User login
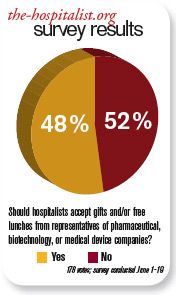
Should hospitalists accept gifts from pharmaceutical, medical device, and biotech companies?

Recent discussions on conflicts of interest in medical publications underscore the significance of the important yet fragile relationship between the pharmaceutical industry and healthcare professionals. Among these is an examination of how academic departments can maintain a relationship with the industry.1 This study suggests that if appropriate boundaries are established between industry and academia, it is possible to collaborate. However, part of the policy in this investigation included “elimination of industry-supplied meals, gifts, and favors.”2
The Institute of Medicine’s “Conflict of Interest in Medical Research, Education, and Practice” included groundbreaking recommendations.3 Among them was a call for professionals to adopt a policy that prohibits “the acceptance of items of material value from pharmaceutical, medical device, and biotechnology companies, except in specified situations.”3
Our nation has been embroiled in a healthcare debate. Questions of right versus privilege, access versus affordability, and, of course, the perpetual political overlay have monopolized most of the discourse. Some contend that healthcare reform will redefine the current relationship between pharma and physicians . . . and not a moment too soon.
Lest there be ambiguity, though, the medical profession remains a noble vocation. This notwithstanding, until 2002, physicians freely participated in golf outings, received athletic tickets, and dined at five-star restaurants. But after the pharmaceutical industry smartly adopted voluntary guidelines that restrict gifting to doctors, we are left with drug samples and, of course, the “free lunch.” Certainly, pharma can claim it has made significant contributions to furthering medical education and research. Many could argue the tangible negative effects that would follow if the funding suddenly were absent.
But let’s not kid ourselves: There is a good reason the pharmaceutical industry spends more than $12 billion per year on marketing to doctors.4 In 2006, Rep. Henry Waxman (D-Calif.) said, “It is obvious that drug companies provide these free lunches so their sales reps can get the doctor’s ear and influence the prescribing practices.”2 Most doctors would never admit any such influence. It would be, however, disingenuous for any practicing physician to say there is none.
A randomized trial conducted by Adair et al concluded the “access to drug samples in clinic influences resident prescribing decisions. This could affect resident education and increase drug costs for patients.”5 An earlier study by Chew et al concluded “the availability of drug samples led physicians to dispense and subsequently prescribe drugs that differ from their preferred drug choice. Physicians most often report using drug samples to avoid cost to the patient.”6
Sure, local culture drives some prescribing practice, but one must be mindful of the reality that the pharmaceutical industry has significant influence. Plus, free drug samples help patients in the short term. Once the samples are gone, an expensive prescription for that new drug will follow. It’s another win for the industry and another loss for the patient and the healthcare system.
Many studies have shown that gifting exerts influence, even if doctors are unwilling to admit it. But patients and doctors alike would like to state with clarity of conscience that the medication prescribed is only based on clinical evidence, not influence. TH
Dr. Pyke is a hospitalist at Geisinger Wyoming Valley Medical Systems in Mountain Top, Pa.
References
- Dubovsky SL, Kaye DL, Pristach CA, DelRegno P, Pessar L, Stiles K. Can academic departments maintain industry relationships while promoting physician professionalism? Acad Med. 2010;85(1):68-73.
- Salganik MW, Hopkins JS, Rockoff JD. Medical salesmen prescribe lunches. Catering trade feeds on rep-doctor meals. The Baltimore Sun. July 29, 2006.
- Institute of Medicine Conflict of Interest in Medical Research, Education and Practice Full Recommendations. 4-28-09.
- Wolfe SM. Why do American drug companies spend more than $12 billion a year pushing drugs? Is it education or promotion? J Gen Intern Med. 2007;11(10):637-639.
- Adair RF, Holmgren LR. Do drug samples influence resident prescribing behavior? A randomized trial. Am J Med. 2005;118(8):881-884.
- Chew LD, O’Young TS, Hazlet TK, Bradley KA, Maynard C, Lessler DS. A physician survey of the effect of drug sample availability on physicians’ behavior. J Gen Intern Med. 2000;15(7):478-483.
Recent discussions on conflicts of interest in medical publications underscore the significance of the important yet fragile relationship between the pharmaceutical industry and healthcare professionals. Among these is an examination of how academic departments can maintain a relationship with the industry.1 This study suggests that if appropriate boundaries are established between industry and academia, it is possible to collaborate. However, part of the policy in this investigation included “elimination of industry-supplied meals, gifts, and favors.”2
The Institute of Medicine’s “Conflict of Interest in Medical Research, Education, and Practice” included groundbreaking recommendations.3 Among them was a call for professionals to adopt a policy that prohibits “the acceptance of items of material value from pharmaceutical, medical device, and biotechnology companies, except in specified situations.”3
Our nation has been embroiled in a healthcare debate. Questions of right versus privilege, access versus affordability, and, of course, the perpetual political overlay have monopolized most of the discourse. Some contend that healthcare reform will redefine the current relationship between pharma and physicians . . . and not a moment too soon.
Lest there be ambiguity, though, the medical profession remains a noble vocation. This notwithstanding, until 2002, physicians freely participated in golf outings, received athletic tickets, and dined at five-star restaurants. But after the pharmaceutical industry smartly adopted voluntary guidelines that restrict gifting to doctors, we are left with drug samples and, of course, the “free lunch.” Certainly, pharma can claim it has made significant contributions to furthering medical education and research. Many could argue the tangible negative effects that would follow if the funding suddenly were absent.
But let’s not kid ourselves: There is a good reason the pharmaceutical industry spends more than $12 billion per year on marketing to doctors.4 In 2006, Rep. Henry Waxman (D-Calif.) said, “It is obvious that drug companies provide these free lunches so their sales reps can get the doctor’s ear and influence the prescribing practices.”2 Most doctors would never admit any such influence. It would be, however, disingenuous for any practicing physician to say there is none.
A randomized trial conducted by Adair et al concluded the “access to drug samples in clinic influences resident prescribing decisions. This could affect resident education and increase drug costs for patients.”5 An earlier study by Chew et al concluded “the availability of drug samples led physicians to dispense and subsequently prescribe drugs that differ from their preferred drug choice. Physicians most often report using drug samples to avoid cost to the patient.”6
Sure, local culture drives some prescribing practice, but one must be mindful of the reality that the pharmaceutical industry has significant influence. Plus, free drug samples help patients in the short term. Once the samples are gone, an expensive prescription for that new drug will follow. It’s another win for the industry and another loss for the patient and the healthcare system.
Many studies have shown that gifting exerts influence, even if doctors are unwilling to admit it. But patients and doctors alike would like to state with clarity of conscience that the medication prescribed is only based on clinical evidence, not influence. TH
Dr. Pyke is a hospitalist at Geisinger Wyoming Valley Medical Systems in Mountain Top, Pa.
References
- Dubovsky SL, Kaye DL, Pristach CA, DelRegno P, Pessar L, Stiles K. Can academic departments maintain industry relationships while promoting physician professionalism? Acad Med. 2010;85(1):68-73.
- Salganik MW, Hopkins JS, Rockoff JD. Medical salesmen prescribe lunches. Catering trade feeds on rep-doctor meals. The Baltimore Sun. July 29, 2006.
- Institute of Medicine Conflict of Interest in Medical Research, Education and Practice Full Recommendations. 4-28-09.
- Wolfe SM. Why do American drug companies spend more than $12 billion a year pushing drugs? Is it education or promotion? J Gen Intern Med. 2007;11(10):637-639.
- Adair RF, Holmgren LR. Do drug samples influence resident prescribing behavior? A randomized trial. Am J Med. 2005;118(8):881-884.
- Chew LD, O’Young TS, Hazlet TK, Bradley KA, Maynard C, Lessler DS. A physician survey of the effect of drug sample availability on physicians’ behavior. J Gen Intern Med. 2000;15(7):478-483.
Recent discussions on conflicts of interest in medical publications underscore the significance of the important yet fragile relationship between the pharmaceutical industry and healthcare professionals. Among these is an examination of how academic departments can maintain a relationship with the industry.1 This study suggests that if appropriate boundaries are established between industry and academia, it is possible to collaborate. However, part of the policy in this investigation included “elimination of industry-supplied meals, gifts, and favors.”2
The Institute of Medicine’s “Conflict of Interest in Medical Research, Education, and Practice” included groundbreaking recommendations.3 Among them was a call for professionals to adopt a policy that prohibits “the acceptance of items of material value from pharmaceutical, medical device, and biotechnology companies, except in specified situations.”3
Our nation has been embroiled in a healthcare debate. Questions of right versus privilege, access versus affordability, and, of course, the perpetual political overlay have monopolized most of the discourse. Some contend that healthcare reform will redefine the current relationship between pharma and physicians . . . and not a moment too soon.
Lest there be ambiguity, though, the medical profession remains a noble vocation. This notwithstanding, until 2002, physicians freely participated in golf outings, received athletic tickets, and dined at five-star restaurants. But after the pharmaceutical industry smartly adopted voluntary guidelines that restrict gifting to doctors, we are left with drug samples and, of course, the “free lunch.” Certainly, pharma can claim it has made significant contributions to furthering medical education and research. Many could argue the tangible negative effects that would follow if the funding suddenly were absent.
But let’s not kid ourselves: There is a good reason the pharmaceutical industry spends more than $12 billion per year on marketing to doctors.4 In 2006, Rep. Henry Waxman (D-Calif.) said, “It is obvious that drug companies provide these free lunches so their sales reps can get the doctor’s ear and influence the prescribing practices.”2 Most doctors would never admit any such influence. It would be, however, disingenuous for any practicing physician to say there is none.
A randomized trial conducted by Adair et al concluded the “access to drug samples in clinic influences resident prescribing decisions. This could affect resident education and increase drug costs for patients.”5 An earlier study by Chew et al concluded “the availability of drug samples led physicians to dispense and subsequently prescribe drugs that differ from their preferred drug choice. Physicians most often report using drug samples to avoid cost to the patient.”6
Sure, local culture drives some prescribing practice, but one must be mindful of the reality that the pharmaceutical industry has significant influence. Plus, free drug samples help patients in the short term. Once the samples are gone, an expensive prescription for that new drug will follow. It’s another win for the industry and another loss for the patient and the healthcare system.
Many studies have shown that gifting exerts influence, even if doctors are unwilling to admit it. But patients and doctors alike would like to state with clarity of conscience that the medication prescribed is only based on clinical evidence, not influence. TH
Dr. Pyke is a hospitalist at Geisinger Wyoming Valley Medical Systems in Mountain Top, Pa.
References
- Dubovsky SL, Kaye DL, Pristach CA, DelRegno P, Pessar L, Stiles K. Can academic departments maintain industry relationships while promoting physician professionalism? Acad Med. 2010;85(1):68-73.
- Salganik MW, Hopkins JS, Rockoff JD. Medical salesmen prescribe lunches. Catering trade feeds on rep-doctor meals. The Baltimore Sun. July 29, 2006.
- Institute of Medicine Conflict of Interest in Medical Research, Education and Practice Full Recommendations. 4-28-09.
- Wolfe SM. Why do American drug companies spend more than $12 billion a year pushing drugs? Is it education or promotion? J Gen Intern Med. 2007;11(10):637-639.
- Adair RF, Holmgren LR. Do drug samples influence resident prescribing behavior? A randomized trial. Am J Med. 2005;118(8):881-884.
- Chew LD, O’Young TS, Hazlet TK, Bradley KA, Maynard C, Lessler DS. A physician survey of the effect of drug sample availability on physicians’ behavior. J Gen Intern Med. 2000;15(7):478-483.
Should hospitalists accept gifts from pharmaceutical, medical device, and biotech companies?

The pharmaceutical industry is big business, and its goal is to make money. If the industry can convince physicians to prescribe its medicines, then it makes more money.
Although pharmaceutical representatives brief physicians on new medications in an effort to encourage the use of their brand-name products, they also provide substantive information on the drugs that serves an educational purpose.
In the past, pharmaceutical companies—along with the medical device and biotechnology industries—showered physicians with expensive gifts, raising ethical questions about physicians’ obligation to the drug companies. Fair enough. These excessive practices were identified and curtailed—to my knowledge—some years ago.
Watchdog groups, however, have continued to call into question every suggestion of “being in the pay” of big pharma. Everything from a plastic pen to a piece of pizza is suspect. There is considerable concern that practicing clinicians are influenced by the smallest gesture, while many large medical institutions continue to accept pharmaceutical-company-funded research grants. If big-pharma investment in research does not corrupt institutions, why is it assumed that carrying a pharmaceutical pen has such a pernicious effect on clinicians?
As a corollary to this question, does anyone really want to discontinue these important research studies just because they are funded by industry dollars?
Listening to drug representatives—even being seen in the vicinity—raises the eyebrows of purists. Do we really want physicians completely divorced from all pharmaceutical company education and communication? Do we feel there is zero benefit to hearing about new medications from the company’s viewpoint?
If physicians completely shut out the representatives, it would be expected that pharmaceutical companies would direct their efforts elsewhere—most likely, to consumers. Is that a better and healthier scenario?
Clearly, there is potential for abuse in pharmaceutical gifts to physicians. The practice should be controlled and monitored. The suspicions raised by purist groups that physicians’ prescribing habits are unalterably biased after a five-minute pharmaceutical representative detail and a chicken sandwich is hyperbole. The voice of reason is silenced in the midst of the inquisition.
In the academic setting, fear of being accused of “bought bias” has physicians clearing their pockets of tainted pens and checking their desks for corrupting paraphernalia. The positive aspects of pharma-sponsored programs and medical lectures are lost for fear of appearing to be complicit with drug companies.
The Aristotelian Golden Mean is superior to extreme positions, and I submit that the best road is the center. Listen to what the drug company representatives have to say, just like you listen to a car salesman: You can learn from both—as long as you research the data and form your own opinion. TH
Dr. Brezina is a hospitalist at Durham Regional Hospital in North Carolina.
The pharmaceutical industry is big business, and its goal is to make money. If the industry can convince physicians to prescribe its medicines, then it makes more money.
Although pharmaceutical representatives brief physicians on new medications in an effort to encourage the use of their brand-name products, they also provide substantive information on the drugs that serves an educational purpose.
In the past, pharmaceutical companies—along with the medical device and biotechnology industries—showered physicians with expensive gifts, raising ethical questions about physicians’ obligation to the drug companies. Fair enough. These excessive practices were identified and curtailed—to my knowledge—some years ago.
Watchdog groups, however, have continued to call into question every suggestion of “being in the pay” of big pharma. Everything from a plastic pen to a piece of pizza is suspect. There is considerable concern that practicing clinicians are influenced by the smallest gesture, while many large medical institutions continue to accept pharmaceutical-company-funded research grants. If big-pharma investment in research does not corrupt institutions, why is it assumed that carrying a pharmaceutical pen has such a pernicious effect on clinicians?
As a corollary to this question, does anyone really want to discontinue these important research studies just because they are funded by industry dollars?
Listening to drug representatives—even being seen in the vicinity—raises the eyebrows of purists. Do we really want physicians completely divorced from all pharmaceutical company education and communication? Do we feel there is zero benefit to hearing about new medications from the company’s viewpoint?
If physicians completely shut out the representatives, it would be expected that pharmaceutical companies would direct their efforts elsewhere—most likely, to consumers. Is that a better and healthier scenario?
Clearly, there is potential for abuse in pharmaceutical gifts to physicians. The practice should be controlled and monitored. The suspicions raised by purist groups that physicians’ prescribing habits are unalterably biased after a five-minute pharmaceutical representative detail and a chicken sandwich is hyperbole. The voice of reason is silenced in the midst of the inquisition.
In the academic setting, fear of being accused of “bought bias” has physicians clearing their pockets of tainted pens and checking their desks for corrupting paraphernalia. The positive aspects of pharma-sponsored programs and medical lectures are lost for fear of appearing to be complicit with drug companies.
The Aristotelian Golden Mean is superior to extreme positions, and I submit that the best road is the center. Listen to what the drug company representatives have to say, just like you listen to a car salesman: You can learn from both—as long as you research the data and form your own opinion. TH
Dr. Brezina is a hospitalist at Durham Regional Hospital in North Carolina.
The pharmaceutical industry is big business, and its goal is to make money. If the industry can convince physicians to prescribe its medicines, then it makes more money.
Although pharmaceutical representatives brief physicians on new medications in an effort to encourage the use of their brand-name products, they also provide substantive information on the drugs that serves an educational purpose.
In the past, pharmaceutical companies—along with the medical device and biotechnology industries—showered physicians with expensive gifts, raising ethical questions about physicians’ obligation to the drug companies. Fair enough. These excessive practices were identified and curtailed—to my knowledge—some years ago.
Watchdog groups, however, have continued to call into question every suggestion of “being in the pay” of big pharma. Everything from a plastic pen to a piece of pizza is suspect. There is considerable concern that practicing clinicians are influenced by the smallest gesture, while many large medical institutions continue to accept pharmaceutical-company-funded research grants. If big-pharma investment in research does not corrupt institutions, why is it assumed that carrying a pharmaceutical pen has such a pernicious effect on clinicians?
As a corollary to this question, does anyone really want to discontinue these important research studies just because they are funded by industry dollars?
Listening to drug representatives—even being seen in the vicinity—raises the eyebrows of purists. Do we really want physicians completely divorced from all pharmaceutical company education and communication? Do we feel there is zero benefit to hearing about new medications from the company’s viewpoint?
If physicians completely shut out the representatives, it would be expected that pharmaceutical companies would direct their efforts elsewhere—most likely, to consumers. Is that a better and healthier scenario?
Clearly, there is potential for abuse in pharmaceutical gifts to physicians. The practice should be controlled and monitored. The suspicions raised by purist groups that physicians’ prescribing habits are unalterably biased after a five-minute pharmaceutical representative detail and a chicken sandwich is hyperbole. The voice of reason is silenced in the midst of the inquisition.
In the academic setting, fear of being accused of “bought bias” has physicians clearing their pockets of tainted pens and checking their desks for corrupting paraphernalia. The positive aspects of pharma-sponsored programs and medical lectures are lost for fear of appearing to be complicit with drug companies.
The Aristotelian Golden Mean is superior to extreme positions, and I submit that the best road is the center. Listen to what the drug company representatives have to say, just like you listen to a car salesman: You can learn from both—as long as you research the data and form your own opinion. TH
Dr. Brezina is a hospitalist at Durham Regional Hospital in North Carolina.
Volume Control, Part II

Last month I began looking at ways hospitalist practices can manage unpredictable increases in patient volume, also known as surge staffing. I provided my view of a “jeopardy” system and a patient volume cap for hospitalists. While both are potentially very effective, they have a high cost and in my view are imperfect solutions. This month I’ll examine some less common strategies to provide surge staffing. Although less popular, I think these options are more valuable.
Schedule More Providers
I’ve worked with a lot of practices and am struck by how patient volume for nearly all of them falls within a reasonably predictable range. While no one can predict with certainty which days will be unusually busy or slow, nearly all practices have a range of daily encounters that is roughly half to 1 1/2 of the mean. For example, if a practice has a mean of 60 billable encounters per day, it probably ranges from about 30 to 90 encounters on any given day. (The larger the practice, the more likely they are to conform to this range. Small practices, with average daily encounters fewer than 20, have a much wider range of daily volumes as a percent of the mean.)
Despite knowing that volumes will vary unpredictably, most practices provide the same fixed “dose” of provider staffing every day—that is, the single most common model for staffing and scheduling is to provide a fixed number of day-shift doctors (“rounders”) who work a fixed number of hours. For example, with an average of 60 billable encounters a day, a hospitalist group might decide to staff with four day-shift rounders working 12-hour shifts. This equates to a fixed 48 hours of daytime staffing. This is reasonable until the busy days arrive. Those four doctors will be much busier than average when there are 90 patients to see in a day, and will probably have a hard time seeing 22 or 23 patients each during their 12-hour shift. If such a busy day occurs more than a couple of times annually, then the practice should probably make some changes.
One approach to solving this type of staffing predicament is to add a fifth day-shift rounder. In other words, when making staffing decisions, consider giving more weight to the busiest days than the average day. This sounds fine until thinking about the practice budget. It will be pretty expensive to add doctors every day just so there are enough on duty when things get really busy. But if the hospitalists are willing to accept reduced compensation, then it might be financially reasonable to go ahead and add staff. This is easiest to do when the hospitalists are paid a significant (e.g. ≥50%) portion of their income based on their productivity, which will enable the hospitalists themselves to have a lot of say about when it is time to add staff. (Being paid on a nearly fixed annual salary means that it is the finance person who usually has the say about when it is time to add staff. And you can bet he’ll be making staffing decisions based on the average daily encounters, rather than the busy days.)
My own preference would be to do just that: Accept a reduction in compensation in return for protection against really busy and stressful days. I’m not suggesting others should agree with me, and in my experience, most don’t. (My own practice partners don’t agree with me on this one.) So I’m not really recommending it as a best practice, but I want to ensure that you don’t forget it is an option. And keep in mind you could adjust staffing by degrees; some settings might add a half-time physician or a nonphysician provider to try to find the sweet spot between having enough staff on duty every day to handle surges in volume and the cost of that staffing to the employer—or the hospitalists themselves.
Of course, if I were willing to reduce my compensation and average daily workload, then I would expect to be freed from the expectation that all rounding doctors work 12-hour shifts. Let’s turn our attention to the interplay between fixed day-shift durations and surge staffing.
Fixed-Shift Schedules Inhibit Surge Capacity
I think it usually is best to avoid fixed durations for day shifts. It might be necessary to require at least one daytime rounder to stay at least until a specified time (e.g. the arrival of the night-shift doctor), but in most cases it is reasonable for some rounders to leave when their work is done. They might need to continue responding to pages until the start of the night shift, but it usually isn’t necessary to have all rounders in the hospital until a predetermined end of the shift.
The problem is that when shifts have a fixed duration, the providers will focus on the start and stop time of their shift and might be unwilling to work beyond it. If instead there are no clearly fixed start and stop times for each day shift, then the hospitalists are likely to be willing to simply work longer on busy days, as long as they can work shorter on slow days. This is probably the most effective method of surge capacity, and it fits well with staffing each day with more providers than are required for the average patient volume.
Simply having the rounding doctors work longer on busy days must be done within reason. And there is a really wide range of opinion about what is reasonable. I think it is reasonable if a hospitalist works two or three hours longer than usual for three or four consecutive busy days, as long as the hospitalist is allowed to work less on days that are not very busy. But just what is a reasonable maximum daily amount of work for even one day is a topic that can lead to passionate debate. You’ll have to decide the details of what is and isn’t acceptable in your group.
Unit-Based Assignments
Aside from fixed-duration day shifts, unit-based assignment of hospitalists is the most common practice inhibiting surge capacity. Not long ago I worked with a practice that followed very strict unit-based assignments, which significantly inhibited “load-leveling,” and thus surge capacity. On any given day the patient volume for the whole practice might be very reasonable, but because it was never distributed evenly among the rounders, there was a very good chance that at least one doctor was drowning in work. And because of the strict approach, the other doctors didn’t come to the rescue.
I think the only reasonable approach is to deviate from such a strict unit-based assignment, at least a little. One rounder could be a utility doctor who doesn’t have her own unit and instead roams throughout the hospital, having been assigned patients based on the workload of each of her unit-based colleagues. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants (www.nelsonflores.com) and codirector and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Last month I began looking at ways hospitalist practices can manage unpredictable increases in patient volume, also known as surge staffing. I provided my view of a “jeopardy” system and a patient volume cap for hospitalists. While both are potentially very effective, they have a high cost and in my view are imperfect solutions. This month I’ll examine some less common strategies to provide surge staffing. Although less popular, I think these options are more valuable.
Schedule More Providers
I’ve worked with a lot of practices and am struck by how patient volume for nearly all of them falls within a reasonably predictable range. While no one can predict with certainty which days will be unusually busy or slow, nearly all practices have a range of daily encounters that is roughly half to 1 1/2 of the mean. For example, if a practice has a mean of 60 billable encounters per day, it probably ranges from about 30 to 90 encounters on any given day. (The larger the practice, the more likely they are to conform to this range. Small practices, with average daily encounters fewer than 20, have a much wider range of daily volumes as a percent of the mean.)
Despite knowing that volumes will vary unpredictably, most practices provide the same fixed “dose” of provider staffing every day—that is, the single most common model for staffing and scheduling is to provide a fixed number of day-shift doctors (“rounders”) who work a fixed number of hours. For example, with an average of 60 billable encounters a day, a hospitalist group might decide to staff with four day-shift rounders working 12-hour shifts. This equates to a fixed 48 hours of daytime staffing. This is reasonable until the busy days arrive. Those four doctors will be much busier than average when there are 90 patients to see in a day, and will probably have a hard time seeing 22 or 23 patients each during their 12-hour shift. If such a busy day occurs more than a couple of times annually, then the practice should probably make some changes.
One approach to solving this type of staffing predicament is to add a fifth day-shift rounder. In other words, when making staffing decisions, consider giving more weight to the busiest days than the average day. This sounds fine until thinking about the practice budget. It will be pretty expensive to add doctors every day just so there are enough on duty when things get really busy. But if the hospitalists are willing to accept reduced compensation, then it might be financially reasonable to go ahead and add staff. This is easiest to do when the hospitalists are paid a significant (e.g. ≥50%) portion of their income based on their productivity, which will enable the hospitalists themselves to have a lot of say about when it is time to add staff. (Being paid on a nearly fixed annual salary means that it is the finance person who usually has the say about when it is time to add staff. And you can bet he’ll be making staffing decisions based on the average daily encounters, rather than the busy days.)
My own preference would be to do just that: Accept a reduction in compensation in return for protection against really busy and stressful days. I’m not suggesting others should agree with me, and in my experience, most don’t. (My own practice partners don’t agree with me on this one.) So I’m not really recommending it as a best practice, but I want to ensure that you don’t forget it is an option. And keep in mind you could adjust staffing by degrees; some settings might add a half-time physician or a nonphysician provider to try to find the sweet spot between having enough staff on duty every day to handle surges in volume and the cost of that staffing to the employer—or the hospitalists themselves.
Of course, if I were willing to reduce my compensation and average daily workload, then I would expect to be freed from the expectation that all rounding doctors work 12-hour shifts. Let’s turn our attention to the interplay between fixed day-shift durations and surge staffing.
Fixed-Shift Schedules Inhibit Surge Capacity
I think it usually is best to avoid fixed durations for day shifts. It might be necessary to require at least one daytime rounder to stay at least until a specified time (e.g. the arrival of the night-shift doctor), but in most cases it is reasonable for some rounders to leave when their work is done. They might need to continue responding to pages until the start of the night shift, but it usually isn’t necessary to have all rounders in the hospital until a predetermined end of the shift.
The problem is that when shifts have a fixed duration, the providers will focus on the start and stop time of their shift and might be unwilling to work beyond it. If instead there are no clearly fixed start and stop times for each day shift, then the hospitalists are likely to be willing to simply work longer on busy days, as long as they can work shorter on slow days. This is probably the most effective method of surge capacity, and it fits well with staffing each day with more providers than are required for the average patient volume.
Simply having the rounding doctors work longer on busy days must be done within reason. And there is a really wide range of opinion about what is reasonable. I think it is reasonable if a hospitalist works two or three hours longer than usual for three or four consecutive busy days, as long as the hospitalist is allowed to work less on days that are not very busy. But just what is a reasonable maximum daily amount of work for even one day is a topic that can lead to passionate debate. You’ll have to decide the details of what is and isn’t acceptable in your group.
Unit-Based Assignments
Aside from fixed-duration day shifts, unit-based assignment of hospitalists is the most common practice inhibiting surge capacity. Not long ago I worked with a practice that followed very strict unit-based assignments, which significantly inhibited “load-leveling,” and thus surge capacity. On any given day the patient volume for the whole practice might be very reasonable, but because it was never distributed evenly among the rounders, there was a very good chance that at least one doctor was drowning in work. And because of the strict approach, the other doctors didn’t come to the rescue.
I think the only reasonable approach is to deviate from such a strict unit-based assignment, at least a little. One rounder could be a utility doctor who doesn’t have her own unit and instead roams throughout the hospital, having been assigned patients based on the workload of each of her unit-based colleagues. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants (www.nelsonflores.com) and codirector and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Last month I began looking at ways hospitalist practices can manage unpredictable increases in patient volume, also known as surge staffing. I provided my view of a “jeopardy” system and a patient volume cap for hospitalists. While both are potentially very effective, they have a high cost and in my view are imperfect solutions. This month I’ll examine some less common strategies to provide surge staffing. Although less popular, I think these options are more valuable.
Schedule More Providers
I’ve worked with a lot of practices and am struck by how patient volume for nearly all of them falls within a reasonably predictable range. While no one can predict with certainty which days will be unusually busy or slow, nearly all practices have a range of daily encounters that is roughly half to 1 1/2 of the mean. For example, if a practice has a mean of 60 billable encounters per day, it probably ranges from about 30 to 90 encounters on any given day. (The larger the practice, the more likely they are to conform to this range. Small practices, with average daily encounters fewer than 20, have a much wider range of daily volumes as a percent of the mean.)
Despite knowing that volumes will vary unpredictably, most practices provide the same fixed “dose” of provider staffing every day—that is, the single most common model for staffing and scheduling is to provide a fixed number of day-shift doctors (“rounders”) who work a fixed number of hours. For example, with an average of 60 billable encounters a day, a hospitalist group might decide to staff with four day-shift rounders working 12-hour shifts. This equates to a fixed 48 hours of daytime staffing. This is reasonable until the busy days arrive. Those four doctors will be much busier than average when there are 90 patients to see in a day, and will probably have a hard time seeing 22 or 23 patients each during their 12-hour shift. If such a busy day occurs more than a couple of times annually, then the practice should probably make some changes.
One approach to solving this type of staffing predicament is to add a fifth day-shift rounder. In other words, when making staffing decisions, consider giving more weight to the busiest days than the average day. This sounds fine until thinking about the practice budget. It will be pretty expensive to add doctors every day just so there are enough on duty when things get really busy. But if the hospitalists are willing to accept reduced compensation, then it might be financially reasonable to go ahead and add staff. This is easiest to do when the hospitalists are paid a significant (e.g. ≥50%) portion of their income based on their productivity, which will enable the hospitalists themselves to have a lot of say about when it is time to add staff. (Being paid on a nearly fixed annual salary means that it is the finance person who usually has the say about when it is time to add staff. And you can bet he’ll be making staffing decisions based on the average daily encounters, rather than the busy days.)
My own preference would be to do just that: Accept a reduction in compensation in return for protection against really busy and stressful days. I’m not suggesting others should agree with me, and in my experience, most don’t. (My own practice partners don’t agree with me on this one.) So I’m not really recommending it as a best practice, but I want to ensure that you don’t forget it is an option. And keep in mind you could adjust staffing by degrees; some settings might add a half-time physician or a nonphysician provider to try to find the sweet spot between having enough staff on duty every day to handle surges in volume and the cost of that staffing to the employer—or the hospitalists themselves.
Of course, if I were willing to reduce my compensation and average daily workload, then I would expect to be freed from the expectation that all rounding doctors work 12-hour shifts. Let’s turn our attention to the interplay between fixed day-shift durations and surge staffing.
Fixed-Shift Schedules Inhibit Surge Capacity
I think it usually is best to avoid fixed durations for day shifts. It might be necessary to require at least one daytime rounder to stay at least until a specified time (e.g. the arrival of the night-shift doctor), but in most cases it is reasonable for some rounders to leave when their work is done. They might need to continue responding to pages until the start of the night shift, but it usually isn’t necessary to have all rounders in the hospital until a predetermined end of the shift.
The problem is that when shifts have a fixed duration, the providers will focus on the start and stop time of their shift and might be unwilling to work beyond it. If instead there are no clearly fixed start and stop times for each day shift, then the hospitalists are likely to be willing to simply work longer on busy days, as long as they can work shorter on slow days. This is probably the most effective method of surge capacity, and it fits well with staffing each day with more providers than are required for the average patient volume.
Simply having the rounding doctors work longer on busy days must be done within reason. And there is a really wide range of opinion about what is reasonable. I think it is reasonable if a hospitalist works two or three hours longer than usual for three or four consecutive busy days, as long as the hospitalist is allowed to work less on days that are not very busy. But just what is a reasonable maximum daily amount of work for even one day is a topic that can lead to passionate debate. You’ll have to decide the details of what is and isn’t acceptable in your group.
Unit-Based Assignments
Aside from fixed-duration day shifts, unit-based assignment of hospitalists is the most common practice inhibiting surge capacity. Not long ago I worked with a practice that followed very strict unit-based assignments, which significantly inhibited “load-leveling,” and thus surge capacity. On any given day the patient volume for the whole practice might be very reasonable, but because it was never distributed evenly among the rounders, there was a very good chance that at least one doctor was drowning in work. And because of the strict approach, the other doctors didn’t come to the rescue.
I think the only reasonable approach is to deviate from such a strict unit-based assignment, at least a little. One rounder could be a utility doctor who doesn’t have her own unit and instead roams throughout the hospital, having been assigned patients based on the workload of each of her unit-based colleagues. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants (www.nelsonflores.com) and codirector and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
"Peel the Onion" to Avoid Common Mistakes With a Hospital's Offer of an Electronic Medical Records System
Large prolapsed fibroid left untreated—despite surgery...and more
Large prolapsed fibroid left untreated—despite surgery
A 48-YEAR-OLD WOMAN PRESENTED to the emergency department (ED) with vaginal pain. A large, prolapsed uterine fibroid was diagnosed. Because she was scheduled for an ObGyn visit 2 days later, she was discharged without any treatment.
The next day, she returned to the ED with vaginal bleeding. Ultrasonography (US) showed multiple fibroids. Physical exam confirmed a prolapsed uterine fibroid extending into the vaginal vault. Her ObGyn performed an open myomectomy a few days later.
She called her ObGyn’s office prior to her scheduled postoperative visit because she still felt something in her vagina, and had pelvic pain and vaginal bleeding. She also reported this at the office visit, where she met with a nurse practitioner.
Two months later, she called the ObGyn’s office to complain of vaginal bleeding, and described passing large clots.
A month later, she saw a surgeon, who determined that the large prolapsed fibroid had never been removed. Surgery was scheduled, during which her uterus was removed. The patient was hospitalized for 11 days.
PATIENT’S CLAIM The ObGyn was negligent in failing to surgically remove the fibroid, perform postoperative US, and properly examine, diagnose, and treat her postoperatively. The ObGyn’s office staff failed to relay her telephone and in-person complaints to the physician.
DEFENDANTS’ DEFENSE The ObGyn and his group denied negligence.
VERDICT A $248,160 Georgia verdict was returned against the group.
Woman claims she was never told mammogram results
AFTER MANY NORMAL MAMMOGRAMS, a woman had an abnormal annual result. However, she claimed the physician did not inform her of the reported results. A year later, she was diagnosed with breast cancer.
PATIENT’S CLAIM The physician was negligent in failing to follow-up on the abnormal mammogram and make a correct diagnosis.
PHYSICIAN’S DEFENSE The woman had refused a recommended biopsy after the abnormal mammogram, and later refused mastectomy and radiation therapy. The patient’s outcome would have been the same even if treatment had begun shortly after the abnormal mammogram.
VERDICT A $175,000 verdict was returned in Indiana.
5,386-g newborn has Erb’s palsy
OXYTOCIN WAS ADMINISTERED after a woman’s labor slowed. During vaginal delivery, the ObGyn encountered and managed shoulder dystocia. The 11-lb, 14-oz infant was later given a diagnosis of Erb’s palsy.
PLAINTIFF’S CLAIM Excessive force during the ObGyn’s management of shoulder dystocia caused the Erb’s palsy. US should have been performed prior to delivery to determine fetal weight. Cesarean section may have prevented the injury.
PHYSICIAN’S DEFENSE Fetal weight was calculated at a time when vaginal delivery could not be safely discontinued. Excessive traction was not used; if it had been used, the injury would have been more significant.
VERDICT A New York jury returned a $485,000 verdict.
Was there delay in recognizing necrotizing fasciitis?
PREGNANT WITH TWINS, a 24-year-old woman was hospitalized at 33 weeks’ gestation, and remained there until delivery. There was no clinical evidence of fever or intrauterine infection during her hospitalization. Her anogenital culture for group B Streptococcus was positive. Clindamycin was begun 11 days prior to delivery, and continued after a successful cesarean delivery by her ObGyn.
Three days later, the mother suffered a high fever and marked elevation of her white blood cell count. The ObGyn reopened and drained the wound incision. Surgical debridement was not performed. The woman continued to deteriorate.
She developed extensive necrosis of the tissue around the abdominal wound, extending to the pannus and mons pubis. The ObGyn performed wide excision of the tissue. Necrotizing fasciitis was confirmed by pathology.
The woman was diagnosed with sepsis, multi-system organ failure, disseminated intravascular coagulopathy, and respiratory dependence. She was transferred to another hospital, where she remained until her death 3 months after delivery.
ESTATE’S CLAIM The ObGyn failed to diagnose and treat the necrotizing fasciitis in a timely manner. He failed to perform emergency surgical debridement when the lesions were first identified.
PHYSICIAN’S DEFENSE Antibiotics were ordered at the first sign of the vaginal strep infection and continued due to postsurgical wound infection.
Consultations with infectious disease specialists were obtained because of the patient’s history of extreme medication reaction and numerous antibiotic allergies. Although testing reported negative results for other infection sources, the patient failed to respond to treatment. Surgical debridement was performed when necessary, and as often as the patient was deemed able to tolerate the procedure.
VERDICT A Georgia verdict of $4,317,495 was returned.
ObGyn at fault for child’s brain injury and vision loss?
AT 22 WEEKS’ GESTATION, a woman presented to the ED with cramping and bleeding. A nurse called the woman’s ObGyn, who was not at the hospital; he ordered monitoring and laboratory tests. Two hours later, the bleeding and pain increased. The ObGyn was notified, although whether he was told about the excessive bleeding or not is in dispute. He ordered morphine. The patient was sent home without being seen by a physician, with instructions to follow-up with her ObGyn.
The woman claimed she called the hospital the next morning to report continued pain and bleeding, and was told to take a bath. She returned to the hospital the next evening. US revealed a dilated cervix with hour-glassing membranes. The child was delivered at 23-weeks’ gestation and suffers from a brain injury and vision loss.
PLAINTIFF’S CLAIM Premature delivery was due to an incompetent cervix, which could have been treated with cerclage. Diagnostic US and a physical examination by the ObGyn were never performed.
DEFENDANT’S DEFENSE Postdelivery evaluation of the placenta indicated that the mother had chorioamnionitis. Cerclage would have been contraindicated; delivery would have occurred despite any efforts to prolong the pregnancy.
VERDICT A Utah defense verdict was returned.
Did untreated hypertension cause mother’s blindness?
A 34-YEAR-OLD PREGNANT WOMAN was admitted to the hospital with new onset hypertension. Three days later her BP increased to 170/98 mm Hg; her ObGyn performed an emergent cesarean delivery. During the procedure, the woman’s BP rose to 203/120, and remained high in recovery. When she awoke, she reported blurred vision, and was later declared to be legally blind.
PATIENT’S CLAIM The physician failed to properly monitor her BP. Failure to use antihypertensive drugs led to an ischemic event, resulting in vision loss.
PHYSICIAN’S DEFENSE The woman’s BP was properly monitored at all times. She had been diagnosed with Purtscher’s retinopathy syndrome, which predisposed her to pregnancy-related vision loss. Her blindness was not BP-related.
VERDICT A Tennessee defense verdict was returned.
Ruptured ectopic pregnancy not treated properly in ED
WHEN BROUGHT TO THE EMERGENCY DEPARTMENT, a 25-year-old woman was found to be in hemorrhagic shock following a ruptured ectopic pregnancy. Her BP was 42/19 mm Hg. She was taken to surgery, where the ruptured fallopian tube was removed.
After surgery, she complained of tremors in her legs and torso, and had difficulty walking unassisted. She was diagnosed with hypoxic ischemic encephalopathy and transferred to a rehabilitation facility.
PATIENT’S CLAIM She was not properly resuscitated in the ED; intravenous fluids and transfusions should have been given immediately. Delayed treatment in the ED caused hypoxic ischemic encephalopathy or a conversion disorder.
PHYSICIAN’S DEFENSE Intravenous fluids and transfusions were started appropriately and promptly in the ED. The patient did not suffer hypoxic ischemic encephalopathy; a conversion disorder could have occurred from the stress of the ruptured ectopic pregnancy.
VERDICT An Illinois jury returned a defense verdict.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
Large prolapsed fibroid left untreated—despite surgery
A 48-YEAR-OLD WOMAN PRESENTED to the emergency department (ED) with vaginal pain. A large, prolapsed uterine fibroid was diagnosed. Because she was scheduled for an ObGyn visit 2 days later, she was discharged without any treatment.
The next day, she returned to the ED with vaginal bleeding. Ultrasonography (US) showed multiple fibroids. Physical exam confirmed a prolapsed uterine fibroid extending into the vaginal vault. Her ObGyn performed an open myomectomy a few days later.
She called her ObGyn’s office prior to her scheduled postoperative visit because she still felt something in her vagina, and had pelvic pain and vaginal bleeding. She also reported this at the office visit, where she met with a nurse practitioner.
Two months later, she called the ObGyn’s office to complain of vaginal bleeding, and described passing large clots.
A month later, she saw a surgeon, who determined that the large prolapsed fibroid had never been removed. Surgery was scheduled, during which her uterus was removed. The patient was hospitalized for 11 days.
PATIENT’S CLAIM The ObGyn was negligent in failing to surgically remove the fibroid, perform postoperative US, and properly examine, diagnose, and treat her postoperatively. The ObGyn’s office staff failed to relay her telephone and in-person complaints to the physician.
DEFENDANTS’ DEFENSE The ObGyn and his group denied negligence.
VERDICT A $248,160 Georgia verdict was returned against the group.
Woman claims she was never told mammogram results
AFTER MANY NORMAL MAMMOGRAMS, a woman had an abnormal annual result. However, she claimed the physician did not inform her of the reported results. A year later, she was diagnosed with breast cancer.
PATIENT’S CLAIM The physician was negligent in failing to follow-up on the abnormal mammogram and make a correct diagnosis.
PHYSICIAN’S DEFENSE The woman had refused a recommended biopsy after the abnormal mammogram, and later refused mastectomy and radiation therapy. The patient’s outcome would have been the same even if treatment had begun shortly after the abnormal mammogram.
VERDICT A $175,000 verdict was returned in Indiana.
5,386-g newborn has Erb’s palsy
OXYTOCIN WAS ADMINISTERED after a woman’s labor slowed. During vaginal delivery, the ObGyn encountered and managed shoulder dystocia. The 11-lb, 14-oz infant was later given a diagnosis of Erb’s palsy.
PLAINTIFF’S CLAIM Excessive force during the ObGyn’s management of shoulder dystocia caused the Erb’s palsy. US should have been performed prior to delivery to determine fetal weight. Cesarean section may have prevented the injury.
PHYSICIAN’S DEFENSE Fetal weight was calculated at a time when vaginal delivery could not be safely discontinued. Excessive traction was not used; if it had been used, the injury would have been more significant.
VERDICT A New York jury returned a $485,000 verdict.
Was there delay in recognizing necrotizing fasciitis?
PREGNANT WITH TWINS, a 24-year-old woman was hospitalized at 33 weeks’ gestation, and remained there until delivery. There was no clinical evidence of fever or intrauterine infection during her hospitalization. Her anogenital culture for group B Streptococcus was positive. Clindamycin was begun 11 days prior to delivery, and continued after a successful cesarean delivery by her ObGyn.
Three days later, the mother suffered a high fever and marked elevation of her white blood cell count. The ObGyn reopened and drained the wound incision. Surgical debridement was not performed. The woman continued to deteriorate.
She developed extensive necrosis of the tissue around the abdominal wound, extending to the pannus and mons pubis. The ObGyn performed wide excision of the tissue. Necrotizing fasciitis was confirmed by pathology.
The woman was diagnosed with sepsis, multi-system organ failure, disseminated intravascular coagulopathy, and respiratory dependence. She was transferred to another hospital, where she remained until her death 3 months after delivery.
ESTATE’S CLAIM The ObGyn failed to diagnose and treat the necrotizing fasciitis in a timely manner. He failed to perform emergency surgical debridement when the lesions were first identified.
PHYSICIAN’S DEFENSE Antibiotics were ordered at the first sign of the vaginal strep infection and continued due to postsurgical wound infection.
Consultations with infectious disease specialists were obtained because of the patient’s history of extreme medication reaction and numerous antibiotic allergies. Although testing reported negative results for other infection sources, the patient failed to respond to treatment. Surgical debridement was performed when necessary, and as often as the patient was deemed able to tolerate the procedure.
VERDICT A Georgia verdict of $4,317,495 was returned.
ObGyn at fault for child’s brain injury and vision loss?
AT 22 WEEKS’ GESTATION, a woman presented to the ED with cramping and bleeding. A nurse called the woman’s ObGyn, who was not at the hospital; he ordered monitoring and laboratory tests. Two hours later, the bleeding and pain increased. The ObGyn was notified, although whether he was told about the excessive bleeding or not is in dispute. He ordered morphine. The patient was sent home without being seen by a physician, with instructions to follow-up with her ObGyn.
The woman claimed she called the hospital the next morning to report continued pain and bleeding, and was told to take a bath. She returned to the hospital the next evening. US revealed a dilated cervix with hour-glassing membranes. The child was delivered at 23-weeks’ gestation and suffers from a brain injury and vision loss.
PLAINTIFF’S CLAIM Premature delivery was due to an incompetent cervix, which could have been treated with cerclage. Diagnostic US and a physical examination by the ObGyn were never performed.
DEFENDANT’S DEFENSE Postdelivery evaluation of the placenta indicated that the mother had chorioamnionitis. Cerclage would have been contraindicated; delivery would have occurred despite any efforts to prolong the pregnancy.
VERDICT A Utah defense verdict was returned.
Did untreated hypertension cause mother’s blindness?
A 34-YEAR-OLD PREGNANT WOMAN was admitted to the hospital with new onset hypertension. Three days later her BP increased to 170/98 mm Hg; her ObGyn performed an emergent cesarean delivery. During the procedure, the woman’s BP rose to 203/120, and remained high in recovery. When she awoke, she reported blurred vision, and was later declared to be legally blind.
PATIENT’S CLAIM The physician failed to properly monitor her BP. Failure to use antihypertensive drugs led to an ischemic event, resulting in vision loss.
PHYSICIAN’S DEFENSE The woman’s BP was properly monitored at all times. She had been diagnosed with Purtscher’s retinopathy syndrome, which predisposed her to pregnancy-related vision loss. Her blindness was not BP-related.
VERDICT A Tennessee defense verdict was returned.
Ruptured ectopic pregnancy not treated properly in ED
WHEN BROUGHT TO THE EMERGENCY DEPARTMENT, a 25-year-old woman was found to be in hemorrhagic shock following a ruptured ectopic pregnancy. Her BP was 42/19 mm Hg. She was taken to surgery, where the ruptured fallopian tube was removed.
After surgery, she complained of tremors in her legs and torso, and had difficulty walking unassisted. She was diagnosed with hypoxic ischemic encephalopathy and transferred to a rehabilitation facility.
PATIENT’S CLAIM She was not properly resuscitated in the ED; intravenous fluids and transfusions should have been given immediately. Delayed treatment in the ED caused hypoxic ischemic encephalopathy or a conversion disorder.
PHYSICIAN’S DEFENSE Intravenous fluids and transfusions were started appropriately and promptly in the ED. The patient did not suffer hypoxic ischemic encephalopathy; a conversion disorder could have occurred from the stress of the ruptured ectopic pregnancy.
VERDICT An Illinois jury returned a defense verdict.
Large prolapsed fibroid left untreated—despite surgery
A 48-YEAR-OLD WOMAN PRESENTED to the emergency department (ED) with vaginal pain. A large, prolapsed uterine fibroid was diagnosed. Because she was scheduled for an ObGyn visit 2 days later, she was discharged without any treatment.
The next day, she returned to the ED with vaginal bleeding. Ultrasonography (US) showed multiple fibroids. Physical exam confirmed a prolapsed uterine fibroid extending into the vaginal vault. Her ObGyn performed an open myomectomy a few days later.
She called her ObGyn’s office prior to her scheduled postoperative visit because she still felt something in her vagina, and had pelvic pain and vaginal bleeding. She also reported this at the office visit, where she met with a nurse practitioner.
Two months later, she called the ObGyn’s office to complain of vaginal bleeding, and described passing large clots.
A month later, she saw a surgeon, who determined that the large prolapsed fibroid had never been removed. Surgery was scheduled, during which her uterus was removed. The patient was hospitalized for 11 days.
PATIENT’S CLAIM The ObGyn was negligent in failing to surgically remove the fibroid, perform postoperative US, and properly examine, diagnose, and treat her postoperatively. The ObGyn’s office staff failed to relay her telephone and in-person complaints to the physician.
DEFENDANTS’ DEFENSE The ObGyn and his group denied negligence.
VERDICT A $248,160 Georgia verdict was returned against the group.
Woman claims she was never told mammogram results
AFTER MANY NORMAL MAMMOGRAMS, a woman had an abnormal annual result. However, she claimed the physician did not inform her of the reported results. A year later, she was diagnosed with breast cancer.
PATIENT’S CLAIM The physician was negligent in failing to follow-up on the abnormal mammogram and make a correct diagnosis.
PHYSICIAN’S DEFENSE The woman had refused a recommended biopsy after the abnormal mammogram, and later refused mastectomy and radiation therapy. The patient’s outcome would have been the same even if treatment had begun shortly after the abnormal mammogram.
VERDICT A $175,000 verdict was returned in Indiana.
5,386-g newborn has Erb’s palsy
OXYTOCIN WAS ADMINISTERED after a woman’s labor slowed. During vaginal delivery, the ObGyn encountered and managed shoulder dystocia. The 11-lb, 14-oz infant was later given a diagnosis of Erb’s palsy.
PLAINTIFF’S CLAIM Excessive force during the ObGyn’s management of shoulder dystocia caused the Erb’s palsy. US should have been performed prior to delivery to determine fetal weight. Cesarean section may have prevented the injury.
PHYSICIAN’S DEFENSE Fetal weight was calculated at a time when vaginal delivery could not be safely discontinued. Excessive traction was not used; if it had been used, the injury would have been more significant.
VERDICT A New York jury returned a $485,000 verdict.
Was there delay in recognizing necrotizing fasciitis?
PREGNANT WITH TWINS, a 24-year-old woman was hospitalized at 33 weeks’ gestation, and remained there until delivery. There was no clinical evidence of fever or intrauterine infection during her hospitalization. Her anogenital culture for group B Streptococcus was positive. Clindamycin was begun 11 days prior to delivery, and continued after a successful cesarean delivery by her ObGyn.
Three days later, the mother suffered a high fever and marked elevation of her white blood cell count. The ObGyn reopened and drained the wound incision. Surgical debridement was not performed. The woman continued to deteriorate.
She developed extensive necrosis of the tissue around the abdominal wound, extending to the pannus and mons pubis. The ObGyn performed wide excision of the tissue. Necrotizing fasciitis was confirmed by pathology.
The woman was diagnosed with sepsis, multi-system organ failure, disseminated intravascular coagulopathy, and respiratory dependence. She was transferred to another hospital, where she remained until her death 3 months after delivery.
ESTATE’S CLAIM The ObGyn failed to diagnose and treat the necrotizing fasciitis in a timely manner. He failed to perform emergency surgical debridement when the lesions were first identified.
PHYSICIAN’S DEFENSE Antibiotics were ordered at the first sign of the vaginal strep infection and continued due to postsurgical wound infection.
Consultations with infectious disease specialists were obtained because of the patient’s history of extreme medication reaction and numerous antibiotic allergies. Although testing reported negative results for other infection sources, the patient failed to respond to treatment. Surgical debridement was performed when necessary, and as often as the patient was deemed able to tolerate the procedure.
VERDICT A Georgia verdict of $4,317,495 was returned.
ObGyn at fault for child’s brain injury and vision loss?
AT 22 WEEKS’ GESTATION, a woman presented to the ED with cramping and bleeding. A nurse called the woman’s ObGyn, who was not at the hospital; he ordered monitoring and laboratory tests. Two hours later, the bleeding and pain increased. The ObGyn was notified, although whether he was told about the excessive bleeding or not is in dispute. He ordered morphine. The patient was sent home without being seen by a physician, with instructions to follow-up with her ObGyn.
The woman claimed she called the hospital the next morning to report continued pain and bleeding, and was told to take a bath. She returned to the hospital the next evening. US revealed a dilated cervix with hour-glassing membranes. The child was delivered at 23-weeks’ gestation and suffers from a brain injury and vision loss.
PLAINTIFF’S CLAIM Premature delivery was due to an incompetent cervix, which could have been treated with cerclage. Diagnostic US and a physical examination by the ObGyn were never performed.
DEFENDANT’S DEFENSE Postdelivery evaluation of the placenta indicated that the mother had chorioamnionitis. Cerclage would have been contraindicated; delivery would have occurred despite any efforts to prolong the pregnancy.
VERDICT A Utah defense verdict was returned.
Did untreated hypertension cause mother’s blindness?
A 34-YEAR-OLD PREGNANT WOMAN was admitted to the hospital with new onset hypertension. Three days later her BP increased to 170/98 mm Hg; her ObGyn performed an emergent cesarean delivery. During the procedure, the woman’s BP rose to 203/120, and remained high in recovery. When she awoke, she reported blurred vision, and was later declared to be legally blind.
PATIENT’S CLAIM The physician failed to properly monitor her BP. Failure to use antihypertensive drugs led to an ischemic event, resulting in vision loss.
PHYSICIAN’S DEFENSE The woman’s BP was properly monitored at all times. She had been diagnosed with Purtscher’s retinopathy syndrome, which predisposed her to pregnancy-related vision loss. Her blindness was not BP-related.
VERDICT A Tennessee defense verdict was returned.
Ruptured ectopic pregnancy not treated properly in ED
WHEN BROUGHT TO THE EMERGENCY DEPARTMENT, a 25-year-old woman was found to be in hemorrhagic shock following a ruptured ectopic pregnancy. Her BP was 42/19 mm Hg. She was taken to surgery, where the ruptured fallopian tube was removed.
After surgery, she complained of tremors in her legs and torso, and had difficulty walking unassisted. She was diagnosed with hypoxic ischemic encephalopathy and transferred to a rehabilitation facility.
PATIENT’S CLAIM She was not properly resuscitated in the ED; intravenous fluids and transfusions should have been given immediately. Delayed treatment in the ED caused hypoxic ischemic encephalopathy or a conversion disorder.
PHYSICIAN’S DEFENSE Intravenous fluids and transfusions were started appropriately and promptly in the ED. The patient did not suffer hypoxic ischemic encephalopathy; a conversion disorder could have occurred from the stress of the ruptured ectopic pregnancy.
VERDICT An Illinois jury returned a defense verdict.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
Delegation
It’s interesting that the more things change, the more they stay the same. The most easily correctable problem I see in private offices today is the same one I saw 30 years ago: underdelegation. (A newer and more alarming problem is overdelegation, but we’ll get to that later.)
Private practitioners famously spend inordinate amounts of time embroiled in minutiae. After all, they are continually hearing the same mantra from know-it-alls like me: The physician is the captain of the vessel, and ultimate responsibility for everyone’s screw-ups rests with you; ergo, as captain, you must run a tight ship.
There is a big difference, however, between maintaining control of your practice’s inner workings and micromanaging the day-to-day details. One never sees a ship’s captain swabbing the decks, cooking the meals, or fixing the engine, and you shouldn’t be billing, purchasing, or arguing with pharmacists when there are patients to see.
Most doctors do delegate, of course, but many don’t do it enough. Try this experiment: For a week, write down everything you do around the office, especially the menial stuff. Then, over the weekend, look at your list. You’ll probably be surprised at how much time you waste on chores that could be delegated.
Handing off tasks can be hard – especially if you have the “nobody does it as well as I do” disease. My rule of thumb: Everything requiring a physician’s license should be done by physicians; everything else should be done by employees or contractors.
I know what you’re thinking: This is going to cost me, and the results won’t be up to my standards. Your overhead may increase while employees learn new duties. You may also need to raise salaries to compensate for the increased workload, or even hire a new person or two. Simple arithmetic, though, will show that in the long run a new employee working at a fraction of your hourly rate will do the job cheaper than you can. Granted, you cannot expect them to immediately do it as well as you do, but with time, proper training, and a bit of patience, employees will nearly always meet, and even exceed, your expectations.
Be alert, however, for something I call reverse delegation. It’s not at all unusual for an employee, faced with a new assignment, to pepper the boss with questions, complaints, and fears about doing it properly. It’s easy, at this point, to yield to the pressure and simply do the job yourself. You have taken the bait: your subordinate has delegated the task back to you!
If you employ nurse practitioners or physician assistants, reassess your options with them as well. Consider additional aspects of examination, diagnosis, testing, and treatment of routine patients that they could be doing, which will in turn free up more of your time for new patients and complex cases.
Remember, though, that state laws vary on who can delegate what to whom. Consult your attorney and local medical association if there is any question about what your state permits, particularly with regard to NPs and PAs.
And that brings us to the disturbing trend of overdelegation. Last year, the Department of Health and Human Services’ Office of Inspector General (a government office you never want to hear from) looked at services billed under Medicare’s “incident-to” rule to determine whether nonphysician billings were appropriate. When suspicious data were identified – for example, when billed services for a single day exceeded 24 hours – the suspect practice was investigated.
The OIG’s report concluded that 21% of services not performed personally by physicians in their selective sample were performed by unqualified nonphysicians.
Offices were found in which Mohs was being delegated to unqualified staff, including, in some cases, untrained medical assistants. The report was based on a relatively small sample, so it is not clear how prevalent such practices are, but, clearly, any prevalence is too high, and you will not fare well with the OIG if you are caught.
Delegating doesn’t mean handing off a task and forgetting about it. Always maintain an open flow of communication with your employees. A good boss does not micromanage, but does remain in the loop.
It’s interesting that the more things change, the more they stay the same. The most easily correctable problem I see in private offices today is the same one I saw 30 years ago: underdelegation. (A newer and more alarming problem is overdelegation, but we’ll get to that later.)
Private practitioners famously spend inordinate amounts of time embroiled in minutiae. After all, they are continually hearing the same mantra from know-it-alls like me: The physician is the captain of the vessel, and ultimate responsibility for everyone’s screw-ups rests with you; ergo, as captain, you must run a tight ship.
There is a big difference, however, between maintaining control of your practice’s inner workings and micromanaging the day-to-day details. One never sees a ship’s captain swabbing the decks, cooking the meals, or fixing the engine, and you shouldn’t be billing, purchasing, or arguing with pharmacists when there are patients to see.
Most doctors do delegate, of course, but many don’t do it enough. Try this experiment: For a week, write down everything you do around the office, especially the menial stuff. Then, over the weekend, look at your list. You’ll probably be surprised at how much time you waste on chores that could be delegated.
Handing off tasks can be hard – especially if you have the “nobody does it as well as I do” disease. My rule of thumb: Everything requiring a physician’s license should be done by physicians; everything else should be done by employees or contractors.
I know what you’re thinking: This is going to cost me, and the results won’t be up to my standards. Your overhead may increase while employees learn new duties. You may also need to raise salaries to compensate for the increased workload, or even hire a new person or two. Simple arithmetic, though, will show that in the long run a new employee working at a fraction of your hourly rate will do the job cheaper than you can. Granted, you cannot expect them to immediately do it as well as you do, but with time, proper training, and a bit of patience, employees will nearly always meet, and even exceed, your expectations.
Be alert, however, for something I call reverse delegation. It’s not at all unusual for an employee, faced with a new assignment, to pepper the boss with questions, complaints, and fears about doing it properly. It’s easy, at this point, to yield to the pressure and simply do the job yourself. You have taken the bait: your subordinate has delegated the task back to you!
If you employ nurse practitioners or physician assistants, reassess your options with them as well. Consider additional aspects of examination, diagnosis, testing, and treatment of routine patients that they could be doing, which will in turn free up more of your time for new patients and complex cases.
Remember, though, that state laws vary on who can delegate what to whom. Consult your attorney and local medical association if there is any question about what your state permits, particularly with regard to NPs and PAs.
And that brings us to the disturbing trend of overdelegation. Last year, the Department of Health and Human Services’ Office of Inspector General (a government office you never want to hear from) looked at services billed under Medicare’s “incident-to” rule to determine whether nonphysician billings were appropriate. When suspicious data were identified – for example, when billed services for a single day exceeded 24 hours – the suspect practice was investigated.
The OIG’s report concluded that 21% of services not performed personally by physicians in their selective sample were performed by unqualified nonphysicians.
Offices were found in which Mohs was being delegated to unqualified staff, including, in some cases, untrained medical assistants. The report was based on a relatively small sample, so it is not clear how prevalent such practices are, but, clearly, any prevalence is too high, and you will not fare well with the OIG if you are caught.
Delegating doesn’t mean handing off a task and forgetting about it. Always maintain an open flow of communication with your employees. A good boss does not micromanage, but does remain in the loop.
It’s interesting that the more things change, the more they stay the same. The most easily correctable problem I see in private offices today is the same one I saw 30 years ago: underdelegation. (A newer and more alarming problem is overdelegation, but we’ll get to that later.)
Private practitioners famously spend inordinate amounts of time embroiled in minutiae. After all, they are continually hearing the same mantra from know-it-alls like me: The physician is the captain of the vessel, and ultimate responsibility for everyone’s screw-ups rests with you; ergo, as captain, you must run a tight ship.
There is a big difference, however, between maintaining control of your practice’s inner workings and micromanaging the day-to-day details. One never sees a ship’s captain swabbing the decks, cooking the meals, or fixing the engine, and you shouldn’t be billing, purchasing, or arguing with pharmacists when there are patients to see.
Most doctors do delegate, of course, but many don’t do it enough. Try this experiment: For a week, write down everything you do around the office, especially the menial stuff. Then, over the weekend, look at your list. You’ll probably be surprised at how much time you waste on chores that could be delegated.
Handing off tasks can be hard – especially if you have the “nobody does it as well as I do” disease. My rule of thumb: Everything requiring a physician’s license should be done by physicians; everything else should be done by employees or contractors.
I know what you’re thinking: This is going to cost me, and the results won’t be up to my standards. Your overhead may increase while employees learn new duties. You may also need to raise salaries to compensate for the increased workload, or even hire a new person or two. Simple arithmetic, though, will show that in the long run a new employee working at a fraction of your hourly rate will do the job cheaper than you can. Granted, you cannot expect them to immediately do it as well as you do, but with time, proper training, and a bit of patience, employees will nearly always meet, and even exceed, your expectations.
Be alert, however, for something I call reverse delegation. It’s not at all unusual for an employee, faced with a new assignment, to pepper the boss with questions, complaints, and fears about doing it properly. It’s easy, at this point, to yield to the pressure and simply do the job yourself. You have taken the bait: your subordinate has delegated the task back to you!
If you employ nurse practitioners or physician assistants, reassess your options with them as well. Consider additional aspects of examination, diagnosis, testing, and treatment of routine patients that they could be doing, which will in turn free up more of your time for new patients and complex cases.
Remember, though, that state laws vary on who can delegate what to whom. Consult your attorney and local medical association if there is any question about what your state permits, particularly with regard to NPs and PAs.
And that brings us to the disturbing trend of overdelegation. Last year, the Department of Health and Human Services’ Office of Inspector General (a government office you never want to hear from) looked at services billed under Medicare’s “incident-to” rule to determine whether nonphysician billings were appropriate. When suspicious data were identified – for example, when billed services for a single day exceeded 24 hours – the suspect practice was investigated.
The OIG’s report concluded that 21% of services not performed personally by physicians in their selective sample were performed by unqualified nonphysicians.
Offices were found in which Mohs was being delegated to unqualified staff, including, in some cases, untrained medical assistants. The report was based on a relatively small sample, so it is not clear how prevalent such practices are, but, clearly, any prevalence is too high, and you will not fare well with the OIG if you are caught.
Delegating doesn’t mean handing off a task and forgetting about it. Always maintain an open flow of communication with your employees. A good boss does not micromanage, but does remain in the loop.
To Discount or Not to Discount
As the “Great Recession” continues, there is much discussion on medical forums about how to increase cash flow, decrease administrative expenses, and deal with ever-increasing numbers of unemployed and uninsured patients.
Extending discounts to patients who pay at the time of service or pay out of pocket is one effective way of addressing all three of these issues. Exercise caution, because discounts can run afoul of federal and state laws. These include state antikickback statutes, the anti-inducement provision of the Health Insurance Portability and Accountability Act, the Medicare exclusion provision, and state insurance antidiscrimination provisions.
From a legal standpoint, any discount is a kickback of sorts—you are returning part of your fee to the patient—and many laws designed to thwart real kickbacks can apply in such situations.
Take the straightforward case of time-of-service discounts for cosmetic procedures and other services not covered by insurance. You would think such transactions are just between you and your patients, but you need to avoid the appearance of using these discounts as marketing incentives (inducements to attract patients).
Also, a shrewd third-party payer could try to pull a fast one on you. Many provider agreements contain what are often called “most favored nation” clauses, which require you to automatically give that provider the lowest price you offer to anyone else, regardless of what they would otherwise pay. In other words, they could demand that you give them the same discount.
My response in that situation would be that a time-of-service discount is exactly that: It is offered only when payment is made immediately. Third parties never pay at the time of service and are not entitled to it.
Things get complicated if you also want to extend discounts for covered services. Be sure that the discounted fee you charge the patient is also reflected on the claim submitted to the insurer. Billing the insurer more than you charged the patient invites a charge of fraud. Avoid discounting so regularly that the discounted fee becomes your new usual and customary rate.
Waiving coinsurance and deductibles can be trouble, too, particularly with Medicare and Medicaid. You might intend it as a good deed, but the Centers for Medicare and Medicaid Services may see it as an inducement or kickback, especially if you do it routinely. The CMS has no problem with an occasional waiver, especially “after determining in good faith that the individual is in financial need” (according to the Office of Inspector General), but thorough documentation is in order in such cases.
Waiving copays for privately insured patients can be equally problematic. Nearly all insurers impose a contractual duty on providers to make a reasonable effort to collect applicable copays and/or deductibles. They view the routine waiver of patient payments as a breach of contract, and there has been litigation against providers who flout this requirement. As with the CMS, accommodating patients with individually documented financial limitations is acceptable, but when there is a pattern of routine waivers and no documentation, you will have difficulty defending it.
In addition to antikickback laws, some states have antidiscrimination laws that forbid either lower charges to any subset of insurance payers or any noninsurance payer than to any insurance payer. Some states make specific exceptions for legitimate discounts—as in cases of financial hardship, or when you are just trying to pass along your lower billing and collections costs—but others do not. Check your state's laws and run everything past your attorney.
As for how much of a discount you can give, I cannot suggest an amount, but if it is completely out of proportion to the administrative costs of submitting paperwork and the hassles associated with waiting for your money, you could, once again, be accused of offering a discount that is a de facto increase to insurance carriers, and that could result in charges of fraud.
In cases of legitimate financial hardship, the most effective and least problematic strategy may be to offer a sliding scale. Many large clinics and community agencies and all hospitals have a written policy for this, often based on federal poverty guidelines. Do a little homework: Contact local social service agencies and welfare clinics, learn the community standard in your area, and formulate a written policy with guidelines for determining a patient's indigence. Once again, consistency of administration, objectivity in policies, and documentation of individual eligibility are essential.
As the “Great Recession” continues, there is much discussion on medical forums about how to increase cash flow, decrease administrative expenses, and deal with ever-increasing numbers of unemployed and uninsured patients.
Extending discounts to patients who pay at the time of service or pay out of pocket is one effective way of addressing all three of these issues. Exercise caution, because discounts can run afoul of federal and state laws. These include state antikickback statutes, the anti-inducement provision of the Health Insurance Portability and Accountability Act, the Medicare exclusion provision, and state insurance antidiscrimination provisions.
From a legal standpoint, any discount is a kickback of sorts—you are returning part of your fee to the patient—and many laws designed to thwart real kickbacks can apply in such situations.
Take the straightforward case of time-of-service discounts for cosmetic procedures and other services not covered by insurance. You would think such transactions are just between you and your patients, but you need to avoid the appearance of using these discounts as marketing incentives (inducements to attract patients).
Also, a shrewd third-party payer could try to pull a fast one on you. Many provider agreements contain what are often called “most favored nation” clauses, which require you to automatically give that provider the lowest price you offer to anyone else, regardless of what they would otherwise pay. In other words, they could demand that you give them the same discount.
My response in that situation would be that a time-of-service discount is exactly that: It is offered only when payment is made immediately. Third parties never pay at the time of service and are not entitled to it.
Things get complicated if you also want to extend discounts for covered services. Be sure that the discounted fee you charge the patient is also reflected on the claim submitted to the insurer. Billing the insurer more than you charged the patient invites a charge of fraud. Avoid discounting so regularly that the discounted fee becomes your new usual and customary rate.
Waiving coinsurance and deductibles can be trouble, too, particularly with Medicare and Medicaid. You might intend it as a good deed, but the Centers for Medicare and Medicaid Services may see it as an inducement or kickback, especially if you do it routinely. The CMS has no problem with an occasional waiver, especially “after determining in good faith that the individual is in financial need” (according to the Office of Inspector General), but thorough documentation is in order in such cases.
Waiving copays for privately insured patients can be equally problematic. Nearly all insurers impose a contractual duty on providers to make a reasonable effort to collect applicable copays and/or deductibles. They view the routine waiver of patient payments as a breach of contract, and there has been litigation against providers who flout this requirement. As with the CMS, accommodating patients with individually documented financial limitations is acceptable, but when there is a pattern of routine waivers and no documentation, you will have difficulty defending it.
In addition to antikickback laws, some states have antidiscrimination laws that forbid either lower charges to any subset of insurance payers or any noninsurance payer than to any insurance payer. Some states make specific exceptions for legitimate discounts—as in cases of financial hardship, or when you are just trying to pass along your lower billing and collections costs—but others do not. Check your state's laws and run everything past your attorney.
As for how much of a discount you can give, I cannot suggest an amount, but if it is completely out of proportion to the administrative costs of submitting paperwork and the hassles associated with waiting for your money, you could, once again, be accused of offering a discount that is a de facto increase to insurance carriers, and that could result in charges of fraud.
In cases of legitimate financial hardship, the most effective and least problematic strategy may be to offer a sliding scale. Many large clinics and community agencies and all hospitals have a written policy for this, often based on federal poverty guidelines. Do a little homework: Contact local social service agencies and welfare clinics, learn the community standard in your area, and formulate a written policy with guidelines for determining a patient's indigence. Once again, consistency of administration, objectivity in policies, and documentation of individual eligibility are essential.
As the “Great Recession” continues, there is much discussion on medical forums about how to increase cash flow, decrease administrative expenses, and deal with ever-increasing numbers of unemployed and uninsured patients.
Extending discounts to patients who pay at the time of service or pay out of pocket is one effective way of addressing all three of these issues. Exercise caution, because discounts can run afoul of federal and state laws. These include state antikickback statutes, the anti-inducement provision of the Health Insurance Portability and Accountability Act, the Medicare exclusion provision, and state insurance antidiscrimination provisions.
From a legal standpoint, any discount is a kickback of sorts—you are returning part of your fee to the patient—and many laws designed to thwart real kickbacks can apply in such situations.
Take the straightforward case of time-of-service discounts for cosmetic procedures and other services not covered by insurance. You would think such transactions are just between you and your patients, but you need to avoid the appearance of using these discounts as marketing incentives (inducements to attract patients).
Also, a shrewd third-party payer could try to pull a fast one on you. Many provider agreements contain what are often called “most favored nation” clauses, which require you to automatically give that provider the lowest price you offer to anyone else, regardless of what they would otherwise pay. In other words, they could demand that you give them the same discount.
My response in that situation would be that a time-of-service discount is exactly that: It is offered only when payment is made immediately. Third parties never pay at the time of service and are not entitled to it.
Things get complicated if you also want to extend discounts for covered services. Be sure that the discounted fee you charge the patient is also reflected on the claim submitted to the insurer. Billing the insurer more than you charged the patient invites a charge of fraud. Avoid discounting so regularly that the discounted fee becomes your new usual and customary rate.
Waiving coinsurance and deductibles can be trouble, too, particularly with Medicare and Medicaid. You might intend it as a good deed, but the Centers for Medicare and Medicaid Services may see it as an inducement or kickback, especially if you do it routinely. The CMS has no problem with an occasional waiver, especially “after determining in good faith that the individual is in financial need” (according to the Office of Inspector General), but thorough documentation is in order in such cases.
Waiving copays for privately insured patients can be equally problematic. Nearly all insurers impose a contractual duty on providers to make a reasonable effort to collect applicable copays and/or deductibles. They view the routine waiver of patient payments as a breach of contract, and there has been litigation against providers who flout this requirement. As with the CMS, accommodating patients with individually documented financial limitations is acceptable, but when there is a pattern of routine waivers and no documentation, you will have difficulty defending it.
In addition to antikickback laws, some states have antidiscrimination laws that forbid either lower charges to any subset of insurance payers or any noninsurance payer than to any insurance payer. Some states make specific exceptions for legitimate discounts—as in cases of financial hardship, or when you are just trying to pass along your lower billing and collections costs—but others do not. Check your state's laws and run everything past your attorney.
As for how much of a discount you can give, I cannot suggest an amount, but if it is completely out of proportion to the administrative costs of submitting paperwork and the hassles associated with waiting for your money, you could, once again, be accused of offering a discount that is a de facto increase to insurance carriers, and that could result in charges of fraud.
In cases of legitimate financial hardship, the most effective and least problematic strategy may be to offer a sliding scale. Many large clinics and community agencies and all hospitals have a written policy for this, often based on federal poverty guidelines. Do a little homework: Contact local social service agencies and welfare clinics, learn the community standard in your area, and formulate a written policy with guidelines for determining a patient's indigence. Once again, consistency of administration, objectivity in policies, and documentation of individual eligibility are essential.
Productivity Capacity

The mark of any great society is balance—balance between the production realized today and the preservation of “production capacity” to ensure the same or greater production in the future. HM is not exempt from this fundamental tenet. What we do now in the way of advancing quality, efficiency, and patient safety will matter little if our contributions are not sustained by the generation that follows us.
It is tempting to think that the issue of how we train residents is germane only to universities, but the reality is that it affects us all. There are 126 “university” medical school programs, but there are 384 residency programs, most of which are within community-based hospitals. The result is that most hospitalists encounter resident physicians in some capacity, and all hospitalists will encounter the results of residency training when they welcome a new recruit to their ranks.
The education and socialization of our residents will define the character of the hospitalists of the future. But the “residency” in which most of us trained does not exist anymore: The duty-hours changes and additional training requirements have dramatically changed the landscape of residency training in the past 10 years, and another series of sea changes is underway. As with all things HM, we again have a choice: Be reactive, wait for the dust to clear, and then lament the results, or be proactive and see this change for what it is—an opportunity to improve healthcare quality now, and in the future.
The ACGME
HM felt the impact of the first wave of duty-hours restrictions beginning in 2003, as many training programs opted to employ hospitalists to provide the coverage that could no longer be maintained by residents working under tighter admission caps and duty-hour restrictions. In doing so, hospitalists have provided a valuable service in preserving the integrity of training environments and fidelity to the Accreditation Council for Graduate Medical Education (ACGME) regulations (more than 85% of training programs have hospitalists working in their systems). But the model of hospitalists working solely as “resident-extenders” is not sustainable.
First, hospitalists who work solely on nonteaching services are at great risk of burning out, especially if the distribution of patients has been manipulated such that the more interesting patients are funneled away from the hospitalist’s service to the teaching service. Second, there is a risk in perception: In models in which the hospitalist is solely the “overflow cap coverage” or the night-float physician (i.e., the resident-extender), residents come to see hospitalists as the “PGY-4, 5, 6 …” physicians—that is, the physician who becomes a resident for life. The result is a serious pipeline issue for us, as the most talented resident physicians are unlikely to forego subspecialty training for a career in HM if hospitalists are perceived as perpetual residents.
The solution is simple: The hospitalist’s role in training environments has to be more than merely solving admission cap or duty-hour issues. It is fine for hospitalists to operate nonteaching services, but the hospitalist also has to be a part of the fulfillment that comes with overseeing teaching services. Further, residents have to see the hospitalist career for what it actually is: Academic or not, HM is much more than merely clinical service. HM is about the value-added services of system interventions to improve quality and patient safety; it is about developing a career as a systems architect. Getting the best and brightest residents to choose HM as a career is contingent upon residents seeing hospitalists in the training environment who are happy and fulfilled in the execution of this career goal.
The hospitalist’s plight was helped substantially on June 23, when ACGME released for comment the revised Common Program Requirements (www.acgme.org). The duty-hours changes are unlikely to substantially alter hospitalists’ lives; the only significant change was a limitation on intern shift durations to fewer than 16 hours in a row (upper-level residents still operate under the 24+6 hour rule, with increased flexibility to stay longer by volition). But the interesting part of the new requirements is an augmented focus on teaching residents transitions-of-care skills, improving direct supervision of residents, and constructing educational systems that minimize handoffs.
There is no specialty that is as suited as HM for fulfilling these unique (and, as of yet, unmet) requirements. Transitions, quality, being present on the hospital wards … this is what we do. And requiring instruction in transitions and quality is an unprecedented leverage point for HM to advance the quality of future physicians. How great it would be to attend HM20 and realize that the attendees had already learned the “Quality 101” lessons (i.e., those we are currently teaching at our annual meeting) as part of their residency? Freed from the need to do basic quality sessions, the content of the annual meeting could escalate to even higher-level principles that would result in substantial and sustainable quality improvement (QI).
MedPAC and GME Funding
Simultaneous with the ACGME changes are changes at the Medicare Payment Advisory Committee (MedPAC), the advisory organization responsible for recommending changes in the distribution of Centers for Medicare and Medicaid Services (CMS) funds to support graduate medical education. CMS is the primary funding agent for residency training. Each hospital receives direct medical expenditures to cover a resident’s salary and benefits. Each hospital has a pre-set per-resident allotment, or PRA. This number varies by hospital, but the average is $100,000 per resident. CMS reimburses the hospital a percentage of this number based upon the percentage of hospital days occupied by Medicare patients (e.g., 35% Medicare days=$35,000 per resident).
The hospital also receives indirect medical expenditures, or IME. IME is not a distinct payment to the hospital, but rather an “inflator” of the clinical-care payments the hospital receives from CMS. IME is paid to the hospital under the presumption that a typical training facility incurs greater cost due to higher patient severity, a higher indigent care percentage, and has higher resource utilization due to residents’ excessive testing, etc. The final presumption is that support is needed for the educational infrastructure (i.e., supervision and teaching).
IME is not inconsequential to a hospital; depending upon the payor mix, a 200-bed hospital might have from $4 million to $8 million in annual IME payments. CMS’ total IME payments to hospitals is more than $6 billion a year. Each hospital’s IME revenue can be found at www.graham-center.org/online/graham/home/tools-resources/data-tables/dt001-gme-2007.html.
The game-changing event occurred in April, when MedPAC announced its intent to reassess the mechanisms of IME funding, with a vision of IME funding eventually being linked to a hospital’s training programs’ ability to demonstrate substantial improvement in quality and patient safety. And here is the leverage point that is a unique opportunity for hospitalists in the training environment. For many hospitalists, especially if employed directly by the hospital, there is little financial incentive to engaging on a teaching service. The ACGME caps limit the service size, and this in turn limits the possible RVUs. Up until now, asking the hospital to compensate for teaching time (i.e., EVUs) was a pipe dream. But the linking of IME funding to quality outcomes (and quality instruction to residents) could change all of that.
If you put the two together: ACGME calling for instruction in quality and transitions, plus MedPAC calling for payments linked to resident outcomes in quality and patient safety, you have one inescapable conclusion—the residency of the future will hinge upon having supervisors with the necessary expertise to ensure that residents participate in, and understand the principles of, patient safety and quality as a part of the residency curriculum. And the people who can ensure that goal are likely to be in a position to warrant compensation for doing so.
Who is better to do this than the hospitalist?
SHM’s Proactive Strategy
This is the opportune time for HM to advance its stature as a profession and to ensure its future via a pipeline of residents adequately training in quality and patient safety. But it is not enough to merely wish for this to happen. There are real barriers that have kept hospitalists from being more intimately involved in physician training, the first of which is age.
HM is a young specialty (the average hospitalist is 37; the average HM leader is 41), and its youth makes it hard to compete with older subspecialists/generalists who have more experience in education. But deficits in experience can be compensated by additional training.
The Academic Hospitalist Academy (AHA)—cosponsored by SHM, the Society of General Internal Medicine (SGIM), and the Association of Chiefs and Leaders of General Internal Medicine (ACLGIM)—is the key to the strategy of catching up quickly. The academy will convene this month outside of Atlanta, and it is very important that each training facility think about sending one of its hospitalists to receive the advanced training in education necessary to compensate for not having years of experience in medical education. Academy details are available at http://academichospitalist.org.
SHM’s initiatives on this front do not stop with the academy. Over the past three months, Kevin O’Leary, MD, and his Quality Improvement Education Committee have been furiously building a “Quality and Patient Safety” curriculum, with a target audience of new hospitalists and resident physicians. The vision is to create a Web-based, interactive curriculum that teaches resident physicians the basics of quality and patient safety, design projects with their colleagues (under the supervision of their hospitalist mentor), and track their data to see real-time results.
Unlike other curricula on the market, the SHM Quality Curriculum for residents will be dynamic, requiring participating institutions commit to SHM’s modus operandi of mentored implementation by sponsoring a hospitalist to receive the training necessary to put the curriculum in motion. To this end, SHM has collaborated with the Alliance for Internal Medicine (AIM) in co-sponsoring the Quality Academy, with a focus on how to teach quality and patient safety. Jen Meyers, MD, FHM, and Jeff Glasheen, MD, SFHM, will be leading the team responsible for the development of this Quality Training Course, which should emerge in the fall of 2011.
As this project proceeds, Paul Grant, MD, chair of the Early Career Hospitalist Committee, and Cheryl O’Malley, MD, chair of the Pipeline Committee, will provide counsel. Both of these groups will continue efforts to improve the process by which residents transition from residency to HM practice, and supporting young physicians with distance mentoring.
The SHM vision of our production capacity is simple: Bring in the best and brightest hospitalists who are interested in teaching quality and patient safety, train them in the fundamentals of medical education, provide them with an “off the net” curriculum for how to teach quality, then return them to their respective training environments to coach residents on the principles of quality.
Training programs that invest in this vision will reap the rewards of fidelity to the new ACGME requirements. Hospitals that support such a vision will receive assurances, should MedPAC’s recommendation come to fruition, that DME and IME funding is secure. Hospitalists investing in this vision will find a fulfilling career in quality education.
And all of us will find assurances that, for as good as things are right now for HM, the future will be even better. TH
Dr. Wiese is president of SHM.
The mark of any great society is balance—balance between the production realized today and the preservation of “production capacity” to ensure the same or greater production in the future. HM is not exempt from this fundamental tenet. What we do now in the way of advancing quality, efficiency, and patient safety will matter little if our contributions are not sustained by the generation that follows us.
It is tempting to think that the issue of how we train residents is germane only to universities, but the reality is that it affects us all. There are 126 “university” medical school programs, but there are 384 residency programs, most of which are within community-based hospitals. The result is that most hospitalists encounter resident physicians in some capacity, and all hospitalists will encounter the results of residency training when they welcome a new recruit to their ranks.
The education and socialization of our residents will define the character of the hospitalists of the future. But the “residency” in which most of us trained does not exist anymore: The duty-hours changes and additional training requirements have dramatically changed the landscape of residency training in the past 10 years, and another series of sea changes is underway. As with all things HM, we again have a choice: Be reactive, wait for the dust to clear, and then lament the results, or be proactive and see this change for what it is—an opportunity to improve healthcare quality now, and in the future.
The ACGME
HM felt the impact of the first wave of duty-hours restrictions beginning in 2003, as many training programs opted to employ hospitalists to provide the coverage that could no longer be maintained by residents working under tighter admission caps and duty-hour restrictions. In doing so, hospitalists have provided a valuable service in preserving the integrity of training environments and fidelity to the Accreditation Council for Graduate Medical Education (ACGME) regulations (more than 85% of training programs have hospitalists working in their systems). But the model of hospitalists working solely as “resident-extenders” is not sustainable.
First, hospitalists who work solely on nonteaching services are at great risk of burning out, especially if the distribution of patients has been manipulated such that the more interesting patients are funneled away from the hospitalist’s service to the teaching service. Second, there is a risk in perception: In models in which the hospitalist is solely the “overflow cap coverage” or the night-float physician (i.e., the resident-extender), residents come to see hospitalists as the “PGY-4, 5, 6 …” physicians—that is, the physician who becomes a resident for life. The result is a serious pipeline issue for us, as the most talented resident physicians are unlikely to forego subspecialty training for a career in HM if hospitalists are perceived as perpetual residents.
The solution is simple: The hospitalist’s role in training environments has to be more than merely solving admission cap or duty-hour issues. It is fine for hospitalists to operate nonteaching services, but the hospitalist also has to be a part of the fulfillment that comes with overseeing teaching services. Further, residents have to see the hospitalist career for what it actually is: Academic or not, HM is much more than merely clinical service. HM is about the value-added services of system interventions to improve quality and patient safety; it is about developing a career as a systems architect. Getting the best and brightest residents to choose HM as a career is contingent upon residents seeing hospitalists in the training environment who are happy and fulfilled in the execution of this career goal.
The hospitalist’s plight was helped substantially on June 23, when ACGME released for comment the revised Common Program Requirements (www.acgme.org). The duty-hours changes are unlikely to substantially alter hospitalists’ lives; the only significant change was a limitation on intern shift durations to fewer than 16 hours in a row (upper-level residents still operate under the 24+6 hour rule, with increased flexibility to stay longer by volition). But the interesting part of the new requirements is an augmented focus on teaching residents transitions-of-care skills, improving direct supervision of residents, and constructing educational systems that minimize handoffs.
There is no specialty that is as suited as HM for fulfilling these unique (and, as of yet, unmet) requirements. Transitions, quality, being present on the hospital wards … this is what we do. And requiring instruction in transitions and quality is an unprecedented leverage point for HM to advance the quality of future physicians. How great it would be to attend HM20 and realize that the attendees had already learned the “Quality 101” lessons (i.e., those we are currently teaching at our annual meeting) as part of their residency? Freed from the need to do basic quality sessions, the content of the annual meeting could escalate to even higher-level principles that would result in substantial and sustainable quality improvement (QI).
MedPAC and GME Funding
Simultaneous with the ACGME changes are changes at the Medicare Payment Advisory Committee (MedPAC), the advisory organization responsible for recommending changes in the distribution of Centers for Medicare and Medicaid Services (CMS) funds to support graduate medical education. CMS is the primary funding agent for residency training. Each hospital receives direct medical expenditures to cover a resident’s salary and benefits. Each hospital has a pre-set per-resident allotment, or PRA. This number varies by hospital, but the average is $100,000 per resident. CMS reimburses the hospital a percentage of this number based upon the percentage of hospital days occupied by Medicare patients (e.g., 35% Medicare days=$35,000 per resident).
The hospital also receives indirect medical expenditures, or IME. IME is not a distinct payment to the hospital, but rather an “inflator” of the clinical-care payments the hospital receives from CMS. IME is paid to the hospital under the presumption that a typical training facility incurs greater cost due to higher patient severity, a higher indigent care percentage, and has higher resource utilization due to residents’ excessive testing, etc. The final presumption is that support is needed for the educational infrastructure (i.e., supervision and teaching).
IME is not inconsequential to a hospital; depending upon the payor mix, a 200-bed hospital might have from $4 million to $8 million in annual IME payments. CMS’ total IME payments to hospitals is more than $6 billion a year. Each hospital’s IME revenue can be found at www.graham-center.org/online/graham/home/tools-resources/data-tables/dt001-gme-2007.html.
The game-changing event occurred in April, when MedPAC announced its intent to reassess the mechanisms of IME funding, with a vision of IME funding eventually being linked to a hospital’s training programs’ ability to demonstrate substantial improvement in quality and patient safety. And here is the leverage point that is a unique opportunity for hospitalists in the training environment. For many hospitalists, especially if employed directly by the hospital, there is little financial incentive to engaging on a teaching service. The ACGME caps limit the service size, and this in turn limits the possible RVUs. Up until now, asking the hospital to compensate for teaching time (i.e., EVUs) was a pipe dream. But the linking of IME funding to quality outcomes (and quality instruction to residents) could change all of that.
If you put the two together: ACGME calling for instruction in quality and transitions, plus MedPAC calling for payments linked to resident outcomes in quality and patient safety, you have one inescapable conclusion—the residency of the future will hinge upon having supervisors with the necessary expertise to ensure that residents participate in, and understand the principles of, patient safety and quality as a part of the residency curriculum. And the people who can ensure that goal are likely to be in a position to warrant compensation for doing so.
Who is better to do this than the hospitalist?
SHM’s Proactive Strategy
This is the opportune time for HM to advance its stature as a profession and to ensure its future via a pipeline of residents adequately training in quality and patient safety. But it is not enough to merely wish for this to happen. There are real barriers that have kept hospitalists from being more intimately involved in physician training, the first of which is age.
HM is a young specialty (the average hospitalist is 37; the average HM leader is 41), and its youth makes it hard to compete with older subspecialists/generalists who have more experience in education. But deficits in experience can be compensated by additional training.
The Academic Hospitalist Academy (AHA)—cosponsored by SHM, the Society of General Internal Medicine (SGIM), and the Association of Chiefs and Leaders of General Internal Medicine (ACLGIM)—is the key to the strategy of catching up quickly. The academy will convene this month outside of Atlanta, and it is very important that each training facility think about sending one of its hospitalists to receive the advanced training in education necessary to compensate for not having years of experience in medical education. Academy details are available at http://academichospitalist.org.
SHM’s initiatives on this front do not stop with the academy. Over the past three months, Kevin O’Leary, MD, and his Quality Improvement Education Committee have been furiously building a “Quality and Patient Safety” curriculum, with a target audience of new hospitalists and resident physicians. The vision is to create a Web-based, interactive curriculum that teaches resident physicians the basics of quality and patient safety, design projects with their colleagues (under the supervision of their hospitalist mentor), and track their data to see real-time results.
Unlike other curricula on the market, the SHM Quality Curriculum for residents will be dynamic, requiring participating institutions commit to SHM’s modus operandi of mentored implementation by sponsoring a hospitalist to receive the training necessary to put the curriculum in motion. To this end, SHM has collaborated with the Alliance for Internal Medicine (AIM) in co-sponsoring the Quality Academy, with a focus on how to teach quality and patient safety. Jen Meyers, MD, FHM, and Jeff Glasheen, MD, SFHM, will be leading the team responsible for the development of this Quality Training Course, which should emerge in the fall of 2011.
As this project proceeds, Paul Grant, MD, chair of the Early Career Hospitalist Committee, and Cheryl O’Malley, MD, chair of the Pipeline Committee, will provide counsel. Both of these groups will continue efforts to improve the process by which residents transition from residency to HM practice, and supporting young physicians with distance mentoring.
The SHM vision of our production capacity is simple: Bring in the best and brightest hospitalists who are interested in teaching quality and patient safety, train them in the fundamentals of medical education, provide them with an “off the net” curriculum for how to teach quality, then return them to their respective training environments to coach residents on the principles of quality.
Training programs that invest in this vision will reap the rewards of fidelity to the new ACGME requirements. Hospitals that support such a vision will receive assurances, should MedPAC’s recommendation come to fruition, that DME and IME funding is secure. Hospitalists investing in this vision will find a fulfilling career in quality education.
And all of us will find assurances that, for as good as things are right now for HM, the future will be even better. TH
Dr. Wiese is president of SHM.
The mark of any great society is balance—balance between the production realized today and the preservation of “production capacity” to ensure the same or greater production in the future. HM is not exempt from this fundamental tenet. What we do now in the way of advancing quality, efficiency, and patient safety will matter little if our contributions are not sustained by the generation that follows us.
It is tempting to think that the issue of how we train residents is germane only to universities, but the reality is that it affects us all. There are 126 “university” medical school programs, but there are 384 residency programs, most of which are within community-based hospitals. The result is that most hospitalists encounter resident physicians in some capacity, and all hospitalists will encounter the results of residency training when they welcome a new recruit to their ranks.
The education and socialization of our residents will define the character of the hospitalists of the future. But the “residency” in which most of us trained does not exist anymore: The duty-hours changes and additional training requirements have dramatically changed the landscape of residency training in the past 10 years, and another series of sea changes is underway. As with all things HM, we again have a choice: Be reactive, wait for the dust to clear, and then lament the results, or be proactive and see this change for what it is—an opportunity to improve healthcare quality now, and in the future.
The ACGME
HM felt the impact of the first wave of duty-hours restrictions beginning in 2003, as many training programs opted to employ hospitalists to provide the coverage that could no longer be maintained by residents working under tighter admission caps and duty-hour restrictions. In doing so, hospitalists have provided a valuable service in preserving the integrity of training environments and fidelity to the Accreditation Council for Graduate Medical Education (ACGME) regulations (more than 85% of training programs have hospitalists working in their systems). But the model of hospitalists working solely as “resident-extenders” is not sustainable.
First, hospitalists who work solely on nonteaching services are at great risk of burning out, especially if the distribution of patients has been manipulated such that the more interesting patients are funneled away from the hospitalist’s service to the teaching service. Second, there is a risk in perception: In models in which the hospitalist is solely the “overflow cap coverage” or the night-float physician (i.e., the resident-extender), residents come to see hospitalists as the “PGY-4, 5, 6 …” physicians—that is, the physician who becomes a resident for life. The result is a serious pipeline issue for us, as the most talented resident physicians are unlikely to forego subspecialty training for a career in HM if hospitalists are perceived as perpetual residents.
The solution is simple: The hospitalist’s role in training environments has to be more than merely solving admission cap or duty-hour issues. It is fine for hospitalists to operate nonteaching services, but the hospitalist also has to be a part of the fulfillment that comes with overseeing teaching services. Further, residents have to see the hospitalist career for what it actually is: Academic or not, HM is much more than merely clinical service. HM is about the value-added services of system interventions to improve quality and patient safety; it is about developing a career as a systems architect. Getting the best and brightest residents to choose HM as a career is contingent upon residents seeing hospitalists in the training environment who are happy and fulfilled in the execution of this career goal.
The hospitalist’s plight was helped substantially on June 23, when ACGME released for comment the revised Common Program Requirements (www.acgme.org). The duty-hours changes are unlikely to substantially alter hospitalists’ lives; the only significant change was a limitation on intern shift durations to fewer than 16 hours in a row (upper-level residents still operate under the 24+6 hour rule, with increased flexibility to stay longer by volition). But the interesting part of the new requirements is an augmented focus on teaching residents transitions-of-care skills, improving direct supervision of residents, and constructing educational systems that minimize handoffs.
There is no specialty that is as suited as HM for fulfilling these unique (and, as of yet, unmet) requirements. Transitions, quality, being present on the hospital wards … this is what we do. And requiring instruction in transitions and quality is an unprecedented leverage point for HM to advance the quality of future physicians. How great it would be to attend HM20 and realize that the attendees had already learned the “Quality 101” lessons (i.e., those we are currently teaching at our annual meeting) as part of their residency? Freed from the need to do basic quality sessions, the content of the annual meeting could escalate to even higher-level principles that would result in substantial and sustainable quality improvement (QI).
MedPAC and GME Funding
Simultaneous with the ACGME changes are changes at the Medicare Payment Advisory Committee (MedPAC), the advisory organization responsible for recommending changes in the distribution of Centers for Medicare and Medicaid Services (CMS) funds to support graduate medical education. CMS is the primary funding agent for residency training. Each hospital receives direct medical expenditures to cover a resident’s salary and benefits. Each hospital has a pre-set per-resident allotment, or PRA. This number varies by hospital, but the average is $100,000 per resident. CMS reimburses the hospital a percentage of this number based upon the percentage of hospital days occupied by Medicare patients (e.g., 35% Medicare days=$35,000 per resident).
The hospital also receives indirect medical expenditures, or IME. IME is not a distinct payment to the hospital, but rather an “inflator” of the clinical-care payments the hospital receives from CMS. IME is paid to the hospital under the presumption that a typical training facility incurs greater cost due to higher patient severity, a higher indigent care percentage, and has higher resource utilization due to residents’ excessive testing, etc. The final presumption is that support is needed for the educational infrastructure (i.e., supervision and teaching).
IME is not inconsequential to a hospital; depending upon the payor mix, a 200-bed hospital might have from $4 million to $8 million in annual IME payments. CMS’ total IME payments to hospitals is more than $6 billion a year. Each hospital’s IME revenue can be found at www.graham-center.org/online/graham/home/tools-resources/data-tables/dt001-gme-2007.html.
The game-changing event occurred in April, when MedPAC announced its intent to reassess the mechanisms of IME funding, with a vision of IME funding eventually being linked to a hospital’s training programs’ ability to demonstrate substantial improvement in quality and patient safety. And here is the leverage point that is a unique opportunity for hospitalists in the training environment. For many hospitalists, especially if employed directly by the hospital, there is little financial incentive to engaging on a teaching service. The ACGME caps limit the service size, and this in turn limits the possible RVUs. Up until now, asking the hospital to compensate for teaching time (i.e., EVUs) was a pipe dream. But the linking of IME funding to quality outcomes (and quality instruction to residents) could change all of that.
If you put the two together: ACGME calling for instruction in quality and transitions, plus MedPAC calling for payments linked to resident outcomes in quality and patient safety, you have one inescapable conclusion—the residency of the future will hinge upon having supervisors with the necessary expertise to ensure that residents participate in, and understand the principles of, patient safety and quality as a part of the residency curriculum. And the people who can ensure that goal are likely to be in a position to warrant compensation for doing so.
Who is better to do this than the hospitalist?
SHM’s Proactive Strategy
This is the opportune time for HM to advance its stature as a profession and to ensure its future via a pipeline of residents adequately training in quality and patient safety. But it is not enough to merely wish for this to happen. There are real barriers that have kept hospitalists from being more intimately involved in physician training, the first of which is age.
HM is a young specialty (the average hospitalist is 37; the average HM leader is 41), and its youth makes it hard to compete with older subspecialists/generalists who have more experience in education. But deficits in experience can be compensated by additional training.
The Academic Hospitalist Academy (AHA)—cosponsored by SHM, the Society of General Internal Medicine (SGIM), and the Association of Chiefs and Leaders of General Internal Medicine (ACLGIM)—is the key to the strategy of catching up quickly. The academy will convene this month outside of Atlanta, and it is very important that each training facility think about sending one of its hospitalists to receive the advanced training in education necessary to compensate for not having years of experience in medical education. Academy details are available at http://academichospitalist.org.
SHM’s initiatives on this front do not stop with the academy. Over the past three months, Kevin O’Leary, MD, and his Quality Improvement Education Committee have been furiously building a “Quality and Patient Safety” curriculum, with a target audience of new hospitalists and resident physicians. The vision is to create a Web-based, interactive curriculum that teaches resident physicians the basics of quality and patient safety, design projects with their colleagues (under the supervision of their hospitalist mentor), and track their data to see real-time results.
Unlike other curricula on the market, the SHM Quality Curriculum for residents will be dynamic, requiring participating institutions commit to SHM’s modus operandi of mentored implementation by sponsoring a hospitalist to receive the training necessary to put the curriculum in motion. To this end, SHM has collaborated with the Alliance for Internal Medicine (AIM) in co-sponsoring the Quality Academy, with a focus on how to teach quality and patient safety. Jen Meyers, MD, FHM, and Jeff Glasheen, MD, SFHM, will be leading the team responsible for the development of this Quality Training Course, which should emerge in the fall of 2011.
As this project proceeds, Paul Grant, MD, chair of the Early Career Hospitalist Committee, and Cheryl O’Malley, MD, chair of the Pipeline Committee, will provide counsel. Both of these groups will continue efforts to improve the process by which residents transition from residency to HM practice, and supporting young physicians with distance mentoring.
The SHM vision of our production capacity is simple: Bring in the best and brightest hospitalists who are interested in teaching quality and patient safety, train them in the fundamentals of medical education, provide them with an “off the net” curriculum for how to teach quality, then return them to their respective training environments to coach residents on the principles of quality.
Training programs that invest in this vision will reap the rewards of fidelity to the new ACGME requirements. Hospitals that support such a vision will receive assurances, should MedPAC’s recommendation come to fruition, that DME and IME funding is secure. Hospitalists investing in this vision will find a fulfilling career in quality education.
And all of us will find assurances that, for as good as things are right now for HM, the future will be even better. TH
Dr. Wiese is president of SHM.
The Devil & the Details

Act I: The Negotiation
(A barren academic office, dimly lit, the pall of difficult negotiations afloat, backlit like dust in the air. Seated, under a strangely intense incandescent bulb, a man, who looks eerily like a good-looking version of me, sits uncomfortably adjusting himself in his seat. His eyes constrict on his counterpart, a miserly sort peering out from behind wire-rim glasses and a shock of hair improbably combed over from ear to ear. The tension crests.)
GOOD-LOOKING ME
(Voice cracking)
I’ve come to ask for a raise for our hospitalist group.
MISER
(Adjusts his clip-on tie)
We just gave you a raise in 2004.
GOOD-LOOKING ME
(Smiles uncomfortably)
That was very gracious, sir, but I think the numbers support another.
MISER
(Incredulous look at his watch)
But your work RVUs are thousands below what I’d like to see.
GOOD-LOOKING ME
(Dabs bead of sweat away from chiseled chin)
That’s because you’ve set your benchmark thousands above a reasonable number.
MISER
(Voice flitting with child-like condescension)
But those are the numbers my finance guy gave me. It’s the benchmark.
(Blackout and end of Act I.)
Mutual Agreement
Tony Award-winning stuff for sure—and based on a true story! In fact, this scene no doubt plays out annually for those of you unfortunate enough to have to negotiate with hospital executives for programmatic support. To be fair, hospital administrators deserve to know that they are getting what they pay for. Thus, the concepts of a benchmark are reasonable. The problem lies in setting mutually-agreed-upon standards.
Act II: Disbelief and Confusion
GOOD-LOOKING ME
(Unsteadily hands document to Miser)
Sir, I’ve highlighted the national benchmarks for you to see. Column four of this 2007-2008 SHM survey clearly shows that the average academic hospitalist should make $168,800 and achieve 2,813 work RVUs. We achieve the latter benchmark but are severely underpaid.
MISER
(Produces a folded cocktail napkin from his shirt pocket)
But look at this: My executive-friends-at-other-medical-centers-who-overwork-and-underpay-their-hospitalists benchmark shows that you should be well over 4,500 work RVUs. And besides, the SHM numbers are skewed; it’s a survey of hospitalists done by a group that represents hospitalists. I don’t believe them.
GOOD-LOOKING ME
(Eyes averted, adopts a tone of trepidation)
But sir, with all due respect, don’t your numbers reflect a survey of hospital administrators who might have a bias toward more expected productivity? Which benchmark should we believe?
(Blackout and end of Act II.)
A New HM Benchmark Arises
It’s all about the benchmark you choose to believe. For years, the best source of data regarding hospitalist compensation and productivity was that published every other year by SHM. It is a fair, but unfounded, concern that these data might tilt toward the benefit of hospitalists. Likewise, the hospital administrator I work most closely with (who, for the record, reads this publication and IS NOT miserly, has a FULL HEAD of hair, and is, for innumerable reasons, a TRULY GREAT man) will produce benchmarks from organizations like the Association of American Medical Colleges (AAMC) or the University HealthSystems Consortium (UHC), all of which show surprisingly disparate numbers dripping with a similar tilt toward the medical center.
Thus, the importance of the 2010 SHM/MGMA report. The Medical Group Management Association (MGMA) consists of administrators and leaders of medical group practices. Since 1926, they’ve been providing accurate, independent data on physician practice metrics. For most hospital administrators, it is the benchmark. The problem is that in the past, MGMA has struggled to identify hospitalists; the MGMA data were always underpowered and, therefore, suspect.
Enter SHM and its large database of HM groups. What has resulted in the new survey rivals those old commercials in which a person walking with a piece of chocolate slams into another with a jar of peanut butter, resulting in the creation of the Reese’s Peanut Butter Cup (apologies to those readers under the age of 35).
Act III: No Raise; Children Go Hungry
GOOD-LOOKING ME
(Unsheathing haloed document from his portfolio)
Perhaps we could agree to use these new SHM/MGMA numbers as our benchmark. It includes data from more than 440 HM groups and 4,200 hospitalists. And it appears to be fair and balanced.
MISER
(Eyes alight, peering through a shroud of compromise)
MGMA, huh? Let’s take a look. Hmmm. Well. But wait—this says the average hospitalist makes $215,000! That’s outrageous.
GOOD-LOOKING ME
(Smugly retorts)
Yes, sir, we are severely underpaid.
MISER
(Reading; a weasel-like countenance overtakes his face)
Let me take a closer look at this. Aha! Here it is. You see, this only included community hospitalist practices. You will be getting no raise!
(Blackout and end of Act III.)
A Cautionary Tale
Alas, the miser is right. It’s not always what the data say but also what they don’t say.
The one snag with the new data is that it only included a handful of academic HM groups (only 1% of respondents). In fact, the survey actively instructed academic HM practices to not complete the survey. Rather, we academic types were instructed to await the MGMA survey of academic practices completed every fall to be reported early next year.
This is emblematic of the need to dig deep when interpreting these data. As tempting as it is to use a sound bite or two of these data to your advantage, the truth lies in the details. It’s easy to say that all hospitalists should make $215,000, see 2,229 encounters, and achieve 4,107 wRVUs annually.
However, just as there is no average hospitalist, there are no average numbers. There are just too many variables (e.g., practice ownership, geography, group size, night coverage, staffing model, compensation structure) to say definitively what an individual hospitalist should look like or achieve. Rather, these numbers should be used as a guide, adapted to each individual situation.
Act IV: See You This Spring
(Standing, Good-Looking Me shakes his foe’s shriveled claw of a hand while looking him intensely in the eye—a look that says, “I’ll see you this spring.” In his rival’s eyes, the Miser sees his future—a future that involves another meeting, more practice-appropriate data, and a dusting off of his checkbook.)
(Blackout and end of Act IV.) TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Act I: The Negotiation
(A barren academic office, dimly lit, the pall of difficult negotiations afloat, backlit like dust in the air. Seated, under a strangely intense incandescent bulb, a man, who looks eerily like a good-looking version of me, sits uncomfortably adjusting himself in his seat. His eyes constrict on his counterpart, a miserly sort peering out from behind wire-rim glasses and a shock of hair improbably combed over from ear to ear. The tension crests.)
GOOD-LOOKING ME
(Voice cracking)
I’ve come to ask for a raise for our hospitalist group.
MISER
(Adjusts his clip-on tie)
We just gave you a raise in 2004.
GOOD-LOOKING ME
(Smiles uncomfortably)
That was very gracious, sir, but I think the numbers support another.
MISER
(Incredulous look at his watch)
But your work RVUs are thousands below what I’d like to see.
GOOD-LOOKING ME
(Dabs bead of sweat away from chiseled chin)
That’s because you’ve set your benchmark thousands above a reasonable number.
MISER
(Voice flitting with child-like condescension)
But those are the numbers my finance guy gave me. It’s the benchmark.
(Blackout and end of Act I.)
Mutual Agreement
Tony Award-winning stuff for sure—and based on a true story! In fact, this scene no doubt plays out annually for those of you unfortunate enough to have to negotiate with hospital executives for programmatic support. To be fair, hospital administrators deserve to know that they are getting what they pay for. Thus, the concepts of a benchmark are reasonable. The problem lies in setting mutually-agreed-upon standards.
Act II: Disbelief and Confusion
GOOD-LOOKING ME
(Unsteadily hands document to Miser)
Sir, I’ve highlighted the national benchmarks for you to see. Column four of this 2007-2008 SHM survey clearly shows that the average academic hospitalist should make $168,800 and achieve 2,813 work RVUs. We achieve the latter benchmark but are severely underpaid.
MISER
(Produces a folded cocktail napkin from his shirt pocket)
But look at this: My executive-friends-at-other-medical-centers-who-overwork-and-underpay-their-hospitalists benchmark shows that you should be well over 4,500 work RVUs. And besides, the SHM numbers are skewed; it’s a survey of hospitalists done by a group that represents hospitalists. I don’t believe them.
GOOD-LOOKING ME
(Eyes averted, adopts a tone of trepidation)
But sir, with all due respect, don’t your numbers reflect a survey of hospital administrators who might have a bias toward more expected productivity? Which benchmark should we believe?
(Blackout and end of Act II.)
A New HM Benchmark Arises
It’s all about the benchmark you choose to believe. For years, the best source of data regarding hospitalist compensation and productivity was that published every other year by SHM. It is a fair, but unfounded, concern that these data might tilt toward the benefit of hospitalists. Likewise, the hospital administrator I work most closely with (who, for the record, reads this publication and IS NOT miserly, has a FULL HEAD of hair, and is, for innumerable reasons, a TRULY GREAT man) will produce benchmarks from organizations like the Association of American Medical Colleges (AAMC) or the University HealthSystems Consortium (UHC), all of which show surprisingly disparate numbers dripping with a similar tilt toward the medical center.
Thus, the importance of the 2010 SHM/MGMA report. The Medical Group Management Association (MGMA) consists of administrators and leaders of medical group practices. Since 1926, they’ve been providing accurate, independent data on physician practice metrics. For most hospital administrators, it is the benchmark. The problem is that in the past, MGMA has struggled to identify hospitalists; the MGMA data were always underpowered and, therefore, suspect.
Enter SHM and its large database of HM groups. What has resulted in the new survey rivals those old commercials in which a person walking with a piece of chocolate slams into another with a jar of peanut butter, resulting in the creation of the Reese’s Peanut Butter Cup (apologies to those readers under the age of 35).
Act III: No Raise; Children Go Hungry
GOOD-LOOKING ME
(Unsheathing haloed document from his portfolio)
Perhaps we could agree to use these new SHM/MGMA numbers as our benchmark. It includes data from more than 440 HM groups and 4,200 hospitalists. And it appears to be fair and balanced.
MISER
(Eyes alight, peering through a shroud of compromise)
MGMA, huh? Let’s take a look. Hmmm. Well. But wait—this says the average hospitalist makes $215,000! That’s outrageous.
GOOD-LOOKING ME
(Smugly retorts)
Yes, sir, we are severely underpaid.
MISER
(Reading; a weasel-like countenance overtakes his face)
Let me take a closer look at this. Aha! Here it is. You see, this only included community hospitalist practices. You will be getting no raise!
(Blackout and end of Act III.)
A Cautionary Tale
Alas, the miser is right. It’s not always what the data say but also what they don’t say.
The one snag with the new data is that it only included a handful of academic HM groups (only 1% of respondents). In fact, the survey actively instructed academic HM practices to not complete the survey. Rather, we academic types were instructed to await the MGMA survey of academic practices completed every fall to be reported early next year.
This is emblematic of the need to dig deep when interpreting these data. As tempting as it is to use a sound bite or two of these data to your advantage, the truth lies in the details. It’s easy to say that all hospitalists should make $215,000, see 2,229 encounters, and achieve 4,107 wRVUs annually.
However, just as there is no average hospitalist, there are no average numbers. There are just too many variables (e.g., practice ownership, geography, group size, night coverage, staffing model, compensation structure) to say definitively what an individual hospitalist should look like or achieve. Rather, these numbers should be used as a guide, adapted to each individual situation.
Act IV: See You This Spring
(Standing, Good-Looking Me shakes his foe’s shriveled claw of a hand while looking him intensely in the eye—a look that says, “I’ll see you this spring.” In his rival’s eyes, the Miser sees his future—a future that involves another meeting, more practice-appropriate data, and a dusting off of his checkbook.)
(Blackout and end of Act IV.) TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Act I: The Negotiation
(A barren academic office, dimly lit, the pall of difficult negotiations afloat, backlit like dust in the air. Seated, under a strangely intense incandescent bulb, a man, who looks eerily like a good-looking version of me, sits uncomfortably adjusting himself in his seat. His eyes constrict on his counterpart, a miserly sort peering out from behind wire-rim glasses and a shock of hair improbably combed over from ear to ear. The tension crests.)
GOOD-LOOKING ME
(Voice cracking)
I’ve come to ask for a raise for our hospitalist group.
MISER
(Adjusts his clip-on tie)
We just gave you a raise in 2004.
GOOD-LOOKING ME
(Smiles uncomfortably)
That was very gracious, sir, but I think the numbers support another.
MISER
(Incredulous look at his watch)
But your work RVUs are thousands below what I’d like to see.
GOOD-LOOKING ME
(Dabs bead of sweat away from chiseled chin)
That’s because you’ve set your benchmark thousands above a reasonable number.
MISER
(Voice flitting with child-like condescension)
But those are the numbers my finance guy gave me. It’s the benchmark.
(Blackout and end of Act I.)
Mutual Agreement
Tony Award-winning stuff for sure—and based on a true story! In fact, this scene no doubt plays out annually for those of you unfortunate enough to have to negotiate with hospital executives for programmatic support. To be fair, hospital administrators deserve to know that they are getting what they pay for. Thus, the concepts of a benchmark are reasonable. The problem lies in setting mutually-agreed-upon standards.
Act II: Disbelief and Confusion
GOOD-LOOKING ME
(Unsteadily hands document to Miser)
Sir, I’ve highlighted the national benchmarks for you to see. Column four of this 2007-2008 SHM survey clearly shows that the average academic hospitalist should make $168,800 and achieve 2,813 work RVUs. We achieve the latter benchmark but are severely underpaid.
MISER
(Produces a folded cocktail napkin from his shirt pocket)
But look at this: My executive-friends-at-other-medical-centers-who-overwork-and-underpay-their-hospitalists benchmark shows that you should be well over 4,500 work RVUs. And besides, the SHM numbers are skewed; it’s a survey of hospitalists done by a group that represents hospitalists. I don’t believe them.
GOOD-LOOKING ME
(Eyes averted, adopts a tone of trepidation)
But sir, with all due respect, don’t your numbers reflect a survey of hospital administrators who might have a bias toward more expected productivity? Which benchmark should we believe?
(Blackout and end of Act II.)
A New HM Benchmark Arises
It’s all about the benchmark you choose to believe. For years, the best source of data regarding hospitalist compensation and productivity was that published every other year by SHM. It is a fair, but unfounded, concern that these data might tilt toward the benefit of hospitalists. Likewise, the hospital administrator I work most closely with (who, for the record, reads this publication and IS NOT miserly, has a FULL HEAD of hair, and is, for innumerable reasons, a TRULY GREAT man) will produce benchmarks from organizations like the Association of American Medical Colleges (AAMC) or the University HealthSystems Consortium (UHC), all of which show surprisingly disparate numbers dripping with a similar tilt toward the medical center.
Thus, the importance of the 2010 SHM/MGMA report. The Medical Group Management Association (MGMA) consists of administrators and leaders of medical group practices. Since 1926, they’ve been providing accurate, independent data on physician practice metrics. For most hospital administrators, it is the benchmark. The problem is that in the past, MGMA has struggled to identify hospitalists; the MGMA data were always underpowered and, therefore, suspect.
Enter SHM and its large database of HM groups. What has resulted in the new survey rivals those old commercials in which a person walking with a piece of chocolate slams into another with a jar of peanut butter, resulting in the creation of the Reese’s Peanut Butter Cup (apologies to those readers under the age of 35).
Act III: No Raise; Children Go Hungry
GOOD-LOOKING ME
(Unsheathing haloed document from his portfolio)
Perhaps we could agree to use these new SHM/MGMA numbers as our benchmark. It includes data from more than 440 HM groups and 4,200 hospitalists. And it appears to be fair and balanced.
MISER
(Eyes alight, peering through a shroud of compromise)
MGMA, huh? Let’s take a look. Hmmm. Well. But wait—this says the average hospitalist makes $215,000! That’s outrageous.
GOOD-LOOKING ME
(Smugly retorts)
Yes, sir, we are severely underpaid.
MISER
(Reading; a weasel-like countenance overtakes his face)
Let me take a closer look at this. Aha! Here it is. You see, this only included community hospitalist practices. You will be getting no raise!
(Blackout and end of Act III.)
A Cautionary Tale
Alas, the miser is right. It’s not always what the data say but also what they don’t say.
The one snag with the new data is that it only included a handful of academic HM groups (only 1% of respondents). In fact, the survey actively instructed academic HM practices to not complete the survey. Rather, we academic types were instructed to await the MGMA survey of academic practices completed every fall to be reported early next year.
This is emblematic of the need to dig deep when interpreting these data. As tempting as it is to use a sound bite or two of these data to your advantage, the truth lies in the details. It’s easy to say that all hospitalists should make $215,000, see 2,229 encounters, and achieve 4,107 wRVUs annually.
However, just as there is no average hospitalist, there are no average numbers. There are just too many variables (e.g., practice ownership, geography, group size, night coverage, staffing model, compensation structure) to say definitively what an individual hospitalist should look like or achieve. Rather, these numbers should be used as a guide, adapted to each individual situation.
Act IV: See You This Spring
(Standing, Good-Looking Me shakes his foe’s shriveled claw of a hand while looking him intensely in the eye—a look that says, “I’ll see you this spring.” In his rival’s eyes, the Miser sees his future—a future that involves another meeting, more practice-appropriate data, and a dusting off of his checkbook.)
(Blackout and end of Act IV.) TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
Surge Protection

Unpredictable workloads and frequent interruptions are the things I regard as the most stressful components of work as a hospitalist. Your list might be very different, but I bet unpredictable workloads ranks at least in the top five of every hospitalist’s list.
I’ve discussed interruptions previously (see “Really, It’s Switch-Tasking,” p. 68, November 2008; “Technological Advance or Workplace Setback?” p. 69, December 2008), but this month and next will turn to unpredictable workloads. In other words, what are the strategies available to a hospitalist practice to provide surge capacity in response to such unpredictable increases in patient volume as an uptick in census or daily admissions 50% to 100% above normal? I’ll leave to others the topic of how hospitals respond to such disasters as terrorist attacks, earthquakes, etc.
The Bottom Line
Sadly, there is no magic bullet for the “surge” problem, and no way to protect on-duty hospitalists from the need to work harder when it gets busy. But we needn’t feel too sorry for ourselves; doctors in most other specialties who practice in the hospital face the same problem and tend to rely heavily on simply working harder and longer when it is unusually busy. Sometimes they couple the “work harder” mantra with other strategies, such as calling another doctor in to help.
Hospitalists have a duty to ensure high patient volume doesn’t lead to deterioration in the quality of patient care, but occasionally working longer days than average probably poses a low risk, and might be less risky than the additional handoffs usually associated with having a doctor on “jeopardy” to be called in when it’s busy. Routinely or frequently working unreasonably long days is another story.
The trick for HM programs is to build some surge capacity into the routine daily staffing 1) without exceeding a reasonable budget, while 2) ensuring that the hospitalists don’t simply become accustomed to light workloads as the only reasonable norm, which could lead to them becoming unwilling to accept higher, but still reasonable, workloads when needed. (More on these issues later.) First, I’ll go through what I see as the pros and cons of several approaches to addressing surges in patient volume. All are in use with variable frequency around the country.
“Jeopardy” System
In its most common form, a jeopardy system has an unscheduled doctor each day who must remain available on short notice by pager. When patient volume surges, the unscheduled doctor is paged to come in and help. In most cases, this doctor focuses primarily—or exclusively—on admitting patients for a few hours. So it is most common for this doctor to be called in late in the afternoon or early in the evening. The jeopardy doctor usually turns over all admitted patients to another hospitalist in the group for all subsequent care. In addition to providing surge capacity, the jeopardy doctor almost always is used to cover unexpected absences of scheduled doctors, including illness-related absences.
Sometimes this doctor is paid extra for each day or week spent being “available” on jeopardy duty (not to be confused with jury duty, though it can be equally difficult to get exempted from). Then again, it is not uncommon to have jeopardy duty included in base compensation. However, once a jeopardy doctor is actually called in to work, most practices pay additional compensation, often based on an hourly rate that usually is higher than the average compensation generated per hour for nonjeopardy work.
There are a number of reasonable ways to compensate the jeopardy doctor. You probably can get some good ideas by talking with others in your hospital who function in a similar capacity, such as cath-lab technicians who get called in on nights and weekends.
No definitive data are available to show how common the jeopardy system is, but my experience is that 30% to 50% of HM groups use some form of it. Its popularity is proof that it is a reasonable system, but I’m not convinced. I think it is in use by a lot of groups not because it is an optimal way to ensure surge capacity, but because it is easy to conceptualize and put in place, and because many hospitalists came from residency programs in which the system was standard.
The gaps between theoretical and realized benefits become evident once a practice implements a jeopardy system. For example, it might be really busy today, but Dr. Stravinsky doesn’t call in Dr. Copeland, who is on jeopardy, because next week their roles will be reversed and Dr. Stravinsky sure hopes he won’t be called in. No one wants to be the weak doctor who calls in the jeopardy doctor and spoils what was otherwise a day off.
I’ve worked with a lot of practices who say they have a jeopardy system in place, but when I ask for the last time the jeopardy doctor was called in, they say it has been more than a year, or in some cases never. So even if the policy manual says they have a jeopardy system, the doctors never activate it, so it provides no benefit.
Practices that do utilize the jeopardy doctor have their own problems, such as assigning that doctor’s admissions the next day. The jeopardy doctor might provide some relief today, but they essentially just delay the work of having to get to know all of those new patients until the morning, when everyone is very busy with rounds. So while there might be significant benefit in activating the jeopardy system today, it could just delay the problem of high workload until the next morning, which isn’t much of a net benefit for the practice.
A small number of practices call in the jeopardy doctor frequently, and sometimes have that doctor continue to round on admitted patients for the next few days. This usage might get the most value out of the system, but the practice should consider if it is more cost-effective, and less stressful for the doctors, if the system were reversed. For example, instead of having the doctor on jeopardy and called in as necessary, the doctor would report to work and be given the day off or let go early when it isn’t busy.
Despite my reservations, if you are convinced the jeopardy system is valuable and cost-effective, keep it in place. However, if your group is thinking about options to handle surge capacity, don’t be too quick to adopt a jeopardy system. It usually falls far short of a perfect solution.
Patient Volume Cap
Another way to address the problem of unpredictable increases in patient volume is to establish a patient volume (e.g., total census) cap for the whole hospitalist practice. Like the jeopardy system, this is an appealingly uncomplicated idea, and hospitalists who have finished residency within the last few years all worked with a cap.
Except for the rarest of exceptions, this is a poor idea and should be avoided if at all possible. I’ll leave for another time a discussion of all the political and financial costs of a cap system, but trust me on this one. It is best to avoid a cap.
Stay Tuned …
Next month, I’ll examine other strategies to provide surge capacity. I think they’re more valuable than the two I’ve mentioned here, but I need to warn you that they aren’t perfect and are more complicated to operationalize. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Unpredictable workloads and frequent interruptions are the things I regard as the most stressful components of work as a hospitalist. Your list might be very different, but I bet unpredictable workloads ranks at least in the top five of every hospitalist’s list.
I’ve discussed interruptions previously (see “Really, It’s Switch-Tasking,” p. 68, November 2008; “Technological Advance or Workplace Setback?” p. 69, December 2008), but this month and next will turn to unpredictable workloads. In other words, what are the strategies available to a hospitalist practice to provide surge capacity in response to such unpredictable increases in patient volume as an uptick in census or daily admissions 50% to 100% above normal? I’ll leave to others the topic of how hospitals respond to such disasters as terrorist attacks, earthquakes, etc.
The Bottom Line
Sadly, there is no magic bullet for the “surge” problem, and no way to protect on-duty hospitalists from the need to work harder when it gets busy. But we needn’t feel too sorry for ourselves; doctors in most other specialties who practice in the hospital face the same problem and tend to rely heavily on simply working harder and longer when it is unusually busy. Sometimes they couple the “work harder” mantra with other strategies, such as calling another doctor in to help.
Hospitalists have a duty to ensure high patient volume doesn’t lead to deterioration in the quality of patient care, but occasionally working longer days than average probably poses a low risk, and might be less risky than the additional handoffs usually associated with having a doctor on “jeopardy” to be called in when it’s busy. Routinely or frequently working unreasonably long days is another story.
The trick for HM programs is to build some surge capacity into the routine daily staffing 1) without exceeding a reasonable budget, while 2) ensuring that the hospitalists don’t simply become accustomed to light workloads as the only reasonable norm, which could lead to them becoming unwilling to accept higher, but still reasonable, workloads when needed. (More on these issues later.) First, I’ll go through what I see as the pros and cons of several approaches to addressing surges in patient volume. All are in use with variable frequency around the country.
“Jeopardy” System
In its most common form, a jeopardy system has an unscheduled doctor each day who must remain available on short notice by pager. When patient volume surges, the unscheduled doctor is paged to come in and help. In most cases, this doctor focuses primarily—or exclusively—on admitting patients for a few hours. So it is most common for this doctor to be called in late in the afternoon or early in the evening. The jeopardy doctor usually turns over all admitted patients to another hospitalist in the group for all subsequent care. In addition to providing surge capacity, the jeopardy doctor almost always is used to cover unexpected absences of scheduled doctors, including illness-related absences.
Sometimes this doctor is paid extra for each day or week spent being “available” on jeopardy duty (not to be confused with jury duty, though it can be equally difficult to get exempted from). Then again, it is not uncommon to have jeopardy duty included in base compensation. However, once a jeopardy doctor is actually called in to work, most practices pay additional compensation, often based on an hourly rate that usually is higher than the average compensation generated per hour for nonjeopardy work.
There are a number of reasonable ways to compensate the jeopardy doctor. You probably can get some good ideas by talking with others in your hospital who function in a similar capacity, such as cath-lab technicians who get called in on nights and weekends.
No definitive data are available to show how common the jeopardy system is, but my experience is that 30% to 50% of HM groups use some form of it. Its popularity is proof that it is a reasonable system, but I’m not convinced. I think it is in use by a lot of groups not because it is an optimal way to ensure surge capacity, but because it is easy to conceptualize and put in place, and because many hospitalists came from residency programs in which the system was standard.
The gaps between theoretical and realized benefits become evident once a practice implements a jeopardy system. For example, it might be really busy today, but Dr. Stravinsky doesn’t call in Dr. Copeland, who is on jeopardy, because next week their roles will be reversed and Dr. Stravinsky sure hopes he won’t be called in. No one wants to be the weak doctor who calls in the jeopardy doctor and spoils what was otherwise a day off.
I’ve worked with a lot of practices who say they have a jeopardy system in place, but when I ask for the last time the jeopardy doctor was called in, they say it has been more than a year, or in some cases never. So even if the policy manual says they have a jeopardy system, the doctors never activate it, so it provides no benefit.
Practices that do utilize the jeopardy doctor have their own problems, such as assigning that doctor’s admissions the next day. The jeopardy doctor might provide some relief today, but they essentially just delay the work of having to get to know all of those new patients until the morning, when everyone is very busy with rounds. So while there might be significant benefit in activating the jeopardy system today, it could just delay the problem of high workload until the next morning, which isn’t much of a net benefit for the practice.
A small number of practices call in the jeopardy doctor frequently, and sometimes have that doctor continue to round on admitted patients for the next few days. This usage might get the most value out of the system, but the practice should consider if it is more cost-effective, and less stressful for the doctors, if the system were reversed. For example, instead of having the doctor on jeopardy and called in as necessary, the doctor would report to work and be given the day off or let go early when it isn’t busy.
Despite my reservations, if you are convinced the jeopardy system is valuable and cost-effective, keep it in place. However, if your group is thinking about options to handle surge capacity, don’t be too quick to adopt a jeopardy system. It usually falls far short of a perfect solution.
Patient Volume Cap
Another way to address the problem of unpredictable increases in patient volume is to establish a patient volume (e.g., total census) cap for the whole hospitalist practice. Like the jeopardy system, this is an appealingly uncomplicated idea, and hospitalists who have finished residency within the last few years all worked with a cap.
Except for the rarest of exceptions, this is a poor idea and should be avoided if at all possible. I’ll leave for another time a discussion of all the political and financial costs of a cap system, but trust me on this one. It is best to avoid a cap.
Stay Tuned …
Next month, I’ll examine other strategies to provide surge capacity. I think they’re more valuable than the two I’ve mentioned here, but I need to warn you that they aren’t perfect and are more complicated to operationalize. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Unpredictable workloads and frequent interruptions are the things I regard as the most stressful components of work as a hospitalist. Your list might be very different, but I bet unpredictable workloads ranks at least in the top five of every hospitalist’s list.
I’ve discussed interruptions previously (see “Really, It’s Switch-Tasking,” p. 68, November 2008; “Technological Advance or Workplace Setback?” p. 69, December 2008), but this month and next will turn to unpredictable workloads. In other words, what are the strategies available to a hospitalist practice to provide surge capacity in response to such unpredictable increases in patient volume as an uptick in census or daily admissions 50% to 100% above normal? I’ll leave to others the topic of how hospitals respond to such disasters as terrorist attacks, earthquakes, etc.
The Bottom Line
Sadly, there is no magic bullet for the “surge” problem, and no way to protect on-duty hospitalists from the need to work harder when it gets busy. But we needn’t feel too sorry for ourselves; doctors in most other specialties who practice in the hospital face the same problem and tend to rely heavily on simply working harder and longer when it is unusually busy. Sometimes they couple the “work harder” mantra with other strategies, such as calling another doctor in to help.
Hospitalists have a duty to ensure high patient volume doesn’t lead to deterioration in the quality of patient care, but occasionally working longer days than average probably poses a low risk, and might be less risky than the additional handoffs usually associated with having a doctor on “jeopardy” to be called in when it’s busy. Routinely or frequently working unreasonably long days is another story.
The trick for HM programs is to build some surge capacity into the routine daily staffing 1) without exceeding a reasonable budget, while 2) ensuring that the hospitalists don’t simply become accustomed to light workloads as the only reasonable norm, which could lead to them becoming unwilling to accept higher, but still reasonable, workloads when needed. (More on these issues later.) First, I’ll go through what I see as the pros and cons of several approaches to addressing surges in patient volume. All are in use with variable frequency around the country.
“Jeopardy” System
In its most common form, a jeopardy system has an unscheduled doctor each day who must remain available on short notice by pager. When patient volume surges, the unscheduled doctor is paged to come in and help. In most cases, this doctor focuses primarily—or exclusively—on admitting patients for a few hours. So it is most common for this doctor to be called in late in the afternoon or early in the evening. The jeopardy doctor usually turns over all admitted patients to another hospitalist in the group for all subsequent care. In addition to providing surge capacity, the jeopardy doctor almost always is used to cover unexpected absences of scheduled doctors, including illness-related absences.
Sometimes this doctor is paid extra for each day or week spent being “available” on jeopardy duty (not to be confused with jury duty, though it can be equally difficult to get exempted from). Then again, it is not uncommon to have jeopardy duty included in base compensation. However, once a jeopardy doctor is actually called in to work, most practices pay additional compensation, often based on an hourly rate that usually is higher than the average compensation generated per hour for nonjeopardy work.
There are a number of reasonable ways to compensate the jeopardy doctor. You probably can get some good ideas by talking with others in your hospital who function in a similar capacity, such as cath-lab technicians who get called in on nights and weekends.
No definitive data are available to show how common the jeopardy system is, but my experience is that 30% to 50% of HM groups use some form of it. Its popularity is proof that it is a reasonable system, but I’m not convinced. I think it is in use by a lot of groups not because it is an optimal way to ensure surge capacity, but because it is easy to conceptualize and put in place, and because many hospitalists came from residency programs in which the system was standard.
The gaps between theoretical and realized benefits become evident once a practice implements a jeopardy system. For example, it might be really busy today, but Dr. Stravinsky doesn’t call in Dr. Copeland, who is on jeopardy, because next week their roles will be reversed and Dr. Stravinsky sure hopes he won’t be called in. No one wants to be the weak doctor who calls in the jeopardy doctor and spoils what was otherwise a day off.
I’ve worked with a lot of practices who say they have a jeopardy system in place, but when I ask for the last time the jeopardy doctor was called in, they say it has been more than a year, or in some cases never. So even if the policy manual says they have a jeopardy system, the doctors never activate it, so it provides no benefit.
Practices that do utilize the jeopardy doctor have their own problems, such as assigning that doctor’s admissions the next day. The jeopardy doctor might provide some relief today, but they essentially just delay the work of having to get to know all of those new patients until the morning, when everyone is very busy with rounds. So while there might be significant benefit in activating the jeopardy system today, it could just delay the problem of high workload until the next morning, which isn’t much of a net benefit for the practice.
A small number of practices call in the jeopardy doctor frequently, and sometimes have that doctor continue to round on admitted patients for the next few days. This usage might get the most value out of the system, but the practice should consider if it is more cost-effective, and less stressful for the doctors, if the system were reversed. For example, instead of having the doctor on jeopardy and called in as necessary, the doctor would report to work and be given the day off or let go early when it isn’t busy.
Despite my reservations, if you are convinced the jeopardy system is valuable and cost-effective, keep it in place. However, if your group is thinking about options to handle surge capacity, don’t be too quick to adopt a jeopardy system. It usually falls far short of a perfect solution.
Patient Volume Cap
Another way to address the problem of unpredictable increases in patient volume is to establish a patient volume (e.g., total census) cap for the whole hospitalist practice. Like the jeopardy system, this is an appealingly uncomplicated idea, and hospitalists who have finished residency within the last few years all worked with a cap.
Except for the rarest of exceptions, this is a poor idea and should be avoided if at all possible. I’ll leave for another time a discussion of all the political and financial costs of a cap system, but trust me on this one. It is best to avoid a cap.
Stay Tuned …
Next month, I’ll examine other strategies to provide surge capacity. I think they’re more valuable than the two I’ve mentioned here, but I need to warn you that they aren’t perfect and are more complicated to operationalize. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.