User login
Managing Your Dermatology Practice: Your 2012 Resolution- Stop Extending Credit!
For as long as I have been writing this column, I have stressed that aggressive management of accounts receivable is the key to any practice’s financial health; and yet, all these years later, accounts receivable is still the subject that generates the most questions.
Okay, folks, let’s go over it one more time: Basically, physicians extend more credit than any business except banks. Despite what you may have read recently, banks are good at it, and they charge interest (and a myriad of fees) to do it. Doctors do it for free. Are we crazy? No business owner in his or her right mind allows customers to take away goods or services without paying for them, but physicians do it every day.
What to do? Common sense tells you to collect everything you can at the time of service, but some patients inevitably brandish the old "I forgot my checkbook" excuse and escape without paying. And the patient-owed portion of most insurance charges is often unknown – and unknowable – at the time of service.
That means you’ll need to send a bill, and every bill you send (or hire somebody to send) costs you a bundle. And when it arrives, it goes right to the bottom of your patient’s payment priority list. That is, each month your patients will pay their electric, water, gas, and telephone bills – and just about any other bill – before getting around to yours. If there is no more money when your bill finally surfaces, that’s just too bad. An unpaid electric company can shut off their power, but what can you do?
What we do in our practice is what every hotel, rental car agency, and many other businesses have done for years: We ask for a credit card number and bill balances to it as they come in. Plastic runs the show everywhere you go – except in most medical offices.
Every new patient in my office receives a letter at their first visit explaining our policy: We will keep a credit card number on file, and use it to bill any outstanding balances. At the bottom is a brief consent for the patient to sign, and a place to write the credit card number and expiration date. (If you would like a copy of my letter as a template for creating your own, e-mail me and I’ll be happy to send you one.)
Do patients object? Some do – mostly older people. But when we explain that we’re doing nothing different from what a hotel does at each check-in, and that it will work to their advantage by decreasing the bills they receive and the checks they must write, most come around. Make it an option at first if you wish; then, when everyone is accustomed, you can make it mandatory.
Do they worry about confidentiality or unauthorized use? They don’t anywhere else. They think nothing of handing a card to servers in restaurant with no thought of what they might do with it in the kitchen. They hand the card to hotel clerks, and never think to ask how long the information is kept or who has access to it. They blithely shoot numbers into black holes on the Internet.
We explain that we guard our patients’ financial information as carefully as we do their medical information. (If you have an EHR, it can go in the chart with everything else; if not, I suggest a separate portable file that can be locked up each night.)
Does it work? In only a year, our accounts receivable totals dropped by nearly 50%; after another year, they stabilized at 30%-35% of previous levels and have remained there ever since. Last year I hired a new accountant. Something must be wrong, he said nervously, after his first look at the books; account receivable totals are "never" that low. His eyes widened as I explained our system. "Why doesn’t every medical office do that?" he asked.
Why indeed? The business of health care delivery will be rocked to its very foundations in the next few years. In my humble opinion, private practice will survive those changes only if physicians learn to do more of what we do best – treating patients – and leave the business of extending credit to the banks.
For as long as I have been writing this column, I have stressed that aggressive management of accounts receivable is the key to any practice’s financial health; and yet, all these years later, accounts receivable is still the subject that generates the most questions.
Okay, folks, let’s go over it one more time: Basically, physicians extend more credit than any business except banks. Despite what you may have read recently, banks are good at it, and they charge interest (and a myriad of fees) to do it. Doctors do it for free. Are we crazy? No business owner in his or her right mind allows customers to take away goods or services without paying for them, but physicians do it every day.
What to do? Common sense tells you to collect everything you can at the time of service, but some patients inevitably brandish the old "I forgot my checkbook" excuse and escape without paying. And the patient-owed portion of most insurance charges is often unknown – and unknowable – at the time of service.
That means you’ll need to send a bill, and every bill you send (or hire somebody to send) costs you a bundle. And when it arrives, it goes right to the bottom of your patient’s payment priority list. That is, each month your patients will pay their electric, water, gas, and telephone bills – and just about any other bill – before getting around to yours. If there is no more money when your bill finally surfaces, that’s just too bad. An unpaid electric company can shut off their power, but what can you do?
What we do in our practice is what every hotel, rental car agency, and many other businesses have done for years: We ask for a credit card number and bill balances to it as they come in. Plastic runs the show everywhere you go – except in most medical offices.
Every new patient in my office receives a letter at their first visit explaining our policy: We will keep a credit card number on file, and use it to bill any outstanding balances. At the bottom is a brief consent for the patient to sign, and a place to write the credit card number and expiration date. (If you would like a copy of my letter as a template for creating your own, e-mail me and I’ll be happy to send you one.)
Do patients object? Some do – mostly older people. But when we explain that we’re doing nothing different from what a hotel does at each check-in, and that it will work to their advantage by decreasing the bills they receive and the checks they must write, most come around. Make it an option at first if you wish; then, when everyone is accustomed, you can make it mandatory.
Do they worry about confidentiality or unauthorized use? They don’t anywhere else. They think nothing of handing a card to servers in restaurant with no thought of what they might do with it in the kitchen. They hand the card to hotel clerks, and never think to ask how long the information is kept or who has access to it. They blithely shoot numbers into black holes on the Internet.
We explain that we guard our patients’ financial information as carefully as we do their medical information. (If you have an EHR, it can go in the chart with everything else; if not, I suggest a separate portable file that can be locked up each night.)
Does it work? In only a year, our accounts receivable totals dropped by nearly 50%; after another year, they stabilized at 30%-35% of previous levels and have remained there ever since. Last year I hired a new accountant. Something must be wrong, he said nervously, after his first look at the books; account receivable totals are "never" that low. His eyes widened as I explained our system. "Why doesn’t every medical office do that?" he asked.
Why indeed? The business of health care delivery will be rocked to its very foundations in the next few years. In my humble opinion, private practice will survive those changes only if physicians learn to do more of what we do best – treating patients – and leave the business of extending credit to the banks.
For as long as I have been writing this column, I have stressed that aggressive management of accounts receivable is the key to any practice’s financial health; and yet, all these years later, accounts receivable is still the subject that generates the most questions.
Okay, folks, let’s go over it one more time: Basically, physicians extend more credit than any business except banks. Despite what you may have read recently, banks are good at it, and they charge interest (and a myriad of fees) to do it. Doctors do it for free. Are we crazy? No business owner in his or her right mind allows customers to take away goods or services without paying for them, but physicians do it every day.
What to do? Common sense tells you to collect everything you can at the time of service, but some patients inevitably brandish the old "I forgot my checkbook" excuse and escape without paying. And the patient-owed portion of most insurance charges is often unknown – and unknowable – at the time of service.
That means you’ll need to send a bill, and every bill you send (or hire somebody to send) costs you a bundle. And when it arrives, it goes right to the bottom of your patient’s payment priority list. That is, each month your patients will pay their electric, water, gas, and telephone bills – and just about any other bill – before getting around to yours. If there is no more money when your bill finally surfaces, that’s just too bad. An unpaid electric company can shut off their power, but what can you do?
What we do in our practice is what every hotel, rental car agency, and many other businesses have done for years: We ask for a credit card number and bill balances to it as they come in. Plastic runs the show everywhere you go – except in most medical offices.
Every new patient in my office receives a letter at their first visit explaining our policy: We will keep a credit card number on file, and use it to bill any outstanding balances. At the bottom is a brief consent for the patient to sign, and a place to write the credit card number and expiration date. (If you would like a copy of my letter as a template for creating your own, e-mail me and I’ll be happy to send you one.)
Do patients object? Some do – mostly older people. But when we explain that we’re doing nothing different from what a hotel does at each check-in, and that it will work to their advantage by decreasing the bills they receive and the checks they must write, most come around. Make it an option at first if you wish; then, when everyone is accustomed, you can make it mandatory.
Do they worry about confidentiality or unauthorized use? They don’t anywhere else. They think nothing of handing a card to servers in restaurant with no thought of what they might do with it in the kitchen. They hand the card to hotel clerks, and never think to ask how long the information is kept or who has access to it. They blithely shoot numbers into black holes on the Internet.
We explain that we guard our patients’ financial information as carefully as we do their medical information. (If you have an EHR, it can go in the chart with everything else; if not, I suggest a separate portable file that can be locked up each night.)
Does it work? In only a year, our accounts receivable totals dropped by nearly 50%; after another year, they stabilized at 30%-35% of previous levels and have remained there ever since. Last year I hired a new accountant. Something must be wrong, he said nervously, after his first look at the books; account receivable totals are "never" that low. His eyes widened as I explained our system. "Why doesn’t every medical office do that?" he asked.
Why indeed? The business of health care delivery will be rocked to its very foundations in the next few years. In my humble opinion, private practice will survive those changes only if physicians learn to do more of what we do best – treating patients – and leave the business of extending credit to the banks.
Does Hospital Medicine Reinforce the Pillars of Career Satisfaction?
Gregory Misky, MD, describes it as a “deer in the headlights” moment. About four years ago, Dr. Misky, assistant professor of medicine at the University of Colorado Denver, and Mark Reid, MD, assistant professor at Denver Health Medical Center, were trying to figure out what being an academic hospitalist was all about. What were the expectations of them, and how could they combine their clinical duties with scholarly work, especially given the significant lack of mentorship?
The duo wondered if other young hospitalists were feeling the same uncertainty about their chosen career, and whether there were any variables that might help predict success or burnout among their fellow doctors.
They haven’t been alone. Regardless of the practice model and location, physicians within the fastest-spreading medical specialty in the U.S. have noted both the promise and unsettled nature of HM. “We are still a relatively young profession, and I think over the past five to 10 years, we’ve been seeing the growing pains of the profession,” says Tosha Wetterneck, MD, MS, FACP, associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
In response to mounting concerns over multiple career-satisfaction-related issues, SHM assembled a Career Satisfaction Task Force that produced a detailed white paper at the end of 2006 (available from the “White Papers” tab under the “Publications” heading at www.hospitalmedicine.org).
One tangible outcome of the paper was the establishment of “Four Pillars of Career Satisfaction” for hospitalists:
- Reward and recognition;
- Workload and schedule;
- Autonomy and control; and
- Community and environment.
The paper included definitions for each pillar, and assembled scorecards, action steps, tools, and recommendations for both HM leaders and individual hospitalists to help shore up perceived weak spots.
So how strong are those pillars in practice? If hospitalists are the future of healthcare, as SHM and other medical groups assert, what do current studies suggest about the prospects of HM solidifying into a satisfying and sustainable career choice?
The Evidence
One outgrowth of Dr. Misky and Dr. Reid’s frustration was a study in which they and their collaborators emailed a 61-question survey to hospitalists at 20 academic medical centers. Among the results, the researchers found that 75% of respondents reported either “high” or “somewhat high” satisfaction with their current job. At the same time, though, 67% felt “high” or “somewhat high” stress levels at work, and nearly 1 in 4 (24%) reported some degree of burnout, based on their own definition of the word.1
As one of the first hospitalists in his group, Dr. Misky recalls the stress he felt over whether the hospital, division, and department would all buy into the idea of an academic hospitalist, and what his role would be. “I think we spent a lot of our early years trying to carve out our niche and proving ourselves and trying to balance the clinical needs that people had for us with other expectations of being an academic,” he says. Dr. Misky likens the experience to the adrenaline rush of mountain-biking straight down a hill. The feeling that too many things are going on at once, though, might also partially explain the apparent dichotomy of high overall satisfaction but a worrisome degree of burnout.
The profession hasn’t been around long enough for good longitudinal studies, and surveys have worded questions on satisfaction and burnout in different ways, complicating attempts at direct comparisons over time. A 2001 study, for example, reported that 12.9% of community and academic hospitalists were burned out, with another 25% at risk, but the survey was limited to dues-paying members of the National Association of Inpatient Physicians, the precursor to SHM.2
Nor has it been easy to compare hospitalist satisfaction and burnout levels to those of other specialists. “We haven’t really defined what a sustained, long-term career in hospital medicine is going to be,” Dr. Wetterneck says. “And in that way, it’s hard to say, ‘Compared to other professions, are we happier or not?’”
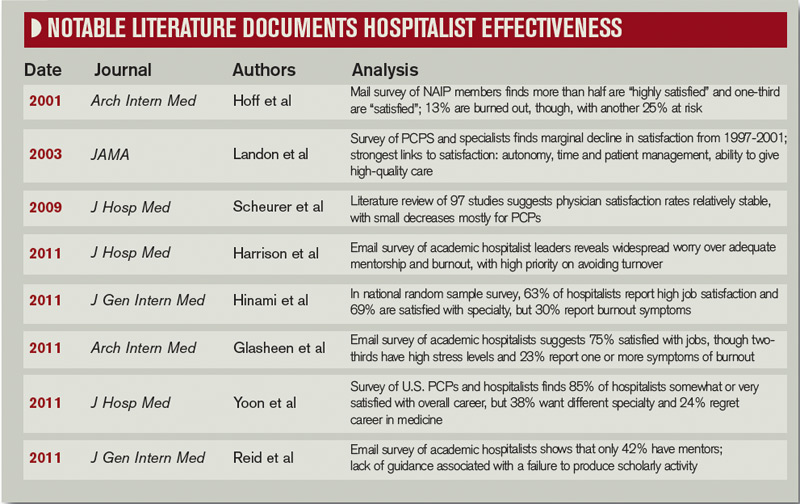
One of her recent studies, however, generally agrees with the handful of surveys addressing satisfaction and burnout among hospitalists. Overall, 63% of respondents reported high satisfaction with their job, while 69% were highly satisfied with their specialty. Roughly 30%, however, also reported feeling symptom of job burnout.3
Kelki Hinami, MD, MS, assistant of professor of medicine at Northwestern University Feinberg School of Medicine in Chicago and a coauthor of the study, says one take-home message is that hospitalists do fairly well in finding jobs that match their individual needs. “To further illustrate this, we found that hospitalists working in various practice models have different ideas about what is most important to their job,” he says.
Autonomy, for example, is considered most important by more local group hospitalists than by those of any other model, while recognition by leaders and having a variety of tasks at work are particularly important to academic hospitalists. Unlike other hospitalists, however, fewer academics consider pay to be the most important job characteristic.
A third study, led by John Yoon, MD, assistant professor in the section of hospital medicine at the University of Chicago, has examined career satisfaction, burnout, and morale among primary-care physicians (PCPs) and hospitalists. So far, the results he reported at HM11 largely agree with the other recent surveys: Combined, 85% of hospitalists report being either somewhat or very satisfied with their overall career. Conversely, 24% of hospitalists regretted choosing medicine as a career and 38% say they would have chosen a different medical specialty if they had to do it over again.4
Dr. Yoon says his data, compiled from two survey samples of about 1,000 generalists each, have revealed few differences between hospitalists and PCPs. “I thought hospitalists would be more satisfied than primary-care physicians, given the declining satisfaction rates of PCPs that we know about, and that students and trainees are less likely to go into primary care,” he says. Even burnout rates are similar, however; Dr. Yoon says he’s noticed a trend toward hospitalists reporting less burnout than PCPs, but the difference is not yet statistically significant.
Choice of a New Generation?
HM’s attractiveness to medical residents offers other clues about its ability to provide a sustainable and satisfying career choice. Salary, part of the “reward and recognition” pillar, has long been one perceived weakness. Anecdotally, however, Dr. Yoon says many general medicine residents see HM as a better financial option than primary care. “Some of the residents I work with, when I asked them, ‘Will you be a primary-care physician or a hospitalist?’ a lot of them say, ‘Probably hospitalist,’” he says. “And generally the reason is because they have to pay off their debt.”
It’s true that hospitalists’ salaries lag behind that of most of other specialists. Nevertheless, researchers like Colin West, MD, PhD, associate professor of medicine and biostatistics at the Mayo Clinic in Rochester, Minn., say many medical residents are prioritizing financial considerations as relatively low on the scale of general preferences.

—John Yoon, MD, assistant professor, section of hospital medicine, University of Chicago
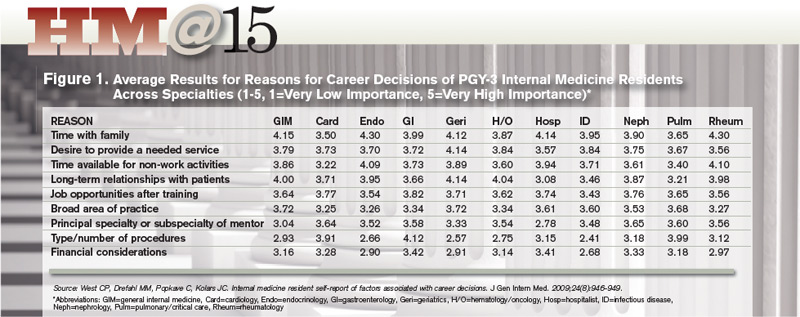
Dr. West, an associate program director for the internal-medicine residency program at Mayo, sees a generational sea change in the career considerations deemed most important. Based on a career decision survey filled out by nearly 15,000 internal-medical residents, he found that roughly 70% of respondents said time with family was of “high” or “very high” importance to their career decisions.5 The category, which relates to SHM’s “workload and schedule” pillar, beat out eight others as the most important factor overall, while global financial considerations scored relatively low.
Residents who placed high value on time with family were more likely to choose careers in more predictable, outpatient-based specialties, such as endocrinology or rheumatology. HM also fared well in this category. Dr. West says the results suggest that residents considering a hospitalist career are attracted to the specialty’s flexibility and predictability of the largely shift-based scheduling.
William Cors, MD, chief medical quality officer at Pocono Health System in East Stroudsburg, Pa., says more physicians are looking for job security, predictable shifts, and a better work-life balance. As HM matures and demonstrates that it can address those needs, Dr. Cors sees it becoming more attractive for medical students and residents.
In practice, though, other research suggests a career in HM doesn’t always meet expectations. Dr. Wetterneck and Dr. Hinami, for example, highlighted both compensation and work-life balance as points of concern in their study: For both factors, only about 30% of hospitalists were optimally satisfied.
Separately, Dr. Misky and his colleagues reported that roughly half of academic hospitalists were satisfied with the ability to control their schedule, and with their amount of personal and family time. Those who were unsatisfied with either of these categories, the survey found, were at higher risk for burnout. Similarly, Dr. Yoon found that physicians who reported having no control over their work hours or their call schedule, part of SHM’s “autonomy and control” pillar, were more likely to report burnout.
So why is HM stumbling on perceived selling points like family friendliness and autonomy? Dr. Wetterneck believes too many unfilled jobs and rapid turnover could be putting more pressure on existing hospitalists and interfering with their ability to balance home and work life. “There’s a huge need for hospitalists everywhere,” she says, and reliance on them has been especially acute at academic centers and large community hospitals contending with the recently imposed limits on residents’ work hours.
The Hospitalist: A People Person
Another shift may be occurring in the types of relationships necessary for a satisfying work environment, a big part of the “community and environment” pillar. Although Dr. Yoon says long-term connections with students and trainees have added meaning to his job, he is mourning the absence of other bonds. “One loss I’m starting to feel keenly as an academic hospitalist, having spent my early training years as a primary-care doc, really is the loss of having long-term relationships with patients,” he says. “My clinical encounters with patients these days as a hospitalist are very intense, but also very brief.”
Dr. Yoon has pondered whether the HM field can rearrange practice settings to promote more satisfying relationships. Such a change, he says, might occur through innovative models that aid coordination with medical homes, or provide more chronic care for high-risk patients. “In my view, the trajectory of hospital medicine is pretty wide open for creativity and new models of care,” he says. “I think it will be partly driven by the need to want to have more meaningful interactions with patients.”
Those relationships need not be long-term, however. One recent study found high satisfaction among hospitalists and laborists working within the fast-growing OBGYN hospitalist field.6
Dr. Hinami says collaborative care that involves close working relationships with specialists and other care providers might help propel the hospitalist movement forward. In his survey with Dr. Wetterneck, hospitalists ranked relationships with staff and colleagues among the most satisfying of any of the domains; hospitalists also indicated high levels of satisfaction with their patient relationships. “Clearly, relationships are critical to overall job satisfaction, and hospitalists, I think, are doing a fairly good job at maintaining those relationships,” Dr. Hinami says.

—Keiki Hinami, MD, assistant professor of medicine, Northwestern University Feinberg School of Medicine, Chicago
A 2002 survey-based study reinforces the importance of such bonds. Job burnout and intent to remain in the hospitalist career, its authors concluded, were more highly influenced by “favorable social relations” involving colleagues, coworkers, and patients than by such factors as reduced autonomy and the use of financial incentives.7
The focus on maintaining multiple relationships fits well with the collaborative approach to care that many hospitalists say they value highly. One big satisfier for hospitalists, Dr. Cors says, will be “a sense that they’re really part of a healthcare team and not just punching the clock and doing their shifts.”
The Verdict
Despite the difficulty in discerning long-term trends, studies suggest that overall satisfaction with the specialty of hospital medicine remains high, a promising sign for the maturing field. Career hospitalists also seem adept at relationships with peers and other providers, a skill that will serve them well as collaborative-care models gain steam.
Nonetheless, surveys also suggest a worrisome rate of burnout and less-than-optimal satisfaction with elements that should be the strong suits of HM, such as work-life balance and autonomy. Academics are searching for their own clinical-research balance. And Dr. West says the jury’s still out on the future pitfalls that might get in the way of a sustainable career path for older practitioners, such as overnight shifts.
Hospitalist-led efforts, however, may be starting to pay dividends. At the University of California at San Francisco, a faculty development program for first-year hospitalists has included a coaching relationship with a senior faculty member, a teaching course, newly established divisional grand rounds, and a framework for meeting scholarly expectations. Upon its implementation, the program has led to higher job satisfaction, skill-set comfort, and academic production among participants.8
Given the expanding range of HM duties and practice models, hospitals, division chiefs, and team leaders cannot rely on a single recipe for happy and productive hospitalists. “I don’t know if there is a cookbook; I think it’s highly variable depending on your institution and the needs of the academic facility where you are,” Dr. Misky says.
SHM’s 2006 white paper stated that the best career satisfaction strategy is to find a job that fits an individual’s preferences and attitudes. “People who are unhappy with their job don’t tend to stay in it, and from what we know about hospital medicine right now, you can find pretty much any type of job anywhere you want, so the job market is very open,” Dr. Wetterneck says.
Ensuring the right fit for doctors within HM, though, will require institutional support. “It’s going to be up to hospitals and hospitalist programs to create jobs that are sustainable that people like,” she says, “so that hospitalists will stay long in their job and in the profession.”
Bryn Nelson is a freelance medical writer based in Seattle.
More Mentorship in Hospital Medicine? It’s Academic

Within the 2011 State of Hospital Medicine report, one statistic in particular points to the youth of the medical specialty: Just over 10% of surveyed hospitalists had reached the rank of associate professor or higher.
How might the potential lack of mentorship within this immature field affect the ability of hospitalists to successfully navigate academia? So asked Gregory Misky, MD, assistant professor of medicine at the University of Colorado Denver, and his colleagues in a survey-based study. The results agree with other recent assessments that mentors are in short supply. “Academic hospital medicine groups have an acute need for mentoring and career development programs,” one study concludes.
The research of Dr. Misky and his collaborators found that only 42% of academic hospitalists could identify a mentor, while only 31% reported that they were mentoring another academic hospitalist.1 Based on sheer numbers and experience, the pool of mentors may significantly expand as the field matures. But Dr. Misky also urges some flexibility, noting that his own mentor is a non-hospitalist.
In his own research, Colin West, MD, PhD, associate professor of medicine and biostatistics at the Mayo Clinic in Rochester, Minn., found that residents considering a career in HM placed less emphasis on the specialty or subspecialty of their mentor.5 Why? Very likely, he says, there just weren’t enough hospitalist mentors around to get a sense of what the career was all about.
Dr. West hopes the numbers suggest otherwise in the near future. “You want to recruit bright people into your specialty, but at the same time, you also want to recruit the right people,” he says. “And that means that you need to be able to expose people to a full breadth of what a decision to pursue a certain specialty really means.”
References
- Glasheen JJ, Misky GJ, Reid MB, Harrison RA, Sharpe B, Auerbach A. Career satisfaction and burnout in academic hospital medicine. Arch Intern Med. 2011;171(8) 782-785.
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers [published online ahead of print July 20, 2011]. J Gen Intern Med. doi:10.1007/s116060-011-1780-z.
- Yoon J, Miller A, Rasinski K, Curlin F. Burnout, sense of calling, and career resilience among hospitalists and primary care physicians: a national survey. J Hosp Med. 2011;6(4):S90-S91.
- West CP, Drefahl MM, Popkave C, Kolars JC. Internal medicine resident self-report of factors associated with career decisions. J Gen Intern Med. 2009;24(8):946-949.
- Funk C, Anderson BL, Schulkin J, Weinstein L. Survey of obstetric and gynecologic hospitalists and laborists. Am J Obstet Gynecol. 2010;203(2):177.e1-177.e4.
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43(1):72-91.
- Sehgal NL, Sharpe BA, Auerbach AA, Wachter RM. Investing in the future: Building an academic hospitalist faculty development program. J Hosp Med. 2011;6(3):161-166.
Gregory Misky, MD, describes it as a “deer in the headlights” moment. About four years ago, Dr. Misky, assistant professor of medicine at the University of Colorado Denver, and Mark Reid, MD, assistant professor at Denver Health Medical Center, were trying to figure out what being an academic hospitalist was all about. What were the expectations of them, and how could they combine their clinical duties with scholarly work, especially given the significant lack of mentorship?
The duo wondered if other young hospitalists were feeling the same uncertainty about their chosen career, and whether there were any variables that might help predict success or burnout among their fellow doctors.
They haven’t been alone. Regardless of the practice model and location, physicians within the fastest-spreading medical specialty in the U.S. have noted both the promise and unsettled nature of HM. “We are still a relatively young profession, and I think over the past five to 10 years, we’ve been seeing the growing pains of the profession,” says Tosha Wetterneck, MD, MS, FACP, associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
In response to mounting concerns over multiple career-satisfaction-related issues, SHM assembled a Career Satisfaction Task Force that produced a detailed white paper at the end of 2006 (available from the “White Papers” tab under the “Publications” heading at www.hospitalmedicine.org).
One tangible outcome of the paper was the establishment of “Four Pillars of Career Satisfaction” for hospitalists:
- Reward and recognition;
- Workload and schedule;
- Autonomy and control; and
- Community and environment.
The paper included definitions for each pillar, and assembled scorecards, action steps, tools, and recommendations for both HM leaders and individual hospitalists to help shore up perceived weak spots.
So how strong are those pillars in practice? If hospitalists are the future of healthcare, as SHM and other medical groups assert, what do current studies suggest about the prospects of HM solidifying into a satisfying and sustainable career choice?
The Evidence
One outgrowth of Dr. Misky and Dr. Reid’s frustration was a study in which they and their collaborators emailed a 61-question survey to hospitalists at 20 academic medical centers. Among the results, the researchers found that 75% of respondents reported either “high” or “somewhat high” satisfaction with their current job. At the same time, though, 67% felt “high” or “somewhat high” stress levels at work, and nearly 1 in 4 (24%) reported some degree of burnout, based on their own definition of the word.1
As one of the first hospitalists in his group, Dr. Misky recalls the stress he felt over whether the hospital, division, and department would all buy into the idea of an academic hospitalist, and what his role would be. “I think we spent a lot of our early years trying to carve out our niche and proving ourselves and trying to balance the clinical needs that people had for us with other expectations of being an academic,” he says. Dr. Misky likens the experience to the adrenaline rush of mountain-biking straight down a hill. The feeling that too many things are going on at once, though, might also partially explain the apparent dichotomy of high overall satisfaction but a worrisome degree of burnout.
The profession hasn’t been around long enough for good longitudinal studies, and surveys have worded questions on satisfaction and burnout in different ways, complicating attempts at direct comparisons over time. A 2001 study, for example, reported that 12.9% of community and academic hospitalists were burned out, with another 25% at risk, but the survey was limited to dues-paying members of the National Association of Inpatient Physicians, the precursor to SHM.2
Nor has it been easy to compare hospitalist satisfaction and burnout levels to those of other specialists. “We haven’t really defined what a sustained, long-term career in hospital medicine is going to be,” Dr. Wetterneck says. “And in that way, it’s hard to say, ‘Compared to other professions, are we happier or not?’”
One of her recent studies, however, generally agrees with the handful of surveys addressing satisfaction and burnout among hospitalists. Overall, 63% of respondents reported high satisfaction with their job, while 69% were highly satisfied with their specialty. Roughly 30%, however, also reported feeling symptom of job burnout.3
Kelki Hinami, MD, MS, assistant of professor of medicine at Northwestern University Feinberg School of Medicine in Chicago and a coauthor of the study, says one take-home message is that hospitalists do fairly well in finding jobs that match their individual needs. “To further illustrate this, we found that hospitalists working in various practice models have different ideas about what is most important to their job,” he says.
Autonomy, for example, is considered most important by more local group hospitalists than by those of any other model, while recognition by leaders and having a variety of tasks at work are particularly important to academic hospitalists. Unlike other hospitalists, however, fewer academics consider pay to be the most important job characteristic.
A third study, led by John Yoon, MD, assistant professor in the section of hospital medicine at the University of Chicago, has examined career satisfaction, burnout, and morale among primary-care physicians (PCPs) and hospitalists. So far, the results he reported at HM11 largely agree with the other recent surveys: Combined, 85% of hospitalists report being either somewhat or very satisfied with their overall career. Conversely, 24% of hospitalists regretted choosing medicine as a career and 38% say they would have chosen a different medical specialty if they had to do it over again.4
Dr. Yoon says his data, compiled from two survey samples of about 1,000 generalists each, have revealed few differences between hospitalists and PCPs. “I thought hospitalists would be more satisfied than primary-care physicians, given the declining satisfaction rates of PCPs that we know about, and that students and trainees are less likely to go into primary care,” he says. Even burnout rates are similar, however; Dr. Yoon says he’s noticed a trend toward hospitalists reporting less burnout than PCPs, but the difference is not yet statistically significant.
Choice of a New Generation?
HM’s attractiveness to medical residents offers other clues about its ability to provide a sustainable and satisfying career choice. Salary, part of the “reward and recognition” pillar, has long been one perceived weakness. Anecdotally, however, Dr. Yoon says many general medicine residents see HM as a better financial option than primary care. “Some of the residents I work with, when I asked them, ‘Will you be a primary-care physician or a hospitalist?’ a lot of them say, ‘Probably hospitalist,’” he says. “And generally the reason is because they have to pay off their debt.”
It’s true that hospitalists’ salaries lag behind that of most of other specialists. Nevertheless, researchers like Colin West, MD, PhD, associate professor of medicine and biostatistics at the Mayo Clinic in Rochester, Minn., say many medical residents are prioritizing financial considerations as relatively low on the scale of general preferences.
—John Yoon, MD, assistant professor, section of hospital medicine, University of Chicago
Dr. West, an associate program director for the internal-medicine residency program at Mayo, sees a generational sea change in the career considerations deemed most important. Based on a career decision survey filled out by nearly 15,000 internal-medical residents, he found that roughly 70% of respondents said time with family was of “high” or “very high” importance to their career decisions.5 The category, which relates to SHM’s “workload and schedule” pillar, beat out eight others as the most important factor overall, while global financial considerations scored relatively low.
Residents who placed high value on time with family were more likely to choose careers in more predictable, outpatient-based specialties, such as endocrinology or rheumatology. HM also fared well in this category. Dr. West says the results suggest that residents considering a hospitalist career are attracted to the specialty’s flexibility and predictability of the largely shift-based scheduling.
William Cors, MD, chief medical quality officer at Pocono Health System in East Stroudsburg, Pa., says more physicians are looking for job security, predictable shifts, and a better work-life balance. As HM matures and demonstrates that it can address those needs, Dr. Cors sees it becoming more attractive for medical students and residents.
In practice, though, other research suggests a career in HM doesn’t always meet expectations. Dr. Wetterneck and Dr. Hinami, for example, highlighted both compensation and work-life balance as points of concern in their study: For both factors, only about 30% of hospitalists were optimally satisfied.
Separately, Dr. Misky and his colleagues reported that roughly half of academic hospitalists were satisfied with the ability to control their schedule, and with their amount of personal and family time. Those who were unsatisfied with either of these categories, the survey found, were at higher risk for burnout. Similarly, Dr. Yoon found that physicians who reported having no control over their work hours or their call schedule, part of SHM’s “autonomy and control” pillar, were more likely to report burnout.
So why is HM stumbling on perceived selling points like family friendliness and autonomy? Dr. Wetterneck believes too many unfilled jobs and rapid turnover could be putting more pressure on existing hospitalists and interfering with their ability to balance home and work life. “There’s a huge need for hospitalists everywhere,” she says, and reliance on them has been especially acute at academic centers and large community hospitals contending with the recently imposed limits on residents’ work hours.
The Hospitalist: A People Person
Another shift may be occurring in the types of relationships necessary for a satisfying work environment, a big part of the “community and environment” pillar. Although Dr. Yoon says long-term connections with students and trainees have added meaning to his job, he is mourning the absence of other bonds. “One loss I’m starting to feel keenly as an academic hospitalist, having spent my early training years as a primary-care doc, really is the loss of having long-term relationships with patients,” he says. “My clinical encounters with patients these days as a hospitalist are very intense, but also very brief.”
Dr. Yoon has pondered whether the HM field can rearrange practice settings to promote more satisfying relationships. Such a change, he says, might occur through innovative models that aid coordination with medical homes, or provide more chronic care for high-risk patients. “In my view, the trajectory of hospital medicine is pretty wide open for creativity and new models of care,” he says. “I think it will be partly driven by the need to want to have more meaningful interactions with patients.”
Those relationships need not be long-term, however. One recent study found high satisfaction among hospitalists and laborists working within the fast-growing OBGYN hospitalist field.6
Dr. Hinami says collaborative care that involves close working relationships with specialists and other care providers might help propel the hospitalist movement forward. In his survey with Dr. Wetterneck, hospitalists ranked relationships with staff and colleagues among the most satisfying of any of the domains; hospitalists also indicated high levels of satisfaction with their patient relationships. “Clearly, relationships are critical to overall job satisfaction, and hospitalists, I think, are doing a fairly good job at maintaining those relationships,” Dr. Hinami says.
—Keiki Hinami, MD, assistant professor of medicine, Northwestern University Feinberg School of Medicine, Chicago
A 2002 survey-based study reinforces the importance of such bonds. Job burnout and intent to remain in the hospitalist career, its authors concluded, were more highly influenced by “favorable social relations” involving colleagues, coworkers, and patients than by such factors as reduced autonomy and the use of financial incentives.7
The focus on maintaining multiple relationships fits well with the collaborative approach to care that many hospitalists say they value highly. One big satisfier for hospitalists, Dr. Cors says, will be “a sense that they’re really part of a healthcare team and not just punching the clock and doing their shifts.”
The Verdict
Despite the difficulty in discerning long-term trends, studies suggest that overall satisfaction with the specialty of hospital medicine remains high, a promising sign for the maturing field. Career hospitalists also seem adept at relationships with peers and other providers, a skill that will serve them well as collaborative-care models gain steam.
Nonetheless, surveys also suggest a worrisome rate of burnout and less-than-optimal satisfaction with elements that should be the strong suits of HM, such as work-life balance and autonomy. Academics are searching for their own clinical-research balance. And Dr. West says the jury’s still out on the future pitfalls that might get in the way of a sustainable career path for older practitioners, such as overnight shifts.
Hospitalist-led efforts, however, may be starting to pay dividends. At the University of California at San Francisco, a faculty development program for first-year hospitalists has included a coaching relationship with a senior faculty member, a teaching course, newly established divisional grand rounds, and a framework for meeting scholarly expectations. Upon its implementation, the program has led to higher job satisfaction, skill-set comfort, and academic production among participants.8
Given the expanding range of HM duties and practice models, hospitals, division chiefs, and team leaders cannot rely on a single recipe for happy and productive hospitalists. “I don’t know if there is a cookbook; I think it’s highly variable depending on your institution and the needs of the academic facility where you are,” Dr. Misky says.
SHM’s 2006 white paper stated that the best career satisfaction strategy is to find a job that fits an individual’s preferences and attitudes. “People who are unhappy with their job don’t tend to stay in it, and from what we know about hospital medicine right now, you can find pretty much any type of job anywhere you want, so the job market is very open,” Dr. Wetterneck says.
Ensuring the right fit for doctors within HM, though, will require institutional support. “It’s going to be up to hospitals and hospitalist programs to create jobs that are sustainable that people like,” she says, “so that hospitalists will stay long in their job and in the profession.”
Bryn Nelson is a freelance medical writer based in Seattle.
More Mentorship in Hospital Medicine? It’s Academic
Within the 2011 State of Hospital Medicine report, one statistic in particular points to the youth of the medical specialty: Just over 10% of surveyed hospitalists had reached the rank of associate professor or higher.
How might the potential lack of mentorship within this immature field affect the ability of hospitalists to successfully navigate academia? So asked Gregory Misky, MD, assistant professor of medicine at the University of Colorado Denver, and his colleagues in a survey-based study. The results agree with other recent assessments that mentors are in short supply. “Academic hospital medicine groups have an acute need for mentoring and career development programs,” one study concludes.
The research of Dr. Misky and his collaborators found that only 42% of academic hospitalists could identify a mentor, while only 31% reported that they were mentoring another academic hospitalist.1 Based on sheer numbers and experience, the pool of mentors may significantly expand as the field matures. But Dr. Misky also urges some flexibility, noting that his own mentor is a non-hospitalist.
In his own research, Colin West, MD, PhD, associate professor of medicine and biostatistics at the Mayo Clinic in Rochester, Minn., found that residents considering a career in HM placed less emphasis on the specialty or subspecialty of their mentor.5 Why? Very likely, he says, there just weren’t enough hospitalist mentors around to get a sense of what the career was all about.
Dr. West hopes the numbers suggest otherwise in the near future. “You want to recruit bright people into your specialty, but at the same time, you also want to recruit the right people,” he says. “And that means that you need to be able to expose people to a full breadth of what a decision to pursue a certain specialty really means.”
References
- Glasheen JJ, Misky GJ, Reid MB, Harrison RA, Sharpe B, Auerbach A. Career satisfaction and burnout in academic hospital medicine. Arch Intern Med. 2011;171(8) 782-785.
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers [published online ahead of print July 20, 2011]. J Gen Intern Med. doi:10.1007/s116060-011-1780-z.
- Yoon J, Miller A, Rasinski K, Curlin F. Burnout, sense of calling, and career resilience among hospitalists and primary care physicians: a national survey. J Hosp Med. 2011;6(4):S90-S91.
- West CP, Drefahl MM, Popkave C, Kolars JC. Internal medicine resident self-report of factors associated with career decisions. J Gen Intern Med. 2009;24(8):946-949.
- Funk C, Anderson BL, Schulkin J, Weinstein L. Survey of obstetric and gynecologic hospitalists and laborists. Am J Obstet Gynecol. 2010;203(2):177.e1-177.e4.
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43(1):72-91.
- Sehgal NL, Sharpe BA, Auerbach AA, Wachter RM. Investing in the future: Building an academic hospitalist faculty development program. J Hosp Med. 2011;6(3):161-166.
Gregory Misky, MD, describes it as a “deer in the headlights” moment. About four years ago, Dr. Misky, assistant professor of medicine at the University of Colorado Denver, and Mark Reid, MD, assistant professor at Denver Health Medical Center, were trying to figure out what being an academic hospitalist was all about. What were the expectations of them, and how could they combine their clinical duties with scholarly work, especially given the significant lack of mentorship?
The duo wondered if other young hospitalists were feeling the same uncertainty about their chosen career, and whether there were any variables that might help predict success or burnout among their fellow doctors.
They haven’t been alone. Regardless of the practice model and location, physicians within the fastest-spreading medical specialty in the U.S. have noted both the promise and unsettled nature of HM. “We are still a relatively young profession, and I think over the past five to 10 years, we’ve been seeing the growing pains of the profession,” says Tosha Wetterneck, MD, MS, FACP, associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
In response to mounting concerns over multiple career-satisfaction-related issues, SHM assembled a Career Satisfaction Task Force that produced a detailed white paper at the end of 2006 (available from the “White Papers” tab under the “Publications” heading at www.hospitalmedicine.org).
One tangible outcome of the paper was the establishment of “Four Pillars of Career Satisfaction” for hospitalists:
- Reward and recognition;
- Workload and schedule;
- Autonomy and control; and
- Community and environment.
The paper included definitions for each pillar, and assembled scorecards, action steps, tools, and recommendations for both HM leaders and individual hospitalists to help shore up perceived weak spots.
So how strong are those pillars in practice? If hospitalists are the future of healthcare, as SHM and other medical groups assert, what do current studies suggest about the prospects of HM solidifying into a satisfying and sustainable career choice?
The Evidence
One outgrowth of Dr. Misky and Dr. Reid’s frustration was a study in which they and their collaborators emailed a 61-question survey to hospitalists at 20 academic medical centers. Among the results, the researchers found that 75% of respondents reported either “high” or “somewhat high” satisfaction with their current job. At the same time, though, 67% felt “high” or “somewhat high” stress levels at work, and nearly 1 in 4 (24%) reported some degree of burnout, based on their own definition of the word.1
As one of the first hospitalists in his group, Dr. Misky recalls the stress he felt over whether the hospital, division, and department would all buy into the idea of an academic hospitalist, and what his role would be. “I think we spent a lot of our early years trying to carve out our niche and proving ourselves and trying to balance the clinical needs that people had for us with other expectations of being an academic,” he says. Dr. Misky likens the experience to the adrenaline rush of mountain-biking straight down a hill. The feeling that too many things are going on at once, though, might also partially explain the apparent dichotomy of high overall satisfaction but a worrisome degree of burnout.
The profession hasn’t been around long enough for good longitudinal studies, and surveys have worded questions on satisfaction and burnout in different ways, complicating attempts at direct comparisons over time. A 2001 study, for example, reported that 12.9% of community and academic hospitalists were burned out, with another 25% at risk, but the survey was limited to dues-paying members of the National Association of Inpatient Physicians, the precursor to SHM.2
Nor has it been easy to compare hospitalist satisfaction and burnout levels to those of other specialists. “We haven’t really defined what a sustained, long-term career in hospital medicine is going to be,” Dr. Wetterneck says. “And in that way, it’s hard to say, ‘Compared to other professions, are we happier or not?’”
One of her recent studies, however, generally agrees with the handful of surveys addressing satisfaction and burnout among hospitalists. Overall, 63% of respondents reported high satisfaction with their job, while 69% were highly satisfied with their specialty. Roughly 30%, however, also reported feeling symptom of job burnout.3
Kelki Hinami, MD, MS, assistant of professor of medicine at Northwestern University Feinberg School of Medicine in Chicago and a coauthor of the study, says one take-home message is that hospitalists do fairly well in finding jobs that match their individual needs. “To further illustrate this, we found that hospitalists working in various practice models have different ideas about what is most important to their job,” he says.
Autonomy, for example, is considered most important by more local group hospitalists than by those of any other model, while recognition by leaders and having a variety of tasks at work are particularly important to academic hospitalists. Unlike other hospitalists, however, fewer academics consider pay to be the most important job characteristic.
A third study, led by John Yoon, MD, assistant professor in the section of hospital medicine at the University of Chicago, has examined career satisfaction, burnout, and morale among primary-care physicians (PCPs) and hospitalists. So far, the results he reported at HM11 largely agree with the other recent surveys: Combined, 85% of hospitalists report being either somewhat or very satisfied with their overall career. Conversely, 24% of hospitalists regretted choosing medicine as a career and 38% say they would have chosen a different medical specialty if they had to do it over again.4
Dr. Yoon says his data, compiled from two survey samples of about 1,000 generalists each, have revealed few differences between hospitalists and PCPs. “I thought hospitalists would be more satisfied than primary-care physicians, given the declining satisfaction rates of PCPs that we know about, and that students and trainees are less likely to go into primary care,” he says. Even burnout rates are similar, however; Dr. Yoon says he’s noticed a trend toward hospitalists reporting less burnout than PCPs, but the difference is not yet statistically significant.
Choice of a New Generation?
HM’s attractiveness to medical residents offers other clues about its ability to provide a sustainable and satisfying career choice. Salary, part of the “reward and recognition” pillar, has long been one perceived weakness. Anecdotally, however, Dr. Yoon says many general medicine residents see HM as a better financial option than primary care. “Some of the residents I work with, when I asked them, ‘Will you be a primary-care physician or a hospitalist?’ a lot of them say, ‘Probably hospitalist,’” he says. “And generally the reason is because they have to pay off their debt.”
It’s true that hospitalists’ salaries lag behind that of most of other specialists. Nevertheless, researchers like Colin West, MD, PhD, associate professor of medicine and biostatistics at the Mayo Clinic in Rochester, Minn., say many medical residents are prioritizing financial considerations as relatively low on the scale of general preferences.
—John Yoon, MD, assistant professor, section of hospital medicine, University of Chicago
Dr. West, an associate program director for the internal-medicine residency program at Mayo, sees a generational sea change in the career considerations deemed most important. Based on a career decision survey filled out by nearly 15,000 internal-medical residents, he found that roughly 70% of respondents said time with family was of “high” or “very high” importance to their career decisions.5 The category, which relates to SHM’s “workload and schedule” pillar, beat out eight others as the most important factor overall, while global financial considerations scored relatively low.
Residents who placed high value on time with family were more likely to choose careers in more predictable, outpatient-based specialties, such as endocrinology or rheumatology. HM also fared well in this category. Dr. West says the results suggest that residents considering a hospitalist career are attracted to the specialty’s flexibility and predictability of the largely shift-based scheduling.
William Cors, MD, chief medical quality officer at Pocono Health System in East Stroudsburg, Pa., says more physicians are looking for job security, predictable shifts, and a better work-life balance. As HM matures and demonstrates that it can address those needs, Dr. Cors sees it becoming more attractive for medical students and residents.
In practice, though, other research suggests a career in HM doesn’t always meet expectations. Dr. Wetterneck and Dr. Hinami, for example, highlighted both compensation and work-life balance as points of concern in their study: For both factors, only about 30% of hospitalists were optimally satisfied.
Separately, Dr. Misky and his colleagues reported that roughly half of academic hospitalists were satisfied with the ability to control their schedule, and with their amount of personal and family time. Those who were unsatisfied with either of these categories, the survey found, were at higher risk for burnout. Similarly, Dr. Yoon found that physicians who reported having no control over their work hours or their call schedule, part of SHM’s “autonomy and control” pillar, were more likely to report burnout.
So why is HM stumbling on perceived selling points like family friendliness and autonomy? Dr. Wetterneck believes too many unfilled jobs and rapid turnover could be putting more pressure on existing hospitalists and interfering with their ability to balance home and work life. “There’s a huge need for hospitalists everywhere,” she says, and reliance on them has been especially acute at academic centers and large community hospitals contending with the recently imposed limits on residents’ work hours.
The Hospitalist: A People Person
Another shift may be occurring in the types of relationships necessary for a satisfying work environment, a big part of the “community and environment” pillar. Although Dr. Yoon says long-term connections with students and trainees have added meaning to his job, he is mourning the absence of other bonds. “One loss I’m starting to feel keenly as an academic hospitalist, having spent my early training years as a primary-care doc, really is the loss of having long-term relationships with patients,” he says. “My clinical encounters with patients these days as a hospitalist are very intense, but also very brief.”
Dr. Yoon has pondered whether the HM field can rearrange practice settings to promote more satisfying relationships. Such a change, he says, might occur through innovative models that aid coordination with medical homes, or provide more chronic care for high-risk patients. “In my view, the trajectory of hospital medicine is pretty wide open for creativity and new models of care,” he says. “I think it will be partly driven by the need to want to have more meaningful interactions with patients.”
Those relationships need not be long-term, however. One recent study found high satisfaction among hospitalists and laborists working within the fast-growing OBGYN hospitalist field.6
Dr. Hinami says collaborative care that involves close working relationships with specialists and other care providers might help propel the hospitalist movement forward. In his survey with Dr. Wetterneck, hospitalists ranked relationships with staff and colleagues among the most satisfying of any of the domains; hospitalists also indicated high levels of satisfaction with their patient relationships. “Clearly, relationships are critical to overall job satisfaction, and hospitalists, I think, are doing a fairly good job at maintaining those relationships,” Dr. Hinami says.
—Keiki Hinami, MD, assistant professor of medicine, Northwestern University Feinberg School of Medicine, Chicago
A 2002 survey-based study reinforces the importance of such bonds. Job burnout and intent to remain in the hospitalist career, its authors concluded, were more highly influenced by “favorable social relations” involving colleagues, coworkers, and patients than by such factors as reduced autonomy and the use of financial incentives.7
The focus on maintaining multiple relationships fits well with the collaborative approach to care that many hospitalists say they value highly. One big satisfier for hospitalists, Dr. Cors says, will be “a sense that they’re really part of a healthcare team and not just punching the clock and doing their shifts.”
The Verdict
Despite the difficulty in discerning long-term trends, studies suggest that overall satisfaction with the specialty of hospital medicine remains high, a promising sign for the maturing field. Career hospitalists also seem adept at relationships with peers and other providers, a skill that will serve them well as collaborative-care models gain steam.
Nonetheless, surveys also suggest a worrisome rate of burnout and less-than-optimal satisfaction with elements that should be the strong suits of HM, such as work-life balance and autonomy. Academics are searching for their own clinical-research balance. And Dr. West says the jury’s still out on the future pitfalls that might get in the way of a sustainable career path for older practitioners, such as overnight shifts.
Hospitalist-led efforts, however, may be starting to pay dividends. At the University of California at San Francisco, a faculty development program for first-year hospitalists has included a coaching relationship with a senior faculty member, a teaching course, newly established divisional grand rounds, and a framework for meeting scholarly expectations. Upon its implementation, the program has led to higher job satisfaction, skill-set comfort, and academic production among participants.8
Given the expanding range of HM duties and practice models, hospitals, division chiefs, and team leaders cannot rely on a single recipe for happy and productive hospitalists. “I don’t know if there is a cookbook; I think it’s highly variable depending on your institution and the needs of the academic facility where you are,” Dr. Misky says.
SHM’s 2006 white paper stated that the best career satisfaction strategy is to find a job that fits an individual’s preferences and attitudes. “People who are unhappy with their job don’t tend to stay in it, and from what we know about hospital medicine right now, you can find pretty much any type of job anywhere you want, so the job market is very open,” Dr. Wetterneck says.
Ensuring the right fit for doctors within HM, though, will require institutional support. “It’s going to be up to hospitals and hospitalist programs to create jobs that are sustainable that people like,” she says, “so that hospitalists will stay long in their job and in the profession.”
Bryn Nelson is a freelance medical writer based in Seattle.
More Mentorship in Hospital Medicine? It’s Academic
Within the 2011 State of Hospital Medicine report, one statistic in particular points to the youth of the medical specialty: Just over 10% of surveyed hospitalists had reached the rank of associate professor or higher.
How might the potential lack of mentorship within this immature field affect the ability of hospitalists to successfully navigate academia? So asked Gregory Misky, MD, assistant professor of medicine at the University of Colorado Denver, and his colleagues in a survey-based study. The results agree with other recent assessments that mentors are in short supply. “Academic hospital medicine groups have an acute need for mentoring and career development programs,” one study concludes.
The research of Dr. Misky and his collaborators found that only 42% of academic hospitalists could identify a mentor, while only 31% reported that they were mentoring another academic hospitalist.1 Based on sheer numbers and experience, the pool of mentors may significantly expand as the field matures. But Dr. Misky also urges some flexibility, noting that his own mentor is a non-hospitalist.
In his own research, Colin West, MD, PhD, associate professor of medicine and biostatistics at the Mayo Clinic in Rochester, Minn., found that residents considering a career in HM placed less emphasis on the specialty or subspecialty of their mentor.5 Why? Very likely, he says, there just weren’t enough hospitalist mentors around to get a sense of what the career was all about.
Dr. West hopes the numbers suggest otherwise in the near future. “You want to recruit bright people into your specialty, but at the same time, you also want to recruit the right people,” he says. “And that means that you need to be able to expose people to a full breadth of what a decision to pursue a certain specialty really means.”
References
- Glasheen JJ, Misky GJ, Reid MB, Harrison RA, Sharpe B, Auerbach A. Career satisfaction and burnout in academic hospital medicine. Arch Intern Med. 2011;171(8) 782-785.
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers [published online ahead of print July 20, 2011]. J Gen Intern Med. doi:10.1007/s116060-011-1780-z.
- Yoon J, Miller A, Rasinski K, Curlin F. Burnout, sense of calling, and career resilience among hospitalists and primary care physicians: a national survey. J Hosp Med. 2011;6(4):S90-S91.
- West CP, Drefahl MM, Popkave C, Kolars JC. Internal medicine resident self-report of factors associated with career decisions. J Gen Intern Med. 2009;24(8):946-949.
- Funk C, Anderson BL, Schulkin J, Weinstein L. Survey of obstetric and gynecologic hospitalists and laborists. Am J Obstet Gynecol. 2010;203(2):177.e1-177.e4.
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43(1):72-91.
- Sehgal NL, Sharpe BA, Auerbach AA, Wachter RM. Investing in the future: Building an academic hospitalist faculty development program. J Hosp Med. 2011;6(3):161-166.
Business Drivers
MIAMI BEACH, Fla.—Muralidharan Reddy, MD, had just finished a five-hour class on the business concepts behind running a hospital and how a hospital CEO thinks—part of the entry-level curriculum at SHM’s Leadership Academy. As he stood up from the round table in a room still buzzing with conversation, he was glad he had signed up—in fact, he had been one of the first to arrive for the 7:30 a.m. session at the Fontainebleau resort.
“It improves my CV, number one,” says Dr. Reddy, a hospitalist at New England Baptist Hospital in Boston. “And it’s not just the CV, but I need the experience to guide me to work as a leader in a hospital group, or even plan on starting a group, or things like that. If I’m going to be a hospitalist, I have to work on trying to get those skills.”
A big plus, he adds, is “you get to learn from experts.”
The four-day academy provides hospitalists an intense learning experience. “Some of these skills, people learn it on the job or you get it through Academy,” Dr. Reddy says. “So I do both.”
Hospitalists who participate in the session repeatedly express concerns that if they don’t hone their understanding of the business aspects of the hospital and refine their skills in interacting with colleagues, they could be left behind in a fast-moving environment.
“I think it’s important,” said Mana Goshtasbi, MD, a hospitalist with Cogent HMG who has worked for two years at St. Joseph’s Hospital in Tampa, Fla. “I think that’s the direction. I think you have to know this stuff because of all the changes.”
Leadership Academy courses come in three levels, which build on one another: Foundations for Effective Leadership, Personal Leadership Excellence, and Strengthening Your Organization. Those who have completed the three levels can apply for certification, which requires completion of a pre-approved leadership project.
Know Your Value, Know Your Customers

In his first-level session, instructor Michael Guthrie, MD, MBA, executive in residence and adjunct professor at the University of Colorado Denver School of Business’ program in health administration, spent most of his presentation on his feet, wending his way among the tables, challenging the physician-students to think differently from the ways they’ve been trained to think about healthcare. That starts with stepping outside of themselves and taking a look at how they are viewed in terms of the hospital they’re working with as hospitalists, says Dr. Guthrie, former CEO of the Good Samaritan Health System in San Jose, Calif., and former COO for the Penrose-St. Francis Healthcare System in Colorado.
“What’s affecting the organization that you operate in, and what does that mean about the kinds of demands that are being made of you and requests that are being made of you?” he asks the attendees. “What does it mean about the value that’s received from the work that you do in that organization?”
A hospitalists’ value is a common theme. “What is it that you offer as hospitalists that has created a group of enthusiasts?” he asks. “What is it that you offer to any customer that’s of value to them that they would give up their hard-earned money in exchange for it? Who are your customers?”
A key “customer” group is primary-care physicians (PCPs) whose patients end up under a hospitalist’s care, he explains. They get value from the hospitalist in a variety of ways.
“That’s a more effective way for them to spend their life [at their own clinic],” he says. “They get to manage their schedule differently, they don’t have to drive. They are all exchange values. … There’s a very definite exchange going on here. If you fail in that exchange, we all know what would happen, right? They’d stop sending you patients.”
A physician chimes in: “If you’re the only hospitalist there, they don’t have a choice.”
Dr. Guthrie, quick to seize upon what he sees as a teaching moment, tells the group to “be careful.”
“In the short term, that’s absolutely true,” he says. “In the long term, there are a lot of other alternatives. And if there aren’t, someone will invent one. You see that’s the thing about our society—if there’s an opportunity with a whole, big, dissatisfied customer segment, somebody will notice and invent the way to satisfy their needs. That’s called capitalism.”
It’s what happened with the late Steve Jobs and the iPod, when he realized customers needed a way to easily access their music collections, Dr. Guthrie points out.
“He understood the dissatisfactions of the market,” he continues. “Before that, they didn’t have any choices.
“Healthcare is the same. But it’s a little more difficult to develop those choices. It’s hard to build a new hospital right in the middle of someplace where there’s only one hospital. So they invent other ways to do it, ways to get their patients taken care of: They travel.”
About 700,000 people flew to Southeast Asia last year for medical procedures, he says, making the point that American patients have options.
“Somewhat difficult, but they do have alternatives,” he says. “Customers will, when pushed hard enough, if dissatisfied enough, leave you, even when you think you have them trapped.”
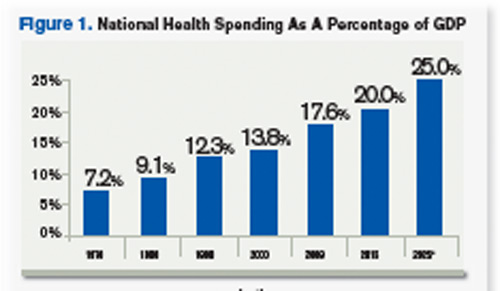
Source: Hartman, M: Martin, A; McDonnell, P et al. (2009). National Helath Spending In 2007: Slower Drug Spending Contributes To Lowest Rate Of Overall Growth Since 1998. Health Affairs, Jan/Feb., p 247. www.healthaffairs.org). See also, Orzag, Peter; Congressional Budget Office (2008). Growth in Health Care Costs, testimony before the Sentae Budget Committee, Jan. 31, p.1. (www.cbo.gov/doc.cfm?index-8948). Center for Medicare & Medicaid Services, January 2011.
Think Tanks
A key part of the session is time set aside for group work, in which Dr. Guthrie gives the class an assignment and attendees tackle it at their tables as a unit. The first task is to identify business drivers at hospitals, what the objectives of the hospital should be in response to those things, and how those objectives affect the work of hospitalists.
Then the groups go to work. A few minutes later, though, Dr. Guthrie speaks up through the chatter.
“Let’s stop for a minute. I want to tell you that most of you are on completely the wrong track,” he says, drawing chuckles. “But this is part of the reason we do it this way. The idea here is to get outside of your head.”
One group lists “profit” as a business driver.
“Profit is not a business driver,” he says. “I know you’re sort of raised to think that way. It isn’t. It’s a measurement. It’s like blood pressure. So it is not a business driver. We use it as a measurement of the success with which we’re synthesizing the business drivers and the environment and meeting the objectives of those drivers, or those trends.”
Business drivers are more along the lines of government mandates and an aging population, which some of the groups had mentioned. “That’s the level of abstraction I want you get to,” he says. “Think out in the marketplace.”
When it comes down to it, Dr. Guthrie explains, the hospitalist plays a role in just about every measurement used to determine excellence at a hospital—from quality to customer loyalty, from retention of patients to productivity.
He also emphasizes the difference between how a doctor has been trained essentially to be an individual expert—patient presents a problem, doctor presents a solution—and how those trained to be managers and leaders operate through other people.
Leaders of the Future
Daniel Duzan, MD, a hospitalist for TeamHealth at Fort Loudoun Medical Center in Lenoir City, Tenn., southwest of Knoxville, says doctors he knows recommended the academy. He says it made sense to him because he’s “migrating toward a leadership role in my own hospital.”
“My goal for coming was to kind of lay some foundation for skills and requirements that it takes to kind of migrate from just being a regular hospitalist to being one that’s got some extra responsibility,” Dr. Duzan says.
He was happy to learn more about “some of the jargon, lingo, that’s getting pushed our direction in terms of business drivers and the objectives” as well as “what would it be like to be the CEO, etc., and kind of putting us in their shoes, hearing things, seeing things and how they think about things, then developing plans.”
Jeet Gujral, MD, a hospitalist at Southside Hospital on Long Island, N.Y., says her motivation to learn about practice management is due in part to the new demands she is feeling because of the business considerations of the hospital. Talking with other hospitalists about their experiences was a big help, she says. In fact, she adds, that was probably even more helpful than the actual content of the session.
“I think what I’m getting more out of it [is that] there are several who are feeling the same heat,” she says. “It’s nice not feeling alone.”
Tom Collins is a freelance writer based in Florida.
MIAMI BEACH, Fla.—Muralidharan Reddy, MD, had just finished a five-hour class on the business concepts behind running a hospital and how a hospital CEO thinks—part of the entry-level curriculum at SHM’s Leadership Academy. As he stood up from the round table in a room still buzzing with conversation, he was glad he had signed up—in fact, he had been one of the first to arrive for the 7:30 a.m. session at the Fontainebleau resort.
“It improves my CV, number one,” says Dr. Reddy, a hospitalist at New England Baptist Hospital in Boston. “And it’s not just the CV, but I need the experience to guide me to work as a leader in a hospital group, or even plan on starting a group, or things like that. If I’m going to be a hospitalist, I have to work on trying to get those skills.”
A big plus, he adds, is “you get to learn from experts.”
The four-day academy provides hospitalists an intense learning experience. “Some of these skills, people learn it on the job or you get it through Academy,” Dr. Reddy says. “So I do both.”
Hospitalists who participate in the session repeatedly express concerns that if they don’t hone their understanding of the business aspects of the hospital and refine their skills in interacting with colleagues, they could be left behind in a fast-moving environment.
“I think it’s important,” said Mana Goshtasbi, MD, a hospitalist with Cogent HMG who has worked for two years at St. Joseph’s Hospital in Tampa, Fla. “I think that’s the direction. I think you have to know this stuff because of all the changes.”
Leadership Academy courses come in three levels, which build on one another: Foundations for Effective Leadership, Personal Leadership Excellence, and Strengthening Your Organization. Those who have completed the three levels can apply for certification, which requires completion of a pre-approved leadership project.
Know Your Value, Know Your Customers
In his first-level session, instructor Michael Guthrie, MD, MBA, executive in residence and adjunct professor at the University of Colorado Denver School of Business’ program in health administration, spent most of his presentation on his feet, wending his way among the tables, challenging the physician-students to think differently from the ways they’ve been trained to think about healthcare. That starts with stepping outside of themselves and taking a look at how they are viewed in terms of the hospital they’re working with as hospitalists, says Dr. Guthrie, former CEO of the Good Samaritan Health System in San Jose, Calif., and former COO for the Penrose-St. Francis Healthcare System in Colorado.
“What’s affecting the organization that you operate in, and what does that mean about the kinds of demands that are being made of you and requests that are being made of you?” he asks the attendees. “What does it mean about the value that’s received from the work that you do in that organization?”
A hospitalists’ value is a common theme. “What is it that you offer as hospitalists that has created a group of enthusiasts?” he asks. “What is it that you offer to any customer that’s of value to them that they would give up their hard-earned money in exchange for it? Who are your customers?”
A key “customer” group is primary-care physicians (PCPs) whose patients end up under a hospitalist’s care, he explains. They get value from the hospitalist in a variety of ways.
“That’s a more effective way for them to spend their life [at their own clinic],” he says. “They get to manage their schedule differently, they don’t have to drive. They are all exchange values. … There’s a very definite exchange going on here. If you fail in that exchange, we all know what would happen, right? They’d stop sending you patients.”
A physician chimes in: “If you’re the only hospitalist there, they don’t have a choice.”
Dr. Guthrie, quick to seize upon what he sees as a teaching moment, tells the group to “be careful.”
“In the short term, that’s absolutely true,” he says. “In the long term, there are a lot of other alternatives. And if there aren’t, someone will invent one. You see that’s the thing about our society—if there’s an opportunity with a whole, big, dissatisfied customer segment, somebody will notice and invent the way to satisfy their needs. That’s called capitalism.”
It’s what happened with the late Steve Jobs and the iPod, when he realized customers needed a way to easily access their music collections, Dr. Guthrie points out.
“He understood the dissatisfactions of the market,” he continues. “Before that, they didn’t have any choices.
“Healthcare is the same. But it’s a little more difficult to develop those choices. It’s hard to build a new hospital right in the middle of someplace where there’s only one hospital. So they invent other ways to do it, ways to get their patients taken care of: They travel.”
About 700,000 people flew to Southeast Asia last year for medical procedures, he says, making the point that American patients have options.
“Somewhat difficult, but they do have alternatives,” he says. “Customers will, when pushed hard enough, if dissatisfied enough, leave you, even when you think you have them trapped.”
Source: Hartman, M: Martin, A; McDonnell, P et al. (2009). National Helath Spending In 2007: Slower Drug Spending Contributes To Lowest Rate Of Overall Growth Since 1998. Health Affairs, Jan/Feb., p 247. www.healthaffairs.org). See also, Orzag, Peter; Congressional Budget Office (2008). Growth in Health Care Costs, testimony before the Sentae Budget Committee, Jan. 31, p.1. (www.cbo.gov/doc.cfm?index-8948). Center for Medicare & Medicaid Services, January 2011.
Think Tanks
A key part of the session is time set aside for group work, in which Dr. Guthrie gives the class an assignment and attendees tackle it at their tables as a unit. The first task is to identify business drivers at hospitals, what the objectives of the hospital should be in response to those things, and how those objectives affect the work of hospitalists.
Then the groups go to work. A few minutes later, though, Dr. Guthrie speaks up through the chatter.
“Let’s stop for a minute. I want to tell you that most of you are on completely the wrong track,” he says, drawing chuckles. “But this is part of the reason we do it this way. The idea here is to get outside of your head.”
One group lists “profit” as a business driver.
“Profit is not a business driver,” he says. “I know you’re sort of raised to think that way. It isn’t. It’s a measurement. It’s like blood pressure. So it is not a business driver. We use it as a measurement of the success with which we’re synthesizing the business drivers and the environment and meeting the objectives of those drivers, or those trends.”
Business drivers are more along the lines of government mandates and an aging population, which some of the groups had mentioned. “That’s the level of abstraction I want you get to,” he says. “Think out in the marketplace.”
When it comes down to it, Dr. Guthrie explains, the hospitalist plays a role in just about every measurement used to determine excellence at a hospital—from quality to customer loyalty, from retention of patients to productivity.
He also emphasizes the difference between how a doctor has been trained essentially to be an individual expert—patient presents a problem, doctor presents a solution—and how those trained to be managers and leaders operate through other people.
Leaders of the Future
Daniel Duzan, MD, a hospitalist for TeamHealth at Fort Loudoun Medical Center in Lenoir City, Tenn., southwest of Knoxville, says doctors he knows recommended the academy. He says it made sense to him because he’s “migrating toward a leadership role in my own hospital.”
“My goal for coming was to kind of lay some foundation for skills and requirements that it takes to kind of migrate from just being a regular hospitalist to being one that’s got some extra responsibility,” Dr. Duzan says.
He was happy to learn more about “some of the jargon, lingo, that’s getting pushed our direction in terms of business drivers and the objectives” as well as “what would it be like to be the CEO, etc., and kind of putting us in their shoes, hearing things, seeing things and how they think about things, then developing plans.”
Jeet Gujral, MD, a hospitalist at Southside Hospital on Long Island, N.Y., says her motivation to learn about practice management is due in part to the new demands she is feeling because of the business considerations of the hospital. Talking with other hospitalists about their experiences was a big help, she says. In fact, she adds, that was probably even more helpful than the actual content of the session.
“I think what I’m getting more out of it [is that] there are several who are feeling the same heat,” she says. “It’s nice not feeling alone.”
Tom Collins is a freelance writer based in Florida.
MIAMI BEACH, Fla.—Muralidharan Reddy, MD, had just finished a five-hour class on the business concepts behind running a hospital and how a hospital CEO thinks—part of the entry-level curriculum at SHM’s Leadership Academy. As he stood up from the round table in a room still buzzing with conversation, he was glad he had signed up—in fact, he had been one of the first to arrive for the 7:30 a.m. session at the Fontainebleau resort.
“It improves my CV, number one,” says Dr. Reddy, a hospitalist at New England Baptist Hospital in Boston. “And it’s not just the CV, but I need the experience to guide me to work as a leader in a hospital group, or even plan on starting a group, or things like that. If I’m going to be a hospitalist, I have to work on trying to get those skills.”
A big plus, he adds, is “you get to learn from experts.”
The four-day academy provides hospitalists an intense learning experience. “Some of these skills, people learn it on the job or you get it through Academy,” Dr. Reddy says. “So I do both.”
Hospitalists who participate in the session repeatedly express concerns that if they don’t hone their understanding of the business aspects of the hospital and refine their skills in interacting with colleagues, they could be left behind in a fast-moving environment.
“I think it’s important,” said Mana Goshtasbi, MD, a hospitalist with Cogent HMG who has worked for two years at St. Joseph’s Hospital in Tampa, Fla. “I think that’s the direction. I think you have to know this stuff because of all the changes.”
Leadership Academy courses come in three levels, which build on one another: Foundations for Effective Leadership, Personal Leadership Excellence, and Strengthening Your Organization. Those who have completed the three levels can apply for certification, which requires completion of a pre-approved leadership project.
Know Your Value, Know Your Customers
In his first-level session, instructor Michael Guthrie, MD, MBA, executive in residence and adjunct professor at the University of Colorado Denver School of Business’ program in health administration, spent most of his presentation on his feet, wending his way among the tables, challenging the physician-students to think differently from the ways they’ve been trained to think about healthcare. That starts with stepping outside of themselves and taking a look at how they are viewed in terms of the hospital they’re working with as hospitalists, says Dr. Guthrie, former CEO of the Good Samaritan Health System in San Jose, Calif., and former COO for the Penrose-St. Francis Healthcare System in Colorado.
“What’s affecting the organization that you operate in, and what does that mean about the kinds of demands that are being made of you and requests that are being made of you?” he asks the attendees. “What does it mean about the value that’s received from the work that you do in that organization?”
A hospitalists’ value is a common theme. “What is it that you offer as hospitalists that has created a group of enthusiasts?” he asks. “What is it that you offer to any customer that’s of value to them that they would give up their hard-earned money in exchange for it? Who are your customers?”
A key “customer” group is primary-care physicians (PCPs) whose patients end up under a hospitalist’s care, he explains. They get value from the hospitalist in a variety of ways.
“That’s a more effective way for them to spend their life [at their own clinic],” he says. “They get to manage their schedule differently, they don’t have to drive. They are all exchange values. … There’s a very definite exchange going on here. If you fail in that exchange, we all know what would happen, right? They’d stop sending you patients.”
A physician chimes in: “If you’re the only hospitalist there, they don’t have a choice.”
Dr. Guthrie, quick to seize upon what he sees as a teaching moment, tells the group to “be careful.”
“In the short term, that’s absolutely true,” he says. “In the long term, there are a lot of other alternatives. And if there aren’t, someone will invent one. You see that’s the thing about our society—if there’s an opportunity with a whole, big, dissatisfied customer segment, somebody will notice and invent the way to satisfy their needs. That’s called capitalism.”
It’s what happened with the late Steve Jobs and the iPod, when he realized customers needed a way to easily access their music collections, Dr. Guthrie points out.
“He understood the dissatisfactions of the market,” he continues. “Before that, they didn’t have any choices.
“Healthcare is the same. But it’s a little more difficult to develop those choices. It’s hard to build a new hospital right in the middle of someplace where there’s only one hospital. So they invent other ways to do it, ways to get their patients taken care of: They travel.”
About 700,000 people flew to Southeast Asia last year for medical procedures, he says, making the point that American patients have options.
“Somewhat difficult, but they do have alternatives,” he says. “Customers will, when pushed hard enough, if dissatisfied enough, leave you, even when you think you have them trapped.”
Source: Hartman, M: Martin, A; McDonnell, P et al. (2009). National Helath Spending In 2007: Slower Drug Spending Contributes To Lowest Rate Of Overall Growth Since 1998. Health Affairs, Jan/Feb., p 247. www.healthaffairs.org). See also, Orzag, Peter; Congressional Budget Office (2008). Growth in Health Care Costs, testimony before the Sentae Budget Committee, Jan. 31, p.1. (www.cbo.gov/doc.cfm?index-8948). Center for Medicare & Medicaid Services, January 2011.
Think Tanks
A key part of the session is time set aside for group work, in which Dr. Guthrie gives the class an assignment and attendees tackle it at their tables as a unit. The first task is to identify business drivers at hospitals, what the objectives of the hospital should be in response to those things, and how those objectives affect the work of hospitalists.
Then the groups go to work. A few minutes later, though, Dr. Guthrie speaks up through the chatter.
“Let’s stop for a minute. I want to tell you that most of you are on completely the wrong track,” he says, drawing chuckles. “But this is part of the reason we do it this way. The idea here is to get outside of your head.”
One group lists “profit” as a business driver.
“Profit is not a business driver,” he says. “I know you’re sort of raised to think that way. It isn’t. It’s a measurement. It’s like blood pressure. So it is not a business driver. We use it as a measurement of the success with which we’re synthesizing the business drivers and the environment and meeting the objectives of those drivers, or those trends.”
Business drivers are more along the lines of government mandates and an aging population, which some of the groups had mentioned. “That’s the level of abstraction I want you get to,” he says. “Think out in the marketplace.”
When it comes down to it, Dr. Guthrie explains, the hospitalist plays a role in just about every measurement used to determine excellence at a hospital—from quality to customer loyalty, from retention of patients to productivity.
He also emphasizes the difference between how a doctor has been trained essentially to be an individual expert—patient presents a problem, doctor presents a solution—and how those trained to be managers and leaders operate through other people.
Leaders of the Future
Daniel Duzan, MD, a hospitalist for TeamHealth at Fort Loudoun Medical Center in Lenoir City, Tenn., southwest of Knoxville, says doctors he knows recommended the academy. He says it made sense to him because he’s “migrating toward a leadership role in my own hospital.”
“My goal for coming was to kind of lay some foundation for skills and requirements that it takes to kind of migrate from just being a regular hospitalist to being one that’s got some extra responsibility,” Dr. Duzan says.
He was happy to learn more about “some of the jargon, lingo, that’s getting pushed our direction in terms of business drivers and the objectives” as well as “what would it be like to be the CEO, etc., and kind of putting us in their shoes, hearing things, seeing things and how they think about things, then developing plans.”
Jeet Gujral, MD, a hospitalist at Southside Hospital on Long Island, N.Y., says her motivation to learn about practice management is due in part to the new demands she is feeling because of the business considerations of the hospital. Talking with other hospitalists about their experiences was a big help, she says. In fact, she adds, that was probably even more helpful than the actual content of the session.
“I think what I’m getting more out of it [is that] there are several who are feeling the same heat,” she says. “It’s nice not feeling alone.”
Tom Collins is a freelance writer based in Florida.
Survey Insights
SHM and the Medical Group Management Association (MGMA) have enjoyed a successful survey collaboration for the past two years. Working together under a survey collaboration agreement to jointly conduct comprehensive annual surveys of HM groups, the two entities have been able to provide an unprecedented amount of high-quality information for members—not only data about hospitalist compensation and productivity, but also about many other aspects of the ways hospitalists and HM groups function.
And while SHM’s relationship with MGMA remains strong, all good things must come to an end—or at least change considerably.
MGMA is headed in new strategic directions that require a reallocation of its existing survey operations department resources. As a result, SHM and MGMA have agreed to change the way they work together, and this will have some important implications for the types of compensation and productivity data that will be available to hospitalists in the future.
MGMA will continue to conduct its regular surveys, including capturing compensation and productivity data for hospitalists. But instead of incorporating a hospital medicine supplement as it has for the last two years, SHM will instead conduct a separate survey each year to collect additional information about the characteristics of HM practices.
The SHM survey will be launched in January to coincide with the launch of MGMA’s Physician Compensation and Production Survey; in fact, academic groups that participated in MGMA’s Academic Practice Compensation and Production Survey for Faculty and Management this fall might already have noticed that the survey no longer included a hospital medicine supplement. SHM is encouraging hospitalists to participate in both the applicable MGMA survey and the companion SHM survey.
SHM will then license MGMA’s compensation and productivity data for both academic and nonacademic hospitalists, then will combine it with the results of its separate SHM survey to create the 2012 State of Hospital Medicine report.
The good news is that this approach will enable SHM to have greater flexibility to design surveys and analyze results in ways that best meet the needs of its constituents, and SHM will also be able to continue to provide survey information annually, rather than going back to the old biannual format.
However, some of the more detailed looks at compensation and productivity data will be lost; those data glimpses only were possible when the supplemental survey was integrated with MGMA’s survey instruments. Such data for 2012 will only be available for national, hospital-employed vs. not-hospital-employed, and geographic region cohorts.
Like the hospitalists it surveys, this report has changed every time it has been conducted. And SHM depends on its members to make sure it is delivering the kind of information that effectively, efficiently, and profitably guides hospitalists’ decisions.
Together, SHM and MGMA have been working to find the right balance that enables MGMA to pursue new strategies and still gives hospitalists the data they need. Ultimately, hospitalists will be the judges of whether the right balance has been struck.
Please send your thoughts and feedback to [email protected].
SHM and the Medical Group Management Association (MGMA) have enjoyed a successful survey collaboration for the past two years. Working together under a survey collaboration agreement to jointly conduct comprehensive annual surveys of HM groups, the two entities have been able to provide an unprecedented amount of high-quality information for members—not only data about hospitalist compensation and productivity, but also about many other aspects of the ways hospitalists and HM groups function.
And while SHM’s relationship with MGMA remains strong, all good things must come to an end—or at least change considerably.
MGMA is headed in new strategic directions that require a reallocation of its existing survey operations department resources. As a result, SHM and MGMA have agreed to change the way they work together, and this will have some important implications for the types of compensation and productivity data that will be available to hospitalists in the future.
MGMA will continue to conduct its regular surveys, including capturing compensation and productivity data for hospitalists. But instead of incorporating a hospital medicine supplement as it has for the last two years, SHM will instead conduct a separate survey each year to collect additional information about the characteristics of HM practices.
The SHM survey will be launched in January to coincide with the launch of MGMA’s Physician Compensation and Production Survey; in fact, academic groups that participated in MGMA’s Academic Practice Compensation and Production Survey for Faculty and Management this fall might already have noticed that the survey no longer included a hospital medicine supplement. SHM is encouraging hospitalists to participate in both the applicable MGMA survey and the companion SHM survey.
SHM will then license MGMA’s compensation and productivity data for both academic and nonacademic hospitalists, then will combine it with the results of its separate SHM survey to create the 2012 State of Hospital Medicine report.
The good news is that this approach will enable SHM to have greater flexibility to design surveys and analyze results in ways that best meet the needs of its constituents, and SHM will also be able to continue to provide survey information annually, rather than going back to the old biannual format.
However, some of the more detailed looks at compensation and productivity data will be lost; those data glimpses only were possible when the supplemental survey was integrated with MGMA’s survey instruments. Such data for 2012 will only be available for national, hospital-employed vs. not-hospital-employed, and geographic region cohorts.
Like the hospitalists it surveys, this report has changed every time it has been conducted. And SHM depends on its members to make sure it is delivering the kind of information that effectively, efficiently, and profitably guides hospitalists’ decisions.
Together, SHM and MGMA have been working to find the right balance that enables MGMA to pursue new strategies and still gives hospitalists the data they need. Ultimately, hospitalists will be the judges of whether the right balance has been struck.
Please send your thoughts and feedback to [email protected].
SHM and the Medical Group Management Association (MGMA) have enjoyed a successful survey collaboration for the past two years. Working together under a survey collaboration agreement to jointly conduct comprehensive annual surveys of HM groups, the two entities have been able to provide an unprecedented amount of high-quality information for members—not only data about hospitalist compensation and productivity, but also about many other aspects of the ways hospitalists and HM groups function.
And while SHM’s relationship with MGMA remains strong, all good things must come to an end—or at least change considerably.
MGMA is headed in new strategic directions that require a reallocation of its existing survey operations department resources. As a result, SHM and MGMA have agreed to change the way they work together, and this will have some important implications for the types of compensation and productivity data that will be available to hospitalists in the future.
MGMA will continue to conduct its regular surveys, including capturing compensation and productivity data for hospitalists. But instead of incorporating a hospital medicine supplement as it has for the last two years, SHM will instead conduct a separate survey each year to collect additional information about the characteristics of HM practices.
The SHM survey will be launched in January to coincide with the launch of MGMA’s Physician Compensation and Production Survey; in fact, academic groups that participated in MGMA’s Academic Practice Compensation and Production Survey for Faculty and Management this fall might already have noticed that the survey no longer included a hospital medicine supplement. SHM is encouraging hospitalists to participate in both the applicable MGMA survey and the companion SHM survey.
SHM will then license MGMA’s compensation and productivity data for both academic and nonacademic hospitalists, then will combine it with the results of its separate SHM survey to create the 2012 State of Hospital Medicine report.
The good news is that this approach will enable SHM to have greater flexibility to design surveys and analyze results in ways that best meet the needs of its constituents, and SHM will also be able to continue to provide survey information annually, rather than going back to the old biannual format.
However, some of the more detailed looks at compensation and productivity data will be lost; those data glimpses only were possible when the supplemental survey was integrated with MGMA’s survey instruments. Such data for 2012 will only be available for national, hospital-employed vs. not-hospital-employed, and geographic region cohorts.
Like the hospitalists it surveys, this report has changed every time it has been conducted. And SHM depends on its members to make sure it is delivering the kind of information that effectively, efficiently, and profitably guides hospitalists’ decisions.
Together, SHM and MGMA have been working to find the right balance that enables MGMA to pursue new strategies and still gives hospitalists the data they need. Ultimately, hospitalists will be the judges of whether the right balance has been struck.
Please send your thoughts and feedback to [email protected].
Exam Guidelines
The extent of the exam should correspond to the nature of the presenting problem, the standard of care, and the physicians’ clinical judgment. Remember, medical necessity issues can arise if the physician performs and submits a claim for a comprehensive service involving a self-limiting problem. The easiest way to demonstrate the medical necessity for evaluation and management (E/M) services is through medical decision-making. It prevents a third party from making accusations that a Level 5 service was reported solely based upon a comprehensive history and examination that was not warranted by the patient’s presenting problem (e.g. the common cold).1
1995 Exam Guidelines
The 1995 guidelines differentiate 10 body areas (head and face; neck; chest, breast, and axillae; abdomen; genitalia, groin, and buttocks; back and spine; right upper extremity; left upper extremity; right lower extremity; and left lower extremity) from 12 organ systems (constitutional; eyes; ears, nose, mouth, and throat; cardiovascular; respiratory, gastrointestinal; genitourinary; musculoskeletal; integumentary; neurological; psychiatric; hematologic, lymphatic, and immunologic).2 Physicians are permitted to perform and comment without mandate, as appropriate, but with a few minor directives:
- Document relevant negative findings. Commenting that a system or area is “negative” or “normal” is acceptable when referring to unaffected areas or asymptomatic organ systems.
- Elaborate abnormal findings. Commenting that a system or area is “abnormal” is not sufficient unless additional comments describing the abnormality are documented.
1997 Documentation Guidelines
The 1997 guidelines are formatted as organ systems with corresponding, bulleted items referred to as “elements.”3 Additionally, a few elements have a numeric requirement to be achieved before satisfying the documentation of that particular element. For example, credit for the “vital signs element” (located within the constitutional system) is only awarded after documentation of three individual measurements (e.g. blood pressure, heart rate, and respiratory rate). Failure to document the specified criterion (e.g. two measurements: “blood pressure and heart rate only,” or a single nonspecific comment: “vital signs stable”) leads to failure to assign credit.
Take note that these specified criterion do not resonate within the 1995 guidelines. Numerical requirements also are indicated for the lymphatic system. The physician must examine and document findings associated with two or more lymphatic areas (e.g. “no lymphadenopathy noted in the neck or axillae”).
In the absence of numeric criterion, some elements contain multiple components, which require documentation of at least one component. For example, one listed psychiatric element designates the assessment of the patient’s “mood and affect.” The physician receives credit for a comment regarding the patient’s mood (e.g. “appears depressed”) without identification of a flat (or normal).

The 1997 Documentation Guide-lines comprise the following systems and elements:
Constitutional
- Measurement of any three of the following seven vital signs:
- Sitting or standing blood pressure;
- Supine blood pressure;
- Pulse rate and regularity;
- Respiration;
- Temperature;
- Height; or
- Weight (can be measured and recorded by ancillary staff).
- General appearance of patient (e.g. development, nutrition, body habitus, deformities, attention to grooming)
Eyes
- Inspection of conjunctivae and lids;
- Examination of pupils and irises (e.g. reaction to light and accommodation, size, symmetry); and
- Ophthalmoscopic examination of optic discs (e.g. size, C/D ratio, appearance) and posterior segments (e.g. vessel changes, exudates, hemorrhages).
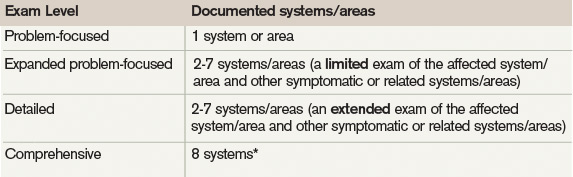
Ears, Nose, Mouth, and Throat
- External inspection of ears and nose (e.g. overall appearance, scars, lesions, masses);
- Otoscopic examination of external auditory canals and tympanic membranes;
- Assessment of hearing (e.g. whispered voice, finger rub, tuning fork);
- Inspection of nasal mucosa, septum, and turbinates;
- Inspection of lips, teeth, and gums; and
- Examination of oropharynx: oral mucosa, salivary glands, hard and soft palates, tongue, tonsils, and posterior pharynx.
Neck
- Examination of neck (e.g. masses, overall appearance, symmetry, tracheal position, crepitus); and
- Examination of thyroid (e.g. enlargement, tenderness, mass).
Respiratory
- Assessment of respiratory effort (e.g. intercostal retractions, use of accessory muscles, diaphragmatic movement);
- Percussion of chest (e.g. dullness, flatness, hyperresonance);
- Palpation of chest (e.g. tactile fremitus); and
- Auscultation of lungs (e.g. breath sounds, adventitious sounds, rubs).
Cardiovascular
- Palpation of heart (e.g. location, size, thrills);
- Auscultation of heart with notation of abnormal sounds and murmurs; and
- Examination of:
- Carotid arteries (e.g. pulse amplitude, bruits);
- Abdominal aorta (e.g. size, bruits);
- Femoral arteries (e.g. pulse amplitude, bruits);
- Pedal pulses (e.g. pulse amplitude); and
- Extremities for edema and/or varicosities.
Chest
- Inspection of breasts (e.g. symmetry, nipple discharge); and
- Palpation of breasts and axillae (e.g. masses or lumps, tenderness).
Gastrointestinal
- Examination of abdomen with notation of presence of masses or tenderness;
- Examination of liver and spleen;
- Examination for presence or absence of hernia;
- Examination (when indicated) of anus, perineum, and rectum, including sphincter tone, presence of hemorrhoids, and rectal masses; and
- Obtain stool sample for occult blood test when indicated.
Genitourinary (Male)
- Examination of the scrotal contents (e.g. hydrocele, spermatocele, tenderness of cord, testicular mass);
- Examination of the penis; and
- Digital rectal examination of prostate gland (e.g. size, symmetry, nodularity, tenderness).
Genitourinary (Female)
- Pelvic examination (with or without specimen collection for smears and cultures), including:
- Examination of external genitalia (e.g. general appearance, hair distribution, lesions) and vagina (e.g. general appearance, estrogen effect, discharge, lesions, pelvic support, cystocele, rectocele);
- Examination of urethra (e.g. masses, tenderness, scarring);
- Examination of bladder (e.g. fullness, masses, tenderness);
- Cervix (e.g. general appearance, lesions, discharge);
- Uterus (e.g. size, contour, position, mobility, tenderness, consistency, descent or support); and
- Adnexa/parametria (e.g. masses, tenderness, organomegaly, nodularity).
- Lymphatic Palpation of lymph nodes in two or more areas: Neck, axillae, groin, other.
Musculoskeletal
- Examination of gait and station;
- Inspection and/or palpation of digits and nails (e.g. clubbing, cyanosis, inflammatory conditions, petechiae, ischemia, infections, nodes);
- Examination of joints, bones and muscles of one or more of the following six areas:
- head and neck;
- spine, ribs and pelvis;
- right upper extremity;
- left upper extremity;
- right lower extremity; and
- left lower extremity.
The examination of a given area includes:
- Inspection and/or palpation with notation of presence of any misalignment, asymmetry, crepitation, defects, tenderness, masses, effusions;
- Assessment of range of motion with notation of any pain, crepitation or contracture;
- Assessment of stability with notation of any dislocation (luxation), subluxation or laxity; and
- Assessment of muscle strength and tone (e.g. flaccid, cog wheel, spastic) with notation of any atrophy or abnormal movements.
Skin
- Inspection of skin and subcutaneous tissue (e.g. rashes, lesions, ulcers); and
- Palpation of skin and subcutaneous tissue (e.g. induration, subcutaneous nodules, tightening).
Neurologic
- Test cranial nerves with notation of any deficits;
- Examination of deep tendon reflexes with notation of pathological reflexes (e.g. Babinski); and
- Examination of sensation (e.g. by touch, pin, vibration, proprioception).
Psychiatric
- Description of patient’s judgment and insight;
- Brief assessment of mental status, including:
- Orientation to time, place, and person;
- Recent and remote memory; and
- Mood and affect (e.g. depression, anxiety, agitation).
Considerations
The 1997 Documentation Guidelines often are criticized for their “specific” nature. Although this assists the auditor, it hinders the physician. The consequence is difficulty and frustration with remembering the explicit comments and number of elements associated with each level of exam. As a solution, consider documentation templates—paper or electronic—that incorporate cues and prompts for normal exam findings with adequate space for elaboration of abnormal findings.
Remember that both sets of guidelines apply to visit level selection, and physicians may utilize either set when documenting their services. Auditors will review documentation with each of the guidelines, and assign the final audited result as the highest visit level supported during the comparison. Physicians should use the set that is best for their patients, practice, and peace of mind.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2010. Northbrook, Ill.: American College of Chest Physicians; 2009:87-118.
- Centers for Medicare & Medicaid Services. 1995 Documentation Guidelines for Evaluation & Management Services. Available at: http://www.cms.gov/MLNProducts/Downloads/1995dg.pdf. Accessed Sept. 12, 2011.
- Centers for Medicare & Medicaid Services. 1997 Documentation Guidelines for Evaluation & Management Services. Available at: http://www.cms.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed Sept. 12, 2011.
- Highmark Medicare Services. Frequently Asked Questions: Evaluation And Management Services (Part B). Available at: http://www.highmarkmedicareservices.com/faq/partb/pet/lpet-evaluation_management_services.html#10. Accessed Sept. 14, 2011.
- Centers for Medicare & Medicaid Services. Transmittal 2282: Clarification of Evaluation and Management Payment Policy. Available at: http://www.cms.gov/transmittals/downloads/R2282CP.pdf. Accessed Sept. 15, 2011.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2011:1-20.
The extent of the exam should correspond to the nature of the presenting problem, the standard of care, and the physicians’ clinical judgment. Remember, medical necessity issues can arise if the physician performs and submits a claim for a comprehensive service involving a self-limiting problem. The easiest way to demonstrate the medical necessity for evaluation and management (E/M) services is through medical decision-making. It prevents a third party from making accusations that a Level 5 service was reported solely based upon a comprehensive history and examination that was not warranted by the patient’s presenting problem (e.g. the common cold).1
1995 Exam Guidelines
The 1995 guidelines differentiate 10 body areas (head and face; neck; chest, breast, and axillae; abdomen; genitalia, groin, and buttocks; back and spine; right upper extremity; left upper extremity; right lower extremity; and left lower extremity) from 12 organ systems (constitutional; eyes; ears, nose, mouth, and throat; cardiovascular; respiratory, gastrointestinal; genitourinary; musculoskeletal; integumentary; neurological; psychiatric; hematologic, lymphatic, and immunologic).2 Physicians are permitted to perform and comment without mandate, as appropriate, but with a few minor directives:
- Document relevant negative findings. Commenting that a system or area is “negative” or “normal” is acceptable when referring to unaffected areas or asymptomatic organ systems.
- Elaborate abnormal findings. Commenting that a system or area is “abnormal” is not sufficient unless additional comments describing the abnormality are documented.
1997 Documentation Guidelines
The 1997 guidelines are formatted as organ systems with corresponding, bulleted items referred to as “elements.”3 Additionally, a few elements have a numeric requirement to be achieved before satisfying the documentation of that particular element. For example, credit for the “vital signs element” (located within the constitutional system) is only awarded after documentation of three individual measurements (e.g. blood pressure, heart rate, and respiratory rate). Failure to document the specified criterion (e.g. two measurements: “blood pressure and heart rate only,” or a single nonspecific comment: “vital signs stable”) leads to failure to assign credit.
Take note that these specified criterion do not resonate within the 1995 guidelines. Numerical requirements also are indicated for the lymphatic system. The physician must examine and document findings associated with two or more lymphatic areas (e.g. “no lymphadenopathy noted in the neck or axillae”).
In the absence of numeric criterion, some elements contain multiple components, which require documentation of at least one component. For example, one listed psychiatric element designates the assessment of the patient’s “mood and affect.” The physician receives credit for a comment regarding the patient’s mood (e.g. “appears depressed”) without identification of a flat (or normal).
The 1997 Documentation Guide-lines comprise the following systems and elements:
Constitutional
- Measurement of any three of the following seven vital signs:
- Sitting or standing blood pressure;
- Supine blood pressure;
- Pulse rate and regularity;
- Respiration;
- Temperature;
- Height; or
- Weight (can be measured and recorded by ancillary staff).
- General appearance of patient (e.g. development, nutrition, body habitus, deformities, attention to grooming)
Eyes
- Inspection of conjunctivae and lids;
- Examination of pupils and irises (e.g. reaction to light and accommodation, size, symmetry); and
- Ophthalmoscopic examination of optic discs (e.g. size, C/D ratio, appearance) and posterior segments (e.g. vessel changes, exudates, hemorrhages).
Ears, Nose, Mouth, and Throat
- External inspection of ears and nose (e.g. overall appearance, scars, lesions, masses);
- Otoscopic examination of external auditory canals and tympanic membranes;
- Assessment of hearing (e.g. whispered voice, finger rub, tuning fork);
- Inspection of nasal mucosa, septum, and turbinates;
- Inspection of lips, teeth, and gums; and
- Examination of oropharynx: oral mucosa, salivary glands, hard and soft palates, tongue, tonsils, and posterior pharynx.
Neck
- Examination of neck (e.g. masses, overall appearance, symmetry, tracheal position, crepitus); and
- Examination of thyroid (e.g. enlargement, tenderness, mass).
Respiratory
- Assessment of respiratory effort (e.g. intercostal retractions, use of accessory muscles, diaphragmatic movement);
- Percussion of chest (e.g. dullness, flatness, hyperresonance);
- Palpation of chest (e.g. tactile fremitus); and
- Auscultation of lungs (e.g. breath sounds, adventitious sounds, rubs).
Cardiovascular
- Palpation of heart (e.g. location, size, thrills);
- Auscultation of heart with notation of abnormal sounds and murmurs; and
- Examination of:
- Carotid arteries (e.g. pulse amplitude, bruits);
- Abdominal aorta (e.g. size, bruits);
- Femoral arteries (e.g. pulse amplitude, bruits);
- Pedal pulses (e.g. pulse amplitude); and
- Extremities for edema and/or varicosities.
Chest
- Inspection of breasts (e.g. symmetry, nipple discharge); and
- Palpation of breasts and axillae (e.g. masses or lumps, tenderness).
Gastrointestinal
- Examination of abdomen with notation of presence of masses or tenderness;
- Examination of liver and spleen;
- Examination for presence or absence of hernia;
- Examination (when indicated) of anus, perineum, and rectum, including sphincter tone, presence of hemorrhoids, and rectal masses; and
- Obtain stool sample for occult blood test when indicated.
Genitourinary (Male)
- Examination of the scrotal contents (e.g. hydrocele, spermatocele, tenderness of cord, testicular mass);
- Examination of the penis; and
- Digital rectal examination of prostate gland (e.g. size, symmetry, nodularity, tenderness).
Genitourinary (Female)
- Pelvic examination (with or without specimen collection for smears and cultures), including:
- Examination of external genitalia (e.g. general appearance, hair distribution, lesions) and vagina (e.g. general appearance, estrogen effect, discharge, lesions, pelvic support, cystocele, rectocele);
- Examination of urethra (e.g. masses, tenderness, scarring);
- Examination of bladder (e.g. fullness, masses, tenderness);
- Cervix (e.g. general appearance, lesions, discharge);
- Uterus (e.g. size, contour, position, mobility, tenderness, consistency, descent or support); and
- Adnexa/parametria (e.g. masses, tenderness, organomegaly, nodularity).
- Lymphatic Palpation of lymph nodes in two or more areas: Neck, axillae, groin, other.
Musculoskeletal
- Examination of gait and station;
- Inspection and/or palpation of digits and nails (e.g. clubbing, cyanosis, inflammatory conditions, petechiae, ischemia, infections, nodes);
- Examination of joints, bones and muscles of one or more of the following six areas:
- head and neck;
- spine, ribs and pelvis;
- right upper extremity;
- left upper extremity;
- right lower extremity; and
- left lower extremity.
The examination of a given area includes:
- Inspection and/or palpation with notation of presence of any misalignment, asymmetry, crepitation, defects, tenderness, masses, effusions;
- Assessment of range of motion with notation of any pain, crepitation or contracture;
- Assessment of stability with notation of any dislocation (luxation), subluxation or laxity; and
- Assessment of muscle strength and tone (e.g. flaccid, cog wheel, spastic) with notation of any atrophy or abnormal movements.
Skin
- Inspection of skin and subcutaneous tissue (e.g. rashes, lesions, ulcers); and
- Palpation of skin and subcutaneous tissue (e.g. induration, subcutaneous nodules, tightening).
Neurologic
- Test cranial nerves with notation of any deficits;
- Examination of deep tendon reflexes with notation of pathological reflexes (e.g. Babinski); and
- Examination of sensation (e.g. by touch, pin, vibration, proprioception).
Psychiatric
- Description of patient’s judgment and insight;
- Brief assessment of mental status, including:
- Orientation to time, place, and person;
- Recent and remote memory; and
- Mood and affect (e.g. depression, anxiety, agitation).
Considerations
The 1997 Documentation Guidelines often are criticized for their “specific” nature. Although this assists the auditor, it hinders the physician. The consequence is difficulty and frustration with remembering the explicit comments and number of elements associated with each level of exam. As a solution, consider documentation templates—paper or electronic—that incorporate cues and prompts for normal exam findings with adequate space for elaboration of abnormal findings.
Remember that both sets of guidelines apply to visit level selection, and physicians may utilize either set when documenting their services. Auditors will review documentation with each of the guidelines, and assign the final audited result as the highest visit level supported during the comparison. Physicians should use the set that is best for their patients, practice, and peace of mind.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2010. Northbrook, Ill.: American College of Chest Physicians; 2009:87-118.
- Centers for Medicare & Medicaid Services. 1995 Documentation Guidelines for Evaluation & Management Services. Available at: http://www.cms.gov/MLNProducts/Downloads/1995dg.pdf. Accessed Sept. 12, 2011.
- Centers for Medicare & Medicaid Services. 1997 Documentation Guidelines for Evaluation & Management Services. Available at: http://www.cms.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed Sept. 12, 2011.
- Highmark Medicare Services. Frequently Asked Questions: Evaluation And Management Services (Part B). Available at: http://www.highmarkmedicareservices.com/faq/partb/pet/lpet-evaluation_management_services.html#10. Accessed Sept. 14, 2011.
- Centers for Medicare & Medicaid Services. Transmittal 2282: Clarification of Evaluation and Management Payment Policy. Available at: http://www.cms.gov/transmittals/downloads/R2282CP.pdf. Accessed Sept. 15, 2011.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2011:1-20.
The extent of the exam should correspond to the nature of the presenting problem, the standard of care, and the physicians’ clinical judgment. Remember, medical necessity issues can arise if the physician performs and submits a claim for a comprehensive service involving a self-limiting problem. The easiest way to demonstrate the medical necessity for evaluation and management (E/M) services is through medical decision-making. It prevents a third party from making accusations that a Level 5 service was reported solely based upon a comprehensive history and examination that was not warranted by the patient’s presenting problem (e.g. the common cold).1
1995 Exam Guidelines
The 1995 guidelines differentiate 10 body areas (head and face; neck; chest, breast, and axillae; abdomen; genitalia, groin, and buttocks; back and spine; right upper extremity; left upper extremity; right lower extremity; and left lower extremity) from 12 organ systems (constitutional; eyes; ears, nose, mouth, and throat; cardiovascular; respiratory, gastrointestinal; genitourinary; musculoskeletal; integumentary; neurological; psychiatric; hematologic, lymphatic, and immunologic).2 Physicians are permitted to perform and comment without mandate, as appropriate, but with a few minor directives:
- Document relevant negative findings. Commenting that a system or area is “negative” or “normal” is acceptable when referring to unaffected areas or asymptomatic organ systems.
- Elaborate abnormal findings. Commenting that a system or area is “abnormal” is not sufficient unless additional comments describing the abnormality are documented.
1997 Documentation Guidelines
The 1997 guidelines are formatted as organ systems with corresponding, bulleted items referred to as “elements.”3 Additionally, a few elements have a numeric requirement to be achieved before satisfying the documentation of that particular element. For example, credit for the “vital signs element” (located within the constitutional system) is only awarded after documentation of three individual measurements (e.g. blood pressure, heart rate, and respiratory rate). Failure to document the specified criterion (e.g. two measurements: “blood pressure and heart rate only,” or a single nonspecific comment: “vital signs stable”) leads to failure to assign credit.
Take note that these specified criterion do not resonate within the 1995 guidelines. Numerical requirements also are indicated for the lymphatic system. The physician must examine and document findings associated with two or more lymphatic areas (e.g. “no lymphadenopathy noted in the neck or axillae”).
In the absence of numeric criterion, some elements contain multiple components, which require documentation of at least one component. For example, one listed psychiatric element designates the assessment of the patient’s “mood and affect.” The physician receives credit for a comment regarding the patient’s mood (e.g. “appears depressed”) without identification of a flat (or normal).
The 1997 Documentation Guide-lines comprise the following systems and elements:
Constitutional
- Measurement of any three of the following seven vital signs:
- Sitting or standing blood pressure;
- Supine blood pressure;
- Pulse rate and regularity;
- Respiration;
- Temperature;
- Height; or
- Weight (can be measured and recorded by ancillary staff).
- General appearance of patient (e.g. development, nutrition, body habitus, deformities, attention to grooming)
Eyes
- Inspection of conjunctivae and lids;
- Examination of pupils and irises (e.g. reaction to light and accommodation, size, symmetry); and
- Ophthalmoscopic examination of optic discs (e.g. size, C/D ratio, appearance) and posterior segments (e.g. vessel changes, exudates, hemorrhages).
Ears, Nose, Mouth, and Throat
- External inspection of ears and nose (e.g. overall appearance, scars, lesions, masses);
- Otoscopic examination of external auditory canals and tympanic membranes;
- Assessment of hearing (e.g. whispered voice, finger rub, tuning fork);
- Inspection of nasal mucosa, septum, and turbinates;
- Inspection of lips, teeth, and gums; and
- Examination of oropharynx: oral mucosa, salivary glands, hard and soft palates, tongue, tonsils, and posterior pharynx.
Neck
- Examination of neck (e.g. masses, overall appearance, symmetry, tracheal position, crepitus); and
- Examination of thyroid (e.g. enlargement, tenderness, mass).
Respiratory
- Assessment of respiratory effort (e.g. intercostal retractions, use of accessory muscles, diaphragmatic movement);
- Percussion of chest (e.g. dullness, flatness, hyperresonance);
- Palpation of chest (e.g. tactile fremitus); and
- Auscultation of lungs (e.g. breath sounds, adventitious sounds, rubs).
Cardiovascular
- Palpation of heart (e.g. location, size, thrills);
- Auscultation of heart with notation of abnormal sounds and murmurs; and
- Examination of:
- Carotid arteries (e.g. pulse amplitude, bruits);
- Abdominal aorta (e.g. size, bruits);
- Femoral arteries (e.g. pulse amplitude, bruits);
- Pedal pulses (e.g. pulse amplitude); and
- Extremities for edema and/or varicosities.
Chest
- Inspection of breasts (e.g. symmetry, nipple discharge); and
- Palpation of breasts and axillae (e.g. masses or lumps, tenderness).
Gastrointestinal
- Examination of abdomen with notation of presence of masses or tenderness;
- Examination of liver and spleen;
- Examination for presence or absence of hernia;
- Examination (when indicated) of anus, perineum, and rectum, including sphincter tone, presence of hemorrhoids, and rectal masses; and
- Obtain stool sample for occult blood test when indicated.
Genitourinary (Male)
- Examination of the scrotal contents (e.g. hydrocele, spermatocele, tenderness of cord, testicular mass);
- Examination of the penis; and
- Digital rectal examination of prostate gland (e.g. size, symmetry, nodularity, tenderness).
Genitourinary (Female)
- Pelvic examination (with or without specimen collection for smears and cultures), including:
- Examination of external genitalia (e.g. general appearance, hair distribution, lesions) and vagina (e.g. general appearance, estrogen effect, discharge, lesions, pelvic support, cystocele, rectocele);
- Examination of urethra (e.g. masses, tenderness, scarring);
- Examination of bladder (e.g. fullness, masses, tenderness);
- Cervix (e.g. general appearance, lesions, discharge);
- Uterus (e.g. size, contour, position, mobility, tenderness, consistency, descent or support); and
- Adnexa/parametria (e.g. masses, tenderness, organomegaly, nodularity).
- Lymphatic Palpation of lymph nodes in two or more areas: Neck, axillae, groin, other.
Musculoskeletal
- Examination of gait and station;
- Inspection and/or palpation of digits and nails (e.g. clubbing, cyanosis, inflammatory conditions, petechiae, ischemia, infections, nodes);
- Examination of joints, bones and muscles of one or more of the following six areas:
- head and neck;
- spine, ribs and pelvis;
- right upper extremity;
- left upper extremity;
- right lower extremity; and
- left lower extremity.
The examination of a given area includes:
- Inspection and/or palpation with notation of presence of any misalignment, asymmetry, crepitation, defects, tenderness, masses, effusions;
- Assessment of range of motion with notation of any pain, crepitation or contracture;
- Assessment of stability with notation of any dislocation (luxation), subluxation or laxity; and
- Assessment of muscle strength and tone (e.g. flaccid, cog wheel, spastic) with notation of any atrophy or abnormal movements.
Skin
- Inspection of skin and subcutaneous tissue (e.g. rashes, lesions, ulcers); and
- Palpation of skin and subcutaneous tissue (e.g. induration, subcutaneous nodules, tightening).
Neurologic
- Test cranial nerves with notation of any deficits;
- Examination of deep tendon reflexes with notation of pathological reflexes (e.g. Babinski); and
- Examination of sensation (e.g. by touch, pin, vibration, proprioception).
Psychiatric
- Description of patient’s judgment and insight;
- Brief assessment of mental status, including:
- Orientation to time, place, and person;
- Recent and remote memory; and
- Mood and affect (e.g. depression, anxiety, agitation).
Considerations
The 1997 Documentation Guidelines often are criticized for their “specific” nature. Although this assists the auditor, it hinders the physician. The consequence is difficulty and frustration with remembering the explicit comments and number of elements associated with each level of exam. As a solution, consider documentation templates—paper or electronic—that incorporate cues and prompts for normal exam findings with adequate space for elaboration of abnormal findings.
Remember that both sets of guidelines apply to visit level selection, and physicians may utilize either set when documenting their services. Auditors will review documentation with each of the guidelines, and assign the final audited result as the highest visit level supported during the comparison. Physicians should use the set that is best for their patients, practice, and peace of mind.
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Pohlig, C. Documentation and Coding Evaluation and Management Services. In: Coding for Chest Medicine 2010. Northbrook, Ill.: American College of Chest Physicians; 2009:87-118.
- Centers for Medicare & Medicaid Services. 1995 Documentation Guidelines for Evaluation & Management Services. Available at: http://www.cms.gov/MLNProducts/Downloads/1995dg.pdf. Accessed Sept. 12, 2011.
- Centers for Medicare & Medicaid Services. 1997 Documentation Guidelines for Evaluation & Management Services. Available at: http://www.cms.gov/MLNProducts/Downloads/MASTER1.pdf. Accessed Sept. 12, 2011.
- Highmark Medicare Services. Frequently Asked Questions: Evaluation And Management Services (Part B). Available at: http://www.highmarkmedicareservices.com/faq/partb/pet/lpet-evaluation_management_services.html#10. Accessed Sept. 14, 2011.
- Centers for Medicare & Medicaid Services. Transmittal 2282: Clarification of Evaluation and Management Payment Policy. Available at: http://www.cms.gov/transmittals/downloads/R2282CP.pdf. Accessed Sept. 15, 2011.
- Abraham M, Ahlman J, Boudreau A, Connelly J, Evans D. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2011:1-20.
Change has come again to ICD-9 diagnostic codes
Did you know? When October 1 rolled around a short time ago, so did new codes for you to learn in the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM).
If you consider that unpleasant news for your billing efforts, I also have what I consider good news: The 2012 fiscal year is the final year for changes to ICD-9-CM codes: On October 1, 2013, the nation switches to 10th Revision (that is, ICD-10-CM) codes. The National Center for Health Statistics has indicated that the only changes to ICD-9 codes permitted from now on are ones describing new diseases that require immediate reporting during this transition/freeze period.
This last set of changes isn’t as massive as what we saw in previous years. Nevertheless, the changes certainly enhance the ability of ObGyn practices to report the reasons for patient encounters.
The major gyn change this year involves reporting vaginal mesh complications. There are several new obstetric codes, too, to enhance reporting of cesarean delivery and management of high-risk OB conditions.
The new codes were added to the national code set on October 1. As in prior years, there is no grace period.
Changes to obstetric codes
ANTIPHOSPHOLIPID ANTIBODY
Antiphospholipid syndrome and lupus anticoagulant are associated with complications of pregnancy that include fetal loss, fetal growth restriction, preeclampsia, thrombosis, and autoimmune thrombocytopenia. Until now, the obstetrician reporting 649.3x (Coagulation defects complicating pregnancy, childbirth, or the puerperium), had only two secondary code options to further describe the patient’s condition: 795.79, used to report a finding of antiphospholipid antibody in a blood specimen, and 289.81, antiphospholipid antibody with hypercoagulable state.
A new code, 286.53 (Antiphospholipid antibody with hemorrhagic disorder), provides a third option when reporting 649.3x.
CHEMICAL PREGNANCY AND BLIGHTED OVUM
Fertility clinics and physicians who specialize in the use of assisted reproductive technology requested a code to identify patients who have what is referred to (imprecisely) as a “false-positive pregnancy,” “chemical pregnancy,” or “biochemical pregnancy.” These terms do not, however, accurately describe a pregnancy achieved using hormone stimulation or other such “chemical” methods.
In some cases, of course, a woman’s pregnancy test comes back positive, indicating a serum human chorionic gonadotropin (hCG) level, but, when she is followed with ultrasonography, no fetus is present—in effect, she has had an early miscarriage. But there has been no ICD-9 code to use at this stage that discriminates between confirmed ectopic pregnancy and confirmed miscarriage—only a code for a laboratory finding.
To improve the specificity of coding, therefore, and to track such pregnancies, existing code 631 (Other abnormal product of conception) has been expanded and divided in two:
| 631.0 | Inappropriate rise (decline) of quantitative hCG in early pregnancy |
| 631.8 | Other abnormal products of conception |
Documentation by the physician that signals that 631.0 should be reported might include a reference to biochemical pregnancy, chemical pregnancy, or an inappropriate level of quantitative hCG for gestational age in early pregnancy. For 631.8 to be reported, documentation might mention such findings as a “blighted ovum” or “fleshy mole.”
Note: Because of this code expansion, the three-digit code 631 will no longer be a valid code for billing purposes.
ELECTIVE CESAREAN DELIVERY BEFORE 39 WEEKS’ GESTATION
ACOG requested new codes for elective cesarean delivery before 39 weeks’ gestation—a scenario that is one of the new markers of quality of care. Whereas ICD-9 has two diagnosis codes that mention cesarean delivery (654.2x, [Previous cesarean delivery not otherwise specified] and 669.71 [Cesarean delivery, without mention of indication]), neither code captures a case in which a woman presents in labor at 37 to 38 weeks’ gestation and the physician determines that it is best to deliver at that time rather than try to take measures that will forestall delivery until the 39th week.
Although ICD-9 already also has a code for early onset of delivery (644.21), it applies only to pregnancies before 37 completed weeks.
The new codes are:
| 649.81 | Onset (spontaneous) of labor after 37 completed weeks of gestation but before 39 completed weeks’ gestation, with delivery by (planned) cesarean section, delivered, with or without mention of antepartum condition |
| 649.82 | Onset (spontaneous) of labor after 37 completed weeks of gestation but before 39 completed weeks’ gestation, with delivery by (planned) cesarean section, delivered, with mention of postpartum complication |
Note: The new code has two options for a fifth digit:
- Reporting a fifth digit 1 indicates that the patient may, or may not, have had a complication in the antepartum period that is related to early onset of labor.
- Reporting a fifth digit 2 indicates that the patient developed a complication after delivery (but before discharge) that is related to the delivery.
For any hospitalization that results in a delivery, you must select a fifth digit 1 or 2; the choice depends on the overriding complication. You may not list code 649.8 twice—i.e., once with a fifth digit 1 and once with a fifth digit 2.
If the patient had a condition that was documented to be why cesarean delivery was medically indicated, list that as a secondary diagnosis—for example, cephalopelvic disproportion (653.4x) or prior cesarean delivery (654.2x).
SUPERVISION OF HIGH-RISK PREGNANCY
Code subcategory V23.4 (Pregnancy with other poor obstetric history) had only two coding options before October 1, 2011: V23.41 (Pregnancy with history of pre-term labor) and V23.49 (Pregnancy with other poor obstetric history).
Ectopic pregnancy. ACOG considers that it is important to track patients who had a prior ectopic pregnancy because such a history gives rise to an increased risk of ectopic pregnancy during the current pregnancy. Therefore, a new code for this status was requested by ACOG, and provided.
Note: Use the new history code only until the patient is confirmed not to have an ectopic pregnancy, if that is the outcome. Once you’ve confirmed that she has only a normal, intrauterine pregnancy, the risk posed by her history no longer has an impact on the current pregnancy. (ICD-9 rules direct you to report conditions that require active intervention or a change in routine care of the pregnancy—not conditions that merely exist without the need for intervention or additional monitoring.)
The new code is:
| V23.42 | Pregnancy with history of ectopic pregnancy |
Fetal viability. There was also no specific code before October 1 to report the need for a sonogram to check fetal viability, especially when a previously confirmed pregnancy comes into question because of the apparent absence of a fetal heartbeat on examination of the mother. In such a case, an additional sonogram might be required beyond the initial scan to confirm fetal demise or a continuing viable pregnancy. Until now, either of these findings could have been reported only with codes that do not accurately describe the situation, such as 659.7 (Abnormality in fetal heart rate or rhythm); V28.89 (Other specified antenatal screening); and V23.89 (Other high-risk pregnancy).
The new code is:
| V23.87 | Pregnancy with inconclusive fetal viability |
Changes to gyn codes
An effective surgical treatment for vaginal vault prolapse is sacrocolpopexy that uses a graft to suspend the upper vagina to the anterior longitudinal ligament of the sacrum. But, regrettably, synthetic graft material has also been associated with erosion of the mesh and subsequent pelvic infection (by erosion into surrounding organs or tissue). Exposure of the mesh in the vagina can also occur (see “Take this simplified approach to correcting exposure of vaginal mesh” in the July 2011 issue, available at obgmanagement.com).
Before October 1, erosion or exposure of mesh (without infection) would have been reported with code 996.39 (Mechanical complication of a genitourinary device, implant and graft) or 996.76 (Other complications due to genitourinary device, implant, and graft). With creation of a new subcategory code, 629.3 (Complication of implanted vaginal mesh and other prosthetic materials), however, these specific complications can be reported and tracked. The new codes also give you a specific linking diagnosis for revision of the mesh.
The two new codes are:
| 629.31 | Erosion of implanted vaginal mesh and other prosthetic materials to surrounding organ or tissue (e.g., into pelvic floor muscles) |
| 629.32 | Exposure of implanted vaginal mesh and other prosthetic materials into vagina (e.g., through the vaginal wall) |
Note: If the patient’s graft material has caused fibrosis, hemorrhage, occlusion, or pain, continue to report 996.76. And, of course, any infection or inflammatory reaction caused by mesh is reported with existing code 996.65.
Because erosion and exposure can occur at the same time, it is proper to report both new codes, if that is the case.
HISTORY OF GESTATIONAL DIABETES
Code V12.2 (Personal history of endocrine, metabolic, and immunity disorders) has been expanded and divided into two five-digit codes:
| V12.21 | Gestational diabetes |
| V12.29 | Other endocrine, metabolic, and immunity disorders |
With this change, four-digit code V12.2 became an invalid diagnosis code; your claim will be denied if you report it as the reason for an encounter.
Note: Code V12.21 may not be reported as a primary diagnosis for an obstetrical patient. Instead, a personal history that may be having an impact on the current pregnancy should be reported with a V23.xx code (Supervision of high risk pregnancy), until (and if) the patient develops a condition.
For example: If a patient had gestational diabetes during a prior pregnancy, she risks developing it again in the current pregnancy. In that case, report V23.49 (Pregnancy with other poor obstetric history) as the primary code and assign V12.21 as the secondary code.
LONG-TERM USE OF BISPHOSPHONATES
In a woman being treated to prevent loss of bone mass, the side-effect profile of the medication and the need to measure its effectiveness require regular follow-up visits. Effective October 1, code V58.68 (Long-term [current] use of bisphosphonates) should be reported for these follow-up visits. The code can be also used to support ordering follow-up bone densitometry.
Medications that might be applicable here are alendronate (Fosamax), ibandronate (Boniva), risedronate (Actonel), and zoledronic acid (Reclast).
Download a free copy of the complete addenda of ICD-9-CM code changes that have been made for fiscal year 2012 at: www.cdc.gov/nchs/icd/icd9cm_addenda_guidelines.htm
We want to hear from you! Tell us what you think.
Did you know? When October 1 rolled around a short time ago, so did new codes for you to learn in the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM).
If you consider that unpleasant news for your billing efforts, I also have what I consider good news: The 2012 fiscal year is the final year for changes to ICD-9-CM codes: On October 1, 2013, the nation switches to 10th Revision (that is, ICD-10-CM) codes. The National Center for Health Statistics has indicated that the only changes to ICD-9 codes permitted from now on are ones describing new diseases that require immediate reporting during this transition/freeze period.
This last set of changes isn’t as massive as what we saw in previous years. Nevertheless, the changes certainly enhance the ability of ObGyn practices to report the reasons for patient encounters.
The major gyn change this year involves reporting vaginal mesh complications. There are several new obstetric codes, too, to enhance reporting of cesarean delivery and management of high-risk OB conditions.
The new codes were added to the national code set on October 1. As in prior years, there is no grace period.
Changes to obstetric codes
ANTIPHOSPHOLIPID ANTIBODY
Antiphospholipid syndrome and lupus anticoagulant are associated with complications of pregnancy that include fetal loss, fetal growth restriction, preeclampsia, thrombosis, and autoimmune thrombocytopenia. Until now, the obstetrician reporting 649.3x (Coagulation defects complicating pregnancy, childbirth, or the puerperium), had only two secondary code options to further describe the patient’s condition: 795.79, used to report a finding of antiphospholipid antibody in a blood specimen, and 289.81, antiphospholipid antibody with hypercoagulable state.
A new code, 286.53 (Antiphospholipid antibody with hemorrhagic disorder), provides a third option when reporting 649.3x.
CHEMICAL PREGNANCY AND BLIGHTED OVUM
Fertility clinics and physicians who specialize in the use of assisted reproductive technology requested a code to identify patients who have what is referred to (imprecisely) as a “false-positive pregnancy,” “chemical pregnancy,” or “biochemical pregnancy.” These terms do not, however, accurately describe a pregnancy achieved using hormone stimulation or other such “chemical” methods.
In some cases, of course, a woman’s pregnancy test comes back positive, indicating a serum human chorionic gonadotropin (hCG) level, but, when she is followed with ultrasonography, no fetus is present—in effect, she has had an early miscarriage. But there has been no ICD-9 code to use at this stage that discriminates between confirmed ectopic pregnancy and confirmed miscarriage—only a code for a laboratory finding.
To improve the specificity of coding, therefore, and to track such pregnancies, existing code 631 (Other abnormal product of conception) has been expanded and divided in two:
| 631.0 | Inappropriate rise (decline) of quantitative hCG in early pregnancy |
| 631.8 | Other abnormal products of conception |
Documentation by the physician that signals that 631.0 should be reported might include a reference to biochemical pregnancy, chemical pregnancy, or an inappropriate level of quantitative hCG for gestational age in early pregnancy. For 631.8 to be reported, documentation might mention such findings as a “blighted ovum” or “fleshy mole.”
Note: Because of this code expansion, the three-digit code 631 will no longer be a valid code for billing purposes.
ELECTIVE CESAREAN DELIVERY BEFORE 39 WEEKS’ GESTATION
ACOG requested new codes for elective cesarean delivery before 39 weeks’ gestation—a scenario that is one of the new markers of quality of care. Whereas ICD-9 has two diagnosis codes that mention cesarean delivery (654.2x, [Previous cesarean delivery not otherwise specified] and 669.71 [Cesarean delivery, without mention of indication]), neither code captures a case in which a woman presents in labor at 37 to 38 weeks’ gestation and the physician determines that it is best to deliver at that time rather than try to take measures that will forestall delivery until the 39th week.
Although ICD-9 already also has a code for early onset of delivery (644.21), it applies only to pregnancies before 37 completed weeks.
The new codes are:
| 649.81 | Onset (spontaneous) of labor after 37 completed weeks of gestation but before 39 completed weeks’ gestation, with delivery by (planned) cesarean section, delivered, with or without mention of antepartum condition |
| 649.82 | Onset (spontaneous) of labor after 37 completed weeks of gestation but before 39 completed weeks’ gestation, with delivery by (planned) cesarean section, delivered, with mention of postpartum complication |
Note: The new code has two options for a fifth digit:
- Reporting a fifth digit 1 indicates that the patient may, or may not, have had a complication in the antepartum period that is related to early onset of labor.
- Reporting a fifth digit 2 indicates that the patient developed a complication after delivery (but before discharge) that is related to the delivery.
For any hospitalization that results in a delivery, you must select a fifth digit 1 or 2; the choice depends on the overriding complication. You may not list code 649.8 twice—i.e., once with a fifth digit 1 and once with a fifth digit 2.
If the patient had a condition that was documented to be why cesarean delivery was medically indicated, list that as a secondary diagnosis—for example, cephalopelvic disproportion (653.4x) or prior cesarean delivery (654.2x).
SUPERVISION OF HIGH-RISK PREGNANCY
Code subcategory V23.4 (Pregnancy with other poor obstetric history) had only two coding options before October 1, 2011: V23.41 (Pregnancy with history of pre-term labor) and V23.49 (Pregnancy with other poor obstetric history).
Ectopic pregnancy. ACOG considers that it is important to track patients who had a prior ectopic pregnancy because such a history gives rise to an increased risk of ectopic pregnancy during the current pregnancy. Therefore, a new code for this status was requested by ACOG, and provided.
Note: Use the new history code only until the patient is confirmed not to have an ectopic pregnancy, if that is the outcome. Once you’ve confirmed that she has only a normal, intrauterine pregnancy, the risk posed by her history no longer has an impact on the current pregnancy. (ICD-9 rules direct you to report conditions that require active intervention or a change in routine care of the pregnancy—not conditions that merely exist without the need for intervention or additional monitoring.)
The new code is:
| V23.42 | Pregnancy with history of ectopic pregnancy |
Fetal viability. There was also no specific code before October 1 to report the need for a sonogram to check fetal viability, especially when a previously confirmed pregnancy comes into question because of the apparent absence of a fetal heartbeat on examination of the mother. In such a case, an additional sonogram might be required beyond the initial scan to confirm fetal demise or a continuing viable pregnancy. Until now, either of these findings could have been reported only with codes that do not accurately describe the situation, such as 659.7 (Abnormality in fetal heart rate or rhythm); V28.89 (Other specified antenatal screening); and V23.89 (Other high-risk pregnancy).
The new code is:
| V23.87 | Pregnancy with inconclusive fetal viability |
Changes to gyn codes
An effective surgical treatment for vaginal vault prolapse is sacrocolpopexy that uses a graft to suspend the upper vagina to the anterior longitudinal ligament of the sacrum. But, regrettably, synthetic graft material has also been associated with erosion of the mesh and subsequent pelvic infection (by erosion into surrounding organs or tissue). Exposure of the mesh in the vagina can also occur (see “Take this simplified approach to correcting exposure of vaginal mesh” in the July 2011 issue, available at obgmanagement.com).
Before October 1, erosion or exposure of mesh (without infection) would have been reported with code 996.39 (Mechanical complication of a genitourinary device, implant and graft) or 996.76 (Other complications due to genitourinary device, implant, and graft). With creation of a new subcategory code, 629.3 (Complication of implanted vaginal mesh and other prosthetic materials), however, these specific complications can be reported and tracked. The new codes also give you a specific linking diagnosis for revision of the mesh.
The two new codes are:
| 629.31 | Erosion of implanted vaginal mesh and other prosthetic materials to surrounding organ or tissue (e.g., into pelvic floor muscles) |
| 629.32 | Exposure of implanted vaginal mesh and other prosthetic materials into vagina (e.g., through the vaginal wall) |
Note: If the patient’s graft material has caused fibrosis, hemorrhage, occlusion, or pain, continue to report 996.76. And, of course, any infection or inflammatory reaction caused by mesh is reported with existing code 996.65.
Because erosion and exposure can occur at the same time, it is proper to report both new codes, if that is the case.
HISTORY OF GESTATIONAL DIABETES
Code V12.2 (Personal history of endocrine, metabolic, and immunity disorders) has been expanded and divided into two five-digit codes:
| V12.21 | Gestational diabetes |
| V12.29 | Other endocrine, metabolic, and immunity disorders |
With this change, four-digit code V12.2 became an invalid diagnosis code; your claim will be denied if you report it as the reason for an encounter.
Note: Code V12.21 may not be reported as a primary diagnosis for an obstetrical patient. Instead, a personal history that may be having an impact on the current pregnancy should be reported with a V23.xx code (Supervision of high risk pregnancy), until (and if) the patient develops a condition.
For example: If a patient had gestational diabetes during a prior pregnancy, she risks developing it again in the current pregnancy. In that case, report V23.49 (Pregnancy with other poor obstetric history) as the primary code and assign V12.21 as the secondary code.
LONG-TERM USE OF BISPHOSPHONATES
In a woman being treated to prevent loss of bone mass, the side-effect profile of the medication and the need to measure its effectiveness require regular follow-up visits. Effective October 1, code V58.68 (Long-term [current] use of bisphosphonates) should be reported for these follow-up visits. The code can be also used to support ordering follow-up bone densitometry.
Medications that might be applicable here are alendronate (Fosamax), ibandronate (Boniva), risedronate (Actonel), and zoledronic acid (Reclast).
Download a free copy of the complete addenda of ICD-9-CM code changes that have been made for fiscal year 2012 at: www.cdc.gov/nchs/icd/icd9cm_addenda_guidelines.htm
We want to hear from you! Tell us what you think.
Did you know? When October 1 rolled around a short time ago, so did new codes for you to learn in the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM).
If you consider that unpleasant news for your billing efforts, I also have what I consider good news: The 2012 fiscal year is the final year for changes to ICD-9-CM codes: On October 1, 2013, the nation switches to 10th Revision (that is, ICD-10-CM) codes. The National Center for Health Statistics has indicated that the only changes to ICD-9 codes permitted from now on are ones describing new diseases that require immediate reporting during this transition/freeze period.
This last set of changes isn’t as massive as what we saw in previous years. Nevertheless, the changes certainly enhance the ability of ObGyn practices to report the reasons for patient encounters.
The major gyn change this year involves reporting vaginal mesh complications. There are several new obstetric codes, too, to enhance reporting of cesarean delivery and management of high-risk OB conditions.
The new codes were added to the national code set on October 1. As in prior years, there is no grace period.
Changes to obstetric codes
ANTIPHOSPHOLIPID ANTIBODY
Antiphospholipid syndrome and lupus anticoagulant are associated with complications of pregnancy that include fetal loss, fetal growth restriction, preeclampsia, thrombosis, and autoimmune thrombocytopenia. Until now, the obstetrician reporting 649.3x (Coagulation defects complicating pregnancy, childbirth, or the puerperium), had only two secondary code options to further describe the patient’s condition: 795.79, used to report a finding of antiphospholipid antibody in a blood specimen, and 289.81, antiphospholipid antibody with hypercoagulable state.
A new code, 286.53 (Antiphospholipid antibody with hemorrhagic disorder), provides a third option when reporting 649.3x.
CHEMICAL PREGNANCY AND BLIGHTED OVUM
Fertility clinics and physicians who specialize in the use of assisted reproductive technology requested a code to identify patients who have what is referred to (imprecisely) as a “false-positive pregnancy,” “chemical pregnancy,” or “biochemical pregnancy.” These terms do not, however, accurately describe a pregnancy achieved using hormone stimulation or other such “chemical” methods.
In some cases, of course, a woman’s pregnancy test comes back positive, indicating a serum human chorionic gonadotropin (hCG) level, but, when she is followed with ultrasonography, no fetus is present—in effect, she has had an early miscarriage. But there has been no ICD-9 code to use at this stage that discriminates between confirmed ectopic pregnancy and confirmed miscarriage—only a code for a laboratory finding.
To improve the specificity of coding, therefore, and to track such pregnancies, existing code 631 (Other abnormal product of conception) has been expanded and divided in two:
| 631.0 | Inappropriate rise (decline) of quantitative hCG in early pregnancy |
| 631.8 | Other abnormal products of conception |
Documentation by the physician that signals that 631.0 should be reported might include a reference to biochemical pregnancy, chemical pregnancy, or an inappropriate level of quantitative hCG for gestational age in early pregnancy. For 631.8 to be reported, documentation might mention such findings as a “blighted ovum” or “fleshy mole.”
Note: Because of this code expansion, the three-digit code 631 will no longer be a valid code for billing purposes.
ELECTIVE CESAREAN DELIVERY BEFORE 39 WEEKS’ GESTATION
ACOG requested new codes for elective cesarean delivery before 39 weeks’ gestation—a scenario that is one of the new markers of quality of care. Whereas ICD-9 has two diagnosis codes that mention cesarean delivery (654.2x, [Previous cesarean delivery not otherwise specified] and 669.71 [Cesarean delivery, without mention of indication]), neither code captures a case in which a woman presents in labor at 37 to 38 weeks’ gestation and the physician determines that it is best to deliver at that time rather than try to take measures that will forestall delivery until the 39th week.
Although ICD-9 already also has a code for early onset of delivery (644.21), it applies only to pregnancies before 37 completed weeks.
The new codes are:
| 649.81 | Onset (spontaneous) of labor after 37 completed weeks of gestation but before 39 completed weeks’ gestation, with delivery by (planned) cesarean section, delivered, with or without mention of antepartum condition |
| 649.82 | Onset (spontaneous) of labor after 37 completed weeks of gestation but before 39 completed weeks’ gestation, with delivery by (planned) cesarean section, delivered, with mention of postpartum complication |
Note: The new code has two options for a fifth digit:
- Reporting a fifth digit 1 indicates that the patient may, or may not, have had a complication in the antepartum period that is related to early onset of labor.
- Reporting a fifth digit 2 indicates that the patient developed a complication after delivery (but before discharge) that is related to the delivery.
For any hospitalization that results in a delivery, you must select a fifth digit 1 or 2; the choice depends on the overriding complication. You may not list code 649.8 twice—i.e., once with a fifth digit 1 and once with a fifth digit 2.
If the patient had a condition that was documented to be why cesarean delivery was medically indicated, list that as a secondary diagnosis—for example, cephalopelvic disproportion (653.4x) or prior cesarean delivery (654.2x).
SUPERVISION OF HIGH-RISK PREGNANCY
Code subcategory V23.4 (Pregnancy with other poor obstetric history) had only two coding options before October 1, 2011: V23.41 (Pregnancy with history of pre-term labor) and V23.49 (Pregnancy with other poor obstetric history).
Ectopic pregnancy. ACOG considers that it is important to track patients who had a prior ectopic pregnancy because such a history gives rise to an increased risk of ectopic pregnancy during the current pregnancy. Therefore, a new code for this status was requested by ACOG, and provided.
Note: Use the new history code only until the patient is confirmed not to have an ectopic pregnancy, if that is the outcome. Once you’ve confirmed that she has only a normal, intrauterine pregnancy, the risk posed by her history no longer has an impact on the current pregnancy. (ICD-9 rules direct you to report conditions that require active intervention or a change in routine care of the pregnancy—not conditions that merely exist without the need for intervention or additional monitoring.)
The new code is:
| V23.42 | Pregnancy with history of ectopic pregnancy |
Fetal viability. There was also no specific code before October 1 to report the need for a sonogram to check fetal viability, especially when a previously confirmed pregnancy comes into question because of the apparent absence of a fetal heartbeat on examination of the mother. In such a case, an additional sonogram might be required beyond the initial scan to confirm fetal demise or a continuing viable pregnancy. Until now, either of these findings could have been reported only with codes that do not accurately describe the situation, such as 659.7 (Abnormality in fetal heart rate or rhythm); V28.89 (Other specified antenatal screening); and V23.89 (Other high-risk pregnancy).
The new code is:
| V23.87 | Pregnancy with inconclusive fetal viability |
Changes to gyn codes
An effective surgical treatment for vaginal vault prolapse is sacrocolpopexy that uses a graft to suspend the upper vagina to the anterior longitudinal ligament of the sacrum. But, regrettably, synthetic graft material has also been associated with erosion of the mesh and subsequent pelvic infection (by erosion into surrounding organs or tissue). Exposure of the mesh in the vagina can also occur (see “Take this simplified approach to correcting exposure of vaginal mesh” in the July 2011 issue, available at obgmanagement.com).
Before October 1, erosion or exposure of mesh (without infection) would have been reported with code 996.39 (Mechanical complication of a genitourinary device, implant and graft) or 996.76 (Other complications due to genitourinary device, implant, and graft). With creation of a new subcategory code, 629.3 (Complication of implanted vaginal mesh and other prosthetic materials), however, these specific complications can be reported and tracked. The new codes also give you a specific linking diagnosis for revision of the mesh.
The two new codes are:
| 629.31 | Erosion of implanted vaginal mesh and other prosthetic materials to surrounding organ or tissue (e.g., into pelvic floor muscles) |
| 629.32 | Exposure of implanted vaginal mesh and other prosthetic materials into vagina (e.g., through the vaginal wall) |
Note: If the patient’s graft material has caused fibrosis, hemorrhage, occlusion, or pain, continue to report 996.76. And, of course, any infection or inflammatory reaction caused by mesh is reported with existing code 996.65.
Because erosion and exposure can occur at the same time, it is proper to report both new codes, if that is the case.
HISTORY OF GESTATIONAL DIABETES
Code V12.2 (Personal history of endocrine, metabolic, and immunity disorders) has been expanded and divided into two five-digit codes:
| V12.21 | Gestational diabetes |
| V12.29 | Other endocrine, metabolic, and immunity disorders |
With this change, four-digit code V12.2 became an invalid diagnosis code; your claim will be denied if you report it as the reason for an encounter.
Note: Code V12.21 may not be reported as a primary diagnosis for an obstetrical patient. Instead, a personal history that may be having an impact on the current pregnancy should be reported with a V23.xx code (Supervision of high risk pregnancy), until (and if) the patient develops a condition.
For example: If a patient had gestational diabetes during a prior pregnancy, she risks developing it again in the current pregnancy. In that case, report V23.49 (Pregnancy with other poor obstetric history) as the primary code and assign V12.21 as the secondary code.
LONG-TERM USE OF BISPHOSPHONATES
In a woman being treated to prevent loss of bone mass, the side-effect profile of the medication and the need to measure its effectiveness require regular follow-up visits. Effective October 1, code V58.68 (Long-term [current] use of bisphosphonates) should be reported for these follow-up visits. The code can be also used to support ordering follow-up bone densitometry.
Medications that might be applicable here are alendronate (Fosamax), ibandronate (Boniva), risedronate (Actonel), and zoledronic acid (Reclast).
Download a free copy of the complete addenda of ICD-9-CM code changes that have been made for fiscal year 2012 at: www.cdc.gov/nchs/icd/icd9cm_addenda_guidelines.htm
We want to hear from you! Tell us what you think.
Gravida in septic shock ... and more

WITH SEVERE ABDOMINAL PAIN AND VOMITING at 14 weeks’ gestation, a 30-year-old woman was brought by ambulance to the hospital. After initial evaluation did not reveal a cause of her symptoms, she was transferred to the antepartum unit for observation.
The mother developed hypotension and a diagnosis of septic shock was made. Fetal cardiac activity ceased and the woman developed intestinal ischemia. She underwent an intestinal transplant several months later.
PATIENT’S CLAIM Both treating physicians and the nursing staff failed to react to her intermittently low blood pressure, and failed to diagnose or treat septic shock in a timely manner.
DEFENDANTS’ DEFENSE The patient was properly monitored and treated.
VERDICT A $11,500,000 Illinois verdict was returned against the hospital. A defense verdict was returned for both physicians.
Lethal outcome of ovarian cystectomy
A WOMAN IN HER 40s underwent ovarian cystectomy. During surgery, her gynecologist encountered dense adhesions that required bowel dissection. Later, the woman complained of severe abdominal pain, despite taking pain medication. A second gynecologist ordered an abdominal scan that showed fluid and possible bowel obstruction. Hospital staff ruled out pulmonary embolism. When her blood pressure dropped to dangerous levels, a surgeon recommended surgery. Preoperative testing found punctures in both large and small intestines. Before she could be given anesthesia, the woman suffered cardiac arrest, and was placed on a ventilator. The family asked that the ventilator be removed after three days, and she died.
ESTATE’S CLAIM The hospital staff and gynecologists were negligent in not ruling out bowel perforation as soon as the woman complained of severe abdominal pain after surgery.
DEFENDANTS’ DEFENSE Bowel perforation is a known complication of the surgery. There was no negligence; it was a complicated problem and the staff had progressively attempted to rule out various postsurgical issues.
VERDICT A $2.5 million Illinois settlement was reached.
Mother’s herpes infection transmitted in childbirth
A BABY BECAME ILL WITHIN 3 DAYS of birth and died several weeks later from a herpes virus infection. The mother had complained of burning pain during the office visits prior to delivery, and during labor and delivery.
PATIENT’S CLAIM Additional testing should have been performed when the mother complained of symptoms prior to birth. The child contracted the herpes virus during vaginal delivery; proper and timely diagnosis would have resulted in a cesarean delivery. The mother denied having sexual partners during her pregnancy.
PHYSICIAN’S DEFENSE Negative results of a Herpes Select Test 6 months before birth made follow-up testing unnecessary. She must have contracted the disease after testing had been performed. She had no symptoms that made the viral disease diagnosable at delivery. The child’s symptoms suggested transplacental transmission of herpes; a cesarean delivery would not have changed the outcome.
VERDICT A Nevada defense verdict was returned.
Home birth emergency
DURING A HOME BIRTH managed by a midwife, the baby was born after the mother pushed for 2 hours and 47 minutes. The child suffered brain damage.
PATIENT’S CLAIM The midwife was negligent in failing to send the mother to the nearest hospital after she had been pushing for 2 hours. The dangers associated with the lack of fetal heart rate monitoring had never been explained to them.
DEFENDANT’S DEFENSE The parents agreed to a home birth without use of fetal heart rate monitoring. They signed a detailed consent form, which advised them that emergencies could occur during delivery, and that the level and type of care would be less than at a hospital.
VERDICT A $1.9 million New Jersey settlement was reached.
APAS causes heart attack; fetal demise
7 MONTHS INTO HER FIRST PREGNANCY, a woman in her 20s suffered intrauterine fetal demise. A perinatologist determined that the mother has antiphospholipid syndrome (APAS), an immune system disorder that can cause excessive blood clotting, premature miscarriage, and heart attack. Although the perinatologist and Dr. A, the woman’s Family Practitioner (FP), received the report, neither told the woman.
When 6-weeks’ pregnant with a second child, the woman awoke with severe, crushing chest pain. Dr. B saw her in the emergency department, but did not order an ECG or cardiac enzyme blood test. After 7.5 hours, Dr. B diagnosed morning sickness or indigestion, or both, and was ready to discharge her. However, the woman, still in intense pain, expressed concern for her fetus. Dr. B sent her to another hospital 2 hours away.
Upon arrival, her chest pain had diminished but she reported radiating back and neck pain. Although the hospital’s protocol required ECG within 10 minutes of presentation with chest pain, no ECG was performed. A diagnosis of “gall bladder problems” was made.
Eighteen hours later, she was sent to a university hospital, where an ECG revealed that she had been experiencing a clot-induced heart attack for 44 hours. Approximately 40% of her heart muscle was damaged, and she was counseled to not continue the pregnancy because of cardiac dysfunction.
PATIENT’S CLAIM The perinatologist and Dr. A were negligent in not telling her that she has APAS. With that information, she could have taken medication to prevent a heart attack during her second pregnancy. Dr. B should have tested her for a heart attack when she reported chest pain. She will require at least two heart transplants during her lifetime.
PHYSICIANS’ DEFENSE The perinatologist claimed that messages were left for the patient on both her work and mobile phones, but she did not return the calls. The perinatologist also mailed a pamphlet on APAS and an additional lab form to the patient. Dr. A claimed that the perinatologist was solely responsible for follow-up regarding the test results. Dr. B claimed that a heart attack is very rare in a 24-year-old woman, and was very difficult to identify; several doctors at two hospitals missed the diagnosis.
VERDICT A New Mexico jury found all parties at fault: Dr. B, 47.5%; Dr. A, 35%; perinatologist, 10%; and patient, 7.5%. The jury awarded $9 million in general damages and established a patient compensation fund for future medical expenses. The plaintiff’s actual recovery was $1.8 million due to a state cap.
Bowel injury after hysterectomy
AN OBGYN PERFORMED laparoscopically assisted vaginal hysterectomy on a 55-year-old woman. After surgery, the woman’s condition deteriorated. The ObGyn consulted with a surgeon, who performed an exploratory laparotomy 2 days after initial surgery; he suspected a bowel perforation, but could not find it.
The patient was transferred to another hospital and 4 days later, an imaging study of the bowel revealed the injury and the bowel was repaired. She developed sepsis and necrosis, and a 44-cm section of bowel was resected. Her recovery was complex.
PATIENT’S CLAIM The ObGyn was negligent in not promptly identifying the bowel injury during the initial surgery. The surgeon was negligent for failing to find the bowel injury during exploratory surgery.
PHYSICIAN’S DEFENSE The injury did not occur during the initial surgery; the perforation found at the second hospital was fresh and unrelated to the previous procedures.
VERDICT A Louisiana defense verdict was returned for the ObGyn. The surgeon was found negligent, and the jury awarded $3,314,801.
Zavanelli maneuver; brachial plexus injury
SHOULDER DYSTOCIA was encountered during delivery, and her ObGyn attempted several procedures, including use of a vacuum extractor. Ultimately, he performed a Zavanelli maneuver, in which the fetal head is pushed back into the birth canal in order to deliver the child by cesarean delivery. The child suffered a brachial plexus injury, and does not have use of her right arm.
PATIENT’S CLAIM The mother was administered too much oxytocin by the delivery nurse, causing contractions to be too strong and come too fast, resulting in fetal distress. The ObGyn applied the vacuum extractor when the fetus was too high in the birth canal, resulting in too much traction on the fetus’ brachial nerves.
PHYSICIAN’S DEFENSE The fetus was in grave danger, and was at the proper stage of delivery when the maneuvers were attempted. The child would have suffered significant brain injury or death if the maneuvers had not been attempted.
VERDICT A Georgia defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
WITH SEVERE ABDOMINAL PAIN AND VOMITING at 14 weeks’ gestation, a 30-year-old woman was brought by ambulance to the hospital. After initial evaluation did not reveal a cause of her symptoms, she was transferred to the antepartum unit for observation.
The mother developed hypotension and a diagnosis of septic shock was made. Fetal cardiac activity ceased and the woman developed intestinal ischemia. She underwent an intestinal transplant several months later.
PATIENT’S CLAIM Both treating physicians and the nursing staff failed to react to her intermittently low blood pressure, and failed to diagnose or treat septic shock in a timely manner.
DEFENDANTS’ DEFENSE The patient was properly monitored and treated.
VERDICT A $11,500,000 Illinois verdict was returned against the hospital. A defense verdict was returned for both physicians.
Lethal outcome of ovarian cystectomy
A WOMAN IN HER 40s underwent ovarian cystectomy. During surgery, her gynecologist encountered dense adhesions that required bowel dissection. Later, the woman complained of severe abdominal pain, despite taking pain medication. A second gynecologist ordered an abdominal scan that showed fluid and possible bowel obstruction. Hospital staff ruled out pulmonary embolism. When her blood pressure dropped to dangerous levels, a surgeon recommended surgery. Preoperative testing found punctures in both large and small intestines. Before she could be given anesthesia, the woman suffered cardiac arrest, and was placed on a ventilator. The family asked that the ventilator be removed after three days, and she died.
ESTATE’S CLAIM The hospital staff and gynecologists were negligent in not ruling out bowel perforation as soon as the woman complained of severe abdominal pain after surgery.
DEFENDANTS’ DEFENSE Bowel perforation is a known complication of the surgery. There was no negligence; it was a complicated problem and the staff had progressively attempted to rule out various postsurgical issues.
VERDICT A $2.5 million Illinois settlement was reached.
Mother’s herpes infection transmitted in childbirth
A BABY BECAME ILL WITHIN 3 DAYS of birth and died several weeks later from a herpes virus infection. The mother had complained of burning pain during the office visits prior to delivery, and during labor and delivery.
PATIENT’S CLAIM Additional testing should have been performed when the mother complained of symptoms prior to birth. The child contracted the herpes virus during vaginal delivery; proper and timely diagnosis would have resulted in a cesarean delivery. The mother denied having sexual partners during her pregnancy.
PHYSICIAN’S DEFENSE Negative results of a Herpes Select Test 6 months before birth made follow-up testing unnecessary. She must have contracted the disease after testing had been performed. She had no symptoms that made the viral disease diagnosable at delivery. The child’s symptoms suggested transplacental transmission of herpes; a cesarean delivery would not have changed the outcome.
VERDICT A Nevada defense verdict was returned.
Home birth emergency
DURING A HOME BIRTH managed by a midwife, the baby was born after the mother pushed for 2 hours and 47 minutes. The child suffered brain damage.
PATIENT’S CLAIM The midwife was negligent in failing to send the mother to the nearest hospital after she had been pushing for 2 hours. The dangers associated with the lack of fetal heart rate monitoring had never been explained to them.
DEFENDANT’S DEFENSE The parents agreed to a home birth without use of fetal heart rate monitoring. They signed a detailed consent form, which advised them that emergencies could occur during delivery, and that the level and type of care would be less than at a hospital.
VERDICT A $1.9 million New Jersey settlement was reached.
APAS causes heart attack; fetal demise
7 MONTHS INTO HER FIRST PREGNANCY, a woman in her 20s suffered intrauterine fetal demise. A perinatologist determined that the mother has antiphospholipid syndrome (APAS), an immune system disorder that can cause excessive blood clotting, premature miscarriage, and heart attack. Although the perinatologist and Dr. A, the woman’s Family Practitioner (FP), received the report, neither told the woman.
When 6-weeks’ pregnant with a second child, the woman awoke with severe, crushing chest pain. Dr. B saw her in the emergency department, but did not order an ECG or cardiac enzyme blood test. After 7.5 hours, Dr. B diagnosed morning sickness or indigestion, or both, and was ready to discharge her. However, the woman, still in intense pain, expressed concern for her fetus. Dr. B sent her to another hospital 2 hours away.
Upon arrival, her chest pain had diminished but she reported radiating back and neck pain. Although the hospital’s protocol required ECG within 10 minutes of presentation with chest pain, no ECG was performed. A diagnosis of “gall bladder problems” was made.
Eighteen hours later, she was sent to a university hospital, where an ECG revealed that she had been experiencing a clot-induced heart attack for 44 hours. Approximately 40% of her heart muscle was damaged, and she was counseled to not continue the pregnancy because of cardiac dysfunction.
PATIENT’S CLAIM The perinatologist and Dr. A were negligent in not telling her that she has APAS. With that information, she could have taken medication to prevent a heart attack during her second pregnancy. Dr. B should have tested her for a heart attack when she reported chest pain. She will require at least two heart transplants during her lifetime.
PHYSICIANS’ DEFENSE The perinatologist claimed that messages were left for the patient on both her work and mobile phones, but she did not return the calls. The perinatologist also mailed a pamphlet on APAS and an additional lab form to the patient. Dr. A claimed that the perinatologist was solely responsible for follow-up regarding the test results. Dr. B claimed that a heart attack is very rare in a 24-year-old woman, and was very difficult to identify; several doctors at two hospitals missed the diagnosis.
VERDICT A New Mexico jury found all parties at fault: Dr. B, 47.5%; Dr. A, 35%; perinatologist, 10%; and patient, 7.5%. The jury awarded $9 million in general damages and established a patient compensation fund for future medical expenses. The plaintiff’s actual recovery was $1.8 million due to a state cap.
Bowel injury after hysterectomy
AN OBGYN PERFORMED laparoscopically assisted vaginal hysterectomy on a 55-year-old woman. After surgery, the woman’s condition deteriorated. The ObGyn consulted with a surgeon, who performed an exploratory laparotomy 2 days after initial surgery; he suspected a bowel perforation, but could not find it.
The patient was transferred to another hospital and 4 days later, an imaging study of the bowel revealed the injury and the bowel was repaired. She developed sepsis and necrosis, and a 44-cm section of bowel was resected. Her recovery was complex.
PATIENT’S CLAIM The ObGyn was negligent in not promptly identifying the bowel injury during the initial surgery. The surgeon was negligent for failing to find the bowel injury during exploratory surgery.
PHYSICIAN’S DEFENSE The injury did not occur during the initial surgery; the perforation found at the second hospital was fresh and unrelated to the previous procedures.
VERDICT A Louisiana defense verdict was returned for the ObGyn. The surgeon was found negligent, and the jury awarded $3,314,801.
Zavanelli maneuver; brachial plexus injury
SHOULDER DYSTOCIA was encountered during delivery, and her ObGyn attempted several procedures, including use of a vacuum extractor. Ultimately, he performed a Zavanelli maneuver, in which the fetal head is pushed back into the birth canal in order to deliver the child by cesarean delivery. The child suffered a brachial plexus injury, and does not have use of her right arm.
PATIENT’S CLAIM The mother was administered too much oxytocin by the delivery nurse, causing contractions to be too strong and come too fast, resulting in fetal distress. The ObGyn applied the vacuum extractor when the fetus was too high in the birth canal, resulting in too much traction on the fetus’ brachial nerves.
PHYSICIAN’S DEFENSE The fetus was in grave danger, and was at the proper stage of delivery when the maneuvers were attempted. The child would have suffered significant brain injury or death if the maneuvers had not been attempted.
VERDICT A Georgia defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
WITH SEVERE ABDOMINAL PAIN AND VOMITING at 14 weeks’ gestation, a 30-year-old woman was brought by ambulance to the hospital. After initial evaluation did not reveal a cause of her symptoms, she was transferred to the antepartum unit for observation.
The mother developed hypotension and a diagnosis of septic shock was made. Fetal cardiac activity ceased and the woman developed intestinal ischemia. She underwent an intestinal transplant several months later.
PATIENT’S CLAIM Both treating physicians and the nursing staff failed to react to her intermittently low blood pressure, and failed to diagnose or treat septic shock in a timely manner.
DEFENDANTS’ DEFENSE The patient was properly monitored and treated.
VERDICT A $11,500,000 Illinois verdict was returned against the hospital. A defense verdict was returned for both physicians.
Lethal outcome of ovarian cystectomy
A WOMAN IN HER 40s underwent ovarian cystectomy. During surgery, her gynecologist encountered dense adhesions that required bowel dissection. Later, the woman complained of severe abdominal pain, despite taking pain medication. A second gynecologist ordered an abdominal scan that showed fluid and possible bowel obstruction. Hospital staff ruled out pulmonary embolism. When her blood pressure dropped to dangerous levels, a surgeon recommended surgery. Preoperative testing found punctures in both large and small intestines. Before she could be given anesthesia, the woman suffered cardiac arrest, and was placed on a ventilator. The family asked that the ventilator be removed after three days, and she died.
ESTATE’S CLAIM The hospital staff and gynecologists were negligent in not ruling out bowel perforation as soon as the woman complained of severe abdominal pain after surgery.
DEFENDANTS’ DEFENSE Bowel perforation is a known complication of the surgery. There was no negligence; it was a complicated problem and the staff had progressively attempted to rule out various postsurgical issues.
VERDICT A $2.5 million Illinois settlement was reached.
Mother’s herpes infection transmitted in childbirth
A BABY BECAME ILL WITHIN 3 DAYS of birth and died several weeks later from a herpes virus infection. The mother had complained of burning pain during the office visits prior to delivery, and during labor and delivery.
PATIENT’S CLAIM Additional testing should have been performed when the mother complained of symptoms prior to birth. The child contracted the herpes virus during vaginal delivery; proper and timely diagnosis would have resulted in a cesarean delivery. The mother denied having sexual partners during her pregnancy.
PHYSICIAN’S DEFENSE Negative results of a Herpes Select Test 6 months before birth made follow-up testing unnecessary. She must have contracted the disease after testing had been performed. She had no symptoms that made the viral disease diagnosable at delivery. The child’s symptoms suggested transplacental transmission of herpes; a cesarean delivery would not have changed the outcome.
VERDICT A Nevada defense verdict was returned.
Home birth emergency
DURING A HOME BIRTH managed by a midwife, the baby was born after the mother pushed for 2 hours and 47 minutes. The child suffered brain damage.
PATIENT’S CLAIM The midwife was negligent in failing to send the mother to the nearest hospital after she had been pushing for 2 hours. The dangers associated with the lack of fetal heart rate monitoring had never been explained to them.
DEFENDANT’S DEFENSE The parents agreed to a home birth without use of fetal heart rate monitoring. They signed a detailed consent form, which advised them that emergencies could occur during delivery, and that the level and type of care would be less than at a hospital.
VERDICT A $1.9 million New Jersey settlement was reached.
APAS causes heart attack; fetal demise
7 MONTHS INTO HER FIRST PREGNANCY, a woman in her 20s suffered intrauterine fetal demise. A perinatologist determined that the mother has antiphospholipid syndrome (APAS), an immune system disorder that can cause excessive blood clotting, premature miscarriage, and heart attack. Although the perinatologist and Dr. A, the woman’s Family Practitioner (FP), received the report, neither told the woman.
When 6-weeks’ pregnant with a second child, the woman awoke with severe, crushing chest pain. Dr. B saw her in the emergency department, but did not order an ECG or cardiac enzyme blood test. After 7.5 hours, Dr. B diagnosed morning sickness or indigestion, or both, and was ready to discharge her. However, the woman, still in intense pain, expressed concern for her fetus. Dr. B sent her to another hospital 2 hours away.
Upon arrival, her chest pain had diminished but she reported radiating back and neck pain. Although the hospital’s protocol required ECG within 10 minutes of presentation with chest pain, no ECG was performed. A diagnosis of “gall bladder problems” was made.
Eighteen hours later, she was sent to a university hospital, where an ECG revealed that she had been experiencing a clot-induced heart attack for 44 hours. Approximately 40% of her heart muscle was damaged, and she was counseled to not continue the pregnancy because of cardiac dysfunction.
PATIENT’S CLAIM The perinatologist and Dr. A were negligent in not telling her that she has APAS. With that information, she could have taken medication to prevent a heart attack during her second pregnancy. Dr. B should have tested her for a heart attack when she reported chest pain. She will require at least two heart transplants during her lifetime.
PHYSICIANS’ DEFENSE The perinatologist claimed that messages were left for the patient on both her work and mobile phones, but she did not return the calls. The perinatologist also mailed a pamphlet on APAS and an additional lab form to the patient. Dr. A claimed that the perinatologist was solely responsible for follow-up regarding the test results. Dr. B claimed that a heart attack is very rare in a 24-year-old woman, and was very difficult to identify; several doctors at two hospitals missed the diagnosis.
VERDICT A New Mexico jury found all parties at fault: Dr. B, 47.5%; Dr. A, 35%; perinatologist, 10%; and patient, 7.5%. The jury awarded $9 million in general damages and established a patient compensation fund for future medical expenses. The plaintiff’s actual recovery was $1.8 million due to a state cap.
Bowel injury after hysterectomy
AN OBGYN PERFORMED laparoscopically assisted vaginal hysterectomy on a 55-year-old woman. After surgery, the woman’s condition deteriorated. The ObGyn consulted with a surgeon, who performed an exploratory laparotomy 2 days after initial surgery; he suspected a bowel perforation, but could not find it.
The patient was transferred to another hospital and 4 days later, an imaging study of the bowel revealed the injury and the bowel was repaired. She developed sepsis and necrosis, and a 44-cm section of bowel was resected. Her recovery was complex.
PATIENT’S CLAIM The ObGyn was negligent in not promptly identifying the bowel injury during the initial surgery. The surgeon was negligent for failing to find the bowel injury during exploratory surgery.
PHYSICIAN’S DEFENSE The injury did not occur during the initial surgery; the perforation found at the second hospital was fresh and unrelated to the previous procedures.
VERDICT A Louisiana defense verdict was returned for the ObGyn. The surgeon was found negligent, and the jury awarded $3,314,801.
Zavanelli maneuver; brachial plexus injury
SHOULDER DYSTOCIA was encountered during delivery, and her ObGyn attempted several procedures, including use of a vacuum extractor. Ultimately, he performed a Zavanelli maneuver, in which the fetal head is pushed back into the birth canal in order to deliver the child by cesarean delivery. The child suffered a brachial plexus injury, and does not have use of her right arm.
PATIENT’S CLAIM The mother was administered too much oxytocin by the delivery nurse, causing contractions to be too strong and come too fast, resulting in fetal distress. The ObGyn applied the vacuum extractor when the fetus was too high in the birth canal, resulting in too much traction on the fetus’ brachial nerves.
PHYSICIAN’S DEFENSE The fetus was in grave danger, and was at the proper stage of delivery when the maneuvers were attempted. The child would have suffered significant brain injury or death if the maneuvers had not been attempted.
VERDICT A Georgia defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
We want to hear from you! Tell us what you think.
Managing Your Dermatology Practice: Work Less
Year’s end is a good time to do your annual maintenance evaluation. Check all of your equipment for malfunctions. Have your curettes and scissors resharpened. Back up your computer files and upgrade software as necessary. And above all, take a good look at the status of your most important asset: yourself.
I write this reminder every couple of years because it’s so easy to lose sight of the big picture among the pressures of our daily routines. Sooner or later, no matter how dedicated we are, the grind gets to all of us, leading to fatigue, irritability, and a progressive decline in motivation. And we are too busy to sit down and think about what we might do to break that vicious cycle. This is detrimental to our own well-being, as well as that of our patients.
There are many ways to maintain your intellectual and emotional health, but here’s how I do it: I work less. Yes, less. I take individual days off (average of one a month) to catch up on journals, take a CME course, or to try something new – something I’ve been thinking about doing "someday, when there is time" – such as a piano or sailing lessons, or a long weekend away with my wife. And I take no less than 4 weeks’ vacation per year.
I know how some of you feel about "wasting" a workday. Vacations are even worse because patients might go elsewhere while you’re gone, and every day the office is idle, we "lose money."
That whole paradigm is wrong. Stop thinking day to day; think year to year instead. You bring in a given amount of revenue per year – more on some days, less on others, and none on weekends and vacation days. It all averages out in the end.
Besides, this is much more important than money. This is breaking the routine, clearing the cobwebs, living your life. And trust me, your practice will still be there when you return.
I am writing this month’s column from Greece. Yesterday, my wife and I, and two of my kids, hiked to the top of the Byzantine ruins of Mystra on the Peloponnese Peninsula; tomorrow we will climb the sanctuary at Delfi. As I huff and puff up the trails, I don’t have the time – or the slightest inclination – to worry about the office. After these 10 days, I will return ready to take on the world, and my practice, anew.
And I will have jotted down some great ideas – practical, medical, and literary. Original thoughts are hard to come by during the daily grind, but they often appear, unannounced, in a new and refreshing environment.
Creative people have long recognized the value of working less. A classic example is the oft-told story of Swiss research scientists Alex Müller and J. Georg Bednorz. In 1986 they reached a major impasse in their superconductivity research; it appeared two decades of work might be for naught. The harder they pressed, the more elusive the answer became. So Müller decided to take time off, put aside his troubles, and research a subject that had always interested him: ceramics.
Nothing could have been further from his research field, of course, since ceramics are among the poorest conductors known. Yet as he relaxed, it occurred to Müller that a unique property of ceramics might apply to their project. Back in the lab, the team created a ceramic compound that became the first successful "high-temperature" superconductor.
The rest, as they say, is history; Müller and Bednorz won a Nobel Prize and triggered an explosion of research leading to breakthroughs in computing, electricity transmission, magnetically-elevated trains, and many other applications that are still being realized.
By working less, you may not change the world, but you will change you; any nudge out of your comfort zone will give you fresh ideas and help you look at the same old problems in completely new ways.
And to those who still can’t bear the thought of taking time off, remember Eastern’s Second Law: Your last words will NOT be, "I wish I had spent more time in the office!"
Year’s end is a good time to do your annual maintenance evaluation. Check all of your equipment for malfunctions. Have your curettes and scissors resharpened. Back up your computer files and upgrade software as necessary. And above all, take a good look at the status of your most important asset: yourself.
I write this reminder every couple of years because it’s so easy to lose sight of the big picture among the pressures of our daily routines. Sooner or later, no matter how dedicated we are, the grind gets to all of us, leading to fatigue, irritability, and a progressive decline in motivation. And we are too busy to sit down and think about what we might do to break that vicious cycle. This is detrimental to our own well-being, as well as that of our patients.
There are many ways to maintain your intellectual and emotional health, but here’s how I do it: I work less. Yes, less. I take individual days off (average of one a month) to catch up on journals, take a CME course, or to try something new – something I’ve been thinking about doing "someday, when there is time" – such as a piano or sailing lessons, or a long weekend away with my wife. And I take no less than 4 weeks’ vacation per year.
I know how some of you feel about "wasting" a workday. Vacations are even worse because patients might go elsewhere while you’re gone, and every day the office is idle, we "lose money."
That whole paradigm is wrong. Stop thinking day to day; think year to year instead. You bring in a given amount of revenue per year – more on some days, less on others, and none on weekends and vacation days. It all averages out in the end.
Besides, this is much more important than money. This is breaking the routine, clearing the cobwebs, living your life. And trust me, your practice will still be there when you return.
I am writing this month’s column from Greece. Yesterday, my wife and I, and two of my kids, hiked to the top of the Byzantine ruins of Mystra on the Peloponnese Peninsula; tomorrow we will climb the sanctuary at Delfi. As I huff and puff up the trails, I don’t have the time – or the slightest inclination – to worry about the office. After these 10 days, I will return ready to take on the world, and my practice, anew.
And I will have jotted down some great ideas – practical, medical, and literary. Original thoughts are hard to come by during the daily grind, but they often appear, unannounced, in a new and refreshing environment.
Creative people have long recognized the value of working less. A classic example is the oft-told story of Swiss research scientists Alex Müller and J. Georg Bednorz. In 1986 they reached a major impasse in their superconductivity research; it appeared two decades of work might be for naught. The harder they pressed, the more elusive the answer became. So Müller decided to take time off, put aside his troubles, and research a subject that had always interested him: ceramics.
Nothing could have been further from his research field, of course, since ceramics are among the poorest conductors known. Yet as he relaxed, it occurred to Müller that a unique property of ceramics might apply to their project. Back in the lab, the team created a ceramic compound that became the first successful "high-temperature" superconductor.
The rest, as they say, is history; Müller and Bednorz won a Nobel Prize and triggered an explosion of research leading to breakthroughs in computing, electricity transmission, magnetically-elevated trains, and many other applications that are still being realized.
By working less, you may not change the world, but you will change you; any nudge out of your comfort zone will give you fresh ideas and help you look at the same old problems in completely new ways.
And to those who still can’t bear the thought of taking time off, remember Eastern’s Second Law: Your last words will NOT be, "I wish I had spent more time in the office!"
Year’s end is a good time to do your annual maintenance evaluation. Check all of your equipment for malfunctions. Have your curettes and scissors resharpened. Back up your computer files and upgrade software as necessary. And above all, take a good look at the status of your most important asset: yourself.
I write this reminder every couple of years because it’s so easy to lose sight of the big picture among the pressures of our daily routines. Sooner or later, no matter how dedicated we are, the grind gets to all of us, leading to fatigue, irritability, and a progressive decline in motivation. And we are too busy to sit down and think about what we might do to break that vicious cycle. This is detrimental to our own well-being, as well as that of our patients.
There are many ways to maintain your intellectual and emotional health, but here’s how I do it: I work less. Yes, less. I take individual days off (average of one a month) to catch up on journals, take a CME course, or to try something new – something I’ve been thinking about doing "someday, when there is time" – such as a piano or sailing lessons, or a long weekend away with my wife. And I take no less than 4 weeks’ vacation per year.
I know how some of you feel about "wasting" a workday. Vacations are even worse because patients might go elsewhere while you’re gone, and every day the office is idle, we "lose money."
That whole paradigm is wrong. Stop thinking day to day; think year to year instead. You bring in a given amount of revenue per year – more on some days, less on others, and none on weekends and vacation days. It all averages out in the end.
Besides, this is much more important than money. This is breaking the routine, clearing the cobwebs, living your life. And trust me, your practice will still be there when you return.
I am writing this month’s column from Greece. Yesterday, my wife and I, and two of my kids, hiked to the top of the Byzantine ruins of Mystra on the Peloponnese Peninsula; tomorrow we will climb the sanctuary at Delfi. As I huff and puff up the trails, I don’t have the time – or the slightest inclination – to worry about the office. After these 10 days, I will return ready to take on the world, and my practice, anew.
And I will have jotted down some great ideas – practical, medical, and literary. Original thoughts are hard to come by during the daily grind, but they often appear, unannounced, in a new and refreshing environment.
Creative people have long recognized the value of working less. A classic example is the oft-told story of Swiss research scientists Alex Müller and J. Georg Bednorz. In 1986 they reached a major impasse in their superconductivity research; it appeared two decades of work might be for naught. The harder they pressed, the more elusive the answer became. So Müller decided to take time off, put aside his troubles, and research a subject that had always interested him: ceramics.
Nothing could have been further from his research field, of course, since ceramics are among the poorest conductors known. Yet as he relaxed, it occurred to Müller that a unique property of ceramics might apply to their project. Back in the lab, the team created a ceramic compound that became the first successful "high-temperature" superconductor.
The rest, as they say, is history; Müller and Bednorz won a Nobel Prize and triggered an explosion of research leading to breakthroughs in computing, electricity transmission, magnetically-elevated trains, and many other applications that are still being realized.
By working less, you may not change the world, but you will change you; any nudge out of your comfort zone will give you fresh ideas and help you look at the same old problems in completely new ways.
And to those who still can’t bear the thought of taking time off, remember Eastern’s Second Law: Your last words will NOT be, "I wish I had spent more time in the office!"
The Earlier, the Better
Every morning at 8 a.m., a multidisciplinary team at Wayne Memorial Hospital in Honesdale, Pa., a rural pocket of about 5,000 people about 30 miles northeast of Scranton, gathers to discuss discharge planning. Representatives from social services, home health, nursing, physical therapy, pharmacy, and the HM group attend the meeting. Each stakeholder weighs in, listens to others, and voices concerns when applicable.
“We go through each patient in the morning, briefly, and go through the plan so that when there’s a discharge coming, everybody is on the same page and can try to get everything organized,” says Louis O’Boyle, DO, FACP, FHM, medical director of Advanced Inpatient Medicine, the hospitalist program contracted by Wayne Memorial, which has 98 acute-care beds. “The hospital has reminded us to be cognizant of getting that early discharge, and it’s become almost so rote now that we don’t even have to worry about it. It’s just a thing we do.”
Better bed management is a new mantra for hospitalists nationwide, because fewer open beds means fewer dollars for both the physician and the hospital. Better bed management also means improved patient satisfaction scores, as most patients would rather be at home (and those scores in the coming years will factor into Medicare reimbursement). And better bed management means reduced backlogs across the hospital, particularly “boarders” in the ED.
“The pressure really is on the hospital for a number of reasons,” says Ken Simone, DO, SFHM, president of Hospitalist and Practice Solutions in Veazie, Maine, and a member of Team Hospitalist. “In terms of reimbursement, the sooner they can get a patient out of the hospital, it opens bed space for patients in the emergency department. It eases up bottlenecks because the patient in the ED may not need the bed that is being opened, but they may need an ICU bed, and the ICU patient is stable enough to be transferred to that medical bed that you’re opening up. So it’s a domino effect, and it certainly helps with creating a better flow within the hospital.”
It sounds simple, of course: Discharge inpatients early in the day and fill that bed with another patient, akin to a busy restaurant flipping tables to reduce the line stretching out the front door. The more customers, the more money made—both for the restaurant (i.e. hospital) and the servers (i.e. providers). And the less potential customers wait, the happier they are with their service.
But adding new beds, at nearly $1 million per bed inclusive of the space, infrastructure, and technology, is unacceptable math for most U.S. hospitals struggling to make ends meet in a tough economy.1 By contrast, an aggressive bed-management approach creates virtual bed capacity that creates more revenue-generating opportunities without those costs. And as Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) surveys tie patient satisfaction more directly to compensation, the more attention that will be focused on the discharge, as it will be the last process the patient experiences, and the one they likely will remember the most.
So if everyone agrees that discharging inpatients earlier in the day is a good idea, what’s the holdup? Interviews with more than a half-dozen hospitalists show a handful of factors that are present in all hospitals, large and small, academic and community:
- Downstream complications. HM is only one piece of the discharge puzzle. Hospitalists might be ready to discharge, but without that last test, or the ability to reach a pharmacist, the process slows. Even when discharge is complete, the room needs to be cleared and cleaned.
- Rounding protocols. Hospital-ists intuitively round on the sickest patients first, but that time-honored tradition has the byproduct of pushing those patients most likely to be sent home to the end of the line, automatically delaying discharges.
- Shift flexibility. Many hospitalist groups have morning shifts that begin at 8 a.m. Given the time it takes to craft discharge orders and deal with inevitable wrinkles in the process, that almost guarantees discharges will be pushed to later in the day.
- Hospital infrastructure. Insti-tutional bed management begins at the top, with a commitment across departments that discharge procedures are a shared priority. Without such across-the-board buy-in, the best hospitalists can do is fight against the tide. For example, a room could be vacated at 10 a.m., but housekeeping isn’t notified (or prepared) to clean the room for two hours because there is no institutional procedure in place to govern that decision.
“It’s harder than you think,” Dr. O’Boyle admits. “There are always extraneous factors that can delay the hospitalists from getting [discharges] done.”
Continued below...

Bed Management
Early-day discharge is just one pathway to improve “patient flow” and, therefore, bed management, according to a recent editorial in Health Affairs jointly penned by executives from the Institute for Healthcare Optimization in Newton, Mass., and the Institute for Healthcare Improvement in Cambridge, Mass.1
Other techniques are:
- Reducing length of stay (LOS): Hospitalists have long focused on keeping patient stays at a minimum, although many researchers have argued that LOS can only be reduced to a point. Quality and patient safety issues in the Affordable Care Act might actually increase LOS, as hospitalists and other physicians work to reduce 30-day readmissions by ensuring everything is done right the first time.
- Expanding capacity: At an estimated cost of $1 million to add one new bed to a hospital, it is simply unlikely that institutions will be in a fiscal position to add physical beds in the next few years.
- Increasing staff: “Here again,” the authors state flatly, “pressures on hospital systems and operating margins make it unlikely that hospitals will dramatically increase their payrolls.”
No Consensus
Although a variety of techniques can help improve early day discharge, all have hurdles. Two of the most common suggestions are geographic rounding and discharge lounges. A third is the active bed-management (ABM) model that hospitalist Eric Howell, MD, SFHM, associate professor of medicine at Johns Hopkins University and director of Johns Hopkins Bayview Medical Center’s HM division, wrote about in the Annals of Internal Medicine in December 2008.2
Geographic rounding, also dubbed unit-based setups, can help improve bed management because all participants are co-located; however, the gains likely are not enough to motivate an institution to implement the model without demonstrated improvements to other systems as well, says John Nelson, MD, FACP, MHM, cofounder and past president of SHM and a principal in the practice management firm Nelson Flores Hospital Medicine Consultants.
Discharge lounges—areas usually administered by a nurse and billed as a place for patients to gather after they’ve been formally discharged but before they have arranged a ride to physically leave the hospital—have been adopted by many hospitals. Dr. Simone and others question the liability issues associated with keeping discharged patients under the watch of hospital staff and also wonder whether the setup can have a negative impact on patient satisfaction. (For more on discharge lounges, check out “Solution of Problem,” at www.the-hospitalist.org.)

—David Bachman, MD, senior medical director for transitions of care, MaineHealth Clinical Integration, Portland, Maine
David Bachman, MD, senior medical director for transitions of care at MaineHealth Clinical Integration in Portland, Maine, and a former hospital administrator in New England, sees hospitalists as a lynchpin to the discharge process, but he also urges them to get the hospital to see them as “change agents” who need institutional support to make significant improvements.
“You’re trying to run cases through and it’s all dependent on downstream activity,” Dr. Bachman says. “If the hospitalist can push back and get this recognized as a hospital issue, that’s the only time when this problem can be solved. Hospitalists are a piece of the puzzle, but it’s not just them.”
Ideas to Chew On
Mitchell Wilson, MD, SFHM, chief medical officer for Eagle Hospital Physicians in Atlanta, agrees that reprioritizing physician rounds to encourage discharges would push patients out earlier, but he wants to see more physician assistants and nurse practitioners (PAs and NPs) blended into those rounds. The partnership would be a relatively simple and direct way for physicians to pass off nonclinical or less-intensive duties that afford them more time to focus on discharge planning. A dedicated nurse for HM service and the use of telemedicine could be folded into HM practices to help.
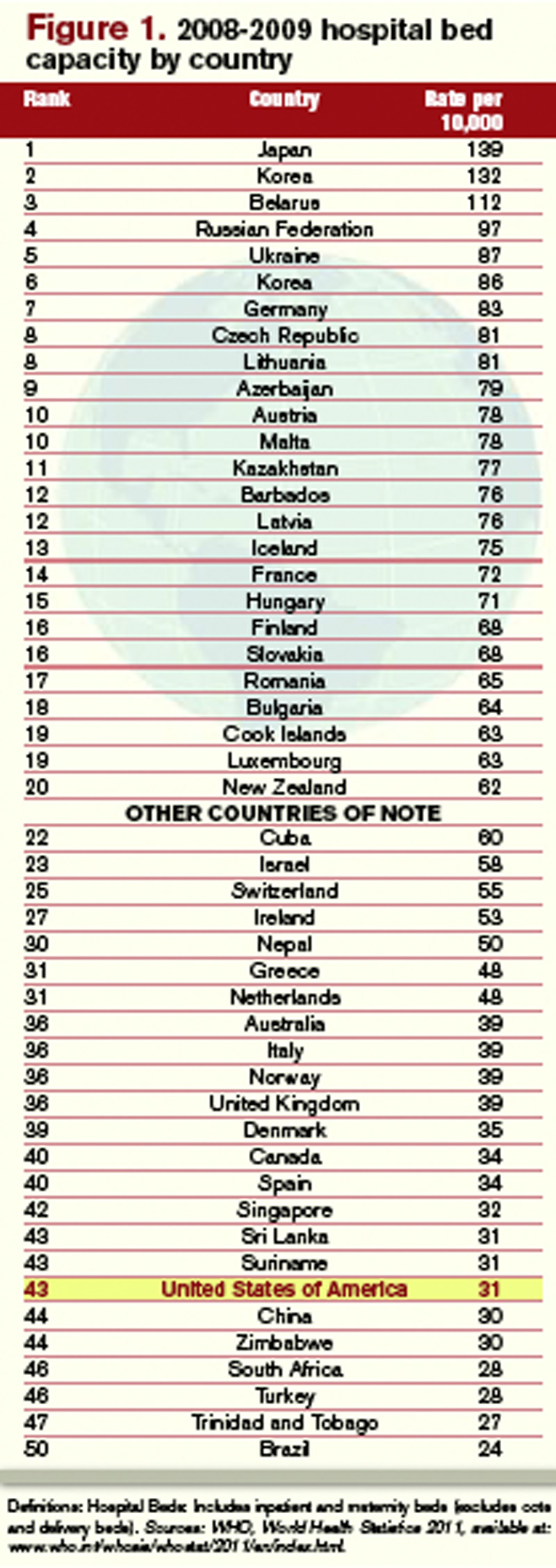
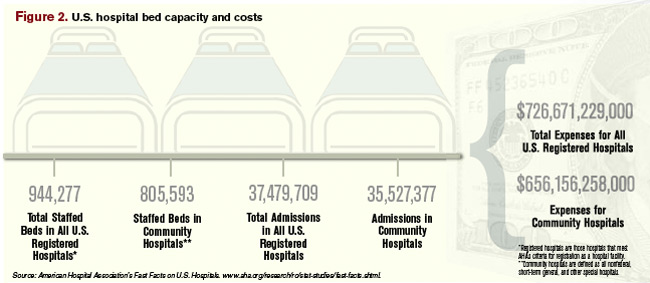
Each of the techniques would serve to get patients out earlier on what is arguably the most costly day of their stay. “Hospitals generally lose money on the last day of a patient’s stay,” Dr. Wilson says. “When appropriate from a patient care standpoint, discharging your patient and getting the bed ready for the next patient sooner is definitely an advantage for the hospital, and for the next patient.”
Dr. Bachman says one of the main hurdles to that process is no single provider “has clear responsibility and oversight. … It’s this diffuse responsibility.” That’s where Dr. Howell and colleagues thought ABM would work well. At Hopkins Bayview, hospitalists staffed an active bed-management program that rounded twice daily in ICUs and visited the ED regularly. The hospitalist on the 12-hour shift had no other duties, a luxury that HM pioneer Robert Wachter, MD, MHM, described at the time as “freeing him or her up to act as a full-time air traffic controller for all medical patients.”
The intervention reduced ED throughput for admitted patients by 98 minutes, to 360 minutes from 458 minutes. It also cut the amount of time the ED diverted ambulances because of overcrowding—the so-called “yellow alert”—by 6%, and the amount of time ambulances were diverted due to a lack of ICU beds—“red alert”—by 27%. Dr. Howell, an SHM board member, says the results showed how hospitalists can lead throughput change through institutions but that more work needs to be done to focus on early-day discharge.
“The hospital medicine side may be incentivized for early discharges,” he says, “but the hospital systems may not.”
Dr. Howell pushes for “2-by-10,” shorthand for identifying two patients daily who could be discharged by 10 a.m. because “the ED doesn’t necessarily need more beds for 24 hours. They need more beds early in the day.” But in keeping with the ABM model, Dr. Howell believes fiscal and personnel resources have to be dedicated to the problem to expect results. In the Hopkins Bayview intervention, Dr. Wachter, professor and associate chairman of the Department of Medicine at the University of California at San Francisco, chief of the division of hospital medicine, and chief of the medical service at UCSF Medical Center, estimated the annual costs of ABM at close to $1 million a year, given the likely need for four to six full-time equivalent hospitalists, according to a post on his Wachter’s World blog (www.wachtersworld. com) after the report was published.
One idea Dr. Howell suggests to push earlier discharges is restructuring physician workweeks, setting aside certain days for admission and certain days for follow-ups. If two shifts of follow-up days are scheduled after two days of admissions, it’s likely a hospitalist could follow a patient through their entire stay, he says. “You have to structure the doctor’s day to focus on discharges first,” he adds.
Dr. Howell also believes multidisciplinary rounds are key to earlier discharges. At Wayne Memorial Hospital and other places that have instituted such teams, discharge usually is just one byproduct of a construct ultimately aimed at quality improvement. Wayne Memorial’s Dr. O’Boyle says that since the team approach was initiated in September 2009, the hospital’s LOS has dropped by 0.75 days and patient satisfaction scores have risen about 25%. Those metrics will be key data points in the years to come as discharges and readmissions become tied to reimbursement via healthcare reform (see “Value-Based Purchasing Raises the Stakes,” May 2011).

“One of the biggest factors for readmissions are things like pharmacy errors, and lack of follow-up, and other loose ends that, if you’re in too much of a hurry to get people out and you don’t have the whole team approach and make sure all your I’s are dotted and T’s are crossed, then they have an increased chance of coming back,” Dr. O’Boyle says. “So we focus on patient satisfaction, and we focus on the discharge day and the discharge time to prevent readmissions and to maximize patient satisfaction. That’s the bottom line for the hospital…It’s interesting how the bottom line seems to follow quality.”
Continued below...
Inherent Conflicts?
Early-day discharge actually can be a bad thing in some cases, Dr. Nelson says. Think of a case in which a patient might be ready for discharge in the late evening or during an overnight. To wait until the morning to send that patient home might not be the best approach.

—Louis O’Boyle, DO, FACP, FHM, medical director, Advanced Inpatient Medicine, Honesdale, Pa.
“The place that manages length of stay most efficiently probably has plenty of late-day discharge,” he says.
Another potential conflict getting in the way of early-day discharge is what Dr. Wilson calls “admission competition.” For example, a hospitalist is working on discharge papers early in the morning but is then called away for a consult on an acute-care case in the ED or elsewhere. Each of the duties is important, but conflicting duties leave the hospitalist having to make choices.
“It’s not all straightforward,” Dr. Nelson says.
Emergency Nurses Association President AnnMarie Papa, DNP, RN, CEN, NE-BC, FAEN, says that collaboration between nurses and physicians is an answer to such competition. Calling the problem a “wrinkle across the system,” Papa says that without hospital administrators taking point and declaring the issue of discharge a priority, little wholesale improvement will be made. Even then, physicians and nurses—as the two main groups interacting with the patient—have to work together, she adds.
“Hospitalists have to partner with nurses,” Papa says, imploring physicians and nurses to work together on discharge decisions. “If the physicians and nurses collaborate on the decision and plans of care for the patients and the care they’re giving them and the discharge instructions, then it’s a win-win for everybody.”
Richard Quinn is a freelance writer based in New Jersey.
Reference
- Litvak E, Bisognano M. More patients, less payment: increasing hospital efficiency in the aftermath of health reform. Health Affairs. 2011;30(1): 76-80.
- Howell E, Bessman E, Kravet S, Kolodner K, Marshall R, Wright S. Active bed management by hospitalists and emergency department throughput. Ann Int Med. 2008;149(11):804-810.
Every morning at 8 a.m., a multidisciplinary team at Wayne Memorial Hospital in Honesdale, Pa., a rural pocket of about 5,000 people about 30 miles northeast of Scranton, gathers to discuss discharge planning. Representatives from social services, home health, nursing, physical therapy, pharmacy, and the HM group attend the meeting. Each stakeholder weighs in, listens to others, and voices concerns when applicable.
“We go through each patient in the morning, briefly, and go through the plan so that when there’s a discharge coming, everybody is on the same page and can try to get everything organized,” says Louis O’Boyle, DO, FACP, FHM, medical director of Advanced Inpatient Medicine, the hospitalist program contracted by Wayne Memorial, which has 98 acute-care beds. “The hospital has reminded us to be cognizant of getting that early discharge, and it’s become almost so rote now that we don’t even have to worry about it. It’s just a thing we do.”
Better bed management is a new mantra for hospitalists nationwide, because fewer open beds means fewer dollars for both the physician and the hospital. Better bed management also means improved patient satisfaction scores, as most patients would rather be at home (and those scores in the coming years will factor into Medicare reimbursement). And better bed management means reduced backlogs across the hospital, particularly “boarders” in the ED.
“The pressure really is on the hospital for a number of reasons,” says Ken Simone, DO, SFHM, president of Hospitalist and Practice Solutions in Veazie, Maine, and a member of Team Hospitalist. “In terms of reimbursement, the sooner they can get a patient out of the hospital, it opens bed space for patients in the emergency department. It eases up bottlenecks because the patient in the ED may not need the bed that is being opened, but they may need an ICU bed, and the ICU patient is stable enough to be transferred to that medical bed that you’re opening up. So it’s a domino effect, and it certainly helps with creating a better flow within the hospital.”
It sounds simple, of course: Discharge inpatients early in the day and fill that bed with another patient, akin to a busy restaurant flipping tables to reduce the line stretching out the front door. The more customers, the more money made—both for the restaurant (i.e. hospital) and the servers (i.e. providers). And the less potential customers wait, the happier they are with their service.
But adding new beds, at nearly $1 million per bed inclusive of the space, infrastructure, and technology, is unacceptable math for most U.S. hospitals struggling to make ends meet in a tough economy.1 By contrast, an aggressive bed-management approach creates virtual bed capacity that creates more revenue-generating opportunities without those costs. And as Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) surveys tie patient satisfaction more directly to compensation, the more attention that will be focused on the discharge, as it will be the last process the patient experiences, and the one they likely will remember the most.
So if everyone agrees that discharging inpatients earlier in the day is a good idea, what’s the holdup? Interviews with more than a half-dozen hospitalists show a handful of factors that are present in all hospitals, large and small, academic and community:
- Downstream complications. HM is only one piece of the discharge puzzle. Hospitalists might be ready to discharge, but without that last test, or the ability to reach a pharmacist, the process slows. Even when discharge is complete, the room needs to be cleared and cleaned.
- Rounding protocols. Hospital-ists intuitively round on the sickest patients first, but that time-honored tradition has the byproduct of pushing those patients most likely to be sent home to the end of the line, automatically delaying discharges.
- Shift flexibility. Many hospitalist groups have morning shifts that begin at 8 a.m. Given the time it takes to craft discharge orders and deal with inevitable wrinkles in the process, that almost guarantees discharges will be pushed to later in the day.
- Hospital infrastructure. Insti-tutional bed management begins at the top, with a commitment across departments that discharge procedures are a shared priority. Without such across-the-board buy-in, the best hospitalists can do is fight against the tide. For example, a room could be vacated at 10 a.m., but housekeeping isn’t notified (or prepared) to clean the room for two hours because there is no institutional procedure in place to govern that decision.
“It’s harder than you think,” Dr. O’Boyle admits. “There are always extraneous factors that can delay the hospitalists from getting [discharges] done.”
Continued below...
Bed Management
Early-day discharge is just one pathway to improve “patient flow” and, therefore, bed management, according to a recent editorial in Health Affairs jointly penned by executives from the Institute for Healthcare Optimization in Newton, Mass., and the Institute for Healthcare Improvement in Cambridge, Mass.1
Other techniques are:
- Reducing length of stay (LOS): Hospitalists have long focused on keeping patient stays at a minimum, although many researchers have argued that LOS can only be reduced to a point. Quality and patient safety issues in the Affordable Care Act might actually increase LOS, as hospitalists and other physicians work to reduce 30-day readmissions by ensuring everything is done right the first time.
- Expanding capacity: At an estimated cost of $1 million to add one new bed to a hospital, it is simply unlikely that institutions will be in a fiscal position to add physical beds in the next few years.
- Increasing staff: “Here again,” the authors state flatly, “pressures on hospital systems and operating margins make it unlikely that hospitals will dramatically increase their payrolls.”
No Consensus
Although a variety of techniques can help improve early day discharge, all have hurdles. Two of the most common suggestions are geographic rounding and discharge lounges. A third is the active bed-management (ABM) model that hospitalist Eric Howell, MD, SFHM, associate professor of medicine at Johns Hopkins University and director of Johns Hopkins Bayview Medical Center’s HM division, wrote about in the Annals of Internal Medicine in December 2008.2
Geographic rounding, also dubbed unit-based setups, can help improve bed management because all participants are co-located; however, the gains likely are not enough to motivate an institution to implement the model without demonstrated improvements to other systems as well, says John Nelson, MD, FACP, MHM, cofounder and past president of SHM and a principal in the practice management firm Nelson Flores Hospital Medicine Consultants.
Discharge lounges—areas usually administered by a nurse and billed as a place for patients to gather after they’ve been formally discharged but before they have arranged a ride to physically leave the hospital—have been adopted by many hospitals. Dr. Simone and others question the liability issues associated with keeping discharged patients under the watch of hospital staff and also wonder whether the setup can have a negative impact on patient satisfaction. (For more on discharge lounges, check out “Solution of Problem,” at www.the-hospitalist.org.)
—David Bachman, MD, senior medical director for transitions of care, MaineHealth Clinical Integration, Portland, Maine
David Bachman, MD, senior medical director for transitions of care at MaineHealth Clinical Integration in Portland, Maine, and a former hospital administrator in New England, sees hospitalists as a lynchpin to the discharge process, but he also urges them to get the hospital to see them as “change agents” who need institutional support to make significant improvements.
“You’re trying to run cases through and it’s all dependent on downstream activity,” Dr. Bachman says. “If the hospitalist can push back and get this recognized as a hospital issue, that’s the only time when this problem can be solved. Hospitalists are a piece of the puzzle, but it’s not just them.”
Ideas to Chew On
Mitchell Wilson, MD, SFHM, chief medical officer for Eagle Hospital Physicians in Atlanta, agrees that reprioritizing physician rounds to encourage discharges would push patients out earlier, but he wants to see more physician assistants and nurse practitioners (PAs and NPs) blended into those rounds. The partnership would be a relatively simple and direct way for physicians to pass off nonclinical or less-intensive duties that afford them more time to focus on discharge planning. A dedicated nurse for HM service and the use of telemedicine could be folded into HM practices to help.
Each of the techniques would serve to get patients out earlier on what is arguably the most costly day of their stay. “Hospitals generally lose money on the last day of a patient’s stay,” Dr. Wilson says. “When appropriate from a patient care standpoint, discharging your patient and getting the bed ready for the next patient sooner is definitely an advantage for the hospital, and for the next patient.”
Dr. Bachman says one of the main hurdles to that process is no single provider “has clear responsibility and oversight. … It’s this diffuse responsibility.” That’s where Dr. Howell and colleagues thought ABM would work well. At Hopkins Bayview, hospitalists staffed an active bed-management program that rounded twice daily in ICUs and visited the ED regularly. The hospitalist on the 12-hour shift had no other duties, a luxury that HM pioneer Robert Wachter, MD, MHM, described at the time as “freeing him or her up to act as a full-time air traffic controller for all medical patients.”
The intervention reduced ED throughput for admitted patients by 98 minutes, to 360 minutes from 458 minutes. It also cut the amount of time the ED diverted ambulances because of overcrowding—the so-called “yellow alert”—by 6%, and the amount of time ambulances were diverted due to a lack of ICU beds—“red alert”—by 27%. Dr. Howell, an SHM board member, says the results showed how hospitalists can lead throughput change through institutions but that more work needs to be done to focus on early-day discharge.
“The hospital medicine side may be incentivized for early discharges,” he says, “but the hospital systems may not.”
Dr. Howell pushes for “2-by-10,” shorthand for identifying two patients daily who could be discharged by 10 a.m. because “the ED doesn’t necessarily need more beds for 24 hours. They need more beds early in the day.” But in keeping with the ABM model, Dr. Howell believes fiscal and personnel resources have to be dedicated to the problem to expect results. In the Hopkins Bayview intervention, Dr. Wachter, professor and associate chairman of the Department of Medicine at the University of California at San Francisco, chief of the division of hospital medicine, and chief of the medical service at UCSF Medical Center, estimated the annual costs of ABM at close to $1 million a year, given the likely need for four to six full-time equivalent hospitalists, according to a post on his Wachter’s World blog (www.wachtersworld. com) after the report was published.
One idea Dr. Howell suggests to push earlier discharges is restructuring physician workweeks, setting aside certain days for admission and certain days for follow-ups. If two shifts of follow-up days are scheduled after two days of admissions, it’s likely a hospitalist could follow a patient through their entire stay, he says. “You have to structure the doctor’s day to focus on discharges first,” he adds.
Dr. Howell also believes multidisciplinary rounds are key to earlier discharges. At Wayne Memorial Hospital and other places that have instituted such teams, discharge usually is just one byproduct of a construct ultimately aimed at quality improvement. Wayne Memorial’s Dr. O’Boyle says that since the team approach was initiated in September 2009, the hospital’s LOS has dropped by 0.75 days and patient satisfaction scores have risen about 25%. Those metrics will be key data points in the years to come as discharges and readmissions become tied to reimbursement via healthcare reform (see “Value-Based Purchasing Raises the Stakes,” May 2011).
“One of the biggest factors for readmissions are things like pharmacy errors, and lack of follow-up, and other loose ends that, if you’re in too much of a hurry to get people out and you don’t have the whole team approach and make sure all your I’s are dotted and T’s are crossed, then they have an increased chance of coming back,” Dr. O’Boyle says. “So we focus on patient satisfaction, and we focus on the discharge day and the discharge time to prevent readmissions and to maximize patient satisfaction. That’s the bottom line for the hospital…It’s interesting how the bottom line seems to follow quality.”
Continued below...
Inherent Conflicts?
Early-day discharge actually can be a bad thing in some cases, Dr. Nelson says. Think of a case in which a patient might be ready for discharge in the late evening or during an overnight. To wait until the morning to send that patient home might not be the best approach.
—Louis O’Boyle, DO, FACP, FHM, medical director, Advanced Inpatient Medicine, Honesdale, Pa.
“The place that manages length of stay most efficiently probably has plenty of late-day discharge,” he says.
Another potential conflict getting in the way of early-day discharge is what Dr. Wilson calls “admission competition.” For example, a hospitalist is working on discharge papers early in the morning but is then called away for a consult on an acute-care case in the ED or elsewhere. Each of the duties is important, but conflicting duties leave the hospitalist having to make choices.
“It’s not all straightforward,” Dr. Nelson says.
Emergency Nurses Association President AnnMarie Papa, DNP, RN, CEN, NE-BC, FAEN, says that collaboration between nurses and physicians is an answer to such competition. Calling the problem a “wrinkle across the system,” Papa says that without hospital administrators taking point and declaring the issue of discharge a priority, little wholesale improvement will be made. Even then, physicians and nurses—as the two main groups interacting with the patient—have to work together, she adds.
“Hospitalists have to partner with nurses,” Papa says, imploring physicians and nurses to work together on discharge decisions. “If the physicians and nurses collaborate on the decision and plans of care for the patients and the care they’re giving them and the discharge instructions, then it’s a win-win for everybody.”
Richard Quinn is a freelance writer based in New Jersey.
Reference
- Litvak E, Bisognano M. More patients, less payment: increasing hospital efficiency in the aftermath of health reform. Health Affairs. 2011;30(1): 76-80.
- Howell E, Bessman E, Kravet S, Kolodner K, Marshall R, Wright S. Active bed management by hospitalists and emergency department throughput. Ann Int Med. 2008;149(11):804-810.
Every morning at 8 a.m., a multidisciplinary team at Wayne Memorial Hospital in Honesdale, Pa., a rural pocket of about 5,000 people about 30 miles northeast of Scranton, gathers to discuss discharge planning. Representatives from social services, home health, nursing, physical therapy, pharmacy, and the HM group attend the meeting. Each stakeholder weighs in, listens to others, and voices concerns when applicable.
“We go through each patient in the morning, briefly, and go through the plan so that when there’s a discharge coming, everybody is on the same page and can try to get everything organized,” says Louis O’Boyle, DO, FACP, FHM, medical director of Advanced Inpatient Medicine, the hospitalist program contracted by Wayne Memorial, which has 98 acute-care beds. “The hospital has reminded us to be cognizant of getting that early discharge, and it’s become almost so rote now that we don’t even have to worry about it. It’s just a thing we do.”
Better bed management is a new mantra for hospitalists nationwide, because fewer open beds means fewer dollars for both the physician and the hospital. Better bed management also means improved patient satisfaction scores, as most patients would rather be at home (and those scores in the coming years will factor into Medicare reimbursement). And better bed management means reduced backlogs across the hospital, particularly “boarders” in the ED.
“The pressure really is on the hospital for a number of reasons,” says Ken Simone, DO, SFHM, president of Hospitalist and Practice Solutions in Veazie, Maine, and a member of Team Hospitalist. “In terms of reimbursement, the sooner they can get a patient out of the hospital, it opens bed space for patients in the emergency department. It eases up bottlenecks because the patient in the ED may not need the bed that is being opened, but they may need an ICU bed, and the ICU patient is stable enough to be transferred to that medical bed that you’re opening up. So it’s a domino effect, and it certainly helps with creating a better flow within the hospital.”
It sounds simple, of course: Discharge inpatients early in the day and fill that bed with another patient, akin to a busy restaurant flipping tables to reduce the line stretching out the front door. The more customers, the more money made—both for the restaurant (i.e. hospital) and the servers (i.e. providers). And the less potential customers wait, the happier they are with their service.
But adding new beds, at nearly $1 million per bed inclusive of the space, infrastructure, and technology, is unacceptable math for most U.S. hospitals struggling to make ends meet in a tough economy.1 By contrast, an aggressive bed-management approach creates virtual bed capacity that creates more revenue-generating opportunities without those costs. And as Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) surveys tie patient satisfaction more directly to compensation, the more attention that will be focused on the discharge, as it will be the last process the patient experiences, and the one they likely will remember the most.
So if everyone agrees that discharging inpatients earlier in the day is a good idea, what’s the holdup? Interviews with more than a half-dozen hospitalists show a handful of factors that are present in all hospitals, large and small, academic and community:
- Downstream complications. HM is only one piece of the discharge puzzle. Hospitalists might be ready to discharge, but without that last test, or the ability to reach a pharmacist, the process slows. Even when discharge is complete, the room needs to be cleared and cleaned.
- Rounding protocols. Hospital-ists intuitively round on the sickest patients first, but that time-honored tradition has the byproduct of pushing those patients most likely to be sent home to the end of the line, automatically delaying discharges.
- Shift flexibility. Many hospitalist groups have morning shifts that begin at 8 a.m. Given the time it takes to craft discharge orders and deal with inevitable wrinkles in the process, that almost guarantees discharges will be pushed to later in the day.
- Hospital infrastructure. Insti-tutional bed management begins at the top, with a commitment across departments that discharge procedures are a shared priority. Without such across-the-board buy-in, the best hospitalists can do is fight against the tide. For example, a room could be vacated at 10 a.m., but housekeeping isn’t notified (or prepared) to clean the room for two hours because there is no institutional procedure in place to govern that decision.
“It’s harder than you think,” Dr. O’Boyle admits. “There are always extraneous factors that can delay the hospitalists from getting [discharges] done.”
Continued below...
Bed Management
Early-day discharge is just one pathway to improve “patient flow” and, therefore, bed management, according to a recent editorial in Health Affairs jointly penned by executives from the Institute for Healthcare Optimization in Newton, Mass., and the Institute for Healthcare Improvement in Cambridge, Mass.1
Other techniques are:
- Reducing length of stay (LOS): Hospitalists have long focused on keeping patient stays at a minimum, although many researchers have argued that LOS can only be reduced to a point. Quality and patient safety issues in the Affordable Care Act might actually increase LOS, as hospitalists and other physicians work to reduce 30-day readmissions by ensuring everything is done right the first time.
- Expanding capacity: At an estimated cost of $1 million to add one new bed to a hospital, it is simply unlikely that institutions will be in a fiscal position to add physical beds in the next few years.
- Increasing staff: “Here again,” the authors state flatly, “pressures on hospital systems and operating margins make it unlikely that hospitals will dramatically increase their payrolls.”
No Consensus
Although a variety of techniques can help improve early day discharge, all have hurdles. Two of the most common suggestions are geographic rounding and discharge lounges. A third is the active bed-management (ABM) model that hospitalist Eric Howell, MD, SFHM, associate professor of medicine at Johns Hopkins University and director of Johns Hopkins Bayview Medical Center’s HM division, wrote about in the Annals of Internal Medicine in December 2008.2
Geographic rounding, also dubbed unit-based setups, can help improve bed management because all participants are co-located; however, the gains likely are not enough to motivate an institution to implement the model without demonstrated improvements to other systems as well, says John Nelson, MD, FACP, MHM, cofounder and past president of SHM and a principal in the practice management firm Nelson Flores Hospital Medicine Consultants.
Discharge lounges—areas usually administered by a nurse and billed as a place for patients to gather after they’ve been formally discharged but before they have arranged a ride to physically leave the hospital—have been adopted by many hospitals. Dr. Simone and others question the liability issues associated with keeping discharged patients under the watch of hospital staff and also wonder whether the setup can have a negative impact on patient satisfaction. (For more on discharge lounges, check out “Solution of Problem,” at www.the-hospitalist.org.)
—David Bachman, MD, senior medical director for transitions of care, MaineHealth Clinical Integration, Portland, Maine
David Bachman, MD, senior medical director for transitions of care at MaineHealth Clinical Integration in Portland, Maine, and a former hospital administrator in New England, sees hospitalists as a lynchpin to the discharge process, but he also urges them to get the hospital to see them as “change agents” who need institutional support to make significant improvements.
“You’re trying to run cases through and it’s all dependent on downstream activity,” Dr. Bachman says. “If the hospitalist can push back and get this recognized as a hospital issue, that’s the only time when this problem can be solved. Hospitalists are a piece of the puzzle, but it’s not just them.”
Ideas to Chew On
Mitchell Wilson, MD, SFHM, chief medical officer for Eagle Hospital Physicians in Atlanta, agrees that reprioritizing physician rounds to encourage discharges would push patients out earlier, but he wants to see more physician assistants and nurse practitioners (PAs and NPs) blended into those rounds. The partnership would be a relatively simple and direct way for physicians to pass off nonclinical or less-intensive duties that afford them more time to focus on discharge planning. A dedicated nurse for HM service and the use of telemedicine could be folded into HM practices to help.
Each of the techniques would serve to get patients out earlier on what is arguably the most costly day of their stay. “Hospitals generally lose money on the last day of a patient’s stay,” Dr. Wilson says. “When appropriate from a patient care standpoint, discharging your patient and getting the bed ready for the next patient sooner is definitely an advantage for the hospital, and for the next patient.”
Dr. Bachman says one of the main hurdles to that process is no single provider “has clear responsibility and oversight. … It’s this diffuse responsibility.” That’s where Dr. Howell and colleagues thought ABM would work well. At Hopkins Bayview, hospitalists staffed an active bed-management program that rounded twice daily in ICUs and visited the ED regularly. The hospitalist on the 12-hour shift had no other duties, a luxury that HM pioneer Robert Wachter, MD, MHM, described at the time as “freeing him or her up to act as a full-time air traffic controller for all medical patients.”
The intervention reduced ED throughput for admitted patients by 98 minutes, to 360 minutes from 458 minutes. It also cut the amount of time the ED diverted ambulances because of overcrowding—the so-called “yellow alert”—by 6%, and the amount of time ambulances were diverted due to a lack of ICU beds—“red alert”—by 27%. Dr. Howell, an SHM board member, says the results showed how hospitalists can lead throughput change through institutions but that more work needs to be done to focus on early-day discharge.
“The hospital medicine side may be incentivized for early discharges,” he says, “but the hospital systems may not.”
Dr. Howell pushes for “2-by-10,” shorthand for identifying two patients daily who could be discharged by 10 a.m. because “the ED doesn’t necessarily need more beds for 24 hours. They need more beds early in the day.” But in keeping with the ABM model, Dr. Howell believes fiscal and personnel resources have to be dedicated to the problem to expect results. In the Hopkins Bayview intervention, Dr. Wachter, professor and associate chairman of the Department of Medicine at the University of California at San Francisco, chief of the division of hospital medicine, and chief of the medical service at UCSF Medical Center, estimated the annual costs of ABM at close to $1 million a year, given the likely need for four to six full-time equivalent hospitalists, according to a post on his Wachter’s World blog (www.wachtersworld. com) after the report was published.
One idea Dr. Howell suggests to push earlier discharges is restructuring physician workweeks, setting aside certain days for admission and certain days for follow-ups. If two shifts of follow-up days are scheduled after two days of admissions, it’s likely a hospitalist could follow a patient through their entire stay, he says. “You have to structure the doctor’s day to focus on discharges first,” he adds.
Dr. Howell also believes multidisciplinary rounds are key to earlier discharges. At Wayne Memorial Hospital and other places that have instituted such teams, discharge usually is just one byproduct of a construct ultimately aimed at quality improvement. Wayne Memorial’s Dr. O’Boyle says that since the team approach was initiated in September 2009, the hospital’s LOS has dropped by 0.75 days and patient satisfaction scores have risen about 25%. Those metrics will be key data points in the years to come as discharges and readmissions become tied to reimbursement via healthcare reform (see “Value-Based Purchasing Raises the Stakes,” May 2011).
“One of the biggest factors for readmissions are things like pharmacy errors, and lack of follow-up, and other loose ends that, if you’re in too much of a hurry to get people out and you don’t have the whole team approach and make sure all your I’s are dotted and T’s are crossed, then they have an increased chance of coming back,” Dr. O’Boyle says. “So we focus on patient satisfaction, and we focus on the discharge day and the discharge time to prevent readmissions and to maximize patient satisfaction. That’s the bottom line for the hospital…It’s interesting how the bottom line seems to follow quality.”
Continued below...
Inherent Conflicts?
Early-day discharge actually can be a bad thing in some cases, Dr. Nelson says. Think of a case in which a patient might be ready for discharge in the late evening or during an overnight. To wait until the morning to send that patient home might not be the best approach.
—Louis O’Boyle, DO, FACP, FHM, medical director, Advanced Inpatient Medicine, Honesdale, Pa.
“The place that manages length of stay most efficiently probably has plenty of late-day discharge,” he says.
Another potential conflict getting in the way of early-day discharge is what Dr. Wilson calls “admission competition.” For example, a hospitalist is working on discharge papers early in the morning but is then called away for a consult on an acute-care case in the ED or elsewhere. Each of the duties is important, but conflicting duties leave the hospitalist having to make choices.
“It’s not all straightforward,” Dr. Nelson says.
Emergency Nurses Association President AnnMarie Papa, DNP, RN, CEN, NE-BC, FAEN, says that collaboration between nurses and physicians is an answer to such competition. Calling the problem a “wrinkle across the system,” Papa says that without hospital administrators taking point and declaring the issue of discharge a priority, little wholesale improvement will be made. Even then, physicians and nurses—as the two main groups interacting with the patient—have to work together, she adds.
“Hospitalists have to partner with nurses,” Papa says, imploring physicians and nurses to work together on discharge decisions. “If the physicians and nurses collaborate on the decision and plans of care for the patients and the care they’re giving them and the discharge instructions, then it’s a win-win for everybody.”
Richard Quinn is a freelance writer based in New Jersey.
Reference
- Litvak E, Bisognano M. More patients, less payment: increasing hospital efficiency in the aftermath of health reform. Health Affairs. 2011;30(1): 76-80.
- Howell E, Bessman E, Kravet S, Kolodner K, Marshall R, Wright S. Active bed management by hospitalists and emergency department throughput. Ann Int Med. 2008;149(11):804-810.
Survey Insights
Those of you who are familiar with Medical Group Management Association’s reports know that MGMA uses medical group “ownership” categories that are similar to, but slightly different from, the employment model categories historically utilized by SHM. This year, we added the question: “Is your practice part of a multistate hospitalist group or management company?” to the SHM-MGMA Hospital Medicine Supplement. This question enables us to crosswalk from MGMA’s ownership categories to SHM’s traditional employment categories:
- Employed by a hospital or integrated delivery system;
- Employed by a multistate hospitalist group or management company;
- Employed by an independent multispecialty or primary-care medical group;
- Employed by an independent hospitalist-only group;
- Employed by an academic entity; and
- Employed by other.
The blue columns in the chart below show median annual direct compensation (light blue) and retirement benefits (dark blue) for all adult hospitalists by employment model, including the data for academic internal medicine hospitalists from the separate SHM-MGMA academic survey conducted in the fall of 2010.1 The median ratio of compensation to work RVUs for each employment type is represented by red squares.
Academic hospitalists report the lowest compensation but the highest compensation per unit of clinical work, even when production data is standardized to 100% billable clinical time.
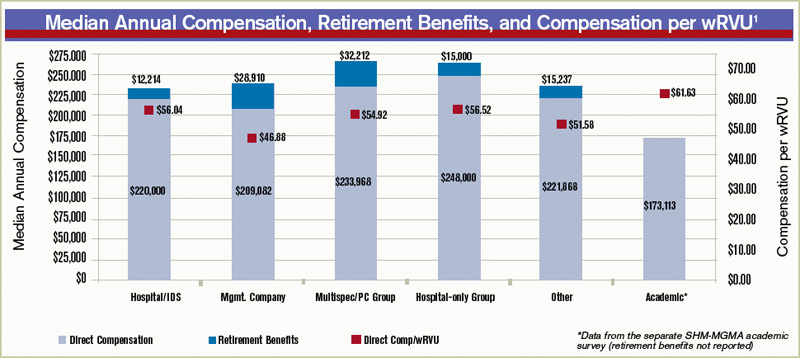
“For most academic hospitalists, teaching and supervising residents is an integral part of our clinical work; this probably impedes our clinical efficiency relative to non-academicians,” explains Grace Huang, MD, a member of SHM’s Practice Analysis Committee (PAC). “On weekends, when only half the residents are present and I don’t spend as much time teaching, I can see two to three times more patients.”
Independent hospitalist-only groups saw both the highest direct compensation and the highest compensation per unit of work, while hospitalists employed by multistate groups and management companies had the second-lowest overall direct compensation and the lowest compensation per wRVU.
When including the value of employer retirement plan contributions, however, hospitalists employed by management companies received a combined total remuneration that was higher than for hospitalists employed by hospitals or “other” employers.
“If I’m a hospitalist working for a multistate group, I want to know I’m getting something good that I might not get working for a hospital,” says PAC member Troy Ahlstrom, MD, SFHM. “A better retirement contribution is an obvious example; a hospital can’t afford to give a high-powered retirement plan to all 5,000-plus employees, while a physician company with all ‘highly compensated’ employees can. It’s a perk of working for an independent company.”
Multispecialty/primary-care medical groups and independent hospitalist-only groups provided the highest direct compensation and total remuneration (including retirement contributions). “Keep in mind, though, that they have different responsibilities that come with the money,” Dr. Ahlstrom says. “Hospitalists in local groups have more management responsibilities and more ownership risk, so they should make more for the extra work of running a business. Hospitalists in multispecialty groups have the benefit of an investment in their salaries by their colleagues, but they also have to answer directly to their colleagues for the privilege.”
Leslie Flores, SHM senior advisor, practice management
Reference

Academic Hospitalists Gear Up for Learning
The challenges of academic HM are different from other sectors of the specialty. Academic hospitalists, division chiefs, and administrators at academic teaching hospitals contend with the pressure of receiving grants, presenting at grand rounds, and reserving time for research and educational projects.
While it can be overwhelming, especially for academic hospitalists early in their careers, the Academic Hospitalist Academy helps untangle those challenges and turn them into long-term professional opportunities. Hosted jointly by SHM, the Society of General Internal Medicine (SGIM), and the Association of Chiefs and Leaders of General Internal Medicine (ACLGIM), the academy is a three-day course dedicated to education, scholarship, and professional success for academic hospitalists.
In addition to helping them become better hospitalists, Academic Hospitalist Academy uses didactic sessions, small-group exercises, and other interactive techniques to help academic hospitalists become better teachers, create and publish scholarly work, and get first in line for promotions.
Now in its third year, Academic Hospitalist Academy is consistently met with rave reviews from attendees. According to evaluations from the 2010 academy, attendees unanimously felt the course was worth their time and money; 99% said they would recommend it to a colleague.
Those of you who are familiar with Medical Group Management Association’s reports know that MGMA uses medical group “ownership” categories that are similar to, but slightly different from, the employment model categories historically utilized by SHM. This year, we added the question: “Is your practice part of a multistate hospitalist group or management company?” to the SHM-MGMA Hospital Medicine Supplement. This question enables us to crosswalk from MGMA’s ownership categories to SHM’s traditional employment categories:
- Employed by a hospital or integrated delivery system;
- Employed by a multistate hospitalist group or management company;
- Employed by an independent multispecialty or primary-care medical group;
- Employed by an independent hospitalist-only group;
- Employed by an academic entity; and
- Employed by other.
The blue columns in the chart below show median annual direct compensation (light blue) and retirement benefits (dark blue) for all adult hospitalists by employment model, including the data for academic internal medicine hospitalists from the separate SHM-MGMA academic survey conducted in the fall of 2010.1 The median ratio of compensation to work RVUs for each employment type is represented by red squares.
Academic hospitalists report the lowest compensation but the highest compensation per unit of clinical work, even when production data is standardized to 100% billable clinical time.
“For most academic hospitalists, teaching and supervising residents is an integral part of our clinical work; this probably impedes our clinical efficiency relative to non-academicians,” explains Grace Huang, MD, a member of SHM’s Practice Analysis Committee (PAC). “On weekends, when only half the residents are present and I don’t spend as much time teaching, I can see two to three times more patients.”
Independent hospitalist-only groups saw both the highest direct compensation and the highest compensation per unit of work, while hospitalists employed by multistate groups and management companies had the second-lowest overall direct compensation and the lowest compensation per wRVU.
When including the value of employer retirement plan contributions, however, hospitalists employed by management companies received a combined total remuneration that was higher than for hospitalists employed by hospitals or “other” employers.
“If I’m a hospitalist working for a multistate group, I want to know I’m getting something good that I might not get working for a hospital,” says PAC member Troy Ahlstrom, MD, SFHM. “A better retirement contribution is an obvious example; a hospital can’t afford to give a high-powered retirement plan to all 5,000-plus employees, while a physician company with all ‘highly compensated’ employees can. It’s a perk of working for an independent company.”
Multispecialty/primary-care medical groups and independent hospitalist-only groups provided the highest direct compensation and total remuneration (including retirement contributions). “Keep in mind, though, that they have different responsibilities that come with the money,” Dr. Ahlstrom says. “Hospitalists in local groups have more management responsibilities and more ownership risk, so they should make more for the extra work of running a business. Hospitalists in multispecialty groups have the benefit of an investment in their salaries by their colleagues, but they also have to answer directly to their colleagues for the privilege.”
Leslie Flores, SHM senior advisor, practice management
Reference
Academic Hospitalists Gear Up for Learning
The challenges of academic HM are different from other sectors of the specialty. Academic hospitalists, division chiefs, and administrators at academic teaching hospitals contend with the pressure of receiving grants, presenting at grand rounds, and reserving time for research and educational projects.
While it can be overwhelming, especially for academic hospitalists early in their careers, the Academic Hospitalist Academy helps untangle those challenges and turn them into long-term professional opportunities. Hosted jointly by SHM, the Society of General Internal Medicine (SGIM), and the Association of Chiefs and Leaders of General Internal Medicine (ACLGIM), the academy is a three-day course dedicated to education, scholarship, and professional success for academic hospitalists.
In addition to helping them become better hospitalists, Academic Hospitalist Academy uses didactic sessions, small-group exercises, and other interactive techniques to help academic hospitalists become better teachers, create and publish scholarly work, and get first in line for promotions.
Now in its third year, Academic Hospitalist Academy is consistently met with rave reviews from attendees. According to evaluations from the 2010 academy, attendees unanimously felt the course was worth their time and money; 99% said they would recommend it to a colleague.
Those of you who are familiar with Medical Group Management Association’s reports know that MGMA uses medical group “ownership” categories that are similar to, but slightly different from, the employment model categories historically utilized by SHM. This year, we added the question: “Is your practice part of a multistate hospitalist group or management company?” to the SHM-MGMA Hospital Medicine Supplement. This question enables us to crosswalk from MGMA’s ownership categories to SHM’s traditional employment categories:
- Employed by a hospital or integrated delivery system;
- Employed by a multistate hospitalist group or management company;
- Employed by an independent multispecialty or primary-care medical group;
- Employed by an independent hospitalist-only group;
- Employed by an academic entity; and
- Employed by other.
The blue columns in the chart below show median annual direct compensation (light blue) and retirement benefits (dark blue) for all adult hospitalists by employment model, including the data for academic internal medicine hospitalists from the separate SHM-MGMA academic survey conducted in the fall of 2010.1 The median ratio of compensation to work RVUs for each employment type is represented by red squares.
Academic hospitalists report the lowest compensation but the highest compensation per unit of clinical work, even when production data is standardized to 100% billable clinical time.
“For most academic hospitalists, teaching and supervising residents is an integral part of our clinical work; this probably impedes our clinical efficiency relative to non-academicians,” explains Grace Huang, MD, a member of SHM’s Practice Analysis Committee (PAC). “On weekends, when only half the residents are present and I don’t spend as much time teaching, I can see two to three times more patients.”
Independent hospitalist-only groups saw both the highest direct compensation and the highest compensation per unit of work, while hospitalists employed by multistate groups and management companies had the second-lowest overall direct compensation and the lowest compensation per wRVU.
When including the value of employer retirement plan contributions, however, hospitalists employed by management companies received a combined total remuneration that was higher than for hospitalists employed by hospitals or “other” employers.
“If I’m a hospitalist working for a multistate group, I want to know I’m getting something good that I might not get working for a hospital,” says PAC member Troy Ahlstrom, MD, SFHM. “A better retirement contribution is an obvious example; a hospital can’t afford to give a high-powered retirement plan to all 5,000-plus employees, while a physician company with all ‘highly compensated’ employees can. It’s a perk of working for an independent company.”
Multispecialty/primary-care medical groups and independent hospitalist-only groups provided the highest direct compensation and total remuneration (including retirement contributions). “Keep in mind, though, that they have different responsibilities that come with the money,” Dr. Ahlstrom says. “Hospitalists in local groups have more management responsibilities and more ownership risk, so they should make more for the extra work of running a business. Hospitalists in multispecialty groups have the benefit of an investment in their salaries by their colleagues, but they also have to answer directly to their colleagues for the privilege.”
Leslie Flores, SHM senior advisor, practice management
Reference
Academic Hospitalists Gear Up for Learning
The challenges of academic HM are different from other sectors of the specialty. Academic hospitalists, division chiefs, and administrators at academic teaching hospitals contend with the pressure of receiving grants, presenting at grand rounds, and reserving time for research and educational projects.
While it can be overwhelming, especially for academic hospitalists early in their careers, the Academic Hospitalist Academy helps untangle those challenges and turn them into long-term professional opportunities. Hosted jointly by SHM, the Society of General Internal Medicine (SGIM), and the Association of Chiefs and Leaders of General Internal Medicine (ACLGIM), the academy is a three-day course dedicated to education, scholarship, and professional success for academic hospitalists.
In addition to helping them become better hospitalists, Academic Hospitalist Academy uses didactic sessions, small-group exercises, and other interactive techniques to help academic hospitalists become better teachers, create and publish scholarly work, and get first in line for promotions.
Now in its third year, Academic Hospitalist Academy is consistently met with rave reviews from attendees. According to evaluations from the 2010 academy, attendees unanimously felt the course was worth their time and money; 99% said they would recommend it to a colleague.