User login
Noted oncologist ponders death, life, care inequities
In 2020, he published a book aimed at cancer specialists and their patients on how to die “with hope and dignity,” titled “Between Life and Death” (Penguin Random House India).

When Dr. Patel, the CEO of Carolina Blood and Cancer Care Associates in Rock Hill, S.C., became president of the Washington-based Community Oncology Alliance 2 years ago, he stepped into a leadership role in community oncology. As an advocate for health care payment reform on Capitol Hill, the South Carolina legislature, and within his own practice, Dr. Patel has long worked to eliminate disparities in U.S. cancer care.
This news organization spoke with Dr. Patel about his unusual career path.
Question: Your father had a great influence on you. Can you tell us more about him?
Answer: My dad was a hermit and a saint. He lost his dad when he was 4 years old and moved to the big city with his cousins. When he was 9 or so, he got a message saying that his mum was very ill. So, he and his cousin raised some money, got a doctor and one of those old, rugged jeeps, and they started driving to the village, but rains had destroyed the road. So, without penicillin, his mum died of pneumonia.
He felt that roads and doctor access were the two big factors that could have saved her life. He eventually became the Superintending Engineer for four districts in Gujarat State, building roads connecting every village, but he never gave up his simplistic, minimalist life.
When I was in elementary school, every other weekend my dad would literally dump me at the Mahatma Gandhi Ashram and come back in 2 hours. So, I’m looking at Gandhi’s cabinets, his pictures, reading about his life. So, my formative years were born in that.
Q: I read that you were intending to become an engineer and join the space race. How did your father nudge you toward medicine?
A: When I was 9 years old, my favorite movie hero died of cancer. To comfort me, my father inserted the idea into my brain: When you grow up, you can become a doctor to cure cancer. So, when I finished high school, I was 24th in the state and had an option to go to the space school in India. On the day when I was going for the interview, I could see tears in my father’s eyes, and he said, You know what, boy? I thought you’re going to become a doctor and cure cancer. So, to honor him, I went to med school instead.
Q: I understand that your father also triggered your interest in photography?
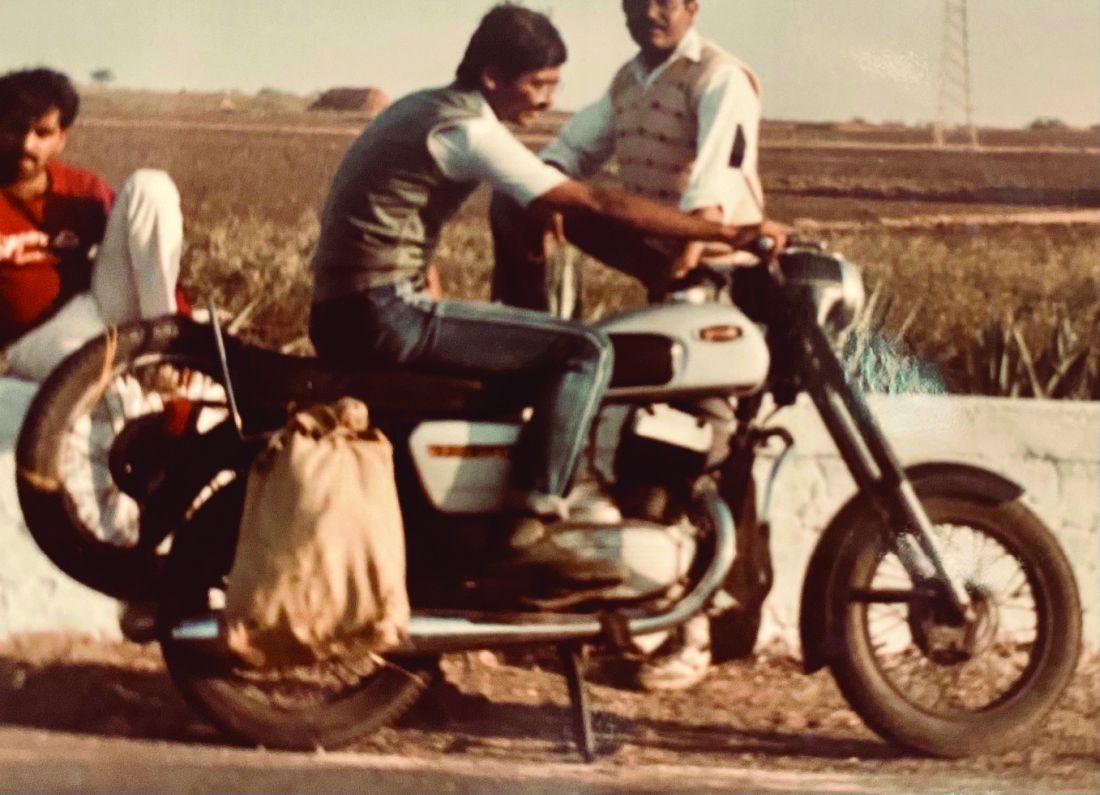
A: I started photographing Kutchi tribal people in 1977, after I bought a camera from a famous architect [Hasmukh Patel], while traveling with my dad. And then my dad bought me a motorcycle, so I started riding myself. From the time I entered med school in 1978 until I finished my residency in 1987, I made several trips following Kutchi migrant families and livestock. They leave their homeland in Kutch [district] during summer in search of grass and water to keep their livestock alive and walk across the state from the desert of Kutch all the way to central Gujarat until monsoon begins. Then they return, only to resume the journey next year. I would catch them along their journey, would talk to them, drink tea and eat millet crepes with them.

In 1984, between Dr. Patel’s medical school and residency, the Lions Club in his hometown, Ahmedabad, India, sponsored him and three buddies to document people and wildlife in Gujarat state. Traveling by motorcycle, the four friends stayed for free with local families by knocking on doors and explaining that they were medical students. Dr. Patel’s photographs were exhibited by the Lions Club of Ahmedabad and at India’s top art institution, the Lalit Kala gallery.
In the 3rd year of his internal-medicine residency in Bombay (now Mumbai), Dr. Patel approached a national newspaper, The Indian Express, for work. He was immediately sent on assignment to cover a cholera epidemic and filed his story and photographs the following day. He worked as a photojournalist and subeditor for a year.

Q: Among all your thousands of pictures, do you have a favorite?
A: There were two photos of Kutchi people that touched me. There was one photo of a lady. All of her worldly belongings were in the picture and a smile on her face showed that we don’t need so many things to be happy. The second photo is of an elderly lady shifting her water pan on her head to a younger family member. And a little girl looks up with a look of curiosity: Will I be doing this when I grow up? We seek so much materialistic happiness. But when you look at the curiosity, smiles, and happiness [in these photos], you realize we could have a lot of happiness in minimalism, as well.
Q: After you finished your residency in Ahmedabad, how did you get started in oncology?
A: In 1986, Ahmedabad City and Gujarat State did not have structured training programs in oncology, so I went to Bombay [Mumbai], where Dr. B.C. Mehta, a true legend and pioneer in India, had started hematology-oncology training. I was a post-doc research fellow with him for a little over a year but when I started seeing patients, I had to answer to myself, Am I doing everything I can to help these people? I saw that the U.K. had one of the best training programs in hem malignancy, so I started applying. Then something happened that was almost like a miracle.
In April 1992, Dr. Patel was working at the Institute of Kidney Diseases in Ahmedabad. One afternoon, just as the clinic was closing for siesta, a family brought in a young girl. She had drug-induced thrombocytopenia and needed an immediate transfusion. The father offered to sell his wedding ring to pay Dr. Patel if he would supervise the treatment and stay by the girl’s side. Dr. Patel told the man to keep his ring, then he remained in the office with the child. At 4 p.m., the office phone rang. It was Dr. H.K. Parikh, an eminent British physician who was wintering in India and needed to make a medical appointment for his wife. On a normal day, Dr. Patel would have missed the call.
“This is how I got to meet Dr. Parikh, out of the blue,” said Dr. Patel. “His wife came to the office for 6 weeks and after 6 weeks, he said, You’re a smart guy; you should come to England. That was in April. I sent a resume and all the usual paperwork. On July 16, 1992, at 2 in the morning, I got a call from the U.K. saying, Your job is confirmed. I’m going to fax your appointment through the Royal College of Physicians, and you’re coming to Manchester to work with us. I’d been sponsored by the Overseas Doctors Training Program.
“So, it turns out that if I’d declined to see that patient and declined to stay in my clinic that afternoon, if I’d declined to see this doctor’s wife, I would never have been in the U.K. And that opened up the doors for me. I like that story because I’ve found that standing up for people who do not have a voice, who do not have hope, always leads to what is destined for me.”
Q: After working as a registrar in the United Kingdom 4 years, you found yourself in the United States and, once again, had to train as an internist. What was new about U.S. oncology?
A: I took 3 years to get recertified in Jamaica Hospital in Queens, then became a fellow in hematology-oncology at the Thomas Jefferson in Philadelphia. My U.K. training was all based on hematological malignancy. In the United States, I shifted into solid tumors.
Q: You have a long history of advocating for affordable oncology at the community, state, and federal level, and you recently launched a disparities initiative in your center called NOLA (No One Left Alone). What was the trigger for NOLA?
A: In the spring of 2020, when we started seeing the COVID surge and the difference in mortality rate between the multiple races, at the same time I saw the AACR [American Association for Cancer Research] 2020 disparity report showing that 34% of cancer deaths are preventable – one in three – if we took care of disparities. The same year, the Community Oncology Alliance asked me to become the president. So, I felt that there is something herding me, leading me, to this position. Eighty percent of cancer patients are treated in community clinics like ours. It put the onus on me to do something.
I learned from Gandhi that I cannot depend on government, I cannot depend on the policy, I have to act myself.
I said, I would not worry about making money, I would rather lose funding on this. So, we started. I read 400+ papers; I spent over 1,000 hours reading about disparities. And I realized that it’s not complicated. There are five pillars to eliminate disparity: access to care for financial reasons, access to biomarker testing or precision medicine, access to social determinants of health, access to cancer screening, and trials. If we focus on these five, we can at least bring that number from 34% to 20%, if not lower.
So, we put that plan in place. I dedicated three employees whose only role is to ensure that not a single patient has to take financial burden from my practice. And we showed it’s doable.
This has now become my mission for the last quarter of my life.
In 2020, Dr. Patel published a book on dying well titled “Between Life and Death.” It’s framed as a series of his conversations with a former patient, Harry Falls. Harry wanted to understand death better, so Dr. Patel narrated five patient stories, drawing the threads together to help Harry face the inevitable. Dr. Patel now uses a similar approach to train clinicians on having meaningful end-of-life conversations with patients.
Q: Why did you feel the need to write a book about dying?
A: The more I’ve witnessed, the more I’m convinced that there are things that we don’t know about this process, which needs to be explored much more. However, I do feel that there’s a power within all of us to steer the process of leaving this world.
Before I sat down with Harry, I loved to counsel patients, but I didn’t have any structural ideas. It was Harry himself who told me that I now had a simple way to explain dying to a much larger audience.
Q: What is your secret for fitting everything into your life?
A: I’ll tell you, it’s very simple. If I put my soul, heart, mind, actions, and language on the one plane and don’t let my brain and conditioning influence my choices, then I live in the moment. Whenever I let my conditioned mind take all the decisions, those are crooked, because you know, we’re selfish creatures – we can use what we call the convenient lie to hide inconvenient truth. And I try not to do that. I mean, it’s been a journey. It didn’t come overnight. I learned. And I feel that over all these years, the only thing that rewarded me, that opened the door of where I am today, was pure, selfless process, whether it’s the act of talking, speaking, or doing.
In 2020, he published a book aimed at cancer specialists and their patients on how to die “with hope and dignity,” titled “Between Life and Death” (Penguin Random House India).
When Dr. Patel, the CEO of Carolina Blood and Cancer Care Associates in Rock Hill, S.C., became president of the Washington-based Community Oncology Alliance 2 years ago, he stepped into a leadership role in community oncology. As an advocate for health care payment reform on Capitol Hill, the South Carolina legislature, and within his own practice, Dr. Patel has long worked to eliminate disparities in U.S. cancer care.
This news organization spoke with Dr. Patel about his unusual career path.
Question: Your father had a great influence on you. Can you tell us more about him?
Answer: My dad was a hermit and a saint. He lost his dad when he was 4 years old and moved to the big city with his cousins. When he was 9 or so, he got a message saying that his mum was very ill. So, he and his cousin raised some money, got a doctor and one of those old, rugged jeeps, and they started driving to the village, but rains had destroyed the road. So, without penicillin, his mum died of pneumonia.
He felt that roads and doctor access were the two big factors that could have saved her life. He eventually became the Superintending Engineer for four districts in Gujarat State, building roads connecting every village, but he never gave up his simplistic, minimalist life.
When I was in elementary school, every other weekend my dad would literally dump me at the Mahatma Gandhi Ashram and come back in 2 hours. So, I’m looking at Gandhi’s cabinets, his pictures, reading about his life. So, my formative years were born in that.
Q: I read that you were intending to become an engineer and join the space race. How did your father nudge you toward medicine?
A: When I was 9 years old, my favorite movie hero died of cancer. To comfort me, my father inserted the idea into my brain: When you grow up, you can become a doctor to cure cancer. So, when I finished high school, I was 24th in the state and had an option to go to the space school in India. On the day when I was going for the interview, I could see tears in my father’s eyes, and he said, You know what, boy? I thought you’re going to become a doctor and cure cancer. So, to honor him, I went to med school instead.
Q: I understand that your father also triggered your interest in photography?
A: I started photographing Kutchi tribal people in 1977, after I bought a camera from a famous architect [Hasmukh Patel], while traveling with my dad. And then my dad bought me a motorcycle, so I started riding myself. From the time I entered med school in 1978 until I finished my residency in 1987, I made several trips following Kutchi migrant families and livestock. They leave their homeland in Kutch [district] during summer in search of grass and water to keep their livestock alive and walk across the state from the desert of Kutch all the way to central Gujarat until monsoon begins. Then they return, only to resume the journey next year. I would catch them along their journey, would talk to them, drink tea and eat millet crepes with them.
In 1984, between Dr. Patel’s medical school and residency, the Lions Club in his hometown, Ahmedabad, India, sponsored him and three buddies to document people and wildlife in Gujarat state. Traveling by motorcycle, the four friends stayed for free with local families by knocking on doors and explaining that they were medical students. Dr. Patel’s photographs were exhibited by the Lions Club of Ahmedabad and at India’s top art institution, the Lalit Kala gallery.
In the 3rd year of his internal-medicine residency in Bombay (now Mumbai), Dr. Patel approached a national newspaper, The Indian Express, for work. He was immediately sent on assignment to cover a cholera epidemic and filed his story and photographs the following day. He worked as a photojournalist and subeditor for a year.
Q: Among all your thousands of pictures, do you have a favorite?
A: There were two photos of Kutchi people that touched me. There was one photo of a lady. All of her worldly belongings were in the picture and a smile on her face showed that we don’t need so many things to be happy. The second photo is of an elderly lady shifting her water pan on her head to a younger family member. And a little girl looks up with a look of curiosity: Will I be doing this when I grow up? We seek so much materialistic happiness. But when you look at the curiosity, smiles, and happiness [in these photos], you realize we could have a lot of happiness in minimalism, as well.
Q: After you finished your residency in Ahmedabad, how did you get started in oncology?
A: In 1986, Ahmedabad City and Gujarat State did not have structured training programs in oncology, so I went to Bombay [Mumbai], where Dr. B.C. Mehta, a true legend and pioneer in India, had started hematology-oncology training. I was a post-doc research fellow with him for a little over a year but when I started seeing patients, I had to answer to myself, Am I doing everything I can to help these people? I saw that the U.K. had one of the best training programs in hem malignancy, so I started applying. Then something happened that was almost like a miracle.
In April 1992, Dr. Patel was working at the Institute of Kidney Diseases in Ahmedabad. One afternoon, just as the clinic was closing for siesta, a family brought in a young girl. She had drug-induced thrombocytopenia and needed an immediate transfusion. The father offered to sell his wedding ring to pay Dr. Patel if he would supervise the treatment and stay by the girl’s side. Dr. Patel told the man to keep his ring, then he remained in the office with the child. At 4 p.m., the office phone rang. It was Dr. H.K. Parikh, an eminent British physician who was wintering in India and needed to make a medical appointment for his wife. On a normal day, Dr. Patel would have missed the call.
“This is how I got to meet Dr. Parikh, out of the blue,” said Dr. Patel. “His wife came to the office for 6 weeks and after 6 weeks, he said, You’re a smart guy; you should come to England. That was in April. I sent a resume and all the usual paperwork. On July 16, 1992, at 2 in the morning, I got a call from the U.K. saying, Your job is confirmed. I’m going to fax your appointment through the Royal College of Physicians, and you’re coming to Manchester to work with us. I’d been sponsored by the Overseas Doctors Training Program.
“So, it turns out that if I’d declined to see that patient and declined to stay in my clinic that afternoon, if I’d declined to see this doctor’s wife, I would never have been in the U.K. And that opened up the doors for me. I like that story because I’ve found that standing up for people who do not have a voice, who do not have hope, always leads to what is destined for me.”
Q: After working as a registrar in the United Kingdom 4 years, you found yourself in the United States and, once again, had to train as an internist. What was new about U.S. oncology?
A: I took 3 years to get recertified in Jamaica Hospital in Queens, then became a fellow in hematology-oncology at the Thomas Jefferson in Philadelphia. My U.K. training was all based on hematological malignancy. In the United States, I shifted into solid tumors.
Q: You have a long history of advocating for affordable oncology at the community, state, and federal level, and you recently launched a disparities initiative in your center called NOLA (No One Left Alone). What was the trigger for NOLA?
A: In the spring of 2020, when we started seeing the COVID surge and the difference in mortality rate between the multiple races, at the same time I saw the AACR [American Association for Cancer Research] 2020 disparity report showing that 34% of cancer deaths are preventable – one in three – if we took care of disparities. The same year, the Community Oncology Alliance asked me to become the president. So, I felt that there is something herding me, leading me, to this position. Eighty percent of cancer patients are treated in community clinics like ours. It put the onus on me to do something.
I learned from Gandhi that I cannot depend on government, I cannot depend on the policy, I have to act myself.
I said, I would not worry about making money, I would rather lose funding on this. So, we started. I read 400+ papers; I spent over 1,000 hours reading about disparities. And I realized that it’s not complicated. There are five pillars to eliminate disparity: access to care for financial reasons, access to biomarker testing or precision medicine, access to social determinants of health, access to cancer screening, and trials. If we focus on these five, we can at least bring that number from 34% to 20%, if not lower.
So, we put that plan in place. I dedicated three employees whose only role is to ensure that not a single patient has to take financial burden from my practice. And we showed it’s doable.
This has now become my mission for the last quarter of my life.
In 2020, Dr. Patel published a book on dying well titled “Between Life and Death.” It’s framed as a series of his conversations with a former patient, Harry Falls. Harry wanted to understand death better, so Dr. Patel narrated five patient stories, drawing the threads together to help Harry face the inevitable. Dr. Patel now uses a similar approach to train clinicians on having meaningful end-of-life conversations with patients.
Q: Why did you feel the need to write a book about dying?
A: The more I’ve witnessed, the more I’m convinced that there are things that we don’t know about this process, which needs to be explored much more. However, I do feel that there’s a power within all of us to steer the process of leaving this world.
Before I sat down with Harry, I loved to counsel patients, but I didn’t have any structural ideas. It was Harry himself who told me that I now had a simple way to explain dying to a much larger audience.
Q: What is your secret for fitting everything into your life?
A: I’ll tell you, it’s very simple. If I put my soul, heart, mind, actions, and language on the one plane and don’t let my brain and conditioning influence my choices, then I live in the moment. Whenever I let my conditioned mind take all the decisions, those are crooked, because you know, we’re selfish creatures – we can use what we call the convenient lie to hide inconvenient truth. And I try not to do that. I mean, it’s been a journey. It didn’t come overnight. I learned. And I feel that over all these years, the only thing that rewarded me, that opened the door of where I am today, was pure, selfless process, whether it’s the act of talking, speaking, or doing.
In 2020, he published a book aimed at cancer specialists and their patients on how to die “with hope and dignity,” titled “Between Life and Death” (Penguin Random House India).
When Dr. Patel, the CEO of Carolina Blood and Cancer Care Associates in Rock Hill, S.C., became president of the Washington-based Community Oncology Alliance 2 years ago, he stepped into a leadership role in community oncology. As an advocate for health care payment reform on Capitol Hill, the South Carolina legislature, and within his own practice, Dr. Patel has long worked to eliminate disparities in U.S. cancer care.
This news organization spoke with Dr. Patel about his unusual career path.
Question: Your father had a great influence on you. Can you tell us more about him?
Answer: My dad was a hermit and a saint. He lost his dad when he was 4 years old and moved to the big city with his cousins. When he was 9 or so, he got a message saying that his mum was very ill. So, he and his cousin raised some money, got a doctor and one of those old, rugged jeeps, and they started driving to the village, but rains had destroyed the road. So, without penicillin, his mum died of pneumonia.
He felt that roads and doctor access were the two big factors that could have saved her life. He eventually became the Superintending Engineer for four districts in Gujarat State, building roads connecting every village, but he never gave up his simplistic, minimalist life.
When I was in elementary school, every other weekend my dad would literally dump me at the Mahatma Gandhi Ashram and come back in 2 hours. So, I’m looking at Gandhi’s cabinets, his pictures, reading about his life. So, my formative years were born in that.
Q: I read that you were intending to become an engineer and join the space race. How did your father nudge you toward medicine?
A: When I was 9 years old, my favorite movie hero died of cancer. To comfort me, my father inserted the idea into my brain: When you grow up, you can become a doctor to cure cancer. So, when I finished high school, I was 24th in the state and had an option to go to the space school in India. On the day when I was going for the interview, I could see tears in my father’s eyes, and he said, You know what, boy? I thought you’re going to become a doctor and cure cancer. So, to honor him, I went to med school instead.
Q: I understand that your father also triggered your interest in photography?
A: I started photographing Kutchi tribal people in 1977, after I bought a camera from a famous architect [Hasmukh Patel], while traveling with my dad. And then my dad bought me a motorcycle, so I started riding myself. From the time I entered med school in 1978 until I finished my residency in 1987, I made several trips following Kutchi migrant families and livestock. They leave their homeland in Kutch [district] during summer in search of grass and water to keep their livestock alive and walk across the state from the desert of Kutch all the way to central Gujarat until monsoon begins. Then they return, only to resume the journey next year. I would catch them along their journey, would talk to them, drink tea and eat millet crepes with them.
In 1984, between Dr. Patel’s medical school and residency, the Lions Club in his hometown, Ahmedabad, India, sponsored him and three buddies to document people and wildlife in Gujarat state. Traveling by motorcycle, the four friends stayed for free with local families by knocking on doors and explaining that they were medical students. Dr. Patel’s photographs were exhibited by the Lions Club of Ahmedabad and at India’s top art institution, the Lalit Kala gallery.
In the 3rd year of his internal-medicine residency in Bombay (now Mumbai), Dr. Patel approached a national newspaper, The Indian Express, for work. He was immediately sent on assignment to cover a cholera epidemic and filed his story and photographs the following day. He worked as a photojournalist and subeditor for a year.
Q: Among all your thousands of pictures, do you have a favorite?
A: There were two photos of Kutchi people that touched me. There was one photo of a lady. All of her worldly belongings were in the picture and a smile on her face showed that we don’t need so many things to be happy. The second photo is of an elderly lady shifting her water pan on her head to a younger family member. And a little girl looks up with a look of curiosity: Will I be doing this when I grow up? We seek so much materialistic happiness. But when you look at the curiosity, smiles, and happiness [in these photos], you realize we could have a lot of happiness in minimalism, as well.
Q: After you finished your residency in Ahmedabad, how did you get started in oncology?
A: In 1986, Ahmedabad City and Gujarat State did not have structured training programs in oncology, so I went to Bombay [Mumbai], where Dr. B.C. Mehta, a true legend and pioneer in India, had started hematology-oncology training. I was a post-doc research fellow with him for a little over a year but when I started seeing patients, I had to answer to myself, Am I doing everything I can to help these people? I saw that the U.K. had one of the best training programs in hem malignancy, so I started applying. Then something happened that was almost like a miracle.
In April 1992, Dr. Patel was working at the Institute of Kidney Diseases in Ahmedabad. One afternoon, just as the clinic was closing for siesta, a family brought in a young girl. She had drug-induced thrombocytopenia and needed an immediate transfusion. The father offered to sell his wedding ring to pay Dr. Patel if he would supervise the treatment and stay by the girl’s side. Dr. Patel told the man to keep his ring, then he remained in the office with the child. At 4 p.m., the office phone rang. It was Dr. H.K. Parikh, an eminent British physician who was wintering in India and needed to make a medical appointment for his wife. On a normal day, Dr. Patel would have missed the call.
“This is how I got to meet Dr. Parikh, out of the blue,” said Dr. Patel. “His wife came to the office for 6 weeks and after 6 weeks, he said, You’re a smart guy; you should come to England. That was in April. I sent a resume and all the usual paperwork. On July 16, 1992, at 2 in the morning, I got a call from the U.K. saying, Your job is confirmed. I’m going to fax your appointment through the Royal College of Physicians, and you’re coming to Manchester to work with us. I’d been sponsored by the Overseas Doctors Training Program.
“So, it turns out that if I’d declined to see that patient and declined to stay in my clinic that afternoon, if I’d declined to see this doctor’s wife, I would never have been in the U.K. And that opened up the doors for me. I like that story because I’ve found that standing up for people who do not have a voice, who do not have hope, always leads to what is destined for me.”
Q: After working as a registrar in the United Kingdom 4 years, you found yourself in the United States and, once again, had to train as an internist. What was new about U.S. oncology?
A: I took 3 years to get recertified in Jamaica Hospital in Queens, then became a fellow in hematology-oncology at the Thomas Jefferson in Philadelphia. My U.K. training was all based on hematological malignancy. In the United States, I shifted into solid tumors.
Q: You have a long history of advocating for affordable oncology at the community, state, and federal level, and you recently launched a disparities initiative in your center called NOLA (No One Left Alone). What was the trigger for NOLA?
A: In the spring of 2020, when we started seeing the COVID surge and the difference in mortality rate between the multiple races, at the same time I saw the AACR [American Association for Cancer Research] 2020 disparity report showing that 34% of cancer deaths are preventable – one in three – if we took care of disparities. The same year, the Community Oncology Alliance asked me to become the president. So, I felt that there is something herding me, leading me, to this position. Eighty percent of cancer patients are treated in community clinics like ours. It put the onus on me to do something.
I learned from Gandhi that I cannot depend on government, I cannot depend on the policy, I have to act myself.
I said, I would not worry about making money, I would rather lose funding on this. So, we started. I read 400+ papers; I spent over 1,000 hours reading about disparities. And I realized that it’s not complicated. There are five pillars to eliminate disparity: access to care for financial reasons, access to biomarker testing or precision medicine, access to social determinants of health, access to cancer screening, and trials. If we focus on these five, we can at least bring that number from 34% to 20%, if not lower.
So, we put that plan in place. I dedicated three employees whose only role is to ensure that not a single patient has to take financial burden from my practice. And we showed it’s doable.
This has now become my mission for the last quarter of my life.
In 2020, Dr. Patel published a book on dying well titled “Between Life and Death.” It’s framed as a series of his conversations with a former patient, Harry Falls. Harry wanted to understand death better, so Dr. Patel narrated five patient stories, drawing the threads together to help Harry face the inevitable. Dr. Patel now uses a similar approach to train clinicians on having meaningful end-of-life conversations with patients.
Q: Why did you feel the need to write a book about dying?
A: The more I’ve witnessed, the more I’m convinced that there are things that we don’t know about this process, which needs to be explored much more. However, I do feel that there’s a power within all of us to steer the process of leaving this world.
Before I sat down with Harry, I loved to counsel patients, but I didn’t have any structural ideas. It was Harry himself who told me that I now had a simple way to explain dying to a much larger audience.
Q: What is your secret for fitting everything into your life?
A: I’ll tell you, it’s very simple. If I put my soul, heart, mind, actions, and language on the one plane and don’t let my brain and conditioning influence my choices, then I live in the moment. Whenever I let my conditioned mind take all the decisions, those are crooked, because you know, we’re selfish creatures – we can use what we call the convenient lie to hide inconvenient truth. And I try not to do that. I mean, it’s been a journey. It didn’t come overnight. I learned. And I feel that over all these years, the only thing that rewarded me, that opened the door of where I am today, was pure, selfless process, whether it’s the act of talking, speaking, or doing.
Community-level actions could mitigate maternal mortality
Maternal mortality in the United States has been rising for several decades, but actions taken at the community level, as well as larger public health initiatives, have the potential to slow this trend, according to experts at a webinar sponsored by the National Institute for Health Care Management.
Maternal mortality in the United States increased by 14% from 2018 to 2020, according to data from the Centers for Disease Control and Prevention’s National Center for Health Statistics.
However, more than 80% of pregnancy-related deaths are preventable, according to 2017-2019 data from the Maternal Mortality Review Committees published online by the CDC. MMRCs include representatives of diverse clinical and nonclinical backgrounds who review the circumstances of pregnancy-related deaths.
In a webinar presented on Sept. 20, the NIHCM enlisted a panel of experts to discuss maternal mortality, the effect of changes to reproductive rights, and potential strategies to improve maternal health outcomes.
Maternal mortality is defined as “death while pregnant or within 42 days of the end of pregnancy, irrespective of the duration and site of pregnancy, from any cause related to pregnancy or its management,” according to the CDC.
Importantly, mortality rates in the United States are approximately three times higher in Black women compared with White women, said Ndidiamaka Amutah-Onukagha, PhD, MPH, of the Tufts University Center for Black Maternal Health & Reproductive Justice. Dr. Amutah-Onukagha addressed some of the potential issues that appear to drive the disparity in care.
The lack of diversity in the health care workforce has a significant effect on patient outcomes, Dr. Amutah-Onukagha said. Overall, Black newborns are more than twice as likely as White newborns to die during their first year of life, but this number is cut in half when Black infants are cared for by Black physicians, she emphasized.
Other factors that may affect disparities in maternal health care include limited access to prenatal care, discriminatory hospital protocols, and mistreatment by health care professionals, said Dr. Amutah-Onukagha. She cited data showing that maternal mortality rates were higher in rural compared with urban areas. “According to the American Hospital Association, half of rural hospitals have no obstetric care, leaving mothers in maternity care deserts; this exacerbates existing disparities,” she said.
In the webinar, Sindhu Srinivas, MD, a maternal-fetal medicine specialist at the University of Pennsylvania, explained how patient, community, and system factors play a role in the disparities in maternal care.
Overall, Black women have to travel further to receive care, which has implications for high-risk pregnancies, and patients on Medicaid have to wait longer for care, and are less likely to be referred, she added. Black women also have higher rates of preexisting conditions compared with other populations that put them in the high-risk category, such as high blood pressure, diabetes, obesity, or being HIV positive, she said.
Other factors contributing to persistent disparities in maternal care include sociodemographics, patient beliefs and knowledge, and psychological issues including stress, said Dr. Srinivas. Community factors, such as social networks, safety, and poverty, also play a role, as do clinician factors of implicit bias and communication skills, she said.
Strategies to reduce disparity
Dr. Srinivas presented several strategies to reduce disparities at various levels. At the policy level, interventions such as establishing a Maternal Mortality Review Committee, establishing a perinatal quality collaborative, and extending Medicaid for a full year postpartum could help improve outcomes, she said. Dr. Srinivas also encouraged clinicians to report maternal mortality data stratified by race and ethnicity, and to participate in the Alliance for Innovation on Maternal Health program (AIM), an initiative in partnership with the American College of Obstetrics and Gynecology.
Dr. Srinivas also proposed maternal health policies to develop payment models “to sustain and scale innovative solutions, and “preserve access to contraception and abortion care.”
For clinicians looking to have an immediate impact, the panelists agreed that working with community health centers can make a significant difference by improving access to maternal care. Consider opportunities for partnership between hospitals and health care delivery centers in the community, said Dr. Srinivas.
Also, don’t underestimate the value of doulas in the birthing process, Dr. Amutah-Onukagha said. She urged clinicians to advocate for doula reimbursement and to take advantage of opportunities for doulas to work with pregnant individuals at the community levels. Data suggest that doulas are associated with increased maternal care visits and with breastfeeding, she noted.
Adam Myers, MD, of the Blue Cross Blue Shield Association, also contributed to the webinar discussion with a key point: Having financial means and commercial coverage is not a buffer against adverse maternal outcomes for racial minorities.
Dr. Myers cited the latest Health of America Report, which included data up to April 2021 with surveys of Medicaid members and their experiences. According to the report, rates of severe maternal mortality (SMM) increased by 9% for commercially and Medicaid-insured women between 2018 and 2020.
Among commercially insured women, SMM was 53% higher among Black women than White women; among Medicaid-insured women, Black women had a 73% higher rate of SMM, compared with White women.
In addition, the report showed that significantly more mothers of color were not able to complete the recommended series of prenatal visits, mainly for reasons of scheduling and transportation, which were greater barriers than COVID-19, Dr. Myers said.
Based on the data, one specific risk profile rose to the top: “We believe women of color aged 35 or higher with comorbid conditions should be treated as very high risk for SMM,” Dr. Myers emphasized. He stressed the need to focus on transportation and scheduling barriers and expressed support for partnerships and health care delivery centers in the community to mitigate these issues.
Finally, Dr. Srinivas encouraged clinicians to have confidence in their expertise and make themselves heard to help their patients and improve maternal health for all. “Use your voice,” said Dr. Srinivas, “As physicians we don’t think of that as an important aspect of our work, or that we can’t articulate, but remember that we are experts, and sharing stories of patients who are impacted is incredibly powerful,” she said.
The presenters had no relevant financial conflicts to disclose.
Maternal mortality in the United States has been rising for several decades, but actions taken at the community level, as well as larger public health initiatives, have the potential to slow this trend, according to experts at a webinar sponsored by the National Institute for Health Care Management.
Maternal mortality in the United States increased by 14% from 2018 to 2020, according to data from the Centers for Disease Control and Prevention’s National Center for Health Statistics.
However, more than 80% of pregnancy-related deaths are preventable, according to 2017-2019 data from the Maternal Mortality Review Committees published online by the CDC. MMRCs include representatives of diverse clinical and nonclinical backgrounds who review the circumstances of pregnancy-related deaths.
In a webinar presented on Sept. 20, the NIHCM enlisted a panel of experts to discuss maternal mortality, the effect of changes to reproductive rights, and potential strategies to improve maternal health outcomes.
Maternal mortality is defined as “death while pregnant or within 42 days of the end of pregnancy, irrespective of the duration and site of pregnancy, from any cause related to pregnancy or its management,” according to the CDC.
Importantly, mortality rates in the United States are approximately three times higher in Black women compared with White women, said Ndidiamaka Amutah-Onukagha, PhD, MPH, of the Tufts University Center for Black Maternal Health & Reproductive Justice. Dr. Amutah-Onukagha addressed some of the potential issues that appear to drive the disparity in care.
The lack of diversity in the health care workforce has a significant effect on patient outcomes, Dr. Amutah-Onukagha said. Overall, Black newborns are more than twice as likely as White newborns to die during their first year of life, but this number is cut in half when Black infants are cared for by Black physicians, she emphasized.
Other factors that may affect disparities in maternal health care include limited access to prenatal care, discriminatory hospital protocols, and mistreatment by health care professionals, said Dr. Amutah-Onukagha. She cited data showing that maternal mortality rates were higher in rural compared with urban areas. “According to the American Hospital Association, half of rural hospitals have no obstetric care, leaving mothers in maternity care deserts; this exacerbates existing disparities,” she said.
In the webinar, Sindhu Srinivas, MD, a maternal-fetal medicine specialist at the University of Pennsylvania, explained how patient, community, and system factors play a role in the disparities in maternal care.
Overall, Black women have to travel further to receive care, which has implications for high-risk pregnancies, and patients on Medicaid have to wait longer for care, and are less likely to be referred, she added. Black women also have higher rates of preexisting conditions compared with other populations that put them in the high-risk category, such as high blood pressure, diabetes, obesity, or being HIV positive, she said.
Other factors contributing to persistent disparities in maternal care include sociodemographics, patient beliefs and knowledge, and psychological issues including stress, said Dr. Srinivas. Community factors, such as social networks, safety, and poverty, also play a role, as do clinician factors of implicit bias and communication skills, she said.
Strategies to reduce disparity
Dr. Srinivas presented several strategies to reduce disparities at various levels. At the policy level, interventions such as establishing a Maternal Mortality Review Committee, establishing a perinatal quality collaborative, and extending Medicaid for a full year postpartum could help improve outcomes, she said. Dr. Srinivas also encouraged clinicians to report maternal mortality data stratified by race and ethnicity, and to participate in the Alliance for Innovation on Maternal Health program (AIM), an initiative in partnership with the American College of Obstetrics and Gynecology.
Dr. Srinivas also proposed maternal health policies to develop payment models “to sustain and scale innovative solutions, and “preserve access to contraception and abortion care.”
For clinicians looking to have an immediate impact, the panelists agreed that working with community health centers can make a significant difference by improving access to maternal care. Consider opportunities for partnership between hospitals and health care delivery centers in the community, said Dr. Srinivas.
Also, don’t underestimate the value of doulas in the birthing process, Dr. Amutah-Onukagha said. She urged clinicians to advocate for doula reimbursement and to take advantage of opportunities for doulas to work with pregnant individuals at the community levels. Data suggest that doulas are associated with increased maternal care visits and with breastfeeding, she noted.
Adam Myers, MD, of the Blue Cross Blue Shield Association, also contributed to the webinar discussion with a key point: Having financial means and commercial coverage is not a buffer against adverse maternal outcomes for racial minorities.
Dr. Myers cited the latest Health of America Report, which included data up to April 2021 with surveys of Medicaid members and their experiences. According to the report, rates of severe maternal mortality (SMM) increased by 9% for commercially and Medicaid-insured women between 2018 and 2020.
Among commercially insured women, SMM was 53% higher among Black women than White women; among Medicaid-insured women, Black women had a 73% higher rate of SMM, compared with White women.
In addition, the report showed that significantly more mothers of color were not able to complete the recommended series of prenatal visits, mainly for reasons of scheduling and transportation, which were greater barriers than COVID-19, Dr. Myers said.
Based on the data, one specific risk profile rose to the top: “We believe women of color aged 35 or higher with comorbid conditions should be treated as very high risk for SMM,” Dr. Myers emphasized. He stressed the need to focus on transportation and scheduling barriers and expressed support for partnerships and health care delivery centers in the community to mitigate these issues.
Finally, Dr. Srinivas encouraged clinicians to have confidence in their expertise and make themselves heard to help their patients and improve maternal health for all. “Use your voice,” said Dr. Srinivas, “As physicians we don’t think of that as an important aspect of our work, or that we can’t articulate, but remember that we are experts, and sharing stories of patients who are impacted is incredibly powerful,” she said.
The presenters had no relevant financial conflicts to disclose.
Maternal mortality in the United States has been rising for several decades, but actions taken at the community level, as well as larger public health initiatives, have the potential to slow this trend, according to experts at a webinar sponsored by the National Institute for Health Care Management.
Maternal mortality in the United States increased by 14% from 2018 to 2020, according to data from the Centers for Disease Control and Prevention’s National Center for Health Statistics.
However, more than 80% of pregnancy-related deaths are preventable, according to 2017-2019 data from the Maternal Mortality Review Committees published online by the CDC. MMRCs include representatives of diverse clinical and nonclinical backgrounds who review the circumstances of pregnancy-related deaths.
In a webinar presented on Sept. 20, the NIHCM enlisted a panel of experts to discuss maternal mortality, the effect of changes to reproductive rights, and potential strategies to improve maternal health outcomes.
Maternal mortality is defined as “death while pregnant or within 42 days of the end of pregnancy, irrespective of the duration and site of pregnancy, from any cause related to pregnancy or its management,” according to the CDC.
Importantly, mortality rates in the United States are approximately three times higher in Black women compared with White women, said Ndidiamaka Amutah-Onukagha, PhD, MPH, of the Tufts University Center for Black Maternal Health & Reproductive Justice. Dr. Amutah-Onukagha addressed some of the potential issues that appear to drive the disparity in care.
The lack of diversity in the health care workforce has a significant effect on patient outcomes, Dr. Amutah-Onukagha said. Overall, Black newborns are more than twice as likely as White newborns to die during their first year of life, but this number is cut in half when Black infants are cared for by Black physicians, she emphasized.
Other factors that may affect disparities in maternal health care include limited access to prenatal care, discriminatory hospital protocols, and mistreatment by health care professionals, said Dr. Amutah-Onukagha. She cited data showing that maternal mortality rates were higher in rural compared with urban areas. “According to the American Hospital Association, half of rural hospitals have no obstetric care, leaving mothers in maternity care deserts; this exacerbates existing disparities,” she said.
In the webinar, Sindhu Srinivas, MD, a maternal-fetal medicine specialist at the University of Pennsylvania, explained how patient, community, and system factors play a role in the disparities in maternal care.
Overall, Black women have to travel further to receive care, which has implications for high-risk pregnancies, and patients on Medicaid have to wait longer for care, and are less likely to be referred, she added. Black women also have higher rates of preexisting conditions compared with other populations that put them in the high-risk category, such as high blood pressure, diabetes, obesity, or being HIV positive, she said.
Other factors contributing to persistent disparities in maternal care include sociodemographics, patient beliefs and knowledge, and psychological issues including stress, said Dr. Srinivas. Community factors, such as social networks, safety, and poverty, also play a role, as do clinician factors of implicit bias and communication skills, she said.
Strategies to reduce disparity
Dr. Srinivas presented several strategies to reduce disparities at various levels. At the policy level, interventions such as establishing a Maternal Mortality Review Committee, establishing a perinatal quality collaborative, and extending Medicaid for a full year postpartum could help improve outcomes, she said. Dr. Srinivas also encouraged clinicians to report maternal mortality data stratified by race and ethnicity, and to participate in the Alliance for Innovation on Maternal Health program (AIM), an initiative in partnership with the American College of Obstetrics and Gynecology.
Dr. Srinivas also proposed maternal health policies to develop payment models “to sustain and scale innovative solutions, and “preserve access to contraception and abortion care.”
For clinicians looking to have an immediate impact, the panelists agreed that working with community health centers can make a significant difference by improving access to maternal care. Consider opportunities for partnership between hospitals and health care delivery centers in the community, said Dr. Srinivas.
Also, don’t underestimate the value of doulas in the birthing process, Dr. Amutah-Onukagha said. She urged clinicians to advocate for doula reimbursement and to take advantage of opportunities for doulas to work with pregnant individuals at the community levels. Data suggest that doulas are associated with increased maternal care visits and with breastfeeding, she noted.
Adam Myers, MD, of the Blue Cross Blue Shield Association, also contributed to the webinar discussion with a key point: Having financial means and commercial coverage is not a buffer against adverse maternal outcomes for racial minorities.
Dr. Myers cited the latest Health of America Report, which included data up to April 2021 with surveys of Medicaid members and their experiences. According to the report, rates of severe maternal mortality (SMM) increased by 9% for commercially and Medicaid-insured women between 2018 and 2020.
Among commercially insured women, SMM was 53% higher among Black women than White women; among Medicaid-insured women, Black women had a 73% higher rate of SMM, compared with White women.
In addition, the report showed that significantly more mothers of color were not able to complete the recommended series of prenatal visits, mainly for reasons of scheduling and transportation, which were greater barriers than COVID-19, Dr. Myers said.
Based on the data, one specific risk profile rose to the top: “We believe women of color aged 35 or higher with comorbid conditions should be treated as very high risk for SMM,” Dr. Myers emphasized. He stressed the need to focus on transportation and scheduling barriers and expressed support for partnerships and health care delivery centers in the community to mitigate these issues.
Finally, Dr. Srinivas encouraged clinicians to have confidence in their expertise and make themselves heard to help their patients and improve maternal health for all. “Use your voice,” said Dr. Srinivas, “As physicians we don’t think of that as an important aspect of our work, or that we can’t articulate, but remember that we are experts, and sharing stories of patients who are impacted is incredibly powerful,” she said.
The presenters had no relevant financial conflicts to disclose.
Dignity
Queen Elizabeth is everywhere. She was even on the last slide of a presentation on COVID, monkeypox, and influenza vaccines given by our physician in charge of quality. This was odd. The presenter wasn’t English. The Queen had nothing to do with vaccines. Nor apparently would she have said even if she did have an opinion about them. But there we were, an audience of physicians and staff pausing for a moment of remembrance of her.
I’m not a Monarchist – except perhaps for the Kennedys. I grew up in New England. I don’t have an opinion on whether or not the British Crown should endure. But I do marvel at the astounding effect Queen Elizabeth’s passing had on so many around the world. Her personal qualities, particularly her steadiness and humane sympathy, might explain why so many are sad hearing the news. But also I think there was something in her role that we all wished for: Not the owning of palaces and sceptres, but rather, the respect that was given to her.

She was a stateswoman of “unmatched dignity,” the White House wrote. That was true, but it seems being the Queen might have been the last job on earth where such dignity is still possible. Certainly in politics, education, and even health care, there doesn’t seem to be much left lately.
The same day of that presentation I walked into the room of a patient 22 minutes late, she held her arm forth tapping her watch to indicate the time and my tardiness. Unnecessary, if not impertinent. Covering for one of my female physician colleagues, I read an email from a patient which began, “Dear Julie, With all due respect …” Another patient submitted a photo for us to review that was clearly taken from her car while waiting at a stop light. Hardly the consideration a clinical encounter should be given.
Much has been lost for patients. too. There are patients trying to make appointments lately who are told: “There are none. Call back later.” . There is no dignified way to remove exam paper stuck to your backside before introducing yourself to the doctor. Maybe that last slide of Her Majesty was in fact for us to have a moment of silence for what we’ve all lost.
Walter Bagehot (pronounce it “Baj-et” if you tell this story to your Harlan wine friends) was a political writer and editor of The Economist in the 1860s. He famously said that the secret to the English government was having two kinds of institutions, the dignified and the efficient. The efficient, Parliament, was responsible for all the work. The dignified, the Crown, gives significance and holds everyone’s respect. If medicine ever once was both dignified and efficient, we aren’t lately. We push to reduce backlogs, offer same-time virtual care, work to reduce costs. We’ve driven medicine to the efficient and left little of the dignity it seems.
The Queen will be remembered for her lifelong dedication to the laborious service of others. Even though each of us in medicine pledges the same, we also mourn this week the loss of dignity that once came with it.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
Queen Elizabeth is everywhere. She was even on the last slide of a presentation on COVID, monkeypox, and influenza vaccines given by our physician in charge of quality. This was odd. The presenter wasn’t English. The Queen had nothing to do with vaccines. Nor apparently would she have said even if she did have an opinion about them. But there we were, an audience of physicians and staff pausing for a moment of remembrance of her.
I’m not a Monarchist – except perhaps for the Kennedys. I grew up in New England. I don’t have an opinion on whether or not the British Crown should endure. But I do marvel at the astounding effect Queen Elizabeth’s passing had on so many around the world. Her personal qualities, particularly her steadiness and humane sympathy, might explain why so many are sad hearing the news. But also I think there was something in her role that we all wished for: Not the owning of palaces and sceptres, but rather, the respect that was given to her.
She was a stateswoman of “unmatched dignity,” the White House wrote. That was true, but it seems being the Queen might have been the last job on earth where such dignity is still possible. Certainly in politics, education, and even health care, there doesn’t seem to be much left lately.
The same day of that presentation I walked into the room of a patient 22 minutes late, she held her arm forth tapping her watch to indicate the time and my tardiness. Unnecessary, if not impertinent. Covering for one of my female physician colleagues, I read an email from a patient which began, “Dear Julie, With all due respect …” Another patient submitted a photo for us to review that was clearly taken from her car while waiting at a stop light. Hardly the consideration a clinical encounter should be given.
Much has been lost for patients. too. There are patients trying to make appointments lately who are told: “There are none. Call back later.” . There is no dignified way to remove exam paper stuck to your backside before introducing yourself to the doctor. Maybe that last slide of Her Majesty was in fact for us to have a moment of silence for what we’ve all lost.
Walter Bagehot (pronounce it “Baj-et” if you tell this story to your Harlan wine friends) was a political writer and editor of The Economist in the 1860s. He famously said that the secret to the English government was having two kinds of institutions, the dignified and the efficient. The efficient, Parliament, was responsible for all the work. The dignified, the Crown, gives significance and holds everyone’s respect. If medicine ever once was both dignified and efficient, we aren’t lately. We push to reduce backlogs, offer same-time virtual care, work to reduce costs. We’ve driven medicine to the efficient and left little of the dignity it seems.
The Queen will be remembered for her lifelong dedication to the laborious service of others. Even though each of us in medicine pledges the same, we also mourn this week the loss of dignity that once came with it.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
Queen Elizabeth is everywhere. She was even on the last slide of a presentation on COVID, monkeypox, and influenza vaccines given by our physician in charge of quality. This was odd. The presenter wasn’t English. The Queen had nothing to do with vaccines. Nor apparently would she have said even if she did have an opinion about them. But there we were, an audience of physicians and staff pausing for a moment of remembrance of her.
I’m not a Monarchist – except perhaps for the Kennedys. I grew up in New England. I don’t have an opinion on whether or not the British Crown should endure. But I do marvel at the astounding effect Queen Elizabeth’s passing had on so many around the world. Her personal qualities, particularly her steadiness and humane sympathy, might explain why so many are sad hearing the news. But also I think there was something in her role that we all wished for: Not the owning of palaces and sceptres, but rather, the respect that was given to her.
She was a stateswoman of “unmatched dignity,” the White House wrote. That was true, but it seems being the Queen might have been the last job on earth where such dignity is still possible. Certainly in politics, education, and even health care, there doesn’t seem to be much left lately.
The same day of that presentation I walked into the room of a patient 22 minutes late, she held her arm forth tapping her watch to indicate the time and my tardiness. Unnecessary, if not impertinent. Covering for one of my female physician colleagues, I read an email from a patient which began, “Dear Julie, With all due respect …” Another patient submitted a photo for us to review that was clearly taken from her car while waiting at a stop light. Hardly the consideration a clinical encounter should be given.
Much has been lost for patients. too. There are patients trying to make appointments lately who are told: “There are none. Call back later.” . There is no dignified way to remove exam paper stuck to your backside before introducing yourself to the doctor. Maybe that last slide of Her Majesty was in fact for us to have a moment of silence for what we’ve all lost.
Walter Bagehot (pronounce it “Baj-et” if you tell this story to your Harlan wine friends) was a political writer and editor of The Economist in the 1860s. He famously said that the secret to the English government was having two kinds of institutions, the dignified and the efficient. The efficient, Parliament, was responsible for all the work. The dignified, the Crown, gives significance and holds everyone’s respect. If medicine ever once was both dignified and efficient, we aren’t lately. We push to reduce backlogs, offer same-time virtual care, work to reduce costs. We’ve driven medicine to the efficient and left little of the dignity it seems.
The Queen will be remembered for her lifelong dedication to the laborious service of others. Even though each of us in medicine pledges the same, we also mourn this week the loss of dignity that once came with it.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
Employers’ self-funded health plans can leave rheumatology patients vulnerable
Health care costs are skyrocketing for everyone! For employers, the cost of health insurance is second only to their payroll expense. Per person spending in employer plans grew by 22% between 2015 and 2019. This outpaced inflation and economic growth. Affording health insurance for business owners has become more and more difficult, bordering on desperation for some. Consequently, they are looking for ways to be more efficient in their health care spending. One way is through self-funding their employees’ health care costs. This means that the employer directly pays for the care of their employees. While it has always been thought this was just for very large employers, it is becoming more common with smaller businesses. There is more flexibility and oversight with self-funded plans, and the employer can dictate exactly what benefits are covered within the bounds of the law. While this can make it easier to exclude certain therapies and even institute site-of-care restrictions, it also can make the employer vulnerable to health insurance companies, pharmacy benefit managers (PBMs), and third-party administrators (TPAs) that promise large discounts in plan and drug spending at the expense of their employees’ health.
Recently enacted state laws often don’t apply
Because employers who self-fund the health care for their employees are increasingly desperate to save money, they will often agree to plans that are less expensive but offer suboptimal care, particularly for patients with chronic diseases requiring expensive medicines. Many employers are not fully informed of the ramifications of these policies, so the Coalition of State Rheumatology Organizations is creating an educational employer tool kit that not only highlights the importance of disease control for their employees with rheumatic conditions but also outlines the pitfalls and misinformation that may be given to them by the insurance companies, PBMs, and other third parties that administer their health plan.

Policies that sacrifice patient care of course are not exclusive to certain self-funded health plans. The CSRO’s Payer Issue Response Team (PIRT) receives complaints daily from rheumatologists around the country regarding both the Employee Retirement Income Security Act and non-ERISA health plan policies that are harmful to their patients. Our PIRT team assesses these complaints and researches solutions that can include writing letters to the health insurance companies, employers, and departments of insurance, as well as applying enacted state legislation that overrides some of the detrimental policies. (Utilization management legislation, which has passed in many states, can be easily found on CSRO’s map tool.) These state laws can help patients with everything from harmful step therapy and nonmedical switching policies to accumulator adjustment programs denying application of copay card value to their deductibles. Unfortunately, these laws do not apply to most self-funded employer health plans, which are preempted by ERISA. Consequently, those employees are not protected from harmful changes in formularies and other policies.
Forced ‘white bagging’ in self-funded plans
Mandated “white bagging” has become a favorite for health plans covered by large insurance companies, which say that the practice is less expensive than what the physician would charge for the medication. White bagging takes away the ability of the physician to “buy and bill” infusibles that are given in their office. While some rheumatologists may accept this, there are many who do not accept infusible medications coming from another source. Often the health plan will tell the rheumatologist they must accept the white bagging or transfer the patient to another rheumatologist who will. Clearly, many health plans and TPAs do not understand the bonds that are created over the years between rheumatologists and their patients. Ironically, the price of the white-bagged medication charged to the employer has been shown often to be higher than what the physician would have charged.
Some TPAs also convince employers to carve out specialty medications from their policy entirely, leaving the employee uninsured for these meds. These TPAs then attempt to obtain the medications from the manufacturers, foundations, compounding pharmacies, and even other countries for free or highly discounted prices. Even if obtained at no cost, the TPA will charge the employer a percentage of the list price or fee for obtaining it. On the surface, this may seem like a good idea, but there are a number of issues with this, including some that are legally suspect. First of all, uninsuring employees for certain medications to take advantage of patient assistance programs from manufacturers and foundations could be viewed as perfectly legal and perfectly unethical. The legality of this practice is questionable when these companies pretend to be the patient when applying for the assistance or present compounded medication as coming from the manufacturer, or if the TPA obtains the medication from outside the country. Additionally, many employers end up paying 20% of the list price of a medication for a service that physicians provide at no cost for uninsured patients.
Educating employers
CSRO’s employer tool kit hopes to educate employers with self-funded health plans about the pitfalls of some of these policies and offers suggestions on how to best navigate these issues for employees with rheumatic diseases. We are hoping to launch this tool kit to small to medium business groups in the near future.
Advocacy is more than just contacting health insurers and those who make our laws and regulations. Although that is important, reaching out to those who employ our patients can be integral to ensuring they get the best care.
Dr. Feldman is a rheumatologist in private practice with The Rheumatology Group in New Orleans. She is the CSRO’s Vice President of Advocacy and Government Affairs and its immediate Past President, as well as past chair of the Alliance for Safe Biologic Medicines and a past member of the American College of Rheumatology insurance subcommittee. You can reach her at [email protected].
Health care costs are skyrocketing for everyone! For employers, the cost of health insurance is second only to their payroll expense. Per person spending in employer plans grew by 22% between 2015 and 2019. This outpaced inflation and economic growth. Affording health insurance for business owners has become more and more difficult, bordering on desperation for some. Consequently, they are looking for ways to be more efficient in their health care spending. One way is through self-funding their employees’ health care costs. This means that the employer directly pays for the care of their employees. While it has always been thought this was just for very large employers, it is becoming more common with smaller businesses. There is more flexibility and oversight with self-funded plans, and the employer can dictate exactly what benefits are covered within the bounds of the law. While this can make it easier to exclude certain therapies and even institute site-of-care restrictions, it also can make the employer vulnerable to health insurance companies, pharmacy benefit managers (PBMs), and third-party administrators (TPAs) that promise large discounts in plan and drug spending at the expense of their employees’ health.
Recently enacted state laws often don’t apply
Because employers who self-fund the health care for their employees are increasingly desperate to save money, they will often agree to plans that are less expensive but offer suboptimal care, particularly for patients with chronic diseases requiring expensive medicines. Many employers are not fully informed of the ramifications of these policies, so the Coalition of State Rheumatology Organizations is creating an educational employer tool kit that not only highlights the importance of disease control for their employees with rheumatic conditions but also outlines the pitfalls and misinformation that may be given to them by the insurance companies, PBMs, and other third parties that administer their health plan.
Policies that sacrifice patient care of course are not exclusive to certain self-funded health plans. The CSRO’s Payer Issue Response Team (PIRT) receives complaints daily from rheumatologists around the country regarding both the Employee Retirement Income Security Act and non-ERISA health plan policies that are harmful to their patients. Our PIRT team assesses these complaints and researches solutions that can include writing letters to the health insurance companies, employers, and departments of insurance, as well as applying enacted state legislation that overrides some of the detrimental policies. (Utilization management legislation, which has passed in many states, can be easily found on CSRO’s map tool.) These state laws can help patients with everything from harmful step therapy and nonmedical switching policies to accumulator adjustment programs denying application of copay card value to their deductibles. Unfortunately, these laws do not apply to most self-funded employer health plans, which are preempted by ERISA. Consequently, those employees are not protected from harmful changes in formularies and other policies.
Forced ‘white bagging’ in self-funded plans
Mandated “white bagging” has become a favorite for health plans covered by large insurance companies, which say that the practice is less expensive than what the physician would charge for the medication. White bagging takes away the ability of the physician to “buy and bill” infusibles that are given in their office. While some rheumatologists may accept this, there are many who do not accept infusible medications coming from another source. Often the health plan will tell the rheumatologist they must accept the white bagging or transfer the patient to another rheumatologist who will. Clearly, many health plans and TPAs do not understand the bonds that are created over the years between rheumatologists and their patients. Ironically, the price of the white-bagged medication charged to the employer has been shown often to be higher than what the physician would have charged.
Some TPAs also convince employers to carve out specialty medications from their policy entirely, leaving the employee uninsured for these meds. These TPAs then attempt to obtain the medications from the manufacturers, foundations, compounding pharmacies, and even other countries for free or highly discounted prices. Even if obtained at no cost, the TPA will charge the employer a percentage of the list price or fee for obtaining it. On the surface, this may seem like a good idea, but there are a number of issues with this, including some that are legally suspect. First of all, uninsuring employees for certain medications to take advantage of patient assistance programs from manufacturers and foundations could be viewed as perfectly legal and perfectly unethical. The legality of this practice is questionable when these companies pretend to be the patient when applying for the assistance or present compounded medication as coming from the manufacturer, or if the TPA obtains the medication from outside the country. Additionally, many employers end up paying 20% of the list price of a medication for a service that physicians provide at no cost for uninsured patients.
Educating employers
CSRO’s employer tool kit hopes to educate employers with self-funded health plans about the pitfalls of some of these policies and offers suggestions on how to best navigate these issues for employees with rheumatic diseases. We are hoping to launch this tool kit to small to medium business groups in the near future.
Advocacy is more than just contacting health insurers and those who make our laws and regulations. Although that is important, reaching out to those who employ our patients can be integral to ensuring they get the best care.
Dr. Feldman is a rheumatologist in private practice with The Rheumatology Group in New Orleans. She is the CSRO’s Vice President of Advocacy and Government Affairs and its immediate Past President, as well as past chair of the Alliance for Safe Biologic Medicines and a past member of the American College of Rheumatology insurance subcommittee. You can reach her at [email protected].
Health care costs are skyrocketing for everyone! For employers, the cost of health insurance is second only to their payroll expense. Per person spending in employer plans grew by 22% between 2015 and 2019. This outpaced inflation and economic growth. Affording health insurance for business owners has become more and more difficult, bordering on desperation for some. Consequently, they are looking for ways to be more efficient in their health care spending. One way is through self-funding their employees’ health care costs. This means that the employer directly pays for the care of their employees. While it has always been thought this was just for very large employers, it is becoming more common with smaller businesses. There is more flexibility and oversight with self-funded plans, and the employer can dictate exactly what benefits are covered within the bounds of the law. While this can make it easier to exclude certain therapies and even institute site-of-care restrictions, it also can make the employer vulnerable to health insurance companies, pharmacy benefit managers (PBMs), and third-party administrators (TPAs) that promise large discounts in plan and drug spending at the expense of their employees’ health.
Recently enacted state laws often don’t apply
Because employers who self-fund the health care for their employees are increasingly desperate to save money, they will often agree to plans that are less expensive but offer suboptimal care, particularly for patients with chronic diseases requiring expensive medicines. Many employers are not fully informed of the ramifications of these policies, so the Coalition of State Rheumatology Organizations is creating an educational employer tool kit that not only highlights the importance of disease control for their employees with rheumatic conditions but also outlines the pitfalls and misinformation that may be given to them by the insurance companies, PBMs, and other third parties that administer their health plan.
Policies that sacrifice patient care of course are not exclusive to certain self-funded health plans. The CSRO’s Payer Issue Response Team (PIRT) receives complaints daily from rheumatologists around the country regarding both the Employee Retirement Income Security Act and non-ERISA health plan policies that are harmful to their patients. Our PIRT team assesses these complaints and researches solutions that can include writing letters to the health insurance companies, employers, and departments of insurance, as well as applying enacted state legislation that overrides some of the detrimental policies. (Utilization management legislation, which has passed in many states, can be easily found on CSRO’s map tool.) These state laws can help patients with everything from harmful step therapy and nonmedical switching policies to accumulator adjustment programs denying application of copay card value to their deductibles. Unfortunately, these laws do not apply to most self-funded employer health plans, which are preempted by ERISA. Consequently, those employees are not protected from harmful changes in formularies and other policies.
Forced ‘white bagging’ in self-funded plans
Mandated “white bagging” has become a favorite for health plans covered by large insurance companies, which say that the practice is less expensive than what the physician would charge for the medication. White bagging takes away the ability of the physician to “buy and bill” infusibles that are given in their office. While some rheumatologists may accept this, there are many who do not accept infusible medications coming from another source. Often the health plan will tell the rheumatologist they must accept the white bagging or transfer the patient to another rheumatologist who will. Clearly, many health plans and TPAs do not understand the bonds that are created over the years between rheumatologists and their patients. Ironically, the price of the white-bagged medication charged to the employer has been shown often to be higher than what the physician would have charged.
Some TPAs also convince employers to carve out specialty medications from their policy entirely, leaving the employee uninsured for these meds. These TPAs then attempt to obtain the medications from the manufacturers, foundations, compounding pharmacies, and even other countries for free or highly discounted prices. Even if obtained at no cost, the TPA will charge the employer a percentage of the list price or fee for obtaining it. On the surface, this may seem like a good idea, but there are a number of issues with this, including some that are legally suspect. First of all, uninsuring employees for certain medications to take advantage of patient assistance programs from manufacturers and foundations could be viewed as perfectly legal and perfectly unethical. The legality of this practice is questionable when these companies pretend to be the patient when applying for the assistance or present compounded medication as coming from the manufacturer, or if the TPA obtains the medication from outside the country. Additionally, many employers end up paying 20% of the list price of a medication for a service that physicians provide at no cost for uninsured patients.
Educating employers
CSRO’s employer tool kit hopes to educate employers with self-funded health plans about the pitfalls of some of these policies and offers suggestions on how to best navigate these issues for employees with rheumatic diseases. We are hoping to launch this tool kit to small to medium business groups in the near future.
Advocacy is more than just contacting health insurers and those who make our laws and regulations. Although that is important, reaching out to those who employ our patients can be integral to ensuring they get the best care.
Dr. Feldman is a rheumatologist in private practice with The Rheumatology Group in New Orleans. She is the CSRO’s Vice President of Advocacy and Government Affairs and its immediate Past President, as well as past chair of the Alliance for Safe Biologic Medicines and a past member of the American College of Rheumatology insurance subcommittee. You can reach her at [email protected].
Family affair: OncBrothers host oncology hangout online
It’s hard out there for a small-town cancer doctor. Just ask Wederson M. Claudino, MD, who serves the town of Paducah in far western Kentucky. The nearest cities with significant numbers of hematologist/oncologists are hours away in cities like St. Louis and Nashville, Tenn., too far to go to talk shop over coffee, drinks, or lunch.
“It’s very challenging in a rural or small community,” he said. “I miss the opportunity to elaborate on a case.”
Now Dr. Claudino and hundreds of colleagues have discovered that useful cancer conversations are just a click away.

Urban and rural oncologists gather there to discuss new research, compare notes about challenging cases, and get to know each other.
“Following their Twitter feed and the comments and discussions make me feel like part of a bigger community,” Dr. Claudino said. And @OncBrothers is indeed a bustling Internet destination: The account’s 4,300 followers include hundreds who participate in discussions and offer perspective.
For instance, the brothers recently posted a poll asking followers how they’d treat a 55-year-old patient with non–small cell lung cancer. Nearly 250 people responded with their preferred approaches, and the survey thread included comments from oncologists from the City of Hope National Medical Center, the University of Florida, UC San Diego, and elsewhere.
In an interview, the Gosain brothers said the Twitter account is an outgrowth of their phone conversations in recent years, as they trained and settled into their early careers as general medical oncologists in smaller communities.
“After our clinic days, we’ll jump on the phone for 30-45 minutes. We’d talk about patients, how he would treat a case, and what I would do,” Rahul said. “We realized that we were living in a bubble, but we also thought that there are a lot more people in the same boat. They might jump at being able to do the same thing.”
Rahul recently became medical director at the new Wilmot Webster Cancer Center in Rochester, N.Y., after working in Corning, a tiny New York town just north of the Pennsylvania border. His brother Rohit is chair of hematology and oncology at the University of Pittsburgh’s Hillman Cancer Center in Jamestown, a small town at the western edge of New York.
“When we initially kicked off the Twitter account in August 2021, we didn’t realize the traction it would get,” Rohit said. “Now we realize that there really is a need for this.”
On an ordinary day, the @OncBrothers account may highlight research presented at a oncology conference, retweet posts by other oncologists about new guidelines or FDA drug approvals, and ask followers to consider how they’d handle a difficult case.
The brothers are especially thrilled when posts spawn discussions that draw voices from leading medical institutions who normally don’t interact much with community oncologists. “You’ll have someone from Sloan Kettering or Dana-Farber saying ‘This is what would do,’ ” Rahul said. “You have the brightest minds pitching in, and we get to learn from them.”
The Gosain brothers were both born in India and immigrated as children to Toronto. They each went to medical school in the Caribbean – for Rohit, it was after a stint as a computer engineer – and they each embraced oncology. “For me, it was about having the right mentors while I was doing my clinical rotations as a medical student and as a resident,” Rahul said. In addition, he said, “this field was moving and is still moving so fast. It really intrigued and excited me and made me want to be at the forefront of it.”
The fast-moving nature of oncology, in fact, was one of the drivers behind the daily conversations between the brothers and the subsequent creation of the @OncBrothers account. “Just last year, in 2021, there were 40 new drugs that were indicated for hematology-oncology,” Rahul said. “To stay on top of that is very, very hard.”
It’s especially difficult to figure out treatment plans when multiple options exist. A 2022 thread on @OncBrothers revealed a wide divergence of opinions about triple therapy in prostate cancer: The 322 respondents to a Twitter poll were sharply divided about the best three-drug combination from these options – docetaxel, daratumumab, abiraterone, androgen deprivation therapy, and alpha-reductase inhibitors.
To make things more challenging, community oncologists often are generalists who treat patients with a wide variety of cancers from prostate and lung to breast and colon. As a result, these oncologists must keep up on developments across the entire cancer field. Rohit highlighted a 2022 thread that polled users about the approach they’d take to another patient with non–small cell lung cancer; 474 people responded. The accompanying discussion emphasized the need for the next-generation sequencing (NGS).
“A significant portion of community oncologists are not even doing NGS testing, which is FDA-approved,” Rohit said. “There’s a huge gap that still exists, and we weren’t even aware of it. We continue to learn from these conversations.”
The brothers contend that there’s a crucial need for education among community oncologists in light of evidence suggesting that some cancer outcomes are worse than those in urban areas.
In fact, Rohit led a 2019 study published in the journal Cancer that found that overall survival in rural patients with neuroendocrine tumors trended toward worse outcomes than in urban patients.
“There are many factors such as financial burden, lack of education, and rural patients not willing to travel to the city,” Rohit said. “We need to be more creative and ask, ‘How can we equip our medical oncologist in rural settings to continue to do better?’ ”
What’s next for the OncBrothers? The Gosains have created a website (www.oncbrothers.com) that highlights their social media work, and they’re exploring options such as podcasts and short videos. “Our goal is to focus on how to continue to keep general medical oncologists up to date, informed, and educated so patients can get the best care close to home,” Rahul said. “We need to do better.”
It’s hard out there for a small-town cancer doctor. Just ask Wederson M. Claudino, MD, who serves the town of Paducah in far western Kentucky. The nearest cities with significant numbers of hematologist/oncologists are hours away in cities like St. Louis and Nashville, Tenn., too far to go to talk shop over coffee, drinks, or lunch.
“It’s very challenging in a rural or small community,” he said. “I miss the opportunity to elaborate on a case.”
Now Dr. Claudino and hundreds of colleagues have discovered that useful cancer conversations are just a click away.
Urban and rural oncologists gather there to discuss new research, compare notes about challenging cases, and get to know each other.
“Following their Twitter feed and the comments and discussions make me feel like part of a bigger community,” Dr. Claudino said. And @OncBrothers is indeed a bustling Internet destination: The account’s 4,300 followers include hundreds who participate in discussions and offer perspective.
For instance, the brothers recently posted a poll asking followers how they’d treat a 55-year-old patient with non–small cell lung cancer. Nearly 250 people responded with their preferred approaches, and the survey thread included comments from oncologists from the City of Hope National Medical Center, the University of Florida, UC San Diego, and elsewhere.
In an interview, the Gosain brothers said the Twitter account is an outgrowth of their phone conversations in recent years, as they trained and settled into their early careers as general medical oncologists in smaller communities.
“After our clinic days, we’ll jump on the phone for 30-45 minutes. We’d talk about patients, how he would treat a case, and what I would do,” Rahul said. “We realized that we were living in a bubble, but we also thought that there are a lot more people in the same boat. They might jump at being able to do the same thing.”
Rahul recently became medical director at the new Wilmot Webster Cancer Center in Rochester, N.Y., after working in Corning, a tiny New York town just north of the Pennsylvania border. His brother Rohit is chair of hematology and oncology at the University of Pittsburgh’s Hillman Cancer Center in Jamestown, a small town at the western edge of New York.
“When we initially kicked off the Twitter account in August 2021, we didn’t realize the traction it would get,” Rohit said. “Now we realize that there really is a need for this.”
On an ordinary day, the @OncBrothers account may highlight research presented at a oncology conference, retweet posts by other oncologists about new guidelines or FDA drug approvals, and ask followers to consider how they’d handle a difficult case.
The brothers are especially thrilled when posts spawn discussions that draw voices from leading medical institutions who normally don’t interact much with community oncologists. “You’ll have someone from Sloan Kettering or Dana-Farber saying ‘This is what would do,’ ” Rahul said. “You have the brightest minds pitching in, and we get to learn from them.”
The Gosain brothers were both born in India and immigrated as children to Toronto. They each went to medical school in the Caribbean – for Rohit, it was after a stint as a computer engineer – and they each embraced oncology. “For me, it was about having the right mentors while I was doing my clinical rotations as a medical student and as a resident,” Rahul said. In addition, he said, “this field was moving and is still moving so fast. It really intrigued and excited me and made me want to be at the forefront of it.”
The fast-moving nature of oncology, in fact, was one of the drivers behind the daily conversations between the brothers and the subsequent creation of the @OncBrothers account. “Just last year, in 2021, there were 40 new drugs that were indicated for hematology-oncology,” Rahul said. “To stay on top of that is very, very hard.”
It’s especially difficult to figure out treatment plans when multiple options exist. A 2022 thread on @OncBrothers revealed a wide divergence of opinions about triple therapy in prostate cancer: The 322 respondents to a Twitter poll were sharply divided about the best three-drug combination from these options – docetaxel, daratumumab, abiraterone, androgen deprivation therapy, and alpha-reductase inhibitors.
To make things more challenging, community oncologists often are generalists who treat patients with a wide variety of cancers from prostate and lung to breast and colon. As a result, these oncologists must keep up on developments across the entire cancer field. Rohit highlighted a 2022 thread that polled users about the approach they’d take to another patient with non–small cell lung cancer; 474 people responded. The accompanying discussion emphasized the need for the next-generation sequencing (NGS).
“A significant portion of community oncologists are not even doing NGS testing, which is FDA-approved,” Rohit said. “There’s a huge gap that still exists, and we weren’t even aware of it. We continue to learn from these conversations.”
The brothers contend that there’s a crucial need for education among community oncologists in light of evidence suggesting that some cancer outcomes are worse than those in urban areas.
In fact, Rohit led a 2019 study published in the journal Cancer that found that overall survival in rural patients with neuroendocrine tumors trended toward worse outcomes than in urban patients.
“There are many factors such as financial burden, lack of education, and rural patients not willing to travel to the city,” Rohit said. “We need to be more creative and ask, ‘How can we equip our medical oncologist in rural settings to continue to do better?’ ”
What’s next for the OncBrothers? The Gosains have created a website (www.oncbrothers.com) that highlights their social media work, and they’re exploring options such as podcasts and short videos. “Our goal is to focus on how to continue to keep general medical oncologists up to date, informed, and educated so patients can get the best care close to home,” Rahul said. “We need to do better.”
It’s hard out there for a small-town cancer doctor. Just ask Wederson M. Claudino, MD, who serves the town of Paducah in far western Kentucky. The nearest cities with significant numbers of hematologist/oncologists are hours away in cities like St. Louis and Nashville, Tenn., too far to go to talk shop over coffee, drinks, or lunch.
“It’s very challenging in a rural or small community,” he said. “I miss the opportunity to elaborate on a case.”
Now Dr. Claudino and hundreds of colleagues have discovered that useful cancer conversations are just a click away.
Urban and rural oncologists gather there to discuss new research, compare notes about challenging cases, and get to know each other.
“Following their Twitter feed and the comments and discussions make me feel like part of a bigger community,” Dr. Claudino said. And @OncBrothers is indeed a bustling Internet destination: The account’s 4,300 followers include hundreds who participate in discussions and offer perspective.
For instance, the brothers recently posted a poll asking followers how they’d treat a 55-year-old patient with non–small cell lung cancer. Nearly 250 people responded with their preferred approaches, and the survey thread included comments from oncologists from the City of Hope National Medical Center, the University of Florida, UC San Diego, and elsewhere.
In an interview, the Gosain brothers said the Twitter account is an outgrowth of their phone conversations in recent years, as they trained and settled into their early careers as general medical oncologists in smaller communities.
“After our clinic days, we’ll jump on the phone for 30-45 minutes. We’d talk about patients, how he would treat a case, and what I would do,” Rahul said. “We realized that we were living in a bubble, but we also thought that there are a lot more people in the same boat. They might jump at being able to do the same thing.”
Rahul recently became medical director at the new Wilmot Webster Cancer Center in Rochester, N.Y., after working in Corning, a tiny New York town just north of the Pennsylvania border. His brother Rohit is chair of hematology and oncology at the University of Pittsburgh’s Hillman Cancer Center in Jamestown, a small town at the western edge of New York.
“When we initially kicked off the Twitter account in August 2021, we didn’t realize the traction it would get,” Rohit said. “Now we realize that there really is a need for this.”
On an ordinary day, the @OncBrothers account may highlight research presented at a oncology conference, retweet posts by other oncologists about new guidelines or FDA drug approvals, and ask followers to consider how they’d handle a difficult case.
The brothers are especially thrilled when posts spawn discussions that draw voices from leading medical institutions who normally don’t interact much with community oncologists. “You’ll have someone from Sloan Kettering or Dana-Farber saying ‘This is what would do,’ ” Rahul said. “You have the brightest minds pitching in, and we get to learn from them.”
The Gosain brothers were both born in India and immigrated as children to Toronto. They each went to medical school in the Caribbean – for Rohit, it was after a stint as a computer engineer – and they each embraced oncology. “For me, it was about having the right mentors while I was doing my clinical rotations as a medical student and as a resident,” Rahul said. In addition, he said, “this field was moving and is still moving so fast. It really intrigued and excited me and made me want to be at the forefront of it.”
The fast-moving nature of oncology, in fact, was one of the drivers behind the daily conversations between the brothers and the subsequent creation of the @OncBrothers account. “Just last year, in 2021, there were 40 new drugs that were indicated for hematology-oncology,” Rahul said. “To stay on top of that is very, very hard.”
It’s especially difficult to figure out treatment plans when multiple options exist. A 2022 thread on @OncBrothers revealed a wide divergence of opinions about triple therapy in prostate cancer: The 322 respondents to a Twitter poll were sharply divided about the best three-drug combination from these options – docetaxel, daratumumab, abiraterone, androgen deprivation therapy, and alpha-reductase inhibitors.
To make things more challenging, community oncologists often are generalists who treat patients with a wide variety of cancers from prostate and lung to breast and colon. As a result, these oncologists must keep up on developments across the entire cancer field. Rohit highlighted a 2022 thread that polled users about the approach they’d take to another patient with non–small cell lung cancer; 474 people responded. The accompanying discussion emphasized the need for the next-generation sequencing (NGS).
“A significant portion of community oncologists are not even doing NGS testing, which is FDA-approved,” Rohit said. “There’s a huge gap that still exists, and we weren’t even aware of it. We continue to learn from these conversations.”
The brothers contend that there’s a crucial need for education among community oncologists in light of evidence suggesting that some cancer outcomes are worse than those in urban areas.
In fact, Rohit led a 2019 study published in the journal Cancer that found that overall survival in rural patients with neuroendocrine tumors trended toward worse outcomes than in urban patients.
“There are many factors such as financial burden, lack of education, and rural patients not willing to travel to the city,” Rohit said. “We need to be more creative and ask, ‘How can we equip our medical oncologist in rural settings to continue to do better?’ ”
What’s next for the OncBrothers? The Gosains have created a website (www.oncbrothers.com) that highlights their social media work, and they’re exploring options such as podcasts and short videos. “Our goal is to focus on how to continue to keep general medical oncologists up to date, informed, and educated so patients can get the best care close to home,” Rahul said. “We need to do better.”
House passes prior authorization bill, Senate path unclear
The path through the U.S. Senate is not yet certain for a bill intended to speed the prior authorization process of insurer-run Medicare Advantage plans, despite the measure having breezed through the House.
House leaders opted to move the Improving Seniors’ Timely Access to Care Act of 2021 (HR 3173) without requiring a roll-call vote. The measure was passed on Sept. 14 by a voice vote, an approach used in general with only uncontroversial measures that have broad support. The bill has 191 Democratic and 135 Republican sponsors, representing about three-quarters of the members of the House.
“There is no reason that patients should be waiting for medically appropriate care, especially when we know that this can lead to worse outcomes,” Rep. Earl Blumenauer (D-Ore.) said in a Sept. 14 speech on the House floor. “The fundamental promise of Medicare Advantage is undermined when people are delaying care, getting sicker, and ultimately costing Medicare more money.”
Rep. Greg Murphy, MD (R-N.C.), spoke on the House floor that day as well, bringing up cases he has seen in his own urology practice in which prior authorization delays disrupted medical care. One patient wound up in the hospital with abscess after an insurer denied an antibiotic prescription, Rep. Murphy said.
But the Senate appears unlikely at this time to move the prior authorization bill as a standalone measure. Instead, the bill may become part of a larger legislative package focused on health care that the Senate Finance Committee intends to prepare later this year.
The House-passed bill would require insurer-run Medicare plans to respond to expedited requests for prior authorization of services within 24 hours and to other requests within 7 days. This bill also would establish an electronic program for prior authorizations and mandate increased transparency as to how insurers use this tool.
CBO: Cost of change would be billions
In seeking to mandate changes in prior authorization, lawmakers likely will need to contend with the issue of a $16 billion cumulative cost estimate for the bill from the Congressional Budget Office. Members of Congress often seek to offset new spending by pairing bills that add to expected costs for the federal government with ones expected to produce savings.
Unlike Rep. Blumenauer, Rep. Murphy, and other backers of the prior authorization streamlining bill, CBO staff estimates that making the mandated changes would raise federal spending, inasmuch as there would be “a greater use of services.”
On Sept. 14, CBO issued a one-page report on the costs of the bill. The CBO report concerns only the bill in question, as is common practice with the office’s estimates.
Prior authorization changes would begin in fiscal 2025 and would add $899 million in spending, or outlays, that year, CBO said. The annual costs from the streamlined prior authorization practices through fiscal 2026 to 2032 range from $1.6 billion to $2.7 billion.
Looking at the CBO estimate against a backdrop of total Medicare Advantage costs, though, may provide important context.
The increases in spending estimated by CBO may suggest that there would be little change in federal spending as a result of streamlining prior authorization practices. These estimates of increased annual spending of $1.6 billion–$2.7 billion are only a small fraction of the current annual cost of insurer-run Medicare, and they represent an even smaller share of the projected expense.
The federal government last year spent about $350 billion on insurer-run plans, excluding Part D drug plan payments, according to the Medicare Advisory Payment Commission (MedPAC).
As of 2021, about 27 million people were enrolled in these plans, accounting for about 46% of the total Medicare population. Enrollment has doubled since 2010, MedPAC said, and it is expected to continue to grow. By 2027, insurer-run Medicare could cover 50% of the program’s population, a figure that may reach 53% by 2031.
Federal payments to these plans will accelerate in the years ahead as insurers attract more people eligible for Medicare as customers. Payments to these private health plans could rise from an expected $418 billion this year to $940.6 billion by 2031, according to the most recent Medicare trustees report.
Good intentions, poor implementation?
Insurer-run Medicare has long enjoyed deep bipartisan support in Congress. That’s due in part to its potential for reducing spending on what are considered low-value treatments, or ones considered unlikely to provide a significant medical benefit, but Rep. Blumenauer is among the members of Congress who see insurer-run Medicare as a path for preserving the giant federal health program. Traditional Medicare has far fewer restrictions on services, which sometimes opens a path for tests and treatments that offer less value for patients.
“I believe that the way traditional fee-for-service Medicare operates is not sustainable and that Medicare Advantage is one of the tools we can use to demonstrate how we can incentivize value,” Rep. Blumenauer said on the House floor. “But this is only possible when the program operates as intended. I have been deeply concerned about the reports of delays in care” caused by the clunky prior authorization processes.
He highlighted a recent report from the internal watchdog group for the Department of Health & Human Services that raises concerns about denials of appropriate care. About 18% of a set of payment denials examined by the Office of Inspector General of HHS in April actually met Medicare coverage rules and plan billing rules.
“For patients and their families, being told that you need to wait longer for care that your doctor tells you that you need is incredibly frustrating and frightening,” Rep. Blumenauer said. “There’s no comfort to be found in the fact that your insurance company needs time to decide if your doctor is right.”
Trends in prior authorization
The CBO report does not provide detail on what kind of medical spending would increase under a streamlined prior authorization process in insurer-run Medicare plans.
From trends reported in prior authorization, though, two factors could be at play in what appear to be relatively small estimated increases in Medicare spending from streamlined prior authorization.
One is the work already underway to create less burdensome electronic systems for these requests, such as the Fast Prior Authorization Technology Highway initiative run by the trade association America’s Health Insurance Plans.
The other factor could be the number of cases in which prior authorization merely causes delays in treatments and tests and thus simply postpones spending while adding to clinicians’ administrative work.
An analysis of prior authorization requests for dermatologic practices affiliated with the University of Utah may represent an extreme example. In a report published in JAMA Dermatology in 2020, researchers described what happened with requests made during 1 month, September 2016.
The approval rate for procedures was 99.6% – 100% (95 of 95) for Mohs surgery, and 96% (130 of 131, with 4 additional cases pending) for excisions. These findings supported calls for simplifying prior authorization procedures, “perhaps first by eliminating unnecessary PAs [prior authorizations] and appeals,” Aaron M. Secrest, MD, PhD, of the University of Utah, Salt Lake City, and coauthors wrote in the article.
Still, there is some evidence that insurer-run Medicare policies reduce the use of low-value care.
In a study published in JAMA Health Forum, Emily Boudreau, PhD, of insurer Humana Inc, and coauthors from Tufts University, Boston, and the University of Pennsylvania, Philadelphia investigated whether insurer-run Medicare could do a better job in reducing the amount of low-value care delivered than the traditional program. They analyzed a set of claims data from 2017 to 2019 for people enrolled in insurer-run and traditional Medicare.
They reported a rate of 23.07 low-value services provided per 100 people in insurer-run Medicare, compared with 25.39 for those in traditional Medicare. Some of the biggest differences reported in the article were in cancer screenings for older people.
As an example, the U.S. Preventive Services Task Force recommends that women older than 65 years not be screened for cervical cancer if they have undergone adequate screening in the past and are not at high risk for cervical cancer. There was an annual count of 1.76 screenings for cervical cancer per 100 women older than 65 in the insurer-run Medicare group versus 3.18 for those in traditional Medicare.
The Better Medicare Alliance issued a statement in favor of the House passage of the Improving Seniors’ Timely Access to Care Act.
In it, the group said the measure would “modernize prior authorization while protecting its essential function in facilitating safe, high-value, evidence-based care.” The alliance promotes use of insurer-run Medicare. The board of the Better Medicare Alliance includes executives who serve with firms that run Advantage plans as well as medical organizations and universities.
“With studies showing that up to one-quarter of all health care expenditures are wasted on services with no benefit to the patient, we need a robust, next-generation prior authorization program to deter low-value, and even harmful, care while protecting access to needed treatment and effective therapies,” said A. Mark Fendrick, MD, director of the University of Michigan’s Center for Value-Based Insurance Design in Ann Arbor, in a statement issued by the Better Medicare Alliance. He is a member of the group’s council of scholars.
On the House floor on September 14, Rep. Ami Bera, MD (D-Calif.), said he has heard from former colleagues and his medical school classmates that they now spend as much as 40% of their time on administrative work. These distractions from patient care are helping drive physicians away from the practice of medicine.
Still, the internist defended the basic premise of prior authorization while strongly appealing for better systems of handling it.
“Yes, there is a role for prior authorization in limited cases. There is also a role to go back and retrospectively look at how care is being delivered,” Rep. Bera said. “But what is happening today is a travesty. It wasn’t the intention of prior authorization. It is a prior authorization process gone awry.”
A version of this article first appeared on Medscape.com.
The path through the U.S. Senate is not yet certain for a bill intended to speed the prior authorization process of insurer-run Medicare Advantage plans, despite the measure having breezed through the House.
House leaders opted to move the Improving Seniors’ Timely Access to Care Act of 2021 (HR 3173) without requiring a roll-call vote. The measure was passed on Sept. 14 by a voice vote, an approach used in general with only uncontroversial measures that have broad support. The bill has 191 Democratic and 135 Republican sponsors, representing about three-quarters of the members of the House.
“There is no reason that patients should be waiting for medically appropriate care, especially when we know that this can lead to worse outcomes,” Rep. Earl Blumenauer (D-Ore.) said in a Sept. 14 speech on the House floor. “The fundamental promise of Medicare Advantage is undermined when people are delaying care, getting sicker, and ultimately costing Medicare more money.”
Rep. Greg Murphy, MD (R-N.C.), spoke on the House floor that day as well, bringing up cases he has seen in his own urology practice in which prior authorization delays disrupted medical care. One patient wound up in the hospital with abscess after an insurer denied an antibiotic prescription, Rep. Murphy said.
But the Senate appears unlikely at this time to move the prior authorization bill as a standalone measure. Instead, the bill may become part of a larger legislative package focused on health care that the Senate Finance Committee intends to prepare later this year.
The House-passed bill would require insurer-run Medicare plans to respond to expedited requests for prior authorization of services within 24 hours and to other requests within 7 days. This bill also would establish an electronic program for prior authorizations and mandate increased transparency as to how insurers use this tool.
CBO: Cost of change would be billions
In seeking to mandate changes in prior authorization, lawmakers likely will need to contend with the issue of a $16 billion cumulative cost estimate for the bill from the Congressional Budget Office. Members of Congress often seek to offset new spending by pairing bills that add to expected costs for the federal government with ones expected to produce savings.
Unlike Rep. Blumenauer, Rep. Murphy, and other backers of the prior authorization streamlining bill, CBO staff estimates that making the mandated changes would raise federal spending, inasmuch as there would be “a greater use of services.”
On Sept. 14, CBO issued a one-page report on the costs of the bill. The CBO report concerns only the bill in question, as is common practice with the office’s estimates.
Prior authorization changes would begin in fiscal 2025 and would add $899 million in spending, or outlays, that year, CBO said. The annual costs from the streamlined prior authorization practices through fiscal 2026 to 2032 range from $1.6 billion to $2.7 billion.
Looking at the CBO estimate against a backdrop of total Medicare Advantage costs, though, may provide important context.
The increases in spending estimated by CBO may suggest that there would be little change in federal spending as a result of streamlining prior authorization practices. These estimates of increased annual spending of $1.6 billion–$2.7 billion are only a small fraction of the current annual cost of insurer-run Medicare, and they represent an even smaller share of the projected expense.
The federal government last year spent about $350 billion on insurer-run plans, excluding Part D drug plan payments, according to the Medicare Advisory Payment Commission (MedPAC).
As of 2021, about 27 million people were enrolled in these plans, accounting for about 46% of the total Medicare population. Enrollment has doubled since 2010, MedPAC said, and it is expected to continue to grow. By 2027, insurer-run Medicare could cover 50% of the program’s population, a figure that may reach 53% by 2031.
Federal payments to these plans will accelerate in the years ahead as insurers attract more people eligible for Medicare as customers. Payments to these private health plans could rise from an expected $418 billion this year to $940.6 billion by 2031, according to the most recent Medicare trustees report.
Good intentions, poor implementation?
Insurer-run Medicare has long enjoyed deep bipartisan support in Congress. That’s due in part to its potential for reducing spending on what are considered low-value treatments, or ones considered unlikely to provide a significant medical benefit, but Rep. Blumenauer is among the members of Congress who see insurer-run Medicare as a path for preserving the giant federal health program. Traditional Medicare has far fewer restrictions on services, which sometimes opens a path for tests and treatments that offer less value for patients.
“I believe that the way traditional fee-for-service Medicare operates is not sustainable and that Medicare Advantage is one of the tools we can use to demonstrate how we can incentivize value,” Rep. Blumenauer said on the House floor. “But this is only possible when the program operates as intended. I have been deeply concerned about the reports of delays in care” caused by the clunky prior authorization processes.
He highlighted a recent report from the internal watchdog group for the Department of Health & Human Services that raises concerns about denials of appropriate care. About 18% of a set of payment denials examined by the Office of Inspector General of HHS in April actually met Medicare coverage rules and plan billing rules.
“For patients and their families, being told that you need to wait longer for care that your doctor tells you that you need is incredibly frustrating and frightening,” Rep. Blumenauer said. “There’s no comfort to be found in the fact that your insurance company needs time to decide if your doctor is right.”
Trends in prior authorization
The CBO report does not provide detail on what kind of medical spending would increase under a streamlined prior authorization process in insurer-run Medicare plans.
From trends reported in prior authorization, though, two factors could be at play in what appear to be relatively small estimated increases in Medicare spending from streamlined prior authorization.
One is the work already underway to create less burdensome electronic systems for these requests, such as the Fast Prior Authorization Technology Highway initiative run by the trade association America’s Health Insurance Plans.
The other factor could be the number of cases in which prior authorization merely causes delays in treatments and tests and thus simply postpones spending while adding to clinicians’ administrative work.
An analysis of prior authorization requests for dermatologic practices affiliated with the University of Utah may represent an extreme example. In a report published in JAMA Dermatology in 2020, researchers described what happened with requests made during 1 month, September 2016.
The approval rate for procedures was 99.6% – 100% (95 of 95) for Mohs surgery, and 96% (130 of 131, with 4 additional cases pending) for excisions. These findings supported calls for simplifying prior authorization procedures, “perhaps first by eliminating unnecessary PAs [prior authorizations] and appeals,” Aaron M. Secrest, MD, PhD, of the University of Utah, Salt Lake City, and coauthors wrote in the article.
Still, there is some evidence that insurer-run Medicare policies reduce the use of low-value care.
In a study published in JAMA Health Forum, Emily Boudreau, PhD, of insurer Humana Inc, and coauthors from Tufts University, Boston, and the University of Pennsylvania, Philadelphia investigated whether insurer-run Medicare could do a better job in reducing the amount of low-value care delivered than the traditional program. They analyzed a set of claims data from 2017 to 2019 for people enrolled in insurer-run and traditional Medicare.
They reported a rate of 23.07 low-value services provided per 100 people in insurer-run Medicare, compared with 25.39 for those in traditional Medicare. Some of the biggest differences reported in the article were in cancer screenings for older people.
As an example, the U.S. Preventive Services Task Force recommends that women older than 65 years not be screened for cervical cancer if they have undergone adequate screening in the past and are not at high risk for cervical cancer. There was an annual count of 1.76 screenings for cervical cancer per 100 women older than 65 in the insurer-run Medicare group versus 3.18 for those in traditional Medicare.
The Better Medicare Alliance issued a statement in favor of the House passage of the Improving Seniors’ Timely Access to Care Act.
In it, the group said the measure would “modernize prior authorization while protecting its essential function in facilitating safe, high-value, evidence-based care.” The alliance promotes use of insurer-run Medicare. The board of the Better Medicare Alliance includes executives who serve with firms that run Advantage plans as well as medical organizations and universities.
“With studies showing that up to one-quarter of all health care expenditures are wasted on services with no benefit to the patient, we need a robust, next-generation prior authorization program to deter low-value, and even harmful, care while protecting access to needed treatment and effective therapies,” said A. Mark Fendrick, MD, director of the University of Michigan’s Center for Value-Based Insurance Design in Ann Arbor, in a statement issued by the Better Medicare Alliance. He is a member of the group’s council of scholars.
On the House floor on September 14, Rep. Ami Bera, MD (D-Calif.), said he has heard from former colleagues and his medical school classmates that they now spend as much as 40% of their time on administrative work. These distractions from patient care are helping drive physicians away from the practice of medicine.
Still, the internist defended the basic premise of prior authorization while strongly appealing for better systems of handling it.
“Yes, there is a role for prior authorization in limited cases. There is also a role to go back and retrospectively look at how care is being delivered,” Rep. Bera said. “But what is happening today is a travesty. It wasn’t the intention of prior authorization. It is a prior authorization process gone awry.”
A version of this article first appeared on Medscape.com.
The path through the U.S. Senate is not yet certain for a bill intended to speed the prior authorization process of insurer-run Medicare Advantage plans, despite the measure having breezed through the House.
House leaders opted to move the Improving Seniors’ Timely Access to Care Act of 2021 (HR 3173) without requiring a roll-call vote. The measure was passed on Sept. 14 by a voice vote, an approach used in general with only uncontroversial measures that have broad support. The bill has 191 Democratic and 135 Republican sponsors, representing about three-quarters of the members of the House.
“There is no reason that patients should be waiting for medically appropriate care, especially when we know that this can lead to worse outcomes,” Rep. Earl Blumenauer (D-Ore.) said in a Sept. 14 speech on the House floor. “The fundamental promise of Medicare Advantage is undermined when people are delaying care, getting sicker, and ultimately costing Medicare more money.”
Rep. Greg Murphy, MD (R-N.C.), spoke on the House floor that day as well, bringing up cases he has seen in his own urology practice in which prior authorization delays disrupted medical care. One patient wound up in the hospital with abscess after an insurer denied an antibiotic prescription, Rep. Murphy said.
But the Senate appears unlikely at this time to move the prior authorization bill as a standalone measure. Instead, the bill may become part of a larger legislative package focused on health care that the Senate Finance Committee intends to prepare later this year.
The House-passed bill would require insurer-run Medicare plans to respond to expedited requests for prior authorization of services within 24 hours and to other requests within 7 days. This bill also would establish an electronic program for prior authorizations and mandate increased transparency as to how insurers use this tool.
CBO: Cost of change would be billions
In seeking to mandate changes in prior authorization, lawmakers likely will need to contend with the issue of a $16 billion cumulative cost estimate for the bill from the Congressional Budget Office. Members of Congress often seek to offset new spending by pairing bills that add to expected costs for the federal government with ones expected to produce savings.
Unlike Rep. Blumenauer, Rep. Murphy, and other backers of the prior authorization streamlining bill, CBO staff estimates that making the mandated changes would raise federal spending, inasmuch as there would be “a greater use of services.”
On Sept. 14, CBO issued a one-page report on the costs of the bill. The CBO report concerns only the bill in question, as is common practice with the office’s estimates.
Prior authorization changes would begin in fiscal 2025 and would add $899 million in spending, or outlays, that year, CBO said. The annual costs from the streamlined prior authorization practices through fiscal 2026 to 2032 range from $1.6 billion to $2.7 billion.
Looking at the CBO estimate against a backdrop of total Medicare Advantage costs, though, may provide important context.
The increases in spending estimated by CBO may suggest that there would be little change in federal spending as a result of streamlining prior authorization practices. These estimates of increased annual spending of $1.6 billion–$2.7 billion are only a small fraction of the current annual cost of insurer-run Medicare, and they represent an even smaller share of the projected expense.
The federal government last year spent about $350 billion on insurer-run plans, excluding Part D drug plan payments, according to the Medicare Advisory Payment Commission (MedPAC).
As of 2021, about 27 million people were enrolled in these plans, accounting for about 46% of the total Medicare population. Enrollment has doubled since 2010, MedPAC said, and it is expected to continue to grow. By 2027, insurer-run Medicare could cover 50% of the program’s population, a figure that may reach 53% by 2031.
Federal payments to these plans will accelerate in the years ahead as insurers attract more people eligible for Medicare as customers. Payments to these private health plans could rise from an expected $418 billion this year to $940.6 billion by 2031, according to the most recent Medicare trustees report.
Good intentions, poor implementation?
Insurer-run Medicare has long enjoyed deep bipartisan support in Congress. That’s due in part to its potential for reducing spending on what are considered low-value treatments, or ones considered unlikely to provide a significant medical benefit, but Rep. Blumenauer is among the members of Congress who see insurer-run Medicare as a path for preserving the giant federal health program. Traditional Medicare has far fewer restrictions on services, which sometimes opens a path for tests and treatments that offer less value for patients.
“I believe that the way traditional fee-for-service Medicare operates is not sustainable and that Medicare Advantage is one of the tools we can use to demonstrate how we can incentivize value,” Rep. Blumenauer said on the House floor. “But this is only possible when the program operates as intended. I have been deeply concerned about the reports of delays in care” caused by the clunky prior authorization processes.
He highlighted a recent report from the internal watchdog group for the Department of Health & Human Services that raises concerns about denials of appropriate care. About 18% of a set of payment denials examined by the Office of Inspector General of HHS in April actually met Medicare coverage rules and plan billing rules.
“For patients and their families, being told that you need to wait longer for care that your doctor tells you that you need is incredibly frustrating and frightening,” Rep. Blumenauer said. “There’s no comfort to be found in the fact that your insurance company needs time to decide if your doctor is right.”
Trends in prior authorization
The CBO report does not provide detail on what kind of medical spending would increase under a streamlined prior authorization process in insurer-run Medicare plans.
From trends reported in prior authorization, though, two factors could be at play in what appear to be relatively small estimated increases in Medicare spending from streamlined prior authorization.
One is the work already underway to create less burdensome electronic systems for these requests, such as the Fast Prior Authorization Technology Highway initiative run by the trade association America’s Health Insurance Plans.
The other factor could be the number of cases in which prior authorization merely causes delays in treatments and tests and thus simply postpones spending while adding to clinicians’ administrative work.
An analysis of prior authorization requests for dermatologic practices affiliated with the University of Utah may represent an extreme example. In a report published in JAMA Dermatology in 2020, researchers described what happened with requests made during 1 month, September 2016.
The approval rate for procedures was 99.6% – 100% (95 of 95) for Mohs surgery, and 96% (130 of 131, with 4 additional cases pending) for excisions. These findings supported calls for simplifying prior authorization procedures, “perhaps first by eliminating unnecessary PAs [prior authorizations] and appeals,” Aaron M. Secrest, MD, PhD, of the University of Utah, Salt Lake City, and coauthors wrote in the article.
Still, there is some evidence that insurer-run Medicare policies reduce the use of low-value care.
In a study published in JAMA Health Forum, Emily Boudreau, PhD, of insurer Humana Inc, and coauthors from Tufts University, Boston, and the University of Pennsylvania, Philadelphia investigated whether insurer-run Medicare could do a better job in reducing the amount of low-value care delivered than the traditional program. They analyzed a set of claims data from 2017 to 2019 for people enrolled in insurer-run and traditional Medicare.
They reported a rate of 23.07 low-value services provided per 100 people in insurer-run Medicare, compared with 25.39 for those in traditional Medicare. Some of the biggest differences reported in the article were in cancer screenings for older people.
As an example, the U.S. Preventive Services Task Force recommends that women older than 65 years not be screened for cervical cancer if they have undergone adequate screening in the past and are not at high risk for cervical cancer. There was an annual count of 1.76 screenings for cervical cancer per 100 women older than 65 in the insurer-run Medicare group versus 3.18 for those in traditional Medicare.
The Better Medicare Alliance issued a statement in favor of the House passage of the Improving Seniors’ Timely Access to Care Act.
In it, the group said the measure would “modernize prior authorization while protecting its essential function in facilitating safe, high-value, evidence-based care.” The alliance promotes use of insurer-run Medicare. The board of the Better Medicare Alliance includes executives who serve with firms that run Advantage plans as well as medical organizations and universities.
“With studies showing that up to one-quarter of all health care expenditures are wasted on services with no benefit to the patient, we need a robust, next-generation prior authorization program to deter low-value, and even harmful, care while protecting access to needed treatment and effective therapies,” said A. Mark Fendrick, MD, director of the University of Michigan’s Center for Value-Based Insurance Design in Ann Arbor, in a statement issued by the Better Medicare Alliance. He is a member of the group’s council of scholars.
On the House floor on September 14, Rep. Ami Bera, MD (D-Calif.), said he has heard from former colleagues and his medical school classmates that they now spend as much as 40% of their time on administrative work. These distractions from patient care are helping drive physicians away from the practice of medicine.
Still, the internist defended the basic premise of prior authorization while strongly appealing for better systems of handling it.
“Yes, there is a role for prior authorization in limited cases. There is also a role to go back and retrospectively look at how care is being delivered,” Rep. Bera said. “But what is happening today is a travesty. It wasn’t the intention of prior authorization. It is a prior authorization process gone awry.”
A version of this article first appeared on Medscape.com.
Horse hockey notwithstanding
He’s 24 years younger than I am, recently married, no kids. Just starting out as a neurologist. He also has a full head of hair, something I’m admittedly jealous of.
He’s always in a sweater, something that seems oddly out of place in Phoenix, Arizona.
He’s the picture on my hospital ID.

I don’t go to the hospital much anymore, but he still sits in my car, greeting me whenever I open the center console to get my sunglasses or phone charger. He looks very enthusiastic about starting his career. I clearly remember the day I had the picture taken, as a newly-minted attending getting his first hospital privileges.
Sometimes I talk to him. Usually it’s just silly advice (“bet on the ’16 Cubs”). Other times I wonder what he’d do in certain situations, with all his youthful enthusiasm. I’m sure he wonders the same about me, with my 24 years of experience.
To a large extent we are the same people we started out as, but time changes us, in ways besides the obvious (like my hairs jumping off like lemmings).
Looking back at him (or even the older pic on my medical school application) I have no complaints about where life and my career have taken me. Would there be a few things I might have changed if I could go back?
Realistically, maybe one or two, both involving my father, but neither of them would likely change where I am.
But as far as medicine goes? Not really. The things I liked then, that got me into the field? I still enjoy them. The horse hockey? Yeah, it’s always there, probably has gotten worse over time, and it still bothers me. But there isn’t a job that doesn’t have its share of cow patties. It’s just a matter of trying not to step in them more than necessary as you do the parts you enjoy.
Sometimes I look at my younger self, and wonder what I’d really say to him if we actually met.
Probably just “good luck, enjoy the ride, and ditch the sweater.”
We measure our gains out in luck and coincidence
Lanterns to turn back the night.
And put our defeats down to chance or experience
And try once again for the light.
– Al Stewart
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
He’s 24 years younger than I am, recently married, no kids. Just starting out as a neurologist. He also has a full head of hair, something I’m admittedly jealous of.
He’s always in a sweater, something that seems oddly out of place in Phoenix, Arizona.
He’s the picture on my hospital ID.
I don’t go to the hospital much anymore, but he still sits in my car, greeting me whenever I open the center console to get my sunglasses or phone charger. He looks very enthusiastic about starting his career. I clearly remember the day I had the picture taken, as a newly-minted attending getting his first hospital privileges.
Sometimes I talk to him. Usually it’s just silly advice (“bet on the ’16 Cubs”). Other times I wonder what he’d do in certain situations, with all his youthful enthusiasm. I’m sure he wonders the same about me, with my 24 years of experience.
To a large extent we are the same people we started out as, but time changes us, in ways besides the obvious (like my hairs jumping off like lemmings).
Looking back at him (or even the older pic on my medical school application) I have no complaints about where life and my career have taken me. Would there be a few things I might have changed if I could go back?
Realistically, maybe one or two, both involving my father, but neither of them would likely change where I am.
But as far as medicine goes? Not really. The things I liked then, that got me into the field? I still enjoy them. The horse hockey? Yeah, it’s always there, probably has gotten worse over time, and it still bothers me. But there isn’t a job that doesn’t have its share of cow patties. It’s just a matter of trying not to step in them more than necessary as you do the parts you enjoy.
Sometimes I look at my younger self, and wonder what I’d really say to him if we actually met.
Probably just “good luck, enjoy the ride, and ditch the sweater.”
We measure our gains out in luck and coincidence
Lanterns to turn back the night.
And put our defeats down to chance or experience
And try once again for the light.
– Al Stewart
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
He’s 24 years younger than I am, recently married, no kids. Just starting out as a neurologist. He also has a full head of hair, something I’m admittedly jealous of.
He’s always in a sweater, something that seems oddly out of place in Phoenix, Arizona.
He’s the picture on my hospital ID.
I don’t go to the hospital much anymore, but he still sits in my car, greeting me whenever I open the center console to get my sunglasses or phone charger. He looks very enthusiastic about starting his career. I clearly remember the day I had the picture taken, as a newly-minted attending getting his first hospital privileges.
Sometimes I talk to him. Usually it’s just silly advice (“bet on the ’16 Cubs”). Other times I wonder what he’d do in certain situations, with all his youthful enthusiasm. I’m sure he wonders the same about me, with my 24 years of experience.
To a large extent we are the same people we started out as, but time changes us, in ways besides the obvious (like my hairs jumping off like lemmings).
Looking back at him (or even the older pic on my medical school application) I have no complaints about where life and my career have taken me. Would there be a few things I might have changed if I could go back?
Realistically, maybe one or two, both involving my father, but neither of them would likely change where I am.
But as far as medicine goes? Not really. The things I liked then, that got me into the field? I still enjoy them. The horse hockey? Yeah, it’s always there, probably has gotten worse over time, and it still bothers me. But there isn’t a job that doesn’t have its share of cow patties. It’s just a matter of trying not to step in them more than necessary as you do the parts you enjoy.
Sometimes I look at my younger self, and wonder what I’d really say to him if we actually met.
Probably just “good luck, enjoy the ride, and ditch the sweater.”
We measure our gains out in luck and coincidence
Lanterns to turn back the night.
And put our defeats down to chance or experience
And try once again for the light.
– Al Stewart
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Physicians can’t be bystanders in ‘silent scourge’ of medical bullying
Maya Iyer, MD, MEd, experienced bullying as a faculty member, and she sensed that she wasn’t alone. “The best ideas for research often come from individual experiences, in both personal and the professional academic medicine setting,” she said in an interview.
“And I was correct. I was not the only one who experienced bullying. In fact, the most severe bullying experiences among ... women physician leaders occurred when they were in leadership positions,” said Dr. Iyer, a pediatric emergency medicine physician at Nationwide Children’s Hospital in Columbus, Ohio.
She is a coauthor of a study that was published in JAMA Network Open in which investigators surveyed the existence of antibullying policies for faculty at almost 100 U.S. medical schools.
The researchers defined bullying as “a severe form of mistreatment [that] occurs in the medical setting when a power differential allows offenders to consciously target individuals through persistent negative actions to impede the education or career of the target.”
The study included 91 medical schools, of which 4 schools had antibullying policies that included the reporting of procedures. Of the 87 medical schools without antibullying policies, 60 had antiharrassment policies; of those schools, 10 of the schools’ websites cited bullying and antiharassment policies. Five schools required a login to access policies, and one school’s website had a broken webpage link, per the study.
“We need to bring the silent scourge of bullying to the forefront because bullying is causing a brain drain on the medical profession,” said Dr. Iyer. “Bullying has numerous downstream negative effects, including depression, anxiety, burnout stress, decreased patient care satisfaction, increased medical errors, and job attrition.”
She added: “Through bullying, we are losing voices in medicine just at that point in time where we are trying to diversify the workforce to improve representation of all physicians.”
Dr. Iyer’s team sampled the top 25 schools for research and the top 25 schools for primary care. They also took a random sampling from 25 schools for research and a random sampling from top 25 schools for primary care. They assessed antibullying policies, antiharassment policies that mentioned bullying, antiharrassment policies that did not mention bullying, and the absence of policies addressing these issues.
Policy comprehensiveness was another focus for the researchers. They evaluated whether the relevant policies included faculty members and articulated the institution’s commitment to providing a safe and healthy workplace. Other factors included defining bullying and the roles and responsibilities of employees and procedures for reporting bullying.
Physicians can’t be bystanders to bullying
This means transitioning from being a bystander to an upstander.”
She doesn’t let medical schools off the hook, however. Instead, she advocated having institutions “provide safe spaces and opportunities for near-peer mentoring so that targets of bullying can share stories.”
Regarding who is responsible for addressing bullying, Dr. Iyer is emphatic. “I do want to be clear that the onus of disrupting does not fall on the targets. Rather, we need to fix the systems in which such behavior is tolerated.”
Her advice to leaders in academic medicine is to create comprehensive, zero-retaliation bullying policies that include detailed reporting procedures. Dr. Iyer advised leaders to partner with colleagues in human resources, offices of equity, and ombudspersons to develop, implement, and enforce these policies.
The study authors reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Maya Iyer, MD, MEd, experienced bullying as a faculty member, and she sensed that she wasn’t alone. “The best ideas for research often come from individual experiences, in both personal and the professional academic medicine setting,” she said in an interview.
“And I was correct. I was not the only one who experienced bullying. In fact, the most severe bullying experiences among ... women physician leaders occurred when they were in leadership positions,” said Dr. Iyer, a pediatric emergency medicine physician at Nationwide Children’s Hospital in Columbus, Ohio.
She is a coauthor of a study that was published in JAMA Network Open in which investigators surveyed the existence of antibullying policies for faculty at almost 100 U.S. medical schools.
The researchers defined bullying as “a severe form of mistreatment [that] occurs in the medical setting when a power differential allows offenders to consciously target individuals through persistent negative actions to impede the education or career of the target.”
The study included 91 medical schools, of which 4 schools had antibullying policies that included the reporting of procedures. Of the 87 medical schools without antibullying policies, 60 had antiharrassment policies; of those schools, 10 of the schools’ websites cited bullying and antiharassment policies. Five schools required a login to access policies, and one school’s website had a broken webpage link, per the study.
“We need to bring the silent scourge of bullying to the forefront because bullying is causing a brain drain on the medical profession,” said Dr. Iyer. “Bullying has numerous downstream negative effects, including depression, anxiety, burnout stress, decreased patient care satisfaction, increased medical errors, and job attrition.”
She added: “Through bullying, we are losing voices in medicine just at that point in time where we are trying to diversify the workforce to improve representation of all physicians.”
Dr. Iyer’s team sampled the top 25 schools for research and the top 25 schools for primary care. They also took a random sampling from 25 schools for research and a random sampling from top 25 schools for primary care. They assessed antibullying policies, antiharassment policies that mentioned bullying, antiharrassment policies that did not mention bullying, and the absence of policies addressing these issues.
Policy comprehensiveness was another focus for the researchers. They evaluated whether the relevant policies included faculty members and articulated the institution’s commitment to providing a safe and healthy workplace. Other factors included defining bullying and the roles and responsibilities of employees and procedures for reporting bullying.
Physicians can’t be bystanders to bullying
This means transitioning from being a bystander to an upstander.”
She doesn’t let medical schools off the hook, however. Instead, she advocated having institutions “provide safe spaces and opportunities for near-peer mentoring so that targets of bullying can share stories.”
Regarding who is responsible for addressing bullying, Dr. Iyer is emphatic. “I do want to be clear that the onus of disrupting does not fall on the targets. Rather, we need to fix the systems in which such behavior is tolerated.”
Her advice to leaders in academic medicine is to create comprehensive, zero-retaliation bullying policies that include detailed reporting procedures. Dr. Iyer advised leaders to partner with colleagues in human resources, offices of equity, and ombudspersons to develop, implement, and enforce these policies.
The study authors reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Maya Iyer, MD, MEd, experienced bullying as a faculty member, and she sensed that she wasn’t alone. “The best ideas for research often come from individual experiences, in both personal and the professional academic medicine setting,” she said in an interview.
“And I was correct. I was not the only one who experienced bullying. In fact, the most severe bullying experiences among ... women physician leaders occurred when they were in leadership positions,” said Dr. Iyer, a pediatric emergency medicine physician at Nationwide Children’s Hospital in Columbus, Ohio.
She is a coauthor of a study that was published in JAMA Network Open in which investigators surveyed the existence of antibullying policies for faculty at almost 100 U.S. medical schools.
The researchers defined bullying as “a severe form of mistreatment [that] occurs in the medical setting when a power differential allows offenders to consciously target individuals through persistent negative actions to impede the education or career of the target.”
The study included 91 medical schools, of which 4 schools had antibullying policies that included the reporting of procedures. Of the 87 medical schools without antibullying policies, 60 had antiharrassment policies; of those schools, 10 of the schools’ websites cited bullying and antiharassment policies. Five schools required a login to access policies, and one school’s website had a broken webpage link, per the study.
“We need to bring the silent scourge of bullying to the forefront because bullying is causing a brain drain on the medical profession,” said Dr. Iyer. “Bullying has numerous downstream negative effects, including depression, anxiety, burnout stress, decreased patient care satisfaction, increased medical errors, and job attrition.”
She added: “Through bullying, we are losing voices in medicine just at that point in time where we are trying to diversify the workforce to improve representation of all physicians.”
Dr. Iyer’s team sampled the top 25 schools for research and the top 25 schools for primary care. They also took a random sampling from 25 schools for research and a random sampling from top 25 schools for primary care. They assessed antibullying policies, antiharassment policies that mentioned bullying, antiharrassment policies that did not mention bullying, and the absence of policies addressing these issues.
Policy comprehensiveness was another focus for the researchers. They evaluated whether the relevant policies included faculty members and articulated the institution’s commitment to providing a safe and healthy workplace. Other factors included defining bullying and the roles and responsibilities of employees and procedures for reporting bullying.
Physicians can’t be bystanders to bullying
This means transitioning from being a bystander to an upstander.”
She doesn’t let medical schools off the hook, however. Instead, she advocated having institutions “provide safe spaces and opportunities for near-peer mentoring so that targets of bullying can share stories.”
Regarding who is responsible for addressing bullying, Dr. Iyer is emphatic. “I do want to be clear that the onus of disrupting does not fall on the targets. Rather, we need to fix the systems in which such behavior is tolerated.”
Her advice to leaders in academic medicine is to create comprehensive, zero-retaliation bullying policies that include detailed reporting procedures. Dr. Iyer advised leaders to partner with colleagues in human resources, offices of equity, and ombudspersons to develop, implement, and enforce these policies.
The study authors reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
EHR: A progress report
I wrote my first column on electronic health records in the mid-1990s. At the time, it seemed like an idea whose time had come. After all, in an era when just about every essential process in medicine had already been computerized, we physicians continued to process clinical data – our key asset – with pen and paper. Most of us were reluctant to make the switch, and for good reason:
Then, the government stepped in. Shortly after his inauguration in 2000, President George W. Bush outlined a plan to ensure that most Americans had electronic health records within 10 years. “By computerizing health records,” the president said, “we can avoid dangerous medical mistakes, reduce costs, and improve care.” The goal was to eliminate missing charts, duplication of lab testing, ineffective documentation, and inordinate amounts of time spent on paperwork, not to mention illegible handwriting, poor coordination of care between physicians, and many other problems. Studies were quoted, suggesting that EHR shortened inpatient stays, decreased risk of adverse drug interactions, improved the consistency and content of records, and improved continuity of care and follow-up.

The EHR Incentive Program (later renamed the Promoting Interoperability Program) was introduced to encourage physicians and hospitals “to adopt, implement, upgrade, and demonstrate meaningful use of certified electronic health record technology.”
Nearly a quarter-century later, implementation is well behind schedule. According to a 2019 federal study, while nearly all hospitals (96%) have adopted a certified EHR, only 72% of office-based physicians have done so.
There are multiple reasons for this. For one thing, EHR is still by and large slower than pen and paper, because direct data entry is still primarily done by keyboard. Voice recognition, hand-held and wireless devices have been developed, but most work only on specialized tasks. Even the best systems take more clinician time per encounter than the manual processes they replace.
Physicians have been slow to warm to a system that slows them down and forces them to change the way they think and work. In addition, paper systems never crash; the prospect of a server malfunction or Internet failure bringing an entire clinic to a grinding halt is not particularly inviting.
The special needs of dermatology – high patient volumes, multiple diagnoses and prescriptions per patient, the wide variety of procedures we perform, and digital image storage – present further hurdles.
Nevertheless, the march toward electronic record keeping continues, and I continue to receive many questions about choosing a good EHR system. As always, I cannot recommend any specific products since every office has unique needs and requirements.
The key phrase to keep in mind is caveat emptor. Several regulatory bodies exist to test vendor claims and certify system behaviors, but different agencies use different criteria that may or may not be relevant to your requirements. Vaporware is still as common as real software; beware the “feature in the next release” that might never appear, particularly if you need it right now.
Avoid the temptation to buy a flashy new system and then try to adapt it to your office; figure out your needs first, then find a system that meets them.
Unfortunately, there is no easy way around doing the work of comparing one system with another. The most important information a vendor can give you is the names and addresses of two or more offices where you can go watch their system in action. Site visits are time-consuming, but they are only way to pick the best EHR the first time around.
Don’t be the first office using a new system. Let the vendor work out the bugs somewhere else.
Above all, if you have disorganized paper records, don’t count on EHR to automatically solve your problems. Well-designed paper systems usually lend themselves to effective automation, but automating a poorly designed system just increases the chaos. If your paper system is in disarray, solve that problem before considering EHR.
With all of its problems and hurdles, EHRs will inevitably be a part of most of our lives. And for those who take the time to do it right, it will ultimately be an improvement.
Think of information technologies as power tools: They can help you to do things better, but they can also amplify your errors. So choose carefully.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
I wrote my first column on electronic health records in the mid-1990s. At the time, it seemed like an idea whose time had come. After all, in an era when just about every essential process in medicine had already been computerized, we physicians continued to process clinical data – our key asset – with pen and paper. Most of us were reluctant to make the switch, and for good reason:
Then, the government stepped in. Shortly after his inauguration in 2000, President George W. Bush outlined a plan to ensure that most Americans had electronic health records within 10 years. “By computerizing health records,” the president said, “we can avoid dangerous medical mistakes, reduce costs, and improve care.” The goal was to eliminate missing charts, duplication of lab testing, ineffective documentation, and inordinate amounts of time spent on paperwork, not to mention illegible handwriting, poor coordination of care between physicians, and many other problems. Studies were quoted, suggesting that EHR shortened inpatient stays, decreased risk of adverse drug interactions, improved the consistency and content of records, and improved continuity of care and follow-up.
The EHR Incentive Program (later renamed the Promoting Interoperability Program) was introduced to encourage physicians and hospitals “to adopt, implement, upgrade, and demonstrate meaningful use of certified electronic health record technology.”
Nearly a quarter-century later, implementation is well behind schedule. According to a 2019 federal study, while nearly all hospitals (96%) have adopted a certified EHR, only 72% of office-based physicians have done so.
There are multiple reasons for this. For one thing, EHR is still by and large slower than pen and paper, because direct data entry is still primarily done by keyboard. Voice recognition, hand-held and wireless devices have been developed, but most work only on specialized tasks. Even the best systems take more clinician time per encounter than the manual processes they replace.
Physicians have been slow to warm to a system that slows them down and forces them to change the way they think and work. In addition, paper systems never crash; the prospect of a server malfunction or Internet failure bringing an entire clinic to a grinding halt is not particularly inviting.
The special needs of dermatology – high patient volumes, multiple diagnoses and prescriptions per patient, the wide variety of procedures we perform, and digital image storage – present further hurdles.
Nevertheless, the march toward electronic record keeping continues, and I continue to receive many questions about choosing a good EHR system. As always, I cannot recommend any specific products since every office has unique needs and requirements.
The key phrase to keep in mind is caveat emptor. Several regulatory bodies exist to test vendor claims and certify system behaviors, but different agencies use different criteria that may or may not be relevant to your requirements. Vaporware is still as common as real software; beware the “feature in the next release” that might never appear, particularly if you need it right now.
Avoid the temptation to buy a flashy new system and then try to adapt it to your office; figure out your needs first, then find a system that meets them.
Unfortunately, there is no easy way around doing the work of comparing one system with another. The most important information a vendor can give you is the names and addresses of two or more offices where you can go watch their system in action. Site visits are time-consuming, but they are only way to pick the best EHR the first time around.
Don’t be the first office using a new system. Let the vendor work out the bugs somewhere else.
Above all, if you have disorganized paper records, don’t count on EHR to automatically solve your problems. Well-designed paper systems usually lend themselves to effective automation, but automating a poorly designed system just increases the chaos. If your paper system is in disarray, solve that problem before considering EHR.
With all of its problems and hurdles, EHRs will inevitably be a part of most of our lives. And for those who take the time to do it right, it will ultimately be an improvement.
Think of information technologies as power tools: They can help you to do things better, but they can also amplify your errors. So choose carefully.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
I wrote my first column on electronic health records in the mid-1990s. At the time, it seemed like an idea whose time had come. After all, in an era when just about every essential process in medicine had already been computerized, we physicians continued to process clinical data – our key asset – with pen and paper. Most of us were reluctant to make the switch, and for good reason:
Then, the government stepped in. Shortly after his inauguration in 2000, President George W. Bush outlined a plan to ensure that most Americans had electronic health records within 10 years. “By computerizing health records,” the president said, “we can avoid dangerous medical mistakes, reduce costs, and improve care.” The goal was to eliminate missing charts, duplication of lab testing, ineffective documentation, and inordinate amounts of time spent on paperwork, not to mention illegible handwriting, poor coordination of care between physicians, and many other problems. Studies were quoted, suggesting that EHR shortened inpatient stays, decreased risk of adverse drug interactions, improved the consistency and content of records, and improved continuity of care and follow-up.
The EHR Incentive Program (later renamed the Promoting Interoperability Program) was introduced to encourage physicians and hospitals “to adopt, implement, upgrade, and demonstrate meaningful use of certified electronic health record technology.”
Nearly a quarter-century later, implementation is well behind schedule. According to a 2019 federal study, while nearly all hospitals (96%) have adopted a certified EHR, only 72% of office-based physicians have done so.
There are multiple reasons for this. For one thing, EHR is still by and large slower than pen and paper, because direct data entry is still primarily done by keyboard. Voice recognition, hand-held and wireless devices have been developed, but most work only on specialized tasks. Even the best systems take more clinician time per encounter than the manual processes they replace.
Physicians have been slow to warm to a system that slows them down and forces them to change the way they think and work. In addition, paper systems never crash; the prospect of a server malfunction or Internet failure bringing an entire clinic to a grinding halt is not particularly inviting.
The special needs of dermatology – high patient volumes, multiple diagnoses and prescriptions per patient, the wide variety of procedures we perform, and digital image storage – present further hurdles.
Nevertheless, the march toward electronic record keeping continues, and I continue to receive many questions about choosing a good EHR system. As always, I cannot recommend any specific products since every office has unique needs and requirements.
The key phrase to keep in mind is caveat emptor. Several regulatory bodies exist to test vendor claims and certify system behaviors, but different agencies use different criteria that may or may not be relevant to your requirements. Vaporware is still as common as real software; beware the “feature in the next release” that might never appear, particularly if you need it right now.
Avoid the temptation to buy a flashy new system and then try to adapt it to your office; figure out your needs first, then find a system that meets them.
Unfortunately, there is no easy way around doing the work of comparing one system with another. The most important information a vendor can give you is the names and addresses of two or more offices where you can go watch their system in action. Site visits are time-consuming, but they are only way to pick the best EHR the first time around.
Don’t be the first office using a new system. Let the vendor work out the bugs somewhere else.
Above all, if you have disorganized paper records, don’t count on EHR to automatically solve your problems. Well-designed paper systems usually lend themselves to effective automation, but automating a poorly designed system just increases the chaos. If your paper system is in disarray, solve that problem before considering EHR.
With all of its problems and hurdles, EHRs will inevitably be a part of most of our lives. And for those who take the time to do it right, it will ultimately be an improvement.
Think of information technologies as power tools: They can help you to do things better, but they can also amplify your errors. So choose carefully.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].

Anesthesiologist arrested, implicated in death of colleague
at Baylor Scott & White Surgicare, a North Dallas surgical center. Raynaldo Rivera Ortiz Jr., MD, 59, is accused of injecting nerve-blocking and bronchodilating drugs into patient IV bags, resulting in at least one death and multiple cardiac emergencies.
In June, an anesthesiologist identified by Dallas ABC affiliate WFAA as Melanie Kaspar, MD, a colleague of Dr. Ortiz’s at the outpatient center, was ill and treated herself for dehydration using an IV bag of saline she had taken home from work. She died immediately after injecting the contents of the bag. According to the autopsy report, she died from a lethal dose of bupivacaine, a nerve-blocking agent often used during the administration of anesthesia. According to WFAA, Dr. Kaspar’s death was initially ruled accidental, but the Dallas County Medical Examiner has since reopened the case.
Then in August, an 18-year-old male patient, identified in court documents as J.A., experienced a cardiac emergency during a scheduled surgery at the clinic. The teen, who according to local press coverage was undergoing nose surgery after a dirt bike accident, was transferred to a local ICU. A chemical analysis of the fluid from the saline bag that was used during his surgery found epinephrine (a stimulant that could have caused his symptoms), bupivacaine, and lidocaine.
According to court documents, an investigation by the surgical center identified about 10 additional unexpected cardiac emergencies that occurred during what should have been unremarkable surgeries, an exceptionally high rate of complications, suggesting a pattern of intentional adulteration of IV bags. These surgeries were performed between May and August.
In addition, the complaint alleges that none of the cardiac incidents occurred during Dr. Ortiz’s surgeries; however, all of the incidents occurred around the time Dr. Ortiz performed services at the facility, and no incidents occurred while he was on vacation. The incidents began 2 days after Dr. Ortiz had been notified that he was the subject of a disciplinary inquiry stemming from an incident in which he allegedly “deviated from the standard of care” during an anesthesia procedure when a patient experienced a medical emergency, according to federal officials.
The complaint also alleges that Dr. Ortiz had a history of disciplinary actions against him, including at the facility, and he complained that the center was trying to “crucify” him.
Surveillance video from the hallway of the center’s operating room shows Dr. Ortiz placing IV bags in the stainless-steel bag warmer shortly before other doctors’ patients experienced cardiac emergencies, according to the complaint. In the description of one instance captured on video, Dr. Ortiz was observed walking quickly from an operating room to the bag warmer, placing a single IV bag inside, visually scanning the empty hallway, and quickly walking away. Just over an hour later, according to the complaint, a 56-year-old woman suffered a cardiac emergency during a scheduled cosmetic surgery after a bag from the warmer was used during her procedure.
The complaint alleges that in another instance, Dr. Ortiz was observed exiting his operating room carrying an IV bag concealed in what appeared to be a paper folder, swapping the bag with another bag from the warmer, and walking away. Roughly 30 minutes later, a 54-year-old woman suffered a cardiac emergency during a scheduled cosmetic surgery after a bag from the warmer was used during her procedure.
“Our complaint alleges this defendant surreptitiously injected heart-stopping drugs into patient IV bags, decimating the Hippocratic Oath,” said Chad E. Meacham, U.S. Attorney for the Northern District of Texas. “A single incident of seemingly intentional patient harm would be disconcerting; multiple incidents are truly disturbing. At this point, however, we believe that the problem is limited to one individual, who is currently behind bars. We will work tirelessly to hold him accountable.”
Dr. Ortiz is charged with tampering with a consumer product and with intentionally adulterating drugs. If convicted, he faces a maximum penalty of life in prison. Dr. Ortiz will make his initial appearance before U.S. Magistrate Judge Renee Toliver in Dallas Sept. 16.
On Sept. 9, the Texas Medical Board suspended Dr. Ortiz’s license in connection with this investigation, noting that the panel found “an imminent peril to the public health, safety, or welfare” and that Dr. Ortiz’s “continuation in the practice of medicine poses a continuing threat to public welfare.”
“It is astounding, stunning [for the victims] to think that anyone did this intentionally,” said Bruce W. Steckler, an attorney for some of the victims, in an interview with WFAA.
Baylor Scott & White Health, which operates the surgical center, said in a statement that the North Dallas facility will remain closed as the investigation continues.
“We actively assisted authorities in their investigation and will continue to do so. We also remain focused on communicating with patients,” the health system said.
A version of this article first appeared on Medscape.com.
at Baylor Scott & White Surgicare, a North Dallas surgical center. Raynaldo Rivera Ortiz Jr., MD, 59, is accused of injecting nerve-blocking and bronchodilating drugs into patient IV bags, resulting in at least one death and multiple cardiac emergencies.
In June, an anesthesiologist identified by Dallas ABC affiliate WFAA as Melanie Kaspar, MD, a colleague of Dr. Ortiz’s at the outpatient center, was ill and treated herself for dehydration using an IV bag of saline she had taken home from work. She died immediately after injecting the contents of the bag. According to the autopsy report, she died from a lethal dose of bupivacaine, a nerve-blocking agent often used during the administration of anesthesia. According to WFAA, Dr. Kaspar’s death was initially ruled accidental, but the Dallas County Medical Examiner has since reopened the case.
Then in August, an 18-year-old male patient, identified in court documents as J.A., experienced a cardiac emergency during a scheduled surgery at the clinic. The teen, who according to local press coverage was undergoing nose surgery after a dirt bike accident, was transferred to a local ICU. A chemical analysis of the fluid from the saline bag that was used during his surgery found epinephrine (a stimulant that could have caused his symptoms), bupivacaine, and lidocaine.
According to court documents, an investigation by the surgical center identified about 10 additional unexpected cardiac emergencies that occurred during what should have been unremarkable surgeries, an exceptionally high rate of complications, suggesting a pattern of intentional adulteration of IV bags. These surgeries were performed between May and August.
In addition, the complaint alleges that none of the cardiac incidents occurred during Dr. Ortiz’s surgeries; however, all of the incidents occurred around the time Dr. Ortiz performed services at the facility, and no incidents occurred while he was on vacation. The incidents began 2 days after Dr. Ortiz had been notified that he was the subject of a disciplinary inquiry stemming from an incident in which he allegedly “deviated from the standard of care” during an anesthesia procedure when a patient experienced a medical emergency, according to federal officials.
The complaint also alleges that Dr. Ortiz had a history of disciplinary actions against him, including at the facility, and he complained that the center was trying to “crucify” him.
Surveillance video from the hallway of the center’s operating room shows Dr. Ortiz placing IV bags in the stainless-steel bag warmer shortly before other doctors’ patients experienced cardiac emergencies, according to the complaint. In the description of one instance captured on video, Dr. Ortiz was observed walking quickly from an operating room to the bag warmer, placing a single IV bag inside, visually scanning the empty hallway, and quickly walking away. Just over an hour later, according to the complaint, a 56-year-old woman suffered a cardiac emergency during a scheduled cosmetic surgery after a bag from the warmer was used during her procedure.
The complaint alleges that in another instance, Dr. Ortiz was observed exiting his operating room carrying an IV bag concealed in what appeared to be a paper folder, swapping the bag with another bag from the warmer, and walking away. Roughly 30 minutes later, a 54-year-old woman suffered a cardiac emergency during a scheduled cosmetic surgery after a bag from the warmer was used during her procedure.
“Our complaint alleges this defendant surreptitiously injected heart-stopping drugs into patient IV bags, decimating the Hippocratic Oath,” said Chad E. Meacham, U.S. Attorney for the Northern District of Texas. “A single incident of seemingly intentional patient harm would be disconcerting; multiple incidents are truly disturbing. At this point, however, we believe that the problem is limited to one individual, who is currently behind bars. We will work tirelessly to hold him accountable.”
Dr. Ortiz is charged with tampering with a consumer product and with intentionally adulterating drugs. If convicted, he faces a maximum penalty of life in prison. Dr. Ortiz will make his initial appearance before U.S. Magistrate Judge Renee Toliver in Dallas Sept. 16.
On Sept. 9, the Texas Medical Board suspended Dr. Ortiz’s license in connection with this investigation, noting that the panel found “an imminent peril to the public health, safety, or welfare” and that Dr. Ortiz’s “continuation in the practice of medicine poses a continuing threat to public welfare.”
“It is astounding, stunning [for the victims] to think that anyone did this intentionally,” said Bruce W. Steckler, an attorney for some of the victims, in an interview with WFAA.
Baylor Scott & White Health, which operates the surgical center, said in a statement that the North Dallas facility will remain closed as the investigation continues.
“We actively assisted authorities in their investigation and will continue to do so. We also remain focused on communicating with patients,” the health system said.
A version of this article first appeared on Medscape.com.
at Baylor Scott & White Surgicare, a North Dallas surgical center. Raynaldo Rivera Ortiz Jr., MD, 59, is accused of injecting nerve-blocking and bronchodilating drugs into patient IV bags, resulting in at least one death and multiple cardiac emergencies.
In June, an anesthesiologist identified by Dallas ABC affiliate WFAA as Melanie Kaspar, MD, a colleague of Dr. Ortiz’s at the outpatient center, was ill and treated herself for dehydration using an IV bag of saline she had taken home from work. She died immediately after injecting the contents of the bag. According to the autopsy report, she died from a lethal dose of bupivacaine, a nerve-blocking agent often used during the administration of anesthesia. According to WFAA, Dr. Kaspar’s death was initially ruled accidental, but the Dallas County Medical Examiner has since reopened the case.
Then in August, an 18-year-old male patient, identified in court documents as J.A., experienced a cardiac emergency during a scheduled surgery at the clinic. The teen, who according to local press coverage was undergoing nose surgery after a dirt bike accident, was transferred to a local ICU. A chemical analysis of the fluid from the saline bag that was used during his surgery found epinephrine (a stimulant that could have caused his symptoms), bupivacaine, and lidocaine.
According to court documents, an investigation by the surgical center identified about 10 additional unexpected cardiac emergencies that occurred during what should have been unremarkable surgeries, an exceptionally high rate of complications, suggesting a pattern of intentional adulteration of IV bags. These surgeries were performed between May and August.
In addition, the complaint alleges that none of the cardiac incidents occurred during Dr. Ortiz’s surgeries; however, all of the incidents occurred around the time Dr. Ortiz performed services at the facility, and no incidents occurred while he was on vacation. The incidents began 2 days after Dr. Ortiz had been notified that he was the subject of a disciplinary inquiry stemming from an incident in which he allegedly “deviated from the standard of care” during an anesthesia procedure when a patient experienced a medical emergency, according to federal officials.
The complaint also alleges that Dr. Ortiz had a history of disciplinary actions against him, including at the facility, and he complained that the center was trying to “crucify” him.
Surveillance video from the hallway of the center’s operating room shows Dr. Ortiz placing IV bags in the stainless-steel bag warmer shortly before other doctors’ patients experienced cardiac emergencies, according to the complaint. In the description of one instance captured on video, Dr. Ortiz was observed walking quickly from an operating room to the bag warmer, placing a single IV bag inside, visually scanning the empty hallway, and quickly walking away. Just over an hour later, according to the complaint, a 56-year-old woman suffered a cardiac emergency during a scheduled cosmetic surgery after a bag from the warmer was used during her procedure.
The complaint alleges that in another instance, Dr. Ortiz was observed exiting his operating room carrying an IV bag concealed in what appeared to be a paper folder, swapping the bag with another bag from the warmer, and walking away. Roughly 30 minutes later, a 54-year-old woman suffered a cardiac emergency during a scheduled cosmetic surgery after a bag from the warmer was used during her procedure.
“Our complaint alleges this defendant surreptitiously injected heart-stopping drugs into patient IV bags, decimating the Hippocratic Oath,” said Chad E. Meacham, U.S. Attorney for the Northern District of Texas. “A single incident of seemingly intentional patient harm would be disconcerting; multiple incidents are truly disturbing. At this point, however, we believe that the problem is limited to one individual, who is currently behind bars. We will work tirelessly to hold him accountable.”
Dr. Ortiz is charged with tampering with a consumer product and with intentionally adulterating drugs. If convicted, he faces a maximum penalty of life in prison. Dr. Ortiz will make his initial appearance before U.S. Magistrate Judge Renee Toliver in Dallas Sept. 16.
On Sept. 9, the Texas Medical Board suspended Dr. Ortiz’s license in connection with this investigation, noting that the panel found “an imminent peril to the public health, safety, or welfare” and that Dr. Ortiz’s “continuation in the practice of medicine poses a continuing threat to public welfare.”
“It is astounding, stunning [for the victims] to think that anyone did this intentionally,” said Bruce W. Steckler, an attorney for some of the victims, in an interview with WFAA.
Baylor Scott & White Health, which operates the surgical center, said in a statement that the North Dallas facility will remain closed as the investigation continues.
“We actively assisted authorities in their investigation and will continue to do so. We also remain focused on communicating with patients,” the health system said.
A version of this article first appeared on Medscape.com.