User login
ONLINE EXCLUSIVE: Audio interview with Troy Ahlstrom, MD, FHM, CFO of Hospitalists of Northern Michigan
SHM Practice Analysis Committee member Troy Ahlstrom, MD, FHM, discusses the new compensation and productivity report, and gives advice on how best to use benchmarking data in your practice.
SHM Practice Analysis Committee member Troy Ahlstrom, MD, FHM, discusses the new compensation and productivity report, and gives advice on how best to use benchmarking data in your practice.
SHM Practice Analysis Committee member Troy Ahlstrom, MD, FHM, discusses the new compensation and productivity report, and gives advice on how best to use benchmarking data in your practice.
Rectal mucosa found in vaginal cuff closure…and more…
Rectal mucosa found in vaginal cuff closure
3 DAYS AFTER A HYSTERECTOMY by her ObGyn, a woman reported increasing pain. At an exploratory laparotomy, surgeons found serosanguineous pelvic fluid, partial dehiscence of the vaginal cuff with necrotic edges, and a suture line incorporating the anterior rectal wall in the vaginal cuff repair. They removed the sutures and repaired the vaginal cuff and several lacerations on the anterior rectal wall.
PATIENT’S CLAIM The ObGyn should have used peritoneal tissue to repair the vaginal cuff. Failure to do so caused lacerations and injuries to the anterior rectal wall and rectum.
PHYSICIAN’S DEFENSE The ObGyn denied negligence.
VERDICT A $3 million Virginia verdict was returned.
Colon injured when trocar is inserted
DIAGNOSTIC LAPAROSCOPY was performed on a 27-year-old woman to find the cause of rectal bleeding and pelvic pain. The ObGyn perforated her colon with the trocar; he immediately converted to laparotomy. The patient had a colostomy for 3 months, then developed paralytic ileus, small bowel obstruction, and incisional hernias. She required surgery for colostomy removal and hernia repair. It was later found that irritable bowel syndrome had caused the bleeding.
PLAINTIFF’S CLAIM Surgery was unnecessary; conservative treatment should have been tried first. The ObGyn blindly inserted the trocar instead of insufflating the abdomen with CO2.
PHYSICIAN’S DEFENSE Laparoscopy was appropriate for the patient’s symptoms; insufflation was used. The patient’s transverse colon was lowlying (below the navel) rather than normal (above the navel), causing it to be in the way of the trocar. The patient had a good recovery and returned to good function.
VERDICT An Illinois verdict of $550,500 was returned.
Late cesarean blamed for newborn’s CP
A WOMAN WITH PREECLAMPSIA was admitted to the hospital. When her membranes ruptured, oxytocin and magnesium sulfate were started. After several hours, she was only dilated to 5 cm. The fetal monitor showed normal baseline, but minimal variability with virtually no accelerations.
Hours later, when she was fully dilated, the ObGyn instructed the nurse to have her push and then went to his office. Immediately upon pushing, late fetal heart rate decelerations developed with every contraction. When the ObGyn returned 30 minutes later, he allowed pushing to continue. A resident attempted forceps delivery, but the forceps slipped several times. The ObGyn reapplied the forceps twice, then allowed the resident to apply vacuum. When the baby presented with shoulder dystocia, the ObGyn stepped in. The child was born with low cord blood pH and multiple skull fractures, and was given a diagnosis of cerebral palsy.
PATIENT’S CLAIM The ObGyn should have performed a cesarean when the fetal heart tracing became nonreassuring.
The child suffered CP because of distress during labor and delivery; a sinus venous thrombosis was never present. The baby’s skull fractures were due to improper use of forceps.
PHYSICIAN’S DEFENSE The skull fractures could have occurred in normal delivery. Because the child did not have spastic quadriplegic CP, the injury was most likely from sinus venous thrombosis.
VERDICT A Wisconsin jury returned a $23.2 million verdict; the court added $187,402 in medical expenses.
OB exonerated following brachial plexus injury
WHEN SHOULDER DYSTOCIA occurred during delivery, the ObGyn performed a McRoberts maneuver and episiotomy; the baby was delivered in 3 minutes. She suffered C5–8 brachial plexus palsy, deformity of the right arm and hand, and limited use of her right hand.
She later had tendon transfer surgery to improve range of motion of her wrist, and tendon release surgery on her shoulder.
PLAINTIFF’S CLAIM Excessive traction to the head and neck and failure to use additional shoulder dystocia maneuvers caused the injury.
PHYSICIAN’S DEFENSE The maneuvers performed were appropriate. The injury was due to natural forces of labor. The baby was delivered easily in less than a minute after using proper techniques. No excessive traction or other maneuvers were needed.
VERDICT An Illinois defense verdict was returned.
Did ovarian remnant + HRT cause DVT and pain?
A 33-YEAR-OLD WOMAN underwent a hysterectomy with salpingo-oophorectomy. Her ObGyn then prescribed hormone replacement therapy (HRT). Although pathology reported the left ovary and fallopian tube were not part of postoperative specimens, the ObGyn maintained that both ovaries and fallopian tubes had been removed. Ten months later, a CT scan revealed a pelvic neoplasm. No mass was found at exploratory surgery, but adhesions were lysed. Eighteen months later, an MRI revealed remnants of the left ovary and fallopian tube. Another gynecologist determined that the ovary was producing estrogen. Two months later, the patient developed deep vein thrombosis (DVT) in her left calf. The obstruction was resolved, but the patient reported residual leg pain.
PATIENT’S CLAIM Excessive levels of estrogen caused the DVT. The ObGyn was negligent in disregarding the initial pathologist’s report. It was inappropriate to prescribe HRT if ovarian function was present after surgery.
PHYSICIAN’S DEFENSE There was no negligence. Dense adhesions and a previous bowel perforation did not allow total ovary removal. The remnant is a known risk of the procedure. Estrogen HRT was appropriately administered.
VERDICT A New York defense verdict was returned.
Severing uterosacral ligament relieved pelvic pain, but…
AFTER CONSERVATIVE THERAPY for several months, a 26-year-old woman underwent exploratory laparoscopy to determine the reason for her severe pelvic pain. Findings were negative, but the physician transected the uterosacral ligament to relieve pain. Four days after surgery, a ureteral injury was diagnosed, and a stent was placed. The patient required complex treatment for her urinary tract injury.
PATIENT’S CLAIM Severing the uterosacral ligament was performed without her consent. The ureter injury was caused by negligent use of electrocauterization. Now the patient was at high risk for future pregnancies.
PHYSICIAN’S DEFENSE The patient’s pain warranted surgery; severing the ligament was appropriate. Injury to the ureter is a known complication.
VERDICT A Tennessee defense verdict was returned.
Why did it take so long to stop her bleeding?
AFTER DELIVERING HER THIRD CHILD, a 34-year-old woman reported significant vaginal bleeding to her ObGyn. Two weeks later, a sonogram was performed but the cause of bleeding was undetermined.
Bleeding continued. Sixteen days later, another sonogram revealed a 2-cm-long mass in the uterine cavity. The ObGyn decided to wait 4 or 5 days for another sonogram to make sure the mass wasn’t a fibroid or placental remnant.
The next evening, the patient was admitted to a hospital with excessive bleeding. The ObGyn performed a hysteroscopy and found a fibroid and a placental remnant. After tissue was removed by dilation and curettage (D&C), the ObGyn reinserted the hysteroscope. She encountered severe bleeding but could not find any other suspicious matter. Pathology reported that the excised material was placental tissue. The patient was hospitalized for 2 more days.
Three days later, she returned to the ObGyn with continued bleeding; the ObGyn determined it was post-D&C bleeding.
Two weeks later, the woman suffered severe vaginal hemorrhage. She went to another hospital where the ED physician felt the woman’s life was in jeopardy. A hysterectomy was performed, including the extraction of a placental fragment determined to be the cause of the hemorrhage.
PATIENT’S CLAIM The ObGyn was negligent in not diagnosing and treating the bleeding in a timely way after the first sonogram. The pathology report after D&C confirmed placental accreta, which should have prompted aggressive evaluation. Hysteroscopy and D&C did not effectively remove the deeply implanted placenta. She should not have been discharged from the hospital until the ObGyn had confirmed full removal of any placental remnants. Continued bleeding after D&C should have elicited further evaluation.
PHYSICIAN’S DEFENSE All the patient’s reports of bleeding were quickly and appropriately addressed. The ObGyn denied being told that the patient was still bleeding heavily until 16 days following the first sonogram. It was reasonable to conclude that the D&C had excised all suspicious matters. Post-D&C bleeding was due to an intraoperative laceration of the cervix; medication and a clamp had halted bleeding. Intraoperative bleeding made failure to remove the placental remnant reasonable. Earlier treatment would not have changed the outcome.
VERDICT A New York jury returned a $625,000 verdict.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
Rectal mucosa found in vaginal cuff closure
3 DAYS AFTER A HYSTERECTOMY by her ObGyn, a woman reported increasing pain. At an exploratory laparotomy, surgeons found serosanguineous pelvic fluid, partial dehiscence of the vaginal cuff with necrotic edges, and a suture line incorporating the anterior rectal wall in the vaginal cuff repair. They removed the sutures and repaired the vaginal cuff and several lacerations on the anterior rectal wall.
PATIENT’S CLAIM The ObGyn should have used peritoneal tissue to repair the vaginal cuff. Failure to do so caused lacerations and injuries to the anterior rectal wall and rectum.
PHYSICIAN’S DEFENSE The ObGyn denied negligence.
VERDICT A $3 million Virginia verdict was returned.
Colon injured when trocar is inserted
DIAGNOSTIC LAPAROSCOPY was performed on a 27-year-old woman to find the cause of rectal bleeding and pelvic pain. The ObGyn perforated her colon with the trocar; he immediately converted to laparotomy. The patient had a colostomy for 3 months, then developed paralytic ileus, small bowel obstruction, and incisional hernias. She required surgery for colostomy removal and hernia repair. It was later found that irritable bowel syndrome had caused the bleeding.
PLAINTIFF’S CLAIM Surgery was unnecessary; conservative treatment should have been tried first. The ObGyn blindly inserted the trocar instead of insufflating the abdomen with CO2.
PHYSICIAN’S DEFENSE Laparoscopy was appropriate for the patient’s symptoms; insufflation was used. The patient’s transverse colon was lowlying (below the navel) rather than normal (above the navel), causing it to be in the way of the trocar. The patient had a good recovery and returned to good function.
VERDICT An Illinois verdict of $550,500 was returned.
Late cesarean blamed for newborn’s CP
A WOMAN WITH PREECLAMPSIA was admitted to the hospital. When her membranes ruptured, oxytocin and magnesium sulfate were started. After several hours, she was only dilated to 5 cm. The fetal monitor showed normal baseline, but minimal variability with virtually no accelerations.
Hours later, when she was fully dilated, the ObGyn instructed the nurse to have her push and then went to his office. Immediately upon pushing, late fetal heart rate decelerations developed with every contraction. When the ObGyn returned 30 minutes later, he allowed pushing to continue. A resident attempted forceps delivery, but the forceps slipped several times. The ObGyn reapplied the forceps twice, then allowed the resident to apply vacuum. When the baby presented with shoulder dystocia, the ObGyn stepped in. The child was born with low cord blood pH and multiple skull fractures, and was given a diagnosis of cerebral palsy.
PATIENT’S CLAIM The ObGyn should have performed a cesarean when the fetal heart tracing became nonreassuring.
The child suffered CP because of distress during labor and delivery; a sinus venous thrombosis was never present. The baby’s skull fractures were due to improper use of forceps.
PHYSICIAN’S DEFENSE The skull fractures could have occurred in normal delivery. Because the child did not have spastic quadriplegic CP, the injury was most likely from sinus venous thrombosis.
VERDICT A Wisconsin jury returned a $23.2 million verdict; the court added $187,402 in medical expenses.
OB exonerated following brachial plexus injury
WHEN SHOULDER DYSTOCIA occurred during delivery, the ObGyn performed a McRoberts maneuver and episiotomy; the baby was delivered in 3 minutes. She suffered C5–8 brachial plexus palsy, deformity of the right arm and hand, and limited use of her right hand.
She later had tendon transfer surgery to improve range of motion of her wrist, and tendon release surgery on her shoulder.
PLAINTIFF’S CLAIM Excessive traction to the head and neck and failure to use additional shoulder dystocia maneuvers caused the injury.
PHYSICIAN’S DEFENSE The maneuvers performed were appropriate. The injury was due to natural forces of labor. The baby was delivered easily in less than a minute after using proper techniques. No excessive traction or other maneuvers were needed.
VERDICT An Illinois defense verdict was returned.
Did ovarian remnant + HRT cause DVT and pain?
A 33-YEAR-OLD WOMAN underwent a hysterectomy with salpingo-oophorectomy. Her ObGyn then prescribed hormone replacement therapy (HRT). Although pathology reported the left ovary and fallopian tube were not part of postoperative specimens, the ObGyn maintained that both ovaries and fallopian tubes had been removed. Ten months later, a CT scan revealed a pelvic neoplasm. No mass was found at exploratory surgery, but adhesions were lysed. Eighteen months later, an MRI revealed remnants of the left ovary and fallopian tube. Another gynecologist determined that the ovary was producing estrogen. Two months later, the patient developed deep vein thrombosis (DVT) in her left calf. The obstruction was resolved, but the patient reported residual leg pain.
PATIENT’S CLAIM Excessive levels of estrogen caused the DVT. The ObGyn was negligent in disregarding the initial pathologist’s report. It was inappropriate to prescribe HRT if ovarian function was present after surgery.
PHYSICIAN’S DEFENSE There was no negligence. Dense adhesions and a previous bowel perforation did not allow total ovary removal. The remnant is a known risk of the procedure. Estrogen HRT was appropriately administered.
VERDICT A New York defense verdict was returned.
Severing uterosacral ligament relieved pelvic pain, but…
AFTER CONSERVATIVE THERAPY for several months, a 26-year-old woman underwent exploratory laparoscopy to determine the reason for her severe pelvic pain. Findings were negative, but the physician transected the uterosacral ligament to relieve pain. Four days after surgery, a ureteral injury was diagnosed, and a stent was placed. The patient required complex treatment for her urinary tract injury.
PATIENT’S CLAIM Severing the uterosacral ligament was performed without her consent. The ureter injury was caused by negligent use of electrocauterization. Now the patient was at high risk for future pregnancies.
PHYSICIAN’S DEFENSE The patient’s pain warranted surgery; severing the ligament was appropriate. Injury to the ureter is a known complication.
VERDICT A Tennessee defense verdict was returned.
Why did it take so long to stop her bleeding?
AFTER DELIVERING HER THIRD CHILD, a 34-year-old woman reported significant vaginal bleeding to her ObGyn. Two weeks later, a sonogram was performed but the cause of bleeding was undetermined.
Bleeding continued. Sixteen days later, another sonogram revealed a 2-cm-long mass in the uterine cavity. The ObGyn decided to wait 4 or 5 days for another sonogram to make sure the mass wasn’t a fibroid or placental remnant.
The next evening, the patient was admitted to a hospital with excessive bleeding. The ObGyn performed a hysteroscopy and found a fibroid and a placental remnant. After tissue was removed by dilation and curettage (D&C), the ObGyn reinserted the hysteroscope. She encountered severe bleeding but could not find any other suspicious matter. Pathology reported that the excised material was placental tissue. The patient was hospitalized for 2 more days.
Three days later, she returned to the ObGyn with continued bleeding; the ObGyn determined it was post-D&C bleeding.
Two weeks later, the woman suffered severe vaginal hemorrhage. She went to another hospital where the ED physician felt the woman’s life was in jeopardy. A hysterectomy was performed, including the extraction of a placental fragment determined to be the cause of the hemorrhage.
PATIENT’S CLAIM The ObGyn was negligent in not diagnosing and treating the bleeding in a timely way after the first sonogram. The pathology report after D&C confirmed placental accreta, which should have prompted aggressive evaluation. Hysteroscopy and D&C did not effectively remove the deeply implanted placenta. She should not have been discharged from the hospital until the ObGyn had confirmed full removal of any placental remnants. Continued bleeding after D&C should have elicited further evaluation.
PHYSICIAN’S DEFENSE All the patient’s reports of bleeding were quickly and appropriately addressed. The ObGyn denied being told that the patient was still bleeding heavily until 16 days following the first sonogram. It was reasonable to conclude that the D&C had excised all suspicious matters. Post-D&C bleeding was due to an intraoperative laceration of the cervix; medication and a clamp had halted bleeding. Intraoperative bleeding made failure to remove the placental remnant reasonable. Earlier treatment would not have changed the outcome.
VERDICT A New York jury returned a $625,000 verdict.
Rectal mucosa found in vaginal cuff closure
3 DAYS AFTER A HYSTERECTOMY by her ObGyn, a woman reported increasing pain. At an exploratory laparotomy, surgeons found serosanguineous pelvic fluid, partial dehiscence of the vaginal cuff with necrotic edges, and a suture line incorporating the anterior rectal wall in the vaginal cuff repair. They removed the sutures and repaired the vaginal cuff and several lacerations on the anterior rectal wall.
PATIENT’S CLAIM The ObGyn should have used peritoneal tissue to repair the vaginal cuff. Failure to do so caused lacerations and injuries to the anterior rectal wall and rectum.
PHYSICIAN’S DEFENSE The ObGyn denied negligence.
VERDICT A $3 million Virginia verdict was returned.
Colon injured when trocar is inserted
DIAGNOSTIC LAPAROSCOPY was performed on a 27-year-old woman to find the cause of rectal bleeding and pelvic pain. The ObGyn perforated her colon with the trocar; he immediately converted to laparotomy. The patient had a colostomy for 3 months, then developed paralytic ileus, small bowel obstruction, and incisional hernias. She required surgery for colostomy removal and hernia repair. It was later found that irritable bowel syndrome had caused the bleeding.
PLAINTIFF’S CLAIM Surgery was unnecessary; conservative treatment should have been tried first. The ObGyn blindly inserted the trocar instead of insufflating the abdomen with CO2.
PHYSICIAN’S DEFENSE Laparoscopy was appropriate for the patient’s symptoms; insufflation was used. The patient’s transverse colon was lowlying (below the navel) rather than normal (above the navel), causing it to be in the way of the trocar. The patient had a good recovery and returned to good function.
VERDICT An Illinois verdict of $550,500 was returned.
Late cesarean blamed for newborn’s CP
A WOMAN WITH PREECLAMPSIA was admitted to the hospital. When her membranes ruptured, oxytocin and magnesium sulfate were started. After several hours, she was only dilated to 5 cm. The fetal monitor showed normal baseline, but minimal variability with virtually no accelerations.
Hours later, when she was fully dilated, the ObGyn instructed the nurse to have her push and then went to his office. Immediately upon pushing, late fetal heart rate decelerations developed with every contraction. When the ObGyn returned 30 minutes later, he allowed pushing to continue. A resident attempted forceps delivery, but the forceps slipped several times. The ObGyn reapplied the forceps twice, then allowed the resident to apply vacuum. When the baby presented with shoulder dystocia, the ObGyn stepped in. The child was born with low cord blood pH and multiple skull fractures, and was given a diagnosis of cerebral palsy.
PATIENT’S CLAIM The ObGyn should have performed a cesarean when the fetal heart tracing became nonreassuring.
The child suffered CP because of distress during labor and delivery; a sinus venous thrombosis was never present. The baby’s skull fractures were due to improper use of forceps.
PHYSICIAN’S DEFENSE The skull fractures could have occurred in normal delivery. Because the child did not have spastic quadriplegic CP, the injury was most likely from sinus venous thrombosis.
VERDICT A Wisconsin jury returned a $23.2 million verdict; the court added $187,402 in medical expenses.
OB exonerated following brachial plexus injury
WHEN SHOULDER DYSTOCIA occurred during delivery, the ObGyn performed a McRoberts maneuver and episiotomy; the baby was delivered in 3 minutes. She suffered C5–8 brachial plexus palsy, deformity of the right arm and hand, and limited use of her right hand.
She later had tendon transfer surgery to improve range of motion of her wrist, and tendon release surgery on her shoulder.
PLAINTIFF’S CLAIM Excessive traction to the head and neck and failure to use additional shoulder dystocia maneuvers caused the injury.
PHYSICIAN’S DEFENSE The maneuvers performed were appropriate. The injury was due to natural forces of labor. The baby was delivered easily in less than a minute after using proper techniques. No excessive traction or other maneuvers were needed.
VERDICT An Illinois defense verdict was returned.
Did ovarian remnant + HRT cause DVT and pain?
A 33-YEAR-OLD WOMAN underwent a hysterectomy with salpingo-oophorectomy. Her ObGyn then prescribed hormone replacement therapy (HRT). Although pathology reported the left ovary and fallopian tube were not part of postoperative specimens, the ObGyn maintained that both ovaries and fallopian tubes had been removed. Ten months later, a CT scan revealed a pelvic neoplasm. No mass was found at exploratory surgery, but adhesions were lysed. Eighteen months later, an MRI revealed remnants of the left ovary and fallopian tube. Another gynecologist determined that the ovary was producing estrogen. Two months later, the patient developed deep vein thrombosis (DVT) in her left calf. The obstruction was resolved, but the patient reported residual leg pain.
PATIENT’S CLAIM Excessive levels of estrogen caused the DVT. The ObGyn was negligent in disregarding the initial pathologist’s report. It was inappropriate to prescribe HRT if ovarian function was present after surgery.
PHYSICIAN’S DEFENSE There was no negligence. Dense adhesions and a previous bowel perforation did not allow total ovary removal. The remnant is a known risk of the procedure. Estrogen HRT was appropriately administered.
VERDICT A New York defense verdict was returned.
Severing uterosacral ligament relieved pelvic pain, but…
AFTER CONSERVATIVE THERAPY for several months, a 26-year-old woman underwent exploratory laparoscopy to determine the reason for her severe pelvic pain. Findings were negative, but the physician transected the uterosacral ligament to relieve pain. Four days after surgery, a ureteral injury was diagnosed, and a stent was placed. The patient required complex treatment for her urinary tract injury.
PATIENT’S CLAIM Severing the uterosacral ligament was performed without her consent. The ureter injury was caused by negligent use of electrocauterization. Now the patient was at high risk for future pregnancies.
PHYSICIAN’S DEFENSE The patient’s pain warranted surgery; severing the ligament was appropriate. Injury to the ureter is a known complication.
VERDICT A Tennessee defense verdict was returned.
Why did it take so long to stop her bleeding?
AFTER DELIVERING HER THIRD CHILD, a 34-year-old woman reported significant vaginal bleeding to her ObGyn. Two weeks later, a sonogram was performed but the cause of bleeding was undetermined.
Bleeding continued. Sixteen days later, another sonogram revealed a 2-cm-long mass in the uterine cavity. The ObGyn decided to wait 4 or 5 days for another sonogram to make sure the mass wasn’t a fibroid or placental remnant.
The next evening, the patient was admitted to a hospital with excessive bleeding. The ObGyn performed a hysteroscopy and found a fibroid and a placental remnant. After tissue was removed by dilation and curettage (D&C), the ObGyn reinserted the hysteroscope. She encountered severe bleeding but could not find any other suspicious matter. Pathology reported that the excised material was placental tissue. The patient was hospitalized for 2 more days.
Three days later, she returned to the ObGyn with continued bleeding; the ObGyn determined it was post-D&C bleeding.
Two weeks later, the woman suffered severe vaginal hemorrhage. She went to another hospital where the ED physician felt the woman’s life was in jeopardy. A hysterectomy was performed, including the extraction of a placental fragment determined to be the cause of the hemorrhage.
PATIENT’S CLAIM The ObGyn was negligent in not diagnosing and treating the bleeding in a timely way after the first sonogram. The pathology report after D&C confirmed placental accreta, which should have prompted aggressive evaluation. Hysteroscopy and D&C did not effectively remove the deeply implanted placenta. She should not have been discharged from the hospital until the ObGyn had confirmed full removal of any placental remnants. Continued bleeding after D&C should have elicited further evaluation.
PHYSICIAN’S DEFENSE All the patient’s reports of bleeding were quickly and appropriately addressed. The ObGyn denied being told that the patient was still bleeding heavily until 16 days following the first sonogram. It was reasonable to conclude that the D&C had excised all suspicious matters. Post-D&C bleeding was due to an intraoperative laceration of the cervix; medication and a clamp had halted bleeding. Intraoperative bleeding made failure to remove the placental remnant reasonable. Earlier treatment would not have changed the outcome.
VERDICT A New York jury returned a $625,000 verdict.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
Negotiation
Negotiation is a fact of life, in and out of the office. Like it or not, we negotiate every day: with patients, employees, pharmacists, insurers, sales people, pharmaceutical reps, family members – everybody.
Unfortunately, most of physicians aren’t very good at it, for a variety of reasons, not least of which is our generally poor concept of compromise: We expect to get our way in the first place. When we don’t, we shy away; we don’t thrive on conflict and adversity, as good negotiators do, and we are not accustomed to rejection. We tend to take issues personally, rather than treating negotiation as an impersonal game.
We are also generally impatient, and often unwilling to listen carefully to what is being said (and not being said). And most of us have little experience with the chesslike discipline of sequential strategy: anticipating the other party’s sequence of moves and planning our own sequence in response.
While I can’t hope to make you a great negotiator in 700 words, I can pass along five essential rules that have stood me in good stead over the years:
– Do your homework. Before negotiating anything of significance, you need to learn everything you can about the issue and context, and whenever possible, about the other negotiating party. You cannot make accurate decisions without understanding the other side’s situation – needs, pressures, options, biases, and circumstances. Good negotiators start with questions, and listen to the answers. Car salespeople, for example, always do their homework: “So what do you do for a living? Are you married? Any kids?” That’s not small talk or idle curiosity; it’s information gathering. Knowledge is power, and frequently your most powerful negotiating tool. If you have left money on the table at negotiation’s end, it’s probably because your information wasn’t as good or thorough as your adversary’s.
– You can always walk away. Be a “reluctant” buyer or seller; make it clear that if a favorable deal cannot be reached, there will be no deal at all. Any time a salesperson senses a hint of emotional attachment – that you “have to have it” or “have to sell it” – your negotiating position falls off a cliff. Don’t be afraid to walk away from a managed care contract if the alternative is signing one that costs you substantial sums of money. Rarely is a bad deal better than no deal at all.
– Learn to “flinch.” Choke, snort, sputter, clutch your chest in pain. However you do it, you are trying to convey a visible sign of shock, and maybe a touch of indignation at the preposterous opening offer from the other side. It’s an essential technique, whether you are actually shocked or not; a buyer or seller who sees no reaction to an outrageous opening price will often conclude it’s not so outrageous after all. Even if flinching isn’t your style, keep in mind that it’s being used against you all the time; don’t mistake such tactics for genuine surprise!
– Beware of “nibbling.” You are most vulnerable to trickery when you think a negotiation is over. Your mind relaxes, and you concede things you otherwise would not. And that is when the other party may try to add or subtract something from the deal you thought was done. Salespeople add expensive options you thought were included; and buyers call back to say the boss “won’t okay it” unless you agree to new conditions, or a lower price. Counter those nibble attempts calmly but firmly: “Come on, we had a deal; you’re not going to kill it over a detail like this, are you?” Of course, turnabout is fair play; for example, remember at your next negotiation for office equipment, before you sign, that nothing prohibits you from saying, “You can give us 60 days on this, right? Your competitor will.”
– Decide when you will not negotiate. Some things are just not negotiable. Employees never stop looking for compromises or exceptions. (“You said we’re only getting cost-of-living raises this year, but that doesn’t include me, does it?”) Patients and pharmaceutical representatives (and kids) often request special treatment as well. If a rule or policy is non-negotiable, make that clear. And stick to your guns
Negotiation is a fact of life, in and out of the office. Like it or not, we negotiate every day: with patients, employees, pharmacists, insurers, sales people, pharmaceutical reps, family members – everybody.
Unfortunately, most of physicians aren’t very good at it, for a variety of reasons, not least of which is our generally poor concept of compromise: We expect to get our way in the first place. When we don’t, we shy away; we don’t thrive on conflict and adversity, as good negotiators do, and we are not accustomed to rejection. We tend to take issues personally, rather than treating negotiation as an impersonal game.
We are also generally impatient, and often unwilling to listen carefully to what is being said (and not being said). And most of us have little experience with the chesslike discipline of sequential strategy: anticipating the other party’s sequence of moves and planning our own sequence in response.
While I can’t hope to make you a great negotiator in 700 words, I can pass along five essential rules that have stood me in good stead over the years:
– Do your homework. Before negotiating anything of significance, you need to learn everything you can about the issue and context, and whenever possible, about the other negotiating party. You cannot make accurate decisions without understanding the other side’s situation – needs, pressures, options, biases, and circumstances. Good negotiators start with questions, and listen to the answers. Car salespeople, for example, always do their homework: “So what do you do for a living? Are you married? Any kids?” That’s not small talk or idle curiosity; it’s information gathering. Knowledge is power, and frequently your most powerful negotiating tool. If you have left money on the table at negotiation’s end, it’s probably because your information wasn’t as good or thorough as your adversary’s.
– You can always walk away. Be a “reluctant” buyer or seller; make it clear that if a favorable deal cannot be reached, there will be no deal at all. Any time a salesperson senses a hint of emotional attachment – that you “have to have it” or “have to sell it” – your negotiating position falls off a cliff. Don’t be afraid to walk away from a managed care contract if the alternative is signing one that costs you substantial sums of money. Rarely is a bad deal better than no deal at all.
– Learn to “flinch.” Choke, snort, sputter, clutch your chest in pain. However you do it, you are trying to convey a visible sign of shock, and maybe a touch of indignation at the preposterous opening offer from the other side. It’s an essential technique, whether you are actually shocked or not; a buyer or seller who sees no reaction to an outrageous opening price will often conclude it’s not so outrageous after all. Even if flinching isn’t your style, keep in mind that it’s being used against you all the time; don’t mistake such tactics for genuine surprise!
– Beware of “nibbling.” You are most vulnerable to trickery when you think a negotiation is over. Your mind relaxes, and you concede things you otherwise would not. And that is when the other party may try to add or subtract something from the deal you thought was done. Salespeople add expensive options you thought were included; and buyers call back to say the boss “won’t okay it” unless you agree to new conditions, or a lower price. Counter those nibble attempts calmly but firmly: “Come on, we had a deal; you’re not going to kill it over a detail like this, are you?” Of course, turnabout is fair play; for example, remember at your next negotiation for office equipment, before you sign, that nothing prohibits you from saying, “You can give us 60 days on this, right? Your competitor will.”
– Decide when you will not negotiate. Some things are just not negotiable. Employees never stop looking for compromises or exceptions. (“You said we’re only getting cost-of-living raises this year, but that doesn’t include me, does it?”) Patients and pharmaceutical representatives (and kids) often request special treatment as well. If a rule or policy is non-negotiable, make that clear. And stick to your guns
Negotiation is a fact of life, in and out of the office. Like it or not, we negotiate every day: with patients, employees, pharmacists, insurers, sales people, pharmaceutical reps, family members – everybody.
Unfortunately, most of physicians aren’t very good at it, for a variety of reasons, not least of which is our generally poor concept of compromise: We expect to get our way in the first place. When we don’t, we shy away; we don’t thrive on conflict and adversity, as good negotiators do, and we are not accustomed to rejection. We tend to take issues personally, rather than treating negotiation as an impersonal game.
We are also generally impatient, and often unwilling to listen carefully to what is being said (and not being said). And most of us have little experience with the chesslike discipline of sequential strategy: anticipating the other party’s sequence of moves and planning our own sequence in response.
While I can’t hope to make you a great negotiator in 700 words, I can pass along five essential rules that have stood me in good stead over the years:
– Do your homework. Before negotiating anything of significance, you need to learn everything you can about the issue and context, and whenever possible, about the other negotiating party. You cannot make accurate decisions without understanding the other side’s situation – needs, pressures, options, biases, and circumstances. Good negotiators start with questions, and listen to the answers. Car salespeople, for example, always do their homework: “So what do you do for a living? Are you married? Any kids?” That’s not small talk or idle curiosity; it’s information gathering. Knowledge is power, and frequently your most powerful negotiating tool. If you have left money on the table at negotiation’s end, it’s probably because your information wasn’t as good or thorough as your adversary’s.
– You can always walk away. Be a “reluctant” buyer or seller; make it clear that if a favorable deal cannot be reached, there will be no deal at all. Any time a salesperson senses a hint of emotional attachment – that you “have to have it” or “have to sell it” – your negotiating position falls off a cliff. Don’t be afraid to walk away from a managed care contract if the alternative is signing one that costs you substantial sums of money. Rarely is a bad deal better than no deal at all.
– Learn to “flinch.” Choke, snort, sputter, clutch your chest in pain. However you do it, you are trying to convey a visible sign of shock, and maybe a touch of indignation at the preposterous opening offer from the other side. It’s an essential technique, whether you are actually shocked or not; a buyer or seller who sees no reaction to an outrageous opening price will often conclude it’s not so outrageous after all. Even if flinching isn’t your style, keep in mind that it’s being used against you all the time; don’t mistake such tactics for genuine surprise!
– Beware of “nibbling.” You are most vulnerable to trickery when you think a negotiation is over. Your mind relaxes, and you concede things you otherwise would not. And that is when the other party may try to add or subtract something from the deal you thought was done. Salespeople add expensive options you thought were included; and buyers call back to say the boss “won’t okay it” unless you agree to new conditions, or a lower price. Counter those nibble attempts calmly but firmly: “Come on, we had a deal; you’re not going to kill it over a detail like this, are you?” Of course, turnabout is fair play; for example, remember at your next negotiation for office equipment, before you sign, that nothing prohibits you from saying, “You can give us 60 days on this, right? Your competitor will.”
– Decide when you will not negotiate. Some things are just not negotiable. Employees never stop looking for compromises or exceptions. (“You said we’re only getting cost-of-living raises this year, but that doesn’t include me, does it?”) Patients and pharmaceutical representatives (and kids) often request special treatment as well. If a rule or policy is non-negotiable, make that clear. And stick to your guns
Dr. Hospitalist

I have been asked to create a proposal for incentive-based reimbursements for our group. One of the more common areas cited in the literature is incentives for “good citizenship.” What exactly constitutes good citizenship and how is it tracked? Thanks.
Lou O’Boyle
Dr. Hospitalist responds:
Congratulations on your new responsibility! Most hospitalist programs in the U.S. have incentive-based compensation as part of their provider compensation plans. While some groups succeed with their incentive-based compensation plans, others fail at what the plan is intended to achieve. In addition to answering your question, I will discuss some keys to developing a successful plan.
From the nature of your question, it sounds as if you are a staff hospitalist or a group administrator who was tasked by the leader or the group to come up with the terms of an incentive-based plan. I am not aware of any guidelines on who is best suited to develop an incentive-based compensation plan, but, in general, I do think it is a mistake for group leaders to unilaterally mandate the terms the of the plan without input from its clinical providers. After all, it seems like common sense to speak with the people who you are trying to motivate before developing an incentive plan. Depending on the size of the group, I think most groups would do well to have a small, representative group of the frontline providers who would work with the leader to develop the plan.
First and foremost, the plan rules must be clear to all participants. Your question is an excellent example. “Good citizenship” probably means different things to different people. For some, it means attending all staff meetings, or active participation on hospital committees. For others, it represents high customer satisfaction or adherence to clinical guidelines. I am not aware of a universal definition for “good citizenship” when it comes to hospitalist incentive-based compensation plans.
After you have determined what you want your plan to motivate the staff to do, I urge you to define the plan rules as clearly as possible; write it down for all providers to see. If the plan rules are vague, opaque, or open to interpretation, participants might not be motivated to reach the goals, because they don’t really understand the plan rules. Even worse, participants might leave with the falsely held belief that someone is trying to mislead them.
Next, figure out a way to easily gather and display the data. Don’t underestimate the amount of work this involves. It is vitally important for everyone to understand who, when, where, and how the data will be gathered and displayed. Needless to say, the process of gathering and displaying the data must be done in a fashion that eliminates questions of validity.
At the core of any incentive-based compensation plan is the actual incentive. The process of determining the actual incentive can be fraught with controversy. I urge all working groups to proceed through this step with caution. What motivates people can vary widely. It is important for participants to view the incentives as sufficiently significant so that they are motivated to take the desired steps to achieve the goal. That said, if participants view the incentive as too large a component of total compensation, they might look for alternative employment with incentive plans they view as “safer” for their personal income.
Most incentive-based compensation plans are from 15% to 25% of total compensation. Again, this is not a fixed rule. Some groups choose incentives that are 5% to 10% of total compensation; others have incentives up to 40% of total compensation. The important takeaway here is to understand what is necessary to motivate your group.
Although most incentives are monetary, I encourage you to think beyond money as the only motivator in your plan. Some examples include time off from work; flat-screen televisions; or all-expenses-paid vacations.
Whether you choose money or nonmonetary items, it is important to be clear on when the payout will occur. Many groups pay the incentive annually. It might be the easy way to do it, but it also doesn’t mean a once-a-year payout is right for your group. The goal of the incentive is to change provider behavior. In order to accomplish this goal, participants must associate their behavior with the incentive-based reward. Paying the incentive-based reward at the right frequency (quarterly, every six months) might increase the chance this will occur. I don’t advise weekly incentives; not only is that process cumbersome, but the rewards also are likely to be small and potentially ineffective. The frequency of payout should be part of the planning discussions.
My last piece of advice is to take steps to help your providers succeed. In addition to telling your providers how to reach their incentives, show them how to succeed. This does not mean setting the bar low. Providers should have to work hard to reach their goals, and there is no reason why you shouldn’t give them the tools to help them succeed. TH
I have been asked to create a proposal for incentive-based reimbursements for our group. One of the more common areas cited in the literature is incentives for “good citizenship.” What exactly constitutes good citizenship and how is it tracked? Thanks.
Lou O’Boyle
Dr. Hospitalist responds:
Congratulations on your new responsibility! Most hospitalist programs in the U.S. have incentive-based compensation as part of their provider compensation plans. While some groups succeed with their incentive-based compensation plans, others fail at what the plan is intended to achieve. In addition to answering your question, I will discuss some keys to developing a successful plan.
From the nature of your question, it sounds as if you are a staff hospitalist or a group administrator who was tasked by the leader or the group to come up with the terms of an incentive-based plan. I am not aware of any guidelines on who is best suited to develop an incentive-based compensation plan, but, in general, I do think it is a mistake for group leaders to unilaterally mandate the terms the of the plan without input from its clinical providers. After all, it seems like common sense to speak with the people who you are trying to motivate before developing an incentive plan. Depending on the size of the group, I think most groups would do well to have a small, representative group of the frontline providers who would work with the leader to develop the plan.
First and foremost, the plan rules must be clear to all participants. Your question is an excellent example. “Good citizenship” probably means different things to different people. For some, it means attending all staff meetings, or active participation on hospital committees. For others, it represents high customer satisfaction or adherence to clinical guidelines. I am not aware of a universal definition for “good citizenship” when it comes to hospitalist incentive-based compensation plans.
After you have determined what you want your plan to motivate the staff to do, I urge you to define the plan rules as clearly as possible; write it down for all providers to see. If the plan rules are vague, opaque, or open to interpretation, participants might not be motivated to reach the goals, because they don’t really understand the plan rules. Even worse, participants might leave with the falsely held belief that someone is trying to mislead them.
Next, figure out a way to easily gather and display the data. Don’t underestimate the amount of work this involves. It is vitally important for everyone to understand who, when, where, and how the data will be gathered and displayed. Needless to say, the process of gathering and displaying the data must be done in a fashion that eliminates questions of validity.
At the core of any incentive-based compensation plan is the actual incentive. The process of determining the actual incentive can be fraught with controversy. I urge all working groups to proceed through this step with caution. What motivates people can vary widely. It is important for participants to view the incentives as sufficiently significant so that they are motivated to take the desired steps to achieve the goal. That said, if participants view the incentive as too large a component of total compensation, they might look for alternative employment with incentive plans they view as “safer” for their personal income.
Most incentive-based compensation plans are from 15% to 25% of total compensation. Again, this is not a fixed rule. Some groups choose incentives that are 5% to 10% of total compensation; others have incentives up to 40% of total compensation. The important takeaway here is to understand what is necessary to motivate your group.
Although most incentives are monetary, I encourage you to think beyond money as the only motivator in your plan. Some examples include time off from work; flat-screen televisions; or all-expenses-paid vacations.
Whether you choose money or nonmonetary items, it is important to be clear on when the payout will occur. Many groups pay the incentive annually. It might be the easy way to do it, but it also doesn’t mean a once-a-year payout is right for your group. The goal of the incentive is to change provider behavior. In order to accomplish this goal, participants must associate their behavior with the incentive-based reward. Paying the incentive-based reward at the right frequency (quarterly, every six months) might increase the chance this will occur. I don’t advise weekly incentives; not only is that process cumbersome, but the rewards also are likely to be small and potentially ineffective. The frequency of payout should be part of the planning discussions.
My last piece of advice is to take steps to help your providers succeed. In addition to telling your providers how to reach their incentives, show them how to succeed. This does not mean setting the bar low. Providers should have to work hard to reach their goals, and there is no reason why you shouldn’t give them the tools to help them succeed. TH
I have been asked to create a proposal for incentive-based reimbursements for our group. One of the more common areas cited in the literature is incentives for “good citizenship.” What exactly constitutes good citizenship and how is it tracked? Thanks.
Lou O’Boyle
Dr. Hospitalist responds:
Congratulations on your new responsibility! Most hospitalist programs in the U.S. have incentive-based compensation as part of their provider compensation plans. While some groups succeed with their incentive-based compensation plans, others fail at what the plan is intended to achieve. In addition to answering your question, I will discuss some keys to developing a successful plan.
From the nature of your question, it sounds as if you are a staff hospitalist or a group administrator who was tasked by the leader or the group to come up with the terms of an incentive-based plan. I am not aware of any guidelines on who is best suited to develop an incentive-based compensation plan, but, in general, I do think it is a mistake for group leaders to unilaterally mandate the terms the of the plan without input from its clinical providers. After all, it seems like common sense to speak with the people who you are trying to motivate before developing an incentive plan. Depending on the size of the group, I think most groups would do well to have a small, representative group of the frontline providers who would work with the leader to develop the plan.
First and foremost, the plan rules must be clear to all participants. Your question is an excellent example. “Good citizenship” probably means different things to different people. For some, it means attending all staff meetings, or active participation on hospital committees. For others, it represents high customer satisfaction or adherence to clinical guidelines. I am not aware of a universal definition for “good citizenship” when it comes to hospitalist incentive-based compensation plans.
After you have determined what you want your plan to motivate the staff to do, I urge you to define the plan rules as clearly as possible; write it down for all providers to see. If the plan rules are vague, opaque, or open to interpretation, participants might not be motivated to reach the goals, because they don’t really understand the plan rules. Even worse, participants might leave with the falsely held belief that someone is trying to mislead them.
Next, figure out a way to easily gather and display the data. Don’t underestimate the amount of work this involves. It is vitally important for everyone to understand who, when, where, and how the data will be gathered and displayed. Needless to say, the process of gathering and displaying the data must be done in a fashion that eliminates questions of validity.
At the core of any incentive-based compensation plan is the actual incentive. The process of determining the actual incentive can be fraught with controversy. I urge all working groups to proceed through this step with caution. What motivates people can vary widely. It is important for participants to view the incentives as sufficiently significant so that they are motivated to take the desired steps to achieve the goal. That said, if participants view the incentive as too large a component of total compensation, they might look for alternative employment with incentive plans they view as “safer” for their personal income.
Most incentive-based compensation plans are from 15% to 25% of total compensation. Again, this is not a fixed rule. Some groups choose incentives that are 5% to 10% of total compensation; others have incentives up to 40% of total compensation. The important takeaway here is to understand what is necessary to motivate your group.
Although most incentives are monetary, I encourage you to think beyond money as the only motivator in your plan. Some examples include time off from work; flat-screen televisions; or all-expenses-paid vacations.
Whether you choose money or nonmonetary items, it is important to be clear on when the payout will occur. Many groups pay the incentive annually. It might be the easy way to do it, but it also doesn’t mean a once-a-year payout is right for your group. The goal of the incentive is to change provider behavior. In order to accomplish this goal, participants must associate their behavior with the incentive-based reward. Paying the incentive-based reward at the right frequency (quarterly, every six months) might increase the chance this will occur. I don’t advise weekly incentives; not only is that process cumbersome, but the rewards also are likely to be small and potentially ineffective. The frequency of payout should be part of the planning discussions.
My last piece of advice is to take steps to help your providers succeed. In addition to telling your providers how to reach their incentives, show them how to succeed. This does not mean setting the bar low. Providers should have to work hard to reach their goals, and there is no reason why you shouldn’t give them the tools to help them succeed. TH
Medical Verdicts
Why wasn’t bloody nipple discharge taken more seriously?
DUE TO BLOODY DISCHARGE from her left nipple, a woman in her thirties had a mammogram; results were suspicious for malignancy. Her surgeon’s examination and biopsy were negative.
Two years later she found a lump in her left breast. Ultrasonography suggested a benign mass at 9 o’clock. Her surgeon could not find a mass at 9 o’clock, but detected a mass at 7 o’clock. He ordered US-guided core biopsy of the 9 o’clock area, but not the 7 o’clock mass—she was instructed to return for removal of the 7 o’clock mass regardless of the biopsy’s outcome. She was impatient for the biopsy, and went to another surgeon. Biopsy results were negative for malignancy.
Months later, during right breast implant replacement, she had the left-sided mass excised. Pathology reported moderate to poorly differentiated infiltrating carcinoma. She underwent a left mastectomy, prophylactic right mastectomy, and chemotherapy.
PATIENT’S CLAIM Further evaluation of her original complaint of bloody nipple discharge by her surgeon would have led to earlier diagnosis.
PHYSICIAN’S DEFENSE The left breast mass was never biopsied because the patient didn’t return as instructed.
VERDICT A Pennsylvania defense verdict was returned.
Uterine artery severed, new mother dies; court mandates changes
THE UTERINE ARTERY WAS SEVERED during cesarean delivery in a 32-year-old woman, causing severe hemorrhage. The ObGyn repaired the uterine vessels in the OR. The patient was sent to the recovery room and then to the surgical ICU, where she was in severe hemorrhagic shock, hypotensive, tachycardic, and had minimal urine output with metabolic acidosis. Exploratory surgery revealed massive blood clots. A trauma surgeon, called in by the ObGyn, found an extensive hematoma and 2 to 3 L of blood in the retroperitoneum. The woman died within 24 hours of delivery.
PLAINTIFF’S CLAIM When repairing injuries that occurred during the cesarean, the ObGyn damaged retroperitoneal uterine arteries. Physicians in the recovery room and surgical ICU informed the ObGyn that the patient appeared to have internal bleeding, but he did not return her to the OR for over 6 hours. After consent for exploratory surgery was signed, the ObGyn left to deliver another baby. The recovery room’s OBIX Perinatal Data System monitors failed to accurately record the patient’s vital signs. Understaffing in the surgical ICU impaired treatment.
DEFENSE CLAIM The ObGyn’s responsibility for the patient was transferred to the recovery room’s attending doctor, who claimed he had discharged his responsibility when he recommended exploratory surgery. After viewing the patient’s chart in the surgical ICU, a surgeon told the ObGyn that immediate treatment was needed for internal bleeding. The hospital claimed staffing issues did not cause the patient’s death.
VERDICT The burden of a $5.2 million settlement was shared by the physicians and hospital. The hospital was mandated to 1) establish an annual lecture on patient safety; 2) purchase a maternal/neonatal simulator to train staff; and 3) change the default settings on all OBIX Perinatal Data System machines to prevent them from defaulting to record normal values for vital signs when the “add” button is pushed.
Severe pain and burns during biopsy and genital wart removal
BIOPSY AND GENITAL WART REMOVAL were performed on a 34-year-old woman without anesthesia. She screamed in pain when the ObGyn biopsied her labia. Pain increased when he removed warts using a trichloroacetic acid mixture. Acid ran into the patient’s vagina and onto her buttocks, causing second-degree burns.
PATIENT’S CLAIM The physician never offered anesthesia, nor did she refuse it. The acid should have been applied more discretely. The paper toweling used to clean up the acid was just moist and could not have caused the acid to spread.
PHYSICIAN’S DEFENSE The ObGyn stated he preferred not to use anesthesia because it might affect the pathology slide quality, but that he offered it to the patient, and she refused. He also claimed that he applied the acid carefully, and attributed the spread and burn to a nurse who brought wet paper towels to dry the patient.
VERDICT A Tennessee defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
Why wasn’t bloody nipple discharge taken more seriously?
DUE TO BLOODY DISCHARGE from her left nipple, a woman in her thirties had a mammogram; results were suspicious for malignancy. Her surgeon’s examination and biopsy were negative.
Two years later she found a lump in her left breast. Ultrasonography suggested a benign mass at 9 o’clock. Her surgeon could not find a mass at 9 o’clock, but detected a mass at 7 o’clock. He ordered US-guided core biopsy of the 9 o’clock area, but not the 7 o’clock mass—she was instructed to return for removal of the 7 o’clock mass regardless of the biopsy’s outcome. She was impatient for the biopsy, and went to another surgeon. Biopsy results were negative for malignancy.
Months later, during right breast implant replacement, she had the left-sided mass excised. Pathology reported moderate to poorly differentiated infiltrating carcinoma. She underwent a left mastectomy, prophylactic right mastectomy, and chemotherapy.
PATIENT’S CLAIM Further evaluation of her original complaint of bloody nipple discharge by her surgeon would have led to earlier diagnosis.
PHYSICIAN’S DEFENSE The left breast mass was never biopsied because the patient didn’t return as instructed.
VERDICT A Pennsylvania defense verdict was returned.
Uterine artery severed, new mother dies; court mandates changes
THE UTERINE ARTERY WAS SEVERED during cesarean delivery in a 32-year-old woman, causing severe hemorrhage. The ObGyn repaired the uterine vessels in the OR. The patient was sent to the recovery room and then to the surgical ICU, where she was in severe hemorrhagic shock, hypotensive, tachycardic, and had minimal urine output with metabolic acidosis. Exploratory surgery revealed massive blood clots. A trauma surgeon, called in by the ObGyn, found an extensive hematoma and 2 to 3 L of blood in the retroperitoneum. The woman died within 24 hours of delivery.
PLAINTIFF’S CLAIM When repairing injuries that occurred during the cesarean, the ObGyn damaged retroperitoneal uterine arteries. Physicians in the recovery room and surgical ICU informed the ObGyn that the patient appeared to have internal bleeding, but he did not return her to the OR for over 6 hours. After consent for exploratory surgery was signed, the ObGyn left to deliver another baby. The recovery room’s OBIX Perinatal Data System monitors failed to accurately record the patient’s vital signs. Understaffing in the surgical ICU impaired treatment.
DEFENSE CLAIM The ObGyn’s responsibility for the patient was transferred to the recovery room’s attending doctor, who claimed he had discharged his responsibility when he recommended exploratory surgery. After viewing the patient’s chart in the surgical ICU, a surgeon told the ObGyn that immediate treatment was needed for internal bleeding. The hospital claimed staffing issues did not cause the patient’s death.
VERDICT The burden of a $5.2 million settlement was shared by the physicians and hospital. The hospital was mandated to 1) establish an annual lecture on patient safety; 2) purchase a maternal/neonatal simulator to train staff; and 3) change the default settings on all OBIX Perinatal Data System machines to prevent them from defaulting to record normal values for vital signs when the “add” button is pushed.
Severe pain and burns during biopsy and genital wart removal
BIOPSY AND GENITAL WART REMOVAL were performed on a 34-year-old woman without anesthesia. She screamed in pain when the ObGyn biopsied her labia. Pain increased when he removed warts using a trichloroacetic acid mixture. Acid ran into the patient’s vagina and onto her buttocks, causing second-degree burns.
PATIENT’S CLAIM The physician never offered anesthesia, nor did she refuse it. The acid should have been applied more discretely. The paper toweling used to clean up the acid was just moist and could not have caused the acid to spread.
PHYSICIAN’S DEFENSE The ObGyn stated he preferred not to use anesthesia because it might affect the pathology slide quality, but that he offered it to the patient, and she refused. He also claimed that he applied the acid carefully, and attributed the spread and burn to a nurse who brought wet paper towels to dry the patient.
VERDICT A Tennessee defense verdict was returned.
Why wasn’t bloody nipple discharge taken more seriously?
DUE TO BLOODY DISCHARGE from her left nipple, a woman in her thirties had a mammogram; results were suspicious for malignancy. Her surgeon’s examination and biopsy were negative.
Two years later she found a lump in her left breast. Ultrasonography suggested a benign mass at 9 o’clock. Her surgeon could not find a mass at 9 o’clock, but detected a mass at 7 o’clock. He ordered US-guided core biopsy of the 9 o’clock area, but not the 7 o’clock mass—she was instructed to return for removal of the 7 o’clock mass regardless of the biopsy’s outcome. She was impatient for the biopsy, and went to another surgeon. Biopsy results were negative for malignancy.
Months later, during right breast implant replacement, she had the left-sided mass excised. Pathology reported moderate to poorly differentiated infiltrating carcinoma. She underwent a left mastectomy, prophylactic right mastectomy, and chemotherapy.
PATIENT’S CLAIM Further evaluation of her original complaint of bloody nipple discharge by her surgeon would have led to earlier diagnosis.
PHYSICIAN’S DEFENSE The left breast mass was never biopsied because the patient didn’t return as instructed.
VERDICT A Pennsylvania defense verdict was returned.
Uterine artery severed, new mother dies; court mandates changes
THE UTERINE ARTERY WAS SEVERED during cesarean delivery in a 32-year-old woman, causing severe hemorrhage. The ObGyn repaired the uterine vessels in the OR. The patient was sent to the recovery room and then to the surgical ICU, where she was in severe hemorrhagic shock, hypotensive, tachycardic, and had minimal urine output with metabolic acidosis. Exploratory surgery revealed massive blood clots. A trauma surgeon, called in by the ObGyn, found an extensive hematoma and 2 to 3 L of blood in the retroperitoneum. The woman died within 24 hours of delivery.
PLAINTIFF’S CLAIM When repairing injuries that occurred during the cesarean, the ObGyn damaged retroperitoneal uterine arteries. Physicians in the recovery room and surgical ICU informed the ObGyn that the patient appeared to have internal bleeding, but he did not return her to the OR for over 6 hours. After consent for exploratory surgery was signed, the ObGyn left to deliver another baby. The recovery room’s OBIX Perinatal Data System monitors failed to accurately record the patient’s vital signs. Understaffing in the surgical ICU impaired treatment.
DEFENSE CLAIM The ObGyn’s responsibility for the patient was transferred to the recovery room’s attending doctor, who claimed he had discharged his responsibility when he recommended exploratory surgery. After viewing the patient’s chart in the surgical ICU, a surgeon told the ObGyn that immediate treatment was needed for internal bleeding. The hospital claimed staffing issues did not cause the patient’s death.
VERDICT The burden of a $5.2 million settlement was shared by the physicians and hospital. The hospital was mandated to 1) establish an annual lecture on patient safety; 2) purchase a maternal/neonatal simulator to train staff; and 3) change the default settings on all OBIX Perinatal Data System machines to prevent them from defaulting to record normal values for vital signs when the “add” button is pushed.
Severe pain and burns during biopsy and genital wart removal
BIOPSY AND GENITAL WART REMOVAL were performed on a 34-year-old woman without anesthesia. She screamed in pain when the ObGyn biopsied her labia. Pain increased when he removed warts using a trichloroacetic acid mixture. Acid ran into the patient’s vagina and onto her buttocks, causing second-degree burns.
PATIENT’S CLAIM The physician never offered anesthesia, nor did she refuse it. The acid should have been applied more discretely. The paper toweling used to clean up the acid was just moist and could not have caused the acid to spread.
PHYSICIAN’S DEFENSE The ObGyn stated he preferred not to use anesthesia because it might affect the pathology slide quality, but that he offered it to the patient, and she refused. He also claimed that he applied the acid carefully, and attributed the spread and burn to a nurse who brought wet paper towels to dry the patient.
VERDICT A Tennessee defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
Dealing With Prior Authorization
Since passage of the health care reform bill in March, there has been considerable discussion in medical periodicals, forums, and blogs about the dramatic changes that will be taking place.
At least one thing—prior authorizations—will not change, because the legislation did not address it.
Lawmakers have offered no public explanation for ignoring such a glaring problem. It should have been obvious, even to them, that requiring physicians to ask permission, over and over, for necessary tests and treatments is senseless and inefficient.
Common sense dictates fixing something so universally hated by doctors and patients alike. One can speculate that the third party in the physician-patient equation—insurers—had a lot to do with this oversight.
Insurers love prior authorization because it saves them money. In fact, it's one of the most effective cost-cutting tools in their box: rationing through inconvenience. So it's logical to speculate that they probably used their considerable input into the reform law's content, via their army of lobbyists, to discourage action.
So, prior authorization will remain a problem for the foreseeable future, and we need to deal with it as best we can.
First and foremost, minimize the wasted time prior authorizations cause you and your staff. My office took a major step toward this goal by banning all submissions by telephone.
A single prior-authorization phone call can easily take 30 minutes of staffers' time as they fight through the automated greetings and category selections, and wait on hold before finally speaking to somebody with a pulse. At that point, since the person is hardly ever authorized to give approval, they get another department's number or a faxed form. It's an inexcusable and outrageously expensive waste of time.
When a request for preauthorization comes in, we call the patient and ask that he or she make the call to the insurance company to request the form.
I have mixed feelings about passing along the automated phone-hoop hassle to patients, but it is their insurance, after all, and this is one area where I simply can't afford the luxury of providing a time-consuming service for free. Plus, it gives patients some understanding of the absurdity of the whole prior-authorization game.
When possible, we enlist the help of any other parties at our disposal. Some insurers will accept prior-authorization requests from pharmacies, which makes a lot of sense. They typically have a complete record of all medications tried and failed, as well as the necessary diagnosis codes.
Unfortunately, many insurers inexplicably insist that only the physician's office submit the request, but it's worth your time to ask if the company in question accepts pharmacy filings, rather than assuming it doesn't.
Also, don't forget that manufacturers of some medications (biologics, for example) will help with some, or all, of the prior-authorization burden. Sometimes they have an auxiliary company set up just for that purpose.
If not, a representative or district manager may be able to help or point you toward someone who can. It never hurts to ask.
Also, most pharmaceutical companies have a “compassion” program that provides medications free when the insurer will not pay and the patient can't afford it.
Other potential allies are the big-box chains that offer selected medications at $4 (or less) per prescription. Sometimes, the most efficient solution is to point the patient toward Walmart, Costco, Target, or another chain in your area, and forget the preauthorization altogether.
The key is to get the insurance company's form. Not only do you avoid the phone runaround, but the form tells exactly what that particular company wants, so your staff won't waste time finding and supplying information that is not needed.
What about patients who request prior authorization for medically unnecessary medications?
In my office, that's usually a retinoid prescription for wrinkles. I tell them it's against the law to say a treatment is necessary when it is not, and that there is zero chance their insurer will pay. (As a diplomatic friend of mine puts it, “Your insurance company barely cares if you are dying, let alone how you look!”) I tell them I will not be able to go to bat for older patients with recalcitrant acne who really need retinoids, if I try to slip cosmetic prescriptions past insurers. Most understand.
Since passage of the health care reform bill in March, there has been considerable discussion in medical periodicals, forums, and blogs about the dramatic changes that will be taking place.
At least one thing—prior authorizations—will not change, because the legislation did not address it.
Lawmakers have offered no public explanation for ignoring such a glaring problem. It should have been obvious, even to them, that requiring physicians to ask permission, over and over, for necessary tests and treatments is senseless and inefficient.
Common sense dictates fixing something so universally hated by doctors and patients alike. One can speculate that the third party in the physician-patient equation—insurers—had a lot to do with this oversight.
Insurers love prior authorization because it saves them money. In fact, it's one of the most effective cost-cutting tools in their box: rationing through inconvenience. So it's logical to speculate that they probably used their considerable input into the reform law's content, via their army of lobbyists, to discourage action.
So, prior authorization will remain a problem for the foreseeable future, and we need to deal with it as best we can.
First and foremost, minimize the wasted time prior authorizations cause you and your staff. My office took a major step toward this goal by banning all submissions by telephone.
A single prior-authorization phone call can easily take 30 minutes of staffers' time as they fight through the automated greetings and category selections, and wait on hold before finally speaking to somebody with a pulse. At that point, since the person is hardly ever authorized to give approval, they get another department's number or a faxed form. It's an inexcusable and outrageously expensive waste of time.
When a request for preauthorization comes in, we call the patient and ask that he or she make the call to the insurance company to request the form.
I have mixed feelings about passing along the automated phone-hoop hassle to patients, but it is their insurance, after all, and this is one area where I simply can't afford the luxury of providing a time-consuming service for free. Plus, it gives patients some understanding of the absurdity of the whole prior-authorization game.
When possible, we enlist the help of any other parties at our disposal. Some insurers will accept prior-authorization requests from pharmacies, which makes a lot of sense. They typically have a complete record of all medications tried and failed, as well as the necessary diagnosis codes.
Unfortunately, many insurers inexplicably insist that only the physician's office submit the request, but it's worth your time to ask if the company in question accepts pharmacy filings, rather than assuming it doesn't.
Also, don't forget that manufacturers of some medications (biologics, for example) will help with some, or all, of the prior-authorization burden. Sometimes they have an auxiliary company set up just for that purpose.
If not, a representative or district manager may be able to help or point you toward someone who can. It never hurts to ask.
Also, most pharmaceutical companies have a “compassion” program that provides medications free when the insurer will not pay and the patient can't afford it.
Other potential allies are the big-box chains that offer selected medications at $4 (or less) per prescription. Sometimes, the most efficient solution is to point the patient toward Walmart, Costco, Target, or another chain in your area, and forget the preauthorization altogether.
The key is to get the insurance company's form. Not only do you avoid the phone runaround, but the form tells exactly what that particular company wants, so your staff won't waste time finding and supplying information that is not needed.
What about patients who request prior authorization for medically unnecessary medications?
In my office, that's usually a retinoid prescription for wrinkles. I tell them it's against the law to say a treatment is necessary when it is not, and that there is zero chance their insurer will pay. (As a diplomatic friend of mine puts it, “Your insurance company barely cares if you are dying, let alone how you look!”) I tell them I will not be able to go to bat for older patients with recalcitrant acne who really need retinoids, if I try to slip cosmetic prescriptions past insurers. Most understand.
Since passage of the health care reform bill in March, there has been considerable discussion in medical periodicals, forums, and blogs about the dramatic changes that will be taking place.
At least one thing—prior authorizations—will not change, because the legislation did not address it.
Lawmakers have offered no public explanation for ignoring such a glaring problem. It should have been obvious, even to them, that requiring physicians to ask permission, over and over, for necessary tests and treatments is senseless and inefficient.
Common sense dictates fixing something so universally hated by doctors and patients alike. One can speculate that the third party in the physician-patient equation—insurers—had a lot to do with this oversight.
Insurers love prior authorization because it saves them money. In fact, it's one of the most effective cost-cutting tools in their box: rationing through inconvenience. So it's logical to speculate that they probably used their considerable input into the reform law's content, via their army of lobbyists, to discourage action.
So, prior authorization will remain a problem for the foreseeable future, and we need to deal with it as best we can.
First and foremost, minimize the wasted time prior authorizations cause you and your staff. My office took a major step toward this goal by banning all submissions by telephone.
A single prior-authorization phone call can easily take 30 minutes of staffers' time as they fight through the automated greetings and category selections, and wait on hold before finally speaking to somebody with a pulse. At that point, since the person is hardly ever authorized to give approval, they get another department's number or a faxed form. It's an inexcusable and outrageously expensive waste of time.
When a request for preauthorization comes in, we call the patient and ask that he or she make the call to the insurance company to request the form.
I have mixed feelings about passing along the automated phone-hoop hassle to patients, but it is their insurance, after all, and this is one area where I simply can't afford the luxury of providing a time-consuming service for free. Plus, it gives patients some understanding of the absurdity of the whole prior-authorization game.
When possible, we enlist the help of any other parties at our disposal. Some insurers will accept prior-authorization requests from pharmacies, which makes a lot of sense. They typically have a complete record of all medications tried and failed, as well as the necessary diagnosis codes.
Unfortunately, many insurers inexplicably insist that only the physician's office submit the request, but it's worth your time to ask if the company in question accepts pharmacy filings, rather than assuming it doesn't.
Also, don't forget that manufacturers of some medications (biologics, for example) will help with some, or all, of the prior-authorization burden. Sometimes they have an auxiliary company set up just for that purpose.
If not, a representative or district manager may be able to help or point you toward someone who can. It never hurts to ask.
Also, most pharmaceutical companies have a “compassion” program that provides medications free when the insurer will not pay and the patient can't afford it.
Other potential allies are the big-box chains that offer selected medications at $4 (or less) per prescription. Sometimes, the most efficient solution is to point the patient toward Walmart, Costco, Target, or another chain in your area, and forget the preauthorization altogether.
The key is to get the insurance company's form. Not only do you avoid the phone runaround, but the form tells exactly what that particular company wants, so your staff won't waste time finding and supplying information that is not needed.
What about patients who request prior authorization for medically unnecessary medications?
In my office, that's usually a retinoid prescription for wrinkles. I tell them it's against the law to say a treatment is necessary when it is not, and that there is zero chance their insurer will pay. (As a diplomatic friend of mine puts it, “Your insurance company barely cares if you are dying, let alone how you look!”) I tell them I will not be able to go to bat for older patients with recalcitrant acne who really need retinoids, if I try to slip cosmetic prescriptions past insurers. Most understand.
Prior Authorization
Since passage of the health care reform bill in March, there has been considerable discussion in medical periodicals, forums, and blogs about the dramatic changes that will be taking place.
At least one thing – prior authorizations – will not change, because the legislation did not address it.
Lawmakers have offered no public explanation for ignoring such a glaring problem. It should have been obvious, even to them, that requiring physicians to ask permission, over and over, for necessary tests and treatments is senseless and inefficient. Common sense dictates fixing something so universally hated by doctors and patients alike. One can speculate that the third party in the physician-patient equation – insurers – had a lot to do with this oversight.
Insurers love prior authorization because it saves them money. In fact, it's one of the most effective cost-cutting tools in their box: rationing through inconvenience. So it's logical to speculate that they probably used their considerable input into the reform law's content, via their army of lobbyists, to discourage action.
So, prior authorization will remain a problem for the foreseeable future, and we need to deal with it as best we can.
First and foremost, minimize the wasted time prior authorizations cause you and your staff. My office took a major step toward this goal by banning all submissions by telephone.
A single prior-authorization phone call can easily take 30 minutes of a staffer’s time as they fight through the automated greetings and category selections, and wait on hold before finally speaking to somebody with a pulse. At that point, since the person is hardly ever authorized to give approval, they get another department’s number or a faxed form. It's an inexcusable and outrageously expensive waste of time.
When a request for pre-authorization comes in, we call the patient and ask that he or she make the call to the insurance company to request the form. I have mixed feelings about passing along the automated phone-hoop hassle to patients, but it is their insurance, after all, and this is one area where I simply can't afford the luxury of providing a time-consuming service for free. Plus, it gives patients some understanding of the absurdity of the whole prior-authorization game.
When possible, we enlist the help of any other parties at our disposal. Some insurers will accept prior authorization requests from pharmacies, which makes a lot of sense. They typically have a complete record of all medications tried and failed, as well as the necessary diagnosis codes.
Unfortunately, many insurers inexplicably insist that only the physician’s office submit the request, but it's worth your time to ask if the company in question accepts pharmacy filings, rather than assuming it doesn’t.
Also, don’t forget that manufacturers of some medications (biologics, for example) will help with some, or all, of the prior-authorization burden. Sometimes they have an auxiliary company set up just for that purpose. If not, a representative or district manager may be able to help or point you toward someone who can. It never hurts to ask.
Also, most pharmaceutical companies have a "compassion" program that provides medications free when the insurer won’t pay and the patient can’t afford it.
Other potential allies are the big-box chains that offer selected medications at $4 (or less) per prescription. Sometimes, the most efficient solution is to point the patient towards Walmart, Costco, Target, or another chain in your area, and forget the pre-authorization altogether.
The key is to get the insurance company's form. Not only do you avoid the phone runaround, but the form tells exactly what that particular company wants, so your staff won’t waste time finding and supplying information that is not needed.
What about patients who request prior authorization for medically unnecessary medications? In my office, that’s usually a retinoid prescription for wrinkles. I tell them it's against the law to say a treatment is necessary when it is not and that there is zero chance their insurer will pay. (As a diplomatic friend of mine puts it, "Your insurance company barely cares if you are dying, let alone how you look!") I tell them I will not be able to go to bat for older patients with recalcitrant acne who really need retinoids, if I try to slip cosmetic prescriptions past insurers. Most understand.
Since passage of the health care reform bill in March, there has been considerable discussion in medical periodicals, forums, and blogs about the dramatic changes that will be taking place.
At least one thing – prior authorizations – will not change, because the legislation did not address it.
Lawmakers have offered no public explanation for ignoring such a glaring problem. It should have been obvious, even to them, that requiring physicians to ask permission, over and over, for necessary tests and treatments is senseless and inefficient. Common sense dictates fixing something so universally hated by doctors and patients alike. One can speculate that the third party in the physician-patient equation – insurers – had a lot to do with this oversight.
Insurers love prior authorization because it saves them money. In fact, it's one of the most effective cost-cutting tools in their box: rationing through inconvenience. So it's logical to speculate that they probably used their considerable input into the reform law's content, via their army of lobbyists, to discourage action.
So, prior authorization will remain a problem for the foreseeable future, and we need to deal with it as best we can.
First and foremost, minimize the wasted time prior authorizations cause you and your staff. My office took a major step toward this goal by banning all submissions by telephone.
A single prior-authorization phone call can easily take 30 minutes of a staffer’s time as they fight through the automated greetings and category selections, and wait on hold before finally speaking to somebody with a pulse. At that point, since the person is hardly ever authorized to give approval, they get another department’s number or a faxed form. It's an inexcusable and outrageously expensive waste of time.
When a request for pre-authorization comes in, we call the patient and ask that he or she make the call to the insurance company to request the form. I have mixed feelings about passing along the automated phone-hoop hassle to patients, but it is their insurance, after all, and this is one area where I simply can't afford the luxury of providing a time-consuming service for free. Plus, it gives patients some understanding of the absurdity of the whole prior-authorization game.
When possible, we enlist the help of any other parties at our disposal. Some insurers will accept prior authorization requests from pharmacies, which makes a lot of sense. They typically have a complete record of all medications tried and failed, as well as the necessary diagnosis codes.
Unfortunately, many insurers inexplicably insist that only the physician’s office submit the request, but it's worth your time to ask if the company in question accepts pharmacy filings, rather than assuming it doesn’t.
Also, don’t forget that manufacturers of some medications (biologics, for example) will help with some, or all, of the prior-authorization burden. Sometimes they have an auxiliary company set up just for that purpose. If not, a representative or district manager may be able to help or point you toward someone who can. It never hurts to ask.
Also, most pharmaceutical companies have a "compassion" program that provides medications free when the insurer won’t pay and the patient can’t afford it.
Other potential allies are the big-box chains that offer selected medications at $4 (or less) per prescription. Sometimes, the most efficient solution is to point the patient towards Walmart, Costco, Target, or another chain in your area, and forget the pre-authorization altogether.
The key is to get the insurance company's form. Not only do you avoid the phone runaround, but the form tells exactly what that particular company wants, so your staff won’t waste time finding and supplying information that is not needed.
What about patients who request prior authorization for medically unnecessary medications? In my office, that’s usually a retinoid prescription for wrinkles. I tell them it's against the law to say a treatment is necessary when it is not and that there is zero chance their insurer will pay. (As a diplomatic friend of mine puts it, "Your insurance company barely cares if you are dying, let alone how you look!") I tell them I will not be able to go to bat for older patients with recalcitrant acne who really need retinoids, if I try to slip cosmetic prescriptions past insurers. Most understand.
Since passage of the health care reform bill in March, there has been considerable discussion in medical periodicals, forums, and blogs about the dramatic changes that will be taking place.
At least one thing – prior authorizations – will not change, because the legislation did not address it.
Lawmakers have offered no public explanation for ignoring such a glaring problem. It should have been obvious, even to them, that requiring physicians to ask permission, over and over, for necessary tests and treatments is senseless and inefficient. Common sense dictates fixing something so universally hated by doctors and patients alike. One can speculate that the third party in the physician-patient equation – insurers – had a lot to do with this oversight.
Insurers love prior authorization because it saves them money. In fact, it's one of the most effective cost-cutting tools in their box: rationing through inconvenience. So it's logical to speculate that they probably used their considerable input into the reform law's content, via their army of lobbyists, to discourage action.
So, prior authorization will remain a problem for the foreseeable future, and we need to deal with it as best we can.
First and foremost, minimize the wasted time prior authorizations cause you and your staff. My office took a major step toward this goal by banning all submissions by telephone.
A single prior-authorization phone call can easily take 30 minutes of a staffer’s time as they fight through the automated greetings and category selections, and wait on hold before finally speaking to somebody with a pulse. At that point, since the person is hardly ever authorized to give approval, they get another department’s number or a faxed form. It's an inexcusable and outrageously expensive waste of time.
When a request for pre-authorization comes in, we call the patient and ask that he or she make the call to the insurance company to request the form. I have mixed feelings about passing along the automated phone-hoop hassle to patients, but it is their insurance, after all, and this is one area where I simply can't afford the luxury of providing a time-consuming service for free. Plus, it gives patients some understanding of the absurdity of the whole prior-authorization game.
When possible, we enlist the help of any other parties at our disposal. Some insurers will accept prior authorization requests from pharmacies, which makes a lot of sense. They typically have a complete record of all medications tried and failed, as well as the necessary diagnosis codes.
Unfortunately, many insurers inexplicably insist that only the physician’s office submit the request, but it's worth your time to ask if the company in question accepts pharmacy filings, rather than assuming it doesn’t.
Also, don’t forget that manufacturers of some medications (biologics, for example) will help with some, or all, of the prior-authorization burden. Sometimes they have an auxiliary company set up just for that purpose. If not, a representative or district manager may be able to help or point you toward someone who can. It never hurts to ask.
Also, most pharmaceutical companies have a "compassion" program that provides medications free when the insurer won’t pay and the patient can’t afford it.
Other potential allies are the big-box chains that offer selected medications at $4 (or less) per prescription. Sometimes, the most efficient solution is to point the patient towards Walmart, Costco, Target, or another chain in your area, and forget the pre-authorization altogether.
The key is to get the insurance company's form. Not only do you avoid the phone runaround, but the form tells exactly what that particular company wants, so your staff won’t waste time finding and supplying information that is not needed.
What about patients who request prior authorization for medically unnecessary medications? In my office, that’s usually a retinoid prescription for wrinkles. I tell them it's against the law to say a treatment is necessary when it is not and that there is zero chance their insurer will pay. (As a diplomatic friend of mine puts it, "Your insurance company barely cares if you are dying, let alone how you look!") I tell them I will not be able to go to bat for older patients with recalcitrant acne who really need retinoids, if I try to slip cosmetic prescriptions past insurers. Most understand.
Observation Care
Many conditions once treated during an “inpatient” hospital stay are currently treated during an “observation” stay (OBS). Although the care remains the same, physician billing is different and requires close attention to admission details for effective charge capture.
Let’s take a look at a typical OBS scenario. A 65-year-old female with longstanding diabetes presents to the ED at 10 p.m. with palpitations, lightheadedness, mild disorientation, and elevated blood sugar. The hospitalist admits the patient to observation, treats her for dehydration, and discharges her the next day. Before billing, the hospitalist should consider the following factors.
Physician of Record
The attending of record writes the orders to admit the patient to observation; indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. The attending reports the initial patient encounter with the most appropriate initial observation-care code, as reflected by the documentation:1
- 99218: Initial observation care, requiring both a detailed or comprehensive history and exam, and straightforward/low-complexity medical decision-making. Usually, the problem(s) is of low severity.
- 99219: Initial observation care, requiring both a comprehensive history and exam, and moderate-complexity medical decision-making. Usually, the problem(s) is of moderate severity.
- 99220: Initial observation care, requiring both a comprehensive history and exam, and high-complexity medical decision-making. Usually, the problem(s) is of high severity.
While other physicians (e.g., specialists) might be involved in the patient’s care, only the attending physician reports codes 99218-99220. Specialists typically are called to an OBS case for their opinion or advice but do not function as the attending of record. Billing for the specialist (consultation) service depends upon the payor.
For a non-Medicare patient who pays for consultation codes, the specialist reports an outpatient consultation code (99241-99245) for the appropriately documented service. Conversely, Medicare no longer recognizes consultation codes, and specialists must report either a new patient visit code (99201-99205) or established patient visit code (99212-99215) for Medicare beneficiaries.
Selection of the new or established patient codes follows the “three-year rule”: A “new patient” has not received any face-to-face services (e.g., visit or procedure) in any location from any physician within the same group and same specialty within the past three years.2 There could be occasion when a hospitalist is not the attending of record but is asked to provide their opinion, and must report one of the “non-OBS” codes.
The attending of record is permitted to report a discharge service as long as this service occurs on a calendar day different from the admission service (as in the listed scenario). The attending documents the face-to-face discharge service and any pertinent clinical details, and reports 99217 (observation-care discharge-day management).
Length of Stay
Observation-care services typically do not exceed 24 hours and two calendar days. Observation care for more than 48 hours without inpatient admission is not considered medically necessary but might be payable after medical review. Should the OBS stay span more than two calendar days (as might be the case with “downgraded” hospitalizations), hospitalists should report established patient visit codes (99212-99215) for the calendar day(s) between the admission service (99218-99220) and the discharge service (99217).3 The physician must provide and document a face-to-face encounter on each date of service for which a claim was submitted.
A more likely occurrence is the admission and discharge from OBS on the same calendar date. The attending of record reports the code that corresponds to the patient’s length of stay (LOS). If the total LOS is less than eight hours, the attending only reports standard OBS codes (99218-99220). The hospitalist does not separately report the OBS discharge service (99217), even though the documentation must reflect the attending discharge order and corresponding discharge plan. If the total duration of the patient’s stay lasts more than eight hours and does not overlap two calendar days, the attending reports the same-day admit/discharge codes:1
- 99234: Observation or inpatient care, same date admission and discharge, requiring both a detailed or comprehensive history and exam, and straightforward or low-complexity medical decision-making. Usually the presenting problem(s) is of low severity.
- 99235: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and moderate-complexity medical decision-making. Usually the presenting problem(s) is of moderate severity.
- 99236: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and high-complexity medical decision-making. Usually the presenting problem(s) is of high severity.
OBS discharge service (99217) is not separately reported with 99234-99236 because these codes are valued to include the discharge component (e.g., the comprehensive service, 99236 [4.26 wRVU, $211], is equivalent to its components, 99220 [2.99 wRVU, $148] and 99217 [1.28 wRVU, $68]). The attending must document the total duration of the stay, as well as the face-to-face service and the corresponding details of each service component (i.e., both an admission and discharge note).3TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:11-16.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.7A. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8C. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8D. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 1, Section 50.3. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c01.pdf. Accessed May 12, 2010.
Many conditions once treated during an “inpatient” hospital stay are currently treated during an “observation” stay (OBS). Although the care remains the same, physician billing is different and requires close attention to admission details for effective charge capture.
Let’s take a look at a typical OBS scenario. A 65-year-old female with longstanding diabetes presents to the ED at 10 p.m. with palpitations, lightheadedness, mild disorientation, and elevated blood sugar. The hospitalist admits the patient to observation, treats her for dehydration, and discharges her the next day. Before billing, the hospitalist should consider the following factors.
Physician of Record
The attending of record writes the orders to admit the patient to observation; indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. The attending reports the initial patient encounter with the most appropriate initial observation-care code, as reflected by the documentation:1
- 99218: Initial observation care, requiring both a detailed or comprehensive history and exam, and straightforward/low-complexity medical decision-making. Usually, the problem(s) is of low severity.
- 99219: Initial observation care, requiring both a comprehensive history and exam, and moderate-complexity medical decision-making. Usually, the problem(s) is of moderate severity.
- 99220: Initial observation care, requiring both a comprehensive history and exam, and high-complexity medical decision-making. Usually, the problem(s) is of high severity.
While other physicians (e.g., specialists) might be involved in the patient’s care, only the attending physician reports codes 99218-99220. Specialists typically are called to an OBS case for their opinion or advice but do not function as the attending of record. Billing for the specialist (consultation) service depends upon the payor.
For a non-Medicare patient who pays for consultation codes, the specialist reports an outpatient consultation code (99241-99245) for the appropriately documented service. Conversely, Medicare no longer recognizes consultation codes, and specialists must report either a new patient visit code (99201-99205) or established patient visit code (99212-99215) for Medicare beneficiaries.
Selection of the new or established patient codes follows the “three-year rule”: A “new patient” has not received any face-to-face services (e.g., visit or procedure) in any location from any physician within the same group and same specialty within the past three years.2 There could be occasion when a hospitalist is not the attending of record but is asked to provide their opinion, and must report one of the “non-OBS” codes.
The attending of record is permitted to report a discharge service as long as this service occurs on a calendar day different from the admission service (as in the listed scenario). The attending documents the face-to-face discharge service and any pertinent clinical details, and reports 99217 (observation-care discharge-day management).
Length of Stay
Observation-care services typically do not exceed 24 hours and two calendar days. Observation care for more than 48 hours without inpatient admission is not considered medically necessary but might be payable after medical review. Should the OBS stay span more than two calendar days (as might be the case with “downgraded” hospitalizations), hospitalists should report established patient visit codes (99212-99215) for the calendar day(s) between the admission service (99218-99220) and the discharge service (99217).3 The physician must provide and document a face-to-face encounter on each date of service for which a claim was submitted.
A more likely occurrence is the admission and discharge from OBS on the same calendar date. The attending of record reports the code that corresponds to the patient’s length of stay (LOS). If the total LOS is less than eight hours, the attending only reports standard OBS codes (99218-99220). The hospitalist does not separately report the OBS discharge service (99217), even though the documentation must reflect the attending discharge order and corresponding discharge plan. If the total duration of the patient’s stay lasts more than eight hours and does not overlap two calendar days, the attending reports the same-day admit/discharge codes:1
- 99234: Observation or inpatient care, same date admission and discharge, requiring both a detailed or comprehensive history and exam, and straightforward or low-complexity medical decision-making. Usually the presenting problem(s) is of low severity.
- 99235: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and moderate-complexity medical decision-making. Usually the presenting problem(s) is of moderate severity.
- 99236: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and high-complexity medical decision-making. Usually the presenting problem(s) is of high severity.
OBS discharge service (99217) is not separately reported with 99234-99236 because these codes are valued to include the discharge component (e.g., the comprehensive service, 99236 [4.26 wRVU, $211], is equivalent to its components, 99220 [2.99 wRVU, $148] and 99217 [1.28 wRVU, $68]). The attending must document the total duration of the stay, as well as the face-to-face service and the corresponding details of each service component (i.e., both an admission and discharge note).3TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:11-16.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.7A. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8C. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8D. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 1, Section 50.3. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c01.pdf. Accessed May 12, 2010.
Many conditions once treated during an “inpatient” hospital stay are currently treated during an “observation” stay (OBS). Although the care remains the same, physician billing is different and requires close attention to admission details for effective charge capture.
Let’s take a look at a typical OBS scenario. A 65-year-old female with longstanding diabetes presents to the ED at 10 p.m. with palpitations, lightheadedness, mild disorientation, and elevated blood sugar. The hospitalist admits the patient to observation, treats her for dehydration, and discharges her the next day. Before billing, the hospitalist should consider the following factors.
Physician of Record
The attending of record writes the orders to admit the patient to observation; indicates the reason for the stay; outlines the plan of care; and manages the patient during the stay. The attending reports the initial patient encounter with the most appropriate initial observation-care code, as reflected by the documentation:1
- 99218: Initial observation care, requiring both a detailed or comprehensive history and exam, and straightforward/low-complexity medical decision-making. Usually, the problem(s) is of low severity.
- 99219: Initial observation care, requiring both a comprehensive history and exam, and moderate-complexity medical decision-making. Usually, the problem(s) is of moderate severity.
- 99220: Initial observation care, requiring both a comprehensive history and exam, and high-complexity medical decision-making. Usually, the problem(s) is of high severity.
While other physicians (e.g., specialists) might be involved in the patient’s care, only the attending physician reports codes 99218-99220. Specialists typically are called to an OBS case for their opinion or advice but do not function as the attending of record. Billing for the specialist (consultation) service depends upon the payor.
For a non-Medicare patient who pays for consultation codes, the specialist reports an outpatient consultation code (99241-99245) for the appropriately documented service. Conversely, Medicare no longer recognizes consultation codes, and specialists must report either a new patient visit code (99201-99205) or established patient visit code (99212-99215) for Medicare beneficiaries.
Selection of the new or established patient codes follows the “three-year rule”: A “new patient” has not received any face-to-face services (e.g., visit or procedure) in any location from any physician within the same group and same specialty within the past three years.2 There could be occasion when a hospitalist is not the attending of record but is asked to provide their opinion, and must report one of the “non-OBS” codes.
The attending of record is permitted to report a discharge service as long as this service occurs on a calendar day different from the admission service (as in the listed scenario). The attending documents the face-to-face discharge service and any pertinent clinical details, and reports 99217 (observation-care discharge-day management).
Length of Stay
Observation-care services typically do not exceed 24 hours and two calendar days. Observation care for more than 48 hours without inpatient admission is not considered medically necessary but might be payable after medical review. Should the OBS stay span more than two calendar days (as might be the case with “downgraded” hospitalizations), hospitalists should report established patient visit codes (99212-99215) for the calendar day(s) between the admission service (99218-99220) and the discharge service (99217).3 The physician must provide and document a face-to-face encounter on each date of service for which a claim was submitted.
A more likely occurrence is the admission and discharge from OBS on the same calendar date. The attending of record reports the code that corresponds to the patient’s length of stay (LOS). If the total LOS is less than eight hours, the attending only reports standard OBS codes (99218-99220). The hospitalist does not separately report the OBS discharge service (99217), even though the documentation must reflect the attending discharge order and corresponding discharge plan. If the total duration of the patient’s stay lasts more than eight hours and does not overlap two calendar days, the attending reports the same-day admit/discharge codes:1
- 99234: Observation or inpatient care, same date admission and discharge, requiring both a detailed or comprehensive history and exam, and straightforward or low-complexity medical decision-making. Usually the presenting problem(s) is of low severity.
- 99235: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and moderate-complexity medical decision-making. Usually the presenting problem(s) is of moderate severity.
- 99236: Observation or inpatient care, same date admission and discharge, requiring a comprehensive history and exam, and high-complexity medical decision-making. Usually the presenting problem(s) is of high severity.
OBS discharge service (99217) is not separately reported with 99234-99236 because these codes are valued to include the discharge component (e.g., the comprehensive service, 99236 [4.26 wRVU, $211], is equivalent to its components, 99220 [2.99 wRVU, $148] and 99217 [1.28 wRVU, $68]). The attending must document the total duration of the stay, as well as the face-to-face service and the corresponding details of each service component (i.e., both an admission and discharge note).3TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Abraham M, Beebe M, Dalton J, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2010:11-16.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.7A. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8C. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8D. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed May 11, 2010.
- Medicare Claims Processing Manual: Chapter 1, Section 50.3. Centers for Medicare and Medicaid Services website. Available at: www.cms.hhs.gov/manuals/downloads/clm104c01.pdf. Accessed May 12, 2010.
Hospitalist Salary Spike

In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
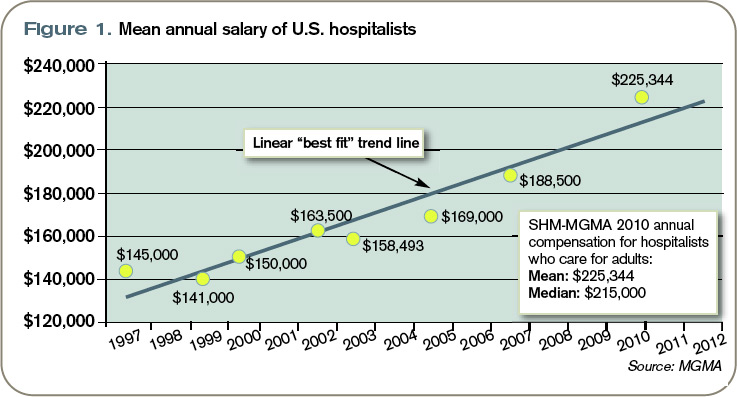
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
In case you haven’t seen it, the latest national survey data on hospitalist production, compensation, and other metrics was released in June.
Just as the Masters golf tournament is promoted as “a tradition like no other,” the combined SHM-MGMA (Medical Group Management Association) survey is without peer. Prior to this year, MGMA and SHM conducted separate surveys annually and biannually, respectively. The organizations chose to do a combined survey to take advantage of MGMA’s size and expertise in survey work (they’ve been conducting an annual survey of every specialty in medicine for decades) as well as SHM’s database of hospitalists and knowledge of the issues unique to HM.
If you want the most reliable data, this is the source you should use. I freely acknowledge my potential conflict of interest, which stems from my history with SHM (as a cofounder of SHM, I feel like a proud parent eager to trumpet all its accomplishments), and my consulting partner, Leslie Flores, was in charge of the survey process and data analysis for SHM. You should consider other sources of hospitalist data that might be available to you, but unless you have an unusually robust local or regional survey, the SHM-MGMA data will be the most valuable.
It’s Just a Survey
This survey provides the best national data, but like all such surveys, it has limitations. First, survey respondents vary in their diligence and accuracy in reporting their own data. It is even likely that some might “sanitize” or adjust the data they report in an effort, usually misguided, to provide a more accurate picture of their practice or cover up what might be for them an embarrassing issue. There is a process in place to catch outlier and inconsistent data submitted by a practice, and such practices are questioned to ensure accurate reporting and clear up any confusion or errors. But even that process is imperfect. There isn’t a team of auditors sent to “look at the books” to independently verify the accuracy of the data reported by each practice; that would be too costly, time-consuming, and even intimidating or annoying to be practical. So keep in mind that there is clearly some unavoidable “noise” or contamination in the data.
People sometimes say “SHM [or MGMA] says that ‘X’ is the right number of encounters for a hospitalist in a year,” where X is a number taken from the survey. Don’t make this mistake. I think it is misleading to think of the survey as establishing optimal or “right” benchmarks for any metric.
In fact, I think of benchmarks being something other than just survey numbers; instead, they’re well-considered data points derived from research showing what is optimal. The average glycohemoglobin of diabetics in the U.S. isn’t a desirable benchmark or goal, but the glycohemoglobin shown by research to be associated with the lowest risk of diabetic complications is. Keep this in mind when thinking about the survey results. There are little or no robust and generalizable research data regarding hospitalist productivity and compensation targets associated with the best performance.
Hospitalist Incomes Surge
Let’s look at one data point: mean salary. The data points in Figure 1 (left) are the average salary going back to the first year the SHM survey was conducted. Note that all historical data points are from the SHM survey only, and thus represent a different population of respondents than the 2010 SHM-MGMA data point. It is important to remember this when looking at any trended hospitalist data.
Perhaps most importantly, previous SHM survey numbers included a significant proportion of academic hospitalist practices, which were largely unrepresented in the new SHM-MGMA survey data because SHM and MGMA will be conducting a separate survey of academic hospitalist practices in the fall.
Since academic hospitalists tend to earn less—and have lower overall productivity—than hospitalists in other settings, their absence from this survey likely results in greater increases in average compensation and production than would otherwise have been the case.
Beginning in about 2001, MGMA began reporting hospitalist compensation, but I have left those numbers off of this figure. And since about 2002, SHM has separated data for hospitalists who care for adults versus those that care for children; when separate data were available, this figure shows the compensation for hospitalists who care for adults and excludes pediatric hospitalists.
Note that the compensation figures include all salary elements, including a “base” or fixed component, productivity component, quality bonus, etc. The numbers exclude such benefits as the cost of health insurance or matching retirement plan contributions.
Inflation and a trend of increased hospitalist productivity are two reasons that hospitalist compensation has been increasing, but neither explains more than a portion of the increase in salary. (According to computational-knowledge engine WolframAlpha.com, inflation in the U.S. averaged 2.3% per year from 1997 to 2002. I’ll talk more about trends in hospitalist productivity in a future column.) I think the principal reason for the rising trend in our pay is “market forces,” primarily demand for hospitalists that has exceeded the supply.
What the Future Holds
It is interesting to speculate whether the historical trend line will accurately predict future increases in salary. At some point, forces will have to “bend the curve” so that it climbs more slowly. It could look like a curve reaching asymptote.
It is anyone’s guess when that might start to happen, but there are two developments over the last couple of years that suggest it might be coming: In some markets, the demand for hospitalists has been met and new candidates can’t find positions, so salaries in those markets might start to level off. And, unlike a few years ago, hospitalists are now competing with nearly every other physician specialty to get financial support from their hospitals, so hospitalists might find their hospital has less money available for them.
But the really big—and unknown—variable that could increase or decrease future hospitalist salaries is the effect of any further national healthcare reform legislation. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelson flores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.