User login
Dos and don’ts of dealing with disruptive behavior
CHICAGO – Dealing with disruptive behavior by staff and colleagues isn’t just about knowing what to do – it’s also about knowing what not to do.
Often, mishandling disruptive behavior can make matters worse and lead to further conflict among physicians and employees, health law experts warn. At a conference held by the American Bar Association, attorneys offered guidance on the dos and don’ts of disruptive behavior management.
Don’t discipline for the wrong reasons
Know what disruptive behavior is not, advised Margo S. Struthers, a Minneapolis-based health law attorney. Criticism offered in good faith with the aim of improving patient care should not be considered disruptive, she said.

“This is a problem that comes up a lot because, often, there is some element of criticism that is offered by the supposed disruptive physician, which may or may not be justified, may or may have been done in good faith, and may or may not have been in a respectful manner.”
An isolated incident of behavior that is not reflective of a pattern of inappropriate, deep-seated, and habitual behavior should not be construed as disruptive, Ms. Struthers added. In addition, disruptive behavior is not respectful disagreement with leadership, presentation of controversial ideas, or the respectful complaining about processes that endanger patient care.
Do address behavior that is truly disruptive
According to the American Medical Association, disruptive behavior is defined as personal conduct, whether verbal or physical, that negatively affects or that potentially may negatively affect patient care, including conduct that interferes the ability to work with members of the health care team. Such behavior can be passive, such as ignoring calls or frequently missing meetings; passive-aggressive, such as excessive sarcasm or veiled threats; or aggressive, such as yelling or bullying.
Don’t focus solely on the behavior
Most disruptive behavior has a root cause, and efforts should be made to get to the bottom of the conduct, according to Sidney Welch, an Atlanta-based health law attorney.

“Often, there’s an underlying frustration in terms of clinical care or what they’re being told to do or the systems and processes [in play],” she said “Where is the sources of the tension that is creating the behavior?”
Do identify contributing factors
Personality characteristics that could lead to hostile behavior include self-centeredness, immaturity, resentfulness, or a need for power and control. Systemic factors could include increased productivity demands, cost-containment requirements, embedded hierarchies, fear of litigation, ineffective or absent conflict-resolution processes, competition between hospitals and medical staff, new care settings, and marketplace demands. Shortages of staff and high work burdens also could fuel disruptive behavior, Ms. Welch said.
“There are situations where there [is] a psychiatric disorder or a personality disorder that’s the root cause of the disruption,” she said. But “sometimes it’s just a stressful situation. A lot of these cases [in which] the physician is the disruption, we’re seeing them in high stakes emergency departments or situations where decisions have to be made very quickly, or fatigue and external stresses may be the source.”
Don’t apply corrective actions inconsistently
Make expectations clear by having a code of conduct supported by policies that apply to every employee, Ms. Welch noted. A lack of fairness among employees can create greater tension and generate increased conflict during a disruptive situation. Ensure that physicians are not be treated differently than nurses or administrators when addressing complaints, she said.
Do implement a graduated set of responses
A tiered response system (informal, formal, disciplinary, regulatory) helps manage disruptive situations based on the extent of conduct, Ms. Welch said.
“The process and disciplinary process [should] to be multileveled so that people know the rules of the road, and the parameters and the bumpers so to speak, are defined.”
Don’t necessarily involve HR
Be cautious of allowing human resource (HR) departments to direct potential disruptive physician issues, Ms. Struthers said.
“I have some concerns about HR getting involved for a couple of reasons,” she said. “If you get nonphysicians involved, it seems to exacerbate the level of tension.”
In addition, if a hospital has a significant number of both employed and independent physicians, HR can sometimes apply different standards and varied courses of action depending on employment status, she said. Of course, if the alleged disrupter is a nonphysician, HR is generally the only route for remedy within a hospital setting, Ms. Welch noted.
Do address the issue through internal processes
Every medical staff should develop and adopt bylaw provisions or policies for intervening in situations in which a physician’s behavior is identified as disruptive, according to AMA policy. Medical staff bylaw provisions or policies should contain procedural safeguards that protect due process.
For doctors in groups or small practices, employment policies and procedures should address protocols when disruption matters arise, Ms. Struthers said.
“The dynamics in a small clinic is that some doctors may more have power than others, so it may be harder in some contexts to treat everyone the same,” she said in an interview. “But that’s a really important thing to do. Any well-advised clinics would have a code of conduct or conduct policy, really to protect the clinic from employee lawsuits.”
Don’t let policies collect dust
“As we all know, you can write the policies, you can put them on the shelf, but if people aren’t reading them and understanding them and aren’t educated on them, then it really does no good,” Ms. Welch said.
Do ensure everyone knows how disruptive behavior is handled
Make certain that all staff review disruptive behavior policies and are adequately trained in how the process works, Ms. Welch added. Employees should know where to seek help if experiencing a disruption matter. Consider having staff members sign or acknowledge a code of conduct upon credentialing or hiring.
“Obviously, disruptive behavior can impact patient care, and it can come from a lot of differ directions; It’s not just physicians,” Ms. Struthers said. “Hospitals [and practices] like other places of business, need to have comprehensive polices and procedures, and they need to follow them.”
On Twitter @legal_med
CHICAGO – Dealing with disruptive behavior by staff and colleagues isn’t just about knowing what to do – it’s also about knowing what not to do.
Often, mishandling disruptive behavior can make matters worse and lead to further conflict among physicians and employees, health law experts warn. At a conference held by the American Bar Association, attorneys offered guidance on the dos and don’ts of disruptive behavior management.
Don’t discipline for the wrong reasons
Know what disruptive behavior is not, advised Margo S. Struthers, a Minneapolis-based health law attorney. Criticism offered in good faith with the aim of improving patient care should not be considered disruptive, she said.
“This is a problem that comes up a lot because, often, there is some element of criticism that is offered by the supposed disruptive physician, which may or may not be justified, may or may have been done in good faith, and may or may not have been in a respectful manner.”
An isolated incident of behavior that is not reflective of a pattern of inappropriate, deep-seated, and habitual behavior should not be construed as disruptive, Ms. Struthers added. In addition, disruptive behavior is not respectful disagreement with leadership, presentation of controversial ideas, or the respectful complaining about processes that endanger patient care.
Do address behavior that is truly disruptive
According to the American Medical Association, disruptive behavior is defined as personal conduct, whether verbal or physical, that negatively affects or that potentially may negatively affect patient care, including conduct that interferes the ability to work with members of the health care team. Such behavior can be passive, such as ignoring calls or frequently missing meetings; passive-aggressive, such as excessive sarcasm or veiled threats; or aggressive, such as yelling or bullying.
Don’t focus solely on the behavior
Most disruptive behavior has a root cause, and efforts should be made to get to the bottom of the conduct, according to Sidney Welch, an Atlanta-based health law attorney.
“Often, there’s an underlying frustration in terms of clinical care or what they’re being told to do or the systems and processes [in play],” she said “Where is the sources of the tension that is creating the behavior?”
Do identify contributing factors
Personality characteristics that could lead to hostile behavior include self-centeredness, immaturity, resentfulness, or a need for power and control. Systemic factors could include increased productivity demands, cost-containment requirements, embedded hierarchies, fear of litigation, ineffective or absent conflict-resolution processes, competition between hospitals and medical staff, new care settings, and marketplace demands. Shortages of staff and high work burdens also could fuel disruptive behavior, Ms. Welch said.
“There are situations where there [is] a psychiatric disorder or a personality disorder that’s the root cause of the disruption,” she said. But “sometimes it’s just a stressful situation. A lot of these cases [in which] the physician is the disruption, we’re seeing them in high stakes emergency departments or situations where decisions have to be made very quickly, or fatigue and external stresses may be the source.”
Don’t apply corrective actions inconsistently
Make expectations clear by having a code of conduct supported by policies that apply to every employee, Ms. Welch noted. A lack of fairness among employees can create greater tension and generate increased conflict during a disruptive situation. Ensure that physicians are not be treated differently than nurses or administrators when addressing complaints, she said.
Do implement a graduated set of responses
A tiered response system (informal, formal, disciplinary, regulatory) helps manage disruptive situations based on the extent of conduct, Ms. Welch said.
“The process and disciplinary process [should] to be multileveled so that people know the rules of the road, and the parameters and the bumpers so to speak, are defined.”
Don’t necessarily involve HR
Be cautious of allowing human resource (HR) departments to direct potential disruptive physician issues, Ms. Struthers said.
“I have some concerns about HR getting involved for a couple of reasons,” she said. “If you get nonphysicians involved, it seems to exacerbate the level of tension.”
In addition, if a hospital has a significant number of both employed and independent physicians, HR can sometimes apply different standards and varied courses of action depending on employment status, she said. Of course, if the alleged disrupter is a nonphysician, HR is generally the only route for remedy within a hospital setting, Ms. Welch noted.
Do address the issue through internal processes
Every medical staff should develop and adopt bylaw provisions or policies for intervening in situations in which a physician’s behavior is identified as disruptive, according to AMA policy. Medical staff bylaw provisions or policies should contain procedural safeguards that protect due process.
For doctors in groups or small practices, employment policies and procedures should address protocols when disruption matters arise, Ms. Struthers said.
“The dynamics in a small clinic is that some doctors may more have power than others, so it may be harder in some contexts to treat everyone the same,” she said in an interview. “But that’s a really important thing to do. Any well-advised clinics would have a code of conduct or conduct policy, really to protect the clinic from employee lawsuits.”
Don’t let policies collect dust
“As we all know, you can write the policies, you can put them on the shelf, but if people aren’t reading them and understanding them and aren’t educated on them, then it really does no good,” Ms. Welch said.
Do ensure everyone knows how disruptive behavior is handled
Make certain that all staff review disruptive behavior policies and are adequately trained in how the process works, Ms. Welch added. Employees should know where to seek help if experiencing a disruption matter. Consider having staff members sign or acknowledge a code of conduct upon credentialing or hiring.
“Obviously, disruptive behavior can impact patient care, and it can come from a lot of differ directions; It’s not just physicians,” Ms. Struthers said. “Hospitals [and practices] like other places of business, need to have comprehensive polices and procedures, and they need to follow them.”
On Twitter @legal_med
CHICAGO – Dealing with disruptive behavior by staff and colleagues isn’t just about knowing what to do – it’s also about knowing what not to do.
Often, mishandling disruptive behavior can make matters worse and lead to further conflict among physicians and employees, health law experts warn. At a conference held by the American Bar Association, attorneys offered guidance on the dos and don’ts of disruptive behavior management.
Don’t discipline for the wrong reasons
Know what disruptive behavior is not, advised Margo S. Struthers, a Minneapolis-based health law attorney. Criticism offered in good faith with the aim of improving patient care should not be considered disruptive, she said.
“This is a problem that comes up a lot because, often, there is some element of criticism that is offered by the supposed disruptive physician, which may or may not be justified, may or may have been done in good faith, and may or may not have been in a respectful manner.”
An isolated incident of behavior that is not reflective of a pattern of inappropriate, deep-seated, and habitual behavior should not be construed as disruptive, Ms. Struthers added. In addition, disruptive behavior is not respectful disagreement with leadership, presentation of controversial ideas, or the respectful complaining about processes that endanger patient care.
Do address behavior that is truly disruptive
According to the American Medical Association, disruptive behavior is defined as personal conduct, whether verbal or physical, that negatively affects or that potentially may negatively affect patient care, including conduct that interferes the ability to work with members of the health care team. Such behavior can be passive, such as ignoring calls or frequently missing meetings; passive-aggressive, such as excessive sarcasm or veiled threats; or aggressive, such as yelling or bullying.
Don’t focus solely on the behavior
Most disruptive behavior has a root cause, and efforts should be made to get to the bottom of the conduct, according to Sidney Welch, an Atlanta-based health law attorney.
“Often, there’s an underlying frustration in terms of clinical care or what they’re being told to do or the systems and processes [in play],” she said “Where is the sources of the tension that is creating the behavior?”
Do identify contributing factors
Personality characteristics that could lead to hostile behavior include self-centeredness, immaturity, resentfulness, or a need for power and control. Systemic factors could include increased productivity demands, cost-containment requirements, embedded hierarchies, fear of litigation, ineffective or absent conflict-resolution processes, competition between hospitals and medical staff, new care settings, and marketplace demands. Shortages of staff and high work burdens also could fuel disruptive behavior, Ms. Welch said.
“There are situations where there [is] a psychiatric disorder or a personality disorder that’s the root cause of the disruption,” she said. But “sometimes it’s just a stressful situation. A lot of these cases [in which] the physician is the disruption, we’re seeing them in high stakes emergency departments or situations where decisions have to be made very quickly, or fatigue and external stresses may be the source.”
Don’t apply corrective actions inconsistently
Make expectations clear by having a code of conduct supported by policies that apply to every employee, Ms. Welch noted. A lack of fairness among employees can create greater tension and generate increased conflict during a disruptive situation. Ensure that physicians are not be treated differently than nurses or administrators when addressing complaints, she said.
Do implement a graduated set of responses
A tiered response system (informal, formal, disciplinary, regulatory) helps manage disruptive situations based on the extent of conduct, Ms. Welch said.
“The process and disciplinary process [should] to be multileveled so that people know the rules of the road, and the parameters and the bumpers so to speak, are defined.”
Don’t necessarily involve HR
Be cautious of allowing human resource (HR) departments to direct potential disruptive physician issues, Ms. Struthers said.
“I have some concerns about HR getting involved for a couple of reasons,” she said. “If you get nonphysicians involved, it seems to exacerbate the level of tension.”
In addition, if a hospital has a significant number of both employed and independent physicians, HR can sometimes apply different standards and varied courses of action depending on employment status, she said. Of course, if the alleged disrupter is a nonphysician, HR is generally the only route for remedy within a hospital setting, Ms. Welch noted.
Do address the issue through internal processes
Every medical staff should develop and adopt bylaw provisions or policies for intervening in situations in which a physician’s behavior is identified as disruptive, according to AMA policy. Medical staff bylaw provisions or policies should contain procedural safeguards that protect due process.
For doctors in groups or small practices, employment policies and procedures should address protocols when disruption matters arise, Ms. Struthers said.
“The dynamics in a small clinic is that some doctors may more have power than others, so it may be harder in some contexts to treat everyone the same,” she said in an interview. “But that’s a really important thing to do. Any well-advised clinics would have a code of conduct or conduct policy, really to protect the clinic from employee lawsuits.”
Don’t let policies collect dust
“As we all know, you can write the policies, you can put them on the shelf, but if people aren’t reading them and understanding them and aren’t educated on them, then it really does no good,” Ms. Welch said.
Do ensure everyone knows how disruptive behavior is handled
Make certain that all staff review disruptive behavior policies and are adequately trained in how the process works, Ms. Welch added. Employees should know where to seek help if experiencing a disruption matter. Consider having staff members sign or acknowledge a code of conduct upon credentialing or hiring.
“Obviously, disruptive behavior can impact patient care, and it can come from a lot of differ directions; It’s not just physicians,” Ms. Struthers said. “Hospitals [and practices] like other places of business, need to have comprehensive polices and procedures, and they need to follow them.”
On Twitter @legal_med
AT THE PHYSICIANS LEGAL ISSUES CONFERENCE

Lesson in Improper Allocations, Unaccounted for NP/PA Contributions
I visited during a hot Florida summer in the mid 1990s and could readily see that the practice was great in most respects. The large multispecialty group had recruited talented hospitalists and had put in place effective operational practices. All seemed to be going well, but inappropriate overhead allocation was undermining the success of their efforts.
The multispecialty group employing the hospitalists used the same formula to allocate overhead to the hospitalists that was in place for other specialties. And compensation was essentially each doctor’s collections minus overhead, leaving the hospitalists with annual compensation much lower than they could reasonably expect. With the group deducting from hospitalist collections the same overhead expenses charged to other specialties, including a share of outpatient buildings, staff, and supplies, the hospitalists were paying a lot for services they weren’t using. This group corrected the errors but not until some talented doctors had resigned because of the compensation formula.
This was a common mistake made by multispecialty groups that employed hospitalists years ago. Today, nearly all such groups assess an appropriately smaller portion of overhead to hospitalists than office-based doctors.
Typical Hospitalist Overhead
It is still tricky to correctly assess and allocate hospitalist overhead. This meaningfully influences the apparent total cost of the program and hence the amount of support paid by the hospital or other entity. (This support is often referred to as a “subsidy,” though I don’t care for that term because of its negative connotation.)
For example, costs for billing and collections services, malpractice insurance, temporary staffing (locums), and an overhead allocation that pays for things like the salaries of medical group administrators and clerical staff may or may not be attributed to the hospitalist budget or “cost center.” This is one of several factors that make it awfully tricky to compare the total costs and/or hospital financial support between different hospitalist groups.
SHM’s State of Hospital Medicine report includes detailed instructions regarding which expenses the survey respondents should include as overhead costs, but I think it’s safe to assume that not all responses are fully compliant. I’m confident there is a meaningful amount of “noise” in these figures. Numbers like the median financial support per FTE hospitalist per year ($156,063 in the 2014 report) should only be used as a guideline and not a precise number that might apply in your setting. My reasoning is that the collections rate and compensation amount can vary tremendously from one practice to another and will typically have a far larger influence on the amount of financial support provided by the hospital than which expenses are or aren’t included as overhead. But I am confining this discussion to the latter.
APC Costs: One Factor Driving Increased Support
SHM has been surveying the financial support per physician FTE for about 15 years, and it has shown a steady increase. It was about $60,000 per FTE annually when first surveyed in the late 1990s; it has gone up every survey since. The best explanation for this seems to an increase in hospitalist compensation while production and revenue have remained relatively flat.
There likely are many other factors in play. One important one is physician assistant and nurse practitioner costs. The survey divides the total annual support provided to the whole hospitalist practice by the total number of physician FTEs. NPs and PAs are becoming more common in hospitalist groups; 65% of groups included them in 2014, up from 54% in 2012. Yet the cost of employing them, primarily salary and benefits, appears in the numerator but not the denominator of the support per physician FTE figure.
This means a group that adds NP/PA staffing, which typically requires an accompanying increase in hospital financial support, while maintaining the same number of physician FTEs will show an increase in hospital support per physician FTE. But this fails to capture that the practice’s work product (i.e., patients seen) has increased as a result of increasing its clinical staff.
This is a tricky issue to fix. SHM’s Practice Analysis Committee, which manages the survey, is aware of the issue and may make future adjustments to account for it. The best method might be to convert total staffing by physicians and NP/PAs into physician-equivalent FTEs (I described one method for doing this in my August 2009 column titled “Volume Variables”) or some other method that clearly accounts for both physician and NP/PA staffing levels. Other alternatives would be to divide the annual support by the number of billed encounters or some other measure of “work output” or to report percent of the total practice revenue that comes from hospital support versus professional fee collections and other sources.
Why Allocation of NP/PA Costs and FTEs Matter
Another way to think of this issue is that including NP/PA costs but not their work (FTEs) in the financial support per FTE figure overlooks the important work they can do for a hospitalist practice. And it can lead one to conclude hospitals’ costs per clinician FTE are rising faster than is actually the case.
This is only one of the tricky issues in accurately understanding hospitalist overhead and costs to the hospital they serve. TH

I visited during a hot Florida summer in the mid 1990s and could readily see that the practice was great in most respects. The large multispecialty group had recruited talented hospitalists and had put in place effective operational practices. All seemed to be going well, but inappropriate overhead allocation was undermining the success of their efforts.
The multispecialty group employing the hospitalists used the same formula to allocate overhead to the hospitalists that was in place for other specialties. And compensation was essentially each doctor’s collections minus overhead, leaving the hospitalists with annual compensation much lower than they could reasonably expect. With the group deducting from hospitalist collections the same overhead expenses charged to other specialties, including a share of outpatient buildings, staff, and supplies, the hospitalists were paying a lot for services they weren’t using. This group corrected the errors but not until some talented doctors had resigned because of the compensation formula.
This was a common mistake made by multispecialty groups that employed hospitalists years ago. Today, nearly all such groups assess an appropriately smaller portion of overhead to hospitalists than office-based doctors.
Typical Hospitalist Overhead
It is still tricky to correctly assess and allocate hospitalist overhead. This meaningfully influences the apparent total cost of the program and hence the amount of support paid by the hospital or other entity. (This support is often referred to as a “subsidy,” though I don’t care for that term because of its negative connotation.)
For example, costs for billing and collections services, malpractice insurance, temporary staffing (locums), and an overhead allocation that pays for things like the salaries of medical group administrators and clerical staff may or may not be attributed to the hospitalist budget or “cost center.” This is one of several factors that make it awfully tricky to compare the total costs and/or hospital financial support between different hospitalist groups.
SHM’s State of Hospital Medicine report includes detailed instructions regarding which expenses the survey respondents should include as overhead costs, but I think it’s safe to assume that not all responses are fully compliant. I’m confident there is a meaningful amount of “noise” in these figures. Numbers like the median financial support per FTE hospitalist per year ($156,063 in the 2014 report) should only be used as a guideline and not a precise number that might apply in your setting. My reasoning is that the collections rate and compensation amount can vary tremendously from one practice to another and will typically have a far larger influence on the amount of financial support provided by the hospital than which expenses are or aren’t included as overhead. But I am confining this discussion to the latter.
APC Costs: One Factor Driving Increased Support
SHM has been surveying the financial support per physician FTE for about 15 years, and it has shown a steady increase. It was about $60,000 per FTE annually when first surveyed in the late 1990s; it has gone up every survey since. The best explanation for this seems to an increase in hospitalist compensation while production and revenue have remained relatively flat.
There likely are many other factors in play. One important one is physician assistant and nurse practitioner costs. The survey divides the total annual support provided to the whole hospitalist practice by the total number of physician FTEs. NPs and PAs are becoming more common in hospitalist groups; 65% of groups included them in 2014, up from 54% in 2012. Yet the cost of employing them, primarily salary and benefits, appears in the numerator but not the denominator of the support per physician FTE figure.
This means a group that adds NP/PA staffing, which typically requires an accompanying increase in hospital financial support, while maintaining the same number of physician FTEs will show an increase in hospital support per physician FTE. But this fails to capture that the practice’s work product (i.e., patients seen) has increased as a result of increasing its clinical staff.
This is a tricky issue to fix. SHM’s Practice Analysis Committee, which manages the survey, is aware of the issue and may make future adjustments to account for it. The best method might be to convert total staffing by physicians and NP/PAs into physician-equivalent FTEs (I described one method for doing this in my August 2009 column titled “Volume Variables”) or some other method that clearly accounts for both physician and NP/PA staffing levels. Other alternatives would be to divide the annual support by the number of billed encounters or some other measure of “work output” or to report percent of the total practice revenue that comes from hospital support versus professional fee collections and other sources.
Why Allocation of NP/PA Costs and FTEs Matter
Another way to think of this issue is that including NP/PA costs but not their work (FTEs) in the financial support per FTE figure overlooks the important work they can do for a hospitalist practice. And it can lead one to conclude hospitals’ costs per clinician FTE are rising faster than is actually the case.
This is only one of the tricky issues in accurately understanding hospitalist overhead and costs to the hospital they serve. TH
I visited during a hot Florida summer in the mid 1990s and could readily see that the practice was great in most respects. The large multispecialty group had recruited talented hospitalists and had put in place effective operational practices. All seemed to be going well, but inappropriate overhead allocation was undermining the success of their efforts.
The multispecialty group employing the hospitalists used the same formula to allocate overhead to the hospitalists that was in place for other specialties. And compensation was essentially each doctor’s collections minus overhead, leaving the hospitalists with annual compensation much lower than they could reasonably expect. With the group deducting from hospitalist collections the same overhead expenses charged to other specialties, including a share of outpatient buildings, staff, and supplies, the hospitalists were paying a lot for services they weren’t using. This group corrected the errors but not until some talented doctors had resigned because of the compensation formula.
This was a common mistake made by multispecialty groups that employed hospitalists years ago. Today, nearly all such groups assess an appropriately smaller portion of overhead to hospitalists than office-based doctors.
Typical Hospitalist Overhead
It is still tricky to correctly assess and allocate hospitalist overhead. This meaningfully influences the apparent total cost of the program and hence the amount of support paid by the hospital or other entity. (This support is often referred to as a “subsidy,” though I don’t care for that term because of its negative connotation.)
For example, costs for billing and collections services, malpractice insurance, temporary staffing (locums), and an overhead allocation that pays for things like the salaries of medical group administrators and clerical staff may or may not be attributed to the hospitalist budget or “cost center.” This is one of several factors that make it awfully tricky to compare the total costs and/or hospital financial support between different hospitalist groups.
SHM’s State of Hospital Medicine report includes detailed instructions regarding which expenses the survey respondents should include as overhead costs, but I think it’s safe to assume that not all responses are fully compliant. I’m confident there is a meaningful amount of “noise” in these figures. Numbers like the median financial support per FTE hospitalist per year ($156,063 in the 2014 report) should only be used as a guideline and not a precise number that might apply in your setting. My reasoning is that the collections rate and compensation amount can vary tremendously from one practice to another and will typically have a far larger influence on the amount of financial support provided by the hospital than which expenses are or aren’t included as overhead. But I am confining this discussion to the latter.
APC Costs: One Factor Driving Increased Support
SHM has been surveying the financial support per physician FTE for about 15 years, and it has shown a steady increase. It was about $60,000 per FTE annually when first surveyed in the late 1990s; it has gone up every survey since. The best explanation for this seems to an increase in hospitalist compensation while production and revenue have remained relatively flat.
There likely are many other factors in play. One important one is physician assistant and nurse practitioner costs. The survey divides the total annual support provided to the whole hospitalist practice by the total number of physician FTEs. NPs and PAs are becoming more common in hospitalist groups; 65% of groups included them in 2014, up from 54% in 2012. Yet the cost of employing them, primarily salary and benefits, appears in the numerator but not the denominator of the support per physician FTE figure.
This means a group that adds NP/PA staffing, which typically requires an accompanying increase in hospital financial support, while maintaining the same number of physician FTEs will show an increase in hospital support per physician FTE. But this fails to capture that the practice’s work product (i.e., patients seen) has increased as a result of increasing its clinical staff.
This is a tricky issue to fix. SHM’s Practice Analysis Committee, which manages the survey, is aware of the issue and may make future adjustments to account for it. The best method might be to convert total staffing by physicians and NP/PAs into physician-equivalent FTEs (I described one method for doing this in my August 2009 column titled “Volume Variables”) or some other method that clearly accounts for both physician and NP/PA staffing levels. Other alternatives would be to divide the annual support by the number of billed encounters or some other measure of “work output” or to report percent of the total practice revenue that comes from hospital support versus professional fee collections and other sources.
Why Allocation of NP/PA Costs and FTEs Matter
Another way to think of this issue is that including NP/PA costs but not their work (FTEs) in the financial support per FTE figure overlooks the important work they can do for a hospitalist practice. And it can lead one to conclude hospitals’ costs per clinician FTE are rising faster than is actually the case.
This is only one of the tricky issues in accurately understanding hospitalist overhead and costs to the hospital they serve. TH
Applying Military Principles to HM Leadership
Hospitalists are more than doctors—they are also leaders in their organizations, which is why a new book by retired Army Lieutenant General Mark Hertling is relevant to what they do every day. Hertling, whose numerous military awards include the Legion of Merit, the Bronze Star, and the Purple Heart, is the author of Growing Physician Leaders: Empowering Doctors to Improve Our Healthcare, which applies his four decades of military leadership to the world of healthcare.
He wrote the book not long after designing the first physician leader course at Florida Hospital in Orlando.
“Many of the administrators and other doctors saw the changes in the doctors, nurses, and administrators who graduated from the course, and they asked me to write down what we had done,” he says. “The book is partially a description of the course, but it’s also a primer on the basics of leadership.”
The book tells readers how to understand what kind of leader they can be as well as how to better understand the motivations of others; it also outlines a variety of influence techniques they can employ to get things done.
“One of the things we drive home is that all physicians are leaders, whether they are in a leadership role or not,” Hertling says.
One of the concepts he outlines is “leading up”—how to influence your bosses to do the things you want them to do. “What we do during this lesson is show readers how they are other people’s bosses, too,” he says, “and that they need to listen to their own people, too, and allow their folks to contribute to the organizational goals.”
Hospitalists are more than doctors—they are also leaders in their organizations, which is why a new book by retired Army Lieutenant General Mark Hertling is relevant to what they do every day. Hertling, whose numerous military awards include the Legion of Merit, the Bronze Star, and the Purple Heart, is the author of Growing Physician Leaders: Empowering Doctors to Improve Our Healthcare, which applies his four decades of military leadership to the world of healthcare.
He wrote the book not long after designing the first physician leader course at Florida Hospital in Orlando.
“Many of the administrators and other doctors saw the changes in the doctors, nurses, and administrators who graduated from the course, and they asked me to write down what we had done,” he says. “The book is partially a description of the course, but it’s also a primer on the basics of leadership.”
The book tells readers how to understand what kind of leader they can be as well as how to better understand the motivations of others; it also outlines a variety of influence techniques they can employ to get things done.
“One of the things we drive home is that all physicians are leaders, whether they are in a leadership role or not,” Hertling says.
One of the concepts he outlines is “leading up”—how to influence your bosses to do the things you want them to do. “What we do during this lesson is show readers how they are other people’s bosses, too,” he says, “and that they need to listen to their own people, too, and allow their folks to contribute to the organizational goals.”
Hospitalists are more than doctors—they are also leaders in their organizations, which is why a new book by retired Army Lieutenant General Mark Hertling is relevant to what they do every day. Hertling, whose numerous military awards include the Legion of Merit, the Bronze Star, and the Purple Heart, is the author of Growing Physician Leaders: Empowering Doctors to Improve Our Healthcare, which applies his four decades of military leadership to the world of healthcare.
He wrote the book not long after designing the first physician leader course at Florida Hospital in Orlando.
“Many of the administrators and other doctors saw the changes in the doctors, nurses, and administrators who graduated from the course, and they asked me to write down what we had done,” he says. “The book is partially a description of the course, but it’s also a primer on the basics of leadership.”
The book tells readers how to understand what kind of leader they can be as well as how to better understand the motivations of others; it also outlines a variety of influence techniques they can employ to get things done.
“One of the things we drive home is that all physicians are leaders, whether they are in a leadership role or not,” Hertling says.
One of the concepts he outlines is “leading up”—how to influence your bosses to do the things you want them to do. “What we do during this lesson is show readers how they are other people’s bosses, too,” he says, “and that they need to listen to their own people, too, and allow their folks to contribute to the organizational goals.”
Recognizing Contributions Physician Personalities Make to the Greater Good
My family and I recently took a spring break trip out west to see a few national parks. During the trip, we stayed on a family ranch in Utah. It had a wide variety of livestock, including a large number of mules and horses.
During our stay at this family-owned ranch, two things really stood out and made me think:
- The guesthouse we stayed in had an inordinate volume of collections dedicated to the science and art of raising horses and mules. Everywhere one looked you could find a wall-mounted picture, poem, or coffee table book about these species. My favorite, written by the owner of the ranch, John Hauer, was The Natural Superiority of Mules.1
- The second thing I noticed was that every member of the ranch-owning family had fairly strong opinions about which was better—horse or mule. Just to recap the biology, a horse is the product of two horses, whereas a mule is the progeny of a male donkey and a female horse. It turns out that their physical structure and demeanors are very different.
One of the oldest members of the ranch family (who I believe was a “distant uncle”) had a very strong opinion about the superiority of the mule. His opinion was based on selected facts, including that mules are “steadier on their feet” in unstable ground, require less volume and less frequent food and water, and very rarely became ill or need costly veterinary care.
Another mule-favoring family member told us how mules get a “bad rap” for being stubborn when they actually are much smarter and better decision makers than horses. She recalled a famous folklore of a farmer who took his mule out to gather materials from across a field. When the farmer and the mule approached a wooden bridge, the mule absolutely refused to cross the bridge. After much back and forth between the farmer and the mule (involving both coaxing and cussing), the farmer gave up and returned to the farm with the mule. He then took his horse on the same errand. When they came to the same bridge, the horse also hesitated but required little bargaining from the farmer to coax it to cross the bridge. When barely halfway across, a rotten board in the bridge gave way, almost sending both the horse and the farmer to their deaths in the ravine below.
The moral of the folklore is that mules cannot be coaxed (or cussed) into performing behaviors that will put themselves or those around them at risk of injury or death. Mules will stop when exhausted or profoundly dehydrated, for example, whereas a horse will continue on if ordered by their farmer, even to the point of running themselves to their eventual demise.
One of the younger members of the family-owned ranch, however, had very strong opinions on the superiority of the horse. Horses are loyal and unwavering in their dedication to please those that they serve. They will put the needs of others before themselves in most situations and therefore almost always “outperform” a mule in all respects. They are willing and (usually) able to perform in uncertain conditions, even despite some reservations. They are loyal and loving, and they have unique and inquisitive personalities, which makes them fun to raise and to ride any day.
Test Drives
Our family of four went on a ride with some of these animals and randomly got two horses and two mules. Interestingly, during our ride, we all did indeed notice the differences between the horses and the mules.
The horses were seemingly easygoing and quick to please, easily following cues to change direction or course. The mules were more hesitant and seemed to need to understand why they were being asked to do something before they acquiesced to the demand.
And when we approached a narrow rocky downslope, the mules were slow, steady, and confident, whereas the horses were seemingly uncomfortable and less agile. And, indeed in researching mules, they seem to have gotten a very bad rap over time (as evidenced by the term “stubborn as a mule”).
Charles Darwin actually categorized mules as an example of “hybrid vigor,” which is a rare example of when an offspring is actually better in most ways than either of its parents. Compared to its parental species, mules have more intelligence, endurance, longevity, health, speed, height, and agility. Also to their advantage, they have harder skin and hooves, allowing them to weather and endure more treacherous conditions.
With all of this newfound knowledge of the mule, it struck me what remarkable similarity some physicians have with mules and the role that these mules are likely serving within our organizations. These physicians are probably labeled as stubborn, obstinate, resistant, or impatient. But maybe they are actually intelligent, agile, and appropriately cautious. Maybe the resistance they express in the organization is serving to warn others about the rotten wooden bridges.
HM Takeaway
Similar to a ranch, most hospitals probably function best with a healthy combination of horses and mules. So if you get an opportunity, next time you encounter physicians at your hospital acting like mules, you should congratulate them and appreciate their mule-like characteristics. Recognize the contribution these types of physicians are making, in their own way, to the greater good of the organization.
After all, we can’t—and shouldn’t—all be horses. TH
Reference
1. Hauer J. The Natural Superiority of Mules: A Celebration of One of the Most Intelligent, Sure-footed, and Misunderstood Animals in the World. New York, NY: Skyhorse Publishing; 2006.

My family and I recently took a spring break trip out west to see a few national parks. During the trip, we stayed on a family ranch in Utah. It had a wide variety of livestock, including a large number of mules and horses.
During our stay at this family-owned ranch, two things really stood out and made me think:
- The guesthouse we stayed in had an inordinate volume of collections dedicated to the science and art of raising horses and mules. Everywhere one looked you could find a wall-mounted picture, poem, or coffee table book about these species. My favorite, written by the owner of the ranch, John Hauer, was The Natural Superiority of Mules.1
- The second thing I noticed was that every member of the ranch-owning family had fairly strong opinions about which was better—horse or mule. Just to recap the biology, a horse is the product of two horses, whereas a mule is the progeny of a male donkey and a female horse. It turns out that their physical structure and demeanors are very different.
One of the oldest members of the ranch family (who I believe was a “distant uncle”) had a very strong opinion about the superiority of the mule. His opinion was based on selected facts, including that mules are “steadier on their feet” in unstable ground, require less volume and less frequent food and water, and very rarely became ill or need costly veterinary care.
Another mule-favoring family member told us how mules get a “bad rap” for being stubborn when they actually are much smarter and better decision makers than horses. She recalled a famous folklore of a farmer who took his mule out to gather materials from across a field. When the farmer and the mule approached a wooden bridge, the mule absolutely refused to cross the bridge. After much back and forth between the farmer and the mule (involving both coaxing and cussing), the farmer gave up and returned to the farm with the mule. He then took his horse on the same errand. When they came to the same bridge, the horse also hesitated but required little bargaining from the farmer to coax it to cross the bridge. When barely halfway across, a rotten board in the bridge gave way, almost sending both the horse and the farmer to their deaths in the ravine below.
The moral of the folklore is that mules cannot be coaxed (or cussed) into performing behaviors that will put themselves or those around them at risk of injury or death. Mules will stop when exhausted or profoundly dehydrated, for example, whereas a horse will continue on if ordered by their farmer, even to the point of running themselves to their eventual demise.
One of the younger members of the family-owned ranch, however, had very strong opinions on the superiority of the horse. Horses are loyal and unwavering in their dedication to please those that they serve. They will put the needs of others before themselves in most situations and therefore almost always “outperform” a mule in all respects. They are willing and (usually) able to perform in uncertain conditions, even despite some reservations. They are loyal and loving, and they have unique and inquisitive personalities, which makes them fun to raise and to ride any day.
Test Drives
Our family of four went on a ride with some of these animals and randomly got two horses and two mules. Interestingly, during our ride, we all did indeed notice the differences between the horses and the mules.
The horses were seemingly easygoing and quick to please, easily following cues to change direction or course. The mules were more hesitant and seemed to need to understand why they were being asked to do something before they acquiesced to the demand.
And when we approached a narrow rocky downslope, the mules were slow, steady, and confident, whereas the horses were seemingly uncomfortable and less agile. And, indeed in researching mules, they seem to have gotten a very bad rap over time (as evidenced by the term “stubborn as a mule”).
Charles Darwin actually categorized mules as an example of “hybrid vigor,” which is a rare example of when an offspring is actually better in most ways than either of its parents. Compared to its parental species, mules have more intelligence, endurance, longevity, health, speed, height, and agility. Also to their advantage, they have harder skin and hooves, allowing them to weather and endure more treacherous conditions.
With all of this newfound knowledge of the mule, it struck me what remarkable similarity some physicians have with mules and the role that these mules are likely serving within our organizations. These physicians are probably labeled as stubborn, obstinate, resistant, or impatient. But maybe they are actually intelligent, agile, and appropriately cautious. Maybe the resistance they express in the organization is serving to warn others about the rotten wooden bridges.
HM Takeaway
Similar to a ranch, most hospitals probably function best with a healthy combination of horses and mules. So if you get an opportunity, next time you encounter physicians at your hospital acting like mules, you should congratulate them and appreciate their mule-like characteristics. Recognize the contribution these types of physicians are making, in their own way, to the greater good of the organization.
After all, we can’t—and shouldn’t—all be horses. TH
Reference
1. Hauer J. The Natural Superiority of Mules: A Celebration of One of the Most Intelligent, Sure-footed, and Misunderstood Animals in the World. New York, NY: Skyhorse Publishing; 2006.
My family and I recently took a spring break trip out west to see a few national parks. During the trip, we stayed on a family ranch in Utah. It had a wide variety of livestock, including a large number of mules and horses.
During our stay at this family-owned ranch, two things really stood out and made me think:
- The guesthouse we stayed in had an inordinate volume of collections dedicated to the science and art of raising horses and mules. Everywhere one looked you could find a wall-mounted picture, poem, or coffee table book about these species. My favorite, written by the owner of the ranch, John Hauer, was The Natural Superiority of Mules.1
- The second thing I noticed was that every member of the ranch-owning family had fairly strong opinions about which was better—horse or mule. Just to recap the biology, a horse is the product of two horses, whereas a mule is the progeny of a male donkey and a female horse. It turns out that their physical structure and demeanors are very different.
One of the oldest members of the ranch family (who I believe was a “distant uncle”) had a very strong opinion about the superiority of the mule. His opinion was based on selected facts, including that mules are “steadier on their feet” in unstable ground, require less volume and less frequent food and water, and very rarely became ill or need costly veterinary care.
Another mule-favoring family member told us how mules get a “bad rap” for being stubborn when they actually are much smarter and better decision makers than horses. She recalled a famous folklore of a farmer who took his mule out to gather materials from across a field. When the farmer and the mule approached a wooden bridge, the mule absolutely refused to cross the bridge. After much back and forth between the farmer and the mule (involving both coaxing and cussing), the farmer gave up and returned to the farm with the mule. He then took his horse on the same errand. When they came to the same bridge, the horse also hesitated but required little bargaining from the farmer to coax it to cross the bridge. When barely halfway across, a rotten board in the bridge gave way, almost sending both the horse and the farmer to their deaths in the ravine below.
The moral of the folklore is that mules cannot be coaxed (or cussed) into performing behaviors that will put themselves or those around them at risk of injury or death. Mules will stop when exhausted or profoundly dehydrated, for example, whereas a horse will continue on if ordered by their farmer, even to the point of running themselves to their eventual demise.
One of the younger members of the family-owned ranch, however, had very strong opinions on the superiority of the horse. Horses are loyal and unwavering in their dedication to please those that they serve. They will put the needs of others before themselves in most situations and therefore almost always “outperform” a mule in all respects. They are willing and (usually) able to perform in uncertain conditions, even despite some reservations. They are loyal and loving, and they have unique and inquisitive personalities, which makes them fun to raise and to ride any day.
Test Drives
Our family of four went on a ride with some of these animals and randomly got two horses and two mules. Interestingly, during our ride, we all did indeed notice the differences between the horses and the mules.
The horses were seemingly easygoing and quick to please, easily following cues to change direction or course. The mules were more hesitant and seemed to need to understand why they were being asked to do something before they acquiesced to the demand.
And when we approached a narrow rocky downslope, the mules were slow, steady, and confident, whereas the horses were seemingly uncomfortable and less agile. And, indeed in researching mules, they seem to have gotten a very bad rap over time (as evidenced by the term “stubborn as a mule”).
Charles Darwin actually categorized mules as an example of “hybrid vigor,” which is a rare example of when an offspring is actually better in most ways than either of its parents. Compared to its parental species, mules have more intelligence, endurance, longevity, health, speed, height, and agility. Also to their advantage, they have harder skin and hooves, allowing them to weather and endure more treacherous conditions.
With all of this newfound knowledge of the mule, it struck me what remarkable similarity some physicians have with mules and the role that these mules are likely serving within our organizations. These physicians are probably labeled as stubborn, obstinate, resistant, or impatient. But maybe they are actually intelligent, agile, and appropriately cautious. Maybe the resistance they express in the organization is serving to warn others about the rotten wooden bridges.
HM Takeaway
Similar to a ranch, most hospitals probably function best with a healthy combination of horses and mules. So if you get an opportunity, next time you encounter physicians at your hospital acting like mules, you should congratulate them and appreciate their mule-like characteristics. Recognize the contribution these types of physicians are making, in their own way, to the greater good of the organization.
After all, we can’t—and shouldn’t—all be horses. TH
Reference
1. Hauer J. The Natural Superiority of Mules: A Celebration of One of the Most Intelligent, Sure-footed, and Misunderstood Animals in the World. New York, NY: Skyhorse Publishing; 2006.
8 steps to avoid legal risks from your practice website
CHICAGO – An inadequately designed medical practice website can pose serious legal dangers, said Michael J. Sacopulos, a medical malpractice defense attorney based in Terre Haute, Ind.
Here is a list of website to-dos that can reduce your legal risks:
• Post emergency information on the website contact page. Unlike the practice’s phone system, the website may fail to include a disclaimer that the patient should call 911 if experiencing a medical emergency.
• Provide disclaimers about doctor-patient relationship. In addition, it’s important that the website includes a warning that communications through the website do not constitute a doctor-patient relationship, Mr. Sacopulos said during an American Bar Association conference. “Most [websites] have a box where you can leave comments. [People need to be told] that it does not create a physician-patient relationship when they describe their medical condition, sometimes even posting photographs.”

• Advise regarding comment security. Under the Health Information Technology for Economic and Clinical Health (HITECH) Act, medical information sent through electronic channels must be encrypted unless a patient consents otherwise. If information can be transmitted through a website’s comment box, patients should be advised that the transmission is not secure before they send their information, Mr. Sacopulos said.
• Secure any online appointment scheduling. Make sure that patients’ names and personal information are not visible to other patients when they schedule appointments, he said. A cardiology practice in Phoenix learned this the hard way when it had to pay the U.S. Department of Health & Human Services $100,000 for lack of HIPAA safeguards online. An investigation by the Office for Civil Rights found the practice was posting clinical and surgical appointments for patients on an Internet-based calendar that was publicly accessible.
• Ensure patient anonymity. The accidental release of private medical information occurred on the website of a St. Louis physician who obtained consent from her patients to include their before and after photos. No names were posted with the photos, but the computer file names of the photos included the patients’ names, and when a person scrolled over a photo with a cursor, the file name popped up. This allowed the public to view the patient name associated with each photo and caused serious problems for the practice, including litigation, he noted.
• Be aware of state board requirements that pertain to physician practice websites. Several state boards do not allow testimonials to be posted on websites. States also differ on the inclusion of before and after photos. New Jersey, for example, allows before and after photos on websites, while New York does not. Some state boards allow doctors to cite that they are board certified on a website without specifics, while states such as Louisiana require that physicians announce the specific certifying board.
“These are ethical and affirmative duties on behalf of physicians that oftentimes come up in websites,” he said.
• Adhere to the Americans With Disabilities Act (ADA). A website is considered real estate for purposes of the ADA, meaning it must include an accessible format to patients with disabilities, Mr. Sacupulos said. Problems arise when certain website features make sites difficult or incompatible with assistance devices that disabled patients require, such as a screen reader or voice interactive software. The National Federation for the Blind has been active in this area and has filed multiple class action lawsuits against companies that did not have compliant websites, he said. An ADA tool kit for best website practices can be found online.
• Hire an experienced Web designer to create the practice’s website. Too often, practices use a family member or friend to set up the company’s page, Mr. Sacupulos said. In one such instance, a young designer became angry at his doctor employer and set up a false website in his name, alleging abuses against patients. “Work with someone credible,” he advised. “Make sure you own your own domain. Many of these Web designers will purchase the domain name and build a site around it, which is great until you want to move to the next Web designer, and then you have to buy your domain back.”
On Twitter @legal_med
CHICAGO – An inadequately designed medical practice website can pose serious legal dangers, said Michael J. Sacopulos, a medical malpractice defense attorney based in Terre Haute, Ind.
Here is a list of website to-dos that can reduce your legal risks:
• Post emergency information on the website contact page. Unlike the practice’s phone system, the website may fail to include a disclaimer that the patient should call 911 if experiencing a medical emergency.
• Provide disclaimers about doctor-patient relationship. In addition, it’s important that the website includes a warning that communications through the website do not constitute a doctor-patient relationship, Mr. Sacopulos said during an American Bar Association conference. “Most [websites] have a box where you can leave comments. [People need to be told] that it does not create a physician-patient relationship when they describe their medical condition, sometimes even posting photographs.”
• Advise regarding comment security. Under the Health Information Technology for Economic and Clinical Health (HITECH) Act, medical information sent through electronic channels must be encrypted unless a patient consents otherwise. If information can be transmitted through a website’s comment box, patients should be advised that the transmission is not secure before they send their information, Mr. Sacopulos said.
• Secure any online appointment scheduling. Make sure that patients’ names and personal information are not visible to other patients when they schedule appointments, he said. A cardiology practice in Phoenix learned this the hard way when it had to pay the U.S. Department of Health & Human Services $100,000 for lack of HIPAA safeguards online. An investigation by the Office for Civil Rights found the practice was posting clinical and surgical appointments for patients on an Internet-based calendar that was publicly accessible.
• Ensure patient anonymity. The accidental release of private medical information occurred on the website of a St. Louis physician who obtained consent from her patients to include their before and after photos. No names were posted with the photos, but the computer file names of the photos included the patients’ names, and when a person scrolled over a photo with a cursor, the file name popped up. This allowed the public to view the patient name associated with each photo and caused serious problems for the practice, including litigation, he noted.
• Be aware of state board requirements that pertain to physician practice websites. Several state boards do not allow testimonials to be posted on websites. States also differ on the inclusion of before and after photos. New Jersey, for example, allows before and after photos on websites, while New York does not. Some state boards allow doctors to cite that they are board certified on a website without specifics, while states such as Louisiana require that physicians announce the specific certifying board.
“These are ethical and affirmative duties on behalf of physicians that oftentimes come up in websites,” he said.
• Adhere to the Americans With Disabilities Act (ADA). A website is considered real estate for purposes of the ADA, meaning it must include an accessible format to patients with disabilities, Mr. Sacupulos said. Problems arise when certain website features make sites difficult or incompatible with assistance devices that disabled patients require, such as a screen reader or voice interactive software. The National Federation for the Blind has been active in this area and has filed multiple class action lawsuits against companies that did not have compliant websites, he said. An ADA tool kit for best website practices can be found online.
• Hire an experienced Web designer to create the practice’s website. Too often, practices use a family member or friend to set up the company’s page, Mr. Sacupulos said. In one such instance, a young designer became angry at his doctor employer and set up a false website in his name, alleging abuses against patients. “Work with someone credible,” he advised. “Make sure you own your own domain. Many of these Web designers will purchase the domain name and build a site around it, which is great until you want to move to the next Web designer, and then you have to buy your domain back.”
On Twitter @legal_med
CHICAGO – An inadequately designed medical practice website can pose serious legal dangers, said Michael J. Sacopulos, a medical malpractice defense attorney based in Terre Haute, Ind.
Here is a list of website to-dos that can reduce your legal risks:
• Post emergency information on the website contact page. Unlike the practice’s phone system, the website may fail to include a disclaimer that the patient should call 911 if experiencing a medical emergency.
• Provide disclaimers about doctor-patient relationship. In addition, it’s important that the website includes a warning that communications through the website do not constitute a doctor-patient relationship, Mr. Sacopulos said during an American Bar Association conference. “Most [websites] have a box where you can leave comments. [People need to be told] that it does not create a physician-patient relationship when they describe their medical condition, sometimes even posting photographs.”
• Advise regarding comment security. Under the Health Information Technology for Economic and Clinical Health (HITECH) Act, medical information sent through electronic channels must be encrypted unless a patient consents otherwise. If information can be transmitted through a website’s comment box, patients should be advised that the transmission is not secure before they send their information, Mr. Sacopulos said.
• Secure any online appointment scheduling. Make sure that patients’ names and personal information are not visible to other patients when they schedule appointments, he said. A cardiology practice in Phoenix learned this the hard way when it had to pay the U.S. Department of Health & Human Services $100,000 for lack of HIPAA safeguards online. An investigation by the Office for Civil Rights found the practice was posting clinical and surgical appointments for patients on an Internet-based calendar that was publicly accessible.
• Ensure patient anonymity. The accidental release of private medical information occurred on the website of a St. Louis physician who obtained consent from her patients to include their before and after photos. No names were posted with the photos, but the computer file names of the photos included the patients’ names, and when a person scrolled over a photo with a cursor, the file name popped up. This allowed the public to view the patient name associated with each photo and caused serious problems for the practice, including litigation, he noted.
• Be aware of state board requirements that pertain to physician practice websites. Several state boards do not allow testimonials to be posted on websites. States also differ on the inclusion of before and after photos. New Jersey, for example, allows before and after photos on websites, while New York does not. Some state boards allow doctors to cite that they are board certified on a website without specifics, while states such as Louisiana require that physicians announce the specific certifying board.
“These are ethical and affirmative duties on behalf of physicians that oftentimes come up in websites,” he said.
• Adhere to the Americans With Disabilities Act (ADA). A website is considered real estate for purposes of the ADA, meaning it must include an accessible format to patients with disabilities, Mr. Sacupulos said. Problems arise when certain website features make sites difficult or incompatible with assistance devices that disabled patients require, such as a screen reader or voice interactive software. The National Federation for the Blind has been active in this area and has filed multiple class action lawsuits against companies that did not have compliant websites, he said. An ADA tool kit for best website practices can be found online.
• Hire an experienced Web designer to create the practice’s website. Too often, practices use a family member or friend to set up the company’s page, Mr. Sacupulos said. In one such instance, a young designer became angry at his doctor employer and set up a false website in his name, alleging abuses against patients. “Work with someone credible,” he advised. “Make sure you own your own domain. Many of these Web designers will purchase the domain name and build a site around it, which is great until you want to move to the next Web designer, and then you have to buy your domain back.”
On Twitter @legal_med
EXPERT ANALYSIS FROM THE PHYSICIANS LEGAL ISSUES CONFERENCE

Prepare early for peer review hearings to avoid negative outcomes
CHICAGO – Being targeted for a peer review can be unnerving for physicians, but proper preparation can help doctors smoothly navigate the process and increase their chances for a favorable outcome.
The first step is taking the situation seriously and remaining calm, said Janet L. Pulliam, a Little Rock, Ark.–based attorney who specializes in health law and employment and labor. Next, hire an experienced attorney and refrain from signing anything without consulting counsel, Ms. Pulliam said at a conference held by the American Bar Association. She also suggested that physicians request an individual meeting with each reviewer before the hearing.

“That’s not to be a lobbying meeting; that’s to be a meeting where you simply, one on one, ask someone who is going to be in judgment of you [to] please keep an open mind until they have heard all of the evidence,” Ms. Pulliam said at the meeting. “Trust me, they’ve already had plenty of information provided to them from the [hospital] administration, so that’s not asking any favors.”
If the peer review stems from a patient interaction or treatment decision, review the patient record in question, but don’t change any documentation, she noted. You can always argue during the hearing that the patient record does not adequately illustrate the encounter or that the charting was inaccurate.
Speak up during peer review meetings and ensure that your case is heard, added Elizabeth A. Snelson, a St. Paul, Minn.–based health law attorney who represents medical staffs, medical societies, and other health professionals.
“Not that it’s easy to put a lawyer in a room and tell her to not talk, but the fact of the matter is that the case will be more successful if it’s the doctor who is addressing the panel, which is usually comprised completely of doctors,” Ms. Snelson said.
Educate the committee, Ms. Pulliam advised. Use the opportunity to explain the protocols specific to your specialty and how they may differ from other specialties.
“It’s your time to educate them,” she said. “The physicians on the committee generally, genuinely want to know what they don’t know, and this is the only shot that you’re going to have to tell them.”

Attend every meeting and be on time. This may sound obvious, but Ms. Pulliam has seen the negative effects a tardy appearance can have on a committee’s perceptions. Making the peer review process a priority and scheduling accordingly is paramount. In addition, ask the hospital for a court reporter to transcribe the hearing. If the hospital refuses, offer to pay for half of the cost, Ms. Pulliam suggested. Accurate documentation is critical and can later be challenged if no record exists. If the hospital declines to share the cost, Ms. Pulliam recommended that doctors foot the entire bill. Make every effort to have a complete transcript, she said.
Be an advocate for a solution when possible, Ms. Pulliam added. Discuss with your attorney potential resolutions, but also know your litigation options. Be prepared to go to court if necessary.
“This is when you need to litigate because procedures and fairness have not been followed in the process,” she said during her presentation. “Courts do allow for equity, declaratory judgments, and injunctions when rights guaranteed to a physician are not followed.”
Knowing those rights and regulations beforehand is key, Ms. Snelson said. States’ peer review laws widely differ. Arkansas law for example, enables physicians to request a hearing officer who is independent and not employed by the hospital and also protects communications by physicians during peer review proceedings. Other states have different features, and some states have nothing regarding peer review on the books, Ms. Snelson said.
“In some states it’s real clear where the peer review requirements are,” she said. “In other states, you really have to go hunting. It could be in the evidence code. It could be all over the place.”
Be aware of appeal rights. Usually, medical staff bylaws allow for an appeal to the governing body of the hospital if a doctor disagrees with a panel’s recommendation. However, sometimes bylaws are silent on appeals, Ms. Snelson said. She noted that the Joint Commission standards refer to peer review hearings and appeals. Thus, if a hospital is accredited by the Joint Commission, and its bylaws do not address appeals, physicians and their attorneys can argue that an appeals process should be in place.
Remember that peer review is not limited to “bad doctors,” and that the process can arise from minor issues, Ms. Snelson said at the meeting.
“Usually when doctors hear ‘peer review,’ they hear ‘discipline,’ ” she said. “[However], It’s not always the ‘bad doctors’; it can be something that is quite minimal that can be escalated. It can be entirely appropriate. What peer review should be is educational ... but sometimes it can be used as a weapon.”
On Twitter @legal_med
CHICAGO – Being targeted for a peer review can be unnerving for physicians, but proper preparation can help doctors smoothly navigate the process and increase their chances for a favorable outcome.
The first step is taking the situation seriously and remaining calm, said Janet L. Pulliam, a Little Rock, Ark.–based attorney who specializes in health law and employment and labor. Next, hire an experienced attorney and refrain from signing anything without consulting counsel, Ms. Pulliam said at a conference held by the American Bar Association. She also suggested that physicians request an individual meeting with each reviewer before the hearing.
“That’s not to be a lobbying meeting; that’s to be a meeting where you simply, one on one, ask someone who is going to be in judgment of you [to] please keep an open mind until they have heard all of the evidence,” Ms. Pulliam said at the meeting. “Trust me, they’ve already had plenty of information provided to them from the [hospital] administration, so that’s not asking any favors.”
If the peer review stems from a patient interaction or treatment decision, review the patient record in question, but don’t change any documentation, she noted. You can always argue during the hearing that the patient record does not adequately illustrate the encounter or that the charting was inaccurate.
Speak up during peer review meetings and ensure that your case is heard, added Elizabeth A. Snelson, a St. Paul, Minn.–based health law attorney who represents medical staffs, medical societies, and other health professionals.
“Not that it’s easy to put a lawyer in a room and tell her to not talk, but the fact of the matter is that the case will be more successful if it’s the doctor who is addressing the panel, which is usually comprised completely of doctors,” Ms. Snelson said.
Educate the committee, Ms. Pulliam advised. Use the opportunity to explain the protocols specific to your specialty and how they may differ from other specialties.
“It’s your time to educate them,” she said. “The physicians on the committee generally, genuinely want to know what they don’t know, and this is the only shot that you’re going to have to tell them.”
Attend every meeting and be on time. This may sound obvious, but Ms. Pulliam has seen the negative effects a tardy appearance can have on a committee’s perceptions. Making the peer review process a priority and scheduling accordingly is paramount. In addition, ask the hospital for a court reporter to transcribe the hearing. If the hospital refuses, offer to pay for half of the cost, Ms. Pulliam suggested. Accurate documentation is critical and can later be challenged if no record exists. If the hospital declines to share the cost, Ms. Pulliam recommended that doctors foot the entire bill. Make every effort to have a complete transcript, she said.
Be an advocate for a solution when possible, Ms. Pulliam added. Discuss with your attorney potential resolutions, but also know your litigation options. Be prepared to go to court if necessary.
“This is when you need to litigate because procedures and fairness have not been followed in the process,” she said during her presentation. “Courts do allow for equity, declaratory judgments, and injunctions when rights guaranteed to a physician are not followed.”
Knowing those rights and regulations beforehand is key, Ms. Snelson said. States’ peer review laws widely differ. Arkansas law for example, enables physicians to request a hearing officer who is independent and not employed by the hospital and also protects communications by physicians during peer review proceedings. Other states have different features, and some states have nothing regarding peer review on the books, Ms. Snelson said.
“In some states it’s real clear where the peer review requirements are,” she said. “In other states, you really have to go hunting. It could be in the evidence code. It could be all over the place.”
Be aware of appeal rights. Usually, medical staff bylaws allow for an appeal to the governing body of the hospital if a doctor disagrees with a panel’s recommendation. However, sometimes bylaws are silent on appeals, Ms. Snelson said. She noted that the Joint Commission standards refer to peer review hearings and appeals. Thus, if a hospital is accredited by the Joint Commission, and its bylaws do not address appeals, physicians and their attorneys can argue that an appeals process should be in place.
Remember that peer review is not limited to “bad doctors,” and that the process can arise from minor issues, Ms. Snelson said at the meeting.
“Usually when doctors hear ‘peer review,’ they hear ‘discipline,’ ” she said. “[However], It’s not always the ‘bad doctors’; it can be something that is quite minimal that can be escalated. It can be entirely appropriate. What peer review should be is educational ... but sometimes it can be used as a weapon.”
On Twitter @legal_med
CHICAGO – Being targeted for a peer review can be unnerving for physicians, but proper preparation can help doctors smoothly navigate the process and increase their chances for a favorable outcome.
The first step is taking the situation seriously and remaining calm, said Janet L. Pulliam, a Little Rock, Ark.–based attorney who specializes in health law and employment and labor. Next, hire an experienced attorney and refrain from signing anything without consulting counsel, Ms. Pulliam said at a conference held by the American Bar Association. She also suggested that physicians request an individual meeting with each reviewer before the hearing.
“That’s not to be a lobbying meeting; that’s to be a meeting where you simply, one on one, ask someone who is going to be in judgment of you [to] please keep an open mind until they have heard all of the evidence,” Ms. Pulliam said at the meeting. “Trust me, they’ve already had plenty of information provided to them from the [hospital] administration, so that’s not asking any favors.”
If the peer review stems from a patient interaction or treatment decision, review the patient record in question, but don’t change any documentation, she noted. You can always argue during the hearing that the patient record does not adequately illustrate the encounter or that the charting was inaccurate.
Speak up during peer review meetings and ensure that your case is heard, added Elizabeth A. Snelson, a St. Paul, Minn.–based health law attorney who represents medical staffs, medical societies, and other health professionals.
“Not that it’s easy to put a lawyer in a room and tell her to not talk, but the fact of the matter is that the case will be more successful if it’s the doctor who is addressing the panel, which is usually comprised completely of doctors,” Ms. Snelson said.
Educate the committee, Ms. Pulliam advised. Use the opportunity to explain the protocols specific to your specialty and how they may differ from other specialties.
“It’s your time to educate them,” she said. “The physicians on the committee generally, genuinely want to know what they don’t know, and this is the only shot that you’re going to have to tell them.”
Attend every meeting and be on time. This may sound obvious, but Ms. Pulliam has seen the negative effects a tardy appearance can have on a committee’s perceptions. Making the peer review process a priority and scheduling accordingly is paramount. In addition, ask the hospital for a court reporter to transcribe the hearing. If the hospital refuses, offer to pay for half of the cost, Ms. Pulliam suggested. Accurate documentation is critical and can later be challenged if no record exists. If the hospital declines to share the cost, Ms. Pulliam recommended that doctors foot the entire bill. Make every effort to have a complete transcript, she said.
Be an advocate for a solution when possible, Ms. Pulliam added. Discuss with your attorney potential resolutions, but also know your litigation options. Be prepared to go to court if necessary.
“This is when you need to litigate because procedures and fairness have not been followed in the process,” she said during her presentation. “Courts do allow for equity, declaratory judgments, and injunctions when rights guaranteed to a physician are not followed.”
Knowing those rights and regulations beforehand is key, Ms. Snelson said. States’ peer review laws widely differ. Arkansas law for example, enables physicians to request a hearing officer who is independent and not employed by the hospital and also protects communications by physicians during peer review proceedings. Other states have different features, and some states have nothing regarding peer review on the books, Ms. Snelson said.
“In some states it’s real clear where the peer review requirements are,” she said. “In other states, you really have to go hunting. It could be in the evidence code. It could be all over the place.”
Be aware of appeal rights. Usually, medical staff bylaws allow for an appeal to the governing body of the hospital if a doctor disagrees with a panel’s recommendation. However, sometimes bylaws are silent on appeals, Ms. Snelson said. She noted that the Joint Commission standards refer to peer review hearings and appeals. Thus, if a hospital is accredited by the Joint Commission, and its bylaws do not address appeals, physicians and their attorneys can argue that an appeals process should be in place.
Remember that peer review is not limited to “bad doctors,” and that the process can arise from minor issues, Ms. Snelson said at the meeting.
“Usually when doctors hear ‘peer review,’ they hear ‘discipline,’ ” she said. “[However], It’s not always the ‘bad doctors’; it can be something that is quite minimal that can be escalated. It can be entirely appropriate. What peer review should be is educational ... but sometimes it can be used as a weapon.”
On Twitter @legal_med
AT THE PHYSICIANS LEGAL ISSUES CONFERENCE

Does U.S. Healthcare Need More Diverse Leadership?
Throughout its history, the United States has been a nation of immigrants. From the early colonial settlements to the mid-20th century, most immigrants came from Western European countries. Since 1965, when the Immigration and Nationality Act abolished national-origin quotas, the diversity of immigrants has increased. “By the year 2043,” says Tomás León, president and CEO of the Institute for Diversity in Health Management in Chicago, “we will be a country where the majority of our population is comprised of racial and ethnic minorities.”

Those changing demographics, cited from the U.S. Census Bureau’s projections, already are evidenced in hospital patient populations. According to a benchmarking survey sponsored by the institute, which is an affiliate of the American Hospital Association, the percentage of minority patients seen in hospitals grew from 29% to 31% of patient census between 2011 and 2013.1 And yet, the survey found this increasing diversity is not currently reflected in leadership positions. During the same time period, underrepresented racial and ethnic minorities (UREM) on hospital boards of directors (14%) and in C-suite positions (14%) remained flat (see Figure 1).

Gender disparities in healthcare and academic leadership also have been slow to change. Periodic surveys conducted by the American College of Healthcare Executives indicate that women comprise only 11% of healthcare CEOs in the U.S.2 And despite the fact that women make up half of all medical students (and one-third of full-time faculty), the Association of American Medical Colleges (AAMC) finds that women still trail men when it comes to attaining full professorship and decanal positions at their academic institutions.3
The Hospitalist interviewed medical directors, researchers, diversity management professionals, and hospitalists to ascertain current solutions being pursued to narrow the gaps in leadership diversity.
Why Diversity in Leadership Matters

Eric E. Howell, MD, MHM, chief of the Division of Hospital Medicine at Johns Hopkins Bayview Medical Center in the Hopkins School of Medicine in Baltimore, believes there is a need to encourage the advancement to leadership positions for female and UREM physicians.
“In medicine, it’s really about service. If we are really here for our patients, we need representation of diversity in our faculty and leadership,” says Dr. Howell, a past SHM president and faculty member of SHM’s Leadership Academy since its inception in 2005. In addition, he says, “Diversity adds incredible strength to an organization and adds to the richness of the ideas and solutions to overcome challenging problems.”
With the implementation of the Affordable Care Act, formerly uninsured people are now accessing the healthcare system; many are bilingual and bicultural, notes George A. Zeppenfeldt-Cestero, president and CEO, Association of Hispanic Healthcare Executives.

“You want to make sure that providers, whether they are physicians, nurses, dentists, or health executives that drive policy issues, are also reflective of that population throughout the organization,” he says. “The real definition of diversity is making sure you have diversity in all layers of the workforce, including the C-suite.”
León points to the coming “seismic demographic shifts” and wonders if healthcare is ready to become more reflective of the communities it serves.
“Increasing diversity in healthcare leadership and governance is essential for the delivery and provision of culturally competent care,” León says. “Now, more than ever, it’s important that we collectively accelerate progress in this area.”
Advancing in Academic and Hospital Medicine
Might hospital medicine offer additional opportunities for women and minorities to advance into leadership positions? Hospitalist Flora Kisuule, MD, SFHM, assistant professor of medicine at Johns Hopkins School of Medicine and associate division director of the Collaborative Inpatient Medicine Service (CIMS) at Johns Hopkins Bayview Medical Center, believes this may be the case. She was with Dr. Howell’s group when he needed to fill the associate director position.
“My advancement speaks to hospital medicine and the fact that we are growing as a field,” she says. “Because of that, opportunities are presenting themselves.”
Dr. Kisuule’s ability to thrive in her position speaks to her professionalism but also to a number of other intentional factors: Dr. Howell’s continuing sponsorship to include her in leadership opportunities, an emergency call system for parents with sick children, and a women’s task force whose agenda calls for transparency in hiring and advancement.
Intentional Structure Change
Cardiologist Hannah A. Valantine, MD, recognizes the importance of addressing the lack of women and people from unrepresented groups in the Science, Technology, Engineering, and Mathematics (STEM) workforce. While at Stanford University School of Medicine, she developed and put into place a set of strategies to understand and mitigate the drivers of gender imbalance. Since then, Dr. Valantine was recruited to bring her expertise to the National Institutes of Health in Bethesda, Md., where she is the inaugural chief officer for scientific workforce diversity. In this role, she is committed “to promoting biomedical workforce diversity as an opportunity, not a problem.”
Dr. Valantine is pushing NIH to pursue a wide range of evidence-based programming to eliminate career-transition barriers that keep women and individuals from underrepresented groups from attaining spots in the top echelons of science and health leadership. She believes that applying scientific rigor to the issue of workforce diversity can lead to quantifiable, translatable, and repeatable methods for recruitment and retention of talent in the biomedical workforce (see “Building Blocks").
Before joining NIH, Dr. Valantine and her colleagues at Stanford surveyed gender composition and faculty satisfaction several years after initiating a multifaceted intervention to boost recruitment and development of women faculty.4 After making a visible commitment of resources to support faculty, with special attention to women, Stanford rose from below to above national benchmarks in the representation of women among faculty. Yet significant work remains to be done, Dr. Valantine says. Her work predicts that the estimated time to achieve 50% occupancy of full professorships by women nationally approaches 50 years—“far too long using current approaches.”
In a separate review article, Dr. Valantine and co-author Christy Sandborg, MD, described the Stanford University School of Medicine Academic Biomedical Career Customization (ABCC) model, which was adapted from Deloitte’s Mass Career Customization framework and allows for development of individual career plans that span a faculty member’s total career, not just a year or two at a time. Long-term planning can enable better alignment between the work culture and values of the workforce, which will improve the outlook for women faculty, Dr. Valantine says.
The issues of work-life balance may actually be generational, Dr. Valantine explains. Veteran hospitalist Janet Nagamine, MD, BSN, SFHM, of Santa Clara, Calif., agrees.
“Nowadays, men as well as women are looking for work-life balance,” she says.
In hospital medicine, Dr. Nagamine points out, the structural changes required to effect a work-life balance for hospital leaders are often difficult to achieve.
“As productivity surveys show, HM group leaders are putting in as many RVUs as the staff,” the former SHM board member says. “There is no dedicated time for administrative duties.”
Construct a Pipeline
Barriers to advancement often are particular to characteristics of diverse populations. For example, the AAMC’s report on the U.S. physician workforce documents that in African-American physicians 40 and younger, women outnumber their male counterparts. Therefore, in the association’s Diversity in Medical Education: Facts and Figures 2012 report, the executive summary points out the need to strengthen the medical education pipeline to increase the number of African-American males who enter the premed track.

Despite the fast-growing percentage of Latino and Hispanic populations in the United States, the shortage of Latino/Hispanic physicians increased from 1980 to 2010. Latinos/Hispanics are greatly underrepresented in the medical student, resident, and faculty populations, according to John Paul Sánchez, MD, MPH, assistant dean for diversity and inclusion in the Office for Diversity and Community Engagement at Rutgers, The State University of New Jersey. Likewise, Zeppenfeldt-Cestero believes that efforts must begin much earlier with Latino and other minority and underrepresented students.
“We have to make sure our students pursue the STEM disciplines and that they also later have the education and preparation to be competitive at the MBA or MPH levels,” he says.
Dr. Sánchez, an associate professor of emergency medicine and a diversity activist since his med school days, is the recipient of last year’s Association of Hispanic Healthcare Executives’ academic leader of the year award. Since September 2014, he has been involved with Building the Next Generation of Academic Physicians Inc., which collaborates with more than 40 medical schools across the country. The initiative offers conferences designed to develop diverse medical students’ and residents’ interest in pursuing academic medicine. Open to all medical students and residents, the conference curriculum is tailored for women, UREMs, and trainees who identify as lesbian, gay, bisexual, or transgender (LGBT), he says. Seven conferences were held in 2015, 10 are planned for this year, and seven for 2017.
Healthcare Leadership Gaps
Despite their omnipresence in healthcare, there is a dearth of women in chief executive and governance roles, as has been noted by both the American College of Healthcare Executives and the National Center for Healthcare Leadership. As with academic leadership positions, the leadership gap in the administrative sector does not seem to be due to a lack of women entering graduate programs in health administration. On the contrary, since the mid-1980s women have comprised 50% to 60% of graduate students.
“This is absolutely not a pipeline issue,” says Christy Harris Lemak, PhD, FACHE, professor and chair of the Department of Health Services Administration at the University of Alabama at Birmingham School of Health Professions and lead investigator of the National Center for Healthcare Leadership’s study of women in healthcare executive positions. Other factors come into play.
In the study, she and her co-authors queried female healthcare CEOs to ascertain the critical career inflection points that led to their success.6 Those who were strategic about their careers, sought out mentors, and voiced their intentions about pursuing leadership positions were more likely to be successful in those efforts. However, individual career efforts must be coupled with overall organizational commitment to fostering inclusion (see “Path to the Top: Strategic Advice for Women").
Hospitals and healthcare organizations must pursue the development of human capital (and the diversity of their leaders) in a systematic way. “We recommended [in the study] that organizations set expectations that leaders who mentor other potential leaders be rewarded in the same way as those who hit financial targets or readmission rate targets,” Dr. Lemak says.

Leadership matters, agrees Deborah J. Bowen, FACHE, CAE, president and CEO of Chicago-based American College of Healthcare Executives.
“I think we’re getting a little smarter. Organizational leaders and trustees have a better understanding that talent development is one of the most important jobs,” she says. “If you don’t have the right people in the right places making good decisions on behalf of the patients and the populations in the communities they’re serving, the rest falls apart.”
Nuances of Mentoring
Many conversations about encouraging diversity in healthcare leadership converge around the role of effective mentoring and sponsorship. A substantial body of research supports the impact of mentoring on retention, research productivity, career satisfaction, and career development for women. It’s important to ensure that the institutional culture is geared toward mentoring junior faculty, says Jessie Kimbrough Marshall, MD, MPH, assistant professor in the Division of General Medicine Hospitalist Program at the University of Michigan Health System in Ann Arbor (UMHS).
Several of our sources pointed out that leaders must learn how to be effective mentors. More attention is being given to enhancing leaders’ mentorship skills. One example is at the Institute for Diversity in Health Management, which conducts an intensive 12-month certificate in diversity management program for practitioners. León says the program fosters ongoing networking and support through the American Leadership Council on Diversity in Healthcare by building leadership competencies.
Dr. Valantine points out that mentoring is hardly a one-style-fits-all proposition but that it is a crucial element to creating and retaining diversity. She says it should be viewed “much more broadly than it is today, and it should focus beyond the trainer-trainee relationship.”

The process is a two-way street. Denege Ward, MD, hospitalist, assistant professor of internal medicine, and director of the medical short stay unit at UMHS, says minorities need to be ready to take a leap of faith.
“Underrepresented faculty and staff should take the risk of possible failure in challenging situations but learn from it and do better and not succumb to fear in face of challenges,” Dr. Ward says.
Although mentoring is one important component in building diversity in academic medicine, Dr. Sánchez asserts that role models, champions, and sponsors are equally important.
“In addition and separate from role models, there must be in place policies and procedures that promote a climate for diverse individuals to succeed,” he says. “What’s needed is an institutional vision and strategic plan that recognizes the importance of diversity. [It] has to become a core principle.”
Dr. Marshall echoes that refrain, noting the recruitment and retention of a diverse set of leaders will take time and intentionality. She is actively engaged in organizing annual meeting mentoring panels at the Society of General Internal Medicine.
“There are still quite a few barriers for women and minorities to advance into hospital leadership roles,” she says. “We still have a long way to go. However, I’m seeing more women and people of color get into these positions. The numbers are increasing, and that encourages me.” TH
Gretchen Henkel is a freelance writer in California.
References
- Institute for Diversity in Health Management. The state of health care diversity and disparities: a benchmarking study of U.S. hospitals. Available at: http://www.diversityconnection.org/diversityconnection/leadership-conferences/Benchmarking-Survey.jsp?fll=S11.
- Top issues confronting hospitals in 2015. American College of Healthcare Executives website. Available at: https://www.ache.org/pubs/research/ceoissues.cfm. Accessed March 5, 2016.
- Association of American Medical Colleges. Diversity in the physician workforce: facts & figures 2014. Available at: http://aamcdiversityfactsandfigures.org/.
- Valantine HA, Grewal D, Ku MC, et al. The gender gap in academic medicine: comparing results from a multifaceted intervention for Stanford faculty to peer and national cohorts. Acad Med. 2014;89(6):904-911.
- Valantine H, Sandborg CI. Changing the culture of academic medicine to eliminate the gender leadership gap: 50/50 by 2020. Acad Med. 2013;88(10):1411-1413.
- Sexton DW, Lemak CH, Wainio JA. Career inflection points of women who successfully achieved the hospital CEO position. J Healthc Manag. 2014;59(5):367-383.
Path to the Top: Strategic Advice for Women
One of the cornerstones of career advancement in healthcare is to stay connected by networking and attending meetings. For women and minorities, the path to leadership may not fit into the traditional linear model of the career ladder.
“For many leadership roles, you have to be visual and present; you have to attend meetings and functions,” says Denege Ward, MD, hospitalist, assistant professor of internal medicine, and director of the medical short stay unit at the University of Michigan Health System in Ann Arbor. “For women, this is difficult. We are still in charge of families and home.”
For some women, it may be more productive to employ the notion of the “leadership labyrinth.” Others refer to a “career lattice” or employ Deloitte’s Mass Career Customization framework.
“For women, the trajectory may include working part-time while their children are small or finding local training opportunities,” says Christy Harris Lemak, PhD, FACHE, professor and chair of the Department of Health Services Administration at the University of Alabama at Birmingham School of Health Professions and lead investigator of the National Center for Healthcare Leadership’s study of women in healthcare executive positions.
Hospitalist Flora Kisuule, MD, assistant professor of medicine at Johns Hopkins School of Medicine and associate division director of the Collaborative Inpatient Medicine Service (CIMS) at Johns Hopkins Bayview Medical Center in Baltimore, is a wife and mother of a 4-year-old. She agrees the leadership path for moms can take unexpected detours. She’s been able to complete some of her administrative tasks at home through the support of her medical director. If pursuing an MBA is too daunting, she encourages her hospitalist peers to take advantage of short courses and programs in leadership.
“As women, we like to do for others,” notes Elizabeth Gundersen, MD, FHM, assistant professor of clinical biomedical sciences at the Charles E. Schmidt College of Medicine at Florida Atlantic University in Boca Raton. While at the University of Massachusetts, she was one of eight physician quality officers and associate division chief of hospital medicine. To counter the impulse to say yes to everything, including roles that distract from ultimate career goals, one of the women leaders at UMass encouraged her mentees to “think of your ideal position—and then when a position is offered, assess that against your criteria.”

Jessie Kimbrough Marshall, MD, MPH, assistant professor in the Division of General Medicine Hospitalist Program at the University of Michigan Health System, seconds that opinion.
“Try to avoid professional commitments and activities that are not aligned to your career trajectory,” Dr. Marshall advises. “You can also identify someone who is in a position that is close to what you envision for yourself and reach out to that person.”
—Gretchen Henkel
Building Blocks: NIH’s Commitment to Enhance Diversity

The National Institutes of Health (NIH) has been committed to enhancing diversity for decades, according to cardiologist Hannah A. Valantine, MD.
“NIH has made considerable investments in programming,” says Dr. Valantine. However, despite these investments, “the change has not been as rapid or sustainable as we would like it to be.”
As a first step, in October 2014, NIH announced a new set of initiatives designed to enhance the ways in which participants are engaged and trained. Three components comprise the Enhancing Diversity in the NIH-Funded Workforce program. The Building Infrastructure Leading to Diversity (BUILD) program was awarded to 10 universities that met eligibility criteria for being under-resourced. The National Research Mentoring Network (NRMN) will recruit mentors and use methods (such as “train the trainer”) to bring a more deliberate and intentional approach to cultivating mentors. The third component, the Coordinating and Evaluation Center (CEC), focuses on evaluation and dissemination of identified best practices and competencies.
“We are moving away from the assumption that just because you are a leader in your research field that that means you are a good mentor,” Dr. Valantine says.
Throughout its history, the United States has been a nation of immigrants. From the early colonial settlements to the mid-20th century, most immigrants came from Western European countries. Since 1965, when the Immigration and Nationality Act abolished national-origin quotas, the diversity of immigrants has increased. “By the year 2043,” says Tomás León, president and CEO of the Institute for Diversity in Health Management in Chicago, “we will be a country where the majority of our population is comprised of racial and ethnic minorities.”
Those changing demographics, cited from the U.S. Census Bureau’s projections, already are evidenced in hospital patient populations. According to a benchmarking survey sponsored by the institute, which is an affiliate of the American Hospital Association, the percentage of minority patients seen in hospitals grew from 29% to 31% of patient census between 2011 and 2013.1 And yet, the survey found this increasing diversity is not currently reflected in leadership positions. During the same time period, underrepresented racial and ethnic minorities (UREM) on hospital boards of directors (14%) and in C-suite positions (14%) remained flat (see Figure 1).
Gender disparities in healthcare and academic leadership also have been slow to change. Periodic surveys conducted by the American College of Healthcare Executives indicate that women comprise only 11% of healthcare CEOs in the U.S.2 And despite the fact that women make up half of all medical students (and one-third of full-time faculty), the Association of American Medical Colleges (AAMC) finds that women still trail men when it comes to attaining full professorship and decanal positions at their academic institutions.3
The Hospitalist interviewed medical directors, researchers, diversity management professionals, and hospitalists to ascertain current solutions being pursued to narrow the gaps in leadership diversity.
Why Diversity in Leadership Matters
Eric E. Howell, MD, MHM, chief of the Division of Hospital Medicine at Johns Hopkins Bayview Medical Center in the Hopkins School of Medicine in Baltimore, believes there is a need to encourage the advancement to leadership positions for female and UREM physicians.
“In medicine, it’s really about service. If we are really here for our patients, we need representation of diversity in our faculty and leadership,” says Dr. Howell, a past SHM president and faculty member of SHM’s Leadership Academy since its inception in 2005. In addition, he says, “Diversity adds incredible strength to an organization and adds to the richness of the ideas and solutions to overcome challenging problems.”
With the implementation of the Affordable Care Act, formerly uninsured people are now accessing the healthcare system; many are bilingual and bicultural, notes George A. Zeppenfeldt-Cestero, president and CEO, Association of Hispanic Healthcare Executives.
“You want to make sure that providers, whether they are physicians, nurses, dentists, or health executives that drive policy issues, are also reflective of that population throughout the organization,” he says. “The real definition of diversity is making sure you have diversity in all layers of the workforce, including the C-suite.”
León points to the coming “seismic demographic shifts” and wonders if healthcare is ready to become more reflective of the communities it serves.
“Increasing diversity in healthcare leadership and governance is essential for the delivery and provision of culturally competent care,” León says. “Now, more than ever, it’s important that we collectively accelerate progress in this area.”
Advancing in Academic and Hospital Medicine
Might hospital medicine offer additional opportunities for women and minorities to advance into leadership positions? Hospitalist Flora Kisuule, MD, SFHM, assistant professor of medicine at Johns Hopkins School of Medicine and associate division director of the Collaborative Inpatient Medicine Service (CIMS) at Johns Hopkins Bayview Medical Center, believes this may be the case. She was with Dr. Howell’s group when he needed to fill the associate director position.
“My advancement speaks to hospital medicine and the fact that we are growing as a field,” she says. “Because of that, opportunities are presenting themselves.”
Dr. Kisuule’s ability to thrive in her position speaks to her professionalism but also to a number of other intentional factors: Dr. Howell’s continuing sponsorship to include her in leadership opportunities, an emergency call system for parents with sick children, and a women’s task force whose agenda calls for transparency in hiring and advancement.
Intentional Structure Change
Cardiologist Hannah A. Valantine, MD, recognizes the importance of addressing the lack of women and people from unrepresented groups in the Science, Technology, Engineering, and Mathematics (STEM) workforce. While at Stanford University School of Medicine, she developed and put into place a set of strategies to understand and mitigate the drivers of gender imbalance. Since then, Dr. Valantine was recruited to bring her expertise to the National Institutes of Health in Bethesda, Md., where she is the inaugural chief officer for scientific workforce diversity. In this role, she is committed “to promoting biomedical workforce diversity as an opportunity, not a problem.”
Dr. Valantine is pushing NIH to pursue a wide range of evidence-based programming to eliminate career-transition barriers that keep women and individuals from underrepresented groups from attaining spots in the top echelons of science and health leadership. She believes that applying scientific rigor to the issue of workforce diversity can lead to quantifiable, translatable, and repeatable methods for recruitment and retention of talent in the biomedical workforce (see “Building Blocks").
Before joining NIH, Dr. Valantine and her colleagues at Stanford surveyed gender composition and faculty satisfaction several years after initiating a multifaceted intervention to boost recruitment and development of women faculty.4 After making a visible commitment of resources to support faculty, with special attention to women, Stanford rose from below to above national benchmarks in the representation of women among faculty. Yet significant work remains to be done, Dr. Valantine says. Her work predicts that the estimated time to achieve 50% occupancy of full professorships by women nationally approaches 50 years—“far too long using current approaches.”
In a separate review article, Dr. Valantine and co-author Christy Sandborg, MD, described the Stanford University School of Medicine Academic Biomedical Career Customization (ABCC) model, which was adapted from Deloitte’s Mass Career Customization framework and allows for development of individual career plans that span a faculty member’s total career, not just a year or two at a time. Long-term planning can enable better alignment between the work culture and values of the workforce, which will improve the outlook for women faculty, Dr. Valantine says.
The issues of work-life balance may actually be generational, Dr. Valantine explains. Veteran hospitalist Janet Nagamine, MD, BSN, SFHM, of Santa Clara, Calif., agrees.
“Nowadays, men as well as women are looking for work-life balance,” she says.
In hospital medicine, Dr. Nagamine points out, the structural changes required to effect a work-life balance for hospital leaders are often difficult to achieve.
“As productivity surveys show, HM group leaders are putting in as many RVUs as the staff,” the former SHM board member says. “There is no dedicated time for administrative duties.”
Construct a Pipeline
Barriers to advancement often are particular to characteristics of diverse populations. For example, the AAMC’s report on the U.S. physician workforce documents that in African-American physicians 40 and younger, women outnumber their male counterparts. Therefore, in the association’s Diversity in Medical Education: Facts and Figures 2012 report, the executive summary points out the need to strengthen the medical education pipeline to increase the number of African-American males who enter the premed track.
Despite the fast-growing percentage of Latino and Hispanic populations in the United States, the shortage of Latino/Hispanic physicians increased from 1980 to 2010. Latinos/Hispanics are greatly underrepresented in the medical student, resident, and faculty populations, according to John Paul Sánchez, MD, MPH, assistant dean for diversity and inclusion in the Office for Diversity and Community Engagement at Rutgers, The State University of New Jersey. Likewise, Zeppenfeldt-Cestero believes that efforts must begin much earlier with Latino and other minority and underrepresented students.
“We have to make sure our students pursue the STEM disciplines and that they also later have the education and preparation to be competitive at the MBA or MPH levels,” he says.
Dr. Sánchez, an associate professor of emergency medicine and a diversity activist since his med school days, is the recipient of last year’s Association of Hispanic Healthcare Executives’ academic leader of the year award. Since September 2014, he has been involved with Building the Next Generation of Academic Physicians Inc., which collaborates with more than 40 medical schools across the country. The initiative offers conferences designed to develop diverse medical students’ and residents’ interest in pursuing academic medicine. Open to all medical students and residents, the conference curriculum is tailored for women, UREMs, and trainees who identify as lesbian, gay, bisexual, or transgender (LGBT), he says. Seven conferences were held in 2015, 10 are planned for this year, and seven for 2017.
Healthcare Leadership Gaps
Despite their omnipresence in healthcare, there is a dearth of women in chief executive and governance roles, as has been noted by both the American College of Healthcare Executives and the National Center for Healthcare Leadership. As with academic leadership positions, the leadership gap in the administrative sector does not seem to be due to a lack of women entering graduate programs in health administration. On the contrary, since the mid-1980s women have comprised 50% to 60% of graduate students.
“This is absolutely not a pipeline issue,” says Christy Harris Lemak, PhD, FACHE, professor and chair of the Department of Health Services Administration at the University of Alabama at Birmingham School of Health Professions and lead investigator of the National Center for Healthcare Leadership’s study of women in healthcare executive positions. Other factors come into play.
In the study, she and her co-authors queried female healthcare CEOs to ascertain the critical career inflection points that led to their success.6 Those who were strategic about their careers, sought out mentors, and voiced their intentions about pursuing leadership positions were more likely to be successful in those efforts. However, individual career efforts must be coupled with overall organizational commitment to fostering inclusion (see “Path to the Top: Strategic Advice for Women").
Hospitals and healthcare organizations must pursue the development of human capital (and the diversity of their leaders) in a systematic way. “We recommended [in the study] that organizations set expectations that leaders who mentor other potential leaders be rewarded in the same way as those who hit financial targets or readmission rate targets,” Dr. Lemak says.
Leadership matters, agrees Deborah J. Bowen, FACHE, CAE, president and CEO of Chicago-based American College of Healthcare Executives.
“I think we’re getting a little smarter. Organizational leaders and trustees have a better understanding that talent development is one of the most important jobs,” she says. “If you don’t have the right people in the right places making good decisions on behalf of the patients and the populations in the communities they’re serving, the rest falls apart.”
Nuances of Mentoring
Many conversations about encouraging diversity in healthcare leadership converge around the role of effective mentoring and sponsorship. A substantial body of research supports the impact of mentoring on retention, research productivity, career satisfaction, and career development for women. It’s important to ensure that the institutional culture is geared toward mentoring junior faculty, says Jessie Kimbrough Marshall, MD, MPH, assistant professor in the Division of General Medicine Hospitalist Program at the University of Michigan Health System in Ann Arbor (UMHS).
Several of our sources pointed out that leaders must learn how to be effective mentors. More attention is being given to enhancing leaders’ mentorship skills. One example is at the Institute for Diversity in Health Management, which conducts an intensive 12-month certificate in diversity management program for practitioners. León says the program fosters ongoing networking and support through the American Leadership Council on Diversity in Healthcare by building leadership competencies.
Dr. Valantine points out that mentoring is hardly a one-style-fits-all proposition but that it is a crucial element to creating and retaining diversity. She says it should be viewed “much more broadly than it is today, and it should focus beyond the trainer-trainee relationship.”
The process is a two-way street. Denege Ward, MD, hospitalist, assistant professor of internal medicine, and director of the medical short stay unit at UMHS, says minorities need to be ready to take a leap of faith.
“Underrepresented faculty and staff should take the risk of possible failure in challenging situations but learn from it and do better and not succumb to fear in face of challenges,” Dr. Ward says.
Although mentoring is one important component in building diversity in academic medicine, Dr. Sánchez asserts that role models, champions, and sponsors are equally important.
“In addition and separate from role models, there must be in place policies and procedures that promote a climate for diverse individuals to succeed,” he says. “What’s needed is an institutional vision and strategic plan that recognizes the importance of diversity. [It] has to become a core principle.”
Dr. Marshall echoes that refrain, noting the recruitment and retention of a diverse set of leaders will take time and intentionality. She is actively engaged in organizing annual meeting mentoring panels at the Society of General Internal Medicine.
“There are still quite a few barriers for women and minorities to advance into hospital leadership roles,” she says. “We still have a long way to go. However, I’m seeing more women and people of color get into these positions. The numbers are increasing, and that encourages me.” TH
Gretchen Henkel is a freelance writer in California.
References
- Institute for Diversity in Health Management. The state of health care diversity and disparities: a benchmarking study of U.S. hospitals. Available at: http://www.diversityconnection.org/diversityconnection/leadership-conferences/Benchmarking-Survey.jsp?fll=S11.
- Top issues confronting hospitals in 2015. American College of Healthcare Executives website. Available at: https://www.ache.org/pubs/research/ceoissues.cfm. Accessed March 5, 2016.
- Association of American Medical Colleges. Diversity in the physician workforce: facts & figures 2014. Available at: http://aamcdiversityfactsandfigures.org/.
- Valantine HA, Grewal D, Ku MC, et al. The gender gap in academic medicine: comparing results from a multifaceted intervention for Stanford faculty to peer and national cohorts. Acad Med. 2014;89(6):904-911.
- Valantine H, Sandborg CI. Changing the culture of academic medicine to eliminate the gender leadership gap: 50/50 by 2020. Acad Med. 2013;88(10):1411-1413.
- Sexton DW, Lemak CH, Wainio JA. Career inflection points of women who successfully achieved the hospital CEO position. J Healthc Manag. 2014;59(5):367-383.
Path to the Top: Strategic Advice for Women
One of the cornerstones of career advancement in healthcare is to stay connected by networking and attending meetings. For women and minorities, the path to leadership may not fit into the traditional linear model of the career ladder.
“For many leadership roles, you have to be visual and present; you have to attend meetings and functions,” says Denege Ward, MD, hospitalist, assistant professor of internal medicine, and director of the medical short stay unit at the University of Michigan Health System in Ann Arbor. “For women, this is difficult. We are still in charge of families and home.”
For some women, it may be more productive to employ the notion of the “leadership labyrinth.” Others refer to a “career lattice” or employ Deloitte’s Mass Career Customization framework.
“For women, the trajectory may include working part-time while their children are small or finding local training opportunities,” says Christy Harris Lemak, PhD, FACHE, professor and chair of the Department of Health Services Administration at the University of Alabama at Birmingham School of Health Professions and lead investigator of the National Center for Healthcare Leadership’s study of women in healthcare executive positions.
Hospitalist Flora Kisuule, MD, assistant professor of medicine at Johns Hopkins School of Medicine and associate division director of the Collaborative Inpatient Medicine Service (CIMS) at Johns Hopkins Bayview Medical Center in Baltimore, is a wife and mother of a 4-year-old. She agrees the leadership path for moms can take unexpected detours. She’s been able to complete some of her administrative tasks at home through the support of her medical director. If pursuing an MBA is too daunting, she encourages her hospitalist peers to take advantage of short courses and programs in leadership.
“As women, we like to do for others,” notes Elizabeth Gundersen, MD, FHM, assistant professor of clinical biomedical sciences at the Charles E. Schmidt College of Medicine at Florida Atlantic University in Boca Raton. While at the University of Massachusetts, she was one of eight physician quality officers and associate division chief of hospital medicine. To counter the impulse to say yes to everything, including roles that distract from ultimate career goals, one of the women leaders at UMass encouraged her mentees to “think of your ideal position—and then when a position is offered, assess that against your criteria.”
Jessie Kimbrough Marshall, MD, MPH, assistant professor in the Division of General Medicine Hospitalist Program at the University of Michigan Health System, seconds that opinion.
“Try to avoid professional commitments and activities that are not aligned to your career trajectory,” Dr. Marshall advises. “You can also identify someone who is in a position that is close to what you envision for yourself and reach out to that person.”
—Gretchen Henkel
Building Blocks: NIH’s Commitment to Enhance Diversity
The National Institutes of Health (NIH) has been committed to enhancing diversity for decades, according to cardiologist Hannah A. Valantine, MD.
“NIH has made considerable investments in programming,” says Dr. Valantine. However, despite these investments, “the change has not been as rapid or sustainable as we would like it to be.”
As a first step, in October 2014, NIH announced a new set of initiatives designed to enhance the ways in which participants are engaged and trained. Three components comprise the Enhancing Diversity in the NIH-Funded Workforce program. The Building Infrastructure Leading to Diversity (BUILD) program was awarded to 10 universities that met eligibility criteria for being under-resourced. The National Research Mentoring Network (NRMN) will recruit mentors and use methods (such as “train the trainer”) to bring a more deliberate and intentional approach to cultivating mentors. The third component, the Coordinating and Evaluation Center (CEC), focuses on evaluation and dissemination of identified best practices and competencies.
“We are moving away from the assumption that just because you are a leader in your research field that that means you are a good mentor,” Dr. Valantine says.
Throughout its history, the United States has been a nation of immigrants. From the early colonial settlements to the mid-20th century, most immigrants came from Western European countries. Since 1965, when the Immigration and Nationality Act abolished national-origin quotas, the diversity of immigrants has increased. “By the year 2043,” says Tomás León, president and CEO of the Institute for Diversity in Health Management in Chicago, “we will be a country where the majority of our population is comprised of racial and ethnic minorities.”
Those changing demographics, cited from the U.S. Census Bureau’s projections, already are evidenced in hospital patient populations. According to a benchmarking survey sponsored by the institute, which is an affiliate of the American Hospital Association, the percentage of minority patients seen in hospitals grew from 29% to 31% of patient census between 2011 and 2013.1 And yet, the survey found this increasing diversity is not currently reflected in leadership positions. During the same time period, underrepresented racial and ethnic minorities (UREM) on hospital boards of directors (14%) and in C-suite positions (14%) remained flat (see Figure 1).
Gender disparities in healthcare and academic leadership also have been slow to change. Periodic surveys conducted by the American College of Healthcare Executives indicate that women comprise only 11% of healthcare CEOs in the U.S.2 And despite the fact that women make up half of all medical students (and one-third of full-time faculty), the Association of American Medical Colleges (AAMC) finds that women still trail men when it comes to attaining full professorship and decanal positions at their academic institutions.3
The Hospitalist interviewed medical directors, researchers, diversity management professionals, and hospitalists to ascertain current solutions being pursued to narrow the gaps in leadership diversity.
Why Diversity in Leadership Matters
Eric E. Howell, MD, MHM, chief of the Division of Hospital Medicine at Johns Hopkins Bayview Medical Center in the Hopkins School of Medicine in Baltimore, believes there is a need to encourage the advancement to leadership positions for female and UREM physicians.
“In medicine, it’s really about service. If we are really here for our patients, we need representation of diversity in our faculty and leadership,” says Dr. Howell, a past SHM president and faculty member of SHM’s Leadership Academy since its inception in 2005. In addition, he says, “Diversity adds incredible strength to an organization and adds to the richness of the ideas and solutions to overcome challenging problems.”
With the implementation of the Affordable Care Act, formerly uninsured people are now accessing the healthcare system; many are bilingual and bicultural, notes George A. Zeppenfeldt-Cestero, president and CEO, Association of Hispanic Healthcare Executives.
“You want to make sure that providers, whether they are physicians, nurses, dentists, or health executives that drive policy issues, are also reflective of that population throughout the organization,” he says. “The real definition of diversity is making sure you have diversity in all layers of the workforce, including the C-suite.”
León points to the coming “seismic demographic shifts” and wonders if healthcare is ready to become more reflective of the communities it serves.
“Increasing diversity in healthcare leadership and governance is essential for the delivery and provision of culturally competent care,” León says. “Now, more than ever, it’s important that we collectively accelerate progress in this area.”
Advancing in Academic and Hospital Medicine
Might hospital medicine offer additional opportunities for women and minorities to advance into leadership positions? Hospitalist Flora Kisuule, MD, SFHM, assistant professor of medicine at Johns Hopkins School of Medicine and associate division director of the Collaborative Inpatient Medicine Service (CIMS) at Johns Hopkins Bayview Medical Center, believes this may be the case. She was with Dr. Howell’s group when he needed to fill the associate director position.
“My advancement speaks to hospital medicine and the fact that we are growing as a field,” she says. “Because of that, opportunities are presenting themselves.”
Dr. Kisuule’s ability to thrive in her position speaks to her professionalism but also to a number of other intentional factors: Dr. Howell’s continuing sponsorship to include her in leadership opportunities, an emergency call system for parents with sick children, and a women’s task force whose agenda calls for transparency in hiring and advancement.
Intentional Structure Change
Cardiologist Hannah A. Valantine, MD, recognizes the importance of addressing the lack of women and people from unrepresented groups in the Science, Technology, Engineering, and Mathematics (STEM) workforce. While at Stanford University School of Medicine, she developed and put into place a set of strategies to understand and mitigate the drivers of gender imbalance. Since then, Dr. Valantine was recruited to bring her expertise to the National Institutes of Health in Bethesda, Md., where she is the inaugural chief officer for scientific workforce diversity. In this role, she is committed “to promoting biomedical workforce diversity as an opportunity, not a problem.”
Dr. Valantine is pushing NIH to pursue a wide range of evidence-based programming to eliminate career-transition barriers that keep women and individuals from underrepresented groups from attaining spots in the top echelons of science and health leadership. She believes that applying scientific rigor to the issue of workforce diversity can lead to quantifiable, translatable, and repeatable methods for recruitment and retention of talent in the biomedical workforce (see “Building Blocks").
Before joining NIH, Dr. Valantine and her colleagues at Stanford surveyed gender composition and faculty satisfaction several years after initiating a multifaceted intervention to boost recruitment and development of women faculty.4 After making a visible commitment of resources to support faculty, with special attention to women, Stanford rose from below to above national benchmarks in the representation of women among faculty. Yet significant work remains to be done, Dr. Valantine says. Her work predicts that the estimated time to achieve 50% occupancy of full professorships by women nationally approaches 50 years—“far too long using current approaches.”
In a separate review article, Dr. Valantine and co-author Christy Sandborg, MD, described the Stanford University School of Medicine Academic Biomedical Career Customization (ABCC) model, which was adapted from Deloitte’s Mass Career Customization framework and allows for development of individual career plans that span a faculty member’s total career, not just a year or two at a time. Long-term planning can enable better alignment between the work culture and values of the workforce, which will improve the outlook for women faculty, Dr. Valantine says.
The issues of work-life balance may actually be generational, Dr. Valantine explains. Veteran hospitalist Janet Nagamine, MD, BSN, SFHM, of Santa Clara, Calif., agrees.
“Nowadays, men as well as women are looking for work-life balance,” she says.
In hospital medicine, Dr. Nagamine points out, the structural changes required to effect a work-life balance for hospital leaders are often difficult to achieve.
“As productivity surveys show, HM group leaders are putting in as many RVUs as the staff,” the former SHM board member says. “There is no dedicated time for administrative duties.”
Construct a Pipeline
Barriers to advancement often are particular to characteristics of diverse populations. For example, the AAMC’s report on the U.S. physician workforce documents that in African-American physicians 40 and younger, women outnumber their male counterparts. Therefore, in the association’s Diversity in Medical Education: Facts and Figures 2012 report, the executive summary points out the need to strengthen the medical education pipeline to increase the number of African-American males who enter the premed track.
Despite the fast-growing percentage of Latino and Hispanic populations in the United States, the shortage of Latino/Hispanic physicians increased from 1980 to 2010. Latinos/Hispanics are greatly underrepresented in the medical student, resident, and faculty populations, according to John Paul Sánchez, MD, MPH, assistant dean for diversity and inclusion in the Office for Diversity and Community Engagement at Rutgers, The State University of New Jersey. Likewise, Zeppenfeldt-Cestero believes that efforts must begin much earlier with Latino and other minority and underrepresented students.
“We have to make sure our students pursue the STEM disciplines and that they also later have the education and preparation to be competitive at the MBA or MPH levels,” he says.
Dr. Sánchez, an associate professor of emergency medicine and a diversity activist since his med school days, is the recipient of last year’s Association of Hispanic Healthcare Executives’ academic leader of the year award. Since September 2014, he has been involved with Building the Next Generation of Academic Physicians Inc., which collaborates with more than 40 medical schools across the country. The initiative offers conferences designed to develop diverse medical students’ and residents’ interest in pursuing academic medicine. Open to all medical students and residents, the conference curriculum is tailored for women, UREMs, and trainees who identify as lesbian, gay, bisexual, or transgender (LGBT), he says. Seven conferences were held in 2015, 10 are planned for this year, and seven for 2017.
Healthcare Leadership Gaps
Despite their omnipresence in healthcare, there is a dearth of women in chief executive and governance roles, as has been noted by both the American College of Healthcare Executives and the National Center for Healthcare Leadership. As with academic leadership positions, the leadership gap in the administrative sector does not seem to be due to a lack of women entering graduate programs in health administration. On the contrary, since the mid-1980s women have comprised 50% to 60% of graduate students.
“This is absolutely not a pipeline issue,” says Christy Harris Lemak, PhD, FACHE, professor and chair of the Department of Health Services Administration at the University of Alabama at Birmingham School of Health Professions and lead investigator of the National Center for Healthcare Leadership’s study of women in healthcare executive positions. Other factors come into play.
In the study, she and her co-authors queried female healthcare CEOs to ascertain the critical career inflection points that led to their success.6 Those who were strategic about their careers, sought out mentors, and voiced their intentions about pursuing leadership positions were more likely to be successful in those efforts. However, individual career efforts must be coupled with overall organizational commitment to fostering inclusion (see “Path to the Top: Strategic Advice for Women").
Hospitals and healthcare organizations must pursue the development of human capital (and the diversity of their leaders) in a systematic way. “We recommended [in the study] that organizations set expectations that leaders who mentor other potential leaders be rewarded in the same way as those who hit financial targets or readmission rate targets,” Dr. Lemak says.
Leadership matters, agrees Deborah J. Bowen, FACHE, CAE, president and CEO of Chicago-based American College of Healthcare Executives.
“I think we’re getting a little smarter. Organizational leaders and trustees have a better understanding that talent development is one of the most important jobs,” she says. “If you don’t have the right people in the right places making good decisions on behalf of the patients and the populations in the communities they’re serving, the rest falls apart.”
Nuances of Mentoring
Many conversations about encouraging diversity in healthcare leadership converge around the role of effective mentoring and sponsorship. A substantial body of research supports the impact of mentoring on retention, research productivity, career satisfaction, and career development for women. It’s important to ensure that the institutional culture is geared toward mentoring junior faculty, says Jessie Kimbrough Marshall, MD, MPH, assistant professor in the Division of General Medicine Hospitalist Program at the University of Michigan Health System in Ann Arbor (UMHS).
Several of our sources pointed out that leaders must learn how to be effective mentors. More attention is being given to enhancing leaders’ mentorship skills. One example is at the Institute for Diversity in Health Management, which conducts an intensive 12-month certificate in diversity management program for practitioners. León says the program fosters ongoing networking and support through the American Leadership Council on Diversity in Healthcare by building leadership competencies.
Dr. Valantine points out that mentoring is hardly a one-style-fits-all proposition but that it is a crucial element to creating and retaining diversity. She says it should be viewed “much more broadly than it is today, and it should focus beyond the trainer-trainee relationship.”
The process is a two-way street. Denege Ward, MD, hospitalist, assistant professor of internal medicine, and director of the medical short stay unit at UMHS, says minorities need to be ready to take a leap of faith.
“Underrepresented faculty and staff should take the risk of possible failure in challenging situations but learn from it and do better and not succumb to fear in face of challenges,” Dr. Ward says.
Although mentoring is one important component in building diversity in academic medicine, Dr. Sánchez asserts that role models, champions, and sponsors are equally important.
“In addition and separate from role models, there must be in place policies and procedures that promote a climate for diverse individuals to succeed,” he says. “What’s needed is an institutional vision and strategic plan that recognizes the importance of diversity. [It] has to become a core principle.”
Dr. Marshall echoes that refrain, noting the recruitment and retention of a diverse set of leaders will take time and intentionality. She is actively engaged in organizing annual meeting mentoring panels at the Society of General Internal Medicine.
“There are still quite a few barriers for women and minorities to advance into hospital leadership roles,” she says. “We still have a long way to go. However, I’m seeing more women and people of color get into these positions. The numbers are increasing, and that encourages me.” TH
Gretchen Henkel is a freelance writer in California.
References
- Institute for Diversity in Health Management. The state of health care diversity and disparities: a benchmarking study of U.S. hospitals. Available at: http://www.diversityconnection.org/diversityconnection/leadership-conferences/Benchmarking-Survey.jsp?fll=S11.
- Top issues confronting hospitals in 2015. American College of Healthcare Executives website. Available at: https://www.ache.org/pubs/research/ceoissues.cfm. Accessed March 5, 2016.
- Association of American Medical Colleges. Diversity in the physician workforce: facts & figures 2014. Available at: http://aamcdiversityfactsandfigures.org/.
- Valantine HA, Grewal D, Ku MC, et al. The gender gap in academic medicine: comparing results from a multifaceted intervention for Stanford faculty to peer and national cohorts. Acad Med. 2014;89(6):904-911.
- Valantine H, Sandborg CI. Changing the culture of academic medicine to eliminate the gender leadership gap: 50/50 by 2020. Acad Med. 2013;88(10):1411-1413.
- Sexton DW, Lemak CH, Wainio JA. Career inflection points of women who successfully achieved the hospital CEO position. J Healthc Manag. 2014;59(5):367-383.
Path to the Top: Strategic Advice for Women
One of the cornerstones of career advancement in healthcare is to stay connected by networking and attending meetings. For women and minorities, the path to leadership may not fit into the traditional linear model of the career ladder.
“For many leadership roles, you have to be visual and present; you have to attend meetings and functions,” says Denege Ward, MD, hospitalist, assistant professor of internal medicine, and director of the medical short stay unit at the University of Michigan Health System in Ann Arbor. “For women, this is difficult. We are still in charge of families and home.”
For some women, it may be more productive to employ the notion of the “leadership labyrinth.” Others refer to a “career lattice” or employ Deloitte’s Mass Career Customization framework.
“For women, the trajectory may include working part-time while their children are small or finding local training opportunities,” says Christy Harris Lemak, PhD, FACHE, professor and chair of the Department of Health Services Administration at the University of Alabama at Birmingham School of Health Professions and lead investigator of the National Center for Healthcare Leadership’s study of women in healthcare executive positions.
Hospitalist Flora Kisuule, MD, assistant professor of medicine at Johns Hopkins School of Medicine and associate division director of the Collaborative Inpatient Medicine Service (CIMS) at Johns Hopkins Bayview Medical Center in Baltimore, is a wife and mother of a 4-year-old. She agrees the leadership path for moms can take unexpected detours. She’s been able to complete some of her administrative tasks at home through the support of her medical director. If pursuing an MBA is too daunting, she encourages her hospitalist peers to take advantage of short courses and programs in leadership.
“As women, we like to do for others,” notes Elizabeth Gundersen, MD, FHM, assistant professor of clinical biomedical sciences at the Charles E. Schmidt College of Medicine at Florida Atlantic University in Boca Raton. While at the University of Massachusetts, she was one of eight physician quality officers and associate division chief of hospital medicine. To counter the impulse to say yes to everything, including roles that distract from ultimate career goals, one of the women leaders at UMass encouraged her mentees to “think of your ideal position—and then when a position is offered, assess that against your criteria.”
Jessie Kimbrough Marshall, MD, MPH, assistant professor in the Division of General Medicine Hospitalist Program at the University of Michigan Health System, seconds that opinion.
“Try to avoid professional commitments and activities that are not aligned to your career trajectory,” Dr. Marshall advises. “You can also identify someone who is in a position that is close to what you envision for yourself and reach out to that person.”
—Gretchen Henkel
Building Blocks: NIH’s Commitment to Enhance Diversity
The National Institutes of Health (NIH) has been committed to enhancing diversity for decades, according to cardiologist Hannah A. Valantine, MD.
“NIH has made considerable investments in programming,” says Dr. Valantine. However, despite these investments, “the change has not been as rapid or sustainable as we would like it to be.”
As a first step, in October 2014, NIH announced a new set of initiatives designed to enhance the ways in which participants are engaged and trained. Three components comprise the Enhancing Diversity in the NIH-Funded Workforce program. The Building Infrastructure Leading to Diversity (BUILD) program was awarded to 10 universities that met eligibility criteria for being under-resourced. The National Research Mentoring Network (NRMN) will recruit mentors and use methods (such as “train the trainer”) to bring a more deliberate and intentional approach to cultivating mentors. The third component, the Coordinating and Evaluation Center (CEC), focuses on evaluation and dissemination of identified best practices and competencies.
“We are moving away from the assumption that just because you are a leader in your research field that that means you are a good mentor,” Dr. Valantine says.
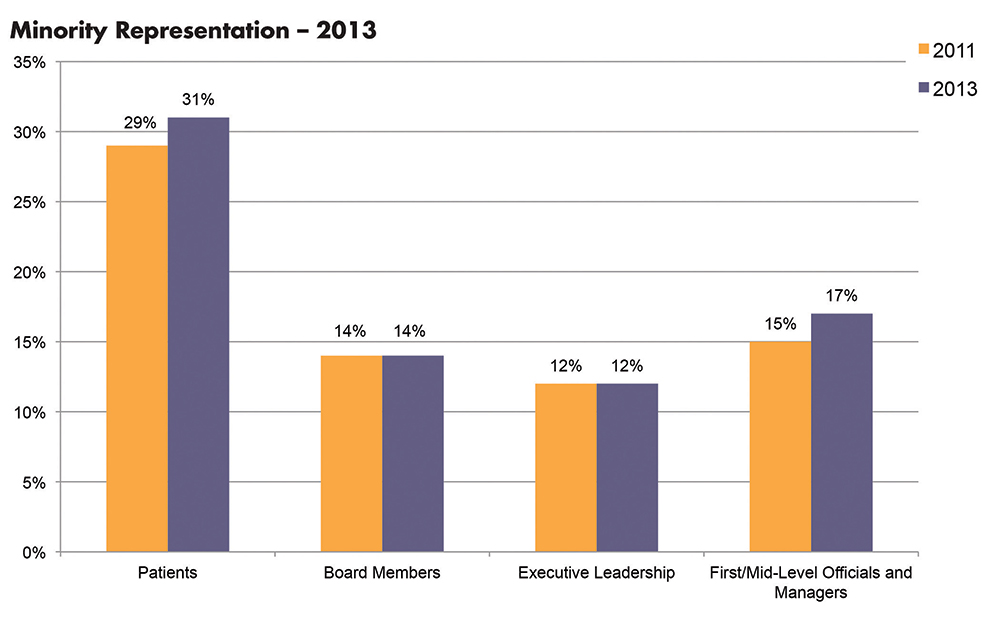
More Hospitals to Be Replaced by FSEDs
If an ED is considered the “front door” to the hospital, how do we regard a free-standing emergency department (FSED) with no hospital attached to it? Fueled by continued hospital closures in the face of steadily increasing demands for emergency care, FSEDs are now replacing hospitals in previously well-served urban areas in addition to serving rural areas lacking alternative facilities.
According to The New York Times (http://nyti.ms/1TB8Z44), since 2000, 19 New York City hospitals “have either closed or overhauled how they operate.” As this issue of Emergency Medicine went to press, plans had been announced to replace Manhattan’s Beth Israel and Brooklyn’s Wyckoff Heights hospitals with FSEDs and expanded outpatient facilities. These hospitals and many others that have recently closed, including St Vincent’s (2010) and the Long Island College Hospital (2014), had been part of the health care landscape in New York for over 125 years.
What do FSEDs mean for emergency medicine (EM) and emergency physicians (EPs), and are they safe alternatives to traditional hospital-based EDs? Newer technologies and treatments, coupled with steadily increasing pressures to reduce inpatient stays, razor-thin hospital operating margins, and the refusal of state and local governments to bail out financially failing hospitals, have created a disconnect between the increasing need for emergency care and the decreasing number of inpatient beds.
On one end of the EM patient care spectrum, urgent care centers (UCCs) and retail pharmacy clinics—collectively referred to as “convenient care” centers—are rapidly proliferating to offer care to those with urgent, episodic, and relatively minor medical and surgical problems. (See “Urgent Care and the Urgent Need for Care” at http://bit.ly/1OSrHSA). With little or no regulatory oversight, convenient care centers staffed by EPs, family practitioners, internists, NPs, and PAs, offer extended hour care—but not 24/7 care—to anyone with adequate health insurance or the ability to pay for the care.
On the other end of the EM patient care spectrum are the FSEDs, now divided into two types: satellite EDs of nearby hospitals, and “FS”-FSEDs with no direct hospital connections. Almost all FSEDs receive 911 ambulances, are staffed at all times by trained and certified EPs and registered nurses (RNs) provide acute care and stabilization consistent with the standards for hospital-based EDs, and are open 24/7—a hallmark that distinguishes EDs from UCCs. FSEDs code and bill both for facility and provider services in the same way hospital-based EDs do. Although organized EM has enthusiastically embraced and endorsed FSEDs, its position on UCCs has been decidedly mixed.
Are FSEDs safe for patients requiring emergency care? The lack of uniform definitions and federal and state regulatory requirements make it difficult to gather and interpret meaningful clinical data on FSEDs and convenient care centers. But a well-equipped FSED, served by state-of-the-art pre- and inter-facility ambulances, and staffed by qualified EPs and RNs, should provide a safe alternative to hospital-based EDs for almost all patients in need of emergency care—especially when no hospital-based ED is available.
Specialty designations of qualifying area hospitals such as “Level I trauma center” will minimize but not completely eliminate bad outcomes of cases where even seconds may make the difference between life and death. In the end though, the real question may be is an FSED better than no ED at all?
Ideally, a hospital-based ED should be the epicenter of a network of both satellite convenient care centers and FSEDs, coordinating services, providing management and staffing for all parts of the network, and arranging safe, appropriate intranetwork ambulance transport.
Should you think that FSEDs are a new phenomenon, you might be surprised to discover that in 1875, after New York Hospital (now part of New York Presbyterian) closed its original lower Manhattan site to move further uptown, it opened a “House of Relief” in its old neighborhood that contained an emergency treatment center, an operating room, an isolation area, a dispensary, a reception area, examination rooms, an ambulance entrance, and wards to observe and treat patients until they could be safely transported to the new main hospital. FSEDs served 19th-century patients well, and in the 21st century may serve as a reminder that sometimes even in medicine, “everything old is new again!” (See http://bit.ly/1NSPlDG.)
Editor’s Note: Portions of this editorial were previously published in Emergency Medicine.
If an ED is considered the “front door” to the hospital, how do we regard a free-standing emergency department (FSED) with no hospital attached to it? Fueled by continued hospital closures in the face of steadily increasing demands for emergency care, FSEDs are now replacing hospitals in previously well-served urban areas in addition to serving rural areas lacking alternative facilities.
According to The New York Times (http://nyti.ms/1TB8Z44), since 2000, 19 New York City hospitals “have either closed or overhauled how they operate.” As this issue of Emergency Medicine went to press, plans had been announced to replace Manhattan’s Beth Israel and Brooklyn’s Wyckoff Heights hospitals with FSEDs and expanded outpatient facilities. These hospitals and many others that have recently closed, including St Vincent’s (2010) and the Long Island College Hospital (2014), had been part of the health care landscape in New York for over 125 years.
What do FSEDs mean for emergency medicine (EM) and emergency physicians (EPs), and are they safe alternatives to traditional hospital-based EDs? Newer technologies and treatments, coupled with steadily increasing pressures to reduce inpatient stays, razor-thin hospital operating margins, and the refusal of state and local governments to bail out financially failing hospitals, have created a disconnect between the increasing need for emergency care and the decreasing number of inpatient beds.
On one end of the EM patient care spectrum, urgent care centers (UCCs) and retail pharmacy clinics—collectively referred to as “convenient care” centers—are rapidly proliferating to offer care to those with urgent, episodic, and relatively minor medical and surgical problems. (See “Urgent Care and the Urgent Need for Care” at http://bit.ly/1OSrHSA). With little or no regulatory oversight, convenient care centers staffed by EPs, family practitioners, internists, NPs, and PAs, offer extended hour care—but not 24/7 care—to anyone with adequate health insurance or the ability to pay for the care.
On the other end of the EM patient care spectrum are the FSEDs, now divided into two types: satellite EDs of nearby hospitals, and “FS”-FSEDs with no direct hospital connections. Almost all FSEDs receive 911 ambulances, are staffed at all times by trained and certified EPs and registered nurses (RNs) provide acute care and stabilization consistent with the standards for hospital-based EDs, and are open 24/7—a hallmark that distinguishes EDs from UCCs. FSEDs code and bill both for facility and provider services in the same way hospital-based EDs do. Although organized EM has enthusiastically embraced and endorsed FSEDs, its position on UCCs has been decidedly mixed.
Are FSEDs safe for patients requiring emergency care? The lack of uniform definitions and federal and state regulatory requirements make it difficult to gather and interpret meaningful clinical data on FSEDs and convenient care centers. But a well-equipped FSED, served by state-of-the-art pre- and inter-facility ambulances, and staffed by qualified EPs and RNs, should provide a safe alternative to hospital-based EDs for almost all patients in need of emergency care—especially when no hospital-based ED is available.
Specialty designations of qualifying area hospitals such as “Level I trauma center” will minimize but not completely eliminate bad outcomes of cases where even seconds may make the difference between life and death. In the end though, the real question may be is an FSED better than no ED at all?
Ideally, a hospital-based ED should be the epicenter of a network of both satellite convenient care centers and FSEDs, coordinating services, providing management and staffing for all parts of the network, and arranging safe, appropriate intranetwork ambulance transport.
Should you think that FSEDs are a new phenomenon, you might be surprised to discover that in 1875, after New York Hospital (now part of New York Presbyterian) closed its original lower Manhattan site to move further uptown, it opened a “House of Relief” in its old neighborhood that contained an emergency treatment center, an operating room, an isolation area, a dispensary, a reception area, examination rooms, an ambulance entrance, and wards to observe and treat patients until they could be safely transported to the new main hospital. FSEDs served 19th-century patients well, and in the 21st century may serve as a reminder that sometimes even in medicine, “everything old is new again!” (See http://bit.ly/1NSPlDG.)
Editor’s Note: Portions of this editorial were previously published in Emergency Medicine.
If an ED is considered the “front door” to the hospital, how do we regard a free-standing emergency department (FSED) with no hospital attached to it? Fueled by continued hospital closures in the face of steadily increasing demands for emergency care, FSEDs are now replacing hospitals in previously well-served urban areas in addition to serving rural areas lacking alternative facilities.
According to The New York Times (http://nyti.ms/1TB8Z44), since 2000, 19 New York City hospitals “have either closed or overhauled how they operate.” As this issue of Emergency Medicine went to press, plans had been announced to replace Manhattan’s Beth Israel and Brooklyn’s Wyckoff Heights hospitals with FSEDs and expanded outpatient facilities. These hospitals and many others that have recently closed, including St Vincent’s (2010) and the Long Island College Hospital (2014), had been part of the health care landscape in New York for over 125 years.
What do FSEDs mean for emergency medicine (EM) and emergency physicians (EPs), and are they safe alternatives to traditional hospital-based EDs? Newer technologies and treatments, coupled with steadily increasing pressures to reduce inpatient stays, razor-thin hospital operating margins, and the refusal of state and local governments to bail out financially failing hospitals, have created a disconnect between the increasing need for emergency care and the decreasing number of inpatient beds.
On one end of the EM patient care spectrum, urgent care centers (UCCs) and retail pharmacy clinics—collectively referred to as “convenient care” centers—are rapidly proliferating to offer care to those with urgent, episodic, and relatively minor medical and surgical problems. (See “Urgent Care and the Urgent Need for Care” at http://bit.ly/1OSrHSA). With little or no regulatory oversight, convenient care centers staffed by EPs, family practitioners, internists, NPs, and PAs, offer extended hour care—but not 24/7 care—to anyone with adequate health insurance or the ability to pay for the care.
On the other end of the EM patient care spectrum are the FSEDs, now divided into two types: satellite EDs of nearby hospitals, and “FS”-FSEDs with no direct hospital connections. Almost all FSEDs receive 911 ambulances, are staffed at all times by trained and certified EPs and registered nurses (RNs) provide acute care and stabilization consistent with the standards for hospital-based EDs, and are open 24/7—a hallmark that distinguishes EDs from UCCs. FSEDs code and bill both for facility and provider services in the same way hospital-based EDs do. Although organized EM has enthusiastically embraced and endorsed FSEDs, its position on UCCs has been decidedly mixed.
Are FSEDs safe for patients requiring emergency care? The lack of uniform definitions and federal and state regulatory requirements make it difficult to gather and interpret meaningful clinical data on FSEDs and convenient care centers. But a well-equipped FSED, served by state-of-the-art pre- and inter-facility ambulances, and staffed by qualified EPs and RNs, should provide a safe alternative to hospital-based EDs for almost all patients in need of emergency care—especially when no hospital-based ED is available.
Specialty designations of qualifying area hospitals such as “Level I trauma center” will minimize but not completely eliminate bad outcomes of cases where even seconds may make the difference between life and death. In the end though, the real question may be is an FSED better than no ED at all?
Ideally, a hospital-based ED should be the epicenter of a network of both satellite convenient care centers and FSEDs, coordinating services, providing management and staffing for all parts of the network, and arranging safe, appropriate intranetwork ambulance transport.
Should you think that FSEDs are a new phenomenon, you might be surprised to discover that in 1875, after New York Hospital (now part of New York Presbyterian) closed its original lower Manhattan site to move further uptown, it opened a “House of Relief” in its old neighborhood that contained an emergency treatment center, an operating room, an isolation area, a dispensary, a reception area, examination rooms, an ambulance entrance, and wards to observe and treat patients until they could be safely transported to the new main hospital. FSEDs served 19th-century patients well, and in the 21st century may serve as a reminder that sometimes even in medicine, “everything old is new again!” (See http://bit.ly/1NSPlDG.)
Editor’s Note: Portions of this editorial were previously published in Emergency Medicine.

Things Hospitalists Want Hospital Administrators to Know
I think it is really cool that this publication has a series of articles on “What Cardiologists [or infection disease specialists, nephrologists, etc.] Want Hospitalists to Know.” I’m always interested to see which clinical topics made the list and which I’m already reasonably familiar with versus know little about. I’ve added this series to my list of things that are always worth the time to read, along with the “What’s New” section in UpToDate, review articles in major journals, and the Cleveland Clinic Journal of Medicine.
Not long ago, I worked with a hospitalist group that had agreed to cardiologists’ request that new hospitalists round with a cardiologist for something like three days as part of their orientation. This seems like they’ve taken the idea of “What Cardiologists Want Hospitalists to Know” a lot further than I had ever considered. I’m sure it would have value on many levels, including positioning the new hospitalist to work more effectively with the cardiologists, but I’m not sure it’s worth the cost. And I’m really concerned it sends a signal that the relationship is one way—that is, the hospitalists need to understand what the cardiologists do and want from them and not the reverse. For many reasons, I think this should be a reciprocal relationship, and it seems reasonable that new cardiologists should orient by rounding with hospitalists.
Same goes for the “… Want Hospitalists to Know” series. I’d like to see articles enumerating what hospitalists want doctors in other fields to know either in this magazine or its counterpart in the other specialty. What follows is the first of these. It is my take on non-clinical topics hospitalists want hospital leaders to know, and I’ll leave it to others to write about clinical topics.
We Aren’t on ‘Vacation’ Every Other Week
If you always think of our days off as a vacation, as in, “Those hospitalists get 26 weeks of vacation a year,” you’re making a mistake. A significant portion of our weekdays off are just like your weekends; they’re days to take a breather.
And you’re likely forgetting how many weekends we work.
And maybe lots of nights also.
You probably work more hours annually, but having more days for a breather are one offset for our weekends and nights.
Insisting Hospitalists Work an Entire Shift (12 Hours) Doesn’t Make a Lot of Sense on Slow Days
Staying around after completing clinical work yields no value. Too often, the time is spent watching YouTube or similar activities. And it means the doctor will be much more frustrated, and more likely to lobby for overtime compensation, when needing to stay beyond the scheduled end of the shift on busy days.
Avoid measuring work effort in hours. And in many cases, it is best to avoid precise determinations of when a day shift ends. At most hospitals, you do need at least one daytime doctor to stay on duty until the next shift arrives, but it rarely makes sense to have all of the hospitalists stay.
Your hospitalists need to be professional enough not to dash out the door the minute they’ve put notes on every patient’s chart. Instead, rather than leaving at the first opportunity on slow days, they could do all of the discharge preparation (med rec, discharge summary, etc.) for patients likely ready for discharge the next day; this can help a lot to discharge patients early the next day. Or they could make “secondary” rounds focused on patient satisfaction, etc.
Obs Patients Usually Are No Less Complicated—or Labor-Intensive—to Care For
It’s best to think of observation as solely a payor classification and not a good indicator of risk, complexity, or work required. Unfortunately “observation” is often thought of as shorthand for simple, not sick, easy to manage, etc. While true for a small subset of observation patients, such as younger people with a single problem such as atypical chest pain, it isn’t true for older (Medicare) patients with multiple chronic illnesses, on multiple medications, and with complex social situations.
Shouldn’t We Measure Length of Stay for All Patients in Hours Rather Than Days?
Then we could better understand throughput issues such as whether afternoon discharges for inpatients are late discharges or really very early discharges that weren’t held until the next morning.
Even High-Performing Hospitalist Groups Are Likely to Have Patient Satisfaction Scores on the Lower End of Doctors at Your Hospital
Don’t decide that just because they have much lower scores than the orthopedists, cardiologists, obstetricians, and other specialties, it is the hospitalists who are falling furthest below their potential. It may be the cardiologists who have a long way to go to achieve great scores for their specialty.
This isn’t an excuse. Just about every hospitalist group can do better and should work to make it happen. And because in nearly every hospital more HCAHPS surveys are attributed to hospitalists than any other specialty by a wide margin, our scores have a huge impact on the overall hospital averages. But you should keep in mind that, for a variety of reasons, hospitalists everywhere have physician communication scores that are lower than many or most other specialties.
To my knowledge, there isn’t a data set that provides patient satisfaction scores by specialty. And scores seem to vary a lot by geographic region, e.g., they’re nearly always higher in the South than other parts of the country. So there isn’t a good way to control for all the variables and know you’re setting appropriate improvement goals for each specialty. But your hospitalists will appreciate it if you acknowledge it may be unreasonable to set the same goals across specialties.
We’d Love Your Help Getting Rid of Pagers
Secure text messaging between all caregivers seems to be the way to go, and we will look to the hospital to make an investment in technology to make it possible and train users to ensure that by making messaging easier the volume of messages (interruptions) doesn’t just skyrocket. We, the hospitalists at your hospital, are happy to help with all of this, from vendor selection to plans for implementation. Please ask! TH
I think it is really cool that this publication has a series of articles on “What Cardiologists [or infection disease specialists, nephrologists, etc.] Want Hospitalists to Know.” I’m always interested to see which clinical topics made the list and which I’m already reasonably familiar with versus know little about. I’ve added this series to my list of things that are always worth the time to read, along with the “What’s New” section in UpToDate, review articles in major journals, and the Cleveland Clinic Journal of Medicine.
Not long ago, I worked with a hospitalist group that had agreed to cardiologists’ request that new hospitalists round with a cardiologist for something like three days as part of their orientation. This seems like they’ve taken the idea of “What Cardiologists Want Hospitalists to Know” a lot further than I had ever considered. I’m sure it would have value on many levels, including positioning the new hospitalist to work more effectively with the cardiologists, but I’m not sure it’s worth the cost. And I’m really concerned it sends a signal that the relationship is one way—that is, the hospitalists need to understand what the cardiologists do and want from them and not the reverse. For many reasons, I think this should be a reciprocal relationship, and it seems reasonable that new cardiologists should orient by rounding with hospitalists.
Same goes for the “… Want Hospitalists to Know” series. I’d like to see articles enumerating what hospitalists want doctors in other fields to know either in this magazine or its counterpart in the other specialty. What follows is the first of these. It is my take on non-clinical topics hospitalists want hospital leaders to know, and I’ll leave it to others to write about clinical topics.
We Aren’t on ‘Vacation’ Every Other Week
If you always think of our days off as a vacation, as in, “Those hospitalists get 26 weeks of vacation a year,” you’re making a mistake. A significant portion of our weekdays off are just like your weekends; they’re days to take a breather.
And you’re likely forgetting how many weekends we work.
And maybe lots of nights also.
You probably work more hours annually, but having more days for a breather are one offset for our weekends and nights.
Insisting Hospitalists Work an Entire Shift (12 Hours) Doesn’t Make a Lot of Sense on Slow Days
Staying around after completing clinical work yields no value. Too often, the time is spent watching YouTube or similar activities. And it means the doctor will be much more frustrated, and more likely to lobby for overtime compensation, when needing to stay beyond the scheduled end of the shift on busy days.
Avoid measuring work effort in hours. And in many cases, it is best to avoid precise determinations of when a day shift ends. At most hospitals, you do need at least one daytime doctor to stay on duty until the next shift arrives, but it rarely makes sense to have all of the hospitalists stay.
Your hospitalists need to be professional enough not to dash out the door the minute they’ve put notes on every patient’s chart. Instead, rather than leaving at the first opportunity on slow days, they could do all of the discharge preparation (med rec, discharge summary, etc.) for patients likely ready for discharge the next day; this can help a lot to discharge patients early the next day. Or they could make “secondary” rounds focused on patient satisfaction, etc.
Obs Patients Usually Are No Less Complicated—or Labor-Intensive—to Care For
It’s best to think of observation as solely a payor classification and not a good indicator of risk, complexity, or work required. Unfortunately “observation” is often thought of as shorthand for simple, not sick, easy to manage, etc. While true for a small subset of observation patients, such as younger people with a single problem such as atypical chest pain, it isn’t true for older (Medicare) patients with multiple chronic illnesses, on multiple medications, and with complex social situations.
Shouldn’t We Measure Length of Stay for All Patients in Hours Rather Than Days?
Then we could better understand throughput issues such as whether afternoon discharges for inpatients are late discharges or really very early discharges that weren’t held until the next morning.
Even High-Performing Hospitalist Groups Are Likely to Have Patient Satisfaction Scores on the Lower End of Doctors at Your Hospital
Don’t decide that just because they have much lower scores than the orthopedists, cardiologists, obstetricians, and other specialties, it is the hospitalists who are falling furthest below their potential. It may be the cardiologists who have a long way to go to achieve great scores for their specialty.
This isn’t an excuse. Just about every hospitalist group can do better and should work to make it happen. And because in nearly every hospital more HCAHPS surveys are attributed to hospitalists than any other specialty by a wide margin, our scores have a huge impact on the overall hospital averages. But you should keep in mind that, for a variety of reasons, hospitalists everywhere have physician communication scores that are lower than many or most other specialties.
To my knowledge, there isn’t a data set that provides patient satisfaction scores by specialty. And scores seem to vary a lot by geographic region, e.g., they’re nearly always higher in the South than other parts of the country. So there isn’t a good way to control for all the variables and know you’re setting appropriate improvement goals for each specialty. But your hospitalists will appreciate it if you acknowledge it may be unreasonable to set the same goals across specialties.
We’d Love Your Help Getting Rid of Pagers
Secure text messaging between all caregivers seems to be the way to go, and we will look to the hospital to make an investment in technology to make it possible and train users to ensure that by making messaging easier the volume of messages (interruptions) doesn’t just skyrocket. We, the hospitalists at your hospital, are happy to help with all of this, from vendor selection to plans for implementation. Please ask! TH
I think it is really cool that this publication has a series of articles on “What Cardiologists [or infection disease specialists, nephrologists, etc.] Want Hospitalists to Know.” I’m always interested to see which clinical topics made the list and which I’m already reasonably familiar with versus know little about. I’ve added this series to my list of things that are always worth the time to read, along with the “What’s New” section in UpToDate, review articles in major journals, and the Cleveland Clinic Journal of Medicine.
Not long ago, I worked with a hospitalist group that had agreed to cardiologists’ request that new hospitalists round with a cardiologist for something like three days as part of their orientation. This seems like they’ve taken the idea of “What Cardiologists Want Hospitalists to Know” a lot further than I had ever considered. I’m sure it would have value on many levels, including positioning the new hospitalist to work more effectively with the cardiologists, but I’m not sure it’s worth the cost. And I’m really concerned it sends a signal that the relationship is one way—that is, the hospitalists need to understand what the cardiologists do and want from them and not the reverse. For many reasons, I think this should be a reciprocal relationship, and it seems reasonable that new cardiologists should orient by rounding with hospitalists.
Same goes for the “… Want Hospitalists to Know” series. I’d like to see articles enumerating what hospitalists want doctors in other fields to know either in this magazine or its counterpart in the other specialty. What follows is the first of these. It is my take on non-clinical topics hospitalists want hospital leaders to know, and I’ll leave it to others to write about clinical topics.
We Aren’t on ‘Vacation’ Every Other Week
If you always think of our days off as a vacation, as in, “Those hospitalists get 26 weeks of vacation a year,” you’re making a mistake. A significant portion of our weekdays off are just like your weekends; they’re days to take a breather.
And you’re likely forgetting how many weekends we work.
And maybe lots of nights also.
You probably work more hours annually, but having more days for a breather are one offset for our weekends and nights.
Insisting Hospitalists Work an Entire Shift (12 Hours) Doesn’t Make a Lot of Sense on Slow Days
Staying around after completing clinical work yields no value. Too often, the time is spent watching YouTube or similar activities. And it means the doctor will be much more frustrated, and more likely to lobby for overtime compensation, when needing to stay beyond the scheduled end of the shift on busy days.
Avoid measuring work effort in hours. And in many cases, it is best to avoid precise determinations of when a day shift ends. At most hospitals, you do need at least one daytime doctor to stay on duty until the next shift arrives, but it rarely makes sense to have all of the hospitalists stay.
Your hospitalists need to be professional enough not to dash out the door the minute they’ve put notes on every patient’s chart. Instead, rather than leaving at the first opportunity on slow days, they could do all of the discharge preparation (med rec, discharge summary, etc.) for patients likely ready for discharge the next day; this can help a lot to discharge patients early the next day. Or they could make “secondary” rounds focused on patient satisfaction, etc.
Obs Patients Usually Are No Less Complicated—or Labor-Intensive—to Care For
It’s best to think of observation as solely a payor classification and not a good indicator of risk, complexity, or work required. Unfortunately “observation” is often thought of as shorthand for simple, not sick, easy to manage, etc. While true for a small subset of observation patients, such as younger people with a single problem such as atypical chest pain, it isn’t true for older (Medicare) patients with multiple chronic illnesses, on multiple medications, and with complex social situations.
Shouldn’t We Measure Length of Stay for All Patients in Hours Rather Than Days?
Then we could better understand throughput issues such as whether afternoon discharges for inpatients are late discharges or really very early discharges that weren’t held until the next morning.
Even High-Performing Hospitalist Groups Are Likely to Have Patient Satisfaction Scores on the Lower End of Doctors at Your Hospital
Don’t decide that just because they have much lower scores than the orthopedists, cardiologists, obstetricians, and other specialties, it is the hospitalists who are falling furthest below their potential. It may be the cardiologists who have a long way to go to achieve great scores for their specialty.
This isn’t an excuse. Just about every hospitalist group can do better and should work to make it happen. And because in nearly every hospital more HCAHPS surveys are attributed to hospitalists than any other specialty by a wide margin, our scores have a huge impact on the overall hospital averages. But you should keep in mind that, for a variety of reasons, hospitalists everywhere have physician communication scores that are lower than many or most other specialties.
To my knowledge, there isn’t a data set that provides patient satisfaction scores by specialty. And scores seem to vary a lot by geographic region, e.g., they’re nearly always higher in the South than other parts of the country. So there isn’t a good way to control for all the variables and know you’re setting appropriate improvement goals for each specialty. But your hospitalists will appreciate it if you acknowledge it may be unreasonable to set the same goals across specialties.
We’d Love Your Help Getting Rid of Pagers
Secure text messaging between all caregivers seems to be the way to go, and we will look to the hospital to make an investment in technology to make it possible and train users to ensure that by making messaging easier the volume of messages (interruptions) doesn’t just skyrocket. We, the hospitalists at your hospital, are happy to help with all of this, from vendor selection to plans for implementation. Please ask! TH
Judge says feds overstepped on ACA cost-sharing subsidies
The Obama administration suffered another legal judgment against the Affordable Care Act when a district court judge ruled that the government has wrongly spent billions of dollars to repay insurers for health insurance provided to certain low-income patients
Congress never appropriated the money for those payments and “no public money can be spent without [an appropriation],” Judge Rosemary M. Collyer of the U.S. District Court for the District of Columbia wrote in her May 12 opinion.

If the ruling stands, the reimbursements could end, making health insurance too expensive for the millions of low-income patients who benefit from the ACA’s cost-sharing subsides, according to Jay Mark Waxman, a Boston-based health law attorney.
“If premiums become too expensive, you have people pulling out, then you have the so-called death spiral,” Mr. Waxman said in an interview. “The law could remain intact, but you could end up with not having very many people taking advantage of the marketplace, particularly the Silver Plan.”
The case in question, U.S. House of Representatives v. Burwell, revolves around two sections of the ACA. Section 1401 provides tax credits to certain patients in order to make insurance premiums more affordable, while Section 1402 requires insurers to reduce copayments, deductibles, and other out-of-pocket costs for certain low-income patients. The health law requires the federal government to reimburse insurers for the cost of these two sections.
While the first section received funding through the congressional appropriations process, the second section did not. In January 2014, HHS started repaying repay cost-sharing subsidies to insurers using federal funds. The House sued, claiming that HHS is illegally spending monies that Congress never appropriated. HHS has argued that other statutory provisions of the ACA authorize expenditures for cost-sharing reimbursements.
Judge Collyer ruled in the House’s favor, writing that paying out reimbursements without an appropriation violates the Constitution.
House members praised the court decision, calling it a victory for “the rule of law and the American taxpayer.”

“We received vindication of what we have known for quite some time – that the administration does not have the authority to spend over $150 billion for payments to insurance companies without an appropriation from Congress,” House Energy and Commerce Committee Chairman Fred Upton (R-Mich.) said in a statement. “The court’s message was clear: Complying with Article I of the Constitution is not optional for President Obama.”
White House Press Secretary Josh Earnest countered that the administration has seen its share of lawsuits over the ACA and that such legal challenges generally end in a government victory.
“This is not the first time that we’ve seen opponents of the Affordable Care Act go through the motions to try to win this political fight in the court system,” Mr. Earnest said during a press conference. “And it’s unfortunate that Republicans have resorted to a taxpayer-funded lawsuit to refight a political fight that they keep losing. They’ve been losing this fight for 6 years. And they’ll lose it again.”

It’s too early to predict how the legal case might be resolved, said Katherine Hempstead, who directs health insurance coverage for the Robert Wood Johnson Foundation.
“There’s a lot of potential endings that don’t lead to people losing their cost-sharing reductions,” Ms. Hempstead said in an interview. “There are a lot of twists and turns ahead, and the probability of people losing their reductions is remote.”
The House could lose the case on appeal, she said. Such a ruling could be made on the merits of the case or on procedural grounds. Whether the House has standing to sue HHS has been questioned as well, she noted. HHS continues to argue that the House has not established a concrete or imminent injury and therefore, the suit should be thrown out. In addition, some have suggested that the federal ruling could be interpreted as requiring Congress to appropriate money to pay for the cost-sharing reductions, she said.
The ultimate resolution could come from the U.S. Supreme Court, Mr. Waxman added. Another possibility is that the next administration will decline to pursue the case.
“Depending on the timing, it could just stop in the court of appeals,” he said. “The next administration could say, ‘We’re happy with where it is and not take it up. You don’t know what’s going to happen.”
Mr. Earnest said the U.S. Department of Justice is reviewing the ruling and will make an announcement about the next step after the analysis.
On Twitter @legal_med
The Obama administration suffered another legal judgment against the Affordable Care Act when a district court judge ruled that the government has wrongly spent billions of dollars to repay insurers for health insurance provided to certain low-income patients
Congress never appropriated the money for those payments and “no public money can be spent without [an appropriation],” Judge Rosemary M. Collyer of the U.S. District Court for the District of Columbia wrote in her May 12 opinion.
If the ruling stands, the reimbursements could end, making health insurance too expensive for the millions of low-income patients who benefit from the ACA’s cost-sharing subsides, according to Jay Mark Waxman, a Boston-based health law attorney.
“If premiums become too expensive, you have people pulling out, then you have the so-called death spiral,” Mr. Waxman said in an interview. “The law could remain intact, but you could end up with not having very many people taking advantage of the marketplace, particularly the Silver Plan.”
The case in question, U.S. House of Representatives v. Burwell, revolves around two sections of the ACA. Section 1401 provides tax credits to certain patients in order to make insurance premiums more affordable, while Section 1402 requires insurers to reduce copayments, deductibles, and other out-of-pocket costs for certain low-income patients. The health law requires the federal government to reimburse insurers for the cost of these two sections.
While the first section received funding through the congressional appropriations process, the second section did not. In January 2014, HHS started repaying repay cost-sharing subsidies to insurers using federal funds. The House sued, claiming that HHS is illegally spending monies that Congress never appropriated. HHS has argued that other statutory provisions of the ACA authorize expenditures for cost-sharing reimbursements.
Judge Collyer ruled in the House’s favor, writing that paying out reimbursements without an appropriation violates the Constitution.
House members praised the court decision, calling it a victory for “the rule of law and the American taxpayer.”
“We received vindication of what we have known for quite some time – that the administration does not have the authority to spend over $150 billion for payments to insurance companies without an appropriation from Congress,” House Energy and Commerce Committee Chairman Fred Upton (R-Mich.) said in a statement. “The court’s message was clear: Complying with Article I of the Constitution is not optional for President Obama.”
White House Press Secretary Josh Earnest countered that the administration has seen its share of lawsuits over the ACA and that such legal challenges generally end in a government victory.
“This is not the first time that we’ve seen opponents of the Affordable Care Act go through the motions to try to win this political fight in the court system,” Mr. Earnest said during a press conference. “And it’s unfortunate that Republicans have resorted to a taxpayer-funded lawsuit to refight a political fight that they keep losing. They’ve been losing this fight for 6 years. And they’ll lose it again.”
It’s too early to predict how the legal case might be resolved, said Katherine Hempstead, who directs health insurance coverage for the Robert Wood Johnson Foundation.
“There’s a lot of potential endings that don’t lead to people losing their cost-sharing reductions,” Ms. Hempstead said in an interview. “There are a lot of twists and turns ahead, and the probability of people losing their reductions is remote.”
The House could lose the case on appeal, she said. Such a ruling could be made on the merits of the case or on procedural grounds. Whether the House has standing to sue HHS has been questioned as well, she noted. HHS continues to argue that the House has not established a concrete or imminent injury and therefore, the suit should be thrown out. In addition, some have suggested that the federal ruling could be interpreted as requiring Congress to appropriate money to pay for the cost-sharing reductions, she said.
The ultimate resolution could come from the U.S. Supreme Court, Mr. Waxman added. Another possibility is that the next administration will decline to pursue the case.
“Depending on the timing, it could just stop in the court of appeals,” he said. “The next administration could say, ‘We’re happy with where it is and not take it up. You don’t know what’s going to happen.”
Mr. Earnest said the U.S. Department of Justice is reviewing the ruling and will make an announcement about the next step after the analysis.
On Twitter @legal_med
The Obama administration suffered another legal judgment against the Affordable Care Act when a district court judge ruled that the government has wrongly spent billions of dollars to repay insurers for health insurance provided to certain low-income patients
Congress never appropriated the money for those payments and “no public money can be spent without [an appropriation],” Judge Rosemary M. Collyer of the U.S. District Court for the District of Columbia wrote in her May 12 opinion.
If the ruling stands, the reimbursements could end, making health insurance too expensive for the millions of low-income patients who benefit from the ACA’s cost-sharing subsides, according to Jay Mark Waxman, a Boston-based health law attorney.
“If premiums become too expensive, you have people pulling out, then you have the so-called death spiral,” Mr. Waxman said in an interview. “The law could remain intact, but you could end up with not having very many people taking advantage of the marketplace, particularly the Silver Plan.”
The case in question, U.S. House of Representatives v. Burwell, revolves around two sections of the ACA. Section 1401 provides tax credits to certain patients in order to make insurance premiums more affordable, while Section 1402 requires insurers to reduce copayments, deductibles, and other out-of-pocket costs for certain low-income patients. The health law requires the federal government to reimburse insurers for the cost of these two sections.
While the first section received funding through the congressional appropriations process, the second section did not. In January 2014, HHS started repaying repay cost-sharing subsidies to insurers using federal funds. The House sued, claiming that HHS is illegally spending monies that Congress never appropriated. HHS has argued that other statutory provisions of the ACA authorize expenditures for cost-sharing reimbursements.
Judge Collyer ruled in the House’s favor, writing that paying out reimbursements without an appropriation violates the Constitution.
House members praised the court decision, calling it a victory for “the rule of law and the American taxpayer.”
“We received vindication of what we have known for quite some time – that the administration does not have the authority to spend over $150 billion for payments to insurance companies without an appropriation from Congress,” House Energy and Commerce Committee Chairman Fred Upton (R-Mich.) said in a statement. “The court’s message was clear: Complying with Article I of the Constitution is not optional for President Obama.”
White House Press Secretary Josh Earnest countered that the administration has seen its share of lawsuits over the ACA and that such legal challenges generally end in a government victory.
“This is not the first time that we’ve seen opponents of the Affordable Care Act go through the motions to try to win this political fight in the court system,” Mr. Earnest said during a press conference. “And it’s unfortunate that Republicans have resorted to a taxpayer-funded lawsuit to refight a political fight that they keep losing. They’ve been losing this fight for 6 years. And they’ll lose it again.”
It’s too early to predict how the legal case might be resolved, said Katherine Hempstead, who directs health insurance coverage for the Robert Wood Johnson Foundation.
“There’s a lot of potential endings that don’t lead to people losing their cost-sharing reductions,” Ms. Hempstead said in an interview. “There are a lot of twists and turns ahead, and the probability of people losing their reductions is remote.”
The House could lose the case on appeal, she said. Such a ruling could be made on the merits of the case or on procedural grounds. Whether the House has standing to sue HHS has been questioned as well, she noted. HHS continues to argue that the House has not established a concrete or imminent injury and therefore, the suit should be thrown out. In addition, some have suggested that the federal ruling could be interpreted as requiring Congress to appropriate money to pay for the cost-sharing reductions, she said.
The ultimate resolution could come from the U.S. Supreme Court, Mr. Waxman added. Another possibility is that the next administration will decline to pursue the case.
“Depending on the timing, it could just stop in the court of appeals,” he said. “The next administration could say, ‘We’re happy with where it is and not take it up. You don’t know what’s going to happen.”
Mr. Earnest said the U.S. Department of Justice is reviewing the ruling and will make an announcement about the next step after the analysis.
On Twitter @legal_med
