be something like the departure (i.e. relocation or retirement) of some of the current doctors, or simply the arrival of someone who has a vision and energy to successfully navigate the obstacles to build one. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.</p>
I think 70% to 80% of U.S. hospitals now have a hospitalist practice. (Some have more than one hospitalist group operating within their walls.) I arrived at this estimate by relying on both my anecdotal experience and on the annual American Hospital Association survey, which in 2009 showed 58% of hospitals have hospitalists, with an ongoing rapid rate of adoption.
No regular reader of The Hospitalist should be surprised that most U.S. hospitals now have hospitalists, but some might be surprised that 20% to 30% don’t. There are about 5,800 hospitals in the U.S. (a ballpark figure), so that means about 1,100 to 1,800 don’t have hospitalists. What is unique about them?
For some hospitals, the answer is easy. For example, the U.S. has something like 450 psychiatric hospitals. They vary a lot, but many simply don’t accept patients with active medical problems, so these facilities would have little need for medical hospitalists.
Variations in how the term “hospitalist” is used probably account for some facilities reporting no hospitalists. For example, long-term acute-care hospitals (LTACs) might have dedicated inpatient providers but simply don’t call them hospitalists.
Even accounting for these things, there are still a lot of “med-surg” hospitals that say they don’t have hospitalists.
The Holdouts
My experience suggests the two most important reasons some hospitals have not yet developed a hospitalist practice are an oversupply of primary-care physicians (PCPs) and an attractive payor mix in the unassigned patient population. In fact, it is hard for me to imagine a hospital that enjoys both of these attributes ever being able to support hospitalists.
Although it isn’t a common problem, an excess of PCPs (or dearth of patients) removes the most universal and powerful stimulus to develop a hospitalist practice: the desire of PCPs to be relieved of hospital work. And in most cases, those PCPs can offset the loss of hospital work and its associated revenue, with more work in the office. This can mean a better lifestyle (e.g. no trips to the hospital on nights and weekends) and the same or higher income. But if there are too many PCPs in the community, they may be unwilling to give up the hospital work, as there might be no way to replace it in the office. End result: no hospitalists.
For the rare hospital that has an attractive ED-unassigned payor mix, PCPs are more likely to want to continue taking ED call and not support a proposal to develop a hospitalist practice. And access to the ED call roster can be important to new PCPs building a community practice. I have seen situations in which a hospital has addressed the poor reimbursement of unattached ED admissions by paying PCPs to provide that care. Even though that same hospital might want a hospitalist practice, the ED call payment it is providing to PCPs may create a barrier that can’t be overcome. Such a hospital will face the very difficult decision of terminating the payments for ED call and redirecting that money to a hospitalist practice—something that is likely to lead to a lot of frustration on the part of PCPs who depend on the pay-for-call arrangement. A common outcome: no hospitalists.
An occasional reason hospitals are late to the hospitalist party is one or two (rarely more than that) of its private PCPs have simply chosen to work heroic amounts, and in addition to office and hospital care of their private patients, they accept referrals from other PCPs. I have met a number of doctors like this. Some are terrific doctors who actively participate in hospital initiatives; many appear chronically tired and harried, and hospital staff express frustration that they do things like make rounds at 3 a.m., take hours to respond to urgent calls, refuse to use protocols, etc. But because they’ve responded to the PCPs’ desire to be relieved of hospital work, other doctors may rally to their support and prevent the hospital from moving forward with a hospitalist program.
Will Every Hospital Have Hospitalists Eventually?
It is really interesting to think about whether every hospital, outside narrow specialty hospitals, will have hospitalists in the future. I wonder what informed people in the 1970s and early 1980s were predicting for emergency medicine’s future. At that point it probably wasn’t clear that, in the future, dedicated ED doctors essentially would staff every ED in the country, but I think that is exactly what has happened. (I once worked with an approximately 100-bed rural hospital that didn’t have ED physicians until 1999. I wonder if they were the last adopter.)
I think hospitalists are critically important for nearly all med-surg hospitals; however, maybe there will always be a small number that either have PCPs continue to practice in the traditional model, working both outpatient and inpatient, or some other effective configuration that makes hospitalists less necessary. We’ll have to wait and see. But I’m pretty confident
that almost no institutions that have hospitalists will ever return to the pre-hospitalist model of care. It seems there is no going back.
For those hospitals without hospitalists currently who will at some future time have hospitalists, the right time for this to happen is dependent on a combination of local factors. It could be something like the departure (i.e. relocation or retirement) of some of the current doctors, or simply the arrival of someone who has a vision and energy to successfully navigate the obstacles to build one. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.</p>
I think 70% to 80% of U.S. hospitals now have a hospitalist practice. (Some have more than one hospitalist group operating within their walls.) I arrived at this estimate by relying on both my anecdotal experience and on the annual American Hospital Association survey, which in 2009 showed 58% of hospitals have hospitalists, with an ongoing rapid rate of adoption.
No regular reader of The Hospitalist should be surprised that most U.S. hospitals now have hospitalists, but some might be surprised that 20% to 30% don’t. There are about 5,800 hospitals in the U.S. (a ballpark figure), so that means about 1,100 to 1,800 don’t have hospitalists. What is unique about them?
For some hospitals, the answer is easy. For example, the U.S. has something like 450 psychiatric hospitals. They vary a lot, but many simply don’t accept patients with active medical problems, so these facilities would have little need for medical hospitalists.
Variations in how the term “hospitalist” is used probably account for some facilities reporting no hospitalists. For example, long-term acute-care hospitals (LTACs) might have dedicated inpatient providers but simply don’t call them hospitalists.
Even accounting for these things, there are still a lot of “med-surg” hospitals that say they don’t have hospitalists.
The Holdouts
My experience suggests the two most important reasons some hospitals have not yet developed a hospitalist practice are an oversupply of primary-care physicians (PCPs) and an attractive payor mix in the unassigned patient population. In fact, it is hard for me to imagine a hospital that enjoys both of these attributes ever being able to support hospitalists.
Although it isn’t a common problem, an excess of PCPs (or dearth of patients) removes the most universal and powerful stimulus to develop a hospitalist practice: the desire of PCPs to be relieved of hospital work. And in most cases, those PCPs can offset the loss of hospital work and its associated revenue, with more work in the office. This can mean a better lifestyle (e.g. no trips to the hospital on nights and weekends) and the same or higher income. But if there are too many PCPs in the community, they may be unwilling to give up the hospital work, as there might be no way to replace it in the office. End result: no hospitalists.
For the rare hospital that has an attractive ED-unassigned payor mix, PCPs are more likely to want to continue taking ED call and not support a proposal to develop a hospitalist practice. And access to the ED call roster can be important to new PCPs building a community practice. I have seen situations in which a hospital has addressed the poor reimbursement of unattached ED admissions by paying PCPs to provide that care. Even though that same hospital might want a hospitalist practice, the ED call payment it is providing to PCPs may create a barrier that can’t be overcome. Such a hospital will face the very difficult decision of terminating the payments for ED call and redirecting that money to a hospitalist practice—something that is likely to lead to a lot of frustration on the part of PCPs who depend on the pay-for-call arrangement. A common outcome: no hospitalists.
An occasional reason hospitals are late to the hospitalist party is one or two (rarely more than that) of its private PCPs have simply chosen to work heroic amounts, and in addition to office and hospital care of their private patients, they accept referrals from other PCPs. I have met a number of doctors like this. Some are terrific doctors who actively participate in hospital initiatives; many appear chronically tired and harried, and hospital staff express frustration that they do things like make rounds at 3 a.m., take hours to respond to urgent calls, refuse to use protocols, etc. But because they’ve responded to the PCPs’ desire to be relieved of hospital work, other doctors may rally to their support and prevent the hospital from moving forward with a hospitalist program.
Will Every Hospital Have Hospitalists Eventually?
It is really interesting to think about whether every hospital, outside narrow specialty hospitals, will have hospitalists in the future. I wonder what informed people in the 1970s and early 1980s were predicting for emergency medicine’s future. At that point it probably wasn’t clear that, in the future, dedicated ED doctors essentially would staff every ED in the country, but I think that is exactly what has happened. (I once worked with an approximately 100-bed rural hospital that didn’t have ED physicians until 1999. I wonder if they were the last adopter.)
I think hospitalists are critically important for nearly all med-surg hospitals; however, maybe there will always be a small number that either have PCPs continue to practice in the traditional model, working both outpatient and inpatient, or some other effective configuration that makes hospitalists less necessary. We’ll have to wait and see. But I’m pretty confident
that almost no institutions that have hospitalists will ever return to the pre-hospitalist model of care. It seems there is no going back.
For those hospitals without hospitalists currently who will at some future time have hospitalists, the right time for this to happen is dependent on a combination of local factors. It could be something like the departure (i.e. relocation or retirement) of some of the current doctors, or simply the arrival of someone who has a vision and energy to successfully navigate the obstacles to build one. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.</p>
Your 2012 Resolution: Stop Extending Credit!
For as long as I have been writing this column, I have stressed that aggressive management of accounts receivable is the key to any practice’s financial health; and yet, all these years later, accounts receivable is still the subject that generates the most questions.
Okay, folks, let’s go over it one more time: Basically, physicians extend more credit than any business except banks. Despite what you may have read recently, banks are good at it, and they charge interest (and a myriad of fees) to do it. Doctors do it for free. Are we crazy? No business owner in his or her right mind allows customers to take away goods or services without paying for them, but physicians do it every day.
What to do? Common sense tells you to collect everything you can at the time of service, but some patients inevitably brandish the old "I forgot my checkbook" excuse and escape without paying. And the patient-owed portion of most insurance charges is often unknown – and unknowable – at the time of service.
That means you’ll need to send a bill, and every bill you send (or hire somebody to send) costs you a bundle. And when it arrives, it goes right to the bottom of your patient’s payment priority list. That is, each month your patients will pay their electric, water, gas, and telephone bills – and just about any other bill – before getting around to yours. If there is no more money when your bill finally surfaces, that’s just too bad. An unpaid electric company can shut off their power, but what can you do?
What we do in our practice is what every hotel, rental car agency, and many other businesses have done for years: We ask for a credit card number and bill balances to it as they come in. Plastic runs the show everywhere you go – except in most medical offices.
Every new patient in my office receives a letter at their first visit explaining our policy: We will keep a credit card number on file, and use it to bill any outstanding balances. At the bottom is a brief consent for the patient to sign, and a place to write the credit card number and expiration date. (The sample text of the letter is at the end of this column.)
Do patients object? Some do – mostly older people. But when we explain that we’re doing nothing different from what a hotel does at each check-in, and that it will work to their advantage by decreasing the bills they receive and the checks they must write, most come around. Make it an option at first if you wish; then, when everyone is accustomed, you can make it mandatory.
Do they worry about confidentiality or unauthorized use? They don’t anywhere else. They think nothing of handing a card to servers in restaurant with no thought of what they might do with it in the kitchen. They hand the card to hotel clerks, and never think to ask how long the information is kept or who has access to it. They blithely shoot numbers into black holes on the Internet.
We explain that we guard our patients’ financial information as carefully as we do their medical information. (If you have an EHR, it can go in the chart with everything else; if not, I suggest a separate portable file that can be locked up each night.)
Does it work? In only a year, our accounts receivable totals dropped by nearly 50%; after another year, they stabilized at 30%-35% of previous levels and have remained there ever since. Last year I hired a new accountant. Something must be wrong, he said nervously, after his first look at the books; account receivable totals are "never" that low. His eyes widened as I explained our system. "Why doesn’t every medical office do that?" he asked.
Why indeed? The business of health care delivery will be rocked to its very foundations in the next few years. In my humble opinion, private practice will survive those changes only if physicians learn to do more of what we do best – treating patients – and leave the business of extending credit to the banks.
PLEASE NOTE:
This generic letter is intended to be used as an example for a letter you might draft for a similar purpose. However, we take no responsibility for your use of its content, either verbatim or altered, or any inappropriate usage.
To Our Patients:
As you know if you have ever checked into a hotel or rented a car, the first thing you are asked for is a credit card, which is imprinted and later used to pay your bill. This is an advantage for both you and the hotel or rental company, since it makes checkout easier, faster, and more efficient.
We have implemented a similar policy. You will be asked for a credit card number at the time you check in and the information will be held securely until your insurances have paid their portion and notified us of the amount of your share. At that time, any remaining balance owed by you will be charged to your credit card, and a copy of the charge will be mailed to you.
This will be an advantage to you, since you will no longer have to write out and mail us checks. It will be an advantage to us as well, since it will greatly decrease the number of statements that we have to generate and send out. The combination will benefit everybody in helping to keep the cost of health care down.
This in no way will compromise your ability to dispute a charge or question your insurance company’s determination of payment.
Co-pays due at the time of the visit will, of course, still be due at the time of the visit.
If you have any questions about this payment method, do not hesitate to ask.
Sincerely yours,
I authorize ********************, PA to charge outstanding balances on my account to the following credit card:
Visa Mastercard American Express Other: __________
Account number ________________
Expiration Date ____________
For as long as I have been writing this column, I have stressed that aggressive management of accounts receivable is the key to any practice’s financial health; and yet, all these years later, accounts receivable is still the subject that generates the most questions.
Okay, folks, let’s go over it one more time: Basically, physicians extend more credit than any business except banks. Despite what you may have read recently, banks are good at it, and they charge interest (and a myriad of fees) to do it. Doctors do it for free. Are we crazy? No business owner in his or her right mind allows customers to take away goods or services without paying for them, but physicians do it every day.
What to do? Common sense tells you to collect everything you can at the time of service, but some patients inevitably brandish the old "I forgot my checkbook" excuse and escape without paying. And the patient-owed portion of most insurance charges is often unknown – and unknowable – at the time of service.
That means you’ll need to send a bill, and every bill you send (or hire somebody to send) costs you a bundle. And when it arrives, it goes right to the bottom of your patient’s payment priority list. That is, each month your patients will pay their electric, water, gas, and telephone bills – and just about any other bill – before getting around to yours. If there is no more money when your bill finally surfaces, that’s just too bad. An unpaid electric company can shut off their power, but what can you do?
What we do in our practice is what every hotel, rental car agency, and many other businesses have done for years: We ask for a credit card number and bill balances to it as they come in. Plastic runs the show everywhere you go – except in most medical offices.
Every new patient in my office receives a letter at their first visit explaining our policy: We will keep a credit card number on file, and use it to bill any outstanding balances. At the bottom is a brief consent for the patient to sign, and a place to write the credit card number and expiration date. (The sample text of the letter is at the end of this column.)
Do patients object? Some do – mostly older people. But when we explain that we’re doing nothing different from what a hotel does at each check-in, and that it will work to their advantage by decreasing the bills they receive and the checks they must write, most come around. Make it an option at first if you wish; then, when everyone is accustomed, you can make it mandatory.
Do they worry about confidentiality or unauthorized use? They don’t anywhere else. They think nothing of handing a card to servers in restaurant with no thought of what they might do with it in the kitchen. They hand the card to hotel clerks, and never think to ask how long the information is kept or who has access to it. They blithely shoot numbers into black holes on the Internet.
We explain that we guard our patients’ financial information as carefully as we do their medical information. (If you have an EHR, it can go in the chart with everything else; if not, I suggest a separate portable file that can be locked up each night.)
Does it work? In only a year, our accounts receivable totals dropped by nearly 50%; after another year, they stabilized at 30%-35% of previous levels and have remained there ever since. Last year I hired a new accountant. Something must be wrong, he said nervously, after his first look at the books; account receivable totals are "never" that low. His eyes widened as I explained our system. "Why doesn’t every medical office do that?" he asked.
Why indeed? The business of health care delivery will be rocked to its very foundations in the next few years. In my humble opinion, private practice will survive those changes only if physicians learn to do more of what we do best – treating patients – and leave the business of extending credit to the banks.
PLEASE NOTE:
This generic letter is intended to be used as an example for a letter you might draft for a similar purpose. However, we take no responsibility for your use of its content, either verbatim or altered, or any inappropriate usage.
To Our Patients:
As you know if you have ever checked into a hotel or rented a car, the first thing you are asked for is a credit card, which is imprinted and later used to pay your bill. This is an advantage for both you and the hotel or rental company, since it makes checkout easier, faster, and more efficient.
We have implemented a similar policy. You will be asked for a credit card number at the time you check in and the information will be held securely until your insurances have paid their portion and notified us of the amount of your share. At that time, any remaining balance owed by you will be charged to your credit card, and a copy of the charge will be mailed to you.
This will be an advantage to you, since you will no longer have to write out and mail us checks. It will be an advantage to us as well, since it will greatly decrease the number of statements that we have to generate and send out. The combination will benefit everybody in helping to keep the cost of health care down.
This in no way will compromise your ability to dispute a charge or question your insurance company’s determination of payment.
Co-pays due at the time of the visit will, of course, still be due at the time of the visit.
If you have any questions about this payment method, do not hesitate to ask.
Sincerely yours,
I authorize ********************, PA to charge outstanding balances on my account to the following credit card:
Visa Mastercard American Express Other: __________
Account number ________________
Expiration Date ____________
For as long as I have been writing this column, I have stressed that aggressive management of accounts receivable is the key to any practice’s financial health; and yet, all these years later, accounts receivable is still the subject that generates the most questions.
Okay, folks, let’s go over it one more time: Basically, physicians extend more credit than any business except banks. Despite what you may have read recently, banks are good at it, and they charge interest (and a myriad of fees) to do it. Doctors do it for free. Are we crazy? No business owner in his or her right mind allows customers to take away goods or services without paying for them, but physicians do it every day.
What to do? Common sense tells you to collect everything you can at the time of service, but some patients inevitably brandish the old "I forgot my checkbook" excuse and escape without paying. And the patient-owed portion of most insurance charges is often unknown – and unknowable – at the time of service.
That means you’ll need to send a bill, and every bill you send (or hire somebody to send) costs you a bundle. And when it arrives, it goes right to the bottom of your patient’s payment priority list. That is, each month your patients will pay their electric, water, gas, and telephone bills – and just about any other bill – before getting around to yours. If there is no more money when your bill finally surfaces, that’s just too bad. An unpaid electric company can shut off their power, but what can you do?
What we do in our practice is what every hotel, rental car agency, and many other businesses have done for years: We ask for a credit card number and bill balances to it as they come in. Plastic runs the show everywhere you go – except in most medical offices.
Every new patient in my office receives a letter at their first visit explaining our policy: We will keep a credit card number on file, and use it to bill any outstanding balances. At the bottom is a brief consent for the patient to sign, and a place to write the credit card number and expiration date. (The sample text of the letter is at the end of this column.)
Do patients object? Some do – mostly older people. But when we explain that we’re doing nothing different from what a hotel does at each check-in, and that it will work to their advantage by decreasing the bills they receive and the checks they must write, most come around. Make it an option at first if you wish; then, when everyone is accustomed, you can make it mandatory.
Do they worry about confidentiality or unauthorized use? They don’t anywhere else. They think nothing of handing a card to servers in restaurant with no thought of what they might do with it in the kitchen. They hand the card to hotel clerks, and never think to ask how long the information is kept or who has access to it. They blithely shoot numbers into black holes on the Internet.
We explain that we guard our patients’ financial information as carefully as we do their medical information. (If you have an EHR, it can go in the chart with everything else; if not, I suggest a separate portable file that can be locked up each night.)
Does it work? In only a year, our accounts receivable totals dropped by nearly 50%; after another year, they stabilized at 30%-35% of previous levels and have remained there ever since. Last year I hired a new accountant. Something must be wrong, he said nervously, after his first look at the books; account receivable totals are "never" that low. His eyes widened as I explained our system. "Why doesn’t every medical office do that?" he asked.
Why indeed? The business of health care delivery will be rocked to its very foundations in the next few years. In my humble opinion, private practice will survive those changes only if physicians learn to do more of what we do best – treating patients – and leave the business of extending credit to the banks.
PLEASE NOTE:
This generic letter is intended to be used as an example for a letter you might draft for a similar purpose. However, we take no responsibility for your use of its content, either verbatim or altered, or any inappropriate usage.
To Our Patients:
As you know if you have ever checked into a hotel or rented a car, the first thing you are asked for is a credit card, which is imprinted and later used to pay your bill. This is an advantage for both you and the hotel or rental company, since it makes checkout easier, faster, and more efficient.
We have implemented a similar policy. You will be asked for a credit card number at the time you check in and the information will be held securely until your insurances have paid their portion and notified us of the amount of your share. At that time, any remaining balance owed by you will be charged to your credit card, and a copy of the charge will be mailed to you.
This will be an advantage to you, since you will no longer have to write out and mail us checks. It will be an advantage to us as well, since it will greatly decrease the number of statements that we have to generate and send out. The combination will benefit everybody in helping to keep the cost of health care down.
This in no way will compromise your ability to dispute a charge or question your insurance company’s determination of payment.
Co-pays due at the time of the visit will, of course, still be due at the time of the visit.
If you have any questions about this payment method, do not hesitate to ask.
Sincerely yours,
I authorize ********************, PA to charge outstanding balances on my account to the following credit card:
Visa Mastercard American Express Other: __________
Account number ________________
Expiration Date ____________